
U.S. Department of Health and Human Services
Important Questions for Hospice in the Next Century
Barbara Gage, Ph.D., Susan C. Miller, Ph.D., MBA, Kristen Coppola, Ph.D., Jennie Harvell, M.Ed., Linda Laliberte, JD, MS, Vincent Mor, Ph.D., and Joan Teno, M.D., MS
March 2000
PDF Version: http://aspe.hhs.gov/daltcp/reports/impques.pdf (191 PDF pages)
This report was prepared under contract #HHS-100-97-0010 between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and the Urban Institute. For additional information about the study, you may visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the ASPE Project Officer, Jennie Harvell, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. Her e-mail address is: Jennie.Harvell@hhs.gov.
This report was prepared for the Office of Disability, Aging and Long-Term Care Policy in the Office of the Assistant Secretary for Planning and Evaluation, US Department of Health and Human Services under contract to the Urban Institute. The project officers were Jennie Harvell, ASPE and Carol Blackford, Health Care Financing Administration.
The authors appreciate the invaluable input of those noted in Appendix E for participating in discussions with us throughout the project. The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
TABLE OF CONTENTS
1. INTRODUCTION
2. THE MEDICARE HOSPICE BENEFIT
History of the Benefit
Today's Medicare Hospice Benefit
3. MEDICARE HMO ENROLLEES AND HOSPICE ELECTION
5. EMPLOYER-BASED HOSPICE BENEFITS
6. MEDICARE HOSPICE BENEFICIARIES
Medicare Hospice Beneficiaries
Medicare Hospice Beneficiaries in Nursing Facilities
Volume and Geographic Distribution
Nursing Facilities with Medicare Hospice Beneficiaries
Contractual Relationships Between Hospices and Nursing Facilities
8. UTILIZATION OF THE MEDICARE HOSPICE BENEFIT
Hospice Lengths of Stay
Office of Inspector General Related Investigations
9. MEDICARE EXPENDITURES AND HOSPICE CARE
Spending on Hospice
End-of-Life Costs and Medicare's Hospice Benefit: Lessons from the Literature
10. ISSUES REGARDING ACCESS TO THE MEDICARE HOSPICE BENEFIT
Geographic Access
Minority Access
Access for Persons Without Caregivers or Eligible for Medicare Skilled Nursing Facility Care
Access to Hospice for AIDS Patients
Access by Diagnosis - Prognosis in Non-Oncologic Disease Models
11. RESEARCH ON THE QUALITY OF HOSPICE CARE
Patient Outcomes and Family Outcomes
12. THE DYING EXPERIENCE OF NURSING FACILITY RESIDENTS
13. RECENT END-OF-LIFE INITIATIVES AND DEMONSTRATION PROJECTS
14. DISCUSSIONS WITH INDUSTRY AND STATE REPRESENTATIVES
Industry and State Certification Representatives
State Medicaid Program Officials
15. A SUMMARY OF ISSUES RELATED TO THE MEDICARE HOSPICE BENEFIT AND ITS USE IN A NURSING FACILITY
16. CONCLUSION
APPENDICES (separate file)
APPENDIX A. Literature Review Methodology
APPENDIX B. National Hospice Organization's Sample Contract
APPENDIX C. Medical Guidelines for Determining Prognosis in Selected Non-Cancer Diseases and Hospice Enrollment Criteria for End-Stage Dementia Patients
APPENDIX D. Wisconsin State Guidelines for Medicare Hospice Care Provision in the Nursing Home
APPENDIX E. Acknowledgement List
LIST OF FIGURES
FIGURE 1. Number of Medicare and Non-Medicare Hospice Patients
FIGURE 2. Number of Medicare and Non-Medicare Certified Hospice Providers
FIGURE 3. Distribution of Medicare Benefit Payments by Type of Service, FY 1997
FIGURE 4. Comparison of Rate of Growth to Projected Rate of Growth in Medicare Benefit Payments per Enrollee by Type of Service
LIST OF TABLES
TABLE 1. Balanced Budget Act of 1997: Provisions Related to Hospice Services
TABLE 2. Hospice Reimbursement Rates From 11/01/83 - 9/30/98
TABLE 3. Medicare Hospice Payments and Use by Level of Care, 1997
TABLE 4. Medicare Hospice Payments and Use by Type of Hospice Affiliation, 1997
TABLE 5. Demographics of Hospice Beneficiaries by Type of Hospice Affiliation, 1987-1990
TABLE 6. Characteristics of Discharged Hospice Patients in the 1994 and 1996 National Home and Hospice Care Surveys
TABLE 7. Number of Medicare-Certified Hospices by Type of Provider Affiliation
TABLE 8. Lengths of Stay by Hospice Provider Affiliation, 1987-1990
TABLE 9. Average Number of Visits per Week by Type of Service
TABLE 10. Adjusted Medicare Reimbursement Saved per Dollar of Hospice Expenditure by Length of Enrollment and Month
TABLE 11. Adjusted Medicare Part A Reimbursement Saved per Dollar of Hospice Expenditures, by Length of Enrollment and Month, 1992
TABLE 12. Adjusted Medicare Part A and Part B Reimbursement Saved per Dollar of Hospice Expenditures, by Length of Enrollment and Month, 1992
AUTHORS
Barbara Gage, Ph.D., The MEDSTAT Group, Cambridge, Massachusetts.
Susan C. Miller, Ph.D., MBA, Brown University, Providence, Rhode Island.
Kristen Coppola, Ph.D., Brown University, Providence, Rhode Island.
Jennie Harvell, M.Ed., ASPE Office of Disability, Aging and Long-Term Care Policy, Washington, D.C.
Linda Laliberte, JD, MS, Brown University, Providence, Rhode Island.
Vincent Mor, Ph.D., Brown University, Providence, Rhode Island.
Joan Teno, M.D., MS, Brown University, Providence, Rhode Island.
EXECUTIVE SUMMARY
This work was conducted under the auspices of the Office of the Assistant Secretary for Planning and Evaluation (ASPE) as part of a larger ASPE study titled Synthesis and Analysis of Medicares Hospice Benefit. The ASPE study goal is to inform policy makers about the role of the Medicare hospice benefit, in general, and specifically about its contribution to end-of-life care for institutionalized beneficiaries.
This report contains six main sections. The first focuses on hospice coverage policies and reviews the history of the Medicare hospice benefit, its current structure, and its influence on care of the dying. Also included is a description of hospice care covered by other insurers including state Medicaid programs and private employers. The second section provides a literature review of the issues surrounding access to hospice and the provision of hospice care in nursing facilities. This is followed by a brief description of current end of life initiatives to improve care of the terminally ill. The next section summarizes discussions with hospice and nursing facility providers, federal and state certification surveyors, and state Medicaid officials regarding overlapping areas in caring for the terminally ill. Last, section 6 summarizes the issues and provides a framework for the four subsequent reports in this study, Medicares Hospice Benefit: Use and Expenditures, Use of Medicares Hospice Benefit Use by Nursing Facility Residents, Outcomes and Utilization for Hospice and Non-Hospice Nursing Facility Decedents, and Hospice Benefits and Utilization in the Large Employer Market.
Congress established the Medicare hospice benefit as both a cost-containment mechanism to limit the programs high costs for beneficiaries in their last year of life and a quality improvement tool to improve care for the dying. Medicare pays hospices a capitated per diem in exchange for delivering almost all services needed in a day to treat the patients terminal illness. Excluded from this payment are room and board costs for a beneficiary who lives in a nursing facility and any costs for attending physicians who are not hospice staff. Hospices coordinate the care of the terminally ill acting as a gatekeeper to manage treatment of the terminal condition. They specialize in pain and symptom management and provide greater levels of aide services than otherwise available under Medicare. In addition, Medicares hospice benefit also covers counseling and bereavement services for beneficiaries family members.1
Medicare is the primary payer for hospice services covering 77 percent of all hospice expenditures. The rest is paid for by Medicaid (4 percent), private insurance (12 percent) or other sources (7 percent). In 1997, Medicare covered 374,723 hospice enrollees at a cost of $2.02 billion (MedPAC, 1998). Average length of coverage was 50 days, although that varied by provider type. For instance, beneficiaries served by free-standing hospices had the longest episodes (53 days per person) in contrast to those treated in skilled nursing facilities (SNFs) whose episodes of care lasted only 39 days per person, on average (HCFA, 1998a). Most hospice enrollees live at home or in a private residence, but an estimated 12 percent may be nursing facility residents (Gage, 1998).
While hospice is a relatively new Medicare benefit, it has been studied extensively. Early research, which focused on the benefits implementation and use, found cancer patients are the most common hospice users (Mor and Kidder, 1985), although people with other terminal illnesses also are choosing hospice as the program matures (Banaszak-Holl and Mor, 1996). The National Hospice Study evaluated the benefits cost effectiveness and found hospice achieved program savings (Kidder, 1992). These lower patient costs were due to patients having lower inpatient hospital costs, particularly in the last months of life. A more recent study which updated the NHS arrived at similar conclusions although this study focused only on cancer patients (Lewin, 1995).
High-cost hospice users -- and the adequacy of Medicares payment rates for their care -- were the focus of yet another study. This study showed that higher expenses were due to longer enrollment periods, not higher daily costs (HCFA, 1993). As a result, the Secretary concluded that the per diem payment rates were adequate for covering this population because they adjusted for volume.
Another study which looked at coverage policies, analyzed the effect of removing the 210-day lifetime limit on Medicare hospice coverage (Banaszak-Holl and Mor, 1996). This study showed that for most cases, length of use did not go up substantially without the limit. However, patients with illnesses other than cancer were most likely to gain from the longer allowable enrollment periods because they tended to have longer episodes of hospice care.
In addition to these national program studies, hospice use is also profiled regularly by the National Center for Health Statistics (NCHS) (NCHS, 1998). These ongoing surveys, which describe hospice use by all insured populations, underscore the important role Medicare plays in covering hospice care. Almost 80 percent of all hospice users are 65 or older, suggesting these probably are Medicare-covered enrollments.
In 1998, the Office of the Inspector General (OIG) in the Department of Health and Human Services (HHS) raised questions about the role of the hospice benefit for dually covered Medicare beneficiaries living in nursing facilities. While Medicare is the primary payer when both programs cover a benefit, the state Medicaid program covers room and board for the nursing facility resident in addition to the Medicare-covered hospice services. The OIG was concerned about the financial relationships between hospices and nursing facilities. Better information was needed about the role of the Medicare hospice benefit, in general, and its contribution to end-of- life care for institutionalized beneficiaries. Specifically, the OIG wanted to know if hospice changed the cost or quality of services provided to dying beneficiaries in nursing facilities. Also at issue was Medicaids role in covering these nursing facility residents. These matters raised additional questions, including how other payers, like Medicaid and private insurers, cover their terminally ill populations and whether their hospice patients had to waive other use of hospital, skilled nursing facility and home health services as required by Medicare (Program manuals, section 144.4).
This study of Medicares hospice benefit addresses these and other questions. Funded by the Office of the Assistant Secretary for Planning and Evaluation (ASPE), this report describes Medicare hospice eligibility, coverage and payment policies, and selected Medicaid (Title XIX) and private insurance programs. It also presents information on costs, utilization, and quality of care in Medicares hospice program. These materials are supplemented with anecdotal reports from hospice representatives, nursing facility providers, and state Medicaid officials. These discussants focused on Medicares hospice benefit in general, and issues around coordinating the staff, services, and payments for hospice enrollees living in nursing facilities. In addition, issues raised by program survey officials are included to describe the problems in assessing quality of care for hospice patients who live in nursing facilities. For example, because the goals of curative and palliative treatment differ, malnourished residents in a nursing facility may be perceived as either neglected or as exercising their right to refuse food, depending on whether they are hospice enrollees.
Hospices influence on the costs and quality of care for dying Medicare beneficiaries is still being debated. Hospice may well save Medicare dollars, but because of inadequate study designs -- including the lack of adequate control for selection bias -- accurate estimates of savings are not available. Studies in the 1980s found few differences in the quality of life or symptoms measured at the end of life between hospice and non-hospice patients. The limited number of studies conducted since the 1980s appear to add very little support to the arguments that hospice care is superior to conventional care for patient and family outcomes. However, the need for better measurement has become evident in the literature, and research efforts are now addressing this need. Further, the changing populations enrolling in hospice raise questions about whether study findings that are largely based on cancer patients are applicable to other terminally ill populations. No study has yet compared the processes and outcomes of care for hospice and non- hospice beneficiaries in nursing facilities. Such research, to the extent possible, is now being conducted as part of this study.
Key questions addressed in this study include:
-
Who uses Medicares hospice benefit? Has this population changed over time? Are enrollees in health maintenance organizations (HMOs) just as likely to use it as those in fee-for-service?
-
How do Medicares eligibility guidelines affect the types of terminally ill patients who enroll in hospice?
-
How do nursing facility residents elect and use hospice? Are their choices affected by their institutional residency?
-
Are there differences in resources used by residents who are on hospice versus terminally ill residents who are not enrolled?
-
Are there differences in the processes of care and the outcomes (e.g., the quality of symptom management) of dying nursing facility residents who have elected hospice compared to those who have not?
-
What can we learn from other hospice benefit programs?
This report is the first in a series which analyze Medicares hospice benefit today and its use in nursing facilities. The other reports in this study for ASPE use Medicare administrative data to analyze total Medicare use and expenditures for hospice patients during, and in the 6 months prior to, enrollment in the benefit in 1996 (Medicares Hospice Benefit: Use and Expenditures). In addition, nursing facility data and Medicare Part A claims data from five states is examined to contrast the enrollees (Medicares Hospice Benefit Use by Nursing Facility Residents) and expenditures, processes, and outcomes for hospice and non-hospice enrollees in nursing facilities (Outcomes and Utilization for Hospice and Non-Hospice Nursing Facility Decedents). And last, administrative data from employer-based insurance claims is used to compare differences in the benefits, use, and cost of covering hospice in the private sector (Hospice Benefits and Utilization in the Large Employer Market). Findings from these analyses will inform the policy debate regarding the provision of hospice care for different types of beneficiaries, including those in nursing facilities. Study conclusions and recommendations reflecting findings from these analyses and this literature review are forthcoming in the final report of this ASPE-funded study.
ACRONYMS
The following acronyms are used in this report.
| AHCPR | Agency for Health Care Policy and Research |
| AIDS | Acquired Immune Deficiency Syndrome |
| ASPE | Office of the Assistant Secretary for Planning and Evaluation |
| BBA | Balanced Budget Act of 1997 |
| CHF | Congestive Heart Failure |
| COPD | Cardiopulmonary Disease |
| COBRA | Consolidated Omnibus Budget Reconciliation Act of 1985 |
| CPT | Current Procedural Terminology |
| FAST | Functional Assessment Staging Criteria |
| GAO | General Accounting Office |
| HAA | Hospice Association of America |
| HCFA | Health Care Financing Administration |
| HHS | Department of Health and Human Services |
| HMO | Health Maintenance Organization |
| IOM | Institute of Medicine |
| MDS | Minimum Data Set |
| MedPAC | Medicare Payment Advisory Committee |
| NAHC | National Association for Home Care |
| NCHS | National Center for Health Statistics |
| NHHCS | National Home and Hospice Care Survey |
| NHO | National Hospice Organization |
| NHOPP | National Hospice Outcomes Planning Project |
| NHS | National Hospice Study |
| OBRA | Omnibus Budget Reconciliation Act of 1987 |
| OIG | Office of the Inspector General |
| OSCAR | Online Survey and Certification Automated Record |
| RWJ | Robert Wood Johnson Foundation |
| SNF | Skilled Nursing Facility |
| TEFRA | Tax Equity and Fiscal Responsibility Act of 1982 |
| VA | Department of Veterans Affairs |
1. INTRODUCTION
Hospice offers palliative care to the terminally ill, focusing on managing pain and other symptoms related to that illness, rather than on providing curative treatments. Congress added a hospice benefit to the Medicare program in 1982 for beneficiaries with six months or less to live.2 Beneficiaries who enroll in Medicare's hospice program waive their right to other inpatient and home health services although they may disenroll from hospice at any time. Still, the benefit is intended to provide better, more cost-effective care to dying beneficiaries.
Medicare's hospice benefit has had a dramatic effect on the provision of hospice care in the United States. Increases in the number of Medicare beneficiaries who elect hospice and the number of participating providers continue into the sixteenth year of the benefit's implementation, with Medicare now paying for 77 percent of all hospice care in the United States. Almost 18 percent of all elderly people who die are enrolled in hospice. Still, concerns abound that the structure of the Medicare benefit and its eligibility requirements may discourage access to hospice care for certain groups of dying persons, particularly those for whom accurate prognoses are difficult to make.
While most hospice is delivered in the community, nursing facility residents are increasingly enrolling in the benefit. The proportion of residents with non-cancer diagnoses who enroll in hospice has been growing although they are still proportionately less likely than cancer patients to choose hospice.
Despite the increased enrollments, nursing facility residents may still have limited access to hospice. According to anecdotal reports, access to hospice care in the nursing facility may have become more difficult since the Office of Inspector General (OIG) of the Department of Health and Human Services questioned the hospice lengths of stay and eligibility of beneficiaries residing in nursing facilities (USDHHS, 1997). In addition, facilities that do not contract with a participating hospice may not make the benefit available to their residents. Access is further contingent on the facility's encouragement of hospice use. And in the case of residents recently discharged from the hospital, nursing facilities have a financial incentive to encourage the beneficiary to use their SNF benefit instead of the hospice benefit. Access to providers also differs dramatically by state and region.
Hospice patients in nursing facilities also encounter other issues because the two types of providers deliver similar services but have very different treatment orientations. Hospice and nursing facility services need to be coordinated yet often lack the benefit of clear guidance and regulation at the federal and state levels. In fact, differences between hospice and nursing facility conditions of participation (and enforcement of such) heighten differences in staff perceptions of what is considered appropriate care. Although individual providers and surveyors seem to address many of these issues and differences, a regulatory and survey environment that fosters the nursing facility-hospice alliance does not yet exist.
Also at issue is the process for paying nursing facilities when dually-covered beneficiaries enroll in Medicare's hospice benefit but reside in a Medicaid-covered nursing facility bed. For these beneficiaries, Medicaid passes the nursing home payment to the hospice which then passes it through to the nursing facility. According to anecdotal reports, this method is problematic and overly burdensome for both hospice and nursing facility providers.
Another important question raised by the OIG is whether hospice costs for routine home care in the nursing facility are lower than when provided in the community (HHS, 1997). Currently, no data are available to examine the difference in hospice costs although hospices are required to submit cost report data for cost reporting periods beginning in 1999 (BBA, 1997). Nonetheless, the overriding question relating to the provision of hospice care in nursing facilities--whether this care reduces costs and improves end-of-life care--has yet to be answered.
This report is the first in this study that considers how hospice is used by the general Medicare population, by nursing facility residents, and by private sector enrollees. This first report will summarize the existing published and anecdotal information on these issues while the remaining reports will present analyses of several data sources. First, this report provides an overview of Medicare, Medicaid and select private insurance policies for hospice coverage. Second, it provides a literature review of hospice use, payments and quality of care issues. Third, a brief description of other end of life initiatives is included. And last, discussions with providers, certification and statistics officials are summarized.
2. THE MEDICARE HOSPICE BENEFIT
History of the Benefit
Hospice was introduced as a Medicare benefit in 1982 under the Tax Equity and Fiscal Responsibility Act of 1982 (TEFRA), about 10 years after hospice had emerged in the United States as a new type of formal service. The first standards for hospice care were formulated in 1974 by a committee of the International Work Group on Death and Dying (Kastenbaum, 1975). At about the same time, hospice also was being introduced in Canada, with the establishment of the Palliative Care Unit at Montreal's Royal Victoria Hospital (Mount, 1976). In 1977, the National Hospice Organization (NHO) was formed in the United States. It advocated for the hospice philosophy of care for the dying, educated the public, and provided a resource and structure for information exchange among the burgeoning number of hospices in this country.
Governmental initiatives and not-for-profit foundation funding bolstered the spread of hospices here. In 1978, the National Cancer Institute awarded grants to three hospices as demonstration projects to investigate the costs associated with care and to describe the actual manner in which care was provided to patients. Shortly thereafter, the Health Care Financing Administration (HCFA) was charged by Congress and the Carter Administration to initiate a research and demonstration study to examine the costs, benefits, and feasibility of having Medicare pay for hospice care. Existing hospice programs were invited to apply. Of 233 applicants, 26 hospices with diverse organizational arrangements were chosen (Greer et al. 1983; Mor et al., 1988; Mor and Masterson-Allen, 1987). The Robert Wood Johnson Foundation (RWJ) and the John A. Hartford Foundation also supported this research project. The W.K. Kellogg Foundation in 1981 awarded a grant to the Joint Commission on the Accreditation of Hospitals to investigate the status of hospice in the United States and to develop standards for accreditation (McCann, 1983).
Congress in 1982 introduced hospice into the Medicare program as a cost-savings provision after a Congressional Budget Office study asserted that hospice would result in sizable savings over conventional hospital care (Mor and Masterson-Allen, 1987). Because the benefit was created so quickly and represented a new area of health care, two special provisions were included in the legislation. First, a sunset provision stipulated that without congressional intervention, the law would expire in November 1986. Second, an evaluation of the impact of the benefit was mandated.
Initially, Medicare's hospice benefit consisted of three benefit periods with a lifetime limit of 210th days of coverage. Patients who lived longer but who still required hospice services were to be cared for by the hospice without charge to Medicare or the patient as a condition of providers' participation in the program. Further, if patients were unable to pay for services, the hospice was not allowed to discharge them on that basis (Hoyer, 1998). Putting the providers at risk for delivering services after the 210th day gave them an incentive to enroll only seriously ill beneficiaries despite the difficulties of predicting survival.
The benefit was limited to 210 lifetime days for several reasons. First, this limit was consistent with results from the National Hospice Study (NHS), which found that more than 95 percent of the 15,000 patients in the study were on hospice for fewer than 210 days. (Fully 90 percent of the participants had a primary diagnosis of cancer, and thus the shorter length of stay is consistent with hospice care for cancer patients.) Secondly, hospice was cost effective for shorter episodes (those lasting up to 100 days) but not for longer ones. That is, savings associated with reduced hospital use in the last weeks of life were offset by the cost of additional services in longer hospice episodes. Recognizing the difficulty of making a prognosis of six months of less, Congress later repealed the 210-day limit for services furnished on or after Jan 1, 1990. Four benefit periods replaced the 210 days: The first two were limited to 90 days each and the third period to 30 days, while the fourth period was unlimited. However, beneficiaries could have no more than four benefit periods.
TEFRA 1982 hospice legislation also established four, graduating levels of hospice care which are still used today. These four levels include routine home care, continuous home care, inpatient respite care, and general inpatient care (see page 6 for a complete description of these levels.) Most covered days are routine home care days except for the days when the enrollee has a higher level of hospice care coverage.
To manage the patient's care, TEFRA also required an interdisciplinary team. That team includes a physician, registered nurse, social worker, and pastoral or other spiritual counselor. Collectively the team--together with the patient, the patient's family, and the patient's primary or attending physician--assesses, coordinates, and provides the appropriate palliative and supportive care to hospice patients and their families. Additionally, the hospice team helps establish the patient's plan of care, providing or supervising hospice care and services, and periodically reviewing and updating the care plan. The team also manages the patient's discomfort and symptom relief. Implicit in the interdisciplinary team concept is the idea that team members will have stable relationships among themselves vis à vis the patient and thereby enhance continuity of care. Unlike multidisciplinary care where each area decides what is best practice in its own discipline, everyone on the hospice interdisciplinary team offers input on all issues facing a patient.
The original hospice legislation not only required hospices to use volunteers, but also mandated records on their use, cost savings, and the expansion of care and services achieved by doing so. Volunteers were considered key to the hospice movement. Although the number of volunteers hospices used varied markedly, proponents thought that their continuous involvement was important to preserving the hospice philosophy. The final hospice regulations contained a requirement that volunteer efforts should account for at least 5 percent of total hospice personnel efforts. This requirement was added because HCFA believed the intent of the law was to develop standards to monitor the level of volunteer activity so to prevent substantial diminution of the proportion of volunteers.
The Title XVIII hospice benefit was designed so that most services were provided in the patient's home. To support this focus, TEFRA contained a 20/80 provision, which limited a provider's total inpatient care days to 20 percent of all care delivered during a year by a given hospice. This provision did not apply to each individual, since some patients might need to stay far longer in an inpatient setting. The provision was intended to control costs, prevent the program from becoming an exclusively inpatient model, and preserve hospice's philosophy of care in a home environment.
Another major provision of the original Medicare hospice legislation was that hospices assess families' bereavement needs. Although Title XVIII payment stops at the time of death, hospice providers must provide bereavement services for up to one year afterwards. Hospice proponents maintained that they made a difference and thus families should continue to receive these services after the patient's death.
In 1986, the Consolidated Omnibus Budget Reconciliation Act (COBRA) of 1985 was signed into law. Besides repealing the sunset provision for Medicare's hospice benefit, it stated that terminally ill patients residing in nursing facilities could elect Medicare hospice care. For every day of care, hospices would be paid Medicare's routine home care rate. COBRA also gave states the option of adding a hospice benefit to their Medicaid programs.
Today's Medicare Hospice Benefit
Today, Medicare Part A insurance provides virtually unlimited hospice coverage to eligible beneficiaries who are terminally ill. Patients must be certified by their physician and the hospice medical director as having a life expectancy of six months or less (if the disease runs its normal course). They must also sign a statement choosing hospice in lieu of standard treatments for their terminal illness, and be treated by a Medicare-certified hospice. Even though they must waive their rights to all other inpatient hospital, skilled nursing facility, and home health services for the terminal illness, beneficiaries may still be treated for other medical problems under the regular Medicare program. For example, if a cancer patient breaks a hip, Medicare will cover hip treatment (and payments) independent of hospice care.
The Balanced Budget Act of 1997 (BBA) established unlimited coverage for beneficiaries by changing the four hospice benefit periods to two 90-day periods, followed by an unlimited number of 60-day periods (Table 1). Benefit periods do not need to be consecutive as long as the patient is certified as terminally ill at the beginning of each one. Hospice election can be canceled at any time and reelected at a later date. Inasmuch as predicting death is difficult and the practice of medicine is changing rapidly, this policy was designed to ensure that access to hospice would always be available. However, so that eligibility would be reviewed more frequently, the law increased the number of times hospice beneficiaries had to be recertified to every 60 days. This change in coverage recognizes that certain conditions may stabilize and that certain complications may require significant medical intervention. Patients can be discharged from hospice during these periods and still be re-admitted into their next hospice benefit period when their condition warrants it.
Medicare's hospice benefit includes services not available under other parts of the program. Among these are extensive coverage of non-IV therapy outpatient prescription drugs for pain relief and symptom management, homemaker services, and bereavement counseling for both the patient and their family members. Although hospices are required to make family counseling available for up to one year after the patient's death, as noted earlier, payment ceases on the patient's death. The hospice benefit also comprises physician management services and nursing care; medical supplies and appliances; short-term inpatient care, including respite care; home health aides; physical and occupational therapy; speech language pathology services; medical social services; dietary and other counseling; and any other Medicare-covered service in the patient's plan of care. Attending physicians who are not associated with the hospice may continue caring for the patient as part of the hospice team, but their visits are not covered by the hospice payment. Instead, they are covered by Medicare's traditional Part B physician benefit. In addition, other physician services may be provided on a consultation basis and paid under Part B.
Generally, a hospice patient's primary caregiver is a family member or "significant other." Each patient has a team consisting of family members, nurses, physicians, social workers, dieticians, counselors, clergy and volunteers who make regular home visits. Speech language pathologists and other therapists are provided on an as-needed basis. Further, the hospice physician and nurse are on-call 24 hours a day, seven days a week to provide advice by phone or visit when necessary.
While most hospice enrollees live at home, an estimated 12 percent live in a nursing facility (Gage, 1998). If a patient lives in a nursing facility, the facility is considered to be the home and the staff members are regarded as family or the patient's primary caregivers. The room and board costs of the nursing facility stay are not included in the hospice benefit.
Medicare uses four payment rates, reflecting different levels of care (Table 2). Payments are capitated, all-inclusive, prospectively set per diems. The amount does not change regardless of the volume or intensity of services provided during the day. These national payment rates are adjusted by the hospital wage index to reflect geographic variations in cost. The four payment levels include:
-
Routine home care. Patients are at home (or living in a nursing facility), under the care of the hospice, receiving fewer than eight hours of care per day. Payments for routine home care in fiscal year 1999 were $97.11 a day. About 87 percent of all payments in 1997 were for routine home care totalling $1.8 billion dollars (Table 3). This is the default payment rate for each day a beneficiary is enrolled in hospice and not receiving a higher level of care.
-
Continuous home care. This care is furnished only during brief periods of crisis and only as necessary to maintain patients at home. A continuous home care day is at least eight hours long and consists predominantly of continuous nursing care, although home health aide and homemaker services may also be provided on a continuous basis. The payment rate is $566.82 for 24 hours of care. These payments accounted for $29 million or 1 percent of the hospice expenditures in 1997.
-
Inpatient respite care. With this care, hospice patients may receive care in approved facilities on a short-term basis (not more than five days at a time) as respite for their caregivers. The payment rate for this level is $100.46 a day. Inpatient respite days represented less than one percent of hospice payments and accounted for only $4.8 million in 1997.
-
General inpatient care. With this care, patients may be admitted to approved facilities for pain control or acute or chronic symptom management that cannot be achieved in other settings. This level of care may be provided in a hospital, a hospice with its own inpatient facility, or a skilled nursing facility. The payment rate for this level is $432.01 a day. General inpatient care is the second most frequently used hospice care accounting for 11 percent of hospice expenditures, or $210 million dollars.
Individual beneficiaries have an unlimited number of inpatient days (including both respite and general inpatient). However, as mentioned earlier, the total inpatient days per year provided by any one hospice can not be greater than 20 percent of all hospice days provided by that facility. Restricting the total share of inpatient days allows providers to give sicker beneficiaries more inpatient days, while offsetting that with patients who use less than 20 percent of days in inpatient care. Hospices are paid a routine home care rate for inpatient days that exceed the 20 percent limit so they have an incentive to limit inpatient use rates.
Total provider payments also are limited to an annual per capita spending cap that is updated annually by the Consumer Price Index. For fiscal year 1999, the cap was $15,313. Facility payments are limited to the product of the cap times the unduplicated number of patients served, although few agencies have ever been restricted by this cap. This cap is essentially a proxy for the cost of care for the last six months of life under the traditional Medicare program (Hoyer, 1998).
Like Medicare hospital payments, hospice payments are updated each year by some portion of the increase in the hospital market basket. For fiscal years 1998 through 2002, the BBA set payments at market basket minus one percentage point for each fiscal year. The BBA also requires hospices to submit cost reports beginning in fiscal year 1999. These data will be important for analyzing the types of costs incurred by hospices. This information will be increasingly important as cancer becomes less dominant in the hospice population. Such information also will be useful to understand differences in costs associated with varying types of hospice ownership and affiliations (for instance, whether the hospice is hospital-based, SNF-based, home-health-agency-based, or free-standing); for various levels of treatment (routine home care, continuous home care, general inpatient, or respite inpatient care); and for various care settings (e.g., home care in a community setting versus in a nursing or assisted living facility).
Beneficiaries have limited copayments for outpatient drugs or biologicals and inpatient respite stays. The drug co-payment is 5 percent of the cost of the drug to the hospice or $5 per prescription item, whichever is less. The inpatient hospital deductible ($764 in 1998) is the annual limit for respite copayments.
To be covered, services must be provided by a Medicare-certified hospice. Certified providers must be engaged primarily in providing hospice care and make services available on a 24-hour basis. About 94 percent of all hospices are certified to participate in Medicare, Medicaid, or both; 89 percent of all hospices are dually certified (NCHS, 1998). Beneficiaries may change providers once during an election period.
3. MEDICARE HMO ENROLLEES AND HOSPICE ELECTION
Beneficiaries enrolled in hospice also may enroll in managed care arrangements. That was not so before the BBA passed in 1997, however, when beneficiaries on hospice could not enroll in an HMO. Also, because of the BBA, HMO enrollees who elected hospice are no longer required to disenroll from the HMO because of their choice.
Medicare payments for HMO enrollees who elect hospice are similar to payments for other hospice cases. When an enrollee elects hospice coverage, the hospice is paid the appropriate per diem amount for the hospice care and the HMO payment is reduced to 1/12 of the prior monthly capitation which covers any additional benefits the HMO offers to its enrollees. As in FFS, the HMO submits fee-for-service bills for costs not related to the terminal illness.
Very few empirical studies have looked at the relationships between HMO and hospice enrollment as they affect cost, utilization or quality of care. Those studies that have been done were based on limited samples -- either members of one specific plan or residents of one limited geographic area -- but they provide some information. One study compared the differences in cost for dying frail elders who were enrolled in an HMO or remained in fee-for-service in California and found no differences in expenditures (Experton, 1996). A second study compared the use of hospice between two groups of Cancer patients in 1992 in South Florida and found that HMO enrollees had a longer length of stay in hospice (20 days compared to 14 days for nonHMO enrollees). Similarly, a larger proportion of HMO enrollees than fee-for-service nonenrollees survived in hospice for longer than 180 days (Vernig, 1999).
More recently, HMO managers were interviewed to find out about their end-of-life care program, including their relationships with hospice providers. While this also was a limited sample -- only 19 managers were interviewed -- the findings may be instructive since they are a geographically mixed group of nonprofit HMOs, for-profit HMOs, IPAs, health systems, and others (Fox, 1999). Most stated that referrals to hospices were "too infrequent and often late only a few days before death." A few of the HMOs owned their own hospices. Some instituted physician education programs to teach physicians about hospice and some have established end of life committees. Others had developed palliative care teams. The interviewees suggested that few HMOs have addressed end of life needs beyond those required by the federal government. Most saw the target population as Cancer patients rather than other terminally ill populations.
Fox found hospices were criticized because of perceptions of poor communications between hospices and plan administrators, physicians, and case managers resulting in poorly coordinated services. The interviewees were concerned about their community image and whether the establishment of end of life programs might be perceived as a means of managing the costs of high cost populations rather than improving the quality of care for dying enrollees. Last, the interviewees were asked whether referring beneficiaries to hospice was financially advantageous. The responses varied widely and only two groups had data - each of which lead to opposite conclusions. Some felt that most of the expensive interventions had already occurred before patients were transferred to hospice.
4. MEDICAID'S HOSPICE BENEFIT
While Medicare pays for most hospice care, Medicaid also may offer hospice coverage as an optional benefit under the Title XIX program. All but 17 states offered this benefit in 1998. State Medicaid hospice programs must include, at minimum, the same services as Medicare, although more types of services may come under the hospice umbrella. Eligibility, payment, and conditions of participation rules mirror Medicare's. As in Medicare, most Medicaid hospice care is routine home care, whether it is actually provided at home or in a nursing facility.
Medicaid per diem payment rates may vary by state and differ from Medicare's. If a Medicaid recipient lives in a nursing facility but enrolls in Medicaid's hospice benefit, Medicaid pays the hospice two amounts -- one for Medicaid hospice coverage and the other for room and board at the nursing facility. For room and board, the state must pay at least 95 percent of the nursing facility rate. Hospices, in turn, must pay nursing facilities at least 95 percent up to 100 percent of Medicaid's room and board rate. (Any amount greater than 100 percent suggests hospices are paying above fair market value (FR, October 1999). If the beneficiary is dually eligible--that is, on Medicaid and Medicare--Medicare pays for hospice care while Medicaid pays the hospice for nursing facility room and board.
Medicaid uses the same program rules for hospice that Medicare uses. A care plan must be established before services are provided. If a state Medicaid program offers hospice, it must cover the same services as Medicare: nursing care; medical social services; physicians' services; counseling services; home health aide; medical appliances and supplies, including drugs and biologicals; and physical and occupational therapy. In general, the services must be related to the palliation or management of the patient's terminal illness, or symptom control, or to enable the individual to maintain activities of daily living and basic functional skills.
In addition, both programs use the same payment methodology as specified in the Social Security Act (section 1907 (a)(13)(D) and cover the same four definitions of care--routine home care, continuous home care for crisis periods, short-term inpatient care if needed, and short-term inpatient respite care to relieve at-home caregivers. As with Medicare's benefit, Medicaid's respite inpatient care is allowable only on an occasional basis and cannot be covered for more than five consecutive days.
Also as in Medicare, Medicaid's inpatient payments to a hospice are limited to 20 percent of the aggregate total number of hospice days provided per facility. The one exception is in the Medicaid program's treatment of the acquired immune deficiency syndrome (AIDS) population. Under Medicaid, AIDS patients may have more than 20 percent of their days as inpatient days. AIDS patients' inpatient days also are excluded from the count of the total inpatient days provided by a hospice. Both these provisions were authorized under the Omnibus Budget Reconciliation Act of 1987 (OBRA 87).
Title XIX has covered hospice services since 1985, when COBRA allowed states to cover hospice as an optional service for Medicaid recipients who waived their rights to other services. OBRA 86 clarified the rules for dually eligible recipients who resided in nursing facilities, elected Medicare hospice coverage, and lived in a state that did not cover hospice services under its optional Medicaid program. In these cases, hospices were still responsible for all costs of hospice enrollees. Medicare would pay them for the hospice benefit coverage, and the state would pay nursing facility room and board plus coinsurance. The state's payment would equal what Medicaid allocated for room and board plus coinsurance amounts. The nursing facility had to have a written agreement with the hospice, identifying the hospice as fully responsible for managing the patient's hospice care while the nursing facility provided room and board.
OBRA 1986 also defined nursing facility room and board to comprise "performance of personal care services, including assistance with activities of daily living, in socializing activities, administration of medication, maintaining the cleanliness of the resident's room, and supervising and assisting in the use of durable medical equipment and prescribed therapies." OBRA 90 (section 4705(a)(4)) deleted this definition.
OBRA 89 added a requirement that the state's payment amount for dual eligibles must equal at least 95 percent of the rate it would have paid the facility if the beneficiary had not elected hospice. This payment is made to the hospice, along with Medicare's per diem for hospice routine care for each day of a nursing home resident's enrollment. Hospices, in turn, must pay nursing facilities for room and board and daily care. That amount must be at least what they receive from the state.
OBRA 90 modified the coverage provisions. Before that legislation, Medicaid-eligible individuals electing the Medicaid hospice benefit waived their right to Medicaid coverage for services other than those described earlier. Under OBRA 90, recipients can receive Medicaid coverage for services related to treating their terminal condition and to other services like personal care that Medicare does not cover.
In general, Medicaid acts as a wraparound benefit for dually covered Medicare beneficiaries, particularly those in nursing facilities. Dually eligible hospice beneficiaries living in the community can use their Medicaid coverage only if the state covers some service, such as personal care or prescription drugs, not covered by Medicare's hospice benefit. By contrast, Medicaid will cover room and board and coinsurance of beneficiaries who live in nursing facilities while Medicare will pay for their hospice services. The exact number of dually-eligible beneficiaries in nursing facilities is unknown.
5. EMPLOYER-BASED HOSPICE BENEFITS
A small proportion of hospice enrollees are privately insured. A recent study of large firms (200 or more employees) found that 83 percent of employees are in firms that offer hospice coverage (Gabel et al., 1998). And the opportunity to choose this benefit increases with firm size--growing from 68 percent of employees in firms with 299-999 employees to 89 percent in firms with 5,000 or more employees.
The availability of hospice benefits also varies by plan type. While 86 percent of conventional fee-for-service, preferred provider organization, and point-of-service plans have hospice as an explicit benefit, only 78 percent of the HMO plans do. Even so, many of the HMOs offer hospice implicitly through their case management programs.
Benefits also vary widely based on geographic region. Whereas about 28 percent of employees in all large firms have dollar caps on their hospice coverage, in the West, 38 percent have caps. By contrast, only 23 percent of the firms located in the northeast and south have caps. Nearly a third (31 percent) of the firms limit length of stay. These limits are found most often in firms located in the northeast and Midwest. Eligibility generally is based on diagnosis of terminal illness by the patient's physician. Nearly half (48 percent) of employees must have a doctor's prognosis of six months or fewer to live, a requirement that varies little by firm size. Less than 1 percent decide eligibility on a case-by-case basis. Little information is available on cost and use of hospice in the private insurance market although some information will be provided by the analyses in the second half of this study.
6. MEDICARE HOSPICE BENEFICIARIES
Medicare Hospice Beneficiaries
Medicare beneficiaries have grown rapidly as a share of the total hospice population, increasing more than seven-fold during the last decade, from 40,356 in 1988 to 302,608, in 1995 (HAA, 1997). In 1995, Medicare covered 78 percent of all hospice users, up from 22 percent in 1988 (Figure 1).
Routine hospice home care is the most widely used benefit. Beneficiaries received 18.2 million days of such care in 1997, accounting for $1.8 billion or 89 percent of total hospice expenditures (Table 3). General inpatient care, by contrast, represented 10 percent of Medicare expenditures (HCFA, 1998a).
