
U.S. Department of Health and Human Services
September 2019
Printer Friendly Version in PDF Format (61 PDF pages)
ABSTRACT
This 2018 report highlights participating states’ CCBHC activities that have been associated with improving access to a comprehensive range of treatment and recovery support services. The range of services includes delivery of mental health, addiction, and either screening for general medical conditions or onsite access to primary care during the first year of the demonstration. It draws on qualitative findings gathered from interviews at the state level and preliminary data from CCBHCs. The report also details how the eight states that were selected to participate in the demonstration are monitoring the CCBHCs for compliance to the certification criteria. Each of the eight demonstration states, Minnesota, Missouri, Nevada, New Jersey, New York, Oregon, Oklahoma, and Pennsylvania is profiled in the report to understand their compliance efforts.
Subsequent annual reports to Congress on this demonstration will include data now being collected and reported by CCBHCs in each of the eight demonstration states as required.
Excerpts of this report were derived from reports delivered under contract #HHSP233201600017I between HHS's ASPE/DALTCP and Mathematica Policy Research to conduct the national evaluation of the demonstration. For additional information about this subject, you can visit the DALTCP home page at https://aspe.hhs.gov/office-disability-aging-and-long-term-care-policy-daltcp or contact the ASPE Project Officer, Judith Dey, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. Her e-mail address is: Judith.Dey@hhs.gov.
DISCLAIMER: The opinions and views expressed in this report are those of the authors. They do not reflect the views of the Department of Health and Human Services, the contractor or any other funding organization. This report was completed and submitted on June 12, 2019.
"
EXECUTIVE SUMMARY
Section 223 of the Protecting Access to Medicare Act (PAMA) of 2014 (Public Law 113-93) is prompting significant improvements in the availability and quality of services to men, women, and children living with mental illness and substance use disorders (SUDs). As authorized by PAMA, eight states are participating in two-year demonstration programs to improve community behavioral health. Throughout these states, certified community behavioral health clinics (CCBHCs) and their designated collaborating organizations (DCOs) are now offering whole-person care, that is, care that is person/family-centered, trauma-informed and recovery-oriented, with the integration of physical and behavioral care serving the "whole-person" rather than simply one disconnected aspect of the individual, regardless of their place of residence or ability to pay (HHS, 2016).
Such care is critical to the health of our communities, many of which are grappling with the ramifications of undertreated or untreated behavioral health issues. Public officials, health care providers, and families are searching for effective responses to serious and complex problems, such as the opioid epidemic that kills an average of 130 people per day in the United States, (HHS, 2019), and in 2015 alone, cost the country $504 billion dollars (Council of Economic Advisers, 2017). Medication-assisted treatment (MAT) is recognized as an effective response to opioid disorder and many of the participating CCBHCs added it as a part of their efforts to incorporate evidence-based practices to earn CCBHC certification. Nearly all CCBHCs provide MAT for opioid or alcohol use disorders; notably, approximately half of these CCBHCs added these services because of the demonstration program.
MAT is but one of the several outpatient mental health and SUD (MH/SUD) services that were added by CCBHCs as they became certified. Sixty-three percent of CCBHCs added some form of MH/SUD service, with 46 percent adding MAT. Fifty-five percent of CCBHCs added psychiatric rehabilitation services; 51 percent added crisis behavioral health services; 49 percent added peer support services; 45 percent added intensive community-based mental health services for members of the armed forces and veterans; and 42 percent added primary care screening and monitoring.
Section 223 mandates specialized services for veterans and also allows states the freedom of prioritizing other subpopulations. Since the start of the demonstration, 81 percent of the CCBHCs have targeted outreach to school-age youth, 67 percent to individuals who were previously incarcerated, 64 percent to individuals experiencing homelessness, and 49 percent to older adults. Other subpopulations identified by states include people with opioid use disorders, youth in state custody, transition-age youth, those involved with juvenile justice, and individuals of all ages with comorbid health conditions.
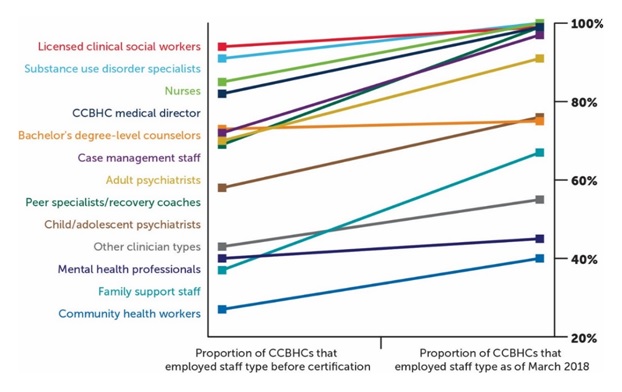
Such a wide diversity of people served with various needs and life experiences calls for credentialed, certified, and licensed staff who can provide person/family-centered, trauma-informed, culturally competent, and recovery-oriented care. By March 2018, staffing among CCBHCs had grown to accommodate this demand, as illustrated by the following chart.
 |
Nationwide, staff offer a wide range of services to a variety of populations at nearly 400 locations. Among CCBHCs that offered services outside of their physical buildings, the most common locations are the homes of people served (84 percent); schools (55 percent); and jails, courts, police offices, and other justice-related facilities (45 percent). This complex network of providers, recipients, services, and locations entails constant and consistent communication.
Toward this end, CCBHCs improved the capacity to share clinical information with DCOs and other external providers by changes to or adoption of new electronic health record (EHR)/health information technology systems. More than half of the CCBHCs reported new quality measure reporting capabilities within the EHR system due to certification. The accuracy of this reporting is vital; many of the CCBHCs' continuous quality improvement (CQI) projects align with the quality measures they are required to report for the demonstration. These projects most commonly focus on assessing risk of and preventing suicide, reducing time between intake and assessment, increasing use of MAT, and preventing unnecessary emergency department visits and hospitalizations. CQI helps maintain fidelity to the CCBHC model, which was carefully established before and during implementation through extensive training and technical assistance.
 |
| Minnesota CCBHC leadership and Department of Human Services representatives receive the 2017 Program Innovation Community Collaboration award from the Minnesota Association of Community Mental Health Programs for their innovative work in promoting health and wellness and/or partnerships to overcome challenges to service delivery for individuals recovering from mental illness and substance use disorders. |
This report discusses the significant progress of CCBHCs thus far, explains the payment system that makes it all possible, and shares state-specific information on monitoring compliance with established criteria and promoting consistent access to quality treatment and support services, in fidelity to the CCBHC model and as intended by Congress.
INTRODUCTION
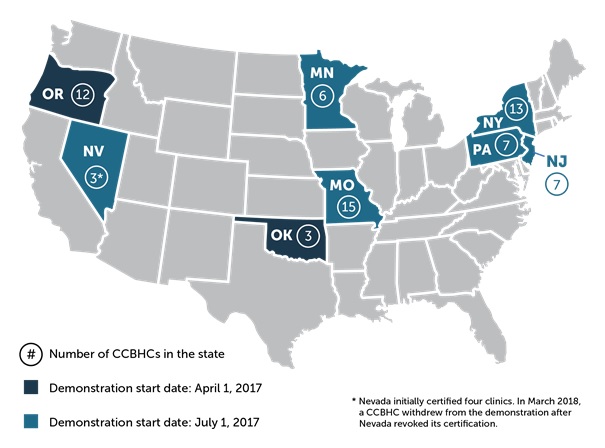
Between April and July 2017, the U.S. Department of Health and Human Services (HHS) provided funding to eight states to operate certified community behavioral health clinic (CCBHC) demonstration programs as called for under Section 223 of the Protecting Access to Medicare Act (PAMA; Public Law 113-93) (as shown in Figure A). In this two-year demonstration, CCBHCs must provide access to a comprehensive range of treatment and recovery support services. The expected costs of demonstration services are reimbursed through a clinic-specific prospective payment system (PPS). The Substance Abuse and Mental Health Services Administration (SAMHSA), the Centers for Medicare & Medicaid Services (CMS), and the Office of the Assistant Secretary of Planning and Evaluation (ASPE) were tasked to implement Section 223, which led to the establishment of 66 CCBHCs with 377 unique service locations providing improved access to a comprehensive range of treatment and recovery support services in urban, rural, and frontier communities. (See Appendix A for a list of CCBHCs.)
| FIGURE A. States Selected to Participate in the CCBHC Demonstration Program |
|---|
 |
The Certified Community Behavioral Health Clinics Demonstration Program, Report to Congress, 2017 (CCBHC Report to Congress, 2017),[1] the precursor to this report, presented the statutory requirements of Section 223 and its implementation. That report also described the planning grant process that helped states prepare for the demonstration program, selection of the states to participate, and activities associated with the launch of the programs. This 2018 report highlights participating states' CCBHC activities that have been associated with improving access to a comprehensive range of treatment and recovery support services. The range of services includes delivery of mental health, addiction, and either screening for general medical conditions or on-site access to primary care during the first year of the demonstration. It draws on qualitative findings gathered from interviews at the state level and preliminary data from CCBHCs.
 |
Subsequent annual reports will include more quantitative information as more data become available from the states. In addition to a detailed accounting of federal funds provided under Section 223, subsequent reports will provide an assessment of the following:
-
Access to community-based mental health services under the state Medicaid program in the area or areas of a state targeted by a demonstration program compared to other areas of the state.
-
Quality and scope of services provided by CCBHCs compared to community-based mental health services provided in states not participating in a demonstration program and in areas within demonstration states that are not participating in the demonstration program.
-
Impact of the demonstration programs on the federal and state costs for the full range of mental health services (including inpatient, emergency, and ambulatory services).
A final report with recommendations for continuation, expansion, modification, or termination of demonstration projects under Section 223 will be submitted to Congress no later than December 31, 2021.
PART I: FIDELITY
Demonstration programs are opportunities to systematically determine the effectiveness of new or innovative approaches to challenging issues. Section 223 of PAMA authorized exploration of the extent to which states can improve mental health and substance use disorder (MH/SUD) services through the establishment and operation of CCBHCs. CCBHCs provide increased access to an array of treatment and recovery support services that include MH/SUD services accessible to all individuals in need of care, regardless of payer or ability to pay, and are paid using a PPS for Medicaid beneficiaries.
In implementing Section 223, HHS recognized that the current status quo is comprised of a patchwork of programs with tremendous variability in access and waiting lists as well as in the range and quality of services available, particularly for those with serious mental illness (SMI) and children with serious emotional disturbance (SED). In fact, many current fee-for-service (FFS) payments result in incentives for patients with low complexity to be prioritized in service and access. To promote quality and access to the range of needed treatment and recovery support services in line with statutory requirements, SAMHSA developed criteria for states to certify CCBHCs.
