
U.S. Department of Health and Human Services
A Literature Review: Psychiatric Boarding
David Bender, Nalini Pande and Michael Ludwig
The Lewin Group
October 29, 2008
PDF Version: http://aspe.hhs.gov/daltcp/reports/2008/PsyBdLR.pdf (30 PDF pages)
This report was prepared under contract #HHS-100-03-0027 between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and and the Lewin Group. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the ASPE Project Officer, John Drabek, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. His e-mail address is: John.Drabek@hhs.gov.
The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
TABLE OF CONTENTS
- I. INTRODUCTION
- III. RESEARCH
- A. Psychiatric Boarding: Existence and Extent
- B. Psychiatric Boarding: Care Delivery
- C. Psychiatric Boarding: Impact
- D. Psychiatric Boarding: Short and Longer Term Practice Improvements
- IV. CONCLUSION
- APPENDIX A: MODELS OF EMERGENCY SERVICES
- LIST OF FIGURES
- FIGURE 1: Model of Emergency Service: General Hospital with Dedicated Psychiatric Unit
- FIGURE 2: Model of Emergency Service: General Hospital without Dedicated Psychiatric Unit or Staff
- FIGURE 3: Model of Emergency Service: Hospital with Dedicated Psychiatric Unit and Psychiatric Staff
I. INTRODUCTION
Boarding, the practice in which admitted patients are held in hallways or other emergency department (ED) areas until inpatient beds become available, has often been suggested as both a cause and effect of ED overcrowding.1 Beginning once a physician in the ED has screened a patient and the decision has been made to admit the patient, boarding can often last for over 24 hours, if not days.2 Boarding inpatients consumes ED resources, prolongs the time all patients wait for services, and reduces the number of ED treatment beds available to accommodate sudden surges in demand.3 For psychiatric patients, boarding occurs when no inpatient psychiatric bed is available, requiring a wait for mental health services, typically in the ED.4 The crowding and lack of space often creates an environment in which a psychiatric patient slowly deteriorates.5 In 2008, 80 percent of ED medical directors reported that their hospital boards psychiatric patients.6 Further, in 2007, 42 percent of hospitals reported an increase in boarding behavioral health patients in the ED.7 More than 90 percent of medical directors indicated that they board psychiatric patients every week with more than 55 percent reporting boarding daily or multiple times per week.8 Flowcharts in Appendix A provide examples of how ED services are delivered in a hospital with and without psychiatric units.
It is important to understand psychiatric boarding within the larger context of the mental health system. First, the mental health system suffers from significant capacity constraints for psychiatric inpatient services. Beginning in the 1960s, deinstitutionalization, defined as placing psychiatric patients in outpatient and community-based treatment facilities, has resulted in significant psychiatric bed shortages.9 Second, demand for psychiatric services is increasing. The annual number of ED visits (medical and psychiatric) from 1996 to 2006 has increased from 90.3 million to 119.2 million.10 Further, there has been a sharp increase in the number of mentally ill persons coming to EDs between 1992 and 2000.11 Third, concerns have been raised about the adequacy of funding for psychiatric services. A 2008 report by the American Medical Association (AMA) states that during the time of deinstitutionalization, necessary services and funding were not put into place for adequate community mental health services.12 The financial strain on hospitals in caring for the uninsured and underinsured is often cited as the primary reason for the closure of psychiatric units and the decline in the number of psychiatric inpatient beds nationally.13
This literature review will explore the relevant literature on several key questions regarding boarding of psychiatric patients in the ED. Is psychiatric boarding a problem? What are the reasons for boarding psychiatric patients? What kind of care is received while patients are boarded? Our review of the literature will delve into these questions as well as the impact of psychiatric patient boarding on others, including the financial impact. We will also discuss how the decisions of key players including ED staff, law enforcement, insurance companies and hospitals have a significant impact on the ED boarding process for psychiatric patients. Where possible, we will provide data to support key findings. Finally, we will highlight best practices and solutions regarding ED psychiatric boarding. We note that current data, although sparse on this topic, is suggestive of an emerging widespread problem causing serious disruption of the service delivery system in a substantial number of communities. However, geographic variation, lack of robust evaluations and data indicate that further academic studies on this topic are needed.
II. PROFILE OF EVIDENCE
In researching this report, we examined several types of literature. First, we reviewed numerous peer-reviewed academic journals. We utilized PubMed (MEDLINE) to identify articles on psychiatric boarding, including those from the Annals of Clinical Psychiatry, Annals of Emergency Medicine, Academic Emergency Medicine, Emergency Psychiatry, Journal of Emergency Medicine, and Psychiatric Services.
Several associations, foundations, and institutes have covered the topics of ED overcrowding, ED boarding and psychiatric boarding in some detail. Publications and press releases by the American College of Emergency Physicians (ACEP), the American Psychiatric Association (APA), the AMA, the Heritage Foundation, the National Mental Health Association, the National Alliance on Mental Illness, the National Association of State Mental Health Program Directors (NASMHPD) and others provided nationwide context for this literature review. Media publications, including mainstream newspapers (i.e., The New York Times, The Washington Post, The Boston Globe, and USA Today) provided additional anecdotal evidence, highlighting instances of boarding at specific hospitals.
While several media publications and associations have written extensively on the topic, perhaps the most notable finding in our review was the lack of academic literature specifically analyzing psychiatric boarding.14 A similar review of the literature on ED overcrowding published in August 2008 found over ninety relevant articles, but only five related to general inpatient boarding.15
III. RESEARCH
A. Psychiatric Boarding: Existence and Extent
1. Definition of Boarding
Before we describe key issues related to boarding, it is important to note that there is no standard definition of boarding in the case of psychiatric patients. Weithorn defines psychiatric boarding as [t]he phenomenon of persons with mental disorders remaining in the hospital emergency rooms while waiting for mental health services to become available.16 Mansbach indicates that psychiatric boarding can include improper placement (i.e., inpatient medical bed instead of an inpatient psychiatric bed).17 In its 2008 survey of ED medical directors, ACEP classifies psychiatric boarding as when a patient remains in the ED for four or more additional hours after the decision is made to admit.18 Finally, Stefan defines psychiatric boarding as a stay in the ED exceeding 24 hours.19
2. Existence and Extent of Boarding
In the most widespread survey on psychiatric boarding to date, ACEP found that roughly 80 percent of ED medical directors believed their hospital boards psychiatric patients in the ED.20 In addition, in a 2007 AHA survey of hospital leaders, 42 percent of hospitals reported an increase in boarding behavioral health patients in the ED.21 While these surveys provide insight into the problem of psychiatric boarding, it is difficult to ascertain whether the problem is concentrated in specific geographic areas or is a nationwide issue.
In most geographic areas, there is clear variability in the amount of boarding from hospital to hospital.22 Bazzoli et al. find that large Metropolitan Statistical Areas have the greatest psychiatric capacity constraints.23 In addition, much of the media coverage concerning severe psychiatric boarding issues comes from major urban centers. This may suggest that populated, urban areas face the most severe cases of ED overcrowding and boarding.
