
Acknowledgements
This paper was prepared for the Office of the Assistant Secretary for Planning and Evaluation (ASPE), U.S. Department of Health and Human Services (HHS), by David Cutler (Harvard University), Amber Jessup (ASPE/HHS), Donald Kenkel (Cornell University), and Martha Starr (U.S. Food and Drug Administration and American University). The contributions of Dr. Cutler and Dr. Kenkel were funded through subcontracts with Mathematica Policy Research. Amber Jessup is the HHS Project Manager.
This paper was informed by reviews of the research literature, discussions with prominent experts on health and behavioral economics, and original research. Valuable feedback on earlier versions of this work came from Frank Chaloupka (University of Illinois at Chicago), James Choi (Yale University), Sherry Glied (New York University), James K. Hammitt (Harvard University), Joseph Newhouse (Harvard University), and Kenneth Warner (University of Michigan), as well as a number of economists from HHS, FDA, Office of Management of the Budget, the Council of Economic Advisors and researchers from the Centers for Disease Control and Prevention. We are also grateful for the contributions of the numerous HHS and FDA staff who supported this effort, and to Lisa Robinson for valuable comments and advice.
Table of Contents
Acknowledgements
Table of Contents
Executive Summary
1.0 Introduction
2.0 Regulatory Context
2.1 Defining Addictive and Habitual Goods
2.2 Previous Analyses of Addictive and Habitual Goods
3.0 Economic Framework
3.1 Defining Rational Behavior
3.2 Conceptual Framework
3.3 Modeling Regulations
3.3.1 Regulations that Affect Information
3.3.2 Withdrawal versus Sustained Utility Losses
3.3.3 Regulations that Affect Price or Product Attributes
3.4 Summary
4.0 An Empirical Approach to Welfare Evaluation
4.1 Impact of Regulations on Cessation
4.2 Valuing Effects on Initiation
4.3 Population Estimates
5.0 Conclusions
References
Appendix 1: Alternative Approaches
A.1 Measuring Willingness to Pay
A.2 Calculating Compensating Differentials
A.3 Directly Measuring Effects of Smoking Cessation on Subjective Well Being
Executive Summary
In analyzing the value consumers place on goods, economic analysis begins with the presumption that consumers reveal their preferences through their consumption behavior. This view is based on the notion that consumers are well informed and well situated to rationally balance the costs and benefits of purchasing a specific good or service. Under these assumptions regulations that reduce consumption of a good or service necessarily result in utility or welfare loss.
There are several reasons to believe that consumption of addictive and habitual goods does not conform to the simple economics of consumer choice. First, consumers may not be fully informed about all costs, benefits and risks associated with such products. Information may be costly to acquire, complex and difficult to interpret. Or it may be deliberately distorted by companies aiming to promote their products. A second set of factors relates to the nature of the addictive and habitually-consumed products and ability to make rational choices. For example in the case of cigarettes young people may systematically misjudge or deny their likelihood of becoming addicted. Regular smokers may misjudge their ability to quit or underweight consequences of their consumption that occur in the distant future. Addiction and habituation will tend to make such errors in choice cumulate over time.
In analyzing economic impacts of regulations aimed at addictive and habitual goods, a particular challenge concerns the issue of lost utility, sometimes referred to as lost consumer surplus. Regulations that induce smokers to quit or that dissuade people from eating foods that are high in calories, fats, sodium, or sugars have health benefits that can be quantified using standard methods of cost-benefit analysis. But should cost-benefit analysis also account for lost satisfactions of consumption people experience when they reduce their intake of such goods? If so on what basis could we value such “utility offsets” to health benefits of regulations?
This paper develops a method for analyzing utility offsets to health benefits of regulations affecting addictive or habitual goods, with special emphasis on the case of smoking. The approach is analytically consistent with up-to-date representations of consumer behavior. It can also be implemented using existing data. The approach rests on identifying consumers most likely to be well-informed and to choose their consumption levels in ways that rationally weigh costs, benefits and risks. Then the values these consumers place on given levels of consumption can be used to estimate losses in utility that may result from regulations. Two different methods of identifying such consumers are used. The first takes smokers who do not meet criteria for nicotine dependence as the rational benchmark, on the grounds their consumption levels are less likely to be biased up by addiction. The second singles out smokers between the ages of 30 and 45 who have 4-year college degrees, on the grounds that they began smoking in an era when its health risks were well-known and that their education provides them with skills and knowledge relevant to accurately assessing benefits, costs and risks of smoking.
Using this framework, we show that utility changes caused by regulations depend in part on the type of regulation, as regulations that primarily increase information work somewhat differently than regulations that raise the cost of smoking. Utility changes also differ across categories of consumers. Existing smokers induced to quit by a regulation experience three potential utility effects: short-term withdrawal costs, utility loss from reduced smoking satisfactions, and money savings. The first two items are subtractions from health benefits; the third adds to them. The analysis is somewhat different for reduced initiation. Potential smokers dissuaded from starting by the regulation realize money savings, but they do not incur withdrawal costs or utility losses, since they never initiate. Finally, existing smokers who continue to smoke or potential smokers who continue to initiate are not affected by regulations that increase information without changing their smoking behavior. But regulations that increase the cost of smoking do reduce their utility because higher costs imply reduced consumption in general.
Our approach differs from two recent lines of work in this area. Unlike Ashley et al. (2015), we specifically analyze how regulations affect smoking initiation, showing that dissuading people from starting to smoke entails no utility offset. Unlike Chaloupka et al (2015), we recognize that existing smokers may experience utility losses even if they wish they had never started to smoke, because the preferences via which they evaluate utility changes reflect their consumption experience.
We use this approach to work through examples of potential regulations, illustrating how estimated utility offsets can be calculated. The empirical analysis shows that the utility cost of smoking cessation is small relative to the health gains in people for whom withdrawal costs are the main utility loss of quitting, and even among people who have some ongoing loss, the utility offsets represent 20-25 percent of the health gains. While marginal smokers induced to quit by regulations can be expected to have low or no steady-state loss, even this higher estimate is far below prevailing estimates of the utility cost of smoking used by FDA and other analysts. The net result is that there are clear offsets to health benefits from reduced consumer utility associated with reduced smoking, but they are far smaller than some recent estimates in the literature.
1.0 Introduction
Consumption of many addictive and habitual goods has significant health costs. In the U.S., smoking accounts for 480,000 premature deaths annually (CDC 2014a). Excess alcohol consumption resulted in approximately 88,000 premature deaths annually from 2006 to 2010 (CDC 2014b). And over 110,000 deaths were linked to obesity in 2000 (Flegal 2005). In this context, would regulations aimed at curbing smoking, drinking, or excess caloric intake be welfare enhancing? There can be substantial health benefits from policies that bring consumption of addictive and habitual goods down to levels consistent with maintaining good health. Yet consumers may also lose some satisfactions from their consumption if they cut back on goods they especially like. This makes it important to examine the extent to which expected health benefits from proposed regulations are offset by lost utility from consumption.
This paper investigates the question of whether there are utility offsets to health benefits of policies addressing consumption of addictive and habitual goods, and if so, how their monetary value can be estimated. We use smoking as an example to illustrate approaches that can be implemented given the data now available, and to identify the areas where more data and research are needed.
Typically, economists assume that consumers reveal their preferences through their actions. If people are well informed about the health risks of a good they consume, to themselves and people around them, and if they fully factor these costs into their consumption decisions, they will incur these health risks only if the ancillary benefits they receive exceed the health loss. 1 In this situation, a regulation that restricts access to a good would necessarily lead to a welfare loss.
However, with addictive and habitually consumed goods, consumption in the absence of regulation may not accurately reflect individual preferences and full and accurately-processed health information. This may occur because the consumer has only partial information or the available information may be inadequate or difficult to interpret, due to intentional distortions by industry or other factors. For example, advertisements that make smoking appear sophisticated, mature, or “cool” might induce people to smoke without fully considering the long-term health costs. It also may occur if consumers find it difficult to act in accordance with their preferences, instead acting impulsively and finding it challenging to exercise self-control, or reacting emotionally without carefully considering the consequences of their behavior. Examples abound – we make numerous decisions in the face of limited information, and often have problems eating less, exercising more, and engaging in other activities that are likely to provide significant benefits in the long run, even as we express a desire to do so.
In some cases, the product itself has attributes that make it difficult to consume in a rational way. This is a particular concern in the case of addictive or habitual goods. Even when people know about the long-term health costs of a product, they may believe that they will not become addicted, that the health harms will happen only to others, or that quitting will be easy when they are eventually motivated to do so. In such cases, regulation may aid individuals in becoming better informed and acting more in accordance with their own preferences.
For addictive or habitual goods, these mistaken understandings and difficulties in decision-making may compound over time. A person may try cigarettes without realizing the long-term health costs of smoking, and only realize those health costs after they have become addicted. The result can be large and growing differences between consumers’ true preferences and their behavior. In this set of circumstances, the utility loss consumers experience from reducing their consumption of the addictive good and replacing it with consumption of other goods may be very small, because the value of the utility they were receiving from consumption of the addictive good was not high to begin with. In this case, regulations aiming to reduce overconsumption of goods with adverse health consequences will be clearly welfare improving, as the health benefits will be large relative to any utility loss.
In this paper, we develop a framework for analyzing the utility consequences of regulations addressing addictive and habitual goods and apply this analysis to the empirical example of smoking regulations. Our preferred approach values the benefits of regulations based on data on individuals who are likely to be well-informed and behaving consistently with their own preferences, on the grounds that their valuation of consumption provides a good approximation to the utility it yields. We also consider ways in which this approach could be improved by further data collection and analysis, and identify other approaches that may be worthy of further development.
Before we present our analysis, we delineate some boundaries. First, our concern is with estimating benefits of regulations to individuals who consume the good or may potentially start to consume the good. Full benefit-cost analyses also consider the external consequences of consumption for non-consumers, such as second hand smoke or insurance costs associated with caring for sicker individuals, as well as costs to industry and government. These are important components of welfare analysis, but not the focus of our paper. Second, we are not centrally concerned with estimating the health gains to individuals of reduced consumption of addictive and habitual goods. Analysis of expected health benefits is best done in the context of specific regulations being considered. Rather our concern is with estimating possible utility offsets to those gains.
We begin in Section 2 with the regulatory context for government intervention. Section 3 lays out the economic framework for welfare changes of regulations affecting addictive or habitual goods. Then, in Section 4, we describe our approach for measuring potential utility offsets to health benefits of proposed regulations. Section 5 concludes and lays out a pathway for implementation. An appendix discusses alternative models that might be used for evaluation of addictive and habitual goods in the future.
2.0 Regulatory Context
HHS and its agencies are authorized to promulgate regulations under numerous statutes. Two are particularly relevant for the regulation of addictive and habitual goods: the Federal Food, Drug and Cosmetic Act (FD&CA) and the Family Smoking Prevention and Tobacco Act (TCA). The FD&CA gives the U.S. Food and Drug Administration (FDA) regulatory authority over most drugs, biological products, medical devices, and cosmetics and certain foods. The TCA gives FDA regulatory authority over the manufacture, distribution, and marketing of tobacco products to protect public health. As part of the federal rulemaking process, HHS and its agencies are required by Executive Orders 12866 and 13563 to analyze the benefits and costs of major proposed and final regulations. When implementing these Executive Orders, HHS and other agencies must follow analytic requirements developed by the U.S. Office of Management and Budget (OMB 2003).
Multiple impacts enter into the analysis of benefits and costs (Table 1). The benefits are the impacts on consumers, which in principle may be positive (like better health) or negative (like lost utility). Negative impacts may be treated as negative benefits or positive costs; it is a matter of convention which method is chosen, as the bottom-line calculation of net benefits to consumers will be the same either way. The current paper treats negative effects on consumers as negative entries on the benefit side.
Traditionally, total net benefits of a regulation are measured by consumers’ willingness to pay for its provisions, which measures what they are willing to give up (in terms of consumption of other goods and services) to gain the benefits of the regulation. For many HHS regulations, a major component of willingness to pay is the health improvements the population can be expected to experience. Health improvements include both increases in life expectancy and reductions in illnesses and chronic conditions that would flow from reducing consumption of the harmful product. Improvements may be experienced by both individuals who have been consuming the product and by others whose health has been adversely affected by being exposed to their consumption (e.g. via secondhand smoke). As noted above, we do not analyze external consequences of improved health associated with reduced use of addictive or habitual goods, and rather focus on individuals who consume the good or are deterred from consuming it.
Consumption decisions are not driven solely by health considerations. Other factors likely to affect willingness to pay include the utility people receive from consuming the product. For cigarettes, these may potentially include relaxation, increased attention, projecting a certain identity, or enjoying the experience of smoking. For foods that are high in calories, fats, or sugar, they may include taste, convenience, or brand loyalty. However, because curbing consumption of a good due to a regulation frees up money for spending on other goods, utility that consumers lose will be offset to some degree by utility gains from increased consumption of other products. The difference between the two is concept of consumer surplus.
The costs of regulations are typically measured as the compliance costs to industry and the monitoring and enforcement costs for government agencies. We do not estimate these costs in this paper. Rather, we focus on the question of how to value lost consumer surplus from policies addressing addictive and habitually consumed goods – the bold parts of Table 1. 2
Table 1: Examples of Benefits and Costs of Regulations
| Benefits | Costs |
|---|---|
| Impacts on consumers: | Companies’ costs of compliance: |
| - Longer life expectancy | - Product approvals and submissions |
| - Better health status | - Product modifications |
| - Reduced externalities (e.g. second-hand smoke) | - Redesigning labels or packaging |
| - Lower medical expenditures | - Product testing |
| - Loss in utility from forgoing consumption of the addictive good | Monitoring and enforcement costs to government |
| - Gain in utility from increased consumption of other goods |
While methods for estimating health benefits are relatively well-established, methods for estimating potential loss in consumer surplus are not. Ordinarily, economists assume that people will take the various attributes of products, including both health and non-health considerations, into account when they make consumption decisions. Health costs are like a non-monetary price paid along with the monetary price of buying the good. Thus, well-informed consumers should consider them the same way, and analysis should be able to use information on market demand for the product to infer the value they place on the good. However, information gaps or decision-making difficulties may break this link, especially for addictive or habitual goods. People may try addictive or habitual goods before they are fully informed about the addictiveness of the product or its health costs, or they may find the short-term withdrawal costs of ceasing consumption overwhelming even if the long-term health benefits are significant. These issues pose notable complications for estimating willingness to pay for addictive and habitually-consumed goods.
Several features suggest that current and potential smokers often do not fully incorporate or accurately value the negative health costs of consuming tobacco products. The first is the importance of decisions made when young. In the case of cigarette smoking, 87 percent of first use of cigarettes occurs by age 18, with nearly all first occurring use by age 26 (98 percent) (CDC 2014a). Research finds that youths are likely to overestimate benefits of risky activities and undervalue their risks more than is true for adults (Reyna and Farley 2006). They may also discount future consequences of their current actions by more than adults (Chabris et al. 2008). Indeed, research establishes the prefrontal cortex of the brain, which is responsible for cognitive analysis and abstract thought, does not fully mature until approximately age 25 (Gogtay et al. 2004; Galvan et al. 2006). Thus, there is an inherent suspicion of the rationality of youth decision making.
A good example of young people underestimating the health risks they run from smoking concerns their predictions of their future smoking. In a study of high school students in the 1996-2007 senior classes, 55 percent of students who were smoking daily said they would not be smoking five years later, but only 24 percent of them had in fact quit five years hence (CDC 2012: 249).
Adult smokers too seem to overestimate the ease of quitting. The 2010-11 Tobacco Use Supplement to the Current Population Survey asked current adult smokers, “If you did try to quit smoking altogether in the next 6 months, how LIKELY do you think you would be to succeed – not at all, a little likely, somewhat likely or very likely?” About 13 percent of everyday smokers chose “not at all”; 25 percent “a little likely”; 39 percent “somewhat likely”; and 24 percent “very likely.” In contrast, only 5-10 percent of cessation attempts are successful. Thus, even the “very likely” share alone overestimates quitting success (24 percent v. 5-10 percent), and the “very likely” and “somewhat likely” shares vastly overestimate it (63 percent vs. 5-10 percent). 3
Taken as a whole, the analysis shows that regulatory analyses need to directly address the degree to which regulatory-induced changes in consumption of addictive or habitual goods add to or subtract from welfare, rather than simply make assumptions based on economic theory.
