
Executive Summary
Changes to the welfare system brought about by the Personal Responsibility and Work Opportunity Reconciliation Act (PRWORA), and state and local welfare reform efforts, carry serious implications for Temporary Assistance to Needy Families (TANF) recipients with disabilities and barriers to employment. Specifically, work participation and time limit requirements are two key provisions of the federal welfare law which provide a new sense of urgency encouraging states to develop strategies to assist clients with their transitions from welfare to work. As a first step in this process, TANF agencies are considering strategies to identify the barriers that are inhibiting or prohibiting this transition. PRWORA offers unprecedented flexibility to develop such strategies and design programs and services to assist with the transition from welfare to work.
As caseloads have declined, there is general agreement among TANF agencies that larger proportions of remaining clients are hard-to-serve. Often this means clients are believed to have substance abuse or mental health problems or learning disabilities, or to be in domestic violence situations referred to collectively in this paper as unobserved barriers to employment. Given the employment focus and time-limited nature of TANF, there is increased interest in screening and assessment approaches that can be used to identify these barriers to employment.
In response to this increased interest, the U.S. Department of Health and Human Services asked The Urban Institute to explore the issues and challenges related to screening and assessment within the TANF context. This paper represents the earliest work under this effort. It identifies ten of the important questions that should be considered by TANF agencies and their partners as they develop approaches to screening and assessing for barriers to employment. By posing these questions, we hope to further the thinking about options for developing approaches to screening and assessment. However, answers to these questions must be developed by TANF agencies and their partners in order to best meet state and local needs and fit within state and local policy guidelines.
This paper is merely a first step in considering some of the many challenges associated with identifying unobserved barriers to employment. In the second phase of this study, we will conduct case studies to further explore how these issues are addressed in a select number of localities. The report based on the case studies will focus specifically on how those localities have answered the questions posed in this report. Regional meetings intended to facilitate discussion among states and localities facing these challenges will also be convened.
Definitions and Context (questions 1-3)
Before moving to the questions of how, when, and by whom TANF clients can be screened or assessed, there are important questions that must be asked that set screening/assessment in its appropriate context. This context is particularly important for TANF agencies just beginning to consider the challenges associated with identifying unobserved barriers to employment, and for partner agencies who may not be familiar with the details of TANF policy. There are a wide range of barriers faced by TANF clients that generally fall under the heading of hard-to-serve. Examining issues related to identifying barriers to employment is complicated by the lack of common terminology. TANF agencies and their partners should take care to ensure they are using terms in the same way to lessen this complication, and in this spirit, Question One notes how terms are used for the purpose of this paper.
Many TANF agencies are already tackling the challenges associated with identifying barriers to employment and need no convincing of the importance of this issue. However, some staff or partner agencies may be less familiar with the objectives of TANF or prevalence of barriers such as substance abuse and mental health problems, domestic violence situations, and learning disabilities. Question Two provides an overview of incentives to screen or assess clients within TANF as well as a review of prevalence estimates for these barriers. Question Three builds on this discussion, outlining key aspects of TANF policy that provide TANF agencies flexibility in how they meet the needs of TANF clients, while also pointing out the requirements that TANF agencies and their partners must consider when developing screening, assessment, and service approaches.
Approaches to SCREENING/ASSESSMENT - How, When, and by Whom? (questions 4-7)
Approaches to screening and assessment are largely defined by how the case management process contributes to identification of barriers, the use of screening or assessment instruments, the timing of identification efforts, and the staffing arrangements used to carry out screening and assessment. Questions Four through Seven address these approaches.
How can the case management process aid in identifying unobserved barriers to employment?
Case management is an ongoing, multi-faceted process of staff interacting with clients, determining needs, establishing goals, addressing barriers, and monitoring compliance with program requirements. Within the case management context, staff may rely on self-disclosure of a barrier or the observation of behaviors that might be indicative of barriers (red flags) for example, bruises or a client who smells of alcohol as methods of identifying barriers to employment. Although inexpensive to implement, and likely already occurring at some level in most TANF agencies, these approaches may be imperfect if they are the only identification strategies undertaken.
The effectiveness of self-disclosure and behavioral indicators as methods of identifying barriers depends heavily on staff's abilities to make clients comfortable disclosing or eliciting disclosure, as well as staff's understandings of different barriers and the behaviors that are indicative of those barriers. In some locations, these less formal methods of identifying barriers are combined with the administration of screening or assessment tools. However, little is known among the TANF community about the tools that are available and their appropriateness for this population.
Are there tools that can be used to identify barriers to employment?
There are several state- and professionally-developed tools being used by TANF agencies (or recommended for use) to identify substance abuse and mental health problems, learning disabilities and domestic violence situations. Tools vary widely with some screening for multiple barriers while also collecting general background information, and others screening for a single barrier. Tools also vary considerably in length, complexity, and cost.
Experts caution that TANF agencies should be careful when selecting or developing tools to ensure that the instrument is methodologically sound. For example, there are a number of tools that have been developed to screen for substance abuse problems, but we were unable to identify such a tool that was designed specifically for use with TANF clients. In contrast, there are two learning disability screening tools that were designed specifically for use with TANF recipients.
When selecting or developing tools, TANF agencies may consider seeking guidance from partner agencies or community-based organizations with experience identifying or addressing a particular barrier. When selecting tools, TANF agencies must not only consider methodological aspects of the instrument but also the cost of the tool and the staff skills necessary to implement the tool and utilize information obtained.
When should screening or assessment occur?
TANF agency administrators interviewed generally considered efforts to identify barriers to employment to be an on-going, dynamic process, noting that there is no singular point in the TANF process when they believe screening or assessment should be carried out. Although the TANF client flow offers a number of opportunities to screen or assess for barriers, staff with whom we spoke noted that they utilize many of these opportunities to further their efforts to identify barriers. For example, TANF program orientations may offer an early opportunity to screen a client for barriers to employment. However, this early screening is often used to determine if a client is eligible for an exemption from participation requirements. The employability planning process offers additional opportunities to uncover barriers and is a common point where formal screening or assessment tools are utilized. As clients participate in work and self-sufficiency activities, re-planning sessions offer further chances to explore the reasons a client has not successfully made the transition from welfare to work.
In some locations, clients are referred to partner agencies for additional services. In some cases, the service received is additional assessment by a subject matter expert or trained clinician. In other situations, clients are referred for work-related services but may receive additional assessment as a part of this process. Finally, some TANF agencies use opportunities presented by non-compliance or lack of success in activities to conduct further assessment. Each of these points in the client flow offer opportunities to further explore barriers to employment. However, there is little information indicating if screening or assessing at any particular point in time yields more accurate information.
Although time limits and work participation requirements provide incentives to conduct screening or assessment early in a clients experience, TANF agencies repeatedly note that they are only concerned with a barrier in so far as it prohibits the client from obtaining or retaining employment. Therefore, even screening or assessment efforts that are conducted up front are conducted within the context of determining services to assist the client with her quest for employment, not based in the belief that the existence of such a challenge necessarily presents a barrier to employment. In some states with a strict work first approach, there is little formal screening or assessment conducted early on and, instead, the labor market is used as the up-front screen to determine job readiness or the existence of a barrier to work.
Who should conduct screening and assessment?
TANF agency officials and subject matter experts generally agree that the most appropriate role for TANF agency staff is to screen clients for barriers to employment and facilitate referrals to organizations with expertise diagnosing and addressing barriers. This belief is based in the fact that many TANF caseworkers are former eligibility or income maintenance workers with little experience with case management and barrier identification. To the extent that this is the case, states may need to consider training existing staff on barriers, screening, or assessment, hiring new staff to conduct screening/ assessment, or creating partnerships with other agencies to assist with screening or assessment efforts.
TANF agencies generally have many partners in the service delivery process. However, for the purpose of identifying and addressing unobserved barriers to employment, TANF agencies may need to develop new relationships or change the nature of existing partnerships. Although resources in communities will obviously vary, other government agencies and communitybased organizations may possess valuable experience identifying and addressing barriers to employment and therefore may be potential partners. Partnerships for the purpose of identifying and addressing barriers to employment faced by TANF clients bring with them many challenges, including understanding respective program philosophies and requirements. For example, partner agencies may not understand the work incentives and work participation rates that exist in PRWORA. In some cases, TANF agencies and their partners may need to consider adaptations in their policies or strategies order to accommodate TANF program requirements such as adapting services to meet shorter time frames or focus more heavily on work-related activities.
Additional Issues (questions 8-10)
Pervading the questions of how, when, and by whom screening and assessment should be conducted are questions relating to staff training and privacy and confidentiality. Although these are two important additional questions, these are merely some of the many questions TANF agencies and their partners must answer.
What training issues are related to screening and assessment?
Regardless of decisions related to the use of tools or informal identification methods, the timing of identification efforts, staffing arrangements and partnerships, it is likely that some training will be necessary. Training may need to be conducted on a wide range of topics including: general awareness of the characteristics of particular barriers, the details of how to administer specific assessment tools, how to determine appropriate services to address barriers once identified, and how to facilitate referrals to partner agencies. Training may also need to be conducted on broader issues of TANF and other program policies as they affect allowable services and the timing of different activities.
Additional training considerations include who to train (including the importance of cross training of partners) and the costs of training (including materials, trainers, and staff time required to attend training). However, there are costs associated with not conducting, or not training, the appropriate staff. Such costs may include inconsistent implementation of screening and assessment approaches, inconsistent information provided to clients by program staff unfamiliar with the program rules or requirements of partner agencies, and unsuccessful program initiatives.
What issues related to privacy and confidentiality should be considered?
Fundamental to the issues of obtaining information about barriers to employment faced by TANF clients and sharing this information with partner agencies in efforts to remove or mitigate such barriers are questions related to privacy and confidentiality. These issues are affected by a variety of laws, perceptions, and individual fears too complex to discuss fully in this report. However, the potential negative consequences of not seriously confronting the importance of these provisions makes the issues worth raising, even briefly. Examples of negative consequences include, but are not limited to: the fear of social stigma, the inability to obtain health insurance, and physical harm (or even death, particularly in the case of sharing information about domestic violence situations). Despite the challenges presented by privacy and confidentiality provisions, states have found ways to address these requirements and meet clients needs.
What other questions should be asked?
Questions One through Nine address some of the common issues that arose during the background research for this paper. However, there are numerous other questions that states and localities should consider. Examples of other important questions include: Should drug testing be used to identify substance use among TANF recipients? What can be done to help medical professionals understand the implications of their assessment or diagnostic findings? Is gaming the system a problem?
Future Directions
The issues raised in this paper suggest that states and localities face a number of decisions in selecting an approach to screening and assessing TANF clients for unobserved barriers to employment. The paper also offers examples of how some states and localities have answered questions related to screening and assessment. However, the issues and discussion presented here generate a number of questions that require additional information to fully address. This suggests that, regardless of the chosen strategy, states, localities, and the federal government should consider incorporating data collection into approaches implemented and plan future research related to strategies for identifying barriers to employment. Perhaps most important among future research questions are those that shed light on the effectiveness of different approaches to screening or assessment of TANF clients for barriers to employment. Additionally, many questions remain regarding the factors that may influence the effectiveness of different approaches.
Introduction
With welfare reform it is now more important than ever to identify and address barriers to employment.
The Personal Responsibility and Work Opportunity Reconciliation Act of 1996 (PRWORA) eliminated the Aid to Families with Dependent Children (AFDC) cash entitlement program and the Job Opportunities and Basic Skills (JOBS) training program, and replaced them with the Temporary Assistance for Needy Families (TANF) block grant. TANF includes both cash assistance and welfare-to-work programs and differs from the former AFDC/JOBS program in that it is a temporary cash assistance program which has the explicit goal of moving families from welfare to work. This employment mission is reinforced by work participation and time limit requirements two key provisions of the federal welfare law which hold important ramifications for welfare recipients, especially those with significant barriers to employment.
Under this system of welfare reform, it is now more important than ever for states to use the flexibility provided under PRWORA to find new ways to help TANF recipients with health conditions, disabilities, or barriers to employment make the transition from welfare to work. To do this, TANF agencies must consider implementing strategies to identify the barriers that are inhibiting or prohibiting this transition. Once barriers are identified, welfare agencies and their partners can develop appropriate service strategies to meet the needs of clients so that they can find and maintain employment and transition off welfare.
Implementing identification and service strategies to address barriers to employment within the complex structure of the welfare systemwhich involves a number of function and partnersis no small task. As welfare agencies consider how best to serve recipients with health conditions, disabilities, or barriers to employment they will likely need to consider the flexibility presented by TANF to develop policies and programs as well as consider how best to use their partners in this endeavor. Partners may include both government entities and the community-based organizations that often serve as the providers of work or barrier-specific services for welfare recipients. When considering partners and service options, TANF agencies may also look to the Welfare-to-Work Grants program. This program, which offers funding to state and local workforce development agencies through the U.S. Department of Labor, is intended to address the needs of the hardest-to-serve TANF clients both while on welfare as well as once they are no longer eligible for cash assistance.1
This report discusses issues related to the development and use of screening and assessment practices (including the use of formal tools) to assist in the identification of disabilities and barriers to employment among TANF recipients. The disabilities and barriers faced by remaining TANF recipients are diverseranging from low basic skills and learning disabilities, to substance abuse and mental health problems, developmental disabilities, and physical disabilities. Although each of these presents challenges for TANF recipients faced with the transition from welfare to work, this report focuses on four of these barriers:
Substance abuse problems;
Mental health problems;
Learning disabilities; and
Domestic violence situations.
This report focuses on this limited list of barriers because prevalence estimates indicate they are common among TANF recipients and because they are often not easily observed by program staff and therefore pose additional identification challenges. However, the lack of discussion of other barriers in this report does not in any way diminish their importance or severity. Additionally, although not addressed specifically here, TANF staff frequently note that many recipients face multiple barriers to employment. Many recipients are believed to face complex situations that may include barriers such as lack of education or work experience along with a less obvious barrier, or the co-occurrence of unobserved barriers such as substance abuse and domestic violence. To the extent that these challenges present barriers to obtaining and maintaining employment, TANF agencies must develop new strategies for identifying these barriers and providing services to assist the client with her quest for self-sufficiency.
This report is organized to address key questions that should be considered as states and localities grapple with the challenge of identifying the unobserved barriers to employment facing TANF recipients remaining on welfare. TANF agencies do not face this challenge alone and may find advantages in involving, or in fact may need to involve, partner agencies. Therefore, this report includes questions that TANF agencies and/or their partners may need to consider. It is structured so as to allow readers to consider either the entire range of questions presented or focus on a particular question of interest. Specifically, the questions addressed here are:
Barriers, Screening, and Assessment: How are we using these terms?
Why should TANF agencies consider screening or assessment?
What policy opportunities and limitations are presented by TANF?
How can the case management process aid in identifying unobserved barriers to employment?
Are there tools that can be used to identify barriers to employment?
When should screening or assessment occur?
Who should conduct screening and assessment?
What training issues are related to screening and assessment?
What issues related to privacy and confidentiality should be considered?
What other questions should be asked?
To varying degrees, states and localities are already in the process of examining these questions and experimenting with different approaches and practices. Examples of these approaches are included throughout the report for illustrative purposes only. They are neither best practices nor suggested approaches. In fact, few have been evaluated and little is known about their effects, intended or unintended. Nonetheless, they provide valuable food for thought as TANF administrators tackle this challenge.
1 The Welfare-to-Work Grants Program was authorized by the Balanced Budget Act of 1997. For additional information about this program see Greenberg 1997 and Perez-Johnson and Hershey 1999.
Methodology
This report reviews issues related to developing and implementing screening and assessment approaches and offers a review of tools that may assist in this process. Identification of the issues to be considered, as well as the tools currently being used to screen or assess for barriers, was primarily based on a series of semi-structured telephone interviews with:
Selected state TANF agency officials, and
"Experts" in particular areas of interest (specifically substance abuse and mental health problems, learning disabilities, and domestic violence).
Respondents were identified through Urban Institute contacts and a review of relevant literature. This process was not intended to systematically uncover screening, assessment, or identification practices used in all states.2 Instead the objective was to identify approaches and tools used in TANF agencies or tools used in other programs that could be used in TANF agencies. (Although other [non-TANF] agencies have been conducting assessments for some time, many experts were hesitant to recommend tools for use by TANF agencies, believing instead that TANF staff should refer clients they suspect may have a particular barrier to a specialized agency that serves such clients for assessment and diagnosis by a trained professional. 3 ) To accomplish this task, we spoke with 65 knowledgeable individuals between December 1999 and April 2000, including TANF and other state and federal government agency officials, researchers, practitioners, and association representatives.
Screening and assessment are on-going and dynamic processes. However, the telephone interviews allowed for a limited review of the range of different points in a TANF client's experience when screening or assessment might occur. For this report, we focused primarily on identification efforts that exist within a TANF agency (although these too may occur at multiple points in time). Where available, information about additional assessment efforts outside of the TANF agency is also included. Further exploration of the complete range of opportunities to conduct screening, as well as in-depth assessment or diagnosis of specific barriers or disabilities, will be a primary objective of the case studies undertaken in the next phase of this project. Services provided in response to assessments will also be a focus of the case studies and are not addressed in this report.
2 The American Public Human Services Association has undertaken a 50-state survey that includes identifying screening and assessment tools used by TANF agencies.
3 See additional discussion of this issue under Question Five.
Question One: Barriers, Screening, and Assessment: How are we using these terms?
Examining issues associated with identifying barriers to employment among TANF recipients is complex in part because there is little common use of terms. Fundamental confusion over the use of terms makes discussing barriers, identifying and designing identification approaches, and delivering services difficult. Clarifying how TANF and other systems define barriers and what is meant by screening and assessment are important first steps in developing effective strategies and partnerships. Given this lack of uniform definitions and terms, this section describes and clarifies our use of the terms "unobserved barriers," "screening," and "assessment" for the purposes of this report. This report does not try to impose standard definitions of these terms or reconcile varying definitions used by others. In discussing barriers it is important to recognize that not every health condition, disability, or personal circumstance presents a barrier to employment and that further, TANF agencies' primary concern lies only with those conditions, disabilities or circumstances that inhibit or prohibit the effect transition from welfare to work and self-sufficiency.
What Barriers do TANF Recipients Face?
TANF recipients continuing to be involved in the welfare system face a range of disabilities and barriers to employment and self-sufficiency. Some of these are barriers with which the TANF system has experience identifying (i.e., lack of transportation or child care, low educational attainment, lack of work experience). However, as TANF caseloads have declined and the more job-ready recipients have left welfare, TANF agencies now face the challenge of identifying and addressing different issues and barriers than they did in the past - health conditions, disabilities, and barriers to employment that are often unobserved. It is this new challenge that has expanded the interest in screening and assessment approaches.
Knowing which barriers should be the focus of identification efforts is an initial challenge faced by states and localities. As will be discussed in Question Two, estimates of the prevalence of different barriers, including substance abuse and mental health problems, domestic violence situations, and learning disabilities, among TANF recipients vary. In fact, many welfare agencies have little specific data indicating the challenges faced by their clients and the extent to which these challenges represent barriers to employment. Despite this, there is a common belief that welfare recipients are "harder-to-serve" than they were in the past and that the challenges they face are in some way prohibiting or inhibiting their transition from welfare to work.
Identifying barriers to employment faced by remaining welfare recipients is a new challenge for TANF agencies.
In many ways, identifying the challenges these remaining welfare clients face represents a new challenge to TANF agencies and their partners. The clients who have been the focus of welfare-to-work programs and who have already left welfare were more likely to have job skills and some work experience than those remaining on welfare. Additionally, although TANF clients with significant barriers to employment were likely to be exempt from participation in the JOBS program, many states have changed their policies to require those formerly exempt recipients to participate in work activities under TANF.4 This challenge to welfare agencies is further compounded by the time-limited nature of federal cash assistance under TANF.
Regardless of specific estimates, or lack thereof, each of the barriers faced by TANF clients is important. They range from lack of adequate transportation and child care, to serious physical disabilities, and caring for children with serious disabilities. TANF agencies vary in their experience dealing with these different barriers. For example, most TANF agencies have historically offered assistance with transportation or child care if they present a barrier to work or participation in required activities. TANF agencies also have experience determining if the lack of education poses a barrier to employment.
As TANF agencies have incorporated methods of identifying barriers that are more obvious, or with which they have experience, they are now beginning to grapple with how to identify the less obvious disabilities or barriers that continue to inhibit TANF recipients' transitions to work and self-sufficiency. Because some barriers - such as substance abuse and mental health problems, domestic violence situations and learning disabilities - are not as obvious to TANF agency staff, or may not be observed, they can be referred to under the broad heading of "unobserved barriers." When TANF agency officials describe clients as "hard-to-serve," these are some of the barriers clients face.
There are a variety of reasons barriers might be unobserved.
Why are some barriers "unobserved?"
Barriers might be less obvious, hidden, or unobserved for a variety of reasons. For example, the recipient may not be aware of or fully understand why she is unsuccessful in her quest to obtain employment. A client might acknowledge that she often feels sluggish or has a hard time arriving at work promptly but be unaware that these are possible symptoms of depression. Additionally, some clients may be in denial regarding a barrier such as substance abuse or domestic violence.
Another reason some barriers are unobserved is that, although a client is aware of the problem, she may be hesitant to disclose it and in fact may make special efforts to keep the problem from being revealed. Examples of this include clients who do not want to be labeled or have the stigma associated with a problem such as substance abuse or who are afraid of additional violence if they reveal a domestic violence situation. Yet another reason a barrier may be unobserved is that clients may be concerned that they are in jeopardy of having their children removed from the household if they disclose a barrier such as substance abuse.
Regardless of the reason, these situations require that TANF agency staff employ different approaches to uncover barriers than they might have employed in the past. Simple reliance on standard past practices of self-dis-closure or medical verification may not be sufficient to identify "unobserved" barriers.
What unobserved barriers are considered in this report?
TANF recipients face a wide range of personal issues and barriers to employment, many of which are unobserved. Although each is important and complex, this report focuses on four commonly unobserved barriers:
Substance abuse problems;
Mental health problems;
Learning disabilities; and
Domestic violence situations.
