
Prepared by:
NORC at the University of Chicago
Dan Gaylin, M.P.A.
Sidra Goldman
Alana Ketchel
Adil Moiduddin, M.P.P.
October 2005
This report is available on the Internet at:
http://aspe.hhs.gov/sp/chc
Executive Summary
The Office of the Assistant Secretary for Planning and Evaluation (ASPE), in close collaboration with the Health Resources and Services Administration (HRSA), contracted with NORC to conduct an assessment of information technology use in ambulatory care health centers whose funding is administered by HRSA’s Bureau of Primary Healthcare (BPHC). As the culmination of that effort, this final report describes how some of the nation’s Federally-funded health centers use information technology (IT), including applications which assist in directly improving the quality, safety, efficiency and effectiveness of health care (health IT). Health centers, which provide a crucial source of medical care for under- and uninsured populations, also represent an early laboratory for health IT implementation, use and impact among ambulatory health care providers. This project assesses the experiences of certain health centers and health center networks implementing IT programs, and describes the challenges faced by both health centers and health center networks in adopting IT, achieving gains from the use of IT and sustaining those gains over time.
Introduction and Importance of the Study
Findings from this study will inform efforts to improve health center use of IT and provide guidance to decision makers interested in understanding the broad potential for health IT to improve the way health care is delivered in the United States. The report begins with a description of NORC’s study methods for the project as well as a detailed background on the project’s purpose and the health center program history and environment.
Study Methods
Project activities were conducted using a tiered-qualitative approach divided into two separate but interrelated phases: 1) an environmental scan, and 2) a series of seven case studies focusing on a set of geographically dispersed health centers and health center consortia with ongoing IT implementation projects. The environmental scan phase involved discussions with 16 thought leaders and key informants knowledgeable about IT and the health care safety net, and a review of published and unpublished documentation. Findings from the environmental scan supplied the basis for setting up the subsequent project activities, including the selection of case study candidates.
The second major phase of the study involved in-depth case studies of seven sites around the U.S. These case studies entailed a series of meetings with stakeholders at health centers and health center networks identified as “leading edge” — those that offered the greatest opportunity for providing policy-relevant lessons learned and informing sustainability and spread of gains from IT implementation. Candidate sites targeted for case study selection were communities maintaining several Section 330 health centers, including IT-savvy health centers and networks. The final sites selected were in the states of Oregon, Virginia, New Hampshire, Florida, and Kentucky, and in the cities of Boston, MA, and Philadelphia, PA. Overall methods included meetings with 120 respondents across 38 health centers and seven health center networks. Meetings covered a range of topics, including health centers’ approaches to and uses of IT, perceived barriers and enablers to technology adoption, participation in networks, and network governance and organization. Detailed case study reports were prepared for each site describing findings and lessons learned from each site visit.
Final analysis activities, which culminated in the current report, drew from findings and themes across all project activities. Findings are discussed at two levels — the health center network level and the individual health center level. We explore health centers’ and networks’ experiences with implementing IT, and describe the different models for IT adoption along with issues relevant to sustainability, replicability and public policy in this area.
Background
The current project will inform policy efforts to encourage the implementation of IT to achieve efficiency and quality of care objectives. Federally sponsored health centers form a key part of the nation’s health care “safety net”, delivering primary care medical services to vulnerable populations. Special data and administrative requirements, including tracking and reporting on their patient populations, maintaining patient-specific data, and supporting disease registries for vulnerable populations, make health centers a prime target for implementing health IT applications. Over the past several years many health centers have chosen to band together to form networks that provide access to these IT applications, business services and technical support. Network development has also been spurred by systems-related grant programs, many of which are funded by the Bureau of Primary Health Care (BPHC), the Agency that provides base funding for the health centers themselves.
Health centers have quickly caught on to technology’s potential for improving efficiency and quality of care. In addition to the factors described above, external trends — such as the increasing rate of IT investment in health care overall and the Bush Administration’s health IT initiatives — have contributed to the fast growth in health centers’ adoption of IT. Electronic Health Record (EHR) adoption has been especially noteworthy. Multiple health centers in three of the seven case studies had implemented an EHR between the start of our study in 2002 and completion of our last site visit in 2004. Findings presented here will assist policy makers as they seek to build on early IT adoption among health centers and other providers.
Case Study Findings
Findings from the case studies are analyzed on two levels: the health center network level and the individual health center level. Overall, the case study findings provide insight into why leading edge health centers and health center networks wanted to invest in IT and what they experienced. In doing so, the findings offer substantive guidance for ASPE and HRSA with regard to policy on IT adoption among health centers. Key themes emerged in several areas.
First, it is clear that several health center networks, formed in response to an increasing emphasis on decreasing the cost of care, have relied on the coordination of IT services as an important strategy for meeting efficiency objectives and providing value-added benefits for their members. Network models, goals, and provision of services differ substantially, with some adopting an incremental approach in rolling out practice management systems for their members and then moving to electronic health records (EHR), while others adopt EHR first or concentrate on building community data warehouses.
Core network functions include convening local stakeholders, directing vendor selections, centralizing IT implementation and support, and administrative management. Many health centers reported receiving considerable benefits from their network membership, but positive experiences were not universal and we observed that networks face ongoing challenges in maintaining buy-in from their stakeholders and ensuring long-term sustainability.
Health centers in general are increasing their centralized planning for and investment in IT systems. Access to systems is widespread, although the majority of health centers we spoke with had acquired such access through their local health center network. The predominant uses of IT include practice management systems, which are perceived to promote financial stability and efficiencies, and EHR systems, which address quality of care, disease management, and practice workflow. Buy-in for adoption of both these technologies is widespread among health centers, and satisfaction with the applications implemented among the health centers we spoke with was overall high.
Conclusions
In synthesizing lessons learned from the case studies, we focus on key issues relevant to the current policy debate, including support for health center networks and EHR adoption. We also describe areas for future research and analysis.
Network Benefits and Challenges. Overall, findings confirm that health center networks can be successful vehicles for the adoption of IT in the safety net. Networks help health centers to finance costly technologies by accessing grant money over and above the Section 330 grants. In addition, we found substantial evidence that health center networks provide human and technology resources through economies of scale that health centers could not afford on their own. Networks offer health centers access to executives skilled at the vendor evaluation, management and procurement processes and are able to leverage market share to hold vendors to a high standard. Finally, networks serve as important forums for sharing best practices among health center members. For communities working to share data through community applications and data warehouses, the network model was particularly suitable to gather buy-in and build infrastructure for such a system. We found that network formation would not be possible without funding specific to encouraging collaboration among health centers.
In addition to these important benefits, networks face a number of difficult challenges in fulfilling their mission. Networks often struggle to meet the diverse requirements of their member health centers in terms of financial resources, IT capacity, infrastructure and vision. Successful networks featured a centralized, collaborative framework that was central to establishing a common vision and strong buy-in among its partners. Networks that focused on building applications to collect store and centrally maintain data from individual health centers faced difficult technical, financial and legal challenges. They were pressed to prove clear benefit to individual health centers in order to ensure participation and realize the goal of data exchange at the network level and beyond.
Rural networks faced especially difficult challenges in building and accessing community-based applications because of resource and infrastructure constraints. Overall, realizing robust, measurable public health and financial benefits from EHR and health data exchange remain opportunities for the future among those health centers consulted. Formal data sharing relationships among hospitals, public health agencies and Medicaid are slow in evolving and networks still require a sustained level of public funding for the training, initial implementation and ongoing support necessary to realize benefits from their software.
EHR-specific Lessons Learned. Successful early adopters of clinical technology offered several lessons for future funders and implementers of EHR. Case studies demonstrated the importance of having not only buy-in, but significant involvement from clinicians at all phases of an EHR implementation to ensure the technology’s smooth integration with clinical work processes thereby allowing clinicians to realize clear benefits from using the system. In order to support the purchase and implementation of such systems, the network required three levels of substantial funds: seed money for start-up, money to build infrastructure and transition workflow, and funds for the ongoing maintenance of technologies. The networks we studied all relied on outside funding to support ongoing maintenance and future systems purchases.
Some health centers that implemented EHR were able to quickly translate resulting improvements in patient outcomes, although the ability to accurately quantify a return on investment on the institutional level is still underdeveloped. Future safety net providers looking to adopt health IT systems may benefit from a riper environment for adoption given its recent emphasis in the policy arena. Adoption efforts would be especially enhanced by the development of data standards, more “usable” software and more available funding to consortia of community providers. However, advances will be balanced by sustained challenges of developing a collaborative and functional network model and overcoming fears of data sharing.
Critical Factors for Success. Despite the many organizational and cultural models employed by these early adopting networks, we did find several factors closely associated with successful adoption of IT among health centers. Networks that understood the relationship between clinical and administrative applications, particularly implementing a robust practice management system as a backbone to implementing an EHR, were more successful in achieving a seamless exchange of information between the two systems.
We found that more integrated networks where there was strong buy-in for shared systems generally managed a smoother implementation of the technology. More decentralized networks sometimes could not achieve consensus necessary to procure shared institution-level applications, focusing instead on combined systems such as data warehouses and external client tracking systems which have proven difficult to implement. Another important aspect determining the networks’ success was the need to build trust through strong leadership. Only those network leaders experienced in large scale IT design and roll out and highly skilled at customer service were able to implement common practice management and EHR applications across centers.
Key Issues for Future Study. This study has elucidated important lessons learned for adoption of IT, including health IT, among health centers and health center networks. A number of areas that merit further investigation to assist policy development include studying the feasibility and sustainability of promoting a network model, analyzing coordination and overlap among health center networks and attempting to quantify the value of health IT systems relative to their costs. In addition, it will be important to follow examples of successful networks as they work to wean themselves from large amounts of outside funding to support ongoing operations.
Introduction
NORC at the University of Chicago (NORC) is pleased to present this Final Report for Community Health Center Information Systems Assessment: Issues and Opportunities to the Office of the Assistant Secretary for Planning and Evaluation (ASPE) at the United States Department of Health and Human Services (HHS). The project applies qualitative methods to describe the use of information technology (IT) among ambulatory health care providers funded by the Health Resources and Services Administration (HRSA), Bureau of Primary Health Care (BPHC) under Section 330 of the Public Health Service Act (hereinafter “health centers”) and health center networks around the nation. NORC conducted this project under contract with ASPE; HRSA and BPHC worked in conjunction with ASPE to guide activities under the project. In this report, we refer both to health centers’ use of IT generally, and, as a subset of IT, to those applications which directly may improve the safety, quality, efficiency and effectiveness of health care delivery, known as health IT.
This report represents a synthesis of several prior deliverables, including an environmental scan and seven interim reports detailing findings from case studies. Overall, we report on findings from discussions with over 120 respondents from health centers (38 total, several with multiple sites), health center networks, public health agencies, associations, foundations and other relevant stakeholders, shedding light on the experiences of health centers and health center networks at various stages of implementing IT programs. We also describe important challenges to the development and long term sustainability of health center network arrangements as well as the obstacles health centers face when initiating IT projects alone or in collaboration with other providers.
Importance of the Current Study
Health centers represent a critical resource for individuals and families who face barriers to securing medical insurance or seeking care through private providers. In FY 2003, health centers provided medical care to approximately 12.5 million Americans, the majority of whom live below the poverty level. In addition to assuring this population access to primary care medicine and ancillary services (such as radiology, clinical laboratories and pharmacy), health centers often link these individuals to Federal, state and local social services programs such as Temporary Assistance for Needy Families (TANF), Medicaid, mental health and substance abuse treatment, and the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC).1
In the past decade many health centers have served the growing national uninsured population comprised increasingly of immigrants and selected minorities while working with reduced Medicaid reimbursement rates and managed care. During this period, health centers have also increased their emphasis on quality improvement for care delivered to patients with chronic illness as well as more effective use of diagnostic and preventive services through participation in a variety of initiatives sponsored by BPHC.
Seeking to achieve administrative efficiencies, optimized reimbursement from third party payers, improvements in clinical decision-making, and better management of chronic illness, many health centers rely on IT applications such as practice management, electronic health records (EHR), disease registries, community-wide client tracking programs and health data repositories. Health centers seek to maximize gains from IT while navigating challenges related to selecting vendors, implementing and customizing the chosen systems, training providers in appropriate use of the systems, and complying with Federal health data standards and privacy rules.
This project is unique in that it provides policy stakeholders with a detailed understanding of health centers’ use of IT — including the challenges related to obtaining systems, funding IT, managing vendor products and relationships, training clinical and administrative staff to use IT, providing user assistance and the technical infrastructure to support IT and using information systems for overall quality improvement. This report comes at an opportune time as the nation’s leading policy makers have identified health IT as an important component to improving the quality and efficiency of care across the health care system. Health centers and health center networks described in this report represent an early laboratory for IT, and specifically health IT, implementation, use and impact among ambulatory health care providers. As such, we anticipate that findings from this study will not only inform efforts to improve health center use of health IT, but will provide guidance to providers, policy makers and other stakeholders interested in understanding the broad potential for IT to improve the way health care is delivered in the United States.
Overall Approach
Given that formal assessment of IT use among ambulatory health care providers is still at its early stages, ASPE specified a multi-tiered qualitative approach to data gathering and analysis for this study beginning with an environmental scan where existing literature was reviewed and thought leaders were consulted. We then conducted detailed case-based data collection among health centers and stakeholders in seven geographic locations and analyzed findings across the entire study.
Because this is a qualitative study of providers and networks at various stages of IT adoption, we emphasize similarities and differences across different models for IT adoption as well as the facilitators, barriers, challenges and opportunities specific to each model and to IT use in general. Findings are framed as potential lessons learned relevant to the desirability, sustainability and replicability of the various approaches encountered in our study. The remainder of this report is organized as follows:
- Study Methods. We begin with a brief discussion of the overall approach and specific methods used to collect and analyze information gathered during the two main phases of the project: the environmental scan, which included in-depth discussions with sixteen thought leaders as well as a review of existing documentation, and seven case studies comprised of telephone and in-person meetings with 120 respondents across 38 health centers and seven health center networks.
- Background. We follow the methods section with a brief overview of the health center landscape, including the health center program’s history, funding structure, special issues and challenges for health centers, and the rise in IT adoption by health centers. We also present key themes and conclusions drawn from the environmental scan, which informed the design of and findings from the seven case studies.
- Health Center Network-Level Findings. We begin our discussion of findings from case studies by presenting findings at the level of the “leading edge” health center networks, including the impetus behind their development, key characteristics and trends, the benefits of network membership for health centers, and ongoing challenges for networks.
- Health Center-Level Findings. Next, we review the IT status and experience of individual health centers, including their approach to IT infrastructure (staffing, resources), uses of IT, including health IT, and participation in health center networks.
- Conclusions. We conclude the Final Report with a discussion of broad conclusions following from the environmental scan activities and the seven case studies. These conclusions include lessons learned from the experience of health centers and health center networks implementing IT and implications of these findings for key stakeholders such as policymakers and other providers.
Footnotes
1 Testimony by Elizabeth M. Duke, Health Resources and Services Administration on “A Review of Community Health Centers: Issues and Opportunities” before the Subcommittee on Oversight and Investigations, Committee on Energy and Commerce, United States House of Representatives. May 25, 2005. Available online from: <http://www.hhs.gov/asl/testify/t050525.html>
Study Methods
As described above, we applied a tiered-qualitative approach described in the original proposal. Overall, our approach hinges on seven detailed case studies conducted in targeted geographic regions where we spoke with health center stakeholders in person and over the telephone regarding their experiences with IT implementation and use. Prior to the case studies we conducted an environmental scan including a review of printed and published materials, discussions with thought leaders, and a detailed summary of practice management systems employed by health centers.
Findings from the environmental scan were used to develop the specific approach for case studies and to identify potential sites. Following each case study we submitted a detailed report outlining major findings and lessons learned. Finally, we conducted an analysis of findings across the environmental scan and all case study reports and synthesized findings and methods in the current report. In the paragraphs below we describe key features of the three project phases.
Environmental Scan
Because the body of literature relevant to IT use and adoption among health centers is relatively limited, we conducted an environmental scan, completed between February and September 2003, which included review of both published and unpublished materials relevant to key study topics. Materials summarized in the environmental scan were gathered through formal searches in health services research databases such as PubMed, paired with searches of popular, non-peer reviewed publications using Internet search engines such as google.com. Searches were conducted using a range of subject-level key words crossing “community health centers” or “FQHC” with words such as “information technology”, “HIPAA”, “practice management”, and “electronic medical or health records”.
Additional sources were identified by contacting individuals at relevant organizations to gain access to unpublished information or publications that were not readily available through public sources. These organizations included HRSA, BPHC, the National Association of Community Health Centers (NACHC), state level primary care associations (PCAs) and others. Overall, we reviewed content from over 100 documents including peer-reviewed articles, market reports, program notices, government evaluations, provider association newsletters, requests for application and other relevant sources.
In addition to review of secondary sources, the environmental scan included loosely structured, one hour discussions with thought leaders in the field of IT and health centers. The 16 thought leaders included consultants working with health centers, health center staff, network representatives, associations and Federal government officials from BPHC and the Veterans Health Administration.
Finally, the environmental scan included a targeted analysis of four practice management systems that cater to the health center market. On direction from ASPE, we focused on practice management because at the time that the environmental scan was conducted in 2003, relatively few health centers or health center networks had made substantial progress with EHR — with increasing EHR activity as the study progressed. Discussion of practice management systems for the environmental scan was based on a detailed review of vendor websites and targeted thought leader discussions. The full environmental scan report is included in this report as Appendix A with key findings highlighted in the Background section of this report.
Case Studies of Leading Edge Health Center Networks
Findings from the environmental scan informed the second major phase of the study involving in-depth case studies. Site visits supporting each case study were conducted at seven communities or states across the nation from October 2003 through September 2004. Each case study entailed a series of in-person and telephone discussions with leadership and staff members at health centers, health center networks and other stakeholder organizations such as PCAs, public health departments and Medicaid offices. Thought leaders consulted for the environmental scan suggested candidate sites based on the presence of Section 330 health centers that had made progress in their use of IT as part of their local or regional network. ASPE and HRSA made the final site visit selections. Each case study represents a somewhat different functional and organizational model to allow for meaningful comparisons.
Prior to site visits, NORC staff conducted preliminary phone conversations with health center and state government stakeholders to introduce the study and identify appropriate respondents. Site visits lasted one or two days and respondents for structured discussions at each site were identified through a combination of government leads, leads from other respondents, and targeted literature and web searches. Teams consisted of at least one senior staff member and one research assistant primarily responsible for taking notes. One of the case studies, in Kentucky, involved a series of detailed telephone calls with key stakeholders but did not include an on-site component. Overall, we conducted discussions with over 120 respondents from among health center staff and other stakeholders.
Data was collected using instruments tailored to each respondent that allowed us to collect detailed, qualitative data on key topics. Each guide included background information on the respondent and highlighted outstanding questions for the team to address. ASPE and BPHC approved the guides prior to initiation of the site visits. In addition, NORC submitted technology inventory forms to health center respondents prior to each site visit as a supplement to data collected through the discussions. The forms consisted of a short table which took a “snapshot” inventory of the health centers’ networking, data and technology capacity. The data collected revealed the degrees of variation in health IT capacity based on differences in size and health IT sophistication among respondent health centers.
Exhibit 1 below lists respondent groups consulted for each case study including health centers, health center networks and other stakeholders. Network leadership generally included the President, Chief Executive Officer (CEO) or Chief Information Officer (CIO) of the network and other network leaders. Health center respondents included administrators such as the Executive Director (ED) or Chief Financial Officer (CFO) as well as information systems staff. In addition, we spoke with clinicians and other end-users of technology, such as billing clerks.
| Case Study Sites | Respondent Characteristics |
|---|---|
| Oregon October 2003 (2 day visit) |
|
| Philadelphia, PA February 2004 |
|
| Virginia February 2004 |
|
| Southeastern Kentucky February-March 2004 |
|
| Boston, MA May 2004 |
|
| Southern New Hampshire May 2004 |
|
| Southern Florida September 2004 |
|
If key respondents were unavailable during the time of the site visit, the team conducted follow-up discussions with the respondent after the site visit was complete. Additional inputs to the findings from each case study included the review of documentation that respondents made available to the team during the discussions.
We queried individual health centers on their overall approach to health IT, technical capacity and systems, major uses of systems and any challenges they face in adopting technologies. Network directors were asked about the origins and organization of the network, how health IT fits into their goals and mission, and any challenges they faced or currently face in adopting systems. Other stakeholders were asked about their involvement with health center IT initiatives, uses of data produced by shared systems, and their role in future safety net health IT initiatives. Themes covered across respondents are described in further detail below.
- Overall approach to health IT. We asked health center directors to discuss the level of resources dedicated to IT (relative to other areas), the process for planning and decision-making around IT and the health center or network’s approach to compliance with privacy regulations.
- IT infrastructure. We asked health centers to describe their hardware capacity, connectivity and data management capability. In addition, we queried on their level of internal staffing, use of vendors and outsourcing of IT functions.
- Major uses of IT. We asked health centers and networks to list major IT applications (from the MS Office suite to disease registries and EHR) used and their primary functions.
- Enablers and barriers to technology adoption. We asked respondents to describe their motivation for adopting health IT, keys to any success, and what challenges they faced in terms of regulatory, organizational, cultural or financial barriers to adoption.
- Participation in networks and vision for the future. Health centers addressed the benefits and challenges of network participation and steps that the health centers planned to take in the future related to health IT and community partnerships.
- Network governance, organization and services. Network leadership specifically were asked to describe how the network was organized and funded, what types of services they provide to member health centers, and the resulting outcomes of these services.
- Technology tools and community health. We queried network and broader community health leaders on their current and future strategies to coordinate care on a community level using IT and health IT.
Data Analysis
After each case study was complete, findings from preliminary phone calls, site visit discussions and follow-up activities were analyzed and written into draft case reports submitted to ASPE and HRSA. Once comments were received, NORC revised each document and submitted it in final form. Each report drew richly detailed findings and lessons learned from stakeholder discussions. These case study reports are included in this report as Appendix B.
Our findings should be interpreted in light of the fact that we focused, by design, on early adopters of IT and health IT among health centers. While some of the barriers encountered by sites visited for this study may be mitigated over time through standards development, increased access to publicly funded capital, a more stable vendor market and better incentives for adoption (e.g., pay for performance), the majority of the challenges described in this report will be encountered by any health center that attempts to enhance their use of IT and health IT. In addition, we note that these challenges may be greater for health centers not studied here because they likely lack the characteristics that made this group early adopters in the first place.
Following a discussion of background, we present findings both at the health center network level and the individual health center level and explore different, but viable models for the adoption of IT in health centers. We describe the health centers’ experiences with implementing and using IT systems, including the various barriers and incentives affecting the implementation of such systems. Our conclusions focus on benefits and challenges associated with health center network activity, critical success factors for health centers implementing IT, special lessons learned from early experience with EHR and issues for future study.
Background
In this section we provide an overview of the Federally sponsored health center landscape, including the health center program’s history, funding structure, special issues and challenges for health centers. We also provide some context on the role of IT and health IT in health centers based on findings from our environmental scan. Much of this section draws from findings elaborated in greater detail in the Environmental Scan report which is Appendix A to this document.
Overview of the Health Center Program
Federally sponsored health centers, authorized under Section 330 of the Health Centers Consolidation Act of 1996 and reauthorized in 2001, are integral parts of the nation’s health care “safety net” (providers who service underserved and uninsured populations) in both rural and urban regions across the United States. Since their inception as a pilot program by the Federal government in 1964, health centers have been instrumental in delivering primary care medical services to vulnerable populations. They represent a critical public resource for individuals and families who face barriers to securing medical insurance or obtaining care from private providers. With expansions in the FY 2005 budget, there will be well over 800 funded Community and Migrant Health Centers and about 3,700 sites by 2006.
Despite some demographic and organizational differences, in recent years health centers have increasingly banded together to form networks or consortia that seek to provide their members with access to sophisticated information systems, business services, IT expertise, and technical support. This trend, spurred by the onset of Medicaid mandatory managed care and the need for health centers to maintain their competitive status, has produced significant organizational and operational changes, including changes in how health centers approach IT. In particular, several grant programs sponsored by the BPHC, described below, have encouraged network development.
Health Center Funding
Since the 1996 passage of the Health Care Consolidation Act, the Federally Qualified Health Center (FQHC) program has grown steadily both in the provision of services to target populations and in funding. Federal appropriations for health centers have risen steadily over the past two decades, an increase that has accelerated over the past several years. For FY 2005, the program was funded at nearly $1.73 billion dollars. Growth in funding has resulted in the increase in health center access points: new health center grantees as well as new health care delivery sites for existing centers. Exhibit 2 below provides a breakdown of estimated actual revenue accrued by health centers from 2002 through 2004. In addition, the table shows the share of total revenue by source of funding (roughly consistent across years).
Funding Source |
2002 Revenues | 2003 Revenues | 2004 Revenues | 2004 % of Total |
|---|---|---|---|---|
| Section 330 | $1,145 | $1,323 | $1,629 | 24 % |
| Medicaid | $1,808 | $2,116 | $2,432 | 36 % |
| Medicare | $299 | $326 | $382 | 6 % |
| SCHIP | $130 | $150 | $145 | 2 % |
| Other 3rd party | $328 | $367 | $418 | 6 % |
| Self Pay | $303 | $352 | $416 | 6 % |
| Other grants (Federal) | $171 | $198 | $196 | 3 % |
| Other grants (State, local, other) |
$171 | $979 | $1,257 | 19 % |
| Total | $5,061 | $5,811 | $6,282 | 100 % |
| * NOTE: All dollar figures in millions2 | ||||
Special Issues and Challenges for Health Centers
As noted in the introduction, health centers have a special set of data and administrative requirements, and these requirements have direct implications for health centers’ needs for IT. Health centers are responsible for providing services to underserved and vulnerable populations, including Medicare and Medicaid recipients, the underinsured, and the uninsured. Health centers must maximize third party payments and collect fees from patients using a sliding fee schedule.
As such, health centers have a specific need to gather socio-economic data from their patients both to assess their eligibility for Medicaid, Medicare or other insurance or health care subsidization programs and to assess patient fees based on ability to pay. This is particularly challenging when working with populations that frequently fall in and out of eligibility for different programs and may seek care only at sporadic intervals and at different locations. Other special features of the context in which health centers operate are described below.
- Reporting and Tracking. Under their Section 330 grants, health centers annually submit Uniform Data System (UDS) reports providing aggregate data on encounters, payer mix, revenues and other key operational and administrative measures. The UDS includes requirements to report encounters by specific diagnosis and procedure and additional information such as birth weight and trimester of first prenatal visit for perinatal care. Other Federal funding programs, such as prevention grants, require health center grantees to submit annual reports describing, for example, utilization of services provided to a given group of patients. In addition, some services provided to special populations — e.g., pediatric immunizations or pregnancy counseling for teenagers — must also be tracked, both for UDS and non-Federal funders.
- Maintaining Patient Data. Health center administrative systems must accommodate the need for double and triple bookings to account for expected no-shows and cancellations which are common with the population they serve, as well as sliding fee schedules for determining patient out-of-pocket costs. In addition, health center providers (like all providers) must schedule and bill patients, and keep separate records of those patients’ appointments, medical histories, test results, orders, diagnoses, therapies and prognoses. This includes protecting individually identifiable health information that is transmitted or maintained by the center in any form per the Health Insurance Portability and Accountability Act (HIPAA) and associated regulations.
- Disease Registries for Vulnerable Populations. Many health centers are actively involved in providing disease management services to chronically ill patients including those with diabetes, asthma, and cardiovascular disease. As of April 2005, more than 600 health centers have participated in the BPHC’s Health Disparities Collaboratives, which were developed using the chronic care model for continuous care quality improvement and eliminating health disparities. An important aspect of participation in the Collaboratives is maintaining patients with specific diagnoses in a registry system that was designed around evidence-based guidelines to drive quality of care improvement. This registry, called the Patient Electronic Care System (PECS), is paired with an electronic management system called the Cardiovascular/Diabetes Electronic Management System (CVDEMS). CVDEMS was designed to assist providers in managing and tracking the quality of care provided to patients with diabetes and cardiovascular disease.
The unique responsibilities Federally-funded health centers face, as described above, place them in a prime position for investment in IT and health IT. Reporting requirements, administrative data management, and public health tracking projects can all be facilitated through the use of applications like practice management, EHRs and data warehouses. Many health centers have accepted the potential for health IT to improve efficiency and quality of care. Even during the relatively short time span of this project, we observed important examples of increased health IT adoption among health centers including use of applications such as EHR. Several factors have contributed to this trend, including various funding programs that have encouraged health center adoption of IT and health IT through participation in networks.
Health Center Investment in Health IT: Preliminary Findings
At the time of the environmental scan, we found that health centers had focused significant investment in practice management systems with some mixed, but overall positive results. Our thought leaders noted that the vast majority of medium-to-large health centers had some form of practice management software and that these applications generally improved basic administrative functions, especially billing. However, they also noted that health centers struggled with using advanced practice management functions, such as reporting, and that very few of these systems were interoperable with other systems used by the health center.
Thought leaders also described a highly fragmented market for practice management software with providers still struggling to understand their requirements and vendors challenged to differentiate themselves. At the time of the environmental scan, several health center-focused vendors were actively engaged in mergers and acquisitions and were still adjusting to clients’ functionality needs, making it difficult to accurately assess differences between products and the long-term stability of vendors. More than one health center we spoke with as part of the case studies had experienced problems when their practice management vendor was bought by another company or discontinued support for their product.
We found that EHRs were (and are) far less common than practice management systems. Thought leaders indicated that health centers were cautious about implementing EHR, due to concerns over provider comfort with the technology, the need for ongoing training, and general reluctance to invest in a technology that is still evolving. As with practice management, our findings revealed that the vendor landscape for EHR is fragmented, with the substantial majority of vendors having fewer than fifty clinic clients.
In general, the vendor landscape for the health center market was found to be still maturing, the largest category of vendors serve a small group of regionally defined customers. Increasingly, we noted that best of breed vendors packaged EHR tools or functionalities with practice management. The most mature use of EHR was found in systems such as the VA, Partners Healthcare or the Regenstrief Institute that had developed their own software for both inpatient and outpatient settings. We found that selected staff model managed care organizations such as Kaiser Permanente were able to work with best in breed vendors such as Epic to implement high end health IT systems, but that these products were out of reach financially for most health centers.
Organization into Health Center Networks
Importantly, the environmental scan pointed to the rising trend of health center participation in community-wide information systems collaborations, which generally took the form of regional health center networks. Funding for health center network activities came from dedicated outside grants, usually from the BPHC. Networks are typically funded through programs such as the Integrated Services Development Initiative (ISDI), Shared Integrated Management Information Systems (SIMIS), and the Healthy Communities Access Program (HCAP). Several Federal funding programs that contributed to the formation of health center networks that are utilizing IT are summarized in the bullets below.
- Integrated Services Development Initiative (ISDI): The Integrated Services Development Initiative (ISDI) is a health center-focused grant that funds implementation of joint practice management systems and EHR across centers in a single area and health center collaborations to form integrated delivery systems designed to increase health center efficiency and effectiveness.
- Shared Integrated Management Information System program (SIMIS). The SIMIS grant program, administered by BPHC, supports inter-center collaboration on systems issues. Funded grantees typically design and implement common platform and tools for centralized billing, utilization review and quality assurance. Another goal of the program is to encourage integration of administrative and clinical information management functions within and across centers. The SIMIS program requires health centers to implement strategic models for community-wide systems decision-making.
- Healthy Communities Access Program (HCAP). HCAP funds models for enhancing integration of safety net services provided in any community. Grant dollars are not restricted to systems-specific initiatives, although nearly all recent grants include substantial allocation of funds for information systems issues. Examples of activities funded under the program include development of client eligibility tracking databases and establishment of a shared EHR system in a community.
- Integrated Communications and Technology (ICT). ICT grants support health centers in fostering the development of a technology infrastructure to integrate uniform clinical information with business systems and care management. In 2004, six ICT grants totaling $4.2 million were awarded.3
- Operational Networks (OPN). OPN grants provide support for existing health center networks by funding ongoing costs associated with the integration of mission-critical functions at the network level. OPN funds may also support comprehensive pharmacy networks in improving access to affordable medications, developing efficient pharmacy management, and improving patient outcomes through pharmaceutical care.4
- Transforming Healthcare Quality through Information Technology (THQIT). The THQIT initiative, launched in 2004 by the Agency for Healthcare Research and Quality (AHRQ), is a set of grant and contract programs aimed at promoting the use of health IT through the development of networks for sharing clinical data as well as projects for planning, implementing, and demonstrating the value of health IT. Several health centers are beneficiaries in the first round of funding under this program beginning in October of 2004.5
Thought leaders reported that, if sustained, networks could enable health centers to overcome the challenges associated with IT adoption and establish a common platform for practice management, EHR and clinical data systems across providers in a community. The environmental scan demonstrated growing interest and capacity of health centers to organize and meet those challenges through network activity. Thought leaders suggested that many health centers represent fertile ground for network-based IT initiatives.
Footnotes
2 Figures drawn from the HRSA/BPHC Section 330 Grantees Uniform Data System Calendar Year 2002, 2003 and 2004 National Rollup Reports. 2004 Report Available Online at: <ftp://ftp.hrsa.gov/bphc/pdf/uds/2004/04Rollup_Nat_01Jul2005.pdf>
3 Press Release, October 2, 2003. Health Resources and Services Administration. “HRSA Awards $10 Million in Grants to Create and Expand Health Center Networks, Improve Information Management Activities”. October 2, 2003. Available online from: <http://newsroom.hrsa.gov/releases/2003/isdi.htm>
4 Preview of HRSA Funding Opportunities. Primary Health Care Summaries. Available online from: <http://www.hrsa.gov/grants/preview/primary.htm#hrsa05109>
5 Press Release, October 13, 2004. “HHS Awards $139 Million To Drive Adoption of Health Information Technology. “Agency for Healthcare Research and Quality, Rockville, MD. Available online from: <http://www.ahrq.gov/news/press/pr2004/hhshitpr.htm>
Health Center Network Findings
As mentioned above, case studies focused largely on the activities of leading edge health center networks that had demonstrated some progress in implementing IT across health centers in a community or region. In this section we describe case study findings on the network level. We begin by providing background on the origin of health center networks, as well as their key characteristics and functions as they relate to IT implementation. We then describe a scheme for categorizing studied networks that demonstrates the link between their structural characteristics and the networks’ functions, successes and challenges.
Health Center Network Background and Objectives
The efforts studied here are part of an ongoing trend toward health center network activity beginning in the mid-1990s. Although health center networks have existed in various forms for decades, several motivating factors have encouraged network formation and activity over the past 10 years. Health system changes such as widespread provider consolidation, the movement towards Medicaid managed care, and policies that require health centers to maximize collection from third party payers have created new incentives for network formation to help health centers adapt, often through collaborative adoption of IT. In addition, several Federally-funded programs, described above, have encouraged network formation and network-level investments in IT. Exhibit 3 found on Page 14 summarizes key activities of health center networks we spoke with for each of the seven case studies.
Given their common origins and requirements, Section 330 health center networks strive to achieve similar goals, ranging from improved operational efficiency on an individual health center level to improved health of the safety net population as a whole. Four of these major goals and their relationship to IT are outlined in the bullets below.
- Financial viability. As described above, health centers face increased pressure to reduce cost of operations, maximize revenue from third party payers and generally exert greater control over their financial status, partly due to the trend towards Medicaid managed care contracting. Networks provide a forum for health center Executive Directors and CFOs to discuss opportunities to save money through collaboration. Some networks have engaged in joint purchasing programs or worked to start Medicaid managed care plans. Establishing robust administrative systems to increase efficiency and third party payments across health centers has been a central focus of many networks, including those investigated as part of this study.
- Administrative reporting. Related to the need to streamline administrative activities is the need for health centers to be able to efficiently and accurately produce a range of reports required for day to day management of their operations as well as those mandated by funding organizations (e.g., the UDS). Helping health enters produce standard and custom reports through use of IT is a central goal for the health center networks investigated as part of this study.
- Disease management and clinical outcomes improvement. Given their role in treating vulnerable populations, health centers have always prioritized quality of care and outcomes improvement. Motivated in part by Federally sponsored programs such as the Health Disparities Collaborative most health center networks studied prioritize the adoption of health IT to improve clinical outcomes. Four of the studied networks use EHR systems (one site rolled out EHR subsequent to our site visit) to enhance the availability of accurate information at the point of care, helping clinicians make informed decisions.
- Coordinated care and public health collaborations. As a coordinating body, several networks seek to coordinate the activities of their member health centers and, in some cases, other providers. Several of the networks seek to collaborate with regional primary care safety net providers in order to promote population-based healthcare, facilitate the secure exchange of patient data across the region to coordinate care, and quickly identify actionable public health issues. None of the networks studied has achieved such a region-wide coordinated system but several indicate that this remains an important goal to pursue in the future.
Although networks by and large form for similar reasons and with similar goals and governance structures, there are important characteristics that distinguish some network models from others. The seven networks we studied represent various organizational and service delivery models. Key areas of variation include horizontal versus vertical collaboration, the extent to which networks have centralized functions previously operated at the health center level and the role of partnering community health stakeholders. We found that these structural components of health center networks often drive prioritization of network objectives as well as key challenges and success factors. An overview of networks investigated and key activities of each are summarized in Exhibit 3 below.
Networks Investigated |
Network Model | Key Partners and Members | Ongoing or Planned Activities | Major Revenue Sources |
|---|---|---|---|---|
| Oregon Community Health Information Network (OCHIN) |
|
|
|
|
| Health Federation of Philadelphia (HFP) |
|
|
|
|
| Community Care Network of Virginia (CCNV) |
|
|
|
|
| Southeastern Kentucky (SKYCAP) |
|
|
|
|
| Boston HealthNet (HealthNet) |
|
|
|
|
| Community Health Action Network of New Hampshire (CHAN) |
|
|
|
|
| Health Choice Network of Florida (HCN) |
|
|
|
|
Basic Network Characteristics
Networks studied exhibited a variety of business and operational models. In the paragraphs below we describe key aspects of network governance and partnership models as well as the major functions health center networks undertook.
Formal governance. We observed a relatively consistent formal governance model across the networks we investigated. These networks are typically governed by a Board of Directors comprised largely of leadership from their member health center organizations. As such, the activities of health center networks, under most circumstances, are controlled by health center Executive Directors. In some cases, respondents indicated that larger health centers that contribute more resources to the network wield greater influence on the Board of Directors than other health centers.
In addition to the Board of Directors, some networks use a series of committees, comprised of both network and health center staff dedicated to specific network priorities or functions. For example, networks that worked on EHR implementation such as Boston HealthNet and the Florida Health Choice Network (HCN) tasked clinical committees and workgroups with reviewing and customizing software prior to roll-out. In addition, networks that provide centrally maintained applications usually have an IT committee where support issues are discussed. In addition to making recommendations to the Board and leadership, committees serve as an important forum for health center staff to provide feedback directly to the network, discuss problems and share lessons learned.
Executive leadership. A feature common to most networks visited is the presence of a single, network-level entrepreneur who served, in name or function, as the network’s CIO. This individual, usually someone with an extensive background in IT from larger provider systems or staff model managed care organizations, provided expertise, leadership and vision around IT not accessible to most independent health centers. In most successful cases, this individual works with health centers to develop a program of collaborative activities, to procure and manage IT vendors, to establish a revenue model using a combination of health center contributions and outside funding, and to attract technical staff necessary to support network activity.
Evidence of strong CIOs was found in the most centralized networks including the Oregon Community Health Information Network (OCHIN), Florida’s HCN and the Community Health Action Network (CHAN) in New Hampshire. Health centers in these networks were very familiar with the CIO and often contacted that person directly when they required assistance. They emphasized that the CIO champion was a crucial factor in providing the impetus to move the group to adopt clinical systems. Typically, health center executives who sit on the Board of Directors are responsible for final sign-off on all network investments. However, these Boards rely heavily on the network leadership to present analyses and recommendations that drive these decisions.
Integration model. We found that health center networks varied considerably in the extent they functioned as integrated decision-making bodies where systems decisions affecting individual health centers were made on the network level. For example, at the Health Federation of Philadelphia (HFP) a process to select a single networked practice management application led only to the selection of a “preferred” application with health centers opting to go on their own rather than give up that level of control to the network. Instead, HFP decided pursue a data warehouse project that would integrate data from individual health center systems.
On the opposite end of the spectrum, HCN in Florida was able to achieve agreement from its core members to hand over control of all of their software applications, data and financial operations (including billing and accounting) to the network and operate under a true shared CFO/CIO model. We found that the level of integration that networks were able to achieve relates to a number of factors, including how they are prioritizing objectives of network formation, the type of partners involved and the historical relationship between partnering organizations. Each of these issues is explored below.
Collaborative history. Well integrated networks were often located in communities that had a more collaborative history than others. CHAN’s health centers, for example, credited their success in adopting a robust system to their small size and highly collaborative environment. Health centers in Boston reported a long history of working together and cooperating with safety net hospitals even while they engage in some competition for patients.
In some cases, such as HFP, networks have been unable to forge member consensus around single applications for practice management or EHR or to convince health centers that these applications are best supported on the network level. Some health centers in Philadelphia acknowledged that there is some reluctance to collaborate because of underlying competition among health centers. In these cases, the networks focus on providing general guidance to health centers and fostering collaboration. Such networks also often work to integrate data from across health centers using interfaces or manual data entry.
Horizontal vs. vertical integration. Most of the networks we visited were horizontal collaborations among ambulatory primary care providers, forming around regionally located health centers, many of which have prior relationships with one another. Within these horizontal collaborations, however, there can often be one member that leads in terms of contribution to the network. This was the case for both OCHIN and HCN. In other cases, regional primary care associations were the convening force that brought health centers together and serve as the center of gravity for the network.
Boston HealthNet and the Southeastern Kentucky Community Action Program (SKYCAP) are key exceptions to the mode of horizontal partnerships. Boston HealthNet is the only true vertically-integrated network we visited, with Boston Medical Center (BMC), the major safety net hospital in Boston that formed after the merger of Boston City Hospital and Boston University Medical Center, providing a strong anchor for the network. BMC, given its resources as a large inpatient institution, often shaped network decisions such as adopting the EHR system being used at the hospital. BMC also has substantial incentive to bring together a coalition of health centers and invest in network development as health center referrals represent a large portion of BMC admissions.
SKYCAP represents a different model where both health and social service providers are connected in a loosely organized structure. Although, the SKYCAP program includes both ambulatory clinics and hospital Emergency Departments, we did not find evidence in this case that including multiple provider types increased incentives for network participation or investment.
Public health involvement. As mentioned in previous sections, several networks forged horizontal partnerships with the wider public health community, such as with Departments of Public Health or Medicaid Managed Care insurance providers. OCHIN and SKYCAP demonstrated the strongest ties to public health stakeholders, attempting to exchange data with these stakeholders with the ultimate goals of improving the tracking of disease outbreaks and other public health trends, and coordinating care among various providers including health centers, hospitals and public health departments. While public health stakeholders were often involved in the consortia of such networks as HCN, OCHIN and CHAN, models of streamlined data exchanged between public health and health centers had not yet been achieved.
Overlapping in networks. In investigating the seven health center networks described in Exhibit 3 above, we came across additional networks engaged in similar activities in the same general geographic area. In some cases, these represented sub-networks or smaller collaborations within networks that were based on historical partnerships among a smaller group of health centers (usually two). This occurred, for example, in Oregon, where two OCHIN health centers were funded by the BPHC for collaborative activities under an organization called Community Health Network of Oregon (CHNO) and some Boston HealthNet health centers located in Boston’s Dorchester community shared a single practice management system.
In other cases, these networks operated on a similar scale as the network we investigated, but in a slightly different geographic region and using a different model. For example, in addition to HCN, we noted the presence of the Community Health Center Alliance (CHCA) in Florida, which provides a networked practice management application and data management capacity for health centers slightly north of HCN’s core health centers. CHCA is a less integrated model for collaboration, offering fewer centralized services to health center members. In the case of Virginia and New Hampshire, other health center networks (the Richmond Enhancing Access to Community Health Project and New Hampshire Community Technology Partnership) had missions that were potentially complimentary to the ones studied, but we found little evidence of collaboration among these networks at the time of the case study.
Core Network Functions
We observed a clear link between network characteristics, described above, and their functionality, with less centralized networks performing fewer services and exhibiting less likelihood of adopting shared systems. For example, less integrated models observed in HFP and SKYCAP faced both financial barriers and lack of buy-in for integration from health centers. These networks served largely as a forum for health centers to convene and communicate with one another. The following paragraphs highlight the many functions that the studied health center networks served, identifying the operational models more or less conducive to specific functions.
Coordinating and convening. As mentioned earlier, many health centers entered into networked relationships to garner better market power for the health center community. Therefore, one of networks’ main functions is to convene leadership across health centers to identify priorities and common needs around IT. Respondents across all sites praised their network’s ability to convene health centers to share best practices in application implementation and use.
Networks also served to represent the needs of their health consortium to negotiate with vendors, to leverage funding opportunities and to lobby resources for health centers in relation to other safety net providers. This is especially applicable in networks which included a large inpatient institution, such as Boston HealthNet, where the network was able to lobby for resources from the safety net hospital using the health centers’ combined leverage. However, we also saw the HFP network take on that function, representing health centers at city-wide coalitions and acting as an advocate for health centers with Federal, state and local governments.
Vendor evaluation and group purchasing. Once networks identified a common need and technology solution, network staff usually initiated the vendor selection and evaluation process. In some cases, such as OCHIN and CCNV, the network determined system requirements and wrote a formal request for proposals, evaluated responses and selected vendor finalists to demonstrate their product. While this process involved input from stand-alone health centers, network staff spearheaded the task using pooled resources. In other cases, the vendor selection process was more informal. For example, staff at SKYCAP worked directly with a local vendor to develop a customized electronic client tracking software.
Network staff often took on negotiations with vendors to secure an affordable and reliable system for their members. Through this method, networks were often able to acquire certain customizations (e.g., interfaces) that member health centers would need due to disparate IT capacity or configurations. In addition, some networks secured training and system maintenance add-ons from vendors based on their size and skill in negotiation. After our visit, OCHIN successfully acquired a state-of-the-art EHR at a price markedly lower than an individual health center could have negotiated.
Centralized IT implementation. Relatively centralized networks initiating shared systems provide a high level of support to health centers during initial startup and in maintaining remote access to network applications. Networks rolling out these systems expressed a great desire to ensure that the systems were implemented successfully. Boston HealthNet and CHAN, for example, deployed their EHRs following large-scale private donations earmarked for the purchase of EHR software licenses. With license costs subsidized, the network targeted its resources towards procuring network staff to manage the implementation of the technology in member health centers, and providing additional staff, training and IT expertise to facilitate a minimally disruptive implementation. Other networks, such as OCHIN, provided some support to their health center members during implementation by sharing network staff among health centers.
Training and user support. Networks provided critical IT support for those centers who did not have their own dedicated IT staff or whose staff were not adequately trained to support some network applications. In two of the networks visited, the vendor agreed to provide support to member health centers by making available their system experts when troubleshooting was necessary. Several networks provided a HelpDesk function to centralize the daily IT support that centers need during and after implementation of a major information system. In two cases, networks purchased staff time from the vendor for a certain period during and after implementation to assist and train health center staff in using the applications.
Hosting networked applications. Often, individual health centers are unable to provide the space and expertise required to store and maintain servers and to host applications. Networks take on this role in a variety of ways. CCNV, for example, relies on a vendor data center while OCHIN and HCN host and maintain their own data servers. This allows the health centers to access vital applications through a desktop PC, with an internet browser and connection, without physically maintaining the servers. The network assumes the burden of ensuring proper maintenance of the central servers. Costs can therefore be spread among multiple parties.
Data management. As mentioned earlier, one of the main goals of all the networks was to facilitate reporting on grant activities as well as to facilitate the production of customized reports on other areas of interest. Networks sought to enhance health centers’ access to their own vital, administrative and clinical data. Networks that administered shared applications made data from these applications available to health centers centrally. In addition, some networks regularly generated standard health center-level and network-level administrative reports and provided these to the centers. To support development of other reports, some networks helped health centers to collect, clean, and transform data housed in disparate applications to develop a common data warehouse. Many of the networks that created data warehouses described this set of activities as among their most complex and time-consuming.
Centralized administrative functions. As mentioned earlier, the networks visited primarily help health centers achieve administrative benefits through the enhanced use of IT. Networks providing centralized practice management applications often expanded their scope of services to include functions such as centralized claims processing. Most networks offer a liaison service to a claims clearinghouse capable of handling electronic claims submissions in a HIPAA-compliant manner. The use of clearinghouses aims to reduce the administrative cost of submitting paper claims and decreases the turnaround time on processing. Of networks investigated in this study, HCN provides the best example of centralized administrative functions, where a network-level executive serves as the centers’ Chief Financial Officer. The Community Care Network of Virginia (CCNV) also provides some centralized administration through a central billing office that several member health centers use.
Variation and Network Types
Although all networks investigated shared similar goals and basic governance models, we observed important variations in the path chosen to achieve network goals. In particular, networks differed widely in terms of their financial and operational model (level of integration, level of financial contribution from health centers) as well as their approach to partnerships. We found that, in many cases, these variations drove the types of functions and services provided by health center networks or the way in which different functions were prioritized.
In order to illustrate important differences among network models and demonstrate the relationship of these differences to actual network function, we divided the seven health center networks investigated as part of this study into three groups described in greater detail in the bullets below. Health center characteristics relevant to each of these models are presented in Exhibit 4 on the following page.
- Incremental adopters refers to the strategy taken by the health center networks in Oregon, Virginia and Florida to incrementally adopt IT systems based on prioritized objectives, beginning with practice management for the purpose of stabilizing health center operations, finances and administrative reporting and then graduating to roll-out of EHR and data warehousing applications on a network level to support quality of care and community health objectives. Key to the success (or non-success) of these networks is their ability to forge some basic consensus among health centers on decisions such as which practice management vendor to select or what type of customizations are appropriate for implementation across health centers. Because these networks provide networked applications, there is some basic level of integrated decision making that health centers must buy into. Finally, in addition to support through grant programs, these networks are funded, in large part, through membership dues and user fees collected from health centers or other providers receiving their services.
Exhibit 4: Dimensions of Network Variation
- Early EHR adopters. We characterize the Boston and New Hampshire networks as early EHR adopters because they rolled out a networked EHR without first establishing a networked practice management system. Reasons for moving directly to EHR were twofold, first that health center members were generally comfortable with the practice management systems they were using and second that the networks both received an infusion of private sector monies tagged for clinical system purchase and rollout. In general, roll-out of EHR occurred successfully for both of these networks that are now moving forward with developing additional reporting and data management functionality to maximize returns from EHR. In the case of CHAN, poor integration between the legacy practice management system and the newly implemented EHR in part prompted the health centers to adopt a new common practice management system that was interoperable with clinical systems. As with the incremental adopters, networks that offer networked EHR are funded, in part, through fees paid by individual health centers and must work to achieve integrated decision making on technology and support issues.
