
U.S. Department of Health and Human Services
The Role of Home and Community-Based Services in Meeting the Health Care Needs of People with AIDS: Final Report
Jennifer Schore, Mary Harrington, and Stephen Crystal
Mathematica Policy Research, Inc.
March 1998
PDF Version: http://aspe.hhs.gov/daltcp/reports/aidsfrpt.pdf (111 PDF pages)
This report was prepared under contract #PHS-282-92-0044 between HHS's Office of the Assistant Secretary for Planning and Evaluation, Office of Disability, Aging and Long-Term Care Policy and Mathematica Policy Research, Inc. For additional information about the study, you may visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the ASPE Project Officer, Gavin Kennedy, at HHS/ASPE/DALTCP, Room 424E, H.H Humphrey Building, 200 Independence Avenue, SW, Washington, DC 20201. His e-mail address is: Gavin.Kennedy@hhs.gov.
The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
TABLE OF CONTENTS
II. THE EVOLUTION OF THE AIDS EPIDEMIC
A. THE CHANGING FACE OF THE EPIDEMIC
B. CHANGING SERVICE NEEDS AND COSTS
C. EFFECTS ON FUNDING SOURCES
III. LESSONS FROM THE FRONT LINES
A. CASE STUDY METHODOLOGY
B. CASE STUDY LESSONS
IV. THE NEED FOR HOME- AND COMMUNITY-BASED SERVICE DATA
A. NATIONAL AND STATE DATABASES
B. PROVIDER DATABASES
C. POTENTIAL USES OF PROVIDER DATA
D. NEXT STEPS
E. CONCLUSION
V. PATTERNS OF UTILIZATION OF HOME CARE SERVICES AMONG MEDICAID RECIPIENTS WITH AIDS IN NEW JERSEY (AIDS Research Group, Institute for Health, Health Care Policy, and Aging Research, Rutgers University)
A. BACKGROUND
B. STUDY POPULATION AND DATABASE DEVELOPMENT
C. FINDINGS
D. CONCLUSION
VI. SYNTHESIS AND IMPLICATIONS
APPENDICES
APPENDIX A: CASE STUDY OF HOME- AND COMMUNITY-BASED SERVICE DELIVERY IN NEW YORK CITY
APPENDIX B: CASE STUDY OF HOME- AND COMMUNITY-BASED SERVICE DELIVERY IN LOS ANGELES
LIST OF FIGURES
FIGURE V.1: Proportion with Any Home Care Use, Waiver/Non-Waiver Combined
FIGURE V.2: Monthly Home Care Spending in Last 6 Months of Life by Waiver Status Among Home Care Users
LIST OF TABLES
TABLE I.1: Overview of Questions Addressed by Project Components
TABLE II.1: Number and Percentage of AIDS Cases, by Selected Characteristics
TABLE II.2: Health and Support Services Used by People with AIDS
TABLE II.3: Public and Private Funding Sources for HIV/AIDS Care
TABLE III.1: Characteristics of Reported AIDS Cases in New York City and Los Angeles
TABLE III.2: Case Study Program Overview
TABLE III.3: The Changing AIDS Environment: Provider Challenges and Responses
TABLE IV.1: Automated Person-Level Data Maintained by Case Study Programs
TABLE IV.2: Tasks for Investigating the Usefulness of Provider Databases
TABLE V.1: Study Population, Compared to NJ and National Registry Data
TABLE V.2: Proportion Using Each Type of Home Care Services, AIDS Diagnosis to Death
TABLE V.3: Average Monthly Expenditures on Home Care Services From AIDS Diagnosis to Death
TABLE V.4: Average Monthly Expenditures on Home Care Services, Among Users of Each Type of Service, From AIDS Diagnosis to Death
ACKNOWLEDGMENTS
Many people have contributed their time, knowledge, and expertise to this report, and we would like to thank them all. The staff of each program in the project's case studies, in addition, generously shared with us their frontline experiences serving people with AIDS every day: AIDS Project LA, AIDS Healthcare Foundation, and AltaMed Health Services Corporation in Los Angeles; and Gay Men's Health Crisis, Visiting Nurse Service of New York, and Village Center for Care in New York City. Medicaid and Ryan White staff for the states of California and New York and cities of Los Angeles and New York provided us with excellent overviews of those programs. Staff with the New York City Division of AIDS Services and federal Health Resources and Services Administration, Health Care Financing Administration, and Centers for Disease Control and Prevention provided us with information not available in the published literature.
We also received invaluable assistance in preparing this report from our project officer in the Office of the Assistant Secretary for Planning and Evaluation, Gavin Kennedy, and his colleagues, as well as from a number of our colleagues at Mathematica. Craig Thornton shared with us his policy expertise and knowledge of service delivery to people with all types of disabilities (in particular, AIDS) throughout the project and provided insightful comments on drafts of this report. Marjorie Mitchell, Cindy Castro, Doreen Ambrose, Besaida Rosado, Jill Miller, and Jennifer Baskwell masterfully word-processed and produced this report. Patricia Ciaccio and Walter Brower provided helpful editorial assistance. We thank each one.
EXECUTIVE SUMMARY
In the early 1980s, when acquired immunodeficiency syndrome (AIDS) made its first appearance, it was an unfailingly acute and fatal disease. Since then, AIDS-specific medical expertise and treatment advances have increased life expectancy for people with AIDS and human immunodeficiency virus (HIV) and shifted AIDS treatment from an acute- to a chronic-care model. Home- and community-based services, such as assistance with daily living activities and the provision of home-delivered meals, have long been an integral part of AIDS care. However, improved health and functioning have broadened the scope of these services to include, for example, assistance returning to work and caring for families.
This is the final report for the project, "The Role of Home- and Community-Based Services in Meeting the Health Care Needs of People with AIDS," conducted by Mathematica Policy Research, Inc. (MPR) for the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation (ASPE). The goal of the project was to assist ASPE in developing a research agenda for studying home- and community-based service use among people with AIDS. The project had three components: (1) a review of the recent literature describing the delivery and financing of home- and community-based services for people with AIDS; (2) case studies of service provision in New York City and Los Angeles; and (3) an analysis of use and reimbursement patterns for New Jersey Medicaid beneficiaries with AIDS (conducted by the AIDS Research Group of the Institute for Health, Health Care Policy, and Aging Research at Rutgers University).
The Evolution of the AIDS Epidemic and Its Financing
In the early days of the epidemic, the typical person with AIDS was recognized as a white man who had contracted HIV through sexual contact with another man. However, the epidemic has increasingly and disproportionately affected women and people who belong to racial or ethnic minorities, and the mode of transmission has increasingly been injection drug use. Meanwhile, improved medical care and pharmaceutical treatment have extended the lives and improved the health of many people with AIDS, leading, in 1996, to the first decline in deaths since the start of the epidemic.
Changes in AIDS treatment and in the characteristics of the AIDS population have had profound and interrelated effects on the use of home- and community-based services by people with AIDS. Increased life expectancy has increased the duration of needed services. Improved treatment has also improved health and decreased levels of functional impairment for many people, which in turn appears to have led to a decrease in their use of traditional home- and community-based services (such as home-delivered meals and personal care). At the same time, this treatment has led to an greater need for other types of support, such as assistance with treatment adherence and return to work. Meanwhile, the increased incidence of AIDS among people with low incomes, people with substance abuse problems, and women with families has led to an increased need for home- and community-based service providers to interact more often and intensively with substance abuse treatment, mental health, family services, and public assistance systems.
Medicaid, Medicare, and the Ryan White Comprehensive AIDS Resources Emergency Act have been the major public funding sources for HIV/AIDS care during the 1990s. Although 1995 Medicaid spending for AIDS care was only about two percent of total Medicaid spending, the increase of AIDS among people with low incomes has placed an increasing burden on the Medicaid (and Ryan White) programs, particularly to fund costly protease combination therapy. The programs also face the challenges of reconsidering eligibility and service coverage criteria to reduce disincentives to work and to increase flexibility in meeting chronic care needs, which typically vary over time in intensity and type.
The recent trend among Medicaid programs to rein in escalating costs by enrolling beneficiaries in managed care plans has had, to date, only a modest effect on people with AIDS, because many states exclude from managed care people with disabilities or chronic illnesses like AIDS. In addition, although Medicaid covers many of the home- and community-based services that people with AIDS need, many Medicaid managed care plans currently exclude these services from capitation arrangements. As a result, little is known about how best to provide the full range of AIDS services in a managed care environment. Increased use of Medicaid managed care also raises questions about whether and how to integrate services currently provided with Ryan White funds to Medicaid beneficiaries who enter managed care.
Lessons from the Front Lines
The project developed case studies to describe current provider approaches to delivering home- and community-based services to a changing AIDS population. The case studies were based on discussions at six large, well-established AIDS providers in Los Angeles and New York City, supplemented by telephone conversations with a small number of Medicaid and Ryan White staff. The New York providers were Gay Men's Health Crisis, the oldest and largest AIDS service organization in the United States; the Visiting Nurse Service of New York, a large, not-for-profit home health agency with a 10-year-old AIDS program; and Village Center for Care, a continuum of AIDS-specific home care, day treatment, case management, and nursing home care. The Los Angeles providers were AIDS Project LA, the second-largest AIDS service organization in the United States; AIDS Healthcare Foundation, an AIDS-specific freestanding outpatient medical provider that operates a Medicaid managed care plan for people with AIDS; and AltaMed Health Services Corporation, a community health center with an HIV/AIDS program that targets the Latino community. In-person discussions with key program staff took place in spring 1997.
Service providers reported that they are changing both the types of services offered and their service delivery approaches in response to growing numbers of disadvantaged clients who are living longer, healthier lives. Providers have found that service delivery models that worked well for earlier clients (namely, end-of-life care for affluent, well-educated gay men) must be modified for newer clients with longer-term and more complex problems (for example, behavioral comorbidities, lifelong poverty, and families also in need of support) and often tenuous informal support systems. Provider response has included broadening the range of services provided in house, increasing referrals to and interactions with providers in other systems, reconfiguring staffing to include more trained professionals and fewer lay staff and volunteers, and developing procedures to provide the most intense services to the clients with the most complex problems. These costly changes have been simultaneous with decreases in private donations and increased pressure to control Medicaid costs.
Only one case study provider had had substantial direct experience with managed care. Nevertheless, all the providers saw Medicaid managed care for their clients just over the horizon and were concerned that many questions about managed care for people with AIDS had not yet been answered: how to set payment rates and manage financial risk in a way that will promote quality medical care (that is, provide specialty care and state-of-the-art treatments); and whether and how to include under capitation home- and community-based care such as that now provided through Medicaid waivers and Ryan White. Providers were concerned that rational planning decisions would be difficult to make because of the scarcity of data on (1) current patterns of service use among different groups of people with AIDS, and (2) the cost-effectiveness of different types of home- and community-based services.
The project also sought information about the feasibility of using provider databases in future research efforts. The case study providers each maintained databases with the capacity to provide detailed sociodemographic and clinical data describing their clients, as well as data describing service use. However, providers noted that while databases contained fields for client characteristics, the fields were frequently not filled in. Providers stated their willingness to consider the inclusion of their databases in future research projects. However, formal permission to gain access to them must be requested and received and data from them examined for completeness and consistency before a research study can be undertaken.
Lessons from the New Jersey Medicaid AIDS Waiver Program
The New Jersey Medicaid waiver program provided an important opportunity to study home- and community-based services for people with AIDS, for several reasons. First, the nation's AIDS population is evolving to look more like New Jersey's. In the early 1990s, of the state's AIDS population nearly one-fourth were females, more than two-thirds were nonwhites, and over half were injection drug users. Second, New Jersey has always emphasized home care in its AIDS services and policies. In 1987 its Medicaid program developed the nation's first home- and community-based service waiver for people with AIDS. Finally, the state has supported the development of a longitudinal research database that links Medicaid claims and AIDS registry data, facilitating analyses of AIDS service use among Medicaid beneficiaries. The portion of the database used for this report included 2,464 people who became eligible for Medicaid between August 1989 and July 1991 and who were diagnosed with AIDS by June 1992. The database describes their service use through June 1994. Of those 2,464 beneficiaries, complete diagnosis-to-death claims data were available for 1,293; this "completely observed" sample was the primary focus of the analysis.
About a third of the 1,293 beneficiaries voluntarily participated in the case-managed AIDS waiver program; the remainder were eligible for more limited home care under the regular Medicaid program. Program eligibility criteria include the need for a nursing home-level of care and either categorical Medicaid eligibility or financial eligibility if the beneficiary were institutionalized. Waiver participants were more likely than nonparticipants to be whites or males but less likely to be injection drug users. Only 20 percent of nonparticipants were whites, 60 percent were males, and 74 percent were injection drug users, as compared with 37, 75, and 62 percent of waiver program participants, respectively. Differences between waiver participants and nonparticipants may have been related to the waiver program's higher income cutoff.
Among nonparticipants, there were substantial disparities among beneficiaries from different racial groups and from transmission risk groups in the use of home care: whites were more likely than blacks, and injection drug users less likely than nonusers, to use home care. These large disparities were not evident among waiver participants. While it is difficult to separate the effects of the ability of the waiver program to improve access to care and the program's self-selection on the findings, they do suggest that case management may hold promise for improving access to home care for groups who make up increasing proportions of the AIDS population.
Planning and Policy Implications
The challenges providers, planners, and policymakers face in the wake of a changing AIDS population and service environment have implications in three areas: (1) development of databases and other types of information to support planning decisions; (2) development of concrete strategies to implement managed care for people with AIDS; and (3) development of a cohesive approach to meeting the needs of people with all types of chronic illness.
In an environment that focuses increasingly on cost control, program planners and policymakers require information to aid in decision making about the provision of home- and community-based services to people with AIDS.
Two broad types of information are needed. The first is basic description of service use and of costs and variations in them over time, by geographic region, and by funding source. Service use and cost patterns should also differentiate among groups of people with AIDS who may be expected to have different use patterns (for example, as defined by HIV risk group, gender, minority status, disease stage, use of particular pharmaceutical treatments, presence of behavioral comorbidities, homelessness, or existence of family affected by HIV). Whereas basic information about service use patterns is sorely needed, more sophisticated analyses--which offer evidence that a particular program, approach, or financing mechanism provides care more cost-effectively--would further rationalize decision making for future programs.
Practice guidelines for home- and community-based services represent a second type of information whose development bears further consideration. Practice guidelines, such as those now widely used in home health care, could clarify the goals and tasks of home- and community-based services (often criticized for their amorphousness). Case management in particular has been faulted for its profusion among people with AIDS, and guidelines could be one part of a strategy to reduce redundancy in case management and help it coordinate services across systems more effectively.
While managed care holds the potential to better coordinate acute care and home- and communitybased services for people with AIDS, its implementation faces challenges beyond those posed by the information gaps just described.
Managed care planners face now well-known challenges in addressing the special medical care needs of people with AIDS: developing both risk management strategies that offer plans incentives to enroll people at risk of high costs and mechanisms to assure high-quality AIDS treatment. However, planners face additional challenges in addressing the needs of people with AIDS for home- and community-based services. If managed care planners decide to include these services under capitation payments, fundamental questions exist as to how to implement and integrate them. For example, who should coordinate and oversee their use: medical or social services providers? Small, neighborhood-based or larger, more comprehensive providers? These and other questions of implementation remain because most of the few managed care plans now serving substantial numbers of people with AIDS currently carve out home- and community-based support services. Even less is known about whether and how to integrate Ryan White funding and services under managed care. This suggests that demonstrations of managed care for people with AIDS must begin to integrate home- and community-based services with medical care.
The problems we face in figuring out whether and how AIDS-specific home- and community-based services should be included in managed care (or in ongoing fee-for-service programs facing costcontrol pressures) are merely special cases of general problems reflecting the need for a cohesive policy to address the needs of people with all types of chronic illnesses.
The health care and support service systems for people with chronic illnesses need to be flexible enough (1) to permit people to vary the intensity with which they receive services in those systems as their needs change over time, and (2) to minimize incentives to provide care at inappropriate levels. The current Medicaid and Medicare systems include perverse incentives that run counter to these goals. In addition, as the number of people with AIDS who are covered by Medicare (but not Medicaid) increases, the funding of support services and medications (not currently covered under Medicare) will be a particular problem, as it is now for all Medicare beneficiaries (and most privately insured individuals) with severe chronic illnesses. Public programs funding medical and support services must also give people with chronic illnesses the flexibility to return to work when they are well enough without jeopardizing access to the very services that make them healthy enough to work. This is a particular dilemma for people with AIDS who are successfully taking protease inhibitors funded by Medicaid or Ryan White.
In addition to providing general assistance with daily living activities or AIDS-specific assistance such as help with adherence to treatment regimens, support services for poor people with chronic illnesses, including AIDS, must mesh more closely with public assistance, family services, and housing providers, because subsistence needs must be met before health and traditional support services can be put in place. Similarly, support services for people with chronic illnesses and behavioral problems must work more closely with mental health and substance abuse treatment providers.
The similarities of the needs of disadvantaged people with AIDS to those of disadvantaged people with other types of chronic illnesses raises a question of equitability in support services funding. The Ryan White program has demonstrated that important service and funding gaps had to be filled for poor people with AIDS. These gaps almost surely exist for all poor people with severe chronic illnesses.
Research Agenda Recommendations
The need for (1) data describing the use and effectiveness of home- and community-based services for people with AIDS, (2) managed care approaches that integrate home- and community-based services for people with AIDS, and (3) a cohesive national chronic-care policy give rise to the following research agenda recommendations:
Database Development. There is a clear need both for large representative databases that can provide timely descriptions of home- and community-based service use among different groups of people with AIDS and for focused data collection to identify and evaluate promising interventions. Large administrative databases are representative and comprehensive, but they lack much data describing individual characteristics and suffer from processing lags that keep them from being as timely as desirable. Provider databases have the potential to add characteristics data and to be more timely, but they describe highly specific populations. Reports concerning the rates at which characteristics data are missing from provider databases lessen their appeal. Nevertheless, research efforts should focus on examining the feasibility of developing combined administrative databases and of using provider data to supplement them.
Practice Guideline and Quality Indicator Development. Although their use is now becoming accepted practice in home health care, practice guidelines and quality indicators have not been used widely for other home- and community-based services. Although provider databases could be useful in developing benchmarks and testing specific approaches, development of guidelines and quality indicators usually relies on panels of experts and consumers. Research efforts should investigate the feasibility of developing such guidelines and indicators. A first step in this effort might include a review of the literature to identify any that already exist, followed by a meeting of experts and consumers to discuss the desirability of developing (or refining) them for specific services (for example, case management or treatment adherence assistance).
Identification of Evaluable Interventions. In the course of its six case study visits, this project identified a number of interventions that could be considered for formal evaluation. However, a more focused approach could be taken to identifying interventions through the release of a request for proposals disseminated widely to AIDS providers. To encourage as many responses as possible by burdening providers as little as possible, the request process could follow a "foundation approach" in which (1) providers were asked to submit two-page letters describing their ideas, (2) a panel reviewed the letters, and (3) selected providers were then asked to submit longer proposals.
Development of Managed Care Demonstrations That Include Home- and Community-Based Services. AIDS-specific demonstrations are needed that include under capitation home- and community-based services (such as those covered under regular Medicaid benefits, Medicaid waivers, and Ryan White funding) in order to fill knowledge gaps about whether and how such arrangements may best be implemented. Such demonstration efforts face a number of nontrivial challenges, including identifying appropriate host organizations, gathering a full range of service providers, and setting payment rates. In addition, any such demonstration should require the collection of encounter data to describe patterns of service use under capitation. Similarly, thought should be given to the design of a Medicare demonstration that provides beneficiaries with AIDS (who do not also have Medicaid) coverage of pharmaceuticals and support services.
Investigation of Return-to-Work Regulations. Although the Supplemental Security Income program contains regulations that provide for the continuation of public benefits for people working with a "severe impairment," it is not clear whether or how these regulations apply to people with AIDS who are being treated successfully with protease or some other therapy. Because AIDS medications are so costly, and thus the disincentive to work particularly strong, this area deserves further investigation and may suggest the need to revise existing regulations to reduce the work disincentives.
Development of Approaches to Better Link AIDS Services to Other Systems. The level of contact between AIDS service providers and providers and entities in other systems--substance abuse treatment, mental health, family services, and public assistance--has increased greatly in recent years, primarily through increased referrals between systems. Yet AIDS providers in our case studies stated that there was not enough sharing of basic knowledge, particularly between AIDS providers and those in the substance abuse treatment and mental health systems. Coordination of efforts between these systems would be particularly important in developing strategies to help people with substance abuse problems or mental illness to adhere to AIDS treatment regimens. Research efforts should thus develop approaches for sharing knowledge and pooling resources between AIDS service providers and those in other systems that serve large numbers of people with AIDS.
Conclusion
As AIDS increasingly becomes a disease of disadvantaged people, medical treatment and health-related support services begin to blend with traditional public assistance programs such as food stamps and housing assistance. Moreover, any changes in service delivery that result from changes in welfare or immigration policy will affect more directly an AIDS population growing poorer. As AIDS increasingly becomes a chronic, rather than an acute and fatal disease, its management resembles more closely that of other serious chronic conditions. Key challenges in developing costeffective models of chronic-disease management include figuring out how to help people take responsibility for their health (adhere to treatment regimens, maintain good self-care practices, and monitor and report symptoms) and how to provide them with the assistance and financial support they need to take this responsibility. Substance abuse treatment, mental health services, assisted or supportive living, interventions with families, assistance returning to work, and help locating safe and secure housing--all may have to play a bigger role in the delivery of home- and community-based services for newer AIDS populations than they did for gay men earlier in the epidemic.
I. INTRODUCTION AND OVERVIEW
In the early 1980s, when acquired immunodeficiency syndrome (AIDS) made its first appearance, it was an unfailingly acute and fatal disease. Since then, accumulation of AIDS-specific medical expertise and pharmaceutical and other treatment advances have increased life expectancy for people with AIDS and human immunodeficiency virus (HIV) and shifted AIDS treatment from an acute to a chronic model of care. Home- and community-based services--skilled home nursing, hospice, personal assistance, and other types of support--have always been an integral part of AIDS care. Advances in home care technology (such as new home infusion methods), the high cost of care delivered in hospitals and nursing homes, and the preferences of many people with chronic illnesses, including AIDS, to be cared for at home all have tended to shift the locus of medical and nursing care from institutions to home and community settings. At the same time, increased life expectancy and improved health and functioning have broadened the scope of home- and community-based care for people with AIDS to include, for example, assistance returning to work and caring for families.
Changes in the prevalence patterns of AIDS have occurred while treatment has improved. In the United States, AIDS originally primarily affected gay men. Today, it affects an increasing number of injection drug users and women with children, hitting particularly hard those who belong to racial or ethnic minorities. The needs, low incomes, and other life circumstances of a growing number of people with AIDS pose special challenges to programs that deliver community-based care and have increased the public burden for that care.
This is the final report for the project, "The Role of Home- and Community-Based Services in Meeting the Health Care Needs of People with AIDS," conducted by Mathematica Policy Research, Inc. (MPR), for the U.S. Department of Health and Human Services (DHHS), Office of the Assistant Secretary for Planning and Evaluation (ASPE). (The project was conducted between September 1996 and April 1998.) The goal of the project was to assist ASPE in developing a research agenda for studying the current status and future of home- and community-based service use among people with AIDS. The project had three analytic components:
- A review of the literature describing the delivery and financing of home- and community-based services for people with AIDS, focusing on literature published within the past five years
- Case studies of current home- and community-based AIDS service delivery in New York City and Los Angeles, based primarily on site visits to three large service providers in each city supplemented by telephone conversations with staff from Medicaid programs and Ryan White grantees and planning councils
- An analysis of patterns of home- and community-based service use and reimbursement for New Jersey Medicaid beneficiaries with AIDS
These components addressed a set of questions whose answers provide the groundwork for setting a research agenda (see Table I.1). How are programs delivering home- and community-based services to people with AIDS organized and operated? What services are used, and by whom? What are the barriers to delivering effective care, and how are those barriers being addressed? How much do services cost? What effect have managed care and changes in AIDS treatment had on service delivery and financing? What type of data are available for following changes in service use and spending over time?
This report summarizes and synthesizes the findings of the project's three components. It identifies in the evolution of the AIDS epidemic three key events that have had profound effects on service providers and thus are likely to shape future policy decisions: (1) changes in the characteristics of the AIDS population; (2) improvements in AIDS treatment; and (3) increased pressures to control the costs of care, particularly in the Medicaid program. Chapter II (summarizing the project's literature review) describes the changing nature of the AIDS epidemic and its effect on service use and funding. Chapter III (presenting lessons from the project's case studies) discusses the challenges that AIDS service providers currently face and the approaches they take to meeting them. (Appendix A and Appendix B contain the descriptive underpinnings of the New York City and Los Angeles case studies, respectively.) Chapter IV discusses the importance of AIDS-specific home- and community-based service databases and approaches to developing them. Chapter V summarizes the findings of the New Jersey Medicaid data analysis (conducted for this project by the AIDS Research Group of the Institute for Health, Health Care Policy, and Aging Research at Rutgers University). Chapter VI discusses the policy implications of the project's findings and makes recommendations for developing an AIDS home- and community-based service research agenda.
| TABLE I.1. Overview of Questions Addressed by Project Components | |||
| Research Questions | Literature Review | Case Studies | New Jersey Data Analysis |
| Program Structure and Service Use Levels | X | X | X |
| How are programs that deliver home- and community-based services to people with AIDS organized and operated? | |||
| How does service use vary by patient population and other key factors? | |||
| Program Costs/Finances | X | X | X |
| What are the costs of care for people with AIDS who use home- and community-based services? How do costs vary by patient population and other key factors? | |||
| The Role of Managed Care | X | X | |
| To what extent, and how, do managed care organizations provide/cover/coordinate home- and community-based services to enrollees with AIDS? | |||
| How are payments to managed care organizations adjusted for the risk of serving enrollees with HIV/AIDS? | |||
| Who is making the payment? Are some services carved out (drugs, long-term care, support for informals, substance abuse treatment)? | |||
| In what ways do capitated care systems change the way services are provided to people with AIDS, including changing the locations where services are provided, the types of staff who deliver services, and the mix of specific services delivered? | |||
| Comparison with Other Long-Term Care Populations | X | ||
| What lessons learned from evaluations of long-term care programs for other populations (for example, frail elderly individuals, people with disabilities) are relevant to those programs for people with AIDS? | |||
| Future Trends | X | X | |
| What factors have contributed to the growth in demand for home- and community-based care for people with AIDS? | |||
| What factors are likely to affect demand in the future? How are they likely to affect demand? | |||
| Availability of Program Databases | X | X | |
| What types of data are maintained by programs that provide home- and community-based services to people with AIDS? | |||
II. THE EVOLUTION OF THE AIDS EPIDEMIC
Home- and community-based services, such as assistance with daily living activities and the provision of home-delivered meals, have always played an important role in AIDS care. As the population living with AIDS has expanded and become more disadvantaged, service needs have changed, and the growing financial burden of AIDS care has fallen increasingly on public programs. At the same time, the Medicaid program, the largest public payer for AIDS care, has come under escalating pressure to move all beneficiaries, including those with disabilities and chronic conditions such as AIDS, into managed care to better coordinate and control the high costs of their care.1
A. THE CHANGING FACE OF THE EPIDEMIC
In the early days of the AIDS epidemic, the typical person with AIDS was recognized as a white man who had contracted HIV through sexual contact with another man. Of the more than 50,000 AIDS cases reported to the CDC between 1981 and 1987, over 90 percent were among men, 60 percent were among non-Hispanic whites, and at least two-thirds were among men whose likely mode of transmission was same-sex contact (see Table II.1).
Since 1981 the epidemic has disproportionately and increasingly affected women and people who belong to racial or ethnic minorities, and the mode of transmission has increasingly been injection drug use. Of 300,000 AIDS cases reported in just the three-and-a-half years between January 1993 and June 1996, 18 percent were among women and nearly 60 percent were among blacks and Hispanics. Fewer than half the cases were among men who had had sex with men. However, 33 percent of cases were among injection drug users (up from 26 percent for cases reported between 1981 and 1987), and 11 percent were among people who had heterosexual contact with someone with AIDS (up from 3 percent during the earlier period). As of June 1996, roughly 200,000 people were living with AIDS, while almost two-thirds of cases reported since 1981 had died (Centers for Disease Control and Prevention 1996a).
