
U.S. Department of Health and Human Services
State Discipline of Physicians: Assessing State Medical Boards through Case Studies
Randall R. Bovbjerg and Pablo AliagaThe Urban Institute, Health Policy Center
Josephine GittlerUniversity of Iowa, College of Law
February 2006
This report was prepared under contract #HHS-100-03-0011 between HHSs ASPE/DALTCP and the Urban Institute. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the ASPE Project Officer, Linda Bergofsky, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. Her e-mail address is: Linda.Bergofsky@hhs.gov.
TABLE OF CONTENTS
- DATA AND METHODS
- Literature Review and Other Early Input
- Case Studies
- National Data
- Overview of Case Study States and Analytic Approach
- THE REGULATORY LOGIC OF STATE MEDICAL BOARDS
- Boards Mission and Activities
- Structural Factors as Enablers or Impediments to Disciplinary Performance
- FINDINGS ON BOARD STRUCTURE AND RESOURCES
- Board Membership, Terms and Remuneration
- Boards Place within State Administrative Operations
- Statutory Support for Board Actions
- Board Funding and Staffing
- COMPLAINT RESOLUTION, THE MAIN DISCIPLINARY PROCESS
- Intake of Complaints
- Investigation
- Pre-Hearing Process: Charging and Settlement or Prosecution
- Adjudicative Hearing
- Imposition of Sanction
- MEASURING DISCIPLINARY PERFORMANCE
- Rates of Sanctioning Physicians
- Throughput of Cases: Backlogs and Speed of Resolution
- IMPEDIMENTS TO DISCIPLINARY PERFORMANCE IN PRACTICE
- Problems at Intake
- Problems in Investigation
- Preparations and Prosecutions
- Costs and Other Cross-Cutting Problems
- IMPROVING DISCIPLINE: EFFECTIVE PRACTICES AND INNVATIONS OF INTEREST
- Process Change and Improved Management
- Medical Expertise
- Efficiency and Targeting Resources
- Innovations Ancillary to Complaint Resolution
- Other Innovations
- APPENDICES
- APPENDIX A: THE TECHNICAL ADVISORY GROUP
- APPENDIX B: DISCUSSION GUIDE, STATE MEDICAL BOARDS AND PHYSICIAN DISCIPLINE
- APPENDIX C: STATE MEDICAL BOARD CASE STUDIES--CORE QUESTIONS ON DISCIPLINARY PROCESS
- APPENDIX D: FSMB MEMBER BOARD ANNUAL SURVEY, 2004
- LIST OF EXHIBITS
- EXHIBIT 1: Case Study Sites, Six State Medical Boards
- EXHIBIT 2: The Simple Logic of Public Protection
- EXHIBIT 3: Concerns from Literature Review
- EXHIBIT 4: Board vs. board: A Note on Nomenclature
- EXHIBIT 5: Administrative Structures in States
- EXHIBIT 6: Ratio of Licensed to Practicing In-State Physicians
- EXHIBIT 7: Budgets per Thousand Physicians
- EXHIBIT 8: Importance of Disciplinary Function, as Perceived over Time
- EXHIBIT 9: Budget Allocation by Function
- EXHIBIT 10: Executives Priorities for Budget Increase
- EXHIBIT 11: Complaint-Driven Discipline
- EXHIBIT 12: Sources of Complaints
- EXHIBIT 13: Complaints per Thousand Physicians
- EXHIBIT 14: Complaints Received per Staff Member
- EXHIBIT 15: Complaint Resolution by Stage of Discipline
- EXHIBIT 16: Availability of Sanctions
- EXHIBIT 17: Sanctions per 1000 Physicians
- EXHIBIT 18: Estimated Costs to Prosecute Fully Contested Quality Case
- EXHIBIT 19: Disciplinary Data Systems and Information Technology
- EXHIBIT 20: Contents of Massachusetts Physician Profiles
ACKNOWLEDGMENTS
The authors would like to thank the many people who contributed to this monograph. First, we thank John Hoff, former Deputy Assistant Secretary, Office of Disability, Aging and Long-Term Care Policy, who saw the need for and took the lead in setting the goals of this study, as well as project officer Linda Bergofsky, who contributed throughout the project, including participation in one site visit and two annual meetings of the Federation of State Medical Boards.
Second, we thank the knowledgeable and helpful members of the projects Technical Advisory Group (TAG) (Appendix A). Before case studies began, they helped shape the issues addressed and overall approach taken, as shown in the concept paper (Bovbjerg and Stockdale 2004). Third, we thank Lisa Robin of the Federation, who served on the TAG and provided automated access to the Federations Exchange data (FSMB 2003b), which provides detailed information about Boards that facilitated case study site selection and contributed to this report. The Federation subsequently also provided access to their most recent member board survey, which has much useful data on Board operations.
Fourth, our special thanks go to the many state officials and others in each case study state that granted us substantial amounts of their time--in many instances during multiple sessions--and supplied numerous documents. Their generous contributions of time, energy, and information made this project feasible. Reasons of confidentiality as well as numbers preclude their being listed by name here. Finally, we thank our colleagues--Holly S. Stockdale, who worked on this project until October 2004; Barbara Ormond and Timothy S. Jost, who reviewed and contributed to the manuscript; and Timothy Waidman, who has managed this and other ASPE projects within the Urban Institutes Health Policy Center.
EXECUTIVE SUMMARY
State Medical Boards that license and discipline physicians play an important and insufficiently studied role in medical quality assurance. This project gathered information on Boards structures, processes for disciplining physicians, especially those relevant to improving medical quality, and methods of self-assessment. The project also identified practices that state Medical Board staff or other experts believe effective or potentially effective in improving their processes or impacts on quality.
Data collection. Issues of interest were framed by the project statement of work and elaborated through literature review, national expert discussions, input from a technical advisory group, and production of a concept paper (Bovbjerg & Stockdale 2004). Information on Board structure and operations came from detailed case study interactions in six states during 2004-05. Descriptive analysis of cross-state structural and performance data was possible based on case study results and national data on Boards for 2003, the most recent available, from the Federation of State Medical Boards, and current licensure requirements came from the compilation of the American Medical Association.
Case studies were conducted in six states: California, Iowa, Massachusetts, Ohio, Virginia, and Washington. They were chosen to include innovations of interest and for reputations of good administration, as well as for some diversity in size and geographic location. Available documentation on Boards was obtained; and open-ended sessions were conducted with physician and non-physician Board members, executive directors and other managers, staff, and outside observers or participants in Board activities. The project focused on current experience, defined as about the last five years, but key informants also referred to prior history.
Board Structure and Resources. Literature suggests that the following factors influence disciplinary performance.
- Some Boards are part of a larger umbrella state agency while others operate more independently.
- Board membership always has a physician majority, but nearly half may be public members.
- Board powers and operations are influenced by specific state enabling legislation, the states law of administrative procedure, and judicial rulings.
- Boards spending per thousand physicians ranges widely, affected by licensure fee levels and state budgetary policies. All six study Boards were in the middle half of budgetary resources nationally in 2003, but the highest state studied still had almost double the funding of the lowest.
Complaint Resolution. Discipline of physicians beyond initial licensure is the Boards main activity. Discipline is largely complaint-driven, and Boards proactively begin few cases.
- Some 60-90% of complaints came from the public in the study states, almost entirely from patients and families. Boards also receive input from other government agencies, hospitals, and malpractice insurers.
- Many complaints at least in part involve allegations of poor quality care--a quarter to half of them, according to executive directors.
- The volume of complaints per thousand physicians varies considerably by state, in part because of differing standards of what constitutes a complaint.
Complaint resolution proceeds through four main stages: intake, investigation, pre-hearing preparations, and hearing. Intake resolves about 14% of cases before investigation, largely because they are minor or complain about unregulated behavior, such as physicians charges. Investigation closes almost two-thirds of cases, typically because there is too little evidence to support formal charges but sometimes with an informal notice of concern or similar communication with the respondent physician. Pre-hearing processes resolve almost 20% of cases, either dropping them after further consideration by staff and prosecuting attorneys or settling them by agreement with the respondent. Only about 1.5% of complaints reach formal hearing.
A final level of process is court appeal after final Board decision. Physicians whose hearing imposed strong sanctions not infrequently appeal, according to case study informants, but appeals constitute a very small share of total disciplinary cases because hearings are so uncommon. In all, almost 5% of complaints result in some level of sanction, which may be negotiated before hearing or imposed after one. Most Boards have authority to take a full range of actions to resolve a complaint. Actions may be informal, such as a confidential letter of education or censure. The most prejudicial formal actions are loss or restriction of license. Other prejudicial actions include fines and reprimands. Some actions are classified as non-prejudicial, often unrelated to sanctions, such as reinstatement of license. Most cases are closed without any action.
Measuring Disciplinary Performance. A key question posed in all case study sites was what outputs Board managers intended to achieve and how they measured them. Only two performance measures were noted in all sites. The first was the number of disciplinary sanctions imposed. The second was timeliness of complaint resolution--and avoidance of a lengthy backlog of open cases.
- The annual rate of prejudicial actions per thousand practicing physicians is not high. Nationally, the average is just under six actions per thousand physicians per year, just under seven in the study states, with substantial variation across states.
- The speed of complaint resolution also varies greatly. For instance, in the typical state only about 10% of cases take more than 360 days to resolve. However, such slow closures constituted 60% or more of closures for about one-fifth of reporting Boards nationally.
- All the study states reported having to address significant backlogs of complaints in some recent period.
Impediments to Disciplinary Performance in Practice. Board members and managers described facing different challenges at different stages of the disciplinary process. At intake, a key issue is conducting reliable triage to set priorities for investigation. During investigation, Board staff must overcome barriers to obtaining medical records from physicians, their own understaffing, and problems discerning whether quality cases were serious enough to receive high priority. Difficulties obtaining sufficient medical and legal expertise were especially problematic. They apply both at screening stages, as Board staff must prioritize investigations or decide whether to charge and prosecute a physician and in preparing for and conducting formal testimony at hearing.
High costs were endemic at all stages, particularly for quality-based cases--starting with the need for early medical screening, more in preparation for hearing, and most of all in fully contested hearings. Where possible, Boards often resolve quality-related concerns against a practitioner by finding an easier-to-prove ground, such as failure to report required information in renewing his or her license. Boards do not track costs by function, but executive directors could provide an approximation of their costs for a recent fully contested quality case that had necessitated expert testimony. Three of the six said such a case had cost $100,000. Costs are high for going to hearing rather than settling because revoking a license requires proof through expert testimony of a continuing pattern of negligence or lack of competence. Board members and managers described wrestling with determinations of just how many instances of negligence are needed to demonstrate incompetence. They confirmed that are no agreed upon, objective standards of competence on which they can rely.
Systemic problems of fragmentation of responsibilities and discontinuities in the disciplinary process were also described. There are typically multiple hand offs among staff as a case progresses through the process, and cases may be sent back for additional investigation once an attorney begins final preparation for hearing.
Board staff also recognized that relying on complaints to find problem physicians is a reactive process with a very narrow focus that generates a large volume of investigation to find a small number of actionable cases, especially starting with complaints from the general public. They expressed desire in better input from expert sources as well as alternatives to conventional discipline. All but one manager complained about the available information technology, although two reported that their states had at least embarked upon major upgrades.
Finally, some noted that decisions on sanctions must weigh not only quality concerns but also competing considerations. For example, whether taking disciplinary action in a marginally troublesome case would curtail physician access in a rural area or reduce patient access to desired pain medication or alternative therapy.
Effective Practices for Improving Complaint-Driven Discipline. Another focus of the project was identifying effective or potentially effective ways to improve Boards quality-related performance. Most input from Board managers involved methods they saw as improvements to conventional discipline, including:
- more effective intake and triage of complaints;
- selective enhancements to staff capacity, especially for investigation and investigative oversight (the stage that resolves most cases);
- improved access to medical expertise throughout the disciplinary process;
- monitoring of throughput of cases in investigation; and
- more modern information technology (IT) including more sophisticated data entry, retrieval, and analysis.
IT was prized partly for its ability to save on costs of paperwork and data sharing and retrieval. For example, managers reported coping with funding shortfalls in part by automating licensure functions and shifting resources to discipline. Even more, better IT and data systems were believed to enable managers to learn much more about their processes and what people and practices work most effectively; over time better tracking capabilities were expected to promote better measures to track. Managers wanted to improve their use of whatever level of funding and staff they have to work with, improving triage and efficiency of throughput in investigation, for example. Experience in two states suggests that better analysis of data on accomplishments and shortfalls can help persuade legislatures to grant more funding as well as Board-desired legal changes.
Two other potentially effective practices sought to enhance medical expertise for conventional discipline:
- One state reported great success in contracting out medical screening reviews to a national peer review organization. Sources there reported not only expanded access to expertise but also improved speed of review.
- Managers in all but the larger states reported interest in regional pooling of experts, as the available in-state expert pool was sometimes very small, especially for subspecialties like pediatric neurology.
Other effective practices were also suggested as improving the efficiency of conventional discipline through cross-cutting interventions:
- reducing handoffs by creating unified teams of investigators, Board managers, and prosecuting attorneys--especially for high-profile cases almost certain to go to hearing;
- more centralization of case oversight to reduce fragmentation of responsibility;
- standardization of sanctions to improve consistency and, by extension, deterrent effect; and
- more active leadership.
Increased budgets were perceived to be necessary to effectuate many of the above noted improvements. All managers believed that improvements in budgetary or IT resources would improve their output. There were suggestive indications that this is so from the increase in cases closed in Virginia, whose budget was significantly increased during the observation period.
Other Innovations Ancillary to Complaint Resolution. Such practices do not directly affect existing conventional processes of disciplinary complaint resolution but rather complement them.
Several Board managers and outside observers suggested that Boards act through rules of general application to head off whole categories of case-by-case complaints. One state cited the example of prompt development of guidelines for bariatric surgery, relatively new as a high-volume procedure. Another cited a collaboration with the pharmacy board to block physicians from filling prescriptions for controlled substances in the names of family members.
Ohios Quality Intervention Program (QIP) is a less formal and faster process that uses two subsidiary panels of volunteer physicians to resolve less serious looking quality cases, typically ones involving a single deficit in a physicians capabilities. Investigators refer quality cases to QIP that are likely to be remediable with re-education but that still might need to be referred back for conventional discipline and stronger action.
A similar alternative to conventional complaint investigation is referral to one of the regional or national clinical assessment centers (CACs) run by medical schools and others. The centers use a variety of hands-on methods to assess any deficiencies a referred physician might have, and can also prepare a program of re-education at the center and continuing back home. California refers many conventionally sanctioned physicians to an in-state center for remediation, but the other states were just beginning to use such centers, mainly earlier in the disciplinary process.
The Massachusetts Boards Patient Care Assessment (PCA) program operates quite separately from conventional, complaint-based discipline. The Boards PCA unit reviews and approves hospitals own PCA safety plans and monitors their operations through several types of required reports. The goal is to promote facilities own efforts and to create safe environments within which physicians can practice, rather than to identify and sanction problem physicians. Managers believe improvements are occurring and also praise the process for quickly uncovering the problems in bariatric surgery noted above, which would have taken far longer to be discovered through conventional complaints.
Another alternative described by case study Board managers and others is to encourage hospitals and other medical institutions to identify physicians with potential quality problems before they hurt patients or generate complaints, referring them to a CAC for evaluation and re-education. A small experiment in several states is attempting to demonstrate the feasibility and utility of this approach; its performance was not part of this case study.
Online physician profiles have been adopted to better inform prospective patients and payers about physician characteristics and thus potentially encourage market responses that promote quality. All the study states make such information available, at varying levels of detail.
Other Innovations. Many Board members and managers wanted to do more for safety than react to complaints. The literature review and case study respondents suggested some other proactive alternatives to complaint-based discipline. These included audits of physician practices, non-disciplinary use of CACs, and efforts to encourage ongoing maintenance of competence. Such approaches not now observable in the field were beyond the scope of this study.
Implications. This case study documented many aspects of Boards structure and operations. It also identified practices considered to make discipline more efficient or effective. Other states could learn from the particular practices recommended by managers and others from these six states. A cross-cutting lesson is that organized assessments of Board performance are useful internally and in seeking a grant of more resources and other Board-desired changes from state legislatures.
Limitations. The six case study states are not nationally representative. They were judgmentally selected to help the project observe innovations. The national survey data available provided comparative perspective, but not fully standardized definitions of data elements. Assessment of the impact of innovations also relied heavily on informed judgment, that of knowledgeable managers and other key informants. It is generally agreed to be beyond the current state of the art to assess performance by measuring any direct impact of Board activities on public health or safety.
Next steps. One near-term development for Boards will likely involve making good use of the new capabilities in IT and data management that managers were actively seeking in every case study state. Beyond the hardware and software, performance improvement was also said to call for: (i) a new approach to data entry and maintenance, (ii) enhanced analytical capabilities, and (iii) standards or comparative benchmarks against which to measure performance. Data from the Federations member board survey already offers Boards some comparative information, but has some limitations, and demand for improved comparative benchmarking seems likely to grow.
For policy research, the next steps may be to more rigorously study existing state interventions or conduct demonstrations to see how well some of them travel to new states. More careful study would be useful for such things as Californias use of clinical assessment centers, Massachusettss physician profiling and unusual relationship with hospital safety efforts (the PCA), Ohios quality improvement program, and efforts in numerous states to form teams of investigators, managers, and lawyers to streamline the handling of important cases. Non-case study states of course also offer opportunities for study.
BACKGROUND AND INTRODUCTION
This project described State Medical Boards disciplinary processes, assessed measurement of disciplinary performance, and identified practices that Boards believe effectively improve their functioning. Finding ways to assess Boards performance is important because states have given them a key role in safeguarding medical quality and patient safety. Boards importance has become apparent again during the recent medical litigation crisis. Many other private and public efforts also attempt to protect quality, but all ultimately rely on Boards to address practitioners who simply cannot or will not meet minimum standards.
The project used case studies and other methods to address such research questions as:
- How do Boards perceive their mission?
- How does discipline relate to licensure and other Board functions?
- What approaches do states use to discipline physicians?
- How is performance assessed--by commentators and by Boards themselves?
- What factors appear to facilitate or impede disciplinary functioning?
- What effective practices have Boards adopted to improve performance that might merit wider adoption?
- How does the work of Boards relate to malpractice litigation and to the new patient safety movement?
More detailed background is provided in the projects prior concept paper (Bovbjerg and Stockdale 2004).
MOTIVATION AND GOALS OF THE PROJECT
State Medical Boards are one of the earliest public interventions in medical quality, dating from the turn of the last century (Ameringer 1999), and have newly attracted attention in the recent surge of interest in medical quality (Bodenheimer 1999), safety (Kohn et al. 2000), and medical litigation reform (Mello et al. 2003). Prior commentary on Boards has long been critical of their performance (Derbyshire 1965), but mainly in very general terms, such as the failure of licensing boards to discipline licensees (Young 2002) or that professional self-policing is inherently unreliable. Others repeat anecdotes of seemingly egregious physician misbehavior that has consistently not been addressed by Boards (Boodman & Davis 2003; Richmond Times-Dispatch 2003; Hall 2004; Thompson 2005a, 2005b) or conclude that states ranking low in disciplinary rates are simply too low (Public Citizen 2005; CJD 2002). Suggestions for improvement are usually general as well.
Substantive analysis is rare, and even careful descriptive documentation of Board activities is unusual (exceptions include R. Fellmeth 1989; Jost et al. 1993; JLARC 2000; J. Fellmeth & Papageorge 2004). In short, the literature is long on opinions about Boards but short on documentation, and there is almost no analysis of disciplinary activities in practice. How best to measure what Boards do is not agreed upon, much less to measure how well they do it, and least of all to assess how disciplinary activities affect health care outcomes.
This projects overall goal, in the words of the Office of the Assistant Secretary for Planning and Evaluation statement of work, was to improve the documenting and measuring of how Boards operate, so as to identify opportunities for improvement. The project was designed to produce descriptive information on Boards structures, their missions and roles, and their operations. It aimed to develop logic models of existing disciplinary processes. Within each model in use, activities and functions were to be cataloged, along with existing and potential measures of performance. The project then intended to identify impediments to and supports for effective performance, as well as effective and potentially effective practices for improving performance. We also sought to identify innovative alternatives to conventional approaches and key informants perspectives on their feasibility and desirability.
DATA AND METHODS
We base the findings presented in this report on information derived from four sources--a review of the literature, discussions with national experts, case studies of State Medical Boards in six states, and analysis of data from national data sets.
Literature Review and Other Early Input
The initial literature reviewed included journal articles as well as web page materials and Board characteristics in The Exchange, produced by the Federation of State Medical Boards or the FSMBa (FSMB 2003b). It provided background on Board structure and characteristics as well as prior evaluations of performance. (Most of the literature reviewed is listed as references at the end of this report.) Following our review of the literature, we held directed discussions with national experts to help identify issues and discuss states to be considered for the case studies. At this stage, a technical advisory group (TAG) was created from among national experts to provide additional background and help develop the projects conceptual review of issues for further investigation (Bovbjerg & Stockdale 2004; see TAG Membership, Appendix A.)
Case Studies
The core of the project was case studies in six states--California, Iowa, Massachusetts, Ohio, Virginia, and Washington. The case studies provided detailed information about each states experiences and approach. Each case study began by reviewing written materials found on the states web page, provided by state officials in advance, or located in news accounts or other sources. Much information came from answers to questions posed during site visits, which took place between June 2004 and May 2005, and from follow-up telephone calls and subsequently provided written materials. Site visits lasting two or three days were made in five of the states. In the sixth state, California, the study relied on the states rich written sources and used only telephone calls.
During the site visits, we met with the Boards Executive Director, typically more than once; if needed, another person with longer historical perspective; staff responsible for the main stages of disciplinary process, including intake and screening, investigation, charging, and prosecution; a person in charge of the automated complaint/case tracking system, if any; an experienced attorney, usually from the attorney generals office; and one or two Board members. For additional perspective, where possible, we also spoke with medical or hospital associations and other outside participants in or observers of disciplinary matters.
Before each visit, state officials were sent a discussion guide in advance to facilitate preparations, including which staffers to meet, and interactions on site. The guide addressed characteristics of Boards and conventional disciplinary process that were expected to be common to all states based on the literature--including Board history, mission, and vision for the future; data on annual expenditures and staffing; description and data on each stage of disciplinary process from intake to resolution and potential follow-up; and explanations of how managers track the process, what barriers they perceive and would like to change, and what standards or rules they use in various parts of the process. (See Discussion Guide, Appendix B.)
For the visits, the discussion guide was augmented with additional questions specific to each state based upon review of supplementary literature and how that states experience related to the research goals identified in the conceptual review:
- to generate relevant background information on Boards structures and roles;
- to describe logic models of how existing disciplinary activities are meant to work;
- to categorize and describe Board activities and functions within each model;
- to identify existing and potential measures of performance, overall and by activity;
- to assess supports for and barriers to good performance, overall and by activity; and
- to describe promising innovative alternatives and their alternative logic.
Each state-level respondent addressed slightly different issues and questions depending upon his or her area of responsibility or expertise in their respective states. This flexible approach resulted in a wide-ranging discussion and allowed us to cover similar issues across states while also giving respondents the opportunity to explain their circumstances, their experiences, areas of concern, and their plans. Post-visit follow-up by telephone and email allowed clarification of the information previously obtained.
Overall, this approach provided a full picture of important developments in each state, although somewhat different information for each one, given the differences in their programs. At the end of the case studies, we spoke again with executive directors in all six states to get contemporaneous responses to a smaller set of core issues that emerged as a result of case study discussions, such as priorities for additional budgeted funds (if they were made available), costs of taking a case to full hearing, and perceptions of effectiveness relative to other Boards.
National Data
Several national data sources supplement the case study information. Three come from the Federation of State Medical Boards and one comes from the American Medical Association:
- The Exchange;
- Member Board Annual Survey;
- Summary of Board Actions; and
- State Medical Licensure Requirements and Statistics.
The Exchange is a compilation of descriptive information by state about Board structure, staffing, and other characteristics (FSMB 2003b). The Member Board Annual Survey is a FSMB database that covers Board budgets, staffing, and detail on licensure and discipline (see Member Board Annual Survey, Appendix D). Boards in 48 states and the District of Columbia responded to the survey, although not to every question.1 We acquired the data for 2003, the most recent available. The Summary of Board Actions provides an annual tally of disciplinary activities and numbers of physicians (FSMB 2005). Again, we used data from 2003. State Medical Licensure Requirements and Statistics is a manual of licensure fees and other requirements by state (AMA 2006). These national sources greatly enrich the case study observations and provide context for interpreting the field observations.