TANF agencies and their partners need to be clear with each other regarding how they define or conceptualize these (and other) barriers. For example, TANF agencies are generally concerned about issues that present barriers to employment. Therefore, although the mere existence of a mental health problem might warrant action by a mental health agency, this problem is primarily important to TANF agencies only in so far as it presents a barrier to employment. Similarly, although substance abuse treatment professionals consider any substance abuse problem deserving of attention, TANF agencies are interested to the extent it presents a barrier to employment.
Additionally, when discussing barriers partner agencies need to be clear about the meaning of different terms. For example, there are several proposed definitions of learning disabilities, yet learning disability experts we spoke to noted that learning disabilities are frequently confused with low educational attainment or literacy problems, as well as mild mental retardation. Further, "mental health problem" is a broad term encompassing a number of specific conditions including depression, anxiety disorders, bi-polar disorder, and post-traumatic stress disorder (PTSD), to name a few. Similarly, what constitutes "domestic violence" varies and may include physical, emotional, and sexual abuse.5
4 Additionally, because of the less stringent participation requirements under JOBS, although not always formally exempt, clients with significant barriers to employment were less likely to be fully engaged in the JOBS program. See also Thompson, et al., State Welfare-to-Work Policies for People with Disabilities: Changes Since Welfare Reform. Washington, DC: US Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, October 1998.
5 Domestic violence experts note that domestic violence differs from the other barriers addressed in this report in that it is a situation imposed on the individual, not an illness, addiction, medical condition, or disability.
What do We Mean by 0 and 0
For the purposes of this report, screening and assessment fall within the broad category of approaches used to identify or uncover barriers to employment. Identification efforts may include the use of case management techniques to elicit disclosure of a barrier, the use of formal or informal screening and assessment tools (discussed in Questions Four and Five), or clinical diagnosis. Because TANF agencies are not expert in diagnosing specific conditions, nor are their staff generally trained as clinicians or social workers, the level of identification undertaken by TANF agencies is likely to fall under the broad headings of screening or assessment. Below we clarify our use of these terms in this report. However, it bears noting that different organizations use these terms differently and, just as TANF agencies and their partners need to clarify how terms used to describe barriers are used, so do they need to clarify terminology used regarding identification.
What do we mean by "screening?"
The use of the term "screening" in this report refers to a process of determining if an individual is "at risk" of a certain condition or barrier. Screenings are intended to determine the likelihood that a person requires additional assessment to uncover a particular barrier. Screening as used here is not considered a definitive decision that a person faces a particular problem or condition - that would be a diagnosis6 - or even a comprehensive attempt to uncover a barrier. Screening tools are often described as inexpensive, requiring no training for staff to administer,7 and requiring little time to implement.
What do we mean by "assessment?"
The term "assessment," as used in this report, includes both specific efforts to identify barriers, as well as an on-going process of determining what barriers an individual faces. Assessment might include using a tool to identify a particular barrier, or could be a more general process of monitoring progress and analyzing (or assessing) why expected progress is not achieved. If a screening determines that an individual is likely to have a substance abuse problem, assessment will help confirm or deny the problem. Assessment for a specific barrier differs from screening in that it is more definitive and likely requires some training to implement and interpret results. However, it does not replace formal diagnosis. Conclusive determination that a problem exists, and determination of its extent, requires clinical assessment or diagnosis by a professional.
6 Diagnosis is a formal medical determination requiring professional training and is often required for insurance purposes or program participation. Given that this level of identification is not likely to occur within TANF agencies, it is not discussed in detail.
7 This does not alleviate the need for training on related issues such as awareness, handling information obtained through screening, or making appropriate referrals based on screening information, discussed further in Question Eight.
Question Two: Why should TANF agencies consider screening or assessment?
While a few states have been screening and assessing clients for health conditions, disabilities, and barriers to work for several years, there are a number of reasons why there is a growing interest in identifying and addressing unobserved barriers to employment. The overarching motivation for uncovering barriers is to fulfill the employment objectives of TANF - if a TANF agency is to fulfill these objectives it likely must identify issues that prohibit clients from making a successful transition from welfare to work. Once barriers to employment are identified, TANF agencies and their partners can develop programs and services to assist clients in their quests to successfully obtain employment, retain jobs, and eventually transition off welfare.
Prevalance estimates indicate high rates of unobserved barriers among TANF clients.
As welfare caseloads have declined, many of the remaining TANF clients are considered hard-to-serve and may require more help to obtain employment. Prevalence estimates presented in this section indicate high rates of unobserved barriers among TANF clients. Additionally, as TANF agencies have successfully moved clients from welfare to work, they are gaining new insights regarding the barriers that inhibit job retention and thus are motivated to address barriers in an effort to promote long-term self-sufficiency and reduce recidivism among clients.
With TANF's emphasis on moving clients from welfare to work and self-sufficiency, TANF agencies have more incentive than in the past to identify and address unobserved barriers to employment. No longer are TANF agencies liberally exempting clients facing obstacles to participation and employment from participation requirements. States we spoke with were acutely aware that participation incentives are reinforced by legislative or policy requirements such as federal work participation requirements, time limits, state TANF policies, and the Family Violence Option. Additionally, civil rights legislation, such as the Americans with Disabilities Act (ADA) of 1990, requires that TANF programs make reasonable accommodations for persons with disabilities, including three of the four unobserved barriers to employment addressed in this report.
Before moving to additional discussion of legislative and policy incentives related to identification of barriers, it is important to note that such efforts should be undertaken with care. Although the incentives to identify barriers to employment are clear, and in many cases early identification allows more time for services to assist clients, welfare agencies and their partners must be cognizant of the potential harm that may result from attempts to identify or mitigate barriers. This is particularly important in the case of domestic violence situations. Although a client may be exempt from certain program requirements if she is a victim of domestic violence, disclosing this fact and taking steps to address this issue must be done in a manner that does not further jeopardize her safety.
How do Legislation and TANF Policies Provide Incentives to Screen and Assess?
Title II of the ADA of 1990 "is intended to protect qualified individuals with disabilities from discrimination on the basis of disability in the services, programs, or activities of all State and local governments."8 The ADA defines "disability" as a physical or mental impairment that substantially limits one or more of the major life activities, and the law specifically requires state and local governments to make reasonable accommodations when necessary to avoid discrimination on the basis of disability.9 Of the four barriers to work considered here, three are disabilities covered by the ADA - substance abuse,10 mental health problems, and learning disabilities.11 States and localities designing and implementing screening and assessment approaches and referrals to services must ensure that they do not discriminate against qualified individuals with disabilities. State and local TANF programs may not use criteria that screen out or tend to screen out an individual with a disability from participating unless such criteria can be shown to be necessary for the service or program. 12 Although the states we spoke to did not specifically identify this as an issue they were grappling with, all states and localities must ensure that their programs meet the guidelines of the ADA. 13
States we spoke to identified several reasons why they developed or were newly developing screening and assessment processes for TANF clients. The reason cited most frequently was meeting the increasing annual federal work participation requirements. In fact, it bears repeating here that welfare agencies are primarily concerned with identifying unobserved disabilities only in so far as they are barriers to employment and participation in work activities. TANF caseload declines are believed to have left many states with an increasing proportion of recipients facing challenges in their efforts to transition from welfare to work. Although states have generally had no trouble meeting work participation rate requirements to date, as increasing proportions of long-term TANF recipients face barriers to work, states are anticipating that meeting federal work requirements will be increasingly difficult.
Time limits provide incentives for TANF agencies to identify unobserved barriers to employment
Many states also indicated that approaching time limits are another reason for increased emphasis on screening and assessing TANF clients for unobserved barriers to employment. Many states, and particularly those with time limits shorter that the federal 60-month limit, are beginning to consider the ramifications of time limits on meeting the needs of clients remaining on TANF. Getting clients screened, assessed, referred, treated, and into work when they have a significant barrier to employment can take time. As the federal 60-month time limit approaches, more and more states will be faced with less and less time to remove or mitigate barriers to work for hard-to-serve TANF clients.
How does the Family Violence Option provide an incentive to screen and assess?
Another reason states mentioned for beginning or enhancing screening and assessment practices specifically related to domestic violence victims receiving TANF is the Family Violence Option (FVO). The FVO enables states that adopt this option to provide temporary waivers from work requirements for domestic violence counseling, safety planning, and other related services. States that adopt the FVO agree to:
Screen and identify individuals who are receiving assistance under TANF and who have a history of domestic violence while maintaining the confidentiality of such individuals;
Make referrals for counseling and supportive services; and
Waive program requirements, pursuant to good cause, such as time limits (for as long as necessary), if complying with the requirements would make it more difficult to escape from domestic violence or unfairly penalize the individual in light of her past or current experience with domestic violence.14
Thirty-two states had adopted the FVO and had all policies and procedures in place as of May 1999.15
8 U.S. Department of Justice. The Americans with Disabilities Act Title II Technical Assistance Manual Covering State and Local Government Programs and Services. Washington, DC: U.S. DOJ, undated.
9 See U.S. Department of Justice. 28 CFR 36.104, Americans with Disabilities Act. Washington, DC: U.S. DOJ, July 26, 1990.
10 Individuals currently using illegal drugs are not protected from discrimination under the ADA, however, the ADA does prohibit denial of health services or rehabilitation services to an individual on the basis of current illegal drug use if the individual is otherwise entitled to such services.
11 U.S. DOJ undated.
12 U.S. DOJ undated.
13 For more information see U.S. Department of Labor. How Workplace Laws Apply to Welfare Recipients. Washington, DC: U.S. DOL, May 1997, U.S. Department of Health and Human Services. Civil Rights Laws and Welfare ReformAn Overview. Washington, DC: U.S. DHHS, August 1999, U.S. Department of Health and Human Services. Technical Assistance for Caseworkers on Civil Rights Laws and Welfare Reform. Washington, DC: U.S. DHHS, August 1999.
14 Public Law No. 104-193, 104th Congress, 2nd Session, Section 402(a)(7). August 22, 1996.
15 Raphael, Jody and Sheila Haennicke. Keeping Battered Women Safe Through the Welfare-to-Work Journey: How are we Doing? Chicago, IL: The Center for Impact Research, September 1999.
How Common are These Barriers?
Yet another reason why TANF agencies who are not already doing so should consider screening and assessing is the prevalence of disabilities and barriers to employment among TANF recipients. A review of several studies with prevalence estimates for substance abuse, learning disabilities, domestic violence, and mental health problems, describe high rates of incidence - a compelling reason for states to enhance or adopt screening and assessment efforts.
Prevalence of Multiple/Co-Occurring Barriers. Many TANF clients face multiple (co-occurring) barriers to employment with some barriers more likely to co-occur than others. Several studies estimate the prevalence of multiple barriers to employment among welfare recipients. Although estimates vary, in part due to differences in definitions of barriers to work, estimates of the co-occurrence are still useful. In a review of several studies, Johnson and Meckstroth (1998) report that nationally 13 to 50 percent of welfare recipients experience multiple barriers - including two or more of the following: lack of child care, disabilities, domestic violence, emergency financial needs, housing instability, lack of health insurance, mental health or substance abuse problems, or lack of transportation - which may impede the ability to work.16
Using administrative data, staff focus groups, and client interviews, a recent study in Utah noted prevalence rates for the following barriers to work:
Clinical depression (42 percent)
Generalized anxiety disorder (7 percent)
Post-traumatic stress disorder (15 percent)
Learning disability (23 percent)
Physical health problems that prevent work (35 percent)
Poor work history (30 percent)
Severe child behavior problems (23 percent)
Severe domestic violence within the last 12 months (12 percent)
The Utah study found that 92 percent of families faced at least one of these barriers to work with many families facing multiple barriers, 26 percent of families faced three barriers, and 37 percent faced four or more barriers to work with longer term welfare recipients reporting more barriers.17
Using the Urban Institute's National Survey of America's Families (NSAF) data for 1997, Loprest and Zedlewski (1999) found that 78 percent of current welfare recipients face one or more barriers to work - including one of the following six barriers:
Very poor mental health or health limiting work;
Education less than high school;
No work experience or having last worked three or more years ago;
Child under age one;
Caring for a child on Supplemental Security Income; or
English-language limitations.
Loprest and Zedlewski further found that 44 percent of current welfare clients face two or more of these barriers, and 17 percent of clients face three or more of these barriers to work.18
Not all barriers are as likely to co-occur as others. Citing a study by Olson and Pavetti (1996), Johnson and Meckstroth (1998) report that among clients with multiple barriers, low basic skills is the barrier most likely to co-occur, with mental illness, housing instability, domestic violence, and substance abuse also likely to co-occur.19 Johnson and Meckstroth (1998) also review past research and report that 42 to 54 percent of domestic violence victims receiving welfare also suffer from depression. Domestic violence is also likely to co-occur with substance abuse with estimates ranging from 19 to 38 percent of domestic violence victims also reporting drug and alcohol abuse or dependency.20
There is little debate that substance abuse is a common barrier faced by TANF recipients.
Prevalence of Substance Abuse. Estimates of the prevalence of substance abuse among welfare recipients vary widely (based on differing data sources and definitions of substance abuse), although there is little debate that this is one of the common barriers faced by TANF clients. A recent report by the National Center on Addiction and Substance Abuse (CASA) notes findings from a recent state survey indicating that "State TANF administrators consistently identified substance abuse among participants as a pervasive problem...."21 Additionally, substance abuse is considered a factor affecting TANF clients' ability to obtain and retain jobs and was included as one of the eligibility factors for the Welfare-to-Work Grants program designed to help hard-to-serve welfare recipients.
One study that reviewed past research reports estimates ranging from two percent for welfare recipients who sought treatment for substance abuse to 20 percent for welfare recipients who self-reported substance use.22
Another review of estimates notes that nationally five to 27 percent of welfare recipients have a substance abuse problem depending on how it is defined - narrowly where the individual is either an alcoholic or drug user or broadly where the individual is a possible alcoholic and/or drug user.23 Yet another summary notes that 6.6 to 37 percent of welfare recipients have a substance abuse problem depending on the measure used.24
Prevalence of Learning Disabilities. Learning disabilities are another commonly cited barrier to employment faced by TANF recipients. However, there is little consensus on a definition of a learning disability. Often issues of low educational attainment, illiteracy, and even developmental disabilities are grouped under the heading of learning disabilities. The lack of a common definition contributes to the range of prevalence estimates available.
Estimates of learning disability prevalence vary with Johnson and Meckstroth (1998) reporting that past national studies found 25 to 40 percent of welfare recipients have a learning disability or low basic skills. The TANF Program Second Annual Report to Congress reports that up to 40 percent of welfare recipients have a learning disability or low basic skills.25 State studies in Kansas, Utah, and Washington report that it is likely that 20 to 33 percent of welfare recipients have a learning disability with Washington suggesting that up to one-half may have a learning disability.26 While these figures seem quite high, Young (1997) suggests that women experience higher rates of learning disabilities as adults due to gender bias in their youth. Lack of diagnosis of a learning disability in youth results in fewer girls receiving the necessary special education, thus lending credibility to higher estimates given the predominance among adult women, who are most commonly the heads of TANF households.27
Estimates of domestic violence situations vary whether based on current or lifetime victimization rates.
Prevalence of Domestic Violence. Domestic violence is a broad term used to describe abusive or aggressive behavior by a person in an intimate relationship with the victim and may be physical, sexual, or emotional.28 Estimates of domestic violence prevalence vary depending on whether current or lifetime victimization rates are measured. The Center for Impact Research - a leading domestic violence advocacy organization - reviewed five major research studies and reports that 20 to 30 percent of welfare recipients are current victims of domestic violence.29 Similarly, in a review of national studies Johnson and Meckstroth (1998) found that 24 percent of welfare recipients have been "physically victimized or threatened by their current partner sometime during the past five years." Yet another summary by Danziger et al. (1999) notes both current and lifetime domestic violence rates ranging from 10 to 31 percent and 48 to 63 percent, respectively. The only other lifetime prevalence rates we identified are state and local estimates reported by Johnson and Meckstroth (1998) with lifetime domestic violence rates ranging from 29 to 65 percent.
Prevalence of Mental Health Problems. Mental health problem is another broad term used to describe what may be a barrier to work for many TANF recipients. Like learning disabilities and domestic violence, the term mental health problem actually encompasses a number of specific conditions including clinical depression, anxiety, post-traumatic stress disorder (PTSD), and others. In estimating prevalence, many studies report about mental health problems or impairments generally while others measure specific mental conditions.
Using the 1997 National Survey of America's Families (NSAF) data, Loprest and Zedlewski (1999) found that 22 percent of current - and 18 percent of former - welfare recipients said they had very poor mental health. Similarly, Sweeney (2000) summarizing recent research, notes that 20 percent of former welfare recipients who are not working have mental health impairments. Other studies estimate different prevalence rates depending on whether welfare clients meet the diagnostic criteria for depression - 6 to 23 percent - or whether welfare clients show symptoms of depression - 13 to 39 percent.30
Estimates of prevalence for specific mental illnesses vary nationally and from state to state. A review of national prevalence rates for specific mental illnesses indicates that the following percentages of welfare clients met definitions of specific mental health problems. 31
Major depression (27 percent)
PTSD (15 percent)
General anxiety disorder (7 percent)
Michigan found 25 percent of welfare recipients - compared to over 40 percent in Utah - had major or clinical depression. Michigan and Utah found similar rates of PTSD and general anxiety disorder at 14 and seven percent, respectively.32
16 Johnson, Amy and Alicia Meckstroth. Ancillary Services to Support Welfare to Work. Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, June 1998.
17 Barusch, Amanda Smith, Mary Jane Taylor, Soleman H. Abu-Bader, and Michelle Derr. Understanding Families With Multiple Barriers to Self Sufficiency. Final Report submitted to Utah Department of Workforce Services. Salt Lake City, Utah: Social Research Institute, February 1999.
18 Loprest, Pamela J. and Sheila R. Zedlewski. Current and Former Welfare Recipients: How Do They Differ? Washington, DC: The Urban Institute, November 1999.
19 Johnson and Meckstroth 1998.
20 Johnson and Meckstroth 1998.
21 The National Center on Addiction and Substance Abuse (in partnership with the American Public Human Services Association). Building Bridges: States Respond to Substance Abuse and Welfare Reform. Washington, DC: CASA, August 1999.
22 Sweeney, Eileen P. Recent Studies Indicate That Many Parents Who Are Current or Former Welfare Recipients Have Disabilities or Other Medical Conditions. Washington, DC: Center on Budget and Policy Priorities, February 2000.
23 Johnson and Meckstroth 1998.
24 Danziger, Sandra, Mary Corcoran, Sheldon Danziger, Colleen Heflin, Ariel Kalil, Judith Levine, Daniel Rosen, Kristin Seefeldt, Kristine Siefert, and Richard Tolman. Barriers to the Employment of Welfare Recipients. Ann Arbor, MI: University of Michigan Poverty Research and Training Center, April 1999.
25 U.S. Department of Health and Human Services, Administration for Children and Families, Office of Planning, Research and Evaluation. Temporary Assistance for Needy Families (TANF) Program: Second Annual Report to Congress. Washington, DC: August, 1999.
26 Sweeney 2000.
27 Young, Glenn, H., Jessia Kim, and Paul J. Gerber. Gender Bias and Learning Disabilities: School Age and Long-Term Consequences for Females. Learning Disabilities: A Multidisciplinary Journal, Vol. 9, No. 3. Pittsburgh, PA: Learning Disabilities Association, 1997.
28 Johnson and Meckstroth 1998.
29 Raphael and Haennicke 1999.
30 Johnson and Meckstroth 1998.
31 Kramer, Fredrica D. Serving Welfare Recipients with Disabilities. Washington, DC: Welfare Information Network, January 1999.
32 Sweeney 2000.
Question Three: What policy opportunities and limitations are presented by TANF?
The devolution of policy making authority granted under PRWORA encourages state and local creativity and flexibility to identify and address unobserved barriers to work among the TANF population. This section discusses the opportunities and limitations presented by federal TANF policies that states face in developing screening and assessment approaches. In particular, we consider four key TANF features - 1) the uses of federal TANF funds and the definition of assistance, 2) time limits, 3) work requirements, and 4) the Family Violence Option.33
When developing screening and assessment policies and approaches state and local TANF agencies and their partners need to clearly understand the intricacies of each policy requirement, and the mix of constraints and opportunities they offer. The intent of this section is to highlight key features of TANF policy that may influence decisions about approaches to screening, assessment, and service provision. In an effort to illustrate some of the program and policy choices states have made, this section offers some examples. However, it is by no means a comprehensive review of the combinations of policies states have adopted, nor does it present the range of combinations states may want to consider.34
33 For a more complete understanding of TANF guidelines, see Public Law 104-193, and TANF regulations at 45 Code of Federal Regulations Parts 260-265. See also regulation summaries prepared by Greenberg and Savner 1999 and Schott, et al. 1999.
34 For additional information on the uses of TANF funds see, U.S. Department of Health and Human Services, Administration for Children and Families, Office of Family Assistance, Helping Families Achieve Self-Sufficiency: A Guide on Funding Services for Children and Families through the TANF Program, www.acf.dhhs.gov/programs/ofa/funds2.htm. Washington, DC: DHHS, undated.
What Opportunities and Limitations are Presented by the Family Violence Option
The Family Violence Option (FVO) may provide states adopting this option protection from penalties that might otherwise be imposed for not meeting work participation requirements or for failing to comply with federal time limits. The FVO provides states with the flexibility to grant families temporary waivers from work and other program requirements without fear of penalties. Waivers may be granted to allow families to pursue domestic violence counseling, safety planning, and other related services.49
However, in order to qualify for this safeguard, states that grant exemptions to domestic violence victims must certify that they have and enforce procedures to screen and identify individuals who have a history of domestic violence and make referrals for counseling services while maintaining confidentiality.50 If a state meets these federal requirements and exceeds the 20 percent limit on the number of clients that can receive federal assistance beyond 60 months because the state is providing waivers to domestic violence victims, the state will not be penalized.51 Similarly, if a state fails to meet the required work participation rate because of good cause waivers to the work requirement granted to domestic violence victims, it will also not be penalized.
49 For the purposes of the FVO, a family must have "...an individual who is battered or subjected to extreme cruelty." See TANF Final Regulations, Section 260.51.
50 See TANF Final Regulations, Section 260.55 for additional details regarding federal recognition of domestic violence good cause waivers.