The criteria establish an expected level of services that CCBHCs will provide, which is critical to determining the effectiveness of the model. Researchers have learned that failing to implement an intervention or policy as intended is a major reason for no-difference or unexpected findings in intervention studies and policy experiments (Walton, Spector, Tombor, & Michie, 2017; Miller & Rollnick, 2014). CCBHC staff received extensive training and technical assistance on all aspects of the CCBHC model in a coordinated federal, state, and local effort to support implementation of the CCBHC criteria noted throughout this report.
|
"[S]ystematic implementation practices are essential to any national attempt to use the products of science--such as evidence-based programs--to improve the lives of its citizens." (Fixsen, Naoom, Blase, Friedman, & Wallace, 2005, p vi) |
Missouri: Statewide Involvement
Missouri: Statewide InvolvementMissouri state officials did not have to be convinced of the merits of the CCBHC demonstration program. "Establishing CCBHCs was the next logical step for Missouri," said Dorn Schuffman, state contact for the demonstration program. "We already had in place many pieces that contribute to greater access to improved care, such as the Health Homes initiative and a crisis response system. It just made sense for us to tap the benefits of moving from a FFS model to a prospective payment system." Years of hard work preceded Missouri's designation as a demonstration state. In October 2011, Missouri became the first state in the nation to receive approval from CMS for Medicaid reimbursement of Health Homes. Community Mental Health Center (CMHC) Healthcare Homes[a] help individuals with SMI more effectively engage with physical health care, MH/SUD care, recovery supports, and social services and other supports. Because of the significant improvement in health outcomes and substantial Medicaid savings the CMHC Healthcare Homes program was able to demonstrate, Missouri received the American Psychiatric Association's 2016 Gold Achievement Award[b] for community-based programs. Fiscal year 2014 marked the start of a multi-year investment in Missouri's Strengthening Mental Health Initiative,[c] which featured several innovations:
Extensive training has been a hallmark of Missouri's journey to better care. By the end of the demonstration, training is expected to raise fidelity-level performance of integrated treatment for co-occurring disorders (simultaneous SUD and mental health treatment rather than fragmented services) among CCBHCs from 57 percent to 100 percent. Senior leadership from all CCBHCs now participate in trauma-informed care and zero suicide learning collaboratives. During Missouri's CCBHC planning process, individuals with lived experience, their family members, and stakeholders from social service and related support organizations expressed a need for additional peer specialists and family support providers. Prior to the launch of the demonstration, fewer than a third of the participating clinics employed family support providers (specially trained parents with lived experience who serve the families of children with SED) and fewer than half employed certified peer specialists. Due to extensive recruitment and training opportunities prompted by the demonstration program, all CCBHCs have started working with family support providers and peer specialists or expanded existing peer specialist and family support staffing.
Having more staff creates the ability to provide more services, and this extends to licensed professionals, as well. Moving to the PPS allowed the clinics to provide competitive salaries for key positions when warranted, thereby attracting more psychiatrists and other licensed professionals. Schuffman noted that the most dramatic improvements were driven by the move from FFS payment for individual services to a bundled encounter rate that is cost-based. He says, "Providers are really excited about this change. It has enabled them to focus differently on the population they serve. Patients, too, are more confident in knowing their provider is there for them." Adopting a PPS may have been more challenging for Missouri than other demonstration states because of its intention, from the beginning of the CCBHC planning process, to include the entire state in the demonstration. This meant a massive, statewide overhaul of all billing and data-reporting systems. Missouri's CCBHCs use Care Manager, a data collection system piloted during the planning grant period, to harness various data feeds. During the first year, Missouri projected serving approximately 130,000 clients. Reflecting 2 percent of its population, this percentage is ten times greater than many of the other demonstration states' projections. Of the 27 potential service areas in Missouri, 19 are included; a state plan amendment is being drafted to maintain the model at the end of the demonstration and add the remaining eight service areas. "We felt empowered to set our sights on the entire state by our level of readiness," reflects Schuffman. "All of our CCBHCs were already serving as Health Homes. Crisis response was operational statewide. No less important, the Department of Mental Health, the Department of Social Services, and the Missouri Coalition for Community Behavioral Healthcare--all key players of the CCBHC project leadership team--have a long history of collaboration. We know how to work together to overcome challenges, to make wellness obtainable for all Missourians." NOTES: |

PART II: FIRST-YEAR IMPLEMENTATION
Section 223 of PAMA requires that states abide by certain criteria and certify clinics to participate in the demonstration program. The CCBHC Report to Congress, 2017 describes the process by which SAMHSA developed criteria for the six statutory requirements: (1) staffing; (2) availability and accessibility of services; (3) care coordination; (4) scope of services; (5) quality and other reporting; and (6) organizational authority.
This report shares activity associated with these areas in the first 9-11 months of the demonstration programs.[2] The 2017 report is based on information and data gathered from interviews with state Medicaid and behavioral health agencies, as well as program reports completed by all CCBHCs, as part of a comprehensive national evaluation of the demonstration managed by ASPE. (For more information on the evaluation process, see CCBHC Report to Congress, 2017.[3])
Requirement 1: Staffing
|
Staff have diverse disciplinary backgrounds, have necessary state-required license and accreditation, and are culturally and linguistically trained to serve the needs of the clinic's patient population. |
Statutory Requirement 1 ensures that CCBHCs are adequately staffed with Medicaid-enrolled providers who are prepared to meet the needs of the population served, which for all demonstration states, includes adults with SMI, children with SED, and anyone with a SUD. States have also prioritized certain subpopulations, such as people with opioid use disorders, individuals experiencing homelessness, veterans, youth in state custody, transition-age youth, people involved in the criminal and juvenile justice systems, and individuals of all ages with comorbid health conditions. Such a wide diversity of people served with intensive needs and varied life experiences requires credentialed, certified, and licensed staff who can provide person/family-centered, trauma-informed, culturally competent, and recovery-oriented care.
Hired Staff
The criteria for CCBHC Certification Requirement 1 include specific staffing requirements, such as a psychiatrist serving in the role of medical director[4] and the following staff:
-
A medically trained behavioral health care provider who can prescribe and manage medications independently under state law.
-
Credentialed SUD specialists.
-
Individuals with expertise in addressing trauma and promoting the recovery of children and adolescents with SED and adults with SMI and those with SUDs.
 |
| Operations staff at Red Rock Behavioral Health Services, one of three CCBHCs in Oklahoma. |
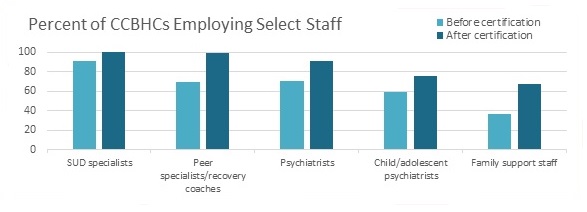
As of March 2018, the majority of CCBHCs reported employing staff to fill the following positions:
-
Ninety-nine percent of CCBHCs reported employing a CCBHC medical director, compared to 82 percent before certification. Ninety-one percent of CCBHCs reported employing a psychiatrist as a medical director. The few clinics that did not have psychiatrists as medical directors hired psychiatric nurse practitioners to fill this role, which CCBHC criteria allows when psychiatrists are unavailable due to workforce shortages.
-
All CCBHCs employed SUD specialists, compared to 91 percent before certification.
-
Ninety-one percent of CCBHCs employed psychiatrists, compared to 70 percent before certification.
-
Seventy-six percent of CCBHCs employed child/adolescent psychiatrists, compared to 58 percent before certification.
CCBHCs also reported hiring specific types of nurses (registered nurses with or without psychiatric experience, nurses with experience in SUDs or providing medication-assisted treatment (MAT) for SUDs, nurse practitioners, psychiatric mental health nurse practitioners, and licensed practical nurses) and other clinical staff (licensed professional counselors, qualified mental health professionals or licensed mental health counselors, and licensed clinical social workers).
The certification criteria allowed states flexibility in developing detailed plans for appropriately staffing CCBHCs according to their existing systems of licensure and accreditation and based on the needs of the populations the CCBHCs serve. Interviews with state officials suggest that variation across CCBHCs and states in the types of staff CCBHCs employed was in part related to the types of services the CCBHCs provided historically. For example, clinics that primarily focused on delivering treatment for SUD before the demonstration found it necessary to hire relatively more mental health providers.
As illustrated in Figure B, a larger proportion of CCBHCs employed peer specialists/recovery coaches, case managers, and family support workers compared with the same clinics before certification. For instance, the percentage of CCBHCs that employed peer specialists/recovery coaches increased from 69 percent before certification to 99 percent by March 2018.
| FIGURE B. Proportion of CCBHCs that Employed Specific Types of Staff Before and After Certification |
|---|
 |
| NOTE: The mental health professional category includes only providers trained and credentialed for psychological testing to align with staff types included in the CCBHC cost report. |
Trained Staff
CCBHCs are required to provide training to new staff that addresses cultural competence; person/family-centered, recovery-oriented, evidence-based and trauma-informed care; and primary care/behavioral health integration at orientation and at reasonable interval thereafter. Other training required at orientation and annuallythereafter includes risk assessment, suicide prevention, and suicide response; the roles of families and peers; and other trainings required by the state or accrediting agency.
As presented in Table 1, CCBHCs have been diligent in providing the required training. Nearly all CCBHCs provided training on risk assessment, suicide prevention and suicide response, evidence-based and trauma-informed care, and cultural competency. More than three-quarters of CCBHCs provided training on each of the other required topics.
| TABLE 1. Number and Proportion of CCBHCs Providing Staff Training in Required Topics since Start of the Demonstration Certification | ||
|---|---|---|
| Required Training | N | % |
| Risk assessment, suicide prevention, and suicide response | 62 | 93 |
| Evidence-based and trauma-informed care | 61 | 91 |
| Cultural competency training to address diversity within the organization's service population | 59 | 88 |
| The role of family and peers in the delivery of care | 52 | 78 |
| Person/family-centered care | 51 | 76 |
| Recovery-oriented care | 51 | 76 |
| Primary and behavioral health care integration | 51 | 76 |
In addition to the required training, CCBHCs provided a range of other training for their staff. The most commonly reported "other" training focused on serving active duty military and veterans, which is consistent with the criteria's call for cultural competency training that includes information related to military culture among those CCBHCs serving this subpopulation. Multiple CCBHCs provided training on specific evidence-based and best practices, including motivational interviewing, cognitive behavioral therapy, and MAT for SUDs.
With respect to the quality measures that are required components of CCBHC certification, staff received training on collecting and using new clinical screening tools, as well as on providing new services implicitly or explicitly required as part of the measurement implementation, such as smoking cessation programs.
States provided support for demonstration clinic staff training during and beyond the initial certification period. Officials from all states held regular meetings with CCBHCs during the early stages of implementation to identify and address CCBHC training and technical assistance needs. Once the types of trainings and knowledge-sharing that would be helpful for clinics were determined, officials in most states used webinars, site visits, regular phone meetings, email and other written communication, or some combination thereof, to assist clinics.
States also leveraged external support to facilitate training. Four states partnered with educational institutions (state or private universities) or other organizations (MH/SUD coalitions) to help provide training opportunities to CCBHCs. Two states used supplementary state or grant funding to help pay for training for the CCBHCs. In addition, multiple states made these trainings accessible throughout the duration of the demonstration. Training sessions are held on an ongoing basis, available ad hoc (e.g., for new staff), or in some instances, saved digitally so that staff can access them as needed.
Identified Challenges
Although nearly all CCBHCs employ the required staff, challenges related to hiring and retaining staff are ongoing. Seventy-two percent of CCBHCs had at least one required staff position vacant for at least 2 months since the start of the demonstration. In six of the eight demonstration states, at least three-quarters of CCBHCs reported having trouble filling staff positions.
CCBHCs most frequently reported vacancies among adult and child/adolescent psychiatrists, peer support staff/recovery coaches, SUD treatment providers, and licensed clinical social workers. Rural or remote CCBHC locations, unworkable salary expectations, and regional and state workforce shortages, were the most commonly cited reasons for hiring and retention difficulties. Demonstration state officials corroborated these findings, noting general mental health and addictions workforce shortages, particularly in rural/frontier areas. Of note, all demonstration states have some CCBHCs in areas designated by the Health Resources and Services Administration as a medically underserved area, medically underserved population, or mental health professional shortage area.