The Member Survey is conducted under promise of confidentiality, and its database was obtained without state identifiers (see Appendix D). We subsequently obtained case study states permission to identify their states, so as to link survey data with other information, but this report maintains the Federations promise of confidentiality. Information specific to individual states is presented where relevant, mainly when available from public sources. Some exhibits identify states only by rank numbers, which differ from exhibit to exhibit.
Because states are identified in Board Actions and The Exchange, measures such as budget per physician can be calculated. Member Survey data are confidential, however, so that disciplinary staffing and complaint data cannot be adjusted for or compared with state characteristics known only from public data, nor can full national totals be computed, as some medical Boards did not respond. The Member Survey also includes an unknown number of responses from the nations 14 osteopathic boards and four territorial boards, which are systematically much smaller than State Medical Boards in licensees and staffing. Although the latter types of boards are likely underrepresented among survey respondents,2 most presentations of data in this report omit extreme values, as a way of focusing more reliably on State Medical Boards--for example, by presenting only a percentile range rather than maximums and minimums.
Overview of Case Study States and Analytic Approach
The six study states were selected for having Boards with reputations for being well administered and to include Board innovations of interest. Selection also sought diversity in geographic location, extent of Board independence as defined by the Federation of State Medical Boards (FSMB 2003b), and other characteristics. Together, the six study states account for about one-quarter of the nations practicing medical doctors (Exhibit 1).
| EXHIBIT 1: Case Study Sites, Six State Medical Boards | ||||||
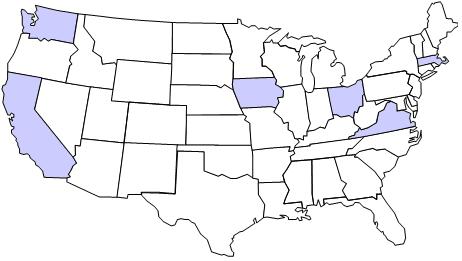 | ||||||
| Attributes | CA | IA | MA | OH | VA | WA |
| Type of Board | Semi-indep. | Semi-indep. | Indep. | Indep. | Semi-indep. | Indep. |
| No. physicians (000s) | 90.0 | 6.0 | 26.2 | 28.0 | 17.7 | 14.5 |
| Ann. Budget ($M) | $38.2 | $1.5 | $5.6 | $6.3 | $5.0 | $4.1 |
| Board size | 19 | 10 | 7 | 12 | 18 | 19 |
| % public members | 37% | 30% | 29% | 25% | 22% | 21% |
| Standard of proof | Clear & convincing evidence | Prepon-derance of evid. | Prepon. | Prepon. | Clear & convin. | Clear & convin. |
| SOURCE: FSMB Exchange, 2003 data; some budgets from interviews. | ||||||
California is the largest of the case study states and has changed board structures several times. Its Board has more written description and data available online than the other study states combined. Not only does the Board compile extensive information, but the legislature also recently funded a separate, temporary office of Discipline Monitor to provide analysis and recommendations (e.g., J. Fellmeth & Papageorge 2004). Iowa is a much smaller state that has recently coped with a large backlog of disciplinary cases. The Massachusetts Board has an apparently unique role in reviewing hospital safety and an evolving relationship with other patient safety efforts within and outside state government. Ohio was an early adopter of formal standards for triaging disciplinary complaints and created an unusual, less formal process for reviewing certain complaints related to medical quality (its Quality Intervention Program). Virginias Board was the subject of an unusually detailed legislative critique in 1999, which prompted numerous changes, including a change in legal standard of proof to facilitate disciplinary prosecutions (JLARC 2000). Washington state is part of an umbrella agency, recently had its standard of proof increased by judicial action, and recently undertook a thorough assessment of its own disciplinary performance.
This report presents descriptive statistics on State Medical Boards, descriptive analyses, and synthesis of respondents expert judgments about problems and performance. It also assesses the logic model of how Boards seek to discipline physicians. The logic-model approach describes the inputs, activities, and regulatory outputs that Boards consider important to their mission, along with the causal links among them, a standard approach to program assessment (Hatry 1999). These foci resemble the quality assessment trilogy of input, process, and outcome (Donabedian 1966, 1972, 1980) but are more practical and measurable.3 Assessing Board activities impacts on ultimate outcomes in health care, like morbidity, mortality and medical injury, would go well beyond current capabilities because outcomes are poorly measured and are affected by so many other factors than Board discipline.
The case studies and this report focus on the last five years. These years differed from the prior five in several respects. First, state budgets were under great strain. Revenues dropped markedly across the nation after fiscal 2001, owing to economic recession and sharp drops in taxpayers capital gains, while Medicaid and some other spending programs rose rapidly (Boyd & Jenny 2003). Significant program cuts were common, as were state hiring freezes or layoffs and across-the-board cuts in some administrative support (Coughlin & Zuckerman 2005; J. Fellmeth & Papageorge 2004). Second, much new publicity about the extent of medical errors was generated by the rise of the patient safety movement and the release of the Institute of Medicine book To Err Is Human (Kohn et al. 2000). Third, starting in 2000, physician malpractice premiums rose rapidly in most states, prompting calls for legal reform and increasing public and legislative concerns about physician competence and extent of negligent behavior (Mello et al. 2003; Blendon et al. 2002).
THE REGULATORY LOGIC OF STATE MEDICAL BOARDS
Boards Mission and Activities
Medical regulation is an exercise of states inherent police power to protect public health and welfare. State enabling statutes, typically called medical practice acts, date from a century ago. Protecting the public is today generally recognized as the main rationale for State Medical Boards (OIG 1986; Finocchio et al. 1998, p.5, FSMB 2003a).4 The logic of public protection is very straightforward: Boards should identify unqualified or unfit doctors and bar them from practice in the state, which directly protects patients from them (Exhibit 2). Indirectly, imposition of sanctions may also lead other physicians to practice more carefully or to tailor their practices to their capabilities. Removal of unsafe physicians from practice has been the most often commented on Board activity (Public Citizen 2005; CJD 2002), but in practice Boards more often impose lesser sanctions, including occasional formal re-education, that aim to keep physicians available to serve patients but with improved future performance.
| EXHIBIT 2: The Simple Logic of Public Protection |
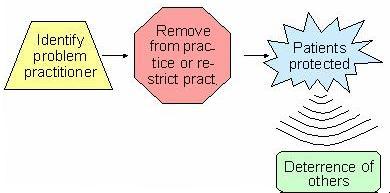 |
Boards exercise two main regulatory functions, licensure and discipline.
Licensure requires a demonstration of educational attainment and knowledge as evidence of competence at the time when doctors first begin practice in a state, whether as a new physician or a mid-career transfer from another state. Over time, requirements for continuing education were added as a condition of licensure renewal. Today, many policy makers are calling for periodic testing of practitioners as a condition of re-licensure, to monitor continuing competence throughout physicians careers (discussed below).
Discipline, in contrast, oversees ongoing practice in a state. Physicians can be disciplined for numerous misbehaviors, from business offenses to problems in the quality of care. Disciplinary actions range in severity from non-public warning letters, to public reprimand, to suspension or revocation of the license to practice. The theory is that discipline protects the public directly by removing some problem physicians from practice, restricting their scope of practice, or improving their practice. The threat of discipline is also meant to deter physicians from practicing beyond their capabilities.
Although discipline is the key method of protecting the public from low quality care,5 most Boards perform three other quality-related functions with regard to practicing physicians: continuing medical education, some quality-relevant rule making (as on use of drugs), and mid-career licensure (as for immigration of out-of-state physicians).
Structural Factors as Enablers or Impediments to Disciplinary Performance
Structural characteristics are often said to influence what approaches are taken to discipline as well as disciplinary effectiveness in practice (Exhibit 3). Some factors are perceived to support Boards and enable them to run effective disciplinary processes. Often cited among these are the following (e.g., Ameringer 1999; Fellmeth 2003; Finocchio et al. 1995; FSMB 1998, 2002; Public Citizen 2005):
- more funding;
- a higher share of public, non-physician membership;
- larger and more professional staffing;
- independence (from state medical societies and other parts of government);
- broader sources of input about physician problems; and
- broader authority, standard of proof, and range of sanctions.
| EXHIBIT 3: Concerns from Literature Review |
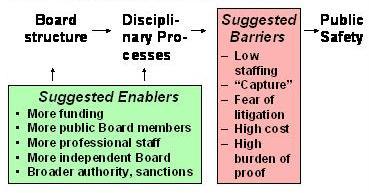 |
Other factors are cited as impediments or barriers to effective discipline (e.g., Brennan 1998; Derbyshire 1965; Cohen & Miike 1974; Grad & Marti 1979; Gross 1984; Miller 1997; Public Citizen 2005)--often the converse of the enablers:
- low funding and staffing;
- capture of Boards by medical interests;6
- insufficient legal framework (e.g., too little statutory priority for public protection, no explicit quality ground for discipline, high legal standards of proof);
- high costs of investigation and formal legal process; and
- fear of litigation by aggrieved doctors.
The case studies and state-specific literature reviews were designed to assess the influence of these structural factors on observed operations of medical discipline. Key concerns were how and how well the Boards logic models of discipline work under various circumstances, what choke points exist in processes and what practices work effectively to alleviate them.
FINDINGS ON BOARD STRUCTURE AND RESOURCES
State medical practice acts establish Boards missions, structures and powers, and administrative procedure acts governs many Board processes, especially for promulgating regulations and holding hearings. Legislation also provides Boards with their budgets and staffing authority. Boards add specificity to general legislative language through regulations, guidelines, and internal practices. Some judicial decisions affect Boards powers and activities as well. This section considers the structural factors that are often said to influence disciplinary activities and that influence perceptions of Boards independence.
Board Membership, Terms and Remuneration
Traditionally, the core of a State Medical Board was its panel of board members (Exhibit 4). All or almost all members were physicians, typically selected by governors from a list submitted by the states medical society or other organized medical group(s). Some medical society influence survives in some states, either by law (as in New York)7 or tradition; but starting in the 1980s, the role of organized medicine has generally been reduced (Adams 2001a).8
| EXHIBIT 4: Board vs. board: A Note on Nomenclature |
| All the observed states have literal boards (small b) as described in this section. These boards are panels that function like a very active board of trustees. Physician and other board members serve part-time, convening periodically to help set general policy and decide on the merits of specific disciplinary cases put to them. These boards roles and level of authority vary by state. Day-to-day administrative operations in the six study states are conducted by a full-time staff of state employees, typically headed by an executive director. In a broader sense, medical Board (capital B) means the collectivity of the board/panel, all board staff, and all other administrative entities responsible for any aspect of physician licensure and discipline. This report mainly describes capital-B Boards, which facilitates making cross-state comparisons. In all states Boards run similar processes for similar reasons, but their component board/panels each play smaller or larger roles according to each states specific legislative design and administrative arrangements. |
Almost every state now requires some number of lay members, on the theory that they are more likely to hold errant physicians accountable (e.g., Robeznieks 2002b; Peters 2005). The typical medical board today has 10-15 members and usually covers osteopathic physicians; stand-alone osteopathic boards are smaller. Some states require geographically representative membership, typically based on Congressional districts. For example, California has 21 members, split between autonomous divisions of licensure and discipline; 14 serve in discipline, functionally split into two panels of seven to decide disciplinary cases (California Board 2003).9 No state has a majority of non-physicians; in the six study states, their share ranges from 21-37% (Exhibit 1). Sometimes other medical practitioners are also represented. Often, the board chair must be a physician.
Board members are appointed by state governors to staggered terms, most commonly of four years (FSMB 2003b). The longest term nationally is 8 years, the shortest is 3 years. Two study states had 3 year terms, three 4 years and one 5 years. Typically, members may be re-appointed to an additional term, but almost all states have 2-term limits; only six states have no limits on number of terms. Four study states had 2-term limits; one had three, and one was unlimited. Payment levels are set at the level of per diem honoraria rather than remuneration for professional time lost from other work. Daily allowances typically range from $50 to $100 (FSMB 2003b); Washington is among the highest states at $250.10 Consequently, Board members generally serve in this capacity on a part-time basis and almost all work full-time in another job.
In practice, Board executives reported that they strive to keep some representation of key medical specialties on the board, including obstetrics. Specialized public member skills, especially those of an experienced attorney, are also valued. Professional skills, however, are not the same as Board member skills needed for disciplinary case review, consideration of new Board rules, and the like. An executive director in a non-case study state suggested having long terms and monthly board meetings more quickly develops a good skill base among members, compared with some states that meet only quarterly and have shorter terms, which does not afford enough time to learn to do the job well. One national advocacy group provides education for new consumer Board members.11 The rationale is that they can be more effective participants if helped to advance up the learning curve and make them comfortable in sitting on a Board with expert professionals.
Staff elsewhere noted the importance of rebuilding institutional memory when members change. Professional Board staff are thus concerned about member recruitment and turnover. In one state, key informants expressed satisfaction with having longer than usual tenure and no problem with turnover. In two others, strong concerns were expressed about inexperienced new Board members and the difficulties of keeping good members to work long hours for little pay (relative to what most physicians earn).
Boards Place within State Administrative Operations
A frequently made structural distinction is whether a Medical Board is free-standing or instead part of an umbrella administrative agency. Umbrella agencies group together various licensing boards, usually in one of two approaches. A department of health may group boards of medicine, nursing, pharmacy and the like. A department of professional licensure typically includes far more occupations.12 Organizational structures in state government vary considerably across states and over time within a state (Exhibit 5).
| EXHIBIT 5: Administrative Structures in States |
| State hierarchies seldom follow standardized, predictable patterns. Over time all have tended to add various departments, divisions, offices, commissions, and boards, as well as quasi-public entities. Reorganizations also occur. In Massachusetts, the State Medical Board in 2003 was moved from an administrative home within the Office of Consumer Affairs and Business Regulation to the Department of Public Health. Public Health also directly licenses a number of other health care professions and institutions, but some remain in Consumer Affairs. Washington state effected a similar reorganization over a decade ago. |
Medical boards also typically act as mini-umbrellas themselves. Most medical boards oversee physician assistants (80% of all boards, nationally, according to calculations from Federation data). Within the six case study states, various boards also covered such other professions as acupuncturists, chiropractors, osteopathic physicians, physical therapists, and respiratory therapists, even massage therapists and naturopaths. Nationally, 14 states have separate osteopathic medical boards.
In a variation on the umbrella/independent typology, the Federation categorizes Board structure as independent, semi-independent, or advisory to a state agency (FSMB 2003b). The Federation typology goes beyond umbrella status to consider the extent to which a Medical Board exercises authority over key functions. It defines independent boards as those that exercise all licensing and disciplinary powers, though some clerical services may be provided by a central agency. Semi-independent means that the board exercises some key powers; central agency may provide clerical and administrative services and make some decisions. Advisory means that the board acts in a purely advisory role to a larger entity (FSMB 2003b). Nationally, the Federation classifies about two-thirds of boards as independent, almost a third semi-independent. Only three Medical Boards are advisory. As already noted, three study states are classified as independent, three as semi-independent (Exhibit 1). Such classifications are useful descriptors, although somewhat subjective.13
Sharing of Functions beyond Medical Boards
All boards, independent or not, are to some extent integrated into state government and rely on other state entities for some functions. Board staff are normally state employees and subject to civil service rules and any applicable union requirements; executive directors may be exempted. Other functions typically handled outside of a Medical Board and its immediate staff include revenue collections and payroll disbursements, acquisition and management of office space, as well as purchase and support for information technology. Most notable among other changes, some Board members and managers described having to cope with new intra-governmental charges imposed by central authorities for such services, which were once provided without charge. Moreover, all the observed Medical Boards had to rely upon state Attorney Generals offices for legal representation in disciplinary cases. All were also subject to general administrative cost-cutting measures imposed by central authority, notably including staff freezes. And in promulgating rules or adjudicating disputes, all had to adhere to the same procedural requirements as other agencies under each states Administrative Procedure Act.14
Because disciplinary functions are shared differently in different states, what the medical boards do is not directly comparable. Hence this paper refers to capital-B Boards to include the totality of a states arrangements for exercising all licensure and disciplinary functions (see Exhibit 4).
Statutory Support for Board Actions
State enabling acts give Boards their mission to protect the public, set statutory grounds for discipline, and establish available sanctions. Contrary to traditional complaints (e.g., Derbyshire 1974, 1979), state officials seldom cited unclear mission or inadequate legal grounds for discipline as a limitation on their ability to take action, perhaps partly because of statutory amendments. California has been the most active of the six case study states, enacting significant legislative reforms in 1990, 1993, 1995, 1997, and 2002. The 1990 act explicitly set protection of the public as the highest priority for the Medical Board and also set investigative priorities, created a new oversight position of independent enforcement monitor, and required specialized medical review of quality of care complaints (California Board 2004; J. Fellmeth & Papageorge 2004). Most boards today can address a broad range of problems--for instance, Ohios statute gives 38 grounds for discipline.15 Key informants also noted that they could often infer authority from general provisions.
Board officials do find it useful to have a broad range of sanctions available. Being able to apply a lesser sanction for a lesser offense (or less readily provable one) enables Boards to negotiate voluntary settlements rather than having to seek a stronger sanction through the much more protracted and expensive process of a full-blown adversarial hearing. Most Boards have such a range of sanctions available. In Virginia, statutory reform in 2003 gave its Board authority to address minor misconduct through a totally confidential consent agreement.16
In practice, however, according to officials in several states, negotiating agreement to even a minor sanction without a hearing is today more difficult than in the past. For example, physicians fear being barred from health plans provider networks for almost any Board action, which reduced willingness to settle and raises the costs of achieving any sanctions.
The standards by which Boards judge potential offenses were mentioned as a substantial issue in two states. In 2001, Washingtons Supreme Court increased the standard of proof by which the Board must make disciplinary findings from mere preponderance of the evidence, that is, that an offense more likely occurred than not, to clear and convincing evidence.17 Nationally and among the case study states, about two-thirds of Boards use a preponderance standard and one-third the higher, clear and convincing rule. Other states have shifted the other way; Maryland by statute adopted the preponderance standard in 2003, although not for discipline based on quality of care concerns.18
In Washington, officials reported that the higher standard made their job more difficult. In Virginia, the traditional standard was gross ignorance or malpractice, that is, persistently outrageous behavior. The standard was reduced to a finding of intentional or negligent conduct likely to cause injury.19 Consequently, workload in Virginia increased and the state raised fees in an effort to compensate.20
The legal authority to subpoena records was cited as very important by managers in Ohio. Traditionally, their Board lacked subpoena power, a basic tool of legal investigation. That power was added by a 1980s reform.
Board Funding and Staffing
The sources and extent of available funding also affect a Medical Boards effective exercise of autonomy.21 In all six case study states, boards are almost exclusively funded from physician licensure fees, as seems to be true for the country at large. Usually fee levels are set by statute, sometimes by regulation. Regardless of the legal arrangements, managers reported that their budgets are effectively subject to legislative control rather than under full control of each Board. Virginia was unusual in that the Board--that is, its umbrella agency--can increase fees by regulation, though within legislative guidelines. In four of the states, physician fees went into a Medical Board trust fund separate from general state revenues. Fines, however, often went to the state treasury. Some commentators and an occasional state-level study participant have cited earmarked physician fee-based funding as evidence of board independence. However, the Boards typically need legislative approval to draw on their funds.22
In practice, how much financial support Medical Boards receive depends both upon the level of licensure and other fees assessed (including whether the Board retains any fines or other monies collected) as well as how much of fees the legislature appropriates. Any mid-year or ongoing cutbacks on spending authority or staffing are also influential. Annual fees range widely, in the case study states from $153 to $300, nationally from $51 to $450 (AMA 2006).
Substantially more physicians obtain licenses--and pay some level of fee--than actively practice in the state. The six study states had from 20% to 73% more licensees than practicing physicians (Exhibit 6), an average of 35% more, slightly below the national average of 44%. It is notable that Virginia and Iowa, the states highest in non-practicing licensees, have sizable river border populations whose metropolitan areas spill into adjoining jurisdictions. The two lowest states, in contrast, have their concentrated populations along their seacoasts. Higher fees may also lower the extent of double licensing by making it more expensive to keeping a little used license in active status.23 More thorough national analyses could improve upon such casual empiricism.
| EXHIBIT 6: Ratio of Licensed to Practicing In-State Physicians | |||
| Per State | Case Study Average | National Average | |
| Virginia | 1.73 | ||
| Iowa | 1.64 | ||
| Ohio | 1.37 | 1.44 | |
| Washington | 1.35 | 1.35 | |
| California | 1.29 | ||
| Massachusetts | 1.20 | ||
| SOURCE: FSMB, 2003 Summary of Board Action http://www.fsmb.org/pdf/FPDC_Summary_BoardActions_2003.pdf>.NOTE: Averages weighted by number of physicians/state. | |||
Because physician fees are set in nominal dollars, fee revenues can rise only as fast as the population of licensees, unless the governor and legislature act to raise them. Fixed fees plausibly keep up with workload driven by the population of physicians overseen, but they generate no additional funding to cope with shifts in workload patterns, nor to meet rising regulatory salaries and other expenses. Officials and other respondents reported great physician resistance to fee increases in all states, and most reported that many years passed between fee increases. Some observers have noted that fees are often raised as part of a legislative reform in response to highly publicized Board shortcomings.
Budgets
Boards annual budgets vary widely across states, even taking into account the variation in number of physicians regulated (Exhibit 7).24 Nationally, the best funded 25% of Boards receive more than double the resources per in-state practicing physician as their lower funded counterparts in the bottom 25%.25 This difference across states seems large, given that Boards perform very similar functions in all states. (Based on knowledge of the case study states, we believe these reported budgets typically cover similar Board functions regardless of whether some spending occurs in an umbrella agency.)
Budgets also ranged broadly in the six case study states--the highest is almost double the lowest. All the case study states, however, lie in the middle half of Boards nationwide; none is a budgetary outlier. The highest case study state is only at the 75th percentile nationally, and the bottom one is just above the 25th percentile nationwide.
Nonetheless, most of the case study states must operate more frugally than average: Five of the six have funding that is below the national average as well as the median. Exactly how frugally depends upon the relative costs of labor and other expenses of operating a regulatory agency in different states, but no adjustment can readily be made for this practical budgetary concern.
| EXHIBIT 7: Budgets per Thousand Physicians(in-state practicing MDs, 2003) | |||
| Case Study States | National | ||
| California | $423,910 | $423,910 | 75th percentile |
| $306,217 | average | ||
| $284,902 | median | ||
| Virginia | $283,222 | ||
| Washington | $281,210 | ||
| Iowa | $255,632 | ||
| Ohio | $226,817 | ||
| Massachusetts | $213,215 | ||
| $191,899 | 25th percentile | ||
| SOURCE: FSMB 2003, Exchange (31 states) + interviews (three states). | |||
All Board managers in the six case-study states reported frequent if not constant budgetary worries; one reported occasional declines in state financial support. All reported that constrained funding or staffing limited their capabilities to discipline doctors, although not necessarily in the same ways. Respondents in all states also reported that their Boards do not receive all fee revenues. Some said that physician fees are intermingled with those of other professions within an umbrella agency.26 Others said that some share of fees has ended up being retained by the state, sometimes as a result of trust fund re-allocations as described above. The Massachusetts Board got an especially low share of fees, only about 40% before 2002 legislation raised fees. The Board got 100% of that increase, which was a condition for the medical societys supporting the fee increase. The increase doubled the Boards available resources, but it still received only 75% of licensure fees paid to the state (Massachusetts 2003).
THE IMPORTANCE OF BOARDS DISCIPLINARY ROLE
Discipline is a key function of Boards and seems to be rising in importance. In the later 1990s, the Pew Trusts commission on workforce reform surveyed medical organizations and individuals about ten areas of workforce policy on which the commission had recommended reforms (Gragnola and Stone 1997). Respondents showed a relatively low level of concern about disciplinary improvement. The top three areas of concern were titles and scopes of practice, redesign of Boards structure and functions, and assuring continuing competence of practitioners--the latter an alternative to case-by-case discipline that also addressed improving quality.
Case study Board executive directors rated recent changes in public perceptions of disciplines importance.27 All but one reported some level of increase (Exhibit 8). One Board manager suggested that attention paid to board discipline is cyclical.
| EXHIBIT 8: Importance of Disciplinary Function, as Perceived over Time | |
| Recent Change in Importance | Number of States |
| More important | 3 states |
| More important to legislators, same to public | 1 state |
| More important to public, same according to disciplinary data | 1 state |
| Same level of importance | 1 state |
| Less important | 0 states |
| SOURCE: Interviews. | |
The importance of discipline shows also in how Boards allocate their funding internally. National survey data do not track discipline as a category in asking Boards how they break out spending by function. The similar category reported is investigation, which is the most expensive part of discipline.
The national median for share of budget spent on investigative functions is 49%, compared with 27% on administrative functions, and 21% on licensing (Exhibit 9). The median for case study states is slightly higher. The full disciplinary share of funding is likely higher than 49%. Some fraction of the spending categorized as administrative probably pays for executives and medical board members involvement in disciplinary activities, up to and including conduct of hearings.