2.1 Defining Addictive and Habitual Goods
According to the National Institute for Drug Abuse, addiction is a “chronic, relapsing brain disease that is characterized by compulsive drug seeking and use, despite harmful consequences. It is considered a brain disease because drugs change the brain; they change its structure and how it works. These brain changes can be long lasting and can lead to many harmful, often self-destructive, behaviors.”4
The concept of “habit” is less clear cut. Scientific and medical researchers tend to understand “habit” as a behavior engaged in automatically, without conscious thought. While habits generally involve compulsive behavior and may be rewarding or reinforcing, unlike addiction they do not typically involve tolerance, psychoactive effects, or withdrawal. Economically, addiction and habit are typically modeled as a situation where the marginal utility (or sense of satisfaction or well-being) associated with current consumption of a good depends on the stock of past consumption.
There are multiple validated measures of nicotine dependence, including the Fagerström Test for Nicotine Dependence (FTND), 5 the Wisconsin Inventory of Smoking Dependence Motives, the Nicotine Dependence Syndrome Scale, and the American Psychiatric Association’s Diagnostic and Statistical Manual (DSM). Analyses using all of these measures suggest that a substantial share of smokers is nicotine dependent. The Substance Abuse and Mental Health Services Administration (SAMHSA) estimates that 57 percent of past 30 day smokers in the National Survey on Drug Use and Health are nicotine dependent (SAMHSA 2013). 6 Further, survey data show that the majority of smokers want to quit but find it very difficult to do so. In 2010, 69 percent of adult smokers in the National Health Interview Survey said they were interested in quitting smoking completely, and 52 percent had a past-year quit attempt (CDC 2011).7 Yet only 6 percent had recently succeeded in quitting.8 Two-thirds of quit attempts were undertaken without smoking-cessation aids. Rates of successful quitting vary strongly with education: they were highest (11 percent) among smokers with an undergraduate degree and lowest (3.2 percent) among smokers with less than 12 years of education. This finding contributes to our definition of rational smoking below.
Although successful quitting is difficult, quitting attempts are frequent enough that a large share of ever smokers have quit. The share of U.S. adults who are former smokers now exceeds the share who currently smoke (21 vs. 18 percent; Blackwell et al. 2014). Among people in a given birth cohort, the prevalence of smoking declines with age, so by age 65 the share still smoking is substantially below its peak (Anderson et al. 2012). Annual probabilities of smoking cessation at any given age are also trending up (CDC 2014a: 729).
2.2 Previous Analyses of Addictive and Habitual Goods
Previous analyses illustrate the difficulty of estimating the changes in consumer surplus associated with regulations of addictive or habitual goods. For example, in 2004, FDA declared dietary supplements containing ephedrine alkaloids “adulterated” because they imposed unreasonable risks, effectively removing those products from the market (FDA 2004). FDA noted that some consumers would experience a loss in utility because the regulation forces them to move from their preferred (ephedrine-containing) product to a substitute (e.g., for weight loss or improved athletic performance). Because willingness to pay estimates were not available, FDA instead tested the sensitivity of its results to different assumptions about the premium consumers might be willing to pay for ephedrine-containing products, testing the impact of estimates ranging from 1 percent to 10 percent of the product’s price.
Another example is FDA’s 2014 proposed regulation revising the nutrition facts panel required on certain food items (FDA 2014a). The supporting analysis considered that, in addition to market failures (such as information gaps) consumers may find it difficult to behave consistently with their preferences, due to the difficulty of self-control and other problems. In such cases, the labeling changes could help consumers by making the nutritional properties of foods more salient at the point of purchase or consumption.
New regulatory authorities under the TCA pose the most significant and relevant challenges for HHS and FDA in measuring consumer surplus changes. Recent rulemaking efforts that addressed these issues include FDA’s analysis of the graphic warnings label rule for cigarettes (FDA 2011)9 and its 2014 proposed rule deeming various types of tobacco products to be subject to the TCA (FDA 2014b). Both rules rely conceptually on the framework set forth by the Australian Productivity Commission (2010) and Weimer et al. (2009). The Australian Productivity Commission addresses the benefits of gambling policies by distinguishing between “recreational” and “problem” gamblers and inferring the welfare benefits from the preferences of recreational gamblers. Weimer et al. apply a similar framework to cigarette smokers, estimating the benefits of tobacco regulations using a contingent valuation survey to elicit smokers’ preferences.
The analysis of Ashley et al. (2015) is most relevant to this paper. Ashley et al. adjust the discounted value of the health benefits of regulation downwards to account for estimated loss of consumer surplus, using parameter values based on simulations in Gruber and Köszegi (2001). They estimate that between 10 and 90 percent of the value of the health gains of reduced smoking is offset
by the consumer surplus loss.
These analyses have generated criticism. In particular, Chaloupka et al. (2015) critique the estimates of consumer surplus in the FDA’s (2011) analysis of graphic warning labels, asserting that analysts should not subtract positive aspects of smoking from health benefits of quitting for smokers who become regular users as minors, because minors have imperfect information and insufficient understanding of the addictiveness of nicotine. For these smokers, Chaloupka et al. suggest that the analysis should consider only the health benefits that accrue to consumers from quitting smoking. For smokers who initiate smoking as an adult, they conclude that there is too much uncertainty to quantify the consumer surplus losses associated with quitting, and the analysis should not include quantitative estimates of these effects.
In the following section, we aim to improve the analytical foundations of approaches used to analyze potential losses in consumer surplus when estimating benefits to consumers of these types of regulations. Our analysis departs in several ways from both FDA’s earlier analyses and the critiques of those analyses. These differences include an evaluation of changes in initiation as well as cessation, and direct consideration of the short-term withdrawal costs associated with cessation, relative to possible ongoing utility losses associated with continuing to smoke.
3.0 Economic Framework
Consumers may experience a number of changes in utility, both positive and negative, when they reduce their consumption of addictive or habitual goods. Table 2 presents some of the effects people experience when they reduce their consumption due to a regulation. People who are affected include both existing users who cut back or quit consuming the good, and people who are deterred from starting to consume it due to the regulation. On the negative side, people who reduce consumption of habitual goods face costs of changing their habits; for example, those who reduce their consumption of foods that are high in calories, sugars, or fat face costs of finding pleasurable alternatives. People who stop consuming addictive goods also bear withdrawal costs. For smokers, withdrawal symptoms include irritability, headaches, anxiety, insomnia, and difficulty concentrating (Hughes 2007); discomforts of withdrawal can be severe and explain the fact that most quit attempts fail within a week. Consumers also lose the satisfactions they received from consumption. In the case of smoking, this may include relaxation, enhanced attention, or weight control. In the case of foods, satisfactions may be pleasing taste, appetizing smell, or appealing appearance. If people value these attributes and are not readily able to find equally satisfying substitutes, then estimates of the effects of the regulation should include this loss. At the same time, consumers may experience gains in utility when they reduce their consumption of addictive or habitual goods. For example, smokers who kick the habit may lose feelings of self-loathing or embarrassment from being a smoker, and improve their sense of self-efficacy from having undertaken a difficult transition. Estimating the effects of regulations on consumers should try to value both negative and positive effects on utility.
Many of the benefits and costs of regulation are difficult to put dollar values on, since they are experienced in utility terms. Is a former smoker who quit because of a regulation that made smoking more costly better off than they would have been in the absence of regulation? Monetizing the net benefit is difficult and depends on how rationally smoking and cessation decisions are made.
Table 2: Examples of Positive and Negative Utility Effects on Individuals who Reduce their Consumption due to a Regulation
| Negative | Positive |
|---|---|
| For existing users: Costs of withdrawal or changing habits | Increased sense of self-efficacy, reduced self-loathing |
| Loss of positive attributes of consumption | Money freed up for spending on other goods |
| Loss of positive identity projection (being cool or defiant) | Loss of social stigma |
3.1 Defining Rational Behavior
Economists define a rational person as one making decisions that are optimal for them, in light of their preferences, information, and budget constraint. This includes rationally evaluating tradeoffs within a period of time (consumption of one good versus another) and tradeoffs over time (preferences for consumption today versus in the future), along with accurately acting on those preferences. This definition of rationality is not necessarily the same as used in other disciplines or everyday discussion. Throughout this paper, we use the economic definition of rationality.
Addiction by itself does not imply that people’s actions are irrational. Becker and Murphy (1988) developed a “rational addiction” model where consumers may choose to use an addictive good if the anticipated lifetime pleasures of the addictive good outweigh the correctly anticipated lifetime expenditures and health risks. Some support for the idea of rational smoking comes from the finding that, when people know cigarette prices will rise in the future, they tend to cut back on their current consumption, which would not be expected if smoking was driven solely by addiction (Chaloupka 1991, Gruber and Köszegi 2001). Thus, even if people are addicted to cigarettes and regret having ever started, their current decisions about continuing or stopping smoking need not necessarily be irrational.
Consistent with this definition, we conceptualize three groups of individuals (Table 3). The first group consists of people who rationally decide to start using the good based on time-consistent preferences and accurate information and expectations, and who also make rational decisions about their consumption levels after they have started. Given the issues associated with decision-making by young people noted above, this group is expected to be a small minority of all people who start smoking. A second group experiments with addictive goods and “accidentally” become addicted, in the sense that their lifetime utility (based on health and longevity as well as consumption) is lower as a smoker than it would have been as a non-smoker. But conditional on having become addicted, this group chooses its current consumption levels rationally. A third group starts using a good accidentally and then smokes “behaviorally.” Some may do so due to time-inconsistent preferences that cause them to wish to quit but find that withdrawal costs always induce them to put off cessation for another day. Others in this group may continue smoking due to inaccurate information, expectations, or beliefs.
Table 3: Groups of Consumers
| Group | Initiation | Subsequent consumption |
|---|---|---|
| * Assumes these people wouldn’t have initiated had they rationally evaluated the difference between their lifetime utility with and without smoking. | ||
| 1 | Rational | Rational |
| 2 | Accidental* | Rational |
| 3 | Accidental* | Behavioral |
In the case of smoking, there are several reasons to think that most initiation falls into the accidental category. First, most youths who start smoking do not initially enjoy the taste of cigarettes (Eissenberg and Balster 2000, O’Connor et al. 2005); enjoyment of smoking comes over time, co-evolving with nicotine addiction. Rather, most people initially begin smoking for attention, to look older, out of curiosity, to flaunt authority, or to fit in (CDC 2012, Chap. 4). Beyond the teenage years, these considerations decline in importance, and smoking initiation drops (recall that nearly 90 percent of smokers start before age 18). There is virtually no smoking initiation after the early 20s. Second, many smokers say they would like to quit, and most adult smokers say they wish they had never started (Fong et al. 2004). This near-universal expression of regret suggests that most smokers took on consumption of an addictive good without rational forward-looking consideration of its costs, benefits and risks. Thus, we expect the vast majority of smokers to be in Groups 2 and 3.
There are a number of economic theories that can explain why consumers may not act in accordance with their true preferences: (1) behavior may be driven by habit and impulse more than rational consideration; (2) preferences may not be consistent over time – for example, consumers may be overly sensitive to short term costs relative to long term gains; (3) consumers face challenges in fully understanding and internalizing the consequences of their consumption decisions; and (4) aggressive marketing may influence behavior. Much of the economics literature has focused on the first two of these.
Bernheim and Rangel (2004) develop a model with “hot” and “cold” states. In the cold state, people behave rationally, consistent with the standard model. They understand the consequences of their behavior and make decisions based on these consequences. When in a “hot” state, however, they respond based on habit and current impulses, which may not be related to rational calculation. Cues often shift people from the cold to the hot state; these may include seeing others using an addictive or habitual good that one once used, or being in a place associated with past use of the good. Because decisions are not consistently rational in this model, regulations can potentially improve welfare even without providing new information.
Other models focus on time-inconsistent preferences. Numerous studies have found that people are overly sensitive to short-term costs over long-term gains, often passing up significant long-term benefits because the short term costs are more salient. 10 For example, people have difficulty with increasing their savings rate despite stating that they should save more, adhering to lower-calorie diets despite a desire to lose weight, exercising at the gym despite paying costly membership fees, and other similar activities. In the classic example, people will continually defer signing up for a 401(k) plan, despite the fact that doing so has very little cost and significant benefits in retirement. People rationalize this behavior by asserting that they are not deciding not to enroll, but are simply putting off the enrollment for a short period of time. Regulation can help correct these behavioral problems – for example, by requiring people to decide on their 401(k) contribution by a certain date.
3.2 Conceptual Framework
We start with a formulation of why there may be excessive consumption of addictive and habitual goods and use that to consider how regulations affect welfare. Our framework applies equally to initiation as to cessation; we indicate in the next section how we implement each decision.
Consider people having a utility function of the form

where W is the discounted value of lifetime utility and Ut is the per-period utility function. We imagine there are two goods: an addictive good, with current consumption at, and all other goods ct, where ct = Y-Paat for constant income Y.11 Pa is the constant real price of the addictive good. St is the stock of addiction entering period t – typically a weighted average of past consumption. We normalize the weights so that at constant a over time (denoted by a̅ ),
 ; that is, the value of the existing stock is equal to the flow of annual consumption. pt+i(a) is the probability of survival to period t+i. It is conditional on the entire past history of consumption of the addictive good, denoted by a. If only the stock of smoking matters, a = St. More generally, smoking may affect health in a different way than it affects addiction. As well as affecting mortality, it also raises morbidity which can reduce per-period utility.
; that is, the value of the existing stock is equal to the flow of annual consumption. pt+i(a) is the probability of survival to period t+i. It is conditional on the entire past history of consumption of the addictive good, denoted by a. If only the stock of smoking matters, a = St. More generally, smoking may affect health in a different way than it affects addiction. As well as affecting mortality, it also raises morbidity which can reduce per-period utility.
For ease, we assume that utility is additively separable in the addictive good and all other goods, and that the marginal utility of all other goods is constant. This implies that Ut = v(at,St) + (Y-Paat). In the Gruber-Köszegi (2001) analysis, v(.,.) is quadratic in the two elements. For presentational simplicity, we assume a simpler formulation where v = v(α1 a t-α2S t). Following standard assumptions, v(.) is assumed to be concave. 12 α1 measures the extent to which consumption of the good increases utility per period. α2 reflects withdrawal. It is the extent to which today’s utility is lower if one consumed more of the good in the past, holding current consumption constant.
The function v(.) embodies the attributes of the product, not necessarily the product itself. In the case of cigarettes, this includes the nicotine it delivers, the relaxation it may convey, the feel in the mouth and hand, and the signals that cigarettes send to others. Empirically, this means that the price elasticity of demand for cigarettes may vary with substitutes for those attributes. For example, if e-cigarettes convey many of the same attributes as combustible cigarettes, the price elasticity of demand for cigarettes will rise when e-cigarettes are available.
The function v(.) may also vary with age. Teens may benefit from the rebellious image that smoking conveys, while adults may not. It is possible that α1 >0 for teens and α1≈0 for adults; this would correspond to a situation where a never-smoking adult may not derive any pleasure from smoking. One important case is where α1 = α2 . If this is true, there is no steady-state benefit to consuming the addictive good. That is, v(.,.) is the same at any constant a̅ , even a̅ =0. But there are withdrawal costs associated with moving from a higher a to a lower a, because reducing a below S would be utility-reducing. To avoid this withdrawal effect , so people may not make the change.
People discount the future in two ways. The first is the standard exponential discount rate, δ. To avoid excess notation, we assume that δ=1. In addition, some people have a preference for current utility over all future utility, captured in the parameter β. If β1, the individual is time inconsistent: they will continually delay making investments with up-front costs, even if they would agree ex ante that the investment is a good idea. Consumers with β=1 apply the same discount between the present and the near-future as they would between two adjacent periods in the future. Consumers with β1 apply an extra discount to all future periods relative to the present, so they will continually delay making investments with up-front costs, even if they would agree when thinking about what would best benefit them in the long-term that the investment is a good idea. Consumers with β1 are commonly referred to as hyperbolic (Laibson 1997).