- Decentralized networks. Networks in Southeastern Kentucky and Philadelphia focused mainly on building systems to collect data on the safety net population and integrate data across individual health center systems in data warehouses. Of the networks visited, these were the most decentralized, with each health center maintaining their own systems and no use of network wide applications for internal functions. Although there have been some important successes in these cases, for the most part respondents indicated that the promise of community-based applications has not yet materialized because of technical difficulty in building interfaces and difficulties with incorporating community based applications into the workflow of individual provider institutions under a loosely connected network.
Networks as Drivers for Health Center IT Adoption
All thought leaders and stakeholders consulted in producing this report agreed on the importance of focusing on health center networks as the locus of advanced health center adoption of IT. While the reviews from health centers regarding their network participation were not uniformly positive, most reported important benefits that networks have over individual health centers in leveraging IT. For example, respondents from HCN indicated that they can relatively easily convene senior executives from WebMD to negotiate around functionality and price, and usually get a swift response from the vendor when problems arise. HCN respondents also noted that they have worked extensively with WebMD to customize the application for health center uses and that the relationship has helped WebMD’s efforts to increase market share among health centers. The health centers involved agreed that it would be difficult to see WebMD developing this same sort of partnership with an individual health center.
Some reviewers have referred to selected health center networks as application service providers (or ASPs). ASPs are third-party organizations that manage and distribute software-based services and solutions to customers across a wide area network from a central data center. Unlike typical ASP’s however, health center networks investigated were in the majority of cases governed by the health centers themselves and did not operate as for profit-enterprises organizationally independent from their customers. While in the private sector market, ASPs are decentralized organizations providing a menu of services at fixed prices remotely, health center networks tend to work very closely with individual health centers and develop user fees and dues that accommodate health centers’ financial circumstances. Finally, beyond providing software and data management services, networks often provide additional services such as billing and accreditation. Among health centers visited for this project, the majority are investing in IT, at least in part, through membership in their local network.
Health Center Level findings
As mentioned above, in conducting case studies, we visited or spoke with a total of 38 centers in seven different locations across the United States. Health centers visited differed substantially in scope of practice (number of patients and sites), management structure, and culture. While some centers we visited were large operations that treat more than 200,000 patient encounters annually and have deployed state-of-the-art practice management and EHR applications, others were small-scale practices supporting a few part-time providers, fewer than 2,000 annual encounters, and basic computing resources.
In this section we present project findings related to 1) health centers’ overall approach to IT, including planning and decision making strategies, resources dedicated by health centers to IT, and HIPAA compliance issues; 2) health centers’ information systems infrastructure, including hardware and software capacities as well as use of vendors; and 3) health centers’ primary uses of IT and health IT systems such as practice management and EHR applications. Before describing findings in each of these areas, in the bullets below we provide some key background information related to illustrate the differences among 38 health centers that were consulted as part of this project.
- Number of Health Center Sites. 23 of the 38 health centers we visited had multiple sites. 20 centers had between two and eight sites, while three centers had nine or more sites.
- Number of Annual Encounters. Half of the health centers we met with (19) have 50,000 or fewer annual patient encounters, with 12 of those 19 seeing fewer than 25,000 encounters per year. Five centers see between 50,000 and 100,000 annual encounters. Seven centers report more than 100,000 encounters per year of which three report more than 220,000 encounters annually.
- Health IT Applications. 92 percent of health centers we visited (35 out of 38) use a practice management application. Nine centers use an EHR, while five others were either in the process of rolling out EHR for their sites or were piloting an EHR system. Three health centers use a dental EHR.
- Network Membership. 33 of the 38 centers we spoke with were members of their regional health center network. The other five had either opted to not join their local network when it formed or had withdrawn from their network when the investment ceased to be regarded as worthwhile.
Overall Approach to IT
We queried health center leadership on how their center made decisions regarding IT and the level of priority afforded to IT in the organization overall. We also asked specifically about trends in IT spending and recent changes in their staffing and organizational approach to IT. Overall, we found that health centers’ approach to IT is evolving along with changes in reimbursement for health care delivery and regulation related to maintaining and exchanging health data. In addition, we found that health centers have increased their focus on disease management and quality improvement leading to increased demand for health IT.
IT Planning and Decision Making. Case study findings indicate that there is substantial variation in the extent to which individual health centers develop strategic plans around IT investment. While nearly all center leadership recognized the need for such processes and noted that a having a strategic vision around these investments was desirable, many smaller or mid-sized providers cited a lack of the resources (both financial and personnel) necessary for such planning. These smaller centers indicated that IT decisions were generally made on an ad-hoc basis, often when they were “forced” to make a change because the vendor discontinued support for the application they were using.
Larger centers were more likely to have developed formal strategic planning and investment initiatives. For example, one large Virginia health center’s Board of Directors had formulated — on the recommendation of the center’s CIO — a strategic plan that prioritized re-allocating budget allotments to permit systems upgrading, staff training in IT, and pursuing investment in EHR. A Philadelphia health center reported going through a lengthy RFP process for selecting a practice management vendor and indicated that IT represented the top budget priority for their center moving forward. Overall, however, we found that this level of planning represented the exception rather than the rule for health centers.
For nearly all the health centers visited, the Board of Directors made the final decisions on IT investments. In health centers with a dedicated CIO or manager-level IT staff (only nine of the 38), recommendations for investment generally came from these staff members and were developed out of some type of systematic planning process. In other centers, recommendations for IT investments were made by committees comprised of the health centers’ administrative, financial and clinical leadership. Increasingly, health centers reported relying on networks to make (or help them make) major IT decisions.
Budget for IT. Health center IT budgets vary substantially. For example, some health centers indicated that IT was the most rapidly growing segment of their annual budgets, while one rural health center in Kentucky reported having no funds to spend on IT and relying on a completely paper-based office. While it was not feasible to systematically collect financial data from each health center, on average, health centers reported spending between two to five percent of their budgets on IT. Respondents frequently indicated that during periods of early ramping-up in information systems investment, IT budgets dramatically increased for a short time.
Funding Sources. We found that health centers fund IT investments from multiple sources. Basic expenditures such as hardware, office software and connectivity come out of the centers’ institutional Section 330 grant, but nearly all of the health centers we spoke with had access to IT-related Federal or state grant money through their regional network. As described in the background section, the Federal government maintains several grant programs aimed at supporting specific aspects of health center information technology service provision, management, and infrastructure and most health centers (33 of 38) consulted took advantage of one or more of these programs. Importantly, in two of the seven case studies, Boston and New Hampshire, private donations have been targeted towards the purchase of software licenses, which was a critical driver for EHR adoption.
Support Staff Resources. Health centers reported that recent investments in IT have largely gone toward improving staffing. Only seven centers reported having no in-house IT expertise. Smaller centers employed only one IT staff person, frequently part-time, to manage technical issues. Nineteen health centers employed between one and three IT staff, while two centers employed 10 or more IT staff.
Three health centers outsourced some or all of their IT support services to local companies, instead of employing internal staff. Some of these centers had long-term relationships with such consultants, who were involved from the beginning of the center’s IT implementations and had worked with the center to develop customizations to its practice management system. Smaller centers generally reported experiencing more problems with systems implementation and ongoing support. IT issues that would have been minor problems for a large center with on-site technical support staff could easily become major stumbling blocks for centers lacking such expertise.
As would be expected given our approach to selecting cases, we found that many health centers counted on networks to supplement their in-house IT expertise. In general, larger centers with their own dedicated IT staff tended to report having better technical support and fewer implementation and maintenance issues with health IT systems, irrespective of whether they also received support from a network.
Chief Information Officers (CIOs). Of the 38 health centers we spoke with, four had an in-house, full-time, dedicated staff member described as a CIO. Dedicated health center CIOs provided vision for prioritizing systems investment, expertise for selecting and managing IT vendors, and managerial experience for the implementation process. Five other centers had senior IT staff with titles such as “IS Coordinator” or “IT Director,” whose duties included managing the two to four support or programming staff and providing some systems investment direction. While these individuals managed other staff they often did not share decision making responsibility on the same level as health center executives. Several of the remaining centers had access to CIOs through their network affiliation.
Technology Infrastructure
With almost no exceptions, health centers we spoke with were working with usable hardware and adequate access to basic software and connectivity. However, reflecting the diversity of health centers’ size, access to funding, and investment priorities, we found that the overall computing environment varied considerably from center to center.
Hardware and Connectivity. In addition to reporting adequate access to hardware, including computers, monitors, hard drives and printers, most health centers we spoke with (75 percent) reported operating in a networked computing environment. Smaller, individual site health centers tended to use basic local area networks (LANs) to allow for networked applications and file sharing with limited file storage and server capacity. In some cases, these health centers were not able to provide many applications over the network and relied instead on installing some types of software locally on user computers (e.g., accounting staff had accounting software installed on their computer). These centers also had basic Internet connectivity and could access applications housed at servers outside their walls through use of virtual private networks (VPNs).
Most centers connected to the Internet or point-to-point shared servers either through a dial-up, cable or broadband connection. Many of the health centers we spoke with upgraded their infrastructure in order to access networked software. In Virginia, for example, several health centers indicated recently upgrading connectivity to the Internet in order to facilitate their use of the practice management software provided through a VPN by their network. Centers that lacked high-speed connectivity tended to be rural or smaller health centers. These centers also tended to experience a higher level of disruption in service compared to others.
Health centers with greater access to resources often used wide area networks (WANs) to create a seamless computing environment across geographically separate sites. With a WAN, health center sites could also access shared applications through their regional health center network. These networks connected to their WAN using dedicated T1 line connections and had adequate server capacity to support administrative applications as well as basic computing needs such as printing and email.
Data Management Capabilities. Several of the health centers we spoke with are maintaining or contributing to master patient indexes (MPIs). Some larger centers with in-house applications expertise were able to build and maintain their own MPI, drawing data from their practice management systems and, in the most sophisticated centers, supplementing administrative data with clinical data from EHRs. Health centers used these sources for querying for UDS reporting and to produce reports used for making management decisions.
Most of the health centers we spoke to were contributing to data warehouses external to their center, housed either in their health center network or a public health stakeholder such as a County Public Health Department. In Philadelphia, for example, the network has developed a community-wide data warehouse which extracts data from the practice management systems of participating health centers. In Boston, members of Boston HealthNet contribute administrative and clinical data to the network through extracts built from their practice management and EHR systems. These warehouses then allow network staff to produce community-level and center-specific reports on cost, utilization or, in some cases, quality of care measures.
As summarized above, we found that health centers we spoke with had a usable IT infrastructure and used a variety of applications. In the remainder of this section, we describe the uses, functionalities, vendors, and health center experiences associated with selected health center computer applications including practice management, EHR and data warehouses.
Health Center Experience with Practice Management
The widespread use of practice management systems stems primarily from the systems’ capacity to improve health centers’ billing capabilities and streamline general day-to-day management operations. Practice management applications are built to increase organization of billing data, catch wrong or missing data elements from encounter records, manage patient scheduling and check-in, facilitate eligibility determination, and coordinate the electronic submission of claims.
As one health center respondent noted, “practice management is all about billing” — the potential for maximizing collections and payment options is key to health centers’ widespread investment in the systems. As discussed earlier, health centers’ reporting requirements (e.g., UDS reports) are also an important impetus for the use of practice management. Most practice management applications marketed directly to health centers have pre-designed reports meant to satisfy UDS reporting requirements.
Practice management vendors. The most commonly utilized products for practice management applications in centers we visited were Epic (eight centers), Medical Manager (nine centers), GE’s Millbrook (four centers), and HealthPro (five centers). Among the few centers that had implemented an EHR, WebMD and Logician were the most frequently used. Consolidation between vendors, detailed in the environmental scan, is common. In the past few years, WebMD has acquired both Medical Manager and HealthPro. Occasionally consolidation creates difficulties for health centers who have invested in one system only to see it bought out and upgraded — sometimes leaving the health centers in a position where they are unable to afford the new version but are without support for their existing system.
Scheduling. Practice management scheduling functionalities were widely reported to be of good quality and extremely valuable to health centers. Many systems allow for double- and triple-bookings to accommodate transient patient populations and health centers were satisfied to have the ability to schedule patients to a specific examining room and provider. Most systems also target concerns specific to health centers. However, some health centers had complaints regarding the usability of the scheduling module included in their practice management application, indicating that it was difficult to view data on missed versus completed visits on the schedule itself.
Billing and accounting. Health centers generally indicated that their system’s billing and accounting modules were a significant improvement over prior systems they used. Claims are typically generated, sent, and reimbursed far more quickly with sophisticated practice management systems. Most applications pre-screen claims before they are sent out in order to catch coding errors — some health centers reported that their systems occasionally fail to catch wrong or missing data, resulting in large increases in accounts receivable and decreased payments until billing glitches were fixed, but most respondents expressed high satisfaction with billing functionalities. One respondent noted that “Commercial payers have never reimbursed as quickly as they do with the [new] system.” In addition, all practice management systems have also been designed by their vendors to streamline compliance with HIPAA Electronic Data Interchange (EDI) regulations.
Electronic claims submission. Some practice management systems also support electronic claims submission capabilities. In the health centers that made use of this functionality, we heard many positive reports about the systems’ success at making accounts receivable and cash flow more predictable, as well as about built-in logic to detect coding errors. However, not all systems’ billing formats accommodate Medicaid or other payers’ electronic submission requirements. Additionally, some payers have not set up a system to receive, process, and remit electronic billing and payments.
Reporting. Reporting capabilities are a key aspect of practice management systems. Health centers generate a wide variety of reports, from the basic to the very complex, and practice management systems are designed to accommodate a range of needs. Although most case study respondents were enthusiastic about the better quality and easy access of data managed in their system, some indicated that the reporting modules are not always user friendly. Designing and generating custom reports requires use of specialized applications such as Crystal Reports, which require a significant level of training to master. Because health centers often do not employ staff with these skills, they rely largely on networks or vendors to design needed reports, at substantial additional cost, delay and inconvenience.
Overall, the role of and rationale for practice management systems is clear: The applications are ubiquitously reported to be superior to the health centers’ prior systems; the return on investment from billing improvements is considerable; and HIPAA compliance is ensured by the vendor. Respondents agree that most functions perform smoothly and that the systems have made a significant difference in their accounts receivable, reporting capabilities, and day-to-day operations.
However, health centers still struggle with some functionalities and interoperability issues. Many cite difficulty with billing formats that accommodate Medicaid or other payers, and reliable, convenient and customized reporting can be difficult to obtain. Those centers with in-house technical staff trained in reporting software, as well as those in highly centralized networks with access to outside reporting expertise, tended to fare better with their systems’ reporting functions. In addition, most practice management systems are not interoperable, creating problems for health centers attempting to build a common data warehouse, given that custom-built interfaces are expensive.
Lastly, health centers respondents emphasized the importance of systems support and vendor management. Health centers that have responsive relationships with their practice management vendor are far better able to customize their systems and address problems, which greatly enhanced their overall implementation and daily use experience. We found that individual health centers often find it difficult to obtain a desired level of service from vendors. The considerable flux among vendors and products, discussed earlier, also presents a challenge.
Health Center Experience with EHR
At the start of this project, EHR was rare in health centers, but we witnessed increases in EHR investment as the study progressed. Three of the seven network sites we visited had begun the process of rolling out EHR systems in 2004 and all other health centers we spoke with expressed support for adopting EHR in the near future.
The EHR systems utilized by case study respondents provide a wealth of valuable clinical functions: the systems facilitate automated clinical assessment with built-in reminders for specified preventive and diagnostic services; allow for electronic communication with pharmacies and clinical laboratories; automate coding of clinical procedures, diagnoses and patient instructions; and support an electronic progress note. Some systems also notify providers of adverse medication interactions and facilitate patient tracking, diagnosis assistance, and electronic document and image management.
Health center respondents we spoke to that had implemented an EHR reported positive experiences with their particular system. For these health centers, the decision to implement EHR was aimed, to some extent, at improving the practice’s efficiency, workflow, and physician productivity. However, health centers focused on mission-related incentives to adopt EHR such as quality of care, effective management of chronic illness, and improved continuity of care. Although financial return on investment (ROI) may come in time, health center staff noted that financial gains, relative to systems costs for EHR, are difficult to demonstrate at the outset of implementation.
EHR vendors. Fewer EHR products are available on the market than are practice management products. The EHR vendor products used by this project’s respondents were GE’s Logician and WebMD’s OmniChart/OmniDoc, as well as the Dentrix oral health EHR. Most EHR systems are built to integrate with a particular practice management system marketed by the same vendor, and do not interface with other systems well. For example, to share data from different proprietary EHR systems or separate EHR and practice management systems, some health centers had resorted to building customized interfaces or re-entering data, both of which are frequently costly approaches.
EHR rollout process and training. Health centers’ approach to user training and EHR implementation varied considerably. Some networks opt for a slower, more deliberate approach than others. In Florida, which has opted for a slower approach, providers begin using the system with a small number of patients per day and gradually add more patients transitioning eventually, to exclusive use of the EHR. They report that this method facilitates take-up and limits productivity loss associated with the transition.
Other networks, where entire health centers were switched from paper to EHR overnight, reported adjustment periods of up to six months and planned for dramatic reductions in productivity during the initial roll-out. In all cases, staff and provider training was intensive early during roll-out and the first several months of using EHR. In some cases, EHRs were rolled out on a site by site basis within a single health center. This would allow each health center to address problems and ensure usability in a single setting prior to moving forward with a broader center-wide implementation. Respondents noted that providers transitioning to EHR almost uniformly grew to appreciate the systems’ benefits over time, in large part because of improved access to key data from the patient chart.
In many cases the roll-out model for EHR was influenced by factors of expediency and feasibility. For example, while the gradual approach employed by health centers in Florida proved beneficial according to respondents, they took this approach, in part, because health centers pulled together funds to buy software licenses one or two at a time (a combination of health center and network money was used to purchase the licenses).
Efficiency and productivity. Increased clinical efficiency and provider productivity were frequently cited as benefits of EHR. New Hampshire respondents reported that the piles of paper records previously taking up space on the physicians’ desks have been eliminated, making workflow more efficient. Transcription costs are also gone. Although New Hampshire and Boston health centers acknowledged experiencing some slowdown in provider productivity during implementation, most centers reported that as providers have gained familiarity with the systems, they have begun seeing similar numbers of patients as pre-implementation. None of the Florida health centers reported major problems with providers becoming comfortable using the EHR system after limited training and use. A provider from one health center noted enthusiastically that EHR has decreased the time it takes for him to review a patient chart.
Access to data and system stability. Both clinical and administrative documentation were reported to have improved dramatically with EHR. Many health centers agreed that EHR has improved the content of their medical records and the accessibility of reliable patient information. The systems allow each provider at a health center, or all health centers in a network, to generate reports assessing the progress of vulnerable patients (such as diabetics). One health center emphasized that the electronic reporting functionality has made it easier to complete and verify UDS reports. Providers in Florida also appreciated the ability to remotely access patient laboratory results and medications. One Florida health center reported that remote access to patient data was especially valuable after a hurricane forced the center to temporarily close. During this time, the health centers’ providers were able to treat their patients from an entirely different provider site with complete access to patient records.
Improvements in patient safety and care processes. Respondents reported important improvements in quality of patient care following EHR implementation. Health centers noted that electronic patient charts are far more legible than handwritten notes, reducing potential for error. For New Hampshire centers, medication management has been enhanced, lab results are now automated and more quickly accessible, the rate of compliance with screening exams for all patient populations has improved, and routine patient follow-ups occur more frequently. EHR systems with a tracking component improved outcomes for some health centers by systematically prompting follow-up for patients with chronic illness or patients indicated for diagnostic screening. At one Boston health center, follow-up features helped bring the mammogram return rate up to 80 percent. Other health centers have benefited from the e-prescribing function, which led to a reduction in the unsafe use of drugs that interact unfavorably with ACE inhibitors.
Links with hospitals and laboratories. EHR-facilitated electronic linkages with labs and hospitals have proven valuable to health centers. In Boston, the EHR has enhanced coordination of care between the hospital and health centers and increased the availability of patient information. In New Hampshire, linkages between the network’s members, local hospitals and a diagnostic testing facility allow the health centers to obtain encounter information when their patients visit one of the participating hospitals or need a routine laboratory test. However, these interfaces currently work only in one direction (the network’s IT system captures electronic data from the hospital and laboratory systems and imports it into the EHR).
Clinical outcomes improvements. Although many respondents were hesitant to point to concrete clinical outcomes improvements stemming from EHR implementation, some reported observing important improvements. For example, one Boston health center cited that after six months of reports and tracking of the diabetic population through their EHR, their HgbAlc measures decreased from 8.6 to 8.01 and the patients’ blood pressures had markedly improved. A Florida health center described a similar experience during the months following implementation. Because all of the EHR implementations studied as part of this project are at their early stages, respondents indicated that they expect to monitor and report on more tangible improvements in clinical outcomes in the coming years.
Barriers and challenges. Costs, training, and provider comfort remain the primary barriers to EHR adoption for most health centers. For all the reasons described above, EHR systems are prohibitively expensive for the average health center and those we spoke with that had implemented EHR noted that they would never have been able to do so individually — network membership provided the financial resources to invest in and support such sophisticated applications. Training providers and other staff to use EHR is an ongoing and costly process, one that networks are generally in a better position to coordinate.
Health centers also report that provider buy-in and the presence of clinician champions are extremely important for successful EHR implementation. Clinician champions at health centers who understand the potential for EHR to greatly improve the efficiency and quality of care and are willing to put in the arduous effort necessary for working with skeptical fellow clinicians to redesign care delivery are invaluable to such efforts. Providers’ learning and productivity curves can be slow during the implementation process, but most see the benefits of using EHR including improved efficiency and decision-support.
Costs and benefits. Health centers implementing EHR reported seeing immediate benefits. Respondents noted improved clinical and administrative documentation, better quality of patient care, greater reliability around patient records and services, and a variety of process and outcome benefits. Health centers also acknowledged the substantial cost associated with EHR. Aside from the financial cost of software licenses, health centers reported other significant start-up costs including procuring appropriate hardware and connectivity, customizing and designing the initial implementation of the software, building clinician buy-in and training users.
In addition, there are the ongoing costs of reporting, analysis and change management necessary for using EHRs to improve care delivered. Even in the most successful implementations, we found that robust buy-in and benefits from EHR implementation were experienced as a result of ongoing, detailed engagement and investment on the part of both IT and clinical staff to design, discuss and refine the EHR functionality and settings. Initial loss of provider productivity during the first six months after an “overnight” implementation is another type of start-up cost associated with EHR.
Respondents also acknowledged the difficulty in quantifying ROI from EHR implementation. While many feel strongly that the systems represent important savings through health benefits and decreased utilization over an extended period of time, health centers typically did not have adequate data to determine whether EHR has resulted in cost savings at an institutional level. Respondents pointed out that it is difficult to tie a dollar amount to some core benefits like the replacement of illegible handwriting with typewritten notes. Some New Hampshire centers reported that quality improvements hastened by the EHR have resulted in increased provision of services for which payers provide little or inadequate reimbursement. Respondents expressed optimism that the ROI was significant, but hard data on whether using EHR saves more than it costs health centers is not available at this time.
Data Warehouses and Other Applications
Two of the case study entities were actively involved in building and populating a data warehouse using practice management and EHR data. Respondents from both sites expressed enthusiasm about the potential of data warehouses for improving provision of diagnostic and preventative services to vulnerable populations, generating reports to inform management decision making, public health policy and research. Some respondents indicated that data warehouses are particularly useful given the lack of other sources on health care utilization and costs specific to the uninsured. However, building and maintaining an effective data warehouse presents difficulties for many health centers: applications across providers are usually not interoperable and developing interfaces between them is expensive and difficult, which poses problems for networks that look to build data warehouses that combine data from several different practice management applications. Other ongoing challenges include assuring data validation/integrity and non-duplication of patient records, as well as the need to program new extracts following practice management system turnover.
In addition to practice management, EHR and data warehouses, we found that health centers used other specialized computerized applications to track specific clients and services. Often, these systems were homegrown databases constructed using Microsoft Access or other common database tools and serving functions associated with specific funder requirements. Health centers involved in the BPHC State and National Health Disparities Collaboratives made use of Federal and state-developed disease registries, including the Patient Electronic Care System (PECS) and the Cardiovascular/Diabetes Electronic Management System (CVDEMS). Centers involved in the Disease Collaboratives are required to enter and submit data on a monthly basis, which they do through PECS, for their population of focus, such as diabetics.
Health centers involved in the Women, Infants and Children Program (WIC) also used specialized software called the Immunization Registry Information System (IRIS) to track immunizations provided and to contribute data to a community-wide registry. Of the health centers visited for this project, four reported using PECS, three used IRIS, and one used CVDEMS. Several health centers also built their own patient information databases using Microsoft Access, to track patients, conditions, and services rendered.
Conclusions
Health centers consulted for this study demonstrated substantial progress in the use of health IT to meet important financial, administrative and clinical goals. Although challenges persist, our findings validated initial observations by some thought leaders that health centers represent fertile ground for health IT adoption among ambulatory providers.
The experience captured in this report represents important lessons learned for future investments in health IT among health centers, health center networks and other ambulatory care providers. We attempt to synthesize these lessons learned focusing on key issues relevant to the current policy debate, including support for health center networks and EHR adoption. We also describe areas for future research and analysis.
Network Benefits and Challenges
Overall, findings confirm that health center networks can be successful vehicles for the adoption of health IT in the safety net. Health center networks successfully acquired systems and innovatively harnessed them for the improvement of operations, both administrative and clinical.
- Access to funding. Individual health centers most often cited cost as the main barrier to purchasing IT. Network formation allows health centers access to grant money above their Section 330 grant. We found that networks often were able to secure a number of Federal grant programs simultaneously, often by having different member organizations take the lead role on different grants. In two cases, networks benefited from private donations that would not have necessarily been made to individual health centers.
- Leveraging resources and expertise. We found substantial evidence that health center networks take advantage of economies of scale to provide resources that health centers could not afford to procure individually. These benefits apply to basic purchases such as software licenses or service time from vendors as well as structural issues such as the ability to attract skilled technical staff. Individual health centers often reported that they found it challenging to find IT staff that had adequate training for complex systems issues. The ability of networks to afford IT staff with the necessary expertise (e.g., on building interfaces, mining practice management and EHR data, building databases, and customizing systems) was critical to individual health center satisfaction with their technology.
- Vendor selection and management. We found that health centers benefited greatly from having access to network executives who were skilled at the vendor evaluation, management and procurement processes. Aided in part by economies of scale, respondents mentioned that network executives were often in a much better position than individual health center Executive Directors to characterize their requirements in an RFP, negotiate favorable terms and hold vendors to a high standard for technical assistance, customizations and other services.
- Collaboration and coordination with other health centers. We found that funding specific to coordination and collaboration across health centers was important to improvements in their use of IT. Several health centers noted that networks offer important forums to share best practices, allowing centers to troubleshoot specific functionalities and share new knowledge relevant to technical, administrative and clinical challenges. Networks brought together providers with similar needs and common goals. In some cases, networks have been able to build an infrastructure for sharing data through community tracking applications and data warehouses. While networks that seek to integrate functionality across centers meet with varying levels of success, it is clear that without funding to promote collaboration and coordination among health centers network development would not be possible.
In addition to these important benefits, we found that health centers faced a number of difficult challenges in fulfilling their mission.
- Meeting diverse requirements of health centers. Because health centers differ substantially operationally and culturally, networks often face the challenge of addressing a diverse set of needs through a single operational model. Network leadership recounted the difficulty in identifying systems and governance structures that met the needs of both larger, more sophisticated centers and smaller centers. More decentralized networks that were unable to build a strong collaborative framework tended to be less successful, as health centers were not fully bought-in and did not share a common vision. These networks were often unable to overcome health centers’ tendency to compete with each other or the fear that their interests would not be addressed in a network structure.
- Building and using community based applications. We noted that networks which focused on building applications to collect, store and maintain data from individual health center applications in a single community faced difficult challenges. The process of building interfaces to allow data exchange across two non-interoperable systems was both time-consuming and costly. Networks reported that vendors were often resistant to release code to interface developers and even when they had access to the right information, turnover in the system of any individual health center meant significant setbacks to these data integration projects.
We found that health center participation in community data warehouses was contingent on some promise of benefit to the individual health center. For example, health centers that felt they could already access and analyze data effectively through their practice management system were unlikely to contribute proprietary data to a warehouse that would only offer slight improvements in ease of reporting. - Setting up networks in rural areas. Rural health centers and networks faced special challenges in building and accessing community-based applications. Rural centers often have limited budgets for IT, less sophisticated IT expertise than urban centers and difficulty in purchasing off-the-shelf systems due to highly specific requirements. In terms of technical challenges, rural initiatives are often unable to access high-speed Internet connectivity needed to use networked applications because of low availability in rural settings. Urban-based networks will likely rely on the improvement of infrastructure in rural areas in order to incorporate rural centers into their network. Progress was being made to this end during the course of the study; for example, SKYCAP’s goal of sharing client tracking data among its community-wide partners recently improved with the spread of high-speed Internet connectivity in that region. In addition, OCHIN leveraged improvements in access to high speed connectivity in rural parts of Oregon to expand its membership.
- Achieving vertically-integrated data sharing model. Most networks in our study were horizontal collaborations among geographically linked ambulatory primary care providers. Only Boston HealthNet formed a true vertical collaboration, revealing both real and perceived barriers to achieving a model shown to be fairly successful for early IT adoption. In order to form a successful vertical relationship among the city’s major safety net hospital and health centers, Boston HealthNet was fortunate to already have an established relationship among these institutions, as the health centers supplied a large portion of the hospital’s patient base. Despite this fortune, the network still had to overcome the barriers of finding interoperable software that met the needs of both the large inpatient institution and ambulatory health centers in addition to mitigating the reluctance on the part of both the health centers and the hospital to share data due to perceived concerns of a breach of privacy and a resulting loss in market competitiveness. Even with its success, Boston HealthNet and other networks attempting to forge a vertical collaboration face the ongoing challenge of prioritizing resources and meeting the technical needs of a very diverse clientele.
- Population health functionality remains a future goal. Health center information sharing initiatives with hospitals, public health agencies and Medicaid are slow in evolving, although most networks felt that building those connections would be an important part of future activities. Networks that had fairly strong ties with public health stakeholders in their region, such as OCHIN, were able to build a collaborative vision for using IT to improve the population’s health and were beginning to work toward a population-wide data warehouse for the safety net population, however formal linkages with Medicaid or state public health information systems had not yet been achieved in any of the networks.
- Achieving sustainability. Network leadership across each case study noted that financial self-sufficiency is not a near-term possibility for their organization. Even in cases where one-time private donations facilitated the purchase of software licenses, networks required a sustained level of public funding for the training, initial implementation and ongoing support necessary to realize benefits from the software.
EHR-specific Lessons Learned
From the health center networks that achieved the implementation of an EHR we drew several lessons for future funders and implementers of technology.
- High level of clinician satisfaction and adoption observed in successful networks. Case studies demonstrated the importance of having not only buy-in, but significant involvement from clinicians at all phases of an EHR implementation. Because EHR implementation changes clinical work flow in profound ways and must be customized across a number of dimensions to support efficiency as well as improved quality of care and safety, clinical leadership must be involved in making core design decisions at the earliest phases. Once systems were implemented, clinicians tended to see clear benefit in using the systems and preferred electronic entry to paper records, citing that they “wouldn’t go back”.
- Three levels of substantial funds are required. Health centers implementing EHR reported three significant investments that accompanied the rollout of their systems: seed money for start-up, money to build infrastructure and transition workflow, and funds for the ongoing maintenance of technologies. Seed money is used to purchase software and licenses, hardware, implementation assistance and technical staffing that health centers reported was as critical as the software application itself. Ongoing funds are critical to help health centers implement and transition smoothly. For example, post-implementation health centers must continue to adjust tools to increase usability and allow centers to leverage the new functionality. None of the networks had achieved self-sustaining funds to pay for ongoing maintenance and future systems purchases, and will rely on outside funding until that is achieved.
- Impacts of technology use can be quickly demonstrated. Respondents suggested that fairly soon after implementation, EHR systems can lead to improvements in patient outcomes. While these benefits have a real impact on an individual health center level, achievement of broader public health benefits is still limited by the absence of robust data sharing with public health agencies, hospitals, Medicaid and other ambulatory care hubs.
- Opportunities and challenges for future initiatives. The health center networks studied here were early adopters of health IT, providing lessons for other networks that will follow suit in adopting technologies to improve operational efficiency and clinical effectiveness. However the challenges these initiatives faced as early adopters may decrease in the near to long term, especially given the recent emphasis of the President in leveraging health IT adoption for the improvement of health care quality.6 Practice management and EHR software will likely become more robust and the adoption of data standards may increase the level of “built-in” system interoperability, eliminating the need for costly customizations and extracts for data exchange. In addition, the success of the network model as a driving force for health IT adoption may spur more funding for new collaborations from Federal and private sources. Despite this ripe environment for adoption, future initiatives may still have to overcome organizational barriers to forging collaboration among health centers and vendors as well as reluctance to data sharing.
Critical Factors for Success
While case studies demonstrated that there is more than one model for successful implementation, we did find several factors closely associated with successful adoption of IT among health centers.
- Understanding the relationship between clinical and administrative applications. Depending on the immediate need articulated by health centers, networks took different approaches towards prioritizing between practice management and EHR. Overall, we found that having a robust practice management application was a necessary first component to implementing an EHR, as the full benefit from both applications comes with the ability to seamlessly exchange information between the two. Even in networks where EHRs were pursued in the absence of networked practice management system, each participating health center did have a successful practice management implementation that they were able to then interface with the EHR.
- Structure of the network impacts function and success. Across the seven sites, we observed a link between the operational model of the network and their success in implementing clinical technologies. We found that more integrated networks where there was strong buy-in for shared systems generally managed a smoother implementation of the technology. Health centers in less integrated networks sometimes could not agree on shared systems, focusing resources instead on systems such as data warehouses and external client tracking systems which have proven very difficult to implement. We illustrate the relationship between network and function and relative success in Exhibit 5 below.
Exhibit 5: Level of Integration and Function
- Building trust through strong leadership. We found that strong, skillful leadership played an indispensable role in building trust and successfully implementing IT on the network level. For example, highly skilled and charismatic network leadership in Boston, New Hampshire and Florida were able to garner trust and buy-in not only for membership into the network but to pool resources for the purchase of common, centrally-housed practice management and EHR systems through which data could be exchanged. These leaders demonstrated not only a strong skill for fostering collaboration but also expertise in key areas such as selecting vendors and building sustainable business models for health center IT investments. Strong leadership was also the keystone to building a vision for systems adoption that facilitated the evolution towards a unified goal of quality improvement for the safety net population both at the network and health center level. In addition to strong leadership, consortia also benefited from a high level of collaboration among consortia partners and public health stakeholders. CHAN, for example, credited a large part of its success to the health centers’ consistent desire to exchange data, overcoming challenges other networks faced in building members’ buy-in and trust.
Key Issues for Future Study
While the current study has elucidated important lessons learned for adoption of health IT among health center and health center networks, we identify a number of areas that merit further investigation to assist policy development moving forward.
- Feasibility and sustainability of promoting a network model. While networks represent an important opportunity for health centers, we found evidence that not all health centers are bought-in to an integrated network approach. For their part, we found that even the most successful networks are not self-sustaining financially and may not be for a significant period of time. Additional work may be required to understand the level of access health centers currently have to health center networks, the issues around health center buy-in for an integrated network model, opportunities for networks to obtain sustainable funding through non-grant sources and the potential role of incentives created by changes in Federal policy.
- Health center network gap and overlap analysis. Health centers around the country currently have different access to networked services depending on geographic location and resources available. While some geographic areas may not have any network activity, in the areas we visited for their study we often found three or more Federally funded health center networks. Although their activities were usually complimentary (and in some cases overlapping), we observed limited coordination and collaboration among networks in the same geographic area. Additional analysis may systematically catalog overlap and gaps in network access for health centers around the nation in an effort to facilitate broader access to networks and optimize future investments.
- Value relative to cost. As in other health care provider settings, health centers implementing health IT, and EHR in particular, struggle with the task of understanding the value of these investments relative to their costs. While health centers, as mission driven organizations may be less concerned with the bottom line for their institution, they are required to make responsible decisions with public resources. Also, understanding value of health IT relative to cost in health centers (where health IT purchases may be subsidized) offers a valuable opportunity to learn about the cost effectiveness of these tools in other ambulatory care settings. As most health centers do not have the resources or expertise to conduct rigorous internal evaluations incorporating initiative costs and comprehensive benefits, external research can play an important role.
- How to foster sustainability. While several health center networks have exhibited important successes in encouraging health center IT adoption, none indicated that they were moving comfortably toward self-sustainability under their current course. Even the most successful networks investigated struggled with the question of how to maintain an adequate level of resources as well as an exclusive focus on health centers while moving towards a self-sustaining financial model. The vision for some has been to expand to include non-health center providers as customers. Future analysis may focus specifically on options for achieving self-sufficiency working within market conditions. Pay for performance or other payer driven incentives specific to the use of EHRs may offer opportunity for these analyses.
- Considerations for future research. Because efforts were made to identify “leading edge” networks for this study, findings presented here do not reflect the state of the “average” health center. However, as the first study focused on health center use of IT generally, we have identified important methodological and substantive considerations. Methodologically, it is clear that any future efforts to assess IT use among health centers should consider an array of relevant respondents, from network leadership and staff, to administrative and clinical leadership at health centers. Because we found that health centers use a variety of models for staffing in IT, with relatively few employing a CIO, identifying appropriate respondents who can speak to how day to day technology decisions are managed will continue to pose a challenge that will need to be addressed on a individual basis with each health center.
Our study also highlights the important issues for focus in future studies of IT use among a representative sample of health centers (e.g., future efforts to survey health centers). For example, it will be critical that any such study consider a wide range of the structural barriers and enablers identified here such as history of network participation and collaboration with other health centers and access to executive level IT management staff. In addition to staffing and capacity, it is clear that gaining clinical benefits from health IT implementation requires sustained investment at multiple stages, from planning, to workflow and culture re-design among clinicians, implementation and ongoing improvement. As such, it will be critical to understand health centers’ plans for financing IT implementation and determining the scope of necessary outside investment. Finally, future research should ask how health centers make IT investment decisions to identify the extent to which health centers are equipped to assess the value of these investments relative to their mission.
Appendix A: Environmental Scan
DRAFT Revised Environmental Scan
Community Health Center Information System Assessment:
Issues and Opportunities
Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services
PREFACE
NORC completed the following environmental scan between February and September 2003, which includes a review of both published and unpublished materials relevant to IT use and adoption among health centers. Materials summarized here were gathered through formal searches in health services research databases such as PubMed, paired with searches of popular, non-peer reviewed publications using Internet search engines. In addition to review of secondary sources, the environmental scan included loosely structured, one hour discussions with thought leaders in the field of IT and health centers. Finally, the environmental scan included a targeted analysis of four practice management systems that cater to the health center market.
NORC at the University of Chicago
Introduction
The Office of the Assistant Secretary for Planning and Evaluation (ASPE) at the U.S. Department of Health and Human Services (HHS) has contracted with NORC at the University of Chicago, a non-profit social science and policy research organization to assess the status of health information systems at the nation’s HHS-funded community health centers (CHCs). The assessment will identify information management issues and opportunities facing CHCs and inform federal initiatives aimed at supporting CHCs in their efforts to more effectively utilize information systems (IS) on a center, community and regional level. A major motivator for the project is the National Health Information Infrastructure (NHII) vision articulated by HHS to maximize availability of health data for improvements in public health, health care financing policies and quality of care. The main purpose of this project is to gather and analyze information from CHCs on the relevant characteristics of their current systems applications, technical infrastructure, data management and transfer practices, processes for systems selection and implementation and the prioritization of information systems related issues within the larger organization. In summary the projects seeks to:
- Assess ongoing information systems related programs and practices employed by CHCs;
- Identify and describe models for successful systems implementation on a CHC and community level;
- Articulate major information systems challenges facing CHCs;
- Describe important barriers to realization of systems-related goals such seamless electronic data transmission to government and health care system partners; and
- Assess findings in relation to ongoing and potential policy initiatives at ASPE and HRSA and across HHS
This report presents results from the initial stage of this study, an environmental scan of the CHC and IS landscape. This environmental scan is based on review and synthesis of existing published and unpublished literature and a small set of discussions with thought leaders in the area of health information technology. The scan is designed to supply general context and background for the project and provide initial results and areas to be further explored during subsequent planned project activities. These activities will include detailed telephone discussions with 25 CHCs, and in-depth site visits with seven of these CHCs. The remainder of this document is organized as follows:
Environmental scan methods. We begin with a brief discussion of the overall approach and specific methods used to collect and analyze the information presented in the environmental scan.
Community health center landscape. We provide a description of CHC characteristics and goals as they relate to health information management activities. In addition to describing basic features of CHC financing and operations, we describe CHC activities that drive health center information system needs and requirements as they relate to administrative, financial and clinical practices.
Health center information systems and vendors. We next describe current resources systems used by health centers for the electronic management and exchange of clinical and administrative information. This discussion provides a description of “state of the art” systems used in larger public and private health centers as well as findings on use of technology such as practice management software and electronic medical records (EMR) more broadly among primary health care providers. The section also includes an overview of major software vendors who typically work with outpatient primary care health centers.
CHC information systems. Following the discussion of the basic CHC environment and the state of current information system technology relating to health centers, we describe the specific experiences of CHCs with information systems. Because this topic represents the main focus of key stakeholder interviews and site visits, this section will provide a very preliminary discussion based on our review of published and unpublished materials and conversations with thought leaders. In particular, we will identify models of innovative management of information systems at CHCs and raise questions for further elaboration with the planned qualitative data collection with CHCs.
Themes for additional study. We conclude the environmental scan report with a summary of key findings and conclusions for the larger study.
Appendices. Appendices 1 and 2 contain supplementary materials on project methods, including a list of printed materials identified for review and the main discussion guide used in conducting thought leader discussions. Next steps, in the form of possible CHCs to include in the next phases of the project and a CHC interview protocol are provided as Appendix 3. Appendix 4 contains a more detailed summary of the health information technology vendor marketplace to supplement the information presented in the main text and Appendix 5 includes an overview of our first planned set of stakeholders and case study involving community health care providers in Indianapolis, IN.
Environmental Scan Methods
As described in above, our environmental scan is based on two major information gathering activities: (1) review of published and unpublished documentation and (2) discussions with a small group of thought leaders and key informants knowledgeable about health information systems (HIS) and CHCs. We note that these discussions (which expanded on the initial activities originally planned at the start of the study) are not intended as substitutes for the series of 25 telephone discussions and seven in-depth site visits that will be undertaken once the environmental scan is complete. Rather, the discussions with key informants were conducted to supplement what was a relatively thin literature (both published and unpublished) on HIS issues confronting CHCs, and to identify relevant information that conventional literature search strategies might miss. Although ASPE, HRSA and NORC anticipated this dearth of relevant literature at the outset, we later determined that it would be important to conduct these initial supplementary discussions in order to ensure that the discussion guides and site selection for the later stages of the project were on target. Accordingly, we note that — as indicated in our original proposal — this environmental scan is more important as a vehicle to set up the subsequent project activities than it is as a mechanism for identifying conclusive results.
In conducting both activities, NORC worked closely with ASPE and representatives from HRSA in order to relate environmental scan process and findings as closely as possible to the goals of the main project sponsors and CHCs themselves. In particular, we were asked to assure complete coverage of the range of current programs related to improving health center information systems, including use of grants sponsored by HRSA and private foundations, the potential use of existing government systems, such as the VA Vista system in community health settings, an overview of private sector advances in health center information systems and promising models for advancement of information systems goals at CHCs.
Preliminary activities and coordination with ASPE. In the weeks following the project kickoff, NORC met with HRSA and ASPE to discuss key study questions and scope out environmental scan activities. At these meetings, ASPE and HRSA underscored the need to think broadly about the systems infrastructure, efficiency and regulatory compliance issues as they related to the mission of CHCs and the environment under which they operate. Furthermore, we were encouraged to look at CHC experiences working on systems projects funding through existing HHS or privately funded programs such as Shared Integrated Management Information Systems (SIMIS) and Community Access Program (CAP). We were also directed to a series of initial thought leader discussants including consultants who regularly work with CHCs on information systems issues. Following this initial meeting and initiation of environmental scan activities, NORC has produced two interim memos outlining progress on key tasks and next steps for completion of the environmental scan and subsequent project phases. Following delivery of each of these memos, NORC met with ASPE and HRSA in order to discuss findings and identify additional avenues for inquiry.
Review of existing documentation. The environmental scan includes review and synthesis of information from existing published and unpublished documents. We used two major approaches in identifying materials for review. First, we conducted a formal search of major social science and health services research databases such as PubMed, HSRProj and PsychInfo, as well as databases such as Lexis-Nexis that may include popular, non-peer reviewed publications. Finally, in order to assure comprehensive coverage of publicly available information, we conducted targeted searches of content available on the Internet using Google.com and other powerful search engines. Searches were conducted using a range of subject-level key words crossing “community health centers” or “FQHC” and “information technology”; “HIPPA”; “practice management”; “electronic medical records”; etc. In addition, we conducted a general literature search on HIS related topics alone to uncover review articles or other publications that characterize the current state of health information management systems as they relate to both public policy and the goals of CHCs.
The second and more fruitful approach, to identifying appropriate information for review included directly contacting individuals at relevant organizations in order to gain access to unpublished information or publications that were not readily available through public sources. These organizations included government Agencies such as the Bureau of Primary Health Care, the Veteran’s Administration and the Indian Health Service; relevant associations such as the National Association for Community Health Centers, the Association of State and Territorial Health Officials (ASTHO), the National Association for City and County Health Officials (NACCHO), the Indiana and Oregon Primary Care Associations (PCAs) and the American Academy of Family Practice (AAFP); charitable foundations such as the Tides Foundation of California and the Robert Wood Johnson Foundation (RWJF); and academic institutions such as the Indiana University’s Regenstrief Center. In many cases, in addition to providing materials for review and synthesis, contacts from these organizations participated in thought leader discussions described in greater detail below. Upon identifying and obtaining these materials NORC reviewed relevant content and important findings were summarized for inclusion in the current report. A comprehensive list of materials identified as part of this scan is included as Appendix 1 to this report.
Thought leader discussions. Thought leaders identified for the environmental scan ranged from independent consultants working with HRSA, individual health centers and networks on systems issues to representatives from relevant associations and foundations such as PCA’s and NACHC, to HRSA and Bureau of Primary Health Care (BPHC) regional staff. Discussions were initiated by telephone or email contact with the discussant or his/her staff. Prior to these discussions, thought leaders were forwarded a set of materials describing the overall project and its methods and providing a preliminary set of topics for discussion in the form of a discussion guide. This guide covered basic questions regarding the current state of CHC information systems including commonly observed challenges and issues as well as examples of how CHCs have leveraged existing sources of funding and expertise to enhance their systems capabilities and the specialized needs of CHCs relative to other providers in this area. Although the discussion guide, included as Appendix 2 to this document, provided an appropriate starting point for many of the thought leader discussions, we did not seek a detailed response to each topic across all respondents. Instead, we encouraged each discussant to provide detailed information on issues of which they had particular experience, knowledge, or interest. In some cases, where the discussants’ expertise focused on a particular area of interest rather than broader issues related to the study, we developed a specialized set of questions. Representatives from ASPE and HRSA were provided an opportunity to participate in each of these discussions. Table 1 below provides a comprehensive list of thought leader discussants, their affiliation and the type of information they were able to provide.
Thought Leader (s) |
Organization | Areas of Contribution |
|---|---|---|
| Steve Dorage, Dennis McMahan, Steve Laslo | HRSA/BPHC |
|
| William Gaud | Independent Consultant |
|
| Marc Wilcox | Independent Consultant |
|
| Carter Crafford | Miterek Systems |
|
| Alice Rae | Indiana Primary Care Association (PCA) |
|
| John Ruiz | National Association of Community Health Centers (NACHC) |
|
| Mike Leahy | Oregon Community Health Information Network (OCHIN) |
|
| Ellen Freedman | Tides Foundation |
|
| David Gans | Medical Group Management Association (MGMA) |
|
| Clem McDonald | The Regenstrief Institute |
|
| Barbara Kelly | The Gartner Group |
|
| Theresa Cullen | Indian Health Service (IHS) |
|
| David Kibbe | American Academy of Family Physicians (AAFP) |
|
| Gary Christopherson | Veterans Health Administration |
|
In addition to the activities described above, NORC has participated in a number of HRSA-sponsored events related to CHC information systems. These include a CAP grantees conference, three sessions with Michael Leahy, Executive Director of the Oregon Community Health Information Network (OCHIN) and HIPPA-compliance related activities with CHCs. Attendance and participation in these meetings have enhanced our understanding of the issues at hand and inform the discussion of project findings provided below.
In the sections that follow, we present the results of all of these environmental scan activities and conclude with a section on how these results will be used to inform the subsequent project activities (telephone discussions with 25 CHCs and in-depth site visits with seven CHCs). It is important to note that, due to the mixed methods used to gather this information, some of the results presented (e.g., those that represent syntheses of information from literature) are more generalizable than others (e.g., an impression or perception reported by one, or even several, of our key informants). We clearly differentiate these different types of results throughout the following sections. Still, it should be emphasized that all of the results presented here — other than basic descriptive information on CHCs and HIS vendors and products — are considered preliminary. As described above, the purpose of this environmental scan is to provide basic context and background on the CHC and HIS landscape, and to use this information, plus initial findings from literature and a relatively few discussions with key informants to illuminate areas for further investigation through a systematic set of interviews and site visits.
Community Health Center Landscape
This section summarizes general information on CHCs as a means of providing context for the specific themes that are the focus of this study — the ways in which CHCs are using health information technology to accomplish their missions. In effect, this document “drills down” to its specific focus by first describing the CHC environment, then describing the health information technology environment, and then describing (to the extent possible) the union of these two areas.
Overview
Federally sponsored health centers are an integral part of the nation’s health care “safety net” (providers who service underserved and uninsured populations) in both rural and urban regions across the United States. Since their inception as a pilot program by the Federal government in 1964, CHCs have been instrumental in delivering primary care medical services to vulnerable populations. They represent a critical public resource for individuals and families who face barriers to securing medical insurance or obtaining care from private providers. Originally supported under the Economic Opportunity Act, the eight inaugural “neighborhood health centers” (NHCs) opened their doors in 1965 as a component of President Johnson’s Great Society plan. With expansions requested in the FY 2004 budget, there will be well over 800 funded Community and Migrant Health Centers with close to 3,700 sites. HHS estimates that CHCs will serve approximately 12.55 million patients during FY 2003 and plans on increasing this number by 1.2 million for FY 2004.
The NHC program was expanded and transferred to the oversight of the Public Health Service in 1969, where it eventually became known as the Community/Migrant Health Center (C/MHC) program. The C/MHC Federal grant program is currently authorized under Section 330 of the Health Centers Consolidation Act of 1996, under the guidance of the Division of Community and Migrant Health Division at the Health Resources and Services Administration’s Bureau of Primary Health Care (BPHC). In its current form, Section 330 governs grants to four types of health centers including community health centers (CHCs); migrant health centers; health care for the homeless clinics; and health care for residents in public housing. Collectively, these grantees are known as Federally Qualified Health Centers (FQHCs). Although the principal subject of the current study are community health centers or CHCs, issues covered will be of general relevance to the broader group of FQHCs and community-based providers.