51 Schott, et al. 1999.
What Opportunities and Limitations are Presented by the Provision of Federal TANF 0
Key to understanding the flexibility offered and constraints imposed by TANF is the concept of TANF "assistance." This is important because two of the more widely talked-about aspects of TANF policy - time limits and work requirements - apply when federal TANF "assistance" is provided. Therefore, decisions about providing services are influenced by whether or not the service falls within the definition of "assistance."
The final TANF regulations provide a fairly narrow definition of "assistance," thus broadening the range of services states and localities can offer clients without subjecting them to time limits and work participation requirements. "Assistance" includes cash payments, vouchers, and other non-cash benefits designed to meet a family's on-going, basic needs. There are specific exclusions from this definition including supportive services to employed families, short-term benefits,35 wage subsidies to employers, and other services that do not provide basic income support.
The federal definition of "assistance" allows states attempting to identify barriers latitude in the services they can offer without subjecting clients to time limits and work participation requirements.
This definition offers states undertaking efforts to identify barriers to employment some latitude in providing a range of services. For example, counseling and case management services - services that do not provide basic income support but that are thought to be important for clients with unobserved barriers to employment - are examples of services excluded from the definition of "assistance." Therefore, states have the flexibility to provide these services without subjecting clients to federal time limits or work participation requirements. However, if for example, federal TANF funds are used to provide a cash benefit while a client is in counseling, time limits and work requirements do apply to that family.
35 States may use TANF funds to provide "short-term" benefits or support "short-term" services for an "episode of need" - defined as four months or fewer - without being considered assistance.
Are services funded by state dollars considered "assistance?"
If a state wants to provide benefits or services that fall within the definition of "assistance," but does not want to subject the family to the consequences of the 60-month federal time limit and federal work requirements, the state may choose to fund benefits and services with state Maintenance of Effort (MOE) dollars. Spending of state funds is explicitly addressed in PRWORA through MOE requirements. In general, states are required to maintain a historic level of spending if they want to receive their maximum TANF block grant. The use of MOE funds separate from federal TANF block grant funds (through Separate State Programs) allows states to provide services, even those that fall within the definition of assistance, but without triggering other requirements. The flexibility offered by Separate State Programs allows states and localities to provide services such as substance abuse or mental health treatment, or educational programs to meet the needs of those with learning disabilities, without subjecting these recipients to federal time limits. While the flexibility exists to create Separate State Programs, states must choose between many competing interests regarding how to spend their state funds.
What Opportunities and Limitations Arepresented by Time Limits?
Both federal and state time limits can affect TANF recipients' opportunities to receive services necessary to successfully transition from welfare to work. Many perceive time limits as a motivating factor for TANF agencies to provide services and clients to undertake steps to change their lives. However, for clients with unobserved barriers to employment, leaving welfare and achieving self-sufficiency within 60 months as required by PRWORA may be a significant challenge.
In some states, clients face the challenge of leaving welfare in less than 60 months. PRWORA allows states to impose time limits shorter than 60 months - an option 23 states have exercised.36 State time limits vary, including being as short as 12 months in Texas (for recipients with 18 or moremonths of recent work experience and a high school diploma, GED, or certificate from a vocational school37 ) and 18 months in Tennessee.38 Both types of time limits increase the urgency around removing or mitigating barriers to work. For instance, a client with a substance abuse problem must have her problem identified, be referred to services, receive and successfully complete services, and ideally leave welfare for work before 60 months has elapsed, or in even less time in many states.
States with shorter time limits might consider making screening and assessment part of initial intake in an attempt to identify and address barriers to employment as soon as possible. For example, concerned about the 36-month state lifetime limit on cash assistance, Utah's state legislature mandated the addition of the four CAGE questions - a common set of questions used to identify substance use problems - to their comprehensive screening tool in an effort to identify clients with substance abuse problems earlier in the process. Officials in Utah said that TANF clients often mask substance abuse problems. However, identifying unobserved barriers as early as possible is very important since the agency has 36 months to treat clients and help them find work.
36 States that established state time limits under a pre-PRWORA federal waiver that differ from the federal time limit defined under PRWORA can continue to operate under the waiver if they choose. For the duration for which the waiver was granted, the state is not required to comply with the provisions of PRWORA that are inconsistent with the waiver (so long as they noted this "inconsistency" in the state TANF plan). When the waiver expires, the state must impose the federal time limit.
37 Gallagher, L. Jerome et al. One Year after Federal Welfare Reform: A Description of State Temporary Assistance for Needy Families (TANF) Decisions as of October 1997. Washington, DC: The Urban Institute, June 1998.
38 After 18 months of assistance in Tennessee, a family must wait at least three months before becoming eligible for another 18 months of assistance. Families in Tennessee are allowed a total of 36 months of TANF assistance.
Can TANF agencies fund services for more than 60 months?
The 60-month limit applies only to clients receiving federal TANF "assistance." Months during which clients receive benefits that fall outside of the definition of assistance, or services that are exclusively state funded, do not count toward the federal time limit. Therefore, the use of separate state funds can serve as a mechanism for effectively "stopping" a client's federal time clock.39 States may provide services for a total of more than 60 months by funding services in some months with federal TANF funds and in others with state dollars. This option may be important as TANF agencies are faced with serving clients with unobserved barriers to employment who may require more than 60 months to make their journey from welfare to work.
Another way to use state funds to offer more than 60 months of services is by supporting clients with state funds once they have reached the federal time limit. States that are willing to use their own funds to provide services can allow families to receive welfare beyond 60 months. For example, Maine, Michigan, and New York have agreed to pay for TANF benefits beyond 60 months using state funds to support families who are unable to transition off of welfare despite participating in required programs or services.
39 Note that the client may still be subject to a shorter, state-imposed time limit which may supercede the federal limit.
What is the 20 percent hardship exemption?
PRWORA allows states to exempt up to 20 percent of its caseload from the federal time limit due to hardship.
In addition to the option of funding services and benefits with state funds, PRWORA also gives states the flexibility to continue to fund services with federal TANF funds beyond 60 months for up to 20 percent of its caseload due to "hardship." PRWORA further gives states the flexibility to define what constitutes a hardship. In other words, 20 percent of TANF families who reach the five-year federal time limit and qualify under state-defined "hardship" criteria may continue to receive federally funded TANF benefits and services.
This provides states the opportunity to determine what disabilities or barriers to employment may exist among the remaining TANF caseload, and define hardship such that these individuals receive a time limit exemption. However, many states have little systematic information about the barriers faced by TANF recipients and must consider which barriers to deem worthy of a hardship exemption, while subjecting other clients to benefit termination. States with 60-month time limits will not have clients who reach this limit until August 2002, and, as a result, it is not surprising that many states are in the early stages of thinking about who should be covered by the federal 20 percent hardship exemption rule.
What other time limit exemptions or extensions exist?
Technically, the only exemption to the federal time limit is the 20 percent hardship exemption mentioned above. However, states have established exemptions to their shorter state time limits. Many of these exemptions are given to clients due to age, disability, or the need to care for a disabled household member. It is important to note that although a person may be exempt from a state time limit, if during this time she receives federally funded TANF "assistance," such as a cash benefit funded by the TANF block grant, the 60-month federal time limit will still apply.
Arkansas offers an example of how a state exempts clients from a shorter state time limit while being assessed. In Arkansas, if a caseworker suspects a client may have a learning disability, the client is placed in deferred status and referred to the Arkansas Rehabilitation Services (ARS) for assessment. While in deferred status, the client's 24-month state time clock is not counting. If the assessment determines that the client is "too impaired" for ARS services, the client remains deferred and her 24-month clock remains stopped. When Arkansas first began TANF, the clock continued to run for those temporarily deferred from the work requirement. However, state officials reported that TANF staff felt this was a poor policy and pushed for a legislative amendment (passed last year) to allow the state time clock to stop and to retroactively reset the clock for those identified with learning disabilities prior to the amendment.
An alternative to exempting recipients from time limits is to offer an extension to the eligibility period. As noted previously, states may effectively extend welfare eligibility by granting a "hardship" exemption or continuing to provide services with state funds. States also have the flexibility to offer extensions to shorter, state time limits. Twenty states offer extensions to time limits when the adults in the family have made a good faith effort to find employment but remain unemployed or underemployed.40 Domestic violence is the most common reason for extensions - unemployment or underemployment are the second.
Utah illustrates how a state with a time limit shorter than 60 months can use extensions to bridge the gap between state and federal time limits. In Utah, the state time limit is 36 months. In January 1997, the state legislature approved a bill that allows 20 percent of TANF recipients, or about 2,000 families, to exceed the state's three-year time limit.41 Therefore, this 20 percent is now eligible for state TANF benefits between 36 and 60 months. 42 Then, after 60 months, this group may also be eligible for the 20 percent federal hardship exemption, should Utah choose to define hardship to include them. Some of the state extension provisions - such as those in Maine, Michigan, and New York - enable TANF recipients to receive benefits beyond five years. However, in making decisions about time limit extensions, states must consider the fact that these extensions may prove costly in the long run.
It is widely assumed that declining caseloads will leave higher proportions of TANF clients with health conditions, disabilities and other circumstances that may negatively affect their ability to find or keep a job, presenting a greater challenge to states to address these issues within the time remaining. Should this assumption prove true, states may need to increasingly seek creative solutions to identify and address unobserved barriers to work using the flexibility allowed through federal and state time limit policies.
40 Center on Law and Social Policy and Center for Budget and Policy Priorities. State Policy Documentation Project, February 2000.
41 State Capitals Newsletters. Utah House Passes Bill Extending Welfare for Violence Victims. Public Assistance and Welfare Trends, Vol. 54, No. 5. Alexandria, VA: State Capitals Newsletters, January 2000.
42 Thus, this law allows 20 percent of recipients to exceed the 36-month time limit.
What Opportunities and Limitations are Presented by Work Requirements?
There are two key aspects of work requirements that must be considered when thinking about how TANF work policies affect clients with unobserved barriers to employment. First, states face work participation rates with strict federal requirements regarding how to calculate the rates. Second, states have the flexibility to allow clients to engage in activities beyond those that count toward the rate calculation. Thus, the list of allowable work activities defined by a state may be broader than the activities defined in PRWORA as countable toward work participation rates.43
States vary in terms of both the types of work requirements they impose on TANF recipients (i.e., how soon client must engage in activities and how many hours they must participate) and the types of work activities that are allowed to show compliance with the work requirement. Under federal law, TANF recipients are required to conduct some work activity within 24 months of receiving TANF, but the definition of the work requirement is left to states, and gives states the discretion to impose requirements sooner than 24 months. Below we discuss factors important to determining what activities TANF recipients may engage in and how this decision is influenced by federal work participation rate requirements.
43 States that defined work activities differently under a pre-PRWORA federal waiver than how they are defined under PRWORA can continue to calculate their work participation rate using the state's definition for the duration of the waiver (so long as they noted this "inconsistency" in the state TANF plan). When the waiver expires, the rate will have to be calculated based on the definition of work discussed in this report.
What is the work participation rate?
Federal law establishes the work participation rates that states must meet or face penalties44 (shown in Table 1). The participation rate calculations are quite complicated, but worth discussing here because they have figured prominently in the specific program and policy choices made by states. The calculation of a state's annual participation rate is based on the average of the state's monthly participation rates in that year and is calculated as the number of families receiving TANF "assistance" that include a working adult or an adult engaged in countable work activities (discussed below) for the required number of hours per week as a percentage of the number of families receiving TANF "assistance" subject to penalty for refusing to work in that month.45
Table 1: Annual Work Participation Requirements Under the TANF Block Grant
| Fiscal Year | All Families a | Two-Parent Families |
|---|---|---|
| 2000 | 40 percent | 90 percent |
| 2001 | 45 percent | 90 percent |
| 2002 | 50 percent | 90 percent |
Source: Greenberg, Mark and Steve Savner 1996.
a Note the all families rate is only for families in which there is an adult.
The required participation rate for each state is reduced by one percentage point for each percentage point the state's average monthly TANF caseload in the prior year is below its FY1995 average monthly AFDC caseload (commonly referred to as the caseload reduction credit).46 Caseload reduction credits have been an important factor in states' early abilities to meet the required participation rates. Because of significant caseload declines, some rates are substantially lower than those established by PRWORA giving states even greater flexibility to assign clients to a broad range of work and self-sufficiency services. However, some states anticipate that meeting participation rates will become more difficult as the participation rates increase over time and as residual caseloads are likely to contain a higher proportion of clients with disabilities and barriers to work.
The work participation requirements for all families allows flexibility in several ways. In FY2000, states must have 40 percent of all families with an adult in countable work activities for 30 hours per week (assuming no caseload reduction credit). However, states can allow alternative activities for all hours for the 60 percent not needed to meet the FY2000 work participation requirements. Additionally, states should consider that some alternative activities or treatment will be short-term, and, as a result, removes clients from the work participation calculation for only a short period of time.
Another source of flexibility in meeting work participation rates stems from the small numbers of recipients who will be participating in alternative activities (e.g., treatment) at any given time. This flexibility may diminish if the percentage of recipients with significant barriers to work increases. Further, states have the flexibility to allow clients to engage in activities that don't count toward the work participation rate, once they have participated in countable activities for the required number of hours per week, thus contributing to the achievement of the participation rate. While some flexibility exists here, many clients with disabilities or unobserved barriers will be unable to meet this 30 hour per week requirement. However, for some clients, treatment may not be full-time, and, as a result, some clients may be able to combine treatment with part-time work or job search.
An example of using the flexibility within the TANF system is the Integrated Resources for Independence and Self-Sufficiency (IRIS) Program in Minneapolis, Minnesota. In Minneapolis, TANF clients who are believed to have a substance abuse or mental health problem are referred to IRIS. While in the IRIS program, a wide variety of activities are considered allowable work activities including: assessment for substance abuse or mental health problems, counseling (individual, family, and group), substance abuse treatment, medical appointments, support groups, basic education, GED, and English-as-a-Second-Language classes.
New Hampshire grants extensions to TANF clients with learning disabilities who were unable to complete education and training programs in the time allotted due to their disability. In the New Hampshire TANF employment program, vocational skills training and post-secondary educational activities are limited to 24 months full-time attendance or 36 months part-time attendance. Basic educational classes are limited to 12 months (extendable by 12 more months if there is a "high likelihood of GED attainment"). New Hampshire grants extensions to the time allowed in these activities (not to the lifetime limit on TANF benefit receipt) to those clients who are diagnosed with a learning disability.47
44 States face a base penalty of five percent of their federal TANF block grant for failing to meet the
work participation rate. The penalty may be increased in subsequent years if the failure to achieve the rate continues. Reductions from the maximum penalty may also be granted depending on the degree of non-compliance.
45 Families that have been sanctioned for three or more of the last 12 months are excluded from the rate calculation.
46 No caseload reduction credit is awarded for caseload declines due to changes in eligibility criteria.
47 To receive an educational/training activity extension clients with a learning disability must have an Individual Education Plan identifying education goals, milestones, accommodations, timeframes and action plans.
What is the difference between allowable and countable activities?
Federal law limits activities that can count toward the participation rate, but leaves states with some flexibility to define these activities. The Congressionally-specified countable work activities that can be used to meet a state's work participation rate are:
Unsubsidized employment
Job search and job readiness
Work experience
Vocational education and training
Community service programs
On-the-job training
Subsidized private employment
Subsidized public employment
Providing child care to community service participants
Satisfactory school attendance
Education related to employment
Job skills training
Additionally, TANF recipients in three activities (all related to education and training) can only be counted towards a state's monthly all-family participation rate after the recipient has engaged in work-related activities in that month for at least 20 hours per week.48
States concerned with screening, assessment, and treatment for clients with disabilities and unobserved barriers to work need not simply adopt the activities in the federal law. Instead they have the flexibility to broadly define allowable work activities to include many services to help disabled recipients or recipients with unobserved barriers to work. States choosing to allow recipients to participate in activities that do not count toward the federal participation rate must determine if they can meet the required rate with the percentage of clients in countable activities, or if they are willing to risk the financial penalties associated with not meeting federal work participation rates.
Some states use PRWORA's flexibility to allow clients to participate in activities that do not count toward federal participation rates.
While some states have adopted only federally countable activities, other states have used the flexibility to include disability screening, assessment, and treatment as allowable activities. Minnesota allows clients in remedial education and working part-time to receive work credit for the hours spent in remedial education. Similarly, officials in Montana said they firmly believe in concurrent "work activities" for clients unable to work full-time and, therefore, allow clients to receive treatment as needed and to engage in employment as possible.
States have considerable flexibility in defining work activities beyond the initial 30 hours per week needed to meet participation rates. The examples above illustrating Minnesota's and Montana's alternative work activities reflect this flexibility. It is important to note that these alternative work activities are allowable in Minnesota and Montana. Clients with barriers to work or disabilities may have difficulty or be unable to participate in 30 hours per week of federally defined countable activities. To the extent that these activities are unrealistic for these clients, states will have to consider whether or not they can meet federal work participation rates and allow participation in non-countable activities. Many states allow participation in non-countable activities, but only in conjunction with participation in a countable activity for the required number of hours. Thus, activities TANF recipients are allowed to engage in are influenced by the state's ability to meet federal work participation rates.
This complicated rate calculation again illustrates the importance of the definition of TANF "assistance" and states' choices regarding what services to provide and how those services are funded. The guidelines around countable activities also demonstrates constraints states face to assure they achieve required rates, yet also provide flexibility as illustrated by the latitude states have to determine allowable activities.
48 It is also important to note that recipients participating in job search or job readiness can be counted towards a state's monthly participation rate only if they have participated in that activity for less than six weeks in any fiscal year (or 12 weeks if the state's unemployment rate is 50 percent higher than the national rate), and have not already been in job search for more than four consecutive weeks. In addition, not more than 30 percent of a state's average monthly participation calculation can include persons in vocational education or school, and individuals who participate in vocational education for more than 12 months do not count toward the rate.
Question Four: How can the case management process aid in identifying unobserved barriers to employment?
The term "case management," as used in the context of TANF, is a multi-faceted process. It is the on-going process of staff interacting with clients, determining needs, establishing goals, addressing barriers, and monitoring compliance with program requirements. Defined this way, case management has always occurred within the welfare system. For example, after an applicant has met the eligibility requirements of TANF, the client is assigned to a case manager.52 Case managers have historically worked with TANF clients and perform a number of functions including conducting orientation and intake, assessing aptitudes and abilities of participants and their families, developing employability plans, identifying, coordinating, and expanding services for participants, and monitoring implementation of the employability plan.53 Similarly, assessment has always been a part of the case management process, although previously it was more focused on identifying recipients who were exempt from work, education, or training programs. As noted previously, with welfare reform and the changing needs of recipients remaining on welfare, the nature of case management has also changed.
Case management - in the era of welfare reform, "harder-to-serve" welfare recipients, and unobserved barriers - has taken on a slightly different meaning. Often terms such as "intensive" or "enhanced" case management are used to describe this new process that contains features always included in case management but that now frequently involves more time identifying and addressing barriers to employment. In so far as this new form of case management involves greater and often more individualized attention to identifying barriers, it may also include several methods of screening and assessment for disabilities or unobserved barriers to work. Included in the case management process are efforts to identify unobserved barriers using approaches relying on self-disclosure, observing "red flags," and professionally- or state-developed tools.
In this section we discuss self-disclosure and red flags as identification methods used within overall case management efforts. The implementation of professionally- and state-developed tools - also implemented as part of the overall case management process - are discussed separately in Question Five. It is important to reiterate here that welfare agencies are screening and assessing for disabilities within the context of the TANF program and to meet the employment objectives of the TANF program - an objective that may differ from those of other organizations. Within the TANF context, the existence of an unobserved barrier is not, in and of itself, an issue of primary concern. This philosophy is consistent with the language of the ADA which stipulates that "a public entity may not make unnecessary inquires into the existence of a disability."54
52 States may use a term other than case manager, such as employment counselor, case coordinator, or caseworker.
53 American Public Human Services Association. Case Management Definitions, Goals, Principles from their Organizational and Professional Development Curriculum. Washington, DC: APHSA, undated.
54 U.S. DOJ undated.
What Should Be Considered About Self-disclosure?
Self-disclosure occurs when a TANF client voluntarily reveals a problem to a TANF worker, often in response to a direct question or prompting. All TANF staff rely on self-disclosure as a method of identification to some extent. Although in some ways a natural part of the case management process, self-disclosure may be limited in its ability to identify barriers to employment. For example, if the unobserved barrier is unknown to the client, or if she does not have an incentive to disclose the problem, agencies may need to combine self-disclosure with other methods. However, if the client is aware of but does not have an incentive to disclose the problem, there are additional steps TANF agencies and staff can take to facilitate self-disclosure.
Much of the discussion around the disclosure of barriers focuses on the environment within which barriers are discussed and uncovered. TANF agencies can create a supportive environment for self-disclosure by making sure staff are prepared to absorb and respond appropriately to information about barriers. In some cases, this means staff need additional training to better understand the barrier, its causes, and consequences. As staff learn more about the characteristics of a barrier, they might also begin to recognize it or a similar problem or experience in their own lives. TANF agencies must acknowledge this possibility and provide a supportive environment for staff, so that staff can, in turn, provide a supportive environment for clients. Whenever possible, conversations should take place in a relatively quiet and private space. Case managers may need to develop trust with clients over time, and should continue to reinforce issues of safety and confidentiality in each meeting with a client. (A separate discussion of privacy and confidentiality is found in Question Nine.)
A common concern among welfare recipients is that disclosing a barrier may result in their children being removed from the home.
Further, TANF staff can alleviate fears clients may have about disclosure by outlining how state or local policies will affect benefit receipt and the services provided. Experts we spoke to emphasized the importance of clearly explaining the consequences of self-disclosure rather than vaguely referencing a policy. Clients must feel confident that disclosing a barrier to work will not have negative repercussions, or be clear about what the repercussions are, so that they can be weighed in the decision to disclose. As noted previously, one common concern by welfare recipients is that disclosing a barrier might result in having their children removed from the home. Other concerns include effects to benefit receipt due to sanctions or other TANF policies. TANF agency staff and their partners should ensure that clients understand expectations related to work, job search, child support enforcement, and the potential for exemptions or extensions, as well as how disclosing a barrier may affect their TANF benefits or their families. Additionally, TANF agencies should have, and should inform clients about, service strategies to address barriers, including referral for further assessment, diagnosis, and treatment for clients who self-disclose.