Demonstration state officials cited long-standing workforce issues, such as staff turnover and low compensation for public sector mental health positions, as challenges to maintaining CCBHC staffing requirements. These officials viewed turnover not only as a challenge to CCBHC implementation, but also as a more general and pervasive issue in the behavioral health field.
Requirement 2: Availability and Accessibility of Services
|
The clinic provides 24-hour crisis management services, a sliding scale for payment, and does not reject or limit services by the patient's ability to pay or place of residence. |
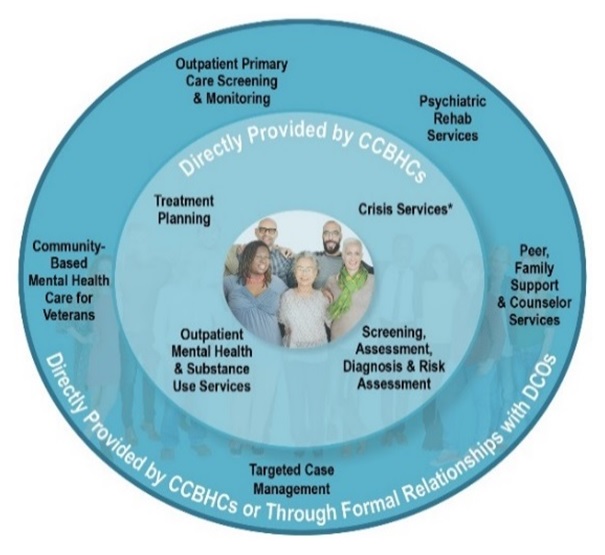
| FIGURE C. Range of CCBHC Services |
|---|
 |
Many people in need of MH/SUD services go without help due to barriers, such as unaffordable services and medicine, lack of insurance coverage, not knowing where to go for help, and inability to get an appointment (Walker, Cummings, Hockenberry, & Druss, 2015). Requirement 2 of the CCBHC demonstration ensures better access to services where and when service recipients need them.
Increased Access
| TABLE 2. Number of CCBHCs, Service Locations, and DCOs (as of March 2018) | |||
|---|---|---|---|
| State | CCBHCs | Service Locations | DCOs |
| Minnesota | 6 | 29[a] | 5 |
| Missouri | 15 | 201[b] | 3 |
| Nevada[c] | 3 | 3 | 1 |
| New Jersey | 7 | 20 | 8 |
| New York | 13 | 77[d] | 4 |
| Oklahoma | 3 | 19 | 2 |
| Oregon | 12 | 21 | 5 |
| Pennsylvania | 7 | 7 | 8 |
|
|||
As depicted in Figure C, CCBHCs are required to provide four core service types: (1) crisis mental health services; (2) screening, assessment, and diagnosis, including risk assessment; (3) patient-centered treatment planning or similar processes; and (4) outpatient MH/SUD services. The remaining services may either be provided directly or by a designated collaborating organization (DCO). These services are: (5) primary care screening and monitoring; (6) targeted case management; (7) psychiatric rehabilitation services; (8) peer support and counselor services and family supports; and (9) services for members of the armed forces and veterans.[5] This network of providers means CCBHC services are available at a multitude of locations, as shown in Table 2.
Among CCBHCs that offered services outside of their physical buildings, the most common locations were the homes of people served, schools, or other community-based settings, as shown in Figure D. Other locations included primary care offices and federally qualified health centers (FQHCs), homeless shelters, public spaces, and on the street. Ninety percent of CCBHCs provided transportation through bus or cab vouchers, by helping those served obtain the Medicaid transportation benefit (if they were eligible and the benefit was available in the state), via care manager or peer support, and directly in CCBHC-owned vehicles.
| FIGURE D. Number and Proportion of CCBHCs that Provide Services Outside of Physical Clinic Space |
|---|
 |
Changes to the physical structure of the clinic have also been needed to facilitate access to care for certain populations, such as those living with physical disabilities. As shown in Table 3, CCBHCs in all states reported renovations to their physical space to meet certification criteria or as a result of their participation in the demonstration. Changes included creating dedicated space for ambulatory detoxification services, adding physical health exam rooms, improving the space for child and adolescent's receiving services, and expanding office space for new staff such as peers and case managers.
| TABLE 3. Number and Proportion of CCBHCs Making Changes to CCBHCs Physical Space to Meet Certification Criteria | ||
|---|---|---|
| Change to Physical Space and Accessibility | N | % |
| Renovations to existing CCBHC facilities | 45 | 67 |
| Expansions or additions to the CCBHC building space | 33 | 49 |
| Improvements to facility safety features | 27 | 40 |
| Other changes to CCBHC physical space | 15 | 22 |
Two-thirds of the CCBHCs offer telehealth, most commonly telepsychiatry, therapy or counseling, and medication management. Those not currently offering telehealth services plan to initiate them to expand access to services.
CCBHCs have made services more convenient by introducing same-day or next-day appointments and accepting walk-in appointments. They have tailored services to the needs of specific populations, such as veterans, school-aged youth, and people experiencing homelessness. For example, more frequent and shorter appointments for high-need individuals is being tested as a strategy for reducing crises and use of emergency services among these populations. CCBHCs have also implemented processes to improve client engagement and retention in services, including monitoring the frequency of phone follow-ups and increasing the number of reminder calls for clients before appointments. Ninety-six percent of the CCBHCs provided translation services, usually through an external interpreter contract.
 |
| Lake Shore Behavioral Health, Inc., a CCBHC in upstate New York. |
Engagement of New Individuals in Service
CCBHCs have been proactive in reaching out to individuals who may need services, such as school-age youth, veterans, individuals transitioning from incarceration, and people experiencing homelessness, as illustrated in Figure E. A CCBHC in Oregon stations a therapist at a nearby U.S. Department of Veterans Affairs (VA) facility to provide screening and monitoring when VA staff are not available or when demand exceeds the VA clinic capacity. Other populations to which CCBHCs have targeted efforts include individuals with SUD, diagnoses of mental illness or comorbid chronic physical health conditions; frequent users of emergency department and inpatient services, and those who identify as sexual or gender minorities, especially youth.
CCBHCs also expanded access to care within their communities by:
-
Initiating new relationships with community-based organizations, including hospital systems, external primary care and mental health or addiction service providers, schools, social service organizations (e.g., shelters), and the criminal justice system (including juvenile justice).
-
Conducting direct outreach to people with mental or substance use disorders and their families through community informational sessions featuring CCBHCs and their service offerings, and through advertising campaigns (including newspaper and television) in their local service areas.
| FIGURE E. Proportion of CCBHCs that Targeted Outreach to Specific Populations since the Start of the Demonstration |
|---|
 |
State agencies have supported targeted outreach efforts by facilitating connections between providers (e.g., assisting CCBHCs in coordinating agreements with provider networks, such as the VA) and providing information on high utilizers of health care services so CCBHCs can target these individuals.
Ensured Affordability
CCBHCs serve people regardless of insurance status or ability to pay. As illustrated in Table 4, almost all CCBHCs reported offering a sliding fee schedule, providing services to people with Medicare and private insurance, and serving people not residing in their catchment area. Among those offering a sliding fee schedule, 73 percent published the fee schedule on their website or provided it to people being served through other means, such as in welcome packets at intake.
| TABLE 4. CCBHC Payment Policies and Service Provision | ||
|---|---|---|
| Payment Policy and Service Provision | Yes Response | |
| N | % | |
| Provide services to consumers unable to pay | 67 | 100 |
| Offer a sliding fee schedule | 66 | 99 |
| Provide services to consumers with Medicare | 66 | 99 |
| Provide services to consumers with private insurance | 66 | 99 |
| Provide services to consumers not residing in clinic catchment area | 65 | 97 |
Some demonstration states have taken additional steps to mitigate the impact of providing services regardless of individual ability to pay. For example, Nevada's Division of Mental Health contracts with clinics to help offset costs of providing services to those who are unable to pay, and Nevada Substance Abuse Prevention and Treatment Block Grants make funds available to serve people with co-occurring mental illnesses and SUDs. The Nevada Division of Welfare embeds staff in CCBHCs to help uninsured clients enroll in Medicaid on-site. Eligibility workers assist with enrollment in Temporary Assistance for Needy Families (TANF) and Women, Infants and Child (WIC) programs, as well.
Requirement 3: Care Coordination
|
Coordinated care across settings and providers promotes seamless transitions for patients across the full spectrum of health services, including physical and MH/SUD needs. The clinics maintain partnerships or formal contracts with the following:
|
Patients, mental health and addiction service providers, physical health providers, and providers of social, housing, educational, and employment services must work together to achieve the objectives of person/family-centered plans of care. Requirement 3 addresses the formal agreements, health information systems, and treatment planning activities necessary for maintaining consistency, clarity, and confidentiality among all partners.
Enhanced Coordination
CCBHCs have leveraged or expanded care management programs through the demonstration program. For example, CCBHCs in Pennsylvania provide targeted case management for all CCBHC patients and use two other models of care coordination: a nurse navigator model in rural areas that utilizes nurses to navigate the health care system and improve access to services, focusing on improving medication adherence for physical conditions and MH/SUDs and a case management model in urban and rural areas focusing on SUD treatment for individuals receiving MAT.
|
"The main difference [between what CCBHCs and other behavioral health providers are providing] is the standards that go along with CCBHC care coordination. We had care coordination before, but now we have the care coordination agreements with the various entities that are required, so it's really an increase in intensity of care coordination." -- Oregon CCBHC Official |
CCBHCs have also engaged in more sophisticated approaches to care coordination. Oklahoma officials cite a client progress dashboard as an example of a CCBHC's transition from a "one-size-fits-all" approach. This one-page tool shows laboratory results, medication compliance, the number of services received, and screenings for a given client. It provides feedback to the agency on not only the extent to which practitioners are providing the services that clients need, but also on how well the services are coordinated. Results are available to all staff involved in the individual's care.
