
U.S. Department of Health and Human Services
The Role of Supports in Successful Labor Force Entry for Youth with Disabilities
David Stapleton, Cornell UniversityMark Nowak, The Lewin GroupGina Livermore, Cornell University
September 2001
PDF Version: http://aspe.hhs.gov/daltcp/reports/2001/youthlfe.pdf (55 PDF pages)
This report was prepared under contract #HHS-100-97-0011 between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and the Lewin Group. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the office at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. The e-mail address is: webmaster.DALTCP@hhs.gov. The Project Officer was Andreas Frank.
The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
TABLE OF CONTENTS
I. INTRODUCTION
II. BACKGROUND
A. Employment of Young Adults with Disabilities
B. Support for Youth and Young Adults with Disabilities
C. The Evolution of Programs and Policies for Youth with Disabilities
III. FOCUS GROUP FINDINGS
A. Introduction
B. Findings
IV. IMPLICATIONS FOR PUBLIC POLICY
A. Importance of Expectations and Motivation
B. Need for Accommodations at School and Work
C. Other Challenging Transitions Accompany the Transition to Work
D. Individualized Services are Highly Valued
ATTACHMENT: Sample List of Educational Accommodations
LIST OF EXHIBITS
EXHIBIT 1. Employment Rates for Young Adults With and Without Disabilities, 1988-1999
EXHIBIT 2: Median Earnings of Young Adults With and Without Disabilities, 1988-1999
EXHIBIT 3: Competitive Post-School Employment Rates by Disability
EXHIBIT 4: SSI Recipients Under Age 18, 1974-2000
EXHIBIT 5: Characteristics of Participants with Disability Onset Before Age 18
EXHIBIT 6: Ranking of Supports Among Participants with Disability Onset Before Age 19
ACKNOWLEDGMENTS
Work on this project was conducted by The Lewin Group and its subcontractors, Berkeley Policy Associates and Cornell University. The study was funded by the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation (ASPE).
Staff from The Lewin Group, under the direction of Gina Livermore, conducted the literature review, developed the data collection methodology and instruments, prepared OMB clearance materials, conducted screening for the Newark, NJ focus groups, developed a database of the focus group findings, and analyzed and prepared the reports of the findings for this project. These staff principally include Mark Nowak, Julie Karp, Elizabeth Eiseman, Jennifer Duffy, and Mark Laidlaw.
Staff from Berkeley Policy Associates, under the direction of Sherry Almandsmith and Kay McGill, assisted in the development of the data collection methodology, pre-tested the data collection instruments, conducted the screening for the Seattle, WA and Los Angeles, CA focus groups, arranged and conducted the focus groups at all sites, and summarized the findings of each focus group session. These staff include Linda Toms Barker, Laurie Posner, Michellana Jester, Christie MacDonald, Susan Haight-Liotta, Laura Ellerbe, and Zinnia Ng.
David Stapleton of Cornell University provided technical guidance throughout the project and co-authored all project reports.
The project has benefited greatly from the input of a number of individuals: Bob Williams, Floyd Brown, and Andreas Frank at ASPE were instrumental in refining the scope and setting the direction for the project, and played important roles in shaping the analysis and presentation of the findings. At the start of the project, the input received from the projects Technical Advisory Group (TAG) greatly influenced the overall direction of the study, the focus group methodology, and the selection of the sites where the focus groups were conducted. The TAG members included: Ruth Brannon, National Institute for Disability and Rehabilitation Research; Henry Claypool, Administration on Developmental Disabilities; Judith Cook, University of Illinois-Chicago; Bruce Flynn, Washington Business Group on Health; Lex Frieden, Institute for Rehabilitation and Research; Claire Ghiloni, Massachusetts Rehabilitation Commission; Allen Jensen, George Washington University; Jennifer Kemp, Presidents Committee on the Employment of Adults with Disabilities; John Kregel, Virginia Commonwealth University; Doug Kruse, Rutgers University; Charlie Lakin, University of Minnesota; Pamela Loprest, The Urban Institute; Bonnie ODay, National Rehabilitation Hospital Research Center; Becky Ogle, Presidential Task Force on the Employment of Adults with Disabilities; Alan Shafer, Social Security Administration; and Ed Yelin, University of California-San Francisco.
We also want to acknowledge the contribution of Michael Collins of the California State Independent Living Council (SILC). His organization funded a study in the Los Angeles area conducted by Berkeley Policy Associates using the focus group methodology developed under this project. The samples and findings of the California SILC study have been integrated with those obtained from the focus groups conducted in Los Angeles for this study.
We greatly appreciate the assistance of the many local disability organizations who provided invaluable assistance in recruiting focus group participants, providing locations to conduct the groups and staff to assist with on-site logistics.
Finally, we would like to thank the nearly 300 individuals who participated in the focus groups and so generously and candidly shared their experiences with us. Without their participation, the study would not have been possible.
The opinions, conclusions, and errors in this report are the sole responsibility of the authors, and do not represent the official views of the U.S. Department of Health and Human Services, the California State Independent Living Council, Berkeley Policy Associates, Cornell University, or The Lewin Group.
FORWARD
This report is one in a series developed by The Lewin Group and its subcontractors, Berkeley Policy Associates and Cornell University, for the Office of the Assistant Secretary for Planning and Evaluation within the U.S. Department of Health and Human Services, in connection with the study, Research on Employment Supports for People with Disabilities. For this project, we reviewed available studies and literature, and collected detailed information on the experiences of people with significant disabilities who are successfully and competitively employed, the events and factors affecting their employment decisions, the relative importance of specific factors, and the reasons for successful and unsuccessful employment attempts.
The goal of the study is to gain a better understanding of the role supports play in the employment of people with disabilities. In particular, the study aims to identify the role(s) supports play in two key areas: providing assistance to people with significant disabilities to participate successfully in competitive employment, and improving employment outcomes for people with disabilities. This project is unique among the many investigations of the factors affecting the employment of people with disabilities in that it focuses on those who have achieved a measure of success in employment, and the factors contributing to their success.
For this study, we defined the term supports very broadly. Supports may include public or private income or in-kind transfers, such as Social Security Disability Insurance (DI), Supplemental Security Income (SSI), and payments for medical care, prescription drugs, medical devices, assistive technology, and personal assistant services. Supports also include employment development programs, such as employment and training programs, job search and retention programs, independent living programs, other housing supports, special education, school-to-work programs, and transportation services. Laws and regulations that encourage behaviors (on the part of firms or individuals) that promote the employment of people with disabilities and informal assistance provided by family members, co-workers, or friends also fall under the definition of supports used in this study.
The study has a number of components: a comprehensive review of the recent literature (since 1990) on issues related to the employment of people with disabilities; the development of an inventory of employment programs serving people with disabilities at the federal, state and local levels; and the conduct of approximately 45 focus groups with working people with significant disabilities in three sites. The findings in this report are based primarily on the information obtained via the literature review, and on the data gathered from 284 focus group participants conducted between April and December 2000 in Seattle/Tacoma, Washington; Newark, New Jersey; and Los Angeles, California. A full description of the focus methodology and summary of the findings are described in other reports in this series.
I. INTRODUCTION
Entry into employment is a major challenge for many people with disabilities, perhaps especially for those who have congenital impairments, or who first experience disability at a young age. The transition to employment can involve a long period of preparation and training, followed by a lengthy job search and, if successful, adaptation and integration into the workplace -- possibly after several unsuccessful placements. Transition can begin in school, with education that has preparation for employment as a key objective, but might also begin during adolescence. It can end when the individual is still a teenager, but might also last until the individual is close to age 30, or even older. During this period, the individual might use a variety of supports. Some of these are specifically designed to support the transition to work (e.g., vocational rehabilitation services), but others provide support to meet the individual's general needs (e.g., income support and health care). Some are designed especially for people with disabilities, but others are not (e.g., general education, training or employment services, and child care). Other significant transitions for people with disabilities are also likely to occur during this period -- in health care providers and insurance coverage, housing and family support, transportation, etc.
In this paper we first summarize programs that provide support during the school-to-work transition period, and how they have evolved in recent years. We then present findings from focus groups conducted with individuals who acquired a significant disability during childhood or prior to gaining significant employment experience and who subsequently achieved a measure of employment success. During these focus groups, we learned about the supports that, in their view, contributed to their success, and about some of the challenges they faced in using them.
Nearly all focus group participants completed their transitions to initial employment ten or more years ago, and, therefore, did so in a program and policy environment that is much different than today's environment. Nonetheless, their experiences are informative about the likely value of policy changes that have occurred recently, and about further changes that might be needed if people who first experience disability at a young age are to become more successful in their efforts to enter employment. We discuss the implications for public policy in the final section.
II. BACKGROUND
A. Employment of Young Adults with Disabilities
As with older adults, employment and earnings among young adults with disabilities are low compared to those for young adults without disabilities, and they have been declining over a long period. According to an analysis of the 1999 Current Population Survey (CPS), the employment rate of men age 25 to 40 with disabilities declined about 10 percentage points between 1988 and 1996 (from 53 percent to 43 percent), while the employment rate of women with disabilities declined six percentage points (from 48 percent to 42 percent). During this same period, the employment rates for men and women without disabilities were about twice as high as those for their counterparts with disabilities, and the rates improved slightly, increasing by about two percentage points for women and remaining virtually unchanged for men (Exhibit 1).1
| EXHIBIT 1. Employment Rates for Young Adults with and without Disabilities, 1988-1999 | |
| Males Age 25-40 | Females Age 25-40 |
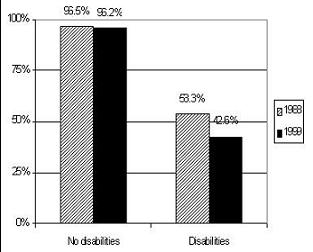 | 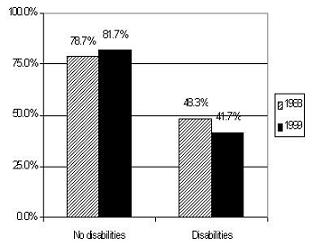 |
Workers with disabilities also earn substantially less than workers without disabilities. In 1988, young men with disabilities earned only about 48 percent as much as young men without disabilities. By 1999, that figure had declined to about 41 percent. In 1988, women with disabilities earned only about 43 percent as much as women without disabilities, but, unlike disabled men, earnings of women with disabilities have improved since 1988. In 1999, women with disabilities earned about 46 percent as much as women without disabilities (Exhibit 2).2
| EXHIBIT 2. Median Earnings of Young Adults With and Without Disabilities, 1988-1999 | |
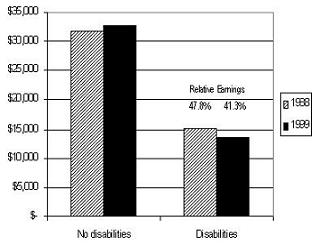 | 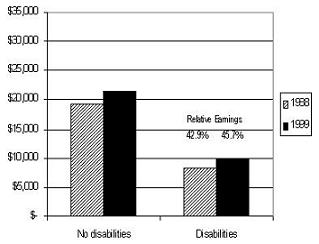 |
| SOURCE: Andrew Houtenville, Cornell University. | |
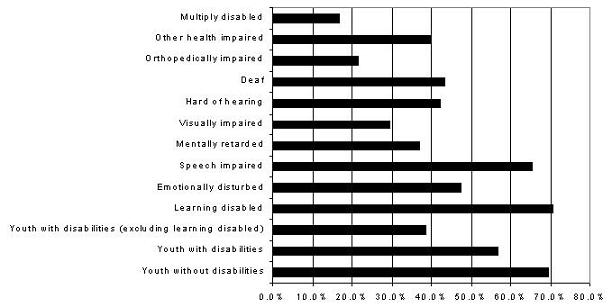
Employment outcomes for youth with disabilities are similarly poor. One analysis examined data on employment outcomes for youth who were enrolled in special education programs during secondary school, collected in the National Longitudinal Transition Study of Special Education Students (NLTS). The NLTS followed a nationally representative sample of 8,000 youths with disabilities ages 15 to 21 in the 1985-1986 school year. Follow-up data were collected in 1987 and 1990. While these data have substantial limitations, they are nonetheless instructive.3 The study found that 57 percent of youths with disabilities were competitively employed three to five years after exiting school (Exhibit 3), compared to 69 percent of youths in the general population. Employment rates were highest for those with learning disabilities (71 percent), the group that also represents the largest share of the survey population. When this group is excluded, the employment rate for the remainder is only 39 percent (Wagner and Blackorby, 1996).
| EXHIBIT 3. Competitive Post-School Employment Rates by Disability Status |
 |
| SOURCE: Wagner and Blackorby (1996). |
B. Support for Youth and Young Adults with Disabilities
Since the 1990 passage of the Americans with Disabilities Act (ADA), there has been an increased focus on engaging people with disabilities, including youth with disabilities, in mainstream work. Several efforts have targeted youth with disabilities specifically, while others provide access to supports for a broad range of disadvantaged individuals. In this section, we briefly review in-school and out-of-school supports for youth with disabilities in transition, as well as more general supports.