A final indicator of the importance of discipline to Boards is executives priorities for use of any revenue increase. In post-case study follow-up discussions with executive directors, the project asked how they would allocate a hypothetical15% budgetary increase. We used the three categories deemed to be standard--discipline, licensure, and administration. We added information technology because some Board staffers had said earlier that it is very important; IT could facilitate activities across all three functions.
| EXHIBIT 9: Budget Allocation by Function | ||||||
| Function | All Boards, Nationwide (Percentile Distribution | 6 Study States | ||||
| 10th | 25th | 50th | 75th | 90th | 50th | |
| % of Dollars Spent | ||||||
| Administrative | 13 | 18 | 27 | 44 | 51 | 15 |
| Investigative | 24 | 37 | 49 | 61 | 67 | 59 |
| Licensing | 6 | 10 | 21 | 34 | 47 | 19 |
| SOURCE: FSMB, Member Board annual survey, 2004.NOTE: Sum of medians is not 100% because distributions are separate. | ||||||
Discipline dominated responses in all but two states (Exhibit 10).28 In one of them, discipline had just received additional staffing; in the other IT needs were more urgent. The state that had previously seen IT as such a high priority no longer did at the time of the second round of case study interaction, as a large expansion of IT capacity was already under way. Two states executives wanted to add other, special initiatives to their priority list--one was an effort to move toward routine clinical skills assessment for re-licensure and the other was higher per diems for board members to assure better access to their expertise while serving and to decrease turnover among members.
| EXHIBIT 10: Executives Priorities for Budget Increase(targeting of a 15% increase across functions) | ||||||
| State | Discipline | Licensure | Administration | IT | Other | Total |
| 1 | - | 25% | - | 25% | 50% | 100% |
| 2 | 33% | 16.5% | 16.5% | 33% | - | 100% |
| 3 | 66% | - | - | - | 33% | 100% |
| 4 | 65% | 11% | 12% | 12% | - | 100% |
| 5 | 95% | - | - | 5% | - | 100% |
| 6 | 33% | - | - | 66% | - | 100% |
| NOTE: Other reflects two state interviewees targeting of special initiatives (see text). | ||||||
COMPLAINT RESOLUTION, THE MAIN DISCIPLINARY PROCESS
The primary Board function of interest is discipline. The primary process by which Boards seek to discipline physicians is investigation of complaints. The case study participants agreed with the literature on the centrality of complaint resolution. Some alternatives are in use or discussed, which are considered separately below.
Each Board handles complaints somewhat differently. Everywhere, cases go through the same basic stages of processing, however. Moreover, all Boards must address very similar issues in deciding what methods and standards to use at each stage of complaint resolution.
The five basic stages are intake, investigation, pre-hearing process, hearing, and action (Exhibit 11). Each stage begins with input of cases from the prior stage and ends either by current resolution or by forwarding the case to the next stage of the process. The diagram shows the full progression of stages, but most cases drop out along the way. States also differ in the number of steps a case may go through within each diagramed stage; Exhibit 12 generalizes and simplifies for clarity of presentation. The diagram also omits the parallel, non-disciplinary rehabilitation process to which physicians may be diverted for problems of mental health or substance abuse.
| EXHIBIT 11: Complaint-Driven Discipline(Simplified Schematic) |
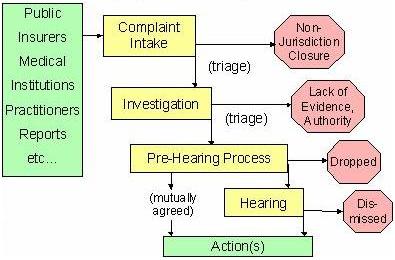 |
Each of the five stages is discussed next, with some descriptive statistics about operations.
Intake of Complaints
Sources of Complaints
Throughout the case study, all Board managers and staff agreed that most complaints come from the public, usually patients or family members. Most states call all disciplinary cases complaints even when there is no complainant.
Five states provided information on sources of complaints (Exhibit 12). The reported public share of complaints ranged from about 60% to 90%.29 The next most common sources are other public agencies and hospitals, accounting for a much smaller share of complaints. Three states received a substantial minority of complaints from other sources, an omnibus category that includes such sources as:
- physicians, nurses, pharmacists, other health personnel;
- Board staff (based on media reports or offshoot of separate investigation), a particularly high source in one state;
- hospital peer review;
- malpractice claims notifications; and
- police or drug enforcement officials.
| EXHIBIT 12: Sources of Complaints | |||||
| State | Public | Government Agencies | Insurers | Hospitals | Other |
| 1 | 90% | - | - | 10% | - |
| 2 | 85% | - | - | - | 15% |
| 3 | 70% | 2.5% | 2.5% | 5% | 20% |
| 4 | 62% | 19% | - | 3% | 18% |
| 5 | 59% | 4% | 1% | 1% | 36% |
| SOURCE: Interviews in case study states.NOTE: State numbering not consistent across tables; other includes Board staff, media, law enforcement, health professionals. | |||||
Many of these other sources come in the form of a standardized report, such as from malpractice insurers or courts, hospital disciplinary authorities, or other agencies taking certain actions, which vary by state. These are typically screened, and only some become complaints, subject to investigation.30 Complainants typically must submit complaints with some degree of formality--on a signed written form, in a similar online form, or by telephone. Ohio is unusual in accepting anonymous complaints (although they represent a negligible proportion of the total); most states ask for names because anonymous complaints are hard to investigate and prosecute. Individual complainants are asked for details of the perceived problem, which become the basis for investigation.
Types of Complaints
Boards do not typically report information on the nature of complaints in annual reports or other regular compilations.31 The categories by which they code cases internally are idiosyncratic, often seeming to relate to the particular statutory listing of sanctionable offenses under which each Board operates. This case study sought information on states top three categories of complaints, with special attention to cases involving clinical quality for which expert reviews could be anticipated. No existing category in any state matched this definition. The categories reported were too disparate to tally for all six study states. One state reported changing its coding of complaints in 2003.32 It can be noted that in California, about 40% of complaints in 2003-04 received a quality review; in Massachusetts about 12% in 2003 (J. Fellmeth & Papageorge 2004; Massachusetts Board 2003). The FSMB Member Survey does not obtain information on types of complaints, possibly because states lack common definitions on which to report. Seeking to create consistency was outside the purview of this project.
Volume of Complaints
The case study Boards varied considerably in number of complaints received, from a low of about 700 to a high of nearly 9,000.33 Larger states naturally generate more complaints than smaller ones, but complaint volume still ranges widely even after accounting for number of practicing physicians. The typical study Board received about 100 complaints per thousand physicians, but the high was one-quarter larger, and the low three-quarters lower (Exhibit 13). Some of this variation may be due to varying definitions of complaint in state intake processes. Board managers and staff uniformly said that they log in almost all public complaints, but many reports from other entities do not become complaints. Officials reported that caseloads are rising over time, but such increases were not uniform.
| EXHIBIT 13: Complaints per Thousand Physicians(in-state practicing MDs, 2003) | |||
| Case Study States | National | ||
| 6 | 126 | ||
| 5 | 121 | ||
| 115 | 75th percentile | ||
| 4 | 105 | ||
| 3 | 93 | ||
| 2 | 75 | ||
| 62 | 50th percentile | ||
| 43 | 25th percentile | ||
| 1 | 29 | ||
| SOURCE: FSMB member survey database, 2003.NOTE: N = 44 (US); 6 (study); means = 92 (study, SD 36), 84 (national, SD 64). State numbering is rank, not consistent across tables. | |||
Importantly for Boards ability to resolve complaints promptly, the volume of complaints received can seem high relative to the staff available to process them. The typical Board in 2003 received 70 complaints for each full-time equivalent investigative staffer; the reporting case study states had lower ratios (Exhibit 14).34 As for other statistics, the range across states is very broadly distributed; one example is the ratio of complaints to total staff, which suggests that the spread across states is not due to differences in the ways states assign investigative functions or interpret survey questions.
| EXHIBIT 14: Complaints Received per Staff Member | |||
| Staffing Category | Percentile Distribution | ||
| 25th | 50th | 75th | |
| All Boards, Nationally | |||
| Investigative Staff | 38 | 70 | 130 |
| Total Staff | 15 | 32 | 60 |
| Case Study Boards | |||
| Investigative Staff | 31 | 46 | 63 |
| Total Staff | 15 | 36 | 38 |
| SOURCE: FCMB, member survey 2004 database.NOTE: Staff is reported full-time equivalents. National N=47; case study N=3, so percentiles are equivalent to lower, middle, and upper values. Means are not presented because skewed by extreme values. | |||
Intake Triage of Complaints
Generally, clerical intake staff log in complaints as they arrive, although in very rare cases, a misdirected communication may not even be logged in. The Boards all use automated systems for docketing and tracking cases, but resulting data are not routinely integrated with other relevant data on operations.
Once logged, cases are screened to determine whether the Board has jurisdiction, that is, whether the Board could legally take action if the complaint is found accurate. Some aspects of triage can be carried out by a paralegal or even by experienced clerical staff who have developed a feel for complaint handling. Intake triage is a modest screening process that avoids expensive investigation of every complaint or communication received.
The main reason for closure without investigation is that a complaint is non-jurisdictional (Exhibit 15). It may be misfiled with the Medical Board and need to be referred to a different agency that has responsibility, such as a Board of Pharmacy or Nursing. Non-jurisdictional closures also occur where a complaint involves physician conduct not constituting an offense, such as refusal to accept Medicare patients, overcharging for services, or failure to provide sufficient patient parking.
Another reason for closure is that the conduct, while potentially actionable, was deemed too minor to warrant action, sometimes referred to as below threshold cases. Such matters include allegedly offensive language (short of sexual harassment) and minor billing disputes (short of fraud). Two states intake and enforcement staff said that they track below threshold closures and occasionally have disciplined a physician for repeated offenses. There appear to be no standardized subcategories for closures at this stage, and the Member Survey codes all such closures as non-jurisdictional.35
| EXHIBIT 15: Complaint Resolution by State of Discipline |
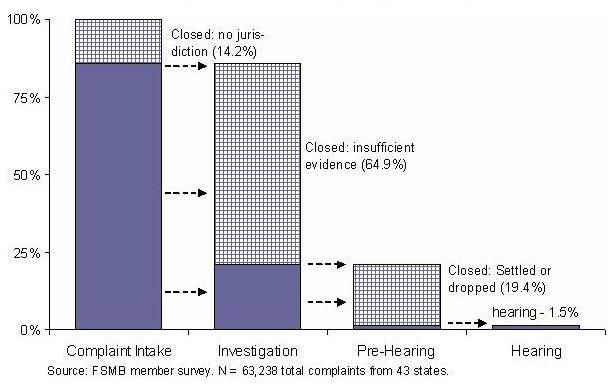 |
Intake triage accomplishes the first winnowing as cases proceed through the disciplinary process. Nationally, about 14% of closures in 2003 occurred before investigation (Exhibit 15). The balance proceeded to some level of investigation.36
Investigation
The investigational stage consists of cases about which Board staff seek more information in order to resolve the complaint. This stage accounts for a large share of states disciplinary effort (accounting for half or more of Boards spending, Exhibit 10 above), and cases are handled in different ways according to their perceived importance. Operational details and the flow of cases through this stage also vary by state. The following description is a general one.
Investigative Triage and Levels of Investigation
Full investigation is very resource intensive, so assignments are typically made by some form of triage team of more senior staff in the Boards investigations or enforcement unit. Depending on the stage of the process and the seriousness of the complained about behavior, different combinations of decision makers may be involved. For significant cases decision making may also involve enforcement attorneys. California conducts unusually extensive triage of quality cases, subjecting all to a medical consultant review before assigning them for investigation in the field (J. Fellmeth & Papageorge 2004). It thus reports a much higher share of cases closed before investigation than is presented in Exhibit 15. Ongoing oversight may also close a case when early investigation is not promising.
The extent of investigation undertaken can vary widely. Some cases are assigned for office based or in house investigation via phone calls or a request for written information from the physician. Some of the states provide for an informal, confidential conference with the respondent physician at this stage. State officials reported, however, that physicians increasingly involve defense attorneys in any interaction they have with their Board.
Other cases are assigned to a field investigator for interviewing of witnesses as well as obtaining medical records and other information at a physicians office, hospital, pharmacy, or other location. What information is needed depends on the nature and severity of the case. Cases alleging substandard clinical care or incompetence require much more effort than those based on criminal conviction or revocation of license in another jurisdiction, for example. It may sometimes be necessary to formally subpoena records, but investigators typically try to obtain voluntary compliance with requests.
A small share of high-priority cases, those posing serious, ongoing threats to patients, are investigated immediately on what many call a fast track basis. Boards usually have authority to impose summary suspensions in such cases, pending final resolution, although it is not clear how often such suspensions occur.37 For fast track or other unusual cases obviously bound for prosecution, staff may constitute a team of complaint, investigative, and legal staff to prepare each case for hand off to prosecutors.
Investigators also must prioritize their own regular caseloads as a matter of routine because more recently received cases may be more important than older pending ones. Caseloads can reach into the hundreds, and backlogs are a common problem at this stage of disciplinary process, one that has drawn considerable managerial attention, as considered more below.
Staffing
Investigators typically work in their own section or department of the Board, or totally separated from other functions in an umbrella agency. Investigative staff account for almost half of Board staff nationally, more in the case study states, much like the investigative share of spending (not presented, similar to Exhibit 10). Investigation does not operate in complete isolation from licensure, however. Some disciplinary complaints are generated by licensure renewal forms that ask physicians to self-disclose such things as malpractice claims and other legal problems. Some initial or endorsement licensure applications may have gaps in histories or other anomalies on which the licensure section may ask for investigative help.
The typical Board nationally received 32 complaints per staff member in 2003, slightly more for the median case study Board. Relative to investigative staff, the ratios are higher--some 70:1 nationally and 46:1 in the case study states reporting. These complaint-volume-to-staff ratios are slightly higher than the actual investigatory caseload, as 14% of complaints are dropped before investigation (Exhibit 15).
Investigators in most states are assigned geographically and spend much of their time alone on the road. This offsite mode of operation complicates record keeping and managerial oversight, although cell phones and computers keep investigators more integrated into home office operations than they once were. Most investigators have prior law enforcement experience rather than nursing or other medical expertise, which was not given high priority by discussants. Today, in most Boards, medical expertise is mainly applied outside the field, through review of records generated or obtained by non-medical investigators. Turnover among investigative staff is frequently said to be a problem, but consistent data are not readily available to support or refute that assertion.
Closures of Investigations
Three-quarters of investigations end with closure during investigation (Exhibit 15). The main reason for closure is that investigation has generated insufficient evidence to support Board action. A small share of closures involve unilateral Board issuance of an informal, minor sanction such as a letter of education or warning (as they are called in Iowa) or a voluntary agreement with the respondent physician to a more significant action. All information gathered typically remains confidential until the Board takes such action. In several states, study participants noted that the process had become less informal over time. Whereas once they could resolve many cases through discussions with a doctor, physicians now much more often involve an attorney even for preliminary interactions with Board staff. Informal or intermediate hearings may be held to determine whether a case should be continued.
Investigators write reports with recommendations, and higher level staff or Board members make the decision whether to proceed. Outside audits of Board practices in two states in earlier periods found shortcomings in extent of investigation before closure.38 If the decision is to close the case, a Board committee or Medical Board member may have to agree. If moved forward, the next stage is further consideration of whether to formally charge a physician and seek a more severe sanction.
Pre-Hearing Process: Charging and Settlement or Prosecution
About 20% of all complaints nationally reached this stage in 2003 (Exhibit 15). In this pre-hearing process, Boards make a final decision on whether to drop an investigated case, to issue a letter of warning or take other non-prejudicial action,39 or instead to bring formal charges, seeking significant sanctions. The decision to bring charges is akin to a probable cause determination in criminal process and may be referred to as such.40
The charge document may have different names, including citation and accusation. Doctors are legally entitled to have formal notice of the charges against them, and issuing charges has significant implications for both the Board and for the respondent physician. Immediately, those charges become a public record, which alone may affect a doctors reputation. Physicians objecting to proposed sanctions are legally entitled to a hearing (next stage, below) and other legal, due process procedural rights at hearing and in pre-hearing preparations. The legal work on both sides requires a substantial commitment of resources.
Boards charging decisions therefore receive senior input, typically involving staff executives, medical board members, and lawyers. In Virginia, for example, the Board president must agree to a staff recommendation to bring charges, although a single board member can authorize dropping a case. Even at this late stage, review of the investigative report may result in sending the case back for further investigation.
Different Board staff than those who investigate may make the final decision whether to prosecute and thereafter to prepare cases for prosecution and present evidence at hearing. Such separation may be said to promote independent exercise of prosecutorial discretion and to avoid any appearance of undue zeal or bias from the investigative stage. Not all states hand over responsibility in this way.
Once a charge is made, cases move on to the most formal stage of the process--usually termed prosecution.41 Board staff make final preparations for presenting the case against the physician at hearing. Prosecutorial staff may be in a separate administrative entity--in California, the Health Quality Enforcement Section of the Attorney Generals Office; in Virginia, the Division of Administrative Proceedings. In almost all states final decisions about prosecutorial strategy involve the Attorney Generals office, whose lawyers actually present cases at hearing.42
Voluntary settlements with respondent physicians may occur at any time during this pre-hearing process. Settlement negotiations may be informal or there may be a formal settlement conference before hearing. Most cases are resolved without a hearing, and most resolutions at this stage involve some level of sanction (discussed further below).
Adjudicative Hearing
Only about 1.5% of all complaints reach a formal hearing (Exhibit 15). At one time, hearings could be quite informal, but today such adjudicative hearings more closely resemble a non-jury trial in a civil court. Administrative procedures and rules of evidence are somewhat less elaborate than judicial ones. States follow one of two basic models for the main adjudicatory hearing, although the details vary considerably across states. In one approach the Medical Board hears evidentiary presentations and legal arguments on each case. In the other, an administrative court, presided over by an administrative law judge separate from the board does this.
Among the six study states, California and Massachusetts send cases to separate hearing agencies. The Massachusetts board formerly held its own hearings, but a legislative initiative generated by the medical society succeeded in moving hearings outside the agency in the late 1980s. The California agency, the Office of Administrative Hearings, has a specialized medical unit called Medical Quality Hearing Panel. The Massachusetts Division of Administrative Law Appeals is unspecialized and hears matters from many other state agencies and Boards. At the close of the evidence in Massachusetts, the hearing officer makes written findings of fact and law and recommends an outcome. The recommendation then goes back to the board, and the parties on both sides can make objections and suggestions. The board then decides whether to accept, reject, or modify the recommendation in issuing a final decision or order.
The other study states hold hearings before the Medical Board, but the board is assisted by a hearing officer with administrative law training. In some states, including Iowa, preliminary proceedings may be presided over by a subset of the board or by an administrative law judge, followed by full hearing before the full Medical Board panel.
Imposition of Sanction
Sanctions include prejudicial actions regarding license, other prejudicial actions and non-prejudicial actions. Sanctions may occur throughout the process, but more serious ones typically come after charging, according to Board managers and staff. In any case, it is the final step in the Board process. If imposed involuntarily after hearing, sanctions must also be upheld against any appeal to court. A sanctioned physician can lodge a judicial appeal to a statutorily designated level of state court, usually a trial court. Appeals are very uncommon--states typically had only a few pending, from multiple years of operations--but any resulting court rulings can be very influential. Appeals are also very costly both to pursue and to defend.
The Federations 2003 tally of available sanctions showed little variation across states (Exhibit 16). All states can impose severe sanctions like license revocations, and all have the power to make stipulations or consent agreements to facilitate case settlements of various types. There is more variation in availability of the lower-level actions, including letters of concern or of censure. As already noted, states often lack authority to collect costs of proceedings.
Available sanctions vary considerably in severity. The most severe type involves loss or restriction of a physicians license, including revocations, suspension, and imposition of mandatory retirement. In the Federations annual tally of Board actions, these are termed prejudicial actions; some national experts and Board members and managers called them actions against the license (FSMB 2004b). Next in severity is what the Federation refers to as other prejudicial actions, such as monetary penalties or reprimands. Reprimands may be made public or kept private, and may vary in degree, for example, from letters of concern to censure. A final category tracked by the Federation is non-prejudicial actions, often not really sanctions, such as denial of a license for lack of qualification and reinstatement of license.
On average, about 10% of initial complaints result in some level of sanction. Rates of sanctioning are discussed further below.
| EXHIBIT 16. Availability of Sanctions(percentage of states with sanctions) | ||
| Type of Sanction | All States | Case Study States |
| Revocation of license | 100% | 100% |
| Suspension of license | 100% | 100% |
| License limitation or restriction | 100% | 100% |
| Stipulations or consent agreements | 100% | 100% |
| Probation | 98% | 100% |
| Summary suspension of license | 96% | 100% |
| Public reprimand | 94% | 100% |
| Collection of fine | 87% | 100% |
| Letter of Concern | 64% | 33% |
| Collection of costs of proceedings | 55% | 50% |
| Letter/decree of censure | 49% | 67% |
| Private reprimand | 43% | 17% |
| SOURCE: FSMB Exchange 2003. | ||
MEASURING DISCIPLINARY PERFORMANCE
The nearly universal mission of Boards is to protect the publics health and safety. There is, however, no feasible way to measure regulations health impacts,43 so this project used the more managerial approach of performance measurement (Hatry 1999, 2002; USGAO 1998). Performance measurement focuses more narrowly on the outputs of discipline, that is, intermediate regulatory outcomes or products.
A key question posed in all case study sites was what outputs Board managers intended to achieve and how they measured them. Two and only two outcomes were noted in all sites. The first was counting disciplinary sanctions. The second was closing open complaints in timely fashion and thus avoiding a lengthy backlog of open cases.44
Rates of Sanctioning Physicians
The main output of discipline is disciplined physicians, and the rate of disciplinary actions is the most publicized measure of Board activity. Board managers universally recognize the importance of sanction counts, and Board reports typically present data on numbers and types of sanctions (Massachusetts 2004). Counts for all states are compiled annually by the Federation (FSMB 2004b). The traditional Federation tabulation lists 16 types of sanction, grouped into two levels of prejudicial action and one level of other actions, as noted above.
Most sanctions taken by Boards in 2003 fell into the most severe category--loss or restriction of license--on average 60% or more of all actions (Exhibit 17). The case study Boards averaged 4.4 such actions per thousand physicians. Nationwide, the average for all Boards was similar, at 4.7 severe actions per thousand. Variation across Boards is wide. The top quarter of states had rates that were more than double those of the bottom quarter, as seen by the percentile spread. The six state study states showed less variation, as measured by the standard deviation of their distribution. (Some variation may come from states using different definitions of whether an informal action, like a mild letter of concern, is counted as an action for reporting purposes.)
| EXHIBIT 17: Sanctions per 1000 Physicians | |||||||
| Type of Action | 6 Study Boards | All Boards, Nationally | |||||
| Percentile Distribution | |||||||
| Mean | Std Dev | Mean | Std Dev | 25th | 50th | 75th | |
| Loss or restriction of license | 4.4 | 1.7 | 4.7 | 2.9 | 2.9 | 3.7 | 6.1 |
| All prejudicial actions | 5.8 | 1.5 | 6.8 | 4.0 | 4.1 | 5.5 | 9.0 |
| Total Actions | 6.8 | 1.8 | 7.9 | 4.7 | 4.5 | 6.6 | 9.7 |
| SOURCE: FSMB 2003 summary of Board actions.NOTE: Physicians = practicing in-state MDs; N = 46 (national), 6 (case study); action counts are cumulative: all prejudicial includes loss or revocation, total includes both others. | |||||||
Non-severe prejudicial actions constituted a lower share of total actions, averaging about 20% in study Boards and 25% nationally. Thus, the study Boards average total of all prejudicial actions was 5.8 per thousand, versus 6.8 nationally (Exhibit 17). Again here, there was less variation across the six study states than nationally.
Other actions were the smallest category, averaging about one per thousand, both in study states and nationally, or about 15% of all actions. Such actions are not mainly disciplinary in character, as described above.
Observing a range of action rates cannot by itself show what level is right, and many key informants noted that a low score does not capture other successes that reduce need for sanctions. Most mentioned that active effort to avoid licensing problem physicians is very important, particularly for doctors seeking to transfer into a state in mid-career. Others noted different efforts to address shortcomings in care, such as encouraging informed consumer choice among practitioners, promoting safe practice through development of practice guidelines and rules (including the aforementioned rule covering narcotic prescribing), and encouraging hospital-based attention to safety--all considered in more detail below. Still, most study state Board members, managers, and staff reported that they are interested in increasing their states rates of discipline.
