
Executive Summary
Welfare reform efforts and significant caseload declines have resulted in a commonly held belief that those remaining on welfare face multiple barriers to employment, or are in some way “hard-to-serve.” Clients with complex barriers to employment, disabilities, or medical conditions, are often grouped under this broad heading. One of the most significant chal-lenges facing states and localities related to serving the hard-to-serve population is identifying the specific conditions and disabilities clients have that may be a barrier to finding and maintaining employment.
In 1999, the U.S. Department of Health and Human Services contracted with the Urban Institute to conduct a Study of Screening and Assessment in TANF/Welfare-to-Work (WtW). The first phase of the study involved a review of the issues and challenges faced by TANF agencies and their partners in developing strategies and selecting instruments to identify substance abuse and mental health problems, learning disabilities, and domestic violence situations among TANF clients. The issues and challenges identified through that review are presented in Ten Important Questions TANF Agencies and Their Partners Should Consider (hereafter referred to as Ten Important Questions). The second phase of the study involved case studies of a limited number of lo-calities to further explore how TANF agencies and their partners responded to the issues and challenges identified during phase one. The findings from the case studies are presented in this report.
Findings are based on discussions held between November 2000 and February 2001 with TANF agency staff and staff of key partner agencies in six localities: Montgomery County, KS, Owensboro, KY, Minneapolis, MN (the IRIS Program), Las Vegas, NV, Arlington, VA, and Kent, WA. Highlights of the insights offered by the case studies are provided below.
Approaches to Identification
The six localities visited represent a diverse mix of locations in which efforts to identify unobserved barriers to employment are merely one aspect of complicated, multifaceted TANF programs.
Identification approaches utilized by the study sites can generally be described under two headings—formal and informal. Formal approaches include the use of a tool, instrument, or test whereas informal approaches rely on discussion, disclosure of barriers by clients, or observation of behaviors that may suggest the existence of a barrier to employment.
The use of formal and informal identification approaches are not mutually exclusive. In fact, many staff responsible for implementing formal identification approaches reported that they use a tool or instrument as a part of a much larger process that includes informal identification strategies as well.
Few tools have been developed for use with TANF clients or are designed to address the multiple barriers many TANF clients face. While many still seek an instrument that would accurately and reliably identify a wide range of issues faced by TANF clients, the reality is no such tool currently exists, or arguably, may ever exist.
Generally, TANF agencies in the study sites use few validated tools to identify unobserved barriers to employment. However, the limited use of validated tools among TANF agencies does not indicate a general lack of use of tools or instruments to collect information and explore barriers. Partner agency staff who frequently possess greater expertise and formal training regarding barrier identification and are able to utilize a wider range of validated tools to uncover unobserved barriers to employment.
Informal efforts to identify barriers occur throughout the case management process. Each interaction with program staff presents an informal identification opportunity where clients can disclose barriers to employment and staff can elicit disclosure or observe behaviors/characteristics that are indicative of the existence of a barrier. The important question is therefore, how TANF agencies should integrate barrier identification into this multi-step process? The answer to this questions must take into consideration the various steps involved, the staff with whom clients interact at each point in the process, and the TANF policy context.
Staff in all sites reported using informal identification approaches throughout an individual’s interaction with the TANF system. These efforts were employed to different degrees across different staff positions, but occurred regardless of the use of a more formal identification instrument or the level of skill or training of the individual staff person. Importantly, even highly specialized staff who possess advanced training related to barrier identification noted the importance of informal strategies.
The majority of staff reported that they believe informal approaches are more effective in uncovering barriers than the completion of a specific screening or assessment tool. However, informal identification efforts rely heavily on clients to disclose a barrier to employment or to exhibit a behavior indicative of a barrier. Reliance on disclosure and behavioral observations presents a particular challenge when considering unobserved barriers to employment because many clients are unaware of their condition or may not consider their condition/situation a barrier to employment. Alternatively, clients may be simply unwilling to disclose a barrier to their case worker and make efforts to conceal the barrier.
The study sites have attempted to maximize the advantages of both formal and informal approaches by using them in combination with one another and expecting no one effort to uncover all barriers to employment.
Staffing Strategies to Identify Barriers to Employment
As TANF agencies and their partners increasingly focus on efforts to identify unobserved barriers to employment, they must consider the roles different staff should play in the barrier identification process. In doing this, they must decide how to best utilize TANF agency staff and staff of partner agencies in this endeavor. In all of the study sites, TANF case managers play an integral role in initial barrier identification efforts, in many cases creating a new role for these staff. However, case managers’ abilities to fulfill barrier identification responsibilities are affected by their other responsibilities, their skills and training, and the size of their caseloads.
The study sites rely on specialized staff to assist in the identification of unobserved barriers to employment to varying degrees. Although TANF case managers bear the primary responsibility for initially detecting the possibility of an unobserved barrier, more specialized workers are responsible for additional assessment or diagnosis. Specialized staff may be social workers employed by the TANF agency or clinicians employed by partner agencies who are co-located in the TANF office. Additionally, in all sites, clients may be referred to partner agencies where specialized staff who have more formal training relating to an unobserved barrier, or experience working with individuals with a particular barrier, are involved in the barrier identification and/or diagnosis process.
Focus groups conducted with TANF clients in each study site indicate that clients give careful consideration to decisions regarding to whom to disclose their barriers, and were generally more comfortable disclosing to specialized workers than staff with responsibility for benefit eligibility determination. Clients are particularly concerned with the possible repercussions of disclosure—including affects to benefits and possible removal of children from the home. Other factors that affect decisions to disclose are the existence of a trusting relationship, understanding the help that is available, and the client’s willingness to accept help.
The coordination and sharing of information among the variety of staff and partners involved in identifying and addressing unobserved barriers to employment is a complicated challenge and requires a significant investment in communication and collaboration at multiple levels. The study sites employed two methods of sharing information among staff—case staffings and a team approach. Generally, staffings are intended to offer the opportunity for a variety of staff to pool information regarding barriers, discuss clients’ situations, and determine appropriate next steps for a client. In sites utilizing team approaches, information is shared on an on-going basis and supported by an understanding of joint responsibility for a case by all members of often interdisciplinary teams.
Sharing information among the variety of staff involved in barrier identification requires that all involved give special attention to issues of confidentiality. A number of different federal and state laws, as well as regulations, guide the protection of privacy, the confidentiality of records, and informed consent. When asked, staff in all of the study sites appeared familiar with their offices’ guidelines regarding confidentiality and information sharing. In some cases, staff of partner agencies appeared more familiar than TANF agency staff with the details of these provisions and the need to obtain informed consent from clients before sharing information with the TANF agency. The experiences of the study sites offers hope that, despite the complexity surrounding issues of privacy and confidentiality, these challenges are not insurmountable and should not prohibit the implementation of proactive strategies to identify and address unobserved barriers to employment.
Identifying and Addressing Barriers to Employment Through Partnerships
TANF agencies in the study sites work with a variety of partners to assist with unobserved barrier identification and to provide services to clients once barriers are identified. Key partners include other government agencies, community mental health centers, substance abuse treatment programs, domestic violence shelters and counseling agencies, educational institutions, and others. In some cases these partners have had longstanding relationships with the TANF agency, while in other cases, new partnerships have formed as efforts to expand the identification of unobserved barriers have grown. In all sites, partnerships offer TANF clients access to staff with skills and expertise related to identifying unobserved barriers and, in some cases, barrier specific services. Thus, partners’ skills and services complement and supplement services provided by the TANF agency.
Partnerships in the study sites were created in a variety of ways. This variation is in part based on the responsibilities maintained at the state level, as compared to those passed to regional or local TANF offices. In some cases, partnerships grew out of past experience working informally with other organizations within a community’s social service system. Overwhelmingly, TANF staff at all levels reported having little difficulty securing services necessary to support efforts to identify and address unobserved barriers. In part this may be a result of the study sites being service rich communities. However, staff commonly attributed this ease to the general availability of TANF funding to purchase or create services.
Forging and maintaining partnerships to provide services to welfare recipients is neither a new nor a simple challenge for TANF agencies. Each of the study sites has faced this challenge and has undertaken different efforts to facilitate partnerships, including taking care to set clear expectations, obtaining support from staff at all levels, and co-locating partners.
In all sites, partners fill multiple roles. Partners typically conduct additional assessment or diagnose a condition and determine the appropriate level or type of treatment or services. In many situations, partners also provide the treatment or services required to address or mitigate barriers. A less formalized although potentially valuable role for partners in some sites is that of educating TANF staff on how toidentify unobserved barriers.
Concluding Observations and a Look to the Future
The case study sites offer a number of lessons regarding the issues and challenges associated with creating strategies to identify substance abuse and mental health problems, domestic violence situations, and learning disabilities. Perhaps one of the most important findings from the case studies is that the study sites have developed approaches that integrate barrier identification throughout a client’s TANF experience rather attempting to identify unobserved barriers at a single point in time. By involving a variety of staff (including staff of partner agencies) and using multiple identification strategies (formal and informal), the study sites have created a variety of opportunities to uncover unobserved barriers to employment while remaining focused on the employment and self-sufficiency goals of welfare reform.
Some welfare agencies that perceive their remaining welfare clients to be hard-to-serve are beginning to rethink their Work First approach. However, the study sites have found ways to maintain a work focus while also incorporating barrier identification strategies. It is important to note that these sites have not reverted to a pre-welfare reform strategy of exempting clients from participation. In all of the study sites, clients may be allowed to engage in non-work related activities in an effort to remove or mitigate barriers. However, these activities are considered a necessary step for a client to ultimately become employable and leave welfare.
TANF clients with substance abuse and mental health problems, domestic violence situations, and/or learning disabilities, will continue to present identification and service delivery challenges to TANF agencies and their partners. The case study sites have made great strides into relatively uncharted territory by developing the identification and service strategies described here. If such strategies are to continue, and new efforts are to be developed, TANF agencies and their partners will require the resources to support staff by maintaining or establishing workloads that facilitate barrier identification efforts, involve specialized staff and/or partner agencies, and provide staff training. If the progress made toward identifying and addressing barriers faced by the hard-to-serve is to be sustained, it will be important for policymakers not to succumb to pressures to reduce funding or limit the flexibility provided to states and localities when considering the reauthorization of TANF in 2002.
Chapter One: Introduction
One of the most significant challenges facing states and localities is identifying specific conditions and disabilities clients have that may be a barrier to finding and maintaining employment.
Nearly five years after federal welfare reform, states and localities have experienced unprecedented caseload declines. With this caseload decline, there has developed a commonly held belief that those remaining on welfare face multiple barriers to employment, or are in some way “hard-to-serve.” Clients with complex barriers to employment, disabilities, or medical conditions, are commonly grouped under this broad heading.
One of the most significant challenges facing states and localities related to serving the hard-to-serve population is identifying specific conditions and disabilities clients have that may be a barrier to finding and maintaining employment. Pressure to address this challenge is increased by the time limited nature of federally funded TANF assistance. This challenge is made more complicated because welfare agencies know relatively little about the specific nature of clients’ disabilities or health conditions. This lack of knowledge is the result of the fact that clients with barriers to employment were exempt from participating in the employment and training program that preceded TANF, the Job Opportunities and Basic Skills (JOBS) training program. Exemptions from participation in JOBS were based on the existence of a condition that fell under the broad headings of illness or incapacity. Federal time limits and work participation rate requirements have led many states to change their exemption policies and require participation in welfare to work programs by clients who were previously exempt, and some states are beginning to collect more specific information about the nature of disabilities and health conditions.1 Nonetheless, states and localities face a number of key challenges including overcoming their general lack of experience with identifying unobserved barriers to employment and developing effective service strategies to address unobserved barriers.2
In 1999, the U.S. Department of Health and Human Services contracted with the Urban Institute to conduct a Study of Screening and Assessment in TANF/Welfare-to-Work (WtW). The first phase of the study involved a review of issues and challenges faced by TANF agencies and their partners in developing strategies and selecting instruments to identify substance abuse and mental health problems, learning disabilities, and domestic violence situations among TANF clients. The issues and challenges identified through that review are presented in Ten Important Questions TANF Agencies and Their Partners Should Consider (hereafter referred to as Ten Important Questions). The second phase of the study involved case studies of a limited number of localities to further explore how these agencies and their partners responded to the issues and challenges identified during phase one. The findings from the case studies are presented here.3
1 See Thompson, et al. State Welfare Reform Policies for People with Disabilities: Changes Since Welfare Reform. October 1998.
2 See Holcomb and Thompson, State Welfare Reform Policies for People with Disabilities: Implementation Challenges and Considerations, August 2000.
3 Another component of the study involved convening a series of three regional discussion meetings. Held in the spring of 2001, these meetings brought together state and local TANF agency representatives from across the country to discuss screening and assessment issues, challenges, approaches, and solutions. Although not discussed separately, key points from the discussion at these meetings are incorporated throughout.
Unobserved Barriers to Employment
Both Ten Important Questions and this report focus on four conditions that are prevalent among TANF clients—substance abuse and mental health problems, domestic violence situations, and learning disabilities.4 These conditions are often not easily detected, and in the case of many welfare recipients, have not been previously diagnosed. They also represent health conditions, disabilities, or situations that clients may be reluctant to disclose—if they are even cognizant that the condition or situation exists. For these reasons, we collectively refer to this group of health conditions, disabilities, and situations as “unobserved barriers to employment.” Identifying these unobserved barriers requires the development of new strategies and practices, in part because they are so difficult to detect and in part because welfare agencies have little experience in this area. Therefore, these strategies are the focus of our case studies.
It should be acknowledged that substance abuse and mental health problems, domestic violence situations, and learning disabilities in and of themselves may not present a barrier to employment or self-sufficiency. Many individuals with these and other disabilities and health conditions work and care for their families every day. To the extent TANF recipients with these issues are able to comply with TANF program requirements, these barriers would likely receive little attention from the TANF system. Unlike other social or health service systems, the TANF system would be typically concerned with these barriers only if they inhibit a client’s participation in required activities and progress toward obtaining employment and achieving self-sufficiency.5 Therefore, for the purposes of both Ten Important Questions and this report, the discussion presented is predicated on the assumption that TANF agencies focus on “unobserved barriers” because these health conditions, disabilities, and situations impede employment and welfare exit.
4 See Question Two in Ten Important Questions for a review of prevalence estimates.
5 These situations would also receive attention from TANF agencies if they jeopardized the safety of children in the household. Such a situation would likely be met with a referral to the local child welfare agency.
Methodology
As noted above, this report presents the findings from phase two of this study. It presents a description and discussion of how TANF agencies in six localities address the issues and challenges associated with identifying clients’ unobserved barriers to employment. Four-day site visits were conducted to each locality between November 2000 and February 2001. During each visit, a team of two researchers met with a wide range of TANF agency staff to discuss how identification efforts were carried out in practice. We also met with staff of key partner agencies who assist with barrier identification and provide services to address unobserved barriers.
Additionally, in each site we conducted a focus group with TANF clients. Focus group participants were recruited by local agency staff. Participants did not have to meet any predetermined criteria and no efforts were made to ensure that participants were representative of clients in that site. While comments from focus group participants should be considered anecdotal, they do provide a sampling of clients’ perspectives on an important dimension of barrier identification—clients’ willingness to disclose their barriers—and raise issues that can be explored in greater depth by future research.
Many factors were considered when selecting sites for inclusion in this study. Most important was the site’s approach to barrier identification, described further in Chapter Two. Potential study sites were initially identified through the course of completing Ten Important Questions. For this more indepth review, we selected sites that were undertaking seemingly proactive and diverse strategies to identify barriers to employment. In reviewing identification strategies, we considered the site’s use of screening and assessment instruments, staffing structure, and the partners involved in identification and service provision. We also sought sites implementing these approaches within diverse TANF policy contexts, across different parts of the country, and in localities of varying sizes. Where approaches were carried out statewide, localities were selected based on input from program managers. The sites included in the study are:
Montgomery County, KS
Owensboro, KY
Minneapolis, MN (the IRIS Program)
Las Vegas, NV
Arlington, VA
Kent, WA
An overview of the TANF policies in each site and approaches to barrier identification are provided in Chapter Two. Figure 1 illustrates the geographical distribution of the study sites. As can be seen from the table in Figure 1, the study sites represent a mix of communities. Montgomery County, KS is a small, rural community containing two welfare offices in the towns of Coffeyville and Independence. Owensboro, KY is also a less urban area. Arlington, VA and Kent, WA both reflect large communities bordering the even larger urban areas of Washington, D.C. and Seattle, Washington, respectively. Minneapolis, MN and Las Vegas, NV are large urban areas.
Figure Figure 1: Location Location of Study Sites
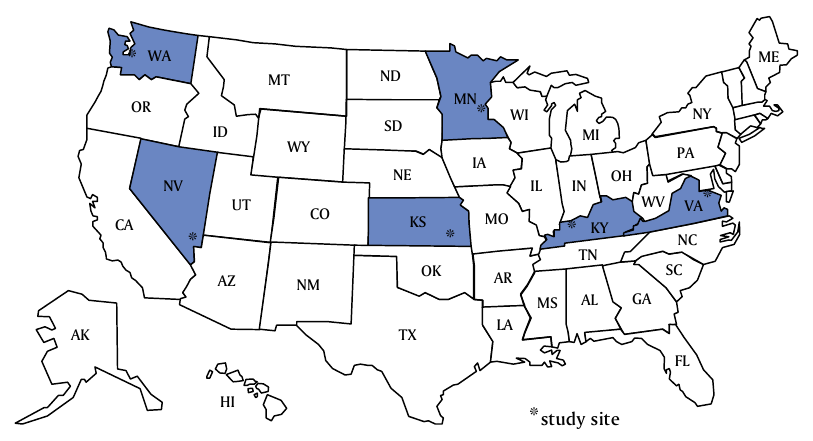
| State | Study Site | Study Site Populationa |
|---|---|---|
| Kansas | Montgomery County (Including the towns of Coffeyville and Independence) | 36,252 (11,021 and 9,846) |
| Kentucky | Owensboro (Daviess County) | 54,067 (91,545) |
| Minnesota | Minneapolis (Hennepin County) | 382,618 (1,116,200) |
| Nevada | Las Vegas (Clark County) | 478,434 (1,375,765) |
| Virginia | Arlington (Arlington County) | 189,753 (189,753) |
| Washington | Kent (South King County) | 79,524 (1,737,034) |
a U.S. Census Bureau http://www.census.gov as of 9/17/01.
A Roadmap to the Report
The issues identified in Ten Important Questions guided the case studies and frame the presentation of case study findings. To remain focused on the questions of interest, the discussion of study sites’ strategies are presented in a topical format, rather than by individual site. However, the strategies discussed throughout must be considered within each site’s local context including each locality’s TANF policies, staffing structures, and partners, that influence how identification strategies were formulated and carried out in practice. Therefore, before moving to a more in-depth discussion of identification strategies, we first present (in Chapter Two) profiles of the localities. Further, it should be noted that the discussion of strategies presented within is not intended to provide a comprehensive review of all services provided by the localities’ TANF programs. For example, the report may not discuss key features of the TANF programs operated by the study sites if they do not directly relate to a barrier identification issue or challenge.
Chapter Three provides a discussion of the types of identification strategies used by study sites. This chapter includes a review of formal strategies, that involve the use of structured tools or instruments, as well as informal strategies, that rely heavily on discussion and disclosure.
Chapter Four emphasizes the on-going nature of barrier identification by highlighting the variety of opportunities to identify unobserved barriers that occur throughout a client’s TANF experience. It also offers a discussion of barrier identification in the context of a Work First philosophy.
Staff roles and responsibilities, including the roles of TANF case managers and more specialized staff in the study sites, are discussed in Chapter Five. This chapter also addresses the challenges related to sharing information among the variety of staff involved in barrier identification efforts.
In Chapter Six, we offer an overview of key partnerships formed in the study sites and the roles partners play in barrier identification, service provision, and education of TANF staff regarding unobserved barriers to employment. Chapter Six also highlights efforts employed to create successful partnerships (Appendix B offers a more detailed description of the services provided by selected partners). Finally, we conclude in Chapter Seven with a summary discussion of key observations from the case studies and a look to the future.
Chapter Two: Profiles of the Study Sites
Efforts to identify unobserved barriers to employment are merely one aspect of the complicated, multi-faceted TANF programs operated by the study sites. To fully understand the identification efforts that are the focus of this report, it is important to understand key contextual features of each site. In this chapter we describe these important features, including the TANF policy context within which efforts to identify barriers are carried out. This chapter also offers an overview of each study site, specifically focusing on the reason the site was included in the study (e.g., use of specialized staff or combinations of staff to assist in barrier identification, use of formal screening tools, use of partners to identify and address barriers). This overview is intended to offer the reader a basic understanding of some of the important features of each site to enhance the crosscutting discussion of issues that comprise the remainder of the report.
TANF Policy Context
Time Limits
Federal law limits the provision of federal TANF assistance to 60 months in an individual’s lifetime, and gives states the flexibility to impose shorter time limits. Moving from welfare to work within 60 months or less may present a particular challenge for clients with unobserved barriers to employment. 6 Time limits thus increase the sense of urgency surrounding the need to develop barrier identification approaches. Table 1 shows that four of the six study states have adopted the 60 month lifetime limit on federal assistance. Nevada and Virginia, impose shorter initial limits on welfare receipt and the first clients had already reached this limit at the time of our site visits. In Nevada, a client may receive welfare for 24 months, but is then ineligible for cash assistance for 12 months. Following this 12 month period of ineligibility, a client may again receive cash assistance up to a lifetime maximum of 60 months. Similarly, Virginia adopted a 24 month initial time limit, followed by 24 months of ineligibility, with a maximum total period of receipt not to exceed 60 months.7
6 States may provide more than 60 months of federally-funded assistance to up to 20 percent of their caseload based on hardship exemption criteria. Although not reviewed here, some of the study sites were reviewing possible criteria upon which to grant hardship exemptions, including the existence of unobserved barriers to employment.
