
U.S. Department of Health and Human Services
State Long Term Care Reform: Development of Community Care Systems in Six States Final Report
Diane Justice, Lynn Etheredge, John Luehrs and Brian Burwell
National Governors' Association
April 1988
PDF Version (167 PDF pages)
This report was prepared under grant #18-C-97923 between the U.S. Department of Health and Human Services (HHS), Office of Social Services Policy (now DALTCP) and the National Governors' Association. Additional funding was provided by the HHS Health Care Financing Administration (now the Centers for Medicare and Medicaid Services). For additional information about the study, you may visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the office at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, SW, Washington, DC 20201. The e-mail address is: webmaster.DALTCP@hhs.gov. The Project Officer was Glen Harelson.
Preparation of this document was supported by a grant from the Office of the Assistant Secretary for Planning and Evaluation through an interagency cooperative agreement with the Office of Research and Demonstrations, the Health Care Financing Administration (HCFA No. 18-C-97923), the Department of Health and Human Services. Mr. Glen E. Harelson is the Project Officer. Printing of this document was supported under a contract with the Health Care Financing Administration, Office of Intergovernmental Affairs (HCFA Contract #500-86-0007). Mr. Richard Chambers is the Project Officer. All opinions expressed herein are those of the authors and do not represent those of the Department of Health and Human Services or the National Governors' Association. Copyright 1988 by the National Governors' Association, Washington, D.C. Reproduction of any part of this volume is permitted for any purpose of the United States Government. Printed in the United States of America.
TABLE OF CONTENTS
- I. STUDY DESIGN
- Major Areas of Inquiry
- Related Research
- II. OVERVIEW OF SIX STATES APPROACHES TO LONG TERM CARE
- Arkansas
- Illinois
- Maine
- Maryland
- Oregon
- Wisconsin
- State Demographic Context for Long Term Care Policy Development
- III. ORGANIZATION OF LONG TERM CARE RESPONSIBILITIES: STATE AND LOCAL ROLES
- Development of State Long Term Care Policy
- State Agency Program Management
- Local Program Management Agencies
- IV. ACCESS TO LONG TERM CARE SERVICES
- Financial Eligibility Criteria
- Functional Eligibility Criteria
- Case Management
- Pre-Admission Screening Programs
- V. SERVICES SUPPORTED BY STATE COMMUNITY CARE PROGRAMS
- Overview of State Service Options
- Home Care Services
- Adult Day Care
- Services Provided in Alternative Living Arrangements
- Quality Assurance
- VI. FINANCING AND MANAGEMENT OF HOME AND COMMUNITY BASED SERVICES
- The Federal Budget and Policy Context
- Overview of State Financing and Management Issues
- Financing Strategies
- Financial Management and Pooling of Funds
- Cost Management
- Management Information Systems
- Budget and Evaluation Processes
- Private Long Term Care Insurance
- APPENDIX I. SUMMARY OF EXPENDITURES FOR LONG TERM CARE SERVICES
- Long Term Care Growth
- APPENDIX II. MEDICAID ELIGIBILITY POLICY AND ITS IMPACT ON HOME AND COMMUNITY BASED SERVICES IN THE SIX CASE STUDY STATES
- Group Coverage Options x Benefit Levels
- Impact of Medicaid Eligibility Options on Coverage of the Elderly
- Eligibility Provisions Unique to Section 2176 Waiver Programs
- LIST OF FIGURES
- FIGURE II-1: Arkansas Organization of Community Care Programs
- FIGURE II-2: Illinois Organization of Community Care Services
- FIGURE II-3: Maine Organization of Community Care Programs
- FIGURE II-4: Maryland Organization of Community Care Programs
- FIGURE II-5: Oregon Organization of Community Care Programs
- FIGURE II-6: Wisconsin Organization of Community Care Services
- FIGURE VI-1: Federal Budget Deficit
- FIGURE VI-2: Federal Medicaid Spending -- Rates of Increase
- FIGURE VI-3: Total State Expenditures for Home and Community Based Care, 1986
- FIGURE VI-4: Percent of Total State Expenditures on Home and Community Based Care Paid by Medicaid
- FIGURE VI-5: Expenditures for Home and Community Based Care as Percentage of Total State Long Term Care Expenditures, 1986
- FIGURE AII-1: Ratio of Non-Institutionalized Elderly on Medicaid to Number of Elderly in Poverty: 1985
- LIST OF TABLES
- TABLE II-1: Poverty Rates
- TABLE II-2: Persons Aged 75+ Living Alone and in Poverty, by State
- TABLE II-3: Population 65 and Over, by State
- TABLE II-4: Growth Rate of Elderly Population 1980-1985
- TABLE III-1: Nursing Home Capacity January 1, 1986
- TABLE III-2: State Agencies Responsible for Long Term Care Programs
- TABLE IV-1: State Supplementation Levels and Medically Needy Levels for an Aged Individual Living Independently in 1986
- TABLE IV-2: Medicaid Coverage of the Elderly in the Six Study States: 1985
- TABLE IV-3: Major State LTC Programs Financial Eligibility Criteria for an Individual in 1986
- TABLE IV-4: Local Agencies Performing Case Management Functions
- TABLE IV-5: Cost Limits on Service Authorization 1986
- TABLE IV-6: Characteristics of Pre-Admission Screening Programs
- TABLE V-1: Major Services Supported by State Community Care Programs
- TABLE V-2: Provider Options
- TABLE AI-1: State Expenditures on Long Term Care Per Individuals Aged 75+
- TABLE AI-2: Other Federal Funds Used for State Long Term Care Programs: Expenditure Trends
- TABLE AI-3: Comparing Rates of Growth in Spending and Population Between the Six Study State and the Nation: Annual Compound Rate of Growth 1982-1986
- TABLE AI-4: Arkansas Expenditures on Long Term Care Programs for the Elderly: 1982-1986
- TABLE AI-5: Summary Table: Arkansas
- TABLE AI-6: Illinois Expenditures on Long Term Care Programs for the Elderly: 1982-1986
- TABLE AI-7: Summary Table: Illinois
- TABLE AI-8: Maryland Expenditures on Long Term Care Programs for the Elderly: 1982-1986
- TABLE AI-9: Summary Table: Maryland
- TABLE AI-10: Oregon Expenditures on Long Term Care Programs for the Elderly: 1982-1986
- TABLE AI-11: Summary Table: Oregon
- TABLE AI-12: Wisconsin Expenditures on Long Term Care Programs for the Elderly: 1982-1986
- TABLE AI-13: Summary Table: Wisconsin
- TABLE AII-1: Coverage of SSI Recipients Under Medicaid
- TABLE AII-2: State Supplementation Levels and Medically Needy Levels for an Aged Individual Living Independently in 1986
- TABLE AII-3: Medicaid Coverage of the Elderly in the Six Study States: 1985
FORWARD
In this country, the public sector responsibility for long term care system development has rested almost entirely at the state level. While federal attention is now being given to proposed financing expansions, long term care has been a significant state policy and budget issue for decades. The state-administered Medicaid program has been the predominant source of third party long term care coverage; therefore, Medicaid's historic bias toward institutional care has significantly influenced the nature and scope of the entire long term care delivery system.
A growing number of states are developing more comprehensive long term care delivery systems that substantially improve the availability of home and community based services. However, state policymakers wishing to develop such systems are often apprehensive over the potential increase in recipients and costs. While demonstration project findings have often shown that such growth is a real possibility, surveys of older persons consistently confirm a strong preference to remain in their homes and community if at all possible. Faced with a growing elderly population in need of these services, the preference for community care, and often severely constrained state resources, state policymakers have frequently expressed the need for affordable strategies to develop and provide community care services.
This study was undertaken to address that state information need by analyzing and comparing the experience and delivery infrastructures in states that have implemented such statewide community care systems. The U.S. Department of Health and Human Services fortunately shared NGA's interest and provided funding for this project. An expert panel selected study states that have made better use of limited resources by integrating multiple long term care programs and services.
The text begins with an Executive Summary and Policy Implications section which provides an overview of the most significant findings from the study. A descriptive analysis of each of the six states' long term care program infrastructures can be found in Chapter II. The remainder of the study presents comparative analysis of the study states' policies, organizational structures, and financing and delivery system characteristics. For readers interested in a quick initial review of the many subissues covered, we have highlighted key observations throughout the text.
The publication of this document is the culmination of an exhaustive effort by Diane Justice, who served as project director. The analysis reflects insights from well over 100 individuals who set policies for, manage, or analyze state community care systems. A wealth of information and experience is presented that we hope will be more broadly applied to better meet the needs of frail elderly persons.
Rick Curtis Director of Health Policy Studies
ACKNOWLEDGEMENTS
State Long Term Care Reform compares and analyzes the approaches undertaken by six states to make their systems more responsive to the needs of older people. The success of these initiatives are in large measure due to the professional expertise and personal dedication of a diverse group of state officials who are intent upon improving the lives of older people in need of long term care. We are deeply indebted to these individuals who willingly participated in time consuming interviews in order to share their insights with other states. They offered candid observations of both the strengths and weaknesses of their state's programs. Over 100 individuals were interviewed during the course of this project.
State officials who served as the primary state contacts for this project deserve special thanks. They not only provided extensive background information but also suggested key state policymakers who should be added to our interview schedule. In addition, they reviewed drafts of this report to ensure its accuracy. Their assistance was invaluable. They are Carol Rasco and Herb Sanderson (Arkansas), Jean Blaser (Illinois), Trish Riley (Maine), Donna Folkemer (Maryland), Dick Ladd (Oregon) and Tom Hamilton and Donna McDowell (Wisconsin).
The identification of policy issues that would be of greatest interest to other states was aided tremendously by the project advisory committee, composed primarily of state officials; the members are listed below. In addition their review of the interview questionnaire helped sharpen our inquiries and elicit more informative responses.
At various points during the project several individuals made unique contributions. As noted on the Title page, Chapter VI and Appendix I and Appendix II were separately authored by Lynn Etheredge, John Luehrs and Brian Burwell, respectively. Bonnie Preston conducted background research on the twelve state long term care systems reviewed in the early stages of this project and coordinated scheduling of the numerous interviews conducted during site visits to the study states. Throughout the duration of the study, John Luehrs generously provided substantive input, guidance on the administrative aspects of the project and unflagging support. Bob Applebaum drafted portions of the interview guide. Special appreciation goes to Janine Breyel, Marie Alcazar, Cindy Wellons and Jennifer Fohs for their tireless work in preparing this document for publication. Felicity Skidmore's extraordinary editing skills significantly improved the format and style of this manuscript.
Appendix I presents comprehensive, longitudinal data and information on state spending for long term care services for the elderly across all programs and funding sources. To our knowledge, this is the first time that such an effort has been made. Completing this task required substantial work by officials in each state to compile the data and respond to numerous questions from NGA staff. Our thanks to the following individuals and their staffs: Herb Sanderson (Arkansas), Jean Blaser (Illinois), Elaine Fuller (Maine), Lillian Moran (Maryland), Dick Ladd (Oregon) and Tom Hamilton (Wisconsin).
This project was made possible by funding from the Office of the Assistant Secretary for Planning and Evaluation (ASPE) granted through the Health Care Financing Administration (HCFA). Glen Harelson of ASPE, who served as the project officer and Leslie Saber (HCFA) were particularly supportive. Their knowledge of long term care issues and experience with other research projects were very helpful.
The National Association of State Units on Aging (NASUA) and the National Governors' Association (NGA) provided substantial financial support for the staff time necessary to conduct this project. Special appreciation is extented to Dan Quirk, Executive Director of NASUA who willingly reorganized staff responsibilities to allow the project director time to conduct this reseach.
Rick Curtis, Director of Health Policy Studies, National Governors' Association, provided invaluable guidance on all aspects of this project. His understanding of how state government works, combined with his substantive knowledge of long term care issues contributed greatly to the quality of this report. His support, enthusiasm and patience made it possible to complete this study within the context of competing time demands on project staff.
Diane Justice Project Director State Long Term Care Reform Study
ADVISORY COMMITTEE FOR THE STUDY OF STATE APPROACHES TO LONG TERM CARE SYSTEM REFORM
| Gerald AdlerOffice of Research DirectorHealth Care Financing AdministrationDepartment of Health and Human Services | Barbara MatulaDirectorDivision of Medical AssistanceRaleigh, North Carolina |
| Thomas Brown, Jr.DirectorOffice of Program ManagementDepartment of Health and Environmental Control | Douglas NelsonDeputy DirectorCenter for the Study of Social PolicyWashington, DC |
| Pam DotyOffice of Legislation and PolicyHealth Care Financing AdministrationDepartment of Health and Human Services | Geoffrey PerselayActing CommissionerDepartment of Human ServicesTrenton, New Jersey |
| Saddia GreenbergOffice of Research and DemonstrationAdministration on AgingDepartment of Health and Human Services | Charles ReedAssistant SecretaryAging and Adult Services AdministrationOlympia, Washington |
| Nellie JohnsonDeputy CommissionerDepartment of FinanceSt. Paul, Minnesota | Scott UmbreitAdministratorOffice of Facility Management and CoordinationSpringfield, Illinois |
EXECUTIVE SUMMARY AND POLICY IMPLICATIONS
The financing and delivery of long term care services for the elderly is one of the most pressing issues facing the states today. For the past two decades, state governments have made major commitments to expand these services. Those commitments are reflected in the expenditure of state matching funds to support services through Medicaid, in the establishment of long term care programs financed totally with state general revenues, and in the development of detailed policies governing the provision of long term care services.
Over the past several years, most states have been faced with severe fiscal constraints due to recession-induced revenue declines and reductions in federally supported domestic programs. At the same time, there has been significant growth in state Medicaid expenditures devoted to nursing home care. Long term care spending now accounts for almost half of all expenditures in Medicaid, which usually is the largest state-administered program in state budgets. These fiscal pressures are compounded by the dramatic rise in the number of persons over age seventy-five, the population group most likely to need long term care services. Since 1980 this group has grown three times as fast as the overall U.S. population.
Until recently long term care services for the elderly were considered synonymous with nursing home care. Public officials, physicians, insurers, and even the elderly shared this perception. Medicaid became, by default, the primary federal and state funding source for long term care services and practically the only source of third party payment. Regulations and limited community service options under that program reinforced the notion that older people needing long term care services by definition needed nursing home care. This resulted in an institution-based delivery system.
A policy revolution now is underway. When state debates focus on long term care system reform, discussions now are likely to highlight ways to expand the availability of community care services rather than emphasize only the detailed nuances of nursing home reimbursement.
Older people strongly prefer to receive long term care services in the community. To date, these strong preferences have been more frequently and forcefully articulated in state capitols than in Washington, D.C. The Medicare and Social Security programs have been the primary focus of elderly advocacy efforts in the nation's capitol; long term care has been the top priority advanced in state capitols.
Faced with the need for long term care services for a growing elderly population, the preference for community based care, and constrained state resources, many states are seeking more affordable strategies for restructuring long term care financing and delivery systems. There is a sense total long term care costs for the elderly are destined to rise if for no other reason than the rapid growth of this population. Therefore, state policymakers are attempting to channel the growth in expenditures to services provided in the community, as the elderly prefer, instead of to continued expansion of nursing home beds.
Important lessons can be learned from those states which have been particularly successful in developing new systems of care. Their experiences certainly are relevant for other states designing similar community care systems. Private insurers also can benefit from state successes in managing total costs while responding to the preferences of older people for care provided in their homes. Federal policymakers, facing increased demands for a national long term care strategy, may find that the structure and operation of large statewide systems provide more pertinent insights than the experiences of individual community projects.
The NGA study provides an in-depth comparative analysis of six states' approaches to long term care system reform. Arkansas, Illinois, Maine, Maryland, Oregon, and Wisconsin were chosen for analysis because of their successful experiences in integrating multiple long term care financing and delivery systems. The study was not designed to formally evaluate these state systems; instead their characteristics were analyzed and compared to identify for other states a broad range of policy options which already have been tested. The study's findings are presented to highlight the range of decisions states must make in designing new approaches. Individual states can combine various system components to reflect their unique demographic, administrative, and political environments.
Major Features of State LTC Systems
Community care systems for the elderly are not developed in a vacuum, but are designed within the context of human services delivery systems developed to address other concerns. In designing new long term care systems, states must integrate existing services for the aged, including social services and health. They cannot start from scratch. In order to overcome the fragmentation of existing service programs and make better use of the new resources being allocated to long term care, states are reorganizing the administrative responsibilities of state and local agencies.
STATE AGENCY ADMINISTRATION. Three basic models of state agency structures have emerged to manage long term care systems. One consolidates all long term care responsibilities covering both institutional and community based care into a single, sole-purpose agency; this involves major reorganization of state government. The Oregon Senior Services Division manages Medicaid payments to nursing homes, Medicaid home and community based services waivers, the Older Americans Act, and state general revenue funds devoted to community care for the elderly. Interestingly, of the six study states, Oregon also has by far the largest proportion (30.1 percent) of its long term care budget going to community care services. Under this organizational model, all long term care expenditures for the elderly are consolidated into one budget, which makes resource allocations between community based care and institutional care a direct and visible trade-off.
A less radical model uses a human services umbrella agency structure, with some internal shifting of responsibilities and increased interdivision coordination. Arkansas, Maine, and Wisconsin use this model.
The third model retains independent, cabinet-level agencies for managing various programs, but establishes an official interagency long term care committee to at least keep agencies informed of each other's activities and, preferably, to coordinate the development of interagency policies as well. Illinois and Maryland use this model.
In all three models, the state office on aging and the Medicaid agency usually have been assigned primary responsibility for long term care program management. Given their respective traditional approaches, compromises are required. Aging agencies have been forced to accept some of the rigidities of the Medicaid program to have access to its funds. Medicaid agencies have had to adjust to programs which are much less standardized than hospital and nursing home care.
The organizational challenge to state governments is to integrate the resource allocation and policy development activities of the various state offices responsible for some aspect of long term care so that a coordinated system of care can be developed, rather than one reflecting a diffuse constellation of individual programs. Regardless of the organizational approaches adopted, the issues which must be examined across various programs are the same. They include: designing a single delivery system supported by multiple funding sources; developing eligibility criteria for individual programs to ensure equitable treatment of persons with similar needs and resources; and examining the mix of community care services supported by each funding stream. Ultimately, the goal of these coordinated efforts is to create the continuum of care which each individual program rhetorically has embraced but cannot by itself achieve.
LONG TERM CARE DELIVERY SYSTEMS. How programs are organized at the local level is even more important than how state responsibilities are organized. Older people come in direct contact with local agencies and their differing eligibility criteria, service packages, and funding sources. If state policies are successful, the elderly will have access to appropriate care without having to contact multiple agencies to receive services for which they are eligible. Therefore, most of the study states have designated a single local agency in each part of the state to serve as the client access point for receipt of all publicly financed community care programs. Centralizing entry helps make the system less fragmented from the perspective of older people in need of assistance, while helping states gain better control of total program costs. Client assessments, pre-admission screening programs, and case management are the key components of access systems for community based care programs. Each are present in the six study states.
Client assessments for community based care focus on an older person's ability to conduct activities of daily living. The results are used by case managers to initially determine if an individual is sufficiently impaired to qualify for long term care programs. Most of the six states' long term care programs provide services only to those older persons who have impairment levels equivalent to those required for nursing home care.
The scope of pre-admission screening programs in the six study states varies substantially. One key difference is the target population group which must be screened--specifically, whether required participation is limited to Medicaid-eligible nursing home applicants or whether a broader group is included, such as persons who are expected to become eligible for Medicaid within a certain time frame after nursing home placement. Another difference is whether the screening process results in a binding decision on placement or is merely advisory. State officials note that since most older people prefer to stay in the community, simply having a process to discuss community care options helps limit nursing home entry even if it only results in an advisory recommendation. And, locating the screening programs in the same local agency which serves as the entry point for community care services increases the potential that clients will receive advice on all the alternatives.
Case management functions are central to the entire community care system, especially when multiple funding sources with differing eligibility criteria and service providers are involved. As a result, state policies on the designation of case management agencies are among the most hotly debated long term care issues. Arkansas, Maine, and Oregon have selected area agencies on aging, while Wisconsin and Maryland have designated county social services departments. Illinois uses local agencies chosen on a competitive basis.
Specific functions assigned by the six states to case management agencies vary. However, general areas of responsibility include developing cost effective individual care plans, authorizing needed services, and following up to ensure needed services actually are provided. Most importantly, case management and assessment agencies are the only client access point for receipt of services financed through the major community care programs in the study states. States have limited the resources which case managers can spend for program participants; this limit either is applied to each client's care plan or is averaged over the case management agency's entire caseload. Usually the limit is tied to the cost of nursing home care.
The scope of services brokered through case management are fairly similar in the various states' long term care systems. The most commonly provided services are personal care, homemaker, and chore services. The assistance provided often includes light housekeeping, meal preparation, and assistance with dressing, bathing, and other aspects of personal care. By specific design, the states' policies allow substantial flexibility in the types of services which can be supported with public funds, consistent with the philosophy of tailoring programs to individual needs.
FINANCING OPTIONS. The six study states each use a combination of funding sources to support community care systems, even though it would be much easier to use only one funding stream and thereby avoid the multiple of rules and restrictions accompanying each individual program. Due to these restrictions, particularly those associated with Medicaid, however, no single source is flexible or large enough to support a comprehensive long term care system. The three major financing sources are state general revenues, Medicaid home and community based services waivers, and the Medicaid optional state plan services of personal care services and adult day care. Each of the study states uses one of these as its primary funding vehicle supplemented by one or more of the other funding sources, along with smaller amounts of the Older Americans Act and the Social Services Block Grant. Wisconsin, Illinois, and Maryland primarily use state funds. Oregon relies chiefly on the Medicaid home and community based services waiver authority to support most long term care services. Arkansas finances its community care system by exercising the option to cover personal care services under the Medicaid state plan. Maine uses a combination of all major funding sources.
Each of these financing sources has advantages and disadvantages. State general revenues offer maximum flexibility in designing community based care systems. The obvious disadvantage is the lack of federal financial participation. All of the study states use state general revenues to some extent, either as the primary vehicle or as a supplement to expand the scope of available services, or to partially or fully subsidize care for persons who are not financially eligible for Medicaid.
The Medicaid home and community based services waiver, established as part of the Omnibus Budget Reconciliation Act of 1981, can provide a broad range of non-medical long term care services. Four of the study states make some use of the waiver authority for providing services to the elderly, with Oregon using the authority most extensively. This state was the first in the country to be granted such a Medicaid waiver, and as a result, its program is substantially larger than most waivers approved in subsequent years. Waiver programs are viewed as a mixed blessing by the study states. The federal financial participation in community care programs is very appealing. Yet, state officials cite changing federal interpretations of program rules, stringent ceilings placed on the number of persons who can be served, and excessive administrative costs as factors limiting the usefulness of this financing source.
Section 4102 of the Omnibus Reconciliation Act of 1987 provides states with a second home and community based services waiver option that will address some of these problems. States using this new option will be able to increase the number of persons served and expenditures for Medicaid waiver services as long as total Medicaid long term care spending (including nursing home outlays) for the elderly does not increase more than a specified percentage above outlays for the base year. The percentage growth limit until October 1, 1989 is 7 percent per year.1 After this date, the rate of increase is the greater of 7 percent or a formula to be developed measuring: the state's age seventy-five and older population growth, plus appropriate indices of goods and services costs facing long term care providers, plus a 2 percent intensity factor. This new option may be a way for those states with adequate base-year Medicaid outlays for total long term care to meet the needs of a growing population by substantially expanding community care while restraining the growth of institutional services. In March 1988, Oregon submitted the first application for a waiver under this new authority.
Exercising the option to cover personal care and adult day care services under the Medicaid state plan is the third major option for financing state community based care initiatives. In contrast to waiver services, no extraordinary administrative requirements are imposed and no ceilings are placed on the number of persons who can receive services. However, since services are provided under the Medicaid state plan, states cannot limit this service to just the elderly long term care population, limit availability to one geographic area, or increase income eligibility thresholds to make them more comparable to nursing home eligibility levels.
Policy Implications
The experiences of the six study states in designing large statewide community care programs have implications for policy development in other states, for the expansion of federal support for community based care systems, and for private insurers responding to the long term care needs of a rapidly expanding older market. Several observations are relevant for all three audiences.
First, all six states have expanded community based care services without generating runaway costs in total long term care spending. While total costs have risen over a five-year period, the increases are modest, averaging 6.2 percent annually per person age seventy-five and older. (See Appendix I, which analyzes long term care expenditure growth in each of the six states.) Fears over uncontrollable costs and increases in service utilization have led states, the federal government, and private insurers to approach expansion of community based care services with great caution. The experiences of the study states indicate that, even when community care services are a benefit under a public entitlement program, overall costs can be contained. Several factors help make community care programs affordable. limiting program eligibility to persons who have multiple limitations in conducting activities of daily living, using a managed care approach to authorize the amount and scope of services needed by individuals, and establishing cost sharing provisions for moderate-income persons all help keep program costs manageable.
Second, the six states have shown that some aspects of community care systems can be tightly structured and uniform statewide without compromising their ability to flexibly respond to individual service needs. Uniform assessment tools, explicit financial eligibility criteria, and system entry channeled through case management agencies have all made access to community care more predictable from a client's perspective and more standardized as viewed by program administrators. Yet, the actual services provided often are very loosely defined, giving local program managers considerable latitude in tailoring service packages to individual needs.
Third, non-medical supportive services form the core of state long term care programs. State officials note that although some limited skilled home nursing care may at times be provided, community based long term care services usually are needed by older people in response to limitations in functional capacity as opposed to specific medical conditions. The services needed most often are non-medical, in-home supports such as homemaker and personal care. Since federal and state officials and private insurers are much more familiar with skilled home health services than with these other services, there may be a tendency to structure supportive services in a medical context. Officials in the six study states believe that would be a mistake.
Some study findings are particularly relevant for other states. The experiences of the six states indicate that some state general revenues are essential for developing a community care system which meets the needs of low- and moderate-income persons. Despite exemplary state efforts to improve coordination and to strengthen management control and allocate resources wisely, rules tied to each federal funding source limit the categories of persons who can be served and the scope of services which can be funded.
Second, containing the growth of Medicaid nursing home expenditures was an explicit component of state strategies to expand community care in four of the six study states. In each case, certificate of need policy was used to limit the number of new beds constructed. State officials found the notion of "reinvesting" into community based care the savings resulting from a freeze on bed expansion to be a useful concept. This policy not only articulates the end goal of long term care system reform, but also actually reduces the rate of growth in Medicaid nursing home expenditures. Curtailing future institutional expenditures will free state resources to expand community based care.
Third, each of the six states developed their systems incrementally. Three of them (Maryland, Wisconsin, and Oregon) phased in statewide implementation of long term care initiatives by geographic area. All added various program components over a period of several years. For example, pre-admission screening programs often were added after the supply of community care services was expanded, enabling screening program staff to offer persons seeking nursing home placement some viable community service options. However, since the various components of community care systems all interrelate, undertaking a comprehensive planning process before major new initiatives are underway makes it easier to add new elements in the future.
The study states found that a broad planning effort achieves other objectives. It helps get multiple agencies and organizations committed to the success of long term care initiatives and fosters consensus on policy goals and objectives. This lays a positive framework for resolving more difficult operational conflicts in the future. Membership organizations of older people often were active participants in state planning processes. Generally they did not press for overly ambitions proposals but rather understood state fiscal limits and worked within them. A consistent concern of these groups in all states but Wisconsin was designing a system which was not identified as being part of the "welfare system." This orientation affected their preferences for the selection of lead management agencies at the state and local level, but did not preclude support for client cost sharing policies and other mechanisms to maximize allocation of available state resources to persons with the least ability to pay.
Other study findings are especially pertinent for the development of federal financing policies for community based long term care. First, one of the most difficult tasks faced by the six study states was linking together separate systems for social services, aging programs, and health care delivery. Decisions had to be made concerning the best local agencies to perform case management, assessment, and direct service delivery. In addition, states had to decide how to expand the capacity of the delivery system to provide an increased supply of services. Sometimes new provider agencies were created, other times new types of services were developed which previously were not available, and frequently existing agencies took on new responsibilities. State activities to build the capacity of local delivery systems necessarily varied with state circumstances. If federal long term care initiatives are to relate to existing state human services delivery systems, states are in a unique position to design approaches that will best build upon the existing infrastructure.
Second, where possible the six study states preferred to hold local long term care systems accountable for end results rather than trying to control every detail of local administration. This approach recognizes differences among communities in local practices and traditions and avoids emphasizing process requirements. As more states adopt new community care programs, diversity among states will increase. This model of accountability used by the study states will be appropriate for federal/state relationships in any new federal community care initiative.
Finally, the six study states have demonstrated to private insurers and other public payers that it is feasible to provide multiple community care services (not traditionally covered by health insurance) if there is a systematic process for assessing client needs, authorizing a package of services, and coordinating multiple providers. Case management systems can perform such functions and allow private or social insurance plans to expand the services covered under long term care policies to include various social supports which are more affordable than medical services traditionally covered by insurance policies. Insurers have been reluctant to offer these services, which typically have low unit costs, in part because they view the administrative costs to be disproportionately high. In addition, insurers are concerned about uncontrollably high utilization rates since they expect older people to actively seek these services while going to great lengths to avoid nursing home placement. The six study states had similar concerns when their programs began but found that improved assessment techniques can effectively limit the eligible population and that case management structures can allocate services to individual clients within overall budget limits.
I. STUDY DESIGN
Major Areas of Inquiry
Important lessons can be learned from states that have made significant progress in developing more balanced systems of care. The purpose of this study is to provide an in-depth analysis of the approaches to long term care system reform adopted by six such states in order to assist other states in developing similar systems. The study focuses primarily on how states have integrated multiple resources and consolidated policy and management control of long term care services at the state and local levels. Since no single state or federal funding source is sufficiently flexible or large enough to support a comprehensive long term care system, states use a patchwork of multiple programs, allocating resources to community care from several funding streams. Each of these programs have their own rules, are frequently administered by different agencies in state government, and may use separate local delivery systems. This study explores how six states have coordinated these federal and state programs to maximize available resources while creating a more rational system of care from the perspective of elderly consumers.
Arkansas, Illinois, Maine, Maryland, Oregon and Wisconsin were chosen for in-depth analysis because of their successful experiences in integrating multiple long term care financing and delivery systems. As the first step in selecting the study states, documents from twenty-one states describing the programmatic and financing features of their long term care systems were reviewed by project staff. Each of these states were measured against the criteria for inclusion in the study established under the grant which supported this research from the U.S. Department of Health and Human Services (HHS). The criteria were three: each potential study state was required to have a statewide community care system for the elderly, multiple funding sources devoted to community based care, and state level organizational structures for consolidating long term care management responsibilities. While an increasing number of states have established statewide community care programs, the three selection criteria together were present only in twelve states. Those states included the six study states plus Colorado, Connecticut, Georgia, Minnesota, South Carolina and Texas.
Project staff prepared a report on the organizational structures and financing mechanisms used by the twelve states for managing state long term care delivery systems. A panel of state and federal officials and researchers convened by HHS used this background information to select the states to be included in the comparative analysis. Since all twelve states met the basic criteria for inclusion, the panel's primary concern was to select a mix of states representing a diverse set of characteristics. Of particular interest was selecting a combination of states with differences in state level organizational structures, local delivery systems, financing mechanisms, geographic location and population size.
In addition to collecting written information on each of the six states' systems, project staff conducted week-long site visits to each of the study states. A structured information collection guide was used to conduct approximately 20 interviews in each state, with a wide range of individuals involved in the development of state long term care policy. Key executive branch respondents in each state included a member of the Governor's staff, the directors of the state aging and Medicaid offices, staff responsible for health planning and the Social Services Block Grant, and an official of the state budget office. Other key contacts included state legislators, local level program managers, advocacy organizations of older people and state associations of nursing home providers and home health agencies. Substantial amounts of time were spent with middle management state staff who have primary responsibility for long term care programs.
Reviewing written materials was the primary vehicle for collecting factual program information; interviews were used to solicit the perspectives of key contacts on why certain strategies were chosen, the major implementation problems faced, and an assessment of both the successes and shortcomings of state policies. Given the diverse group of individuals interviewed within each state, the level of consensus on key points was remarkable. State officials also provided candid assessments of their systems' limitations, reflecting in part the continual process of long term care system reform.
Related Research
Federally supported research and demonstration projects conducted over the past decade have made significant contributions to the knowledge base needed to establish community care systems. Many of these projects have been undertaken in partnership with state governments through experimentation with Medicaid policy changes. Such efforts -- conducted in the late 1970s and early 1980s in limited geographic areas of New York, Georgia, South Carolina, Connecticut, California and Oregon -- identified improved ways of organizing and managing community care services as alternatives to institutional care.
The largest research effort undertaken in this area was the National Long Term Care Channeling Demonstration, begun in 1980 and completed in 1986. The demonstration states applied for and won contracts from the U.S. Department of Health and Human Services to conduct demonstrations in designated local sites to test the effects of using case management systems to improve the provision of community care services. States participating in the research include Florida, Kentucky, Maine, Maryland, Massachusetts, New Jersey, New York, Ohio, Pennsylvania and Texas. The final report on the Channeling Demonstration reports notes "the channeling evidence indicates that expansion of case management and community services beyond what already exists does not lead to overall cost savings. But it does yield benefits in the form of increased in-home care, reduced unmet need, and improved satisfaction with life for clients and the informal caregivers who bear most of the care burden. Whether these benefits are commensurate with its costs is a decision for society to make."2
In addition to the awards made to the 10 states for multi-year channeling demonstration projects, 15 other states received one-year systems development grants to formulate state strategies for improving the coordination and management of long term care services. States receiving these federal grants include Arkansas, California, Colorado, Delaware, District of Columbia, Idaho, Illinois, Minnesota, New Hampshire, North Carolina, Oregon, Rhode Island, South Dakota, Washington and Wisconsin. These grants were awarded through a competitive process at the same time that the other 10 states were selected for channeling demonstrations. These grants helped to further support existing state interests in improving the delivery of long term care services.
Knowledge about long term care continues to grow as research produces new findings. To date, most long term care research has focused on program design and implementation within individual communities; minimal attention has been given to research on statewide programs. This void has left states with limited experience to draw upon in developing complex large scale systems. Certainly the results of long term care research based on individual community programs can give states guidance in designing components of statewide systems such as individual client assessments and case management functions. However, more than just structuring individual program components, states must consider how to combine these components to foster community care systems that can fit diverse local delivery systems. Often states face the trade off between the desirability of flexible programs with significant local discretion in implementation and the need for tightly managed cost effective systems. This study analyzes the approaches used by six states in addressing this dilemma.
II. OVERVIEW OF SIX STATES APPROACHES TO LONG TERM CARE
The approaches to long term care system reform in the six states included in this overview share the same fundamental goal: to create a more rational allocation of public resources between community based and institutional care. They share other similarities as well. They have all developed managed systems of care which coordinate services needed by frail older people through a central access point. They have all used state funds to greatly expand the scope of available community based services to meet these needs. And regardless of their current program structure, they have all built their systems incrementally, on foundations laid in the late 1970s.
There are also significant differences, however. In some states, for example, nursing home capacity controls are integral components of larger strategies for increasing community care options. In other states, growth in nursing home expenditures has never been considered a deterrent to the expansion of home and community based services. Some states have targeted assistance primarily to Medicaid eligible individuals. Other states have subsidized care for moderate income older people as well.
This chapter reviews the evolution of each state's long term care initiatives, beginning with a brief summary of the long term care system currently in place and highlighting major milestones. These experiences make it clear that lasting change does not come easily or quickly.
Arkansas
Personal care services financed through the state's Medicaid program constitute the core of Arkansas' community based long term care system. By exercising the option to cover personal care services under the authority of the Medicaid state plan, Arkansas has not needed a Home and Community Based Services waiver to expand in-home services for the elderly. In fiscal year 1986, $10 million in Medicaid funds were spent in Arkansas for this purpose.
Medicaid state plan services are augmented by the state-funded Supplemental Personal Care Program, serving lower-income older people whose incomes are higher than the Medicaid eligibility ceiling but below 125 percent of poverty. State funds also finance the Alternative Care Program, which supports a variety of services such as day care, chore and respite services, informal caregiver training and support groups. In addition, the Social Services Block Grant and the Older Americans Act both fund some community care services.
Under contract with the state Department of Human Services, locally based Client Assessment Teams conduct functional assessments of all clients seeking Medicaid personal care services, authorize the amount of care to be paid by Medicaid, and refer clients to personal care providers. In one quarter of the state, these Client Assessment Teams also conduct pre-admission screening for Medicaid clients seeking nursing home care. In the rest of the state, determination of need for Medicaid funded nursing home care is performed at the state level through a paper review of client information. Local offices of the Department of Human Services determine whether a client meets the financial eligibility criteria for Medicaid.
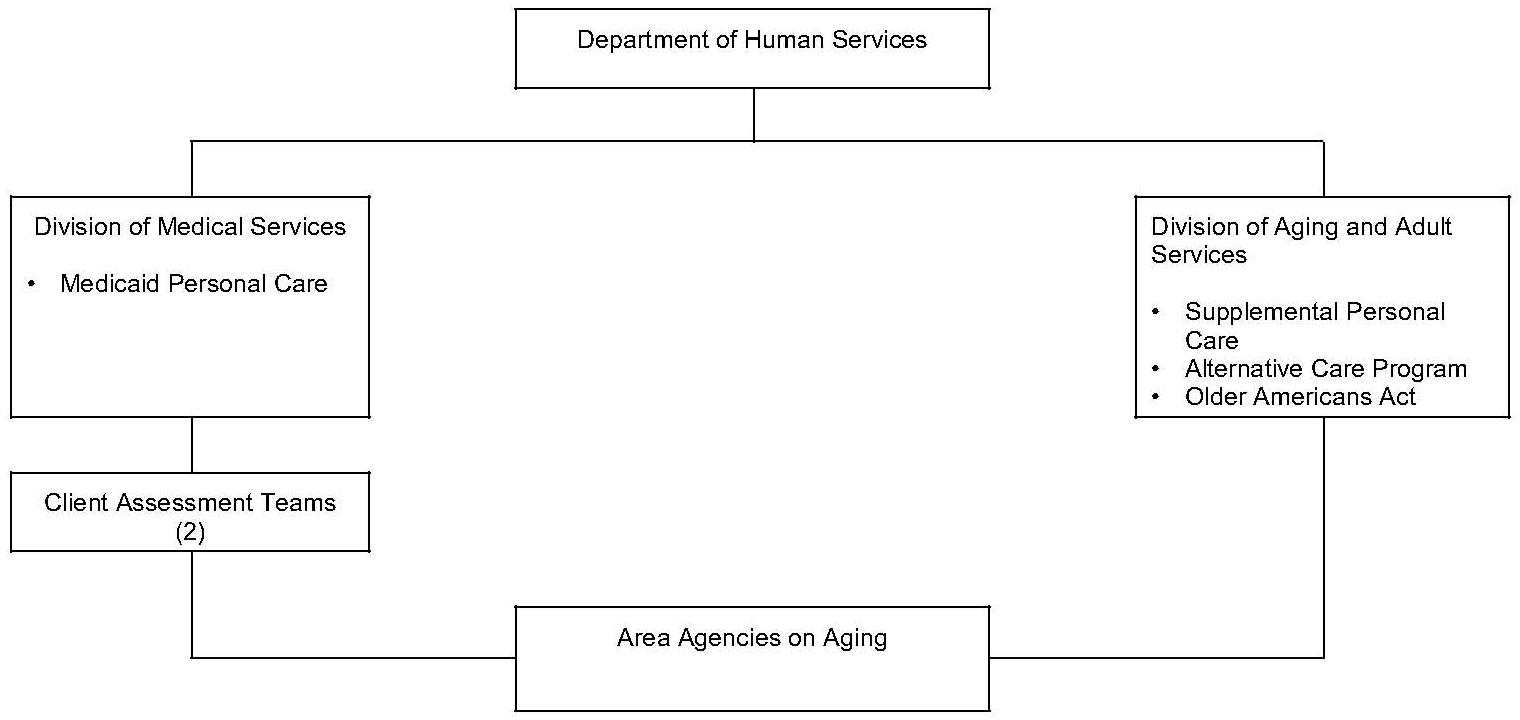
Within state government, administrative responsibility for community based care programs is shared by two components of the Department of Human Services -- the Division of Aging and Adult Services and the Division of Economic and Medical Services. In most parts of the state, area agencies on aging actually provide the personal care services. In two areas of the state, however, these agencies are precluded from direct service delivery because they have statewide responsibility for the Client Assessment Teams and would face potential conflicts on interest. A community action agency and a local health department provide personal care services in those two regions. Figure II-1 depicts the organization of community care programs in Arkansas.
| FIGURE II-1: Arkansas Organization of Community Care Programs |
 |
DEVELOPMENT OF STATE POLICY INITIATIVES. Arkansas' initial efforts to establish community based care can be traced back to 1977, when an area agency on aging in one region of the state initiated a small demonstration project providing in-home services to persons at risk of entering a nursing home. This effort was funded in part by state funds and in part through the Older Americans Act. The following year, with a $110,000 grant from the Administration on Aging, a case management system was implemented to better coordinate the provision of in-home services.
Since funding for this initiative was only temporary, state officials and project staff focused on securing more permanent financing. An agreement was developed among the state Medicaid division, the state aging division and the area agencies on aging to amend the Medicaid state plan to include personal care as a covered service. With little fanfare or debate the legislature approved a proposal to allow state funds which previously had been spent for in-home services to match Medicaid expenditures for personal care. Area agencies on aging became the only certified providers of personal care services, with the state office on aging playing a major role in establishing service standards and operating procedures.
Three years later, in 1982, the legislature passed a bill which reflected support for further development of community based care as well as concern about accessibility and coordination of existing services. The legislation mandated the various divisions and agencies involved in long term care to establish assessment agencies on a demonstration basis in limited parts of the state to test procedures for conducting client assessments and making referrals to appropriate care providers.
The executive branch's response was the creation of two pilot Client Assessment Teams (CAT) to conduct individual client functional assessments in one quarter of the state. The CAT teams also served as the state's agent in authorizing the provision of Medicaid funded long term care services -- including personal care, home health and nursing home care -- in those regions. Area agencies on aging were selected in each of the two regions to carry out the CAT functions; a local health department and a community action agency became personal care providers in those regions since the CAT agencies were precluded from direct service delivery.
The expansion of community care stimulated policymakers to undertake an intense examination of Medicaid institutional expenditures, particularly as they related to the supply of nursing home beds. In 1983 a two-year moratorium was placed on nursing home construction, during which the State Health Coordinating Council conducted an in-depth review of the existing criteria used for certificates of need and developed a long term care need methodology. Working through a study committee comprising representatives of other state agencies, consumers and providers, the council applied the new methodology to an examination of the supply of nursing homes, board and care facilities and in-home services. The resulting projections called for major increases in personal care and board and care facilities with very minimal, selective additions to the nursing home bed supply. Since that time there have been no certificates of need approved for nursing home construction.
To bring about an increased supply of personal care, one of the major recommendations of this study committee was that the availability of personal care services be expanded beyond the Medicaid-eligible population and that other types of services be developed. In his 1985 legislative budget request, Governor Clinton proposed and received funding for a new two-part program. The first part is the Supplemental Personal Care Program which, as noted, serves older people whose incomes are higher than the Medicaid eligibility ceiling but below 125 percent of poverty. The second component is the Alternative Care Program which funds one Community Based Care Developer in each area agency to identify unmet needs and develop new services to meet those needs. The Alternative Care Program also supports a variety of activities and services for family caregivers.
With the advent of these two programs and the growth of the Medicaid personal care program, the state Department of Human Services decided to gain more control over the authorization process for personal care services. The Client Assessment Teams which covered two regions of the state were expanded to have statewide responsibility for conducting client assessments to determine eligibility for personal care and home health. Nursing home pre-admission screening was not expanded beyond the pilot two regions.
FACTORS SHAPING ARKANSAS' APPROACH. Arkansas has one of the oldest populations in the country, ranking third in the nation in the percentage of its population age 65 and over. It also has one of the highest poverty rates in the country; in 1980, 55 percent of Arkansas' population age 75+ living alone had incomes below the poverty level. This combination makes the use of Medicaid to fund community care services a very viable approach for Arkansas. Despite stringent Medicaid eligibility criteria (federal SSI income and asset standards, no medically needy program) the high poverty rate results in many older people qualifying for care under Medicaid. And the low per capita income level results in a very favorable ratio of federal financial participation (75 percent).
The possibility of using Medicaid waivers has been consistently rejected as a funding alternative in Arkansas. The high investment of state staff time required and the multitude of federal policy constraints are frequently cited as reasons for this decision.
There is no single major initiative or event which dramatically shaped the service delivery system in Arkansas. The milestones are subtle, building gradually and steadily on current or previous activity. State officials note that this incremental approach is a major factor in their state's success. With no dramatic new initiatives there have also been no major system upsets.
