
State and Community Efforts to Address Stimulant Use
Rebecca L. Haffajee and Sara Heins
RAND Corporation
May 2021
Link to Printer Friendly Version in PDF Format (48 PDF pages)
ABSTRACT: As the rate of stimulant-involved overdose deaths has risen in recent years, policymakers have expressed increasing interest in public health interventions to support individuals with stimulant use disorder and prevent overdose deaths. ASPE conducted this study to inform policymaking by gaining a better understanding of the landscape of efforts to address stimulant-related concerns nationwide. Our methods consisted of semi-structured discussions with subject matter experts and leaders from across the country to uncover themes related to program activities, funding, barriers, and facilitators. We found a variety of similarities across efforts, such as public health/public safety and other cross-sector partnerships and a focus on recovery support services, as well as differences, such as the treatment models being emphasized and implemented.
This report was prepared under contract between HHS's ASPE/BHDAP and RAND Corporation. For additional information about this subject, you can visit the BHDAP home page at https://aspe.hhs.gov/bhdap or contact the ASPE Project Officer, at HHS/ASPE/BHDAP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201; Daniel.Schwartz@hhs.gov.
DISCLAIMER: The opinions and views expressed in this report are those of the authors. They do not reflect the views of the Department of Health and Human Services, the contractor or any other funding organization. This report was completed and submitted on February 22, 2021.
TABLE OF CONTENTS
1. INTRODUCTION AND BACKGROUND
- Stimulant Use in the United States
- Treatment of Stimulant Use Disorder
- Funding for Programs That Address Stimulant Use
- Study Purpose
2. METHODS
- Identifying Stakeholders
- Discussion Methodology
- Overview of State and Community Efforts
- Stakeholder Initiatives and Implementers
- Summarizing Discussion Data
3. RESULTS
- Topics and Themes
4. DISCUSSION
- Summary of Key Findings
- Limitations
- Policy Options
- Research and Funding Considerations
APPENDICES
- APPENDIX A: Stakeholder Discussion Guide
- APPENDIX B: Summary of Discussants
- APPENDIX C: Summary of Topics Discussed, Themes Identified, and Supporting Quotes
LIST OF FIGURES
- FIGURE 1.1: Percentage of People Aged 12 or Older Who Used Methamphetamine in the Past Year
LIST OF TABLES
- TABLE 2.1: Information About Stakeholders
PREFACE
The United States is experiencing a growing drug overdose crisis and is on track to reach a record number of drug overdose deaths in 2020. Although the majority of attention has been focused on opioid overdoses, overdose deaths involving illicit stimulants--namely cocaine and methamphetamines--also have increased dramatically over the past decade. Stimulant use is a long-standing problem in some areas of the country, whereas in others it is an emerging concern. Addressing problematic stimulant use is challenging, particularly due to the absence of medications approved to treat stimulant use disorder. Funding for substance use disorders, especially at the federal level, has centered on the opioid crisis in recent years, despite the growing magnitude of stimulant-related harms. Recently, however, permissible uses of federal State Opioid Response grants have expanded to include initiatives that target stimulant use.
To better understand available strategies to tackle stimulant use concerns and how to target newly available funds towards them, state and community stakeholders need to be aware of the existing efforts being pursued. Questions of interest to these stakeholders are as follows: Which efforts are being pursued to address stimulant use? How should activities be prioritized? Where should additional funds be directed? What barriers and facilitators are likely to be encountered?
This report analyzes discussions with diverse stakeholders--including multisector coalitions, government health agencies/departments, law enforcement agencies, health care providers, and community groups/nonprofit organizations--who are currently working or worked in the recent past to address stimulant use in their states and communities. It identifies common activities, sources of funding, barriers, and facilitators. Policy options for stakeholders at the community, state, and federal levels are also included.
This research was sponsored by the Office of the Assistant Secretary for Planning and Evaluation in the U.S. Department of Health and Human Services and was carried out within the Payment, Cost, and Coverage Program in RAND Health Care.
RAND Health Care, a division of the RAND Corporation, promotes healthier societies by improving health care systems in the United States and other countries. We do this by providing health care decisionmakers, practitioners, and consumers with actionable, rigorous, objective evidence to support their most complex decisions.
For more information, see https://www.rand.org/health-care.html, or contact
RAND Health Care Communications
1776 Main Street
P.O. Box 2138
Santa Monica, CA 90407-2138
(310) 393-0411, ext. 7775
RAND_Health-Care@rand.org
ACKNOWLEDGMENTS
We wish to acknowledge stakeholder representatives who participated in discussions with our research team and thank them for their willingness to share their time and expertise. We would also like to thank Shoshanna Shelton for her assistance on the project. We thank internal advisers and staff at RAND Corporation for their assistance and reviews of this report, including Christine Eibner, Paul Koegel, and Ryan McBain. Finally, we thank Rachel Winograd for her valuable reviews and suggestions.
ACRONYMS
The following acronyms are mentioned in this report and/or appendices.
| ASAP | Arizona Substance Abuse Partnership |
|---|---|
| ASPE | Office of the Assistant Secretary for Planning and Evaluation |
| CBT | Cognitive Behavioral Therapy |
| CDC | Centers for Disease Control and Prevention |
| CM | Contingency Management |
| COVID-19 | Coronavirus Disease 2019 |
| FDA | Food and Drug Administration |
| HIDTA | High Intensity Drug Trafficking Area |
| HOPE | Heroin, Opiate Prevention and Education |
| KDADS | Kansas Department for Aging and Disability Services |
| LEAD | Law Enforcement Assisted Diversion |
| NEON | Needle and Sex Education Outreach Network |
| OUD | Opioid Use Disorder |
| SABG | Substance Abuse Prevention and Treatment Block Grant |
| SAMHSA | Substance Abuse and Mental Health Services Administration |
| SOR | State Opioid Response |
SUMMARY
The United States is experiencing a growing drug overdose crisis and is on track to reach a record number of drug overdose deaths in 2020.[1] Although the majority of recent attention has been focused on opioid overdoses, overdose deaths involving illicit stimulants--namely cocaine and methamphetamines--also have increased dramatically over the past decade. From 2012 through 2018, the age-adjusted rate of drug overdose deaths involving cocaine more than tripled.[2] Over that same time period, the age-adjusted rate of drug overdose deaths involving psychostimulants with abuse potential (including methamphetamine, amphetamine, and methylphenidate) increased by a factor of 4.9.[2] Increases in stimulant potency, more than increases in use, have contributed to rises in deaths in recent years, highlighting the importance of interventions that aim to reduce harms.
Stimulant use is a long-standing problem in some areas of the country, whereas in others it is an emerging topic of concern. For example, in 2016, the Western United States had more than double the age-adjusted rate of overdose deaths involving psychostimulants with abuse potential as other census regions, but from 2016 to 2017, these overdose deaths increased at the highest rate in the Midwest and the lowest rate in the West.[3] In contrast to opioid use disorder (OUD), there are no approved medications for stimulant use disorder, making its treatment challenging. Despite this barrier, a number of evidence-based behavioral health treatments for stimulant use disorder exist, including contingency management (CM), community reinforcement approach, motivational interviewing, and cognitive behavioral therapy. However, additional detail about their effectiveness and implementation in practice is needed.[4]
Funding stimulant use prevention, treatment, and recovery efforts is also a continuing challenge, although the recent expansion of State Opioid Response (SOR) grants to cover stimulant-related activities presents new opportunities for states. To better tackle problematic stimulant use and understand how funds can be used to address this issue, state and community stakeholders need to be aware of existing efforts already being pursued.
Toward this end, we identified and conducted semistructured discussions with stakeholders--who included individuals in leadership positions at government agencies, organizations, and coalitions--working to address stimulant use in their states and communities. These stakeholders represent different geographic areas and work in a range of sectors such as public health, health care, and law enforcement. We analyzed discussions for key themes related to program activities, funding, barriers, and facilitators.
Based on our discussions with stakeholders, we found that program activities often involved coordination across multiple sectors or types of care. For example, some programs involved connecting individuals from the criminal justice system into treatment or from treatment to longer-term peer support networks. We also found that program activities collectively spanned a continuum from stimulant exposure to long-term recovery. For instance, some targeted educating youth about stimulants to prevent initiation, others focused on treatment engagement for persons with stimulant use disorder, and many focused on various forms of inpatient and outpatient treatment. Multiple programs represented recognized that full recovery can be a years-long to lifetime prospect and emphasized ongoing peer, housing, and employment supports. Widespread polysubstance use also influenced program activities. Even when activities focused on people using stimulants, stakeholders noted the importance of preparing staff to recognize and address substance use more broadly.
Discussion participants identified several funding sources. In most states represented, stakeholders stated that Medicaid was the largest funder of treatment for stimulant use disorder. However, funding provided by state legislatures and federal substance use disorder grants also helped support prevention and treatment activities; in particular, these sources can help fill gaps in funding for treatment among the uninsured or underinsured.
Discussants noted several facilitators to addressing stimulant use. Participants expressed appreciation that SOR grants could now be applied to stimulants. More broadly, they noted that access to multiple funding mechanisms increased the range of activities that they could support, including innovative practices. They also noted that peer support systems and the broader inclusion of people with lived experiences in stimulant use in recovery activities were key to successfully engaging people with stimulant use disorder. Use of telehealth and technology was frequently cited as a facilitator for expanding the reach of program activities, particularly to rural areas.
A key barrier noted by discussants was the lack of medication-assisted treatment and other therapies supported by robust research for stimulant use. This gap resulted in greater reliance among stakeholders on recovery supports to address stimulant use. Other stakeholders noted that coronavirus disease 2019 impeded interpersonal interaction and regularly scheduled activities (e.g., peer support group meetings) that are critical to recovery for persons using stimulants. Lack of flexibility in how certain funds could be spent--for example, limits on using certain funds for housing and perceived restrictions on annual CM payments[5]--were cited as significant barriers. Even when flexibility in funding was available, stakeholders noted that the need for substance use treatment often still outpaced available funding.
Based on our discussions with a diverse group of stakeholders, we identified the following policy options for states and communities to consider in addressing stimulant-related concerns:
-
Pursue innovative uses of grant funds to address stimulants, like the SOR funds that can newly be directed toward stimulant use responses. For example, grant funds earmarked for OUD could be put toward interventions that address co-occurring OUD and stimulant use disorder.
-
Diversify funding sources, including from federal sources (Medicaid, Section 1115 Waivers, SOR, Substance Abuse Prevention and Treatment Block Grant [SABG]), state and local government sources, and philanthropic funders, to help cover the varied activities required to address stimulant use. For instance, local and philanthropic funds could supplement services not robustly covered by federal funding sources, such as long-term housing and more generous CM incentives.
-
Disseminate information on evidence-based treatment for stimulant use disorder to clinical providers.
-
Consider Medicaid expansion and Section 1115 substance use disorder waivers as vehicles for expanding more generous coverage of stimulant use disorder treatment, including residential treatment, to a larger proportion of a state's population.
-
Leverage and enhance existing OUD/substance use disorder infrastructure to treat stimulant use disorder.
-
Consider comprehensive care models, like the Hub-and-Spoke system, to provide coordinated services along the treatment continuum (e.g., inpatient to outpatient, linking persons with stimulant use disorder to long-term treatment and support services).
-
Pursue recovery supports for those with stimulant use disorder, including housing, peer support, employment assistance, and child care.
-
Evaluate stimulant use disorder treatment models implemented, to contribute to the evidence base on effective strategies to address this disorder.
-
Form multisector coalitions on stimulant use or drug use more generally, to bring together stakeholders from complementary areas and facilitate collaborations across sectors (e.g., law enforcement, public health, housing services).
-
Pursue programs and strategies to divert individuals using stimulants to treatment settings instead of criminal justice settings.
-
Innovate telemedicine and workforce initiatives to augment services available to address stimulant use and disorder in rural areas.
-
Engage in education campaigns to reduce stigma around stimulant use and disorder.
Based on our discussions, we additionally identify the following potential considerations for federal, state, and local policymakers in structuring funding and research in ways that can help states and communities best address stimulant use:
-
Provide flexibility in permissible allocation of funds related to substance use disorders, including stimulant use disorder. Flexibility in funding that would be particularly valuable when addressing stimulant use could involve residential treatment, coverage of CM, housing and employment supports, peer support, and harm reduction services.
-
Avoid earmarking funds for initiatives related to specific drugs, given the increasing frequency of polysubstance use and co-occurring health conditions with stimulant use disorder.