7 In Virginia, clients are eligible for 12 months of transitional assistance following their 24 months of cash assistance. The 24 month period of ineligibility begins following the receipt of transitional assistance, effectively leaving clients without cash assistance for 36 months before being eligible for additional cash assistance.
Table 1: Selected TANF Policy Characteristics
| Study state | Characteristic | ||||||
|---|---|---|---|---|---|---|---|
| Year Welfare Reform Began in Study State | TANF Caseload as of 9/00 a | TANF Caseload Decline 1/95-9/00 b | Maximum Monthly TANF Benefit Level for a 3 Person Family c | Exempt from Work Participation Due to Disability? d | Time Limit (in months) e | Date First Family Reaches Time Limit f | |
| Kansas | 1995 | 12,713 | 56% | $403 | No | 60 | 10/01 |
| Kentucky | 1996 | 37,249 | 51% | $262 | No | 60 | 11/01 |
| Minnesota | 1997 | 39,005 | 36% | $801 g | Yes | 60 | 7/02 |
| Nevada | 1995 h | 6,473 | 60% | $348 | No | 24 followed by 12 months of ineligibility; 60 total | 01/00 |
| Virginia | 1996 | 29,939 | 59% | $320 | Yes | 24 followed by 24 months of ineligibility; 60 total | 10/99 |
| Washington | 1997 | 53,759 | 48% | $546 | No | 60 | 8/02 |
a U.S. Department of Health and Human Services, Administration for Children and Families, Office of Planning, Research and Evaluation. www.acf.dhhs.gov/news/stats/welfare.htm as of 11/1/01.
b Urban Institute calculations based on Department of Health and Human Services caseload statistics reported at www.acf.dhhs.gov/news/stats/welfare.htm and www.acf.dhhs.gov/news/stats/case-fam.htm as of 11/1/01.
c Monthly cash assistance for a single-parent family with no earnings as of 2001. Center on Law and Social Policy and Center for Budget and Policy Priorities. State Policy Documentation Project at www.spdp.org as of 12/11/01.
d Ibid.
e Ibid.
f Ibid.
g Minnesota provides a cash grant that combines cash assistance and Food Stamp benefits.
h Official welfare reform policy was not implemented until January 1998 and federal time limits began counting in Nevada in January 1997.
Work Participation Rates
Although all of the study sites are focused on moving clients from welfare to work as quickly as possible, they all give staff the flexibility to determine the appropriate service strategies based primarily upon indi- vidual needs.
Another TANF policy requirement which has had an impact on how states decide to serve clients with barriers is the TANF work participation rate. Activities that “count” in the rate calculation are defined by federal law and include, but are not limited to, job search and job readiness activities, subsidized and unsubsidized employment, vocational education and training, and on-the-job training.8 Services to address unobserved barriers to employment, such as substance abuse treatment or mental health counseling, do not count toward the federal participation rate. Although federal law defines the activities that count toward the participation rate, states are not required to achieve 100 percent participation following this definition. Therefore, states have some flexibility to determine the activities in which clients are “allowed” to participate. States do not necessarily have to restrict participation to the federally defined activities, as long as they meet the required work participation rate, currently set at 50 percent for all families for fiscal year 2002.
Although all of the study sites are focused on moving clients from welfare to work as quickly as possible, they all give staff the flexibility to determine the appropriate service strategies based primarily upon individual needs. For example, in all of the study sites, clients with barriers to employment were typically not required to immediately participate in activities that count toward the federal participation rate. Clients with barriers were commonly allowed to participate in non-countable activities such as drug/alcohol treatment, domestic violence services, or mental health programs. Although aware of the work participation rate requirements and which activities counted toward achieving the rates, TANF staff consistently reported that choices regarding services for clients were primarily guided by the individual’s needs, not the work participation rates. Partner agency staff varied in their understanding of TANF work requirements and did not report facing pressure to modify their approaches or alter recommended services in response to TANF requirements.
8 See Question Three in Ten Important Questions for a discussion of opportunities and limitations presented by TANF requirements. See the Personal Responsibility and Work Opportunity Reconciliation Act of 1996 and final TANF regulations for a complete detailing of TANF work participation rate requirements.
Work Participation Exemptions
In addition to defining activities in which clients may participate, states and localities may also grant exemptions from participation. The most common exemption, granted by 44 states, is for the need to care for a young child. However, 34 states also exempt disabled adults from work requirements.9 As shown in Table 1, only two of the six case study states allow work participation exemptions due to a disability.
It is also important to note that unobserved barriers such as substance abuse and mental health problems, learning disabilities, and domestic violence situations are not necessarily considered “disabilities” in the TANF system. Often, to be exempt due to a disability, TANF clients must produce a medical report verifying the condition. If an unobserved barrier has not been previously diagnosed or the client is not aware that the condition exists, she is unlikely to be given a work participation exemption. 10
Although not granted a formal exemption, some states have other mechanisms to excuse clients from participating in work activities. In Washington, for example, clients may be granted a “deferral” from work activities. Deferring a client consists of granting a temporary reprieve from work participation. Deferring a client differs from exempting a client in that a deferral is granted for a short period of time at the discretion of the worker, whereas exemption criteria are clearly defined in policy and their durations are determined by medical reports. Although exemptions or deferrals may offer a reprieve from participating in work programs, it is important to note that an exemption from work participation does not necessarily mean that the client is not subject to the time limit.
9 Center on Law and Social Policy and Center for Budget and Policy Priorities. State Policy Documentation Project at www.spdp.org as of 11/5/01.
10 The overwhelming majority of TANF recipients are women. Therefore, for ease of discussion clients will be referred to using the feminine pronoun.
Site Profiles
Each of the study sites has undertaken a proactive approach to identifying unobserved barriers to employment. Strategies include a mix of different identification methods, including informal and formal screenings or assessments, a mix of staff involved in barrier identification, and a variety of partners to assist with identification and service provision. Although many of these features are discussed in the remaining chapters of the report, this section provides a brief overview of the identification approaches undertaken by each site that led to their inclusion in the study.
TANF clients encounter many different staff persons as they progress through the TANF system. Staff may include TANF eligibility workers and case managers, specialists such as social workers, and staff of partner agencies. 11 The site profiles below provide an overview of the key staff involved in the process of identifying barriers to employment. The roles and responsibilities of these staff will be discussed in greater detail in later chapters (see Table 2).
TANF agencies can benefit from the expertise and services offered by a wide range of partners in their efforts to identify and address unobserved barriers to employment. Each of the study sites utilizes a wide range of government and community-based partners to assist in their barrier identification approaches. These partner organizations, such as local community mental health centers and domestic violence shelters, will be referenced and discussed repeatedly throughout the report. The profiles below provide a brief overview of the key partner organizations in each site (see Table 3).
11 TANF case managers are also called employment case managers and employment and training specialists. For ease of discussion, TANF staff responsible for employability and service planning will be generally referred to as case managers.
Table 2: Key TANF Agency Staff Involved in Identifying Unobserved Barriers by Site
| Function | Kansas | Kentucky | Minnesota | Nevada | Virginia | Washington |
|---|---|---|---|---|---|---|
| Financial Eligibility Determination | Case Manager | Case Manager | Intake Eligibility Worker; On-going Eligibility Worker | Intake Eligibility Worker; On-going Eligibility Worker | Intake Eligibility Worker; On-going Eligibility Worker | Case Manager |
| Case Management/ Service Planning | Employment Service Providersa | Employment and Training Specialist | Employment Case Manager | |||
| Additional In - depth Services/ Specialized Barrier Identification | N/A | N/Ab | Social Worker | Crisis Assistance Bureau Social Worker; c Substance Abuse/Mental Health Therapist | Social Worker |
a The staffing structure of employment service providers varies from provider to provider. There are more than 30 employment service providers in Minneapolis.
b Targeted Assessment Project (TAP) assessors are co-located in the TANF office but are employed by the University of Kentucky, Institute on Women and Substance Abuse.
c TANF clients may also be referred to a social worker in the Crisis Assistance Bureau. These social workers assist clients with emergency situations such as rent, utilities, and homeless services/shelters.
Table 3: Selected Key Partners by Site
| Study Site | TANF | Mental Health | Substance Abuse | Domestic voilence | Learning Disabilities |
|---|---|---|---|---|---|
| Montgomery County, KS | Kansas Department of Social and Rehabilitation Services (SRS) | Four County Mental Health | Regional Alcohol and Drug Assessment Center (RADAC) and treatment facilities | Safe House | SRS/ Vocational Rehabilitation Services |
| Pittsburg State University | |||||
| Four County Mental Health, Extra Effort Program | |||||
| Owensboro, KY | Kentucky Cabinet for Families and Children (CFC)/Department of Community Based Servicesa | University of Kentucky TAP Project | |||
| River Valley Behavioral Health | Owensboro Area Shelter and Information Services (OASIS) | Kentucky Cabinet for Workforce Development/ Department of Vocational Rehabilitation | |||
| Minneapolis, MN | Hennepin County Department of Economic Assistanceb | Integrated Resources for Independence and Self-Sufficiency (IRIS) | Harriet Tubman Centerc | Minnesota Department of Economic Security/ Rehabilitation Services Branch | |
| Las Vegas, NV | Nevada Department of Human Resources (DHR)/Nevada State Welfare Division (NSWD) | Local providers coordinated by Health Maintenance Organizationsd | DHR/Nevada Health Division/Contract service providers of the Bureau of Alcohol and Drug Abuse (BADA) | Safe Houseе | Nevada Department of Employment, Training, and Rehabilitation/ Bureau of Vocational Rehabilitation |
| Arlington, VA | Arlington County Department of Human Services (DHS)f | DHS/Department of Mental Health, Mental Retardation, and Substance Abuse Services (DMHMRSAS) | DHS/Department Children and Fam ily Services/ Victims of Violence Program Safe House | DHS/ Aging and Disability Servicesg | |
| Sheltered Occupational Center (SOC) Enterprises | |||||
| Kent, WA | Washington Department of Social and Health Services (DSHS)/ Economic Services Administration | Independent psychologist | King County Department of Community and Human Services/ Mental Health, Chemical Abuse, and Dependency Services Division | Domestic Violence Women's Network (DAWN) | Seattle-King County Workforce Development Council, Learning Disability Project |
| Northwest Counseling | YWCA | ||||
a Within the Department of Community Based Services the Division of Family Support provides TANF cash assistance and employment services, Medicaid, and Food Stamps. The Division of Protection and Permanency provides child welfare services.
b At the state level, MFIP is administered by the Minnesota Department of Human Services. Employment services are provided through a joint effort of the Department of Human Services and the Department of Economic Security.
c The Harriet Tubman Center is one of a number of domestic violence service providers in Hennepin County.
d Outside of Las Vegas, mental health services are provided according to an agreement with DHR/NSWD/Division of Mental Health and Developmental Services.
e Safe House is one of a number of domestic violence service providers in Las Vegas.
f Arlington is unique in Virginia in that the TANF program is operated by the Department of Human Services which also provides mental health, substance abuse, and vocational rehabilitation services. At the state level, TANF is administered by the Department of Social Services. Mental health, substance abuse, and other services are provided by different state level agencies.
g Operates the Vocational Rehabilitation program. Managed by Department of Rehabilitation Services at the state level.
Montgomery County, Kansas
Kansas has a history of using screening tools to assess the needs, experiences, and
interests of its welfare recipients.
Kansas has a history of using screening tools to assess the needs, experiences, and interests of its welfare recipients. Several years into its welfare reform effort, Kansas changed its work exemption policy. As of April 1999, having a disability no longer warrants an exemption from participation in the Kansas Works program. To effectively implement this policy and serve these formerly exempt clients, Kansas developed an Assessment Guide for case mangers to assess the goals, strengths, and barriers of TANF recipients. Case managers have also been provided with a protocol to use to determine if additional assessment or testing is needed based on the information collected through the completion of the Assessment Guide. Additionally, Kansas has long been recognized for its involvement in efforts to develop an instrument to screen for learning disabilities among TANF clients, the Adult Learning Disability Screen.
The Kansas Works Program is operated by the Kansas Department of Social and Rehabilitation Services (SRS) through the Economic and Employment Service Division. Montgomery County is unique in that it has two SRS offices, one in Coffeyville and one in Independence, whereas other counties in Kansas typically have one SRS office. In Montgomery County, eligibility and case management functions are both carried out by a case manager. Clients with unobserved barriers to employment in Montgomery County may be referred to a number of community partners. The primary partners in this site include, Safe House (the local domestic violence shelter), the Regional Alcohol and Drug Assessment Center (RADAC) which provides on-site substance abuse assessments, and Four County Mental Health Center. Four County Mental Health provides mental health counseling, job readiness services, and operates the pilot program, Extra Effort. Extra Effort is designed to identify TANF clients who are at risk of becoming involved in the child welfare system. These clients often face unobserved barriers to employment, and once identified, are provided intensive services. Two partners are involved in addressing learning disabilities in Montgomery County, SRS’s Vocational Rehabilitation Services and Pittsburg State University.
Owensboro, Kentucky
Although Kentucky’s welfare-to-work program, the Kentucky Works Program, focuses on moving clients to employment as quickly as possible, there is a recognition that some barriers to employment make it harder for TANF recipients to find and keep a job. Building on earlier efforts to identify substance abuse among TANF clients, in 1999 the Kentucky Cabinet for Families and Children (CFC) partnered with the University of Kentucky’s Institute on Women and Substance Abuse to operate a pilot project called the Targeted Assessment Project (TAP). The TAP places experienced clinicians (TAP assessors) who are employees of the University of Kentucky in welfare offices to assist in screening and assessing barriers to employment, facilitating appropriate referrals to partner agencies, and involving community agencies in further assessing and serving TANF recipients.12 Owensboro was included in the study because it was the first of eight communities where the TAP was implemented and was therefore furthest along in its implementation.13
In Kentucky, TANF is administered locally through the CFC’s Department of Community Based Services. Case managers in the Department of Community Based Services, Division of Family Support are responsible for determining financial eligibility for TANF and other programs, as well as employment service planning and monitoring compliance with program requirements. Staff of the Divisions of Child Support and Protection and Permanency are also commonly involved with TANF clients.
In addition to services provided directly by the Department of Community Based Services, TANF clients have access to several barrier-removal services that are located in Owensboro. Some key partners in this site include, the Owensboro Area Shelter and Information Services (OASIS) which provides services to domestic violence victims, the Cabinet for Workforce Development, Department of Vocational Rehabilitation, and River Valley Behavioral Health (the local community mental health center). As noted earlier, the University of Kentucky’s Institute on Women and Substance Abuse, a service arm of the University, operates the Targeted Assessment Project.
12 TAP assessors are placed in both the Division of Family Support which administers TANF and the Division of Protection and Permanency which is responsible for child welfare. Although the assessors fill similar roles, for the purposes of this study, we focused on the assessor placed within the Division of Family Support.
13 Since our site visit the TAP pilot has expanded to serve 17 communities in Kentucky. For more information see: http://www.kentuckyconnect.com/heraldleader/news/062701/statedocs/27Welf...
Minneapolis, Minnesota
The Minnesota Family Independence Program (MFIP), Minnesota’s TANF program, involves a variety of service providers to assist with the transition of recipients from welfare to work. In Minneapolis, service planning, job readiness, and job search services are provided under contract by more than 30 employment service providers. Employment service providers employ case managers and other staff to assist in this endeavor. MFIP clients also meet with an MFIP eligibility worker who is employed by Hennepin County to determine financial eligibility for benefits.
In addition to employment service providers, there are a number of partner agencies in Minneapolis to which clients with unobserved barriers to employment may be referred. One such provider is the Integrated Resources for Independence and Self-sufficiency (IRIS) Program—the focal program for this study. IRIS, which is a part of Hennepin County’s Children, Family, and Adult Service Department, Vocational Services Program, began serving Welfare-to-Work (WtW) clients in 1999.14 In 2000, IRIS expanded to serve MFIP and WtW clients having trouble fulfilling work requirements because of chemical and/or mental health barriers. Clients referred to IRIS receive vocational, social, and clinical services to assist them with their transitions from welfare to work. Services are provide by a staff team consisting of a social worker, a vocational counselor, and a therapist. In addition to IRIS, other partners include domestic violence shelters such as the Harriet Tubman Center, and the Vocational Rehabilitation program operated by the Department of Economic Security.
14 The Welfare-to-Work grants program was created under the 1997 Balanced Budget Act and is administered nationally by the U.S. Department of Labor. The program is intended to provide job opportunities, employment preparation, and job retention services for welfare recipients who are the hardest to employ. See Nightingale, et al. Early Implementation of the Welfare-to-Work Grants Program: Findings from Exploratory Site Visits and Review of Program Plans. February 2000.
Las Vegas, Nevada
Managers in Nevada realized that some welfare clients have multiple and complicated barriers to employment that require different strategies than those that had been the focus of early welfare reform efforts.
Nevada got an early start on welfare reform by implementing its welfare employment program, New Employees of Nevada, in July of 1995, 18 months before federal welfare reform began. This early start led managers in the Department of Human Resources, Nevada State Welfare Division to realize that some welfare clients have multiple and complicated barriers to employment that require different strategies than those that had been the focus of early welfare reform efforts. In the mid-1990s, TANF managers requested that the state legislature fund social worker positions to assist in serving clients with barriers to employment. Social workers provide an additional resource to clients who also work with an eligibility worker and a case manager.
In addition to this new staffing strategy, the Nevada State Welfare Division has developed partnerships with several state agencies and local service providers in an effort to enhance and provide services to recipients with unobserved barriers to employment. Many of these partnerships are based on formal agreements between state agencies that clarify the expectations and responsibilities of each organization. For example, the TANF agency has formal partnerships with the Division of Mental Health and Developmental Services and contracts with Bureau of Alcohol and Drug Abuse contractors for substance abuse treatment. Furthermore, the TANF agency partners with the Vocational Assessment Center and the Department of Employment, Training, and Rehabilitation, Rehabilitation Division for vocational assessment and rehabilitation services, as well as domestic violence service providers.
Arlington, Virginia
The state of Virginia gives counties wide latitude to determine how to operate the TANF employment program, Virginia Initiative for Employment not Welfare. In supporting this locally-operated system, the state has offered a variety of resources to assist with identifying barriers to employment among TANF clients. Among these are a compendium of tools that could be used to identify barriers to employment, and support for involvement in the National Institute for Literacy’s “Bridges to Practice” training. 15 The state also invested in services jointly provided by the Departments of Social Services (DSS) and Rehabilitation Services (DRS).
The state identified Arlington as a county that has implemented efforts to enhance its focus on barrier identification. Arlington has engaged in an effort to train staff to identify learning disabilities following the “Bridges to Practice” model, including using a formal screening tool for learning disabilities. Their efforts to support hard-to-serve recipients also include developing a team approach to working with welfare clients. The core team consists of an eligibility worker, a case manager, a job developer, and a social worker from the Crisis Assistance Bureau. Depending on the needs of the client, the team may be expanded to include the on-site substance abuse/mental health therapist. In addition, Arlington also partners with the Department of Rehabilitation Services (DRS) and Sheltered Occupational Center (SOC) Enterprises to assist clients suspected of having a learning disability. If a client is referred for these services, she would also work with a team of staff consisting of a DRS counselor, a case manager from SOC Enterprises, and a psychologist.
15 The National Institute for Literacy’s (NIFL) “Bridges to Practice” guide is a research-based guide for practitioners serving adults with learning disabilities. This guide includes topics such as, ‘Understanding Learning Disabilities’ and ‘Creating an Appropriate Learning Environment.’ For more information see www.nifl.gov.
Kent, Washington
Washington has invested in a structured, computerized, multi-barrier assessment instrument to uncover barriers to employment. The Virtual Interactive Employability Worksheet (VIEW) is used with all TANF clients and addresses a range of barriers to employment such as, mental health and substance abuse problems, domestic violence situations, and learning disabilities. If case managers (who are responsible for financial eligibility and service planning) determine that a client has a barrier to employment based on a response to the VIEW questions or other information obtained by the case manager, she may be referred to a social worker.
Social workers are employed by the Department of Social and Health Services (the TANF agency) and are located in local welfare offices. Social workers may subsequently refer clients to a wide range of partners. In the Kent office, many of these partners are co-located. For example, the Economic Security Department provides fast track job search and other job readiness services. Also co-located are a public health nurse, an independent psychologist, and an assessor from the state substance abuse agency. Washington also provides a number of services through contractual or other partnership arrangements. One such service is called Intensive In-Home Services. These services are provided under contract (one local provider in Kent is Rainier Case Management) and are intended to serve clients who are sanctioned or about to be sanctioned due to non-compliance with TANF work requirements. Other partners include Northwest Counseling, the Domestic Violence Women’s Network (DAWN), the YWCA (a domestic violence service provider), and the Seattle-King County Workforce Development Council’s Learning Disability Project.
Chapter Three: Approaches To Identification— Formal and Informal
This study looked at a wide range of identification efforts to uncover unobserved barriers to employment.