Several factors help to explain the gradual nature of Arkansas' system development. First, until 1986 the Governor was elected to only a two-year term. The shortness of the term had two disadvantages. It allowed minimal time to accomplish any major initiative. It also led to instability in the state's leadership -- when the Governor changes, so do most of the top level management staff in state agencies. Nonetheless, the strong support for community care by Governor Clinton and, in the early years, Governor Pryor, is frequently cited as one reason for the program's success. The second factor restricting rapid policy change is the particularly difficult state fiscal climate, although fiscal stringency has not prevented the Governor from proposing and the legislature from approving a commitment of new state funds for services provided to low income older people above the Medicaid eligibility limit. The third factor contributing to the incremental growth of home care services is the political strength of the nursing home industry. This is cited repeatedly by state officials and advocacy groups as a deterrent to more dramatic program expansion. Recognition of the industry's power, in fact, is one of the major reasons that the pre-admission screening functions of the client assessment teams were not extended statewide along with personal care authorizations.
The American Association of Retired Persons and the area agencies on aging are the primary advocate groups pushing for an expansion of community care services. In fact they share an office in Little Rock during the legislative session. There is a strong perception of legislative support for home care. But the nursing home lobby is stronger than the community care lobby. This seems to be because the nursing industry has a clear sense of what they want, whereas there is still an experimental aura about home care, with uncertainty about where the system is headed.
State officials share these concerns and frequently mention that no interagency long range planning effort has yet been undertaken. A major goal of these officials is to enhance their policy analysis and planning capacity over the next several years.
Illinois
The major components of Illinois' community long term care system are under the umbrella of the state's large Community Care Program (CCP). In response to a class action suit brought against the Department on Aging in 1982, the CCP functions as an entitlement program with a budget of $72 million in FY 1986. Although most of the funding for this program is from state sources, about 30 percent of the total budget reflects payment for services to clients financially eligible for Medicaid waiver services.
All program participants must be assessed as meeting the functional and medical criteria for nursing home admission. Non-Medicaid clients must have less than $10,000 in liquid assets in order to be eligible. And a client co-payment is required which is set according to an individual's income and level of service needed.
CCP provides three direct services -- adult day care, homemaker and chore services. In addition it pays for assessments, care planning and ongoing case management.
As in most of its other human services programs, Illinois uses a state centralized form of administration with state government contracting directly with providers. State administrative responsibility for the program belongs to the Department on Aging. The Department of Rehabilitation is responsible for a similar program for the physically disabled. Both agencies work with the Department of Public Aid in developing program rules which meet Medicaid requirements in order to receive some federal funds to support community programs.
All assessment and case management functions are performed by Community Care Units (CCUs) under contract with the Department on Aging. They are prohibited from direct delivery of CCP services. About one third of the 63 CCUs are home health agencies; another third are senior service agencies; the remaining third are a mix of other agency types, mainly family social service agencies, health clinics, and mental health centers. In addition to assessing client for functional levels in determining eligibility for community care, the CCUs also conduct pre-admission screening for nursing home care. Medicaid clients and persons expected to be eligible for Medicaid within 60 days of nursing home entry are required to participate. Financial eligibility for Medicaid is determined by local offices of the state Department of Public Aid. The CCUs also use Older Americans Act funds to do assessments and care plans for persons who do not meet the CCP eligibility criteria.
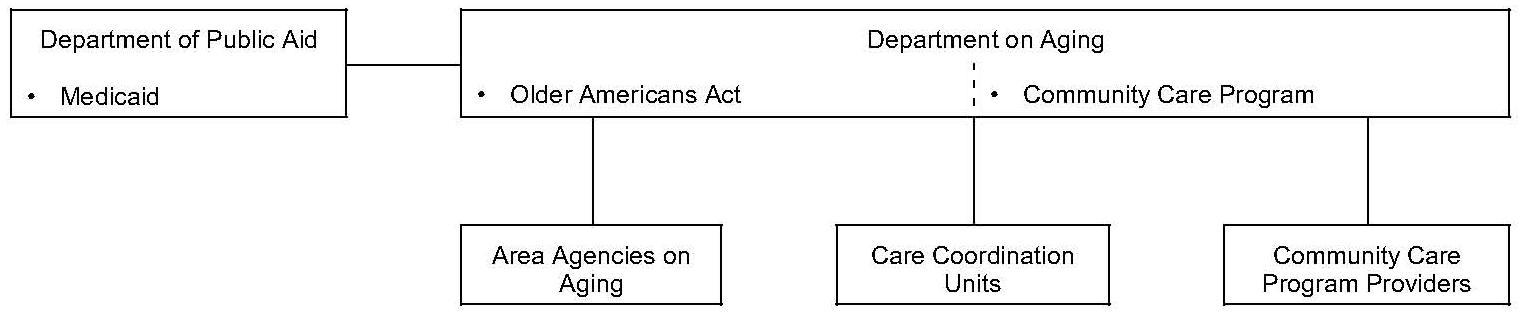
Until 1986, service providers were chosen by a competitive bid process focusing on price. They are now chosen on the basis of quality and paid a fixed rate for each service. Illinois' 13 area agencies on aging provide administrative support to CCP. Under contract with the Department on Aging, area agencies help CCUs resolve billing problems and develop new services not covered by the CCP. Figure II-2 depicts the organization of community care programs in Illinois.
| FIGURE II-2: Illinois Organization of Community Care Services |
 |
DEVELOPMENT OF STATE POLICY INITIATIVES. Illinois' state funded Community Care Program (CCP) was first established in 1978 as an income tested program and placed in the Department of Public Aid. The in-home services program was transferred to the Department on Aging the following year, however, in response to aging advocacy group objections that the program as currently administered carried a welfare stigma. The income eligibility criteria were also eliminated. The Department allocated the funds through a state formula to the area agencies on aging, who performed case management and then awarded funds to local service providers.
After one year of operation under the Department on Aging, the decision was made to centralize program administration and allocation of funds to area agencies on aging was discontinued. Also eliminated were the case management functions performed by area agencies. Instead the state contracted directly with service providers who also were responsible for client assessment and case management. Despite the apparent conflict in combining service authorization with service provision, the care plans were in fact low-cost ones, due to the tremendous pressure from the community to stretch the funds over large numbers of clients. Even with low-cost plans, in a short period of time the program had a full enrollment and providers had extensive lists of persons waiting to receive services. Those on the waiting lists, of course, could only receive program services through natural attrition of program clients.
In 1982 a class action suit was filed on behalf of clients who had been placed on waiting lists. This court case is the key factor shaping Illinois' current community care policy. The suit argued that those who had applied later for services were being discriminated against. Negotiations with the plaintiff attorney resulted in a court decree which eliminated waiting lists, in effect making the CCP an entitlement program. The decree also required the Department to report on the time elapsed between making an application and determining need, and between determination of need and receipt of services.
Major changes resulted, including a more stringent review of functional capacity, a limit on the liquid assets program participants could have, and a sliding fee scale for client cost sharing. In addition, because the new entitlement nature of the program contained an implicit incentive to expand services, the state separated the assessment and case management functions from service provision. Care Coordination Units (CCUs) were designated to conduct client assessments, authorize the provisions of service and perform on-going case management. Because of the mandated separation of case management from service, most of the participating agencies had to decide whether to provide assessment and case management (and apply to become a CCU), or to provide direct services. By July 1983, the CCUs had been selected, awards had been made to service vendors and the pre-admission screening program was in place.
Until this point state general revenues had provided all the CCP funding. The new entitlement aspects of the program required so much expansion that it made sense to seek a 2176 waiver to fund services for Medicaid-eligible clients. In July of 1983 the waiver program began.
CCP is now a mature program. Thus, the state is no longer dealing with basic structural issues, but rather with fine tuning various components, in particular the rates paid to and selection of providers. Over the last several years, the state's large and politically well connected private nonprofit service providers have been increasingly underbid by proprietary agencies. This led to the creation of a task force chaired by the Governor's office, to review the current system and to recommend changes. As a result, providers will now be competitively selected based on quality measures identified through compliance monitoring, and each of the three direct services funded by the program will be reimbursed at a fixed rate. Of this rate, 73 percent must be passed on to direct salaries and benefits for workers. This provision was adopted in response to charges that workers' salaries and benefits were being adversely affected by rate competition.
FACTORS SHAPING ILLINOIS' APPROACH. The primary factor shaping Illinois' current policies, as noted, was the 1982 court case defining the CCP as an entitlement program. A tightly run program with a strong cost containment focus resulted. In fact, this emphasis on keeping costs down led eventually to major political problems due to the competitive bid process for selecting providers and setting rates. At the same time, the legislature has wanted to spend more money on the program than the executive branch has requested. In fiscal 1986, in fact, the legislature appropriated more state funds than the Department could use.
CCP has broad based political support. As a state legislator noted, with a Republican Governor and a Democratic Legislature few programs escape detailed criticism but this one does. During the most difficult fiscal times, while other programs were cut back and taxes were raised, this program grew. Aging advocates now take the program for granted; although they were very influential in getting the program established there is little organized advocacy needed now.
The administrative structure of the CCP follows the pattern used for most other state human services functions in Illinois -- a centralized form of administration, using a state contracting system to award service funds to a well established private nonprofit delivery system. While several state agencies may be direct providers of service through local offices of state government, there is no significant human services role for county government. Therefore the administrative structure of the Community Care Program is similar to that used for other state human services functions.
Many state officials emphasized that the program was transferred from the Department of Public Aid because the elderly would have objected to the "welfare" image. However, the assets test and the required client cost sharing seem to stimulate only minimal objections since these policies were adopted as part of the major program expansion.
Finally, Illinois is the only state of the six studied that was not concerned about a growth in nursing home beds. Their 1986 bed ratio was 70/1000, significantly higher than the national average. Even so, nursing home capacity controls are clearly not a component of their approach to expand community care options. In fact several state officials express the view that excess nursing home capacity is an advantage in that it helps keep costs down due to competition among facilities.
Maine
Maine's long term care system has been primarily built upon the Home Based Care Program. HBC provides a broad range of services to older people who are assessed as meeting the medical and functional criteria for nursing or boarding home care. Although it was originally initiated as a totally state funded program, by fiscal year 1986 about two thirds of the $2.6 million program was supported by state revenues and one third was supported by state and federal Medicaid funds authorized under a 2176 waiver. There are few specifically defined services, leaving substantial flexibility for local program managers to decide on and fund the types of assistance needed. Personal care assistance is the most frequently used service, often provided by a neighbor or someone known to the client. In 8 percent of the state-funded cases, family members are paid providers -- which requires state agency approval. Payment to families is not allowed in those cases supported by the Medicaid waiver.
A small amount of Social Services Block Grant (SSBG) funds are available for impaired older persons receiving agency-provided homemaker services. The Older Americans Act funds case management services conducted for clients of the HBC. It also funds case management for the Congregate Housing Program. This is a small ($100,000 a year) state-funded program providing meals, housekeeping and personal care services for low and moderate income elderly living in subsidized housing. Eligibility for it is determined through individual client assessments reviewed by the housing manager, the area agency case manager and a home health agency nurse.
At the state level all of these programs are supervised by the Department of Human Services. The Bureau of Maine's Elderly administers HBC and, cooperatively with the Bureau of Medical Services, shares supervision of the Medicaid waiver component. The Bureau of Maine's Elderly also administers the Congregate Housing Program.
At the local level, area agencies on aging administer HBC (including the Medicaid waiver component) and the Congregate Housing Program; and they have access to a negotiated number of SSBG-funded homemaker slots for priority clients. A regional plan is required every two years and is reviewed in a public meeting to which a state-specified list of local providers are invited. A regional Quality Assurance Review Committee is also required, comprising representatives of home health agencies, hospitals, homemaker agencies, nursing homes and consumers. The committee, which must be chaired by a health professional not employed by the area agency, is required to review all program policies and procedures of the area agency; participate in the development of the annual report submitted to the state agency; and review randomly selected cases to note any policy or operational changes that should be made by the area agency. The Committee must meet at least bi-monthly and minutes of the meeting must be sent to the Bureau of Maine's Elderly.
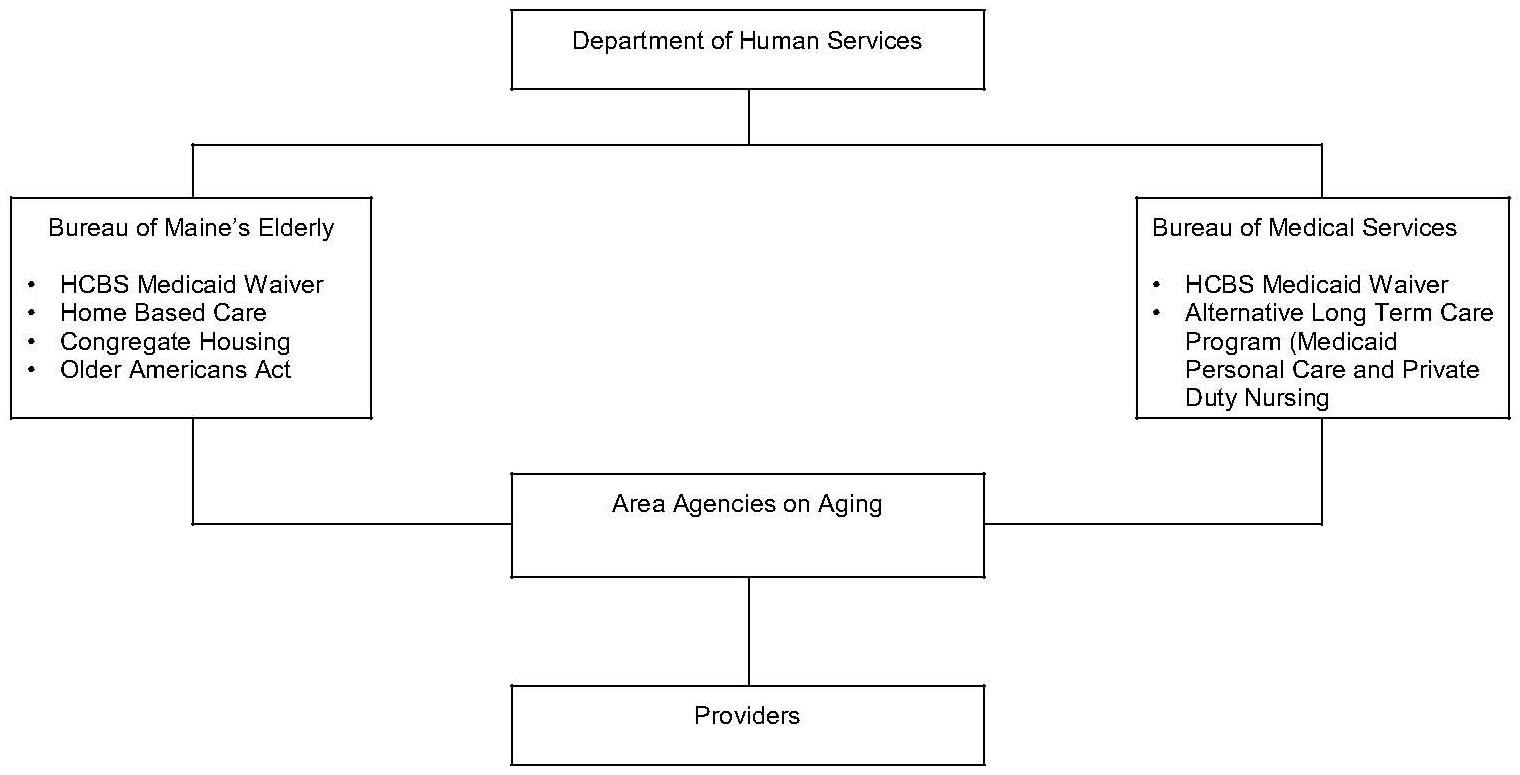
Area agency on aging staff perform individual client assessments, develop care plans and serve as case managers. The Department of Human Services has developed a standardized assessment tool which is used for all clients seeking home care services through HBC and congregate housing. It is used also by hospital discharge workers in making a referral to either HBC or a nursing home, and by area agencies in pre-admission assessments of Medicaid eligible clients who are currently living in their own homes and are seeking nursing home admission. Local offices of the Department of Human Services determine financial eligibility for Medicaid. Figure II-3 depicts the organization of community care programs in Maine.
| FIGURE II-3: Maine Organization of Community Care Programs |
 |
DEVELOPMENT OF STATE POLICY INITIATIVES. Development of Maine's long term care policy initiatives started with two events in 1979. The first was imposition of a one-year moratorium on new nursing home bed construction, following rapid expansion of nursing home beds in the 1970s. The second was creation by the governor of a task force of consumers, legislators, state agency staff and providers to develop a report on the long term care needs of the state's elderly. The task force report resulted in administrative policies to further constrain the growth of institutional expenditures. It also served as the impetus for the state-funded HBC established in 1981.
During the same period Maine was selected as one of the states participating in the National Channeling Demonstration. As part of its planning for the channeling demonstration, the Bureau of Maine's Elderly held meetings across the state to solicit input on long term care policies. In the process it helped to build a statewide constituency for creating a home care program to serve the whole state, not just the part covered by channeling. At a legislative hearing in 1981, for example, over 1,000 older people attended to show their support of new state funding for home care -- those parts of the state not covered by channeling wanted a home care program too.
Thus the state began implementing HBC at the same time the local channeling site began operation. As in many states, the local turf issues were especially thorny, with the Medicare certified home health agencies and the area agencies on aging in direct competition for lead agency status in both programs. This represented a significant change in the home health agencies' stated position. Several years before, the Bureau of Maine's Elderly had approached the home health agencies to generate interest in providing non-health-related long term care services. At that time they were not willing to change their medical focus. When funds became available, however, they wanted part of the action. Competition was most heated over the case management function, with home health agencies claiming it on the grounds that they already did case management. Ultimately area agencies were designated as the lead local agencies, in part due to state rules (no longer in effect) that identified case management as a mandated function but prohibited the use of HBC funds for this purpose. Area agencies had other resources under the Older Americans Act funds, and chose to use them for case management.
The other components were added to the long term care delivery system incrementally. The state-funded Congregate Housing Program began operation in 1982. In 1983 the Bureau of Maine's Elderly began a series of demonstrations involving nursing homes in the provision of community care services. Specific grants were given to nursing homes for adult day care, respite care and some in-home services. In partial response to the limited entry of nursing homes into the home care field, home health agencies pushed for and received legislation which required state licensure for home heath agencies.
In 1984, the state applied for and received approval of a 2176 waiver request. Some of the state general revenues previously devoted to HBC became matching funds for the Medicaid component. State officials emphasize that an initial use of state funds to develop a program resulted in a better system for Maine than would have resulted had they built their system around the requirements of the waiver.
The most recent addition to Maine's system is the Alternative Long Term Care Program. This program combines the optional Medicaid state plan services of private duty nursing, personal care and traditional home health services and bills them at an hourly rate. Prior authorization is required from the Bureau of Medical Services. This packaging is an attempt to control what had been runaway costs for these services while at the same time meeting medical long term care needs. Clients receiving Alternative Long Term Care services must be nursing-home eligible and the costs of their service packages may not exceed nursing home costs.
One of the most unique aspects of Maine's long term care strategy is its approach to determining nursing home bed needs. The 1979 moratorium resulted in a strategy of planned growth. Since then beds have increased by approximately 7 percent, most of which is attributable to beds that were authorized in 1979 but not yet built. The legislature has the annual responsibility of determining the state's bed needs, with recommendations from the health planning agency. The rationale for the legislature's involvement is that since such a high proportion (80 percent) of nursing home residents are Medicaid recipients, the approval of new beds is a de facto Medicaid expenditure. Therefore since only the legislature can appropriate funds, then the legislature should approve the number of new beds. The geographic location of these new beds, however, is left up to the health planning agency.
FACTORS SHAPING MAINE'S APPROACH. The Maine program is based on a strongly held state philosophy of building on informal supports for the provision of publicly financed care. It is for this reason, combined with its rural nature, that personal care assistance by a neighbor or friend is the most commonly used service.
Other major factors shaping Maine's approach are the early battles between the home health industry and area agencies on aging for lead agency designation. These have resulted in compromises that give home health agencies a larger role in the long term care system than they have in the other five states studied. Home health agencies, for example, usually chair the Quality Assurance Review Committees. They are also the providers of care under the Alternative Long Term Care Program. In fact this program was created as part of a compromise between the home health industry and the state over the designation of area agencies as case management organizations.
Maryland
Responsibility for long term care programs for the elderly is divided among three state agencies: the Department of Health and Mental Hygiene, the Department of Human Resources and the Office on Aging. The directors of these three agencies constitute the Interagency Committee on Aging Services (IAC), created by the legislature to improve state level coordination.
The Department of Health and Mental Hygiene administers Medicaid personal care services at a level of $3 million in FY 1986, state general revenue grants and Medicaid reimbursement for adult day care at a level of $3.5 million, and state funded geriatric evaluation services consisting of both pre-admission screening and community care evaluations funded at a level of 1.2 million. The Department also manages Medicaid nursing home payments. At the local level, Medicaid personal care services are provided by independent contractors supervised by a nurse who is frequently employed by a home health agency. The day care centers have a variety of organizational affiliations. The geriatric evaluation service is part of the county health department.
The Department of Human Resources is responsible for social services and income maintenance programs. Specifically the Department manages In Home Aides Services, funded at $5.7 million in FY 1986 from the Social Services Block Grant and state general revenues. Also funded with state general revenues (at $2.9 million annually) are case management services and (at $.6 million) in subsidies for domiciliary care for older people. Those programs are all administered through local social services offices of the Department of Human Resources.
The Office on Aging administers the Older Americans Act of which $1.5 million is devoted to home delivered meals. Locally, Older Americans Act funds are administered by area agencies on aging, which are part of county government. The Office on Aging also administers the state-funded sheltered housing program, which provides $1 million for personal care and chore services on a sliding fee basis to frail residents of subsidized housing. Grants are made to housing facilities on behalf of the elderly recipient. The Gateway II program ($1.1 million in state general revenues) is also administered by the Office on Aging in collaboration with the other two members of the IAC. This program provides case management and gap filling funds to counties for services to older persons assessed as being at risk of nursing home placement. County officials decide whether the local lead agency will be the health department, the area agency on aging or the social services department. Counties also are required to establish a local Interagency Committee on Aging Services and develop a plan for the coordination of all publicly financed services. Figure II-4 depicts the organization of community care programs in Maryland.
Development of Maryland's Policy Initiatives. Coordination of long term care services has been a long standing concern in Maryland. From the mid 1970s to the early 1980s, aging advocacy organizations were pressing for the creation of a Department on Aging under which all resources devoted to serving older people could be consolidated. Ultimately this approach was rejected; however this pressure has led the three state agencies responsible for aging services to approach coordination efforts cautiously.
In 1980, Maryland expanded its focus on long term care in several ways. The Department of Health and Mental Hygiene amended the Medicaid State Plan to begin covering personal care services and adult day care. At the same time, the Office on Aging received two grants for community care demonstrations. The first, funded as part of a multi-state effort by the Robert Wood Johnson Foundation, led to a long term care coordination project administered in Baltimore County. The second was for the National Channeling Demonstration to be implemented in the city of Baltimore. Federal requirements for channeling mandated that a state level working group comprising at a minimum the three state agencies administering Medicaid, the Social Service Block Grant and the Older Americans Act, be established to prepare a state long term care plan and to establish policies for the new demonstration.
| FIGURE II-4: Maryland Organization of Community Care Programs |
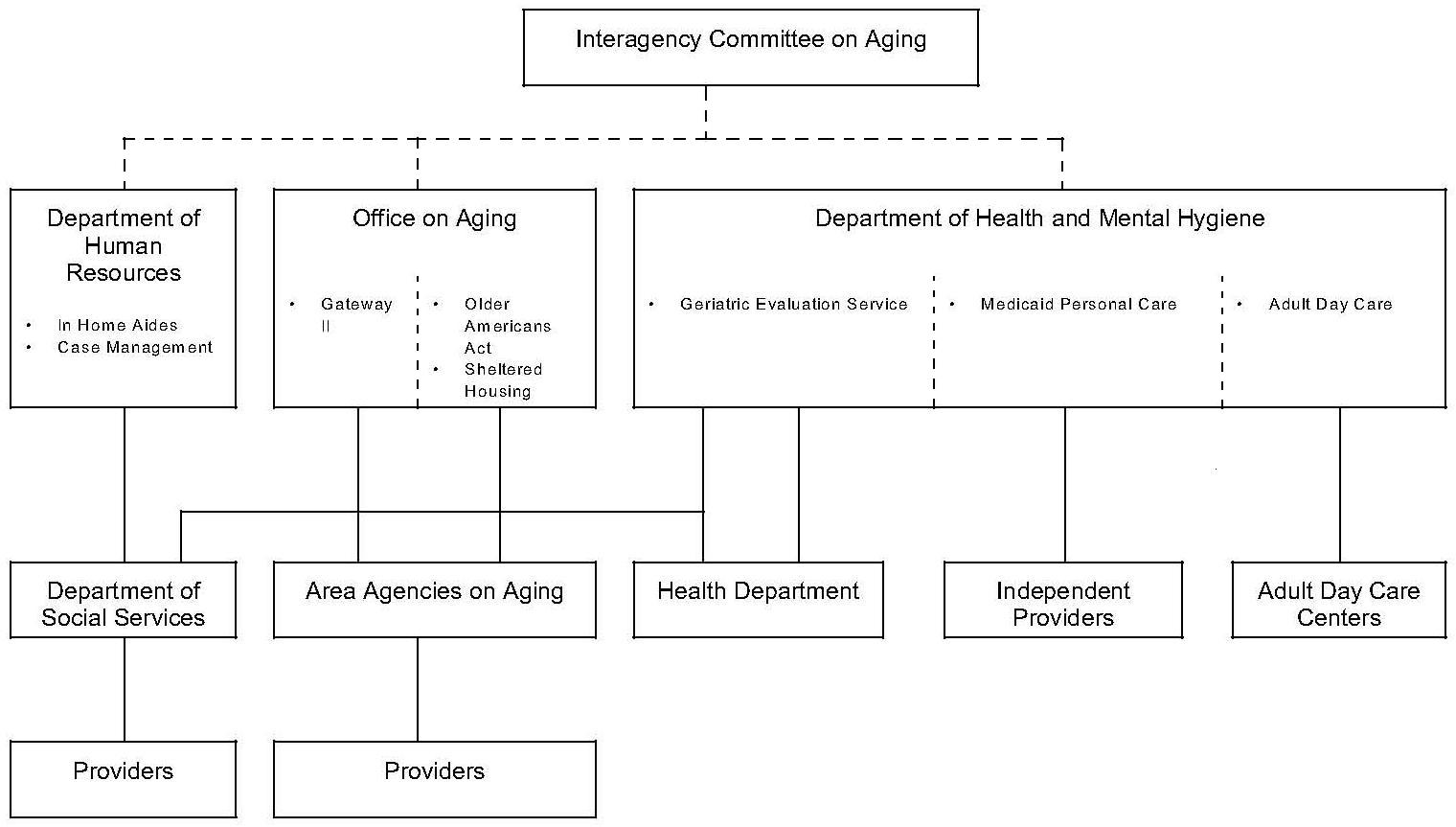 |
A year and a half later, former Governor Hughes decided to make services to the elderly a major priority within his 1982 legislative package. The interagency task force had just completed its state long term care plan and had several new proposals waiting. These included Gateway I, designed to improve service access for older people through strengthening statewide information and referral services. The second proposal, Gateway II, called for local demonstrations in pilot counties to better organize the delivery of long term care services.
Both Gateway proposals also reflected the concerns of the major membership organizations of older people that services be better coordinated. While advocates wanted more money, their foremost concern was that older people were falling through the cracks of the various state and federal programs. Both Gateway I and II were adopted by the legislature. Advocate groups again raised the issue of consolidating the state's various long term care programs in a new Department on Aging. As a compromise, the legislature addressed the coordination concerns by creating an Interagency Committee on Aging Services (IAC) comprising the three state agencies involved in long term care services for the elderly, with lead responsibility assigned to the Office on Aging. By statute, this committee is responsible for setting policy for the Gateway II program, addressing coordination problems across the three agencies, and developing an interagency annual budget request for aging services.
In the fall of 1984, the Department of Budget and Fiscal Planning released a study undertaken at the direction of the legislature to examine the various programs financing in-home services in Maryland. The three state agencies responded by making a number of changes in their programs. One of the major findings was that much of the gap filling funds of the Gateway II program were being spent for in-home services that could have been funded under other programs. Specifically, Gateway II funds were being spent because workers could not be recruited to deliver Medicaid personal care services and funds for the Department of Human Resources' in home aides had been exhausted. The report recommended that the traditional programs be fully funded before support for Gateway II was expanded. It also proposed changes in the personal care program to decrease the likelihood that either in-home aides or Gateway II services would be provided to clients who are Medicaid eligible.
Finally, the report recommended that the IAC establish more uniformity in the way Gateway II is administered across the state. In many ways this recommendation is counter to the program's original purpose -- of providing flexible funds to counties to increase service coordination. However, the IAC agreed that since the legislature had appropriated funds to achieve statewide coverage by July 1986, the time had come for more uniformity. Several important policies were adopted, including standardized financial eligibility criteria and a methodology for allocating funds to counties. One of the most controversial proposals -- which would have designated the local offices of the Department of Human Resources as the primary agencies to perform case management -- was not adopted.
In order to minimize the start-up difficulties faced by the Gateway II pilot counties, the three state agencies have developed a systematic process for bringing new counties on board. Some of these efforts, like providing more lead time to counties in developing their plans and conducting county meetings attended by each of the three state agencies on the IAC, were designed to obtain better coordination from the start.
The most recent addition to Maryland's long term care initiatives is preadmission screening, which began July 1986. Screening is required for all persons who are currently eligible for Medicaid as well as those who would be financially eligible within 6 months of nursing home placement. The Geriatric Evaluation Service in each local Health Department administers the screening program. Staff of the three state agencies serving on the IAC have developed a single assessment tool which will now be used for pre-admission screening and all the community care programs of the IAC agencies.
FACTORS SHAPING MARYLAND'S APPROACH. Maryland's policy initiatives over the years have assured that each of the three relevant state agencies has a carefully negotiated role in long term care programs for the elderly. Each state agency acknowledges the difficult task of achieving three-way cooperation while at the same time maintaining the current division of responsibilities. Coordination has become increasingly effective over the past several years, in part because of the personal commitment of the three agency heads to improving the system. Many sources noted the symbolic importance of the three secretaries testifying together at a budget hearing in 1986 on behalf of all aging programs -- with moderate increases for each agency.
Each of the three state agencies have their own local delivery systems. The Department of Health and Mental Hygiene has local health departments; the Office on Aging has area agencies on aging. Both are part of county government. The Department of Human Resources local offices are part of state government. In addition, independent personal care contractors and their supervisors relate directly to the Department of Health and Mental Hygiene or the Department of Human Resources depending on the funding source. Some state officials note that their increased commitment to work together filters down to the local level; others believe that coordination is, in any case, more effective at the local level than at the state level.
Maryland has made an explicit choice not to pursue a 2176 waiver to serve the elderly (they are already administering a waiver program for the developmentally disabled population). State officials are unanimous in their reasons for rejecting the waiver approach. They note that Maryland wants to see community based care services grow substantially. With limits on the number of people that can be served by waiver programs and limits on total expenditures, Maryland feels that expansion will be more substantial and reliable if it comes about by encouraging greater use of Medicaid personal care services and adult day care provided under the state plan.
Oregon
Oregon bas consolidated all components of its long term care programs into a single administrative structure at the state level and a highly integrated delivery system at the local level. A single state agency, the Division of Senior Services, manages all of the state's community and institutional long term care programs. These include Medicaid, a Home and Community Based Services Waiver, the state funded Oregon Project Independence and the Older Americans Act. In addition to developing community care systems, the Division licenses and certifies nursing homes, reimburses them for the care of Medicaid clients, and develops policies governing the participation of nursing homes in Medicaid. This administrative structure is the most consolidated of any of the long term care policy approaches included in this study.
The Medicaid Home and Community Based Services waiver is the core of Oregon's community care system. In 1986 over $19 million was spent under the waiver for community care services provided to Medicaid eligible persons assessed to need institutional care. Individual client assessments and case management services are financed through Medicaid administration funds. In addition Oregon Project Independence, funded with state general revenues provides similar services to persons who have the same functional impairments as waiver clients but who do not meet Medicaid financial eligibility criteria. These persons receive services based on a sliding fee scale, which starts at an income level of 125 percent of poverty.
Major components of the service delivery system include case management, relocation planning, risk intervention and pre-admission screening. All these functions are performed by case managers who assess client needs, develop a care plan authorizing the provision of services, and establish financial eligibility for Medicaid and income maintenance programs.
Case managers assigned to relocation planning help institutionalized older people return to the community. Since 1982 over 5000 nursing home residents have been relocated to community settings. Risk intervention case managers develop care plans for persons who do not meet the functional or financial criteria for the waiver program or Oregon Project Independence. Services are privately purchased and/or provided by neighbors and voluntary organizations. Pre-admission screening is conducted for persons who are currently Medicaid eligible or will be within three months of nursing home placement. Staff also identify persons who might require only a short placement, so relocation case managers can follow up.
| FIGURE II-5: Oregon Organization of Community Care Programs |
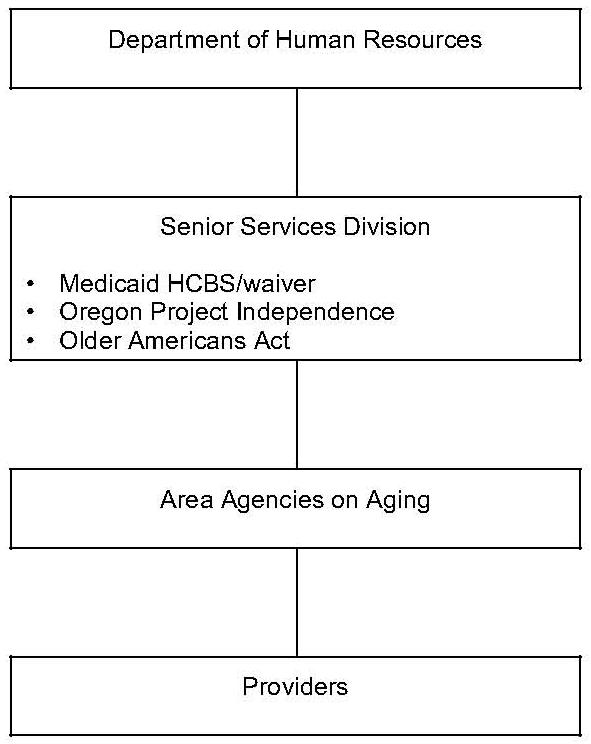 |
Local administration of Oregon's community care system is the responsibility of the area agencies on aging, with the scope of responsibility dependent upon their type of governing structure. The vast majority (90 percent) of clients are in jurisdictions where the area agencies are part of local government (counties or councils of government). These agencies administer all funding sources and programs including Medicaid waiver services, OAA, and Project Independence. They also conduct case management, relocation planning, risk intervention and pre-admission screening.
In the remainder of the state, the area agencies on aging are private non-profit organizations. They administer the OAA and Project Independence programs. In these jurisdictions, district offices of the state Senior Services Division manage the waiver program, and perform case management and pre-admission screening. Figure II-5 depicts the organization of community care programs in Oregon.
DEVELOPMENT OF STATE POLICY INITIATIVES. Like many other states, Oregon's emphasis in the 1970s was on building new nursing homes. In an attempt to reverse that trend, Oregon Project Independence, a state funded Community Care Program, was created in 1975. In addition, the state in 1979 received approval from the Administration on Aging and the Health Care Financing Administration to undertake a demonstration in several geographic areas, using Medicaid funds for community care services and setting up a formal process to improve coordination of service delivery. At approximately the same time Oregon began a statewide pre-admission screening program. These efforts laid the groundwork for a more comprehensive long term care initiative.
Planning for the new approach was facilitated by a federal Long Term Care Systems Development Grant. Concurrently the Governor gave the Commission on Aging the responsibility of formulating proposals to reorganize the way services to older people are administered. A wide range of interests were represented on the planning committee, including state officials, service providers, community planners and older people themselves. There were two major results.
The first was state legislation enacted in 1981 which dramatically reorganized the state and local administrative structures for long term care services. The Division of Senior Services was created by merging the functions of the previous state aging agency with the long term care unit of the state Medicaid agency. At the local level, the new legislation also changed the role of state government's district offices. In those parts of the state where area agencies are part of local government, they could choose to perform their traditional functions as well as assuming the responsibilities of the state's district offices. Most area agencies chose this expanded role which included determining both functional and financial eligibility for Medicaid, as well as conducting case management and pre-admission screening.
The second was development of an application for a waiver for Home and Community Based Services. The request was granted and, with the new reorganization in place, Oregon became the first state to receive a waiver. In implementing the waiver program, Oregon not only attempted to divert new nursing home admissions by providing community services; it also embarked on an effort to relocate existing nursing home residents to community settings. Due to state budget constraints in the early 1980s and federal reductions in Social Services Block Grant funds, some of the state's programs serving less frail persons were terminated. Oregon's response was the risk intervention initiative which provides case management assistance to persons ineligible for publicly financed services.
The dramatic changes in Oregon's long term care system in such a relatively short time, not surprisingly, led to significant tensions among the state agency, area agencies on aging, service providers and aging advocacy groups. To address the major disagreements that arose, a process called the Negotiated Investment Strategy was undertaken. The interests of the state, area agencies, service providers and elderly advocate groups were each represented by their own five member team. These four teams met for a full day every other week for more than six months, at the end of which agreements were reached that successfully clarified the roles and expectations of all parties.
A major outgrowth of the Oregon change from central office control of state district offices to a state supervised locally managed program was a new program monitoring system. It changed from a concern for structural and process measures of quality of care, to a system that focuses on client outcomes. State teams look at a sample of case files and interview individual clients in their own homes to review appropriateness of care. This approach was seen by state staff as the final step in the transition from state to local program management begun in 1981.
By 1985 there were only two long term care activities which the Senior Services Division did not manage, both of which are now under the Division. One was Inspection of Care -- a federally mandated process of reviewing service provision and utilization as part of the certification process for nursing homes participating in Medicaid; the second was nursing home licensure. The Division became responsible for Inspection of Care in 1985 and the state survey and licensure functions in 1987.
With the expansion of community care options during the late 1970s, the health planning agency began tightening nursing home bed need criteria. Although Oregon never implemented an official moratorium on approval of certificates of need, the bed need criteria was so stringent that it achieved the same result with only 300 new beds authorized since 1981. Health planning officials note the importance of limiting bed expansion in conjunction with the Senior Services Division's emphasis on controlling nursing home utilization and keeping occupancy rates down. As a result, there has been minimal demand for new construction.
FACTORS CONTRIBUTING TO OREGON'S APPROACH. Both state officials and older people themselves played an active role from the late 1970's on in Oregon's planning for long term care policy change. Passage of the 1981 state legislation which dramatically reorganized the community care delivery system coincided with Congressional enactment of the Omnibus Budget Reconciliation Act of 1981, which included authorization for the Medicaid Home and Community Based Services waivers. The newly developed state long term care plan was translated into a waiver request -- and Oregon was granted the first waiver in the country.
Being first has not always been advantageous, however. Oregon's waiver program is among the country's largest. At least in part for this reason it has faced extensive federal pressure to reduce the number of persons served. In addition, the program was in full operation before the federal requirements governing the waivers were in place. Waiver policies were constantly evolving for the first several years of state program operation, necessitating constant program changes.
Another major influence on Oregon's long term care initiative was the severe economic recession which developed as Oregon began program implementation. The recession, combined with the major reduction in federal funds flowing to states led to a strong emphasis on cost control. Keeping down Medicaid nursing home case loads became a major objective leading to more pressure on community care services. Functional impairment levels for waiver services eligibility also were tightened; and the same tightened eligibility levels were applied to the previously flexible Oregon Project Independence.
It is noteworthy that aging services are the only component of human services in Oregon not directly managed by state government. The sharing of responsibility with the area agencies on aging led to major frictions. While state officials were accustomed to tightly controlling all aspects of policy implementation, area agencies on aging were accustomed to having substantial flexibility and autonomy. They did not easily adapt to fairly rigid Medicaid rules.
The combination of difficulties that the Oregon long term care initiative faced during the first several years of operation -- unpredictable federal waiver policy, strong state cost control pressures, changing relationships between state and local government in human services management, and new agencies at the state and local level learning to cope with the complexities of Medicaid -- could easily have caused Oregon's system to topple. Instead, Oregon has created a strong well managed community care system that many states would like to emulate. A good deal of the credit goes to state officials who were willing to take risks and to persevere.
Wisconsin
The Community Options Program is the focal point for the coordination of all federal, state and local resources devoted to community care services. The Community Options Program, (COP) like initiatives in a number of states, was created in response to a crisis -- that of rapidly escalating Medicaid expenditures for nursing home care. Unlike the responses in other states, however, Wisconsin responded with a program that did not focus only on the elderly. The state funded COP is designed to serve all populations needing long term care, including the elderly, physically disabled, developmentally disabled, chronically mentally ill and chemically dependent. Both children and adults are served. In addition to supportive services, COP also funds individual client assessments, care planning and on-going case management. State government has not defined a particular group of services which must or can be funded; nor has it prescribed extensive administrative procedures which must be followed in implementing the program locally. Rather, state guidelines concentrate on developing county plans for coordinating existing service programs, and involving the client and family in developing individual care plans.
With a funding level of $17 million in 1986, approximately half of COP's expenditures are spent on the elderly. The resources coordinated with COP include Supportive Home Care funded at approximately $11 million for FY 1986 with state funds comprising 80 percent of the total and the Social Services Block Grant comprising 20 percent. They also include special supplements to the Federal Supplemental Security Income (SSI) payment to older people for persons with special needs. (These payments are in addition to a basic state supplement to SSI for all older people meeting SSI income and assets criteria). As in a number of other states, these payments help finance the costs of board and care. However, Wisconsin also provides these special supplements to persons receiving more than 40 hours of publicly funded home care services a month, with the assumption that these individuals are likely to incur other additional living expenses due to their frailty. Recent state initiatives to support families of persons with Alzheimer's disease resulted in several major program thrusts -- including an expansion of COP eligibility for those with Alzheimer's disease, and a state appropriation of $1.2 million for cash grants of up to $4,000 a year to Alzheimer's family caregivers.
Finally Wisconsin has four 2176 Medicaid waivers. Two waivers serve developmentally disabled persons and two serve the elderly and physically disabled. The largest waiver is entitled the Community Integration Program. Counties may access the Community Integration waiver on behalf of older people when there has been a reduction of licensed nursing home beds in the county, either due to a public or private facility closing or a decrease in the number of licensed beds in an individual nursing home. Wisconsin's payment system contains provisions which help nursing homes maximize Medicaid reimbursement if a certain occupancy level is maintained; this provides an incentive for a facility to reduce licensed beds in order to maintain high occupancy levels.