1. In-School Supports
The Individuals with Disabilities Education Act of 1994 (IDEA), the major legislation addressing in-school supports for youth with disabilities, requires states to provide free and appropriate public education for students with disabilities at the elementary and secondary level. The Act provides funding to school districts for transition and other education and support services, and requires states to identify, locate, and evaluate all children with disabilities in the state in need of special education and related services. The Act identifies transition services as a coordinated set of activities for a student with a disability that promotes the student's movement from school to post-school activities, such as post-secondary and adult education, vocational training, employment, and independent or community living. Service delivery is organized through the development of an Individualized Education Program (IEP), which is provided for each participating student, and includes an assessment of the student's needs, a statement of measurable annual goals, and a statement of the special education and related services to be provided to the child. Transition planning begins for each student no later than age 16. Students are to be educated in the least restrictive environment possible, and to be provided appropriate accommodations to ensure access to full participation in education and transition activities. The nature of accommodations received depends, in part, upon the nature of the disability.
Such accommodations might include alternative exam formats or additional time, tutors to assist with coursework, readers or classroom notetakers, registration assistance or priority class registration, textbooks on tape, assistive listening devices, talking computers, sign language interpreters, and course substitutions or waivers.
The School to Work Opportunities Act of 1994 authorized development grants ("seed money") to states to create systems that prepare all students for the transition from school to work. These training systems are designed to teach young Americans marketable skills, to prepare them for their first job in a high-skill, high-wage career, and to increase their opportunities for further education, such as at a four-year college or university. The law also requires each local program that receives a grant to establish a work-based learning component, including work experience, workplace mentoring, and broad instruction in "all aspects of an industry." Moreover, the law requires that all school-to-work programs funded under the act be open to all youth, with particular emphasis on ensuring opportunities for disadvantaged youth and school dropouts (Brown, 2000). Under a sunset provision within the legislation, authority for the Act terminates October 1, 2001. It is anticipated that school-to-work programs developed in many states through the development grants will continue to operate in various forms after federal grant making authority expires. Starting in October, the major federal legislation governing funding for school-to-work activities will be the Workforce Investment Act of 1999, which we describe in the next section.
2. Out-of-School Supports
The principal out-of-school programs that provide transition supports to youth with disabilities include employment support programs, income support programs, health-related and technology programs, and a number of in-kind support programs such as housing, transportation and food stamps. Many of these programs are means-tested. Employment support programs include vocational rehabilitation (VR) and workforce investment systems. VR programs, which are funded through a combination of federal and state funds, provide therapeutic services, counseling, education, training, work-related placement assistance and other services. The 1999 Workforce Investment Act (WIA) provides assistance to states interested in establishing integrated statewide and local workforce investment systems to increase employment, retention and earnings of participants.4 The goals of WIA include improving the quality of the workforce to sustain economic growth, improving productivity and competitiveness, and reducing dependency on welfare.
Under WIA, states are required to create workforce development plans that describe how the state will meet the needs of major customer groups, including individuals and youth with disabilities, and show how the plans will ensure nondiscrimination and equal opportunity. Services are to be provided through One-Stop delivery systems, under which separate workforce investment, education and human service programs are linked (physically or technologically) to provide coordinated service delivery. Some of the partners in this system include employment services, adult education, post-secondary vocational education, VR, Welfare-to-Work, and Community Services Block Grants. In many states, these systems are directly linked to VR and/or Temporary Assistance for Needy Families (TANF) services. Local workforce investment boards (WIB) coordinate WIA service delivery, and each WIB includes a Youth Council to coordinate youth services.
The Social Security Administration's (SSA) Supplemental Security Income (SSI) program provides cash benefits to low-income families with disabled children. Children qualifying for SSI are also eligible for Medicaid coverage. Students under age 22 who are regularly attending school may exclude up to $1,290 of earned income a month (and $5,200 annually) for the purpose of determining SSI eligibility. The means test for child recipients (those under 18) counts parental income deemed available to support the child after considering the financial need of other family members. Child recipients must re-qualify for SSI as adults when they reach age 18. As of December 2000, there were approximately 850,000 children and youth (i.e., under 18) receiving SSI. Such recipients make up about 13 percent of the total SSI caseload (Pickett, 2000).
SSA recently developed a Youth Continuing Disability Initiative, which is currently being implemented in Florida and Maryland. Under the pilot project, state Disability Determination Service (DDS) staff screen SSI recipients ages 15 to 17 for return-to-work potential during regularly scheduled continuing disability reviews. Those determined to have such potential are referred to the state VR agency for screening and enrollment in transition programs where they have access to information on skill assessments, career aspirations, educational goals, health care needs, reasonable accommodations, employment supports, and community and governmental transition services. The pilot will provide individual assessments, information about employment development opportunities, and linkages to services. SSA is examining the feasibility of implementing the initiative nationally.
SSA has also awarded cooperative agreements to 12 states to conduct State Partnership Initiatives (SPIs) with the goal of developing innovative projects to increase employment of people with disabilities who want to work. At least one of the SPIs is developing a transition services component for youth who are high-school age. SSA has also developed a Youth Employment Strategy that includes a demonstration transition program for individuals ages 11 to 30, designed to improve employment outcomes. SSA has also launched a research project with the Children's National Medical Center in Washington, D.C. and the American Academy of Pediatrics to benefit SSI beneficiaries ages 11 to 21 through the development of transition plan training for health care providers, beneficiaries, parents, and the school system.
TANF provides support to low-income families with children. TANF replaced the Aid to Families with Dependent Children (AFDC) program in 1996. While TANF is not designed primarily to serve people with disabilities, a substantial share of families receiving TANF have an adult or child family member with a disability. States receive block grants to provide cash benefits to needy families with children. Benefits are subject to federal time limits, and adults must meet work requirements in order to continue to receive benefits, although the work requirements for people with disabilities vary across states. During transition, only a small percentage of youth with disabilities (i.e., teenage parents) would be subject to such requirements.
Medicaid, which pays for medical care, is the major public health insurance program available to youth with disabilities. Eligibility and benefits vary by state. Benefits are generally available to recipients of SSI and TANF, as well as to many other children in low-income families. The 1997 Balanced Budget Act (BBA) established the State Children's Health Insurance Program (SCHIP), which further expanded Medicaid eligibility to children, regardless of disability, in low-income families. Medicaid funds are also used to reimburse schools for medically necessary services provided under IDEA; in fact, available Medicaid funds must be used before any funds available under IDEA for such purposes are expended. Such services might include transportation, speech and audiology services, psychological services, and physical and occupational therapy. Under the BBA, states may also extend Medicaid benefits (or the option to "buy in" to Medicaid) to working individuals who meet the medical eligibility criteria for SSI, but fail to qualify because of earnings. Under the Ticket to Work and Work Incentives Improvement Act of 1999 (TWWIIA), states have the option to allow people with disabilities that are sufficiently severe to meet SSI criteria to buy in to Medicaid, without restrictions on earnings.5
Other health-related programs include mental health services and mental retardation/developmental disabilities (MR/DD) services. Mental health services provided to youth with disabilities include school-based counseling services, residential rehabilitation services, and services within the child welfare and juvenile justice systems. One of the main providers of these services are Comprehensive Community Mental Health Services programs available in a number of states and administered by the Center for Mental Health Services within the Substance Abuse and Mental Health Services Administration (SAMHSA). Of school children nationwide, 16 percent use school mental health services (U.S. Department of Health and Human Services, 1999).
The state MR/DD systems fund services for people with mental retardation or developmental disabilities. State MR/DD agencies provide a range of services, including employment supports, traditional facility-based options such as sheltered workshops and non-work day habilitation programs, and community integration services. The Administration on Developmental Disabilities within HHS administers the State Councils on Developmental Disabilities Program to increase the independence, productivity, inclusion and integration into the community of people with developmental disabilities. The program funds systemic change, capacity building, and advocacy efforts, including training and public education. The Maternal and Child Health Services Programs, created in 1935 under Title V of the Social Security Act, provides funding to states for preventive health and primary care services for women and children.
The Maternal and Child Health Bureau within the Health Resources and Services Administration of HHS administers the $3 billion federal/state program. The Division of Services for Children with Special Health Care Needs funds hearing screening for newborns prior to departure from the hospital, routine health care for children with disabilities, and research regarding genetic screening. The Healthy and Ready to Work program, begun in 1996, funds a national center and nine grantees to assist youth with disabilities in the transition to adulthood through demonstration and other projects.
The Technology-Related Assistance for Individuals with Disabilities Act Amendments of 1994, administered by the National Institute on Disability and Rehabilitation Research (NIDRR) within the U.S. Department of Education's Office of Special Education and Rehabilitative Services (OSERS), provides grants to establish a program of statewide, comprehensive, technology-related assistance for individuals with disabilities of all ages, with special emphasis on children. The State Technology Assistance Program, funded under the Act, provides up to ten years of funding to applicant states to support program development. Authorization for the Act expired in 1999.
Other supports available to youth with disabilities include food stamps, housing support, independent living services, transportation services, and personal assistance services. Each of these supports has complex eligibility criteria and, with the exception of food stamps, eligibility varies across states and localities.
Food stamps are available to low-income households and are designed to increase the food purchasing power of such households by subsidizing food purchases through coupons that can be used like cash at the grocery store. The federal Housing Choice Voucher system ("Section 8" housing) provides housing assistance payments to participating owners on behalf of eligible tenants. The Centers for Independent Living program (administered by the Rehabilitation Services Administration and funded with federal and state money) provides independent living skills training, peer counseling, community outreach, and employment services. Transportation services include funding from VR to modify vehicles, and public transportation subsidies. Personal assistance services (PAS) include help from another person in accomplishing basic and other activities of daily living, such as eating, dressing, bathing, shopping and preparing meals. Publicly-financed programs that deliver PAS are typically designed and implemented at the state level, and there is a good deal of variation in eligibility requirements. Most youth with disabilities receive help from informal care givers, and do not rely heavily on public or private PAS programs (Adler, 1994 cited in Doty, et al., 1994).
Finally, youth with disabilities receive a wide range of private and informal supports provided by family, friends and community or advocacy organizations, to varying degrees. For example, families and friends might pay for or provide personal care services, transportation, housing, and private health insurance, and they can serve as important sources of emotional support. Family and friends can also serve to motivate individuals. Community and advocacy groups might provide benefit planning, assistance and outreach services; advocacy and protection services; case management services; transportation services; housing services; and funding for medical and assistive devices (e.g., prosthetics, text-to-speech converters, wheelchair lifts, etc.).
C. The Evolution of Programs and Policies for Youth with Disabilities6
Until recently, disability policy for adults in the U.S. has focused on conducting eligibility determinations, and providing cash and in-kind benefits to those determined unable to participate in the labor force and vocational rehabilitation services to others. There has been, however, a gradual shift toward the prevention and management of disabilities, with a focus on increased independence. Policy makers are currently trying to develop and implement policies that encourage individuals with disabilities to work and to live independently. For working-age adults, this shift has been reflected in policies that emphasize the right to work (e.g., the Americans with Disabilities Act), and address work disincentives and access to employment supports (e.g., the Ticket to Work and Work Incentives Improvement Act).