-
Invest in research on how SOR and SABG funds, including increased flexibility in SOR grants, are being used to address stimulant use and associated health outcomes.
-
Invest in research on how Medicaid expansion and Section 1115 substance use disorder waivers affect access to treatment and outcomes related to stimulant use disorder.
-
Invest in research on evidence-based treatments for stimulant use disorder, including effective medications and behavioral therapy protocols.
-
Invest in research to better understand the characteristics and predictors of co-use of stimulants with other substances and co-occurrence of stimulant use with mental disorders.
1. INTRODUCTION AND BACKGROUND
Stimulant Use in the United States
Drug use and overdose are significant public health problems affecting communities across the United States. Although recent attention and efforts have focused on combating the opioid crisis, the misuse of stimulants--notably cocaine and methamphetamine--is a growing concern. Provisional data for June 2019 through May 2020 indicated that 23.2 percent of drug overdose deaths involved cocaine and 24.2 percent involved other stimulants. From 2012 through 2018, the age-adjusted rate of drug overdose deaths involving cocaine more than tripled.[2] Over that same time period, the age-adjusted rate of drug overdose deaths involving psychostimulants with abuse potential (including methamphetamine, amphetamine, and methylphenidate) increased by a factor of 4.9.[2] Data from a nationwide public health surveillance system indicated that from April 2019 through October 2020, methamphetamine was the most common type of substance involved in substance use-related emergency department visits, accounting for 33.7 percent of such visits.[6] Males and patients aged 26-45 accounted 71.8 percent and 62.5 percent of methamphetamine-related emergency department visits, respectively.[6]
Despite the marked increase in and high prevalence of harms involving stimulants, self-reported use of cocaine and methamphetamine nationally has not increased dramatically. Past-year use of cocaine was relatively stable from 2015 to 2019 and even decreased slightly since 2006.[7] Past-year use of methamphetamines also has remained relatively stable, increasing only slightly from 0.6 percent of the population in 2006 to 0.7 percent in 2019, according to the National Survey on Drug Use and Health. However, methamphetamine use has increased significantly among those aged 26 and older, from 0.5 percent of the population in 2016 to 0.8 percent in 2019.[7] Cocaine and methamphetamine use are likely underreported in surveys,[8] and more comprehensive methods generally produce higher risk estimates.[9] However, even when these refined estimates are used, the pattern of increases in overdose deaths outpacing use persists.
Several important factors may contribute to the rise in stimulant-related harms, notwithstanding relative stability in use rates. One potential factor is that the potency of methamphetamine has increased over time.[10] Methamphetamine use also has increased among groups already at high risk of drug harms, notably among people who inject heroin.[11] People who use methamphetamines are more likely to inject the drug (as opposed to engaging in other forms of administration) if they also inject heroin.[12] Methamphetamine injection also is associated with other risky behaviors, such as needle sharing.
Co-use of stimulants with other drugs is a significant concern. In 2019, individuals who used methamphetamine in the past year were more than twice as likely to engage in heavy alcohol use, more than four times as likely to use marijuana, more than ten times as likely to misuse opioids, and more than 17 times as likely to use cocaine compared with those who did not use methamphetamine in the same timeframe.[7] Concomitant use of opioids with stimulants has increased dramatically and is substantially more risky than using either substance alone.[13, 14] Persons who co-use stimulants and opioids (which suppress central nervous system functioning) may mistakenly believe that doing so will reverse the effect of the other drug or do so in an effort to self-treat and lessen negative withdrawal symptoms.[15] In one large-scale study, the rates at which individuals who use cocaine or methamphetamine tested positive for nonprescribed fentanyl increased 20-fold and 8-fold, respectively, from 2013 to 2018.[16] Law enforcement seizures indicate that contamination of illicit stimulants with fentanyl is on the rise.[17] This evidence suggests opioids contribute to the increases in stimulant-related deaths. However, they are not the sole drivers, and obtaining precise information about the primary cause of death in overdoses involving stimulants and opioids is challenging.[3]
Although stimulant misuse is widespread, certain demographic groups and geographic areas are disproportionately affected. In 2016, the West experienced over twice the age-adjusted rate of overdose deaths involving psychostimulants with abuse potential than did other census regions.[3] More recently, however, stimulant-involved deaths are devastating other areas of the country. From 2016 to 2017, rates of stimulant-involved overdose deaths increased by 63.2 percent in the Midwest, 50.0 percent in the Northeast, and 42.9 percent in the South, whereas only increasing 20.5 percent in the West.[3] In 2016-2017, past-year methamphetamine use was markedly higher in the Western and Midwestern United States than in states in other regions (Figure 1.1).[18]
| FIGURE 1.1. Percentage of People Aged 12 or Older Who Used Methamphetamine in the Past Year |
|---|
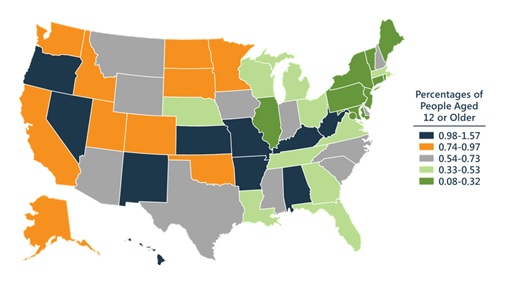 |
| SOURCE: SAMHSA. The National Survey on Drug Use and Health: 2018. Presentation of NSDUH data and webcast slides presented by Dr. Elinore F. McCance-Katz. Center for Behavioral Health Statistics and Quality, Rockville, MD. 2019. |
Meanwhile, the Northeast has experienced the highest prevalence of past-year cocaine use.[19] New Hampshire and Vermont had the highest rates of past-year cocaine use among young adults ages 18-25 (2013-2015 data, 10.54 percent and 9.33 percent, respectively).[19]
In terms of racial and ethnic groups, the age-adjusted rate of overdose involving psychostimulants with abuse potential in 2017 was highest among Native Americans (8.3 deaths per 100,000 population). The overdose death rate in 2017 involving cocaine was highest among African Americans (8.3 deaths per 100,000 population).[3] Death rates are elevated among Native American and African American populations despite evidence that their rates of stimulant use are comparable to those among other racial and ethnic groups,[20] suggesting that structural disadvantages may increase their vulnerability to negative outcomes.
The supply of stimulants used in the United States has evolved in recent decades. In the 1990s and early 2000s, methamphetamine was commonly produced in domestic laboratories--environments also associated with additional risks of fires, explosions, and chemical exposures.[21] Domestic methamphetamine production decreased significantly following enactment of the Combat Methamphetamine Epidemic Act of 2005, which set legal requirements for the production and sale of a key ingredient, pseudoephedrine, and led to a small and short-lived decrease in methamphetamine use.[22] These decreases have since been offset by increases in Mexican production of methamphetamine. Methamphetamine seizures at the Southwest border more than tripled between 2013 and 2018.[21] Although domestic clandestine methamphetamine laboratories have decreased overall, low production capacity laboratories still maintain a presence in the Midwest, Southeast, and Northeast, perhaps because of the lower availability of methamphetamine imported over the Southwest border.[21] Colombia is the largest producer of cocaine used in the United States, and the Southwest border is the primary route of entry.[21]
Treatment of Stimulant Use Disorder
In contrast to other substances such as opioids, nicotine, and alcohol, there are no Food and Drug Administration (FDA)-approved medications to treat stimulant use disorder. However, certain evidence-based treatments are available, and there is ongoing study of pharmacological interventions.[23, 24] The goals of treatment for stimulant use disorder vary by person and program and may range from harm reduction (e.g., using clean needles for injection drug use) to reduction in frequency or quantity of use, to abstinence.[4]
A recent Substance Abuse and Mental Health Services Administration (SAMHSA) report on the treatment of stimulant use disorder highlights four major categories of evidence-based practices: motivational interviewing, contingency management (CM), community reinforcement approach, and cognitive behavioral therapy (CBT).[4] Motivational interviewing is a type of treatment in which providers help patients overcome internal barriers and become motivated to limit or abstain from stimulant use. CM involves reinforcing positive behaviors such as attending treatment sessions or outcomes such as negative drug tests through provision of incentives, including opportunities to win prizes or direct cash payments. Systematic reviews have found sufficient evidence to support the efficacy of CM for the treatment of stimulant use disorder.[23] The community reinforcement approach focuses on mitigating behaviors that reinforce stimulant use and building an environment that encourages a stimulant-free lifestyle. This goal may be accomplished through reinforcing positive behaviors, developing new social networks, engaging in new types of activities, and employment training or assistance. The community reinforcement approach is often implemented alongside CM, with evidence of effectiveness.[23] CBT, a type of psychotherapy, helps individuals understand their current experiences and barriers to change to develop strategies for reducing stimulant use.
Another common approach for treating stimulant use disorder is the Matrix Model, which includes aspects of the community reinforcement approach and CBT. The Matrix Model is a 16-week program that consists of relapse prevention activities, social support groups, one-on-one counseling, family involvement, and drug testing.[25] This model was originally developed to address cocaine use disorder and has since been applied with some success to treatment of methamphetamine use disorder.[26]
Treatment for stimulant use disorder has evolved over time. Some treatment approaches were originally developed for treatment of other substances and were later adapted for and validated among individuals with stimulant use disorder. For example, the community reinforcement approach was originally developed for alcohol use disorder and was later adapted for stimulant use disorder.[4] Other programs, particularly CBT, have been adapted for digital delivery, which can help extend their outreach to rural areas.[4] Providers and policymakers have employed CM with increasing frequency in recent years, although there is still some resistance around providing incentives--especially cash--as part of substance use treatment and uncertainty around the appropriate size of incentives remains.[27, 28]
Although many efforts included in this report focus on treatment for stimulant use disorder, various stakeholders emphasize related efforts that may not fit within a treatment model or be provided in health care settings to address stimulant use. These include prevention, recovery supports, harm reduction, and improving social determinants of health. For example, a group may develop media campaigns targeted at the general public or youth, or help link those who use stimulants with peers in recovery, to housing or to employment. Other groups have strong partnerships with the law enforcement community, which can be instrumental in both reducing the available supply of stimulants and diverting individuals who use stimulants from the criminal justice system into treatment.
Funding for Programs That Address Stimulant Use
There are multiple funding sources available at the local, state, and federal levels to address stimulant use. These include funding from local and state health departments, Medicaid coverage for treatment of stimulant use disorder, grants from nonprofit organizations, and federal grants. Medicaid expansion and Section 1115 waivers can provide additional funding opportunities to cover treatment and recovery supports for stimulant use disorder. Of specific interest for this report, Congress recently made changes to expand the allowable uses of State Opioid Response (SOR) grants.[29] SOR grants were originally established to provide funding to states and territories to address prevention, treatment, and recovery activities for opioid use disorder (OUD). Beginning in 2020, money from the grants could also be put toward funding activities related to stimulant use disorder, allowing states more flexibility. For instance, grant funds may be used to address stimulant use disorder by supporting evidence-based clinical treatment, CM strategies (maximum value per contingency of $15, totaling not more than $75 in value per patient per year in treatment), and innovative telehealth strategies in rural and underserved areas.[30] Another major source of federal funding available to address stimulant-related concerns are the Substance Abuse Prevention and Treatment Block Grants (SABGs) administered by SAMHSA. U.S. states and territories can use these noncompetitive, formula-based funds to plan, implement, and evaluate substance use prevention and treatment activities.
Study Purpose
This report presents the results of our discussions with stakeholders that address stimulant use in their states and communities across the United States. We focus on the following research questions:
-
How are states and communities addressing stimulant-related concerns?
-
What programs or initiatives exist to address stimulant-related concerns?
-
Who implements them?
-
What are their activities?
-
How do they decide what activities to prioritize?
-
What barriers and facilitators have they faced?
-
-
How are efforts to address stimulant-related concerns funded and how would additional funds be used?
We address Question 1 in the Methods section that follows, under the "Overview of State and Community Efforts" subheading. We address Questions 2 and 2(a) in the Methods section under the "Stakeholder Initiatives and Implementers" subheading. We address the remaining research questions in the Results section, most directly under subheadings "Program Activities and Priorities" (Questions 2[b], 2[c]), "Funding Sources" (Question 3), and "Facilitators" and "Barriers" (Question 2[d]). Based on what we learned about these topics from stakeholders, we crafted a set of policy options for states and communities as they consider how to address stimulant use within their populations. We also suggest priorities for funding and research to best support and inform responses to stimulant use in communities.