Creating this ideal environment for self-disclosure may require training of staff and significant changes to the existing TANF office environment. Such a situation requires that staff utilize interpersonal skills to create relationships with clients that foster trust. In many localities, or for some specific workers, this may be a significant departure from existing relationships with clients that are focused on accurate benefit determination, monitoring, and sanctioning. Facilitating such relationships may require substantial training efforts, or even the hiring of staff with different skills or qualifications. However, this level of training or staffing changes may be more than the TANF agency can or will accept.55 In such situations, non-TANF staff might be needed to perform this function. (See Question Seven for further discussion of who should be involved in identifying unobserved barriers.) Finally, creating such an environment may require structural changes to the welfare office (i.e., creating private offices instead of large rooms housing multiple workers) that in some cases are beyond the agency's control.
In some cases, regardless of attempts to create supportive environments or clearly explain the consequences of self-disclosure, clients might not feel comfortable disclosing barriers to any staff within the TANF agency. Combining self-disclosure with other methods of identification, such as red flags or professionally- or state-developed tools in enhanced case management, may increase the likelihood that barriers to work will be correctly identified.
55 For example, some states face hiring freezes and strict state hiring guidelines. Another challenge to
such a change may be union negotiations regarding changes in job responsibilities for some staff.
What Should Be Considered About Red Flags?
Another method of identifying potential barriers to employment within the case management context is the reliance on clues or "red flags." Red flags are verbal or behavioral cues a TANF caseworker observes that may indicate a disability or barrier to work. For example, some examples of red flags include a client who smells of alcohol when arriving for appointments, has unexplained bruises, or has trouble distinguishing letters such as "p" and "q." For states that have not developed screening and assessment approaches per se, self-disclosure and red flags are a means of identifying clients with disabilities or barriers to work.
Observing red flags is a very inexpensive policy for TANF agencies to implement and a technique used commonly by experienced caseworkers. However, red flags alone are unreliable measures and present many opportunities for caseworkers to incorrectly identify barriers (including by relying on stereotypes or personal biases). Although from the TANF agency's perspective it might be more advantageous to refer clients to further assessment based on red flags, this option must be weighed against the financial and time costs associated with the possibility of sending a client down the wrong path based on a "clue." Some localities have addressed this by educating staff about the behaviors associated with particular barriers and some use formal behavioral checklists to document these "clues."
Observing "red flags" can be a method used to decide who gets screened or assessed.
For states who do not screen every TANF client, red flags are often a method of deciding who gets screened or referred for further assessment. Using red flags in conjunction with self-disclosure or professionally- or state-developed tools is more likely to correctly identify TANF clients with disabilities or unobserved barriers to work. Officials in Minnesota reported shifting from relying on behavioral indicators in an effort to identify clients with problems towards developing a more structured approach to screening and assessment because they wanted a more objective approach. Similarly other states noted that more formal screening efforts were implemented in response to caseworkers' reports about recipients' behavior.
Question Five: Are there tools that can be used to identify barriers to employment?
As noted in Question Four above, the case management process offers a number of opportunities to incorporate efforts to identify unobserved barriers. In addition to relying on self-disclosure and red flags, available screening and assessment tools or instruments can also be implemented as part of the case management process. In this section, we review some of the available screening and assessment tools, followed with a discussion of issues that should be considered when using screening or assessment tools generally.
Although other (non-TANF) agencies have been conducting assessments for problems such as substance abuse and mental health problems for some time, many experts we interviewed were hesitant to identify instruments that could be used by TANF agencies. Instead, many believed strongly that TANF agency staff should refer any clients they suspect are facing barriers to an agency that specializes in that issue. For example, if a TANF case manager suspects a client faces a mental health problem, that client should be referred to the local mental health treatment agency for assessment. This preference is based on the common belief that most TANF case managers do not have the training necessary to conduct assessment and that such assessment should be conducted by staff with appropriate skills and training. Despite this preference, many TANF agencies have demonstrated increased interest in using screening and assessment tools to guide such referrals.
In this section, we discuss tools used to identify multiple barriers to work, as well as standalone or targeted tools intended to identify a single barrier - substance abuse, learning disabilities, domestic violence, and mental health problems. The discussion includes examples of states that have adopted these tools, provided for illustrative purposes. Although we highlight some key features of each tool presented, this section is not intended to promote or suggest the use of any instrument. Instead, it is intended to offer TANF administrators and their partners additional information about tools that are currently used in a TANF agency, or that were suggested for use by subject-matter experts. State and local staff can then use this information to consider the use of tools in the context of their screening and assessment needs and objectives.
What Screening Tools are Used to Identify Disabilities OR Unobserved Barriers to Work?
Although screening and assessment are on-going and dynamic processes (as discussed further in Question Six), our efforts to identify tools focused on those that are currently being used, or that can be used, by TANF agency staff. Additionally, it bears repeating that this review of tools is not intended to be an exhaustive review of screening, assessment, or identification tools used in all states.56 It is also not intended to suggest the use of particular tools. Instead the objective was to identify examples of tools used in TANF agencies and to expand thinking by states and localities that have not established or are considering changes to their screening or assessment approaches. Overall, there are few studies and even fewer evaluations of these tools' effectiveness, particularly when used in welfare to work programs.57
Appendix A provides profiles of the screening and assessment tools we identified. The actual instruments are not included because many tools are copyrighted or, in some cases, our state contacts were not comfortable with the distribution of their state-developed tool.58 For each instrument identified, the profile notes the following key features:
barriers identified;
number and types of questions (form and content);
target population;
methodological information;
notes about implementation (i.e., time required, self-administered, administered in an interview setting);
cost (of purchasing necessary tools);
source or publisher; and
states known to be using.
While the profiles describe key features of the instruments, they do not fully capture the variation in wording of the questions, perhaps one of the more distinctive features of each instrument. Some questions carefully inquire about the experiences considered characteristic of an individual with a particular barrier. Others simply ask whether or not a barrier exists. Still others do not include questions at all. Instead, they provide a topical interview guide, leaving it to the interviewer to determine appropriate questions given the client and the ensuing conversation. Such a guide may or may not be considered a screening or assessment tool by its users and other observers but is included here.
The tools we identified also vary in how they are administered. The majority are designed as paper and pencil instruments and are meant to be self-administered (with some offering computer administration options). Others are meant to be completed in an interview setting, where a staff person poses questions and records responses. The paper and pencil tools often include 'yes' or 'no' or scaled questions ranging in length from one question to more than 75 questions. Tools designed to be completed in an interview setting may be 'yes' or 'no' or scaled questions but are also more likely to be short-answer, open-ended questions. We also identified a couple of tools that are notifications to clients about their rights that require an affirmative acknowledgement of a barrier and, in so doing, serve as a screening tool.
Each state or locality must determine which tool best meets their needs.
We present this diverse set of tools to document the array of screening and assessment tools that exist and so that states may consider which approach best meets their needs. Although, as illustrated in this section, some tools are more widely used than others, this should not be considered an endorsement of a particular tool or approach. Each state or locality must determine which particular barrier (or combinations of barriers) they wish to identify and consider tools or approaches that best meet the needs of their clients and capacity of their staff.
56 The American Public Human Services Association has undertaken a 50-state survey that includes identifying the screening and assessment tools in use in TANF agencies.
57 We also present a few screening and assessment tools that were recommended for use with TANF recipients by subject matter experts, although like the examples of tools used by states, little is known about their ability to accurately identify barriers among TANF clients.
58 In some cases, this was because the state is in the process of revising its tool.
What tools are used to identify multiple barriers to work?
Because many clients face multiple barriers to employment, some states have developed tools intended to identify several barriers.
Although TANF agencies have always screened for barriers, there is now greater interest in tools to assist in identifying a wider range of barriers to employment than might have been included in existing assessment tools. Because many welfare clients do not face a single barrier to work, some states have developed a single tool that is intended to identify several different barriers. In some cases, states are adding questions that probe for the existence of a possible barrier to employment but do not go so far as to incorporate questions from a targeted screening tool or questions commonly used by experts in a specific field. Other states are incorporating questions from a separate, targeted screening instrument into their existing employability assessment tool.
For example, Rhode Island's "Family Needs Assessment" collects information about immediate subsistence needs (i.e., housing, utilities, food, health-care needs). This tool also includes an item requiring the Social Caseworker to indicate whether or not a client uses alcohol or drugs and if such use prevents successful participation in required activities (in this case the worker is instructed to refer the client for professional/medical evaluation to determine the best treatment plan). As discussion points, this document lists the four questions from the CAGE, a well-known substance abuse screening tool. The Family Needs Assessment also has discussion questions
regarding the need for mental health services.
Montana also uses a single assessment tool to collect information on a variety of different barriers to employment including substance abuse and mental health problems, learning disabilities, limited English proficiency, legal issues, health conditions, availability of transportation and child care, and existence of an employment goal.59 Although this tool collects information about employment experience and the client's ability to search for work, it differs from Rhode Island's tool in that it is much shorter and collects responses to only 'yes' or 'no' questions, not detailed information about past employment or educational levels.
Washington uses a combination of tools that address a range of issues. During the initial intake interview with Department of Social and Health Services (DSHS) WorkFirst case managers, clients not only complete eligibility related requirements, but are also asked a number of questions regarding their ability to participate in Washington's WorkFirst program. Questions range from basic employment and education histories and child care and transportation needs, to questions about physical, emotional, or behavioral barriers to obtaining and maintaining a job. Barriers might include health conditions, domestic violence (discussed under the heading of "Family Support"), substance abuse problems, and literacy or learning problems. Based on responses to these questions, the case manager offers follow up questions and can also choose to involve a DSHS social worker.60 Social workers use a different tool that covers many of the same issues and is also administered in an interview setting. This "Intensive Services Assessment" is divided into 16 sections that collect information ranging from basic information about the client, how to contact her, and her education and employment history to detailed questions about her health, family planning, parent-child relationships, domestic violence, and other issues.
59 As of March 2000, Montana was in the process of revising this tool.
60 "Social worker" is the term that is used; however, individuals are not required to be licensed social workers or hold Master's of Social Work degrees.
What tools are used to identify substance abuse?
By far, the most commonly noted specialized tools used to identify substance abuse problems are the CAGE and the Substance Abuse Subtle Screening Inventory (SASSI). These tools were most commonly mentioned by both TANF agencies screening for substance abuse problems as well as substance abuse experts. The CAGE's popularity is likely due to its ease of administration. A short tool, it consists of only four questions that require no training to administer. Not surprisingly, the CAGE was found to be used widely both as a stand-alone tool and incorporated into tools designed to identify multiple barriers to employment. Originally developed for individuals already known to be drinking, the CAGE is designed to assess whether alcohol use is a problem. The CAGE is currently being used more broadly in welfare offices and by others to identify whether or not an individual is using alcohol or drugs. Some in the substance abuse field expressed concern about TANF agencies using the CAGE this way, given this was not its intended purpose.
The SASSI is also popular for its ease of administration. Although the SASSI (78 questions) is a longer tool than the CAGE (four questions), it can be administered quickly and easily. Unlike the CAGE, administration of the SASSI requires training and comes at a cost to agencies.
Despite the popularity of the CAGE and SASSI, there are a number of other tools that can be used to identify substance use. The U.S. Department of Health and Human Services, Center for Substance Abuse Treatment created the Simple Screening Instrument for Alcohol and Other Drug Abuse.61 The Simple Screening Instrument is 16 'yes' or 'no' questions regarding consumption, problem recognition, experience with adverse consequences, and awareness of a past or present problem with alcohol and other drugs, among other things. According to the implementation guidelines, it can be used by a diverse group of outreach workers, paraprofessionals, and professionals in the fields of both alcohol and drug abuse and infectious diseases.
According to the recent report by the National Center on Addiction and Substance Abuse (CASA), the State of North Carolina is actively attempting to identify substance abusers from among the TANF population. The North Carolina Department of Social Services has entered into a process of using both TANF staff and Qualified Substance Abuse Professionals62 to assist with the identification of substance abuse problems. All TANF applicants and recipients are supposed to be screened for alcohol and substance abuse problems. County offices determine which staff will conduct the initial screening (either Department of Social Services staff or Qualified Substance Abuse Professionals) and the procedures that work best for their office. The initial screen can be conducted using one of two other types of substance abuse tools: the Alcohol Use Disorder Identification Test (AUDIT) or the Drug Use Questionnaire (DAST-10). If either of these tools indicates a problem, the client is referred to the QSAP for in-depth assessment using the Substance Use Disorder Diagnostic Schedule (SUDDS-IV).63
61 More recently, the Center for Substance Abuse Treatment has undertaken an effort to prepare a Technical Assistance Publication addressing screening and assessing for substance abuse problems among TANF clients (forthcoming).
62 Qualified Substance Abuse Professionals are employed by local mental health authorities but in some cases are located in DSS offices.
63 National Center on Addiction and Substance Abuse August 1999, pp. 39-40.
What tools are used to identify learning disabilities?
Washington and Kansas stand on the forefront of state efforts to develop and rigorously test screening tools that can be used to identify the possibility of a learning disability among TANF clients.64 The Kansas tool has been validated for use with TANF clients, and, although it contains more questions than the Washington tool, it requires relatively little time to implement and score. In Kansas, all TANF clients who are work program participants are screened for learning disabilities. If the screen indicates the likelihood of a learning disability, the individual is referred for further assessment, often by the Vocational Rehabilitation program or in some cases through a local mental health or education provider.
We identified two tools designed to screen for learning disabilities among TANF clients.
The Washington tool is a short, 13-item screen that was validated for use with TANF clients. It is intended to identify individuals who potentially have a learning disability but is neither an assessment nor a diagnostic tool. A number of states have adopted Washington's tool due to its ease of administration. For example, Minnesota was attracted to Washington's tool because it had been rigorously tested and would be easy for contractors to implement. Services in Minnesota, including case management, employability planning, and screening for learning disabilities, are provided through a number of decentralized service contractors.65
64 The National Institute for Literacy (NIFL) has also undertaken an effort to assist literacy programs enhance services to adults with learning disabilities. Although not specifically targeted for TANF recipients, NIFL's series Bridges to Practice offers a review of tools used to identify learning disabilities and offers a training curriculum for literacy professionals.
65 However, TANF officials in Minnesota indicated problems with inconsistent implementation of the tool, given the number of service contractors and their varying processes. This is but one challenge associated with working with partners, discussed further in Question Seven.
What tools are used to identify victims of domestic violence?
Many states are developing tools and other methods to screen for domestic violence, perhaps in part due to prevalence estimates regarding domestic violence and the adoption of the Family Violence Option.66 However, our review did not identify any non state-developed tools intended to screen or assess for the existence of a domestic violence situation in a TANF family.
For example, Louisiana uses a one-page document to notify welfare recipients of their right to claim "good cause" due to domestic violence. In claiming good cause, TANF recipients not only disclose their domestic violence situation but can then receive an exemption from work requirements. Filling out the form is voluntary and confidential. The form also gives examples of abuse and tells the client to ask the case manager for more information about services.
Montana requires clients to fill out a multi-barrier tool (described earlier) and if the results of this screen are positive, they are asked to complete a more detailed tool - the Domestic Violence Screening Questionnaire. This tool was developed by the state's Domestic Violence Coalition for use in TANF offices and focuses specifically on domestic violence. If a welfare client answers 'yes' to one or more questions on this specialized tool, they are referred to a DVC counselor for appropriate services.
Oregon's system of identifying domestic violence is quite extensive and Oregon was called a "model state" by one expert. Oregon has a comprehensive system including several tools that utilize different approaches to screen and assess welfare clients for domestic violence issues - three are profiled here.67 Domestic violence is discussed several times throughout the application process and each of the tools has a different purpose and is used at a different point in the process. There is a Reference Card for the caseworkers to use with brief information about how and where to screen a client, safety questions, the referral services available, and behavioral clues to observe. An Interview Questions tool provides caseworkers with suggested questions to ask at each stage of a conversation regarding how to: establish trust, broach the subject, identify patterns of abuse, assess the level of risk to the children, and establish the woman's history of seeking help. Finally, an optional Safety Assessment was designed to make a general determination about the safety of the client and her children. It provides caseworkers with suggested questions meant to be asked in the office when the abuser is not around.
Domestic violence experts emphasized the importance of the environment in which screening is conducted.
Domestic violence experts interviewed did not recommend any tools for use with TANF clients but emphasized that the environment in which screening is done is very important. One expert said that the environment in which domestic violence issues are addressed should be a safe environment where clients are informed about what happens if they decide to disclose domestic violence. Caseworkers, in turn, need to know what to do if a client confides that they are a victim of domestic violence.
66 For additional information on state approaches to identifying and addressing domestic violence, see Burt, Martha, Janine M. Zweig and Kathryn Schlichter. Strategies for Addressing the Needs of Domestic Violence Victims within the TANF Program. Washington, DC: U.S. Department of Health and Human Services, June 2000.
67 Virginia is working to publish a collection of screening tools including Oregon's. See State of Virginia, Department of Human Services. Compendium of Screening Tools (Draft), undated.
What tools are used to identify mental health problems?
Several states screen welfare clients for mental health problems as part of a multi-barrier screening tool. Among the states reviewed, we found only two states or localities using separate, targeted tools to screen for mental health problems. Mental health experts we interviewed identified several standard tools that are used by trained, clinical professionals to assess people for mental health problems.However, none of the mental health experts we interviewed believed these tools should be used by laypersons in a TANF agency. In fact, experts said that standard tools should only be used by clinically trained professionals. Examples of these may include, but are not limited to the Beck's Depression Inventory-II (BDI-II), the Posttraumatic Stress Diagnostic Scale, and the Zung Depression Scale.
Some mental health tools must be administered by trained professionals.
The BDI-II has 21 scaled questions, must be administered by someone with a Master's degree, and be scored and interpreted by someone with a Ph.D./Ed.D. The Zung Depression Scale is 20 scaled questions and also requires a clinical professional or licensed social worker to administer. The Posttraumatic Stress Diagnostic Scale, on the other hand, is 49 'yes' or 'no' and scaled questions and requires only that it be administered by someone with a Bachelor's degree in psychology or education or a closely related field.
In New Jersey the Divisions of Family Development and Mental Health Services within the Department of Human Services, have initiated a pilot program funded with TANF dollars to identify TANF recipients in one county who have mental illnesses and need related services to help them enter the workforce. The pilot program involves the county welfare agency and two mental health providers who work as a team to identify TANF recipients who have mental illnesses, assess their clinical needs, and to link them to mental health services and a supported employment program to facilitate entry into the workforce. A twelve-item instrument was developed for use by county welfare case managers to assist them in identifying customers who could benefit from the pilot program.
In Portland, Oregon all new TANF applicants screened for mental health and substance abuse problems through participation in an "Addiction Awareness Class." During this class, TANF clients are asked to complete the Zung Depression Scale. The results of the Zung are scored by an onsite alcohol and drug clinical assessment specialist. The specialist informs both the client and the client's caseworker in writing about the test results and the next steps to take.68
68 National Center on Addiction and Substance Abuse 1999.
What are the DSM IV and the Asam Criteria and How are They Used?
In our review of screening and assessment tools, we found two diagnostic criteria manuals - the Diagnostic and Statistical Manual - IV (DSM IV) and the American Society of Addiction Medicine (ASAM) Patient Placement Criteria - 2. The DSM IV and the ASAM criteria are not tools per se and are applicable to both mental health and substance abuse problems. Experts indicated that the DSM IV and ASAM criteria should only be used by a trained clinician and not by a layperson.
The DSM IV is a descriptive classification system published by the American Psychiatric Association and, as a system, is used to assess clients (but it is not an assessment tool per se). It provides clinical guidelines to tell the clinician whether symptoms are present and provides a list of symptoms. Clinicians rely on these guidelines in making diagnoses, often for medical insurance purposes. However, the application of these guidelines may vary their application by clinicians.
The ASAM criteria provides two sets of guidelines, one for adults and one for adolescents, and five levels of service for each group. The levels of service are:
Early Intervention
Outpatient Services
Intensive Outpatient/Partial Hospitalization Services
Residential/Inpatient Services
Medically-Managed Intensive Inpatient Services69.
For each level of care, a brief overview of the services available by severity of addiction/illness and related problems is presented. Also presented is a structured description of the settings, staff and services, admission, continued service, and discharge criteria. The terminology used in ASAM has been updated to be consistent with the most recent language of the American Psychiatric Association's DSM IV.
In some states, the DSM IV and ASAM criteria are being used in relation to TANF either onsite or offsite. Clinically trained professionals - such as staff holding Masters of Social Work degrees - co-located onsite in TANF offices may use the DSM IV or ASAM criteria after clients have positively screened for mental health or substance abuse problems using one of the multi-barrier tools. Alternatively, a TANF client who is referred for services may receive a further diagnosis from an offsite clinical professional using the DSM IV and ASAM. Finally, the DSM IV or ASAM could be used as the foundation or guidelines for developing screening or assessment tools.
Officials in Utah specifically mentioned the use of DSM IV and ASAM criteria when the initial, multi-barrier screening tool suggests the possibility of a mental health problem. If a TANF client screens positive for mental health issues from the multi-barrier tool, the client is referred to a credentialed social worker. Social workers are located throughout the state in TANF offices and apply the DSM IV and the ASAM criteria. If a client is diagnosed as positive for substance abuse or a mental health disorder, they are referred to an offsite provider for further assessment and treatment.
69 American Society of Addiction Medicine (ASAM). Second Edition of Patient Placement Criteria, Annapolis Junction, MD, 1996.
What Else Should Be Considered About Tools ?
Several issues should be considered when developing a screening or assessment approach for TANF recipients. Many of these are mentioned in other sections of this report. Here we revisit some issues and raise others associated with developing, selecting, and using screening and assessment tools.
Where should we seek information and what partners should be involved?
As discussed in greater detail in Question Seven, other state and local government agencies or community-based organizations that specialize in a particular barrier to work provide a valuable source of expertise to TANF agencies. Partnerships between TANF agencies and other organizations or experts can yield information about both a particular barrier to work (e.g., substance abuse) or tools that can be adapted for a TANF agency's use.
Partnerships with other agencies can be a valuable source of information for TANF agencies considering developing a screening tool.