Most patients received services from free-standing hospice programs or from hospice programs based in home health agencies (52 percent and 29 percent, respectively).3 These patients also have the most days on hospice, on average, and account for 82 percent of the expenditures (Table 4). The highest average costs per case are for patients treated by free-standing facilities ($5,796, on average, per beneficiary) or by providers based in SNFs ($5,079). Only 17 percent of the hospice expenditures were for patients treated by hospital-based hospices (HCFA, 1998a). (Hospices affiliated with nursing facilities and hospitals deliver hospice care in home and institutional settings. The level of care specifies whether the patient was treated as an inpatient.)
Banaszak-Holl and Mor (1996) examined characteristics of Medicare hospice enrollees between 1987 and 1990. They were in a variety of settings: free-standing hospices as well as in hospitals, SNFs, and home health agencies (Table 5). Nearly half (47 percent) were female, 90 percent were white, and 16 percent had non-cancer diagnoses. The average age at hospice enrollment was 75.6 years.
Across hospice provider types, SNF-based hospices enrolled the highest percentage of females (53 percent), whereas free-standing facilities had the fewest (45 percent). Hospital-based and SNF-based hospices had the largest share of non-whites (13 percent), and free-standing facilities the least (9 percent). Hospital- and SNF- based hospices had fewer enrollees with non-cancer diagnoses (15 percent and 13 percent respectively). Of enrollees in home-health-agency-based and in free-standing hospices, 16 percent had diagnoses other than cancer. Mean ages did not differ significantly by hospice provider type (Table 6).
As discussed earlier, the National Center for Health Statistics (NCHS) profiles hospice users across all insured populations in its National Home and Hospice Care Survey (NHHCS). These data are useful in comparing hospice patient characteristics across all insured populations with those of Medicare hospice patients. The sample universe for the NHHCS is home care and hospice agencies classified by the (updated) 1991 National Health Provider Inventory (10,900 total home and hospice agencies in 1992 and 13,500 in 1996). For each provider chosen, a random sample of six current and six discharged patients in a randomly selected designated month are chosen. Table 6 shows national estimates from the 1994 and 1996 surveys of characteristics of discharged hospice patients.
Besides providing data for comparisons, the NHHCS highlights the importance of the public payer. In both the 1994 and 1996 surveys, at least 90 percent of the patients received care from a hospice certified by Medicare or Medicaid or both (NCHS, 1996 and 1998). Almost 70 percent of all hospice enrollees were 65 or older in 1996, although this represents a decline from the 1994 survey, when 72.9 percent of discharges were 65 or older.
The survey found that regardless of insurer, hospice patients are less likely to be "White" (80 percent of hospice enrollees compared to 85 percent in total Medicare population) and of different ages than Medicare hospice enrollees. Additionally, among survey participants one finds a much higher percentage of hospice discharges with non-cancer diagnoses (32.7 percent in 1994 and 30.3 percent in 1996), compared with Medicare hospice enrollees (16 percent overall in 1987-90) (Banaszak-Holl and Mor). These differences may be due either to changes in diagnosis mix over time, inasmuch as the 1994 and 1996 NHHCS represent four to eight years, respectively, after Banaszak-Holl's and Mor's study, or to the different diagnosis mix among younger hospice patients seen across all provider types. That a smaller share of Medicare hospice patients have diagnoses other than cancer may also reflect restricted access (see the section titled "Diagnosis").
As Banaszak-Holl and Mor suggest, hospice care in nursing facilities is particularly important for females. Because women generally outlive their husbands, or if not married have no children, they are more likely to lack the social support to remain in the community as their health fails. Therefore, females make up a disproportionate share of nursing facility residents. Without the availability of hospice in nursing facilities this benefit would not be available to a significant proportion of older women. When compared to Medicare hospice enrollees (in the 1996 Banaszak-Holl and Mor study), the NHHCS estimates of hospice discharges show that hospice patients across all payer sources seem quite comparable to Medicare hospice patients in terms of the percentage of female hospice patients. However, Medicare SNF-based hospice providers still appear to provide hospice care to the highest percentage of female hospice patients.
Medicare Hospice Beneficiaries in Nursing Facilities
Medicare hospice beneficiaries residing in nursing facilities have been the fastest-growing hospice population since OBRA 89 was passed. Indeed, these residents accounted for up to 35 percent of all hospice beneficiaries in some markets (Petrisek and Mor, 1998). Banaszak-Holl and Mor (1996) examined Medicare claims between 1986 and 1991. They found a statistically significant increase in the proportion of hospice beneficiaries who were receiving nursing facility-based services between 1987 and 1990 (6.6 percent versus 9.9 percent). Furthermore, this increase was concentrated in certain markets and community based hospices. By 1997, an estimated 12 percent of Medicare hospice beneficiaries were living in nursing facilities while receiving hospice care (Gage, 1998). Still, only a fraction (about 1 percent) in each facility were on hospice (Petrisek and Mor, 1998). The percentage of nursing home decedents who received the hospice benefit is unknown, but will be examined in five states in the next phase of the ASPE project.
The growth in the number of nursing facility residents receiving hospice care is changing the profile of the traditional Medicare hospice patient. Unlike hospice patients enrolled from the community, hospice beneficiaries in long-term care settings often include patients with lower functional status, dementia, and chronic illnesses (e.g., congestive heart failure, chronic obstructive lung disease). Also found among this group are patients without available caregivers in the community (Banaszak-Holl & Mor, 1996) a recognized deterrent to hospice admission for African Americans and Hispanics (Gordon, 1995).
Such diversity was seen in a study of hospice patients in a nursing facility served by the Hospice of Washington (a hospice in a long-term care setting). In that study, major changes in patient sociodemographic characteristics, diagnoses, and payer and referral sources were observed over a 10-year period from 1978 to 1988 (Infeld et al., 1990). Specifically, by 1988 a much higher percentage of hospice patients were unmarried (46.2 percent versus 23.5 percent), non-white (49.5 percent versus 17.6 percent), had non-cancer diagnoses (24.8 percent versus 0 percent), and were enrolled in managed care (36.8 percent versus 0 percent). The investigators saw hospice care in long-term care settings as providing an option for elderly people living alone who have no available caregiver--a growing population among Medicare beneficiaries. And like Infeld, Banaszak-Holl and Mor found that an increasing share of hospice beneficiaries in nursing facilities had diagnoses other than cancer, 12 percent in 1987 versus 17 percent in 1990.
7. HOSPICE PROVIDERS
Volume and Geographic Distribution
Even before Medicare's hospice benefit was enacted in 1982, the number of organizations furnishing hospice care had grown substantially. The General Accounting Office (GAO) identified 59 operational hospices in 1978 (GAO, 1979). A National Hospice Organization survey counted 235 hospices by 1980. The Joint Commission on the Accreditation of Hospitals in 1981 received 650 responses to a national survey of hospices; by 1982, the National Hospice Organization had 464 provider program members. By 1984, McCann (1985) estimated there were 1,694 hospices. Yet despite their proliferation, as of January 1986, only 245 hospice programs were Medicare-certified. Since then, however, that number has increased ten-fold (Table 7). The distribution of Medicare-certified hospices by provider type has changed as well, with free-standing and hospital based providers growing most rapidly. In 1996, 38 percent of Medicare-certified hospice programs were based in home health agencies and 37 percent were free-standing, 24 percent were hospital-based, and 1 percent was SNF-based.
Over time, Medicare-certified hospices have increased as a share of all hospice providers and now represent the majority (Figure 2). Of 2,722 hospice programs in the United States in 1996, 79 percent (2,154) were certified by Medicare (NHO, 1998a).
Nursing Facilities with Medicare Hospice Beneficiaries
Petrisek and Mor (1998) not only documented the distribution of hospice beneficiaries in nursing facilities, but also examined how facility type, market, and environmental factors affected provision of hospice services to residents. They found that 30 percent of nursing facilities had at least one Medicare hospice beneficiary and that the proportion of residents on the Medicare hospice benefit differed substantially within and across states. Only 4.2 percent of the nursing facilities studied had 5 percent or more of their residents on the hospice benefit, but these nursing facilities served approximately 34 percent of all hospice beneficiaries in nursing facilities.
Organization and market-area characteristics also seem to influence whether nursing facilities offer hospice. When comparing nursing facilities with at least a 5 percent concentration of Medicare beneficiaries on hospice to those with less than 5 percent concentration, the researchers found that facilities with a small share were more likely to be hospital-based, to have fewer Medicare and Medicaid residents, and to have lower nurse staffing levels. Additionally, all else equal, nursing facilities in counties with greater hospice penetration (i.e., where there were more total hospices altogether, and where most were for-profit, institutional-based, and larger) were more likely to have at least a 5 percent concentration. The distribution of hospice beneficiaries in nursing facilities follows an economically motivated path, Petrisek and Mor suggest. State Medicaid policies, such as the services that must be included in daily Medicaid rates, may also partly account for variation among states in the use of Medicare's hospice benefit in nursing facilities.
Similarly, Jones and colleagues (1997) found that factors besides patient need or demand influenced whether hospice was available in nursing facilities. In 23 nursing facilities owned by the same company whose hospice use rates ranged from 2 percent to 39 percent, for instance, the administrator's attitude influenced whether the facilities used such services. Usage rates were three times higher in nursing facilities where administrators were "most sympathetic" to hospice than in those where they were "least sympathetic." The administrators' discretionary power thus seemed to influence hospice enrollment options. This finding is consistent with program implementation theory, which describes how the power of local administrators can limit access to new programs they find problematic.
Contractual Relationships Between Hospices and Nursing Facilities
The HHS Office of Inspector General, which examined the contractual arrangements between hospices and nursing facilities, identified opportunities for fraud, waste, and potential abuse in implementing the Medicare hospice benefit in nursing facilities. The OIG's study was conducted to determine whether hospice contracts in nursing facilities lead to inappropriate or excessive payments to nursing facilities (HHS, 1997a). Of the 31 responding hospice programs, 22 had patients residing in nursing facilities and 17 had contracts with information sufficient to determine the payments made to nursing facilities. Medical and financial records of 208 patients residing in the 22 hospices in December 1995 were reviewed, as were the 17 contracts. Nearly all 17 hospices paid the nursing facilities the same or more than the state Medicaid agency would have paid if the resident had not opted for hospice care (10 paid 100 percent, 5 paid 105 percent, 1 paid 120 percent, and 1 paid less than 100 percent).
It was unclear to OIG whether additional services were provided by the nursing facility to warrant the increase in payment over what the State would have provided. The hospices paying over 100 percent had a high percentage of their patients in nursing facilities (on average, 49 percent with two hospices having close to 100 percent of patients residing in nursing facilities) when compared to the hospices paying 100 percent or less had (on average, 24 percent of patients in nursing facilities). Additionally, three contracts suggested that kickbacks were provided for hospice referrals, leading the OIG to voice concern that some hospices may be violating Medicare-Medicaid anti-kickback laws. The OIG also speculated that financial incentives, rather than patient care, might sometimes have influenced hospice referrals.
Since OIG released its findings and recommendations, HCFA has worked with hospice associations to educate hospices about how to avoid potential fraud and abuse--or the appearance of such in inappropriately worded contracts. The OIG also recommended that HCFA work with states to develop regulations specifying what room and board payments include, but such regulations are yet to be released.
The OIG study noted that hospices and nursing facilities alike can benefit financially by enrolling patients in hospice. Indeed, in some instances they have a strong financial incentive to enroll residents prematurely (that is, when life expectancy is longer than six months). The report spelled out potential financial benefits as follows:
For hospices, these benefits were seen as:
- additional income if Medicaid payment to the hospice exceeds the hospice payment to nursing facility;
- increase in average length of stay of patients resulting in more potential profit per patient; and
- increase in efficient use of staff, since several patients may be at one geographic location.
For nursing facilities, these benefits were seen as:
- increase in reimbursement if the nursing facility receives more than the 100 percent daily rate it would have received from Medicaid;
- additional staff at no extra cost and reductions in supply and medication costs when provided or paid for by the hospice; and
- increase in patient census by admitting hospice patients to the nursing facility.
The OIG based its conclusions on its study, Hospice Patients in Nursing Homes (HHS, 1997b). The study's findings about average length of stay are most likely biased, as will be discussed later. The true average hospice length of stay in a nursing facility is probably much shorter than the OIG observed.
8. UTILIZATION OF THE MEDICARE HOSPICE BENEFIT
Hospice Lengths of Stay
Banaszak-Holl and Mor (1996), who studied hospice enrollees between 1987 and 1990, found average stays longest in free-standing hospices and shortest in SNF-based ones (Table 8). In fiscal year 1995, free-standing hospices still had the longest stays on average, at 62.9 days. By comparison, stays averaged 56.7 for hospital-based hospices, 53.8 days for those based in home health agencies, and 49.3 days for those in SNFs. For residents receiving the Medicare hospice benefit, NHO estimated average length of stay at 56.3 days in 1995, in contrast to the OIG, which estimated average stays of 181 days (HHS, 1997b). However, as detailed in the next section, the OIG figure is probably too high.
Office of Inspector General Related Investigations
In 1995, Operation Restore Trust was established to identify areas in the Medicare program that might be vulnerable to fraud, waste, and abuse. The initiative was a joint project of the OIG, HCFA, and the Administration on Aging. Audits were conducted in five states (California, Florida, Illinois, New York, and Texas) where Medicare spending represents 40 percent of total program expenditures. Hospice care was one of three areas being investigated. In-depth audits revealed problems related to both the certification of nursing facility residents as hospice patients and the services the received. Certain provisions in the Balanced Budget Act of 1997 partly responded to some of the OIG's concerns. One, for instance, mandated more frequent physician certifications of patient eligibility after 180 days of hospice care.
Hospice Patients in Nursing Homes examined the eligibility, services, and growth in numbers of hospice patients living in nursing facilities (HHS, 1997b). Specifically, hospice and nursing facility records were reviewed to determine: (1) whether patients were eligible for the Medicare hospice benefit at hospice admission, (2) the frequency, type and nature of services hospice provided, and (3) whether services changed after patients elected hospice. Additionally, a medical reviewer was asked if staff members could have furnished the same services hospice did.
Six hospices were selected from each of the five states where Operation Restore Trust was under way. Six others were randomly selected from the nonparticipating states. The sampling frame was patients receiving routine home care during December 1995. A sample of 262 hospice nursing facility beneficiaries was selected from the 22 hospices with patients living in nursing facilities. If a hospice had fewer than 35 patients in a nursing facility, all were included in the study. Otherwise, 35 patients were chosen on a random basis. In the end, 200 Medicare nursing facility beneficiaries remained in the sample.
Two levels of hospice and nursing facility medical record review were conducted, the first by nurse reviewers with experience in hospice or nursing facilities and the second by physician reviewers in specialties related to a patient's diagnosis and who had referred their own patients for hospice care. If the first medical reviewer questioned hospice eligibility, another one responsible for hospice services at a Medicare Regional Home Health Intermediary performed a second review.
The OIG estimated that 16 percent of hospice patients living in nursing facilities did not actually qualify for the Medicare hospice benefit upon enrollment. Some enrollments were considered premature--though patients had a terminal illness, the condition was not deteriorating per NHO's Medical Guidelines for Determining Prognosis in Selected Non-Cancer Diseases (NHO,1995a). Of the questionable enrollments, many involved dual eligibles, most of whom went on hospice after being admitted to the nursing facility.
As NHO noted in responding to the OIG hospice report, to be eligible for Medicare's hospice benefit, patients do not have to show signs of decline when they choose the benefit. Nor do they have to be in an unstable condition or on the brink of death. The NHO also criticized the OIG for using NHO's medical guidelines to determine eligibility since they postdated the OIG's study and thus probably were unavailable to hospices and physicians in the period being reviewed.
Patients the OIG found ineligible when they chose hospice had much longer average lengths of stay (369 days) than those found to be eligible (145 days). Average length of hospice stay overall was 181 days, which was longer than the 58.8-day average stay found in fiscal year 1995 (HHA, 1997). It also exceeded the average of 56.3 days estimated by NHO for hospice beneficiaries in nursing facilities in 1995 (HHS, 1998).
Although OIG's estimates are compelling and raise concerns about possible abuse of the benefit, they are based on an extremely small sample and are most likely influenced by incidence- prevalence bias. (Especially in a nursing facility setting, prevalent cases represent more long- stay patients with chronic conditions than do incident cases.) Further, given that OIG sampled active beneficiaries in December 1995, rather than sampling incident admissions or deaths per discharge across a longer time period, the probability of oversampling residents with longer lengths of stays (i.e., prevalent cases) is high. This oversampling of prevalent cases is especially likely since individual hospices had so few nursing facility residents included in the study (reducing the likelihood of capturing incident cases). (Of the 22 hospices studied, 15 had 9 or fewer nursing facility patients, while 11 had 4 or fewer.) With the probable sampling of beneficiaries with longer lengths of stays, it follows that the estimation of the percentage of questionable admissions would be high. (Beneficiaries with longer lengths of stay are more likely to have conditions more difficult to accurately prognosticate, such as non-cancer diagnoses.)
The incidence-prevalence bias discussed above is documented by results from the National Hospice and Home Care Survey, which samples both hospice discharges (i.e., incident patients) and current patients (i.e., prevalent patients). Three major differences between the current and discharged patient samples in the 1996 NHHCS are noteworthy. First, current patients are likelier than discharged ones to have a diagnosis other than cancer (40.4 percent versus 30.3 percent in 1996). Current patients are also more apt to be 85 or older (21.3 percent versus 16.4 percent) and female (55.1 percent versus 49.7 percent in 1996). In a nursing facility population, these contrasts are probably even sharper. Because current patients in the NHHCS had not been discharged from hospice when the survey was conducted, it is spurious to use NHHCS data to compare current and discharged patients.
Another possible shortcoming of the OIG study is the difficulty of making an accurate six-month prognosis (and agreeing on it) for most nursing facility residents, the majority of whom are dying from chronic conditions like congestive heart failure, Alzheimer's disease, or chronic obstructive pulmonary disease. Further, the OIG hospice audits were performed on hospice admissions that occurred before fiscal intermediaries introduced more stringent requirements for documenting a terminal illness (Texas Association for Home Care, 1997). Thus, although the number of hospice beneficiaries retrospectively deemed ineligible through the OIG study provides some support that a problem exists, the culprit may be poor documentation practices or actual difficulty in predicting death rather than faulty admission practices.
According to OIG, hospice workers saw beneficiaries living in nursing facilities less frequently than NHO guides recommended (Table 9) (HNO, 1995b). Also, even though hospice patients in nursing facilities received fewer services than those living in the community, hospices were paid at the same level for care in both settings. That finding raised concerns that hospices were being overpaid for services provided in nursing facilities. Consequently, the OIG recommended that HCFA seek legislation to modify Medicare and Medicaid payments for hospice patients living in nursing facilities. The OIG recommended reducing the hospice payments for beneficiaries in nursing facilities or revising the benefit requirements for nursing facility residents.
But before concluding that fewer hospice services actually are provided to hospice beneficiaries in nursing facilities, the validity of OIG's comparisons must be considered. In fact, the data may not be comparable. For example, OIG observed hospice services provided in nursing facilities only during December 1995, not across the entire hospice episode. NHO, on the other hand, derived the average number of visits per week from staffing ratios (ratio of visits per week to patient caseload) based on a survey of providers. NHO's figures thus reflect visits made to patients over time and throughout their hospice episode, including when they were close to death (NHO, 1995b). Since the number of hospice visits increases as death approaches, the OIG average is likely to be too low. This possibility warrants serious attention when considering the validity of the OIG's findings on service use. It also underscores the need for other studies that examine provision of hospice care to nursing facility residents.
OIG also reported that although regulations may have made it hard for nursing facility staff to provide certain hospice services, most hospice patients received only basic nursing and aide visits. Recall, however, that these findings are based on medical reviewers' opinions rather than on empirical data. No comparable group of dying nursing facility residents was examined to determine if, in fact, similar services were or could be provided by nursing staff. Thus, it seems premature to conclude that they could duplicate all hospice services.
The OIG also addressed hospice eligibility for Medicare hospice beneficiaries in Medicare Hospice Beneficiaries: Services and Eligibility (HHS, 1998). Although this study concluded that Medicare's hospice program seemed to be working as intended, it raised questions about possible ineligibility of a large percentage of hospice beneficiaries in nursing facilities.
Besides using methodology similar to that in the Operation Restore Trust study, this analysis also sampled hospice beneficiaries enrolled as of June 14, 1996. Nurses reviewed 236 beneficiary hospice records, 102 of which were referred for physician review. The records were for beneficiaries in nursing facilities (all were referred) or other beneficiaries for whom nurses questioned eligibility. (Documentation in 27 records was not sufficient to determine eligibility.) In the 209 medical records in which documentation allowed for determination of eligibility, 10 of the 19 beneficiaries found ineligible were in nursing facilities. Using weighted averages, the OIG found 7.21 percent of the total sample ineligible for hospice: 29.3 percent of community-dwelling hospice beneficiaries (10 of 39) and 2 percent of nursing facility hospice beneficiaries (9 of 197).
These findings are influenced by the incidence-prevalence bias described earlier. Because of this, the ineligibility percentages may be overestimates. Since there are well-known differences in diagnosis and length of stay among nursing facility residents, depending on whether they are incident cases (admissions or discharges) versus prevalent cases (current residents), this overestimation is likely to be greater for the nursing facility hospice beneficiaries. In addition, all nursing facility hospice beneficiary records were referred for physician review, whereas referrals occurred for other Medicare hospice beneficiaries only when nurses questioned eligibility. For the 10 ineligible nursing facility residents, 7 had non-cancer diagnoses, 1 had prostate cancer, and 2 had lung cancer. Other than the lung cancer, all of these diagnoses represent a significantly reduced risk of death, and thus a longer hospice stay (Christakis and Escarce, 1996).
In relation to the above ineligibility findings, NHO disputed what in its view were differences in medical opinion used to determine ineligibility. The NHO thinks OIG's "intense scrutiny" of hospices has led to underutilization of the benefit. It was disappointed that OIG failed to comment on that possibility (HHS, 1998). The Hospice Association of America (HHA), while not expressing specific concerns about OIG's methodology, thought it would be inhumane to "support a system that focuses on error-free prognoses of six months or less." HHA also said that Medicare's requirement of a prognosis of six months or less to live, "in reality translates to the last few days or weeks of life" (HHS, 1998).
9. MEDICARE EXPENDITURES AND HOSPICE CARE
Spending on Hospice
In 1997, Medicare spent $2.7 billion (1 percent of total program expenditures) on hospice care (Figure 3). Over half of the program's hospice expenditures (53.4 percent) went to free-standing hospices, 27.8 percent to home-health-agency-based hospices, 17.4 percent to hospital-based hospices, and 1.4 percent to SNF-based hospices (HCFA, 1998a).
Medicare hospice payments grew rapidly between fiscal years 1990 and 1996. However, the projected growth per hospice enrollee in fiscal years 1997 to 2002 is less than the average for all other Medicare benefits (Figure 4). This growth reflects increases in average lengths of stay, and heavier utilization of more costly levels of hospice care. For example, between fiscal years 1994 and 1995 total hospice continuous care hours climbed by 73 percent and inpatient respite days by 60 percent, while total hospice routine care days rose by 36 percent and general inpatient days by 39 percent. Average length of stay actually fell slightly (from 58.9 days to 58.8 days) (Hospice Association of America, 1997).
End-of-Life Costs and Medicare's Hospice Benefit: Lessons from the Literature
Although this review found few new studies of patient and family outcomes relating to hospice, the debate over whether hospice is more economical than conventional care continues in the literature. This dialog is not surprising, given that the amount of health care resources consumed in the last year of life has become a significant national concern. Lubitz and Riley (1993), who examined Medicare data for 1976, 1980, 1985, and 1988, found that almost a third of program payments (27 percent to 30 percent) each year were for the small percentage (5 percent to 6 percent) of beneficiaries who died in a year.
Studies of Medicare's hospice benefit in the early 1990s showed that expenditures varied by type of hospice -- those affiliated with a hospital, SNF, home health agency, or free-standing (Banaszak-Holl and Mor, 1996). They found significant differences in costs, depending on the setting. SNF-based hospice programs were costliest, while those in free-standing facilities were the least expensive. They also found that hospices based in SNFs and hospitals attracted more non-white, female beneficiaries and fewer beneficiaries with non-cancer diagnoses, suggesting that spending differences may be related to what types of patients choose a particular hospice program. In SNF-based hospices, for example, the study data suggested that hospice patients had lower functional status--or at least a more complex cancer diagnosis--than patients who used other types of hospice programs.
The National Hospice Study (NHS) was the first examination of the difference in end of life costs for those dying with or without hospice care (Greer, et al. 1983). The study, which consisted primarily of cancer patients, evaluated hospital-based and home-based hospice care. The latter appeared to save money by substituting home care for inpatient hospital care. Occurring largely in the last months of life, these savings offset higher costs incurred by patients served in hospice for longer than two months (Mor and Kidder, 1985; Birnbaum and Kidder, 1984). Mor and Kidder (1985) comment that the savings estimates may be sensitive to any shifts in time of entry into hospice or to the mix of patients admitted to hospice. Considering this, the NHS findings may not be generalizable to hospice beneficiaries in nursing facilities.
Legislative changes in hospice care financing and their cost effectiveness have also been examined. In 1988, HCFA sponsored what became an influential study of Medicare's hospice benefit during its first three years of the program (Kidder, 1992). Multivariate analyses matched hospice and non-hospice decedents by length of enrollment, controlling for geographic access to certified hospice programs. For hospice users the enrollment period was the length of hospice enrollment. For non-users, it was the time that elapsed between the first claims with a diagnosis of cancer and the date of death. Based on comparisons of Medicare Part A expenditures in the last seven months of life for hospice and non-hospice decedents with at least one diagnosis of malignant cancer (90 percent had cancer as a primary diagnosis), Kidder estimated that Medicare Part A saved 26 cents for every dollar it spent on hospice patients. Much of the savings occurred during the last month of life, largely due to home care being substituted for inpatient care. Importantly, the study also found that savings were associated with length of enrollment in hospice, decreasing the longer a beneficiary is enrolled. An exception was hospice patients with the longest length stays (180-210 days) whose hospice care still resulted in savings, a net of 6 cents on every dollar spent for hospice care (Table 10). These savings were greatest--$2.77 for every dollar spent -- in the last month of life.
In addition, although Medicare Part A expenditures generally were lowest in free-standing hospice programs, long-stay enrollees in hospices based in home health agencies, hospitals, and nursing facilities also saved Medicare dollars during the last month of life. For example, Medicare Part A saved one dollar for every dollar spent in the last month of life for hospice patients in hospital and skilled nursing facility based hospices with enrollments of at least 150 days. Similar long-enrollment hospice patients (controlling for demographic factors and medical conditions) in free-standing facilities represented dollar losses to Medicare Part A in the last month of life.
Despite cost savings, Kidder concluded that Medicare's hospice benefit is not likely to be "an important tool for containing costs of terminally ill Medicare beneficiaries." Hospice reimbursement rate increases and preliminary evidence at the time of the study that lengths of hospice enrollment were increasing influenced Kidder's thinking. In addition, both Kidder and Scitovsky (1994) thought that estimated savings associated with hospice care might be too high due to selection bias. That is, people who choose hospice probably would have declined expensive, invasive care even if they had not enrolled in the palliative treatment program. Presumably, hospice enrollees differ from patients who choose not to enroll in hospice in the first place (assuming the option is available). (Because of data limitations, Kidder's analysis could not optimally control for selection bias. Thus, some of his estimated savings could be too high.)
In 1994, HCFA submitted to Congress a report, High Cost Hospice Care, in response to OBRA 89, which mandated an examination of costly hospice care provided to Medicare beneficiaries and an evaluation of the adequacy of payment to cover these cases (HCFA, 1993). HCFA found that high-cost cases were more likely to be associated with unusually long lengths of stay in hospice care rather than expensive medical intervention. Since Medicare pays for hospice on a per diem basis and since per diem rates vary for each level of care, the study concluded that hospices were already receiving appropriately higher payment for these long-stay patients and recommended continuing the current payment system.
In 1995, the National Hospice Organization (Lewin-VHI, INC., 1995) sponsored a study to determine if the cost savings Kidder (1992) had observed earlier had persisted, given the health care environment of the 1990s. The research design was similar to Kidder's: All Medicare enrollees who had died between July 1 and December 31, 1992, and who had a primary diagnosis of cancer on at least one claim were studied. (By contrast, only 90 percent of Kidder's sample had cancer as a primary diagnosis.) While Kidder examined Medicare Part A expenditures only, the Lewin study compared Medicare Part A and B spending. Decedents with one or more hospice claims were classified as hospice users; those with no such claims were designated as non-users.
A variable called "length of illness" was created and used for matching. This variable represented the time between the first claim with the primary diagnosis of cancer and the date of death. (The comparable variable in the Kidder study represented time between the first claim with any diagnosis of cancer and the date of death.) For hospice users the enrollment period was the length of hospice enrollment; for non-users, it was the length of illness. As in Kidder's study, multivariate regression analyses were performed separately for seven groups of decedents who were matched by length of enrollment. Also, as in Kidder's study, variables reflecting geographic access to Medicare-certified hospices were included in multivariate models. Analyses by Medicare-certified hospice provider type (i.e., free-standing or home-health-agency, hospital or SNF-based hospice organization) were not performed.
Overall, whether examining Medicare Part A expenditures alone or combined with B spending, hospice beneficiaries cost Medicare less in the last month of life (Table 11 and Table 12). Like Kidder's study, Lewin's found that Medicare Part A savings fell the longer patients were enrolled in hospice before dying (with no savings for patients in hospice 120 days or longer) (Table 11). Unlike patients in the Kidder study, hospice patients with the longest stays (180 to 209 days) did not save Medicare Part A dollars. However, Lewin's study did not calculate Medicare Part A savings for long-stay patients by hospice provider type, in contrast to the Kidder study. Because of that, it is possible that Medicare Part A savings accrue for long-stay patients enrolled by a certain type of hospice provider, such as a SNF.
Looking at Medicare Part A and B spending by length of hospice enrollment, on average, hospice saved Medicare dollars, regardless of length of stay (Table 12). These savings accrued in the last two months of life, regardless of category. The authors concluded that despite longer stays, a shift to unlimited days of coverage under, and the rapid growth in hospice enrollment for beneficiaries with cancer, hospice would still save Medicare money.
Like the Kidder study, Lewin's work may be affected by inadequate control for selection bias. However, as the Lewin investigators argued, even if selection bias were better controlled, one still would find Medicare savings associated with hospice enrollment because of the size and significance of the hospice effect. (This observation is likely applicable to the Kidder study as well.) Both studies thus provide some evidence that Medicare's hospice benefit saves the program money. However, since both included primarily hospice patients with cancer diagnoses, such savings for Medicare hospice patients with other diagnoses cannot be inferred.
Although the literature suggests that, for dying patients, hospice care is a cost-effective alternative to conventional care, some have challenged these findings. Emanuel and Emanuel (1994), for instance, called the cost savings associated with advance directives and hospice care at the end of life an illusion. The researchers point to the fact that savings cannot be generalized beyond cancer patients because data are limited and there are too few randomized studies. They also cite the higher socioeconomic status of hospice patients as enabling them to get additional services not included in cost estimates, and point out the fact that if overall rates of hospitalization at the end of life decline, so will the savings seen from hospice.
Emanuel's meta-analysis of cost savings from hospice care (1996) concluded they were far lower than most people had anticipated. In the last year of life, for example, he found very little savings (zero to 10 percent of costs). In the last six months, savings rose to 10 percent to 17 percent, reaching 25 percent to 40 percent for care in the last month of life. This review also outlined methodological difficulties that make it hard to assess some of the existing studies of cost savings related to hospice. These problems include selection bias, time frame of assessment, types of medical costs assessed, reporting of savings, and generalizability.
On the basis of current evidence, hospice seems to provide cost savings over conventional care for at least the last one to two months of life. However, controversy persists. The literature continues to call for a large-scale, randomized study of costs lasting longer than six months. Emanuel (1994) has argued that a prospective cohort study of terminally ill patients that assesses preferences for life-sustaining treatments and social support and follows the patients until death is a more feasible undertaking. Using these data, patient preferences and other factors can be controlled for and information about cost, choice of hospice and other factors can be examined.
10. ISSUES REGARDING ACCESS TO THE MEDICARE HOSPICE BENEFIT
Georgraphic Access
As Petrisek and Mor (1998) documented, the percentage of nursing facility residents enrolled in Medicare's hospice benefit varies substantially by state and by regions within states. The extent to which the geographic availability of Medicare-certified hospice providers versus the individual characteristics of nursing facilities and their case-mix affects the individual nursing facility's choice to offer hospice care to its residents has not been documented. The researchers found that in counties with greater hospice penetration, nursing facilities were more likely to have at least 5 percent of their residents on the hospice benefit. Furthermore, both Petrisek and Mor (1998) and Jones and colleagues (1997) showed that a nursing facility's characteristics and its staff influence its decision to offer Medicare hospice care.
Brown University's Center for Gerontology and Health Care Research is currently conducting research to measure the importance of geographic availability relative to facility factors in a nursing facility's decision to offer hospice care. Research to date clearly shows that availability varies substantially geographically, for reasons besides beneficiary demand.
The influence of factors other than patient need in determining whether certain services are provided is not unique to hospice. For example, the Dartmouth Atlas of Health Care (1998), shows Medicare beneficiaries' utilization of health care resources at the end of life and site of death vary considerably depending on where they live. In the Dartmouth study, a community's supply of hospital resources (i.e., beds), rather than patient demand, was the strongest predictor of dying in a hospital. In other words, the more inpatient beds in a community, the more likely was death to occur in a hospital. Petrisek and Mor's work (1998) suggests that the same type of relationship exists between a community's hospice penetration and the proportion of nursing facilities in the community with at least 5 percent concentration of hospice beneficiaries. The greater a community's total number of hospices and the greater the percentages of for-profit, institution based and larger hospices, the more likely a nursing facility resident will enroll in Medicare's hospice benefit. The question raised in the Dartmouth study and relevant for hospice care in nursing facilities is which rate is the right one?
Using NHO's 1997 National Hospice Census and the 1989 Area Resource File, Hamilton (1993) examined the sensitivity of hospice certification to changes in fixed-price reimbursement. After simulating certification decisions, outcomes of alternative reimbursement methodologies were assessed. Of primary interest was whether the Medicare hospice benefit increased access to hospice care by enabling a hospice to serve more patients than it would if it were not certified.
Hamilton found that the Medicare hospice and home care reimbursement rates played a significant role in a hospice's decision on whether to become Medicare-certified. A one dollar increase in the hospice payment rate resulted in a 1.7 percent increase in the probability of certification, while a one dollar increase in the home health agency payment rate resulted in a 1.9 percent decrease in the probability of certification. Also, the Medicare hospice benefit was found to increase access to hospice care by enabling Medicare-certified hospices to serve more patients. In her work, Hamilton noted that the wage indices HCFA uses to adjust hospice reimbursement rates did not fully reflect actual variations in labor costs across regions and thus failed to adjust reimbursement rates correctly for the real cost of certification across region. Hamilton speculated that these disparities resulted in differential access to hospice care for Medicare beneficiaries.
To our knowledge, whether such disparities are associated with the current geographic availability of Medicare certified hospices has not been studied. Nor have researchers looked at whether reimbursement mechanisms compensate hospice providers equally across geographic regions for the differential costs of providing Medicare hospice care in a nursing facility. However, Hamilton's work suggests that differences in geographic access to Medicare hospice in nursing facilities (not associated with Medicare beneficiary demand or facility factors) can be modified by adjusting the reimbursement structure and rates. These questions may be addressed better in the future as hospices begin submitting cost reports to the Medicare program.
Minority Access
There is some evidence that minorities experienced differences in access to Medicare hospice depending on provider type and payer. As discussed previously, hospital-based and SNF-based Medicare-certified hospices enrolled higher percentages of non-whites (13 percent) than did free-standing facilities and hospices based in home health agencies based facilities (9 percent and 10 percent) (Banaszak-Holl and Mor, 1996). Access to Medicare hospice by Latinos and African Americans may be limited by the need for continuity of care and the resulting (implicit) requirement for a primary caregiver (Gordon, 1995).
The higher percentages of minorities cared for in institution-based hospice programs may reflect the lower need for a primary caregiver in these settings. Indeed, hospice patients are more apt to be non-white than their non-hospice Medicare counterparts (9 to 13 percent versus 21 percent) (NCHS, 1996 and 1998; Petrisek and Mor, 1998). Whether this difference is due to greater variation in age and casemix for hospice patients across all payer types, to time period differences, or to the design of the Medicare hospice benefit itself is unknown.
In its resolution on access to hospice care, the National Hospice Organization states its "support [of] the principle of access to hospice care for all terminally ill individuals regardless of age, gender, nationality, race, creed, sexual orientation, disability, diagnosis, availability of primary caregiver, or ability to pay" (Harper, 1995). A national task force on minorities' access to hospice care, convened by NHO in 1987, concluded that data were inadequate and outlined actions plans. Since then, awareness about access problems for minorities has grown. The Hospice Journal, for example, devoted an entire issue to this subject, most of which consisted of editorials and descriptive research reports (NHO, 1995c).
Access for Persons Without Caregivers or Eligible for Medicare Skilled Nursing Facility Care
Primary caregivers provide direct patient care and support, or, alternatively, assume responsibility for arranging whatever care hospice does not provide directly. (NHO, 1997b). Although Medicare does not require a primary caregiver to ensure continuity of care, beneficiaries who want to be cared for at home need such a person (or a group of committed caregivers). In nursing facilities, staff members act as surrogates. That setting, then, may be the only feasible hospice option for beneficiaries who lack other caregivers. Banaszak-Holl's and Mor's (1996) observation that beneficiaries enrolled in Medicare-certified, SNF-based hospice programs are less likely to be have caregivers in the community supports this notion.
Second, beneficiaries discharged from the hospital to a nursing facility may have problems accessing the hospice benefit. According to anecdotal reports, nursing facility administrators "discourage" Medicare hospice enrollment for dual-eligible beneficiaries who qualify for Medicare's SNF coverage because Medicare 's SNF benefit has a higher room and board payment rate than does the typical Medicaid nursing facility benefit. Since Medicare's hospice benefit does not include room and board coverage, dual-eligible enrollees on hospice would have their NF costs paid by Medicaid. If a beneficiary enrolls in hospice, the NF would receive only the Medicaid residential rate while the hospice would be paid for the hospice care. Similarly, Medicare-only beneficiaries who have just been discharged from a hospital also have a disincentive to enroll in hospice rather than be admitted to a SNF because the latter covers room and board while hospice does not provide that type of coverage. Although there are no hard data, anecdotal reports suggest that beneficiaries have less access to hospice care if no caregiver is available at home. The implication for quality of care for these beneficiaries is unknown.
Access to Hospice for AIDS Patients
This literature review also found many articles on access to hospice care among persons with AIDS. Although in principle hospice programs accept these patients, in practice that is problematic. The key issues for AIDS patients relate to difficulties in prognostication about their illness, rapid development of new treatments, the view of HIV as a chronic condition, and questions about reimbursement for hospice care (von Gunten, et al., 1991; Tehan, 1991). Buchanon's research (1995-96) on Medicaid recipients with AIDS indicated that the range of services, including hospice care, differed among states. (Medicaid's hospice benefit to persons with AIDS is optional.) Buchanon speculated AIDS patients might be more expensive to treat than other hospice patients. Of the six states with a high incidence of AIDS (all of which offered Medicaid hospice), only New Jersey and New York made allowances for Medicaid payment rates for AIDS patients in hospice.
Nonetheless, persons with AIDS seem to have more access to hospice than do patients with other non-cancer diagnoses (NHO, 1996). Data from the NHO showed that one in three persons who died of AIDS in 1995 was in hospice. That figure is comparable to people who died of cancer, but is a much higher share than for those succumbing to chronic heart disease (one in 10 of whom die in hospice). New treatments, however, have changed the disease trajectory for AIDS; it has now become a chronic illness with a mortality that is hard to predict. This changed disease trajectory is thought to have resulted in a smaller hospice enrollment of AIDS patients and in much shorter hospice lengths of stay for AIDS patients. Both of these effects presumably are related to the difficulty in predicting mortality for AIDS patients (NHO, 1998b). Considering this, the following discussion may be appropriate for the diagnosis of AIDS as well.
Access by Diagnosis -- Prognosis in Non-Oncologic Disease Models
A final issue related to access is whether Medicare's hospice benefit is as available to beneficiaries with terminal diagnoses other than cancer. At issue is that accessibility is driven by a physician's ability to make a definitive, six-month terminal prognoses (if the illness runs its normal course), rather than by the beneficiary's needs. The imprecision of survival prognoses for people with chronic illnesses like dementia, congestive heart failure, and chronic lung disease may limit accessibility to this benefit for most nursing facility residents (Christakis and Escarce, 1996; Luchins et al., 1997; Lynn et al., 1997). The ability of doctors to predict the course of a patient's terminal illness accurately became an important consideration when Medicare's hospice benefit was established. The inherent difficulties in making such predictions have caused confusion about timing patient referrals to hospice as well as the appropriateness of patients for the Medicare hospice benefit.