People who are currently infected with HIV but who do not yet have AIDS represent the AIDS cases of the next decade. The reporting of HIV cases has not been systematic. However, estimates of the number of HIV cases range from just under two to three-and-a-half times the number of AIDS cases (Centers for Disease Control and Prevention 1996a; and Flaskerud 1995).2 Among reported HIV cases are even larger proportions of women and members of minority groups than among reported AIDS cases, which suggests that the increasing incidence of AIDS among women and minority group members of the 1980s and 1990s will continue into the next decade (Centers for Disease Control and Prevention 1995b).
| TABLE II.1. Number and Percentage of AIDS Cases, by Selected Characteristics(1981 TO June 1996, United States) | |||
| Cases During the Period | 1981 to 1987 | 1988 to 1992 | 1993 to June 1996 |
| Number of AIDS Cases | 50,352 | 203,217 | 294,533 |
| Number of AIDS Deathsa | 41,027 | 157,295 | 144,678 |
| Percentage of AIDS Cases, by Sex | |||
| Male | 92.0 | 87.5 | 82.1 |
| Female | 8.0 | 12.5 | 17.9 |
| Percentage of AIDS Cases, by Transmission Risk Group | |||
| Men who have sex with men | 64.0 | 54.6 | 44.5 |
| Injection drug users | 17.2 | 24.2 | 27.2 |
| Men who have sex with men and inject drugs | 8.3 | 7.0 | 5.7 |
| Heterosexual | 2.5 | 6.1 | 10.7 |
| Others | 8.0 | 8.2 | 12.0 |
| Percentage of AIDS Cases, by Raceb | |||
| Non-Hispanic white | 59.8 | 50.5 | 42.0 |
| Non-Hispanic black | 25.4 | 31.1 | 38.3 |
| Hispanic | 14.0 | 17.3 | 18.5 |
| Percentage of AIDS Cases, by Regional Areac | |||
| Northeast | 38.8 | 30.7 | 30.3 |
| Midwest | 7.5 | 10.0 | 10.1 |
| South | 25.7 | 32.4 | 35.0 |
| West | 26.9 | 23.0 | 21.4 |
SOURCE: Centers for Disease Control and Prevention 1995a and 1996a.
| |||
B. CHANGING SERVICE NEEDS AND COSTS
People with AIDS use a wide range of health and health-related services, because AIDS gives rise to a staggering array of opportunistic infections, and AIDS treatment is geared both to treating these infections and to providing complex antiretroviral therapy to minimize the likelihood of future infection. The opportunistic illnesses brought about by AIDS appear as acute and often recurrent episodes (Ungvarski and Staats 1995). Common opportunistic illnesses among people with AIDS include Pneumocystis carinii pneumonia and other types of recurrent pneumonia, HIV wasting syndrome, a variety of cancers (including Kaposi's sarcoma), and bacterial and fungal infections rarely seen in people with healthy immune systems. Therapies to control opportunistic illnesses are complex and usually must be long term; moreover, people with AIDS may experience several illnesses at once. The incidence of opportunistic infection may be sharply reduced when antiretroviral medications are successful. The regimens for these medications, however, are complex, their side effects must be carefully monitored, people taking the medications need to make sure their nutritional intake is adequate, and they must practice good self-care (Ungvarski et al. 1995). Thus, treatment regimens and symptom monitoring become complex tasks that may require ongoing assistance from a nurse or other health professional.
As people with AIDS experience opportunistic illnesses, they may suffer some level of functional impairment for which they require support services. Usually, functional limitations are assessed in terms of a person's ability to carry out the activities of daily living (dressing, bathing, toileting, eating, and so on) and instrumental activities of daily living (taking medications, handling finances, shopping, preparing meals). The most obvious example of an AIDS-related opportunistic illness that leads to loss of functioning is HIV-related encephalopathy, or AIDS dementia. As with Alzheimer's disease, AIDS dementia initially affects memory and concentration, making it increasingly difficult, for example, to adhere to medication regimens and remember medical appointments. Later, motor impairment limits the person's ability to carry out daily living activities (Ungvarski and Staats 1995). Even people with AIDS who do not have dementia or an opportunistic disease may experience debilitating levels of fatigue that lead them to require some help with daily living activities (Shilts 1988). Such assistance may come from friends or relatives or from formal agencies or volunteer organizations.
Empirical studies have shown that both specific functional limitations and fatigue have been associated with the use of home care (Wilson and Cleary 1996; and Fleishman 1997). However, the level of need may change frequently, especially regarding assistance with work and child care (Crystal and Sambamoorthi 1996). Moreover, people with chronic illnesses like AIDS constantly vary the intensity with which they use services in the acute medical and support services environments.
Thus, for many people with AIDS, effective and efficient home- and community-based service delivery requires the kind of coordinated effort among medical, nursing, and support services providers that has been difficult to achieve for groups with other chronic illnesses or disabilities. The literature describes a wide range of medical, institutional, residential, and home- and community-based services used by people with AIDS (see Table II.2). The focus of this project has been home- and community-based services: the many types of services included in the center and rightmost panels of the table. These include home- and community-based services traditionally used by frail elders and other people with disabilities, such as case management (needs assessment and service planning, public assistance advocacy, and counseling), skilled home health care, paraprofessional home care (for example, assistance with personal care and housekeeping), home-delivered meals, transportation, and adult day health care.
Home- and community-based care for people with AIDS has come to include an additional group of services, for two reasons. First, people with AIDS as a group are more likely than frail elders to be of working and childbearing age, and when they are ill, they may need help finding ways to continue, to the extent possible, working or caring for children. In addition, they seem to be more likely than older people to make use of peer assistance such as buddy programs and support groups, partly because they are younger and have had more exposure to these types of help. Second, because people with AIDS are increasingly likely to have behavioral comorbidities such as serious mental illness or substance abuse problems, home- and community-based services for them have come to include mental health and substance abuse treatment services.
| TABLE II.2. Health and Support Services Used by People with AIDS | ||
| Medical, Institutional, and Residential Services | "Traditional" Home- and Community-Based Services | "AIDS-Specific" Home- and Community-Based Services |
| Inpatient hospital acute | Case management | Information hotline |
| Subacute/step down | Home health/skilled nursing | Counseling/education |
| Skilled nursing facility | In-home hospice | Support groups/buddy programs/peer counseling |
| Inpatient hospice | Home infusion therapy | Legal services |
| Inpatient/residential substance abuse treatment | Private duty nursing | Financial management services |
| Psychiatric care/other mental health services | Rehabilitative services | Protective services |
| Attendant care facility | Homemaker/housekeeper | Employment assistance and counseling |
| Board and care home | Personal care/attendant care | Assistance in purchasing pharmaceuticals |
| Adult/child foster care | Respite care | Assistance with medication adherence/directly observed therapy |
| Congregate housing | Home-delivered meals/congregate meals | Child care |
| Primary and specialty medical | Home modifications/assistance moving | Nutrition services |
| Outpatient clinic | Adult day health care | Housing |
| Dental | Transportation to medical care/other | In-home/outpatient substance abuse treatment |
| Vision | Supplies and durable medical equipment | Social day care/recreation programs |
| Massage therapy/acupuncture | ||
| SOURCES: Benjamin 1989; Cowart et al. 1994; Cowart and Mitchell 1995; Katoff 1992; Master et al. 1996; Merzel et al. 1992; Schultz et al. 1994; and personal communication with HCFA Medicaid long-term care staff.NOTE: Home- and community-based services refer to health-related support care provided with both public and private funding and by volunteers. | ||
If pharmaceutical treatments for AIDS continue to help people regain (or maintain) their ability to function, a whole new range of community-based services is needed, such as assistance adhering to treatment regimens, assistance returning to (or beginning) work, and legal assistance with problems encountered when returning to work or becoming bankrupt while ill.3 Important policy issues arise concerning the ability of people to retain public benefits for medical insurance (particularly Medicaid) and for the purchase of pharmaceuticals (through the Ryan White AIDS Drug Assistance Programs) even if they do return to work. The decision to return to a productive work life presents a dilemma if people must choose between work and the medications and services that give them the ability to work.
However, recent studies suggest that protease combination therapy may be effective for only half the people who try it (New York Times, September 30, 1997). Nor do all people with AIDS choose to take this therapy or have the opportunity to take it. Moreover, some functional deficits that result from infections that occurred before taking protease therapy cannot be reversed even when protease therapy is successful (for example, blindness resulting from cytomegalovirus retinitis). Thus, for many people, health problems and functional deficits will continue to give rise to traditional home- and community-based service needs.
Uncompensated care (often referred to as informal care) has been a cornerstone of home-based AIDS care, and its presence often affects formal service needs (Crystal and Sambamoorthi 1996). Although there appear to be no reliable estimates of the extent to which people with AIDS use informal care or of the monetary value of such care, some research suggests that the use of informal care has been extensive among gay men with AIDS. Caregivers frequently have been partners or (less often) family members (Institute of Medicine 1994). Evidence also exists of significant family caregiving among injection drug users with AIDS (Crystal and Schiller 1993). The importance of informal caregiving in AIDS care is underscored by the fact that AIDS service organizations have traditionally included volunteer buddy programs to provide informal care when no family or friends are available.
Despite anecdotally high levels of home- and community-based service use, and perhaps because the range of these services has changed dramatically since the start of the epidemic, very little comprehensive data exist describing use levels (and costs) for specific types of home- and community-based services and how use may vary by category of people with AIDS or by geography. AIDS-specific cost-effectiveness studies for specific groups of services (or funding approaches) are nonexistent.
Studies of the cost-effectiveness of home- and community-based services for frail elders suggest that the provision of these services does not reduce overall spending for health care but does reduce unmet need and increase well-being and satisfaction with care (see, for example, Kemper et al. 1987; and Weissert 1985). Studies among elders of the cost-effectiveness of treatment adherence assistance through high-cost case management approaches have yielded mixed conclusions (see for example, Schore et al. 1997; Rich et al. 1995; and Weinberger et al. 1996). However, these interventions tend to encounter three types of problems: (1) it is difficult to design interventions that can improve self-care behavior; (2) it is necessary, but not sufficient, to identify clients who have high rates of inpatient use to reduce those rates; and (3) the intervention can be so costly that very large reductions in inpatient and other service use are required to produce overall cost savings (Schore et al. 1997).
Estimates of the lifetime costs of care for people with HIV/AIDS vary according to assumptions concerning life expectancy (which has increased over time), the inclusion of specific services (for example, support) or expensive medications, trends in the use of inpatient hospital care, the use of informal assistance, and other factors. The experience of Kaiser-Permanente in the mid-1980s demonstrated that lifetime costs after an AIDS diagnosis for private, prepaid health plan members amounted to $32,816, including inpatient and outpatient care, home health, counseling, and pharmaceuticals--assuming a life expectancy of just over a year following AIDS diagnosis (Hiatt et al. 1990). Data from the 1992 AIDS Cost and Service Utilization Survey (ACSUS) were the basis for a lifetime estimate of $119,274, assuming more than 10 years of HIV infection before the onset of AIDS, and just over 2 years following the onset of AIDS. The $119,274 included inpatient care (accounting for 52 percent of the cost estimate), outpatient care (27 percent), home health (6 percent), prescriptions (14 percent), and long-term care (1 percent) (Hellinger 1993). A study of Medicaid beneficiaries receiving AIDS care from the Johns Hopkins University AIDS Program between 1991 and 1994 estimated that a patient who began care with a CD4 count of at least 500 would live about eight years and accumulate $150,000 in Medicaid payments (Kaiser Family Foundation 1996). It is noteworthy that none of these studies provides information on the use and costs of specific types of home- and community-based services.
Pharmaceuticals have accounted for a significant proportion of lifetime HIV/AIDS costs. Two primary types of drugs--antiretroviral drugs and drugs to treat AIDS-related conditions--are used in current therapies. Antiretroviral medications are taken to reduce the amount of HIV in the blood; these drugs work by blocking the viral enzymes needed to replicate the HIV. An additional set of medications exists to prevent or suppress AIDS-related infections and conditions. The first decline in deaths since the start of the epidemic (13 percent nationwide) was observed between 1995 and 1996. These declines were attributed to life-lengthening treatments developed in the early 1990s, as well as to greater access to medical care as a result of an influx of government funding in 1994 (Medicine and Health 1997; and Altman 1997).
Protease inhibitors, available since late 1995, seem an even more promising, though costly, class of antiretroviral drugs. Protease inhibitors are prescribed in combination with older antiretroviral medications like zidovudine (AZT). Cost estimates for protease inhibitors alone range from $6,000 to $14,000 a year (Gilden 1996; AIDS Treatment Data Network 1996; TennCare News 1996; and Bartlett and Moore 1996). Combination therapies, including one of the three currently available protease inhibitors, can cost up to $18,000 a year (American Public Health Association 1996). As noted, additional medications often are needed to prevent or suppress AIDS-related infections and conditions. Thus, the already high cost of pharmaceutical treatment for AIDS has recently grown substantially.
Finally, there is a notable lack of literature discussing approaches to assessing the quality of home- and community-based services for people with AIDS and even fewer rigorous, comprehensive assessments of the quality of specific programs. This is likely due to the fact that, despite the growth of home care over the past 10 to 20 years, development of quality assurance procedures for home care is still in its infancy. Kane et al. (1994) provide a conceptual framework for assessing the quality of home- and community-based services along four dimensions: (1) structure (for example, whether workers have adequate knowledge and are in sufficient supply), (2) process (whether assessment and care plans are adequate and implemented appropriately), (3) outcome (whether care recipients are unintentionally injured or intentionally abused or whether they experience adverse events associated with particular types of care), and (4) enabling (whether care recipients are confident that workers will be available when and for as long as needed and whether care recipients have adequate control of selection, training, and retention of workers).
Some inroads have been made toward developing measures of home care quality. HCFA has devoted considerable effort to developing guidelines to assess the quality of home health care (see, for example, Shaughnessy et al. 1994), but home health is only a part of home- and community-based services. Case managers for Medicaid home- and community-based waiver programs often monitor the quality of direct services, and many states independently review care plan design and implementation (Laudicina and Burwell 1988). The literature describing the quality of home- and community-based service programs for people with AIDS is limited and often includes only the results of client satisfaction surveys. For example, Cowart and Mitchell (1995) and Master et al. (1996) both reported that surveyed clients were satisfied with program services. However, Master et al. also monitored the incidence of Pneumocystis carinii pneumonia as a quality indicator and reported that it had decreased among clients after enrollment in the program. Thus, comprehensive quality assurance procedures and indicators for home- and community-based services for people with AIDS (and other populations) have yet to be fully developed.
Changes that have occurred in AIDS treatment and in the characteristics of the AIDS population have had profound and interrelated effects on the type and level of home- and community-based services that people with AIDS need.
-
Improved AIDS treatment (increased medical expertise and the development of antiretroviral medications such as AZT and protease inhibitors) has increased life expectancy, which in turn has increased the duration of needed services.
-
Improved treatment has also improved health and decreased levels of functional impairment among many people living with AIDS, which in turn appears to have led to a decrease in their use of traditional home- and community-based services (such as home-delivered meals and personal care). At the same time, this treatment has led to an increased need for other types of support, such as assistance with adhering to regimens and returning to work. Those who do not receive treatment or for whom it is ineffective, however, continue to require traditional services.
-
Meanwhile, the increased incidence of AIDS among people with low incomes, people with substance abuse problems, and women with families suggests an increased need for a mix of home- and community-based services that more often than previously must mesh with medical, substance abuse treatment, mental health, family services, and public assistance systems.
C. EFFECTS ON FUNDING SOURCES
Medicaid, Medicare, and the Ryan White Comprehensive AIDS Resources Emergency (CARE) Act have been the major public funding sources for HIV/AIDS since 1991 (see Table II.3). For fiscal year 1996, their combined spending totaled more than $4.9 billion.4 Private insurance has accounted for only a small proportion of overall spending (although the private insurance data in Table II.3 are incomplete) and may be expected to account for even less as the AIDS population becomes more disadvantaged. Yet spending by federal and state governments and by private insurers does not describe the full burden of the costs of HIV/AIDS care to society. It does not account for public spending at the county or city level, out-of-pocket spending, charity care, spending for medications in clinical trials or drug company indigent care programs, or the value of informal care giving.
1. Medicaid and Managed Care
Medicaid is the largest public funder of AIDS-related care, not only because the epidemic disproportionately affects individuals with low incomes, but also because many people with AIDS with higher incomes eventually spend down so that they become eligible for Medicaid (Markson et al. 1994). Between 1991 and 1996, annual Medicaid spending for people with AIDS more than doubled, to more than $3.5 billion; this is five times the estimated 1996 spending levels of Medicare or the Ryan White CARE Act (see Table II.3). In 1995, spending on AIDS-related care, however, was only about two percent of the total Medicaid spending of $156.3 billion, and beneficiaries with AIDS represented just under two percent of all Medicaid beneficiaries (U.S. House of Representatives 1996).
Medicaid covers many of the health and health-related services people with AIDS need, although specific services vary by state. Federally mandated services include inpatient and outpatient hospital services, ambulatory care, long-term institutional care, and skilled home health care (U.S. House of Representatives 1996). States have the option to cover additional services such as prescription drugs, personal care, hospice care, and mental health and substance abuse treatment. State Medicaid programs may also provide additional services under 1915(c) home- and community-based waivers (either for beneficiaries with AIDS only or for beneficiaries more generally at risk of institutional care). The most commonly provided waiver services have been case management, personal care and homemaker services, respite care, psychosocial care, counseling and education, and nursing care, including skilled and private duty nursing (Klein and Thornton 1994).5
| TABLE II.3. PUBLIC AND PRIVATE FUNDING SOURCES FOR HIV/AIDS CARE(In Millions of Dollars) | ||||||
| 1991a | 1992 | 1993 | 1994 | 1995 | 1996 | |
| Medicaid Cost Estimatesb | ||||||
| Federal | 870 | 1,080 | 1,290 | 1,490 | 1,640 | 1,800 |
| State | 820 | 1,020 | 1,220 | 1,410 | 1,560 | 1,710 |
| Total | 1,690 | 2,100 | 2,510 | 2,900 | 3,200 | 3,510 |
| Medicare Cost Estimatesb | 180 | 280 | 385 | 500 | 600 | 690 |
| Ryan White CARE Act Funding Levels | ||||||
| Title I | 87.8 | 121.7 | 184.8 | 325.5 | 356.5 | 391.7 |
| Title II | 87.8 | 107.7 | 115.3 | 183.9 | 198.1 | 260.8 |
| Title III(b) | 44.9 | 49.9 | 48.0 | 48.0 | 52.3 | 56.9 |
| Title IV | 0.0 | 0.0 | 0.0 | 22.0 | 26.0 | 29.0 |
| Total | 220.5 | 279.3 | 348.1 | 579.4 | 632.9 | 738.4 |
| Private Insurance Claimsc | 206.2 | 282.1 | 229.5 | 197.0 | 146.3 | NA |
SOURCES: For Medicaid and Medicare estimates, personal communication with HCFA Office of Actuary staff. For Ryan White appropriations, personal communication with HRSA Division of HIV Services staff. For private insurance claims, American Council of Life Insurance and Health Insurance Association of America (1996).
NA = not available. | ||||||
As of early 1998, only 16 states had active, approved AIDS waivers.6 Klein and Thornton (1994) concluded, from conversations with state and federal staff involved with waiver programs, that states might be discouraged from applying for AIDS waivers in the future because of a general trend away from institution-based AIDS care. These trends would make it more difficult to demonstrate that it would be no more expensive to care for people with AIDS in the community than in an institution, a federal requirement for waiver approval.
The recent trend among Medicaid programs to rein in escalating costs by enrolling beneficiaries in managed care plans under Section 1115 waiver authority has had only a modest effect so far on people with AIDS.7 As of February 1996, only 17 states had implemented prepaid managed care programs for beneficiaries with disabilities, and only six of these programs were mandatory for some or all beneficiaries (U.S. General Accounting Office 1996).8 For example, Tennessee's prepaid managed care program, TennCare, has enrolled all people with disabilities (including people with AIDS) into state-approved managed care organizations. However, only 2,000 (less than one percent) of TennCare members have AIDS.9 The other 11 states offer voluntary programs to beneficiaries with disabilities, including those with AIDS. Massachusetts Medicaid specifically targets people with severe disabilities and people with AIDS to enroll in three prepaid health plans; the Community Medical Alliance (CMA) was the first of these health plans to contract with the state (Master et al. 1996; and U.S. General Accounting Office 1996). California offers voluntary prepaid managed care to the categorically eligible Medicaid population (excluding those who meet the Medicaid medically needy criteria). For example, MediCal contracts with Positive Healthcare, a Primary Care Case Management plan affiliated with AIDS Healthcare Foundation, to serve Medicaid beneficiaries with AIDS in the Los Angeles area (Reis 1996). In addition, New York is currently developing a Special Needs Plan for people with AIDS under its Section 1115 waiver that initially will enroll Medicaid beneficiaries voluntarily but eventually will be mandatory (Kaiser Family Foundation 1997). The states with the largest number of AIDS cases are not among those that currently mandate managed care enrollment for beneficiaries with disabilities.
Moreover, even among the existing managed care plans that serve people with AIDS, most appear to carve out support services usually covered under fee-for-service Medicaid. Of the 17 states with prepaid managed care programs for beneficiaries with disabilities, only 7 (Arizona, Colorado, Massachusetts, Oregon, Pennsylvania, Tennessee, and Utah) include beneficiaries receiving long-term home- and community-based services. Even in Arizona and Tennessee, prepaid plans cover primary and acute care but provide long-term care under separate arrangements (U.S. General Accounting Office 1996). Similarly, capitation payments to CMA exclude personal care and transportation, and those to Positive Healthcare include only primary and specialty medical care.
Including beneficiaries with AIDS in managed care plans poses some serious challenges to Medicaid programs and providers but also holds some promise for coordinating care better. The challenges include:
- Limiting financial risk and setting payment rates to compensate plans adequately for all needed services, including state-of-the-art pharmaceutical treatment and medical care
- Developing a network of AIDS specialty providers
- Covering the full range of medical and support services that people with AIDS require, including, but not limited to, those currently covered by fee-for-service Medicaid
- Coordinating resources with other programs that fund services for people with AIDS, like Ryan White and Medicare
Nevertheless, Medicaid managed care has the potential to monitor care quality better, to coordinate care across the acute- and chronic-care settings better, and to provide support and preventive services that may reduce the risk of costly acute episodes. However, because Medicaid managed care has been primarily voluntary for people with AIDS, and because managed care plans tend to carve out home- and community-based services, there has been little actual experience providing these services under capitation. As a result, we have no evidence concerning the ability of managed care to live up to this potential for people with AIDS.
Experiences with frail elders suggest that it is difficult to realize this potential. For example, the evaluation of the first Social/Health Maintenance Organization (S/HMO) demonstration found that although medical providers and case managers were located in the same place, and efforts were made to integrate service provision, the coordination of medical and home- and community-based services was limited because communication between medical providers and case managers was limited. In addition, they found that the S/HMOs failed to offer special geriatric medical services, employed few geriatricians, and failed to account for the special needs of frail enrollees (such as the need for longer physician appointments) (Harrington et al. 1993). Perhaps as a result, enrollees who had disabilities or chronic illnesses experienced greater functional decline than Medicare beneficiaries in the evaluation's fee-for-service comparison group (Manton et al. 1993).
2. Ryan White
The Ryan White CARE Act, initiated in 1991, provides federal funds for states and localities for HIV/AIDS-related health care and support services with the goal of supplementing existing service and funding systems. Congress enacted the CARE Act because certain cities and states were overburdened with the cost of AIDS-related care for low-income people with little or no insurance. Local communities set service priorities. CARE Act programs (1) serve people with low incomes who are not eligible for Medicaid, and (2) provide Medicaid beneficiaries with services that are not covered by Medicaid. In instances where a person with low income has Medicaid (or private insurance), Ryan White may fund needed noncovered services as a payer of last resort. CARE Act funds have increased from $220.5 million in 1991 to $807.5 million as budgeted for fiscal year 1997.10
The CARE Act provides assistance through four titles:
-
Title I funds go to metropolitan areas. Funds may be used to provide outpatient and ambulatory health and support services, including case management and comprehensive treatment services for people with HIV. As of 1996, 49 eligible metropolitan areas received Title I funding.
-
Title II provides funds to states to (1) establish and operate HIV care consortia that provide a comprehensive continuum of care to people with HIV, (2) deliver home- and community-based care, (3) continue health insurance coverage, and (4) provide treatments and pharmaceuticals that prolong life or prevent serious deterioration of health.
-
Title III(b) funds are awarded competitively to public or nonprofit entities providing comprehensive primary care service to populations at risk for HIV infection. Services may include HIV risk reduction counseling and testing, partner notification/risk reduction, transmission prevention, and counseling and education on living with HIV disease.
-
Title IV, funded beginning in fiscal year 1994, awards competitive demonstration grants to community health centers and other appropriate public and nonprofit entities to support research and health care services for pediatric HIV patients and their families (U.S. Department of Health and Human Services 1994).
Title II also funds AIDS Drug Assistance Programs (ADAPs) to subsidize the cost of medications for people with AIDS who are uninsured or underinsured; some of the larger states match federal ADAP funds. From 1987 to 1990, ADAP was an independent program created solely to provide AZT, but in 1991, ADAP funding was folded into Title II. Because of the increased use of combination therapies and additional antiretroviral medications, ADAPs have begun to experience problems serving everyone eligible for drug assistance. During 1996, the first year following approval of protease inhibitors, 34 state ADAPs were able to cover at least one protease inhibitor. However, because of the cost, ADAPs have had to limit the number of recipients of protease therapy. To administer protease inhibitors to more people with AIDS, 1996 Title II funding contained an additional $167 million earmarked for drug assistance. ADAPs and Medicaid prescription benefits have been estimated to pay for two-thirds of all antiretroviral prescriptions (American Public Health Association 1996).
The Ryan White program faces additional challenges as more Medicaid beneficiaries with AIDS move into managed care. A fundamental question exists as to how much and what type of integration is needed between the Ryan White program and Medicaid managed care plans to ensure Ryan White's ongoing role as a safety net provider to Medicaid beneficiaries in managed care and to ensure a measure of care continuity across services covered by each program. Little (possibly nothing) has been published describing ongoing or planned responses of the Ryan White program (or providers receiving substantial Ryan White funding) to the coming increased enrollment of Medicaid beneficiaries with AIDS in managed care.
3. Medicare
In 1996, Medicare was estimated to spend about $690 million for HIV/AIDS care. Medicare provides medical insurance for people 65 or older and younger people with permanent disabilities. People in both groups must have a substantial work history, have paid Federal Insurance Contributions Act (FICA) taxes into social security trust funds, and have undergone a two-year waiting period. (People with end-stage renal disease are eligible for Medicare regardless of their work history.) People with AIDS primarily receive Medicare coverage on the basis of permanent disability. Medicare has not been a major payer for AIDS-related care, because until recently most people with AIDS have not survived long enough to become eligible. However, as the life expectancy of people with AIDS has increased, Medicare's proportion of AIDS-related care has increased, and future costs for AIDS care are expected to increase further.
Medicare primarily covers acute-care services, such as inpatient and outpatient hospital care, skilled nursing facility care, home health care, hospice care, and physician services. Thus, it does not cover some health services important to people with AIDS, perhaps most notably prescription drugs (other than those provided in an inpatient setting). In addition, Medicare covers home health services for homebound people who require intermittent or part-time skilled nursing or therapy, but it does not cover home health in the absence of a skilled need, case management, home- and community-based services or other health-related support services, or long-term nursing home care.
As the number of people with AIDS who qualify for Medicare increases, so too will the number who are dually eligible for Medicare and Medicaid. They will enter the same system(s) of care as other dual eligibles, systems that generally have been recognized as hindering the efficient and coordinated delivery of services. For example, because Medicare is the primary payer for dual eligibles and because states must contribute to the Medicaid program, states have a financial incentive to use Medicare services inappropriately to avoid Medicaid expenditures. HCFA is currently operating demonstrations in several states to test a managed care approach to coordinating services for primarily elderly dual eligibles (HCFA 1997: and Mollica and Riley 1997).
Increases in the incidence of AIDS among people who must rely on public programs for medical care and support services and the growth of managed care in the public sector pose serious challenges to planners who must decide how to finance health-related services for people with AIDS.