2. METHODS
Identifying Stakeholders
We began with the goal of speaking with at least nine state and community groups that are leading efforts to address stimulant use to gain insight into policy initiatives and emerging best practices. We sought to contact a diverse group of organizations, coalitions, and agencies (collectively, "stakeholders") with representation from multiple states and regions of the country. We targeted stakeholders who focus on methamphetamine, cocaine, or multiple substances (defined to include methamphetamine or cocaine). In our discussant selection, we emphasized work around methamphetamine, given its greater contribution to mortality in recent years than cocaine. We surveyed stakeholders drawn from a variety of domains, including state and local government, treatment providers, nonprofit organizations, and law enforcement agencies. We also attempted to speak with individuals leading stakeholder efforts, to ensure their comprehensive knowledge on the topics discussed and broad awareness of ongoing stimulant-related activities.
As a selection starting point, we consulted with the Office of the Assistant Secretary for Planning and Evaluation (ASPE) and conducted an Internet search of prominent efforts to address stimulant use in the United States. Through these efforts, we identified two key stakeholders to contact: the San Diego Methamphetamine Strike Force and the San Francisco Methamphetamine Task Force. From the San Francisco Methamphetamine Task Force report,[12] we identified two other key groups to contact: the Colorado Substance Abuse Trend and Response Task Force and the Wisconsin kNOw Meth Campaign. We subsequently identified additional stakeholders through snowball sampling--that is, asking for referrals from discussants. When snowball sampling failed to identify appropriate targets, we identified additional potential government stakeholders through review of state SABG recipients and state treatment coordinators with a specific focus on cocaine and/or methamphetamine. Among these additional potential stakeholders identified, we selected discussants based on our goals for representation listed above. For instance, we sought to speak with at least one stakeholder from each geographic region substantially affected by methamphetamine use and cocaine use.
Discussion Methodology
Prior to our first discussion, we developed a stakeholder discussion guide that included a list of questions and optional follow-up prompts based on overarching research questions (Appendix A). We used this guide to conduct semistructured interviews, which varied based on context and range of expertise. These discussions took place with organization, coalition, and agency representatives over Microsoft Teams, either by video or audio-only conference, depending on the discussant's preference. All discussions lasted approximately one hour and were attended by a RAND Corporation researcher who led the discussion, a second RAND researcher who took notes, and the ASPE project officer who posed follow-up questions as relevant. All discussions were recorded and summarized. After the first three discussions, we updated our discussion guide to obtain consent for transcription; all subsequent discussions were transcribed. All discussion protocols were approved by RAND's Internal Review Board.
Overview of State and Community Efforts
We provide a complete list of the stakeholder discussants, along with summaries of program activities, funding sources, and websites, in Appendix B. For almost half of the discussions, there were at least two individual participants representing a given stakeholder who were involved in the discussion together (i.e., together, this constituted a single discussion).
States and communities engaged in a variety of efforts to address stimulants, varying from state and local government programs, to coalitions formed across various sectors, to grassroots efforts that were organized into nonprofit or community groups. The stakeholders with whom we spoke represented a range of activities along the continuum of support and care for people who use stimulants, including prevention, treatment, recovery, law enforcement, and harm reduction. Individual discussion participants often were involved in multiple groups and roles, giving them diverse perspectives into activities addressing stimulant use in their states and communities. For instance, discussants from many coalitions and organizations actively participated in legislative activities in their states, whether formally on committees or in an advisory capacity, specific to stimulants and substance use.
Stakeholder Initiatives and Implementers
In Table 2.1, we summarize stakeholder characteristics, including their region, sector, state or substate level, substance focus (i.e., methamphetamine, cocaine, or multiple substances), and how we identified the stakeholder. We identified 47 percent of stakeholders through discussant referrals and 53 percent through independent research methods.
The organizations, coalitions, and agencies that took part in our discussions represented seven states, with most stakeholders located in the West (n=12), followed by the Midwest (n=2), and Northeast (n=1). Because the West has had long-standing methamphetamine use, our snowball sampling approach frequently identified subsequent targets in this region. The stakeholders represented a range of sectors including departments of health/public health (n=6), multisector coalitions (n=5), community nonprofits (n=2), law enforcement (n=1), and health care providers (n=1). Stakeholders were nearly evenly split between the state (n=8) and substate/local (n=7) levels. Eight stakeholders primarily focused on methamphetamine use, whereas the other seven focused on substance use more generally. Although no stakeholders focused specifically on cocaine use, one agency (Vermont Department of Health) noted that more of their efforts were targeted toward cocaine as compared with methamphetamine given the relative prevalence of use of each drug in their state.
Summarizing Discussion Data
Shortly following each discussion, a RAND researcher produced a summary document containing synopses of answers to each question asked. We generated recordings and transcriptions for reference and use in developing this report. Two RAND researchers reviewed the discussion summaries and identified key topics, themes, and supporting quotes. The researchers consulted the discussion recordings and transcripts as necessary to confirm the accuracy of information reported and quotes provided. The RAND researchers, in consultation with the ASPE project lead, discussed and iterated on key themes that emerged from the discussions until all were satisfied with the content captured.
| TABLE 2.1. Information About Stakeholders | |
|---|---|
| Stakeholder Characteristic | Number of Stakeholders (%) |
| Region | |
| Midwest | 2 (13) |
| Northeast | 1 (7) |
| South | 0 (0) |
| West | 12 (80) |
| Sector | |
| Department of Health/Public Health | 6 (40) |
| Law enforcement | 1 (7) |
| Multisector coalitions | 5 (33) |
| Health care providers | 1 (7) |
| Community/nonprofits | 2 (13) |
| Intrastate Level | |
| State | 8 (53) |
| Local | 7 (47) |
| Primary Substance Focus | |
| Methamphetamine | 8 (53) |
| Cocaine | 0 (0) |
| Multiple substances | 7 (47) |
| Means of Identification | |
| Researcher identified | 8 (53) |
| Discussant referral | 7 (47) |
3. RESULTS
Topics and Themes
Based on our study goals and research questions, we expected discussion themes to fall within four broad topical areas: program activities, funding sources, facilitators, and barriers. Within these topics, we identified 24 themes that emerged over the course of our discussions. These topics and identified themes, along with supporting quotes, are summarized in Appendix C. The themes are italicized and discussed in detail below.
Program Activities and Priorities
The diverse group of stakeholders we spoke with engaged in a wide variety of program activities along the support continuum. Many common themes emerged about these activities and which are prioritized. First, engagement and coordination of stakeholders across multiple sectors was a cornerstone of many programs. The five coalition stakeholders with whom we spoke were formed with the intention of bringing multiple sectors together to address stimulant use collaboratively in their communities. These sectors often included health agencies, health care treatment providers, the judiciary, public safety and law enforcement, supportive housing and homelessness services, child welfare agencies, and people with lived experiences using drugs. We also heard from health departments that their work relied on collaborations with law enforcement to help connect people involved in the criminal justice system with treatment.
Programs engaged in diverse treatment practices for stimulant use disorder.[4] Commonly employed treatment modalities included CM and CBT. Questions about the appropriate incentive and costs involved with the CM approach were common. Some stakeholders employed the Matrix Model, usually in a variant form from that originally developed, so that they could cater it to specific population characteristics. For example, the version adopted in parts of one state focuses on social/emotional needs, community reinforcement, and family engagement. Many stakeholders focused on expanding forms of residential treatment.
Stakeholders reported that other key components to program activities were facilitating social support systems and creating environments for recovery. Individuals involved in various stages of stimulant use treatment and recovery were connected to supports in the forms of recovery housing and peer-based activities. Program planning often involved those with lived experience of stimulant use, because these individuals could best relate to those currently using stimulants. Community groups, in particular, recognized the importance of surrounding individuals with positive social influences rather than situations resembling those in which they used stimulants, to improve the prospects for recovery.
Although some stakeholders focused solely on one aspect of stimulant use, such as prevention or treatment, multiple stakeholders provided or linked services across the care continuum. For example, Vermont employs the "Hub-and-Spoke" program to engage individuals in higher levels of residential care (Hubs) and link those to lower levels of care provided in outpatient settings (Spokes). Although this program was devised to respond to OUD, it is increasingly being used for persons with co-occurring OUD and stimulant use disorder. San Francisco is working to focus on the immediate needs of people who use stimulants by admitting them to inpatient treatment, later connecting them with outpatient or longer-term residential services, and finally referring them to recovery support services. Several stakeholders saw the need to connect certain individuals to residential step-down programs that provide long-term residential treatment to aid in sustained recovery. Yavapai County in Arizona has employed a "Reach Out" program that links sectors and levels of care. Law enforcement in this county provide a "warm hand-off" for first-time offenders to wraparound support services that can include a mental health assessment, treatment, employment, transportation, day care, and housing.
Programs often engaged in activities to address polysubstance use, because this behavior is increasingly common among people using stimulants. For example, representatives from Vermont noted the importance of addressing stimulant use within existing Hub-and-Spoke treatment settings, which focus on providing medication-assisted treatment for OUD, given the prevalence of polysubstance use and risks associated therewith. Increasing co-use of methamphetamine or cocaine with opioids--often fentanyl--was noted by several stakeholders, demonstrating the need to have OUD treatment and naloxone (an opioid overdose reversal drug) available to persons using stimulants. Another stakeholder noted the prevalence of individuals in the community who injected both heroin and methamphetamine and that syringe services programs were important for harm reduction, regardless of substance.
Finally, multiple stakeholders conveyed that treatment and public health/public safety partnerships are increasingly preferred over law enforcement approaches when responding to stimulant use in their communities. Whereas many communities historically responded to methamphetamine use with criminal justice responses, we observed growing appreciation that treatment would better serve affected individuals. Because law enforcement is often the first line of intervention or contact with persons using stimulants, some communities have trained these officers to divert individuals to services instead of jail, such as in the Law Enforcement Assisted Diversion (LEAD) Program. In California, their Section 1115 waiver for Medicaid has resulted in a large number of persons being diverted from the criminal justice system into residential treatment centers.
Funding Sources
Stakeholders noted that treatment for stimulant use disorder was funded by a hierarchy of sources, starting with the Federal Government. Most government and health care providers indicated that Medicaid was the primary funder of stimulant use disorder treatment in their states. The generosity of coverage varied depending on whether a state had expanded Medicaid or not. Medicaid coverage also varied for residential treatment. All states in our project had an approved Medicaid Section 1115 waiver for substance use disorder treatment, except for Colorado, whose pending waiver application was approved in November 2020, and Arizona, whose application is still pending. These waivers allow states to receive federal matching funds for services that are typically subject to the Institution for Mental Diseases exclusion. The waivers have helped or will imminently help facilitate short-term inpatient and residential treatment for stimulant use disorder. In states like Kansas that have not expanded Medicaid (and therefore limit coverage to individuals at lower income levels), SABG and, more recently, SOR grants are necessary to fill in the gaps as primary funders for treatment of stimulant use disorder. Expansion states also have drawn upon SABG and SOR funds to fill critical funding gaps.
State funds earmarked for addressing substance use can help fund activities other than prevention or treatment. For example, one stakeholder indicated that appropriations from the state legislature helped fund a pretrial diversion program for individuals arrested for drug possession.
Facilitators
Several stakeholders valued flexibility in funding applications, particularly the new ability to use SOR funds for activities addressing stimulant use, and hoped this practice could extend into the future. This flexibility allows states to provide stimulant use disorder treatment to individuals who might not qualify for Medicaid or who do not have an OUD. In areas more affected by stimulant use than opioid use, like Northern Wisconsin, this type of flexibility is critical to address prominent and emerging drug-related concerns, given that many funding sources have been restricted to opioid-related programs in recent years.
Similarly, diversification of funding sources helped stakeholders overcome restrictions on how certain funding sources could be used. For instance, philanthropic funding allows San Francisco to fund innovative CM programs in ways that state Medicaid dollars do not allow.
Medicaid expansion and Section 1115 substance use disorder waivers have been a direct facilitator to providing more generous stimulant use disorder treatment. Colorado described Medicaid expansion as "essential" to increasing access to behavioral health care and recovery support services. Section 1115 waivers have been particularly instrumental in expanding access to residential treatment for stimulant use disorder.
According to various stakeholders, provision of coordinated and continuous services along the care continuum is critical to addressing stimulant use disorder. Given that stimulant use disorder recovery can be a long-term prospect--in part because stimulant use can cause extensive neurobiological changes--stepped-down care is critical. As well, the comorbid presentation of stimulant use disorder with other substance use disorders and/or mental health disorders highlights the challenges of treating any mental health condition. These individuals have complex needs that require coordinated clinical care and support services, which can extend to housing and employment assistance.