Strengthened Treatment Planning and Teams
More than three-quarters of CCBHCs reported that treatment teams have changed because of the certification process. The addition of care coordinators, case managers, peer support staff, SUD providers, psychiatrists, and primary care staff has prompted more frequent treatment team meetings and "huddles." These regular meetings allow team members to share information about clients, which reduces "silo-ing" and facilitates treatment planning. Table 5 presents the types of providers who participate in CCBHC treatment planning and treatment teams. Per responses to an open-ended question in CCBHCs' progress reports, other providers who participate in treatment planning include nurses, peer support staff, vocational or employment specialists, care coordinators, nurse care managers, and family support providers.
| TABLE 5. Number of Proportion of CCBHCs that include Types of Providers... | ||||
|---|---|---|---|---|
| Type of Provider | in Developing and Updating a Comprehensive Treatment Plan |
on Treatment Teams | ||
| N | % | N | % | |
| Mental health clinicians | 67 | 100 | 67 | 100 |
| SUD providers | 66 | 99 | 66 | 99 |
| Consumers/clients | 65 | 97 | 62 | 93 |
| Consumer/client family members | 64 | 96 | 52 | 78 |
| Case managers | 62 | 93 | 67 | 100 |
| Psychiatrists | 59 | 88 | 63 | 94 |
| Primary care physicians | 27 | 40 | 36 | 54 |
| Other | 29 | 43 | 31 | 46 |
| Community support and social service providers | NA | NA | 56 | 84 |
| NOTE: Columns are not mutually exclusive; CCBHCs could select that a provider participated in treatment planning and/or the treatment team. NA = Not applicable (question was not asked). |
||||
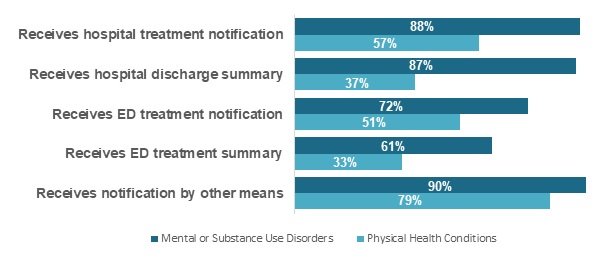
With respect to information-sharing, 72 percent of CCBHCs reported receiving notification about their clients' use of emergency department services when the emergency department visit was for a mental or substance use disorder. In contrast, only 51 percent of CCBHCs reported receiving such notifications from an emergency department for the treatment of physical health conditions (Figure F).
| FIGURE F. Proportion of CCBHCs that Receive Notification about Treatment for Physical Conditions and MH/SUDs |
|---|
 |
Expanded Care Provider Networks
Establishing partnerships with external providers and support services in the community has been another important strategy for improving care coordination. CCBHCs most often developed relationships with FQHCs (to provide primary care), family support service organizations, and hospitals but also established relationships with a wide variety of external providers. Nearly all reported an informal or formal relationship with the providers listed in Table 6, with the following exceptions: 72 percent have a relationship with an urgent care center, 58 percent with a school-based health center, 48 percent with a rural health center, and 40 percent with IHS or tribal programs.
As presented in Table 6, DCOs, organizations providing required CCBHC services through a formal relationship, are most frequently used to provide suicide/crisis services. Officials from the four demonstration states in which CCBHCs established DCO relationships with suicide/crisis hotlines and warmlines commented that using a DCO to provide this service made sense, because it is a specialized service. In explaining why CCBHCs prefer to provide services directly rather than establish a formal relationship with a DCO, state officials cited CCBHCs' concerns about: (1) legal requirements for DCO agreements (preferring informal relationships and/or more flexible partnership arrangements that existed before the demonstration); (2) information sharing; and (3) lack of experience with the PPS. New York State resolved the issue of "lack of experience with the PPS" by hiring staff from a DCO through a contract and building this cost into the cost report, thus eliminating DCO billing and a DCO payment agreement.
| TABLE 6. Number and Proportion of CCBHCs that have Relationships with Other Facilities and Providers | ||||||||
|---|---|---|---|---|---|---|---|---|
| Facility/Provider Type | DCO | Other Formal Relationship | Other Informal Relationship | Any Relationship[a] | ||||
| N | % | N | % | N | % | N | % | |
| FQHCs | 2 | 3 | 40 | 60 | 19 | 28 | 58 | 87 |
| Rural Health Clinics | 0 | 0 | 21 | 31 | 12 | 18 | 32 | 48 |
| Primary care providers | 2 | 3 | 48 | 72 | 25 | 37 | 66 | 99 |
| Inpatient psychiatric facilities | 1 | 1 | 52 | 78 | 19 | 28 | 67 | 100 |
| Psychiatric residential treatment facilities | 1 | 1 | 40 | 60 | 28 | 42 | 64 | 96 |
| SUD residential treatment facilities | 3 | 4 | 43 | 64 | 28 | 42 | 67 | 100 |
| Medical detoxification facilities | 2 | 3 | 42 | 63 | 23 | 34 | 64 | 96 |
| Ambulatory detoxification facilities | 1 | 1 | 32 | 48 | 26 | 39 | 55 | 82 |
| Post-detoxification step-down facilities | 0 | 0 | 31 | 46 | 24 | 36 | 52 | 78 |
| Residential (non-hospital) crisis settings | 3 | 4 | 35 | 52 | 24 | 36 | 57 | 85 |
| MAT providers for substance use | 2 | 3 | 43 | 64 | 20 | 30 | 61 | 91 |
| Schools | 0 | 0 | 51 | 76 | 19 | 28 | 65 | 97 |
| School-based health centers | 0 | 0 | 21 | 31 | 20 | 30 | 39 | 58 |
| Child welfare agencies | 0 | 0 | 43 | 64 | 26 | 39 | 66 | 99 |
| Therapeutic foster care service agencies | 0 | 0 | 31 | 46 | 31 | 46 | 56 | 84 |
| Juvenile justice agencies | 0 | 0 | 38 | 57 | 26 | 39 | 60 | 90 |
| Adult criminal justice agencies/courts | 0 | 0 | 51 | 76 | 19 | 28 | 65 | 97 |
| Mental health/drug courts | 0 | 0 | 52 | 78 | 15 | 22 | 62 | 93 |
| Law enforcement | 0 | 0 | 36 | 54 | 32 | 48 | 64 | 96 |
| IHS or other tribal programs | 0 | 0 | 10 | 15 | 18 | 27 | 27 | 40 |
| IHS youth regional treatment centers | 0 | 0 | 4 | 6 | 13 | 19 | 17 | 25 |
| Homeless shelters | 0 | 0 | 28 | 42 | 33 | 49 | 59 | 88 |
| Housing agencies | 0 | 0 | 40 | 60 | 30 | 45 | 64 | 96 |
| Suicide/crisis hotlines and warmlines | 19 | 28 | 38 | 57 | 15 | 22 | 65 | 97 |
| Employment services/supported employment | 2 | 3 | 35 | 52 | 29 | 43 | 63 | 94 |
| Older adult services | 0 | 0 | 27 | 40 | 30 | 45 | 56 | 84 |
| Other social and human service providers | 2 | 3 | 38 | 57 | 35 | 52 | 65 | 97 |
| Consumer-operated/peer service provider organizations | 3 | 4 | 26 | 39 | 31 | 46 | 55 | 82 |
| VA treatment facilities | 0 | 0 | 37 | 55 | 32 | 48 | 66 | 99 |
| Urgent care centers | 0 | 0 | 21 | 31 | 29 | 43 | 48 | 72 |
| EDs | 2 | 3 | 45 | 67 | 26 | 39 | 66 | 99 |
| Hospital outpatient clinics | 0 | 0 | 29 | 43 | 37 | 55 | 62 | 93 |
NOTE: Columns are not mutually exclusive.
|
||||||||
Requirement 4: Scope of Services
|
CCBHCs provide, in a manner reflecting person-centered care, the following services:
CCBHCs also provide directly, or through referral with DCOs, the following services:
|
A hallmark of this demonstration program is its capacity to offer recipients a comprehensive range of high-quality services, delivered directly by the CCBHC or through DCOs. Recognizing the inherent complexity of providing such a range, states were permitted flexibility in aligning the scope of services with their Medicaid State Plans and other state regulations. Requirement 4 also calls for the continuous integration of evidence-based practices (EBPs).
 |
| Demonstrating the spectrum of whole-person health care, clients participate in services at Grand Lake Mental Health Center, Inc., a CCBHC serving rural populations of Oklahoma. |
Added Services
Eighty-four percent of CCBHCs made changes to the range of services they provide. They most often added services within the categories of outpatient MH/SUD services, psychiatric rehabilitation services, and crisis behavioral health services. (See Figure G.) Responding to a write-in question on the progress report, CCBHCs reported providing "other" CCBHC services, including emergency room enhancement services, CMHLs, and withdrawal management services.
| FIGURE G. Proportion of CCBHCs that added Services within Each Service Category as a Result of Certification |
|---|
 |
| NOTE: CCBHCs may have provided services within each of the service categories illustrated in Figure G prior to CCBHC certification. For example, all CCBHCs provided some type of outpatient mental health and/or SUD treatment prior to certification. However, 63 percent of CCBHCs added some type of outpatient mental health and/or SUD treatment as a result of certification. The service categories illustrated in this figure correspond to the service categories described in the CCBHC certification criteria. |
Table 7 presents the availability of services in CCBHCs and DCOs. 24-hour mobile crisis teams and MAT for alcohol and opioid use are the services most often added as a result of CCBHC certification. Eighty-four percent of CCBHCs provide MAT for alcohol and opioid use; among the 11 CCBHCs that did not provide MAT either directly or through a DCO, nine had either a formal (four) or informal (five) relationship with a MAT provider.
In addition to MAT, other services frequently added because of certification include targeted case management (40 percent) and illness management and recovery (31 percent). State officials attributed variability in the proportion of CCBHCs providing certain EBPs (e.g., MAT, multi-systemic therapy, assertive community treatment, supported education) to a combination of perceived population needs, state priorities and ongoing state initiatives, and workforce shortages.
| TABLE 7. Required Services Provided by CCBHCs and/or DCOs | ||||||||
|---|---|---|---|---|---|---|---|---|
| Service | CCBHC Directly Provided Service |
DCO Provided Service | Either CCBHC and/or DCO Provided Service[a] |
Added as a Result of CCBHC Certification |
||||
| N | % | N | % | N | % | N | % | |
| Crisis behavioral health services | ||||||||
| 24-hour mobile crisis teams | 49 | 73 | 23 | 34 | 65 | 97 | 31 | 46 |
| Emergency crisis intervention | 59 | 88 | 20 | 30 | 67 | 100 | 21 | 31 |
| Crisis stabilization | 60 | 90 | 14 | 21 | 66 | 99 | 21 | 31 |
| Screening, assessment, and diagnosis | ||||||||
| Mental health | 67 | 100 | 4 | 6 | 67 | 100 | 9 | 13 |
| SUD | 67 | 100 | 3 | 4 | 67 | 100 | 15 | 22 |
| Person/family-centered treatment planning services | 66 | 99 | 5 | 7 | 66 | 99 | 12 | 18 |
| Outpatient mental health and/or SUD services | ||||||||
| First episode/early intervention for psychosis | 40 | 60 | 0 | 0 | 40 | 60 | 9 | 13 |
| MAT for alcohol and opioid use[b] | 55 | 82 | 2 | 3 | 56 | 84 | 31 | 46 |
| Outpatient SUD treatment | 67 | 100 | 0 | 0 | 67 | 100 | 13 | 19 |
| Specialty MH/SUD services for children and youth | 58 | 87 | 0 | 0 | 58 | 87 | 15 | 22 |
| Community wraparound services for youth/children[b] | 50 | 75 | 2 | 3 | 51 | 76 | 10 | 15 |
| Psychiatric rehabilitation services | ||||||||
| Illness management and recovery | 62 | 93 | 4 | 6 | 65 | 97 | 21 | 31 |
| Medication education | 65 | 97 | 3 | 4 | 66 | 99 | 14 | 21 |
| Self-management | 63 | 94 | 5 | 7 | 65 | 97 | 16 | 24 |
| Skills training | 64 | 96 | 5 | 7 | 66 | 99 | 14 | 21 |
| Supported employment | 45 | 67 | 5 | 7 | 50 | 75 | 18 | 27 |
| Supported education | 33 | 49 | 5 | 7 | 36 | 54 | 11 | 16 |
| Wellness education services (diet, nutrition, exercise, tobacco cessation, etc.) | 65 | 97 | 6 | 9 | 67 | 100 | 24 | 36 |
| Peer support services | ||||||||
| For consumers/clients | 66 | 99 | 4 | 6 | 67 | 100 | 29 | 43 |
| For families | 48 | 72 | 4 | 6 | 49 | 73 | 23 | 34 |
| Targeted case management | 62 | 93 | 1 | 1 | 63 | 94 | 27 | 40 |
| Primary care screening and monitoring | 63 | 94 | 3 | 4 | 65 | 97 | 28 | 42 |
| Community-based mental health care for armed forces and veterans | 47 | 70 | 1 | 1 | 48 | 72 | 30 | 45 |
NOTE:
|
||||||||
To facilitate crisis planning, CCBHCs used best practices such as psychiatric advance directives, and safety/crisis plans, as presented in Table 8. "Other" strategies listed include suicide assessments such as the Columbia Suicide Severity Rating Scale (C-SSRS), relapse prevention and planning, critical intervention planning, and working with external partners and stakeholders to provide patient-centered services in crisis planning.
| TABLE 8. Number and Proportion of CCBHCs using Specific Crisis Planning Strategies | ||
|---|---|---|
| Strategy | N | % |
| Wellness recovery action plan | 49 | 73 |
| Psychiatric advance directives | 46 | 69 |
| Develop a safety or crisis plan | 29 | 43 |
| Other | 37 | 55 |
Resolved Challenges
State officials described overcoming the following initial barriers to implementing a full scope of services:
-
State credentialing and licensure requirements. State officials worked with state licensure offices and CCBHCs to obtain licensure for certain required services (e.g., ambulatory withdrawal management [AWM]) or hiring staff with the credentials necessary to provide required services (e.g., peer support).
