
Regular physical activity, fitness, and exercise are critically important for the health and well being of people of all ages. Research has demonstrated that virtually all individuals can benefit from regular physical activity, whether they participate in vigorous exercise or some type of moderate health-enhancing physical activity. Even among frail and very old adults, mobility and functioning can be improved through physical activity.1 Therefore, physical fitness should be a priority for Americans of all ages.
Regular physical activity has been shown to reduce the morbidity and mortality from many chronic diseases. Millions of Americans suffer from chronic illnesses that can be prevented or improved through regular physical activity:
- 12.6 million people have coronary heart disease2;
- 1.1 million people suffer from a heart attack in a given year2;
- 17 million people have diabetes; about 90% to 95% of cases are type 2 diabetes, which is associated with obesity and physical inactivity3; approximately 16 million people have pre diabetes;
- 107,000 people are newly diagnosed with colon cancer each year4,5;
- 300,000 people suffer from hip fractures each year6;
- 50 million people have high blood pressure2; and
- Nearly 50 million adults (between the ages of 20 and 74), or 27% of the adult population, are obese; overall more than 108 million adults, or 61% of the adult population are either obese or overweight.7,8
In a 1993 study, 14 percent of all deaths in the United States were attributed to activity patterns and diet.9 Another study linked sedentary lifestyles to 23 percent of deaths from major chronic diseases.10 For example, physical activity has been shown to reduce the risk of developing or dying from heart disease, diabetes, colon cancer, and high blood pressure. On average, people who are physically active outlive those who are inactive.11-16
Despite the well-known benefits of physical activity, most adults and many children lead a relatively sedentary lifestyle and are not active enough to achieve these health benefits. A sedentary lifestyle is defined as engaging in no leisure-time physical activity (exercises, sports, physically active hobbies) in a two-week period. Data from the National Health Interview Survey shows that in 1997-98 nearly four in 10 (38.3 percent) adults reported no participation in leisure- time physical activity.17
| Figure 1: Physically inactive |
|
|
| SOURCE: 1997-98 National Health Interview Survey |
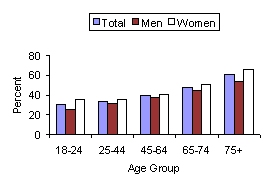
Approximately one-third of persons age 65 or older lead a sedentary lifestyle. Older women are generally less physically active than older men. Fifty-four percent of men and 66 percent of women age 75 and older engage in no leisure-time physical activity.17 In general, African American older adults are less active than white older adults. In the mid 1990's, 37 percent of white men age 75 and older reported no leisure-time physical activity, compared to 59 percent of African American men age 75 and older; 47 percent of white women age 75 and older reported no leisure-time physical activity, compared to 60 percent of African American women age 75 and older.18
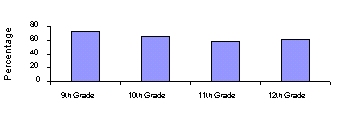
More than one-third of young people in grades 9-12 do not regularly engage in vigorous physical activity. Furthermore, 43 percent of students in grades 9-12 watch television more than two hours per day.19 Physical activity declines dramatically over the course of adolescence, and girls are significantly less likely than boys to participate regularly in vigorous physical activity.
| Figure 2: Vigorous Physical Activity of Adolescentsby Grade Level, 1999 |
|
|
| Vigorous physical activity is defined as exercise that made the respondent sweat and breathe hard for at least 20 minutes on 3 or more of the 7 days preceding the survey.SOURCE: Youth Risk Behavior Surveillance System (YRBSS), CDC, NCCDPHP |
Economic Consequences of Inactivity
Physical inactivity and its associated health problems have substantial economic consequences for the U.S. health care system. In the long run, physical inactivity threatens to reverse the decades-long progress that has been made in reducing the morbidity and mortality associated with many chronic conditions such as cardiovascular disease. A physically inactive population is at both medical and financial risk for many chronic diseases and conditions including heart disease, stroke, colon cancer, diabetes, obesity, and osteoporosis.