-
The increase of AIDS among people with low incomes will place an increasing burden on state Medicaid and state and local Ryan White programs and particularly on resources for pharmaceuticals if demand for protease combination therapy increases. In addition, eligibility and service coverage criteria need to be reconsidered in order to reduce disincentives to return to work and increase provider flexibility in meeting fluctuating chronic-care needs.
-
As state Medicaid programs increasingly adopt managed care approaches that include people with AIDS and other disabilities, there will be a growing need for data accurately describing the level and cost of the full range of services used by different groups of people with AIDS to ensure that managed care plans receive payments adequate to provide high-quality AIDS care (including access to AIDS specialty care, support services, and cutting-edge medications). Cost-effectiveness studies of specific home- and community-based interventions or alternative financing approaches would also provide planners with sorely needed information.
-
Increased use of managed care for Medicaid beneficiaries with AIDS raises questions about whether and how to integrate services currently provided with Ryan White funds to Medicaid beneficiaries to those who will enter managed care. Should Ryan White funds be combined with Medicaid funds under capitated arrangements? If so, how will this be done? If not, how can we minimize incentives for managed care plans to shift costs to the Ryan White program?
-
As people with AIDS live longer, and as more qualify for Medicare coverage, questions arise as to both how to pay for medications and support services (neither of which Medicare covers) and how to integrate Medicare and Medicaid funding for those who are dually eligible so that incentives to provide services at inappropriate levels are reduced.
III. LESSONS FROM THE FRONT LINES
The project developed case studies to describe current provider approaches to delivering home- and community-based services to people with AIDS. The case studies were based on in-person discussions with staff at six large and well-established AIDS service providers in Los Angeles and New York City and were supplemented by telephone conversations with state Medicaid and Ryan White Title I and II representatives. It was evident from these discussions that the AIDS service environment is currently in an extremely fluid state as providers seek efficient and effective responses to changes in the AIDS population, new treatments, and increased cost-control pressures. Thus, the challenges and approaches described by providers in this chapter are but a snapshot of a rapidly changing landscape. Moreover, some of the challenges providers currently face stem from problems in the larger health service delivery and funding systems and thus lie beyond their ability to address directly. The chapter begins with an overview of the methodology followed in developing the case studies.11
A. CASE STUDY METHODOLOGY
The project case studies are the end product of a process that included developing criteria for selecting programs to visit, developing a list of site visit candidate programs, choosing six programs, setting up and conducting visits, reviewing program documentation, telephoning staff with key public funders, and synthesizing the information gathered from all sources. In this section, we briefly describe key steps in this process.
We developed a set of selection criteria to ensure that the six programs visited would provide as broad a perspective as possible, with the understanding that the experiences of just six providers could not be considered truly representative of those of all AIDS service providers. Selection was based on the following provider characteristic classification scheme: principal focus of service delivery (support services, nursing, or medical care); primary funding source (Medicaid, Ryan White, or private sources) and funding mechanism (fee-for-service or capitation); primary transmission risk group served; affiliation (free-standing or affiliated with an organization likely to bring its own perspective and financial imperatives to bear); and geography.
To concentrate project resources, we chose two cities with different AIDS populations and service environments: New York and Los Angeles. The AIDS population in Los Angeles remains largely one of white men who have had sex with men, but it includes more and more women, injection drug users, and minority group members. By contrast, the New York City AIDS population includes a substantial proportion of injection drug users, women, and minority group members--as it has for some time (see Table III.1). As the proportions of people with AIDS in these groups increase nationally, providers in other cities are likely to encounter problems meeting their special needs, problems that have existed in New York for some time.
While the New York City AIDS population may look more like the national AIDS population of the future, the Los Angeles service environment may look more like the national environment of the future. The Los Angeles service environment is much more heavily dominated by managed care than many other areas, including New York City. In 1994, approximately 40 percent of Los Angeles residents received their health care from some type of managed care organization, compared with only 17 percent of New York City residents (InterStudy 1995). As Medicaid managed care becomes more widespread, AIDS service providers across the country are likely to have to find ways to work with managed care organizations and support clients who are managed care enrollees, as they may currently be doing in Los Angeles.
| TABLE III.1. Characteristics of Reported AIDS Cases in New York City and Los Angeles(Percentages of Total Cases Reported Through 1996, Except As Needed) | |||
| New York City | Los Angeles | United States | |
| Sex | |||
| Male | 79.0 | 94.0 | 84.7 |
| Female | 21.0 | 6.0 | 15.3 |
| Race | |||
| Black | 40.3 | 18.9 | 35.0 |
| Hispanic | 30.8 | 25.3 | 17.7 |
| White and other | 28.9 | 55.8 | 47.3 |
| Transmission/Exposure Category | |||
| Among Men | |||
| Male-to-male sexual contact | 43.6 | 79.8 | 58.4 |
| Injection drug use and injection drug use/ male-to-male sexual contact | 45.9 | 12.4 | 29.5 |
| Among Women | |||
| Heterosexual contact | 29.6 | 44.7 | 36.7 |
| Injection drug use | 56.9 | 27.6 | 43.2 |
| Total Number of Cases Reported | 92,253 | 34,615 | 581,429 |
| Total Number of Cases Living | 29,169 | 12,418a | 219,425 |
SOURCES: New York City statistics from personal communication with New York City Office of AIDS Surveillance 1997. Los Angeles statistics from personal communication with County of Los Angeles HIV Epidemiology Program 1997. U.S. statistics from Centers for Disease Control and Prevention 1996b.
| |||
We then judgmentally selected three providers in each city to get broad representation of provider types. In New York City, these were Gay Men's Health Crisis (GMHC), the oldest and largest AIDS service organization in the United States; the Visiting Nurse Service of New York (VNSNY), a large, not-for-profit home health agency with a 10-year-old AIDS program; and Village Center for Care, a continuum of AIDS-specific home care, day treatment, case management, and nursing home care. In Los Angeles, we chose AIDS Project LA (APLA), the second largest AIDS service organization in the United States; AIDS Healthcare Foundation, an AIDS-specific freestanding outpatient medical provider that also operates a Medicaid managed care plan for people with AIDS; and AltaMed Health Services Corporation, a community health center with an HIV/AIDS program targeting the Latino community. Table III.2 provides an overview of basic characteristics of these six programs.
| TABLE III.2. Case Study Program Overview | |||||
| Program | Nursing/Support Services/Medical Focus | Primary Funding Sources | Affiliation | Services Provided | Client Characteristics |
| Los Angeles | |||||
| AIDS Healthcare Foundation/Positive Healthcare | Medical/nursing | AIDS Healthcare Foundation: Medicaid/other third party and Ryan White Positive Health Care: Medicaid | Freestanding residential and outpatient AIDS medical services organization; MediCal-financed capitated health plan for primary medical care | Residential hospice, transitional, skilled nursing, and treatment adherence care; home health; outpatient medical; medical case management; clinical trials; prescription drugs (pharmacy benefits management and ADAP dispenser) | 3,000 clients in 1996; 360 in Positive Health Care: 10% female; 60% nonwhite; 10% injection drug users; 45% uninsured |
| AIDS Project LA | Support services | Private donations 80% | Freestanding AIDS service organization | Case management, dental, home health, housing assistance, food bank, mental health, buddy services, legal and treatment advocacy, living skills, nutrition, HIV prevention and education, transportation | 6,100 clients in 1997: 9% female; 57% nonwhite; 5% injection drug users; 16% uninsured |
| AltaMed Health Services Corporation/HIV Services | Medical | HIV Services: Ryan White | Part of comprehensive community health centera | HIV prevention and testing; primary medical care; case management; home health; mental health; treatment advocacy; prescription drug program (ADAP dispenser) | 600 clients in 1997: 10% female; 89% nonwhite; 2% injection drug users; 83% uninsured |
| New York City | |||||
| Visiting Nurse Service of New York, AIDS Services | Nursing | Medicaid fee-for-service | Part of home health agency | Home health care (skilled nursing, rehabilitation, home health aide, personal care), counseling | 37,000 AIDS patients in 1996: 40% female |
| Village Center for Care | Nursing/support | Medicaid fee-for-service | Freestanding network of long-term care providers | Skilled nursing facility, home health, adult day care, case management | 1,600 clients with AIDS in 1996: 25% female; 75% nonwhite; 33-50% injection drug users |
| Gay Men's Health Crisis | Support | Private donations 75% | Freestanding AIDS service organization | Case management, health care and legal advocacy, legal services, mental health services, recreation, nutritional counseling, meals, buddy services, HIV prevention and education | 8,000 in client services in 1997: 19% female; 60% nonwhite; 20% injection drug users |
| |||||
Site visit discussions, which took place between April and June 1997, were primarily with key informants to gain a broad overall perspective on the service delivery system in each city. Informants included the chief executive officer (or program director), the chief financial officer (or staff knowledgeable about program revenue sources and costs), a clinical supervisor, the data manager, and one or two staff working directly with clients.
The following conceptual framework, which describes how organizations make key service provision decisions, was developed to provide a uniform structure with which to collect and integrate disparate pieces of information from site visit discussions:
| Factors that lead to the development of the program | How consensus has been built in the host organization (or among freestanding founders) for program parameters (whom to serve, how to do outreach, what services to provide, how to fund, etc.) | Barriers to and facilitators of program development | Current program parameters, challenges, delivery approaches, and environmental factors that may lead to change |
Information about why a program was initially conceived and how its key features were designed provides insights into program goals and the motivation for current program activities and decision making. Information about factors that either helped or hindered program development provides insights into problems future programs may encounter and strategies for avoiding or overcoming them. Information about current program parameters and challenges builds our understanding of the kinds of people currently using services and the types and amounts of the services they use. This creates a profile of current service delivery that, together with provider insights into expected changes in the service environment, helps identify service delivery problems, assess where service gaps (or redundancy) may occur in the future, and describe how providers address these problems and gaps.
B. CASE STUDY LESSONS
Consistent with reported demographic trends, case study providers reported that the characteristics of their clients have changed dramatically since the 1980s, when most of their clients were affluent, well-educated gay white men whose sense of community provided a measure of support during their illness. The service needs of gay men differ markedly from those of the more recent clients: increasing numbers of women, many of whom have families that are also directly or indirectly affected by AIDS; members of racial or ethnic minorities; people with behavioral comorbidities; and people who are homeless.
Providers are finding that the approaches they had developed, while effective for serving gay men, often do not work well for other clients. Some providers, at least initially, have felt overwhelmed and inadequately staffed to help the newer population. In some instances, providers have undergone what could be termed "culture shock" in serving more disadvantaged clients. Take for example, GMHC's experience with its Meals Program. This program, which serves more than 50,000 meals each year on site as an opportunity for socialization and good nutrition to maintain health, was originally conceived as a service for people who were accustomed to dining out but no longer felt well enough to do so. Some of GMHC's newer, more disadvantaged clients had never had a meal served to them before coming to the Meals Program.
These fundamental changes in client characteristics have served as important reminders to providers to rethink their models of outreach and service delivery, the types of services they provide, and the qualifications of staff who provide the services. Table III.3 provides an overview of the many challenges providers described and their responses to them. However, some of the challenges they face (for example, shortages of substance abuse treatment programs or uncertainties surrounding managed care) clearly lie beyond the ability of individual providers to address directly, but instead pose challenges to policymakers and planners.
1. Women with Families
Providers have found serving women with families to be complicated for a number of reasons. First, most women with AIDS put their own, usually extensive, health care needs after those of family members. Cultural norms may exacerbate this problem. Los Angeles providers noted that Latinas are not traditionally encouraged to be assertive in addressing or even discussing their needs. Second, when women come in for services, the "client" is actually the entire family--a group of people with numerous, different types of needs. Other family members may be infected but may not seek care. Potential care partners (spouses and other companions), when women have them, may provide assistance, but often they do not. In fact, they may erect barriers to formal care providers by aggravating already chaotic living conditions. Third, children and adolescents, in particular, need to deal physically and emotionally with their mothers' inability to provide expected care and with the grief associated with the loss of one or both parents. Children need assistance in staying in school and in avoiding drugs and risky sex; adolescents need serious and useful AIDS-prevention advice. (Providers noted that the sense of invulnerability most adolescents normally experience tends to undermine any message from a relative with AIDS about avoiding risky behaviors.) If the mother dies (or if both parents die), children may need to be adopted or placed in foster care. This may be complicated to arrange as well as difficult for children to adjust to. Finally, safe, secure housing is more difficult for families than for individuals without children to find.
| TABLE III.3. The Changing AIDS Environment: Provider Challenges and Responses | |
| Challenges Faced by Providers/Gaps Faced by People with AIDS | Approaches Taken by Case Study Programs |
| Increased Numbers of Infected Women/Families | |
|
|
| Increased Numbers of Poor People from Racial/Ethnic Minorities | |
|
|
| Increased Numbers of People with Behavioral Comobidities | |
|
|
| Increased Number of Complex Cases More Generally | |
|
|
| Changing Service Needs as a Result of Improved Treatment | |
|
|
| Pressures to Control Costs | |
|
|
| SOURCE: Project case study discussions conducted in New York City and Los Angeles between April and June 1997. | |
The primary approaches providers are taking to serving women with AIDS has been to increase their linkages to family service organizations and housing providers and to develop or expand in-house specialized programs for women and families. For example, it is outside the mandate of VNSNY, as a provider of Medicaid home health care, to furnish extensive counseling to children of infected mothers or to spend substantial time locating appropriate housing or getting women placed on public assistance. VNSNY refers women with these needs to other agencies but provides additional support directly through several programs funded by public and private grants, including Community Outreach to Adolescents of Parents with HIV/AIDS, which provides a short-term intervention to help adolescents understand and accept their parent's illness, resolve issues related to death and dying, adjust to new surroundings, and resolve behavior difficulties; the Pediatric Respite Program, which gives parents caring for children with HIV/AIDS respite by providing in-home care by specially trained staff; and the AIDS Mental Health Program, which provides licensed therapists to perform mental health assessments and provide in-home counseling to individuals who are homebound or in crisis.
GMHC has been increasing its outreach to women in recent years, having introduced support groups for lesbians and heterosexual women with HIV/AIDS and holding forums on research, prevention, and treatment issues specific to women. Enrollment in GMHC's Child Life Program increased by 50 percent in 1996, and the program extended its babysitting hours to better accommodate parents using other GMHC services.
The AIDS Healthcare Foundation in Los Angeles has teamed up with a specialized women's health and social services program, Prototypes, to deliver HIV-related medical care at the Prototypes center. Prototypes provides a range of support services for women and families (with and without HIV/AIDS). AIDS Healthcare Foundation staff reported that the collaboration was working well but that as yet few of them were involved.
2. Poor Members of Minority Groups
Poor minority group members with AIDS face other types of problems. First, they have difficulty gaining access to a full range of needed services, because not all types of services are available in all neighborhoods. This problem was noted repeatedly in both cities, where services tend to be clustered in central and more prosperous areas and less available in poor areas, which often contain large minority populations. Second, some minority group members do not trust nonminority providers or "establishment" medical interventions. Several providers noted that many black men and women resist enrolling in clinical trials or trying new pharmaceutical treatments because of incidents like the Tuskeegee syphilis experiments. Third, cultural differences between workers (particularly, home care workers) and clients from different ethnic groups can lead to disagreements over meal preparation or the appropriate role of a spouse as caregiver, among other conflicts. Finally, the stigma associated with homosexuality and AIDS, particularly among Hispanic people, has made it especially difficult for them to seek and obtain adequate care, in part because they often keep their HIV status a secret even from other household members. This secrecy often results in even greater obstacles to adhering to complex treatment regimens.
Providers have taken a number of approaches to increase outreach to and improve services in minority communities. GMHC has increased educational forums in minority communities, helps smaller AIDS service organizations in minority neighborhoods to apply for grants, and contributes financially to a pool that provides resources to smaller organizations. Village Center for Care expanded the catchment area of its home health agency to include Brooklyn in addition to Manhattan. All providers have become more sensitive to cultural differences, and some, like VNSNY, have attempted to match workers and clients more carefully to minimize conflict. AltaMed staff emphasized how important it has been to use indirect or subtle language and approaches with its Latino/a clients to elicit full participation in their own care. They noted that support groups often provide a more comfortable setting than one-on-one counseling sessions to confront issues concerning HIV and sexuality.
3. People with Behavioral Comorbidities
Providers have found that people with AIDS who also have behavioral comorbidities (most notably those who have problems with substance abuse or who have serious mental illness) have particular difficulty showing up for regular medical appointments and adhering to treatment regimens (whether or not the latter include protease inhibitors). In the face of behavioral problems, providers who formerly used service provision models with the goal of empowering clients to advocate and arrange for services for themselves find this strategy unworkable, so they have adopted a more "hands-on" approach. Staff from the GMHC and Village Center case management programs (which both serve high proportions of clients with behavioral comorbidities) arrange services for clients and provide intensive followup. They will also escort clients to appointments with physicians and public assistance agencies to make sure that clients make scheduled appointments and interactions go as smoothly as possible. Programs that provide, as does GMHC, emergency cash grants or tickets to entertainment events consider, more often and more carefully, whether clients will sell the tickets and use the cash or grants to purchase alcohol or drugs.
Clients with behavioral problems are more likely to be abusive to or threaten staff and are more likely to have dangerous living situations that pose a threat to staff safety. Safety is a particular problem for home care workers. APLA staff noted that it had to deal with its first incidents of violence and threats to staff only in the last year and developed written policies to address these problems. VNSNY and the Village Center home health agency reported taking an incremental approach to worker safety. Most frequently they send workers in pairs if there is a concern about safety and conduct visits in the morning when the likelihood of dangerous confrontations seems to be minimized. If this is not sufficient, VNSNY sends security guards along with its nurses. (Each of these remedies adds substantially to the cost of a visit.) In the worst case, clients are discharged from home care and referred (or referred back) to the criminal justice or mental health systems.
As a greater number of people with AIDS also have behavioral problems, providers also reported a need for increased interaction and shared knowledge between traditional AIDS service providers and mental health and substance abuse treatment providers. In particular, they noted the paucity of research about the interaction between psychotropic medications and AIDS medications, and whether specific psychological disorders in people with AIDS (for example, depression) are best treated with medication or with counseling. They also noted an overall shortfall in the availability of mental health services and substance abuse treatment. Because of these perceived inadequacies of mainstream mental health providers, two of the providers we spoke with are developing (or expanding) mental health expertise in house. Village Center is considering opening its own AIDS-specific mental health program. APLA is increasing the number of social workers and planning to increase the number of mental health professionals on staff. (Interestingly, developing partnerships with mental health and substance abuse treatment providers were not mentioned as an approach to filling this service gap.)
AIDS service providers have long been frustrated in their attempts to stop clients from engaging in risky behaviors (unsafe sex or needle sharing). These efforts seem even more futile with clients who also have behavioral problems. This frustration, which becomes demoralizing to program staff who believe they should be able to change harmful client behaviors, has led New York providers to adopt an approach they refer to as "harm reduction." Harm reduction establishes criteria for acceptable behavior that clients must meet as a condition of receiving services (for example, requiring that the client not use or purchase drugs while the worker is present). This approach also allows workers to acknowledge that they may not be able to change all undesirable client behaviors. Both VNSNY and Village Center staff mentioned adopting a harm reduction approach; GMHC describes harm reduction approaches in training materials it distributes to other providers. VNSNY's client education materials specifically state that clients may not take drugs or drink when staff are present, nor may they ask staff to purchase drugs or alcohol for them. Village Center case management staff noted that they time contacts with clients who are substance abusers so that they see them each month only after Supplemental Security Income (SSI) checks have been spent on drugs. When clients are at least temporarily without the distraction posed by drugs, they can turn more of their attention to their health and subsistence needs.
4. Complex Cases More Generally
Increased numbers of complex cases of all types have led to a number of general challenges. First, AIDS service organizations, with roots in the early days of the epidemic, have traditionally included many nonprofessional volunteers. Such volunteers, sometimes referred to as "buddies," are invaluable to clients who only have a few months to live and require companionship and assistance with daily living tasks. As just described, however, many newer clients have multiple social, economic, and psychological problems and are not terminally ill. Providers have found that buddies and other nonprofessional staff, while excellent sources of end-of-life care, are simply not equipped to help clients with complex problems and chaotic lives. It is noteworthy that GMHC's case management program (which serves clients with the most complex problems) uses nonprofessional staff only in clerical positions. Similarly, APLA has increased the educational and experience requirements for its case managers and has introduced trained, designated case managers for handling the needs of increasing numbers of homeless clients. The sheer numbers of such complex clients have also strained case management resources. Village Center's case management program and APLA use a multitiered system to assign the most dysfunctional clients to higher levels of case management. AltaMed is considering a similar strategy.
Second, as a corollary to the increase in clients with more complex problems, there is an increase in clients who are homeless or living in shelters or single room occupancy hotels. Staff remarked that such clients are among the most disenfranchised and distrustful they serve. Village Center found engaging them usually requires visiting with them in their homes (that is, in shelters and hotels) rather than requiring them to come to program offices. AltaMed uses a mobile van to provide outreach to homeless people at high risk of becoming HIV-infected and has recently seen an increase in the number of substance abusers who come to them through this type of outreach. GMHC has increased outreach in drug treatment centers, homeless shelters, and prisons.
Finally, clients who are very poor and disenfranchised must have their subsistence needs met before they can begin to address their health care needs. This has required AIDS providers to interact more frequently and more intensely with public assistance and housing programs. Providers in both cities noted that publically funded housing assistance programs did a good job as far as they went (for example, the federal Department of Housing and Urban Development program, Housing Opportunities for People with AIDS [HOPWA] and New York City-funded housing programs for people with AIDS). However, a severe shortage of affordable, secure housing is a serious problem for all New Yorkers and Los Angelinos with low incomes and is particularly acute for people with AIDS who have families, behavioral comorbidities, or other complex problems.
5. Improved Treatment and Changing Services Needs
Improved medical and pharmaceutical treatment has led to increased life expectancy and improved health for people with HIV and AIDS. Providers noted that they feel compelled to address social, economic, and behavioral problems that were largely tangential to AIDS care when the average time between their first client contact and the client's death was six months. In addition, as pharmaceutical treatment has grown more complicated, the need for assisting clients involved in making treatment decisions has grown, and the knowledge base needed to provide this assistance has also expanded rapidly. Treatment advocacy programs, which originally had the goals of increasing access to clinical trials and advocating for better treatment options, now must also provide information to clients and medical providers about a complicated array of medications, now including the protease combination therapies. The technical complexity of this information has led APLA to consider adding nurses to its lay treatment advocacy staff.
Individuals receiving treatment for AIDS, particularly with protease inhibitors, need assistance adhering to what is currently a very complicated treatment regimen and monitoring carefully what can be life-threatening side effects. AIDS Healthcare Foundation has planned transitional residential support to stabilize some clients on protease combination therapy to maximize the likelihood that they successfully adhere to the regimen when they return home. APLA is considering providing special training to buddy volunteers so that they can assist clients with treatment adherence.
Finally, many people who thought they were going to die have been successful with the new combination therapies and now find themselves likely to live. Many require vocational rehabilitation because they have been out of the workforce and highly debilitated for so long. Some have never held jobs before and now desire employment training. Those who return to work, however, worry about the loss of public assistance, and they face a particular dilemma if they lose eligibility for Medicaid, which pays for the medications that are keeping them healthy. Others accumulated high levels of debt when they expected to die. GMHC and APLA have developed new return-to-work programs and have stepped up their legal assistance programs in response.
6. Pressures to Control Costs
Pressures on AIDS providers to control costs come from the growing role of managed care in health service delivery, from efforts to control public fee-for-service spending, from the high cost of new pharmaceutical treatments, and from a decrease in private donations. At present, New York AIDS service providers have had little direct experience with managed care because most of their clients are covered by the Medicaid program, which has not yet started enrolling beneficiaries with AIDS in managed care. Even in Los Angeles, where Medicaid managed care penetration is greater, enrollment of beneficiaries with AIDS in managed care is not mandatory, and home- and community-based services tend not to be included in capitation payments. Furthermore, APLA and AltaMed have not been greatly affected by managed care because their funding is primarily from grants and donations. Medicaid managed care for people with AIDS in New York has been in the planning stages for several years and will eventually arrive in the form of Special Needs Plans for people with AIDS and for people with serious mental illness (as a condition of the state's 1115 waiver). Both Village Center for Care and VNSNY are considering different partnering arrangements with large medical providers for Special Needs Plans. All three New York providers were considering marketing (or were currently trying to market) different service packages to managed care organizations (for example, mental health and counseling, disease management, specialty long-term AIDS care).
Providers noted that quantitative data and other needed information is largely lacking to answer key questions about providing managed care for people with AIDS and that this lack of information, combined with the expectation (particularly in New York) that managed care will eventually be the norm for Medicaid beneficiaries with AIDS, has brought with it a measure of anxiety. Providers were concerned about a lack of information to make rational decisions concerning how payments would be adjusted and financial risk managed to ensure that managed care organizations have financial incentives to provide high-quality care, including AIDS specialty care and cutting-edge pharmaceutical treatments; and whether and how home and community-based services would be included under capitation arrangements.
Developing a comprehensive network of AIDS specialists was not a problem for Positive Healthcare, the Medicaid managed care plan of the AIDS Healthcare Foundation, because Positive Healthcare relies on AIDS Healthcare Foundation's already well-developed network. However, Positive Healthcare has had its share of financial difficulties. Risk/profit-sharing arrangements were one source of lower-than-expected revenue. Positive Healthcare receives a capitation payment for outpatient medical care but also has prior approval authority over inpatient services. It believed that its risk-sharing arrangement applied only to those services over which it had authority--inpatient hospital and medical specialty care--whereas the state reportedly included some services Positive Healthcare does not control (like home- and community-based waiver services). Positive Healthcare had also decided to cover protease combination therapy, although its high cost was not figured into its capitation payment, which contributed further to their financial loss. (They no longer cover these medications under capitation.) Both Positive Healthcare and the Medicaid program agree that the methodology used to develop Positive Healthcare's capitation payment was imperfect. As is typical in Medicaid and Medicare managed care, the methodology relies on historical fee-for-service spending, discounted for expected managed care savings. However, this approach may miss certain types of costs, such as disproportionate share payments to hospitals and spending associated with increases in service use as a result of improved access to services under managed care.
In the meantime, in the face of anecdotes about the catastrophic consequences of primary care gatekeepers who lacked sufficient AIDS expertise to make appropriate referrals, GMHC has stepped up efforts to teach clients already in managed care how to negotiate the system and intensified its lobbying efforts with the state and HMOs to ensure that Special Needs Plans and private managed care provide the appropriate range and quality of care for people with AIDS.
Concern over future pressures to control public AIDS spending in the fee-for-service sector have heightened tensions that tend to stay just below the surface when funding seems more secure. The provider communities in New York City and Los Angeles were described as generally collaborative and cooperative, but this was attributed at least in part to AIDS service-funding levels having been generous over the last few years. Nonetheless, in New York there appeared to be some tension between large providers who offer a range of services and smaller, neighborhood-based providers who offer just one or two services. Some staff at GMHC stated that smaller providers were less efficient and that people with AIDS preferred a one-stop-shopping approach to care. (In this spirit, later in 1997 GMHC planned to open an HIV testing center in conjunction with an outpatient clinic to be operated by New York Hospital.) These factors notwithstanding, there is a measure of cooperation between large and small organizations, most visibly in referrals of clients between providers of different sizes, and GMHC, in particular, has a long history of providing technical assistance to smaller organizations.
More prominent in Los Angeles were long-standing tensions between medical and social services providers concerning who had the best interests of the clients at heart and who should oversee service coordination. Medical providers tend to believe they should be given control over care coordination in light of the complexity of the new pharmaceutical treatments. Social services providers typically worry that this control would inappropriately medicalize support services.
Joint ventures between medical and social services providers have not been the norm and appear to be difficult to implement successfully. For example, AIDS Healthcare Foundation had subcontracted with APLA for case management services and agreed to pay APLA $55 per member per month. AIDS Healthcare Foundation also expected APLA to "market" Positive Healthcare and make referrals to the plan. When referrals were not forthcoming, the subcontract was terminated. Providers noted the increased presence of managed care, and any future reductions in fee-for-service Medicaid and Ryan White funding could heighten existing tensions and reduce levels of cooperation in the future.