For youth with disabilities, this shift in perspective is reflected in policy changes that emphasize access to mainstream education, access to other supports that promote independence and educational attainment, and access to school-to-work transition services. One of the first major pieces of legislation reflecting this emerging change in emphasis was the Vocational Rehabilitation (VR) Act of 1973, which prohibited discrimination and provided for equal opportunity in educational settings for people with disabilities. The Act required schools to develop Individualized Written Rehabilitation Plans (IWRPs) that would specify rehabilitation goals and identify types of services to be provided to meet those goals. The Act also guaranteed access to reasonable accommodations within the educational setting. Subsequent amendments provided access to supported employment for people with severe disabilities (1986), and increased emphasis on self-determination regarding service receipt as well as receipt of community-based services (1992).
The Education for All Handicapped Children Act of 1975 (EAHCA) reinforced the early provisions of the VR Act. EAHCA required states receiving federal financial assistance to provide all children with disabilities a free and appropriate public education in the least restrictive setting possible ("mainstreaming").7 The Carl D. Perkins Vocational Education Act of 1984 sought to improve access to vocational rehabilitation services for students with disabilities who had historically been underrepresented in such programs. The Act specified that the majority of funds allocated to states for vocational education were to be spent to provide supplemental services, such as needs and interest assessments, career development activities, and counseling services to facilitate the transition from school to work. Subsequent amendments to the Act integrated academic instruction into vocational coursework and increased emphasis on applied technology education (1990 and 1998).
IDEA, described earlier, evolved from the EAHCA and retains its basic provisions. To assist states regarding implementation of IDEA, the legislation authorized the creation of five-year system change grants, administered by OSERS in the U.S. Department of Education, to fund the overhaul and expansion of state transition services to youth with disabilities.
In 1989, the Omnibus Budget Reconciliation Act required states to provide and promote family-centered and community-based care for children with disabilities and to recognize the right of families to take lead roles in directing care and service provision. The creation of the Healthy and Ready to Work program within HRSA provides services to prepare youth for the transition to adulthood, and emphasizes the right of youth with disabilities to participate in their own health care, to choose career and other goals, and to select services designed to help meet those goals.
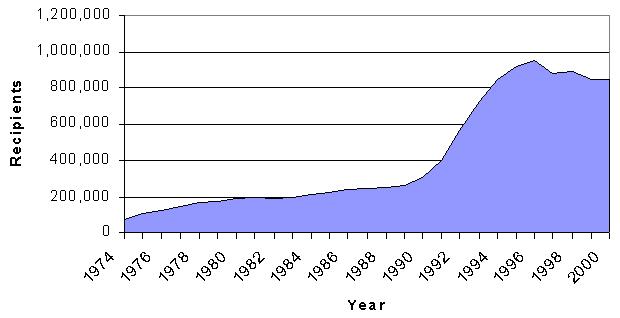
During the early 1990s, several policy changes significantly expanded the medical and non-medical criteria for child SSI eligibility. These changes produced substantial increases in the number of children receiving SSI during the early 1990s. In February 1990, the United States Supreme Court, in Sullivan v. Zebley, ruled against SSA's policy of requiring a stricter definition of disability for children than adults.8 Consequently, SSA issued regulations in February 1991 that required children who did not meet SSA's medical eligibility requirements to undergo a second stage evaluation, called an individualized functional assessment (IFA). SSA also expanded the mental impairment category for children to include additional developmental, behavioral, and emotional disorders, and changed the deeming rules so that the amount of family income considered available to support the child in many cases was reduced. Effectively, these changes expanded eligibility and increased the value of the benefit for some families. Between December 1989 and December 1996, the number of child SSI recipients increased by over 250 percent, from 309,000 to 955,000 (Exhibit 4).
| EXHIBIT 4. SSI Recipients Under Age 18, 1974-2000 |
 |
| SOURCE: Pickett (2000). |
Accompanying expanded access to SSI were efforts to increase access to home and community-based services. The first Home and Community-Based Services (HCBS) waiver (under Section 1915(c) of the Social Security Act) was established in 1981. HCBS waivers give states flexibility in providing needed services to Medicaid-eligible individuals at home, rather than placing such individuals in hospitals, nursing facilities or intermediate care facilities (for persons with mental retardation). Waiver expenditures have risen from $290 million in 1985 to almost $10.4 billion in 1999 (Lutzky et al., 2000). Services provided under the waiver include assistive technology, adaptive equipment, case management, personal care attendants, homemaker services, personal care services, and vocational services. The primary recipients of waiver services are individuals with MR/DD, and the aged with disabilities.
The Social Services Block Grant program (authorized in 1975 under Title XX of the Social Security Act), provides another source of federal funding for community-based services. Services to adults and children with disabilities comprise the largest share of program funding, and include transportation services and residential treatment. The grant also funds services to promote self-sufficiency, such as education and training services, and independent living services (Administration for Children and Families, 1998).
Expanded access to SSI may have initially created an expectation of future income support among youth with disabilities. It was several years before policy changes started to emphasize work preparation and reduced access to benefits. The School to Work Opportunities Act of 1994 (described earlier), for example, authorized funding for the development of state school-to-work systems, and the 1996 Personal Responsibility and Work Opportunity Reconciliation Act (PRWORA) required child SSI recipients to reapply for benefits upon reaching adulthood. The reapplication requirement serves as an opportunity to assess work readiness of individuals, and effectively requires youth to make affirmative choices regarding benefit receipt and work. PRWORA also created work requirements and time limits for TANF and food stamp benefits, which could encourage employment among those with disabilities. However, these programs continue to give people with severe disabilities special status with respect to such requirements.9 Finally, PRWORA significantly reversed the child SSI eligibility expansion by eliminating the IFA in the evaluation of child disability.
III. FOCUS GROUP FINDINGS
A. Introduction
The findings in this paper are from focus groups conducted in three cities (Seattle, Washington; Newark, New Jersey; and Los Angeles, California) between April and December 2000. All focus group participants were 18 years old or older, had a significant disability with onset prior to first substantial employment, and had annual earnings of at least $8,240 before taxes and transfers. At the time of the focus groups, the latter was the federal poverty line for a family of one.10 It is approximately equivalent to working 30 hours a week at the federal minimum wage. A total of 284 individuals participated in focus groups and individual interviews for the study, and among these, 156 experienced disability onset prior to the age of 18.11 We focused on the latter group for this paper. Basic socio-demographic, disability, and employment information was collected via a telephone screening instrument and a pre-focus group registration form. Exactly half of those reporting disability onset prior to age 18 was of each gender, and their average age was 37 at the time of interview (Exhibit 5). A large majority (78 percent) experienced disability onset before age 13. Just over half were single, 78 percent were white, 11 percent were African-American, and five percent were Hispanic.
While all had earnings, 23 percent had annual earnings below $10,000. Median earnings were under $20,000.12 Only five percent had earnings above $50,000. Many lived in households with other income; median household income was about $40,000. The largest impairment category was cognitive (31 percent), followed by communication (25 percent) and mobility (22 percent).
Focus group participants were asked to rank on a scale of 1 (very important) to 5 (not important) the importance of various supports in helping them find and maintain employment. More than 75 percent of participants who experienced disability onset during youth assigned a rank of 1 or 2 to each of five supports: employer accommodations; public income support programs; job search assistance; family/peer encouragement; and health insurance (Exhibit 6). These rankings are generally consistent with the bulk of comments made during the focus groups, although job search services ranked more highly than was generally reflected in the discussions. Vocational rehabilitation services rank lowest by both indicators.
| EXHIBIT 5. Characteristics of Participants with Disability Onset Before Age 18 | |||
| Characteristic | Percent | Characteristic | Percent |
| DEMOGRAPHIC | PERSONAL INCOME | ||
| Female | 50.0 | Less Than $20,000 | 53.3 |
| Married | 29.1 | $20,001-$35,000 | 23.4 |
| White | 78.2 | $35,001-$50,000 | 16.2 |
| Black | 10.6 | More Than $50,000 | 5.8 |
| PRIMARY IMPAIRMENT | HOUSEHOLD INCOME | ||
| Cognitive | 30.6 | Less Than $15,000 | 23.5 |
| Communication | 25.2 | $15,001-$37,500 | 24.5 |
| Mobility | 21.8 | $37,501-$52,500 | 29.4 |
| Mental Illness | 14.9 | $52,501-$75,000 | 17.7 |
| Other Chronic Illness | 7.5 | More Than $75,000 | 2.9 |
| EDUCATION | PARENT'S EDUCATION | ||
| Less Than High School | 10.5 | Less Than High School | 16.5 |
| High School Graduate | 26.8 | High School Graduate | 23.5 |
| Some College | 24.2 | Some College | 27.8 |
| Four-Year College or More | 37.3 | Four-Year College or More | 30.4 |
| EMPLOYMENT | CHILDREN IN HOUSEHOLD | ||
| Mean Age at First Work | 20.9 | 0 | 85.3 |
| Mean Hours Worked per Week | 30.6 | 1 | 7.3 |
| Mean Months Worked per Year | 9.0 | 2 or more | 7.4 |
| Mean Number of Job Interruptions | 0.9 | 3 | |
| AGE AT ONSET OF DISABILITY | AVERAGE AGE | 37.1 | |
| 0-12 | 78.2 | ||
| 13-18 | 21.8 | ||
Support rankings vary by impairment, as well. For example, the supports with the largest proportion of participants with cognitive impairments ranking them as "very important" included job search assistance (75 percent and access to health insurance (71 percent), while the most important supports to participants with mobility impairments included access to health insurance (68 percent)13 and family/peer non-financial support (63 percent). We further discuss the variation across individuals with different types of impairments in another report in this series.14
| EXHIBIT 6. Ranking of Supports Among Participants with Disability Onset Before Age 16 | |||||||
| Support | Number of Responses | Percent in Category | Median | ||||
| 1 | 2 | 3 | 4 | 5 | |||
| Employer Accommodations | 86 | 59.1 | 25.0 | 6.8 | 3.4 | 5.7 | 1 |
| Public Income Assistance/Entitlement Programs (SSI, DI, TANF) | 78 | 61.0 | 20.7 | 12.2 | 2.4 | 3.7 | 1 |
| Job Search Assistance | 82 | 68.2 | 12.5 | 11.4 | 2.3 | 5.7 | 1 |
| Family/Peer Non-Financial Support and Encouragement | 80 | 65.0 | 13.8 | 12.5 | 1.3 | 7.5 | 1 |
| Access to Health Insurance/Medical Care | 88 | 60.5 | 16.3 | 10.5 | 2.3 | 10.5 | 1 |
| Family Financial Support or Income Other than Work Earnings | 88 | 46.3 | 18.3 | 20.7 | 6.1 | 8.5 | 2 |
| Job Coach | 65 | 58.3 | 6.0 | 7.1 | 6.0 | 22.6 | 1 |
| Assistive Devices/Technology | 77 | 49.3 | 13.3 | 9.3 | 5.3 | 22.7 | 2 |
| Personal Assistance Services | 72 | 44.4 | 16.1 | 9.9 | 11.1 | 18.5 | 2 |
| Special Skills or Other Training | 82 | 48.1 | 10.4 | 6.5 | 7.8 | 27.3 | 2 |
| Special Education as a Youth | 74 | 42.2 | 14.5 | 10.8 | 6.0 | 26.5 | 2 |
| Transportation Services | 84 | 42.5 | 13.8 | 13.8 | 10.0 | 20.0 | 2 |
| College Education | 80 | 38.5 | 12.3 | 9.2 | 6.2 | 33.9 | 2 |
| Specific Drugs or Treatments | 83 | 33.3 | 14.1 | 6.4 | 7.7 | 38.5 | 3 |
| Public In-Kind Assistance Programs (Food Stamps, Housing) | 75 | 41.9 | 4.1 | 14.9 | 10.8 | 28.4 | 3 |
| Vocational Rehabilitation | 81 | 26.4 | 8.3 | 11.1 | 6.9 | 47.2 | 4 |
| 1 = Very Important; 5 = Not important Sorted by support receiving highest proportion of "1" and "2" responses. | |||||||
B. Findings
Our analysis of the focus group data revealed four major findings:
- Employment and other success requires strong motivation;
- Participants strongly favor mainstream education over segregated special education;
- The transition-to-work period was a time of many challenging transitions in participants' lives; and
- Participants highly value supports and services that were individualized, and that enabled them to participate more fully in mainstream society.