For example, in Tennessee the state TANF agency collaborated with four other agencies in developing their multiple barrier screening tool. The YWCA provided input on domestic violence issues. The Bureau of Drug and Alcohol Service within the State Department of Health offered substance abuse expertise. Community mental health centers were involved as contractproviders, and the University of Tennessee's Center for Literacy Studies provided input on learning disabilities. Collaborating with four additional agencies is a challenging prospect, requiring five different agencies to "speak the same language" and make decisions jointly. While Tennessee has made this five-way partnership work for them, even partnerships with one other agency are likely to be a valuable source of information for states and localities considering developing a screening tool.
What barriers should a tool screen for?
Although in this report we focus on substance abuse and mental health problems, learning disabilities and domestic violence situations, states and localities must decide which health conditions, disabilities or personal circumstances (or combinations of these issues) that inhibit clients' transitions from welfare to work they wish to address in their screening or assessment efforts. As discussed in more detail in Question Two, some states receive guidance from the state legislature or from other organizations specializing in a particular issue area. For example, New York law requires that the TANF system screen for substance abuse problems. Several states we spoke with noted that state and local domestic violence coalitions actively encouraged the TANF agency to develop approaches to screening or assessing for domestic violence situations.
While states and localities often must respond to these influences, any data that states may have about prevalence of disabilities or barriers to work among the TANF population in their state, locality, or nationally may help them decide which barriers should be the focus of identification efforts. In addition to prevalence estimates and state or local data, anecdotal evidence from caseworkers or other front line staff about prevalence might provide useful guidance about what issues are preventing people from obtaining work within the required time limits.
In any case, states must proceed cautiously, being sure to consider how a new screening tool will fit into their TANF client flow and what necessary services must follow the identification of a barrier to work or a disability. Some individuals interviewed for this study indicated that screening for a particular barrier should only be conducted if the TANF agency can subsequently offer services to address the problem. The length and format of the tool should also be considered. For example, using shorter tools or interviews may save time and resources. On the other hand, caseworkers may find that taking the time to establish a rapport initially will save the system time in the long run by preventing client barriers from being identified later in the process of moving to work.
How should the questions be worded and in what context should they be asked?
States and localities can get many ideas for questions and wording from existing tools. We heard varying opinions about whether clients should be asked directly about a problem or asked about how a problem impacts the ability to function. For instance, a question could be worded: Do you have a drinking problem? or Have you ever been late for a job because of drinking? Some experts we interviewed said, if asked about an activity directly, many people will be less likely to be truthful because they are used to being asked the question in this form. However, it was also noted by one expert that asking questions directly is more likely to elicit a truthful response in situations where the respondent believes there is nothing wrong or atypical about her behavior.
In general, experts we spoke to favored asking questions in the context of moving TANF clients to work rather than gathering unnecessary details about a disability or barrier to work. In particular, domestic violence experts suggest that domestic violence questions should be asked only as they pertain to the ability to obtain employment, child support, transitional housing, or education.70 They suggest avoiding asking about specific aspects of the violence such as punching, slapping, or kicking. As stated earlier, asking only about barriers as they limit or prevent work is consistent with the language of the ADA which stipulates that "a public entity may not make unnecessary inquires into the existence of a disability."71
Welfare clients should also be encouraged to self-disclose a problem at any point during the process of receiving welfare. Providing a private space, although difficult in many offices, may make a client more likely to reveal a problem more easily. Experts also emphasized the importance of trust and developing rapport with a client. While this may not always be possible when caseworkers have high caseloads, repeating a screening tool later on in the process may make clients more likely to reveal a problem.
70 Raphael and Haennicke 1999.
71 U.S. DOJ undated.
What resource implications should be considered?
For a state not currently screening and assessing TANF clients for barriers to work, developing its own tool is a considerable undertaking. States will have to estimate the additional resources that will be required to design, develop, and validate a tool that might not be required if a state uses a professionally developed tool or relies substantially on input from partners or other states. Using a professionally developed tool likely requires fewer resources than developing a new tool from scratch. That said, although the staff and coordination resources will certainly be fewer, some standard tools are copyrighted and must be purchased or require investments in training and scoring materials as well as the tools themselves.72
TANF and partner agency staff training requirements (discussed in Question Eight) will vary depending on the tool selected and may not differ significantly from the training costs associated with a state-developed tool. Nonetheless, resources associated with training efforts can be considerable and should be a part of the decision process. Additionally, some standard tools are designed to be administered or scored by a professional with clinical training. In this case, the TANF agency may need to invest significantly in the upgrading of staff skill levels or purchase this expertise through contracts or other means, if adopting this approach.
72 Where this information is available, we have incorporated it into the tool profiles in Appendix A.
What methodological considerations exist?
Several methodological considerations bear mentioning in the use of screening and assessment tools. For example, to achieve the best results it is important to ensure that the questions are designed for the population being screened or assessed. This is particularly important if adopting professionally- or externally-developed tools as many of these were not originally designed specifically for welfare recipients.73
Although concepts such as validity and reliability of instruments may be more meaningful to researchers and test designers than TANF agency staff, they should also be considered if TANF agencies place high expectations on the ability of screening and assessment tools to identify barriers.74 To the extent such tools are used as a preliminary screen, expectations may not be high (however, this approach does carry other implications, such as resources expended to assess based on inaccurate screening mechanism and time spent being assessed for a barrier that may not exist).
Consideration should be given to methodological aspects of tools if high expectations are placed on the tool's ability to identify barriers.
Although few TANF agency officials we spoke to mentioned validity and reliability, some suggested that their existing efforts to identify barriers were not yielding expected results. While this could be attributed to a wide range of causes, using a tool that is not designed for use with TANF clients may be one such reason. This should be of concern to TANF agencies expending funds on screening and assessment efforts and points to the need for evaluation of these approaches.
Administering tools as designed is another methodological consideration. For example, some tools are intended to be implemented in an interview setting, with the interviewer obtaining a response to the question posed before moving on to the next question. This allows the interviewer to ensure answers are obtained and that the respondent cannot look ahead at subsequent questions that may affect the way she answers the current question. If a tool intended to be administered through an interview is self-administered, the respondent may observe in subsequent questions
incentives to provide inaccurate responses. The environment in which a tool is administered is also a consideration. For example, if the tool was designed to be administered one-on-one, altering this setting (for example, administering during a group orientation) may affect assessment outcomes.
73 In the tool profiles in Appendix A we have indicated the target population for the professionally-developed tools.
74 Reliability is whether a tool will give the same scores when administered twice to the same person (before the measured traits have changed), and validity is whether a tool actually measures the characteristics it is designed to measure.
Question Six: When should screening or assessment occur?
There are a number of points in a client's TANF experience when screening and assessment can occur. However, most TANF agency officials we spoke to noted that despite these discrete events, barrier identification is an on-going process. In addition to specific points in time when attempts are made to uncover barriers, the employment objectives of TANF encourage TANF agencies to continue focusing on barriers to employment until each barrier is identified and addressed (or the individual leaves welfare).
Early identification of barriers allows more time to be spent addressing such barriers.
Time limits and work participation requirements provide incentives for screening to be conducted as early in a client's experience as possible. By identifying barriers early, agencies can spend more time and resources focusing on assisting a client address or overcome her barrier as she attempts to transition to work. Earlier identification can also save valuable resources otherwise expended if a client is referred to activities she cannot successfully complete because of an unobserved barrier. Substance abuse experts note that identifying this barrier early in a client's TANF experience may allow the agency to address the problem in its early stage, possibly before it develops into an addiction. TANF agencies must weigh these advantages against the cost of referrals of individuals who are ultimately determined to not have a barrier (referred to as "false positives").
Of course, efforts to identify a barrier early in a client's TANF experience do not guarantee that the client will successfully address the barrier or obtain and maintain employment. Many unobserved barriers cannot be easily overcome and require on-going efforts to accommodate the challenge. Additionally, clients must be willing and able to participate in services designed to address their barriers and follow through on prescribed courses of action. Finally, transitions to work are challenging for any welfare client and particularly so for a client facing one or more of the unobserved barriers to employment discussed here. Therefore, program administrators and staff may need to prepare strategies that allow time for small steps toward progress as well as set-backs.
"Work First" approaches rely on the labor market as the first screen of a client's job readiness.
It should be noted that "Work First" program approaches adopted by many states may not be consistent with early identification of barriers. Such approaches rely on the labor market to be the first screen of whether or not a client is job-ready instead of incorporating formal screening or assessment early-on. In these situations, clients are likely to be required to participate in work or job search activities, and assessment may be conducted if they fail to find or keep a job.
Below we describe common steps in a generic, TANF client flow process (see Figure One) and note how screening or assessment might be conducted at these points. These steps include intake/eligibility determination, employability planning, and referrals to assessment and services (including non-compliance with program requirements). However, Figure One does not represent all of the possible steps in a TANF clients' experience, nor does it illustrate all of the possible combinations of these generic steps. States and localities use these steps in different sequences, depending on local policies and program approaches. Further, many localities individualize services such that no two clients follow exactly the same path. This discussion is intended to illustrate how screening may occur at these points, with examples of how some states or localities we talked to implement their screening and assessment approaches across these steps.
Figure 1: Possible Screening or Assessment Points in the General TANF Client Flow
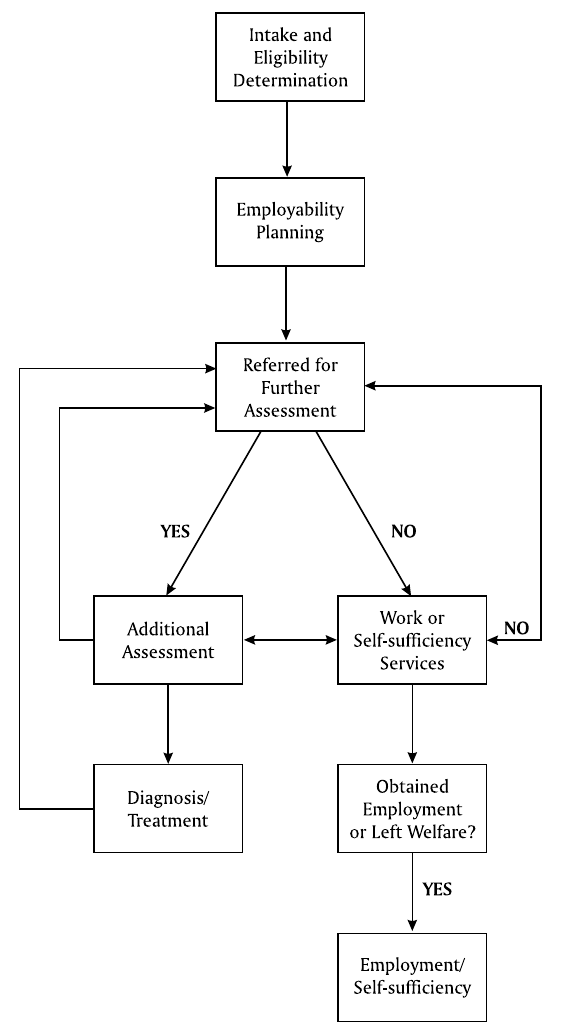
What are the Common Pointsin a Client's TANF Experience Where Screening OR Assessment Could Occur?
Intake/Eligibility Determination. Generally, a client's first interaction with the TANF program occurs at the point of application and eligibility determination. In some states, there are pre-eligibility requirements - often related to job search or diverting clients from public assistance to other services. These pre-eligibility activities might result in the identification of barriers to successful job search or might also include screening for specific, unobserved barriers. It is also possible that applicants, or new TANF recipients, are required to attend an orientation.
Orientations typically include an overview of program requirements and may offer clients an opportunity to disclose barriers to participation. Orientations might also include the collection of additional information about the individual and her family, but it may or may not include an assessment of barriers to employment. It is sometimes at this step that information is collected to determine if the client should be exempt from work participation requirements. Because the focus of this step in the process is eligibility determination, any information gathered at this point is generally provided as input into the employability planning process.
TANF Employability Planning. The next phase of a non-exempt client's TANF experience is usually focused on employability and service planning. Generally, at this point the client is assigned a case manager who retains ongoing responsibility for service planning and monitoring the client's progress toward meeting the goals outlined in a service plan (sometimes called an employability development plan, self-sufficiency plan, or individual responsibility plan). 75 It is during the employability planning process that the bulk of information about the individual - including education and work history, family supports, and barriers to employment - is collected. If a state or locality is using a screening or assessment tool in an effort to collect information and uncover barriers to employment, it is likely completed at this step in the process.
During the employability planning process, the TANF case manager is developing a relationship with the client. The client and case manager generally have on-going discussions about establishing and meeting, as well as barriers to achieving, work and self-sufficiency goals. Throughout this process, the case manager continues to observe behavior, noting clues to unobserved or previously unidentified barriers. It is also throughout this process that clients have opportunities to self-disclose barriers. If behavior or disclosure indicates a potential barrier, it is at this point that the case manager might use a specialized tool designed to assess a particular unobserved barrier. A screening tool used with all clients is likely to be administered during the employability planning process, as well. It is also at this point that the case manager may rely on specialists to provide further insights into barriers to employment.
Case managers use information during the employability planning process to develop service plans.
Using the information collected through the employability planning process, case managers work with clients to develop service plans that guide future steps. Referrals to additional assessment services or work and self-sufficiency services are outlined in these plans.
Service Referral. Employability plans commonly outline referrals to other services clients are supposed to pursue. In some situations, the plan might indicate that the client is to obtain further assessment or diagnosis of a potential barrier to employment. For example, if screening conducted during the employability planning process indicates the possibility of a substance abuse problem, the client may be referred for more in-depth assessment or diagnosis. If barriers to employment such as substance abuse and mental health problems, domestic violence situations, and learning disabilities are not identified (or not considered to be a barrier to employment), the client is likely to be referred to work-related services such as a job search workshop or a subsidized work activity.
Although the primary purpose of work-related services is not to conduct further assessment, these services might include a formal assessment for barriers to employment. Participation in these work-related services might also serve as a screening mechanism to uncover unobserved barriers. As program staff monitor participation and assess clients' abilities to fulfill program requirements or obtain employment, they may find that the client faces a previously unobserved barrier. Where the client is unable to successfully complete the assigned activity or is non-compliant due to the existence of an unobserved barrier, program staff are likely to refer the client back to the TANF case manager for additional assessment or for referral to another organization that can provide further assessment. This feedback continues the on-going assessment process, guided by the TANF case manager.
Non-Compliance with Service Referral/Program Requirements. As illustrated with the generic client flow described above, there are numerous steps that clients follow as they progress through the TANF system. If at any point they fail to complete a required step (i.e., attend a mandatory orientation, keep an appointment for an assessment), or participate in a required activity (i.e., job search or work readiness workshop) the client may face a sanction. Although sanction policies vary across states, generally, this financial penalty is intended to motivate a client to change her behavior and comply with program requirements. Non-compliance may also serve as a clue or red flag that an unobserved barrier is prohibiting compliance. When considered in this way, non-compliance offers another opportunity at which TANF and partner agency staff can screen or assess for a potential barrier to employment.
75 Some states have moved to an integrated worker model in which eligibility determination and employability planning functions are performed by the same staff person. In these states, eligibility and orientation functions described above might be integrated with the employability planning process.
How do States and Localities Conduct Screening and Assessment at These Different Points in the TANF Client Flow?
States and localities combine these general steps differently, often tailored to the needs of each client. Below we provide a few examples to illustrate how some of the states and localities we reviewed incorporate screening and assessment into the general client flow. However, each state or locality must consider its own client flow, and how to effectively incorporate screening or assessment efforts within the particular combination of steps that comprise their TANF client flow.
Washington has combined eligibility and employment planning functions with a single staff person, a WorkFirst case manager. During the process of working with the case manager, clients are screened for a range of barriers to employment using the Virtual Interactive Evaluation Worksheet (VIEW). If, through self-disclosure or completion of the VIEW, the client indicates she has a disability, barrier to employment, or is considered "hard-to-serve" by the case manager, a social worker may be assigned to the case.76 The social worker will conduct further assessment using the Intensive Services Assessment and recommend referrals to appropriate services. If the case manager does not identify barriers to employment that cannot be overcome by job seeking assistance, the client is referred to a job search workshop. If a barrier is uncovered during the job search workshop, the client may be referred back to the case manager for additional assessment or with the suggestion that the client be referred to specialized services to address her barrier (i.e., mental health counseling or substance abuse treatment). If a client fails to participate in prescribed activities and is sanctioned, a social worker is assigned to the case to conduct further assessment of the barriers to participation.
Washington and Utah use specialized staff within the TANF agency to assist with barrier identification.
In Utah, Employment Counselors administer the Assessment Interview Guide (AIG) during the employment planning process. The AIG is an 8-page tool that explores a range of issues including an employment goal, work history, education and training, family situation, domestic violence, emotional or psychological issues, drug or alcohol use, legal issues, physical health, and resources. Similar to Washington, Utah has another classification of specialized staff in the TANF agency to assist with barrier identification. If, based on the AIG, the employment counselor determines the client can benefit from further assessment, the client may be referred to a social worker.
Social workers in Utah, who have Masters of Social Work degrees, rely on their clinical interviewing skills to elicit self-disclosure of barriers. Social workers may also use other assessment tools such as the SASSI or rely on their understanding of diagnostic criteria from the ASAM or DSM-IV. Officials in Utah noted that using credentialed social workers for this additional assessment provided several advantages. First, social workers have more training on assessment than employment counselors and can better determine barriers to employment. Second, social workers "speak the same language" as many of the organizations or treatment facilities to which clients are subsequently referred so they can effectively communicate with partners about services for TANF clients. Finally, the social workers help to facilitate a continuum of services bridging the gap between employment counselors and service providers.
Other states use experts from outside of the TANF agency to assist with assessment and service planning.
Kentucky and Tennessee also have specialized staff who assist TANF staff in identifying barriers and facilitating referrals. In these states efforts are underway to hire experts from outside the TANF agency to assist with assessment and service planning. Kentucky has established pilot sites in eight designated counties under its Targeted Assessment Project that are provided with Assessors who are experienced masters-level clinicians. The assessors are employees of the University of Kentucky, Institute on Women and Substance Abuse which has a contract with the State of Kentucky for this pilot effort. Assessors serve as advisors on screening and assessment processes, assess clients referred by TANF staff, and help establish community linkages to facilitate services to TANF clients with barriers such as mental health and substance abuse problems, among others.
Tennessee has established a Family Counseling Program through which 11 contractors provide specialty workers - Family Service Counselors (FSCs) - to TANF offices. This program was developed because of a recognition that the existing mix of services might not meet the needs of recipients remaining on Families First, the Tennessee TANF program. That is, Tennessee decided it needed to provide additional counseling and assessment services to address the needs of less job-ready TANF recipients. The FSCs are intended to alleviate the burden of screening and assessment from TANF caseworkers who are not trained on how to conduct in-depth assessments. Although TANF caseworkers will continue to observe behavioral clues and ask questions that elicit self-disclosure, they may refer clients on to FSCs if additional assessment seems warranted. A client will also be referred to an FSC if she is unable to complete work activities, cannot retain employment once placed, or is determined to need further assessment by a service provider (such as an adult basic education instructor). FSCs will conduct further assessment for substance abuse, domestic violence, mental health problems, learning disabilities, child health or behavior problems, and/or other family relationship problems.
Other states rely on contract agencies as a referral resource for clients who need additional assessment. For example, in Arkansas, after financial eligibility is determined by an eligibility worker, clients are screened by TANF caseworkers for barriers to employment using the Transitional Employment Assistance Skills, Employability & Intake Assessment Background Information form. Staff also use a "desk guide" to assist in the identification of behaviors or characteristics associated with substance abuse. If during this screening process a substance abuse or mental health problem is identified, the client is referred to the Department of Health or other local providers for additional assessment or services. Caseworkers also use the Learning Needs Assessment developed in Washington State to screen for learning disabilities. If the learning disability screen is positive, the client would be referred to Rehabilitation Services (the Vocational Rehabilitation program).
In Denver, Colorado, caseworkers screen clients using a multi-barrier tool as part of the Family Counseling Program within the county TANF agency. If a client is thought to have a disability or an unobserved barrier to work based on the screening, the client is referred to one of 13 different community-based organizations with contractual relationships with the Denver County TANF agency. Services available to referred clients include: mental health counseling services for individuals and families, substance abuse treatment, and legal advocacy, shelter, and non-residential services for victims of domestic violence.
76 "Social worker" is the term that is used; however, individuals are not required to be licensed social workers or hold Master's of Social Work degrees.
Question Seven: Who should conduct screening and assessment?
Based on the interviews conducted with TANF agency officials and subject matter experts, there seems to be a consensus that, generally, the most appropriate role for TANF agencies is to screen for barriers to employment and facilitate referrals to organizations with expertise diagnosing and addressing that barrier. Because TANF agency staff experience levels vary, few believe that TANF agency staff should be primarily responsible for determining that an unobserved barrier exists. For example, experts strongly believe that the diagnosis of a mental health or substance abuse problem should be conducted by a trained clinician or medical professional. However, TANF agency staff can play a pivotal role by screening for such barriers and referring those who screen positive for further assessment and diagnosis.
What Role Can TANF Agency Staff Play?
Observers are quick to note that, in many states, TANF caseworkers are former eligibility or income maintenance workers with little experience with case management and barrier identification. Staff hired to perform eligibility functions are required to have high levels of attention to detail and an understanding of the complex budgeting requirements required to determine if a family is eligible for TANF. This differs markedly from the skills required to conduct case management, including developing relationships with clients that foster trust and facilitate disclosure of barriers.
The challenges associated with former eligibility workers assuming new responsibilities for case management and employment planning are significant and common across states. For these staff, their focus has historically been determining accurate benefit amounts and in some cases processing sanctions for non-compliance. Assuming barrier identification and service planning responsibilities is a dramatic change.
As discussed in Question Four, because screening relies heavily on obtaining honest information from recipients, staff conducting screening must be able to establish rapport and a trusting relationship with the client, sufficient to allow for self-disclosure or honest responses to screening or assessment questions. If staff are primarily focused on accurate eligibility determination or sanction processing, they may have established a different (and in some cases punitive) relationship with clients that does not facilitate effective screening for barriers. Where this is the case, agency managers should consider whether or not screening for barriers is an appropriate responsibility for these staff and if so, what training or professional development opportunities should be offered.