Finally, the decrease in the population of gay men with AIDS has led to a decrease in private donations among traditional contributors who were part of or sympathetic to the gay community. Similarly, the favorable publicity protease therapy has received has also dampened private donations among individuals who view it as heralding "the end of the epidemic." This has been a particular problem for APLA and GMHC, which rely on private donations for more than 70 percent of their revenue. In response, APLA has reduced its staff by 15 percent and is currently evaluating its programs and scope of services using surveys of clients and reviews of program records to identify high-priority services and unmet needs. Additionally, GMHC has stepped up its fundraising efforts from institutional donors because the cost of generating contributions from individuals is so high. Providers also fear that as the epidemic moves away from the politically cohesive and affluent gay community, AIDS service delivery will receive less attention and thus less public and private funding.
7. Summary
Home- and community-based AIDS service providers are changing both the types of services they offer and their service delivery approaches in response to growing numbers of disadvantaged clients who are living longer, healthier lives as a result of improved AIDS treatment. Providers have found that service delivery models that worked well for earlier clients (namely, end-of-life care for relatively affluent and well-educated gay men) must be modified for newer clients with longer-term and more complex problems (for example, behavioral comorbidities, lifelong poverty, and families also in need of support). Provider response to increasing numbers of multiproblem clients has included broadening the range of services they provide in house, increasing referrals to and interactions with providers in other systems (mental health, substance abuse treatment, housing, and public assistance), reconfiguring staffing to include more trained professionals and fewer lay staff and volunteers, and developing procedures to identify clients with the most complex problems for the most intense services. Thus, the combination of more program clients living longer and with more complex problems increases service costs to providers and the Medicaid and Ryan White programs just when pressures to control or reduce spending are mounting.
Very few home- and community-based service providers have had substantial direct contact with managed care, because most Medicaid managed care plans have so far either carved out people with disabilities and chronic illnesses like AIDS or have carved out home- and community-based services.12 Nevertheless, providers see Medicaid managed care for their clients just over the horizon and are concerned that many important questions about managed care for people with AIDS (and other chronic illnesses) have not yet been answered: how to set payment rates and manage financial risk in a way that will promote quality medical care (that is, provide specialty care and state-of-the-art treatments); and whether and how to include under capitation home- and community-based care such as that now provided through Medicaid waivers and the Ryan White program. Providers are concerned that they will have difficulty making rational decisions about key managed care parameters because not enough data exist describing current patterns of service use among different groups of people with AIDS and not enough is known about the cost-effectiveness of different types of home- and community-based services. The experiences of the one Medicaid managed care provider in our case study only underscore the difficulties of setting payment rates and developing risk-sharing procedures.
IV. THE NEED FOR HOME- AND COMMUNITY-BASED SERVICE DATA
An important lesson from the case studies, and one that is underscored by the literature, is that there is urgent need for data describing the use and costs of home- and community-based services by people with AIDS. These data are needed to support key decisions about managed care and to help planners and providers identify and implement cost-effective interventions as financial resources grow tighter. Two broad types of data are needed. The first type comprises representative time-trend databases that can describe patterns of service use and mortality, variations in them over time, and variations across different groups of people with AIDS. Such databases track the course of the epidemic and provide data that describe service supply and demand and that can be the basis of use and cost benchmarks. The second type of data come from focused data collection efforts to support the development and testing of hypotheses concerning effective interventions. Such evaluation data need to track evaluation sample members for a period long enough to assess intervention outcomes.
Ideally, both types of databases would include person-level descriptors of the following:
- Demographic and socioeconomic data and clinical information to identify particular groups of people with AIDS and to control for key differences in individuals that affect service use
- Service use and expenditure data (service type, duration, intensity, location, charge/reimbursement) from all public and private sources, as well as from unpaid sources
- Medication use (type and dates used) to track the effect of treatments (like protease combination therapy) on service use
- Participant outcomes, such as satisfaction, health, well-being, mortality, and other quality indicators.
A. NATIONAL AND STATE DATABASES
Administrative service-use and financial data from payers (such as Medicaid, Medicare, and Ryan White) and surveillance data from the Centers for Disease Control and Prevention have been used to develop the first type of database, (see, for example, the analysis of New Jersey Medicaid data in Chapter V of this report, Fasciano et al; 1997; and Anderson and Mitchell 1997). Payer data sets provide a comprehensive and reasonably accurate picture of use and spending for services covered by the payer. Payer data contain only limited sociodemographic and clinical data, which makes it difficult to describe service use for particular subgroups of people with AIDS, particularly subgroups defined by risk group or level of informal care. When data come from payers that finance care to people in addition to those with AIDS, developing an AIDS-specific database requires identifying people with AIDS within the larger population. Typically, such identification relies on case-finding algorithms based on diagnosis codes (as in Thornton et al. [1997], which identifies Medicare beneficiaries with AIDS) or matching administrative service use records to an AIDS registry (as in the case of the New Jersey Medicaid analysis in the following chapter).
The Agency for Health Care Policy and Research has contracted for two surveys to assemble comprehensive databases describing the characteristics of and services used by people with HIV and AIDS. Although the surveys address some aspects of home health care and long-term care, they do not address home- and community-based services in detail. The first survey, the AIDS Cost and Service Utilization Survey (ACSUS), was conducted over an 18-month period in 1991 and 1992. The second survey, the HIV Cost and Services Utilization Study (HCSUS), commenced in early 1996 and is scheduled for completion in 1998. In addition to service use and spending, HCSUS will examine quality of care, access to care, unmet health needs, quality of life, social support, knowledge of HIV, and clinical outcomes for 3,700 adults with HIV. HCSUS currently includes only a limited number of questions about home- and community-based services, but these could be supplemented for later waves of the survey.
National and state databases such as these have been the source of much of what is currently known about changes in service use, population characteristics, and mortality over the course of the AIDS epidemic. Service use and spending estimates from these databases have served, and will continue to serve, as benchmarks for emerging provider-specific interventions and evolving managed care plans for people with AIDS. Correlations between service use, individual characteristics, and mortality derived from large, representative databases (for example, correlations between pharmaceutical treatment and service use) suggest hypotheses that deserve formal testing.
B. PROVIDER DATABASES
Provider databases, although more narrowly defined, may offer an opportunity to observe service use trends over time for special AIDS populations (namely, clients of specific providers), as well as to develop hypotheses about and support evaluations of promising interventions. For both operational and financial purposes, AIDS service providers often maintain extensive databases that clearly identify people with AIDS. The site visits conducted as part of this project's case studies collected information describing the databases of the selected providers by speaking with data managers and by reviewing database documentation. Table IV.1 provides an overview of the findings from this investigation.13
The six providers have databases that can collect extensive client-level sociodemographic and clinical data at intake or other points in time. In addition to basic demographic data (sex, race, and date of birth), they collected information on important predictors of home- and community-based service use, such as transmission risk group and potential level of informal care (as captured by marital status and household composition). All had information on type of insurance (including Medicaid). Several providers also collected information about level of education and employment status. Providers collected different types of information that could be used to describe AIDS stage of illness: diagnosis date, AIDS-related illnesses, and CD4 counts. Most also collected information describing functional and cognitive status.
The six provider databases collected extensive information describing service use, but only three collected information about spending (billed amount or paid amount). Service use data included date of a service encounter, type of service provided, and units of service. (Four of the six collected all three data items describing service use; two collected only date and type of service.) Although provider databases contain some of the same service use information as payer files, they also contain information on the use of services not documented elsewhere (for example, legal and employment services provided by APLA or GMHC or residential treatment adherence services provided by AIDS Healthcare Foundation). For those databases that include no spending data, it seems likely that researchers or providers could estimate unit prices for most services. If databases were to be combined across providers, and if some had spending data but others did not, it might be desirable to use estimated, rather than actual, spending for all providers as a matter of comparability.
The six providers also collected identifiers that could allow information in their databases to be linked to Medicaid and Medicare eligibility and claims files. (One provider also maintained a Ryan White identifier, potentially allowing a link to client-level Ryan White administrative files.) Linking home- and community-based provider databases to Medicaid and Medicare data files would be useful for studying the relationship between the use of home- and community-based services and medical care and other reimbursable services delivered by other providers. Linked payer/provider databases also allow for the study of administrative use and spending data in the context of sociodemographic and clinical characteristics. Payer/provider linkages could be made, however, only if they did not violate provider/client confidentiality agreements.
| TABLE IV.1. Automated Person-Level Data Maintained by Case Study Programs | ||||||
| Types of Data Available | Gay Men's Health Crisis | Village Center for Care | Visiting Nurse Service of New York | AIDS Healthcare Foundation | AIDS Project LA | AltaMed |
| Sociodemographic Characteristics | Sex, race, date of birthEducation, languageMarital statusHousehold compositionTransmission mode InsurancePublic assistance eligibilityVeteran status | Sex, race, date of birthEducation, languageMarital statusHousehold compositionTransmission mode Insurance | Sex, race, date of birthaLanguage Marital statusInsurance | Sex, race, date of birthCitizenship, languageMarital statusNumber of dependent childrenSexual orientation InsurancePublic assistance eligibilityEmployment status | Sex, race, date of birthLanguage Living arrangementSexual orientationTransmission modeInsurancePublic assistance eligibilityb | Sex, ethnicity, date of birthLanguage Marital statusFamily and household sizeSexual orientationHIV risk factorsHomeless statusInsuranceEmployment statusIncome |
| Clinical Information | AIDS diagnosis dateAIDS-related illnessesImpaired vision, hearing, mobilityWhether homeboundReferral source | AIDS-related illnessesTB or heart conditionPhysical disabilityMental statusLab test resultsReferral source | Primary and secondary diagnosesSurgical procedures preceding admissionMedicationsFunctional statusMental status Referral source | AIDS and HIV diagnosis datesMost recent CD4 countHospitalization/ associated diagnosisCurrent medicationsSubstance abuse | AIDS and HIV diagnosis datesCD4 count, viral loadFunctional status | AIDS and HIV diagnosis datesCDC disease stageTB, STD statusPregnancySubstance abuseMental illness |
| Program Service Use | Date of serviceType of serviceNumber of contactsDuration of contactsAmount of cash grants | Date of serviceType of serviceVisitsMedications | Date of serviceNumber of visits/hoursType of service | Date of serviceProcedure codeProvider | Date of serviceType of serviceUnits of serviceProvider | Date of serviceProcedure codeProvider |
| Program Service Cost/Reimbursement | No | Billed amountPaid amount | Billed amountPaid amount | Billed amount | No | No |
| Linking Identifiers | Social Security numberMedicaid numberMedicare number | Social Security numberMedicaid numberMedicare number | Social Security numberMedicaid numberMedicare number | Social Security numberMedicaid numberMedicare number | Social Security numberMedicaid numberMedicare numberRyan White number | Social Security numberMedicaid numberMedicare number |
| Cases or Data Items Excluded | Clients only in education programs | None | None | Positive Healthcare clients do not have service use data | Clients only in education programs | None |
| History Versus Snapshot | Sociodemographic and clinical data are snapshots at intake; service use data are historical dating to the start of the GMHC database and are not currently being archived | Sociodemographic and clinical data are current snapshots; all diagnoses are maintained; service use data are historical dating to the start of the VCC database and are not archived | Sociodemographic and clinical data are snapshots at intake (updated in comment screens); service use data are historical and are archived to tape periodically | Sociodemographic data are snapshots at intake; clinical data are current snapshots; service use data are historical | Clinical data are current snapshots; service use data are historical | Sociodemographic and clinical data are current snapshots; service use data are historical |
| Reported Problems | None | Non-billing-related data may be supplied in only 50 to 75% of cases | None | Many data items not consistently collected; databases cannot be linked across sites | None | None |
SOURCE: Project site visit discussions and documentation.
| ||||||
Provider database managers noted several known problems or shortcomings of the databases. First, like many managed care plans, Positive Healthcare, the Medicaid managed care plan operated by AIDS Healthcare Foundation, does not maintain client-level service use data. This is unfortunate because Positive Healthcare is one of only a few Medicaid managed care plans currently serving people with AIDS. Village Center staff reported that individual data items not directly related to billing could be missing in from half to three-quarters of their records. (Presumably this would include primarily sociodemographic and clinical data that staff keep in client charts but fail to enter into the database.) Similarly, AIDS Healthcare Foundation staff noted that not all data items are collected consistently. It seems likely that all six databases would have some degree of missing data. Thus, the databases of these six organizations have the potential to provide extensive clinical and sociodemographic data, but in practice these data may not be present. Provider staff might not enter these data into automated systems, because their data-keeping orientation remains geared toward client charts and other types of hard-copy documentation.
Assessing the extent and seriousness of missing data would necessarily be a crucial component of testing real data from any provider database being considered for a research project. Providers selected for research projects that included retrieving information from their databases could be requested to take steps to minimize missing data (and perhaps be offered a financial incentive to do so), particularly data items normally available in hard copy. It might even be possible, but more expensive, to retrieve such missing data for historical case records. On the other hand, developing programs and procedures to maintain person-level service use would likely be a very costly undertaking for a managed care plan such as Positive Healthcare, since it involves redesigning databases and changing recording procedures.
All providers stated that they would be willing to share databases with government-sponsored research projects if confidential data could be adequately protected. We found this encouraging, but somewhat surprising, since AIDS service providers have traditionally been reluctant to participate in such endeavors at all because of concerns about client confidentiality. However, the case study providers may have been unique in that many have a longstanding interest in conducting research. Staff from some providers publish articles containing quantitative information generated from the databases; all generate end-of-year descriptions of clients and service use, among other reports.
C. POTENTIAL USES OF PROVIDER DATA
Provider data have the potential (1) to address issues concerning levels of use and spending for a particular set of home- and community-based services (namely, the services offered by individual providers or a group of providers), and (2) to answer questions about the effectiveness of specific provider interventions. Clearly, provider databases are likely to describe not the full range of AIDS-related home- and community-based services used by clients, but only those services the provider offers. Even very large provider caseloads are unlikely to be entirely representative of the larger AIDS population in a city or state. Nonetheless, provider data could be a useful source of specialized service use and spending information.
In addition to offering overviews of service use, provider databases have the potential to generate data to evaluate the cost-effectiveness of specific interventions (for example, the AIDS-specific mental health program Village Center is considering or the AIDS Healthcare Foundation's residential program for stabilizing multiproblem clients on medication regimens). If providers had enough clients who were eligible and interested in trying the interventions, they could be randomly assigned either to the new intervention or to services provided in the conventional way (for example, mental health services from a generic mental health provider in the case of the former, community-based medication adherence assistance in the case of the latter).14
The available provider data combined with program expertise could also play a role in developing practice guidelines and creating quality assurance procedures and indicators for interventions shown to be effective. Practice guidelines usually include a structure for identifying client needs, steps clients and providers can take to meet identified needs, a schedule for carrying out those steps, and expected client outcomes indicating that needs have been met.15 Quality assurance procedures and indicators provide a framework for systematically comparing service interventions. Provider databases can play an important role in the development of practice guidelines and quality assurance procedures and indicators (either by themselves or linked to payer data) by serving as the basis for benchmark estimates of overall service use patterns (for example, number of visits per month, duration of treatment, and duration and timing of followup), of service use by subgroups of clients, and of potential quality indicators (such as levels of unmet need for assistance with medication adherence or daily living tasks or rates of hospitalization for Pneumocystis carinii pneumonia). However, while data analysis can support the development of guidelines and quality assurance procedures, their actual development relies primarily on the efforts of panels of providers, consumers, and other experts.
D. NEXT STEPS
A number of tasks must be undertaken before provider databases can be used either for basic descriptive service-use analysis or to evaluate the cost-effectiveness of a specific intervention (see Table IV.2). The first set of tasks concerns selecting databases to meet specific research study goals. For example, if the goal of the study is to provide timely, descriptive analyses of overall and subgroup-specific service use, one might consider combining the databases of a number of providers into a quick-turnaround data system. One approach would be to select cities (or other communities) regarded as barometers of AIDS service delivery and to then select within these cities providers to that already have well-developed, roughly comparable data systems. (This approach is similar to the Sentinel Communities approach taken by the Center for Studying Health Systems Change and the approach used to develop the ACSUS sample.) Quantitative data and focused qualitative information from these providers could then be used to describe service-use patterns, population characteristics, and emerging practice approaches for different groups of people with AIDS.
A second set of tasks further investigates the procedures through which access could be gained to provider databases for a given research project. First among this set of tasks is verifying that the provider databases are in fact available for the envisioned research project. As noted, site visitors for this project were told that, in principle, databases could be made available for government-sponsored studies. However, a formal request stating the purpose of the research would have to be made to providers, and confidentiality procedures would govern the use of the data. Providers might have to clear such requests with their institutional review boards.
| TABLE IV.2. Tasks for Investigating the Usefulness of Provider Databases |
| Identify research study questions and provider databases that have the potential to address the questions either alone or in combination with payer or additional provider databases |
Investigate procedures to access selected databases and to link to other databases, if necessary
|
Test provider data and design research database
|
The second step in this task is deciding whether the envisioned research project requires linking provider records with Medicaid, Medicare, or Ryan White administrative files. The provider must then be asked whether such a link can be carried out without violating provider/client confidentiality agreements, and permission must be granted by the relevant public program(s). If it is feasible to link provider and administrative records, a process must be set up for doing so that includes the relevant public payers. Providers may prefer to do the linking themselves and then delete identifying information from records before turning them over to a research contractor. On the other hand, providers are unlikely to have the programming resources for such an undertaking.
The third step is deciding whether it is desirable to include the databases of other providers from the same cities as those included in the case studies or from other cities. If so, exploratory discussions with providers (such as those undertaken for this project) need to be conducted for assessment of the content and accessibility of their databases for the envisioned research, followed by detail-oriented discussions. Similarly, further investigation of the contents and accessibility of the new New York State AIDS Institute database might be warranted.
The final step is identifying whether there was a need for primary data collection to support database analysis (for example, client surveys to obtain additional client outcomes or to follow up with clients after they left the provider program, or site visits to better understand specific interventions). Furthermore, if it was necessary to track client service use and outcomes over time, a process for receiving data at intervals would have to be developed with providers. If it was necessary to track clients after they left a program (for example, as part of a cost-effectiveness analysis), a survey to obtain follow-up information directly from individuals might have to be developed.
A third set of tasks concerns testing data from provider databases and designing a research database that integrates them (if the research project will combine data from more than one provider or from some other source). The first step here involves getting test data files and assessing any differences between program data documentation and actual data, then assessing the extent of missing information and whether missing data might be retrieved from hard copy. (As noted, database managers mentioned that some fields were more consistently filled in than others.) Second would be investigating how specific data items are coded and developing an approach for making coding as uniform as possible (again, if the goal is to integrate databases across providers). The third step would be determining whether it was possible to build and how to build key constructed variables from provider databases. For example, if CD-4 count or AIDS-related illness snapshots were chosen to identify groups of people at different stages of AIDS, some judgment (based on input from physicians familiar with AIDS staging) would be needed in defining the period of service use to which the recorded CD-4 counts or illnesses could reasonably be applied.
E. CONCLUSION
There is a clear need both for large representative databases that can provide timely descriptions of home- and community-based service use trends among people with AIDS and for focused data collection to identify and evaluate promising interventions. In Chapter V, we describe an approach to linking Medicaid and AIDS Registry data to create the former type of database. Provider data systems have the potential to be the basis of the latter type used for highly focused analysis and for quick-turnaround systems. The databases of the six case study providers appear to hold the potential to support interesting research studies. However, before a research study can be undertaken, in addition to identifying and designing research projects for which these databases might be appropriate, formal permission to gain access to them must be requested and received from providers, and data must be examined for completeness and consistency.
V. PATTERNS OF UTILIZATION OF HOME CARE SERVICES AMONG MEDICAID RECIPIENTS WITH AIDS IN NEW JERSEY16
In framing the overall research questions for this study (see Chapter I), ASPE noted the need for information on (1) what home- and community-based services are used by which individuals within the population of people with AIDS; (2) the costs of care for people with AIDS who use home- and community-based services, and (3) variations in costs by patient population and other key factors. The New Jersey analyses were undertaken to address these questions. Specifically, the aims of these analyses were:
- To identify the characteristics of users of home care services in a diverse statewide population of people with AIDS on Medicaid
- To analyze patterns of use of particular types of home care services (such as skilled nursing services and paraprofessional services)
- To estimate total Medicaid expenditures associated with home care use and the breakdown of these costs by type of home care service
- To determine the variation in service use and cost patterns across different AIDS subpopulations (for example, by HIV risk group, minority status, geography, and gender)
- To estimate multivariate models to identify factors that predict home and community-based service use and costs
- To explore the association between home- and community-based care and inpatient hospital use
A. BACKGROUND
New Jersey provides an important opportunity for the study of home- and community-based care for AIDS patients. The state has a large and diverse AIDS population, with good representation of major subgroups but a higher proportion of minorities, injection drug users, and women than the national AIDS population (see Table V.1). The national AIDS population is evolving to look more like New Jersey's AIDS population, as discussed in Chapter II, with increasing numbers of injection drug users, blacks, and women. Therefore, in many respects New Jersey's AIDS population can be seen as a leading indicator of the future of AIDS care.
New Jersey is a major epicenter of the epidemic, ranking fifth among states in cumulative AIDS cases. The state has emphasized home care services in its development of HIV/AIDS care policies and programs and was a recognized innovator in developing the nation's first AIDS-specific, statewide Medicaid home- and community-based waiver program. New Jersey is also an appropriate setting for study because a research database has been developed that links Medicaid claims and AIDS Registry data, facilitating analyses of HIV health services use.
Utilizing this research database, the analyses in the present study were aimed at providing basic descriptive data on the extent to which people with AIDS in New Jersey use HIV home care services and on the cost of these services. In addition, a particular concern for the study was to explore issues of access to home- and community-based services for minorities, injection drug users, and women. Prior studies often have found that members of these subgroups tend to use less outpatient care and more inpatient care than other people with AIDS, suggesting that they may experience more barriers to outpatient care. Equity of access is an important goal for HIV health policy. Therefore, assessing group differences in use of particular services is an important first step in identifying special outreach and other needs to make home- and community-based services available to all segments of the AIDS population.
| TABLE V.1. Study Population (ACCAP and Non-ACCAP Samples), Compared to New Jersey and National Registry Data | |||||
| New Jersey Medicaid Completely Observed Sample | All People with AIDS, New Jersey and National Registry | ||||
| All (n=1,293) | Non-ACCAP (n=866) | ACCAP (n=427) | New Jerseya (n=8,060) | Nationalb (n=203,217) | |
| Female | 0.350 | 0.400** | 0.251 | 0.235 | 0.125 |
| Black | 0.577 | 0.625** | 0.480 | 0.531 | 0.311 |
| Hispanic | 0.166 | 0.172 | 0.155 | 0.144 | 0.173 |
| Injection Drug User | 0.697 | 0.736** | 0.618 | 0.564 | 0.312 |
| Near New York City | 0.715 | 0.771** | 0.600 | 0.663 | n.a. |
| Age | 36.0 | 36.2 | 35.6 | 37.0 | n.a. |
| Survival/Follow-Up Months | 12.992 | 11.133** | 16.763 | n.a. | n.a. |
* Significantly significant difference between ACCAP and non-ACCAP samples at the 5 percent level. ** Significantly significant difference between ACCAP and non-ACCAP samples at the 1 percent level. n.a. = not applicable. | |||||
Another concern in understanding access to home care services involves patterns of service provision in areas where HIV prevalence is the highest. These often are areas in which health care resources are strained by high HIV caseloads and high rates of poverty. These factors may affect access to home care and other services. In New Jersey, the high-prevalence part of the state is the area nearest New York City, made up of Essex, Hudson, Passaic, Bergen, and Union Counties. These counties include such inner-city areas as Newark, Jersey City, and Paterson. The present analysis explores the extent to which use of home care services in this area differs from use patterns in the rest of the state.
An important feature of HIV care under Medicaid in New Jersey is that, while all people with AIDS have access to at least some home care services, about a third participate in an HIV-specific, case-managed Medicaid home- and community-based waiver program in which case management is characterized by relatively small caseloads, monthly home visits, and case managers who typically are registered nurses (Merzel et al. 1992). Comparing patterns of home care utilization both within and between the waiver and nonwaiver populations was an important opportunity and a particular concern for the study. Such data provide information on the utilization and cost patterns associated with a "package" of home- and community-based services provided through a waiver mechanism. Of particular interest was the extent to which any intergroup differences in home care utilization among nonwaiver participants were reduced (or increased) among waiver participants. A more equal pattern of utilization across subgroups within the waiver program than among nonwaiver clients would suggest that packaging services through this type of case-managed service structure might be an effective way to overcome the barriers to care that less advantaged subgroups disproportionately experienced, thus "leveling the playing field" in terms of access to HIV home care services.
1. Home Care Services Available to All New Jersey Medicaid Participants
Home care services people with HIV in New Jersey receive include regular state plan Medicaid services and waivered services. State plan services include skilled nursing, home health aides, and medical social services, provided through state-licensed home health agencies. Additional services are provided within a case-managed structure through an HIV-specific Medicaid waiver program, as described next.
2. New Jersey's Medicaid Waiver for Home- and Community-Based Care for People with HIV Disease
In March 1987, New Jersey introduced a case-managed home- and community-based care waiver program under Section 1915c of the Social Security Act. The AIDS Community Care Alternatives Program (ACCAP) provides home- and community-based services to people with HIV/AIDS who would otherwise require institutional care. ACCAP was the nation's first homeand community-based care program to focus exclusively on people with HIV disease. Program eligibility criteria include the need for a nursing home level of care and either categorical Medicaid eligibility or financial eligibility if the beneficiary were institutionalized.
By 1991, a total of 14 states had developed HIV-specific waiver programs (Miller 1992), but growth in this service delivery modality appears to have leveled off in recent years; as Chapter II notes, only 16 states were operating active AIDS waivers as of early 1998. A variety of factors may have contributed to the lack of waiver implementation in other states. Some states perceived difficulty with demonstrating the cost-neutrality of waiver services (see Chapter II). Anderson and Mitchell (1997) state that reasons for reluctance to enact such programs include (1) the administrative burden of applying for and monitoring the waivers, and (2) administrators' fears of constraints on state flexibility (although the availability of waivers is intended precisely to provide more flexible options for the states). States that already were offering liberal "personal care" benefits as state plan services may have perceived less need to apply for waivers. In New Jersey, however, the decision was made to develop an HIV-specific home- and community-based waiver program that would provide access to a relatively intensive form of case management, an expanded range of home care services, and broader financial eligibility.
ACCAP is available on a voluntary basis to people with HIV disease who are deemed to have medical and social needs that would otherwise require care in a skilled nursing or other long-term care facility. To encourage participation, the waiver program is available to individuals with income levels above the regular Medicaid income threshold, up to the income level at which they would become financially eligible if institutionalized. (This was $1,158 per month in 1990, at about the midpoint of the 1989-1991 Medicaid participation "time window" for the match, as discussed below.)
A central component of ACCAP is mandatory case management, wherein case managers are required to maintain weekly contact with their clients and make monthly home visits. Case managers, who are typically registered nurses, are responsible for planning, coordinating, monitoring, and securing the services needed to maintain clients at home. Arranging and securing home care services is a major part of their workload. In addition to case management, adult clients are eligible to receive five other waivered services: (1) private duty nursing by a registered nurse or licensed practical nurse, (2) personal care assistance, (3) specialized medical day care for people with HIV, (4) home-based narcotic and drug abuse treatment, and (5) home-based hospice service (implemented in 1992). As we discuss below, ACCAP participation influences home care use both because ACCAP participants have access to home care services not available to non-ACCAP participants and because the case management component of ACCAP facilitates access to home care services, including state plan (nonwaivered) services.
As of August 1997, there were 1,000 approved slots in ACCAP statewide, of which 83 percent (834) were filled. Each county has a separate allocation of slots. Most counties had significant numbers of unfilled slots; among the high-prevalence counties, however, Hudson (at 94 percent) and Union (at 97 percent) were close to their caps. High-prevalence counties averaged 87 percent of slots filled, while lower-prevalence counties averaged 80 percent.
B. STUDY POPULATION AND DATABASE DEVELOPMENT
The study population used in these analyses reflects the population of people with AIDS participating in Medicaid in New Jersey. This includes Medicaid participants in New Jersey's HIV-specific Medicaid waiver program for home- and community-based care and participants in the traditional Medicaid program. This population is estimated to represent about 60 percent of the total number of people with AIDS in the state (Crystal et al. 1997).