Certain regions of the country have been highlighted as areas with severe cases of psychiatric boarding. Clark County, Nevada declared a state of emergency in July 2004 because individuals with symptoms of mental disorders were flooding hospital emergency rooms.24 Boarding times for psychiatric patients in Georgias emergency rooms average 34 hours, with many waiting several days for an inpatient bed in one of seven state-run psychiatric hospitals.25 In Maryland, many EDs see and treat over a dozen psychiatric patients daily and may board up to a dozen for days at a time. Media publications often highlight boarding at individual hospitals. For example, an article in The Washington Post stated that 80 percent of children for whom staff recommended inpatient mental health treatment ended up boarding at Yale-New Haven Children's Hospital.26
To date, no comprehensive academic evaluation on psychiatric boarding detailing the extent of the problem exists. Much of the information on the prevalence of psychiatric boarding comes from individual hospital analyses, association surveys or anecdotal media publications. However, two Massachusetts studies on pediatric psychiatric boarders provide primary empirical data on psychiatric boarding at individual hospitals.27 In an analysis of Boston Medical Center, Sharfstein found that 34 percent of children with acute psychiatric needs were admitted to inpatient pediatric service, awaiting a psychiatric bed.28 Similarly, Mansbach and colleagues found that 33 percent of patients who needed psychiatric admission were boarded on the medical floor.29 It is unclear whether these studies can be generalized given their focus on psychiatric boarding of children at individual hospitals in Massachusetts.
3. Reasons for Psychiatric Boarding
The Subcommittee on Acute Care to the President's New Freedom Commission reported in 2003 that the total number of inpatient psychiatric beds per capita had declined dramatically (62 percent) since 1970.30 Over this same period, state and county psychiatric hospital beds per capita decreased even more sharply (89 percent).31 The Committee concluded that the decline in the supply of most types of beds for short-term inpatient psychiatric care has led to a serious disruption of the service delivery system in a substantial number of communities.32 Meanwhile, from 2000 to 2006, the percentage of cases presenting to the ED with a mental disorder as the primary diagnosis increased from 3.2 percent to 3.6 percent.33
While lack of inpatient capacity is a direct cause of psychiatric boarding, it is important to delve into the reasons why there is a lack of capacity. Further, it is important to understand why there has been an influx of psychiatric patients into the ED and the root causes of this influx.34
Capacity Issues
Hospital Capacity Issues. Beginning in the 1960s, a trend toward placing psychiatric patients in outpatient and community-based treatment facilities, or deinstitutionalization, has resulted in a decrease in the number of inpatient and residential psychiatric beds for state and county mental health hospitals from approximately 400,000 nationwide in 1970 to 50,000 in 2006.35 While this was partially offset by an increase of 50,000 private and general hospital psychiatric beds during this time, a large gap remains in the treatment of the mentally ill.36 Psychiatric hospital closures and bed reductions nationwide have strained access to psychiatric acute care.37
The shortage of inpatient psychiatric beds is a nationwide occurrence, according to a survey by the ACEP.38 The California Institute for Mental Health documents a shortage of psychiatric inpatient beds in California and inadequate capacity of the existing mental health system to provide alternative care for those with more severe and urgent needs.39 The November/December 2001 issue of the APA newsletter, Psychiatric Practice and Managed Care, provided accounts of psychiatric bed shortages in 16 states. The newsletter reported that Hawaii was limited to admitting patients who have been court ordered for commitment.40 Further, delays in discharging children from inpatient beds prevent boarded patients from accessing these beds.
Lack of Outpatient Resources and Coordination. The rise in emergency visits by psychiatric patients is often seen as a proxy measure for failure of the outpatient mental health system to accommodate their needs.41 While research has demonstrated that community-based approaches to treatment of mental illness yield high levels of success, the presence of community-based services continues to be limited.42
Community-based services are often unavailable or unaffordable to many mentally ill individuals, forcing many psychiatric patients to present to the ED as their last attempt to obtain care.43 Documented increases in psychiatric patients to the ED, particularly children have been noted at both Childrens Hospital of New York-Presbyterian and Yale-New Haven Childrens Hospital.44 During one fiscal year, children in Massachusetts spent 20,811 days in psychiatric wards, waiting for community-based mental health services to become available.45 Similarly, a Boston Globe article documented children staying in hospitals long after their discharge date due to lack of sufficient alternatives.46 The 2008 ACEP survey of ED medical directors indicated that 23 percent have no community psychiatric resources available.47 Rural areas have more severe access issues, with many critical access hospitals (CAHs) being forced to transfer patients to facilities outside the community.48 According to the Maine Rural Health Research Center, nearly half (43 percent) of CAH ED managers have no access to local mental health providers of any kind. CAHs are forced to transfer patients to medical detoxification and inpatient psychiatric services, with mean travel times averaging one hour.49
Given the unavailability and lack of affordability of community-based mental health services, patients may use the emergency room as a last resort. Further, care in the ED must be provided regardless of a patients ability to pay under the Emergency Medical Treatment and Labor Act (EMTALA) requirements.50 This places excessive strain on ED capacity, and is a significant contributor to psychiatric boarding. Thus, the ED has become a safety-net when other alternatives are unavailable.51
Additionally, the lack of coordination between the mental health system and the ED creates a lack of shared responsibility and accountability between the mental health system and the ED. In fact, the states mental health agency often has little or no relationship with EDs. This is despite the states role in licensing, accreditation and, in the case of Medicaid services, reimbursement of the ED.52 We note that in some communities, hospitals have begun joint actions with state and local authorities to target specific psychiatric emergency cases and identify potential solutions. In addition, local emergency medical services agencies are working with hospitals and ambulance service providers to improve local communications and coordination of ED services.53
Lack of funding. While capacity issues are a key reason for boarding, it is important to analyze the root cause of these capacity constraints. A 2008 report by the AMA states that necessary services and funding were not put into place for adequate community mental health services during the trend of deinstitutionalization since the 1960s.54 Further, Bazzoli indicates that there are few financial incentives for hospitals to build new units to meet the demand for inpatient psychiatric services, contributing to a bed shortage.55 One article explains, in an era when revenues are tightening, hospitals are looking for where to cut expenditures [and] any service not profitable and not required is on the chopping block.56 The article notes that psychiatric services are not a required service for an acute hospital.57 Appelbaum explains that the costs of hospitalizing Medicaid patients and the uninsured have been shifted from the public sector to private hospitals.58 Appelbaum points to a progressive and systematic defunding of psychiatric services and indicates that mental health services provided in hospitals and clinics have become a money-losing proposition.59
Unnecessary Inpatient Admission
Legal and Liability Issues. Several authors cite legal and liability issues as a factor contributing to inpatient admission and, in turn, higher boarding rates due to the general lack of inpatient capacity. Upon presenting to the ED, psychiatric patients often provide clinicians with extremely difficult decisions concerning admission. Having to decide whether to admit a mentally ill patient often within five minutes, ED physicians typically choose to err on the side of caution in order to avoid potential liability issues, according to anecdotal evidence.60 If a patient later attempts or commits suicide after an examination, mental health clinicians can face legal repercussions.61 Consideration of liability issues often leads to increased admission of mentally ill patients.62 In addition, contingent suicidality exists, where an individual reports being suicidal just to gain admission, and then rescinds the statement after being admitted. Even if staff believe there are no suicidal or homicidal tendencies, staff members perceive the need to admit patients in this instance given potential liability.63 Stefan recommends that hospital administrators support clinically-based, rather than liability-based decisions. She encourages careful assessment, including review of collateral information, and legible, conduct-based documentation to reduce inappropriate inpatient admission as well as liability.64