All of these long term care programs are supervised by the Community Services Division of the Department of Health and Social Services. Local implementation is through county government, a strong and long-standing pattern of human service administration in Wisconsin. In most cases, County Social Services Departments are responsible for program planning and coordination, eligibility determination, and individual case management. Frequently counties subcontract with other agencies for service delivery; in some cases county government directly provides services or uses independent contractors. Figure II-6 depicts the organization of community care programs in Wisconsin.
| FIGURE II-6: Wisconsin Organization of Community Care Services |
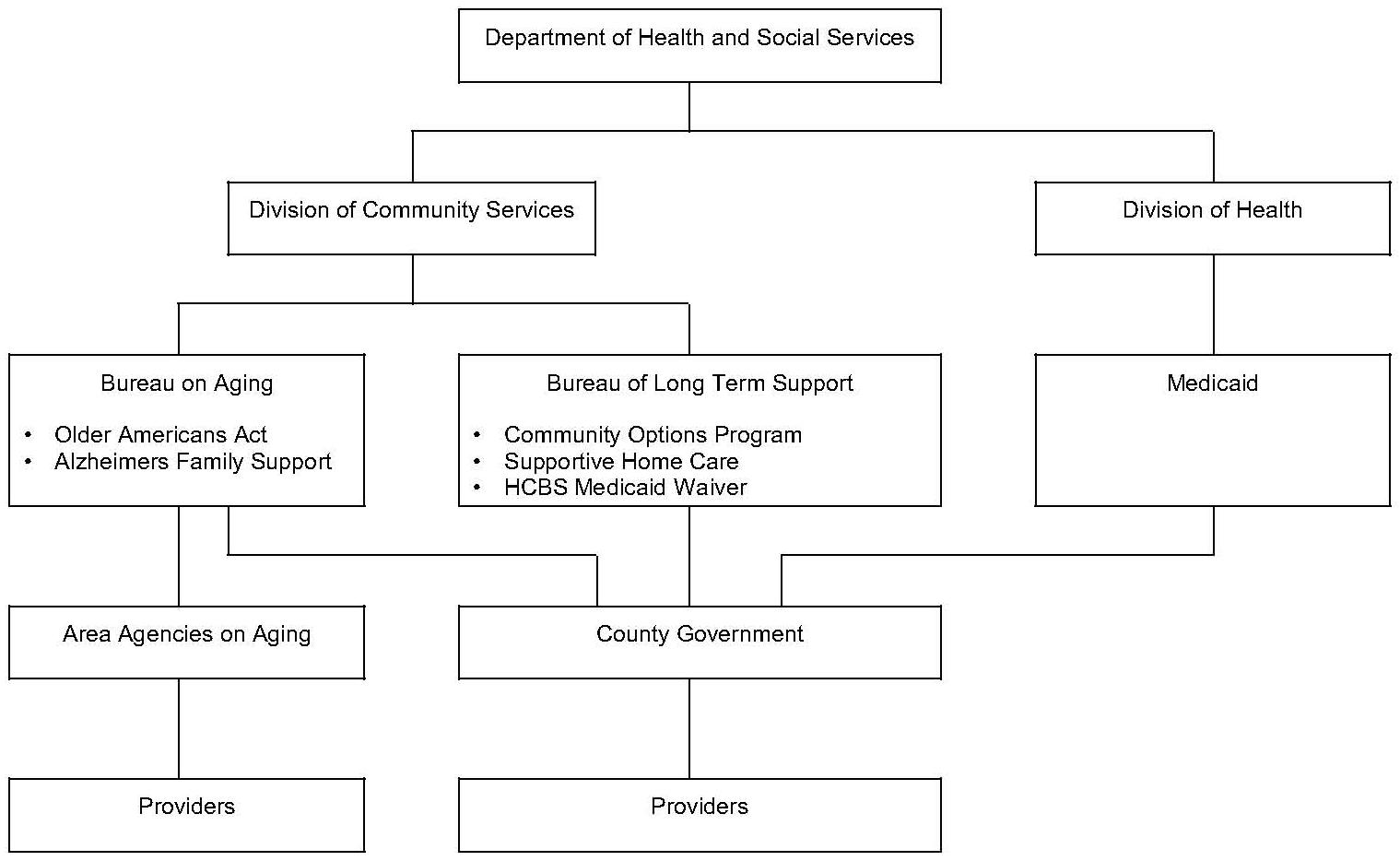 |
DEVELOPMENT OF STATE POLICY INITIATIVES. Wisconsin has a long history of leadership in human services programs. In 1980, Wisconsin had the nation's second highest number of nursing home beds in relationship to their elderly population. In the 1970s that was an indication of a responsive, caring, human services policy. As priorities changed, however, the large nursing home capacity became a liability in attempting to direct more resources to community care. This factor, along with a tradition of strong advocacy groups and a willingness to experiment with new approaches, converged in the late 1970s to result in major policy changes.
From the late 1960s on, the major funding source in Wisconsin for community services for persons of all ages has been Community Aids, which is an allocation of both federal and state appropriated funds awarded to counties on a formula basis. Counties have substantial discretion in determining how funds are spent, except that a portion of each county's allocation is earmarked for state mandated expenditures. Supportive home care provided to the elderly is one of those mandated program areas and until the creation of COP, was the major source of community care for the elderly.
In 1976 Wisconsin pilot-tested four demonstration projects to provide comprehensive community care as alternatives to nursing homes. Established with an 1115 Medicaid waiver, this Community Care Organization (CCO) demonstration covered four counties and provided assessments, case management and services to allow older people to stay in the community. The general consensus in the state is that the project was somewhat of a failure, in part because it was managed through the Lt. Governor's office, instead of being part of the long term care system under the Department of Health and Social Services. At the local level the project was similarly unconnected to the primary administrator of all human services programs, county government. This isolation from the state's well established delivery system resulted in neither state nor county government being willing to continue the project at the end of the federal demonstration period. However, the CCO project did familiarize policymakers and advocates with the notion of providing comprehensive packages of long term care services in the community and helped change perceptions of who needs nursing home care.
In the late 1970s, the state's substantial investment in nursing home care began to sky rocket, stimulating considerable support for seeking new approaches. In 1979 alone total Medicaid expenditures increased by $100 million due to increased nursing home costs. Advocates for the developmentally disabled and the physically handicapped were well organized and had been urging the expansion of home care services for several years. The aging groups also began calling for alternatives to nursing home care. Ultimately a coalition of various groups helped to generate legislative support for policy change.
The Department of Health and Social Services had in fact been planning for change, officially beginning in mid-1979 with the establishment of an ad hoc planning group of upper level managers. The result was a package of policies presented to the legislature in early 1981. This package had two major components. First, due to the extremely high proportion of nursing home beds in relationship to the state's elderly population, the legislature adopted a moratorium on nursing home bed expansion, which is still in place today. Secondly they approved as a pilot program the Community Options Program (COP), to begin in eight counties in 1982, with eventual statewide coverage in 1986. The authorizing legislation specified that program participants must be assessed as requiring nursing home care and that on average, COP service expenditures per person could not exceed the state's share of Medicaid expenditures (42 percent) for an individual's monthly nursing home costs. The moratorium on nursing home construction was central to financing COP. State funds which would have been devoted to matching Medicaid for increased nursing home care were to be spent instead on community care.
Wisconsin was awarded its Long Term Care Systems Development Grant about the same time that the COP program was created. This grant provided the state with supplemental staff to develop an implementation plan, including a phase-in timetable for achieving statewide coverage. As part of the phase-in plan, the nursing home pre-admission screening component in each county's program was scheduled to cover all nursing home admissions during the fifth year of COP operation in that county. The program did, in fact, become statewide on schedule.
Other programs were subsequently developed to supplement COP. In 1984 a new component was added to the state supplement to SSI. Older people receiving more than 40 hours of publicly supported home care services are entitled to an extra SSI supplement designed to address the higher living costs encountered by the frail elderly. In 1985, a state funded program for support to family caregivers of persons with Alzheimers Disease was established.
Also in 1985, the state applied for and received a 2176 waiver to support a small proportion of new elderly COP clients with Medicaid funds. Wisconsin had deliberately delayed seeking a Medicaid waiver until all of the basic components of their system were in place. While the waiver brings a small amount of federal funds to a system which is otherwise state funded, state officials question the value of the federal contribution in relation to the high investment of time required in developing the waiver application, implementing the program and monitoring the results. They note that their waiver request by design insured cost effectiveness since a waiver slot would not be activated unless a nursing home bed was removed from the supply. Even so, it still took almost two years to obtain approval. Late in 1986 Wisconsin received approval for its second Medicaid waiver for the elderly; this one is not dependent on the closure of existing nursing home beds.
FACTORS CONTRIBUTING TO WISCONSIN'S APPROACH. A significant factor which shaped Wisconsin's approach was the availability of state general revenue funds as the primary financing source for their community care system. The strong principle of client choice in developing individual care plans, and the flexibility given to local administrators to implement those plans, is in large part possible because of the state's ability to totally finance the program. This brings with it a flexibility in program design that is hard to achieve under the constraints of federal program regulations.
In deference to Wisconsin's long tradition of a state supervised/county administered human services delivery system, state officials consciously avoided detailed prescriptions of local administrative structures for community care programs in the design of COP. A local planning committee including at least five consumers of services is required to develop a county COP plan. State decisions regarding state and county roles were primarily those on the margin -- like how much flexibility should counties have in structuring their delivery system rather than a basic yes/no decision on whether the system should be standardized in all 72 counties. Instead of concentrating on the issue of administrative structures, state officials focused on clearly defining program values and outcomes. There are no disallowed services, only disallowed settings (i.e., settings which are not small and community-integrated).
Finally, Wisconsin's community care system serves all populations requiring long term care services. This can be done effectively due to the enormous flexibility of the program. Even after five years of operation, there is very little debate on whether separate systems should be established for each population group. In part the generic approach has been preserved by the advocate groups who believe that the program is more likely to grow if the various interests all unite. At the same time, however, there is some discussion of earmarking portions of the state's large community aids grants to counties, with designated amounts to be spent on social services for certain client groups.
State Demographic Context for Long Term Care Policy Development
The characteristics of the elderly population in the six study states seemed to influence the choice of financing mechanisms for long term care services. As noted in Table II-1, the percentage of Arkansas' 65+ population that falls below the poverty rate is substantially larger than in the other five states. Consequently Arkansas has targeted its long term care assistance to persons qualifying for Medicaid personal care services and, in state funded home care programs, to persons with incomes below 125 percent of poverty. State funds are not used to partially subsidize services for moderate income persons through sliding fee scales. Wisconsin, in contrast, has an elderly poverty rate far below the national average of 14.9 percent. The state's Community Options Program supports individual assessments and care planning for all older people needing long term care. Services, however, are provided with clients sharing in the cost of their care based upon ability to pay. Approximately 75 percent of all Wisconsin long term care clients contribute to the cost of their care, with one quarter paying for the full amount. Both Arkansas and Wisconsin have responded to the unique characteristics of their elderly populations, resulting in very different approaches.
| TABLE II-1: Poverty Rates | ||
| State | Number of PersonsBelow Poverty | Percent of PersonsBelow Poverty |
| AR | 83,524 | 28.16 |
| IL | 140,985 | 11.87 |
| MD | 47,375 | 12.66 |
| ME | 21,553 | 16.37 |
| OR | 34,031 | 11.82 |
| WI | 49,787 | 9.57 |
| NATIONAL AVERAGE | 14.9 | |
The percentage of persons age 75 and over living alone who have incomes below the poverty line pinpoints the population which is usually the target of publicly assisted long term care programs. Table II-2 includes these figures for the six study states. Again, Arkansas and Wisconsin represent the two extremes.
| TABLE II-2: Persons Aged 75 + Living Alone and in Poverty, by State | |||
| Persons 75 and Over(Thousands) | Persons 75 andOver Living Alone(Thousands) | Percentage of Persons 75+Living Alone WhoAre Below Poverty | |
| AR | 120 | 41 | 55 |
| IL | 497 | 172 | 26 |
| ME | 58 | 19 | 37 |
| MD | 147 | 44 | 28 |
| OR | 118 | 43 | 28 |
| WI | 223 | 79 | 22 |
The study states also differ in the size of their elderly populations. Table II-3 shows the size of each state's elderly population in both absolute numbers and as a percentage of the state's total population. The absolute numbers vary widely, matching differences in state size. The percent of persons age 65 and over within each state's total population varies less. Arkansas has the highest percentage, which is frequently cited by state officials as one reason for their early involvement in long term care program development.
| TABLE II-3: Population 65 and Over, by State | ||||
| Number in Thousands | U.S. Rank | Percent of State'sTotal Population | U.S. Rank | |
| AR | 312 | 27 | 13.7 | 2 |
| IL | 1,262 | 6 | 11.0 | 29 |
| ME | 141 | 36 | 12.5 | 11 |
| MD | 396 | 23 | 9.4 | 42 |
| OR | 303 | 30 | 11.5 | 22 |
| WI | 564 | 14 | 12.0 | 16 |
Finally, the rate of increase in the elderly population differs among the study states (see Table II-4). Even the more modest increases are dramatic, however, particularly among those aged 75 and over, leading all six states to address the increasing need for long term care services.
| TABLE II-4: Growth Rate of Elderly Population | ||||||
| 65 and Over | 75 and Over | |||||
| 1980000's | 1985000's | 1980-85% inc. | 1980000's | 1985000's | 1980-85% inc. | |
| AR | 312 | 338 | 8.3 | 120 | 140 | 16.6 |
| IL | 1,261 | 1,368 | 8.4 | 500 | 555 | 11.0 |
| ME | 141 | 154 | 9.2 | 59 | 67 | 13.5 |
| MD | 395 | 459 | 16.2 | 148 | 176 | 18.9 |
| OR | 304 | 354 | 16.4 | 119 | 143 | 20.1 |
| WI | 564 | 617 | 9.3 | 234 | 264 | 12.8 |
III. ORGANIZATION OF LONG TERM CARE RESPONSIBILITIES: STATE AND LOCAL ROLES
Long term care initiatives in each of the six states have focused on investing public funds in new approaches to meet the needs of older people. This chapter identifies the long term care strategies adopted and the state and local administrative structures responsible for implementing those new policies. Those policies were shaped by the context of their initial adoption and the differing objectives of state long term care initiatives. This chapter begins with a brief outline of the demographic context of the six study states.
Development of State Long Term Care Policy
The six states included in the study fall into two distinct groups, according to whether they made plans for explicit long term care system reform from the start, or whether their system evolved out of more modest objectives pursued without major system reform in mind. Arkansas, Maryland and Illinois began funding community care services gradually in the late 1970s without a conscious attempt to achieve reform in their overall long term care systems or to reduce the growth of Medicaid nursing home expenditures. Their objective was simply to enable older people to remain in their own homes a little longer. With little fanfare or advance planning Arkansas and Maryland added personal care to the services covered by their Medicaid state plan and Illinois established a modest state funded home care program.
The other three states in the study -- Maine, Oregon and Wisconsin -- set out to deliberately control long term care expenditures through system changes. Each began with an extensive planning process, and in each case, the resulting initiatives reflected assessments of the prevailing problem that were unique to each state's particular circumstances. Oregon, for example, in response to coordination barriers identified through a broad based public planning process, consolidated responsibility for all long term care programs in a single state agency and a single entry point at the local level. Wisconsin created its Community Options Program as a response to rapidly escalating nursing home costs and a serious overall budget deficit. For this reason COP was accompanied by a freeze on nursing home construction, with the estimated savings to be funneled into the Community Options Program. Maine responded to a perceived lack of non-medical services, establishing a program that could be flexibly run using a wide variety of providers. While the state funded Home Based Care program was implemented in a time of great fiscal constraint, cost containment never became a primary thrust.
Several factors distinguish the group of states that undertook a comprehensive approach from the group that followed an evolutionary one. First, the incremental states began their initiatives before major state budget crises hit. The other three states were forced to take a broader view; as a result, nursing home capacity controls became integral components of strategies to expand community care. Second, the three evolutionary initiatives started from the efforts of a single individual or a small group. States setting out to completely change their systems involved numerous participants in major planning efforts.
The issues each state had to face were similar, whether the initial approach was incremental or comprehensive. States that undertook a comprehensive approach, however, emphasize that their planning activities in the 1970s laid a solid foundation for more substantial efforts in the 1980s -- a foundation that they feel greatly improved the effectiveness of their current long term care system over what would have been possible without extensive prior planning.
STATE AGENCY COLLABORATION IN POLICY DEVELOPMENT. Interagency collaboration was important in all states for both initial policy development and ongoing program management. However, the coordination structures created, the specific participants involved and the duration of the effort depended on whether the structures were established for policy development or for actual policy implementation. This section explores collaboration on policy development; later in this chapter, state level management integration will be discussed.
All the states included in the study emphasized that coordination among state agencies and the programs they administer is necessary to develop a continuum of care capable of offering a range of health and social services to persons with diverse needs. Such a continuum of care typically necessitates a combination of policies cutting across various state agencies if lasting change is to be achieved. Each agency affected by these changes has different expertise and resources; collaboration helps to maximize both. This is not an easy task, as years of turf battles indicate. However, in these six states and across the country, resource constraints, pressures from interest groups and strong gubernatorial leadership have forced more collaboration, and the results have been invariably positive in reducing turf battles.
Coordinating committees are frequently established to develop new state approaches to meeting the long term care needs of older people. The evolution of these policy work groups shared several major similarities across the six states.
First, in their initial phase, planning groups typically include participants from both inside and outside state government. Aside from the substantive benefits of broad based input, multiple interests are more likely to support policy change if they are identified with its success.
Second, in contrast to structures established for ongoing coordination of interagency program management, policy work groups tend to have higher level state officials as members. This is important both symbolically and substantively. When representation gets assigned to lower level state staff, the issues addressed tend to change from broad policy issues to narrower issue of program operation.
Third, in the six states studied, policy development efforts often were part of an official research or planning effort. Five of the six states were recipients in 1980 of either Channeling awards or State Systems Development Grants. While some of these states had already designed the basic structure of their initiatives, these federally financed planning grants helped in further refining approaches. If a state level coordinating committee did not already exist, recipients of both types of awards were required to establish one that included at a minimum the Medicaid, aging and social services agencies.
In Oregon and Maine, even before the federal planning grants had been awarded, the governors had appointed committees with broad based membership to study long term care and make recommendations for change. The Oregon planning group's recommendations were later adopted by the legislature, including a consolidation of all state responsibilities into one agency, thereby eliminating the need for future state level coordinating committees. In Maine the Governor's task force on long term care had almost completed its work and had achieved consensus on major directions for policy change by the time it received a Channeling award. A smaller group began implementing those changes at the same time as the channeling demonstration was begun.
In Illinois and Maryland interagency policy development was particularly important since both states have multiple independent cabinet level agencies responsible for some aspect of long term care. Illinois' policy group included the directors of the departments of public aid, aging, mental health, rehabilitation and budget, and a representative of the Governor's office. Within a year, this group had successfully addressed most of the policy, planning and budget issues surrounding the establishment of a new long term care system. Since then most major policy issues have been resolved during meetings of Cabinet officers who head the various state agencies responsible for human service programs; a working group of midlevel staff meets regularly to resolve implementation problems. In Maryland, a policy group was established similar in composition to Illinois' committee. After adopting a package of proposals recommended by the policy group, the legislature formally established the Interagency Committee on Aging Services (IAC) comprising the Department of Human Resources, the Department of Health and Mental Hygiene and the Office on Aging. This committee still exists.
While its primary focus has been implementation of the Gateway II community care program, the IAC has a broader mandate to improve coordination among the three agencies' programs and to develop a coordinated annual budget request for aging services across state agencies. As the state begins new initiatives like pre-admission screening, the IAC has provided a forum for working out policy differences. Last year the IAC submitted to the legislature a consolidated budget request for aging services. It was not a unified budget, but rather a compilation of budget decisions made by each department; yet, as noted elsewhere in this report, the symbolism was considered important by both state officials and advocacy groups. It is the only example in the six states of a single public document aggregating all state expenditures on behalf of the elderly.
Wisconsin has devoted extensive time and effort to policy planning, retaining and expanding its planning committee established under the systems development grant. The committee, called the Long Term Support Management Reference Group, includes directors of the offices of Medicaid, aging, health planning, state institutions, vocational rehabilitation, community services, policy and budget, program initiatives and the deputy secretary of the Department of Health and Social Services. The group meets every two weeks and rarely do members send substitutes. Policy issues that might be decided in a single division in another state are addressed through a team approach here. Since counties make the detailed administrative decisions governing all of the state's community care programs, developing state policies that help coordinate Wisconsin's multiple programs at the local level is a major priority.
Arkansas is the only one of the six state that has not undertaken a major interagency effort to develop state long term care policy. The nearest thing to it is a report prepared by the health planning agency with input from the other state agencies on future long term care needs. As part of an effort to develop a methodology for determining the need for new nursing home beds, the plan examined the supply of both nursing home care and home care, recommending that the availability of home care be significantly expanded. Arkansas state officials have been frustrated by their lack of staff to conduct long range strategic planning. Their recent receipt of a long term care planning grant, however, has now enabled them to initiate Project 2000, the goal of which is to develop a long term care plan for the state.
The experiences of these six states in developing a coordinated package of state policies offer two major development lessons for other states. First, where collaboration was most successful, substantial blocks of time during the initial planning stages were devoted to discussing philosophy and goals. This emphasis was displayed constantly in Wisconsin where, in response to interview questions, state officials invariably began by discussing the state's value system. And that perspective was identical regardless of whether the Medicaid director, the director of the Bureau on Aging or the deputy director of the Department of Health and Social Services was expressing an opinion. Other states also noted the importance of obtaining consensus on goals and expectations, perhaps since they had to revisit this issue during their program implementation. While it may seem extravagant to spend substantial amounts of time on clarifying intentions instead of resolving "real" operational issues, in the long run it pays off in a common understanding among all the actors.
Second, especially during the early stages, it is important to get people at the highest level involved. While mid-level staff may actually do most of the work, the visible commitment to change and to interagency cooperation that is provided by top level participation lays a positive framework for resolving more difficult operational conflicts in the future.
GENERIC OR CATEGORICAL: POPULATIONS COVERED BY LONG TERM CARE POLICIES. Several population groups in addition to the elderly have long term care needs, including the developmentally disabled, mentally ill, and physically handicapped. Although these populations have different characteristics, they share similar objectives: to receive needed care in their own homes when possible and maximize their own independence. In designing long term care systems, states must decide whether they will address only the needs of the elderly; whether they will establish similar yet separate delivery systems for older people and other populations; or whether they will design a generic system to serve all populations needing long term care.
The way this decision has been made in the study states depends in part on the type of advocacy group activity in the state -- if there is a coalition of different groups it is more likely that a generic approach will be taken, or at least a parallel approach for various populations. It depends also in part on historical considerations -- if community care services are already in place for one population group such as the developmentally disabled, programs for the elderly may develop separately as well. Finally, it depends in part on the organization of state government; the existence of a human services umbrella agency tends to lead to a more generic approach.
The six states approached this question in various ways. With its high proportion of older people, Arkansas focused primarily on the elderly. Some of Maryland's programs serve all long term care populations, particularly Medicaid personal care; however, Maryland has enough coordination problems with three state agencies involved in providing services to the elderly; there are different systems for other groups.
Illinois, Oregon and Maine have separate but parallel systems for the different populations. Illinois' Community Care Program initially served both the elderly and physically handicapped. After one year advocacy groups for both populations achieved a program split, with the Department on Aging administering the program for the elderly and the Department of Rehabilitation Services managing the program for the physically disabled. These two populations are now served through two state-funded programs and two 2176 waiver programs administered through the two departments' delivery systems. Oregon's state reorganization affected only the management of services to the elderly; however, its first waiver application included the developmentally disabled as well as the elderly. Waiver services for these two groups were always separately managed and delivered. Now, as required by federal regulations, Oregon submits one waiver request for services to the elderly and another one for the developmentally disabled.
Maine's Home Based Care program was established to serve several populations. Five percent of program funds are used for non-elderly populations who are chronically or terminally ill. The remaining funds are allocated to three groups: the elderly who receive 75 percent of the funds, the physically handicapped who receive 20 percent, and adult protective services clients who receive the remaining 5 percent. While some generic program rules apply to all populations, separate state and local delivery systems manage the program for each population group.
Wisconsin's system is generic, with the Community Options Program serving five population groups -- the elderly, physically disabled, developmentally disabled, chronically mentally ill and chronic substance abusers -- through the same state and local delivery system. Several factors influenced this approach. First, there is a long history of program integration as reflected by the broad scope of both the Department of Health and Social Services and the Community Aids fund (which provides a flexible allocation of state funds to counties for social services directed to all needy populations). Second, the strong philosophy of stressing client choice, enhancing independence and strengthening the informal support system was sufficiently general to apply to all groups. Third, program designers wanted to create a very flexible program; by including five population groups, the resulting structure by necessity was not rigidly defined. While some support is growing for earmarking the Community Aids allocation to counties for expenditures devoted to each population group, there is minimal discussion of earmarking the Community Options Program. One of the main factors is political. In difficult fiscal times, would budgets closely identified with specific populations fare better in the legislature than a generic allocation to counties? To date Wisconsin has felt that the answer to this question is no.
Advice on this topic offered to other states by officials in the study's six states varied dramatically. As one would expect, Wisconsin advised integration. Oregon recommended separation by client group. Maine is in the middle, having created separate delivery systems for different population groups and now wondering if some integration might be in order. The answer seems to be based more on the previous patterns of providing services to various populations and political alliances than on inherent advantages to a particular program design.
NURSING HOME CAPACITY CONTROLS: RELATIONSHIP TO COMMUNITY BASED CARE POLICY. Faced with the rapid growth of the elderly population, states expect their expenditures for long term care to grow. However, in the past decade they have attempted to channel that growth into services provided in the home -- as the elderly usually prefer -- instead of supporting the continued expansion of nursing home beds. An on-going concern is the current and future cost of maintaining the institutional expenditure base, which ultimately affects the amount of remaining state resources for expanding community based care.
Initiatives to slow the growth of Medicaid nursing home expenditures frequently focus on using certificate-of-need (CON) policy to limit the number of new beds constructed. Most of the study states subscribe to the philosophy that a bed built is a bed filled and have taken strong measures to limit growth.
Health planning agencies in each of the six states have devoted at least one chapter of their state health plan to community based care. Most have tightened their criteria for determining nursing home bed need. Three of the six have placed a moratorium on nursing home construction at some point during the last several years. Moratoriums adopted in conjunction with an expansion of community care frequently provide a planning period for developing and implementing new approaches and serve to place these new initiatives in a context of fiscal responsibility and cost containment. "Reinvesting" the savings resulting from moratoriums into community based care has become a major component of some states' policy packages.
Wisconsin, Arkansas, Maine and Oregon have severely limited the growth of the nursing home bed supply. Wisconsin has the longest running moratorium, begun in 1981 and renewed in each subsequent legislative session; it is currently extended through fiscal year 1989. Faced in 1981 with the nation's second highest ratio of nursing home beds per 1000 elderly, policy makers received widespread support for taking this action.
Arkansas had a two-year moratorium on nursing home expansion (1983 and 1984). During this period an interagency task force was appointed to review the existing supply of long term care services, including both community based and nursing home care. Its final report recommended tightening nursing home bed need criteria and greatly expanding community care. Since then only 300 beds have been authorized and new state funded community services have been initiated to supplement Medicaid personal care.
Maine also adopted a two-year moratorium on nursing home construction (1979-1980). Like Arkansas, a gubernatorial task force appointed in 1979 proposed tightly constrained bed growth and a substantial increase in community care. With Medicaid recipients comprising 75 percent of all Maine nursing home residents, the state legislature assumed responsibility for approving any additional nursing home beds. Authorizing new beds in essence commits state matching funds for future Medicaid expenditures, and only the legislature has the authority to appropriate state revenues. This policy very visibly links nursing home capacity to state long term care expenditures.
Oregon never adopted a moratorium, but it did significantly tighten its methodology for determining nursing home bed needs while expanding community care. Few beds have been approved since then, and officials note that, with the state's low bed occupancy rate, there is no pressure for more construction.
Each of these four states perceive a strong relationship among nursing home bed growth, Medicaid institutional expenses and funds remaining for community care. They have generally found collaborative interagency policy development very fruitful. Health planning officials are pleased with their role in advancing their state's objectives of shifting long term care growth to community care. And Medicaid directors emphasize the importance of nursing home capacity controls in containing the growth of their institutional expenditures.
The experience of Maryland and Illinois is in sharp contrast. Policymakers in those two states do not perceive a strong relationship between community care growth and institutional expansion. In fact in Illinois both Medicaid officials and health planning staff see bed expansion as a way to increase competition and thereby contain nursing home rate increases. Health planning officials have, however, established policies to encourage nursing home providers to become involved in community care by giving such facilities an advantage in CON approval.
Unlike the other states, Maryland has not encountered a major budget crisis over nursing home expenditures. Instead, rising hospital costs have been their major concern. As a result Maryland developed one of the first hospital prospective payment systems. The health planning agency has undertaken several endeavors to give community care more visibility, while favoring a simultaneous expansion of both nursing home and community care. State officials note, however, that nursing home costs are rising rapidly and may lead to a future budget crisis.
Table III-1 displays data on each of the six states' nursing home capacity as of January 1, 1986. The number of beds added in each state since 1982 reflects differences among the states in the extent to which nursing home capacity controls have been adopted in conjunction with an expansion of community care services.
| TABLE III-1: Nursing Home CapacityJanuary 1, 1986 | |||
| State | Beds Per 1000Persons Age 65+ | Number of New BedsApproved Since 19821 | Occupancy Rate |
| AR | 62.4 | 366 | 92% |
| IL | 70.4 | 2100 | 90% |
| ME | 60.8 | 400 | 95% |
| MD | 52.3 | 1700 | 87% |
| OR | 42.7 | 300 | 88% |
| WI | 73.1 | 0 | 93% |
| |||
Freezing the existing bed supply has not been strongly opposed by the nursing home industry in any of the study states. As Douglas Nelson, former Wisconsin official noted at a recent NGA conference, "Wisconsin's moratorium created a regulated public monopoly that guaranteed existing nursing home operators a market and a monopoly that greatly increased the value of certificates of need and the facilities that they covered."3
Neither does the nursing home industry, except in Arkansas, appear to oppose the expansion of community based care. Almost all nursing home spokespersons note, however, that they resent the rhetoric used to advocate for increased public funds for in-home services. Especially resented are arguments that people do not want to enter a nursing homes and that home care will save money.
Some nursing homes have also become community care providers, but most have not. The low payment level for community care services seems to be the major stumbling block to greater participation. As one would expect, the nursing home industry usually strongly opposes pre-admission screening programs. This opposition has kept both Maine and Arkansas from implementing pre-admission screening programs statewide and has resulted in a screening program in Maryland with non-binding recommendations to clients.
Nursing home payment policies do not seem to be related directly to community care policies. Maryland and Illinois adopted case mix reimbursement systems in 1983. While their payment systems make it less profitable than it used to be for nursing homes to accept residents with lower care needs, the primary motivation was to make sure that heavier care persons would not be turned away and that these persons would receive the intensified services they needed. Oregon and Wisconsin are currently (1987) implementing case mix systems. Maine also is developing a case mix system and has over the past several years adjusted payments to accommodate changes in the severity of patients served. Arkansas uses flat rates. With freezes on the nursing home bed supply, the initiation of pre-admission screening programs and the expansion of community care options, the study states have found that on the average clients entering a nursing home are more impaired than in the past. In light of these changes states can expect to face pressures for increased per diem rates.
ROLE OF ADVOCACY GROUPS IN SHAPING STATE POLICY. In each of the six study states, membership organizations of older people were very influential in the adoption of new state long term care policies. In Washington, D.C. most of the attention of these groups is focused on Social Security and Medicare. In state capitols their top concerns relate to long term care.
State officials in governors' offices and in numerous state agencies remarked on the symbiotic relationships established with advocacy groups as policy initiatives were advanced. Their experiences offer other states valuable lessons. Strong support by older people for community care was no accident, but rather the result of concerted efforts by state officials to make activists more realistically informed about long term care options. While these relationships facilitated the creation of new programs, they also shaped advocacy groups' perceptions of state limits in the amount of resources available for long term care. The recognition of overall cost constraints led to support on the part of advocacy groups for cost sharing and other attempts to target resources to persons who, because of income or functional impairment, are most in need of services.
In Maine, Illinois, Oregon and Wisconsin organized advocacy efforts were critical factors in achieving long term care system reform. In the other two states support of older people, although less organized, was also important in adopting some of the incremental measures. When the new systems are firmly established, organized advocacy groups become less involved. As legislators in some states noted, these programs appeal to a large constituency and do not need organized advocacy efforts to support program expansion. Older people continue to be involved in ongoing policy discussions, however. Because older people themselves actively participated in designing Oregon's system, for example, they remained actively invested in its implementation. In particular, when the tensions of rapid change became a threat to the system's continued existence Oregon embarked on its Negotiated Investment Strategy. Older people formed one of the negotiating teams along with separate teams of providers, area agency staff and state staff. State officials note the value of involving older people themselves in both soliciting their input and giving advocates a better understanding of management issues.
In Wisconsin, advocacy groups have also had an active role in overseeing program implementation. The Community Options Program serves all populations needing long term care including the elderly, developmentally disabled, physically handicapped and the chronically mentally ill. Organizations representing these groups formed a coalition to push for the program's enactment and now maintain that coalition for program oversight. Since official state policy emphasizes the involvement of client groups in serving as members of state and local advisory committees, the advocacy coalition has numerous individual members actively engaged in program operational issues.
The six states' experiences illustrate several principles related to the role of advocacy organizations. First, they are extremely influential in pressing for the adoption of state long term care initiatives. Second, in cooperation with state officials, they can understand states' fiscal limits and work within them. Finally, a long range strategy of supporting community care stimulates so much popular support that the role and influence of organized advocacy generally tends to decline as programs become more stable.
State Agency Program Management
At a recent NGA conference, Charles Reed, Assistant Secretary for Aging and Adult Services in Washington State noted that it would be easier to start from scratch in designing a long term care system than to try to put together a number of health, social services and aging systems that are already in place.4 States, however, do not have that luxury.
Most state level human services agencies were created to address other issues, such as income maintenance, acute health care for poor families and children, food programs for low income persons of all ages, mental health, etc. Only recently has long term care policy for the elderly become a major issue for state government.
As a result, long term care programs and policies for the elderly tend to be scattered throughout various agencies in state government. These include the separate agencies or divisions administering Medicaid, the Older Americans Act, and the Social Services Block Grant, with the state Medicaid agency focusing on health care and the other two agencies dealing with supportive services. Health planning agencies, budget offices and policy research bureaus may also have a role. The challenge to state officials is to find a way to integrate the resource allocation and program management activities of these various offices so that a coordinated system of care can be developed rather than a diffuse constellation of individual programs. Ultimately, the goal of these coordination efforts is to create the continuum of care that each individual agency rhetorically has embraced but cannot by itself achieve.
In order to achieve this goal, a number of systems development issues must be considered: designing a single delivery system supported by multiple funding sources; developing eligibility criteria for individual programs to ensure equitable treatment of all clients according to their needs and resources; and examining the mix of community care services supported by each funding stream. Perhaps the most challenging aspect of systems development is addressing the relationship between community and institutional expenditures in order to strike an appropriate balance between the two models of care. This requires the intensive involvement of Medicaid agencies and budget offices in conjunction with the state agencies responsible for various social services programs.
Three basic models of state agency structures have emerged to manage long term care systems. One consolidates all long term care responsibilities covering both institutional and community based care into a single sole purpose agency; this involves major reorganization of state government. Another, somewhat less radical, model uses a human services umbrella agency structure, with some internal shifting of responsibilities and increased inter-division coordination. Frequently the State Unit on Aging and the Medicaid division share major responsibilities for managing long term care programs. The third, least radical, model retains independent cabinet level agencies for managing various programs, but establishes an official inter-agency long term care committee to at least keep agencies informed of each other's activities and preferably, to coordinate the development of interagency policies as well. Table III-2 summarizes the management responsibilities of state agencies in the six study states.
Oregon has created a single agency, the Senior Services Division (SSD), within the Department of Human Resources to administer all long term care programs. Under the structure adopted in 1981, Medicaid long term care services, eligibility determination for income maintenance programs and adult protective services were transferred out of the Adult and Family Services Division (AFS) to SSD and combined with the agency on aging that was handling Older Americans Act programs and Project Independence. AFS central office staff managing these functions were transferred to the SSD central office; AFS district office staff were transferred to area agencies on aging. Responsibility for nursing home licensure and certification was transferred to SSD from the Health Division in 1987.
| TABLE III-2: State Agencies Responsible for Long Term Care Programs |
| ARKANSAS(Umbrella Agency Model) |
| Department of Human Services Division on Aging and Adult Services: State Funded Home Care Older Americans Act Division of Economic and Medical Services Office of Long Term Care: Medicaid funding for nursing homes; nursing home licensure and certification Office of Medical Services: Medicaid funding for personal care services Office of Purchased Services: Social Services Block Grant |
| State Health Planning and Development Agency Health Planning, Certificate of Need |
| ILLINOIS(Cabinet Agencies Model) |
| Department of Aging Community Care Program Older Americans Act |
| Department of Public Aid Medicaid Medicaid Certification of Nursing Homes (Inspection of Care) |
| Department of Health Licensure of nursing homes Health Planning, Certificate of Need |
| MAINE(Umbrella Agency Model) |
| Department of Human Services Bureau of Maine's Elderly: Home Based Care, Older Americans Act Bureau of Medical Services: Medicaid, Health Planning, Licensure and Certification Bureau of Social Services: Social Services Block Grant |
| MARYLAND(Cabinet Agency Model) |
| Department of Health and Mental Hygiene Medicaid Adult Day Care, Geriatric Evaluation Services Division of Licensing and Certification Health Resources Planning Commission: Health Planning, Certificate of Need |
| Department of Human Resources Social Services Block Grant In-Home Aides Case Management Foster Care |
| Office on Aging Gateway II Continuing Care Facilities Sheltered Housing Older Americans Act |
| OREGON(Consolidation Model) |
| Department of Human Resources Senior Services Division Medicaid Payments (nursing homes and Home and Community Based Services Waiver) Licensure and Certification Project Independence Older Americans Act |
| State Health Planning and Development Agency Health planning, certification of need |
| WISCONSIN(Umbrella Agency Model) |
| Department of Health and Social Services Division of Community Services Bureau of Long Term Support: Community Options Program, Supportive Home Care, Medicaid Waivers, SSI Bureau on Aging: Alzheimer's Family Support Program, Older Americans Act Program offices for developmental disabilities, physical disabilities, mental health, drug and alcohol Division of Health Medicaid Licensure and Certification Health planning, certificate of need Division of Policy and Budget Centralized Agency Budgeting |
Under this consolidation model, all long term care expenditures are placed in one budget, making resource allocations between community based and institutional care a direct and visible trade-off. This provides program managers with an incentive to give their nursing home caseloads as much scrutiny as their community based expenditures. (In fact local program managers suggest that too much emphasis is placed on keeping institutional expenditures down in relationship to expanding community care.) From a programmatic perspective this organizational structure also enhances linkages among various programs. For example, there are no inter-agency battles over which assessment form to use for determining eligibility for institutional and community care.
Oregon officials caution that this approach may not be right for every state.5 Such a major reorganization requires the strong support of the affected state agencies, the local delivery system and older people themselves.
Arkansas and Maine have human services umbrella agencies encompassing the major long term care programs serving the elderly. They are both small states with small bureaucracies, which undoubtedly facilitates coordination. In both states the Aging division and the Medicaid division are the major actors. In both states the Aging agency and the Medicaid agency use the same delivery system for their long term care services and any serious disagreements between the two agencies have long since been resolved.
In Arkansas, until recently the Medicaid division provided all the funding for community care, with the aging division addressing most of the program development and operational issues. When state funds were appropriated to supplement Medicaid personal care services, the Aging division became responsible for managing the new program and adopted the Medicaid rules as operating policy. Arkansas created an intradepartmental long term care committee of mid-level staff chaired by the Division on Aging and Adult Services to address on-going operational issues. This committee has now been replaced by a working group created as part of Arkansas Project 2000, a recently initiated long term care planning project.
The Bureau of Maine's Elderly was both the leading advocate within state government for establishing the Home Based Care (HBC) program and was its major architect. As a result the Bureau became responsible for its implementation. Several years later a 2176 waiver program was developed jointly by the Medicaid and Aging agencies to secure Medicaid funding to expand the HBC program. This waiver program is administered by the Bureau of Medical Services, in coordination with the HBC program administered by Bureau of Maine's Elderly. Maine also has an intradepartmental long term care committee chaired by the Deputy Commissioner of the Department of Human Services, with the directors of the Bureau of Maine's Elderly, Bureau of Medical Services, and the Bureau of Rehabilitation as members. Placed outside the Department of Human Services yet within state government, the Maine Committee on Aging has been created to serve as an internal and external advocate. Most other states have an advisory committee on aging whose members are appointed by the governor; usually this group is staffed by the state aging agency. The Maine Committee on Aging has its own staff, who administer the long term care ombudsman program and hold an annual statewide conference for older people, co-sponsored by the Bureau of Maine's Elderly, to develop a legislative advocacy agenda for the following year.
Wisconsin also has a human service umbrella agency which administers all of its long term care programs. However, Wisconsin is a much larger state than Maine and Arkansas, with a significantly larger state bureaucracy. Several other factors also complicate state level coordination. First, Wisconsin's human services agency is the most comprehensive in the country -- it even includes the state correctional system. As a result many individual divisions and bureaus have responsibilities comparable to those of separate agencies in other states. Simply locating all these programs in one single department does not in any way guarantee coordination. Second, Wisconsin has created a generic long term care system serving many different populations. Therefore, not only is coordination needed among the Medicaid, aging, health planning, and social services block grant programs, but also with the program offices for mental health, developmental disabilities, the physically handicapped and drug and alcohol abuse.
Wisconsin has deliberately not created a singular entity with consolidated authority over all long term care services. In fact numerous state officials emphasize that decentralization of responsibility at the state level is a factor contributing to the state's success. Having many persons involved in decision-making, they argue, helps to take advantage of differing expertise, enables more people to claim ownership of new policies, brings divergent viewpoints to the table, and stimulates greater creativity. However, the agency did create a new Bureau of Long Term Support to administer the generic Community Options Program and to serve as a focal point for coordination of all community long term support services.
Because of its reliance on coordination rather than consolidation, Wisconsin makes extensive use of its Long Term Care Support Management Reference Group and associated work groups. With Wisconsin's multi-population approach to long term care systems development, this seems essential. The members of the Management Reference Group include the directors of the offices of Medicaid, aging, health planning, state institutions, vocational rehabilitation, developmental disabilities, community services, policy and budget, program initiatives and the Deputy Director of the Department of Health and Social Services. The directors rarely send substitutes.
While the amount of time devoted to this process seems excessive, the results are impressive. All individual program decisions which might possibly have an effect on related community care programs are brought to the group such as changes in eligibility criteria, scope of services or reporting requirements. Subgroups have studied such questions as whether the state should amend its Medicaid state plan to include case management as a covered service, whether to apply for Medicaid waivers, and whether the state should adopt a case mix nursing home reimbursement system.
The group is chaired by the Department's Director of Policy and Budget and meets every two weeks. The day before each meeting, the directors of the Community Services Division's program offices meet to formulate the Division's position on issues to be resolved during the Reference Group meeting and to discuss any management problems encountered with counties. The program directors also share expertise and contribute specialized knowledge to the implementation of COP. All of these coordination activities obviously consume a great deal of senior state officials' time. However, no one identified this as a problem or felt that it was time not well spent.
Illinois and Maryland have separate cabinet level agencies responsible for various aspects of their long term care programs. Like the other states, however, they have created structures to enhance the coordination of program management.
Two agencies in Illinois are responsible for long term care programs for the elderly. The Department of Public Aid manages the state's Medicaid program, including payments to nursing homes and handles all contacts with HCFA regarding federal reporting and claims processing for the 2176 Waiver Program. The Department on Aging manages the state's Community Care Program, which is partly funded through state general revenues and partly through the Medicaid waiver. Within Medicaid rules, the Department on Aging develops the program's operational policies, monitors service providers and processes provider payments for both state funded and Medicaid funded services.
State officials note that an unexpected benefit of the Medicaid waivers has been greater cooperation among state human services agencies. The Department of Public Aid, the Department on Aging and the Department of Rehabilitation (which manages a waiver program for the physically handicapped) have formed a work group to address ongoing waiver implementation. Issues addressed include responses to HCFA assessments, waiver applications and renewals, joint training sessions for state and local staff, and state budget requests.
Medicaid program staff began involving staff from the other agencies in conference calls to the HCFA regional office when seeking clarification on Medicaid rules, following up on HCFA assessments and responding to federal questions regarding waiver renewals and amendments. Each Department noted the positive effect of this practice on interagency relationships in reducing misunderstandings, avoiding paranoia and giving the operating agencies a direct opportunity to follow-up on policy interpretations.
No serious consideration has been given to reorganizing state government to consolidate the separate departments responsible for various human services functions. The relevant departments appear to have few turf battles and are able to resolve policy differences. This process has undoubtedly been helped by the governor's office and the Bureau of the Budget, both of which place great emphasis on the importance of cooperation.
In Maryland things are more complicated. The Department of Health and Mental Hygiene administers the Medicaid program which funds nursing home care, personal care and adult day care; it funds and supervises the pre-admission screening program through the geriatric assessment service; and it licenses and certifies nursing homes. The Department of Human Resources administers the In-Home Aides program and provides case management through its local offices. The Office on Aging administers the Older Americans Act, manages the Gateway II program and staffs the IAC. These three state agencies have a long history of disagreements over the division of responsibilities and authority.
In the late 1970's and early 1980's aging advocates were pressing for the creation of a single department where all long term care resources and other programs for the elderly could be consolidated. Instead the legislature created the Interagency Committee on Aging in 1982.
To address coordination problems across the three agencies, the IAC was given a broad mandate, including developing an interagency annual budget request for aging services and setting policy for the Gateway II program. Most of its activities to date have centered on Gateway II, but it has also consolidated the three agency budgets for services to the elderly into one request that all three agencies support. As the Gateway II program becomes fully operational, the IAC has the potential to address other issues.
Coordination has improved, as evidenced by the successful implementation of a new pre-admission screening program, and development of a standard assessment tool not only for pre-admission screening but for all community care programs. But the difficulty with which related issues were resolved (such as selecting which local agencies would administer the screening program) indicates the need for further coordination.