1. Key Issues in Research Database Development
In using state-level administrative data to study use of health care services (such as home care) among people with AIDS, several important methodological issues must be addressed. These include methods for:
- Identifying people with AIDS within a larger population
- Identifying key "staging" dates during the illness (such as dates of AIDS diagnosis)
- Determining important respondent characteristics needed as covariates (such as risk group)
- Dealing with incompletely observed or "censored" observations, for example, those for individuals whose full diagnosis-to-death services use is not observed because they enroll in Medicaid only after their diagnosis or they are still alive as of the most recent date for which utilization information is available).
In research using large administrative data sets such as Medicaid files, the two principal methods that have been used to identify people with AIDS are (1) coding nets (case-finding algorithms based on diagnostic codes), and (2) file matching. The coding net approach involves screening Medicaid claims or other encounter data to identify cases with HIV-related ICD-9 diagnostic codes. This approach has often been combined with case identification based on use of HIV-specific treatments such as zidovudine. The file-matching approach, used in the present research, involves linking Medicaid eligibility files with AIDS Registries maintained for surveillance. In New Jersey, under the auspices of a cooperative agreement between the State Department of Human Services (which manages the Medicaid program) and the State Department of Health and Senior Services (which manages the AIDS Registry), the AIDS Registry and Medicaid eligibility files have been matched on two occasions (once in 1992 and once in 1996). Analysis files with claims information on the population identified by the 1996 match were not yet ready for use in time for this initial analysis; therefore, results are based on the population identified by the 1992 match.
The creation of a research file on health services use by people with AIDS on Medicaid helped to address each of the four issues listed earlier. Several factors facilitated the creation and usefulness of such a file. One important circumstance was the existence of a statewide confidential registry based on provider reports of individuals in the state with AIDS and, more recently, those with HIV infection. (Although HIV reporting was not used in the 1992 match on which the present analysis is based, it was used in the 1996 match and will contribute in a major way to the usefulness of subsequent studies.) AIDS registries exist in all states; they usually are based on name reporting, although a few places use unique identifiers without names. However, of the 10 states with the highest rates of reported AIDS cases in 1996, only New Jersey and Louisiana conduct HIV case surveillance (Gostin et al. 1997). A second critical factor was the existence of a cooperative effort among state agencies and between such agencies and university-based researchers, which made it possible for research purposes to match cases between the Registry and Medicaid eligibility files and use the results for research on HIV-related health care utilization in the Medicaid program. Because of the complexity of databases created through such matching procedures and the numerous methodological issues that arise in longitudinal analyses of health care use over time with such data, an extended time commitment to such research efforts is needed to make the most effective use of them. The research data set developed by the Rutgers researchers and used in the present study has also been extremely useful in providing information on a range of HIV health care utilization and access issues in the state. For example, it has been used to analyze incidence and persistence of antiviral treatment (Crystal et al. 1995).
The AIDS Registry and Medicaid eligibility files were the two key data systems used to identify cases for inclusion in the research data set. The AIDS Registry is a confidential disease surveillance system initiated in 1985 to monitor the incidence and prevalence of the disease in the state. Use of these data to build knowledge about access to care, health care utilization, survival, and other characteristics of the HIV-infected population (including their use in carefully controlled file linkages) for those reasons is considered part of the public health purpose for which the Registry exists. For example, they are periodically matched with vital statistics files to improve understanding of trends in HIV/AIDS survival. Matching with Medicaid eligibility files is conducted, under an interagency memorandum of understanding, under the auspices of the state surveillance staff.
The Registry matching procedure, in contrast to coding nets that use ICD-9 codes in Medicaid claims to identify cases of treated HIV disease, has many advantages. Since AIDS surveillance reports generally are based on reports from medical providers, they are highly specific (that is, there are few false positives). Case identification does not depend on the use of particular services, so that case identification is not confounded with utilization. Information on risk group from the AIDS Registry is more precise than such information in studies that use coding nets (in which, for example, information on injection drug use history may be available only if the individual uses drug abuse-related health care services). Of particular importance is the availability of information on the date of AIDS diagnosis from the Registry. Utilization patterns during the period from AIDS diagnosis to death differ considerably from those among HIV-positive people without AIDS. Therefore, these dates provide essential staging information that enables comparisons of utilization at comparable stages of illness. Finally, vital status information merged into the AIDS Registry, through file matching, makes it possible to accurately determine vital status and dates of death, which are essential to compare service use across comparable stages of illness. These data elements frame the AIDS diagnosis- to-death period that is the focus of the present analyses.
2. Creation of 1992 Match File
The 1992 match, conducted under the auspices of the Department of Health and Senior Services, used the Medicaid eligibility file as of July 1991, which was matched with the AIDS Registry as of June 30, 1992. Identifying information used to match cases included name, birth date, gender, and social security number. Since cases remain on the eligibility file for about two years after death or Medicaid case closing, the match represented the population of individuals who were eligible for Medicaid during the period from August 1989 to July 1991 and who were diagnosed with AIDS by mid-1992. For the population identified by the match, the Division of Medical Assistance and Health Services of the New Jersey Department of Human Services then extracted and subsequently updated claims histories for the people with AIDS identified in the Registry match; in this analysis, we used data on services received between January 1988 and June 1994. The original match identified 4,398 people with AIDS in the Medicaid eligibility file. Cases were carefully checked for completeness of information and for consistency between information reported from the merged data sources. The use of health services by individual people with AIDS is tracked throughout the claims histories with a unique person-level identifier provided in the claims files. The identifier allows for longitudinal analysis of health services utilization during the progression of the disease.
As with all large claims databases, extensive data cleaning is necessary with data of the type used in this study to eliminate inconsistencies and questionable cases from the analysis file. In this study, adult cases who received medical care through the Medicaid program for at least some part of the AIDS diagnosis-to-death period were the population of interest. Therefore, cases that appeared on the eligibility and Registry files but had no paid claims were excluded, since they were not actually receiving medical care through the Medicaid program. Similarly, cases in which the amount paid on all claims was zero were excluded. Cases were also excluded in the cleaning process if they had no services of any kind in the last 30 days of life, because they may have been receiving services outside the state or outside the Medicaid program (Crystal et al. 1997). Also excluded were cases under age 18 (since patterns of services utilization for children are likely to be quite different from those for adults), cases with no claims after AIDS diagnosis, cases determined to represent duplicate records, cases with medical service dates after death dates, cases in which all claims were prior to 1988, and cases of individuals who died on the day of their AIDS diagnosis. Remaining in the sample were 2,464 adult people with AIDS who were diagnosed with AIDS prior to June 1992 and receiving services between January 1988 and June 1994. Of these, 1,293 were observed during the entire period from diagnosis to death.
The completely observed sample of 1,293 was the primary focus of the analyses because it offered the opportunity to explore the full extent of home- and community-based care use over the full course of AIDS, including the often costly last months of life. Because the incompletely observed groups may differ in some respects from the completely observed groups, a series of comparisons were made between results for the censored groups and the fully observed group (Crystal et al. 1997). In general, differences in utilization across the subgroups examined were similar for the fully observed and the censored populations.
3. Characteristics of Study Population
As Table V.1 shows, among the fully observed sample 35 percent were female, 58 percent were black, and 70 percent were injection drug users; 33 percent were ACCAP participants, and 72 percent lived in the high-HIV-prevalence area of the state. Table I.1 compares the study population (both ACCAP and non-ACCAP) to the total population of people with AIDS in New Jersey (as reflected in Registry data) and to the national AIDS population, at approximately the time of the study. Overall, the ACCAP population was fairly similar demographically to the statewide AIDS population (with the largest difference being a modest underrepresentation of individuals living in the counties near New York City). The non-ACCAP Medicaid population included a higher proportion of women, blacks, injection drug users, and people living near New York City. The New Jersey study populations, like the New Jersey Registry population, included more women, blacks, and injection drug users than were characteristic of people with AIDS nationally. However, the national AIDS population is also moving toward greater representation of these demographic groups. For example, the proportion of women among adult/adolescent AIDS cases reported nationally in 1996 reached 20 percent, and the proportion of blacks reached 41 percent (Centers for Disease Control 1996).
C. FINDINGS
1. Use of Home Care Services
Approximately 40 percent of Medicaid beneficiaries with AIDS used home care services at some point during their illness. Overall, home care services were more likely to be used by Medicaid participants who lived in areas of the state less heavily affected by the HIV epidemic, by those who were not drug users, and by whites. Figure V.1 provides bivariate comparisons of the proportion of subgroups with any home care use, within the overall Medicaid AIDS population (ACCAP and non-ACCAP). Only 36 percent of blacks, versus 50 percent of whites, used home care. Similarly, 37 percent of injection drug users versus 52 percent of non-injection drug users, used any home care. Women were also less likely overall to use home care.
While both ACCAP and non-ACCAP participants use home care, the proportion with any use was much higher among those in ACCAP. Roughly one-third of Medicaid beneficiaries were enrolled in ACCAP at some point between AIDS diagnosis and death. Eighty-three percent of ACCAP participants and 21 percent of non-ACCAP participants used home care services at some point between AIDS diagnosis and death. In addition to their use of waivered services, ACCAP participants were substantially more likely to use traditional Medicaid home care services for which all Medicaid participants are eligible.
| FIGURE V.1: Proportion with Any Home Care Use, Waiver/Non-Waiver Combined(n = 1,293) |
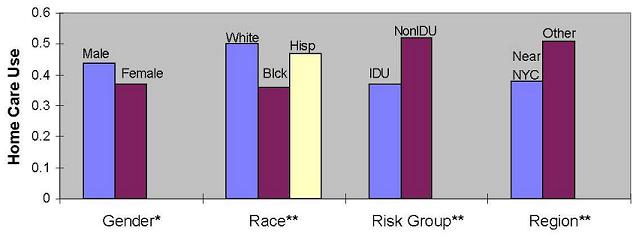 |
| * p .05, ** p .01 |
Detailed analyses were conducted of utilization patterns for each type of home care service, including both waivered services and nonwaivered services (Crystal et al. 1997). These breakdowns are complex since they involve a diversity of services (as described above), and services by similar types of personnel may be delivered either as waivered or nonwaivered services. In this report, to provide overall comparisons of types of service used, consolidated measures of services use by discipline of provider are used. A "home nursing" category groups ACCAP RN and LPN services with traditional Medicaid skilled nursing services, and a "paraprofessional home care services" category groups personal care assistants provided as a waivered service with home health aide services provided as a state plan service. These represent the most widely used services and most of the expenditures. A small third group of specialty services, not shown here, included the ACCAP services of home drug treatment, medical day care, and hospice, as well as the traditional Medicaid home medical social services (Crystal et al. 1997). Table V.2 provides comparisons of types of services used, based on the consolidated measures.
Overall, 76 percent of the ACCAP participants used home nursing services and 53 percent used paraprofessional home care services. In contrast, 19 percent of non-ACCAP participants used home nursing services, and 11 percent used paraprofessional services (as state plan services). In addition to their use of waivered services, ACCAP participants were much more likely than non-ACCAP participants to use state plan home care services; 71 percent of them used skilled nursing services, and 29 percent used home health aide services.
Within the ACCAP sample, women and residents of the high-prevalence area of the state were more likely than others to use paraprofessional services, and injection drug users were less likely than others to use home nursing services. The bivariate analyses indicated that there were significant racial differences in use of both home nursing and paraprofessional services among non-ACCAP participants but not among ACCAP participants. Multivariate regressions of use/nonuse of home care services confirmed the bivariate findings, suggesting that waiver participation does tend to level racial differences in the proportion using home care services.
| TABLE V.2. Proportion Using Each Type of Home Care Services, AIDS Diagnosis to Death | |||||
| Non-ACCAP Participants(n=866) | ACCAP Participants(n=427) | ||||
| Home Nursing | Paraprofessional | Home Nursing | Paraprofessional | ||
| All | 0.19 | 0.11 | 0.76 | 0.53 | |
| Gender | |||||
| Male | 0.19 | 0.11 | 0.76 | 0.49* | |
| Female | 0.19 | 0.12 | 0.79 | 0.64 | |
| Race | |||||
| White | 0.23* | 0.13* | 0.74 | 0.47 | |
| Black | 0.16 | 0.09 | 0.76 | 0.55 | |
| Hispanic | 0.26 | 0.17 | 0.83 | 0.59 | |
| Risk Group | |||||
| Injection Drug User | 0.17* | 0.09** | 0.73* | 0.50 | |
| Non-Injection Drug User | 0.25 | 0.17 | 0.82 | 0.58 | |
| Region | |||||
| Near New York City | 0.18 | 0.12* | 0.75 | 0.59** | |
| Elsewhere | 0.22 | 0.08 | 0.78 | 0.44 | |
| * p.05, ** p.01 | |||||
2. Home Care Expenditures
The above analyses show subgroup differences in the proportion of respondents with any use of services but do not address differences in the quantity of services used. Differences in amounts of home care resources used overall and across groups are reflected in differences in expenditures on their behalf for home care services; thus, bivariate and multivariate analyses of average monthly home care expenditures were performed. On average, combining both ACCAP and non-ACCAP cases, Medicaid enrollees used approximately $300 per month in home care services, about 57 percent of which was for home nursing services. Total monthly expenditures for home care were 53 percent as high for injection drug users as non-injection drug users, 52 percent as high for blacks as for whites, 59 percent as high for Hispanics as for whites, and 50 percent as high for residents of the high-prevalence area as for the rest of the state. The geographic difference was even larger for home nursing services, which were used in the high-prevalence area at less than one-third the rate at which they were used in the rest of the state.
It was expected that ACCAP participants would use more home care services, since eligibility for ACCAP requires the presence of functional limitations that would qualify people with AIDS for care in an intermediate-care facility or skilled nursing facility, and ACCAP participants have access to a broader array of home care services. The magnitude of this difference, however, was striking, reflecting the fact that expenditures for state plan home care services among non-ACCAP people with AIDS were quite limited (Crystal et al. 1997). As Table V.3 shows, total spending on home care services for ACCAP enrollees (about $800 per person per month) was 16 times higher than for traditional Medicaid enrollees (about $50 per person per month). Home nursing services made up the majority of expenditures for ACCAP enrollees (61 percent), while paraprofessional services made up the majority of expenditures for non-ACCAP enrollees (59 percent).
| TABLE V.3. Average Monthly Expenditures on Home Care Services From AIDS Diagnosis to Death | |||||
| Non-ACCAP Participants(n=866) | ACCAP Participants(n=427) | ||||
| Home Nursing | Paraprofessional | Home Nursing | Paraprofessional | ||
| All | $19.88 | $28.57 | $477.93 | $307.49 | |
| Gender | |||||
| Male | 19.11 | 20.52* | 485.72 | 267.86 | |
| Female | 21.03 | 40.65 | 454.61 | 399.10 | |
| Race | |||||
| White | 26.90* | 30.75* | 613.70 | 273.78 | |
| Black | 14.07 | 19.60 | 391.90 | 359.21 | |
| Hispanic | 36.69 | 58.55 | 424.18 | 226.52 | |
| Risk Group | |||||
| Injection Drug User | 16.10** | 21.19** | 411.67 | 282.69 | |
| Non-Injection Drug User | 30.39 | 49.08 | 585.24 | 347.66 | |
| Region | |||||
| Near New York City | 18.82 | 35.96** | 325.76** | 342.04 | |
| Elsewhere | 23.45 | 3.62 | 705.73 | 255.77 | |
| * p.05, ** p.01 | |||||
There were substantial and significant racial and risk group disparities in use of home nursing and paraprofessional services among non-ACCAP participants, but no such significant disparities among ACCAP participants. Expenditures both for home nursing and for paraprofessional services were less than two-thirds as much for non-ACCAP blacks as for non-ACCAP whites. Among non-ACCAP cases, expenditures for injection drug users, both for home nursing and paraprofessional services, were only about half as large as for non-injection drug users, while risk group differences were not significant among ACCAP cases.
Geographic differences were apparent both for non-ACCAP and ACCAP participants. For non-ACCAP participants, more paraprofessional services were used in the high-prevalence area than elsewhere, although amounts of service used were much smaller than for ACCAP participants. A much larger geographic difference existed among ACCAP participants: mean expenditures for home nursing were much higher in the lower-prevalence area (at $706 per person per month) than in the high-prevalence area (at $326 per person per month).
Multivariate analyses of monthly expenditures for home nursing and paraprofessional services were performed (Crystal et al. 1997). These findings generally confirmed the bivariate results, indicating the presence of substantial race, risk group, and gender differences in home care use within the non-ACCAP population that were substantially reduced or eliminated within the ACCAP population.
Table V.4 displays mean monthly expenditures among people with AIDS who use home care services. The results show that, once disadvantaged subgroups initiate use of services, their use patterns are similar to those of other people with AIDS, regardless of waiver status. Among users of each type of service, amounts used did not vary significantly by gender, race, or risk group. However, there were marked differences in service provision patterns by region of the state. Within the non-ACCAP sample, residents of the high-prevalence area tended to use paraprofessional services much more intensively than residents of the low-prevalence region. Within the ACCAP sample, residents of the low-prevalence area tended to use nursing services much more intensively than residents of the high-prevalence area.
| TABLE V.4. Average Monthly Expenditures on Home Care Services, Among Users of Each Type of Service, From AIDS Diagnosis to Death | |||||
| Non-ACCAP | ACCAP | ||||
| Home Nursing | Paraprofessional | Home Nursing | Paraprofessional | ||
| All | $105.62 | $252.44 | $626.38 | $581.27 | |
| Gender | |||||
| Male | 102.46 | 194.04 | 642.28 | 560.73 | |
| Female | 110.27 | 327.13 | 579.09 | 627.99 | |
| Race | |||||
| White | 118.36 | 246.02 | 825.33 | 577.17 | |
| Black | 89.54 | 212.06 | 518.32 | 651.66 | |
| Hispanic | 128.20 | 335.52 | 509.02 | 383.33 | |
| Risk Group | |||||
| Injection Drug User | 95.85 | 228.79 | 566.04 | 569.69 | |
| Non-Injection Drug User | 124.29 | 288.21 | 711.90 | 596.51 | |
| Region | |||||
| Near New York City | 105.67 | 289.41** | 434.35** | 583.74 | |
| Elsewhere | 105.50 | 47.84 | 900.59 | 575.48 | |
| n | 163 | 98 | 326 | 226 | |
| * p.05, ** p.01 | |||||
3. Use of Services Over Time
As anticipated, use of home care services was considerably higher in the later stages of illness and particularly immediately preceding death. Among ACCAP enrollees, 32 percent of men and 26 percent of women used home care during the three months following their AIDS diagnosis, while 78 percent of men and 81 percent of women used home care during the three months preceding death. Among non-ACCAP clients, 5 percent of men and 9 percent of women used home care during the three months following diagnosis, while these proportions increased to 22 percent of men and 27 percent of women during the three months preceding death.
Most ACCAP enrollees used home care during the terminal period of life, although there was a significant difference by risk group (73 percent of injection drug users versus 84 percent of non-injection drug users). Among non-ACCAP enrollees, this difference was larger (20 percent of injection drug users versus 34 percent of non-injection drug users). Although ACCAP participation did not eliminate the risk group difference, most ACCAP participants, across demographic and exposure categories, received home care services during the terminal period of life. Use of home care services by ACCAP participants during the terminal period of life was intensive, amounting to more than $2,000 per month among home care users during the last 30 days of life. Figure V.2 illustrates trajectories of monthly home care spending among home care users during the last six months of life for ACCAP participants and nonparticipants.
| FIGURE V.2: Monthly Home Care Spending in Last 6 Months of Life by Waiver Status Among Home Care Users |
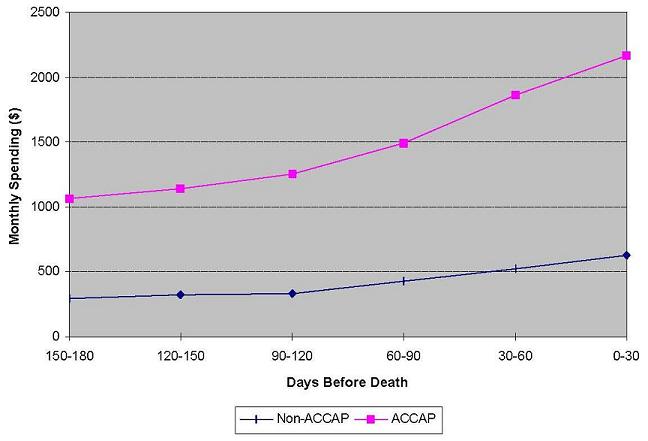 |
4. Home Care and Inpatient Utilization
Many studies of home care use in other populations (such as the elderly) have attempted to find a relationship between home care use and inpatient hospital use. Because inpatient hospital expenditures are very high for people with AIDS, we attempted to learn more about the association between home care use and hospitalizations. Causal relationships between home care use and hospital use are difficult to determine using observational administrative data of this type, but our results at least provide suggestive correlations between home care use and inpatient hospital use. These results are summarized briefly below.
The average length of hospital stay for AIDS patients in our data set was approximately 17 days. In general, hospital stays tended to be somewhat shorter for ACCAP participants than non-ACCAP cases (by about three days). Although ACCAP participants survived longer and spent more total days in the hospital, ACCAP participants used half as many hospital days per month as non-ACCAP participants (6 days versus 13 days). Among non-ACCAP participants, average length of hospital stays was somewhat shorter for people who used home care services (16 days versus 20 days).
ACCAP enrollees had a lower rate of terminal hospitalization than non-ACCAP enrollees (46 percent versus 61 percent). They experienced fewer days of hospitalization in the last 30 and the last 60 days of life, but there was no clear relationship within ACCAP between use of home care services and terminal hospital days. These analyses suggest that ACCAP participation is associated with less hospitalization, but within the ACCAP program there is no clear relationship between home care use and hospitalization. Within the non-ACCAP population, there appeared to be an association between use of home nursing services and lower hospital use. However, it is not clear whether these differences are truly program effects or reflect unmeasured differences between users and nonusers of home nursing services. These analyses, described in more detail in the project report, are probably best viewed as inconclusive. However, they do suggest that the relationship between home care use and hospitalization in HIV disease deserves further exploration.
D. CONCLUSION
This analysis set out to explore whether home care utilization on the part of minorities, injection drug users, and women differed from that of other people with AIDS; to investigate whether participation in a case-managed, HIV-specific Medicaid waiver program (ACCAP) reduced such differences; and to analyze geographic differences in the use of home care services. Results indicated that the size of racial, risk group, gender, and geographic differences among all Medicaid participants was substantial: approximately two to one for non-injection drug users, as compared with injection drug users; for whites, compared with blacks; and for residents of the lower-prevalence areas of the state as compared with the high-prevalence area. The most important factor shaping these differences appeared to be differences in waiver program participation by sociodemographic characteristics and region. These ACCAP participation rates are the most crucial determinant of home care use rates across groups; although all people with AIDS are eligible for some home care services, most home care services were used by ACCAP enrollees. Injection drug users, blacks, and women were less likely to be enrolled in ACCAP, leading in turn to substantially lower rates of home care use among those groups. In addition, the differences in ACCAP participation rates were exacerbated by differences in services use that existed even controlling for waiver status, particularly among nonwaiver participants.
In addition to using large amounts of waivered home care services, ACCAP participants use substantial amounts of state plan (nonwaivered) home care services, while non-ACCAP participants, although they are eligible for these services, use much less of them (Crystal et al. 1997). The greater use of traditional Medicaid home health services by ACCAP enrollees may reflect the impact of the case management component of ACCAP in overcoming barriers to home care use. The importance of ACCAP as the major gateway for access to home care services in New Jersey is indicated by the finding that ACCAP participants averaged in total about $800 per month in home care services versus $50 per month for non-ACCAP participants. Given this important "gateway" role, the lower rate of ACCAP enrollment by minorities, women, and injection drug users is of concern. Fewer than 20 percent of nonwaiver participants used any home care services, although it is likely that many of them experienced need for such services at some point, given the episodic nature of HIV disease and the fact that functional status in HIV disease varies greatly over time, even from month to month (Crystal and Sambamoorthi 1996; and Fleishman and Crystal, in press). The results suggest that there is a need for increased efforts to enroll into waiver programs the most disadvantaged demographic subgroups among Medicaid beneficiaries, including minorities and injection drug users, and to develop new ways to link these services with treatment for substance abuse and other behavioral comorbidities that are increasingly prevalent among people with HIV.
The analyses suggested that ACCAP participation is associated with mitigation of sociodemographic differences in utilization of home care services. Within the nonwaiver population, there were significant and substantial differences by race, risk group, and gender in home care utilization. Within the ACCAP population, these differences were reduced or eliminated. These findings suggest that waiver program participation reduces barriers to access to these services and "levels the playing field" between demographic and risk groups in use of home care. Addressing such barriers is especially important given the increasing proportions of disadvantaged subgroups in the AIDS population nationally.
Because newer data were not yet available within the original time frame of the study, results from this study represent utilization patterns in the early 1990s but do not necessarily reflect more recent patterns. These data provide little ability to identify trends in home care use. Since patterns of HIV care have changed markedly in the 1990s, it will be important to compare the patterns observed in the cohort defined by the 1992 match with results from the now available utilization data on the 1996 match population. There is also a need to explore the experience of policy planners and providers in delivering services to the diverse subgroups that make up the population of people with HIV and AIDS in the state and the access barriers and other factors that may underlie and explain utilization differences across subgroups. In addition, data on institutional long-term care were not available for the 1992 cohort; thus, the extent to which subgroups lower in home care use meet their long-term care needs through institutional channels is not known. There is a need to explore patterns and costs of institutional home care use in the state and the relationship of these patterns to home care use. Another subject not explored in the present study, the relationship between psychiatric comorbidity and home- and community-based care in HIV disease, also should be a high priority for investigation with more recent data. However, the present results are of interest in highlighting access and outreach issues to specific subpopulations that deserve further attention.
A variety of HIV health services studies, such as analyses from the AIDS Cost and Services Utilization Survey (ACSUS), show that whites and non-injection drug users with AIDS tend to use more outpatient and ambulatory care than do nonwhites and injection drug users. However, these differences have seldom been observed to be on the order of magnitude of two to one, as with the overall AIDS population in the present study. These results suggest that home care may be a service particularly vulnerable to access differentials, unless special efforts (such as broader use of case-managed service packages like the ACCAP waiver program) are made to overcome these barriers. Broader use of such strategies--including additional efforts to bring services similar to the waiver program's relatively intensive, nursing-oriented case management component to more individuals among all subgroups of the AIDS population--might further help improve access to home care services for the state's full AIDS population.
For waiver programs, the changing face of the AIDS epidemic and AIDS care has brought new challenges, including the need for increased attention to meeting needs related to behavioral comorbidities. Issues of eligibility and of the mix of services needed also need to be considered. Most HIV-specific waiver programs currently in place, including ACCAP, were designed from the mid-1980s to early 1990s. In the newer era of combination therapy with protease inhibitors, fewer individuals among the HIV population may need extensive paraprofessional assistance with activities of daily living, and fewer may qualify for nursing home or intermediate care. However, important home health care needs remain, particularly related to adherence, monitoring, and management of pharmaceutical regimens. Indeed, given the complex and demanding nature of current combination therapy regimens and the severe individual and public health consequences of nonadherence, access to nursing-oriented case management and to in-home health care services, across all subgroups of the patient population, may be even more important. In-home visits by nurses or other health care providers could be particularly helpful in facilitating appropriate and consistent use of these complex regimens, particularly for individuals with limited education, concomitant substance abuse, or psychiatric problems. Considering the extent to which the waiver program has become the "gateway" to home care services in New Jersey, however, it is ironic that improvements in health status resulting from the effectiveness of newer treatment regimens may also limit the number of individuals eligible for waiver programs that, like ACCAP, require that participants be eligible for institutional long-term care. Given the major changes in the HIV/AIDS care landscape documented in other chapters of this report, it may be time to consider "reinventing" the design of waiver and other programs for home- and community-based HIV/AIDS care in order to reach a broader spectrum of the HIV/AIDS population.