Throughput of Cases: Backlogs and Speed of Resolution
Rates of actions taken at the end of disciplinary process may get more public attention, but Board managers express more concern about regularly moving all cases through to some resolution, often called their throughput. Unresolved cases can build up at various stages of disciplinary process.
Backlogs are a major concern to Board management. Boards are seen as not fulfilling their primary mission to protect the public if they do not take prompt action on a respondent physician who is perceived as not practicing safely. Moreover, if a patient is harmed by a physician on whom one or more complaints is stuck in a backlog, a Board faces very unpleasant media and legislative response. Even absent a scandal, backlogs may be indicative of underperformance obvious to any outside observer. Inquiries found that Boards do not generate consistent data across states on backlogs at various points in process. But backlogs have consistently caused problems in all states within the recent memory of Board managers. For example: In California in the 1990s, a large backlog of uninvestigated complaints led to controversial administrative closures without investigation (J. Fellmeth & Papageorge 2004). In Iowa, by 2004 the backlog had reached about two years worth of investigations (Iowa 2004), and ultimately led to substantial changes in case handling procedures. Massachusettss large backlog of cases by 1999 generated bad publicity, a crash program of catch-up review, and a change in administrative leadership (Massachusetts 1999).
Speed of completion of cases is related to successful throughput, and critiques of Board performance have often cited long delays before closure (JLARC 2000). Closure times vary considerably according to how far through the disciplinary process a case proceeds. Nationally, cases resolved before or during investigation averaged 180 days from intake to closure in 2003, 425 days for cases closed after investigation but before hearing, and 675 days to reach hearing (FSMB member survey, not presented).
As for other measures, speed of case resolution varies greatly within and across states. Most states closed a large majority of their cases quickly in 2003, according to their reports for the Federation's member survey. The typical Board's share of "quick" closures (under 180 days) was about 70% of total closures. However, the range was great. About a fifth of states closed only 20% or less of their caseload faster than 180 days. At the slower end of the spectrum, the typical state took longer than 360 days to close about 10% of its cases. For about one-fifth of reporting Boards, however, such slow closures constituted 60% or more of all closures. The typical Board closed about 20% of cases at intermediate speed (between 180 and 360 days).
IMPEDIMENTS TO DISCIPLINARY PERFORMANCE IN PRACTICE
One area of inquiry for this project was what factors might inhibit Boards functioning (Exhibit 3), and thus act as barriers to better Board performance or bottlenecks or chokepoints in the flow of cases through Boards disciplinary process. Board members and managers identified a variety of concerns, some specific to particular stages of disciplinary process and others more cross-cutting.
Problems at Intake
Key respondents expressed some frustration that Board complaint intake was not finding enough of what might be termed problem physicians or not finding them soon enough. Views differed on whether the issue was generating more complaints or getting different types of referrals. Some saw the level of complaints as too low and actively sought to stimulate more complaints by better informing the public and medical audiences about the Board and its complaint resolution role, but most did not. Nor do all have 800 numbers or take anonymous complaints to stimulate submissions.
A contrasting view was that the important shortfall was in complaints or referrals from sources more expert than the general public. Respondents almost universally noted that most public complaints, while surely indicative of real consumer dissatisfaction, were inadequate indicators of quality problems and other failings on which Boards could take action. Acting on complaints from the general public, especially after alleged mistreatment or injury, also necessarily puts the Board in a reactive position.
Many key informants stated that physicians, nurses, hospitals, and other providers have the best information about quality problems and problem practitioners, and also should theoretically be able to refer a practitioner for discipline before patients are injured. However, it was widely believed that hospitals and fellow professionals underreport disciplinary or peer review actions taken against practitioners, and greatly underreport problems that have not received peer review attention. These beliefs are consistent with the observation that that 70% of reports to the National Practitioner Data Bank come from malpractice payouts rather than Medical Board or hospital adverse actions, and that about half of US hospitals had never reported a single clinical privileges action (suspension of 30 days or more) from the Banks inception in 1989 through 2003 (NPDB 2004).45
One aspect of the underreporting problem is that legal mandates have not worked. All six case study states and almost all states nationally mandate reporting of possible violations of the medical practice act including incompetence along with all the other grounds for discipline noted above (FSMB 2003b). About half of states provide for some level of confidentiality for whistle blowers who report problems, as suggested by an analysis of Boards published in 1987 (Kusserow et al. 1987), although in some states including two case study states confidentiality applies only for investigations, not if the physician is charged with a violation. A few states provide civil penalties for failure to report.
Nonetheless, medical professionals remain reluctant to report possible quality issues with one of their colleagues for a number of reasons, said case study respondents (see also Terry 2002a). Some mentioned medical culture or reluctance to conclude incompetence from observing one mistake or injury. It has also been suggested that fear of professional retaliation may deter some practitioners from reporting (Twedt 2003), while desire to retaliate may prompt others to report (Fellmeth 1989 suggested that Boards may receive as many reports based on personal animosity and hospital politics, as on medical performance). Similarly, hospitals are often said to be reluctant to conduct peer reviews or formally to discipline physicians, preferring to accept a voluntary departure, and even more reluctant to inform state authorities (e.g., Heisel and Saar 2002a, 2002b).46 Both whistleblowers and institutions may fear litigation by reported physicians.
It should also be noted that Board managers and staff also described underreporting from police departments and the courts.
Boards themselves seem not to seek out intake from one potentially relevant source, federal Quality Improvement Organizations (QIOs, formerly known as PROs) that perform quality reviews for Medicare. Case study respondents did not suggest this, and only a few Boards in 2003 had formal information sharing agreements with QIOs (FSMB 2003b).
Boards do get information about malpractice claims. Liability carriers are required to report paid claims to Boards in most states, and in all but one of the case study states (FSMB 2003b). In California, attorneys are required to notify the Board even before filing a malpractice lawsuit, sending it the same notice of intent to sue that they must send defendants, and insurers notify the state Board at the time they file paid-claims reports nationally (J. Fellmeth & Papageorge 2004). The Massachusetts Board has worked with plaintiffs attorneys to receive regular notification of the subset of cases that may involve the type of gross negligence that warrants Board action for a single incident (Massachusetts Board 2004).
Since 1989, Boards have also been entitled to obtain a physicians record of paid malpractice claims from the federal National Practitioner Data Bank. Nationally, Boards make over 5,000 such queries a year (Jones 2005). However, each query costs five dollars, and case study respondents said that they could not afford to query on a routine basis.47 A national survey of Boards conducted by the Health Resources and Services Administration (an agency in HHS) found that they would have made 70% more queries if querying were free of charge, but it is unlikely that the fee will be waived for Boards (Jones 2005; Pincus 2006).
As with consumer complaints, getting more complaints seemed less of an issue than knowing how to identify which are worth detailed investigation; many Board managers suggested that they received far too many reports of malpractice payouts to investigate them all. They also noted that malpractice, even with patient injury, is not the same thing as incompetence. Malpractice is a conclusion about physician behavior in a single accident or incident, whereas incompetence is a continuing status of incapacity or inability. Most case study Boards did not even list malpractice reports as complaints, and California, for example, appears to close most reports routinely without investigation (J. Fellmeth & Pagageorge 2004). When it comes to the utility of malpractice reports as a source of insight into physician competence, the perspective of those outside the Board (e.g., legislators, can be decidedly different) (JLARC 2000; Public Citizen 2003a).
Problems in Investigation
Every state reported having some recent problem with backlogs of cases at the investigatory stage of discipline, as already noted. Given that it is during this stage that Boards close about two-thirds of all cases opened, at some times investigators cannot close cases as fast as more are assigned to them.
Staffing and Flow of Complaints
One contributor to investigatory backlog is simple volume of cases per investigator, especially when the volume of complaints jumps or the number of investigators falls. One executive director noted that many cases receive preliminary review, perhaps including an initial interview with the doctor, then are set aside into a low priority queue. Another source of backlog is the difficulty investigators have in determining investigative priority order, as well as how much time each case is worth. Individual investigator preferences and practices also influence work flow.
Most cases in most states appear to be handled on a one-on-one basis. Each investigator decides what information is needed--from office records to interviews with former employees, colleagues, or neighbors--then personally tracks down each piece of evidence and assembles a report. Investigators must constantly juggle moving forward on their stock of existing cases as new ones arrive, some of which need to go to the head of the queue. High priority cases include those with significant potential for ongoing patient harm, but also often licensure derived cases, where a binding deadline may require a prompt decision. The level of oversight and coordination of investigations varies across states.
Investigators must also spend some time searching for other leads in the field, working from pending cases or developing new ones by following leads from news accounts, listening to medical personnel, or to police and other justice system sources. Investigators geographic assignments facilitate their knowing the territory in these ways. From most reports, investigators tasks appear to be relatively unstructured and call for exercising a good deal of discretion, which contributes to differences in approach and in activities across people and areas. Investigators need to be able to investigate on ones own in the field, independently seeking out and following leads, is one reason that executives value prior investigative experience in hiring new investigators. The frequent field travel also poses problems of managerial oversight, according to a number of Board managers.48
Staffers at Medical Boards that must share investigators with other licensing entities often noted that investigations of physicians required different skills than for other licensees or that medical investigations were not getting sufficient attention. Few managers thought that lack of formal medical training was an obstacle to investigations, although some would have liked additional medical training for investigators. Managers mainly wanted investigators to obtain and bring in material for evaluation and looked to hire former police officers in preference to nurses, for example, in support of their primary roles as fact finders and not decision makers. Resource constraints are always perceived as an obstacle. In every state, managers felt shorthanded and under-funded for investigations, even though the median case study state devoted 59% of its resources to investigation in 2003, 10 points above the national median (Exhibit 9). In California, the Enforcement Monitor reported that the long-lasting personnel freeze was particularly damaging to that Boards disciplinary capacity (J. Fellmeth & Papageorge 2004)--even though California has the highest funding and most staff per licensee of any of those studied and might be expected to achieve some economies of scale. At the small end of the study scale, in Iowa, a 2005 budgetary shortfall came on the heels of a 2004 across-the-board state cut and translated into the loss of 38 hours a week of compliance and supporting staff time--a substantial impact for a Board with only 16 employees in 2003 (Iowa Board 2004; FSMB 2003b).
There was little agreement about appropriate levels of staffing or case loads and standards do not exist. For example, Californias Auditor General asserted in 1991 that a caseload of 20 cases per investigator was reasonable, drawing an analogy to law enforcement agencies. The Board went on record in mid-decade that a caseload of 26 cases per investigator was unreasonably heavy (as quoted by J. Fellmeth & Papageorge 2004, pp. 42, 44). Managers in Iowa, in contrast, thought that 60 cases per person was quite manageable. (As noted above, California triages quality complaints through medical record screening and drops many quality complaints without sending them for field investigation, so its quality cases on average are presumably more consequential than those in Iowa.)
Difficulties in Obtaining Medical Records
Record acquisition is a constant challenge for external investigation. Almost any quality-related case requires records review, and Board managers and staff typically said that investigators request needed records on a voluntary basis, often with the patient-complainants authorization, but that compliance was often delayed. One Board manager described the problem as having been worse before the Board had obtained subpoena power to compel delivery of requested records, which was seen as a basic regulatory need. There are three problem aspects of record acquisition: (i)unwillingness of complainants and other patients to share information and of respondents to cooperate with the investigative process; (ii)involvement of attorneys who encourage clients and staff not to assist in the investigation; and (iii)that many facilities have contracted out the preparation of record copies, which results in increased costs and delays.
Problems accessing medical records were cited by external reviews of Board processes in California and Virginia (California Joint Committee 2005; JLARC 2000).
Preparations and Prosecutions
Another key focus in this project was to examine the role of physician discipline in quality-related cases. For these types of cases, a major hurdle is good access to medical expertise when Boards must make judgments about whether to proceed. Usually, this need arises after investigation, but California performs an initial medical review for potential quality-related cases even before field investigation. Different reviewers later advise on whether to prosecute a case and help prepare for prosecution. Informants reported backlogs at the point of expert physician review, citing insufficient peer review capability.
Some Boards use physician or nurse staffers or Board physicians for reviews at earlier stages of disciplinary process in lieu of outside experts, although outside experts are needed for actual hearing testimony.49 This approach, applying medical expertise, makes Board decision-making very dependent upon key staff and Board members. In Ohio the Board Secretary (the physician chair) and Supervising Member (a senior lay member) read every case file and must agree on all prosecutions. In Virginia, any one Board member may agree to close a case, as already noted, but only the Chair must agree to take a case forward. This reliance on key members suggests that leadership is important to Board performance. In several states key informants noted the importance of having talented and engaged Board members, particularly since Board service is a part time position, and the workload can be substantial. A number of study participants noted that members face a steep learning curve to operate effectively in a regulatory setting. Some felt that turnover among Board members was too frequent, so that much time was spent bringing new members up to speed.
As a Board moves to charge and prosecute a case after investigation, the disciplinary process becomes much more formal. Many key informants noted that the involvement of lawyers slows the process. Generally, Boards are reliant on assistant attorneys general (AAGs) from a different state office; in some states the AAGs are dedicated to the Medical Board, but in others they serve many boards. In a number of states, disciplinary hearings are under the purview of agencies outside of the Board. From the perspective of several key informants, this involvement of other actors may delay the process. However, the Federation member survey does not track times past the initiation of hearing, so documentation of comparative times under different arrangements for hearing and prosecution is not available.
Costs and Other Cross-Cutting Problems
The High Cost of Proving Low Competence
High costs are a major obstacle to disciplinary throughput and, ultimately, prosecutions. Cost is especially high for investigation and prosecution of quality-related cases. Board members and managers reported that it is difficult to prove persistently unacceptable quality or physician incompetence because there are no objective, readily applicable standards to imply, only implicit standards that must be established and applied through expert peer review. One key informant noted that Boards have no objective tool to decide medical competence. The reason is that, with few exceptions, the science to develop standards to measure medical performance has been largely unavailable, according to the American Board of Medical Specialties (ABMS 2001). Thus, in order to take strong disciplinary action a Board must document a continuing problem or series of related problems that suggest a pattern of low quality. Thus the challenge, as well described by one participant, is distinguishing between an isolated incident and a pattern or way of doing business in standard of care cases. All discussants noted the difficulty and expense of proving substandard care through expert review and testimony.50
Given the difficulty of proving low quality, Board managers and staff say that they often pursue other grounds for discipline that are easier to prove. One example cited was sanctioning a physician for not following his own practices established standards for prescription of pain medication. Another was concealing a prior hospital staff privileging action in submitting an application for relicensure; it was said to be easier to discipline for the concealment than for the underlying competence problem. Just how often such shifts in grounds for discipline occur is not clear.
A member of the projects TAG noted that Boards essentially have to win multiple malpractice actions simultaneously to revoke a medical license. Boards cannot simply rely on the fact of liability settlements or even of peer-review based hospital discipline, but must re-prove each case used to justify any disciplinary holding. Even when hospitals notify the Board of disciplinary action taken against a physician, they may provide little information other than the fact of having taken action. The Board therefore has to start its own case from scratch. Boards can use proceedings in other jurisdictions as evidence for action in their own state, but even then, a new hearing is typically required, in the study states as in almost all others (FSMB 2003b).
The lack of a clear standard complicates the efforts of Boards, which must face the issue of how many individual instances of substandard conduct they need to prove to impose a severe sanction like license revocation. Several states reported that staff at least until very recently often felt the need to prove the validity of ten or more complaints; one AAG recalled a decade old case with 40 complaints and another instance in which the hearing officer had limited presentation to 15. Many managers said they had sought to develop internal guidelines on the number of cases sufficient to support action. One states managers reported judicial guidance on this issue, that revocation was justified by a single instance of gross negligence or more than three instances of simple negligence. The applicable legal standard for gross negligence, however, called for a physicians conscious wrongdoing, so that in practice it was easier to wait to accumulate three instances of simple negligence.
High Costs of Legal Process
Many Board members and managers commented that over time their disciplinary process has become more legalistic. That is, staff perceive more need for documentation, for outside medical opinions, for having more formal stages in process, and above all for more frequent, earlier, and more thoroughgoing participation by attorneys on both sides. The participation of lawyers, in the view of many Boards, injects a lot of legal formality even into early, informal conferences meant to speed the process. Another states staff observed that respondents attorneys often press to have the Boards administrative processes resemble the more extensive procedural traditions of criminal law. These developments are perceived as burdensome in staff time and calendar time. At the same time, staff often noted that respondent physicians are entitled to traditional due process protections against arbitrary decisions and that taking extra effort can improve the visible quality of evidence and create a record available for external accountability. Clearly, both sides perceive that high stakes are involved in any disciplinary action.
Sometimes, more elaborate process has resulted from legislative enactments. Most notably, the California legislature has passed numerous strictures over time, in a way seeking to impose more discipline on a disciplinary agency perceived not to be pushing cases hard enough. Rarely, a court decision changes how Boards operate. The notable example for these states was a Washington Supreme Court decision that put a higher burden of proof on that states disciplinary process.51
Moreover, the regulatory environment has changed substantially in the last decade, giving discipline a much higher profile than it traditionally had. This is literally true since almost all states have posted physician profiles on the internet starting with Massachusetts in 1996, on which more below. Patients have also become much more sensitized to potential physician problems (Blendon et al. 2002), in part because of the publicity generated by the patient safety movement (Leape et al. 1996) and the recent medical litigation crisis (Albert 2002). Moreover, health insurers have moved to coverage favoring a network of preferred providers (Gabel et al. 2000), and the risk of delisting raises the stakes for respondent physicians facing disciplinary inquiries. Finally, the Boards themselves have come under considerable public scrutiny amidst concerns that too few doctors are disciplined; pushing for stronger sanctions naturally moves disciplinary cases further along the spectrum toward more formal legal process.
As one administrative law judge explained, medical cases are fully litigated, and respondent counsel often come in with plans for rehabilitation and new support systems for respondent doctors to propose in lieu of disciplinary sanction. They also bring in outside experts, prompting AAGs to respond in kind. More formal legal process creates direct costs in the form of higher attorneys' fees, which are untabulated. An observed indirect effect is the tendency for both sides to more closely hold onto available information, making disciplinary processes slower and more costly in staff time and other resources.
Dollar Estimates
Reliable information on just how much per case Boards must spend to prosecute quality-related disciplinary actions is not available. Executive directors all reported that they could not track costs per case, although most expressed interest in generating such management information. Such expenses are spread across two or more administrative entities (the Board itself and the Attorney Generals office, plus additional divisions for umbrella Boards) and relevant information resides on multiple data bases. Moreover, their accounting systems typically do not track staff time or other expenses by case.
Directors were asked instead to describe one or more recent fully contested cases involving clinical quality and to estimate the costs involved. Three respondents gave the round figure of $100,000 as an estimate (Exhibit 18).52 Other estimates were substantially lower. As one respondent noted, costs vary all over the place depending on the precise circumstances of a case.
| EXHIBIT 18: Estimated Costs to Prosecute Fully Contested Quality Case | ||
| State | Amount | Comments |
| 1 | -- | Unable to determine; one recent case involved 10 patients, 2 weeks of hearing testimony; assistant Attorney General in this state said could only prepare 2 such contested cases in a year. |
| 2 | $15,000 | Estimate covers bills for hearing only, not including lawyers; case involved 30 patients, took a year to work up. |
| 3 | $37,000 | Case went to hearing. |
| 4 | $100,000 | Precise totals for cases are unknown; costs easily reach 100K; if case goes to judicial appeal all bets are off. |
| 5 | $100,000+ | Case started with 10-20 patients, narrowed to 10 for 5 day hearing. Investigator spent entire year preparing. |
| 6 | $100,000 | Case had 3 doctors, with 10 patients each, ran several years. |
| SOURCE: Case study executive directors.NOTE: Estimates did not include any post-hearing appeal. | ||
Many managers and other participants commented on the cost of hiring outside experts, several noting an hourly fee in their state of about $150, well below rates in medical litigation cases. In another state the Board evidently had a worse problem, in one recent year being unable to afford any payment whatsoever for outside experts. Other cost drivers include internal legal and other staff time, which runs into weeks and months as well as substantial staff down time waiting for reviews.
Some managers said that quality-related cases were becoming more complex over time, often because the medical procedures were new or more practitioners were involved. Occasionally they involved multiple medical partners as respondents and needed reviewers from multiple specialties--a very expensive occurrence.
High expense for proving low quality practice is not unique to medical boards. Legal and associated costs related to medical litigation account for over half of all claims costs, counting both sides together. Nationwide payouts in 2003 averaged some $295 thousand per paid physician claim (NPDB 2003), implying total investigational/prosecution/defense expenses of well over $100 thousand per case. Discussions with hospital executives suggest that the costs of contested hospital disciplinary actions are also very high.
Access to Medical Expertise
In four of the six states, executive directors named prompt access to expert physicians one of the top three factors impeding effective discipline. High costs were noted as the main reason. Boards can no longer rely on inexpensive access to their own members for all or most medical input. Outside peer reviewers are needed because the volume of cases and number of specialties involved is so great, and attorneys and courts prefer to see outside input. Peer reviewers are expensive if a Board tries to come close to prevailing rates, and where payment is small or lacking, timeliness is a problem. In California, for example, it was reported that the Board often ran short of pre-qualified experts, and cited low payment rates, which affect the Boards ability to compete for the best experts. (J. Fellmeth & Papageorge 2004, p.ES-28). Other states pay even lower rates than California; one Board reported frequent reliance on volunteer reviewers. In at least one state, peer reviewers must be in active medical practice, although managers believe that they can use recently retired physicians for screening reviews.
Moreover, cost is not the only reason that Boards have difficulties accessing sufficient numbers of medical experts. As a number of staff and observers noted, many professionals still feel reluctant to investigate much less testify against a colleague or even fellow physician. The difficulty is most severe in smaller jurisdictions and smaller subspecialties, such as pediatric neurosurgery or pain management. Boards can face the problem that no in-area reviewer is available with the same expertise as a respondent physician who does not know or have business relations with that respondent. Moreover, some medical experts are not adept at interfacing with the legal system.
Difficulties in Finding and Prosecuting Quality of Care Cases
Outside observers have long complained that very few Board sanctions address lack of competence (Derbyshire 1974, 1979; USDHHS 1986).53 Most Board sources also acknowledged that quality problems in the field went far beyond the complaints they received, most of which do not support any action. The quality-related share of sanctions has risen over time, according to the Federation. Project staff asked state Boards executive directors what share of complaints were related to clinical quality, defining them as standard of care cases that usually involve expert medical witnesses.
Five states were able to respond, citing figures from 25% to 51%. These levels were surprisingly high, given the prior literature. Comparisons across states are not presented, as some informants were citing specifics from their published reports, whereas others were estimating. Moreover, as already noted, states differ in their categorizations of complaints and of grounds for discipline.
Three states also provided information on what share of sanctions related to quality. Here the range was lower, from 7% to 19%.54 There is not a one to one correspondence between complaints and sanctions. Multiple complaints may be consolidated into a single case against the respondent physician, and one case can result in more than one sanction.
One reason that quality cases constitute a lower share of sanctions than of complaints might be that it is harder to prove quality deficiencies, so that quality cases are disproportionately dropped or resolved with a minor action. Also, as noted previously, Boards often try to discipline a physician perceived to have quality problems on a different ground that is easier to prove. Another plausible explanation for the drop off in quality percentage is that patient complainants are not able to discern poor clinical quality or incompetence as readily as other physician performance issues.
Quality of Staff
One experienced state official observed that recruitment and retention problems plague personnel management, especially in that experienced investigators leave for better paying positions (J. Fellmeth & Pagageorge 2004). None of the executive directors cited such personnel problems as a key barrier or chokepoint, but some did mention occasional difficulties. Some noted problems in staffing or maintaining productivity of investigators in the field. One noted that the office of the Attorney General has a staff turnover problem because of its high work load. It should also be noted that in two of the six study states executive directors left their positions during the two years of the study.
Several managers operating within umbrella boards noted that the larger scale of operations from combining many boards gave staff more options for advancement, a career ladder lacking within the typical sized Medical Board. Larger entities can also create specialized positions like research analyst. Half of the countrys Medical Boards have 14 or fewer staff, according to 2003 Federation data (2003b).
Weak Data Systems
Most managers identified limitations of the data systems on which they had to rely for tracking disciplinary cases and other management purposes. In only one state did the executive director express full satisfaction with the existing system. Identified weaknesses included the following:
- Boards data systems are simply too old, often referred to by users as obsolete.
- Boards have to rely on multiple legacy systems for different purposes. Information is not integrated across various regulatory functions or across time. Quantitative questions posed during this project were usually answerable, but only through mini-research projects by a user knowledgeable about all the systems. Managers want integrated data that combines licensure and disciplinary information and also includes management information such as operational status of a complaint, which staff member is handling it, staffing time spent, and expenses.
