
Randall Blair, Junqing Liu, Miriam Rosenau, Michael Brannan, Natalie Hazelwood, Kelsey Farson Gray, Jonathan Brown, Eric Morris, Alyssa Hart, Kenneth Jackson, Angela Schmitt, Katherine Sobel, Mary Barton, Milesh Patel, Allison Siegwarth, Xiao Barry, and Stephanie Rodriguez
Mathematica Policy Research
Abstract
As part of its National Quality Strategy, the U.S. Department of Health and Health Services (HHS) Office of the Assistant Secretary for Planning and Evaluation (ASPE) and the HHS Centers for Medicare and Medicaid Services (CMS) are committed to developing and implementing measures that can be used for behavioral health care quality improvement. To further the implementation of such measures, and as mandated in Section 3401, Subsection 10322 of the Patient Protection and Affordable Care Act of 2010, CMS developed the Inpatient Psychiatric Facility (IPF) Quality Reporting (IPFQR) program, a pay-for-reporting program that went into effect for fiscal year 2014. Under this program, IPFs must report their performance on a set of quality measures or face a two percentage point reduction to the update of their Medicare standard federal rate for that year. Funded through an inter-agency agreement between ASPE and CMS, the goal of this project was to develop and test measures that may be incorporated into the IPFQR program; these included four chart-based measures that assess screening for risk of suicide, risk of violence, substance use, and metabolic conditions, and one claims-based measure that assesses whether Medicare beneficiaries receive follow-up care after IPF hospitalization.
DISCLAIMER: The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
Printer friendly version in PDF format (122 PDF pages)
TABLE OF CONTENTS
A. Project Overview
B. Report Roadmap
A. Evidence Review
B. Reviewing Specifications of Similar Measures
C. Defining Data Sources, Denominators, and Numerators
III. RESEARCH METHODS
A. Quantitative Approach to Chart-Based Measure Testing
B. Quantitative Approach to Claims-Based Follow-Up Measure Testing
C. Qualitative Approach to Measure Testing
IV. TESTING RESULTS FOR SCREENING MEASURES
A. IPFs and Denominator Population
B. Quantitative Testing Results
C. Qualitative Testing Results
D. Summary of Findings and Proposed Revisions
V. TESTING RESULTS FOR THE FOLLOW-UP AFTER IPF HOSPITALIZATION MEASURE
A. Characteristics of Medicare Beneficiaries Who Used IPFs
B. Performance by Numerator Options
C. Impact of Measure Exclusions on Follow-Up Measure Performance
D. Follow-Up after IPF Hospitalization by Beneficiary Characteristics and Geographic Location
E. Reliability Analysis
F. Stakeholder Feedback on the Follow-Up Measure
G. Summary and Revisions to Follow-Up Measure Specification
VI. FOLLOW-UP MEASURE PERFORMANCE USING MERGED MEDICARE-MEDICAID CLAIMS
A. Methods
B. IPFs' Efforts to Encourage and Track Follow-Up Care
C. IPF Perspectives on a Chart-Based Approach to Measuring Follow-Up Care
D. Analysis of Insurance Coverage, Patient Demographics, and Sample Sizes
E. Conclusion
VIII. CONCLUSIONS AND LESSONS
APPENDICES
APPENDIX A: IPF Technical Expert Panel Members
APPENDIX B: Screening Measure Specifications
APPENDIX C: Follow-Up after IPF Hospitalization Measure Specifications
APPENDIX D: Supplemental Tables for Screening Measures
APPENDIX E: Summary of State Selection Process for Follow-Up Measure Analysis with Medicaid Claims
LIST OF FIGURES
FIGURE IV.1: Average Screening Performance Rates across 6 IPFs
FIGURE IV.2: Suicide Risk Screening Performance across 6 IPFs
FIGURE IV.3: Violence Risk Screening Performance across 6 IPFs
FIGURE IV.4: Substance Use Screening Performance across 6 IPFs
FIGURE IV.5: IPF Screening Performance, by Measure Specification
FIGURE IV.6: Metabolic Screening Performance across 6 IPFs
FIGURE IV.7: Performance on Screening Measures, by Primary Payer
FIGURE V.1: 30-Day Follow-Up Rates by IPF Diagnosis, among Non-Dual FFS Medicare Beneficiaries
FIGURE V.2: 30-Day Follow-Up Rate by Patient Ethnicity, among Non-Dual FFS Medicare Beneficiaries
FIGURE V.3: 30-Day Follow-Up after IPF Hospitalization by Region, among Non-Dual FFS Medicare Beneficiaries
FIGURE VII.1: Primary Payer for IPF Stays in 6 IPFs, 2013
LIST OF TABLES
TABLE ES.1: Measures Tested, Performance
TABLE I.1: Measures Developed for the IPFQR Program, 2012-2014
TABLE I.2: Timeline of IPFQR Program Measure-Development Activities
TABLE II.1: Comparison of New Measures and Similar Existing Measures
TABLE III.1: Quantitative Analyses for Chart-Based Measures
TABLE III.2: IPFs Represented in Measure Testing, 2014
TABLE III.3: Quantitative Analysis of Follow-Up after IPF Hospitalization Measure
TABLE IV.1: Number of Discharged and Sampled Patients, by IPF
TABLE IV.2: Characteristics of Denominator Population for Screening Measures, by IPF
TABLE IV.3: Screening Performance Rates, by IPF
TABLE IV.4: Suicide Risk Screening Performance, by IPF
TABLE IV.5: Violence Risk Screening Performance, by IPF
TABLE IV.6: Substance Use Screening Performance, by IPF
TABLE IV.7: Performance Rates across Screening Measures
TABLE IV.8: 1-Day versus 3-Day Measure Performance
TABLE IV.9: Metabolic Screening Performance, by IPF
TABLE IV.10: Screening Measure Exclusions
TABLE IV.11: Screening Measures Performance Before and After Exclusions
TABLE IV.12: Performance on Screening Measures across Demographic Characteristics
TABLE IV.13: Inter-Rater Agreement on Screening Measures
TABLE IV.14: Summary of Testing Results, Stakeholder Feedback, and Proposed Revisions for Screening Measures
TABLE V.1: Characteristics of FFS Medicare Beneficiaries with At Least One Mental Health IPF Hospitalization in Calendar Year 2008
TABLE V.2: Numerator Options for Follow-Up Measure
TABLE V.3: Follow-Up within 7 and 30 Days of IPF Hospitalization, among Non-Dual FFS Medicare Beneficiaries
TABLE V.4: Performance among Numerator Options: Follow-Up within 30 Days of IPF Hospitalization, among Non-Dual FFS Medicare Beneficiaries
TABLE V.5: Proportion of Eligible Discharges Excluded from the Follow-Up Measure Denominator, among Non-Dual FFS Medicare Beneficiaries
TABLE V.6: Impact of Measure Exclusions on Follow-Up Rates, among Non-Dual FFS Medicare Beneficiaries
TABLE V.7: Follow-Up after IPF Hospitalization by Patient Characteristics, among Non-Dual FFS Medicare Beneficiaries
TABLE V.8: Follow-Up after IPF Hospitalization by State, among Non-Dual FFS Medicare Beneficiaries
TABLE V.9: Follow-Up after IPF Hospitalization by Number of Discharges per Facility, among Non-Dual FFS Medicare Beneficiaries
TABLE V.10: Testing Results, Stakeholder Feedback, and Proposed Revisions to the Follow-Up after IPF Hospitalization Measure
TABLE VI.1: Facility Performance by Numerator Option: Follow-Up within 30 Days of IPF Hospitalization among Dual and Non-Dual Eligible Beneficiaries
TABLE VI.2: Follow-Up within 30 Days of IPF Hospitalization among All Medicare Beneficiaries, by Data Source
TABLE VII.1: IPFs Represented in Focus Groups and Debriefing Sessions, 2014
TABLE VII.2: Commonly Cited Facilitators to Tracking Follow-Up Care
TABLE VII.3: Commonly Cited Constraints to Tracking Follow-Up Care
TABLE VII.4: Comparison of Patient Demographics for FFS Medicare IPF Discharges versus All IPF Discharges
TABLE VII.5: Quarterly Sample Sizes for the Follow-Up after IPF Hospitalization Measure
TABLE VII.6: Advantages and Disadvantages of Chart and Claims-Based Approaches to the Follow-Up after IPF Hospitalization Measure
TABLE A.1: IPF Technical Expert Panel Members
TABLE B.1: Measure Specifications: Screening for Risk of Suicide
TABLE B.2: Measure Specifications: Screening for Risk of Violence
TABLE B.3: Measure Specifications: Screening for Substance Use
TABLE B.4: Measure Specifications: Metabolic Screening
TABLE C.1: Codes to Identify IPF Discharges
TABLE C.2: Codes to Identify Principle Mental Health Diagnosis
TABLE C.3: Codes to Identify Acute Care Facilities
TABLE C.4: Codes to Identify Admission to Non-Acute Care
TABLE C.5: Codes to Identify Patient Deaths and Transfer/Discharge to Another Institution
TABLE C.6: Codes to Identify Outpatient Visits, Intensive Outpatient Encounters, and Partial Hospitalizations
TABLE C.7: Codes to Identify Mental Health Practitioners in Medicare
TABLE C.8: Codes to Identify Mental Health Practitioners in Medicaid
TABLE C.9: Codes to Identify Outpatient Visits
TABLE C.10: Additional Resource: HEDIS Definition of Mental Health Practitioner
TABLE D.1: Average Performance on Screening Measures, Including and Excluding IPF
TABLE D.2: Number and Proportion of Patients Excluded from Screening Measures, by IPF
TABLE D.3: Percent Agreement on Screening Measures, by IPF
TABLE E.1: Results of State Selection Process for Merged Medicare-Medicaid Analysis
Mathematica Policy Research and the National Committee for Quality Assurance prepared this report under contract to the Office of the Assistant Secretary for Planning and Evaluation (ASPE), U.S. Department of Health and Human Services (HHS) (HHSP23320100019WI/HHSP23337001T). The authors appreciate the guidance of D.E.B. Potter, Joel Dubenitz, and Kirsten Beronio (ASPE), Elizabeth G. Ricksecker and Jeff Buck (HHS Centers for Medicare and Medicaid Services [CMS]), and Lisa Patton (HHS Substance Abuse and Mental Health Services Administration [SAMHSA]).
The views and opinions expressed here are those of the authors and do not necessarily reflect the views, opinions, or policies of ASPE, CMS, SAMHSA, HHS, or the technical expert panel. The authors are solely responsible for any errors.
Summary: As part of its National Quality Strategy, the U.S. Department of Health and Health Services (HHS) Office of the Assistant Secretary for Planning and Evaluation (ASPE) and the HHS Centers for Medicare and Medicaid Services (CMS) are committed to developing and implementing measures that can be used for behavioral health care quality improvement. To further the implementation of such measures, and as mandated in Section 3401, Subsection 10322 of the Patient Protection and Affordable Care Act of 2010, CMS developed the Inpatient Psychiatric Facility (IPF) Quality Reporting (IPFQR) program, a pay-for-reporting program that went into effect for fiscal year 2014. Under this program, IPFs must report their performance on a set of quality measures or face a two percentage point reduction to the update of their Medicare standard federal rate for that year. Funded through an inter-agency agreement between ASPE and CMS, the goal of this project was to develop and test measures that may be incorporated into the IPFQR program; these included four chart-based measures that assess screening for risk of suicide, risk of violence, substance use, and metabolic conditions, and one claims-based measure that assesses whether Medicare beneficiaries receive follow-up care after IPF hospitalization.
Major Findings: Among the six inpatient psychiatric facilities (IPFs) that piloted the chart-based measures, performance was generally high on the suicide, violence, and substance use screening measures. In contrast, there was wide variation in metabolic screening rates across IPFs. All chart-based measures demonstrated good inter-rater reliability and had moderate to strong stakeholder support. The claims-based follow-up measure demonstrated wide variation across IPFs and very strong reliability, but received mixed stakeholder support.
Purpose: This project developed measures that may be incorporated into the IPFQR program, including four chart-based screening measures (risk of suicide, risk of violence, substance use, and metabolic conditions) and a claims-based measure to assess whether individuals discharged from the IPF receive follow-up care. The measures were tested using quantitative and qualitative methods to assess attributes consistent with National Quality Forum endorsement criteria -- importance, feasibility, usability, and scientific acceptability (reliability and validity).
Methods: This project first reviewed existing measures and gathered input from consumers, IPFs, IPFQR program vendors, state agencies, and performance measurement experts to identify opportunities for new measures. Based on the evidence to support measure concepts, measure specifications were developed and pilot tested. The follow-up measure was tested using Medicare claims data for over 1,600 IPFs. The chart-based measures were piloted at six IPFs. Quantitative testing for all measures involved calculating performance rates to examine variation across IPFs, differences in performance among subpopulations, and reliability. For all measures, qualitative data collection included focus groups with a range of stakeholders to get input on the measure specifications and understand whether the measures yield findings that could be used to inform quality improvement efforts. A technical expert panel provided input throughout the project.
The following acronyms are mentioned in this report and/or appendices.
| ACRONYMS | |
|---|---|
| ADA | American Diabetes Association |
| APA | American Psychiatric Association |
| ASPE | HHS Office of the Assistant Secretary for Planning and Evaluation |
| ASSIST | Alcohol, Smoking and Substance Involvement Screening Test |
| AUDIT | Alcohol Use Disorders Identification Test (screen) |
| AUDIT-C | Alcohol Use Disorders Identification Test Consumption (screen) |
| BETOS | Berenson-Eggers Type of Service |
| BMI | Body Mass Index |
| BVC | Broset Violence Checklist |
| CAGE | Cut down, Annoyed, Guilty, and Eye-opener (questionnaire) |
| CAH | Critical Access Hospital |
| CHP | Child Psychiatrist |
| CMS | HHS Centers for Medicare and Medicaid Services |
| CHN | Child Neurologist |
| CPT | Current Procedural Terminology |
| CRAFFT | Car, Relax, Alone, Forget, Friends, Trouble (screen) |
| DAST-10 | Drug Abuse Screening Test-10 items |
| DO | Doctor of Osteopathy |
| DUA | Data Use Agreement |
| EDB | Enrollment Data Base |
| ER | Emergency Room |
| FACTYP | Facility Type |
| FFS | Fee-For-Service |
| FUH | Follow-up After Hospitalization for Mental Illness |
| FY | Fiscal Year |
| G-MAST | Geriatric version-MAST |
| GAIN-SS | Global Appraisal of Individual Needs Short Screener |
| HbA1c | Glycated Hemoglobin |
| HBIPS | Hospital-Based Inpatient Psychiatric Services |
| HCPCS | Healthcare Common Procedure Coding System |
| HEDIS | Healthcare Effectiveness Data and Information Set |
| HHA | Home Health Agency |
| HHS | U.S. Department of Health and Human Services |
| HMO | Health Maintenance Organization |
| ICD-9-CM | International Classification of Disease, 9th revision, Clinical Modification |
| ICF | Intermediate Care Facility |
| IPF | Inpatient Psychiatric Facility |
| IPFQR | Inpatient Psychiatric Facility Quality Reporting |
| IQR | Interquartile Range |
| MAST | Michigan Alcohol Screening Test |
| MAX | Medicaid Analytic eXtract (files) |
| MCO | Managed Care Organization |
| MD | Medical Doctor |
| MSIS | Medicaid Statistical Information System |
| MSSI | Modified Simple Screening Instrument |
| NCQA | National Committee for Quality Assurance |
| NPI | National Provider Identification |
| NQF | National Quality Forum |
| OP | Outpatient |
| OT | Medicaid Other Services/Therapy File |
| PA | Physician Assistant |
| POS | Place of Service |
| SAFE-T | Suicide Assessment Five-Step Evaluation and Triage |
| SAMHSA | HHS Substance Abuse and Mental Health Services Administration |
| SBQ-R | Suicide Behaviors Questionnaire-revised |
| SNF | Skilled Nursing Facility |
| SSI-SA | Simple Screening Instrument for Substance Abuse |
| SSRI | Suicide Screening Risk Inventory |
| SUB | Substance Use |
| TAP | Technical Advisory Panel |
| TEP | Technical Expert Panel |
| TJC | The Joint Commission |
| TOS | Type of Service (in Medicaid files) |
| TPBBEG | Part B Enrollment -- Beginning Date |
| TPBEND | Part B Enrollment -- End Date |
| TWEAK | Tolerance Worried Eye-opener Amnesia K/cut down |
| TYPSVC | Type of Service (in Medicare files) |
| UB | Uniform Billing |
| VERDICT | Veterans Evidence-based Research, Dissemination, and Implementation Center |
| V-RISK | Violence Risk Screening |
Despite improvements in behavioral health treatments, gaps remain between evidence-based care and the care provided to millions of individuals living with mental health problems (Institute of Medicine 2006). As part of its National Quality Strategy, CMS is committed to reducing this gap by developing and implementing measures that can be used for quality improvement within inpatient psychiatric facilities (IPFs). To further the implementation of such measures, and as mandated in Section 3401, Subsection 10322 of the Patient Protection and Affordable Care Act of 2010, CMS developed the Inpatient Psychiatric Facility Quality Reporting (IPFQR) program, a pay-for-reporting program that went into effect for fiscal year 2014. Under this program, IPFs must report their performance on a set of quality measures or face a 2 percentage point reduction to the update of their Medicare standard federal rate for that year.
Over 1,800 IPFs (both freestanding psychiatric hospitals and psychiatric units of general hospitals) reported their performance on several measures in the first year of the IPFQR program. These measures include six chart-based process measures that address patient safety, care coordination, and medication use.1 Although the six measures currently included in the IPFQR program provide a strong foundation for improving the quality of inpatient behavioral health care, gaps in measurement persist.2
In September 2012, the Office of the Assistant Secretary for Planning and Evaluation, with support from CMS, modified an existing contract with Mathematica Policy Research and its subcontractor -- the National Committee for Quality Assurance (NCQA) -- to develop measures for the IPFQR program. The goal of this new component of the project was to develop and test four chart-based measures that assess screening for risk of suicide, risk of violence, substance use, and metabolic conditions, and one claims-based measure that assesses whether Medicare beneficiaries receive follow-up care after IPF hospitalization.
The first phase of work under this contract involved conducting a targeted review of evidence to support the selected measure concepts; this review was completed in late 2012. Next, the team held several meetings with IPF staff and other subject matter experts to obtain input and guidance on the technical specifications of these measures. In September 2013, the team presented draft specifications for the five measures to a technical expert panel (TEP), and the TEP provided the team with useful feedback on ways to further refine and strengthen the specifications prior to measure testing.
In early 2014, the team pilot tested the chart-based measures at six IPFs and began testing the claims-based measure using Medicare claims data. Starting in April 2014, Mathematica and NCQA staff also gathered qualitative feedback on the performance and usability of the measures through debriefing sessions with IPFs that participated in testing, as well as focus groups with state policymakers, consumer and advocacy groups, measure experts, IPFQR program vendors, and additional IPF staff. The results of quantitative measure testing are summarized in Table ES.1.
| Measure | Variation in Measure Performance Across IPFs (number of IPFs)1 | Mean Measure Performance1 | Reliability2 |
|---|---|---|---|
NOTES:
| |||
| Screening for risk of suicide | 67.6-99.4% (6 IPFs) | 93.4% | 0.65 |
| Screening for risk of violence | 47.7-99.1% (6 IPFs) | 89.0% | 0.63 |
| Screening for substance use | 51.4-96.4% (6 IPFs) | 85.8% | 0.49 |
| Metabolic screening | 6.2-98.6% (6 IPFs) | 41.5% | 0.93 |
| Follow-Up after IPF hospitalization (30 days)3 | 0-100% (1,669 IPFs)25th percentile: 42.375th percentile: 67.3 | 53.5% | 0.93 |
Measure Testing Results
Admission Screening Measures. The three admission screening measures -- screening for risk of suicide, risk of violence, and substance use -- require that IPF staff collect information on core screening elements within one day of patient admission. Performance was quite high across IPFs on these measures, with average performance on the measures ranging from 86 percent (in the case of substance use) to 93 percent (in the case of suicide). Reliability was moderate for the substance use measure and substantial for the suicide and violence measures. Stakeholders were generally supportive of the measures and thought they represented an improvement over existing screening measures used in an inpatient psychiatric setting, including HBIPS-1: Admission Screening for Violence Risk, Substance Use, Psychological Trauma History and Patient Strengths, a TJC measure reported by a large portion of IPFs throughout the country.
Regarding changes to measure specifications, stakeholders generally recommended that the final specification of the substance use, violence, and suicide screening measures use a three-day time frame to allow for complete and accurate screenings. Obstacles to performing accurate screenings within one day of admission include staff shortages, patient uncooperativeness, and lack of patient lucidity. Some stakeholders noted that the suicide and violence measures should be conducted within a one-day time frame, given the clinical importance of obtaining that information quickly. Based on this feedback, the research team recommends changing the time frame for the substance use screening measure from one day to three days, and keeping the suicide and violence screening specifications at one day (as specified prior to testing). The additional two days for the substance use measure will facilitate the capture of complete and accurate information regarding patients' alcohol and drug use, without compromising the need to capture important information on suicide and violence risk in the first day of admission.
Metabolic Screening Measure. The metabolic screening measure requires that the following four screenings are documented in the patient record for all individuals discharged on antipsychotic medications: (1) body mass index (BMI); (2) blood pressure; (3) glucose or glycated hemoglobin (HbA1c); and (4) a full lipid panel. Performance on the metabolic screening measure was low, on average, across the six IPFs. The measure's average performance rate of 42 percentage points highlights a sizable performance gap on the measure. The metabolic screening measure also demonstrated non-trivial variation in performance among IPFs as well as by patient characteristics. In addition, it demonstrated near-perfect agreement between chart abstractors (kappa of 0.93 for the measure numerator).
Overall, stakeholders found the metabolic screening measure to be important for addressing a notable gap in psychiatric care. However, focus group participants and TEP members were divided over whether to keep the requirement of a full lipid panel, as some felt that blood pressure, BMI, and glucose/HbA1c tests were sufficient screening requirements. In particular, three of nine TEP members expressed concern that the measure might inadvertently encourage IPFs and other clinicians to conduct unnecessary tests -- namely a full lipid panel in instances in which there is no clinical need. However, given the preponderance of clinical evidence supporting a full lipid panel on an annual basis for patients taking regularly prescribed antipsychotic medications, we suggest that the full lipid panel remain a screening element in the metabolic screening measure.
Follow-Up Measure. The claims-based follow-up measure calculates the proportion of patients that had an outpatient visit with a mental health practitioner within seven and 30 days following IPF hospitalization. The measure demonstrated strong quantitative performance; there was good variation in measure performance across IPFs and among demographic subgroups. In addition, IPFs' low average performance on the measure on a national scale highlights room for improvement. The measure also had very good reliability (beta-binomial statistic of 0.93 for the 30-day measure).
Stakeholder support for the follow-up measure was mixed. Three of the six IPFs involved in testing, and at least 11 of the 28 focus group participants expressed concern that the measure may inappropriately hold IPFs solely accountable for follow-up care, despite the range of community-level factors that may influence performance on the measures. However, at least five focus group participants -- primarily policymakers and measurement experts -- noted that this measure could help to drive innovative partnerships between facilities, community mental health agencies, health plans, and providers to improve follow-up care for IPF patients. Likewise, TEP members were divided in their support for the follow-up measure. Two TEP members were concerned that the measure would unfairly hold IPFs accountable for factors outside of their control, whereas two other TEP members expressed strong support for the follow-up measure, arguing that it could identify opportunities for quality improvement among facilities with low rates of follow-up care.
Despite improvements in behavioral health treatments, gaps remain between evidence-based care and the care provided to millions of individuals living with mental health problems (Institute of Medicine 2006). As part of its National Quality Strategy, the U.S. Department of Health and Human Services (HHS) Centers for Medicare and Medicaid Services (CMS) is committed to reducing this gap by developing and implementing measures that can be used for quality improvement within inpatient psychiatric facilities (IPFs). To further the implementation of such measures, and as mandated in Section 3401, Subsection 10322 of the Patient Protection and Affordable Care Act of 2010, CMS developed the Inpatient Psychiatric Facility Quality Reporting (IPFQR) program, a pay-for-reporting program that went into effect for fiscal year (FY) 2014. Under this program, IPFs must report their performance on a set of quality measures or face a 2 percentage point reduction to the update of their Medicare standard federal rate for that year.
Over 1,800 IPFs (both freestanding psychiatric hospitals and psychiatric units of general hospitals) reported measures in the first year of the IPFQR program. These measures include performance rates on six chart-based process measures that address patient safety, care coordination, and medication use.3 Although the six measures currently included in the IPFQR program provide a strong foundation for improving the quality of inpatient behavioral health care, gaps in measurement persist.4
In September 2012, the HHS Office of the Assistant Secretary for Planning and Evaluation (ASPE), with funding from CMS, modified an existing contract with Mathematica Policy Research and its subcontractor, the National Committee for Quality Assurance (NCQA), to support the development of measures for the IPFQR program. Prior to the modification, the contract supported the development of behavioral health quality measures for health plans with funding from ASPE and the HHS Substance Abuse and Mental Health Services Administration. The goal of this new component of the project was to develop and test four chart-based measures that assess screening for risk of suicide, violence, substance use, and metabolic conditions, and one claims-based measure that assesses whether Medicare beneficiaries receive follow-up care after IPF hospitalization (Table I.1).
Under a separate contract in 2012, a technical expert panel (TEP) prioritized these screening measure concepts as the most clinically relevant and feasible to measure among a set of nearly 20 promising measurement concepts. These new measures were intended to strengthen the standards of existing psychiatric inpatient screening measures by requiring specific screening elements that were recommended by the TEP and supported by the evidence, and requiring screening within one day of admission (as opposed to within three days of admission). In late 2012, CMS and ASPE prioritized the adaptation of an existing Healthcare Effectiveness Data and Information Set (HEDIS) follow-up measure (NQF #0576) for use in IPFQR program.
| Measure Concept | Primary Data Source* |
|---|---|
| * The data for the screening measures primarily derive from medical records. However, other data sources could be used to populate the measure numerator, such as administrative data or laboratory data that are not integrated with the medical record. | |
| Screening for risk of suicide | Medical record |
| Screening for risk of violence | Medical record |
| Screening for substance use | Medical record |
| Screening for metabolic conditions | Medical record |
| Follow-up after IPF hospitalization | Medicare claims |
A. Project Overview
Building on work that Mathematica and NCQA completed under a previous contract with CMS (HHSP23320100019WI), the first phase of work under this contract involved conducting a targeted review of evidence to support the selected measure concepts; this review was completed in late 2012. Mathematica and NCQA staff then used that evidence to develop measure specifications throughout 2013. In addition, the team held several meetings with IPF staff and other subject matter experts to obtain input and guidance on the technical specifications of these measures. The team presented draft specifications for the five measures to a TEP at its September 2013 meeting, and the TEP provided the team with useful feedback on ways to further refine and strengthen the specifications prior to measure testing. (A full list of TEP members is provided in Appendix A.)
In early 2014, the team pilot tested the chart-based measures at six IPFs and began testing the claims-based measure using Medicare claims data. Starting in April 2014, Mathematica and NCQA staff also gathered qualitative feedback on the performance and usability of the measures through debriefing sessions with IPFs that participated in testing and focus groups with state policymakers, consumer and advocacy groups, measure experts, IPFQR program vendors, and additional IPF staff. In late 2014, the team revised the measure specifications based on qualitative and quantitative testing results, as well as input from the final TEP meeting. (Full measure specifications for the screening measures and the follow-up measure are provided in Appendix B and Appendix C, respectively.)