The increasing prevalence of chronic medical conditions and diseases related to physical inactivity are associated with two types of costs. First, there are health care costs for preventative, diagnostic, and treatment services related to these chronic conditions. These costs may include expenditures for physician visits, pharmaceuticals, ambulance services, rehabilitation services and hospital and nursing home care. In addition, there are other costs associated with the value of lost wages by people unable to work because of illness and disability, as well as the value of future earnings lost by premature death. In 2000, the total cost of overweight and obesity was estimated to be $117 billion.7 In addition, the total estimated cost from chronic diseases is substantial.
| Table 1: National Cost of Illness for Selected Diseases(in billions) | |
| Disease | Cost |
| Heart Diseases | $183 |
| Cancer | 157 |
| Diabetes | 100 |
| Arthritis | 65 |
| SOURCE: National Institutes of Health, 2000 | |
Individuals suffering from chronic diseases bear a substantial portion of these medical costs. A recent study demonstrated that obese individuals spend approximately 36 percent more than the general population on health services and 77 percent more on medications.20 Furthermore, the study found that the effects of obesity on health spending were significantly larger than effects of current or past smoking.
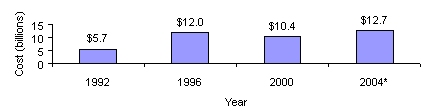
The Medicare and Medicaid programs currently spend $84 billion annually on five major chronic conditions that could be significantly improved by increased physical activity, specifically diabetes, heart disease, depression, cancer, and arthritis. Medicare spent $10.4 billion on diabetes treatment and services in 2000 and is estimated to spend $12.7 billion in 2004.
| Figure 3: Estimated Direct and Indirect Medicare Program Payments forDiabetes Treatments and Services |
|
|
| *Projected data NOTE: These estimates include only Medicare program payments for direct and indirect costs. Therefore, they do not reflect payments by beneficiaries for co-payments and deductibles.SOURCE: Office of the Actuary, June 2002 |
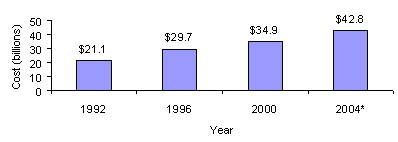
In addition, Medicare spending on heart disease treatment and services has grown from $21.1 billion in 1992 to $34.9 billion in 2000 and is expected to reach $42.8 billion in 2004.
| Figure 4: Estimated Direct Medicare Program Payments forHeart Disease Treatments and Services |
|
|
| *Projected data NOTE: These estimates include only Medicare program payments for direct costs. Therefore, they do not include any indirect costs of the disease, which may be significant, and do not reflect payments by beneficiaries for co-payments and deductibles.SOURCE: Office of the Actuary, June 2002 |
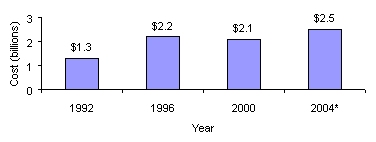
Medicare spending on depression treatment and services has grown from $1.3 billion in 1992 to $2.1 billion in 2000 and is estimated to increase to $2.5 billion in 2004.
| Figure 5: Estimated Direct Medicare Program Payments forDepression Treatments and Services |
|
|
| *Projected data NOTE: These estimates include only Medicare program payments for direct costs. Therefore, they do not include any indirect costs of the disease, which may be significant, and do not reflect payments by beneficiaries for co-payments and deductibles.SOURCE: Office of the Actuary, June 2002 |
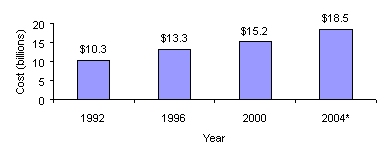
Medicare spending on cancer treatment and services has grown from $10.3 billion in 1992 to $15.2 billion in 2000 and is expected to increase to $18.5 billion in 2004.
| Figure 6: Estimated Direct Medicare Program Payments forCancer Treatments and Services |
|
|
| *Projected data NOTE: These estimates include only Medicare program payments for direct costs. Therefore, they do not include any indirect costs of the disease, which may be significant, and do not reflect payments by beneficiaries for co-payments and deductibles.SOURCE: Office of the Actuary, June 2002 |
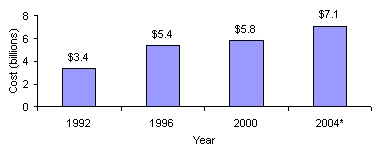
Medicare spending on arthritis treatment and services has grown from $3.4 billion in 1992 to $5.8 billion in 2000 and is estimated to be $7.1 billion in 2004.