Stakeholders viewed peer supports as critical to long-term recovery. Peer support specialists bring expertise derived from lived experience and success in the recovery process to support those currently facing stimulant use disorder. Many stakeholders noted the importance of peer support--either individually or in group settings--for individuals with stimulant use disorders to establish connections with trained specialists and see a path to recovery modeled. Many states have developed certification programs for peer support specialists.
Several stakeholders discussed the importance of low barrier harm reduction approaches to addressing stimulant use in their communities. Many recognized and supported that the path to recovery varies by individual and that harm reduction measures can be particularly helpful in engaging with people who use stimulants. Discussants emphasized the need to "meet people where they are" and pursued activities that could offer significant health benefits, like reduced overdoses or spread of infectious diseases, even if abstinence from stimulant use was not the immediate goal. One nonprofit that focuses on men who have sex with men in Washington educates volunteers on sexually transmitted infections, safer drug use, and safer sex and provides them with supplies, including clean needles, that the volunteers then deliver to hard-to-reach communities (e.g., commercial sex workers).
Finally, the availability of telemedicine and other digital communications was an important facilitator of stimulant use disorder recovery. Some stakeholders had long-standing telehealth programs, particularly to reach residents in rural areas. Other stakeholders moved activities such as counseling or group meetings online in response to the coronavirus disease 2019 (COVID-19) pandemic and subsequently realized unanticipated benefits. Stakeholders noted that moving activities to virtual platforms helped individuals without reliable access to transportation attend more easily and allowed programs to expand their services outside their standard catchment areas. But broadband accessibility was critical to the success of these endeavors, and coverage is inconsistent in many rural areas.
Barriers
A commonly cited barrier was the lack of well-researched, gold standard treatments for stimulant use disorder. Unlike OUD, which can be treated with FDA-approved medications including methadone, buprenorphine, and naltrexone, stimulant use disorder lacks established pharmacotherapy options. Although some evidence-based behavioral treatments exist for stimulant use disorder, stakeholders often were unsure about which treatments were most effective or how to prioritize treatment resources. For instance, stakeholders were uncertain of the clinically effective threshold for incentives in CM. The need for additional research on and development of effective treatments was noted by many.
Stakeholders also noted that COVID-19 disrupted stimulant use disorder treatment and recovery, particularly in-person therapy. Some planned innovations, such as a methamphetamine sobering center or expanded drug testing as part of CM, were delayed. Others suggested that increased isolation and economic instability from COVID-19 might lead to increased drug use or make recovery more challenging. Lockdowns hindered the ability of programs to provide in-person services, like education and counseling about safer injection drug use. A law enforcement representative noted that reductions in vehicle traffic due to COVID-19 resulted in more ambitious attempts to get methamphetamine across the Mexico/United States border in bulk shipments.
Although stakeholders were overwhelmingly grateful for the new flexibility to apply SOR grants toward addressing stimulant use, they noted that not all funding sources had sufficient flexibility, including to address social determinants of health. For example, representatives of one group noted that a lot of funding from the state legislature was earmarked for opioid-related activities, despite low levels of opioid use relative to methamphetamine use in one region of the state. However, they did note that this was gradually changing, and funds were increasingly available for substance use in general, allowing communities to address their individual needs. Disaggregating funding streams by drug type was seen by many as counterproductive, given co-occurring drug use and common social determinants of health (e.g., housing) that affect people using any drug type.
As a whole, stakeholders felt that current funding frameworks provided inadequate flexibility to adequately address stimulant use disorder, including social determinants of health, such as housing and employment. For example, multiple stakeholders noted that limited federal dollars are available for housing after completion of residential treatment. Stakeholders commonly viewed stable housing as critical to helping individuals maintain recovery. They also noted that individuals experiencing homelessness may use stimulants to stay awake and protect their possessions, with one discussant noting, "What people will say when you interview them is that you can't let your guard down and you can't sleep when you're homeless." Another restriction that concerned several stakeholders was the perceived $75 per person annual limit on CM payments made by Medicaid and SOR. Stakeholders did not seem aware of the nuances in federal interpretation of limitations around CM incentives, suggesting a need for additional education around these parameters.
Even when funding was highly flexible, absolute levels of funding for substance use treatment remained a constraint. One stakeholder noted that the state's overall SOR grant award level had been cut from the previous year, so they felt unable to use the new flexibility to expand stimulant-related activities. This state felt torn between drawing from much-needed SOR funds for OUD activities to address stimulant use disorder concerns, which were also in need of funding. Another discussant observed that his state's choice to not expand Medicaid, along with increased need and unchanged SABG funding, resulted in significantly more treatment need than availability relative to states that did expand Medicaid.
Stakeholders noted that rural areas were particularly affected by stimulant use disorder and that insufficient infrastructure and workforce development in these locales were barriers to delivering care. The difficulties in reaching rural, remote areas and the lack of services in these locales hindered stimulant use responses. Stakeholders noted that rural areas frequently lack specialized treatment services, making consistent use of outpatient treatment or recovery support services challenging. Attracting and retaining substance use treatment professionals has proven challenging in rural areas, resulting in some innovative recruitment approaches like tuition reimbursement and social marketing counseling to teens for these vocations. Discussants noted high turnover because staff often left for higher paying jobs in correctional or private mental health settings. Multiple stakeholders noted that workforce development was an area where additional funding could be utilized.
Stigma towards individuals who use stimulants was another commonly cited barrier to effective treatment and recovery. Although stigma is an important issue for all types of substance use, those who use stimulants face unique challenges. First, stigma may be heightened because of the frequently illicit nature of stimulant use. Stakeholders noted that episodes of psychosis were common among those with long-term stimulant use and could elicit fear in the general public and negative interactions with law enforcement. Furthermore, instances where individuals who use stimulants have caused damage to housing units could result in challenges for finding and maintaining housing. To tackle stigma, one coalition has worked with communities to implement initiatives like recovery-friendly workplaces and street cleanup. Groups also noted that some public messaging has been alienating, using terms like "addict" to describe those with stimulant use disorder, which can hinder efforts to reach and provide services to individuals with stimulant use disorder.
Finally, stakeholders noted that potent stimulants, particularly methamphetamines, were widely available in many parts of the country, making prevention and recovery efforts challenging. The influx of Mexican cartels as major methamphetamine suppliers has contributed to this increase in supply, compared with when the drug was predominantly produced by local laboratories. In addition, they noted that methamphetamines have increased in purity and potency in recent years, making the consequences of use more deadly. For both methamphetamine and cocaine, contamination with fentanyl was another worrying trend in multiple communities, leading to innovative approaches like providing testing of drug supplies at syringe services programs and making naloxone more widely available, even to those who primarily use stimulants.
4. DISCUSSION
To better understand available community strategies to address stimulant use concerns, we conducted key stakeholder discussions with representatives drawn from diverse sectors, including state and local departments of health, multisector coalitions, community nonprofit organizations, health care providers, and law enforcement.
Summary of Key Findings
Stakeholders engaged in a wide variety of program activities along the care and support continuum to address stimulant use. Engagement of multiple sectors in the work facilitated a more comprehensive understanding of the variety of challenges encountered by those with stimulant use disorder and facilitated collaborative strategies. Indeed, this is perhaps why many communities that have been facing stimulant concerns for decades, most notably in the West, have formed coalitions to tackle the issue. These collaborative relationships have fostered momentum around efforts to address stimulant use and coordination between sectors (e.g., law enforcement to treatment services).
Among stakeholders we spoke with, treatment for individuals with stimulant use disorder was generally preferred to law enforcement approaches--responses favored in past decades that have not demonstrated sustained success in deterring stimulant use or promoting long-term recovery. A number of discussants noted that illicit stimulant availability, particularly of methamphetamine, has increased in recent years with the rise in Mexican cartel production. Therefore, law enforcement interdiction of stimulant shipments is important to addressing overall supply. In addition, methamphetamine supply has become purer and more potent. Because stimulants are increasingly mixed with other drugs (namely fentanyl) and because individuals regularly co-use stimulants and other drugs, individual treatment and recovery approaches need to consider multiple substances and engage in widespread harm reduction.
At the same time, discussants regularly noted that the use of stimulants is unique from other drugs in important ways. The lack of a gold standard of care that includes effective medications makes treating stimulant use disorder more difficult than other substance use disorders, such as OUD. Because stimulant use can cause long-term cognitive impairment and define individual lifestyles (e.g., people experiencing homelessness using stimulants to stay awake during the night), breaking away from use patterns can be particularly challenging. Stigma toward individuals who use stimulants--perhaps rooted in the illicit nature of use and its associations with violence, homelessness, and distinct physical characteristics (e.g., tooth decay)--is unique and can obfuscate successful treatment and recovery. Chronic stimulant use is also associated with psychotic symptoms including delusions, hallucinations, and paranoia. Many stakeholders said that stimulant use disorder is the most difficult substance use disorder to treat and that it takes individuals substantial periods of time to achieve sustained recovery. In short, stimulant use disorder recovery can be complex, individualized, long-term, and require addressing multiple life domains.
Treatment along the health care continuum is important in addressing stimulant use disorder, in part because it commonly co-occurs with other mental health and substance use disorders. Targeted forms of treatment engaged in by stakeholders typically fell within two evidence-based categories--CM and CBT--or involved some combination of components from the Matrix Model. However, the details of these programs and how they were implemented differed, with little common understanding expressed about the core components that would render these programs most effective. Instead, most communities adapted these treatment models to suit their population needs, for instance, by engaging families in therapy where these networks were close and available to support recovery. Virtually all stakeholders desired more research on effective treatments for stimulant use disorder and thought funding should be devoted to this undertaking.
Stakeholder activities also demonstrated that long-term recovery from stimulant use disorder relies on social supports beyond traditional health care settings. Housing, in particular, was viewed as critical. Discussants repeatedly emphasized that sustained recovery will rarely be achieved by accessing acute care, for instance, through a visit to the emergency department. In order for persons with stimulant use disorder to modify and discontinue their use patterns, changes in environment and life activities are critical. Having peers, particularly those with lived experience, to model positive behavior was considered very helpful. Having employment and consistency in daily schedules, as well as regular interpersonal interactions, were viewed as important elements to recovery.
Funding for treatment of stimulant use disorder was primarily drawn from federal sources, according to the stakeholders with whom we spoke. Medicaid was a primary funder, particularly for acute and residential treatment. More Medicaid funds were available to a larger proportion of the population in states that had expanded Medicaid. SABG and, more recently, SOR funds filled some of the gaps left by Medicaid, for instance, by covering the underinsured and uninsured. Increased flexibility in applying federal and state funds to the use of multiple drugs, not just opioids, was seen as helpful, particularly in states more heavily affected by stimulant use than other drugs. State, local, and philanthropic funds provided flexibility to support activities not necessarily allowable under certain federal funding mechanisms and beyond the scope of traditional health care, such as housing, CM, pretrial diversion programs, and harm reduction services. Overall funding levels were seen as insufficient to tackle all activities necessary to effectively address stimulant-related concerns in the communities with which we spoke.
Reaching and providing care to populations with concerning stimulant use patterns was often a challenge for stakeholders. The lack of health care facilities and specialized services, transportation barriers, and workforce shortages all made reaching rural communities--often heavily affected by stimulant use--difficult. Telemedicine, including in the age of COVID-19, has improved these efforts to a degree. However, COVID-19 has compromised in-person contact important to stimulant use disorder treatment and recovery, such as peer support groups and counseling about safe injection drug use.
Limitations
Our study has limitations. Our sample was not designed to be representative of all state and community efforts to address stimulant use, because our sampling scheme was mainly based on convenience. Thus, our results may suffer from selection bias. Most individuals we contacted were responsive to our request for discussion. However, three groups contacted did not follow-up or declined to speak with us because they did not have sufficient information to contribute on the topics of focus. Our results may also reflect reporting bias. Stakeholders were aware that this study was being conducted on behalf of ASPE and that an ASPE representative was present during discussions, which could have incentivized them to respond in ways they believed were desirable to the Federal Government.
Our discussants were drawn predominantly from the West. Although this region has historically been the most heavily affected by methamphetamine use, the Midwest has more recently seen substantial increases in use prevalence and overdose deaths. Programs focused on cocaine use were underrepresented in our sample, as was the Northeast region most affected by use of this drug. Our discussions did not focus on racial and ethnic minority groups who are particularly affected by stimulant use.