Table I.2 provides a timeline of testing activities performed under this contract. At the time of this report, CMS has not made final decisions about the measure specifications or inclusion of these measures in IPFQR program. As of late 2014, these measures have not been submitted to the NQF for endorsement.
| Date | Activities |
|---|---|
| September 2012 | TEP meeting to receive feedback on measure concepts |
| December 2012 | Updated evidence review focused on selected measure concepts |
| Early to mid-2013 | Specified measures |
| September 2013 | Obtained TEP input on draft measure specifications. |
| January-April 2014 | Tested chart-based measures in 6 IPFs and obtained input through stakeholder focus groups |
| January-July 2014 | Conducted analysis of claims-based follow-up measure and obtained input through stakeholder focus groups |
| October 2014 | Obtained final TEP input on measures |
B. Report Roadmap
This report presents final testing results for the four chart-based screening measures and the claims-based follow-up measure developed and tested under this contract. Chapter II describes the process for specifying the measures; Chapter III describes the methods used to test the measures; and Chapter IV, Chapter V, and Chapter VI present the findings. The final chapter (Chapter VII) offers a summary of findings and lessons learned from this project that may be applicable to future measure-development and implementation efforts for inpatient psychiatric populations.
The specification of the measures consisted of three overarching steps: (a) conducting an evidence review; (b) reviewing specifications of similar measures; and (c) identifying feasible data sources that could be used to construct the denominator and numerator for each measure. These steps are discussed below.
A. Evidence Review
In early 2013, Mathematica and NCQA staff updated evidence reviews that were completed under the previous contract with CMS (HHSP23320100019WI) for all five measure concepts in development. In all evidence reviews, the team attempted to assess whether there was clear guidance to specify the denominator and numerator of each measure. The evidence reviews also addressed a critical component of NQF review -- the importance of each measure, including the evidence base supporting the measure and the extent to which it reflects a high-impact aspect of the national health care system. The reviews drew on clinical guidelines, systematic reviews (including meta-analyses), and the recommendations of authoritative government agencies and task forces, including the U.S. Preventive Services Task Force, the HHS Centers for Disease Control and Prevention, and others.
The review identified several guidelines that informed measure specifications, particularly regarding necessary tests to screen for metabolic conditions, as well as the frequency with which metabolic screening should occur.5 However, the review provided no clear guidance regarding the content of screenings for suicide, substance use, and violence -- that is, the screening elements that constitute a high quality suicide, violence, or substance use screening. For this reason, the team conducted an analysis of screening elements in validated screening tools, and identified a core set of screening elements that appeared across screening tools. This analysis of screening elements informed the specifications for these three screening measures.
B. Reviewing Specifications of Similar Measures
Next, the team reviewed specifications of similar screening measures to determine potential areas for improvement. Several screening measures developed as part of this project are conceptually similar to existing screening measures currently reported by IPFs. Specifically, three of the four chart-based screening measures are similar to two existing screening measures developed by TJC for inpatient populations (see Table II.1). Below is a comparison between the measures in development under this contract and similar TJC measures.
| New Measure | Description | Similar To: | Key Difference |
|---|---|---|---|
| Suicide risk screening | Percentage of admissions for which a detailed screening for risk of suicide was completed within 1 day of admission. Screening must include inquiry into: (1) suicidal ideation; (2) plans or preparations; (3) intent; (4) past suicidal behavior; and (5) risk and protective factors. | HBIPS-1 Violence Risk to Self screening component | The new measure requires screening elements, whereas HBIPS-1 only requires documentation of a screening. The new measure requires a completed screening within 1 day of admission versus 3 days for HBIPS-1. |
| Violence risk screening | Percentage of admissions for which a detailed screening for risk of violence was completed within 1 day of admission. Screening must include inquiry into: (1) threats of violence; and (2) lifetime history of violent episodes. | HBIPS-1 Violence Risk to Others screening component | The new measure requires screening elements, whereas HBIPS-1 only requires documentation of a screening. The new measure requires a completed screening within 1 day of admission versus 3 days in the case of HBIPS-1. |
| Substance use (alcohol and drug) screening | Percentage of admissions for which a detailed screening for drug use was completed within 1 day of admission. Screening must include inquiry into: (1) type, frequency, and amount of alcohol and substance use in the past 12 months; (2) adverse effects of this use (if use is reported); (3) dependence upon these substances (if use is reported); and (4) any lifetime history of drug/alcohol abuse. | HBIPS-1 Substance Use screening component SUB-1: Alcohol Use Screening | The new measure requires specific alcohol and drug screening elements, whereas HBIPS-1 only requires documentation of drug and alcohol screening. SUB-1 screens only for alcohol use. The new measure requires a completed screening within 1 day of admission versus 3 days for HBIPS-1 and SUB-1. SUB-1 is specified for a general inpatient population, whereas the new measure and HBIPS-1 are specified for an inpatient psychiatric population. SUB-1 requires screening with a validated instrument, whereas HBIPS-1 and the new measure do not. |
Three of the screening measures under development in this contract are similar to components of TJC's HBIPS measure titled "Admission Screening for Violence Risk, Substance Use, Psychological Trauma History and Patient Strengths" (HBIPS-1).6 TJC-accredited IPFs -- more than one-fourth of all IPFs included in the IPFQR program -- currently report HBIPS-1 to TJC (NRI 2012). HBIPS-1 reports whether screenings for suicide, violence, and substance use (among other assessments) were completed; IPFs earn credit on the measure only if all screenings were completed within three days of patient admission. In this contract, Mathematica and NCQA developed and tested individual screening measures for suicide, violence, and substance use. Based on the guidance from the TEP, these new measures were intended to strengthen the screening standards of HBIPS-1 by requiring specific screening elements that were recommended by the TEP and supported by the evidence, and requiring screening within one day of admission (as opposed to within three days in the case of HBIPS-1).
In addition, the newly developed substance use screening measure is conceptually related to TJC's SUB-17 (Alcohol Use Screening), which will be included the IPFQR program in FY 2015.8 The primary distinction between SUB-1 and the substance use screening measure developed under this contract is that the new measure requires the documentation of specific drug and alcohol screening elements recommended by the TEP (for example, inquiry into negative consequences of alcohol use), whereas SUB-1 requires an alcohol screening with a validated instrument, but no drug screening. The new substance use screening measure also requires that the screening be completed within one day of admission, versus within three days in the case of SUB-1.9
As described in Chapter III, during measure testing, the research team compared IPFs' performance on the newly specified screening measures to their performance on the relevant components of HBIPS-1 and SUB-1. The goal of these comparisons was to better understand how alternate specifications for screening measures affect IPF performance. We present these results in Chapter IV.
C. Defining Data Sources, Denominators, and Numerators
Next, the research team determined the appropriate data sources for the: (1) admission screening measures; (2) metabolic screening measure; and (3) follow-up measure, discussed below.
1. Admission Screening Measures
Identification of Data Sources. Admission screening measures include the suicide, violence, and substance use screening measures. Based on feedback from stakeholder focus groups and our TEP, we determined that patient record review was necessary to accurately capture the numerator of the admission screening measures, given that claims and administrative data would not have complete information on individual screening elements. However, as described below, administrative data were used to identify the measure denominator and exclusions, as they provide reliable information regarding patients' length of stay and age.
Defining the Denominator. We sought screening measures that would be broadly applicable to all IPFs and their full patient populations. As such, we defined the denominator for admission screening measures as all discharged IPF patients. In the interest of comparing measure performance with existing measures, we aligned these measures' denominators with existing HBIPS sampling methods (TJC 2012), which use IPF administrative data (not claims) to draw sufficiently large sample sizes across five age groups to generate performance rates for each of these groups. This sampling approach slightly oversamples patients under 18 and patients over 64, but largely yields a random sample of at least 20 percent of each IPF's entire patient population on a monthly or quarterly basis.
Refining Admission Screening Numerator Time Frame to Require Completion of Screening within One Day of Admission. We specified the admission screening measures to require completion of each screening within one day of admission. We made this decision based on initial input from the TEP, which reasoned that these screenings must occur within one day, given that screening results -- particularly for suicide and violence -- are necessary early in the inpatient stay to inform subsequent care. This approach differs from similar measures (including HBIPS-1 and SUB-1), which require that screening be completed within three days of admission.10 As part of measure testing, the research team documented whether all screening elements were completed within 1-3 days of admission, to compare performance.
Strengthening Numerator Requirements to Reflect a Higher Standard of Quality. Based on stakeholder feedback, guidance from the TEP, and the evidence review and subsequent analysis, the admission screening measures require the documentation of specific screening elements. For example, a patient record must include documentation on the presence or absence of suicidal ideation, plans, intent, history of suicidal behavior, and risk and protective factors in order for the facility to receive credit for completing the suicide screen. We identified these screening elements through a systematic review of evidence, analysis of validated screening tools, and consultation with the TEP. Generally, these core elements reflect screening elements that are common across validated screening tools and relevant clinical guidelines.11
As discussed above, this element-centered approach differs from similar measures, which require only documentation that screening was completed (in the case of HBIPS-1) or that screening was completed using a validated instrument (SUB-1).12 The TEP and other stakeholders perceived that requiring core screening elements represented a higher standard of quality than merely documenting presence or absence of a completed screening (as in the case of HBIPS-1). Furthermore, the TEP and other stakeholders asserted that requiring a core set of screening elements for each measure would have more clinical value than requiring the use of a validated screening tool. However, the TEP and stakeholders reported that the use of validated instruments that contain the specific screening elements was acceptable in order for an IPF to receive credit for the measure.
2. Metabolic Screening Measure
Identification of Data Sources. Based on feedback from stakeholder focus groups and the TEP, we determined that patient record review was necessary to accurately capture the numerator of the metabolic screening measure, which requires a series of measurements and tests. This is because: (1) data elements to examine all aspects of metabolic screening (like a blood pressure measurement or a full lipid panel) are not captured in claims; and (2) only a portion of all IPF stays are captured in claims. Similar to the admission screening measures, administrative data from the IPFs were also vital to determining the metabolic screening measure denominator and exclusions -- including patients' length of stay and whether patients were discharged from IPFs on antipsychotic medications.13
Defining the Denominator. Consistent with clinical research (Marder et al. 2004), TEP input, and an existing HEDIS diabetes screening measure,14 we defined the denominator as all patients discharged on antipsychotic medications. We selected patients discharged on any antipsychotic medication -- as opposed to patients discharged on second-generation antipsychotic medications -- for the measure denominator because there is evidence that both first-generation and second- generation antipsychotics can contribute to weight gain, dyslipidemia, and type 2 diabetes (Marder et al. 2004; ADA 2006; Roohafsza et al. 2013).15 In light of this risk, relevant consensus statements recommend a full metabolic screening for patients discharged on any antipsychotic medication. Most notably, in a consensus statement on antipsychotic drugs and obesity and diabetes, the ADA, the APA, the American Association of Clinical Endocrinologists, and the North American Association for the Study of Obesity stated, "The panel recommends that baseline screening measures be obtained before, or as soon as clinically feasible after, the initiation of any antipsychotic medication (ADA-APA 2004)."
In addition, the selection of any antipsychotic medication for the measure denominator was influenced by feasibility concerns, given that TJC-accredited IPFs currently track the number of patients discharged on any antipsychotic medication for HBIPS-4: Patients discharged on multiple antipsychotic medications. Drawing the distinction between first-generation and second-generation antipsychotic medications for this metabolic screening measure would require IPFs to construct new data elements, which IPFs described as quite burdensome. Therefore, basing this measure denominator on the HBIPS-4 denominator was an appropriate option. No distinction is made in the measure specifications between patients who initiated antipsychotic treatment during the IPF stay versus those who continued an antipsychotic treatment regimen during the IPF stay, as guidelines state that a full metabolic screening is necessary for both populations (ADA-APA 2004).
Defining the Numerator. The metabolic screening measure requires that the following four screenings were documented in the patient record: (1) body mass index (BMI); (2) blood pressure; (3) glucose or glycated hemoglobin (HbA1c); and (4) a full lipid panel. These requirements were largely based on clinical guidelines for individuals taking antipsychotic medications, as well as data elements included in the HEDIS diabetes screening measure and similar measures designed for alternate health care settings and populations. Experts agree that the combination of these tests, as opposed to any individual test, provides more accurate information about patients' risk for diabetes and cardiovascular disease (ADA-APA 2004).
Related to the high risk of diabetes among individuals on antipsychotics, an HbA1c or glucose test plays a vital role in assessing diabetes risk before and after initiation of an antipsychotic medication regimen. One evidence review (Marder et al. 2004) states, "A baseline measure of plasma glucose should be collected for all patients before starting a new antipsychotic. Measurement of the fasting plasma is preferred, but measurement of HbA1c is acceptable if a fasting plasma glucose tests is not feasible." A full lipid panel is also an integral component of metabolic screening, given that antipsychotics may be associated with hyperlipidemias, which can increase the risk of coronary heart disease (Marder et al. 2004; ADA-APA 2004; Casey 2004). In addition, at least one guideline supported regular blood pressure and BMI measurement for individuals with serious mental illness, due to these measurements' low cost and high utility in identifying hypertension and obesity, respectively (Marder et al. 2004).
Defining the Numerator Time Frame. Consistent with the ADA-APA guideline (2004) and TEP input, we determined that the measure should require a complete metabolic screening at least once a year for all patients discharged on antipsychotics.16 To receive credit for the screening, each component must be completed during the index IPF stay or in previous IPF stays or outpatient visits in the 12 months preceding the IPF discharge.17 If completed at IPFs, this screening could serve as a baseline for patients that began antipsychotics during the IPF stay, or it could serve to monitor for metabolic conditions among patients who were taking antipsychotic medications at the time of IPF admission.
3. Follow-up after IPF Hospitalization Measure
The follow-up measure calculates the proportion of patients that received outpatient mental health care within seven and 30 days following IPF discharge. This measure is calculated using only Medicare claims data. The follow-up measure specification was modeled on the NQF-endorsed Follow-up After Hospitalization for Mental Illness (FUH) measure (NQF #0576), for which NCQA is the steward.
Identification of Data Source. Although the other measures we tested rely mostly on chart data, claims data were the only suitable data source for the follow-up measure at this time. This is because IPFs have very limited access to information regarding their patients' follow-up care, either in patient charts or administrative data. As such, claims data offer more complete information on patients' follow-up. However, the primary limitation of claims data is that they are available only for Medicare beneficiaries, who comprise a subset of IPF patients that may not be representative of all patients.
Defining the Denominator. We sought for this measure to be broadly applicable to IPF patients. Based on feedback we received from CMS and an analysis of claims data, we limited the denominator to IPF stays with a principal mental health diagnosis.18 These mental health diagnosis codes are fully aligned with the HEDIS FUH measure. We excluded dually eligible Medicare and Medicaid ("dual") beneficiaries from the denominator, because Medicaid claims data are not available on a timely basis in each state to examine Medicaid-reimbursed follow-up services for this population, and there may be systematic differences in their access to follow-up care relative to non-dual beneficiaries. However, as a sensitivity analysis for the specification that uses only Medicare data, we tested an alternate version of the measure that tabulates dual beneficiaries' receipt of follow-up care using merged Medicare and Medicaid data from calendar year 2008.
Defining the Numerator. The numerator for the measure requires an outpatient or partial hospitalization visit with a mental health practitioner, and specifies both a seven-day follow-up rate and a 30-day follow-up rate for each IPF. However, in specifying this measure as a Medicare claims-based measure, we identified and tested alternate numerator options, including an outpatient visit or partial hospitalization with a mental health diagnosis. Testing these alternate numerator specifications allowed us to examine the extent to which IPF performance would change using different numerator options.
The testing protocol was designed to assess the psychometric properties and performance of the measures and to gather information to inform their eventual implementation. Moreover, the goal of testing was to gather information about the importance, scientific acceptability, usability, and feasibility of the measures, as defined in the following NQF measure criteria:
-
Importance. Strength of evidence supporting the measure concept that promotes high quality care and allows for differentiation in performance.
-
Scientific Acceptability. Verification that the psychometric properties of the measure -- validity and reliability -- are strong enough to justify its use to assess quality of care.
- Validity. The correct data elements are included in the measure, and the final measure score promotes correct conclusions regarding measured entities' quality of care.
- Reliability. The ability of measure specifications to promote consistency in data collection and aggregation to ensure that variability in measure score reflects actual variation in performance.
-
Usability. The value of the measure in informing quality improvement activities.
-
Feasibility. The availability of data elements required for the calculation of the measure, whether the measure is susceptible to human error, and the level of effort involved in collecting and calculating the measure.
The following overarching questions guided measure testing:
-
Do the measures assess quality of care and do they address a priority condition? Is there room for improvement and are there gaps in care?19 (importance)
-
As specified, can the data elements and measures be calculated consistently (reliability) and capture the intended information? (validity)
-
Are measure exceptions or exclusions necessary and appropriate? (validity)
-
Can the measures be calculated accurately and without undue burden? (feasibility)
-
Can stakeholders use performance results for quality improvement and decision making? (usability)
In addition to these overarching questions, measure testing answered more specific questions about the denominator and numerator specifications, as described in Table III.1.
| NQF Criterion | Testing Question(s) | Data Source | Data Analysis |
|---|---|---|---|
| * The research team also assessed measure feasibility and validity with qualitative methods, as discussed in the next chapter. | |||
| Importance/performance gap |
|
|
|
| Feasibility* |
|
|
|
| Reliability (inter-rater) |
|
|
|
| Validity (content)* |
|
|
|
| Validity (content)* |
|
|
|
We used qualitative and quantitative methods to test the four chart-based screening measures and the claims-based measure of follow-up after IPF hospitalization. Quantitative data collection largely informed our analyses of measure validity, reliability, and importance -- namely gaps in care -- whereas qualitative data collection largely informed our analyses of measure validity, feasibility, and usability. Below is a brief summary of these methods.
A. Quantitative Approach to Chart-Based Measure Testing
Quantitative testing of the measures focused on demonstrating the importance of the measures, based on the evidence of performance gaps and disparities in care, reliability between chart abstractors in obtaining data from patient records, and validity of the specifications, especially the measure numerator and exclusions.
Quantitative testing was divided into five phases: (1) site selection; (2) developing data collection instruments and protocols; (3) IPF staff training; (4) chart-abstraction and data collection; and (5) analysis.
-
Site Selection. We recruited a total of six IPFs to participate in testing the measures; this was the maximum number of facilities the project could support while offering a sample size that would allow the detection of variation in measure performance across IPFs. Each IPF was offered $25,000 as an honorarium to participate.20 Potential partner IPFs were identified through conversations with the CMS and ASPE, existing relationships with IPFs, and other data sources, including HBIPS performance statistics compiled by TJC. After a list of potential partner IPFs was compiled, we attempted to select IPFs that represented a mix of facility types and facility ownership. This included a combination of freestanding facilities and psychiatric wards, as well as public and private IPFs. Site outreach activities occurred from August 2013 to October 2013. The six IPFs selected for testing included three freestanding facilities (two public and one private) and three psychiatric wards (all private); see Table III.2.
| Freestanding Facilities | Psychiatric Wards | |
|---|---|---|
| Private facilities | 1 | 3 |
| Public facilities | 2 | 0 |
-
Developing Data Collection Instruments and Protocols. Parallel to conducting IPF recruitment, we developed a data collection tool for chart-abstraction in participating IPFs. We developed a Microsoft Access-based tool that contained all of the necessary data elements to calculate measure performance. The tool had pre-programmed skip logic and error checking to ease the burden of data collection while ensuring high quality data. Abstractors followed the instructions included in the tool's user interface to review each patient record and answer a set of questions about the information provided in it. Abstractors completed one electronic form per patient, which populated a back-end spreadsheet. In addition to collecting data with the chart-abstraction tool, IPFs also extracted administrative data on patient demographics, insurance status, length of stay during the visit selected for abstraction, number of stays during the past year, and other relevant data elements.
All IPFs obtained the appropriate authorizations (in some cases institutional review board approval) to participate in measure testing. IPFs submitted all relevant administrative and abstracted data using a secure password-protected encrypted website accessible only to immediate project staff. Mathematica and NCQA did not have any direct access to patient medical records and did not receive any personally identifiable information such as patient birthdates, Social Security numbers, or insurance identifiers. Rather, IPFs generated and employed random patient numbers that were not linked to other identifiers. All data were housed on Mathematica's secure servers.
-
IPF Staff Training. Before chart-abstraction began, all IPFs participated in training sessions that presented the testing methodology, introduced the measures, reviewed the structure and process for completing data collection instruments, and informed IPFs of the global testing timeline. A Mathematica senior researcher who was familiar with IPF services, chart-abstraction, testing protocol, and data collection instruments led the sessions. Participants in the training included chart abstractors, quality improvement staff, and any necessary administrative staff. Abstractors had multiple options to ask for clarification and additional guidance. The project team held biweekly check-in calls with all IPFs or with individual facilities as needed.
-
Chart-Abstraction and Data Collection. Chart-abstraction took place from January 2014 to April 2014 in all six participating IPFs. During this time, experienced chart abstractors from each IPF abstracted at least 115 patient charts corresponding to one month of discharges in larger facilities and three months of discharges in smaller facilities. Patient charts were randomly sampled from a universe of discharges from previous months, corresponding to October, November, and December 2013 for facilities participating in testing. Following HBIPS-1 sampling procedures, sampling was stratified by the four age strata, which were: (1) younger than age 13; (2) ages 13-17; (3) ages 18-64; and (4) ages 65 and older. This sampling approach was sufficient to detect differences in performance on the measures between the IPFs participating in testing, as well as differences in performance by age group and other patient characteristics.
Two staff at each testing site conducted chart-abstraction: a primary abstractor, who collected data from all sampled charts, and a secondary abstractor, who collected data from a subset of ten charts to allow for assessment of inter-rater reliability.21 During the first week of testing at all six IPFs, primary and secondary abstractors each abstracted ten charts and then reviewed them with the research team. During this review, the team discussed any discrepancies between the primary and secondary abstractors, and reached consensus regarding the correct abstraction of records. This review allowed us to ensure that the abstractors understood the specifications and data collection protocol before proceeding with full record abstraction.
-
Chart-Based Measure Analysis. We used the data from chart-abstraction and administrative data sources to summarize the demographic characteristics of the population, analyze IPF performance on each measure, examine performance rates for subgroups, determine the sensitivity of performance rates to alternate numerator specifications and exclusions, and calculate inter-rater reliability. Each analysis was designed to investigate one or more issues related to the importance, reliability, and validity of the measures. We discuss these analyses in more depth below:
-
Validity. To estimate the measures' validity, we conducted tests to determine whether measure exceptions altered performance rates, and how alternate numerator specifications altered IPF performance rates. In particular, we tested how performance varied across individual screening elements. In addition, we disaggregated alcohol and drug use screening rates within the substance use screening measure to assess potential differences in IPF performance between rates. We also conducted some validity and reliability tests for the alcohol and drug components separately; we report the results of these tests in Chapter IV.
-
Room for Improvement/Performance Gap. We calculated a score for each IPF, as well as the average across IPFs, to determine if there was room for improvement and variation in performance rates. We also explored performance rates by patient diagnosis and age to determine if disparities in screening for specific subpopulations were present.
-
Measure Reliability. As described above, this analysis answered the question of whether the data collected by two abstractors at the same IPF were comparable. To do this, we generated kappa statistics, or indicators of the measures' inter-rater reliability.
-
Comparison with Existing Measures. During measure testing, we also compared IPFs' performance on the newly specified screening measures to their performance on the relevant components of HBIPS-1 and SUB-1. The goal of these comparisons was to determine the extent to which stronger requirements regarding screening elements and screening time frames (within one day versus three days of admission) would affect IPFs' performance on violence, suicide, and substance use screening, and the extent to which the requirement of screening with a validated instrument would affect IPFs' performance on alcohol screening.
-
B. Quantitative Approach to Claims-Based Follow-Up Measure Testing
Our primary follow-up measure analysis used Medicare claims to assess facility performance and measure reliability. However, we also assessed facility performance using a file that contained Medicare and Medicaid Analytic eXtract (MAX) claims data. Although the IPFQR program is a Medicare quality reporting program, over half of patients discharged from IPFs are eligible for both Medicare and Medicaid, according to information from MedPac (2012). Because these "dual eligible" beneficiaries could access additional outpatient mental health services through Medicaid, using only Medicare data to assess measure performance may undercount these beneficiaries' receipt of follow-up care.22 Therefore, we created a file that linked Medicare and MAX data at the beneficiary level to enable more accurate calculation of the measure for dual eligible beneficiaries.
Quantitative testing for the follow-up measure was divided into five components: (1) preparation, including development of a data use agreement (DUA); (2) receipt and preparation of claims data; (3) descriptive analyses and detailed data review; (4) performance and reliability analyses; and, (5) supplementary analysis of a chart-based versus claims-based approach to measuring follow-up care.
-
Preparation. We initiated a DUA to obtain 2008 Medicare claims and MAX data. We used data from 2008 because this was the latest year of MAX data available at the contract start date. We obtained DUA approval and received these data in early 2013.
-
Preparation and Analysis of Claims Data. We linked the Medicare and MAX claims at the beneficiary level. We followed the linking protocol developed by Prela et al. (2009) to link Medicaid and Medicare databases for dual eligible beneficiaries. This protocol used health insurance claim numbers, patient gender, and date of birth.
In addition, we investigated the completeness of MAX data to determine whether any states should be excluded from the dual eligible beneficiary analysis due to potential missing data. MAX data contains information on FFS Medicaid encounters in all states and managed care Medicaid encounters in some states. This analysis of dual eligible beneficiaries is limited to FFS Medicaid data because managed care encounters are not reliably captured in MAX data for every state.23 Thus, if a substantive proportion of dual eligible beneficiaries in a state are enrolled in Medicaid managed care, these analyses would likely underestimate the receipt of outpatient care. To avoid this potential bias, states with more than 25 percent of dual eligible beneficiaries enrolled in Medicaid managed care were excluded from the analyses. In addition,states that did not have complete 2008 MAX data -- generally related to the availability of data elements to identify mental health practitioners -- were excluded from the dual eligible beneficiary analysis. In total, we excluded 24 states from our analysis of MAX claims, leaving an analysis sample of 26 states for the dual eligible beneficiary analysis.24 Additional details of this state selection process are provided in Appendix E.
| Analysis | Testing Question(s) | Data Source | Data Analysis |
|---|---|---|---|
| Facility performance |
|
|
|
-
Performance Analyses. After generating descriptive statistics and analyzing MAX data completeness, we calculated measure performance for each IPF -- expressed as a rate (percentage) for each facility -- and tested the reliability of the follow-up measure. Table III.3 presents the details of each of these analyses, including relevant testing questions and a brief description of the approach.
-
Testing Alternative Numerators. We explored IPF performance on the measure using four alternative methods of calculating the numerator:
- The first method follows the original HEDIS specification, which defines an outpatient mental health visit as a visit to a mental health practitioner (specified using provider specialty or National Provider Identification [NPI] codes) for a specific mental health treatment (specified using Current Procedural Terminology [CPT] and Healthcare Common Procedure Coding System [HCPCS] codes).
- The second method defines an outpatient mental health visit as the presence of a designated mental health CPT/HCPCS code in combination with a primary mental health diagnosis code. Unlike the first calculation method, visits with non-mental health providers count toward the numerator under this method.
- The third method defines outpatient mental health care as any outpatient visit with a primary mental health diagnosis code, regardless of the provider or specific procedural code.
- The fourth method defines follow-up care as any outpatient visit, regardless of diagnosis. This option is not a viable measure of outpatient mental health care; rather, it was calculated to provide context for the other numerator options.
These numerators were developed in consultation with CMS, ASPE, and claims measurement experts. The primary rationale for the second numerator option was to determine the viability of identifying follow-up care using patient diagnosis, as opposed to provider specialty. The primary rationale for the third numerator option was to test specifications of follow-up care that could be accurately measured with Medicare as well as Medicaid claims, given the high proportion of dual eligible beneficiaries using IPFs. All of these options are feasible with Medicare data, but the third option may be the most feasible with Medicaid data, given the inconsistency of Medicaid data across states.25
-
Sensitivity Tests, Disparities, and Room for Improvement. Next, we tested the sensitivity of measure performance to proposed exclusions. Most of the proposed exclusions are related to admission to an IPF or another inpatient setting within the follow-up period, as this admission could preclude beneficiaries' access to outpatient care. In addition, we examined facility performance according to various facility and beneficiary characteristics including geographic location and size of IPFs, as well as patients' principal diagnosis, type of insurance coverage, age, gender, and race.