| Figure 7: Estimated Direct Medicare Program Payments forArthritis Treatments and Services |
|
|
| *Projected data NOTE: These estimates include only Medicare program payments for direct costs. Therefore, they do not include any indirect costs of the disease, which may be significant, and do not reflect payments by beneficiaries for co-payments and deductibles.SOURCE: Office of the Actuary, June 2002 |
Since regular physical activity helps prevent disease and promote health, it may actually decrease health care costs. A study performed by researchers at the Centers for Disease Control and Prevention found that physically active people had, on average, lower annual direct medical costs than did inactive people. The same study estimated that increasing regular moderate physical activity among the more than 88 million inactive Americans over the age of 15 years might reduce the annual national direct medical costs by as much as $76.6 billion in 2000 dollars.21 Further, it found that physically active people had fewer hospital stays and physician visits and used less medication than physically inactive people. The cost savings were consistent for men and women, for those with and without physical limitations, and even for smokers and nonsmokers. In this study, the biggest difference in direct medical costs was among women 55 and older, supporting the belief that the potential gain associated with physical activity is especially high for older women. The researchers concluded that adoption of a population-wide physical activity strategy might produce health care cost savings among most adult age groups.
Employers can benefit too. Workplace physical activity programs can reduce short-term sick leave by six to 32 percent, reduce health care costs by 20 to 55 percent, and increase productivity by 2 to 52 percent. 22 In 1998, 93 percent of employers had programs that fostered employee health, up from 76 percent in 1992, according to Hewitt Associates. Such wellness programs typically offer help in smoking cessation, managing stress, prenatal care, nutrition, and fitness.23
Physical Activity and Good Physical Health
Participation in regular physical activity at least 30 minutes of moderate activity on at least five days per week, or 20 minutes of vigorous physical activity at least three times per weekis critical to sustaining good health. Youth should strive for at least one hour of exercise a day. Regular physical activity has beneficial effects on most (if not all) organ systems, and consequently it helps to prevent a broad range of health problems and diseases. People of all ages, both male and female, derive substantial health benefits from physical activity.
Regular physical activity reduces the risk of developing or dying from some of the leading causes of illness in the United States. Regular physical activity improves health in the following ways22:
- Reduces the risk of dying prematurely from heart disease and other conditions;
- Reduces the risk of developing diabetes;
- Reduces the risk of developing high blood pressure;
- Reduces blood pressure in people who already have high blood pressure;
- Reduces the risk of developing colon and breast cancer5;
- Helps to maintain a healthy weight;
- Helps build and maintain healthy bones, muscles, and joints;
- Helps older adults to become stronger and better able to move about without falling;
- Reduces feelings of depression and anxiety; and
- Promotes psychological well-being.
Regular physical activity is associated with lower mortality rates for both older and younger adults.22 Even those who are moderately active on a regular basis have lower mortality rates than those who are least active. Regular physical activity leads to cardiovascular fitness, which decreases the risk of cardiovascular disease mortality in general and coronary artery disease mortality in particular. High blood pressure is a major underlying cause of cardiovascular complications and mortality. Regular physical activity can prevent or delay the development of high blood pressure, and reduces blood pressure in persons with hypertension.
Regular physical activity is also important for maintaining muscle strength, joint structure, joint functioning, and bone health.22 Weight-bearing physical activity is essential for normal skeletal development during childhood and adolescence and for achieving and maintaining peak bone mass in young adults. Among post-menopausal women, exercise, especially muscle strengthening (resistance) activity, may protect against the rapid decline in bone mass. However, data on the effects of exercise on post-menopausal bone loss are not clear-cut and the timing of the intervention (e.g., stage of menopausal transition) can influence the response. Regardless, physical activity including muscle-strengthening exercise appears to protect against falling and fractures among the elderly, probably by increasing muscle strength and balance.22 In addition, physical activity may be beneficial for many people with arthritis.
Regular physical activity can help improve the lives of young people beyond its effects on physical health. Although research has not been conducted to conclusively demonstrate a direct link between physical activity and improved academic performance, such a link might be expected. Studies have found participation in physical activity increases adolescents self-esteem and reduces anxiety and stress.22 Through its effects on mental health, physical activity may help increase students capacity for learning. One study found that spending more time in physical education did not have harmful effects on the standardized academic achievement test scores of elementary school students; in fact, there was some evidence that participation in a two-year health-related physical education program had several significant favorable effects on academic achievement.24
Participation in physical activity and sports can promote social well-being, as well as good physical and mental health, among young people. Research has shown that students who participate in interscholastic sports are less likely to be regular and heavy smokers or use drugs25, and are more likely to stay in school and have good conduct and high academic achievement.26 Sports and physical activity programs can introduce young people to skills such as teamwork, self-discipline, sportsmanship, leadership, and socialization. Lack of recreational activity, on the other hand, may contribute to making young people more vulnerable to gangs, drugs, or violence.