Inappropriate Deference to "Secondary Utilizers" of ED Service and Inadequate Assessments. Stefan notes that EDs are places where secondary utilizers such as police, group home operators, and family resolve conflicts with the psychiatric patient. In fact, Stefan cites research indicating that when an individual is accompanied to the ED, the patient is more likely to be admitted as an inpatient, regardless of symptoms or perceived risk. Stefan also notes that there are few incentives to conduct a thorough assessment of a psychiatric patient in the ED, contributing to increased admission and consequently, increased boarding.65
Additional Reasons
Transfer Issues. The EMTALA Technical Advisory Group notes that there is often confusion with EMTALA transfer requirements. Given such confusion, hospitals will admit the psychiatric patient to avoid a possible inappropriate EMTALA transfer violation.66 This contributes to increased admission and consequently, increased boarding. Further, a lack of ambulances willing to transport psychiatric patients to outpatient facilities has also been cited as a reason for boarding.67
Iatrogenic Crisis in the ED Setting. Stefan argues that it is rarely recognized how often an individual arrives at the ED in a state that would not necessitate inpatient admission and escalates in the ED into uncontrollable agitation. The crowding, lack of space and delays due to medical tests and assessments create an environment in which a psychiatric patient slowly deteriorates, requiring inpatient admission and consequently, increased boarding.68
Other Reasons. Additional reasons for psychiatric boarding cited throughout the literature include limited psychiatric staff, such as case workers and psychiatrists, the need for medical clearance, the need to wait for a patient to be sober before evaluation, and time spent handling pre-certification issues from insurance carriers.69 Stefan cites the link between the increase in ED presentations (and inpatient psychiatric admissions of people in psychiatric crisis) with cuts in specific mental health programs, and decisions to deny coverage for certain medications under Medicaid.70 She also cites the lack of ED staff training, which can lead to inappropriate inpatient admissions.71
B. Psychiatric Boarding: Care Delivery
1. Quality of Care Received
In 2003, the Subcommittee on Acute Care to the President's New Freedom Commission reported on communities where emergency departments are overwhelmed with patients in extreme psychiatric distress who have nowhere else to go.72 Over the last few years, several incidents of patients waiting and even dying in the ED have prompted media coverage highlighting the crowding of EDs and the crisis in treatment of psychiatric patients.73
Upon boarding, psychiatric patients are often placed in extremely loud, hectic environments that may exacerbate many of their pre-existing conditions. Emergency physicians at major medical centers have been documented as stating there is no real therapy going on. They [psychiatric patients] languish there for days.74 Often, hospitals do not have the staffing or capabilities to treat psychiatric patients.75 What staff is present is typically dedicated to inpatient psychiatric patients, leaving mentally ill and substance abuse patients in the ED lacking services. Patients with mental illness are boarded longer than medical patients, which can be both uncomfortable and frightening for individuals with psychosis or severe depression.76 Additionally, the literature has documented instances where emergency nurses have viewed psychiatric patients as frustrating, puzzling and even scary, contributing to disrespect and hostility by staff toward psychiatric patients.77
Inadequate Assessments. First and foremost, any review of quality of care should not only analyze the care received while boarded, but also whether a patient is getting a sound assessment in the ED. ED physicians spend as little as 5-15 minutes evaluating patients, creating incentives to admit. Stefan suggests that improved evaluation techniques can offset poor quality of care and prevent many inappropriate inpatient admissions which contribute to boarding.78
Inadequate Services. Sharfstein et al find that not one boarded child in their sample of ten children covered by Medicaid received any of the services that Medicaid requires to be available in psychiatric hospitals while boarding.79 Similarly, the 2008 ACEP psychiatric boarding survey found that 61 percent of hospitals do not have psychiatry staff caring for ED patients while they wait.80
Iatrogenic Effect of Boarding. Stefan explains that the iatrogenic effect of boarding can worsen the patients condition. She writes:
[i]t is not hard to imagine that an individual in psychiatric crisis, forced to wait alone for many hours in a small unfurnished room, which is sometimes locked, or on a narrow gurney, might lose the control that he or she possessed upon arrival at the ED. That loss of control, in turn, will result in the use of force, often by security guards, and imposition of restraint and seclusion. An individual who arrived at the ED with no need for inpatient admission has been transformed by the ED experience into someone who needs an inpatient bed.81
We describe in the law enforcement section how physical and chemical restraints are used on psychiatric patients, often with serious consequences.
2. Repeat ED Users
As detailed in the previous section, a lack of comprehensive mental health services within the community forces some psychiatric patients to present to the ED, often on multiple occasions. A revolving door syndrome ensues, where the same psychiatric patients repeatedly return to the emergency room for care -- never obtaining the extent of the care that is needed.82 In addition, boarding can be attributed to increased walkouts, with a number of patients subsequently returning to the ED and using duplicative services.83 Health professionals have acknowledged that few efforts have been made to identify frequent users and understand the underlying causes of their repeat visits.84 Further, Stefan notes that repeat psychiatric users are often blamed by ED staff members for taking staff time away from real patients, resulting in punitive actions and inadequate care of psychiatric patients. Also, hospitals often are at a loss in identifying past problems of repeat users due to the Health Insurance Portability and Accountability Act requirements, where medical information is kept private.85
Several studies have identified particular social, clinical, and demographic characteristics which serve as predictors of repeat psychiatric emergency use. Younger, non-White, unemployed, and unmarried males have the highest rates of repeat use, with homelessness serving as a strong indicator of high utilization.86 These individuals typically have a history of psychotic disorder or schizophrenia, substance abuse, prior hospitalization and a need for medication.87 A study conducted in Washington noted that 56 percent of individuals who visited the ED 31 times or more in a year had diagnoses of both alcohol or drug disorder and mental illness.88 However, one author notes that recidivism is not necessarily a bad marker when psychiatric patients are being served, as patients are recognizing their need for help and the hospital is meeting a need which community mental health services are not providing.89
3. Law Enforcement
Law enforcement often plays an extensive role in the care and commitment of mental health patients. Each state has varying laws and requirements surrounding commitment, forced hospitalization of mentally ill individuals, and the use of law enforcement.90 Typically, the commitment process involves law enforcement officers taking mentally ill individuals directly to the ED or hospital for evaluation, avoiding arrest.91 A person with a mental illness can be committed in most of the 37 states that have Involuntary Outpatient Commitment (IOC) laws with a finding of imminent danger to self or others.92
A number of states explicitly allow police forcibly to pick up and detain individuals for mental evaluations if they have failed to comply with any provision in an IOC order.93 In Maryland, law enforcement has the right to petition to take an individual to the ED against the individuals will for examination by a physician. A physician must evaluate the patient within six hours of arrival and be discharged from the ED within 30 hours.94 In California, Section 5150 of Californias Welfare and Institutions Code allows an officer to involuntarily confine a person deemed to be a danger to himself/herself or others.95 In Pennsylvania, any person taken involuntarily to an ED for psychiatric evaluation must be examined within two hours.