Time inconsistent discounting will lead to suboptimal outcomes. Incomplete information about future consequences of current actions will as well. People may not understand the health costs of the addictive good (pt+i(a)) or how addictive the good is (α2 ). For simplicity, we assume people understand the addictiveness of cigarettes (i.e., perceptions of α2 are accurate) and examine the impact of inadequate understanding of the health cost of smoking – for example, the evidence that people do not appreciate how sick they will be at the end of life. We denote the perception of this variable p̃t+i(a). The individual’s optimal consumption of the addictive good can be found by maximizing utility.
This yields the first order condition:
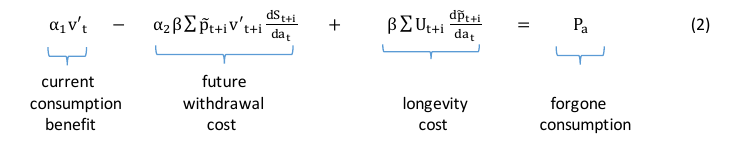
The first term on the left hand side of equation (2) is the current marginal benefit of consumption. That may involve direct consumption benefits or indirect benefits such as relaxation or weight loss. It also includes the change in health within a year – that is, health-related quality of life. The second term is the discounted value of the future withdrawal cost that will be caused by consuming more of the addictive good in the current period. These costs are only born for users of the good as they reduce consumption These costs decay in the future as the impact of current consumption on the future stock of addictive capital declines (i.e.,  declines with increasing i). The third term is the mortality impact – the reduction in lifetime utility from premature mortality due to smoking in period t. Note that
declines with increasing i). The third term is the mortality impact – the reduction in lifetime utility from premature mortality due to smoking in period t. Note that  so this term is negative.
so this term is negative.
At the optimum, the consumer will trade off the sum of these impacts against the cost of increasing consumption. This cost is the marginal utility of other consumption forgone, which is given by Pa.
Figure 1 shows a graphical version of this model that underlies the framework for valuing benefits and costs of regulations. As is the norm, we include the monetary price and health and longevity costs as costs, and the consumption benefits net of withdrawal as the value to the individual, though no practical difference in results depends on whether a health harm is termed a cost or a negative benefit. The demand curve thus reflects the first two terms on the left hand side of equation (2), and the remaining two terms are built into the cost. Because withdrawal costs vary with past consumption, so too will the value of current consumption. We start by assuming the individual has some addictive stock and draw the demand curve corresponding to that addictive stock. We return to the dynamics below.
The model can be applied for both existing users of the good and for potential initiators, although the implementation differs between the two cases. Considering existing users first, we delineate two types of individuals with otherwise similar characteristics (age, gender, etc.): type I consumers who make smoking decisions in a way that is fully rational and fully informed (β=1 and p̃t+i=pt+i); and type II consumers who have time inconsistent preferences (β1) or misperceive how their current actions will affect their future choices and health risks (p̃t+i≠pt+i). Relative to Table 3, both group 1 and group 2 consumers fall in the type I category; group 3 consumers are all type II.
The demand curves of the two types of consumers are shown by DI and DII respectively; these demand curves can reflect either the share of people who use the good or the total number of units used by those individuals, each of which will vary with price. For type I individuals, the demand curve reflects the value of consumption to the individual – the first two terms on the left hand side of equation (2). For type II individuals, the demand curve may differ from the true value to the extent that people have difficulty making their actions match their intentions. If type II individuals find it hard to reduce consumption when that is desired, DII will be farther out than DI .
There are two prices to consumption: the health cost, which we denote Ph, and the market price of the good, Pa. For example, Gruber and Köszegi (2001) estimated that the health cost far exceeded the monetary cost -- $30 per pack in health cost versus $5 per pack in monetary cost at that time.13 Given these prices, consumers from the two groups will choose to consume QI and QII respectively. QI and QII would also differ if type II individuals misperceive the full health cost to using the good. For example, if type II consumers do not perceive any health cost to using the good, the equilibrium will be where their valuation of the good is equal to the monetary price of the good, Pa. This result is shown as QII in Figure 1. If they misperceive some of the cost, QII will be lower, but still above QI.
Figure 1. Equilibrium with two types of consumers
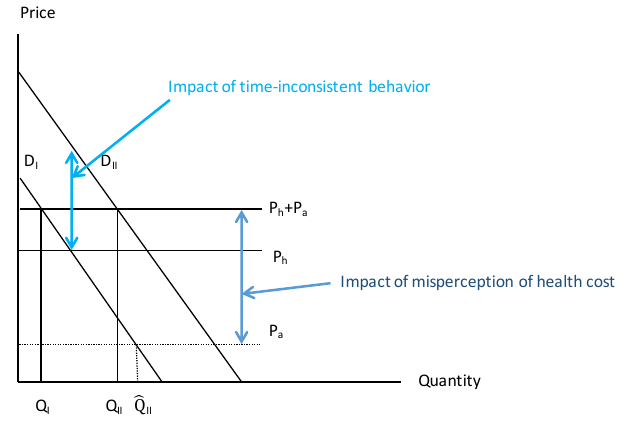
With some change in interpretation, Figure 1 also models the smoking initiation decision. DI corresponds to group 1 in Table 3 – the (presumably very small) group of people who start smoking rationally; DII reflects demand from groups 2 and 3. The figure would then show the share of people in each group who choose to smoke, or equivalently the number of cigarettes among each type of potential smoker.
Regulations induce some individuals to stop smoking and others to avoid initiation. The longevity benefits of this regulation are picked up by the third term in equation (2), corresponding to Ph in Figure 1. The relevant issue for our analysis is how to value the offset from lost pleasure of smoking. We discuss this in the context of Figure 1.
3.3 Modeling Regulations
In carrying out its responsibilities for regulating food, tobacco, drugs, and other products, FDA may issue several types of regulations that could affect consumers. First, some regulations change the information available to consumers (as with ingredient labels), or the salience of the information (as with graphic warning labels), in the interest of fostering well-informed consumer choice. Second, regulations may require producers to change how they manufacture, distribute, or market their good, usually aiming to better satisfy public-health or safety concerns. If such a change increases producers’ costs, the higher costs may be passed through to consumers in the form of higher prices. Third, regulations that change how products are marketed, distributed, or sold may require consumers to spend more time or money acquiring goods. For example, limiting vending machine sales of cigarettes reduces the density of
potential places to buy cigarettes, so consumers have to spend more time finding an alternative outlet. This is in effect an increase in the implicit price of the good, because the total cost to the consumer of acquiring it (the money cost plus the time cost of acquiring it) has increased.
Fourth, some regulations may require companies to alter or eliminate product attributes that people value, such as flavors or packaging, perhaps in the interest of reducing smoking initiation by youth. Conceptually a reduction in valued attributes can also be understood as an implicit price increase for the good. For example, if a regulation requires companies to remove flavors from cigarettes, and people who liked flavors switched over to electronic cigarettes to continue smoking flavored products, the implicit price of smoking rises for them, as they would now have to consume two different products (non-flavored combusted cigarettes plus flavored e-cigarettes) to get the same cluster of attributes they previously consumed in one.
Finally, FDA may issue jurisdictional or administrative regulations that clarify regulatory procedures or formalize the scope of its regulatory authority (like the deeming rule). Regulations in this category will usually have relatively small direct effects on consumers, as they usually intend to facilitate implementation of other regulations or enable smooth functioning of regulatory processes broadly, rather than altering consumption experiences of end-users of the product.
Economically, these regulatory activities fit into two groups: those that affect information and those that affect prices, where the price increase may be explicit (e.g., higher manufacturing costs that are passed along to consumers) or implicit (higher search or acquisition costs to achieve the same benefits). We discuss each of these below. We further differentiate between the impact of regulations on existing users and on potential new users.
3.3.1 Regulations that Affect Information
We start with regulations that increase the amount or salience of information about health effects. Information about some of the major harms of smoking, such as risks of lung cancer and heart disease, has been widely available for some time, making it tempting to ignore this issue in the case of cigarettes. An important line of economics research suggests that consumers accurately perceive the mortality risks of cigarette smoking, if not over-estimate them.14 However, it is not clear that current regulations can be interpreted as occurring in a context of full information. Even if consumers are aware of the major health risks associated with cigarette smoking, it is more difficult to assess whether they understand the severity of health risks, or whether information they know remains salient enough to affect their choices. Consumers also may not understand how population risks associated with smoking apply to them.15 Finally, the scientific research on the health risks of tobacco products is evolving, especially for novel products like e-cigarettes, and consumer knowledge may not fully reflect the evolving understanding.16
Suppose that type II consumers have a difficult time giving up cigarettes or not initiating smoking, but regulations help them do that (perhaps by highlighting the salience of poor health outcomes later in life). Also suppose that after the regulation comes into effect, type II consumption is denoted Q'II. The welfare of type II consumers would be affected in three ways. First, they would save money on the packs of cigarettes they no longer buy. This is the right hand side of equation 2 and is shown as the green rectangle in Figure 2 – the retail price per pack times the reduction in consumption. The entirety of the green rectangle is a benefit to consumers, but not all of it is a social benefit. Notably, the reduction in demand reduces tax payments to governments and sales revenues for producers, so that part of the saving by consumers comes from a transfer of resources away from governments and producers. While a full regulatory impact analysis would subtract losses to governments and producers from the benefits to consumers to derive the social benefit, the full amount of the savings to consumers is of interest here due to our focus on the benefits part of the analysis.
Figure 2. Welfare with a Salience-Based Regulatory Intervention
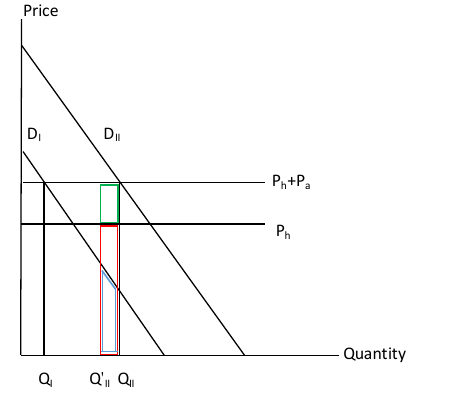
Second, there is the health benefit of reduced consumption. This is the expected health cost per unit consumed times the reduction in units consumed, the red box in Figure 2. Third, there is a utility change associated with reduced consumption. This includes the first two terms on the left hand side of equation (2). Graphically, this change in utility corresponds to the blue area under the type I demand curve for the addictive good between QII and the new level of consumption. The key is that the demand curve to use to value this change is that of the rational consumer (type I), not the consumer with behavioral difficulties (type II). The reason is that the rational consumer’s demand reflects the true value of smoking to the individual.
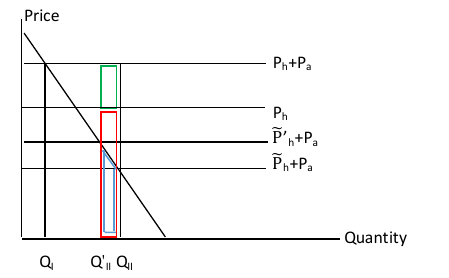
Figure 2 shows a situation where the regulation affects consumption by encouraging consumers to shift their smoking towards the rational standard. We can alternatively model the regulation as affecting the information that consumers have. Figure 3 shows the situation where all intentions are accurately acted upon, but type II consumers do not appreciate the full health cost of smoking – they perceive health costs to be  rather than Ph. With only an informational problem, there is only a single demand curve. But there are two equilibrium quantities, QI, which reflects demand among those who correctly perceive the health cost of smoking, and QII, which reflects demand among those with inaccurate perceptions. A regulation that increases the information available to type II consumers – for example, increasing their perception of health costs to
rather than Ph. With only an informational problem, there is only a single demand curve. But there are two equilibrium quantities, QI, which reflects demand among those who correctly perceive the health cost of smoking, and QII, which reflects demand among those with inaccurate perceptions. A regulation that increases the information available to type II consumers – for example, increasing their perception of health costs to  – will reduce their consumption to Q'II. The welfare calculation will be quantitatively the same as the previous case because the market price is the same and the correct health benefit to consider is the true health cost (Ph), not the inaccurate initial impression of health costs.
– will reduce their consumption to Q'II. The welfare calculation will be quantitatively the same as the previous case because the market price is the same and the correct health benefit to consider is the true health cost (Ph), not the inaccurate initial impression of health costs.
Figure 3. Welfare with a Regulation that Affects Knowledge of Health Harms
3.3.2 Withdrawal versus Sustained Utility Losses
Figures 2 and 3 are set in a single time period. The dynamics are more complex than this static analysis, however, because the utility consequences of changing consumption vary over time. In the short run, the biggest utility consequence of reduced consumption is withdrawal costs, which are high at first but smaller in later years. Over time, the costs are more heavily focused on foregone consumption value, which are initially lower but need not decline.
Analytically, this distinction is seen in the first two terms in equation (2). Imagine a consumer who has been consuming ahigh for a number of years – long enough for the stock of past consumption (St) to equal ahigh . The annual benefit of consumption is then v((α1 -α2 )*ahigh ). Now suppose regulation induces the individual to switch to a low. The steady-state benefit of consumption is v((α1 -α2)*alow). The loss in steady-state utility from the reduction in smoking is approximately (α1 -α2)*v'*(alow -ahigh). If α1≈α2 – that is, the major benefit of continuing to smoke is avoiding the withdrawal cost – there is very little steady-state loss to reduced consumption. But moving to that point involves withdrawal costs, which are given by ∑ v (α1 alow − α2 St+i). These costs may be significant.
To understand the situation graphically, we need to consider the dynamics of demand. If a person stops or cuts back on smoking, their stock of addictive capital declines in the future. This will lead to a shift down in the demand curve (the same utility is achieved at lower consumption). This process continues until the addictive stock reaches its new, lower level.
Figure 4 shows the new equilibrium. The demand curve D’I is the value of cigarette consumption in steady state, when the stock of addictive capital has declined to its long-run level. The downward slope to the demand curve is consistent with α1 >α2; some type I individuals value the addictive or habitual good, even beyond avoiding withdrawal. Even still, the value of consumption is lower than in the short-run demand curve, DI because in the long-run there are no withdrawal costs. As is apparent, the steady-state welfare loss is much smaller than the short-run welfare loss, because withdrawal costs are only experienced in the short-run.
Figure 4. Welfare Accounting for Withdrawal Costs
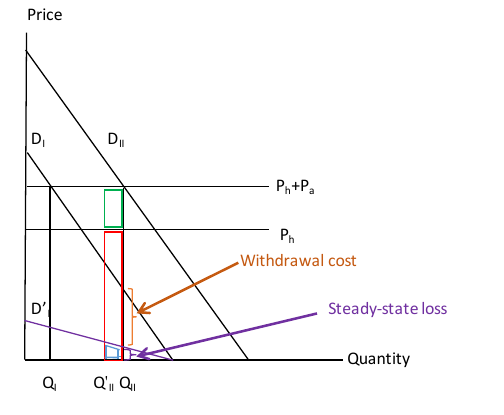
Distinguishing between withdrawal costs and steady-state welfare losses cannot be done without knowing α1, α2 , and the evolution of St. Theoretically, we might expect that the division between withdrawal costs and long-run utility offset would differ across addictive and habitually consumed goods. In the case of smoking, a natural benchmark for the long run is that the only cost of regulatory-induced smoking reduction is the withdrawal cost, and that smoking itself conveys no utility benefit (α1 =α2 ). Thus, the long-run per-period utility offset is zero. This is consistent with the view that few people ever start smoking as adults – the benefits are not sufficient to warrant it. 17 Another rationale for this benchmark is that some people may benefit from regulatory induced-changes in consumption even more than the health consequences suggest. Many smokers who quit experience improvements in self-worth or reductions in self-loathing after they quit (Piper et al. 2012). These costs are not shown in Figure 4 but are real. It is unknown how many people experience improvements in self-regard relative to the share that experiences losses from not smoking at their former level.
In practice, we use several methods to approximate the short run utility loss of reduced consumption of cigarettes, including using physiological and psychological data on the process of withdrawal to estimate the quality of life implications of changes in smoking and examining long-run shares of type I and type II consumers who smoke.
3.3.3 Regulations that Affect Price or Product Attributes
A second category of regulations is those affecting the product price, explicitly or implicitly. As mentioned, regulations that affect producers’, distributors’ or retailers’ costs may increase the explicit price of the product paid by consumers. Regulations that restrict marketing channels for tobacco products or remove valued product attributes implicitly increase the price consumers pay to acquire the same product as before or to acquire the same bundle of product attributes as they did previously. Thus, the point of departure for analyzing this category of regulation is to estimate how the regulation affects the product’s effective price.