Physical Activity and Good Mental Health
Regular physical activity reduces morbidity and mortality from mental health disorders.27 Mental health disorders pose a significant public health burden in the United States and they are a major cause of hospitalization and disability. Mental health disorders cost approximately $148 billion per year.22 Potentially, increasing physical activity levels in Americans could substantially reduce medical expenditures for mental health conditions.
In adults with affective disorders, physical activity has a beneficial effect on symptoms of depression and anxiety.27 Animal research suggests that exercise may stimulate the growth of new brain cells that enhance memory and learningtwo functions hampered by depression. Clinical studies have demonstrated the feasibility and efficacy of exercise as a treatment for depression in older men and women. Currently, National Institute of Mental Health (NIMH) investigators are conducting research comparing the effectiveness of home-based and supervised aerobic exercise to the use of antidepressants in relieving depression in these groups, and reducing relapse rates. Other NIMH researchers are studying whether greater exercise levels result in more symptom improvement. Regular physical activity also appears to enhance well-being.
The preventive effects of physical activity on mental disorders are less well studied. Some studies suggest physical activity prevents depressive illness. Future research will clarify the extent to which physical activity may actually protect against the development of depression.
Regular physical activity may also reduce risk of cognitive decline in older adults, though more research is needed to clarify the mechanism of this possible effect. Among people who suffer from mental illness, physical activity appears to improve the ability to perform activities of daily living.27
Physical Activity (Along with a Nutritious Diet) is Key to Maintaining Energy Balance and a Healthy Weight
Regular physical activity along with a nutritious diet is key to maintaining a healthy weight. In order to maintain a healthy weight, there must be a balance between calories consumed and calories expended through metabolic and physical activity. Although overweight and obesity are caused by many factors, in most individuals, weight gain results from a combination of excess calorie consumption and inadequate physical activity.
Even though a large portion of a persons total caloric requirement is used for basal metabolism and processing food, an individuals various physical activities may account for as much as 15 to 40 percent of the calories he or she burns each day. While vigorous exercise uses calories at a higher rate, any physical activity will burn calories. For example, a 140-pound person can burn 175 calories in 30 minutes of moderate bicycling, and 322 calories in 30 minutes of moderate jogging. The same person can also burn 105 calories by vacuuming or raking leaves for the same amount of time.
The Epidemic of Overweight and Obesity
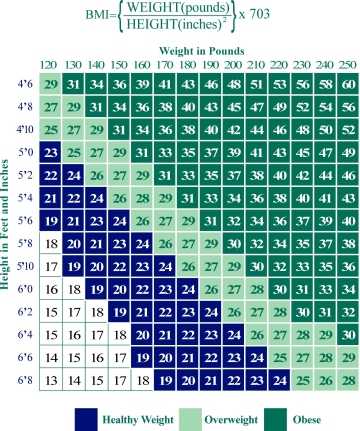
As a result of lifestyle and dietary changes, overweight and obesity have reached epidemic proportions in the United States. The Body Mass Index (BMI) is the most commonly used measure to define overweight and obesity. BMI is a measure of weight in relation to height. BMI is calculated as weight in pounds divided by the square of the height in inches, multiplied by 703.
According to the National Institutes of Health Clinical Guidelines, overweight in adults is defined as a BMI between 25 lbs/in2 to 29.9 lbs/in2; and obesity in adults is identified by a BMI of 30 lbs/in2 or greater.28 These definitions are based on evidence that suggests that health risks are greater at or above a BMI of 25 lbs/in2 compared to those at a BMI below that level. The risk of premature death increases with an increasing BMI. This increase in mortality tends to be modest until a BMI of 30 lbs/in2 is reached.