Once placed on involuntary holds, patients are monitored by police officers and security guards for violent and destructive behavior. The process of using seclusion or restraints on psychiatric patients may involve severe force and/or chemical sedation. Several instances of patient deaths and injuries by security guards have been reported.96 Additionally, seclusion and restraint provides a hostile environment for patients who are already unstable.97 The use of restraints and seclusion has been cited as a sign of treatment failure, and many organizations have taken formal positions against their use.98
C. Psychiatric Boarding: Impact
1. Financial Impact
Psychiatric patients are typically uninsured or enrolled in Medicaid, which may provide inadequate reimbursement to the hospital.99 Currently under EMTALA, hospitals must screen and stabilize patients who present to the ED regardless of ability to pay.100 For individuals who are uninsured or underinsured, the financial burden of treatment of the psychiatric patient falls on the hospital unless it can transfer the patient to a public facility or alternative outpatient facility that takes patients who do not have insurance.101 In addition, in some states, hospitals are not reimbursed for patients waiting for transfer. In Massachusetts, once application for transfer from an inpatient acute care bed is made, private payers consider patients as no longer in need of acute care, and therefore do not reimburse the hospital and physicians for care provided.102 The financial strain on hospitals is often cited as the primary reason for the closure of psychiatric units and the decline in the number of psychiatric inpatient beds nationally.103
There are very few studies on the financial impact of psychiatric boarding. One financial study on the cost of psychiatric boarding estimated that additional patient services (if provided in lieu of inpatient boarding) could have generated median net revenues of $3,960,264, and increased FY2005 net revenue from ED operations by 13 percent, for a 450-bed non-profit community teaching hospital in South Central Pennsylvania.104 We note that this study makes the assumption that there are insured patients in need of these services in order to substantiate the opportunity cost estimates provided.
2. Impact of Insurance Status
In one study, Medicaid patients had double the rate of psychiatric-related ED visits compared with the uninsured and almost eight times the rate of those privately insured.105 It has also been suggested that homeless and uninsured individuals represent a disproportionate share of psychiatric emergency services (PES) users.106 Mansbach et al find that Medicaid patients were equally likely to board as other non-capitated insurance plans.107 This may indicate that a patients insurance status may not be indicative of whether he/she boards.
Although insurance status may not be a factor in whether a patient boards, it may be a factor in how long the patient boards. For example, Appelbaum indicates that Massachusetts community mental health centers (CMHCs) previously received direct state support for treatment of the uninsured. However, today, the state does not provide such funding for CMHC outpatient care, causing CMHCs to turn away uninsured patients, since even they have to limit the losses incurred in rendering outpatient treatment.108 Additionally, the responsibility of treating psychiatric patients who are uninsured or underinsured falls on the hospital unless it can transfer the patient to a public facility or alternative outpatient facility that takes patients who do not have insurance.109 Thus, it is possible to conclude that uninsured, boarded patients may indeed board longer than their insured counterparts given difficulties in finding private, outpatient facilities that are willing to take them. Further studies on this topic are needed to make a definitive conclusion.110
3. Impact of Psych Boarding on Other ED Services and Patients
While psychiatric boarding has documented impacts on the financial health of the hospital, the treatment of psychiatric patients, and the capacity of the ED, it also has overarching effects on other ED patients and the hospital staff, resulting in an impact on the ED services provided.
The 2004 ACEP Psychiatric Survey of emergency physicians found boarding individuals with mental illness resulted in the following staff and patient well being issues:
- Reduced availability of emergency staff (90 percent of respondents);
- Longer waits for patients in the waiting room (85 percent);
- Patient frustration (89 percent);
- Negative effect on the care of other patients (80 percent).111
Another negative externality of boarding is the toll that high patient volume and boarding has on nursing staff. Due to an already overwhelming work load, nurses may participate in bed hiding, a situation where rooms are not cleaned rapidly, and beds are hidden to reduce the number of patients seen.112 Psychiatric patients intensify high stress situations for nursing staff; due to frequent substance abuse and complex mental issues, psychiatric patients are often the most difficult cases to treat. Many psychiatric patients present to the ED with assaultive behavior that may be harmful to themselves and/or others.113 The disturbances and disruption creates tension for staff and other patients.114
D. Psychiatric Boarding: Short and Longer Term Practice Improvements
Despite budget constraints and systemic problems within the mental health system, some communities and hospitals have been successful at designing and implementing practices to improve the psychiatric boarding issues described in this literature review. For instance, since 2004, Clark County, Nevada has implemented several policies to address the shortage of psychiatric beds and psychiatric boarding. The Governor of Nevada released $100,000 in emergency funds to divert psychiatric patients to other treatment resources. Additionally, the state instituted Legal 2000, a system to expedite the transfer of psychiatric patients who appear to be in danger of harming themselves or someone else to psychiatric facilities rather than boarding them in EDs. In 2008, Clark County reopened a 50-bed community triage center at WestCare, a non-profit mental health and drug rehabilitation clinic in Las Vegas.115
Below are details of the short-term practice improvements and longer term system-level changes most commonly cited in the literature in relation to reducing psychiatric boarding in EDs. Short-term practice improvements include a focus on quality of care and coordination regarding inpatient bed availability. The longer term proposals, referenced in the literature and reviewed for this paper, focus on large, systemic issues such as improving, quality, capacity, reimbursement, training and implementing legislative reforms, including national standards.
1. Short-Term Practice Improvements
ED PES. Several sources supported the implementation of PES. PES focuses on providing high quality and effective ED assessments which can reduce psychiatric boarding. Developed over 40 years ago, PES is now recognized as an essential component of comprehensive mental health services for ambulatory patients with psychiatric emergencies. The concept of PES includes several different models:
- The psychiatric consultant to the ED is called when needed;
- A self-contained PES within the main ED; and/or
- A separate psychiatric ED in the general hospital or the ED of a freestanding psychiatric hospital.116
While a growing number of hospitals are creating psychiatric consultation services within hospital EDs, PES models vary widely among hospitals. In-house PES is recommended for hospitals with a high frequency of ED psychiatric cases.117
Separate psychiatric EDs or holding areas have also been suggested by some experts as part of the PES model or as stand-alone best practices. Schenkel recommends the creation of a separately staffed 6-10 bed holding unit, staffed with a nurse and technician.118 This removes the psychiatric patient from the commotion of the ED, and allows for proper treatment. An alternative practice (if a separate holding area is not feasible) is a quiet room or separate waiting area for psychiatric patients within the ED.119 Often termed special needs areas, these rooms are specifically dedicated for psychiatric emergencies.120 Further, the Maryland Health Care Commission recommends establishing a diversion center in the ED to triage and care for psychiatric patients.121