Early literature suggested that prognostication for terminally ill cancer patients was an inexact science and that performance scales (e.g., the Karnofsky scale) might be helpful in making these assessments (e.g., Yates et al., 1980; Forster and Lynn, 1988; Reuben et al., 1988). Indeed, the Institute of Medicine's book, Approaching Death: Improving Care at the End of Life, reaffirmed difficulties in making prognoses for patients with cancer and non-cancer diagnoses (IOM, 1997).
In a pilot project, Christakis (1994) examined the timing of referral to an outpatient hospice and possible predictors of that referral. The researcher found that 15 percent of patients died "early" (within seven days) and 12 percent died "late" (after 180 days). Although many of the variables Christakis studied were not related to length of hospice stay, clinical factors like depression and whether the patient was mentally oriented were related to lower death rates. So, too, were prostate cancer and cardiovascular disease. The author concluded that making accurate prognoses for different types of terminal illnesses called for more study and that results might lead to more timely referral to hospice programs.
On examining length of survival in 1990 among Medicare hospice patients in California, Florida, New York, Pennsylvania and Texas, Christakis and Escarce (1996) found the median survival time was 36 days. The researchers considered 15 percent of the referrals to be early and 14.9 percent to be late. Additionally, survival time varied markedly, depending on diagnosis (i.e., survival was longer in people with more chronic terminal illnesses) and by type of hospice provider. For instance, patients being cared for by newer, for-profit, larger, hospices that were not based in hospitals lived longer than their counterparts in other types of facilities. As for survival times, patients with renal failure, leukemia or lymphoma, and liver or biliary cancer did not live as long as those with dementia, chronic lung disease and breast cancer. Looking at gender, men on hospice died before women (10 percent increased risk of death) while non- Latino whites died before non-whites (11 percent increased risk of death).
Christakis and Escarce speculate that given the short lengths of many hospice stays, the high up-front costs associated with evaluating newly admitted hospice patients, and the hospice per diem payment system, some hospices may "encourage the early enrollment of patients as a way to recoup the high up-front costs associated with admission." Even so, they are not certain whether hospices having a higher share of long-stay patients are eliminating barriers or whether patients whose life span is expected to exceed six months are being enrolled inappropriately. As for short lengths of stay, the authors theorize that Medicare's hospice benefit requirement of a six-month terminal prognosis, together with the imprecision of terminal prognoses for those with chronic terminal illness, may lead to late referral to hospice. However, they also point out that late referral is a cultural phenomenon not unique to the United States, noting that it may reflect more fundamental factors related to how physicians and patients confront terminal illness.
The researchers maintain that more study is needed on characteristics of physicians, patients, and hospice providers as these relate to timing of enrollment in hospice programs. They conclude that earlier referral to hospice may enhance outcomes for patients and families, as well as reduce the cost of end-of-life care.
The Christakis-Escarce study was limited by its inadequate controls for clinical severity. Because claims data were used for analysis, a Charlson score reflecting diagnosis mix was the only severity measure used. Reuben and others (1988) documented that functional performance (using the Karnofsky Performance Scale) is the most important clinical factor in estimating cancer patients' survival time. They also found, however, that the clinical symptoms of shortness of breath, problems with eating or anorexia, trouble swallowing, dry mouth, and weight loss were independently predictive of survival. When they controlled for patient functioning and symptomatology, neither gender nor site of cancer was associated with length of survival. Although the Christakis and Escarce study observed survival in hospice (and thus also reflects referral patterns), rather than survival overall, the work by Reuben and colleagues suggests that observed differences by gender and diagnosis (especially by site of cancer) may be overestimates.
To help overcome problems with prognostication, NHO published guidelines for identifying patients with non-oncologic terminal illness who are likely to have significantly decreased prognosis if the illness were to follow its normal course (NHO, 1995a and 1996). Besides general non-cancer guidelines, NHO also publishes more specific guidelines and worksheets for heart, pulmonary, liver, renal, and HIV disease, as well as for dementia, stroke and coma, and amyotrophic lateral sclerosis. NHO's most recent general non-cancer and end-stage dementia guidelines are in Appendix C.
One barrier to utilization of the hospice benefit has been difficulty with prognostication, even though early pilot hospice programs for at least dementia patients were both feasible and ethical. For example, Luchins and colleagues (1997) published the first study of the utility of the NHO guidelines in evaluating the prognosis of dementia patients. In that study, the researchers also developed and evaluated eligibility criteria for the Medicare hospice benefit for patients with advanced dementia and related medical complications (see Appendix C for criteria). Their criteria predicted a median survival time of 4 months and a mean survival of 6.9 months. Of the patients in their sample, 38 percent lived more than 6 months. Conversely, NHO guidelines identified patients who had high mortality and a short time to death. The authors caution that using NHO guidelines might decrease access to hospice for many dementia patients.
According to Volicer (1997), the Luchins study suggests that the NHO end-stage dementia guidelines can predict who will not die within six months, but not who will. This poor sensitivity in detecting who will die within a 6 month period results in lack of hospice access for dying patients who do not satisfy the NHO guidelines (see Appendix B). Notably, however, sensitivity vastly improved when the Functional Assessment Staging criteria (FAST) could be applied (which was possible for only about half the patients studied). NHO states that its 1996 guidelines have made changes to the FAST criteria so that they are applicable to many more patients (NHO, 1996).
Commenting further on the Luchins study, Volicer observes that the findings cannot be generalized. Luchins's patient population was limited by enrollment criteria (those persons with current or recent history of serious complications), whereas NHO guidelines only require the presence of a co-morbid condition in the last year. Also, the Luchins study compared its criteria with NHO dementia guidelines using FAST criteria only, whereas NHO's guidelines also contain alternative criteria on medical complications.
Medicare fiscal intermediaries now use adaptations of NHO guidelines to review eligibility for hospice admission. One proposed revision was evaluated to determine whether the criteria could pinpoint patients with fewer than six months to live (Schonwetter et al., 1998). This study applied the criteria to 104 hospice patients who died within six months of being admitted to a Florida hospice. The criteria identified only 35 percent of these patients as meeting hospice eligibility criteria. While 94 percent of the decedents with the diagnosis of stroke and coma were identified as eligible for hospice, only zero to 44 percent of decedents with the diagnoses of dementia, cardiac disease, amyotrophic lateral sclerosis, liver disease, renal disease, pulmonary disease or HIV were identified as eligible for hospice. The average lengths of hospice stay for those decedents determined to be ineligible for hospice ranged from 16 to 48 days.
The researchers noted that the criteria they studied were more restrictive than NHO's guidelines. However, they did not compare eligibility determinations using the NHO guidelines. Although the study population was small and included decedents at just one hospice, the findings raise concerns about how Medicare fiscal intermediaries' use of eligibility criteria affects access to Medicare hospice for beneficiaries with terminal diagnoses other than cancer.
11. RESEARCH ON THE QUALITY OF HOSPICE CARE
Hospice is one of the few innovative health care services introduced in the United States that was evaluated extensively before being adopted as a Medicare benefit. The largest, most comprehensive study of hospice care was the National Hospice Study (NHS), which evaluated the impact of a federally funded hospice demonstration program introduced by the Health Care Financing Administration (Mor et al., 1988). The NHS study included primarily people with a diagnosis of cancer and evaluated two hospice options -- hospital-based hospice (i.e., hospice had inpatient beds) and home care based hospice (i.e., hospice had no inpatient beds). Patients served by home-based hospice programs received substantially more care at home and were in the hospital for fewer days in the last month of life than hospice patients cared for by hospital-based programs or patients receiving conventional non-hospice care (Greer et al, 1986). Patients served in any type of hospice were significantly less likely than conventional care patients to receive diagnostic testing or intensive therapies such as surgery, chemotherapy, radiation therapy, transfusions, and intravenous lines in the last weeks of life.
Another study, funded by the Department of Veterans Affairs (VA) evaluated an inpatient hospice program in a single VA hospital, using a randomized trial approach (Kane et al., 1984). Both the National Hospice Study and the VA analysis found that in terms of quality, outcomes in good hospice programs were comparable to those with good conventional care. These observations suggest that an individual and his or her family should be able to choose the style of care they prefer.
This section reviews current literature on whether hospice as a model of terminal care maximizes quality of life for patients and families and whether outcomes differ for hospice and non-hospice patients. In examining the effectiveness of hospice, patient outcomes (e.g., pain and symptom control), family member outcomes (e.g., grief), and persistent measurement issues are discussed.
Patient Outcomes and Family Outcomes
Findings from the National Hospice Study suggested that patients served by home-based hospices received substantially more care at home and were hospitalized for fewer days in their last months than those in hospital-based programs or those receiving conventional non-hospice care (Greer et al., 1986). Patients in any type of hospice were significantly less likely than those getting conventional care to receive diagnostic testing or intensive therapies like surgery, chemotherapy, radiation, therapy transfusions, and intravenous lines in the last weeks of life.
There were few differences in quality of life or symptom management between hospice and non- hospice patients, a National Hospice Study finding corroborated by Kane and others (1984). However, in the NHS study, patients in hospital-based hospices were significantly less likely to be "in persistent severe pain" than patients who received conventional care at both three weeks (3 percent versus 14 percent) and one week (5 percent versus 22 percent) before death. Non-significant differences were also seen for patients treated in hospital-based hospices rather than home-based hospice programs (Morris et al, 1986). The researchers speculated that these observed differences might result in part from the ability of a hospital-based program to more closely monitor pain and calibrate treatment in a controlled environment.
A related finding was that patients in hospital-based hospices were more likely to have an analgesic prescription and to have consumed analgesics than patients in the conventional or home-based hospice setting (Goldberg et al, 1986). For example, 91.3 percent of the hospital- based patients had an analgesic prescription compared to 66.1 percent of the home-care based and 69.7 percent of the conventional care patients. Additionally, both hospital-based and home-based hospice patients were significantly more likely than conventional care patients to receive medications orally, rather than by more invasive methods such as intramuscularly or parenterally. Hospice patients were also significantly less likely to receive analgesics on a prn (as necessary) basis rather than on a scheduled basis (Goldberg et al, 1986). These findings suggest hospice is superior for managing pain. However, since a randomized control trial by Kane and colleagues (Kane et al, 1984; Kane et al, 1985) failed to replicate these pain management findings their generalizability should be viewed with caution.
The study by Kane and colleagues was funded by the Veteran's Administration and used a randomized trial approach to evaluate the impact of an inpatient hospice program in a single VA hospital. The study sample was predominantly male. The trial showed no difference in pain control, symptoms, or levels of depression or anxiety for hospice and nonhospice patients. However, hospice patients were more satisfied than non-hospice patients. Measurement in the Kane and colleagues study differed from the NHS study in two important ways: (1) Kane only used patient reports while the NHS study used patient and caregiver reports, especially near the end of life when a large proportion of patients were nonresponsive) and (2) it made no attempt to measure pain and symptom levels at comparable time periods prior to death as did the NHS study (Masterson-Allen and Mor, 1988).
In a 1987 review, Mor and Masterson-Allen concluded there was too little evidence to support the claim that hospice care was more effective than conventional care in treating patients' physical or psychological symptoms or in improving overall quality of life. Hospice did, however, seem to facilitate patient choice in location of death. Control over that aspect of dying was related to hospice patients' having greater satisfaction with care than non-hospice patients.
Very little research has been added to the literature regarding the influence of hospice on patient outcomes. One study examined site of death for cancer patients. It confirmed that hospice patients with cancer were more apt to die at home than cancer patients who were not on hospice (McMillen 1996; Moinpour and Polissar, 1989). Two other studies compared outcomes of hospice patients with those of non-hospice patients, while two more looked at quality-of-life issues in hospice patients.
Wallston and his colleagues (1988) used data from the National Hospice Study to examine "quality of death" for hospice and non-hospice cancer patients. They developed this measure for the study and defined it as "experiencing in the last three days of life feelings and events that terminally ill patients reported they desired." Patients' primary care providers perceived quality of death was higher for hospice patients than for those who had received conventional care. Although the components of the researchers' quality of death scale were not analyzed individually, the largest difference was seen in the reports of "patient able to stay home as long as he/she wanted." Fully three-quarter (76 percent) of primary care providers for hospice patients agreed, in contrast to 53 percent of those caring for non-hospice patients. The study results appear to be a promising development in measurement, although further research is needed to determine the reliability and validity of the researchers' scale.
Hendon and Epting (1989) examined depression, hopelessness, and death threat in hospice patients, cancer patients with remission, and patients with a temporary illness. Though hospice patients were more depressed than the patients with a limited illness, they were no more depressed than cancer patients. Hospice patients were as optimistic as those with a limited illness, but less optimistic than cancer patients in remission. As predicted, the hospice patients were the least threatened by their own death in comparison to the other patients. The authors suggest that hospice patients had integrated their death into their daily existence because they were in an environment that facilitates coming to terms with death.
Two studies focused on the quality of life of cancer patients receiving hospice services. The first evaluated patients' quality of life as perceived by patients and caregivers at admission, and three weeks after hospice services had commenced (McMillan and Mahon, 1994). There was no significant difference in patients' own ratings on the overall quality of life scale, although some individual items suggested improvement. Caregivers, by contrast, perceived that patients' quality of life was significantly better. The authors suggested that hospice services may be considered as effective since there was no great decline in quality-of-life scores, an observation supported by other studies of patients near the end of life. However, the sample size here was quite small. Further, although quality-of-life scores improved for half the patients, they fell for the other half. McMillan (1996) later replicated the stability of quality of life scores in cancer patients receiving hospice services.
Since hospice services focus on the patient and the family as the unit of care and target their services as such, outcomes experienced by family members are equally important in evaluating the effectiveness of hospice. Most research has focused on a family's experiences during bereavement rather than while the patient is still alive. Mor and Masterson-Allen (1987) document only a handful of studies that compared hospice caregivers' anxiety and depression reactions with those of conventional care providers. The results of these studies were mixed. The National Hospice Study, for example, found no differences in anxiety, depression, or an array of other indicators of distress. On the other hand, a few studies found some evidence that hospice caregivers were less anxious than conventional care providers. Much more attention has been given to bereavement outcomes of family members who received hospice care, with no conclusive evidence supporting the superiority of hospice over conventional care.
Since Mor and Masterson-Allen's 1987 review, only a few studies have addressed family outcomes. One looked at family needs during a member's final days and death from cancer. Two others examined the bereavement experience. Dawson (1991) compared how well hospice and conventional care met the emotional needs of families whose loved one was dying from cancer. Although overall satisfaction with hospice care was consistent among the hospice groups, family members of those who had home hospice care reported the highest level of satisfaction with both the nurse and meeting basic needs.
Ransford and Smith (1991) explored the grief experience of surviving spouses of patients who died in a hospice or a hospital acute care oncology ward. At six months after the patient's death, differences were reported between the two groups, with surviving spouses of hospice patients being better adjusted on depression and orderly physical appearance scales but not on a measure of anxiety. At 12 months, the differences were even greater: Those whose spouse had hospice care scored significantly better on most measures of grief resolution than those whose spouse died in the hospital. Speer and others (1995) reported no differences in the bereavement adjustment of caregivers based on their spouses' length in hospice before death.
It is clear from reviewing the literature that patient and family outcomes have become less of a research focus. The limited number of studies add little to support the contention that hospice care produces better care for patient and family outcomes than conventional care could, although better measurement tools are needed. When examining both quality of life and quality of care while dying, most researchers choose from limited existing measures, each of which seems to capture a different aspect of care. Two conferences have been convened to address the measurement problem for those who study end-of-life care. These meetings will likely change the face of hospice and palliative care research in the coming years. (See http://www.chcr.brown.edu for information on the palliative care outcomes collaborative.)
12. THE DYING EXPERIENCE OF NURSING FACILITY RESIDENTS
No population-based, empirical study has described the dying experience of nursing facility residents. In the SUPPORT study, seriously ill patients who died in hospitals often had severe pain and dyspnea in their final days (The SUPPORT Investigators, 1995). Two out of three dying persons found it difficult to tolerate emotional symptoms in the last days of life, according to family members. Other studies by nursing facilities show that physicians often fail to identify pain as a problem (Ferrell, 1995; Sengstaken, 1993), to reassess pharmacologic interventions (Wagner et al., 1996), or to prescribe adequate pharmacologic treatment for nursing facility residents (Bernabei et al., 1998; Ferrell, 1995; Wagner, 1996). Ferrell and colleagues (1995) found that most nursing facility patients were given only acetaminophen. In five states, Bernabei and colleagues found that only 26 percent of those nursing facility residents with cancer and daily pain received any analgesic agent, and only 26 percent of those patients with cancer received morphine. Presence of pain was associated with age, gender, race, physical function, depression, and cognitive impairment. It was prominent among older and minority patients.
Hanson and colleagues (1997) studied deaths of 461 older adults across sites of death in North Carolina central and eastern counties having no university medical centers. Bereaved family members were asked about their perceptions and satisfaction with terminal care, as well as for recommendations to improve it. While family perceptions and satisfaction with care were not reported separately for 28 percent of the deaths occurring in nursing facilities, those facilities had the smallest share of positive comments (51 percent) when compared with hospitals, the decedent's home, or other locations.
These findings reconfirm the opinion of an expert panel convened by the Agency for Health Care Research (AHCPR). The panel concluded that the frail elderly--especially those in nursing facilities--need special attention for pain management (AHCPR, 1994). The findings also raise concerns about possible nursing facility shortcomings in all the major health care quality problem areas identified by the Institute of Medicine (IOM) (Lohr, 1990). The IOM's study found that (1) care may be underutilized (i.e., poor symptom assessment and management and inaccessibility to palliative care); (2) care may be overutilized (i.e., unwanted interventions and hospitalizations); (3) technical performance may be poor (i.e., inadequate medical management of symptoms); and (4) interpersonal performance may be inadequate (i.e., failure to fully inform patients and families regarding care and to ascertain and adhere to patient and family preferences). Clearly, study is needed to elucidate the dying experience of nursing facility residents. Also, study is needed to document the "value added" of providing hospice care in these nursing facilities.
13. RECENT END-OF-LIFE INITIATIVES AND DEMONSTRATION PROJECTS
The National Institutes of Health have funded a variety of research projects (related to cancer, Alzheimer's disease, and AIDS), 'educational efforts,' 'demonstration projects,' and clinical trials. One AHCPR-funded dissertation grant (R03HS06619), "The Impact of the Medicare Hospice Benefit on Hospices," which produced the article, "The Impact of Ownership Form and Regulatory Measures on Firm Behavior: A study of Hospices," was applicable to the current review (Hamilton, 1994). In addition, AHCPR has supported work conducted by Christakis and Escarce (Survival of Medicare Patients After Enrolling in Hospice Programs, 1996; NRSA training grant T32 HS00009) and is supporting a new study (HS08691) that is examining the adoption of AHCPR's cancer pain guidelines, a project that will inform the referral and timing of referrals to hospice care.
The Robert Wood Johnson Foundation's Last Act Initiative has funded a variety of grants aimed at improving care at the end of life. It has also supported conferences, educational efforts, and basic research on this topic. One grant partially supported the IOM's (1997) book, Approaching Death: Improving Care at the End of Life. A second is examining care of the dying in managed care settings (Fox, 1999). A third is studying the impact of a palliative care team on end of life care in nursing homes (Genesis, 1999).
Another RWJ-funded research effort is the development of a Toolkit of Instruments to Measure End-of-Life care (TIME, see http://www.chcr.brown.edu). A central goal of TIME is that measures incorporate perspectives of both patients and their loved ones; are clinically meaningful; and strive for high standards of reliability, validity, and responsiveness.
The National Hospice Organization has received funding through the RWJ's Chronic Care Initiatives for a planning grant to establish the scope of a National Hospice Outcomes Planning Project (NHOPP). The objective of the planning grant is to determine the scope and design of a NHOPP to assess the impact of various treatment strategies on outcomes of hospice care using the Clinical Practice Improvement study methodology. The project will also create a large, national, integrated database to determine what works best and when for the management of hospice patients.
RWJ and other foundations, such as the Archstone and Andrus Foundations, have also funded demonstration projects examining alternative terminal care models under the "MediCaring" concept (http://www.Medicaring.org). Demonstration projects under MediCaring combine capitated financing and palliative care models for people with chronic and eventually terminal illness. Participating providers will include various health care systems, including VA, several managed care organizations, and some of the larger hospices. The national project will target alternative service packages for seriously ill populations, particularly COPD and CHF patients. The demonstration differs from Medicare's hospice benefit because eligibility is not based on a prognosis of six months survival. Outcomes like costs, satisfaction, and symptom management, will be measured. The demonstrations are in the initial development stage.
One project already completed is the development and test marketing of a supportive care benefit for elderly Medicare beneficiaries. Focus groups, expert panels, and telephone surveys were used to assess beneficiaries' understanding and preferences for an alternative benefit that enhanced the availability of home-based nursing services, maintenance rehabilitation, symptom relief, and terminal care at home without making surgery, intensive care, and hospitalization more difficult to access. Unlike Medicare's hospice benefit, under this proposed benefit package no specific treatment was made unavailable, and beneficiaries did not have to be certified within six months of death. However, there was a greater focus on pain control and provider continuity of care. This study showed that even though beneficiaries understood the issues, many would prefer staying at home with significant illness and disability (Lynn, 1999).
The Department of Veterans Affairs (VA) also has several important end-of-life initiatives under way. In May 1998, the department sponsored a national strategy summit to discuss ways to improve care for terminally ill veterans. In addition, with RWJ's support VA has incorporated end-of-life care issues into its physician training programs. The VA also developed a Palliative Care Index to measure the proportion of patients with advanced, progressive, incurable illnesses who have discussed options other than aggressive curative treatments and been given psychological, social and spiritual support. Cancer, AIDS, chronic renal failure, congestive heart failure, and chronic obstructive pulmonary disease patients with two or more hospitalizations were randomly sampled to measure the proportion who were receiving individualized plans for comprehensive, coordinated, palliative services.
The VA is also collaborating with the Center to Improve Care for the Dying at George Washington University and the Institute for Healthcare Improvement in a Medicaring project targeting end-of-life care for CHF and COPD patients. About 50 health care providers will participate in this nine-month project to improve care for these patients. In addition, VA recently completed a congressionally mandated study of hospice care that described the numbers and types of veterans using hospice, where they were receiving it, whether patients and families were satisfied with it, estimated costs, and potential barriers and solutions to accessing hospice in the VA system (Hickey et al., 1998).
The Open Society Institute also has funded several major initiatives on end of life issues, including co-supporting the Institute of Medicines's 1997 efforts. OSI's Project on Death in America Campaign has funded projects aimed at understanding and affecting the culture and experience of dying in the United States. One area of attention is financing options and costs of end-of-life care. OSI has sponsored meetings and supported educational materials on this issue. Two other projects are in the early stages. One will focus on educating long-term care providers in the care of the dying, while the second will compare outcomes of end-of life care (e.g., access to hospice, pain and suffering, satisfaction) in three settings (acute care hospital, nursing facility, and home/hospice) in Oregon.
Other initiatives to improve end of life are described in IOM's Approaching Death: Improving Care at the End of Life (1997). More recent initiatives also are summarized in "New Endeavors and Innovative Programs in End of Life Care" in a recent issue of The Hospice Journal (Wilkinson, 1998).
14. DISCUSSIONS WITH INDUSTRY AND STATE REPRESENTATIVES
Representatives from the nursing facility and hospice industries, state survey and certification officials, and state Medicaid officials were asked to discuss the different roles of the Medicare and Medicaid programs in covering dual-eligible beneficiaries residing in nursing facilities. Representatives from the provider industries were chosen by staff at the National Hospice Organization, the American Health Care Association, and the American Association of Homes and Services for the Aging. In addition, staff at the Hospice Association of America were included in these discussions. The goals of these discussions were to understand the relative contributions of nursing facilities and hospices in caring for the terminally ill in nursing facilities and the differences in quality of care for residents enrolled in hospice versus those who were not enrolled.
Medicare is the primary payer for hospice services for the dual-eligible because it covers hospice care. States may supplement the Medicare benefit with other medical services not covered by Medicare, such as personal care. In addition, Medicaid may cover room and board costs for dual-eligible hospice enrollees who live in nursing facilities. (States may also provide their own hospice services to Medicaid eligible persons who do not qualify for Medicare.) As noted earlier, the two public programs together, cover the medical and residential costs of dual-eligible beneficiaries living in nursing facilities.
Industry and State Certification Representatives
This section summarizes the issues raised by nursing home and hospice providers, and survey and certification officials (Appendix E). These groups often raised similar issues and shared recommendations as to how the two types of providers could promote better care for the dying, and better integrate and monitor their services. These issues and alternatives for resolving them are discussed here.
Divergent Goals
One problem that underlaid other difficulties in coordinating the care of dual-eligible nursing facility residents on hospice was the divergent goals and perceptions of nursing facilities (either skilled or residential) and hospices. Nursing facility staff and state surveyors view the facility's role as one of restoring health or providing rehabilitation services. This orientation makes it difficult for nursing facility staff to switch between providing restorative/rehabilitative care and palliative care. This issue was mentioned by both the nursing facility and hospice professionals and was complemented by the survey and certification officials' perception that nursing homes are expected to restore function and that death in the nursing homes may often be perceived as a situation requiring greater review. While the state operations manual provides guidance on evaluating whether assessments and care plans are coordinated, the discussants thought this remained a confusing area.
Different "Treatments"
In concert with these viewpoints, respondents also distinguished differences in how dying residents were treated by hospice staff (including physicians and nurses) and nursing facility staff. Hospice professionals specialize in palliative care and are reported to have a particular expertise in caring for dying patients that nursing facility staff do not possess. For example, hospice physicians regard narcotics as pain management tools. They review care plans to ensure that patients are not being excessively drugged but managed with a level of medication that may be greater than the average resident receives. This is a sensitive issue since NFs can be cited for quality of care issues if a resident is perceived to be overmedicated. Similarly, hospice nurses recognize an unwillingness to eat as a dying patient's right to refuse food rather than a difficulty to be overcome. The NF, on the other hand, is concerned with possibly being cited for substandard care if a resident is malnourished or dehydrated. These citations are less likely since interpretive guidelines were developed for surveyors (Appendix PP in the State Operations Manual) but remain an issue.
Discussants further distinguished the types of services provided by hospice from those provided by nursing home staff. Both agreed that hospice staff spend their time with patients differently than do nursing facility staffs. They may hold a patient's hand or help him or her achieve inner peace prior to death--services that a typical nursing facility staff does not have the resources to provide. In addition, hospices reported regularly providing bereavement counseling for the patient and family (including nursing home staff and residents) in the year following the patient's death. While religious personnel tend to visit in nursing facilities, and some facilities may have a rabbi or pastor on staff, the hospice team consistently includes this type of professional to assist in caring for the dying and their family.
In view of the nursing facility's emphasis on restorative care rather than palliative care, all informants agreed that hospice in the nursing facility improves the quality of care and psychosocial support provided to terminally ill residents and their families or significant others. Participants in these discussions generally indicated that nursing home residents receiving hospice often had more comprehensive assessments and better symptom, pain, and psycho-social management than terminally ill residents not receiving hospice services.
Dying without Hospice in Nursing Facilities
Despite these observations, and perhaps because of them coupled with the recognition that hospice is not available in all communities, most discussants recommended that nursing homes need to recognize that caring for the dying is also an important part of their mission. The State of Colorado has dealt with this issue by developing "comfort measures" that address the quality of care provided to nursing home residents who die without the support of the hospice benefit. These guidelines require that each nursing facility establish policies for caring for terminally ill residents who lack hospice. In addition, this state requires that the facilities supplement the minimum data set with a pain assessment tool to monitor the "comfort" of the dying patient.
Who Is Responsible?
One theme that emerged with most informants (including surveyors) was that nursing facilities are held responsible for their residents' care, regardless of whether another entity is coming into the facility to treat them. While Medicare rules require both parties to enter into a contract for service delivery and to develop a coordinated plan of care maintained in each patient's records at the hospice and nursing facility, nursing homes perceive these requirements as inadequate for relieving them from responsibility if problems arise. Some states, including Wisconsin, Colorado, and Kansas, have handled this problem by establishing state guidelines that nursing facilities and hospices must use when treating these patients. (See Appendix D for Wisconsin's guidelines.) These guidelines require that the contracting providers (i.e., the nursing facility and hospice) clearly spell out each provider's responsibilities in the contract. Including these guideline requirements in the contract also addresses payers' concerns that costs (and responsibilities) are being inappropriately shifted between providers for these patients.
Palliative Care Training Needs
All informants, including the state certification officials, agreed that both nursing facility staff and state surveyors would benefit from training regarding hospice and the needs of terminally ill nursing facility residents, in general. Since health care professionals are not routinely trained in providing palliative care, hospices often educate nursing facility staff so they can better respond to dying patients' special needs. Some hospice and survey officials indicated that the role of hospice as educator was one of the most important functions of hospice in nursing homes.
They respondents also suggested that health care providers would benefit from more training in palliative care, and, more specifically, that initial and on-going training in the care of dying residents was needed for professional and paraprofessional nursing home staff. They noted that on-going training was needed because of the high turnover in nursing facility staff, particularly among aides. Also suggested were broader medical educational reforms to teach physicians how to identify dying patients, listen to family members and patients in their choices for care, and train them in appropriate pain and symptom management. All informants recommended training for surveyors in what constitutes proper care (with and without hospice) for the dying nursing home residents and how to monitor this care.
Payment Issues
Because two payers are involved in reimbursing for services to the dually-eligible dying resident, questions about the relative costs and payments for each type of service arise. One question targets the appropriateness of requiring the hospice to manage the residential costs while the other focuses on whether two different payment rates are needed for the institutional and community-based populations.
Room and Board Payments. Both hospice and nursing facility representatives raised questions about the payment procedures for dual-eligible nursing facility residents. Currently, hospices are responsible for all costs of the dying patient. If the patient is dual-eligible, the hospice receives two sets of payments. First, Medicare pays the capitated per diem for hospice care. Second, Medicaid pays (1) the per diem rates for room and board and (2) personal care costs for nonMedicare services provided by the nursing facility. The hospice, in turn, is responsible for paying all providers, including the nursing facility.
Respondents thought that having the hospices receive the state payment, and in turn, pay the nursing facility creates unnecessary problems. First, it gives the hospice an opportunity to reimburse the nursing facility at some agreed-upon rate which may differ from the state's room and board rate. This issue has been quite controversial, as the OIG study demonstrated (HHS, 1997). In fact, the OIG issued guidelines (FR Oct 5 1999) that room and board payments that exceed what the NF would have received under Medicaid without hospice and hospice payments for "noncore" NF services that are above fair market value would raise anti-kickback concerns. Effectively, this maintains the pass-through nature of the Medicaid room and board payment. Second, having to bill Medicaid for room and board payments adds an administrative burden to hospices' billing and cost management, and is perceived to delay final payments to nursing facilities for occupied beds. Interestingly enough, however, is that anecdotal reports indicate that many hospices reimburse nursing facilities for the per diem within 30 to 60 days (per a negotiated contract). In these cases, it is the hospice that suffers if the Medicaid payments are delayed.
Hospice Payment Levels. A second payment issue is whether Medicare should use different rates for hospice services delivered in nursing facilities than for those delivered in the community. The OIG's report suggests that hospice patients in nursing facilities receive fewer hours care per day than those living in the community. They argue that nursing facility staff, who are considered family according to the rules, provide care that reduces the need for nursing services to be provided by the hospice. The OIG suggested modifying the hospice per diem rates to reflect this perceived difference in resource costs for the two populations. This concern was echoed by state survey officials who expressed concern that the level of hospice care to nursing home residents was less than the level of care provided to community-based hospice beneficiaries. However, it is difficult to verify this without cost report information.
State Medicaid Program Officials
We also contacted Medicaid program officials in the five states (Kansas, Maine, Mississippi, New York, and North Dakota) whose nursing facility data will be used in this project. We reviewed with them the operational issues related to use of Medicare's hospice benefit by dual-eligible nursing facility residents. Kansas, Mississippi, and New York each have a hospice benefit in their Medicaid programs, while Maine was planning to implement one in the fall of 1998.
In terms of administrative processes, officials said that hospices are responsible for obtaining documentation regarding a beneficiary's election of hospice and forwarding it to Medicaid. The methods and time periods for doing so vary by state. In New York, for instance, hospices must inform the local Medicaid Social Services office of the date hospice was chosen. In Mississippi, the appropriate Medicaid Regional office must receive documentation of the nursing facility's discharge of the resident from Medicaid coverage on the same date that the hospice admits the patient to its service.
Upon receiving the appropriate notification from the hospice, state Medicaid agencies change their payment databases, and the hospice is designated as the provider-recipient of the Medicaid room and board and personal care service reimbursement for that patient. Because all payment systems are automated, the database must be updated to stop payments to the nursing facility before the hospice files a claim. In one state, although the payment system was automated, officials indicated that there was no formal notification process.
"Our system just indicates what nursing facility an elder is in and we automatically pay the nursing facility unless the nursing facility tells us otherwise, which then opens the door for the hospice provider... We simply react when a claim comes in from hospice to pay them when we have already paid the nursing facility. In this case, the nursing facility has not contacted us, so they have to fill out a void for their claim so that Medicaid can then pay hospice only after the void has gone through."
According to Medicaid officials, timely Medicaid payments to the hospice depend on three steps occurring in the proper sequence. First, the hospice must submit information regarding the date the resident elected hospice care. Second, the Medicaid payment system must be updated. Third, the hospice must file a claim with Medicaid for the patient. Most billing problems reportedly were due to missing steps or performing them out of sequence. For example, a hospice may have submitted a claim along with the notification, or the nursing facility had already been paid for the resident's "hospice days" when the payment system was updated.
Because of the OIG's concern that NFs were being paid too much for room and board once a beneficiary enrolled in hospice, we asked Medicaid officials to define room and board as it applied to dual-eligible residents on the hospice benefit. One state referred to the definition contained in its program information for the Medicaid hospice benefit, which was identical to the federal definition, cited the first section of this review (the definition contained in OBRA 85 but deleted by OBRA 90). Other responses were nonspecific, ranging from "everything it takes to care for that resident" to "meals, room, and facility use."
We also asked officials about their Medicaid payment policies for services not included in the hospice benefit, specifically for beneficiaries or services not covered by Medicare. All states indicated that the hospice would submit a claim for these services. The only exception mentioned was for a physician claim from a non-hospice physician; the physician would bill Medicaid directly if the patient was not dually-eligible. When we asked about mechanisms to determine whether such claims were allowable or appropriate, Kansas representatives indicated that prior authorization by Medicaid was required for non-terminal care services used by hospice patients. New York officials indicated that the state's payment system would screen out claims for inappropriate (i.e., terminal) services. No states had a schedule of non-terminal reimbursable services and none of the informants had information regarding the rate of denials of such claims.
In the context of the Medicare hospice benefit for dual-eligible beneficiaries, nearly all billing disputes resulted from failing to follow administrative procedures. These disputes were handled quite consistently across states. Medicaid staff members, usually someone with a clinical background, and a fiscal representative, review the claim. Their findings are submitted to the provider who may appeal.
15. A SUMMARY OF ISSUES RELATED TO THE MEDICARE HOSPICE BENEFIT AND ITS USE IN A NURSING FACILITY
Much research is needed to understand the role hospice plays for patients living in nursing facilities. Nursing facilities are increasingly becoming the site of death for the elderly, with one in five dying in this setting (NCHS, 1996). However, the ability of nursing facility staff to manage terminal symptoms and provide adequate levels of psychosocial support to individuals and their families may not be equal to that of the hospice staff. Yet, relatively few residents -- less than one percent (0.9 percent) -- enroll in hospice (Petrisek and Mor, 1998).
These low enrollment rates may be related to several issues. First, Medicare's enrollment rules require patients to acknowledge they are dying and no longer want curative or heroic efforts but instead are opting for comfort and palliation. Because this is a difficult step, many physicians hesitate to raise the issue of hospice, or for that matter, the issue of advance directives. In fact, one recent study showed that only 12 percent of the subjects who had advance directives in place had been counseled by a physician about writing the directive (The SUPPORT Investigators, 1995).
Second, physicians must certify patients as having only 6 months or less to live for them to qualify for Medicare's hospice benefit. Because of the intense scrutiny of the OIG's office in recent years, physicians may be hesitant to predict death unless the patient has one of the more predictable diseases, such as cancer. While cancer still dominates the types of patients enrolling in hospice, other chronic terminal conditions, such as congestive heart failure and chronic obstructive pulmonary disease, whose survival rates are more difficult to predict also are occurring more frequently. Questions have been raised about whether better methods for determining hospice eligibility benefit are needed in order for hospice to continue affecting costs and quality of care at the end of life. Analyses in the second part of this project will help clarify whether the eligibility requirements are creating barriers to access.
Terminally ill residents who do not enroll in hospice may be using more hospital and SNF services in place of palliative care. These patients are more likely to be admitted to a hospital and then discharged to a SNF where they may stay until their health improves or they die. Beneficiaries who live in nursing facilities have a financial incentive to choose the more intensive acute care treatments because the more aggressive SNF benefit covers their room and board. Because Medicare's hospice benefit does not cover room and board costs, a beneficiary who lives in a nursing facility and opts for hospice care incurs additional charges for room and board. Medicaid covers these charges for the dual-eligible population, but other patients must pay for them out of pocket or through private insurance coverage. If, instead of hospice, beneficiaries use the skilled nursing facility benefit, Medicare will cover their room and board and treatment costs for a limited time. But these residents will be given more aggressive care and may not receive comparable symptom management and psychosocial support that would be available through the Medicare hospice benefit.
If, instead, a nursing home resident elects hospice, other problems may occur because of the divergent goals and conditions of participation for the two types of providers. Because the dividing line for services is sometimes unclear, there may be confusion regarding which provider will be held accountable for various services. As a result, even if a beneficiary has elected hospice they may not be allowed to refuse food or have unusually high levels of pain medication. As noted in the discussions, nursing facility staffs view their primary role as being restoration and rehabilitation. By contrast, hospice staff members view themselves as providing palliative and supportive care, as prescribed in their conditions of participation.
Many of these potential problems can be managed through explicit contract provisions between providers and a patient's care plan, as is being done in Wisconsin, Colorado, and Kansas. But, this level of coordination and alternative responses requires clear guidance and staff acceptance, knowledge, and cooperation. Nursing facility staff and survey and certification staff need greater education regarding the needs of the dying patients.
On a related note, some have suggested that hospices provide fewer hours of care to patients in nursing facilities than to those living in the community because the nursing facility staff can supplement their work. Because of this perception, the appropriateness of paying hospices the same per diem rate when care is provided in a nursing facility has been questioned (HHS, 1998). In contrast, others have suggested that hospice staff and volunteers appropriately supplement the number of hours otherwise provided by nurses, social workers, clergy, and aides to meet the more intensive needs of dying patients (and their families or significant others) in nursing facilities. In the past, it has been difficult to measure whether these differences exist. As mentioned earlier, the newly required hospice cost reports may shed some light on this issue in the future.
Confusion about expectations of hospice and nursing home providers is exacerbated by the lack of federal regulations specifying what services are included in the nursing facility per diem. The current payment system for dual eligibles, which pays hospices directly for both the hospice and nursing facility room and board is problematic. As discussed earlier, the Office of Inspector General found problems in contracts between hospices and nursing facilities, with some hospices paying nursing facilities a per diem amount greater than they would have received from the state, and with no apparent additional services being provided. Also, there have been many anecdotal reports that this payment mechanism has increased the administrative burden for both hospices and nursing facilities. Both industries advocated dropping the hospice from the nursing facility reimbursement process. This would also eliminate any possibility of "kick-back" payments which the OIG had been concerned about.
Some of these issues have been raised by The National Hospice Organization in its reports on the Medicare Hospice Benefit and End-of-Life Care and their Nursing Home Task Force report (NHO, 1998c and 1998d). These reports make recommendations to reduce the barriers to hospice care. Many of the recommendations address issues discussed in this review, some target nonregulatory changes needed in practice and some target program policies. For example, some of the NHO's recommendations include:
-
Addressing the problems created by the six-month prognosis requirement by changing the eligibility requirement from an expected death in 6 months to 12 months
-
Improving the quality of life at the end of life by increasing access to hospice and developing outcome measures and criteria to help providers know when to refer a patient to hospice.
-
Addressing inadequacies in Medicare payment for hospice services by analyzing the variation in costs for different types of patients and hospice providers.
-
Clarifying the role of hospice in NFs and improving the coordination of hospice and nursing facilities.
-
Educating the public and professionals on the value of hospice care.