| Figure 8: BMI Weight Chart |
|
|
| SOURCE: Surgeon Generals Call to Action to Prevent and Decrease Overweight and Obesity, 2001 |
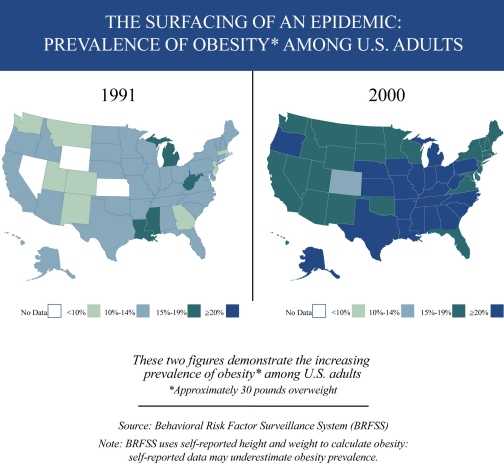
Overweight and obesity are increasing in both genders and among all population groups. In 1999, an estimated 61 percent of adults in the U.S. were overweight or obese; this contrasts with the late 1970s, when an estimated 47 percent of adults were overweight or obese.7 Figure 9 demonstrates the increasing prevalence of obesity among adults throughout the United States.
| Figure 9 |
|
|
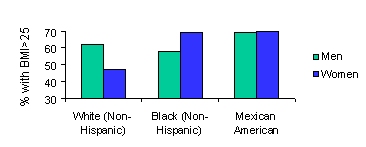
Among women, the prevalence of overweight and obesity generally is higher in women who are members of racial and ethnic minority populations than in non-Hispanic white women.7 Among men, Mexican Americans have a higher prevalence of overweight and obesity than non-Hispanic whites or non-Hispanic blacks. For non-Hispanic men, the prevalence of overweight and obesity among whites is slightly greater than among blacks.
| Figure 10: Age-adjusted prevalence of overweight or obesityin selected groups, 1988-1994 |
|
|
| SOURCE: Surgeon Generals Call to Action to Prevent and Decrease Overweight and Obesity, 2001 |
Disparities in prevalence of overweight and obesity also exist based on socioeconomic status.7 For all racial and ethnic groups combined, women of lower socioeconomic status (income 130 percent of the poverty threshold) are approximately 50 percent more likely to be obese than those with higher socioeconomic status (income > 130 percent of the poverty threshold). Men are about equally likely to be obese whether they are in a low or high socioeconomic group.
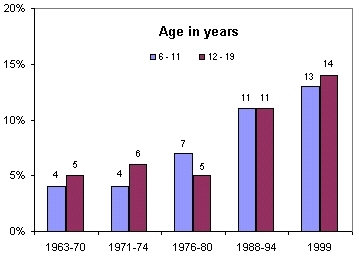
The overweight and obesity epidemic is not limited to adults. What is particularly alarming is that the percentage of young people who are overweight has almost doubled in the last 20 years for children aged 6-11 and almost tripled for adolescents aged 12-19. In children and adolescents, overweight has been defined as a sex- and age- specific BMI at or above the 95th percentile for a reference population, based on Centers for Disease Control and Prevention (CDC) growth charts
| Figure 11: Prevalence of Overweight in Children and Adolescents ages 6-19 |
|
|
| NOTES: Excludes pregnant women starting with 1971-74. Pregnancy status not available for 1963-65 and 1966-70. Data for 1963-65 are for children 6-11 years of age; data for 1966-70 are for adolescents 12-17 years of age, not 12-19 years.SOURCE: CDC/NCHS, NHES and NHANES. |
Associated Health Risks of Not Maintaining a Healthy Weight
Epidemiological studies show an increase in mortality associated with overweight and obesity. Approximately 300,000 deaths a year in this country are currently associated with overweight and obesity.29 Morbidity from obesity may be as great as from poverty, smoking, or problem drinking.20 Overweight and obesity are associated with an increased risk for developing various medical conditions including cardiovascular disease, certain cancers (endometrial, colon, postmenopausal breast, kidney, and esophageal)5, high blood pressure, arthritis-related disabilities and type 2 diabetes.7
| Table 2: Health risks associated with obesityObesity is Associated with an Increased Risk of: | |
|
|
| SOURCE: Surgeon Generals Call to Action to Prevent and Decrease Overweight and Obesity, 2001 | |
It is also important for individuals who are currently at a healthy weight to strive to maintain it since both modest and large weight gains are associated with significantly increased risk of disease. For example, a weight gain of 11 to 18 pounds increases a persons risk for developing type 2 diabetes to twice that of individuals who have not gained weight, while those who gain 44 pounds or more have four times the risk of type 2 diabetes.30
Recent research studies have shown that a gain of 10 to 20 pounds resulted in an increased risk of coronary heart disease (which can result in nonfatal heart attacks and death) of 1.25 times in women31 and 1.6 times in men.32 In these studies, weight increases of 22 pounds in men and 44 pounds in women resulted in a increased coronary heart disease risk of 1.75 and 2.65, respectively. In one study among women with a BMI of 34 or greater, the risk of developing endometrial cancer was increased by more than 6 times.33 Overweight and obesity are also known to exacerbate many chronic conditions such as hypertension and elevated cholesterol. Overweight and obese individuals also may suffer from social stigmatization, discrimination, and poor body image.