- Data entry is inflexible. For example, data fields were often too small and automated categories too constraining; sometimes typographical errors could not be corrected locally, only centrally. Working with systems could require brute force workarounds. Similarly, another state had no edits for quality control, and, for example, any date entered is accepted. Others said that it was difficult to enter data on a case that moved forward toward resolution then back into investigation rather than only forward. Another weakness was lack of cross-references between related entries, across types of reporters or across time.
- Users have limited ability to query for information. Traditional data bases do not facilitate simple phrasing of data queries or ad hoc specifications of information requests as distinct from standardized ones; thus, special programming was get needed to get information out of the system.
Different states emphasized slightly different issues (Exhibit 19). Several states were moving to better systems as of the last round of case study interaction in mid-2005. Over time, several have found that making upgrades for data systems is challenging. One system typically has to serve multiple boards, even multiple agencies, causing delays in decision making and compromises about capabilities and features. Typically, a separate administrative entity makes the final decisions about IT purchases and also manages the upgrade. One states managers reported that a new IT system was supposed to have been completed by the end of calendar 1999, but the first set of vendors failed, and a second upgrade was in process. The California Boards Consumer Affairs System mainframe computer program has been described as so antiquated that the Board is forced to track some information manually or with additional small database programs (J. Fellmeth & Papageorge 2005, p. 45).55
| EXHIBIT 19: Disciplinary Data Systems and Information Technology | |
| State | Comments |
| 1 | CAS - consumer affairs system, used throughout Department of Consumer Affairs. Very labor intensive, does not allow for ad hoc management queries; 22 years old, runs on mainframe; fields are very small, unable to manipulate data well. |
| 2 | IFMC License Tracker 1.2d. It does discipline and licensure. For some years have worked with another company to redo all of computer systems. |
| 3 | Now moving to CLARIS (consolidated licensure and regulatory information system) with fully electronic imaging. CLARIS is a quasi-relational data system, can answer queries like how many cases are older than X, of which Y are of category Z. Last of legacy systems being integrated as of 2005. |
| 4 | Ancient, antique system on VAX computer; staff have added all the fields they can, still drowning in paper. As of 2005, moving in concert with other state boards to CAVU software package (relational database for regulation and revenues) used in other states. |
| 5 | Umbrella department maintains system, can track many measures for any particular case after docketing. Can do queries in almost any way queriers desire. |
| 6 | ASI (15 year old commercial licensing database no longer available), with BATS disciplinary tracking add-on that ties to images. No edits or quality control. Moving to integrated system to serve multiple agencies; vendor to be selected by end of 2005. |
| SOURCE: Case study key informants. | |
Fragmentation and Discontinuities in Disciplinary Process
Many entities are involved in the course of discipline. Experience in two states illustrated some problems that can result. A detailed examination of the California Board in the 1980s cited this fragmented and cumbersome structure as a key weakness (R. Fellmeth 1989). In most case study states, operations remain somewhat fragmented, in every case because of the separate organization of the Attorney Generals office, and often because investigations or hearings are held separately (in California, investigations are run out of regional district offices). Fragmentation complicates orderly progress of disciplinary process, creates delays as one actor must wait for another to act, impedes unified management of case flow, and raises costs.
Washington State (2004b) had just completed an internal review of its own disciplinary process at the time of this study. A key observation was that many hands had to handle a case from inception to completion, which dilutes any staffers sense of ownership of a case and also diminishes accountability for case management. Some re-learning has to occur after each handoff of responsibility, and multiple handoffs increase the likelihood that someone will lose track of a case or omit some action that will later require patching up. Further, although the process is meant to be linear (as presented above), in fact numerous circularities are built in. Newly responsible staff at a later stage not uncommonly ask for more or different information than was generated by a predecessor. Requests for more information were found to be especially likely once a case was assigned to an AAG for final preparation for hearing.
The Reactiveness and Narrow Focus of Complaint-Driven Discipline
Managers frequently noted the issue of always having to react to complaints rather than take systematic action to promote the safe and effective medical practice they saw as their mission. The limitations of this approach are numerous, most notably that it is not an efficient way of addressing poor quality (or the converse, ensuring good quality). Furthermore, it is resource intensive and often the complainants and the issues they raise do not reflect typical practice. The narrow focus of complaint resolution also drew mention. For example, it was observed that trying to establish a causal connection between an individual practitioner and untoward outcomes makes it very hard to understand the larger context of the apparent problem, including the practitioners history within a hospital, or the insurance plan applicable to care.
Regulatory Capture of Boards by the Regulated Profession
Another commonly cited barrier to effective discipline is that professional influence, especially by state medical societies might prevent boards from taking effective action or may appear to make board members or staff more practitioner-friendly than patient-oriented. This perspective was, understandably, more commonly expressed by outsiders than by Board staff or members. Outside analysis of the California Board suggests that it has changed from an old boys club to a more willing regulator (compare R. Fellmeth 1989 with J. Fellmeth & Papageorge 2004).
Discussants recognized the difficulties of resisting political pressure and maintaining regulatory autonomy for a Board and staff, which are viewed as crucial to regulatory success. While there may be many reasons why the organized medical community in any given state is not supportive of strong discipline, it was hypothesized by participants that medical society leadership composition and philosophy differ radically from the broad population of physicians. By expressing dislike of any incursion into professional autonomy, including state regulation, managed care, or malpractice liability, organizations in this view have become more trade associations than professional societies devoted to education or advancement of professional norms.
One point of influence of the organized medical community is the nominating process for Board members, in which medical societies retain some role, though much less than historically.56 Another is the legislative battle over Boards budgets or other statutory change (J. Fellmeth & Papageorge 2004; Robeznieks 2002a). Less direct influence may occur through cooperation on obtaining peer review, running a diversion program, or disseminating educational materials.
Competing Goals
A final reason that a Board may be less than maximally assertive in disciplining doctors is that Boards must consider countervailing concerns. Their need to provide due process to respondent doctors has already been mentioned. This requirement may be written into a Boards mission, but in any case American legal norms call for due process as a matter of fairness and promoting accountability by regulators. Indeed, some courts may even make a physicians right to practice a more fundamental right than public protection.57
Other competing interests have more practical or policy related roots. Patients may see regulatory intervention as reducing their access to care. Many key informants cited this consideration in discussing the tradeoff between zealously enforcing narcotics laws and allowing efficacious pain management for severely ill patients. Others noted that the same issue arises for alternative therapies, which have earned differing degrees of acceptance by mainstream practitioners; patients may actively seek out such alternatives even though overall clinical support for them is limited. Still others noted the use of nurse practitioners or other limited practitioners who might be seen as pushing the boundary of their scope of practice in order to bring some care to rural patients.
IMPROVING DISCIPLINE: EFFECTIVE PRACTICES AND INNOVATIONS OF INTEREST
The literature review and case studies sought to identify practices that many key informants and others cited as effective or potentially effective in achieving improvements in discipline. The main benchmark of effectiveness was the informed opinions of case study participants, along with some internal measures of performance. External benchmarks are lacking, as noted above, as are good ways to measure health or safety impacts, much less to tie them to particular practices or innovations of Boards. The literature and case study participants also discussed some innovations of some interest but not in general use.
Process Change and Improved Management
Intake
Almost all case study managers and staff thought that the intake of complaints could be improved. Some spoke of outreach to consumers through such means as having a toll free phone line or giving presentations around the state. A number of people noted that better web pages and physician profiling online had increased public awareness about their Board. One state reported having done a survey.
Board respondents felt even more strongly that intake would be improved if hospital staff and others with better knowledge about medical quality were to file more reports on problem physicians. No one, however, had a good way to improve on what they perceived as a low level of compliance with mandatory reporting statutes. One executive director described spending a year educating physicians, nurses, and hospital staff. That effort did succeed in quadrupling the number of reports; however it was only a modest increase from eight to 32 reports a year.
Triage and Prioritization for Investigation
Good prioritization of complaints was very frequently cited as an effective practice. Most states created ways to drop low-priority cases, to fast-track high-priority cases, and to assign a priority level to those in the middle for standard investigation. Managers perceived it especially important to identify quality-related cases quickly, as they are both important and resource intensive.
It is not practical to investigate every complaint, and investigative staff benefit from being able to focus on more serious cases. All the study states concluded that effective practice calls for dropping some cases as below the threshold needed to justify investigation before they can accumulate into a backlog. Among the case study states, Iowa was the last to develop a mechanism for such administrative closure. There, historical practice was to investigate every case, a practice evidently thought appropriate by the Attorney Generals office. This view shifted before this projects last case study interaction, by which time the Board had created a new pre-investigation screening committee of a medical person, a lawyer/negotiator, and the head of investigations. All the states now have some such mechanism.
Closure is not the only alternative to field investigation. California attempts to handle some complaints by immediate cease and desist orders or citations and others, for example involving criminal convictions, by immediate referral to the Attorney Generals office (California Board 2004).
At the other end of the spectrum, all the states have some mechanism for fast-tracking certain complaints, which all see as an important public protection in obviously high-profile cases with potential for ongoing harm to the public. These mechanisms vary by state, and it is unclear what share of cases qualify or how much more quickly they are handled. For ordinary investigations, three states sought to improve consistency and efficiency by formally assigning priority levels for investigation. California, Ohio, and Washington have such procedures, which they believed helpful. Some level of medical screening for quality cases is effectively a form of triage as well.
All these triage methods rely on complaint review by an individual or committee to categorize a complaint according to how its circumstances match the applicable verbal formulae. The California Monitor has proposed also giving weight to the source of the complaint; that is, seeking to emphasize investigations of types of complaints found most likely to yield results.
Management Timelines and Other Protocols
Half of the study states have formal management timelines by which Boards can measure the progress of cases through disciplinary process--for example, 60 days for intake and screening or 180 to complete a routine investigation. In California, investigatory target times are directed by statute; in Virginia and Washington State by the umbrella board for all covered professions discipline. The other states use only internal rules of thumb and seek to promote timeliness mainly though hands-on management of investigations and other components of disciplinary process. Investigators may have to file a case management plan for each case, for example, which then benchmarks performance. One state manager described weekly meeting between the director of enforcement and each investigator attorney team, also monthly meetings on very old cases, for example. The management timelines are seen as somewhat artificial but still useful markers for internal management and external accountability. In terms of effectiveness, it bears noticing that times are conceded often to exceed the guidelines.
States also typically face legal timelines set by statute or regulation as part of due process protections for doctors being prosecuted, for instance that a physician must have 30 days to respond to a charge. Some legal timelines are perceived as unrealistic and in one state are often waived by agreement of the parties.
In addition to timelines, some Boards have developed protocols to identify and resolve certain high-volume types of minor cases without field investigation. For example, one state reported that medical records release complaints are handled in house by communications staff. Some Boards use informal protocols to guide decisions; one executive director noted as an example of an automatic close that a complaint file was opened only because Medicaid had sanctioned a provider--but that Medicaid itself based its action on prior Board action.
Coordination across Stages of Discipline
Investigator Attorney Teamwork
An essential element for coordination in a discipline case is the relationship between the investigators and managers who decide what cases to advance into prosecution and the lawyers who must prepare and present any prosecutorial case at hearing. Almost all senior managers supported closer relationships at an earlier stage than prosecution, working across the traditionally separate stages of disciplinary process.
Massachusetts, for example, often uses a team approach for investigations, particularly on complicated or emergency cases (Massachusetts Board 2003, p. 15). Teams may include investigators, nurse investigators, and their supervisors along with paralegals and in-house lawyers. Investigator lawyer teams are immediately assigned for all allegations of sexual misconduct. Other states also attempt to form integrated teams--sometimes referred to as SWAT or rapid response teams58--for challenging cases. Involving the attorney as soon as the matter is referred to investigation is meant to avoid duplication of effort or the need for subsequently referring a matter back for further investigation that could have been more efficiently conducted the first time.
Teamwork is more difficult to achieve across the line of demarcation between Boards and offices of the Attorney General, even though individual Assistant Attorneys General are often assigned in whole or in part to the Medical Board. In one state an AAG reported positive results from earlier involvement in disciplinary investigations, noting that preparatory time was cut from over a month to under a week. In 1997 California moved some dedicated AAGs into field offices to help during investigations, called the Deputy in District Office (DIDO) system. DIDO improved upon the prior handoff model of investigation and prosecution, and the state is moving toward even closer coordination (J. Fellmeth & Papageorge 2004).
Administrative Centralization
Managers in several states spoke in favor of more centralized management of cases as a way to reduce fragmentation of responsibility and a large number of handoffs as a case moves through traditional disciplinary stages of process. This approach appears to be most advanced in Washington State, building upon its internal disciplinary process review (Washington 2004b). The managerial goal is functional coordination of all disciplinary activities--including investigative, legal, and compliance work. As an umbrella agency for multiple boards, the agency wants to create common practices and depth of staff across professional boards to respond to major caseload increases or staffing issues. This larger scope also permits managers to cross train staff and to create teams of various specialists, which can be particularly important where a respondent holds multiple credentials. Larger scope also offers a larger and more diverse career ladder for staff that is not available in a very small Board. Senior managers at umbrella boards say that this approach facilitates achieving consistent results and allows them to set more measurable performance objectives; they believe that they are making progress in process improvement. Unfortunately, the problems of poor coordination are better documented than the success of better coordination (e.g., J. Fellmeth & Papageorge 2004). While centralization might appear easier with an umbrella agency, both Virginia and Washington State report ongoing challenges with coordination.
Managerial Capacity
A related practice is expanding managerial staff to oversee the key processes of investigation and peer review for quality-related cases. Board managers found this approach useful for avoiding backlogs and assuring that higher priority cases are identified and pursued. Iowa, Massachusetts, and Virginia all hired new staff to oversee investigations or peer review. Ohio did not increase staff but in recent years, its Medical Board secretary (physician chair) and supervising member (layperson) reportedly made themselves more available to Board staff, reading every case file. Their coordination with staff provided real-time training and managerial oversight for staff and also expanded medical capacity.
Guidelines for Sanctions
Many case study participants spoke in favor of making sanctions more consistent through guidelines. In California disciplinary guidelines are required by statute59 and govern the recommendations of hearing judges. In Washington State, case disposition criteria apply across professions and are used after investigation to determine appropriate action, including notice of correction, informal disposition and formal charges (Washington State 2004a). In Ohio, standards are embodied in a non-binding position statement (Ohio Board 2002).
Virginia appears to have a well-developed scheme. Its Board scores both the seriousness of offense (including nature of offense, extent of harm done, and continuing risk of further harm) as well as respondent factors (such as prior record). Scoring is based on weights developed through analysis of prior decision making. The scores are entered into a matrix that generates a single value, which is then subject to adjustment based on aggravating or mitigating circumstances. Where the Board decides to vary from the scheduled sanction, it provides an explanation that can be used for later reevaluation of the scaling factors (Virginia Board 2004; see also Kauder & Carter 2004). Another state decides on the level of sanctions separately from finding disciplinary violations, in order to facilitate consistency across cases.
Assessing Quality of Boards Decision-Making
One executive director suggested that a Boards biggest challenge is to measure its quality of decision-making, for example, in triaging complaints and deciding on prosecution and sanctions, a sentiment echoed by another states executive director. They and others elsewhere spoke of the need for self-evaluation, but also its difficulty. There was, however, little active review of cases, no consensus about the most effective approach, and little managerial time available to devise approaches. The Washington Board does conduct random internal audits of its credentialing, a far more routinized process than discipline.
Some Board members and managers recognized value in having to undergo sunset review before their legislatures, which brought new perspectives on efficiency and effectiveness of operations. In two states, outsiders audited case files for quality of decision making. California conducted a very thoroughgoing assessment of performance through its Enforcement Monitor. The California Board faced two audits of its case closures in the early 1990s, and significant deficiencies were found (J. Fellmeth & Papageorge 2004). Virginia faced similar investigation by a legislative audit committee in the late 1990s (JLARC 2000).
Another form of feedback was a consumer satisfaction survey done in California as part of sunset review (J. Fellmeth & Papageorge 2004). Massachusetts also conducted a customer satisfaction survey of physicians about its licensure process and did usability studies of its website, which was a pioneer of physician profiling.
Medical Expertise
Effective processing of quality-related complaints calls for sufficient access to medical expertise, according to all Board managers and observers. All thought that more support for additional medical expertise is an effective use of resources. Medical capacity was described as particularly important at two stages. The first is screening and oversight of complaints and investigations, usually done in house. The second is peer review of cases for active prosecution, usually done by outside consultants.
In-House Capacity
Virginia was unique among the six states in having a physician as executive director of its Medical Board, under the umbrella Department of Health Professions.60 In recent years, the board added a second physician as medical review coordinator. They agreed that it is very useful to have two sets of physician eyes on staff even before drawing upon their Medical Board President. Having a colleague creates a synergistic effect, and an extra person helps cope with sheer volume. Iowa managers said that even a lay coordinator could effectively monitor and cajole peer review physicians, and that this new position was very productive. One other states executive director was giving consideration to hiring a physician, funds permitting.
Massachusetts and Ohio use staff nurse reviewers to screen cases for potential referral to peer review. Iowa, however, has rejected nurse reviewers on the ground that their reviews could not be kept confidential; the state peer review shield law would not prevent litigants from obtaining copies for use in malpractice or other lawsuits, unlike physician peer reviews. California relies on in-house medical consultants and sometimes external expert consultants to screen quality cases, even before going to field investigation. Washington at the time of the case study similarly used physician assistants to screen complaints through medical records review; that practice was halted in the wake of an August 2005 judicial decision.61
Most states also appear to rely on their board members for at least some medical screening. Most managers noted that winning active participation of board members was important, especially for screening, allowing a greater volume of cases to be screened.62 Indeed, many executive directors described relations with a few key board members as functioning much like an executive committee between meetings of the full board. Ohio has standardized this relationship through heavy reliance on its secretary and supervising member, who by statute oversee enforcement activities. They have for some years made themselves readily available to staff, meeting twice a month for two days each time, and make decisions at key points. This interaction not only provides staff with expert medical help but also increases accountability for their staff work. Some managers asserted that better Board pay or additional members would support more reviews as well as more frequent meetings.
Contracting Out
Massachusetts began outsourcing screening of most quality cases to cope with an emergency backlog of cases in 2000. Through a competitive process, managers selected the Center for Health Dispute Resolution (CHDR) to review cases alleging substandard care.63 CHDR is paid per case for expert peer reviews and liaises with the senior Board nurse. CHDR supplies only the expertise needed when it is needed, without the possible down time of in-house staff. The contract calls for each case to be reviewed by a nurse, then a physician within the specialty. A named signatory takes responsibility for each review. Occasionally, CHDR has provided expert witnesses for a prosecuted case, for which it receives additional payment, but the Board much prefers to use in-state experts. Board members and managers were very satisfied with this arrangement. It avoids potential conflicts of interest, holds down costs, provides timely response, and very coherent case summaries. This contracting out for quality screening turned the tide for the Board in terms of efficiency and case flow, according to the executive director.
Regional Pools of Experts
States could also deal with occasional difficulties finding a specialist peer reviewer in state--which sometimes occurred even in the larger states--by forming a regional pool with their neighbors. No state had participated in one, but a number of case study participants thought a pool was a good idea; some non-study state managers at the 2005 Federation annual meeting reported that pooling was under consideration. Some participants reported informal ways of finding experts through sister Boards in other states, including use of Exec Net, a broadcast email service of Administrators in Medicine, the association of executive directors. In one state, however, there was resistance to any use of hired guns who cross borders to testify.
Efficiency and Targeting Resources
Most Boards in this era were striving to improve regulatory outputs even as staff cuts were required (Washington 2004a). Better information technology was universally seen as a key to improving efficiency. All managers strongly believed that better IT would allow them to improve performance through ongoing monitoring and feedback. As already noted, no state had operational IT systems that fully met their regulatory needs as executive directors and other users saw them. Two states were in advanced stages of implementing improvements.
Better IT was a high priority use for any available new funding, as already noted (Exhibit 11). What managers all described, in varying ways, was a form of relational data base with several key attributes:
- integrated across all Board activities;
- user friendly;
- flexible enough for various types of data to be entered--including information that does not fit predefined categories;
- easily searchable with simple query language rather than detailed programming; and
- able to generate various types of output for multiple uses.
Electronic complaint records were expected to improve quality of performance, much as electronic patient records can enhance clinical care and public health (Gingrich and Merritt 2005). Having more data handling capacity is expected to encourage keeping and tracking more types of data, such as information on below threshold complaints that are routinely closed without investigation, but a pattern of which might indicate a larger problem. Managers and staff in one state with a recently improved IT system said that they did track such cases.
Indicators of Effectiveness
IT was expected to improve performance across stages of disciplinary process, from targeting investigations to post-disciplinary monitoring of licensee compliance, and improved computer hardware and software were clearly central to various other performance management improvements also noted.
Economies Achieved through Automation
The most frequently mentioned example of the virtues of automation was computerization of licensure tasks. Most of the Boards in recent years have automated routine activities of licensure and have encouraged licensees to submit applications online rather than by paper documents that require that Board staff input the information, which adds cost and some errors. As noted above, Iowa even lowers fees for online applicants.
Several informants also praised the practice of scanning documents that they must file and of sending pre-meeting paperwork to board members by compact disc rather than in hard copy. Even though such CDs are only scans, not fully searchable documents, noted one states executive director, the CDs can have bookmarks that facilitate finding material within them.
All described such automation as an efficient method of data storage and retrieval, which freed up staff, storage, and postage budgets for reallocation, mainly to disciplinary tasks. In other cases, managers anticipated useful outputs not yet readily available. For example, managers were keenly aware of the constant need to hold down costs and operate more efficiently. They generally regretted their current inability to track costs per case in real time, for example.
Targeted Enforcement
Many key informants anticipated that better IT would enable them to track trends in existing data so as to target available resources where they could do the most good. They felt that they could address many issues of interest with existing capabilities, but not easily or in real time. More data capacity was expected to allow more benchmarking, so as to target outliers for investigation or other action. The leading example cited was focusing on repeat offenders, physicians with multiple malpractice or disciplinary activity over a period of years. The Massachusetts Board has begun to compile information across multiple disciplinary complaints (or malpractice claims) to find patterns of a problem when no one complaint in isolation would appear serious. It has published a compilation of data suggesting that three paid malpractice claims in ten years is a good indicator of a problem physician. In response, it has adopted a policy of automatically performing a clinical review of such physicians (Massachusetts Board 2004). Other case study informants recommended such activity as well.
The California Enforcement Monitor analyzed the extent to which different categories of complaints or reports led to action. The analysis found that consumer initiated complaints were rarely even referred for field investigation (unlike in other states). In contrast, several other types of reports were much more likely to have been found worthy of follow-up--including those from hospital peer review, malpractice carriers, coroners, self-reporting by physicians, medical and osteopathic boards in other states, other government agencies, and local police or sheriffs departments. The latter type of high yield complaints was urged to get more attention (J. Fellmeth & Pagageorge 2004).
It should be noted that additional IT capabilities in the absence of other important resources might not generate the same results. As one example, the California analysis was more recently advanced in large part because the state funded the position of an external Enforcement Monitor who had long experience with regulatory boards and good cooperation in accessing information from within the various components of Californias process (J. Fellmeth & Papageorge 2004, 2005).
Persuasiveness of Data Analysis
The California Monitors report highlighted the availability of analyzable data as a major reason that its 2004 report could improve upon its predecessors efforts of 15 years before (J. Fellmeth & Papageorge 2004; R. Fellmeth 1989). In 1989, the Board had not maintained good data nor automated what it did have.64 More recently, even the rather primitive data capabilities available to the Monitor allowed that office to generate numerous useful recommendations. Moreover, the recommendations carried great weight not only within the Board and the office of the Attorney General but also in the state legislature, and a great many recommendations made in late 2004 became official practice or state law by the next fall (J. Fellmeth & Papageorge 2005).
Massachusettss recent success in raising its budget also came after the Board undertook higher tech and more analytical approaches to the problem of frequent offenders, as noted above, and to online profiling (considered below). More prosaic successes were also involved--closing backlogged cases and getting support from the medical society.
Staffing and Leadership
Many case study participants spoke of the need to attract and retain good quality staff, which was a focus for the California Monitors writing as well (J. Fellmeth & Papageorge 2004).65 Most managers felt generally successful in their staffing, though many commented on the challenges of managing within public sector personnel practices.
Maintaining or increasing investigative staff was identified as a particular need in many states. A frequent goal was to return to earlier ratios of staff to workload (J. Fellmeth & Papageorge 2004; Washington State 2004a). Having field investigators with full medical credentials in nursing or another health profession was not generally seen as an effective practice. Most but not all key informants emphasized medical capacity at a supervisory or review level instead. Similarly, some but not all thought that additional medical training for investigators would pay off in better performance.
All Board managers, however, believed that more staff would aid productivity. Of course, almost any manager would like to have more staff, but the case study found some indications of improved performance from enhanced staffing. Almost all the case study states successfully reduced backlog with greater dedication of resources, sometimes with a temporary push by senior management, either during the study period or in prior years. Some non-case study states in this era also added resources and staff to reduce backlogs (Adams 2003, 2004b).