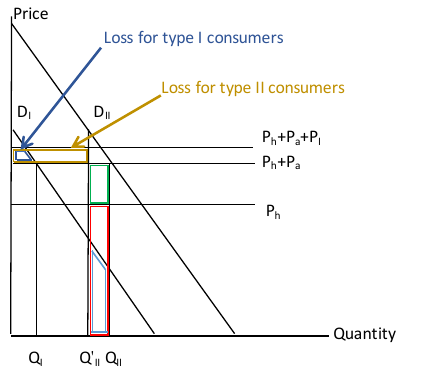
The economics of an implicit price increase are shown in Figure 5. Suppose that a regulation increases the implicit price of the product from Ph+Pa to Ph+Pa+PI. The welfare consequences for those who choose to stop consuming are the same as in Figure 3: there are cost savings, health benefits, and a utility loss. There is an additional cost, however, corresponding to the higher implicit prices paid by the type I and type II consumers who continue to use the good. For example, if regulations require people to smoke outdoors, the cost of being outdoors in cold climates is a cost that needs to be counted. Both groups suffer a loss equal to the implicit price increase multiplied by the number of units they consume in the new equilibrium. Here there is also a loss for type I smokers, who forgo utility benefits for the units of the good they no longer consume because of the higher price.
Figure 5. Welfare with Regulatory Intervention that Increases the Product Price
One case of particular note is regulations that affect the attributes of goods, for example those changing flavors like menthol or other characterizing flavors.18 The effective price increase from such a regulation can be determined by the change in demand combined with the demand elasticity; alternatively the effective price may be estimated directly then used to project the change in demand expected to be caused by the regulation. This price increase would then be applied to people for whom the flavor was a key part of the value of consumption. Whether such regulations are beneficial or harmful on net depends on the benefits of reduced consumption relative to the cost of raising prices for goods that people would otherwise consume.
3.4 Summary
There have been a variety of estimates of the welfare consequences of regulations affecting addictive and habitual goods, particularly tobacco use. On the one hand, FDA (2011) and Ashley et al. (2015) argue that 10 to 90 percent of the health benefits of smoking could be offset by the lost pleasure from smokers consuming less. On the other hand, Chaloupka et al. (2015) argue that because most smoking is initiated while people are teens, when decisions are unlikely to be rational, there should be no utility offset for smoking reduction.
Our analysis shows that neither of these analyses is complete. Relative to the approaches in the literature, we make three innovations. First, we show that reduced spending on smoking should be included in the benefits to consumers along with health benefits. Reducing consumption of addictive and habitual goods saves consumers a significant amount of money that would otherwise have been spent on the addictive or habitual good. Not all of this saving is a social benefit because it comes out of sales revenues of companies and tax revenues of governments. But the money savings properly belong in the benefits to consumers.
Second, we divide the utility offsets of reducing consumption into two components: the short-term costs of withdrawal, and the steady-state benefits of not consuming a good. The withdrawal costs are real; most smokers make several attempts before they quit the habit. After withdrawal has been achieved, however, the losses from not smoking on an ongoing basis may be much smaller. It is important to estimate both the short-term and the steady-state utility costs of regulatory-induced changes in consumption.
Third, there may be additional costs for people who continue to consume the addictive or habitual good even after the regulatory intervention. Regulations that increase the cost of the addictive good – for example, making it less attractive or more difficult to obtain – impose real costs on these individuals and these costs need to be counted. Not all regulations affect cost for continuing users, and some impose costs for only some individuals. But costs that are imposed on consumers need to be understood and evaluated.
4.0 An Empirical Approach to Welfare Evaluation
Modeling the impact of regulations empirically is complex when observed behavior is not a full guide to utility. Chetty (2015) lays out three approaches to welfare analysis in such a setting. First, analysts can measure actual utility as it is experienced (termed ‘experienced utility’) and use that instead of the more conventional ‘decision utility.’ For example, an individual may believe they will be worse off if they stop smoking, but in actuality may be better off. The actual experience will measure this better than pre-cessation predictions. Some research examines how smokers’ subjective well-being changes when they quit – an approach that could potentially be useful for directly measuring utility offsets to health benefits of regulations.19 However, methods of quantifying changes in subjective well-being and translating them into monetary values are not sufficiently well-developed at present to be able to use results from existing work in cost-benefit analysis.20
Second, analysts can parameterize an explicit model of utility and use that to estimate welfare losses. This is the approach taken in Gruber and Köszegi (2001) and approximated in Ashley et al. (2015). A key problem with this approach is that calculations that result from it are highly sensitive to the parameterization of the time consistency problem and to assumptions about smokers’ expectations and beliefs.21 It also analyzes utility losses of existing smokers only; if a regulation works in part by deterring initiation, and utility losses of deterred initiators are small compared to those of existing smokers,
analyzing the latter only may overstate utility loss in the full pool of people affected by the rule.
Third, analysts can find groups of people believed to be making rational decisions and compare their behavior to that of the entire population. The difference in behavior between these groups is then a guide to the impact of regulations that encourage people to shift their behavior towards the rational benchmark. Largely for data reasons, we focus on the third of these methodologies in this paper. The appendix discusses other approaches that could also be used to quantify non-health effects in a cost-benefit context.
4.1 Impact of Regulations on Cessation
In this section, we address the empirical question: if some smokers are induced by regulation to stop smoking, how do we measure the utility consequences of the consumption change other than those associated with better health and longer life expectancy?
Our analysis is based on the demand curves analyzed above, so we start with empirical formulations of those curves. The data on smoking that we employ are from the 2010-11 Tobacco Use Supplement to the Current Population Survey (CPS-TUS), conducted by the U.S. Census Bureau. These data contain information on adults’ current and former smoking status, and various measures of addiction and desire to quit smoking.
We start with the short-run demand curves – demand curves among those who are current smokers of cigarettes. The average smoker in the CPS-TUS consumed 230 packs of cigarettes annually, and the average retail price of cigarettes in 2010-2011 was $5.43 (Orzechowski and Walker 2012). Thus, the demand curve for the average smoker must pass through this point. Consistent with existing research on the elasticity of demand for cigarettes (Chaloupka and Warner 2000, Gallet and List 2003), we assume a price elasticity of -0.3. As in our theoretical description, we linearize the demand curve around the equilibrium values. This implies a slope of dP/dQ = -0.079. We assume this slope applies for both type I and type II smokers.
Delineation of type I and type II consumers
To measure the utility cost of smoking, we need to differentiate between type I and type II smokers. There is no perfect division of the population into these two groups, since we do not know whose smoking behavior is rational or not (in an economic sense) for large segments of the population. In the absence of better information, we make two main cuts at the delineation between type I and type II smokers, shown in Table 4, with some additional insights from a third. Our first distinction is between those who have clear addiction to cigarettes and those who do not. This division of the population is consistent with the methodology of the Australian Productivity Commission (2010), which compared gambling rates among problem gamblers and non-problem gamblers. A widely used measure of nicotine addiction is whether the person has their first cigarette within one-half hour of waking (CDC 2000). We define type I smokers as those who do not have their first cigarette within one-half hour of waking, and type II smokers as those who do.
By this definition, 56 percent of current smokers are type I and 44 percent are type II. 22 Type I and II smokers differ in systematic ways. Compared to type II smokers, type I smokers are younger (average age of 41 vs. 45), better educated (15 percent with a college degree vs. 9 percent), and higher income (18 percent with a family income above $60,000 vs. 14 percent). Type I smokers also consume fewer cigarettes than type II smokers: 152 packs per year compared to 327 packs per year. Some of this difference is due to differences in demographics between the two groups, but not the bulk of it; for example, using a Tobit model to control for differences in demographics across groups, the unadjusted difference of 175 packs per year corresponds to 154 packs per year (results not shown).
Our second empirical proxy for type I and type II smokers uses demographic information that is generally associated with more rational economic behavior. We consider type I smokers to be people age 30-45 having a college degree or more, and type II smokers as those over age 45 or age 30-45 without a college degree.23 Age and education pick up both access to information and the ease of acting on that information. Individuals in the 30-45 age range began smoking well after the health risks of smoking became well-publicized and thus had better information with which to make decisions.24 Further, having a college education correlates with the time and ability to process scientific information about risks and with greater resources enabling people to carry through on forward-looking decisions.25 Since education decisions are not yet final for much of the population below age 30 and full economic rationality for part of that group is suspect (as noted above), we omit them from this analysis. Not surprisingly, smoking decisions vary greatly across these groups. Type I smokers smoke 162 packs per year, compared to 250 packs for type II smokers.26 Type I smokers are only 6 percent of the smoking population age 30 and above. Clearly this delineation does not fully reflect the type I population but rather captures a segment whose behavior may best approximate the rational benchmark. To the extent that many other people are rational smokers but are grouped as not fully rational, this will bias us away from finding any large difference between the groups, thus overstating the potential losses from smoking cessation.
Table 4: Alternative Delineations of Type I and Type II Smokers
| Degree of Addiction | Age and Education | Quit Intentions | ||||
|---|---|---|---|---|---|---|
| Type I | Type II | Type I | Type II | Type I | Type II | |
| Not nicotine dependent | Nicotine dependent | Age 30-45 and 4-year college degree or more | Age>45 or age 30-45 and less than 4-year college | Quit smoking or smoking without trying to quit | Trying to quit | |
| Current smokingstatus | ||||||
| % in current smoking population | 55.9% | 44.1% | 5.6% | 94.4% | --- | --- |
| # packs per current smoker | 152 | 327 | 162 | 250 | --- | --- |
| Long-run cessation | ||||||
| % of ever smokers who currently smoke | --- | --- | 34.4% | 42.0% | 32.4% | 100% |
| # packs per ever smoker | --- | --- | 56 | 105 | 89 | 173 |
| Initiation | ||||||
| % ever smoker | 19.9% | 39.8% | ||||
| % with sustained initiation | --- | --- | 6.9% | 16.7% | --- | --- |
| # packs per potential initiator | --- | --- | 11 | 42 | --- | --- |
We now consider two types of regulatory interventions: a first which helps smokers align their actions with their preferences but without affecting cigarette prices (perhaps increasing the salience with which health information is conveyed); and a second that can be thought of as imposing an implicit tax on smoking. For concreteness, we assume that each intervention reduces demand among smokers by 10 percent -- for example, by leading 10 percent of existing smokers to quit. In the case of a salience intervention, all of the reduction in demand would occur from type II individuals. In the case of an implicit price increase, both type I and type II individuals would be affected.
Impact of a salience-based intervention
The welfare effects of a policy that helps type II smokers align their behavior with their true preferences can be measured in three steps, which are shown in the top left panel of Table 5. The first impact is the health benefits, including both improvements in morbidity and mortality. A large research literature shows that smoking adversely affects length and quality of life (CDC 2014a). As a basis for gauging how the magnitude of utility offsets compare to health benefits, we compute standard estimates of benefits to a smoker of quitting now relative to continuing to smoke, in terms of both reduced mortality only and mortality and morbidity together.27 Valuing health benefits in dollar terms requires two additional parameters: the discount rate and the value per quality-adjusted life year (QALY). We use the two discount rates, 3 percent and 7 percent, recommended by OMB (2003) in its guidelines for conducting cost-benefit analyses of federal regulations. In line with a recent review of high-quality research on values per statistical life (VSL) (Robinson and Hammitt 2015), we anchor our estimates of the value per QALY in VSLs of $4.3 million and $9.3 million; accounting for age-related changes in the health-related quality of life, these estimates imply values per QALY of $220,000 and $480,000 at a 3 percent rate, and $370,000 and $790,000 at a 7 percent rate. For a 35-year old smoker, the results (in the first row of Table 5) show that continuing to smoke has health costs of about $200,000 to nearly $1.5 million for a 35-year old smoker, depending on the assumptions used.
Second, there is the money saved. Smokers who quit save $5.43 for every pack they do not buy. Multiplying times the average packs per type II smoker in Table 4, the money savings is $1,776 per yearin the addiction-based delineation and $1,358 per year in the age/education delineation. For simplicity, we take the central value to be about $1,500 per year.
Finally, there is the utility offset from reduced smoking. The first step in estimating the utility offset from the demand curve is to estimate the implied value of cigarettes for type I consumers. Recall that our goal here is to measure the value of smoking to type I individuals at the current level of consumption of type II individuals (see Figure 2). We can calculate this using the slope of the demand curve and the gap in cigarettes consumed between type I and type II consumers. Because cigarettes consumed differ in the addiction and age/education frameworks, the implicit valuation for the type I consumers at that point is slightly different.
The exact dollar value depends on the health costs that type I smokers perceive. To approximate expectations of the health cost per pack for type I smokers, we use estimated effects on longevity and health described above, divided by the average number of packs smoked per year computed from the 2010-11 CPS-TUS. As shown in Table 5, when both mortality and morbidity costs are taken into account, estimates of the health cost per pack range from $48 to $174, depending on assumptions about the discount rate and value per QALY. Given the slope of the demand curve, we can determine how much lower prices would need to be for type I consumers to smoke at the level of type II consumers.28 We estimate the price reduction to be $7-14 per pack. Multiplying the implied value of a pack of cigarettes by the number of packs given up yields utility losses ranging from $5,500 to $54,000 for smokers who quit (the middle block of table 5). Focusing on results with both morbidity and mortality costs of smoking, we take the central value to be $25,000.
Table 5. Estimated utility losses from quitting using the demand approach for a 35-year old smoker
| VSL of $4.3 million | VSL of $9.3 million | |||||||
|---|---|---|---|---|---|---|---|---|
| 3% discount rate | 7% discount rate | 3% discount rate | 7% discount rate | |||||
| Notes: Values per statistical life are from Robinson and Hammitt (2015). Values per quality-adjusted life year (QALY) are adjusted to reflect age-related changes in health-related quality of life (Hanmer et al. 2006). In analyses including morbidity, smoking is assumed to reduce the QALY by .05 (from Jia and Lubetkin 2010); after a person quits, the discount is assumed to fade out over the next 5 years. Expected lifetime health benefits of quitting are co mputed by taking the difference between the expected present discounted value of future QALYs if the person quits, to that if the person continues to smoke until death. Data on mortality risks are taken from Arias (2014, Table 1); data on relative risks for current and former smokers are from Vugrin al. (2015, Appendix). To compute implied health cost per pack, we divide the expected lifetime health benefits of quitting (i.e. the cost the person would incur by continuing to smoke) by the expected number of packs the person would smoke: this is the expected additional number of years the person would smoke, times 232 packs per year (average packs per year, computed from the CPS-TUS). In estimates allowing for the possibility of ongoing utility losses from quitting, the loss is assumed to be 100% of the dollar value in the year when the smoker quits, 50% the next year, and 25% thereafter. | ||||||||
| Health benefits includedin estimate | ||||||||
| Mortality | yes | yes | yes | yes | yes | yes | yes | yes |
| Morbidity | no | yes | no | yes | no | yes | no | yes |
| Estimated health benefits of quittingnow | ||||||||
| Expected lifetime health benefits | $462,400 | $669,400 | $209,000 | $403,900 | $1,008,800 | $1,460,500 | $446,300 | $862,300 |
| Implied health cost per pack | $55 | $80 | $25 | $48 | $120 | $174 | $53 | $103 |
| Utility loss of existing smokers who quit | ||||||||
| Addicted v. not | $15,300 | $23,400 | $5,400 | $13,000 | $36,500 | $54,200 | $14,600 | $30,900 |
| Age/education | $13,400 | $19,600 | $5,900 | $11,600 | $29,600 | $43,100 | $12,900 | $25,400 |
| Utility loss as % of lifetime health benefit | ||||||||
| One-year loss: | ||||||||
| Addicted v. not | 3% | 4% | 3% | 3% | 4% | 4% | 3% | 4% |
| Age/education | 3% | 3% | 3% | 3% | 3% | 3% | 3% | 3% |
| Ongoing loss of 25% of first-year value | ||||||||
| Addicted v. not | 23% | 24% | 18% | 22% | 26% | 25% | 23% | 24% |
| Age/education | 20% | 20% | 20% | 19% | 21% | 20% | 20% | 20% |
Withdrawal costs and steady-state utility loss The component of the utility offset due to withdrawal will decline over time, as the stock of addictive capital declines. Estimating the component of this cost which is due to withdrawal is difficult. We make several passes at this.