The second NHO report which specifically targeted hospice care in nursing homes (NHO, 1998d) repeated many of these concerns. They further emphasized the problems generated by the difference in terminology, language, regulation and culture between the two industries. They call for better pathway guidelines for treating these populations and better training for staff working in this environment.
Much of the discussion thus far has focused on improving the Medicare hospice benefit to make it more accessible to nursing facility residents since so many are terminally ill. Yet, nursing facilities are required by law to make appropriate services available to their patients (CFR 483.25). Nursing facility staff and state and federal regulators need to recognize that caring for the dying is part of the nursing facility's mission and that these populations require different services than those receiving custodial care. Nursing facility staff, both professional and paraprofessional, and regulators need to be trained in appropriate means of caring for the dying. Many of the discussants, including representatives of nursing facilities, hospices, and regulators agreed that the training provided by hospice staff when they are in a facility was invaluable both for the hospice patient and others in the facility.
Better clarification of the roles and responsibilities of multiple providers treating the dying patient are needed. While program rules currently require each resident who is enrolled in hospice to have a care plan documenting the respective services provided, all discussants agreed that better definition of these contracts is needed. Specific responsibilities need to be documented and kept in the patients' records.
Better methods for measuring the quality of care provided to the dying NH resident are also needed. Information on the differences in services provided to hospice and nonhospice residents is needed before we can measure the impact of hospice services for nursing facility residents. Some of this is available in the minimum data sets collected by the nursing facilities and more will be in the future. The second part of this project will provide some information using these data. Additional information will be available as the hospice cost reports become standard submissions. Understanding the differences in resources used for the two types of patients and their respective impact on pain and symptom management will be extremely important for understanding the impact of hospice in treating the terminally ill.
Last, the procedures for Medicaid room and board payments for dual-eligible enrollees need to be reconsidered in order to minimize opportunities for fraud and abuse. New systems are needed to minimize the hospices' involvement in costs not associated with the terminal illness. Both nursing home and hospice informants concurred that having Medicaid pay the hospice, so that it in turn, could pay the nursing facility, was administratively burdensome, costly, and caused delays in the timely payment for room and board. Paying the nursing facility directly would be consistent with the payment methods for other providers involved in treating the patient for conditions that are not associated with the terminal illness. This would also require a new method for notifying state Medicaid agencies that their recipient qualifies for the reduced Medicaid coverage and no longer needs full nursing care coverage.
16. CONCLUSION
Provision of the Medicare hospice benefit in nursing facilities appears to have extended the benefit to a higher percentage of populations than were previously receiving it. However, access to the benefit does not appear to be equitable across geographic settings, nursing facilities, and perhaps across nursing facility residents with diverse terminal illnesses. An optimal model for care of the terminally ill in nursing facilities would provide quality terminal care and support to residents and their families or significant others needing this level of care on an equitable basis, while not increasing the costs of care.
Information on whether hospice improves outcomes for beneficiaries living in nursing facilities is needed. This project will be analyzing Medicare claims to identify changes in the types of populations enrolling in Medicare, the types of services used under Medicare's hospice benefit, and to the extent possible, the outcomes of hospice enrollees in nursing facilities relative to other residents. This work will provide policymakers with information to address the issues being raised in the field.
In summary, policymakers should consider how high quality of care can be provided to the dying nursing home resident, and whether and at what level hospice services are needed to achieve that outcome. Some refinements to the service delivery system that will promote high quality care to dying nursing home residents and will allow for future analysis of the outcomes of care for dying nursing home residents who receive and do not receive hospice are as follows:
-
Educate health care professionals and paraprofessionals, including nursing home staff, about the needs of and care for the dying
-
Provide clear guidance and regulation at the federal and state level regarding appropriate care, with and without hospice, for dying nursing home residents. Guidelines clarifying the need for nursing facilities to provide palliative care, the roles and responsibilities of hospices and nursing facilities when treating a hospice patient, and the minimal contract provisions affecting hospices and nursing facilities when treating these patients.
-
Define and measure outcomes of care provided to terminally ill nursing home residents, distinguishing between those who are receiving hospice services and those who are not.
-
Simplify the room and board payment systems for dually-covered nursing facility residents who choose hospice.
While these refinements will promote the efficient delivery of high quality care to dying nursing home residents, for both those who receive hospice services and those who do not, they will also permit a study of different models of terminal care delivery in nursing facilities. Measuring outcomes for the two groups will help document the effectiveness of hospice and nursing homes in caring for terminally ill persons. Only then can the public and policymakers have an informed debate about maintaining the hospice benefit as an alternative to traditional care, and effectively managing and monitoring the quality end-of-life care in nursing facilities.
Finally, simplifying the payment system for dually eligible nursing facility residents who enroll in Medicare's hospice benefit will reduce provider burden and minimize opportunities for fraud. This could be an important contribution to improving the administrative systems related to benefits for the terminally ill.
REFERENCES
AHCPR. (1994): Cancer pain. Clinical management panel. Management of cancer pain. Clinical practice guideline no. 9. Publication no. 940592. Rockville, MD: U.S. Department of Health and Human Services Public Health Service.
Banaszak-Holl J, Mor V. (1995): Hospice report: The impact of changing Medicare coverage on hospice beneficiaries. Report prepared in connection with HCFA contract #500-89-0063 to Abt Associates, Inc.
Banaszak-Holl J, Mor V. (1996): Differences in patient demographics and expenditures among Medicare hospice providers. The Hospice Journal, 11(3):1-19.
Bernabei R, Gambassi G, Lapane KL, et al. (1998): Management of pain in patients with cancer. Journal of American Medical Association, 279:1877-1882.
Birnbaum HG, Kidder D. (1984): What does hospice cost? American Journal of Public Health, 74(7):689-697.
Brooks CH, Smyth-Staruch K. (1984): Hospice home care cost savings to third-party insurers. Medical Care, 22(8):691-703.
Buchanon, RJ. (Winter 1995/1996). Medicaid policies for home care and hospice care provided to Medicaid recipients with AIDS. AIDS & Public Policy Journal, 10(4): 221-237.
Christakis NA, Escarce JJ. (1996): Survival of Medicare patients after enrollment in hospice programs. The New England Journal of Medicine/Special Article, 335:172-8.
Christakis NA. (1994): Timing of referral of terminally ill patients to an outpatient hospice. Journal of General Internal Medicine, 9:314-320.
Consolidated Omnibus Budget Reconciliation Act of 1989 (OBRA-89), Pub. L.
Dawson NJ. (1991): Need satisfaction in terminal care settings. Soc. Sci. Med., 32(1):83-87.
Emanuel EJ, Emanuel LL. (1994): The economics of dying: The illusion of cost savings at the end of life. The New England Journal of Medicine/Special Articles, 540-544.
Emanuel EJ. (1996): Cost savings at the end of life. Journal of the American Medical Association, Special Communication, 275:1907-1914.
Experton, Bettina et al (1996): A Comparison of Payor/Provider Type of the Cost of Dying Among Frail Older Adults. Journal of the American Geriatrics Society, 44(9): 1098-1107.
Federal Register, Publication of the OIG Compliance Program, Guidance for Hospices, Vol.64, No. 192, October 5, 1999, 54031-54049.
Ferrell BA. (1995): Pain evaluation and management in the . Annals of Internal Medicine, 123:681-687.
Field MJ, Cassel CK, eds. (1997): Approaching Death: Improving Care at the End of Life. Washington, D.C.: National Academy Press.
Forster LE, Lynn J. (1988): Predicting life span for applicants to inpatient hospice. Archives of Internal Medicine, 148:2540-2543.
Fox, Peter, (1999): End of Life Care in Managed Care Organizations. American Association of Retired Persons, Public Policy Paper. Washington, DC.
Gabel J, Hurst K, Hunt K, Kim J. (1998, January): Health benefits for the terminally ill: Coverage, understanding and attitudes. Report to the Robert Wood Johnson Foundation.
Gage, B. (1998): Estimates of Medicare Hospice Users in Nursing Facilities. Memo prepared for HCFA under ASPE contract # HHS-100-97-0070.
General Accounting Office (GAO). (1979): Hospice care: A growing concept in the United States. Report to the Congress.
Gordon, AK. (1995) Deterrents to access and service for Blacks and Hispanics: the Medicare hospice benefit, healthcare utilization, and cultural barriers. The Hospice Journal, 19(2):65-83.
Greer DS, Mor V, Morris JN, Sherwood S, et al. (1986): An alternative in terminal care. Results of the national hospice analysis plan. Journal of Chronic Diseases, 36(11):737-780.
Greer DS, Mor V, Sherwood S, Morris JN, Birnbaum H. (1983): National hospice study analysis plan. Journal of Chronic Diseases, 36(110):737-780.
Hamilton V. (1993, Winter): The Medicare hospice benefit: the effectiveness of price incentives in health care policy. RAND Journal of Economics, 24(4): 605-624.
Hanson, LC, Danis M, Garrett, J. (1997): What is wrong with end-of-life care? Opinions of bereaved family members. Journal of American Geriatric Society, 45:1339-44.
Harper BC. (1995): Report from the National Task Force on Access to Hospice Care by Minority Groups. The Hospice Journal, 10(2):1-9.
Health Care Financing Administration. (1993): High cost hospice care.
Health Care Financing Administration. (1998a): Personal communication from C. Blackford, CHPP, HCFA based on data from the standard analytic files.
Health Care Financing Administration. (1998b): A profile of Medicare: chart book.
Hendon MK, Epting FR. (1989): A comparison of hospice patients with other recovering and ill patients. Death Studies, 13:567-578.
Hickey E, Berlowitz D, Anderson J, Hankin C, Hendricks A, Lehner, L. (1998): The Veterans Hospice Care Study: An Evaluation of VA Hospice Programs. VA Center for Health Quality, Outcomes and Economic Research.
Hospice Association of America. (1997): Hospice Facts and Statistics.
Hoyer, T. (1998): A History of the Medicare Hospice Benefit. The Hospice Journal. 13(1/2):6169.
Infeld DL, Crum GE, Koshuta MA. (1990): Characteristics of patients in a long-term Care hospice setting. The Hospice Journal, 6(4): 81-104.
Institute of Medicine. (1997). Approaching death: Improving care at the end of life, Field MJ, Cassel CK, Eds. Washington, DC: National Academy Press.
Jones B, Nackerud L, Boyle D. (1997): Differential utilization of hospice services in Nursing Homes. The Hospice Journal, 12(3): 41-55.
Kane R.L., Wales J., Bernstein L., Leibowitz A., et al. (1984): a randomized controlled trial of hospice care. Lancet, 1(8382):890-894.
Kastenbaum R. (1975): Toward standards of care for the terminally ill, Part 1: What standards exist today? Omega, 6:289-290.
Kidder, D. (1992): The effects of hospice coverage on Medicare Expenditures. Health Services Research, 27:195-217.
Lohr KN (ed). (1990):Institute of Medicine: Medicare: a strategy for quality assurance. Washington, DC: National Academy Press.
Lubitz JD, Riley GF. (1993): Trends in Medicare payments in the last year of life. The New England Journal of Medicine/Special Article, 328:1092-6.
Luchins DJ, Hanrahan P, Murphy K. (1997): Criteria for enrolling dementia patients in hospice. Journal of the American Geriatrics Society, 45:1054-1059.
Lynn J, Harrell FE Jr., Cohn F, et al. (1997): Prognoses of seriously ill hospitalized patients on the days before death: Implications for patient care and public policy. New Horizons, 5:5661.
Lynn J, O'Connor M, Dulac J, Roach MJ, Ross C, Wasson J. (1999): Medicaring: Development and Test Marketing of a Supportive Care Benefit for the Older Elderly," Draft Project Report.
McCann B. (1983): JCAH hospice project: Proposed standards. Caring, 2(6):15-27.
McCann B. (1985): The hospice project report. Chicago: Joint Commission on Accreditation of Hospitals.
McMillan, SC, Mahon M. (1994): A study of quality of life of hospice patients on admission and at week 3. Cancer Nursing, 17(1):52-60.
McMillan, SC. (1996): The quality of life of patients with cancer receiving hospice care. Oncology Nursing Forum, 23(8):1221-8.
Medicare Payment Advisory Committee. (1998): Care for people at the end of life. Report to the Congress: Context for a changing Medicare program. Washington, DC. June:157-166.
Moinpour CM, Polissar L. (1989): American Journal of Public Health, 79(11):1549-1551.
Mor V, Greer D, Kastenbaum R, (eds). (1988): The hospice experiment. Baltimore, MD: Johns Hopkins University Press.
Mor V, Kidder D. (1985): Cost savings in hospice: final results of the national hospice study. Health Services Research, 20(4):407-421.
Mor V, Masterson-Allen S. (1987): Hospice care systems: Structure, process, costs, and outcome. New York: Springer Publishing Company.
Mount BM. (1976): The problem of caring for the dying in a general hospital: The palliative care unit as a possible solution. Canadian. Medical Association Journal, 115(2):119-21.
National Center for Health Statistics. (1996): An overview of home health and hospice care patients: 1994 national home and hospice care survey. (Advance Data from Vital and Health Statistics: No. 274). Hyattsville, MD: Strahan G.
National Center for Health Statistics. (1998): An overview of home health and hospice care patients: 1996 National Home and Hospice Care Survey. (Advance Data from Vital and Health Statistics: No. 297). Hyattsville, MD: Haupt, B.
National Hospice Organization. (1994): Hospice Bibliography. Arlington, VA.
National Hospice Organization. (1995a): Medical guidelines for determining prognosis in selected non-cancer diseases edition. Arlington: VA.
National Hospice Organization. (1995b): Hospice services guidelines and definitions. Arlington, VA.
National Hospice Organization. (1995c):Hospice care and cultural diversity. The Hospice Journal, 19(2).
National Hospice Organization. (1996): Medical guidelines for determining prognosis in selected non-cancer diseases, 2nd edition. Arlington: VA.
National Hospice Organization. (1997a): National Hospice Census for 1995. Arlington, VA.
National Hospice Organization. (1997b): Hospice operations manual: Hospice for the next century. Arlington, VA. Kiburn, Linda
National Hospice Organization. (1997c): Hospice Fact Sheet. Arlington, VA.
National Hospice Organization. (1998a): NHO unpublished estimates.
National Hospice Organization. (1998b): Personal communication, S. Connor.
National Hospice Organization. (1998c): National Hospice Organization Committee on Medicare Hospice Benefit and End-of-Life Care: Highlights of the final report. Arlington, VA.
National Hospice Organization. (1998d): National Hospice Organization: Nursing Home Task Force Report. Arlington, VA.
Petrisek, AC, Mor V. (Submitted for publication, 1998): Hospice in s: A facility level analysis of the distribution of hospice beneficiaries. Providence, Rhode Island: Brown University, Center for Gerontology and Health Care Research.
Pevrone C, Manard B, Hogan P. (1995): An analysis of the cost savings of the Medicare hospice benefit. Report #712901. Arlington, VA: National Hospice Organization.
Ransford HE, Smith ML. (1991): Grief resolution among the bereaved in hospice and hospital wards. Soc. Sci. Med., 32(3):295-304.
Reisberg, B. (1988): Functional assessment staging (FAST). Psychopharmacology Bulletin, 24:653-659.
Reuben DB, Mor V, Hiris J. (1988): Clinical symptoms and length of survival in patients with terminal cancer. Archives of Internal Medicine, 148:1586-1591.
Schonwetter RS, Teasdale TA, Storey P, Luchi RJ. (1990): Estimation of survival time in terminal cancer patients: An impedance to hospice admissions? The Hospice Journal, 6(4): 65-79.
Schonwetter RS, Soendker S, Perron V, Martin B, Robinson BE, Thal AE. (1998): Review of Medicare's proposed hospice election criteria for select noncancer patients. The American Journal of Hospice and Palliative Care, May/June, 155-158
Scitovsky AA. (1994). The high cost of dying revisited. Milbank Quarterly, 72(4):561-591.
Secretary of Health and Human Services. (1993): Report to Congress: High cost hospice care. Washington, D.C.: Donna E. Shalala.
Sengstaken, EA, King SA. (1993): The problems of pain and its detection among geriatric residents. Journal of the American Geriatrics Society, 41:541-44.
Spector WD, Mor V. (1984): Utilization and charges for terminal cancer patients in Rhode Island. Inquiry, 21(4):328-337.
Spear DC, Robinson BE, Reed MP. (1995): The relationship between hospice length of stay and caregiver adjustment. Hosp-J, 10(1):45-58.
Tax Equity and Fiscal Responsibility Act of 1982, Pub. L. No. 97-248, 96 Stat. 324-707 (1982).
Tehan C. (1991): "The cost of caring for patients with HIV infection in hospice." AIDS and the Hospice Community. The Haworth Press, Inc.
Texas Association for Home Care. (1997):TAHC Library, Hospice, http://www.tahc.org.
The SUPPORT Investigators. (1995): A controlled trial to improve outcomes for seriously ill hospitalized patients: The Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatment (SUPPORT). Journal of the American Medical Association, 274:1591-1598.
U.S. Department of Health and Human Services. (1997/October): Hospice and contractual relationships. (DHHS Publication No. OEI-05-95-00251): June Gibbs Brown, Inspector General.
U.S. Department of Health and Human Services. (1997/September): Hospice patients in nursing homes. (DHHS Publication No. OEI-05-95-00250): June Gibbs Brown, Inspector General.
U.S. Department of Health and Human Services. (1998/April): Medicare Hospice Beneficiaries: Services and Eligibility. (DHHS Publication No. OEI-04-93-00270): June Gibbs Brown, Inspector General.
Vernig, Beth et al, (1999): Do Medicare HMOs and Medicare FFS Differ in Their Use of the Medicare Hospice Benefit, Hospice Journal, (In Press).
Volicer L. Hospice care for dementia patients. Journal of American Geriatric Society, 45(9):1147-1149.
Von Gunten CF, Martinez J, Weitzman SA, Von Roenn J. (1991, July/August): AIDS and hospice. The American Journal of Hospice & Palliative Care, 17-19.
Wagner, AM, Baker M, Campbell B, et al. (1996): Pain prevalence and pain treatments for residents of Oregon's long-term care facilities. Prepared for the state of Oregon Senior Disabled Services Division, client care monitoring unit.
Wallston KA, Burger C, Smith RA, Baugher RJ. (1988): Comparing the quality of death for hospice and non-hospice cancer patients. Medical Care, 26(2):177-182.
Wennberg JE, McAndrew-Cooper M., Eds. (1998): The Dartmouth atlas of health care in the United States. Chicago: American Hospital Publishing.
Wilkinson, AM. (1998): New Endeavors and Innovative Programs in End of Life Care. The Hospice Journal, 13(1/2):165-180.
Yates JW, Chalmer B, McKegney FP. (1980): Evaluation of patients with advanced cancer using the Karnofsky performance status. Cancer, 45(8): 2220-2224.
NOTES
-
Although health maintenance organizations may cover some outpatient drugs, this benefit varies by plan and generally is more limited than the pain medications covered under hospice.
-
The hospice benefit was established under the Tax Equity and Fiscal Responsibility Act of 1982.
-
This reference is to the four types of Medicare-certified hospice providers, not to the level of hospice care. Medicare-certified hospice providers that are not an organizational entity of a hospital, SNF, or home health agency are classified as free-standing hospice providers. Other Medicare-certified hospices are classified as either hospital-, SNF-, or home-health-agency-based providers. All Medicare certified hospice providers deliver the four different levels of hospice care.
| FIGURE 1. Number of Medicare and Non-Medicare Hospice Patients |
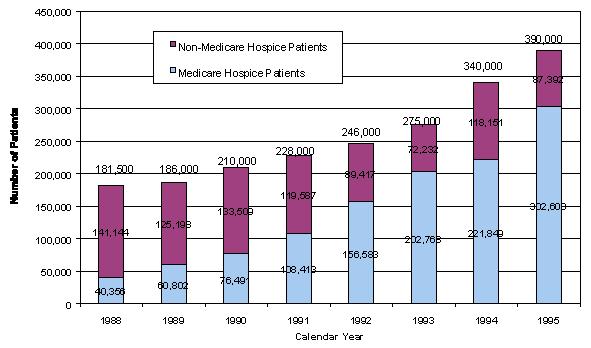 |
| Source for total hospice patients: NHO (1998a), Totals used for 1998 and 1991 represented averages between 2 years. Source for hospice Medicare beneficiaries: HCFA, BPD (10/96) from Hospice Association of America (1997) |
| FIGURE 2. Number of Medicare and Non-Medicare Certified Hospice Providers |
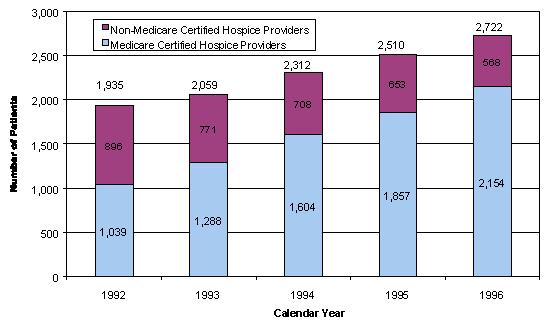 |
| Source for Total Hospice Providers in U.S.: National Hospice Organization, (1998a)Source for Total Medicare-Certified Hospices: HCFA, HSQB (12/98), from Hospice Association of America |
| FIGURE 3. Distribution of Medicare Benefit Payments by Type of Service, FY 1997 |
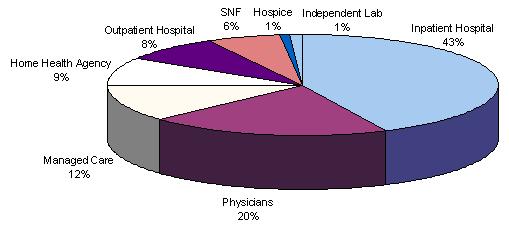 |
| SOURCE: HCFA/Office of the Actuary. In: A Profile of Medicare: Chart Book (HCFA, 1998) |
| FIGURE 4. Comparison of Rate of Growth to Projected Rate of Growth in Medicare Benefit Payments per Enrollee by Type of Service |
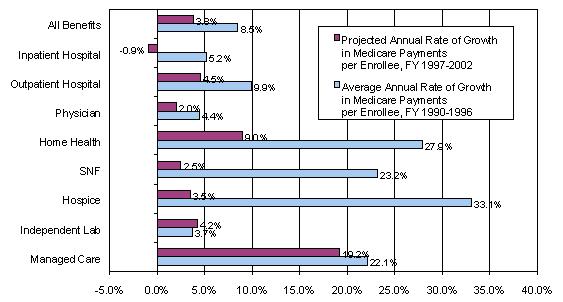 |
| SOURCE: A Profile of Medicare: Chart Book (HCFA, 1998). Based on estimates of incurred benefits from the 1998 Annual Report of the Board of Trustees of the Federal Hospital Insurance Trust Fund and Federal Supplementary Medical Insurance Trust Fund. |
| TABLE 1. Balanced Budget Act of 1997: Provisions Related to Hospice Services | ||
| Section | Provision | Effective Date |
| 4441.Payments for Hospice Services | The hospice prospective payment rates will be updated by the hospital market basket minus 1 percentage point for each of the fiscal years 1998 through 2002. In addition, the hospices will be required to submit such data as the Secretary requires on the costs of the care they provide for each fiscal year beginning with fiscal year 1999. | as stated |
| 4442.Payment for Home Hospice Care Based on Location of Service | Hospice services will be paid based on the location where the service is provided, rather than where the service is billed (typically the urban location of the hospice agency.) | for cost reporting periods beginning on or after 10/1/97 |
| 4443.Hospice Care Benefits Period | Restructures the hospice benefit periods to include two 90-day periods, followed by an unlimited number of 60-day periods. The medical director or physician member of the hospice interdisciplinary team would have to re-certify that the beneficiary is terminally ill at the beginning of each benefit period. | upon enactment 8/5/97 |
| 4444.Other Items and Services included in Hospice Care | Amends the definition of hospice care to include the existing enumerated services as well as any other item or service which is specified in a patient's plan of care and for which Medicare may pay. (Existing services include nursing care: physical, occupational and speech therapy; medical social services; home health aide and homemaker services; medical supplies and appliances; physician services, short-term patient care; and counseling.) | for items and services furnished on or after April 1, 1998 |
| 4445.Contracting with Independent Physicians or Physician Groups for Hospice Services | Deletes physician services from a hospice's core services and allows hospices to upon enactment: employ or contract with physicians for their services. (Currently, hospices are required to provide directly for certain core services, including physician services.) | 8/5/97 |
| 4446.Waiver of Certain Staffing Requirements for Hospice Care Programs in Non-urbanized Areas | The Secretary is allowed to waive requirements with regard to hospices upon enactment: being required to provide certain services, as long as they are not located in urbanized areas and can demonstrate to the satisfaction of the Secretary that they have been unable, despite diligent efforts, to recruit appropriate personnel. For these hospices, the Secretary could waive (1) the requirement that dietary counseling be provided directly by the hospice and (2) the requirement that physical or occupational therapy or speech-language pathology services be made available on a 24-hour basis to the extent necessary to meet the needs of the patient. | upon enactment: 8/5/97 |
| 4447.Limitation on Liability of Beneficiaries for Certain Hospice Coverage Denials | Medicare's limitation of liability protection is extended to determinations that an individual is not terminally ill. (Limitation on liability: Medicare provides financial relief to beneficiaries and providers for certain services for which payment would otherwise be denied, if the beneficiary or provider did not know, and could not reasonably have known, that services would not be covered.) | upon enactment: 8/5/97 |
| 4448.Extending the Period for Physician Certification of an Individual's Terminal Illness | The specific, statutory time frame for completion of physicians' certification for admission to a hospice are eliminated. Physicians now will be required to certify that a beneficiary is terminally ill at the beginning of the initial 90-day period. | upon enactment: 8/5/97 |
| TABLE 2. Hospice Reimbursement Rates From 11/01/83 - 9/30/98 | |||||||||||||
| Level of Care | 11/01/83 12/31/84 | 01/01/85 03/31/86 | 04/01/86 12/31/89 | 01/01/90 09/30/90 | ** 10/01/90 | 10/01/91 09/30/92 | 10/01/92 09/30/93 | 10/01/93 09/30/94 | 10/01/94 09/30/95 | 10/01/95 09/30/96 | 10/01/96 09/30/97 | 10/01/97 09/30/98 | 10/01/98 09/30/99 |
| Routine | $46.25 | 53.17 | 63.17 | 75.80 | 79.74 | 83.25 | 86.66 | 88.65 | 90.51 | 92.32 | 94.17 | 95.77 | 97.11 |
| Continuous | $358.67 | 358.67 | 368.67 | 442.40 | 465.40 | 485.88 | 505.88 | 517.43 | 528.30 | 538.87 | 549.65 | 558.99 | 566.82 |
| Inpatient Respite | $55.33 | 55.33 | 65.33 | 78.40 | 82.48 | 86.11 | 89.64 | 91.70 | 93.63 | 95.50 | 97.41 | 99.07 | 100.46 |
| General Inpatient | $271.00 | 271.00 | 281.00 | 337.20 | 354.73 | 370.34 | 385.52 | 394.39 | 402.67 | 410.72 | 418.93 | 426.05 | 432.01 |
| ** NOTE: These payment rates were effective for services provided on or after October 1, 1990 through October 20, 1990 and January 1, 1991 through September 1, 1991. Hospice payments for the period beginning on October 21, 1990 through December 31, 1990 are the same as the 1990 rates. The return to the FY 1990 rate for the period October 21 through December 31 is the result of the freeze in Part A payments provided in Section 4007 of the Omnibus Budget Reconciliation Act of 1990. | |||||||||||||
| TABLE 3. Medicare Hospice Payments and Use by Level of Care, 1997 | |||||
| Medicare Use and Expenditures | Total Use | Levels of Care | |||
| Routine Home Care | Continuous Home Care | Inpatient Respite | General Inpatient | ||
| Use Levels (In 1,000s)a | N.A. | 18,190 | 1,191 | 48 | 471 |
| Medicare ExpenditureIn Millions (In percent) | $2,025 (100 percent) | $1,770 (87 percent) | $29 (1 percent) | $4.8 (>1 percent) | $210 (11 percent) |
SOURCE: Unpublished data from HCFA, 1998a
| |||||
| TABLE 4. Medicare Hospice Payments and Use by Type of Hospice Affiliation, 1997 | |||||
| Medicare Use and Expenditures | Total | Type of Hospice Affiliation | |||
| Free-standing | Hospital Based | SNF Based | HHA Based | ||
| Number of Users | 374,723 | 193,765 | 68,688 | 2,547 | 109,723 |
| Medicare ExpendituresIn Millions (In percent) | $2,025 (100 percent) | $1,123 (55 percent) | $345 (17 percent) | $13 (1 percent) | $543 (27 percent) |
| Average Dollars per Beneficiary | $5,402 | $5,796 | $5,026 | $5,079 | $4,949 |
| Average Days per Beneficiary | 50 | 53 | 48 | 40 | 46 |
| SOURCE: Unpublished data from HCFA, 1998a. | |||||
| TABLE 5. Demographics of Hospice Beneficiaries by Type of Hospice Affiliation, 1987-1990 | ||||||||||
| Beneficiary Characteristics | All Providers | Type of Hospice Affiliation | ||||||||
| Hospital | SNF | HHA | Free-standing | |||||||
| Number | Percent | Number | Percent | Number | Percent | Number | Percent | Number | Percent | |
| Sex | ||||||||||
| Female | 5,545 | 47 | 958 | 47 | 487 | 53 | 2,168 | 49 | 2,195 | 45 |
| Age Entered Hospice | ||||||||||
| Mean | 75.6 years | 75.6 years | 75.2 years | 75.6 years | 75.6 years | |||||
| (SD) | (8.5) | (8.6) | (8.4) | (8.6) | (8.6) | |||||
| Race | ||||||||||
| White | 10,553 | 90 | 1,751 | 87 | 308 | 87 | 3,974 | 90 | 4,441 | 91 |
| Black | 776 | 7 | 169 | 8 | 38 | 11 | 296 | 7 | 269 | 6 |
| Other | 179 | 1 | 49 | 2 | 3 | 1 | 60 | 1 | 66 | 1 |
| Unknown | 242 | 2 | 50 | 3 | 5 | 1 | 84 | 2 | 102 | 2 |
| Diagnoses | ||||||||||
| Cancer: | ||||||||||
| Colon | 2,596 | 24 | 437 | 24 | 100 | 30 | 962 | 24 | 1,052 | 23 |
| Lung | 2,551 | 23 | 437 | 24 | 70 | 21 | 937 | 23 | 1,086 | 24 |
| Breast | 644 | 6 | 104 | 6 | 27 | 8 | 254 | 6 | 254 | 6 |
| Reproductive | 1,163 | 11 | 207 | 11 | 45 | 13 | 411 | 10 | 491 | 11 |
| Urinary | 420 | 4 | 64 | 3 | 11 | 3 | 147 | 4 | 194 | 4 |
| Leukemia | 141 | 1 | 23 | 1 | 3 | 1 | 52 | 1 | 62 | 1 |
| Other | 1,643 | 15 | 292 | 16 | 36 | 11 | 641 | 16 | 664 | 15 |
| Non-Cancer | 1,699 | 16 | 278 | 15 | 44 | 13 | 663 | 16 | 702 | 16 |
| SOURCE: From Banaszak-Holl & Mor, 1996. | ||||||||||
| TABLE 6. Characteristics of Discharged Hospice Patients in the 1994 and 1996 National Home and Hospice Care Surveys | ||||
| Beneficiary Characteristics | 1993-1994 Discharges(n=328,000) | 1995-1996 Discharges(n=393,200) | ||
| Number | Percent | Number | Percent | |
| Sex | ||||
| Female | 156,500 | 47.7 | 195,500 | 49.7 |
| Race | ||||
| White | 260,400 | 79.4 | 310,000 | 78.9 |
| Black | 24,000 | 7.3 | 43,900 | 11.2 |
| Other or unknown | 43,600 | 13.3 | 39,100 | 9.9 |
| Age | ||||
| Under 45 years | 18,600 | 5.7 | 31,700 | 8.1 |
| 45-64 years | 69,900 | 21.3 | 89,400 | 22.7 |
| 65 years and older | 239,100 | 72.9 | 265,200 | 67.5 |
| Marital Status | ||||
| Married | 160,300 | 48.9 | 190,300 | 48.4 |
| Widowed | 97,300 | 29.7 | 115,600 | 29.4 |
| Not married | 48,300 | 14.7 | 62,000 | 15.8 |
| Unknown | 22,2002 | 6.82 | 25,300 | 6.4 |
| Diagnoses (at admission)1 | ||||
| Neoplams (malignant) | 220,900 | 67.3 | 274,000 | 69.7 2 |
| Diseases of Circulatory System | 36,100 | 11.0 | 37,600 | 9.6 |
| Diseases of Respiratory System | 7,300 | 2.2 | 20,500 | 5.2 |
| Diseases of Nervous System & Sense Organs | 8,3002 | 2.52 | 12,5002 | 3.22 |
| Diseases of GU System | 10,7002 | 3.32 | 9,3002 | 2.42 |
| Infectious & Parasitic Diseases | 9,500 | 2.9 | 15,2002 | 3.92 |
SOURCE: National Center for Health Statistics, 1996 & 1998
| ||||
| TABLE 7. Number of Medicare-Certified Hospices by Type of Provider Affiliation | |||||
| Year | HHA | HOSP | SNF | FSTG | TOTAL |
| 1984 | n/a | n/a | n/a | n/a | 31 |
| 1985 | n/a | n/a | n/a | n/a | 158 |
| 1986 | 113 | 54 | 10 | 68 | 245 |
| 1987 | 155 | 101 | 11 | 122 | 389 |
| 1988 | 213 | 138 | 11 | 191 | 553 |
| 1989 | 286 | 182 | 13 | 220 | 701 |
| 1990 | 313 | 221 | 12 | 260 | 806 |
| 1991 | 325 | 282 | 10 | 394 | 1011 |
| 1992 | 334 | 291 | 10 | 404 | 1039 |
| 1993 | 438 | 341 | 10 | 499 | 1288 |
| 1994 | 583 | 401 | 12 | 608 | 1604 |
| 1995 | 699 | 460 | 19 | 679 | 1857 |
| 19961 | 815 | 526 | 22 | 791 | 2154 |
SOURCE: Hospice Association of America, 1997 based on HCFA data.
| |||||
| TABLE 8. Lengths of Stay by Hospice Provider Affiliation, 1987-1990 | ||||||||
| Length of Coverage1 | Hospital | SNF | HHA | Free-standing | ||||
| Number | Percent | Number | Percent | Number | Percent | Number | Percent | |
| 15 days | 821 | 41.4 | 163 | 46.4 | 1,845 | 42.3 | 1,915 | 39.7 |
| 15-29 days | 349 | 17.6 | 63 | 17.9 | 805 | 18.5 | 849 | 17.6 |
| 30-89 days | 520 | 26.2 | 86 | 24.5 | 1,060 | 24.3 | 1,269 | 26.3 |
| 90-149 days | 162 | 8.2 | 18 | 5.1 | 340 | 7.8 | 383 | 7.9 |
| 150-209 days | 76 | 3.8 | 10 | 2.8 | 189 | 4.3 | 237 | 4.9 |
| 210+ days | 57 | 2.9 | 11 | 3.1 | 118 | 2.7 | 171 | 3.5 |
| Mean Length of Coverage (in days) | 45.1 | 39.5 | 45.3 | 51.5 | ||||
| (SD) | (73.0) | (68.4) | (75.4) | (90.9) | ||||
| Median Length of Coverage (in days) | 21.0 | 17.0 | 20.0 | 22.0 | ||||
| SOURCE: Banaszak-Hall and Mor, 1996Statistically significant at p.05 | ||||||||
| TABLE 9. Average Number of Visits per Week by Type of Service | ||||
| Service | NHO Staffing Ratios1 | Nursing Home Patients2 | Home Patients3 | Percent Difference4 |
| Nurse | 2.0 | 1.5 | 2.7 | -.44 percent |
| Aide | 1.5 | 1.3 | 2.5 | -.48 percent |
| Social Worker | .8 | .42 | .53 | -.21 percent |
| Spiritual/Pastoral | .4 | .28 | .16 | 75 percent |
SOURCE: USDHHS, Office of the Inspector General, 1997
| ||||
| TABLE 10. Adjusted1 Medicare Reimbursement Saved per Dollar of Hospice Expenditure, by Length of Enrollment and Month3 | |||||||
| Enrollment Month | Length of Enrollment2 | ||||||
| 1 Month | 30-59 Days | 60-89 Days | 90-119 Days | 120-149 Days | 150-179 Days | 180-209 Days | |
| Last month of life | 1.32* | 1.49* | 1.48* | 1.42* | 1.50* | 0.93 | 3.77* |
| Month 2 | 0.82* | 0.91 | 0.88 | 0.88 | 0.67 | 1.35 | |
| Month 3 | 0.73* | 0.72 | 0.71 | 0.61 | 0.86 | ||
| Month 4 | 0.84 | 0.71 | 0.46 | 0.73 | |||
| Month 5 | 0.83 | 0.65 | 0.61 | ||||
| Month 6 | 0.92 | 0.56 | |||||
| Month 7 | 0.75 | ||||||
| Total for all months after hospice entry | 01.32* | 1.14* | 1.04 | 0.99 | 0.96 | 0.72* | 1.06* |
SOURCE: Kidder, 1992; AAI/HCFA Hospice Benefit Monthly File.* Ratio is significantly different from 1 at p.10 level of significance.
| |||||||
| TABLE 11. Adjusted Medicare Part A Reimbursement Saved per Dollar of Hospice Expenditures, by Length of Enrollment and Month, 1992* | |||||||
| Enrollment Month | Length of Enrollment1 | ||||||
| 1 Month | 30-59 Days | 60-89 Days | 90-119 Days | 120-149 Days | 150-179 Days | 180-209 Days | |
| Last month of life | 1.65 | 2.13 | 2.08 | 1.96 | 1.98 | 1.89 | 0.86 |
| Month 2 | 0.91 | 1.07 | 1.00 | 0.91 | 0.90 | 0.95 | |
| Month 3 | 0.88 | 0.76 | 0.69 | 0.68 | 0.66 | ||
| Month 4 | 0.62 | 0.62 | 0.55 | 0.52 | |||
| Month 5 | 0.57 | 0.51 | 0.47 | ||||
| Month 6 | 0.48 | 0.46 | |||||
| Month 7 | 0.45 | ||||||
| Total for all months after hospice entry | 1.65 | 1.48 | 1.29 | 1.09 | 0.98 | 0.86 | 0.82 |
SOURCE: Lewin-VHI Analysis of 1991-1992 Medicare Part A claims from the National Claims History File.* Reprinted with permission of the National Hospice Organization, all rights reserved.
| |||||||
| TABLE 12. Adjusted Medicare Part A and Part B Reimbursement Saved per Dollar of Hospice Expenditures, by Length of Enrollment and Month, 1992* | |||||||
| Enrollment Month | Length of Enrollment1 | ||||||
| 1 Month | 30-59 Days | 60-89 Days | 90-119 Days | 120-149 Days | 150-179 Days | 180-209 Days | |
| Last month of life | 1.68 | 2.46 | 2.39 | 2.25 | 2.34 | 2.17 | 1.06 |
| Month 2 | 1.35 | 1.22 | 1.17 | 1.16 | 1.22 | ||
| Month 3 | 0.84 | 0.99 | 0.91 | 0.91 | 0.89 | ||
| Month 4 | 0.72 | 0.83 | 0.76 | 0.72 | |||
| Month 5 | 0.67 | 0.70 | 0.67 | ||||
| Month 6 | 0.57 | 0.65 | |||||
| Month 7 | 0.56 | ||||||
| Total for all months after hospice entry | 1.68 | 1.64 | 1.49 | 1.29 | 1.19 | 1.06 | 1.03 |
SOURCE: Lewin-VHI Analysis of 1991-1992 Medicare Part A and Part B claims from the National Claims History File.* Reprinted with permission of the National Hospice Organization, all rights reserved.
| |||||||
TABLE OF CONTENTS
APPENDIX A. Literature Review Methodology
APPENDIX B. National Hospice Organization's Sample Contract
APPENDIX C. Medical Guidelines for Determining Prognosis in Selected Non-Cancer Diseases and Hospice Enrollment Criteria for End-Stage Dementia Patients
APPENDIX D. Wisconsin State Guidelines for Medicare Hospice Care Provision in the Nursing Home
APPENDIX E. Acknowledgement List
APPENDIX A. LITERATURE REVIEW METHODOLOGY
OVERVIEW
The purpose of the literature review was to update Mor and Allen's 1987 hospice review (Mor & Allen, 1987) by identifying subsequent completed and ongoing hospice research, and by documenting research findings relating to the utilization, cost and quality of hospice care. A focus of the review was the Medicare hospice benefit in the nursing facility. An extensive search was conducted utilizing online databases and Internet resources. Additionally, unpublished work was solicited from leading health services researchers. The complete methodology including search strategies and subsequent results are detailed below.