-
Workforce shortages. As noted previously, several states experienced challenges in recruiting and hiring certain types of staff, such as peer support staff in rural areas. Strategies to attract and retain employees included offering competitive salaries and leveraging professional networks within the state to advertise CCBHC positions.
-
Inexperience in providing specific services to certain populations. CCBHCs in some states were required to add new service lines, to fulfill demonstration criteria. CCBHCs in other states needed to expand certain services to new populations, such as youth in order to become a CCBHC.
-
Billing and claims/encounter data. States supported CCBHCs in administering PPS claims and recording encounters during the planning phase and the initial months of the demonstration. In the March 2018 interviews, officials from all states reported that the CCBHCs were using the systems they had put in place, the payment and encounter information was being appropriately recorded and submitted, and the PPS claims were being paid. However, most state officials also noted that they have not yet conducted detailed audits, so early impressions are subject to change. For instance, detailed audits of the data would be required to identify gaps in the encounter data or systematic errors in PPS claims.
Requirement 5: Quality and Other Reporting
|
The clinic reports encounter data, clinical outcomes data, quality data, and such other data as the Secretary requires. |
The criteria through which CCBHCs become certified include 21 quality measures. CCBHCs are required to report on nine of these measures; the respective state entity reports on the other 12. (See Figure H.) The measures reported by CCBHCs rely on data typically derived from electronic health records (EHRs) or other electronic administrative sources. The measures reported by the states use data from Medicaid claims and encounter data, among other sources. Appendix B presents demonstration state information on the state entity for monitoring compliance with the criteria, the monitoring instrument, method and frequency of monitoring, and additional safeguards put in place to promote consistency in accessible and quality treatment and support services, in fidelity to the CCBHC model and as intended by Congress.
| FIGURE H. Required Quality Measures | |
|---|---|
| 9 Clinic-Reported CCBHC Quality Measures | 12 State-Reported CCBHC Quality Measures |
|
|
Changes Made to Data Collection Systems
States and CCBHCs invested considerable time ensuring that participating CCBHCs had data systems in place to meet the reporting needs of the demonstration. Extensive training and technical assistance were provided on preparing EHR/health information technology (HIT) systems, facilitating information exchange between disparate data systems, and streamlining the reporting process.
As part of the CCBHC certification process, 97 percent of CCBHCs changed their EHR/HIT systems, and 33 percent adopted a new EHR/HIT system. Among those CCBHCs that reported implementing new EHR features, the most commonly added features were allowance of electronic exchange of clinical information with DCOs and other external providers, as well as quality measure reporting capabilities, reflecting the importance of these features to the CCBHC care model, as shown in Table 9. All CCBHCs reported that their EHRs include mental health, SUD, and case management or care coordination records. (For most CCBHCs, these features were not new per CCBHC certification.) Quality measure reporting capability, generation of electronic care plans, and electronic prescribing were also available in more than 90 percent of CCBHCs.
| TABLE 9. Number and Proportion of CCBHCs that Reported Function of CCBHC EHR and HIT Systems | ||||
|---|---|---|---|---|
| Function | CCBHCs Reporting EHR Function |
New Due to CCBHC Certification[a] |
||
| N | % | N | %[b] | |
| EHR contains mental health records | 67 | 100 | 6 | 9 |
| EHR contains SUD records | 67 | 100 | 8 | 12 |
| EHR contains case management or care coordination records | 67 | 100 | 16 | 24 |
| EHR has quality measure reporting capabilities | 63 | 94 | 34 | 54 |
| EHR generates electronic care plan | 62 | 93 | 8 | 13 |
| Use any form of electronic prescribing | 61 | 91 | NA | NA |
| EHR incorporates laboratory results into health record | 55 | 82 | 12 | 22 |
| EHR provides clinical decision support | 52 | 79 | 15 | 29 |
| EHR contains primary care records | 41 | 61 | 11 | 27 |
| EHR communicates with laboratory to request tests or receive results | 38 | 57 | 8 | 21 |
| EHR allows electronic exchange of clinical information with other external providers | 31 | 46 | 16 | 52 |
| EHR allows electronic exchange of clinical information with DCOs | 26 | 39 | 16 | 62 |
NOTE: Columns are not mutually exclusive.
|
||||
Facilitated Reporting
Challenges associated with CCBHCs' lack of familiarity with the required measures and difficulty in obtaining certain variables, such as new service codes or new population subgroups, from clinic EHRs were typically resolved through training webinars and direct technical assistance that was provided through multiple channels (phone, online, or in-person) to:
-
Explain the measures and the information needed to produce each metric from the CCBHCs.
-
Provide examples of how to extract information and create measures from the EHR data (e.g., what queries to run; the numerators and denominators to use).
-
Explain how to complete the reporting template.
States continued to provide support as the year progressed and the process unfolded. For example, they worked with state Medicaid agencies to conduct "test" data collections with the CCBHCs that may reveal missing or inaccurate data for CCBHC-reported measures. As of March 2018, several states were in the process of reviewing preliminary submissions of test data from CCBHCs to conduct validation and quality assurance prior to the formal reporting deadline.
Pursued Quality Improvement Initiatives
CCBHCs are measuring the degree to which clients are receiving required services; tracking clients' appointment wait time and symptoms over time; developing alerts for screening or follow-up service; and standardizing treatment protocols. Nearly 80 percent of the CCBHCs reported using the quality measures as an opportunity to change and improve the services they offer.
All but one of the CCBHCs described the continuous quality improvement (CQI) projects they are conducting. The focus of these projects frequently aligns with the quality measures the CCBHCs are required to report for the demonstration. Specific examples include:
-
Twenty-six percent of these CCBHCs used suicide risk assessment and prevention measures, such as the C-SSRS, in routine practice and provided staff training on the measures.
-
Nineteen percent more consistently used measures to screen for depression (especially the Patient Health Questionairre-9) and more regularly conducted follow-up with those served.
-
Seventeen percent used measures related to reducing time between intake and assessment to ensure timely care.
Other CQI initiatives focus on safety planning and risk assessment, increasing use of MAT, and preventing unnecessary emergency department visits and hospitalizations. CCBHCs also implemented new internal performance improvement processes to ensure better CQI, such as conducting more frequent measurement and reporting of data, holding regular review meetings, hiring dedicated quality assurance staff, providing staff trainings, and aligning demonstration-focused CQI initiatives with state and other reporting requirements and programs.
The methods CCBHCs used to implement changes in response to the measures have been diverse and include hiring more providers, improving intake and assessment processes, and hiring external consultants to help implement changes.
CCBHCs have informally shared information regarding quality measures during collaborative meetings and have expressed interest in reviewing aggregate data regarding performance on quality measures across CCBHCs within a state to better understand their performance relative to the larger group. Several demonstration states are planning to implement systems for sharing aggregate quality measures data with the CCBHCs, which will provide CCBHCs with benchmarks for different measures and help them identify specific quality improvement and technical assistance needs.
State CCBHC leaders collaborated closely with the CCBHCs to develop and support CQI initiatives by providing clinics with tools to facilitate internal performance monitoring and staff development. They also engaged with the CCBHCs in regularly scheduled webinars, conference calls, site visits, and in-person work groups or training workshops on targeted subjects, such as data system buildout, metric development, and reporting processes. At the time of the interviews, Minnesota officials were planning a CCBHC learning collaborative to assist CCBHCs in sharing "lessons learned" and "best practices" in direct response to requests from the CCBHCs for this type of resource.
New Jersey: Embracing Change
New Jersey: Embracing ChangeThe potential for effecting positive change attracted New Jersey to the CCBHC demonstration program. Assistant Division Director at the Division of Mental Health and Addiction Services (DMHAS) and state point of contact for the CCBHC demonstration program Suzanne Borys shared, "In New Jersey, we have separate licenses for providing MH/SUD treatment. We required our CCBHCs to have both licenses. The demonstration program provided an opportunity for people with addictions to get the same level of care as those with mental illness, and it brings us a step closer to our long-term goal of an integrated licensure structure for both physical health and behavioral health." Director of Care Management Vicki Fresolone added, "Many of the professional staff at the CCBHCs are mental health providers, and the requirement that they provide AWM was a real challenge for them. Once trained on and experienced with it, they wholeheartedly embraced it." Prior to the CCBHC demonstration program, withdrawal management was typically delivered "unbundled" from other treatment services in residential settings and AWM was limited to very few providers, most of which did not accept Medicaid. Now, it is an allowable service within the CCBHC's outpatient addiction treatment license, which has significantly increased access to this level of care. Another significant change in New Jersey is the increase in availability of MAT for service recipients with SUDs. Formerly, unless licensed as opioid treatment programs, most outpatient SUD treatment providers did not provide MAT. The seven CCBHCs, however, are required to offer naltrexone or buprenorphine and to establish referrals for clients who need methadone. Building on the success of the CCBHCs, the state is creating a buprenorphine network through which all outpatient settings can offer MAT and counseling. CCBHCs play a significant role in New Jersey's Opioid Overdose Recovery Program (OORP), as well. OORP's recovery specialists help individuals in emergency departments who have received a naloxone reversal accept treatment or recovery support and connect them to service providers. The first five counties to offer OORP (now available statewide) also hosted a CCBHC. Connections were made between OORP and CCBHC providers that enabled individual referrals from the OORPs to CCBHC services. Leveraging partnerships such as this has been key to the success of the CCBHC program. One very important relationship is between DMHAS and the state's Medicaid agency, the Division of Medical Assistance and Health Services. Borys commented, "We've always worked well together. We were equal partners during the Medicaid expansion, and that laid the groundwork for jointly pursuing the CCBHC demonstration program. We had a better understanding of how each division worked and the needs of the population." The third state partner is the Department of Children and Families' Children's System of Care, which contributes its expertise and resources on delivering mental health services to children and SUD services to adolescents. Rutgers University's School of Social Work (SSW) rounds out the CCBHC project team. SSW played a significant role in preparing the state to become a CCBHC planning and demonstration grantee in the areas of outcome collection and EBP. Dr. Robert Eilers, DMHAS Medical Director and CCBHC Project Director, explains, "Several years ago, Rutgers' Center for State Health Policy secured a Center for Medicare and Medicaid Innovation State Innovation Model (SIM) design award for New Jersey. Goals for this SIM award included advancing behavioral and physical integration strategies and addressing Medicaid cost and value, especially for patients generating high costs. This led to a landscape survey, which, in turn, led to a comprehensive review of related regulations by the Seton Hall Center for Health and Pharmaceutical Law and Policy. Truly, Rutgers helped get the ball rolling and, then, paved the way with technical assistance and training on evaluation, data collection, reporting, and EBPs." Extensive technical assistance and training have paid off, helping providers adjust to significant changes in practice that ranged from adjusting to a new funding methodology--the CCBHC PPS-2--to connecting with emergency departments and other providers through a health information exchange. As noted by Fresolone, "CCBHCs have lifted morale among provider staff. Historically, clinicians faced client needs for which they had no means to help. The scope of services available with the CCBHC enables them to meet client needs, resulting in much happier staff!"