Although Section 330 mandates certain common elements and requirements for CHCs (see below), they differ substantially in terms of their organization and size. While some operate as primary care physician group practices with a large professional staff scattered around several sites within a community and serving tens of thousands of patients, others operate as single clinician offices with a handful of full-time employees and serving a much smaller population. Furthermore, CHCs exist within a range of larger organizational settings. While all are non-profit organizations, some are church or Foundation sponsored charity clinics, while others have relationships with Universities, non-profit hospitals or other community stakeholders. Given this diversity of organizational partners and size, CHCs differ substantially in terms of their internal management structure. For example, smaller clinics often have a single professional manager who serves as the primary clinician and administrator, whereas larger CHCs often have a Chief Executive Officer (CEO) or Executive Director, a Medical Director and a Chief Financial Officer, each with responsibilities over specific aspects of center administration, clinical services and finances.
Federal Requirements
The Health Centers Consolidation Act and associated regulations lay out minimum requirements for qualification as a FQHC. These qualifications include issues of governance, populations to be served, services provided and administrative reporting requirements. Each of these requirements is described in greater detail below.
Service and operational requirements. FQHCs must provide services to underserved populations or be located in a medically underserved area (MUA) as designated by HHS and provide services to all residents within that area without regard to income or insurance status. They are also required to provide comprehensive primary care and ancillary services including clinical care by physicians and nurses; diagnostic laboratory and radiology services; perinatal services; immunizations; well-child exams; pediatric eye, ear and dental screening; family planning; and, pharmacy services. Finally, FQHCs are required to maximize patient payments (using an income-based sliding fee schedule) and third party payments, using the Section 330 grant, only to cover deficits after other sources of funding have been exhausted.
Health center governance. In addition to the basic requirements described above, CHCs, like all FQHCs, are subject to federally defined governance requirements. Specifically, HRSA rules require full authority and oversight responsibility for the center to rest with a governing board of 9-25 members, the majority of whom must have actually used clinic services in the last two years or be the legal guardians of CHC clients. Non-client members must represent the area served by the center and have expertise in community affairs. Half of these non-client members cannot earn more than 20 percent of their income from the health care industry and, overall, board members must demographically reflect the group of individuals served by the center. Finally, center staff and their spouses are not eligible for the governing board. Board responsibilities include meeting at least once a month, selecting the services to be provided by the center, scheduling the hours during which services will be provided, approving the center’s budget and leadership and establishing general policies for the center.
Reporting requirements. CHCs are required to annually submit data to the national Uniform Data System (UDS). Data for this annual submission includes basic information on the center finances, staffing and resources as well as encounter and patient based information. The list of items for submission includes:
- contact information for center grantee and service delivery sites;
- services offered and delivery methods;
- center staffing;
- encounter based information including frequency of selected diagnoses and utilization of selected services (e.g., pregnancy and prenatal care, mental health services, etc.);
- demographic information on health center users including age, gender, race/ethnicity, languages spoken, socioeconomic characteristics and insurance status; and
- center revenues broken out by patient related revenue (managed care and non-managed care) and other sources of revenue
Because centers are required to provide these data electronically, the ability to accurately and efficiently manage this information is an important feature of CHC information systems. In addition to federal reporting requirements related to the UDS, many CHCs fulfill requirements for accreditation by the Joint Commission on the Accreditation of Health Care Organizations (JCAHO).
Funding
Since the 1996 passage of the Health Care Consolidation Act, the C/MHC program has grown steadily both in terms of provision of services to target populations and funding. For FY 2003, the program was funded at over $1.45 billion dollars. This funding includes all center grants included under Section 330: CHCs, MHCs, public housing clinics and Health Care for the Homeless Sites. Growth in funding has resulted in the increase in health center access points: new health center grantees and new health care delivery sites that expand the reach of existing center grantees. The President’s budget FY 2004 increases requested appropriations for the Community and Migrant Health Centers to $1.627 billion, a figure that was recently approved by Congress. Table 2 below, provides a breakdown of estimated actual revenue accrued by C/MHCs in 2002 as well as planned revenue for 2003 and 2004. In addition, the Exhibit 1 shows the share of total revenue by source of funding (roughly consistent across years).
| Estimated 2002 Revenues (in millions) |
Planned 2003 Revenues (in millions) |
Proposed 2004 Revenues (in millions) |
% | |
|---|---|---|---|---|
| Section 330 | 1,328 | 1,433 | 1,582 | 25% |
| Medicaid | 1,660 | 1,800 | 1,950 | 31% |
| Medicare | 300 | 325 | 350 | 6% |
| SCHIP | 90 | 100 | 110 | 2% |
| Other Third Party | 430 | 470 | 510 | 8% |
| Self Pay | 305 | 330 | 360 | 6% |
| Other Federal Grants | 150 | 160 | 175 | 3% |
| State/Local/Other | 1,020 | 1,100 | 1,200 | 19% |
| Total | 5,283 | 5,718 | 6,237 | 100% |
Priority Initiatives
The BPHC’s 2004 budget justification emphasizes the importance of HIS to overall health center effectiveness. In particular, the budget justification describes systems efforts related to the Bureau’s Health Disparities Collaboratives program and promotion of systems issues through the Integrated Services Delivery Initiative (ISDI). Information on other HIS support initiatives is provided in Section 5 of this report.
Health Center Information Systems and Vendors
This section presents high level trends in the use of information systems across the range of primary health care providers in the United States. This information was obtained from a review of recent publications in the area of health information technology as well as detailed conversations with thought leaders on the major systems related issues facing primary health care providers. In particular, we queried industry thought leaders on aspects of information systems most relevant for CHCs including implementation of practice management and electronic medical records systems and HIPAA compliance. We also include information on selected vendors in this area. Because thought leaders estimate that there are over 1,000 current vendors of electronic health record or practice management applications, it was beyond the scope of this study to exhaustively list and describe these vendors. In sections that follow we present information from our more detailed research using company websites, on vendors identified as particularly relevant to community-based providers such as CHCs.
Background
Over the past several years information systems (IS) and health care experts alike have reflected on the relatively slow pace of adoption of information technology in the health care industry compared to many other industries. Although specific sectors within health care, such as the hospital supply and pharmaceutical industry, have been using advanced electronic information management and data interchange for decades, other segments of the health care marketplace, physicians in particular, have been cautious about introducing even basic information management technologies such as email or networked computers. Recent estimates indicate that the health care organizations make approximately one fifth of the investment in information technology (as a percentage of their overall operating budget) compared to industries with similar information needs. Another trend of note is the lack of commonly accepted and utilized standards for health information management and transfer. Such standards would facilitate the important goal of efficient and secure exchange of electronic health data among providers and between providers and other entities. This is a particular challenge in light of HIPAA data standards and privacy requirements.
There are, however, important exceptions to the overall trend of relative underutilization of information technology and systems by providers. Key among these is the increasing prevalence of electronic submission of claims to Medicare and other large health care purchasers, although these submissions are largely mediated by third-party clearinghouses that take data produced through hospital and or physician office systems and convert it to meet purchaser standards. In addition, there are examples of larger public and private providers such as Kaiser Permanente, Partners Healthcare System and the U.S. Veterans Administration that have successfully used information system technology to implement electronic medical records, enhanced communication with patients, greater access to medical knowledge resources, electronic order entry and clinical decision support tools. Because the recent focus of health centers in this area has been to implement tools related to more efficient administrative management of center activities and, in some cases, employment of electronic systems for electronic capture of clinically relevant information, we focused our environmental scan around these two broad issues. In the sections that follow we discuss concepts and tools involved in enhanced practice management and use of EMR or electronic health records.
Practice Management
Practice management systems generally deal with appointment scheduling, billing and accounting, enrollment and eligibility, coding and claims processing, patient demographics information management, master patient index, and, in some cases, recordkeeping functionality (i.e.: encounter documentation). According to industry sources the vast majority of large to medium sized physician group practices have implemented some form of practice management software to handle basic administrative and office management tasks such as scheduling, billing and resource management. Still, thought leaders indicated that the majority of clinics are running multiple systems for administrative record keeping and that these systems are not meaningfully integrated and are running at less than full efficiency. For example, many clinics combine use of dedicated practice management tools with generic tools such as the MS Office Suite (e.g., Outlook, Word, Access, etc.) to manage and track the wide range of administrative functions central to the operations of a clinic. Very few clinics under 10-15 physicians have dedicated IT staff or a conscious strategic plan to systematically integrate practice management tools into their operations.
Interviewees described a highly fragmented market for practice management software, both in terms of demand from clinics and the landscape of vendors. Customers are gradually developing sharper preferences regarding requirements and service providers are slowly adapting to these preferences and growing smaller through mergers, acquisitions and closings, making it difficult to get an accurate sense of the core differences between providers. Most providers offer the same basic functionalities: patient appointment scheduling, tracking of patient insurance plan status and terms, patient billing/claims submission and financial systems and inbound and outbound referrals. Many products also include advanced features such as capitated billing and financial management and allow for easy exchange of data with managed care and major insurer information systems to facilitate overnight verification of eligibility and automated electronic claims submission and payment.
Because practice management marketing efforts primarily target administrators rather than clinicians the most sophisticated products include tools to help identify and address opportunities to recover lost revenue including electronic submission of all insurance claims, claims editing and tools to facilitate analysis of revenue and claims by payment source and other relevant variables. Another relatively new, advanced functionality is combining resource management (both plan and labor) with scheduling. Finally, looking forward, thought leaders indicated that the major distinguishing feature among practice management vendors is their ability to offer products that easily integrate all administrative, financial and resource management aspects of clinic operations and that effectively sync data from those functions with patient-level electronic medical records or electronic health records. Relatively sophisticated vendors that currently offer combined practice management and electronic health record products include Medic computer systems and Mysis LTD of the UK.
Electronic Health Records and Electronic Medical Records
Electronic Medical Records (EMR) systems are multi-functional. EMRs typically document patients’ past clinical history and family history; capture encounter information; create prescriptions and track current/past medications, allergies; act as a repository for laboratory and other diagnostic data and, in some cases, varying degrees of clinical decision support tools, such as checking for medication interactions or some practice management functionality, such as appointment scheduling and master patient index. In recent years, a broader model for implementing these systems has been referred to as electronic health record (EHR) systems. According to one of our thought leaders, David Kibbe of the AAFP, EHR refers to an integrated system that makes an appropriate level of medical or clinical data available to both providers and patients, facilitates reporting of medical events for public health purposes, includes a secure messaging system for placing pharmacy or laboratory orders and integrates with a health center’s practice management system.
In contrast to practice management, there are very few stand alone outpatient clinics that have any form of EMR. A recent survey of 6,000 members by the AAFP revealed that only 3-5 percent of their members have any type of electronic health record while between 10 and 24 percent have some form of electronic medical record. As with practice management, the vendor landscape for electronic health records and electronic medical records is fragmented, with the substantial majority of regional vendors having fewer than fifty clinic clients.
Vendor Landscape
On the vendor side, interviewees indicated that there are between 1,000-2,000 total practice management vendors on the market in the U.S. This estimate suggests substantial but unrefined demand and a maturing vendor landscape. Thought leaders also acknowledge that the market is consolidating and the total number of vendors will likely markedly decline over the next several years. The majority of these vendors are considered regional players, providing basic administrative software to a limited number of small or medium sized clinics in a defined geographic area. Many of these vendors are small companies that promise to custom design software and provide support services to meet the specific needs of their client clinics. Interviewees indicated that these vendors develop systems and services of inconsistent quality, with a common difficulty being the ability to create useful interfaces with other systems both existing and anticipated (e.g., an electronic health record system or community-wide eligibility tracking system for low income individuals), facilitate the use of data standards for reporting and exchange and build in the flexibility to accommodate compliance with regulatory provisions such as those imposed by HIPAA.
The AAFP survey showed approximately 256 different EMR or e-health record software vendors, the largest being Medicalogic with 148 clients out of the approximately 1,440 clinics who indicated having some type of software in this area. Thought leaders describe the vendor landscape for the this market as similar to that of practice management applications with the bulk of vendors being regional players and with a few of the larger HIT and health care companies packaging EMR tools or functionalities with a full suite of practice management and clinical decision support applications.
Thought leaders identified four general groups of IT vendors in terms of market orientation and product focus:
- Regional players. As described above, the bulk of organizations currently developing and marketing physician office practice management software are small to medium sized regional players with 10-20 clients. Interviewees indicated that they often caution physicians who are tempted by the customization and low cost offered by many of these companies because of their lack of stability (most will either go out of business or be purchased by larger vendors over time) and their tendency to oversell the virtues of their customizations relative to the need to install systems that are easily integrated and designed to accommodate relevant data standards and regulatory requirements. One advantage to these systems may be in the area of support services because they deal with a smaller number of clients and support is provided, in many cases, by individuals who were involved in design and initial software installation.
- Application service providers (ASP). There are a growing number of dot.net organizations selling rights and support services for practice management software that they make available for installation and operations via the Internet. These organizations also tend to be smaller and offer the advantage of, in many cases, being focused exclusively on designing, improving and supporting a single package of practice management (and increasingly electronic medical record) software.
- Enterprise vendors. Interviewees indicated that there is a growing group of health care and health information technology corporations that combine practice management and electronic medical records functions with comprehensive offerings for health care information applications across all types of providers and settings. Prominent among this group of vendors are Epic, Mckesson and Cerner. Larger IT companies such as IBM also fall into this category.
- Best of breed vendors. Interviewees identified a number of vendors considered best of breed. These vendors have developed and marketed products with high-end functionality and performance in one particular aspect of practice management or electronic health record application. Examples include: AthenaHealth a partner of Siemans; Amico, a three-way partnership between IBM, Microsoft and Pfizer; Nexgen, Microsyst, GE Medical and Vitalworks.
Some thought leaders felt that the ASP model is a particularly promising mechanism for developing electronic records capabilities in individual physician clinics because it offers a low cost option for accessing and implementing the software in a particular clinic and an easily accessed platform in the Internet for data exchange between network providers and other community and policy stakeholders. Other thought leaders expressed skepticism that these products can be successfully integrated with a clinic’s locally operated system(s) for practice management functions.
In addition to the general information on the scope of the overall vendor landscape for practice management and electronic health records our environmental scan activities revealed the following, more generic findings on the nature of product offerings in this market:
- Modular product formats. In general, in most cases vendors do not market a single system that claims full services practice management or electronic health records functionalities. Instead, practice management or electronic health records (or, more often EMR) is used by vendors to describe a package of their products (called “modules”) that perform specific functions.
- Product modality. Most of the companies researched offer access to their data using multiple modalities, e.g., clinical workstation, handheld computer and web site.
- Clinical data repositories. Every product must store its data somewhere, more than likely in a relational database management system. It is also likely that this data has some degree of structure that can be used for analysis or other types of intelligent processing (e.g., alerts). In this sense, every vendor has what could be called a “clinical data repository.” However, only one or two products contain a sophisticated, fully integrated data repository by general IT industry standards
The cost of implementing and maintaining practice management systems vary widely depending on the nature of the application and services acquired and the particular clinic setting and requirements. Thought leaders indicated that, on average, physicians spend approximately 15 percent of revenues on health information management tools and applications and related applications over a fixed period of time that includes a major purchase or upgrade with approximately about one fifth of that amount being spent ongoing user support and technical assistance services. One interviewee indicated that this substantial investment in information technology has not reaped commensurate benefits in terms of efficiency or improved patient care. He attributed this to the lack of integration among different information management systems within the same clinic and the lack of attention to health information technology purchases as core strategic investments that will determine the success of the clinic in achieving clinical, operational and financial goals.
CHC Information Systems
Like other members of the provider community, CHCs face opportunities and challenges related to their approach to accessing, producing, reporting and storing information. As core safety net providers, serving, according to the BPHC, approximately 11.3 million Americans in 2002 and as publicly sponsored centers with ties to the public health infrastructure, CHCs represent critical consumers and producers of health data for patient care and public policy purposes. For these reasons, CHCs play an important role in achieving a National Health Information Infrastructure. As described above, CHCs vary substantially in terms of their size and organizational characteristics. Still, there are shared information systems needs across CHCs and other community-based primary health care centers and many CHCs have made substantial strides in this area.
Support for CHC Information Systems
In recent years, the federal government have directed additional funding towards advancing CHC information management goals. In addition to programs focused exclusively on specific information management issues, CHCs have made use of more general grants to make important advances in IT. The main focus of these programs, described below, has been to encourage community-wide collaborations on systems issues. This type of collaboration helps pool costs to accommodate the substantial fixed costs of operating and maintaining systems and helps facilitate the important goal of seamless exchange of data across all relevant health care stakeholders.
Integrated Services Development Initiative (ISDI). The Integrated Services Development Initiative (ISDI) is a CHC focused grant that funds two major activities: (1) implementation joint practice management systems and EMR systems across centers in a single area and (2) to work with (or establish) managed care networks to maintain CHC share of clients eligible for Medicaid coverage. Since its initiation in 1994, the ISDI program has awarded approximately 70 grants (ranging from $250,000 to $400,000) for up to four years.
Shared Integrated Management Information Systems (SIMIS). The Shared Integrated Management Information Systems (SIMIS) grant administered by BPHC supports inter-center collaboration on systems issues. Funded grantees typically design and implement common platform and tools for centralized billing, utilization review and quality assurance. Another goal of the program is to encourage integration of administrative and clinical information management functions within and across centers. In addition to joint purchasing of HIS resources, the SIMIS program requires health centers to implement strategic model for community-wide systems decision-making including: fulfilling IT staffing needs, conducting employee trainings, optimizing use of software licenses and support contracts, planning for regulatory compliance and mapping out future systems-related investments.
Community Access Program (CAP). The Community Access Program (CAP) funds models for enhancing integration of safety net services provided in any community. Unlike the SIMIS program, CAP is not designed to exclusively support systems initiatives. Examples of activities funded under CAP include development of client eligibility tracking databases to be used by a range of community social service providers and establishment of a shared electronic medical records (EMR) system public health plans and safety net providers in a community. Although, not restricted to systems-specific initiatives, nearly all recent CAP grants include substantial allocation of funds for information systems issues. The Oregon Health Information Network’s (OCHIN) use of CAP to establish a common, state-wide system for practice management including safety-net health care providers and health plans represents a leading case of the use of a CAP grant for an information system enhancement and integration. CAP grants are currently found in 158 communities around the U.S. in urban, rural, and tribal areas.
HIPAA-related support from HRSA. A major regulatory compliance issue facing CHCs and other primary health care centers involved in electronic transfer of health care related information is adherence to Health Insurance Portability and Accountability Act (HIPAA) requirements for Standard Transactions and Code Sets, Privacy and Security. In an effort to assist CHCs in moving with the development and implementation of HIPAA compliant electronic data systems, HRSA has contracted with MGMA to conduct a series of technical assistance audio conferences. As an initial phase, MGMA conducted a focus group with CHC grantees to determine HIPAA implementation status and common problems. Focus group participants revealed that many vendors were not planning on developing HIPAA compliant software, instead directing clients to use data clearinghouses at extra cost. Based on this feedback, HRSA incorporated management and negotiation with vendors as an important aspect of the audio conference curriculum. To date, three audio conferences have been presented. The first audio conference on Standard Transactions and Code Sets drew 420 registrants and 1,500 listeners. Subsequent audio conferences focused on the privacy rule and drew over 1,000 listeners. Future audio conferences are being planned to cover the security rule as well as additional information on later stages of standard transactions and code set implementation, including testing systems with payers. Although thought leaders knowledgeable on CHC issues related to HIPAA compliance expressed support for the technical assistance effort, some expressed concern regarding CHC access to technical resources to implement recommendations provided as part of this effort.
Electronic Medical Records Resources Project. BPHC is currently working on an initiative to assist CHCs in developing effective Electronic Medical Records (EMR) and Disease Management (DM) systems to enhance the quality of care. This effort hopes to identify the functional role that EMR and DM systems would ideally play for CHCs and help determine how CHCs can reach this ideal with their systems. The project includes: in-depth research of EMRs history, goals, current status, and future direction; identifying current EMR vendors; interviewing health care providers as well as Health Information Management professionals to assess their Medical Record needs in addition to their opinion of currently available systems; and creating a set of functional specifications to establish a standard for ambulatory care EMR. BPHC is currently funding an EMR pilot program involving three California CHCs and provides extensive guidance on its website for CHCs interested in using EMR technology in their clinic. The project’s website also includes information on basic functional requirements for EMR vendors appropriate for community-based health centers, vendor assessments and guidance related to planning EMR projects.
Veterans Health Information Systems and Technology Architecture (VISTA). VISTA is a federally-run, publicly-owned health information software system administered by the Department of Veterans Affairs that has become available for use by some community-based providers. First implemented in 1996, VISTA is a comprehensive system supporting all sizes of health care providers ranging from small community-based clinics to community hospitals to tertiary facilities, covering virtually all aspects of care. Currently, VISTA is undergoing a number of modifications to enhance and improve its capabilities with the aim of forming both a next-generation VISTA system for the VA, Healthe-Vet VISTA, as well as a public version, Healthe- People VISTA, which will be made available to such entities as state departments of health, medical schools and physician group and solo practices and individual practices. Currently VISTA automates patient records and provides VA clinicians with patient level information during encounters using a graphical user interface (GUI). The VISTA system has been incorporated by community health providers in Washington, DC, who received a grant from the Department of Commerce to fund the purchase and implementation of the software. In addition, a new project will look at using VISTA in a number of community health settings in West Virginia, possibly hosted by one of the state’s universities or major hospitals in the area. We note that while many observers consider VISTA a strong model for health center information management, others note the challenge of adopting VISTA for non-VA use. Important requirements include development of clinical modules not relevant to the VA population such as pediatric care as well as recording and coding encounter data for billing purposes.
Indian Health Service. Finally, the Indian Health Service also implements a computer-based health system known as Resource and Patient Management System (RPMS) to meet their health center management needs. Because IHS clinics are largely, rural and modestly staffed, the IHS currently does not use a GUI front end for data entry and clinical information dissemination (though IHS is in the process of developing a GUI). Instead, clinic staff enter data from a specifically designed encounter form into the RPMS system. This data entry includes comprehensive therapeutic and diagnostic information including CPT codes for billing. Specific information entered varies by diagnostic module. In addition to allowing for automated billing based on the encounter specific data entered into the system, for subsequent patient visits the encounter form can be printed out to include information on prior visits and serves as a clinical tool. Notably, a number of IHS tribal clinics, particularly those in Alaska and California are also designated as FQHCs eligible for Section 330 funding and so some FQHCs currently use the RPMS system.
Tides Foundation. In addition to public sector funders, some community providers receive support for technical infrastructure from charitable foundations. Most notably in partnership with the California Endowment, The Tides Foundation has granted approximately $30 million to help develop basic health infrastructure (i.e. automated accounting, practice management) for community-based safety net providers in California since 1999. Tides reports that 80% of funding has gone to individual primary care clinics with the remaining amount going to regional provider networks in California. The program targets funds towards centers that lack basic electronic resources such as Internet access or any form of automated information system. According to Tides much of the funding under this initiative goes toward planning and training health center staff. Specific grants have also gone toward implementation of practice management and EMR systems in community based health settings.
CHC Use of Information Systems
Generally speaking, the needs of CHCs are quite similar to mainstream, private practices: both have significant practice management and record-keeping needs. As a result, the most prevalent applications in use at CHCs are practice management and EMR systems. As expected, we also discovered that CHCs have some unique characteristics that complicate their needs when compared with private practices. These needs include special reporting needs (i.e. the uniform data set) and eligibility/coverage determination. In the paragraphs below we briefly describe the two prominent applications that are currently in use, or are being contemplated by CHCs, as well as CHC-specific data needs.
Practice Management Systems. From discussion with thought leaders and review of environmental scan materials, it appears that practice management systems are the most widely implemented recent infrastructure enhancement at many CHCs and networks and, as described above, are a focus of many grantees to the SIMIS or CAP programs. Furthermore, tailoring practice management systems for CHC-use has been a focus of some software vendors, most notably Medical Manager.
Electronic Medical Records. Like other providers, CHCs are cautious in adopting EMR software and integrating its use into every day practice. Thought leaders cite multiple specific challenges. These include the computer literacy of the providers and their overall comfort with using the technology; staff turnover that necessitates an ongoing training plan; the inefficiency of information transfer from existing medical records; and a hesitance on the part of some administrative staff and providers to invest in technologies that are still evolving and might quickly become obsolete or unsupported. However, once the EMR has been implemented, doctors and administrative professionals tend to be highly satisfied with the system, and especially appreciate EMR for preventing lost medical records and making the effort associated with losing this information a thing of the past, as well as the constant availability of organized, current information. There some CHCs that are working with EMR software both through the grant programs described above and through an EMR pilot study involving three California CHCs. A pilot study for EMR systems is currently being conducted by the Central Valley Health Network in Central San Joaquin, California. Three of the Networks 12 health centers, are participating in the pilot study: the Darin M. Camarena Health Centers; the Family Healthcare Network; and the Golden Valley Health Centers.
In addition to the pilot study in California, thought leader discussions revealed that other CHCs are also planning EMR system implementations. One example of this is planned implementation of an EMR program by the Oregon Community Health Information Network (OCHIN), a network of CHCs and other community provider stakeholders in Oregon, which they are attempting to fund, partially, through a SIMIS grant application.
CHC Information Systems Needs and Challenges
Environmental scan activities have revealed substantial activity in the implementation of health center information systems. Advances identified to date in locations such as Oregon, Miami-Dade County, Washington D.C. and other locations reflects both strong vision on the part of community leadership timely, well-focused support by key federal stakeholders such as HRSA and the VA. However, as with other health care providers, CHCs vary dramatically in terms of their approach to health information systems. Thought leaders indicated that many CHCs still rely on long outdated methods for basic administrative tasks and that most CHCs face an uphill struggle with respect to issues such as assuring HIPAA compliance without the use of clearinghouses. We note that this situation is not different from that of most small to medium size primary care health clinics and group practices. Some of the key challenges and barriers related to design and implementation of health information systems in CHCs are described below.
CHC-specific Needs. As community-based safety net providers, CHCs have a special set of data and administrative needs that may be addressed using health center and community based information systems. For example, CHCs are typically required to assess the eligibility of clients for Medicaid, Medicare or other insurance or health care subsidization programs to ensure maximum reimbursement from third party payers. This is particularly challenging when working with a population that frequently falls in and out of eligibility criteria and may seek care only at sporadic intervals and at different locations. Community-wide tracking eligibility systems have been offered as a solution to this need. In addition, CHC administrative systems must accommodate the need for double and triple bookings and sliding fee schedules for determining patient out of pocket costs. Finally, the requirement that CHCs submit data on UDS means that CHCs must have an efficient way to tabulate encounters by diagnosis and procedure and provide additional information such as birth weight and trimester of first prenatal visit for specific types of visits.
Procedural Challenges. Overall, thought leaders indicated that the majority of the IT challenges facing CHCs seem to fall into the area of CHC organization and administrative procedures used in decision-making, design, and implementation activities related to their systems. These challenges include those related to application/system implementation (i.e., project management, skills for proper configuration); vendor performance against contract requirements; user training and issues related to “homegrown” systems solutions. Of these, thought leaders emphasized the concept of poor vendor management and relationship building leading to the inefficiencies and failure to meet important project objectives. Some specific deficiencies cited included the vulnerability of CHCs to unfavorable contracts due to lack of appropriate technical knowledge and also varying levels of assertiveness from leadership. In addition to lacking the appropriate technical knowledge, thought leaders indicated that CHCs face difficulties related to negotiating major vendor contracts generally. Finally, CHCs entering into systems decisions are especially vulnerable, not only because they are more likely to lack appropriate contract and technical expertise, but also because they receive none of the benefits available from group price negotiation. We note that HRSA has acknowledged the importance of vendor relations and provides CHC with substantial guidance on procurement and contract management issues.
Other challenges stem from the lack of knowledge among vendors regarding CHC operations. While there are specific examples of CHCs working with vendors to familiarize themselves with their specific challenges, many of these relationships encounter difficulties because of a lack of understanding of CHCs among vendors. One common refrain is that vendors tend to underestimate the level of support CHC users will require relative to users with their traditional customers.
Organizational Challenges. Environmental scans and thought leader discussions in particular, have elucidated a number of organizational challenges related to issues and opportunities for CHCs in regard to information systems development and implementation. For example, our discussions suggested that strong leadership from a Chief Information Officer (or similar individual) with an accurate sense of organizational mission and culture is an important element to progress on systems issues both for individual CHCs and networks. CHCs and networks that lack strong systems expertise suffer from implementation of systems that are consistent with the expertise and biases of existing staff, rather than those representing the optimal solution given the organization’s mission and constraints. Perhaps most telling is the notion reported by thought leaders that primary care providers including CHCs generally invest too much of their information management resources on specific applications and systems, rather than developing and implementing a strategic plan for procuring and using information technology for their clinic. Again, this is a challenge that HRSA has addressed to some extent by emphasizing the importance of CHC-investments in HIS strategy and dedicated leadership to follow through on HIS objectives.
Finally, there exist challenges related to funding and resources. These include a lack of knowledge or a failure on the part of CHCs to take advantage of all funding sources and other support mechanisms. Conversely, some have expressed concern that the multiple funding sources and programs are too small and seem uncoordinated. Additionally, thought leaders mentioned that individual CHCs that are not in States with strong networks are often ineligible for systems-specific grant funding and that the levels of funding available are not adequate to support necessary improvements even among network CHCs with good management practices. Finally, while CHCs are encouraged to form networks and consortiums to take advantage of funding opportunities or respond to changes in the reimbursement environment, some thought leaders indicated that CHCs are provided relatively little guidance on how to operate successfully as members of a consortium or network.
CHC-Specific Vendor Overview
As described in this earlier, there exist a number of serious barriers to implementation and maintenance of advanced information management applications in CHCs as well as the difficulties in CHC relationships with vendors and in compliance with regulatory requirements on health data exchange mandated via HIPAA. We have found that most of the sophisticated practice management applications on the market can accommodate special CHC-requirements related to administrative and financial management applications (e.g., sliding fee schedules, robust patient scheduling capabilities, tracking of specific clinical outcomes and UDS reporting) In the bullet list below we describe vendors identified by thought leaders as being of particular relevance to CHCs. We note that more detailed information on these vendors and others is provided as Appendix 2 to this document. Finally, we note that the descriptive information provided here is taken from both thought leader discussions and the vendors own websites. We plan to obtain independent confirmation in subsequent key stakeholder interviews or case studies involving CHCs currently using these systems.
- Epic. Epic is one of the largest and most respected enterprise applications vendors. Epic’s clients are typically very large healthcare provider organizations such as Cleveland Clinic, Northwestern University Medical Center and other large healthcare enterprises. Epic is relevant to CHCs because the Oregon Community Health Information Network (OCHIN) chose to use its software as the basis for its networked practice management system. Part of OCHIN’s success story is the collaboration between OCHIN and Epic to create customized software based on CHC needs and requirements such as family planning and sliding fee scales. OCHIN noted that it would not have been feasible for Epic to have designed CHC-specific customizations had it not been for the aggregated buying power of the OCHIN network.
- Medical Manager. Medical Manager is a product that has historically been used and well-liked by CHCs. Nearly every thought leader we interviewed mentioned the use of Medical Manager at CHCs, and it has been known as one of the small handful of vendors who is receptive to the special needs and challenges of the CHC community. Perhaps the best example of a CHC network using Medical Manager is the Health Choice network in Miami, FL. The company was recently acquired by WebMD who is now marketing the former company’s products as the “Medical Manager System”. Signs of strain between the CHCs and WebMD have begun to show as a result of the transition, according to our thought leader interviews. One thought leader stated that Medical Manager was now becoming too expensive and noted that he encourages CHCs to network in order to be able to purchase it (although he did not make a recommendation as to whether or not they should purchase Medical Manager). Another thought leader stated that “HealthPro, WebMD, and Medical Manager have approximately 65 percent of the market . . . their growth is beginning to show in negative ways as many complaints are coming in from the field.” WebMD has also acquired many other healthcare vendors relevant to CHC HIT including HealthPro, Resource America, Calyx, and Envoy. Resource America and Calyx are not discussed because it appears that WebMD is no longer marketing any of the products that those companies produced. Envoy (now “WebMD Envoy”) is perhaps the most notable of these purchases as Envoy is “one of the largest electronic claims and electronic payments transactions processor in the country” according to one thought leader.
- MDExchange. MDExchange is building what one thought leader termed a “community [master] patient index.” According to literature received from the vendor, MDExchange is a central repository in which care providers (e.g., hospitals, clinics) are able to register the presence of records related to an individual. When a physician accesses the MDExchange system, he/she can query all of the registered records and create a summary patient chart that combines information from multiple care providers.
- MDServe. While not primarily geared towards CHCs (as was the case with Medical Manager), MDServe has worked successfully with CHC networks in Maryland and Texas to create custom functions based on the needs of CHCs. In addition to advertising that the company’s product is “endorsed by the Technology Support Program of the NACHC.” The company offers its own success stories in the version of case studies of three implementations (Arizona, Georgia, and Texas).
- Healthcare Data Systems. One thought leader stated that CHCs in Indiana use one of two vendors: Healthcare Data Systems and HealthPro (see next bullet). While the thought leader praised Healthcare Data Systems’ “knowledgeable and helpful staff,” she indicated that the company may not remain in the market due to market forces (e.g., consolidations and closures).
- HealthPro. HealthPro is an example of one of the best of breed companies that was created specifically to meet the needs of CHCs; the general consensus was that this was good company to do business with because the people who worked there cared about CHCs. HealthPro no longer exists as a company due to being acquired by WebMD. Its product is being produced and marketed by WebMD as “HealthPro XL”. It remains to be seen how long that will be the case as WebMD is said to be steering its customers towards using the new version of Medical Manager. One thought leader indicated that when HealthPro was still in business that they had an unreliable track record with respect to providing quality training and that training costs were high.
- AAFP Open source EMR. The Open source EMR project is being sponsored by AAFP in order to test the hypothesis that an open-source web accessible model for electronic patient record software will markedly increase the use of this technology by clinicians. If successful, the Open source EMR would be made available to anyone who wished to implement it. If such a model is successful, it would likely be an idea candidate for use at CHCs. The most likely way for it to be successfully used at CHCs is in a networked environment; the CHC community could also combine its resources to create a specialized version of the product that incorporated special CHC requirements. At the time of our discussion with AAFP, they were in the process of bringing on practice management vendor partners to develop customized interfaces allowing integration of clinical and administrative data in settings using the Open Source EMR product. Notably, they had not been able to reach such an agreement with Medical Manager.
Themes for Additional Study
This document has presented findings from the first of three main project activities -- a comprehensive environmental scan including review of available printed materials and discussions with a limited group of thought leaders. Because of the unstructured nature of information in this area, we note that environmental scan findings are not intended to identify and definitively characterize all aspects of CHC experience with information systems. Instead, we have attempted to synthesize the background information on the characteristics of CHCs and health information systems as well as the easily available information on the success and challenges with design and implementation of health information systems in community health center settings. We have also characterized the overall vendor environment for clinic based health information systems and particularly those of specific relevance to CHCs. One of the main purposes of this environmental scan was to identify specific themes for further exploration during upcoming telephone interviews with 25 CHC and in-depth site visits with 7 of the 25 centers. We describe topics for additional study below.
Medical Manager/WebMD and vendor relationships generally. While there are a number of companies that CHCs have used for systems issues, the dominant vendor of practice management software to CHCs has been Medical Manger. This seems to be a result of a conscious effort to acquire competitors and develop customizations, such as automatic UDS reporting. Though they have achieved a substantial market share the future for product upgrades and support services for Medical Manager remains unclear. Thought leaders indicate that Medical Manager is not planning on developing a HIPAA compliant upgrade to their existing system for CHCs. There is also speculation that WebMD’s goal is to move CHCs (and other customers) to web-based software platforms - this will likely pose a problem for many current Medical Manager clients with limited access to high-speed Internet connectivity. The CHC experience with Medical Manager may reflect the larger challenges inherent in building relationships with vendors, including the impact of market and vendor volatility and the difficulty involved in procuring and managing vendors in areas where CHC staff traditionally have little expertise. Assisting CHCs in the vendor procurement and relations process has been a priority of HRSA. Our environmental scan findings confirm the importance of expanding CHC capabilities in this area and, in subsequent phases of this study, we will investigate CHC-vendor relationships and produce recommendations to inform current federal policies and programs in this area.
Models for community collaboration on health information management. HHS’ vision for a National Health Information Infrastructure (NHII) requires CHCs to work closely with other community health and social service stakeholders. Use of a common platform for practice management and clinical data systems across providers in a community provides economies of scale and facilitates generation of aggregate data for administrative, public health and public policy purposes. Obstacles to this type of coordination include the challenge of determining how to equitably share management and cost burden of such a system across providers and instituting effective user-training across multiple settings and user types. Although the CAP and SIMIS programs have encouraged the growth of collaborative systems investment and planning, many thought leaders indicate that coordination in developing proposals and securing grant money through these programs, does not always translate into effective collaboration the programs themselves. One notable exception to this trend is the Oregon Community Health Information Network (OCHIN). OCHIN has been able to leverage affiliations with prominent Oregon CHCs and the State’s primary care association to forge a State-wide information management program for community health care delivery, including use of a CAP grant for implementation of a community-wide practice management program and well developed plans to apply for a SIMIS grant to implement a common EMR across the same group of providers. Findings from the environmental scan confirm that OCHIN has been able to establish a unique level of collaboration across community health center stakeholders. Subsequent activities including stakeholder interviews and case studies will assess CHC involvement in community-wide information systems initiatives, strategies used by CHCs to overcome the challenges of community wide or regional collaboration and opportunities to replicate success models for collaboration such as OCHIN in other locations.
Challenges and opportunities related to HIPAA compliance. As described above, CHCs face a substantial challenge related to compliance with HIPAA administrative data standards. Results from the environmental scan indicate that almost all CHCs requested extensions for the compliance deadline. Furthermore, Medical Manager’s CHC practice management software does not accommodate HIPAA requirements and there is no apparent effort underway to upgrade the software for HIPAA compliance. Policy makers at HHS face the difficult task of attempting to encourage and ultimately mandate compliance with HIPAA-related data standards, while supporting the efforts of community-safety net providers to enhance their use of electronic data systems generally. While HIPAA presents a daunting challenge for those CHCs who already use electronic data transfer for billing and reporting purposes, it may serve as an impetus for achieving common (compliant) data format and standards across health care providers. Furthermore, HHS efforts to support the use of HIPAA compliant data exchange models may facilitate the use of electronic data systems among CHCs that still rely on paper-driven processes for administration and billing. Subsequent phases of this project will include detailed investigation of CHCs plans related to HIPAA including strategies for overcoming barriers to compliance and new systems related opportunities that emerge from HIPAA compliance related efforts.
Wide disparities in use of information systems. Findings from the environmental scan confirm that there exist large disparities in the use of information systems for administrative and clinical functions at CHCs. While a main focus of this project will be to identify successful models of CHC systems design and implementation that may be replicable in other settings, the goals of the project also require some investigation of a representative group of CHCs. This group will include those CHCs, that, similar to other providers, demonstrate relatively limited use of electronic systems. Looking at these centers will allow us to describe in detail the basic resource and knowledge constraints facing small- to medium-sized community-based health care providers, including those rural CHCs that are not able to pool resources across a network of providers. In order to provide both a broad picture of CHC experience and opportunities with information systems anda thorough understanding of leading models for integration of systems into the management of CHCs, we plan on using a two-pronged strategy for selecting CHCs for the next stages of the project: we will set aside some (e.g., 8-10) of the interviews to speak with a relatively representative group of CHCs, including those with relatively little access to advanced systems technologies. This will allow appropriate and accurate characterization of the overall CHC experience. With the remaining CHC interviews and subsequent case studies, we will focus on those CHCs, urban and rural, that have some demonstrated successes in information management. This will enable us to characterize various models of CHC IT experience and to compare these models in terms of consistency with the NHII vision, sustainability of progress and replicability in other settings. Furthermore, in looking closely at these CHCs and, in many cases, their networks, we will have the opportunity to assess the impact the various BPHC and privately funded efforts in this area and identify opportunities to enhance these programs over time. A table of potential sites for future study is included as Appendix 3 to this report. Appendix 5 outlines our plans for conducting the CHC interviews and provides information on Community HealthNet and other community providers in Indianapolis, IN the setting identified early in the project as a key target for a site visit.
Endnotes
HRSA, Budget Justification for the President’s 2004 Budget to Congress
Recent summary on legislative activity http://www.nachc.org/
Starr P. Smart Technology, Stunted Policy: Developing Health Information Networks. Health Affairs, May/June 1997.
DK Francies et al. Health Care Information Technology (New York: JC Bradford, 1999).
Bush, J. Open-Source Software: Just What the Doctor Ordered? Family Practice Management, June 2003. < http://www.aafp.org/fpm/20030600/65open.html#box_a>
EHR Interest Survey Results. American Academy of Family Practice, January 2003. < http://www.aafp.org/x19997.xml?printxml>
National Summary of 2002 UDS data from <www.hrsa.gov>
National Summary of 2002 UDS data from <www.hrsa.gov>
Recent summary on legislative activity http://www.nachc.org/
HRSA, Budget Justification for the President’s 2004 Budget to Congress
Appendix B: Case Study Reports
Community Health Center Information Systems Assessment: Issues and Opportunities
Findings from Oregon Site Visit
Submitted to the Office of the Assistant Secretary for Planning and Evaluation and Health Resources and Services Administration, US DHHS
NORC at the University of Chicago
January 2004
Oregon
1.0 Introduction and Background
NORC at the University of Chicago (NORC) is pleased to present this site visit report describing methods, key findings and conclusions from Oregon for “Community Health Center Information Systems Assessment: Issues and Opportunities.” This project is sponsored by the Office of the Assistant Secretary for Planning and Evaluation (ASPE) at the U.S. Department of Health and Human Services (HHS) and will assess the status of health information systems (IS) at the nation’s HHS-funded consolidated health centers (hereafter referred to as “consolidated health centers”). Results from this study will help guide a range of HHS projects focused on infrastructure at consolidated health centers and, more broadly, HHS policy relating to the United States health care safety net. The study will also help identify research and development priorities as they relate to consolidated health center use of IS. The project involves collection and analysis of information on the characteristics of systems applications and technical infrastructure currently in place at consolidated health centers. Findings from the project will focus on unmet IS related needs and models for successful use of IS within consolidated health centers and the communities they serve.
Site visits to seven communities with consolidated health centers around the country form the major data gathering activity of the assessment. Additional assessment activities include a comprehensive environmental scan summarizing findings from available published and unpublished sources on issues related to consolidated health center use of IS, discussions with a series of 15 experts (or “thought leaders”) with experience in the financing, development, support or design of health center IS and structured interviews with a set of 25 consolidated health centers across the United States.
1.1 Site Visit Objectives
The Oregon site visit involved telephone, email and in person exchanges with 30 respondents representing 18 institutions involved in the primary health care safety net in the State of Oregon. Findings from these activities help identify issues and opportunities facing health centers in Oregon, particularly with respect to the activities of the Oregon Community Health Information Network (OCHIN), an independent non-profit consortium of safety net health centers and stakeholders founded in the year 2000 and supported to date through short term grants awarded by the Bureau of Primary Healthcare (BPHC) and other federal sources. OCHIN’s mission is to improve health centers’ use of IS for clinical and administrative purposes and to facilitate dissemination of high quality health care and public health data on a community, State and Regional level. Overall, the site visit explored two main themes: (1) the state of IS use among consolidated health centers in the State of Oregon, and (2) the sustainability, replicability and effectiveness of OCHIN as a model for maximizing benefits of IS for health centers and other stakeholders in a particular State or region.
This report is organized into three main sections:
- Introduction and background. In addition to introducing the purpose of the project and current site visit, we begin with an overview of safety net programs in Oregon including the OCHIN initiative.
- Site visit findings. The main section of the report summarizes key findings from the site visit, including a discussion of the development and organization of OCHIN; an overview of the current IS infrastructure, practices, and needs of the Oregon consolidated health centers; and an assessment of safety net stakeholders’ satisfaction with OCHIN.
- Conclusions. We end the report with a set of analytic conclusions that explore issues related to the sustainability and replicability of the OCHIN model, challenges facing consolidated health centers and other safety net stakeholders in Oregon, and issues for future study in subsequent site visits.
1.2 Oregon Safety Net Programs
Site visits such as this one represent an important opportunity to guide HHS efforts to maximize benefits from use of IS in primary health care settings. Oregon presents a particularly interesting setting for our first site visit due to the State’s history of progressive thinking and organization around health care and public health issues. The State Primary Care Office and the Office of Medical Assistance Programs have worked closely with the consolidated health centers and the Oregon Primary Care Association (OPCA) to address issues of health care access, cost and quality of care for Oregon’s safety net community. The formation of CareOregon, the State’s largest Medicaid managed care provider, in the 1990’s represents a recent example of safety net stakeholders working together in Oregon. CareOregon, formed through a cooperative venture involving safety net providers in the State, has assisted consolidated health centers work with the State’s Office of Medical Assistance Programs (OMAP) to continue serving low-income populations following adoption of Medicaid managed care. More recently a range of senior State health officials have shown strong interest and involvement both in OCHIN and in other infrastructure-related initiatives affecting the State’s consolidated health centers. CareOregon has also played an important role in the early development of OCHIN by serving as the consortium’s first organizational home.
Safety net providers and the populations they serve in Oregon. The 30-plus consolidated health centers comprise the major portion of safety net providers in Oregon. These include community health centers, health care for the homeless centers, Indian/tribal health centers, rural health centers and school-based health centers. While many of consolidated health centers are located along the Western edge of the State, a number of consolidated health centers are located in rural parts of the state south and east of Portland. The populations served by these health centers differ substantially in terms of insurance status, demographics and chronic disease prevalence. The consolidated health centers also vary significantly by number of sites, dedicated clinical and administrative staff, total clients and total encounters per year.
Oregon’s consolidated health centers and their associated networks fulfill their mission by serving the State’s uninsured, underinsured, Medicaid beneficiaries and other vulnerable populations. In 2002, approximately 14 percent or nearly one half million Oregonians were without health insurance. According to a 2002 OPCA report on safety net gaps, primary care safety net clinics in Oregon serve 27 percent of the uninsured population and 15 percent of the Medicaid population over the course of a year. Over 60 percent of Oregon’s Medicaid population are enrolled in one of the state’s 14 fully capitated managed care plans.
1.3 The OCHIN Initiative
OCHIN is a non-for-profit consortium of health centers and health safety net stakeholders created in 2000 following a state-sponsored study that recommended enhanced use of IS to improve the organization, coordination, financial stability and management of safety net health centers. OCHIN is governed through its Board by the directors of participating consolidated health center organizations as well as the directors of the Oregon Primary Care Association (OPCA) and State Primary Care Office. OCHIN’s partnering consolidated health centers reflect the full diversity of health safety net providers in Oregon described above. All of these centers receive funding under Section 330 of the Public Health Service Act.
The full OCHIN membership currently includes 23 organizations and agencies that serve Oregon’s safety net population. As described above, OCHIN describes its mission as increasing access to IS to improve administrative and clinical functions at primary care safety net health settings and to increase access to high quality information on the populations served by the safety net for planning and policy. OCHIN’s primary accomplishment to date has been to design, develop, and maintain a regional, HIPAA-compliant, high-speed data network for its member health centers. As part of maintaining this network, OCHIN administers a system of central servers using an application service provider (ASP) type model to provide full featured practice management to a growing number of consolidated health centers throughout the State and region. To provide this software, OCHIN has partnered with Epic Systems, Inc., a health information software vendor whose products are typically used in high-end health care provider settings such as elite academic medical centers. In addition to the practice management software, OCHIN plans to implement an electronic medical records (EMR) software system to allow systematic tracking of clinical data as well as a comprehensive data warehouse that will allow policy makers, providers and other stakeholders to access near real-time data on the health status and health care utilization of the safety net population. OCHIN’s development and technical infrastructure, as well as other issues relevant to the initiative’s sustainability, replicability and overall effectiveness, will be described in later sections of this report.
2.0 Site Visit Methods
This case study involved a series of preliminary phone conversations and subsequent on-site structured interviews with key stakeholders in the Oregon safety net. We contacted consolidated health centers in and around Portland, identifying senior leadership and IS staff to query on administrative, management, clinical and technical issues related to IS use at their health centers. We also contacted stakeholders who could provide distinct perspectives on Oregon’s legislative, governmental, and cultural environment relevant to the safety net and OCHIN, including key leadership at OCHIN itself. We list key respondent organizations and their role in the State in Table 1 below. Our respondents included:
- Oregon health centers (including consolidated health centers) of various sizes, both OCHIN participants as well as non-participants
- Oregon state health officials
- OCHIN leadership
- Representatives from CareOregon
- Members of the OCHIN leadership
- Out-of-state OCHIN participants located in Seattle, Washington and Santa Cruz, California.
We spoke with stakeholders in the two largest population centers with in the state, Portland and Salem, as well as stakeholders in the more rural areas of Oregon. To streamline logistics, we organized our site visit to coincide with the Northwest Primary Care Association (NWPCA) conference in Portland on October 18th through 22nd. This allowed us to speak in person with leadership from health centers across a larger geographic spread than originally anticipated.
2.1 Site Visit Process and Logistics
In the preliminary phases of the site visit planning, we contacted OCHIN leadership to describe the goals of the study and secure their assistance with identifying respondents and developing a data collection approach. These contacts provided key background materials on OCHIN’s efforts and assisted in identifying a wide range of relevant potential respondents. We also made extensive use of State websites and contacts provided by ASPE, HRSA and Oregon state officials to ensure the site visit would capture the full range of health center and stakeholder experience and knowledge.
Preliminary phone conversations. Prior to the site visit itself, NORC conducted approximately 20 half-hour telephone conversations with a range of health center and state government stakeholders. For many of these respondents, the initial telephone conversations served as an important opportunity to introduce the study and help focus the development site visit instruments. In other cases, initial telephone conversations were conducted with key officials or stakeholders who provided important context and background for this report independent of data gathered during the site visit itself.
Site visit activities. The site visit itself was conducted by six NORC staff on October 21st and 22nd, 2003. Each team of two staff members consisted of a senior staff lead (either a NORC Senior Vice President, Project Manager or Systems Expert) and a project Research Assistant. The site visit team consisted of two members of NORC’s Information Technology Department who have extensive experience in health IS, and four members of NORC’s former Health Studies Department1 who have broad expertise in health care and public health issues related to vulnerable populations. During the site visit, the NORC team conducted 17 total interviews involving 28 respondents. The interview localities were primarily in or around Portland, but we also talked with respondents in Salem, Tillamook County (near the Oregon shore), Oregon City, and Cornelius (several miles west of Portland). Two interviews were conducted by telephone with OCHIN partner consolidated health centers outside of Oregon: one with Pike Market Health Center in Seattle, WA and another with Santa Cruz County Health Department in Santa Cruz, CA.
2.2 Respondent Characteristics
Table 1 below describes the respondents interviewed during the site visit and provides some brief background on each organization that participated in the study. We have categorized health center respondents using OCHIN’s terminology:
- “Integrated Practice Management (IPM) Partners” are health centers that have a legal agreement with OCHIN to utilize the Epic practice management software and its related connectivity, user support and data management services;
- “Collaborators” are health centers that do not yet use the Epic software but may submit data for the data warehouse initiative or enter into formal service arrangements with OCHIN once the network rolls out an electronic medical record product.