Public hospitals in Louisiana are implementing a new mental health emergency room extension (MHERE) model to provide a more therapeutic environment for psychiatric patients waiting in the ED. The model moves psychiatric patients out of the ED to designated stabilization units that provide patients with a more controlled and quiet environment. Within this extension area of the acute ED, nurses, counselors and social workers provide comprehensive care to the patient during his or her stay in the unit. Some patients can be released from the units after several hours and others who need to be placed in psychiatric inpatient care appear more calm given that therapy has started in the extension unit. Public and private hospitals in Louisiana plan to implement additional MHERE models through partnerships with the Louisiana Office of Mental Health.122
The University of Alabama, Birmingham (UAB) Department of Psychiatry, through a partnership with the Jefferson, Blount, St. Clair Mental Health Authority, is working to develop a PES as part of a Comprehensive Emergency Program for the Birmingham metropolitan area. The PES will follow guidelines established by the APA for a full continuum of psychiatric emergency services. UAB believes that although funding is necessary to establish the PES, cost savings will be realized in other agencies such as jails, police departments, EDs elsewhere, paramedics and inpatient hospitalization.123
Guidelines for Psychiatric Emergency Care and Use of Restraints. Several organizations, including the APA Task Force, the Center for Public Representation, the Substance Abuse and Mental Health Services Administration (SAMHSA) and the Joint Commission, have also developed guidelines relating to particular aspects of emergency psychiatric care, such as seclusion and restraint.124
Use of Inpatient or Acute Care Hallway Instead of an ED. It has been suggested that psychiatric patients be boarded in a separate psychiatric wing. If this is not feasible, emergency physicians support bed location outside of the ED.125 In addition, several surveys have been conducted indicating inpatient hallways are the preferred boarding location for patients, if boarding is necessary.126
Advanced Discharge Planning /Bed Czar. Better management of inpatient capacity has been cited as a way of reducing boarding. Some hospitals have put together teams of utilization review staff, social workers and physicians to assess inpatient bed utilization and help plan more timely discharges. It has been reported that some hospitals appoint bed czars who are often given the authority to transfer and discharge patients, and cancel or hold elective procedures in order to more effectively manage inpatient capacity.127 Additionally, computerized bed management systems have been shown to improve hospital flow.128
2. Longer Term System-Level Changes
Reimbursement for Psychiatric Services. Several organizations have suggested that additional reimbursement of PES could reduce boarding if such reimbursement reduced the financial burden on hospitals and led to an increase in inpatient capacity. For example, the 2008 AMA Report recommends providing adequate reimbursement for the care of patients with mental illness, which is currently not provided under EMTALA.129 In addition, the House Bill The Medicaid Emergency Psychiatric Care Act of 2007, also recommended altering hospital reimbursement for treatment of psychiatric patients for care required under EMTALA.130 Further, the Maryland Health Care Commission also suggests pursuing funding opportunities and study options for improving access to community-based mental health services to reduce improper use of the ED.131
Regional PES. Due to limited staffing of mental health professionals, a regional PES, which handles all psychiatric emergencies in a particular geographic area, may shift the burden of care for psychiatric patients from the hospital to an organized group of psychiatric professionals.132 Eighty percent of respondents in the 2008 ACEP survey agreed that regional, dedicated emergency psychiatric facilities nationwide would work better than the current system for dealing with psychiatric emergency patients.133
Improved Coordination between EDs and Community-Based Mental Health Services. It has been suggested that improved coordination between EDs, state mental health agencies, and community-based mental health services could assist in reducing inpatient admissions, and thus inpatient boarding. In addition, frequent users often return to the ED because of a lack of community mental health services. Linking these individuals with a triage nurse on an as-needed basis and scheduled contacts with an identified staff member, coupled with a proactive community approach in identifying these individuals, has been proposed as a strategy for reducing ED use for repeat users.134 Further, mobile crisis teams that treat emergencies in the community have been cited as a way to reduce the number of psychiatric cases arriving at a hospital.135 In addition, the Maryland Health Care Commission recommends increased case management for chronically homeless individuals to avoid presentation at the ED.136
Inpatient Capacity. Certain commentators argue that increasing the number of psychiatric beds may be an effective means of reducing psychiatric boarding, absent other changes in the mental health system.137 Nationwide, in 1955, there were 340 public psychiatric beds per 100,000 population but only 17 public psychiatric beds per 100,000 population in 2005.138 Some states have begun to develop projections of future inpatient psychiatric bed needs. One study found that 11 states used statewide proactive planning for psychiatric beds. These states typically have formulas based on population and target occupancy rates.139 In addition, some hospitals have begun joint actions with state and local authorities to provide alternative types of care.140
Mental Health Training to Physicians, Nurses and Law Enforcement. Commentators have suggested that qualified mental health professionals could provide training to police officers regarding identification of psychiatric emergencies given that law enforcement often brings the patient to the ED.141 Further, continuing education for ED staff in the care of psychiatric patients has also been suggested.142
IV. CONCLUSION
To date, no comprehensive, nationwide academic evaluation of psychiatric boarding detailing the extent of the problem exists. Much of the information on the prevalence of psychiatric boarding comes from individual hospital analyses, association surveys or anecdotal media publications.
The existing literature indicates that psychiatric boarding can lead to serious consequences, both for psychiatric patients and ED staff as well as other patients in the ED. Boarding has also been reported to have a significant financial impact on hospitals. It appears that the decisions of key players including ED staff and law enforcement have a significant impact on the ED boarding process for psychiatric patients. Existing evidence indicates that a lack of training in the care and management of psychiatric patients among ED physicians and the relatively short time an ED physician is able to spend with psychiatric patients during assessment can create inappropriate patient admission as well as poor quality of care while boarding. Suggested practice improvements address capacity constraints, quality of care improvements, training of ED staff and law enforcement, and the coordination of ED care with community mental health services.
Limited data on this topic is suggestive of a widespread problem causing serious disruption of the service delivery system in a substantial number of communities. However, geographic variation, lack of robust evaluations and data indicate that further academic studies on this topic are needed.
APPENDIX A. MODELS OF EMERGENCY SERVICES
The Illinois Hospital Associations Behavioral Health Steering Committee, Best Practices Taskforce developed a report on best practices for the treatment of patients with mental and substance use illnesses in the ED. The report included the following flowcharts on models of emergency services.
| FIGURE 1. Model of Emergency Service: General Hospital with Dedicated Psychiatric Unit1 |
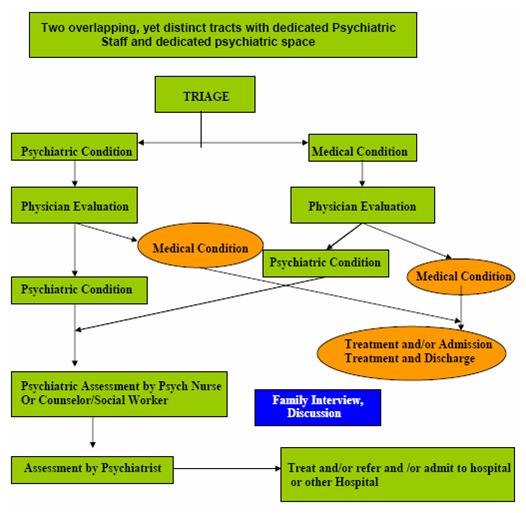 |
| Illinois Hospital Association, 2007. |
| FIGURE 2. Model of Emergency Service: General Hospital with Dedicated Psychiatric Unit or Staff1 |
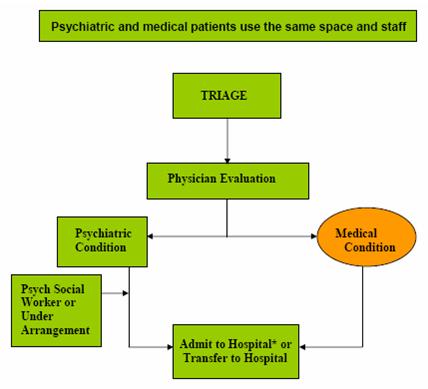 |
| Illinois Hospital Association, 2007.* Refer up to three days. |
| FIGURE 3. Model of Emergency Service: Hospital with Dedicated Psychiatric Unit and Psychiatric Staff1 |
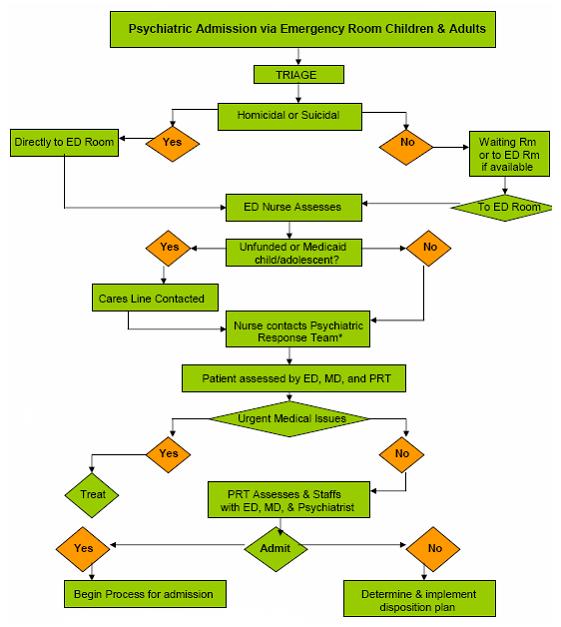 |
| Illinois Hospital Association, 2007.* PRT also serves as SASS Team & CHIPS Team. |
NOTES
-
Young, Donna. ED Physicians Offer Solutions for Boarding. American Journal of Health System Pharmacy. Vol. 64, June 15, 2007. OShea, John. The Crisis in Americas Emergency Rooms and What Can be Done. The Heritage Foundation. No. 2092, December 28, 2007. Olshaker, Jonathan. Emergency Department Overcrowding and Ambulance Diversion: The Impact and Potential Solutions of Extended Boarding of Admitted Patients in the Emergency Department. Administration of Emergency Medicine. 30(3): 351-356, May 2005.