Moreover, two of the six study states, Massachusetts and Virginia, had notable increases of resources during the timeframe of this study, and their experiences lend support to the efficacy of increased resources. The evidence from Massachusetts is qualitative. After licensure fees were increased in 2002, the Board could expand its use of external peer reviewers. Virginia tracked output more directly. The Board planned for an increase in complaints in 2003-04 above 2001-02 levels because of a legislated change in the standard of proof. The state increased staff full-time equivalents (FTEs) for medicine by 28%. Complaint closures in this biennium increased slightly more--by 31%, or 2% more cases per FTE. The average time to closure was also reduced by 7% (Virginia DHP 2004, appendix G).
Innovations Ancillary to Complaint Resolution
Promulgation of Rules in Lieu of Case-by-Case Enforcement
A non-disciplinary alternative to complaint resolution is to try to improve medical practices through education or guidelines. Washington State, for example, has listed as a formal goal moving From Reaction to Prevention through Education (2002, p. 8). Like any administrative agency, Medical Boards can not only make decisions through adjudicatory, case-by-case proceedings but also through legislative style rule making to govern frequently arising cases. The case study Boards tried to make rules both to protect public safety in advance and to reduce their own burden of resolving multiple similar complaints.
Ohio managers credited the states advance rules on over-prescribing as being very helpful in addressing a recurring category of cases involving physicians who abused drugs by writing prescriptions in the names of relatives. The Board cooperated with the pharmacy board not only to ban such physicians prescriptions but also to ban pharmacists from filling them--with the result that such cases disappeared from regulatory dockets. In another example, the Massachusetts Boards review of confidential, non-disciplinary hospital reports made an early discovery of emerging problems from bariatric surgery, a newly popular type of procedure. The Board issued an emergency rule to govern such practices, and managers believe they avoided problems as a result.
Other rule making followed more general trends; changes often reacted to national shifts in medical practice or new media attention to problems (Adams 2001b). The rise of outpatient surgery provides one example. Virginia, like many other Boards nationally, assessed general information about anesthesia and sedation, including the statutes and regulations of other state boards, and convened an expert advisory panel before establishing minimum standards through regulation. Such a response is akin to scope of practice regulation for licensure, and can draw complaints of over regulating legitimate new practices desired by consumers. Rules on pain medications illustrate a similar dilemma, where protection against abuses needs to be weighed against strong demand for more effective pain relief than is conventionally supplied (Kaufman 2003).
A New Process for Some Quality Complaints
Ohio has created an alternative process that diverts some quality-related complaints from conventional disciplinary process into its QIP.66 QIP uses less formal, non-adversarial administrative evaluation to quickly resolve quality-related cases that do not look serious but might prove to be (Ohio Board 2004). It was developed in the mid-1990s to cope with a growing backlog of cases that investigators were reluctant to close without any inquiry but were constantly postponing to cope with the constant flow of newer, clearly more serious cases. Many involved a practitioners poor practice patterns or failure to keep up with current practice standards that did not actively endanger patients but that might worsen without intervention. Such problems were believed to be remediable with a modest amount of retraining, often focused on a single practice deficit rather than across-the-board problems.
Cases are referred to QIP before formal charges are brought. Hence confidentiality protections apply as during conventional investigation, and full legal requirement of due process are not yet applied. QIP is run by two parallel panels, each with six physicians representing key specialties and one lay member. The physicians are not Board members, so they constitute a new source of expertise, and the time burden on members is kept down because the two panels alternate sessions, each meeting every other month.
The panels each review medical records and other submissions in the manner of peer review rather than adversarial hearing, which permits peer discussions with the licensee. QIP panels may close a case without action, send a caution letter to the physician, refer the physician to a remedial educational program, or return the case to conventional discipline if irreparable and serious problems seem likely.
QIP effectively eliminated the backlog of low-quality cases, according to managers. In 2003, the panels resolved 103 cases, simply closing almost 60% of cases, sending letters for 20%, and sending about 10% each to re-education or back to discipline. This throughput is of similar scope to conventional process, which in that year held 49 hearings and took 153 actions (Ohio Board 2003). One board member especially liked that QIP has a foundation in medical theory because it is grounded in peer review. Another wanted to expand the number of panels available to incorporate more medical specialties.
QIPs confidentiality, use of the panels own medical expertise to reach judgments, and emphasis on remediation makes it resemble a prior eras informal Board practice. It marks a sharp departure from the formal adjudicative model universally used for todays discipline. One outside observer suggested that over use of QIP could present opportunity for abuse as well as to do good, as there is a real danger in returning to informal, secret disciplinary practices.
External, Educational Assessments of Physician Competence
Key informants in multiple states explained that it is always difficult to evaluate physician competence or to re-educate physicians with a quality deficit, especially through the fact-finding and formal orders of adversarial disciplinary process.67 Yet many practitioners over time are believed to develop particularized deficits in competence such as those targeted by QIP. The mismatch between one-time testing of competency and lifetime medical practice has created interest in other methods, although these are not yet much used.68
There was interest among case study respondents in referring physicians for assessment at private educational entities, often termed clinical assessment centers (Prager 2000). Such centers can undertake thoroughgoing, hands-on assessments using a variety of mechanisms, and also typically offer additional retraining as needed. Techniques include structured clinical interviews by expert physicians based on actual patient charts from the doctors own practice as well as hypothetical charts, simulated patient encounters, interpretation of diagnostic tests, objective answer written tests, computer-based assessment of cognitive skills, and review of documentation. A number of such programs exist across the country (Prager 2000; Terry 2002b; CAC 2003; FSMB 2005a). Among the best known are the PACE program at the University of San Diego School of Medicine (Physician Assessment and Clinical Education), CPEP in Aurora, Colorado (private non-profit Center for Personalized Education for Physicians), and the Physician Assessment and Individualized CME program at the University of Wisconsin Medical School.69 The Federation has begun working with multiple such programs; one goal is more standardization (FSMB 2005b).
Managers in all of the case study states were aware of such programs, yet most of the study states made few such referrals. The only large user of such services was California, which now often makes sanctioned physicians undergo remedial training at PACE (J. Fellmeth & Papageorge 2005). CAC (2003) also found only one large user Board nationally. Board managers and staff often noted the high costs to physicians, about $5,000 in tuition plus costs of absence from practice, a factor also mentioned in the literature (Prager 2000). Of course, costs are also very high on both sides even for Board investigation of quality cases and can be especially high for prosecuted quality cases, as noted above. Physicians must typically pay for the programs themselves; one Board manager particularly emphasized that there no state resources could be made available for such costs.70
Disseminating Physician Information: A Complementary Approach
One new approach is to give consumers information before they use medical services as well as to respond to any complaints they may have afterward. The world wide web gave Boards a cost-effective means to help patients become better consumers by providing more information about physicians, including information about their disciplinary and malpractice history. Massachusetts was the first state to create and maintain physician profiles, starting in 1996 (Sullivan 2000).
The Massachusetts approach served as a model that numerous other states have followed (Exhibit 20). States postings typically include background data of general interest to consumers, such as a physicians insurance plan participation, hospital affiliation, and medical specialties. Also generally provided are past sanctions against each physician and often malpractice payments as well.71 Malpractice information is controversial, as many physicians believe that many or most payouts are little related to past medical negligence, much less to ongoing competence. Pending complaints and past ones closed without public sanction are typically not included.
| EXHIBIT 20: Contents of Massachusetts Physician Profiles |
|
| SOURCE: http://profiles.massmedboard.org. |
The Massachusetts website has proven very popular. In 2003 it totaled over 16 million hits (Massachusetts Board 2003)--or about 600 per licensed physician. Web-posting can also make information about Board sanctions more readily available to interested consumers than does the traditional form of disclosure through periodic Board newsletters. Those mailings themselves may have more durable impact because they are also commonly posted online. Conceptually, greater visibility through online postings could increase the deterrence effect of Board activities, as health care plans, individual consumers, and the media have ready access to the sites. However, evidence is lacking.
Beneficial side effects of public disclosure on Board performance are also cited, resulting from disclosure and some new public feedback. As a result of profiling, the Massachusetts executive director has argued, Our data quality is better, our staff is sharper, and our closeness to the public and its concerns has never been more intimate (Sullivan 2000).
Quality-Diversion Models
One potentially effective idea discussed by some case study participants is for Boards to cooperate more with hospitals and other front-line facilities to find doctors with remediable quality problems early on, then intervene with education rather than punishment. Such practitioners could be diverted away from discipline into re-education, following the precedent set by physician assistance programs for impaired doctors.72 Another precedent in the case study states is Ohios QIP process for certain quality complaints, which also takes a non-disciplinary approach to quality concerns.
Every case study state and almost every state nationwide has such a physician assistance program, a 1980s innovation designed as a more productive alternative to discipline for doctors with treatable substance abuse or mental or physical impairment. Funding comes partly from the Medical Boards (in Washington State with a dedicated share of physician licensure fees), partly from participants, who typically pay for their own treatment, meetings expense, and compliance costs. Quality diversion could readily use the same types of national clinical assessment centers noted above.
Under quality diversion, physicians could self-refer (possibly encouraged by colleagues or hospital officials) or Board staff could send some disciplinary cases for the type of assessment and re-education to which QIP and some other states already refer some physicians. The goal would be early intervention and prevention of harm, using the educational alternative not as an adjunct to completed discipline as in California today but instead in place of discipline altogether.
To be effective, such programs would need to motivate provider institutions to provide more referrals of physicians with quality problems than the institutions historically have referred to discipline. Todays impairment diversion programs are also small; California, for example, had only about 250 participants in its 5 year program as of mid-2004 (J. Fellmeth & Papageorge 2004). Eliciting more referrals would likely require persuading health care institutions that the Board program is a trustworthy partner in re-education.
Another challenge for effectiveness is ongoing monitoring. One shortcoming of relying on clinical assessment centers for quality oversight is rather weak follow-up through applied education in a practitioners home area. Some respondents noted that effective monitoring requires that local entities need to be involved as well a national center especially local medical schools or medical societies. The effectiveness of compliance monitoring for impairment diversion has also sometimes been questioned (J. Fellmeth & Papageorge 2005; Thompson 2005a).
One small national effort to get institutions and Boards to cooperate on quality diversion began in 2002 to encourage Boards of medicine and nursing to take this re-educational approach for a much larger number of cases. This Practitioner Remediation and Enhancement Partnership (PREP) is run by a nongovernmental organization to promote patient safety by helping medical and nursing boards work with hospitals and other providers to identify, remediate, and monitor caregivers with deficiencies that are cause for concern yet do not rise to the level of precipitating disciplinary action (CAC 2002, p.1)--a standard similar to that of Ohios QIP. The program refers such people for assessment and re-education to facilities like Colorados CPEP (described above). PREPs operations were beyond the scope of this project.
Patient Care Assessment in Massachusetts
The Massachusetts Board runs a safety-oriented, hospital-focused system of physician oversight quite apart from discipline. The Board describes its authority as unique, deriving from legislation that gives it authority to require most health care facilities to run systems of quality assurance, risk management, peer review, and credentialing known as PCA programs. The enactment dates from 1986, responding to a prior liability insurance crisis. The rationale for involving the physician Board was that physician leadership is needed for quality assurance to succeed and that physicians should have to practice only in safe institutional environments.
The Board reviews and approves facilities PCA plans and monitoring their operations through three types of required reports. Two types of mandatory reports on progress implementing plans are submitted semi-annually and annually. A third requirement is reporting of major incidents, that is, serious, unexpected patient outcomes, somewhat similar to the sentinel events that JCAHO requires to be investigated within hospitals. PCA reports to the Board are due within about three months (to allow time for investigation and action); they are entirely confidential and undiscoverable in legal actions. Each contains narrative about the case, explaining what happened, how the hospital investigated, and what changes were later made to prevent recurrence.73 Other matters may also be sent to the PCA committee from within the medical Board if they seem to involve matters of facility safety.
The Board PCA committee operates separately from licensure and discipline, not sharing any identified information with them. The committee reviews the submissions to see how well hospitals in-house programs are working. In particular, they assess whether changes made in response to problems were appropriate and sufficient. Board members and managers believe that the PCA program has positive impacts on helping create a general climate supportive of safety. They cite the discovery of problems in bariatric surgery and ensuing standards (above) as a key success that prevented problems rather than disciplining them after the fact.
As of 2004-05, the states policy on sanctioning and safety appeared to be in evolution, as officials and stakeholders were sorting out what entities would have what responsibilities. It was as yet unclear what roles were to be played by physicians, by hospitals, and by hospital and physician regulators. Also being debated were what one key informant called the tensions between the blaming culture of discipline and the reporting culture of patient safety that calls for a non-disciplinary blame free approach to medical error that promotes disclosure and learning from problems (see also Bovbjerg et al. 2001). Some in the state had begun promoting a new approach to accountability that charges institutions with avoiding most problems including ordinary errors but holds individuals accountable for knowing misconduct or disregard of safety strictures. The state health department, within whose umbrella the Medical Board operates, also created a new Patient Safety center in 2004, with an agenda that overlaps with the Boards PCA program.74 A public-private coalition is also considering the allocation of safety and monitoring authority.75
Other Innovations
Many Board members and managers expressed a desire to do more for safety than react to complaints. The literature review and case study respondents suggested some other pro-active alternatives to complaint-based discipline. These included audits of physician practices, non-disciplinary use of CACs, and efforts to encourage ongoing maintenance of competence.76 Such approaches not now observable in the field were beyond the scope of this study.
CONCLUDING DISCUSSION
State Medical Boards play an important role in American health care quality assurance because these licensing agencies are the only entities with the authority to completely stop practitioners from practicing beyond their level of competence (Jost 2002). Other entities also affect clinical performance, often on a more day-to-day basis: For example, hospitals employ some practitioners, grant staff privileges to non-employees, conduct internal peer reviews, and may run patient safety systems. Medical groups influence their physicians activities. Private medical specialty boards credential specialists. Health plans admit practitioners to their provider networks and may review the appropriateness and quality of care. Other practitioners refer patients to particular practitioners or do not. Patients also play a role in selecting they practitioners they see, the facilities they use, and the therapies they receive. However, only State Medical Boards have ultimate legal authority over all ways and areas in which physicians practice--inside or outside of hospitals, cooperating or not with safety or quality protocols, and keeping up with evolving standards of practice or not.
By statute and stated mission, State Medical Boards activities and their budgets are driven by the need to resolve public complaints. Thus, complaint resolution is the core of traditional Board quality assurance beyond initial licensure. What matters to success (or failure) in this key function is finding and appropriately sanctioning substandard physicians. This in turn requires sufficient intake of complaints, well targeted processing of complaints, and effective Board review of allegations--all accomplished within an adversary legal process. Success results when a Board can move cases quickly and efficiently through multiple stages, from complaint intake to discipline and follow-up (Exhibit 15); failure is visible in large backlogs of cases and inability to prioritize so as to address those with the most serious implications for safe patient care.
This project found that cases readily back up in investigation, in peer review, and in administrative proceedings. It identified a number of key features and strategies that Boards employ, to varying degrees, to fulfill their required functions, including:
- using initial triage to drop cases of low importance;
- monitoring of throughput of cases in investigation;
- enhancing peer review capacity for quality cases, including contracting out for reviews;
- coordinating and collaborating between hearing attorneys and investigators, especially on serious cases;
- applying sanctions for substandard physician practice more promptly and consistently across cases; and
- improved managerial capacity to track cases, along with self-monitoring of performance to continuously develop and perpetuate improvements.
Almost all Board members and managers believed that better IT is needed to improve efficiency, target resources, develop better tools for spotting and managing problem cases, and meet higher standards of accountability. A key issue was perceived to be focusing resources on high-value cases, ones most likely to call for disciplinary action in the end. Improving performance with IT calls not just for acquiring computer capabilities but also for using them effectively. A number of other requisites to maximizing a Boards functional performance were noted by case study participants: (i) inputting all relevant information--not only on licensure and disciplinary status but also on associated staffing, hours, expenses, and other managerial information; (ii) having analytical capability to use the information once it is made available; and (iii) accessing or developing standards by which to measure performance. Moving to more automated and analytical approaches calls for different staffing than traditional clerical input for paper files; experience in automating licensure suggests than some staffing shifts can be achieved. Larger Boards appear to be at an advantage in creating fulltime new specialists.77
As for standards of comparison, analysts within Boards and external reviewers like the California Enforcement Monitor mainly relied upon comparisons with prior times and common sense assessment. Umbrella Boards also often compared statistics across different health professions. Enhancing Boards abilities to make comparisons across states and with regulatory activities in other areas would likely be helpful. The Federation offers Boards that complete its member survey comparisons with similar states responses (without identifying states), but there is interest in doing more. The development of benchmarks on costs per activity, timeliness, and other measures may be helpful based on the experience of State Medical Boards that have access to such information.
All senior managers believed they could accomplish more with better tools and staff, and there was suggestive evidence of such improvements in the experience of two Boards that received marked budget increases during the case study period observed. A generation ago, leaders of the Federation of State Medical Boards wrote in a leading medical journal, The success of boards to improve medical discipline will finally depend, of course, on the funding, staffing, and authority of state boards. These can only come from state legislatures willing to "act responsibly (Breaden & Galusha 1987). To this assessment today must be added the observation that in order to command additional resources in an era of constraint Boards must better document their performance needs and their achievements. Board budgets in the past have been boosted mainly in response to failure--a highly publicized case detailing backlogged complaints or a clearly errant physician whom the Board had neglected to discipline. Hopeful signs are visible from California, Massachusetts, and Virginia that better analysis documenting performance achievements and needs can also encourage better budgetary and other forms of support from the rest of state government.
Traditional forms of complaint-driven discipline and mechanisms for improvement were necessarily the focus of this case study, for that is what Boards mainly do to protect medical quality and safety beyond initial licensure. Complaint investigation and resolution respond to acute problems, risks that have already affected patients, at least as perceived by patients themselves. Board members and managers participating in this case study were acutely aware of the shortcomings of their traditional approach--its reactive nature and inherently high costs and low speed. High costs come both from having to find a small number of substandard needles in a large haystack of somewhat haphazard consumer complaints and from the need to conclusively prove unacceptable quality through expert testimony within an adversarial process of administrative law that protects physicians rights and the legal integrity of fact finding.
These managers and members of State Medical Boards were also very interested in finding more proactive and preventive ways to meet their statutory role of protecting the public. Case study participants described some alternative mechanisms already in use in some places, including:
- establishing advance rules where possible to improve practice without waiting for complaints;
- a special review process by Board subpanels to resolve a subset of quality-related complaints;
- use of national clinical assessment centers as an adjunct to discipline;
- patient education through physician profiles posted online;
- board review of hospital incidents and responsive safety mechanisms, wholly separate from discipline; and
- cooperation with hospitals for early detection of physician with deficits in capabilities, for remediation in place of discipline.
Many Board members and managers also expressed a desire to do more for safety than react to complaints. The literature review and case study respondents suggested some other proactive alternatives to complaint-based discipline. These included audits of physician practices, non-disciplinary use of CACs, and efforts to encourage ongoing maintenance of competence. Such approaches not now observable in the field were beyond the scope of this study.
Implications. This case study documented many aspects of State Medical Boards structure and operations. It also identified practices considered to make discipline more efficient or effective. The extent of variation observed across Boards in terms of such factors as rates of sanctions, timeliness of case closure, investigatory staffing ratios, budgetary support, and many other outputs and inputs suggests that Boards may have much to learn from one another. Such learning seemed possible based on interest of managers and others from these six states. A cross-cutting lesson from all is that some organized assessments of Board performance using data on problems and accomplishments were followed by the grant of more resources and other Board-desired changes from state legislatures in at least Virginia, Massachusetts, and California. Managers from case study states consistently pushed for more IT and data capabilities as IT was described as facilitating such analyses.
Limitations. This study focused mainly on experience in six case study states, although it also drew upon comparative national data to describe many elements of Board structure, operations, and performance. The six states are not representative but rather were judgmentally selected to be likely to show innovations in approach. The comparative data available lacked fully standardized definitions, which makes cross-state comparisons imperfect, for example on the number and nature of complaints. Another measure tabulated, elapsed time to case resolution, is incomplete in that a state can have quick resolution of cases actually closed but a growing backlog of very old cases; conversely, a state improving by closing out its backlog thereby raised the average time to closure. Finally, the literature, Board managers and members, and other observers agreed that it is impossible to measure any direct impact of Board activities on public health or safety, although most Board personnel felt that their activities had beneficial impacts.
Next steps. One major near term development for Boards will likely be acquiring and using new IT and data management capabilities to improve effectiveness and efficiency of disciplinary performance. Such improvement was being actively sought in every case study state. It was suggested that working toward performance improvement calls for not only new IT hardware and software but also: (i) a new approach to tabulating all relevant information in one database--on licensure and disciplinary status and also on associated staffing, hours, expenses, and other managerial information; (ii) having analytical capability to use the information once it is made available; and (iii) accessing or developing standards by which to measure performance. Data from the Federations member board survey is already made available to states for certain comparisons with de-identified other states, which has the strengths and limitations already noted. Demand for comparative capabilities and benchmarks may well grow. Performance standards for physicians or more objective definitions of competence are also of great interest to many Board managers.
For policy research, the next steps may be to more rigorously study existing state interventions or conduct demonstrations to see how well some of them travel to new states. More careful study would be useful for such things as Californias use of clinical assessment centers, Massachusettss physician profiling and unusual relationship with hospital safety efforts (the PCA), Ohios quality improvement program, and efforts in numerous states to form teams of investigators, managers, and lawyers to streamline the handling of important cases. Non-case study states of course also offer opportunities for study.
REFERENCES
ABMS (American Board of Medical Specialties). 2001. Physician Performance Outcomes, featured article (October-November) http://www.abms.org/Downloads/Monthly_Articles/Physician%20Performance%2... cited with approval by Administrators in Medicine, association of executive directors of state medical boards http://www.docboard.org/>.
-----. 2005. Maintenance of Certification (MOC) (current webpage with link to explanatory materials, including published articles) http://www.abms.org/MOC.asp>.
AMA (American Medical Association). 2006. State Medical Licensure Requirements and Statistics 2006.
Adams, Damon. 2001a. Maryland examines doctors influence: How close is too close? Thats a question a state legislature is asking about the relationship between state medical boards and state medical associations, American Medical News, October 15.
-----. 2001b. Some States Take Prevention Tactic on Doctor Discipline: Disciplinary Actions against Doctors Increased Last Year, But Some Medical Boards Are Turning to Education and Practice Guidelines to Keep Physicians out of Trouble, American Medical News, May 7.
-----. 2003. Texas Medical Board Funding Will Help Root out Bad Doctors, American Medical News, July 21.
-----. 2004a. Judging and Being Judged: The Thankless Job of Doctor Discipline: Physicians Who Serve on State Medical Boards Arent Always Popular, but Theyre Necessary, American Medical News, April 12.
-----. 2004b. North Carolina Board Claims Boost in Doctor Discipline, American Medical News, March 8.
Albert, Tanya. 2002. Liability insurance crisis: Bigger awards just one factor, American Medical News, April 15.
Ameringer, Carl F. 1999. State Medical Boards and the Politics of Public Protection (Baltimore, MD: Johns Hopkins).
Apple, Kathy. 2005. Evidence-Based Regulation: A Regulatory Performance Measurement System, Presentation to Citizen Advocacy Center Annual Meeting Denver, CO on behalf of National Center of State Boards of Nursing, November http://www.cacenter.org/Kathy%20Apple%27s%20Evidence%20Based%20Regulatio....
Bodenheimer, Thomas. 1999. The American Health Care System--The Movement for Improved Quality in Health Care, N Engl J Med. 340:488-92.
Boodman, Sandra G. and Patricia Davis. 2003. Va. Doctors Misconduct Left Trail of Broken Lives: Medical System Failed To Protect Patients, Washington Post, September 28, page A01 http://www.washingtonpost.com/wp-dyn/articles/A10967-2003Sep27.html>.
Bovbjerg, Randall R. 2004. Malpractice and Discipline--Claims and Competence: Evidence from Research, Presentation for session Malpractice Claims and Competence Is there a Relationship? presentation to the Annual Meeting of the Federation of State Medical Boards, May 1, Arlington, VA, slides available at http://www.fsmb.org/education/AM_Pages/2004_AMPRES/bovbjerg.pdf>.
----- and Robert A. Berenson. 2006. Enterprise Liability in the 21st Century, in Medical Malpractice and the U.S. Health Care System: New Century, Different Issues, edited by William M. Sage and Rogan Kersh, Cambridge University Press (forthcoming).