Respondent Organization |
Type |
Description |
|---|---|---|
|
Consolidated Health Center Respondents |
||
| Multnomah County Health Department | IPM partner | Multnomah County Health Department is both a county health department and consolidated health center located in Portland, OR. It is the largest consolidated health center in the state. In 2002, the consolidated health center served 52,569 patients in 233,342 annual visits. |
| Klamath Open Door Clinic | IPM partner | Klamath Open Door Clinic is a stand-alone rural community health center and consolidated health center located approximately 280 miles south of Portland in Klamath Falls, Oregon. It has two sites that service around 4,500 patients annually and saw 17,230 encounters in 2001. |
| Tillamook County Health Department | IPM partner | The Tillamook County Health Department is both a rural county health department and consolidated health center located in Tillamook County, Oregon. Its five sites served around 6,000 patients with 20,437 encounters in 2001. |
| Virginia Garcia Memorial | IPM partner | Virginia Garcia Memorial Health Center is a stand-alone consolidated health center centered in rural Cornelius, Oregon. Their five sites serve 15,000 patients annually with 48,402 visits in 2001. |
| Pike Market Medical Clinic | IPM partner | Pike Market Medical Clinic is a stand-alone consolidated health center located in Seattle, WA. The site provides around 25,000 visits to 3,500 patients annually. |
| Ochoco Community Clinic | IPM partner | Ochoco Community Clinic is a small-sized stand-alone consolidated health center located in central Prineville, Oregon, making it the Eastern-most IPM partner. Its rural site provided 1,900 patient visits in 2002 and is expanding. |
| Clackamas County Health Division | IPM partner | The Clackamas County Health Division is a public health division that also provides primary care services and is located in Oregon City, OR. The site served 11,070 patients in 2002 in 29,230 visits. |
| La Clinica del Valle | Collaborator | La Clinica del Valle is a federally supported stand-alone community/migrant health center located in rural Medford, Oregon. Its three sites service around 7,800 patients annually with 25,137 encounters in 2002 and it is expanding. |
|
Respondent Organization |
Type |
Description |
|
|---|---|---|---|
|
Consolidated Health Center Respondents (continued) |
|||
| Outside In | Collaborator | Outside In is a stand-alone consolidated health center serving primarily homeless youth, located in Portland, Oregon. Its one site saw 7,700 patient visits last year. It is a member of the Coalition of Community Clinics, a network of 11 small, community-based providers that serve the needs of vulnerable populations in the Portland metropolitan area. | |
| Santa Cruz County Health Services Agency | Collaborator | The Santa Cruz County Health Services Agency is a large department in the county of Santa Cruz, California which houses two consolidated health centers. The Agency is in the process of becoming an IPM partner. | |
| Northwest Human Services | Outside OCHIN | Northwest Human Services is a stand-alone consolidated health center located in Salem, OR. The two health center sites served 10,000 patients in 38,959 visits in 2002. | |
|
Non-Consolidated Health Center Respondents |
|||
| Oregon Community Health Information Network | State — leadership | The Oregon Community Health Information Network (OCHIN), is an independent non-profit collaborative of consolidated health centers and other stakeholders that works to strengthen the health care safety net through improved IS and management services. | |
| CareOregon | Medicaid Managed Care Plan | CareOregon, a (501(c)3) is Oregon’s largest Medicaid managed care plan with over 80,000 members. It served as OCHIN’s administrative home until September 2003. | |
| Oregon Primary Care Association | State — Public Health | The Oregon Primary Care Association (OPCA) is a non-profit advocacy and member association that offers technical assistance to its safety net consolidated health center members to increase their efficiency and quality and to help them operate as a business. OPCA had a role in writing the original Community Access Program (CAP) grant for OCHIN’s initial funding. | |
| State Primary Care Office | State — Public Health | The State Primary Care Office (State PCO), and specifically its health systems planning division, helps determine where shortages of health professionals exist in the state as well as where under-served populations exist. | |
| Office of Medical Assistance Programs | State — Medicaid | The Office of Medical Assistance Programs (OMAP) manages the medical and dental services of the Oregon (Medicaid) Health Plan. OMAP helped develop the data infrastructure and helped to finance the OCHIN program. | |
| Office for Oregon Health Policy and Research | State — Public Health | The Office for Oregon Health Policy and Research (OHPR) is a state agency that provides health research, health policy analysis and technical expertise to the Governor, legislators and communities. | |
| Oregon Department of Human Services | State — Public Health | The state Department of Human Services (DHS) sets public health policy and provides administrative and technical assistance to county health departments and other local collaborators who deliver services in the community. | |
| Wallace Medical Concern | Urgent Care Center | Wallace Medical Concern is a private, non-profit clinic that caters urgent care services to low-income, uninsured populations. The clinic is located in Portland, OR. The clinic receives no federal funding, provides only urgent care services, and does not bill for its services, and is therefore being treated as an outlier for the purposes of this summary. | |
2.3 Site Visit Tools
We developed structured but open ended data gathering tools for the site visit to (1) allow for targeted, systematic collection of relevant information and (2) capture the overall richness of respondent experiences. Telephone discussions and in-person interviews with respondents were conducted using discussion guides and a tabular form was emailed to IS staff at respondent health centers to facilitate collection of standard information relating to infrastructure and technical capacity.
Discussion guides. Preliminary versions of the discussion guides used for the site visit followed from a generic site visit protocol developed earlier in the study and reviewed, modified and approved by ASPE and HRSA. As noted above, informal pre-site visit conversations with respondents allowed us to incorporate information gathered during those conversations into tailored discussion guides for each interview. For each scheduled interview, the NORC team prepared materials that outlined our preliminary knowledge of the respondent and highlighted outstanding questions to address during the interview. Respondents who had experience with OCHIN were asked about the impetus behind OCHIN, the characteristics of the participating health centers versus the non-participating centers, the stakeholders’ experiences with OCHIN and Epic, and the potential for replicating a system like OCHIN in other regions of the country. Examples of discussion guides and preparation materials used in the site visit are included as Appendix A.
Gathering data on health center IS.To gather information about the health centers’ IS infrastructure; we designed a short table with fields relevant to various aspects of a health center’s network, data and technology. This table was distributed to the various health center respondents prior to the site visit. Several of the sites returned very helpful information, including diagrams of their local or wide area networks (LANs or WANs), examples of written policy statements, a classification of support issues compiled by the center’s help desk, examples of paper-based records, and information about applications used to manage clinical and practice management data. The table used to gather these data is provided as Appendix B.
3.0 Key Site Visit Findings
This section summarizes major findings from information gathered as part of the site visit. Because of OCHIN’s importance in ongoing systems-related improvements among consolidated health centers in Oregon, much of this section is dedicated to describing the development, administrative processes and technical characteristics of the OCHIN network. This section also describes the IPM partner and collaborator consolidated health centers’ experiences with OCHIN. Finally, the section includes an extensive discussion of our findings related to the technical and operational characteristics of IS at the health centers themselves, including software, hardware, networking, procedures and staff resources. This discussion is based on reports from health centers that are not current OCHIN IPM partners as well as those that are OCHIN-affiliated.
3.1 OCHIN Development and Early History
We begin by describing the environment from which OCHIN emerged and key aspects of OCHIN’s early history, including the impetus behind the development of the collaborative. We focus also on the organizations that helped establish initial goals, direction, and a longer term vision for the consortium.
Early leadership. Key stakeholders in the creation of OCHIN included the OPCA, CareOregon and consolidated health centers in the State of Oregon, notably the health center run through the Multnomah County Department of Health. These organizations headed the development of a steering committee composed of themselves as well as leadership from relevant offices within State government. Several members of this steering committee were interviewed as part of our site visit. Under the organizational umbrella of CareOregon, the steering committee applied for and secured a Community Access Program (CAP) grant that allowed them to hire staff and begin the process of developing the consortium in late 2000. In addition to citing the need for improvements in safety net health center administrative systems, the original CAP application emphasized OCHIN’s potential to collect and distribute high quality information on the health status and health care experience of vulnerable populations through a coordinated central data warehouse.
Organizational goals and focus. OCHIN’s original steering committee believed that it was important to maintain the consortium’s non-profit status and to focus on reaching out to different primary care safety net providers across the State and region. OCHIN sought to collaborate with consolidated health centers rather than other providers such as hospitals or private group physician practices. After securing CAP funding, the OCHIN steering committee brought on Mike Leahy (then a consultant with the Tillamook County Health Department’s consolidated health center) as Executive Director. The steering committee also prioritized the procurement and implementation of a sophisticated practice management system that could improve administrative efficiency and facilitate HIPAA compliant data exchange for the State’s 30-plus consolidated health centers and other safety net providers. The decision to prioritize practice management coincided with Multnomah County’s ongoing independent effort to select a practice management system vendor for their own consolidated health center. Over time, Multnomah County merged these activities with those of the health centers represented in the original OCHIN steering committee.
Vendor selection and initial implementations. After gathering the initial IPM partners and deciding to prioritize the procurement of a practice management vendor, the new OCHIN staff developed a request for proposals and evaluated the 25 responses they received. The first tier of evaluation focused primarily on functionality and workability of proposed solutions. The question of affordability was reserved for subsequent phases of the selection. Following an initial review of proposals, three vendors were selected as finalists including Epic (the ultimate winner) and NextGen.
The final selection process involved a live product demonstration by the three finalists, after which each consolidated health center in Oregon was given the chance to hear presentations from the finalists and fill out score cards. This process resulted in Epic’s selection as OCHIN’s software vendor. Several respondents mentioned that Epic was selected primarily for its extensive experience with marquee private group practices such as Kaiser Permanente and the Cleveland Clinic and because it would be able to provide an electronic medical records (EMR) system, which remained one of OCHIN’s goals. It should be noted that some of the OCHIN leadership was familiar with Epic from previous experiences and actively sought out Epic’s bid and was instrumental in capturing the software company’s attention. To date, seven IPM partners have “gone live” with the new integrated practice management platform in over 50 clinic sites and the partnership continues to expand within and beyond Oregon. Multnomah County Health Department plays a central role in hosting and supporting the main OCHIN server.
Plans for expansion. While the group of initial IPM partners allowed OCHIN to begin operations and secure additional funding, OCHIN’s leadership and current IPM partners acknowledge the need for further expansion to ensure an independently sustainable model capable of financing access to software and associated services. The current scope of the practice management initiative (involving seven IPM partners and more than 500,000 encounters per year) is substantially subsidized through temporary grant funding from HHS. At the time of vendor selection the OCHIN Board understood that — given the cost of the Epic product — longer term viability of the network would require establishing partnerships with safety net health centers outside of Oregon. At the time of the site visit OCHIN had one out of state IPM partner (Pike Market Health Center in Seattle, WA) and another implementation was planned for late 2003 (in Santa Cruz, CA).
Future direction and funding. The consortium is continuing to expand service and product offerings to individual health centers. In addition to two years of initial funding through the CAP program, OCHIN recently secured three additional grants, each focused on an important component of the consortium’s practice management and anticipated EMR offerings. In particular, immediate plans include at least doubling the annual volume of practice management visits managed by the Epic software by 2006 and developing an EMR product to be rolled out to alpha and beta sites in FY 2005. Early indications suggest that it will be possible to work with OCHIN to incorporate the existing BPHC software used in monitoring care delivered as part of the Health Disparities Collaborative project into a comprehensive EMR.
OCHIN continues to work towards implementing a safety net data warehouse for Oregon, but the consortium does not currently have adequate funding or resources to develop or manage the systems necessary for collecting patient data from the non-partner health centers that do not use the Epic software and integrating these data with that of the IPM partner health centers to form the basis of a patient- or encounter-level data warehouse. Currently, administrative data on patient encounters from IPM partner health centers is captured in a master patient index (MPI), which OCHIN leadership describes as a precursor to the data warehouse and a potentially rich source of utilization and administrative data related to safety net care in Oregon. The MPI currently includes data on the approximately 400,000 patients who obtained care via IPM partner consolidated health centers over the last two years.
Organizational affiliation and governance. CareOregon served as the administrative home for OCHIN in its initial two years of existence. In particular, CareOregon served as the grantee organization for the original CAP grant that supported OCHIN. At the time of its creation and subsequently, both CareOregon and OCHIN agreed that the formal legal relationship between the two organizations was a temporary arrangement that would last only long enough for OCHIN to become a viable, independent entity. At the time of our site visit, OCHIN was going through a legal separation with CareOregon that has subsequently been finalized.
Separation from CareOregon was possible at this time because of additional grants secured for the consortium through other IPM partner consolidated health centers and organizations. In conversations following separation, OCHIN leadership indicated that their new independent status will result in greater freedom for OCHIN as it seeks to establish its own viability as a financially independent safety net provider network. As before, OCHIN is governed by a board of directors including leadership from State officials, consolidated health centers, the OPCA and CareOregon. In addition to being one of OCHIN’s IPM partners with representation on the Board of Directors, the Multnomah County Health Department houses OCHIN’s centrally located servers and support staff. Many of OCHIN technical staff are former employees of either CareOregon or Multnomah County.
3.2 Motivation of Early OCHIN Partnerships
As described above, OCHIN commenced practice management software “go-lives” with several consolidated health centers in late 2002 and early 2003. OCHIN established independent service agreements with these “integrated practice management (IPM) partner” health centers. These agreements describe the Epic-related implementation services that are to be provided by OCHIN, including:
- access to the centrally maintained practice management software application as users under an ASP model
- consultation with health centers on necessary technology upgrades
- provision of ongoing training and user support for health centers
- administration of automated electronic claims submission through OCHIN and McKesson, a data clearinghouse vendor selected by Epic.
In addition to shouldering the cost of start-up at their site(s), under these agreements, individual IPM partner health centers are required to pay a $1.04 per-encounter fee for use of OCHIN services. This is a subsidized rate; the actual estimated cost per visit is $1.75 per-encounter.
The current IPM partners are comprised of four smaller stand-alone consolidated health centers and three clinics affiliated with county health departments. These IPM partner clinics differ substantially across important characteristics such as total number of annual encounters, demographic characteristics of patients served and payer mix. The largest health center, Multnomah County based in Portland, experiences close to a quarter million encounters per year, while the smallest health center — Ochoco Community Health Services, located in the rural geographic center of the State — experiences fewer than 2,000 encounters per year. Although each of these IPM partner health centers came to OCHIN with different technical infrastructure characteristics, varying levels of systems expertise, and distinct support needs, they had similar reasons for partnering with the consortium including those described in the bullets below.
- Billing. According to our respondents, the single most important factor motivating their decision to join OCHIN was having access to the reliable billing component of the Epic practice management software. As one center’s Executive Director phrased it, “practice management is all about billing.” The need for streamlined, reliable billing processes is particularly critical in light of expectations from BPHC that health centers maximize revenue generated through billing payers wherever possible.
- Reporting. Consolidated health centers benefit substantially from grants administered by government and charitable foundations that require regular reporting on grant activities. To maintain Section 330 grants for example, consolidated health centers are required to submit Uniform Data System (UDS) reports providing aggregate data on encounters, payer mix, revenues and other key operational and administrative measures. For this reason access to practice management software such as Epic with expanded, customizable reporting functionalities was a draw for health centers who decided to participate in OCHIN.
- Local Training, Support and Collaboration. Many of the respondents reported problems with using regional or national practice management vendors that provided no local access to user support and training. OCHIN offered local and on-site training opportunities and better responsiveness through a team of locally-based technical staff.
- Future EMR Prospects. Many consolidated health centers mentioned their interest in OCHIN is related to its planned implementation of an EMR system. Several health centers were especially pleased with the idea that Epic would be the EMR provider because of compatibility with Epic’s practice management software.
Several of the health centers that chose not to become IPM partners were still interested in some form of collaboration, especially with the data warehouse and the EMR. Non-Partner respondents highlighted several reasons for deciding not to participate, including satisfaction with existing systems and costliness of Epic. Some health centers expressed concerns regarding the long-term viability of OCHIN. Many of the non-IPM partners are still involved in the OCHIN collaboration and have some input on the direction of future OCHIN ventures such as the data warehouse or EMR. The few centers we spoke with who were not involved with OCHIN at all were very small or were located in the less densely populated Eastern portion of the state.
3.3 Health Center IS Capacity
One of the central project goals is to learn more about the IS-related expertise and infrastructure at HHS funded consolidated health centers. Oregon is a particularly interesting case because of the role OCHIN has played in providing previously unavailable opportunities for consolidated health centers to access state-of-the-art practice management software.
3.3.1 Ochin is Infrastructure Characteristics: the ASP Model
As described in the introduction, OCHIN currently delivers the Epic practice management software and related services to its IPM partners via the application service provider or “ASP” model. Under this model one central vendor, OCHIN in this case, maintains and hosts all of the hardware and software necessary to support a complex application, such as the Epic Practice management system. Users, such as consolidated health centers, access the software using a web browser on the user’s desktop or another user-friendly “thin client” application2. The application that OCHIN’s IPM partners use to access the Epic software is a Citrix thin client. IPM partners access the application over T1 lines that allow for high-speed network connection. Through the thin client application, users at consolidated health centers can enter data relevant for each encounter to their health center and generate/access reports, bills and schedules based on data previously entered.
The use of thin clients in the ASP model minimizes technical support and maintenance requirements at the health centers themselves. The multiple high-speed connections to and from the host (i.e., the OCHIN data center) create a Wide Area Network (WAN) that gives consolidated health centers ready access to the Epic practice management application and provides for efficient transfer of data from a desktop at the health center to the central location where it is securely stored and maintained. The health center can then access the same data in the form of reports or other materials. We note that the centralization offered by the ASP model provides important benefits in the case of OCHIN. For example, it facilitates for collaboration across consolidated health centers and access to resources that a single health center would not be able to amass on its own. However, there are some downsides to the ASP model particularly in situations where each user site has substantially different needs or inadequate connectivity. We provide more detail on opportunities and challenges posed by the ASP model later in this report.
3.3.2 Systems Infrastructure at OCHIN IPM Partner Health Centers
Although the ASP model reduces requirements for the procurement, management, and maintenance of technology at each health center site, it does require health centers to purchase and maintain (with the help of OCHIN) some key internal technical components. In addition, most IPM partner health centers also maintain a systems infrastructure independent of their use of the Epic Systems practice management application supplied through OCHIN. Systems infrastructure characteristics at IPM partner health centers are described below.
Infrastructure related to the ASP connection to OCHIN: Wide Area Networks (WANs).The ASP model arrangement requires some level of technical capacity on the part of each health center. For example, site workstations have to be configured with the Citrix clients, secure connectivity has to be procured and maintained, and the site must be able to maintain a good working relationship with their Internet service provider (ISP). In many cases, OCHIN has been able to provide technical support to health centers that needed assistance with initial startup desktop and connectivity configurations.
All of the IPM partner health centers maintain a high-speed, secure connection to OCHIN which includes necessary security technology in addition to the high-speed T1 connection lines. In addition to being on the OCHIN WAN, most of the IPM partner consolidated health centers have multiple sites which are networked together using the building blocks of network connectivity: high-speed lines, routers, firewalls, virtual private network (VPN) technology (for secure networking using the public Internet), and some form of remote access. A subset of the sites belong to a collaborative named Community Health Network of Oregon (CHNO), which is also funded via an HHS grant and provides network application services such as Internet connectivity, email services and clinical indicator tracking to its safety net clinic collaborators.
Infrastructure related to internal connectivity: Local Area Networks (LANs) and basic communication services.Within the four walls of a site, the IPM partner health centers typically operate LANs which connect file servers, email servers, and other networked applications detailed in the following section. In order to manage basic center communication and file sharing, each IPM partner operates these LANs along with certain communication systems such as telephone services. If the health center is part of a county health department, such as the Multnomah County consolidated health center, the health center can sometimes “piggyback” on the county infrastructure for these services, thus reducing the center’s responsibility for their construction and maintenance. Although, some health centers report that the requirement to use a county network infrastructure can present a burden. Other health center respondents that were not affiliated with a health department demonstrated a high level of sophistication in this area. For example, the Klamath Open Door Clinic operates its own WAN to connect two sites, participates in the OCHIN WAN, and maintains a LAN and several servers as well as networked applications. We note that prior to practice management implementation, OCHIN did assist some IPM partner health centers with their internal network setup this service was particularly valuable for rural health centers.
3.3.3 Applications & Data Management Systems
In this section we describe applications typically used at IPM partner health centers to collect, manage, and use clinical and practice management data. Discussion includes both software maintained through OCHIN and software developed or procured independently by IPM partner health centers.
Practice Management Application Functionality.All of OCHIN’s IPM partner health centers use the Epic practice management application, which is tailored to meet practice management needs of the health care safety net as recommended by the Bureau of Primary Health Care (BPHC). Especially useful functions included billing and claims management, scheduling, reporting, and the MPI described above. As the Epic practice management system was not designed to address clinical data acquisition or management functions such as immunization tracking, additional technology solutions will be necessary to meet these goals.Many IPM partners have been able to use different applications to track encounter results, send lab orders and receive lab results, and maintain disease registries.
Health Center Custom-Developed Applications.Many Oregon health centers create custom applications to meet their individual needs, either by programming entirely new software, as in the case of Multnomah County, or by creating custom versions of databases using widely available software. Smaller consolidated health centers reported using Microsoft Access to create applications that manage discrete clinical data items such as obstetrics care, screening interventions, or to track inventory of donated pharmaceuticals dispensed to uninsured clients. Also, health centers in Oregon often develop interfaces (described below) to integrate data from Epic and their custom-developed databases to produce reports that combine clinical and practice management data.
Federal and State-based Software Applications.A number of health centers reported that they manage clinical data items as part of the BPHC’s Health Disparities Collaborative, using the Patient Electronic Care System (PECS) and Cardio Vascular & Diabetes Electronic Management System (CVDEMS) software provided by the BPHC. These systems allow each health center to create and maintain registries of patients with specific chronic illnesses; the data is used for monitoring and informing the care of individual patients, supporting continuous quality improvement efforts at the health center level and for reporting purposes to the Collaborative.
Several centers also use state-based tracking programs that are unaffiliated with the Epic practice management suite. Two of the most common were the Immunization and Record Information System (IRIS), which is used to record immunization services provided by health departments across the state; and The Women, Infants and Children Information System Tracker (TWIST), which offers scheduling, paperless charts, and case management modules in order to collect data and coordinate services provided to clients in the Women, Infants and Children (WIC) Program.
Epic interfaces.A significant area of application development is the building of interfaces from Epic to other systems, whether they are in-house systems or third-party systems. For example, health centers may use an interface to transfer billing data into specific formats for electronic claims that are not handled via Epic/McKesson. Other health centers required interfaces to be built for reporting to local health departments or other funding sources. Multnomah County has developed software that interfaces with Epic in part to replace functionality that was lost when the county discontinued use of a mainframe-based application that integrated management and clinical data that they had developed in house. Part of this effort was to develop an interface to Epic that allows for data exchange between Epic, a nursing triage system, and a reporting system.
Other applications. While the applications and data management processes described above are those most relevant to the current project and site visit, respondents also reported use of certain applications to aid in general management. Particularly, a number of the health centers are using Micro Information Processing (MIP) accounting software as their primary financial package. Sites also generally use Microsoft Office applications such as Word or Excel (or equivalent applications) for general productivity purposes.
Overall, we find that health centers in Oregon engaged in significant application development to support various clinical and administrative data needs. Much of the relevant data resides in disparate systems where integration with Epic is not possible without significant effort; and it is clear that the existing applications do not contain all of the clinical data being managed with paper records. Many informants expressed a strong desire to have an EMR integrated with the practice management system which would give them greater support with their clinical data needs and quality improvements needs.
3.3.4 Health center IS decision-making process
In addition to gathering and reviewing information on systems capacity and infrastructure at consolidated health centers, site visit activities focused around understanding organizational decision making processes and tools used by consolidated health centers to guide their systems investment and maintenance activities. We found that consolidated health centers were aware of the need for better planning around systems at their health center, but had not yet adopted specific policies or tools. Most health centers indicated that their thinking in this area is evolving in tandem with increasing opportunities to collaborate with neighboring health centers on application acquisition and infrastructure through OCHIN. Specific findings with respect to budget and application selection issues are described below.
Budget decisions.Overall, our findings suggest that health centers spend less than five percent of their total annual expenditures on IS. This figure is lower than those seen in many comparable primary care health settings that serve the general population. We note, however, that some IPM partners indicated a dramatic (one year) increase in percent spending on systems in 2003 as they had to invest in hardware and connectivity upgrades necessary for the practice management implementation.
Notably, respondents suggested a link between their organizational affiliation and willingness to invest in systems resources. Consolidated health centers that are part of the county infrastructure may benefit because county governments often operate a single information system that works across all administrative and service agencies. Under this scenario, the cost of system maintenance and support is spread across a wider group of organizations is often funded out of central county budgets rather than out of individual agencies. While access to the county infrastructure may be more efficient, in some cases we found evidence that this connection to the county government IS may not be functionally useful, such as when there is insufficient county level investment in systems. Additionally, independent consolidated health centers face much greater incentive than county-based health centers to actively to monitor their bottom line and assure against write-offs at the end of a fiscal year. This often leads to a more frugal approach by these health centers to investments not directly related to revenue generation.
Applications decisions. While most health center Executive Directors we interviewed acknowledge the need for systematic, strategic thinking at their health center around systems issues, including decisions regarding applications investments, most reported no formal processes currently in place to facilitate this. IPM partners report learning a great deal about vendor procurement and evaluation practices following their experience with the practice management procurement and ongoing discussion regarding EMR. Health centers also report that regulatory (e.g., HIPAA) and reporting requirements (e.g., UDS) drive many application implementation activities.
3.4 OCHIN Non-Partner IS Characteristics
In this section we focus on the IS characteristics of non-OCHIN partner health centers that we interviewed. As the needs of non-partners and IPM partners are quite similar, we focus here on key differences between the IS characteristics of non-partners and the IPM partners.
Northwest Human Services (NWHS).NWHS in Salem, Oregon has developed a similar practice management system to the OCHIN/Epic solution in terms of functionality. Like Epic, their system includes scheduling, billing/claims, reporting, and accounts receivable. While there were several reasons that they decided not to implement Epic’s IPM software, one was that they believed that NextGen, their alternative practice management software vendor, could be better tailored and customized for their health center. The center’s executive director along with the IS staff and the board selected NextGen based on an extensive proposal review process including discussions with vendors, consultants, and an attorney for contract negotiations. They experienced a successful rollout to multiple sites, including trainings for IS staff and users. NWHS reports satisfaction with the support, cost and on-going relationship with the NextGen vendor. However, the respondents noted that they still appreciate the benefits of collaborating with the OCHIN members.
Coalition of Community Clinics.Two of our health center respondents, Outside In and the Wallace Medical Concern, are part of the Coalition of Community Health Clinics, a network of 11 small, community-based providers that serve the needs of vulnerable populations in the Portland metropolitan area and its suburbs at low or no charge to clients or outside payers. While some of the coalition members are consolidated health centers, most are smaller “free clinics” funded through local sources. Of key interest to our discussion is the Coalition’s use of a system of Microsoft Access-based databases created by its database administrator. Each clinic has an Access-based database system, tailored to their organization’s needs, that has common data features which enable to health centers to produce annual reports and other necessary functions. The Access-based system at Outside In provides the primary functions of billing, claims processing, and reporting (including the UDS reporting capability). Respondents at this clinic, while seeing the value in the collaborative nature of OCHIN, feel that using Epic is not feasible for the smaller clinics that make up the Coalition.
3.5 Stakeholder Experience with OCHIN
As part of the site visit we sought to gather and assess objective information on the satisfaction of consolidated health centers with applications, services and administrative procedures developed and implemented by OCHIN’s board. We note that many of the findings included in this section are taken from the comments of operational or administrative staff that have direct experience working with OCHIN software applications and processes. We also include the experience of non-provider based stakeholders within the State.
3.5.1 Collaboration with the Larger Oregon Safety Net Community
Stakeholders from various State government agencies, the OPCA and CareOregon consistently expressed enthusiasm for OCHIN’s existence and accomplishments to date. Overall, non-provider stakeholders indicated that OCHIN’s approach to collaboration among safety net providers in the State serves an important, previously unmet function. In particular, respondents from OMAP, the State’s Medicaid Office for health care services, and CareOregon complemented OCHIN and credited the network for improvements in the quality and efficiency of Medicaid billing in the State. Payer respondents also indicated that OCHIN can act as a useful liaison between payers and the providers to clarify issues related to how services were recorded in the system for a particular encounter.
Respondents from the State Office of Primary Care and OMAP agreed that the availability of a data warehouse populated by combined practice management and EMR data and covering primary care safety net providers in the State would be invaluable to public health policy. In Oregon, as in that nation as a whole, understanding the health and health care utilization characteristics of low income clients is a central challenge facing policy makers. In particular, the ability to track safety-net users across primary care encounters would allow for better targeting of outreach and provider resources to increase quality and minimize the costs associated with providing primary and preventive care for this population. Depending on how well OCHIN is able to integrate data from other government-funded service providers the data warehouse may be able to enhance officials’ ability to understand the extent of uninsurance or underinsurance in the State on a local level. Because representatives from these organizations have been involved in OCHIN from the start and continue to be involved in the consortium, they expressed a strong belief that the direction and goals of the network are consistent with the priorities and requirements of safety net health care providers in the State and of the larger public health, public policy and research community. Stakeholder respondents also expressed confidence in the motivation, ability and dedication of OCHIN staff.
3.5.2 Important Systems Functionalities and Satisfaction
Scheduling. The scheduling functionality of Epic was generally thought to be an improvement over the legacy practice management systems. Our respondents were especially pleased at enhanced functions like a module that allows patients to be scheduled to a specific room and care provider at the center. The software was also praised for its sensitivity to concerns specific to consolidated health centers, such as a mechanism that verifies that each patient has a paying agency affiliated with them (if applicable). None of the centers we spoke with had major complaints regarding this aspect of Epic’s functionality.
Electronic Claims Submission. Many centers using the Epic suite reported that their accounts receivable and cash flow are now more predictable due to the standardization of electronic claims submission. Respondents praised special features of the system such as built-in logic that allow identification of potential coding errors. We were told that the Epic software permits better identification of coding inaccuracies before the claims are mailed, increases the likelihood that insurance claims are mailed at all, and improves the centers’ chances of receiving grants because grantors take the centers’ robust infrastructure as a signal that the practice is managed effectively.
Although respondents recognized that the ability to submit claims electronically is a great improvement from the centers’ legacy systems, certain respondents desired a more streamlined billing process. Some reported that having OCHIN as an intermediary (between health centers and claims clearinghouses/payers) tends to slow the process down and that in the past OCHIN has not always submitted claims to payers or McKesson on a standard, predictable schedule.
Issues with custom billing. Because there are so many variations in how centers bill their patients and payers, Epic has had to customize its system to accommodate centers’ individual needs, such as adding different modules for sliding fee schedules. This customization process presented occasional difficulties during its implementation. For example, one consolidated health center reported problems with the sliding scale system they use to accommodate their vulnerable patient population. Because they did not have time to adequately test the application during Epic’s implementation at their center, there were some gaps left in the system relative to their needs and the center experienced financial setbacks as a result. These issues have now reportedly been resolved. Other clinics have experienced some problems with electronic claims submission to Aylers, which is the contractor the Oregon Public Health Department uses to distribute payments specific to the Family Planning Expansion Project (FPEP). In these cases as well, the respondents indicated that they would have liked more time to assess the requirements of the health centers pre-implementation.
It should be noted that billing complications were not attributed solely to the Epic system. One respondent noted that providers do not always fill out the paperwork correctly (for example, certain items are not always coded properly), which results in delayed or insufficient payment. Also, several of the billing issues mentioned by respondents were attributed to the process of implementing a system of Epic’s capacity in health centers. In general, respondents recognized that billing problems were often not the result of poor management on OCHIN’s part or inferior quality of the software: they assumed that the difficulties the health centers had experienced would inevitably arise in the course of launching a specialized IS collaborative.
Out-of-State issues. Some OCHIN centers, especially the out-of-state IPM partner in Seattle, WA, experienced difficulties when billing claims to Medicaid programs. In customizing the system for use by the Pike Market Medical Clinic of Seattle, OCHIN was not always able to identify potential problems or differences in the Medicaid billing office requirements or processes ahead of time in order to avoid delays or complications. For example, in Oregon, procedure codes must be bundled to be submitted to their Medicaid office for payment. Washington’s Medicaid office, however, does not recognize bundling. Early on this issue resulted in some payment denials for the health center. Although this problem has largely been resolved, Pike Market still reports issues with the billing component of the practice management system, which has resulted in declining cash collections and rising accounts receivables. Currently, Epic is customizing its system for use in the California consolidated health center and may be able to avoid some the complications it has faced in its implementation in Washington.
Networking with OCHIN. Initially, establishing and maintaining a secure, efficient connection with OCHIN posed an important challenge, particularly for smaller health centers with little existing systems infrastructure and no in-house technical expertise. One site reported some initial difficulty in setting up Citrix clients during Epic’s implementation in their center, but that issue has apparently been resolved. Likewise, some sites reported initial difficulty configuring connectivity with the OCHIN WAN, but they attributed this difficulty to typical start-up difficulties with a new service initiative and did not report serious ongoing incidents.
Reporting. While many health centers indicated that ease of reporting was an important consideration in their decision to join OCHIN, health centers meet with mixed results when using Epic to report. When probed on the issue, most centers indicated that they found the software complicated to use but were able to produce more accurate and tailored reports than with their previous system. Centers that lacked a dedicated technical staff reported the most problems. For example, one center trained three staff members to use the Clarity reporting system, but due to its complicated structure, these staff are often still not able to generate even simple reports that are used system-wide. If the center needs to produce more complicated reports, it is completely dependent on OCHIN staff and technical support. Additionally, the Pike Market Medical Clinic in Washington reported that the data requirements differ by state or locality and often the information that is compiled for Epic’s canned reports is not the information that is required by the State of Washington or City of Seattle. Other centers had concerns with Epic’s canned reports as well, stating that they do not cover all the necessary data requirements.
Centers that did have IS staff knowledgeable about Epic’s Crystal reporting system experienced fewer setbacks when producing reports and often saved time on presenting the data they need to get funding. For example, the Tillamook County Health Department has a reporting group composed of members who each have experience generating a specific type of report, so that when that type of report is needed the job is assigned smoothly. Several centers employing staff with some technical expertise observed that Epic’s reports offered more flexibility than their legacy reporting system did, so that they could choose to submit higher quality, more accurate and tailored data to the county or state. This level of accuracy often helped centers in receiving valuable wrap-around payments designed to fill the gap between the capitated payments and the actual cost of managed care patients served by the health center.
HIPAA compliance. Although the HIPAA compliance aspect of the Epic system was not generally a driving force behind the IPM partners’ decisions to join OCHIN, it was often noted as an attractive feature. Utilization of the McKesson Clearinghouse relieved the pressure on health centers to develop a solution around HIPAA data exchange procedures with their payers. This relationship ensures that centers are compliant with HIPAA standards relating to transactions and codes sets. Respondents at the Klamath Open Door Clinic also noted that many of the legacy software vendors were unable to provide documentation of HIPAA compliance to the health centers, so the Clinic felt greatly relieved to be working with OCHIN, Epic, and McKesson, who have supplied such documentation.
In-house IS resources. It should be noted that many of the health centers best satisfied with the Epic system and its technical functionality were also centers who had some internal IS staff (or at least staff who were knowledgeable about IS systems). While the OCHIN and Epic support staff were able to help centers take full advantage of the functionality of the software, the process was greatly expedited if there was a member of the health center team who was knowledgeable and capable of manipulating the system and fixing simple problems. While some of the smaller centers (such as Klamath Open Door Clinic) had qualified and expert individuals that facilitated their use of Epic, other smaller centers who did not have staff dedicated to working with the Epic software were less satisfied with both the technical aspects of OCHIN as well as the organizational and process aspects detailed below.
3.5.3 Organizational and Process Experiences with OCHIN
Collaboration. Overall health centers were very pleased at opportunities for collaboration afforded through OCHIN. Many stated that prior to OCHIN there was little exchange related to IS between health centers in different counties. OCHIN provides ample opportunities to network with other health centers and share best practices. For example, OCHIN organizes specialty workgroups where representatives from different health centers and technology experts participate in regular conference calls. These forums allow health centers to joint troubleshoot over specific functionalities and regularly share new knowledge on a range of technical issues. The OCHIN Board of Directors, where health center executives can discuss current issues as well as the future path of OCHIN, provides another opportunity for collaboration.
Not all centers were entirely satisfied with the collaboration process. One of the smaller IPM partners remarked that they were not as influential in the Board’s decision-making process as were the larger consolidated health centers. Another IPM partner located far away from Portland noted the difficulty of collaborating on the Board through phone conferencing.
Training and support. The quality of training and support provided by OCHIN was reportedly mixed. During Epic’s implementation stage, many of the stakeholders appreciated having OCHIN/Epic technical support included in the package, and felt confident that this support would be responsive to their needs. Several health centers noted that OCHIN was doing as much as it could in terms of providing adequate support to its existing IPM partners and that its “track-it” system and helpdesk were effective and very responsive. Others believed that they were being left behind due to OCHIN focus on expanding to other centers.
In the months following the implementation of the Epic suite, more issues with the quality and availability of support and training surfaced. IPM partners that do not staff a systems expert and rely exclusively on OCHIN for support can face substantial delays in service. As a result, smaller size clinics such report relying on temporary staff to fix problems that they had anticipated OCHIN support staff would handle. Even larger centers often complained that the support process was not always as accelerated as they had hoped. Also, certain respondents noted that the differences between centers, such as those that are stand-alone versus affiliated with a local health department, were not always taken into account in the training modules. While several centers were dissatisfied with the delays in the OCHIN support process and the necessity for continuous training, the centers did appreciate their ability to support each other though networking and workgroups involving IPM partner consolidated health centers.
Customizations. As with similar ASP models, OCHIN requires payment from individual health centers for specific customizations they request. Once the customization is paid for by one health center all IPM partners can access its benefits. Under this scenario, smaller health centers have a strong disincentive to request customizations they believe will be requested by larger health centers down the road. Respondents from some health centers reported that they sometimes did without necessary customizations, waiting until Multnomah County decided that it needed the customization and was willing to pay for it. Several respondents agreed that it has been important for the success of OCHIN to have an IPM partner consolidated health center as large as the Multnomah County Health Department, which is able to invest significant resources towards customizing Epic’s software towards the needs of the participating consolidated health centers. Problems arise where customizations for the smaller health centers do not mirror those for Multnomah County. For example, the mix of managed care and private payers at smaller, rural health centers in the Eastern portion of the State is very different from Multnomah County’s leading to different billing format or reporting requirements.
Connectivity. Some respondents raised concerns related to connectivity. Rural health centers occasionally experience minor disruptions in their T1 connection to OCHIN. While many of these problems are now being addressed, it is important to note that connectivity was a barrier to satisfaction for certain health centers during the beginning of the implementation process.
Cost. In the start-up phases of OCHIN, most of the IPM partner respondents realized that the costs of using Epic would be significant but chose to invest the money anyway, and now believe they receive good value for their investment. There were some concerns reported with unexpected fees, such as the software licensing fees that OCHIN required its IPM partners to pay during the implementation process. Others expressed concern about the rise in per-encounter costs for existing IPM partners, which have been implemented in order to bring other centers into the collaborative. For most of the IPM partners, however, fluctuating costs did not seem to lower the health centers’ satisfaction with their participation in OCHIN in the long run. Other centers noted that the per encounter cost of Epic for smaller or rural health centers may become prohibitive over time as these centers expand their encounters. We also note that cost was an important reason for non-participation in OCHIN cited by those health centers that are not part of OCHIN.
3.5.4 Perspectives on Next Steps: Data Warehouse and EMR
All stakeholders report they eagerly anticipate the implementation of both the EMR system and the data warehouse. Health centers are interested in the EMR because the many types of software that they use to track patients and services could be consolidated into a single EMR system, facilitating administrative duties. The centers are also excited by the prospect of coordinating a clinically-based, uniform set of data that they can supply to legislatures and the state and federal Departments of Health and Human Services. They believe this data system will help them improve the quality of care they give to patients on a regional scale, and will help them direct resources to where they will make the most impact.
Other stakeholders from state agencies and the Medicaid managed care plan expressed their interest in and anticipation of the EMR system. Members of the State Primary Care Organization as well as CareOregon indicated that the EMR system and the data warehouse would allow them to more accurately track and collect data about their low-income and uninsured patient populations, which tend to be very mobile. The ability to track these patients would help the agencies set better standards of care for this population, providing improvements not only in quality of patient care but also in cost efficiency.
3.6 Challenges Moving Forward
The following paragraphs highlight challenges identified for OCHIN and health centers from the discussion above. In addition to operational challenges we describe those challenges related to their perception by the larger safety net and public health policy community in Oregon.
Supplementing and enhancing existing application functionality. While most the Oregon health centers indicated that the Epic application provides them with the important functionalities required for compliance with federal rules and efficient administrative management, many report that important enhancements to existing functionalities are required. In particular, health centers with no dedicated IS staff reported an interest in seeing a more user-friendly reporting and billing systems, that would allow non-technical health center staff to more independently create specialized reports and billing formats as necessary. In addition, almost all health centers indicated being ready and willing to move forward with EMR and clinical decision support applications, stating that clinicians for the most part were eager to begin using these types of systems.
Capacity of data storage and WAN infrastructure. OCHIN has made substantial investments in server and network technology to secure data storage and transfer capacity that exceeds current requirements. However, expansions to additional IPM partners and addition of applications may, at any time, lead to steep increases in capacity requirements. This is a particular challenge because, to date, OCHIN has successfully acquired adequate technology and communications services at discounted pricing because of active planning on their part and their ability to “sell” vendors on the importance of their mission. There is no guarantee that these types of arrangements will be available moving forward.
Collaboration under the ASP model. As mentioned above, the ASP model offers both substantial benefits and some potential problems for collaborations like OCHIN. The two primary pitfalls are processes surrounding customization and release strategies. ASPs work best when all of their customers’ needs are identical; this keeps custom application development to a minimum. When customers require customizations, as the health centers have, one of two approaches can be taken. The ASP can either build customizations on a per-customer basis, or the ASP can require that all customers agree to the customizations (in essence, treating all customers’ needs as identical).
OCHIN has elected to work with the latter approach requiring “free” customizations to be agreed upon by all IPM partners. In the event that one IPM partner requires specialized customizations that are not relevant to a broader group of stakeholders, they must fund the customization on their own. This is particularly difficult for smaller health centers that have needs distinct from larger centers, limited internal systems resources to implement reporting customizations on their own, and fewer resources to draw on to fund special customizations.
Cost of OCHIN to health centers. Most health centers that decided not to become IPM partners in OCHIN cited cost as the largest barrier to joining. Both the start-up cost and the per-encounter cost required by OCHIN were especially burdensome for smaller health centers. The start-up costs include Epic’s fees, licensing costs and any necessary hardware upgrades, which can cost centers anywhere from $50,000 to $100,000 depending on how many licenses are needed and how many upgrades need to be performed. The centers also have to pay a $1.04 per patient encounter fee. This per encounter cost can increase during periods when OCHIN is expanding to another health center.
Some, such as La Clinica del Valle, a consolidated health center in Medford, OR, stated that their concerns about joining OCHIN were partially related to the per-encounter costs, which created a disincentive for their goals of expansion. While this is a typical pricing scheme for ASP models such as OCHIN, it is one that health centers are unfamiliar with and which can become a barrier to participation. Even larger-size health centers that had more resources, such as Northwest Primary Care in Salem, OR, had reservations about participating in OCHIN because they believed there was no way to ensure that costs would stay below a certain threshold. In other words, being a part of the collaborative forced them to lose total control over their cost structure and they would be unable to control overall costs individually.
Future expansion and solvency.OCHIN’s structure necessitates that the program expand substantially to maintain financial viability and achieve independence over time. Ideally for OCHIN, the total patient population served by their IPM partners (existing and new) would at least double its current numbers. This expansion will require working with health centers both outside of the state and potentially outside of the entire Northwest region. However, this expansion is not guaranteed: OCHIN has accrued a substantial and early market share, but Oregon’s second largest consolidated health center has declined to participate in the network. Furthermore, as the experience from Seattle demonstrates, out of State providers pose special challenges to OCHIN because of differences in Medicaid billing requirements by State as well as problems with establishing a healthy collaborative atmosphere when IPM partners are too geographically distant for regular, in person meetings. Some health centers felt that the current model for achieving financial solvency through expansion is not realistic and leaves the network financially exposed in the medium to long term.
Service delivery (e.g., training).Although feedback about OCHIN from participating health centers was generally positive, several raised concerns about the organization’s record of providing program support and training to center staff. This was particularly an issue among smaller health centers, which tend to have little internal systems expertise and depend heavily on OCHIN’s IS staff. Reports indicated that key services, such as training, are of mixed quality and in need of improvement. At the same time, OCHIN will need to expand their business in the future to provide EMR to the IPM partners and collaborators, putting stress on their in-house systems personnel and financial resources.
Support from non-provider safety net stakeholders. Although by and large complimentary, stakeholders from government, payer organizations and associations were acutely aware of challenges facing OCHIN related to expansion to smaller health centers and maintaining a balance between a robust system and a costly system. They acknowledge a tension within OCHIN in terms of how best to simultaneously achieve a stable financial model, robustly meet the disparate operational needs of safety net providers in the State and support public health policy. One respondent expressed the sentiment that OCHIN’s longer term success depends on its ability to hold and consolidate gains as they are made in addition to looking ahead towards their next project.
4.0 Conclusions
In this section we briefly summarize key conclusions following from this report with an emphasis on areas relevant for federal funding and policy making. Additional conclusions related to the replicability of the OCHIN model, challenges facing Oregon consolidated health centers and OCHIN moving forward will be discussed at more length after subsequent site visits and other project activities have shed more light on these issues.
Overall IS infrastructure among consolidated health centers in Oregon. The consolidated health centers visited as part of this case study all demonstrated substantial use of IS and systems for key functions. All those included had ample access to desktop hardware and basic software used in most professional settings. There were substantial differences in terms of connectivity, access to networks and data maintenance capabilities across consolidated health centers. Beyond the obvious factors such as total patient served, number of sites and annual revenue, we found that a few key factors can affect the type of infrastructure at a health center and their ability to make use of what they have.
As described above, affiliation with a county health department allows some health centers to more efficiently access some level of technical infrastructure and networking, though the level of function provided by counties, particularly in rural areas, may fall short of the consolidated health centers needs. Furthermore, health centers that staff or have some access to even one dedicated IS employee report far fewer problems with use of networked applications such as Epic compared to those who rely on outside vendors or ASP-providers (e.g., OCHIN) to trouble-shoot and handle connectivity or applications related problems from a distance. In particular, we found that technology solutions for safety-net providers in Oregon often relied on the idea of collaboration and leveraging technical resources and expertise across providers. Aside from OCHIN, we see this with CHNO and the efforts of the Coalition of Community Clinics described above.
Vision and acceptance of OCHIN from relevant stakeholders. One of the striking features of the materials provided by OCHIN (mostly applications for HHS grants) and generally validated through discussions with health centers and other safety net stakeholders in the State was the network’s strong vision around which all stakeholders could take part and organize. All respondents agreed with OCHIN’s approach of addressing systems needs of health centers while simultaneously addressing information needs of public health stakeholders. This agreement around vision has led to good, active collaboration from both the health center and public health community. Although some respondents questioned specific aspects of the network’s decision making processes and pricing policies, all agreed on the importance of a comprehensive, collaborative vision for improving using health IS to improve the health and health care of vulnerable populations.
Satisfaction with existing products and services. Although, overall IPM partners indicated satisfaction with their organization’s participation in OCHIN, particularly from the perspective of enhanced opportunities for collaboration and the prospect of a centrally administered EMR, the preceding section’s discussion clearly demonstrates some lack of satisfaction with specific aspects of the practice management software and services provided by OCHIN. One common theme was that operations staff at health centers felt that OCHIN needs to do a better job of understanding existing workflows and requirements at IPM partner health centers and, particularly, how the needs of smaller, stand-alone or rural health centers differ from the needs of larger, county-based health centers such as Multnomah County. These issues may be indicative of the early stages of a complex implementation. One positive sign, according to OCHIN respondents, was the lack of connectivity problems during the start-up of their newest IPM partner health center in recent weeks.
Integration with Medicaid or public health systems. Although OCHIN has spent considerable effort reaching out to State Medicaid and public health officials and complies with accepted transfer standards (e.g., HL7), as of yet, there has not been a successful initiative to link the 400,000 MPI with Medicaid or state public health systems. This is in part due to the fact that they currently collect only administrative data, with very limited and incomplete information on procedures and diagnoses. In addition, there is some evidence that Medicaid systems in Oregon, and other States, are outdated and significant upgrading will be necessary before data can be integrated in a useful way with outside databases. Still, this is an issue that is of importance both to OCHIN and State officials with whom we spoke, particularly as OCHIN moves toward rolling out a data warehouse and EMR application.
Sustainability. The issue of OCHIN’s long to medium term sustainability remains open. To date, they have been largely financed through HHS grant programs designed to provide start-up costs for community-based consortia to improve quality and efficiency of health care delivery, with the idea that over time the activities of the consortia will be self-sustaining. Although OCHIN has shown strong motivation in leveraging start-up financing from a number of federal grant programs (often by having different IPM partners take the lead role on different grants), achieving longer term financial viability through expansion of partnerships exclusively among safety-net primary health care providers is clearly a more difficult challenge.
Importantly, OCHIN has and continues to make important strategic decisions that will influence their ability to meet this challenge. For example, by selecting a higher end vendor they have effectively priced out some of the smaller and rural safety net providers in the State. OCHIN acknowledges this and has considered development of an “Epic-lite” package that could be offered to these health centers at lower cost. Additionally, because OCHIN has made the decision not to accept partnerships from private group practices, they will need to continue to effectively build partnerships with out of State health centers. Aside from the challenges of inter-state collaboration described earlier in this report is the issue that OCHIN will not be able to count on the automatic buy-in and support from non-provider safety net stakeholders in other States unless they actively pursue this end.
Replicability. OCHIN’s success in dealing with challenges associated with building a broad-based coalition of disparate health centers and stakeholders around a comprehensive safety net health information system is encouraging with respect to replicability of this model in other settings. It is important to note, however, that Oregon was somewhat ideally positioned for a network of this type because of the state’s long history of partnership across the safety net and between the safety net and state/local health departments. The best example of this was the establishment of CareOregon in the 1990s to help consolidated health centers continue to serve vulnerable populations that were moved to Medicaid managed care. In addition, the time was ripe for a solution such as Epic in Oregon given that there were a number of consolidated health centers concurrently looking to replace an existing system or establish a robust practice management system.
A fair amount of resource investment from the local safety net community itself (e.g., Multnomah County, CareOregon and OPCA) was necessary before the network could secure start-up funding from the federal government and OCHIN benefited by finding an early organizational home within CareOregon. Finally, all respondents complimented OCHIN’s early leadership and attribute much of the network’s success to the efforts of individuals to see the project through. In particular, respondents felt that OCHIN is aided by its staff’s ability to find “next best” or good solutions when the optimal route is ruled out for one reason or another. As the network moves forward, it will be important to assess the extent to which early service and functionality problems reported by out-of-state or rural partners are resolved in the near future, as this will inform the federal government’s understand of the feasibility of implementing this type of network across a demographically diverse group of providers.