VI. SYNTHESIS AND IMPLICATIONS
Three important, interrelated forces are shaping the evolution of the AIDS epidemic and AIDS-related home- and community-based services: (1) improvements in AIDS treatment; (2) changes in the characteristics of the AIDS population; and (3) pressures to control spending, particularly as Medicaid increasingly moves beneficiaries into managed care. As illustrated below, these events converge to change the service delivery model for people with AIDS while increasing the public burden for financing services.
| KEY FORCES IN THE EVOLUTION OF THE AIDS EPIDEMIC | ||
Improved Treatment
| More People with Complex Problems
| Increased Cost-Control Pressures
|
 | | |
| CHANGES IN SERVICE DELIVERY AND FINANCING | ||
Provider Responses
| Increased Public Burden
| |
IMPROVED AIDS TREATMENT
Improved AIDS treatment (increased medical expertise and the development of antiretroviral medications such as AZT and protease combination therapy) has increased life expectancy, which in turn has increased the duration of needed services. Improved treatment has also decreased levels of functional impairment among people living with AIDS, which in turn (according to project site visit discussions) appears to have led to a decrease in the use of traditional home- and community-based services (such as home-delivered meals and personal care) and skilled home health care. However, increased life expectancy has led to an increase in the need for other types of support (such as assistance with adherence to complex treatment regimens and with return to work).
MORE PEOPLE WITH COMPLEX NEEDS
Meanwhile, the increased incidence of AIDS among people with low incomes, people without safe and secure housing, people with substance abuse problems and serious mental illness, and women with families has led to the need for a new mix of home- and community-based services that, more often than previously, must be meshed with the medical, mental health, substance abuse treatment, family services, and public assistance systems. Providers have moved to more hands-on approaches from models of service delivery that had the goal of empowering clients to advocate for themselves. They have had to consider reducing the proportion of lay volunteers on staff (who over the years have provided compassionate end-of-life care) and increasing the proportion of professionals trained to address the more complex needs of the newer populations who must learn to live with AIDS. Providers have also broadened the range of services they provide in house, increased referrals to providers in other systems, and developed procedures to deliver the most intense services to the clients with the most complex problems. Case management (such as that delivered under Medicaid waiver programs) appears to be one approach to reducing barriers to care that women, minority group members, and people with behavioral comorbidities have historically experienced.
INCREASED COST-CONTROL PRESSURES
The increase of AIDS among people with low incomes and complex problems, combined with increased life expectancy, is placing a growing burden on Medicaid and Ryan White programs, especially on resources for pharmaceuticals as the demand for protease combination therapy grows. State Medicaid programs are moving increasingly toward managed care approaches that include people with AIDS (and other disabilities) to control the high costs of their care, while looking for mechanisms to ensure that payments to managed care plans are adequate to provide high-quality AIDS care, including access to AIDS specialty care and cutting-edge medications. To date, few if any managed care plans receive capitation payments that include home- and community-based services for people with AIDS. Thus, questions about which services to include and how to pay for them remain unanswered. Whether and how to include under managed care services currently funded through Ryan White are also unanswered. As people with AIDS live longer, and as more qualify for Medicare coverage, questions arise about how to pay for their medications and support services (neither of which Medicare covers) and how to integrate Medicare and Medicaid funding for those who are dually eligible, so that incentives to provide services at inappropriate levels are reduced. In addition, private donations to AIDS service organizations have recently declined because the epidemic has been moving away from the relatively affluent gay community to more disadvantaged groups and because protease therapy has received favorable publicity.
The 1990s have confronted AIDS home- and community-based service planners and providers with dramatic changes in population characteristics and needs and heightened pressures to control costs. Providers have modified their service delivery approaches in response, although some of the challenges they face are clearly beyond their direct control (for example, how to meet the subsistence needs of increasingly disadvantaged clients, which must be done before clients can turn their attention to their health). Providers and planners alike have had to formulate responses to these changes and pressures in what is a nearly total information vacuum. Few data exist describing basic levels of home- and community-based service use and costs among different groups of people with AIDS; almost none exist assessing the cost-effectiveness of specific interventions or groups of services.
PLANNING AND POLICY IMPLICATIONS
The challenges that providers, planners, and policymakers face in the wake of a changing AIDS population and service environment have implications in three broad policy areas: (1) the development of databases to support planning decisions, (2) the development of concrete strategies to implement managed care for people with AIDS, and (3) the development of a cohesive approach to meeting the needs of people with all types of chronic illness.
In an environment that focuses increasingly on cost control, program planners and policymakers in both the managed care and the fee-for-service sectors require information to aid in decision making about the provision of home- and community-based services to people with AIDS.
Two broad types of information are needed. The first is a basic description of service use, costs by funding source, and mortality patterns, including variations in them over time, by geographic region, and across different groups of people with AIDS. Descriptions of service patterns should differentiate between those who take protease and those who do not, as well as among other personal characteristics found to affect use, such as HIV risk group, gender, minority status, disease stage, presence of behavioral comorbidities, homelessness, and existence of family affected by HIV. Whereas basic information about service use patterns for different groups of people with AIDS is sorely needed, more sophisticated analyses--which offer evidence that a particular program, approach, or financing mechanism provides care more cost-effectively--would further rationalize decision making for future programs. Chapter IV discussed approaches to developing these data using administrative and, potentially, provider databases.
In discussing with providers their approaches to addressing the changing AIDS service environment, we identified a number of interventions that might merit formal evaluation (for example, the development of AIDS-specific mental health programs or short-term residential treatment adherence assistance). It seems likely that the interventions discussed in response to site visit questions may be only the "tip of the iceberg" of all interventions providers believe to hold promise for newer AIDS clients and changing financing mechanisms. If providers were explicitly solicited for evaluable interventions and offered seed money for startup costs, they would likely generate additional ideas.
When home- and community-based services for people with AIDS are evaluated, the frail elderly literature provides an important caution concerning the goals of such services. This literature demonstrates that home- and community-based services that attempt to lessen nursing home use seldom reduce overall health and health-related spending, although they do decrease unmet need and increase well-being. AIDS service planners of the late 1980s and early 1990s nevertheless believed that home- and community-based services could reduce overall spending for people with AIDS, because these services were meant to reduce inpatient hospital use, a much more costly and commonly used service. However, medical services in the 1990s in general, and for people with AIDS in particular, have moved away from inpatient care. Thus, it seems that a reduction in overall spending may not be a realistic goal for home- and community-based services for people with AIDS. Improved quality of life, reduced unmet need, and increased satisfaction with care at modest costs might be more attainable objectives for many interventions.
Practice guidelines for home- and community-based services represent a second type of information whose development bears further consideration. Practice guidelines, such as those now widely used in home health care, could clarify the goals and tasks of home- and community-based services (often criticized for their amorphousness) and would be an effective way for providers with extensive experience in serving newer AIDS populations to communicate what they have learned to those who are just starting to serve these populations. Quality indicators offer providers a means to assess their effectiveness. Case management in particular has been criticized for its profusion among people with AIDS, and guidelines could be one part of a strategy to reduce redundancy in case management and help it coordinate services across systems.
While managed care holds the potential to better coordinate acute care and home- and community-based services for people with AIDS, its implementation faces challenges beyond those posed by the information gaps just described.
Managed care planners face now well-known challenges in addressing the special medical care needs of people with AIDS: developing risk management strategies (risk adjusters and risk-sharing arrangements) that offer managed care plans incentives to enroll people at risk of high costs and developing mechanisms to assure quality AIDS care (specialty medical care and cutting-edge pharmaceuticals). However, planners face additional challenges in addressing the needs of people with AIDS for home- and community-based services. If funders decide to include these services under capitation payments (or if the managed care plans themselves view them as approaches to controlling costs), fundamental questions must be answered as to how to implement and integrate them. For example, who should coordinate and oversee their use: medical or social services providers? Small, neighborhood-based or larger, more comprehensive providers? These and other questions of implementation remain, because even the few managed care plans now serving substantial proportions of people with AIDS (for example, Positive Healthcare and Community Medical Alliance) currently carve out home- and community-based support services (although Community Medical Alliance covers home health care.) The first generation S/HMO evaluation demonstrates the difficulties coordinating acute and traditional home- and community-based services under a capitated, case-managed system even when providers are co-located. Even less is known about how to integrate Ryan White funding and services under managed care. This suggests that demonstrations of managed care plans for people with AIDS must begin to integrate home- and community-based services with medical care and must collect encounter data to provide insights into changes in service use over time and across different groups of people. Evaluations of and practice guidelines for home- and community-based services in the fee-for-service sector could also help managed care plans and payers decide whether and how to include these services.
The problems we face in trying to figure out whether and how AIDS-specific home- and community-based services should be included in managed care (or in ongoing fee-for service programs facing cost-control pressures) are merely special cases of general problems reflecting the need for a cohesive policy to address the needs of people with all types of chronic illnesses.
The health care and support service systems for people with chronic illnesses need to be flexible enough to permit people to vary the intensity with which they receive services in those systems as their needs change over time and to minimize incentives to provide care at inappropriate levels. The current Medicaid and Medicare systems include perverse incentives that run counter to these goals. HCFA's current dual eligible demonstrations should shed some light on how managed care may reduce such incentives (although these demonstrations tend to focus on frail elders). In addition, as the number of people with AIDS with Medicare (but not Medicaid) increases, funding support services and medications (not currently covered under Medicare) will be a particular problem, as it currently is for Medicare beneficiaries (as well as most privately insured individuals) with severe chronic illnesses.
Public programs funding medical and support services must also give people with chronic illnesses the flexibility to return to work when they are well enough without jeopardizing access to the very publicly funded services that make them healthy enough to work. This is a particular problem for people with AIDS who are successfully taking protease inhibitors funded by Medicaid or ADAPs. The concept of working with a disability while retaining a measure of income and insurance security is not without precedent. The Supplemental Security Income (SSI) program's 1619 regulations currently provide a model under which recipients who "work with severe impairment" continue to receive cash benefits and Medicaid coverage until their earnings exceed a specified level. However, it is unclear whether a person receiving successful treatment with protease combination therapy or other AIDS treatments, for example, would be considered to have a "severe impairment" under these regulations.
In addition to providing general assistance with daily living activities or AIDS-specific assistance such as help with adherence to treatment regimens, support services for poor people with chronic illnesses, including AIDS, must mesh more closely with public assistance, family services, and housing providers, because subsistence needs must be met before health and traditional support services can be put in place. Similarly, providers of support services for people with chronic illnesses and behavioral problems must work more closely with mental health and substance abuse treatment providers. Although these linkages are needed for all poor people with severe chronic illnesses, they play a particularly important role in AIDS service delivery, because AIDS is increasingly a disease of highly disadvantaged people.
Finally, the similarities of the needs of disadvantaged people with AIDS to those of disadvantaged people with other types of chronic illnesses raises a question of equitability in support services funding. The Ryan White program has demonstrated that important service and funding gaps had to be filled for poor people with AIDS. These gaps almost surely exist for all poor people with severe chronic illnesses.
RESEARCH AGENDA RECOMMENDATIONS
The need for (1) data describing the use and effectiveness of home- and community-based services for people with AIDS, (2) managed care approaches that integrate home- and community-based services for people with AIDS, and (3) a cohesive national chronic-care policy gives rise to the following research agenda recommendations:
-
Database Development. There is a clear need both for large representative databases that can provide timely descriptions of home- and community-based services among different groups of people with AIDS and for focused data collection to identify and evaluate promising interventions. Large administrative databases (such as Medicaid and Medicare claims systems and Ryan White records) are representative and comprehensive (within the realm of each program), but they lack much data describing sociodemographic and clinical characteristics found to affect service use and suffer from processing lags that keep them from being up to date. Provider data have the potential to add characteristics data and are more timely but describe highly specific populations (namely, provider clients), and reports concerning the rates at which characteristics data are missing from provider databases lessen their appeal. Nevertheless, research efforts should focus on examining the feasibility of developing combined administrative databases and of using provider data to supplement them.
-
Practice Guideline and Quality Indicator Development. Although their use is now becoming accepted practice in home health care, practice guidelines and quality indicators have not been used widely for other home- and community-based services. Although provider databases could be useful in developing benchmarks and testing specific approaches, development of guidelines and quality indicators usually relies on panels of experts and consumers. Research efforts should investigate the feasibility of such development. A first step in this effort might include a review of the literature to identify any existing guidelines and indicators, followed by a meeting of experts and consumers to discuss the desirability of developing (or refining) them for specific services (for example, case management or treatment adherence assistance).
-
Identification of Evaluable Interventions. In the course of its six site visits, this project identified a number interventions that could be considered for formal evaluation. However, a more focused approach could be taken to identifying interventions through the release of a request for proposals disseminated widely to AIDS providers. To encourage as many responses as possible by burdening providers as little as possible, the request process could follow a "foundation approach" in which providers were asked to submit two-page letters describing their ideas, a panel reviewed the letters, and selected providers were then asked to submit longer proposals. It would be important for the request to ask providers to describe data that could be used for evaluation and if their own databases were mentioned, how data completeness would be assured.
-
Development of Managed Care Demonstrations That Include Home- and Community-Based Services. AIDS-specific demonstrations are needed that include under capitation payments home- and community-based services (such as those covered under regular Medicaid benefits, Medicaid waivers, and Ryan White funding) in order to fill knowledge gaps about whether and how such arrangements may best be implemented. Such demonstration efforts face a number of nontrivial challenges, including identifying appropriate host organizations and a full range of service providers and setting payment rates. In addition, any such demonstration should require the collection of encounter data to describe patterns of service use under capitation. Similarly, thought should be given to the design of a Medicare demonstration that provides beneficiaries with AIDS (who do not also have Medicaid) coverage of pharmaceuticals and support services.
-
Investigation of Return-to-Work Regulations. Although the Supplemental Security Income program contains regulations that provide for the continuation of public benefits for people working with a "severe impairment," it is not clear whether or how these regulations apply to people with AIDS who are being treated successfully with protease or some other therapy. Because AIDS medications are so costly, and thus the disincentive to work particularly strong, this area deserves further investigation and may suggest the need to revise existing regulations to reduce the work disincentives.
-
Development of Approaches to Better Link AIDS Services to Other Systems. The level of contact between AIDS service providers and providers and entities in other systems--substance abuse treatment, mental health, family services, and public assistance--has increased greatly in recent years, primarily through increased referrals between systems, as the proportion of disadvantaged people with AIDS has increased. Yet AIDS providers in our case studies stated that there was not enough sharing of basic knowledge, particularly between AIDS providers and those in the substance abuse treatment and mental health systems. Coordination of efforts between these systems would be particularly important in developing strategies to assist people with substance abuse problems or mental illness to adhere to AIDS treatment regimens. Case study providers also stated that not enough was known about interactions between AIDS and psychotropic medications. Research efforts should thus develop approaches for sharing knowledge and pooling resources between AIDS service providers and those in other systems that serve large numbers of people with AIDS. Efforts might begin with a literature review and informal conversations with providers from systems of interest, followed by a meeting of experts and consumers to identify concrete strategies for increasing coordination between the systems.
CONCLUSION
As AIDS increasingly becomes a disease of disadvantaged people, medical treatment and health-related support services begin to blend with traditional public assistance programs such as food stamps and housing assistance. In addition, any changes in service delivery that result from changes in welfare or immigration policy will affect more directly an AIDS population growing poorer. As AIDS increasingly becomes a chronic, rather than an acute and fatal disease, its management has come to resemble more closely that of other serious chronic conditions. Key challenges in developing cost-effective models of chronic disease management include figuring out how to help people take responsibility for their health (adhere to treatment regimens, maintain good self-care practices, and learn to monitor and report symptoms) and how to provide them with the assistance and financial support they need to take this responsibility. Substance abuse treatment, mental health services, assisted or supportive living, interventions with families, assistance returning to work, and help locating safe and secure housing--all may have to play a bigger role in the delivery of home- and community-based services for newer AIDS populations than they did for gay men earlier in the epidemic.
REFERENCES
AIDS Treatment Data Network. "Paying for Protease Inhibitors." Treatment Review, no. 22, August 1996.
Altman, Lawrence. "Deaths from AIDS Decline Sharply in New York City." The New York Times, January 25, 1997.
American Council of Life Insurance and Health Insurance Association of America. "AIDS-Related Claims Survey: Claims Paid in 1995." Washington, DC: ACLI and HIAA, 1996.
American Public Health Association. "Costly Drugs Bring Hope to AIDS Patients but Strain State Budgets." The Nation's Health, October 1996, p. 10.
Anderson, Kathryn, and Jean Mitchell. "Expenditures on Services for Persons with Acquired Immunodeficiency Syndrome Under a Medicaid Home- and Community-Based Waiver Program." Medical Care, vol. 35, no. 5, 1997, pp. 425-439.
Bartlett, J.G., and R.D. Moore. "Are Protease Inhibitors Cost Effective?" The Hopkins HIV Report, vol. 8, no. 4, November 1996.
Benjamin, A.E. "Perspectives on a Continuum of Care for Persons with HIV Illnesses." In Conference Proceedings May 17-19, 1989: New Perspectives on HIV-Related Illnesses: Progress in Health Services Research, edited by W. LeVee. Rockville, MD: National Center for Health Services Research and Technology Assessment, September 1989, pp. 145-158.
Centers for Disease Control and Prevention. HIV/AIDS Surveillance Report, 1996a, vol. 8, no. 1.
Centers for Disease Control and Prevention. HIV/AIDS Surveillance Report, 1996b, vol. 8, no. 2.
Centers for Disease Control and Prevention. "First 500,000 AIDS Cases--United States, 1995." Morbidity and Mortality Weekly Report, vol. 44, no. 46, November 24, 1995a, pp. 849-853.
Centers for Disease Control and Prevention. HIV/AIDS Surveillance Report, 1995b, vol. 7, no. 2.
Cowart, M.E., and J.M. Mitchell. "Florida's Medicaid AIDS Waiver: An Assessment of Dimensions of Quality." Health Care Financing Review, vol. 16, no. 4, summer 1995, pp. 141-153.
Cowart, M.E., et al. "Project AIDS Care: Florida's Home- and Community-Based Waiver for Persons with AIDS." AIDS & Public Policy Journal, vol. 9, no. 4, winter 1994, pp. 189-197.
Crystal, Stephen, and Usha Sambamoorthi. "Functional Impairment Trajectories Among Persons with HIV Disease: A Hierarchical Linear Models Approach." Health Services Research, vol. 31, no. 4, October 1996, pp. 469-488.
Crystal, Stephen, and N.G. Schiller. "Stigma and Homecoming: Family Caregiving and the 'Disaffiliated' Intravenous Drug User." In The Social and Behavioral Aspects of AIDS: Advance in Medical Sociology, edited by R. Zimmerman and G. Albrecht. Greenwich, CT: JAI Press, 1993, pp. 165-184.
Crystal, Stephen, Anthony LoSasso, Usha Sambamoorthi, and Richard Johnson. "Patterns of Utilization of Home Care Services Among Medicaid Recipients with AIDS in New Jersey." Final Report. New Brunswick, NJ: AIDS Research Group, Institute for Health, Health Care Policy, and Aging Research, 1997.
Crystal, Stephen, Usha Sambamoorthi, and C. Merzel. "The Diffusion of Innovation in AIDS Treatment: Zidovudine Use in Two New Jersey Cohorts." Health Services Research, vol. 30, no. 4, 1995, pp. 591-612.
Fasciano, Nancy, Ann Cherlow, Barbara Turner, and Craig Thornton. "Profile of Medicare Beneficiaries with AIDS: Application of an AIDS Casefinding Algorithm." Princeton, NJ: Mathematica Policy Research, Inc., June 1997.
Flaskerud, J.H. "Overview of HIV Disease and Nursing." In HIV/AIDS: A Guide to Nursing Care, edited by J.H. Flaskerud and P.J. Ungvarski. Philadelphia, PA: W.B. Saunders Company, 1995.
Fleishman, John. "Utilization of Home Care Among People with HIV Infection." Health Services Research, vol. 32, no. 2, June 1997, pp. 155-175.
Fleishman, John, and Stephen Crystal. "Functional Status Transitions and Survival in HIV Disease: Evidence from the AIDS Cost and Services Utilization Survey." Medical Care. In press.
Gilden, D. "Protease Inhibitor New Math." GMHC Treatment Issues, August 1996.
Gostin, L.O., J.W. Ward, and A.C. Baker. National HIV Care Reporting for the United States: A Defining Moment in the History of the Epidemic. New England Journal of Medicine, vol. 337, no. 16, October 16, 1997, pp. 1162-1167.
Harrington, C., et al. "Medical Services in Social Health Maintenance Organizations." The Gerontologist, vol. 33, no. 6, December 1993, pp. 790-800.
Health Care Financing Administration. "Multi-State Evaluation of Dual Eligibles Demonstrations." RFP #97-015. U.S. Department of Health and Human Services press release, June 12, 1997.
Hellinger, F.J. "The Lifetime Cost of Treating a Person with HIV." Journal of the American Medical Association, vol. 270, no. 4, July 28, 1993, pp. 474-478.
Hiatt, R.A., et al. "The Cost of Acquired Immunodeficiency Syndrome in Northern California." Archives of Internal Medicine, vol. 150, April 1990, pp. 833-838.
InterStudy. Competitive Edge: Regional Market Analysis. St. Paul, MN: Decision Resources, Inc., 1995.
Institute of Medicine. AIDS and Behavior: An Integrated Approach. Washington, DC: National Academy Press, 1994.
Kaiser Family Foundation. "HIV Capitation Risk Adjustment Conference Report, May 28-29, 1997." Prepared by Diane Aschman et al. Chicago, IL: Health Research Network, 1997.
Kaiser Family Foundation. "Delivering HIV Care in a Managed Care Environment: Issues and Strategies." Prepared by Lawrence Bartlett and Patricia Hitz. Menlo Park, CA: Kaiser Family Foundation, January 17, 1996.
Kane, R., et al. "Perspectives on Home Care Quality." Health Care Financing Review, vol. 16, no. 1, fall 1994, pp. 69-89.
Katoff, L. "Community-Based Services for People with AIDS." Primary Care, vol. 19, no. 1, March 1992, pp. 231-243.
Kemper, Peter, et al. "Community Care Demonstrations: What Have We Learned?" Health Care Financing Review, vol. 8, no. 4, 1987, pp. 87-100.
Klein, A., and C. Thornton. "Profile of the Medicaid Home- and Community-Based Care Waivers for People with AIDS or HIV Infection." Report submitted to the Health Care Financing Administration. Princeton, NJ: Mathematica Policy Research, Inc., April 15, 1994.
Laudicina, S., and B. Burwell. "A Profile of Medicaid Home- and Community-Based Care Waivers, 1985: Findings of a National Survey." Journal of Health Politics, Policy and Law, vol. 13, no. 3, fall 1988, pp. 525-647.
Manton, Kenneth, et al.. "Social/ Health Maintenance Organization and Fee-for-Service Health Outcomes Over Time." Health Care Financing Review, vol. 15, no. 2, 1993, pp.173-202.
Markson, L.E., et al. "Pattern of Medicaid Expenditure After AIDS Diagnosis." Health Care Financing Review, vol. 15, no. 4, summer 1994, pp. 43-59.
Master, R.T., et al. "The Community Medical Alliance: An Integrated System of Care in Greater Boston for People with Severe Disability and AIDS." Managed Care Quarterly, vol. 4, no. 2, 1996, pp. 26-37.
Medicine and Health. "HHS: First-Ever Drop in AIDS Deaths Shouldn't Cut Efforts Against Disease." Medicine and Health, March 3, 1997.
Merzel, C., et al. "New Jersey's Medicaid Waiver for Acquired Immunodeficiency Syndrome." Health Care Financing Review, vol. 13, no. 3, spring 1992, pp. 27-44.
Miller, N.A. Medicaid 2176 Home and Community-Based Care Waivers. Health Affairs, vol. 11, no. 4, winter 1992, pp. 162-171.
Mollica, Robert, and Trish Riley. "Managed Care for Low Income Elders Dually Eligible for Medicaid and Medicare." Portland, ME: National Academy for State Health Policy, June 1997.
New York Times. "Setbacks for Many on Drugs for AIDS." September 30, 1997.
Reis, P. "Positive Healthcare." Paper presented at Beyond Water's Edge: Charting the Course of Managed Care for People with Disabilities, sponsored by the Office of Disability, Aging and Long-Term Care Policy, Assistant Secretary for Policy and Evaluation, U.S. Department of Health and Human Services, November 20-22, 1996. [http://aspe.hhs.gov/daltcp/reports/96cfpkes.htm]
Rich, Michael, Valerie Beckham, Carol Wittenberg, Charles Leven, Kenneth Freedland, and Robert Carney. "Multidisciplinary Intervention to Prevent the Readmission of Elderly Patients with Congestive Heart Failure." New England Journal of Medicine, vol. 333, no. 18, November 2, 1995, pp. 1190-1195.
Schoff, Jennifer, and Jennifer Schore. "The Role of Home- and Community-Based Services in Meeting the Health Care Needs of People with AIDS: Literature Review." Princeton, NJ: Mathematica Policy Research, Inc., January 1997. [http://aspe.hhs.gov/daltcp/reports/aidslit.htm]
Schore, Jennifer, Randall Brown, Valerie Cheh, and Barbara Schneider. "The Costs and Consequences of Case Management for Medicare Beneficiaries." Princeton, NJ: Mathematica Policy Research, Inc., April 1997.
Schultz, B.M., et al. "Improving Access to Long-Term Care for Persons with AIDS: Contrasting the Need for Acute Care with the Need for Functional Assistance." AIDS & Public Policy Journal, vol. 9, no. 1, spring 1994, pp. 49-52.
Shaughnessy, P., et al. "Measuring and Assuring the Quality of Home Health Care." Health Care Financing Review, vol. 16, no. 1, fall 1994, pp. 35-68.
Shilts, Randy. And the Band Played On. New York: Penguin Books, 1988.
TennCare News. "Cost of AIDS Drugs." Vol. 1, no. 8, October 1996, p. 5.
Thornton, Craig, Nancy Fasciano, Barbara Turner, Ann Cherlow, and Deo Bencio. "Methods for Identifying AIDS Cases in Medicare and Medicaid Claims Data." Princeton, NJ: Mathematica Policy Research, Inc. March 1997.
Ungvarski, P.J., et al. "HIV/AIDS Self-Care Guide." Visiting Nurse Service Of New York, 1995.
Ungvarski, P.J., and J.G. Staats. "Clinical Manifestations of AIDS in Adults." In HIV/AIDS: A Guide to Nursing Care, edited by J.H. Flaskerud and P.J. Ungvarski. Philadelphia, PA: W.B. Saunders Company, 1995.
U.S. Department of Health and Human Services. Information About: The Ryan White Comprehensive AIDS Resources Emergency Act of 1990. Washington, DC: DHHS, August 1994.
U.S. Food and Drug Administration. The Protease Inhibitors Backgrounded. Washington, DC: FDA, September 1996.
U.S. General Accounting Office. Medicaid Managed Care: Serving the Disabled Challenges State Programs. Publication no. GAO/HHS-96-136. Washington, DC: GAO, July 1996.
U.S. House of Representatives. 1996 Green Book: Background Material and Data on Programs Within Jurisdiction of the Committee on Ways and Means. Washington, DC: U.S. Government Printing Office, 1996.
Weinberger, Morris, Eugene Oddone, and William Henderson. "Does Increased Access to Primary Care Reduce Hospital Readmissions?" New England Journal Of Medicine, vol. 334, no. 22, May 30, 1996, pp. 1441-1447.
Weissert, William. "Seven Reasons Why It Is So Difficult to Make Community-Based Long-Term Care Cost-Effective." Health Services Research, vol. 20, no. 4, October 1985, pp. 423-433.
Wilson, Ira, and Paul Clearly. "Clinical Predictors of Functioning in Persons with Acquired Immunodeficiency Syndrome." Medical Care, vol. 34, no. 6, 1996, pp. 610-623.
APPENDIX A. CASE STUDY OF HOME- AND COMMUNITY-BASED SERVICE DELIVERY IN NEW YORK CITY
The New York City AIDS service delivery system appears to provide a full range of services, largely because of the state's expansive Medicaid program and generous Ryan White funding. In particular, the New York Medicaid program covers a wide range of home- and community-based services: post-hospital home health services (skilled nursing, therapy, and the assistance of home health aides); long-term home health services; home-based personal care services; and, under its waiver for elderly people and people with disabilities at risk of nursing home placement, medical social services, social day care, home modifications and maintenance, home-delivered meals, and nutritional counseling. In addition, the New York Medicaid program covers targeted case management for people who are HIV-positive or in a high HIV risk group, which links clients to medical, social, and educational services.