We oversampled stakeholders from departments of health and multisector coalitions. Thus, our conclusions about law enforcement agencies, health care providers, and nonprofit organizations are more limited. Given our discussions with many coalitions, our findings that collaborations were important to addressing stimulant use may have been biased, although this theme was regularly repeated by stakeholders from other sectors. We did not speak with people who use drugs or their family members, so their perspectives are not explicitly represented in our results. We also were constrained by time (one-hour discussions), making it challenging to delve deeply into a number of topics relevant to stimulant use challenges and responses, such as specifics about affected subgroup populations, budgets, and treatment protocols.
Policy Options
This report is intended to provide information about efforts of states and communities to address stimulant use. The themes we describe are intended to represent the perspectives of some prominent stakeholders leading efforts in the area, including among groups and communities that have been dealing with stimulant use concerns for some time. States and localities facing stimulant-related concerns and looking to implement programs can learn from these existing and past efforts, including about their activities, funding sources, barriers, and facilitators.
As generated from our discussions with leaders in this domain, the following are 12 policy options for states and communities to consider when addressing stimulant-related concerns:
-
Pursue innovative uses of grant funds to address stimulants, like the SOR funds that can newly be directed toward stimulant use responses. For example, grant funds earmarked for OUD could be put toward interventions that address co-occurring OUD and stimulant use disorder.
-
Diversify funding sources, including from federal sources (Medicaid, Section 1115 waivers, SOR, SABG), state and local government sources, and philanthropic funders, to help cover the varied activities required to address stimulant use. For instance, local and philanthropic funds could supplement services not robustly covered by federal funding sources, such as long-term housing and more generous CM incentives.
-
Disseminate information on evidence-based treatment for stimulant use disorder to clinical providers.
-
Consider Medicaid expansion and Section 1115 substance use disorder waivers as vehicles for expanding more generous coverage of stimulant use disorder treatment, including residential treatment, to a larger proportion of a state's population.
-
Leverage and enhance existing OUD/substance use disorder infrastructure to treat stimulant use disorder.
-
Consider comprehensive care models, like the Hub-and-Spoke system, to provide coordinated services along the treatment continuum (e.g., inpatient to outpatient, linking persons with stimulant use disorder to long-term treatment and support services).
-
Pursue recovery supports for those with stimulant use disorder, including housing, peer support, employment assistance, and child care.
-
Evaluate stimulant use disorder treatment models implemented, to contribute to the evidence base on effective strategies to address this disorder.
-
Form multisector coalitions on stimulant use or drug use more generally, to bring together stakeholders from complementary areas and facilitate collaborations across sectors (e.g., law enforcement, public health, housing services).
-
Pursue programs and strategies to divert individuals using stimulants to treatment settings instead of criminal justice settings.
-
Innovate telemedicine and workforce initiatives to augment services available to address stimulant use and disorders in rural areas.
-
Engage in education campaigns to reduce stigma around stimulant use and disorders.
Research and Funding Considerations
Our stakeholder discussions revealed a number considerations for federal, state, and local policymakers in structuring funding and research in ways that can help states and communities best address stimulant use. They include the following:
-
Provide flexibility in permissible allocation of funds related to substance use disorders, including stimulant use disorder. Flexibility in funding that would be particularly valuable when addressing stimulant use could involve residential treatment, coverage of CM, housing and employment supports, peer support, and harm reduction services.
-
Avoid earmarking funds for initiatives related to specific drugs, given the increasing frequency of polysubstance use and co-occurring health conditions with stimulant use disorder.
-
Invest in research on how SOR and SABG funds, including increased flexibility in SOR grants, are being used to address stimulant use and associated health outcomes.
-
Invest in research on how Medicaid expansion and Section 1115 substance use disorder waivers affect access to treatment and outcomes related to stimulant use disorder.
-
Invest in research on evidence-based treatments for stimulant use disorder, including effective medications and behavioral therapy protocols.
-
Invest in research to better understand the characteristics and predictors of co-use of stimulants with other substances and co-occurrence of stimulant use with mental disorders.
ENDNOTES
-
Stephenson J. Drug Overdose Deaths Head Toward Record Number in 2020, CDC Warns. JAMA Health Forum, 2020.
-
Hedegaard H, Minino AM, Warner M. Drug Overdose Deaths in the United States, 1999-2018. NCHS Data Brief, 2020; 356: 1-8.
-
Kariisa M, Scholl L, Wilson N, Seth P, Hoots B. Drug Overdose Deaths Involving Cocaine and Psychostimulants with Abuse Potential--United States, 2003-2017. Morbidity and Mortality Weekly Report, 2019; 68: 388-395.
-
Substance Abuse and Mental Health Services Administration (SAMHSA). Treatment of Stimulant Use Disorders. Publication No. PEP20-06-01-001. National Mental Health and Substance Use Policy Laboratory, Rockville, MD. 2020.
-
The Office of Inspector General's guidance on the permissibility of CM payments is nuanced. CM program incentives consisting of in-kind items or services with a retail value of no more than $15 per item or $75 in the aggregate per beneficiary per year may fall within the patient engagement and support safe harbor of the federal Anti-Kickback Statute, assuming all other safe harbor conditions are met. The lawfulness of in-kind items and services of greater values, as well as any cash or cash-equivalent payments for CM, are evaluated on a case-by-case basis, including consideration of the intent of the parties. The purpose behind these rules is to protect vulnerable patients from fraud (Medicare and State Health Care Programs: Fraud and Abuse; Revisions to Safe Harbors Under the Anti-Kickback Statute, and Civil Monetary Penalty Rules Regarding Beneficiary Inducements, 85 Fed. Reg. 77,791 [December 2, 2020]).
-
SAMHSA. DAWN and Methamphetamine. Center for Behavioral Health, Rockville, MD. 2020.
-
SAMHSA. Key Substance Use and Mental Health Indicators in the United States: Results from the 2019 National Survey on Drug Use and Health. HHS Publication No. PEP20-07-01-001, NSDUH Series H-55. Center for Behavioral Health Statistics and Quality, Rockville, MD. 2020.
-
Johnson TP. Sources of Error in Substance Use Prevalence Surveys. International Scholarly Research Notices, 2014; 2014: 923290.
-
Midgette G, Davenport S, Caulkins JP, Kilmer B. What America's Users Spend on Illegal Drugs, 2006-2016. RAND Corporation, Santa Monica, CA. 2019.
-
Centers AA. Neighborhood Drug Dens: Identifying Meth Lab Locations over Time. https://www.rehabs.com/explore/neighborhood-drug-dens/.
-
Jones CM, Underwood N, Compton WM. Increases in Methamphetamine Use Among Heroin Treatment Admissions in the United States, 2008-17. Addiction, 2020; 115(2): 347-353.
-
San Francisco Department of Public Health. San Francisco Methamphetamine Task Force. Final Report. San Francisco, CA. 2019.
-
Timko C, Han X, Woodhead E, Shelley A, Cucciare MA. Polysubstance Use by Stimulant Users: Health Outcomes over Three Years. Journal of Studies on Alcohol and Drugs, 2018; 79: 799-807.
-
Nolan ML, Shamasunder S, Colon-Berezin C, Kunins HV, Paone D. Increased Presence of Fentanyl in Cocaine-Involved Fatal Overdoses: Implications for Prevention. Journal of Urban Health, 2019; 96(1): 49-54.
-
Ellis RJ, Childers ME, Cherner M, et al. Increased human immunodeficiency virus loads in active methamphetamine users are explained by reduced effectiveness of antiretroviral therapy. Journal of Infectious Disease, 2003; 188(12): 1820-1826.
-
LaRue L, Twillman RK, Dawson E, et al. Rate of Fentanyl Positivity Among Urine Drug Test Results Positive for Cocaine or Methamphetamine. JAMA Network Open, 2019; 2(4): e192851.
-
U.S. Drug Enforcement Administration. Cocaine/Fentanyl Combination in Pennsylvania. Philadelphia, PA. 2018.
-
SAMHSA. Key Substance Use and Mental Health Indicators in the United States: Results from the 2018 National Survey on Drug Use and Health. HHS Publication No. PEP19-5068, NSDUH Series H-54. Center for Behavioral Health Statistics and Quality, Rockville, MD. 2019.
-
Hughes A, Williams MR, Lipari RN, Van Horn S. State Estimates of Past Year Cocaine Use Among Young Adults: 2014 and 2015. The CBHSQ Report. December 20, 2016. Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration, Rockville, MD.
-
SAMHSA. 2019 National Survey of Drug Use and Health (NSDUH) Releases. 2020.
-
U.S. Department of Justice, Drug Enforcement Administration. National Drug Threat Assessment. Washington, DC. 2019.
-
Cunningham JK, Liu LM, Callaghan RC. Essential/Precursor Chemicals and Drug Consumption: Impacts of US Sodium Permanganate and Mexico Pseudoephedrine Controls on the Numbers of US Cocaine and Methamphetamine Users. Addiction, 2016; 111(11): 1999-2009.
-
Ronsley C, Nolan S, Knight R, et al. Treatment of Stimulant Use Disorder: A Systematic Review of Reviews. PLoS One, 2020; 15(6): e0234809.
-
Trivedi MH, Walker R, Ling W, et al. Bupropion and Naltrexone in Methamphetamine Use Disorder. New England Journal of Medicine, 2021; 384(2): 140-153.
-
Obert JL, McCann MJ, Marinelli-Casey P, et al. The Matrix Model of Outpatient Stimulant Abuse Treatment: History and Description. Journal of Psychoactive Drugs, 2000; 32(2): 157-164.
-
Rawson RA, Marinelli-Casey P, Anglin MD, et al. A Multi-Site Comparison of Psychosocial Approaches for the Treatment of Methamphetamine Dependence. Addiction, 2004; 99(6): 708-717.
-
Hartzler B, Donovan DM, Tillotson CJ, Mongoue-Tchokote S, Doyle SR, McCarty D. A Multilevel Approach to Predicting Community Addiction Treatment Attitudes About Contingency Management. Journal of Substance Abuse Treatment, 2012; 42(2): 213-221.
-
Aletraris L, Shelton JS, Roman PM. Counselor Attitudes Toward Contingency Management for Substance Use Disorder: Effectiveness, Acceptability, and Endorsement of Incentives for Treatment Attendance and Abstinence. Journal of Substance Abuse Treatment, 2015; 57: 41-48.
-
Further Consolidated Appropriations Act, 2020, 133 STAT. 2534, §II. 2020.
-
SAMHSA. Funding Opportunity Announcement (FOA) No. TI-20-012: State Opioid Response Grants. Department of Health and Human Services, Rockville, MD. 2020.
APPENDIX A. STAKEHOLDER DISCUSSION GUIDE
-
Could you please identify the program that addresses stimulant use in your community with which you are involved? What is your role in leading or overseeing that program?
-
How long have you been with this program or organization? How long have you been in your current role?
-
What is the nature of the program you lead or oversee, as it relates to cocaine or methamphetamine? What policy levers do you employ? What prompted these efforts? [Optional follow-ups: What are your program activities? How did you decide on those activities?]
-
What population(s) does your program primarily serve? [Optional follow-ups: Do most people your program helps live in rural areas? Urban areas? Do you serve a large homeless population?]
-
What does the stimulant use disorder treatment and support services infrastructure look like in your community? What role does your program play in delivering these services?
-
What program areas or investments have been most impactful?
-
What barriers have you encountered in addressing stimulant-related concerns? What would help you to overcome prominent barriers?
-
What facilitators have helped you in addressing stimulant-related concerns?
-
How is your program currently funded? How have these funds been allocated? What program areas are priorities for funding and why?
-
How would additional funds (e.g., from the SOR grants) be used by your program or in your community for stimulant-focused efforts?
-
How do other actors within your state (localities, state governance) affect your capacity to act on stimulant-related concerns? [Optional follow-ups: Are there any specific policies that interfere with the services your organization can provide? Do you get help and resources from other actors in your state?]
-
How does the Federal Government impact your capacity to act on stimulant-related concerns? [Optional follow-ups: Are there any specific federal policies that interfere with the services your organization can provide? Do you get help and resources from certain federal programs; if so, which ones?]
-
How have population health crises (e.g., COVID-19; natural disasters like fires, hurricanes) impacted your program operations and ability to serve your target population(s)? [Optional follow-ups: How have physical distancing measures during COVID-19 affected your program activities and populations served? How are your program's activities and populations served affected by business closures, high unemployment, and unaffordable housing costs? What do you think these effects will mean for methamphetamine and/or cocaine-related concerns in your community in the future?]