Maryland's situation is unique among the six study states. Maryland's three state human services agencies are all equally involved in community care services. In the other five states, one agency (or at most two) dominates. In addition, each state agency in Maryland has its own local delivery system and all three local systems want a role. Also there is no one single program or financing source dominating the community care system in Maryland, so there is no automatic presumption about which should be the lead state agency. Instead Medicaid, the Social Service Block Grant, state general revenue funds and the Older Americans Act form a delicate balance. In summary, Maryland's coordination problems seem to result from the strengths of three separate systems, each created for purposes other than delivering long term care services to the elderly, and each anxious to maintain and expand their current role.
The organizational approaches used by these six states can provide some guidance to other states. The structure of agencies in state government is not easily changed to respond to new issues, particularly in the management of human services. Traditional ways of administering programs significantly shape the approach used to organize and manage community care programs.
Oregon has taken the most dramatic step and reorganized major parts of state government to create an agency whose sole purpose is to manage all of the state's long term care programs. Of equal importance is Oregon's decision to reorganize their local delivery system to create one local agency responsible for long term care. Without reorganization at both levels, significant consolidation would not have been achieved. The advantages of this option are significant, primarily in being able to mesh policy and resource allocation for both community and nursing home care. However, states considering it should recognize that such a dramatic change makes it imperative to have the broad support of most or all of the affected organizations. Even with that support, as was present in Oregon, be prepared for several rocky years.
Arkansas, Maine and Illinois without any major reorganization have achieved good management coordination at the state level. In each of the three, the aging and Medicaid agencies have jointly developed their community care systems and use the same local delivery system for their programs. In contrast to Oregon, the main component missing in Arkansas, Maine and Illinois is consolidated control over both institutional and community care programs. Wisconsin's management model is based on coordination rather than consolidation, which is probably essential given its policy goals. With so many different programs and population groups comprising Wisconsin's institutional and community based long term care systems, one single sole purpose entity is not feasible. Wisconsin's state organizational structure seems to work well for two reasons. First, all the relevant senior level officials are highly committed to improving community care systems and therefore willingly devote substantial time to this issue -- reflecting a high priority sustained over several years. Second, for all age groups and all programs, Wisconsin uses a single delivery system at the local level --county government. Other states attempting to replicate Wisconsin's generic approach will have a much more difficult time if both of these factors are not present.
For states with structures similar to Maryland where reorganization may not be politically or administratively feasible, establishing an interagency coordinating committee is useful. In contrast to other models, this one requires more active involvement of the Governor's staff and the staff of the Budget Office in sorting out priorities.
The agencies in the six study states that administer the Social Services Block Grant (SSBG) had varying involvement in community care systems development. In Oregon and Illinois, state general revenues rather than SSBG funds support services for older people, so in those two states, the social services agency was not a key player. In Wisconsin and Maryland, however, substantial amounts of SSBG are used for in-home services for the target populations, and as a result, the agencies responsible for those programs exerted great influence. In Arkansas and Maine, SSBG is divided at the state level among programs for eligible populations. Planning for the use of those funds is undertaken by the aging system with the state SSBG agency managing provider payments. The SSBG agencies in these two states have a peripheral role in community care systems development.
The six states offered several pieces of advice to others:
- Assign your best staff to community care systems development.
- Maintain the ongoing involvement of senior state officials in both policy development and program management. This involvement sends a message about the importance of long term care; assigning lower level staff to interagency management committees can trigger lower level participation among all agencies, running the risk of committee members lacking the necessary status to make final decisions.
- Involve all relevant agencies; if a system is being designed exclusively for older people, at a minimum Medicaid, aging, and the budget office must be included. If nursing home capacity controls are part of the policy package, health planning and agencies managing state institutions have a role. If substantial amounts of Social Services Block Grant (SSBG) Funds are used for older people, the social services agency is also important.
- Despite exemplary efforts to improve coordination, to strengthen management control and to allocate resources wisely, a comprehensive system cannot be built with federal funds alone. State funds are needed to cover either clients or services that fall between the cracks of federally financed programs.
Finally, state officials offer divergent views on how ambitiously and comprehensively states should approach management changes. From Oregon: Get as much as possible under control from the start. From Wisconsin: If you get all participants to embrace the same philosophy, effective coordination will follow. Both views describe the two states' successes.
Local Program Management Agencies
A major goal of state long term care initiatives is to overcome the fragmentation of existing programs while making better use of new resources for community care. In many states, this will require a reorganization of local human service delivery systems. Like human services agencies at the state level, local service delivery systems were created for a myriad of purposes; administering community based long term care programs for the frail elderly is not their sole responsibility. And those local agencies that do manage community care programs are frequently responsible for only one part of the picture.
How programs are managed at the local level is perhaps even more important than bow state responsibilities are organized. Older people come in direct contact with local agencies -- and their differing eligibility criteria, service packages and funding sources. If state policies are successful, older people will have access to appropriate care without having to contact multiple agencies to receive services for which they are eligible. Therefore, state long term care policies frequently designate a single local agency in each part of the state to manage all publicly financed community care programs. Usually these local agencies conduct client assessments, administer pre-admission screening programs and provide case management.
STATE DESIGNATION OF LOCAL AGENCIES. This designation is likely to be one of the most hotly debated decisions made by states. Three of the states studied --Arkansas, Oregon, and Maine -- chose area agencies on aging. Wisconsin and Maryland required the lead local agency to be part of county government, but left the specific choice up to county elected officials. Illinois selected its local lead agencies through a competitive bidding process. In each of the six states, decisions were based on both an assessment of the strengths of one agency's capacities to carry out a lead agency role and of the weaknesses of others.
Although Arkansas, Oregon and Maine all chose area agencies on aging, they had different reasons for doing so. In Arkansas in the late 1970s, there were no other local agencies serving older people. Local offices of the State Health Department were focused mainly on maternal and child health care; local offices of the State Department of Human Services were primarily intake points for income maintenance programs; there were few private nonprofit Medicare certified home health agencies; and there were no proprietary home health agencies. The State Office on Aging and the area agencies on aging were strong advocates for home care services and as a result became responsible for the system's development.
In Oregon, the state and local delivery system was designed by a commission appointed by the Governor. Its recommendations, adopted by the legislature, gave area agencies two options for their administrative structures. If an area agency was a part of local government, it could choose to manage all long term care programs, including Medicaid, state funded Project Independence and the Older Americans Act. In addition, the area agency would be responsible for eligibility determination, service authorization, case management and pre-admission screening. If an area agency on aging was not part of local government, it could seek administrative attachment to a governmental unit or could opt to maintain its current responsibilities (OAA and Project Independence) without adding Medicaid, case management, pre-admission screening, etc. District offices of the state Senior Services Divisions would continue performing the functions not assumed by area agencies. The area agency/local government link was a compromise between the elderly constituencies' preference for the area agencies on aging as the lead agency and government's need for Medicaid accountability. Most of Oregon's area agencies have opted to attach to a local government unit and assume the full set of responsibilities.
The other alternative available to the state was to designate district offices of the state as lead local managers, leaving area agencies on aging with only the Older Americans Act. This alternative was not supported by older people, who preferred the area agency structure with its history of involving the elderly in advisory committees and advocacy initiatives. Since, however, area agencies would be managing a large and complex program (namely Medicaid), the state insisted on accountability through local government.
In Maine area agencies on aging were chosen as the lead agencies after heated turf battles with the Medicare certified home health agencies. Area agencies were given an edge due to a state requirement that mandated case management functions but prohibited Home Based Care funds to be used for this purpose. With their Older Americans Act funds, area agencies on aging had other resources that could be allocated to case management.6
Wisconsin and Maryland have given county government lead responsibility, with locally elected officials choosing the specific agency. Wisconsin gives counties two choices. They can select either the Social Services Department, which administers Supportive Home Care, special supplements to SSI for persons requiring extensive home care services and most income maintenance programs, or they can choose the County "51" Boards administering programs for the developmentally disabled, the mentally ill, and the chemically dependent. Eighty percent of the counties chose the Social Services Department. Wisconsin's state funded grants to family caregivers of persons with Alzheimer's Disease are also administered by county government. One third of the counties use Social Services Departments; another one third use "51" boards; and in another one third the program is managed by county aging units. Wisconsin has six private non-profit area agencies on aging covering multi-county areas and county aging units in all 72 counties. County aging units are funded by both area agencies and the state Bureau on Aging with funds from Older Americans Act and state general revenues.
Maryland has three human service delivery systems. The Department of Human Resources has local Departments of Social Services in each county, staffed by state employees. The Department of Health and Mental Hygiene has local Departments of Health, staffed by county employees. And the Office on Aging has designated county government to be the home for area agencies on aging, also staffed by county employees. The Department of Social Services provides case management and administers the in-home aides program. The Health Department includes the Geriatric Assessment Service, which conducts assessments of older people for community care services and pre-admission screening. Area agencies on aging manage Older Americans Act programs.
County officials designate one of these three agencies to serve as the lead for managing Gateway II. Of Maryland's 24 counties, 17 have chosen area agencies on aging, 4 have chosen health departments and 3 have chosen departments of social services. The two local agencies not chosen as lead are members of the County Interagency Committee on Aging.
Illinois selected its local agencies, Care Coordination Units (CCUs), through a joint designation process with the area agencies. Operating in 63 subdivisions of the state, the CCUs are prohibited from being direct providers of Community Care Program services. About one third of the CCUs are home health agencies; another one third are senior services agencies; and the remaining third are a mix of family service agencies, health clinics, mental health centers, etc. The CCUs are the local entry point for all older people seeking publicly funded community care. County government in Illinois does not have a role in managing human services and the area agencies have been given a program support role, functioning under contract on behalf of the state.
States seem generally satisfied with their decisions. Oregon officials noted that at first area agencies had a difficult time managing the state's Medicaid waiver program since they were accustomed to the flexibility of the Older Americans Act. In retrospect, they recommend that other states following a similar course give more attention in the early stages to intensive training seminars on Medicaid management. Maine experienced similar but less major problems since Maine's area agencies began with smaller programs. Arkansas' area agencies have been the state's only Medicaid personal care providers since the program began and therefore were able to become gradually accustomed to the Medicaid rules. All three states noted that area agencies had proven to be cost-effective managers; yet some state officials question whether it is wise for the area agencies to potentially jeopardize their advocacy mission by devoting most of their time and attention to program management.
Two of the three states using area agencies on aging (Oregon and Maine) and the two states using counties (Maryland and Wisconsin) are sometimes frustrated by what they perceive to be a lack of sufficient control over local management agencies. State officials have obviously given this issue a good deal of thought, and are torn in two directions. On the one hand, they believe localities should have substantial flexibility to shape community care services to respond to individual client needs. On the other band, states are under tremendous pressure to run tightly managed, cost effective programs. Some commented that a state run system would be ideal while at the same time saying that one of their system's strengths is the latitude given to localities.
The power of persuasion is identified as one of the best tools available to state officials in convincing local entities to comply with their policies. In Wisconsin state officials note that county governments have significant influence in the state legislature; it is, therefore, difficult to establish policies with tough enforcement provisions. In Maryland the perceived independence of local agencies makes coordination at the state level more difficult, since each agency questions whether their state counterparts will be able to get agreements carried out across the state.
Oregon and Maine have similar perceptions of their relationships with their local agencies. In those states, area agencies on aging are conducting some functions that have traditionally been responsibilities of state government such as authorizing the expenditure of Medicaid funds on behalf of individual clients. Oregon's long term care legislation gives the Senior Services Division the power to fire (but not hire) an area agency director and to also to withdraw all program funds. Other states may not even have those options; usually the only option is to de-designate the organization operating as the area agency and appoint a new agency -- a process that can be tied up in appeals for months. State officials suggest that less drastic measures need to be available as intermediate courses of action if state government continues to turn over more authority to local agencies, especially to those whose private non-profit status removes them from direct accountability to local publicly elected officials.
RESPONSIBILITIES ASSIGNED TO LOCAL AGENCIES. State Officials agree that a local administrative structure is necessary for the management of long term care programs. At the very least, a local agency is needed to serve as an entry point to the long term care delivery system. Conducting client assessments, providing case management and administering pre-admission screening programs are the primary responsibilities of local lead agencies in all the study states. Beyond these basic functions, however, there is significant variation in the roles assigned to local agencies by state government. Each of the six study states began with the philosophy that older people would be better served if maximum flexibility was given to local agencies in developing community care programs. Yet over time, each state has gradually taken steps to tighten its control of program management. In some cases, significant flexibility was deliberately given to local agencies in order to experiment with new approaches. Most frequently this demonstration mentality was present when pilot programs were established with less than statewide coverage. But in some places local decision making was fostered because there was limited experience across the country that could provide models for operating large statewide community care systems. Now states are examining and re-examining how much responsibility should be delegated to local agencies and under what conditions.
At one extreme are Illinois and Oregon, which have exerted very strong state control over many aspects of their systems. Since these two states operate the largest elderly community care entitlement programs of the six study states, the significant level of state authority is perhaps expected. Equally important, however, is their tradition of centralized human services administration. Ironically, officials in Oregon who were not directly involved in program management frequently commented on the local flexibility built into their community care system, and wondered if the state should have more control. Given that most other human service functions are performed directly by state staff in Oregon, long term care programs appear by comparison to be very autonomous.
At the other extreme is Wisconsin, with a structure designed to give maximum discretion to county government in managing community care services. State human services officials want a system that could provide almost any assistance needed by an individual to remain living at home. This philosophy meshes well with the state legislature's desire to avoid placing any undue burden on counties by adopting uniform state rules.
Arkansas, Maine and Maryland are in between, tightening their control over time yet remaining committed to local flexibility. A review of selected functions which could be performed by either state or local agencies illustrates variations across states in delegating management responsibilities.7
Long term care planning and systems coordination. The relative emphasis placed on reviewing local service capacity, identifying service gaps and planning for future needs was highly related to the authority given to local agencies in deciding which services should be financed with public funds. If those decisions are made by state government, as in Illinois and Oregon, less attention was given to this local planning function. Likewise, since these same states used a consolidation model with one or two large programs financing community based care, coordination among various local agencies and programs was less problematic. The other states, however placed a substantial emphasis on these functions.
Maryland's Gateway II program, for example, gives counties some flexible service funds in exchange for achieving better coordination among existing programs. Each year counties submit to the state a coordination plan which also serves as the application for Gateway II funds. The county Inter-agency Committee on Aging, consisting of the Area Agency on Aging, the Social Service Department and the Health Department identify which agency will provide case management, client assessment and overall fiscal management for the Gateway II program. In addition, the plan specifies how client referral and service provision are to be coordinated.
In Maine, in order to receive Home Based Care funds area agencies on aging in Maine prepare a regional plan and hold a public hearing to which a state specified list of agencies must be invited. A description of the case management process, types of services offered, provider selection process and methods for coordinating with other programs are components of the plan. This process solicits feedback on the current operation of the Home Based Care Program and identifies needed improvements.
In Arkansas, beginning in 1985, state resources are used to fund a planning staff position called Community Based Care Developer for each of the state's eight area agencies on aging. These staff determine service gaps in the community and stimulate new programs to fill those gaps. In contrast to Maryland and Wisconsin, Arkansas' concern is to create new services as opposed to coordinating a fairly well established infrastructure of existing providers. The state Division on Aging and Adult Services has prepared technical assistance manuals and conducted training programs to help the Community Based Care Developers develop plans for supportive housing, family caregiver training and Alzheimer's support groups.
Wisconsin places a great deal of importance on county plans to implement the Community Options Program, with the plan serving as the county's application for state funds. A county Long Term Support Planning Committee must be established with its core membership including representatives of various agencies and population groups specified by state policies. The plan reflects coordination agreements with relevant public and private agencies administering community care services, with particular emphasis on specifying how the client assessment and case management functions will be carried out. In keeping with its philosophy of designing individually tailored care plans, the state does not request a proposed annual budget from counties for specific service expenditures; such a requirement state officials believe would limit the creativity of counties to respond to specific client needs. To assure that services to older people are adequately addressed, the county long term care committee must include an older consumer and a representative of the county commission on aging. In addition, the state Bureau on Aging has prepared guidelines for area agencies on aging to use in reviewing plans from counties in their regions prior to state approval.
While many state officials continue to strongly support a required local planning process, they note that its usefulness decreases as programs mature. Soon what were once innovative program initiatives become permanent, and new coordination approaches become routine.
Selecting and contracting with providers. States use a variety of processes to select service providers. In Wisconsin, counties select all providers. In Illinois, the state selects all providers of Community Care Program services through a competitive bidding process. Oregon, Arkansas, Maine and Maryland use a combination of processes.
In Oregon, area agencies have the option of managing their own competitive bidding process for Medicaid waiver services and Oregon Project Independence, or they may ask the state to include bids for their area in a statewide announcement handled by the state agency. In Arkansas, the state has designated area agencies to be the direct providers of Medicaid personal care services in six of the state's eight geographic districts. For the Social Services Block Grant, the Department of Human Services gives each division a planning allocation for negotiating contracts to serve certain population groups. The Division of Aging and Adult Services divides its allocation among the state's eight districts, giving area agencies on aging the responsibility of determining how funds will be spent in their area and selecting the providers. The actual service contract is written between the provider and the Department of Human Services. Maine follows a similar procedure for managing its Social Services Block Grant. The Department of Human Services negotiates service contracts, but allocates to aging a designated number of homemaker service units. Area agencies on aging select providers for both the state funded Home Based Care program and Medicaid Waiver services. Maryland uses three different processes. For Medicaid personal care services, individual providers are located by a nurse who is under contract with the state. For in-home aides, local offices of the Department of Human Resources select providers from a list of vendors approved by the state. For Gateway II, providers are selected locally.
In five of the six states, there is some local discretion in selecting service providers but there is no clear cut distinction related to funding source. For example in three states -- Oregon, Maine and Wisconsin -- Medicaid providers are chosen by localities. Again, the procedures followed at the two extremes, Illinois (state centralization) and Wisconsin (county management), are largely determined by tradition and political culture.
Service authorization. Under a community care program, authorizing the provision of services is equivalent to spending public funds. As will be discussed in greater detail in Chapter IV, all states have separated service authorization from most service delivery but have vested the local management agency with the ability to authorize service provision.
In summary, states have delegated significant authority to local management agencies, including some areas like service authorization and provider selection that have been traditional functions of state government. It should not be surprising, therefore, that developing and maintaining cooperative relationships between state and local agencies is a topic of some concern.
Advice from all six states focused on maintaining active formal and informal lines of communications with local agencies. State agencies in Arkansas and Maine hold monthly meetings with area agencies to review operational issues. In Maryland the local lead agencies designated under the Gateway II program meet with staff of the IAC every two months. Illinois and Wisconsin hold several training sessions a year for local management agency staff.
Oregon has the most unique approach to state/local relationships. In 1984 serious tensions erupted throughout Oregon's state and local service delivery system. With such rapid and far reaching changes in the organization and delivery of long term care programs, the state agency, area agencies, providers and the advocacy groups were all engaged in major battles with each other. Oregon took a drastic step; a consultant was hired to mediate a Negotiated Investment Strategy -- a process for identifying major disagreements and attempting to reach some resolution. Four teams of five members each were formed, representing the state agency, area agencies, service providers and elderly advocate groups. These teams met for a full day every other week for more than six months. During that time, major state policies covering a range of topics such as reimbursement systems, monitoring, provider selection, financial audits, etc. were developed through the negotiations of the four teams. In the end, a report titled "Shared Roles and Responsibilities for Delivery of Services Through the Oregon Senior Services System" was prepared to document all policies adopted through the mediation process.
Although the undertaking was risky for the state agency, since in effect it was relinquishing significant policymaking authority to a mediation process, the Division of Senior Services notes that the process was a major success. It gave all participants a better understanding of the federal constraints placed on the system and a common set of goals and expectations.
Established as an outgrowth of that mediation process, the Program Management Council, composed of five Senior Service Division staff and five area agency directors meets every six weeks to discuss new policies and program requirements. While the group tries to operate on a consensus basis, all final policy decisions are the responsibility of the director of the Senior Services Division.
Officials from other states also emphasize the importance of actively soliciting the advice of local program agencies in developing operating policies. Maine's Medicaid director, who was formerly the state's aging director, suggested that this advice is especially pertinent to Medicaid programs. Often operating with state centralized authority, seeking out local input may not be the norm for Medicaid agencies.
Another recommendation offered to other states is -- don't try to control every detail of local administration. Instead of worrying about process, hold the local delivery system accountable for client outcomes. To be effective, however, this approach requires the establishment of a monitoring system that will measure outcomes rather than program requirements.
IV. ACCESS TO LONG TERM CARE SERVICES
In designing community based care systems, states are of necessity dealing with multiple programs. In order to overcome the fragmentation of these existing programs as well as make better use of new resources being allocated to long term care, states are changing how older people enter the long term care system and how they become eligible for services. This chapter will explore four major aspects of client access to care including:
- Financial eligibility determination -- Client financial eligibility criteria are a direct function of the amount of program funds available for long term care services. In all states client income is used to limit the number of persons receiving fully subsidized public services, thereby allocating resources to those least able to pay for care. Most states also use cost-sharing policies to identify how much eligible individuals are expected to contribute to the cost of their care.
- Functional eligibility determination -- Most of the six states' long term care programs provide services to only those older persons who have impairment levels equivalent to those required for nursing home placement.
- Case management -- Developing individual care plans is particularly important when there are multiple programs with differing eligibility criteria and service providers. In all the states local case management agencies serve as agents of state government in authorizing payment for the specific type and amount of services in individual care plans.
- Pre-admission screening -- Increasingly states are trying to make sure that only older persons who cannot be served in the community enter a nursing home. One effective way to do so is to integrate access to institutional and community based care creating a single entry point for both. This helps older people learn about services that could defer nursing home entry.
All these functions, with the frequent exception of financial eligibility determination, are carried out in the six study states by the state-designated local management agencies. The previous chapter discussed state considerations in selecting case management agencies and their management responsibilities extending beyond their core functions. This chapter addresses their core functions.
Within the context of this analysis, eligibility determination, case management and pre-admission screening programs are examined as integral components of statewide service delivery systems. In particular, emphasis is placed on how states use case management agencies to translate state policies into service provision. Since this study is a comparative analysis, not an outcomes evaluation, judgments cannot be made about which state's assessment tool most effectively identifies persons at risk of institutionalization or which pre-admission screening program keeps more people out of nursing homes. Extensive studies have been conducted on these and other similar topics. Instead, this study compares and contrasts how six states have designed large statewide systems of care, integrating major program components such as client assessment, case management and pre-admission screening. Service access mechanisms are integral components of community based care systems. In an institutional setting all services are provided under one roof, and after entering a nursing home, older people are usually eligible for all available services. In a community based care system needed services are often delivered by a variety of different providers. By establishing care management systems, a package of community care services can be provided which is almost as comprehensive as care provided in a nursing home.
In addition to helping older people link up with needed community care, service access mechanisms serve a second important function -- controlling utilization of publicly financed programs. Unlike nursing home care, community based services are not packaged and paid for by one comprehensive fee -- unless capitated financing mechanisms are used. Also older people actively seek community based care services, while going to great lengths to avoid nursing home placement. The combination of these two factors -- piecemeal financing of community services and strong preferences of older people to remain in their own homes -- stimulates service demand, pointing to the need for prioritizing individual access to care, controlling service utilization and thereby containing overall public cost.
Thus, access mechanisms both help older people enter the system and also keep out persons not meeting the functional or financial criteria for program participation. Despite a significant expansion of state revenues devoted to community based services, public funds are still inadequate to address all long term care needs. Therefore states have had to make painful choices in selecting population groups to cover.
Financial Eligibility Criteria
Financial eligibility criteria are one policy tool used by states to prioritize the population to receive publicly supported long term care services. These criteria are a function of three variables. The first is the amount of state resources available. The second is a perception of the scope of the state's responsibility for financing long term care services. The third is a policy decision as to whether to create a system which can be accessed by all persons, with higher income persons paying a large share (or all) of their support costs.
In none of the six states was there a philosophical inclination to provide universal public support for community based care without regard to a client's income. Rather, all six states viewed their role as strengthening the ability of families to care for their older relatives; expanding the service delivery infrastructure so that moderate income persons would have improved access to partially subsidized care; and finally financing care for persons with low incomes. There were no protracted debates over whether services should be provided on an ability to pay basis; the only question was how to translate this philosophy to operational policy.
There are two ways of using financial criteria to define target populations. One is to establish an eligibility ceiling, with persons having incomes above the specified level prohibited from receiving any program benefits. The second is to use client cost sharing provisions to set sliding fee scales based on income. The six study states used a combination of the two.
MEDICAID ELIGIBILITY CRITERIA. For Medicaid funded services, persons who are categorically eligible are subject to an income ceiling; persons who qualify for Medicaid as a result of medically needy provisions are, in principle, subject to cost sharing since they are required to spend down to medically needy income levels. In addition to the eligibility policies adopted for coverage of medical services, there is a multitude of technical provisions relating only to Medicaid eligibility for nursing home care. Individually these technicalities may not have much effect on eligibility determination; however their combined effect can be substantial. An in-depth review of all states' Medicaid eligibility policies has recently been conducted by the National Governors' Association.8 Since the primary focus of this study is on building community care systems, only those provisions relevant to eligibility for care provided outside of a nursing home are examined here.
In addition to nursing home coverage, the Medicaid program finances some community based services in each of the six states. Personal care services provided under the Medicaid state plan are used extensively in Arkansas and Maryland; 2176 waivers finance some services for the elderly in Illinois, Oregon, Maine, and Wisconsin. (For a more detailed analysis of Medicaid eligibility criteria applicable to community based care in each of the six states, see Appendix II.) Several key points are summarized here to illustrate how Medicaid eligibility criteria relate to eligibility rules established for state funded programs. General revenues are used in each of the six states to finance care of persons who are above Medicaid eligibility levels but below a specified income ceiling. State Medicaid policies therefore influence eligibility criteria used for other programs.
States have three options in covering SSI cash recipients under Medicaid. They can automatically cover all SSI recipients without requiring them to make a separate application for Medicaid. Arkansas, Maine, Maryland, and Wisconsin all use this option. The second option, used by Oregon, extends Medicaid eligibility to all SSI cash recipients but requires them to make a separate application for Medicaid. Since two application processes are required, this option may reduce the number of SSI recipients enrolled in Medicaid. The third option, used by Illinois, is to take advantage of Section 209(b) to establish more restrictive criteria for Medicaid than for SSI. As a result, only 69 percent of SSI recipients in Illinois are enrolled in Medicaid.
Whether a state supplements SSI also affects Medicaid eligibility, since persons receiving state supplements are generally eligible for Medicaid. Arkansas and Maryland do not supplement SSI payments; Oregon and Maine supplement them only minimally ($1.70 and $10 a month, respectively). Illinois supplements on a case by case basis and Wisconsin's supplement is $101.70. Each of the six states has a medically needy program. SSI payment levels and medically needy income levels by state are illustrated in Table IV-1.
| TABLE IV-1: State Supplementation Levels and Medically Needy Levels for an Aged Individual Living Independently in 1986 | |||
| State | Total SSI/SSPBenefit Level | State Supplementation | Medically NeedyLevel |
| AR | $336.00 | $0.00 | $108 |
| IL | Variable | Variable | 267 |
| ME | 336.00 | 0.00 | 325 |
| MD | 346.00 | 10.00 | 336 |
| OR | 338.70 | 1.70 | 355 |
| WI | 438.70 | 101.70 | 438 |
| SOURCES: Social Security Administration, The Supplemental Security Income Program for Aged, Blind, and Disabled. Characteristics of State Assistance Programs for SSI Recipients, and Commerce Clearinghouse, Medicare and Medicaid Guide. All data are for 1986. Prepared by Brian Burwell. | |||
| TABLE IV-2: Medicaid Coverage of the Elderly in the Six Study States: 1985 | |||
| State | Percent Elderlyon Medicaid | Percent Elderlyin Poverty | Ratio on Non-InstitutionalizedElderly on Medicaid toElderly in Poverty |
| AR | 18.7 | 28.2 | 0.47 |
| IL | 7.0 | 9.9 | 0.32 |
| ME | 11.0 | 12.0 | 0.45 |
| MD | 15.3 | 16.4 | 0.56 |
| OR | 6.4 | 11.8 | 0.28 |
| WI | 13.6 | 9.4 | 0.57 |
| SOURCES: HCFA 2082 data, Bureau of Data Management and Strategy; U.S. Bureau of the Census; and 1985 March Current Population Survey. Percent Elderly on Medicaid includes nursing home recipients. Data include adjustments to HCFA 2082 data for disabled Medicaid recipients over age 65. Prepared by Brian Burwell. | |||
The combination of these and other Medicaid eligibility policies shape the extent to which older persons living in the community can qualify financially for Medicaid. Table IV-2 illustrates the proportion of low income persons living in the community who received medical assistance from Medicaid in 1985. This proportion is an indicator of how broadly the Medicaid program covers the low income elderly population in each state as a result of state specific Medicaid eligibility criteria. It does not measure the proportion of low income older persons who received Medicaid community based services. It does, however, indicate how effective each state's Medicaid program would be in reaching the elderly low income population in need of community based care without a waiver of any Medicaid eligibility criteria. It is interesting that Oregon and Illinois, with the smallest percentages of their low income elderly enrolled in Medicaid, make such extensive use of Medicaid waiver programs in comparison to other states. However, Illinois compensates for its stringent Medicaid eligibility criteria by investing significantly more state resources in their Community Care Program than in services under the Medicaid waiver. Oregon has extended eligibility for waiver services to persons with incomes up to 300% of SSI as illustrated in Table IV-3. Under this option older people can buy into the waiver by paying the difference between their monthly income and the SSI level -- as one half of Oregon's case load has done. Therefore, Oregon has been able to expand the number of persons which can be served due to unique eligibility criteria available for waiver programs.
Wisconsin and Maine have also adopted the 300% of SSI eligibility option. In addition, they have received a waiver of Medicaid deeming rules allowing them to count only the income and assets of the applicant in determining Medicaid eligibility for waivered services (rather than having to include those of the applicant's spouse).
ELIGIBILITY FOR STATE FUNDED PROGRAMS. State Medicaid eligibility criteria are usually not developed with an explicit consideration of the unique affects on older people needing community care services. Eligibility criteria for state funded programs are, however. As noted earlier there are two methods for using financial criteria to define target populations. One is establishing an eligibility ceiling, with persons having incomes above the specified level prohibited from receiving any program benefits. The second method is using cost sharing provisions to set sliding fee scales based on income. State funded programs use cost sharing in five of the six study states. Arkansas is the exception, using an eligibility ceiling of 125 percent of poverty as the income cut off for receiving state financed personal care. Table IV-3 summarizes the eligibility criteria and cost sharing scales for the major long term care programs in each of the six states.
Under cost sharing policies, clients having incomes above a certain threshold are required to pay a percentage of their total service costs. The percentage usually increases with higher income levels until the client is fully responsible for the entire cost. This method is used for the In-Home Aides Program in Maryland, Home Based Care in Maine, Oregon Project Independence and in Wisconsin for the Community Options Program. Usually the income level at which cost sharing begins is tied to a general principle (i.e., 80 percent of the state's median income) so that the actual income amount can change every year, without changing the standard.
Illinois uses a variation of these cost sharing principles. A portion of a client's income over $426 a month is applied to the cost of the approved care plan. The actual percentage varies with client impairment levels and service utilization. Persons who use substantial amounts of services in relation to their impairment level will have a higher percentage of their income above $426 a month devoted to the cost of their care.
| TABLE IV-3: Major State LTC Programs Financial Eligibility Criteria for anIndividual in 1986 | ||||||
| Arkansas | Illinois | Maine | Maryland | Oregon | Wisconsin | |
| Medicaid: SSI Recipients | $336 | Variable | $346 | $336 | $338 | $438 |
| Medicaid: Medically Needy Level | $108 | $267 | $336 | $325 | $355 | $438 |
| Medicaid: Waiver Criteria* | NA | NA | $1,008 | NA | $1,008 | $1,008 |
| State Funded: Eligibility Ceiling | 125% poverty ($573 month) | NA | NA | NA | NA | NA |
| SSBG: Eligibility Ceiling | 80% of State Median Income ($779 month) | NA | 80% of State Median Income($661 month) | In-Home Aides: ($1230) (Income Level for Start of Cost Sharing) | NA | Supportive Home Care: Income($789) |
| State Funded: Income Level for Start of Cost Sharing | NA | Community Care Program: $426 month | Home Based Care: $600 minimum; higher depending on medical expenses | Gateway II: ($15,863) Eligibility Ceiling: Not Cost Sharing | Oregon Project Independence: 125% Poverty($573 month) | Community Options Program: $463; can be higher depending on individual medical expensesAlzheimers Caregiver Grants: $760 month family income |
| Not included in the chart is the Older Americans Act (OAA) which finances some community care services for the elderly, although at a significantly lower funding level than programs in the six states supported with state general revenues. Federal policies explicitly prohibit the use of income eligibility criteria or client cost sharing in administration of the OAA program, yet the Act is laced with directives to target services to low income and minority older people. State officials have actively and unsuccessfully sought federal policy changes which would provide them with increased authority to use income criteria to better target services.* Maine, Oregon and Wisconsin use the special option for waiver programs which allows persons with incomes up to 300 percent of SSI to buy into the waiver by paying the difference between their monthly income and the SSI level.** Social Services Block Grant Programs in Maryland and Wisconsin include substantial amounts of state general revenues. The federal and state funds are co-mingled and amdinistered as one program. | ||||||
Arkansas's financial criteria exemplify the interface between available state resources and eligibility decisions. State funds finance personal care services for persons with incomes above the Medicaid eligibility level (SSI-$336 month) and below 125 percent of poverty ($573 month). State officials would like to initiate cost sharing through a sliding fee for persons with incomes above 125 percent of poverty; however, due to the large size of Arkansas' low income population, state funds are currently not sufficient both to cover personal care for persons below 125 percent of poverty and to partially subsidize care for persons above that amount.
Interestingly, leaders of state membership organizations of older people in the study states affirmed their support for cost sharing policies in interviews with project staff. In fact advocacy groups in Arkansas volunteered a desire for a sliding fee home care program in order to reach older people with moderate incomes.
Cost sharing policies are favored by state officials over eligibility cut offs for several reasons. First, cost sharing policies give a visible program priority to lower income persons by setting a floor below which services are fully subsidized while still permitting persons with moderate incomes to participate in the program and receive some partial public subsidy for services. Second, sliding fee scales can counter the images of "welfare" that are so resisted by older people; having lived through the depression they take pride in paying some portion of service costs themselves. Third, as in private insurance and Medicare, even nominal cost sharing makes the beneficiary more aware of the actual costs of care. Fourth, cost sharing policies are used in a variety of state human services programs; applying the same principles to programs for the elderly can promote equity across these programs, providing similar treatment of persons receiving publicly financed services, regardless of age. Finally, and most importantly, state officials have for the past 20 years lived with Medicaid rules which make program eligibility an all or nothing proposition. They want to prevent older people from becoming destitute and thus dependent upon Medicaid for the rest of their lives. Cost sharing policies do not require persons to relinquish all of their resources before receiving services.
Each state has developed a continuum of financial eligibility criteria with one program's income ceiling reached as another begins. Medicaid, of course, serves the poorest clients, with state funds reaching the near poor. State general revenues are essential to developing a long term care system that meets the needs of the elderly with low and moderate incomes; theoretically, the Older Americans Act can finance services for this population, but the program's small size limits its role as a major financing source. In the absence of state funds, individuals receiving publicly funded services in each of the study states except Wisconsin would have to be capable of living alone in the community on $350 a month or less while being sufficiently frail to need nursing home care.
Wisconsin is the exception in that, besides having a higher income threshold for Medicaid eligibility, it provides SSI recipients with an income supplement over the basic state SSI supplement for those persons receiving 40 hours of home care services a month. This special supplement is not used to finance community care services; rather it is provided for living expenses, based on the assumption that these clients are likely to incur increased living expenses due to their extreme frailty.
State approaches to setting income eligibility criteria reflect the same dilemma encountered in other human services programs. States with higher proportions of low income persons are the least able to finance needed services. Therefore, financial eligibility criteria becomes a function of both the size of the population who meet the criteria and the amount of available resources to finance care.
Functional Eligibility Criteria
Most community care programs have been established with the goal of providing in home services to persons who would otherwise require nursing home care. Therefore, program participation is often limited to persons who are at risk of nursing home placement. This criterion may seem rather straight forward. However, community care demonstrations and other research have shown the difficulty of developing assessments -- however precisely drawn -- that can identify those persons whose impairment levels indicate a need for nursing home care in the absence of community services -- in other words, that can predict actual nursing home utilization.
Officials in the six study states acknowledge this problem, have repeatedly redesigned their assessment tools to sharpen their targeting capabilities, and now think they are targeting as tightly as possible. In the end though, they agree that it is, practically speaking impossible to accurately measure client "intent" to enter a nursing home. Some older persons who by any objective standard need nursing home care and lack formal services will remain in their own homes with the extensive assistance from families and friends. Therefore, the creation of community care programs, will itself increase the demand for care, because some older people with significant levels of impairment will be eligible for services in their home that were not previously available.
Access to community care programs in each of the six study states is based on a functional assessment of client limitations in activities of daily living. Since the assessment process leads to service authorization, the study states have consciously placed this function in agencies that do not directly provide publicly financed long term care services.9 In four of the six states, assessments are performed by the same agency (and sometimes by the same staff) that provide ongoing case management. In Illinois, for example, these agencies are Case Coordination Units; in Maine and Oregon, they are area agencies on aging; in Wisconsin they are County Social Service Departments or (less frequently) Mental Health Boards.
In Arkansas assessments are handled by two area agencies on aging designated by the state through a competitive process. These projects assess client needs for Medicaid funded personal care services and authorize Medicaid payment. The two area agencies on aging serving as assessment agencies do not provide personal care services; the other six area agencies are the direct providers.
In Maryland the Geriatric Evaluation Service of local health departments usually conduct the assessments; however in a few counties, area agencies on aging and departments of social services may perform some assessments as well. Case management is usually provided by departments of social services.
All the study states except Wisconsin use a standard assessment tool to determine eligibility for most community care programs. Using a standardized assessment tool to determine need for community long term care services may seem rather straightforward. However, its development generally entails months of disagreement among health professionals, social workers, and various program administrators over the factors that are most likely to indicate need for their individual programs.
In Wisconsin the state has developed a recommended assessment form, but counties are free to use their own. There is a standardized screening tool, however, which sorts out those persons with more routine service needs who could be helped through information and referral services from those needing detailed assessments. The standardized screening tool provides some statewide uniformity. The screen determines eligibility; the assessment is used for developing individual care plans. Assessment tools primarily measure client functional impairments, mental health status, and informal support systems, while giving less emphasis to medical conditions. Consistent with that focus, states are placing less importance on requiring a registered nurse to participate in assessments. Illinois, Maryland and Oregon allow assessments to be performed solely by social workers. Maine's Home Based Care Program uses assessments performed by social workers, but the waiver component requires that a nurse review the assessment results; Wisconsin requires a nurse/social work team, but grants exceptions. In contrast, Arkansas uses registered nurses instead of social workers and requires physician review. Since the personal care program in Arkansas is financed through the Medicaid state plan rather than a 2176 waiver, federal rules require a more medical orientation, with services ordered by a physician. States with the flexibility to decide whether this requirement makes sense (under waiver programs and those funded with state general revenues) have not chosen to adopt it.
The results of client assessments determine whether an individual's impairment level meets nursing home admission criteria, thereby indicating eligibility for community care services. Some factors, such as the strength of a person's informal supports, may not explicitly be used to deny program eligibility; but the presence of informal supports most certainly will shape the type and amount of care which case managers authorize.
An interesting dilemma arises in considering the presence of a family caregiver as a factor in program eligibility. Research has definitively identified the lack of an informal support system as a major determinant of whether an older person is likely to enter a nursing home. Since many state community care programs attempt to serve only persons who would otherwise need institutional care, should they restrict participation to only those persons without any family caregivers? Or should services be provided to supplement the assistance of family caregivers in order to prevent family burn out and eventual nursing home placement? A further consideration is whether public agencies should make ethical decisions about the appropriate contribution of family caregivers. Should an older person without a nearby family receive services while someone with similar impairments having a daughter in close proximity be refused care? These moral judgments are often skirted by granting eligibility while limiting the services authorized.
Oregon and Illinois, the two states exerting the strongest centralized control over their community care systems, are the most specific in their measures used to determine client functional eligibility. Assessment tools in these two states are structured to produce a numerical score. If the score is below a certain cutoff individuals are not eligible. This permits the eligibility cutoff to be adjusted depending on availability of care. Oregon raised the score needed for eligibility in 1986, for example, in response to limited funds and growing case loads.
Wisconsin has explicitly rejected imposing a numerical assessment score out of concern that case managers would lose a measure of creativity and begin developing standardized care plans for certain scores. Having invested substantial effort in creating a very flexible program, officials did not want to lose the emphasis placed on individually tailored care plans. It is instructive to note in this context that Oregon's scoring system, although it has somewhat diminished the latitude given to case managers, has not prevented care plans from being individualized, as discussed in the next section.
In Arkansas assessment staff also use a standardized tool, although eligibility is not determined solely on the basis of a numerical score. Since Arkansas' community care system is built primarily on personal care services provided under the Medicaid state plan "medical necessity" for long term care services must be demonstrated in addition to limited functional capacity.
Arkansas' experience in conducting client assessments for persons seeking personal care services provided under the Medicaid state plan has great relevance for other states considering the same approach. One of the drawbacks states have perceived in going the state plan route is the entitlement nature of Medicaid services. Unlike waivered services, state plan services must be available on a statewide basis and cannot be restricted to just the elderly. However, by requiring recipients to participate in a formal assessment process, Arkansas has been able to place some controls on program utilization -- a major concern faced by other states in financing personal care under the state plan.
As the need for long term care services grows, states may be faced increasingly with the prospect of directing all community services to the care of the most impaired and the poorest, while lacking adequate resources to also maintain programs designed to keep older people healthy and living independently. For example, Oregon Project Independence had been providing services to persons with functional limitations who were not as impaired as the long term care population. Last year state policies were changed to require OPI program participants to meet the same functional criteria as Medicaid waiver clients. Wisconsin's Supportive Home Care Program still serves some persons with impairment levels lower than those required for participation in the Community Options Program, although Supportive Home Care is frequently used at the local level to supplement services to COP clients.
Using tightly drawn functional assessment tools will become increasingly important in containing overall costs as the need for long term care services expands. The continuing dilemma is balancing stringent functional eligibility criteria with the ability to assist older people before they become too impaired to continue living independently in the community.
Case Management
Case management has emerged as a critical process to effectively guide the use of limited public and private resources for the support of vulnerable older persons. Developing flexible systems of service for the elderly is the primary objective of state long term care initiatives. Case management is one vehicle for achieving this objective. Statewide service delivery systems coordinated through case management are in place in each of the six study states.
Although specific functions assigned by states to case management agencies vary, general areas of responsibility include developing cost effective individual care plans, authorizing needed services and following up to ensure that needed services are actually provided. In each state significant emphasis is placed on building the formal plan of care around the core supports provided by families and friends. Usually policies require that older persons and their informal caregivers be active participants in the care planning process, although several state officials noted that the lack of family supports is the primary reason clients seek formal services.
The scope of case management activities within each state is affected by 1) the locus of responsibility for financial and functional eligibility determination; 2) the range of existing services and providers; 3) the emphasis placed on utilization controls through service authorization; and 4) whether case management is explicitly defined as a universal benefit for all older people with long term care needs or is limited to those persons financially eligible for publicly funded services. A review of each of these four factors serves to highlight differences and similarities in case managers' responsibilities across the six study states.