-----, Robert H. Miller, and David W. Shapiro. 2001. Paths to Reducing Medical Injury: Professional Liability and Discipline vs. Patient Safety--and the Need for a Third Way, Journal of Law, Medicine and Ethics 29(3and4, Fall and Winter):369-380.
----- and Holly S. Stockdale, 2004. Conceptual Review of Issues: Assessing State Medical Boards Performance in Disciplining Physicians--Limitations and Potential Improvements, project report to DHHS/ASPE, revised, April 27.
Boyd, Donald J. and Nicholas W. Jenny. 2003. State Fiscal Crisis Far Worse Than Economy Would Suggest, The Rockefeller Institute State Fiscal News, Vol. 3, No. 4, May.
Breaden, Dale G. and Bryant L. Galusha. 1987. State Medical Discipline: Defects and Hindrances, JAMA 257:828-29.
Brennan, Troyen A. 1998. The Role of Regulation in Quality Improvement, Milbank Quarterly 76:709-31.
CAC (Citizen Advocacy Center). 2002. Practitioner Remediation and Enhancement Partnership (PREP): Improving Patient Safety and Healthcare Quality, Washington, DC: CAC, report to Health Resources and Services Administration, Bureau of Health Professions, Division of Quality Assurance, Department of Health and Human Services, April http://www.4patientsafety.net/PREPYearOne.pdf>.
-----. 2003. PREP 4 Patient Safety [Practitioner Remediation and Enhancement Partnership], Assessment and Remediation Resource Manual. Washington, DC: CAC, report to HRSA, contract #230-03-0004 [report undated, with internal evidence of year of creation] http://www.4patientsafety.net/assessmentandremediationmanualfinal.pdf>.
California Board (Medical Board of California). 2003. Manual of Model Disciplinary Orders and Disciplinary Guidelines, 9th ed. Sacramento, CA: Board Division of Medical Quality, State and Consumer Services Agency http://www.medbd.ca.gov/Pubs_Disciplinaryguide.htm>.
-----. 2004. 2003-2004 Annual Report. Sacramento, CA: Medical Board of California http://www.medbd.ca.gov/Pubs_Annualrept_2003-2004.pdf>.
California Joint Committee on Boards, Commissions, and Consumer Protection. 2005. Medical Board of California: January 2005 Hearing on the Initial Report of the Medical Board Enforcement Monitor, Background Paper http://www.sen.ca.gov/jlsrc/2005_Backgrounder_MEDICAL_BOARD.doc>.
CJD. 2002. A Short Guide to Understanding Todays Medical Malpractice Insurance Crisis (and Useful Questions to Ask) NY: Center for Justice and Democracy, September 25 http://www.centerjd.org/MediaGuide.pdf>.
Cohen, Harris S. and Lawrence H. Miike. 1974. Toward a More Responsive System of Professional Licensure, International Journal of Health Services 4:265-72
Coughlin, Teresa A. and Stephen Zuckerman. 2005. Three Years Of State Fiscal Struggles: How Did Medicaid And SCHIP Fare? Health Affairs, Web Exclusive, August 16 http://www.healthaffairs.org>.
CPEP, 2002. A National Leader in Evaluating and Enhancing Physician Performance Aurora, CO: Center for Personalized Education for Physicians http://www.cpepdoc.org/assessment.htm>.
Derbyshire, Robert C. 1979. Physician Competence: What is the problem? What are the answers? New York State Journal of Medicine 7:1028-31.
Derbyshire, Robert C. 1974 Medical Ethics and Discipline, JAMA 228: 59-63
Derbyshire, Robert C. 1965. What Should the Profession do about the Incompetent Physician? JAMA 194(12):1287-90
Donabedian, Avedis. 1980. The Definition of Quality and Approaches to its Assessment (Ann Arbor, MI: Health Administration Press).
Donabedian, Avedis. 1966. Evaluating the Quality of Medical Care. Milbank Memorial Fund Quarterly: Health and Society 44(3; pt. 2):166-203.
Donabedian, Avedis. 1972. Models for Organizing the Delivery of Personal Health Services and Criteria for Evaluating Them, Milbank Memorial Fund Quarterly 50(part 2):120-22.
Epstein, Ronald M. and Edward M. Hundert. 2002. Defining and Assessing Professional Competence, JAMA 287:226-235.
Fellmeth, Julianne DAngelo. 2003. Effective Disciplinary Programs, Journal of Medical Licensure and Discipline 89(3):109-116.
----- and Thomas A. Papageorge. 2004. Initial Report: Medical Board of California, Enforcement Program Monitor, November 1 accessible from http://www.medbd.ca.gov/Pubs_Enforcementrept.htm>.
----- and Thomas A. Papageorge. 2005. Final Report: Medical Board of California, Enforcement Program Monitor, November 1, accessible from http://www.medbd.ca.gov/Pubs_Enforcementrept.htm>.
Fellmeth, Robert C. 1989. Physician Discipline in California: A Code Blue Emergency - An Initial Report on the Physician Discipline System of the Board of Medical Quality Assurance (San Diego, CA: Center for Public Interest Law, University of San Diego School of Law, April 5) http://www.cpil.org/download/Code_Blue_Report.pdf>.
Finocchio, Leonard J., Catherine M. Dower, Theresa McMahon, Christine M. Gragnola and the Taskforce on Health Care Workforce Regulation. 1995. Reforming Health Care Workforce Regulation: Policy Considerations for the 21st Century (San Francisco, CA: Pew Health Professions Commission, December) http://www.futurehealth.ucsf.edu/pdf_files/reforming.pdf>.
Finocchio, Leonard J., Catherine M. Dower, Noelle T. Blick, Christine M. Gragnola and the Taskforce on Health Care Workforce Regulation. 1998. Strengthening Consumer Protection: Priorities for Health Care Workforce Regulation (San Francisco, CA: Pew Health Professions Commission, October) http://www.futurehealth.ucsf.edu/pdf_files/RTF.PDF>.
FSMB (Federation of State Medical Boards). 1998. Elements of a Modern State Medical Board, May http://www.fsmb.org/pdf/1998_grpol_Modern_Medical_Board.pdf>.
-----. 2003a. A Guide to the Essentials of a Modern Medical Practice Act, 10th Edition [initial version 1986] http://www.fsmb.org/pdf/2003_grpol_Modern_Medical_Practice_Act.pdf>.
-----. 2003b. The Exchange, vol. 1. Licensing Boards, Structure and Disciplinary Functions (Euless, TX: FSMB, looseleaf compilation).
-----. 2004a. Interim Report of Special Committee on Maintenance of Licensure. Dallas: Federation of State Medical Boards of the United States, May.
-----. 2004b. Summary of Board Actions, annual release of prior years actions, accessible in Federation Physician Data Center http://www.fsmb.org/m_fpdc.html>.
-----. 2005a. Directory of Physician Assessment and Remedial Education Programs, last updated January 27 http://www.fsmb.org/pdf/IPE_Directory_AssessmentRemedial_Programs.pdf>.
-----. 2005b. Post-Licensure Assessment System (webpage for Special Purpose Examination [SPEX] and the Institute for Physician Evaluation [IPE], undated but regularly updated) http://www.fsmb.org/m_plas.html>.
-----. 2005c. Annual Meeting of the House of Delegates: Report of the Reference Committee http://www.fsmb.org/pdf/GRPOL_2005_HOD_Rpt_Ref_Committee.pdf>.
Gabel, Jon R., Paul B. Ginsburg, Heidi H. Whitmore, and Jeremy D. Pickreign. 2000. Withering on the vine: the decline of indemnity health insurance, Health Affairs 19(5, Sep-Oct):152-7.
Gaul, Gilbert M. 2005. Once Health Regulators, Now Partners: Private Groups Limit Patient Access to Medical Files, Rarely Punish Doctors, Washington Post, July 26, A01.
Gingrich, Newt and David Merritt. 2005. Rx for America: A Healthy Dose Of Information Technology, The Forward, June 3 http://www.forward.com/articles/3270>.
Grad, Frank P. and Noelia Marti. 1979. Physicians Licensure and Discipline: The Legal and Professional Regulation of Medical Practice (Dobbs Ferry, NY: Oceana Publications).
Greiner Ann C. and Elisa Knebel, eds. 2003. Health Professions Education: A Bridge to Quality. Washington, DC: National Academies Press (for the Committee on the Health Professions Education).
Gross, Stanley J. 1984. Of Foxes and Henhouses: Licensing and the Health Professions (Westport, CT: Quorum).
Hall, Sheri. 2004. Doctors records go unchecked in U.S.: Beaumont Issues Highlight Piecemeal Reviews, The Detroit News, February 16.
Hatry, Harry P. 1999. Performance Measurement: Getting Results (Washington, DC: The Urban Institute Press).
Hatry, Harry P. 2002. What Types of Performance Information Should Be Tracked? chapt.2, pp. 17-34 in Dall Forsythe, ed., Quicker, Better, Cheaper? Managing Performance in American Government (Albany, NY: Rockefeller Institute Press) http://www.rockinst.org/publications/federalism/QuickerBetterCheaperChapter2.pdf>.
Heisel, William and Mayrav Saar. 2002a. Doctors without discipline--Medical Board allows doctors to practice despite litany of complaints, Orange County Register, April 7 (first in long series of articles, all accessible from http://www.ocregister.com/features/doctor/>).
-----. 2002b. Doctor discipline faulty: Hospitals policing yields few reports to Medical Board--and sometimes years later, Orange County Register, September 22 http://www2.ocregister.com/ocrweb/ocr/article.do?id=3882>.
Iowa BME (Board Of Medical Examiners). 2004. News Update, May 24 http://www.docboard.org/ia/PDF_Files/05ImpactStatements.pdf>.
-----. 2005. Disciplinary Process, webpage (undated, downloaded 2005) http://www.docboard.org/ia/DisciplinaryProcess.htm>.
JLARC (Joint Legislative Audit and Review Commission of the Virginia General Assembly). 2000. Final Report: Review of the Health Regulatory Boards, House Document No. 5 http://leg2.state.va.us/dls/handsdocs.nsf/By+Year/HD052000/$file/HD5_2000.PDF>.
Jones, Shirley. 2005. Presentation to NPDB Executive Committee Meeting, November 17. U.S. Department of Health and Human Services, Health Resources and Services Administration, Bureau of Health Professions, Practitioner Data Banks Branch.
Jost, Timothy S., ed. 2002. Regulation of the Health Care Professions (Ann Arbor, MI: Health Administration Press).
Jost, Timothy S., Linda Mulcahy, Stephen Strasser, and Larry A. Sachs. 1993. Consumers, Complaints, and Professional Discipline: A Look at Medical Licensure Boards, Health Matrix: Journal of Law-Medicine 3(2):309-38 (Summer).
Kauder, Neal B. and Elizabeth A. Carter, 2004. An Empirically Based Structured Sanctioning System, Journal of Medical Licensure and Discipline 90(4):8-17.
Kaufman, Marc. 2003. Worried Pain Doctors Decry Prosecutions, Washington Post, December 29, p. A01.
Kohn, Linda T., Janet M. Corrigan, and Molla S. Donaldson, eds. (for an Institute of Medicine committee). 2000. To Err Is Human: Building a Safer Health System (Washington, DC: National Academy Press).
Kusserow, Richard P., Elisabeth A. Handley, and Mark Yessian. 1987. An Overview of State Medical Discipline, JAMA 257:820-24.
Leape, Lucian L., David D. Woods, Martin J. Hatlie, Kenneth W. Kizer, Steven A. Schroeder, and George D. Lundberg. 1998. Promoting Patient Safety by Preventing Medical Error, JAMA 280: 1444-47 (founding and principles of National Patient Safety Foundation).
Marx, David. 2001. Patient Safety and the Just Culture: A Primer for Health Care Executives (New York, NY: Columbia University) http://www.mers-tm.net/support/Marx_Primer.pdf>.
Maryland Board of Physicians. 2004. Senate Bill 500 Makes Changes to Physician Licensing and Discipline in Maryland, MBP Newsletter, Winter https://www.mbp.state.md.us/forms/winter04.pdf>.
Massachusetts Board (of Registration in Medicine). Annual Report 1999 http://www.massmedboard.org/public/pdf/announcements/arweb.pdf>.
-----. Annual Report 2003 http://www.massmedboard.org/public/pdf/announcements/ar2003.pdf>.
McAuley RG, Paul WM, Morrison GH, Beckett RF, Goldsmith CH. 1990. Five-year results of the peer assessment program of the College of Physicians and Surgeons of Ontario, Canadian Medical Association Journal 143(11):1193-9.
Mello, Michelle M., David M. Studdert, and Troyen A. Brennan. 2003. The new medical malpractice crisis. N Engl J Med; 348:2281-2284.
Miller, Frances H. 1997. Medical Discipline in the Twenty first Century: Are Purchasers the Answer? Law and Contemporary Problems 60(1):31-58.
Norcini, John J. 1999. Recertification in the United States, British Medical Journal 319:1183-1185.
Norton PG, Dunn EV, Beckett R, Faulkner D. 1998. Long-Term Follow-Up in the Peer Assessment Program for Nonspecialist Physicians in Ontario, Canada, Joint Commission Journal on Quality Improvement 24(6):334-41.
NPDB (National Practitioner Data Bank). 2004. 2003 Annual Report. Rockville, MD: USDHHS, Health Resources and Services Administration http://www.npdb-hipdb.com/pubs/stats/2003_NPDB_Annual_Report.pdf>.
Ohio Board (State Medical Board of Ohio). 2003. Annual Report 2003 http://med.ohio.gov/pdf/Annual%20reports/2003report.pdf>.
-----. 2002. Disciplinary Guidelines. Columbus: State Medical Board of Ohio, Revised, April http://med.ohio.gov/pdf/meddis.pdf>.
-----. 2004. The Quality Intervention Program, program description provided by Board.
OIG (US Department of Health and Human Services, Office of the Inspector General, Office of Analysis and Inspections). 1986. Medical Licensure and Discipline: An Overview (Washington, DC: USDHHS, Control No. P-01-86-0064, June).
-----. 2005. HHS Agencies Compliance With the National Practitioner Data Bank Malpractice Reporting Policy, OEI-12-04-0031O, October 11 http://oig.hhs.gov/oei/reports/oei-12-04-00310.pdf>.
Pawlson, L. Gregory and Margaret E. OKane. 2004. Malpractice Prevention, Patient Safety, and Quality of Care: A Critical Linkage, American Journal of Managed Care 10:281-284 http://www.ajmc.com/files/articlefiles/AJMC2004AprlPawlson281_284.pdf>.
Peters, Charles. 2005. Tilting at Windmills: Doctors without Borders Washington Monthly, May.
Pincus, Mark S. 2006. Letter to American Association of Dental Examiners, re Free Queries for Medical and Dental Boards, January 30.
Prager, Linda O. 2000. Licensing Officials Launch Clinical Assessment Center: State Medical Licensing Boards Are Expected to Refer 200 Physicians to a Denver-Area Evaluation Center over the Next 12 Months for Scrutiny of their Competence, American Medical News, May 1.
Public Citizen, Health Research Group. 2003a. New 2002 Government Data Dispute Malpractice Lawsuit Crisis in Rhode Island, press release, July 8 http://www.citizen.org/documents/RI_NPDB.pdf>.
-----. 2005. Ranking of the Rate of State Medical Boards Serious Disciplinary Actions: 2002-2004 (HRG Publication #1737), April 19 [date of web posting, document undated] http://www.publiccitizen.org/publications/release.cfm?ID=7380>.
-----. 2004. Medical Malpractice Briefing Book: Challenging the Misleading Claims of the Doctors Lobby. Congress Watch, Rev. August http://www.citizen.org/documents/MedMalBriefingBook08-09-04.pdf>.
Richmond Times-Dispatch. 2003. Patients at Risk (multi-part series), January http://www.timesdispatch.com/news/patientsatrisk/> (Last Updated Tue Jan 28, 2003 11:39 AM ET)
Robeznieks, Andis. 2002a. California Medical Assn., Medical Board Reach Compromise: A Bill Calls for the State Medical Board to Release More Settlement Information, Add Public Members and Be Watched More Closely, American Medical News, September 2.
-----. 2002b. Public Active on Medical Boards, But Not Always Tougher on Doctors: Having Nonphysicians on State Medical Boards, However, Is Seen as a Credibility-Builder for Panels Seeking More Public Trust, American Medical News, November 11.
Schmitt, Kara and Benjamin Shimberg. 1996. Demystifying Occupational and Professional Regulation: Answers to Questions You May Have Been Afraid to Ask (Lexington, KY: Council on Licensure, Enforcement and Regulation).
Shimberg, Benjamin. 1982. Occupational Licensing: A Public Perspective (Princeton: Princeton Educational Testing Service).
Shimberg, B. 1991. Regulation in the Public Interest: Myth or Reality? Resource Brief. Lexington, KY: Council on Licensure Enforcement and Regulation.
St. George, Ian M. 2004. Assessing Performance 1: There but for the Grace of God Go I, New Zealand Family Physician 31(February 1):45-47 (1st of 8 articles, ending in 32(April 2), 2005) http://www.rnzcgp.org.nz/news/nzfp/Feb2004/StGeorgeISSUES_Feb04.pdf>.
-----. 2003. Doctors whose Competence Has Been Reviewed under the Medical Practitioners Act 1995, Journal of the New Zealand Medical Association, 116(1175):U459 http://www.nzma.org.nz/journal/116-1175/459/>.
Steinbrook, Robert. 2005. Renewing Board Certification, New England Journal of Medicine 353:1994-1997.
Sullivan, Nancy Achin [now Audesse]. 2000. Testimony before the House Commerce Committee on the Matter of HR5122 (Patient Protection Act) [for the Massachusetts Board of Registration in Medicine], September 20 http://www.massmedboard.org/public/pdf/announcements/othertestimony.pdf>.
Svorny, Shirley. 1987. Physician Licensure: A New Approach to Examining the Role of Professional Interests, Economic Inquiry 25:497-509.
Terry, Ken. 2002a. Impaired Physicians: Speak No Evil?--Ethics sometimes takes a back seat to inertia, fear, or empathy for a fellow doctor, but patients may pay the price, Medical Economics 19:110, Oct. 11.
-----. 2002b. When Doctors Put Patients at Risk, Medical Economics 22:25, Nov. 22.
Thompson, Cheryl W. 2005a. Medical Boards Let Physicians Practice Despite Drug Abuse, Washington Post, April 10, p. A01.
-----. 2005b. D.C. Board Rarely Punishes Physicians, Washington Post, April 11, 2005; Page A01 http://www.washingtonpost.com/wp-dyn/articles/A42456-2005Apr10.html>.
Twedt, Steve. 2003. The Cost of Courage: How the tables turn on doctors, Pittsburgh Post-Gazette, October 26, (First of a series) http://www.post-gazette.com/pg/03299/234499.stm>.
USGAO (United States Genera1 Accounting Office). 1989. VA Health Care: Improvements Needed in Procedures to Assure Physicians Are Qualified (Publication No. GAO/HRD-89-77, August).
-----. 1998. Performance Measurement and Evaluation: Definitions and Relationships (Publication No. GAO/GGD 98-26, April).
Virginia DHP (Department of Health Professions). 2004. Biennial Report for the Fiscal Years 2003 and 2004: Regulating Healthcare Professionals http://leg2.state.va.us/dls/handsdocs.nsf/By+Year/RD1162004/$file/RD116.pdf>.
Virginia Board of Medicine. 2004. Sanctioning Reference Points, Instruction Manual, prepared by VisualResearch, Inc. for the Virginia Department of Health Professions, July http://www.dhp.state.va.us/Medicine/guidelines/85-11-SRPManual-revised6-21-05.pdf>.
Washington State Department of Health, Health Systems Quality Assurance. 2004a. 2001-2003 Biennial Report: Health Professions Quality Assurance Regulatory Activities, July https://fortress.wa.gov/doh/hpqa1/Publications/documents/uda2001-2003.pdf>.
-----. 2002. 1999-2001 Biennial Report, Health Professions Quality Assurance and Regulatory Activities, June https://fortress.wa.gov/doh/hpqa1/Publications/documents/uda1999-2001.pdf>.
-----. 2004b. Disciplinary Process Review, Report to the Secretary, June.
Young, S. David. 2002. Occupational Licensing in The Concise Encyclopedia of Economics. Indianapolis: Liberty Fund, Inc., ed. David R. Henderson [online], http://www.econlib.org/library/Enc/OccupationalLicensing.html>.
NOTES
- The Federation of State Medical Boards is the national association of medical and osteopathic boards.
ENDNOTES
-
Two of the six case study states did not complete the Federations survey. For some survey-based presentations, we added data for them from other sources (e.g., Exhibit 1).
-
These other types of boards disproportionately do not provide information for The Exchange (FSMB 2003b), where respondents are identified, and similar response rates likely for the Member Survey.
-
Interestingly, Donabedian (1972) also developed six criteria of an effective operational control system that resembles performance measurement described here. His first three criteria are: (1) it provides continual monitoring and reporting of data; (2) it functions regularly, not ad hoc; (3) both outcomes of services and processes are monitored.
-
In Washington State, two Supreme Court decisions show evolving views. A 1958 decision cited the standing of the medical profession in the eyes of the public as a goal coequal with pub protection, whereas a 2001 See In re Revocation of License of Kindschi, 52 Wn.2d 8, 319 P.2d 824 (S.Ct WA 1958) and Bang D. Nguyen v. The Department of Health, Medical Quality Assurance Commission, 144 Wn.2d 516, 29 P.3d 689 (2001). [accessible at http://www.mrsc.org/mc/courts/supreme/052wn2d/052wn2d0008.htm>].
-
The key focus here is discipline related to physician competence because that most plausibly affects medical quality. Discipline for other failings (e.g., fiscal improprieties or moral turpitude) is less directly relevant.
-
This same complaint is also made about medical peer review and Medicare quality review, (e.g., Gaul 2005).
-
NY Public Health Law Section 230 (1).
-
The non-case study state of Maryland provides a recent example. In 2003 legislation reduced the large traditional role its medical society had played in board member selection and peer review. MD Code of Health Occupations, §14-101 et seq. (added by Acts of 2003, c.252, §1 eff. July 1, 2003).
-
New York has the largest number of members, at 159, of whom over a third are public members, the statutory maximum. In number of members the state is an outlier, in part owing to having different boards for licensure and discipline and also to an extensive committee system. The next largest board is New Jerseys, with 21 members.
-
Delaware seems to be lowest at $50 per meeting, to a maximum of $500 per year.
-
The organizations self-description: The Citizen Advocacy Center (CAC) is a unique training and support program for public members serving on health care regulatory and oversight agencies, governing boards and advisory bodies as representatives of the consumer interest. http://www.cacenter.org/about.htm>.
-
Missouri's Division of Professional Registration covers 39 professional licensing boards and commissions responsible for 240 different trades and professions. See the Divisions webpage at http://pr.mo.gov/>.
-
For example, the FSMB (2003b) categorizes Washington State as having an independent Board, although the medical board there operates within the Department of Healths Division of Health Professions Quality Assurance; Washington sources consider semi-independent to be more accurate.
-
See for example, Iowa Administrative Procedure Act, Iowa Code, chapt. 17A. For the national model APA, see National Conference of Commissioners on Uniform State Laws, Model State Administrative Procedures Act. The 1981 model act is online at http://www.nmcpr.state.nm.us/acr/presentations/1981MSAPA.htm>. For the 2005 draft, see http://www.law.upenn.edu/bll/ulc/msapa/2005AprMtgDraft.htm>.
-
OH Code sect. 4731.22. The Federation model medical practice act recommends 43 grounds for discipline (FSMB 2003a). These include business-related offenses (false or misleading advertising, fee splitting), unethical behavior (willful betrayal of professional confidence, any violation of professional code of ethics), criminal behavior (any felony conviction, non-therapeutic drug prescribing, misdemeanors of moral turpitude), quality problems (substandard care even without injury, noncompliance with body fluid safety standards), or demonstrated impairment or incompetence (including mental or physical problems, substance abuse).
-
The reform is known as House Bill 1441.
-
Bang D. Nguyen v. The Department of Health, Medical Quality Assurance Commission, 144 Wn.2d 516, 29 P.3d 689 (2001).
-
Maryland Board 2004.
-
§54.1-2915 House Bill 1441, 2003.
-
Virginia DHP 2004.
-
For this reason, another well known typology expands to five types of board in order to categorize states by each Boards control over licensure fees as well as by its extent of administrative autonomy (Shimberg, 1982, 1991; Schmitt and Shimberg 1996). As of 1996, most states 21 of 50 had boards with shared authority, meaning that a central agency oversees budget, staff, and may also investigate complaints and hold hearings, but boards make final decisions on disciplining doctors. Next most common (17/50) were autonomous boards that hire staff, investigate complaints, discipline licenses, collect fees and maintain their own budget. Small numbers of states had boards that shared administrative functions with a central agency, had limited authority, or where the state operated a centralized licensing authority.