Even more to the point of the CCBHC demonstration program, clients are benefitting from improved access to and a higher quality of community-based mental health services and from the enhanced capability of CCBHCs to coordinate care. Case in point? "Marcus" is a veteran who struggles with post-traumatic stress disorder (PTSD), childhood trauma, and addiction. Through the CCBHC AWM program, he detoxified from heroin. He embarked on MAT for long-term opioid dependence under the guidance of an outpatient psychiatrist and a therapist trained in PTSD and veteran's issues. Marcus' therapist, case manager, nurse, and psychiatrist worked closely together throughout Marcus' treatment to help him navigate each phase of care. He has been sober for several months and is learning to manage his anxiety and trauma. He has not had any suicidal ideations in more than 6 months, nor exhibited any violent behavior since entering the program. He has reconnected with family and secured employment as a union carpenter. The CCBHC program worked with Marcus in an open-minded, empathetic, and non-judgmental manner, helping him creatively overcome obstacles that prior traditional treatment programs were unable to help him circumvent. |
PART III: PROSPECTIVE PAYMENT SYSTEM
CCBHCs participating in the demonstration receive Medicaid payment for services delivered to Medicaid beneficiaries through a PPS. States receive federal matching funds at an enhanced rate for CCBHC expenditures. In accordance with Section 223 of PAMA, CMS developed guidance for states on how to determine rates when using a PPS methodology. The agency provided extensive technical assistance to states, offering webinars on various topics and responding to numerous questions from states. CMS issued an Office of Management and Budget-approved cost report to assist states in setting PPS rates and for CCBHCs to report actual cost incurred during the demonstration. States had to choose one of the following PPS methodologies:
-
Certified Clinic Prospective Payment System (CC PPS-1) uses a daily PPS methodology, in which CCBHCs receive a fixed daily, clinic-specific rate that is based on the expected cost of care for each day services are provided to a Medicaid enrollee. This rate is paid when at least one of the nine required demonstration services has been provided to a Medicaid beneficiary. A state may choose to offer a quality bonus payment (QBP) to CCBHCs that demonstrate achievement of required quality measures. The state may issue QBPs using additional measures, but only after the certified clinic has met state-determined performance goals for the required set of bonus measures.
-
CC PPS Alternative (CC PPS-2) uses a monthly PPS methodology that is paid to a CCBHC when at least one of the nine demonstration services has been provided to a Medicaid beneficiary during the month. The monthly rate is clinic-specific and is based on the expected cost of care. Each clinic is assigned at least two monthly rates: (1) a monthly PPS rate for demonstration services provided to clinic users who are not necessarily part of a higher need population; and (2) a monthly PPS rate to reimburse CCBHCs for the increased costs associated with providing services to higher need/special populations (i.e., adults with SMI, children with SED, those with long-term and serious substance misuse, and those with mental disorders and SUDs). Under the CC PPS-2 model, the state may determine more than two rates for each clinic, depending on the populations served by the clinic. The state is required to incorporate a QBP into the overall CC PPS-2 methodology and to make a separate outlier payment for reimbursement of costs more than the state-identified threshold.
The demonstration allows payment to be made through FFS or managed care. CMS provided guidance and technical assistance to states on how to incorporate such payments in managed care systems: building PPS rates into managed care rates and contracts; avoiding duplication of payment, data, and reporting; and claiming the enhanced federal medical assistance percentage(FMAP) for the portion of the managed care payment attributable to CCBHC services. States electing to build CCBHC PPS rates into managed care capitation payments chose one of the two payment options represented below.[6]
-
Missouri and Pennsylvania chose to fully incorporate the CCBHC PPS payment into the managed care capitation rate and require the managed care plans to pay the full CCBHC PPS or its actuarial equivalent.
-
Minnesota, Nevada, New York, and Oregon require managed care plans to pay a rate to the CCBHCs that other providers would receive for similar services and then use a supplemental payment (wraparound) to ensure the total payment is equivalent to the CCBHC PPS.
Prospective Payment System Rates
States set clinic-specific rates based on the expected cost of providing demonstration services divided by the expected total number of demonstration visits, regardless of payer. In evaluating the expected cost of care, states and the CCBHCs reported that their costs took into consideration factors such as the expected number of demonstration encounters, the populations served, and new costs to be assumed. For example, some CCHBHCs hired new staff or trained existing staff to provide care consistent with the CCBHC model of care specified in the program criteria. The amount paid through the rate was also affected by the location of the individual clinics: urban, rural, or frontier areas. Some rural clinics directors reported the need to incur higher staffing costs under the demonstration to attract qualified providers.
One state attributed variation in their rates across clinics to the different needs and circumstances of the clinics' respective communities. Each clinic has evolved to fill a different role in their community, depending on the presence or absence of other providers. For example, a CCBHC may provide crisis services for two other CCBHCs within the same service area. Connected to that are variations in the severity and acuity of individual needs and the level of care provided in response to need. The two clinics with the lowest rates are in areas with few other providers, which means they serve a broader range of people with varying severity and acuity levels. The higher rates are in areas where other providers (including many private providers) serve lower-cost individuals, so the CCBHC works with proportionally more clients with more complex needs. The clinics with the lowest rates are in relatively rural areas, which lowers facility costs, but limits available labor.
Demonstration Year One
Table 10 presents PPS rates for Demonstration Year One (DY1). If a state pays a CCBHC more than its actual cost of care through the DY1 rate, it cannot require the certified clinic to return any portion of the demonstration payment; retrospectively adjust the CCBHC PPS; or recoup such payment through adjustment to the following year's rate.
| TABLE 10. States' Selected Methodology, QBP Provision, and Range of DY1 PPS Rates among CCBHCs | |||
|---|---|---|---|
| State | Methodology | Offering QBP | Range of DY1 PPS Rates Among CCBHCs |
| Minnesota | PPS-1 | Yes | $253.35-$666.91 (daily rate) |
| Missouri | PPS-1 | Yes | $165.46-$252.26 (daily rate) |
| Nevada | PPS-1 | Yes | $181.53-$214.40 (daily rate) |
| New York | PPS-1 | Yes | $172.00-$380.00 (daily rate) |
| Oregon | PPS-1 | No | $185.31-$324.48 (daily rate) |
| Pennsylvania | PPS-1 | Yes | $150.72-$393.86 (daily rate) |
| New Jersey | PPS-2 | Yes | $480.72-$1,151.22 (monthly rate) |
| Oklahoma | PPS-2 | Yes | $532.73-$1,264.39 (monthly rate) |
| SOURCE: State officials and demonstration grant applications. | |||
Demonstration Year Two
Using cost report data, state officials can compare the actual cost of care in DY1 with payments to adjust the Demonstration Year Two (DY2) PPS rate. States may trend the DY1 rates by the Medicare Economic Index and are not required to adjust the DY2 rate to reflect DY1 cost.
-
Nevada and Oklahoma are rebasing their rates for DY2. They anticipate that the costs of care reflected in the cost reports will differ enough from the original estimates used to set the DY1 PPS rates such that an adjustment will be needed.
-
In DY2, Missouri, New York, and Oregon will continue to pay the rates established for services delivered in DY1. These states believe the DY1 Rates are adequate to cover DY2 costs. Officials in these states expressed concerns about the variability in costs over time and the limited experience the clinics had after one year of operation.
-
At the time of the March 2018 interviews, the remaining three states (Minnesota, New Jersey, and Pennsylvania) had not decided about rebasing their rates.
Paying for Services Provided to Dually Eligible Beneficiaries
Certain Medicare beneficiaries are eligible for some level of Medicaid assistance. These individuals are often referred to as "dually eligible" beneficiaries. Section 223 requires states to pay up to the PPS rate for demonstration services provided to dually eligible beneficiaries for whom the state must share in the cost of direct services, rather than just Medicare cost sharing for all demonstration services delivered to Medicaid beneficiaries. Specifically, CMS guidance[7] states the following:
-
There are two types of dually eligible beneficiaries--Qualifying Individuals (QI), and Qualified Disabled and Working Individuals (QDWI)--for whom Medicaid pays some or all of their Medicare premiums, but does not pay for services. Under a demonstration, no Medicaid payment would be made for services furnished to such individuals by certified clinics.
-
For Qualified Medicare Beneficiaries (QMBs), states must pay Medicare cost sharing, but may adopt a methodology paying the lesser of Medicare cost sharing or the amount that would result in total payment equal to the PPS.
-
Specified Low-Income Medicare Beneficiaries (SLMB) are generally eligible only for payment of Medicare premiums, but there is a state option to pay Medicare Part B cost sharing. To the extent the state elects this option, demonstration services for SLMBs would be treated the same way as services for QMBs otherwise, no Medicaid payment would be due for demonstration services. For full-benefit dual-eligible individuals, the statute requires payment up to PPS (after accounting for the Medicare payment).
-
Thus, PPS is not required to be paid for services provided to the following dually eligible beneficiaries: QI, QDWI and SLMB only.
Matching Rates for Demonstration Expenditures
Under this demonstration, a state may only claim expenditures for services provided to Medicaid beneficiaries. Consistent with Section 223(d)(5) of PAMA, the matching rates for demonstration expenditures are as follows:
-
For services provided to newly eligible Medicaid beneficiaries enrolled in the New Adult Eligibility Group as described in paragraph (2) of Section 1905(y) of the Social Security Act (42 U.S.C. 1396(y)), expenditures are matched at the newly eligible FMAP rate applicable under paragraph (1) of that section.
-
For demonstration services provided by CCBHCs that are IHS or tribal facilities and furnished to American Indian and Alaskan Natives, the expenditures are matched at 100 percent.
-
For services provided to targeted low-income children in a Children's Health Insurance Program (CHIP) Medicaid expansion program, expenditures are matched at the enhanced FMAP at Section 2105(b), including the 23-percentage-point increase in effect October 1, 2015-September 30, 2019. (Of note: These expenditures are also applied against the state CHIP allotment.) Reporting will only affect the Maternal and Child Health Integrated Program (CMS-64.21) for CHIP. It does not apply to the CMS-21 standalone CHIP.
-
For all other services, expenditures are matched at the CHIP enhanced FMAP at Section 2105(b), without applying the 23-percentage-point increase in effect October 1, 2015-September 30, 2019.
Fast Facts: Demonstration Claiming
Fast Facts: Demonstration Claiming
|
APPENDIX A: Certified Community Behavioral Health Clinics by State
| MINNESOTA |
|---|
|
| MISSOURI |
|
| NEVADA |
|
| NEW JERSEY |
|
| NEW YORK |
|
| OKLAHOMA |
|
| OREGON |
|
| PENNSYLVANIA |
|
NOTE: CCBHCs by State as of August 2018.