RESPONSIBILITIES FOR FUNCTIONAL AND FINANCIAL ELIGIBILITY DETERMINATION. Assigning these two functions to case management agencies creates a single service entry point for older people in need of long term care. Only in Oregon and Wisconsin has this been done for all long term care clients, irrespective of funding source. Illinois and Maine have placed responsibility for client functional assessments with the care management agency, but another agency certifies Medicaid financial eligibility. Maryland has a unified entry point for some clients, but multiple agencies for others. Arkansas has a different agency for each function except for clients receiving state funded services, for whom case management and financial eligibility are combined. Table IV-4 shows the local agencies in each state that have been assigned responsibility for case management, financial eligibility determination and functional eligibility determination.
| TABLE IV-4: Local Agencies Performing Case Management Functions | ||||
| Case ManagementAgencies | Local Agencies Conducting | |||
| Functional Assessments | Financial Eligibility(State Programs) | Financial Eligibility(Medicaid) | ||
| AR | Area Agencies on Aging (AAA) | Client Assessment Teams | AAA | Dept. of Human Services |
| IL | Case Coordination Units (CCU) | CCU | CCU | Dept. of Publi Aid |
| MD | AAA | AAA | AAA | |
| Dept. of Social Serivces | DSS | DSS | DSS | |
| Health Dept. | HD | |||
| ME | AAA | AAA | AAA | Dept. of Human Services |
| OR | AAA | AAA | AAA | AAA |
| WI | County Depts. of Social Services (usually) | DSS | DSS | DSS |
Medicaid financial eligibility determination seems to be the function which is the most difficult to integrate with other access activities. In state funded programs, usually the local agencies assigned to assess clients' functional capacities and provide case management also set client cost sharing amounts. Thus in state funded programs, financial and functional eligibility criteria are usually reviewed by the same agency. Medicaid rules, however, limit the agencies that can handle financial eligibility determination. Only in Oregon and Wisconsin, the two states with a single entry point can older people go to the same agency for Medicaid financial and functional eligibility. And in Oregon, lengthy discussions with HCFA were necessary to achieve this single entry point since normal Medicaid rules permit a state to either determine eligibility through state employees or through local governmental employees, but not through a combination of both. With the Medicaid program being administered through local offices of the state for all other populations, the case management agencies (part of local government) would not be permitted to determine financial eligibility for the elderly long term care population. Ultimately, Oregon was allowed to create a single entry point, but had to agree to a state level paper review of eligibility decisions conducted retroactively.
This dichotomy between financial eligibility determination for state funded programs and Medicaid complicates case managers' roles. When computing client cost sharing amounts for state funded services, case managers must request the same type of financial information needed for Medicaid determination. In addition, to maximize the use of state funds every effort is made to obtain Medicaid payment when clients appear to be Medicaid eligible. In states with multiple entry points this means that clients must be referred by the case manager to another agency for Medicaid eligibility determination. In making this referral, one aspect of a case manager's job is frequently seen as assisting older people, if necessary, to complete the required paperwork for Medicaid enrollment. Depending on the complexity of the eligibility process, significant amounts of a case manager's time can be expended on this task.
Other options for determining Medicaid financial eligibility need to be explored. Older people themselves are the most negatively affected by these multiple referrals in most of the study states. Elderly long term care clients have already been assessed as needing nursing home care and as a result have limited capacities to maneuver through the process.
RANGE OF SERVICES AND PROVIDERS. The service options available to case managers in developing individual care plans can vary widely. Maine and Wisconsin very consciously have avoided specifying the scope of services that can be provided under the Home Based Care Program and the Community Options Program. Thus services can be combined in any number of ways, requiring and encouraging significant creativity by case managers.
Other states have tightly constrained service options. Illinois case managers, for example, can draw upon homemaker, chore and day care services. Arkansas case managers can only draw on personal care services, although the tasks performed by the worker are fairly broad and tailored to individual needs. Maryland's case managers primarily use in-home aides and personal care; however, under the Gateway II program, the choices are as broad as in Maine and Wisconsin. Oregon, like Arkansas, provides most of its community long term care services under the general term of home care, although adult foster care provided in family type settings for up to five older persons is growing in importance.
Unlike in the other five states, Oregon case managers are assigned to handle nursing home case loads as well as clients living in the community. As part of relocation planning case managers conduct a systematic review of all Medicaid nursing home residents within 30, 60, and 90 days of admission to assess whether their needs could be met in a less restrictive setting. If so, a plan is developed for transition to community care. In urban areas of the state, certain case managers' case loads may be entirely made up of nursing home residents. In rural areas an individual case manager may have clients in both institutional and community settings. Oregon state officials credit part of their success in reducing the size of Medicaid nursing home caseloads to their emphasis on relocation planning. Local program managers, however, sometimes see this activity as diverting staff attention from the community care case load.
In addition to the scope of services covered by a state's long term care program, characteristics of the service provider system affect case managers' roles. The most basic distinction is one of supply. Are there multiple agencies providing different services and therefore requiring significant coordination? Or are there only one or two agencies that are stretched to their capacity? Or, more importantly, are services delivered by independent providers rather than through agencies? If so, more time will be spent by case managers in locating individual providers, scheduling their visits and authorizing their payments. Maine, Oregon, Maryland and Wisconsin make extensive use of independent providers, particularly in rural areas. In contrast, agency providers are used in Illinois almost exclusively for services for the elderly, although similar services provided to the developmentally disabled are delivered by independent contractors. Arkansas case management agencies are also direct providers of services. Chapter V analyzes in greater detail state experiences with different types of providers. This discussion merely notes the effects of different arrangements on case management systems.
SERVICE AUTHORIZATION. All six study states have empowered local case management agencies to authorize the use of long term care funds for individual client services. In fact, the only way a person can receive services under the major state programs is through authorization of a case manager. Arkansas is an exception in that the Client Assessment Team rather than the case managers authorizes the provision of services, since the case managers and personal case workers are both employed by the area agencies on aging. Even so, Arkansas shares with the other five study states two important principles. First, an agency outside of state government has been given responsibility for service authorization, which in long term care systems is equivalent to allocating public resources; and second, service authorization has almost always been separated from service delivery.
As previously discussed, one responsibility of case managers in all six states is managing and coordinating needed services on behalf of elderly clients. This might be described as an advocacy function. However, case managers are also gatekeepers, controlling client utilization of community based services. Although case managers have both responsibilities, emphasis on the gatekeeping function is increasing as cost effectiveness concerns intensify.
The parameters of utilization control activities conducted by case managers vary based on other long term care policies, in particular ceilings on the allowable cost of individual care plans. Table IV-5 illustrates state established cost limits on individual community care plans, which are usually tied to the monthly cost of nursing home care in each state. Medicaid waiver policy specifies that for the entire program clientele, community care services can be no more costly than nursing home care. Besides limiting the average cost per case, some waiver programs also place a ceiling on expenditures for individual care plans. Limits on the cost of individual care plans have also been adopted by several of the state funded programs. As Medicaid nursing home rates vary dramatically across the country, so do the cost limits applied to publicly funded individual community care plans.
In Maine case managers authorize service provision under both the state funded Home Based Care Program and the Medicaid waiver component. In both cases, ceilings on the cost of individual care plans are placed at the cost of nursing home care. State officials note that since the inception of the Home Based Care Program, case managers roles have increasingly focused on cost containment, especially with the advent of the Medicaid waiver component. In order to obtain approval of their waiver request, Maine was required to limit per case expenditures to 75 percent of nursing home costs. A year later through the Consolidated Omnibus Budget Reconciliation Act of 1985, Congress prohibited HCFA from requiring states to meet a community care cost standard more stringent than "equal to or less than" the costs of care provided in a nursing home. During the interim period, however, case managers transferred Medicaid clients with severe impairments (and therefore higher service costs) from the waiver program to the state funded case load to avoid exceeding the 75 percent limitation.
Personal care services in Arkansas are subject to a limitation of 72 hours per month, which at $6.00 an hour now equals $432. Originally the cap was pegged to 80 percent of nursing home costs; however that percentage has declined with increased nursing home rates and stable rates for personal care. Since the personal care program is a state plan service and therefore a Medicaid entitlement, there is no ceiling on the number of persons that can be served (as in waiver programs) and no limit on total program expenditures (as in legislative appropriations for state funded programs). As a result, a well-managed process for client assessment and service authorization is especially important to control utilization.
| TABLE IV-5: Cost Limits on Service Authorization 1986 | |
| AR | Medicaid Personal Care Services$432 month |
| IL | Community Care Program (Medicaid waiver component)$980 month (average cost of nursing home care) |
| MD | Gateway IIAverage cost of nursing home care varies by geographic area |
| In-Home Aides$640 month (2/3 of average cost of nursing home care) | |
| ME | Home Based Care and Medicaid waiver component$915 month (cost of ICF care) |
| OR | Medicaid WaiverNo individual case limit$833 month limit on the average for all clients (cost of ICF care) |
| WI | Community Options ProgramNo individual case limit$550 month limit on the average for all clients (equal to the state share -- 42% of nursing home care) |
| Medicaid waiverNo individual case limit$1280 month on average for all clients (average cost of nursing home care) | |
| Alzheimer's Family Caregiver Grants$4000 year | |
Similarly in Illinois, significant emphasis is placed on assessment and service authorization. Prior to the 1983 court ruling that interpreted the program to be an entitlement, local service providers could determine the amount and scope of services provided within state specified cost caps. Now, with the program having entitlement status, assessment and service authorization have been separated from providers and lodged with Case Coordinating Units. Medicaid waiver clients can receive a service package with a total monthly cost no greater than a limit related to the average cost of institutional care. For non-Medicaid clients, Illinois' cost sharing provisions explicitly encourage minimal intervention.
Oregon shares Illinois' concern for appropriately limiting the package of services authorized. For both the large Medicaid waiver program and the smaller state funded Oregon Project Independence, state officials have developed a computer program for case managers use in developing care plans and authorizing services. Client assessment data are entered into the computer, producing a numerical score and a recommended level of service. Although the case manager is not required to accept the recommended care plan, state officials believe this system balances any tendency to authorize more services than needed. Like the other states using Medicaid waivers, the average cost per case cannot exceed the cost of nursing home care. However, Oregon does not limit each care plan to that standard.
Maryland has three service authorization processes depending on which program is used. In-home aide services are authorized by case managers in County Departments of Social Services. Medicaid personal care services are authorized by nurses under contract with the Department of Health and Mental Hygiene and Gateway II services are authorized by the local lead agency chosen by county officials. The total public cost for services provided to Gateway II clients must be less than the average cost of nursing home care. In-home aides clients are limited to services costing up to two-thirds of average nursing home rates. There is no upper limit on personal care services, although low provider rates keep down total costs.
In Wisconsin almost all publicly financed community care services are authorized by case managers in county Departments of Social Services (DSS). Occasionally counties have chosen the agency managing mental health and developmental disabilities programs as the lead agency for the Community Options Program (COP) instead of DSS; however most often county DSS offices authorize services provided under COP, Supportive Home Care and the Medicaid waiver, and determine the size of individual Alzheimer's Family Caregiver grants. There is no official limit on the number of supportive home care hours that can be authorized, although these clients are usually less impaired than persons served under COP. Grants to Alzheimer's family caregivers are limited to $4,000 a year per family.
The Community Options Program does not limit the cost of services to an individual, but requires within each county that on the average, program expenditures per client not exceed the state share of Medicaid nursing home costs. When COP was created the Medicaid waivers did not exist. For this and a variety of programmatic and policy reasons, state funds have continued to be used instead of Medicaid. Connecting a limit on expenditures under the state funded community care program to the state share of Medicaid nursing home costs, along with the multi-year freeze on nursing home certificates of need has helped make the Community Options Program budget neutral. With Wisconsin's relatively generous nursing home reimbursement rates, 42 percent of nursing home costs (the state share) is still adequate to finance the care of most community clients.
Wisconsin's approach provides an interesting perspective on issues faced in service authorization under a county formula grant program in contrast to an individual entitlement program. When a local case management agency has been granted a finite amount of program funds, it may attempt to serve as many persons as possible by providing a lower level of care than is actually needed by some clients. State officials are concerned that eventually this can result in clients with higher impairment levels being unable to remain in the community.
Other study states also observed that formula allocation programs may create local incentives to reduce needed levels of care. Illinois, for example, found that prior to the court case changing its program from a formula grant to an individual entitlement, local agencies responded to community pressures to serve as many persons as possible by funding very limited care plans, perhaps to an extent that was detrimental to older people. A study of in-home service programs conducted by the Maryland Department of Budget and Fiscal Planning also found that local Departments of Social Services have at times responded to excess demand by reducing the type and intensity of services authorized.10 As that study noted, a fundamental policy question is whether services should be limited to the most impaired or whether a broader group of persons should receive services that only partially meet their needs.11 Long term care programs in the six study states have usually opted for meeting the more intensive needs of the most impaired, recognizing that those persons not served may also have significant functional limitations. With a growing population in need of long term care and constrained program budgets, incentives to spread service funds thinly still remain.
To address this dilemma, Wisconsin state officials, after several years of operational experience, now require counties serving more than 25 persons to reserve a minimum of 20 percent of their case load for high cost cases, defined as persons needing a care plan costing twice the allowable average. In 1986 this amount was $1100. For the balance of their caseloads, counties are required to set ceilings on the maximum cost of individual care plans at least as high as $800 a month.
State officials note that case managers in entitlement systems may have the opposite incentives, resulting in a tendency to authorize more services than needed. State sponsored training programs can help case managers be more aware of cost containment concerns. Staff of Illinois' Case Coordinating Units report that case managers have slowly become more comfortable with limiting services instead of authorizing a complete package of all potentially available services. As they gain more experience in monitoring the implementation of care plans, case managers get firsthand feedback on the scope of services needed and can make any necessary adjustments.
Service authorization responsibilities set case managers in the study states apart from those in some other localities across the country where case managers arrange for client services without the authority to order service provision. In managed systems of care financed by state resources and state administered federal funds such as Medicaid, state government can designate case management agencies to act as agents of the state in authorizing needed services. Without an explicit delegation of this authority, case management agencies can help older people locate services but cannot directly allocate public resources to individual care plans.
CASE MANAGEMENT FOR PRIVATE PAY CLIENTS. The study states have in varying degrees considered the appropriate role of public case management systems in arranging community care for persons not financially eligible for state subsidized services. Numerous issues are involved. What is government's responsibility for linking consumers with services purchased in the private market? Do state initiatives to make publicly financed systems more responsive to low and moderate income elderly logically extend to helping higher income persons gain better access to needed care? More practically, can governments currently afford to provide care planning services as a public entitlement to all persons needing long term care?
There are distinct advantages to expanding the role of state designated case management systems to assist older people in all income levels. First, these systems can link family caregivers to a limited set of formal services designed to help sustain their informal assistance and delay the need for more intensive care. Second, by directing the state designated case management system to serve as an access point for all persons needing care planning, states can minimize the development of two-class service systems where publicly assisted clients enter through one door and private pay clients enter through another.
It is, of course, true that some components of case management services for publicly assisted clients are not applicable for private pay clients (for example, financial eligibility criteria are not relevant and services are not formally authorized). But case managers can act as valuable counselors, helping older people and their families identify potential sources of assistance.
The six study states differ substantially in how private pay clients are handled. From their inception some state programs included the provision of case management services, supported with public funds, for persons not meeting the income criteria for services. In some programs resources are explicitly allocated to this purpose; in others care planning assistance is handled more informally. Some states, however, limit case managers' roles to assisting clients financially eligible for services.
Of the six states, Wisconsin has made by far the most explicit commitment to providing care planning assistance to private pay clients. From the start, the Community Options Program was designed to offer assessments and care planning to all functionally impaired persons as a public entitlement, with direct services provided on a sliding fee basis. In fact counties are given two separate allocations of funds, one for assessments and care planning and another for direct services. Asserting that all long term care clients need some help in sorting out the service delivery system, the original architects created a program with broad based appeal.
Two factors shaped their approach. One was a fairly widespread philosophy in Wisconsin that state government has a role in strengthening informal systems of care (the state funded Alzheimer's grants are another indication of that perception). Second, Wisconsin has one of the lowest percentages of older people with incomes below the poverty level, partly due to high SSI state supplements. As a result many people are able to pay for at least part of their service package, freeing more public funds for care planning.
One quarter of all persons receiving state funded assessments and care planning assistance under the Community Options Program in 1986 fully paid for all needed direct services. This indicates, state officials assert, that their publicly funded access system does not have a "welfare" image but is rather seen as an acceptable and appropriate way to link all impaired persons to services.
Illinois has also provided some case management services through Case Coordinating Units to private pay clients, although not to the same degree as Wisconsin. Case Coordinating Units were originally designated jointly by the state Department on Aging and by Area Agencies on Aging, with the rationale that Community Care Program funds allocated by the state would support case management for persons meeting program eligibility criteria, while Older Americans Act funds administered by the area agencies would be used for all other long term care clients.
Oregon funds risk intervention case managers who help arrange services for persons who due to either impairment levels or income are not eligible for services financed through public programs. This approach was adopted in response to cutbacks in state and federal programs which provided less intensive services. However, as the private pay clientele expands, risk intervention case managers are able to assist a shrinking percentage of the total.
Maryland's Gateway II program serves some "case management only" clients, consistent with its purpose of helping to better coordinate existing services while funding gap filling services as a last resort. Care planning has always been seen as a program component not subject to client financial eligibility criteria, although with limited program funds, the primary focus is on persons with low incomes.
Maine limits the percentage of Home Based Care funds which can be spent on case management primarily out of a concern for allocating as many resources as possible to direct care. The state also explicitly prohibits the use of HBC funds for case management assistance to persons ineligible for the program. Area agencies on aging have been pushing for approval to provide case management for a fee to persons ineligible for state supported services. However, the state is concerned that this would divert attention from the most needy populations, and since Older Americans Act funds are frequently used for some case management services, the prohibition on charging a fee under the OAA would greatly limit the ability to pool funds for case management.
Arkansas' case managers view themselves as a general resource to a wide range of older people; however state case management funds are directed to persons with low incomes.
The most significant factor distinguishing the state with the greatest emphasis on assisting private pay clients (Wisconsin) from the state with the least emphasis (Arkansas) is the percentage of the older population with incomes below poverty. Wisconsin bas the lowest percentage of older people with incomes below poverty and, of the states in this study, Arkansas has the highest. Like its effect on financial eligibility criteria, a state's income characteristics shape the percentage of its population's needs which can be met through public programs, the size of the private pay market and the available state resources which can be devoted to long term care programs.
Pre-Admission Screening Programs
Pre-admission screening programs, are the entry points in state long term care systems for persons seeking nursing home care. For the purpose of this analysis, pre-admission screening is defined as "an assessment used to determine the need or appropriateness of nursing home care that goes beyond financial eligibility determination and physicians' certification of need to include an on-site evaluation of many aspects of a client's status."12 Instead of using a rather loose consideration of "medical necessity" for nursing home care (as is done in the absence of screening programs), a comprehensive examination is made of a person's functional, psychological and medical status with a bias toward determining whether informal supports combined with formal community services could meet the individual's long term care needs.
Besides being part of an organized access point for long term care services, pre-admission screening programs are a logical component of state policies designed to curb the growth of Medicaid institutional expenditures and apply the cost savings to an expanded community care system. Since a significant proportion of older people entering a nursing home become Medicaid eligible within a short period, the need for cost control has stimulated increased attention to potential "inappropriate placements." This concern is heightened by the realization that once an individual enters a nursing home, community supports erode, a residence and other possessions may be liquidated and return to the community -- even for someone inappropriately placed to begin with -- becomes unlikely. In addition, as discussed in Chapter III, most of the study states have placed strict limits on the construction of new nursing home beds. Tightening up on client access to institutional care through pre-admission screening programs complements efforts to control bed supply. Viewed as integral components of state community based care systems, pre-admission screening programs can link persons seeking nursing borne care with in-home services instead. Thus, in addition to having a cost containment focus, pre-admission screening programs are a vehicle for integrating client access to both institutional and community care.
In all six states, pre-admission screening programs are carried out by the same agencies that conduct assessments for clients initially seeking community care. Beyond these general parameters, state screening programs vary in significant ways.
STATE PROGRAM CHARACTERISTICS. Table IV-6 illustrates some of the major state differences. Some states include only Medicaid recipients in their programs; others include persons who, based on an assessment of their income and resources, are likely to become Medicaid eligible within 60, 90 or 180 days of nursing home placement. In most cases, participation of the target population is mandated in order to receive Medicaid payment for care. However, mandatory participation in the screen does not necessarily entail a binding decision on placement. Medicaid is the payment source for pre-admission screening programs in all six states.
| TABLE IV-6: Characteristics of Pre-Admission Screening Programs | |||
| AR(one quarter of state) | Medicaid | Mandatory | Binding |
| IL | Medicaid and eligibles | Mandatory | Binding |
| MD | Medicaid and 180 day eligibles | Mandatory | Advisory |
| ME | Medicaid | Mandatory | Binding |
| OR | Medicaid and 90 day eligibles | Mandatory | Binding |
| WI | Medicaid | Mandatory | Advisory |
| All | Voluntary | Advisory | |
Oregon and Illinois have the most rigorous programs. Both include potential Medicaid clients as well as current eligibles; both mandate participation of the target population and result in a binding decision on placement. In 1986 21 percent of persons seeking nursing home entry in Oregon were diverted to home care and Illinois diverted 18 percent. Since screening programs in the other four states either are not statewide or have been only recently initiated, comparable figures are not available. Even if the data were available, however, its relevance is questionable since there are so many factors that affect the rate of nursing home applications. For example several state officials noted that demand for pre-admission screening has declined as physicians and hospital discharge planners become more aware of community options.
Arkansas' program was established in 1983 through pilot projects covering one quarter of the state. These projects conducted nursing home pre-admission screening and assessments for clients seeking Medicaid funded personal care and home health. In 1986 the projects assumed statewide responsibility for assessing the need for and authorizing the provision of personal care. Nursing home pre-admission screening and assessments for home health were not expanded beyond the original geographic area, however.
Maine, Maryland and Wisconsin have created screening programs even more recently -- each having less stringent provisions than those of the other three states. Maine began on a small scale using assessments for only Medicaid clients seeking nursing home entry directly from the community, based on the theory that persons currently living in the community have the best chance of remaining. Now hospitalized Medicaid clients applying for nursing home admission are also included. The Maryland program was started too recently for any information on its operations to be available.
Wisconsin's Community Options Program requires counties to initiate pre-admission screening for Medicaid clients during their first year and then expand screening to cover all nursing home admissions by their fifth year of program operation. Since new counties were added to the COP program over a four year period, screening requirements have become effective at different times throughout the state. Counties are also required in their fifth year of COP implementation to screen all current Medicaid nursing home residents to determine whether relocation to the community might be possible. Neither counties nor nursing home providers are very happy with this requirement, arguing (1) that since most counties have waiting lists for services, it would be undesirable to raise nursing home residents' expectations and (2) that most nursing home residents have lost their community supports, their home and other possessions, making return to the community unlikely. Oregon's experience, however indicates that relocation may be achieved in some instances. Case managers assigned to monitor nursing home clients have in the past five years placed over 5,000 nursing home residents in community care settings.
NURSING HOME INDUSTRY ROLE IN SHAPING STATE SCREENING POLICY. Certain state screening program characteristics often result from political constraints rather than deliberate policy design; examples include the limited population groups covered, and the advisory nature of staff conclusions. Such limitations in scope and authority reflect the influence of the nursing home industry on state legislatures. Arkansas, Illinois, and Maine all began their programs by an administrative directive. Any further expansion they assert, would need legislative approval and would be fiercely fought by the industry. Interviews with nursing home representatives confirmed their strong opposition to any changes.
Arkansas state officials would like to expand their program statewide; Maine wants to include a broader population group; the executive branch in Oregon proposed to expand their program to private pay applicants, but has been stymied by the legislature; Maryland officials were forced to accept an advisory finding from screening results due to successful attempts by the industry to amend the authorizing legislation for pre-admission screening.
Various reasons are cited for nursing home opposition to program expansion. As one would expect, the appropriateness of state government being able to prohibit the entrance of private pay persons to nursing homes is questioned. In addition nursing home representatives maintain that decisions to enter a nursing home are not made lightly and usually few options remain; therefore the cost of administering the program would exceed the resulting benefit to the state Medicaid budget. State officials counter that a major benefit of pre-admission screening is the knowledge older people gain of other alternatives.
INTEGRATING ACCESS TO COMMUNITY BASED AND INSTITUTIONAL LONG TERM CARE. One of the most important features of state pre-admission screening programs, at least in principle, is the links created among community care, nursing home care and acute care. Since all six study states have assigned primary responsibility for screening programs to the agencies conducting client assessments for community care, a central entry point for non-institutional and institutional long term care services has been created. In addition, most of the study states use the same assessment tool for both functions. While states would like stronger pre-admission screening programs, they note that simply making people aware of their community care options can go a long way in deferring nursing home entry. A single access point enhances the potential that clients will receive information on an entire range of possible alternatives.
The link between acute care and long term care has been less satisfactorily made. When linking community based care with nursing home care, states can control access to the delivery system, since long term care is financed mostly through state resources and the state administered Medicaid program. Acute care is controlled primarily by physicians and hospitals -- both paid by Medicare. Since states cannot mandate cooperation, they have to use their powers of persuasion with physicians and hospital discharge planners. Convincing them of the value of skilled home care is difficult; encouraging them to make referrals to non-medical state community care programs is even more challenging.
Pre-admission screening programs face predictable resistance from physicians and hospital discharge planners, who initially view the process as one more layer of bureaucracy. Also, doctors resent intrusions into their authority and discharge planners claim that some form of pre-admission screening is already part of their ongoing responsibilities. In order to solicit the cooperation of discharge planners, Maine and some Wisconsin counties contract with them for assessments of hospital patients seeking nursing home care. With the same purpose, Illinois encourages hospital discharge planners to work with their pre-admission screening staff and has adopted presumptive eligibility provisions for hospital discharges.
Local managers of pre-admission screening programs emphasize the importance of state leadership in providing needed public information and education in combating resistance from physicians and other health professionals. In particular, they believe that strong communications from state government to providers underscoring the permanence of the screening program and its authority to determine care needs would enhance the success of initial program implementation.
V. SERVICES SUPPORTED BY STATE COMMUNITY CARE PROGRAMS
States have designed new systems of care which have dramatically reorganized state and local management of long term care services to establish a single entry point for client services. The creation of uniform assessment tools, explicit financial eligibility criteria and case management services all make access to community care more predictable from a client's perspective and more standardized as viewed by program administrators. In contrast, the approach used for the actual provision of services frequently places a high value on diversity and informality, giving long term care consumers a substantial role in directing the way in which care is provided.
Community long term care services, which rely extensively on social supports to deal with chronic conditions, are vastly different from the acute care focus of more traditional Medicare funded skilled home health services. Long term care services are intended to compensate for limitations in an individual's ability to carry out normal activities of daily living; assistance is likely to be needed for an extended period of time. In contrast, skilled home health services address an individual's medical needs; they are frequently provided on a short term basis following hospital discharge, are prescribed by a physician, and delivered by a health care professional using a clinical focus. The provision of skilled home health services is triggered by a medical diagnosis; long term chronic care is based on functional need.
The primary or acute health care needs of long term care clients are addressed by Medicare and Medicaid funded physician services, hospital care and/or short term skilled home nursing. Since these services can be supported under existing federal and state programs, they are not usually covered by state long term care programs.
Establishing a new system of non-professional social supports to meet the long term care needs of the elderly demands a new way of conceptualizing home care. While various communities across the country have successfully undertaken small scale projects, building large statewide delivery systems is much more complicated. The challenge to states is to place some parameters around publicly financed services to make them cost effective and manageable without compromising the character of flexible, non-medical services which respond to individualized needs.
This chapter analyzes the scope of community based services supported by state systems and the developmental efforts undertaken to expand their supply. These efforts have focused on three types of care: in-home services, adult day care and services provided in alternative living arrangements. Approaches used by the six study states used to deliver these three types of care are explored in depth. Finally, new methods for assuring quality care are required to complement the non-medical nature of these services. State efforts to grapple with appropriate consumer safeguards are reviewed, and several methods having potential for replication by other states are discussed.
Overview of State Service Options
Service delivery systems for community care services respond to an array of client needs. In all six states these needs are addressed primarily through in-home services, which are considered to be the core of any community care program. There is, however, considerable variation among the six states in the extent to which they specify other allowable services that can be provided within the overall budget ceiling.
Maine and Wisconsin have deliberately avoided defining the services that can be supported under the Home Based Care Program and the Community Options Program. In these two states almost any service package is possible and officials in both states have their favorite anecdotes describing off-beat service packages uniquely designed for program participants. Wisconsin's program guidelines caution counties to avoid approaching care planning with the attitude of "what you need is what we have." They also explicitly state that there are no disallowed services; only disallowed settings (i.e., services provided in an institution).
The largest community care programs in Maryland and Arkansas have explicitly defined allowable services; yet both states have smaller, very flexible state funded programs which finance any service a client needs. Oregon's two programs delineate a half-dozen permissible services. Illinois represents the other end of the continuum from Maine and Wisconsin, using a tightly defined list of three services supported by its Community Care Program; however senior companion and home health are also provided on a very limited basis as part of demonstrations funded with state general revenue funds.
In spite of the fact that states vary in the extent to which they explicitly define permissible services, there are many similarities in the services actually provided. Categorizing state service options first requires some common definition of terms. Each state uses different names to describe essentially identical in-home services (such as personal care, supportive home care, homemaker, in-home aides). Differences in service titles in part reflect state traditions and in part are tied to funding streams used to finance the services. These services are typically defined to encompass a wide range of activities from heavy to light housekeeping and from minimal to substantial assistance with bathing, dressing, eating and other activities of daily living. Regardless of the service name, the focus and intensity of the service varies within states according to client need. It would therefore be a mistake to assume that a personal care worker in Arkansas performs a different range of activities than a homemaker in Illinois.
Adult day care is financed in Maryland with state general revenues and Medicaid, in Illinois as part of the Community Care Program, and in several geographic areas of Maine and Arkansas, as part of programs financed with state general revenues. Maryland and Maine both finance services for impaired older persons living in congregate housing. Through a special state supplement to SSI, Maine also supports the costs of board and care for low income older persons.
Oregon funds a limited amount of adult day care services through Oregon Project Independence, but does not include this service in its waiver program. However, providing care to persons in alternative living arrangements is a major service strategy in Oregon through the use of adult foster homes and residential care facilities.
Table V-1 illustrates the major service options available through state community care programs. While there are substantial similarities among states in the primary service strategies used (home care, adult day care and services in alternative living arrangements) there are significant differences in their implementation.
Home Care Services
A variety of factors influence how home care services are delivered within each state including the supply of formal providers, the philosophy and goals articulated during the creation of community care programs, and historical traditions in delivering similar services to other populations.
There are three basic vehicles for delivering home care services: agency providers, client employed providers and family caregivers. Most of the states use a combination of the three options, with the exception of Illinois which relies exclusively on agency providers.
| TABLE V-1. Major Services Supported by State Community Care Programs | |||
| Home Care | Adult Day Care | Services in AlternativeLiving Arrangements | |
| AR | Personal Care | Limited Supply | Board and Care |
| IL | Housekeeping/ChoreHomemaker | Allowable Service | |
| MD | Personal CareIn-Home Aides | Major Emphasis | Congregate Housing Services |
| ME | Personal Care Assistance | Demonstrations | Congregate Housing ServicesBoard and Care |
| OR | Home Care | Limited Emphasis | Adult Foster CareResidential Care Facilities |
| WI | Supportive Home Care | Allowable Service | Adult family HomesCommunity-Based Residential Facilities |
Regardless of the manner in which home care services are delivered, state officials express concern over the low wages paid to home care workers and the frequent lack of health insurance or pension benefits. Yet, with constrained budgets, the obvious trade off is to serve fewer older persons in need of care-also an unsatisfactory decision. Shortages of home care workers are also reported, usually in states with the strongest economies.
Table V-2 illustrates the provider options adopted by each state's home care program.
| TABLE V-2. Provider Options | ||
| Service | Provider Types | |
| AR | Personal Care | Area Agencies on AgingPublic and Private Agencies in CAT regions |
| IL | Housekeeping/ChoreHomemaker | Agency Providers: 60% Proprietary 40% Non-Profit |
| MD | Personal Care | Client Employed |
| In-Home Aides | Public and Private AgenciesClient Employed | |
| Gateway II | All the above and families | |
| ME | Personal Care Assistance | Client Employed Families |
| OR | Home Care | Client EmployedPrivate AgenciesFamilies |
| WI | Supportive Home Care | Client EmployedPublic and Private AgenciesFamilies |
AGENCY PROVIDERS. Of the six study states, only Illinois uses agency providers exclusively to deliver services. Chosen by a competitive bid process, about 60 percent of the providers in Illinois are proprietary agencies; the other 40 percent are private non-profit organizations such as Catholic Charities and Lutheran Social Services.
The cost containment features of Illinois' competitive bid process have created political tensions with the large and influential private non-profit providers since they were increasingly being underbid by proprietary agencies. In addition labor unions representing service workers objected to the bidding process since salary increases and fringe benefits were curtailed due to competition based on cost. As a result, the payment system and the selection process have been revised with providers now selected on the basis of performance measures, and the rates uniformly set by the Department on Aging. In response to the workers' concerns, providers must document that 73 percent of the payment rate is devoted to worker wages and benefits.
Other states have a much lower reliance on agency providers than Illinois. This difference seems to be attributable to several factors. First, Illinois manages a very large state-administered program with all provider payments issued at the state level. The sheer magnitude of direct payments which would be made under an independent contractor model would be administratively infeasible. Second, as a result of smaller programs preceding Illinois' current efforts, a large pool of provider agencies had been developed; re-enrolling them in the new program was relatively easy. Finally, and probably most importantly, using agency providers is consistent with other Illinois community care policies which result in a tightly managed, formalized service delivery system.
The other five study states use agency providers more selectively. Oregon uses a mix of provider types with agency providers being the most frequent form in urban areas. Area agencies on aging have the option of managing their own competitive bid process or requesting the state agency to include bids for their area in a statewide announcement. Maryland and Wisconsin also deliver services through various types of providers including independent contractors. Arkansas' area agencies on aging directly provide personal care services, having formerly managed the program through client employed workers. Maine uses home health agencies to administer the Alternative Long Term Care Program, which packages Medicaid home health with private duty nursing services and Medicaid personal care. These services are provided to a specialized population group with intensive medical needs.
Medicare certified home health agencies are generally not used to provide long term care services. While state officials praise their excellent post-acute skilled nursing care, they note that home health agencies' philosophies generally do not mesh with community based care, even when these agencies have expanded their service coverage beyond the traditional package of Medicare reimbursed services. Specifically noted is a tendency to respond in a way that is more medically related than necessary, desirable, or affordable. Even when the response is not over-professionalized, their Medicare mandated administrative processes produce overhead costs that result in high unit costs, making their services more expensive than comparable services provided by other agencies. Home health agencies counter that state systems are too informal; they insist that a stronger health focus is required, with all home care provided under the direction of registered nurses.
CLIENT EMPLOYED PROVIDERS. Independent contractors are the predominant provider type in Oregon, in the Maine Home Based Care Program and and in the Maryland personal care program. They are also extensively used in Wisconsin. They were the major provider type in Arkansas' personal care program until several years ago when the client employed workers were taken off independent contracts and put on the staff of area agencies on aging.
Complicated legal issues surround the definition of a client employed worker and the responsibilities of the employer (in this case the client) for handling such matters as social security taxes and coverage for workers compensation. The following discussion of these federally adopted legal provisions and resulting administrative responsibilities is drawn from an excellent technical assistance document prepared for county departments of social services by the Wisconsin Bureau of Long Term Support.13
Client employed workers are not part of an agency but are rather independent contractors who work directly for individuals. Administrative agencies responsible for setting generic employment standards and the courts have both used a test of "direction and control" to determine who is the legal employer of a worker. The practical implications of this test are that in order to establish a employer/employee relationship, the employer (in this case the client) must have the right to hire, supervise and fire a worker and to substantially determine the tasks to be performed. While case managers finalize a client's plan of care and authorize the amount of needed services, clients must be given the authority to control how their care plans are implemented.
Besides directing work performance, an employer must also comply with various provisions of laws governing minimum wage and payment of social security taxes. Federal income tax withholding is not required; participation in workers compensation varies from state to state; and rarely must unemployment compensation tax be paid. States using client employed providers often serve as fiscal agents for clients and handle payment of the various required taxes. State government directly performs this role in Oregon and sometimes in Maryland; area agencies on aging serve as fiscal agents in Maine; county departments of social services assume this responsibility in Wisconsin. With or without a fiscal agent, clients as employers must finalize all paperwork and certify the hours of service provided.
Procedures for recruiting workers are fairly consistent from state to state. Usually case managers ask clients whether someone they already know would be able and willing to serve as a paid provider, such as a friend or a worker who has successfully delivered care to an acquaintance. If no such person is available, an employee will be selected from a screened list of workers recruited by case managers. Case managers are responsible for ensuring that the provider is able to perform the assistance needed by the client. Wisconsin counties often contract with independent vendors (e.g., Independent Living Centers) to screen potential providers; to train recipients in hiring, firing, and supervising attendants; and to assist the recipient in various other employer duties.
Wisconsin, Maine and Oregon encourage the use of independent providers for philosophical reasons. Empowering clients to direct and manage their own care is consistent with their explicit emphasis on enhancing the independence of older people. Program guidelines and technical assistance materials prepared by these three states emphasize these values throughout. While independent providers may be less expensive than agency providers, potential cost savings do not seem to be the primary factor influencing the choice of this provider type in Wisconsin and Maine. Oregon emphasizes both cost advantages and program philosophy in encouraging the use of independent providers.
In the case of Maryland's Medicaid personal care program, the use of independent providers seems to be based largely on cost containment concerns. Interviews with state staff and state program documents do not reflect the philosophical emphasis present in Maine, Oregon and Wisconsin.
A management structure which can routinely handle payments to thousands of individuals is necessary to effectively administer an independent provider program. In particular state administrators recommend that the agency managing the community care program (either at the state or local level) assume the role of fiscal agent on behalf of the client. Under this model some of the administrative tasks performed by provider agencies must be handled at the local level by case management agencies or by state government. For example, the required paperwork for payment of social security taxes and workers compensation taxes must be filed; management information systems must be in place to handle payments to each individual provider rather than issuing one check to a provider agency; and payments must be made promptly in order to retain a large lower income work force. The costs of these types of management functions are normally part of provider agencies' overhead charges. Under an independent provider model the costs of these functions are assumed by state government or local case management agencies. Therefore a simple comparison of differences in unit costs for independent providers and agency providers will understate the expenses related to performance of fiscal agent responsibilities under the independent provider model.
Some orientation must be given to clients on how to handle their employer responsibilities; this task is normally assumed by case managers. Materials designed to assist in this orientation process have been prepared by state program staff. Maine has developed a clearly written consumer handbook titled "You and Your Personal Care Assistant" which gives clients guidance on managing the paperwork aspects of their employer responsibilities and offers advice on how to direct and supervise worker performance.
The use of client employed providers can be controversial. Critics (mainly agency providers) charge that the quality of care is lower, although state experiences with systems using a combination of provider types do not seem to support this theory. It is questionable whether a worker known to the client and/or screened by a case manager represents any greater risk to a client than a worker hired by an agency, although quality complaints may underestimate problems, since clients may be less likely to complain about someone known to them personally. Legitimate concerns are the low wages paid to workers and the absence of any employee benefits such as health care coverage; but these concerns often apply to homemakers and personal care workers employed by agency providers as well.
A mix of various agency providers and client employed providers is by far the most prevalent situation to be made by state community care systems. Thus the real decision is the relative emphasis to place on the use of each option.
FAMILY CAREGIVERS. Family caregivers are recognized as the primary provider of long term care services, and as such are the target for increased state efforts to provide them with non-monetary support in order to sustain their efforts. State policies explicitly establish linkages between informal supports and several aspects of formal service delivery systems. For example, family supports are one factor-used in assessing an individual's need for publicly assisted community care services. They are also acknowledged in the frequently articulated care planning goals of "building the formal system of care around existing informal supports." And their views are solicited as part of the pre-admission screening process. All of these policies relating to informal supports have become universally accepted principles that are relatively easy to implement.
Paying family caregivers, however, is another matter. Most state administrators seem to agree that paying family caregivers to be formal service providers is at times the most practical option. They note, however, that state and local elected officials are frequently uncomfortable with this approach because of philosophical concerns over using public funds to subsidize what are believed to be family obligations. Where such payment is made it is unvariably the option of last resort. Usually payments are linked to financial hardships resulting from caregiver activities, such as being unable to seek paid employment.
Paying families as caregivers is in some ways an extension of the independent provider concept since client employed workers are frequently persons previously known to clients such as neighbors or friends. Some legal requirements relating to independent providers, however, do not apply for family members -- such as making payments for social security taxes and meeting minimum wage standards.
In four of the six study states family caregivers can be paid as providers under some of the major long term care programs. These programs include the Community Options Program in Wisconsin, the Home Based Care Program in Maine, Gateway II in Maryland and both Oregon Project Independence and the waiver program in Oregon. In all these states, officials estimate that family caregivers are used in these programs in less than 10 percent of all cases. Maine and Maryland require prior state approval of all payments made to family members. Wisconsin allows payment to family members subject to each county's policy. Most counties permit payment if it does not reduce normal caregiving and is more cost-effective than using other providers. Some counties limit payments to situations where the caregiver foregoes outside employment in order to care for their relative. Of the four states permitting payments to families, only Oregon prohibits payment to spouses under its regular community care programs. However, the Oregon Senior Services Division does manage a specially appropriated account of $125,000 for state authorized spousal payments.
Wisconsin also has a specially designated appropriation for grants of up to $4,000 per year to family caregivers of Alzheimer's victims. In 1986 this program was funded at a level of $1.3 million. In commenting on this program at a NGA conference Wisconsin's aging director noted, "The public will to directly pay families seems to be aroused only in regard to dramatic situations of tragic disabling conditions. It is hard to get the same level of support for victims of strokes, for example."14
Adult Day Care
Adult day care services are expanding as increased emphasis is placed on supporting family caregivers. Not only does day care function as a respite service, particularly for families caring for an Alzheimer's victim; it also can offer active therapeutic treatment or simply socialization. It is not inexpensive, however, making state officials cautious about initiating the service as a regular program benefit. (They do note that with rates from $20-$35 a day it is less costly than eight hours of homemaker service).
In Maryland state general revenues are awarded to day care centers through an annual request for proposal process. In 1986 almost $1 million was allocated to 26 centers. These funds help defray initial start-up costs as well as subsidize sliding fee scales for persons who are not eligible for Medicaid. Adult day care is also a covered service under the Maryland Medicaid state plan with $4 million expended in 1986. State officials emphasize that without grant funds to cover some developmental costs, day care would not be as widely available since programs must, of course, be operational before any Medicaid support can be obtained.
Illinois' Community Care Program also finances adult day care delivered in a variety of locations including nursing homes, hospitals, senior centers and free standing sites. In 1986 $3.6 million was expended for day care services. Unlike Maryland, state funds are not available to new vendors to offset initial program costs. State officials identify the lack of start up assistance as a major deterrent to program development.
In Arkansas the state funded Alternative Care Program has provided the ability to expand the supply of adult day care by awarding small start-up grants. Oregon also funds limited amounts of day care under Oregon Project Independence and is currently examining whether day care is a cost effective service which should be provided across the state under its waiver program.
In Maine, as part of a general strategy to solicit nursing home support for community based care, a state funded demonstration project has provided developmental funds and some operational support for adult day care provided in several nursing homes. Further expansion has been stymied for several reasons, however, including a competitive posture by area agencies (which has limited client referrals) and nursing home dissatisfaction with community based reimbursement rates. Similar observations were made by nursing home representatives in other states -- unless community care rates increase, there will be minimal interest in service provision. Adult day care programs with a more social service orientation have been established across the state in several locations, including congregate meal sites.
Wisconsin takes an opposite strategy, explicitly prohibiting the use of Community Options Program funds for adult day care provided in nursing homes. This approach is consistent with the intent of COP, which is to expand non-institutional services in order to create more balance in the types of care available. In explaining this adult day care policy, state guidelines document the disparity between public expenditures for nursing home and community care and note that "COP funds were appropriated as gap-filling resources of last resort to be used in concert with other monies. It is neither plausible nor desirable that the gaps filled by COP funds should be in the relatively well-developed and well financed institutional sector."15
While most state officials support the development of adult day care as a component of a larger long term care system, obstacles to further expansion were identified fairly consistently in all states. Funding is a predictable problem. Beside the need for start up funds (which some of the states have addressed to a degree), ongoing financing sources are difficult to secure. While Medicaid payment is available in Maryland and the Community Care Program will support care for eligible clients in Illinois, economies of scale indicate a need for expanded participation of private pay individuals. One factor limiting private pay involvement is minimal community awareness of the service concept and its availability. Illinois notes that a major state initiative to expand assistance to Alzheimer's victims and their families has promoted adult day care as a potential source of family support; resulting publicity has led to an increase in the number of private pay persons seeking services.
Services Provided in Alternative Living Arrangements
Increasingly the lack of supportive housing options is viewed as a major gap in community care delivery systems. Without a place to live frail older people cannot remain in the community regardless of how well the long term care system is organized. The study states have finally bridged the barriers between health and social service systems in their development of integrated community care programs. The next frontier is to establish better linkages between housing policies and long term care.
In many ways this linkage will be more difficult. Not only do the two systems have distinct programs, administrative structures and financing mechanisms, they also have different vocabularies that make communication more problematic. In addition, the appropriate locus of coordination efforts is elusive since most housing programs are federally administered while long term care systems are managed by states.
The study states have each considered these problems and have had varying success in grappling with housing options. Maryland and Maine have made the strongest inroads into the housing field with the development of congregate housing programs. Oregon has made significant strides in the development of foster care homes, an approach which addresses supportive housing from the perspective of a social services model. Finally, some of the study states have supported care provided in more traditional residential care facilities and board and care homes.