A first pass is to see whether there are significant numbers of type II individuals for whom the marginal value of smoking seems to be entirely to avoid withdrawal. Evidence suggests this is the case. As noted above, two-thirds of current smokers say they want to quit, and 52 percent have made a quit attempt in the past year. Likely because of high withdrawal costs, most of these attempts have been unsuccessful. One interpretation of this evidence is therefore that about half the current smokers smoke only because the cost of withdrawal is high.
A second way to estimate the withdrawal cost is to estimate the QALY losses from symptoms frequently encountered during nicotine withdrawal and value those QALY losses in dollars. People who quit smoking may have a combination of anxiety, depression, headache, insomnia, and other symptoms. Research suggests that symptoms are most acute in the first month, and then decline progressively for most of a year (Hughes 2006). By one year post-quitting, there are few physiological symptoms of withdrawal. Since anxiety is among the most common side effects, we parameterize the utility loss as equivalent to a clinical case of anxiety. Sullivan et al. (2005) estimate a decrement of 0.0421 in health-related quality of life resulting from anxiety. We assume the full decrement occurs in the first month of smoking cessation, then it gradually phases out over the next year.29 Adding up over a year, this implies that the QALY loss from a single successful quit attempt is 0.0087.
Quitting smoking often takes multiple attempts. The majority of smokers (75-80 percent) attempting to quit relapse within 6 months, and relapses may continue to occur even after years of abstinence (Zhou et al. 2009). Hughes et al. (2004) estimate 10 to 14 attempts to quit based on a 5 percent or 3 percent success rate, with 50 percent of smokers quitting at some point. Data from the 2010-11 CPS-TUS show that 60 percent of everyday smokers who had made a quit attempt in the past year made two or more attempts.30 We thus assume two attempts per year and a total of 10 attempts before a successful quit, so that the average successful quit occurs over 6 years.
Failed quit attempts are likely to be shorter and less distressing than an eventual successful quit. Using data on the length of unsuccessful quit attempts (Hughes 2006), the average failed quit is assumed to involve approximately one-fourth of the QALY loss smokers experience from a successful quit. We assume this value applies to all failed quit attempts. The combined QALY loss from the sequence of failed attempts before a successful quit is thus .02175 (undiscounted).31
Using the values per QALY discussed above, the net result is that the cost of withdrawal symptoms from smoking cessation ranges from $6,200 with a $220,000 value per QALY and 3 percent discount rate, to $20,100 for $790,000 value per QALY and a 7 percent discount rate. Given the shortness of the time period, the discount rate matters less than the VSL used. We take the central value of the withdrawal cost to be $12,500. By comparison, if we had assumed that withdrawal was equivalent to depression rather than anxiety, the utility cost of withdrawal would be about $18,600.32 A reasonable estimate is likely in this range.
Table 6. QALY loss due to withdrawal, by VSL and discount rate
| VSL of $4.3 million | VSL of $9.3 million | |||
|---|---|---|---|---|
| 3% discount rate | 7% discount rate | 3% discount rate | 7% discount rate | |
| Value per QALY | $220,000 | $480,000 | $370,000 | $790,000 |
| QALY loss in years of unsuccessful quit attempts (years 1-5) | $965 | $2,105 | $1,625 | $3,464 |
| th QALY loss in year of successful quit (6 year) | $1,930 | $4,210 | $3,245 | $6,929 |
| QALY loss of full sequence of quit attempts | $6,755 | $11,665 | $14,735 | $24,250 |
| Present discounted value of full QALY loss from withdrawal | $6,200 | $9,700 | $13,560 | $20,100 |
This estimate of QALY losses due to withdrawal symptoms is close to our estimates of lost utility from the demand-curve approach. At our central estimates, the withdrawal symptoms ($12,500-$18,600) are about one-half to three-quarters of the utility loss of smoking cessation ($25,000). Some part of the remaining one-quarter to one-half may represent other transitory utility costs of quitting smoking (for example, missing the sensory experience of smoking at accustomed times and places; Piasecki et al. 2010), and another part may constitute a steady-state loss for people who continue to miss smoking after they quit.
Economic theory suggests that the people most likely to quit in response to regulation are those for whom the steady-state loss is smallest. All else equal, people with the lowest cumulative costs are most likely to withdraw when given an incentive to do so. Thus, our expectation is that the remaining one-quarter to one-half of the utility loss will typically be over when withdrawal has run its course. As a sensitivity test, though, below we consider the impact if one-quarter of the utility loss reflects steady- state loss.
A third way to examine the importance of withdrawal costs is to examine the long-run smoking behavior of type I and type II individuals. To the extent that the steady-state value of smoking is low, the divergence between type I and type II consumers should grow over time, as type I individuals should reduce smoking at a greater rate than type II individuals. In fact, this is true. Using our age/education delineation of the type I and type II populations, only 34 percent of ever smoking type I individuals currently smoke, compared to 42 percent of type II ever smokers (Table 4). When combined with the smaller number of cigarettes smoked, average current consumption is half as large for type I ever smokers compared to type II ever smokers.
A final way to gauge the value of steady-state utility loss is to measure the smoking rate among those for whom the health costs are low. If smoking has high implicit value, such individuals should be particularly likely to smoke. An example of this approach comes from the work of Oster et al. (2013), who study the behavior of people at high risk for Huntington’s disease. People who have a parent with Huntington’s have a 50 percent chance of inheriting the disease. Those with the disease are extremely unlikely to survive to old age; thus, the health consequences of smoking for this group are lower. Oster et al. examine the subsequent smoking behavior of people with ex ante identical risk, some of whom learn they have Huntington’s and others who learn they do not. They show that among ever-smokers, the smoking rate of those who learn they have the disease is 69 percent higher than the rate among those who learn they do not have the disease. This finding suggests some ongoing utility loss for former smokers, though it is clouded by the fact that smoking is viewed as reducing anxiety, which is likely to be higher among those who test positive.
Given this range of data, we present several estimates of the share of the utility loss due to withdrawal relative to health benefits of quitting. Our first estimate is the most straightforward: a large number of people report wanting to quit smoking but are unable to overcome the withdrawal cost; we assume that the marginal quitter who quits as a result of a new regulation is one for whom the utility loss ends after withdrawal is complete. In this case, the full utility loss occurs in the year when the smoker quits and is zero thereafter. This is not true for all individuals. Thus, we also consider a situation where one-quarter of the initial loss persists in the steady-state as a bound on what the extent of the loss could be if some people who quit continue to miss smoking after withdrawal has passed.
The last part of Table 5 shows the ratio of the utility costs of quitting relative to estimates of the morbidity and mortality benefits from quitting for a 35-year old smoker. Although utility losses from quitting are relatively large in the short-run, they wind up being small relative to estimated benefits from improved health and longer life expectancy. When utility costs are assumed to be entirely due to withdrawal, the utility losses represent about 3 percent to 4 percent of lifetime health benefits. Under the assumption that one-quarter of the value of the initial loss is ongoing, the offsets would represent 20 to 25 percent of the value of the lifetime health benefits. Whether a given regulation would result in an expected offset ratio towards the lower or higher end of this range depends on characteristics of the regulation; only if the regulation cuts fairly deeply into the smoking population would we expect to see an offset ratio towards the higher end of the range. Even in the case where a regulation induces non-marginal quitting, the ratio of utility loss to health benefits falls at the low end of the 10 to 90 percent range given in previous work.
Impact of implicit price increases
A regulation that also affects price would have an additional utility offset for existing smokers who continue to smoke, because they will pay higher prices for those cigarettes. Using the demand curves above, reducing demand by 10 percent would require an effective price increase of $1.78 per pack in the addiction-based delineation or $1.93 in the age/education delineation. We calculate the welfare loss from this by assuming that all continuing smokers pay the higher price – though the extent to which this is true for all smokers, as opposed to some smokers, is an empirical question. For type II consumers, the welfare loss is the price increase times the equilibrium number of packs smoked (225 or 304 per year per continuing smoker after the price increase, depending on the delineation method used), so total losses sum to $435 or $543 per continuing smoker per year. For type I consumers, the loss is analogously defined but also includes a loss associated with the decline in packs consumed (23-24 packs), together amounting to approximately $251 or $289 per smoker per year. Taking weighted averages across the two groups, this increased spending amounts to $375 or $427 per continuing smoker per year, or approximately $400.
Table 7. Impact of implicit price increases on continuing smokers
| Delineation method | ||
|---|---|---|
| Addiction-based | Age/education | |
| Price increase associated with 10% decrease in demand | $1.78 | $1.93 |
| Type I | $251 per year (129 packs) | $289 per year (137 packs) |
| Type II | $543 per year (304 packs) | $435 per year (225 packs) |
| Average | $375 per year | $427 per year |
4.2 Valuing Effects on Initiation
The analysis of initiation is conceptually similar to that of cessation: we estimate the cost savings and utility offsets to those who are deterred from initiating, along with any additional costs to those who initiate even after the regulation. The difficult question is whether people who are deterred from smoking experience any utility loss.
We can gain insight into this question by examining differences in smoking initiation and cessation between type I and type II consumers as identified from the demographic delineation. To focus on initiation, we consider in both cases the population aged 30-45, who came of age when health risks of smoking were well-known and thus had better information from which to make decisions. Thus, we can approximate the informed-population’s smoking decisions. We can only estimate initiation rates by demographics, since we do not know initiation rates by potential to become addicted.
As shown in Table 4, these two groups have very different initiation patterns. Eighty percent of type I individuals never smoked, compared to only 60 percent of type II individuals. Further, most of the type I individuals who started smoking subsequently quit; less so among type II individuals. The rates of current smoking are about 7 percent for type I individuals and 17 percent for type II individuals. As the subsequent decision to quit probably better aligns behavior better with underlying preferences than the decision to ever initiate, we estimate that the population smoking initiation rate that accurately reflects underlying well-informed standard preferences is about 7 percent annually. As noted above, even this estimate may be too high, since some of the highly educated young smokers may have initiated “accidentally” in their teens and now would prefer to quit – group 2 in Table 3. Fifty percent of type I smokers in the 30-45 age range say that they are seriously considering quitting within the next 6 months, and 33% report a high overall interest in quitting (8-10 on a scale of 1-10). Thus, the “rational” smoking rate not conditional on having started may be much below 7 percent.
Since there is no withdrawal for non-initiators, the relevant cost is the steady-state loss from not consuming cigarettes. That is, given that 7% of type I individuals currently smoke, what can we infer about the value of smoking for the person who would be the 17th percentile of type I smokers?
This difference is again very large. To match the smoking share of type II individuals, demand among type I individuals would need to rise by 140%. There are differing estimates in the literature about the price elasticity of youth initiation, with studies ranging from essentially 0 to as high as -0.8 (DeCicca et al. 2002; Carpenter and Cook 2008; Nonnemaker and Farrelly 2011). If we assume that the demand elasticity is the same as for our cessation analysis, the monetary price would have to be significantly negative for type I consumers to match the initiation rate of type II consumers. If the “content” quit rate is only half as high as the actual quit rate, the required price would fall even more. And if the youth smoking elasticity is even lower, as recent studies suggest, the required price would be lower still.
Given these estimates, it seems implausible that people far from the margin of smoking value cigarettes highly. This is consistent with the prediction that, because people deterred from starting to smoke never develop a special taste for tobacco products, they are able to get equal or better satisfactions from consuming other products, so a regulation that deters them from starting to smoke entails no utility loss. Therefore, the weight of the evidence suggests that analyses should assume no lost utility for prevented initiation among type II individuals. The health benefit and money saved would then be the full benefit.
Table 8 summarizes the estimated effects of the two types of regulations on potential initiators. Again the information-related regulation affects potential type II smokers only, while regulations that change the effective price of smoking affect both groups. As before, the health benefits per deterred initiator would be estimated using projections of reduced mortality and morbidity (along with other factors like reduced secondhand smoke). The money savings from reduced spending on cigarettes is again $5.43 per pack, or about $1,350 per deterred initiator per year.
Table 8. Estimated effects on potential initiators
| Deterred initiator | People who still initiate | |
|---|---|---|
| Information-based regulation | ||
| Money savings | $1,350 per year | 0 |
| Lost utility | 0 | 0 |
| 10% increase in effective price | ||
| Money savings | $1,350 per year | 0 |
| Lost utility | 0 | -$275 per year |
The analysis of how a price- or attribute-based regulation would affect initiation also requires accounting for the higher price that people who choose to smoke even in the face of higher prices will pay. A price increase of $1.40 is needed to reduce quantity of cigarettes consumed by potential initiators by 10 percent. %.33 The welfare loss from this would be about $275 for each continuing initiator each year ($1.40 x ~200 packs), assuming all continuing initiators paid the higher cost. This offsets some, but not all, of the health benefits and cost savings.
4.3 Population Estimates
Table 9 provides a summary of the non-health benefits of the two types of regulations for the specific types of people who may be affected. The total benefits of a regulation are given by these amounts, multiplied by the number of people affected in each category, summed across people for each year of the time horizon of the analysis, then discounted to the present using appropriate discount rates (3 percent or 7 percent). Total non-health benefits are computed by summing the annual benefits over the relevant time horizon (e.g. which may be 10- or 20-years for a jurisdictional or administrative regulation, or 20- to 100-years for a regulation that would significantly affect smoking rates).
For either information-based or price-based regulations, smokers who quit realize money savings of about $1,500 per year and dissuaded initiators have savings of about $1,350 per year, occurring on an ongoing basis. Smokers who quit experience a one-time utility loss of $12,500 to $25,000 in present value terms, depending on the approach we use. We expect most smokers who quit as a result of a regulation to have utility losses that run their course after withdrawal is over. However, if a regulation cuts further into the pool of existing smokers, some may experience ongoing utility losses; our estimates of QALY losses from withdrawal symptoms suggest ongoing utility losses of less than one-quarter of the initial loss. For regulations that increase the explicit or implicit price of smoking, smokers who continue to smoke or initiate smoking have ongoing utility losses of $400 or $275 per year respectively.
Table 9: Summary of utility offsets for existing smokers and potential initiators*
| Regulation Type | ||||
|---|---|---|---|---|
| Information or salience intervention only | Regulation that increases effective cigarette price | |||
| Existing smokers | Induced quitters | Smokers who continue to smoke | Induced quitters | Smokers who continue to smoke |
| Health benefits | yes | no | yes | some |
| Money saving | ~$1,500 per year | --- | ~$1,500 per year | --- |
| Utility loss (gain) | ||||
| One-time | $12,500 to $25,000 | --- | $12,500 to $25,000 | --- |
| Ongoing | Possible loss of $6,250 | --- | Possible loss of $6,250 | -$400 per year |
| Potential initiators | Dissuaded initiators | People who still initiate | Dissuaded initiators | People who still initiate |
| Health benefits | yes | no | yes | some |
| Money saving | ~$1,350 per year | --- | ~$1,350 per year | --- |
| Utility loss (gain) | ||||
| One-time | --- | --- | --- | |
| Ongoing | --- | --- | --- | -$275 per year |
| * Regulation assumed to reduce consumption of existing smokers by 10% and reduces initiation by 10%. | ||||
Tables 10-13 illustrate how to use the estimated offsets per person to compute population-level estimates of health benefits and utility offsets. Because health benefits of quitting smoking or avoiding initiation depend on smoking history, it is valuable to analyze health benefits and utility offsets for different age cohorts, then aggregate estimated benefits and offsets across cohorts at given points in time or over time.34 For illustrative purposes, Tables 10-11 analyze how a regulation that reduces smoking by 10% affects a cohort of 35-year old smokers. Tables 12-13 analyze effects of a regulation that reduces the smoking initiation rate by 10 percent (2 percentage points) for a cohort of 18-year old potential initiators.
As shown in Table 10, the total value of offsets for existing 35-year old smokers is derived by multiplying the number of smokers induced to quit by the regulation by the estimated values for money savings and utility loss per smoker, and multiplying the number of continuing smokers by the extra spending per smoker caused by the increase in price. Then for each year the total offset is found by summing these three components; the total is then discounted to the present using an appropriate discount rate (3 percent in this example).
The total value of offsets is substantial in the first few years – as much as a billion dollars – due to utility losses from having 100,000 smokers in the age cohort quit. Withdrawal is costly, and that is reflected in the table. In the case where utility costs for smokers who quit are primarily withdrawal costs, the utility losses trail down to $364 million (undiscounted), reflecting costs to continuing smokers of paying higher prices for cigarettes.