SEARCHES CONDUCTED
Initial online research databases searched for this review included Medline (medical research), Psychlit (psychological research), Sociofile (sociological research), Econlit (economic research) and ERIC (reports). First, a search using the key word "hospice" was employed yielding nearly 3,000 records. This search was refined using the following set of key words in addition to the key word hospice: Medicare, Medicaid, cost, utilization, expenditure, quality of care, quality of life, outcome, grief or bereavement, depression, pain or symptom control, patient or family satisfaction, and. All abstracts found with these key words were reviewed and articles were selected based on their relevance to the goals of the current project and the following criteria: (1) research published after Mor and Allen's 1987 review; (2) research conducted in the U.S.; (3) analytic methods were employed.
The National Hospice Organization (NHO) also provided us with a 1994 bibliography of all identified literature from a variety of databases. Bibliographies from databases that were not initially searched were examined. These databases included Ageline, Cancerlit, Family Resources, CINAHL, Health Periodicals, Religion Index, Sociological Abstracts and Dissertation Abstracts. Finally, a HealthSTAR search (policy and administrative issues in health care) was conducted using hospice and economics cost savings, health expenditures, health care costs, reimbursement mechanisms and cost-benefit analysis.
In addition to online database searches, Internet searches were performed. First, searches were conducted in government web sites for relevant reports, publications, research or demonstration projects. These sites included the Health Care Financing Administration and the Office of the Inspector General. Second, research funded from the following agencies were searched using "hospice" as a keyword: National Institute of Health (NIH), Agency for Health Care Policy and Research (AHCPR), The Robert Wood Johnson Foundation Last Act Initiative, and the Open Society's Project on Death in America Campaign. When relevant research projects were found, the principal investigator was contacted and asked to describe the purpose, current status and findings of the project if available.
Finally, after reviewing the current abstracts and also the previous references reported in Mor and Allen's review, a list of 20 leading health services researchers in hospice care were identified. These researchers were contacted by letter and asked to provide information about any current research (funded or not funded) that they were pursuing relating to hospice care.
RESULTS OF SEARCHES
The results of the online database search are shown below ( Table A.1). Because no program was used to sort the abstracts and identify duplicates, the number of abstracts identified for each category may be an overestimate. The limited number of articles identified for inclusion in the literature review was not surprising given the criterion employed. Indeed, in their final bibliography, Mor and Allen reported only 13% of their total bibliography contained analytic papers and only 7% were based on outcomes of hospice care. Additional references (10) were found in the NHO bibliography and 3 were subsequently used in the review. Similarly, HealthSTAR search yielded an additional meeting abstract and one article.
| Key Word(s) | Hits | Articles Reviewed | Met Criteria |
|---|---|---|---|
| NOTE: Online databases included Medline, Psychlit, Sociofile, Econlit and ERIC. Some "hits" may be duplicated due to the use of multiple databases. | |||
| Hospice and | 2,915 | N/A | N/A |
| Cost | 155 | 16 | 11 |
| Utilization | 124 | 11 | 8 |
| Expenditures | 14 | 2 | 1 |
| Outcome | 91 | 2 | 2 |
| Quality of Care | 127 | 7 | 5 |
| Medicare | 155 | 36 | 23 |
| Medicaid | 22 | 9 | 6 |
| 114 | 5 | 5 | |
| TOTAL | 802 | 88 | 61 |
Internet searches provided varied materials including reports, background information and funded grants. The numbers of identified grants are shown on Table A.2 below. Under the Department of Health and Human Services, the Office of the Inspector General search yielded information on three relevant audits that were conducted under Operation Restore Trust. These audits and their findings were included and discussed in the literature review.
| Funding Agency | Reviewed | Met Criteria for Inclusion |
|---|---|---|
| National Institute of Health | 72 | 1 |
| Agency for Health Care Policy & Research | 10 | 3 |
| The Robert Wood Johnson Foundation Last Act Initiative | 27 | 3 |
| Open Society's Project on Death in America Campaign | 81 | 4 |
Finally, of the 20 health researchers that were contacted by letter, 10 return letters were received. Of these, 2 researchers gave us additional information to include in the review on recent research they were conducting.
APPENDIX B. NATIONAL HOSPICE ORGANIZATION'S SAMPLE CONTRACT1
INTRODUCTION
Attached you will find a sample nursing home contract. Please be aware that this document is meant to be utilized after your organization has made the decision to deliver hospice care in nursing homes.
BACKGROUND INFORMATION
There are currently more than 1.5 million persons living in nursing homes across the United States. One in four women age 85 or older lives in a nursing home, compared to one in seven men in the same age group. Of Americans age 65 and older, 43% will spend some time in a nursing home before death.
In the past few years, increasing attention has been focused on establishing relationships between hospices and nursing facilities. The Omnibus Reconciliation Act (OBRA) of 1986 first established that hospice care could be provided in a nursing home under the routine home care level. With the passage of OBRA '89, the financial disincentives were removed. The regulatory environment improved with OBRA '90, known as the Nursing Home Reform Act, when nursing homes were required to meet standards similar in philosophy to hospice.
As these changes have occurred, the National Hospice Organization has received an increased number of requests for a sample nursing home contract. Medicaid requires that a contract is in place before hospice services are provided. In response to the needs of its membership, NHO sought legal assistance in developing a generic contract. Providers are advised to utilize this tool as a guide and to make modifications in relation to state laws and their individualized needs under the direction of local legal counsel.
FACILITATING WORKING TOGETHER
Although the pieces have now fallen into place from a financial, regulatory, and legal standpoint, establishing a mutually beneficial relationship is still difficult. Procedures need to be agreed upon for the following areas:
- Obtaining and recording physician orders
- Maintenance of medical records
- Scheduling and coordinating hospice visits
- Defining role of each hospice team member
- Developing and updating a coordinated Plan of Care
- Referral of patients
- Provision of continuous care and general in-patient care
- Notifying hospice of changes in a patient's condition
The above list of issues to be considered in negotiating relationships with nursing facilities is not all inclusive, but rather a sample of the types of issues to be examined.
The intent of this guide to implementing a nursing facility contract was to focus the hospice provider on issues of primary concern. Additional important considerations are your state nursing home regulations and, where applicable, the hospice licensing law.
There are many hospices throughout the United States that have successful programs in place and are willing to provide technical assistance. It is through the sharing of experiences that we will be able to refine the integration of hospice services within this health care setting.
NATIONAL HOSPICE ORGANIZATION ("NHO")
SAMPLE
SERVICE AGREEMENT BY AND BETWEEN A HOSPICE AND A NURSING FACILITY*
NOTICE
THIS FORM OF AGREEMENT IS MADE AVAILABLE TO NHO MEMBERS SOLELY AS AN ILLUSTRATION AND EXAMPLE OF A SERVICE AGREEMENT BETWEEN A HOSPICE AND A NURSING FACILITY. NO REPRESENTATIONS OR WARRANTIES ARE MADE BY NHO OR BY ANY NHO REPRESENTATIVES OR AFFILIATES AS TO THE APPROPRIATENESS, ACCURACY, OR COMPLETENESS OF THE TERMS AND CONDITIONS INCLUDED IN THIS FORM OF AGREEMENT. THIS FORM OF AGREEMENT AND THE TERMS AND CONDITIONS CONTAINED HEREIN MAY NOT BE SUITABLE DOCUMENTATION FOR EVERY CONTRACTUAL ARRANGEMENT BETWEEN A HOSPICE AND A NURSING FACILITY. SHOULD AN NHO MEMBER DESIRE TO UTILIZE THIS FORM OF AGREEMENT, IN WHOLE OR IN PART, IN CONTRACTING WITH ANY NURSING FACILITY, REVIEW OF THIS FORM OF AGREEMENT AND APPLICABLE FEDERAL AND STATE LAW AND REGULATIONS BY SUCH MEMBER'S LEGAL COUNSEL IS ADVISED. PROVISIONS OF THIS FORM OF AGREEMENT THEN SHOULD BE MODIFIED, BY OR IN CONSULTATION WITH LEGAL COUNSEL, TO REFLECT SUCH REVIEW AND THE PARTICULAR CIRCUMSTANCES AND NEEDS OF THE NHO MEMBER.
*This service agreement incorporates provisions of the nursing facility regulations that went into effect October 1, 1990.
Table of Contents
I. Recitals
II. Definitions
III. Services to Be Provided by Hospice
IV. Services to Be Provided by Nursing Facility
V. Records
VI. Designation of Liaison; Administrative Appeals
VII. Representations, Warranties and Covenants of Hospice
VIII. Representations, Warranties and Covenants of Nursing Facility
IX. Quality Assurance
X. Confidentiality
XI. Use of Name or Marks
XII. Reimbursement
XIII. Insurance and Indemnification
XIV. Term and Termination
XV. General Provisions
THIS AGREEMENT (the "Agreement") is made and entered into this ___day of _______, 19__, by and between [ full legal name of hospice], a [ insert state of incorporation] corporation (" Hospice") and [ full legal name of nursing facility], a [ insert state of incorporation] corporation (" Nursing Facility").
1.1 Hospice is a patient-and family-centered program engaged in the provision of interdisciplinary services for the palliation and management of terminal illness.
1.2 Nursing Facility is skilled and experienced in the operation of a nursing facility and in the provision of long term care services to its residents, including certain assistance with activities of daily living. Nursing Facility is certified to participate in the Medicaid program and has established policies and protocols for the care of terminally ill patients consistent with those of Hospice.
1.3 The parties contemplate that from time to time individuals residing in Nursing Facility will need Hospice Services as defined in Section 2.6, and individuals previously accepted into Hospice will need care in Nursing Facility. Hospice and Nursing Facility desire by entering into this Agreement to make it possible for individuals with terminal illness to receive needed Hospice Services in conjunction with Nursing Facility Services (as defined in Section 2.10).
2.1 " Attending Physician" means a doctor of medicine or osteopathy, duly licensed under applicable state and local law and regulations, who, upon the election of Hospice Services, is identified by a Hospice Patient (or such patient's legal representative) as having the most significant role in the determination and delivery of such Hospice Patient's medical care.
2.2 " Effective Date" means the date of execution of this Agreement.
2.3 " HCFA" means the Health Care Financing Administration.
2.4 " Hospice Patient" means an individual who elects, directly or through such individual's legal representative, to receive Hospice Services and is accepted by Hospice to receive Hospice Services.
2.5 " Hospice Physician" means a duly licensed doctor of medicine or osteopathy employed by Hospice to render physician services to each Hospice Patient, as necessary, in accordance with the applicable Plan of Care.
2.6 " Hospice Services" means those services provided to a Hospice Patient for the palliation and management of such Hospice Patient's terminal illness, either directly or under arrangement by Hospice, as specified in the Plan of Care. Hospice Services include nursing care and services by or under the supervision of a registered nurse; medical social services provided by a qualified social worker under the direction of a physician; physician services to the extent that these services are not provided by the Attending Physician; counseling services (including bereavement, dietary and spiritual counseling); physical therapy, occupational therapy and speech-language pathology services; home health aide/homemaker services; medical supplies; drugs and biologicals; use of medical appliances; and inpatient care when needed for pain control, symptom management and respite purposes.
2.7 " Interdisciplinary Group" means the Attending Physician and certain Hospice employees which employees shall include, without limitation, the following individuals: (a) a doctor of medicine or osteopathy, (b) a registered nurse, (c) a social worker, and (d) a pastoral or other counselor.
2.8 " Medicaid Eligible Residential Hospice Patient" means a Residential Hospice Patient who either (a) is eligible for Medicaid benefits in a state which has a hospice benefit and who has elected to receive the state's Medicaid hospice benefit or (b) is eligible for both Medicaid and Medicare Part A benefits and who has elected the Medicare hospice benefit.
2.9 " Medicare Eligible Residential Hospice Patient" means a Residential Hospice Patient who is eligible for Medicare Part A benefits and who has elected to receive the Medicare hospice benefit.
2.10 " Nursing Facility Services" means collectively Nursing Facility Room and Board Services and Other Nursing Facility Services.
2.11 " Nursing Facility Room and Board Services" means those personal care services provided by Nursing Facility as specified in the Plan of Care for a Residential Hospice Patient, including, but not limited to, providing food (including individualized requests); assisting in activities of daily living, socializing activities, and in the administration of medicine; providing and maintaining the cleanliness of the Residential Hospice Patient's room; supervising and assisting in the use of any durable medical equipment and therapies included in the Plan of Care; providing laundry and personal care supplies; and providing the usual and customary room furnishings provided to Nursing Facility Residents, including, but not limited to, beds, linens, lamps, and dressers.
2.12 " Other Nursing Facility Services" means all items and services provided by Nursing Facility which are not related to treatment of the Residential Hospice Patient's terminal illness but specified in the Plan of Care.
2.13 " Plan of Care" means a written care plan established, maintained, reviewed and modified, if necessary, at intervals established by the Interdisciplinary Group, which includes (a) an assessment of each Hospice Patient's needs, (b) an identification of the Hospice Services, including management of discomfort and symptom relief, needed to meet such Hospice Patient's needs and the related needs of the Hospice Patient's family, (c) details concerning the scope and frequency of such Hospice Services, and (d) details concerning the Nursing Facility Services to be provided to the Hospice Patient. The Hospice and Nursing Facility will jointly develop and agree upon a coordinated Plan of Care which is consistent with the hospice philosophy and is responsive to the unique needs of the Residential Hospice Patient and his/her expressed desire for hospice care.
2.14 " Private Pay Residential Hospice Patient" means a Residential Hospice Patient who is not eligible for the Medicare hospice benefit or the Medicaid hospice benefit or, if so eligible, has revoked or elected not to receive the Medicare hospice benefit and/or the Medicaid hospice benefit, as the case may be.
2.15 " Purchased Hospice Services" means those Hospice Services specified in Exhibit B that Hospice has contracted with Nursing Facility to provide.
2.16 " Residential Hospice Care Day" means a day on which a Residential Hospice Patient receives Nursing Facility Room and Board Services.
2.17 " Residential Hospice Patient" means a Hospice Patient who resides in Nursing Facility.
2.18 " Uncovered Items and Services" means those services provided by Nursing Facility which are not Hospice Services, Nursing Facility Room and Board Services or Other Nursing Facility Services, including, but not limited to, telephone, guest trays, and television hookup.
III. SERVICES TO BE PROVIDED BY HOSPICE.
3.1 Admission to Hospice Program.
-
If a resident of Nursing Facility requests the provision of Hospice Services, Hospice shall perform an assessment of such resident and shall notify the Nursing Facility, either orally or in writing, whether such resident is authorized for admission as a Residential Hospice Patient. Hospice shall maintain adequate records of each authorization of Hospice admission.
-
On or prior to the execution of this Agreement, Hospice will provide Nursing Facility with its current criteria for admission. Hospice will promptly provide Nursing Facility with any modification to these criteria.
3.2 Design and Maintenance of Plan of Care.
-
Nursing Facility Residents. In accordance with applicable Federal and state laws and regulations, Hospice shall coordinate with Nursing Facility to develop a Plan of Care for each new Residential Hospice Patient. Hospice shall furnish Nursing Facility with a copy of the Plan of Care.
-
Non-residential Hospice Patients. Promptly upon admission of Hospice Patient, who has not been residing in a nursing home, to the Nursing Facility and consent of the Hospice Patient (or his/her legal representative), Hospice will furnish Nursing Facility with a copy of the then-current Hospice Plan of Care. In coordination with the Nursing Facility, Hospice shall promptly modify the Plan of Care, as necessary, to accommodate Hospice Patient's change in residence.
-
Modifications. At intervals established by the Interdisciplinary Group, the Interdisciplinary Group will review and modify, if necessary, the Plan of Care. The Hospice will consult and coordinate with Nursing Facility, as reasonably necessary, with respect to any modification to the Plan of Care, and will provide the Nursing Facility with any modification to the Plan of Care.
-
Monitoring. Hospice will promptly inform Nursing Facility of any identified change in the condition of a Residential Hospice Patient which requires supplementation, modification or alteration of the Plan of Care.
-
Physician Orders. All physician orders communicated to Nursing Facility on behalf of Hospice in connection with Plan of Care shall be in writing and signed by the applicable Attending Physician or Hospice Physician; provided, however, that in the case of urgent or emergency circumstances, such orders may be communicated by the Attending Physician or the Hospice Physician orally and confirmed in writing thereafter. Hospice shall maintain adequate records of all physician orders communicated in connection with the Plan of Care.
3.4 Notification of Hospice Services. Hospice shall fully inform Residential Hospice Patients of the Hospice Services to be provided by Hospice and the Nursing Facility Room and Board Services and Purchased Hospice Services, if any, to be provided by Nursing Facility.
3.5 Provision of Hospice Services. Hospice shall be available to provide Hospice Services, as required by applicable Federal and state laws and regulations, twenty-four (24) hours a day, seven (7) days a week. Hospice will provide Hospice Services to each Residential Hospice Patient in accordance with the Plan of Care for that patient.
3.6 Supervision of Hospice Plan of Care. Hospice will be responsible for the professional management of the Plan of Care, including any Purchased Hospice Services.
IV. SERVICES TO BE PROVIDED BY NURSING FACILITY.
4.1 Admission to Nursing Facility.
-
Request for Admission. In the event that a pre-existing Hospice Patient requests admission to the Nursing Facility, Nursing Facility shall admit such Hospice Patient, subject to Nursing Facility's admission policies and procedures and the availability of beds. Nursing Facility shall notify Hospice, either orally or in writing, whether such Hospice Patient is authorized for admission as a Residential Hospice Patient. Nursing Facility shall maintain adequate records of all such authorizations of admission.
-
Admission Policies. On or prior to the execution of this Agreement, Nursing Facility will provide Hospice with its current admission policies and procedures. Nursing Facility will promptly provide Hospice with any modification to these policies and procedures.
4.2 Notification of Nursing Facility Residents. Nursing Facility shall inform each terminally ill resident of the Nursing Facility of that resident's option to elect to receive Hospice Services, subject to such resident's meeting the Hospice's criteria for admission.
4.3 Notification of Services. Nursing Facility shall fully inform Residential Hospice Patients of the Other Nursing Facility Services and Uncovered Items and Services to be provided by Nursing Facility.
4.4 Coordination with Hospice Regarding Plan of Care.
-
Design of Plan. In accordance with applicable Federal and state laws and regulations, Nursing Facility shall coordinate with Hospice in developing a Plan of Care for each new Residential Hospice Patient.
-
Modification. The Nursing Facility will assist with periodic review and modification of the Plan of Care. Nursing Facility will consult with Hospice, as reasonably necessary, with respect to any modification of the Plan of Care.
-
Monitoring of Residential Hospice Patient. Nursing Facility shall immediately inform Hospice of any change in the condition of a Residential Hospice Patient.
4.5 Provision of Nursing Facility Services. Nursing Facility shall be available to provide Nursing Facility Room and Board Services, as necessary or as appropriate, twenty-four (24) hours a day, seven (7) days a week. Nursing Facility will provide Nursing Facility Room and Board Services and Purchased Hospice Services, if any, to each Residential Hospice Patient in accordance with the Plan of Care for that Residential Hospice Patient.
4.6 Facility Requirements.
-
Patient Room. Nursing Facility shall provide each Residential Hospice Patient with a clean, home-like room, designed and equipped for the comfort, privacy and safety of the Residential Hospice Patient and his/her personal belongings, which will accommodate visitors as contemplated by Section 4.5(b) hereof.
-
Visiting Privileges. Nursing Facility shall permit free access and unrestricted visiting privileges (including, but not limited to, visits by children of any age) on a twenty-four (24) hours a day basis, each day of the calendar year.
-
Visitor Accommodations. Nursing Facility shall provide adequate space, located conveniently to the Residential Hospice Patient, for private visiting among the Residential Hospice Patient, the Residential Hospice Patient's family members and any other visitors. Nursing Facility shall provide adequate accommodations for the Residential Hospice Patient's family members to remain with the Residential Hospice Patient up to twenty-four (24) hours a day and to permit family members privacy following the death of the Residential Hospice Patient.
-
Hospice Access to Facility. Nursing Facility shall permit employees, contractors, agents and volunteers of the Hospice free and complete access to the Nursing Facility twenty-four (24) hours per day, as necessary, to permit Hospice to counsel, treat, attend and provide services to each Residential Hospice Patient.
-
Personnel and Training. Upon Hospice's request, Nursing Facility shall cause Nursing Facility personnel who provide Nursing Facility Services to Residential Hospice Patients under this Agreement (i) to attend, at reasonable times and locations, training provided by Hospice in the care of Hospice Patients and (ii) to attend meetings and conferences of the Interdisciplinary Group. Nursing Facility personnel who provide Nursing Facility Services to Hospice Patients shall be reasonably acceptable to Hospice.
4.7 Facility Protocols. Nursing Facility shall institute, maintain and conduct administrative procedures and patient care protocols which are (a) consistent with the procedures and protocols of Hospice, including, but not limited to, Hospice protocols relating to resuscitation, nutrition and hydration, (b) in accordance with recognized professional standards of care for terminally ill patients and (c) reasonably necessary to implement the provisions of this Agreement. Upon the execution of this Agreement, Nursing Facility shall provide Hospice with Nursing Facility's established policies and protocols and shall promptly provide Hospice with any amendments or modifications thereto.
4.8 Patient Care. Nursing Facility shall provide care to each Residential Hospice Patient to keep him/her comfortable, clean and well groomed and protected from accident, injury or infection.
4.9 Patient Transfer. Nursing Facility agrees not to transfer any Residential Hospice Patient to another care setting without the prior approval of Hospice. If Nursing Facility fails to obtain the necessary prior approval, Hospice bears no financial responsibility for the costs of transfer and the costs of care provided in another setting.
5.1 Compilation of Records.
-
Preparation. Nursing Facility and Hospice shall each prepare and maintain complete and detailed clinical records concerning each Residential Hospice Patient receiving Nursing Facility Services and Hospice Services under this Agreement in accordance with prudent record-keeping procedures and as required by applicable Federal and state law and regulations and applicable Medicare and Medicaid program guidelines. Each clinical record shall completely, promptly and accurately document all services provided to, and events concerning, each Residential Hospice Patient (including evaluations, treatments, progress notes, authorizations to admission to Hospice and/or Nursing Facility and physician orders entered pursuant to this Agreement). Nursing Facility and Hospice shall cause each entry made for services provided hereunder to be signed by the person providing the services.
-
Storage. Nursing Facility and Hospice shall each retain such records for five (5) years from the date of discharge of each Residential Hospice Patient or such other time period as required by applicable state law. Each such record [shall document that the specified services are furnished in accordance with this Agreement and] shall be readily accessible and systematically organized to facilitate retrieval by either party.
5.2 Access. Subject to any required authorization by the subject Residential Hospice Patient (or his/her legal representative), Nursing Facility and Hospice shall each permit the other party or its authorized representative, upon reasonable notice, to review and make photocopies of records maintained by Nursing Facility or Hospice, as the case may be, relating to the provision of services under this Agreement, including but not limited to, the Plan of Care, medical records and records relating to billing and payment.
5.3 Inspection. To the extent required by applicable Federal or state law and regulations, Nursing Facility and Hospice and any respective agents thereof shall make available, upon written request by the Secretary of the United States Department of Health and Human Services, the Comptroller General of the United States, or any other authorized Federal or state official, or the duly authorized representative of the foregoing, their respective books, documents, and records necessary to verify the nature and extent of costs of Nursing Facility Services or Hospice Services until the expiration of four (4) years after the Nursing Facility Services or Hospice Services provided under this Agreement are furnished.
5.4 Destruction of Records. Nursing Facility and Hospice shall take reasonable precautions to safeguard records against loss, destruction, and unauthorized disclosure.
VI. DESIGNATION OF LIAISON; ADMINISTRATIVE APPEALS
6.1 Liaison. On or prior to the execution of this Agreement, Hospice and Nursing Facility shall each designate [a [number]] representative(s) to serve as liaison between them and to facilitate cooperative efforts in performance of their respective obligations under this Agreement. Thereafter, each of Hospice and Nursing Facility will promptly notify the other party of any change in its representative(s).
6.2 Resolution. Within [sixty (60)] days of execution of this Agreement, Hospice and Nursing Facility shall develop, maintain, and conduct, as necessary, clearly articulated dispute resolution procedures and shall act promptly to mediate any disputes with respect to the appropriateness of the Plan of Care, Hospice Services or Nursing Facility Room and Board Services.
VII. REPRESENTATIONS, WARRANTIES AND COVENANTS OF HOSPICE.
Hospice hereby represents, warrants and covenants to Nursing Facility as follows:
7.1 Organization. Hospice is a corporation duly organized, validly existing and in good standing under the laws of the state of [ specify state] and has all requisite corporate power to conduct its business as presently conducted. [Hospice is duly qualified to do business as a foreign corporation in the state of [ specify state].]
7.2 Authorization of this Agreement. The execution, delivery and performance of this Agreement has been duly authorized by all requisite corporate action on the part of Hospice. This Agreement has been duly executed and delivered by Hospice and constitutes a valid and binding obligation of Hospice.
7.3 Compliance. Hospice has materially complied with, and in performing this Agreement shall comply, in all material respects with all Federal, state and local laws and regulations applicable to it, its business and operations, including, without limitation (i) all applicable Federal, state and local laws and regulations relating to health and safety and (ii) all applicable Federal, state and local laws and regulations relating to hospice care.
7.4 Licensure. Hospice is duly certified as a Medicare provider under Title XVIII of the Social Security Act [and as a Medicaid provider under TitleXIX of the Social Security Act.] Hospice possesses all Federal, state and local licenses and permits material to and necessary in the conduct of its business as presently conducted. Such licenses and permits are in full force and effect, no violations are or have been recorded in respect of any such licenses or permits, and no proceeding is pending or, to the knowledge of Hospice, threatened to revoke or limit any thereof. Upon request of Nursing Facility, Hospice shall furnish true and complete copies of any of the aforementioned licenses or permits.
[7.5 No Litigation. [There is no action, suit, investigation or proceedings pending or, to the knowledge of Hospice, threatened against Hospice before any court or by or before any governmental or administrative body or arbitration board or tribunal.] Hospice shall promptly notify Nursing Facility of the commencement of any action or proceeding against Hospice with respect to any of its licenses, permits or other legal authorizations, including, but not limited to any sanctions, intermediate or otherwise, administrative or judicial fines, penalties, investigations or reports of action by Federal or state officials against Hospice pursuant to Federal or state laws or regulations.]
7.6 Insolvency. Hospice shall inform Nursing Facility in the event that any proceeding shall be instituted by or against Hospice in bankruptcy, or seeking liquidation, winding up, reorganization, protection, relief or composition of its debts under any law relating to bankruptcy, insolvency, reorganization or relief of debtors or seeking the appointment of a receiver or trustee.
7.7 Adequate Staffing and Facilities. As of the date hereof, Hospice has, and will maintain throughout the term of this Agreement, a sufficient number of medical, nursing and other staff to permit Hospice to perform its obligations hereunder. Such staff will be duly licensed, certified or registered in accordance with applicable Federal and state laws.
VIII. REPRESENTATIONS, WARRANTIES AND COVENANTS OF NURSING FACILITY.
Nursing Facility hereby represents, warrants and covenants to Hospice as follows:
8.1 Organization. Nursing Facility is a corporation duly organized, validly existing and in good standing under the laws of the state of [ specify state] and has all requisite corporate power to conduct its business as presently conducted. [Nursing Facility is duly qualified to do business as a foreign corporation in the state of [ specify state].]
8.2 Authorization of this Agreement. The execution, delivery and performance of this Agreement has been duly authorized by all requisite corporate action on the part of Nursing Facility. This Agreement has been duly executed and delivered by Nursing Facility and constitutes a valid and binding obligation of Nursing Facility.
8.3 Compliance. Nursing Facility has materially complied with, and in performing this Agreement shall comply, in all material respects with all Federal, state and local laws and regulations applicable to it, its business and operations, including, without limitation (i) all applicable Federal, state and local laws and regulations relating to health and safety and (ii) all applicable Federal, state and local laws and regulations, including, but not limited to, the Patient Self-Determination Act, relating to nursing facilities.
8.4 Licensure. Nursing Facility is duly certified as a Medicaid provider under Title XIX of the Social Security Act. Nursing Facility possesses all Federal, state and local licenses and permits material to and necessary in the conduct of its business as presently conducted. Such licenses and permits are in full force and effect, no violations are or have been recorded in respect of any such licenses or permits, and no proceeding is pending or, to the knowledge of Nursing Facility, threatened to revoke or limit any thereof. Upon request of Hospice, Nursing Facility shall furnish true and complete copies of any of the aforementioned licenses or permits.
[8.5 No Litigation. [There is no action, suit, investigation or proceedings pending or, to the knowledge of Nursing Facility, threatened against the Nursing Facility before any court or by or before any governmental or administrative body or arbitration board or tribunal.] Nursing Facility shall promptly notify Hospice of the commencement of action or proceeding against Nursing Facility with respect to any of its licenses, permits or other legal authorizations, including, but not limited to any sanctions, intermediate or otherwise, administrative or judicial fines, penalties, investigations or reports of action by Federal or state officials against Nursing Facility pursuant to Federal or state laws or regulations.]
8.6 Insolvency. Nursing Facility shall inform Hospice in the event that any proceeding shall be instituted by or against Nursing Facility in bankruptcy, or seeking liquidation, winding up, reorganization, protection, relief or composition of its debts under any law relating to bankruptcy, insolvency, reorganization or relief of debtors or seeking the appointment of a receiver or trustee.
8.7 Adequate Staffing and Facilities. Nursing Facility has, and will maintain throughout the term of this Agreement, a sufficient number of nursing and other staff who have the requisite training, skills and experience to permit Nursing Facility to perform its obligations hereunder. Such staff will be duly licensed, certified or registered in accordance with applicable Federal and state laws. Nursing Facility has, and will maintain, adequate facilities and equipment throughout the term of this Agreement to perform its obligations hereunder.
[8.8 Care of Hospice Patients. Nursing Facility has familiarized itself with the administrative, recordkeeping and personal care needs of Hospice Patients and the Nursing Facility is, and will be, fully competent and able to perform its obligations under this Agreement in accordance with recognized professional standards for the care of terminally-ill patients.]
Hospice shall develop, maintain, and conduct an ongoing, comprehensive assessment to evaluate the quality and appropriateness of Hospice Services and Nursing Facility Room and Board Services, as set forth and described in Exhibit A attached hereto and made a part hereof (" Quality Assurance Program"). Nursing Facility shall cooperate with Hospice in the conduct of the Quality Assurance Program and facilitate the administration of such program in relation to Purchased Hospice Services and Nursing Facility Room and Board Services performed by Nursing Facility. Hospice shall cooperate with Nursing Facility in the conduct of Nursing Facility's quality assessment and assurance committee as it relates to Residential Hospice Patients.
10.1 Confidentiality of Hospice Information. In the performance of its obligations under this Agreement, Hospice shall be required to disclose to Nursing Facility certain information pertaining to Hospice Patients (including, but not limited to, assessments, medical records, patient and family histories and the Hospice Plan of Care (collectively " Patient Information")) and may be required to disclose certain business or financial information of the Hospice (collectively, with the Patient Information, the " Hospice Confidential Information"). Nursing Facility agrees that it shall treat the Hospice Confidential Information with the same degree of care Nursing Facility affords to its own similar confidential information and shall not, except as specifically authorized in writing by Hospice or as otherwise required by law, reproduce any Hospice Confidential Information or disclose or provide any Hospice Confidential Information to any person.
10.2 Confidentiality of Nursing Facility Information. In the performance of its obligations under this Agreement, Nursing Facility shall be required to disclose to Hospice certain Patient Information (as defined in Section 10.1) pertaining to Nursing Facility residents (including the Plan of Care) and may be required to disclose to Hospice certain business or financial information of the Nursing Facility (collectively, with the Plan of Care and the Patient Information, the " Nursing Facility Confidential Information"). Hospice agrees that it shall treat the Nursing Facility Confidential Information with the same degree of care Hospice affords to its own similar confidential information and shall not, except as specifically authorized in writing by Nursing Facility or as otherwise required by law, reproduce any Nursing Facility Confidential Information or disclose or provide any Nursing Facility Confidential Information to any person.
XI. USE OF NAME OR MARKS. Neither Nursing Facility nor Hospice shall have the right to use the name, symbols, trademarks or service marks of the other party in advertising or promotional materials or otherwise without receiving the prior written approval of such other party; provided, that one party may use the name, symbols or marks of the other party in written materials previously approved by the other party for the purpose of informing prospective Residential Hospice Patients and Attending Physicians of the availability of the services described in this Agreement.
12.1 Medicaid Patients. Nursing Facility agrees to bill Hospice a fixed payment rate for each Residential Hospice Care Day provided to a Medicaid Eligible Residential Hospice Patient as set forth in Exhibit C and to accept such payment as payment in full for Nursing Facility Room and Board Services provided such Medicaid Eligible Residential Hospice Patient; provided, however, that Nursing Facility may bill such Medicaid Eligible Residential Hospice Patient for any items or services set forth in Section12.4. For Medicaid Eligible Residential Hospice Patients, Nursing Facility also agrees to bill Hospice for any Purchased Hospice Services provided to a Medicaid Eligible Residential Hospice Patient and to accept such payment as payment in full for such services.
12.2 Medicare Patients. Nursing Facility agrees to bill Hospice for any Purchased Hospice Services provided to a Medicare Eligible Residential Hospice Patient, as set forth in Exhibit B. Nursing Facility will accept such payment as payment in full for Purchased Hospice Services provided under this Agreement to such Medicare Eligible Residential Hospice Patient. Nursing Facility shall bill each Medicare Eligible Residential Hospice Patient (or the Medicare Eligible Residential Hospice Patient's third-party payor, if applicable), for Nursing Facility Room and Board Services provided such Patient and accept such payment as payment in full for Nursing Facility Room and Board Services.
12.3 Private Pay Residential Hospice Patients. With respect to any Private Pay Residential Hospice Patient, Nursing Facility agrees to bill [ select one: Hospice or Private Pay Residential Hospice Patient] for any Purchased Hospice Services provided to that Private Pay Residential Hospice Patient, as set forth in Exhibit B, and to accept such payment as payment in full for such Purchased Hospice Services. Nursing Facility shall bill each Private Pay Residential Hospice Patient (or the Private Pay Residential Hospice Patient's third-party payor, if applicable), for Nursing Facility Room and Board Services provided such Patient and accept such payment as payment in full for Nursing Facility Room and Board Services. Neither party shall seek reimbursement from the other in the event of default of financial obligations on the part of the Private Pay Residential Hospice Patient.
12.4 Other Services. Nursing Facility shall bill any Residential Hospice Patient (or the Residential Hospice Patient's third party payor, if any) for (a)Other Nursing Facility Services, (b)Uncovered Items and Services, and (c)care provided by Nursing Facility upon the advance written request of a Residential Hospice Patient which is not reasonable or necessary for palliation or management of terminal illness and not rendered in accordance with the applicable Plan of Care. Hospice shall bear no responsibility, obligation, or other liability to reimburse Nursing Facility for the cost of these services.
12.5 Billing. Within [thirty (30)] days after the provision of Nursing Facility Room and Board Services or Purchased Hospice Services, Nursing Facility shall submit to Hospice all bills issued pursuant to Section 12.1, 12.2 or 12.3 on forms acceptable to Hospice that include information usually provided to third party payors to verify the services and charges reflected in such billings. Hospice shall pay Nursing Facility either [(a)] within sixty (60) days after receipt of each Nursing Facility bill [or (b) if applicable, upon payment by Medicaid to Hospice, whichever is later.] Payment by Hospice in respect of such bills shall be considered final, unless adjustments are requested in writing by Nursing Facility within [thirty (30)] days of receipt of payment.
12.6 Financial Recordkeeping. Nursing Facility will keep accurate books of account and records (the " Financial Records") at its principal place of business covering all transactions relating to this Agreement. [Not more than once a year, Hospice may, at its expense, retain an independent public accountant or other auditor to review the Financial Records and prepare a detailed statement showing the charges made to Hospice by Nursing Facility.] Hospice and its duly authorized representatives, including any [such] independent public accountant or other auditor, shall have the right during regular business hours and on reasonable written notice to Nursing Facility to examine Nursing Facility's Financial Records and to make copies thereof.
XIII. INSURANCE AND INDEMNIFICATION
13.1 Nursing Facility Insurance. Nursing Facility shall obtain and maintain, at its sole cost and expense, professional liability insurance, including coverage for any acts of professional malpractice, covering Nursing Facility, its directors, officers, employees, or agents in an amount not less than $_____ per claim and $_____ in the aggregate and comprehensive general liability insurance in an amount not less than $_____ in the aggregate and shall name Hospice as an additional insured party. At the request of Hospice, Nursing Facility shall furnish to Hospice satisfactory evidence of its liability insurance coverage and shall notify Hospice thirty (30) days prior to any material change in or termination of insurance coverage.
13.2 Hospice Insurance. Hospice shall obtain and maintain, at its sole cost and expense, professional liability insurance, including coverage for any acts of professional malpractice, covering Hospice, its directors, officers, employees, volunteers, and agents in an amount not less than $_____ per claim and $_____ in the aggregate and comprehensive general liability insurance in an amount not less than $_____ in the aggregate and shall name Nursing Facility as an additional insured party. At the request of Nursing Facility, Hospice shall furnish to Nursing Facility satisfactory evidence of its liability insurance coverage and shall notify Nursing Facility thirty (30) days prior to any material change in or termination of insurance coverage.
13.3 Indemnification.
-
Nursing Facility agrees to indemnify and hold harmless and defend Hospice, its directors, officers, employees, volunteers, and agents from and against any and all claims, suits, damages, fines, penalties, liabilities and expenses (including reasonable attorney's fees and court costs) resulting from or arising out of, any claimed [willful or negligent?] act or omission by Nursing Facility or any of its directors, officers, employees, agents or volunteers pertaining to the services hereunder.
-
Hospice agrees to indemnify and hold harmless and defend Nursing Facility, its directors, officers, employees, volunteers, and agents from and against any and all claims, suits, damages, fines, penalties, liabilities and expenses (including reasonable attorney's fees and court costs) resulting from or arising out of, any claimed [willful or negligent?] act or omission by Hospice or any of its directors, officers, employees, agents, or volunteers, pertaining to the services hereunder.
-
For purposes of such indemnification, the following provisions shall apply. A person or entity entitled to be indemnified under paragraph (a) or (b) above (an " Indemnified Person") shall promptly notify the party having the obligation under this Agreement to indemnify the Indemnified Person (the " Indemnifier") with respect to any notice of a claim, threat to institute a proceeding or the commencement of an action. The Indemnifier will, if requested by the Indemnified Person, assume the defense of any litigation or proceeding for which indemnity hereunder is available, including the retention of counsel and payment of reasonable fees of such counsel, in which event, except as provided below the Indemnifier will not be responsible for any other fees or expenses of any other counsel retained by the Indemnified Person. However, if the Indemnified Person and Indemnifier reasonably conclude that the representation of both parties by the same counsel may involve a conflict due to actual or potential differing interests between them, the Indemnifier shall pay the reasonable fees of counsel for the Indemnified Person. The Indemnifier shall not be liable for any settlement of any litigation or proceeding effected without its written consent, which shall not be unreasonably withheld. If the Indemnifier assumes the defense of any litigation or proceeding, the Indemnifier will not settle such litigation or proceeding without the Indemnified Person's written consent, which shall not be unreasonably withheld.
14.1 Term of Agreement. The initial term of this Agreement shall be [one year] beginning with the Effective Date, with automatic [one year] renewals, unless sooner terminated as provided in this Article XIV of this Agreement.
14.2 Termination Without Cause. Either party may terminate this Agreement for any or no reason prior to the expiration of its term by providing at least [ninety (90)] days written notice of termination to the other party prior to the date of such termination. Such termination shall be effective without prior notice or consent of any Residential Hospice Patient, Attending Physician, or other third party.
14.3 Termination for Cause.
Either party shall have the right to terminate this Agreement for the following reasons:
-
In the event that the Nursing Facility does not provide a material portion of the Nursing Facility Room and Board Services or Purchased Hospice Services, if any, to be provided under this Agreement for a period of thirty (30) consecutive days, upon ten (10) days written notice given prior to the effective date of such termination;
-
In the event that the Hospice does not provide a material portion of the Hospice Services to be provided under this Agreement for a period of thirty (30) consecutive days, upon ten (10) days written notice given prior to the effective date of such termination;
-
If any license, certification or accreditation of a party which is material to the performance of this Agreement is suspended or revoked;
-
If any administrative or judicial fines, penalties or sanctions in excess of [$1,000] are imposed on one of the parties;
-
If one of the parties commences or has commenced against it proceedings to liquidate, wind-up, reorganize or seek protection, relief or a composition of its debts under any law relating to insolvency, reorganization or relief of debtors or seeking the appointment of a receiver or trustee;
-
If Hospice fails to develop and maintain a Plan of Care pursuant to applicable Federal, state or local law and regulations and in accordance with this Agreement;
-
If Nursing Facility fails to assist in developing and maintaining a Plan of Care pursuant to applicable Federal, state or local law and regulations and in accordance with this Agreement; or
-
If an action is prosecuted to final judgment against a party for violation of Federal or state laws or regulations.