Efforts to identify barriers to employment faced by TANF clients are described and discussed using various terminology. Common terms such as “screening” and “assessment” are sometimes used interchangeably. However, the term screening is also used to describe a less rigorous effort to determine the possible existence of a barrier, while assessment often connotes a more structured, in-depth approach to barrier identification. Still others use the term assessment to describe the on-going process of uncovering barriers that occurs throughout a client’s experience with the TANF system. For the purposes of this report, distinguishing between efforts to screen as compared to efforts to assess is not as valuable as understanding how identification approaches are carried out in practice. Therefore, this study looked at a wide range of identification efforts—including those that may be described as either screening or assessment—to uncover unobserved barriers to employment.
Identification approaches utilized by the study sites can be generally described under two headings—formal and informal. Formal approaches include the use of a tool, instrument, or test. Informal approaches rely on discussion, disclosure of barriers by clients, or observation of behaviors that may suggest the existence of a barrier to employment. The use of formal and informal identification approaches are not mutually exclusive. In fact, many staff responsible for implementing formal identification approaches reported that they implement a tool or instrument as a part of a much larger process that includes informal identification strategies as well.
The primary goal of identification approaches employed by TANF agencies is to provide an initial indication of the likelihood that a barrier to employment exists. Generally, this information is used to refer a client to a more highly trained specialist for additional assessment and confirmation of the existence of this barrier. In some cases, these more specialized partners undertake more detailed assessments that may guide treatment or service strategies, but generally do not include a formal diagnosis. However, in some situations TANF agency staff refer clients to partner agencies where staff can assess, diagnosis, and treat a particular barrier.16 In the next sections, we examine both formal and informal approaches to barrier identification and conclude with a discussion of the advantages and disadvantages of each approach.
16 Efforts undertaken by barrier-specific experts to formally diagnose conditions were not reviewed as a part of this study.
Formal Approaches
Many who are interested in identifying unobserved barriers to employment—such as substance abuse and mental health problems, domestic violence situations, and learning disabilities—among the TANF population, are in search of a formal tool or instrument to identify barriers. However, few tools have been developed for use with TANF clients or designed to address the multiple barriers many TANF clients face.17 Where instruments are available, they are often state or locally-developed and have rarely been validated for use with the TANF population.
While many still seek an instrument that would accurately and reliably identify a wide range of issues faced by TANF clients, the reality is no such tool currently exists, or arguably, may ever exist. Those working in the trenches on this issue are far more concerned with developing a process that helps identify the likelihood that a barrier exists. Their challenge extends beyond the selection of a specific instrument, to determining how to integrate identification efforts into the existing TANF eligibility determination and service planning process, how best to utilize existing staff and partner agencies in this endeavor, and how to establish new partnerships where existing expertise or capacity is insufficient.
Within this larger process, formal tools do have a role and the study sites use a variety of tools or instruments to assist in identifying barriers.18 Tools used in the study sites can be divided into two categories—validated tools and non-validated tools. We define validated tools as those which were developed for use with a specific population and have been rigorously tested to determine their validity and/or reliability. Non-validated tools refer to those tools which are state or locally-developed and have not been rigorously tested.
Minneapolis, Minnesota is an example of a study site that is making a concerted attempt to use tools to specifically identify mental health and substance abuse barriers. At the time of our visit, the Minnesota Department of Human Services was in the process of attempting to validate a screening tool. This tool, which was being piloted in several areas around the state, including with some employment service providers in Minneapolis, is intended to guide TANF case managers’ decisions to refer clients for mental health and/or substance abuse assessments. This self-administered screening tool consists of sixteen “yes” or “no” questions—12 questions relating to mental health and four questions about substance abuse. The latter questions are similar in wording to those found in the CAGE, a substance abuse tool. Once a client completes the screening tool, the case manager scores the results. A client receives one point for every ‘yes’ response to questions, one through six of the mental health questions and a score of two points for every “yes” response for questions seven through 12. Clients that score a two or higher are recommended for referral. For the substance abuse questions, a client receives one point for every ‘yes’ questions and is recommended for substance abuse assessment if she scores one point or higher. The implementation of the mental health and substance abuse screening tool pilot was still in progress and the tool had yet to be validated at the time of our site visit.
17 For a more detailed discussion of the availability of tools, see Question Five in Ten Important Questions.
18 Although below we highlight several tools that the study sites use, this is in no way intended to promote the use of any instrument.
Validated Tools Used by TANF Agencies
Generally, TANF agencies in the study sites use few validated tools to identify unobserved barriers to employment. This is due in part to the general lack of availability of validated tools designed for use with the TANF population.19 While none of the TANF agencies in the study sites relied on validated domestic violence or mental health screening tools, we found that several of the study sites did use validated tools to help identify substance abuse and learning disabilities.
Across the sites the most commonly used substance abuse tools were the CAGE and the Substance Abuse Subtle Screening Inventory (SASSI). It is important to note that, although commonly used in a variety of settings, neither of these tools were designed specifically for use with TANF clients. Each of these tools is described further below.
CAGE:
A short, self-administered tool used in three sites—Montgomery County,KS, Owensboro, KY, and Minneapolis, MN.
Consists of four “yes” or “no” questions.
Comes at no cost and requires no specialized training for staff to administer or score.
CAGE questions can be incorporated into tools or forms that are collecting other information or attempting to uncover additional barriers.
Substance Abuse Subtle Screening Inventory(SASSI):
A longer tool used in Montgomery County, KS and is an option for usein Las Vegas, NV.
Consists of seventy-eight questions.
Must be purchased and requires some training to administer and score.
Two learning disability screening tools have been developed and validated for use with TANF clients. The Adult Learning Disability Screen (ALDS) was developed at the University of Kansas, and the Learning Needs Screening tool, was developed by the State of Washington. These tools are used in a total of four of the six sites and are described further below.
Learning Needs Screening:
Used in Arlington, VA, Las Vegas, NV, and is an option in Kent, WA.
A short, 13 question tool.
Comes at no cost and requires little if any training to administer.
Adult Learning Disability Screen (ALDS):
Used in only one study site—Montgomery County, KS.
A three part tool—Part 1 of the ALDS is a self-rating scale that has twenty five questions about social, spelling, reading, and organizational skills. Part 2 is a self-administered inventory that has questions on learning problems, fraction skills and mathematical operations, educational experience, and mental health. Part 3 is an interview where there are questions on topics such as family history, learning problems, and comprehensive skills.
Must be purchased and requires some training to administer and score.
19 It is important to note that measures determined valid or reliable for other populations may not generate the same results when used with TANF clients.
Non-Validated Tools Used by TANF Agencies
The limited use of validated tools does not indicate a general lack of use of tools or instruments to collect information and explore barriers.
The limited use of validated tools among TANF agencies does not indicate a general lack of use of tools or instruments to collect information and explore barriers. On average, TANF clients in the study sites typically encounter four or more non-validated tools that include questions regarding unobserved barriers to employment. Some of the sites use state or locally-developed tools that identify multiple barriers to employment while others rely on separate, barrier-specific tools.
The non-validated tools used in the study sites vary widely across many dimensions. For example, they vary in the number of questions asked and the type of questions (i.e., open or closed-ended). TANF case managers in Las Vegas, NV use the Post-Approval Assessment to identify a wide range of barriers early in a client’s interaction with the welfare system. This state-developed tool is a topical interview guide that requires the interviewer to formulate specific questions rather than presenting a series of structured questions to be read to clients. The topics covered include the client’s physical condition, mental condition, family relationships, housing/living relationships, and social issues. TANF case managers in Montgomery County, KS use a similar guide to assess clients. Kansas’ Assessment Guide is a multi-barrier tool that includes a mix of “yes” and “no” and open-ended questions. The instructions for this instrument explicitly state that the text is designed to serve as a guide and that questions may be added or changed depending on an individual’s circumstances. Questions inquire about a variety of topics such as education, work history, health information, domestic information, and support services. Within each topicthere are questions that inquire specifically about unobserved barriers. Additionally, this tool includes a section for workers to note observations of the client’s attitude and behavior.
Not all of the non-validated tools used in the study sites address as many barriers to employment as those described above. Many of the study sites’ “assessment” forms are centered around collecting employment and financial information and have integrated only a few “yes” or “no” barrier identification questions. For example, one tool includes the question “Have you experienced alcohol/substance abuse?” after asking “Have you experienced any difficulties finding or keeping a job?”
How Tools are Used — Two Examples
Validated Tools at Orientation
In Montgomery County, KS several validated tools are used during client orientation to identify barriers including substance abuse and learning disabilities (see additional discussion of client orientations in Chapter Four). Decisions about additional referrals are based on the results of the tools implemented during orientation. These decisions are guided by a state-developed protocol that outlines when referrals should be made and to which partners. During orientation, clients complete the SASSI as well as the CAGE questions (which are incorporated into an interest inventory). Additionally, clients complete the Comprehensive Adult Student Assessment System (CASAS) appraisal, a fifty-question test that examines basic reading and math skills related to the work environment. Finally, staff also administer the Adult Learning Disability Screen to identify possible learning disabilities.
After orientation, clients meet with their TANF case manager and review the results from their screening and assessment tools. During this time, clients also complete the state-developed Assessment Guide. As mentioned earlier, this comprehensive assessment inquires about various barriers to employment. Staff use the results of the tools administered during orientation, responses to the Assessment Guide, and additional information from the interview with the case manager, to determine appropriate next steps for the client. Next steps are guided by an assessment referral protocol that instructs staff on appropriate referrals in response to results of various screening instruments.
Automated Screening
Kent, Washington is another example of a study site’s specific effort to use tools to identify unobserved barriers to employment. In each of the local welfare offices in Washington, including Kent, case managers use a state-developed, automated screening tool called the Virtual Interactive Employability Worksheet (VIEW).20 The VIEW is a multi-barrier tool that uses a progressive series of questions on a number of different issues including: domestic violence, current employment, child care, transportation, housing, listening and learning, substance abuse, criminal history, pregnancy, family planing, health, and clothing needs. Under each heading there are a number of questions that probe the issue in greater detail. For example, under the broad heading of domestic violence a “family violence screening script” is provided for case managers. This script gives several examples of opening lines to use when talking about a sensitive topic such as domestic violence. These “ice-breakers” set the stage for the case manager to ask a series of seven questions which inquire about family violence.
If a client answers “yes” to any of the questions, the computer screen indicates that a client should be referred to a social worker or family violence counselor. From the results of the VIEW, case managers then decide whether to refer the client to job search, bundle services like treatment and counseling with work activities, or defer the client from job search and refer the client to a social worker for additional assessment and services.
20 In mid-April 2000, the automated VIEW replaced the paper forms that were used as the initial screen for barriers to job search.
Partner Agencies and Tools
Decisions to use tools within TANF agencies may depend in part upon the skills and training of staff. Because TANF staff do not generally have advanced training, or expertise in barrier identification, TANF agencies often rely on specialists employed by partner agencies to further the identification process. Partner agency staff frequently possess greater expertise and formal training regarding barrier identification, and are able to utilize a wider range of validated tools to uncover unobserved barriers to employment. For example, therapists might use the Beck Depression Inventory-II (BDI-II), the Minnesota Multiphasic Personality Inventory (MMPI), or an intelligence test in their efforts to diagnose a mental health problem or disability. Addiction counselors employed by substance abuse partners may use additional tools developed to determine the extent of a substance abuse problem and the appropriate treatment.
In Montgomery County, Kansas, Regional Alcohol and Drug Assessment Center (RADAC) assessors use the Michigan Alcohol Screening Test (MAST) and the Kansas Client Placement Criteria (KCPC).21 The MAST is a simple self-scoring test. This twenty-five question tool inquires not only about an individual’s drinking habits, but also about any history of mental illness. After the MAST, the RADAC assessors administer the automated KCPC. This state-developed tool requires approximately an hour to complete and is conducted through an interview with responses recorded on a laptop computer. Questions on the KCPC range from the client’s employment history, to household members’ histories of substance abuse or mental health problems. Scoring the assessment and interpreting the results requires the application of clinical knowledge by a substance abuse professional.
Specialists from partner agencies rely heavily on psycho-social assessment interviews to explore unobserved barriers. Although many psycho-social interviews are guided by a form that outlines the topics to be covered, this was considered merely a guide by those conducting interviews. Across the study sites, specialists noted that the psychosocial form is used as a springboard for a conversation and that strong interpersonal or “soft” skills were as important as clinical training when conducting this interview. However, psycho-social interviews differ from other in-depth interviews in that they require advanced training to administer and interpret the results.
Psycho-social interviews are conducted by clinically trained Targeted Assessment Project (TAP) assessors in Owensboro, KY, therapists at River Valley Behavioral Health in Owensboro, KY, therapists at Four County Mental Health in Montgomery County, KS, as well as the on-site therapist at the IRIS Program in Minneapolis, MN. Generally this assessment is conducted as an in-depth interview covering topics such as: medical history, family history of physical/psychiatric illness, chemical (alcohol/drug) history, gambling history, sexual history, domestic violence history, education/learning, social history, measures of functioning (e.g., activities of daily living) employment history, legal involvement, interactions with family/household members, history of previous treatment, recent stressful life situations, mental status, client’s strengths, and clinical impression.
21 The state of Kansas requires that two tools be used to diagnose an addiction.
Informal Approaches
The majority of staff reported that they believe informal approaches are more effective in uncovering barriers than is the completion of a screening or assessment tool.
Tools play an important role, both within the TANF agency and as used by partners. However, the use of interviews as a way to administer questions from a tool highlights the fact that tools are merely one part of a larger assessment process. Informal efforts to identify unobserved barriers are discussed further below.
Informal efforts to identify barriers occur throughout the case management process. By case management we mean the multi-faceted, on-going process that takes place between staff and clients in order to determine needs, establish goals, identify and address barriers, and monitor compliance with program requirements. Each interaction with program staff presents an informal identification opportunity where clients can disclose barriers to employment and staff can elicit disclosure or observe behaviors/characteristics that are indicative of the existence of a barrier. Staff in all sites reported using informal identification approaches throughout an individual’s interaction with the TANF system. These efforts were employed to different degrees across different staff positions, but occurred regardless of the use of a more formal identification instrument or the level of skill or training of the individual staff person. Importantly, even highly specialized staff who possess advanced training related to barrier identification noted the importance of informal strategies.
Although not evaluated as a part of this study, the majority of staff reported that they believe informal approaches are more effective in uncovering barriers than is the completion of a screening or assessment tool. Several staff noted that these informal mechanisms are more successful because clients are more willing to offer personal information in the course of a conversation than if a worker asks about a situation for the purpose of completing a form. The majority of TANF staff interviewed were confident that they are able to initiate discussions and observe behaviors that lead to barrier identification through their one-on-one interactions with clients. This does not imply that TANF agency staff determine with specificity the conditions faced by clients. Rather, they believe that they are able to rely on informal identification strategies to indicate that the client could benefit from a referral for additional assessment or services by a specialist or partner agency.
TANF agency staff rely heavily on their past experiences working with clients and their interpersonal skills to elicit disclosure or recognize behaviors indicative of unobserved barriers to employment. Although TANF agency staff reported that they had received training on a wide variety of issues, including barriers to employment, in many cases they found it difficult to recall the details or content of the training. Some staff did note that training on a particular barrier (e.g., substance abuse, domestic violence) was offered and contributed to their overall understanding of the barrier, its characteristics, and effects. This general training assisted in their use of informal strategies including eliciting disclosure and recognizing characteristics or statements made by clients as possible indicators of the existence of an unobserved barrier.
Disclosure
Informal identification efforts rely heavily on clients to disclose a barrier to employment. By disclosure we mean acknowledgment of the existence of a barrier, or comments that lead staff to suspect the existence of a barrier. Reliance on disclosure presents a particular challenge when considering unobserved barriers to employment. Because of the nature of the disabilities, health conditions, and barriers to employment considered here, many clients are unaware of their condition or may not consider their condition/situation a barrier to employment. Alternatively, clients may be simply unwilling to disclose a barrier to their case worker. Not surprisingly, staff reported that clients are most likely to report a condition that was previously diagnosed.
All staff who are responsible for identifying barriers reported making attempts to elicit disclosure of barriers, or information that may indicate the existence of a barrier, from clients. Staff frequently mentioned that establishing a trusting relationship and good rapport are essential if clients are to feel comfortable disclosing. For many staff, this was a natural and integral part of the case management process—so common that in some cases they had trouble describing their approaches. Many staff noted that they rely heavily on their interpersonal or “soft” skills to make clients feel comfortable. Managers also frequently noted that these soft skills were important for staff responsible for identifying barriers. Based on our interviews it appears that, among other techniques, workers make efforts to establish rapport with clients and develop trust by:
asking general questions about the client, her family, and her employment or interests before delving into personal topics such as substance abuse or domestic violence;
exploring past experiences that clients are more comfortable discussing that may provide insights into current situations or behaviors (e.g., past substance use, experiences with family or sexual violence in childhood);
telling clients something about his/her own experience—particularly when the worker is a single parent or former welfare recipient—in an effort to gain credibility with the client; and/or
normalizing a client’s situation or feelings (e.g., by indicating that anyone in the client’s situation would feel depressed or stressed and could benefit from counseling; by indicating that seeking mental health treatment does not mean the client is “crazy;” or by explaining that being assessed for substance abuse does not mean the client is an alcoholic).
Some staff reported using the provision of supportive services such as transportation assistance, clothing, or dental assistance as a way to develop trust. By providing these services, staff were able to tangibly demonstrate that they intend to help the client. This reportedly encouraged some clients to subsequently disclose additional barriers or be willing to follow through with more formal assessments for unobserved barriers. Many workers acknowledged that building a trusting relationship with clients takes time. Some workers believed they were able to establish a trusting relationship sufficient for clients to feel comfortable disclosing by the completion of the initial interview, while other workers reported that it may take several interactions with the client before such rapport was established.
Behavioral Observations
In addition to efforts to elicit disclosure of unobserved barriers by clients, staff universally reported relying on behavioral observations—commonly described as “red flags” or “clues”—to assist in the barrier identification process. For the majority of staff interviewed, these efforts were undertaken informally and were based heavily on past experience. Some staff indicated that they attended training sessions on topics such as substance abuse or domestic violence that included discussion of behaviors staff might observe that may indicate a client has an unobserved barrier to employment. None of the study sites systematized the documentation of behavioral observations, for example through the use of a behavioral observation checklist that are used in some other states.22
Common examples of behaviors said to be indicative of barriers to employment include clients:
being jumpy, fidgety, or nervous;
slurring speech or smelling of alcohol;
having glazed eyes or dilated pupils;
avoiding eye contact; and/or
overreacting to questions.
Despite the common reliance on the observation of behaviors described above, staff noted that clients are generally very good at hiding these clues from the welfare system. As such, staff reported that they sometimes rely on more general behavioral clues to indicate that the client may have an unobserved barrier to employment. For example, staff indicated that changes in behavior or offering inconsistent answers to questions are more general indicators of the possible presence of a barrier to employment. However, such behaviors offer little indication as to specific nature of the barrier.
For many TANF staff, the mere suspicion that the client is grappling with issues beyond the need for standard supportive services (e.g., transportation or child care) or motivation to work, is often enough to warrant a referral to more specialized staff who can begin to discern the exact nature of the client’s disability, health condition, or barrier to employment. For example, a case manager in Owensboro, KY offered the example of a client who was initially very enthusiastic about participation in job readiness training and the possibility of obtaining employment. The client reportedly initially participated in required activities but then unexpectedly changed her attitude and abruptly stopped participating. This change in behavior was an indicator to the case manager that the client was likely to have an unobserved barrier such as a substance abuse problem or domestic violence situation and the client was referred to the TAP assessor for additional assessment.
22 For example, see discussion of North Carolina’s use of behavioral observation checklists in National Center on Addiction and Substance Abuse (CASA) at Columbia University (in partnership with the American Public Human Services Association). Building Bridges: States Respond to Substance Abuse and Welfare Reform. New York, New York: CASA, August 1999.
Challenges to Establishing Trust and Rapport
Many believe that clients may be more comfortable disclosing barriers to staff who do not control their benefits.
Workers who are responsible for determining benefit levels or imposing sanctions understood that these responsibilities may make it more difficult to establish a trusting relationship. All staff interviewed acknowledged their responsibilities to report child abuse or neglect, but generally did not believe that their status as “mandatory reporters” affected clients’ willingness to disclose unobserved barriers to employment.
Staff of partner agencies reported, and many TANF agency staff agreed, that clients may be more comfortable disclosing barriers to staff who do not control their benefits. Partner agency staff reported this despite their status as mandatory reporters. TAP assessors in Owensboro, KY, as well as staff of the IRIS Program in Minneapolis, MN and Rainier Case Management in Kent, WA reported that they regularly try to distinguish themselves from welfare agency staff in an effort to build trust with clients and elicit disclo- sure. By being able to honestly report that they have no direct control over benefit termination or the imposition of sanctions, and that they are not bound by the same rules or program requirements as TANF staff, these workers believed that they were able to gain a higher level of trust than TANF agency staff could achieve and serve as a mediator between the client and TANF agency staff.
A less commonly used technique to establish trust and elicit disclosure is to explain to clients how information will be used. Although TANF staff indicated their awareness of confidentiality guidelines and the need for signed releases from clients before sharing information, few seemed to take care to explain how information would be used or the implications of failure to sign an authorization to release information. For example, staff did not commonly explain that information could be used to make a referral to other services, how participation in a barrier-specific service would affect requirements to participate in work-related services, or what information would lead to a referral to the child welfare agency. The extent to which TANF agency staff reported making efforts to indicate—prior to disclosure—the range of services available, or the possible negative repercussions of disclosing a substance abuse problem or other barrier to employment, varied widely.