Table 11 shows cumulative changes in health and monetary gains and utility offsets for this cohort over the first 50 years after the regulation takes effect. In the first decade, utility losses are large relative to health and monetary benefits. But over time, utility costs taper off while health and monetary benefits rise, so that the ratio of the two steadily declines. In the 50 th year after the regulation takes effect, utility losses represent 8 percent of health and monetary benefits if all utility loss experienced by quitters is withdrawal. The share would be higher if some quitters experience ongoing loss but even in the outside case that all of them do, the loss would not exceed 20 percent of health and monetary gains. In either case, the offset rate is higher here than in the computations in Table 5, because utility losses include those of continuing smokers who pay higher prices as well as those who quit.
Tables 12 and 13 provide similar analysis for potential initiators. Here also the total money savings for dissuaded initiators is smaller than the total utility loss due to higher prices for those who continue to initiate, resulting in a negative offset of $101 million per year (undiscounted). Because deterred initiators experience no utility loss, even in the early decades after the regulation comes into effect, the utility offset ratio is relatively low -- around 12 percent after the 10 th year. This rate falls to 7.5 percent by the 50th year and 5 percent by the 80th. The much lower offset ratio among initiators, compared to existing smokers, underlines that methods for computing utility losses computed from losses of existing smokers only will usually overstate utility offsets to health benefits of regulations. Given the focus in the TCA on reducing youth initiation, this illustrates the importance of distinguishing between reductions in smoking due to cessation versus those due to decreased initiation when estimating utility offsets.
Table 10. Example of total offsets from a regulation that increases the effective price of cigarettes: Cohort of 35 -year old existing smokers
| Numbers of people affected by the regul ation (‘000) | Millions of dollars (undiscounted) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| year | Continuing smokers | Smokers who quit | Total utility losses (continuing smokers and quitters) if loss of quitters is: | ||||||
| Smokers | Newly induced quitters | Cumulative # of quitters | Lost utility from higher price per pack (a) x $400 | Money saving (c) x $1,500 | Lost utility frassuming t | om quitting he loss is: | |||
| All withdrawal (d) x $25,000 | 25% steady state* | All withdrawal | 25% steady state | ||||||
| 0 | 1,012 | ||||||||
| 1 | 1,002 | 10 | 10 | -$401 | $15 | -$253 | -$253 | -$654 | -$654 |
| 2 | 986 | 15 | 25 | -$395 | $38 | -$379 | -$506 | -$774 | -$900 |
| 3 | 961 | 25 | 51 | -$384 | $76 | -$632 | -$885 | -$1,017 | -$1,270 |
| 4 | 946 | 15 | 66 | -$378 | $99 | -$379 | -$854 | -$758 | -$1,232 |
| 5 | 936 | 10 | 76 | -$374 | $114 | -$253 | -$759 | -$627 | -$1,133 |
| 6 | 926 | 10 | 86 | -$370 | $129 | -$253 | -$790 | -$623 | -$1,161 |
| 7 | 921 | 5 | 91 | -$368 | $137 | -$126 | -$727 | -$495 | -$1,095 |
| 8 | 916 | 5 | 96 | -$366 | $144 | -$126 | -$727 | -$493 | -$1,093 |
| 9 | 911 | 5 | 101 | -$364 | $152 | -$126 | -$759 | -$491 | -$1,123 |
| 10 | 911 | 0 | 101 | -$364 | $152 | $0 | -$664 | -$364 | -$1,028 |
| * $25,000 in the first year, $12,500 in the second, and $6,250 thereafter. Number of 35-year old smokers is from the IPUMs version of the National Health Interview Survey, 2013 (Ruggles et al. 2015). Health benefits do not count gains to continuing smokers from consuming a lower number of packs per year. | |||||||||
Table 11. Cumulative benefits and costs of a regulation that increases the effective price of cigarettes: Cohort of 35-year old existing smokers
| Present value in milli ons (3% discount rate) | Utility offset to health & monetary benefits if losses of quitters are: | ||||
|---|---|---|---|---|---|
| Utility losses of continuing smokers + quitters if losses of quitters are | Health & monetary benefits | Total net benefits | |||
| Years since the regulation took effect: | Withdrawal 25% steady only state | Withdrawal only | 25% steady state | ||
| Values are adjusted for mortality risks specific to smokers and nonsmokers. See notes to Table 5 for explanation of data sources and derivation of health benefits. | |||||
| 10 | -$5,589 -$9,262 | $9,984 | -$4,866 | 56% | 93% |
| 20 | -$7,826 -$15,487 | $32,188 | $8,875 | 24% | 48% |
| 30 | -$9,267 -$19,708 | $58,182 | $29,206 | 16% | 34% |
| 40 | -$10,027 -$22,269 | $91,522 | $59,226 | 11% | 24% |
| 50 | -$10,293 -$23,504 | $125,982 | $92,186 | 8% | 19% |
Table 12. Example of total offsets from a regulation that increases the effective price of cigarettes: Cohort of 18-year old potential initiators
| Numbers of peoplregulatioe affected by the n (‘000) | Millions of dollars (undiscounted) | ||||
|---|---|---|---|---|---|
| year | Continuing initiators | Deterred initiators | Continuing initiators | Deterred initiators | |
| Lost utility from higher price per pack (a) x $275 | Money savings (b) x $1,350 | Lost utility | |||
| 1 | 808 | 90 | -$222 | $121 | 0 |
| 2 | 808 | 90 | -$222 | $121 | 0 |
| 3 | 808 | 90 | -$222 | $121 | 0 |
| 4 | 808 | 90 | -$222 | $121 | 0 |
| 5 | 808 | 90 | -$222 | $121 | 0 |
| 6 | 808 | 90 | -$222 | $121 | 0 |
| 7 | 808 | 90 | -$222 | $121 | 0 |
| 8 | 808 | 90 | -$222 | $121 | 0 |
| 9 | 808 | 90 | -$222 | $121 | 0 |
| 10 | 808 | 90 | -$222 | $121 | 0 |
| Number of 18-year olds is taken from the IPUMs version of the National Health Interview Survey, 2013 (Ruggles et al. 2015). Health benefits do not count gains to continuing smokers from consuming a lower number of packs per year. | |||||
Table 13. Cumulative benefits and costs of a regulation that increases the effective price of cigarettes: Cohort of 18-year old potential initiators
| Present value in millions (3% discount rate) | Utility offset to health & monetary benefits | ||||
|---|---|---|---|---|---|
| Utility losses | Health & monetary benefits | Total net benefits | |||
| Continuing initiators | Deterred initiators | ||||
| Values are adjusted for mortality risks specific to smokers and nonsmokers. See notes to Table 5 for explanation of data sources and derivation of health benefits. | |||||
| Years since the regulation took effect: | |||||
| 10 | $1,951 | 0 | $15,895 | $13,944 | 12.3% |
| 20 | $3,382 | 0 | $31,092 | $27,710 | 10.9% |
| 30 | $4,421 | 0 | $43,768 | $39,347 | 10.1% |
| 40 | $5,141 | 0 | $57,128 | $51,986 | 9.0% |
| 50 | $5,585 | 0 | $74,323 | $68,739 | 7.5% |
| 60 | $5,797 | 0 | $94,796 | $88,999 | 6.1% |
| 70 | $5,852 | 0 | $111,876 | $106,024 | 5.2% |
| 80 | $5,855 | 0 | $117,846 | $111,991 | 5.0% |
5.0 Conclusions
Incorporating preferences inconsistent with standard economic models due to addictive and habitual goods raises significant analytical challenges for HHS and FDA in meeting the requirements to assess the costs, benefits, and other impacts of major regulations. The expectation from standard economic theory that consumers choose to consume only those products where the benefits they get from consumption outweigh the costs and risks appears not to hold for these goods. However, issues of market failure associated with addiction and habit do not warrant disregarding altogether the utility losses people may experience from regulations aimed at curbing consumption of products with health risks. Rather, the question is how to value these losses when consumers’ preferences, beliefs and/or decision-making practices differ from the standard model.
Relative to the approaches in the literature, we make several innovations. First, we explicitly delineate the money savings from reduced consumption of health-harming goods and place those alongside the health benefits. Second, we show that the utility offsets of reducing consumption have both short-term withdrawal costs and longer-term steady-state utility costs. Each cost is important in the short run, but withdrawal costs decline over time. Third, there may be additional costs for people who continue to consume the addictive or habitual good even after the regulatory intervention, if regulations change the explicit or implicit price of the good.
Empirically, we measure the utility offsets of regulations using information on consumption of rational individuals to value utility losses of individuals whose consumption is too high relative to their preferences. Our estimates of utility losses or withdrawal costs from quitting smoking are meaningful in the short-run. That said, they are small relative to the lifetime health benefits of quitting: below 5% for regulations that induce quitting only among smokers who experience no steady-state loss, and no higher than 20-25% in the outside case that all of them do. Regulations that increase prices for continuing smokers will lead to somewhat higher offset ratios because of the additional utility losses they induce. Still, even these higher estimates are well below those reported in previous work. The size of the offset depends on the discount rate, time frame of the analysis, whether there are ongoing utility losses, and if the regulation deters initiation or induces quitting. Because most regulations will induce quitting among smokers who will not miss smoking in the long term, and because people deterred from starting to smoke have no utility loss, we expect the population-level estimate of the offset ratio will be closer to 5 percent.
We also find that considering initiation separately from cessation is important in considering consumer surplus changes from policy interventions. For those who are addicted, withdrawal costs are substantial, while non-initiation avoids these costs.
The current paper focuses on the case of cigarette smoking. That said, the approach developed here can be extended to analysis of regulations in other areas where there are concerns about whether observed consumption levels of some segment of consumers may exceed their desired levels. This situation may characterize a variety of food and tobacco products that have adverse health consequences when consumed habitually, where issues of addiction, incomplete or non-salient information, time-inconsistency, inaccurate expectations, and related problems may drive a wedge between consumers’ decision utility and the experienced utility that will result from their actions.
Future research is needed to lower the ranges of uncertainty in the approach we recommend, as well as to consider other approaches that show promise. These needs are pressing as HHS and its agencies may well need to conduct regulatory analyses for a range of addictive and habitual goods. HHS committed in its strategic plan to prevent and reduce tobacco use, and the passage of the TCA in 2009 gives FDA a wide range of new authorities to regulate tobacco. This paper provides a methodology for evaluating regulations affecting tobacco products and other addictive and habitual goods.
References
Anderson, C., D. Burns, K. Dodd, and E. Feuer. 2012. “Birth-Cohort-Specific Estimates of Smoking Behaviors for the U.S. Population.” Risk Analysis 32(Suppl 1): S14-24.
Angeletos, G-M., D. Laibson, A. Repetto, J. Tobacman, and S. Weinberg. 2001. “The Hyperbolic Consumption Model: Calibration, Simulation, and Empirical Evaluation.” Journal of Economic Perspectives 15(3): 47-68.
Arias, E. 2010. “United States Life Tables, 2009.” National Vital Statistics Reports 62(7). Centers for Disease Control and Prevention, U.S. Department of Health and Human Services.
Ashley, E., C. Nardinelli, and R. Lavaty. 2015. “Estimating the Benefits of Public Health Policies that Reduce Harmful Consumption.” Health Economics 24(5): 617–624.
Australian Productivity Commission. 2010. Gambling: Productivity Commission Inquiry Report. http://www.pc.gov.au/inquiries/completed/gambling-2009/report/gambling-…
Baker, T. B. et al. 2007. “Time to First Cigarette in the Morning as an Index of Ability to Quit Smoking: Implications for Nicotine Dependence.” Nicotine and Tobacco Research 9(Suppl 4): S555–S570.
Becker, G. and K. Murphy. 1988. "A Theory of Rational Addiction." Journal of Political Economy 96: 675-700.
Bernheim, B.D. and A. Rangel. 2004. “Addiction and Cue-Triggered Decision Processes.” American Economic Review 94(5): 1558-1590.
Blackwell, D., J. Lucas, and T. Clarke. 2014. “Summary Health Statistics for U.S. Adults: National Health Interview Survey, 2012.” National Center for Health Statistics, Vital and Health Statistics 10(260): 1-171.
Borland R., T. Partos, H-H. Yong, M. Cummings, and A. Hyland. 2012. “How Much Unsuccessful Quitting Activity Is Going on Among Adult Smokers? Data from the International Tobacco Control Four Country Cohort Survey.” Addiction 107:671-682.
Carpenter, C., and P. Cook. 2008. “Cigarette Taxes and Youth Smoking: New Evidence from National, State, and Local Youth Risk Behavior Surveys.” Journal of Health Economics 27: 287–299.
Chabris, C., D. Laibson and J. Schuldt. 2008. "Intertemporal Choice." New Palgrave Dictionary of Economics, 2nd edition. Eds. S. Durlauf and L. Blume. New York: Palgrave Macmillan.
Chaloupka, F. 1991. “Rational Addictive Behavior and Cigarette Smoking.” Journal of Political Economy 99(4): 722-742.
Chaloupka, F. 2011. FDA Public Comment. Docket: FDA-2010-N-0568.
Chaloupka, F. and K. Warner. 2000. “The Economics of Smoking.” In Handbook of Health Economics, Vol. IA, eds. A. Culyer and J. Newhouse, 1539-1627. Amsterdam: North Holland/Elsevier.
Chaloupka, F., K. Warner, D. Acemoglu, J. Gruber, F. Laux, W. Max, J. Newhouse, T. Schelling, and J. Sindelar. 2015. “An Evaluation of the FDA's Analysis of the Costs and Benefits of the Graphic Warning Label Regulation,” Tobacco Control 24: 112-119.
Chetty, R. 2009. “Sufficient statistics for welfare analysis: a bridge between structural and reduced-form methods.” Annual Review of Economics 1: 451–488.
Chetty, R. 2015. “Behavioral Economics and Public Policy: A Pragmatic Perspective.” American Economic Review Papers and Proceedings 105(5): 1-33.
Choi, S., S. Kariv, W. Müller, and D. Silverman. 2014. "Who Is (More) Rational?" American Economic Review 104(6): 1518-50.
Cook B., G. Wayne, E. Kafali, Z. Liu, C. Shu, and M. Flores. 2014. “Trends in Smoking among Adults with Mental Illness and Association between Mental Health Treatment and Smoking Cessation.” Journal of the American Medical Association 311(2):172-182.
Cutler, D. 2002. “Health Care and the Public Sector.” In Handbook of Public Economics, Vol. 4, eds. A. Auerbach and M. Feldstein, 2143-2243. Amsterdam: Elsevier/North Holland.
DeCicca, P., D. Kenkel, and A. Mathios. 2002. “Putting Out the Fires: Will Higher Cigarette Taxes Reduce the Onset of Youth Smoking?” Journal of Political Economy 110: 144–169.
DellaVigna, S. 2009. “Psychology and Economics: Evidence from the Field.” Journal of Economic Literature 47(2): 315-372.
DellaVigna S. and M.D. Paserman. 2005. “Job Search and Impatience.” Journal of Labor Economics 23(3): 527-588.
Eissenberg, T. and R. Balster. 2000. “Initial Tobacco Use episodes in Children and Adolescents: Current Knowledge, Future Directions.” Drug and Alcohol Dependence 59:41-60.
Fiore, M., C. Jaén, T. Baker, et al. 2008. Treating Tobacco Use and Dependence: 2008 Update. Clinical Practice Guideline. Rockville, MD: U.S. Department of Health and Human Services, Public Health Service.
Flegal, K., B. Graubard, D. Williamson, and M. Gail. 2005. “Excess Deaths Associated With Underweight, Overweight, and Obesity.” Journal of the American Medical Association 293: 1861–67.
Fong, G., D. Hammond, F. Laux, M. Zanna, K. Cummings, R. Borland, and H. Ross. 2004. “The Near-Universal Experience of Regret among Smokers in Four Countries: Findings from the International Tobacco Control Policy Evaluation Survey.” Nicotine and Tobacco Research 6 (Suppl 3): S341-S351.
Frederick S., G. Loewenstein, and T. O’Donoghue. 2002. “Time Discounting and Time Preference: A Critical Review.” Journal of Economic Literature 40: 351-401.
Fujiwara, D. and R. Campbell. 2011. “Valuation Techniques for Social Cost-Benefit Analysis: Stated Preference, Revealed Preference and Subjective Well-Being Approaches.” Report Prepared for the UK Treasury and Department for Works and Pensions.