-
Comparing Medicare-Only Rates to Merged Medicare-Medicaid Rates. Another key sensitivity test was determining the extent to which performance rates were affected by excluding Medicaid claims from the calculation. For this test, we compared performance rates calculated using linked Medicare and Medicaid claims to performance rates calculated using only Medicare claims data.26 The extent to which these rates differed provided insight into the additional follow-up care captured through Medicaid claims.
-
Testing Variation in Performance. In addition, we examined the distribution of facilities' performance. We calculated the minimum, maximum, median, mean, and interquartile range (IQR) for the follow-up measure. The IQR is demarcated by the values at the 25th and 75th percentiles of a distribution. Generally speaking, measures with a broader IQR are preferable to those with a narrowly distributed IQR or those with an IQR at the very low or very high end of the distribution. Based on our past experience with quality measure testing, we consider measures with an IQR of at least 10 percentage points to have the strongest evidence of importance for quality measurement purposes.
-
-
Reliability Analyses. Next, we tested the reliability of the follow-up measure. This involved a beta-binomial test and an analysis of the stability of IPF performance across quarters.
-
Beta-Binomial Test. We conducted a beta-binomial test to examine how well the measure as specified can distinguish performance between IPFs (the ratio of signal to noise). The signal in this case is the proportion of the variability in measured performance that can be explained by real differences in IPF performance. The beta-binomial approach is appropriate for measures like this one, where each denominator event represents a binary opportunity to pass or fail the measure (Adams 2009). The approach assumes that the performance measure score (pass/fail rate) across IPFs has a flexible beta distribution, characterized by a signal variance. Based on the performance measure score, the observed data (number of passes/failures) for each IPF has a binomial distribution, which provides the noise (measurement error) variance. From the beta-binomial model, the signal and noise variances are used to calculate reliability as follows: Signal variance / (signal + noise variance).
-
Stability of IPF Performance Across Quarters. We also examined the stability of facility performance over three quarters during 2008. We compared each facility's performance quartile in the first quarter with its performance in the other quarters, and examined whether facilities remained in the same quartile throughout all three quarters. In addition, we examined these changes in performance by facility size in an effort to determine whether large facilities were less likely to experience shifts in performance from one quarter to the next.
-
-
Supplementary Analysis of the IPF Follow-Up Measure. In March 2013, ASPE and CMS expressed interest in exploring the relative merits and drawbacks of a claims-based approach versus a chart-based approach to measuring follow-up care after IPF hospitalization. This included an analysis of patient characteristics, sample sizes, IPF capacity, and data availability related to patient follow-up. To explore this issue in more depth, we used administrative data provided by the six IPFs that participated in measure testing to conduct some preliminary quantitative analysis on the potential implications of insurance coverage, patient demographics, and sample size constraints associated with a chart-based versus claims-based approach to follow-up care. We present the results of this analysis in Chapter VII.
C. Qualitative Approach to Measure Testing
Qualitative testing spanned chart-based and claims-based measures, and comprised four components: (1) debriefing with IPFs; (2) focus groups with stakeholders; (3) TEP consultation; and (4) consultation with TJC.
-
Debriefings with IPFs. In mid-2014, we held a debriefing meeting with each of the six IPFs after we calculated facility performance on the measures. These debriefing sessions provided us with an opportunity to share preliminary results with IPFS, assess the total amount of time and effort associated with collecting the data, and to document the IPFs' final conclusions and perspectives on the measures. We also used these debriefings as an opportunity to gather input for the supplementary follow-up analysis discussed above. During these conversations, we gathered stakeholder feedback on IPFs' efforts to promote and track follow-up care, including factors that facilitate recording accurate data on patients' care following their IPF stay. In addition, we asked stakeholders about the feasibility of a chart-based approach to the follow-up measure, including data collection and reporting burden, as well as infrastructure and resources that would be necessary to support reporting.
-
Focus Groups with Stakeholders. In late 2014, we held focus groups with additional stakeholders including quality measure experts, consumers/advocacy organizations, state policymakers, and IPFs that did not participate in our chart-abstraction work. Below is a brief description of the stakeholder groups involved in focus groups and their value in providing feedback on the measures.
-
Quality Measurement Experts. Measurement experts provided feedback on the measure specifications, strength of evidence supporting the measures, and practical considerations in implementing the measures.
-
Consumers and Advocacy Organizations. Consumers and behavioral health advocacy organizations provided feedback on the saliency of measure concepts and the usefulness of performance on the measures for decision making and improving the quality of care.
-
State Policymakers. Although IPFQR program is a Medicare quality reporting program, the existing IPFQR measures (and those under development in this contract) are reported for both Medicare and Medicaid beneficiaries; therefore, state Medicaid agencies have an interest in performance on these measures. State mental health and substance abuse agencies also have an interest in the performance, given that IPFs play a central role in the state mental health system and some IPFs are state-operated. These stakeholders provided insight into the importance and usability of the measures within the larger context of the mental health service system.
-
IPF Representatives. In part due to the diversity of IPF resources and services at the national level, IPF representatives have varying perspectives on the proposed measures. Holding separate focus groups for different types of IPFs provided critical insight into the feasibility, usability, and importance of each measure from the perspective of each type of facility. We recruited a mix of freestanding facilities and psychiatric units within general medical hospitals for these focus groups. During these focus groups, we asked IPF staff about the feasibility of a chart-based approach to the follow-up measure, including data collection and reporting burden, as well as infrastructure and resources that would be necessary to support reporting.
-
IPFQR Program Vendors. Vendors contracted by IPFs to assist with IPFQR program reporting have an in-depth understanding of reporting burden and IPF capacity to sample patients, abstract patient records, and aggregate relevant information for measure reporting.
-
-
TEP Consultation. We met with the TEP throughout the testing process. Three key TEP meetings took place from 2012 to 2014 with regard to measure testing. In late 2012, we met with the TEP to secure their approval for the screening measure concepts and their guidance regarding the measure specifications. In late 2013, we shared our specifications with the TEP to obtain their approval on all measures before testing began. In late 2014, we shared our final performance and reliability estimates with the TEP once testing was complete. This meeting allowed the TEP to conduct a final analysis of the measures' properties -- including their importance, reliability, validity, usability, and feasibility -- with the full set of testing results. (See Appendix A for a list of all TEP members.)
-
Consultation with TJC. Similar to consultations with the TEP, we consulted with TJC staff at three key points in the testing process. First, we shared our specifications with TJC in an August 2013 meeting, before pilot testing began. Next, we shared our final performance and reliability estimates with TJC staff once analysis was complete in late 2014. In addition, we shared testing results with TJC's technical advisory panel (TAP) for the HBIPS measure set in September 2014. This ongoing communication with TJC and its TAP was intended to share testing results among interested parties, particularly given commonalities between the new screening measures and TJC's HBIPS-1 and SUB-1 measures.
IV. TESTING RESULTS FOR SCREENING MEASURES
This chapter summarizes the quantitative and qualitative results of measure testing for the admission screening measures -- suicide risk, violence risk, and substance use screening -- as well as the metabolic screening measure. Section A describes how the measure denominator population was selected, and summarizes patient characteristics in the IPFs that participated in testing. Section B and Section C summarize measure performance, inter-rater reliability, and stakeholder feedback on the measures. Section D discusses changes to final measure specifications based on testing results.
A. IPFs and Denominator Population
The six IPFs that participated in measure testing are diverse in both structure and size. Three IPFs are private psychiatric wards with fewer than 50 patient beds, two are public freestanding facilities with over 100 beds, and one is a private freestanding facility with 400 beds. The IPFs are located throughout the country, with representation in the Mid-Atlantic, Northeast, Mid-West, South, and West. Four of the six IPFs employ a vendor to tabulate and report quality measures for the IPFQR program.
A total of 1,857 patients were discharged from the six IPFs between October 1, 2013, and December 31, 2013 (with the exception of one large IPF [IPF 6], for which only one month's data were necessary, corresponding to December 2013).27 We implemented an approach that mirrored the HBIPS sampling procedure, sampling at least 20 percent of patients in each of four age strata, with a minimum of 120 sampled patients in each IPF. This resulted in a total of 825 patients selected for manual chart-abstraction across the six IPFs, with sample sizes ranging from 120 patients in IPFs 1 and 2 to 176 patients in IPF 3.
As illustrated in Table IV.1, the suicide, violence, and substance use screening measures used the full denominator of 825 sampled patients. In contrast, the metabolic screening measure included only sampled patients discharged on antipsychotic medications, resulting in a smaller denominator for the six sites combined (506 patients; 61 percent of patients in the full sample).
| Total Discharges | Final Sample Size for Suicide, Violence, and Substance Use Screening | Final Sample Size for Metabolic Screening | |||
|---|---|---|---|---|---|
| N | % of Total Discharges | N | % of Total Discharges | ||
| SOURCE: Administrative data and medical records from 6 IPFs, corresponding to all discharges from October 1, 2013, to December 31, 2013. * Discharges in IPF 6 are all discharges from December 1 to December 31, 2013. | |||||
| All IPFs | 1857 | 825 | 44.4 | 506 | 27.2 |
| IPF 1 (private psychiatric unit) | 172 | 120 | 69.8 | 56 | 32.6 |
| IPF 2 (private psychiatric unit) | 382 | 176 | 46.1 | 118 | 30.9 |
| IPF 3 (private psychiatric unit) | 409 | 120 | 29.3 | 85 | 20.8 |
| IPF 4 (public freestanding hospital) | 152 | 120 | 78.9 | 79 | 52.0 |
| IPF 5 (public freestanding hospital) | 272 | 118 | 43.4 | 78 | 28.7 |
| IPF 6* (private freestanding hospital) | 470 | 171 | 36.4 | 90 | 19.1 |
The overall patient population used for measure testing was diverse in terms of age, gender, race, diagnosis, and type of insurance coverage (Table IV.2). The majority of patients were between the ages of 27 and 64 at discharge, with approximately 17 percent of patients over age 64. Roughly half were female. The most common primary diagnoses were bipolar disorder (42 percent across IPFs) and schizophrenia (19 percent across IPFs). Patients were most likely to be insured with Medicare FFS coverage (23 percent across IPFs), private or commercial insurance (21 percent across IPFs), or state or county insurance (17 percent across IPFs).
We observed important differences in patient characteristics between IPFs, particularly with respect to patient length of stay, ethnicity, diagnosis, and age. Notably, there were pronounced differences in length of stay between psychiatric units (IPFs 1, 2, and 3) and freestanding hospitals (IPFs 4, 5, and 6) involved in measure testing. Average length of stay at freestanding hospitals ranged from 15 to 82 days, whereas average length of stay at psychiatric units ranged from five to nine days.28 In addition, over 80 percent of patients in two psychiatric units were White, compared to less than 50 percent of patients at two public freestanding hospitals. Also, a larger share of psychiatric units' patients had primary diagnoses of bipolar disorder (38-76 percent) relative to freestanding hospitals (18-25 percent). Also notable is that over 75 percent of patients in IPF 4 were male; a large portion of these patients were transferred directly from correctional facilities whose populations were predominantly male.
| Patient Characteristics | All IPS | Psychiatric Units | Freestanding Hospitals | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IPF 1(private) | IPF 2(private) | IPF 3(private) | IPF 4(public) | IPF 5(public) | IPF 6(private) | |||||||||
| N | % | N | % | N | % | N | % | N | % | N | % | N | % | |
| Total Patients | 825 | 100.0 | 120 | 100.0 | 176 | 100.0 | 120 | 100.0 | 120 | 100.0 | 118 | 100.0 | 171 | 100.0 |
| SOURCE: Administrative data and medical records from 6 IPFs, corresponding to all discharges from October 1, 2013, to December 31, 2013. * The high proportion of missing data on patient insurance in IPF 5 was due to hospital staff's inability to fully merge administrative files with financial records. | ||||||||||||||
| Age at the Time of Discharge | ||||||||||||||
| Average (in years) | 42.1 | 38.5 | 51.7 | 50.3 | 36.7 | 38.0 | 35.6 | |||||||
| Younger than 13 | 23 | 2.8 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 23 | 13.5 |
| 13-17 | 39 | 4.7 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 6 | 5.0 | 0 | 0.0 | 33 | 19.3 |
| 18-26 | 146 | 17.7 | 22 | 18.3 | 32 | 18.2 | 23 | 19.2 | 27 | 22.5 | 23 | 19.5 | 19 | 11.1 |
| 27-44 | 276 | 33.5 | 59 | 49.2 | 35 | 19.9 | 28 | 23.3 | 55 | 45.8 | 58 | 49.2 | 41 | 24.0 |
| 45-64 | 203 | 24.6 | 36 | 30.0 | 44 | 25.0 | 29 | 24.2 | 30 | 25.0 | 35 | 29.7 | 29 | 17.0 |
| 65 and older | 138 | 16.7 | 3 | 2.5 | 65 | 36.9 | 40 | 33.3 | 2 | 1.7 | 2 | 1.7 | 26 | 15.2 |
| Primary Diagnosis | ||||||||||||||
| Bipolar disorder | 346 | 41.9 | 76 | 63.3 | 133 | 75.6 | 45 | 37.5 | 22 | 18.3 | 27 | 22.9 | 43 | 25.1 |
| Schizophrenia | 154 | 18.7 | 14 | 11.7 | 11 | 6.3 | 44 | 36.7 | 38 | 31.7 | 38 | 32.2 | 9 | 5.3 |
| Alcohol/drug | 68 | 8.2 | 18 | 15.0 | 2 | 1.1 | 3 | 2.5 | 14 | 11.7 | 15 | 12.7 | 16 | 9.4 |
| Psychosis | 61 | 7.4 | 2 | 1.7 | 3 | 1.7 | 10 | 8.3 | 22 | 18.3 | 15 | 12.7 | 9 | 5.3 |
| Major depressive disorder | 45 | 5.5 | 2 | 1.7 | 5 | 2.8 | 3 | 2.5 | 3 | 2.5 | 6 | 5.1 | 26 | 15.2 |
| Alzheimer's/dementia | 34 | 4.1 | 0 | 0.0 | 17 | 9.7 | 7 | 5.8 | 2 | 1.7 | 0 | 0.0 | 8 | 4.7 |
| Delusional disorder | 2 | 0.2 | 0 | 0.0 | 1 | 0.6 | 0 | 0.0 | 0 | 0.0 | 1 | 0.8 | 0 | 0.0 |
| Other | 86 | 10.4 | 8 | 6.7 | 2 | 1.1 | 8 | 6.7 | 19 | 15.8 | 15 | 12.7 | 34 | 19.9 |
| Missing | 29 | 3.5 | 0 | 0.0 | 2 | 1.1 | 0 | 0.0 | 0 | 0.0 | 1 | 0.8 | 26 | 15.2 |
| Race/Ethnicity | ||||||||||||||
| Caucasian | 541 | 65.6 | 106 | 88.3 | 145 | 82.4 | 75 | 62.5 | 56 | 46.7 | 50 | 42.4 | 109 | 63.7 |
| African American | 217 | 26.3 | 4 | 3.3 | 23 | 13.1 | 13 | 10.8 | 61 | 50.8 | 63 | 53.4 | 53 | 31.0 |
| Other | 23 | 2.8 | 3 | 2.5 | 8 | 4.5 | 5 | 4.2 | 1 | 0.8 | 5 | 4.2 | 1 | 0.6 |
| Missing | 44 | 5.3 | 7 | 5.8 | 0 | 0.0 | 27 | 22.5 | 2 | 1.7 | 0 | 0.0 | 8 | 4.7 |
| Gender | ||||||||||||||
| Female | 415 | 50.3 | 65 | 54.2 | 113 | 64.2 | 74 | 61.7 | 29 | 24.2 | 50 | 42.4 | 84 | 49.1 |
| Male | 410 | 49.7 | 55 | 45.8 | 63 | 35.8 | 46 | 38.3 | 91 | 75.8 | 68 | 57.6 | 87 | 50.9 |
| Insurance Coverage | ||||||||||||||
| Medicare FFS | 192 | 23.3 | 20 | 16.7 | 73 | 41.5 | 35 | 29.2 | 33 | 27.5 | 15 | 12.7 | 16 | 9.4 |
| Private/commercial insurance | 172 | 20.8 | 46 | 38.3 | 63 | 35.8 | 14 | 11.7 | 6 | 5.0 | 0 | 0.0 | 43 | 25.1 |
| State/county | 139 | 16.8 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 66 | 55.0 | 0 | 0.0 | 73 | 42.7 |
| Medicaid FFS | 53 | 6.4 | 0 | 0.0 | 12 | 6.8 | 19 | 15.8 | 0 | 0.0 | 22 | 18.6 | 0 | 0.0 |
| Self-pay | 41 | 5.0 | 0 | 0.0 | 25 | 14.2 | 9 | 7.5 | 0 | 0.0 | 0 | 0.0 | 7 | 4.1 |
| Medicare managed care | 36 | 4.4 | 0 | 0.0 | 0 | 0.0 | 11 | 9.2 | 0 | 0.0 | 0 | 0.0 | 25 | 14.6 |
| Medicaid managed care | 32 | 3.9 | 0 | 0.0 | 0 | 0.0 | 20 | 16.7 | 12 | 10.0 | 0 | 0.0 | 0 | 0.0 |
| Other | 46 | 5.6 | 23 | 19.2 | 3 | 1.7 | 12 | 10.0 | 1 | 0.8 | 0 | 0.0 | 7 | 4.1 |
| Missing* | 114 | 13.8 | 31 | 25.8 | 0 | 0.0 | 0 | 0.0 | 2 | 1.7 | 81 | 68.6 | 0 | 0.0 |
| Length of Stay | ||||||||||||||
| Average (in days) | 29.0 | 5.1 | 9.1 | 7.9 | 81.8 | 70.8 | 15.2 | |||||||
| 0 or 1 days | 41 | 5.0 | 12 | 10.0 | 3 | 1.7 | 13 | 10.8 | 2 | 1.7 | 8 | 6.8 | 3 | 1.8 |
| 2 or 3 days | 125 | 15.2 | 40 | 33.3 | 13 | 7.4 | 38 | 31.7 | 8 | 6.7 | 20 | 16.9 | 6 | 3.5 |
| 4 to 7 days | 249 | 30.2 | 45 | 37.5 | 60 | 34.1 | 38 | 31.7 | 18 | 15.0 | 40 | 33.9 | 48 | 28.7 |
| 8 to 14 days | 216 | 26.2 | 20 | 16.7 | 75 | 42.6 | 15 | 12.5 | 14 | 11.7 | 30 | 25.4 | 62 | 36.3 |
| 15 to 21 days | 62 | 7.5 | 2 | 1.7 | 20 | 11.4 | 4 | 3.3 | 9 | 7.5 | 7 | 5.9 | 20 | 11.7 |
| 22 to 30 days | 34 | 4.1 | 1 | 0.8 | 5 | 2.8 | 5 | 4.2 | 9 | 7.5 | 1 | 0.8 | 13 | 7.6 |
| >30 days | 98 | 11.9 | 0 | 0.0 | 0 | 0.0 | 7 | 5.8 | 60 | 50.0 | 12 | 10.2 | 19 | 11.1 |
B. Quantitative Testing Results
This section provides quantitative testing results for the suicide, violence, substance use, and metabolic screening measures. In addition to presenting overall performance statistics, we describe any variation in performance across facilities, as well as IPF performance on individual screening elements. Performance rates discussed below are the proportion of patients that met each measure numerator requirement, after accounting for exclusions.
| Screening Measure | All IPS | Psychiatric Units | Freestanding Hospitals | ||||
|---|---|---|---|---|---|---|---|
| IPF 1 (private) | IPF 2 (private) | IPF 3 (private) | IPF 4 (public) | IPF 5 (public) | IPF 6 (private) | ||
| % | % | % | % | % | % | % | |
| SOURCE: Administrative data and medical records from 6 IPFs, corresponding to all discharges from October 1, 2013, to December 31, 2013. | |||||||
| Suicide risk | 93.4 | 67.6 | 97.1 | 98.1 | 98.2 | 94.9 | 99.4 |
| Violence risk | 89.0 | 47.7 | 97.1 | 86.8 | 99.1 | 94.2 | 98.8 |
| Substance use | 85.8 | 51.4 | 89.6 | 80.4 | 94.4 | 94.8 | 96.4 |
| Metabolic | 41.5 | 16.3 | 13.9 | 51.7 | 98.6 | 6.2 | 59.8 |
Table IV.3 and Figure IV.1 provide an overview of IPF performance on the screening measures. As illustrated, IPF performance on the admission screening measures (suicide, violence, and substance use) was generally strong, with average performance above 85 percent on all three measures. In contrast, performance on the metabolic screening measure was generally poor, at 42 percent across IPFs on average.
FIGURE IV.1. Average Screening Performance Rates across 6 IPFs
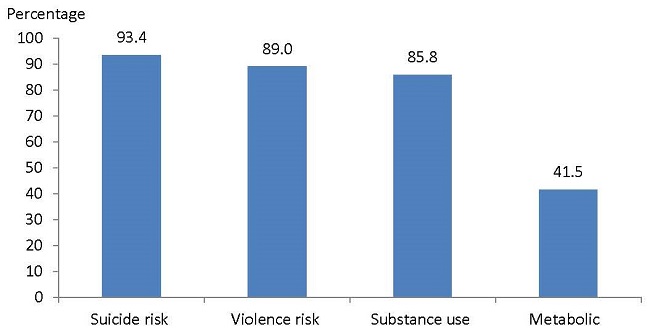
Admission Screening Measures. In general, IPFs that performed well on one admission screening measure also performed well on the other two measures. One private freestanding facility (IPF 6) had the highest or second-highest performance on all three admission screening measures, with performance ranging from 96 percent to 99 percent. Four other facilities, representing a mix of freestanding hospitals and psychiatric units, did consistently well on admission screening measures, with performance in the 80 percent to 99 percent range for all three measures. One private psychiatric unit (IPF 1) had the lowest performance on all three measures, with performance ranging from 48 percent to 68 percent. If this IPF were excluded from the analysis, average performance across the remaining five IPFs would be 97.7 percent for suicide, 95.7 percent for violence, and 91.5 percent for substance abuse. (See Table D.1 in Appendix D for additional details.)
Metabolic Screening Measure. IPF performance on the metabolic screening measure exhibited similar trends, in that IPF 6 had relatively high performance (at 60 percent) and IPF 1 had relatively low performance (at 16 percent). However, a public freestanding IPF (IPF 5) had the lowest performance (at 6 percent) and another public freestanding IPF (IPF 4) had the highest performance (at 99 percent). Consistent with these findings, clinical staff from the lowest-performing site noted that they do not perform a full metabolic screening on their patients as a general practice, whereas staff from the highest performing IPF noted that they provide all their patients -- regardless of their use of antipsychotic medications -- with a full metabolic screening at least once during their stay.
1. Suicide Risk Screening
In order for the IPF to meet the numerator requirement for the suicide screening measure, the medical record must contain documentation that all five screening elements were completed within one day of admission -- either through use of a validated screening tool or a non-validated assessment protocol.29 These screening elements are listed below.
Suicide Risk Screening Numerator Requirement
The medical record must provide documentation that all five of the following screening elements were completed within one day of admission:
- Presence or absence of suicidal ideation.
- Extent of plans or preparation (if ideation is reported).
- Intent to act on those plans (if plans are reported).
- Any history of suicidal behavior.
- Risk and protective factors related to suicide.
Overall Performance. Five of the six IPFs had relatively high performance on the suicide screening measure, with performance rates ranging from 95 percent to 99 percent of patients screened within one day of admission (Figure IV.2 and Table IV.4). However, one psychiatric unit (IPF 1) had a relatively poor performance rate of 68 percent. In a debriefing session following chart-abstraction, clinical staff from this psychiatric unit noted that they consistently ask patients about each of these suicide screening elements upon admission. However, patient records do not systematically reflect the information provided by patients on these elements, thus generating relatively poor performance on the measure. Aggregating performance among all six IPFs, average performance on the measure was 93 percent.
FIGURE IV.2. Suicide Risk Screening Performance across 6 IPFs
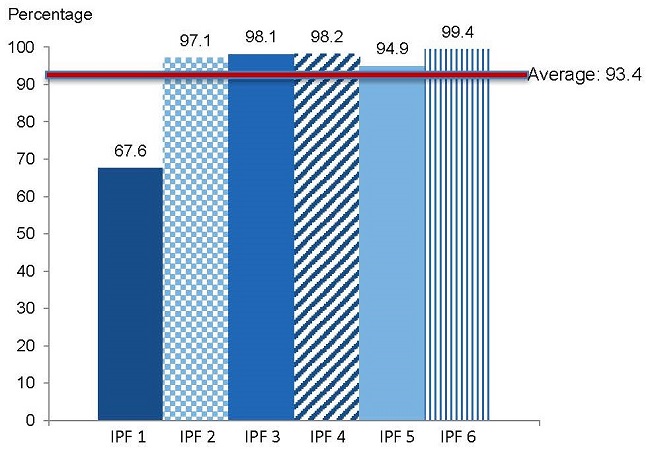
SOURCE: Administrative data and medical records from 6 IPFs, corresponding to all discharges from October 1, 2013, to December 31, 2013.
NOTE: Performance rates also presented in Table IV.4.
Performance on Individual Elements. Average performance on individual screening elements was relatively uniform and high across IPFs, ranging from 97 percent completion for past suicidal behavior to 98 percent completion for suicidal ideation. However, one IPF (IPF 1) had relatively low performance on two screening elements: 82 percent completion of past suicidal behavior, and 90 percent completion of intent to act on suicide plans. These element-level performance rates contributed to the IPF's relatively low performance rate on the measure of 68 percent.
Use of Standard Screening Tools. Standard instruments were used to conduct suicide risk screening for only 5 percent of patients across all IPFs. For these patients, IPFs generally used the SAFE-T or the Suicide Screening Risk Inventory (SSRI) tool.
| All IPS | Psychiatric Units | Freestanding Hospitals | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IPF 1(private) | IPF 2(private) | IPF 3(private) | IPF 4(public) | IPF 5(public) | IPF 6(private) | |||||||||
| N | % | N | % | N | % | N | % | N | % | N | % | N | % | |
SOURCE: Administrative data and medical records from 6 IPFs, corresponding to all discharges from October 1, 2013, to December 31, 2013.
| ||||||||||||||
| Denominator (after exclusions) | 761 | 100.0 | 108 | 100.0 | 172 | 100.0 | 106 | 100.0 | 109 | 100.0 | 99 | 100.0 | 167 | 100.0 |
| Overall rate (met numerator requirement) | 711 | 93.4 | 73 | 67.6 | 167 | 97.1 | 104 | 98.1 | 107 | 98.2 | 94 | 94.9 | 166 | 99.4 |
| 1 element missing | 26 | 3.4 | 21 | 19.4 | 1 | 0.6 | 2 | 1.9 | 1 | 0.9 | 0 | 0.0 | 1 | 0.6 |
| 2 or more elements missing | 24 | 3.2 | 14 | 13.1 | 4 | 2.4 | 0 | 0.0 | 1 | 0.9 | 5 | 5.0 | 0 | 0.0 |
| Screening elements met within 1 day of admissiona | ||||||||||||||
| Suicidal ideation | 749 | 98.4 | 103 | 95.4 | 168 | 97.7 | 106 | 100.0 | 108 | 99.1 | 97 | 98.0 | 167 | 100.0 |
| The extent of plans or preparation | 748 | 98.3 | 100 | 92.6 | 170 | 98.8 | 106 | 100.0 | 108 | 99.1 | 97 | 98.0 | 167 | 100.0 |
| The intent to act on those plans | 745 | 97.9 | 97 | 89.8 | 171 | 99.4 | 106 | 100.0 | 108 | 99.1 | 97 | 98.0 | 166 | 99.4 |
| Past suicidal behavior | 734 | 96.5 | 89 | 82.4 | 169 | 98.3 | 105 | 99.1 | 109 | 100.0 | 95 | 96.0 | 167 | 100.0 |
| Risk factors and protective factors | 738 | 97.0 | 94 | 87.0 | 169 | 98.3 | 105 | 99.1 | 108 | 99.1 | 95 | 96.0 | 167 | 100.0 |
| Standard screening tools administered within 1 day of admissionb | ||||||||||||||
| SAFE-T | 18 | 2.4 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 18 | 16.5 | 0 | 0.0 | 0 | 0.0 |
| SSRI | 17 | 2.2 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 17 | 15.6 | 0 | 0.0 | 0 | 0.0 |
| Any standard tool | 35 | 4.6 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 35 | 32.1 | 0 | 0.0 | 0 | 0.0 |
2. Violence Screening
To meet the numerator requirement for the violence screening measure, the medical record must contain documentation that both screening elements were completed within one day of admission -- either through use of a validated screening tool or a non-validated assessment protocol.30 These screening elements are listed below.