Appendix A. Examples of site visit discussion guide and preparation materials
Tillamook County Health Department
9th Street and Laurel Avenue, Tillamook, OR
Phone: (503) 842-3900
Respondents
John Robinson, Executive Director
-Mr Robinson also sits on the OCHIN Advisory Board.
Ron Wallace, Assistant Administrator
Jeff Underwood, IS Coordinator
Interviewers: Mike Tilkin and Alana Ketchel
Logistics
We will be meeting with John Robinson and Ron Wallace, an assistant administrator at Tillamook County Health Department as well as Jeff Underwood, the IS contact for the center. We will meet with them at their building on the corner of 9th St. and Laurel in Tillamook, OR. We were instructed to leave approximately 1 hour and a half for travel. John Robinson warned us that he might be called away for another meeting he might have to attend but we will at least be meeting with Ron Wallace and Jeff Underwood. We previously spoke with Darlene Dannis, finance manager, via phone.
Further directions: Take Highway 6 into Tillamook, come to the 101 and hang a left at the 2nd stop light. We will be coming into town one-way and will watch on the left for 9th St. where we will hang another left. After we pass the 101 coming the other way, their building will be on the next block at the corner of 9th St. and Laurel.
What we know
- Tillamook County Health Department is both a county health department and community health center located in Tillamook County, OR. They are an IPM partner in the OCHIN System.
- Prior to OCHIN, the Tillamook County Health Department was having difficulties maintaining a practice management system because software companies were not able to stay in business. They started out with MDX Software and moved onto the Physicians Computing Network (PCN) which was then bought out by Medical Manager. They were having concerns about continued support for the software given how often it changed hands.
- Also previous to OCHIN, they had trouble b/c all the health centers were providing different information in different formats to the State and Feds. Now, as one unified network, they all can share the same language with the State.
- Besides the EPIC practice management system, the clinic is currently utilizing separate care management/tracking systems. One relates to the Diabetes Collaborative and the other relates to Evidence-Based Data (the PECS Software).
- They interviewees identified several critical functions they perform as a CHC for which the OCHIN system provides support. The first was that OCHIN simplifies the process of producing the UDS report. Also, being able to go through the OCHIN clearinghouse for direct billing allows them to bill in a way that is less expensive with a faster turnaround. Finally, they are looking forward to the prospect of an EMR system which, without the financial backing of OCHIN, they could not develop alone.
- Ron Wallace noted that as a county health department, the IS infrastructure at Tillamook (e.g. e-mail systems, etc.) must fall under county standards which can be handicapping. To enroll in the EPIC system, they had to pay for some changes in the EPIC program such as extra software training and systems upgrades b/c their system wasn’t up to par with the requirements of EPIC
- The health department offers the perspective of an IPM partner that is affiliated with a local health department. We have contacted Jeff Underwood to obtain basic information on their non-OCHIN related network and system resources. Please refer to the summary of OCHIN and their network which the Tillamook County Health Department and CHC has access to as an IPM partner.
Basic Information
Tillamook County Health Department
Clinic Address: 801 Pacific Ave., PO Box 489, Tillamook, OR 97141
Phone: 503-842-3900
Web Site: www.co.tillamook.or.us/gov/health
Additional Sites: Rockaway; Dental Clinic, Tillamook; Cloverdale
Clinic Type: Federally supported Community Health Center
Services Provided:
- Comprehensive primary medical and dental care services for acute and chronic disease management, public health and preventive services
- Women's Health Care
- Dental Care
- WIC
- Home Nurse Visits
- Teen Clinic
- School Nurses
- Public Health Services e.g., immunizations, environmental health, vital statistics, family planning clinics, TB screening and treatment, HIV/AIDS case management, etc.
- Enabling Services including: Outreach, transportation vouchers, OHP eligibility assistance, interpretation/translation, special education program
Patient Profile
| Patient Profile | |
|---|---|
| Patients 2001: | 6,086 |
| Number of visits: | 20,437 |
| Ethnicity | |
| Hispanic | 15% |
| White | 83% |
| Amer Indian/Alaska Native | 1% |
| Asian | 1% |
| Payment | |
| Medicaid | 20% |
| Medicare | 9% |
| Uninsured/private pay | 45% |
| Commercial Insurance | 26% |
Staffing
Total Staff: 35
Clinical Staff
2 Physicians
2 Nurse Practitioners
1 Dentist
1 Dental Hygienist
What we want to learn
- We will query them extensively on their center’s IS resources, management and longer term strategy and the role of OCHIN.
- Also, we will query on the their experience with using the EPIC suite of practice management software and the gains they expect through using this system and participating in other planned OCHIN initiatives such as data warehousing and electronic medical records.
- Specifically, we want to find out more about the experience of being a health department and CHC in terms of their ability to become a partner in OCHIN’s practice management system and other ventures given the county standards they must adhere to. What exactly did it take for them to sign onto be an IPM partner? What did they gain/sacrifice?
- We would also like to find out more about the non-EPIC patient care tracking software they are using such as the Diabetes Collaborative. Find out more about the PECS (sp?) software they referenced above.
- Note: Mr. Wallace wanted to make sure that if we had input on their infrastructure and what it might be lacking in comparison to other health centers/ health departments, we would let them know.
PROTOCOL
Note: skip questions answered above such as those in italics
Center/Systems Background Information
- What is your organization’s mission and how do IS play a role?
- What is your center’s systems related budget?
- As a percentage of your overall budget?
- How much of this are costs associated with OCHIN participation?
- Has OCHIN increased or decreased your investment in systems?
- How are financial decisions related to IS made at your center?
- How does your clinic finance OCHIN related expenses?
- Please describe your decision to participate as a IPM partner
- How is your center different from other primary health care providers or CHCs, and how what IS needs follow from those differences?
Applications Dimension
- What are the major benefits of the OCHIN software applications to your center, how would you prioritize their importance to overall center objectives?
[PLEASE QUERY SPECIFICALLY ON EACH OF THESE…]
- scheduling and resource management
- claims submission, billing — including under capitated arrangements
- tracking eligibility and insurance status and verification
- administrative reporting to HRSA and other federal agencies
- tracking payments and accounts receivable
- other administrative and financial functions
- Eligibility tracking for Medicaid/SCHIP
- Tracking of specific outcomes or exposures (e.g., birth weight, exposure to environmental hazards)
- Availability and utilization of specific “free” resources (e.g., pharmaceuticals)
- Other features?
Which of these practice management functionalities are currently not available, but needed? Which ones do you have access to but don’t use?
- Are there other systems applications that you would like to see initiated? How would you prioritize these?
- electronic medical record or e-health record
- clinical decision support applications
- others?
- Are you currently, part of the Health Disease Collaborative or any other disease management or quality improvement program based on electronic tracking of patient care? Please describe the applications used for those programs (e.g., PECS or CV-DEMS for the Collaborative) and how they might interface with an EMR.
- What application development technologies and methodologies does your organization use? What systems have you developed vs. bought off-the-shelf? How was this decision made?
- What is the future plan for the application architecture (individual applications as well as integrated systems)? How are future plans made and then revised over time? How much of this is driven by OCHIN decisions?
- How do you use/plan on using data resources available through your participation such as the Master Patient Index or data warehouse reports?
Technology Domain
- To what extent has OCHIN standardized hardware used at your center?
- What are your strategic plans for updating it, assuming more applications will operate in a more broadly networked environment?
- Describe any integration challenges/successes across the consortium with respect to networking and infrastructure.
Process Domain
- In general how are technology decisions made at your center? How is the process consistent with center goals?
- How are requirements collected, technologies or vendors selected, and “build vs. buy” determined?
- Specifically what do you rely on vendors or consultants to provide in this area? What do you rely on OCHIN to provide?
- IS strategy, technology selection
- implementation, systems support
- How would you characterize your relationship w. vendors and OCHIN?
- What has been your experience working within the OCHIN network to access/use Epic practice management software? (e.g., ease of connectivity, benefits from enhanced functionality, support, initial start-up etc.)
- Describe process for supporting user community (help desk, on call system administrators, ad hoc)? How much of this function does OCHIN or EPIC provide?
- How would you rate your satisfaction to date with OCHIN/EPIC, why?
- Describe how you learn about new technologies and technology best practices. How do you share this knowledge with your colleagues within the CHC and the broader consortium?
- What kind of training occurs to help keep your IS staff current?
- Describe any formal processes your organization has for insuring that policy and clinical procedures are working in concert with and are appropriately balanced with healthcare IS.
- Please describe the organizational relationship between the key actors in your organization (e.g., clinicians, administrators, patients, technology professionals, decision makers and policy makers) with regards to healthcare IS as related to the business process of clinical care.
- Please describe to what extent healthcare IS in your organization is able to be measured against key desirable outcomes (e.g., reduced costs, improved efficiency, high quality of care, improved patient safety).
Location Domain
- What technologies (e.g. web) are used to mitigate the challenges of distance? Do you feel that technology is adequately able to mitigate these challenges? Can you please describe why or why not?
Organization Domain
- Describe your Center’s organizational structure as a whole.
- Describe your overall health information vision and strategy:
- How is health information used in the organization?
- How does this information and the IS used to manage it contribute to accomplishing the organization’s overall mission?
- How are technology decision made at your center? For example, please describe how you arrived at your decision to participate in OCHIN as an IPM partner.
- What are the organization’s goals for improving the use/management of health information? How has this changed after OCHIN?
- Please describe the nature of the IS unit of your organization:
- How is it funded and staffed?
- What is its level of expertise?
- What is its capability to provide end-user support alongside “back office” support?
- How is it perceived by the users?
- What is the current use of or need for outside technical assistance?
- What is the organization’s IS staffing capacity to meet its technology goals? Do you outsource? If yes, what tasks?
- How much do you rely on OCHIN for IS expertise? Has OCHIN increased/decreased the IS staffing in your center?
Environment Domain
- How do you, with OCHIN and EPIC manage to comply with regulatory requirements (especially HIPAA privacy and transaction standards)?
- How do you understand the regulations and the impact they have on your organization?
- How do you stay informed of changes?
- How does the consortium deal with HIPAA specifically?
- Who is responsible for monitoring/auditing HIPAA compliance?
- What challenges does HIPAA present vis-à-vis the consortium?
- Do you feel that there are adequate resources available for understanding and complying with HIPAA? If not, who do you feel would be the best provider of this type of guidance?
- Please describe other regulatory elements that drive technological decisions.
- Please describe any local, regional, or national cultural enablers or hindrances to healthcare IS and to community-based healthcare in general.
- Please describe any local, regional, or national political enablers or hindrances to healthcare IS and to community-based healthcare in general.
- Please describe any local or regional enablers or hindrances to healthcare information
- State and federal government payment policies
- Private sector payment policies
- Resources
- Interactions with other providers
Items for Follow-up, If we don’t already have them.
Center/Systems Background Information
- What is your center’s federal designation … CHC? M/RHC? SBHC? HCH?
- How many sites does your center have?
- How many patients do you see on an annual basis, what are the characteristics of your patients in terms of case mix and payor?
- Please describe overall how you access health information system resources …
- What do software/resources do you get through your relationship with OCHIN and access to the OCHIN WAN?
- What do you do in house?
Applications Dimension
- What Non-OCHIN software do you currently use? For example, what commercial general productivity software (e.g. desktop applications such as MS Word) does your center use on a regular basis?
Data Domain
- What are your major domains of data (e.g., clinical, financial)? What data is created in the course of your In what ways to you share/exchange data with OCHIN? Other sources? By what means?
- In what ways do you use interoperability standards to exchange information (e.g. HL7 and other messaging standards)?
- In what ways do you ensure confidentiality/privacy with regard to your data? (See also “External Factors and Environment” Domain.)
- Please describe how data is stored operationally (e.g. database platform(s)).
- Please describe how data is archived and stored so that an electronic record is preserved. Are the policies and procedures in place with regards to data archives to guard against technology obsolescence and the preservation of knowledge over time
Technology Domain
- What type of hardware (e.g., servers, PCs, laptops, PDAs) is typically used at your center?
- What type of operating systems?
- Please describe your physical plant (e.g. cabling)
- Describe your non-OCHIN network (LAN, WAN) architecture.
- What kind of connectivity do you provide to the Internet (in terms of bandwidth and access points)?
- Do you have a strategy related to wireless communications?
- Do you provide any other connectivity options (e.g., proprietary networks, local modem pool)?
- Please describe your technical security architecture and disaster recovery capabilities:
- Processes, Policies, Procedures
- Technology (e.g. firewalls, Internet VPNs, storage/archival systems for electronic records)
OCHIN Integrated Practice Management Centers
Note: skip questions answered above
Information System Characteristics
- What is your organization’s mission and how do IS play a role?
- What is your center’s systems related budget?
- As a percentage of your overall budget?
- How much of this are costs associated with OCHIN participation?
- Has OCHIN increased or decreased your investment in systems?
- How are financial decisions related to IS made at your center?
- How does your clinic finance OCHIN related expenses?
- Please describe your decision to participate as a IPM partner
- How is your center different from other primary health care providers or CHCs, and how what IS needs follow from those differences?
- Please describe overall how you access health information system resources …
- What do software/resources do you get through your relationship with OCHIN and access to the OCHIN WAN?
- What do you do in house?
Applications Dimension
- What are the major benefits of the OCHIN software applications to your center, how would you prioritize their importance to overall center objectives?
[PLEASE QUERY SPECIFICALLY ON EACH OF THESE…]
- scheduling and resource management
- claims submission, billing — including under capitated arrangements
- tracking eligibility and insurance status and verification
- administrative reporting to HRSA and other federal agencies
- tracking payments and accounts receivable
- other administrative and financial functions
- Eligibility tracking for Medicaid/SCHIP
- Tracking of specific outcomes or exposures (e.g., birth weight, exposure to environmental hazards)
- Availability and utilization of specific “free” resources (e.g., pharmaceuticals)
- Other features?
- Are there other systems applications that you would like to see initiated? How would you prioritize these?
- electronic medical record or e-health record
- clinical decision support applications
- others?
- What Non-OCHIN software do you currently use? For example, what commercial general productivity software (e.g. desktop applications such as MS Word) does your center use on a regular basis?
- What application development technologies and methodologies does your organization use? What systems have you developed vs. bought off-the-shelf? How was this decision made?
- What is the future plan for the application architecture (individual applications as well as integrated systems)? How are future plans made and then revised over time? How much of this is driven by OCHIN decisions?
- How do you use/plan on using data resources available through your participation such as the Master Patient Index or data warehouse reports?
Technology Domain
- What type of hardware (e.g., servers, PCs, laptops, PDAs) is typically used at your center?
- What type of operating systems?
- Please describe your physical plant (e.g. cabling)
- Describe your non-OCHIN network (LAN, WAN) architecture.
- To what extent has OCHIN standardized hardware used at your center?
- What has been your experience working within the OCHIN network to access/use Epic practice management software? (e.g., ease of connectivity, benefits from enhance functionality, support, initial start-up etc.)
- What are your strategic plans for updating it, assuming more applications will operate in a more broadly networked environment?
- Describe any integration challenges/successes across the consortium with respect to networking and infrastructure.
- What kind of connectivity do you provide to the Internet (in terms of bandwidth and access points)?
- Do you have a strategy related to wireless communications?
- Do you provide any other connectivity options (e.g., proprietary networks, local modem pool)?
- Please describe your technical security architecture and disaster recovery capabilities:
- Processes, Policies, Procedures
- Technology (e.g. firewalls, Internet VPNs, storage/archival systems for electronic records)
Process Domain
- In general how are technology decisions made at your center? How is the process consistent with center goals?
- How are requirements collected, technologies or vendors selected, and “build vs. buy” determined?
- Specifically what do you rely on vendors or consultants to provide in this area? What do you rely on OCHIN to provide?
- IS strategy, technology selection
- implementation, systems support
- How would you characterize your relationship w. vendors and OCHIN?
- Describe process for supporting user community ( help desk, on call system administrators, ad hoc)? How much of this function does OCHIN provide?
- Describe how you learn about new technologies and technology best practices. How do you share this knowledge with your colleagues within the CHC and the broader consortium?
- What kind of training occurs to help keep your IS staff current?
- Describe any formal processes your organization has for insuring that policy and clinical procedures are working in concert with and are appropriately balanced with healthcare IS.
- Please describe the organizational relationship between the key actors in your organization (e.g., clinicians, administrators, patients, technology professionals, decision makers and policy makers) with regards to healthcare IS as related to the business process of clinical care.
- Please describe to what extent healthcare IS in your organization is able to be measured against key desirable outcomes (e.g., reduced costs, improved efficiency, high quality of care, improved patient safety).
Data Domain
- What are your major domains of data (e.g., clinical, financial)? What data is created in the course of your In what ways to you share/exchange data with OCHIN? Other sources? By what means?
- In what ways do you use interoperability standards to exchange information (e.g. HL7 and other messaging standards)?
- In what ways do you ensure confidentiality/privacy with regard to your data? (See also “External Factors and Environment” Domain.)
- Please describe how data is stored operationally (e.g. database platform(s)).
- Please describe how data is archived and stored so that an electronic record is preserved. Are the policies and procedures in place with regards to data archives to guard against technology obsolescence and the preservation of knowledge over time?
Location Domain
- What technologies (e.g. web) are used to mitigate the challenges of distance? Do you feel that technology is adequately able to mitigate these challenges? Can you please describe why or why not?
Organization Domain
- Describe your Center’s organizational structure as a whole.
- Describe your overall health information vision and strategy.
- How is health information used in the organization?
- How does this information and the IS used to manage it contribute to accomplishing the organization’s overall mission?
- How are technology decision made at your center? For example, please describe how you arrived at your decision to participate in OCHIN as an IPM partner.
- What are the organization’s goals for improving the use/management of health information? How has this changed after OCHIN?
- Please describe the nature of the IS unit of your organization:
- How is it funded and staffed?
- What is its level of expertise?
- What is its capability to provide end-user support alongside “back office” support?
- How is it perceived by the users?
- What is the current use of or need for outside technical assistance?
- What is the organization’s IS staffing capacity to meet its technology goals? Do you outsource? If yes, what tasks?
- How much do you rely on OCHIN for IS expertise? Has OCHIN increased/decreased the IS staffing in your center?
Environment Domain
- How do you manage to comply with regulatory requirements such as HIPAA?
- How do you understand the regulations and the impact they have on your organization?
- How do you stay informed of changes?
- How does the consortium deal with HIPAA specifically?
- Who is responsible for monitoring/auditing HIPAA compliance?
- What challenges does HIPAA present vis-à-vis the consortium?
- Do you feel that there are adequate resources available for understanding and complying with HIPAA? If not, who do you feel would be the best provider of this type of guidance?
- Please describe other regulatory elements that drive technological decisions.
- Please describe any local, regional, or national cultural enablers or hindrances to healthcare IS and to community-based healthcare in general.
Appendix B. Health Center Technology Domain and Data Domain Data Set Table
| Domain Component | Site Information |
|---|---|
|
1. Network Operating Software; Resource Management |
|
|
2. Network Resources Inventory (eg, file, print servers, connected PCs) |
|
|
3. LAN / WAN Architecture (including any logical and/or physical diagrams that are available) |
|
|
4. Network Security and Disaster Recovery - Processes, Policies, Procedures, Technology (eg, firewalls, VPN) |
|
|
5. Internet Connectivity (eg, ISP) |
|
|
6. Other Connectivity (eg, local modem pool) |
|
|
7. Storage (eg, file servers, storage area network, optical jukebox) |
|
|
8. Telecommunications (hardware, provider(s)) |
|
|
9. Future Plans / Initiatives |
| Domain Component | Site Information |
|---|---|
|
1. Major domains of data managed (eg, financial / administrative, clinical) |
|
|
2. Means of ensuring data confidentiality / privacy. |
|
|
3. Use of interoperability standards for data communications between clinical applications; between clinic partners (eg, outside labs) |
|
|
4. Method for storing data operationally (eg, database platform(s)) |
|
|
5. Method for storing data for archival purposes (eg, off-site tape storage) |
|
|
6. Data reporting / decision support capabilities |
|
|
7. Future Plans / Initiatives |
Philadelphia
1. Introduction
NORC at the University of Chicago (NORC) is pleased to present this report detailing findings from our recent site visit to Philadelphia, PA for “Community Health Center Information Systems Assessment: Issues and Opportunities.” NORC conducted this site visit under contract with the Office of the Assistant Secretary for Planning and Evaluation (ASPE) at the U.S. Department of Health and Human Services (HHS). The Health Resources and Services Administration (HRSA) and the Bureau of Primary Healthcare (BPHC) work in conjunction with ASPE to guide activities under this project.
The current site visit focuses on an ongoing initiative in the County of Philadelphia to support enhancements in information systems capacity at BPHC-funded consolidated health centers. Findings presented here describe information systems capacity as well as systems related challenges facing consolidated health centers in Philadelphia. In particular, we focus on health center experiences working with a data warehouse initiative managed by the Health Federation of Philadelphia (HFP), a federally-funded consortium of safety net ambulatory health care providers. The report is organized as follows.
- Background and Methods. We begin with background on the ambulatory care safety net in the County of Philadelphia and details on the organizations we spoke with as part of the site visit.
- Key Findings. In this section we summarize findings from in person interviews and other site visits activities conducted in Philadelphia, including HFP activities focusing on information systems. We also describe features of the information systems infrastructure at ambulatory health care providers interviewed in Philadelphia.
- Conclusions. Here we present conclusions and lessons learned from the site visit, with particular emphasis on issues related to long term sustainability and replicability of models used to promote health center use of information systems in Philadelphia.
2. Background and Methods
The County of Philadelphia (which shares boundaries with the City of Philadelphia) has a population of over 1.5 million more than half of which is made up of ethnic minority groups. 23 percent of the city’s population is below poverty, and approximately 94,000 Philadelphia residents lacked health insurance in 2000. Statewide, the level of uninsurance was 11 percent, a total of 1.38 million people.3 A total of 468,843 Philadelphians were enrolled in Medicaid in 2003.4 Uninsured and low income populations in Philadelphia are served by two types of ambulatory care providers: those operated by the Philadelphia Department of Public Health’s Ambulatory Health Services (AHS) office and stand alone consolidated health centers supported primarily by BPHC. Although, the health department-run clinics are federally qualified health center (FQHC) look-alike clinics, they are supported primarily through local government dollars.
City-wide, AHS operates eight health care centers annually serving 100,000 patients who produce 330,000 visits. The majority of these patients are uninsured. The seven stand-alone health centers (many with multiple sites) in Philadelphia are all HFP members. Patient demographics and payor mix differ by health center and site. Generally, Medicaid beneficiaries make up more than half of the patient population at HFP consolidated health centers and another 24-40 percent of these individuals are uninsured. HFP and AHS collaborate on many fronts including the data warehouse. Stakeholders describe HFP as a de facto Primary Care Association for Philadelphia’s safety net health centers.
Methods. The site visit to Philadelphia, which took place on February 27, 2004, involved initial telephone and email contacts followed with in-person interviews with 24 respondents representing 7 institutions involved in the primary health care safety net in the city. Table 1 below lists all health centers and other stakeholders interviewed as part of the site visit and follow-up telephone calls.
Respondent Organization |
Description |
|---|---|
|
Consolidated HealthCenter Respondents |
|
| Greater Philadelphia Health Action | GPHA is the largest member of the HFP, with 7 sites across Philadelphia. It is a CHC and serves 48,000 patients through over 110,000 billable encounters per year. |
| Delaware Valley Community Health | DVCH is the second largest member CHC, with 3 sites serving 26,978 patients over 112,611 encounters in 2003. The center is currently implementing a pilot electronic medical record (EMR) program. |
| Covenant House Health Services | Covenant House saw 7,100 patients in 2003 and is planning to expand. The center is the only CHC in the northwest section of Philadelphia. |
| Spectrum Health Services | Spectrum Health operates 2 sites and serves around 7,000 patients annually. It is a CHC and was one of the HFP’s founding members. |
| Quality Community Care | Quality Community Care is a CHC operating four sites around Philadelphia, 2 of which are school based. They serve 12,000 patients annually. |
|
Other Stakeholders |
|
| The Health Federation of Philadelphia | The HFP is a member organization for safety net health centers in the Philadelphia area. It currently has seven member consolidated health centers and works closely with the city’s Department of Health. |
| Philadelphia Department of Public Health, Office of Ambulatory Health Services (AHS) | AHS operates 8 safety net Health Centers located in Philadelphia, which combined serve 100,000 people annually. AHS is planning on contributing its patient data to the Health Federation’s data warehouse. |
Telephone and in-person interviews with respondents were conducted using open-ended discussion guides, providing for a consistent structure to each exchange while allowing sufficient flexibility to capture all relevant information from respondents. In addition, a table shell was emailed to information systems staff at respondent health centers prior to the site visit to facilitate collection of standard information relating to infrastructure and technical capacity. For each scheduled site visit interview, the NORC team prepared materials that outlined our preliminary knowledge of the respondent and highlighted outstanding questions to address during the interview. Examples of discussion guides, other data gathering tools and preparation materials used in the site visit are included as Appendices A and B.
3. Key Findings
Health center collaborative information systems activities in Philadelphia follow a different model than those observed in other sites in that key stakeholders made an active decision not to implement a community-wide practice management application. While respondents at HFP and consolidated health centers acknowledged the importance of practice management as the core application necessary for effective health center administration, they decided against the feasibility and desirability of implementing a community-wide solution. We describe the approach that lead to this decision and the model ultimately adopted by the HFP in the paragraphs that follow.
3.1 The Health Federation of Philadelphia
As described above, this site visit focuses on health center experience working with the Health Federation of Philadelphia (HFP), a private, non-profit membership organization which provides shared services to a consortium of consolidated health centers in the Philadelphia area. All consolidated health centers in the Greater Philadelphia Region are eligible to be members of HFP. As mentioned above, HFP currently has seven member community health centers as well as a collaborative relationship with the City of Philadelphia’s AHS clinics.
Background on HFP. HFP was founded in 1983 as a non-profit corporation and federation of Philadelphia region consolidated health centers. The federation’s leadership consists of a dedicated Chief Executive Officer (CEO) and a contracted Chief Information Officer (CIO) who report to a Board of Directors which consists primarily of the executive directors of member health centers. Overall, HFP provides the following types of services to member health centers
- Representation and advocacy. HFP represents health centers at city-wide coalitions and acts as an advocate for health centers with federal, state and local governments.
- Collaboration. The HFP provides a forum where health centers can come together to address common administrative and operational issues.
- Program coordination. HFP assists with centralized program development and implementation. For example, HFP often contributes services necessary for applying for grants such as those offered by BPHC and managing activities funded under those grants.
In recent years, the HFP has focused attention around supporting health center needs in the area of health information systems. HFP is operating a data warehouse and is facilitating a pilot EMR program being initiated in a HFP member health center. To support its information systems programs HFP receives funding from the Administration for Children, Youth, and Families; the Department of Housing and Urban Development; the Philadelphia Departments of Public Health and Human Services; AmeriCorps; and various foundations. The data warehouse is paid for partially by a BPHC SIMIS grant acquired in 1999 as well as from an initial contribution by the member health centers. We end our discussion of HFP with a description of an ongoing electronic medical record (EMR) pilot project being run through the federation.
Data warehouse history and vision. The HFP’s data warehouse project grew out of an initial focus around helping health centers make the most out of available practice management applications. Initially, the HFP facilitated a community-wide evaluation of practice management vendors to identify a “best in class” product and encourage use of that product on a community level. Having conducted the evaluation, however, they found that a common implementation was not feasible given the varied experiences and needs of member health centers. Instead, HFP and member health centers decided on developing a community-level solution to enhance access to practice management data on a health center and consortium level.
While practice management products typically include some reporting function including the ability to create standard reports required for UDS, some health centers describe problems with data reliability and significant burden associated with developing custom reports. For the most part, these applications allow users to program reports through a technical process after reviewing a complex set of database specifications. In most cases, practice management system databases are designed with to promote administrative efficiency rather than full-featured reporting. For example data may be stored in a “flat” rather than a relational format ideal for producing reports. Additionally, most operational databases are geared towards transactions, e.g., updating data, and retrieving discrete data elements, such as the time of an appointment, to be displayed on an application screen. To answer reporting questions, such as the number of appointments scheduled during one year broken down months, would require additional queries and/or views to group and summarize data. Health centers often lack the expertise and resources to take full advantage of this less than ideal reporting capacity and are left wanting for more flexible, user-friendly tools for accessing and analyzing their practice management data.
The HFP’s data warehouse addresses this concern by integrating practice management data across health centers into a community-wide data format designed to facilitate flexible reporting and data dissemination on both a community and health center level. The new data warehouse would store and maintain data using a sophisticated structure and, importantly, provide access to these data via a user-friendly interface that allowed non-programmers to access manipulate and analyze data in real time from their own desktop. In theory, the data warehouse would add value in a number of ways. First, it would allow more convenient and reliable access to data on the health center level. Second, it would allow an assessment of safety net ambulatory health center experience on a community-level and identify differences in practice patterns across centers. Finally, the data warehouse represents and important public health tool for enhancing understanding of insurance status, health status and health care experience of indigent populations living in Philadelphia.
Vendor Selection and System Installation Process. HFP contracted with Ingenix, a subsidiary of United Health Care, to support the data warehouse project, in part because Ingenix had an existing warehouse architecture that could serve as a shell for the new project. Working with Ingenix, HFP identified data requirements and built interfaces to extract these data from various practice management systems. These requirements expand on data elements present in UDS and HCFA 1500 reports.
Following identification of data requirements, HFP faced the challenge of building interfaces to facilitate transfer of data from individual health center systems. This was a particular challenge because of the proprietary nature of these databases. Two practice management vendors agreed to provide Ingenix with the details that allowed Ingenix to program data extracts to pull data appropriate data from the vendor systems. In other cases, Ingenix provided the data warehouse architecture to the practice management vendors who then developed programs to produce extracts from their own databases at significant additional cost to the project.
HFP supplied all the hardware and supportive network infrastructure for the data warehouse using SIMIS funds and set up internet communication linkages. The extraction process took two years to finalize, after which health centers sent their extracted data to the centralized database as a trial run. Currently, the system holds this data from 2002 and HFP is in the process of running accuracy and quality assurance checks to eliminate any errors caused during data transfer or coding.
It is important to note that once data from 2002 are validated, HFP will face the additional cost of creating new extracts for health centers that changed practice management vendors between 2002 and 2003. In some cases health centers had to turnover practice management systems unexpectedly because of vendor decisions to upgrade and discontinue support of older products. One important challenge facing HFP and member health centers, especially given the turnover in practice management systems, is streamlining data extraction and validation. The goal over time will be to facilitate regular transfer of data from health centers to the data warehouse to minimize time it takes for events to be reflected in data warehouse output.
Ongoing data warehouse support activities. HFP support for the individual centers’ data warehousing efforts is provided by the two IT staff at the consortium, the part-time CIO and the Network Administrator. The Network Administrator runs a basic or “level one” helpdesk, which the centers can call if they experience problems accessing their data warehouse information or generating reports. Ingenix, which provides the data warehouse software through a yearly license, also operates a helpdesk for more complicated user support. Additionally, the HFP has made some efforts to facilitate collaborative support groups involving information technology staff from various health centers participating in the data warehouse project.
EMR pilot. In 2002 the HFP arranged to conduct a pilot EMR project across several health centers using CliniFlow’s EMR product, which was compatible with Medical Manager and HealthPro, two practice management vendors used by area consolidated health centers. Although the original grant provided funding for the four data warehouse participants to do the pilot, further investigation revealed that available funds would support only one health center’s participation in the pilot program. Additionally, agreements between CliniFlow and the two key practice management vendors broke down during early stages in the project. This left HFP and the pilot health center to come up with an alternate approach, still in development, involving the use of a WebMD EMR product called “Intergy”. We describe health center progress related to EMR in greater detail below.
3.2 Health Center Information Systems Capacity and Experience
In addition to consulting with HFP staff, we conducted interviews with major consolidated health center respondents in Philadelphia. Each of these health centers were HFP members though they differed in their levels of participation and attitude toward the data warehouse project. Health centers interviewed also differed in terms of in-house investment in information systems expertise and their level of sophistication in their use of practice management applications.
Health center governance. Each of the BPHC funded consolidated health centers we interviewed relied on a community Board of Directors for overall governance. An Executive Director (ED) typically managed the center, assisted by senior staff including a chief medical officer and administrative or financial lead. We also interviewed one of the HSA’s, FQHC “look alike” clinics. These clinics are governed by the City of Philadelphia rather than a Board of Directors.
Information systems staffing. Most of the health centers we interviewed reported having some knowledgeable and dedicated information systems staff. For one of the largest center (three sites and more than 100,000 encounters), this staff consisted of about three full time equivalents (FTE), a manager or coordinator level lead supported by an applications development specialist with some programming expertise and a technical support specialist focused on responding to support requests from individual users.
Lead information systems staff at the larger health centers indicated having some experience, approximately 5-8 years, in information systems development and support roles in health care provider settings (e.g., hospitals) prior to working for the CHC, but none had the title of Chief Information Officer (CIO) or experience with directing large scale health information systems as would be typical of health systems leads in large private health care provider settings.
In smaller health center with fewer resources, information systems activities were handled either by a single, less experienced employee, often with some formal training in information systems, or by two or three employees with other administrative responsibilities. In one health center, the information systems lead doubled as the human resources coordinator. Importantly, most of health center respondents indicated that dedicated information systems staff reported to department heads responsible for finance or administration rather than directly reporting to the ED.
Information systems decision making. Smaller centers with fewer resources tended to make these decisions on an ad hoc level, relying substantially on guidance provided by Marc Wilcox a part-time CIO who provides services under contract with the HFP. Many of the larger health centers did have sufficient expertise in house to make strategic decisions regarding information systems and use standard operating procedures for day to day systems activities. Although, even these health centers report that needs assessment and planning activities occur on a relatively informal basis.
Hardware and connectivity. Health centers interviewed in Philadelphia generally reported operating in a networked computing environment. Smaller, individual site health centers use local area networks (LAN) to allow for shared use of network applications. Larger, multi-site health centers generally operated wide area networks (WAN), maintained T1 line connections across disparate sites and adequate server capacity to support administrative applications for billing and accounting as well as basic computing needs such as printing and email. One health center in an infrastructure-poor area of North Philadelphia has not yet purchased a T1 line and does not have access to broadband. As such this health center relies on a dial-up Internet Service Provider (ISP) for connectivity to the Internet. Health centers generally reported having adequate access to computing hardware.
Core applications. Health centers interviewed indicated using a wide array of software applications, including applications related to practice management, tracking of care for populations with specific chronic conditions, electronic billing, accounting and interfacing with laboratory providers. For practice management, health centers reported using products designed specifically for CHC use including those developed by HealthPro and Medical Manager. In addition, some health centers reported supporting programs that facilitated communication with clinical laboratory services vendors or specialized applications to support provision of mental health or dental services.
- Larger centers with in-house applications development expertise report having developed a number of data tracking tools using commercial database software such as MS Access to track care delivered and cost associated with treating specific populations. In many cases, these specialized databases draw a baseline level of data from the practice management system and then supplement these data with clinical data. Several centers we interviewed participate in the BPHC-sponsored Health Disparities Collaborative program, these centers report using the either CV-DEMS or PECS software developed as a part of this program to track care and outcomes for clients with ambulatory care sensitive conditions. Finally, all health centers reported using the standard MS Office Suite for general productivity software.
- Three of the health centers interviewed are actively taking part in the community-wide data warehouse initiative coordinated by HFP and have gone through the process of transferring data from their practice management system to the community wide data warehouse using the extracts described above. Health clinics governed by the City of Philadelphia Health Department, have the benefit of the City’s relationship with Siemens, Inc which handles issues related to their network and access to practice management data. These health centers use a practice management product called Signature developed by Shared Medical Systems a system typically used in private sector group practices.
Electronic Medical Records. While we did not speak with any providers in Philadelphia who are currently using electronic medical records, all health centers indicated a strong interest in pursuing EMR implementation in the coming years. Several health centers have said that it is an internal priority to investigate EMR options and come up with a development plan. The HFP is supporting a federally funded EMR pilot in one of the consolidated health centers. This health center is currently closely investigating a new product being marketed by WebMD. This product, called Intergy, is a combined EMR/practice management system with a menu-driven interface designed to streamline clinical evaluation and chart writing. The interface walks clinicians through a series of closed-ended questions regarding an individual patient evaluation and, based on answers, produces a standard preliminary write-up of the clinical evaluation.
3.3 Stakeholder Experiences with Current Resources
In this section we summarize the Philadelphia health centers’ experiences with their practice management systems, other features of their information systems, and the HFP consortium. In particular, we focus on the centers’ perspectives on the data warehouse project and their general organizational interactions with HFP.
Practice Management Functionalities and Satisfaction. As described above, there is no consistent practice management software system utilized across all Philadelphia health centers. When deciding to implement a data warehouse, the network made a conscious decision to forego standardizing the practice management systems and instead to develop extracts for each system that would then deposit each center’s data into the warehouse. Two of the centers use Medical Manager, two use HealthPro, and one uses GE’s Centricity system.
Access to data and reporting. As described above, HFP has sought to enhance health centers’ access to their own vital administrative and clinical data. Four of the nine health providers currently extract their data to the data warehouse, and a fifth (the local health department, which operates its own health centers) hopes to contribute its data in the coming few years. The HFP data warehouse is not completely functional at this stage. Due to the ongoing data validation and need to program new extracts following practice management system turnover. As such, participating health centers still predominantly rely on their respective practice management systems to gain access to their data, but at least five health centers reported looking forward to the enhanced access to data they feel will follow from the data warehouse initiative.
The two health centers we spoke with do not plan to involve themselves in the data warehouse — one of which uses Medical Manager; the other has the Centricity system. These health centers report relatively few problems accessing and manipulating their data. One respondent indicated that she had been successfully manipulating her practice management data for seventeen years and didn’t understand why a common data warehouse was necessary. Respondents at another center expressed similar views, indicating that they easily extracted the data they needed from Medical Manager. As would be expected, health centers that have not “bought in” to the usefulness of the data warehouse tend to be the larger health centers and those with the expertise necessary to support development of custom reports.
The centers we interviewed who participate in the data warehouse reported experiencing significant problems accessing and manipulating their data through their practice management systems. Center respondents indicated that their practice management system reports rarely produced reliable figures and that they were not user-friendly or flexible. For example, one health center executive using HealthPro reported that while she could access necessary encounter data for the center as a whole, she did not have access to this data not broken down by the health centers’ sites. In the bullets below we summarize health center comments on ease of reporting with specific practice management applications.
- HealthPro. Health centers described HealthPro’s reporting functionality as adequate, but indicated that center staff had spent considerable time and resources to validating data and revising reports. The two health centers interviewed that use HealthPro independently reported that they had done extensive manual comparison and “hand-counting” of reports to make sure that the data was correct One center indicated that half of the “canned” reports provided by HealthPro needed to be revised in order to be useful. Both centers look forward to full implementation of the HFP data warehouse.
- Medical Manager. The two centers using Medical Manager generated reports in different ways. The smaller of the centers could not afford to purchase the system’s report-generating module and paid the vendor to produce all of their reports. This center eagerly anticipates having new reporting functions through the HFP data warehouse. The larger center used the report module and indicated that it was relatively satisfactory, although the staff did not completely trust the report data and checked their accuracy before sending UDS reports to BPHC.
- GE Centricity. The health center using GE’s Centricity practice management system indicated that it worked adequately for their purposes and they had experienced few problems. This health center is not participating in the data warehouse project.
Billing. All of the centers reported that their respective billing and claims submission modules generally worked well. A few indicated that their billing systems were a significant improvement over those of their old practice management software products, and had increased accuracy of claims and reporting requirements fulfillment while reducing paperwork. Electronic claims submission is not ubiquitous; even the centers that submit some claims electronically noted that not all payors are set up to receive the claims and remit payments electronically.
Scheduling. Three out of the five health centers reported no problems with their systems’ scheduling modules. Of the other two centers, one center’s respondents indicated that staff had experienced considerable initial difficulties with the Medical Manager scheduling module, but that many of the problems were due to a lack of initial training on how to use the system. This center, which is quite large and had three dedicated IT staff, had also custom-built a second scheduling model to deal with walk-in appointments. The second health center, which is using an older, currently unsupported version of HealthPro, indicated that the system lacks desired functions such as being able to see appointments by specific provider and that appointments often got erased while staff manipulated data to produce desired information.
Organizational Experiences with the Health Federation. The participating health centers reported that the HFP’s IT staff was responsive and quick to resolve routine problems. There is also evidence that HFP works collaboratively with health centers with special needs. For example the HFP has agreed to assist the Philadelphia’s AHS clinics set up an interface between their practice management system managed by Siemens and the warehouse. Connectivity between the centers and the data warehouse has not been an issue for the network. The health centers dial directly in to the system via high-speed T-1 lines, or in one case a 56K dial-up, and reported no problems with downtime.
Challenges associated with data warehouse implementation. Although participating health centers reported a generally favorable view of services received through the HFP, it is clear from our interviews that the network encountered various problems during the first phase of the warehouse development. First it took two years before agreements were worked out for producing data extracts and the various vendors had completed programming. After the programs were written, important differences in key data definitions were identified, creating some concern regarding data quality and significantly complicating the task of correcting and validating data.
For example, depending on their internal policy, some sites recorded a client visit as a single encounter, whereas other centers defined encounters in terms of billable procedures that were provided during the visit. Some respondents said that, at the onset, they were not aware of the level of health center staff time that would be dedicated to running extracts and validating warehouse data. One larger participating health center had enough IT staff to dedicate to the program, but other centers employed staff who had no background in data validation and were then required to spend many hours doing hands-on tasks that they thought, at the outset of the project, would be automated.
Finally, while the prospect of sharing proprietary data did not discourage the four providers we spoke with from participating in the warehouse; it has proved a barrier to two of the network’s other centers, which so far have refused to contribute their information. These centers indicated that they were reluctant to allow others to view their data in a safety net provider environment which both described as competitive. Respondents from one of these centers noted that they already shared their data at the Federal level and saw no need to do so at the regional level. These respondents felt that the HFP should be focusing its IT efforts in other areas, such as developing an Internet site allowing the health centers to view announcements, share documents, and post to electronic message boards. They also felt that grant money related to IT infrastructure was better allocated on the health center, rather than consortium, level.
4. Conclusions
Acknowledging health center arguments that “one size does not fit all” in the case of practice management as well as the understandable reluctance on the part of health centers with an established practice management system to change to a different community-wide application, the HFP decided to focus community-level information systems efforts around developing a data warehouse which pulls data from individual health center systems into a common format to facilitate assessment of health care experience on a community or health center level. While some health centers eagerly await the enhanced data access and reported functionalities promised by the data warehouse project, some remain skeptical of the merits of the project.
Multiple hurdles to interfacing practice management systems. The experience in Philadelphia highlights the substantial challenges associated with developing and using data tools that pull data from disparate systems into a single database. First, the design of the database structure and the knowledge embedded in the structure may be considered the intellectual property of, not the health center. As such, obtaining specifications necessary to implement interfaces across practice management systems requires extensive negotiation with each vendor. In some cases, vendors simply refuse to provide access to these specifications regardless of the proposed application. In addition, health centers often use their practice management systems idiosyncratically. Under these circumstances, developing standard data requirements and developing extracts to pull consistent data across systems requires significant investment to investigate and reconcile each health centers data management practices.
Changing vendor landscape. Fluidity in the products and services available to health centers from information systems vendors also contributes to the challenge of implementing community-wide data projects. Rapid consolidation among practice management vendors has led to discontinuation of support for many practice management products causing unpredictable changes in the software a health center will use from one year to the next. Programs designed to extract data from one health center practice management system will not be useful in subsequent years if the health center switches systems or if the existing product is modified in such a way in which the database design changes.
Data access and reporting issues are key. Despite the delays in fully implementing the data warehouse, the four participating health centers we spoke with indicated that they were very excited at the warehouse’s potential. Although none of these centers have used the system to generate reports to date, they have been able to identify errors and missing elements in their records and in some cases correct the problems. The drill-down capabilities of the software are extensive and will allow the centers to locate bad data as well as to perform detailed manipulations. In addition, respondents anticipated the ability to share information and best practices across individual sites as well as health centers. This enthusiasm reflects a common complaint regarding poor access to data and reporting flexibility using commonly available practice management products.
Health center organizational orientation and approach differs. Interestingly, larger consolidated health centers interviewed in Philadelphia took different positions with respect to their willingness to share their practice management data on a community level. Some health centers participating in the data warehouse indicated going through a process where at first they were worried about the implications of sharing data that could be used to compare health centers on quality of care issues, but slowly bought into the idea because of the promise of having access to data that they could readily use to support robust continuous quality improvement efforts. These health centers generally warmed up to the idea that the data warehouse would provide them with a valuable opportunity to learn from others. Other health centers candidly expressed that there was some degree of competition within the city among consolidated health center providers and that they didn’t understand the benefit to their health center in participating in the data warehouse.
Defining the role for public health. In some ways the ultimate success of the data warehouse project in Philadelphia may hinge on the successful integration from the single largest ambulatory care safety net provider in the area, the Department of Health’s AHS clinics. Integration of the AHS clinics’ would not only substantially expand the data available for analysis within the data warehouse, it might signal the potential public health applications of the data warehouse. Experience has shown that appeals to collaborate based on the project providing necessary services to individual health centers does not always work in situations where health centers feel comfortable with their in house capacity and expertise. Instead, endorsement from the public health department and their clinics may establish a feeling that participation in the data warehouse is the “right thing to do” from a public health perspective regardless of gains for individual centers. To do this, HFP would have to continue working with AHS, not only to integrate data from the AHS clinics, but also establish an analytic program where data warehouse output could meaningfully inform local and regional public health policy on an ongoing basis.
Boston
1. Introduction
NORC at the University of Chicago (NORC) is pleased to present this report detailing findings from our recent site visit to Boston, MA for “Community Health Center Information Systems Assessment: Issues and Opportunities.” NORC conducted this site visit under contract with the Office of the Assistant Secretary for Planning and Evaluation (ASPE) at the U.S. Department of Health and Human Services (HHS). The Health Resources and Services Administration (HRSA) and the Bureau of Primary Healthcare (BPHC) work in conjunction with ASPE to guide activities under this project.
The current site visit focuses on an ongoing initiative in Boston to support enhancements in information systems capacity at BPHC-funded consolidated health centers. Findings presented here describe the information systems capacity of consolidated health centers and safety net hospitals in Boston focusing on health centers affiliated with the Boston Medical Center, the area’s largest safety net provider. The report is organized as follows:
- Site Background and Methods. We begin by describing the safety net health care landscape in Boston, focusing on health centers and health information systems (IS) initiatives affiliated with Boston Medical Center (BMC) and its health center network, Boston HealthNet (BHN). These initiatives include the work of the Community Health Automated Record Technology (CHART) project, Boston CareNet and a related HCAP program operated out of BHN.
- Key Findings. In this section we summarize findings from in person interviews and other site visits in Boston. This section includes discussion of each BHN IS initiative and health centers’ experiences working with these initiatives.
- Conclusions. Here we present conclusions and lessons learned from the site visit, with particular emphasis on issues related to long term sustainability and replicability of models used to promote and enhance health center use of health information systems.
2. Site Background and Methods
The Boston area is a major center for health care and medicine, with an unusually high concentration of medical schools and teaching hospitals to serve the area’s 4 million residents. As with the rest of the health care system in Boston, the area’s health care safety net includes a large, varied landscape of providers with shifting organizational affiliations. The area includes 25 consolidated health centers and numerous free clinics as well as major public hospitals that provide care to the underserved population. Given the overall size of the safety net in Boston, we focus our site visit on a major subset of consolidated health centers in Boston — those affiliated with the BMC and the BHN network.
Boston Medical Center and the Health Care Safety Net. Boston’s health care safety net environment changed significantly in 1994 as a result of a major hospital merger between Boston City Hospital and the Boston University Medical Center. Prior to the merger, each of these hospitals provided care to underserved populations, with Boston City Hospital serving as the largest inpatient safety net provider in the City. Boston City Hospital had long fostered relationships with many of the consolidated health centers in Boston. The merger created a new institution, the Boston Medical Center (BMC). Currently BMC is the largest single safety net institution in Boston, providing approximately $300 million of free care in 2003.
BMC also serves as the base institution for the Boston HealthNet network (BHN), a network of 15 consolidated health centers in the Boston area that had strong relationships with Boston City Hospital prior to the merger. BHN acts as a convening body, providing coordination, logistical and organizational support for initiatives to help health centers make the most of their affiliation with BMC and access government and private grant funds. Several of these initiatives including Boston CareNet, the BHN HCAP project and CHART focus on designing, implementing and supporting community level health information systems (IS) including a community-wide electronic medical record (EMR) and data warehouse. In this report we describe the work of these initiatives and the related experience of Section 330 supported health centers.
Characteristics of the BHN health centers. As described above, BHN includes 15 of the Boston area’s approximately 25 consolidated health centers. Of these 15, seven are community health centers (CHCs), one is a Health Care for the Homeless Center and the rest are Federally Qualified Health Center (FQHC) “look alike” centers. The other health centers in the Boston area do not share a strong referral link with BMC and do not participate in BHN.5 Referrals from the 15 BHN health centers provide nearly one quarter of BMC’s annual inpatient volume of 27,500 admissions. The network’s partners provide primary and specialty care, outreach, prevention, and dental services to their patients. The health centers enjoy a strong relationship with BMC and have set up a range of programs that facilitate patient transitions between primary care and hospital stays, provide the partner health centers with greater access to capital and medical personnel resources and enhance the ability of members to work with managed care. The affiliation with BHN also affords these centers benefits related to the IS initiatives introduced in the following section.
Respondent Organization |
Description |
|---|---|
|
Consolidated HealthCenter Respondents |
|
| Dorchester House Multi-Service Center | Dorchester House is a CHC founding member of BHN and is closely affiliated with Codman Square Health Center. The CHC had 89,458 encounters in 2003. Dorchester house has implemented the Logician EMR system. |
| Harvard Street Community Health Center | Harvard Street is a CHC and BHN partner. In 2003 the health center saw 30,000 encounters. The center recently implemented the Logician EMR system. |
| Whittier Street Health Center | Located in Roxbury, WSHC saw 32,614 encounters in 2003. It is a BHN partner and has fully implemented the Logician EMR system. |
| East Boston Neighborhood Health Center | EBNHC is the largest CHC in Massachusetts, seeing over 250,000 encounters annually. It is a BHN partner but implemented the EpiCare EMR system years prior to the HealthNet EMR initiative. |
|
Other Stakeholders |
|
| Boston Medical Center (BMC) | BMC is the largest safety net provider in New England. It is a private, nonprofit hospital formed by a merger of Boston University Medical Center and Boston City Hospital in 1994. It had more than 854,000 encounters and provided more than $300 million of free care in 2003. |
| Boston HealthNet | BHN is a loose provider network comprised of BMC, Boston University School of Medicine, and 15 consolidated health centers around Boston. The network coordinates care for the underserved population of Boston and leads several IS initiatives. We spoke with BHN leadership, as well as BHN affiliated staff who run key IS programs such as CHART and the HCAP project. |
| BMC CareNet Plan | CareNet is a BHN collaboration that allows uninsured city residents to maintain a relationship with a primary care provider throughout changes in insurance status. CareNet also houses and maintains the community data warehouse server and individual CHC EMR servers. |
Site Visit Methods. The site visit to Boston, which took place on May 12 and 13, 2004, involved initial telephone and email contacts followed with in-person interviews with eighteen respondents representing seven institutions involved in the city’s primary health care safety net. Table 1 above lists all health centers and other stakeholders interviewed as part of the site visit and follow-up telephone calls. Telephone and in-person interviews with respondents were conducted using open-ended discussion guides, providing a consistent structure to each exchange while allowing sufficient flexibility to capture all relevant information from respondents. In addition, a table shell was emailed to information systems staff at respondent health centers prior to the site visit to facilitate collection of standard information relating to infrastructure and technical capacity. For each scheduled site visit interview, the NORC team prepared materials that outlined our preliminary knowledge of the respondent and highlighted outstanding questions to address during the interview. Examples of the discussion guides and other materials can be found in previous site visit reports.