1. Employment and Other Success Requires Strong Motivation
The transition from school to work poses a challenge for most individuals, regardless of background, skills or characteristics. It is a complex period that requires individuals to call upon the vocational, social, and cognitive skills learned during school, and to apply those skills to the unfamiliar environments of work and adulthood. New challenges include finding transportation, securing housing, and managing self and home care, and financial responsibilities. These endeavors are daunting for all youth making the transition from school to work, but can be particularly difficult for individuals with disabilities who face additional challenges in gaining access to appropriate accommodations and in securing and managing needed benefits and services.
We found that focus group participants pointed to a high degree of motivation as key to achieving their diverse goals. This finding was consistent across all disability types, sites, and support use. Most traced the origins of their motivation to childhood experiences, in their family or home -- in many instances to the expectations of parents, teacher or other role models. Many indicated that motivation was key to obtaining needed accommodations in school, in obtaining their first job, obtaining accommodations on the job, and managing their benefits and supports.
a. Origins of Motivation
Many participants traced their motivation to the positive expectations or supports of their parents:
-
"Where I think my parents really helped was that I was required to be a responsible person in the household. I had my own chores. I didn't get any special treatment and I started learning how to make money early. My parents would take me down the highway [in our rural area] when the walnuts started dropping, and say, Here are some gunny sacks,' and I'd have to fill them. I'd make money that way. They weren't going to hand it to me for nothing, so I had to earn it like my other siblings earned their money."
-
"I've had a very supportive family, even though I had several challenges when I was younger. I have now overcome them partly because I'm a very, very hard worker and the fact that I have a very supportive family, teachers, and other support systems around me that help me strive for the very, very best."
In other cases, individuals had access to teachers and other role models who encouraged them. Regardless of educational environment (special education or mainstream), participants reported that the high expectations of their teachers and others were instrumental in their success.
-
"The teacher I had from day one just kept saying -- we, all of us, knew that we would be in college. We knew there wasn't any other choice and she'd shoot us if we didn't go. It was just a given from the time I was-well, about six years old. I had her starting in first grade."
-
"My elementary school teacher. He was the kind of teacher [who] kind of knew your limitations. And if he knew you could do it, he made you do it. He told me, Either you do it yourself or don't expect [it]. Don't depend on anybody. If you can do it, do it.'"
-
"I had an art teacher in high school [and] she was kind of Bohemian, you know, a Carol King kind of woman. [Some of the students not in wheelchairs] were going on a school trip, and she was like, Oh no, you're going. We'll find a way. Even if the boys carry you up on the bus, we'll find a way to get you [there].' She took me to games and things in New York City, and the guys carried me on the bus and everything. I always just admired her."
While positive expectations and support were often cited as the origin of motivation, a number of participants discussed how, in early childhood or at disability onset, they developed a strong determination to succeed despite the low expectations of others. Rather than accepting the low expectations of others, including parents and teachers, they became intent on proving them wrong:
-
"My family was basically [thinking that] I'm going to be bedridden for the rest of my life. My parents said, You can stay here, we'll take care of you, you don't have to ever work again.' I was still in the hospital, and I told them, There's no way I'm allowing this. I have to take care of myself.' So I did. It did drive me, when I did start working, to go harder, and make sure that I achieved it. I know my life's a lot harder, so I gotta work harder. [We have to start getting ready] a couple of hours [early just] to have a nine-to-five job. But, I'm willing to make the adjustments. Just gotta adapt. It takes time to get used to a new way of life, but it can be done."
-
"[My parents told me,] I don't know why you're going to school. You're never going to get a job.' [So] those were the spots where defiance was the mode."
-
"[My parents] were in a lot of denial. They were supportive [and] they would say, You know what you can do,' [but] deep inside I felt the doubts and everything. [They were just saying what they felt they should be saying]. I just felt like they're full of it . . . but that just gave me more motivation. I'm going to prove them wrong, and to this date, I have."
-
"[I learned to believe] that I have to be better than other people, because it's important because people look down on people with disabilities already."
-
"I had to get away from my family because if I'd stayed I'd have a sighted guide forever. Couldn't walk down the street by myself or couldn't do anything, basically. [According to them,] I always had to have somebody."
b. Gaining Accommodations in School
Many indicated that motivation was key to obtaining accommodations in school:
-
"I was actually the only one with a physical disability on campus. I was the only person in a wheelchair. Back then in high school, I started to do my own advocating None of my classrooms were equipped with wheelchair ramps, so I [told] the principal that I would go to the city college. In other words, I was blabbering a lot of things in order to get action or to see some results I saw results. They started building ramps. I just started telling them I probably won't be the only person who uses a wheelchair attending your school, and it helped."
-
In the city that I lived in there were several high schools, most of which were two-story high schools and I used crutches at the time. I had a counselor at the high school who said, Why don't you go to the school [that's] a single story? You won't have to climb the stairs.' I said, No, this is the neighborhood I live in, this is where my friends go, and this is where I will go.' And so I used to climb the stairs. Then I got a little bit smarter and [when] they'd say, You can't take this class because it's offered upstairs,' I'd say, Move the classroom,' and they did."
-
"Whatever it took, I was going to attend that school. And, again, determination is what got me there, and giving the administration pressure. It was more convenient for them to bus me out of the city, for them not to build a ramp. By me deciding to go to this campus it ruined their routine, the route that they had. The bus [driver] actually had to wake up an hour earlier. [But] I would get picked up at 6:30, two hours before starting school so in other words, it was for their convenience, not for mine. It was never for my convenience until I started fighting back."
-
"I wanted to make a real effort to completely graduate from my class, and I think it's now what we call mainstreaming, but the high school was not accessible and they [had to] make provisions to make [it so]."
In some cases, parental motivation was key:
-
"I had a teacher who always wrote equations on the board and didn't bother, unless he was asked two or three times, to [say] them out loud. So my mother calls to arrange for me to have a tutor the last six weeks. [The vice-principal] said, basically, Well, what's the problem, your son is blind, he's not going to college anyway.' And my mother went off on him like Cher went off on the poor principal in Mask,' and said my son will either have a tutor or I will go to [the media]. Needless to say, I got a tutor."
-
"When we first started...public school, it was only the second year of the program and there was no money for blind kids so our parents went out and raised money to buy the first Braille writer to teach us because the teacher they hired didn't know Braille-one lesson ahead of the blind kids. And then the parents got together and beat up the school district until they started funding and getting us the equipment and then the money just rolled in like water."
c. Seeking and Maintaining Employment
Numerous participants said they relied on themselves in seeking and finding first employment out of school or subsequent to a disability, and many said that obstacles early in life had only made them more determined to succeed. An individual who acquired a disability as the result of a car accident said that his determination and desire for independence helped him overcome challenges:
-
"When I left [the hospital] it was different, definitely different. But there was a motivation that's always been in me. I refuse to quit. I'm always on the go. I carry my regular forty-hour job, I have an Internet business now. I'm a wheelchair referee for able-bodied basketball with the LA high schools, and I also play wheelchair basketball. My belief is if I can't be happy at what I'm doing then I won't do it. I'll change jobs and right now I have a great job."
Another said that understanding his strengths and limitations within the labor market motivated him to develop more marketable skills:
-
"I went with most of my buddies, they were transitioning from school into jobs which I really knew I couldn't have. Be realistic, certain jobs you might as well scratch off your list. That alone just gave me the motivation to start researching what worked for me. I went a year to vocational school, mostly in clerical, computer classes. Crappy skills which probably six months after I got the certificate were [obsolete] in the real world. You couldn't challenge [yourself] with those skills. So I went back to school. I went to college and started as a full-time student."
Numerous others described the importance of self-reliance during the transition to employment:
-
"My first job, I applied at a heating and cooling company, and I did that on my own."
-
"[VR provided me with] training into a job but I had possessed the skills as an advocate myself. For [my current job], I did my own job development."
-
"I was very aggressive and persistent all the time "
-
"Independence, I think, is the most important factor to me. I don't really want to have to depend on anybody."
d. Gaining Job Accommodations
As described above, motivation was cited as key to obtaining accommodations in school. Similarly, participants often said that motivation was key to obtaining job accommodations:
-
"I wanted to get into high tech [but] I could not find any college that would put in the [accessible] computers and teach [the accessible] software. I approached the Braille Institute to tour training centers, and attended a seminar where they had the vice president of EarthLink's Customer Service come in. And at that time they were hiring. They accommodated me by giving me a workstation training, office accommodations and software."
-
"I had an issue with my previous boss where he actually called me into his office and said, I'm becoming very concerned about your many absences.' And, I looked straight at him and said, All of my absences are just for a few hours every couple of weeks or so and they're all for medical appointments. I have no choice but to go to my doctor.'"
Among participants who related stories about successfully requesting accommodations, many were in reference to employment at jobs subsequent to first employment. In some cases, participants who demanded appropriate accommodations did so because of previous experiences not receiving needed support.
e. Managing a Complex Benefit Structure
Numerous participants described the challenge in learning the complex set of benefits available to adults with disabilities. For many, success in navigating the system was due to their persistence:
-
"I just started making phone calls that would lead to another phone call and another. Coming from a small city there's just not the resources and you don't hear about them. I think what drove me was that I couldn't pay $500 per month [for medications], so I was going to find different options."
-
"You do what you've got to do."
-
"You know how to be creative. Whereas somebody else may look at what the procedure is, you're looking more at, How can we make this happen?' It's just a matter of at some point you have to kind of take responsibility and just kind of go after it."
-
"I was depending on public transportation, which we all know is the worst, especially if you're a wheelchair user. I would go to school. It started at nine o'clock, [so] I would leave home at seven o'clock in the morning, get passed up by several busses; [the driver would say,] Sorry, buddy, my lift doesn't work.' I got to the point where I was so damn frustrated I [decided] to try to get my own car. So I started hustling. I was going to get a car; I was determined. Once again, my determination [paid off, and] my financial aid money backed my loans and I had a car."
2. Participants Favor Mainstream Education Despite Tradeoffs
Most participants who had educational experiences in both segregated and integrated settings believed they benefited more from the integrated. In particular, participants said that educational opportunities were more diverse within the mainstream educational system and often of higher quality. Many participants also favored mainstream education because they could be schooled within the general community, rather than separated from it.
-
"When I started school, mainstreaming was the thing. It is good for yourself and good for the rest of the school [for you] to be part of things, not stuck outside the rest of the school and doing your own thing, it's not good. It's the key to accepting how you fit in society, and having society accept you as well."
-
"[As] I got older I sort of hated it because we had to go [to] a school away from our house and I always thought, You know if I went to school right in my neighborhood, then people would be more accepting.'"
-
"In high school I went into a self-contained classroom where I was in that classroom for the first five periods of the day and then mainstreamed for the other three. [This was] very beneficial because it helped me learn skills that I needed to join the workforce [and for] life in general."
According to some, the disadvantages of segregated education were striking. Several people said that their segregated programs provided no vocational classes or job opportunities; others said that their programs lacked basic instructional materials and teacher expertise, or that the programs did not otherwise meet their basic needs.
-
"They were putting me in classes that I didn't belong in. They'd associate physical disability with someone who is mentally disabled."
-
"I went to a school that was just for the handicapped [around eighth grade]. I felt that I didn't come away by learning a lot that I wanted to learn. Like [t]hey just kind of failed to work with me on reading. I was lucky to learn how to tell time and count money, things like that . Back then, they had to graduate you whether you wanted to graduate or not."
-
"[I also] went to a [segregated] school and it was horrible. I did not get an education there. I went there from first grade through high school, and I hated every minute of it because most of the kids were -- I'm not sure how to put it -- severely emotionally disabled. I did not belong there. The teachers they pretty much coddled us and would pat our heads a lot, you know, that kind of an attitude."
While a majority favored integrated over segregated settings, some did not. This might reflect the nature of their impairment and/or some especially positive aspect of their experience in a segregated setting. Among those reporting positive experiences in segregated educational settings, most attributed their experiences to special education teachers that challenged them, were intent on seeing the participant succeed, and were even willing to break rules to provide unconventional or additional supports or accommodations:
-
"I had a wonderful teacher [in a segregated setting] who emphasized the need for reading and educating yourself. Certain teachers along the way were challenging."