Violence Risk Screening Measure Numerator Requirement
The medical record must provide documentation that both of the following screening elements were completed within one day of admission:
- Presence or absence of threats of violence.
- Any history of violence.
Overall Performance. Overall, 89 percent of patients in the denominator received a full violence risk screening. Performance varied across IPFs; four IPFs had performance rates ranging from 94 percent to 99 percent, one IPF had a performance rate of 87 percent, and one IPF had a performance rate of only 48 percent (Figure IV.3 and Table IV.5). In most cases of incomplete screenings, only one of the two required elements was missing in the patient record.
FIGURE IV.3. Violence Risk Screening Performance across 6 IPFs
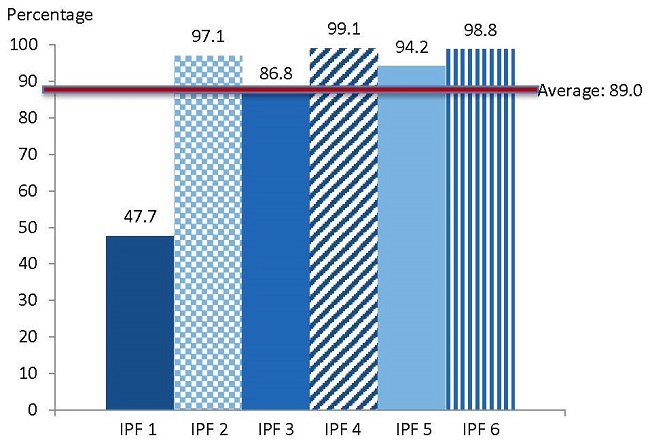
SOURCE: Administrative data and medical records from 6 IPFs, corresponding to all discharges from October 1, 2013, to December 31, 2013.
NOTE: Performance rates also presented in Table IV.5.
| All IPS | Psychiatric Units | Freestanding Hospitals | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IPF 1(private) | IPF 2(private) | IPF 3(private) | IPF 4(public) | IPF 5(public) | IPF 6(private) | |||||||||
| N | % | N | % | N | % | N | % | N | % | N | % | N | % | |
| SOURCE: Administrative data and medical records from 6 IPFs, corresponding to all discharges from October 1, 2013, to December 31, 2013. NOTE: Totals for individual tools do not always sum to any standard tool, given that more than 1 tool could have been used for a patient.
| ||||||||||||||
| Denominator (after exclusions) | 765 | 100.0 | 107 | 100.0 | 173 | 100.0 | 106 | 100.0 | 109 | 100.0 | 103 | 100.0 | 167 | 100.0 |
| Overall rate (met numerator requirement) | 681 | 89.0 | 51 | 47.7 | 168 | 97.1 | 92 | 86.8 | 108 | 99.1 | 97 | 94.2 | 165 | 98.8 |
| 1 element missing | 66 | 8.6 | 49 | 45.8 | 0 | 0.0 | 14 | 13.2 | 0 | 0.0 | 1 | 1.0 | 2 | 1.2 |
| Both elements missing | 18 | 2.4 | 7 | 6.5 | 5 | 2.9 | 0 | 0.0 | 1 | 0.9 | 5 | 4.9 | 0 | 0.0 |
| Screening elements met within 1 day of admissiona | ||||||||||||||
| Threats of violence | 731 | 95.6 | 98 | 91.6 | 168 | 97.1 | 92 | 86.8 | 108 | 99.1 | 98 | 95.1 | 167 | 100.0 |
| Any history of violent episodes | 697 | 91.1 | 53 | 49.5 | 168 | 97.1 | 106 | 100.0 | 108 | 99.1 | 97 | 94.2 | 165 | 98.8 |
| Standard screening tools administered within 1 day of admissionb | ||||||||||||||
| V-RISK-10 | 27 | 3.5 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 27 | 24.8 | 0 | 0.0 | 0 | 0.0 |
| BVC | 1 | 0.1 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.9 | 0 | 0.0 | 0 | 0.0 |
| Any standard tool | 27 | 3.5 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 27 | 24.8 | 0 | 0.0 | 0 | 0.0 |
Performance on Individual Elements. Examining performance on individual screening elements, screening for threats of violence was common (average of 96 percent across all IPFs), with performance ranging from 87 percent to 100 percent of patients. Similarly, five IPFs screened between 94 percent and 100 percent of patients for history of violence. However, one psychiatric unit (IPF 1) screened only half of its patients for history of violence. In a debriefing session, clinical staff from this psychiatric unit stated that they do not systematically inquire into patients' history of violence, and that their measure performance likely reflects this fact. This stands in contrast to the same IPF's statement regarding suicide screening -- namely that their suicide screenings cover all required elements, but patients' responses are not necessarily reflected in the patient record.
Use of Standard Screening Tools. The use of standardized screening tools for violence screening was rare. IPF staff used standard tools to conduct violence screenings for only 4 percent of patients across all six IPFs. For these patients, IPFs generally used the V-RISK-10 to administer the screening.
3. Substance Use
In order for the IPF to meet the numerator requirement for the substance use screening measure, the medical record must contain documentation that all four screening elements were completed within one day of admission -- either through use of a validated screening tool or a non-validated assessment protocol.31 Because each element pertains to both alcohol and drug use, they can be interpreted as eight screening elements -- four for alcohol and four for drug use. All screening elements are listed below.
Substance Use Screening Measure Numerator Requirement
The medical record must provide documentation that all four of the following screening elements were completed within one day of admission:
- Type, frequency, and amount of alcohol and drug use.
- Adverse effects of this use (if use is reported).
- Dependence upon these substances (if use is reported).
- Any history of drug and alcohol abuse.
First, we summarize IPF performance on alcohol and drug screening as separate components; then we discuss performance on the full measure, which requires a complete alcohol and drug screening within one day of admission.
a. Alcohol Screening
Overall Performance. Average performance on the alcohol screening component of the measure was 90 percent across all six IPFs. However, there was variation among IPFs. Four IPFs had similar performance, with between 93 percent and 96 percent of patients meeting the numerator requirement. Of the remaining two IPFs, IPF 5 had a performance rate of 84 percent and IPF 1 had a performance rate of 66 percent (Table IV.6).
Performance on Individual Elements. Average IPF performance on the measure's four screening elements was uniformly high, ranging from 93 percent on any history of alcohol abuse to 96 percent on frequency and amount of alcohol use. Across all IPFs, most incomplete screenings had only one of four screening elements missing. At the IPF that had the lowest alcohol screening rate (IPF 1: 66 percent performance), element-level performance was lowest for any history of alcohol abuse (78 percent).
b. Drug Screening
Overall Performance. Average performance on the drug screening component of the measure was 90 percent across six IPFs. Four IPFs screened patients for drug use at similar rates, with between 93 percent and 98 percent of patients screened (Table IV.6). Similar to their performance on the alcohol screening component, IPFs 3 and 1 screened the lowest proportion of patients for drug use, with performance rates of 85 percent and 65 percent, respectively.
Performance on Individual Elements. Average IPF performance on the measure's four drug screening elements was somewhat uniform, ranging from 94 percent on adverse effects of reported substance use to 96 percent on type, frequency, and amount of substance use. Most incomplete screenings had only one screening element missing. At the IPF that had the lowest drug screening rate (IPF 1: 65 percent across all elements), individual-level performance was lowest for adverse effects of drug use (79 percent). As with the suicide screening measure, this IPF reported that it routinely gathers this information from patients, but that some of its records fail to reflect information provided by patients on these screening elements.
c. Combined Alcohol and Substance Use Screening
Overall, 86 percent of patients at the six IPFs received a full screening for substance use -- including all four elements for alcohol use and all four elements for drug use. The proportion of patients screened for all elements varied notably by IPF, from 51 percent at IPF 1 to 96 percent at IPF 6 (Figure IV.4 and Table IV.6).
| All IPS | Psychiatric Units | Freestanding Hospitals | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IPF 1(private) | IPF 2(private) | IPF 3(private) | IPF 4(public) | IPF 5(public) | IPF 6(private) | |||||||||
| N | % | N | % | N | % | N | % | N | % | N | % | N | % | |
| SOURCE: Administrative data and medical records from 6 IPFs, corresponding to all discharges from October 1, 2013, to December 31, 2013. NOTE: Totals for individual tools do not always sum to any standard tool, given that more than 1 tool could have been employed for 1 patient.
| ||||||||||||||
| Denominator (after exclusions) | 754 | 100.0 | 107 | 100.0 | 173 | 100.0 | 102 | 100.0 | 108 | 100.0 | 97 | 100.0 | 167 | 100.0 |
| Overall rate: alcohol and drugs | 647 | 85.8 | 55 | 51.4 | 155 | 89.6 | 82 | 80.4 | 102 | 94.4 | 92 | 94.8 | 161 | 96.4 |
| Overall rate: alcohol | 675 | 89.5 | 71 | 66.4 | 160 | 92.5 | 86 | 84.3 | 105 | 95.4 | 92 | 94.8 | 161 | 96.4 |
| 1 element missing | 50 | 6.6 | 23 | 21.5 | 7 | 4.1 | 13 | 12.8 | 3 | 2.8 | 1 | 1.0 | 3 | 1.8 |
| 2 or more elements missing | 29 | 3.9 | 13 | 12.1 | 6 | 3.5 | 3 | 2.9 | 0 | 0.0 | 4 | 4.1 | 3 | 1.8 |
| Alcohol screening elements met within 1 day of admissiona | ||||||||||||||
| Frequency and amount of alcohol use | 723 | 95.9 | 101 | 94.4 | 164 | 94.8 | 92 | 90.2 | 107 | 99.1 | 95 | 97.9 | 164 | 98.2 |
| Adverse effects of reported alcohol use | 720 | 95.5 | 95 | 88.8 | 163 | 94.2 | 93 | 91.2 | 108 | 100.0 | 94 | 96.9 | 167 | 100.0 |
| Dependence upon alcohol | 716 | 95.0 | 90 | 84.1 | 165 | 95.4 | 92 | 90.2 | 108 | 100.0 | 94 | 96.9 | 167 | 100.0 |
| Any history of alcohol abuse | 706 | 93.6 | 83 | 77.6 | 169 | 97.7 | 94 | 92.2 | 106 | 98.1 | 93 | 95.9 | 161 | 96.4 |
| Overall rate: drugs | 678 | 89.9 | 70 | 65.4 | 160 | 92.5 | 87 | 85.3 | 103 | 95.4 | 94 | 96.9 | 164 | 98.2 |
| 1 element missing | 46 | 6.1 | 22 | 20.6 | 6 | 3.5 | 13 | 12.8 | 5 | 4.6 | 0 | 0.0 | 0 | 0.0 |
| 2 or more elements missing | 30 | 4.1 | 15 | 14.0 | 7 | 4.1 | 2 | 2.0 | 0 | 0.0 | 3 | 3.0 | 3 | 1.8 |
| Drug screening elements met within 1 day of admissiona | ||||||||||||||
| Type, frequency, and amount of substance use | 725 | 96.2 | 102 | 95.3 | 166 | 96.0 | 90 | 88.2 | 108 | 100.0 | 95 | 97.9 | 164 | 98.2 |
| Adverse effects of reported substance use | 711 | 94.3 | 85 | 79.4 | 165 | 95.4 | 91 | 89.2 | 108 | 100.0 | 95 | 97.9 | 167 | 100.0 |
| Dependence upon substances | 717 | 95.1 | 89 | 83.2 | 167 | 96.5 | 91 | 89.2 | 108 | 100.0 | 95 | 97.9 | 167 | 100.0 |
| Any history of substance abuse | 713 | 94.6 | 87 | 81.3 | 168 | 97.1 | 97 | 95.1 | 103 | 95.4 | 94 | 96.9 | 164 | 98.2 |
| Standard screening tools administered within 1 day of admissionb | ||||||||||||||
| CAGE (alcohol) | 18 | 2.4 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 18 | 16.7 | 0 | 0.0 | 0 | 0.0 |
| AUDIT (alcohol) | 11 | 1.5 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 5 | 4.6 | 0 | 0.0 | 6 | 3.6 |
| Other standard tool | 9 | 1.2 | 9 | 8.4 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| DAST-10 (drugs) | 6 | 0.8 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 6 | 5.6 | 0 | 0.0 | 0 | 0.0 |
| Any standard tool | 40 | 5.3 | 9 | 8.4 | 0 | 0.0 | 0 | 0.0 | 25 | 23.2 | 0 | 0.0 | 6 | 3.6 |
FIGURE IV.4. Substance Use Screening Performance across 6 IPFs
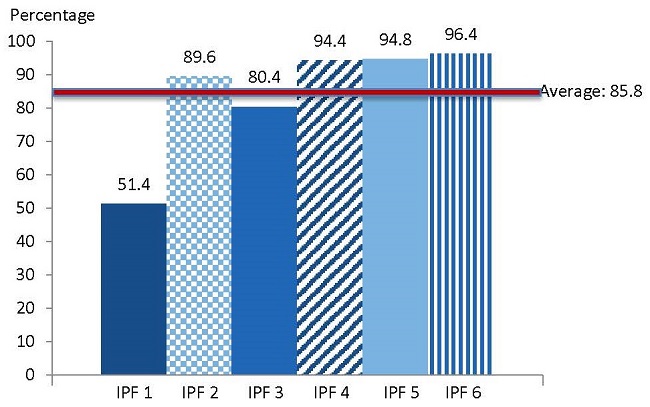
SOURCE: Administrative data and medical records from 6 IPFs, corresponding to all discharges from October 1, 2013, to December 31, 2013.
NOTE: Performance rates also presented in Table IV.6.
Use of Standard Screening Tools. Standard screening tools were used to conduct alcohol or drug screenings for just over 5 percent of patients sampled. These tools included the AUDIT for alcohol use, and the CAGE and the DAST-10 for drug use. Three of the six IPFs did not use any standardized instruments to screen patients for alcohol or drug use.
Screening Results
Throughout the chart-abstraction process, abstractors noted patients' responses to screening questions in cases in which these responses would determine if additional screening elements were necessary. For example, information on suicide plans was required only in cases in which patients reported suicidal ideation. The following screening results reflect data collected on patients' responses to screening questions, averaged across all IPFs:
- 50% of patients reported suicidal ideation, and 76% of patients who reported suicidal ideation also reported making plans or preparations for suicide.
- 31% of patients reported drug use.
- 28% of patients reported alcohol use.
4. Comparisons with Existing Screening Measures
Table IV.7 and Figure IV.5 compare performance on these admission screening measures with performance on similar existing measures, including HBIPS-1and SUB-1. As described earlier, the major difference between these new measures, HBIPS-1, and SUB-1 is that these screening measures require screening within one day of admission (whereas HBIPS-1 and SUB-1 require screening within three days of admission), and these new measures require all designated screening elements to be completed (whereas HBIPS-1 requires only that a screening be completed, and SUB-1 requires that a validated tool be used to screen for alcohol use).
| Suicide | Violence | Substance Use | Alcohol Component of Substance Use* | |
|---|---|---|---|---|
| SOURCE: Administrative data and medical records from 6 IPFs, corresponding to all discharges from October 1, 2013, to December 31, 2013. * This is the alcohol screening component of the substance use screening measure, which comprises an alcohol screening component as well as a drug screening component. This alcohol screening component is the closest analogue to SUB-1, which measures completion of an alcohol use screening. | ||||
| New IPF measure performance(screening within 1 day that meets all required elements) | 93.4% | 89.0% | 85.8% | 89.5% |
| HBIPS-1 PERFORMANCE(screening within 3 days with no specific element requirements) | 99.7% | 98.9% | 99.5% | NA |
| SUB-1 PERFORMANCE(screening within 3 days with no specific element requirements) | NA | NA | NA | 9.5% |
| Difference in performance rates(average across 6 IPFs) | 6.3 points higher on HBIPS-1 | 9.9 points higher on HBIPS-1 | 13.7 points higher on HBIPS-1 | 80 points loweron SUB-1 |
The six IPFs that participated in testing scored, on average, between 6 and 14 percentage points lower on the new measures compared to their analogue components in HBIPS-1, predominantly due to the new measures' stricter requirements regarding screening elements that must be documented in patient charts.32 One average, the six IPFs involved in testing had performance rates of nearly 100 percent for the Risk to Self component of HBIPS-1 (comparable to the suicide screening measure) and 99 percent for the Risk to Others component (comparable to the violence screening measure). However, their performance on the new suicide and violence risk screening measures was lower at 93 percent and 89 percent, respectively. Similarly, average IPF performance on the Substance Use screening component of HBIPS-1 was nearly 100 percent, compared to 86 percent on the new substance use screening measure.
In contrast, across the six IPFs, only 10 percent of patients met the numerator requirement for SUB-1. However, there was substantial variation across sites on SUB-1 performance. For example, IPF 2 had a 23 percent performance rate on the measure, whereas three sites had performance rates of around 0 percent (not shown). IPFs performed much higher on the alcohol screening component of the new substance use measure than on SUB1, due primarily to SUB-1's requirement of a validated screening tool.
FIGURE IV.5. IPF Screening Performance, by Measure Specification
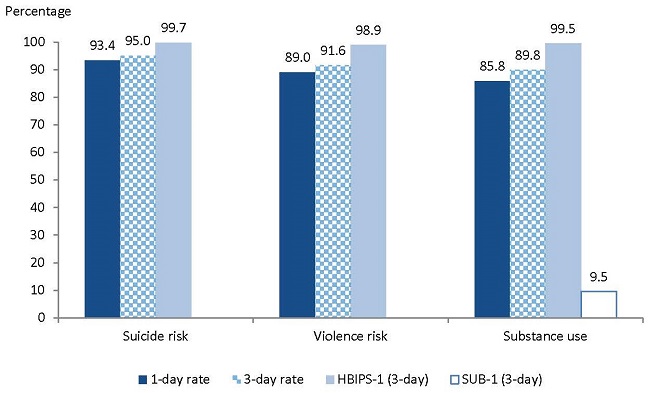
SOURCE: Administrative data and medical records from 6 IPFs, corresponding to all discharges from October 1, 2013, to December 31, 2013.
5. One-Day Versus Three-Day Performance
Another objective of measure testing was to determine the extent to which IPF performance varied using a one-day versus a three-day version of these screening measures. The three-day version of the measures tabulated the proportion of patients who were screened within three days of admission (as opposed to within one day of admission).33
There was little change in average measure performance when screening within three days was required rather than screening within one day. Average performance on the substance use measure was four points higher when a three-day requirement was used versus a one-day requirement (89.8 percent versus 85.8 percent, respectively). This trend was also evident in the substance use measure's two components: for the alcohol component, performance on the three-day measure was around 3 percentage points higher than performance on the one-day measure (92.6 percent versus 89.5 percent, respectively). For the drug component, performance on the three-day measure was around 3 percentage points higher than performance on the one-day measure (92.6 percent versus 89.9 percent, respectively). For the suicide and violence measures, performance was 2 and 3 percentage points higher, respectively, when a three-day requirement was used compared to a one-day requirement (see Table IV.8 and Figure IV.5).
| Suicide | Violence | Substance Use | |
|---|---|---|---|
| SOURCE: Administrative data and medical records from 6 IPFs, corresponding to all discharges from October 1, 2013, to December 31, 2013. NOTE: Denominator size for the 1-day measure is 761, 765, and 754 for the suicide, violence, and substance use measures, respectively. Denominator size for the 3-day measure is 642, 646, and 637 for the suicide, violence, and substance use measures, respectively. | |||
| 1-day specification (after exclusions) | 93.4 | 89.0 | 85.8 |
| 3-day specification (after exclusions) | 95.0 | 91.6 | 89.8 |
| Difference in performance rates | 1.6 points higher on 3-day version | 2.6 points higher on 3-day version | 4.0 points higher on 3-day version |
6. Performance on the Metabolic Screening Measure
Next, we summarize testing results for the metabolic screening measure. As illustrated below, the medical record must contain documentation that all four of the following tests were completed at least once in the 12 months preceding IPF discharge for patients discharged on antipsychotic medications, either during or prior to the index IPF stay. Either an HbA1c or glucose test meets the requirement in the third element. For the fourth element, a lipid panel must be a full panel, as no credit is given for a partial panel.
- BMI.
- Blood pressure.
- HbA1c or glucose.
- Lipid panel (includes total cholesterol, triglycerides, high-density lipoprotein, and low-density lipoprotein).
Overall Performance. Across all sites, approximately 42 percent of all patients discharged on antipsychotic medications received complete metabolic screenings in the 12 months prior to their IPF discharge. Performance rates on metabolic screening differed greatly between sites; the percentage of patients screened ranged from 6 percent to 99 percent (Figure IV.6 and Table IV.9). In nearly half of all denominator-eligible patient stays (46 percent across all sites), patients received all but one screening measurement or test.
| Patient Characteristics | All IPS | Psychiatric Units | Freestanding Hospitals | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IPF 1(private) | IPF 2(private) | IPF 3(private) | IPF 4(public) | IPF 5(public) | IPF 6(private) | |||||||||
| N | % | N | % | N | % | N | % | N | % | N | % | N | % | |
| SOURCE: Administrative data and medical records from 6 IPFs, corresponding to all discharges from October 1, 2013, to December 31, 2013. NOTE: Of the 180 patients with a completed metabolic screening in the 12 months prior to discharge, only 3 (1% of patients screened) had the screening completed prior to the index discharge, but within 12 months of discharge. Only 5 patients (or 1.2% of the denominator population) completed a partial lipid panel, as opposed to a full lipid panel.* IPFs did not change their screening or admission processes to test these measures. | ||||||||||||||
| Denominator (after exclusions) | 434 | 100.0 | 43 | 100.0 | 108 | 100.0 | 58 | 100.0 | 73 | 100.0 | 65 | 100.0 | 87 | 100.0 |
| Overall rate (met numerator requirement) | 180 | 41.5 | 7 | 16.3 | 15 | 13.9 | 30 | 51.7 | 72 | 98.6 | 4 | 6.2 | 52 | 59.8 |
| 1 element missing | 197 | 45.4 | 29 | 67.4 | 88 | 81.5 | 22 | 37.9 | 1 | 1.4 | 29 | 44.6 | 28 | 32.2 |
| 2 or more elements missing | 57 | 13.1 | 7 | 16.3 | 5 | 4.6 | 6 | 10.3 | 0 | 0.0 | 32 | 49.2 | 7 | 8.1 |
| Screening elements met within 1 year prior to discharge* | ||||||||||||||
| BMI | 345 | 79.5 | 36 | 83.7 | 104 | 96.3 | 41 | 70.7 | 73 | 100.0 | 21 | 32.3 | 70 | 80.5 |
| Blood pressure | 431 | 99.3 | 43 | 100.0 | 106 | 98.1 | 58 | 100.0 | 73 | 100.0 | 64 | 98.5 | 87 | 100.0 |
| Glucose or HbA1C | 407 | 93.8 | 40 | 93.0 | 105 | 97.2 | 58 | 100.0 | 73 | 100.0 | 51 | 78.5 | 80 | 92.0 |
| Glucose | 405 | 93.3 | 40 | 93.0 | 104 | 96.3 | 58 | 100.0 | 73 | 100.0 | 50 | 76.9 | 80 | 92.0 |
| HbA1C | 151 | 34.8 | 11 | 25.6 | 18 | 16.7 | 13 | 22.4 | 73 | 100.0 | 12 | 18.5 | 24 | 27.6 |
| Full lipid panel | 220 | 50.7 | 8 | 18.6 | 14 | 13.0 | 40 | 69.0 | 72 | 98.6 | 19 | 29.2 | 67 | 77.0 |
Performance on Individual Elements. Although a large majority of patients discharged on antipsychotic medications received a blood pressure measurement (99 percent), a glucose/HbA1c test (94 percent), and a measurement of their BMI (80 percent), only around half of all patients received a complete lipid panel (51 percent).34 IPFs were much more likely to measure patients' glucose than HbA1C; however, as noted above, either test satisfied the element requirement.
FIGURE IV.6. Metabolic Screening Performance across 6 IPFs
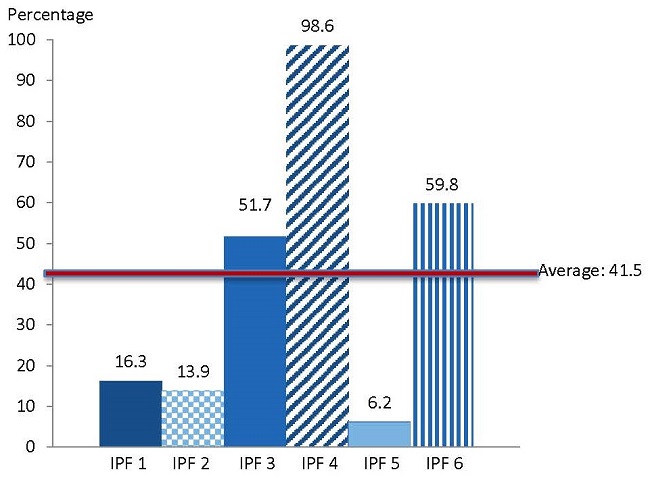
SOURCE: Administrative data and medical records from 6 IPFs, corresponding to all discharges from October 1, 2013, to December 31, 2013.
NOTE: Performance rates also presented in Table IV.9.