3. Site Visit Findings
We begin discussion of findings by presenting the structure of major IS initiatives coordinated through BHN and the role of each initiative as described by their leadership. We then go on to describe findings from detailed interviews with four health centers that actively participate in these initiatives. Given that Boston is one of two sites investigated as part of this project that have implemented a community-level EMR, we allocate a substantial portion of our discussion to health center experience implementing and using EMR.
3.1 Boston HealthNet Organizational Structure and Roles
As described above, this site visit focuses on health center experience working with the BHN network of BMC affiliated health centers. BHN serves primarily as a coordinating body. Each of the BHN health centers operate as stand alone institutions, supported through Section 330 provisions and private donations. Consistent with Section 330 rules, each health center is governed by a board of directors that oversees the activities of an executive director and senior management team. Following the merger that created BMC, BHN was created to bring together the 15 health centers that enjoyed strong institutional relationships with the old Boston City Hospital. In this convening and coordinating role, BHN manages projects funded through corporate donations and federal grants to assist BMC and its health center partners. In the decade since its formation as a subsidiary of BMC, BHN has successfully initiated and maintained a series of programs related to improving access to care, health care quality and efficiency among its 15 health centers and BMC. In the bullets below, we describe BHN initiatives that relate to IS development and support.
- Community Health Automated Record Technology (CHART). The CHART program grew out of a major, one-time corporate donation to BMC and BHN to support implementation of Logician electronic medical records (EMR) software in 8 of the 15 BHN consolidated health centers. Following the announcement of this donation, CHART was created to acquire and implement the EMR applications in health centers across BHN and then foster use of the EMR to support community-level improvements in health care.
- Boston Healthy Community Access Project (HCAP). Concurrent with the EMR donation, BMC and BHN applied for a BPHC HCAP grant. The grant outlined opportunities to support, enhance and leverage the burgeoning IS resources at BHN consolidated health centers, notably EMR, to improve quality and efficiency of care provided to uninsured patients. In practice, activities of the HCAP project have focused on helping BHN health centers manage diabetes care, reduce inappropriate ED utilization, improve mammography screening rates and generally maximize benefits from having EMR. HCAP funds have also supported the development of a data warehouse which includes claims-based data on 80,000 uninsured, or recently uninsured, individuals to support the mission of the CareNet initiative described below.
- BMC CareNet Plan. CareNet is a program developed out of BHN that tracks care received by uninsured individuals in BHN health centers. CareNet works to assure that each patient maintains a primary care “medical home” and that BHN centers are appropriately reimbursed for care to the uninsured from the state’s uncompensated care pool. Following the award of the Boston HCAP grant, described above, CareNet has served as the organizational home for BHN-wide data warehouse project.
- BMC HealthNet Plan. BMCHP is an independent Masscheusettes Medicaid managed care organization operated through BMC and BHN. BMCHP facilitates care for over 100,000 Medicaid recipients throughout Massachusetts. Because of ongoing shifts in eligibility among families, there is substantial overlap between patients whose care is tracked by CareNet and patients enrolled in the BMCHP health plan.
We should note that although each of these bullets represent distinct initiatives or organizations from the funding and operational perspective, BHN and BMC work to assure appropriate coordination and collaboration across programs. For example, while CHART had primary responsibility for implementation of the EMR, funding from the HCAP program played in instrumental role in incorporating EMR use in everyday practice of the health centers and ensuring a smooth transition from paper to electronic records. Also, although the CareNet plan pre-dates the HCAP initiative as the entity responsible for monitoring care to uninsured populations, this activity has been considerably aided by the data warehouse established and maintained using HCAP funding.
In addition to serving as the organizational home for the CHART project and fostering the development of each of these initiatives and affiliated organizations, BHN maintains an overall Board of Directors comprised of leadership from BMC, affiliated health centers, CareNet, Boston HCAP and the BMCHP. This board effectively brings leadership together to maintain a robust, coordinated program of initiatives and organizations to enhance safety net care provided by BMC and its affiliated health centers.
3.2 Development of Boston HealthNet Information Systems Initiatives
Since its inception, BHN has leveraged funds from federal grants and private donations directed to BMC to support improvements in IS infrastructure and applications available to affiliated health centers. In 1997, BHN received a three-year $250,000 ISDI grant that supported specific improvements to the consolidated health center IS infrastructure. Subsequently, in 2001, BHN (through BMC) received a $6 million grant from a private corporation to implement a common EMR system in eight partnering CHCs. That same year, BHN received their first HCAP grant geared towards the construction of a broader and more comprehensive infrastructure for gathering and analyzing data related to uninsured patients. The two major products of these initiatives, a data warehouse and EMR system, are described below.
Data warehouse and HCAP initiatives. The data warehouse project, spearheaded by staff from CareNet and the Boston HCAP project, compiles data on care delivered to the uninsured across health centers and the BMC (inpatient). The data warehouse allows BMC and health center leadership to identify utilization and cost trends and enhance services across the continuum of care. Specifically, the project seeks to reduce inappropriate use of Emergency Departments and to foster appropriate management of ambulatory care sensitive conditions such as diabetes. The project focused exclusively on the uninsured because of the dearth of knowledge on this population relative to BHN’s Medicaid population many of whom were covered by BMCHP which monitors utilization and costs for their population separately.
The preliminary form of this warehouse was a Master Patient Index (MPI) that simply compiled and updated demographic information on uninsured patients seeking care at BHN institutions. A later version, implemented in 2003, provides CHCs with timely information on the CareNet populations’ inpatient encounters such as the top diagnoses, patients whose costs have exceeded $100,000, and the number of diabetic patients that are inappropriately admitted. In recent months, CareNet and HCAP have begun disseminating center-specific reports highlighting key cost and utilization measures relevant to uninsured patients treated at each health center. The warehouse currently contains nearly four years of data on the target population — the nearly 80,000 uninsured individuals who are enrolled in the CareNet Plan.
While the majority of data included in the warehouse comes from interfaces developed to extract data from health center practice management systems and BMC’s administrative systems (for inpatient care), HCAP and CareNet staff have begun to include EMR data specific to diabetes patients in the data warehouse to support the HCAP project’s goal of improving management of diabetes care. In order to assess diabetes care and patient outcomes, HCAP staff worked with health center and BMC physicians and nursing staff to identify 10 EMR-based measures of diabetic care adequacy and four measures of disease control. These include checking HgbA1C levels and blood pressure at least once in 7 months, checking BMI, LDL, monofilament, microalbumin, and eyes at least once in 15 months, among other such “best practices”. HCAP staff are currently developing periodic reporting mechanisms for these performance measures at the individual clinician (PCP and nurse) and CHC level, as well as at the HealthNet community level (by geographic, socioeconomic and ethnic groupings). HealthNet has already collected baseline data on hemoglobin levels and found health improvements over the course of one year, such as that 69% of patients with A1C levels >8.5 had a reduction of at least 1 point. More complex reports are still pending adequate data and EMR template revision.
The CHART project and EMR implementation. In 2001, a strategic planning committee from the BHN Board proposed moving to electronic records in health centers as an important next step in developing the IS capacity of the network. After garnering approval from participants at their annual retreat, BHN leadership brought this idea to BMC’s development office who then met with a private corporation that agreed to fund the initiative. This corporation gifted $5.9 million to BMC to implement EMR systems in eight partnering CHCs. This grant supported the purchase of PCs, licenses for General Electric’s (GE) Logician EMR, implementation assistance from GE and staffing. The donor channeled the funds through BMC, and consequently BHN, to coordinate and facilitate implementation in health centers and provide oversight. The initiative was titled the Community Health Automated Record Technology “CHART” Project. Implementation across 8 CHCs began in 2001 and is still ongoing, though mostly complete. HCAP funds supplemented resources available through the donation during critical phases of implementation.
While CHART was initially geared towards implementation, the project’s focus has now shifted to maintaining the technology and enhancing its use. Several committees within BHN support the CHART project. The CHART working-group consists of a subcommittee of BHN leadership and IS representatives from each of the eight CHCs who discuss overarching issues such as implementation budgeting, planning and allocation. The Clinical Computing Collaborative, chartered by BMC’s Division of Community Medicine, convenes CHC medical directors and other staff to discuss specific end-user issues and discuss the use of technology in the HCAP initiatives described above.
3.3 Health Center Information Systems Capacity
In this section we describe the IS capacity across the BHN health centers interviewed highlighting both shared, network resources and areas where health centers use dedicated in-house resources. Although they are convened together through affiliation with BMC and BHN, each of the 15 BHN primary and secondary partner health centers retain a distinct IS infrastructure reflecting their individual needs and the development of their internal IS operations over time. While eight health centers are using the Logician EMR system implemented as part of the CHART project, two others are using EMRs by a different vendor. Similarly, all 15 health centers maintain their own practice management systems, with the majority using either HealthPro or Medical Systems Incorporated (MSI) products.
Vision and decision-making. Interviews conducted with health center leadership demonstrated large variation in the extent to which health centers developed and refined a specific vision and strategy for IS decision making. One larger health center that had implemented an Epic Care EMR system independent of the CHART project, indicated that they developed and worked from a five year strategic plan to guide their decision making including the extent to which they leveraged BHN resources for their systems needs. Other health centers indicated that they lacked resources and expertise for this type of planning and instead relied heavily on BHN initiatives to identify and pursue new IS programs.
Although all health centers interviewed indicated that they participate actively in IS discussions on the BHN level, most reported that final decision making on IS issues was handled by their own Board of Directors and Executive Director in consultation with committees and IS staff internal to their health center. Health centers that implemented EMR reported that they based this decision on several factors including the potential for improving patient safety, efficiency of care, and compliance.
In the network context, decisions that affect all of the health centers using the Logician application are brought up through BHN in working groups and discussions. Proposed enhancements and new functionality are assessed based on their cost, available resources and the breadth of benefit. For example, the CHART project will prioritize the development of specific Logician reports if there is a critical mass of health centers requesting that particular report. However, if one center needs an interface from Logician to a specific application, not used by other health centers, this request will be given relatively lower priority.
Staffing and technical expertise. Health centers we spoke also varied greatly in the extent of their internal IS staff resources. One center had an IS staff of five including a network manager, PC and phone support staff, and data managers all reporting to a CIO. Another had a staff of three relatively junior IS support staff. For health centers using Logician, the network provides “Logician Analysts” for two years after implementation. These staff provide technical support and training for the EMR as well as infrastructure support. The BHN also maintains a CIO responsible for managing the Logician analysts assigned to each health center and a CHART help desk. In addition, the HCAP project works with health center medical directors and IT staff to identify and support specific data and reporting needs. For example, they will pull data on specific diseases and utilization patterns from the data warehouse for center specific analysis. HCAP staff also worked extensively with health center IS leads to design and implement data extracts for the data warehouse.
Infrastructure and connectivity. While most CHCs fund hardware, connectivity and basic systems
applications from their internal operating budgets, there are targeted areas where BHN provides
infrastructure support. For example, through a $50,000 grant in 2001 from the National Institutes of Health National Library of Medicine, BHN secured a shared Internet service provider for all 15 health centers. In addition, the private donation of Logician software included funds for some hardware purchases and upgrades. Logician health centers also benefit from use of dedicated EMR servers that are all located and maintained centrally by BHN and connected to health centers via T1 lines. Finally, health centers also have a Citrix-based connection to BMC’s inpatient medical record data. By clicking on a Logician desktop icon and entering an individual password, appropriate users can gain access to BMC clinical systems such as laboratory and radiology to access test results anytime, from any location within the BHN network. By being able to quickly “cut and paste” hospital test results directly into the CHC database, one physician reported that he has become less dependent on his colleagues for important patient information. In addition, the physician’s ability to access the full patient record at all hours has allowed him to avoid unnecessary hospital admissions that previously used to occur due to a lack of information. Specialists do not currently share such a link with the Logician system but BHN is working on achieving that capability.
3.4 Stakeholder Experience with Boston HealthNet Information Systems Initiatives
As with all IS implementation projects in “real world” health care settings, health center respondents described mixed experience with initial implementation and use of both the EMR and the data warehouse applications. Overall, however, health centers were very satisfied with the technology they are using and highly value having the EMR and data warehouse resources. Because work with these applications has just begun, stakeholders were enthusiastic about opportunities to enhance functionality and use of these tools moving forward.
4. Conclusions
Overall, our site visit to BHN revealed the operation of a complex, but largely coordinated, set of initiatives to improve quality of care and efficiency that focused significantly on the promise of enhanced information systems and technical resources. Although they have made significant strides over the past several years, all respondents in Boston candidly discussed limitations of their current activities and their enthusiasm for building on these projects moving forward. In particular, the experiences described in this report inform policy and planning related to community-level EMR implementation among a set of diverse, mostly independent urban health centers. We end the report with the following set of analytic conclusions highlighting aspects of site visit findings.
BMC leadership. Although the hospital merger that created BMC is now nearly 10 years old, respondents made it clear that the success of the initiatives discussed largely leveraged the early momentum from this event and BMC’s leadership. Respondents cited several specific reasons why their model of vertical collaboration, with a safety net hospital at the head, contributed to their ability to acquire sophisticated health information systems. First, BMC (BHN) proved to be an effective platform for applying for federal grants and attracting private donations to support IS initiatives. In addition, BMC’s experience with large scale systems implementations and resource management, led to very effective planning and project implementation processes with an appropriate emphasis on standardization and adherence to deadlines. Finally, the BMC’s participation, allowed health centers to benefit from grand economies of scale for hugely expensive, core activities such as housing and maintaining servers and securing back-up technical support. Because BMC’s own operations require large scale systems administration and support resources, they were able to contribute to health center-focused initiatives at little additional cost.
Vertical collaboration among heterogeneous institutions. The success of IS initiatives in Boston is particularly surprising considering the number and diversity of independent health centers in collaboration. For the most part, BHN health centers are entrenched institutions with long histories and close ties to their community. In addition, prior to the BMC merger, each health center worked relatively independently to fund, develop and implement IS projects. Bringing health centers together in this environment required the BMC and BHN leadership to walk a fine line between building systems to meet the unique needs of individual health centers and maintaining a basic level of standardization necessary for efficient centralized maintenance and administration. While some health centers did note typical criticisms, e.g., larger health centers having greater leverage to influence group decision making, overall all, health centers reported positive experiences working with the central BHN/BMC programs. Respondents acknowledge that institutional incentives also helped shape the collaboration. BHN health center referrals represent the majority of BMC admissions and health centers benefited greatly from the extraordinary levels of uncompensated care that BMC provides to their patients.
Clinician buy-in for EMR. As with new EMR implementation, the CHART and HCAP groups in Boston had to contend with the difficult process of securing clinician buy-in for using an EMR. Although, this process was aided somewhat due to the relatively sophisticated health care environment in Boston relative to other parts of the country, many respondents still noted clinician buy-in as a significant challenge. Respondents noted two major strategies for securing buy-in. First, they made sure to include clinical representation in the earliest work group discussions related to design and implementation of the EMR. This allowed clinical interests to weigh-in on issues such as template design, application set up and functionality. In addition, the HCAP program in particular, has focused on quickly leveraging the EMR to support difficult aspects of clinical care, such as management of chronic illness, streamlining referral and follow-up and designing an appropriate level of clinical decision support (e.g., automated reminders that are useful not burdensome). The guiding philosophy has been that once clinicians see improvements in care and outcomes as a result of EMR use, their buy-in is permanently secured. Another key aspect of achieving and maintaining clinical buy-in is buy making sure the system works to enhance clinician access to key data by allowing them to electronically query lab results and inpatient records.
Need for substantial initial and ongoing investments. The experience in Boston demonstrates the need for two significant types of investment to implement and sustain a community-wide EMR. Clearly the $6 million in seed money that was privately donated was the critical, initial investment required to get the project off the ground. More than just allowing access to the software and licenses, the seed money supported costly hardware purchases, implementation assistance from the vendor and technical staffing that were as important as the application itself. While the large bolus was necessary to get the system up and running, continuous and ongoing investments provided through the HCAP grant were critical to helping health centers transition smoothly and leverage the new functionality to quickly achieve improvements in care delivery and outcomes. Without this ongoing centralized investment in reporting, customization and clinical enhancement, enthusiasm for the technology would have likely waned leading to only piece-meal improvements in service delivery. Finally, obstacles to the success of the EMR and data warehouse remain. For example, as health centers replace core applications such as practice management or accounting systems, they will need to find resources and time to plan and develop new interfaces. Again, there will be risk that buy-in and collaboration will falter because of these new costs. As such, respondents emphasize that ongoing investment in using EMR and data warehouse resources to assess and improve care will be critical to the ongoing success of the initiative.
Community cost savings and return on investment. Several respondents indicated that use of EMR has led to a series of cost savings. One health center reported that Logician has enhanced revenue capture by facilitating more accurate, comprehensive recording and coding of procedures. Another center immediately noticed cost savings in terms of the reduced medical records staff time and the restructuring of their work to remove some of the burden off of the front line nursing staff. Users also noticed that the time delay that was present with faxing and locating paper records is eliminated with the EMR since information may be accessed immediately from any BHN provider site.
Still, respondents acknowledge that they could never have justified the required initial and ongoing investments described above without the upfront gift and ongoing support through BHN and federal grants. As with other cases, we found that measurable cost savings to individual institutions did not meet the costs associated with purchasing and maintaining an EMR. However, community-level, vertical collaborations such as BHN represent strong model for understanding the system-wide benefits of using EMR to improve quality and efficiency of care. For example, the network has already prioritized efforts to measure savings due to reductions in inappropriate ED admissions for ambulatory care sensitive conditions that affect BMC. In addition, by providing patient-level data to state health care financing and public health officials, through the data warehouse, BHN, and specifically the HCAP project is making an important stride toward turning the EMR initiative into a true patient electronic health record as envisioned by the National Health Information Infrastructure.
Kentucky
1. Introduction
NORC at the University of Chicago (NORC) is pleased to present this report detailing findings from our recent case study looking at use of health information systems by rural ambulatory care safety net providers in and around Hazard, Kentucky. This case study is part of “Community Health Center Information Systems Assessment: Issues and Opportunities” a project being conducted by NORC under contract with the Office of the Assistant Secretary for Planning and Evaluation (ASPE) at the U.S. Department of Health and Human Services (HHS). In collaboration with ASPE, the Health Resources and Services Administration (HRSA) and its Bureau of Primary Healthcare (BPHC) provide technical direction for this project.
The Kentucky case study involved telephone and e-mail exchanges with 14 respondents representing nine institutions involved in the primary health care safety net in Southeastern Kentucky. Overall, the site visit explored two main themes: (1) the state of information systems use among ambulatory care safety net providers in southeastern Kentucky, and (2) stakeholder experience with the Southeastern Kentucky Community Access Program (SKYCAP) a community-based rural health outreach and client tracking system initiated as a rural demonstration project in September 2000. SKYCAP aims to improve access to health care, social services, and housing for the underinsured and uninsured residents of Harlan, Perry, Knott and Leslie Counties in Kentucky. Findings presented here will be combined with those from other case studies and site visits to inform a final report on the use of information systems in community health centers and other ambulatory care settings. The remainder of this report is organized into four main sections:
- Background and Methods. This section describes key features of the site visit including background on the safety net in the State of Kentucky and the four-county SKYCAP service area along with a description of the stakeholders who contributed to our findings.
- Consortium Activity. This section describes the development and organization of SKYCAP including an overview of the information systems currently used by the consortium.
- Provider Information Systems (IS) Capacity and Experience. This section summarizes findings relevant to the overall state of health information system use among safety net ambulatory care providers interviewed for this study. We will also review the provider experience working with the SKYCAP program.
- Conclusions. Finally, we present a set of conclusions that explore issues related to the sustainability and replicability of the SKYCAP model and challenges facing consolidated health centers and other safety net stakeholders in Kentucky.
2. Background and Methods
In the following paragraphs we provide relevant context and describe the methods employed for the case study. We begin by describing relevant characteristics of the ambulatory care safety net in Kentucky with an emphasis on areas of Southeastern Kentucky serviced by SKYCAP. As with other regions investigated as part of this study, we used a variety of email and telephone communication with local providers and organizers to gather the information summarized in this report.
2.1 Kentucky Safety-Net Characteristics
One of the key challenges facing consortium activity in Southeastern Kentucky is the relative lack of federally sponsored consolidated health centers that serve this area. While there are 14 consolidated health centers in Kentucky overall, only one of these, a health care for the homeless (HCH) center, is located within the four-county region served by SKYCAP (the majority of Kentucky’s consolidated health centers are located in or near Louisville). The only 330 grantee FQHC in the Southeastern region sits outside the SKYCAP service area. Some of its satellite clinics are located within the SKYCAP region but are generally too small to participate in the consortium. Aside from these satellite clinics, several free clinics, other primary care clinics and two public hospitals serve the uninsured and underinsured within the SKYCAP service area. Two of these clinics are considering applying for consolidated health center status.
Demographic data from the SKYCAP service area demonstrates the extent of the poverty and health problems affecting this region. In 2003, between 20 and 40 percent of the population was without insurance in the four-county target area. It is estimated that 24 to 45 percent of the population in Harlan and Perry counties live in poverty compared to the state average of 16 percent6. These counties also have the highest rates of asthma, diabetes, heart disease, hypertension and severe mental illness in the state. Hospitalizations for these diseases exceed the rates in the rest of the state by 2 to 10 times7.
2.2 Methods
The SKYCAP/Kentucky Case Study involved a series of initial e-mail and telephone contacts followed by telephone-based structured interviews with 14 key stakeholders in the Southeastern Kentucky safety net. Stakeholders included senior leadership in SKYCAP, staff at the Kentucky Primary Care Association, and directors and IT staff at consolidated health centers, clinics, and area hospitals. Providers interviewed included both participants of SKYCAP and non-participants. All respondent organizations are listed below in Table 1. The majority of the stakeholders we spoke with were located in Harlan and Perry counties near Hazard, KY.
Respondent Organization |
Description |
|---|---|
|
Consolidated Health Center Respondents |
|
| Mountain Comprehensive Health Corporation | MCH comprises Kentucky’s largest CHC network, serving approximately 33,000 clients in 190,000 encounters in 2002. MCH is an CHC located in Whitesburg, KY. The main clinic site sits outside the SKYCAP service area. |
| Harlan/Perry Health Care for the Homeless Center | Harlan/Perry HCH is located in Hazard, KY and is the only primarily BPHC funded center squarely within the SKYCAP service area. They provide primary care through contracts with clinics, volunteer physician networks and on-site at area shelters. |
|
Non-Consolidated Health Center Respondents |
|
| Hazard Appalachian Regional Healthcare (ARH) Medical Center | Both of the hospitals in the SKYCAP region are owned by ARH. We spoke to a physician and administrator who practice at these hospitals and who were involved in the planning stages of SKYCAP. |
| Clover Fork Clinic | Clover Fork Clinic is a primary care community clinic located in Evarts, KY (in Harlan County). The clinic describes itself as being close to a look-alike FQHC and sees 18,000 annual visits in the medical unit. |
| East Kentucky Family Practice Clinic | EKFPC is a rural health and primary care clinic affiliated with the University of Kentucky Center for Excellence in Rural Health (UKCRH). They are applying for FQHC status in the next grant cycle. The clinic sees around 5,000 annual client visits. |
| SKYCAP Program | The SKYCAP program is a rural health outreach and client tracking program serving the underinsured and uninsured of Perry, Harlan, Knott and Leslie counties in Southeastern Kentucky. |
| Kentucky Primary Care Association | KPCA is the statewide primary care association. Based in Frankfurt, it provides its members with services related to provider recruitment, cooperative purchasing, consulting, information, and training. |
| Data Futures, Inc. | Data Futures, Inc. is a Hazard-area software vendor that developed the SKYCAP MIS software. |
| Harlan Countians for a Healthy Community, Inc. | One of the co-administrators of the SKYCAP Program, Harlan Countians for a Healthy Community is a coalition of health care providers, consumers, and other interested agencies formed to improve the health care system in Harlan county. |
Structured interviews with respondents were conducted using open-ended discussion guides. In addition, a tabular form was emailed to information technology staff at 5 respondent health centers prior to the site visit to facilitate collection of standard information relating to infrastructure and technical capacity. For each structured interview, the NORC team prepared materials that outlined our preliminary knowledge of the respondent and highlighted outstanding questions to address during the interview. Examples of discussion guides and preparation materials used in the site visit are included as Appendix A. The table used to gather data on clinic technical infrastructure is provided as Appendix B.
3. Consortium Activity
As noted above, this case study sought to investigate state and local initiatives to improve use of information systems among ambulatory safety net providers. Besides the Kentucky e-Health network, a program (currently in early development) to establish a statewide health information infrastructure, SKYCAP was the only such initiative in the Hazard, KY area that emerged from our interviews. In this section we present more details on SKYCAP including its early development, characteristics of its electronic client tracking system and a description of services provided.
3.1 SKYCAP Development and Early History.
We begin by describing the environment from which SKYCAP emerged and key aspects of SKYCAP’s early history, including the impetus behind the development of the program, its organizational structure, and the core functions it now provides to the community.
Impetus for SKYCAP Development. The rationale for creating SKYCAP stemmed from two trends identified by public health stakeholders in Southeastern Kentucky. First observers noted extensive, inappropriate use of area emergency rooms as first line providers for low income individuals seeking routine primary care services. Secondly, the region lacked a social services support system to serve the low-income clients affected by mental illness or other ambulatory care-sensitive conditions. Community organizations observed that these clients experienced several serious barriers to adequate care including lack of access to needed medications, problems scheduling appointments with ambulatory care providers, poor access to transportation and a lack of awareness around self management of chronic illnesses. Particularly problematic were those elderly or disabled low income individuals without adequate care support through family or other social networks.
Early History. Citing these trends, in 2000, the Hazard-Perry County Community Ministries invited the University of Kentucky Center for Rural Health and a community organization called the Harlan Countians for a Healthier Community to lead a social services program targeting underserved populations in Harlan and Perry Counties. The vision of SKYCAP evolved into two main components. First, the program would include an electronic client tracking system that allows service providers to record and share data on clients to facilitate community-wide tracking, continuity of care and provision of basic chronic care case management services for the uninsured and underinsured populations. The second activity, to be facilitated largely by this tracking system, is a health navigation program where “lay” Family Health Navigators (FHNs) would be hired and trained to work with clients individually to help them navigate the safety net and access social services available in the community.
While several counties in Kentucky had been collecting data on uninsured clients since 2001, SKYCAP’s goal was to track those data elements specifically requested by community providers and then to share that data across providers by deploying the system in ambulatory health care and social service settings. In planning data needs, SKYCAP sought input from a wide range of service providers from lab technicians, nurses, physicians to social workers and mental health counselors. Upon classifying appropriate data elements, they began to seek out vendors to create a client tracking system based on the needs identified. Data Futures, Inc., a local vendor, was selected to develop the system.
Mission and Goals. The overarching goal of the SKYCAP program is to provide a multi-dimensional (or “holistic”) approach to improving and managing health status for underinsured and uninsured clients by encouraging well timed use of available social services including mental wellness services, health care, and housing and transportation services. A key feature of this goal is to ensure that all clients have a medical home. Through the use of case management and navigation, SKYCAP hopes to benefit the community by reducing unnecessary hospitalizations and inappropriate emergency room usage for underserved individuals, particularly those with ambulatory care sensitive conditions. The client tracking system is seen as an integral part of this goal, by giving providers in the community, including FHNs, nurses, physicians, pharmacists and social workers access to the demographic, administrative and clinical information to help coordinate care and services provided to individual clients. The tracking system also holds the potential for providing policy makers and other stakeholders with a community-level overview of care provided to underserved individuals in the targeted counties.
3.2 SKYCAP Organizational Structure and Operations Model
SKYCAP is not a single organization with a dedicated set of staff or resources. Key activities are governed and managed by staff from several community partners. The University of Kentucky Center for Rural Health administers the project and provides key staff including a Program Director and Educational Coordinator. In addition to leadership staff from the University of Kentucky, navigation activities and clinical programs are developed and managed by a consortium of health care providers, faith based organizations and health-focused foundations. FHNs represent the majority of SKYCAP’s labor. Other community institutions that are considered partners in SKYCAP include academic institutions, public hospitals, health departments, community-based services, faith-based services, pharmacies, and others.
SKYCAP Participants. The SKYCAP administration and its partners work to add as many providers as possible to the network in order to reach the greatest base of uninsured and underinsured clients and to manage the activities of FHNs. Fifty safety net medical providers currently participate in SKYCAP, meaning they refer clients to the program and have the ability to access and modify records recorded in SKYCAP’s client tracking system. These providers operate out of public hospitals, health departments, an HCH, primary care clinics, emergency shelters, housing developments, and other clinics in the four-county SKYCAP target area. In order to share and store client data gathered from the client tracking system in a central database, SKYCAP entered a data sharing agreement between hospitals, physicians and other partners.
Exhibit 2: SKYCAP Structure
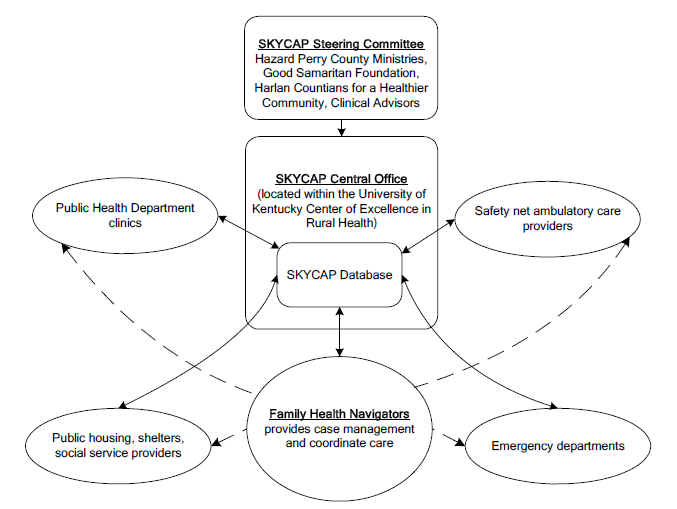
Note: solid lines indicate data transfer; dotted lines indicate referral or other case management contact.
Funding. SKYCAP received initial funding from the three-year CAP grants. It also received funding from a local foundation to expand its services from two to four counties in 2002. Additional funding was received through a federal Healthcare for the Homeless grant provided to a key partner along with several in-kind contributions from local hospitals, clinics, and health departments. At the current time, SKYCAP’s main funding sources will run out in August of 2004.
Core Activities. As described above, SKYCAP consists of two basic activities (1) maintaining a client tracking system to follow key health and social status variables as well as utilization for clients using safety net health care and social services and (2) empowering a cadre of FHNs to follow the progress of individual clients and provide basic case management or disease management services as necessary. Residents of Harlan, Perry, Leslie and Knott counties who are uninsured and underinsured are eligible to participate in the program.
Person-level records are initiated in the tracking system when an individual is referred to SKYCAP from any source in the community, usually clinics or hospital physicians. Each client is provided with their individual identification number which is attached to their record. Once they are referred, the program uses the FHNs to assist these clients in receiving care in the most appropriate settings. FHNs are randomly assigned to new clients who are referred to the system. They conduct an initial interview either at the client’s home or another setting where they query the client about demographic information, access to housing and transportation, chronic disease status (e.g., diabetes, heart disease, hypertension, or asthma), emergency room utilization or hospitalizations within the last year and other basic health status issues. FHNs then enter this baseline information into the client tracking system, as close to real time as possible. After this initial interview, FHNs also enter and update client-level information as they see clients in the field. Individual clinical providers are also able to use the client tracking system to access client level data and update information relevant to a client’s medical history, diagnosis and treatment. Thus, when all parties who interact with the client enter client-level data into the tracking system, the record holds an integrated and complete patient history, including any medical treatments received across the span of providers as well as case management services provided.
Client records currently held in the system are divided into three levels, depending on their level of need determined from the initial interview. Clients who do not have any of the targeted illnesses, do not require follow-up and require only a minimal coordination and delivery of services are considered to fall under Level 3. Level 2 clients have one or more of the target illnesses and are less able to obtain medications. These clients require a clinical review and at least two contacts per month. Level 1 clients are the highest priority, in that they have the least access to medical and social services and their illness is out of control. These clients require at least four contacts a month along with regular intensive, long term case management.
Record types |
Description |
|---|---|
| Level 1 | Client has uncontrolled chronic illness, often with very little family support. FHNs contact client on a weekly basis. |
| Level 2 | Client has one or more chronic illness, with some difficulty accessing appropriate treatment and medications. FHNs contact client twice a month. |
| Level 3 | Client is relative stable without targeted chronic illness and do not require regular follow-up. |
Depending on their need for services (i.e., their “level”), FHNs will continue to interact with clients on a regular basis by providing disease management education and linking them to needed services such as free medical services and pharmaceuticals. In addition to telephone contact, these interactions can involve in-person visits to the client’s home. The goal for clients at all three levels is to establish a primary provider or a medical home, provide access to necessary medications, and educate clients about their illness. Determining a client’s eligibility for free or subsidized drugs is determined using built-in system features. In the first three years of the program, SKYCAP reports helping more than 9,000 clients and facilitating 87,000 interactions between those clients and health or social service providers. Because the largest health center (and Section 330 funded FQHC) in the region lies outside of SKYCAP’s service area, SKYCAP’s client intake seems small when compared to the entire Southeastern Kentucky region’s service base. In addition, SKYCAP does not include a comprehensive record of all FQHC encounters in its service area. However, SKYCAP has fairly extensive penetration in the region it directly serves and in its specific patient population of the uninsured and underinsured.
3.3 Potential Uses for Community Providers
SKYCAP’s client tracking system supports a range of services that are available for use by different members of the community. Its main function is as a data collection tool and community resources databank. As discussed above, various levels of information are input by FHNs, providers and other SKYCAP staff in the community and are stored in a central server. The data in the system generally covers demographic information, where clients received care, whether they can pay for care and whether they have adequate housing, along with other relevant information for effective case management. FHNs are the most common user of the system, entering and accessing data to facilitate the coordinated case management process. In the paragraphs below, we describe potential uses of the SKYCAP database.
Master Client Index. Since every client who is eligible is automatically referred to SKYCAP and receives an individual identification number and corresponding record, the system database serves as a Master Client Index. Baseline information on every SKYCAP client is entered by FHNs and can be searched for under various parameters to identify prior encounters. The data stored in the Master Client Index can be used to track trends in care and disease incidence and utilization management in one segment of the target population or in the community as a whole. The system also allows for systematic tracking of program enrollment, eligibility for drug access programs, as well as referrals to specialists or inpatient providers.
Common Electronic Client Record. The SKYCAP tracking system may also be used as a shared electronic client record. From their base ambulatory care setting, community physicians may gain access to the system to gauge if any changes, for example, in the clients’ home environment, may affect their access to pharmaceuticals or compliance with other therapies. The system may also hold clinical information entered by a physician or clinical team leader on individual clients such as diagnoses, medications prescribed, as well as notes to other professionals who may provide services to the client. Client records may be accessed from a number of different sites where patients may receive care and social services in the community, making client information transportable across their continuum of care. For example, one respondent noted that emergency room staff often calls the SKYCAP office to get the latest medications or dosages that a client was prescribed by another physician as it is quicker to pull information off the database than for the staff to retrieve the patients’ paper charts.
Reporting. The client tracking system includes a report function for clinics and physicians who wish to analyze information about their client population or utilization of services. Data can be pulled from the general database to find out what services clinics provided to the SKYCAP population. The system’s data may also be extracted for use by consolidated health centers to complete UDS reports. The HCH, for example, pulled demographic data about their client base from the SKYCAP system, in combination with other systems, in order to complete a UDS report.
Case Management. FHNs use the data entered within the SKYCAP system to help with case management and some limited disease management with their clients. For example, the system prompts the FHN to enter such information as appointment status, type of appointment as well as the services and medications clients received at each appointment. By tracking this information FHNs can remind the client of any necessary follow-up as well as maintain a schedule of regular contact with clients. The tracking system also provides FHNs with disease management protocols which serve to educate the client on how they can receive care and self-manage their illness adequately in order to reduce long term complications. Links to social service providers including those in charge of state and community housing, meals and mental health services had been mostly informal but are now becoming more formally integrated. For example, the executive director of one of the founding SKYCAP organizations, Harlan Countians for a Healthier Community, now sits on the local housing board. Also, the baseline information collected within SKYCAP’s MIS system offers the housing programs a tailored client base, resulting in a more institutionalized and streamlined link from SKYCAP patients to needed services. The vignette presented below illustrates how SKYCAP can identify and help address a wide range of social service needs beyond health care.
In Harlan County, a male presented to the emergency room for diabetic services. He had no insurance, no medicines and was unable to read. The emergency room staff referred the patient to the SKYCAP Program. A FHN who was assigned to the case observed the client’s need for mental health services and diabetes case management. In conducting the preliminary home visit and interview, the FHN discovered that the client had no refrigeration or running water. The FHN coordinated an interdisciplinary team of Housing and Urban Development staff, mental health specialists and health care providers to provide the client with needed social services such as low-income housing, transportation and mental health counseling as well as a primary care home to control his diabetes. By entering the client’s data into the SKYCAP tracking system, and checking in on a regular basis, the FHN could follow future appointments to arrange for adequate transportation and could track progress to make sure the client was able to comply with the treatment. The man is now living independently and his illness is under control.
Pharmaceutical Discount Program. Many providers emphasize the importance of increased access to benefits afforded through use of SKYCAP. The program links specific clients with free or reduced-price prescription drugs negotiated with local pharmacies, pharmaceutical companies and other indigent drug programs. Using the tracking component, clinics may view client prescription information to gauge which clients are eligible for this program as well as what drugs they have received at a discounted rate.
Overall Provider use of SKYCAP. From our interviews, it is clear that providers have come to use the system in a variety of ways, reflecting their individual needs and priorities. For example, one clinic uses SKYCAP essentially as a complete client tracking system, entering clinical information (e.g., client diagnoses and prescribed medications) after each appointment. Physicians at another clinic that already has an electronic medical record system separate from SKYCAP use the SKYCAP terminal in their office, although inconsistently, to pull up information on their SKYCAP patients, identified by a code on the front sheet of their electronic record, to look up information about what social/environmental conditions may be affecting their patients’ adherence to treatment. They also use SKYCAP’s patient record to view any treatment the patient may have received in other settings so they can communicate with other providers if they have a question or consultation and are able to anticipate any potential drug-drug interactions. Other clinics use SKYCAP solely to assess eligibility for ancillary benefits (e.g., donated pharmaceuticals) for their clients. Still others use it to review information about the clients’ ability to pay or their access to adequate housing or other environmental resources. Most users take advantage of and contribute to the MIS system in pieces, only using the one or two functionalities that benefit them the most.
3.4 Technical Infrastructure and Services
SKYCAP’s technical infrastructure is designed to accommodate challenges associated with supporting networked health care applications in a rural environment, including relative lack of reliable, high-speed data transfer capabilities and lack of IT resources and expertise on the part of health care providers. The following section describes basic technical aspects of SKYCAP’s network model, including the means by which health care providers or FHNs create or modify records and access information from the master client index.
Provider Integration Model. SKYCAP used grant money to purchase and network dedicated workstations at each participating provider site to allow data entry and reporting. Data is entered through a total of eight SKYCAP workstations located at provider sites around the service area. At least one terminal sits in the emergency room of each of the two area public hospitals. The other six terminals are located in clinics in a separate office designated for SKYCAP use. Each terminal is networked to the central SKYCAP server via a frame relay connection. Once entered, client data resides in the central server maintained at the University of Kentucky Center for Rural Health. As of March 2004, this model will change to a virtual private network (VPN) model where providers have access to SKYCAP via the Internet. This platform will offer substantial reduction in cost relative to maintaining a separate frame relay connection and paying telecommunication charges for each health center.
User Access and Privacy. Users access the system using an individual password that is encrypted upon transmission to insure that client records are protected from unauthorized use. Under a roles-based access model, physicians have more access to the system than social workers so that each user is only able to see client information pertinent to their site and realm of activity. Everyone who uses the system receives confidentiality training for interacting with patients. Access is determined on an individual basis, with the executive director maintaining control over what information each individual should be able to access. Each client is provided with a consent form which is completed and verified before any data is entered in their record.
Support and Training. Data Futures, Inc., the local vendor of SKYCAP, provides support for the SKYCAP staff. If individual users experience a problem with the system, they call the SKYCAP’s technical staff that provides basic support (for example issues related to system connectivity). If their information technology staff can not help the user, calls go to Data Futures for more advanced support regarding use of specific application functions. Data Futures handled the majority of information technology implementation and support up until mid-2003; SKYCAP is now trying to take over more of that role. Since they also have access to the information technology department at the University of Kentucky, they are able to save money by using resources internally. Data Futures, Inc. trained the SKYCAP administrative staff how to use the system and they, in turn, trained other users including FHNs and clinicians.
System Upgrades. Data Futures currently updates the SKYCAP program’s client tracking software that is hosted at the main SKYCAP offices, and the SKYCAP technician updates the workstations at individual physician sites and at other sites. The SKYCAP database resides in a Microsoft SQL Server 2000 database that is running on a server that SKYCAP paid for but is now aged. New hardware was purchased upon their move to a new building in March 2004. Data backup and disaster recovery processes are in place and have been tested. The University of Kentucky provides and updates general productivity software such as the Microsoft Office Suite.
Relationship with Data Futures, Inc. After completing an informal vendor search, SKYCAP eventually selected Data Futures, Inc. mainly because they were willing to create a system customized to SKYCAP’s needs rather than using an already-made system and because of their local presence in Harlan county. The company was thought to be interested in working with SKYCAP as they hoped to develop a program that they could market in other communities. Data Futures has implemented a similar software in 11 networks around the nation so far comprised of over 100 sites who are now vested partners in assuring success of the system. Other networks that selected Data Futures were interested in having a combination patient record/case management software that was able to be used as a community-wide solution to coordinate care among a variety of partners. One network with a regional access program was in the process of implementing the Data Futures software in order to perform case management and disease tracking among their uninsured and underinsured patients so that they could ensure that this population was able to gain access to necessary healthcare, including hospital care, primary care, and mental health and other social services. They stated that Data Futures was available at a lower cost than other electronic medical records software and was less clinical-based making it easier to share across a variety of users.
Interfaces with Existing Systems. There are currently no interfaces with existing data collection systems. Future plans are to interface the system with programs that track eligibility as well as other software that
contains useful client data that SKYCAP may not currently track or track as consistently. By integrating data held in other medical and administrative databanks, the SKYCAP database could increase in value as it would hold a greater amount of standardized information to better inform health center participants of their client population and patterns of care they provide. Interoperability with existing provider systems would also potentially encourage greater use of the SKYCAP application as it reduces or eliminates the need for double entry of data, a common complaint among current users.
4. Health Center and Clinic Capacity and Experience
As in other regions investigated as part of this study, safety net ambulatory health care providers in Southeastern Kentucky enjoy varying levels of access to health information technologies and applications. In this section we describe systems capacity at community health centers interviewed in Southeastern Kentucky. We also describe their experience using both internal systems and consortium-based systems such as the client tracking function of SKYCAP.
4.1 Health Center and Clinic Infrastructure
Most of the clinics we interviewed in the Southeastern Kentucky region did not have a robust technical infrastructure or support staff, although access to information technology resources and staff expertise varied significantly across the region. Some of the region’s larger health centers and primary care clinics have a more sophisticated level of information technology either due to personal motivation on the part of center leadership, greater access to financial resources such as a higher proportion of commercial clientele, or both. Key aspects of technological infrastructure are discussed below to provide a general sense of the capacity of health centers and clinics in the safety net varying by size and other circumstances.
Organization and Governance. Given the relative lack of consolidated health centers in rural Southeastern Kentucky, the clinics we spoke to tended to have a less consistent organization and governance model. Most of the clinics were led by an Executive Director who often doubled as the Medical Director and chief clinician. Instead of a Board of Directors made up largely of clients, many of the clinics we interviewed were governed by a parent provider or by a group of community leaders. Decision making, including technology decision making, is often left to the health center’s administrative and clinical leadership.
Systems Leadership and Vision. Two of the larger health centers and clinics seemed to have a well developed vision around the importance of information technology in their everyday management as well as a structure built around information technology decision-making. These centers reported having had a dedicated Chief Information Officer, network administrator or an individual with some technical knowledge acting in that role. Other health centers did not share such a vision around information technology, but rather made do with what resources they had since many of these clinics report having no funds to invest in information technology expertise and infrastructure, relying on SKYCAP or using a purely paper-based system.
Staffing. Most of the clinics we interviewed acquired technical support from their relationship with community resources such as the University of Kentucky or through the various vendors of the software they use. The larger clinics and University-affiliated clinics tended to have network administrators and other staff that could aid them in terms of answering basic technical questions. However, most of the centers did not have a dedicated Chief Information Officer.
Hardware and Applications. Most of the clinics had access to basic computer hardware and productivity software such as the Microsoft Office Suite. The use of other software varied based on the clinics’ client volume and access to resources. For example, two of the clinics we spoke to were using specialized practice management systems, Medical Manager and Megawest, that allowed for scheduling, reporting and eligibility tracking functionalities and one health center had successfully initiated an electronic medical record system. Other clinics and health centers depended entirely on SKYCAP for administrative data, meaning that they used no other practice management system. However, some of these clinics reported using software designated by various grants that required them to enter data similar to the data elements in SKYCAP. Notably, since SKYCAP services are provided through a terminal workstation distinct from the information technology infrastructure of individual providers, none of the clinics or health centers acquired new hardware or software or performed upgrades specifically to participate in the program.
Networking and Internet Connectivity. A few clinics and health centers managed a LAN or WAN networking multiple sites. Almost all of the clinics we spoke to were able to gain access to the Internet, although assumedly the smallest and more remote partners in SKYCAP would be less likely to have adequate infrastructure to access SKYCAP through the Web. These centers may or may not be able to upgrade their connectivity to the Internet to in order to achieve the high speed connection needed to facilitate their use of the SKYCAP database.
4.2 Organizational Participation in SKYCAP
As with other community provider networking activities, the success of SKYCAP depends largely on active participation from community-based providers. In addition to technical challenges related to provider participation, network organizers face the challenge of assisting local providers to incorporate use of their application into the daily routine of administrative and clinical staff. In this section we summarize health center experience using the SKYCAP navigation services and client tracking systems both technically and on an organizational level.
Community Partnerships. Stakeholders generally reported that SKYCAP fostered a greater level of communication between hospitals, physicians and FHNs in the community. Most stakeholders felt that the human component fulfilled a need for greater communication between these parties in their care of a common client population. For example, participants noted that FHNs can pass on valuable information to physicians about a client’s home environment such as their need for transportation, housing or treatment they received from another provider. One respondent offered that the electronic tracking component facilitated this inter-provider communication by revealing within a client’s record all their previous episodes of care, in emergency room, mental health and primary care settings, so that providers who saw the same patient could consult each other about the most effective treatment strategy.
Provider Buy-In. Most physicians initially bought-in and continued to believe that SKYCAP provided benefits in terms of increased provider communication and networking. They also believed that viewing information in the SKYCAP client record before seeing patients had the potential to improve care and coordination. However, many providers noted that the latter goal has been a challenge to pursue in practice due to the system’s incompatibility with workflow. Since physicians had to note that their patient was a SKYCAP client and then go to a separate office to pull information from the terminal, the process became too time intensive and inconvenient to perform on a regular basis. One physician who did use the system on a regular basis found it useful to have access to the client information before the appointment so that he could anticipate any potential drug interactions or other conditions that might affect his treatment plan. Most of the respondents recognized the population-level data possibilities that the MIS system could contribute in theory, however, with the exception of FHNs, they rarely made use of the system to its full potential in practice. SKYCAP leadership recognized this as a “lesson learned” and hopes to increase provider use of the system by making it internet accessible in the future.
4.3 Satisfaction with Client Tracking Components
As described above, provider use of SKYCAP varies substantially. Interviews with various providers highlighted specific issues and concerns with respect to tracking clients under SKYCAP, relating both to the general user-friendliness of the system and to specific functionalities of the database and tracking application. In this section we describe provider reports regarding their use of the SKYCAP client tracking system.
Ease of Use. Most users felt that the system was easy to use once they were trained and that data entry did not require a high level of technological sophistication. Generally, SKYCAP reported that participant complaints related to loose cables or incorrect system hook-ups rather than issues with the software itself. However, participants did note the inconvenience of using a system that did not communicate with other software they used. Physicians and nurses, as well as FHNs in the field, were also inconvenienced by having to enter data from a separate SKYCAP terminal in a designated office rather than from desktop computers or laptops that they used for regular work activities. Most participants cited these two items as the greatest barriers to their full participation in the program.
Most of the clinics believed that system utilization would increase if the system could be accessed through the internet using a standard browser versus using a dedicated application on a stand-alone terminal. This change was proposed to be implemented in March of 2004 so it is too early to gauge its success. Since clinics had such varied technological capacity, it was often hard for the limited SKYCAP staff to be able to accommodate the clinics’ various needs or desires in terms of service provision. Different computer versions created a difficulty for SKYCAP staff to easily bring all clinics up to full participation in a timely manner.
Reporting. Stakeholders felt that SKYCAP’s reporting capacity was still in early development and did not yet met their needs. Often, clinics complained that it was labor intensive to pull data adequate for a comprehensive report. In particular, the HCH reported that they could not rely solely on the SKYCAP database to provide all the information they needed to complete a UDS report given the data’s inconsistency and the effort required to pull useful data. Users observed that baseline information entered by FHNs was usually complete across all clients but health information was less complete, forcing clinics to draw from various sources to get a complete set of information needed for a comprehensive report. SKYCAP is still working on improving this function as the vendor completed the front end and left the back end for SKYCAP to develop internally.
Duplication of Services. Several clinics were already using practice management software or internal electronic medical records systems that tracked some of the same elements as SKYCAP. These clinics found that it was less optimal for them to double-enter data into both programs as they would get the same benefit if they entered client information into their internal system only. At least one health center reported that they were unlikely to continue their use of the SKYCAP system since it duplicates services they already gain through an existing software program. They believed that the software could be much more effective if it was interfaced with other existing software in the community or if its use was more standardized across all parties.
Case Management/Disease Education. Many clinics indicated that case management and disease self-care education was the core service that SKYCAP provided. While clinics did not directly speak to their experience with this portion of the tracking system, certain stakeholders felt that this element had benefited the community by providing information which allowed FHNs to efficiently distribute care for low-income clients across the community so as not to overburden a single provider. Others praised the system for providing clear benefits in terms of lower unnecessary emergency room utilization.