Currently, relatively few city residents with AIDS and Medicaid coverage are enrolled in managed care plans. In July 1997, however, the state's application for a 1115 waiver was accepted, which, for most beneficiaries, will make enrollment in managed care mandatory. The state expects that by 2000, 2.4 million of its 3.1 million Medicaid beneficiaries will be enrolled in managed care plans. While the 1115 waiver currently excludes people with AIDS (and those with serious mental illness), special needs managed care programs for these populations are planned.
The Ryan White CARE Act is the other major source of funding for AIDS home- and community-based services in New York City. Ryan White funds pay for home- and community based services (as well as outpatient and ambulatory care and comprehensive treatment services) for people without insurance or who are underinsured. In 1995, New York City received $94 million in Title I funds, and New York State received $29 million in Title II funds. New York State also maintains a pool (which draws on Title I, Title II, and county funds) to pay for medications, primary care, and home care for people with AIDS who do not have insurance.
The city Division of AIDS Services helps people with symptomatic HIV infection or AIDS in applying for public assistance; it also provides financial assistance for housing, food, and transportation. As of the end of 1996, Division of AIDS Services clients made up just under two-thirds of 29,169 people living with AIDS in New York City. Virtually all Division of AIDS Services clients receive Medicaid benefits or are spending down to Medicaid.
AIDS services in New York City are generally viewed as comprehensive (although shortages of particular services were reported in particular neighborhoods); on an organizational level, the provider community is generally collaborative and cooperative. This level of collaboration has been facilitated by generous service-funding levels, but the spirit of collaboration might suffer in the future, as a result of pressures generated by the increasing presence of managed care in New York City and potential cost-cutting in the Medicaid program.
On the other hand, there appeared to be some coordination gaps. Some case study participants noted a lack of coordination between the Ryan White Title I (city) Planning Council and the Title II (state) consortium networks. Oddly, the lack of coordination among these groups was attributed to the Title II consortium networks being neighborhood-based, while the Title I Planning Council takes a citywide approach. There also appeared to be long-standing, but fairly common, tension between medical and social service providers. The tension often stems from disagreements about who truly has a client's best interest at heart (for example, a home health agency that is required to discharge the client when services are no longer medically necessary or a social service case manager who wants to continue agency visits to reduce the social isolation of a homebound client). People with AIDS in New York were also described as having too many case managers with different types of providers and programs (medical, home health, Division of AIDS Services, mental health, substance abuse, supported housing, and so forth), with too little coordination and cooperation among them.
The major service gaps for people with AIDS in New York City were: safe and secure housing, mental health services, substance abuse treatment, and vocational rehabilitation, as well as specialized services for women, newborns, and adolescents. It is noteworthy that housing, mental health services, and substance abuse treatment are in short supply in New York for all people with low incomes, not just those with AIDS. Over the past few years these service gaps have become more serious problems for AIDS providers as the time from an AIDS diagnosis to death has increased and the epidemic has increasingly affected people with substance abuse problems or serious mental illness or people with no homes or substandard homes and those living in single-room-occupancy hotels. In addition, as the number of infected women with children has increased, lack of adequate, affordable housing has become a more serious problem. Furthermore, families affected by AIDS require such specialized services as assistance planning for the care of children whose parent or parents have died. Children whose parent(s) are ill or deceased require emotional support, support to help them stay in school, and AIDS-prevention education. Adolescent children of parent(s) who have AIDS tend to engage in risky behaviors, in spite of their family's experiences with AIDS.
Our New York City case study included three relatively large, well-established providers of AIDS services of different types: Gay Men's Health Crisis, an AIDS service organization; Visiting Nurse Service of New York, a home health agency; and Village Center for Care, a neighborhood-based network that includes residential, home-based, and community-based services.
A. GAY MEN'S HEALTH CRISIS
Gay Men's Health Crisis (GMHC), founded in 1981 shortly after the first CDC reports of Pneumocystis carinii pneumonia and Kaposi's sarcoma among gay men in New York City, is the oldest and largest AIDS service organization in the United States. GMHC was founded by six gay men in response to their frustration over the inability of the medical establishment to explain these deaths and the disease that caused them. The founders were all financially successful and understood the need to use power to effect change. The organization began with an AIDS hotline in an apartment, but over the years it has developed different programs to assist people with AIDS negotiate the health care system and fill gaps in education and support services. In 1982, with an all-volunteer staff, GMHC set up its formal hotline and volunteer buddy programs. The next program added was Client Advocacy, which initially addressed problems of discrimination against people with AIDS by health care workers. In 1983-84, GMHC started its safer sex and education programs; in 1986 its public policy department. GMHC is incorporating HIV testing into its continuum of support services to assist uninfected individuals remain so, assist infected individuals avoid transmission, and provide a range of information about treatment and health care. The GMHC HIV-testing center is expected to open in 1997 in conjunction with a clinic operated by New York Hospital.
The early days of GMHC were contentious as the organization tried to balance its primary goal of client care with the goals of education and policy change. GMHC views itself as a strong, conservative organization that is also flexible and able to adapt to change. It enjoys a high level of community ownership, but community involvement has also made it a difficult organization to manage. For many years the board of directors, originally made up of volunteer staffers, was heavily involved in the day-to-day management of the organization, but it has since moved away from this type of involvement. Current board members include "stakeholders" from New York's power elite (who made up the original board), people with AIDS who are clients or volunteers, community activists, and health and social service professionals.
1. Client Characteristics
GMHC currently serves about 10,000 people; 8,000 of whom are in client service programs. Referral tends to be through word-of-mouth and health and social service providers. GMHC's roots are in the gay community, and gay men are still a strong presence. However, it was clear from site visit discussions and GMHC documents that GMHC is making a concerted effort to provide outreach to effectively serve other people with AIDS and that it has been working with neighborhood organizations to reach them. In 1995, 19 percent of GMHC clients were women, about 60 percent were nonwhite, and half had contracted AIDS other than through homosexual contact. These figures reflect a clear departure from a strictly gay white male client base and are very roughly in line with the proportion of city residents with AIDS. Fewer than a fifth of GMHC clients, however, contracted AIDS through injection drug use, which is less than half the rate for the city as a whole.
2. Service Provision and Coordination
GMHC provides a number of one-on-one client services, as well as providing prevention and wellness education and public policy advocacy. One-on-one client services include: intensive case management, group therapy, the buddy program, mental health assessment/referral/crisis intervention, therapeutic recreation, complementary therapies (such as massage and acupuncture), nutritional counseling, meals, support for families in which children or parents are infected, and client advocacy and legal services.
Coordination with medical and nursing service providers appeared to be minimal, as most of the programs provided by AIDS service organizations such as GMHC are oriented more toward providing social services and other nonmedical support. Health service providers, however, were noted as an important source of referrals for GMHC. The level of coordination with medical providers may increase when GMHC's HIV testing center and clinic open.
We briefly describe four key GMHC programs: Intensive Case Management, Health Care Advocacy, Financial Advocacy, and Legal Services. Intensive Case Management, which is primarily a Medicaid-targeted case management program for people with AIDS, provides needs assessment, service planning, arranging or referral, and followup. The program also has one case manager position funded by Ryan White. Intensive Case Management clients tend to have substance abuse problems or are people with serious mental illness. The program has four case management teams (consisting of case managers and case management technicians), with 40 clients per team. Case managers and technicians must have college degrees in social work or a related field. If a client has a case manager with another organization, the Intensive Case Management case manager is usually designated as primary.
GMHC operates two client advocacy programs, Health Care Advocacy and Financial Advocacy. The Health Care Advocacy program, began in 1982 as a traditional ombudsman program, investigates and resolves complaints about health care (for example, service gaps or denial of equal access to care), provides information and referral to clients, and works for system change. Now the program receives fewer complaints about discrimination by health care workers, but more about the city Division of AIDS Services and about problems concerning discrimination and housing adequacy. With two coordinators and nine advocates, the program serves about 500 clients and has several volunteers who provide clerical support. The Health Care Advocacy program anticipates having to provide more client education to help clients advocate for themselves with HMOs as managed care begins to affect people with AIDS in New York City more directly.
The Financial Advocacy program provides information and referral about entitlements, as well as performing financial assessment for public assistance and providing Medicaid-reimbursable health insurance grants. (These grants allow GMHC to pay premiums for private health insurance for eligible Medicaid beneficiaries; Medicaid later reimburses GMHC for this payment.) Financial Advocacy also provides emergency cash grants for food, bills, and some travel. Recently, this program has been addressing issues concerning return to work and public benefits retention. The program staff consists of eight advocates who work with 160 clients. Three volunteers perform assessments and provide follow-up monitoring by telephone.
The Legal Services program also started in 1982. Disputes brought to this program tend to concern landlord-tenant disagreements; housing, employment, and public accommodation discrimination; wills and planning for children; immigration; bankruptcy; and employment/disability problems. The program currently has 10 to 12 paid lawyers and 10 to 12 support staff. It has seen more immigration cases lately concerning deportation of individuals who are likely to receive inadequate AIDS care in their country of origin.
GMHC client programs formerly used an "empowerment model," which taught clients to advocate for themselves; but staff have found this model does not work well for clients with mental illness or substance abuse problems. This is particularly true for clients of the Intensive Case Management program. In addition to changing their approach to serving clients, GMHC has found it difficult to integrate some newer clients who may not be respectful of differences in sexual orientation. Another problem has emerged: providing cash grants or entertainment tickets to substance abusers, who use the money (or sell tickets) to purchase drugs or alcohol. Requests for cash grants now receive much closer scrutiny. As an example of the type of changes in organizational culture that GMHC has had to undergo to serve newer AIDS populations, consider GMHC's experience with its Meals Program. The Meals Program, serving more than 50,000 meals each year on-site to provide an opportunity for socialization as well as good nutrition to maintain health, was originally conceived as a service for people who felt they could no longer go out to restaurants. Some newer clients have never been to restaurants or had a meal served to them.
Total staff size is 270 paid staff and 6,500 volunteers. It is noteworthy that most staff assigned to the four client programs described above are paid and must have relevant college degrees, with only a small number of volunteers providing clerical assistance. On the other hand, volunteers make up the bulk of the staff for GMHC's buddy, therapeutic recreation, and complementary therapy programs.
3. Revenue Sources
GMHC's 1996 operating budget was $26.1 million. Revenue was primarily from private donations (77 percent) and government funds (19 percent, including Medicaid and Ryan White). Medicaid funds only the case management program; Ryan White funds can be used only for clients with AIDS, thus are used only for one-on-one programs, not prevention education or other programs that may serve clients with asymptomatic HIV. Volunteer time was valued at $2.5 million. GMHC currently charges no client fees, but the new HIV testing center will use a sliding scale fee system. (GMHC currently receives fees for corporate HIV education and training.) In 1996, 47 percent of its operating budget was spent on client services, 17 percent on education, 12 percent on advocacy and public policy; management consumed 6 percent and fund-raising, 19 percent. GMHC is trying to reduce the cost of fund-raising by encouraging more corporate giving and large donations.
B. VISITING NURSE SERVICE OF NEW YORK
The Visiting Nurse Service (VNS), founded in 1893, provided 5.2 million home visits for 103,000 patients in 1995. VNS started its AIDS Services program in 1986 in response to an RFP from the city to become a preferred provider of home care to city Medicaid beneficiaries. That same year, the city Human Resources Administration instituted the Division of AIDS Services to coordinate applications to public assistance programs (including Medicaid) for city residents with AIDS. Under its ongoing contract with the city, the VNS receives referrals for home care from the Division, retaining some and disseminating others in neighborhoods where VNS does not have sufficient capacity to handle them. The Division of AIDS Services contract became VNS's AIDS Project. VNS's AIDS Services program includes the AIDS Project and other initiatives for patients with AIDS who are not Medicaid beneficiaries. The AIDS Project was also the basis of VNS's AIDS Center of Excellence, which promotes clinical expertise in AIDS care and disseminates expertise to other city providers.
The AIDS Services program is at present part of the agency's Acute Care unit, but will soon be moved to its Long Term Care unit, reflecting the agency's view that AIDS care is now more closely related to long-term chronic care than to post-hospital acute care. Early in the planning of the AIDS Project, the agency decided to provide all staff with a basic level of competence in AIDS care, rather than educate only a subset of its staff to provide AIDS care. This decision was due primarily to the very high number of AIDS cases in the city (as compared with the VNA of San Francisco, which adopted an AIDS-team approach) and the fact that cases were spread across the entire city (though not evenly). Thus, nurses do not report to the AIDS Services program, but instead receive education and support from the program. (AIDS program staff occasionally accompany nurses into the field to address specific problems.) Because nurses are assigned to cases geographically, and because AIDS is more prevalent in some parts of the city than others, in practice, some of its nurses are more experienced than others in providing AIDS care.
1. Client Characteristics
In 1996, 3,736 people with AIDS were referred to VNS. AIDS patients make up about 10 percent of overall agency census. Staff believe that they see about 75 percent of New York City's AIDS patients who require home care. The average daily census of patients with AIDS in early 1997 was 1,700, down only slightly from 1,800 for the previous year or so. The average length of a home health episode for a patient with AIDS is seven months, although most AIDS patients receive home health for only three months.
In 1996, 68 percent of VNS's referrals for AIDS patients came from hospitals--3 percent from physicians; and the rest from a variety of sources, including clinics and self-referrals. In that year, just over 40 percent of the patients were women, about twice the proportion of women with AIDS citywide. (VNS has only just started tracking patients by race and does not keep automated data on transmission risk group.)
2. Service Provision and Coordination
VNS provides nursing and medical social work services directly but contracts for rehabilitative services, home health aides, and personal care. For homemaker and housekeeper services, it refers patients to the Division of AIDS Services. The most heavily used services among their patients with AIDS are skilled nursing, home health aide, personal care, and rehabilitation. In 1996, VNS provided 110,000 nursing visits, 205,000 home health aide visits, just under 10,000 personal care visits, and 6,000 rehabilitation visits to its patients with AIDS.
All registered nurses (RNs) with VNS receive an initial two-day HIV orientation and continuing in-service training. The RNs assess patients, develop plans of care, and provide all hands-on care using clinical pathways for AIDS care and patient education materials developed by the VNS. In addition, the RN is the agency point of contact for patient physicians and coordinates aide and therapist contractors, private duty nurses, and laboratory services. Nurses have 25 to 30 patients and are expected to make six to seven visits per day. Frequency of contact ranges from daily (or twice a day) to every two weeks.
Family members and other care partners are both pluses and minuses in the delivery of home health care. Because of the limited number of visits allowed for teaching and direct care, care partners can be particularly important for patients in managed care. However, half of their patients with AIDS live alone, and of those many have no other family or friend to act as care partners; women patients are less likely than men to have care partners. Some (mostly male) partners refuse to provide care. Other care partners give up when they become overwhelmed by the reality of caregiving activities. Some care partners are abusive to the patient or staff; others sell the patient's medications. (This is also true of some patients.) Some care partners are representative payees (receiving a patient's public assistance benefit checks) but do not fulfill their obligation to pay the patient's bills.
New York City's unusually diverse population has led to conflicts between patients and agency staff that further complicate service provision. Conflict often erupts around meal preparation, due to differences in food preferences and preparation styles. The following factors were cited as the basis for disagreements concerning food or personality conflicts: sexual orientation, socioeconomic status, and specific nationality within a racial group (for example, Caribbean versus U.S. black, Puerto Rican versus Dominican Hispanic, Asians, Russians). To minimize conflict, VNS has attempted to identify more home care workers from specific minority groups and generally attempts to match patients and staff.
In addition to the AIDS Project, VNS has several other AIDS programs: Community Outreach to Adolescents of Parents with HIV/AIDS (funded through private donations, grants, and VNS); Supportive Services for People Living with the Impact of AIDS, which provides counseling and pastoral care (funded through Ryan White Title I and private foundations); the Pediatric Respite Program (funded through the Community Development Agency, AIDS Institute, and private foundations); and the AIDS Mental Health Program, providing licensed therapists in Brooklyn and Manhattan (funded through private foundations).
3. Revenue Sources
In 1995, VNS had a total operating budget of just under $500 million and revenue just above that. Most revenue for patients with AIDS comes from Medicaid. VNS's contract with Medicaid for the AIDS Project was $22 million in 1995. Medicaid paid for nearly 80 percent of all professional visits to patients with AIDS (nursing, therapy, nutritional counseling, and social work) and 92 percent of paraprofessional hours (home health aide, personal care attendant, housekeeper and homemaker). As noted above, special AIDS programs are funded primarily by Ryan White and various foundations.
VNS has contracts with all the major managed care providers in the city. HIP is the oldest contract (starting in 1993); Oxford and US Healthcare are the largest contracts. However, less than five percent of 1996 visits and hours to patients with AIDS were paid by managed care organizations. Payment to the agency under its managed care contracts is on a discounted fee-for-service basis; none of VNS's managed care contracts are capitated. Managed care contracts tend to exclude home health aide services. Patients in managed care with low incomes requiring aide services can receive them with Ryan White funding.
C. VILLAGE CENTER FOR CARE
Village Center for Care is located, and strongly rooted, in the Greenwich Village and Chelsea neighborhoods of Manhattan. Village Center began when, in 1977, community residents purchased the Village Nursing Home, the only residential geriatric facility in this part of Manhattan as it was about to be closed. When AIDS hit the community in the 1980s, community members wanted to respond with a continuum of services to meet the special needs of people with AIDS located in their own community. The continuum began first with the AIDS Day Treatment Program, which opened in 1988, followed by an AIDS-specific certified home health agency (1991), a Medicaid targeted Community Case Management program (1995), and Rivington House, an AIDS-specific nursing home (also 1995). (The site visit included day treatment, home care, and case management programs, but was too short to include a visit to Rivington House.) Changes in the AIDS population from relatively affluent gay white men with fairly stable lives to poorer people, people of color, more women, and people with relatively chaotic lives have not changed Village Center's basic client- and community-centered model of care (which accepts clients as they are and allows clients to set many of the parameters of their own care), but they have led Village Center to adapt the way it delivers care.
1. Client Characteristics
In 1996, Village Center served just under 1,600 clients with AIDS, roughly three-quarters of whom were not white and about a quarter of whom were women. One-third to one-half of all clients (depending on program) contracted AIDS through injection drug use. Thus, Village Center clients are roughly typical of New York City's AIDS population.
Historically, St. Vincent's Hospital has been, and continues to be, Village Center's largest single referral source. Over the past few years, however, it has been receiving relatively fewer referrals from St. Vincent's and other hospitals. In part, this is because inpatient use among people with AIDS has declined and in part because hospitals are increasingly opening up their own home care agencies to make up for that shortfall.17 Village Center has been getting an increasing number of referrals from the Department of AIDS Services for clients living in single-room-occupancy hotels, particularly to the Community Case Management Program. These clients are particularly difficult to work with, not just because of their living environment but because they are disenfranchised and distrustful of all providers; thus, it is difficult to get them to seek primary care and public assistance and difficult to engage them in problem solving. In the first six months of 1997, all Village Center programs had seen a marked increase in the number of clients with serious mental illness and problems with substance abuse.
2. Service Provision and Coordination
Services vary by program and seem relatively well coordinated within Village Center, as would be expected from an organization with the goal of providing a continuum of services to meet changing care needs. Referrals between Village Center programs are common, and Village Center's data system permits the sharing of key client data across programs. Changes are being made to the organization's database and to the procedures for increasing the efficiency of data sharing for clients who use multiple programs.
Serving clients who continue to abuse drugs or alcohol or who engage in risky sexual practices has posed a serious challenge to Village Center staff (as well as staff of the other two organizations we visited). Staff have been particularly frustrated by their inability to stop clients from injecting drugs or otherwise engaging in risky behavior. Village Center (and VNS) staff noted that they now follow a "harm reduction" model of service provision. This model provides staff with an approach that allows them to continue serving clients who exhibit counterproductive behaviors, without becoming totally burned out in a short time. It allows staff to acknowledge that some clients may engage in risky behaviors despite the best efforts of staff members. Under this model, however, clients may not use, buy, or sell drugs when staff are present, or they will be discharged. Clients are also discharged if they abuse staff or seriously threaten them with abuse. Clients discharged for these reasons are referred back to the Division of AIDS Services, to parole officers, or to psychiatric providers.
Village Center's certified home health agency serves clients in Manhattan and, more recently, Brooklyn. A special needs home health agency serving only people with AIDS, it currently serves 350 clients (down from 400 in 1995). The average length of stay is just over six months; most clients are terminally ill by the time they use the agency (rather than the day treatment program). The agency uses a geographically assigned team approach to delivering care. Teams include a supervisor, clinical coordinator, five primary nurses, and a clinical assistant. Clinical coordinators respond to client telephone calls when primary nurses are out in the field, which is most of the time. Primary nurses assess clients, develop care plans, and coordinate with mental health services, AIDS service organizations, and Village Center's Community Case Management program, as well as providing hands-on care. They have caseloads of 20 to 25 clients, whom they contact at least once a week. Care partners (spouses, significant others, and other informal caregivers) are included in care plans, but many are ill themselves or find they cannot assume as much care as originally promised.
The AIDS Day Treatment Program was, at its inception in 1988, a day program primarily for gay men with AIDS dementia. The program had the goals of providing the same type of support to Medicaid beneficiaries that more affluent people can afford to pay for (for example, medical and psychiatric care, alternative medicine, nutrition, rehabilitation, recreation, and entitlement advocacy); and a one-stop-shopping approach to receiving this care while also attending to ancillary medical problems associated with AIDS (such as skin and gastrointestinal problems). Program staff quickly discovered that not many of their clients had dementia (as a result of treatment with AZT), nor were that many gay men. Clients of the AIDS Day Treatment Program tend to have no family or friends to care for or help them; so, the program becomes a surrogate family for most day treatment program clients. It uses a client-centered model of care that allows clients to define their own needs; clients are accepted as they are, and the program tries to eliminate barriers between staff and clients. Some 50 to 60 clients per day are seen, and clients must attend for at least three hours a day. The program is open six days a week. The average length of stay for clients enrolled in 1996 was about two years. Each client goes through a two-day intake assessment and develops a plan of care in conjunction with a social worker and nurse, which the client signs and can change as needed. Clients pick the days they will visit. On a typical day, a client sees his or her case manager, has two meals, visits the clinic, and receives some type of alternative therapy. Although there is van pickup for the program, most clients are given tokens and arrive via public transportation.
The Community Case Management Program (begun in January 1995) is a Medicaid-targeted case management program for people who are HIV positive or in a high HIV risk group (as is GMHC's Intensive Case Management program). This program operates under state guidelines governing assessment, frequency of contact, and care delivery, and the state AIDS Institute trains the program's workers. The Village Center program varies from those of other organizations in that it provides more home visits rather than requiring clients to come to the office (this is viewed as less intimidating and more likely to engage the client). The program conducts assessments of needs and develops worker/client goals. Clients with relatively simple needs are referred to the Division of AIDS Services for public assistance or to other organizations. Clients with more complicated needs are often escorted by program staff to medical appointments or to the Division of AIDS Services to provide assistance filling out forms and interacting with city workers. Recently, the program's caseload of clients living in single-room-occupancy hotels has increased dramatically. Clients addicted to crack are especially difficult to work with; case managers usually wait until after the 10th of the month, when SSI checks have been spent on drugs, to contact them. A team approach is used, including case managers, case management technicians, and community follow-up workers. (Case managers must have a bachelor's degree; technicians and follow-up workers must be high school graduates and have some experience serving people with AIDS. Follow-up workers must also come from the communities they serve.) Each team has 40 to 50 clients. Some clients are seen two to three times a week, but at a minimum must have at least nine contacts every 90 days, of which at least two are in person.
3. Revenue Sources
The Village Center AIDS programs are almost entirely funded by Medicaid. All funding for the day treatment and community case management programs is from Medicaid; 90 percent of the funding for the home health agency is from Medicaid. Most other home health funding is from Medicare, although a small amount of funding comes from Ryan White. Private fund-raising has played a small role in revenue and has been used only for special purposes. For example, there was a lot of fund-raising to build Rivington House. Village Center is trying to expand its fund-raising activities.
The Village Center programs have very few clients in managed care. The programs negotiate fees and service authorization individually with the managed care organizations for clients who are in managed care. Village Care management, however, believes that managed care will become more important for its clients and is aggressively positioning itself to participate in the managed care market. It has plans to apply to be a Medicaid managed care Special Needs Plan in collaboration with St. Vincent's and Beth Israel hospitals and has been marketing specific service packages to private managed care organizations.
APPENDIX B. CASE STUDY OF HOME- AND COMMUNITY-BASED SERVICE DELIVERY IN LOS ANGELES
Key attributes of the HIV/AIDS delivery system in Los Angeles are that (1) it covers a very large geographic area; (2) there are many medical and social/support service providers (more than 100 AIDS service organizations), which are more concentrated in certain neighborhoods than others; and (3) a centralized county-based system exists for providing all secondary and tertiary care to low-income uninsured people. In contrast to San Francisco, the Los Angeles public sector was reportedly slower to act and generally less supportive in the epidemic's early years. This early weakness in the county system, combined with concerns about widespread homophobia and discrimination toward people with AIDS, provided the impetus for development of private community-based medical programs for people with AIDS. Gradually the county programs grew and became more sophisticated; but the community-based system has also prevailed and flourished, so that now the two operate alongside one another.
California's Medicaid program (Medi-Cal) has, since 1989, operated a home- and community-based waiver program for people with AIDS or symptomatic HIV; since 1986, the state has operated a similar program with state-only funds. The waiver program serves Medi-Cal eligibles with mid- to late-stage AIDS who have a safe home setting and who require a nursing home level of care or higher, and have functional limitations. The older state-only program, known as the Case Management Program, currently serves HIV-positive children and adults who have AIDS or symptomatic HIV and functional limitations. (The functional limitation criterion for the state-only program is somewhat less stringent than that of the Medi-Cal program.) Although there are no income eligibility criteria for the Case Management Program, most clients are either spending down for Medi-Cal eligibility or are Medi-Cal beneficiaries who do not yet meet the waiver program's more stringent functional status criterion. Both programs provide case management, attendant care, homemaker services, psychosocial counseling, in-home skilled nursing and infusion therapy, nonemergency medical transportation, durable medical equipment and supplies, minor home modifications, nutrition supplements and home-delivered meals, and nutrition counseling. The Case Management Program also provides housing assistance, food subsidies, and hospice care; Medi-Cal provides hospice care outside the waiver program. In 1996, each program served roughly 3,100 people. There are per-person expenditure caps for both programs: $13,209 annually for the Medi-Cal waiver program (annual costs average $3,273 per client), and $536 per month for the Case Management Program. For 1997, the Case Management Program is financed with $6.4 million in state funds and $1.3 million in Ryan White Title II dollars.
The state has fairly generous income eligibility criterion for the ADAP (up to $50,000 adjusted gross annual), but timely access to prescription drugs is limited. HIV/AIDS-related prescription drugs are currently covered by Medi-Cal as soon as they receive FDA approval, whereas, under California's ADAP program, new drugs are not added to the formulary until they are recommended by a medical advisory board and approved by the state. Because the ADAP advisory board meets only twice a year, and because not enough funds are available to support all new drugs, there are greater delays and gaps in drug coverage under ADAP.
Although neither the state nor the county has a recent estimate for the magnitude of Medi-Cal spending on HIV/AIDS care, Medi-Cal is believed to be the largest single payor for this care in the state. Ryan White grants also contribute a substantial share. In fiscal year 1996/97, California received a total of roughly $135 million in Ryan White funds. Of that, $87 million went to the nine qualifying Title I metropolitan areas; Los Angeles received more than $30 million. The ADAP program is financed with Ryan White money ($17.8 million), state funds ($15.6 million), and $3.5 million from a special drug reimbursement authority.
Among people with private insurance, managed care penetration rates in California have been high for years and are rapidly growing among the publicly insured. Medicaid managed care is being implemented differently in each county; and in Los Angeles, AFDC-related beneficiaries are gradually being required to choose between two HMO-style plan options. Managed care is still voluntary for people with disabilities, including AIDS. Medically needy populations are excluded from joining an HMO, primarily because of problems with intermittent eligibility and cost-sharing requirements. In Los Angeles, Medi-Cal eligibles with AIDS have the option of joining a special capitation program for people with AIDS that is operated by the AIDS Healthcare Foundation.