-
Are you aware of other notable program efforts to address stimulant-related concerns? Can you recommend programs and key informants within them that we could speak with on this topic?
Questions if time/more relevant to public health officials/law enforcement:
-
What data or information do you use to track stimulant use, stimulant use disorder, or stimulant-involved overdoses? [Optional follow-ups: Where do you get this data/information? Who collects this data/information?]
-
Have patterns of stimulant use changed in your community? If so, have you changed any aspects of your program in response?
-
How do you evaluate or measure your program outcomes? [Optional follow-ups: How did you select those measures? Who in your organization is responsible for evaluating or measuring these outcomes?]
APPENDIX B. SUMMARY OF DISCUSSANTS
| Stakeholder Name | Program Activities | Funding Sources | Website |
|---|---|---|---|
| Multisector Coalitions | |||
| San Diego Methamphetamine Strike Force | Strike Force serves as facilitator to connect different state agencies on issues of methamphetamine use. | Strike Force funded by small facilitation contract from County of San Diego Health and Human Services Agency. Specific projects funded by various agencies in San Diego County. | https://www.no2meth.org/ |
| Colorado Substance Abuse Trend and Response Task Force | Task Force tracks data on substance use in Colorado on an annual basis, collects qualitative data from network and coalition partners, recommends legislation and other policy action to the state. | Task Force funded by Colorado state and nonprofit sources. | https://coag.gov/task-force/ |
| Arizona Substance Abuse Partnership (ASAP) | ASAP oversees community efforts related to different substances. Discussants also held roles on MATFORCE, an organization that brings different stakeholders together to address substance use in Yavapai County, and the Arizona Health Care Cost Containment System, which is the Medicaid Agency of Arizona. | Treatment primarily funded through fee-for-service and managed care Medicaid and providers primarily contracted through a provider network. Appropriation from state legislature and SOR grants fund other program activities. | https://goyff.az.gov/councils-commissions/arizona-substance-abuse-partnership |
| kNOw Meth campaign | Campaign was created in partnership between the Northwoods Coalition, Marshfield Clinic, and Department of Justice to develop and support methamphetamine prevention efforts in Wisconsin. | Partners work funded by federal and state block grants. For example, Heroin, Opiate Prevention and Education (HOPE) legislation (2015) eventually funded methamphetamine issues in North and Northeast Wisconsin. | https://knowmethwi.org/ |
| Health Agency/Department | |||
| Mental Health Reform in San Francisco | Mental Health Reform in San Francisco was launched by the city's mayor to identify solutions for substance use and behavioral health challenges faced by the city, particularly among those experiencing homelessness. | The Mental Health Reform group funded by and sits within the San Francisco Department of Public Health. Initiatives promoted by group funded by state Medicaid dollars and philanthropic donations. | https://www.sfdph.org/dph/comupg/knowlcol/mentalhlth/default.asp |
| Coloradoa Department of Human Services, Office of Behavioral Health | The Office of Behavioral Health is the single state agency to address substance use prevention and treatment for the state and to fund services. | The Office of Behavioral Health supports and helps to administer treatment under Medicaid and administers the SAMHSA SABG. | https://www.colorado.gov/pacific/cdhs/behavioral-health |
| Californiaa Department of Health Care Services Behavioral Health Division | The Department of Healthcare Services is the single state agency responsible for California's Medicaid program and oversight of several grants. | State Medicaid program primarily funds treatment of substance use disorder. Department oversees several grants that address substance use such as the SABG, the Mental Health Services Block Grant, and SOR grants. | https://www.dhcs.ca.gov/services/Pages/MentalHealthPrograms-Svcs.aspx |
| Division of Drug and Alcohol Abuse Programs at the Vermonta Department of Health | Division oversees statewide network of treatment and a variety of programs focused on substance use treatment, prevention, recovery, and provider workforce development. | Division sits within and funded by the Vermont Department of Health. Division oversees grantee activities funded by federal block grant; treatment largely funded by Medicaid. | https://www.healthvermont.gov/alcohol-drugs |
| Washingtona State Health Care Authority | Washington State contracts with behavioral health and managed care plans to treat substance use disorders. | Primarily funded by Medicaid for treatment of substance use disorder. SOR grants fund activities related to methamphetamine. | https://www.hca.wa.gov/ |
| Kansas Department for Aging and Disability Services (KDADS) | KDADS oversees the SABG and Mental Health Block Grant and the SOR grants. Also sets certification and credentialing standards for addiction professionals. | Medicaid and grants fund substance use treatment in the state. State has special funding for substance use treatment for first-time teen offenders in juvenile justice system. | https://www.kdads.ks.gov/ |
| Law Enforcement Agency | |||
| San Diego-Imperial High Intensity Drug Trafficking Area (HIDTA) | San Diego-Imperial HIDTA detects, deters, and dismantles drug trafficking organizations operating within San Diego and Imperial counties in California. | San Diego-Imperial HIDTA funded by a federal grant program. | https://sdihidta.org/ |
| Health Care Provider | |||
| Centennial Mental Health Center | Centennial Mental Health provides treatment for substance use disorder and has specific programs for stimulant use disorder, including enhanced outpatient programs for stimulant use and methamphetamine use. | Primarily funded by Medicaid. Also received federal rural expansion grant to allow purchase of property for sober homes. | https://www.centennialmhc.org/ |
| Community Group/Nonprofit Organization | |||
| Advocates for Recovery Colorado | Advocates provides peer support groups, coaches people in all stages of use and recovery, and conducts advocacy work. | Organization receives state funding and reimbursement for services provided through a managed service organization. | https://advocatesforrecovery.org/about-advocates-for-recovery-colorado/ |
| Project NEON (Needle and Sex Education Outreach Network) | Project NEON focuses on men who have sex with men and methamphetamine use in Washington State. Educates a group of volunteers on issues facing the community and provides them with materials for safer sex and safer drug use. | Funded by Washington State. | https://seattlecounseling.org/project-neon/ |
| |||
APPENDIX C. SUMMARY OF TOPICS DISCUSSED, THEMES IDENTIFIED, AND SUPPORTING QUOTES
| Themes Identified | Supporting Quotes |
|---|---|
| 1. Program Activities | |
| Program activities involve coordination across multiple sectors. | [The Task Force] was a convening of treatment providers, city staff from public defenders, district attorneys to public health, homelessness and supportive housing, some representatives of the user community or former user community ... folks who work in the jails. The Methamphetamine Strike Force ... is the collaboration comprised of public safety, health and human services, nongovernmental community groups that has been in existence now nearly 25 years. It is the group and body that represents for the entire county of San Diego in our response to methamphetamines. A variety of partners take what they're hearing and learning from the Task Force and integrate it into their work. It could be child welfare, it could be prevention work, it could be treatment work, and law enforcement work as well. |
| Programs engage in a variety of treatment modalities. | I've been very much impressed with programs that offer really innovative strategies, such as what's called contingency management, which is essentially when you offer someone an incentive to help them ... change their use of substances. And so, you can offer an individual an incentive and it's important to clarify what that is. In many cases, it might be a financial incentive but not in all of the cases, to be able to help them to change their behavior and change their relationship with street drugs. And so, there are organizations in San Francisco that offer that particular service to our clients. [W]e have a Hub-and-Spoke program here which, for instance, a Hub distributes methadone or buprenorphine and a Spoke might do other medication-assisted treatment. Also, some of my grantees are residential programs and they treat people with various substance use disorders. I also have different preferred providers who provide outpatient treatment for people with various substance use disorders. ... Most of our Hubs [also] do some sort of contingency management looking at cocaine use and other stimulant use within their populations. ... And a lot of contingency management research has occurred right here in Vermont, so we have some very heavy hitters here in the research world. [We have an] Enhanced Outpatient Program which is designed to provide between two-to-five hours per week of outpatient treatment for those individuals. And there's a number of components to that. There's a relapse prevention component, which is based upon the SAMHSA Matrix Model. Then there's also a component of [CBT] treatment, group treatment. And then individual, including family, also, as needed, concurrent with substance use monitoring. A lot of our work right now is helping to move [treatment providers] into the current century of thinking. They're very abstinence-based focused, which 20 years ago with alcohol was appropriate. And so we've really spent a lot of time in the last couple of years really trying to help them understand the current science and ways to do things. ... They've never had to contract with healthcare plans, so a lot of this is just helping them understand how to negotiate in the current world. Some of them offer contingency management, we don't yet have the ability to really see if how they're implementing it is appropriate. So right now, a lot of our work at the agency is this huge transition, and then working to see what specific programs are offered. |
| Programs emphasize recovery and social supports. | We're in the process right now of opening up two sober living homes, which should be a great recovery support service [for] anybody who is showing a willingness to try for recovery and to agree to the rules of participating in the home and being an active peer member, supporting the other group members and participating in treatment. ... Traditionally a lot of times sober living homes have been available for people after they're coming out of some higher level of care ... but also we'll probably be seeing folks ... that are just engaged in outpatient therapy and just need additional support and accountability and structure that living in a sober living home would give them, too. Our program is a peer-run, peer-led, authentic Recovery Community Organization. ... All of our services are peer-based. We provide peer recovery coaching and we do that both to individuals as well as in group settings. ... We absolutely believe that the opposite of addiction is connection. And so, it provides an opportunity for people to be able to connect with each other and really build support outside of a treatment agency and in their own community. |
| Programs provide or link services across the health care and recovery continuum. | San Francisco has a really robust substance use disorder care continuum, encompassing from what we would consider very low barrier, low threshold services ... and onward to residential treatment and withdrawal management programs ... on through residential treatment that lasts 90 days. And we also have what's called residential step-down, which are year-long programs for people, to help them maintain or sustain the gains from their recovery experience and the residential treatment programs. For every individual that comes into our jail, we try to do an assessment and connect that individual to services out in the community. So that when they get released we're not just releasing them to the street but we are releasing them--we call it a warm hand-off--we're trying to release them directly to services. ... Our hope is that that individual, rather than going back to the street, the same folks that they were hanging out with that got them into trouble in the first place, that, while the criminal case is moving through the system, that they are taking advantage of that opportunity to connect to services. |
| Activities often engage with polysubstance use. | Vermont's perspective is that most people are not using just one substance, that poly-substance use really is the issue. And so, our expectation with all of our grantees, including our Hub-and-Spoke system, which they are focused on medication for OUD, the expectation is they are addressing all substance use across the board. So, all of our programs are addressing stimulant use as appropriate, based on the person's [health] assessment. In San Francisco, what we are seeing is a pattern of mixed drug use. Meaning that often times, when people are using opioids like heroin, it is often intermixed with methamphetamine, and often times when they're using methamphetamine, it's intermixed with opioids. And specifically, unfortunately, it's also intermixed often with fentanyl, and we are seeing more and more individuals who are suffering the consequences of this mixed drug use. It's unclear yet whether this is really intentional or is this just a contaminant, where someone is inadvertently experiencing being exposed to fentanyl as they're using what they thought was purely methamphetamine. And so, it's important to us to have medications like suboxone, buprenorphine disseminated in the community and readily available as much as possible just one, to help protect individuals who might be using one substance and finding that they're actually coming in contact with another, and to help further reduce the overall harms of drug use. |
| Treatment and public health/public safety partnerships are increasingly preferred to law enforcement approaches in responding to stimulant use. | Of course, a lot of our folks are overlapped with justice-involved. And there's another funding stream that our providers have that's usually referred to as Senate Bill 123 that sits under the Sentencing Commission. And it has been probably there for about 10 years and the providers contract directly with the Sentencing Commission on this source of funding and it is mainly made for stimulant ... first-time offenders ... to put them into treatment and they use the cognitive model. And they have been ... instrumental in really moving that model into Kansas. The idea right from the get-go was the importance of linking people into treatment and preventing people from getting into use of meth. It was this broader end-to-end approach from the prevention side all the way to the incarceration side ... our waiver for Drug Medi-Cal has afforded us the ability for the first time to build out and organize drug treatment system because I don't believe those exist in our country. With our justice partners we focus on alternatives to [incarceration] ... we've been able to provide resources to folks to get into rehab and recovery, that was much more difficult ten years ago. Both in our civilian and correctional populations having a much more robust delivery system has been a focus for us. San Francisco has multiple programs that are focused on collaboration with law enforcement entities to help navigate people into care, instead of incarceration, when it is appropriate. ... Our Crisis Intervention Teams, where the San Francisco Police Department and those teams of individuals receive extensive multiple hours of training in how to engage, assess, and offer services to individuals who are experiencing a mental illness or substance use-related concern. And so, that team of officers often are our first line, in terms of when a person is encountering the community with one of those two concerns, to help intervene. And help give thought to where we might direct this person next, instead of going to jail, if it's not appropriate, to a treatment setting. And the other program that has been really interesting has been the development of our Law Enforcement Assisted Diversion Program, our LEAD Program, which again offers an opportunity for people with nonviolent drug possession offenses an opportunity to be navigated into treatment services, as opposed to being sent to the local jail with the expectation that they will engage with the social workers or case workers, as well as law enforcement, in helping them get into treatment services. I would say in general, yes, law enforcement is invested in getting people to treatment versus into the criminal justice system. Vermont is fairly diverse and so there are certainly pockets of very liberal communities and then pockets of much more conservative areas in the state. And so, there has been definitely a shift over time in some of those more conservative areas from the punitive perspective to the treatment perspective. So it has been an evolution. |