CONGREGATE HOUSING. Both Maryland and Maine have appropriated state funds for congregate housing programs which finance a package of services provided to frail residents of (usually federally assisted) housing. Both programs are managed by state offices on aging and are considered to be integral parts of state long term care systems. Maryland's program is older and larger, established in 1976 and serving approximately 1,000 persons, while Maine's program was begun in 1980 and serves approximately 170 persons. In contrast to board and care homes, residents in congregate housing have their own apartments with a kitchen and bath. Rents are federally subsidized for low income persons, so state outlays are only for services, which include meals, personal care and housekeeping.
In both states the target population is persons who have moderate impairments but are not candidates for nursing home placement. In Maryland, the housing manager and/or staff determine individual eligibility. In Maine a Professional Assessment Committee -- consisting of the project's housing manager, a case manager from the area agency on aging and a nurse from a home health agency -- select program participants. The same functional assessment tool used for determining eligibility for the Home Based Care Program and for pre-admission screening is used to determine the need for congregate housing services.
The service package in both states costs approximately $250 a month. In Maine the total cost is fully paid by the congregate housing program since all recipients must have low incomes. In Maryland both low and moderate income persons can participate through the use of a sliding fee scale used to partially finance services for moderate income elderly. In 1986, Maryland's program received a state appropriation of $1 million while the Maine program was funded at $100,000. An additional $360,000 was appropriated in Maryland to fund service packages for persons living in group settings of four to fifteen residents; in this model, as contrasted with congregate housing, an older resident may share a room and bath with another resident.
Congregate housing programs offer states a vehicle for supporting services within an existing supply of housing facilities. Increasingly housing projects that were once inhabited by a younger, mobile elderly population are now occupied by more frail and impaired older persons as the initial residents "age in place." These residents, therefore, are likely to have growing long term care needs.
ADULT FOSTER HOMES. Oregon has actively encouraged the development of adult foster homes as a major service strategy under its Medicaid waiver program. Now serving over 1,900 waiver clients, adult foster homes provide personal care services in a residence of up to five clients, in addition to the operator's family. The development of this service option has been a crucial component of Oregon's strategy to relocate current nursing home residents to community settings.
Adult foster care homes are licensed locally by area agencies on aging and are paid directly by the client, who receives Medicaid waiver funding for the service aspects of foster care. As the availability of this service has increased for publicly assisted clients, it has also become an attractive option for private pay clients, 5,000 of whom now reside in adult foster homes.
BOARD AND CARE HOMES/RESIDENTIAL CARE FACILITIES. States have mixed reactions to the development of these types of facilities. While they offer an alternative to nursing home care, they are still "institutional" in nature, lacking the privacy and familiarity provided by one's own home. Maine is currently spending $4.5 million annually on special state SSI supplements to support care provided to older people in board and care facilities. The state approves client placements, sets a rate unique to each client and facility and makes payment directly to the facility after providing the client with a personal needs allowance.
Through its Medicaid waiver, Oregon finances care provided to clients living in residential care facilities. The state pays the facility directly for the cost of the service package, while the client pays for the room and board component. Residential care facilities are licensed by the Oregon Senior Services Division. State officials note that with the increase in the availability of adult foster homes, the use of residential care facilities has declined. Adult foster homes are seen as a more attractive option due to their smaller size and family-like environment.
Arkansas has 102 residential care facilities. The state provides a fixed supplement directly to residential care providers for recipients determined to be at risk of entering a nursing home. Supplemental payments were made on behalf of approximately 200 clients in fiscal year 1986. In an attempt to expand the availability of this service option, the state has proposed an amendment to its Medicaid state plan to add residential care facilities as a setting in which personal care services can be provided. To date this amendment has not yet been approved. In essence this proposal is similar to Oregon's approach, in which the Medicaid waiver pays for services in residential care facilities while a client's SSI check is used for room and board costs.
Wisconsin does not finance services provided in residential care facilities unless the total number of residents is less than four or six people, or in some exceptional circumstances less than eight. This limit reflects Wisconsin's program philosophy of expanding supports to help people remain in their own homes in order to balance its very large supply of nursing home beds.
Quality Assurance
Statewide community based care systems have been established with the goal of creating new approaches to meeting the long term care needs of older people. By design, these systems promote diverse and flexible community responses, drawing primarily upon non-medical social supports to complement existing health care services. Unlike the traditional physician ordered and nurse supervised acute care system, older consumers themselves are actively involved in developing their own community care plans and in supervising the plan's implementation. These program attributes provide the context for state approaches to assuring that older people receive appropriate care.
None of the six study states have applied Medicare's quality assurance procedures for skilled home care to their community care programs. A comparison of several features of community care programs with skilled nursing services highlights differences in program characteristics which shape state quality assurance initiatives.
First, states have created managed systems of care relying heavily on case managers to assess a client's needs, authorize a package of services and monitor, on an individual basis, the extent to which the client's needs are being met. With the exception of Arkansas, the study states either discourage or prohibit case managers from providing direct services under state community care programs. This policy not only separates service authorization from service delivery, but also establishes a point for ongoing oversight of client care independent of the service provider. This case management responsibility is applied to care provided by all types of providers, but is particularly important in a system using independent providers. In fact, the presence of a strong independent case management system makes the use of client employed providers possible. No similar mechanism exists outside of the provider agency for ongoing monitoring of individual care under the Medicare home health benefit.
A second feature distinguishing state community care programs from the Medicare home health benefit is the emphasis on client empowerment and consumer control, both in the development of individual care plans and in the design of overall program policies. As discussed earlier in the report, older people were key actors in the establishment of community care programs and the development of implementation policies. Their collective input and oversight continues through state and local committees established to give ongoing implementation advice.
Finally and most obviously, the services provided under the two programs are different. Medicare's home health benefit covers skilled nursing, physical, occupational and speech therapy, medical social work and, only in conjunction with one of the other services, home health aide services. Community care programs complement acute care services by providing generally non-medical services delivered by professionals and non-professionals. Medicare's services respond to an acute care need which can be successfully treated over three to four weeks; community care services respond to client functional limitations that are likely to be present for an extended period of time, perhaps for the remainder of one's life. Therefore the measures of successful client outcomes are different; home health focuses on restorative and rehabilitative care, whereas long term care services seek to maintain current levels of functioning.
Perhaps the main similarity between the two programs is that they both provide care in the home. As a result, states have determined that new ways of assuring the delivery of appropriate home care need to be applied to these emerging service delivery systems. Developing new quality assurance mechanisms has been difficult, however.
Some traditional mechanisms are used in all of the six states to provide quality assurance. These include promulgating service standards and using state or local staff to conduct on site reviews of provider performance. For example, Maryland Department of Human Resources staff conduct annual reviews of the county department of social services' management of the in-home aides programs. Other states have refined their approaches to training workers to address quality control concerns. For example, in order to efficiently train personal care workers, area agencies on aging in Arkansas have pooled their resources to jointly conduct a 40 hour training course. The course is offered for new staff every two months. In addition to assigning case management agencies ongoing responsibility for client based monitoring, the study states have adopted four different approaches to quality assurance: assessing program performance based on client outcome measures; quantifying quality measures for competitive provider selection; establishing external quality assurance committees; and formalizing client grievance mechanisms. Each approach, adopted by one or more of the study states, has potential for replication in other states.
ASSESSING PROGRAM PERFORMANCE BASED ON OUTCOME MEASURES. Oregon's current approach to program monitoring was developed out of a process discussed earlier in this report called the Negotiated Investment Strategy. That process developed rules covering a multitude of program issues through the negotiation of four teams representing the Oregon Senior Services Division, the area agencies on aging, organizations of older people and providers. In fact tensions arising specifically from the previous monitoring process contributed to the need for negotiations.
Under the system that has been in place since 1985, a team of state staff conduct annual on site reviews of all area agency operations from fiscal management to client care. Although Oregon has numerous service standards, operational rules and fiscal requirements, the emphasis of annual reviews is on client outcomes not administrative process. In reviewing client care, a sample of clients is drawn and records on intake, eligibility determination, assessment, care planning, and service provision are reviewed. Then state staff conduct interviews with clients in their own homes to assess whether appropriate services were authorized and delivered in a manner that meets the clients' needs. State officials note that local agencies may not be managing programs exactly as the state would like, but if clients are well served, then the system is achieving its objective.
COMPETITIVE PROVIDER SELECTION BASED ON QUALITY MEASURES. Illinois has the most formalized service delivery system of the six states and the most standardized assessment process. One of the most unique aspects of Illinois' quality assurance efforts is the effect that past performance has on provider selection. Beginning in 1988, providers will be competitively selected on the basis of quality rather than price. The results of compliance reviews and documented complaints filed against an agency will be compared to the same measures averaged for all other contractors operating across the state. A service history score will be assigned to each provider, either giving them an advantage or disadvantage in the provider selection process. This approach makes weeding out agencies with poor performance easier than terminating provider certification under Medicare and Medicaid.
EXTERNAL QUALITY ASSURANCE COMMITTEES. Maine requires the area agencies on aging to establish a Quality Assurance Committee for the Home Based Care program and the Medicaid waiver component. The committees are usually chaired by home health agencies -- originally the major competitors with the area agencies for state designation as case management agencies. Other state mandated committee members include a physician, a nursing home representative, a hospital discharge planner, an adult protective services manager, and a representative of the state office on aging. During its monthly meetings, the committee conducts random reviews of client cases and also serves as an advisor to area agency staff in resolving difficult problems with care plans. This committee is also required to submit an annual report to the Bureau of Maine's Elderly that comments on the quality of local program efforts.
CLIENT GRIEVANCE MECHANISMS. Consistent with the emphasis on empowering individual consumers to take an active role in directing their care, formalized grievance mechanisms have been established in Illinois, Maine and Wisconsin. In all three states clients are given information explaining the community care programs and describing how to place a complaint.
Maine and Wisconsin use a complaint resolution system that is external to the agencies managing community based care programs. The state long term care ombudsman program, which in most states handles only complaints regarding nursing home care and board and care, has in these states been expanded to address home care as well. It is usually managed by the state office on aging, but in Wisconsin and Maine is placed with a staffed advocacy board whose members are appointed by the Governor. The ombudsman programs have no enforcement authority, but rather attempt to mediate a resolution of complaints between client and providers. The Maine program just began receiving home care complaints in July 1986, so there is little experience to report. Wisconsin's program has been covering home care since 1985 and reports that the number of complaints average from 15-20 per month for community based care as opposed to 75-80 per month for nursing home care. Interestingly, some home care complaints are not over the quality of service provided but deal with the responsibilities of case managers in developing and authorizing service packages. Ombusdman staff believe these types of complaints usually reflect an incomplete understanding how the community care system operates.
Illinois' grievance mechanism is managed internally by the Department on Aging. Complaints and actual violations are received through a state toll free line and are classified into three categories, depending upon the extent to which they pose an immediate threat to the client's health and safety.
To obtain information about the affected client's plan of care state staff work with the case management agency and the vendor directly providing services. Unlike the ombudsman model, this internal complaint mechanism triggers the involvement of enforcement staff who have the authority to mandate immediate resolution of program violations.
All the new approaches to quality assurance being implemented by the study states need to be used in combination with other strategies. Standing alone these mechanisms have some inherent weaknesses. For example grievance mechanisms, although they offer a structured vehicle for expressing complaints, place the burden on clients to improve the quality of their care. And the external quality assurance committees that rely upon staff time donated by various community agencies may require more staff volunteer contributions than are feasible as case loads grow.
State officials in the six study states are keenly aware of the need to establish consumer safeguards in the delivery of community services. Based on their experiences, these officials advise other states to look at quality concerns in the early stages of program development. The challenge to states is to develop methods for enhancing quality care without making standards so inflexible and rigid that delivery systems cannot respond optimally to the diverse needs of individual older people. Quality assurance mechanisms are the most underdeveloped areas of community care. Meaningful quality assurance is expected in many states to be a major issue as community care is expanded and reliance or institutions is lessened.
VI. FINANCING AND MANAGEMENT OF HOME AND COMMUNITY BASED SERVICES
The Federal Budget and Policy Context
In the first half of the 1980s, the Federal budget and policy context for state long term care initiatives was shaped by:
- Federal budget deficits of unprecedented size;
- Restraints on federal domestic program spending;
- Reforms to allow states to develop home and community based alternatives in their Medicaid programs; and
- Increasing policy concern for evaluation of home and community based care and for development of private long term care insurance financing.
Federal Budget Deficit. As shown in the following figure, the federal government's budget deficits reached unprecedented levels in the mid1980s. Initially, the rising deficits resulted from the worst economic conditions in half a century and large tax cuts. Even with a recovering economy, however, the deficits continued on an upward trend through 1985. (See Figure VI-1.) For state governments, these large deficits meant that their policies had to be shaped in the face of continuing national budget battles and the resulting uncertainty about federal financial support.
Medicaid and Other Federal Spending. In both its first and second terms, the Reagan administration proposed to cap federal Medicaid spending and to limit future increases by the medical CPI or other index. Congress did not adopt permanent Medicaid spending limits. Temporary reductions in federal matching payments were enacted, however, for 1982-84.16 During this restraint period, states needed to be particularly concerned about the use of Medicaid funds for expanded long term care initiatives. By 1985, however, the Medicaid program's basic provisions for open-ended federal matching payments had been restored and Congress had started adding requirements and options for expanded Medicaid eligibility for coverage of pregnant women and young children. As shown in the following figure, Medicaid's spending trends have been lower than its annual 17% increases in the 1970s, but the federally-imposed restraints of 1982-84 have now given way to a higher growth rate. (See Figure VI-2.)
| FIGURE VI-1: Federal Budget Deficit |
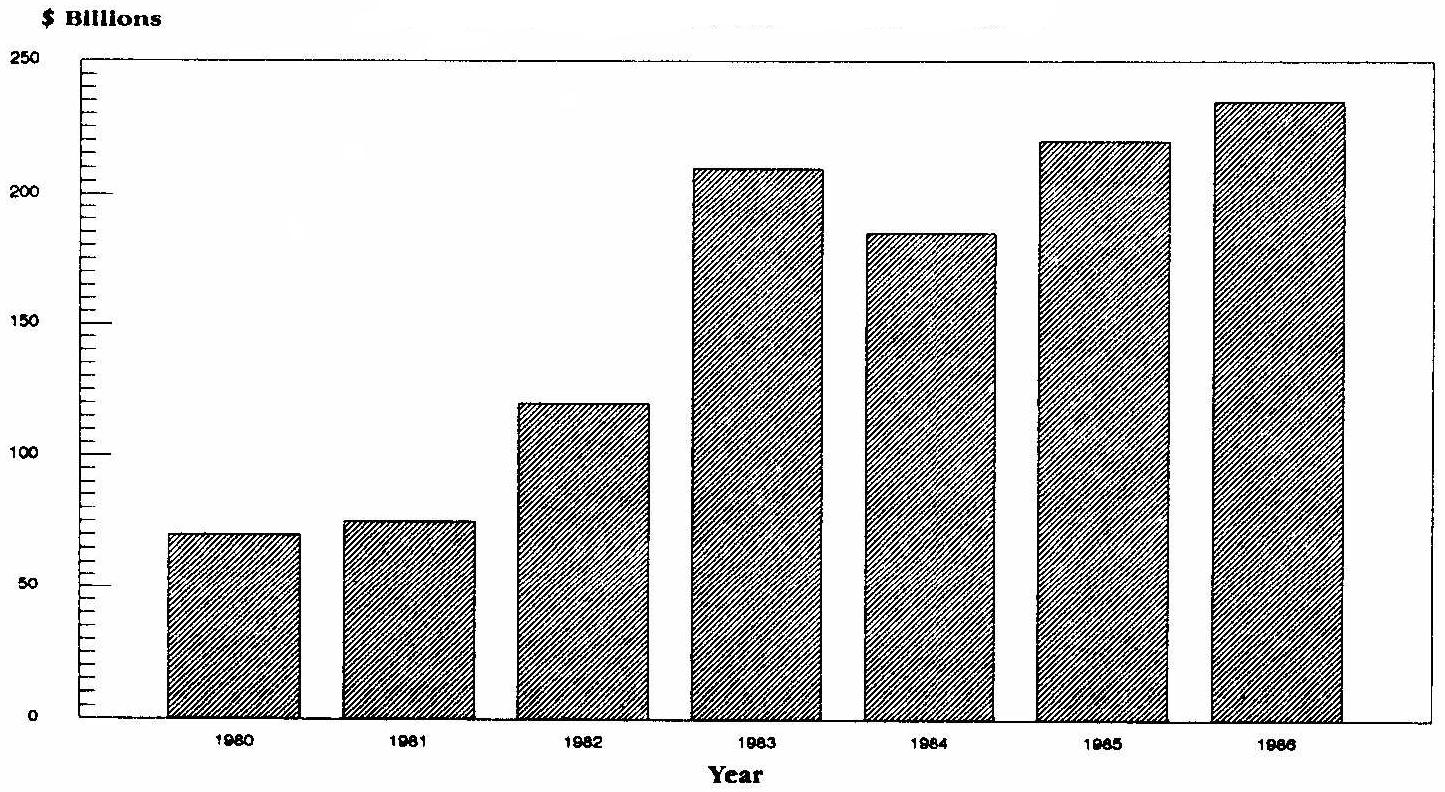 |
| SOURCE: Budget of the United States Government, FY 1988 and Congressional Budget Office. |
Other federal grant programs that could be used for financing home and community based services were more sharply affected by budget restraint. Appropriations for social services block grants grew less than 2% per year, and Older Americans Act social service funding rose less than 2.5% per year over the 1982-86 period. Such increases did not keep pace with inflation.
| FIGURE VI-2: Federal Medicaid Spending -- Rates of Increase |
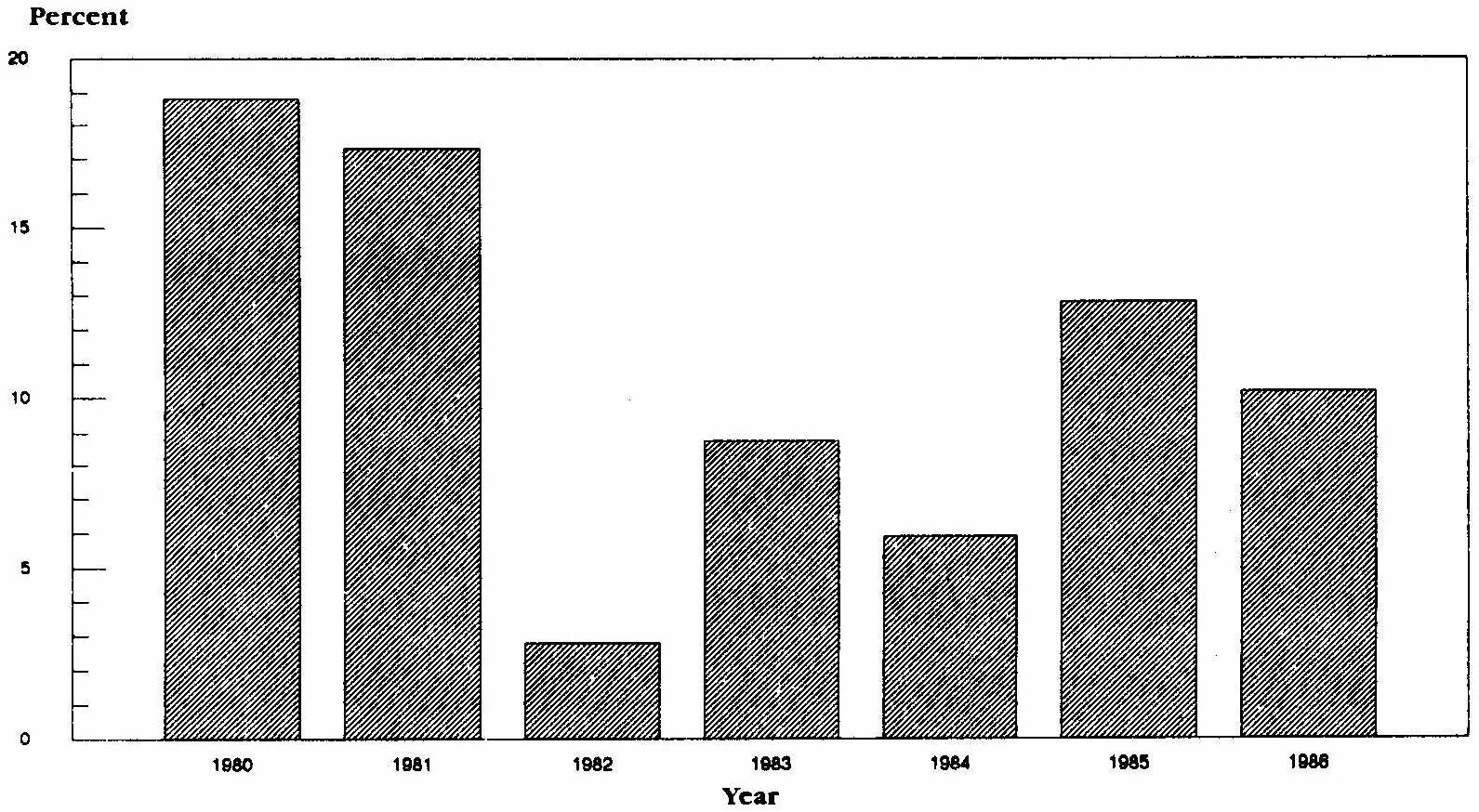 |
| SOURCE: Background Material and data on Programs Within the Jurisdiction of the Committee on Ways and Means, WMCP 100-4, p. 307. |
Expanded State Discretion for Medicaid Home and Community Based Care but with Tight Budget Controls. A major federal policy redirection in the early 1980s was to provide states greater Medicaid flexibility to develop home and community based alternatives to institutional care of dependent populations. These reforms, enacted in 1981, permitted states to receive Medicaid matching funds for a broad range of non-medical services, e.g., personal care and adult day care for long term care populations (Section 2176 waivers). As of mid-1986, forty-seven states had filed waiver requests (for 188 waivers), and forty states were operating a program under such waivers.17 About half of the waivers dealt with mentally retarded and mentally ill populations, and about half with the elderly and disabled populations. In light of the federal budget deficit, these waivers have been tightly administered, and states are required to demonstrate that no additional federal spending will result from such services.
Research and Policy Concerns. Finally, the early 1980s saw an intensified federal research interest in evaluating alternatives to nursing home care and in private insurance financing of long term care services. During the first half of the 1980s, the federal government undertook its most extensive, carefully evaluated national effort to date on home and community based care in the "channelling" demonstration.18 In 1985, Congress broadened previous policy research efforts by mandating a stud of the expansion of private insurance financing of long term care services.19 Increased policy interest in new delivery and financing options for long term care services was also reflected in support for several studies of state Medicaid 2176 waiver initiatives, as well as in this study.
Overview of State Financing and Management Issues
States that expanded home and community based care programs in the first half of the 1980s needed to consider a series of financing strategy and cost management issues. The six states in this study were selected, in part, for their diversity, so they often reflect different responses to these issues. These experiences illustrate several successful ways to finance and manage the costs of home and community based care programs. Where there was common ground, such policies and design elements suggest a common core of proven experience.
The following sections review the financing strategy and cost management issues faced by these six states and the similarities and differences in how they dealt with them. These issues can be grouped into six areas:
- States must choose a funding strategy for expanding home and community based services. Among the major options to be considered are whether and how to make use of basic Medicaid authorities, Medicaid section 2176 waivers, and state-sourced funds.
- States must design a financial management system for implementing their funding through an administrative structure. Such efforts must reconcile the differing roles of state government, local government and private agencies in determining what funds will be spent; they must also resolve the issues of authority, discretion and accountability in expenditure decisions by these different actors. A particular concern is how to coordinate state Medicaid programs, which are centrally administered and designed for reimbursement of providers' bills, with local management agencies for home and community based services.
- There must be cost management of home and community based services. States must assure that funding is targeted to those most in need, that services are delivered in an efficient manner, and that program growth is subject to policy control. Lessons learned in these six states demonstrate a number of key elements of effective cost management.
- States which fund major home and community based care programs need management information systems for these efforts. Such systems should be designed for program managers and reflect the state's priority objectives(s). These systems need to be separate from, but coordinated with, financial accounting and budgeting for home and community based care services.
- States must consider whether or not to change their normal budget and evaluation processes to assure sound decision-making for home and community based care programs. These issues arise, in particular, where several different funding sources and state agencies are involved in financing services to the target population.
- Finally, states need to consider the potential role of private long term care insurance to reduce the financial burdens on their Medicaid programs and allow affluent elderly persons to finance their own care needs. The following sections discuss these issues and how each of the six states deals with them.
Financing Strategies
A broad range of federal, state and local government programs can provide some assistance to elderly persons in need of home and community based care services. Such programs include social security, Medicare, Medicaid, food stamps, Supplemental Security Income (SSI), social services (Title XX), Older Americans Act (OAA) programs, various housing programs, low income energy assistance, veterans benefits, general assistance and other local programs. An evaluation of Wisconsin's home and community based care program found that more than 35 different federal, state, and local program sources and private funds were involved in financing services to its beneficiary population.
This multitude of sources can make it complicated for states and local agencies to design and coordinate financial aid and service packages for each client. Nevertheless, the financial options for coming up with a substantial and growing sum of money for a major state-based initiative in the current federal fiscal and policy environment are limited. Two major funding sources which can pay for home and community based care services (Older Americans Act (OAA) and Social Services Block Grant (Title XX)), for example, are dependent on federal appropriations and are thus not now a source for funding growth. Other programs involved also have clearly limited purposes (e.g., Medicare, SSI, housing). Our interviews showed that a state's basic choices for substantially increasing funds for home and community based care services are few.
The six states in the study were selected to provide case study material for three basic funding strategies of home and community based care initiatives:
- current Medicaid authorities;
- Medicaid Section 2176 waivers; and/or
- state-generated funds.
The states used these financing strategies in various combinations. Among the six states studied, there were two notable examples of each of the three strategies. General factors which entered into state considerations are discussed first, followed by a review of each state's major initiatives.
CURRENT MEDICAID AUTHORITIES. The current Medicaid statute provides states with the authority to include case management, personal care services, day care, private duty nursing, and home health services in their Medicaid programs. Most importantly for a state's financial strategy on how to finance home and community based care, Medicaid spending benefits from open-ended federal matching funds. The federal matching percentage is higher the lower the per capita income of the state. Among the six states studied, the federal match rate for services ranged from 50% (Illinois and Maryland) to 58% (Wisconsin), 62% (Oregon), 68% (Maine) and 73% (Arkansas). Medicaid programs are also generally targeted at the lowest income elderly populations and those in need of nursing home financing. The matching rates and targeting potential mean that use of the Medicaid program is an attractive option for many states that want to expand home and community based services for the elderly.
States that did not choose to build their financing strategies on basic Medicaid authorities viewed this mechanism as having some liabilities. Among the Medicaid statute's requirements, one of the most consequential is that covered services must normally be provided, on a statewide basis, at least to the entire categorically eligible population. The potential costs and management difficulties of such a broad scale program can be a deterrent to states that have not already built the infrastructure for such a broad effort. There are also distinct differences among Medicaid's long term care populations (e.g., developmentally disabled, chronically mentally ill, adult disabled and elderly) which have mitigated against across-the-board service entitlements. Also important in some states was concern about limitations of Medicaid eligibility to only a fraction of the elderly poverty population and limitations on the types of services that could be offered. States wanting to launch a broad program for the elderly and disabled population found it necessary to consider supplemental financing sources.
MEDICAID SECTION 2176 WAIVERS. Officials interviewed in the six states viewed financing strategies built on Medicaid 2176 waivers as offering states a different mix of advantages and drawbacks. A state may use one (or more) 2176 waivers to target different Medicaid population subgroups within a state or to limit the number of persons who will receive home and community based services under the waiver. In this way, a state can have a great deal of flexibility to proceed at its own pace and to limit financial risks while learning how to manage and control the costs of a home and community based care program. A financing strategy using waivers can also allow a state to offer a much wider potential range of home and community based services than can be provided by the basic Medicaid options. States may also use 2176 waivers options to increase the number of potentially eligible persons beyond normal Medicaid criteria, e.g., to use 300% of normal income standards and waive some income deeming rules in order to reach persons who are at substantial risk of spending down to Medicaid eligibility levels if they are forced to enter a nursing home.
From a state perspective, however, officials reported in interviews that there are two limitations to extensive use of the 2176 waiver. First, states that adopt this strategy have to demonstrate, by tightly drawn and interpreted "no additional cost" rules, that Medicaid expenses have not increased for the waivered populations. Second, the reporting and compliance requirements are a fairly heavy burden. States' concerns about their ability to comply with changing rules, reporting and documentation requirements, facing the risk of federal financing disallowances, were reported to be a significant factor for those who decided not to pursue the 2176 option.
STATE-ONLY FUNDS. The third basic strategy available to states wanting to expand home and community based services for the elderly is to do so with their own funds. Such spending has the principal liability of not qualifying for federal matching payments and thus is much more costly for a state than a Medicaid-based financing strategy, for a given amount of services. But most states made some funding increases for such programs an integral part of their financing strategy, and several states gave them the primary role.
Three factors were involved in such choices. First, the state-only approach allows states flexibility to design their own programs, e.g., by providing "gap filling" money or starting a program without having to meet federal Medicaid requirements. Secondly, state funds allow use of the existing infrastructure of programs and institutions that provide assistance for the elderly outside the Medicaid program. Some expanded role for these activities, as part of an overall strategy, can have both practical and political attractions. Finally, this policy emphasis is essential for states that decide, as a matter of state policy, to make home and community based services available to the majority of elderly persons who need home and community based services but do not qualify for the Medicaid program or 2176 options.
The major characteristics of the financing initiative of each of the six study states are discussed below.20
Two of the states -- Arkansas and Maryland -- are using their statutory options for Medicaid state plan design as major financing for expanding home and community based services for the elderly.
The Arkansas financing strategy emphasizes expansion of Medicaid personal care services for the elderly. In FY 1986, such spending came to $10 million and was supplemented by $4.8 million in Medicaid funding for home health care. Medicaid funds contributed 74% of Arkansas's total spending on home and community based services for the elderly (see Figure VI-3). Arkansas also provides some state money ($1.0 million in 1986) as secondary financing for alternative and supplemental personal care and day care services which can expand upon Medicaid services and eligibility levels.
| FIGURE VI-3: Total State Expenditures for Home and Community Based Care, 1986 |
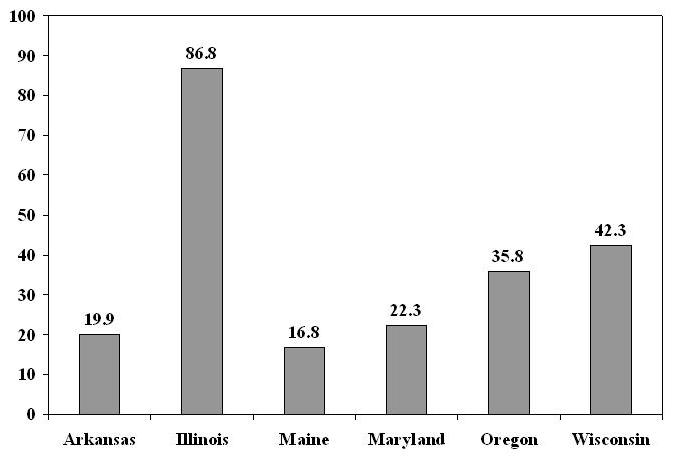 |
| SOURCE: State-reported expenditures, See Appendix I. |
Maryland's Medicaid-based initiative also includes spending for personal care services and adult day care, supplemented by home health for the elderly. In FY 1986 such spending came to $5.3 million. At the time of our study, Maryland had a base of in-home aides services, funded by social services grants and state funds, which together were larger than its Medicaid spending ($5.7 million in FY 1986). State-only funds are also available for "gap filling" grants (Gateway II, $1.1 million), for county geriatric assessment units/STEPS ($1.7 million) and other services. Overall, Maryland's Medicaid funding provided 24% of total state home and community based care spending (see Figure VI-3). State officials (Department of Health and Mental Hygiene) described plans, however, for Maryland to make increasing use of Medicaid reimbursement initiatives to finance these in-home aides and the STEP activity.
Two other states, Oregon and Maine, have developed financing structures that exemplify statewide initiatives based on use of Medicaid 2176 waivers.
The Oregon program provides the most Medicaid spending for home and community based care services relative to nursing home spending of the six states. In FY 1986, Oregon made very broad use of Medicaid 2176 waiver authority (foster care, residential care, home care), plus non-waivered home health and personal care, to finance over $27 million of home and community based services. These funds are about 25% of Oregon's spending on nursing home care for the elderly which was reported as $79 million. Medicaid spending constitutes 76% of Oregon's financing for home and community based care services (see Figure VI-3). Oregon uses state-sourced funds as a secondary strategy to supplement Medicaid waiver funds.
Maine's small home and community based care initiative is based on a Medicaid 2176 waiver which emphasizes personal care, homemaker services and adult day care. Approximately $0.8 million of such services were provided to Maine's elderly through the waiver in 1986. Another $5.4 million of home and community based services were still financed under the basic Medicaid program and an alternative long term care program using personal duty nurses and home health aides. In total, Maine's Medicaid spending came to 37% of its total funding for home and community based care services (see Figure VI-4).
The last two states -- Illinois and Wisconsin -- have built their major financing initiatives for home and community based care through state-sourced funds.
Illinois's extensive home and community based care program is the largest of the six states studied. Spending under the Community Care Program has been growing rapidly, from $9.4 million in 1980 to $22.5 million in 1982, to $36 million in 1984, to an estimated $72 million in 1986 -- over 80% of the state's home and community based care spending of $87 million (see Figure VI-4). The program's size and growth rate can be attributed in substantial measure to judicial rulings that home and community based care is an entitlement for all elderly persons in Illinois. Approximately 30% of CCP clients are Medicaid eligible and 70% are financed from state only funds. Illinois's statewide. 2176 waiver thus assures Medicaid financing for part of this much broader state initiative but is not the central element in its design. Services provided include chore, homemaker, and adult day care.
The Wisconsin Community Options Program (COP) is an example of a state funded initiative designed to support home and community based care through formula grant funds to local governments. For FY 1986, the COP program provided $8 million for the elderly. COP has grown rapidly from a $0.2 million level for FY 1982, as more counties are phased in to participate. The COP initiative is still relatively small, however, in comparison to Wisconsin's total $42 million of home and community based care spending (see Figure VI-4). Wisconsin officials report that the COP program initiative has been developed because of the advantages of flexible administration and local discretion in providing the core of a system suited to Wisconsin's state/local traditions. Wisconsin also has a small Medicaid 2176 waiver.
| FIGURE VI-4: Percent of Total State Expenditures on Home and Community BasedCare Paid by Medicaid |
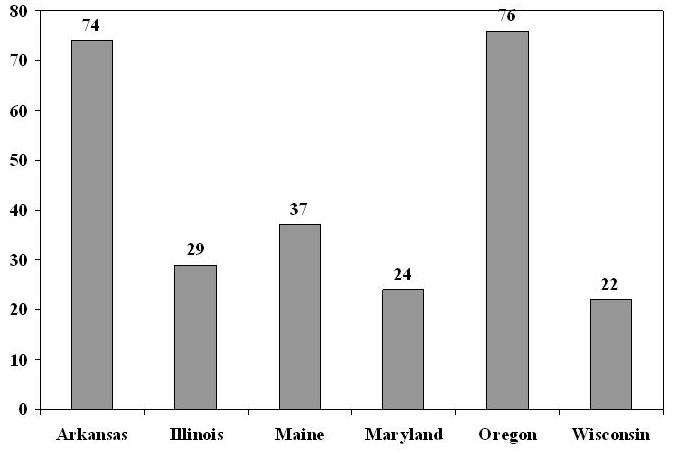 |
| SOURCE: State-reported expenditures, See Appendix I. |
In sum, the six states adopted widely different strategy mixes for financing major expansions of their home and community based services. These strategies usually involved some initiative for use of the Medicaid program (basic program authorities and/or section 2176 waivers) to take advantage of the federal matching available for covered services to the Medicaid-eligible elderly. In only two states, however, did states use Medicaid funds for more than half of their total spending. State-only funds, as well as the large base of social service and Older Americans Act grants, still had (cumulatively) the primary role in most states. Even where Medicaid programs had more important roles in state's future plans, state funding also had vital roles to fill in or extend the financing which could be provided through the Medicaid program.
Financial Management and Pooling of Funds
States must establish a financial management system that will implement their financing strategy and resolve issues of policy control, authority for obligation of funds, reporting and financial accountability among the state government, local government, and private sector actors involved.
Among the six states studied, each state accomplished this coordination in a somewhat different fashion. In general, however, states built on existing financial management arrangements for similar programs. The basic financial management choices for the home and community services initiatives -- which parallel program administration options -- can be viewed as a continuum which includes three basic models:
- a state government operated financing system with direct state-provider dealings and little autonomous role for other actors;
- a mixed state government/local government financial management system with substantial roles for each level;
- a fully local system with state funds block-granted to localities.
The Illinois system comes closest to the unified, central financial management model. In Illinois, state government rather than local government has been the major provider of social services. This tradition has also been adopted for in-home and community based care for the elderly. Illinois' 63 local case coordination units (CCUs) receive their funds through direct contracts with the state's Department on Aging and are paid on a fee-for-service basis for carrying out specified assessments, authorization and reauthorization, and case management under the contract's terms. Service vendors are also under direct contract to the state's Department on Aging. All service bills are sent to the Department on Aging for payment.
These arrangements result in a unified system in which the Community Care Program is a single pool of funds and determinations of service needs are made without distinctions between Medicaid and non-Medicaid eligibility. The Medicaid financial participation is handled centrally. At the end of each month, the Department of Aging runs a tape-to-tape match of its payments file against the Medicaid program's eligibility file, and federal financial participation is requested for the expenditures for covered services that the Community Care Program has made on behalf of Medicaid-eligible persons.
Arkansas, like Illinois, also has a primarily state-run financial management system for home and community based services. This reflects Arkansas's tradition and circumstances as a rural, relatively poor state in which few social services are available except those funded by the state either wholly or with Medicaid matching funds. The financial management of home and community based services is through direct arrangements. The Medicaid program is the primary funding source and the six area agencies on aging (AAA), plus a health department and CAP agency, have been the state's primary providers of personal care services. The AAAs are paid directly by the state Medicaid program for their Medicaid reimbursable claims. The AAAs also receive most of the state's discretionary funds for services to the elderly through budget allocations from the state's Division of Aging and Adult Services (in its Department of Human Services). This Department is also the cognizant agency for approving AAA cost allocation rates to their different budget activities, provides monthly allocations of grant funds to the agencies, and assures that their personal care service charges to the Medicaid program are acceptably cost-based. Similarly, Arkansas also has only two Client Assessment Team (CAT) agencies, one for northern and one for southern Arkansas. Both agencies are funded directly through Medicaid for their specific activities on behalf of the home and community based care program.
Maine, like Illinois and Arkansas, has a primary state government role because it has almost no county government. But its state-level managerial control is not as strong as in the two other states. In Maine, social services are usually provided by state funding for private, non-profit agencies which undertake a number of administrative tasks. Under the statewide Medicaid 2176 waiver, Maine allocates waiver slots to local AAAs based on their projected caseload. The AAAs do case management, arrange for services and, for Medicaid waiver clients, pay providers' bills for those services. In turn, the AAAs then bill the state Medicaid program. For non-waiver clients, the home and community based care providers bill the state Medicaid program directly.
Oregon's financial management system combines a strong state government role in policy direction and funding control with a substantial and semi-autonomous role for local government agencies. The Senior Services Division (SSD) has centralized control over all major state funds for the elderly, including Medicaid institutional and home and community based service funds, social services block grant funds, Older Americans Act funds, and SSI. In areas with over 90% of the state's elderly population, SSD works through counterpart local AAAs which are part of local government (counties or councils of government). The AAAs also provide pre-admission nursing home screening and case management for home and community based care. Of the six states studied, Oregon thus comes closest to having organized its state and local government services to serve the elderly through an integrated "one stop shopping" agency. Medicaid spending which AAAs authorize, is projected and carefully monitored by the state's Senior Services Division, which pays the bills submitted by service providers.
As noted elsewhere, Oregon did not develop this state-local financial management system for long term care services without difficulty. In particular, local AAAs had been used to grant funding and considerable autonomy vis-a-vis the state government. The AAAs undertaking of Medicaid program-related tasks required sharply different operating procedures, standardization and reporting, cultural changes and much less autonomy than previously. As a result of the difficulties involved in working out these relations, Oregon adopted for a time a highly structured, formal negotiation process between SSD and the local AAAs to implement its program management system.
Of the six states studied, Maryland has the most complex state and local financial management, which it is still trying to rationalize. At the state level, three largely autonomous cabinet agencies have roles in the overall services system: the Department of Health and Mental Hygiene (Medicaid and geriatric assessment grants to local governments (STEPS)), the Department of Human Resources (state funded in-home aides), and the Office of Aging (general policy coordination responsibilities, Gateway II gap-filling funds). Each of these three agencies also has largely independent counterparts at the county level in local health and social services departments and AAA agencies. Under Maryland's Gateway II concept, there is a designated "lead" local agency which is charged with coordination of the other local agencies. There were concerns expressed in several interviews about the coordination of state and local agencies; and the Maryland General Assembly had requested a study of the overlap, duplication and coordination among the state programs. The state's strategy (at least as represented by several DHMH officials), is to take maximum advantage of Medicaid matching funds, and use the financial management requirements of the Medicaid program to impose greater policy direction and coordination. The STEPS initiative would shift some funding of local geriatric evaluation units from state formula allocations to Medicaid fee-for-service reimbursement. This would become a vehicle for standardized assessments, reporting and greater state policy control. An expanded Medicaid role would also make the DHR/social services agencies Medicaid providers, subject to Medicaid's prospective rates and other requirements. Such efforts, were they to occur, would bring greater management and state financial accountability to what is now a complex and fragmented home and community based initiative.
The Oregon experience and Maryland policy thinking highlight a potential financial management issue for states with mixed state government-local government responsibilities: Can states allow local administrators to commit Medicaid funds and still assure the financial accountability, program standardization and budget control required of state Medicaid programs? In systems like Illinois, the use of Medicaid funds is subject to strong state management roles or oversight of local agencies. The Oregon and Maryland experiences demonstrate that Medicaid funds cannot be "pooled" as an undifferentiated source of funds to be used at the full discretion of local governments. The Medicaid program, even with a 2176 waiver, has precise eligibility rules. Medicaid-covered services must be defined with standardized measures recognizable for payment by the state's Medicaid computer. Payment rates must be established, services authorized, bills filled out completely, accurately and on time. Local agencies which anticipate that an expanded Medicaid home and community based care program will mean expanded autonomy and additional discretionary funds also find their responsibility for Medicaid spending involves expanded administrative and procedural requirements and more demands for standardization, regulations, paperwork and accountability.
These administrative requirements are not, of course, necessarily undesirable for states venturing into mixed state-local financial management roles for home and community based care. As reflected in Oregon and Maryland, the Medicaid program's payment requirements can be a useful vehicle for states to establish program policies and procedures on a statewide basis, and result in an ability to assure cost-effective program management and standardization of operations. Such policies and procedures can also be established in state funded programs.
The Wisconsin COP initiative comes closest to the "local government" financial management model. The COP funds (which are state-generated) are formula-granted to local units of government, which then are responsible for determining needs for services and spending the funds for home and community based services at their discretion. Thus, COP is not an entitlement program. The state also gives major grants to localities from its funds for other supportive services for the elderly.
In summary, two major findings stand out from the study about financial management arrangements for home and community based care initiatives:
- The six states -- selected for their leadership in long term care initiatives -- adopted three different state, local and private agency models. These were state-operated, state-local, and locally run systems for the financial management of home and community based services. Financial management systems logically follow and implement program administration structure and roles.
- Broader use of Medicaid funds for home and community based care can break new ground in requiring coordination of this state-operated payment system with a locally administered service authorization and case management system. The issues involved in working out financial accountability, administrative policies and procedures, and budget control involve power relations and cultural differences. These can be resolved, but they are potential sources of tension in implementing effective financial management systems.
Cost Management
A third basic design issue for a system of home and community based care services is to identify and incorporate key program elements which allow the programs to be managed in a cost-effective manner.
The six study states faced this issue and developed a number of ways for dealing with these problems. One of the most important common features of the six state systems is that they are all managed systems of care. They do not follow the traditional open-ended health insurance reimbursement model in which providers prescribe the need for their own services and are reimbursed for whatever they spend or charge (e.g., through "usual, customary, and reasonable" reimbursement rates).