7. Screening Measure Performance With and Without Exclusions
The methodology used to exclude patients from the final denominator for all screening measures was modeled after the HBIPS measure set, which excludes patient stays of less than three days, stays of greater than one year, and patient inability or unwillingness to complete screenings. We applied these exclusions as well, in addition to exclusions related to multiple admissions during the same hospitalization, as psychiatric units could not be expected to re-screen patients who transferred out of their units for a brief period of time, and then returned during the same hospital stay. However, we modified the HBIPS exclusion of a patient stay of less than three days to be a patient stay of less than one day, to accommodate the admission screening measures' one-day time frame.
| Suicide | Violence | Substance Use | Metabolic | |||||
|---|---|---|---|---|---|---|---|---|
| N | & | N | & | N | & | N | & | |
| SOURCE: Administrative data and medical records from 6 IPFs, corresponding to all discharges from October 1, 2013, to December 31, 2013. NOTE: Totals for individual tools do not always sum to any standard tool, given that more than 1 tool could have been employed for 1 patient.
| ||||||||
| Denominator before exclusions | 825 | 100.0 | 825 | 100.0 | 825 | 100.0 | 506 | 100 |
| Exclusions Identified | ||||||||
| Patients with a length of stay less than 1 day | 41 | 5.0 | 41 | 5.0 | 41 | 5.0 | NA | NA |
| Patients with a length of stay less than 3 days | NA | NA | NA | NA | NA | NA | 63 | 12.5 |
| Patients with a length of stay equal to or greater than 365 days | 10 | 1.2 | 10 | 1.2 | 10 | 1.2 | 6 | 1.2 |
| Patients who had previous admissions to psychiatric units during a single hospitalization | 2 | 0.2 | 2 | 0.2 | 2 | 0.2 | 2 | 0.4 |
| Patient inability or unwillingnessb | 11 | 1.3 | 7 | 0.8 | 20a | 2.4 | 1 | 0.2 |
| Total exclusions | 64 | 7.8 | 60 | 7.3 | 71 | 8.6 | 72 | 14.2 |
| Denominator after exclusions | ||||||||
| Denominator for screening within 1 day of admission | 761 | 92.2 | 765 | 92.7 | 754 | 91.4 | 434 | 85.8 |
Admission Screening Measures. As shown in Table IV.10, exclusions did not have a major impact on the size of the denominator population for the three admission screening measures. Across the six IPFs, the admission screening measures excluded 41 patients for lengths of stay of less than one day, ten patients for lengths of stay equal to or greater than 365 days, and two patients who had previous admissions to psychiatric units during a single hospitalization. The denominator used by each measure differed only by the number of patients excluded due to inability or unwillingness to complete the screening within one day admission. Notably, 20 patients were excluded from the substance use measure due to patient unwillingness or inability to complete the screening, 11 were excluded from the suicide screening measure, and seven were excluded from the violence measure for this reason. (See Appendix Table D.2 for the number of patients who met measure exclusions at each IPF, presented for each screening measure.)
Metabolic Screening Measure. Patients with stays of fewer than three days were excluded from the metabolic screening measure based on the rationale that IPFs could not be expected to complete all metabolic screening tests (or verify that they were completed elsewhere within the previous 12 months) within that short time period. As a result, exclusions had a more substantial impact on the size of the denominator population of the metabolic screening measure relative to the admission screening measures; exclusions totaled 14 percent of discharges for the metabolic screening measure, versus less than 9 percent of discharges for the admission screening measures.
Performance rates were slightly higher among the denominator population after exclusions, compared with the population before exclusions were applied (Table IV.11). However, these differences were not large in magnitude (ranging from one point on the violence screening measure to 2 percentage points on the substance use screening measure) and were not statistically significant. We found similar results for the alcohol and drug components of the substance use measure: for the alcohol component, performance increased by 2 percentage points once exclusions were applied. For the drug component, performance increased by 1 percentage point once exclusions were applied.
| Suicide | Violence | Substance Use | Metabolic | |
|---|---|---|---|---|
| SOURCE: Administrative data and medical records from 6 IPFs, corresponding to all discharges from October 1, 2013, to December 31, 2013. * A t-test of means was conducted to determine if performance before exclusions was statistically different from performance after exclusions. These tests found no statistically significant differences (all p-values > 0.10). | ||||
| Performance before exclusions | 92.0 | 88.1 | 83.8 | 40.3 |
| Performance after exclusions | 93.4 | 89.0 | 85.8 | 41.5 |
| Difference in performance rates* | 1.4 points higher after exclusions | 0.9 points higher after exclusions | 2.0 points higher after exclusions | 1.2 points higher after exclusions |
8. Performance by Patient Characteristics
Admission Screening Measures. There were some statistically significant differences in measure performance across patient subgroups. When data were combined across IPFs, there were no statistically significant differences in performance on the admission screening measures (suicide, violence, and substance use) by patient gender (Table IV.12). However, overall screening rates for patients between the ages of 18 and 64 (ranging from 84 percent to 92 percent) were lower than for other age groups, and these differences were statistically significant for the suicide and substance use measures.
FIGURE IV.7. Performance on Screening Measures, by Primary Payer
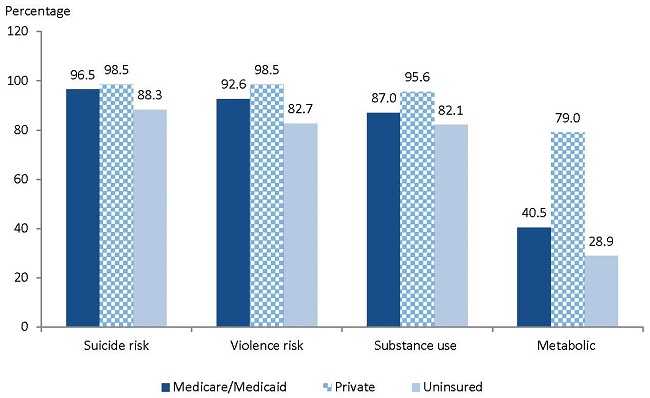
SOURCE: Administrative data and medical records from 6 IPFs, corresponding to all discharges from October 1, 2013, to December 31, 2013.
There were statistically significant differences in overall performance rates by race for all three admission measures. In each case, measure performance was highest among African American patients (with a minimum performance rate of 95 percent across all measures) and lowest among White patients (with a minimum performance rate of 82 percent across all measures). These differences in performance likely reflect the underlying differences in patient demographics across the six IPFs. The African American patient population was concentrated in IPFs 4, 5, and 6 -- the three IPFs with the highest performance on most of these measures.
| Suicide | p-Value | Violence | p-Value | Substance Use | p-Value | Metabolic | p-Value | |
|---|---|---|---|---|---|---|---|---|
| SOURCE: Administrative data and medical records from 6 IPFs, corresponding to all discharges from October 1, 2013, to December 31, 2013. NOTE: Statistically significant differences at 5% are in bold. Readers should be cautious interpreting these differences given that there are multiple comparisons; these bivariate differences may not hold when controlling for other patient or facility characteristics. | ||||||||
| Gender | ||||||||
| Female | 95.0 | 0.07 | 88.1 | 0.40 | 86.4 | 0.67 | 37.8 | 0.11 |
| Male | 91.8 | 90.0 | 85.3 | 45.5 | ||||
| Race | ||||||||
| White | 91.8 | 0.05 | 85.5 | 0.01 | 82.4 | 0.01 | 37.3 | 0.01 |
| African American | 96.5 | 97.5 | 94.9 | 53.7 | ||||
| Other | 96.6 | 90.0 | 84.7 | 24.1 | ||||
| Age | ||||||||
| Under 13 | 100.0 | 0.02 | 95.7 | 0.06 | 82.6 | 0.04 | 22.2 | 0.26 |
| 13-17 | 100.0 | 100.0 | 100.0 | 41.2 | ||||
| 18-64 | 91.8 | 87.5 | 84.3 | 44.0 | ||||
| Greater than 64 | 97.7 | 91.7 | 89.3 | 34.4 | ||||
| Insurance Coverage (primary payer) | ||||||||
| All Medicare and Medicaid | 96.5 | 0.01 | 92.6 | 0.01 | 87.0 | 0.01 | 40.5 | 0.01 |
| Dually eligible | 100.0 | 87.0 | 90.5 | 57.1 | ||||
| Medicare-only | 97.2 | 93.0 | 90.0 | 40.5 | ||||
| Medicaid-only | 94.3 | 91.7 | 77.9 | 36.0 | ||||
| Private insurance | 98.5 | 98.5 | 95.6 | 79.0 | ||||
| Uninsured | 88.3 | 82.7 | 82.1 | 28.9 | ||||
| Primary Diagnosis | ||||||||
| Schizophrenia | 95.7 | 0.02 | 91.5 | 0.03 | 88.1 | 0.34 | 51.2 | 0.01 |
| Bipolar disorder | 90.1 | 84.0 | 83.0 | 30.8 | ||||
| Depression | 97.6 | 95.2 | 90.5 | 69.2 | ||||
| Other | 95.5 | 92.9 | 86.9 | 40.8 | ||||
In addition, admission screening measure performance varied by patient insurance; patients with private insurance and Medicare generally had higher screening rates than uninsured patients and Medicaid-only beneficiaries (Figure IV.7). Also notable, performance was highest among patients with a depression diagnosis and lowest among patients with a bipolar disorder diagnosis; these differences were statistically significant for the suicide and violence screening measures.35
Metabolic Screening Measure. Similar to the admission screening measures, performance on the metabolic screening measure was lowest among patients in the bipolar disorder diagnoses (31 percent versus over 40 percent for other diagnoses). In addition, performance varied by patient insurance; patients with private insurance had much higher screening rates than patients with alternate insurance or no insurance (Figure IV.7). As noted later in this report, several stakeholders noted that this finding may reflect that some types of private insurance provide more generous coverage of lab tests compared with public insurance programs.
Also similar to the admission screening measures, there were significant differences in metabolic screening rates in our sample by race, with highest performance among African Americans patients (54 percent compared to 37 percent among Whites and 24 percent among other ethnicities). These differences in performance likely reflect the higher concentration of African American patients in IPFs 4 and 6; these two IPFs had the highest performance on the metabolic screening measure.
9. Inter-Rater Agreement for Screening and Monitoring Measures
Inter-rater reliability assesses whether two chart abstractors independently reviewing data from the same record agreed on whether the patient met the requirements for the numerator, denominator, and/or exclusions for the measure. In order to assess inter-rater reliability, each IPF had two abstractors independently abstract the same record for a sample of charts. We used Cohen's kappa statistic, a measure of agreement adjusted for chance, to quantify agreement among these abstractors.
Inter-rater reliability was moderate to high for all measures. Percentage agreement ranged from 93 percent to 98 percent across measure elements (Table IV.13). The kappa coefficients for measure exclusions were 0.85 or above for all three admission screening measures, which is considered near-perfect agreement (Landis and Koch 1977). For the numerator, element kappa coefficients ranged from 0.49 (substance use) to 0.93 (metabolic screening). In addition, we calculated a kappa coefficient for each of the alcohol and drug screening components of the substance use measure. Kappa for the alcohol screening numerator was 0.99 whereas kappa for the drug screening numerator was 0.49. As such, the drug screening component is responsible for the lower overall kappa coefficient for the substance use screening measure.
| Number of Patient Charts Double Extracted Across All IPFs | Percent Agreement | Kappa Coefficient | 95% Confidence Interval | |
|---|---|---|---|---|
| SOURCE: Administrative data and medical records from 6 IPFs, corresponding to all discharges from October 1, 2013, to December 31, 2013. NOTE: A kappa of 0.21-0.40 indicates fair agreement; a kappa of 0.41-0.60 indicates moderate agreement; a kappa of 0.61-0.80 indicates substantial agreement; a kappa of 0.81 or higher indicates almost perfect agreement. | ||||
| Suicide | ||||
| Exclusions | 58 | 98.3 | 0.85 | 0.56-1.00 |
| Numerator | 58 | 96.6 | 0.65 | 0.20-1.00 |
| Violence | ||||
| Exclusions | 58 | 98.3 | 0.85 | 0.56-1.00 |
| Numerator | 58 | 93.1 | 0.63 | 0.31-0.96 |
| Substance Use | ||||
| Exclusions | 58 | 98.3 | 0.85 | 0.56-1.00 |
| Numerator | 58 | 96.6 | 0.49 | -0.11-1.00 |
| Metabolic | ||||
| Exclusions | 58 | 98.3 | 0.95 | 0.84-1.00 |
| Numerator | 58 | 96.5 | 0.93 | 0.83-1.00 |
Interpreting these scores, the substance use numerator exhibits moderate agreement, the suicide and violence numerators exhibit substantial agreement, and the metabolic screening numerator exhibits near-perfect agreement. This near-perfect agreement on the metabolic screening measure likely reflects the non-subjective nature of the numerator, which required explicit tests to have been performed, as opposed to the admission screening measures, which required a higher level of abstractor interpretation of written notes in the patient record documenting clinical interviews. See Appendix Table D.3 for percentage agreement at each IPF, presented for each screening measure.
C. Qualitative Testing Results
Feedback from stakeholders -- including IPF staff, measure experts, policymakers, consumer and advocacy group representatives, and TEP members -- focused on the importance of the measures, the face validity of measure elements, the required time frame for completion of screening, and the measures' usability and feasibility. This feedback is summarized below.
1. Admission Screening Measures
Importance. Focus group participants and IPFs involved in measure testing acknowledged the importance of all three screening measures as the starting point for high quality care in IPFs. However, many thought CMS should also place a strong measure focus on whether patients receive appropriate treatment and demonstrate positive outcomes. The TEP underscored the importance of screening in IPF populations and was supportive of all three screening measure concepts. Some TEP members pointed to higher screening rates among African Americans compared to White and Latino patients as evidence of disparities in care.
Validity. Overall, focus group participants and IPFs involved in testing supported the validity of all three screening measures. Notably, five of the six IPFs that participated in the testing reported that the measures accurately captured their completion of screenings within one day of patient admission.36 Most participants viewed the measures' required screening elements (for example, the suicide screening measure's required documentation of ideation, plans, intent, and so on) as an improvement over HBIPS-1 in terms of mandating a high quality screening. A majority of participants preferred requiring these screening elements over requiring the use of validated instruments for all three measures. However, several participants voiced support for validated suicide screening tools, given their usefulness in treatment planning.
At least three of nine TEP members were surprised at the high average performance rates for the screening measures (performance of between 85 percent and 95 percent for all three measures), and noted that the measures might be "topped out." Overall, however, the TEP was supportive of the screening elements, and four out of five TEP members37 preferred individual screening elements over the required use of validated screening instruments.
Time Frame. At least 13 of the 25 focus group participants expressed concern about IPFs' capacity to gather accurate or complete information from screenings within one day of admission, due to patients' medical status on admission, IPF staffing constraints, or the difficulty of obtaining collateral information within one day. However, three focus group participants favored a one-day time frame for the suicide and violence risk measures -- given the clinical importance of such screening immediately upon admission -- and a three-day timeline for the substance use screening measure.
Three of nine TEP members preferred a three-day time frame over a one-day time frame for all three measures, citing the importance of allowing sufficient time to complete comprehensive and accurate screenings, as well as the need to incentivize IPF staff to re-screen patients within the first three days of their stay to complete and refine initial assessments.38 Although one TEP participant suggested using non-uniform time frames across screening measures (for example, one day for violence and suicide risk screening, and three days for substance use screening), two participants noted that it would be more feasible to use a standard time frame across all three screening measures. One TEP member argued for a one-day time frame for all three screening measures.
Usability. The majority of the 25 focus group participants and the six IPFs involved in testing generally agreed that these screening measures would be useful to inform quality improvement activities. However, some thought that the value of the measures would be stronger in the short term as IPFs would modify their screening and tracking practices to fully comply with the measures. Consumer advocates mentioned that although consumers generally have little choice in IPFs, advocacy groups have a strong interest in examining publicly available performance rates, and calling attention to poor IPF performance if necessary. Such efforts could motivate IPFs to improve their performance on these screening measures, among others.
The majority of TEP members agreed that the screening measures could contribute to quality improvement. However, given the high performance rates on these measures, two TEP members questioned whether further improvement on these measures would be possible for a subset of high-performing IPFs. These participants suggested that future IPFQR program measures be oriented toward processes and outcomes with more sizable gaps in performance.
Feasibility and Burden. The majority of focus group participants and IPFs involved in testing agreed that the burden of abstracting and reporting these three screening measures was manageable. In particular, the six IPFs that piloted the measures noted that the full abstraction of a patient's record for all three screening measures took 10-15 minutes, on average, as required data elements were readily available in records. However, representatives of three of 11 IPFs, one consumer representative, one quality measurement expert, and one IPFQR program vendor noted that if IPFs choose to integrate new screening tools into their electronic medical record to ensure reliable data capture for the measures, the transition could take at least six months to implement.
The TEP agreed that the task of abstracting and reporting the suicide, violence, and substance use screening measures was manageable. However, three TEP members strongly recommended that the measures be harmonized with HBIPS-1 to decrease IPF burden and redundancy across psychiatric inpatient measures.
2. Metabolic Screening Measure
Importance. Representatives from IPFs, IPFQR program vendors, policy experts, and consumer groups agreed that monitoring patients' metabolic functioning is extremely important, given the psychiatric inpatient population's high risk for metabolic conditions, and expressed strong support for CMS's focus on the issue. TEP members also supported the importance of the metabolic screening measure, citing large performance gaps across IPFs that participated in testing.
Validity. Focus group participants generally supported the measure concept and its elements. However, some IPFQR program vendors, measurement experts, and consumer representatives were unsure if all of the required elements were clinically relevant -- particularly a full lipid panel. One vendor and a clinician expressed concern that the measure might inadvertently encourage IPFs and other clinicians to conduct unnecessary tests, and that test results might not be transmitted to patients' next level of care. Three of six IPFs involved in measure testing expressed some resistance to the measure's full lipid panel requirement. According to these IPF representatives, clinicians generally used their judgment in determining whether a panel was necessary. As such, requiring a full panel for all patients on antipsychotics might "over treat" patients.
Three of nine TEP members expressed similar concern over the measure requirement of a full lipid panel. One TEP member stated that lipid panels were relatively expensive lab tests, and that some IPFs serving patients with state or county insurance could not get adequate compensation for a full lipid panel for all patients on antipsychotics. Two participants suggested excluding the lipid panel requirement, or structuring the measure such that IPFs are required to complete blood pressure, BMI, and glucose tests, and then proceed to a full lipid panel if necessary. However, one TEP member strongly disagreed, citing the strength of scientific evidence in support of a full lipid panel at least once per year for individuals on antipsychotics.
Usability. Representatives from IPFs, IPFQR program vendors, policy experts, and consumer groups generally supported the potential usability of the metabolic screening measure, reasoning that poor performance could help IPFs identify gaps in care and areas for improvement. However, one IPF representative noted that some hospitals with poor performance on the measure may face cost constraints -- particularly related to reimbursement from some payers for a full lipid panel -- that might preclude their improvement on the measure.
TEP members supported the measure's usability, noting that IPFs' low performance on the measure (around 42 percent performance across six IPFs, on average) suggests strong potential for quality improvement efforts around metabolic screening. However, two participants noted that screening could contribute to improved quality only if it informs care beyond screening (such as treatment options).
Feasibility and Burden. Focus group participants expressed concern that the metabolic screening measure would place a large burden on IPF staff, as they must search patient records to determine whether required tests were completed within the past year. IPFs involved in measure testing verified that chart-abstraction of this measure was more labor-intensive than the other screening measures, but generally did not exceed 20 minutes for any given discharge. One IPF involved in testing stated that chart abstractors often did not have access to relevant lab test results due to data sharing restrictions. However, the other five IPFs involved in testing mentioned that abstractors have easy access to relevant lab records. Only one of nine TEP members explicitly expressed concerns about the burden of abstracting or reporting the metabolic screening measure.
D. Summary of Findings and Proposed Revisions
Admission Screening Measures. Measure performance was quite high across IPFs on the suicide, violence, and substance use screening measures, with average performance on the measures ranging from 86 percent (in the case of substance use) to 93 percent (in the case of suicide). Reliability was moderate for the substance use measure and substantial for the suicide and violence measures. In addition, IPF performance on the measures was not substantively affected by exclusions or specification as one-day versus three-day measures, thus providing support for the measures' face validity. Stakeholders were generally supportive of the measures and thought their screening element requirements represented an improvement over existing screening measures used in an inpatient psychiatric setting, including HBIPS-1.
Regarding changes to measure specifications, stakeholders generally recommended that the final specification of the substance use, violence, and suicide screening measures use a three-day time frame to allow for complete screening. Obstacles to performing accurate screenings within one day of admission include staff shortages, patient uncooperativeness, and lack of patient lucidity. Citing harmonization needs, the TEP also noted that a three-day version of this measure would be consistent with HBIPS-1. Some stakeholders noted that the suicide and violence measures should be conducted within a one-day time frame, given the importance of obtaining that information quickly. Based on this feedback, the research team recommends changing the time frame for the substance use screening measure from one day to three days, and keeping the suicide and violence screening specifications at one day (as currently specified; see Table IV.14). The additional days will facilitate the capture of complete and accurate information regarding patients' alcohol and drug use, without compromising the need to capture important information on suicide and violence risk in the first day of admission.
Metabolic Screening Measure. Performance on the metabolic screening measure was low, on average, across the six IPFs. The measure's average performance rate of 42 percentage points signals strong room for improvement on the measure. The metabolic screening measure demonstrated non-trivial variation in performance among IPFs as well as by patient characteristics. In addition, it demonstrated near-perfect agreement between chart abstractors (kappa of 0.93 for the measure numerator).
Overall, stakeholders found the metabolic screening measure to be important for addressing a notable gap in psychiatric care. However, focus group participants and TEP members were divided over whether to keep the requirement of a full lipid panel, as some felt that blood pressure, BMI, and glucose/HbA1c tests were sufficient screening requirements. In particular, one of the six IPFs that participated in pilot testing and two of nine TEP members expressed concern that the measure might inadvertently encourage IPFs and other clinicians to conduct unnecessary tests -- namely a full lipid panel in instances in which there is no clinical need. However, given the preponderance of clinical evidence supporting a full lipid panel on an annual basis for patients taking regularly prescribed antipsychotic medications, we suggest that the full lipid panel remain a screening element in the metabolic screening measure (see Table IV.14).
| Measure | Quantitative Testing Results | Stakeholder Input | Revisions to SpecificationFollowing Testing |
|---|---|---|---|
| Suicide screening |
|
|
|
| Violence screening |
|
|
|
| Substance use screening |
|
|
|
| Metabolic screening |
|
|
|
V. TESTING RESULTS FOR THE FOLLOW-UP AFTER IPF HOSPITALIZATION MEASURE
We used Medicare and Medicaid claims data from calendar year 2008 to test the measure of follow-up after IPF hospitalization. This measure is closely based on the HEDIS FUH measure (NQF #0576). As part of quantitative testing, we examined measure performance across various numerator options, as well as measure reliability. In addition, we held stakeholder focus groups and debriefing sessions to gather qualitative input on the validity, credibility, and representativeness of the measure. In the next section, we present the results of quantitative measure testing.
A. Characteristics of Medicare Beneficiaries Who Used IPFs
Across all 50 states in this analysis, roughly 210,000 FFS Medicare beneficiaries had an IPF stay with a mental health diagnosis from January 1, 2008, to December 1, 2008 (Table V.1). These beneficiaries were almost equally divided between male and female, and most were over 50 years old. The majority of beneficiaries were White; approximately half received a principal diagnosis of bipolar disorder and one-third a diagnosis of schizophrenia during their IPF stay.
The denominator for the measure is based on discharges rather than individual patients. The 210,326 FFS Medicare beneficiaries in the denominator population had a total of 321,454 IPF discharges during 2008, generating an average of around 1.5 IPF stays per beneficiary over the calendar year. A total of 1,702 IPFs had at least one FFS Medicare discharge during 2008 (not shown). On average, each IPF had 189 FFS Medicare discharges during the year, but this varied significantly (range = 1-1,300 discharges; median of 139 FFS Medicare discharges).
Our primary quantitative analyses used Medicare claims data to examine measure performance among non-dual eligible beneficiaries. At the outset of the project, CMS determined that, due to feasibility issues and data limitations, the follow-up measure would be calculated using only Medicare data.39 Including dual eligible beneficiaries in the denominator of a measure that relies solely only on Medicare data would be problematic because these data would not capture dual eligible beneficiaries' receipt of Medicaid-financed services. For this reason, we excluded dual eligible beneficiaries from the measure denominator prior to conducting most validity and reliability analyses.
As illustrated in Table V.1, the non-dual eligible population represented 37 percent of all FFS Medicare beneficiaries who had at least one IPF hospitalization in 2008. The remainder of this chapter summarizes measure performance among this non-dual eligible population, using only FFS Medicare claims. Chapter VI presents supplemental analyses of measure performance among all FFS Medicare beneficiaries, including dual eligible beneficiaries, using a combination of Medicare and Medicaid claims.
| Characteristic | Number of FFS Medicare Beneficiaries | Percentage of FFS Medicare Beneficiaries (%) |
|---|---|---|
| SOURCE: FFS Medicare claims from calendar year 2008. NOTE: Counts in this table are Medicare FFS beneficiaries discharged from IPFs with a mental health diagnosis. Sample size is 321,454 discharges at 1,702 IPFs that had at least 1 FFS Medicare discharge during 2008. | ||
| All beneficiaries | 210,326 | 100.0 |
| Age | ||
| Under 27 | 8,897 | 4.2 |
| 27-39 | 36,355 | 17.3 |
| 40-49 | 48,429 | 23.0 |
| 50-64 | 56,002 | 26.6 |
| 65-79 | 42,889 | 20.4 |
| 80 or older | 17,745 | 8.4 |
| Gender | ||
| Male | 98,186 | 46.7 |
| Female | 112,140 | 53.3 |
| Race | ||
| White (non-Hispanic) | 161,436 | 76.8 |
| African American (non-Hispanic) | 36,227 | 17.2 |
| Asian/Pacific Islander | 2,044 | 1.0 |
| Hispanic/Latino | 5,910 | 2.8 |
| American Indian/Alaskan Native | 1,290 | 0.6 |
| Other | 2,870 | 1.4 |
| Unknown | 549 | 0.3 |
| Primary Diagnosis | ||
| Schizophrenia | 69,764 | 33.2 |
| Bipolar disorder | 109,769 | 52.2 |
| Major depressive disorder | 8,448 | 4.0 |
| Psychosis | 12,720 | 6.1 |
| Other | 9,625 | 4.6 |
| Insurance Coverage | ||
| Medicare FFS only | 77,928 | 37.1 |
| Medicare/Medicaid dual beneficiary | 132,398 | 62.9 |
B. Performance by Numerator Options
We tested four numerator options (Table V.2) for the follow-up measure. These options define a follow-up mental health visit in four slightly different ways:
Option 1 uses a definition of outpatient follow-up care that closely follows the HEDIS FUH measure: a mental health procedure (identified by CPT/HCPCS codes) provided by a mental health practitioner, who is a psychiatrist, psychologist, social worker, psychiatric nurse or physician assistant with a psychiatric specialty.40 This option does not use diagnosis codes to define follow-up mental health services.
Option 2 uses the same CPT/HCPCS codes used in option 1, but requires that these codes be accompanied by a principal mental health diagnosis instead of requiring that the procedure be performed by a mental health practitioner (as in option 1). Following the HEDIS FUH measure specification, diagnoses of schizophrenia, depression, bipolar disorder, stress, and personality disorders are considered mental health diagnoses, but diagnoses of alcohol and drug dependency, as well as some anxiety disorders, are not.41
It should be noted that CPT/HCPCS codes used in options 1 and 2 include services that are explicitly behavioral health care (such as a psychiatric evaluation and psychotherapy), as well as services that are not exclusively behavioral health care (such as office visits and home visits). However, procedure codes that are not explicitly for behavioral health care only count toward the numerator if they are either provided by a mental health practitioner (option 1) or provided in conjunction with a principal mental health diagnosis (option 2).
Option 3 requires a mental health diagnosis, but does not require a specific CPT/HCPCS procedure code. Rather, it requires that the service was billed as an outpatient service. This less-restrictive definition of mental health care -- any outpatient visit accompanied by a principal mental health diagnosis -- captures mental health services performed by primary care providers and other practitioners who are not mental health practitioners according to the HEDIS FUH definition.
Option 4 requires only an outpatient visit, regardless of diagnosis or provider. This is not a viable option for measuring follow-up mental health care. However, we included it in our analysis to provide context for the other three numerator options.