To the extent TANF staff have experience performing needs assessments and service planning responsibilities (i.e., former JOBS case managers or staff hired with these skills), they might be well positioned to screen for unobserved barriers. Often these staff are already engaged in the case management process and have developed a relationship with recipients focused on meeting needs and service planning. In many states, such staff are responsible for collecting information about the recipient and her circumstances including barriers to employment. For these workers, the added responsibility of screening for unobserved barriers might be a natural fit.
The size of workers' caseloads may effect their ability to conduct screening and assessment.
TANF staff's ability to screen and assess for unobserved barriers may be affected by the size of their individual caseloads. Although nationwide TANF caseload declines have been dramatic, these declines often mask high individual worker:caseload ratios. The number of cases each individual worker is responsible for becomes increasingly important to consider when staff must assume new responsibilities (i.e., case management, service planning, and monitoring in addition to eligibility determination). If individual caseloads are high, it may not be possible for TANF staff, even with training, to provide the level of case management services or conduct the formal or informal assessment necessary to identify unobserved barriers to employment.
As noted in Question Six, Utah and Washington offer examples of ways TANF agencies can use their staff to conduct not only initial screening as part of employability planning, but also more in-depth assessment guided by that screening. However, despite smaller caseloads and a windfall in TANF funding, many states face hiring freezes that do not allow state government agencies to add staff with the skills necessary to identify the barriers faced by remaining TANF recipients. Still others must undertake complicated and time consuming union negotiations in order to implement changes to staff responsibilities. In this situation, states and localities may need to offer additional training or seek assistance from partner agencies.
How Can Other Organizations Assist with Screening and Assessment?
Other organizations - including other public agencies and community-based organizations - have valuable expertise that can help TANF agencies conduct or augment quality screening, assessment, and service delivery. For example, the substance abuse community has invested substantially in developing screening and assessment tools to identify substance abusers. They have worked with this population and are familiar with the issues of denial that make identification difficult. Instead of starting from scratch, there are likely valuable lessons a TANF agency can learn from the state or local substance abuse agency or local treatment facilities. Additionally, the TANF agency may be able to use welfare funds to purchase staff time or treatment services for TANF clients, thereby providing a higher level of access to expertise and services than exist solely within the welfare agency. Similar arguments can be made for the other barriers considered in this report.
What resources are available in the community?
Understanding what possible partners exist in a community requires an understanding of the community and its service infrastructure. When considering screening or assessment options, TANF agencies should assess the availability of assessment resources and barrier-specific expertise that already exist within their communities. Because TANF agencies often rely heavily on community-based organizations as service providers, they may already possess this knowledge.77 Further, other government sponsored programs also serve clients with similar barriers and may serve as a resource for TANF agencies. It goes without saying that resources in each community will vary but it should be noted that rural areas may face a greater challenge in this regard than urban areas.
In addition to identifying organizations with the desired expertise, TANF agencies must also consider the capacity of these organizations to serve as a partner. In some cases, community-based organizations are small and have few staff resources to dedicate to on-going supervision and reporting. Additionally, many organizations face limited funding, or specific program eligibility requirements, that affect service capacity and renders them unable to accept additional service referrals from the TANF agency. For example, Kansas used to rely on its Vocational Rehabilitation (VR) program to receive referrals for assessment of learning disabilities. However, because VR instituted an order of selection process that slowed the response time for some referrals, Kansas chose to contract directly with local psychologists for this service. Before assuming a partner agency can receive and serve TANF referrals, the TANF agency should explore these capacity issues with administrators and consider funding requirements associated with additional referrals, including using TANF funds to support services.
77 For many TANF agency staff, being aware of community resources is an implicit job requirement. For new staff, or where this understanding does not exist, often communities have developed resource guides, or state agencies can assist in identifying local resources.
What other agencies may be involved?
Other government agencies or providers of publicly funded services may be natural partners for TANF agencies.
Other Government Agencies. TANF agencies may find natural partners in the other parts of state government or among entities that administer publicly funded programs. For example, VR and the Department of Labor's Welfare-to-Work (WtW) grants programs offer examples of other programs with which TANF agencies may consider partnering. Both VR and laborrelated programs have considered these and similar challenges in so far as they present barriers to employment. In fact, the WtW program is not only intended to serve hard-to-serve TANF clients, but includes TANF recipients with substance abuse problems as one of its eligibility criteria.
In some cases such programs are housed within the same department or division within a state agency. Where this is the case, the fact that multiple agencies answer to the same boss and share similar objectives(albeit at a high level), potentially encourages and facilitates collaboration. In Arkansas and some other states, mental health functions are housed in the same part of the state government as public assistance. In Missouri, the Governor issued an Executive Order that requires the Department of Social Services (which houses TANF) and the Department of Mental Health (DMH; which houses both substance abuse and mental health services) to work together because of common interests and objectives. Therefore, when Missouri's TANF program administrators sought assistance in identifying substance abuse problems among TANF recipients, they turned to DMH. Because DMH includes both substance abuse and mental health services, they were able to assist in the development of a tool that screens for both barriers.
In Arizona and Rhode Island, the TANF and VR programs are housed within the same state government department. In Rhode Island, the VR program has worked with TANF to incorporate questions to screen for learning disabilities into the TANF employability planning process. If a client screens positively for a learning disability, she is referred to VR for additional services. In Phoenix, Arizona, TANF funds are used to support VR staff who work exclusively with TANF recipients. TANF recipients who are deferred from Arizona's welfare to work program are screened for VR eligibility, and if eligible, offered the same array of assessment and other services available to VR clients.78
CBOs under contract to provide employment services may also have expertise identifying or addressing barriers.
Community-Based Organizations. In addition to government agencies, non-governmental and community-based organizations (CBOs) also offer expertise with barriers to employment. Many TANF programs already rely heavily on CBOs for contracted employment services. In some cases, these same CBOs may have expertise identifying or addressing a particular barrier, and may be a valuable resource to the TANF agency. For example, homeless service providers, domestic violence shelters or coalitions, community mental health treatment facilities, substance abuse treatment organizations, adult and secondary education providers, faith-based service organizations, and others may offer TANF agencies assistance.
For example, Kansas relies on non-profit Regional Alcohol and Drug Assessment Centers for additional assessment services. Kentucky is relying on the expertise of staff the University of Kentucky to assist with the identification of barriers among TANF recipients. Through its Targeted Assessment Project, the University of Kentucky has hired highly experienced assessors who are place in TANF offices to assist with barrier identification issues.
78 Holcomb, Pamela A. and Terri S. Thompson. State Welfare-to-Work Policies for People with Disabilities: Implementation Challenges and Considerations. Washington D.C.: U.S. Department of Health and Human Services, August 2000.
What are the implications of different program philosophies or requirements?
Regardless of the type of agency, all partnerships must contend with inherent challenges. These include fostering effective communication across agencies and between staff, ensuring that program objectives and requirements are understood, and addressing differences in organizational cultures or program philosophies that affect service delivery. These differences may require TANF agencies to use some of the flexibility granted by PRWORA and may require partner agencies to adjust their approaches when serving TANF clients.
The use of different language and terminology create challenges to effective collaborative efforts.
The challenges associated with speaking the same language pervade collaborative efforts. As noted at the outset of this report, even seemingly simple terms like "barriers" and "screening" may be subject to differing interpretations. Misunderstandings or miscommunication about program requirements can also impede effective collaborations. Cross-training, discussed in Question Eight, can assist in educating staff about program requirements and philosophies and can also serve to open the lines of communication across agencies or organizations.
New Jersey offers an example of the challenges of inter-governmental collaboration. In New Jersey, the Divisions of Family Development (DFD) and Mental Health Services (DMHS) are collaborating to implement a pilot to screen TANF recipients for mental health problems. In discussing this effort, officials in New Jersey noted that the challenges arising from the fact that the two Divisions have different objectives - specifically that DFD is focused on resolving issues so that clients can obtain employment, whereas DMHS seeks longer term solutions to mental health problems. A long-term approach is not well-suited for clients facing time-limited benefits and strict work requirements, an issue that DMHS recognizes and is addressing.
Another example of agencies and programs with differing goals and not bound by similar programmatic requirements is offered by looking at TANF and VR. Although VR programs share the common goal with TANF of helping clients obtain (or return to) work, VR is a voluntary program that is not bound by limits on the duration of service or "allowable" activities. Further, eligibility for VR programs is not based on income and the program has neither the resources nor the mandate to serve everyone that is eligible for services. Working intensively with TANF recipients may require adjustments on the part of VR staff and program. The VR assessment process is much more lengthy and thorough than typically found in TANF welfare-to-work programs and there is no time limit on services. Moreover, a VR client's service package (i.e., types of services, duration, and intensity) is not shaped or constrained by considerations that are central to TANF programs such as time limits, work requirements, and sanctions for failure to meet program demands. For example, the VR program in Rhode Island is trying to accommodate TANF policies by developing service plans for TANF recipients that are considerably shorter than the typical four years for traditional VR clients.
Question Eight: What training issues are related to screening and assessment?
Regardless of the chosen approach to screening and assessment, caseworkers and other staff can likely benefit from increased awareness about disabilities and unobserved barriers to work. Despite varying progress on establishing policies and procedures, every state we spoke to has considered the issue of training caseworkers or has implemented some form of training. TANF agencies must consider training needs in light of the screening or assessment approach being undertaken, the skills of existing staff, and resources required. States and localities should also consider who needs training, whether to make training mandatory, and what incentives may be available to encourage staff to obtain training.
What Kinds of Training Should States and Localities Consider?
The kind of training needed to screen and assess for barriers to employment depends on the types and methods of screening and assessment and the skills of existing staff. By its nature, a screening tool is generally sufficiently brief and self-explanatory that it requires little or no training to use. To the extent that TANF case managers are responsible for administering assessment tools, they will likely require training on the instrument, how it should be administered, how it is scored, and how data are to be used (i.e., interpreting test scores, understanding diagnostic information).
We spoke to many states who developed training programs - generally referred to as "domestic violence 101" or "substance abuse 101" - to make caseworkers and other frontline staff aware of barriers to work. The "101" programs vary but often include teaching caseworkers what visible signs or "red flags" may indicate a problem. For instance, caseworkers may be asked to look for "red flags" such as lack of energy or feelings of hopelessness as signs of a mental health problem. Red flags for learning disabilities may be confusing similar letters such as "p" and "q," or the client misspelling common words, being easily distracted, or unable to pay attention. Red flags for substance abuse may include alcohol on the breath, slurred speech, or evidence of needle tracks, among others. This introductory training also provides an opportunity for staff to become aware of the characteristics associated with particular barriers, while also recognizing stereotypes or biases. Because few states had engaged in complicated assessment or testing processes, we heard little about training on the administration of specific tools. However, if states or localities choose to use a formal assessment tool, they should consider the training requirements associated with administering the tool.
Training can help staff become aware of characteristics associated with barriers, while also recognizing stereotypes or biases.
State TANF officials and subject-matter experts also discussed the need for training to help caseworkers who, once trained to screen or work with TANF recipients with barriers, realize they have a similar problem. Some states indicated that caseworkers who are exposed to "domestic violence 101," or have a client who is a victim of domestic violence, may realize that they have also experienced domestic violence. Thus, some states are designing part of their training to helping caseworkers deal with their own history with domestic violence, substance abuse, or another issue that may arise when they are working with recipients.
Finally, information obtained through screening and assessment efforts should also be used to determine appropriate services and/or treatment for recipients. Therefore, caseworkers need to be well informed about how to respond to a client disclosing a problem. Specifically, the TANF agency needs to have clearly outlined policies and procedures for referrals to services and/ or treatment, effects on benefit receipt and time limits, and confidentiality (discussed in more detail under Question Nine). This allows caseworkers to clearly relay these policies to the recipient before screening or disclosure so that TANF clients are fully informed of their rights and are clear about the incentives and disincentives associated with self-disclosure. Having such policies and procedures in place also allows staff to respond to identified barriers with service or treatment options.
The cost of training is an obvious consideration for states adopting screening and assessment approaches. In Missouri, a national training organization provided one pilot site mental health and substance abuse awareness training. However, the cost of this training required the state to consider conducting regional training to reach staff in rural areas in a more cost-effective manner. Other states have done this sort of professional training in one site and then have designed "train the trainer" programs where TANF staff from the original site travel around the state repeating the training for other local offices. Other states find that partnering with a local community-based organization or service providers offers a knowledgeable, inexpensive source of training.
WHO Should Be Trained?
Training is one way of ensuring that all involved in screening or assessment efforts are presented necessary information about the approach. Therefore, it is likely that TANF staff and staff of partner agencies should be trained. Several states we spoke to said that training, to the extent that it is presenting new policies, procedures, and issues, should not only be incorporated into new worker training, but that it should also be provided for experienced caseworkers as well as supervisors. While it was not the norm among states we reviewed, some states require and many experts recommend that caseworkers repeat training at periodic intervals as a refresher.
Although staff often express a desire for additional training, they also note concern regarding the time training requires, noting that lengthy training can make it difficult to keep up with their workload. However, to ensure that all staff receive important information, some states have made training mandatory for caseworkers. For example, Utah has mandatory training for all employment counselors that includes information about assessment. In fact, to encourage everyone to participate in training, Utah has tied completion of the training to promotions of their employment counselors and to pay raises. States and localities will need to decide for themselves the relative importance of training on screening and assessment issues and weigh this against the costs associated with mandatory training for all staff involved.
To the extent a state or locality is working with other organizations to implement its screening or assessment approach, it is important that all staff involved be trained. Training for partner agencies may include information about TANF policies, the opportunities and limitations these policies hold for case managers, and the obligations TANF recipients face. Cross-training on procedures can also assist with the implementation of collaborative efforts. In some cases, partner agencies who have greater expertise identifying and addressing barriers might serve as a training resource for TANF agencies.
Question Nine: What issues related to privacy and confidentiality should be considered?
In considering how to screen or assess for unobserved barriers, TANF agencies and their partners must consider the complex issues around privacy and confidentiality of information obtained through the identification process. A detailed assessment of these issues is beyond the scope of this report,79 but, because of the importance of the issue, we provide an overview of the legal underpinnings for privacy and confidentiality of information handling. Although issues related to confidentiality are complex, many states have found effective ways to address these requirements in order to meet clients' needs. Experts emphasize that concerns about or initial struggles with privacy and confidentiality requirements should not inhibit states and localities from providing services to address clients' needs.
As noted throughout this report, screening and assessment for unobserved barriers and the provision of services to address barriers requires that programs serving TANF recipients share individual data with welfare case managers (and sometimes vice versa) about clinical assessments, program participation, and client progress. Such data sharing raises complex issues around privacy and confidentiality. These issues include the fear of social stigma, inability to obtain health insurance, and physical harm or even death (in the case of sharing information about domestic violence situations).
For example, if the whereabouts of a woman who has suffered domestic violence were revealed to another program, it could inadvertently become known to the batterer and imperil her life. In some states, knowledge obtained by a child welfare agency that a parent is addicted to illicit drugs can be grounds for a finding of child neglect and removal of children from the home (in all states, welfare workers are mandatory reporters of suspected child abuse or neglect to the child welfare agency). In other instances, a client found to have learning disabilities, and provided appropriate accom-
modations in order to take a GED exam, might wish her disability to be kept confidential from prospective employers so as to avoid the inappropriate but all too common stigma of being perceived as "dumb." Yet, her welfare case manager might encourage her to reveal the learning disability to the employer in order to obtain accommodations in the work place.
Federal and state law and regulation abound on the protection of privacy, the confidentiality of records, and informed consent. At the federal level, generic laws include the Privacy Act of 1974, the Right to Financial Privacy Act of 1978, the Freedom of Information Act, the Data Matching and Privacy Protection Act of 1988, and their associated federal agency regulations. In addition, specific laws (and associated regulations) address confidentiality involving information about the disabilities or barriers covered in this report, including the:
Comprehensive Alcohol Abuse and Alcoholism Prevention, Treatment and Rehabilitation Act of 1970;
Drug Abuse Prevention, Treatment and Rehabilitation Act of 1972;
Americans with Disabilities Act (ADA) of 1990;
Individuals with Disabilities Education Act (last amended in 1997);
Health Insurance Portability and Accountability Act of 1996;80 and
Section 188 of the Workforce Investment Act (WIA) of 1998.
Moreover, States have enacted their own laws on these issues, some of which may go beyond federal law and regulation in restricting access to personal information. In some states, privacy protections are embedded in their constitution. This whole body of federal and state law and regulation are premised on serving several critical purposes. As stated by Brady, Powell, and Schink (1999):
"Confidentiality rules ensure that people's preferences are considered when deciding who will obtain their personal data. They also serve a pragmatic function, encouraging participation in activities that involve the collection of sensitive information.... Guarantees of confidentiality are also considered essential in encouraging participation in potentially stigmatizing programs, like mental health and substance abuse treatment services. Confidentiality laws are legislative responses to the pervasive stigma associated with many public programs and services."81
We would add that, in some cases, confidentiality laws are legislative responses to real financial, personal, or physical threats to safety.
Welfare case managers must be cognizant and well-trained about the conflict that arises between the need to share program and service information among partner agencies, and the need to maintain client privacy and confidentiality. Failure to maintain the proper balance can lead to real harm to clients. Failure to obtain written informed consent to disclose information can lead to lawsuits against the agency. Yet, failure to lawfully obtain vital information on a client's progress in program services can result in ineffective case management, inappropriate service planning, or inappropriate case closure. In order for case managers to be cognizant and well-trained, policy makers and other state officials must inform themselves of the laws, regulations, and issues, in order to pass on appropriate information and safeguards to case managers.
79 Much of the information from this section was taken from, and further detail can be found in, the U.S. Department of Health and Human Services, Center for Substance Abuse Treatment. Technical Assistance Publication Series (TAP) Series #24. Welfare Reform and Substance Abuse Treatment Confidentiality: General Guidance for Reconciling Need to Know and Privacy. Washington, DC: DHHS, 1999.
80 This law contains language specifically requiring the Secretary of HHS to develop and issue regulations governing the privacy and confidentiality of mental health patients' records. HHS issued proposed regulations for public comment in November, 1999; final regulations await incorporation of commenters' suggestions for revision.
81 Brady, Henry E. et al. Access and Confidentiality Issues with Administrative Data. UC DATA, Draft for discussion purposes only. Berkeley, CA: University of California, Berkeley, Data Archive and Technical Assistance, December 9, 1999.
Question Ten: What other questions should be asked?
Questions one through nine address some of the most common issues that arose when discussing screening and assessment with TANF agency officials and subject matter experts. However, these generate any number of additional and equally important questions. Below, we briefly touch on some additional questions that bear consideration.
Should Drug Testing Be Used to Identify Substance Use Among TANF Recipients ?
Drug testing is an emerging, controversial issue in the TANF community. Drug testing - through urinalysis, blood, or hair testing - has been used as a part of the substance abuse treatment and criminal justice systems for some time and is increasingly being used by employers. The goals of drug testing in these settings are to determine if an individual is following a required treatment plan or to screen out drug users as a step in the hiring process.
The uses of drug testing in TANF programs are not as clear. They include identifying substance use problems as a potential barrier to employment or monitoring compliance with treatment required as part of a TANF client's service plan. Drug testing might also serve as a screen for TANF work programs referring clients to job opportunities with employers known to drug test applicants. More punitive uses, such as denying benefits to recipients who refuse random drug tests, are controversial. A federal court in Michigan indicated that the use of drug testing in this manner may be unconstitutional, influencing other states potentially interested in adopting this type of policy, at least for the time being, to hold off on adopting this approach.82
In addition to the legal implications of the uses of drug testing, states should carefully consider the limitations that come with this form of identification. For example, drug testing identifies recent drug use, not substance abuse or addiction. Given TANF agencies' focus on barriers to employment, they may be more interested in on-going addiction or abuse problems, not usage. Among other limitations, drug testing can:
be expensive;
be considered unethical if used in situations where drug use is not suspected (i.e., such as the case of random or universal testing); and
create an environment of confrontation or suspicion that prohibits the development of a positive relationship between case managers and TANF clients, thus inhibiting other barrier identification and constructive service planning.
Although many questions remain regarding drug testing, this is an emerging issue in the area of barrier identification that TANF agencies may choose to monitor.83
82 American Civil Liberties Union (ACLU). Judge Blocks First-Ever Mandatory Drug Testing of Michigan Welfare Recipients. Press Release. November 10, 1999.
83 See also the forthcoming Technical Assistance Publication by the U.S. Department of Health and Human Services, Public Health Service, Substance Abuse and Mental Health Services Administration, Center for Substance Abuse Treatment, Identifying Substance Abuse Among TANF Eligible Families.
What Can Be Done to Help Medical Professionals Understand the Implications of Their Assessment OR Diagnostic Information?
As noted throughout this report, one reason TANF agencies may want to involve other organizations in their efforts to identify unobserved barriers to employment is that TANF agency staff often do not have the skills or training to conduct such assessment or diagnosis. This being the case, they must still be able to understand and act on the assessment and diagnostic results from medical professionals. While this is, on the one hand, an issue of training TANF staff, it can also be considered within the context of outreach to partners.
For example, several states have already undertaken efforts to revise their forms used for medical verification of a disability or barrier to employment to provide information not only about the client's limitations, but also her capabilities. However, TANF staff offer examples of situations where doctors' concerns about liability issues affects how they complete the forms. For example, because of liability concerns associated with indicating that an individual can participate in work activities, doctors take what some TANF staff consider a "conservative" approach in indicating a client cannot participate.
Some TANF staff are concerned that medical professionals do not understand how assessment information they provide interacts with TANF policies.
While TANF staff generally acknowledge that they do not have the medical training to question an assessment or diagnosis, they are concerned that medical professionals do not understand how this assessment information interacts with TANF polices - specifically time limits - to produce what may be a negative result for the client. Consider the example of a client who has a serious back problem that affects her ability to work. A doctor might indicate that the condition should preclude participation in any work activity, while not understanding that a deferral will cause the client to use valuable time on her time clock while not progressing toward finding a work situation that accommodates her condition. If the doctor were instead to indicate that the individual can work, but for limited hours or in certain conditions (i.e., work must be conducted sitting, no heavy lifting should be required), the client could then receive employment services to assist her on her path to self-sufficiency.