In characterizing relationships among AIDS service organizations, most of the case study participants thought that direct provider staff collaborate well but that there has been significant tension and "turf concern" at the executive and organizational levels. Tensions have reportedly been greatest between medical and social service organizations; but tension also exists between some of the larger service organizations, which tend to serve primarily gay men, and the numerous smaller organizations that provide a few services or serve particular populations (other than gay men). Some of this tension has arisen because funding priorities are being reevaluated in light of changing demographics and advances in medical treatments, but personality conflicts also play a role. Among recent efforts to improve coordination and representation among AIDS programs and providers are: combining the Title I planning council with local Title II consortium bodies, to form a joint "LA County HIV Health Services Commission"; changing the mix of planning commission members to better represent consumers and changing demographic and service use trends; and increasing the extent to which focus group and statistical data support decisions about funding priorities. Final decisions about spending are made by the Los Angeles County Board of Commissioners, an elected body.
Despite the large number of case management providers and agencies in the community, reportedly few people are assigned more than one case manager. As case management funding has become scarcer in recent years, efforts to eliminate multiple case managers have intensified.
As in New York City, housing tops the list of unmet needs for people living with AIDS. This need is expected to intensify as more and more very poor and disenfranchised people become infected. Homelessness is a large and growing problem, too, and there is a growing need for emergency/crisis shelter, transition housing, and assisted-living alternatives. The demand for available services from programs--such as the federal Department of Housing and Urban Development Housing Opportunities for People with AIDS (HOPWA) program, which provides short-term assistance with rent, moving and utility expenses--far exceeds available resources. Because Los Angeles is so large, and because facility-based services tend to be clustered in the central parts of the city, transportation is another big unmet need. Some other service gaps are the need for more mental health and substance abuse treatment services, appropriate programs for women and families (especially blacks and Latinas), and services geared to helping people return to work.
The three Los Angeles organizations included in the case study represent important facets of the local AIDS delivery system: AIDS Project Los Angeles, a large HIV/AIDS social services organization; AIDS Healthcare Foundation, a residential and outpatient medical provider that also operates a specialized Medicaid managed care plan; and AltaMed Health Services Corporation, a community health center with a dedicated HIV/AIDS program targeting the Latino/a community.
A. AIDS PROJECT LOS ANGELES
AIDS Project Los Angeles (APLA) is the second-largest AIDS service organization in the United States, with a total client caseload equal to nearly 50 percent of the current AIDS population in Los Angeles. Formed one year after, and in many ways modeled after GMHC, APLA was also started by a group of gay men as a hotline operated out of a small apartment. Over the years it has blossomed, now providing more than 30 different services to 6,100 clients. A buddy program was added in 1983 and mental health and case management services were soon thereafter. The organization has long had strong ties to the Hollywood community; its fund-raising efforts include high-profile annual events involving Hollywood celebrities. Like most AIDS service organizations formed in the early 1980s, APLA began serving mostly gay men (many of the founding board members still see this as the organization's primary mission). With client demographic trends shifting away from gay men, tensions have developed within the organization as it reevaluates the organization's mission as the epidemic evolves.
1. Client Characteristics
Of APLA's 6,100 active clients, most (91 percent) are men, the majority of whom are gay or bisexual (67 percent). Notably, more than 50 percent are nonwhite--a proportion that reportedly is increasing; the percentages of APLA clients who are black or Latino/a are higher than the citywide figures for the epidemic. Other significant trends include a growing number of clients who are homeless (now 13 percent of the caseload), poor, and/or dealing with substance abuse and serious mental health problems. Only nine percent of APLA's clients are women, but the proportion is on the increase. Most clients (84 percent) are insured, about half through Medicaid and/or Medicare.
For most APLA programs, clients must reside in Los Angeles County and have symptomatic HIV infection. A few programs also have income restrictions or are limited to people with full-blown AIDS. Prevention and education services (including counseling about benefits, nutrition, and HIV/AIDS treatments) are generally available to anyone affected by HIV in the community.
Because APLA is large and well known within the Los Angeles community, the organization does little in the way of outreach. Most clients self-refer, based on word-of-mouth, or are referred by another AIDS service organization. Food pantry and case management programs attract clients from all over the city. Some outreach is conducted for their prevention programs, which primarily target adolescents and young adults.
2. Service Provision and Coordination
APLA's major service divisions are client services, education, and policy and planning. Client services programs, as the name suggests, deal mostly with registered clients (all of whom are at least HIV positive and symptomatic), whereas education and policy and planning focus on the overall community. Client services encompass mental health (including the buddy program), case management, home health and dental care, food pantry, nutrition counseling, transportation, living skills, benefits and legal counseling, and housing assistance. Major education efforts include the hotline, treatment advocacy, and outreach/prevention programs for adolescents and young adults.18 Overall, APLA employs 230 staff and utilizes between 2,00 and 3,000 volunteers.
Case management is a core service at APLA. Over 70 percent of the active caseload currently receives some form of case management. Recognizing that caseloads were too high and that many clients were functioning reasonably well, APLA several years ago created a new program, which it calls Clientline, that uses a telephone-based model to serve clients with less intensive needs. The face-to-face case management program is then aimed at clients who need more intensive support. Of 4,300 clients currently being case managed, fewer than one-fifth are in the face-to-face program. Nearly half of these clients are homeless and are served by designated, specially trained staff. In Clientline, clients call their case manager when they have a problem or question, and a trained, supervised group of 40 volunteers provides backup to case managers by calling clients who have not been in touch with their case manager in the past three months. Case managers for both programs receive extensive on-the-job training. Several years ago, APLA began upgrading the education/skill requirements for its case managers because client needs were becoming more complex and treatment issues more sophisticated. APLA now requires staff to have at least a bachelor's degree and, preferably, previous case management experience.
APLA administers home care programs under both the Medi-Cal waiver program and the state's Case Management Program. With a staff of seven nurses and four social workers, it currently serves 230 clients across the two programs. When the programs began, the typical patient was a gay white male, bedridden and needing hospice-oriented assistance. The current caseload is more stable medically, but staff report that clients have more complex psychosocial needs stemming from poverty, criminal justice involvement, mental illness, substance abuse, and a host of other factors. Major recent changes experienced by the home care programs include fewer client deaths, decreased demand for attendant care services, and greater need for skilled social workers and staff with mental health training.
APLA provides a full range of mental health services ranging from the buddy program, which links clients to volunteer companions for support/friendship, to one-on-one counseling by licensed clinical psychologists and family therapists. As in other APLA programs, mental health staff have seen an increase in the number of clients exhibiting more complex mental illnesses and other comorbidities, especially substance abuse. Many clients are also struggling with issues related to the new treatments--difficulties with adherence and other factors affecting whether they can tolerate the new therapies and become healthier under them. Because adherence to the complicated regimens for the new therapies is so demanding, APLA is thinking about training volunteers in the buddy program to assist clients.
Additional assistance with the pharmaceutical treatments is provided through the treatment advocacy program. Offered by many Los Angeles AIDS service organizations, this program began as an effort to influence the direction of, and access to, clinical trials for people with HIV and AIDS. It also advocates getting new treatments approved by the Food and Drug Administration, gathers extensive information on available therapies, and helps clients decipher complex, sometimes conflicting, information about the pros and cons of various alternative therapies. Because the new protease-combination therapies are so complex, demand for treatment advocacy services has grown at the same time that the service has become more difficult to provide. APLA is now considering whether to hire nurses to help its lay treatment advocates.
Among numerous other direct client services, APLA staff counsel clients about public and private assistance and assist with legal matters. The latter program is being expanded to focus more on employment-related issues, benefits law, and guardianship, in addition to the more traditional services related to wills, estate planning, and bankruptcy. APLA also operates a food pantry program, in which low-income clients "shop" for groceries and other items that have been donated or deeply discounted, and nutrition counseling is provided. A life skills program was recently added when staff began to worry that many clients needed help getting out and living actively again after focusing for so long on preparing to die.
3. Revenue Sources
APLA's 1996 operating budget was $20.1 million. Like GMHC in New York, APLA relies heavily on fund-raising and private donations to finance its programs. Roughly 70 percent of its operating revenue comes from these sources; another 20 percent is from grants through Ryan White programs and other state and local sources. Less than 10 percent of its revenue is from insurers, primarily for services provided through home and dental care programs. With all the publicity and optimism surrounding the new treatments, APLA has begun to experience a decline in revenue from fund-raising and donations. (Staff attribute some of this decline to a natural drop-off that occurs after donors give over many years.) Staff are worried, too, that the changing face of the AIDS epidemic may take its toll on fund-raising efforts--many of their traditional donors were drawn to the organization because of its role in serving the gay community.
For the most part, fund-raising shortfalls to date have been offset by reserves; at the same time, APLA has reduced its operating budget by cutting roughly 15 percent of its staff positions. It is currently in the process of evaluating its programs and scope of services. Two years ago, APLA initiated a strategic planning and needs assessment process that uses survey input from clients and program records to identify high-priority services and unmet needs. This information will help APLA management determine changes that may be necessary in the mix of services, and guide decisions about program and service priorities, should the organization face continued funding cuts.
B. AIDS HEALTHCARE FOUNDATION
AIDS Healthcare Foundation (AHF) was founded in 1987 to fill a perceived gap in medical care for people with AIDS. Initially, AHF operated one 25-bed hospice facility in a former nurses' dormitory. In 1991, the first of four outpatient medical clinics was added, all to be located on the campuses of major tertiary care hospitals. Two more hospice/residential care facilities were added, one in 1992, the other in 1996. In addition, AHF collaborates with another organization to operate a specialized program for women. In 1995, under a contract with the state Medicaid program, AHF began operating one of this country's few capitated managed care plans for people with AIDS.
In addition to the provision of state-of-the-art medical care, AHF's mission has long included a strong emphasis on advocacy. Specialized AIDS medical programs were reportedly slower to develop in Los Angeles than in other U.S. cities with large AIDS caseloads. Although the county's programs have since improved and are now viewed as first-rate by many providers, by all accounts the county system was inadequate in the epidemic's early years. Hostility toward homosexuals and people with AIDS among many private providers helped create further barriers. AHF's founder and executive director has, from the beginning, been an outspoken critic of perceived problems and injustices with the AIDS delivery system. He has spoken out against the county and other AIDS service organizations when he believed doing so was in the best interest of AHF's clients and other people with AIDS. This strategy has placed AHF at odds with various AIDS service organizations in the county, as well as with the county Board of Supervisors (which makes the final decisions about Ryan White spending).
1. Client Characteristics
AHF served nearly 3,300 clients in 1996, most of whom are symptomatic or have full-blown AIDS. Forty percent of AHF's clients are insured through Medicaid, a small percentage are privately insured (5 percent), and the rest are uninsured. Although the proportion of clients who contracted the virus through male-to-male sex matches the proportion in Los Angeles overall (roughly 80 percent), AHF serves a greater number of women (11 percent), blacks (23 percent), and Latino/as (36 percent) than reflected in community-wide figures (6 percent women, 19 percent black, and 25 percent Latino/a). Staff expect the growth in black, Latino/a, and female clients to accelerate. Despite this trend, AHF physicians and staff noted that they have much to learn in serving these newer populations. As one physician put it, "We know that we have a model that works well for gay men, but we really don't have a clue about how best to serve some of these other groups." As an example, a year or two ago, AHF opened a new clinic in a predominantly black area. AHF staff expected to see mainly gay black men, but in fact most of the clients were women with complex medical and social problems. AHF staff were not well prepared to deal with their problems and eventually decided to close the clinic. (Cost pressures also played a significant role.)
All of the roughly 360 clients in AHF's Medicaid managed care product, Positive Healthcare, are Medicaid-eligible. They are between the ages of 21 and 65, and meet the CDC's definition for AIDS. Enrollment into this program is voluntary. People who qualify for Medicaid under the medically needy (or spend-down) rules are prohibited from joining any managed care plan, including Positive Healthcare.
2. Service Provision and Coordination
AHF provides a continuum of AIDS-specific medical care, including outpatient primary and specialty care, outpatient prescription drugs, inpatient physician services, transitional and assisted residential care, and residential hospice care. It also has a small, though shrinking, home care program which is operated under a subcontract to the Visiting Nursing Association of Los Angeles. While, in the past, AHF offered more support services, it has had to cut back, and now provides only a limited amount of medically oriented case management. (Clients are referred to other AIDS service organizations for additional support services.)
Since its inception as a 25-bed hospice program, AHF has added two new 25-bed residential facilities and recently expanded the residential model to include transitional/skilled nursing care and assisted-living programs, in addition to traditional hospice care. In recognition of changing needs, AHF recently began calling these facilities "houses" rather than "hospices." The shift away from hospice care to less intensive forms of residential care has been driven primarily by advancements in treatment. Demand for intensive inpatient care and hospice services has fallen dramatically. Yet, while many clients are leaving the hospital sooner and healthier, some still require skilled nursing care during a transition period until they are ready to be cared for on an outpatient basis. Also, the new combination drug treatments have given rise to new service needs: assistance in adhering to the complicated mediation regimens. AHF staff have found that clients who lack stable support systems and who are experiencing multiple problems and generally more complicated lives benefit from more intensive support when they begin the treatment regimen. Only 30 percent of AHF's residential beds are now being used for hospice care; in the future, AHF anticipates needing only 20 percent for this level of care. The rest of the beds will be split between intensive nursing and treatment adherence, with an average length of stay for these programs of four to six weeks (compared with four to six months for hospice care).
In developing its outpatient medical programs, AHF aimed to create state-of-the-art programs that would employ the very best physicians and most up-to-date medical advances. To facilitate access to top-notch specialists and inpatient care, all the clinics are located on the campuses of major hospitals or are adjacent to them. Except for low-income, uninsured patients, who are referred to the county, AHF physicians follow their patients during hospitalization.19 AHF is also directing 25 clinical trials of antiretroviral therapies funded by pharmaceutical and biotechnology firms. Two additional studies are being sponsored by the federal government. One is looking at women's health needs and service use; the other is trying to identify the factors that most influence adherence to the new therapies. Research staff report much greater difficulty recruiting women and black men for the clinical trials. They have found that many women, particularly Latinas, are hesitant to put their needs above those of their spouse or family, while black men often do not trust the medical establishment because of incidents such as the Tuskegee experiment. Adding to the continuum of outpatient care, AHF is a certified ADAP provider and recently began operating the only AIDS-specific Pharmacy Benefits Management program in the country.
In keeping with its track record of developing cutting-edge programs, AHF has one of the few operational AIDS-specific managed care plans. Development of the plan, known as Positive Healthcare, was supported in part by a Special Projects of National Significance grant under the Ryan White CARE Act. In April 1995, AHF signed a $26 million contract with the Medi-Cal program to operate as a Primary Care Case Management plan. Medicaid eligibles enroll voluntarily, and AHF is paid a capitation amount that covers primary and specialty care. Inpatient care is paid for outside the capitation, as are home- and community-based waiver services and (in the current contract) prescription drugs approved after 1995. AHF is eligible for a "savings share" if its enrollees use less inpatient, skilled nursing, and hospice care than their fee-for-service counterparts, but, to date, it has received no payments from this pool. AHF is currently protesting the state's method of computing both the savings share and the capitation payment.
At 360 clients, enrollment in Positive Healthcare has been lower than expected. (By mid-1997, they hoped to have 1,000 clients.) Staff attribute the enrollment problems to two major factors: (1) many AHF clients are prohibited from joining the plan because they qualify under the medically needy program, and (2) AHF has not received many referrals from other AIDS service organizations. About a year ago, AHF subcontracted to AIDS Project Los Angeles for case management services and agreed to pay APLA $55 per member per month. In addition to providing social case management, AHF expected APLA to "market" Positive Healthcare and make referrals to the plan. Referrals were not forthcoming, so AHF stopped paying APLA and will not be renewing the latter's contract.
3. Revenue Sources
Roughly half of AHF's current $28 million dollar operating budget is expected to be financed with revenue from public and private insurers. The other substantial proportion (34 percent) will come from Ryan White and other grants. Only eight percent of its revenue will come from donations and fund-raising. Remaining revenue comes from proceeds from eight thrift stores that AHF operates throughout the county.
By all accounts, AHF has experienced financial difficulties because of its commitment to provide equal access to medical care regardless of cost or ability to pay. The financial crunch has been especially acute since FDA approval of the protease-combination therapy in December 1995. AHF experienced major losses for both its Positive Healthcare and its ADAP clients. Rather than make the ADAP clients wait for the drugs to be added to the formulary, AHF decided to provide access equally to ADAP clients and absorb the financial loss. Similarly, AHF provided the new drugs to its Positive Healthcare clients even though its capitation payments would not cover these costs fully. (AHF subsequently negotiated a contract that carves out from the capitation payment all prescription drugs released after 1995, and pays for them separately.)
AHF may experience further financial problems resulting from changes in the way outpatient medical care will be paid under the Ryan White program. Rather than issuing grants, the local Title I grantee will soon begin paying for these services on a fee-for-service basis. This will put pressure on organizations with higher costs and could result in shortfalls, at least in the short term.
Another challenge involves getting insurance coverage for the nonhospice residential services, which currently are paid for out of grants and general operating revenue. AHF has succeeded in getting legislation passed that will allow Medicaid to pay for transitional/skilled nursing care if AHF gets the facilities certified by both Medicare and Medicaid (Medicare certification is still pending). There are no provisions in place at this time for Medicaid or Medicare reimbursement of care related to treatment adherence.
C. ALTAMED HEALTH SERVICES CORPORATION
Whereas the other two Los Angeles providers we visited focus exclusively on HIV/AIDS, AltaMed is a comprehensive community health center formed in the late 1960s, which subsequently developed an HIV/AIDS division in response to growing need among its patients. In addition to HIV services, the organization operates four primary care sites, a methadone maintenance program, a large health and social support service program for the elderly, and several teen prevention and education programs. Both AltaMed and its HIV division are dedicated to serving Latino/as, and the HIV program is recognized as a major provider serving Latino/as in Los Angeles.
The HIV program, formally established in 1991 with a caseload of about 25 clients and 7 staff, has grown steadily each year to its current size of 600 clients and 53 staff. The program is located within AltaMed's Sunol site in a predominantly Latino/a area of East Los Angeles. In 1995, AltaMed began providing HIV services at a second location, in Pico Rivera, a mostly middle-class community; currently, about 100 of AltaMed's 600 clients are served at this location. The Sunol site is co-located with several local health department programs and a child care facility. Initially, these neighbors were opposed to an identified HIV program because they thought it would scare away their clients. HIV/AIDS and homosexuality are not well accepted in Latino/a communities. Staff report that greater stigma is associated with these than with being a prostitute or a thief. Intense efforts early on to educate staff from these other programs reportedly helped resolve many misconceptions and paved the way for greater acceptance and smooth-working relationships that have persisted.
The building that houses the Sunol site is old, and space is tight for both the regular primary care and the HIV programs. AltaMed corporate leaders recently decided to move the Sunol programs to a larger, more modern facility nearby; but HIV program staff worry that the move will erode their efforts to integrate HIV care with other community programs and reduce the stigma of HIV and AIDS. Being housed in a separate and newer facility, however, may help attract more clients who are insured and help AltaMed increase the site's involvement in managed care.
1. Client Characteristics
Like the other two programs we studied, AltaMed's HIV program serves primarily gay men; at AltaMed, however, most are Latino. Although the proportion of clients reporting use of intravenous drugs is very low (two percent), recent trends suggest that the proportion using other drugs may be growing. Nearly all have incomes under 300 percent of the federal poverty level, and 83 percent are uninsured. The percentage without insurance is expected to grow as welfare reform further reduces access to Medicaid and other public insurance among more recent immigrants.
Latino/a culture erects special barriers for people living with AIDS, and staff have worked hard to create a comfortable environment for clients. Many clients, especially those still living with their families, are not open about their sexuality or their HIV status in the home. In addition, Latino/as reportedly are uncomfortable talking openly about sex and sexuality--which means that materials and discussions must be indirect and subtle. Women are especially hesitant to speak openly about sexual issues or to make demands of their partners, in part because "machismo" is both accepted and widespread. It is not generally acceptable, for example, for women to ask their partners to use condoms. Finally, because family is so important in Latino/a culture, program brochures were designed to focus on how the HIV program was like a family that supports and embraces its clients.
2. Service Provision and Coordination
The HIV program provides a full continuum of primary care and related support services, including prevention and testing, specialized medical care, mental health, home care, and case management. Most of the staff are bilingual and bicultural, but it has been difficult finding enough mental health/social work staff with these attributes. Prevention and testing services are provided through a mobile van program that targets homeless people and those with substance abuse problems. Another prevention program targets gay/bisexual Latino men, and it seeks to change attitudes and misconceptions that drive high-risk behaviors.
The medical program focuses only on primary care. AltaMed has a staff of four physicians, one nurse, and three medical assistants. Almost all specialty and inpatient care for its HIV clients is provided by the county, in part because, in Los Angeles, Ryan White programs fund specialty and inpatient care only if it is provided by county programs. Also, AltaMed is one of the few authorized ADAP providers in the county and so may dispense ADAP-approved drugs to its clients. (Last year, the total budget for the ADAP program was $2 million, two-thirds of the HIV medical services budget.) A treatment advocacy program was added last year to help both clients and physicians keep up with all the new therapies, as well as the pros and cons of various treatment alternatives.
The home care program, certified under the state-funded Case Management Program, currently serves 32 clients with a nurse, social worker, and case aide. AltaMed staff assess clients, develop care plans, and provide case management, homemaker and attendant care services. They contract with the Visiting Nurses Association of Los Angeles for skilled nursing and other home health care services as needed. Demand for these formal home care services has declined since fall 1996, and staff attribute this to the new pharmaceutical treatments. Although the home care program still has a full caseload, its waiting list has grown much shorter.
About a third of AltaMed's HIV clients (230) receive case management services provided by two case managers. Face-to-face contacts take place in the clinic roughly once a month, with additional contacts by phone. Case managers are not required to have a bachelor's degree; instead, staff are selected based on their experience and bilingual/bicultural capabilities. Because current caseloads are high (more than 100 per case manager) and client needs vary, AltaMed is considering the introduction of a new multilevel case management approach that would deal with some clients more intensively than others.
The HIV program's mental health staff provide individual and group counseling, crisis intervention, and peer support groups. The support groups are well attended, in part because they provide a less threatening alternative for clients who are uncomfortable with more formal counseling services. Mental health staff estimate that about 20 percent of the people they see in the counseling programs have a diagnosable condition, whereas most are dealing with adjustment problems related to their HIV status and issues that revolve around sexuality.
AltaMed staff report having a good working relationship with most other AIDS service organizations in the county, and the HIV program is very active in the local Ryan White HIV planning commission. Clients reportedly receive most of their care from AltaMed; major outside referrals are for psychiatric care and specialty/inpatient care. Many AltaMed clients also access food pantry services through organizations like APLA and Bienestar.
3. Revenue Sources
Virtually all of AltaMed's HIV-related revenue is from Ryan White. This year, AltaMed expects to receive a total of $5 million from the various Ryan White programs ($3 million for medical services, and $2 million for prescription drugs). It also expects to receive roughly $40,000 in Medicaid revenue, a tiny amount ($200) from client fees, and $1,200 from private donations. The biggest problem to date has been running the program within the limited administrative expenditures allowed under the Ryan White grants (capped at no more than 10 percent of the grant award). AltaMed corporate staff estimate that they subsidize the HIV program at a level of about 15 percent each year for administrative costs.
NOTES
-
This chapter is based on the project's literature review (Schoff and Schore 1997).
-
Also, personal communication with CDC staff, 1997.
-
Treatment regimens for protease combination therapy (approved by the Food and Drug Administration at the end of 1995) are particularly complex and total adherence to them crucial. Protease combination therapy includes numerous medications taken on different schedules--some with food, others on an empty stomach, some that need refrigeration, others that must be kept at room temperature. Adherence is made more difficult by frequent side effects such as diarrhea, nausea, and abdominal pain (U.S. Food and Drug Administration 1996). In mid-1997, diabetes was flagged as an infrequent but significant complication of their use. Nonadherence to a regimen renders medications ineffective and can result in the development of HIV strains resistant to all protease inhibitors.
-
Personal communication with HCFA staff, and personal communication with Health Resources and Services Administration (HRSA) staff.
-
Also, personal communication with Health Care Financing Review Medicaid long-term care staff.
-
Personal communication with HCFA Division of Benefits, Coverage, and Payment staff.
-
Under the 1997 Balanced Budget Act, states can require managed care enrollment of adult Medicaid beneficiaries with disabilities who are not dually eligible for Medicare. The ability of states to require such enrollment is likely to increase the number of Medicaid beneficiaries with AIDS enrolled in managed care plans.
-
The 17 states include (1) mandatory programs for all Medicaid eligibles (Arizona, Delaware, Oregon, Tennessee, Utah, and Virginia), (2) voluntary programs that target only people with disabilities (District of Columbia, Ohio, and Wisconsin), (3) voluntary programs for the general Medicaid population (California, Colorado, Florida, Maryland, Michigan, New Jersey, and Pennsylvania) and (4) both types of voluntary programs (Massachusetts).
-
Personal communication with TennCare staff.
-
Personal communication with HRSA, Bureau of Health Resources Development, Division of HIV Services staff.
-
Descriptions of the New York and Los Angeles service environments and the organization and operations of individual providers appear in Appendix A and Appendix B, respectively.
-
Private insurance and managed care almost never include home- and community-based services; they also cover a decreasing proportion of people with AIDS.
-
During site visits, we also learned that the New York State AIDS Institute is implementing a uniform reporting system for all providers serving people with AIDS with Ryan White or Medicaid funding. The AIDS Institute offers providers a Windows application that lets them collect and report person-level sociodemographic, clinical, and service use data in a uniform format and with uniform coding. The institute also assists providers in purchasing hardware. The program began in 1996 and is expected ultimately to include as many as 300 New York City providers (personal communication with New York AIDS Institute staff).
-
Client samples for evaluating interventions expected to have relatively small impacts must be relatively large. This suggests that a single provider might not have enough interested, eligible clients to test certain interventions. For development of client samples of sufficient size, such interventions would have to be implemented by several providers.
-
Disease-specific practice guidelines (or clinical pathways) are routinely used by home health agencies. VNSNY developed its own clinical pathway for AIDS care.
-
This chapter was prepared under subcontract to Mathematica Policy Research, Inc. by Stephen Crystal, Anthony LoSassa, Usha Sambamoorthi, and Richard Johnson of the AIDS Research Group of the Institute for Health, Health Care Policy, and Aging Research at Rutgers University.
-
The Village Center home health staff also noted a marked decline in the need for home health care, particularly high-tech care and skilled nursing as a result of decreases in the incidence of opportunistic infections that require infusion therapy, but a greater need for homemakers and personal care attendants. The decline led them to lay off some staff and expand their service area into Brooklyn.
-
The state recently decided to consolidate its hotline programs, and the San Francisco hotline won the competition to be the sole provider. Thus, the APLA hotline was expected to end in June or July of 1997.
-
Outpatient medical providers in Los Angeles are not permitted to use their Ryan White grant funds for specialty and inpatient care; instead, they must refer low-income, uninsured patients needing such care to the county's AIDS program.
REPORTS AVAILABLE
Serving A Changing Population: Home- and Community-Based Services for People With AIDS
HTML http://aspe.hhs.gov/daltcp/reports/aidssum.htm
PDF http://aspe.hhs.gov/daltcp/reports/aidssum.pdf
The Role of Home and Community-Based Services in Meeting the Health Care Needs of People with AIDS: Final Report
HTML http://aspe.hhs.gov/daltcp/reports/aidsfrpt.htm
PDF http://aspe.hhs.gov/daltcp/reports/aidsfrpt.pdf
The Role of Home and Community-Based Services in Meeting the Health Care Needs of People with AIDS: Literature Review
HTML http://aspe.hhs.gov/daltcp/reports/aidslit.htm
PDF http://aspe.hhs.gov/daltcp/reports/aidslit.pdf
To obtain a printed copy of this report, send the full report title and your mailing information to:
U.S. Department of Health and Human ServicesOffice of Disability, Aging and Long-Term Care PolicyRoom 424E, H.H. Humphrey Building200 Independence Avenue, S.W.Washington, D.C. 20201FAX: 202-401-7733Email: webmaster.DALTCP@hhs.gov
RETURN TO:
Office of Disability, Aging and Long-Term Care Policy (DALTCP) Home [http://aspe.hhs.gov/_/office_specific/daltcp.cfm]Assistant Secretary for Planning and Evaluation (ASPE) Home [http://aspe.hhs.gov]U.S. Department of Health and Human Services Home [http://www.hhs.gov]