Many advocates for TANF clients take issue with this approach and encourage TANF agency staff to fully inform clients regarding how information will be used so that clients can make informed decisions regarding disclosure. As will be noted in Chapter 5, clients who participated in focus groups also reported that not knowing how information would be used affects their decisions to disclose.
Advantages and Disadvantages
Both formal and informal identification strategies carry advantages and disadvantages. Because many involved in identifying unobserved barriers are in search of a tool to assist in this process, there has been relatively little discussion of informal strategies. However, the discussion below of the advantages and disadvantages of both strategies, as well as descriptions of the study sites’ approaches, illustrate that perhaps the most comprehensive approach to uncov- ering unobserved barriers involves the integration of both strategies.
The use of formal screening or assessment tools or instruments has the advantage of providing staff with a structured approach that may provide greater consistency regarding who is screened and what information is collected. Formal tools are often forms that collect information that can be used by TANF agencies and their partners to determine the prevalence of different barriers. If the data are collected and analyzed it can then be used to more accurately determine the level and scope of service responses that are warranted.
To the extent that tools used have been methodologically tested, the use of such instruments may provide some greater assurance that the barriers will be identified. However, as noted above, few such tools exist, and regardless of methodological rigor, even the best tools rely on some level of disclosure from clients. Most of the tools used by the study sites are not validated and many provide merely a place to record information collected through a conversation or interview.
Many indicated that regardless of the instrument used, if it is not implemented within a context of safety and trust, it will fail to uncover the desired information.
Many state or locally-developed instruments used by the study sites require relatively little skill or formal training to utilize and interpret. By posing specific questions regarding the existence of unobserved barriers to employment, these tools provide a straightforward way for staff who are not comfortable with personal or sensitive topics to explore these issues with clients. However, when utilized by staff who are not comfortable with the topic, the use of a more structured and straightforward approach may detract from the staff person’s ability to establish a trusting relationship or good rapport with the client. Many staff interviewed indicated that regardless of the instrument used, if it is not implemented within a context of safety and trust, it will fail to uncover the desired information. Further, tools or instruments not completed in a personal, sensitive manner could be perceived as just another form that must be completed in order for the client to obtain benefits. Where this is the case, such tools are less likely to capture the true nature of the client’s unobserved barriers.
If staff are only looking for information on which to base a referral for more in-depth or formalized assessment, investing in validated tools or creating validated tools for the purpose may not be necessary. Informal strategies may be equally or more effective in achieving this goal.
The on-going process of staff interacting with clients throughout their TANF experience lends itself to the use of informal identification strategies. Therefore, it is not surprising that all staff rely on informal identification strategies, including disclosure, efforts to elicit disclosure, and behavioral observations, as integral parts of their overall barrier identification process. In many ways, what is described here as an identification strategy are techniques that would be expected to be employed by experienced case managers. Informal strategies offer an inexpensive, more personal approach to exploring clients’ needs that require little formal training and build on a worker’s past experience. Use of informal strategies allow staff to develop the trusting relationship and positive rapport reported as essential to identifying unobserved barriers to employment. Additionally, the on-going use of informal approaches offers multiple opportunities to uncover barriers (as opposed to the one time implementation of a tool) thus decreasing the likelihood that a client would be sanctioned or have her benefits terminated without several efforts to uncover barriers and several opportunities for clients to disclose barriers or pursue additional assessment.
Informal strategies, particularly to the extent they are not employed by specialized staff or used in conjunction with other strategies, present a number of pitfalls.
However, informal strategies, particularly to the extent they are not employed by specialized staff or used in conjunction with other strategies, present a number of pitfalls. First, the unstructured nature of informal identification offers a wealth of opportunity for staff to apply biases or stereotypes when interpreting clients’ comments or behaviors. To the extent staff have not been trained regarding the characteristics of individuals likely to have different barriers, they may make incorrect referrals for additional assessment or services or fail to make referrals when appropriate.
Staff also have varying experiences and levels of formal training on which to base their efforts to elicit disclosure and understand of clients’ responses. Staff who are uncomfortable discussing personal or sensitive issues are less likely to employ informal identification techniques or establish the level of comfort or trust necessary for this technique to be effective. The use of behavioral observations also requires that staff know the client well enough, or interact frequently enough, that they can accurately interpret what are perceived as changes in behavior.
The study sites have attempted to maximize the advantages of both formal and informal approaches by using them in combination with one another and expecting no one effort to uncover all barriers to employment. As will be illustrated in the next chapter, the on-going nature of barrier identification provides multiple opportunities for TANF agency staff and partners to identify unobserved barriers to employment using both formal and informalstrategies.
Chapter Four: When Identification Occurs
An important question facing TANF agency administrators and staff is when to undertake efforts to identify unobserved barriers to employment. Some argue that because a primary objective of TANF is to assist clients in obtaining employment, clients should first attempt to find a job thus allowing the labor market to determine if they are employable. Following this Work First philosophy, barrier identification would not take place until after the client has attempted to find a job and failed. Others believe that because of declines in caseload, remaining welfare clients may have a variety of barriers to employment and thus be “hard-to-serve.” In an effort to alleviate these barriers so that clients can successfully obtain and retain jobs, some argue that identifying barriers early in a client’s experience is the best approach. Early identification of barriers allows staff to direct clients to resources to alleviate or mitigate barriers prior to job entry.
The case studies indicate that attempting to establish a single point when barrier identification should occur may be shortsighted. The study sites illustrate that a client’s experience in the TANF system offers a variety of opportunities to identify unobserved barriers to employment. These range from the initial intake/eligibility interview, through service planning, and referrals to partner agencies for work-related or other services. The important question is therefore, how TANF agencies should integrate barrier identification into this multi-step process, taking into consideration the various steps involved, the staff with whom clients interact at each point in the process, and the TANF policy context. In this section we discuss when barrier identification occurs in the study sites.
Barrier Identification and Work First : Can They Co-exist?
Several sites have modified their Work First approaches for clients who disclose barriers.
Decisions about the timing of efforts to uncover barriers to employment are affected by the welfare reform philosophy of the state and/or locality. By its strictest definition, a Work First approach to welfare reform rests on the belief that any job is a good job, and that the labor market should determine whether or not a welfare recipient is employable. Several of the study sites reported that they employ a Work First approach. However, reflecting the sites’ commitment to barrier identification, this approach has been modified such that if a client discloses a barrier, she may not be required to engage in job search immediately. Nonetheless, given the issues noted above regarding clients’ willingness to disclose barriers early in her TANF experience, it is likely that some clients with barriers to employment will be referred to job search activities as a first step in their service plan. In such a situation, the client’s success or failure in job search would be another way in which barriers are identified.
Applicant job search requirements are one way TANF agencies pursue a Work First approach. By requiring a client to look for a job while her application is pending, staff can determine which clients are employable, despite any substance abuse or mental health problems, domestic violence situations, or learning disabilities. The TANF programs in Las Vegas, NV and Montgomery County, KS require that TANF applicants participate in job search while their applications are being processed. However, in both sites if barriers are revealed, the client may be exempt from this requirement.
In the early days of its welfare reform effort, the state of Kansas required all TANF applicants to participate in job search while eligibility was being determined. As the TANF caseload declined and it seemed to agency officials that remaining clients were harder-to-serve and faced barriers to immediate job entry, this policy changed. At the time of our visit, TANF workers in Montgomery County used a formal screening tool with applicants. The Temporary Assistance to Families Applicant Job Search/Employability Assessment Process Initial Screening Guide is used to determine whether or not barriers exist that would make applicant job search more likely to be a frustrating or disheartening experience, as opposed to a productive step toward finding a job. If the screen indicates that clients meet certain conditions, such as being currently involved in the Vocational Rehabilitation program, having difficulty getting hired or keeping a job, or having a mental health, domestic violence, or substance
abuse problem that interferes with looking for work, they would not be required to fulfill applicant job search requirements.
The study sites have found ways to maintain a work focus while also incorporating barrier identification strategies.
While maintaining a strong work focus, Kent, WA has also slightly modified its Work First strategy for clients who disclose personal barriers that would prohibit obtaining employment. Clients who disclose an unobserved barrier to employment while completing the Virtual Interactive Employability Worksheet (VIEW) with their case manager can be referred directly to a social worker instead of to the Employment Security Department (ESD) for job search services. However, if a barrier was not uncovered at this early point in the client flow, the client would be referred to ESD and be required to engage in job search as her first step toward obtaining employment and leaving welfare. This initial job search period lasts for 12 weeks during which the client is assisted by ESD job counselors. If after approximately nine weeks the client is not making progress toward finding a job, ESD and TANF agency staff meet to discuss the client’s situation. This “staffing” may result in the client being referred to a social worker or other partners for additional assessment.
Of the sites visited, Minneapolis, MN maintains the strictest Work First approach. Although service strategies vary widely across contract employment service providers, generally clients who do not initially disclose barriers are required to engage in eight weeks of job search. If the client is not successful in obtaining employment, she would complete a “secondary assessment” with her employment service provider. The results of the sec ondar y assessment may indicate that the client could benefit from barrier-specific assessment or referral to other services such as the IRIS Program.
Some welfare agencies that perceive their remaining welfare clients to be harder-to-serve, or face unobserved barriers to employment, are beginning to rethink their Work First approach and, as in the study sites, have found ways to maintain a work focus while also incorporating barrier identification strategies. Some study sites still rely on the labor market to be an early determinant of a client’s employability, but also provide an opportunity for clients who are aware of barriers to employment to reveal them and thus not be required to engage in job search activities immediately.
While some might argue that these sites no longer employ a Work First approach, staff in the study sites were clear that helping clients leave welfare for work remained a top priority. It is important to note that these sites have not reverted to a pre-welfare reform strategy of exempting clients from participation. In all of the examples above, clients may be allowed to engage in non-work related activities in an effort to remove or mitigate barriers. However, these activities are considered a necessary step for a client to ultimately become employable and leave welfare.
On-going Opportunities to Identify Unobserved Barriers
In the study sites barrier identification is on-going throughout a client’s TANF experience.
Perhaps one of the most important findings of this study is that barrier identification as carried out by the study sites is an ongoing process, not a single event. Universally, respondents indicated that there is no single point when barrier identification occurs. Rather, they indicated that barrier identification is on-going throughout a client’s TANF experience, including while being served by partner agencies. As various staff interact with clients attempting to make the transition from welfare to work, efforts to identify barriers to this transition are undertaken, both formally and informally.
In all sites, there are specific points in a client’s TANF experience when efforts to identify barriers using a particular tool are undertaken—some of these were noted in earlier chapters. In addition, staff universally employ informal strategies to identify barriers during nearly every interaction with clients. Staff who rely heavily on informal strategies generally consider each interaction with a client as an opportunity to uncover possible barriers to employment, thereby reinforcing the on-going nature of barrier identification. Within this ongoing process, there are specific points when efforts are made to identify barriers. Common points utilized across the study sites are presented in Figure 2 and are further described below. These opportunities to identify barriers seem to vary in part based on the responsibilities of the staff involved, activities that normally occur early in a client’s TANF experience in each locality, and the TANF policy context.
Figure 2: Possible Opportunities to Identify Barriers to Employment
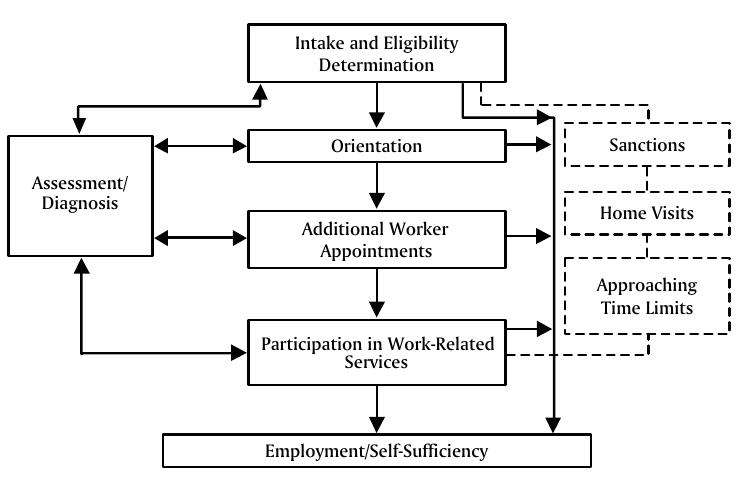
Intake/Eligibility Determination
Sites vary in the extent to which identification occurs at a client’s initial intake/ eligibility determination appointment. In part, whether a locality uses this step in the client flow to identify barriers depends on whether or not the site has adopted a Work First philosophy and the responsibilities of staff involved. In some sites, such as Minneapolis, MN and Arlington, VA, separate staff perform eligibility and service planning/ case management functions (recall Table 2). In these sites eligibility workers are not as integrally involved in the barrier identification process as other workers.23
However, barrier identification at the intake/eligibility determination appointment is not precluded by the focus of a staff person’s responsibility being financial eligibility determination. For example, in Las Vegas, NV, eligibility workers who are not responsible for ongoing case management perform an initial screen for barriers and may identify barriers that warrant a referral to an in-house social worker.
In other sites, such as Owensboro, KY, Montgomery County, KS, and Kent, WA, eligibility and case management functions are integrated under one worker. This worker is responsible for both eligibility determination as described above, and developing a service plan that will guide the steps a client will take on her path to self-sufficiency. In these sites, the worker’s case management responsibilities require that she or he also engage in barrier identification. Because this worker wears multiple hats and is expected to identify barriers to employment, barrier identification begins with his or her first interaction with the client—the intake/eligibility determination interview.
The IRIS program in Minneapolis, MN specifically decided to conduct barrier assessment early in a client’s interaction with the program. IRIS staff have found that clients often require immediate barrier removal assistance in order to be successful in IRIS’s vocational services. Therefore, when clients first enter the IRIS Program, they meet with a social worker who is responsible for “social stabilization” (i.e., taking care of immediate needs such as housing, food, or child care). The IRIS Program also requires that clients take part in formal psychological assessment with an on-site psychologist. Clients are required to attend six sessions with the psychologist with the first session beginning soon after intake and before involvement in vocational services. Although some clients have failed to complete these required sessions, staff believe that by engaging clients in this process as early as possible, they are better able to uncover and assist clients with their substance abuse or mental health problems.
During their interviews with clients, these integrated workers not only collect information about household composition, income, and assets, but they also explore the reasons the client is applying for or remains on public assistance, and determine the steps she should take to transition from welfare to work. For example, in Owensboro, KY, staff complete the Targeted Assessment Project Orientation Screen at the initial eligibility interview to determine if the client should be referred to the University of Kentucky TAP assessor as part of the service plan. This opportunity to identify barriers at the intake and eligibility stage is illustrated in Figure 2 where a two way arrow links the Intake and Eligibility Determination box to the Assessment/
Diagnosis box. Similarly in Kent, WA, staff complete the VIEW assessment to determine if a client should be referred to an in-house social worker for a more intensive assessment or service referrals.
In Las Vegas, NV the orientation sessions vary across local offices. In one office visited, the orientation is a week-long session used to both provide information about the New Employees of Nevada program requirements and as an opportunity to identif y barriers to employment. The session was described as involving a significant amount of discussion of barriers, particularly domestic violence and substance abuse. It was also reported that the orientation facilitator uses the session to explore clients’ situations and to observe behaviors that may indicate the existence of a barrier to employment. Further, the interaction among orientation participants was believed to facilitate disclosure as clients bond with each other and become comfortable disclosing barriers to a group of their peers. Information gathered during the orientation in this office is passed on to the TANF case manager responsible for developing a service plan, which may include a referral to an in-house social worker for additional assessment or barrier-specific services.
23 However, in all sites if a client discloses a barrier or a worker suspects the existence of a barrier, this information would be relayed to staff who are more involved in barrier identification or alleviation.
Orientation
Another early point in the client flow where barrier identification may occur is during TANF orientation. Typically client orientations offer the opportunity to provide clients information about program services and requirements. Five of the six study sites conduct a group orientation for TANF clients, but they vary in the extent to which they use this as an opportunity to identify barriers. As noted previously, in Montgomery County, KS, the primary function of the orientation is the implementation of several formal assessment tools. Similarly, in Arlington, VA, clients must attend an orientation session at which three screening forms are completed. These forms collect a wide range of information including indications of the existence of unobserved barriers. Further, the mental health/substance abuse therapist who is co-located in the TANF office attends this portion of the orientation to discuss barriers and services available.
Additional Worker Appointments
TANF clients meet with their various workers periodically following initial eligibility determination—whether it be for eligibility redetermination or service planning. In Montgomery County, KS, Arlington, VA, and Las Vegas, NV, clients have a meeting with their case workers following orientation that serves as a primary opportunity to identify barriers. In Montgomery County, KS, clients meet with their worker for an initial assessment appointment following orientation. It is at this appointment that the worker reviews the results of structured assessments which were the primary purpose of the orientation. This is the second meeting with the case manager in this site and staff use assessment information from the orientation to build on what was learned at the intake/eligibility appointment and work with clients to develop a service plan.
It is also at this point that workers in Montgomery County, KS screen clients to determine whether they are at risk of becoming involved in the child welfare system and could be better served by the Extra Effort pilot program. If, at this appointment, the worker determines that assessment results indicate the likelihood of a substance abuse problem, the client would be referred for additional assessment. Similarly, if the client discloses a domestic violence situation, she would be referred to the local domestic violence shelter.
In Arlington, VA, clients meet with their employment case manager following orientation. At this first meeting with the case manager (like in Las Vegas, earlier meetings were with the eligibility worker), the case manager reviews the forms completed at orientation and completes additional screening tools including substance abuse, domestic violence, and learning disability screening instruments. At this meeting, the case manager also works with the client to develop an employability plan. If the client indicates the existence of a substance abuse or mental health problem during this meeting, she would be referred to the on-site substance abuse/mental health therapist. If a learning disability was suspected, the client would be referred to the joint Department of Rehabilitation Services/SOC Enterprises program to obtain additional assessment, rehabilitative services, and/or accommodations.
Participation in Work-Related Services
In some cases, barriers are not disclosed or otherwise identified early-on, and the client is referred to standard work-related services such as a job search workshop. Commonly, services related to job readiness include the use of assessment tools or the opportunity for clients to disclose barriers. As shown in Figure 2, a client may be referred for additional assessment/diagnosis if a barrier is identified while participating in work-related services. For example, if a client is not referred to the TAP assessor in Owensboro, KY, she would likely be referred to the six-week Project LIFE job readiness workshop. Although only one barrier-related assessment form is completed as part of the workshop, staff reported that barriers are commonly uncovered or disclosed during the workshop. Additionally, many partner agency staff in Owensboro indicated that although a client may be referred to them because of a specific barrier, they may conduct additional assessment for other, co-occurring barriers.
Sanctions, Home Visits, and Approaching Time Limits
Figure 2 illustrates three additional opportunities to identify barriers—sanctions, home visits, and approaching time limits—that apply to some clients depending on their individual situations. One such opportunity is the imposition of financial penalties, called sanctions, for failure to comply with TANF program requirements. In the majority of sites, non-compliance is one of many behaviors that may indicate to workers that the client has a barrier to employment. Often, this prompts workers to contact the client to further explore, often through an interview, why the client is non-compliant and if there are additional or different services required.
In Kent, WA, case managers have the option to refer sanctioned clients to Intensive In-Home Services, provided locally under contract by Rainier Case Management. Rainier conducts home visits with sanctioned clients in an effort to determine the cause of non-compliance and establish a plan for reconnecting clients with services. Staff of Rainier Case Management conduct intensive interviews with sanctioned clients to determine if the cause of noncompliance may be an unobserved barrier and encourage clients to comply with TANF program requirements (see additional discussion of Rainier CaseManagement’s services in Chapter Six).
Home visits also provide an opportunity to identify unobserved barriers. Visiting a client in her home offers staff the opportunity to identify the possibility that a client faces an unobserved barrier to employment. By observing the home environment staff noted that they can gain a richer picture of the client’s situation than is apparent through interviews in an office. Home visits reportedly offer insights into the existence of barriers such as substance abuse or domestic violence situation (i.e., by noting empty alcohol bottles or drug paraphernalia or observing a room in disarray due to violence). Staff in a number of sites who conduct home visits reported home visits as a helpful opportunity to explore barriers.24 Staff reported that visiting clients in their home or a neutral site, or spending time with clients going to appointments, provides the opportunity to continue building a trusting relationship that may lead to the disclosure of a barrier.
Finally, time limits are a primary motivating factor behind developing barrier identification strategies. Some sites use approaching time limits as an opportunity to reexamine the possible existence of barriers. For example, at the time of our visit, staff in Montgomery County, KS were beginning a preliminary review of the caseload in preparation for the imposition of federal time limits and the need to determine who will be granted a hardship exemption. Staff were reviewing long-term recipient cases to determine what services had been provided and if additional assessment could uncover barriers that could be addressed before clients faced benefit termination.
Similarly, the TANF agency in Minneapolis, MN was in the process of implementing new services for long-term TANF recipients. These services, called Tier II services, are to be targeted to long-term TANF clients who have been unsuccessful in finding a job through the existing employment service providers. Although exact service approaches to be implemented through Tier II providers had not been determined, one anticipated component is additional, in-depth barrier assessment.
24 Home visits are conducted by social workers in Las Vegas, NV, Extra Effort case managers in Montgomery County, KS, IRIS social workers in Minneapolis, MN, and TAP assessors in Owensboro, KY.