Illinois has addressed this problem by creating a form letter that is attached to medical verification forms to be completed by doctors. Not only does the form ask for additional information about the individual's capabilities as well as her limitations, but the form letter explains TANF rules and the implication of a client unnecessarily delaying efforts toward self-sufficiency. The letter also clarifies that nothing about the medical diagnosis will affect the client's receipt of medical assistance which pays for the doctor's services. 84
84 Holcomb 2000.
Is Gaming the System a Problem?
A few states we spoke to said that in designing and implementing screening and assessment programs and services some state legislators or system observers expressed concern about whether welfare clients would "game the system." That is, clients would respond incorrectly or dishonestly to screening and assessment questions to achieve a result desired by the client but often inconsistent with the objective of the policy. In Tennessee, fears about clients gaming the system to forestall work was briefly raised but was not enough of a concern to prevent them from going ahead with implementation. A more extreme example, and certainly an atypical one, came from two Utah senators who argued against a bill extending welfare for domestic violence victims claiming the bill would open up a new form of welfare fraud.85
While each of these examples indicates a concern about screening and assessment initiatives, we did not speak to any states where fears about recipients gaming the system stopped or slowed implementation. However, it raises an important point that states must periodically review their policies and procedures and monitor clients receiving services to ensure that those recipients who need help are getting it and those who do not are not using the system to prolong their TANF receipt.
85 State Capitals Newsletters 2000.
Directions for Future Research: Where do we go from here?
The issues presented in this report suggest that states and localities face a number of decisions when selecting an approach to screening or assessing TANF clients for unobserved barriers to employment. In fact, this paper merely scratches the surface, presenting some of the questions to be considered. Each question prompts a number of sub-questions, only some of which are addressed here.
Although some states and localities have been screening or assessing for unobserved barriers for some time, few of these methods have been studied and little is known about their effectiveness. These outstanding questions suggest that, regardless of the chosen strategy, states, localities, and the federal government should consider incorporating evaluation into approaches implemented and research related to TANF.
Further, there is much that can be learned from studying approaches in different states and localities to determine the contextual factors that contribute to successful outcomes. Just as no two TANF clients face the same circumstances, no two states or localities face the same policy environment, service delivery structure, or service mix. These dimensions present a number of questions regarding what factors influence the effectiveness of different screening and assessment methods. Below we offer a few of the possible questions that may guide future research.
Research Questions Regarding Screening and Assessment Methods
Does a particular screening or assessment effort yield desired results? States and localities are actively considering what screening or assessment approach to adopt. However, few efforts to screen or assess for unobserved barriers to employment have been rigorously evaluated. Without this information, it will remain unclear how states and localities can most effectively identify the challenges TANF recipients continue to face.
How effective are approaches that rely on self-disclosure or red flags alone? Although relatively easy to implement and low-cost approaches, relying on red flags or self-disclosure may or may not identify barriers as effectively as more formal approaches. These approaches should be examined to determine their effectiveness.
Does the use of formal screening tools enhance a TANF agency's ability to identify unobserved barriers to employment? To some degree, all TANF agencies rely on case management, self-disclosure, and red flags to uncover barriers to employment. Does the addition of a formal screening or assessment tool more effectively uncover barriers? Few tools have been designed or tested for use with TANF recipients. Given this, there is little known about their effectiveness. To understand if the use of formal instruments is more effective than less formal approaches, further study is necessary.
Is it more effective to assess for and address a single barrier or address multiple barriers at once? The research available and caseworker anecdotes indicate that few clients face a single barrier to employment. Yet, little study has focused on the most effective approaches to identifying and addressing multiple barriers. Outstanding questions include: Should services be designed to address a single barrier at a time, or should the approaches be comprehensive attempting to simultaneously address several issues? Can clients effectively participate in services addressing more than one barrier at a time? More information about the co-occurrence of barriers and service approaches is also necessary.
Research Questions Regarding Key Dimensions That May Influence the Effectiveness a Screening OR Assessment Method
Which barriers are most prevalent among remaining TANF cases? Despite the range of prevalence estimates offered in Question Two, there is actually little known - particularly at the local level - about the specific challenges faced by remaining TANF recipients. Further, what data are available is based on differing methodologies and definitions resulting in wide-ranging estimates. For policy makers and program administrators to determine how to allocate resources and make service delivery decisions, more precise data about prevalence of, and circumstances surrounding the existence of, barriers is needed.
What staffing requirements are associated with each approach? In many states and localities, TANF agency staff have seen significant shifts in their responsibilities. In some cases, former eligibility staff are now responsible for case management. In others, what was formerly a program geared toward education and training now has a Work First focus. Given these changes TANF staff are already facing, is it realistic to expect them to assume responsibility for, and effectively carry out, screening and assessment? Do TANF agencies need to reconsider skill requirements for TANF staff or purchase expertise from another source?
What training approaches are effective? If staff requirements change due to the adoption of a screening or assessment approach, training will be necessary. Some argue that training to raise awareness of barriers also enhances identification efforts. However, little is known about what training approaches are effective.
What partnerships are most effective in identifying unobserved barriers? Non-TANF agencies have been serving clients with unobserved barriers to employment for some time. Much can be learned from these agencies regarding identifying and serving TANF clients facing these barriers. However, this requires new partnerships and an understanding by all partners regarding different program requirements and philosophies. How should such partnerships be structured to facilitate effective cooperation and collaboration? Are formal partnerships (i.e., contracts or memoranda of understanding) more effective than informal collaborations? Does co-location significantly enhance partnerships?
Are there unintended consequences of assessment efforts? While few argue that identifying barriers is the first step in determining how best to serve TANF clients, little is known about unintended effects of assessment. For example, are "false negatives" costly to agencies or clients? Does assessment label or stigmatize clients? Does it divert clients from services from which they could benefit?
References
Allen, J.P., M.H. Eckardt, and J. Wallen. Screening for Alcoholism: Techniques and Issues. Public Health Reports 103:586-592, 1988.
American Civil Liberties Union. Judge Blocks First-Ever Mandatory Drug Testing of Michigan Welfare Recipients. Press Release. November 10, 1999.
American Public Human Services Association. Case Management Definitions, Goals, Principles from their Organizational and Professional Development Curriculum. Washington, DC: APHSA, undated.
American Society of Addiction Medicine (ASAM). Second Edition of Patient Placement Criteria. Annapolis Junction, MD. 1996.
Baldwin, Joyce and Staff. Questionnaire Helps Primary Care Physicians Detect Mental Disorders. Psychiatric Times, Vol. XII, Issue 2, February 1995.
Barusch, Amanda Smith, Mary Jane Taylor, Soleman H. Abu-Bader, and Michelle Derr. Understanding Families With Multiple Barriers to Self Sufficiency. Final Report submitted to Utah Department of Workforce Services. Salt Lake City, Utah: Social Research Institute, February 1999.
Beck, Aaron T., M.D. and R. A. Steer. Beck Depression Inventory. Psychological Corporation.San Antonio, TX. 1996.
Brady, Henry E. et al. Access and Confidentiality Issues with Administrative Data. UC DATA, Draft for discussion purposes only. University of California, Berkeley: Data Archive and Technical Assistance, December 9, 1999.
Burt, Martha R., Janine M. Zweig and Kathyrn Schlichter. Strategies for Addressing the Needs of Domestic Violence Victims within the TANF Program. Washington D.C.: U.S. Department of Health and Human Services, June 2000.
Center on Law and Social Policy and Center for Budget and Policy Priorities. "State Policy Documentation Project," February 2000.
Danziger, Sandra, Mary Corcoran, Sheldon Danziger, Colleen Heflin, Ariel Kalil, Judith Levine, Daniel Rosen, Kristin Seefeldt, Kristine Siefert, and Richard Tolman. Barriers to the Employment of Welfare Recipients. Ann Arbor, MI: University of Michigan Poverty Research and Training Center, April 1999.
Foa, Edna B. PDSтм (Posttraumatic Stress Diagnostic Scale). Http://www.ncs.com/assessments/tests/pds.htm. 1996.
Gallagher, L. Jerome et al. One Year after Federal Welfare Reform: A Description of State Temporary Assistance for Needy Families (TANF) Decisions as of October 1997. Washington, DC: The Urban Institute, June 1998.
Gerry, Martin, and Candace Shively. The Kansas Learning Disabilities Initiative. Kansas Department of Social and Rehabilitative Services, January 1999.
Greenberg, Mark and Steve Savner. A Detailed Summary of Key Provisions of the TemporaryAssistance for Needy Families Block Grant of H.R. 3734: The Personal Responsibility and Work Opportunity Reconciliation Act of 1996. Washington, DC: Center for Law and Social Policy, August 1996.
Greenberg, Mark. Welfare to Work Grants and Other TANF-Related Provisions in the Balanced Budget Act of 1997. Washington, DC: Center for Law and Social Policy, August 1997.
Greenberg, Mark and Steve Savner. The Final TANF Regulations: A Preliminary Analysis. Washington, DC: Center for Law and Social Policy, May 1999.
Holcomb, Pamela A. and Terri S. Thompson. State Welfare-to-Work Policies for People with Disabilities: Implementation Challenges and Considerations. Washington, D.C.: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, August 2000.
Impara, James C. and Barbara S. Plake, editors. The Thirteenth Mental Measurements Yearbook. The Buros Institute of Mental Measurements. Lincoln, NE: University of Nebraska Press. 1998.
Jackson, Gregg B. Measures for Adult Literacy Programs. A joint publication of the Association for Community Based Education and The ERIC Clearinghouse on Tests, Measurements, and Evaluation. Washington, DC: American Institutes for Research, August 1990.
Johnson, Amy and Alicia Meckstroth. Ancillary Services to Support Welfare to Work. Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, June 1998.
Keyser, Daniel J. and Richard C. Sweetland, editors. Test Critiques: Volume III. Kansas City, MO: Test Corporation of America. 1985.
Kramer, Fredrica D. Serving Welfare Recipients with Disabilities. Washington, DC: Welfare Information Network, January 1999.
Lazowski, L.E., F.G. Miller, M.W. Boye, and G.A. .Miller. Efficacy of the Substance Abuse Subtle Screening Inventory - 3 (SASSI-3) in Identifying Substance Dependence Disorders in Clinical Settings. Journal of Personality Assessment, 71(1): 114-128, 1998.
Loprest, Pamela J. and Sheila R. Zedlewski. Current and Former Welfare Recipients: How Do They Differ? The Urban Institute, Washington, DC., November 1999.
National Center on Addiction and Substance Abuse (in partnership with the American Public Human Services Association). Building Bridges: States Respond to Substance Abuse and Welfare Reform. New York, New York: CASA, August 1999.
National Institute for Literacy. Bridges to Practice: A Research-based Guide for Literacy Practitioners Serving Adults with Learning Disabilities. Washington, DC: The National Institute for Literacy and Learning Disabilities Center. 1999.
National Partnership for Women and Families. Preventing Discrimination: A Guide for Caseworkers and Others Helping Welfare Recipients Enter the Workplace, as posted at www.nationalpartnership.org, August 2000.
Olson, Krista and LaDonna Pavetti. Personal and Family Challenges to the Successful Transition from Welfare to Work. Washington, DC: The Urban Institute, May 1996.
Perez-Johnson, Irma and Alan M. Hershey. Early Implementation of the Welfare-to-Work Grants Program Report to Congress. Princeton, NJ: Mathematica Policy Research. March 1999.
Personal Responsibility and Work Opportunity Reconciliation Act of 1196. U.S. Public Law 104-193. 104th Congress, 2nd Session, Sections 402(a)(7) & 408, August 22, 1996.
Raphael, Jody and Sheila Haennicke. Keeping Battered Women Safe Through the Welfare-to-Work Journey: How are we Doing? Chicago, IL: The Center for Impact Research, September 1999.
Russell, M. and J.B. Skinner. Early Measures of Maternal Alcohol Misuse as Predictors of Adverse Pregnancy Outcomes. Alcoholism Clin Exp Res 12(6): 824-830, 1988.
Saunders, J.B., O.G. Aasland, T.F. Babor, J.R. de la Puente, and M. Grant. Development of the Alcohol Use Disorders Screening Test (AUDIT). WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol Consumption, Part II. Addiction 88: 791-804, 1993.
Schott, Liz, Ed Lazere, Heidi Goldberg, and Eileen Sweeney. Highlights of the Final TANF Regulations. Washington DC: Center for Budget and Policy Priorities, www.cbpp.org, April 29, 1999.
State Capitals Newsletters. Utah House Passes Bill Extending Welfare for Violence Victims. Public Assistance and Welfare Trends, Vol. 54, No. 5. Alexandria, VA: State Capitals Newsletters, January 2000.
State of Virginia, Department of Human Services. Compendium of Screening Tools (Draft), undated.
State of Washington, Department of Social and Health Services. Economic Services Administration, Work First Division. Learning Disabilities. September 29, 1998.
Sweeney, Eileen P. Recent Studies Indicate That Many Parents Who Are Current or Former Welfare Recipients Have Disabilities or Other Medical Conditions. Washington, DC: Center on Budget and Policy Priorities, February 2000.
"Temporary Assistance for Needy Families Program (TANF), Final Rule" Federal Register 64:69 (12 April 1999) p. 17720.
Thompson, Terri S., Pamela A. Holcomb, Pamela Loprest, and Kathleen Brennan. State Welfare-to-Work Policies for People with Disabilities: Changes Since Welfare Reform. Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, October 1998.
U.S. Department of Health and Human Services. Civil Rights Laws and Welfare Reform - An Overview. Washington, DC: U.S. DHHS, August 1999.
U.S. Department of Health and Human Services. Technical Assistance for Caseworkers on Civil Rights Laws and Welfare Reform. Washington, DC: U.S. DHHS, August 1999.
U.S. Department of Health and Human Services. Administration for Children and Families, Office of Planning, Research and Evaluation. Temporary Assistance for Needy Families (TANF) Program: Second Annual Report to Congress. Washington, DC: USOHHS, August 1999.
U.S. Department of Health and Human Services. Administration for Children and Families, Office of Family Assistance. Helping Families Achieve Self-Sufficiency: A Guide on Funding Services for Children and Families through the TANF Program, www.acf.dhhs.gov/programs/ofa/funds2.htm, undated.
U.S. Department of Health and Human Services. Public Health Service. Substance Abuse and Mental Health Services Administration. Center for Substance Abuse Treatment. Treatment Improvement Protocol (TIP) Series #11. Simple Screening Instruments for Alcohol and Other Drug Abuse and Infectious Diseases. 1994.
Appendix A: Tool Profiles
Section I: General Employability Assessment/Multiple Barriers
Family Needs Assessment (Rhode Island)
Barriers Identified
| Substance Abuse | Transportation | Utilities |
| Mental Health | Housing/Shelter | Physical Health |
| Child or Elder | Food Availability | Child Development |
Number and Types of Questions
Nine topical headings with additional discussion points under each
Target Population
TANF clients statewide
Methodological Information
Not available
Implementation
Completed in an interview setting at first appointment after eligibility determination
Cost
None
Source or Publisher
Rhode Island Department of Human Services
State(s) Believed to be Using
Rhode Island
Pathways/Community Service Screening Guide (P/CSSG) (Montana)
Barriers Identified
| Substance Abuse | Work Experience | Legal Issues |
| Learning Disabilities | English Proficiency | Physical Health |
| Low Educational Attainment | Transportation | Child Care |
Number and Types of Questions
Fifty 'yes' or 'no' questions
Target Population
TANF clients statewide
Methodological Information
Not available
Implementation
Self-administered paper and pencil tool
Cost
None
Source or Publisher
Montana Department of Public Health and Human Services
State(s) Believed to be Using
Montana
Virtual Interactive Evaluation Worksheet (VIEW) (Washington)
Barriers Identified
| Substance Abuse | Substance Abuse | Legal Issues |
| Learning Disabilities | Family Planning | General Health |
| Mental Health | Child Health/Nutrition | Housing |
| Employment History | Child and Dependent Care | Family Support/ Domestic Violence |
| Other Agency Involvement | Parent/Child Development |
Number and Types of Questions
Computer screens that present 23 questions to WorkFirst case managers
Target Population
TANF clients statewide
Methodological Information
Not available
Implementation
Completed by case mangers at initial interview. Depending on responses, Case Managers are instructed with prompts or suggestions for further evaluation, including referral to a social worker responsible for more in-depth assessment.1
Cost
None
Source or Publisher
Washington Department of Social and Health Services (DSHS)
State(s) Believed to be Using
Washington
1 The term "social worker" refers to individuals who may or may not be licensed or hold Master's of Social Work degrees.
Intensive Services Assessment (Washington)
Barriers Identified
| Substance Abuse | Pregnancy | Transportation |
| Domestic Violence | Family Planning | Legal Issues |
| Mental Health | Child Health/Nutrition | Housing |
| Educational History | Parent/ChildDevelopment | Child Care |
| Employment History | General Health | |
| Other Agency Involvement |
Number and Types of Questions
Eighteen pages, 138 questions; many 'yes' or 'no' or checklists
Target Population
TANF clients statewide who are referred for additional assessment (i.e., because determined to have barriers or be "hard-to-serve" by a case manager, in sanction status, or are a pregnant or parenting teen).
Methodological Information
Not available
Implementation
Interview administered by a DSHS social worker
Cost
None
Source or Publisher
Washington Department of Social and Health Services
State(s) Believed to be Using
Washington
Transitional Employment Assistance (TEA) Skills, Employability & Intake Assessment Background Information (Arkansas)
Barriers Identified
| Substance Abuse | Work Experience | Domestic Violence |
| Occupational Skills | Child Care | Transportation |
| Educational Attainment | General Health |
Number and Types of Questions
Fifteen 'yes' or 'no,' check list, and open-ended questions
Target Population
TANF clients statewide
Methodological Information
Not available
Implementation
Self-administered paper and pencil tool
Cost
None
Source or Publisher
Arkansas Department of Human Services Division of County Operations
State(s) Believed to be Using
Arkansas
Feelings and Behavior Inventory (Missouri)
Barriers Identified
| Substance Abuse | Mental Health | Gambling |
Number and Types of Questions
Eleven 'yes' or 'no' questions organized into three sets addressing the three barrier areas; substance abuse questions are the CAGE questions
Target Population
TANF clients in three pilot areas of metropolitan Kansas City
Methodological Information
One or more 'yes' response to a set of questions indicates need for referral for further assessment for a probable problem.
Implementation
Could be self-administered but more likely completed in an interview setting. Interviewer is also given a behavioral observation checklist to assist with determining the possible existence of a problem.
Cost
None
Source or Publisher
Missouri Department of Public Health and Human Services
State(s) Believed to be Using
Missouri
Assessment Interview Guide (Utah)
Barriers Identified
| Substance Abuse | Work Experience | Legal Issues |
| Domestic Violence | Physical Health | Resources |
| Mental Health | Family Situation | Educational Attainment |
| Job Seeking/Keeping Skills | Occupational Skills/Training |
Number and Types of Questions
Eight-page interview guide with approximately 40 topics
Target Population
TANF, General Assistance, and other clients requiring an employment plan statewide
Methodological Information
Not available
Implementation
Interview guide used by caseworkers during initial interview with clients
Cost
None
Source or Publisher
Utah Department of Workforce Services and other state government agencies
State(s) Believed to be Using
Utah
Adult Psychological Assessment (Tennessee)
Barriers Identified
| Substance Abuse | Educational Background | Legal Issues |
| Learning Disabilities | Physical Health | Resources |
| Domestic Violence | Work History | Mental Health |
| Family Situation |
Number and Types of Questions
Twelve pages, 90 questions; primarily 'yes' or 'no' with space for additional explanation; substance abuse questions are the CAGE questions
Target Population
TANF clients statewide
Methodological Information
Not available
Implementation
Conducted by a Family Service Counselor after either
referral from caseworkers or ABE instructor;
caseworker notices a red flag indicating further screening required or
client unable to complete work requirements or retain employment.
Cost
None
Source or Publisher
Tennessee Department of Human Services in collaboration with
YWCA
Department of Health, Bureau of Drug and Alcohol Services
Community Mental Health Centers
University of Tennessee Center for Literacy Studies
State(s) Believed to be Using
Tennessee
Section II: Substance Abuse
Cage
Barriers Identified
Alcohol Use Problems (modified CAGE can be used for other drug use problems)
Number and Types of Questions
Four 'yes' or 'no' questions
Target Population
Adults and Youth
Methodological Information
Sources differ on the methodological assessment of the CAGE. Although one source reports the CAGE's sensitivity and specificity levels as acceptable (at cut-score of two affirmative responses, 75 percent of alcoholics are correctly identified as alcoholics and 95 percent of non-alcoholics are identified correctly), another source indicates that the reliability and validity have been demonstrated in clinical settings but are untested with a general population.2
Implementation
The tool can be completed individually or as part of a group. It can be self-administered and self-reported or it can be conducted by a clinician. It takes approximately one minute to complete. It should be completed as part of the individuals general history. A total of two or more positive answers indicates a history of alcoholism.
Cost
None
Source or Publisher
Dr. John Ewing
Bowles Center for Alcohol Studies
University of North Carolina at Chapel Hill
Chapel Hill, NC
State(s) Believed to be Using
Alabama, Kansas, New Jersey (CAGE aid), California, Utah, Minnesota,
New York (CAGE aid), Delaware (CAGE aid), Maryland (modified CAGE)
2 See Allen, JP, M.H. Eckardt, and J. Wallen. Screening for Alcoholism Techniques and Issues. Public Health Reports 103 586-592, 1988 and State of Virginia, Department of Human Services, undated.
Substance Abuse Subtle Screening Inventory (SASSI)
Barriers to be Identified
Alcohol or Drug Problems
Number and Types of Questions
Seventy-eight true/false and scaled questions
Target Population
Adults and adolescents ages 12-18
Methodological Information
The SASSI is an empirically validated screening and is effective as an aid in treatment planning. The instrument correctly classified substance dependent people in about 93 percent of all cases with approximately seven percent error in classifying nondependent people as dependent (false positives) and six percent error in classifying dependent people as nondependent (false negatives). 3
Implementation
Self-administered, paper and pencil or computerized test that takes 10-15 minutes to take and less than five minutes to score. Must be scored by a trained caseworker. Caseworkers are trained by a SASSI consultant.