For each of the 1,669 IPFs that treated at least one non-dual FFS Medicare beneficiary in 2008, we calculated the proportion of patients that received follow-up care within seven days and within 30 days of their IPF discharge.42 For example, an IPF with ten FFS Medicare discharges in 2008, in which four of these stays were accompanied by a follow-up visit within the month, would have a performance rate of 40 percent for the year. In the tables below, we present pooled results, or the average of IPF performance rates for 2008 on all four numerator options.
| TABLE V.2. Numerator Options for Follow-Up Measure | |
|---|---|
| Option 1 | An outpatient visit, an intensive outpatient encounter or partial hospitalization with a mental health practitioner within 30 or 7 days of discharge. (Uses CPT/HCPCS codes and NPI/Taxonomy codes.) (This definition most closely aligns with the HEDIS FUH measure.) |
| Option 2 | An outpatient visit, an intensive outpatient encounter or partial hospitalization (with any provider) with a principal mental health diagnosis within 30 or 7 days of discharge. (Uses CPT/HCPCS codes and mental health diagnosis codes.) |
| Option 3 | Any outpatient visit with a principal mental health diagnosis within 30 or 7 days of discharge (excluding emergency department, ambulance, lab, and other non-ambulatory claims). |
| Option 4 | Any outpatient visit, regardless of diagnosis or provider. |
Overall IPF Performance. On average, numerator options 1, 2, and 3 yield similar estimates of follow-up care: slightly less than one-third of non-dually eligible FFS Medicare beneficiaries received follow-up mental health care within seven days, whereas slightly more than 50 percent received such follow-up care within 30 days (Table V.3). Seven-day rates are between 28 percent and 30 percent for all three options, and 30-day rates are between 52 percent and 55 percent for all three options. Among the first three numerator options, option 3 has the highest average performance on both the seven-day and 30-day measures; this is not surprising given that it has the least restrictive definition of follow-up care among the three options. Also notable, option 1 has slightly higher performance than option 2 (30-day follow-up rate of 54 percent for option 1 versus 52 percent for option 2). This difference is due to option 2's requirement that the outpatient visit have a principal mental health diagnosis, which identified slightly less numerator hits than option 1's requirement that the visit take place with a mental health practitioner.
| Mean | Min | 25th Percentile | Median | 75th Percentile | Max | IQR | |
|---|---|---|---|---|---|---|---|
| SOURCE: FFS Medicare claims from calendar year 2008. NOTE: Sample size 61,871 index discharges among 1,669 facilities with at least 1 non-dually eligible FFS Medicare discharge in 2008. | |||||||
| Option 1 | |||||||
| 7-day follow-up | 28.7 | 0 | 16.7 | 27.8 | 39.5 | 100 | 22.8 |
| 30-day follow-up | 53.5 | 0 | 42.3 | 55.0 | 67.3 | 100 | 25.0 |
| Option 2 | |||||||
| 7-day follow-up | 28.2 | 0 | 16.7 | 27.3 | 38.5 | 100 | 21.8 |
| 30-day follow-up | 52.0 | 0 | 40.0 | 53.1 | 65.9 | 100 | 25.9 |
| Option 3 | |||||||
| 7-day follow-up | 30.3 | 0 | 18.8 | 29.3 | 40.9 | 100 | 22.2 |
| 30-day follow-up | 54.5 | 0 | 42.9 | 55.9 | 67.7 | 100 | 24.8 |
| Option 4 | |||||||
| 7-day follow-up | 50.3 | 0 | 40.0 | 50.0 | 60.6 | 100 | 50.3 |
| 30-day follow-up | 80.4 | 0 | 73.7 | 83.3 | 90.2 | 100 | 80.4 |
Variation in Performance. As shown below, all numerator options demonstrate wide variation in performance across IPFs, with IQRs of greater than 21 for all numerator options.43 The follow-up measure's relatively large IQR -- indicative of a large distribution of performance among IPFs -- suggests widespread opportunities for improvement on the measure.
In addition, there is large dispersion of IPF performance on the measure, with a minimum of zero and a maximum of 100 percent performance for the seven-day and 30-day versions of the measures for all numerator options. However, some of the extremes in these minima and maxima reflect instances of small sample sizes -- generally IPFs that had fewer than ten FFS Medicare-paid discharges in 2008.
Stability of Performance Across Numerator Options. To determine the extent to which IPFs' performance under one numerator option is correlated with performance under other numerator options, we tabulated the portion of IPFs that score within the same decile -- or within 10 percentile points -- on any combination of options. For this analysis, we converted each IPF's score for each numerator option into a percentile score, reflecting that IPF's performance relative to other IPFs in the sample. Next, we determined the portion of IPFs whose percentile scores for two numerator options were within ten points of each other. For example, if an IPF's score on option 1 is the 87th percentile and its score for option 2 is the 93rd percentile, the IPF would qualify as remaining in the same decile in a comparison of options 1 and 2.
There is considerable consistency in IPF performance across numerator options 1, 2, and 3. As illustrated in Table V.4, at least 73 percent of IPFs score within the same decile between any two numerator options. In addition, the median percentile difference between numerator options was relatively small, ranging between 3 and 5 percentile points. These results illustrate that IPFs have similar performance relative to other IPFs under all three numerator options -- essentially that a high-performing IPF under any option would likely be high-performing under the other two options.
| Options 1 and 2 | Options 1 and 3 | Options 2 and 3 | |||
|---|---|---|---|---|---|
| Median Percentile Difference | IPFs That Remained in the Same Decile(%) | Median Percentile Difference | IPFs That Remained in the Same Decile(%) | Median Percentile Difference | IPFs That Remained in the Same Decile(%) |
| SOURCE: FFS Medicare claims from calendar year 2008. NOTE: Sample size 61,871 index discharges among 1,669 IPFs. | |||||
| 4 | 77.1 | 5 | 72.8 | 3 | 94.4 |
Final Numerator Selection. In consultation with CMS, ASPE, and the TEP during the measure testing process, we determined that numerator option 1could be accurately calculated using only Medicare claims. As mentioned above, option 1 closely adheres to the NQF-endorsed HEDIS approach, which allows for a direct comparison with health plan performance on the FUH measure. Because option 1 has similar performance relative to the other two numerator options for non-dual beneficiaries, and has the additional advantage of closely following FUH measure specifications, stakeholders viewed it as the most appropriate numerator option. For this reason, we used numerator option 1 to conduct the remaining analyses of measure exclusions, variation in performance by IPF size and demographics, and reliability.
C. Impact of Measure Exclusions on Follow-Up Measure Performance
Measure exclusions for the follow-up measure align with those of the HEDIS FUH measure, which excludes IPF discharges followed by acute care and non-acute care during the 30-day follow-up period.44 The rationale for exclusions related to acute and non-acute care is that an inpatient or institutional stay could interfere with the ability of the beneficiary to seek and obtain follow-up care after an IPF hospitalization. We examined the impact of these measure exclusions on the denominator size and measure performance.
| Exclusion | Rationalefor Exclusion | Proportion of IPF Discharges (%) | Number of Discharges |
|---|---|---|---|
| SOURCE: FFS Medicare claims from calendar year 2008. NOTE: Sample size is 106,139 index discharges among 1,669 IPFs. The exclusions presented in this table are not mutually exclusive. For example, exclusions 1 and 2 may both apply to the same discharge and would be counted toward the proportion reported for each exclusion. Exclusions apply to both 7-day and 30-day versions of the measure. | |||
| 1. Death within 30 days of IPF discharge | Death within the follow-up period does not allow for follow-up care | 0.6 | 718 |
| 2. For an IPF discharge where the patient visited an IPF in the previous 30 days, exclude the previous IPF discharge | Including these IPF discharges would influence the number of discharges in the denominator and measure performance | 17.8 | 18,787 |
| 3. IPF discharges with a non-IPF inpatient or other residential stay during follow-up period | An inpatient or otherwise residential stay may interfere with patients' receipt of follow-up care | 38.0 | 40,374 |
| All exclusions (proportion excluded for any of the exclusions above) | 41.7 | 44,268 | |
Roughly 42 percent of IPF discharges are excluded from the denominator after all exclusions are implemented (Table V.5). One percent of IPF discharges were followed by death within 30 days (exclusion 1), approximately 18 percent of IPF discharges were followed by another IPF stay within 30 days (exclusion 2), and 38 percent of IPF discharges were followed by a (non-IPF) inpatient or other residential stay during the 30-day follow-up period (exclusion 3; Table V.5).
After implementing these exclusions, average performance is about 5 points higher for sevenday follow-up (29 percent versus 24 percent) and average performance was about 10 points higher for the 30-day follow-up measure (54 percent versus 44 percent; Table V.6).These differences are largely attributable to exclusion 3, in which IPF discharges are excluded if they are followed by a non-IPF inpatient or other residential stay within 30 days.
| Exclusions | Average 7-Day Follow-Up Rate (%) | Average 30-Day Follow-Up Rate (%) |
|---|---|---|
| SOURCE: FFS Medicare claims from calendar year 2008. NOTE: Follow-up rates use numerator option 1. Sample size is 106,139 index discharges among 1,669 IPFs. | ||
| No exclusions | 24.0 | 43.8 |
| All exclusions | 28.7 | 53.5 |
| Exclusion 1: Death | 24.1 | 44.0 |
| Exclusion 2: Exclude readmission to IPF | 25.1 | 47.0 |
| Exclusion 3: Exclude admission to non-IPF inpatient care or other residential stay | 28.6 | 52.7 |
Although these exclusions result in a substantial decrease in the denominator size, the TEP considered all exclusions to be necessary for the face validity of the measure and to maintain consistency with the NQF-endorsed HEDIS measure (which may facilitate more accurate comparison between IPF and health plan performance).
D. Follow-Up after IPF Hospitalization by Beneficiary Characteristics and Geographic Location
IPF performance on the follow-up measure varies significantly according to patient characteristics. On average, seven-day and 30-day follow-up rates are lower for adults ages 18-26 relative to other age groups (Table V.7). In addition, males have lower average rates of follow-up care compared to females, as do African Americans and patients with IPF diagnoses of depression and psychosis (Figure V.1 and Figure V.2). All these differences are statistically significant (however, we are likely to detect some spurious bivariate relationships, given the large sample size).
| Characteristic | Average 7-Day Follow-Up | p-Value | Average 30-Day Follow-Up | p-Value |
|---|---|---|---|---|
| SOURCE: FFS Medicare claims from calendar year 2008. NOTE: Follow-up rates use numerator option 1. Sample size 61,871 index discharges among 1,669 IPFs. The average rate presented here is a pooled average across patients, based on their demographic characteristics. Performance can be interpreted as IPF performance for each subpopulation. Statistically significant differences at 5% are in bold. | ||||
| All beneficiaries | 28.7 | 53.5 | ||
| Age | ||||
| 18-26 | 24.7 | 0.01 | 42.6 | 0.01 |
| 27-39 | 30.9 | 52.9 | ||
| 40-49 | 30.3 | 53.3 | ||
| 50-64 | 30.0 | 53.8 | ||
| 65-79 | 31.0 | 58.9 | ||
| 80+ | 23.3 | 50.6 | ||
| Gender | ||||
| Male | 26.3 | 0.01 | 48.9 | 0.01 |
| Female | 30.7 | 57.6 | ||
| Race | ||||
| White | 29.5 | 0.01 | 55.1 | 0.01 |
| African American | 22.5 | 42.5 | ||
| Asian/Pacific Islander | 28.5 | 49.0 | ||
| Hispanic/Latino | 27.9 | 50.8 | ||
| American Indian/Alaskan Native | 35.3 | 50.6 | ||
| Other | 31.7 | 57.6 | ||
| Unknown | 31.0 | 59.2 | ||
| Primary Diagnosis | ||||
| Schizophrenia | 26.7 | 0.01 | 50.9 | 0.01 |
| Bipolar disorder | 30.7 | 56.9 | ||
| Major depressive disorder | 22.6 | 44.3 | ||
| Psychosis | 21.3 | 43.0 | ||
| Other | 22.7 | 45.4 | ||
FIGURE V.1. 30-Day Follow-Up Rates by IPF Diagnosis, among Non-Dual FFS Medicare Beneficiaries
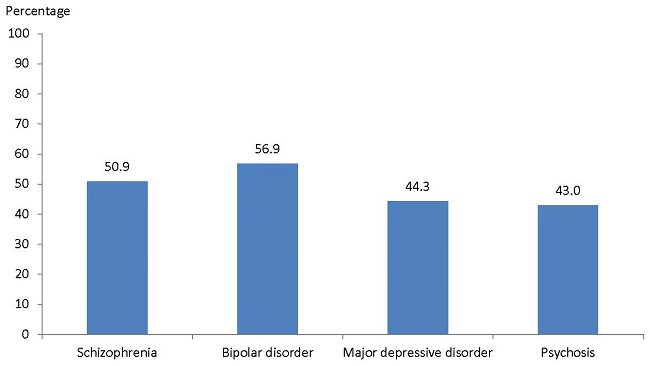
SOURCE: FFS Medicare claims from calendar year 2008.
NOTE: Follow-up rate uses numerator option 1.
FIGURE V.2. 30-Day Follow-Up Rate by Patient Ethnicity, among Non-Dual FFS Medicare Beneficiaries

SOURCE: FFS Medicare claims from calendar year 2008.
NOTE: Follow-up rate uses numerator option 1.
IPF performance on the follow-up measure also varies by state and region (Table V.8 and Figure V.3). On average, seven-day and 30-day follow-up rates are lower in Southern and Western states relative to Eastern and Mid-Western states. States with particularly high follow-up rates include New Hampshire and Vermont, with 74 percent and 72 percent follow-up on the 30-day measure, respectively. States with particularly low rates of follow-up care include Idaho and Alaska, with 36 percent and 37 percent follow-up on the 30-day measure, respectively. However, most of these highest and lowest-performing states had fewer than ten IPFs with FFS Medicare beneficiaries in 2008; therefore, these state-level averages should be interpreted with caution.
| Characteristics | Number of Facilities | Average Number of Discharges Per Facility in 2008 | Average 7-Day Follow-Up | Average 30-Day Follow-Up |
|---|---|---|---|---|
| SOURCE: FFS Medicare claims from calendar year 2008. NOTE: Follow-up rates use numerator option 1. Sample size 61,871 index discharges among 1,669 IPFs. Within each region, states are arranged from highest to lowest performance on the 30-day measure.cs = Suppressed in adherence to CMS DUA governing use of Medicare data. | ||||
| All facilities | 1,669 | 37.1 | 28.7 | 53.5 |
| East | 398 | 37.5 | 36.0 | 59.0 |
| New Hampshire | 12 | 36.3 | 50.0 | 73.7 |
| Vermont | 4 | 28.3 | 53.8 | 71.5 |
| Maine | 7 | 21.9 | 41.7 | 65.8 |
| Massachusetts | 55 | 31.5 | 40.9 | 67.3 |
| Connecticut | 33 | 34.1 | 39.4 | 64.0 |
| Pennsylvania | 100 | 32.6 | 30.3 | 57.2 |
| Rhode Island | 6 | 57.8 | 30.3 | 55.8 |
| New Jersey | 52 | 46.4 | 33.3 | 55.3 |
| New York | 129 | 41.6 | 36.6 | 55.1 |
| Delaware | 4 | 80.3 | 32.9 | 53.2 |
| Mid-West | 429 | 34.2 | 29.3 | 58.6 |
| Michigan | 62 | 53.8 | 37.2 | 65.1 |
| Iowa | 28 | 17.4 | 33.5 | 62.9 |
| North Dakota | 10 | 24.3 | 30.0 | 62.6 |
| Wisconsin | 32 | 32.2 | 32.5 | 61.4 |
| South Dakota | 4 | 41.0 | 23.9 | 60.1 |
| Indiana | 50 | 20.6 | 32.1 | 59.0 |
| Nebraska | 9 | 23.4 | 35.8 | 58.8 |
| Minnesota | 29 | 26.2 | 23.1 | 58.7 |
| Missouri | 44 | 42.7 | 26.7 | 57.1 |
| Kansas | 26 | 21.2 | 28.2 | 56.7 |
| Illinois | 64 | 37.9 | 27.0 | 55.4 |
| Ohio | 71 | 35.8 | 23.6 | 53.6 |
| South | 620 | 41.4 | 24.6 | 49.1 |
| West Virginia | 14 | 36.4 | 30.5 | 61.2 |
| Virginia | 39 | 44.4 | 28.4 | 58.3 |
| North Carolina | 41 | 48.6 | 27.0 | 54.7 |
| South Carolina | 21 | 59.2 | 23.0 | 54.5 |
| Florida | 61 | 70.3 | 28.4 | 52.7 |
| Kentucky | 27 | 31.3 | 23.5 | 52.2 |
| Texas | 86 | 53.5 | 26.4 | 51.0 |
| Tennessee | 49 | 34.4 | 20.8 | 50.8 |
| Alabama | 41 | 32.3 | 18.0 | 47.3 |
| Louisiana | 76 | 21.0 | 33.2 | 46.3 |
| Georgia | 37 | 68.3 | 19.2 | 43.6 |
| Maryland | 8 | 49.5 | 28.5 | 43.5 |
| Arkansas | 34 | 19.6 | 17.4 | 42.6 |
| Mississippi | 49 | 18.1 | 20.6 | 40.8 |
| Oklahoma | 33 | 30.9 | 16.3 | 40.0 |
| West | 210 | 29.4 | 25.6 | 46.2 |
| Montana | 3 | 26.3 | 30.2 | 64.2 |
| Wyoming | 6 | cs | 17.2 | 64.2 |
| Utah | 11 | 25.1 | 33.3 | 57.9 |
| New Mexico | 10 | 27.3 | 26.7 | 54.7 |
| Colorado | 20 | 28.4 | 31.7 | 52.6 |
| Washington | 20 | 25.8 | 27.3 | 52.3 |
| Arizona | 18 | 45.0 | 27.6 | 47.0 |
| Hawaii | 4 | cs | 35.5 | 45.8 |
| Oregon | 10 | 28.1 | 24.2 | 43.9 |
| California | 88 | 28.6 | 24.0 | 41.1 |
| Nevada | 10 | 60.9 | 21.0 | 40.0 |
| Idaho | 8 | 16.6 | 15.3 | 36.9 |
| Alaska | 2 | cs | 17.9 | 35.7 |
| Other | 12 | 39.3 | 25.5 | 44.2 |
| District of Columbia | 6 | 26.3 | 31.4 | 46.7 |
| Puerto Rico | 6 | 52.3 | 19.7 | 41.7 |
FIGURE V.3. 30-Day Follow-Up after IPF Hospitalization by Region, among Non-Dual FFS Medicare Beneficiaries
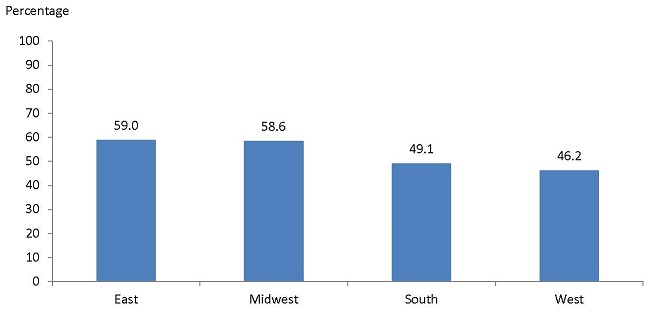
SOURCE: FFS Medicare claims from calendar year 2008.
NOTE: Follow-up rate uses numerator option 1.
E. Reliability Analysis
We conducted a beta-binomial test to examine the reliability of the measure specification using numerator option 1. This test estimates the measure's ratio of "signal to noise." The "signal" is the proportion of the variability in measured IPF performance that can be explained by actual differences in performance between IPFs, whereas "noise" is any measurement error due to sampling in the time period of interest. This test produces a reliability score ranging from 0 to 1: a score of 0 implies that all the variability in the measure is attributable to measurement error; a score of 1 implies that all the variability is attributable to actual differences in performance.
The measure demonstrated high reliability: 0.94 for the seven-day measure and 0.93 for the 30day measure. This suggests that the measure can strongly detect actual variation in IPF performance. (We note that beta-binomial statistics are generally high with large sample sizes -- in this case, a large number of facilities.)
Next, we calculated reliability estimates for subgroups of IPFs, based on their number of FFS Medicare discharges per year (Table V.9). Only IPFs with fewer than 11 discharges per year had reliability estimates that dropped below the lower limit of 0.70 that is considered necessary to distinguish the quality of care at one facility from that at another (Adams 2009). This is consistent with CMS rules regarding public reporting, which require that measures based on a sample size of fewer than 11 discharges not be publicly reported.45
| Facility Characteristic | Average 7-Day Follow-Up Rate | Reliability | Average 30-Day Follow-Up Rate | Reliability | Number of Facilities |
|---|---|---|---|---|---|
| SOURCE: FFS Medicare claims from calendar year 2008. NOTE: Follow-up rates use numerator option 1. Sample size 61,871 index discharges among 1,669 IPFs. Reliability rates below the lower limit of 0.7 are shaded above. | |||||
| All facilities | 28.7 | 0.94 | 53.5 | 0.93 | 1,669 |
| By number of Medicare FFS discharges per year: | |||||
| 0-10 | 19.5 | 0.72 | 41.3 | 0.65 | 75 |
| 11-20 | 24.1 | 0.91 | 49.8 | 0.88 | 122 |
| 21-30 | 22.4 | 0.93 | 45.5 | 0.91 | 112 |
| 31-40 | 26.3 | 0.94 | 50.9 | 0.93 | 113 |
| 41-50 | 27.5 | 0.95 | 53.1 | 0.94 | 118 |
| 51-60 | 29.6 | 0.95 | 54.8 | 0.94 | 108 |
| 61-70 | 33.2 | 0.93 | 59.4 | 0.93 | 85 |
| 71-80 | 28.8 | 0.95 | 54.2 | 0.95 | 98 |
| 81-90 | 30.4 | 0.96 | 54.4 | 0.96 | 92 |
| 91-100 | 31.6 | 0.95 | 56.9 | 0.96 | 86 |
| 101-125 | 31.4 | 0.98 | 56.6 | 0.98 | 177 |
| 126-150 | 31.2 | 0.98 | 58.8 | 0.98 | 123 |
| 151-200 | 29.4 | 0.98 | 53.8 | 0.98 | 130 |
| 201 or more | 30.7 | 0.99 | 54.6 | 0.99 | 230 |
In addition, we examined the follow-up measure's stability across quarters -- or the extent to which IPFs maintained their performance relative to other IPFs throughout the course of the year. We found that approximately 54 percent of all IPFs remained in the same performance quartile during the first three quarters of 2008.46 However, performance rates were more stable in IPFs with a substantial number of FFS Medicare patients during the year. Approximately 80 percent of IPFs with at least 50 FFS Medicare discharges in 2008 remained in the same performance quartile during all three quarters. These findings support the measure's reliability, in that IPF performance is generally stable throughout the calendar year, particularly among IPFs with at least 50 FFS Medicare discharges.
F. Stakeholder Feedback on the Follow-Up Measure
Stakeholder support for the follow-up measure was mixed. Three of the six IPFs involved in testing, and at least 11 of the 25 focus group participants expressed concern that the measure may inappropriately hold IPFs accountable for patient behavior and system inadequacies that are outside of facilities' control, including limited provider availability and long wait-times in some regions. However, at least five focus group participants -- primarily policymakers and measurement experts -- noted that this measure could help to drive innovative partnerships between facilities, community mental health agencies, health plans, and providers to improve follow-up care for IPF patients.
Although the TEP generally agreed that follow-up for IPF patients was important to measure, two TEP members were quite vocal in expressing the concern that the measure would unfairly hold IPFs accountable for factors outside of their control -- particularly the availability of follow-up care in their community and patients' disposition to keep follow-up appointments. Two other TEP members expressed strong support for the follow-up measure, arguing that it could identify opportunities for quality improvement. One TEP member suggested that this measure should not be publicly reported, given that it could have the unintended consequence of diverting patients from IPFs that provide high quality inpatient services, but have poor performance on the measure due to factors outside their control.
Regarding the measure numerator, focus group participants and TEP members supported specifying follow-up care as services provided by licensed behavioral health practitioners (numerator option 1). They favored this numerator because it closely adheres to the NQF-endorsed HEDIS measure (and would therefore better facilitate comparisons with health plan follow-up rates) and because they felt that patients discharged from an IPF require follow-up care from a mental health professional rather than from a primary care or other provider.
Regarding the measure denominator, focus group participants and TEP members noted that limiting the denominator to non-dual Medicare beneficiaries would exclude a large proportion of IPF patients; therefore, measure performance may not be representative of all patients discharged from IPFs. However, TEP members agreed that non-dual Medicare beneficiaries still represent a sizable portion of all IPF patients and thus constitute "a good place to start" for measuring follow-up care. TEP members stated that IPF patients without a principal mental health diagnosis should be excluded from the measure, given the lack of consensus regarding what follow-up services are most appropriate for patients with dementia, Alzheimer's, or substance abuse diagnoses. This feedback is consistent with the current denominator specification.
G. Summary and Revisions to Follow-Up Measure Specification
The claims-based follow-up measure demonstrated strong quantitative performance; there was good variation in measure performance across IPFs and among patient characteristics. In addition, IPFs' relatively low average performance for all numerator options highlights room for improvement on the measure. The measure also demonstrated very good reliability. Nonetheless, many stakeholders were opposed to the implementation of this measure because they did not think IPFs should be solely accountable for the performance it measures, given the many other community-level factors that could influence patients' receipt of care.
If this measure is to be implemented with Medicare claims, we recommend using numerator option 1 -- an outpatient visit or partial hospitalization with a mental health professional -- to determine the proportion of non-dual Medicare beneficiaries who receive follow-up care (Table V.10). This numerator option most closely adheres to the NQF-endorsed measure from which this measure was adapted and is consistent with stakeholder and TEP support for follow-up care provided by mental health specialists.
| Testing Results | Stakeholder Input | Revisions to Specifications |
|---|---|---|
|
|
|
To maintain consistency with the NQF-endorsed measure and maintain the face validity of the measure, we recommend no changes to the measure exclusions. However, in combination with the exclusion of dual eligible beneficiary stays, these exclusions substantially reduce the measure denominator to a fraction of all FFS Medicare-paid stays. We discuss this issue in more depth in Chapter VII, which presents a comparison of a chart-based and claims-based version of the follow-up after IPF hospitalization measure.
VI. FOLLOW-UP MEASURE PERFORMANCE USING MERGED MEDICARE-MEDICAID CLAIMS
Given that more than 65 percent of Medicare IPF discharges are dual eligible beneficiaries, we completed a supplemental analysis of the follow-up measure performance using both Medicare and Medicaid claims from calendar year 2008 to calculate follow-up care among all Medicare beneficiaries, including dual eligible beneficiaries. Using both Medicare and Medicaid claims allows us to more accurately calculate follow-up care among dual eligible beneficiaries.
In this chapter, we present analyses of merged Medicare and Medicaid data for dual eligible beneficiaries discharged from an IPF in 2008. In contrast to the analysis in Chapter V, which uses Medicare data from all 50 states, this analysis uses Medicare and Medicaid data from only those states that had: (1) at least 75 percent of dual eligible beneficiaries enrolled in Medicaid FFS in 2008; and (2) provider Specialty codes in 2008 MAX data that could be used to identify outpatient services provided by mental health practitioners. A total of 26 states met these criteria. (See Appendix E for details on the selection of these 26 states.)
In Table VI.1, we present 30-day follow-up rates for dual eligible beneficiaries (using merged Medicare and Medicaid claims) versus non-dual eligible beneficiaries (using only Medicare claims). As illustrated, dual eligible beneficiaries have higher average rates of follow-up care compared with non-dual eligible beneficiaries on all numerator options. However, differences in performance are most pronounced for options 2 and 3; follow-up rates among dual eligible beneficiaries are approximately six points higher than Medicare-only beneficiaries when outpatient care is defined with a principal mental health diagnosis (as opposed to a mental health practitioner in option 1). This higher rate likely reflects the fact that dual eligible beneficiaries have access to a wider range of services under their Medicaid benefits compared with Medicare-only beneficiaries.