Chapter Five: Staffing Strategies To Identify Barriers To Employment
As TANF agencies and their partners increasingly focus on efforts to identify unobserved barriers to employment, they must consider the roles different staff should play in the barrier identification process. In doing this, they must decide how to best utilize TANF agency staff and staff of partner agencies in this endeavor. In all of the study sites, TANF case managers play an integral role in initial barrier identification efforts. In many cases this is a new role for these staff. However, the abilities of TANF case workers to fulfill barrier identification responsibilities are affected by their other responsibilities, their skills and training, and the size of their caseloads. Each of these dimensions is discussed below.
Case managers in several study sites are supported by specialized workers or through partnerships with organizations that employ specialized workers. While staff of partner agencies—such as substance abuse treatment facilities, community mental health centers, Vocational Rehabilitation programs, or domestic violence shelters—likely have greater expertise or more formal training related to identifying or addressing barriers within their area of expertise, they may not have the ready access to TANF clients that workers in the TANF system possess and therefore must coordinate with the TANF system in order to fully address the needs of welfare recipients. The use of specialists in the study sites, and efforts to coordinate identification and service efforts carried out by the variety of staff involved, are also discussed below.
TANF Case Managers: Responsibilities, Skills and Training, and Caseload Sizes
In the study sites, primary responsibility for initially determining that a client may have an unobserved barrier to employment rests with TANF case managers. Although many other staff may be involved in the barrier identification process, it is the case manager who is typically responsible for conducting a preliminary assessment or utilizing assessment information to develop a service plan for the client. Often it is the case manager who refers a client to a specialized worker or partner agency for services to remove or mitigate a barrier. Case managers are also generally responsible for monitoring a client’s compliance with her service plan and progress toward achieving self-sufficiency.
Financial Eligibility Responsibilities Responsibilities of Case Managers
The dual responsibility for eligibility determination and service planning may make it difficult for case managers to identify unobserved barriers to employment.
As noted above, the responsibilities of case managers are multi-faceted and commonly include service planning, monitoring, and making referrals. Some case managers are also responsible for determining financial eligibility for TANF, Food Stamps, and Medicaid (this was the case in Montgomery County, KS, Kent, WA, and Owensboro, KY). In other sites (Minneapolis, MN, Las Vegas, NV, and Arlington, VA), clients meet with a separate eligibility worker to determine financial eligibility for TANF before being referred to a case manager for service planning.25
The dual responsibility for eligibility determination and service planning may provide a TANF case manager the opportunity to begin the barrier identification process early in a client’s TANF experience and provide more holistic services. However, this dual responsibility may also make it difficult for case managers to identify unobserved barriers to employment. The TANF, Food Stamp, and Medicaid programs place a high priority on accurate and timely eligibility determination that may detract from efforts to identify barriers during the eligibility interview. The completion or collection of often voluminous eligibility-related paperwork may detract from efforts to establish rapport and encourage disclosure of barriers. For example, the completion of formal assessment tools may be perceived as just another form to be completed to be deemed financially eligible. Additionally, as indicated by focus group respondents, clients may be hesitant to disclose their barriers to this worker for fear that it will affect their eligibility for benefits.
In two of the study sites (Montgomery County, KS and Kent, WA), eligibility determination and case management functions were combined to create an integrated worker when welfare reform was implemented. While such integration was intended to provide more holistic services to clients, some staff reported that this dual responsibility makes it difficult for them to carry out their case management and barrier identification responsibilities. In part, this challenge was created because the priority and workload associated with timely and accurate eligibility determination did not diminish even though integrated staff assumed new and very different responsibilities.
At the time of our visit, one office in Montgomery County, KS was attempting to address the challenge integrated workers face. In this office, an eligibility worker was paired with case managers who had the dual responsibility of eligibility determination and service planning. Although the case manager collected documentation related to financial eligibility when interviewing clients, the eligibility worker entered the data in the computer system and conducted other eligibility-related tasks. It was hoped that this structure would allow the case managers to focus more on developing service plans, uncovering barriers, and monitoring progress toward achieving self-sufficiency. In two other study sites (Owensboro, KY, and Kent, WA) where eligibility and case management are integrated under one worker, the challenge of these combined responsibilities is addressed by involving specialized staff to assist with barrier identification and service referrals (discussed further below).
25 In Minneapolis, MN, employment service provider staff are contracted to provide case management/ service planning function in addition to other employment-related functions. In Las Vegas, NV and Arlington, VA the case manager is an employee of the TANF agency.
Skills and Training
The skills most valued in eligibility workers stand in contrast with the “soft” or interpersonal skills reported as the most important skill required of staff responsible for barrier identification.
In many TANF agencies, case manager positions are filled by former eligibility workers. While an in-depth understanding of eligibility rules may benefit case managers and their clients, the skills required to be an eligibility worker are quite different from those required to be a case manager. Program eligibility determination requires attention to detail and an understanding of, and strict adherence to, complex program rules. Case managers may also be required to have an understanding of program eligibility rules, but focus more on rules related to program participation and non-compliance.
The skills most valued in eligibility workers stand in contrast with the “soft” or interpersonal skills reported as the most important skill required of staff responsible for barrier identification. These interpersonal skills are credited with generating the trust and safety considered key for clients to disclose information about barriers to employment. Further, the ability to identify barriers to employment requires—at a minimum—the ability to recognize characteristics of barriers, conduct interviews with clients to discuss and elicit disclosure, and provide appropriate responses, both verbally and through service referrals. A case manager’s ability to develop service plans and make referrals also requires a knowledge of state and/or local work participation policies and the availability of services in the community. Such knowledge is not necessary to determine financial eligibility.
Case managers in the study sites often possess little formal training as counselors and vary in their possession of the strong interpersonal skills reported as essential to successful barrier identification. TANF case managers in the study sites are generally required to hold a Bachelor’s degree in a social science field and complete training on TANF policies. 26 This contrasts with the skills of specialized staff who are required to have strong interpersonal skills and often more formal education or training.
The extent to which TANF case managers are able to undertake efforts to identify barriers to employment is affected by the size of their overall workload.
All TANF staff interviewed had received some formal training from the TANF agency, although they were frequently unable to recall when the training had occurred or the details of the information provided. Most commonly, staff recalled training related to TANF policy changes, although some noted having received training related to the identification of characteristics, or general understanding, of one or more unobserved barrier to employment. Few staff had received formal training regarding the use of screening or assessment instruments, with the exception of training required to implement or score validated tools (such as the SASSI or ALDS). In carrying out their case management and barrier identification responsibilities, case managers in the study sites rely heavily on their past experiences with other TANF clients and their own life experiences. Therefore their abilities to identify unobserved barriers varied widely, were often based on little formal education regarding characteristics of barriers, and may have been influenced by personal biases or stereotypes.
26 Arlington, VA is an exception. In this site it is common for employment case managers to exceed the educational requirements with some holding Masters degrees in social work, counseling, or education.
Caseload Size
The extent to which TANF case managers are able to undertake efforts to identify barriers to employment is affected by the size of their overall workload. Although staff consistently reported that each case requires a different level of attention and involvement, caseload size can serve as a proxy for understanding individual workloads. In four of the six study sites case managers were responsible for 80-100 or in some sites even more cases.27 Commonly, staff reported that they do not have the time necessary to explore barriers or develop relationships with all of their clients. Given this, in-depth efforts to identify barriers may require smaller caseloads that allow more time to be spent with each client. Smaller caseloads were incorporated into special efforts to identify barriers that were carried out in the study sites. For example, Extra Effort pilot staff in Montgomery County, KS each work with five to six families, IRIS social workers are assigned ten clients and vocational counselors work with 20 clients, and social workers in Kent, WA ideally work with 60-80 clients.28
Workers responsible for both eligibility determination and case management/service planning functions may have a difficult time integrating efforts to identify barriers to employment into an already heavy workload. Staff in these positions reported feeling on-going pressure to fulfill the functions associated with benefit eligibility determination—including timely eligibility redetermination and imposing financial sanctions for non-compliance—and some noted that this may inhibit disclosure of barriers by clients. If remaining TANF clients have multiple barriers to employment, there are several drawbacks to relying on integrated workers to identify barriers. If staff are to retain both eligibility and case management responsibilities, including barrier identification, they may need to be responsible for smaller caseloads or receive significant support from more specialized staff. Given the complex nature of many unobserved barriers to employment, even TANF case managers who are not responsible for eligibility determination may benefit from the support of additional identification efforts carried out by specialists and having responsibility for smaller caseloads.
27 The two sites with smaller caseloads are Montgomery County, KS, which is the smallest rural community in the study with a smaller overall TANF caseload, and Arlington, VA, which has a small proportion of TANF clients required to participate in work activities due to more liberal application of exemption policies.
28 At the time of our visit, the social work unit in Kent had recently been reorganized and had a staff vacancy resulting in higher than planned caseloads.
Clients Willingness to Disclose to TANF Workers
Focus groups conducted with TANF clients in each study site offer interesting, albeit anecdotal, insight into clients’ views on disclosing barriers to employment. Clients who participated in focus groups were asked about their decisions to disclose unobserved barriers to employment and specifically their relationships with different staff members and whether or not these relationships impacted their willingness to disclose.
“When I call my eligibility worker, it takes her a week to get back to me. I could have an emergency, but do you think she cares? No. All she feels is like I’m looking for some money, Food Stamps.”
“They’re like robots. They’re not people people. Sometimes they’re flat-out rude. They make you feel small. Like ‘We’re helping you so you should deal with however I treat you.’”
“They don’t care. They’re just doing data entry.”
“She has an attitude. She looks down at you like you’re dirt. If she was asking me the questions, I’d just say no.”
Focus group respondents generally reported being less willing to disclose their unobserved barriers to employment to eligibility workers. Typically, eligibility workers were perceived to not be interested in helping clients with their needs beyond the receipt of cash, food, or medical assistance. Clients acknowledged that an eligibility worker’s primary responsibility is determining and monitoring eligibility for benefits, but noted that in carrying out these responsibilities workers often fail to create relationships that encourage or facilitate disclosure. Focus group respondents also reported frustration with frequent worker reassignments that made it difficult to interact with the same worker over time and develop a relationship. Finally, clients noted that many eligibility workers are responsible for large caseloads which inhibit workers’ abilities to develop relationships with individual clients.
Specialized Staff Involved in Barrier Identification
The study sites rely on specialized staff to assist in the identification of unobserved barriers to employment to varying degrees. Although TANF case managers bear the primary responsibility for initially detecting the possibility of an unobserved barrier, more specialized workers are responsible for additional assessment or diagnosis. In all sites, staff of partner agencies who have more formal training relating to an unobserved barrier, or experience working with individuals with a particular barrier, are involved in the barrier identification and/or diagnosis process. Many of these staff also work with clients to determine appropriate strategies for addressing barriers and may provide individual treatment or accommodations.
Clients who participated in the focus groups indicated that they were more comfortable disclosing to specialized workers (both specialized workers within the TANF office and staff of partner agencies), where they had such interactions. In three of the six study sites, a specialized staff person is located within the TANF agency specifically to assist with barrier identification and the development of service strategies. In two sites (Las Vegas, NV and Kent, WA) the specialists carry the title social worker and are employed by the TANF system, and in the third (Owensboro, KY), the specialist is the TAP assessor employed by the University of Kentucky. Below we describe how these three sites utilize specialists to aid in the barrier identification process.
Use of Specialists—Three Specialists—Three Examples
L as Vegas, Nevada
In response to the concern that clients remaining on welfare have a wide range of serious barriers that inhibit employment and welfare exit, the Nevada Welfare Division proposed reintroducing social worker positions into the agency staffing structure.29 The state legislature supported the request providing funding for more social worker positions than were requested. At the time of our visit in late 2000, there were five or six
social workers in each of the two offices we visited in Las Vegas. Social workers are required to have a Bachelor’s degree in social work and hold a state license (which requires social workers to complete continuing professional education requirements). They work with small caseloads of approximately 25-30 cases referred to them either by TANF eligibility workers or case managers. Unlike case managers in Las Vegas, social workers are not bound by the federally-defined countable work activities. This provides them greater flexibility to design service plans tailored to address the unobserved barriers of their clients. Social workers have frequent interactions with their clients, including in-person and telephone contact, as well as quarterly (or more frequent) home visits.
Social workers rely on their formal training as well as strong interpersonal skills to conduct a psycho-social evaluation, exploring topics such as household composition, educational background and work history, medical history, childhood background, issues with children, support systems, as well as domestic violence, mental health and substance abuse problems, and relationship issues. These social workers may utilize other tools, such as the SASSI, the Learning Needs Screening tool, a domestic violence screen, or the South Oaks Gambling Screen. Based on this assessment, they refer clients to partners to address the barriers uncovered or provide one-on-one counseling. If, through working with the social worker and partner agencies, the client’s barriers are alleviated or mitigated, she would return to working with the case manager to pursue employment and self-sufficiency.
29 Social workers existed within the welfare system in the 1970s, but later focused primarily on child welfare cases not families receiving cash assistance.
Owensboro, Kentucky
In addition to formal training and credentials, TAP assessors must also have experience working with low-income women with multiple barriers to employment and be familiar with the communities in which they work.
As in Las Vegas, case managers in Owensboro are also supported by more highly trained specialists. The Targeted Assessment Project (TAP) co-locates TAP assessors, who are experienced clinicians, in the welfare office to assist with barrier identification. Assessors are employees of the University of Kentucky, Institute on Women and Substance Abuse. The Institute has a contract with the Kentucky Cabinet for Families and Children to operate the Targeted Assessment Project which is designed to take a holistic approach to identifying and addressing TANF clients’ barriers. To accomplish this objective, TAP designers believe that assessors must have advanced formal training (i.e., hold a Masters of social work, counseling, or education degree, be a Certified Addictions Counselor, or have other clinical training). In addition to formal training and credentials, TAP assessors must also have experience working with low-income women with multiple barriers to employment and be familiar with the communities in which they work. In Owensboro, the TAP assessors are very experienced. They each have multiple of the required credentials, had both previously worked in the local mental health services community, and have relationships with staff at key partner agencies to which TANF clients are referred.30
TANF clients may be referred to the TAP assessor in a number of ways. During the initial assessment interview, case managers complete a screening form with clients to determine if she should be referred to the TAP assessor. Case managers reported that they also refer clients who are not making progress toward self-sufficiency or are generally “difficult” cases. Additionally, clients who do not initially disclose barriers and are referred to the Project LIFE job readiness workshop, but who later disclose a barrier, may be referred. TAP assessors rely on both their clinical training, as well as their interpersonal skills, to develop a rapport with clients and conduct a psycho-social interview. In some cases, this assessment is conducted over the course of several interviews and may involve the TAP assessor visiting the client in her home or meeting the client at a neutral site. Based on this assessment, the TAP assessor makes recommendations to the case manager regarding changes or additions to the client’s service plan to include referrals to address unobserved barriers, as appropriate. To ensure that clients do not fall through the cracks of a complicated social service system, TAP assessors often call theirpeers in other agencies to personally arrange appointments. In some cases the TAP assessors even accompany clients to the first appointment with a partner agency to ensure follow-through and make sure the client is comfortable with the new specialist.
30 To assure that everyone in the community accepts the individual hired as the assessor, applicants are screened and interviewed by a group of community social service representatives.
Kent, Washington
Case managers in Kent are also supported by social workers. Unlike the social workers in Las Vegas and the TAP assessors in Owensboro, these staff have the title social worker but are not required to have advanced formal education or training or be licensed. However, social workers in Kent can be considered specialists because they carry a specialized caseload of TANF clients with significant barriers to employment. Social workers may have advanced training or be pursuing other professional development opportunities which allow them to better serve their clients, but this is not required. Social workers also work with relatively smaller caseloads than case managers, which further facilitates their ability to focus on barriers such as domestic violence, substance abuse, mental health problems, and learning disabilities.31 Social workers in Kent, as in the other sites, may also assist with crisis needs such as lack of housing, emergency payment of utility bills, or problems with children in the household.
Social workers in Kent, WA, take an individualized approach to exploring barriers.
Case managers in Kent use the VIEW screening tool to guide referrals to social workers. In addition to clients with unobserved barriers to employment, case managers may refer TANF clients who are not progressing in their work-related activities, are sanctioned, or are parenting teens. Case managers have a fair amount of discretion in deciding who to refer to a social worker. As a guideline it is suggested that case managers refer clients who have barriers that will not be resolved within three to six months. Once a client is referred, social workers take an individualized approach to exploring barriers. They often review information in the case record, including responses to the VIEW screening questions. Although there are some formal tools available, social workers reportedly rely primarily on discussion to uncover the issues preventing clients from achieving or progressing toward self-sufficiency. Once a client is referred, social workers assume responsibility for creating and monitoring the client’s service plan which will likely include referrals to partner agencies that provide additional assessment or barrier-specific services. Because, Washington maintains a strong focus on work, social workers are encouraged to combine services to eliminate or mitigate barriers with other work-related activities when possible.
31 As noted previously, the social work units in the Kent office has recently been reorganized at the time of our visit. The goal in Kent is for two social workers to focus on serving TANF clients and carry caseloads of approximately 60 individuals.
Additional Specialists
In addition to the specialized workers mentioned above, all sites rely on experts from partner agencies to further the identification process or diagnose conditions and provide services to clients with unobserved barriers to employment. For example, staff in all sites refer clients to community mental health centers, local substance abuse treatment agencies, domestic violence shelters, and/or Vocational Rehabilitation programs that employ staff who have the skills and tools to determine with certainty that a barrier exists. Specialized staff in these organizations have the formal training required to work with these clients and administer barrier-specific tools. Specialists at community mental health centers commonly hold Master’s or Ph.D. degrees, while staff of substance abuse treatment organizations are commonly Certified Addictions Counselors or have other specialized training. Domestic violence service providers who are partners in the study sites employ an interdisciplinary staff, some of whom are advocates, counselors, or have other specialized training.
Vocational counselors involved in Vocational Rehabilitation (VR) programs typically must possess a degree in vocational counseling. VR programs also work with other vocational evaluators and diagnosticians, depending on the client’s specific disability.
The VR pilot program co-located with one of the employment service providers in Minneapolis, MN initially sought to employ staff who had experience with both vocational counseling and social service provision. This joint requirement was considered important because TANF clients were believed to require a different level of need for support than other VR clients. Thus staff would have to address not just the vocational evaluation and counseling needs of the client, but those needs that affect their ability to participate in or complete VR services. This joint requirement was difficult to fulfill and managers resorted to hiring staff with some social service experience and who would commit to completing their vocational counseling course of study after employed.
Additional Client Thoughts on Disclosing Barriers to Staff
In addition to the comments provided earlier, focus groups participants indicated that they take a variety of factors into consideration when making decisions regarding disclosing unobserved barriers to employment. Although some clients have distinct concerns about disclosing barriers to eligibility workers, they did note some additional factors—that may apply equally to eligibility workers, case managers, or other staff—that contribute to their decisions to disclose.
The Importance of Trust and Relationships
“It’s important for your worker to know you personally. Not as a stereotype, not as a number.”
“He listens and he doesn’t judge you for the things that happen.”
“They keep on you. They come to your house. It helps keep you going. Financial workers don’t care. They just tell me my case is closed.”
“The social worker showed up at my house to see if I was okay. My family doesn’t even do that.”
“She doesn’t talk at me, she talks with me. Like she may be able to understand
some of the things you’re going through.”
Clients clearly stated that they were more likely to disclose to someone they trust and with whom they have established a personal relationship.
Clients clearly stated that they were more likely to disclose to someone they trust and with whom they have established a personal relationship. Clients noted a number of characteristics of staff with whom they were more likely to develop a trusting relationship and thus to whom they are comfortable disclosing unobserved barriers to employment. Staff considered trustworthy, and to whom clients would or could confide, were commonly described as respectful, responsive, caring, down-to-earth, interested, nonjudgmental, compassionate, and supportive.
When pressed about how they came to determine staff to be trustworthy, many clients indicated that trust was gained when staff demonstrated their willingness and ability to help, for example through the provision of supportive services or a helpful referral. Home visits were mentioned by some clients as being evidence of a worker’s caring or interest in helping. On the other hand, some believed that home visits, particularly when unannounced or when their intent was not understood, were off-putting and an invasion of privacy. Several clients noted that determining that an individual was trustworthy or developing a trusting relationship requires time. However, examples provided indicate that there is no fixed period of time required to develop a relationship, and that some relationships form more quickly, whereas others may take some time.
Fears of Repercussions
“The eligibility tech, I wasn’t honest with her. I needed money. I needed Food Stamps. I was not going to sit there and say I’m an active alcoholic. I wasn’t going to do anything to disrupt that money coming.”
“You can’t tell them. They come take your kids.”
“It’s always a threat that they’re going to take your kids. A threat is close enough for me.”
“Even though we have a good relationship, I wouldn’t tell her. Because of
the position they hold, they’ve got the power.”
Clients’ decisions to disclose to barriers are significantly affected by their fears of
repercussions.
Clients overwhelmingly reported that their decisions to disclose barriers to employment are significantly affected by their fears of repercussions. The most common repercussions that clients fear, and which reportedly deter disclosure, are the involvement of child protective services or child welfare agencies, and the potential loss of benefits. Clients noted giving careful consideration to what information they would provide and the possibility that disclosure would result in having their children removed from the home. Clients reported that some concerns about repercussions could be alleviated if they were told how information would be used and with whom it would be shared, before being asked to disclose.
Focus group respondents reported that the fear of repercussions applied equally to different forms of disclosure, including discussions with workers as well as completing screening or assessment instruments. The foundation beneath the fear of repercussions related to disclosing barriers is the belief that TANF staff have “power” over clients’ situations insofar as they can initiate actions to remove children from the home or impose financial sanctions (i.e., reduce or terminate benefits). Some clients acknowledged that this control of benefits is a fundamental part of the worker’s job that cannot be changed, and as such some clients associate these responsibilities more with eligibility workers than case managers or specialized workers.32
32 However, where eligibility and service planning functions are combined, the concerns about disclosure would diminish the likelihood of the client disclosing to this integrated worker.