Each of the programs differ but all of them include three basic elements:21
- Pre-admission Screening. Before a patient can be admitted to a nursing home at Medicaid expense, states screen to determine if a nursing home admission is necessary. If home and community based services are a viable alternative, the patient is advised of these options. This preadmission process helps target programs to those at risk of being placed in a nursing home and to save what would otherwise be spent on nursing home care for those who are appropriate for home and community based services. This certification process may also be extended to non-Medicaid patients, based on the reasoning that nearly all nursing home admissions could lead to Medicaid spending, and that the most cost-effective time for a state to offer home and community based alternatives is prior to such admissions.
- Patient Assessment and Care Planning. An individual receiving home and community based care has a service plan developed, typically using standardized, quantitative assessment instruments. Such plans specify the amount of home and community based care which the person will need, how it will be managed and paid for. Such assessments and plans provide a way of prospectively managing case costs and service use.
- A Case Management System. One function of a case manager is to assist clients in obtaining needed services, e.g., by providing a list of potential providers from whom a person may select, and/or making arrangements for the services. A case manager may also be responsible for seeing that services are provided within a defined budget limit.
For several states, the designation of a case management agency was a critical question because of concerns about conflicts of interest and states' ability to control costs. In particular, states need to resolve whether AAAs, which were established legislatively to be advocates for the elderly, should also be case managers. States also must resolve whether case managers should be different from service providers. In Arkansas, for example, case management and provision of services were both AAA functions, but the assessment of service needs and plans of care were restricted to CAT agencies (AAAs which had relinquished their direct service functions). Illinois limits AAAs to a program support function without a direct role in needs assessment or case management. On the other hand, Oregon relies on AAAs (when they are units of local government) for eligibility, assessment, care plans and case management for the home and community based care program. Maine allows AAAs to be both case managers and service providers for personal care assistants and home delivered meals only. Thus, there was no consensus on this issue or its implications for program costs among the six states.
In addition to these common cost management elements, states' home and community based care programs also made use of one (and usually more) of the following program elements:
Limited Population Eligibility. Limiting the population which is potentially eligible for home and community based services provides a clear upper limit on one of the most important cost-driving factors. A state program limited to Medicaid eligibles automatically restricts the service population to the categorically eligible population, with state options for the medically needy. A section 2176 waiver or state-financed program can also be used to limit eligibility to a population defined by age or other criteria. Among the six states, Illinois and Wisconsin were the only two without clearly limited population eligibility, although both had functional eligibility criteria and cost-sharing requirements.
Payment Methods and Rates. Establishing economical unit service prices is also a key element in cost control. Such measures are necessary because of the wide variations in potential prices for home and community based care services. Under open-ended Medicare cost-based reimbursement, time limited medical home health services provided during a recuperative period maybe paid for at $40-60 dollars per visit. The six states in this study established prospective prices for longer-term home-based support services, usually provided by non-medical personnel, which were far lower than these rates. The range for personal care services, for example was $5-$10 hour. The services covered under Medicare and these programs differ quite substantially; cost-management requires that such differences be reflected in payment rates.
States and local agencies established their rates through a combination of competitive bidding, fixed rates, cost audits, and prior experience. Rates are not directly comparable across states because of differences in service definitions, provider types and qualifications, and general price levels. Examples of several methods are discussed below.
In Illinois, the state government used to contract from Springfield for all CCP services on a competitive basis for each service area. About 60 percent of the home care services were contracted from for-profit home service agencies and four vendors had about one-half of the market. Under this system the state had obtained rates which had declined for five years in a row. The state's rates declined to the point that major non-profit, religiously affiliated providers complained that they were too low to adequately pay for full time, well qualified staff at rates which included normal fringe benefits (such as health insurance). As a result, Illinois ended the competitive bid process and replaced it with a negotiated payment rate process. In Illinois, competition for who will be a service provider is now determined, from among those willing to accept these prices, on the basis of service quality. In 1985, Illinois' statewide averages were $5.80 per hour for chore services, $6.51 per house for homemaker services, and $20 per day for adult day care. Case monitoring was paid at $10/client per month. Initial face-to-face assessment by CCUs (case coordination units) were paid at a $65 rate, and the fee for their periodic client reassessments was $42. Assessments which involved only phone screening were paid at a $10 fee.
In Oregon, provider payment rates are normally set (for agencies) by competitive Requests for Proposals (RFPs) (for agencies) or (for independent providers) as a flat rate. These rates were reported to range between $3.45 per hour and $5.53 per hour for personal care services. Foster care, the key out-of-nursing home service which Oregon has developed using the section 2176 waiver, is paid on a statewide fixed fee basis, plus add-on amounts for specific services. The basic foster care service rate (not including room and board) is $150/month, which compared to state costs of about $750/month for nursing home care.
In Arkansas, the AAAs are the primary providers of Medicaid personal care services. The reimbursement rates are cost based and developed from Department of Human Services supervised cost allocation and audits of the AAAs' budgets. These costs now average about $6 per hour. A limited number of home health aide services are paid at a $22/visit rate (no minimum time), a differential compared to personal care services which state officials say needs to be examined. Chore services were reported to be paid in the range from $3.35/hr to $8.45/hr across the state, homemaker services from $3.55 to $6.40 per hour, and adult day care from $6-$10 for a 1/2 day to $20 for a full day. The CAT agencies were reported to be paid $60 per assessment and reassessment.
Maryland has a more complex rate structure than the other states because of the several different departments involved in home and community based care. The Department of Health and Mental Hygiene has revised prospective payment rates for its Medicaid program based on the program's experience. The personal care service rate under Medicaid, which had been a flat $10 per visit, was revised in 1986 to become a graduated system paying $10 per visit (for a visit of up to 3 hours), $20 per visit (for 3-4 hour visits), and $25 for two visits per day. Similar prospective rate reviews were reported underway for home health, physical and occupational therapy, and home aides, with variations by geographic region. Medical day care rates are derived from daily nursing homes rates; the $35 per day payment is now pegged to 75% of the daily nursing home rate. In-home aides provided by the Department of Human Resources cost $6 to $11 per visit depending on the cost accounting technique used. Nurse managers of personal care services are paid $37-40 per month per worker supervised. Geriatric evaluations by the different county health departments, which are not now standardized, were paid prior to 1987 on a cost basis reported to range from $60 to $180 per evaluation. At the time of this study, the state was in the process of trying to negotiate a more uniform rate and standardized geriatric assessments with the counties (the STEPS initiative).
Another rate-setting option for states involves leaving rate negotiations for personal care workers to individuals and their families. Client-negotiated rates (at least in some instances) are used in Wisconsin. Under these arrangements, clients may be able to negotiate some packages of care directly at costs which are below what states would have to pay. Such arrangements, for example, may be made when a neighbor helps out on a part-time basis.
Cost sharing. Patient cost sharing is an effective way to reduce third-party payments of health care costs, and states also have some options for use of cost sharing for home and community based care services. Such measures are useful primarily in state-financed systems which expand on Medicaid's coverage, since cost sharing is not permitted for Medicaid services for the categorically eligible population. Cost sharing possibilities also arise in meeting Medicaid spend-down eligibility requirements.
In Illinois's program, cost sharing features are particularly important since home and community based care is an entitlement for all elderly persons. Illinois has designed its cost sharing system to encourage patients to use only what services are really needed, rather than all for which they could qualify on the basis of determination of need scores. In making a client's cost sharing calculation, the first $426 per month of income is protected. Thus if a client has an income of $626 per month, the total funds available for cost sharing is calculated to be $200 per month. The cost sharing actually required will be $200 times the ratio of actual service costs to the maximum amount for which the client is eligible, up to a cost sharing rate of 90%. In this example, if a client were eligible for $450 per month of services, and made arrangements with relatives, neighbors and informal caregivers so that only half this potential maximum ($225) were provided by CCP, the cost sharing for the CCP services would be $100 (1/2 of $200). Illinois officials believed the cost sharing did result in service cost reductions. Average case cost sharing was reported to be $28/month, compared to individual care cost limits of $750/month.
The Wisconsin COP program provides an example of how cost sharing can be used in a home and community based care program for populations near Medicaid-eligibility levels. There is almost no COP cost sharing for the Medicaid-eligible categorically or medically needy populations There is cost sharing, however, for the "six-month" Medicaid eligible population (i.e., those who are deemed to be eligible for in-home or community based services because, if they entered a nursing home, they would "spend down" their income and assets to Medicaid eligibility within 6 months), as well as for all higher income patients. At county option, the six-month eligible population can be charged cost sharing of 50% to 100% of the care costs they receive under the COP program.
Costing sharing is also used in Maryland (state funded programs), Maine (state home-based care) and in Oregon (state funded Project Independence).
Client Spending Limits. Several of the states in the study made use of explicit client spending limits to control costs. Typically, such limits are established in setting up a plan of care. States may establish limits on maximum payable amounts in relation to explicit disability ratings and/or in relation to what would have been spent on nursing home care for a client. Per client spending limits can also be used in establishing local agency funding allocations and, by such agencies, in setting spending targets for individual case managers for their group of clients.
Maine has one of the most explicit spending limits for administration of its 2176 waiver program. Each AAA has a budget allocation target, which is calculated as a per client cap equal to the state's potential expense of providing ICF care for that person. In turn, each case manager has this financing allotment provided for his or her caseload. This maximum amount is also programmed into the state's Medicaid computer so that spending for a client may not exceed this amount. Through these spending limits, Maine is able to assure that its waiver spending will be less than institutional care costs for the covered population. Illinois is similar. Each client has a cap equal to group care costs for his or her level of impairment.
Oregon does not establish absolute limits for each area, but does use a sophisticated system of forecasting target nursing home spending and tracking expenditures. Areas which run over projections may be able to get approved reallocations of budget targets from other areas; but there is a strong emphasis on dealing with excess costs by improving local administrative performance in keeping individuals out of nursing homes. In Oregon, the determination of how many service hours each client will receive is calculated by formula based on ADL functional scores, and is not limited to cost per case for nursing home equivalent service levels.
Arkansas currently limits its personal care services to a maximum of 72 hours per client per month ($442/month). Arkansas also is developing options to expand its ability to control per client spending through prepaid plan options. This approach would capitate a residential care facility or boarding home as a personal care provider for a defined group of individuals (Medicaid-eligible residents). The facility will receive a flat capitation payment of $180/month per client to cover all of their personal care needs (a service average of about 6 hours per week). In addition, the individual's SSI check, less personal allowance, will add about $342 per month ($367-$25) of income for the facility.
Wisconsin does not set any maximums for individuals. The state sets an average payment level for the counties and counties are not reimbursed if their average cost for all recipients exceeds the contract level. In CY 1987, the county average was $603 per month (actual spending was below that level). The county average is adjusted each year and represents the average amount of state Medicaid funds that would be incurred if the program participants entered nursing homes. Counties may set service maximums for individuals served, so long as those maximums are not below $800/month. About 20% of the counties established such maximums in CY 1986.
Limit State Appropriation. All states in our sample had state constitutional prohibitions on overspending and all spending -- including Medicaid expenditures -- had to be appropriated. Statutory language, appropriations structure and state administrative practices, however, determined whether and how tightly each individual program element was controlled. Spending limits could apply specifically to line-item appropriations for home and community based care programs or (more usually) to broader categories, such as a department's total appropriation. When included in broader control totals, home and community based programs can be at risk of being reduced because of overruns in other spending; but they also can be assisted, of course, by the potential for offsetting their overruns (if any) through other program reductions.
Management Accountability and Performance. Systems that provide home and community based care need to be managed care systems. Financial management systems (discussed previously) and management information systems (discussed in the next section) thus have important roles and need to be used for cost control. States also found that training sometimes needed to be provided for the key administrative and cost management functions (particularly related to Medicaid requirements and procedures), performance needed to be monitored, and administrative follow-ups were required when cost problems arose.
Conclusion. The various mechanisms described above provide a potentially broad and effective set of tools for the cost effective management of home and community based care programs. States may face many pressures to expand these programs. Indeed, if these approaches for meeting long term care needs come to replace a majority of institutional care spending they would be at least two to five times larger than they are today in these six states. But rapid program growth seems more likely to result from policy-level funding decisions or from unwillingness to take cost containing measures than from inherent lack of technical tools for program management.
In the concern with such technical details of how to manage costs for home and community based care programs, however, it may be too easy to overlook the critical importance of having qualified people to start and run new home and community based care programs for the elderly. Regardless of the system, the individuals working in a program are responsible for its successes. Among these six leadership states, we found that their programs were run by an exceptional group of individuals, committed both to improving services for the elderly population and to good public administration.
Management Information Systems
A fourth major element needed for successful home and community based care programs is a management information system (MIS). Such systems -- intended to assist program managers in daily operations -- differ from (but need to be related to) other data and information-based activities which states also require, such as budget development, financial accounting, and evaluation studies.
There were major differences among the six states in their MIS systems design, reflecting their varying policy objectives, funding strategies, financial management arrangements, and other program characteristics. Two generalizations applicable to all six states are discussed first. Three of the state MIS systems are then discussed in greater detail as representative of state-government run, state-local, and local-operated systems.
The first general observation is that the Medicaid program's basic Management Information System (MMIS) is inadequate for the day to day management of home and community based care programs. MMIS provides a retrospective accounting of Medicaid bills paid which meets federal requirements for matching funds. Its principal drawbacks for a managed care system for Medicaid clients are that key management-relevant information is not reported (e.g., ADL scores), the data reports are generated after events have occurred, and MMIS files are frequently so large and cumbersome that they cannot be easily analyzed. Managers need systems that allow for timely tracking and management intervention (e.g., at a point when a person applies for a nursing home admission or when service costs are authorized) and analysis which provides key performance indicators for how well the program is operating.
The second general observation is that none of these states operated total client-based management information systems which tracked all federal, state and local assistance received by a recipient of home and community based services. Such comprehensive management and tracking systems are complex and expensive. Among these six states, only Wisconsin had developed such a system, and it had been dropped after a year. Comprehensive client information may be critical for local assessment and case management agencies. To initiate a home and community based care program, however, it is not necessary to have comprehensive state-level reporting of all of the programs benefiting a client. State management information systems for home and community based care can be designed for what state managers need for management of their own funds and monitoring results for which they are accountable.
Three of the states -- Illinois, Oregon and Wisconsin -- have management information systems that provide useful examples of operating systems for different models of home and community based care programs.
The Illinois MIS is designed for a system which is run almost entirely by a state government agency through direct contracts with assessment agencies, case managers and service providers. Since a court case has established that such services are a statewide entitlement -- and have to be provided in a timely manner -- the Illinois MIS tracks clients from their initial application for the program and reports data on the number of days before such applications are resolved. The key management control point in the Illinois system is prior authorization of services. The MIS thus emphasizes extensive reporting on patient assessments and care plans. Each CCU (case coordination unit) files a report containing patient demographic and economic data and quantified scores from the ADL/determination of need assessments. These reports also include a summary plan of care showing how many services, by which providers, have been authorized for each client. Actual expenditures are checked against the service maximums in the service authorization reports. This basic data set then becomes the basis of generating a number of management analyses (e.g., determination of need (DON) scores), authorized and actual spending and service patterns by different agencies in relation to client DON score, client use profiles, living arrangements and economic status of clients, etc.
The Oregon Senior Services Division oversees most state spending for senior citizens, including both nursing home and home and community based care. The primary SSD management objective is to keep elderly individuals out of nursing homes if they can be served in the community. Oregon's MIS emphasizes this objective and the information needed for 2176 waiver reports.
The Oregon MIS has two subsystems. One focuses on nursing home-related placements. Each area of the state is tracked on projected vs. actual numbers of nursing home admissions, discharges, and relocations. To provide timely monitoring of system performance, most of these statistics are gathered each week by telephone. This is the state's primary information tool for "real time" monitoring and management intervention. The second system integrates expenditure data from financial draws and Medicaid program data to track actual vs projected long term care expenditures in each area. These figures come in more slowly from financial and bill-paying reports. For preparing management analyses and 2176 waiver reports, Oregon officials also emphasize the need for creative programming in order to use Medicaid data as a client-based tracking system. For some purposes (e.g., budget), it is desirable to have data on a full-time equivalent or "slots" basis; for other purposes actual expenditures per client are needed. For some purposes, simple service counts are adequate; to answer other questions it is necessary to know the distribution of such services and how many clients are receiving several different types of services. Without investing in a client-based Medicaid analysis capability, such tracking capacity from routine MMIS reports is limited.22
Wisconsin's management information system for its largely county-run system program, is based on reports the counties file each month on the type and number of service units received by each client. Since the state program is intended to provide maximum flexibility to local governments, subject to an overall spending constraint, most services are reported under a general "supportive home care" label. At the end of each year, the state sends each county a summary of the service units which they have reported providing to each client, and the county fills in the payment rates and total spending and returns the completed form. This becomes the state's basic expenditure record for how the formula grant funds were spent. Counties also file reports on client assessments and case plan developments. These reports are, in effect, payment vouchers since counties are reimbursed separately for each of these services. Several different management reports are then generated from these basic records, e.g., average client costs, trends in expenditures per case, characteristics of high and low cost clients. Wisconsin's reporting system thus provides summary spending information for state officials and recognizes county government's role as the day to day program managers.
In 1985, Wisconsin implemented a more extensive computerized Client Services Information System (CSIS) in which counties reported on all clients for state funded programs. The Community Options Program (COP) reporting was one of the modules in this integrated statewide information system. As noted, the CSIS was dropped after one year. The CSIS has now been replaced by another client-based, on-line information system. Under the new system, units of service are obtained for all persons but financial data is obtained only for COP funds. The new state system collects total COP funds expended for each COP recipient but breaks down those costs into each service component only for persons who are on Medicaid waiver funding.
Arkansas was in the process of designing a state MIS system in 1986. The central Medicaid role in financing and the established state fiscal management system vis-a-vis local AAA are precedents for such a state-operated system.
Maryland's multi-agency, multi-government level roles make an integrated state MIS system at best an unlikely and problematic undertaking. More limited efforts at state standardization, e.g., of geriatric assessments (STEPS), were immediate priorities. Local MIS efforts had been demonstrated in Baltimore.
Maine's delegation of responsibilities to local agencies did not have a comprehensive management information system as a prerequisite, although work on an MIS system also was underway in 1986.
In summary, the lesson from the study states is that an MIS system is necessary for states that wish to manage their home and community based care system. The state MIS can start as a basic reporting system designed in light of the state's administrative role and focus on key operating data needed by state program managers.
Budget and Evaluation Processes
States need to consider whether to develop new budget and evaluation processes for home and community based care programs. As discussed below, most (though not all) of the six states found that existing budgetary processes could accommodate these new efforts. However, separate evaluation studies are necessary for some program assessments.
BUDGET DEVELOPMENT FOR HOME AND COMMUNITY BASED CARE SERVICES. The six states shared basic similarities in budgeting and appropriations processes. Executive branch departments prepared initial budget requests. Governors, working with their budget offices, personal advisors and department heads, reviewed these requests and proposed budgets to the legislative branch. Legislatures reviewed these requests, held hearings and enacted appropriations.
Despite these similarities, the respective role and authorities of the actors varied. Maryland, for example, has a strong role for the governor in fiscal affairs. Under Maryland's Constitution, the legislature may not increase any line item in the governor's budget request. In contrast, Arkansas has a legislature-dominated budget process and its legislative council is involved in many operational details of programs, including regulations, contracts, and personnel. The respective role of state budget offices also varied. In Wisconsin, for example, the state budget office analyzed and projected various program options, whereas in Maine such issues were mostly deliberated between the governor and agency head.
In five of the six states, the state's home and community based care initiative was handled within the state's normal budgetary processes. This was facilitated by the broad responsibilities of the agency in which the program was housed. Four of the states (Arkansas, Oregon, Maine, and Wisconsin) had a broad Department of Human Resources, Department of Human Services, or Department of Health and Social Services which included the major home and community based care program, Medicaid and other social services programs. The fifth, Illinois, centralized its home and community based services in the Department of Aging, also making for a relatively integrated budget process. Issues raised by a home and community based care program are similar to many other human resources, social service and Medicaid program issues. Developing funding strategies, fiscal management and controlling costs for such programs are normal government budget activities.
Maryland, with three cabinet agencies involved in home and community based care efforts, is the major exception. The state's Interagency Committee on Aging Services, chaired by the Office on Aging (a small cabinet department), was tasked to develop an integrated budget request for the Department of Health and Mental Hygiene, Department of Human Resources, and Office on Aging programs. Its initial effort, however, simply consolidated the agency budget requests and transmitted them to the the governor's office. In a similar effort to develop a cross-agency funding strategy, Maryland's legislature also went outside the budgetary process and required a separate study from the state budget office (the Duchez report).
None of the states developed unified state budgets covering all spending on behalf of the elderly. Most state appropriations that benefit the elderly are not exclusively "elderly" programs. Only Maryland had a supplementary budget analysis that estimated state spending on the elderly. A copy of this table has been published for several years as part of the governor's overall budget request.
A final common finding about budget-making for home and community based care services was the importance of developing broad consensus on the program's philosophy and purposes in providing elderly persons services which they wanted as an alternative to nursing home care. In all six states the key budget actors interviewed were well-versed about what the program was trying to do, as well as its problems. In initial years of a program, when reliable data and formal evaluations can be difficult to provide, such understandings, often a result of informal discussions among program personnel, decision-makers, and interested state, local and private sector persons, seemed to provide a context in which the formal budget process occurred.
PROGRAM EVALUATION. States cannot answer all important questions concerning home and community based care through normal financial, budgetary, and program management systems. Some key data can be provided by such systems, however. Oregon, for example, can demonstrate the decline in its nursing home census. As illustrated in Figure VI-5 of the six study states Oregon has the highest proportion of total long term care spending going to community care. Illinois can track spending trends for clients with different characteristics on a very sophisticated basis. Arkansas can document that the nursing home population has remained constant since 1979.
A comprehensive program evaluation needs to include the effects of home and community based care programs on nursing home placements, on many different federal, state and local programs, and on individuals and their families. Such assessments require so many resources that they can only be done periodically; in addition, they do not make much sense during the first few years of a program until it has gone through an implementation and start-up phase and is operating well.
| FIGURE VI-5: Expenditures for Home and Community Based Care as Percentage ofTotal State Long Term Care Expenditures, 1986 |
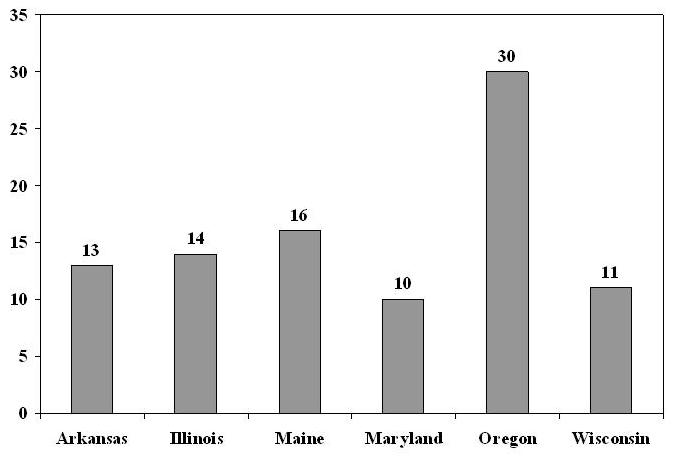 |
| SOURCE: State-reported expenditures, See Appendix I. |
Several states were in the process of initiating or undertaking broad studies of targeting, cost-effectiveness and other key effects of their home and community based care programs during the study period. Wisconsin, however, was the only state to have completed a comprehensive cost study.23 For this study, a structured sample of about 200 cases had been taken and, for each of these clients, a detailed record was developed of all the government (federal, state and local) assistance and non-government income which those individuals had received (approximately 35 different sources). Each of the clients was also independently assessed as to whether or not they needed to be in a nursing home. Expenditures were analyzed for impacts on federal and state governments, counties and other government units, and individuals. Overall, the evaluation concluded that COP reduced total expenditures for all public payers. Nevertheless, state government expenditures rose because state funds paid 59% of community care compared to only 42% of nursing home care, some COP-funded services went to persons not at imminent risk of entering nursing homes and some COP clients would not have been Medicaid-eligible immediately upon entering a nursing home. Assistance by friends, neighbors and. relatives was not affected by the receipt of COP-funded services.
This type of extensive client-based, multiple-program, multiple-government level evaluation is not necessary for states to be well-informed about many aspects of their home and community based care programs. Much program information is generated by financial, MIS and other reporting systems; periodic budget and appropriations processes assess program performance measures; and ad-hoc evaluations are also made through the feedback from citizens, local government officials and interest groups to state program managers and decision-makers. If necessary, formal arrangements for ongoing monitoring can also be established for home and community based programs, such as Maine's quality assurance committees and client satisfaction survey. Nevertheless, if states wish to thoroughly assess impacts on clients and the benefits and costs of their systems, such broad evaluation studies are necessary.
Private Long Term Care Insurance
Less than 3% of the elderly's nursing home expenses are now covered by Medicare or by private long term care insurance. As a result, almost the full burden of financing services that the elderly cannot pay for themselves falls on state Medicaid programs, which now account for nearly one-half of national nursing home expenses. If a viable insurance market can be developed, such policies might extend to home and community based care services, allow a substantial number of elderly persons to finance long term care insurance needs from their own resources, and reduce fiscal pressures on state Medicaid programs.
The six states studied faced similar problems of trying to foster private insurance company interest in offering long term care insurance, while also protecting consumers from the potential for deception, fraud and unsound policies which could result from a completely uncontrolled market.
All of the states had some form of private long term care insurance initiative in 1986. These efforts can be seen as early or interim steps toward a private insurance financing base for long term care. Nevertheless, there is still a great deal of uncertainty about how effective these measures will be -- and about how far and fast private long term care insurance can develop. As well, these initiatives dealt far more with coverage of institutional long term care services -- a leading cost concern -- than with home and community based alternatives.
The state initiatives fell into three broad categories: (1) studies; (2) consumer protection standards; and (3) mandated insurance benefits.24
Three states -- Wisconsin, Oregon, and Illinois -- had formal government-mandated studies in 1986. In Wisconsin, a study by the legislature's staff was focusing on how to encourage the sale and purchase of private long term care insurance. In Oregon, an advisory committee to the legislature's health care committee had been established to report on long term care issues. Illinois's task force on long term care insurance, enacted in 1985, was still in its formative stage. None of these studies had been completed at the time of this survey.
Consumer protection appeared to be the major intent of actions by Maine and Arkansas. In 1986, Maine enacted legislation which expanded regulatory authority over nursing home policies, with a particular emphasis on such issues as financial disclosure, cancellation, and marketing practices. Maine had also participated on planning groups for LTC insurance with Blue Cross/Blue Shield of Maine. Arkansas had issued minimum nursing home policy standards dealing with concerns such as amount and duration of benefits.
Maryland and Wisconsin were pursuing strategies which included mandating private insurance benefits. In 1986, Maryland enacted legislation to require all health insurance (as of mid-1987) to offer nursing home and custodial care options, although insurance companies were allowed to include cost sharing, benefit limitations and other risk-management features. Wisconsin statutes have required nursing home coverage as part of health insurance since 1975, but attempts to enforce these provisions through state-established minimum requirements in 1981 led to most insurance companies withdrawing their policies. Revised regulations were issued in 1986 designed to meet private insurors' concerns (e.g., by allowing three-day prior hospitalization requirements). In addition to these requirements, Maine, Maryland and Wisconsin also have longstanding requirements that health insurance policies include home health benefits.
In summary, while state officials were aware of the need for private long term care insurance -- and searching for ways to expand such coverage -- government actions to develop this financing base for home and community based care had not yet become a major policy theme.
APPENDIX I. SUMMARY OF EXPENDITURES FOR LONG TERM CARE SERVICES
This Appendix contains information on services and expenditures for long term care in each of the six study states during the period from 1982 through 1986. The information depicts total expenditures on long term care services for the elderly across all funding sources: Medicaid, Social Services Block Grants, Older Americans Act appropriations, and programs supported by state General Revenue Funds. The data were collected from a number of sources. First, published state documents and reports were collected and reviewed. Second, data were collected during the site visits to each state. Third, responsible officials in each state were asked to verify information and reconcile discrepancies between sources. These efforts were undertaken to develop a database for each state that was both comprehensive and accurate. In addition, efforts were made to collect the data according to a general framework that would allow intra- and inter-state comparisons.25
The focus of the overall study is reform of state long term care systems emphasizing the development of home and community based services. The data in this Appendix reflects that emphasis. Data are presented and formatted to illustrate trends in state spending for noninstitutional services. It should be noted, however, that expenditures for long term care are dominated by Medicaid spending for nursing home care. As shown in the summary tables for each of the six study states, only Oregon spends less than eighty-four cents of every long term care dollar on nursing homes.
The Appendix presents the data in the following manner. Table AI-1 provides information on Medicaid and total spending for long term care services and the population most at risk of long term care. Table AI-2 shows the national expenditures for the other two significant sources of federal LTC funds to states: the Social Services Block Grant and the Older Americans Act. Table AI-3 compares the rates of growth on selected expenditure and population variables for each of the six states, compared to the six states in aggregate, and, where data are available, to national trends. The rest of the material consists of pairs of state-specific tables, arranged alphabetically by state. The first of each pair of state tables lists expenditures by program and/or funding stream for the period 1982-1986. The second of each pair is a summary table that applies the same data to show year-to-year fluctuations and overall trends for the 1982-1986 study period.
Long Term Care Growth
The increase in expenditures for long term care over the five year period from 1982 to 1986 showed significant, but not exceptional, growth. The average compound rate of growth over the period as a whole was in the 5 percent to 12 percent range, depending on the state. Growth has not been steady, however. The highest growth rates for most states took place from 1982-1984, slowing by 1986. This may indicate that growth will level off in the next few years.
HOME AND COMMUNITY BASED SERVICES (HCBS) GROWTH. As could be expected of the states chosen for this study, the growth rate for HCBS from all funding sources outstripped that of total long term care (LTC) expenditures. In all the study states except Oregon, the difference was substantial. The lower rate of growth in Oregon's spending on HCBS services compared to LTC expenditures as a whole can be explained by its relatively high base year (1982) expenditures on these services. Oregon's HCBS expenditures were already 25 percent of total LTC expenditures in 1982, whereas in the other five states HCBS spending ranged from about 4 percent to 10 percent of total LTC spending in that year. This reflects the fact that Oregon had substantially expanded HCBS before the study period; the other five states began significant expansion during the period from 1982 to 1986. As with LTC expenditures generally, the growth in HCBS expenditures was not steady. There was a good deal of volatility from year to year. In three of the study states (Illinois, Oregon, and Wisconsin) growth rates peaked in the middle of the period. In the other three states the fastest growth in HCBS expenditures occurred at the beginning of the period and declined relatively steadily thereafter.
| TABLE AI-1. State Expenditures on Long Term Care Per Individuals Aged 75+ (1986) | ||||||||
| AR | IL | ME | ME | OR | WI | National1 | National ExceptNew York2 | |
| MEDICAID: | ||||||||
| LTC* | 1051.05 | 998.42 | 1459.70 | 1087.85 | 751.02 | 1240.00 | 913.73 | 766.00 |
| HCBS** | 103.50 | 44.01 | 92.54 | 29.28 | 185.71 | 34.82 | 64.66 | 22.49 |
| TOTAL:*** | ||||||||
| LTC* | 1086.71 | 1107.21 | 1608.96 | 1181.77 | 808.84 | 1396.30 | N/A | N/A |
| HCBS** | 139.16 | 152.81 | 253.73 | 123.20 | 243.54 | 156.30 | N/A | N/A |
* LTC = Long Term Care. LTC includes institutional expenditures for SNF and ICF services and home- and community-based long term care services, such as personal care, home health, adult day care, and servies available under Section 2176 waiver authority.** HCBS = Home- and Community-Based Services. HCBS includes all non-institutional long term care services, such as: personal care, home health, adult day care, and services under Section 2176 waiver authority.*** Total includes expenditures on long term care services from all funding sources; Medicaid, state general funds, Social Services Block Grant, and Older Americans Act. | ||||||||
| TABLE AI-2. Other Federal Funds Used for State Long Term Care Programs:Expenditure Trends(1982-1986) | ||||||
| 1982 | 1983 | 1984 | 1985 | 1986 | ACRG | |
| SSBG* | $2.400b | $2.675b | $2.700b | $2.725b | $2.584b | 1.9% |
| Percent Change | ||||||
| 82-3 | 83-4 | 84-5 | 85-6 | |||
| 11.5% | 0.9% | 0.9% | -5.2% | |||
| Percent Change: 1982-1986 | ||||||
| OAA** | Title IIB (Social Services) | 10% | ||||
| Title IIIC2 (Home Delivered Meals) | 20% | |||||
| NOTES: * Social Services Block Grants appropriated funds.** Older Americans Act. | ||||||
| TABLE AI-3. Comparing Rates of Growth in Spending and Population Between the Six Study State and the Nation: Annual Compound Rate of Growth 1982-1986 | ||||||||
| AR | IL | ME | MD | OR | WI | 6 StateAggregate | National | |
| MEDICAID | ||||||||
| Total Long Term Care | 5.8 | 9.6 | 8.9 | 11.9 | 8.5 | 8.0 | 7.9 | 8.61 |
| HCBS | 17.0 | 72.9 | 72.5 | 48.15 | 19.8 | 47.2 | 33.4 | N/A |
| Nursing Home | 4.9 | 8.6 | 7.4 | 11.3 | 5.7 | 3.4 | 6.9 | 7.2 |
| POPULATION | ||||||||
| Total | 0.7 | 0.2 | 0.7 | 1.1 | 0.3 | 0.2 | 0.4 | 1.0 |
| Age 75+ | 2.6 | 2.0 | 2.0 | 3.0 | 3.5 | 2.3 | 2.4 | 2.8 |
| SPENDING PER PERSON AGE 75+ | ||||||||
| Total long term care | 3.3 | 8.5 | 8.9 | 8.9 | 3.8 | 2.8 | 6.2 | N/A |
| Total Medicaid LTC | 3.1 | 7.4 | 7.1 | 8.6 | 4.8 | 1.6 | 5.3 | 5.7 |
SOURCE OF NATIONAL DATA: Medicaid Expenditures: Division of Medicaid Cost Estimates Office of Actuarial Analysis HCFAPopulation Information: State Population and Household Estimates With Age, Sex, and Components of Change: 1981-1986 Current Population Reports, Series P-25, No. 1010 U.S. Bureau of the Census
| ||||||||
HCBS EXPENDITURES BY FUNDING SOURCE.
Medicaid. Medicaid is the predominant public payer for long term care services. The overwhelming bulk of Medicaid expenditures for long term care for the elderly is for institutional services provided in skilled nursing facilities (SNFs) and intermediate care facilities (ICFs). Medicaid also covers HCBS through two separate mechanisms -- the state plan and Section 2176 waivers. The state plan must cover home health services and, at state option, personal care. State officials indicate that most home health expenditures under the state plan are related to acute care rather than long term care. It is not possible to disaggregate expenditures for home health vis-a-vis personal care, but since they are such a small proportion of total Medicaid expenditures, this does not affect the overall Medicaid LTC expenditure trends. Under the Section 2176 waiver authority, states receiving approval from the U.S. Department of HHS may provide a range of HCBS services.
Of the six states, only Oregon used both the personal care option and Section 2176 waivers over the past five years. Arkansas and Maryland cover personal care, but do not have a waiver. Illinois has a waiver, but does not cover personal care. Wisconsin does not offer personal care, but has recently implemented a Medicaid waiver. Maine added personal care in 1986 and has a Medicaid waiver.
In four of the six states Medicaid HCBS spending is a relatively small percentage of total Medicaid LTC expenditures. Oregon, primarily due to the Section 2176 waiver, spent proportionately more on Medicaid HCBS in each of the five years than any of the other six states. The state of Arkansas spent the next highest proportion of its Medicaid LTC budget on HCBS, primarily through the personal care service option.
Three of the six states -- Illinois, Maine and Maryland -- had an annual compound rate of growth for total Medicaid LTC spending greater than the national average (8.6%) from 1982-1986. Two states (Arkansas and Wisconsin) had Medicaid LTC spending growth rates below the national average, while Oregon essentially matched the national average.
Though these six states have increased their Medicaid dollars for HCBS, institutional spending continues to greatly outstrip HCBS. In all the study states except Oregon, institutional expenditures totaled between 90 percent to 97 percent of Medicaid long term care in 1986. In Oregon, due primarily to the Section 2176 waiver, institutional expenditures totaled 75 percent of Medicaid long term care expenditures.
Growth rates in Medicaid institutional spending over the study period differed by state. Three states had compound rates of growth lower than the national average of 7.2 percent during the period.. In four of the six states the rate of growth slowed in the last two years. For all six states annual changes in rates of growth showed wide fluctuations.
Other HCBS. Non-Medicaid HCBS includes all other programs providing HCBS to the elderly. It should be noted that these programs include those with federal funds other than Medicaid -- such as Social Services Block Grant (SSBG) and Older Americans Act (OAA) -- as well as programs funded solely by state general funds. These federal funds are grouped with state funded programs for two reasons. First, states devote a substantial amount of general revenue funds to supplement federal SSBG and OAA dollars. Second, these funding streams do not have to be used for services to the elderly (except OAA) or devoted to HCBS. Whether they are so used is a state decision.
The Social Services Block Grant (SSBG) provides funding for states to provide social services. States are not required to match federal funds, but many states provide supplemental funds at their own discretion. In 1983, according to the American Public Welfare Association, home-based services under SSBG accounted for about $555 million, though no data specific to the elderly are available. Home-based services usually include homemaker, chore, home health, companion, and home maintenance.26
The Older Americans Act provides funding to states to support a number of services to the elderly. States are required to provide at least 15 percent state matching funds to receive federal funds. National or state data are not available to determine spending for particular services. However, in-home services are a priority under OAA. In-home services usually include housekeeping, personal care, chore, and telephone reassurance services.
In four of the six states non-Medicaid HCBS expenditures constitute the predominant proportion (between 63 percent and 97 percent) of Total HCBS spending. As mentioned in the previous section, Arkansas and Oregon are the exceptions.
Funding LTC Reform: Medicaid HCBS v. Other HCBS. States trying to reform their LTC systems by expanding HCBS can choose to do so through Medicaid, other programs, or a combination. The six states in this study are using a combination approach, with Oregon and Arkansas placing a greater emphasis on Medicaid, an emphasis that could have been expected for two reasons. First, Medicaid's financial participation is attractive. Four of the six states have federal matching rates of approximately 60 percent and above. This means that a state investment of $4 generates an additional $6 in federal funds. Second, authority for Section 2176 waivers was enacted in 1981. This authority made it possible for states to develop Medicaid HCBS programs targeted to specific eligibles for different services than were available under the traditional Medicaid program. Four of the six states have taken advantage of Section 2176 waiver authority. In three of these four states, Medicaid HCBS expenditures grew more than forty-five percent over the study period.
While Medicaid IICBS have grown rapidly, as mentioned earlier, other HCBS expenditures have also experienced substantial increases. In four of the six states, other HCBS rates of growth from 1982 to 1986 were greater than that of total LTC expenditures and total Medicaid LTC expenditures.
The combination approach prevalent in these six states indicates that these six states are expanding their investments in HCBS for the elderly across funding streams. Trends in from four of the six states suggest that the emphasis on long term care and home- and community based services may be reaching a plateau where rates of increase will slow.