-
ACEP Psychiatric and Substance Abuse Survey 2008. 2008. http://www.acep.org/uploadedFiles/ACEP/Advocacy/federal_issues/PsychiatricBoardingSummary.pdf. Mansbach, Jonathan et al. Which Psychiatric Patients Board on the Medical Service? Pediatrics 111(6): e693-e698, June 18, 2003. In addition to boarding wait time, psychiatric patients often wait prior to be screened and again wait during the evaluation process.
-
Falvo, Thomas. The Opportunity Loss of Boarding Admitted Patients in the Emergency Department. Academic Emergency Medicine. 14(4): 332-337, April 2007.
-
Weithorn, Lois. Envisioning Second-Order Change in Americas Responses to Troubled and Troublesome Youth. Hofstra Law Review. 33: 1305, 2005.
-
Stefan, Susan. Emergency Department Assessment of Psychiatric Patients: Reducing Inappropriate Inpatient Admissions, August 2006. http://www.medscape.com/viewprogram/5768.
-
ACEP Psychiatric and Substance Abuse Survey 2008. 2008.
-
American Hospital Association. The 2007 State of Americas Hospitals -- Taking the Pulse: Findings from the 2007 Survey of Hospital Leaders. http://www.aha.org/content/2007/PowerPoint/StateofHospitalsChartPack2007....
-
ACEP Psychiatric and Substance Abuse Survey 2008. 2008.
-
Tuttle, Georgia A. AMA. Report to the Council on Medical Service. August 2008. The Medicaid Institutions for Mental Disease (IMD) exclusion bars federal reimbursement for the cost of medically necessary inpatient care incurred in treating Medicaid beneficiaries ages 21-64 who receive care in certain institutions that fall within the definition of an institution for mental disease. This exclusion creates for states a significant financial incentive to limit treatment in psychiatric hospitals. The IMD exclusion is often seen as the largest factor behind deinstitutionalization, as states seek to steer patients into Medicaid-eligible services where the Federal Government pays for the majority of the services. Treatment Advocacy Center. Fact Sheet. http://www.gwumc.edu/sphhs/departments/healthpolicy/chsrp/downloads/beha....
-
Pitts, Stephen R. et al. Centers for Disease Control and Prevention. National Hospital Ambulatory Medical Care Survey: 2006 Emergency Department Summary. National Health Statistics Report, No. 7, August 6, 2008. McCaig, Linda, Burt, Catharine. National Hospital Ambulatory Medical Care Survey: 2000 Emergency Department Summary. Advance Data from Vital and Health Statistics. National Center for Health Statistics, No. 355, 2003. From 2000 to 2006, the percentage of cases presenting to the ED with mental disorder as the primary diagnosis increased from 3.2 percent to 3.6 percent.
-
APA. Psychiatric News. 39(21): 13, November 5, 2004.
-
Tuttle, 2008.
-
Kowalczyk, L. Romneys Medicaid Cuts Hit Hard, Hospitals Say. The Boston Globe. February 3, 2003.
-
Sharfstein, J. et al. Clinical and Fiscal Implications of Using a Pediatric Inpatient Service as a Psychiatric Unit. Presented at the 2000 Ambulatory Pediatric Association Meeting. Boston, MA, May 14, 2000. Mansbach, 2003.
-
Hoot, Nathan, Aronsky, Dominik. Systematic Review of Emergency Department Crowding: Causes, Effects, and Solutions. Annals of Emergency Medicine. 52(2): 126-136, August 2008.
-
Weithorn, 2005.
-
Mansbach, J et al. A New Problem in Pediatric and Adolescent Medicine: The Psychiatric Boarder. National Association of Inpatient Physicians. Fifth Annual Meeting. April 9-10, 2002.
-
ACEP Psychiatric and Substance Abuse Survey 2008. 2008.
-
Stefan, Susan. Emergency Department Treatment of Psychiatric Patient: Policy Issues and Legal Requirements. Oxford University Press: United States, 2006.
-
ACEP Psychiatric and Substance Abuse Survey 2008. 2008.
-
American Hospital Association, 2007. http://www.aha.org/content/2007/PowerPoint/StateofHospitalsChartPack2007....
-
Schenkel, Stephen. Maryland Patient Safety Center. Strategies for Handling the Psychiatric Patient Population. July 2006.
-
Bazzoli, Gloria et al. Does U.S. Hospital Capacity Need to be Expanded? Health Affairs. (22)6: 40-54, November/December 2003.
-
Mental Health Crisis Needs a Permanent Fix. Las Vegas Sun. July 13, 2004.
-
Tuttle, 2008. In Georgia, the conditions are reportedly so unacceptable that the U.S. Department of Justice is investigating whether the hospital conditions violate patients civil rights.
-
Trafford, Abigail. Boarder Kids -- On the Edge. The Washington Post. June 27, 2000.
-
Mansbach, 2003. Sharfstein, 2000.
-
Sharfstein, 2000.
-
Mansbach, 2003.
-
President's New Freedom Commission on Mental Health. Report of the Subcommittee on Acute Care. March 5, 2003. http://www.mentalhealthcommission.gov/minutes/march03.htm.
-
Pitts, 2008.
-
Although people whose complaints primarily arise from psychological/mental disorders constitute only 3-4 percent of all visitors to EDs, they are presenting at the ED at an increasing rate. Stefan, 2006.
-
Tuttle, 2008.
-
Tuttle, 2008.