Fujiwara, D. and P. Dolan. Forthcoming. “Happiness-Based Policy Analysis.” In Oxford Handbook of Well-Being and Public Policy, eds. M. Adler and M. Fleurbaey. Oxford, UK: Oxford University Press.
Gallet, C. and J. List. 2003. “Cigarette Demand: A Meta-Analysis of Elasticities.” Health Economics 12(10): 821–835.
Galvan, A, T. Hare, C. Parra, J. Penn, H. Voss, G. Glover, and B. Casey. 2006. “Earlier Development of the Accumbens Relative to Orbitofrontal Cortex Might Underlie Risk-Taking Behavior in Adolescents.” Journal of Neuroscience 26(25): 6885-6892.
Gogtay, N., J. Giedd, L. Lusk, K. Hayashi, D. Greenstein, and A. Vaituzis. 2004. “Dynamic Mapping of Human Cortical Development during Childhood through Early Adulthood.” Procedures of the National Academy of Science 101: 8174-8179 Gruber, J. 2002-2003. “Smoking’s ‘Internalities’.” Regulation 25(4): 52–57.
Gruber, J. and B. Köszegi. 2001. ‘‘Is Addiction ‘Rational’? Theory and Evidence.” Quarterly Journal of Economics 116(4): 1261-1303.
Gruber, J. and B. Köszegi. 2004. “Tax Incidence When Individuals are Time Inconsistent: The Case of Cigarette Excise Taxes.” Journal of Public Economics 88(9-10): 1959-1988.
Gruber, J.H., and S. Mullainathan. 2005. “Do Cigarette Taxes Make Smokers Happier?” B.E. Journal of Economic Analysis & Policy 5(1).
Hanmer, J., W. Lawrence, J. Anderson, R. Kaplan, and D. Fryback. 2006. “Report of Nationally Representative Values for the Noninstitutionalized US Adult Population for 7 Health-Related Quality-of-Life Scores.” Medical Decision Making 26(4): 391-400.
Hughes, J.R. 2006. “Clinical Significance of Tobacco Withdrawal.” Nicotine and Tobacco Research 8(2): 153-156.
Hughes, J.R. 2006. “Clinical Significance of Tobacco Withdrawal.” Nicotine and Tobacco Research 8(2): 153-156.
Hughes, J.R. 2007. “Effects of Abstinence from Tobacco: Valid Symptoms and Time Course.” Nicotine and Tobacco Research 9(3): 315-327.
Hughes, J.R., J. Keely, and S. Naud. 2004. “Shape of the Relapse Curve and Long-term Abstinence among Untreated Smokers.” Addiction 99(1): 29-38.
Jia, H. and E. Lubetkin. 2010. “Trends in Quality-Adjusted Life-Years Lost Contributed by Smoking and Obesity.” American Journal of Preventive Medicine 38(2): 138-144.
Kahneman, D. and A. Deaton. 2010. “High Income Improves Evaluation of Life but not Emotional Well-Being.” Proceedings of the National Academy of Sciences 107(38): 16489-16493.
Kenkel, D. 2000. “Prevention.” In Handbook of Health Economics, Vol. IA, eds. A. Culyer and J. Newhouse, 1675-1720. Amsterdam: North Holland/Elsevier.
Kenkel, D. and L. Chen. 2000. “A Consumer Information and Tobacco Use.” In Tobacco Control in Developing Countries, eds. P. Jha and F. Chaloupka, 177-214. Oxford, UK: Oxford University Press.
Laibson, D. 1997. “Golden Eggs and Hyperbolic Discounting.” Quarterly Journal of Economics 112(2): 443-477.
Lasser, K., J. Boyd, S. Woolhandler, D. Himmelstein, D. McCormick, and D. Bor. 2000. “Smoking and Mental Illness: A Population-Based Prevalence Study.” Journal of the American Medical Association 284(20): 2606-2610.
Mullainathan S., J. Schwartzstein, and W. Congdon. 2012. “A Reduced-Form Approach to Behavioral Public Finance.” Annual Review of Economics 4: 511-40.
National Research Council. 2013. Subjective Well-Being: Happiness, Suffering, and Other Dimensions of Experience. Washington, DC: National Academies Press.
Nonnemaker, J. and M. Farrelly. 2011. “Smoking Initiation among Youth: The Role of Cigarette Excise Taxes and Prices by Race/Ethnicity and Gender.” Journal of Health Economics 30: 560-567.
O'Connor, R., L. Kozlowski, D. Vandenbergh, A. Strasser, M. Grant, and G. Vogler. 2005. “An Examination of Early Smoking Experiences and Smoking Status in a National Cross-sectional Sample.” Addiction 100: 1352–1357.
Oncken, C., S. McKee, S. Krishnan-Sarin, S. O’Malley, and C. Mazure. 2005. “Knowledge and Perceived Risk of Smoking-related Conditions: A Survey of Cigarette Smokers.” Preventive Medicine 40(6): 779–84.
Organization for Economic Cooperation and Development. 2013. OECD Guidelines on Measuring Subjective Well-Being. Paris: OECD Publishing. http://dx.doi.org/10.1787/9789264191655-en.
Orzechowski and Walker. 2012. The Tax Burden of Tobacco. Historical Compilation. Vol. 42. http://www.taxadmin.org/fta/tobacco/papers/tax_burden_2012.pdf.
Oster, E., E. Dorsey, and I. Shoulson. 2013. “Limited Life Expectancy, Human Capital and Health Investments,” American Economic Review 103(5): 1977-2002.
Paterson R., K. Boyle, C. Parmeter, J. Neumann, and P. De Civita. 2008. “Heterogeneity in Preferences for Smoking Cessation.” Health Economics 17(12): 1363-77.
Piasecki, T., M. Piper, and T. Baker. 2010. “Tobacco Dependence: Insights from Investigations of Self-Reported Motives,” Current Directions in Psychological Science 19(6): 395-401.
Piper, M., S. Kenford, M. Fiore, and T. Baker. 2012. “Smoking Cessation and Quality of Life: Changes in Life Satisfaction Over 3 Years Following a Quit Attempt.” Annals of Behavioral Medicine 43: 262-270.
Reyna, V. and F. Farley. 2006. “Risk and Rationality in Adolescent Decision Making: Implications for Theory, Practice, and Public Policy.” Psychological Science in the Public Interest 7(1): 1-44.
Robinson, L. and J. Hammitt. 2013. “Skills of the Trade: Valuing Health Risk Reductions in Benefit-Cost Analysis.” Journal of Benefit-Cost Analysis 4(1): 107-130.
Robinson, L. and J. Hammitt. 2015. “Valuing Reductions in Fatal Illness Risks: Implications of Recent Research,” Health Economics. Published online: 30 JUN 2015 (DOI: 10.1002/hec.3214).
Ruggles, S., J. Alexander, K. Genadek, R. Goeken, M. Schroeder, and M. Sobek. 2015. Integrated Public Use Microdata Series: Version 5.0 [Machine-readable database]. Minneapolis: University of Minnesota.
Saad, Linda. 2002. “Tobacco and Smoking.” Gallup Brief, http://www.gallup.com/poll/9910/tobacco-smoking.aspx#risks.
Schauffler, H., S. McMenamin, K. Olson, G. Boyce-Smith, J. Rideout, and J. Kamil. 2001. “Variations in Treatment Benefits Influence Smoking Cessation: Results of a Randomized Controlled Trial.” Tobacco Control 10: 175-180.
Shahab, L. and R. West. 2009. “Do Ex-Smokers Report Feeling Happier Following Cessation? Evidence from a Cross-Sectional Survey.” Nicotine and Tobacco Research 11(5): 553-557.
Shahab, L. and R. West. 2012. “Differences in Happiness between Smokers, Ex-Smokers and Never Smokers: Cross-Sectional Findings from a National Household Survey. Drug and Alcohol Dependence 121(1): 38-44.
Shiffman S., M. Dunbar, X. Li, S. Scholl, H. Tindle, S. Anderson, and S. Ferguson. 2014. “Smoking Patterns and Stimulus Control in Intermittent and Daily Smokers.” PLoS One 9(3), e89911.
Skiba P. and J. Tobacman. 2008. “Payday Loans, Uncertainty, and Discounting: Explaining Patterns of Borrowing, Repayment, and Default.” Vanderbilt Law and Economics Research Paper No. 08-33.
Sloan, F., J. Ostermann, C. Conover, D. Taylor and G. Picone. 2004. The Price of Smoking. Cambridge, MA: MIT Press.
Sloan, F. and A. Platt. 2012. “Information, Risk Perceptions, and Smoking Choices of Youth.” Journal of Risk and Uncertainty 42: 161-193.
Sloan, F. and Y. Wang. 2008. “Economic Theory and Evidence on Smoking Behavior of Adults.” Addiction 103: 1777–1785.
Sullivan P., W. Lawrence, and V. Ghushchyan. 2005. “A National Catalog of Preference-Based Scores for Chronic Conditions in the United States.” Medical Care 43:736-749.
Taylor, D., V. Hasselblad, S. Henley, M. Thun, and F. Sloan. 2002. “Benefits of Smoking Cessation for Longevity.” American Journal of Public Health 92(6): 990-996.
Taylor, G., A. McNeill, A. Girling, A. Farley, N. Lindson-Hawley, and P. Aveyard. 2014. “Changes in Mental Health after Smoking Cessation: Systematic Review and Meta-Analysis.” British Medical Journal 348: 1-22.
Tóbiás, Á. 2014. “Optimal Taxation of Addictive Goods Consumed by Naïve Hyperbolic Discounters.” Mimeo, Yale University.
U.S. Centers for Disease Control and Prevention. 1990. The Health Benefits of Smoking Cessation: A Report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services. http://www.surgeongeneral.gov/library/reports/index.html
U.S. Centers for Disease Control and Prevention. 2000. Reducing Tobacco Use: A Report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services. http://www.cdc.gov/tobacco/data_statistics/sgr/2000/complete_report/ind…
U.S. Centers for Disease Control and Prevention. 2002. Women and Smoking: A Report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services. http://www.cdc.gov/tobacco/data_statistics/sgr/2001/complete_report/
U.S. Centers for Disease Control and Prevention. 2003. “Prevalence of Current Cigarette Smoking among Adults and Changes in Prevalence of Current and Someday Smoking: United States, 1996–2001.” Morbidity and Mortality Weekly Report 289(18): 2355–2356
U.S. Centers for Disease Control and Prevention. 2010. How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease: A Report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services. http://www.ncbi.nlm.nih.gov/books/NBK53018/
U.S. Centers for Disease Control and Prevention. 2011. “Quitting Smoking among Adults: United States, 2001-2010.” Morbidity and Mortality Weekly Report 60(44): 1513-1519.
U.S. Centers for Disease Control and Prevention. 2012. Preventing Tobacco Use among Youth and Young Adults: A Report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services. http://www.surgeongeneral.gov/library/reports/preventing-youth-tobacco-…
U.S. Centers for Disease Control and Prevention. 2014a. The Health Consequences of Smoking: 50 Years of Progress: A Report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services. http://www.surgeongeneral.gov/library/reports/50-years-of-progress/
U.S. Centers for Disease Control and Prevention. 2014b. “Alcohol-Attributable Deaths and Years of Potential Life Lost -- 11 States, 2006-2010” Morbidity and Mortality Weekly Report 63(10): 213-216.
U.S. Centers for Disease Control and Prevention. 2014c. “Current Cigarette Smoking Among Adults: United States, 2005–2013.” Morbidity and Mortality Weekly Report 63(47): 1108-12.
U.S. Food and Drug Administration. 2004. “Final Rule Declaring Dietary Supplements Containing Ephedrine Alkaloids Adulterated Because They Present an Unreasonable Risk.” Federal Register 69: 6788-6854.
U.S. Food and Drug Administration. 2011. “Required Warnings for Cigarette Packages and Advertisements, Final Rule.” Federal Register 76: 36628-36777.
U.S. Food and Drug Administration. 2014a. “Analysis of Impacts: Nutrition Facts/Serving Sized Combined Preliminary Regulatory Impact Analysis”. http://www.fda.gov/downloads/Food/GuidanceRegulation/GuidanceDocumentsR….
U.S. Food and Drug Administration. 2014b. “Deeming Tobacco Products to Be Subject to the Federal Food, Drug, and Cosmetic Act, as Amended by the Family Smoking Prevention and Tobacco Control Act (Proposed Rule) – Preliminary Regulatory Impact Analysis.” http://www.fda.gov/downloads/AboutFDA/ReportsManualsForms/Reports/Econo…
U.S. Office of Management and Budget. 2003. Circular A-4: Regulatory Analysis.
U.S. Substance Abuse and Mental Health Services Administration. 2010. Results from the 2009 National Survey on Drug Use and Health: Volume II. Technical Appendices and Selected Prevalence Tables (Office of Applied Studies, NSDUH Series H-38B, HHS Publication No. SMA 10-4856). Rockville, MD.
U.S. Substance Abuse and Mental Health Services Administration. 2013. Results from the 2012 National Survey on Drug Use and Health: Detailed Tables. http://archive.samhsa.gov/data/NSDUH/2012SummNatFindDetTables/DetTabs/N…
Vugrin, E., B. Rostron, S. Verzi, N. Brodsky, T. Brown, C. Choiniere, B. Coleman, A. Paredes, and B. Apelberg. 2015. “Modeling the Potential Effects of New Tobacco Products and Policies: A Dynamic Population Model for Multiple Product Use and Harm,” PlosOne, March 27.
Wang, M., X. Wang, T. Lam, K. Viswanath, and S. Chan. 2014. “Ex-Smokers are Happier than Current Smokers among Chinese Adults in Hong Kong.” Addiction 109: 1165-1171.
Weimer, D., A. Vining, and R. Thomas. 2009. “Cost-Benefit Analysis Involving Addictive Goods: Contingent Valuation to Estimate Willingness to Pay for Smoking Cessation.” Health Economics 18: 181-202.
Weinhold, D. and F. Chaloupka. 2014. “Happiness and Smoking.” Unpublished manuscript, London School of Economics.
Zhou X., J. Nonnemaker, B. Sherrill, A. Gilsenan, F. Coste, and R. West. 2009. “Attempts to Quit Smoking and Relapse: Factors Associated with Success or Failure from the Attempt Cohort Study.” Addictive Behaviors 34:365-373.
Appendix 1: Alternative Approaches
The approach presented above is not the only way that utility offsets to health benefits of regulations affecting consumption of other addictive or habitual goods could be evaluated. In this section, we present three other approaches that have been suggested in the literature. They are not specifically concerned with measuring utility offsets to health benefits, but rather offer ways of measuring benefits of proposed regulations more generally. Each is promising, but all have significant theoretical and empirical issues that need to be addressed before they can be implemented.
A.1 Measuring Willingness to Pay
In many contexts, economists use willingness to pay estimates to infer the value of changes in consumption. In many contexts, economists use willingness to pay estimates to infer the value of changes in consumption. In this section, we consider how data on purchases of cessation products canbe used to estimate this willingness to pay. As we discuss, the results raise many questions that cannot be resolved without more research. Thus the approach described in the prior section appears preferable at this time.
Consider a current smoker contemplating quitting. Denote the self-assessed value of quitting smoking as V. This is what we wish to measure. There are products that people can buy that increase the probability of successfully quitting, including counseling, nicotine replacement products (patches, lozenges, gum) and prescription medications like Chantix and Zyban. Assume that the probability ofsuccessfully quitting smoking is dn without aids and dw with aids, so that ∆d=(dw-d n) is the impact of using aids on the probability of cessation. Empirically, the incremental effectiveness of smoking aids is about 5 percent to 20 percent,35 though we consider what smokers believe below. Finally, suppose that the monetary cost of these aids is p and the withdrawal cost of quitting smoking is the same with or without aids. The person will purchase the aid provided the additional benefit to using the product is greater than the monetary cost: ∆d∙V > p. If we know the price at which people will buy cessation aids, p, and how consumers perceive the effectiveness of aids, ∆d, we can use this equation to calculate V: V = p/∆d.