The higher performance of options 2 and 3 relative to option 1 among dual eligible beneficiaries is likely attributable, in part, to the fact that several states do not provide sufficient information in Medicaid claims to identify all mental health providers (relevant to option 1). Similarly, option 3 likely has slightly higher average performance than options 1 and 2 due to the fact that state Medicaid programs use many procedure codes besides those in the HEDIS FUH measure to reimburse outpatient behavioral health care (relevant to options 1 and 2); outpatient visits using state-specific procedure codes that do not appear in the FUH measure could qualify as follow-up care under option 3, provided that they have a principal mental health diagnosis. Given that option 3 is not affected by the two primary data concerns related to Medicaid -- a lack of complete information on providers, as well as state-specific procedure codes -- it is likely the most attractive numerator option for measuring follow-up care among all FFS Medicare beneficiaries with combined Medicare and Medicaid claims.
| Numerator Option | Dual Eligible (%) | Non-Dual Eligible (%) | Difference |
|---|---|---|---|
| SOURCE: Medicare and Medicaid claims from calendar year 2008. NOTE: The sample of IPF stays is restricted to those 26 states with complete and reliable MAX data and at least 75% of dual eligible beneficiaries enrolled in FFS Medicaid. | |||
| Option 1: Mental health practitioner + CPT/HCPCS Code (HEDIS approach) | 54.7 | 54.3 | 0.4 |
| Option 2: Principal mental health diagnosis + CPT/HCPCS Code | 58.7 | 52.9 | 5.8 |
| Option 3: Principal mental health diagnosis + Outpatient visit | 61.6 | 55.4 | 6.2 |
| Option 4: Any outpatient visit | 84.3 | 80.0 | 4.3 |
We also conducted an analysis of the stability of performance rates when Medicaid claims are used to supplement Medicare claims for all beneficiaries, including dual eligible and non-dual eligible beneficiaries.47 This analysis is also based on Medicare and Medicaid data from the 26 states that had at least 75 percent of dual eligible beneficiaries enrolled in FFS Medicaid and MAX data that could be used to identify outpatient services provided by mental health practitioners. As shown in the Table VI.2, performance rates for all four numerator options were between 1 and 4 percentage points higher when the measure numerator was calculated using Medicaid claims in addition to Medicare claims. This increase in performance is due solely to additional follow-up services provided to dual eligible beneficiaries, as measured by Medicaid claims.
| Numerator Option | All Beneficiaries | Difference | |
|---|---|---|---|
| Using Only Medicare Claims | Using Medicare and Medicaid Claims | ||
| SOURCE: Medicare and Medicaid claims from calendar year 2008. NOTE: The sample of IPF stays is restricted to those 26 states with complete and reliable MAX data and at least 75% of dual eligible beneficiaries enrolled in FFS Medicaid. | |||
| Option 1: Mental health practitioner + CPT/HCPCS Code (HEDIS approach) | 54.3 | 55.0 | 0.7 |
| Option 2: Principal mental health diagnosis + CPT/HCPCS Code | 53.5 | 57.2 | 3.7 |
| Option 3: Principal mental health diagnosis + outpatient visit | 56.7 | 59.9 | 3.2 |
| Option 4: Any outpatient visit | 81.2 | 83.3 | 2.1 |
Although CMS anticipates implementing the claims-based follow-up measure as part of IPFQR program in 2015, the measure may be transitioned to draw on other data sources in future years, including patient medical records or other administrative data sources (such as electronic patient tracking systems or registries). We conducted an exploratory analysis to examine the feasibility of measuring follow-up care using other data sources. Our analysis included comparing denominator sample sizes if different data sources were used, and gathering qualitative feedback on the strengths and limitations of different data sources and measurement approaches. This analysis is designed to provide CMS and other stakeholders with insights into the advantages and disadvantages of a chart-based approach to the follow-up measure, relative to a claims-based approach. In this chapter, we use the term "chart-based" to refer to a range of data sources available to IPFs, including electronic records, patient charts, and administrative data. These analyses should be interpreted with caution, given the limited number of stakeholders and IPFs included in the analysis.
A. Methods
In 2014, Mathematica and NCQA held three focus groups with administrative staff from nine IPFs, as well as debriefing sessions with each of the six IPFs that piloted the four chart-based measures (Table VII.1). During these conversations, we gathered feedback on IPFs' efforts to encourage and track follow-up care, including factors that facilitate and constrain IPFs' ability to capture accurate data on their patients' follow-up care. In addition, we asked about the feasibility of a chart-based approach to the follow-up measure, including data collection and reporting burden, as well as infrastructure and resources that would be necessary to support reporting. Finally, we asked participants questions about their patients' insurance coverage and demographics to provide additional context for quantitative analyses discussed below.
| Freestanding Facilities | Psychiatric Wards | |
|---|---|---|
| Private facilities | 8 | 3 |
| Public facilities | 4 | 0 |
In addition, we used administrative data provided by the six IPFs that participated in measure testing to conduct a quantitative analysis of patient characteristics and IPF discharges, with the goal of comparing and contrasting the denominator sizes and characteristics of a chart-based versus a claims-based approach to the follow-up measure. These six IPFs included one private freestanding hospital, two public freestanding hospitals, and three private psychiatric wards (included in Table VII.1). Below we present our qualitative and quantitative findings of this analysis.
B. IPFs' Efforts to Encourage and Track Follow-Up Care
Encouraging Follow-Up Care. Many of the IPFs that participated in focus groups and debriefing sessions have basic processes in place to facilitate patients' follow-up care after they are discharged. Nearly all of the 15 participating IPFs stated that they schedule patients' follow-up appointments prior to discharge, and five IPFs noted that they coordinate with outpatient providers on a regular basis to encourage patients' continuity of care. However, IPFs vary considerably in the level of effort and resources allocated to such efforts. For example, one IPF schedules follow-up appointments for all psychiatric patients, but makes no additional efforts to encourage or track follow-up care. Other IPFs reported much more labor-intensive processes, in which IPF staff schedule aftercare appointments prior to patient discharge, arrange for patients to meet aftercare providers directly preceding or following discharge, and then contact patients by phone to remind them of upcoming appointments.
- Representative of a public freestanding IPF
Around half of IPFs indicated some effort to contact patients after discharge, generally by phone, to check on their status and encourage them to attend follow-up appointments. IPF staff noted that these follow-up efforts require a large investment of staff time and resources. For example, one facility is working to dedicate a full-time staff person to making calls to patients in advance of their scheduled follow-up appointments. Although a small number of IPFs attempt some follow-up with all discharged patients, other facilities' social work teams focus their limited resources more narrowly on contacting individuals most likely to miss follow-up appointments or be readmitted to the IPF.
Examples of IPFs' Efforts to Coordinate Follow-Up Care
As part of its quality improvement strategy, one IPF has entered into a partnership with a local university to develop and implement a pilot project that uses innovative technologies such as instant phone messaging to remind discharged patients about upcoming aftercare appointments. The hospital also employs certified peer specialists to conduct follow-up outreach by phone, primarily to encourage high-risk patients to keep follow-up appointments. In addition, a private freestanding IPF recently opened a transitional outpatient clinic to promote its patients' continuity of care. The clinic uses motivational interviewing to identify and mitigate patients' barriers to outpatient care -- including transportation difficulties and motivational constraints. The IPF noted a substantial improvement in follow-up care linked to patients' engagement with clinic staff.
Tracking Follow-Up Care. Although most IPFs reported having processes in place to schedule follow-up appointments or track whether patients received reminder calls prior to their scheduled appointments, it was much less common for IPFs to track whether or not patients actually received follow-up care. Five out of 15 IPFs reported using simple information systems to track whether follow-up care occurred, based on information provided by patients, community partners, managed care organizations (MCOs), or some combination of these sources. One public hospital, for example, has built a form into its electronic medical record to capture who was contacted and what information was gathered regarding each patient's follow-up status. In contrast, two public IPFs mentioned that although their social workers schedule aftercare appointments for patients prior to discharge, the IPFs are not permitted to access patients' files after discharge, thereby eliminating opportunities for patient follow-up and tracking.48
- Representative of a private freestanding IPF
IPFs mentioned partnerships with external providers and stakeholders as a key facilitator of tracking patient follow-up (see Table VII.2 for a summary of all facilitators mentioned by more than one IPF). In particular, public IPFs noted strong working relationships with community providers, and mentioned that such relationships enable them to follow discharged patients closely. Private IPFs noted that data sharing with partner organizations was critical to their efforts to track patients' care. Three IPFs mentioned collaborating with MCOs to receive and share data related to follow-up care. IPFs also indicated the necessity of well-established patient consent or release processes to allow IPF staff to contact patients and share information with providers.
Examples of IPFs' Efforts to Track Follow-Up Care
One IPF works closely with the largest outpatient providers and MCOs in its region to construct follow-up and readmission rates for a subset of patients. The goal of these analyses is to identify high-risk and high-utilizing IPF patients and to focus staff resources on encouraging these patients to keep follow-up appointments. Another IPF systematically tracks whether patients readmitted to the hospital kept their initial follow-up outpatient appointments as planned. The representative reported that most patients readmitted to the IPF within 30 days did not keep their follow-up appointment. In both cases, IPFs track only a subset of their full patient population -- namely those individuals for whom data on follow-up care is available.
| Comment | Frequency Mentioned |
|---|---|
| Partnerships with external providers, particularly community mental health care providers | 9 |
| Collaborations with MCOs and other payers | 5 |
| Well-established patient consent and release process | 3 |
| Information-sharing systems with in-network providers | 3 |
C. IPF Perspectives on a Chart-Based Approach to Measuring Follow-Up Care
IPFs participating in focus groups were strongly opposed to a chart-based approach to measuring follow-up care, citing sizable obstacles related to data availability and human resources, discussed below and summarized in Table VII.3.
| Comment | Frequency Mentioned |
|---|---|
| Tracking and reporting would require hiring or dedicating additional staff | 7 |
| Patient consent/release process would be burdensome, or privacy would be a concern | 7 |
| Obtaining complete data would be difficult due to patient non-response | 4 |
| Monitoring patients outside of IPF networks would be challenging | 4 |
| Tracking would require changes to electronic health records or other systems | 3 |
| Tracking via telephone would impose a considerable time burden on IPF staff | 2 |
| Tracking via telephone would require significant expense | 2 |
Data Availability. More than half of IPFs reported that they do not have a data collection infrastructure to accurately capture the actual receipt of follow-up care in the community, and that creating such an infrastructure would require substantial financial resources. In particular, staff from several IPFs stated that accessing and tracking data on patients that are outside their network would be extremely difficult. IPFs noted that changes to existing data systems and administrative procedures would be necessary to accommodate a chart-based follow-up measure, as patient records or other data tracking systems would require new data elements and modified processes to remind staff to populate these elements following patient discharge. IPF staff noted that these modifications are not trivial, and would likely be expensive to implement, both in terms of information technology investments and staff training.
- Representative of a private psychiatric ward
Also related to data availability, several IPFs noted that some patients refuse to sign information release forms upon discharge. As such, IPFs cannot contact these patients or their outpatient providers to determine whether follow-up care occurred.
Human Resources. More than half of IPF respondents noted that tracking and reporting follow-up care for the full patient population would require a significant investment of staff time, particularly to determine if scheduled follow-up appointments were kept. IPFs cited the transient nature of their patient populations as a major barrier to locating them in the community, and noted that some patients do not have phones or are reluctant to maintain contact with the IPF. Three facilities mentioned that they would likely have to hire additional staff to conduct systematic patient follow-up by phone if a chart-based follow-up measure were introduced to the IPFQR program.
- Representative of a public freestanding hospital
The IPFs that already conduct patient and provider outreach indicated that obtaining follow-up information is labor-intensive and requires a considerable amount of staff time and effort. One IPF noted that follow-up calls to patients do not generate a strong return in terms of the amount of information gained per hour of staff time devoted to the task. Commonly, IPF staff will make multiple phone calls over the course of several days to determine if a patient attended a single follow-up appointment.
Citing these feasibility concerns, IPF staff heavily favored a claims-based approach over a chart-based approach to the follow-up measure. IPFs overwhelmingly viewed the claims-based measure's minimal burden (to IPFs) as a primary advantage over a chart-based follow-up measure, which several IPFs viewed as "impossible" to implement under current conditions. However, as described below, some IPFs had concerns about the representativeness of a claims-based approach that uses only FFS Medicare beneficiaries as the measure denominator.
D. Analysis of Insurance Coverage, Patient Demographics, and Sample Sizes
In this section, we present analyses of patient characteristics and IPF discharges, with the goal of comparing and contrasting the denominator sizes and characteristics of a chart-based versus a claims-based approach to the follow-up measure. For this analysis, we use administrative data from the six IPFs that participated in measure testing under the contract, corresponding to all discharges at these IPFs from October 1, 2013, to December 31, 2013.
FIGURE VII.1. Primary Payer for IPF Stays in 6 IPFs, 2013
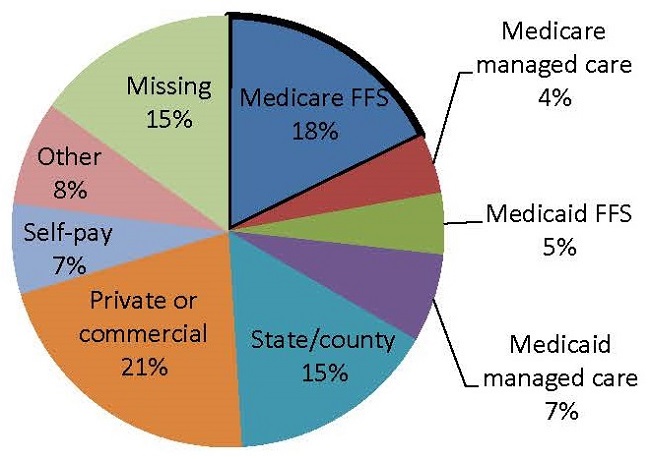
NOTE: Sample size is 1,857 patients discharged from 6 IPFs from October 2013 to December 2013. Missing data on primary payer reflects 1 IPF's unavailability of data on the primary payer for a majority of patients.
Insurance Coverage. We collected information regarding patients' insurance coverage from the six IPFs that participated in chart-based measure testing. Three of these IPFs were private psychiatric wards with fewer than 50 beds, two were public freestanding facilities with over 100 beds, and one was a private freestanding facility with 400 beds.49 As illustrated in Figure VII.1, FFS Medicare was the primary payer for only 18 percent of patient stays at the six IPFs. Because dually eligible Medicare-Medicaid beneficiaries account for over half of FFS Medicare-paid stays,50 we can estimate that non-dual FFS Medicare beneficiaries accounted for less than 10 percent of stays at these IPFs.51 This is an important statistic, because a claims-based approach to measuring follow-up care will likely rely on claims for non-dual FFS Medicare patients -- a relatively small portion of IPFs' total patient population. In contrast, a chart-based approach to the measure would potentially draw from all patients, including patients covered by FFS Medicare, Medicare managed care, Medicaid, state or county payment sources, private insurance, and the uninsured. This stronger representativeness -- or "generalizability" of the chart-based follow-up measure to the entire IPF population -- represents a potential advantage of a chart-based specification versus a claims-based specification that uses only FFS Medicare data. However, if FFS Medicare beneficiaries are not systematically different from IPFs' total patient population, a claims-based approach would likely yield similar performance results to a chart-based measure that draws on a broader denominator population. Below, we examine potential differences between FFS Medicare beneficiaries and IPFs' total patient population in more depth.
| Characteristics | Stay Covered by FFS Medicare | All IPF Discharges | ||
|---|---|---|---|---|
| NOTE: Sample size is 1,857 patients discharged from 6 IPFs from October 2013 to December 2013. | ||||
| N | % | N | % | |
| Age at Discharge | ||||
| Under 18 | 0 | 0 | 103 | 5 |
| 18-26 | 15 | 5 | 388 | 21 |
| 27-44 | 86 | 26 | 630 | 34 |
| 45-64 | 135 | 41 | 589 | 32 |
| 65 and older | 93 | 28 | 147 | 8 |
| Primary Diagnosis | ||||
| Schizophrenia | 107 | 33 | 361 | 19 |
| Bipolar disorder | 109 | 33 | 704 | 38 |
| Delusional disorder | 29 | 9 | 134 | 7 |
| Major depressive disorder | 4 | 1 | 90 | 5 |
| Psychosis | 19 | 6 | 111 | 6 |
| Alcohol or drug dependency | 11 | 3 | 151 | 8 |
| Alzheimer's/dementia/degeneration | 20 | 6 | 37 | 2 |
| Other | 18 | 5 | 206 | 11 |
| Missing | 12 | 4 | 63 | 3 |
| Race/Ethnicity | ||||
| African American | 65 | 20 | 389 | 21 |
| Caucasian | 234 | 71 | 1,120 | 60 |
| Other | 5 | 2 | 57 | 3 |
| Missing | 25 | 8 | 291 | 16 |
| Gender | ||||
| Male | 166 | 50 | 964 | 52 |
| Female | 163 | 50 | 893 | 48 |
| Length of Stay | ||||
| 0, 1, or 2 days | 25 | 8 | 248 | 13 |
| 3 or 4 days | 43 | 13 | 320 | 17 |
| 5, 6, or 7 days | 77 | 23 | 454 | 24 |
| 8 to 14 days | 82 | 25 | 466 | 25 |
| 15 to 21 days | 37 | 11 | 129 | 7 |
| 22 to 30 days | 20 | 6 | 70 | 4 |
| >30 days | 45 | 14 | 170 | 9 |
| Sample Size | 329 | 100 | 1,857 | 100 |
Patient Demographics. Table VII.4 presents a comparison of beneficiary demographics for patients whose IPF stays were paid by FFS Medicare versus IPFs' full patient populations. As illustrated, patients with FFS Medicare stays were different from IPFs' total patient population in several respects. First, they are generally older than the full patient population, with nearly 70 percent of FFS Medicare patients over the age of 43, compared to 40 percent among all IPF patients. FFS Medicare patients are also more likely to have schizophrenia as a principal diagnosis than the full patient population (33 percent versus 19 percent in the full population), and more likely to have IPF stays of over two weeks (31 percent versus 20 percent of all patients). These data suggest that FFS Medicare patients are systematically different from the full IPF patient population. As such, it is possible that FFS Medicare patients could have different rates of follow-up care than non-FFS patients, related to demographic characteristics or length of stay. (For example, it is possible that IPFs may have more opportunities to arrange follow-up care for FFS Medicare patients with longer lengths of stay if discharge planning begins upon admission). If this were the case, a claims-based follow-up measure would either underestimate or overestimate follow-up care among IPFs' full patient population.
Stakeholder Feedback on Medicare Beneficiaries
Qualitative input from IPFs involved in focus groups and debriefing sessions suggests potential systematic differences between patients covered by Medicare and patients with other forms of insurance, as well as the potential for these differences to affect rates of follow-up care -- although the direction of the potential bias is unclear. One IPF stated that Medicare patients tend to have more co-morbidities than other patients, and these co-morbidities could serve as obstacles to outpatient follow-up care. In addition, representatives from one IPF expressed concern that many outpatient providers do not accept Medicare patients, potentially generating lower follow-up rates for a claims-based measure specification (drawing only from Medicare beneficiaries) versus a chart-based specification (drawing from all IPF patients). Staff from another two IPFs could not estimate whether Medicare patients would have higher or lower rates of follow-up care compared with other patients, but they conjectured that Medicare patients would likely have more outpatient visits and thus higher rates of follow-up care than uninsured patients.
Sample Sizes. We analyzed IPF administrative data to estimate the number of IPFs for which a chart-based approach to calculating the follow-up measure would result in larger sample sizes than those generated under a claims-based approach that only uses non-dual FFS Medicare patients as the denominator. A chart-based follow-up measure would likely use a sampling method that is similar to chart-based measures in the HBIPS measure set.52 Under this method, IPF staff or an IPFQR program vendor would select a random sample of discharged patients as the measure denominator. Following the HBIPS algorithm, a chart-based sampling approach to the follow-up measure would require that a minimum of 20 percent of patients with a mental health diagnosis be sampled on a quarterly basis.53 We compared this minimum chart-based sample to the estimated sample size for a claims-based follow-up measure corresponding to the same time period: one-half of the total number of FFS Medicare beneficiaries with a mental health diagnosis that were served by IPFs. We divide the total number of FFS Medicare beneficiaries in half because an estimated 50 percent of these patients are likely dually eligible beneficiaries and would thus be excluded from the claims-based measure denominator.54
| All Sites | IPF 1 | IPF 2 | IPF 3 | IPF 4 | IPF 5 | IPF 6 | |
|---|---|---|---|---|---|---|---|
NOTE: Sample size is 1,857 patients discharged from 6 IPFs from October 2013 to December 2013.
| |||||||
| All discharges | 1,857 | 152 | 272 | 172 | 382 | 409 | 470 |
| All discharges with a mental health diagnosis | 1,400 | 109 | 203 | 136 | 347 | 365 | 240 |
| Minimum chart-based sample sizea | 280 | 22 | 41 | 27 | 69 | 73 | 48 |
| FFS Medicare discharges | 329 | 42 | 15 | 28 | 94 | 106 | 44 |
| FFS Medicare discharges with a mental health diagnosis | 268 | 34 | 14 | 26 | 75 | 101 | 18 |
| Estimated claims-based sample sizeb | 134 | 17 | 7 | 13 | 38 | 51 | 9 |
| Percentage of all patients covered by FFS Medicare | 18% | 28% | 6% | 16% | 25% | 26% | 9% |
As illustrated in Table VII.5, sample sizes for a chart-based follow-up measure are larger than projected sample sizes for a claims-based follow-up measure for all six IPFs, particularly for two IPFs that had less than 10 percent of stays covered by FFS Medicare (IPF 2 and IPF 6). For these two IPFs, the quarterly sample size for a claims-based measure is less than ten patients, whereas the sample size for a chart-based version of the measure is more than 40 patients. This illustrates a primary disadvantage of a claims-based follow-up measure, in that IPFs serving a small number of FFS patients relative to their full patient population can generate quarterly sample sizes that do not meet minimum CMS requirements for public reporting.
Stakeholder Feedback Related to Follow-Up Measure Sample Size
IPF staff who participated in focus groups -- representing freestanding hospitals and psychiatric wards, as well as public and private facilities -- confirmed that FFS Medicare beneficiaries represent a minority of their full patient population. A private hospital noted that approximately 10-12 percent of its patient population has Medicare coverage, saying, "It's only a sliver of the individuals we work with." Most IPFs involved in focus groups made similar statements regarding the proportion of their full patient population covered by Medicare.
E. Conclusion
Based on this qualitative and quantitative analysis, a chart-based approach to tracking and reporting follow-up care would be difficult for IPFs to implement in the short term, given the constraints they noted related to data availability and IPF human and financial resources. However, a chart-based approach to the follow-up measure could be more generalizable to the full IPF patient population, assuming that data on follow-up care could be collected for in-network as well as out-of-network patients. In addition, a chart-based follow-up measure would likely generate fewer instances in which small sample sizes preclude public reporting.
A claims-based approach to follow-up care would be more feasible in the short term, primarily because it imposes no burden on IPFs. In addition, a claims-based follow-up measure can precisely measure follow-up care among FFS Medicare beneficiaries, as it draws from all Medicare claims.55Table VII.6 provides a high-level summary of the relative advantages and disadvantages of these two approaches to the follow-up measure.
| Approach | Advantages | Disadvantages |
|---|---|---|
| Chart-based |
|
|
| Claims-based |
|
|
The measures developed in this project are an attempt to fill gaps and improve upon existing screening measures for an inpatient psychiatric setting. At the time of this report, CMS has not made final decisions about these measures' inclusion in IPFQR program, and none of the measures has been submitted to NQF.
Of the screening measures, the one with the most potential for improving the quality of IPF care appears to be the metabolic screening measure, which has average performance of 42 percent across IPFs. Although the suicide, violence, and substance use screening measures had generally high performance among the six IPFs in which they were piloted, they also exhibit potential to standardize screening elements across IPFs. CMS may collaborate with TJC to harmonize these screening measures with HBIPS-1. Such harmonization efforts would ensure that new measures do not place undue burden on IPFs.
This analysis found substantial room for improvement with respect to follow-up after IPF hospitalization, with 30-day follow-up rates below 55 percent. In its current specification as a Medicare claims-based measure, the follow-up measure poses some concerns regarding its generalizability to the full IPF population. However the alternative of a chart-based specification does not appear feasible to implement in the short term, due to data availability and human resource constraints.
Together with existing IPFQR program measures, these new measures provide a strong foundation for monitoring and improving the quality of inpatient behavioral health care; however, some gaps persist, particularly between the care patients experience and the outcomes they report. Unlike screening measures (that assess a specific process of care within the IPF), some of these measurement concepts (like the follow-up measure) may require some type of shared accountability between actors because they deal with system-level issues of access to care, insurance coverage, and the care continuum spanning inpatient and outpatient care. There is a tension associated with developing new measures that are premised upon this shared responsibility, particularly because measures are often confined to one unit of analysis.
Future measure-development efforts for the IPFQR program should attempt to involve as many IPFs and different types of stakeholders as possible, to understand variation in performance across different types of facilities, patient populations, and in different community contexts. Measure-development should also draw on the latest studies and clinical guidelines, as substantive advancements in the field occur on a regular basis.
Adams, John (2009). The Reliability of Provider Profiling. RAND.
American Diabetes Association (2006). Antipsychotic Medications and the Risk of Diabetes and Cardiovascular Disease. Available at: http://professional.diabetes.org/admin/UserFiles/file/CE/AntiPsych%20Meds/Professional%20Tool%20%231(1).pdf.
Casey, D.E. "Dyslipidemia and atypical antipsychotic drugs." J Clin Psychiatry, 2004; 65 Suppl(18): 27-35.
American Diabetes Association and American Psychiatric Association. "Consensus development conference on antipsychotic drugs and obesity and diabetes." Diabetes Care, February 2014, 27(2).
Institute of Medicine, Committee on Crossing the Quality Chasm: Adaptation to Mental Health and Addictive Disorders (2006). Improving the Quality of Health Care for Mental and Substance-Use Conditions. Washington, DC: National Academies Press.
Landis J.R., and G.G. Koch. "The measurement of observer agreement for categorical data." Biometrics, 1977, 33: 159-174.
Marder. S.R., S.M. Essock, A.L. Miller, R.W. Buchanan, D.E. Casey, J.M. Davis, J.M. Kane, et al. "Physical health monitoring of patients with schizophrenia." American Journal of Psychiatry, August 2004, 161(8): 1334-1349.
MedPac (2012). A Data Book: Health Care Spending and the Medicare Program, Section 6. Available at: http://www.medpac.gov/chapters/Jun12DataBookSec6.pdf.
NRI's Behavioral Healthcare Performance Measurement System (2012). History of HBIPS Core Measure Set. 2012. Available at: http://www.nri-inc.org/projects/bhpms/docs/HBIPSHistory.pdf. Accessed on July 1, 2013.
Prela, C., G. Baumgardner, G. Reiber, L. McFarland, C. Maynard, N. Anderson, and M. Maciejewski. "Challenges in merging Medicaid and Medicare databases to obtain healthcare costs for dual-eligible beneficiaries." PharmacoEconomics, 2009, 27(2): 167-177.
Roohafsza, H, A. Khani, H. Afshar, A. Garakyaraghi, and B. Ghodsi. "Lipid profile in antipsychotic drug users: A comparative study." ARYA Atheroscler. May 2013; 9(3): 198-202.
TJC (2012). Specifications Manual for Joint Commission National Quality Measures. Available at: https://manual.jointcommission.org/releases/TJC2013A/HospitalBasedInpatientPsychiatricServices.html. Accessed on January 1, 2015.