Cost
$75.00 for a manual, 25 questionnaires and profiles, scoring key, and a sample scored questionnaire with profile
Source or Publisher
The SASSI Institute
Route 2, Box 134
Springville, IN 47462
State(s) Believed to be Using
| Florida | Nevada | Oklahoma |
| Kansas | North Carolina | Tennessee |
| New Jersey | Oregon | Utah |
| New Mexico |
3 See Lazowski, L.E., F.G. Miller, M.W. Boye, and G.A. Miller. Efficacy of the Substance Abuse Subtle Screening Inventory - 3 (SASSI-3) in Identifying Substance Dependence Disorders in Clinical Settings. Journal of Personality Assessment, 71(1) 114-128, 1998.
Simple Screening Instrument for Alcohol and Other Drug (AOD) Abuse
Barriers Identified
Substance Abuse
Number and Types of Questions
Sixteen questions 'yes' or 'no' questions regarding consumption, problem recognition, experience with adverse consequences (including symptoms, preoccupation, loss of control), feelings of guilt, family history, and awareness of past or present problem.
Target Population
Adults and adolescents at risk of having an AOD abuse problem
Methodological Information
Measurement scope intended to be limited to screening for potential problems, not establishing a diagnosis. Questions answered 'yes' are scored as '1.' A score of 0-1 indicates no to low risk of AOD abuse, 2-3 minimal risk, and greater than or equal to 4 moderate to high risk; possible need for further assessment.
Implementation
Two forms are available, one for use in an interview setting, the other can be self-administered. Each takes no more than 10-15 minutes. Can be used by a diverse group of outreach workers, paraprofessionals and professionals in the fields of both AOD abuse and infectious diseases. The clinical decision for individuals who score positive on the instrument would be referred for a more comprehensive assessment or for a complete diagnostic evaluation.
Cost
None
Source or Publisher
Treatment Improvement Protocol (TIP) Series #11
U.S. Department of Health and Human Services, Public Health Service
Substance Abuse and Mental Health Services Administration
Center for Substance Abuse Treatment
Rockwall II, 5600 Fishers Lane
Rockville, MD 20857
State(s) Believed to be Using
None identified
Alcohol Use Disorder Identification Test (AUDIT)
Barriers Identified
Alcohol Use and Problems
Number and Types of Questions
Eight scaled questions, two 'yes' or 'no' questions. There are three questions on the amount and frequency of drinking, three questions on alcohol dependence, and four on problems caused by alcohol
Target Population
Not specifically designed for use with TANF recipients. Appropriate for use with primary care, emergency room, surgery, and psychiatric patients; DWI offenders, criminals in court, jail, and prison; enlisted men in the Armed Forces; and workers encountered in employee assistance programs and industrial settings.
Methodological Information
Reliability studies conducted test-retest, internal consistency. Measures of validity derived content, criterion (predictive, concurrent, postdictive), and construct. 4
Implementation
AUDIT is a self-report paper and pencil or interview tool. Time required to complete is two minutes. Training is required for administration. The AUDIT is available in Japanese, Romanian, and Norwegian. Time required for scoring is one minute.
Cost
Free with $75.00 training fee
Source or Publisher
Program on Substance Abuse
World Health Organization
211 Geneva, Switzerland
or
Thomas F. Babor
Alcohol Research Center
University of Connecticut
Farmington, CT 06030-1410
State(s) Believed to be Using
North Carolina
4 Saunders, J.B., O.G. Aasland, T.F. Babor, J.R. de la Puente, and M. Grant. Development of the Alcohol Use Disorders Screening Test (AUDIT). WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol Consumption, part II. Addiction 88791-804, 1993.
Drug Abuse Screening Test-20 (DAST-20)
Barriers Identified
Substance Abuse (drugs not including alcohol)
Number and Types of Questions
Twenty 'yes' or 'no' questions
Target Population
Clients of Addiction Treatment
Methodological Information
This tool was found to be correct about 75 percent of the time, according to one study. No validity data is available for the DAST-20 at this time. One review finds that the DAST - 20 is very useful for identifying minimal and heavy substance users; however, this same review states that the DAST - 20 is probably not the best option for screening individuals with moderate substance abuse issues.5
Implementation
While no training is needed to administer this paper and pencil tool, it is recommended that it be administered by experienced workers or professionals.
Cost
None
Source or Publisher
Dr. Harvey Skinner
Addiction Research Foundation
33 Russell St., Toronto
Canada, M5s 2s1
State(s) Believed to be Using
Louisiana (DAST 10) North Carolina
5 Impara, James C. and Barbara S. Plake, editors. The Thirteenth Mental Measurements Yearbook. Lincoln, NE University of Nebraska Press 1998, pp. 379-381.
Substance Use Disorders Diagnostic Schedule (SUDDS-IV)
Barriers Identified
Substance Abuse and Dependence (also screens for depression and anxiety indicators)
Number and Types of Questions
Sixty-four multiple choice and frequency scaled questions. Covers general information, stress, anxiety, depression, smoking, specific drug and alcohol use, and effects of substance use.
Target Population
Developed for arrestees; considered appropriate for general population suspected of substance abuse or dependence
Methodological Information
Described as providing "definitive support" for substance-specific abuse or dependence diagnosis based on DSM-IV criteria.6
Implementation
Can be used as a routine part of clinical intake or part of a substancerelated diagnostic workup. Can be administered in a comprehensive interview or in segments. Requires 35-45 minutes to complete; scoring can be completed within five minutes.
Cost
$23.00 for an Administration Guide plus five interviews; $62.50 for additional sets of 25 interviews
Source or Publisher
Norman G. Hoffman, Ph.D.
Patricia A. Harrison, Ph.D.
Evince Clinical Assessments
P.O. Box 17305
Smithfield, RI 02917
State(s) Believed to be Using
North Carolina
6 The DSM-IV is a diagnostic criteria manual discussed in Question Five.
Alcohol/Substance Abuse Screening Instrument (New York)
Barriers Identified
Substance Abuse (drugs and alcohol)
Number and Types of Questions
Nine 'yes' or 'no' questions about alcohol/substance abuse in the last 12 months
Target Population
TANF clients
Methodological Information
Not available
Implementation
All TANF applicants are screened for the possibility of drug and alcohol using this one-page tool. Training for staff administering the tool is not mandatory, but is provided through workshops, seminars, and teleconferences.
Cost
None
Source or Publisher
New York Office of Alcoholism and Substance Abuse Services (OASAS)
State(s) Believed to be Using
New York
Uncope
Barriers Identified
Substance Abuse and Dependence (alcohol and drug)
Number and Types of Questions
Six 'yes' or 'no' questions (similar to CAGE)
Target Population
Developed for arrestees; considered appropriate for general popula-
tion suspected of substance abuse or dependence
Methodological Information
Two or more positive responses indicate possible abuse or dependence. Using this cut score produces sensitivities in a clinical population for alcohol, cocaine and marijuana of 93 percent, 94 percent, and 82 percent respectively. Specificities for this cut-off are 97 percent, 99 percent, and 97 percent respectively. Four or more positive responses strongly indicate dependence.
Implementation
Not available
Cost
None
Source or Publisher
Norman G. Hoffman, Ph.D.
Evince Clinical Assessments
P.O. Box 17305
Smithfield, RI 02917
State(s) Believed to be Using
None identified
Tweak
Barriers Identified
Alcohol Use
Number and Types of Questions
Five questions; four 'yes' or 'no' questions (similar to UNCOPE and CAGE)
Target Population
Pregnant women
Methodological Information
Validated among women. 7 'Tolerance' and 'Worried' questions each contribute two points; other three items contribute one point each. Tolerance score of two given if applicant reports being able to hold six or more drinks. A total score of two indicates that obstetric patients are likely to be risk drinkers. Cut-points of three and four are better than two for identifying harmful drinking and alcoholism.
Implementation
Paper and pencil; self-administered or interview setting; computer administration also available. Requires less than two minutes to complete. No training is required for administration.
Cost
Not available
Source or Publisher
Marcia Russell, Ph.D.
Research Institute on Addictions
1021 Main Street
Buffalo, NY 14203
State(s) Believed to be Using
None identified
7 Russell, M. and J. B. Skinner. Early Measures of Maternal Alcohol Misuse as Predictors of Adverse Pregnancy Outcomes. Alcoholism Clin Exp Res 12(6)824-830, 1988.
Section III: Learning Disabilities
Learning Needs Screening Tool
Barriers Identified
Learning Disabilities
Number and Types of Questions
The tool uses open-ended questions to collect information on the types of educational degrees obtained, job experience, and aspirations. It includes 13 'yes' or 'no' questions designed to identify potential learning disabilities.
Target Population
TANF clients
Methodological Information
The first five items are weighted times one, the next two items are weighted times two, the next three items are weighted times three, and the last three items are weighted times four. A total of 12 or more indicates the need for further assessment. One study states that this tool classified 74 percent of the participants as LD or non - LD, positively identifying 70 percent of the participants with LD and correctly ruling out 79 percent of those without an identified special learning need.8
Implementation
Implementation varies across states
Cost
None
Source or Publisher
Washington Department of Social and Health Services
States Believed to be Using
| Alaska | Gergia | New Hampshire |
| Arkansas | Minnesota | Oregon |
| Florida | Missouri | Washington |
8 State of Washington, Department of Social and Health Services, Economic Services Administration, WorkFirst Division. Learning Disabilities. September 29, 1998.
Adult Learning Disability Screening (ALDS)
Barriers Identified
Learning Disabilities
Number and Types of Questions
In addition to collecting descriptive, demographic information, the tool is divided into three parts. Part One is a 25-item Self-Rating Scale of frequency of difficulty performing "activities of daily living." Part Two is a 19-item Self-Administered Inventory requiring 'yes' or 'no' responses on an inventory of family and educational history. Part Three includes follow-up questions that probe further on previous responses. Additionally, the tool includes questions to the examiner as a procedural and administration validity check.
Target Population
Adults age 16 - 64
Methodological Information
Self-Rating Scales were found to be 85 percent accurate in predicting the existence of a learning disability and the Self-Administered Inventory was 90 percent accurate in predicting the existence of a learning disability.9
Implementation
The first and second parts of the ALDS are designed to be completed by the participant (self-administered), while part 3 is comprised of follow-up questions which the examiner asks the client. Each part of the battery is completed in less than 8 minutes for most examiners.
Cost
$5.00 for Manual; $7.00 for Technical Report; $3.00 each for tool and scoring sheet
Source or Publisher
University of Kansas, Cntr for Research on Learning
Attention: Daryl Mellard or Sean Lancaster
3061 Dole Center, Lawrence, KS 66045
State(s) Believed to be Using
Kansas
9 Gerry, Martin and Candace Shively. The Kansas Learning Disabilities Initiative. Kansas Department of Social and Rehabilitative Services, January 1999.
Section IV: Domestic Violence
Notification of Right to Claim Good Cause (Louisiana)
Barriers Identified
Domestic Violence
Number and Types of Questions
One 'yes' or 'no' question asking if the client wants to claim family violence exemption based on the information about what is required to claim exemption and examples of abuse.
Target Population
TANF clients statewide
Methodological Information
Not available
Implementation
This flyer is given to TANF clients (and may also be read to them), but they are not required to fill it out.
Cost
None
Source or Publisher
Louisiana Department of Social Services
Office of Family Support
State(s) Believed to be Using
Louisiana
Domestic Violence Screening Questionnaire (Montana)
Barriers Identified
Domestic Violence
Number and Types of Questions
Six 'yes' or 'no' questions asking about physical or sexual harm, fear of partner, restrictions on working or money, threats to the client or children, and past history in a shelter.
Target Population
TANF clients statewide
Methodological Information
Not available
Implementation
It is a self-administered paper and pencil tool. The tool is only used if a concern about domestic violence is detected from the initial multibarrier Pathways/Community Service Screening Guide (P/CSSG). One or more 'yes' answer requires a referral to the Domestic Violence Coalition Counselor AND a Family Strengthening Activity coded on the participant's Family Investment Agreement.
Cost
None
Source or Publisher
Montana Department of Health and Human Services
Child and Family Services Division
State(s) Believed to be Using
Montana
Domestic Violence Screening Form (New York)
Barriers Identified
Domestic Violence
Number and Types of Questions
Six 'yes' or 'no' questions about physical, sexual, and emotional abuse, fear of partner, threats to the client or children, and stalking.
Target Population
TANF clients statewide
Methodological Information
Not available
Implementation
It is a self-administered paper and pencil tool. The tool is given to all clients at intake and mentioned verbally, however, clients are not required to fill it out. One or more 'yes' answers lead to a referral to the Domestic Violence Specialist where the client will be expected to provide more detailed information about their situation.
Cost
None
Source or Publisher
New York State Department of Family Assistance (DFA)
Office of Temporary and Disability Assistance in coordination with
Office of Children and Family Services,
New York State Domestic Violence Coalition, and
legal experts
State(s) Believed to be Using
New York
Reference(Oregon) Card
Barriers Identified
Domestic Violence
Number and Types of Questions
The reference card provides brief information about how and where to screen a client, safety questions, the referral services available, developing a self-sufficiency plan, availability of financial resources, and behavioral clues to observe.
Target Population
TANF clients statewide
Methodological Information
Not available
Implementation
The reference card is a two sided card give to all reception staff and caseworkers as a brief reference to use while screening and assessing clients suspected of suffering from domestic violence.
Cost
None
Source or Publisher
Oregon Adult and Family Services
State(s) Believed to be Using
Oregon
Interview(Oregon) Questions
Barriers Identified
Domestic Violence
Number and Types of Questions
Thirty-five open-ended suggested questions to ask at each stage of a conversation on how to establish trust, how to broach the subject, how to identify patterns of abuse, how to assess the level of risk to the children, and the woman's history of seeking help.
Target Population
TANF clients statewide
Methodological Information
Oregon workers have found a disclosure rate of close to 50 percent, depending on where the client is in the domestic violence cycle.
Implementation
Typically caseworkers use this as a guide to interview the client. Questions and comments listed in the guide are used by the interviewer to establish a trusting relationship with the client.
Cost
None
Source or Publisher
Adapted for use by Oregon Adult and Family Services staff from a handout from Bradley Angle House, Portland, OR after consulting with staff at the Mid-Valley Women's Crisis Services, Salem, OR
State(s) Believed to be Using
Oregon
Safety Assessment (Oregon)
Barriers Identified
Domestic Violence
Number and Types of Questions
Eleven 'yes' or 'no' suggested questions about physical and emotional abuse, fear of partner, threats to the client or children, and stalking.
Target Population
TANF clients statewide
Methodological Information
Not available
Implementation
The Safety Assessment provides caseworkers with suggested questions meant to be asked in the office when the abuser is not around. The form is not placed in any packet a woman would take home due to the risk of abuse. The Safety Assessment is designed to make a general determination about the safety of the client and her children and is optional.
Cost
None
Source or Publisher
Oregon Adult and Family Services
State(s) Believed to be Using
Oregon
Rhode Island Assessment Tool
Barriers Identified
Domestic Violence
Number and Types of Questions
Fourteen open-ended questions about threats to the client or family members, sexual abuse, fear of partner, ability to participate in education and work requirements, residency, child support, paternity, location of absent parent, and hiding from absent parent.
Target Population
TANF clients statewide
Methodological Information
Not available
Implementation
All TANF clients a required to sign a written notification at initial contact. If a client discloses a problem with domestic violence, a domestic violence specialist meets with the client in the TANF office and uses this paper and pencil screening form to evaluate the client.
Cost
None
Source or Publisher
Rhode Island Department of Human Services in coordination with
- State(s) Believed to be Using
- community groups
State(s) Believed to be Using
Rhode Island
Section V: Mental Health
Beck Depression Inventory - II (BDI-II)
Barriers Identified
Mental Health - specifically depression
Number and Types of Questions
Twenty-one scaled questions
Target Population
Individuals ages 13 through 80
Methodological Information
The BDI-II has a reliability of 92 percent.10
Implementation
The BDI-II is a paper and pencil test that takes five minutes to complete. The test must be administered by person with a Master's degree and scored and interpreted by someone with a Ph.D./Ed.D.
Cost
$120.00 for a package of 100
Source or Publisher
The Psychological Corporation
555 Academic Court
San Antonio, TX 78204
State(s) Believed to be Using
New Jersey
10 Beck, Aaron T., M.D. and R.A. Steer. Beck Depression Inventory. Psychological Corporation. San Antonio, TX. 1996.
Posttraumatic Stress Diagnostic Scale (PDS)
Barriers Identified
Mental Health - specifically Post Traumatic Stress Disorder (PTSD)
Number and Types of Questions
Forty-nine 'yes' or 'no' and scaled questions
Target Population
Individuals ages 18 through 65 with at least an 8th grade reading level
Methodological Information
Subjects were recruited for the normative sample from a number of treatment and research centers that have a high frequency of PTSD among their patient populations. A total of 248 valid tests were collected.11
Implementation
The PDS is a 49 item paper and pencil instrument that can be administered in 10-15 minutes by someone with a Bachelor's degree in psychology, education, human relations, or a closely related field and courses in the use of psychological assessment instruments (graduate or undergraduate) or participation in an NCS approved workshop. The structure and content of the PDS assessment mirrors the DSM-IV diagnostic criteria for PTSD. The PDS can be used by psychologists, social workers and counselors to help 1) screen for the presence of PTSD in large groups with people who have identified themselves as victims of a traumatic event, and 2) gauge symptom severity and functioning in patients already identified as suffering from PTSD.
Cost
$51.00 for PDS manual, 10 answer sheets, 10 scoring worksheets, and 1 scoring sheet; $120.00 for reorder kit with 50 answer sheets, 50
scoring worksheets, and 1 scoring sheet
Source or Publisher
NCS Federal Government Sales Organization & Services Division
4301 Wilson Boulevard, Suite 200, Arlington, VA 22203-4196
State(s) Believed to be Using
New Jersey
11 Foa, Edna B. PDSTM (Posttraumatic Stress Diagnostic Scale). 1996.
Primary Care Evaluation of Mental Disorders (PRIME - MD)
Barriers Identified
Mental Health - specifically mood, anxiety, alcohol, and eating disorders
Number and Types of Questions
Twenty-six 'yes' or 'no' questions and a 12-page clinical evaluation guide for physicians
Target Population
Not available
Methodological Information
The validity of the diagnoses was compared to that of mental health professionals who interviewed the same patients; the accuracy rate was 88 percent. Prevalence of psychiatric disorders detected by the PRIME-MD in the 1,000 patients was as follows: any mood disorder, 26 percent; any anxiety disorder 18 percent; any eating disorder, three percent; and probable alcohol abuse/dependence, five percent.12
Implementation
The patient completes the one-page questionnaire prior to meeting with the clinician. The clinician uses the 12-page clinical evaluation guide to follow up on the patient's positive responses to the patient questionnaire.
Cost
None
Source or Publisher
Pfizer Inc.
235 East 42nd Street
New York, NY 10017-5755
State(s) Believed to be Using
New Jersey
12 Baldwin, Joyce and Staff. Questionnaire Helps Primary Care Physicians Detect Mental Disorders. Psychiatric Times, Vol. XII, Issue 2, February 1995.
Zung Depression Scale
Barriers Identified
Mental Health - depression
Number and Types of Questions
Twenty scaled questions
Target Population
Adults between the ages of 20 and 65 who may be suffering from depression13
Methodological Information
Studies have found that the Zung Depression Scale is a reliable method of discerning between normal and psychologically depressed individuals. The test has been criticized for placing equal weight on each question it asks. This means that a highly significant symptom of depression, such as sadness, carriers no more weight in this index than a less significant symptom of depression.14
Implementation
The Zung Depression Scale is a paper and pencil tool requiring 5-10 minutes to administer. It should be administered by professionally trained clinicians or licensed social workers and should be used as a complement rather than a substitute for an in-depth interview.15
Cost
None
Source or Publisher
William K. Zung
State(s) Believed to be Using
Oregon
13 Keyser, Daniel J. and Richard C. Sweetland, editors. Test Critiques. Kansas City, MO Test Corporation of
America, 1984 - 1994, p. 596.
14 Keyser pp. 599-601.
15 State of Virginia, Department of Human Services, undated.
About the Study
The Urban Institute
The Urban Institute is a nonprofit policy research organization established in Washington, D.C. in 1968. Its objectives are to sharpen thinking about society's problems and efforts to solve them, improve government decisions and their implementation, and increase citizens' awareness about important public choices. Institute researchers identify and measure the extent of social problems, assess developing trends and solutions to those problems, evaluate existing social and economic programs and policy options, and offer conceptual clarification and technical assistance in the development of new strategies. In pursuit of broader research and educational goals, Institute staff present their analysis and research to members and staff of the executive and legislative branches, the media, and other interested groups.
The Authors
The report was prepared by Terri S. Thompson and Kelly S. Mikelson, Research Associates at the Urban Institute.
Funders
This study was funded by the U.S. Department of Health and Human Services, Administration for Children and Families (ACF) and the Office of the Assistant Secretary for Planning and Evaluation (ASPE).
Acknowledgments
This study could not have been completed without the cooperation and assistance of many individuals. Most importantly, our thanks go to TANF agency officials and subject matter experts who assisted us with our research on screening and assessment tools and practices. We also thank Pamela Holcomb of The Urban Institute for her support and guidance throughout the project. We further recognize the invaluable contributions of project team members Lynne Fender, Jesse Valente, Pamela Loprest, and Sabina Taj. David Peabody produced the design and desktop publishing for this report. Finally, we are indebted to our two Project Officers, Jamie Kendall of ACF and William Marton of ASPE, for their commitment to the project.
How to Get the Report
A free copy of the report can be obtained from
Marie Belt
U.S. Department of Health and Human Services
Office of the Assistant Secretary for Planning and Evaluation
Hubert H. Humphrey Building, Room 424E
200 Independence Avenue, S.W.
Washington D.C. 20201
Fax (202) 401-7733
DALTCP2@osaspe.dhhs.gov
Copies may also be accessed through the websites of the Administration for Children and Families (www.acf.dhhs.gov), Office of the Assistant Secretary for Planning and Evaluation (www.aspe.hhs.gov), and the Urban Institute (www.urban.org).