Perspectives on the Future of the System. Many of the stakeholders we spoke with were optimistic about the sustainability of the navigation portion of SKYCAP. However, stakeholders expressed concern over the future of the patient tracking system portion, describing it as the part of SKYCAP that is most in jeopardy of disappearing. It has been a problem to secure funding the information systems portion through community resources. For example, area hospitals are willing to fund an FHN to be staffed at each hospital unit but not the community-wide tracking effort. Although the hospitals recognize that they are saving funds in uncompensated care due to their participation in SKYCAP, they claim that the savings do not amount to a large enough incentive for substantial investment in the MIS system given that the hospital does not generate much revenue.
A group of respondents indicated that the elimination of the electronic patient tracking system would severely impede data sharing and access to care for SKYCAP clients would suffer. Providers would lack real time data, services would be duplicated, and FHNs would not be able to evaluate and coordinate clients’ care and services as effectively as they could using the electronic tracking system. Future potential endeavors described by SKYCAP leadership include a “next generation” SKYCAP which will expand on the current model and will extend to additional counties. While this is not yet fully developed or funded, it is clear that SKYCAP continues to seek greater participation among providers as well as a wider client base. Also, while broader dissemination of SKYCAP data and use for research or policy purposes has been contemplated there is currently no funding available for furthering these ideas.
5. Conclusions
Information provided by SKYCAP suggest that the case management portion of the initiative has substantially helped low income or uninsured residents navigate health and social safety net services available in the four county service area. The findings from this case study suggest that the use of lay health workers accessing a community-wide tracking database is a useful model for consideration in other settings. The main challenge for SKYCAP has been creating a culture where all relevant providers including hospital emergency departments and safety net ambulatory care providers regularly access, update and use the software and data structure available through the system. Our conclusions focus on the specific aspects of this challenge and how they may be addressed moving forward and in other settings.
Comprehensive Approach. Unlike previous cases studied under this project, SKYCAP offers an opportunity to learn about how an electronic data repository can facilitate the provision of a wide range of social services to low income and underserved populations. In particular, interviews with the stakeholders in Kentucky has demonstrated the potential improvements for identifying and addressing social service needs through use of dedicated health navigators aided by a means for electronic client tracking. Because this model incorporates a range of providers, the potential impact on population health status are substantially greater than programs focused exclusively on improving access to health care. In particular, the SKYCAP program has helped underserved individuals in Southeastern Kentucky access the appropriate social service at the appropriate time, thereby fostering health improvement and maintenance in a multi-dimensional or “holistic” manner.
Organizational Presence. One of the remarkable aspects of SKYCAP has been the initiative’s ability to operate without a single organization dedicated to its success and without a significant administrative incentive for participation on the part of providers. SKYCAP is operated out of the University of Kentucky Center for Rural Health and is led by an Executive Director, an Educational Coordinator, and several clinical and educational team leaders. With no single entity responsible for assuring buy in, SKYCAP’s leadership worked to create initial buy-in and participation from a wide range of community providers each with different organizational structures and incentives. In particular, because of the lack of substantial consolidated health center presence in the target area, SKYCAP is unable to encourage participation by providing services that are key to consolidated health center operations such as competent billing systems and consistent ability to produce UDS reports.
It is clear from our interviews that each provider approaches their participation in SKYCAP differently, fulfilling their own internal data and care management needs as the system allows. This has produced some clear benefits for individual clinics, for example, allowing them to track various services they have provided patients, or to be aware of other medications their patients might be prescribed. However, this has also led to inconsistencies in the types of data being entered for each individual across the community. Because providers are not bound by specific reporting or administrative requirements, desired data formats and reports vary across providers. In sum, SKYCAP’s implementation faced greater resistance than other network implementations since there was no dedicated organization behind the initiative and that there was substantial heterogeneity in the needs and orientation of the providers it aimed to serve.
Structural Incentives. Although stakeholders believed in the potential community-wide value that widespread use of the SKYCAP electronic client tracking system could produce, users did not always feel they could contribute to this potential due to the system’s incompatibility with specific work processes. Incorporating use of the application into FHN, clinic and provider culture and workflow represents an important next step in the application’s development. The current SKYCAP infrastructure asks providers to perform data entry tasks unrelated to their prior workflow and, in many cases, using a separate terminal not used for any other purpose. This approach presents important challenges including requiring double entry of administrative data on clients, incurring costs related to a system that is not yet related to the health center’s core operation and, most importantly, requiring a change in the work processes used by busy clinical staff (e.g., emergency room staff). We note that, at the time of this case study, SKYCAP was working to address these problems, to some extent, by implementing virtual private network-based access to their database. Data entry can also be greatly facilitated by developing specialized interfaces or processes that allow the transfer of data from existing to new systems with limited (or no) additional effort on the part of the users.
Demonstrating Data Value. One of the important challenges facing SKYCAP is the lack of specific institutional requirements that can be met by data produced via the system. While data tracked using SKYCAP is very useful particularly for supporting community-based case management, maximizing benefits from these data requires more complete participation from ambulatory care providers and hospital emergency rooms. Initiatives like SKYCAP may facilitate their own success by developing specific functionalities around administrative or financial needs faced by health centers on an ongoing basis. For example, by developing modules or reports that automatically highlight a specific provider’s clients who are eligible for insurance but remain un-enrolled, SKYCAP may be able to assist providers in increasing revenue from client visits. Developing these types of reports will ultimately create a dependency between the provider and the initiative that will sustain and improve the initiative over time. Enriching the data held in SKYCAP could also attract resources from researchers or other granting bodies who are interested in the SKYCAP model as a mechanism to provide reliable, population-level data on their target population. For example, one respondent reported that the State of Kentucky was looking at the SKYCAP model to manage the Medicaid population but that initiative has been delayed. Other entities have shown an interest in the SKYCAP model but nothing concrete has surfaced as of yet.
Strategies for Rural Areas. Rural Southeastern Kentucky area health centers faced some of the same major challenges that were uncovered in previous site visits to CHCs located in urban areas: low budgets for IT resources (including technical and management staff), lack of IT expertise, difficulty purchasing off-the-shelf systems due to highly customized needs, and an increasing client load. But, they also face a set of challenges specific to their rural environment. First, in terms of technical challenges, it may be difficult to procure the high-speed Internet connectivity that is needed to use networked applications because of low availability in rural settings. This will become less of a problem as broadband connections such as DSL become more widespread. For example, the SKYCAP program is in the process of moving from a frame-relay connection to a high-speed Internet connection.
Another technical challenge faced by rural areas is the lack of a concentration of talented IT professionals. Networking and using browser-based applications (as with SKYCAP) should reduce the need for in-person technical support visits to remote sites. Finally, being in a rural center may substantially reduce access to vendors. This challenge could be mitigated by the rural CHCs joining more broad-based consortia, including those based in urban areas, where there is a greater likelihood of having a wider selection of vendors.
Virginia
I. Introduction
NORC at the University of Chicago (NORC) is pleased to present this report detailing findings from our recent site visit to Virginia for “Community Health Center Information Systems Assessment: Issues and Opportunities.” NORC conducted this site visit under contract with the Office of the Assistant Secretary for Planning and Evaluation (ASPE) at the U.S. Department of Health and Human Services (HHS). In coordination with ASPE, the Health Resources and Services Administration (HRSA) and its Bureau of Primary Healthcare (BPHC) provide technical direction for this project.
The current site visit focuses on ongoing efforts in the State of Virginia and, in particular, the Richmond metropolitan area to support enhancements in information systems capacity at BPHC-funded consolidated health centers. We began the site visit with the goal of understanding the information systems capacity at consolidated health centers in Virginia, systems related issues and challenges faced by health centers, and their experience working with two prominent federally funded consortia focused on specific information systems-based projects. Findings presented here will be combined with findings from other site visits and related project activities to help elucidate the current state of health information system use by consolidated health centers, challenges facing health centers in this area, the context of health center information systems activities and models for successful collaboration around health center information systems issues. We organize the site visit report as follows.
- Background and Methods. This section describes key features of the site visit including background on the ambulatory care safety net in the city of Richmond and State of Virginia and details on who we met with as part of the site visit.
- State and Local Initiatives. This section describes the activities and infrastructure of two collaborations investigated as part of this site visit: the Community Care Network of Virginia (CCNV) and the Richmond Enhancing Access to Community Health Care (REACH) consortium. Both of these efforts are funded through grants provided by BPHC.
- Health Center Capacity and Perspectives. Because the project focuses on consolidated health centers and their experiences with use of health information systems, this section presents findings from our interviews with seven ambulatory care safety net providers in Richmond and other parts of Virginia. The majority of these providers are consolidated health centers funded primarily through Section 330 grants administered by BPHC.
- Conclusions. This section presents conclusions and lessons learned from the site visit.
II. Background and Methods
Twenty-seven consolidated health centers currently operate within the State of Virginia and three more will go live in the coming months. The majority of these centers are in rural locations scattered throughout Virginia, with heavier concentrations in the southeast and southwest areas of the state. Four health centers, including two CHCs, support the Richmond population, 21 percent of which is below 100 percent FPL. Statewide, more than one million people — 14.9 percent of the population — are uninsured; the most current estimates for Richmond indicate that 8,265 of the city’s children were uninsured as of February 2003 (there are no estimates for number of uninsured adults).8 As of 1998, 689,571 Virginians were enrolled in the state Medicaid program, 61.7 percent of which were covered through a managed care plan.9
In addition to receiving core funding through the federal BPHC, consolidated health centers in Virginia interact with and are supported by a number of Government and association entities. In particular, the Virginia Primary Care Association (VPCA) has provided technical assistance and advocacy support for ambulatory care safety net providers in Virginia for several decades. In addition to the VPCA, health centers are supported by the State’s primary care office (PCO) housed in the Virginia Department of Health Office of State Health Planning and Policy. Consolidated health centers in Virginia also interact with various Medicaid payers. Distinct from many States, Virginia’s Medicaid office sits in a separate Department of Medical Assistance, not within the Department of Health with the State’s PCO.
Consolidated health centers also work with each other through various State and community-level consortia. Two of these consortia, REACH and the CCNV, are featured in this report. Our discussions with stakeholders suggest that government and association support for health centers is largely distributed among distinct organizations and that coordination between offices is sporadic, though there is some evidence of increased communication and coordination over the past year.
Methods. The site visit to Virginia involved initial telephone and email contacts followed with in-person interviews with 22 respondents representing 10 institutions involved in the primary health care safety net in the State of Virginia. Because of the concentration of both community health centers and BPHC-funded consortia in Richmond, we focused our site visit around health centers and stakeholders located in this area. To assure that we received a variety of perspectives capturing health center systems resources and experience, we conducted telephone interviews with a number of non-Richmond area health centers following the main site visit. Table 1 below lists all health centers and other stakeholders interviewed as part of the site visit and follow-up telephone calls.
Telephone discussions and in-person interviews with respondents were conducted using open-ended discussion guides that provided some structure to each exchange while allowing sufficient flexibility to capture all relevant information from each respondent. In addition, a table shell was emailed to information systems staff at respondent health centers prior to the site visit to facilitate collection of standard information relating to infrastructure and technical capacity. For each scheduled site visit interview, the NORC team prepared materials that outlined our preliminary knowledge of the respondent and highlighted outstanding questions to address during the interview. Examples of discussion guides, other data gathering tools and preparation materials used in the site visit are included as Appendices A and B.
Respondent Organization |
Description |
|---|---|
|
Consolidated HealthCenter Respondents |
|
| Daily Planet Homeless Health Center | Daily Planet is a HCH located in Richmond. In 2002 they served 2300 patients over 3900 encounters. They are not a CCNV shareholder but are a participating provider. |
| Vernon J. Harris East End Community Health Center | Vernon J. Harris is a CCNV shareholder and a CHC. It is located in Richmond and served 3300 patients in 2002, with 7000 encounters. |
| Kuumba Community Health & Wellness Center | Kuumba Health Center is a CCNV shareholder CHC located in Roanoke, VA. |
| Peninsula Institute for Community Health | PICH is a CHC and CCNV shareholder located in Newport News, VA. In 2003 they had 20,473 users over 77,600 encounters. |
| Eastern Shore Rural Health System | ESRHS is a CHC and CCNV shareholder. They operate several sites in Nassawadox, VA. In 2001 they had 61,229 patient encounters. |
|
Other Stakeholders |
|
| Irvin Gammon Craig Health Center | Craig Health Center is a CCNV shareholder, and is in the process of applying for CHC status. It is located in Richmond and served around 1849 patients in 2001, with 3075 total encounters. |
| Hayes E. Willis Health Center of South Richmond | Hayes E. Willis is a Richmond clinic affiliated with Virginia Commonwealth University Health System. They do not participate in CCNV and are applying for CHC status. |
| Richmond Enhancing Access to Community Healthcare | The REACH consortium provides its health stakeholder members with technological (through the MORE Access system) and non-technological services related to data storage, report generation, eligibility tracking, needs assessment, and general support. |
| Community Care Network of Virginia | CCNV is a for-profit, CHC-owned health management services company. Based in Richmond, VA, CCNV provides practice management software, billing, reporting, credentialing, training, and other services to all consolidated health centers in the state. |
| Virginia Primary Care Association | The VPCA is the statewide CHC association. Based in Richmond, it provides its 27 members with services related to provider recruitment, cooperative purchasing, consulting, information, and training. |
| Virginia DOH Office of Health Policy and Planning | The Office of Health Policy and Planning oversees Virginia’s Health Workforce Advisory Committee, the Board of Health, the Primary Care Office (PCO), rural and minority health, and the designation of medically underserved areas. |
III. State and Local Initiatives
As mentioned above, site selection for the current project depends largely on the presence of ongoing activity related to building health information system capacity and infrastructure among consolidated health centers. As such, many of the sites selected are States or local areas where consolidated health centers and other safety net stakeholders are collaborating around community, State or regional approaches to enhancing information system capacity. This site visit focused on two of these collaborations: CCNV, a for profit management services organization providing business and systems support to consolidated health centers and other providers throughout the State, and REACH, a smaller initiative focused on supporting safety net care in the Richmond metropolitan area. This section of the report describes both of these initiatives in greater detail.
3.1 The Community Care Network of Virginia
This site visit focuses primarily on health center experience working with the Community Care Network of Virginia (CCNV), a for-profit provider network of safety net health centers and small private practices incorporated in 1996 and supported through federal grants and revenue-generating services. CCNV’s activities range from provider credentialing to establishment of a central billing office and, importantly for the current project, the establishment of a common platform for accessing practice management software through a subsidiary called Comcare, LLC. Although the consortium has considered the potential for implementing an electronic medical record (EMR) as well, they indicate that their current funding cannot support such an initiative. The organization is owned and managed by 17 consolidated health center shareholders, who elect CCNV’s Board of Directors. In addition to these 17 shareholder consolidated health centers, the network includes three participating providers or smaller private primary care practices that are customers of CCNV services. Three of the four consolidated health centers in Richmond are members of CCNV.
Organizational structure and staffing. In 1996, CCNV was governed by a nine-person Board of Directors. VPCA staff played a prominent role in early organizational activities, but after grant funds were secured the search for full-time CCNV staff began. A Chief Executive Officer was hired in 1997. Currently CCNV supports 21 full-time employees (FTEs) and three independent contractor staff. The Board of Directors is still made up of nine members who are all shareholders and serve for three year terms with staggered classes. Bylaws require 51 percent governance 4by health centers, but so far health centers have maintained 100 percent control. The remaining shareholders who do not have a representative elected to the Board are assigned to the Board member from their region for direct representation.
CCNV’s corporate senior staff members include a CEO, a CIO, and the Directors of the major programs: medical management, contracting, credentialing, and the central business office. A compliance analyst ensures that the network members are in compliance with government mandates and provides coding audits, training, and development activities. Currently, CCNV serves 19 health centers. The 3 additional participating providers are private physician practices or clinics that are located outside the service areas of the owner health centers and have hired CCNV to manage their practices — a funding source that contributes to CCNV’s outside income stream. By adding these participating providers, CCNV hopes to create economies of scale, further spreading the fixed cost of application services, and increasing savings for member centers.
CCNV Origins. In 1994, Virginia applied for and received a federal waiver to transition their fee-for-service Medicaid program to a mandatory managed care model. Through the VPCA, health centers in the State sought to organize around meeting the administrative and policy requirements of their new environment. The substantial resources and expertise needed to deal with these changes went beyond those currently available through the VPCA or the health centers themselves, so the steering committee decided to establish a separate health center network which became CCNV.
In preparation for starting the network, each participating health center contributed $1,500 of seed money. After organizational structuring and marketplace analysis, the centers reached the conclusion that they needed to form a new corporation, separate from the non-profit VPCA entity, which would give health centers corporate flexibility in the marketplace. This decision resulted in the formation and incorporation of CCNV as a Virginia stock organization in November 1996. All of the Section 330 health center grantees in the state purchased stock in the organization.
Funding sources. Once CCNV was incorporated, all 17 community health centers in the State became owners of the organization, contributing $6,000 in stock options as start-up money to pay for the shares. CCNV received an ISN grant in 1995, which added $217,000 to CCNV’s capital base. Their annual operating budget has grown from $122,000 in 1996 to its current level of around $1.5 million. Revenue is 17 percent grant-driven, 37 percent driven by user fees, and the remaining 46 percent stems from commercial activities. Since its inception, the organization has received continued grant support from the Bureau of Primary Health Care including the ISDI and SIMIS developmental network grants and their predecessors. Outside income is drawn from credentialing activities, financial management activities, and practice management technology provided to health centers and private physician practices. These activities are described in greater detail in the following sections.
State-wide practice management history. During CCNV’s early development, many of the state’s major health centers were using stand-alone practice management software owned and managed by a local vendor, Monet. In late 1998, Monet notified the health centers that it would be pulling out of the market due to issues surrounding Y2K, leaving the centers faced with the need for an alternate practice management vendor. Although Monet recommended that health centers use Medical Manager as their new practice management provider, CCNV leadership decided to conduct a vendor scan and selection based on the centers’ perceived needs. The network decided to take advantage of the federal government’s growing interest in health centers’ use of information technology and, in talks with the BPHC, laid out a plan for acquiring technology as an integrated network.
Vendor selection process. Initially, CCNV used consultants to learn about different applications and to develop criteria for evaluating options. CCNV sent out 27 RFPs to targeted vendors and received 14 proposal responses. A steering committee of health centers that did national review work scored every RFP against the evaluation criteria to narrow down the potential candidates. Four potential vendors conducted demonstrations of their products concurrently on both ends of the state, rotating between Richmond and Roanoke, Virginia. The health centers then scored each vendor and requested Best and Final Offers asking each of the four finalists to address specific questions. After extensive negotiation, Companion Technologies (with its practice management software suite Megawest) was selected as the winning vendor.
Following the acquisition of the software, in 1999, the decision was made to set up a subsidiary limited liability company (LLC) called ComCare to acquire, house and manage the statewide practice management system. This decision was made in order to protect the grant assets from any risks associated with supporting practice management, as CCNV would be its sole member and all assets would flow through CCNV. CCNV, via ComCare (with assistance and services provided by Companion Technologies), has implemented the MegaWest practice management suite at health centers in Virginia and Georgia. The MegaWest application is accessed via the Internet via a virtual private network (VPN) connection to a central server where the application and associated data are stored and maintained.
Non-Virginia Activities. CCNV provides credentialing and network services support to several health centers and one network in six other states. Credentialing services are provided to health centers in four of these states, including New Mexico, Delaware, Iowa, and Kentucky. These activities represent a major business line for the network. CCNV also provides training and Level 1 Help Desk Support for the Georgia Primary Care Association Management Information System Network. This strategy allows CCNV to use the business-related services they provide for their health center members and expand that model to out-of-state health centers and networks to generate revenues and keep costs to shareholder health centers low down.
ComCare Technical Infrastructure and Services. The ComCare approach is built on the application service provider (ASP) model in which an application and its associated data is hosted and maintained at a central location. This system allows health centers access to the practice management application and data using a virtual private network without having to install and maintain software and data at their own site. In the case of CCNV, there are some nuances to this model: Companion Technologies is the ASP vendor, and MegaWest is the hosted application. ComCare procures and manages the services received from Companion Technologies, and in delivers the services to the centers. This arrangement was designed so that ComCare could add value as an intermediary between the centers and the vendor itself.
The value added extends to both the centers and to Companion Technologies, as the centers are able to focus on their mission (while receiving assistance from ComCare) and Companion Technologies is able to take advantage of the many centers being represented by a single entity. As Companion Technologies is the ASP vendor, health centers using MegaWest access the vendor’s server via the Internet — hosted at a Companion Technologies site — using a virtual private network (VPN) connection. Approximately 20 health centers, over 48 individual clinic sites (including 2-3 health centers located outside the State of Virginia) and 400 users are provided with access to MegaWest using this system.
In addition to providing access to the practice management system, ComCare provides some support to health centers in ensuring connectivity to the Internet. Health centers we interviewed typically access the Internet (and, thus, the ComCare VPN) via T1 or DSL connections with local providers. All CCNV connections to the MegaWest server are routed through a central communications hub in Richmond allowing for a single circuit for communication with the vendor’s main South Carolina server. In many cases, shareholder health centers initiated the creation of a high speed Internet connectivity infrastructure specifically to access MegaWest software. ComCare is responsible for managing telecommunications costs associated with use of the software and typically helps health centers ramp up for enhanced connectivity if necessary. The telecommunications fees and maintenance costs are passed on to health centers. Health centers also pay for any upgrades to operating systems, desktops or network hardware necessary for building out their high speed Internet connectivity infrastructure.
In addition to securing access to the application and associated data, ComCare also provides one level of user support to health centers using the MegaWest software. ComCare mans a “Level 1” Help Desk to assist users with basic software and hardware issues related to their connectivity to the MegaWest server and use of the software. Under current staffing, one technician employed by ComCare is responsible for responding to inquiries coming into this line from all 400 users. In many cases, advanced questions regarding software functionality are referred to a “Level 2” Help Desk that is provided by Companion Technologies.
Relationship with Companion Technologies. While CCNV understands that the level of customization that can be provided by outside vendors is limited, they expect Companion Technologies to act as “a partner.” Overall, CCNV characterizes the relationship as mutually beneficial, noting that the initiative provided Companion Technologies with a valuable entrée into the community health center market. However, there was also a general feeling among CCNV respondents that Companion viewed the Megawest software (which was created by a separate company later acquired by Companion) as a relatively minor product and not a priority for internal research or marketing investment. We discuss the implications of this perception in greater detail under Conclusions.
3.2 Richmond Enhancing Access to Community Health Care
“Richmond Enhancing Access to Community Healthcare,” or REACH, is a partnership between more than 13 public and private health stakeholders in Richmond, including safety net health centers (both CHCs and free clinics), an academic health center, the City Health Department, the Bon Secours Richmond Health System, HCA Healthcare, the Central Virginia Health Planning Agency, and the Richmond City Department of Social Services. REACH’s stated mission is to increase access to a comprehensive continuum of quality healthcare services for persons who are uninsured or underinsured. The consortium, which was incorporated in 2002, provides a resource for data about health care for uninsured people, assesses community health needs, assists low-income individuals in applying for low cost health care options, and coordinates both non-technological and technological efforts across its partnering providers. Services provided to REACH partners include site-specific training, user groups hosting, limited on-site technical support, maintenance and software upgrades of software, and booster trainings. The majority of these services are coordinated through the MORE Access software system.
MORE Access. REACH’s MORE Access (Medical Online Resource Enhancing Access) system, which was described by REACH respondents as the “hub” for the organization’s IT initiatives, was designed to facilitate eligibility assessment and patient information sharing, provide a foundation for data warehouse, and serve as a communication tool. MORE Access was built for REACH by a local vendor, XPerts that was selected during a competitive procurement process in 2001 following the consortium’s reception of an HCAP grant. The software collects and maintains data on clients and encounters, including demographic and financial information (including client tax forms). It also supports automated eligibility determination for Medicaid and other State and local assistance programs. Like CCNV, REACH provides its partners with access to the MORE Access software via the Internet using VPN connections.
Although MORE Access is primarily a data entry system for patient financial and demographic information, it also contains built-in applications for data warehousing, GIS mapping, document imaging, financial screening, eligibility determination, and limited report generation. REACH staff anticipate that the system will improve collaboration between providers, for instance by enhancing understanding of patient utilization across different health centers.
Interfaces. Important features of MORE Access that enhance the potential for its use among a wide range of community providers are built in interfaces that allow the online system to “talk” with health center practice management systems. To date, REACH has developed two specific interfaces. One is with ComCare’s Megawest system, as many REACH partners are also CCNV participants; the other is with a separate practice management program used by a health center that is part of the Virginia Commonwealth University Health System (VCUHS), where the MORE Access servers are housed.
The need for the Megawest interface was recognized early on in the program’s development, as one of REACH’s main goals is to reduce duplication of efforts across the region’s health center networks. ComCare participated in some of the discussions around this interface. REACH paid Companion Technologies to design the actual system, which creates a text file incorporating the data elements from Megawest that is then uploaded into MORE Access. This process is not seamless: the text file must be extracted and made available on the ComCare server, then copied to a ComCare staff member’s PC, then transferred via SSH Secure File Transfer Client to the ftp server at Virginia Commonwealth University, where it can finally be uploaded to MORE Access. Although there has been some discussion about a more direct interface (one that does not require multiple active processes), this has not yet been designed.
Data entered by health centers is stored and maintained in an Oracle database. REACH leadership envisions the database and reporting infrastructure as a precursor to a community level data warehouse that could produce basic encounter and client level information from across the community, as well as support individual health center UDS reporting.
Early Experience. REACH is in the process of re-implementing health center utilization of the system this spring, having experienced problems with the eligibility determination function during the initial rollout in 2002. The revamped MORE Access system is currently being rolled out at the consortium’s three participating health systems and will soon go live at the community-based health centers across Richmond, as well as the Richmond City Department of Public Health. REACH respondents explained that their go-live strategy called for implementing the new MORE Access at the health systems first to facilitate the development of a training package for the centers that would correspond exactly with the needs and requirements of the health systems. They have encountered a few setbacks with one of the health systems, but anticipate bringing the health centers on-line towards the end of April.
Interestingly, REACH respondents indicated that they had had no knowledge of CCNV during their consortium’s initial stages. They felt that this was in part due to the high staff turnover among the local health centers. The respondents regretted not having known about CCNV’s existence during the start-up, but they thought that the two consortiums would be collaborating more in the future. REACH does currently work with the VPCA and the state Primary Care Office. In the section that follows, we present an overview of health center experiences working with both CCNV and REACH. Exhibit 1 below provides an overview of State and local initiatives described above and their relationship with CHCs in Richmond and statewide.
Exhibit 1. Overview of State/Local CHC-focused IT Initiatives
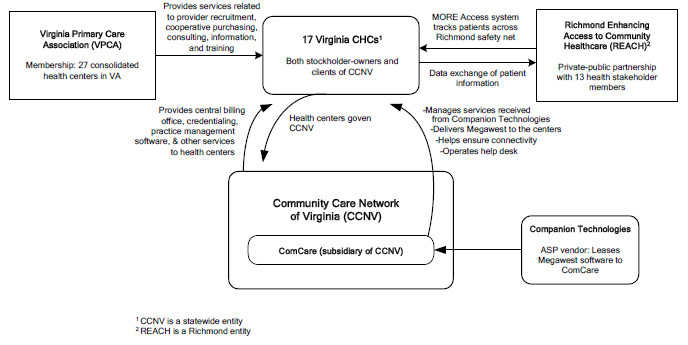
IV. Health Center Experience and Capacity
In addition to extensive discussions with leadership at CCNV/ComCare, the VPCA, and REACH, core site visit activities included in person or telephone meetings with seven community-based ambulatory care safety net providers in Richmond and other parts of Virginia. Overall, we found that health centers interviewed in Virginia differ substantially in terms of their access to information systems resources. As expected, we found that larger health centers have greater ability to acquire resources using general revenues and are more likely to have dedicated systems staff and ongoing planning around systems issues. We also found that health centers with affiliations to a larger health system such as an academic medical center benefit from increased access to systems resources. For example, we spoke with one center affiliated with the Virginia Commonwealth University health system, which provides all its centers with access to Cerner practice management software, 24-hour IT support, and plans to implement an electronic medical record.
4.1 Health Center Infrastructure
In this section we describe the information systems capacity at each of our interviews with consolidated health centers and other primary care safety net providers in Virginia, as well as their experience and perceptions from working with CCNV/ComCare and REACH on systems priorities.
Health Center Organization and Governance. As BPHC-funded consolidated health centers, the majority of ambulatory care providers we spoke with were governed by a Board of Directors who select and retain an Executive Director and other senior staff responsible for ongoing management of the health center. Stakeholders note that there has been considerable turnover in leadership at Virginia health centers over the last 2-4 years, leading to some important challenges for community and State collaboration. The majority of health centers interviewed are stand-alone organizations with a long history of serving low income residents in their communities. Unlike other States, there are no consolidated health centers in Virginia that are housed within county or local health departments. One of the health centers we interviewed is part of a larger academic health care system in the State and is currently in the process of applying for CHC status.
Systems Leadership and Vision. Some of the State’s larger health centers have made recent efforts to improve their level of expertise by bringing on experienced technical managers to serve as Chief Information Officers. These centers have typically been going through a re-assessment process and are making improvements to technical resources and information management processes. Other health centers report having no financial flexibility to invest in information technology expertise and infrastructure and rely heavily on CCNV. Still other health centers are part of larger provider systems, including inpatient providers, where technology decisions and resources are governed at a corporate level. In the paragraphs below we describe key features of the technical infrastructure at health centers we interviewed, summarizing the differences in key domains according to the health centers circumstances.
Staffing. Even the largest health centers we interviewed (some with more than 50,000 annual encounters) rarely had more than 2-3 dedicated information technology staff. For the most part, health centers in Virginia — including most of the CCNV shareholders — rely substantially on consultants or vendors to support their requirements around hardware acquisition, networking set up and support. In addition, several indicate relying extensively on CCNV and Companion for all access and functionality issues relating to the use of the MegaWest software. Health centers with the greatest access to systems expertise and support were those connected with larger health systems where these services are provided on a system-wide level.
Networking and Internet Connectivity. A few of the health centers interviewed maintained local or wide area networks (LAN/WAN) connecting different sites. In one case the WAN was supported not through the health center but by their parent health system. Health centers that were networked generally reported adequate access to network technology including high end servers, routers and platforms for managing use of applications across the network. Other health centers operating out of a small number of sites with limited access to resources report very little networking activity outside of Internet-based connectivity to the virtual private network used to access MegaWest. As described above, several health centers we interviewed indicated recently upgrading connectivity to the Internet in order to facilitate their use of the MegaWest software.
Software. With one exception, all the health centers we interviewed used the MegaWest product developed and maintained by Companion Technologies, Inc. for practice management. Furthermore, the majority of health centers accessed this software via Comcare. We found that health centers in the Richmond area have begun use of the REACH MORE Access software which is interfaced with MegaWest, providing a direct link between each health center’s practice management system and a community-wide client tracking and eligibility determination program. In addition, some health centers mentioned ongoing initiatives to integrate their practice management system with commercial laboratory information systems to allow automated tracking of clinical laboratory results. Commercial laboratories whose software is involved in these ventures include LabCorp and Quest Diagnostics.
A few respondent health centers also report participating in a pharmacy application coordinated by the Mountain Empire Older Citizens organization and the Virginia Healthcare Foundation. This program, Pharmacy Connect, provides health centers with a soon-to-be Web-based application for linking specific patients with free or reduced-price prescription drugs provided by pharmaceutical companies’ patient assistance foundations. The program also stores patient prescription information. Participating health centers praised the program, but noted that the software system did not interface with MegaWest. Finally, most CHCs interviewed reported using separate financial software and general productivity software such as the Microsoft Office Suite.
4.2 Health Center Perspectives
In this section we summarize health center experience using software and other systems resources currently available in Virginia. In particular, we describe their experience using the MegaWest practice management software, their very early experience using REACH’s MORE Access, and overall organizational interactions with CCNV, ComCare and REACH. We begin with discussion of health centers’ experience with CCNV and ComCare on an organizational level.
CCNV/ComCare Participation. Despite recent turnover in leadership at some health centers, many of the centers’ leadership, particularly for those centers that are CCNV shareholders, were very familiar with the history and evolution of CCNV and ComCare. Many small to mid size health centers interviewed credit the presence of the consortium as the primary reason they currently have an adequate platform for conducting basic practice management functions such as administrative reporting, scheduling and billing. While these health centers report having substantial challenges associated with their use of MegaWest (described in greater detail below), they attribute these problems primarily to a lack of adequate resources for the consortium.
Importantly, however, some health centers interviewed expressed substantial concern with the organizational orientation of CCNV and the usefulness of the services it provides. In particular, one of the larger consolidated health centers in the State reported recently discontinuing use of ComCare for access to practice management software, citing escalating costs to participating health centers, inadequate responsiveness around core issues such as reporting customizations and too much system downtime. This health center, and another larger health center that we did not interview, are both currently working directly with Companion Technologies for access to the same MegaWest software instead of using ComCare as an intermediary.
The health center we spoke with indicated their current arrangement affords them greater control over data maintenance, reporting and connectivity issues. While this has required substantial investment by the health center (they recently created the position of CIO), they sees it as a necessary step for assuring return on investment in information systems resources over time. Leadership from this center believes there are important efficiency concerns in Virginia where distinct entities with separate leadership, direction and funding seek to provide services to health centers. They suggested that, under this model, the health center community spends too many resources on defining organizational and legal boundaries or dealing with administrative issues and not enough time on addressing their own needs.
Experience with MegaWest. Many health centers interviewed suggested the importance of having access to a practice management platform to facilitate basic administrative activities and reporting to federal sponsors. While all stakeholders (including CCNV leadership) acknowledged that MegaWest was not an ideal solution, the majority of health centers interviewed felt that the MegaWest system was adequate in meeting these basic needs at an affordable price. In the bullets below we summarize health center experiences with using MegaWest for basic practice management functions. We note that these comments come largely from the health centers that access MegaWest using the circuit to the central software server maintained by ComCare.
- Scheduling. Most health centers report that the MegaWest system is used for scheduling patient visits at their health center and that it performs this function adequately. One important critique offered by health centers was that summary schedule data is not readily available from the system. While there is a process for pulling up a presentation of all appointments scheduled for a particular time, the process is clumsy and requires a non-trivial level of training in order to master. Many of the health centers report having inadequate resources to afford training offered through ComCare and Companion Technologies.
-
Billing. In Virginia, like elsewhere, having a systematic and automated process for developing encounter-specific reports and generating bills is the critical reason for information systems investments. All of the CCNV partners who access Megawest through ComCare utilize the software’s billing component; the majority reported satisfaction with the module’s performance. Three centers felt that the Megawest billing component worked “as well as any other system” and had experienced no problems with delayed payments. These centers were grateful that CCNV handles the billing, since they no longer had to dedicate a full FTE to that task. Another center, although generally quite pleased with the billing component, expressed the desire for an electronic payment posting functionality.
In addition to using MegaWest as their billing platform, some health centers completely outsource their billing function through CCNVs Central Billing Office. An executive director from one of these centers reported dissatisfaction with the necessity of outsourcing billing functions (this arrangement was in place prior to his heading the health center) and noted that Medicare and Medicaid payments sometimes took 80 or 90 days to arrive “when it should only take 60.” In addition, this center’s respondent reported that the system occasionally failed to catch wrong or missing data elements, leading to inaccurate claims submissions. - Reporting. Reporting capabilities, especially around UDS reports, are vital to all safety net health care providers. The Virginia health centers we spoke with indicated that reliable reporting functionality was one of their top priorities for practice management systems and information systems in general. According to most of the ComCare-affiliated centers, the Megawest system does not always perform as well at reporting as it does with scheduling and billing functions. These centers rely solely on Megawest to do UDS programming, and a few described the system as “not user friendly” and difficult to manipulate. These comments are likely related to the fact that data on the MegaWest server is not stored in a relational database format, substantially increasing the complexity reporting tasks.
One rural health center reported having problems identifying the relevant “dictionary” fields to pull specific information from, and another related that identical reports run at different times occasionally produce non-identical output. Two health centers indicated that they had no problems with their UDS reporting other than the minor issues arising every year when the report specifications are changed, but had trouble with more advanced reporting functions. One rural center sometimes relied on other health centers with more in-house expertise to run these reports for them. Training on these advanced capabilities is available but involves large fees that smaller centers are often reluctant to pay.
Experience with MORE Access. REACH experienced a few problems throughout its development, but it appears that its stakeholders now generally believe it is on track to provide useful and desirable functions. Early problems stemmed from a number of resource issues related to health center involvement in the initiative. For example, health centers were not always fully involved in the software development process. In addition, the initiative was hindered by recent changes in leadership at 50 percent of the core provider partners — a massive turnover that affected CCNV activities as well. This turbulence resulted in a decrease of health center knowledge about REACH and MORE Access, and the organizational leaders had to devote extra time and resources to re-educating health center staff about the REACH initiative and its IT project.
However, the MORE Access project seems to now be on firmer ground and working to establish itself in the Richmond safety net community. REACH leaders are planning to expand to additional organizations in need of eligibility determination systems and other components of the MORE Access software, but as of yet are only in the preliminary discussion stages with the interested entities. While our REACH respondents declined to comment extensively on partner satisfaction with MORE Access because the system is still being implemented, they thought that satisfaction levels were generally high and that the participating providers were optimistic about the program’s potential. This impression was confirmed by the health centers we spoke to who participated in REACH — they believed that REACH’s activities would be extremely useful to the centers’ functioning, and praised the “niche application” model of REACH as an “instant benefit” that would help both the uninsured population and the centers themselves.
V. Conclusions
Findings from Virginia illustrate important opportunities and challenges facing consortia that work with health centers to maximize benefits from administrative and clinical information systems. Many of the conclusions presented here highlight challenges owed to the rapidly changing context for safety net activities in Virginia and elsewhere.
Network participants have diverse needs which are not always met. While the health centers generally applauded CCNV’s efforts to address the need to support a basic platform for practice management, many centers indicated that they continue to face important unmet needs. For example, most health centers we spoke with lacked confidence that they were gaining the full benefits from their use of the MegaWest system due to lack of in-house IT expertise. On the other extreme, health centers that enjoyed ample resources for hiring senior information systems staff have been opting out of participation in CCNV for practice management, citing greater flexibility and efficiency from setting up individual relationships with practice management vendors.
This situation highlights the importance of and the challenges associated with meeting the broad spectrum of needs facing health centers of all sizes and levels of access. Less sophisticated health centers expressed the desire for services such as basic technical support (e.g., network connectivity), training, user support (e.g., helpdesk) and application services (e.g., a hosted application), but larger health centers with an existing systems infrastructure believed they would benefit more from interfaces linking their existing tools to community or State-wide systems. In all cases, the ability to customize services to meet diverse health center needs was seen as an important capability.
A changing environment poses special challenges. As in other areas, the ambulatory safety net provider landscape in Virginia has changed rapidly over the last four years. Health center and consortia are at risk for losses resulting from prior infrastructure investments that leave them with limited ability to adapt to these changes. As such, the ability to anticipate these changes and actively assist health centers avoid this potential danger is crucial. For example, some consortia have established efficient exit procedures allowing health centers to opt out of specific aspects of collaborative activities, recognizing that the needs and resources of health centers are likely to evolve. Furthermore, several centers mentioned that they would like to conduct regular vendor evaluation and re-assessment, but did not have the resources to do so themselves and therefore saw CCNV as a potential agent for this kind of activity. Having exit procedures and ongoing vendor assessment emphasize the flexibility of the consortium and its focus on meeting health centers’ evolving needs.
The need for ongoing vendor re-evaluation is particularly critical in light of the perception that MegaWest is not a priority product for Companion. CCNV regards MegaWest and Companion as a viable solution at this time, but if it is truly the case that the MegaWest application is not a priority for Companion, then it is likely that its viability as a solution will degrade over time and CCNV would find itself in the position of needing to migrate to another solution in order to provide current levels of service. This is not an unusual situation in that all software products and services solutions have known lifecycles which include migration to new products and technologies. However, it highlights the need to build in flexibility to any model for procuring and managing vendors.
Consortia can leverage sophistication of high end health centers. In trying to assure that the needs of all health centers are accommodated, the larger, more sophisticated health centers can provide an invaluable source of leadership and direction. Gains from systematic thinking on the part of those health centers with more resources to hire management staff with technical backgrounds can be spread to all consortium members through regular and open communication regarding system performance, unmet needs and strategies that can be implemented on health center or consortium-wide level. For example, several smaller health centers in Virginia appreciated the casual communication between themselves and larger, more sophisticated partners, but thought that a more extensive collaboration process would be of benefit to both parties. Existing solutions should be open to review and reconsideration.
Financial constraints contribute to the unequal status and lesser potential of smaller centers. While large, well-established safety net providers have the financial viability and resources to implement solutions independently if need be, smaller centers rarely have this option and must rely on consortium activities or outside funding to address their needs. This situation can result in two “tiers” of network partners, with the potential to adversely affect potential for collaboration. The specific challenge for policy makers and consortia leadership is to develop mechanisms that allow smaller health centers to benefit from the sophistication of those health centers with greater access to resources, while giving the larger centers a strong incentive to provide that assistance.
Coordination of support activities between regional health stakeholders is vital. One important frustration voiced by health centers in Virginia and elsewhere focuses around less than appropriate coordination and communication around ongoing grants, administrative, and support activities between the key players. For example, while stakeholders suggested collaboration, we found limited evidence of interaction on health systems issues between key organizations such as CCNV, the VPCA, REACH, the DOH Office of Primary Care, and the State Medicaid office. In addition to missing out on some opportunities to capitalize on collaboration, the distributed support atmosphere puts additional burden on health center leadership looking for involvement and support from each of these separate entities.
New Hampshire
1. Introduction
NORC at the University of Chicago (NORC) is pleased to present this report detailing findings from our recent site visit to New Hampshire for “Community Health Center Information Systems Assessment: Issues and Opportunities.” NORC conducted this site visit under contract with the Office of the Assistant Secretary for Planning and Evaluation (ASPE) at the U.S. Department of Health and Human Services (HHS). The Health Resources and Services Administration (HRSA) and the Bureau of Primary Healthcare (BPHC) work in conjunction with ASPE to guide activities under this project.
The current site visit focuses on an ongoing initiative in the State of New Hampshire to support enhancements in information systems capacity at BPHC-supported consolidated health centers. Findings presented here describe the information systems (IS) capacity of consolidated health centers in the southern half of New Hampshire, and focus on health center experiences working with a provider network headed by the Community Health Access Network (CHAN), a federally-funded consortium of safety net ambulatory health care providers. The report is organized as follows:
- Background and Methods. We begin with background on the ambulatory care safety net in New Hampshire and details on the organizations we spoke with as part of the site visit.
- Key Findings. In this section we summarize findings from in person interviews and other site visits activities conducted in New Hampshire. This includes features of the information systems infrastructure at consolidated health center providers interviewed in New Hampshire, health center experience with CHAN initiatives and CHAN’s relationship to other public health programs.
- Conclusions. Here we present conclusions and lessons learned from the site visit, with particular emphasis on issues related to long term sustainability and replicability of models used to promote health center use of information systems in New Hampshire.
2. Site Background and Methods
The State of New Hampshire, with its population of approximately 1.3 million, includes a relatively even mix of smaller urban, suburban and rural settings for the delivery of safety net health care. Although the State lacks significant county-level public health resources, it supports a substantial public health care system. New Hampshire also has seven Federally-funded Section 330 ambulatory care health centers. Five southern New Hampshire health centers make up the membership of CHAN, a not-for-profit organization that relies primarily on grants from the BPHC and other funders to operate. CHAN’s primary purpose is to support the mission of the health centers themselves. To do this, CHAN provides technical assistance and develops standard policies related to clinical, administrative, financial and technical aspects of health center operations. In recent years, the network has developed its own IS infrastructure and launched use of shared applications for EMR and practice management among member health centers.
Four of CHAN’s member health centers are community health centers (CHCs) and the fifth is a 330-funded Health Care for the Homeless center. Collectively, the CHAN members, all of whom provide comprehensive primary health care as well as some specialty services, have more than 136,000 patient encounters per year. Some centers provide health care to nearly 15 percent of their local population. Although patient and payor mix vary by health center, approximately 45 percent of CHAN patients are below 200 percent FPL and pay either on a sliding scale or through Medicaid; 7 percent are Medicare enrollees; 30 percent are commercially insured; and 15 percent self-pay the full cost of their care. Only one center, Nashua Area Health, serves a large minority (predominantly Hispanic) population.
The site visit, which took place on May 11, 2004, involved initial telephone and email contacts followed with in-person interviews with 15 respondents representing 5 institutions involved in the State’s primary health care safety net. Table 1 below lists all health centers and other stakeholders interviewed as part of the site visit and follow-up telephone calls.
Respondent Organization |
Description |
|---|---|
|
Consolidated HealthCenter Respondents |
|
| Lamprey Health Care | Lamprey is NH’s oldest and largest community health center (CHC), and one of CHAN’s founding members. Located in Raymond, NH, it operates 3 sites and serves 16,500 patients per year. |
| Manchester Community Health Center | MCHC is a CHC and CHAN partner located in Manchester, NH. It currently has one site and sees over 7,000 patients per year. |
| Health First Family Care Center | Health First is a CHC and CHAN member based in Franklin, New Hampshire. The center operates one site and serves 3,000 patients annually. |
|
Other Stakeholders |
|
| Community Health Access Network (CHAN) | CHAN is a not-for-profit network of health centers in southern New Hampshire. It provides shared information systems, IT infrastructure, training, clinical programs and other integrated services to its five members. |
| New Hampshire Department of Health and Human Services, Office of Community and Public Health (OCHP) | OCPH supports the state’s public health entities through grants, policy decisionmaking, technical assistance and education, and quality assurance activities. It works in collaboration with CHAN on various initiatives. |
Telephone and in-person interviews with respondents were conducted using open-ended discussion guides, designed to support a consistent structure for exchange while allowing sufficient flexibility to capture all relevant information. In addition, a table shell was emailed to information systems staff at respondent health centers prior to the site visit to facilitate collection of standard information relating to infrastructure and technical capacity. For each scheduled site visit interview, the NORC team prepared materials that outlined our preliminary knowledge of the respondent and highlighted outstanding questions to address during the interview. Examples of the discussion guides and other materials can be found in previous site visit reports.
3. Findings
In presenting findings from interviews and other site visit activities we begin with an overview and history of CHAN. We then go on to describe the current information systems capability and resources at CHAN health centers and provide details regarding the recent roll-out of EMR and practice management software. We end the section with discussion of CHAN’s role within the larger public health context in the state.
3.1 The Community Health Access Network
CHCs in Southern New Hampshire organized CHAN in 1995 to strengthen their collective ability to provide comprehensive primary care to underserved populations. As we’ve seen with the formation of CHC networks in other sites, CHAN developed, partially, in anticipation of Medicaid managed care. Overall, respondents indicated that CHAN’s formation was aimed at:
- expanding health center capacity by hiring more physician staff and broadening services offered;
- ensuring implementation of health care “best practices” across all centers;
- preparing the health centers to deal effectively with the administrative and financial challenges of impending mandatory managed care; and
- improving the centers’ ability to track patient care and enhance quality of care.
Defying some predictions, NH Medicaid did not go to mandatory managed care in the mid-1990s. Even without substantial pressures related to managed care, however, CHAN members decided that collaboration was the best method to remain competitive and solvent. In particular, they saw great value in using the network to support, plan and implement improvements in IS used by health centers. Beginning in 1997 CHAN took advantage of state funds set aside to encourage community interagency collaboration. Two years later CHAN secured its first BPHC SIMIS grant allowing the organization to purchase centralized servers and other components of a network systems infrastructure. Subsequently, CHAN obtained additional grants from the state and BPHC as well as from private donors including corporations and local foundations.
While CHAN has long prioritized development of networked EMR and practice management applications, this goal has become a reality only in the last few years with the roll-out of GE’s Logician package for the EMR system and Millbrook for practice management. Currently, the services CHAN provides to its member health centers include:
- access to shared applications for practice management, EMR and accounting accessed through a Wide Area Network/virtual private network (WAN/VPN);
- technical and user support to health centers using shared applications;
- standardized care management for chronic illnesses including diabetes, asthma and hypertension;
- development of a triage support through a phone notes tool for use in all sites;
- annual survey of patient perceptions regarding quality of care and services provided;
- development of shared corporate management services including compliance and accreditation.
We discuss these services and the health centers’ experiences participating in CHAN in subsequent sections of this report.
3.2 Health Center Information Systems Characteristics, Capacity and Resources
In addition to talking with CHAN staff, we interviewed the directors and lead IT staff from three of the five CHAN network health centers. Network participation and collaboration over the last eight years have succeeded in substantially improving the technical infrastructure and capacity at each of the five health centers. All centers have both the Logician EMR and Millbrook practice management systems up and running (except for one site that will implement Millbrook over the next few months), provide a similar set of services to their patients, and participate in network directives like electronic linkages with local hospitals and the BPHC-sponsored Health Disparities Disease Collaboratives.
Health center governance. Each of the BPHC funded consolidated health centers we interviewed relies on a community Board of Directors for overall governance. An Executive Director (ED) typically manages the center and is assisted by senior staff including a chief medical officer and senior administrative or financial officers. The CHAN member health centers have experienced low rates of staff turnover; most of the EDs have held their positions for many years and buy in to the potential offered by CHAN. In addition, all site visit respondents indicated that the level of cooperation between New Hampshire safety net providers in general, and CHAN members in particular, is exceptionally high.
Health center information system staffing. Although each health center does employ some dedicated IS staff, CHAN and member health centers significantly share staff resources. CHAN itself employs 8 FTEs (including both IS and non-IS staff), spread out over fifteen people. Six of these fifteen work exclusively for the network, totaling 4.5 FTE; the remainder are “shared staff” based at one or more of the member health centers whose responsibilities include IS duties for both CHAN and the staff person’s base health center. For example, the CFO/CIO of the CHAN network is also the IT Director for Lamprey Health Care. These shared staff operate the network’s help desk, which is available five and a half days a week and is based at the CHAN central offices. The health centers’ dedicated IS staff is primarily responsible for general office support, such as assisting end users with hardware, database, and minor connectivity issues. They have formal training in information systems but are typically not qualified to do end user support for the Logician EMR system. Specific support related to Logician is provided through the CHAN Logician specialists and from Logician directly.
Information system decisionmaking. CHAN health center IS decisions are worked out through a highly collaborative process. Most of the member health centers have informal internal IS committees made up primarily of their IS staff. These committees assess needs and make suggestions to the wider CHAN IS committee, which is composed of network and health center IS staff, led by the CHAN CIO. This committee receives significant input from the centers’ clinical and administrative leadership. Once a consensus has been reached within committee that an initiative should be pursued following a specific implementation strategy, the proposal is presented to the CHAN Board of Directors (made up of the health center Executive Directors) which then decides whether to go ahead. CHAN’s CIO/CFO noted that since nearly everyone involved in the process wears two hats — health center and network — decisions are made with both responsibilities in mind. CHAN is the source of all IS components of the network, so any changes affect all five centers. The CHAN CIO could not recall a major systems decision being made that was not universally agreed upon by the committee members.