-
National Association of Psychiatric Health Systems. Challenges Facing Behavioral Health Care. 2003. http://www.naphs.org/news/WhitePaper4031.pdf. Appelbaum, Paul. The Quiet Crisis in Mental Health Services. Health Affairs. 22(5): 110-116, September/October 2003. Appelbaum notes specific cases in Michigan, Minnesota, Massachusetts, and South Carolina. Ohio Department of Mental Health. The Crisis in Ohios Acute Mental Health Care: A Mental Health and Overall Health Problem. April 2004. Ohio has also witnessed a steady decline not only in the number of available private and public hospital beds, but also in the actual number of psychiatric hospitals or hospital psychiatric units. Thirteen private psychiatric units closed between 1997 and 2002, representing a 13 percent decrease in beds from 3,456 to 2,842.
-
ACEP Psychiatric Emergencies Survey 2004.
-
California Institute of Mental Health. Psychiatric Beds in California: Reduced Numbers Create System Slow-down and Potential Crisis. 14, 2001. http://www.cimh.org/downloads/Acute_Services_Report_Final.pdf. The California Institute of Mental Health also found that children and adolescents has a significant increase in admissions over the course of the study as compared to adults.
-
Ohio Department of Mental Health. The Crisis in Ohios Acute Mental Health Care: A Mental Health and Overall Health Problem. April 2004. http://www.mh.state.oh.us/medicaldirdiv/documents/acutecare.report.pdf.
-
Pasic, Jagoda et al. High Utilizers of Psychiatric Emergency Services. Psychiatric Services. 56(6): 678-684, June 2005.
-
Weithorn, 2005.
-
Bazelon Center for Mental Health Law. Olmstead Planning for Children with Serious Emotional Disturbance: Merging System of Care Principles with Civil Rights Law.
-
At Childrens Hospital of New York-Presbyterian, the number of children arriving at its emergency room with psychiatric symptomatology jumped from around 200 in 1994 to 800 in the year 2002. A Yale-New Haven Childrens Hospital study found a 59 percent increase in children in psychiatric crisis visiting its emergency room between 1995 and 1999.
-
Weithorn, 2005.
-
Knox and Demner. Trapped in a Mental Ward: State Lacks Programs for Troubled Youth. The Boston Globe. June 4, 2000.
-
ACEP Psychiatric and Substance Abuse Survey 2008.
-
Maine Rural Health Center. Smallest Rural Hospitals Treat Mental Health Emergencies. http://muskie/usm.maine.edu/Publications/rural/wp32pdf.
-
Final Report of the Emergency Medical Treatment and Labor Act Technical Advisory Group to the Secretary, U.S. Department of Health and Human Services. April 2, 2008. http://www.cms.hhs.gov/FACA/Downloads/EMTALA_Final_Report_Summary.pdf. EMTALA requires certain hospitals receiving federal funds to screen individuals presenting to the ED, evaluate whether an emergency is occurring, and if a condition exists, to stabilize the individual prior to transfer, regardless of the individuals ability to pay.
-
Illinois Hospital Association. Behavioral Health Steering Committee Best Practices Task Force. Best Practices for the Treatment of Patients with Mental and Substance Use Illnesses in the Emergency Department. Naperville, IL: Illinois Hospital Association. 2007.
-
Stefan, 2006.
-
Bazzoli, 2003.
-
Tuttle, 2008.
-
Bazzoli, 2003. A St. Cloud, Minnesota hospital built a new adolescent unit in 1998, and expected to lose $6 million on mental health services.
-
Chong, Jia-Rui. County Lacks Beds for Mental Patients. Los Angeles Times. November 23, 2004.
-
Appelbaum, 2003.
-
Stefan, 2006.
-
Lampert, Kristen. Risk Management Issues in Assessing Suicidal and Homicidal Patients. Journal of Healthcare Risk Management. 27(3), 2007.
-
Stefan, 2006.
-
Final Report of the Emergency Medical Treatment and Labor Act Technical Advisory Group to the Secretary, U.S. Department of Health and Human Services. 2008. Passed by Congress in 1986, EMTALA requires a psychiatric patient to be stable for discharge -- when [a] patient is protected and prevented from injuring himself or others. CMS notes that confusion exists surrounding the use of chemical and/or physical restraints necessary to ensure the patient is stable for transport.
-
ACEP Psychiatric and Substance Abuse Survey 2008.
-
Stefan, 2006.
-
ACEP Psychiatric and Substance Abuse Survey 2008. Howard, Patricia. Psychiatric Care in the Emergency Department -- Chaos or Crisis? Emergency Medicine and Critical Care Review. 41-42, 2006.
-
Stefan, 2006.
-
President's New Freedom Commission on Mental Health. Report of the Subcommittee on Acute Care. March 5, 2003. http://www.mentalhealthcommision.gov/minutes/march03.htm.
-
Katz, Abram. Patients Wait for Hours in Hallways: Strain Felt Throughout State. New Haven Register. April 16, 2006. Holmberg, David. The Patients in the Hallways. New York Times. June 10, 2007. Smith, Scott. Take a Number: Getting One of Minnesotas Inpatient Beds Is Still a Waiting Game. Minnesota Medicine. January 2007. The case of Esmin Green at Kings County Hospital received the most prominent national media attention, as it involved a death of a patient in a waiting room. Media publications have also written on psychiatric boarding issues at Boston Medical Center, Yale-New Haven Hospital, Johns Hopkins Hospitals in Baltimore, Harbor-UCLA, and Hennepin Count Medical Center in Minnesota among many others.
-
Trafford, 2000.
-
Howard, 2006. Howard notes that fewer than 20 percent of EDs have a mental health center.
-
ACEP Psychiatric Emergencies Survey 2004.
-
Hart, Beverly. ENA: Advocating Care for Psychiatric Emergency Patients. Journal of Emergency Nursing. 34(4), August 2008. Stefan, 2006.
-
Stefan, Emergency Department Treatment of Psychiatric Patient: Policy Issues and Legal Requirements. 2006.
-
Sharfstein, 2000. These Medicaid requirements include, among other things, staffing requirements and maintaining clinical records on all patients.
-
ACEP Psychiatric and Substance Abuse Survey 2008.
-
Stefan, 2006.
-
Tuttle, 2008.
-
Richardson, DB, Bryant, M. Confirmation of Association between Overcrowding and Adverse Events in Patients who Do Not Wait To Be Seen. Academic Emergency Medicine. 11(5): 462, 2004.
-
Stefan, 2006.
-
McNeil et al. Psychiatric Emergency Service Use and Homelessness, Mental Disorder, and Violence. Psychiatric Services. 56(6): 699-704, June 2005. One study of San Francisco General Hospital found that homeless individuals accounted for 30 percent of the episodes of service in the psychiatric emergency service and were more likely to account for multiple episodes of service. Another study divided high utilization by quarter and by standard deviation, with homelessness serving as a high utilizer by quarter buy not by quarter but not by standard deviation. Pasic, 2005. Arfken C et al. Case-control Study of Frequency Visitors to an Urban Psychiatric Emergency Service. Psychiatric Services. 55: 295-301, 2004. Sullivan, P et al. Characteristics of Repeat Users of a Psychiatric Emergency Service. Hospital and Community Psychiatry. 44: 376-380, 1993. Dhossche, D, Ghani, S. A Study on Recidivism in the Psychiatric Emergency Room. Annals of Clinical Psychiatry. 10: 59-67, 1998.
-
Mancusco, David et al. Washington State Department of Social and Health Services. Frequent Emergency Room Visits Signal Substance Abuse and Mental Illness. June 2004.
-
Stefan, 2006.