| 2. Funding Sources | |
| Medicaid is a primary funder for treatment of stimulant use disorder. | The mental health and the SABG grant, those funds are payer of last resort, so ... in the state of California, you would have to utilize Medi-Cal [California Medicaid] dollars first. So, if those services are available and billable under Medi-Cal then that's ... the hierarchy. And then we utilize our block grant funding. We were a Medicaid expansion state before Medicaid expansion existed. So, a lot of what we've been able to do is because of our historical Global Commitment Waiver, which allowed a huge leveraging of Medicaid dollars. ... We have a large Medicaid fee-for-service carve-out. We also have some other types of Medicaid-related investments that fund, for example, our recovery services or some of our intervention program, like, public inebriate services In 2018, we saw really significant increases in the amount of money going into treatment, into our Medicaid behavioral health system through our single state authority substance use treatment centers. ... There's been a pretty high increase ... in the number of people who have accessed treatment with a stimulant use disorder. |
| Federal grant funding, particularly SOR grants and SABGs, helps address stimulant use. | We have several demonstration grants that are related to prevention, opioid use disorder, which now includes allowances for stimulants. We have overdose prevention grants, so we have a variety of standalone demonstration grants from the Substance Abuse and Mental Health Services Administration as well as the [Centers for Disease Control and Prevention] CDC. When somebody presents for block grant funding, you know, that would be your uninsured or underinsured, when they present we can either pull from the block grant funding because they have substance use or what we can do is if they happen to have opioids at this time, because using the SOR I dollars was only designated for opioids, then we could pull from that funding stream. So, that is kind of seamless for that person--we were able to pull funding depending upon their diagnosis, basically. So, what we're doing with SOR II for our treatment dollars, just kind of a bigger picture, is that if someone should present and now if they have opioids or if they have stimulants, we can pull from that funding to serve those folks and then if they don't have that diagnosis, they would fall under the block grant. This has really helped our state. The mental health and the SABG grant, those funds are payer of last resort, so ... in the state of California, you would have to utilize Medi-Cal [California Medicaid] dollars first. So, if those services are available and billable under Medi-Cal then that's ... the hierarchy. And then we utilize our block grant funding. |
| Funding earmarked by state legislatures for substance use programs facilitates addressing stimulant use. | I think investment in diversion programs similar to the one that we have at the Yavapai County Attorney's Office would pay off. Those programs are not inexpensive. We had received an appropriation from our state legislature a couple of years ago and that's the funding that we are using to support our program. A little bit about the HOPE legislation that came through from Representative Nygren, and he started all of that HOPE legislation probably in 2015 when it was at the peak of the opioid epidemic. But in the Northern to Northeastern part of Wisconsin there was a HOPE grant that was received or like ten community agencies that covered five counties and three tribes. And the very first thing that they identified was, yes, this is great that we have opioid funds to focus on treatment and recovery, but we can't just do this with opioids. And so that group ... made some noise about that and kind of got it passed right away to address methamphetamine as well, which kudos to them because they recognized the need for that right away. And it seemed like it went through the grant officers quickly. So that was one mini win, I would say. |
| 3. Facilitators | |
| Flexibility in applying federal funds is useful. | We're dedicating a good chunk of money from our SOR grant to make sure that people with stimulant use disorders who need residential care based on clinical criteria are able to get it. The other thing around the recovery realm is some direct investments in recovery community organizations to offer peer-delivered services. So, you know, we've had a strong grassroots kind of recovery movement in Colorado. You've got Advocates for Recovery which is an affiliate of Faces and Voices of Recovery. And they're doing various self-help groups, peer-delivered services, peer-to-peer services throughout the state. ... So, those sorts of organizations throughout Colorado, we want to do some direct investment out of our SOR grant to support the peer services that they're offering. And obviously, that grant will focus on opioids and stimulants, so we really want to make sure that they develop some specific outreach efforts related to those populations. We want them to continue to serve anybody in recovery or seeking recovery, but we'll make sure that they develop some specific outreach efforts for that population. |
| Diversification of funding mechanisms enhances capabilities. | Our treatment services in San Francisco, a significant portion of those are funded by state Medicaid dollars. ... But we also have very deep relationships with the philanthropic community, which helps us to bridge the gap between what the state regulations allow us to do and what we know is helpful for the San Franciscans. The relationships there are strong and important for us to be able to offer innovations, such as contingency management. (Mental Health Reform in San Francisco) Our funding in general is more based on population than substance, unless you start moving out towards our demonstration grants. So, we have our core funding, which is the Medicaid and the block grant, some state funds but then we have several demonstration grants that are related to prevention, opioid use disorder, which now includes allowances for stimulants ... so we have a variety of standalone demonstration grants from the Substance Abuse and Mental Health Services Administration as well as the CDC. |
| Medicaid expansion and Section 1115 substance use disorder waivers have supported more comprehensive stimulant use disorder treatment. | And we're a Medicaid expansion state, which is essential for any behavioral health services because it means the people that might be unemployed or have jobs that don't come with insurance and don't make that much, the working poor, they have access to healthcare in Colorado. And that is tremendously helpful. ... Our office's money has supported the people who don't have Medicaid insurance. And that includes residential treatment, which is not yet covered by Medicaid in Colorado. So, that's one of the areas that we're really focusing on is making sure that there's adequate residential coverage for people with methamphetamine or cocaine use disorders. ... If you look at everyone with addiction, only a small percentage will ever need to be in residential treatment, but some people will one be able to attain recovery if they have access to that level of care. It's not as prevalent as we'd like. We've been doing some other things to ramp up care and again, that's going to help anyone with any substance use disorder. ... We are hoping for Medicaid to expand its residential benefits, January 1. And again, that's going to relieve a lot of pressure since we're covering treatment for people with both Medicaid and those up to 300% of poverty who don't have insurance. Come January, our funds will stretch farther, because Medicaid will take care of their share and we'll hopefully be able to help even more people. And that's our threshold, up to 300% of federal poverty is typically where we want our funds to be dedicated. Kansas doesn't happen to be a Medicaid expansion state. So, we generally have more need than we have funding available and the block grant has stayed even for at least probably about the last decade of the funding being there. [In] 2015, the Centers for Medicaid/Medicare Services approved California's 1115 Demonstration Waiver. And basically under the Drug Medi-Cal program nonwaiver, the Drug Medi-Cal program covers approximately four to five [treatment] services; so it was somewhat limited. What we call the Drug Medi-Cal Organized Delivery System Waiver really allowed counties who opted in ... it really expanded the level of service, all of which is under the [Administrative Case Management] ACM criteria and different levels of care, and broadened length of stay for residential treatment. It offered more access to medication, such a buprenorphine, and the coverage in that, ... which went beyond just traditional medications. So the waiver really broadened and enhanced the level of service. The [Medi-Cal] waiver is a significant portion of the organized long-term treatment delivery system. ... [The Medi-Cal waiver has enabled us to pursue] treatment over jail. ... Over the years, in working with the bench (they've been great partners), they have developed more of a partnership with the clinical assessment of where an individual is and their drug addiction ... where we've been able to allow people to be placed into residential treatment. But it was very difficult when we didn't have the robust residential treatment and the type of services they wanted in those treatments prior to Drug Medi-Cal. ... It was a sizable number over the last two years that we have now diverted from jail directly into residential drug treatment. ... [To pursue] the drug Medical [waiver], it was a significant amount--over $100 million of local funding we had to put up to be a part of that waiver; so there is a tremendous amount of local commitment to expand drug treatment. It was with the intent to create truly not just more capacity ... but really a lot of culture change in the way that we were working with folks that were dealing with addiction. So that was and still is a transformative aspect of the Drug Medi-Cal success we've seen. [The SUD waiver for payment of residential treatment in Medicaid will] be a big step for us ... we were very pleased to get support. That came out of the interim substance use disorder committee, where the legislators were willing to push this forward to basically force our Medicaid folks to apply for that waiver. ... The provider network has been asking for this. ... It's going to make a big difference in our state. |
| Coordinated and continuous care is critical to treating stimulant use disorder. | The Matrix Model is an intensive community engagement-focused model. It's really structured on relationships and shared accountability. And it is quite effective when deployed. ... The challenge for why it's often difficult to help the methamphetamine users is because ... the methamphetamine, in particular, hijacks the brain's craving centers. Whereas many of us experience an increase in certain hormones in the brain response to a pleasurable stimulus, methamphetamine intensifies those hormonal releases by five as much a 10 to 20 times. And so, you have an intense surge of this pleasurable, pleasure-inducing hormone in the body at that time. ... The unfortunate consequence is that they also, even in single use, can deplete those pleasure-filling hormones, and so ... after a methamphetamine user uses the substance, they often have this phase of protracted depression and increased need for sleep. It makes the engagement process difficult, because they often are very much agitated and restless when they're high, and then they need a few day to recover once they come down. In the context of people who are going in and out of emergency room settings, it's not the ideal place for engagement, because the emergency room visits are only on the order of hours and sometimes these people need days, in order to start to feel better ... when those particular substances that cause them to feel otherwise normal are depleted, it can take up to six months for those chemicals to rebalance in the brain and for their brain chemistry to return to normal. In the intervening period, they have the difficulty that you might associate with someone who has attention deficit disorder. They may be impulsive. They can't focus and concentrate. It's hard to navigate things. And so, it becomes even more important that they have appropriate care navigation and care coordination with the intensive case managers if they're going to be successful. So, for Hub-and-Spokes ... we do have a number of Spokes that sit actually within in our preferred provider network. So, the connections between the Hub-and-Spokes and the larger preferred provider network exist. Could we leverage it more? Yes. And that is something that as state we are talking about and exploring as kind of healthcare evolves nationwide, how we would leverage the Health/Home Model that is our Hub-and-Spoke system to potentially better serve individuals who either don't have a primary opioid use disorder or have a very stable opioid use disorder, but again, are continuing to struggle with other substances. |
| Peer support facilitates long-term recovery. | As the client gets further into it and has a period of nonuse under their belt, then there's a social support group that some of them would participate in. Which is peer-run but also facilitated by a therapist, to engage in different activities and explore different topics within the context of learning about each other and being comfortable together without using, kind of familiarizing themselves with that. I definitely think having staff with lived experience, and recovery specifically from stimulants, is really helpful in working with people with those issues. I think that that connection, that real feeling of this person knows where I've been because they've lived it is a big deal. Certainly, I believe the connections are really important. In my life coming out of my own addiction, I think about the lifestyle because it's very specific and to get people to sort of break out of that lifestyle and begin to bond with people who are, for example, sleeping at night and working during the day instead of staying up days and days at a time, I think that that's important. We've added money through the legislature for people who want to be certified as a peer specialist. We have a model in two emergency rooms in Colorado--we're starting a peer support model for people to work in emergency rooms, for people who come in that may have an addiction they are dealing with. So we are trying to increase that workforce through a certification model for peer support services. |
| Harm reduction is necessary to reach certain persons with stimulant use disorder. | So, it is a harm reduction program in its truest form. So, we support recovery in all of its forms, but it's not our main focus. We like to get people healthy and then get them to come to that as they see fit. We also do a lot of drug management, so we teach people how to--if you're going to do them, pay rent and then go buy drugs; not the other way around, things like that. So we get involved a little bit in their ... life skills and managing their circumstances the best way possible for them at that particular moment. Low barrier or harm reduction ... is really important. People do want care, they do want to connect, but our systems don't want that. And our Syringe Exchange survey very clearly shows that; 60 percent of people in the Syringe Exchange survey said they needed healthcare in the last year and did not get it, mostly because of how they were treated by providers. |