Although obesity-associated morbidities occur most frequently in adults, important consequences of excess weight as well as antecedents of adult disease occur in overweight children and adolescents. Overweight children and adolescents are more likely to become overweight or obese adults. As the prevalence of overweight and obesity increases in children and adolescents, type 2 diabetes, high blood lipids, and hypertension as well as early maturation and orthopedic problems are occurring with increased frequency. A common consequence of childhood overweight is psychosocialspecifically discrimination.34
Call to Action
Because physical inactivity is a risk factor for many diseases and conditions, making physical activity an integral part of daily life is crucial. Physical activity need not be strenuous to be beneficial. People of all ages benefit from moderate physical activity, such as 30 minutes of walking five or more times a week. In addition, physical activity does not need to be sustained for long periods of time in order to provide health benefits. Repeated shorter bursts of moderate-intensity activity also yield health benefits. In other words, walking in two 15-minute segments or three 10-minute segments is beneficial.
This report makes clear the pressing need to encourage a more active lifestyle among the American people. Clearly, the goal of a more active population will be a challenge, requiring a commitment to change on the part of individuals, families, work places, and communities. Both the public and private sectors will need to band together to promote more healthy habits for those of all ages.7 Encouraging more activity can be as simple as establishing walking programs at schools, worksites and in the community. Some communities have an existing infrastructure that supports physical activity, such as sidewalks and bicycle trails, and work sites, schools, and shopping areas in close proximity to residential areas. In many other areas, such community amenities need to be developed to foster walking, cycling, and other types of exercise as a regular part of daily activity. Schools provide many opportunities to engage children in physical activity as well as healthy eating. For adults, worksites provide opportunities to reinforce the adoption and maintenance of healthy lifestyle behaviors. Perhaps the most important change, however, is at the individual and family level. Each person must understand the value of physical activity for his or her health and well-being and commit to a lifestyle that is truly active.
References
1. Butler RN, Davis R, Lewis CB, et al. Physical fitness: benefits of exercising for the older patient. Geriatrics 53(10):46-62. 1998.
2. American Heart Association. 2002 heart and stroke statistical update. Dallas, TX: American Heart Association, 2001.
3. Centers for Disease Control and Prevention. National diabetes fact sheet: general information and national estimates on diabetes in the United States, 2000. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, 2002.
4. American Cancer Society. Cancer facts & figures 2002. Atlanta, GA: American Cancer Society. Inc, 2002.
5. Vainio H, Bianchini F, Eds. Weight control and physical activity. IARC Handbooks of Cancer Prevention. IARC Press Vol 6, 2002.
6. Popovic JR. 1999 National Hospital Discharge Survey: Annual summary with detailed diagnosis and procedure data. National Center for Health Statistics. Vital Health Statistics 13(151). 2001.
7. U.S. Department of Health and Human Services. The Surgeon Generals call to action to prevent and decrease overweight and obesity. Rockville, MD: U.S. Department of Health and Human Services, Public Health Service, Office of the Surgeon General; 2001. (Available from US GPO, Washington)
8. U.S. Census Bureau. Resident population estimates of the United States by age and sex, July 1, 1999. Accessed on June 17, 2002, on the Internet at: http://eire.census.gov/popest/archives/national/nation2/intfile2-1.txt
9. McGinnis JM, Foege WH. Actual causes of death in the United States. JAMA 270(18):207-12.1993.
10. Hahn RA, Teuesch SM, Rothenberg RB, et. al. Excess deaths from nine chronic diseases in the United States, 1986. JAMA 264(20):2554-59. 1998.