14.4 Effect of Termination on Availability of Service.
In the event that this Agreement is terminated pursuant to Section 14.2 or 14.3, each of Nursing Facility and Hospice may negotiate separately with any former Residential Hospice Patient (or such patient's legal representative) to contract for the continuation of care. Nursing Facility agrees not to discharge any former Residential Hospice Patient until an alternative placement is found that is mutually agreeable to Nursing Facility, Hospice, and former Residential Hospice Patient.
14.5 Termination of Hospice Services by Residential Hospice Patient
-
A Residential Hospice Patient may terminate receipt of Hospice Services and/or any Nursing Facility Services provided pursuant to this Agreement by written notice, including, but not limited to, use of Hospice's revocation form, given by the Residential Hospice Patient (or his/her legal representative) to Hospice and Nursing Facility. Such termination shall be effective upon delivery of such notice to both Nursing Facility and Hospice or upon such time as specified in the written notice.
-
Termination of the receipt of Hospice Services and/or Nursing Facility Services by an individual Residential Hospice Patient shall not constitute a termination of this Agreement as a whole.
-
In the event that a Residential Hospice Patient terminates receipt of Hospice Services and Nursing Facility Services pursuant to this Agreement, each of Hospice and Nursing Facility may negotiate separately with such former Residential Hospice Patient (or such patient's legal representative) to contract for the continuation of care.
[APPLICABLE STATE OR LOCAL LAWS AND REGULATIONS MAY AFFECT THIS CONTRACT. THE NHO MEMBER'S LEGAL COUNSEL SHOULD BE CONTACTED REGARDING APPROPRIATE MODIFICATIONS.]
15.1 Notices. Except as otherwise specified herein, all notices, demands, requests, or other communications which may be or are required to be given, served, or sent by any party to any other party pursuant to this Agreement shall be in writing and shall be delivered personally, mailed by first-class, registered or certified mail, return receipt requested, postage prepaid, or transmitted by facsimile transmission, addressed as follow:
-
If to Hospice:______________________________Attention: __________Fax No.: __________
with a copy (which shall not constitute notice) to:______________________________
-
If to Nursing Facility:______________________________Attention: __________Fax No.: __________
with a copy (which shall not constitute notice) to:______________________________
Each party may designate by notice in writing a new address to which any notice, demand, request or communication may thereafter be so given, served or sent. Each notice, demand, request or communication which shall be mailed, delivered or transmitted in the manner described above shall be deemed sufficiently given, served, sent and received for all purposes at such time as it is (a) delivered personally to the addressee, (b) received in the mail by the addressee (with the return receipt, the delivery receipt or the affidavit of messenger being conclusive evidence of its receipt), (c)with respect to a facsimile transmission, the machine confirmation being deemed conclusive evidence of such delivery or (d) at such time as delivery is refused by the addressee upon presentation.
15.2 Severability. If any part of any provision of this Agreement or any other agreement, document or writing given pursuant to or in connection with this Agreement shall be invalid or unenforceable under applicable law, said part shall be ineffective to the extent of such invalidity or unenforceability only, without in any way affecting the remaining parts of said provision or the remaining provisions of said agreement.
15.3 Survival. It is the express intention and agreement of the parties hereto that Articles V, X, XI, XII, XIII, and XIV of this Agreement shall survive the termination of this Agreement for any reason and that the covenants contained in Articles VII and VIII shall survive the execution of this Agreement until they are no longer effective by their terms.
15.4 Waiver. Neither the waiver by either of the parties hereto of a breach of or a default under any of the provisions of this Agreement, nor the failure of either of the parties, on one or more occasions, to enforce any of the provisions of this Agreement or to exercise any right or privilege hereunder shall thereafter be construed as a waiver of any subsequent breach or default of a similar nature, or as a waiver of any such provisions, rights or privileges hereunder.
15.5 Binding Effect. Subject to provisions hereof restricting assignment, this Agreement shall be binding upon and shall inure to the benefit of the parties hereto and their respective successors and permitted assigns.
15.6 Non-assignability. This Agreement shall not be assignable, in whole or in part, by either party without the prior written consent of the other party hereto. If Nursing Facility is duly permitted by Hospice to assign or subcontract any obligation or obligations under this Agreement, Nursing Facility shall cause any such permitted assignee or subcontractor to agree to applicable provisions of this Agreement, including, but not limited to, Articles V, X, XI and XIII.
15.7 Limitation on Benefits of this Agreement. It is the explicit intention of the parties hereto that no person or entity other than the parties hereto is or shall be entitled to bring any action to enforce any provision of this Agreement against either of the parties hereto, and that the covenants, undertakings, and agreements set forth in this Agreement shall be solely for the benefit of, and shall be enforceable only by, the parties hereto or their respective successors and assigns as permitted hereunder.
15.8 Amendment. This Agreement shall not be amended, altered, or modified, except by an instrument in writing duly executed by the parties hereto.
15.9 Entire Agreement. This Agreement, including Exhibits A, B, and C hereto, constitutes the entire agreement between the parties hereto with respect to the subject matter hereof, and it supersedes all prior oral or written agreements, commitments or understandings with respect to the matters provided for herein.
15.10 Headings. Article and Section headings contained in this Agreement are inserted for convenience of reference only, shall not be deemed to be a part of this Agreement for any purpose, and shall not in any way define or affect the meaning, construction or scope of any of the provisions hereof.
15.11 References. Except as otherwise specified, references to Articles and Sections contained in this Agreement shall be to the correspondingly numbered Articles and Sections as set forth in this Agreement.
15.12 Governing Law. This Agreement, the rights and obligations of the parties hereto, and any claims or disputes relating thereto, shall be governed by and construed in accordance with the laws of the state of __________ (but not including the choice of law rules thereof).
IN WITNESS WHEREOF, the undersigned have duly executed this Agreement, or have caused this Agreement to be duly executed on their behalf, as of the day and year first here in above set forth.
HOSPICE: Attest: [full legal name of hospice] _______________ By: _______________ its authorized agent
NURSING FACILITY: Attest: [full legal name of nursing facility] _______________ By: _______________ its authorized agent
Exhibit A. [Hospice Quality Assurance Program to be set forth and described as Exhibit A]
Exhibit B. PURCHASED HOSPICE SERVICES [Service/Charge]
Exhibit C. [Reimbursement Agreements to be set forth as Exhibit C]
APPENDIX C. MEDICAL GUIDELINES FOR DETERMINING PROGNOSIS IN SELECTED NON-CANCER DISEASES AND HOSPICE ENROLLMENT CRITERIA FOR END-STAGE DEMENTIA PATIENTS
MEDICAL GUIDELINES FOR DETERMINING PROGNOSIS IN SELECTED NON-CANCER DISEASES
Second Edition
Published by The National Hospice Organization
Copyright 1996, by the National Hospice Organization. All rights reserved.
The National Hospice Organization
1901 North Moore Street, Suite 901
Arlington, VA 22209
Written by
Standards and Accreditation Committee
Medical Guidelines Task Force
Brad Stuart, MD
Carla Alexander, MD
Cheryl Arenella, MD
Stephen Connor, PhD, Medical Guidelines Task Force Chair
Laurel Herbst, MD, American Academy of Hospice and Palliative Medicine
Diane Jones, MSW, Hospice Association of America
Barry Kinzbrunner, MD
Paul Rousseau, MD
True Ryndes, ANP, MPH, Standards and Accreditation Committee Chairperson
Michael Wohlfeiler, MD, JD
Chris Cody, RNC, MSN, Staff Liaison
Susan Buckley, CRNH, MS, Staff Liaison
©Copyright 1996, by the National Hospice Organization. All rights reserved. No portion of this publication may be duplicated without the written permission of the National Hospice Organization. Printed in the United States of America. These documents also are available at http://www.guideline.gov.
Item Number 713008
ISBN 0-931207-50-9
TABLE OF CONTENTS
General Guidelines for Determining Prognosis
Appendices:
APPENDIX I: Type, Strength and Consistency of Evidence
APPENDIX II: Karnofsky Performance Status Scale
APPENDIX III: New York Heart Association Functional Classification
APPENDIX IV: Functional Assessment Staging (FAST) Scale: Dementia
APPENDIX V: Typical Time Course of Alzheimer’s Disease*
APPENDIX VI: Diagnostic Imaging Factors Indicating Poor Prognosis After Stroke
Worksheets*
* These sections were not included as part of Appendix C.
INTRODUCTION AND OVERVIEW
This document is written to help identify which patients with non-oncologic terminal illness are likely to have a significantly decreased prognosis if the disease runs its normal course. These Guidelines may also be helpful in determining patient eligibility under the Medicare/Medicaid Hospice Benefit by defining a population that may have a life expectancy of approximately six months.
Increased access to hospice services for patients with diagnoses across the medical spectrum is also a goal of this effort. Until recently, hospice in the US has been identified with care of the end-stage cancer patient. 1 Dissemination of these Guidelines to hospice programs and the medical community should facilitate hospice referrals for patients with heart, lung, liver, Alzheimer's dementia, HIV and other non-cancer diseases.
Recent studies support this effort as timely and relevant. Earlier this year, Christakis and Escarce 2 reported that in 1990, less than twenty percent of hospice referrals in five major states carried a non-cancer diagnosis. Since that time, the proportion of hospice admissions for diseases other than cancer has risen steadily. However, because of inherent challenges in predicting prognosis in non-cancer disease, a large proportion of patients surviving longer than six months are in this category. In the Christakis and Escarce cohort, for example, hospice patients with dementia had a median survival of 74 days, and 34.7 percent of these patients survived for longer than six months. These findings suggest that physicians and hospice programs might benefit from help in determining which non-cancer patients are likely to have a prognosis of approximately six months.
These Guidelines are a starting point, both for hospice programs evaluating patients for admission and recertification, and for critically-needed research on prognosis in end-stage disease. Pending confirmation and refinement through ongoing research with hospice patients, they provide a set of working criteria to use in determining prognosis. The Guidelines do not pretend to predict prognosis exactly in each case. In fact, even if based directly on clinical research, any set of criteria defines a range of probabilities for mortality in a specific population. Prediction of prognosis in individual cases cannot be expected; clinical judgment is always required on the original assessment and throughout the admission.
As of this writing, research is underway to assess the accuracy of existing Guidelines, and to amend them based on new findings. For example, one group has already documented that the previously-published NHO Guidelines 3 for Alzheimer's disease do indeed predict six-month mortality in about 85% of patients who fit previous Guideline criteria. 4 This is an improvement over Christakis and Escarce's findings from 1990 data, where only about 65% of hospice patients with dementia died within six months. Recent findings also have allowed us to refine the criteria for severity of dementia past Stage 7 of the FAST criteria. 5 These changes have been included in this edition.
The Medical Nature of the Guidelines
These Guidelines are based on medical findings. However, decisions to admit patients to hospice are often not based on medical factors alone. They are routinely influenced by nonmedical factors which would generally be reflected in the treatment plan, e.g. patient decisions to receive strict symptom control rather than life-prolonging care, or selection of "optimal" rather than "maximal" treatment regimens tempered by intolerance or refusal of medication due to side-effects.
In addition, it is important to make a distinction between admitting a patient to the hospice program and certifying a patient for the Medicare Hospice Benefit. Individual hospice programs may establish admission criteria that reflect the unique characteristics and values of their communities. This may mean that some patients could be admitted to hospice care prior to an estimated six months before death. However, care must be taken to certify patients for the Benefit only when it is reasonable to conclude that their prognosis is six months or less. In other cases alternative modes of reimbursement, often provided through community support, can be sought outside the Medicare Hospice Benefit.
Emphasis should be placed on evaluating the whole person and the entirety of the illness. It is important to note, for example, that a patient may have multiple medical problems, none of which individually amount to a terminal diagnosis, but when taken together indicate a terminal condition. In short, clinical judgment that takes both medical and nonmedical factors into account is necessary for accurate estimation of prognosis.
Potential Limitations
Several caveats are in order when using these Guidelines for prognostic purposes. They are a first attempt at extrapolating a large amount of heterogeneous evidence from many studies to predict survival in non-cancer diseases (see Appendix I). Their accuracy will need to be validated by further research. These Guidelines should be applied to individual cases very cautiously, for at least the following reasons:
-
Many of the studies referenced here indicate an increased likelihood of death, sometimes within an uncertain time frame. The six month definition of terminal illness adopted for the Medicare Hospice Benefit has rarely been used as a specific outcome measure in most of this research. Further studies with larger populations of hospice patients are needed to determine median survival accurately with reference to the six month standard.
-
Clinical judgment must always be applied in each individual case to supplement these Guidelines. All studies are performed on large enough populations to attain statistical significance, so that individual differences in disease progression are averaged and lost to view. An individual patient who may meet Guideline criteria that were significant in a study of a large cohort might respond in unpredictable ways and have unexpected outcomes as his or her disease runs its own unique course. Therefore the Guidelines must be applied to patients not only on admission, but at intervals throughout the patient's course in hospice.
-
Many of the studies referenced here were done in institutionalized populations. They may or may not be generalizable to patients living at home with family caregivers.
-
Many studies pool patients at all stages of disease. Studies done with selected cohorts of end-stage patients might yield different conclusions. For instance, for a large population of patients with dementia at all stages of severity, antibiotics may be shown to postpone mortality. However, the same drugs have not been shown to lengthen survival in the subpopulation with very end-stage dementia. 6 Again, further research is needed in the terminal population.
-
Almost all studies have been done with patients who received standard medical therapy when they became acutely ill, thus prolonging the course of the illness. Little recent research has been done to study the natural course of untreated end-stage disease. Thus, much of the literature may be defining length of life as inappropriately long for patients who choose a non-curative approach.
-
The course of most non-cancer disease is inherently difficult to predict. The natural history of most non-cancer diseases is characterized by periods of relative stability punctuated by acute downturns, as opposed to the comparatively relentless, and thus more predictable, downhill course in cancer. This natural tendency toward stabilization in non-cancer disease may be augmented by hospice intervention, which may bring about a prolongation of the terminal phase due to improved patient compliance, symptom control and prevention of complications.
-
This difficulty in predicting mortality in non-cancer disease is compounded by the fact that palliation of non-cancer disease is frequently similar, and sometimes identical, to standard medical treatment. Therefore hospice can and frequently does coincidentally extend the life of the non-cancer patient in the act of palliating symptoms. This situation is new to many hospices, who have been trained to treat cancer pain but to leave treatment of cancer itself to the oncologist. To palliate cancer symptoms, hospice employs medications and other interventions which in most cases do not prolong life. Chemotherapy or radiation for palliation are generally used by hospices only when pain and symptoms can not be managed by other interventions. On the other hand, hospice frequently uses the same medications and interventions to palliate non-cancer symptoms that the primary physician or medical specialist uses for active treatment. For instance, skillful palliation of end-stage congestive heart failure requires not only morphine for dyspnea, but also judicious use of diuretics and vasodilators. But these drugs do more than make the patient comfortable -- it is well established that they also prolong life significantly. 7 Thus good hospice care can stabilize patients with non-cancer disease, creating a dilemma for the program if the patient survives for longer than six months without evidence of serious clinical decline.
Fiscal intermediaries and hospice programs alike would benefit from a thorough awareness of these factors. These Guidelines are just a starting point in decision making in non-cancer disease. It is clear that they must be supplemented by clinical judgment at the time of admission. But frequent clinical reassessment, decisions concerning recertification versus possible discharge from the Medicare/Medicaid Hospice Benefit, thorough documentation of medical evidence of continued disease progression and cooperative review of appropriateness of care with intermediaries are all important ongoing considerations.
Acknowledgment
Recognition should be given to other systems of prognostication already devised for use in advanced medical illness. 8 However, these Guidelines were developed de novo for several reasons. First, previous systems were developed for predicting prognosis in seriously ill hospitalized patients who were all receiving aggressive medical therapy. This is a different population than those who are generally considered hospice candidates, although this situation could change. Also, prior prognostic systems require large amounts of detailed clinical and laboratory data. This quantity and quality of information is primarily utilized in research studies, and generally unavailable to providers in the field. Additionally, unlike other systems, these Guidelines were designed for ease of application by the average hospice program, whose staff may not have access to the computer hardware, software and programming expertise needed to use more sophisticated prognostic systems. The medical knowledge and clinical experience needed to understand and apply these Guidelines should be well within the existing capabilities of the hospice staff, ideally under the active leadership of a qualified and enthusiastic Medical Director.
GENERAL GUIDELINES FOR DETERMINING PROGNOSIS
The following parameters may be used to help determine whether a patient is appropriate for hospice care and/or eligible for the Medicare/Medicaid Hospice Benefit. These General Guidelines apply to all patients referred to hospice. However, they may be specifically applied to patients who do not fall under any of the specific diagnostic categories for which disease-specific Guidelines have been written. An example might be the elderly debilitated patient whose intake of food and fluid has declined to the point where weight loss has become significant, although no specific disease predominates in the clinical picture.
The patient should meet all of the following criteria:
-
The patient's condition is life limiting, and the patient and/or family have been informed of this determination.
-
A "life limiting condition" may be due to a specific diagnosis, a combination of diseases, or there may be no specific diagnosis defined. 9
-
-
The patient and/or family have elected treatment goals directed toward relief of symptoms, rather than cure of the underlying disease.
-
The patient has either of the following:
-
Documented clinical progression of disease, which may include:
-
Progression of the primary disease process as listed in disease-specific criteria, as documented by serial physician assessment, laboratory, radiologic or other studies.
-
Multiple Emergency Department visits or inpatient hospitalizations over the prior six months. 10
-
For homebound patients receiving home health services, nursing assessment may be documented.
-
For patients who do not qualify under 1, 2 or 3, a recent decline in functional status may be documented.
-
Functional decline should be recent, to distinguish patients who are terminal from those with reduced baseline functional status due to chronic illness. Clinical judgment is required for patients with a terminal condition and impaired status due to a different non-terminal disease, e.g., a patient chronically paraplegic from spinal cord injury who is recently diagnosed with cancer.
-
Diminished functional status may be documented by either:
-
Karnofsky Performance Status of less than or equal to 50%, 11, 12, 13 (see Appendix II) or
-
Dependence in at least three of six Activities of Daily Living (ADL's). 14, 15, 16, 17, 18, 19, 20, 21, 22
"Activities of Daily Living" are:-
Bathing
-
Dressing
-
Feeding 23
-
Transfers
-
Continence of urine and stool
-
Ability to ambulate independently to bathroom.
-
-
-
-
-
Documented recent impaired nutritional status related to the terminal process.
-
MEDICAL GUIDELINES FOR DETERMINING PROGNOSIS: HEART DISEASE
This section is meant to assist in the determination of prognosis for patients with end-stage heart disease. It is important to remember that with skillful palliation including judicious use of diuretics and vasodilators, particularly angiotensin-converting enzyme (ACE) inhibitors, some patients may survive for long periods with extremely severe symptoms. These drugs definitely promote patient comfort, but they also prolong life. 31 On the other hand, some patients with advanced coronary disease may die suddenly and unexpectedly from acute ventricular arrhythmias.
The likelihood of early mortality is increased in patients who show all of the following characteristics:
-
Symptoms of recurrent congestive heart failure (CHF) at rest.
-
These patients are classified as New York Heart Association (NYHA) Class IV 32 (see Appendix III).
-
Ejection fraction of 20% or less is helpful supplemental objective evidence, but should not be required if not already available. 33
-
-
Patients should already be optimally treated with diuretics and vasodilators, preferably angiotensin-converting enzyme (ACE) inhibitors.
-
The patient experiences persistent symptoms of congestive heart failure despite attempts at maximal medical management with diuretics and vasodilators.
-
"Optimally treated" means that patients who are not on vasodilators have a medical reason for refusing these drugs, e.g. hypotension or renal disease.
-
Although newer beta blockers with vasodilator activity, e.g. carvedilol, have recently been shown to decrease morbidity and mortality in chronic CHF, 34 they are not included in the definition of "optimal treatment" at this time.
-
-
In patients with refractory, optimally treated CHF as defined above, each of the following factors have been shown to decrease survival further, and thus may help in educating medical personnel as to the appropriateness of hospice for cardiac patients.
MEDICAL GUIDELINES FOR DETERMINING PROGNOSIS: PULMONARY DISEASE
Determining prognosis in end-stage lung disease is extremely difficult. There is marked variability in survival. 41 Physician estimates of prognosis vary in accuracy, even in patients who appear end-stage. 42 Even at the time of intubation and mechanical ventilation for respiratory failure from acute exacerbation of chronic obstructive pulmonary disease (COPD), six-month survival cannot be predicted with certainty from simple data easily available to the clinician. 43 Far less information than this is available to most hospice programs at the time of referral.
Patients who fit the following parameters can be expected to have the lowest survival rates. Although the end stages of various forms of lung disease differ in some respects, most follow a final common pathway leading to progressive hypoxemia, cor pulmonale and recurrent infections. Thus, these Guidelines refer to patients with many forms of advanced pulmonary disease. At the present time, it is uncertain what number or combination of these factors might predict six-month mortality; clinical judgment is required.
-
Severity of chronic lung disease documented by:
-
Disabling dyspnea at rest, poorly or unresponsive to bronchodilators, resulting in decreased functional activity, e.g., bed-to-chair existence, often exacerbated by other debilitating symptoms such as fatigue and cough.
Forced Expiratory Volume in One Second (FEV1), after bronchodilator, less than 30% of predicted, 44, 45, 46 is helpful supplemental objective evidence, but should not be required if not already available.
-
Progressive pulmonary disease.
-
-
Presence of cor pulmonale or right heart failure (RHF). 50, 51, 52
-
These should be due to advanced pulmonary disease, not primary or secondary to left heart disease or valvulopathy.
-
Cor pulmonale may be documented by:
-
Echocardiography.
-
Electrocardiogram.
-
Chest x-ray.
-
Physical signs of RHF.
-
-
-
Hypoxemia at rest on supplemental oxygen.
-
pO2 less than or equal to 55 mm Hg on supplemental oxygen.
-
Oxygen saturation less than or equal to 88% on supplemental oxygen.
-
-
Hypercapnia.
-
pCO2 equal to or greater than 50 mm Hg.
-
-
Unintentional progressive weight loss of greater than 10% of body weight over the preceding six months. 53, 54
-
Resting tachycardia greater than 100/minute in a patient with known severe chronic obstructive pulmonary disease. 55, 56, 57, 58
MEDICAL GUIDELINES FOR DETERMINING PROGNOSIS: DEMENTIA
This section is meant to assist in determining whether a patient with end-stage dementia is appropriate for hospice care and/or eligible for the Medicare/Medicaid Hospice Benefit. Although dementia shortens life independent of culture or ethnicity, 59 prediction of six-month mortality is challenging. Severity of dementia alone correlates with poor survival in studies of institutionalized 60 and outpatients, 61 but patients with very advanced dementia can survive for long periods with meticulous care as long as they do not develop lethal complications. Death usually occurs, in fact, as a result of comorbid conditions. 62
The term "dementia" refers here to chronic, primary and progressive cognitive impairment of either the Alzheimer or multi-infarct type. Although most research on prognosis in dementia is done with Alzheimer's patients, the vascular (multi-infarct) dementias appear to progress to death more quickly. 63, 64, 65 These guidelines do not refer to acute, potentially reversible or secondary dementias, i.e., those due to drug intoxication, cancer, AIDS, major stroke, or heart, renal or liver failure.
-
Functional Assessment Staging
-
Even severely demented patients may have a prognosis of up to two years. Survival time depends on variables such as the incidence of comorbidities and the comprehensiveness of care.
-
The patient should be at or beyond Stage Seven of the Functional Assessment Staging 66 Scale (see Appendix IV). The factors listed below should be understood explicitly, since many patients do not progress in an orderly fashion through the substages of Stage 7. Also see Appendix V, "Typical Time Course of Alzheimer's Disease," for a pictorial representation of the continuum of dementia. 67
-
The patient should show all of the following characteristics:
-
Unable to ambulate without assistance.
This is a critical factor. Recent data indicate that patients who retain the ability to ambulate independently do not tend to die within six months, even if all other criteria for advance dementia are present. 68
-
Unable to dress without assistance.
-
Unable to bathe properly.
-
Urinary and fecal incontinence.
-
Occasionally or more frequently, over the past weeks.
-
Reported by knowledgeable informant or caregiver.
-
-
Unable to speak or communicate meaningfully.
-
Ability to speak is limited to approximately a half dozen or fewer intelligible and different words, in the course of an average day or in the course of an intensive interview.
-
-
-
-
Presence of Medical Complications.
-
The presence of medical comorbid conditions of sufficient severity to warrant medical treatment, documented within the past year, whether or not the decision was made to treat the condition, decrease survival in advanced dementia. 69, 70
-
Comorbid Conditions associated with dementia:
-
Aspiration pneumonia.
-
Pyelonephritis or other upper urinary tract infection.
-
Septicemia.
-
Decubitus ulcers, multiple, stage 3-4.
-
Fever recurrent after antibiotics
-
-
Difficulty swallowing food or refusal to eat, sufficiently severe that patient cannot maintain sufficient fluid and calorie intake to sustain life, with patient or surrogate refusing tube feedings or parenteral nutrition.
-
Patients who are receiving tube feedings must have documented impaired nutritional status as indicated by:
-
-
MEDICAL GUIDELINES FOR DETERMINING PROGNOSIS: HIV DISEASE
With the introduction of new classes of anti-retroviral therapy such as protease inhibitors (PI's), and better control of opportunistic infections, the perception of HIV may be changing from that of inexorably fatal disease to that of chronic illness. 78 The ability to measure the amount of circulating virus (viral load, HIV RNA) 79, 80 has dramatically changed both the management of disease 81 and the ability to predict survival. Previously published data using the CD4+ cell count 82 alone as a prognostic marker will not be as helpful in determining appropriateness for hospice care.
With the announcement that viral load could be suppressed to undetectable levels for at least a year in 90% of treated patients by a combination of AZT, 3TC and indinavir, a PI, 83 a new air of hopefulness exists in AIDS treatment. Although authorities now discuss the possibility of eradicating HIV from patients, it is far from certain that new drugs will result in complete reconstitution of the immune system, 84 or in recovery of other organ systems already seriously damaged by HIV. Therefore, at this time these Guidelines must reflect past literature until newer studies are available.
HIV mortality is influenced by new and changing therapies, practitioners' skill and experience in management, and individual patient tolerance for treatment. Other factors contribute to the difficulty of prognosis in this disease. It occurs predominately in the young, who are both constitutionally better able to withstand a heavy burden of disease, and less likely to forego intensive therapies, than the more elderly populations typical of other end-stage illnesses. Because of improved prophylactic regimens, most deaths from AIDS are now caused by opportunistic infections, persistent wasting, or neoplasm.
It is important to discuss a patient's clinical course with a physician who is experienced in caring for persons with HIV disease 85, 86 or with one who is experienced in Palliative Medicine. As in any end-stage disease, optimum therapy should have been exhausted or refused by the patient. The course over the previous month may reflect the patient's prognosis.
Concerning protease inhibitors, unless patients taking these medications fit the CD4+ and viral load criteria listed below, they may have a prognosis considerably longer than six months. Thus these drugs may be considered life-prolonging, not palliative, in the hospice setting. Additionally, patients already enrolled in hospice who decide to start these medications may lengthen their prognosis considerably. Programs will have to take these issues into account when deciding whether to cover PI's under the Medicare/Medicaid Hospice Benefit.
The following factors are correlated with early mortality and therefore may be helpful when evaluating a patient for terminal care or for coverage by the Medicare/Medicaid Hospice Benefit:
-
CD4+ Count
-
Patients whose CD4+ count is below 25 cells/mcL, measured during a period when patient is relatively free of acute illness, may have a prognosis less than six months, but should be followed clinically and observed for disease progression and decline in recent functional status.
-
Patients with CD4+ count above 50 cells/mcL who are followed by an experienced AIDS practitioner probably have a prognosis longer than six months unless there is a non-HIV-related co-existing life-threatening disease. In one study of CD4+ counts and mortality, median survival of the entire population of patients with CD4+ 50 was 11.9 months. 87
-
-
Viral Load
-
Patients with a persistent HIV RNA (viral load) of >100,000 copies/ml may have a prognosis less than six months.
-
Patients with lower viral loads may have a prognosis of less than six months if. 88
-
They have elected to forego antiretroviral and prophylactic medication.
-
Their functional status is declining.
-
They are experiencing complications listed in IV below.
-
-
-
Life-threatening complications with median survival:
The following HIV-related opportunistic diseases all are associated with prognosis less than six months. Note that prognosis may be longer for certain conditions if patient elects treatment:
HIV-related opportunistic diseases. A. CNS lymphoma 89 2.5 months B. Progressive multifocal leukoencephalopathy 90 4 months C. Cryptosporidiosis 91 5 months D. Wasting (loss of 33% lean body mass) 92 6 months E. MAC bacteremia, untreated 93 6 months F. Visceral Kaposi's sarcoma unresponsive to therapy 94 6 month mortality 50%. G. Renal failure, refuses or fails dialysis 95, 96 6 months H. Advanced AIDS dementia complex 97 6 months I. Toxoplasmosis 98 6 months -
The following factors have been shown to decrease survival significantly and should be documented if present:
MEDICAL GUIDELINES FOR DETERMINING PROGNOSIS: LIVER DISEASE
Prognosis in advanced liver disease has been widely studied to assess readiness for liver transplantation. 109, 110 Clinical symptoms and signs and laboratory values contained within the Child-Turcotte classification 111 as modified by Pugh, 112 not included here, have been shown to correlate significantly with early mortality. 113, 114 Some of these variables, with the addition of other clinical syndromes associated with mortality, are shown below.
Although accurate, albeit complex, prognostic indices based on multivariate analyses have been developed, 115 they are still controversial. They are not recommended here since:
-
All the required elements may not be available to hospice programs at the time of referral.
-
The computing power needed to calculate these scores may not be available to many hospice admissions staff.
-
Nearly every study on prognosis in advanced liver disease has been done outside the US, and World Health Organization data reveals that patterns of death from liver disease, as well as risk factors such as alcoholism and hepatitis B, can differ widely among countries. 116
The following factors have been shown to correlate with poor short-term survival in advanced cirrhosis of the liver due to alcoholism, hepatitis, or uncertain causes (cryptogenic). Their effects are additive; i.e. prognosis worsens with the addition of each one. Clinical judgment is vital. The following factors should be followed and reviewed over time. Patients should have end-stage cirrhosis; those who are newly decompensated, i.e. in their first hospitalization, may improve dramatically with treatment compared to those who are in the terminal phase of a chronic process. 117
The patient should not be a candidate for liver transplantation.
-
Laboratory indicators of severely impaired liver function:
Patients with this degree of impairment have a poor prognosis. The patient should show both of the following:
-
Prothrombin time prolonged more than 5 sec. over control.
-
Serum albumin 2.5 gm/dl.
-
-
Clinical indicators of end-stage liver disease:
The patient should show at least one of the following:
-
Ascites, refractory to sodium restriction and diuretics, or patient non-compliant.
-
Maximal diuretics generally used: Spironolactone 75-150 mg/day plus furosemide >40 mg/day. 118
-
Spontaneous bacterial peritonitis. 119
-
-
Median survival 30% at one year; 120 high mortality even when infection cured initially if liver disease is severe or accompanied by renal disease. 121
-
Hepatorenal syndrome. 122
-
-
In patient with cirrhosis and ascites, elevated creatinine and BUN with oliguria (400 ml/da) and urine sodium concentration 10 mEq/l.
-
Usually occurs during hospitalization; survival generally days to weeks.
-
-
Hepatic encephalopathy, refractory to protein restriction and lactulose or neomycin, 123 or patient non-compliant.
-
Manifested by: decreased awareness of environment, sleep disturbance, depression, emotional lability, somnolence, slurred speech, obtundation. 124
-
Physical exam may show flapping tremor of asterixis, although this finding may be absent in later stages. 125
-
Stupor and coma are extremely late-stage findings.
-
Recurrent variceal bleeding. 126
-
-
Following initial variceal hemorrhage, one third died in hospital, one third rebled within six weeks; two thirds survived less than 12 months. 127
-
Patient should have rebled despite therapy, or refused further therapy, which currently includes: 128, 129
-
-
-
The following factors have been shown to worsen prognosis and should be documented if present:
MEDICAL GUIDELINES FOR DETERMINING PROGNOSIS: RENAL DISEASE
This section is meant to assist in determining whether a patient with end-stage renal disease is appropriate for hospice care and/or eligible for the Medicare/Medicaid Hospice Benefit. Absent other comorbid conditions, the patient should not be seeking dialysis or renal transplant. Patients who do refuse dialysis or transplant are generally appropriate for hospice services if they fit dialysis criteria. 140, 141 When evaluating patients with end-stage renal disease (ESRD), 142 a nephrology consultation may be helpful since individual patient variables can influence longevity. 143
Hospitalized patients may develop acute renal failure (ARF) following trauma or major surgery. Short-term survival may be difficult to predict during initial evaluation and treatment. However, factors listed in III. below may be helpful in evaluating these acutely-ill patients for hospice admission. 144
Chronic renal failure (CRF) can be treated with either hemo- or chronic ambulatory peritoneal dialysis (CAPD), which prolongs survival indefinitely. If dialysis is discontinued, the chance of early death is greatly increased. An occasional patient with residual renal function after dialysis is discontinued may remain alive for a period of time, but survival beyond six months is highly unlikely.
Care should be taken in assessing patients with nephrotic syndrome. This illness often follows a protracted course; nephrology consultation can assist with prognosis.
-
Laboratory criteria for renal failure.
These values may be used to assess patients with renal failure who are not dialyzed, as well as those who survive more than a week or two after dialysis is discontinued. Patients with this degree of renal failure can be expected to die shortly without dialysis. Bearing in mind individual differences in tolerance for very elevated creatinine levels, critical renal failure is defined (HCFA form #2728) as:
-
Creatinine clearance of less than 10cc/min (less than 15 cc/min for diabetics) AND
-
Serum creatinine greater than 8.0 mg/dl (greater than 6.0 mg/dl for diabetics).
Notes:
-
Creatinine clearance may be estimated by using the following formula, thus avoiding a 24-hour urine collection:
Ccreat = (140 - age in yrs.) (body wt. in kg); multiply by 0.85 for women. (72) (serum creat in mg/dl) -
Blood urea nitrogen (BUN) values are not used in the determination of critical renal failure, since they can be extremely elevated from prerenal azotemia due to dehydration, hypovolemia or other causes.
-
-
-
Clinical signs and syndromes associated with renal failure.
The following clinical signs are used as criteria for beginning dialysis. For patients with end-stage renal disease who are not to be dialyzed, the following may help define hospice appropriateness:
-
Uremia: clinical manifestations of renal failure.
-
Confusion, obtundation
-
Intractable nausea and vomiting
-
Generalized pruritis
-
Restlessness, "restless legs"
-
-
Oliguria: Urine output less than 400cc/24 hrs.
-
Intractable hyperkalemia: persistent serum potassium >7.0 not responsive to medical management.
-
Uremic pericarditis.
-
Hepatorenal syndrome.
-
Intractable fluid overload.
-
-
In hospitalized patients with ARF, these comorbid conditions predict early mortality:
MEDICAL GUIDELINES FOR DETERMINING PROGNOSIS: STROKE AND COMA
After stroke, patients who do not die during the acute hospitalization tend to stabilize with supportive care only. Continuous decline in clinical or functional status over time means that the patient's prognosis is poor.
Conversely, steady improvement in the patient's functional or physiologic status may indicate that the patient is not terminally ill. Care should be taken to distinguish true recovery of performance and physiologic function from the improvement in symptoms and subjective well-being that can accompany hospice intervention.
-
During the acute phase immediately following a hemorrhagic or ischemic stroke, any of the following are strong predictors of early mortality:
-
Coma or persistent vegetative state secondary to stroke, beyond three days' duration. 169, 170, 171, 172, 173, 174, 175
-
In post-anoxic stroke, coma or severe obtundation, accompanied by severe myoclonus, persisting beyond three days past the anoxic event. 176, 177, 178
-
Comatose patients with any 4 of the following on day 3 of coma had 97% mortality by two months: 179
-
Abnormal brain stem response
-
Absent verbal response
-
Absent withdrawal response to pain
-
Serum creatinine >1.5 mg/dl
-
Age >70
-
-
Dysphagia severe enough to prevent the patient from receiving food and fluids necessary to sustain life, in a patient who declines, or is not a candidate for, artificial nutrition and hydration.
-
If computed tomographic (CT) or magnetic resonance imaging (MRI) scans are available, certain specific findings may indicate decreased likelihood of survival, or at least poor prognosis for recovery of function even with vigorous rehabilitation efforts, which may influence decisions concerning life support or hospice. Please see Appendix VI for a list of these diagnostic imaging factors. It should be borne in mind that clinical variables, not imaging studies, are the primary criteria for hospice referral.
-
-
Once the patient has entered the chronic phase, the following clinical factors may correlate with poor survival in the setting of severe stroke, and should be documented. The referenced factors have been studied in relation to prognosis in stroke, whereas others may be found elsewhere in these Guidelines where they relate to declining patients in general, or to comparable conditions such as dementia.
-
Poor functional status, as evidenced by Karnofsky score of 50%. See Appendix II.
-
Post-stroke dementia, as evidenced by a FAST score of greater than 7. See Appendix IV.
-
Poor nutritional status, whether on artificial nutrition or not:
-
Medical complications related to debility and progressive clinical decline. It is assumed that these patients are in chronic care situations similar to those with end-stage dementia. 191 Although studies are not available to relate these directly to six-month prognosis in stroke, their presence should be documented.
-
Aspiration pneumonia.
-
Upper urinary tract infection (pyelonephritis).
-
Sepsis.
-
Refractory stage 3-4 decubitus ulcers.
-
Fever recurrent after antibiotics.
-
MEDICAL GUIDELINES FOR DETERMINING PROGNOSIS: AMYOTROPHIC LATERAL SCLEROSIS (ALS)
Amyotrophic lateral sclerosis (ALS) is a progressive neurologic disease that is fatal in about three fourths of patients within one to five years after symptom onset, 192 with median survival of 4 years or less, 193 although some studies indicate longer survival in some patients with symptom onset before age 45. 194 The cause is unknown in 90% of cases, and at present there is no effective treatment. 195, 196 Crude mortality rates from ALS have risen about 50% in the last fifteen years, 197, 198 but this appears due to declining competitive mortality from ischemic heart disease and stroke rather than rising incidence of ALS. 199
Although the disease usually starts with focal involvement, patients become quadriplegic and unable to speak, swallow and ultimately to breathe. 200, 201 A small percentage of patients may survive beyond five years, 202 particularly with ventilators and feeding tubes, although centers specializing in the care of patients with advanced ALS report that with counseling, very few of them choose assisted ventilation. 203
For predicting prognosis in ALS, several characteristics of the disease are important to remember:
-
ALS tends to progress in a linear fashion over time. Thus the overall rate of decline in each patient is fairly constant and predictable, unlike many other non-cancer diseases.
-
However, no single variable deteriorates at a uniform rate in all patients. 204 Therefore, multiple clinical parameters are required to judge the progression of ALS.
-
Although ALS usually presents in a localized anatomical area, the location of initial presentation does not correlate with survival time. 205 By the time patients become end-stage, muscle denervation has become widespread, affecting all areas of the body, and initial predominance patterns do not persist. Bulbar presentation, for example, was thought to correlate with relatively poor prognosis, but more recent studies have shown that bulbar cases present with later age of onset, which does correlate with more rapid progression.
-
Progression of disease differs markedly from patient to patient, as much as 60-fold in one series. 206 Some patients decline rapidly and die quickly; others progress more slowly. For this reason, the history of the rate of progression in individual patients is important to obtain to predict prognosis.
-
In end-stage ALS, two factors are critical in determining prognosis: ability to breathe, and to a lesser extent ability to swallow. The former can be managed by artificial ventilation, and the latter by gastrostomy or other artificial feeding, unless the patient has recurrent aspiration pneumonia.
Numerous ALS rating scales have been developed to help predict ALS prognosis for use in drug intervention trials. 207, 208, 209, 210, 211, 212 Although the predictive value of some are excellent, they are meant to grade patients in all stages of the disease. Their clinical complexity precludes their use by most hospice staffs, and many medical directors, without special training. 213 More importantly, the only factor that is critical in end-stage ALS is respiratory function. The other variables considered in these rating systems, e.g. muscle strength, bulbar function other than swallowing, and upper and lower extremity function, are irrelevant in predicting six-month prognosis.
Examination by a neurologist within three months of assessment for hospice is advised, both to confirm the diagnosis and to assist with prognosis.
The following factors may define those ALS patients with expected survival of approximately six months. These patients generally fit one of the following categories
-
Both rapid progression of ALS and critically impaired ventilatory capacity.