APPENDIX B: State Snapshots--Compliance Monitoring
NOTE: Information provided in state snapshots was gathered from demonstration grant applications and conversations with state officials.
Minnesota
|
|||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||
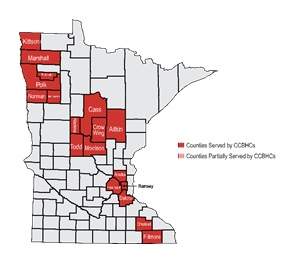
State Entity Responsible for Monitoring Compliance
Minnesota Department of Human Services with support from Department of Human Services' Licensing Division
Monitoring Instrument
SAMHSA Certification Guide, supplemented by a state-designed checklist for monitoring compliancewith care coordination standards.
Method and Frequency of Monitoring
-
Following initial certification at launch, thestate conducts at least one site visit, including client record reviews,during the 2-year demonstration period.
-
CCBHC reports on quality measure performanceand state impact measures are verified every 3 months.
-
Medicaid Department of Human Services fiscal policy/rates staff review monthly reports of paid claims for CCBHC servicesto ensure that the full breadth of CCBHC services is offered.
Additional Safeguards
-
State CCBHC staff review Department of Human Services Licensing Division's bi-weekly publications regarding agencies with violations and follow up when a CCBHC has a violation or receives a correction order. Corrective actions are coordinated between state CCBHC staff and Department of Human Services Licensing Division licensors.
-
State CCBHC staff review notification of changes that could impact certification status, such as adding, closing, ormoving program locations or making changes to services/programming, certifications, licenses, National Provider Identifiers, or provider identification, through a standardized form and submission process.
-
Consumer survey results are reviewed annually.
-
Department of Human Services provides individualized technical assistance as requested by CCBHCs.
-
CCBHC staff participate 2-3 times per month in Department of Human Services-facilitated learning collaboratives focusing on CCBHC-specific billing policies, quality measures, and service standards.
Missouri
|
|||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||

State Entity Responsible for Monitoring Compliance
Missouri Division of Behavioral Health (DBH)
Monitoring Instrument
Demonstration Application Guidance, State's Compliance with CCBHC Criteria Checklist
Method and Frequency of Monitoring
-
Based on quarterly reports, CCBHC practice coaches conduct site visits to review progress and provide technical assistance onissues relevant to implementation of the demonstration program. Practice coaches submit written reports of their site visits to DBH and meet regularly with DBH staff to share progress of their assigned CCBHCs.
-
CCBHCs submit quarterly reports on thefollowing:
-
Aggregated Daily Living Activities.
-
Numberof contacts categorized as urgent and routine.
-
Percentage of urgent contacts in which an initial evaluation was completed within 1 business day.
-
Percentage of routine consumer contacts in which an initial evaluation was completed within 10 business days.
-
Mean number of days from first contact to completion of an initial evaluation forurgent and routine contacts.
-
Mean number of days before comprehensive diagnostic and planning evaluations are completed.
-
Number of peer specialists, family support providers, and Missouri Recovery Support Specialist Peers employed.
-
-
Other quarterly reports are generated and reviewed by DBH in collaboration with the Coalition for Community Behavioral Healthcare:
-
Participation in required governing board and consumer/family member leadership training.
-
Outpatient SUD services and MAT provided.
-
Participation in required EBPs training and learning collaboratives (e.g., trauma, suicide prevention).
-
Tobacco cessation services provided.
-
Documentation of client's military service.
-
Accreditation/certification status.
-
Additional Safeguards
-
CCBHCs are required to submit their proposed health screen for approval by DBH and to submit reports and data required for various DBH programs. They also submit performance measure and program evaluation data, an annual staffing plan, and an annual cost report.
-
Practice coaches trained on the objectives of the demonstration program and the SAMHSA CCBHC certification criteria are assigned to CCBHCs to detect and resolve implementation problems, identify and share best practices for implementation, and promote consistency.
-
Technical assistance is provided through regularly scheduled conference calls and webinars.
Nevada
|
|||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||
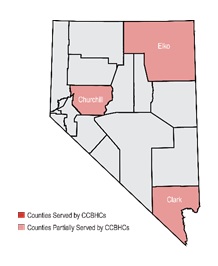
State Entities Responsible for Monitoring Compliance
-
The Nevada Department of Health and Human Services (DHHS) CCBHC Executive Committee oversees monitoring and oversight.
-
The Division of Health Care Financing and Policy (DHCFP), in conjunction with the Center forHealth Information Analysis (CHIA), monitors data and utilization compliance.
-
The Bureau of HealthCare Quality and Compliance (BHCQC) reviews certification compliance.
Monitoring Instrument
Demonstration Application Guidance, State's Compliance with CCBHC Criteria Checklist
Method and Frequency of Monitoring
-
The CCBHC Executive Committee reviews all data and reports as part of its mission to maintain CCBHC compliance during the 2-year demonstration program. The committee includes the DHHS director and staff representatives; division administrators for the Division of Public and Behavioral Health (DPBH), Division of Child and Family Services, Division of Welfare and Supportive Services, and DHCFP; and the CCBHC project director.
-
CHIA and DHCFP's Data Analytics Unit collect and analyze CCBHC-led and state-led measures quarterly to ensure CCBHCs are meeting goals for process and outcome data. A summary of the CQI quality measures is provided to each CCBHC quarterly to review progress over time, alignment with goals, and opportunity to address areas in need of improvement. CQI plans include suicide deaths or attempts, 30-day readmissions, and all CCBHC-led quality measures.
-
DHHS' Surveillance and Utilization Review (SUR) Unit conducts fiscal reviews to identify and recover overpayments made to Medicaid providers due to potential fraud, waste, abusive billing, and other improper payments. Review occurs bi-annually or more frequently if warranted. The SUR Unit also reviews any complaints or referrals received.
-
BHCQC provides on-site compliance reviews twice per year throughout the duration of the demonstration program. On-site reviews include staff who can provide on-site and off-site technical assistance to CCBHCs should the need arise. Should deficiencies be identified on these visits, formal remediation efforts occur and include letters of deficiencies and plans of correction. Should a CCBHC require a plan of correction, additional monitoring of plan and agency, including furtheron-site review, is conducted as needed until the situation is resolved.
Additional Safeguards
-
A summary of all 21 quality measures for each CCBHC is provided to the executive committee to identify successes and areas in need of technical assistance. These data are reported to SAMHSA annually and used to determine achievement of benchmarks established for QBPs.
-
CCBHCs meet with the core team (representatives from DPBH and DHCFP) twice a month to discuss a variety of topics and to engage in cooperative learning. The core team provides technical assistance through learning communities to support CCBHCs in maintaining and reporting fidelity to specific EBPs.
-
DPBH assigned a program monitor to each CCBHC to assist in the review of fidelity measures and data related to the CQI plan. The program monitor works with the CCBHC to review results and develop plans, as needed, to ensure CQI. The program monitor is available to provide training or technical assistance when deemed appropriate.
New Jersey
|
|||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||

State Entity Responsible for Monitoring Compliance
A CCBHC monitoring team involving staff from New Jersey FamilyCare (Medicaid), the Department of Children and Families, and the Department of Human Services' DMHAS.
Monitoring Instrument
Demonstration Application Guidance, State's Compliance with CCBHC Criteria Checklist, modified to include a provider self-assessment.
Method and Frequency of Monitoring
-
The CCBHC monitoring team monitors compliance with program requirements through annual on-site monitoring visits and review of an annual self-administered assessment tool.
-
Billing through the Medicaid Management Information System is reviewed quarterly. "Numbers served" are requested two times per month. The first full data submissions were submitted in January 2018 for state review.
Additional Safeguards
-
New Jersey's Department of Human Services contracted with Rutgers University to assess and monitor the implementation of EBPs among CCBHC providers.
New York
|
|||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||
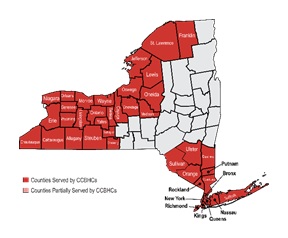
State Entity Responsible for Monitoring Compliance
New York State Office of Alcoholism and Substance AbuseServices, Office of Mental Health, and Department of Health
Monitoring Instrument
New York State CCBHC Demonstration Program Monitoring Tool (modified version of the Demonstration Application Guidance,State's Compliance with CCBHC Criteria Checklist).
Method and Frequency of Monitoring
-
Each CCBHC receives a non-site monitoring visit at least quarterly. To maintain consistency during site visits, the CCBHC team uses a standardized programmatic monitoring tool. The accompanying chart review ensures services provided are following certification and record-keeping standards.
Additional Safeguards
-
Each CCBHC has periodic individual conference calls with the state CCBHC team to discuss any concerns or challenges encountered.
Oklahoma
|
|||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||
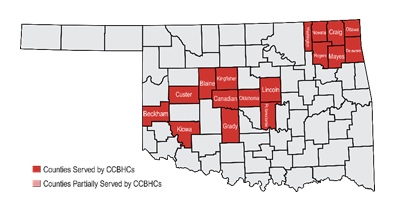
State Entity Responsible for Monitoring Compliance
Oklahoma Department of Mental Health and Substance AbuseServices (ODMHSAS)
Monitoring Instrument
SAMHSA Certification Guide and Demonstration Application Guidance, State's Compliance with CCBHCCriteria Checklist
Method and Frequency of Monitoring
-
ODMHSAS' Decision Support Services division monitors the evaluation criteria required for the demonstration period. It reports any deficiencies in data-reporting and provides technical assistanceto ensure data are entered.
-
ODMHSAS' integrated services manager and systems of care senior director monitor the clinical and recovery support activities required by CCBHC standards. Technical assistance is provided as necessary.
-
Methods of monitoring include site visits, monthly data review (such as agency staff-to-client ratio), chart reviews, desk reviews, video conferencing, client interviews, and surveys.
-
The two individuals designated to oversee the demonstration program requirements per ODMHSAS do so quarterly during the demonstration period and yearly thereafter.
-
ODMHSAS' provider certification division reviews the CCBHC checklist criteria during site visits conducted within 6 months of CCBHC operation. Deficiencies require a correction plan and follow-up until improvement is sufficient. Based on the score the CCBHC earnsat the 6-month certification review, recertification takes place yearly or every 3 years. The provider certification division routinely makes at least one unannounced visit prior to recertification.
Additional Safeguards
-
Monthly, ODMHSAS analyzes data, identifies areas in need of improvement, and holds meetings with CCBHC staff to share data analysis, discuss implications,and plan for CQI.
-
Oklahoma's contract monitoring team provides ongoing support and technical assistance related to the CCBHC contract.
-
ODMHSAS created a CCBHC scope of work (SOW) for each state fiscal year. SOWs are also createdfor innovative and EBPs disseminated through grants and other funding. Based on deliverables within these various SOWs, ODMHSAS works with contracted agencies to improve the access and quality of services.
Oregon
|
|||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||

State Entity Responsiblefor Monitoring Compliance
Oregon Health Authority (OHA)
Monitoring Instrument
SAMHSA Certification Guide in conjunction with state CCBHC standards, other guidance on CCBHC requirements, and state administrative rules.
Method and Frequencyof Monitoring
-
Each CCBHC participates in two formal check-in conversations per year during the demonstration period, as well as one formal on-site visit occurring between 2017 and 2019.
-
Formal reviews include the completion of a CCBHC checklist aligning with state and federal standards. Reviews occur no more often than every 6 months, unless concerns are expressed by CCBHC project staff, consulting parties, or a request is made by the CCBHC or licensing and certification staff.