Accepting Help and Understanding What’s Available
“The one that helped the most gave me a lot of information.”
Finally, clients reported that their willingness to disclose barriers to employment was affected by their readiness to accept help and their understanding of their barriers. Several respondents noted that prior to their disclosure they were in denial and therefore would have indicated to a worker that they faced no barriers to employment. Others noted that it was not until they were ready to accept help that they informed workers of their need for assistance. Some clients indicated that their willingness to disclose could be encouraged by understanding the range of services available to them.
Information Sharing
The coordination and sharing of information among the variety of staff and partners involved in identifying and addressing unobserved barriers to employment is a complicated challenge and requires a significant investment in communication and collaboration at multiple levels. In this section, we discuss the efforts to facilitate communication between individual workers involved in the barrier identification process undertaken by the study sites.
Communication among the various individuals involved in barrier identification in the study sites takes several forms. In all sites, staff engage in informal discussions with peers and supervisors on a regular basis. In Montgomery County, KS, TANF case managers served as a clearinghouse of information. They used information from partners to update clients’ service plans and make additional referrals. However, specialized staff of partner agencies did not appear to communicate with each other directly. TANF case managers in the other sites served a similar function.
In addition to centralized communication through case managers, in three of the sites (Kent, WA, Owensboro, KY, and Las Vegas, NV), case managers and other staff convened meetings, sometimes called staffings, to discuss clients’ progress, or lack thereof. In two sites (Minneapolis, MN and Arlington, VA), TANF agency staff or staff of a partner organization communicated more frequently, operating as a team that regularly shared information in an effort to jointly assist TANF clients. The use of staffings and communication among teams of staff are both discussed below.
Staffings
Staffings provide an opportunity for staff to share information regarding a client and receive input from others regarding possible strategies for addressing the client’s needs.
As TANF agencies tackle the challenge of addressing unobserved barriers to employment—and in many cases, multiple or co-occurring barriers—some have introduced or reintroduced case staffings. Staffings are a common tool used among those in the social work field to share information and brainstorm solutions. Generally, staffings provide an opportunity for staff to share information regarding a client and receive input from others regarding possible strategies for addressing the client’s needs. Their primary purpose, as used in the study sites, is to exchange information regarding barriers, discuss a client’s situation, and determine the appropriate next step for a client. The composition of staff involved in the staffings varies from site to site, as well as by individual meeting, that are often are called in response to specific events in a client’s TANF experience.
For example, in Kent, WA, staffings are often called when a client fails to make progress toward finding a job. If the Employment Security Department (ESD) job counselor determines that, after engaging in job search for approximately nine weeks, the client is not likely to obtain employment, he or she may call a staffing. Likely participants at this staffing are the ESD job counselor, TANF case manager, a DSHS social worker, and the client. If the client is involved with other organizations, staff of those partners may also be invited. At this meeting, staff explore the reasons the client is not making the expected progress and determine appropriate next steps, which may include additional assessment for, or diagnosis of, a possible unobserved barrier. Staffings may also be called by social workers or staff of other agencies involved with the client in response to barriers faced by clients or the need to coordinate service strategies.
As noted earlier, staffings in Owensboro, KY are also called in response to an event. In Kentucky, clients who are sanctioned six out of 24 months face benefit termination. Prior to this, staff involved in the client’s case meet with the client to attempt to uncover the reasons for non-compliance and offer the client one more opportunity to avoid benefit termination. Along with the client, staff who participate in such meetings include the TANF case manager, the TAP assessor, and staff of partner agencies who work with the client. If, at this meeting, the client agrees to take the steps necessary to come into compliance, she can avoid benefit termination. Formal staffings are not the only way staff share information in Owensboro. Staff also reported frequent interaction between the TAP assessors and case managers in an effort to share information about clients’ barriers and needs.
In Las Vegas, Nevada, staffings are referred to as Individual Disciplinary Team (IDT) meetings and are convened by social workers for clients determined to be in need of this type of intensive, focused look at their specific situation and service needs. For example, an IDT might be conducted for a client who is not progressing with her assigned plan of action for reasons that were not clear. In addition to the social worker, the meeting might include the social work supervisor, staff from other agencies who have worked with the client (e.g., substance abuse counselor, mental health counselor), and the client. Generally, no more than three other partner agencies are represented at a single meeting. During the IDT meeting, staff discuss and explore the client’s specific situation and determine appropriate steps to be taken. These meetings are not convened for every client; rather, they are called at the discretion of the social worker.
In some sites, the opportunity to discuss cases and strategies also serves a cross-training purpose. As staff who have less formal training or who are less involved in barrier identification have the opportunity to review specific cases or situations with more specialized staff, they often obtain important information about characteristics or indicators of barriers. These staff also further their understanding of appropriate responses to such barriers and thus believe they are better able to identify and address barriers when they work with other clients.33
33 It is important to note that such cross-training does not only occur during formal staffings. Staff reported that the opportunity to work with specialists on an on-going basis furthered their understanding of barriers to employment. Further, in some sites, specialists conducted more formal training session for TANF agency staff regarding barriers to employment.
Team Approaches
Two of the study sites go beyond informal communication among staff or even the sharing of information through staffings. In the IRIS Program in Minneapolis, MN and in Arlington, VA, staff operate as a team. In these sites, information is shared on an on-going basis and supported by an understanding of joint responsibility for a case.
The IRIS Program is designed to assist welfare recipients who have trouble fulfilling their Minnesota Family Investment Program (MFIP) employment plan requirements due to a mental or chemical health problem. IRIS takes a multi-disciplinary approach to these issues by assigning each client to a team of specialists. Each team consists of a social worker, a vocational counselor, and a therapist. When it was originally designed, the IRIS Program used a single staff person—a vocational counselor—to work with clients to address their unobserved barriers to employment. However, approximately eight months into the implementation of IRIS, staff realized that clients faced a complex array of issues that require more support than a vocational counselor alone could provide. In response to this need, the IRIS Program sought and obtained additional funding to create a team staffing structure that includes social worker and therapist in additional to the vocational counselor.34
The IRIS staffing structure assigns staff in teams with relatively small caseloads—each vocational counselor carries a caseload of 20 and works with two social workers who carry caseloads of ten each.35 The team works with the client to develop an individualized plan that will assist the client in overcoming social and employment-related barriers. IRIS team members reported regular, on-going interaction among team members. Social workers and vocational counselors conduct a joint assessment which provides both members of the team critical information regarding the client’s situation. Additionally, social workers meet with the vocational counselor throughout the initial period of social stabilization (prior to involvement in vocational services) to keep the vocational counselor apprised of progress and additional issues that arise. Finally, the therapist also communicates with the social worker and vocational counselor, sharing (as appropriate) information from her sessions with clients.
IRIS team members provided positive feedback regarding this team structure. The team approach reportedly allows each staff member to focus on a more narrow range of issues drawing on his or her own area of expertise while providing a comprehensive set of services to meet clients’ needs. There appeared to be little confusion regarding roles or information sharing, and staff reported appreciating the contribution made by other members of the team. All members of the IRIS team were committed to working with the client to identify and address her needs through a supportive and caring approach. They also collectively believed that there was no client need that the team, individually or collectively, could not address.
In Arlington, VA, team members work with a specified group of clients and work together closely to ensure that the client is fulfilling participation requirements and obtaining necessary services.
Arlington, Virginia also utilizes a team approach to coordinate the efforts of the various types of staff who may be involved in an individual client’s case. At the time of welfare reform, Arlington recognized the need for linking the work done by eligibility workers with that done by the staff known at the time as JOBS workers. While other counties in Virginia decided to assign both eligibility and employment program duties to eligibility workers, officials in Arlington believed that eligibility workers already had multiple programs to learn and administer and would not be able to manage the additional responsibility of the employment services required by TANF. Instead, they chose to create a team consisting of the ongoing financial eligibility worker, the TANF employment case manager, the job developer, and the Crisis Assistance Bureau social worker. The latter is not as intensively involved compared to the other member of the team, unless the client has been referred to the social worker for help with immediate needs.36 A substance abuse/mental health therapist, a co-located partner, would be a member of the team if a client had been specifically referred to him or her or if other team members were unsure of the specific barriers that were preventing clients from getting or keeping jobs and wished to draw on the therapist’s expertise.
Team members work with a specified group of clients and work together closely to ensure that the client is fulfilling participation requirements and obtaining necessary services. In addition to frequent, on-going communication among the members of the core team (who are housed in the same physical location), the team meets monthly to discuss issues, problems, and concerns related to specific cases facing crucial needs (e.g., nearing the end of the time limit or encountering a crisis that might cause them to lose their job). Individual case staffings can also be convened and may include team members, staff from relevant partner providers, and clients themselves.
If a client is referred to the Vocational Rehabilitation program operated by the Department of Rehabilitation Services (DRS), a second team is formed. In such a situation, the team consists of the DRS employment counselor, staff from Sheltered Occupational Center (SOC) Enterprises and a psychologist. These team members coordinate with each other to complete additional evaluations and/or provide diagnoses, develop an employment plan, and secure appropriate services or accommodations for the client. The second team also meets with members of the core team, (usually the TANF employment case manager and the job developer), thus linking the members of the two teams, all of whom work together to address the needs of the client.
Team members in Arlington were, in general, very positive about the team approach to case management and service provision that had been implemented. Staff believed that the team approach was particularly helpful in providing multiple opportunities for different types of staff to develop a relationship with and identify barriers faced by individual clients. For example, a job developer in the course of weekly job search meetings with the participant, might identify a potential barrier that the case manager had missed. The two workers would immediately consult with each other, and other team members as appropriate, to discuss the situation and make necessary referrals. Staff reported that the physical co-location of the primary team members, as well as the regular presence of the substance abuse/ mental health therapist and staff from DRS and SOC Enterprises, contributed to the successful operation of the team concept.
34 Prior to this professional mental health services were purchased from outside agencies. It was noted that bringing this service in-house provided more immediate access to psychological services necessary to meet clients’ needs.
35 Therapists work with varying numbers of clients depending on clients’ need for on-going therapy.
36 Crisis Assistance Bureau Social Workers are social workers with Masters-level degrees and at least two of years of relevant experience who assist clients with emergency needs such as shelter, utility bills or food assistance. In the course of addressing these emergency needs, unobserved barriers may be identified.
Confidentiality
Sharing information among the variety of staff involved in barrier identification requires that all persons involved give special attention to issues of confidentiality. As noted in Ten Important Questions, developing strategies for identifying unobserved barriers brings to the forefront questions regarding what information can be shared, under what conditions information can be shared, and how information should be shared. A number of different federal and state laws, as well as regulations, guide the protection of privacy, the confidentiality of records, and informed consent.
When asked, staff in all of the study sites appeared familiar with their offices’ guidelines regarding confidentiality and information sharing. Staff could easily and quickly produce the forms clients were asked to sign to facilitate information sharing. In many cases, TANF agency staff asked clients to sign these forms very early in the process to allow greater latitude to share information as it was uncovered.37 In some cases, staff of partner agencies appeared more familiar than TANF agency staff with the details of these provisions and the need to obtain informed consent from clients before sharing information with the TANF agency.
Generally, specialists reported sharing only the information they believed was relevant with TANF staff. TANF staff occasionally reported frustration regarding obtaining information from specialists—particularly those in the substance abuse and domestic violence fields. This appears to be due to several factors including the special confidentiality provisions that guide sharing of information regarding substance abuse, and the fact that many domestic violence service providers also serve as advocates for their clients and place clients’ interests above those of the TANF system. TANF case managers’ frustration appeared to be rooted in the fact that, in accepting responsibility for the case, case managers often believe that they should have the broadest set of information available, whether or not it related to TANF eligibility or service strategies.
The study sites illustrate that the challenges associated with ensuing privacy and confidentiality are not insurmountable.
Staff reported that clients rarely objected to signing release or informed consent forms. In a few cases, staff attributed this to their strategy of informing clients how the information would be used, with whom it would be shared, and under what conditions. More commonly, staff asked clients to sign release forms as part of a process that requires the completion of many forms. Staff acknowledged that clients may not fully understand the implications of signing different forms. It is unclear from these staff reports if clients are willing to sign the forms because they have no concerns about how information will be used or with whom it will be shared, or, if as indicated in the focus groups, clients sign the required forms so as not to jeopardize their eligibility for benefits and consider these confidentiality issues when deciding what to disclose and to whom.
Although confidentiality provisions and agreements deserve a more detailed review than offered by this study, it is clear that the challenges associated with ensuring privacy and confidentiality are not insurmountable. States and localities engaged in developing unobserved barrier identification strategies should not view issues of confidentiality as a barrier to the implementation of proactive screening and assessment strategies.
37 Our exploration of this issue did not include a detailed review of the forms, time period specified for allowable information sharing, or other details related to the use of these signed consent forms.
Staffing Conclusions
In all sites, TANF case managers play a key role in initially determining that a client may face an unobserved barrier to employment. TANF agencies must consider the extent to which such key TANF staff will be responsible for further assessing barriers and making appropriate referrals. Such decisions need to take into consideration the skills and training of these staff members, their workloads, and the availability of specialists to provide additional identification services.
Staff overwhelmingly believed that strong interpersonal and good communication skills are most critical for staff responsible for identifying barriers to employment.
It is worth noting again that staff and managers overwhelmingly believed that strong interpersonal and good communication skills are most critical for staff responsible for identifying barriers to employment. Although formal, clinical training may assist in the identification of barriers it may not be necessary to have clinically trained staff within the welfare agency, if this skill is available through partnerships. If the primary responsibility is to determine with reasonable likelihood that a barrier to employment exists and make an appropriate referral to a specialist, formal education or training may not be required and informal identification strategies may be adequate. Staff with strong interpersonal skills that allow clients to feel comfortable disclosing barriers, or who have received enough training to be aware of the general characteristics of barriers, may be wholly capable of obtaining enough information to make an initial referral to more specialized staff or partners. Specialists and staff of partner agencies in the study sites reported that, in general, referrals they received from TANF case managers were appropriate.
TANF agency staff in the study sites consistently commented that they were pleased to have the support of individual specialists in their offices, as well as more specialized staff from partner agencies. Although clarifying respective roles and responsibilities, establishing effective referral protocols, and making appropriate referrals may take time, each of the study sites had addressed these challenges and were utilizing specialists to further the barrier identification process.
Finally, because TANF clients—particularly those with multiple barriers to employment—are likely to become involved with a number of different staff persons, efforts must be made to keep the lines of communication open. Communication and clarification of respective roles and responsibilities among staff and with clients can minimize potential confusion for clients. Communication within the bounds of confidentiality guidelines can also result greater levels of barrier identification, better services to clients, further education of staff regarding barriers, and knowledge of services available to address barriers.
Chapter Six: Identifying and Addressing Barriers to Employment Through Partnerships
TANF agencies in the study sites work with a variety of partners to assist with identifying unobserved barriers and to provide services to clients once barriers are identified. Key partners include other government agencies, community mental health centers, substance abuse treatment programs, domestic violence shelters and counseling agencies, educational institutions, and others. In this chapter we briefly describe how some of the partnerships were established, the role of partner organizations, the services they provide, and strategies used by the study sites to strengthen partnerships.
Partner Organizations and Efforts to Establish Partnerships
TANF agencies in the study sites have a wide range of partners. In some cases these partners have had longstanding relationships with the TANF agency, while in other cases, new partnerships have formed as efforts to identify unobserved barriers have expanded. Although the capacity to meet all clients’ needs was not sufficient in every site, no site reported difficulty identifying potential partners. Some relationships between agencies were so longstanding that staff could not easily recall how partners were initially identified. In many sites, TANF agency staff were aware of organizations in the community with expertise addressing unobserved barriers to employment but had not worked closely with them. As efforts to identify the diverse needs of the TANF population have evolved, existing partnerships have expanded to include new partners, as well as the utilization of existing partners in new ways. In this section we discuss some skills and experiences partners offer and ways in which the study sites facilitate partnerships.
Skills and Experiences of Partners
In all sites, partnerships offer TANF clients access to staff with skills and expertise related to identifying unobserved barriers and, in some cases, barrier specific services. Thus, partners’ skills and services complement and supplement services provided by the TANF agency. Common partners include other government agencies and community-based organizations, often specializing in one or two specific unobserved barriers.
Mental health organizations that have experience working with severely and persistently mentally ill (SPMI) adults noted that they have a long history of working with persons with the types of barriers characterized by TANF agencies as “hard-to-serve.”
Community mental health centers are common partners because they have experience diagnosing and addressing the wide range of mental health problems some TANF clients may have. Mental health organizations that have experience working with severely and persistently mentally ill (SPMI) adults noted that they have a long history of working with persons with the types of barriers characterized by TANF agencies as “hard-to-serve.” For example, staff at Four County Mental Health in Montgomery County, KS believe working with TANF clients with unobserved barriers was a natural extension of their services to SPMI adults. By drawing on their experience with these clients and applying lessons learned, they were able to develop services to address the challenges faced by TANF clients. Similarly, staff of the IRIS Program in Minneapolis, MN believe they are able to apply their experience working with SPMI clients through sheltered workshops and other strategies to effectively serve TANF clients with mental or chemical health problems that inhibit fulfilling their Minnesota Family Investment Program employment plans.
Vocational Rehabilitation (VR) programs offer another source of expertise to TANF agencies. In four of the six study sites, the VR program was a primary source for obtaining the diagnosis of and services for learning disabled TANF clients.38 VR programs share a common overarching goal with TANF of helping clients with disabilities return to work and become self-sufficient. VR programs focus on moving clients with disabilities to work by providing appropriate training and accommodations. Although their primary expertise generally rests in serving clients with physical disabilities, many VR agencies also have experience dealing with mental health problems and learning disabilities.
Relationships with VR agencies varied across the study sites, in part due to sites’ varied focuses on learning disabilities as an unobserved barrier to employment. VR partnerships were also affected by funding availability. For example the VR agency in Kent, WA was in “order of selection.” This means that they only had funding available to serve the most severely disabled clients which often did not extend to TANF clients with unobserved barriers to employment. However, staff in Kent, WA rely on an alternative partnership, with the Seattle-King County Workforce Development Council, to provide additional assessment and arrange for the diagnosis of learning disabilities. Similarly, Montgomery County, KS used a partnership with the local VR agency to assist with some barriers but also established a relationship with Pittsburg State University to obtain learning disability diagnoses. Finally, the Targeted Assessment Project in Kentucky has served as a catalyst for developing a stronger relationship between the TANF agency and the VR program.
Substance abuse treatment organizations are another key partner in all of the study sites. Although in some sites, other partners participate in determining the level of treatment a client may require, treatment agencies ultimately provide necessary services. For example, in Montgomery County, KS, the Regional Alcohol and Drug Assessment Center (RADAC) serves as a gatekeeper to substance abuse treatment. RADAC assessors use formal assessment tools and their training as certified addictions counselors to determine the level of treatment a client requires (e.g., group meetings such as Alcoholics Anonymous, outpatient therapy, inpatient or residential treatment). Based on this assessment, clients are referred to a treatment facility that can meet their needs. Staff from the Department of Community and Human Services/Mental Health, Chemical Abuse, and Dependency Services Division fill a similar role in Kent, WA.
All six study sites have also created partnerships with domestic violence counseling organizations and/or shelters. In Arlington, VA and Minneapolis, MN domestic violence victims may also be assisted by a domestic violence liaison housed within the welfare agency. These liaisons assist clients in obtaining services from a shelter or counseling agency.
38 In Kent, WA, clients thought to face a learning disability are referred to the Seattle-King County Workforce Development Council Learning Disabilities Project (SKCWDC/LD). The SKCWDC/LD is one of the nation’s leaders is developing strategies to address learning disabilities among TANF clients.
Mechanisms for Establishing Partnerships
Partnerships in the study sites were created in a variety of ways. In some cases, partnerships grew out of past experience working informally with other organizations within a community’s social service system. In Kentucky, the University of Kentucky’s Targeted Assessment Project (TAP) is based on a previous relationship between the University’s Institute on Women and Substance Abuse and the Kentucky Cabinet for Families and Children. Prior to the TAP effort, the Women’s Institute had worked with the Cabinet to provide training on substance abuse identification and referrals. The Women’s Institute built on this relationship with the Cabinet to encourage a more holistic approach to barrier identification, out of which the TAP effort grew.
Approaches to establishing relationships varied across the sites, in part based on the responsibilities maintained at the state level, as compared to those passed to regional or local TANF offices. In the example above, the State of Kentucky initiated the TAP effort with the University of Kentucky. In Arlington, VA and Minneapolis, MN, the devolved nature of responsibility for TANF operations has resulted in relationships being established primarily between local-level agencies.39
Alternatively, Nevada is a state administered TANF system and as such the state welfare agency took the lead in establishing relationships in support of identifying and addressing unobserved barriers. Memoranda of understanding between organizations outline the expectations of each agency relative to barrier identification, referrals, and services, and serve as the foundation for local level operations. In Washington, service contracts are established regionally so that they can be more closely tailored to local needs. However, local office directors in Washington have the latitude to establish additional partnerships and can even initiate additional local contracts if regionally-secured services do not meet local needs.
Overwhelmingly, TANF staff at all levels reported having little difficulty securing services necessary to support efforts to identify and address unobserved barriers.