SUMMARY. The expenditure trend data presented here illustrate how these six states have funded reforms in their long term care systems. Though the data are not directly comparable across states and across programs, some general summary statements can be made. First, all six study states have devoted substantial proportions of their total LTC expenditures to HCBS. Second, increases in spending on HCBS have occurred across programs and funding streams. Third, while expenditures on HCBS has increased greatly, long term care remains heavily dominated by institutional expenditures in all but one of the study states. Fourth, the growth in HCBS was marked by wide fluctuations from year to year. Even though these six states were selected for the study because of their early development of comprehensive statewide community based services programs, long term care spending in the six study states paralleled national trends.
| TABLE AI-4. Arkansas Expenditures on Long Term Care Programs for the Elderly: 1982-1986(millions of dollars) | |||||
| Program | 1982 | 1983 | 1984 | 1985 | 1986a |
| MEDICAIDa | |||||
| SNF/ICF | 112.1 | 122.5 | 134.5 | 134.2 | 135.5 |
| Home Health | 0.9 | 1.7 | 2.5 | 3.2 | 4.8 |
| Personal Care | 7.0 | 9.0 | 9.1 | 9.8 | 10.0 |
| HOME DELIVERED MEALSb | |||||
| (OAA) | 0.7 | 1.0 | 0.9 | 1.1 | 1.1 |
| (SSBG) | 1.0 | 1.1 | 1.2 | 1.2 | 0.9 |
| ADULT DAY CAREb | |||||
| (SSBG) | 0.02 | 0.02 | 0.05 | 0.1 | 0.05 |
| CHORE SERVICESb | |||||
| (SSBG) | 0.1 | 0.2 | 0.3 | 0.3 | 0.2 |
| (OAA) | 0.1 | 0.1 | 0.1 | 0.1 | 0.1 |
| SGFb | |||||
| Case Management | 0.9 | 0.9 | 1.1 | 1.7 | 1.5 |
| Personal Care | 0.5 | 0.1 | |||
| Alternate Care | 0.2 | 0.2 | 0.5 | 0.5 | 0.5 |
| Comm-Based Developers | 0.2 | 0.2 | |||
| Adult Day | 0.4 | ||||
| BOARDING HOMESb | 0.1 | 0.1 | 0.1 | 0.1 | 0.1 |
KEY: OAA = Older Americans ActSGF = State General FundsSSBG = Social Services Block GrantSOURCE: Data received from Arkansas Department of Human Services.NOTES:
| |||||
| TABLE AI-5. Summary Table: Arkansas | ||||||
| 1982 | 1983 | 1984 | 1985 | 1986 | % Change1982-86 | |
| EXPENDITURES ON LTC AND, WITHIN LTC, ON HCBS | ||||||
| Expenditures (in millions) | ||||||
| Total: | ||||||
| LTC | 123.1 | 136.8 | 150.3 | 153.0 | 155.4 | 26.5 |
| HCBS | 11.0 | 14.3 | 15.8 | 18.8 | 19.9 | 80.9 |
| Ratio of: | ||||||
| HCBS/Total | 8.9% | 10.5% | 10.5% | 12.3% | 12.8% | |
| Expenditures (in millions) | ||||||
| Medicaid LTC | 120.0 | 133.2 | 146.1 | 147.2 | 150.3 | 25.3 |
| HCBS | 7.9 | 10.7 | 11.6 | 13.0 | 14.8 | 87.3 |
| SNF/ICF | 112.1 | 122.5 | 134.5 | 134.2 | 135.5 | 20.9 |
| Ratio of: | ||||||
| HCBS/Medicaid | 6.6% | 8.0% | 7.9% | 8.8% | 9.8% | |
| SNF-ICF/Medicaid | 93.4% | 92.0% | 92.1% | 91.2% | 90.1% | |
| Expenditures (in millions) | ||||||
| State HCBS | 3.1 | 3.6 | 4.2 | 5.8 | 5.1 | 64.5 |
| Ratio of: | ||||||
| Other HCBS/T HCBS | 28.2% | 25.2% | 26.6% | 30.9% | 25.6% | |
| Other HCBS/T LTC | 2.5% | 2.6% | 2.8% | 3.8% | 3.3% | |
| 1982 | 1983 | 1984 | 1985 | 1986 | ACRGa(percent)82-86 | |
| POPULATION (in thousands) | ||||||
| Total Population | 2308 | 2326 | 2347 | 2360 | 2372 | 0.7 |
| Age 75 & Older | 129 | 133 | 136 | 140 | 143 | 2.6 |
| EXPENDITURES PER PERSON AGE 75+ (dollars) | ||||||
| Total LTC | 954.26 | 1028.57 | 1105.15 | 1092.86 | 1086.71 | 3.3 |
| Medicaid LTC | 930.23 | 1001.50 | 1074.27 | 1051.43 | 1051.05 | 3.1 |
| 82-83 | 83-84 | 84-85 | 85-86 | ACRGa(percent)82-86 | ||
| ANNUAL PERCENT CHANGE IN EXPENDITURES | ||||||
| Total LTC | 11.1 | 9.9 | 1.8 | 1.6 | 6.00 | |
| HCBS | 27.3 | 12.9 | 16.9 | 5.9 | 16.00 | |
| Medicaid LTC | 11.0 | 10.2 | 1.8 | 1.5 | 5.79 | |
| HCBS | 35.4 | 8.4 | 12.1 | 13.8 | 16.99 | |
| SNF/ICF | 9.3 | 9.8 | -0.2 | 1.0 | 4.85 | |
| Other HCBS | 16.1 | 16.7 | 38.1 | -12.1 | 13.25 | |
| ||||||
| TABLE AI-6. Illinois Expenditures on Long Term Care Programs for the Elderly: 1982-1986(dollars in millions) | |||||
| Program | 1982 | 1983 | 1984 | 1985 | 1986a |
| MEDICAIDa | |||||
| SNF/ICF | 390.6 | 445.1 | 437.9 | 492.6 | 543.1 |
| Home Health | 2.8 | 2.4 | 3.0 | 4.4 | 6.0 |
| Waiver/CCP | N/A | N/A | 9.8 | 15.0 | 19.0 |
| GENERAL FUNDS/CCPa (SGF) | 22.5 | 25.5 | 25.8 | 38.6 | 53.2 |
| HOME DELIVERED MEALS | |||||
| (OAA) (SGF) | 2.7 | 3.2 | 3.5 | 3.8 | 4.2 |
| Home Health (SGF) | 0.0 | 0.04 | 0.08 | ||
| HOMEMAKER (OAA) | N/A | 0.3 | 0.3 | 0.3 | 0.3 |
| CASE MANAGEMENT (OAA) | N/A | N/A | 2.1 | 5.4 | 4.0 |
SOURCE: Data received from Division of Long Term Care, Illinois Department on Aging.NOTES: All data are for state fiscal year. Medicaid data include federal matching funds.
| |||||
| TABLE AI-7. Summary Table: Illinois | ||||||
| 1982 | 1983 | 1984 | 1985 | 1986 | % Change1982-86 | |
| EXPENDITURES ON LTC AND, WITHIN LTC, ON HCBS | ||||||
| Expenditures (in millions) | ||||||
| Total: | ||||||
| LTC | 481.6 | 476.5 | 482.4 | 560.1 | 628.9 | 50.2 |
| HCBS | 28.0 | 31.4 | 44.5 | 67.5 | 86.8 | 210.0 |
| Ratio of: | ||||||
| HCBS/Total | 6.7% | 6.6% | 9.1% | 12.1% | 13.8% | |
| Expenditures (in millions) | ||||||
| Medicaid LTC | 393.4 | 447.5 | 450.7 | 512.0 | 567.1 | 44.2 |
| HCBS | 2.8 | 2.4 | 12.8 | 19.4 | 25.0 | 792.9 |
| SNF-ICF | 390.6 | 445.1 | 437.9 | 492.6 | 543.1 | 39.0 |
| Ratio of: | ||||||
| HCBS/Medicaid | 0.7% | 0.5% | 2.8% | 3.8% | 4.4% | |
| SNF-ICF/Medicaid | 99.3% | 99.5% | 97.2% | 96.2% | 95.6% | |
| Expenditures (in millions) | ||||||
| State HCBS | 25.2 | 29.0 | 31.7 | 48.1 | 61.8 | 145.2 |
| Ratio of: | ||||||
| Other HCBS/T HCBS | 90.0% | 92.4% | 71.2% | 71.3% | 71.2% | |
| Other HCBS/T LTC | 6.0% | 6.1% | 6.6% | 8.6% | 9.8% | |
| 1982 | 1983 | 1984 | 1985 | 1986 | ACRGa(percent)82-86 | |
| POPULATION (in thousands) | ||||||
| Total Population | 11,479 | 11,492 | 11,524 | 11,537 | 11,552 | 0.2 |
| Age 75 & Older | 524 | 535 | 545 | 556 | 568 | 2.0 |
| EXPENDITURES PER PERSON AGE 75+ (dollars) | ||||||
| Total LTC | 798.86 | 890.65 | 885.14 | 1007.37 | 1107.21 | 8.5 |
| Medicaid LTC | 750.76 | 836.45 | 817.98 | 920.86 | 998.42 | 7.4 |
| 82-83 | 83-84 | 84-85 | 85-86 | ACRGa(percent)82-86 | ||
| ANNUAL PERCENT CHANGE IN EXPENDITURES | ||||||
| Total LTC | 13.8 | 1.2 | 16.1 | 12.3 | 10.71 | |
| HCBS | 12.1 | 41.7 | 51.7 | 28.6 | 32.69 | |
| Medicaid LTC | 13.8 | 0.7 | 13.6 | 10.8 | 9.57 | |
| HCBS | -14.3 | 433.3 | 51.6 | 28.9 | 72.86 | |
| SNF-ICF | 14.0 | -1.6 | 12.5 | 10.3 | 8.59 | |
| Other HCBS | 15.1 | 9.3 | 51.7 | 28.5 | 25.14 | |
| ||||||
| TABLE AI-8. Maryland Expenditures on Long Term Care Programs for the Elderly: 1982-1986(dollars in millions) | |||||
| Program | 1982 | 1983 | 1984 | 1985 | 1986a |
| MEDICAIDa | |||||
| SNF/ICF | 124.7 | 147.2 | 178.8 | 184.4 | 191.6 |
| Personal Care | 0.4 | 1.1 | 1.8 | 2.9 | 3.3 |
| Home Health | 0.2 | 0.2 | 0.2 | 0.4 | 0.5 |
| Adult Day Care | 0.1 | 0.5 | 0.7 | 1.2 | 1.5 |
| IN-HOME AIDES | |||||
| In-Home Aideb | 3.5 | 4.1 | 5.1 | 4.9 | 5.7 |
| Home Meals (OAA) | 1.3 | 1.4 | 1.5 | 1.6 | 1.5 |
| COMMUNITY-BASED | |||||
| Day Care (SGF) | 0.7 | 0.8 | 0.8 | 0.8 | 1.0 |
| Protective (SGF/SSBG) | 0.8 | 0.7 | 0.7 | 1.0 | 1.3 |
| ASSISTED HOUSING | |||||
| Sheltered (SGF) | 0.5 | 0.6 | 0.6 | 0.7 | 1.0 |
| Domiciliary (SGF) | 0.2 | 0.3 | 0.6 | 0.6 | 0.6 |
| SCREENING (SGF) | |||||
| Geriatric Evaluation | 0.7 | 0.9 | 1.3 | 1.1 | 1.2 |
| Coordinated Services | N/A | 0.4 | 0.4 | 0.5 | 0.5 |
| COMMUNITY PLACEMENT (SGF) | 0.2 | 0.2 | 0.3 | ||
| STEPSc | N/A | N/A | N/A | 0.5 | 0.2 |
| CASE MANAGEMENT (SGF/SSBG) | 1.5 | 2.0 | 2.5 | 2.9 | 2.9 |
| GAP-FILLING (SGF) | 0.1 | 0.4 | 0.5 | 0.8 | 1.1 |
Data are for state fiscal years. Based on estimated number of elderly enrolled in each program.SOURCE: Annual State Budget, Chart 13: Major Publicly Funded Programs for the Aged Administered by the State of Maryland.
| |||||
| TABLE AI-9. Summary Table: Maryland | ||||||
| 1982 | 1983 | 1984 | 1985 | 1986 | % Change1982-86 | |
| EXPENDITURES ON LTC AND, WITHIN LTC, ON HCBS | ||||||
| Expenditures (in millions) | ||||||
| Total: | ||||||
| LTC | 135.5 | 161.6 | 197.1 | 209.2 | 213.9 | 57.9 |
| HCBS | 10.6 | 13.6 | 17.0 | 19.9 | 22.3 | 110.4 |
| Ratio of: | ||||||
| HCBS/Total | 7.8% | 8.4% | 8.6% | 9.5% | 10.4% | |
| Expenditures (in millions) | ||||||
| Medicaid LTC | 125.8 | 149.0 | 181.5 | 188.9 | 196.9 | 56.5 |
| HCBS | 1.1 | 1.8 | 2.7 | 4.5 | 5.3 | 381.8 |
| SNF-ICF | 124.7 | 147.2 | 178.8 | 184.4 | 191.6 | 53.6 |
| Ratio of: | ||||||
| HCBS/Medicaid | 0.8% | 1.2% | 1.5% | 2.4% | 2.7% | |
| SNF-ICF/Medicaid | 99.2% | 98.8% | 98.5% | 97.6% | 97.3% | |
| Expenditures (in millions) | ||||||
| State HCBS | 9.5 | 11.8 | 14.3 | 15.4 | 17.0 | 78.9 |
| Ratio of: | ||||||
| Other HCBS/T HCBS | 89.6% | 86.8% | 84.1% | 77.4% | 76.2% | |
| Other HCBS/T LTC | 7.0% | 7.3% | 7.3% | 7.4% | 7.9% | |
| 1982 | 1983 | 1984 | 1985 | 1986 | ACRGa(percent)82-86 | |
| POPULATION (in thousands) | ||||||
| Total Population | 4272 | 4299 | 4348 | 4393 | 4463 | 1.1 |
| Age 75 & Older | 161 | 166 | 171 | 176 | 181 | 3.0 |
| EXPENDITURES PER PERSON AGE 75+ (dollars) | ||||||
| Total LTC | 841.62 | 973.49 | 1152.63 | 1188.64 | 1181.77 | 8.9 |
| Medicaid LTC | 781.37 | 897.59 | 1061.40 | 1073.29 | 1087.85 | 8.6 |
| 82-83 | 83-84 | 84-85 | 85-86 | ACRGa(percent)82-86 | ||
| ANNUAL PERCENT CHANGE IN EXPENDITURES | ||||||
| Total LTC | 19.3 | 22.0 | 6.1 | 2.2 | 12.09 | |
| HCBS | 28.3 | 25.0 | 17.1 | 12.1 | 20.43 | |
| Medicaid LTC | 18.4 | 21.8 | 4.0 | 4.2 | 11.85 | |
| HCBS | 63.6 | 50.0 | 66.7 | 17.8 | 48.15 | |
| SNF-ICF | 18.0 | 21.5 | 3.1 | 3.9 | 11.34 | |
| Other HCBS | 24.2 | 21.2 | 7.7 | 10.4 | 15.66 | |
| ||||||
| TABLE AI-10. Oregon Expenditures on Long Term Care Programs for the Elderly: 1982-1986(millions of dollars) | |||||
| Program | 1982 | 1983 | 1984 | 1985 | 1986a |
| MEDICAIDa | |||||
| SNF/ICF | 66.5 | 69.3 | 72.1 | 80.3 | 83.1 |
| Home Health | 0.4 | 0.6 | 0.7 | 0.8 | 0.7 |
| Personal Care SER. | 1.4 | 2.0 | 2.1 | 1.6 | 1.5 |
| Waiverb | 11.5 | 15.9 | 19.8 | 24.3 | 25.1 |
| HOME DELIVERED MEALSc | |||||
| (SGF) | 0.1 | 0.2 | 0.3 | 0.3 | 0.3 |
| ADULT FOSTER CAREc | |||||
| (SSBG & SGF) | 1.3 | 0.6 | 0.7 | 0.8 | 0.8 |
| RESIDENTIAL CAREc | |||||
| (SSBG & SGF) | 1.7 | 0.8 | 0.9 | 1.0 | 1.0 |
| HOME CARE | |||||
| (SSBG & SGF)c | 3.0 | 1.5 | 1.7 | 1.8 | 1.9 |
| SOCIAL SERIVCES (OAA)c | 2.6 | 2.7 | 3.3 | 3.2 | 3.4 |
| HOME DELIVERED MEALSc (OAA) | 0.7 | 0.8 | 1.0 | 1.0 | 1.1 |
KEY: OAA = Older Americans ActSGF = State General Funds (Oregon Project Independence)SSBG = Social Services Block GrantSOURCE: Senior Services Division Long Term Care Chart Book for Long Term Care
| |||||
| TABLE AI-11. Summary Table: Oregon | ||||||
| 1982 | 1983 | 1984 | 1985 | 1986 | % Change1982-86 | |
| EXPENDITURES ON LTC AND, WITHIN LTC, ON HCBS | ||||||
| Expenditures (in millions) | ||||||
| Total: | ||||||
| LTC | 89.1 | 94.2 | 102.6 | 114.0 | 118.9 | 33.2 |
| HCBS | 22.6 | 24.9 | 30.5 | 33.8 | 35.8 | 58.5 |
| Ratio of: | ||||||
| HCBS/Total | 25.4% | 26.5% | 29.7% | 29.6% | 30.1% | |
| Expenditures (in millions) | ||||||
| Medicaid LTC | 79.8 | 87.7 | 94.7 | 106.0 | 110.4 | 38.4 |
| HCBS | 13.3 | 18.4 | 22.6 | 25.7 | 27.3 | 105.7 |
| SNF-ICF | 66.5 | 69.3 | 72.1 | 80.3 | 83.1 | 24.9 |
| Ratio of: | ||||||
| HCBS/Medicaid | 16.6% | 21.0% | 23.9% | 24.3% | 24.7% | |
| SNF-ICF/Medicaid | 83.4% | 79.0% | 76.1% | 75.7% | 75.3% | |
| Expenditures (in millions) | ||||||
| State HCBS | 9.3 | 6.5 | 7.9 | 8.0 | 8.5 | -8.4 |
| Ratio of: | ||||||
| Other HCBS/T HCBS | 41.3% | 26.0% | 25.9% | 23.8% | 23.9% | |
| Other HCBS/T LTC | 10.5% | 6.9% | 7.7% | 7.1% | 7.2% | |
| 1982 | 1983 | 1984 | 1985 | 1986 | ACRGa(percent)82-86 | |
| POPULATION (in thousands) | ||||||
| Total Population | 2669 | 2660 | 2676 | 2686 | 2698 | 0.3 |
| Age 75 & Older | 128 | 133 | 138 | 142 | 147 | 3.5 |
| EXPENDITURES PER PERSON AGE 75+ (dollars) | ||||||
| Total LTC | 696.09 | 708.27 | 743.48 | 802.82 | 808.84 | 3.8 |
| Medicaid LTC | 623.44 | 659.40 | 686.23 | 746.48 | 751.02 | 4.8 |
| 82-83 | 83-84 | 84-85 | 85-86 | ACRGa(percent)82-86 | ||
| ANNUAL PERCENT CHANGE IN EXPENDITURES | ||||||
| Total LTC | 5.7 | 8.9 | 11.1 | 4.3 | 7.5 | |
| HCBS | 10.3 | 22.4 | 10.7 | 6.1 | 12.2 | |
| Medicaid LTC | 10.0 | 8.0 | 11.9 | 4.1 | 8.5 | |
| HCBS | 39.0 | 22.6 | 13.8 | 6.1 | 19.8 | |
| SNF-ICF | 4.2 | 4.1 | 11.3 | 3.5 | 5.7 | |
| Other HCBS | -30.5 | 21.7 | 1.7 | 6.4 | -2.2 | |
| ||||||
| TABLE AI-12. Wisconsin Expenditures on Long Term Care Programs for the Elderly: 1982-1986(millions of dollars) | |||||
| Program | 1982 | 1983 | 1984 | 1985 | 1986a |
| MEDICAIDa | |||||
| SNF/ICFa | 285.0 | 306.3 | 317.1 | 334.0 | 325.4 |
| Home Healtha | 2.0 | 2.8 | 4.0 | 7.1 | 8.9 |
| Waiverb | N/A | N/A | N/A | 0.1 | 0.5 |
| COMMUNITY OPTIONS PROGRAMb | |||||
| (SGF) | 0.2 | 1.4 | 3.0 | 7.0 | 8.1 |
| COMMUNITY AIDS (SSBG & SGF)b,c | |||||
| Supportive Home Care | 10.1 | 10.1 | 10.6 | 11.0 | 11.3 |
| Case Management | 1.5 | 1.5 | 1.5 | 1.6 | 1.6 |
| Alzheimer's | N/A | N/A | N/A | N/A | 1.2 |
| Other | 5.1 | 5.1 | 5.2 | 5.4 | 5.5 |
| OLDER AMERICANS ACTb,d | |||||
| Personal & Adult Day | N/A | N/A | N/A | 0.3 | 1.0 |
| Home Delivered Meals | 3.2 | 3.4 | 3.9 | 4.3 | 4.2 |
KEY: OAA = Older Americans Act.SGF = State General Funds.SSBG = Social Services Block Grant.SOURCE: Data received from Bureau of Long Term Support.NOTES:
| |||||
| TABLE AI-13. Summary Table: Wisconsin | ||||||
| 1982 | 1983 | 1984 | 1985 | 1986 | % Change1982-86 | |
| EXPENDITURES ON LTC AND, WITHIN LTC, ON HCBS | ||||||
| Expenditures (in millions) | ||||||
| Total: | ||||||
| LTC | 309.1 | 333.4 | 349.3 | 377.9 | 377.1 | 22.0 |
| HCBS | 22.1 | 24.3 | 28.2 | 36.7 | 42.3 | 91.0 |
| Ratio of: | ||||||
| HCBS/Total | 7.2% | 7.3% | 8.1% | 9.7% | 11.2% | |
| Expenditures (in millions) | ||||||
| Medicaid LTC | 287.0 | 309.1 | 321.1 | 341.2 | 334.8 | 16.7 |
| HCBS | 2.0 | 2.8 | 4.0 | 7.2 | 9.4 | 370.0 |
| SNF-ICF | 285.0 | 306.3 | 317.1 | 334.0 | 325.4 | 14.2 |
| Ratio of: | ||||||
| HCBS/Medicaid | 0.7% | 0.9% | 1.2% | 2.1% | 2.8% | |
| SNF-ICF/Medicaid | 99.3% | 99.1% | 98.8% | 97.9% | 97.2% | |
| Expenditures (in millions) | ||||||
| State HCBS | 20.1 | 21.5 | 24.2 | 29.5 | 32.9 | 63.2 |
| Ratio of: | ||||||
| Other HCBS/T HCBS | 91.0% | 88.5% | 85.8% | 80.4% | 77.7% | |
| Other HCBS/T LTC | 6.5% | 6.4% | 6.9% | 7.8% | 8.7% | |
| 1982 | 1983 | 1984 | 1985 | 1986 | ACRGa(percent)82-86 | |
| POPULATION (in thousands) | ||||||
| Total Population | 4747 | 4749 | 4764 | 4776 | 4785 | 0.2 |
| Age 75 & Older | 247 | 253 | 258 | 264 | 270 | 2.3 |
| EXPENDITURES PER PERSON AGE 75+ (dollars) | ||||||
| Total LTC | 1251.42 | 1317.79 | 1353.88 | 1431.44 | 1396.30 | 2.8 |
| Medicaid LTC | 1161.94 | 1221.74 | 1244.57 | 1292.42 | 1240.00 | 1.6 |
| 82-83 | 83-84 | 84-85 | 85-86 | ACRGa(percent)82-86 | ||
| ANNUAL PERCENT CHANGE IN EXPENDITURES | ||||||
| Total LTC | 7.8 | 4.8 | 8.2 | -0.2 | 5.09 | |
| HCBS | 10.0 | 16.1 | 30.1 | 15.0 | 17.55 | |
| Medicaid LTC | 7.7 | 3.9 | 6.3 | -1.9 | 8.01 | |
| HCBS | 40.0 | 42.9 | 80.9 | 30.6 | 47.24 | |
| SNF-ICF | 7.5 | 3.5 | 5.3 | -2.6 | 3.37 | |
| Other HCBS | 7.0 | 12.6 | 21.9 | 11.2 | 13.02 | |
| ||||||
APPENDIX II. MEDICAID ELIGIBILITY POLICY AND ITS IMPACT ON HOME AND COMMUNITY BASED SERVICES IN THE SIX CASE STUDY STATES
Although the details of Medicaid eligibility policy are complex, three components of Medicaid eligibility policy have the greatest potential impact on providing elderly persons with Medicaid-funded home and community based services in the six case study states. These are:
- Group coverage options;
- Treatment of SSI cash recipients for Medicaid
- Coverage of the medically needy
- Benefit levels; and
- State Supplementation Program (SSP) benefit levels
- Medically needy income levels
- Eligibility Provisions unique to Section 2176 waiver programs
Group Coverage Options
Two important eligibility decisions which states make in extending Medicaid coverage to its elderly citizens are: 1) how the state elects to cover persons receiving SSI cash assistance; and 2) whether the state elects to cover the medically needy. States have three options regarding how they cover SSI recipients. First, states can elect to automatically cover all SSI cash recipients without requiring them to make a separate application for Medicaid. These states are commonly referred to as "1634 States," since this option relates to Section 1634 of the Social Security Act. Most states (30) have elected this option and four of the six case study states (Arkansas, Maine, Maryland and Wisconsin) are 1634 States, as shown in Table AII-1.
| TABLE AII-1. Coverage of SSI Recipients Under Medicaid | ||||
| State | 1634 | StateDetermination | 209(b) | Ratio of MedicaidCash Recipients toSSI Recipients |
| AR | X | 1.09 | ||
| IL | X | 0.69 | ||
| MD | X | 1.21 | ||
| ME | X | 1.17 | ||
| OR | X | 0.93 | ||
| WI | X | 1.18 | ||
| SOURCES: HCBA 2082 data, Bureau of Data Management and Strategy; and Social Security Administration, Office of Research and Statistics. Data are for 1985. The ratio of Medicaid cash recipients to SSI recipients exceeds 1.0 in some States because the former includes all aged persons who received Medicaid during 1985, while the latter includes only the number of elderly persons who received an SSI cash payment in the month of December 1985. | ||||
Second, states can extend Medicaid eligibility to all SSI cash recipients, but require them to make a separate application for Medicaid eligibility. Nationwide, six states have elected this option, one of which is Oregon. States generally choose this option in order to retain total control over the Medicaid eligibility determination process, rather than relinquishing this role to the Social Security Administration. From the applicant's perspective, however, this option serves as an administrative barrier to Medicaid enrollment, since it requires an applicant to go through both the SSI eligibility process with the Social Security Administration and the Medicaid eligibility process with the state.
Third, states can elect the Section 209(b) option, and impose more restrictive eligibility criteria for Medicaid than are used in determining eligibility for SSI, so long as the criteria applied were part of the state's Medicaid plan in January 1972, prior to enactment of the federal SSI program. 209(b) states may be more restrictive in their definition of blindness or disability, and/or more restrictive than SSI in their financial requirements for Medicaid. It is generally regarded as the most conservative SSI option. Fourteen states currently elect the 209(b) option, one of which is the state of Illinois.
Table AII-1 shows which option each of the six study states has elected, and how these options affect Medicaid enrollment of aged beneficiaries. This was done by calculating the ratio of aged Medicaid recipients receiving SSI cash assistance to the number of aged SSI recipients in the state in 1985. The data clearly show that Oregon and Illinois, which have elected the more restrictive options, have lower coverage of their SSI populations than the four "1634" states. Illinois' election of the Section 209(b) option particularly appears to have had a substantial impact on limiting Medicaid enrollment of aged SSI beneficiaries.
Of all Medicaid eligibility options, a state's decision of whether or not to cover the "medically needy" probably has the greatest impact. In electing a medically needy program, states can extend eligibility to persons who are not eligible for SSI/SSP due to excess income or assets, but who have large medical expenses. Under the medically needy option, applicants may "spend down" to Medicaid eligibility levels by deducting their medical expenses from their countable income. After an applicant has met the spend-down requirement (i.e. the difference between the applicant's countable income and the medically needy income level), he/she becomes eligible for Medicaid for the remainder of his/her medical expenses. In effect, aged persons of all income levels are potentially eligible for Medicaid in states that have medically needy programs, if their medical bills are large enough.
All of the six study states have medically needy programs. However, Oregon's medically needy program for the aged, blind and disabled only became effective in 1986. Prior to 1986, the only way in which an elderly person outside of a nursing home could become eligible for Medicaid in Oregon was to be eligible for SSI cash assistance and/or a state supplementation payment, or fall under 300% of the SSI standard for institutional and waiver clients.
Benefit Levels
Benefit levels are also extremely important in determining the extent of Medicaid coverage for the elderly. The higher the benefit level, the more elderly persons who are potentially eligible for Medicaid. The first benefit level of importance is whether or not a state chooses to supplement the federal SSI benefit, since persons who receive state supplementation payments are generally eligible for Medicaid as well. Of course, the level at which a state chooses to supplement the SSI benefit level is also important.
Another benefit level of importance is the medically needy income level. As previously discussed, this is the income level which medically needy applicants must "spend down" to before they are eligible for Medicaid. The medically needy level, ironically, is not tied to the SSI/SSP level, but to benefit levels established for the AFDC program. States may elect to set their medically needy income levels anywhere between the AFDC benefit level and 133 1/3% of that level.
Table AII-2 shows SSI/SSP levels and medically needy income levels in the six study states for a single aged person living independently. Two states, Arkansas and Maryland, provide no state supplements for aged persons living alone, although Maryland does provide supplementation payments to certain persons living in specially licensed board-and-care homes. Oregon only provides a very small state supplementation payment of $1.70 per month. Illinois' State Supplementation Program is unique among states in that it is the only state which determines the SSP benefit level on a case-by-case basis. Functional status is one of the factors used in determining the benefit level, so that Illinois' SSP program is one which is specifically oriented towards persons with long term care needs. Wisconsin's SSP level is by far the most generous of the six states, increasing the federal SSI benefit level by 31%.
Medically needy levels also vary considerably across the six states, depending upon where each state has set its benefit levels for the AFDC program. In three of the states, medically needy levels and the SSI/SSP levels are the same or almost the same, but in two states -- Arkansas and Illinois -- the medically needy levels are below the SSI/SSP levels (we know it is below the SSI/SSP level in Illinois because even though the state supplementation benefit varies from case to case, it cannot be below the federal SSI level of $336). This means that persons who do not qualify for SSI/SSP due to excess income must nevertheless spend down to an income level below the SSI/SSP level in order to become eligible for Medicaid. This phenomenon is referred to as "negative bands," and relates to the differences between benefit levels for the AFDC program and for the SSI/SSP program.27 It is an inequity which has always existed in the Medicaid program, but one which has grown in magnitude as the difference between AFDC and SSI/SSP benefit levels has increased in many states.
| TABLE AII-2. State Supplementation Levels and Medically Needy Levels for an Aged Individual Living Independently in 1986 | |||
| State | Total SSI/SSPBenefit Level | StateSupplementation | Medically NeedyLevel |
| AR | $336.00 | $0.00 | $108 |
| IL | Variable | Variable | 267 |
| MD | 336.00 | 0.00 | 325 |
| ME | 346.00 | 10.00 | 336 |
| Oregon | 338.70 | 1.70 | 355 |
| Wisconsin | 438.70 | 101.70 | 438 |
| SOURCES: Social Security Administration, The Supplemental Security Income Program for Aged, Blind, and Disabled. Characteristics of State Assistance Programs for SSI Recipients, and Commerce Clearing House, Medicare and Medicaid Guide. All data are for 1986. | |||
Another option which states have under their medically needy programs is to establish higher resource limits for medically needy applicants than are used in the SSI program. It is another strange twist of Medicaid eligibility policy that income levels for the medically needy can be below SSI/SSP levels, while the resource limits can be higher. However, of the six states, only Maryland has set higher resource limits for the medically needy ($2,500 for an individual), while the remaining five states use the SSI limits ($1,600).
Impact of Medicaid Eligibility Options on Coverage of the Elderly
What impact do these state eligibility options regarding group coverage and benefit levels have on the degree to which Medicaid covers the elderly poor in the six study states? Simply calculating the percentage of all elderly persons in a particular state who are eligible for Medicaid is a misleading statistic, because Medicaid enrollment is related to overall poverty trends as well as to the expansiveness or restrictiveness of Medicaid eligibility options. An alternative is to measure the ratio of elderly Medicaid recipients to the number of elderly persons living below the poverty line in a particular state. However, this statistic is also misleading because poverty data for the elderly do not include persons in nursing homes or other group quarters. Therefore, a better measure of Medicaid's coverage of the elderly is to calculate the ratio of non-institutionalized elderly on Medicaid to the number of elderly persons in poverty.
These data are presented in Table AII-3 and Figure AII-1. Table AII-3 shows the percentage of all elderly persons in each state who received medical assistance from Medicaid in 1985; the percentage of all elderly persons living in poverty in each state; and the ratio of non-institutionalized elderly on Medicaid to the number of elderly poor. Figure AII-1 illustrates this last statistic in a bar graph. The table shows the wide variation in poverty rates across the six states -- the poverty rate among elderly persons in Arkansas (28.2%) was about three times the poverty rate in Illinois (9.9%) and Wisconsin (9.4%). Thus, a much higher proportion of elderly in Arkansas are potentially eligible for Medicaid.
Regarding Medicaid's coverage of the non-institutionalized elderly poor, the six states fall into three groups. Wisconsin and Maine provide the broadest coverage, covering between 56-57 percent of the elderly poor who are not institutionalized. Arkansas and Maryland fall into the middle group, covering between 45 percent and 47 percent. The states with the most restrictive eligibility provisions are Oregon and Illinois, which cover only 27-32 percent of the non-institutionalized elderly poor.
It is clear that Medicaid eligibility decisions are major factors in the variation in coverage across the six states. Wisconsin, with the most liberal eligibility policies, has the broadest coverage. Of the six states, it has the highest state supplementation level, the highest medically needy level, and it is a 1634 state. Data show that Wisconsin's SSP program increases the number of SSI/SSP recipients by 58% over the number who would be eligible if the state provided no supplement to federal SSI benefits.
Maine's SSP program also plays an important role in broadening Medicaid coverage of the elderly. Although its supplementation level for aged individuals living alone is by no means generous ($10 per month), Maine has a much broader supplementation program for elderly persons in licensed board-and-care facilities. Some elderly persons receive state supplements of up to $234 per month in these facilities. Overall, Maine's SSP program increases its pool of Medicaid eligibles by 33 percent over those who would be eligible if the state provided no state supplements to SSI.
| TABLE AII-3. Medicaid Coverage of the Elderly in the Six Study States: 1985 | |||
| State | Percent Elderlyon Medicaid | Percent Elderlyin Poverty | Ratio on Non-institutionalizedElderly on Medicaid toElderly in Poverty |
| AR | 18.7% | 28.2% | 0.47 |
| IL | 7.0% | 9.9% | 0.32 |
| MD | 11.0% | 12.0% | 0.45 |
| ME | 15.3% | 16.4% | 0.56 |
| OR | 6.4% | 11.8% | 0.28 |
| WI | 13.6% | 9.4% | 0.57 |
| SOURCES: HCFA 2082 data, Bureau of Data Management and Strategy; U.S. Bureau of the Census; and 1985 March Current Population Survey. Percent Elderly on Medicaid includes nursing home recipients. Data include adjustments to HCFA 2082 data for disabled Medicaid recipients over age 65. | |||
Maryland's and Arkansas' coverage of the elderly poor falls into the intermediate range. Maryland has a very small SSP program, and Arkansas does not supplement SSI at all. Although they both have medically needy programs, Arkansas' medically needy income level is so low ($108 per month) that it is almost impossible to qualify for Medicaid outside of a nursing home and still have enough money to live on. However, both states are 1634 states, and thus extend Medicaid eligibility to all SSI/SSP recipients automatically.
| FIGURE AII-1. Ratio of Non-Institutionalized Elderly on Medicaid to Number of Elderlyin Poverty: 1985 |
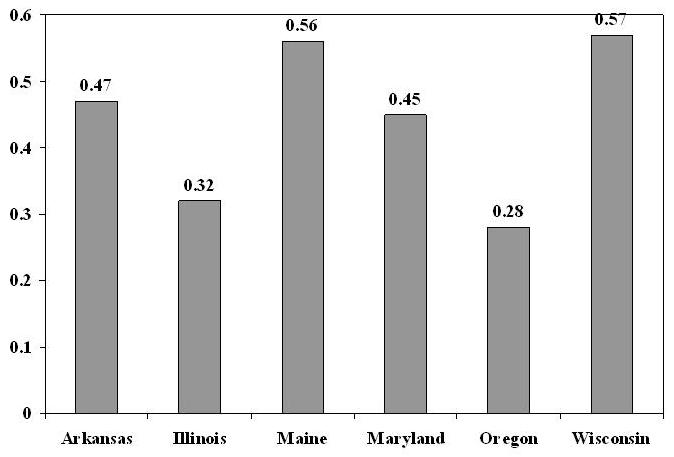 |
| SOURCES: HCFA 2082 data, Bureau of Data Management and Strategy; U.S. Bureau of the Census; and March 1985 Current Population Survey. |
It is clear that Oregon's and Illinois' decision to not be 1634 states has limited their coverage of their elderly populations under Medicaid. Illinois' election of the Section 209(b) option is more restrictive than Oregon's decision to require SSI recipients to undergo a separate application process for Medicaid. On the other hand, Illinois has a more extensive State Supplementation Program than Oregon, and prior to 1986, Oregon had no medically needy program. Thus, prior to 1986, about the only way an elderly person not in a nursing home could get on Medicaid in Oregon was to be an SSI recipient. Even then it was necessary to go through a separate application process in order to get a Medicaid card.28
It is noteworthy that in all six states, there are many elderly persons living in poverty who are not Medicaid eligible. Even Wisconsin, which had the broadest coverage, still covered only 57 percent of the non-institutionalized elderly poor, according to these measures. There are a number of reasons for this apparent low coverage. First, excluding aged Medicaid recipients who are nursing home recipients biases these statistics somewhat, since many nursing home recipients are institutionalized for only part of the year, and are non-institutionalized for the rest of the year.29 Second, the data presented include only aged persons who receive services reimbursed by Medicaid; they do not include persons who were enrolled in Medicaid but received no services.30 Data on the proportion of Medicaid recipients relative to the number of elderly poor therefore underestimate Medicaid's coverage of the elderly somewhat. Third, poverty data are based solely on income, not assets. However, SSI and Medicaid applicants must not only meet income requirements, but fairly restrictive asset requirements (in most cases, Medicaid recipients could have no more than $1,600 in liquid assets in 1985). Thus, while many elderly poor persons may qualify for SSI or Medicaid on the basis of income, they may be excluded on the basis of excess resources.
Eligibility Provisions Unique to Section 2176 Waiver Programs
All states which had medically needy programs extended eligibility for waiver services to the medically needy as well. However, Oregon had also elected the option of extending eligibility to persons with incomes up to 300% of the federal SSI benefit level. Under this option, elderly persons who are otherwise eligible for waiver services may "buy in" to the waiver, by paying the difference between their monthly income and the SSI/SSP level. Approximately half of Oregon's caseload of 6,000 waiver recipients are not SSI/SSP recipients, but persons who have chosen to "buy into" eligibility for waiver services under this option.
Two states -- Maine and Wisconsin -- had received a waiver of Medicaid deeming rules. This waiver permits these states to only count the income and assets of the applicant in determining Medicaid eligibility for waiver services, without taking into account the income and assets of the applicant's spouse. Thus, some persons in these states are eligible for waiver services who would otherwise not be eligible for Medicaid outside a nursing home.
BIOGRAPHICAL SKETCHES
Diane E. Justice served as the Director of this study. In addition to authoring most of this publication, she was responsible for the design and implementation of the study. Ms. Justice prepared the background analysis used by the advisory committee to select the study states, coordinated the work of consultants, and developed and administered the interview schedule used in the site visits.
To conduct this study, Ms. Justice was on leave from her permanent position as the Deputy Director of the National Association of State Units on Aging (NASUA). At NASUA, Ms. Justice provides guidance to staff in designing and implementing projects that analyze and report on a wide range of state management, program and policy initiatives. Her functions also include providing primary staff support to the NASUA Board of Directors in developing the organization's public policy agenda, emphasizing health and long term care issues. Prior to her service at NASUA, Ms. Justice was the Director of Planning for the Minnesota Board on Aging.
Lynn Etheredge, who authored Chapter VI, "Financing and Management of Home and Community Based Services," is a principal with the Consolidated Consulting Group and a researcher whose work deals primarily with public and private health care financing, government health and income security policies, and the growing elderly population. He served with the U.S. Office of Management and Budget (OMB) for many years as a senior executive and as principal analyst for Medicare and Medicaid, national health insurance proposals, and welfare reform. Mr. Etheredge has been particularly concerned with the implications of an aging society for both the public and private sectors.
John E. Luehrs, who authored Appendix I, "Summary of Expenditures for Long Term Care Services," is Project Director for the State Medicaid Information Center within the National Governors' Association's Health Policy Studies unit. In this capacity, he monitors and maintains a data base of state Medicaid and health care cost containment activities, and participates in research and preparation of analyses of selected health care cost containment issues. His major areas of interest have included long term care and home and community based waivers, indigent care, and Medicaid coverage for AIDS patients.
Brian O. Burwell, who authored Appendix II, "Medicaid Eligibility and Its Impact on Home and Community Based Services in the Six Study States," is a Senior Research Analyst at Systemetrics/McGraw-Hill in Lexington, Massachusetts. His research interests include long term care financing, home and community based services, and financing services for the developmentally disabled. He is currently working on a study of how nursing home residents spend-down their income and resources for Medicaid eligibility.
RELATED HEALTH POLICY PUBLICATIONS AVAILABLE FROM THE NATIONAL GOVERNORS' ASSOCIATION
State Long Term Care Reform: Development of Community Care Systems in Six States is one of a series of publications on state long term care policy issues published by the Health Policy Studies unit within NGA's Center for Policy Research. Other recent publications addressing long term care issues are:
Using State-Developed Case-Management Systems and Concepts for Privately Financed Long Term Care: A Preliminary Analysis of Issues and Potential Applications by R. Curtis, D. Justice, and E. Neuschler Forthcoming. April 1988. 80 pages. $12.50
This report assesses whether and how the insurance industry could benefit from the extensive state experience in developing and implementing home-based long term care. The report summarizes a day-long symposium of insurance industry, state and research community experts on this topic and includes a case study of a Washington State initiative, under which Blue Cross has contracted with that state's network of local case management agencies to perform client assessment care planning and coordination.
Medicaid Eligibility for the Elderly in Need of Long Term Care by E. Neuschler Pub. No. 3835. September 1987. 160 pages. $17.50
Based on a detailed survey of 50 states' Medicaid programs, this report discusses the basic eligibility criteria elderly people must meet to obtain Medicaid coverage of nursing home care or community based care. The book outlines the basic eligibility factors for the general reader, includes a detailed appendix for the technically oriented reader, and displays state program standards and requirements in 30 tables.
Prepaid Health Plans for the Aged That Include Long Term Care: New Policy Options for Medicaid by J. Malone, J. Greenberg, P. Farseth, and C. Harrington Pub. No. 3167. June 1987. 70 pages. $12.50
Prepaid long term care plans for the elderly hold great promise as comprehensive delivery systems that emphasize care in the most cost-effective setting appropriate to individual need. This document discusses the major issues involved in developing a capitation approach to long term care for Medicaid recipients, closely examines capitation methods and risk-sharing alternatives, and details the steps necessary to develop rates using data from the state Medicaid claims payment system.
Building Affordable Long Term Care Alternatives: Integrating State Policy R Curtis, D. Justice and J. Luehrs, editors. Pub. No. 3072. April 1987. 260 pages. $27.50
This publication draws on the proceedings of a conference held in July, 1986 and is divided into three sections: the first assesses demographic trends, changes in financing and delivery systems, and state and federal budget concerns; the second describes and analyzes the state role in developing an affordable continuum of long term care services; the third discusses potential private financing options.
Additional copies may be purchased from:
Publications Office National Governors' Association 444 North Capitol Street, Suite 250 Washington, D.C. 20001 (202) 624-7880
NOTES
-
This limit could be lower if a special Index, measuring the state's age sixty-five and older population growth plus inflation facing long term care providers plus a 2 percent intensity factor, yields less than 7 percent. This is highly unlikely.
-
U.S. Department of Health & Human Services. National Long Term Care Channeling Demonstration: The Evaluation of the National Long Term Care Demonstration: Final Report. Mathematica Policy Research, Inc., Princeton, New Jersey 08540, May, 1986. P. [http://aspe.hhs.gov/daltcp/reports/chanfr.htm]
-
National Governor's Association, Building Affordable Long Term Care Alternatives Integrating State Policy, April, 1987, p. 113.
-
Ibid. p. 61.
-
Texas and Washington have also created a consolidated state agency to handle all long term care programs. While there are slight variations in the composition of each agency's responsibilities, the objective is the same -- to achieve better management control over long term care resources.
-
A limited amount of HBC funds can now be used for case management.
-
Since local agencies in all six states conduct client assessments, case management and pre-admission screening, a comparison of state and local roles is not applicable. These responsibilities will be reviewed in depth in Chapter IV.
-
Neuschler, Edward. Medicaid Eligibility for the Elderly in Need of Long Term Care, National Governors' Association, September 1987.
-
One exception is the Maryland In-Home Aides program, where assessments are performed by local Departments of Social Services and services are sometimes provided by the same agencies' staff.
-
State officials note that current policy is to meet the full range of needs for persons accepted into the program.
-
Maryland Department of Budget and Fiscal Planning, Review and Comparison of Four In-Home Service Programs, September 1984.
-
Iverson, Laura Hines. A Description and Analysis of State Pre-Admission Screening Programs, Interstudy, 1986.
-
Glenn Silverberg, Technical Assistance on the Consumer as Employer and Other Employer/Employee Options in Supportive Home Care, Bureau of Long Term Support, Wisconsin Department of Health and Social Services, November, 1985.
-
National Governors' Association, Building Affordable Long Term Care Alternatives: Integrating State Policy, April 1987, p. 88.
-
Wisconsin Department of Health and Social Services, Program Guidelines for the Community Options Programs, 1985.
-
P.L.97-35 (OBRA 1981) reduced federal matching payments to which a state was entitled by 3% in 1982, 4% in 1983 and 4% in 1984. These reductions were partially offset in some circumstances e.g., if a state had a high unemployment rate, or if its Medicaid program growth was less than pre-set target rates.
-
J. Greenberg et al. An Analysis of Responses to the Medicaid Home and Community Based Long Term Care Waiver Program, National Governors Association (1983) and S. Tames "Protecting Home and Community Based Waivers," Medicine and Health (16 June 1986).
-
Mathematica Policy Research. The Evaluation of the National Long-Term Care Demonstration: Final Report, Report to DHHS, May 1986. These efforts tested two different models of home and community based care, each in five different sites, and randomly assigned over 6,300 extremely frail elderly persons to these different arrangements. [http://aspe.hhs.gov/daltcp/reports/chanfr.htm]
-
Report to Congress and the Secretary by the Task Force on Long Term Health Care Policies. September, 1987, HCFA #87-02170. [http://aspe.hhs.gov/daltcp/reports/lthcpes.htm]
-
Details of state expenditures are reported in Appendix I.
-
For a comprehensive analysis of screening, assessment and case management as well as client eligibility, cost sharing and client spending limits, the reader is referred to Chapter IV.
-
Oregon's management information system is summarized in Building Affordable Long Term Care Alternatives: Integrating State Policy, National Governors Association, 1987.
-
The Community Options Program -- An Evaluation of Program Operations During 1982 and 1983. Wisconsin Department of Health and Social Services (Division of Policy and Budget, Bureau of Evaluation), December, 1984.
-
D. Lipson State Legislation and Regulations Related to Long-Term Care Insurance, Intergovernmental Health Policy Project, Washington DC, February 1987. This document provides a broad overview of state initiatives and was useful in the preparation of this material.
-
Unfortunately, the latter objective was not fully achievable. As shown on the attached charts, some data are for federal fiscal years, while other data are for state fiscal year or calendar year. Medicaid data include federal funds and may include data for the disabled as well as the elderly. State program data typically are limited to the elderly over age 60, but may include some federal funds. As a result, these data should be viewed with caution. While every attempt was made to include all programs providing home and community based services (HCBS) to the elderly, there are undoubtedly some omissions. For example, state and local general assistance programs may pay for HCBS provided to recipients, some of whom may be elderly. Furthermore, data reporting varies widely from program to program. Medicaid has stringent federal reporting requirements which entail the collection of detailed data on services, expenditures, and recipients. Other programs, especially those funded by state general revenues, do not have such directly comparable detailed data sets. As a result, it is very difficult to disaggregate expenditures for these programs by a particular category of service (e.g., HCBS) or recipient (e.g., the elderly). The data contained in the following tables, however, are useful in making general comparisons of six state long term care expenditures and, in particular their spending on HCBS.
-
Report to the Secretary on Private Financing of Long Term Care for the Elderly. November 1986 pp. 2-42 to 2-45.In all the six states except Oregon, spending on State HCBS grew at a fairly rapid rate from 1982 to 1986, ranging from about 13 percent in Wisconsin to 52 percent in Maine. These rates exceed increases in federal SSBG and OAA funding, indicating that these states are continuing to invest their own dollars in HCBS programs despite the lack of federal funding increases. [http://aspe.hhs.gov/daltcp/reports/pfltce.htm]
-
For a fuller discussion of "negative bands," see Rymer M., Oksam G., Bailis L. and Ellwood D.: Medicaid Eligibility: Problems and Solutions. Westview Press, 1979.
-
Unless the elderly person was enrolled in Oregon's Section 2176 Medicaid waiver program.
-
In effect, we are comparing longitudinal and cross-sectional data in these measures in that HCFA 2082 data include all recipients of Medicaid service over a particular year, while poverty data estimate the number of poor persons at a particular point in time.
-
Data from the Medicaid Tape-to-Tape data set indicate that approximately 85 to 90 percent of all aged Medicaid enrollees in a particular year are users of Medicaid-funded services.