-
Both rapid progression of ALS and critical nutritional impairment, with a decision not to receive artificial feeding.
-
Both rapid progression of ALS and life-threatening complications.
-
Rapid progression of disease and critically impaired ventilatory capacity.
-
Rapid progression of ALS.
The patient should have developed most of their disability within the past 12 months. Patients with slow progression may survive for longer periods, although clinical judgment may still indicate they may be within six months of death.
Examples would include, within the past year:
-
Progressing from independent ambulation to wheelchair- or bed-bound.
-
Progressing from normal to barely intelligible or unintelligible speech.
-
Progressing from normal to blenderized diet.
-
Progressing from independence in most or all Activities of Daily Living (ADL's) to needing major assist by caretaker in all ADL's.
-
-
Critically impaired ventilatory capacity.
The patient should have, within the past 12 months, developed extremely severe breathing disability. Examples include:
-
Vital Capacity (VC) less than 30% of predicted.
-
Significant dyspnea at rest.
-
Requiring supplemental oxygen at rest.
-
Patient declines intubation or tracheostomy and mechanical ventilation.
Note: Patients who are already on assisted ventilation, whether by negative-pressure external means (e.g. Cuirass) or positive-pressure through tracheostomy, may survive for periods considerably longer than six months unless there is a life-threatening comorbid condition, e.g. recurrent aspiration pneumonia.
-
-
-
Rapid progression of ALS and critical nutritional impairment.
-
Rapid progression of ALS. Please see I.A. above.
-
Critical nutritional impairment.
Most ALS patients develop swallowing difficulties early in the illness, so that gastrostomy feeding is reasonable.
However, some patients with end-stage or rapidly-advancing ALS may choose not to undergo artificial feeding.
These patients may have a prognosis of less than six months if their oral intake of nutrients and fluids is insufficient to sustain life.
Nutritional impairment may be documented by:
-
Continued weight loss.
-
Dehydration or hypovolemia.
-
-
-
Rapid progression of ALS and life-threatening complications.
-
Rapid progression of ALS. Please see I.A. above.
-
Life-threatening complications.
-
Recurrent aspiration pneumonia.
This may occur whether or not the patient is receiving tube feedings.
-
Decubitus ulcers, multiple, Stage 3-4, particularly if infected.
-
Upper urinary tract infection, e.g. pyelonephritis.
-
Sepsis.
-
Fever recurrent after antibiotics.
-
-
REFERENCES
-
Callahan D. Frustrated mastery -- The cultural context of death in America, in Caring for Patients at the End of Life [Special Issue]. West J Med 1995; 163:226-30.
-
Christakis NA et al. Survival of Medicare patients after enrollment in hospice programs. New Eng J Med 1996;335:172-8.
-
Stuart B et al. Medical Guidelines for Determining Prognosis in Selected Non-Cancer Diseases. Arlington, VA: National Hospice Organization, 1995.
-
Luchins DJ et al. Criteria for enrolling dementia patients in hospice programs. In preparation.
-
Reisberg, B. Functional assessment staging (FAST). Psychopharmacology Bulletin, 1988; 24:653-659.
-
Fabiszcewski KJ et al. Effect of antibiotic treatment on outcome of fevers in institutionalized Alzheimer patients. JAMA 1990; 263:3168-72.
-
Giles TD. Optimizing the treatment of heart failure. Curr Opin Cardiol 1994;9 Suppl 1:S21-7.
-
Lynn, J et al. Accurate prognostication of death: opportunities and challenges for physicians. West J Med 1995;163:250-7.
-
Kinzbrunner, BM et al. Debility, unspecified: a terminal diagnosis. Abstract, J Palliat Care 1994; vol. 10:4:58.
-
Kinzbrunner BM. Non-malignant terminal diseases: criteria for hospice admission. Hospice Update 1993; 3:3-6.
-
Karnofsky DA et al. The use of nitrogen mustards in the palliative treatment of cancer. Cancer 1948; 1(4):634.
-
Mor V et al. The Karnofsky Performance Status Scale: an examination of its reliability and validity in a research setting. Cancer 1984; 53:2002.
-
Evans C et al. "Prognostic uncertainty in terminal care: can the Karnofsky index help?" Lancet 1985; 1:1204.
-
Katz S et al. Studies of illness in the aged. The index of ADL: a standardized measure of biological and psychosocial function. JAMA 1963;185:914.
-
Donaldson LJ et al. The elderly in residential care: mortality in relation to functional capacity. J Epidemiol and Comm Health 1980; 34:96.
-
Rudman D et al. Antecedents of death in the men of a Veteran's Administration nursing home. J Am Geriatr Soc 1987; 35:496.
-
Wolinsky FD et al. Changes in functional status and the risks of subsequent nursing home placement and death. J Gerontol and Soc Sci 1993; 48(3):S94.
-
Narain F et al. Predictors of immediate and 6-month outcomes in hospitalized elderly patients: the importance of functional status. J Am Geriatr Soc 1988; 36:775.
-
Goldfarb AI et al. Predictors of mortality in the institutionalized aged. Dis Nerv System 1966; 27(1):21.
-
Lichtenstein MJ et al. Factors associated with early demise in nursing home residents: a case control study. J Am Geriatr Soc 1985; 33:315.
-
Reuben DB et al. Value of functional status as a predictor of mortality: results of a prospective study. Am J Med 1992; 93:663.
-
Clark LP et al. Taking to bed: rapid functional decline in an independently mobile older population living in an intermediate-care facility. J Am Geriatr Soc 1990; 38:967.
-
This may be a factor that independently determines early mortality in selected patients. See Siebens H et al. Correlates and consequences of eating dependency in institutionalized elderly. J Am Geriatr Soc 1986; 34:192.
-
Murden RA et al. Recent weight loss is related to short-term mortality in nursing homes. J Gen Int Med 1994; 9:648.
-
Dwyer JT et al. Changes in relative weight among institutionalized elderly adults. J Gerontol 1987; 42(3):246.
-
Marton KI et al. Involuntary weight loss: diagnostic and prognostic significance. Ann Int Med 1981; 95:568.
-
Rudman D, op. cit.
-
Corti M-C et al. Serum albumin level and physical disability as predictors of mortality in older persons. JAMA 1994; 48:1173.
-
Agrawal N et al. "Predictive ability of various nutritional variables for mortality in elderly people." Am J Clin Nutr 1988; 48:1173.
-
Phillips P et al. "Grip strength, mental performance and nutritional status as indicators of mortality risk among female geriatric patients." Age and Aging 1986; 15:53.
-
Reyes AJ. Angiotensin-converting enzyme inhibitors in the clinical setting of chronic congestive heart failure. Am J Cardiol 1995;75:50F-55F.
-
From Nomenclature and Criteria for Diagnosis of Disease of the Heart and Great Vessels, 9th Ed., Little Brown & Co., 1993.
-
Marantz PR et al. "Prognosis in ischemic heart disease: can you tell as much at the bedside as in the nuclear laboratory?" Arch Int Med 1992; 152:2433-2437.
-
Packer M et al. Effect of carvedilol on morbidity and mortality in patients with chronic heart failure. US carvedilol heart failure study group. New Eng J Med 1996;334:1349-55.
-
Landry FJ et al. "Outcome of cardiopulmonary resuscitation in the intensive care setting." Arch Int Med 1992 Nov; 152(11):2305-8.
-
Middlekauff HR et al. "Syncope in advanced heart failure: high risk of sudden death regardless of origin of syncope." J Am Coll Cardiol 1993 Jan; 21(1):110-6.
-
Maggiorini M. "Indications for heart transplantation: preoperative assessment and treatment." Ther Umsch 1993 Jun; 50(6):434-41.
-
Kapoor WN. "Evaluation and outcome of patients with syncope." Medicine (Baltimore) 1990 May; 69(3):160-75.
-
Hornig CR et al. "Early outcome and recurrences after cardiologic brain embolism." Acta Neurol Scand 1993 Jul: 88(1):26-31.
-
Currie PF et al. "Heart muscle disease related to HIV infection: prognostic implications." Brit Med J 1994 Dec 17; 309(669):1605-7.
-
Burrows B et al. "Course and prognosis of chronic obstructive pulmonary disease." N Eng J Med 1969; 280:397-404.
-
Pearlman RA. "Variability of physician estimates of survival for acute respiratory failure in chronic obstructive pulmonary disease.>" Chest 1987; 91(4):515-521.
-
Kaelin RM et al. "Failure to predict six-month survival of patients with COPD requiring mechanical ventilation by analysis of simple indices." Chest 1987; 92(6):971-978.
-
Anthonisen NR. "Prognosis in chronic obstructive pulmonary disease: results from multicenter clinical trials." Am Rev Resp Dis 1989; 140:S95-S99.
-
Hodgkin JE. "Prognosis in chronic obstructive pulmonary disease." Clin Chest Med 1990; 11:555-569.
-
Traver GA et al. "Predictors of mortality in chronic obstructive pulmonary disease." Am Rev Resp Dis 1979; 119:895-902.
-
Diener CF et al. "Further observations on the course and prognosis of chronic obstructive lung disease." Am Rev Resp Dis 1975; 111:719-724.
-
Kanner RE et al. "Predictors of survival in subjects with chronic airflow limitation." Am J Med 1983; 74:249-255.
-
Postma DS et al. "Prognosis of chronic obstructive pulmonary disease: the Dutch experience." Am Rev Resp Dis 1989; 140 (Suppl):S100-S105.
-
Boushy SF et al. "Factors affecting prognosis in emphysema." Dis Chest 1964; 45:402-411.
-
France AJ et al. "Does right ventricular function predict survival in patients with chronic obstructive lung disease?" Thorax 1988; 11:423-434.
-
Kawakami Y. "Prognostic factors in COPD: the importance of pulmonary hemodynamic variables." Pract Cardiol 1985; 11:124-137.
-
Braun SR et al. "Predictive clinical value of nutritional assessment factors in COPD." Chest 1984; 85:353-357.
-
Braun SR et al. "Predictive clinical value of nutritional assessment factors in COPD." Chest 1984; 85:353-357.
-
Shih H et al. "Frequency and significance of cardiac arrhythmias in chronic obstructive lung disease." Chest 1988; 94:44-48.
-
Sahn SA et al. "Ten-year follow up of a comprehensive rehabilitation program for severe COPD." Chest 1980; 77(suppl):311-314.
-
Postma DS et al. "Prognosis in severe chronic obstructive pulmonary disease." Am Rev Resp Dis 1979; 119:357-367.
-
Anthonisen NR et al. "Prognosis in chronic obstructive pulmonary disease." Am Rev Resp Dis 1986; 133:14-20.
-
Katzman R et al. "The malignancy of dementia: Predictors of mortality in clinically diagnosed dementia in a population survey of Shanghai, China." Arch Neurol 1994; 51(12):1220-5.
-
Drachman DA et al. "The prognosis in Alzheimer's disease: 'how far' rather than 'how fast' best predicts the outcome." Arch Neurol 1990; 47(8):851-6.
-
Walsh JS et al. "Survival of outpatients with Alzheimer-type dementia." Ann Int Med 1990; 113(6):429-34.
-
Volicer BJ et al. "Predicting short-term survival for patients with advanced Alzheimer's disease." J Am Geriatr Soc 1993; 41:535-540.
-
Koopmans RT et al. "Multi-infarct dementia in nursing home patients: more comorbidity and shorter life expectancy than in Alzheimer's disease." Ned Tijdschr Geneeskd 1992; 136(45):2223-7.
-
Reding MJ et al. "Follow up of patients referred to a dementia service." J Am Geriatr Soc 1984; 32(4):265-8.
-
Brodaty H et al. "Time until institutionalization and death in patients with dementia." Arch Neurol 993; 50(6):643-50.
-
Reisberg B. "Functional Assessment Staging (FAST)." Psychopharmacology Bulletin, 1988; 24:653-659.
-
Reisberg B et al. "Dementia staging in chronic care populations." In Alzheimer's Disease and Associated Disorders. 1994; 8(Suppl.) S188-S205.
-
Luchins DJ, Hanrahan P and Murphy K, personal communication. Manuscript in preparation.
-
Hanrahan P et al. "Survival time among end-stage demented hospice patients." NR253, presented at annual conference of American Psychiatric Association, Miami, Florida, 1995.
-
Alexakos MJ et al. "Criteria to enroll end-stage dementia patients into hospice." NR516, presented at annual conference of American Psychiatric Association, Philadelphia, Pennsylvania, 1994.
-
Murden RA et al. Recent weight loss is related to short-term mortality in nursing homes. J Gen Int Med 1994; 9:648.
-
Dwyer JT et al. Changes in relative weight among institutionalized elderly adults. J Gerontol 1987; 42(3):246.
-
Marton KI et al. Involuntary weight loss: diagnostic and prognostic significance. Ann Int Med 1981; 95:568.
-
Rudman D et al. Antecedents of death in the men of a Veteran's Administration nursing home. J Am Geriatr Soc 1987; 35:496.
-
Corti M-C et al. Serum albumin level and physical disability as predictors of mortality in older persons. JAMA 1994; 48:1173.
-
Agrawal N et al. "Predictive ability of various nutritional variables for mortality in elderly people." Am J Clin Nutr 1988; 48:1173.
-
Phillips P et al. "Grip strength, mental performance and nutritional status as indicators of mortality risk among female geriatric patients." Age and Aging 1986; 15:53.
-
Volberding PA. Improving the outcomes of care for patients with human immunodeficiency virus infection. New Eng J Med 1996;334(11):729-31.
-
Mellors JW et al. Prognosis in HIV-1 infection predicted by the quantity of virus in plasma. Science 1996;272:1167-1170.
-
Saag, MS et al. HIV viral load markers in clinical practice. Nature Med 1996;2(6):625-629.
-
Carpenter, CCJ, et al. Antiretroviral Therapy for HIV Infection in 1996: Recommendations of an international panel. JAMA 1996;276(2):146-154.
-
Mills,CD, Jones PD. Relationship between CD4 lymphocyte count and AIDS mortality, 1986-1991. AIDS 1993;7:1383-1386.
-
Gulick R et al. 3rd national conference on human retroviruses and related infections, Washington DC, 29 Jan 96 (abstract), p. 162.
-
Pennisi E et al. Eradicating HIV from a patient: not just a dream? Science 1996;272:1884.
-
Stone, VE et al. Relation between hospital experience and mortality for patients with AIDS. JAMA 1992;268(19):2655-2661
-
Kitahata, MM et al. Physicians' experience with the acquired immunodeficiency syndrome as a factor in patient's survival. New Eng J Med 1996;334(11):701-706.
-
Mills GD & Jones PD. Relationship between CD4 lymphocyte count and AIDS mortality, 1986-1991. AIDS 1993;7:1383-6.
-
Mellors JW et al, op. cit.
-
Neaton et al. Statistics in Medicine 1994; 13:2107-2125.
-
Neaton et al. Op. cit.
-
Moore RD et al. Natural history of opportunistic disease in an HIV-infected urban clinical cohort. Ann Int Med 1996;124:633-42.
-
Chin DP et al. Impact of mycobacterium avium complex bacteremia and its treatment on survival of AIDS patients: a prospective study. J Infect Dis 1994; 170-578-84.
-
Neaton et al., op cit.
-
Rao TK et al. Outcome of severe acute renal failure in patients with acquired immunodeficiency syndrome. Am J Kidney Dis 1995;25:390-8.
-
Stone HD et al. Human immunodeficiency virus-associated nephropathy: current concepts. Am J Med Sci 1994;307:212-7.
-
Moore RD et al, op. cit.
-
Sanchez-Mejorada G. Clinical patterns of diarrhea in AIDS: etiology and prognosis. Rev Invest Clin 1994;46:187-96.
-
Herrmann FR et al. Serum albumin level on admission as a predictor of death, length of stay and readmission. Arch Int Med 1992; 152:125-30.
-
Guenter P et al. Relationships among nutritional status, disease progression and survival in HIV infection. J Acq Immun Defic Synd 1993; 6:1130.
-
Chlebowski RT et al. Nutritional status, gastrointestinal dysfunction and survival in patients with AIDS. Am J Gastroenterol 1989;84:1288-93.
-
Alcabes P et al. Injection drug use and human immunodeficiency virus infection. Clin Infect Dis 1995;20:1467-79.
-
Operskalski EA et al. Human immunodeficiency virus type 1 infection: relationship of risk group and age to rate of progression to AIDS. Transfusion Safety Study Group. J Infect Dis 1995;172:648-55.
-
Martin JN et al. Effect of older age on survival in human immunodeficiency virus (HIV) disease. Am J Epidemiol 1995;142:1221-30.
-
Santagostino E et al. Factors associated with progression to AIDS and mortality in a cohort of HIV-infected patients with hemophilia followed up since seroconversion. Cell Mol Biol 1995;41:371-80.
-
Diamondsstone LS et al. Prognostic factors for all-cause mortality among hemophiliacs infected with human immunodeficiency virus. J Infect Dis 1995;142:304-13.
-
Currie PF et al. "Heart muscle disease related to HIV infection: prognostic implications." Brit Med J 1994 Dec 17; 309(669):1605-7.
-
Keefe, EB. Selection of patients for liver transplantation. In Maddrey WC and Sorrell MF, eds. Transplantation of the Liver, 2nd Ed. Norwalk, CT:Appleton and Lange,1995;13-60.
-
Christensen E et. al. Updating prognosis and therapeutic effect evaluation in cirrhosis with Cox's multiple regression model for time-dependent variables. Scand J Gastroenterol 1986;21:163-74.
-
Child CG and Turcotte JG. In: Child CG. ed. The Liver and Portal Hypertension. Philadelphia: WB Saunders Co., 1964:50.
-
Pugh RNH et al. Transection of the oesophagus for bleeding oesophageal varices. Br J Surg 1973;60:646-649.
-
Albers I et al. Superiority of the Child-Pugh classification to quantitative liver function tests for assessing prognosis of liver cirrhosis. Scand J Gastroenterol 1989;24:269-76.
-
Infante-Rivard C et al. Clinical and statistical validity of conventional prognostic factors in predicting short-term survival among cirrhotics. Hepatology 1987;7:660-4.
-
Christensen E et al. Prognostic value of Child-Turcotte criteria in medically treated cirrhosis. Hepatology 1984;4:430-5.
-
LaVecchia C et al. Worldwide patterns and trends in mortality from liver cirrhosis, 1955 to 1990. Ann Epidemiol 1994;4:480-6.
-
Christensen E et. al. Updating prognosis and therapeutic effect evaluation in cirrhosis with Cox's multiple regression model for time-dependent variables. Scand J Gastroenterol 1986;21:163-74.
-
Rector WG Jr. Sodium retention and ascites formation. In: Rector WG Jr., ed. Complications of Chronic Liver Disease. St. Louis, MO:Mosby-Year Book Inc.,1992;68-84.
-
Runyon BA. Spontaneous bacterial peritonitis: an explosion of information. Hepatology 1988;8:171-5.
-
Tito L et al. Recurrence of spontaneous bacterial peritonitis in cirrhosis: frequency and predictive factors. Hepatology 1988;8:27-31.
-
Toledo C et al. Spontaneous bacterial peritonitis in cirrhosis: predictive factors of infection resolution and survival in patients treated with cefotaxime. Hepatology 1993; 17:251-7.
-
Gines A et al. Incidence, predictive factors and prognosis of the hepatorenal syndrome in cirrhosis with ascites. Gastroenterology 1993;105:229-36.
-
Trey C et al. Treatment of hepatic coma by exchange blood transfusion. N Eng J Med 1966;274:473-81.
-
Gitlin N et al. The diagnosis and prevalence of subclinical hepatic encephalopathy in apparently healthy, ambulant, nonshunted patients with cirrhosis. J Hepatol 1986;3:75-82.
-
Vierling JM. Epidemiology and clinical course of liver disease: identification of candidates for liver transplantation. Hepatology 1984;4:84S-94S.
-
D'Amico G et al. Survival and prognostic indicators in compensated and decompensated cirrhosis. Dig Dis & Sci 1986;31:468-75.
-
Graham DY et al. Course of patients after variceal hemorrhage. Gastroenterology 1981;80:800-9.
-
Terblanche J et al. Controversies in the management of bleeding esophageal varices. N Eng J Med 1989;320:1393-8, 1469-75.
-
Lebrec D. Portal hypertension. In: Rector WG Jr, Ed. Complications of Chronic Liver Disease. St Louis, MO:Mosby-Year Book Inc; 1992:24-67.
-
Davis TV et al. Update on managing bleeding esophageal varices. JOM 1992;6:16-21.
-
Stiegmann GV et al. Endoscopic sclerotherapy as compared with endoscopic ligation for bleeding esophageal varices. N Eng J Med 1991;326:1527-32.
-
Lebrec D. Op. cit.
-
Zemel G et al. Percutaneous transjugular portosystemic shunt. J Am Med Assoc 1991;266:390-3.
-
Qiao Z-K et al. Relationship between liver cirrhosis death rate and nutritional factors in 38 countries. Int J Epidemiol 1988;17:414-8.
-
Borowsky SA et al. Continued heavy drinking and survival in alcoholic cirrhosis. Gastroenterol 1981;104:1755-61.
-
Pande NY et al. Cirrhotic portal hypertension: morbidity of continued alcoholism. Gastroenterol 1978;74:64-9.
-
Powell WJ et al. Duration of survival in patients with Laennec's cirrhosis. Am J Med 1968;44:406-20.
-
D'Amico G et al., op. cit.
-
D'Amico G et al., op. cit.
-
Brenner BM. Brenner and Rector's The Kidney. Philadelphia, PA: WB Saunders, 1996.
-
Bonomini V. Timing dialysis in chronic uraemia. Life Support Syst 1987;5:1.
-
Port FK. End-stage renal disease: magnitude of the problem, prognosis of future trends and possible solutions. Kidney Int 1995;48:S3-S6.
-
Khanna R et al. Choosing a dialysis therapy: introduction to a mini-symposium. Am J Kidney Dis 1984;4:217.
-
Schaefer JH et al. Outcome prediction of acute renal failure in medical intensive care. Intensive Care Med 1991;17:19-24.
-
Chertow GM et al. Prognostic stratification in critically ill patients with acute renal failure requiring dialysis. Arch Int Med 1995;155:1505-11.
-
Brenner BM, op.cit.
-
Chertow GM et al, op. cit.
-
United States Renal Data System. Comorbid conditions and correlations with mortality risk among 3399 hemodialysis patients. Am J Kidney Dis 1992;20:32-8.
-
Chertow GM et al, op. cit.
-
Brenner BM, op.cit.
-
Chertow GM et al, op. cit.
-
Groeneveld ABJ et al. Acute renal failure in the medical intensive care unit: predisposing and complicating factors and outcome. Nephron 1991;59:602-10.
-
United States Renal Data System, op. cit.
-
Chertow GM et al, op. cit.
-
McCarthy JT. Prognosis of patients with acute renal failure in the intensive care unit: a tale of two eras. Mayo Clin Proc 1996;71:117-26.
-
Groeneveld ABJ et al, op. cit.
-
United States Renal Data System, op. cit.
-
Chertow GM et al, op. cit.
-
Port FK, op. cit.
-
Mc Carthy JT, op. cit.
-
Groeneveld ABJ et al, op. cit.
-
United States Renal Data System, op. cit.
-
Salomone M et al. Dialysis in the elderly: improvement of survival results in the eighties. Nephrol Dial Transplant 1995;10:60-4.
-
Chertow GM et al, op. cit.
-
Shabar E et al. Improved survival of stroke patients during the 1980's: The Minnesota Stroke Survey. Stroke 1995;26:1-6.
-
Gladman J et al. Predicting the outcome of acute stroke: prospective evaluation of five multivariate models and comparison with simple methods. J Neurol Neurosurg Psych 1992;55:347-51.
-
Chambers et al. Prognosis of acute stroke. Neurology 1987;37:221-5.
-
Viitanem M et al. Determinants of long-term mortality after stroke. Acta Med Scand 1987;221:349-56.
-
Howard G et al. Community hospital-based stroke programs: North Carolina, Oregon and New York III. Factors influencing survival after stroke: proportional hazards analysis of 4219 patients. Stroke 1986:17:294-9.
-
Henley S et al. Who goes home? Predictive factors in stroke recovery. J Neurol Neurosurg Psych 1985;48:1-6.
-
Allen CMC. Predicting the outcome of acute stroke: a prognostic score. J Neurol Neurosurg Psych 1984;47:475-80.
-
Base E. Cardiopulmonary arrest: pathophysiology and neurologic complications. Ann Int Med 1985;103:920-7.
-
Dougherty J et al. Hypoxic-ischemic brain injury and the vegetative state: clinical and neuropathologic correlation. Neurology 1981;31:991-7.
-
Widjicks E et al. Prognostic value of myoclonus states in comatose survivors of cardiac arrest. Ann Neurol 1994;35:239-43.
-
Hamel MB et al. Identification of comatose patients at high risk for death or severe disability. JAMA 1995;273:1842-8.
-
Barnford J et al. The frequency, causes and timing of death within 30 days of a first stroke: The Oxfordshire Community Stroke Project. J Neurol Neurosurg Psych 1990;53:824-9.
-
Dennis M et al. Long-term survival after first-ever stroke: The Oxfordshire Community Stroke Project. Stroke 1993;24:796-800.
-
Turney T et al. The natural history of hemispheric and brainstem infarction in Rochester, Minnesota. Stroke 1984;15:790-4.
-
Wade D et al. Recovery after stroke: the first 3 months. J Neurol Neurosurg Psych 1985;48:7-13.
-
Murden RA et al. Recent weight loss is related to short-term mortality in nursing homes. J Gen Int Med 1994; 9:648.
-
Dwyer JT et al. Changes in relative weight among institutionalized elderly adults. J Gerontol 1987; 42(3):246.
-
Marton KI et al. Involuntary weight loss: diagnostic and prognostic significance. Ann Int Med 1981; 95:568.
-
Rudman D et al. Antecedents of death in the men of a Veteran's Administration nursing home. J Am Geriatr Soc 1987; 35:496.
-
Corti M-C et al. Serum albumin level and physical disability as predictors of mortality in older persons. JAMA 1994; 48:1173.
-
Agrawal N et al. "Predictive ability of various nutritional variables for mortality in elderly people." Am J Clin Nutr 1988; 48:1173.
-
Phillips P et al. "Grip strength, mental performance and nutritional status as indicators of mortality risk among female geriatric patients." Age and Aging 1986; 15:53.
-
Hanrahan P et al. "Survival time among end-stage demented hospice patients." NR253, presented at annual conference of American Psychiatric Association, Miami, Florida, 1995.
-
Caroscio JT et al. Amyotrophic lateral sclerosis: its natural history. Neurol Clinics 1987;5:1-8.
-
Ringel SP et al. The natural history of amyotrophic lateral sclerosis. Neurology 1993;43:1316-22.
-
Norris F et al. Onset, natural history and outcome in idiopathic adult motor neuron disease. J Neurol Sci 1993;118:48-55.
-
Haverkamp LJ et al. Natural history of amyotrophic lateral sclerosis in a database population. Brain 1995;118:707-19.
-
Smith RA et al. Recombinant growth hormone treatment of amyotrophic lateral sclerosis. Muscle Nerve 1993;16:624-33.
-
Lilienfeld DE et al. Rising mortality from motoneuron disease in the USA, 1962-1984. Lancet 1989;1:710-12.
-
Durrleman S et al. Increasing trends of ALS in France and elsewhere: are the changes real? Neurology 1989;39:768-73.
-
Riggs JE et al. Rising mortality due to Parkinson's disease and amyotrophic lateral sclerosis: a manifestation of the competitive nature of human mortality. J Clin Epidemiol 1992;45:1007-12.
-
Bonduelle M. Amyotrophic lateral sclerosis. In Vincken PJ & Bruyn GW, Eds. Handbook of Clinical Neurology. New York, Elsevier, 1973:22:281-338.
-
Appel SH et al. Amyotrophic lateral sclerosis associated clinical disorders and immunological evaluations. Arch Neurol 1986;43:234-8.
-
Mulder DW et al. Patient resistance and prognosis in amyotrophic lateral sclerosis. Mayo Clin Proc 1976;51:537-41.
-
Jablecki, CK, Personal communication.
-
Rosen AD. Amyotrophic lateral sclerosis. Arch Neurol 1978;35:638-42.
-
Haverkamp LJ et al. Op. cit.
-
Jablecki CK et al. Survival prediction in amyotrophic lateral sclerosis. Muscle Nerve 1989;12:833-41.
-
Norris FH et al. The administration of guanidine in amyotrophic lateral sclerosis. Neurology 1974;24:721-8.
-
Olarte MR. Therapeutic trials in amyotrophic lateral sclerosis. Adv Neurol 1982;36:555-7.
-
Andres PL et al. Quantitative motor assessment in amyotrophic lateral sclerosis. Neurology 1986;36:937-41.
-
Appel V et al. A rating scale for amyotrophic lateral sclerosis: description and preliminary experience. Ann Neurol 1987;22:328-33.
-
Jablecki CK et al, op. cit.
-
Eisen A et al. Duration of amyotrophic lateral sclerosis is age dependent. Muscle Nerve 1993;16:27-32.
-
Jablecki CK et al, op. cit.
-
Adapted from Jacox A et al, Management of Cancer Pain.. US Department of Health and Human Services, AHCPR Publication No. 94-0592, March 1994.
APPENDIX I. MEDICAL GUIDELINES FOR DETERMINATION OF PROGNOSIS: TYPE, STRENGTH AND CONSISTENCY OF EVIDENCE
These guidelines were constructed whenever possible on the basis of evidence from the medical literature concerning early mortality in non-cancer diseases. This evidence may be grouped in the following categories: 214
-
Meta-analysis of multiple, well-designed controlled studies.
-
At least one well-designed experimental study.
-
Well-designed, quasi-experimental studies:
-
Nonrandomized controlled.
-
Single group pre/post.
-
Cohort.
-
Time Series.
-
Matched case-controlled.
-
-
Well-designed non-experimental studies.
-
Comparative and correlational descriptive and case studies.
-
-
Case reports and clinical examples.
Strength and consistency of evidence may then be sorted as follows:
-
There is evidence of Type I or consistent findings from multiple studies of Types II, III or IV.
-
There is evidence of Types II, III or IV, and findings are generally consistent.
-
There is evidence of Types II, III or IV, but findings are inconsistent.
-
There is little or no evidence, or there is Type V evidence only.
-
There has been no attempt in these Guidelines to classify each recommendation individually. In general, most of these Guidelines would be classified as within Group B, with a number in Groups A and C. With further more targeted research on mortality in end-stage non-cancer disease, it would be expected that Guidelines would evolve upward in this classification to Categories A or B.
APPENDIX II. KARNOFSKY PERFORMANCE STATUS SCALE DEFINITIONS RATING (%) CRITERIA
| Karnofsky Performance Status Scale Definitions Rating Criteria | ||
|---|---|---|
| Oxford Textbook of Palliative Medicine, Oxford University Press. 1993;109. | ||
| Able to carry on normal activity and to work; no special care needed. | 100 | Normal no complaints; no evidence of disease. |
| 90 | Able to carry on normal activity; minor signs or symptoms of disease. | |
| 80 | Normal activity with effort; some signs or symptoms of disease. | |
| Unable to work; able to live at home and care for most personal needs; varying amount of assistance needed. | 70 | Cares for self; unable to carry on normal activity or to do active work. |
| 60 | Requires occasional assistance, but is able to care for most of his personal needs. | |
| 50 | Requires considerable assistance and frequent medical care. | |
| Unable to care for self; requires equivalent of institutional or hospital care; disease may be progressing rapidly. | 40 | Disabled; requires special care and assistance. |
| 30 | Severely disabled; hospital admission is indicated although death not imminent. | |
| 20 | Very sick; hospital admission necessary; active supportive treatment necessary. | |
| 10 | Moribund; fatal processes progressing rapidly. | |
| 0 | Dead | |
APPENDIX III. NEW YORK HEART ASSOCIATION (NYHA) FUNCTIONAL CLASSIFICATION
| New York Heart Association Functional Classificaiton | |
|---|---|
| Class I. | Patients with cardiac disease, but without resulting limitation of physical activity. Ordinary physical activity does not cause undue fatigue, palpitation, dyspnea, or anginal pain. |
| Class II. | Patients with cardiac disease resulting in slight limitation of physical activity. They are comfortable at rest. Ordinary physical activity results in fatigue, palpitation, dyspnea, or anginal pain. |
| Class III. | Patients with marked limitation of physical activity. They are comfortable at rest. Less than ordinary activity causes fatigue, palpitation, dyspnea, or anginal pain. |
| Class IV. | Patients with cardiac disease resulting in inability to carry on any physical activity without discomfort. Symptoms of heart failure or of the anginal syndrome may be present even at rest. If any physical activity is undertaken, discomfort is increased. |
APPENDIX IV. FUNCTIONAL ASSESSMENT STAGING (FAST)
(Check highest consecutive level of disability.)
-
No difficulty either subjectively or objectively.
-
Complains of forgetting location of objects. Subjective work difficulties.
-
Decreased job functioning evident to co-workers. Difficulty in traveling to new locations. Decreased organizational capacity.*
-
Decreased ability to perform complex tasks, e.g., planning dinner for guests, handling personal finances (such as forgetting to pay bills), difficulty marketing, etc.
-
Requires assistance in choosing proper clothing to wear for the day, season or occasion, e.g., patient may wear the same clothing repeatedly, unless supervised.*
-
-
Improperly putting on clothes without assistance or cueing (e.g., may put street clothes on over night clothes, or put shoes on wrong feet, or have difficulty buttoning clothing) occasionally or more frequently over the past weeks.
-
Unable to bathe properly (e.g., difficulty adjusting bath-water temperature) occasionally or more frequently over the past weeks.*
-
Inability to handle mechanics of toileting (e.g., forgets to flush the toilet, does not wipe properly or properly dispose of toilet tissue) occasionally or more frequently over the past weeks.*
-
Urinary incontinence (occasionally or more frequently over the past weeks).*
-
Fecal incontinence (occasionally or more frequently over the past weeks).*
-
-
-
Ability to speak limited to approximately a half a dozen intelligible different words or fewer, in the course of an average day or in the course of an intensive interview.
-
Speech ability is limted to the use of a single intelligible word in an average day or in the course of an intensive interview (the person may repeat the word over and over).
-
Ambulatory ability is lost (cannot walk without personal assistance).
-
Cannot sit up without assistance (e.g., the individual will fall over if there are not lateral rests [arms] on the chair).
-
Loss of ability to smile.
-
Loss of ability to hold up head independently.
-
* Score primarily on the basis of information obtained from acknowledgeable informant and/or category.
Reisberg, B. Functional assessment staging (FAST). Psychoparamacology Bulletin, 1988; 24:653-659.
APPENDIX VI. DIAGNOSTIC IMAGINGFACTORS INDICATING POOR PROGNOSIS AFTER STROKE
-
For non-traumatic hemorrhagic stroke:
-
For thrombotic/embolic stroke:
APPENDIX D. WISCONSIN STATE GUIDELINES FOR MEDICARE HOSPICE CARE PROVISION IN THE NURSING HOME1
| Tommy G. Thompson Governor | State of Wisconsin Department of Health and Social Services | Division of Health |
| Joe Leean Secretary | 1 West Wilson Street P.O. Box 309 Madison, WI 53701-0309 |
| Date: | January 19, 1996 | |
| To: | Hospices Nursing Homes | BQC-96-002 HSPCE _2_ NH _1_ |
| From: | Judy Fryback, Director Bureau of Quality Compliance |
Guidelines for Care Coordination for Hospice Patients Who Reside in Nursing Facilities
Regulatory concerns have resulted about the appropriate application of nursing home and hospice regulations to nursing home residents who have elected hospice services. To respnd to these concerns, and to promote compliance with both the nursing home and hospice requirements, representatives from the Wisconsin Health Care Association (WHCA), the Wisconsin Association of Homes and Services for the Aging (WAHSA), the Hospice Organization of Wisconsin (HOW) and the Bureau of Quality Compliance (BQC) met as a workgroup to assess these concerns and to develop a protocol to resolve them. The protocol that was developed is attached for your review.
One of the most significant problems identified was the nursing home regulation that requires a new Resident Assessment Instrument (RAI) when there are significant changes in a resident's or patient's condition. The workgroup developed a document called "MDS/RAP--Change of Condition," to guide care planning and to address the RAI requirements for hospice residents/ patients residing in nursing homes. This document is intended to be a tool to facilitiate the provision and coordination of care in a consistent manner, while meeting the intent of hospice and long term care regulatory requirements.
The use of this comprehensive document as a tool in planning services for hospice patients residing in nursing facilities should facilitate the coordination of care and benefit patient care.
The Bureau of Quality Compliance, along with the three associations, is planning a statewide training the implementation of these guidelines in the spring of 1996.
Please share this information with your staff. Questions regarding this information can be directed to either Barbara Woodford, Nurse Consultant, Provider Regulation Section at (608) 264-9896; or Richard Cooperrider, Supervisor, Community Based Provider Program, at (608) 267-7389.
JF/RC/BW/jh 96002.nm
NURSING HOME/HOSPICE INTERFACE
Guidelines For Care Coordination
For
Hospice Patients Who Reside in Nursing Facilities
This document was jointly produced by representatives of the Wisconsin Health Care Association (WHCA), the Wisconsin Association of Homes and Services for the Aging (WAHSA), and the Hospice Organization of Wisconsin (HOW). All rights reserved. No portion may be reproduced without written permission of these organizations.
October 1995
CONTENTS
SECTION I. Introduction and Background
SECTION II. Regulatory References
SECTION III. Contract Considerations for Hospices and Nursing Homes
SECTION IV. Clinical Protocol Development
- Priority Areas
- Plan of Care
- MDS Care Plan Process
- Examples
- Exhibit A
- Exhibit B
SECTION V. Guidelines for Inservice/Education Planning
SECTION VI. Conclusion and Acknowledgments
SECTION I. INTRODUCTION AND BACKGROUND
Persons who are eligible to access their hospice entitlement have the right to receive those services in their primary place of residence. For some individuals, their place of residence may be a nursing home. In order to protect access to hospice care for nursing home residents in Wisconsin, a statewide task force was formed in June of 1994. This task force consisted of representatives of the hospice and nursing home industries across the state.
Initially, representatives from WHCA, WAHSA, and HOW met to discuss problems arising in the interface between hospice and nursing homes. Most of these problems result from differences in the application of both nursing home and hospice regulations to those nursing home residents who have elected hospice services.
A clinical workgroup was appointed to address what many considered the most pressing problem in the hospice/nursing home interface: anticipated changes in patient condition which could potentially trigger the need for a new Minimum Data Set (MDS), as required by nursing home regulations. This workgroup developed a draft MDS/RAP change of condition document to guide care planning and address MDS regulatory requirements for nursing home residents who elect hospice services. The draft was presented to representatives from the Wisconsin Division of Health, Bureau of Quality Compliance, who were favorably impressed and recommended field testing of the document. Field testing commenced in the fall of 1994 following distribution of the document to all Wisconsin hospices and nursing homes that are members of the three statewide organizations. It concluded six months later. Minor changes recommended as a result of the field testing were incorporated into Section IV.B. (MDS Care Plan Process).
Concurrent with field testing, this work group continued to meet to address other clinical issues. Two additional work groups were formed to address other significant issues impacting coordination of hospice care in the nursing home. One work group was given the task of developing guidelines to deal with contractual issues; the other work group dealt with educational issues. These three work groups' efforts comprise the Clinical Protocols, Contract, and Education sections of the guidelines.
This comprehensive document is not intended to be a "blueprint" for providers, but rather a tool to facilitate care coordination in a consistent manner, while maintaining regulatory compliance. Nursing homes and hospices engaging in collaborative arrangements are encouraged to structure their individual relationships in a manner that reflects their unique mission, community needs, and patient populations.
The Bureau of Quality Compliance reviewed this document in October of 1995 and determined that it meets both hospice and nursing home regulations in the State of Wisconsin.
SECTION II. REGULATORY REFERENCES
Protocols and guidelines outlined in this document were developed with consideration for existing state and federal regulations. References include:
42 CFR Part 418, Hospice
Health Care Financing Administration (HCFA), State Operations Manual and Hospice Interpretive Guidelines
Chapter HSS 131, Hospices, Wisconsin Administrative Code
Chapter HSS 132, Nursing Home Rules, Wisconsin Administrative Code
42 CFR Part 483, Medicare and Medicaid; Requirements For Long Term Facilities
SECTION III. CONTRACT CONSIDERATIONS FOR HOSPICES AND NURSING HOMES
Introduction
The following list of key considerations during hospice/nursing home contract negotiations is meant to assist providers in effectively coordinating provider services to the hospice patient receiving routine home care who resides in a nursing home. While by no means all-inclusive, these factors reflect many provisions found in the hospice and nursing home regulations and were compiled from comments and guidance distributed by authoritative state (Bureau of Quality Compliance) and federal (Health Care Financing Administration) sources.