Overwhelmingly, TANF staff at all levels reported having little difficulty securing services necessary to support efforts to identify and address unobserved barriers. In part this may be a result of the study sites reflecting service rich communities. However, staff commonly attributed this ease to the general availability of TANF funding to purchase or create services. For example, in Kent, WA, TANF funds were used to support additional beds in substance abuse treatment facilities, thus ensuring that TANF clients have access to required treatment. In Minneapolis, MN the IRIS Program was initially funded with Welfare-to-Work grant funds and later received funding from the TANF system to allow access to IRIS services by a broader range of TANF clients. In Nevada, TANF funds were used to expand mental health services to ensure TANF clients would not face long waiting lists and risk running out of months on TANF before receiving necessary services.
39 An important exception is the Department of Social Services/Department of Rehabilitation Services jointly funded project that facilitates services by SOC Enterprises.
Strategies to Facilitate Partnerships
Forging and maintaining partnerships to provide services to welfare recipients is not a new challenge to TANF agencies. However, few believe that creating and maintaining effective partnerships is easy. Each of the study sites has faced this challenge and offers some lessons and options regarding facilitating partnerships. Below we highlight selected strategies including co-locating partners, setting clear expectations, and obtaining support from staff at all levels.
Co-location
Offerring services in the same location was considered advantageous for clients and a way to strengthen relationaships.
A strategy to facilitate partnerships undertaken in some study sites is the co-location of partner agency staff in the welfare office. Physically offering services in the same location was not only considered advantageous for clients, but was considered another way to strengthen relationships between partner and TANF agency staff. In Arlington, VA, staff of SOC Enterprises, a contract psychologist, and the Department of Rehabilitation Services have offices and regular hours during which they see TANF clients at the Arlington Employment Center (AEC). Also in Arlington, staff reported that much of the success of the partnership with the substance abuse/mental health therapist is a result of this specialist being co-located in the AEC.
Initially efforts to facilitate this partnership included educating TANF staff about identifying substance abuse and mental health problems and how to make referrals. This effort was followed by the assignment of one person as the single point of contact in the partner agency. Neither of these efforts resulted in the expected number of referrals. Finally, funding was secured to support a dedicated worker and managers of both agencies agreed that colocating a staff person in the AEC may be a better approach to meeting staff and client needs. With the co-location of this specialist, referrals have increased and a strong partnership has developed.
The Kent, WA office also co-locates a number of partners including representatives of the Employment Security Department who conduct same day job search; a public health nurse who provides parenting, pregnancy prevention, and health services; a substance abuse assessor who conducts same day assessments, if scheduling permits; and an independent psychologist (available several days a week) for clients who may require counseling or mental health assessments. Kent was planning to co-locate a domestic violence advocate in the welfare office, at the time of our visit. This co-location creates a one-stop shopping environment for clients and allows TANF case managers and social workers to consult with specialists on an ongoing basis and become increasingly knowledgeable regarding how to recognize and address unobserved barriers to employment.
Setting Clear Expectations
Setting clear expectations for all involved can form a solid platform on which to build a partnership. For example, service contracts in Washington outline the services to be provided by contract agencies and the populations to be served. Further, by basing payments on performance outcomes, the Washington Department of Social and Health Services clearly communicates its expectations of its service contractors. Contracts also clarify how long clients may be engaged in services and the reporting requirements of the contract agency.
As mentioned earlier, the formal memoranda of understanding used in Nevada establish clear expectations on the parts of the agencies involved. By putting in writing the list of services to be provided or functions to be carried out by each organization, agency managers in Nevada clarified for each other, and the staff in local offices, what was to be expected. While these expectations were written at a broad level and did not replace the need to establish local operating procedures, they did give staff the foundation on which to build referral and reporting procedures.
Support From All Levels
One key to a successful partnership is support from upper level managers as well as front line staff.
Partner agencies in several sites noted that one key to a successful partnership is support from upper level managers as well as front line staff. For example, in Montgomery County, KS, managers and line staff in both the TANF agency and at their partner Four County Mental Health noted strong support for the Extra Effort pilot program. This support was considered essential to facilitate the development and refinement of this new program, as well as the implementation of referral procedures.
Referrals to partner agencies rely heavily on front-line staff ’s understanding of the services available and their willingness to refer clients. Although some sites reported concerns about roles and responsibilities when some partnerships were established, many of these concerns seemed to dissipate with time. Time spent working together allowed TANF case managers to gain a better understanding of the services offered by partners and to understand how these services complemented, rather than replaced services they provide. At the time of our visits, most TANF agency staff reported a strong appreciation for the services offered by specialized staff and partners, particularly given the large and multifaceted workloads faced by many TANF case managers.
Staff of the Targeted Assessment Project operating in Owensboro, KY also noted the importance of support and buy-in, not just from multiple levels within the TANF organization but from the entire community. University of Kentucky TAP managers established early-on that operating a project in multiple communities requires strong working relationships with each local TANF agency, as well as partner agencies that address unobserved barriers to employment. To obtain this support staff of the University of Kentucky convened meetings of key stakeholders to discuss the TAP and how it should operate in the community. This group formed a local advisory board that provides feedback on the effort and is even involved in hiring local TAP assessors.
The Roles of Partners in the Study Sites
In all sites, partners serve multiple purposes. Partners typically conduct additional assessment or diagnose a condition and determine the appropriate level or type of treatment or services required. In many situations, partners also provide treatment or services to address or mitigate barriers. A less formalized although potentially valuable role for partners in some sites is that of educating TANF staff on how to identify unobserved barriers. Each of these roles is discussed in greater detail below.
Furthering the Identification of Unobserved Barriers to Employment
Most TANF agencies make referrals to partners based on information that leads them to suspect that a client may have an unobserved barrier to employment. Even where sites utilize formal assessment tools, these assessments determine that an unobserved barrier to employment likely exists, but does not constitute a diagnosis or definitive determination of a condition.
Partner agencies are in many cases better positioned to identify unobserved barriers to employment than TANF agencies because their staff possess the skills, tools, and expertise to diagnose barriers to employment and determine the exact nature of the barrier. For example, mental health partners in the study sites typically conduct a series of in-depth interviews, and may utilize formal psychological tests, to determine the exact nature of the suspected barriers. Screening conducted by TANF agency staff may indicate that a client shows signs of depression or an anxiety disorder, but this cannot be confirmed without further assessment by professionals trained in applying clinical criteria.
Similarly, TANF agency staff who learn that a client occasionally uses drugs or alcohol would use this as the basis for a referral to a substance abuse partner agency. Substance abuse partners would engage in further assessment to determine the extent of the substance abuse problem, if the usage level constitutes abuse, and the level or type of treatment required. For example, in Kent, WA, TANF clients suspected of having a substance abuse problem based on the VIEW questions or behavioral observations are referred to the on-site substance abuse specialist who conducts a thorough assessment to determine the extent of the problem and recommends an appropriate course of treatment.
In the case of domestic violence situations, referrals are often the result of a victim’s disclosure and willingness to seek assistance. Therefore, domestic violence partners are not typically required to determine if the barrier exists, rather they move immediately to exploring the specific nature of the situation and assisting the victim in developing an appropriate safety plan.
Services to Address Barriers
Many partner agencies in the study sites not only assist in diagnosing barriers but also provide services to address or mitigate the barrier. Although this study did not attempt to undertake a comprehensive review of the variety of service strategies employed, we did have the opportunity to explore some of services provided by key partners that led us to include certain sites in the study. Below we provide a brief overview of selected programs. Each is discussed in greater detail in Appendix B.
The IRIS Program in Minneapolis, MN and SOC Enterprises in Arlington, VA both utilize an interdisciplinary team to address the varied needs of clients with unobserved barriers to employment. Both provide vocational assessment, job readiness services, and psychological assessments. In addition, some clients may participate in sheltered workshops or subsidized employment as they prepare for unsubsidized positions.
Services offered by both the IRIS Program and the Extra Effort program in Montgomery County, KS are based on the agencies’ experiences serving severely and persistently mentally ill (SPMI) adults, who have many of the same barriers as hard-to-serve TANF clients. Both programs keep staff-to-client ratios low so as to facilitate individualized and intensive services. Both provide social stabilization or support services as well as job readiness services.
Finally, Rainier Case Management’s Intensive In-Home Services in Kent, WA is also an individualized, intensive approach to assisting clients with unobserved barriers to employment. Unlike the services described above, Rainier’s services are offered to clients who are non-compliant with TANF program requirements, or at risk of being sanctioned for non-compliance. Rainier case managers conduct in-depth assessments to determine if an unobserved barriers is the cause of the non-compliance and attempt to connect clients with services that will bring them back into compliance. Although Rainier staff offer some informal, one-on-one counseling, their primary service is convincing the client to come back into compliance and working with TANF agency staff to modify service plans to address clients’ needs.
Partners as Educators
In several sites, partner agencies not only assist with identification and service provisions, but they also fill an educational role. By sharing their expertise, consulting on specific cases, participating in staffings, and conducting more formal training, partner agency staff help educate TANF staff about recognizing and addressing unobserved barriers to employment. For example, TAP assessors in Owensboro, KY:
consult frequently with TANF case managers about cases;
educate TANF staff on unobserved barriers through informal discussions;
conduct training sessions for TANF staff on topics such as the characteristics associated with depression and substance abuse, and anger management;
educate community partners on TANF program requirements by serving as a bridge between the TANF agency and barrier-specific service providers.
Like the TAP assessors in Owensboro, many partner agency staff are colocated in the TANF office in Kent, WA. Staff of the Employment Security Department, the state substance abuse agency, a public health nurse, and an independent psychologist are co-located in the Kent welfare office.40 By having the opportunity to interact with these partners on a daily basis, TANF agency staff have more immediate access to services for clients and can use this frequent, often informal consultation, as an educational tool.
Partner staff in Las Vegas, NV have also conducted training for TANF agency staff. For example, staff from local domestic violence shelters and substance abuse treatment programs provided training to help TANF staff improve their abilities to recognize these potential barriers to employment. Educational sessions were also held with staff of the Vocational Assessment Center to educate case managers and social workers on how to interpret the results of vocational assessments. Similarly, staff of Four County Mental Health and RADAC in Montgomery County, KS also conducted training for TANF
agency staff to help raise awareness of the characteristics of mental health and substance abuse problems.
In addition to conducting training sessions, partners in Las Vegas, NV also help to educate each other about service availability and strategies through Multi-Disciplinary Team (MDT) meetings. These meetings allow community partners to share information about resources and services available generally, but they also provide a forum for brainstorming about specific, difficult case situations, within the bounds of confidentiality guidelines. While the format and composition of these meetings may vary from office of office, MDTs are usually organized by TANF social workers and may include up to 25 partners agencies representing a wide range of service providers such as transportation, housing, utility, substance abuse, domestic violence, vocational rehabilitation, health and counseling services. At the time of welfare reform implementation, MDTs were held in the local offices monthly, but as the partners have learned how to best share resources and become more familiar with each others’ services and staff, the frequency of these meetings was reduced and they are now held on a quarterly basis.
40 The psychologist was co-located 2-3 days/week. At the time of our visit, plans were underway to colocate staff of a domestic violence partner agency as well.
Chapter Seven: Concluding Observations and a Look into the Future
Concluding Observations
The case studies illustrate that perhaps the most comprehensive barrier identification strategies do not rely on screening or assessment tools.
The case study sites offer a number of lessons regarding the issues and challenges associated with creating strategies to identify substance abuse and mental health problems, domestic violence situations, and learning disabilities. Perhaps one of the most important findings from the case studies is that the study sites have developed approaches that integrate barrier identification throughout a client’s TANF experience, rather attempting to identify unobserved barriers at a single point in time.
Barrier identification as carried out in the study sites is a process, not an event. These processes are complicated and incorporate multiple identification strategies. Further, the case studies illustrate that perhaps the most comprehensive barrier identification strategies do not rely on screening or assessment tools to uncover barriers. In part, this is because few tools have been created and validated that fill this need. However, staff who have spent time addressing the challenge of barrier identification emphasize that informal strategies (carried out by knowledgeable staff with strong interpersonal skills) may be equally if not more effective. This is particularly true if the objective is to identify the likelihood of the existence of a barrier upon which to base a referral for additional assessment or diagnosis.
As noted above, the choice of barrier identification strategies is dependent in part upon the skills and training of staff involved in the process. The use of specialists contributes significantly to barrier identification efforts in some sites. These specialist typically have more formal training regarding barrier identification and can use a wider array of validated tools than can TANF case managers. However, the case studies indicate that it may not be necessary to involve staff with extensive formal education or credentials. Staff who have a basic understanding of the characteristics indicative of unobserved barriers, and who can develop a trusting relationship with clients, may be equally effective in this role. However, a staff person’s ability to be effective in this endeavor is also affected by his or her mix of responsibilities and overall workload.
The case studies also show that efforts to identify unobserved barriers do not necessarily have to replace a program’s emphasis on obtaining jobs and becoming self-sufficient. Some might argue that the study sites do not employ a Work First approach by its strictest definition. However, the study sites have found ways to implement barrier identification efforts while remaining focused on the programs’ ultimate objective of helping clients leave welfare for work. This being said, a focus on barrier identification may require TANF agencies and their partners to allow clients more time to obtain treatment or accommodations for unobserved barriers as a step on their journey to employment.
Another important finding from the case studies is that TANF agencies do not have to singularly bear the burden of identifying unobserved barriers to employment. In all of the study sites, partner agencies and their staffs play an essential role by helping TANF agencies identify or confirm the existence of unobserved barriers to employment. The study sites have also demonstrated the value the expertise contributed by a wide range of partners including other government agencies and community-based organizations.
Finally, the study sites have utilized the resources and flexibility provided by federal welfare reform and the TANF block grant structure to create proactive strategies for identifying unobserved barriers to employment. These aspects of the existing welfare system may be debated as Congress undertakes TANF reauthorization and raise important questions for the future.
A Look to the Future
TANF clients with substance abuse and mental health problems, domestic violence situations, and/or learning disabilities, will continue to present identification and service challenges to TANF agencies and their partners. The case study sites have made great strides into relatively uncharted territory by developing the identification and service strategies described here. If such strategies are to continue, and new efforts are to be developed, TANF agencies and their partners will require the resources to support staff by maintaining or establishing workloads that facilitate barrier identification efforts, involve specialized staff and/or partner agencies, and provide staff training. If the progress made toward identifying and addressing barriers faced by the hard-to-serve is to be sustained, it will be important for policymakers not to succumb to pressures to reduce funding or limit the flexibility provided to states and localities when considering the reauthorization of TANF in 2002.
For example, the case study sites reported little difficulty identifying and establishing partnerships to assist in barrier identification efforts and to provide barrier-specific services, at least in part because TANF funds were available to support these partnerships. Some sites were even able to use TANF funds to ensure that welfare clients would not face long waiting lists for barrier-specific services. If TANF funding levels are reduced, such efforts may not be possible.
It will be important to guard against the possible erosion of the progress made in developing strategies to help the hardest-to-serve clients and a return to a focus on more job-ready clients.
Further, flexibility to determine the activities that contribute to federal work participation rates also supports state and local efforts to treat or mitigate unobserved barriers to employment. The flexibility provided by the lower actual participation rate requirement (resulting from the caseload reduction credit) has given states and localities the latitude to allow participation in a wider range of services by hard-to-serve clients—flexibility embraced by the study sties. If caseloads continue to increase, TANF agencies will increasingly face pressure to meet work participation rates and may return to a focus on participation in work-related activities defined strictly by law. It will be important to guard against the possible erosion of the progress made in developing strategies to help the hardest-to-serve clients and a return to a focus on more job-ready clients. Legislative changes to TANF work participation rates or definitions of countable activities may provide this safeguard and support the expansion of barrier identification efforts and barrier-specific services.
The future also holds a number of unanswered questions about how non-discrimination laws will be applied to TANF barrier identification strategies and the provision of barrier-specific services. To the extent unobserved barriers are covered by the Americans with Disabilities Act (ADA) and other non-discrimination laws, TANF agencies and their partners have an obligation to provide services and accommodations and utilize non-discriminatory methods of administration. However, the application of these laws to TANF practices has not been widely explored. As additional consideration is given to this issue, more issues are tested in the courts, and practices are reviewed by oversight organizations, questions may be answered. This process is likely to be lengthy and uncertainty will remain while these questions are being answered.
The case study sites offer a number of potentially promising approaches to identifying unobserved barriers to employment. However, answers to the multitude of questions surrounding how best to identify unobserved barriers to employment will have to be continually reassessed and developed within the context of a changing policy environment and economy. States and localities will need to continue to develop approaches to serving clients with disabilities, medical conditions, and unobserved barriers to employment, while balancing competing demands for state and federal funds and taking into account differing local policies, practices, and priorities.
References and Resources
American Public Human Services Association. Charting the Path to
Employment: States’ Client Assessment Policies and Practices to Support
Welfare Reform. Washington, D.C. June 2001.
Derr, Michelle K., Sarah Douglas, and LaDonna Pavetti. Providing Mental
Health Services to TANF Recipients: Program Design Choices and
Implementation Challenges in Four States. Washington, D.C.: U.S.
Department of Health and Human Services, Office of the Assistant
Secretary for Planning and Evaluation. August 2001.
Center on Law and Social Policy and Center for Budget and Policy Priorities.
“State Policy Documentation Project,” http://www.spdp.org/tanf
(Accessed November 5, 2001).
California Institute for Mental Health. “The CalWORKS Project: Six County
Case Study Project Report,” April 2000. http://www.cimh.org
“Temporary Assistance for Needy Families Program (TANF), Final Rule”
Federal Register 64:69 (12 April 1999) p. 17720.
Holcomb, Pamela A. and Terri S. Thompson. State Welfare-to-Work Policies for
People with Disabilities: Implementation Challenges and Considerations.
Washington, D.C.: U.S. Department of Health and Human Services, Office
of the Assistant Secretary for Planning and Evaluation. August 2000.
LaCheen, Cary. 2001. “Using Title II of the Americans with Disabilities Act
on Behalf of Clients in TANF Programs,” Georgetown Journal on Poverty
Law & Policy, Volume II, Number 1.
Lennon, Mary Clare, Juliana Blome, and Kevin English. Depression and Low-
Income Women: Challenges for TANF and Welfare-to-Work Policies and
Programs. New York, New York: Research Forum on Children, Families,
and the New Federalism. April 2001.
McDonald, Tom, Terry Moore, and Peggy Billings. Extra Effort: Pilot Project in
Montgomery County Kansas, SRS Chanute Area Office. Lawrence, Kansas:
University of Kansas, School of Social Work. July 2000.
Nakashian, Mary. Identifying Substance Abuse Among A Better Chance Families in
Delaware: A Review of the State’s Model and Referral Processes. Washington,
D.C.: U.S. Department of Health and Human Services, Administration for
Children and Families, Office of Family Assistance. July 2001.
National Center on Addiction and Substance Abuse (CASA) at Columbia
University (in partnership with the American Public Human Services
Association). Building Bridges: States Respond to Substance Abuse and
Welfare Reform. New York, New York: CASA, August 1999.
National Institute for Literacy. www.nifl.gov
Nightingale, Demetra Smith, Terri Thompson, Nancy Pindus, Pamela
Holcomb, Edgar Lee, Jesse Valente, and John Trutko. Early
Implementation of the Welfare-to-Work Grants Program: Findings from
Exploratory Site Visits and Review of Program Plans. Washington, D.C.:
U.S. Department of Health and Human Services, February 2000.
Personal Responsibility and Work Opportunity Reconciliation Act of 1196.
U.S. Public Law 104-193. 104th Congress, 2nd Session. August 22, 1996.
Sections 402(a)(7) & 408.
Richardson, Monica. “UK Welfare-to-Work Institute Gets $3.2 Million from
State.” Lexington Herald-Leader, June 27, 2001.
Thompson, Terri S., Pamela A. Holcomb, Pamela Loprest, and Kathleen
Brennan. State Welfare-to-Work Policies for People with Disabilities:
Changes Since Welfare Reform. Washington, D.C.: U.S. Department of
Health and Human Services, Office of the Assistant Secretary for
Planning and Evaluation. October 1998.
Thompson, Terri S. and Kelly S. Mikelson. Screening and Assessment in TANF/
Welfare-to-Work: Ten Important Questions TANF Agencies and Their Partners
Should Consider. Washington, D.C.: U.S. Department of Health and
Human Services, Office of the Assistant Secretary for Planning and
Evaluation and Administration for Children and Families. March 2001.
U.S. Department of Commerce. U.S. Census Bureau. www.census.gov
U.S. Department of Health and Human Services. Administration for
Children and Families. Office of Planning Research and Evaluation.
Temporary Assistance for Needy Families (TANF) 3rd Annual Report to
Congress. Washington, D.C.: DHHS, August 2000.
U.S. Department of Health and Human Services. Administration for
Children and Families. Office of Family Assistance. Addressing Substance
Abuse Problems Among TANF Recipients: A Guide for Program
Administrators. Washington, D.C.: DHHS, August 2001.
U.S. Department of Health and Human Services. Office for Civil Rights.
Prohibition Against Discrimination on the Basis of Disability in the
Administration of TANF (Temporary Assistance for Needy Families), Summary
Policy Guidance. Washington, D.C.: DHHS, January 19, 2000. http://
www.hhs.gov/ocr/prohibition.html.
U.S. Department of Health and Human Services. Substance Abuse and Mental
Health Services Administration. Center for Substance Abuse Treatment.
Technical Assistance Publication Number 26: Identifying Substance Abuse Among
TANF-Eligible Families. Washington: D.C.: DHHS, 2001.