-
Janofsky, Jeffrey, Tamburello, Anthony. Diversion to the Mental Health System: Emergency Psychiatry Evaluations. Journal of American Academic Psychiatry Law. 34(3): 283-291, 2006.
-
Dupont, R, Cochran, S. Police Response to Mental Health Emergencies: Barriers to Change. Journal of American Academic Psychiatry Law. 28: 338-344, 2000.
-
Judge David L. Bazelon Center for Mental Health Law. Involuntary Outpatient Commitment: Summary of Statutes, April 2000.
-
Judge David L. Bazelon Center for Mental Health Law, 2000.
-
Janofsky, 2006.
-
Los Angeles County Department of Mental Health, LPS Designation Handbook. http://dmh.lacounty.gov/cms1_055116.pdf.
-
Stefan, 2006.
-
Currier, Glenn, Allen, Michael. Physical and Chemical Restraint in the Emergency Department Emergency Service. Emergency Psychiatry. 51(6): 717-719, June 2000.
-
Stefan, 2006. The Presidents New Freedom Commission on Mental Health, JCAHO, SAMHSA, the Bazelon Center, and NASMHPD have all taken stances against seclusion and restraint in the ED.
-
Appelbaum, 2003.
-
Final Report of the Emergency Medical Treatment and Labor Act Technical Advisory Group to the Secretary, U.S. Department of Health and Human Services. 2008.
-
Weithorn, 2005.
-
Appelbaum, 2003.
-
Kowalczyk, L. Romneys Medicaid Cuts Hit Hard, Hospitals Say. Boston Globe. February 3, 2005.
-
Falvo, 2007. The study does note that from a strictly financial perspective, reserving inpatient beds for more predictable (and profitable) uses than unscheduled admissions from the ED may indeed be the most cost-effective strategy to follow. This would concur with the research claiming hospitals have a financial incentive to board patients if not for the opportunity cost and financial cost lost to the inefficiencies of inpatient boarding.
-
APA. Psychiatric News. 39(21): 13, November 5, 2004.
-
McNeil et al. Psychiatric Emergency Service Use and Homelessness, Mental Disorder, and Violence. Psychiatric Service. 56(6): 699-704, June 2005.
-
Mansbach, 2003. McNeil, 2005.
-
Appelbaum, 2003.
-
Weithorn, 2005.
-
We note, however, that although the ED may be the only source available for psychiatric care for the uninsured, even those with insurance may face challenges. The exhaustion of coverage maximums, low rates of reimbursement, and limitations on types of covered services place them in the same position as the uninsured. Weithorn, 2005.
-
ACEP Psychiatric Emergencies Survey 2004.
-
Katz, 2006.
-
Zun, Leslie. Evidence-Based Treatment of Psychiatric Care. Journal of Emergency Medicine. 28(3): 277-283, April 2005.
-
Bazzoli, 2003.
-
Ryan, Cy. New Plan Could Shorten ER Waits. Las Vegan Sun. July 31, 2008. http://www.lasvegassun.com/news/2008/july/31/new-plan-could-shorten-er-w....
-
Evaluation of the Quality of Care and Process Improvement in Psychiatric Emergency Services: An Informatics Perspective. Fall 2003. http://www.emergencypsychiatry.org/PDF/AAEP_Fall2003.pdf.
-
Brown, Jennifer. Emergency Department Psychiatric Consultation Arrangement. Health Care Management Review. 30(3): 251-261, July 2005.
-
Schenkel, 2006.
-
Illinois Hospital Association, 2007.
-
Maryland Health Care Commission. Use of Maryland Hospital Emergency Departments: An Update and Recommended Strategies to Address Crowding. January 1, 2007.
-
Stills, Marsha. Mental Health Emergency Room Extension Creates Model. Louisiana Medical News. 2008.
-
UAB. UAB Psychiatry. Vol. 2,4, Winter 2008.
-
Stefan, 2006. Curie, Charles. SAMHSAs Commitment to Eliminating the Use of Seclusion and Restraint. Psychiatric Services. 56(9): 1139-1140, September 2005.
-
Morrissey, John. Gong with the (Patient) Flow. Modern Healthcare. 34(6): 6-8, February 9, 2004. Katz, 2006.
-
Garson, Chad et al. Emergency Department Patient Preferences for Boarding Locations with Hospitals Are at Full Capacity. Annals of Emergency Medicine. 51(1): 9-12e, January 2008. McNamee, CS et al. Emergency Department Overcrowding: Patient Preference for Boarding Hallway. Annals of Emergency Medicine. 44(4): S115, October 2004. Walsh, Paul. Patients Would Prefer Ward to Emergency Department Boarding while Awaiting an Inpatient Bed. Journal of Emergency Medicine. 34(2): 221-226, October 2007.
-
ACEP. Emergency Department Crowding: Information Paper. April 2004.
-
Katz, 2006.
-
Tuttle, 2008.
-
The Medicaid Emergency Psychiatric Care Act of 2007 was introduced in the House (with a similar bill in the Senate) to address this issue. It would require the Medicaid program to reimburse institutions for care and services required to stabilize an emergency medical condition of an individual between ages 21 and 65, if the treatment is within the range of services that such institution typically provides. HR 2050 IH. Medicaid Emergency Psychiatric Care Act of 2007. http://thomas.loc.gov/cig-bin/query/D?c110:1:./temp/~c1102pIPig.
-
Maryland Health Care Commission. January 1, 2007.
-
Evaluating the Quality of Care and Process Improvement in Psychiatric Emergency Service: An Informatics Perspective. Emergency Psychiatry, Fall 2003. https://www.emergencypsychiatry.org/PDF/AAEP_Fall2003.pdf.
-
ACEP Psychiatric and Substance Abuse Survey 2008.
-
Stefan, 2006.
-
Moran, Mark. AMA. As Insurance Coverage Wanes, Psychiatric ERs Get Busier. Psychiatric News. 39(21): 12, November 5, 2004.
-
Maryland Health Care Commission, January 1, 2007.
-
Torrey, E. Fuller et al. The Shortage of Public Hospital Beds for Mentally Ill Persons. Treatment Advocacy Center. http://www.treatmentadvocacycenter.org/Reportbedshortage.htm.
-
Ibid. Nevada, Arizona and Arkansas have the lowest number of psychiatric beds per capita, with less than seven per 100,000 population in 2006. (Nevada opened a new state mental hospital not accounted for in this study in 2007.)
-
Bryan, T., Pathak, D. An Evaluation of Methodologies Used in Developing a Statewide Proactive Acute Care Bed Plan: A National Survey. 2003. http://gateway.nlm.nih.gov/MeetingAbstracts/102275622.html.
-
Bazzoli, 2003.
-
Janofsky, 2006.
-
Illinois Hospital Association, 2007.
To obtain a printed copy of this report, send the full report title and your mailing information to:
U.S. Department of Health and Human ServicesOffice of Disability, Aging and Long-Term Care PolicyRoom 424E, H.H. Humphrey Building200 Independence Avenue, S.W.Washington, D.C. 20201FAX: 202-401-7733Email: webmaster.DALTCP@hhs.gov
RETURN TO:
Office of Disability, Aging and Long-Term Care Policy (DALTCP) Home [http://aspe.hhs.gov/_/office_specific/daltcp.cfm]Assistant Secretary for Planning and Evaluation (ASPE) Home [http://aspe.hhs.gov]U.S. Department of Health and Human Services Home [http://www.hhs.gov]