The information which follows is specifically pertinent to the routine home care contract. It is not intended to comprehensively address considerations for inpatient and respite care, which hospices and nursing homes may elect to include as part of the same contract or as separate contracts. Providers are encouraged to review the following contract considerations, but since the listing is not exhaustive, are cautioned to also review their respective regulations, insurance and liability concerns, financial position and attorney's advice prior to entering into any formal contract.
* * * * * *
CONSIDERATIONS FOR THE HOSPICE "ROUTINE HOME CARE" CONTRACT
-
Administrative Concerns and Core Services Requirements
-
The hospice/nursing home agreement must be in writing.
-
The written agreement must specify that (1) the hospice takes full responsibility for professional management of the patient's hospice care, and (2) the nursing home provides room and board.
-
Hospice must provide the same services otherwise offered if the patient was in a private residence, including necessary medical services and inpatient care arrangements.
-
Identify a dispute resolution mechanism to be utilized in the event of disputes.
-
Hospice may not discharge a hospice patient at its discretion, even if care promises to be costly or inconvenient.
-
Statute/regulation prohibits a hospice from discontinuing care due to inability of the patient to pay for care.
-
References to specific government agencies can often be misleading and should be omitted from contract language. Refer more generally to "state" (or "federal") regulations, rather than "HCFA," "BQC," etc.
-
Admission criteria and requirements must be identical for all individuals regardless of pay source.
-
Specify the exact services, and extent of services, that will be provided individually by the hospice and nursing home.
-
Specify the exact responsibilities of each provider in the provision, and coordination, of care and services.
-
Substantially all core services must be routinely provided "directly" by hospice employees, and must not be delegated. (Interpretation of "directly" is that the person providing the service for the hospice is a hospice "employee." "Employee" includes paid staff and volunteers under the jurisdiction of the hospice (see 42CFR 418.3).
-
Hospice must provide the following core services through its own employees:
- physician services
- nursing services
- medical social services
- counseling services
-
Hospice may not contract with the nursing home to provide core services.
-
The nursing home may provide non-core services, if hospice assumes management responsibility for these services, and, assures that these services are performed in accord with hospice policy and the plan of care.
-
Room and board services to be provided by the nursing home include:
- personal care services
- assistance with ADLs
- administration of medications
- social activities
- room cleanliness
- supervision/assistance with DME use and prescribed therapies
-
Hospice must include the patient's primary physician in the care planning process.
-
Hospice certification and licensure does not require designation of a primary caregiver, although individual hospices can require this as a prerequisite to admission.
-
Identify the terms and procedure for formal review and renewal of the hospice/nursing home relationship on a regular basis.
-
-
Coordination of Services
-
At the time each hospice patient/resident is admitted to the facility, the nursing home must have physician orders for the person's immediate care.
-
Both providers must specify who obtains, and who retains, the supply of emergency medications.
-
All information relevant to the patient's care must be shared and contained in the medical records compiled by both the hospice and nursing home. (Caution: The term "relevant" must be interpreted broadly enough to avoid inadvertently failing to share marginally relevant information.)
-
Except where dictated by state or federal regulations, identify which provider will retain "originals" and which provider will retain "copies" of pertinent documents in the medical record.
-
Specify a procedure for the prompt and orderly relay of general information, MD orders, etc., between the providers.
-
Specify a procedure that clearly outlines the chain of communication between the hospice and nursing home in the event a crisis or emergency develops.
-
Identify who will be responsible for completing various parts of the MDS document. (It is, ultimately, the responsibility of the nursing home to make sure the MDS is completed, signed and dated.)
-
Indicate whether hospice patients will be allowed to use their own medications. If so, the expiration date and labelling requirements of HSS 132 must be satisfied.
-
The hospice and nursing home must jointly coordinate, establish, and agree upon a single plan of care to be used by both providers. This coordinated single plan of care must be implemented according to accepted professional standards of practice.
-
The coordinated plan of care must specifically identify the respective care and services which the nursing home and hospice will provide.
-
Aside from responsibilities that are part of the core requirements, include a statement that the plan of care must specify who is responsible for carrying out various patient interventions.
-
Specify the chain of communication to be followed between the hospice and nursing home whenever a change of condition occurs and/or changes to the plan of care are indicated.
-
All changes in the plan of care must be immediately communicated to the other provider.
-
Each provider must be aware of the other's responsibilities in implementing the plan of care.
-
Hospice must ensure that hospice services are always provided in accordance with the plan of care, in all settings.
-
Hospice may involve nursing home personnel in administration of prescribed therapies in the patient's plan of care only to the extent that hospice would routinely utilize the patient's family/caregiver in implementing the plan of care.
-
Hospice is responsible for making all inpatient care arrangements.
-
-
Employment Issues
-
A key consideration for both the hospice and nursing home is the extent to which services will be directly provided by hospice with its own staff, since hospice receives the payment.
-
A hospice may use contracted employees for core services only during:
- periods of peak patient load
- extraordinary circumstances
-
Nursing home employees may also be employed by the hospice to serve hospice patients.
-
For purposes of a hospice, "employee" is defined in 42 CFR 418.3.
-
Essential requirements for nursing home employees who are also employed by hospice to perform core services include:
- accurate time records
- clear delineation of responsibilities (intent is to avoid allegations of dual reimbursement.)
-
-
Reimbursement Issues
The following chart briefly summarizes various reimbursement mechanisms for hospice care provided in a nursing home:
Medicaid Reimbursement Medicare/Medicaid
(Dual Entitlees)Medicare Private Pay/ Insurance * In rare cases, if it can be demonstrated that skilled nursing care as defined by Medicare is needed for care not related to the terminal illness, Medicare Part A will pay for nursing home care under normal Part A Medicare and hospice care under the Medicare Hospice Benefit. T.19 pays hospice rate for routine home care plus room and board at 95% of nursing home's Medicaid rate. Hospice reimburses nursing home in accordance with contract. (NOTE: Hospice may contract with nursing home for services covered by hospice (e.g., supplies, pharmacy, DME, OT, PT, speech, CNAs). T.18 pays hospice rate for routine home care. T.19 pays hospice at 95% of nursing home's Medicaid rate. Hospice reimburses nursing home in accordance with contract. (NOTE: Hospice may contract with nursing home for services covered by hospice (e.g., supplies, pharmacy, DME, OT, PT, speech, CNAs).
Patient must either* Elect the Medicare Hospice Benefit (Medicare pays hospice routine home care, and nursing home bills patient or private insurance);
or,
Elect normal Medicare (revoke hospice benefit). Nursing home bills Medicare. Hospice may provide service and bill patient or private insurance.
Nursing home bills patient or private insurance. Hospice bills patient or private insurance.
***************
SAMPLE PROVISIONS FOR INCLUSION
IN A
HOSPICE/NURSING HOME CONTRACT
Developed by Jan A. Erickson, Director of Legal Services,
Wisconsin Health Care Association; and Mary H. Michal, Shareholder,
Reinhart, Boerner, Van Deuren, Norris & Rieselbach, S.C.
On behalf of the Hospice/Nursing Home Task Force, the following sample contract provisions have been compiled for review or use by providers when developing the format of a hospice-nursing home contract. Since it is essential that the contract process be individualized to best meet the particular circumstances of the contracting parties, these sample provisions are intended for general reference only.
This document does not purport to be all-inclusive or "model" in nature. It will likely need to be changed in at least several respects to accurately conform to the intentions of each party. For example, exact terms used in the "Definitions" section will probably vary among providers and certain other sections might be more easily addressed in combination under one general topic heading. In addition, providers may prefer to include additional provisions and sections which are not included among the samples in order to provide greater detail and clarity to their agreement. Therefore, while providers should feel free to review these sample provisions (as well as others) during preliminary contract negotiations, the format of their actual contract should always reflect the individuality of their specific relationship.
***************
RECITALS
Definitions (particularized to individual needs and terminology):
Attending Physician
Care Manager
Covered Services
Facility
Hospice
Hospice Care
Hospice Medical Director
Hospice Services
- Routine Home Care
- Inpatient Respite Care
- Continuous Care
- Inpatient Acute Care
Informed Consent
Interdisciplinary Group
Non-covered Services
Nursing Home Medical Director
Patient Care Management
Plan of Care
Residential Hospice Patient
Respite Care
Room and Board Services
Other Pertinent Definitions as Identified by the Parties
Eligible Residents (criteria):
Medicaid Eligible
Medicare Eligible
Medicaid/Medicare (Dual Entitlees)
Private Insurance or HMO
Private Pay
Other Pertinent Sections As Identified By The Parties
Coordination of Services:
Admission Procedures (general process, written orders, authorizations)
Patient Care Management (decision process, delegation of responsibility)
Continuity of Care (transfers between levels of care, actions requiring patient notice)
Communication Process (detail the process generally and for emergencies)
- notification of MD (change of condition, death, etc.)
- notification of hospice
Interdisciplinary Team Meetings
Quality Assurance Program
Drugs and Pharmaceuticals
Medical Equipment and Medical Supplies
Transportation and Ambulance
Family Services and Bereavement Care
Other Pertinent Sections As Identified By The Parties
Hospice Duties, Responsibilities and Services:
Hospice Services (general coverage under Routine Home Care)
Provision of Core Services
Compliance with Law (including licensure, staff qualifications)
Hospice Patient Care Management
Management of the Terminal Illness: Plan of Care
Medical Orders: Responsibilities of Attending Physician
Medical Order Procedures
Documentation (clarification of respective duties, location of original medical record)
Confidentiality of Medical Record
Orientation and Education
Other Pertinent Sections As Identified By The Parties
Facility Duties, Responsibilities and Services:
Facility Services (generally, room and board, specific services, plan of care, cooperation with hospice in identified areas, bedhold policy)
Compliance with Law (including licensure, staff qualifications)
Availability of Nursing Home Care (hours of care, adequate services, personnel)
Documentation (clarification of respective duties, location of original medical record)
Facility Staff Privileges: Hospice Medical Director
Access to Documents (medical/business records, federal record retention requirements for facility, subcontractors)
Orientation and Education
Other Pertinent Sections As Identified By The Parties
Financial Responsibility:
Responsibility of the Hospice
Responsibility of the Facility
Reimbursement
- Medicaid Patients
- Medicare Patients
- Medicaid/Medicare Patients
- Private Pay/Insurance Patients
Purchase of Services by the Hospice from the Facility
Other Pertinent Sections As Identified By The Parties
Insurance and Indemnification
Joint Review of Hospice Services (quality, appropriateness)
Compliance with Government Regulations
Relationship Between the Parties
Conflict Resolution Process
Term of the Agreement (length, renewals)
Termination of the Agreement (for cause/without cause, events precipitating, regulatory implications, resident transfers and single-case continuation agreements, resident notice timeframes)
Amendments to the Agreement
Notice Requirements (form, method, delivery)
Miscellaneous (including Non-discrimination Policy)
Other Pertinent Sections As Identified By The Parties
Appendices (if desired, may include references to provider policies, clinical protocols and procedures; see also: "Clinical Protocols" and "Educational Planning" documents for possible policies and protocols.)
The preceding information and documents were developed and compiled by Attorney Jan A. Erickson, Director of Legal Services for Wisconsin Health Care Association, and Attorney Mary H. Michal, a Partner in the law firm of Reinhart, Boener, van Deuren, Norns & Rieselbach, S.C., for the Wisconsin Hospice Nursing Home Task Force. These items may not be reproduced without the express written consent of either one of the authors, Hospice Organization of Wisconsin, or Wisconsin Health Care Association.
SECTION IV. CLINICAL PROTOCOL DEVELOPMENT
Effective coordination of care that assures patient needs as well as regulatory requirements are met, necessitates careful planning by both the nursing home and the hospice. The development of policies and protocols that define care coordination issues is essential to ensure consistent quality.
A. PRIORITY AREAS
Priority areas have been identified for consideration in the development of clinical protocols:
Admission process
Physician orders
Supplies and Medications
Medical Record Management
Hospice Core Services
Death Event
Quality Assurance
Emergency Care
Admission Process:
Protocols should be developed that clarify the process of admitting a current nursing home resident to the hospice program, a current hospice patient to the nursing home, and lastly for the simultaneous admission of a patient that is new to both the hospice and the nursing home.
ADMISSION: REFERRAL OF NURSING HOME RESIDENT TO HOSPICE
- Referral of resident made to Hospice
- Consult/information provided by Hospice
- Agreement obtained to pursue admission to Hospice care
- Hospice secures orders from the physician and manages orders from this point
- Change of condition MDS and RAP are completed. Hospice and nursing home begin care planning jointly.
- Nursing home applies from HSS 132 waiver.
ADMISSION: REFERRAL OF HOSPICE PATIENT TO NURSING HOME
- Referral to nursing home: the hospice may initiate contact with the nursing home and facilitates communication between the patient/family and the nursing home representative.
- Hospice and the nursing home coordinate securing required admission paperwork (i.e.: history and physical, TB screening, physician orders, etc.)
- Nursing home applies for HSS 132 waiver
- Transfer to patient to nursing home: hospice involvement begins on day of transfer
- MDS and revision of care plan initiated jointly by nursing home/hospice
ADMISSION: SIMULTANEOUS REFERRAL TO NURSING HOME/HOSPICE
- Referrals made to hospice and nursing home
- Hospice and nursing home coordinate the admission process and required paperwork
- Nursing home applies for HSS 132 waiver
- Transfer of patient to nursing home. Hospice involvement begins on day of transfer.
- MDS and initiation of joint care plan by hospice and nursing home
Physician Orders:
Hospice is responsible for securing medical orders and assuring they are consistent with the hospice philosophy.
- Standing orders are obtained by the hospice and provided to the nursing home. These orders are initiated by the hospice according to patient need.
- Nursing home standing orders may be utilized (based on contract), provided they are consistent with the hospice philosophy and specified on the plan of care.
- All verbal, phone and written orders must be preauthorized by hospice before initiated.
- Lab tests or other diagnostics related to terminal illness must be approved by hospice and specified on the plan of care
- Nursing home coordinates the scheduling of routine physician visits (and/or nurse practitioner visits). Under state and federal law applicable to nursing homes, a nurse practitioner may be utilized after 30 days of the first 90 days, and after 60 days thereafter. "Certified Registered Nurse Hospice" (CRNH) does not qualify as an advanced practice nurse.
- Nursing home nurse may accept orders from a hospice nurse as prescribed by the physician.
Supplies and Medication/Contracted Services:
Supplies and medications related to the management of the terminal illness are the responsibility of the hospice. The nursing home and hospice shoudl coordinate obtaining and monitoring the following supplies and services according to the terms of their contract:
- Prescription medications related to the terminal illness (medications supplied by hospice must meet nursing home pharmacy labeling requirements)
- Durable medical equipment (DME), i.e. W/C, walker, bath bench, commode, oxygen, etc.
- Disposable medical supplies related to the terminal illness, as specified in the plan of care.
- Provision of contracted services such as physical therapy, occupational therapy, speech therapy, dietary, etc., should be specified on the plan of care and clarified in the contract.
Medical Record Management:
- Copies of physician orders and coordinated plan of care should be on medical records of both organizations. The location of the original orders should be based on the contract.
- Copies of hospice informed consent and current physician certification must be on nursing home chart.
- Original MDS/RAP stays with nursing home record.
- The patient's record in the nursing home will be identified as a hospice patient.
- If specified in contract, both the hospice and nursing home retain copies of the other's record following death or discharge of a hospice patient.
- All clinical information (orders, data assessments, etc.) obtained by both providers that is relevant to the hospice patient's care while a resident must be on both patient's records.
Hospice Core Services:
Core services as defined in the Federal Register includes nursing services, medical social services, physician services (medical director), and counseling services. These services are to be provided routinely by the hospice employees.
Nursing services
- Nursing care is a core service of hospice for assessment, intervention, and evaluation.
- The hospice of prescribed interventions if specified in the plan of care.
Medical Social Services
- Social services is a core service of hospice for assessment, intervention, and evaluation related to the terminal illness.
- Other social service interventions may be provided collaboratively by hospice and nursing home social workers based on the plan of care.
Counseling Services
- Counseling is a core service of hospice for assessment, intervention, and evaluation related to the terminal illness (type of counseling is defined by individual hospice).
- Additional counseling interventions may be provided collaboratively by the hospice and nursing home staff based on the plan of care.
Physician Services
- Physician Services is a core service of hospice for assessment and evaluation.
- Physician participation may be provided by the medical director, the attending physician, a consulting physician, or their designees.
Other (non-core) services
- CNA/HHA services should be provided collaboratively by the hospice and nursing home based on patient need and specified in the plan of care (clarify in contract).
- Volunteer services are to be coordinated by the hospice but may be provided collaboratively by the hospice and nursing home as specified in the plan of care (clarify volunteer role in contract, especially related to hands-on care).
Death Event:
Protocols should be established that define mutual responsibilities at the time of death:
- The hospice must be notified.
- Review state and facility guidelines regarding coroner involvement, and follow protocol specified in contract for notification.
- Nursing home and hospice coordinate notification of physician for release of body when heart rate and respirations have ceased.
- Medication disposal.
Quality Assurance:
- The nursing home and hospice are required to implement quality assurance activities per respective regulations.
- A collaborative approach to problem solving and outcome monitoring is encouraged for inter-related issues.
Emergency Care:
Emergency care is defined as unexpected and may be related or unrelated to the terminal illness.
- Care should be consistent with the patient's stated wishes in the advance directive, and the physician's order with regard to code status.
- Nursing home staff provide immediate care in conjunction with facility policy and/or based on plan of care.
- Nursing home staff to call hospice immediately for change of condition and further assessment and revision of plan of care.
B. PLAN OF CARE
The nursing home and hospice must coordinate, establish, and agree upon one plan of care for both providers which reflects the hospice philosophy, and is based on the inidividual's needs and unique living situation in the nursing home. Each nursing home and hospice should develop policies and protocols to accomplish the MDS/RAP care plan process.
1. MDS CARE PLAN PROCESS
General Framework for Decision-Making:
Nursing homes are required to complete a minimum data set (MDS) for residents upon admission to the nursing facility. The MDS is to be reviewed and updated quarterly and annually. In addition, a new MDS is to be generated upon a change of patient condition. There are a series of criteria which, when present in a patient in various combinations or alone, can trigger the need to generate a new MDS.
Recommendation #1:
The task force recognized the importance of the initial MDS, as well as the quarterly and annual reviews of the MDS, and strongly encouraged that this information be shared, if not jointly developed, by the hospice and nursing home. It is essential that the hospice core team and the nursing home staff both device patient care decisions from the same core set of patient data.
The task force reviewed the fact that many of the patient-change criteria that can trigger the need for generation of a new MDS for a terminally ill or dying patient are, in fact, changes that are a natural, expected outcome of the progression of a terminal illness and/or the dying process. In these situations, the patient care benefits of generating a new MDS are minimal at best, and are far outweighed by the intrusion to the patient that the process of developing a new MDS entails. To address this fact, the task force developed the following statement to govern the decision-making process relating to a change-of-condition MDS.
Recommendation #2:
When a patient changes from a maintenance/curative course of care to hospice palliative, the initial change-of-condition minimum data set (MDS) is the final change of condition are anticipated and documented as part of the progression of the terminal illness and/or dying process. Quarterly and annual reviews are still required.
Illustrated as a process, this statement would look as follows:
| TRIGGER | Change in Patient Condition (after hospice election) | |
| NOTIFY AND REVIEW | Nursing home reports change to hospice and initiates a RAP review jointly with hospice staff | |
| DECISION | The hospice and nursing home staffs make a two-fold determination: (a) is the change in condition related to the progression of the terminal illness?, and (b) was the change already anticipated and documented on the MDS? | |
| If "YES" to both questions: | If "NO" to one or both questions: | |
| ACTION | No new MDS generated; hospice and nursing home staff address change through plan of care | New MDS must be generated by the nursing home staff and/or hospice and shared by the two agencies |
It was the consensus of the task force that revisions could be made in a provider's approach to the MDS process that would protect quality of care for patients by forcing a review of the patient condition against the changes expected and documented as part of the progression of the terminal illness and/or dying process, without triggering in a rote manner an intrusive MDS that, in many instances, is of little value in the care of the terminally ill patient electing hospice.
Patient Change of Condition:
The task force reviewed, in the context of the hospice philosophy and experience, various elements of the nursing home MDS and discussed how each one relates to the progression of the terminal illness and/or dying process. Elements subject to a change in condition were divided into three categories, detailed below. Guidelines to govern the decision-making process for determination of whether a new MDS is to be generated are outlined in the following paragraphs.
| Category | Problem Areas |
|---|---|
| Potential expected outcomes of the progression of the terminal illness and/or dying process | Delirium Use of psychotropic drugs Pressure ulcers Dental care Urinary incontinence (including catheter) Behavior Problems Falls (patient at risk for) Cognitive loss/dementia Communication |
| Expected outcome of the progression of terminal illness and/or dying process | Deydration and fluid maintenance Psychosocial changes Activities of daily living (ADL) Mood states Activities Nutritional status Visual function |
| Specials | Physical restraints Feeding tubes |
Potential, Expected Outcomes:
Certain changes in patient condition are potential, expected outcomes of the progression of the terminal illness and/or dying process. That is, while they may not be present in every terminally ill or dying patient, these changes are not unexpected and are routinely addressed by hospice personnel in the regular course of care. The fact that one of these changes should not, in the opinion of the task force, trigger a change of condition MDS provided that the change is related to the terminal illness and/or dying process, is anticipated and is documented. The value of the information generated through a change of condition MDS is of very limited value in reshaping care provided to the terminally ill or dying patient.
At the time the change in condition presents in the hospice patient residing in the nursing home, a determination should be made as to whether the change is related to the terminal illness or dying process, and whether it has been documented. If so, then a new MDS would not be triggered but, rather, the change of condition would be addressed by the hospice interdisciplinary team through the plan of care.
In evaluating the change of condition, the elements of the change as set out in Appendix F of the HCFA Nursing Home Manual should be reviewed by the nursing home staff with the hospice staff. It was understood by the task force that the hospice staff will not have working familiarity with the Manual or its criteria; this process will necessarily involve the expertise of the nursing home staff and underscores the importance of the review being a joint effort. The following grid provides sample statements that include the minimum elements to be reviewed under each RAP problem area listed. Additional elements for review may be included based on an assessment of individual patient circumstances.
| RAP Problem Area | Elements of Review |
|---|---|
| Delirium | Assess medication, psychosocial state and sensory loss. |
| Use of psychotropic drugs | Assess medications (drug review) and side effects of medication. Adjuvant drug therapy will be utilized to provide palliative symptom management. The risk-benefit ratio evaluation regarding drug initiation and continued use, including use outside the guidelines, will be assessed by the hospice IDT/IDG and nursing home staff and documented on the clinical record by the nursing home staff. |
| Pressure ulcers | Assess pressure ulcer versus stasis, review skin integrity. |
| Dental care | Dental care to increase comfort may be undertaken; preventive dental care not an unexpected part of the plan of care. |
| Urinary incontinence (including catheter) | Reduced output is a given in the progression of the terminal illness and dying process. Assess UTI, fecal impaction, CUA, diabetes, medication. |
| Behavior problems | Assess volatility of mood, medications, and cognitive status. |
| Falls (patient at risk for) | Safety issues can be anticipated because of physical deterioration with a terminal illness and associated adjuvant drug therapy. Assess medications, appliances, and environment. |
| Cognitive loss/dementia | Assess functional limitations, sensory impairment, medication involvement factors, and failure to thrive. |
| Communication | Assess components of communication, including strengths and weaknesses, and medication. |
Expected Outcomes:
Certain changes in patient condition are not only expected but are a given outcome with a high probability of occurring as part of the progression of the terminal illness and/or dying process. There are no identifiable benefits of triggering a change-of-condition MDS on these criteria, provided that the hospice and nursing home staffs (1) have jointly reviewed the criteria and determined that the change of condition is linked to the terminal illness and/or dying process, and (2) this review and determination has been documented in the clinical records.
Seven of the RAP problem areas are believed by the task force to be given outcomes of the progression of the terminal illness and/or dying process. The task force discussed each area and the following sample statements were developed to address the respective RAP problem areas listed.
Dehydration and fluid maintenance - Changes in hydration status and fluid balance will occur as part of the progression of the terminal illness and/or dying process; so long as the change noted in the patient is related to that progression, the benefits of generating a change- of-condition MDS are minimal in terms of patient care and do not outweigh the intrusion of conducting the MDS.
Psychosocial changes - Changes in lifestyle and interactions will occur as part of the progression of the terminal illness and/or dying process.
Activities of daily living (ADL) - The hospice patient residing in the nursing home will become progressively more dependent on his or her activities of daily living as part of the progression of the terminal illness and/or dying process.
Mood states - The person experiencing a terminal illness, from diagnosis to death, is anticipated to have emotional fluctuations.
Activities - A decrease in or non-involvement in activities is an expected outcome of the progression of the terminal illness and/or dying process.
Nutritional status - Declining nutritional status with progressive weight loss is expected in a terminal illness.
Visual function - A decrease in visual function is anticipated with the dying process.
Special Circumstances:
Changes in patient condition which present the potential need for feeding tubes or physical restraints warrant special consideration in the judgment of the task force. Both can be classified as potential expected outcomes of the progression of the terminal illness and/or dying process; yet they are of such a nature as to merit different elements of review.
Physical restraints - The least restrictive use of physical restraints only is to be applied to enable the resident to maintain his or her highest level of functioning. This is consistent with the guidelines set forth in the HCFA Nursing Home Manual, Appendix F.
Feeding tubes - The hospice will discuss the use of feeding tubes with the patient/family as the terminal illness progresses and initiate enteral/perenteral feeding at patient/family request as consistent with the philosophy of the individual hospice.
Provided that the need for use of physical restraints or feeding tubes is driven by the progression of the terminal illness and/or dying process, it is the belief of the task force that these changes should not alone trigger a change-of-condition MDS.
2. EXAMPLES
Exhibit A:
Subject: Nursing Home Setting
Title: Plan of Care
Policy: Hospice and nursing home will establish one individualized Plan of Care for the hospice patient/family in the Nursing Home Setting.
Purpose: To plan for quality hospice care.
Special Instructions:
-
Upon admission to hospice, the initial Plan of Care will be developed by hospice and charted.
-
Nursing home resident to hospice:
Hospice will do assessment and gather information from existing Plan of Care and nursing home staff. Hospice and nursing home will jointly establish the Plan of Care. Nursing home staff will initiate change-of-condition MDS/RAP as care changes focus from curative/maintenance to palliative.
Hospice patient to nursing home:
Hospice/nursing home will develop a Plan of Care. Nursing home will initiate change-of-care focus MDS/RAP and gather information from hospice.
-
At initial interdisciplinary team conference after nursing home admission, hospice will address the RAP problem areas and document anticipated potential patient outcomes based on terminal disease progression and dying process on form NH 021. A copy will be placed on nursing home chart.
-
Hospice will attend 14-day MDS/RAP review after notification by nursing home.
-
At interdisciplinary team meeting following MDS/RAP review, the triggered RAP areas will be addressed by hospice interdisciplinary/nursing home team meeting with problems opened or rationale for not opening documented on form NH 021 with copy on nursing home chart.
-
When a new problem is opened, hospice will document on interdisciplinary team minutes form if anticipated and related to terminal illness or if unrelated to terminal illness and provide a copy for nursing home chart.
-
Hospice will participate in nursing home quarterly review of MDS and Care Plan.
| Hospice Executive Director _________________________ | Date __________ |
| Nursing Home CEO _________________________ | Date __________ |
* Example reproduced with permission of Hospice of Portage County.
Exhibit B:
Care Plan Process
Purpose: To delineate responsibility for development of one plan of care in order to meet federal regulations of both nursing home and hospice.
Policy: Hospice patient residing at the nursing home will have one plan of care developed jointly by both staffs.
Procedure:
-
Three Different Categories of Patients
-
NEW PATIENT TO BOTH HOSPICE AND NURSING HOME
-
Nursing home does initial nursing plan of care within 24 hours.
-
Hospice-assessing RN writes on nursing home initial plan of care and brings copy back to hospice.
-
If hospice social worker has plan of care completed, assessing hospice RN brings copy of plan of care to nursing home to be filed with initial plan of care.
-
Proceed with MDS on Tuesday and care planning meetings on Thursday. Nursing home resident care coordinator to coordinate time with hospice patient care coordinator.
-
Hospice social worker to complete MDS form and patient care coordinator to bring to MDS meeting.
-
-
NEW PATIENT TO HOSPICE (NURSING HOME RESIDENT)
-
Hospice-assessing RN to review nursing home plan of care; make changes on nursing home plan of care and bring copy back to hospice.
-
Proceed with MDS on Tuesday and care planning meetings on Thursday. Nursing home resident care coordinator to coordinate time with hospice patient.
-
Hospice social worker to coordinate MDS with nursing home social worker and patient care coordinator to bring to MDS meeting.
-
-
NEW PATIENT ONLY TO NURSING HOME (CURRENT HOSPICE PATIENT)
-
Hospice to provide a copy of plan of care and assessments.
-
Nursing home to use hospice plan of care.
-
Hospice social worker to do MDS form and patient care coordinator to bring to MDS meeting.
-
Proceed with MDS on Tuesday and care planning meetings on Thursday. Nursing home resident care coordinator to coordinate time with hospice patient care coordinator.
-
-
-
MDS AND CARE PLAN MEETING
-
MDS to be done on Tuesday - hospice RN and patient care coordinator; nursing home resident care coordinator and RN to attend.
-
Hospice social worker will contribute to MDS meeting with written form.
-
Care planning meeting will be on Thursday. Family, hospice SW, RN, patient care coordinator and nursing home RN, SW and resident care coordinator will attend.
-
NH - SW to invite family to meeting.
-
NH - RCC to contact hospice patient care coordinator to coordinate time for meeting.
-
MDS and care planning meetings will be done every three months.
-
-
PLAN OF CARE
-
Changes will be made on plan of care to reflect appropriate hospice care.
-
Changes will be entered into computerized plan of care and one plan of care will be filed into both charts.
-
-
IDG MEETINGS (INTERDISCIPLINARY GROUP)
-
Nursing home will attend IDG meetings at hospice offices approximately one month after the care planning at nursing home.
-
Patient care coordinator to coordinate and inform nursing home for attendance.
-
Plans of care which are updated every two weeks at IDG meetings will be Xeroxed and brought to nursing home.
-
All telephone calls to patient and families will be documented and copies provided to nursing home.
-
* Example reproduced with permission of Grancare Nursing Center of Green Bay.
SECTION V. GUIDELINES FOR INSERVICE/EDUCATION PLANNING
Clear communication of the basic components of the contract, the policies and protocols that guide care coordination, and the key regulations that govern both providers is essential for a successful nursing home/hospice partnership. Achieving quality outcomes for patients and their families should be the focus of all staff efforts.
Assuring effective participation by all levels of staff requires careful planning of the initial orientation following the establishment of a contract, as well as ongoing educational efforts aimed at improving efficiencies and understanding of experienced and new staff.
Suggested content for these educational efforts are separated into "Initial Orientation" and "Ongoing Education."
Initial Orientation
Introducing the hospice concept to nursing home staff may be most effectively accomplished by using an interdisciplinary approach. Representation from each of the core disciplines is ideal to establish trusting relationships and encourage professional interaction. Recommendations for inclusion in the initial orientation process are listed below.
*Note: It may be useful to group the topic areas according to individual roles of Nursing Home staff (i.e., meeting with business office and clerical staff separately from direct patient care staff to allow for questions and discussion specific to the expertise of the group.)
- Discussion of hospice concept and philosophy, including reference to patient's entitlement.
- Informed consent and corresponding expectations/accountabilities.
- Services available - delineation of benefits.
- Introduction of core team members/roles.
- Terminology - definition of terms as specified in the contract.
- How/when to notify hospice.
- On call availability
- Discussion of mutual roles and responsibilities as outlined in the contract
- Communication and collaboration relating to care planning, ongoing patient needs, family support, record maintenance.
- Symptom management practices common for hospice patients.
- Securing and processing of physician orders (including utilization of standing orders, if applicable).
- Reimbursement scenarios.
- Bereavement services available.
- Location of resource materials such as a hospice manual with accompanying quick references.
- DME, disposable supplies, oxygen, and ancillary services to be supplied by the hospice.
- Provision of pharmacy services.
Clarifying the role of the hospice team in the nursing home needs to be balanced by a corresponding effort to educate hospice staff on the regulations and protocols of the nursing home. Information to be included in this effort might include the following:
- Tour of the facility, with introductions of key personnel, location of records, security system operation, and any information specific to the physical layout and daily routine.
- Discussion of Resident Rights.
- Life Safety Code, including fire/emergency procedures, exits, etc.
- Key terminology - definition of terms, including terms specified in the contract.
- Comprehensive assessment process and requirements.
- Care planning process, including conferences, family involvement, etc.
- Record keeping practices.
- Infection control issues, especially including biohazard waste disposal, location of PPE and blood spill clean-up kit, etc.
- Chemical/Physical restraints.
- Medication management, including regulations governing use of psychotropics, "unnecessary medications", self-medication, etc.
- Patient levels of care and reimbursement scenarios.
- Pertinent facility policies (i.e., CPR, hydration, RN coverage, including any policies that explore ethical issues).
Ongoing Education:
Many hospices provide periodic updates for their contracted nursing homes to review practical issues related to mutual roles and responsibilities. This provides an opportunity for dialogue, problem solving, feedback, and recognition of the cooperative relationships and the impact this collaboration has on quality care for patients. Suggested topics to include in these periodic updates:
- Inservices on pain control and other symptom management protocols commonly used for hospice patients.
- Inservices on loss, grief and bereavement care.
- Quality assurance/improvement study results and recommendations.
- Practical issues related to communication with physicians, management of orders, etc.
- Care plan coordination process.
- Volunteer involvement and utilization.
- Review and discuss mutual roles and responsibilities as appropriate.
Some hospices hold regular conferences in the nursing home on a prearranged schedule (weekly to monthly) to communicate on patient related issues. Others conduct occasional IDG meetings in the nursing home and encourage nursing home staff participation.
These suggestions, as well as the guidelines for initial orientation, are not intended to be all-inclusive. Creative approaches that foster improved understanding and communication between the nursing home and hospice providers are encouraged. The use of various "mediums" is helpful to have available in the nursing home for staff who are unable to attend scheduled inservices. These might include audio/video tapes, self-learning modules, quick reference materials, and a manual containing pertinent hospice protocols/policies.
SECTION VI. CONCLUSION AND ACKNOWLEDGEMENTS
The Wisconsin Health Care Association, Wisconsin Association of Homes and Services for the Aging, and the Hospice Organization of Wisconsin have undertaken this statewide joint venture for the purpose of protecting access to quality hospice care for eligible nursing home residents.
Through the combined efforts of the initial task force and the associated work groups, the intended outcome has been to develop guidelines and protocols for nursing homes and hospices that are:
- flexible enough to meet individual patient needs;
- predictable enough to ensure quality of care; and
- consistent with the requirements that govern patient care as set forth in HSS 131, HSS 132, and federal regulations for hospices and nursing homes.
The measure of success for this collective effort is the question of access. It is hoped that access to hospice care for nursing home residents may be protected and expanded through diligent efforts to maintain clear communication while striving to meet the unique needs of patients and their families.
WHCA, WAHSA, and HOW gratefully acknowledge the contributions of the numerous individuals who have participated in this process and the support of their organizations. The shared commitment of the statewide nursing home and hospice industries has set the tone for continued success in this collaborative process.
APPENDIX E. ACKNOWLEDGMENT LIST
| Hospice of Metro Denver Denver, CO | VISTA Southfield, MI |
| San Diego Hospice San Diego, CA | Hospice of Palm Beach County West Palm Bech, FL |
| Hospice of North Central Florida Gainesville, FL | Hospice of the North Shore Evanston, IL |
| Hospice Association of Western NY Cheektowaga, NY | Hospice of the Grand Valley Grand Function, CO |
| VITAS Healthcare Corporation Miami, FL | Hospice of the Blue Grass Lexington, KY |
| Hospice of the Florida Suncoast Largo, FL | Cabrini Center for Nursing and Rehabilitation New York, NY |
| Parker Jewish Institute for Health Care and Rehabilitation New Hyde Park, NY | Jennings Hall Garfield Heights, OH |
| Frankfort Community Care Home Kansas | Clara Baldwin Stocker Home and Convalescent Hospital West Covina, CA |
| Laguna Honda Hospital and Rehabilitation San Francisco, CA | Bethany Medical Center Kansas City, KS |
| Terence Cardinal Cooke Health Center New York, NY | Catholic Care Center Wichita, KS |
| Menorah Park Center for Aging Cleveland, OH | Montefiore Home Beachwood, OH |
| Jewish Home for the Aged San Francisco, CA | Oklahoma State Department of Health Oklahoma City, OK |
| South Dakota Department of Health Pierre, SD | Agency for Health Care Health Facilities Compliance Tallahassee, FL |
| Colorado Department of Public Health and Environment Denver, CO | Genesis ElderCare Rehabilitation Tampa, FL |
| National Hospice Organization Washington, DC | Hospice Association of America Washington, DC |
| American Association of Homes and Services for the Aging Washington, DC | American Health Care Association Washington, DC |
| Robert Wood Johnson Foundation Princeton, NJ | HCFA/Center for Medicaid and State Operations Baltimore, MD |
| Wisconsin Department of Health and Family Services Madison, WI | New Jersey Department of Health and Senior Services Trenton, NJ |
NOTES
-
Reprinted with permission of the Hospice Organization of Wisconsin, all rights reserved.
| Report Files: | |
|---|---|
| MAIN REPORT | http://aspe.hhs.gov/daltcp/reports/impques.htm |
| APPENDIX A. Literature Review Methodology | http://aspe.hhs.gov/daltcp/reports/impquesa.htm#appendA |
| APPENDIX B. National Hospice Organization's Sample Contract | http://aspe.hhs.gov/daltcp/reports/impquesa.htm#appendB |
| APPENDIX C. Medical Guidelines for Determining Prognosis in Selected Non-Cancer Diseases and Hospice Enrollment Criteria for End-Stage Dementia Patients | http://aspe.hhs.gov/daltcp/reports/impquesa.htm#appendC |
| APPENDIX D. Wisconsin State Guidelines for Medicare Hospice Care Provision in the Nursing Home | http://aspe.hhs.gov/daltcp/reports/impquesa.htm#appendD |
| APPENDIX E. Acknowledgement List | http://aspe.hhs.gov/daltcp/reports/impquesa.htm#appendE |
PROJECT REPORTS AVAILABLE
The goal of ASPE's Medicare Hospice Benefit study was to provide general information on the role of the Medicare hospice benefit and more specific information about how end of life care is provided to institutionalized beneficiaries. Six reports wereproduced from this study:
Synthesis and Analysis of Medicare's Hospice Benefit: Executive Summary and Recommendations (report 1) briefly summarizes the methods used for each report and the findings and recommendations that emerged from each of the following reports under this study.
HTML http://aspe.hhs.gov/daltcp/reports/samhbes.htm
PDF http://aspe.hhs.gov/daltcp/reports/samhbes.pdf
Important Questions for Hospice in the Next Century (report 2) synthesizes the literature related to the Medicare hospice benefit and summarizes discussions with key informants on the use of hospice in nursing homes.
Executive Summary http://aspe.hhs.gov/daltcp/reports/impquees.htm
HTML http://aspe.hhs.gov/daltcp/reports/impques.htm
PDF http://aspe.hhs.gov/daltcp/reports/impques.pdf
Medicare's Hospice Benefit: Use and Expenditures, 1996 Cohort (report 3) analyzes Medicare utilization and payments for hospice users in 1996.
HTML http://aspe.hhs.gov/daltcp/reports/96useexp.htm
PDF http://aspe.hhs.gov/daltcp/reports/96useexp.pdf
Use of Medicare's Hospice Benefit by Nursing Facility Residents (report 4) examines differences in hospice utilization and expenditures as a function of when nursing facility residents started using hospice services (i.e., before or during a nursing home stay).
HTML http://aspe.hhs.gov/daltcp/reports/nufares.htm
PDF http://aspe.hhs.gov/daltcp/reports/nufares.pdf
Outcomes and Utilization for Hospice and Non-Hospice Nursing Facility Decedents (report 5) compares pain management and types of services provided to dying nursing home residents receiving hospice compared to other dying residents who did not receive hospice.
HTML http://aspe.hhs.gov/daltcp/reports/oututil.htm
PDF http://aspe.hhs.gov/daltcp/reports/oututil.pdf
Hospice Benefits and Utilization in the Large Employer Market (report 6) reports on how hospice services are provided by 52 large employers and used by their employees, and identifies alternative approaches to designing and administering hospice benefits.
Executive Summary http://aspe.hhs.gov/daltcp/reports/empmktes.htm
HTML http://aspe.hhs.gov/daltcp/reports/empmkt.htm
PDF http://aspe.hhs.gov/daltcp/reports/empmkt.pdf