-
"There were these two social workers [on the school's Child Study Team]. They kind of adopted me. They said, If you're not going to come to school, then just come to see us at the Board of Ed office and we'll go over all the subjects with you.' They knew I was really smart, so they just gave me the homework . . . . [I wouldn't have made it] if it wasn't for the diligence of this lady, who would basically say, Just come over and bring a lunch.'"
-
" ...I eventually did go back to school and finished, [but it was] with these people's help... They broke every rule in the book and I loved them. They were not supposed to take me out to lunch and to come over to my house. [Also, there's a limit on the] number of days that you could be out of school but they said no, he's got some kind of doctor's note or something."
-
"I went to orthopedic school,' [where] the teachers were role models [who] taught you the way society thought about disabled people. [It was] for people who were physically challenged, not [kids with] learning disabilities. You had to keep up with the other kids. They didn't think about your disability, they just saw you keeping up."
Those who had experiences in segregated settings also reported having greater access to physical accommodations in those settings and difficulty in obtaining them in integrated settings.
-
"I started special ed at age 10 until graduation. Instead of assisting me in mainstreaming me, they kept me in courses that did repetitive training instead of supporting me in areas that I was lacking. In college I had assistance, I had my books-on-tape, I had someone helping me take notes. If I had had that in grade school, I could have been mainstreamed."
-
"I started out going to a cerebral palsy school, actually, when I was a kid, for kindergarten, because they didn't know where else to put me. But after we moved [from] New York to New Mexico, they went ahead and put me into totally mainstream classes and worked with me. I didn't need any extra help as far as learning. I was actually advanced for school. But I couldn't go out, I couldn't play at recess, I couldn't walk far enough to get to the lunch room and stuff."
-
"I had problems with putting things on paper [from] my head. I had to use a tape recorder, I had to take physical therapy, speech, and my mom had me take dancing with my classes and stuff like that. It was the teacher's idea [to use the tape recorder]."
-
"I had a sign-language interpreter and I had my textbooks in Braille."
3. Other Challenging Transitions Accompanying the Transition to Work
Other challenging transitions often accompany the transition to work. As with any individual, the transition to work period is a transition from the familiar surroundings of school to the less familiar surroundings of work. In addition, for many people, the transition to work signifies a move to increased independence in housing and finances. People with disabilities often face special challenges with these transitions. Concurrently, the individual with disabilities might face significant transitions in formal supports.
Access to health care is especially likely to change. If the individual receives Medicaid, continued coverage might be threatened as the individual ages out of covered groups. At age 18, child SSI recipients must re-apply for SSI (which may be an intimidating prospect), and learn how work choices may affect disability payments and Medicaid receipt. Others who might have Medicaid coverage as children in low-income families could simply lose that coverage. Employers may offer private health care coverage, and some youths will need to assess the availability and sufficiency of such coverage. Some may need to change health care providers because of insurance changes, because of a change in residence, or because they have moved out of the age range served by pediatric specialists.
Youth must also face an uncertain job market where success might depend, in part, on disability type and education experience. Some will experience employment discrimination. For those who do, learning and understanding their rights and responsibilities under the law will be necessary. Throughout this period the youth is learning to accept responsibilities that may have been handled by parents in the past. Therefore, obtaining useful information and making good choices are critical.
The need for consistent health care was a dominant theme in focus group discussions. Some participants reported loss of health care or loss of specific coverage (pre-existing conditions) when parents changed jobs. Others described parents who made employment decisions based in large part on access to health care for a child. When transitioning to work, many participants described a strong desire to make employment choices that ensured continuity of coverage, which most deemed as extraordinarily important to ensuring independence. A few participants reported loss of Medicaid coverage when they began to work. A number of participants described the tension between securing employment and retaining access to health insurance.
One participant sought assistance in retaining access to public health insurance while working:
-
"The Community Health Law Project [was] helpful in me getting my disability benefits, because the first time I was denied, and so they were able to help me get them, and even now, [they] help me to keep my medical benefits while I'm working, so I can get work."
Other participants described concerns about loss of health insurance coverage as the result of employment:
-
"[I had] the best doctor in town at [the mental health center, paid by] Medicaid up until the point I got my job. It was a long time before I realized that [the MH center] was not covered by my insurance, [and] my doctor wasn't being paid by my insurance agency. So I lost my doctor as a result of me getting my job, [and] I've not had as good a doctor ever since. I have group health. I get a new doctor every six months, [and] with my particular illness, I have to retrain a physician almost every time I have a new doctor. The logical conclusion is, if I wanted good health, I would have stayed unemployed."
-
"A lot of us are not really pursuing that because when you think about it, [if] I lose my Medi-Cal how much is going to be my monthly income? $1000. OK. Fine. [With my] kind of expenses [I'm] going to end up with maybe with $700.00, which is what I'm getting now from my SSI. So, [should] I stay there? I stay with them [SSI] instead of pursuing employment, because if you are one of those that needs a lot of health care, and you lose your Medi-Cal, that's it."
-
" I knew that as soon as I went to work somewhere that I would be off [Social Security]. So it was real scary because it's kind of like having a rug come out from under you. I thought if I can't make it on my own But I just started earning more than $500 a month. I always report my earnings, and one day I got a notice saying it had been discontinued. But the nice thing was they let me keep my [Medicare] benefits, as long as I paid the premium."15
Many participants reported expending substantial effort in retaining access to health care during their transition to work. Some participants reported turning down employment when private coverage was inferior to public coverage, or choosing to work only part-time to keep earnings low:
-
"I was able to work part-time by joggling the figures, so I was able to go to work at the college. Then I reached a point where I was making too much, but by then [my employer's] Basic Health was available and then eventually I got on as a permanent classified employee, so I have my health benefits through the college."
A number of participants reported negotiating successfully with employers (and others) to prevent loss of Medicaid benefits due to earnings. Participants reported using a number of strategies, including taking time off, shifting responsibilities, working without pay, shifting to part-time employment, and turning down promotions. For example, a participant with chronic back problems said she had delayed getting a job in order to maintain her benefits. Another participant, with multiple sclerosis, said that she works less than she would like because she does not want to exceed the earnings limit for fear of losing her benefits.
For youth with disabilities, making a successful transition to work depends, in part, on understanding the benefit landscape facing adults. For instance, SSI receipt is re-evaluated upon turning 18. SSI can change depending upon work activity, and receipt of some public supports (e.g., welfare) is dependent upon work. Many found the loss of benefits just as they started to work discouraging and unfair:
-
"With SSI, you can make some arbitrary amount [that] you keep.[Then,] every month, you've got to report how much you made. You give the federal government a dollar back for every two dollars you make. Where is the incentive in that? What person is going to go out and work [at] something and have to give half of [their earnings] away?"
-
"It seems as though when you do work, you're penalized for it. They cut your monies and I don't understand it. It really puts a damper on getting better."
Navigating the new benefit landscape can be difficult and can also be demoralizing when program features create obstacles to employment. Several expressed frustration regarding the level of knowledge of SSA staff regarding program rules related to employment. For example, one participant said:
-
"I went down there with a case manager and we reported everything. And they said, Okay, everything's fine.' It's like, you should be getting that money. And like a year or something goes by, and another case manager says, Wait a minute. You're being overpaid. You're going to have to pay all that money back.' And so I start to go, Oh my God, it's going to be thousands of dollars.' And so we went down to SSI and they said, Well, there's nothing we can do about it. You [should have] put that money all in an account and just saved it.' But we came to the conclusion [that] if I had saved all that money, then they would have taken my medical benefits away from me because Id have too much money [in savings]. They do it to everybody. I've worked very hard to get where I am, and I really don't think it's fair that I have a $7,000 debt that I have to pay back."
Participants across focus groups related numerous stories about SSI overpayments, including difficulty in identifying and resolving them. In some cases, participants were aware that they were receiving overpayments (due to eligibility or earnings), but they were unsuccessful in resolving the issue quickly, or at all, until the Social Security Administration eventually and independently identified the overpayment, and requested that the money be returned:
-
"I'm paying $10 a month for the next 19 years to pay back $2,300. They're taking it out of my Social Security."
-
"I was misled by some of the rules, some of the things they were telling me, so actually, right now I owe $5,000."
-
"[SSI] kept sending me checks after I started working even after I had informed them I had been working. I knew they were going to ask for it back at some point. All those checks I received from them, I just put them in the bank and drew interest on them. When they asked for them back, I said, fine. It wasn't my fault they kept sending me checks."
Several participants briefly referred to having received personal assistance services at the time they were seeking their first jobs. Two received in-home support services through SSI but lost these services once they began working, because they were no longer eligible for disability benefits. The services remained valuable but out of reach, which one participant described as "unfair and infuriating."
A number of participants related their experiences in seeking housing assistance during the transition to work. One was pleased with successful participation in independent living programs:
-
"I got independent living skills through my worker at South Central Regional Center. He helped me with getting to work, learning how to get there on the bus, and help with my SSA, so I know how much I can make. And I had mobility training through Regional Center."
Another said:
-
"I got help through the Independent Living Center in Van Nuys. They helped me quite a bit and had me come back and forth to their facility to undergo learning type stuff. [It was like] a training house for disabled students, to help you become independent."
One participant noted the importance of housing when seeking employment:
-
"If you don't have a place to live, it's pretty hard to get yourself together to look decent for work."
Participants also discussed their varied experiences searching for Section 8 housing. Several reported success in qualifying for the program and finding housing, while others reported difficulties in securing housing after completing the application process. Several participants indicated that they had been on an eligibility list for Section 8 housing assistance, but never actually received it. As one participant said:
-
"I've tried to get on Section 8 and the [waiting] list is so long [that] it was non-existent for a while."
Another participant described her difficulties in finding a place to live because "the government does not have much housing for single people."
Many participants reported the need for reliable transportation in seeking and maintaining employment. One participant used specialized paratransit to get to job interviews. A second participant relied upon her family for transportation to potential employers. Others mentioned receiving cab vouchers and bus passes during their job searches, and they discussed other subsidized transportation services available to people with disabilities, such as discounted license and registration fees. Many participants described difficulties maintaining and securing necessary transportation.
For example, one woman said that while seeking employment she "discovered" ACCESS-Link, but was not permitted to use it because she lived outside the service area. She went through a two-year legal battle in order to obtain access. Another participant said that she took public transportation to her first job, which was extremely difficult "I had to leave about 5:30 in the morning just to get to work by 8:30," she said. "Getting back and forth was an issue."
Those who reported the most satisfaction with transportation services typically received funding or otherwise found the means to purchase or modify a private vehicle.
4. Individualized Services that Support Mainstream Participation are Highly Valued
Participants highly valued supports and services that were individualized, and that enabled them to participate in "mainstream" activities -- i.e., enabled independent participation in activities in integrated settings. For example, participants were most pleased with VR providing or paying for equipment and services, such as computers, assistive technologies, transportation, and third-party training. Such supports targeted specific needs and promoted independence. They were less satisfied with services received in a "sheltered" or segregated environment, such as job training provided through the state VR system.
-
"DVR is a very, very, very, very good organization. It's been really good with me. They paid for classes [and] class fees [and] they paid for my books. They gave me transportation, supplied me with transportation, gas."
-
"DVR, about five or six years ago, also bought me a computer with voice recognition technology so that I could do my current job using computer technology."
-
"They paid for all my supplies for school. I think that's the best part about it."
-
"They helped purchase a hard drive for my computer one time. They've helped me a lot with supplies for school for the last several years."
Participants with MR/DD were particularly pleased with job coaches for the same reason. Job coaches promote independence by providing motivation and support, serving as a source of information about services, mentoring and counseling individuals, in some cases accompanying individuals on job interviews, and even helping resolve employment disputes and difficulties.
Participants spoke less favorably about VR job training and job search services. In some cases, participants were dissatisfied with the quality of the services. Predominantly, participants were discouraged by the extent to which they had to accommodate the VR agency's timetable, rather than the agency accommodating their timetable.
-
"I tried Rehab. I did their job club and the whole bit, but it was a joke. I mean, you went in there and you did cold calling. It wasn't worth my time "
-
"When you go to VR they require you to do a job search you call them back a couple days later, and say, I put an application in there, how come you guys never called me?' [They say they'll] call you back in a couple days and you never hear from them. That makes your confidence low, go even lower."
-
"When it came to getting the training I went to one class and jumped into the vocational program class. [But then they said,] This is what we can do, but let's wait and see.' I was in a situation where I could not wait and see. It was either employed or not. That's why it works for some and doesn't for others."