U.S. General Accounting Office. More Coordinated Federal Effort Could Help
States and Localities Move TANF Recipients with Impairments Toward
Employment. Washington, D.C.: GAO-02-37, October 2001.
Appendix A: Selected Tools Used by the Study Sites to Screen for Unobserved Barriers
| Question Characteristics | Validated ? | Topics covered | Mothod of Administration | Notes About Implementation | |
|---|---|---|---|---|---|
| Kansas | |||||
| TANF AJS/EAP Initial Screening Guide | 7 Yes/No questions | No | Education, employment history (mental health concerns, domestic violence, and substance abuse). | Administered by a case manager. | |
| KSRS-EES Screening Guide and Assessment | 63 Yes/No and open-ended questions | No | Substance abuse, mental health, domestic violence, learning disabilities, education, work history, health information, domestic information, support services, and staff observations. | Administered by a case manager. | The instructions for this instrument state that the text is designed to serve asaguideandthatquestions may be added or deleted depending on an individual's circumstance. |
| SASSI | 78 True/False and scales | Yes | Substance abuse | Self-administered paper and pencil test. | Staff must be trained to administer and score. |
| CAGE | 4 Yes/No questions | Yes | Substance abuse | Questions are asked as apart of the KSRS-EES Guide and Assessment. | Two or more positive answers indicates a history of alcoholism. |
| Adult Learning Disabilities Screen (ALDS) | The tool is divided into three parts. Part I is a 25 item Selfrating Scale of frequency of difficulty performing "activities of daily living." Part II is a 19-item Self-Administered Inventory requiring yes or no responses on an inventory of family and educational history. Part III includes follow-up questions that probe previous questions. | Yes | Learning disabilities | Part I and Part II are selfadministered and Part III is administered by the case manager. | Staff must be trained to administer and score. |
| Michigan Alcohol Screening Test (MAST) | 25 Yes/No questions | Yes | Alcohol problems and mental health history. | Self-administered paper and pencil test. | Self-scoring test. |
| Kansas Client Placement Criteria (KCPC) | Yes/ No questions and open ended questions | No | Employment, substance abuse, and mental health history. | Automated series of screens; Indepth interview conducted by a RADAC assessor. | The RADAC assessor is free to adapt the wording of the questions as he or she moves through the assessment. |
| FCMH Psycho-Social Assessment | Topical interview guide | No | Medical history, family history, of physical/ psychiatric illness, chemical (alcohol/ drug) history, gambling history, sexual history, domestic violence history, education/ learning, social history, activities of daily living, employment, legal involvement, family participation, history of previous treatment, recent stressful life situations, mental status, client's strengths, and clinical impression. | In-depth interview conducted by a therapist. | Results determined by applying clinical criteria. |
| FCMH Extra Effort Assessment | Topical interview guide | No | Housing, daily living, employment/ vocation, education, finance, insurance, credit/ budget, social supports, affection/ affirmation, health/ insurance, drug/ alcohol issues, leisure/ recreation, personal safety, stresses/ coping skills, and goals/ needs. | In-depth interview conducted by the FCMH case manager. | |
| Kentucky | |||||
| KY Works Assessment Form | 26 Yes/No questions and 4 CAGE adapted questions | No | Basic skills, education, training, employment history, employment goals, and concerns/ barriers (disabilities substance abuse, family violence, transportation, clothes, lack of housing, and health care). | Administered by a case manager. | Receive form at orientation. |
| Transitional Assistance Self-Assessment | Yes/No and Check all that apply | No | Client Information (marital status, drug/ alcohol abuse, health problems, abuse, housing, money problems), family information, employment information, and financial information. | Self-administered | Receive form at orientation. |
| UK TAP Orientation Screen | 15 Yes/No questions | No | Substance abuse, mental health, domestic violence, and learning disabilities | Self-administered | Receive form at orientation. |
| UK Targeted Assessment and History | Topical interview guide | No | Medical history, family history, of physical/ psychiatric illness, chemical (alcohol/ drug) history, gambling history, sexual history, domestic violence history, education/ learning, social history, activities of daily living, employment, legal involvement, family participation, history of previous treatment, recent stressful life situations, mental status, client's strengths, and clinical impression. | In-depth interview conducted by a TAP Assessor. | Results determined by applying clinical criteria. |
| RVBH Psycho-Social Evaluation | Topical interview guide | No | Medical history, family history, of physical/ psychiatric illness, chemical (alcohol/ drug) history, gambling history, sexual history, domestic violence history, education/ learning, social history, activities of daily living, employment, legal involvement, family participation, history of previous treatment, recent stressful life situations, mental status, client's strengths, and clinical impression. | In-depth interview conducted by a RVBH therapist. | Results determined by applying clinical criteria. |
| Minnesota | |||||
| MFIP Secondary Assessment (West-Metro) | 37 Yes/No questions | No | Family status, program involvement, education, health (mental health, substance abuse problems, and learning disabilities), work history, work experience, military service, legal, and economic status. | Administered by a employment service provider case manager. | |
| MFIP Secondary Assessment-Mental Health and Substance Abuse Screening Pilot | 16 Yes/No questions | Validation effort in progress | Mental health and substance abuse | Administered by a employment service provider case manager. | |
| Self-Administered Alcohol and Drug Screening Self-Assessment | 4 CAGE questions | Yes | Substance abuse | Self-administered | Handed out at orientation. |
| IRIS Intake Application | 48 Yes/No questions | No | Transportation, family status, medical history, activities (learning disabilities), psychological history (mental health and substance abuse), and criminal history. | Administered by a vocational counselor. | |
| IRIS Social Needs Assessment | 30 Yes/No questions | No | Housing, day care, child protection issues, health issues, domestic abuse, budgeting, support system, criminal history, and clothing/food. | Administered by a social worker. | |
| IRIS Diagnostic Assessment | Topical interview guide | No | Medical history, family history, of physical/ psychiatric illness, chemical (alcohol/ drug) history, gambling history, sexual history, domestic violence history, education/ learning, social history, activities of daily living, employment, legal involvement, family participation, history of previous treatment, recent stressful life situations, mental status, client's strengths, and clinical impression. | In-depth interview conducted by in-house psychologist. | |
| Nevada | |||||
| NSWD Post-Approval Assessment | Topical interview guide | No | Physical condition (substance abuse), mental condition(mental health), family relationships (domestic violence), housing/living arrangements, social issues, transportation, education (learning disabilities), and employment. | Administered by a case manager. | Results determined by applying clinical criteria. |
| SASSI | 78 True/False and scales | Yes | Substance abuse | Self-Administered with guidance from social worker, paper and pencil test. | Staff must be trained to administer and score. Optional; Administered if a substance abuse problem is suspected. |
| South Oaks Gambling Screen (SOGS) | 16 Yes /No questions | Yes | Gambling problems | Self administered | If you answer yes to 3 or 4 there may be a problem and if 5 or more are answered than there is a problem. Optional; Administered if a gambling problem is suspected. |
| Domestic Violence Screen | No | Domestic violence | Administered by a social worker | Optional; Administered if domestic violence is suspected. | |
| Learning Needs Screening Tool | Includes 13 yes/no questions designed to identify potential learning disabilities. | Yes | Learning disabilities | Administered by a social worker. | Optional; Administered to all TANF clients receiving social worker intervention. |
| Psycho-Social Assessment | Topical interview guide | No | Medical history, family history, of physical/ psychiatric illness, chemical (alcohol/ drug) history, gambling history, sexual history, domestic violence history, education/ learning, social history, activities of daily living, employment, legal involvement, family participation, history of previous treatment, recent stressful life situations, mental status, client's strengths, and clinical impression. | In-depth interview is conducted by a social worker in the client's home. | Results determined by applying clinical criteria. |
| Virginia | |||||
| Substance Abuse Pre-Screening Tool | 10 Yes/No questions | No | Substance Abuse | Administered by a case manager. | If a client answers yes on one, two, or three of the questions, a referral should be considered. If a client answers yes to four or more than an automatic referral to the local substance abuse counselor is in order. |
| Domestic Violence Questionnaire | 13 Yes/No questions | No | Domestic violence | Administered by a case manager. | |
| Learning Needs Screening Tool | Includes 13 yes/no questions designed to identify potential learning disabilities. | Yes | Learning disabilities | Administered by a case manager. | |
| Washington | |||||
| Virtual Integrated Employability Worksheet (VIEW) | Progressive series of yes or no and open-ended questions | No | Domestic violence, current employment, child care, transportation, housing, listening and learning, substance abuse, criminal history, pregnancy, family planning, health, and clothing. | Automated series of screens; questions asked by a case manager. | If a client answers yes to any of the questions, the computer screen indicates that a client should be referred to a social worker or family violence counselor. |
| Learning Needs Screening Tool | Includes 13 yes/no questions designed to identify potential learning disabilities. | Yes | Learning disabilities | Administered by a case manager or social worker. | Optional; Administered if learning disability is suspected. |
Appendix B: Descriptions of Selected Services to Address Unobserved Barriers to Employment
Integrated Resources for Independence and Self-sufficiency(iris)
The IRIS Program in Minneapolis, MN is a WtW and MFIP funded program designed to assist welfare clients with chemical or mental health problems that inhibit employment and self-sufficiency. IRIS uses a team approach to barrier identification, and offers social supports, individual and group therapy, and vocational services. IRIS services are built on the experience of the Hennepin County Children, Families, and Adult Services Department, Vocational Services Program, serving severely and persistently mentally ill (SPMI) adults. It is this experience which shapes the vocational services offered by IRIS. However, IRIS staff learned early-on that MFIP clients also face a variety of social needs and therefore, vocational services are supplemented by social stabilization services and substance abuse or mental health therapy. IRIS’s program follows five stages intended to lead to competitive employment, described below.
Stage 1 involves comprehensive assessments, therapy, and family stabilization provided by the IRIS staff team. Every IRIS client is required to go through this stage of the program. As the name implies, family stabilization involves ensuring that the client’s basic needs are met. This includes food, shelter, child care and clothing, as well as domestic violence and substance abuse services. The IRIS social worker will do whatever is necessary to meet the client’s needs, including accompanying the client to a homeless shelter or food bank. Clients also must attend a women’s support group and a life skills group. The life skills group involves weekly meetings that cover topics such as budgeting, the importance of work, and appropriate work attire.
Stage 2 involves participation in Steps to Success. Steps to Success involves 15 hours per week of psycho-social programming that consists of classes that attempt to psychologically prepare clients for work, as well as offers very basic training in keyboarding. Classes include employer site visits and classes on selfesteem, the reality of working, grooming, coping with anxiety, parenting concerns, nutrition, and budgeting. Clients generally participate in this stage until employment is obtained. Stage 3 offers an on-site vocational assessment as an evaluation tool for clients with limited work experience, chemical, or mental health problems. In Stage 3, clients also take part in job readiness classes including assistance in preparing resumes and refining interviewing skills, additional computer training, and other vocational training offered through TANF training programs (such as those preparing clients for jobs as nursing assistants, telephone operators, carpenters, or auto mechanics).
Clients who progress to Stage 4 (meaning their mental and chemical health challenges are becoming more stable, clients are taking their prescribed psychiatric medications, or have completed a drug treatment program) work intensively with a vocational counselor in locating job leads, preparing specific resumes, attending job fairs, and attending interviews. The goal for all clients is unsubsidized employment. However, some clients are assisted in locating positions within the community that may offer additional supports such as job coaching or a subsidized internship to provide on-the-job experience. The vocational counselor and client work together closely to find a job that meets the clients needs and interests. Once employed, all IRIS clients are provided job retention services. The level of job coaching or other job retention services is tailored to the individual client’s needs. Typically, the vocational counselor meets daily with the client during the first two weeks of employment, if the client and employer are amenable to this arrangement. Visits with the client away from the
worksite are also common.
Although there is a natural progression to the IRIS Program as indicated by the stages described above, client participation in IRIS services are highly individualized and depend on client needs, choices, and priorities. Each client progresses toward unsubsidized employment differently, but all clients receive a diagnostic assessment and some vocational services. Consistent with this individualized approach, clients spend varying lengths of time in the IRIS Program.
Rainier Case Management – Intensive In-home Services
Rainier Case Management has a long history of working with injured workers and has worked with TANF clients in Kent, WA providing job retention services. In August 2000, Rainier began providing Intensive In-Home Services for clients who are sanctioned or about to be sanctioned for not fulfilling their TANF obligations. The purpose of Intensive In-Home Services is to identify barriers that are preventing participation and to facilitate the reconnection to services. Staff work with relatively small caseloads of 30-35 clients for a short period of time, usually not longer than three months.
Clients referred to Rainier’s Intensive In-Home Services are first contacted either by telephone, letter, or home visit. Once contact is made, an initial interview is conducted wherever the client desires (including at her home, at the welfare office, or another location) and covers a variety of topics including substance abuse and mental health problems and domestic violence. During this interview staff observe behaviors that might indicate a problem (e.g., noting if clients seem fidgety, clients who don’t read forms that are handed to them) and, if the interview is conducted in the home, review the environment for evidence of a barriers (i.e., to see if there is drug paraphernalia around the house). During this interview, staff are not trying to diagnose problems but to obtain enough of an indication of the existence of a barrier to help connect the client to services. For example, if staff of Rainier Case Management suspect a mental health problem, they would make a referral to a mental health professional for a diagnosis.
Staff noted that building a trusting relationship is an essential part of the Intensive In-Home Services. Clients who come to understand that Rainier staff are dedicated to helping them are reportedly more likely to open up, disclose barriers, and consider steps required to come back into compliance. Once a relationship is established, staff begin to work with the client to develop a service plan. The plan is intended to include what the TANF case manager indicates needs to be done to fulfill TANF requirements, as well as incorporate additional services to address previously unidentified barriers. The goal is to bring the client back into compliance without them feeling like they are forced to something they do not want to do.
Department of Rehabilitation SERVICES/SOC Enterprises
At the state level, the Virginia Departments of Social Services (DSS) and Rehabilitation Services (DRS) have funded a small number of jointly-administered projects intended to assist TANF clients with disabilities that may be barriers to employment. One project is being implemented in Arlington, VA through a partnership between the local DHS and DRS offices with a contract with SOC Enterprises. This project is intended to assist clients suspected of having a learning disability or other disabilities requiring rehabilitation or accommodations and requiring intensive one-on-one services.
Under this three-way collaboration, TANF employment case managers screen all clients for learning disabilities using a learning disability screening tool. If the employment case manager suspects that a client has a learning or other disability, she meets with both the DRS counselor assigned to work with TANF clients, and the SOC Enterprises case manager, to discuss the case. If appropriate, the case manager makes a written referral for services provided by DRS/SOC Enterprises. The SOC Enterprises case manager then schedules an intake and assessment meeting and meets with the referred client. If the client is agreeable, she is referred to DRS for a vocational assessment and eligibility determination.1 Once DRS eligibility is determined, DRS works with the client and the TANF case manager to develop an employment plan and to coordinate the services required to carry out the goals outlined in the employment plan.
For example, if a client had not had a recent psychological evaluation, and further assessment is needed, the client may be referred to a clinical psychologist who works with DRS and SOC Enterprises for additional psychological testing and evaluation. The psychologist meets with clients in the TANF office on a regular basis, therefore alleviating the problem experienced earlier in the project by clients who fail to keep scheduled offsite appointments with psychologists. During this assessment meeting, the psychologist may administer a variety of assessment instruments such as mental health/ personality screens, intelligence tests, and other assessments to identify the presence of learning disabilities and/or cognitive issues. Once a formal diagnosis is made, the psychologist meets with the client, the case manager, the Substance Abuse/Mental Health therapist, and other team members as needed, to explain the results and the implications of the testing process. If warranted, it may be recommended that the client engage in individual counseling. Additional referrals, for hearing, vision, or speech and language problems or for individualized tutoring may also be made.
Once DRS eligibility is confirmed, an SOC Enterprises case manager specifically assigned to work with TANF clients facilitates the provision of many employment-related services. The SOC Enterprises case manager generally carries a smaller caseload of about 25 clients and is able to augment the work done by the TANF employment case manager by providing more intensive, one-on-one services. Services provided by SOC Enterprises may include individual counseling, career exploration and development, skills training, work assessment (short-term try-out employment which may lead to permanent employment), job development with the SOC onsite job developer, job retention services, and/or employment at the SOC facility (e.g., jobs in the company mailroom or copy center).
The key to services provided by SOC Enterprises is that the case manager provides the client with very hands-on, intensive service and support. For example, it would not be unusual for the case manager to drive to the client’s home to pick her up, take her to the bus stop and help her master the transportation system. Additionally, the case manager might work closely with a try-out employer to stay on top of any job-keeping issues the client might have (e.g., attendance) and work quickly with both to address this or other problems.
1 A client must have an open DRS case in order to work with the SOC Enterprises program.
Four County Mental Health (FCMH)/EXTRA Effort
The Department of Social and Rehabilitation Services (SRS; the TANF agency) in Montgomery County, KS has developed a partnership with the local community mental health center to provide a wide range of services to TANF clients. FCMH has a history of providing services to severely and persistent mentally ill (SPMI) adults under contract to the Vocational Rehabilitation (VR) program within SRS. These services involve barrier resolution, supported work, and employment placement. When SRS was seeking job preparation services for TANF clients, FCMH believed its experience and employer contacts developed through its SPMI services could be applied to TANF clients. FCMH applied and was awarded contracts to provide job club and life skills group services and individual job development and job retention services. Through these TANF and VR contracts, SRS and FCMH have developed a strong working relationship. Therefore, when SRS sought to develop additional services to prevent TANF clients from becoming involved in the child welfare system—they turned to FCMH for assistance with the pilot effort. What resulted was the Extra Effort Pilot Program.
Extra Effort is a program designed to address TANF clients’ multiple, often unobserved barriers to employment that are believed to result in not only continued welfare receipt, but possible involvement with the child welfare system. In an effort provide more enhanced services to these at-risk families, FCMH case managers work closely with small caseloads (approximately five families per case manager) to identify and address unobserved barriers to employment. Barriers are identified through the combined use of formal and informal identification strategies. Case managers noted that although they complete a number of assessment tools, including a strengths assessment and a family risk scale, they also rely heavily on their interpersonal skills to build a positive and trusting relationship with clients.
Once identified, FCMH case managers work closely with clients to assist them in addressing barriers. FCMH staff noted that there is almost nothing that Extra Effort will not address, although they take care to empower clients to help themselves so that they can build problem solving skills to be used in the future. In some respects, the case managers serve as mentors or coaches, getting to know clients and their families very well and visiting their homes. In addition to these one-on-one informal counseling services, Extra Effort also helps clients by providing a wide range of services including scheduling appointments with other social service agencies, providing transportation to appointments, assisting with dental needs, housing searches, and legal matters, and assisting clients in addressing behavior issues with children in the family, or providing supportive services.
Appendix C: Site Contacts
Montgomery County, Kansas
Katie Evans
Research and Special Projects Manager
Kansas Department of Social and Rehabilitation Services
Economic and Employment Support Division
681-West, Docking State Office Building
915 SW Harrison
Topeka, Kansas 66612
Phone: (785) 296-6756
Owensboro, Kentucky
Alayne White or Barbara Ramlow
University of Kentucky
Institute on Women and Substance Abuse
Targeted Assessment Project
1151 Red Mile Road, Suite 1B
Lexington, Kentucky 40504
Phone: (859) 257-6441
Minneapolis, Minnesota
Reese Erdner
Acting Program Supervisor
Children, Families, and Adult Services Department
Vocational Services Program—IRIS
219 North Second Street, Suite 407
Minneapolis, Minnesota 55401
Phone: (612) 596-7589
Las Vegas, Nevada
Rota Rosaschi
Chief of Benefits and Support
Nevada State Welfare Division
1470 East College Parkway
Carson City, NV 89706-7924
Phone: (775) 684-0610
Arlington, Virginia
Suzanne Eisner
Division Director
Economic Independence Division
Arlington County Department of Human Services
3033 Wilson Boulevard, Suite 700-A
Arlington, Virginia 22201
Phone: (703) 228-1350
Kent, Washington
Rick Krauss
WorkFirst Program Coordinator
Region 4/King County
Washington Department of Social and Health Services
400 Mercer Street, Suite 600
Seattle, Washington 98109
Phone: (206) 272-2160
About the Study
The Urban Institute
The Urban Institute is a nonprofit policy research organization established in Washington D.C. in 1968. Its objectives are to sharpen thinking about society’s problems and efforts to solve them, improve government decisions and their implementation, and increase citizens? awareness about important public choices. Institute researchers identify and measure the extent of social problems, assess developing trends and solutions to those problems, evaluate existing social and economic programs and policy options, and offer conceptual clarification and technical assistance in the development of new strategies. In pursuit of broader research and educational goals, Institute staff present their analysis and research to members and staff of the executive and legislative branches, the media, and other interested groups.
Funders
This study was funded by the U.S. Department of Health and Human Services, Administration for Children and Families (ACF) and the Office of the Assistant Secretary for Planning and Evaluation (ASPE).
Acknowledgments
This study could not have been completed without the cooperation and assistance of many individuals. Most importantly, we are indebted to the state and local TANF agency officials and their partners who allowed us to visit their offices and conduct interviews with staff. Without their permission and support, this study could not have been completed. We also thank the other members to of the project team at the Urban Institute for their invaluable contributions—particularly, Pamela Holcomb, Jeffrey Capizzano, and Kelly Mikelson. Finally, we are indebted to our Project Officers, William Marton of ASPE, K.A. Jagannathan of ACF, and Jamie Kendall formerly of ACF, for their commitment to the project.