11. Paffenbarger RS, Hyde RT, Wing AL, et al. The association of changes in physical-activity level and other lifestyle characteristics with mortality among men. N Engl J Med 328(8):538-45. 1993.
12. Sherman SE, DAgostino RB, Cobb JL, et al. Physical activity and mortality in women in the Framingham Heart Study. Am Heart J 128(5):879-84. 1994.
13. Kaplan GAA, Strawbridge WJ, Cohen RD, et al. Natural history of leisure-time physical activity and its correlates: Associations with mortality from all causes and cardiovascular diseases over 28 years. Am J Epid 144(8):793-97. 1996.
14. Kushi LH, Fee RM, Folsom AR, et al. Physical activity and mortality in postmenopausal women. JAMA 277:1287-92. 1997.
15. Lee CD, Blair SN, Jackson AS. Cardiorespiratory fitness, body composition, and all-cause and cardiovascular disease mortality in men. Am J Clin Nutr 69 (3):373-80. 1999.
16. Wei M, Kampert JB, Barlow CE, et al. Relationship between low cardiorespiratory fitness and mortality in normal-weight, overweight, and obese men. JAMA 282(16):1547-53. 1999.
17. U. S. Department of Health and Human Services. Leisure-time physical activity among adults: United States, 1997-98. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics, 2002.
18. Centers for Disease Control and Prevention. CDC Surveillance Summaries, December 17, 1999. MMWR 48(no.SS-8). 1999.
19. Kann L, et al. Youth risk behavior surveillanceUnited States, 1999. In: CDC Surveillance Summaries, June 9, 2000. MMWR 49(No. SS-5):1-96. 2000.
20. Strum R. The effects of obesity, smoking and problem drinking on chronic medical problems and health care costs. Health Affairs 21(2):245-253. 2002.
21. Pratt M, Macera CA, Wang G. Higher direct medical costs associated with physical inactivity. The Physician and Sportsmedicine 28:63-70. 2000.
22. U.S. Department of Health and Human Services. Physical activity and health: a report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, 1996.
23. Freudenheim M.. Employers focus on weight as workplace health issue. New York Times. Sept. 6, 1999.
24. Sallis JF, McKenzie TL, Kolody B, Lewis M, Marshall S, Rosengard P. Effects of health-related physical education on academic achievement: project SPARK. Research Quarterly for Exercise and Sport 70(2):127-34. 1999.
25. Escobedo LG, Marcus SE, Holtzman D, Giovino GA. Sports participation, age at smoking initiation and the risk of smoking among US high school students. Journal of the American Medical Association 269:1391-5. 1993.
26. Zill N, Nord CW, Loomis LS. Adolescent time use, risky behavior and outcomes: an analysis of national data. Rockville, MD: Westat, 1995.
27. U.S. Preventive Services Task Force. Guide to Clinical Preventive Services, 2nd ed. Baltimore: Williams and Wilkins, pages 611-624. 1996.
28. U.S. Department of Health and Human Services, National Institutes of Health, National Heart, Lung, and Blood Institute. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults; evidence report. HHS, PHS; Pub No.98-4083. 1998.
29. Allison DB, Fontaine KR, Manson JE, Stevens J, VanItallie TB. Annual deaths attributable to obesity in the United States. JAMA Oct 27;282(16):1530-8. 1999
30. Ford ES, Williamson DF, Liu S. Weight change and diabetes incidence: Findings from a national cohort of US adults. Am J Epidemiol 146(3):214-22. Aug 1, 1997.
31. Willett WC, Manson JE, Stampfer MJ, et al. Weight, weight change and coronary heart disease in women. Risk within the normal weight range. JAMA 273(6):461-65. Feb 8 1995.
32. Galanis DJ, Harris T, Sharp DS, et al. Relative weight, weight change, and risk of coronary heart disease in the Honolulu Heart Program. Am J Epidimiol 147(4):379-86. Feb 15, 1998.
33. Weiderpass E, Persson I, Adami HO, et al. Body size in different periods of life, diabetes, hypertension, and risk of postmenopausal endometrial cancer. Cancer Causes Control 11(2):185-92. Feb 2000.
34. Dietz WH. Health consequences of obesity in youth: Childhood predictors of adult disease. Pediatrics 101(3)Supp:518-525. Mar 1998.