-
"[It was] three months before [they] would even get somebody to see if [I] was eligible. [So I] put my wheels down, and just went out and got a job. I figured it'd take them another year before they could ever help get me in school and go through the training and take the testing."
Participants looking for specialized work were displeased with state workforce development systems, primarily because they were not able to receive needed services.
-
"I learned some good things about resumes, job interviewing techniques, etc., but they didn't really have anything in the social services field."
-
"I hooked up with the Department of Labor program for people with disabilities in New York City. They were not helpful at all [beyond my] getting evaluated, [and] my husband's insurance actually paid for [that]. Basically what they had was low, meager jobs to offer and that wasn't the stuff that I was looking for. They didn't have anything [for someone with] a college degree in psychology. So they really didn't help. I mean, they did [provide] a computer to do my resume but I had already secured [that for] myself."
Participants with the fewest skills, and consequently those looking for basic skills training and entry-level positions, were most satisfied with these services.
Participants typically reported positive experiences with school-based work preparation programs. Many seemed particularly pleased that the programs gave them an alternative to school, and allowed them to pursue a vocational interest. For example, instead of going full time to a regular school, one participant took a 60-credit childcare class that helped prepare her for a career. Other participants said:
-
"When I was going to school, they started putting handicapped kids into [a school/vocational program] and I [learned about] painting, spray painting cars, or a bumper, and it was real interesting. They put you out in the community where you're helpful and the guy was there with me, making sure I did it right. That was the neatest thing I ever did."
-
"In high school I got trained in how to be a maintenance [worker] you know, [the] whole summer. I start at 3:00 o'clock in the morning and I don't get off until 2:30 [pm]. Those are long hours. And they pay me for it, because that's during school hours."
Participants said that the variety of skills developed in these programs (e.g., janitorial skills, public speaking, basic medical skills) led directly to later employment.
IV. IMPLICATIONS FOR PUBLIC POLICY
Each of the findings regarding youth in transition has important implications for public policy. In this section, we discuss those implications and the relevance of recent legislation.
A. Importance of Expectations and Motivation
Expectations and motivation played a critical role in the employment success of those we interviewed. This does not mean, of course, that those who have not achieved a similar measure of employment success are not highly motivated -- the most highly motivated individuals might be unable to overcome the barriers and disincentives to employment that are faced by many people with disabilities. Yet the fact that motivation was key to the success of those we interviewed, and in particular, helped them persist in their efforts to navigate a complex support system, does have two important policy implications. First, policy changes that motivate people to work and promote work expectations are more likely to be successful than others. Second, policy changes that help people navigate the support system or make the system less difficult to navigate are likely to improve employment outcomes.
We would expect policies that promote work expectations and motivate people to work be critical for the improvement of employment outcomes for people with disabilities. Conversely, policies that promote the expectation of dependence and create work disincentives are likely an important cause of low employment rates for this population. The most obvious of the latter are that income and many types of in-kind support are linked negatively to earnings, directly or indirectly.
Based on the findings, it appears that the educational reforms embodied in IDEA and the School to Work Opportunities Act are an important step in the right direction for those whose impairments begin at birth, in early childhood or adolescence. Bringing children and youth with disabilities into the least restrictive educational setting possible and working on vocational plans with them by age 16 is likely to enhance work expectations. Of course, success will depend on how these programs are implemented by local school systems. This is a difficult challenge because it must overcome the inertia of past policies and attitudes, which embody low work expectations.
This finding also argues well for recent policy changes that seek to increase work incentives or reduce disincentives, such as the increase in the SSI student child earned income exclusion. Under the exclusion, youth under age 22 and attending school are able to exclude earnings from income. In January 2001, the exclusion was increased from $400 to $1,290 per month, with a yearly limit of $5,200 (increased from $1,620). The value of the exclusion will increase annually based on increases in the cost-of-living index.
Other recent policy changes that seek to increase work incentives or reduce disincentives include the expansion of access to Medicaid, most recently through the Medicaid buy-in and extended Medicare eligibility provisions under TWWIIA. The Ticket to Work program itself also provides an incentive to work, because the full value of the Ticket to SSI (and DI) beneficiaries and their providers is only realized if the beneficiary achieves significant earnings goals. The fact that Ticket participants are exempt from continuing disability reviews also removes a work disincentive. The legislation also addresses the substantial risk that beneficiaries who exit SSI/DI must take when they leave the rolls -- the risk that they will not be able to return if they lose their job -- through provisions that would make it easier to return.
The mandatory re-determination of SSI eligibility at age 18, required by PRWORA, might encourage or discourage work, depending on the beneficiary's circumstances and perspective. As a child or youth, the beneficiary might be less likely to assume that SSI will be available in adulthood, and therefore be more motivated to pursue efforts leading to employment and independence. From that perspective, the new policy seems in line with other policy changes for children and youth with disabilities. However, at age 18, youth near the margin of adult SSI eligibility might have a strong incentive to demonstrate inability to work, as eligibility requires, rather than pursue work. This problem is exacerbated by the lengthy initial determination and appeals process. The Ticket program may further add to this problem because eligibility for the Ticket, as currently proposed, will be withheld until adult SSI status is obtained.
The problem with re-determinations at age 18 is not the child SSI policy, but the adult policy. That is, despite the reforms in the Ticket legislation, it will still be the case that income support for adults is conditioned on inability to work, and many other benefits are still linked negatively to work. Put differently, it will still be true that, for people with disabilities, the economic gain from work will be much less than the compensation they might command from employers because of benefits that are linked to earnings. Achieving significant progress in improving adult employment outcomes for youth with disabilities might require policies that do not undermine the economic gain from work, or even policies that enhance it. The Presidential Task Force on Employment of Adults with Disabilities has recommended that the age for mandatory re-determination be raised in order to postpone the decision regarding SSI re-determination and encourage a transition to work or pursuit of additional education. The Task Force has also recommended the creation of additional private-public internships as well as an expansion of the National Youth with Disabilities Leadership Development Program to increase access to opportunities for employment and leadership development for youth with disabilities (Swenson and Richards, 1999).16
While the expansion of the availability of home and community based services through Medicaid HCBS waivers is a positive development in many respects for people with disabilities who need such services, the way they are financed, via Medicaid, could significantly undermine incentives to work. Because for most people with disabilities the best way to obtain Medicaid eligibility is via SSI, the provision of these services via Medicaid increases the value of not working. While the services provided under HCBS waivers might make it more feasible for users to work, the way they are provided might significantly undermine the motivation to work. Medicaid expansions, such as the Buy-in, that weaken the link between SSI and Medicaid eligibility will help address this issue.
An example of a policy that would enhance the gain from work is the Disability Earned Income Tax Credit (DEITC), proposed by the National Academy of Social Sciences' Disability Policy Panel (NASI, 1996). A DEITC would pay a tax credit to disabled workers with sufficiently low earnings, through the federal income tax system. The DEITC would be "refundable," meaning that the worker would receive the payment even if the worker's tax liability was lower than the credit. The amount of the credit would increase as earnings increase, up to a point, then gradually decline as earnings increase further. This would create a positive incentive to work for those who can only command low starting wages in the competitive labor market. An EITC already exists for all workers, but is very small unless the worker is a parent. In 1999, the maximum credit for non-parents was $347. For parents with two or more children, the credit was 40 percent of income up to $9,540, at which point the credit was $3,816. The credit stayed constant from that point up to income of $12,460, and was then phased out, reaching zero at an income of $30,580. The EITC paid out $31.9 billion in benefits in 1999 (Hotz and Sholtz, 2000a and 2000b).
The main beneficiary of the EITC has been families headed by unmarried mothers. Their recent experience suggests that such a policy would significantly improve adult employment outcomes for youth with disabilities. Strong evidence attributes a large share of recent increases in employment of unmarried mothers and declines in TANF participation to the early 1990s expansion of the Earned Income Tax Credit that is available to low-income families with children (Hotz and Sholtz, 2000a and 2000b). It might also be necessary to base income support on some criterion other than "inability to work," such as some measure of the cost of supports that an individual with a significant impairment needs to function at a reasonable level.17
The importance of reducing bureaucratic barriers within the support system is evident. Currently, people must navigate a complex system in order to receive benefits and services; the system is even more complex for those who simultaneously pursue work. TWWIIA includes benefits, planning, assistance and outreach (BPAO) grants to fund state and local organizations to provide counseling, planning and related information for people with disabilities. We address this issue further in another paper in this series.18 See also the discussion of other challenging transitions faced by youth with disabilities, below.
B. Need for Accommodations at School and Work
While most participants favored education in integrated, rather than segregated, settings, many reported difficulty in receiving necessary accommodations outside special education classrooms. Participants also described difficulties in receiving reasonable accommodations in the workplace, despite the requirements to provide such accommodations under the ADA.
Most participants attended secondary school 20 or more years ago, when less emphasis was placed on accommodating students with disabilities in the least restrictive environment. The implementation of IDEA and other initiatives has no doubt increased the number of students with disabilities who are in the least restrictive environment and who receive appropriate accommodations. As noted earlier, through IDEA, students receive a variety of services intended to support the transition from primary school to secondary school or independent living. In a recent summary of available research on school programs, the U.S. Department of Education (1996a) identified longitudinal planning, work-based learning, sustained employer involvement, emphasis on career development, and access to ancillary services (such as housing and independent living) as features common to successful transition programs. In general, the summary suggested that transition programs should link school, work, and human service systems to ensure access and coordination of needed services. The development of One-Stop centers under WIA might have important implications for integrating such service delivery and improving access to accommodations for youth, both in school and during the transition to work.
Access to accommodations within post-secondary institutions may gain importance as a policy issue in the near future as the percentage of students with disabilities attending post-secondary institutions continues to increase. Between 1986 and 1994, the percentage of students with disabilities over age 16 who had attended at least some college rose from 29 percent to 45 percent (U.S. Department of Education, 1996b). In 1996, approximately nine percent of entering college freshman reported a disability (Henderson, 1998).
While nearly 62 percent of focus group participants reporting disability onset before age 18 attended at least some college, they spoke little about post-secondary accommodation receipt (or non-receipt). Additional attention to this issue may be warranted, however. A recent effort to systematically collect national data regarding the availability of educational accommodations within post-secondary educational institutions found that 98 percent of post-secondary institutions that enrolled student with disabilities in 1996 and 1997 provided at least one support service or accommodation. Provision of accommodations, however, varied considerably by institution type and size, with large institutions (10,000 or more students) far more likely to provide accommodations than small institutions (fewer than 3,000 students). Public institutions were also more likely than private institutions to provide accommodations (Lewis and Farris, 1999). Historically, post-secondary graduation rates for people with disabilities have been lower than among the general population, and accommodation issues might contribute to this difference. Further, timely accommodations might play a key role in improving matriculation.19
A list of example educational accommodations, identified through a review of educational institution surveys and policies, is provided as an Attachment to this report.
Participant experiences with employment accommodations are more contemporary. These experiences highlight the importance of accommodation policy in employment outcomes for people with disabilities. The findings also suggest a need for additional effort to make workplace accommodations available, although existing need is difficult to ascertain from a study of this nature. At a minimum, the study points to the potential value of existing efforts in this area, which are substantial.
One federal program already provides technical assistance to employers: the Job Accommodation Network (JAN). Created by the President's Committee on Employment of People with Disabilities, JAN provides a toll-free information and referral service to employers seeking information on job accommodations, employers' responsibilities under the ADA, and technical assistance. Projects with Industry (PWI), administered by the Rehabilitation Services Administration (RSA), might also contribute significant support to facilitation of accommodations. This program links receptive employers and qualified workers with disabilities, and does so in the competitive labor market. Through job matching and follow-up services provided by the 99 programs nationally, PWI facilitates the exchange of information between workers and employers, including information about accommodations. Providing such information could also become a significant activity of One-Stop service centers, the Employment Networks of the Ticket program.