Willingness to pay for cessation aids can be estimated using either revealed- or stated-preference methods (e.g., Paterson et al. 2008, Weimer et al. 2009).36 Paterson et al. (2008, Table V) estimate that heavy smokers who wish to quit would be willing to pay about $145 (Canadian $2004) for a nicotine patch that would increase their probability of successfully quitting from 1.5 percent to 6 percent. This implies a typical value of quitting of $145/4.5% = $3,200 (Canadian). Schauffler et al. (2001) report that the fraction of smokers in the treatment group of a randomized controlled trial who used nicotine gum or patches increased from 14 percent to 23 percent when the cost of these products to them was reduced from the market price to zero (through health-insurance coverage). Assuming the cost to control-group subjects of these products is $25037 and assuming a linear demand curve implies that the average WTP among the 23 percent who would use the products if they were free is $320. 38 Schauffler et al. report that 13 percent of subjects in their control group and 18 percent in the treatment group quit smoking, implying an average incremental effectiveness of 5 percent. Taking this as an estimate of perceived effectiveness and combining it with average WTP yields a typical value of quitting of $320/5% = $6,400. Volpp et al. (2009) consider the impact of financial incentives to stop smoking. The authors conduct a randomized control trial where participants in the treatment group received up to $750 to quit smoking. They found that rates of prolonged abstinence from smoking after 9 or 12 months of follow-up were 9.7 percent higher in the group that was eligible for financial incentives than in the control group. Dividing the total incentive payments by the difference in successful abstinence yields an estimate of $750/9.7% = $7,700. The illustrative values of cessation thus range from about $3,200 to $7,700.
There are two major difficulties with relying on data on cessation products that FDA will have to address before it can be implemented. First, one needs to decide what to make of the 77 percent of smokers who decline to use the cessation aids when free. In practice, this group includes both smokers who do not wish to quit and smokers who wish to quit but do not purchase cessation aids. About two-thirds of smokers say they wish to quit. We suspect that the non-takers are more similar to those who take up the cessation aids than to those who do not wish to quit. As a result, it is reasonable toattribute the value of cessation estimated for smokers who do purchase cessation aids to smokers who wish to quit but do not purchase such aids (e.g., $6,400).
The second problem is that these values seem far too low to be plausible. Indeed, the implied value of cessation is far below what most smokers spend on cigarettes in a year. It is not entirely clear what explains this discrepancy. It may be that such people perceive ∆d as smaller or the full price p as larger than used above. Alternatively, they may incorrectly believe they will quit in a future period at lower cost. Before using this method, FDA would need to obtain survey evidence of existing smokers to measure their perceived ∆d and p.
Willingness to pay estimates can be extended to non-initiators as well. For a non-smoker, the benefit of not initiating is the expected value of a lottery that reflects uncertainty about whether or not the smoker will wish to quit at some time after initiation.39 If he smokes and wishes to quit, the harm from having initiated is the withdrawal costs of cessation.
In principle, withdrawal costs can be estimated using the willingness to pay approach, by considering an aid that virtually eliminated these costs and comparing that to an aid that does not. Weimer et al. (2009) elicited smokers’ willingness to pay for a hypothetical drug “that would completely block your craving for cigarettes.” The drug would be administered by injection; it would work for one year and could be renewed with another injection. Estimated mean willingness to pay for this drug is roughly $300 - $350 (depending on model specification). As these values are smaller than the estimates of willingness to pay that do not eliminate the physical and psychic costs, they are not plausible estimates of the value of quitting if there were no physical and psychic costs. An alternative is to estimate withdrawal costs by matching withdrawal symptoms to quality-of-life disutilities in the literature, as was done above.
The cost of non-initiation is the harm from preventing initiation for those smokers who never regret initiation. As we argue below, very few rational individuals initiate smoking. Thus, we suspect that these costs are small.
A.2 Calculating Compensating Differentials
A second approach to valuing the costs of smoking changes is to evaluate the benefits of regulation with an assumed utility function.40 In equation (1), W is consumer welfare without a regulatory intervention; denote this Wwithout. Welfare with a regulatory intervention is denoted Wwith. The welfare benefit of a regulation to consumers is given by C, where Wwith(Y-C) = Wwithout(Y). The goal is to calculate C for different policies.
Gruber and Köszegi (2001) make a start on this for the utility function in equation (1), estimating the optimal tax needed to counter time inconsistency. They limited their analysis to ‘sophisticated’ hyperbolic discounters – those who are aware of their time inconsistency. Sparked by this panel, the solution to this problem has been solved for ‘naïve’ hyperbolic discounters – those who do not recognize their time inconsistency – by Áron Tóbiás of Yale University (Tóbiás 2014), who worked under James Choi. Both the Gruber-Köszegi solution and the Tóbiás solution are derived for a steady state – a person who will smoke the same amount over time. That is relevant for existing smokers but clearly not relevant for potential initiators. Thus, this approach is only relevant for the cessation margin.
In practice, the calculations that result from this are extremely sensitive to the parameterization of the time inconsistency problem that consumers face. To see this, note that the optimal tax to correct time inconsistency is given by
Optimal taxi ≡ τi = θi∙(1- β)∙HS ,
where HS the discounted lifetime value of the health costs of smoking 41 and θi is a parameter that takes on two values, one for naïve hyperbolic consumers and a second for sophisticated hyperbolic consumers.
Figure A-1 shows the optimal corrective tax as a function of β using parameters similar to those chosen in Gruber and Köszegi (2001).42 In this example, the present value of the health harm from cigarettes is assumed to be $30.45 per pack. At β=0, none of this cost is internalized, and so the optimal
corrective taxation is that amount. At β=1, the full cost is internalized, and so the optimal corrective tax
is zero.
A general consensus is that the average β in the population is likely about 0.7 (Angeletos et al. 2001), in which case the optimal corrective tax is about $8 per pack. However, there is almost certainly heterogeneity in β, and this will be important. For example, studies show that current smokers, problem gamblers, and children have lower β’s (Chabris et al. 2008). Additionally, given the widespread knowledge about the harms of smoking and the dramatic reduction in smoking over time, one expects that shortsighted people are overly represented in the smoking population. Added to this is the fact that adults with mental illness are more likely to be smokers than the rest of the population. Estimates of β in the literature range from as low as 0.4 (DellaVigna and Paserman 2005) to as high as 0.9 (Skiba and Tobacman 2008). Further research on discounting among current smokers would be valuable.
Figure A-1: Variation in Optimal Corrective Taxation with β
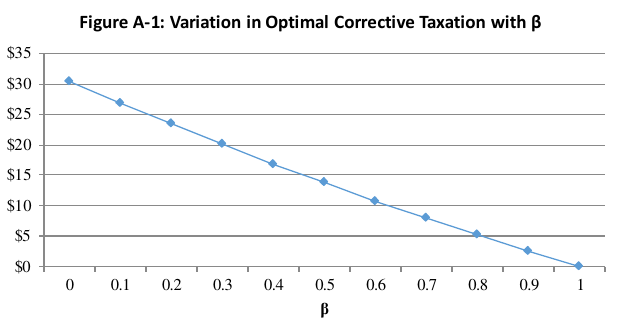
A.3 Directly Measuring Effects of Smoking Cessation on Subjective Well Being
Information on subjective well-being (or “happiness”) is an additional way to measure the impact of regulations. If one interprets measures of self-reported happiness as experienced utility, this method can indicate how regulations affect the utility of those they influence.
Measures of subjective well-being are derived using surveys to ask questions about “how happy” or “how satisfied” respondents are with their lives. Answers can then be translated into monetary values by estimating the change in income that provides the same change in subjective well-being as the event of interest.
An increasing number of studies have looked at the relationship between smoking and measures of subjective well-being.43 It is clear that many smokers are unhappy with their smoking, and former smokers are happy with their decision to quit (Shahab and West 2009, Kahneman and Deaton 2010, Piper et al. 2012, Taylor et al. 2014, Wang et al. 2014, Weinhold and Chaloupka 2014). In a cost-benefit context, it is a question whether regulatory-induced changes in smoking have the same effect on well-being as people who quit for other reasons. Gruber and Mullainathan (2005) find that higher cigarette excise taxes are associated with greater subjective well-being among those with a propensity to smoke in the U.S. and Canada. More systematic review is needed to evaluate existing research and its applicability to the specific types of policies HHS is likely to pursue, and more work is needed to determine the relationship of empirical measures of subjective well-being to monetary values.
1 Externalities are a major issue with many addictive and habitual goods, including tobacco use (Cutler 2002: 2156-62). Because this paper’s concern i s with the issue of utility offsets, for simplicity it does not address the question of external effects of consumption on others, which would lead to welfare losses even if individuals make fully informed decisions.
2 HHS and FDA do not include improved productivity among the benefits of regulations that improve health, because doing so would double-count the benefits of better health status.
3 Authors’ computations from the CPS-TUS data using sample weights provided by the U.S. Census Bureau.
4 http://www.drugabuse.gov/publications/media-guide/science-drug-abuse-ad….
5 The Fagerström Test measures tobacco dependence using multiple factors like time from awakening to the first cigarette, number of cigarettes smoked, and compulsion to use, but most of its ability to predict ability to quit is from the time to the first cigarette after waking measure (Baker et al. 2007).
6 This estimate considers a smoker to be nicotine dependent if the first cigarette is smoked within 30 minutes of waking (a key measure from the FTND) or the person scores 2.75 or more on the 19-item Nicotine Dependence Syndrome Scale (SAMHSA 2010).
7 This rate is based on former smokers who had stopped smoking in the past year and current smokers who had refrained from smoking for one or more days in the past year because they wanted to quit.
8 Quitting is defined here as not having smoked at all in the 6 months preceding the interview.
9 The graphic warning labeling final rule was not implemented as a result of court rulings that its requirements violated the first amendment.
10 For reviews, see Frederick et al. (2002) and DellaVigna (2009).
11 The fact that all income is spent on the addictive and non-addictive goods implies that there is no saving or borrowing.
12 Addiction is modeled empirically as adjacent complementarity – the value of consumption today is higher if consumption was greater in the past. We capture adjacent complementarity in a slightly non-standard way. If aincreases, then St+1 increases as well. Because higher St+1 leads to greater withdrawal costs, utility is lower in t+1. Given the concavity of the utility function, this increases the return to a t+1. An alternative way of capturing adjacent complementary would be to include a term α3a t St , where α 3>0 reflects adjacent complementarity. Adding such a term would not materially affect our analysis.
13 Gruber and Köszegi (2001). Their estimate factors in health costs of reduced life expectancy only, not reduced health during the lifetime.
14 As a review of research by Sloan and Wang (2008) concludes, “The economic literature lends no empirical support to the view that mature adults smoke because they underestimate the probability of harm to health from smoking.” See also Kenkel (2000, 1697-1699), Kenkel and Chen (2000) and Chaloupka and Warner (2000, 1595).
15 For review, see Reyna and Farley (2006).
16 For example, Oncken et al. (2005) found that over 90 percent of smokers had good knowledge of risks of cardiovascular, pulmonary, and oral problems due to smoking, but only 40-60 percent had good knowledge of other types of risks (cancers other than lung, reproductive problems, smoking-related disabilities).
17 Note that this is not definitive, however. It may be that all the people who would want to smoke initiate as teens. Empirical evidence about whether people deterred by tobacco-control interventions from smoking as teens have risks of taking up smoking as young adults is limited.
18 The 2009 TCA banned cigarettes with characterizing flavors (clove, chocolate, pineapple, grape, etc.). FDA has also considered whether to ban menthol cigarettes.
19 Relevant studies include Shahab and West (2009, 20120), Piper et al. (2012), Taylor et al. (2014), Wang et al. (2014), and Weinhold and Chaloupka (2014).
20 A question of concern in a cost-benefit context is whether changes in subjective well-being associated with self-initiated voluntary quits may not accurately represent quits induced by regulations. In part to address this concern, Gruber and Mullainathan (2005) examined how increases in cigarette excise taxes affected subjective well-being among those with a propensity to smoke in the U.S. and Canada, finding a positive effect.
21 Explicit models of addictive consumption are also highly stylized and hard to distinguish between empirically, so that the appropriateness of the model to the issue at hand is an untestable maintained hypothesis.
22 When more detailed measures of nicotine dependence are used, the share of smokers categorized as nicotine dependent is higher (e.g. SAMHSA 2013).
23 For evidence on relationships between age, education, and decision-making, see Choi et al. (2014).
24 In 2010, for example, people in this age range turned 16 in the years between 1981 and 1996. According to Gallup poll data, 45 percent of the adult population believed smoking was a cause of lung cancer in 1958. By 1969, the share had increased to 71 percent. It has been above 90 percent since the early 1990s (Saad 2002).
25 Because the vast majority of smokers begin smoking while still in their teens, this ability may affect choices about cessation more than choices about initiation. Nonetheless, if teens who eventually obtain college degrees begin to acquire this ability as teens, their choices related to smoking initiation may also have been relatively well-informed and forward-looking compared to other teens.
26 Because we omit the population under age 30, the overall average of cigarettes smoked is slightly higher using this methodology than in sorting people by the degree of addiction: 245 vs. 230 packs annually. These are sufficiently close that we assume the same demand elasticity in both settings.
27 Notes to Table 5 give data sources and methods.
28 The necessary price change is given by dP/dQ * (Q II-QI).
29 We assume the full QALY loss occurs in the first month of cessation and phases down over the next 11 months, taking one-half of its initial in the second month, one-quarter in the third month, one-eighth in months four through six, and one-sixteenth in months 7 through 12.
30 Authors’ calculations using sample weights.
31 Five years of two attempts per year, with each failed attempt entailing a QALY decrement of (.25)*.0088
32 Depression is estimated to have a quality of life decrement of 0.0625.
33 From Table 1, average packs per year are 11 and 42 for type I and type II potential initiators respectively; with the two group’s shares of potential initiators being about one-third and two-thirds, average packs for all potential initiators is about 33. Again taking the demand elasticity to be -0.3, the fact that the demand curve passes through the point {p=$5.43,q=42} implies dq/dp=-2.33. Then the price increase that would decrease average packs per potential initiator by 10% (3.33 packs) is 3.33/2.33 =$1.40.
34 Formally, for a regulation adopted at time 0, for people of a given age j, the expected discounted benefits of the regulation would be

where d is the discount rate (3 percent or 7 percent), njdis the number of people of age j who are deterred from smoking by the regulation (either induced to quit or dissuaded from initiating), n jc is the number who continue smoking or initiating, and b jt d and b jt Ic are the benefits in the tth year after the regulation takes effect for people in these two groups respectively. Then the aggregate benefits of the policy can be computed as the sum of the benefits across the age groups.
35 Fiore et al. (2008), Table 6.26, p. 109.
36 Revealed-preference methods use actual purchase behavior. Stated-preference methods rely on smokers’ responses to survey questions asking if they would take a specific action to increase their chance of quitting.
37 Schauffler et al. report the cost of the treatment as $32,487 for the 124 subjects who used gum or patches and 6 who used behavioral therapy. Assuming the 6 are not included in the 124 implies an average cost of $250 (≈$32,487/130) per subject who used the cessation products.
38 The estimated inverse demand is p = 640 – 28 q where p is WTP ($) and q is the percentage purchasing the cessation product; mean WTP = $640/2.
39 In this section, “wish to quit” means the smoker would quit if there were no physical, psychic, or financial costs of quitting. Given that there are large physical and psychic costs, many smokers who “wish to quit” may choose not to attempt to quit.
40 Chetty (2009) and Mullainathan, Schwarstzstein and Congdon (2012) review the theory and practice of reducedform versus structural approaches to standard and behavioral welfare economics.
41 Formally,  where δ=1/(1+ρ), ρ is the discount rate for a non-hyperbolic consumer, and d is the rate at which stock of past consumption declines over time (e.g., how rapidly the harmful stock of past cigarette consumption changes).
where δ=1/(1+ρ), ρ is the discount rate for a non-hyperbolic consumer, and d is the rate at which stock of past consumption declines over time (e.g., how rapidly the harmful stock of past cigarette consumption changes).
42 Specifically, we assume d=0.8, λ=0.7, and δ=1.
43 A useful survey is Fujiwara and Dolan (forthcoming). The field increasingly emphasizes development of best practices for use in policy analysis and other settings, including recent U.S., U.K., and OECD recommendations (National Research Council 2013, Fujiwara and Campbell 2011, Organization for Economic Cooperation and Development 2013). The U.S. recommendations developed by the National Research Council focus primarily on measuring subjective well-being, while the U.K. and OECD guidance also address the use of these measures in benefit-cost analysis.