Health center IS infrastructure. Even prior to the development of CHAN, member health centers maintained relatively robust hardware and software to support a range of administrative applications including practice management and in some cases EMR. Under the current model where practice management and EMR applications are housed on a central CHAN-administered server and provided to health centers via a VPN/WAN connection, member health centers still maintain their own servers and support general productivity software such as the Microsoft Office Suite. Each health center connects to the CHAN server and Internet via T1 lines purchased, installed and supported in collaboration with CHAN.
3.3 CHAN Information Systems Implementations
In this section we summarize the two primary information systems implementations coordinated by CHAN for the benefit of its member health centers: the Logician EMR system and the Millbrook practice management software suite, both of which are now owned by GE and marketed together as the Centricity Information Systems package. We focus in particular on 1) issues related to implementation of these applications and 2) key functionality and benefits offered by these systems based on health center experiences to date. We note that both initiatives grew out of the perceived need to develop a model for sharing access to and support for mission critical applications across health centers. Both of these activities were accelerated by the initiation of the BPHC’s SIMIS grant program.
3.4 CHAN and the Public Health Environment in New Hampshire
CHAN stakeholders attributed the network’s success, in part, to a statewide cultural mindset that favors the sharing of information, resources, and assistance among public health entities trying to build themselves up. This section outlines the public health safety net environment in New Hampshire and discusses a selection of other initiatives going on in the State and their relationship with CHAN.
The OCPH. The Office of Community and Public Health in the N.H. Department of Health and Human Services (DHHS) provides leadership and a core public health capacity for New Hampshire. The Office is organized into five major program divisions, comprised of the Divisions of Family and Community Health, Chronic Disease Prevention, Laboratory Sciences and Environmental Health, Epidemiology and Vital Statistics, and Health Services Planning and Review. The OCPH collects information on pre-natal care, family planning, diabetes, and cancer screening performance measures from consolidated health centers in New Hampshire, including the member centers of CHAN, and provides funding and support to safety net providers. Respondents indicated that the Office works closely with CHAN on issues related to reportable conditions, chronic disease management and public health education among low income populations. CHAN has been the administrative contractor for the NH Diabetes Prevention and Control Program since 1999. Similar developments are underway in NH for Asthma, also through CDC funding support. Although there is no automated electronic reporting between Logician and the OCPH, this functionality has been discussed.
Bi-State PCA. Through a Memorandum of Agreement (MOA), the first of its kind nationally, CHAN also collaborates closely with the Bi-State Primary Care Association, a private, not-for-profit organization with a membership of forty entities in Vermont and New Hampshire that provide and support community-based primary care services. These member organizations include community health centers, rural health clinics, private and hospital-supported primary care practices, health care for the homeless programs, clinics for the uninsured and social service agencies. To assure sensible division of goals and services between the PCA and CHAN, there is overlap between the board of directors of the two organizations and regular communication among leadership regarding new and ongoing initiatives.
Southern NH AHEC. A separate MOA is with the Southern NH Area Health Education Center, a non-profit program dedicated to the development of health professions. CHAN collaborates with the AHEC on the identification of staff development needs and the provision of a range of continuing education services for the health center staff. Training topics range from clinical competencies to cultural and leadership skills. Specifically for CHAN, the AHEC provides education credits for the EMR training curriculum.
New Hampshire Logician User Group. An informal group of health centers have been collaborating on the deployment of EMR since 1997. The agencies work together primarily on the development of end-user tools, which are shared between the organizations, thereby capitalizing on limited resources and technical talent with experience in Logician. CHAN has been an active collaborator of this group; giving and receiving tools and developing the collective intellectual capital. The User Group sponsors an annual regional workshop, named “AutumnLogic”, that showcases the work in New Hampshire and provides opportunity for potential EMR users to interface with EMR pioneers and observe new vendor developments.
The New Hampshire Community Technology Partnership. The N.H. Community Technology Partnership is a collaborative of six regional partnerships, representing more than 50 health and social service agencies in New Hampshire. The partnership’s goal is to implement a statewide, online service that provides clients access to health and human services programs and allows service providers to coordinate delivery of services online. Funded primarily through a BPHC HCAP grant, the coalition is working on developing an electronic “tool box” of program eligibility screening and care coordination tracking software with a central data base for all clients. Currently, the eligibility screening and care coordination modules are online and the central database prototypes are being delivered. Overall, the project seeks to (1) provide a network that connects participating agencies to a wide range of health care providers and human services agencies; (2) streamline intake processes across services and systems by providing a single point of entry; and (3) host a centralized database that maintains client-level information for program eligibility, care history and demographics.
Of the CHAN members, only Health First Family Care (HFFC) is currently involved in the Technology Partnership, although all are eligible. Our HFFC respondent explained that the current tracking software allows secure, confidential, centralized sharing of key data on safety net clients online. In Health First Family Care’s region, network agencies have agreed to create a joint disease management and treatment program that is managed electronically through the Partnership’s IS tools. Although CHAN has not been formally involved to date in the eligibility screening and care tracking initiative, CHAN respondents indicated that they are looking forward to a demonstration of the system scheduled for September 2004 and may play an active role in the project.
Medication Bridge Program. The New Hampshire Medication Bridge Program, a private-public partnership that helps eligible uninsured and underinsured patients obtain prescription medications from pharmaceutical companies’ Patient Assistance Programs, is the fourth prominent state health initiative. Participating sites include hospitals, community health centers, physician offices, senior housing, and non-profit organizations. All five CHAN members participate in the program, which has provided over 200,000 prescriptions for over 14,000 individuals throughout the state since January 2001.
4. Conclusions
The CHAN collaboration’s progress towards a fully integrated, technologically sophisticated network focused on meeting its membership’s information systems needs is (to date) the most advanced of any site’s yet visited for this project. A centralized and interoperable practice management/EMR system is fully functional in four out of the five network members, with plans to go live in the last site within the next few months. The organization’s health centers cooperate closely and share uniform goals for CHAN’s future. They have already seen benefits from the utilization of the Logician EMR and Millbrook practice management system, including improved medical outcomes, data of better quality and accessibility, more efficient physician workflow, fewer claim denials, and cost reductions. In the paragraphs below we outline key conclusions from the site visit.
Successful collaboration. A key theme to emerge from the New Hampshire site visit was the unusually high degree of collaboration practiced by CHAN members. The network goes to great lengths to obtain member input for all decisions and most votes are unanimous. Lamprey Health Care respondents described the organization as “great to work with…it’s like a big user group.” Stakeholders agreed that problems are approached from a collaborative angle; the attitude of “How can we fix this together?” prevails. There is a strong organizational commitment to advancing the network’s goals and mission jointly, even when it has meant that one entity (e.g., Lamprey Health Care) must disproportionately bear the risks and sacrifices.
Site visit respondents noted that this organizational cohesion and trust is owed in large part to the wider New Hampshire health care environment. New Hampshire is a small state, sparsely populated, and continually short of funds. Relative to other states, there is little money in New Hampshire’s Medicaid and other safety net programs to compete over. The uninsured and underinsured population is large and geographically dispersed, so CHAN members do not consider themselves to be in competition. Instead, the network health centers report that their best chance for long-term success is to make a joint case that the health care provided by FQHCs is high quality and should be reimbursed by all available funding sources. As one respondent noted, “It’s a small state, so we all see each other on a regular basis…you don’t want enemies, so we all help each other.”
Expanding collaboration. Within New Hampshire, the network will have to continue to collaborate with various public health entities. For example, CHAN may consider a network approach to participation in the New Hampshire Community Technology Partnership as a means to communicate more effectively with non-CHAN health care and social service providers and enhance the level of services available to their clients. In addition, there exists the powerful potential in New Hampshire to streamline and automate reporting conditions of public health importance through the infrastructure developed both by CHAN and the Technology Partnership. Finally, CHAN may expand to include the two consolidated health centers located in the northern half of the state, which have opted out of participating in CHAN. Technological limitations and geographical distance prevented these centers from joining the network during its inception — their IS infrastructure is less sophisticated than that of the other members, which would have meant poorer system performance, and their location hampers the staff sharing made easy by the south’s short distances. However, these centers still participate in CHAN’s clinical best practices projects and other collaborations. “We keep having discussions with them,” said one CHAN respondent, “and maybe in the future it will work out.”
Moving away from grant dependency. CHAN currently subsists on federal, state, and local foundation grants (which comprise 80% of the total budget), as well as annual member dues and shared fees (which make up the remaining 20%). However, grants are a tenuous and energy-intensive source of funds, and frequently pay for specific initiatives rather than broad overhead costs. Like similar organizations, CHAN applies for grants to conduct projects of interest to network members, but this necessitates a lot of “patch work” budgeting. Member fees are not used for the network’s developmental efforts. “The worst thing about CHAN is the need to constantly try and dig up funds,” said one respondent. “We want to get our message out and help others, but we need money to do that.”
Following from the model in other successful networks, CHAN is fostering consulting and technical assistance relationships with other health center consortia seeking to implement a shared systems infrastructure and applications. CHAN has recently begun work under a contractual agreement with a large CHC network in the Midwest to help with their EMR implementation. CHAN respondents described this initiative as “new turf,” but they indicated that there was great excitement through the network over the project. The partnership is designed, in part, to help CHAN grow its capacity. CHAN staff will assist the Midwest network by sharing their knowledge and experience in successfully implementing a centralized EMR system. Once that network’s system is fully operational, the two organizations will move forward with joint data reporting, sharing best practices, and other initiatives.
Enhancing functionality and customer service. As with any forward-looking organization, CHAN’s leadership is engaged in developing new avenues for program enrichment and revenue generation. CHAN’s philosophy is to use cutting-edge technology as a tool for survival — avant-garde computer applications that improve patient care and cut costs can leverage success with funding agencies. One of the network’s planned endeavors is to involve the patients in their own medical records: Using Kryptiq Corporation’s web-based ChartCatalyst software, patients are able to view their personal file and enter in information about their demographics, medical history, and current health status. The program then transfers the information to the EMR database, reducing redundant patient interviewing.
CHAN respondents noted that all of the network’s needed systems improvements are either currently offered by GE and other vendors, or are scheduled to be released in the near future. In terms of user issues, respondents agreed that decreasing provider workload while maintaining patient care quality was an important goal. As described above, entering patient information through Logician’s desktop protocols during an encounter can be cumbersome for the providers, and CHAN staff are seeking ways to make this process more efficient.
Florida
1. Introduction
NORC at the University of Chicago (NORC) is pleased to present this report detailing findings from our recent site visit to Florida for “Community Health Center Information Systems Assessment: Issues and Opportunities.” NORC conducted this site visit under contract with the Office of the Assistant Secretary for Planning and Evaluation (ASPE) at the U.S. Department of Health and Human Services (HHS). The Health Resources and Services Administration (HRSA) and the Bureau of Primary Healthcare (BPHC) work in conjunction with ASPE to guide activities under this project. Findings presented in this report describe the information systems capacity of consolidated health centers and safety net hospitals in Florida focusing on health centers affiliated with the Health Choice Network (HCN), a consortium of independent Community Health Centers and affiliates.
Site Visit Methods
With a diverse population of approximately 16 million, Florida is the nation’s fourth most populous state. The state has numerous community health centers, many of which belong to one of two major consortia, the Health Choice Network (HCN) and the Community Health Centers Alliance (CHCA). This report focuses on HCN, the larger of these two consortia, which serves pproximately 350,000 patients annually at 10 centers across Florida and at affiliated centers in Utah (7) and New Mexico (6). HCN is a non-profit health center governed network that provides information systems (IS) and administrative services to its member health centers using a centralized model.
The site visit to Florida, which took place on September 8th and 9th, 2004, involved initial telephone and email contacts followed by in-person interviews with eighteen respondents representing six institutions involved in the state’s primary health care safety net, as well as telephone meetings with two representatives from a seventh institution on October 6th. Table 1 below lists all health centers and other stakeholders interviewed as part of the site visit and follow-up telephone calls.
Respondent Organization |
Description |
|---|---|
| Health Choice Network (HCN) | HCN is a network of 10 health centers in FL, plus 7 in UT and 6 in NM. The network provides a centralized IS and administrative services to member health centers. |
| Community Health of South Dade (CHI) | CHI provides comprehensive primary and behavioral health services, including pediatrics, dental, vision, lab and pharmacy services. It served approximately 40,000 patients in 2003 at its 12 sites. |
| Camillus Health Concern (CHC) | Sponsored by the US Catholic Church, CHC has been a BPHC Healthcare for the Homeless grantee since 1989, and provides services at four sites, seeing approximately 5,200 patients in 2003. |
| Helen B. Bentley Family Health Center (HBB) | HBB provides primary and some specialty services, including pediatrics, dental care, vision, and social services at its 2 sites, seeing approximately 12,500 patients in 2003. |
| Economic Opportunity Family Health Center (EOFHC) | EOFHC provides primary care services, including dental and vision, at its 19 sites serving approximately 26,000 patients in 2003. |
| Broward Community & Family Health Centers (BCFHC) | BCFHC provides primary care, including pediatric, geriatric, lab and pharmacy services, at its 2 locations and approximately 3,000 patients in 2003. |
| Family Health Centers of Southwest Florida (FHC) (Interviewed by telephone conference) | FHC provides family health services, including OB-GYN, dental pediatrics, vision and social services at its 12 sites for approximately 46,500 patients (2003). |
Telephone and in-person interviews with respondents were conducted using open-ended discussion guides, providing a consistent structure to each exchange while allowing sufficient flexibility to capture all relevant information from respondents. In addition, a table shell was emailed to information systems staff at respondent health centers prior to the site visit to facilitate collection of standard information relating to infrastructure and technical capacity. For each scheduled site visit interview, the NORC team prepared materials that outlined our preliminary knowledge of the respondent and highlighted outstanding questions to address during the interview.
The remainder of this report is organized around findings from site visit activities related to HCN evolution, activities and governance model as well as the IS infrastructure and experience of health centers in South Florida. We end the report with a series of conclusions highlighting issues relevant to the effectiveness, sustainability and replicability of the approach represented by HCN.
2. Health Choice Network Overview
Health Choice Network (HCN) is a community-based, not for profit 501(c)(3) organization representing a group of BPHC supported (330) community health centers and other health care providers and organizations in South and Central Florida, plus affiliated centers in Utah and New Mexico. Although HCN shares some characteristics with other health center networks investigated as part of this study, it represents a distinctly comprehensive approach to network functionality and operations.
Under other models health center networks serve as an application services provider for targeted applications or, in less centralized models, networks collect and manage data derived from applications administered by individual health centers. By contrast, HCN comprehensively administers all of their health centers’ computing. HCN provides, supports and administers a full set of clinical and administrative IS applications, centralized billing, centralized accounting and general productivity software. In addition, HCN plays a substantial leadership role for its member health centers, with a network Senior Vice President serving both Chief Information Officer (CIO) and Chief Financial Officer (CFO) for several health center members of the network.
Understanding that its member centers were in many different situations in terms of needs and funds, HCN has a tiered membership system in place. All Network ‘Affiliated Members’ participate in the centralized IT and Fiscal services and may elect to participate in other integrated functions such as centralized billing, , managed care, and program development. ’Network level only’ Members may contract for some of the affiliated services (e.g. IT), and also may participate in group purchasing and other network activities, and are represented on the Board. There are also the NM and Utah networks, each of which have a service contract with HCN for provision of IS services.
Health Choice Network History
HCN, headquartered in Miami, Florida, originated in 1994 as health centers in and around Miami became increasingly concerned about provider consolidation and the movement towards mandatory Medicaid managed care. In addition, health centers were motivated by sharp increases in immigration from Latin America and in the prevalence of HIV/AIDS, which placed growing demand on their services even as they operated in an increasingly difficult business environment.
Developing the network model. The original HCN membership consisted of three health centers in the Miami metropolitan area: Community Health Center of South Dade, Inc., Economic Opportunity Family Health Center, Inc., and Family Health Center, Inc. Camillus Health Concern, Inc., joined within the first year of operation. This original group prioritized fiscal consolidation and joint investments in IS. The network also began exploring the possibility of forming a managed care organization. The network’s original IS strategy involved providing only direction and management on a network level, allowing each health center to maintain their existing administrative applications. Following the resignation of the network’s IS director in 1996 and a subsequent independent assessment, the network decided that true improvements and economies of scale could only be achieved through a broader approach including the use of common, centrally administered applications for accounting and practice management.
Also in 1996, Family Health Centers of Southwest Florida (FHC) in Fort Myers joined the network, expanding the reach of the network beyond Miami and bringing the network a new senior executive, Kevin Kearns, who had served as the Director of Finance & MIS since 1992. Kearns became the network’s new CIO/CFO and quickly moved to implement a networked accounting and financial system based around Best Software’s Platinum for Windows, as well as the Medical Manager practice management system. The network’s new IS strategy, implemented by Kearns, involved the expansion of network-based applications to include all health center software, including email and general productivity software. Also, in 1996, the network decided against forming a managed care organization, opting instead to negotiate a risk contract with an existing Medicaid managed care organization.
Maturity and expansion. Concurrent with changes in the level of centralization and support, the network decided to establish affiliation agreements with member health centers that formally recognized HCN, and specifically Kevin Kearns, as their shared CIO and CFO. Under these affiliation agreements, health centers signed on to participation in an integrated delivery system (IDS), agreeing to consolidate their financial and administrative operations even as they remained distinct institutions. To improve financial stability, the network’s fiscal department implemented a centralized billing system in 2001. This system serves members of the IDS Affiliated Members as well as Network only members.
In 1998, HCN met with the CEO of the New Mexico Integrated Services Network, a group of 6 health centers, who wanted to save costs by outsourcing IS systems and services rather than building them internally. The New Mexico centers could not effectively run their billing and tracking systems, nor attract staff who could, and had heard of HCN’s successful IS services, and felt that contracting out would be easier than building their own. The New Mexico ISN health centers agreed to engage HCN through “purchase of service” contracts for the purpose of administering their IS systems. There are four other health centers in New Mexico that are not part of the ISN. The two biggest centers in the New Mexico network did not participate because they wished to develop their own systems, and the two smallest could not afford to join. HCN entered into a similar arrangement with a health center network in Utah around two years later. Working with these two remote partners posed some initial challenges to HCN’s IS team, including how to reach such remote locations in the New Mexico desert, and hiring additional support staff to cover the time differences, but on the whole has shown that geography is at most a minor limitation in today’s technology marketplace.
Faith-Based Initiatives. Health Body, Health Soul is a combined faith-and-community-based program working to promote healthcare and disease prevention in African-American and Hispanic communities, particularly those with lower incomes, operated by HCN and six member centers, with participation from ten ‘lead-faith’ partners and over 100 Florida churches. HBHS currently targets pediatric asthma, diabetes and lung, prostate, breast and cervical cancer, and has partnered with member centers to provide pneumococcal and influenza vaccinations for seniors in Florida.
Formal partnerships with academic institutions, including Florida International University and University of Miami Medical School, are being explored for possible collaboration on research activities, in addition to ones already in place with the H. Lee Moffit Comprehensive Cancer Center and University of Miami Sylvester Cancer Center.
Moving to clinical applications. Today, HCN has ten network member health centers in Florida as well as contractual relationships with health center networks in New Mexico and Utah. Network health centers treat over 346,000 patients annually, including over 200,000 in the Florida centers, over 100,000 in the New Mexico centers, and over 46,000 in Utah centers. Over the past three years, the network has successfully pilot tested an EHR system, secured grant funding to support a wider roll-out, and begun implementation of the full-featured EHR (WebMD’s OmniChart Suite) in several Florida and New Mexico health centers.
To facilitate EHR adoption and implementation, the network has recently brought on a part time Medical Director who works closely with existing clinical quality committees. In addition, respondents noted that the network has renewed its focus on public health priorities including educational efforts around prevention and elimination of racial and ethnic disparities through partnership with the State, faith-based organizations and commercial entities.
Network Governance, Operations and Infrastructure
The network operates under a flexible but relatively formal model. Permanent governance derives from a Board of Directors, whose makeup is described below. A standing Integrated Delivery System (IDS) committee oversees issues specific to the nine health centers that have fully devolved their fiscal and IS functions to the network and are therefore considered IDS members. An additional set of topic-specific committees allow member health centers to make collaborative decisions and recommendations, which are reported either to the IDS standing committee or the Board of Directors.
Board of Directors and IDS Committee. The HCN Board of Directors is comprised of representatives from member health centers and health center networks. Founding members, including Family Health Centers of Southwest Florida (who were grandfathered in as a Founding member in 1996) have two representatives on the Board, while all other Florida health centers have one representative. Health centers contracting with HCN from Utah and New Mexico are represented on the board through their respective local networks. The HCN Board also includes a clinical representative and consumer Board members of its health centers.
The IDS standing committee governs business relationships between the network and 9 member health centers that have entered into agreement to share access to centralized core business functions through the network. This standing committee closely oversees these integrated functions and makes recommendations to the full Board of Directors.
Decision Making and HealthCenter Relations. A critical aspect of the network’s organization is its committee structure. Committees that report either to the full Board of Directors or the IDS standing committee are responsible for recommending policies specific to a wide range of network activities. In addition to making policy recommendations, the committees serve as an important forum for health centers’ staff to provide feedback directly to the network, discuss common problems and share lessons learned. Current committees include Finance, IS, Human Resources, Grants, Clinical and Dental.
Importantly, these committees cover topics of ongoing interest to health centers, regardless of the level of formal network involvement. For example, the committee on clinical issues had been in existence prior to the start of the EHR initiative and became a natural forum for introducing the EHR concept and customizing the EHR application once it was introduced. The committee system was widely praised by both network and health center staff regardless of the size of their health center.
Membership tiers and fee structure. Site visit respondents noted that HCN dues are relatively high. Network members pay annual fees of $15,000 for founding centers and $20,000 for new ones. There are also cost-based usage fees for using Medical Manager, frame relay lines, Platinum Support, and maintenance fees. These additional fees are loosely based on the size of a health center and average 1.5% of the overall health center budgets.. Finally, health centers obtaining other services through the network (including centralized billing or membership in risk contracting with Medicaid managed care organizations) pay an additional fee.
Network and health center staff indicated that this fee structure is considered very fair, as the services that come with IDS membership would cost centers between $600,000 and $700,000 per year to procure independently. Health centers disinclined to become full members of the Affiliated IDS have the option of joining as Network level member only, which have access to selected services based on payment of fees for those services. The health centers in Utah and New Mexico with contractual relationships with HCN mediated through their local networks form a third membership tier.
HCN Staffing. HCN currently has 85 network staff including approximately twelve on Florida’s West coast. IT staffing includes several executives and managers as well as a large cadre of billing specialists, programmers, technical support staff and trainers. The executive team includes a President and CEO, Senior Vice President for Development, a Medical Director, a Senior Vice President for managed care operations, and Kevin Kearns, the joint CIO/CFO for the network. Kearns supervises two Vice Presidents, one for finance and one for IT, as well as a Director of Reimbursement and Director of Implementations.
Infrastructure, Connectivity and Security. HCN operates a highly consolidated systems infrastructure. All systems including production servers are housed at HCN headquarters, and networked computers at individual centers can act simply as terminals, running all their applications over the network. HCN has partnerships with two major telecommunications providers, with whom they have negotiated pricing and service contracts: BellSouth in Florida and QWEST in New Mexico and Utah. In Florida, the network uses BellSouth T-1 lines with ADSL backup connections in all large facilities on a secure, high-speed wide area network (WAN). BellSouth provides both routers and WAN lines, all of which terminate at HCN headquarters in Miami.
For enhanced security, all connections are point-to-point, with no connection to the public internet. The connections are additionally secured by IP-level access control — only users at a given center can see that center’s data. All practice management and accounting data as well as some EHR data is downloaded nightly into a SQL server database and backed up. In case of disasters, HCN maintains capability to completely restore data and services within 24 hours for all centers. This system is tested twice annually. HCN maintains a 50KW generator at their headquarters that can keep systems running for 7 days independently. In addition, the network has contracted with a mobile backup unit which can provide change-over generator coverage in case the generator at HCN headquarters is compromised.
Administrative Applications
HCN provides network members access to centrally administered applications for practice management and accounting. The two primary applications selected by HCN include Platinum and WebMD’s Medical Manager. Kearns has implemented the Platinum financial system successfully at Family Health Centers in Fort Meyers prior to that health center joining the network. The Medical Manager application was selected by the HCN MIS Committee and had not been running previously in any of the centers. Medical Manager is currently owned and operated by WebMD, and provides health centers with typical practice management functionality including patient scheduling, resource management and billing.
Data management and reporting. Data downloaded nightly to HCN’s SQL Server database from Medical Manager is available to health centers for query using InfoPoint or Crystal reports. Platinum data is directly accessible via Crystal. In addition, HCN itself employs programmers and regularly provides standard center- and network-level accounting and practice management reports to the health centers.
Medicaid billing formats. HCN has worked extensively with Medical Manager and their corporate parent, WebMD, to accommodate health center needs around Medicaid billing. Member health centers successfully bill to numerous Medicaid managed care organizations (including through direct billing) and other payers, each of which typically require a different format for billing. Respondents indicated some difficulty in using Medical Manager to efficiently produce billing formats consistent with HIPAA requirements for electronic data interchange.
This limitation posed an immediate problem when Utah and New Mexico health centers began using the Medical Manager product as the Medicaid offices in these States, unlike Florida’s, has moved to requiring HIPAA-compliant formats. Although these problems have largely been addressed, Kearns indicated that the introduction of a new managed care organization or other type of payer will often require special effort to further customize billing templates.
Relationship with WebMD. HCN, which administers Medical Manager to support over 1 million encounters over a wide geographic range, enjoys an atypical level of responsiveness from Medical Manager’s parent company, WebMD. While health centers from other site visits using Medical Manager reported inconsistent customer service from WebMD, Kearns indicated that he can relatively easily convene senior executives from WebMD to negotiate around functionality and price and is generally able to get a swift response from the vendor when problems arise.
Although there have been some reported problems with Medical Manager, the stability the network has achieved using the system exceeds the typical health center experience with this product. HCN respondents indicated that they have worked extensively with WebMD to customize the application for health center uses and that the relationship has helped WebMD’s efforts to increase market share among health centers.
As the network’s experience with WebMD has developed, the likelihood of the consortium changing vendors has decreased — particularly because there is high overall health center satisfaction with the tool. Additional findings related to health center experience with using Medical Manager are provided in the section discussing health center experiences below.
Electronic Health Records and Electronic Oral Health Records
In 2002, the BHPC funded a pilot program to help HCN implement EHRs at 4 Florida centers. The pilot program met with mixed success, and important lessons learned. Based on their experience from the pilot, HCN received a four year, $4.4 million Information and Communication Technology (ICT) project award from HRSA to roll out EHR and Electronic Oral Health Records at all Florida centers. HRSA funded this and five other ICT projects to support health center participation in the development of integrated business and medical technology systems. HCN bolstered these funds with a commitment of $8 million from participating centers.
Pilot experience. The Board of Directors and Clinical Committee identified centers and providers appropriate and willing to serve as pilot sites. All pilot providers are champions of EHR and now help with training in their respective centers. The initial pilot test involved four providers, three tech-savvy and one technologically inexperienced, across three Florida health centers. Although HCN did conduct a limited assessment of vendors prior to conducting the pilot, it was clear, given their existing relationship with WebMD and the potential for integrating the EHR with Medical Manager, that WebMD’s Omni Chart system represented the best business fit for the network.
Omni Chart provides a suite of EHR functionality including electronic prescription writing, clinical task management functions and electronic lab orders and results. Additional EHR functionality is provided through OmniDocs, a system for electronic capture of open ended progress notes. In addition, HCN has worked with the WebMD’s Document Image Manager for document and image management and Dentrix Systems for electronic oral health records. A full description of the EHR functionality available through HCN is provided in Table 2 below.
| Application | Functionality |
|---|---|
| Rx-Writer * | Allows electronic prescription writing and transmission to pharmacies |
| Clinical Task Manager * | Tracks items requiring follow-up (e.g., labs, patient instructions) |
| Transcription Manager * | Stores transcribed notes in patient’s electronic charts |
| E-Encounter | Allows electronic selection of visit procedure and diagnosis code(s) |
| WebMD’s OmniDocs | Provides user friendly graphical user interface for progress notes |
| Document & Image Management System | Stores scanned clinical images for inclusion in patient record |
| Dentrix | Electronic Oral Health Record system |
| * Each of these functionalities is included in the WebMD OmniChart Suite | |
As preparation for the pilot began, it became clear that key features of the software were not ready for implementation. Although the backbone of the software was written; WebMD had very little experience supporting the tool in real world settings. For example, there were very few default forms available and standard drop down menus and templates were cumbersome and inappropriate for use in a health center setting without further customization. As a result, the pilot began with limited roll-out of the prescription writing functionality.
After several months of working with WebMD and a new Medical Director hired by the vendor to handle customization of the OmniChart product, templates were developed that enhanced the usability of the system and gradually additional functionality was added. Overall, the pilot experience highlighted the importance of conducting extensive assessment of usability by working directly with providers, identifying physician champions who would be willing to “tough it out” in the early stages of an implementation, and connecting providers directly to staff at the vendor to tailor applications.
Ongoing roll-out. In 2004, having secured funding for a broader EHR implementation through the ICT grant, HCN began working closely with WebMD on additional customizations. As with Medical Manager, HCN’s significant market share allowed the network to negotiate a strong partnership with WebMD around EHR. WebMD has subsequently used customizations developed in conjunction with HCN to expand the scope of functionality it can make available to the wider health center and private provider market.
Over the past year, HCN has gradually increased the scope of its EHR activities, steadily adding to the number of providers using EHR, as well as the functionalities used by those providers. As in the pilot, providers and health centers tend to start with limited functionality in order to gain facility with the initial user interface. Providers then move on to using the task manager and computerized progress note applications. Table 3 below highlights the status of EHR roll-out at several of the health centers visited as part of the study.
| HealthCenter | EHR Status |
|---|---|
| Community Health of South Dade (CHI) | Six providers are live on the full HCN EHR package (including OmniDoc), and four more are up to the Rx-writer stage. Ten more medical providers will be added in the future, but CHI’s 20 behavioral health providers are not currently slated to join the EHR until 2006. |
| Camillus Health Concern (CHC) | All providers at CHC are currently using Medical Manager’s administrative and practice management functions, and the center was just beginning to implement EHR at the time of visit. |
| Helen B. Bentley Family Health Center (HBB) | All 20 of HBB’s providers are using Rx-writer, and are at various stages in adopting the full EHR. |
| Economic Opportunity Family Health Center (EOFHC) | 3 medical providers are fully live on the EHR, and all 5 dentists are fully live on Dentrix, with the rest coming on shortly. |
| Broward Community & Family Health Centers (BCFHC) | All 3 providers are using Rx-writer and are in the process of going live with the rest of the EHR components. |
| Family Health Centers of Southwest Florida (FHC) (Interviewed by telephone conference) | This center participated in the Pilot program of HCN’s EHR system, and all of its providers use some aspect of it, including 20 providers fully live on all components. 47 total providers, including six dentists, use some modules of EHR. |
Although the systems can be installed on stationary terminals in exam rooms, most health centers are implementing the system using the Lifebook wireless tablet PCs that their providers carry. The cost of purchasing this hardware falls largely on the health centers. These computers connect to the HCN network through secure wireless network access points (WAPs) installed at each health center site.
Training model. While specific training programs vary from center to center, the basic approach is the same across HCN. First, the network works with health centers to select the providers that will participate in the initial roll-out. The goal is to start with at least two or three patient and enthusiastic providers simultaneously at any give site. Once providers are selected, they attend an intensive training either at HCN headquarters or on-site. After the initial training, local IS staff are supplemented by a dedicated on-site HCN trainer who comes to the center for several days to help providers transition to using the system.
Depending on a given center’s needs and logistical considerations, follow-up training may be conducted online using WebEx (online training software) or subsequent visits back at HCN. In addition to training activities coordinated through HCN, each health center has identified physician champions and peer trainers (generally highly respected colleagues) who continue to support use of the application by their fellow providers. At one center, the physician champion meets with providers over a series of dinners to discuss their experiences with EHR.
Phased-approach. Unlike other networks implementing EHR, where a large infusion of private sector dollars led to relatively rapid implementation of EHR across a series of health centers, HCN has slowly phased in EHR use among health centers and providers. Health centers can take advantage of having the network infrastructure to support electronic records for some patients even as most of their patient records continue to be paper-based. In addition, HCN does not ask providers to switch exclusively to using the EHR “over night.” Instead, providers begin by using the system for a limited number of their patient visits in a given week (e.g., one or two visits per day out of a total of six).
Most providers begin by using only the Rx-Writer and clinical task manager for lab orders and results. These modules are simple to use, and their benefits are immediately clear. HCN finds that starting with these modules promotes initial buy-in and interest among providers. HCN is now in the process of moving to full EHR — all providers using all functionality — in several of its centers. The overall goal is to implement the full system with all 200 Florida providers by December 2007.
Clinician Involvement. Key to HCN’s success in implementing EHR has been clinician involvement at all levels of the process. The initial discussions around EHR implementation during the pilot phase prominently featured the clinical committee, composed of the medical directors from each member center. These clinical leaders were involved at all steps of EHR selection, customization and implementation. In addition, the use of clinician champions across health centers has markedly enhanced take-up.
In addition to allaying concerns and encouraging clinicians through difficult steps, medical directors and champions, through the clinical committee, regularly report challenges or issues with EHR use back to the CEO, CIO, and EHR project managers at HCN for quick resolution. The consistent level of buy-in from clinical leadership across health centers has greatly mitigated physician resistance to EHR in the health centers. The general experience is that once a few providers at a given center go live on the EHR, the others — including many of those initially most resistant — become very interested, and want to get on board.
Importantly, clinician input drives all customizations of EHR tools, including setting “pop-up” reminders to encourage appropriate delivery of diagnostic or preventive services as well as other clinical decision-making features. Recently, a network-level medical director has been hired to coordinate quality improvement and prevention programs that leverage the availability of EHR and build close relationships with other community stakeholders.
3. Health Centers’ Experience with HCN and the EHR
Health center respondents uniformly praised their experience with HCN, citing major improvements in their overall operations following establishment of the network. One center CEO said that his center is “not the same entity” it was before HCN, indicating that the organization would either not be in existence or be operating on a very limited scale were it not for the network’s support. These comments are motivated primarily by the health centers’ experience with administrative and financial improvements facilitated by use of HCN accounting and practice management systems. However, it is clear that the trust and comfort level generated from HCN’s strong support of health centers’ administration have enhanced the network’s ability to successfully navigate the difficult process of EHR implementation.
Health Center Infrastructure and Staffing
As typical in other networks visited, the in-house administrative and IS infrastructure at HCN health centers varies considerably. Some HCN health centers employ dozens of providers across up to 15 sites and manage between 40,000 and 50,000 patient encounters each year. Others are much smaller health centers, with one site that sees barely 5,000 encounters per year. HCN’s approach accommodates these differences very well; respondents from centers of all sizes said they felt more than adequately supported.
Hardware and connectivity. Access to hardware differs considerably across the network. While some centers are able to regularly upgrade their computers and purchase hand-held devices or Lifebooks as necessary to support EHR roll-out, other health centers work with relatively outdated computers and have begun implementing EHR using stationary terminals. Because all HCN-supported software is run over the WAN, centers can use older computers, which would otherwise be obsolete and need replacement, as ‘dummy terminals,’ saving precious capital funds. Smaller centers visited remarked that this flexibility was a major benefit for them.
Staffing and user support. With one exception, all health centers visited had personnel resources dedicated to supporting computing. At the larger health centers, the in-house computing personnel typically total three staff: an administrative manager, an operations hardware expert and a programmer or applications expert. These staff worked closely with staff from HCN to review infrastructure and hardware specifications needed to support HCN applications and maintain compliance with HCN’s guidance (e.g., regarding access to back-up hardware). In addition, health center IS staff work closely with HCN technical service personnel to respond to service requests from clinicians and other users.
Typically, staff at the health center will handle relatively minor requests for assistance, including any request involving faulty hardware or connectivity setup. Simple guidance regarding how to use HCN applications may also be provided by the health center IS staff, although the HCN help desk is required to deal with any request that requires changes to settings or permissions as in-house staff have no administrator rights for HCN applications. A key benefit of HCN membership, according to health centers, is the ability to maintain a relatively limited group of in-house systems staff even as the center continues to upgrade software and roll-out new functionality.
Software applications. HCN’s IDS member health centers typically restrict themselves to use of HCN supported applications available through the HCN network including Microsoft Office (including email), Medical Manager, the various EHR applications and Platinum. In addition, HCN provides health centers access to their practice management or EHR data for the purpose of producing custom reports using Info point or Crystal Reports.
In some cases, we found that health centers were using additional, non-HCN applications “off line,” including database software customized to tracking specific procedures or conditions linked to maintaining non-BPHC funding. Respondents indicated that HCN staff tries to help as much as possible with these applications, though their use is not officially supported or condoned by the network. Health center staff reports that they strive to use HCN supported software whenever possible.
Experiences with Medical Manager
Staff at health centers reported overwhelmingly positive experiences using Medical Manager. The most effusive comments were made when comparing current use of Medical Manager to the systems for practice management and billing they had in place prior to HCN. Health centers uniformly noted improvements in operational and administrative efficiency. While there were some functionalities that people indicated could be improved, most were satisfied with the application as implemented by HCN. Furthermore, most health centers believe that their satisfaction with Medical Manager was largely a result of HCN’s buying power and ability to work effectively with WebMD on customizations and problem resolution.
Billing and administrative simplicity. Respondents consistently indicated that the implementation of Medical Manager through HCN has allowed them to more effectively collect from payers with less investment on their part. In many cases, this enhanced efficiency followed not only on the use of Medical Manager but the outsourcing of their entire billing operation through HCN. In particular, health centers noted that Medical Manager does a better job than other applications in supporting sliding-scale billing. Health center networks have indicated that billing errors have been greatly reduced using Medical Manager and, when they occur, they are largely the result of inadequate user training rather than an application issue. While some health centers did suggest that more flexibility around billing formats would be desirable given evolving payer requirements, overall satisfaction was very high.
Reporting functionality. Health centers also indicated satisfaction with reporting capabilities provided through HCN and supported by Medical Manager. In particular, health centers noted that Medical Manager facilitates development of required reports such as the UDS and helps with tracking specific disease populations and procedures as required by some funders. While health centers indicate that the reporting capabilities provided through Info point and Crystal Reports are robust, many do not have the in-house expertise to produce custom reports and rely instead on standardized reports produced by HCN.
These standard reports are useful, particularly because some of them elucidate utilization and management trends associated with specific diseases. However, some health centers note that they would like to see better reporting from Medical Manager around administrative or business issues, including reports that assess health center productivity, reports tracking use of volunteer hours and reports describing experience with specific high cost diagnoses and procedures.
Ease of use. Some health center respondents reported problems with making full use of the Medical Manager application. Many health centers indicated that their staff was routinely unable to use the system to realize specific functionality that they were told the application supports. For example, respondents indicated that they have had difficulty using Medical Manager to track instances where patients do not show up for scheduled appointments or to track which user (health center staff member) was responsible entering data for a particular encounter. Other health centers indicated that they would like to use Medical Manager to “flag” veterans, school-aged children or patients who have been seen at another of the health center’s sites, a function they have not been able to make work.
Some health centers felt that these problems were a result of inadequate training, other cited lack of appropriate skill among some of their health center employee users. HCN is able to address these issues through the development of standardized reports or functionalities where they “do the work” for the health centers. However, HCN is not able to satisfy all of these requests, especially when the demand for them is restricted to one or two health centers.
Experiences with EHR
Health centers reported positive experiences with initial roll-out of EHR in Florida and a high level of enthusiasm in expanding take-up of EHR within their center with the goal of improving the quality of care as well as the overall efficiency. After some struggles at the pilot sites, center staff all report being very pleased with the system and multiple respondents reported that interest grows with each additional provider who goes live. In the paragraphs below we highlight significant aspects of health center experiences with EHR in Florida as recorded during our site visit.
Clinical decision making tools and patient safety. Clinical staff interviewed indicated a high level of comfort with the customization of clinical decision support functionality. Many mentioned that “pop up” notification of laboratory results in a problematic range has allowed for quicker clinical response. They also praised the usefulness of drug interaction and allergy warnings. In addition, several respondents mentioned having an increased level of comfort with prescriptions that are electronically prescribed due to the elimination of legibility issues.
One clinician noted that his health center has benefited specifically from the reduction in unsafe use of drugs that interact unfavorably with ACE inhibitors. Health centers are involved in ongoing customization of the pop up message functionality so that it provides appropriate levels of clinical decision support with out overburdening the provider. Clinical leadership across the health centers indicated that HCN has used these tools effectively to date, working closely with clinicians to adjust settings over time. Finally, health centers noted the safety benefits of having easy access to patient-level medication data. For example, following the recall of Vioxx, health centers using EHRs were able to query their EHR data to quickly identify and notify affected patients.
Quality of care benefits. Although most health centers are early on in their implementation of EHR some did indicate that they are already able to see outcomes and process improvements. In particular, one health center noted that their average HbA1c for diabetic patients went from 8.5 to 7 during the months immediately following implementation of EHR. Currently, HCN only maintains a limited set of the EHR data in a format available for query by health centers and use of EHR data to monitor and support quality of care occurs largely on a center by center basis. At this time, a limited percentage of patient encounters across the HCN network are facilitated by EHR. The HCN medical director is working with clinical leadership across health centers to develop HCN-wide disease management and quality of care programs to be rolled-out as use of EHR expands across the network.
EHR effects on productivity. Unlike other settings where an “overnight” approach to EHR implementation results in substantial decreases in productivity over the course of several months, HCN’s approach of incremental roll-out results in relatively small, short term reductions in productivity at the time of implementation. HCN recommends that centers plan for about 90 days of decreased productivity; so far they have mainly seen 5-10% reductions for 60-90 days, after which productivity returns to and, in some cases, exceeds previous levels.
Usability and patient response. Although clinical leaders indicated some apprehension on the part of clinicians, none reported major problems with providers becoming comfortable with using the EHR system after limited training and use. Health center staff reported that even the least computer savvy clinicians have adjusted to using the application after overcoming the initial fear of not being able to adopt. Several clinicians noted that the electronic record was more usable than the paper system. For example, the application allows them to review multiple parts of a patient’s record on the same screen reducing the time it takes to “flip back and forth” in a paper chart. One clinician indicated that using the EHR has dramatically decreased the time it takes for him to review a patient chart.
In addition, health centers note that patient response has been positive. Clinicians introduce and explain the EHR concept to patients during the first encounter facilitated by the application. Many indicated that patients take comfort in observing that their physicians are using advanced computing. Some clinicians indicated that the Lifebooks offer a wonderful opportunity to educate patients in the exam room — by pulling up graphics of key clinical indicators or diagnostic images at the point of care. However, some clinicians indicated this type of patient education was not possible given the current setup in their health center. Overall, there were no indications from our interviews that use of EHR has detracted from patient satisfaction with the quality of patient/clinician interactions.
System stability and access to data. Because the HCN envisions a completely paperless environment in all health centers following complete roll out of all EHR functionality, great care has been taken to assure system stability and reliability. These investments are particularly important in Florida where during hurricane season, health care providers often scramble to provide care after a portion of their facilities have been destroyed. During the 2004 hurricane season, the HCN network stayed functional with no downtime. The only downtime was experienced at the centers directly affected by the storms). After having to temporarily shutdown specific health center sites with EHR, patients who served at those sites were treated seamlessly at other network sites where providers had complete access to their EHR. This experience increased enthusiasm for EHR across the network and motivated health centers to step-up their plans for investment and implementation.
Supporting various care needs. HCN health centers have successfully customized the applications they use to facilitate specific primary care services, including pediatrics and chronic care management. Current efforts are directed towards Network-wide implementation of quality care guidelines, case management systems, disease management initiatives, and network-wide quality improvement. Health centers have also considered instituting use of the EHR among their behavioral health providers. Although health centers indicated that these providers would be able to use EHRs to an extent, there is some skepticism regarding the ability to customize forms and templates to deliver behavioral health care. Individual centers participate in a number of disease management collaboratives of their own choosing, including a Diabetes Consortium, Cancer, Depression, Asthma, Medicaid/Medicare, and BPHC performance benchmarking, and HCN has developed customized forms for a few of the more common ones within Medical Manager. Some centers use stand-alone PECS, but they have moved to a new network version which allows HCN to support the databases. HCN staff report that their long-range plan is to create the collaborative reports from Medical Manager and submit them electronically, eliminating the need for PECS and CV DEMS. They are currently testing an export program that will take lab results from Medical Manager and export them to a file that is then imported into the PECS software.
HCN’s system is able to track patients who are seen at various participating centers, and the EHR has been able to identify patients who move from center to center “drug seeking.” Presently, they do not share EHR or administrative data for security reasons, but in the long-term they plan to share data not only between centers, but with hospitals and private practices, creating a “true continuum of care” for patients.
Costs and future uses. HCN health centers were overall very positive regarding EHR use citing the cost of licenses and hardware being the greatest barriers to adoption. Although there are still some reluctant providers, there was an overall willingness and enthusiasm to learn. Critique of the EHR centered on unrealized potential benefits. For example, although some health centers are able to access inpatient data on their clients through Jackson Memorial Hospital, there is no two-way electronic communication on client issues across non-HCN health care providers. In addition, some indicated that they would like to see greater compatibility between Medical Manager and the progress note functionality of the EHR. Finally, some health centers indicated that the Rx-writer’s formulary functionality was not compatible with the format in which several health plans provide their formulary data. HCN continues with its implementation of the EHR products, and respondents say they plan to have 200 providers in Florida live on the full EHR by 2007.
4. Conclusions
Findings from our site visit demonstrate the potential of a centralized network to serve health center needs through substantial integration financial and information systems. The site visit shows, that when appropriately pursued, such integrations allow health centers to enjoy a much higher level of service than they could afford on their own. Key conclusions are highlighted in the paragraphs below.
Serving and leading. Respondents made it clear that HCN has worked hard to simultaneously serve and lead health centers. Kearns and other HCN staff take their role of systems administrators very seriously, asking health centers to comply with extensive guidelines related to systems use and maintenance making it very clear to health centers that compliance with these guidelines is necessary to achieve full benefits from their investment in HCN. In addition, HCN is firm on not allowing staff from individual health centers to have administrator rights over their applications, as they believe that centralized control is essential for maintaining a highly secure, highly reliable network.
At the same time, HCN has shown great flexibility in working to meet the specific service needs of a wide variety of health centers. Unlike in other networks, respondents from the smallest health centers did not notice any lack of responsiveness to their needs. Although all acknowledged resource limitations, there was consensus that HCN has done an effective job of maintaining a customer orientation with senior staff working creatively, often on a one to one level, to understand each health centers’ environment and to provide an appropriate level of service.
Incremental approach to meeting health center needs. HCN pursued an incremental approach, focusing first on “righting” the health centers’ administrative and financial position before moving on to EHR. All indications suggest that they met the first objective very well, providing a robust set of services delivering their members huge economies of scales and improvements in core functions such as billing, reporting and accounting. In doing so, HCN has built the trust among members necessary for encouraging health centers investments in EHR.
While other networks have successfully implemented EHR in the absence of networked practice management, it is clear that HCN’s EHR agenda would not be possible without their initial success in helping health centers address threats to their fiscal survival. Unlike other networks, HCN has been able to successfully roll-out EHR in health centers without a very large, one time private sector donation, relying instead on piece-meal funding from the ICT-grant, network revenues and the health centers themselves.
Slow, but steady goals for EHR. Consistent with the considered incremental, approach to overall systems design and implementation, HCN’s EHR roll-out is occurring deliberately with a focus on understanding and applying lessons learned at the early stages to subsequent stages of implementation. For example, early experience in the EHR pilot phase highlighted the downsides of beginning EHR using “out of the box” templates. As a result, HCN works very closely with clinician leaders, allowing them to drive customization and functionality for the EHR and to build buy-in and confidence in the usefulness of the system among their clinician colleagues. To some extent the slow, phased approach to implementation is a benefit of the funding model which requires health centers to find resources internally to incrementally fund a portion of necessary hardware and licensing costs to bring each provider live.
Effective vendor management strategies. HCN enjoys a much closer relationship with its major practice management and EHR vendor, Medical Manager/WebMD, than typically experienced by health centers. The network has worked very closely with the vendor over the years in setting up health center specific customizations and helping Medical Manager effectively market itself to other health centers. HCN has successfully leveraged their strategic position as a high volume purchaser and early adopter to obtain products highly tuned to the requirements of their health center members.
More importantly, HCN’s relationship with Medical Manager results in significantly enhanced responsiveness when issues arise. Kearns indicated that he can easily get a meeting with Medical Manager and WebMD executives around the need to address problems. This level of access was particularly instrumental following the addition of out of state health centers when HIPAA-compliance became an issue for the first time. Purchasing power aside, it is clear that the vendor management and negotiation skills of HCN leadership have served its health centers very well. As a result, users report far fewer problems and frustrations compared with other health centers.
Return on Investment for EHR. Health centers acknowledge that it is too early in the implementation to make many concrete statements about return on investment for EHR; however they state that early indications are positive. Providers who are fully integrated into the system have seen some increased productivity with easier access to prescriptions, laboratory results and patient charts. Interviewees agreed that results have been largely positive from an ROI standpoint with reduced errors, fewer lost files, and increased revenues due to more accurate billing. Health centers also anticipated increased cost savings as use of EHR broadens.
Because the vision is for a paperless system across health centers, there are some costs that can be eliminated all together including medical records staff and basic purchases such as prescription pads and paper charts. HCN staff emphasized the need to consider and track societal returns from investing in EHR as use of this system begins contributing to better management of chronic illness and enhances the effectiveness of public health programs targeting the population served by the health centers.
Endnotes
1 NORC’s Health Studies Department was recently renamed the Department of Health Survey, Program, and Policy Research to reflect its merger with the former Project Hope Center for Health Affairs group.
2 The term thin client generally refers to a very light-weight software application installed on a user's desktop that allows users to access networked applications. The advantage of a thin client is that they require little memory to run, require little storage space to install, and are easy to maintain in that they require little maintenance or upgrades after installation. In a thin client architecture, the client is used primarily to send requests for data to a server where all of the processing is done; the client receives the results and displays them to the user. The most ubiquitous example of a thin client is the web browser.
3 <http://www.healthpolicy.ucla.edu/pubs/files/DifferencesInAccessPolicyBrief.pdf>
4 Data obtained from the Pennsylvania Department of Public Welfare, Office of Medical Assistance Program
5 Several of these additional health centers, including those in the Boston area’s Northeastern region belong to the Cambridge Health Alliance, which is not covered as part of this site visit.
6 Bureau of Primary Health Care CAP Grant Data, 2003
7 HRSA CAP Spotlight. Website on the Internet. Available from: http://www.capcommunity.hrsa.gov/uk_center_spotlight.htm
8 Virginia Coalition for Children’s Health. 2003. “Updating the Estimates: Uninsured Children Eligible for Virginia’s Child Health Insurance Programs.” <http://www.signupnowva.org/In%20Depth.pdf>
9 Kaiser Family Foundation State Health Facts Online. <http://www.statehealthfacts.kff.org/cgi-bin/healthfacts.cgi?> Retrieved March 8, 2004.