In addition to responsibilities under the ADA to provide accommodations, several provisions (e.g., credits and deductions) in the U.S. tax code provide incentives to employers to hire persons with disabilities by reducing the employer's tax burden and compensating for the potential or realized costs of hiring individuals with disabilities.20 Among these are the Work Opportunity Tax Credit (WOTC), enacted in 1996, which provides a tax credit of up to $2,400 for employers who hire SSI recipients and vocational rehabilitation referrals. Small businesses (those with fewer than 30 employees and less than $1 million in gross receipts) are eligible for the Section 44 Credit (also known as the Disabled Access Credit), which provides a credit equivalent to 50 percent of all eligible access expenditures that exceed $250 but do not exceed $10,250. The deduction is intended to cover the expenses incurred by small businesses complying with the ADA, for whom the cost of compliance is likely to be particularly burdensome. The Section 190 Deduction (also called the Deduction of Costs of Removing Architectural or Transportation Barriers to the Disabled or Elderly) allows businesses to deduct expenses incurred while removing barriers to persons with disabilities from the location of the business. The maximum deduction is $15,000.
Increased public support for accommodations might also be warranted. A mail survey of employers who contacted JAN revealed that 40 percent had made an accommodation based on information provided during the contact (JAN, 1999).21 Among employers making the accommodation, 82 percent rated the accommodation as "very effective" or "effective," citing a number of beneficial outcomes including increased worker productivity (cited by 54 percent of employers) and ability to hire or retain a qualified employee (cited by 56 percent of employers).
C. Other Challenging Transitions Accompany the Transition to Work
The finding that young adults transitioning to work often face other challenging transitions contemporaneously has important implications for public policy. First, there might be substantial payoffs to providing such individuals with assistance in managing all of their transitions, not just the transition from school to work. For instance, youth/young adults with disabilities could be provided with counseling services by individuals who were trained to assist them over a period of time in which they started work, moved to a new residence, determined how to meet transportation needs, changed health insurance and providers, entered support systems or networks (e.g., a peer support group), and became involved in other adult activities. Designing and implementing such a system would be a significant challenge. One way to do it would be to enlist the services of peer support groups, because they already have substantial familiarity with the issues and are more likely to be trusted than a government agency. Second, efforts to facilitate other transitions (e.g., in health care or housing) could have the additional benefit of facilitating work.
Recent policy developments have addressed this issue to a degree. IDEA provides for multi-year, individually-tailored support services (through the development of IEPs) from childhood through secondary school, which ensures access to appropriate accommodations and helps reduce discontinuities in support receipt. Eligible youth in all states may receive services until age 19, and some states permit receipt of supports through age 21. Individuals who have not completed the transition to work prior to attaining age 19 (or in some states, age 21), however, may experience discontinuities in support receipt. IDEA also provides grants to states to fund changes in the systems that provide services to youth with disabilities, for the purpose of shifting service delivery from segregated to community settings. These objectives of the grants are to help states substantially increase the number of youth who are served in general education and neighborhood environments, and to reduce gaps in service.
State VR programs can provide some limited assistance in providing broad supports during the transition period. For example, VR may pay for assistance devices, including computers, which can provide support both for employment and daily activities. VR can also provide transportation assistance, including assistance in purchasing and modifying vehicles and providing funding for gas.
SSA is implementing a benefits planning and assistance program, as authorized under TWWIIA. This program has the potential for providing transition counseling to youth and young adults who are SSI recipients. The Act's Ticket to Work program also has the potential to help eligible SSI recipients with transitions in areas other than the transition to work, provided the assistance ultimately leads to employment with sufficient earnings to meet Ticket requirements. That is, the Employment Networks that provide services to Ticket users could provide the needed assistance. As noted above, however, proposed regulations would not allow young SSI recipients to become eligible until they attain adult SSI eligibility. The focus group findings suggest that extending eligibility to older child SSI recipients would be very desirable.
In states that adopt it, the Medicaid buy-in option will help SSI youth as they transition to adulthood by providing assurance that continued Medicaid coverage will likely be available when they start work, regardless of the outcome of the SSI eligibility re-determination.
Of course, the Ticket and Medicaid Buy-in will not be available to those whose disability is not sufficiently severe for SSI eligibility. Many non-SSI youth with disabilities who benefit from Medicaid, TANF, and possibly other programs as children likely lose this assistance when they become adults.22 Efforts by the CMS23 and SSA to expand access to health care for individuals with disabilities who are working reflect the role of health care as a key employment support. We discuss this issue in greater detail in another paper in this series.24 It will be important for evaluations of the Medicaid buy-in and other state Medicaid initiatives to examine whether their programs support or create a barrier to the continuity of health care for youth who are transitioning to adulthood.
The frequency of problems that focus group participants had with SSI overpayments and subsequent repayments, usually as they exited SSI, is surprising. It is not possible for us to differentiate between problems that result from a flawed payment determination process, clerical errors committed by SSA employees, and errors committed by the recipients. While many of the participants insisted that SSA staff misled them or otherwise made errors, we have no way to verify that. Most of the experiences reported took place many years ago, and it might be that more recent experiences have been better. It might be important, however, for SSA to examine this process, always keeping in mind that many beneficiaries might have substantial difficulty understanding the rules. Ensuring that this transition is a smooth one will become even more important if current policy initiatives are successful in improving employment outcomes.
It might be worthwhile to conduct a comprehensive review of how public policy supports or hinders the entire array of challenging transitions faced by youth with disabilities as they enter adulthood. While individual programs consider transitions in areas that are pertinent to their own programs, we are not aware of any efforts to look at the combined challenges of these transitions and their many possible interactions.
D. Individualized Services Are Highly Valued
The finding that participants highly value individualized services that support independent, mainstream participation substantiates the argument that supports need to address the unique needs of each youth with disabilities as he or she attempts to succeed in the labor force. While "one-size-fits-all" supports might be easier to provide, they are not as highly valued by the users.
Over the last three decades, disability policy has increased emphasis on individualized services, in part through increased emphasis on consumer choice and self-determination regarding vocational goals, living arrangements, and selection of support services. Consumer choice and self-determination are critical to the provision of individualized services because it is in the consumers' self interest to obtain the services that will best meet their own needs. While they might benefit from counseling and other assistance in obtaining services, their ability to make decisions is critical to achieving an outcome that meets their needs.25
Many recent policy changes have moved public policy toward more individualized services. This is clearly the intent of the recent history of legislation in the area of education, culminating in IDEA. The same intent is reflected in the School to Work Opportunities Act, the One Stops of the Workforce Investment Act, and the Ticket legislation, all of which seek to support individualized services offered in mainstream settings where appropriate. The Rehabilitation Act Amendments of 1992 and 1998 emphasize efforts to ensure that clients are able to exercise informed choice throughout the rehabilitation process. In exercising informed choice, the client works with the VR counselor to match the client's strengths, interests and abilities to a vocational goal and a set of services designed to achieve that goal. The process is intended to provide the client with sufficient information so that he or she is able to select from a range of vocational options and services, and is able to weigh the benefits and costs of various choices. The 1992 Amendments authorized funding for the Demonstration Projects to Increase Client Choice Program. This program funded efforts that demonstrate ways to increase client choice during the rehabilitation process, including in the selection of vocational goals, providers and services. The program was targeted at individuals with disabilities who are not currently receiving VR services. Seven demonstrations were developed and evaluated under the program, which ended in 1999.
The less-than-satisfactory experiences that several participants had in obtaining accommodations in integrated school settings, and difficulties some encountered in obtaining accommodations at work are an important reminder that accommodations are not easy to obtain. Although JAN finds that most accommodations actually provided by employers appear to be inexpensive, this might not be true for a significant number of workers, or potential workers. The need for schedule changes to accommodate individuals with mental or other chronic illnesses might be especially problematic, depending on the setting. One reason is that it can be difficult for other workers, or the organization as a whole, to cope with unanticipated or prolonged absences. Another reason is that other workers might think they are being treated unfairly, especially if the accommodations (or the reason for them), is undisclosed to protect the accommodated worker's privacy. Employer accommodation also requires workers and job applicants to disclose their conditions to the employer, and many individuals may decide that it is not in their best interest to do so.
While these developments appear to be in the right direction, more could be done. One area for further consideration is how public policy can encourage the use and availability of supports that are not directly provided by the government. It is clear from the focus groups that many participants relied significantly on significant supports from others in childhood and as they entered adulthood -- families, friends, co-workers, peer support organizations, advocacy groups, independent living centers, faith-based organizations, and others. Compared to government or government-supported providers, these sources seem likely to provide support in a way that is more personal, tailored to the individual's needs, and supportive of their participation in integrated activities. Policies that encourage the use of such supports might significantly improve adult employment outcomes for youth with disabilities, as well as the overall quality of their lives.
The current Administration's initiative to increase the availability of federal support for social services when they are provided by faith-based organizations might be one small step in this direction. Policymakers might also want to consider contracting with peer support organizations and independent living centers to provide services in a variety of areas. Opportunities for such organizations to do so already exist (e.g., as an Employment Network for the Ticket to Work program), but it might be necessary to encourage those organizations to get involved, and perhaps modify the opportunities in ways that would make it more attractive for them to do so.
It might also be worthwhile to review how existing policies encourage or discourage the individual's use of informal support from families, friends and co-workers. For instance, to what extent do programs that pay for personal assistance services allow the individual to use a family member, friend or co-worker to provide the services, rather than somebody who formally works as a personal assistant but might be a complete stranger to the individual? Could a program pay for assistance by others without making the program exceedingly costly or providing substantial opportunity for fraud and abuse? In general, fixed stipends paid to the beneficiary, with the amount based on estimated cost of needed services, given the individual's health conditions, might be a more efficient and effective way to finance services than fee-for-service payments to vendors. A key issue is the potential cost of such programs, because they would start to pay for services that, in many instances, are provided without pay.
NOTES
-
The "percentage point" difference is a reflection of absolute change and is calculated by subtracting one figure from the other (e.g., 53 percent minus 43 percent equals a 10 percentage point difference). The "percent" difference (versus percentage point difference) is a reflection of relative change (e.g., how much did one rate change relative to its previous value), and in this case is calculated by dividing the original rate by the percentage point difference between the two rates. For example, the percent decline in employment for young men with disabilities is expressed as (0.533 - 0.426)/0.533 = .200, meaning that the employment rate for young men with disabilities declined 20 percent between 1988 and 1999.
-
These statistics were generated and provided by Andrew Houtenville of Cornell University. The analysis sample included only those who worked at least 52 hours per month and used the methods described in Burkhauser et al., 2000.
-
The first limitation is that they are somewhat dated. The Department of Education is currently conducting the second NLTS. A second limitation is that they exclude people who did not participate in special education, including those who became disabled in their late teens or early twenties (e.g., through onset of a chronic physical or mental illness, or because of injury). Third, they only follow students for three years.
-
The WIA replaces the Job Training Partnership Act (JTPA), passed in 1982, which authorized funding for programs to prepare youth (and adults) for entry into the labor force. Under JTPA, state programs were established and administered by Private Industry Councils (PICs) comprised of employers and education personnel. Services varied by state, but generally included job search, basic skills training, labor market information, occupational skills training, work experience, literacy training, job placement assistance, and summer youth employment.
-
Although Buy-in programs under TWWIIA do not restrict income, most current state Medicaid Buy-in programs were developed under the Balance Budget Act of 1997 authorization, which imposes a family income eligibility limit of 250 percent of the federal poverty line.
-
For a lengthier discussion of transition education and transition services available to adolescents with disabilities, see Neubert (2000).
-
The term "mainstreaming" is colloquial and does not appear in controlling statutes or regulations. As it is commonly understood, mainstreaming refers to the process of moving individuals with disabilities from a segregated (people with disabilities only) environment into an integrated, inclusive environment (people with and without impairments) where they have access to a full range of services. IDEA requires states to provide to children a "free and appropriate public education," and the IDEA regulations require that this education be provided in the "least restrictive environment" possible (which is to be determined on a case-by-case basis). For some, the least restrictive environment consistent with the receipt of an appropriate education might be a fully integrated setting. For children with severe disabilities, the least restrictive environment might be a supported or segregated environment. The IDEA statute and regulations require modifications to the educational environment, including wheelchair access and specialized educational services, when needed, to ensure that students are served in as integrated an environment as feasible.
-
Sullivan v. Zebley, 493 US 521.
-
This varies by state for TANF, but DI and SSI beneficiaries are typically exempt from work requirements.
-
Source: Federal Register (1999).