-
One states interviewees described in detail how cutbacks were imposed during administrative preparation of budgets even before any request was made to the legislature. Others said that legislatures sometimes reallocated monies from Boards and others trust funds to other purposes.
-
This point comes from Timothy Jost.
-
We adjust by practicing physicians rather than licensed ones, as we expect non-practicing physicians to generate little regulatory work and therefore to impose very modest budgetary burdens.
-
The national data are presented by percentile because a few extreme values appear implausible and may be artifacts of reporting.
-
In Virginia, for example, the medical board spends only about 40% of the Board total, with the balance allocated to the umbrella Department of Health Professions performs many Board functions, including disciplinary and preparation of cases for hearing, as well as automated systems and staff for budgetary, financial, and human resources management (Virginia DHP 2004).
-
The question: Is the amount of public attention paid to discipline related to medical quality presently less, the same or more than it was a few years ago:
-
This table and others number states to maintain confidentiality of data; the numbers are not consistent across tables.
-
Two states data were estimates from executive directors; two were provided by directors from internal data sources.
-
Massachusetts has a separate section, its Data Repository Unit, which indicates the state received 6280 such reports in 2003, of which 236 reports were forwarded to the Enforcement Division for further investigation, and 196 statutory reports relating to potential impairment issues were forwarded to the Physician Health and Compliance Unit Annual Report 2003.
-
California is an exception; see Fellmeth and Papageorge 2004.
-
One category of complaint almost never mentioned by managers was unlicensed practice of medicine. In contrast, early commentators often complained that medical boards were more eager to prosecute unlicensed practice by physicians competitors than to discipline errant physicians (e.g., Gross 1984). Only Washington State tabulated such complaints. One reason may be that Boards refer such cases to other authorities.
-
Data compiled from state documents.
-
Case study reporting is quite incomplete, however, as only half of the six states are represented in this data field. Moreover, some states reported such low staffing (owing partly to drawing staff from other parts of state government), that the extremes of the distribution are very skewed. The very low staffing reported by a few makes the complaint per staff huge and the mean implausible.
-
Jost et al. (1993) reviewed a random sample of Ohio cases from 1990 and reported that very few non-jurisdictional closures consisted of below threshold complaints.
-
The extent of pre-investigatory closure varies by state. California is unusual in doing much more in-office triage than the other states observed. It closes some 90% or more of consumer-initiated complaints without a field investigation (Fellmeth and Pagageorge 2004). This figure is not directly comparable to other states because California sends quality-related cases to medical screening without field investigation, whereas other states handled such reviews through investigation. Note: Exhibit 15 shows closed complaints, so each successive stage come from an earlier time period. Not truly a flow of cases.
-
In Iowa, any summary suspensions occur at the end of the investigation (Iowa BME 2005).
-
A 1993 outside audit and a 2001-02 sunset review of the California Boards closures found insufficient investigation or follow up for hundreds of cases. See Fellmeth and Papageorge 2004, pp. 33 and 83. In Virginia, an audit committee review found that quality of care cases were few and closed with insufficient investigation. JLARC 2000, pp 71-72. Such an investigation of the completeness of documentation was beyond the scope of this project.
-
States make varying use of letters or notices of education, warning, correction, or deficiency--the nomenclature also varies by state--but the exact extent of use if often not reported. Washington State (2004a) reports that such actions are rare, resolving only three complaints against physicians and physicians assistants during the 2001-03 biennium, out of 2,031 received. It is unclear to what extent these occur during investigation or only at the immediate pre-charging stage.
-
Ohio Code chapt 4730 §4730.33.
-
The process is almost always called prosecution, although it adheres to administrative rather than criminal standards.
-
The Massachusetts Board has its own legal staff; the AGs office only represents the Board on judicial appeals.
-
The Pew taskforce, for example, called for Boards to promote effective health outcomes (Finocchio et al. 1998, p.5), but gave little guidance on implementation of this lofty goal.
-
The National Center for State Boards of Nursing has run a project on evidence-based regulation for some years. In a presentation, its executive director recently cited two examples of performance measures used, timeliness of complaint handling and number of complaints resolved in a fiscal year (Apple 2005).
-
According to the Bank, state Boards also somewhat underreport actions. According to the HHS Office of the Inspector General, from 1997-2004, federal agencies reported only about one-third as many malpractice payments as they should have (OIG 2005).
-
According to USGAO (1989, p.4) VA [Veterans Affairs] is reluctant to send to the federation the names of physicians who resign or retire before receiving a hearing because an opportunity for such a hearing is a due process right. As a result, some problem physicians are allowed to leave VA with no indication on their records of prior problems.
-
Boards also made little use of information from another federal source as of 2003--the Quality Improvement Organizations--formerly, Professional Review Organizations--that oversee quality of care under Medicare and Medicaid. Only 12 Boards have QIO formal agreements, and 12 more report getting some other form of assistance, usually on request, only occasionally on routine basis (FSMB 2003b, Table 29).
-
Board managers clearly perceived that some investigators were more productive and capable than others, but the general managerial problem how to make people more productive in their jobs goes beyond the scope of this report.
-
One administrative law judge explained that because respondents lawyers bring in outside experts, assistant attorney generals want to do so, too. They very reluctant to rely on board members for expert opinion testimony.
-
One assistant attorney general said, based on qualitative evidence, that medical quality cases are the most complex, requiring heavy engagement in pre-hearing discovery, and are therefore very costly, but that the overall difficulty is higher in sexual conduct cases. The reason for this is the amount of support needed to keep the complainant able to testify well. Because of the social stigma of such a case, respondents fight harder and are likely to attack the victim, it was said.
-
Bang Nguyen v. Department of Health, 144 Wn.2d 516, 29 P.3d 689 (2001) (due process of law requires proof by clear and convincing evidence before a physician can be deprived of his medical license, not mere preponderance of the evidence).
-
The typical figure of $100,000 suggests the power of a large, round number. For the same figure, see the marketing brochure for an educational alternative to discipline (CPEP 2002) (Defense of a licensure to practice medicine can exceed $100,000).
-
Most sanctions traditionally addressed inappropriate prescriptions or substance abuse; however, such problems certainly could also affect the quality of care delivered.
-
It is not clear that these counts of quality cases are limited to those in which quality is the main or only ground for complaint. The legislative audit review in 2000 found that only 3% of cases were solely concerned with standards of care. JLARC 2000 p.v. and Exhibit 11. (Board staff disagreed with this assessment, but noted that the Board did not track cases well at that time.)
-
Data system problems were also described at some length in numerous portions of Board operations in the prior years report (Fellmeth and Papageorge 2004, e.g., at p.94, n. 114, p.288 n.352). In spite of this major weakness, the Monitor was able to produce much more quantification about Board performance than is readily available in other states.
-
FSMB 2003b (appointment of members, showing a role for medical society in many states).
-
Bang Nguyen v. Department of Health, 144 Wn.2d 516, 29 P.3d 689 (2001).
-
The Enforcement Monitor called these rapid response teams Fellmeth and Papageorge 2004, p. ES25.
-
Fellmeth and Pagageorge 2004 (n. 235) cites Government Code sect. 11425.50 guidelines in licensing boards regulations. The medical Board adopted sect 1361, Title 16 of the California Code of Regulations, which incorporates by reference the 2003 version of the Boards disciplinary guidelines.
-
Nationally, at least 40 state Boards lack a physician on staff. The Federations Exchange shows that 11 jurisdictions reported having a full time physician on staff or assigned to them. Some of these reports are probably miscoded for physicians with standing agreements to serve on request, rather than working full-time. The highest state reported having 65 full-time physicians, but its web page lists only 20 staff, none with a medical degree, and no position of medical director. This state was not among the six in this case study. The Federation suggests that a modern Boards staff may include, but need not be limited to c. one or more medical consultants. FSMB 1998 (sect. I. Staff, Special Personnel).
-
A state appellate court ruled in Clients A & B v. Yoshinaka,128 Wn. App. 833, 116 P.3d 1081 that the Psychology Board had engaged in illegal delegation of authority (absent formal rulemaking) by having DOH staff use board guidelines to authorize an investigation.
-
The Massachusetts board chair personally led a 2003 effort to eliminate a backlog in the states Patient Care Assessment (PCA) program, within which serious hospital incident reports had gone unreviewed in some cases for years. From May to the end of the year, the chair and the PCA committee cleared 512 of the 584 pending reports, also uncovering what proved to be a serious patient care pattern that until then had gone unnoticed--deaths following gastric bypass surgery (Massachusetts Board 2003).
-
CHDR is best known for providing independent appeals for health plan disputes and has subsequently been acquired by MAXIMUS. See Center for Health Dispute Resolution (webpage self-description, undated) http://www.maximus.com/corporate/pages/CHDR.asp>.
-
Fellmeth and Papageorge (2004) noted that no one kept systematic records of the throughput or output of the enforcement program as of the late 1980s, thus inhibiting informed, data-based enforcement policymaking by either the Board or the Legislature (p. 25).
-
Public Citizen proffers that excellent leadership is one determinant of the extent of discipline achieved in a state (e.g., Public Citizen 2005).
-
The approach was allowed by legislation in the 1999-2000 session. See OH Rev. Stat. Sect. 4731.22.
-
See also Epstein and Hundert (2002).
-
One little used approach was a type of written continuing-competency exams called the Special Purpose Examination. SPEX is a multiple-choice test developed by the Federation and the National Board of Medical Examiners in the 1980s (FSMB 2005b) and completed on an automated basis. FLEX and similar exams were seldom mentioned by case study interviewees; FLEX itself seemed to be used mainly for physicians applying to move from another state, and a recent national survey of Boards confirmed that few states used this or similar tests more than a few times a year (CAC 2003).
-
See their respective homepages: PACE http://www.paceprogram.ucsd.edu/index2.html>; CPEP http://www.cpepdoc.org/>, and Wisconsin http://cme.wiscedu.com/$spindb.query.courses.cmeview.4>. The cited programs offer full range assessments; many other programs offer only specialized assessments or education, for example, in appropriate prescribing, medical ethics, medical recordkeeping, or improved patient communication. For listings, see CAC (2003) and FSMB (2005).
-
Another factor may be the perceived strength of legal authority to order a range of examinations for doctors as part of investigation rather than in conjunction with imposing a sanction by settlement or decision after hearing (including QIP proceedings, above). This legal issue was not addressed with interviewees. The Federations Exchange (2003b), Table 32 suggests that almost all Boards may require examinations; OH Revd Stat. sect. 4731.22 that authorizes the QIP says that it may offer an educational and assessment program.
-
For state-specific examples, see Massachusetts Board of Registration in Medicine, On-Line Physician Profile Site http://profiles.massmedboard.org/Profiles/MA-Physician-Profile-Find-Doctor.asp>, Ohio License Center (covering a number of medical professions) https://license.ohio.gov/lookup/default.asp?division=78>; Virginia Board of Medicine, Practitioner Information Website http://www.vahealthprovider.com>.
-
Today's impairment programs are run by an arm of Boards themselves (as in two thirds of study states, one third of all states) or by state medical societies or other contractors (FSMB 2003b).
-
Not dissimilar hospital reports on severe patient injuries must be made to the Department of Health, but these are public documents.
-
Betsy Lehman Center for Patient Safety and Medical Error Reduction http://www.mass.gov/dph/betsylehman>.
-
The Massachusetts Coalition for the Prevention of Medical Errors http://www.macoalition.org>.
-
Examples from the literature include: McAuley et al. 1990 and Norton et al. 1998 (Ontario audits of physician practice); St. George 2003, 2004 (strengths and weaknesses of similar New Zealand audits); Marx 2001, Pawlson and OKane 2004 (relation of patient safety efforts to discipline and other interventions); Norcini 1999, Steinbrook 2005 (ongoing competence approaches to certification by medical specialty boards); FSMB 2004a, 2005b, 2005c (post-licensure assessment approaches).
-
The California analysis was possible only because a knowledgeable and talented Enforcement Monitor could be attracted to make good analytic use. Half of all Boards had 14 or fewer full time staff in 2003, according to Federation statistics (FSMB 2003b).
APPENDIX A. THE TECHNICAL ADVISORY GROUP
(affiliations listed as of the February 2004 TAG meeting)
Geraldine Bednash, PhD, RN, FAAN, Executive Director, American Association of Colleges of Nursing, Washington, DC.
Troyen A. Brennan, MD, JD, MPH, Professor, Law and Public Health, Harvard School of Public Health, Boston, MA.
Catherine Dower, JD, Associate Director, Health Law and Policy, Center for the Health Professions, San Francisco, CA.
James Frogue, Director of the Human and Health Services Task Force, American Legislative Exchange Council, Washington, DC.
Margaret Garikes, JD, Director for the Division of Federal Affairs, American Medical Association, Washington, DC.
Martin J. Hatlie, JD, President, Partnership for Patient Safety, Chicago, IL.
John Horty, JD, Horty, Springer, and Mattern, P.C., Pittsburgh, PA.
Ron Joseph, Former Executive Director, Medical Board of California, Sacramento, CA.
Timothy S. Jost, JD, Professor, School of Law, Washington and Lee University, Lexington, VA.
Lucian L. Leape, MD, Adjunct Professor of Health Policy, Harvard School of Public Health, Boston, MA.
Lisa Robin, Vice President, Leadership and Legislative Services, Federation of State Medical Boards, Euless, TX.
Lawrence E. Smarr, President, Physician Insurers Association of America, Rockville, MD.
Mark R. Yessian, PhD, Regional Inspector for Evaluation and Inspections, U.S. Department of Health and Human Services, Office of Inspector General, Boston, MA.
APPENDIX B. DISCUSSION GUIDE, STATE MEDICAL BOARDS AND PHYSICIAN DISCIPLINE
Discussion will vary slightly depending on the case study participant.
I. Board Structure
- Describe the mission of the Board in your state.
- History of the Board and any major changes in its mission or structure.
- If there have been changes, the impact on Board operations, etc.
- Number of board members and method of selection.
- Monthly time commitment of Board members to discipline-related activities.
- Annual budget for the Board, and allocation across functions.
- Number of staff their responsibilities.
- Vision for the future.
II.Process
Intake
- Approximate number of complaints received annually, and sources (compare to data stats in annual report).
- Who may make a complaint and how.
- Other sources of intake used besides voluntary individual complaints.
- Roles of Boards in stimulating complaints.
- Describe the complaint tracking process and use of data systems.
- Overview of the barriers to this process that you would like to change.
Screening
- Level of screener expertise used.
- Standards in use.
- Use of information beyond the complaint.
- How cases are prioritized by urgency.
- Overview of the barriers to this process that you would like to change.
Investigation
- Who conducts investigations.
- Specialization of investigators by type of complaint or seriousness.
- Levels or intensity of investigation for different types of cases.
- Overview of any barriers to this process that you would like to change.
Charging
- Who decides whether investigated physician should be charged for prosecution and on what basis.
- Overview of any barriers to this process that you would like to change.
Prosecution
- Description of prosecution process.
- Who hears the case at each stage, e.g., administrative law judge followed by full Board.
- Review of standards of proof at each stage.
- How cases are presented and proven.
- Use of Board substantive rules to simplify determinations.
- How the need for medical judgment/expertise is assessed and how the Board obtains expert witnesses and evaluates evidence submitted.
- Burden of proof.
- Overview of any barriers to this process that you would like to change.
Intervention
- Levels of sanctions that are applied (including negotiated sanctions).
- How physicians are notified of the sanctions against them.
- How information is communicated to physicians.
- Overview of any barriers to this process that you would like to change.
Appeal
- Number of cases that are appealed, types of cases and outcomes.
- Overview of any barriers to this process that you would like to change.
Follow-up
- How Boards follow up on compliance with sanction or negotiated agreement and frequency of follow up.
APPENDIX C. STATE MEDICAL BOARD CASE STUDIES--CORE QUESTIONS ON DISCIPLINARY PROCESS
Our goal here is to revisit our case-study states to generate information consistently for all six states at the same time. Please help us with the following key questions.
A. Budget
A1. If you saw a 15% increase in the budget, what proportion of this increase would go towards
| Discipline ..................................... | |
| Licensure ..................................... | |
| Administrative ............................. | |
| Information & Technology .......... | |
| Other ............................................ | |
| 100% |
A2. We are interested in the cost and difficulty of disciplining physicians mainly on the grounds that they have exercised or lack sufficient clinical competence. Our perception is that such standard of care cases usually involve expert medical witness. Can you recall such a case or cases that were fully contested and estimate the total cost and time it took to close the case? Would you also quantify the number of patient cases that were at issue in the particular case or cases that you are reporting?
| Approximate Total Cost | $________________ |
| Approximate Total Time | ________________ (in days) |
| # of patients at issue | ________________ |
| Did the case go to hearing or was it settled prior to hearing by agreement? | Hearing ________________ Settlement ________________ |
[If the case chosen consisted of multiple complaints combined into one proceeding, please indicate whether the total time indicated runs from the date of earliest case filing or is estimated on some other basis.]
A3. Approximately what share of disciplinary cases is related to clinical competence (quality)?
B. Disciplinary Intake
B1. Is the amount of public attention paid by discipline related to medical quality presently less, the same or more than it was a few years ago? (Please check one box)
| Less |  |
| Same | |
| More | |
B2. What data system(s) do you use to track complaints? ________________
B2a. Do you have statutory or internal policy based timelines establishing when a complaint must be closed or disciplinary action be initiated? If so, what are those timelines and are they statutory or internal policy based?
B3. What proportion of disciplinary complaints comes from:
| Public | |
| Government Agencies | |
| Insurers | |
| Hospitals | |
| Other | |
| Total | 100% |
B4. What are the top five disciplinary complaints reported to your board (and their percentage share of the total complaint population if it is known)?
1.__________________________________
2.__________________________________
3.__________________________________
4.__________________________________
5.__________________________________
C. Barriers to and Enablers of Good Practice
C1. Are there identifiable barriers or choke points of cases at any stage of the investigative or disciplinary process? What are they?
C2. Please list three major factors that have at any time in the last 5 years hampered your ability to handle disciplinary complaints effectively.
1.__________________________________
2.__________________________________
3.__________________________________
C3. Please list major practices that you feel have improved efficiency or effectiveness in handling complaints and disciplinary actions.
1.__________________________________
2.__________________________________
3.__________________________________
C4. Among performance statistics tracked, number or rate of disciplinary actions and length of time to resolve complaints appear frequently. What other indicators of performance does your Board use? What other ones would you like to see used?
D. Looking to the Future
D1. How would you rank your board against other boards in your effectiveness to handle disciplinary complaints?
D2. Please explain how your decision was formed above?
D3. Looking into the future, what would you say are your top three priorities in terms of improving efficiencies as they relate to handling disciplinary cases?
1.__________________________________
2.__________________________________
3.__________________________________
APPENDIX D. FSMB MEMBER BOARD ANNUAL SURVEY, 2004
Note: For purposes of this survey, use data from the most recent fiscal year for which financial records have been closed.
1. What were the total dollars expended to fulfill the duties of your board: (Regulation of MDs, DOs and/or PAs)?
Include amounts spent on investigators, board counsel, hearing costs, etc., and contracted services. (Do not include expenditures for professions other than MDs, DOs and/or PAs.)
* Note: For purposes of the question below, functions are described as follows: Administrative--Human resources, education, legislative, budgeting, accounting, payroll, public affairs, administrative support staff, information systems support and executive management; Investigative/Disciplinary--Investigations, legal counsel, legal support staff, prosecution, disciplinary monitoring, information systems support and investigative/disciplinary management; Licensing--Credentialing, license verification, license renewal, licensure support staff, information systems support and licensure management.
a. Dollars expended on administrative functions $__________
b. Dollars expended on investigative/disciplinary functions $__________
c. Dollars expended on licensing functions $__________
d. Total dollars expended (add lines 1a, 1b and 1c)
Total dollars expended may not equal the total budget due to one-time appropriations for particular projects or for other expenses not included above, etc. If you had a one-time appropriation in the fiscal year for regulation in this area, add it to line d. $__________
e. Has your board been given a mandate within the most recent fiscal year which was not funded, requiring you to re-direct resources from an existing program? Yes ____ No ____
2. Does your board have regulatory and licensing authority over PAs? Yes ____ No ____
3. How many applications for licensure in the following categories did you receive? Include all complete and incomplete applications received.
a. Initial and Endorsement licensure: __________
b. Re-registration/Renewal: __________
c. Total applications for licensure received: (add lines 3a and 3b) __________
d. Do you charge a fee to send a licensure application package to an applicant? Yes ____ No ____
4. How many applications for licensure were approved/granted?
a. Initial and Endorsement licensure: __________
b. Re-registration/Renewal: __________
c. Total applications approved/granted: (add lines 4a and 4b) __________
5.
a. How many licensure applications were denied (as opposed to just being withdrawn)? __________
b. How many licensure applications were withdrawn? __________
c. How many submitted licensure applications were abandoned or lapsed? __________
d. Total of all applications not approved (add lines 5a, 5b and 5c). __________
6. How many licensure verification requests/queries
a. did your staff process in writing (by fax or mail)? __________
b. did your staff process by phone? __________
c. were processed electronically? __________
d. Total licensure verifications processed by staff: (add lines 6a and 6b). __________
7. How many Full-Time equivalent (FTE) staff were being paid for by your board at the end of the previous fiscal year to support the following functions? (Include ALL staff categories as they relate to MDs, DOs and or PAs.) If your board contracted out its investigative and/or attorney services, or shared investigators with other agencies under an umbrella organization, calculate the number of hours actually worked during the year and divide by 2,080 hours. Report ALL personnel employed by, assigned to, or used by your board.
* See the note on Question # 1 for definition of functions.
Example 1: If you shared 1 FTE investigator equally with three other agencies, then you should report having 0.25 FTE investigator (1 investigator divided by four agencies).
Example 2: If you contracted for 208 hours of investigations, then you should report having 0.1 FTE investigator (208 hours divided by 2,080 hours).
| Administrative: | ____ FTEs |
| Investigation/Discipline: | ____ FTEs |
| Licensure: | ____ FTEs |
8. How many complaints concerning medical licensees did you receive? For purposes of this question, a complaint should be defined as any allegation of misconduct.
a. MD, DO complaints: __________
b. PA complaints: __________
c. Total complaints (add lines 8a and 8b): __________
9.
a. How many complaints concerning medical licensees did you investigate? __________
b. How many complaints were closed due to lack of appropriate jurisdiction over the complaint (Non-jurisdiction Closure)? __________
c. Total complaints (add lines 9a and 9b): __________
10. For all investigated complaints (from the point of receiving the complaint):
a. How many were dismissed* due to lack of statutory authority or lack of evidence of Physician wrongdoing? __________
How many were dismissed* due to lack of statutory authority or lack of evidence of Physician Assistant wrongdoing? __________
b. On average, how many calendar days did it take to dismiss* complaints? __________
c. How many resulted in a mutually agreed disposition without the necessity of a formal hearing? (e.g., consent order/agreement, stipulated order, etc.) __________
On average, how many calendar days did it take to reach a mutually agreed disposition? __________
d. How many resulted in a formal hearing? __________
e. On average, how many calendar days did it take to complete the investigation and hold a formal hearing? __________
*The term dismissed may be defined differently by member boards; for example, to some it may be synonymous with closure or it may refer to complaints that did not proceed to adjudication.
f. I) How many resulted in a prejudicial disciplinary action before or after a formal hearing? Prejudicial Action is defined as: 1.) Modification of a physicians license, or the privileges granted by that license, 2.) that results in a penalty or reprimand, etc., to the physician. Such action is specific to the individual physician as opposed to a group of physicians (example: denial of a license due to adverse information concerning an individual as opposed to a denial based on lack of qualification that would apply to a large group of people).
Prejudicial Actions taken against a license that include: revocation, suspension, surrender or mandatory retirement of license, loss of privileges afforded by that license, probation, limitation or restriction of license or of licensed privileges, letters of reprimand or warning, and or fines
II) How many resulted in a non-prejudicial disciplinary action before or after a formal hearing? Non-Prejudicial Action is defined as: actions not included in the above prejudicial actions. These actions are frequently administrative in nature, such as a license denial due to lack of qualification, a reinstatement following disciplinary action, probation termination, license issued following a previous denial or vacating a prior order of the board.
III) Total number of complaints that resulted in a prejudicial or a non-prejudicial disciplinary action (add lines h.I and h.II). __________
g. On average, how many calendar days did this outcome take? __________
Overall, what percentage of complaints received by your board were resolved
| within 0 - 180 days? | ____ % |
| within 180 - 360 days? | ____ % |
| within 360 days or more? | ____ % |
11. List any changes or initiatives that positively or negatively affected the boards workload as well as any significant economic impacts.
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
_____________________________________________________________
| ______________________________ Executive Directors signature | ____________ Date |
| _______________________________________________________ Name of Board | |
[report authors note: formatting condensed for presentation here]