| Use of telehealth and technology has the potential to expand program reach. | Right now in the age of COVID, a lot of [outpatient substance use treatment] is happening through telemedicine. A lot of our rural communities had already embraced telemedicine, just because of access. They've got two psychiatrists to cover 10 counties. ... We have a lot of land mass to cover, and so they've been embracing telemedicine for a long time. COVID has forced me to kind of think about this--just like [Alcoholics Anonymous] AA and [Narcotics Anonymous] NA meetings and other support meetings ... there's not a lot of options in the North for people in recovery to engage in those types of support services. And so when they are available, you know, you may need to travel like a half hour or 45 minutes to get to the closest one. And so we've been engaging in technology. We have our recovery core program which is basically just recovery coaches helping people in recovery navigate things like this. And so we have been trying to find different apps and other things that they can engage maybe as a national forum of people in recovery that just kind of lean on each other for support. But one thing we're also finding out in the Northwest is the broadband is really bad, so we don't have the type of Wi-Fi that we need necessarily to engage in those types of things. So we're trying to find solutions to our problems but it's not working because another issue comes up or another issue comes up. We had to learn Zoom really fast. We've continued to provide the peer coaching using the Zoom platform to be able to do that. And we've had pretty good luck with people participating. ... In Sterling, they've got good Internet and stuff. I am aware that there are some communities that don't have that. I think that Zoom did a good job of setting that up so that people could join with their ... cell phone, and not have to have computers. ... We've actually been able to serve people outside of our usual area. So ... people ... have made contact with us and said, "I would love to have a coach," and we have that ability to do that using the Internet and taking away that transportation barrier or the distance barrier. |
| 4. Barriers | |
| Lack of medication-assisted treatment and other therapies supported by robust research hinder treatment for stimulant use disorder. | That's obviously a barrier that there's no medication that can be covered or prescribed for [methamphetamine]. So, that's why we're looking at CBT and we're looking into CMs for those areas. One of the challenges with managing the needs of individuals facing methamphetamine addiction is that we don't have well-researched medication treatment options for methamphetamine use. This is in contrast to when you consider alcohol use disorder, for which we have Food and Drug Administration approved medications which are shown to decrease the use and the craving for that substance. We also have similar FDA-approved medications for opioid use, and even for tobacco, nicotine use. But we don't yet have an option for the methamphetamine user as a substitution therapy or as a craving reduction therapy. So, that really limits our ability to respond to their needs. |
| COVID-19 has disrupted stimulant use disorder treatment and recovery. | The drug sobering center is one where the funding has been allocated. But in the midst of the coronavirus response, the full process to deploy that is delayed, unfortunately, because of the limitations on the ability to gather the people that are necessary to provide the appropriate inputs to roll the program forward. [COVID] had a huge impact on the community I work with. ... For instance, a lot of my volunteers used to work in several of the buildings here in town that are transitional housing. ... Because all the buildings went on lockdown none of my volunteers could get in. ... Then we've been delivering supplies directly to the building and just handing them cases of syringes and things like that so the staff can pass it out. Overdose death has been a big issue and a big focus of the SOR grants. And opioid overdose was starting to decline, and I think COVID has unfortunately turned things the wrong way. ... But what we'd already been seeing is while opioid overdose deaths were declining before COVID, we were seeing an increase in overdose deaths related to methamphetamine and cocaine. And part of the things that we're concerned about and that we're hearing more anecdotally ... and actually, seeing some, because some of the syringe access programs have been providing testing kits to their clients, so that they can test their drug samples ... that fentanyl is involved or is in a decent amount of the cocaine drug supply and the methamphetamine drug supply. So, while Narcan cannot reduce an overdose that is cocaine or methamphetamine-related, if the person who is taking methamphetamine is taking it that's tainted with fentanyl and it's truly an opioid overdose, even though their drug of choice is stimulants, we've been investing heavily to make sure that there's naloxone access throughout the state. ... So, while naloxone prevents opioid overdose, we do know that the population using cocaine and methamphetamine are at-risk because the drug supply is tainted. |
| Lack of flexibility in how certain funds may be spent, including to address social determinants of health, is limiting. | We really worked with our legislators and elected officials to say, "Stop earmarking money just for opioids." You know, could you maybe earmark it for drug prevention, whether that be opioids or stimulants or whatever it is in your community? Because we can meet any threshold you need for methamphetamine. ... You can give us money for opioids and we can't even spend it, because it's just not an issue here yet, knock on wood, but we can burn through all your money in a day working on methamphetamine. So we really tried to reach out and get at that state level and just let them know the way you're currently doing it is not working for local communities. [In reference to housing and employment supports for people in recovery] There are none in our area. And I would echo that for most of the Northwoods, there's not. It's something that we really, really, really struggle with. We have a few larger employers that maybe offer some small programs, but housing specifically is something that we've been looking at and trying to figure out because we just have none of it. Fundamentally, you don't have anything as potent as housing. ... We see a lot of prolonged residential [treatment] stays and ... the reason in part ... is people do not have a place to go. And you don't want them very fragile early in recovery to go back to where they came from and just not have a hope of succeeding. And we're challenged by that because Medicaid, by law, can't pay for housing ... we're trying to figure out how can we rethink residential care in a way that maybe supports housing in a different way than Medicaid dollars, but prolongs the ability for people to access that substance-use disorder care after 30, 60, 90 days. |
| Overall funding for addressing stimulant use is inadequate. | Kansas doesn't happen to be a Medicaid expansion state. So, we generally have more need than we have funding available and the block grant has stayed even for at least probably about the last decade of the funding being there. The challenge is that the models that they have researched and promoted are very expensive and not workable for most of our clinics. ... We're really struggling with how you put together a practice that you can sustain over time with limited resources. Most of our Hubs are doing some sort of contingency management and we do have some [Intensive Outpatient Programs] IOPs who are doing contingency management. I think any of them would say that to be able to have more funding to find that right prize, you know, obviously, contingency management is about what that thing is that reinforces behavior. And I think any of our providers would say just having a little extra funding to kind of be able to figure out what that prize cabinet should have in it, you know, would be something that they would be looking for. The standard treatment program now is a 90-day program. It can be longer, but the base that MediCal pays for is a 90-day program. Well that's a real problem if a lot of the people going into residential treatment are going in because they are homeless. They might not need residential treatment if they had a place to live. And they might be able to do an outpatient program, which would be less expensive. And then at the end of that 90 days, ... some very large number of people (I think last year the statistic was ∼40%) of unhoused people who go into a residential treatment program are released to a shelter or the streets. So some of what we funded [out of city general funds] last year was more housing options for people coming out of treatment programs to make it more likely that their sobriety would stick. So more money to support people coming out of treatment [is needed]. |
| Rural areas are heavily challenged by stimulant use and disorders. | I think historically with California being so diverse in the makeup of our counties, geographically, we do struggle and we do have predominate problems in our rural Northern counties where sometimes it's geographically hard to get places or funding opportunities as opposed to your larger cities, like San Diego. ... So, we always try to focus on these small and rural counties when we're looking at how we can better assist our partners. In our rural communities, it's very difficult to have specialized groups by substance. So, you're going to have people where alcohol is primary mixed together with people with marijuana that might be primary or methamphetamine that's primary. Most of our cocaine use tends to be much more in the metro areas, whereas methamphetamine is both in the metro areas, as well as in our rural communities. And specifically Northeast Colorado while methamphetamine seemed to decline a little bit as we got into 2010 or so, it never went away in Northeast Colorado. So, you know, while it looked like hey we're past this methamphetamine crisis, other parts of our state it never went away. And it's still been critical, even as we were ramping up opioid response which has very specific approaches around medication. We're seeing that obviously those communities were crying for help related to methamphetamine. I think all services ... the whole array is more challenging ... in our rural and frontier areas. ... When you go out West, there really just isn't a whole lot out there to help people, or they have to drive a huge distance. |
| There is insufficient infrastructure, including an inadequate workforce, to treat stimulant use disorder. | We have real workforce shortage issues where we live. Trying to get people to come work in these tiny little towns is tough. And so, you know, we've always had that, that kind of workforce shortage and workforce challenges, that come with working in rural communities. That's just sort of the norm. Currently we do have a legislative committee working right now on modernization and a focus of that has also come in with the workforce in mental health and ... we're hoping to look at that through the legislature also to ... get more promotion of some tuition reimbursement-type things. They do have in the rural and frontier areas some incentive zones where they will do tax reductions and some things like that, but that still doesn't seem that it's brought these type workers to those communities yet. And what I'm pushing right now ... is that there become more efforts to really social market behavioral health services and addiction counseling, those type of things to the 12 to 18-year-olds. ... But, like I said, I've been working in this field for 40 years and it's been an issue for 40 years. I think like most states, workforce is a challenge and certainly we see decent turnover in our workforce within our preferred provider network; it's hard work, you know, working for treatment providers. And so, folks do kind of move on to easier, better paying jobs. We have unique challenges here in Northern Wisconsin where transportation becomes an issue and you can't cross county lines to get certain treatment because of insurance and all those fun things to work through. ... We're considered a clinical shortage area. |
| Stigma toward individuals who use stimulants hinders effective treatment. | There are many people providing supportive housing services, including for people with methamphetamine use disorder and it is really hard. Folks with methamphetamine use disorder are really struggling, they could be very physically destructive to their housing units. Housing providers are saying they're having a hard time keeping insurance because their buildings keep being damaged. So, it's very, very tough. ... A lot of training that we're working on isn't just about helping providers know how to treat stimulant-use disorder ... but it also is trying to help the service providers not give up as well because they really just throw their hands up in the air. In general, the campaign is to really trying to get the community behind this because a big piece of this is stigma. They don't want to help those "junkies"--those awful things that they say. And so it's really just trying to get buy-in from the community to understand that this is a problem that needs to be solved at the community level. I think stigma is still a real issue. I'm much more pleased the way we've dealt with the opioid crisis because we've tried to destigmatize getting help and the people that provide the help and the people that need the help. I think the way we responded in the late 1990s and early 2000s to the stimulant use problem, unfortunately, was the wrong way. We tried to kind of scare people straight and completely stigmatize it, you know? Showing people the before and after pictures of someone who has had long-term methamphetamine use, and they've lost their teeth and those sorts of things, I think is destructive and it's not good prevention messaging. ... And remember, only about 10 percent of the population who uses any given substance will develop a substance use disorder to it. So, people know people that use methamphetamine that don't look like that, then they don't trust any of the messaging coming from government ... I think the messaging, the much better messaging shows the before and after, that shows the person that was able to attain recovery. And the Lift the Label campaign ... was focused on prescription drug abuse. That was the kind of play on words with the label. But also saying let's move away from the label of addict or some of those other pejorative terms we use for people struggling with a substance use disorder. And we're going to double down on that and really look at an anti-stigma campaign that more broadly addresses all substance use. I still feel that one of the primary barriers with methamphetamine and other substance use disorders is the significant amount of stigma and perception of communities. I've experienced that in regards to sitting down at neighborhood meetings in regards to neighborhoods not wanting, for example, a treatment center within their community, because they refer to individuals in very derogatory terms that have substance-use conditions. ... And then, because of that stigma, navigating to services makes it all the more challenging. |
| Increase in stimulant potency, fentanyl contamination, and availability of supply have contributed to increased stimulant-related harms in recent years. | [Drug trafficking organizations] can purchase fentanyl pretty inexpensively. It comes in from China and India into Mexico, and they cut [methamphetamine with fentanyl] to increase their profit margin. But the meth that we're seeing right now is some of the purest meth that we have ever seen. It's like 80% to 90% pure and you only need microgram quantities of fentanyl, we're talking a grain of salt, to cut and to have an effect on it. We've seen that the price of methamphetamine has increased. We're still on pace to have more seizures as far as finished product at the ports of entry than we were last year. We're seeing that the drug trafficking organizations are taking advantage of the market being more difficult to smuggle into the United States. ... Since COVID-19, there's been about a 75% decrease in vehicle traffic coming North. ... So we're seeing that they're having massive loads of meth come across because they're desperate to try to get it across to the market. And as far as the demand, where there's demand you're going to see a supply. ... They're putting through big seizures to try and get it across. If they can get it in the vehicles, you know, it's 50, 60 pounds. I mean, actually, we just had a seizure the other day that was astronomical. With methamphetamine in Kansas it used to be most of it was homegrown industry with the shake-and-bakes. And Kansas sits on several major East-West and North-South corridors of interstate. And so, currently now probably the main part of methamphetamine coming in is Mexican cartel ... and prices are very cheap and purity is very high. And so, it has really ... gone and exploded in Kansas over the last two to three years because of the availability of the substances. |