-
At each site, a number of individuals who were screened in as focus group participants but who could not attend a focus group were interviewed by phone.
-
All earnings and income medians reported are approximate because participants reported income in ranges.
-
Rankings are based on the full sample (versus the sub-sample of individuals with disability onset before age 19 presented in Exhibit 6).
-
See Stapleton et al. (2001).
-
A number of focus group participants, such as this one, referred to having received DI and Medicare prior to first employment. Because DI is contingent upon prior work history, it may be that some participants confused SSI/Medicaid with DI/Medicare. It is also possible that some participants received Social Security and Medicare benefits as dependents of Social Security beneficiaries, and therefore had been in receipt of Social Security benefits and Medicare prior to first employment. Also, some could have been referring to DI and Medicare benefits received somewhat later in life, after they had met DI work history requirements. Because we do not have specific information on this, we have placed the references to DI, Social Security, and Medicare in brackets to indicate that these programs may be incorrectly identified.
-
In 1999, the Task Force also recommended that the value of the student child earned income exclusion be increased. (The exclusion was increased in 2001 as described previously in the paper.) The Task Force was integrated into the Office of Disability Employment Policy within the U.S. Department of Labor in 2000.
-
In the conceptual framework of disability developed by Nagi (1965), disability results when an individual is unable to perform socially defined roles or tasks (e.g., work) due to impairment. In this framework, supports that allow the individual to function at a reasonable level in their environment would reduce or eliminate disability, even though the impairment would remain.
-
See Livermore et al. (2001).
-
Among students beginning post-secondary education in 1989-1990, 27 percent of students without disabilities earned a Bachelor's degree, while 16 percent of students with disabilities did so. Students with disabilities were more likely to receive a vocational certificate, or to receive no degree, than students without disabilities (Horn and Berktold, 1999).
-
A tax credit differs from a deduction in that tax credits are calculated against the tax burden, while deductions are calculated against taxable income.
-
Of the remaining 60 percent, half decided not to make the accommodation and the remainder had not made a final determination at the time the survey was conducted.
-
Important exceptions are those who become teenage parents. Young women with disabilities are particularly at risk of early parenthood. Based on NLS data, Wagner et al. (1993) found that 41 percent of young women with disabilities are mothers within three to five years after leaving school. This figure is significantly higher than that of young women without disabilities (28 percent) and is more than double the parenting rate of young men with disabilities (16 percent). Twenty percent of single young women with disabilities, and 54 percent of female dropouts with disabilities are mothers. Parenting rates are highest for young women who have learning disabilities (50 percent), serious emotional disturbance (48 percent), and hearing impairments (48 percent). Others might maintain Medicaid eligibility under medically needy programs, state-only programs, or other categories that vary by state.
-
Formerly the Health Care Financing Administration (HCFA).
-
See Livermore et al. (2001).
-
Individuals with significant cognitive impairments are an exception. A difficult challenge is to develop public policies that allow appropriate levels of consumer choice for those with varying degrees and types of cognitive impairments.
REFERENCES
Adler, M. (1994). Analyses of the 1990 Survey of Income and Program Participation. Intramural research for the Office of the Assistant Secretary for Planning and Evaluation. Washington, DC: Unpublished.
Administration for Children and Families (1998). Annual Report on Expenditures and Recipients. Washington, DC: Department of Health and Human Services.
Brown, D.E. (2000). The Role of Job Training Partnership Act Programs in School-to-Work Transition. Washington, DC: National Governor's Association. http://old.nga.org/Pubs/OnlinePubs/STWOA.htm.
Burkhauser, R.V., Daly, M. and Houtenville, A.J. (2000). How Working Age People with Disabilities Fared Over the 1990s Business Cycle. Paper presented at the National Academy of Social Insurance Conference on Ensuring Health and Income Security for an Aging Workforce, January 26-27, 2000. Washington, DC.
Doty, P., Eustis, N.N. and Lindsay, B.E. (1994). Research Agenda: Personal Assistance Services and Related Supports. Washington, DC: Department of Health and Human Services, Office of Disability, Aging and Long-Term Care Policy. [http://aspe.hhs.gov/daltcp/reports/resagpas.htm]
Federal Register (1999). Volume 64, Number 52 (13428-13430). From the Federal Register Online via GPO Access [wais.access.gpo.gov] [DOCID:fr18mr99-84]. March 18, 1999.
Henderson, C. (1998). "Profile of 1996 College Freshmen with Disabilities," HEATH Electronic Newsletter, Volume 1, E1. Washington, DC: American Council on Education.
Horn, L. and Berktold, J. (1999). Students with Disabilities in Postsecondary Education: A Profile of Preparation, Participation and Outcomes (NCES 1999-187). Washington, DC: Department of Education, National Center for Education Statistics.
Hotz, V.J. and Sholz, T.K. (2000a). The Earned Income Tax Credit. Working Paper, University of California at Los Angeles and University of Wisconsin.
Hotz, V.J. and Sholz , T.K. (2000b). The Earned Income Tax Credit and Labor Market Participation of Families on Welfare. Working Paper, University of California at Los Angeles and University of Wisconsin, Madison.
Job Accommodation Network (1999). Accommodation Benefit/Cost Data. Morgantown, WV: West Virginia University. http://www.jan.wvu.edu/media/Stats/BenCosts0799.html. Access date: March 28, 2001.
Lewis, L. and Farris, E. (1999). An Institutional Perspective on Students with Disabilities in Postsecondary Education (NCES 1999-046). Washington, DC: Department of Education, National Center for Education Statistics.
Livermore, G.A., Nowak, M.W. and Stapleton, D.C. (2001). The Role of Health Insurance in Successful Labor Force Entry and Employment Retention. Washington, DC: Office of the Assistant Secretary for Planning and Evaluation. [http://aspe.hhs.gov/daltcp/reports/lfentry.htm]
Lutzky, S., Alecxih, L.M.B., Duffy, J. and Neill, C. (2000). Review of the Medicaid 1915(c) Home and Community Based Services Waiver Program Literature and Program Data. Washington, DC: Health Care Financing Administration.
Nagi, S. (1965). "Some Conceptual Issues in Disability and Rehabilitation." In: Sussman, M.B., ed. Sociology and Rehabilitation. Washington, DC: American Sociological Association.
National Academy of Social Insurance (NASI), Disability Policy Panel (1996). Balancing Security and Opportunity: The Challenge of Disability Income Policy, National Academy of Social Insurance.
Neubert, D.A. (2000). "Transition Education and Services Guidelines," Transition Education and Services for Adolescents, Sitlington, P.L., Clark, G.M. and Kolstoe, O.P., eds. (Third Edition). Boston, MA: Allyn and Bacon.
Pickett, C. (2000). Children Receiving SSI: December 2000. Washington, DC: Social Security Administration, Office of Research, Evaluation and Statistics.
Swenson, S. and Richards, C. (1999). Report from the Subcommittee on Expanding Employment Opportunities for Young People with Disabilities. Washington, DC: Presidential Task Force on Employment of Adults with Disabilities, Committee on Access to Employment and Lifelong Learning.
Stapleton, D.C., Nowak, M.W. and Livermore, G.A. (2001). Meeting the Diverse Needs of People with Disabilities. Washington, DC: Office of the Assistant Secretary for Planning and Evaluation.
U.S. Department of Education (1996a). "Servicing Youth with Disabilities Within School-to-Work System," Resource Bulletin. [On-Line]. Available: http://www.stw.ed.gov/factsht/bull0696.htm.
U.S. Department of Education (1996b). Eighteenth Annual Report to Congress on the Implementation of the Individuals with Disabilities Education Act. Washington, DC.
U.S. Department of Health and Human Services (1999). Mental Health: A Report of the Surgeon General--Executive Summary. Rockville, MD: Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Mental Health Services, National Institutes of Health, National Institute of Mental Health.
Wagner, M., Blackorby, J., Cameto, R., Hebbeler, K. and Newman, L. (1993). The Transition Experiences of Young People with Disabilities: A Summary of Findings from the National Longitudinal Study of Special Education Students. Menlo Park, CA: SRI International.
Wagner, M. and Blackorby J. (1996). "Transition from High School to Work or College: How Special Education Students Fare." Special Education for Students with Disabilities, Vol.6, No.1 (Spring).
SAMPLE LIST OF EDUCATIONAL ACCOMMODATIONS
Academic and Administrative Flexibility and Support
- Allow extra time for exams, tests, quizzes, and assignments
- Permit exams to be individually proctored (including in hospital)
- Permit exam responses to be verbal, dictated, scribed, or typed
- Provide tests in alternative formats (e.g., essay versus multiple choice)
- Increase frequency of tests and exams
- Administer tests in segments with breaks between segments
- Decrease weight of spelling mistakes
- Allow hand-written papers to accommodate students who do not type
- Provide substitute assignments (e.g., written exercises or other out-of-class exercises may be necessary for a student with a psychiatric disability to best demonstrate grasp of the subject)
- Permit assignments to be produced in alternative formats (e.g. narrative tape instead of written journal)
- Delay assignment due dates to accommodate hospital stays or time off for medical treatment
- Permit incomplete (rather than a failing grade) for students who are unable to complete course requirements in scheduled time due to hospital stays or time off for medical treatment
- Allow course substitutions or waivers
- Provide adaptive physical education courses or sports
- Provide priority seating in a classroom (e.g., near door or near front of room)
- Have teachers face the class while lecturing
- Provide copies of lecture overheads and notes; provide advance copy of syllabus; allow student to photocopy another student's notes
- Move class to better-suited classroom
- Permit beverages in class (helps alleviate dry mouth or fatigue caused by some medications)
- Allow for pre-arranged breaks
- Provide parking passes
- Have school staff administer medication and/or provide reminder to take medication
- Provide assistance with organizational skills
- Assist parents in monitoring homework
- Provide advance notice of assignments (allow students to plan time, energy, and workload and arrange for any needed support in advance)
- Provide orientation and assistance with administrative procedures, registration, financial aid, and course selection
- Allow priority registration
- Allow flexibility in determining "full time" status (for purposes of financial aid and health insurance)
Provision or Allowance of Special Equipment or Technology
- Allow student to use a computer to take exams
- Provide elevator keys
- Provide materials in alternative formats (e.g., enlarged text, Braille)
- Allow student to tape record exam questions and/or answers
- Allow use of calculator and spell checker
- Remove architectural and structural barriers
- Provide or allow textbooks on tape
- Provide or allow TDD or TTY
- Provide or allow assistive listening devices
- Provide or allow talking computers
- Provide paratransit for on-campus mobility
Provision or Allowance of Personal Assistants
- Assign another person (support staff or another student) to accompany the student
- Provide or allow assistant for tasks such as note taking and reminders to assist concentration during lectures
- Provide or allow signers, interpreters
- Provide or allow tutors to assist with classwork
- Provide or allow special lighting or acoustic equipment
ALL REPORTS AVAILABLE
Research on Employment Supports for People with Disabilities: Summary of the Focus Group Findings
Executive Summary: http://aspe.hhs.gov/daltcp/reports/fgfindes.htm
Full HTML Version: http://aspe.hhs.gov/daltcp/reports/fgfind.htm
PDF:
The Role of Health Insurance in Successful Labor Force Entry and Employment Retention
Full HTML Version: http://aspe.hhs.gov/daltcp/reports/lfentry.htm
PDF:
The Role of Supports in Successful Labor Force Entry for Youth with Disabilities
Full HTML Version: http://aspe.hhs.gov/daltcp/reports/2001/youthlfe.htm
Full PDF Version: http://aspe.hhs.gov/daltcp/reports/2001/youthlfe.pdf
To obtain a printed copy of this report, send the full report title and your mailing information to:
U.S. Department of Health and Human ServicesOffice of Disability, Aging and Long-Term Care PolicyRoom 424E, H.H. Humphrey Building200 Independence Avenue, S.W.Washington, D.C. 20201FAX: 202-401-7733Email: webmaster.DALTCP@hhs.gov
RETURN TO:
Office of Disability, Aging and Long-Term Care Policy (DALTCP) Home [http://aspe.hhs.gov/_/office_specific/daltcp.cfm]Assistant Secretary for Planning and Evaluation (ASPE) Home [http://aspe.hhs.gov]U.S. Department of Health and Human Services Home [http://www.hhs.gov]