-
Monitoring is conducted during key billing and data-reporting periods.
-
OHA's Division of Licensing and Certification sets the schedule for recertification reviews (approximately once every 3 years).
Additional Safeguards
-
CCBHCs informally participate in check-in meetings, site visits, and every-other-month CCBHC demonstration calls.
-
Time is reserved in each CCBHC meeting to discuss any broad compliance issues that may be applicable to all participating CCBHCs.
Pennsylvania
|
|||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||
|
|||||||||||||||||||||||||||||
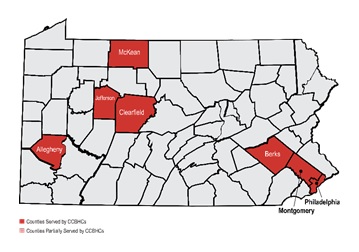
State Entity Responsible for Monitoring Compliance
Pennsylvania Department of Human Services' Office of Mental Health and Substance Abuse Services (OMHSAS)
Monitoring Instrument
SAMHSA Certification Guide, modified for the state certification process.
Method and Frequency of Monitoring
-
OMHSAS conducts an annual on-site review ateach clinic to determine that the clinic continues to meet CCBHC criteria.
-
The Finance Department monitors quarterly financial reports from the managed care plans, as well as all available encounter data.
-
In the first 6 months of demonstration program implementation, monitoring focused on the ability of the clinics to submit required data elements, including:
-
Weekly submissions of patients' and families' experience of care reports by each CCBHC.
-
Monthly data submission into the quality dashboard.
-
Accuracy of claims submission.
-
-
Interim cost reports were required for the first 6 months of the demonstration program (July-December 2017).
-
A report of activity from the FFS program was requested.
Additional Safeguards
-
All CCBHCs must maintain valid licensing for the services provided under the demonstration program. These licensing processes occur annually to comply with current Pennsylvania regulations.
-
Discussions occur with individual clinics regarding their data, as well as with all clinics regarding the overall results of the various evaluation findings.
-
After the completion of the first year of the demonstration program, a critical review will explore the results of all the quality metrics being collected, including the six which can result in a QBP.
GLOSSARY OF ACRONYMS
| ADHD | Attention Deficit/Hyperactivity Disorder |
|---|---|
| ASAM | American Society of Addiction Medicine |
| ASPE | HHS Office of the Assistant Secretary for Planning and Evaluation |
| AWM | Ambulatory Withdrawal Management |
| BHCQC | Nevada Bureau of Health Care Quality and Compliance |
| C-SSRS | Columbia Suicide Severity Rating Scale |
| CC PPS | Certified Clinic Prospective Payment System |
| CCBHC | Certified Community Behavioral Health Clinic |
| CHIA | Nevada Center for Health Information Analysis |
| CHIP | Children's Health Insurance Program |
| CMHC | Community Mental Health Center |
| CMHL | Community Mental Health Liaisons |
| CMS | HHS Centers for Medicare & Medicaid Services |
| CQI | Continuous Quality Improvement |
| DCO | Designated Collaborating Organization |
| DHCFP | Nevada Division of Health Care Financing and Policy |
| DHHS | Nevada Department of Health and Human Services |
| DMHAS | New Jersey Division of Mental Health and Addiction Services |
| DPBH | Nevada Division of Public and Behavioral Health |
| DY | Demonstration Year |
| EBP | Evidence-Based Practice |
| ED | Emergency Department |
| EHR | Electronic Health Record |
| FFS | Fee-For-Service |
| FMAP | Federal Medical Assistance Percentage |
| FQHC | Federally Qualified Health Center |
| HHS | U.S. Department of Health and Human Services |
| HIT | Health Information Technology |
| IHS | HHS Indian Health Service |
| MAT | Medication-Assisted Treatment |
| MCHIP | Maternal and Child Health Integrated Program |
| MH/SUD | Mental Health and Substance Use Disorder |
| ODMHSAS | Oklahoma Department of Mental Health and Substance Abuse Services |
| OHA | Oregon Health Authority |
| OMHSAS | Pennsylvania Office of Mental Health and Substance Abuse Services |
| OORP | New Jersey Opioid Overdose Recovery Program |
| PAMA | Protecting Access to Medicare Act (Public Law 113-93) |
| PPS | Prospective Payment System |
| PTSD | Post-Traumatic Stress Disorder |
| QBP | Quality Bonus Payment |
| QDWI | Qualified Disabled and Working Individuals |
| QI | Qualifying Individuals |
| QMB | Qualified Medicare Beneficiaries |
| SAMHSA | HHS Substance Abuse and Mental Health Services Administration |
| SED | Serious Emotional Disturbance |
| SIM | State Innovation Model |
| SLMB | Specified Low-Income Medicare Beneficiaries |
| SMI | Serious Mental Illness |
| SOW | Scope of Work |
| SSW | School of Social Work |
| SUD | Substance Use Disorder |
| SUR | Surveillance and Utilization Review |
| TANF | Temporary Assistance for Needy Families |
| VA | U.S. Department of Veterans Affairs |
| WIC | Women, Infants and Child nutrition program |
REFERENCES
Advocates for Human Potential, Inc.. (2018). Certified Community Behavioral Health Clinics Demonstration Program, Report to Congress, 2017. Rockville, MD: Substance Abuse and Mental Health Services Administration. Retrieved from https://www.samhsa.gov/sites/default/files/ccbh_clinicdemonstrationprogram_071118.pdf.
Bellg, A.J., Borrelli, B., Resnick, B., Hecht, J., Minicucci, D.S., Ory, M., Ogedegbe, G., Orwig, D., Ernst, D., & Czajkowski, S. (2004). Enhancing treatment fidelity in health behavior change studies: Best practices and recommendations from the NIH Behavior Change Consortium. Health Psychology, 23(5), 443-451. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/15367063.
Cummings, J., Allen, L., Clennon, J., Ji, X., & Druss, B. (2017). Geographic access to specialty mental health care across high- and low-income US communities. JAMA Psychiatry, 74(5), 476-484. doi:10.1001/jamapsychiatry.2017.0303.
Council of Economic Advisers. (2017). The underestimated cost of the opioid crisis. Retrieved from https://www.whitehouse.gov/briefings-statements/cea-report-underestimated-cost-opioid-crisis/.
Dobson, D., & Cook, T. (1980). Avoiding type III error in program evaluation: Results from a field experiment. Evaluation and Program Planning, 3, 269-276. doi: 10.1016/0149-7189(80)90042-7.
Fixsen, D., Naoom, S., Blase, K., Friedman, R., & Wallace, F. (2005). Implementation research: A synthesis of the literature. Tampa, FL: University of South Florida, Louis de la Parte Florida Mental Health Institute, National Implementation Research Network (FMHI Publication #231). Retrieved from http://ctndisseminationlibrary.org/PDF/nirnmonograph.pdf.
Fukui, S., Goscha, R., Rapp, C., Mabry, A., Liddy, P., & Marty, D. (2012). Strengths model case management fidelity scores and client outcomes. Psychiatric Services, 63(7), 708-710. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/22752035.
Horner, S., Rew, L., & Torres, R. (2006). Enhancing intervention fidelity: A means of strengthening study impact. J Spec Pediatr Nurs, 11(2), 80-89. doi: 10.1111/j.1744-6155.2006.00050.x.
McHugo, G., Drake, R., Teague, G., & Xie, H. (1999). Fidelity to Assertive Community Treatment and client outcomes in the New Hampshire dual disorders study. Psychiatric Services, 50 (6), 818-824. doi: 10.1176/ps.50.6.818.
Miller, W., & Rollnick, S. (2014). The effectiveness and ineffectiveness of complex behavioral interventions: Impact of treatment fidelity. Contemporary Clinical Trials, 37(2), 234-241. doi: 10.1016/j.cct.2014.01.005.
Rossi, P., & Freeman, H. (1985). Evaluation: A Systemic Approach (3rd ed.). Beverly Hills, CA: Sage.
Teague, G., Mueser, K., & Rapp, C. (2012). Advances in fidelity measurement for mental health services research: Four measures. Psychiatric Services, 63(8), 765-71. doi: 10.1176/appi.ps.201100430.
U.S. Department of Health and Human Services. (2019). The Opioid Epidemic by the Numbers. Retrieved from https://www.hhs.gov/opioids/sites/default/files/2019-01/opioids-infogra….
U.S. Department of Health and Human Services. (2016). Criteria for the Demonstration Program to Improve Community Mental Health Centers and to Establish Certified Community Behavioral Health Clinics. Retrieved from https://www.samhsa.gov/sites/default/files/programs_campaigns/ccbhc-criteria.pdf.
Walker, E., Cummings, J., Hockenberry, J., & Druss, B. (2015). Insurance status, use of mental health services, and unmet need for mental health care in the United States. Psychiatric Services (Washington, DC), 66(6), 578-584. doi: 10.1176/appi.ps.201400248.
Walton, H., Spector, A., Tombor, I, & Michie, S. (2017). Measures of fidelity of delivery of, and engagement with, complex, face-to-face health behaviour change interventions: A systematic review of measure quality. Br J Health Psychol, 22, 872-903. doi:10.1111/bjhp.12260.
NOTES
-
See https://www.samhsa.gov/sites/default/files/ccbh_clinicdemonstrationprogram_071118.pdf.
-
Oklahoma and Oregon launched their CCBHC programs statewide on April 1, 2017, and the remaining six states launched theirs on July 1, 2017.
-
See https://www.samhsa.gov/sites/default/files/ccbh_clinicdemonstrationprogram_071118.pdf.
-
In cases where a CCBHC is unable to employ a psychiatrist as medical director (e.g., due to a documented behavioral health professional shortage in its vicinity), the criteria specify that "a medically trained behavioral health care provider with appropriate education and licensure with prescriptive authority in psychopharmacology who can prescribe and manage medications independently pursuant to state law" can serve as a CCBHC medical director.
-
Crisis behavioral health services may be provided by a DCO if the DCO is an existing state-sanctioned, certified, or licensed system or network. DCOs may also provide ambulatory and medical detoxification in American Society of Addiction Medicine Criteria (ASAM) categories 3.2-Withdrawl Management and 3.7-Withdrawl Management. The ASAM criteria provide a comprehensive set of guidelines for placement, continued stay, and transfer/discharge of patients with addiction and co-occurring conditions.
-
Oklahoma does not currently have managed care arrangements in its Medicaid program. At the start of the demonstration, New Jersey did not include MH/SUD services in most managed care contracts. Medicaid enrollees who received MH/SUD benefits through managed Long Term Services and Supports or the Division of Developmental Disabilities in New Jersey who did receive services through managed care represented less than 0.5 percent of Medicaid enrollees and were thereby excluded from the CCBHC demonstration.
-
See https://www.medicaid.gov/medicaid/finance/223-demonstration/index.html.
INFORMATION ON PROJECT AND REPORTS
This report was prepared under contract #HHSP233201600017I between HHS's ASPE/DALTCP and Mathematica Policy Research. For additional information about this subject, you can visit the DALTCP home page at https://aspe.hhs.gov/office-disability-aging-and-long-term-care-policy-daltcp or contact the ASPE Project Officer, Judith Dey, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. Her e-mail address is: Judith.Dey@hhs.gov.
Reports Available
Certified Community Behavioral Health Clinics Demonstration Program, Report to Congress, 2017
Certified Community Behavioral Health Clinics Demonstration Program: Report to Congress, 2018