APPENDIX A. IPF TECHNICAL EXPERT PANEL MEMBERS
| Name | Title | Organization/Agency |
|---|---|---|
| * Did not attend final TEP meeting. | ||
| Frank Ghinassi | Vice President, Quality and Performance Improvement | Western Psychiatric Institute |
| Eric Goplerud | Senior Vice President and Director of Substance Abuse, Mental Health, and Criminal Justice Studies | NORC |
| Richard Hermann | Director, Center for Quality Assessment and Improvement in Mental Health | Institute for Clinical Research and Health Policy Studies, Tufts |
| Mary E. Johnson | Professor | Rush University/American Psychiatric Nurses Association |
| Kathleen McCann | Director, Quality and Regulatory Affairs | National Association of Psychiatric Health Systems |
| Lucille Schacht | Senior Director of Performance and Quality Improvement | National Association of State Mental Health Program Directors Research Institute |
| Elizabeth Stallings | Former Chief Operating Officer | John Muir Behavioral Health Center |
| Ann Watt | Associate Director, Department of Quality Measurement, Division of Quality Measurement and Research | The Joint Commission |
| Richard Wohl | President, Princeton House Behavioral Health | Princeton HealthCare System |
| Joel Streim* | Professor | Department of Psychiatry, University of Pennsylvania School of Medicine |
| Alice Lind* | Senior Clinical Officer | Center for Health Care Strategies |
APPENDIX B. SCREENING MEASURE SPECIFICATIONS
| Measure Dimension | Description |
|---|---|
| Description | Percentage of discharges from an IPF for which a structured suicide screening for 5 elements was completed. |
| Denominator | Psychiatric inpatient discharges during the measurement period. |
| Numerator | Suicide risk screening completed within the first day of admission. |
| Numerator Details | Screening ContentThe medical record must provide documentation that information was obtained--either from the patient or from a collateral source--regarding the following 5 topic areas: (1) suicidal ideation; (2) the extent of plans or preparation (if ideation is reported); (3) the intent to act on those plans (if plans are reported); (4) past suicidal behavior; and (5) risk factors and protective factors.Timing of ScreenAll screening content must be obtained within the first day of admission (any time on the day of admission or the following day).Screening AdministrationScreening must be completed by a qualified psychiatric practitioner. The titles of qualified psychiatric practitioners may vary from state to state. Written and electronic collateral information and information provided by the patient in intake forms is acceptable if it has been reviewed by a qualified psychiatric practitioner. |
| Exclusions | Patient stays for which a screening could not be completed within the first day of admission due to the patient's enduring unstable medical or psychological condition. Patient stays with a length of stay equal to or greater than 365 days, or less than 1 day. Patient stays with multiple admissions to psychiatric units during a single hospitalization. |
| Stratification and Risk Adjustment | The measure is currently stratified by age in to 4 categories: children (age 1-12), adolescents (age 13-17), adults (age 18-64) and older adults (age 65+). No risk adjustment is planned. |
| Sampling | These measures will rely on a sampling methodology, by which cases are sampled quarterly or monthly. Facilities will be required to sample at least 20% of each stratum population for the quarter or month, with a minimum of 15 cases in each stratum per month. (Sampling will follow HBIPS-1 sampling guidelines.) |
| Measure Dimension | Description |
|---|---|
| Description | Percentage of discharges from an IPF for which a structured violence screening for 2 elements was completed. |
| Denominator | Psychiatric inpatient discharges during the measurement period. |
| Numerator | Violence risk screening completed within the first day of admission. |
| Numerator Details | Screening ContentThe medical record must provide documentation that information was obtained--either from the patient or from a reliable source--regarding the following 2 topic areas: (1) threats of violence; and (2) any history of violent episodes.Timing of ScreenAll screening content must be obtained within the first day of admission (any time on the day of admission or the following day).Screening AdministrationScreening must be completed by a qualified psychiatric practitioner. The titles of qualified psychiatric practitioners may vary from state to state. Written and electronic collateral information and information provided by the patient in intake forms is acceptable if it has been reviewed by a qualified psychiatric practitioner. |
| Exclusions | Patients stays for which a screening could not be completed within the first 3 days of admission due to the patient's enduring unstable medical or psychological condition. Patient stays with a length of stay equal to or greater than 365 days, or less than 1 day. Patient stays with multiple admissions to psychiatric units during a single hospitalization. |
| Stratification and Risk Adjustment | The measure is currently stratified by age in to 4 categories: children (age 1-12), adolescents (age 13-17), adults (age 18-64) and older adults (age 65+). No risk adjustment is planned. |
| Sampling | These measures will rely on a sampling methodology, by which cases are sampled quarterly or monthly. Facilities will be required to sample at least 20% of each stratum population for the quarter or month, with a minimum of 15 cases in each stratum per month. (Sampling will follow HBIPS-1 sampling guidelines.) |
| Measure Dimension | Description |
|---|---|
| Description | Percentage of discharges from an IPF for which a structured substance use screening for 4 elements was completed. |
| Denominator | Psychiatric inpatient discharges during the measurement period. |
| Numerator | Alcohol AND drug use screening completed within the first day of admission. |
| Numerator Details | Screening ContentThe medical record must provide documentation that information was obtained--either from the patient or from a collateral source--regarding the 4 key topic areas: (1) type, frequency, and amount of alcohol AND substance use; (2) adverse effects of this use (if use is reported); (3) dependence upon these substances (if use is reported); and (4) any history of drug/alcohol abuse.Timing of ScreenAll screening content must be obtained within the first day of admission (any time on the day of admission or the following day).Screening AdministrationScreening must be completed by a qualified psychiatric practitioner. The titles of qualified psychiatric practitioners may vary from state to state. Written and electronic collateral information and information provided by the patient in intake forms is acceptable if it has been reviewed by a qualified psychiatric practitioner. |
| Exclusions | Patients stays for which a screening could not be completed within the first 3 days of admission due to the patient's enduring unstable medical or psychological condition. Patient stays with a length of stay equal to or greater than 365 days, or less than 1 day. Patient stays with multiple admissions to psychiatric units during a single hospitalization. |
| Stratification and Risk Adjustment | The measure is currently stratified by age in to 4 categories: children (age 112), adolescents (age 13-17), adults (age 18-64) and older adults (age 65+). No risk adjustment is planned. |
| Sampling | These measures will rely on a sampling methodology, by which cases are sampled quarterly or monthly. Facilities will be required to sample at least 20% of each stratum population for the quarter or month, with a minimum of 15 cases in each stratum per month. (Sampling will follow HBIPS-1 sampling guidelines.) |
| Measure Dimension | Description |
|---|---|
| * Medications that fall under this classification are identical to medications identified in HBIPS-4 "Multiple Antipsychotic Medications at Discharge." | |
| Description | Percentage of discharges from an IPF for which a structured metabolic screening for 4 elements was completed in the past year. |
| Denominator | Psychiatric inpatient discharges with 1 or more routinely scheduled antipsychotic medications during the measurement period.* |
| Denominator Details | PRN antipsychotic medications or short-acting intramuscular antipsychotic medications do not count towards the denominator of this measure. |
| Numerator | The total number of patients who received a metabolic screening in the 12 months prior to discharge--either prior to, or during the index IPF stay. (If no record of a complete metabolic screening prior to the stay is found, the IPF must conduct the screening.) |
| Numerator Details | Screening ContentThe medical record must provide documentation of the completion of all 4 of the following tests/measurements: (1) BMI; (2) blood pressure; (3) glucose or HbA1c; and (4) a lipid panel (which includes total cholesterol, triglycerides, high density lipoprotein, and low density lipoprotein).Timing of ScreenScreenings must have been completed at least once in the 12 months prior to the patient's date of discharge. Screenings can be conducted either at the reporting facility or another facility for which records are available to the reporting facility. |
| Exclusions | Patients stays for which a screening could not be completed due to the patient's enduring unstable medical or psychological condition. Patient stays with a length of stay equal to or greater than 365 days, or less than 3 days. Patient stays with multiple admissions to psychiatric units during a single hospitalization. |
| Stratification and Risk Adjustment | The measure is currently stratified by age in to 4 categories: children (age 1-12), adolescents (age 13-17), adults (age 18-64) and older adults (age 65+). No risk adjustment is planned. |
| Sampling | These measures will rely on a sampling methodology, by which cases are sampled quarterly or monthly. Facilities will be required to sample at least 20% of each stratum population for the quarter or month, with a minimum of 15 cases in each stratum per month. |
APPENDIX C. FOLLOW-UP AFTER IPF HOSPITALIZATION MEASURE SPECIFICATIONS
Measure Specifications: Follow-Up after IPF Hospitalization
| Eligible Population | |
|---|---|
| Data Sources |
|
| Ages | No Restriction on Age |
| Continuous Enrollment |
|
| Event/Diagnosis |
|
| Exclusions | |
| IPF Readmission or Direct Transfer |
|
| Non-IPF Admission or Direct Transfer |
|
| Exclusions Related to Discharge Status or Death |
|
Description
The percentage of discharges from an IPF that had a follow-up outpatient visit, intensive outpatient encounter or partial hospitalization for their mental disorder after discharge. Two rates are reported:
-
The percentage of discharges that received follow-up within 30 days of discharge.
-
The percentage of discharges that received follow-up within seven days of discharge.
There are two approaches to calculating the measure numerator: (A) Using only Medicare claims to calculate follow-up care for non-dual eligible beneficiaries; and (B) using Medicare and Medicaid claims to calculate follow-up care for all Medicare beneficiaries, including dual eligibles.
| TABLE C.1. Codes to Identify IPF Discharges |
|---|
| NOTE: A stay in any facility that meets 1 of the 3 criteria above constitutes an IPF stay. |
| Inpatient claim lists the following facility codes (Medicare inpatient file) |
|
| TABLE C.2. Codes to Identify Principle Mental Health Diagnosis |
|---|
| NOTE: Diagnosis codes are uniform across Medicare and Medicaid. Additional codes related to substance abuse diagnoses, particularly 303-305, can be included if the measure is intended to capture related services. |
| ICD-9-CM diagnosis (Medicare carrier/outpatient and Medicaid OT files) |
| 295-299, 300.3, 300.4, 301, 308, 309, 311-314 |
| Description(Medicare inpatient files) | Provider Number |
|---|---|
| NOTE: Medicare files are used to identify all exclusions. Any acute care stay during the 30-day period following IPF discharge constitutes an exclusion. | |
| Provider number corresponding to acute care facilities | 5th thru 8th digit (0001-0899) |
| Description | HCPCS(Medicarecarrier file) | UB Revenue(Medicare SNF, hospice,outpatient, and HHA files) | UB Type of Bill(Medicare SNF, hospice, outpatient, and HHA files) | POS(Medicare carrier files) |
|---|---|---|---|---|
| NOTE: Medicare files are used to identify all exclusions. Any code corresponding to the 30-day period following IPF discharge constitutes an exclusion. | ||||
| Hospice | 0115, 0125, 0135, 0145, 0155, 0650, 0656, 0658, 0659 | 81x, 82x | 34 | |
| SNF | 019x | 21x, 22x, 28x | 31, 32 | |
| Hospital transitional care, swing bed or rehabilitation | 18x | |||
| Comprehensive inpatient rehabilitation facility | 0118, 0128, 0138, 0148, 0158 | 61 | ||
| Respite | 0655 | |||
| ICF | 54 | |||
| Residential substance abuse treatment facility | 1002 | 55 | ||
| Psychiatric residential treatment center | T2048, H0017-H0019 | 1001 | 56 | |
| Description | Discharge Code(Medicare inpatient file) |
|---|---|
| NOTE: Medicare files are used to identify all exclusions. Any code corresponding to the 30-day period following IPF discharge constitutes an exclusion. | |
| Discharged/transferred to other short-term general hospital for inpatient care. | 02 |
| Discharged/transferred to SNF with Medicare certification in anticipation of covered skilled care--for hospitals with an approved swing bed arrangement, use Code 61--swing bed. For reporting discharges/transfers to a non-certified SNF, the hospital must use Code 04--ICF. | 03 |
| Discharged/transferred to ICF | 04 |
| Discharged/transferred to another type of institution for inpatient care | 05 |
| Expired | 20 |
| Discharged/transferred to a federal hospital | 43 |
| Hospice--home | 50 |
| Hospice--medical facility | 51 |
| Discharged/transferred within this institution to a hospital-based Medicare approved swing bed | 61 |
| Discharged/transferred to an inpatient rehabilitation facility including distinct parts units of a hospital | 62 |
| Discharged/transferred to a long-term care hospitals | 63 |
| Discharged/transferred to a nursing facility certified under Medicaid but not under Medicare | 64 |
| Discharged/transferred to a psychiatric hospital or psychiatric distinct unit of a hospital | 65 |
| Discharged/transferred to a CAH | 66 |
| Discharged/transferred to another type of health care institution not defined elsewhere in code list | 70 |
| Died during the 30-day follow-up period | Death_DT from Medicare Enrollment File |
Administrative Specification
| Denominator | Medicare discharges from IPFs that are not excluded due to the rules above.Below we outline 4 potential options for identifying follow-up care: option 1 uses a combination of provider codes and procedural codes; options 2 and 3 use a combination of diagnosis codes and place/type of service and procedural codes; and option 4 uses only general place/type of service and procedural codes to identify follow-up care. |
| Numerator Option 1 | An outpatient visit, an intensive outpatient encounter or partial hospitalization with a mental health practitioner within 30 or 7 days of discharge. (Uses CPT/HCPCS/POS/Revenue/FACTYP/TOS codes in Table C.6 and NPI/Taxonomy codes in Table C.7; this definition most closely aligns with the HEDIS follow-up after mental health hospitalization measure.) Consult Table C.8 for a list of Medicaid Specialty codes that can be used to determine whether Medicaid-paid services were provided by a mental health practitioner--only applicable if using Medicaid claims to determine follow-up among dual eligible beneficiaries. |
| Numerator Option 2 | An outpatient visit, an intensive outpatient encounter or partial hospitalization (with any provider) with a principal mental health diagnosis within 30 or 7 days of discharge (Uses CPT/HCPCS/POS/Revenue/FACTYP/TOS codes in Table C.6 and diagnosis codes in Table C.2) |
| Numerator Option 3 | Any outpatient visit with a principal mental health diagnosis within 30 or 7 days of discharge. (Uses general outpatient codes in Table C.9: POS and FACTYP/TYPSVC in Medicare claims and TOS and PLC_OF_SRVC codes in Medicaid claims, and diagnosis codes in Table C.2.) |
| Numerator Option 4 | Any outpatient visit with any principal diagnosis within 30 or 7 days of discharge. (Uses general outpatient codes in Table C.9: POS and FACTYP/TYPSVC in Medicare claims and TOS and PLC_OF_SRVC codes in Medicaid claims.) |
| NOTE: It is important to note that Numerator options 1 and 2 use a narrow definition of outpatient care --generally assessment, management, and therapy provided by mental health specialists--whereas options 3 and 4 use a more general definition of outpatient care that can be provided in a variety of settings and by a larger range of providers. | |
| CPT (Medicare carrier/outpatient and Medicaid OT files) | HCPCS (Medicare carrier/outpatient and Medicaid OT files) | |
|---|---|---|
| NOTE: A claim meeting any of the requirements above constitutes an outpatient visit. | ||
| 90804-90815, 98960-98962, 99078, 99201-99205, 99211-99215, 99217-99220, 99241-99245, 99341-99345, 99347-99350, 99383-99387, 99393-99397, 99401-99404, 99411, 99412, 99510 | G0155, G0176, G0177, G0409-G0411, H0002, H0004, H0031, H0034-H0037, H0039, H0040, H2000, H2001, H2010-H2020, M0064, S0201, S9480, S9484, S9485 | |
| CPT with POS (Medicare carrier and Medicaid OT files) | ||
| 90801, 90802, 90816-90819, 90821-90824, 90826-90829, 90845, 90847, 90849, 90853, 90857, 90862, 90870, 90875, 90876 | with | 03, 05, 07, 09, 11, 12, 13, 14, 15, 20, 22, 24, 33, 49, 50, 52, 53, 71, 72 |
| 99221-99223, 99231-99233, 99238, 99239, 99251-99255 | with | 52, 53 |
| CPT with TYPSVC/FACTYP (Medicare outpatient files) | ||
| 90801, 90802, 90816-90819, 90821-90824, 90826-90829, 90845, 90847, 90849, 90853, 90857, 90862, 90870, 90875, 90876 99221-99223, 99231-99233, 99238, 99239, 99251-99255 | with | TYPSVC of 2 or 3 if FACTYP = 1-6 or 9 FACTYP = 7 FACTYP = 8 |
| UB Revenue (Medicare outpatient and Medicaid OT files) | ||
| 0513, 0900-0905, 0907, 0911-0917, 0919--does not have to be with mental health practitioner for option 10510, 0515-0517, 0519-0523, 0526-0529, 077x, 0982, 0983--must be with either a principal mental health diagnosis or practitioner for option 1 | ||
| ER visits cannot count toward numerator (Medicare carrier/outpatient and Medicaid OT files) | ||
| No line-level claim information related to ER services can count as a numerator hit. These are defined as [revenue center code values of 0450-0459 (ER) or 0981 (Professional fees-ER) or HCPCS codes associated with ER use (99281, 99282, 99283, 99284, 99285) in the OP file] OR [Place of Service code (23=ER-hospital) or BETOS code (M3 = ER visit) in the carrier file] | ||
| HEDIS Definition of Mental Health Practitioner | SpecialtyCode | Taxonomy(linked to NPI) |
|---|---|---|
| NOTE: All codes are found in Medicare outpatient/carrier files. Either a Medicare Specialty code OR Taxonomy code qualifies as a numerator hit. Specialty codes and Taxonomy codes are the best match with mental health practitioners defined in HEDIS specifications (see additional resource table below). NPI codes and Specialty codes in Medicare claims can be used to determine provider taxonomy and type, respectively. Specialty codes in Table C.9 should be used to identify mental health providers in Medicaid claims. | ||
| An MD or DO who is certified as a psychiatrist or child psychiatrist | 26 | 2084P0800X; 2084P0804X |
| Neurologist (not in original HEDIS specification) | 13 | 2084V0102X; 2084N0400X; 2084N0402X |
| An MD or DO who successfully completed an accredited program of graduate medical or osteopathic education in psychiatry or child psychiatry and is licensed to practice patient care psychiatry or child psychiatry | 86 | 2084A0401X; 2084P0802X; 2084B0002X; 2084N0600X; 2084D0003X; 2084F0202X; 2084P0805X; 2084H0002X; 2084P0005X; 2084N0008X; 2084P2900X; 2084P0015X; 2084S0012X; 2084S0010X |
| Licensed Psychologist | 62 | 103T00000X; 103TA0400X; 103TA0700X; 103TC0700X; 103TC2200X; 103TB0200X; 103TC1900X; 103TE1000X; 103TE1100X; 103TF0000X; 103TF0200X; 103TP2701X; 103TH0004X; 103TH0100X; 103TM1700X; 103TM1800X; 103TP0016X; 103TP0814X; 103TP2700X; 103TR0400X; 103TS0200X; 103TW0100X |
| Certified in Clinical Social Work | 80 | 1041C0700X |
| Psychiatric Nurse, Physician Assistant, or Occupational Therapist | not applicable | 364SP0808X; 364SP0809X; 364SP0807X; 364SP0810X; 364SP0811X; 364SP0812X; 364SN0800X; 364SP0813X; 363LP0808X; 225XM0800X |
| State | Physician/ Neurology | MD or DO Certified as Psychiatrist or Child Psychiatrist | MD or DO Completed Accredited Program in Psychiatry or Child Psychiatry | Licensed Psychologist | Certified in Clinical Social Work | Psych Nurse, Psych Physician Assistant, or Occupational Therapist |
|---|---|---|---|---|---|---|
| NOTE: Any of these codes qualifies as a numerator hit. State-specific Specialty codes and Taxonomy codes are the best match with mental health practitioners defined in HEDIS specifications (see Table C.10 below). Data source is states' initial MSIS applications. Any Specialty code qualifies as a numerator hit for the claim in question. All codes can be found in Medicaid OT file. Codes are subject to change over time. | ||||||
| Alaska | 13 | 26, 27 | 69 | |||
| Arkansas | 13 | 26 | P5 | 62 | ||
| California | 13, 79 | 26 | 27, 36 | |||
| Connecticut | 26 | 92 | 26 | |||
| Delaware | N040 | P080 | M080 | |||
| Florida | 22 | 23 | 42, 43 | 44 | ||
| Illinois | CHN, N | CHP, P | PYA | |||
| Indiana | 326 | 339 | 112 | 113 | 117 | |
| Louisiana | 13 | 26 | 27 | 62 | ||
| Maryland | 050 | 051, 052 | 196 | |||
| Massachusetts | 144 | 153, 154 | 186 | |||
| Michigan | 0708 | 0290-0295 | ||||
| Missouri | 17 | 27 | 45 | 42, 43, A2, A3 | ||
| Nebraska | 13 | 26 | 62 | 80 | ||
| New Hampshire | 13 | 26,27 | 69 | |||
| New Jersey | 130 | 260 | 270 | 610 | 262 | |
| New Mexico | 013 | 026, 027 | 062 | |||
| New York | 193, 194 | 191,192, 195, 931, 945, 946, 964 | 780 | 781 | ||
| North Carolina | 13 | 26 | 109 | 110 | 112 | |
| North Dakota | 13 | 26 | 62 | |||
| Oklahoma | 326 | 339 | 112 | 116 | ||
| South Carolina | 22 | 48, 49 | 82 | |||
| Texas | 13 | 26 | 27 | 62 | A7 | |
| Virginia | 71 | 77 | ||||
| West Virginia | N1 | R5 | W8 | |||
| Wisconsin | 13 | 26 | 62 | 78 | ||
| Codes | Files |
|---|---|
| NOTE: A claim meeting any of the requirements above constitutes an outpatient visit. | |
| No line-level claim information related to ER services can count as a numerator hit. These are defined as [revenue center code values of 04500459 (ER) or 0981 (Professional fees-ER) or HCPCS codes associated with ER use (99281, 99282, 99283, 99284, 99285) in the OP file] OR [Place of Service code (23=ER-hospital) or BETOS code (M3 = ER visit) in the carrier file] | Medicare Outpatient and Carrier; Medicaid OT |
| The following POS codes count as a numerator hit if they appear in any line-level claim: 03, 05, 07, 09, 11, 12, 13, 14, 15, 20, 22, 24, 33, 49, 50, 52, 53, 71, 72 | Medicare Carrier |
| The following codes count as a numerator hit: TYPSVC of 2 or 3 if FACTYP = 1-6 or 9 OR FACTYP = 7 or 8 | Medicare Outpatient |
Numerator hit in Medicaid if 1 of 2 conditions are present as defined by TOS and/or POS codes:
| Medicaid OT |
| TABLE C.10. Additional Resource: HEDIS Definition of Mental Health Practitioner |
|---|
| Use HEDIS Definition: |
A mental health practitioner is a practitioner who provides mental health services and meets any of the following criteria:
|
APPENDIX D. SUPPLEMENTAL TABLES FOR SCREENING MEASURES
| Screening Measure | Average Among All 6 IPFs (including IPF 1) | Average Among 5 IPFs (excluding IPF 1) |
|---|---|---|
| SOURCE: Administrative data and medical records from 6 IPFs, corresponding to all discharges from October 1, 2013, to December 31, 2013. | ||
| Suicide risk | 93.4 | 97.7 |
| Violence risk | 89.0 | 95.7 |
| Substance use | 85.8 | 91.5 |
| Metabolic | 41.5 | 44.3 |
| All IPS | Psychiatric Units | Freestanding Hospitals | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IPF 1(private) | IPF 2(private) | IPF 3(private) | IPF 4(public) | IPF 5(public) | IPF 6(private) | |||||||||
| N | % | N | % | N | % | N | % | N | % | N | % | N | % | |
| SOURCE: Administrative data and medical records from 6 IPFs, corresponding to all discharges from October 1, 2013, to December 31, 2013. NOTE: Totals for individual tools do not always sum to any standard tool, given that more than 1 tool could have been employed for 1 patient.
| ||||||||||||||
| Suicide denominator before exclusions | 825 | 100.0 | 120 | 100.0 | 176 | 100.0 | 120 | 100.0 | 120 | 100.0 | 118 | 100.0 | 171 | 100.0 |
| Suicide screening exclusions | ||||||||||||||
| Patients with a length of stay less than 1 day | 41 | 5.0 | 12 | 10.0 | 3 | 1.7 | 13 | 10.8 | 2 | 1.7 | 8 | 6.8 | 3 | 1.8 |
| Patients with a length of stay equal to or greater than 365 days | 10 | 1.2 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 7 | 5.8 | 3 | 2.5 | 0 | 0.0 |
| Patients who had previous admissions to psychiatric units during a single hospitalization | 2 | 0.2 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.8 | 0 | 0.0 | 1 | 0.6 |
| Patient unwillingness or inabilitya | 11 | 1.3 | 0 | 0.0 | 1 | 0.6 | 1 | 0.8 | 1 | 0.8 | 8 | 6.8 | 0 | 0.0 |
| Suicide denominator after exclusions | 761 | 92.2 | 108 | 90.0 | 172 | 97.7 | 106 | 88.3 | 109 | 90.8 | 99 | 83.9 | 167 | 97.7 |
| Violence denominator before exclusions | 825 | 100.0 | 120 | 100.0 | 176 | 100.0 | 120 | 100.0 | 120 | 100.0 | 118 | 100.0 | 171 | 100.0 |
| Violence screening exclusions | ||||||||||||||
| Patients with a length of stay less than 1 day | 41 | 5.0 | 12 | 10.0 | 3 | 1.7 | 13 | 10.8 | 2 | 1.7 | 8 | 6.8 | 3 | 1.8 |
| Patients with a length of stay equal to or greater than 365 days | 10 | 1.2 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 7 | 5.8 | 3 | 2.5 | 0 | 0.0 |
| Patients who had previous admissions to psychiatric units during a single hospitalization | 2 | 0.2 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.8 | 0 | 0.0 | 1 | 0.6 |
| Patient unwillingness or inabilitya | 7 | 0.8 | 1 | 0.8 | 0 | 0.0 | 1 | 0.8 | 1 | 0.8 | 4 | 3.4 | 0 | 0.0 |
| Violence denominator after exclusions | 765 | 92.7 | 107 | 89.2 | 173 | 98.3 | 106 | 88.3 | 109 | 90.8 | 103 | 87.3 | 167 | 97.7 |
| Substance use denominator before exclusions | 825 | 100.0 | 120 | 100.0 | 176 | 100.0 | 120 | 100.0 | 120 | 100.0 | 118 | 100.0 | 171 | 100.0 |
| Substance use screening exclusions | ||||||||||||||
| Patients with a length of stay less than 1 day | 41 | 5.0 | 12 | 10.0 | 3 | 1.7 | 13 | 10.8 | 2 | 1.7 | 8 | 6.8 | 3 | 1.8 |
| Patients with a length of stay equal to or greater than 365 days | 10 | 1.2 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 7 | 5.8 | 3 | 2.5 | 0 | 0.0 |
| Patients who had previous admissions to psychiatric units during a single hospitalization | 2 | 0.2 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 0.8 | 0 | 0.0 | 1 | 0.6 |
| Patient unwillingness or inabilitya,b | 20 | 2.4 | 1 | 0.8 | 0 | 0.0 | 5 | 4.2 | 3 | 2.5 | 11 | 9.3 | 0 | 0.0 |
| Substance use denominator after exclusions | 754 | 91.4 | 107 | 89.2 | 173 | 98.3 | 102 | 85.0 | 108 | 90.0 | 97 | 82.2 | 167 | 97.7 |
| Metabolic screening denominator before exclusions | 506 | 100.0 | 56 | 100.0 | 118 | 100.0 | 85 | 100.0 | 79 | 100.0 | 78 | 100.0 | 90 | 100.0 |
| Metabolic screening exclusions | ||||||||||||||
| Patients with a length of stay less than 1 day | 63 | 12.5 | 13 | 23.2 | 10 | 8.5 | 27 | 31.8 | 2 | 2.5 | 9 | 11.5 | 2 | 2.2 |
| Patients with a length of stay equal to or greater than 365 days | 6 | 1.2 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 3 | 3.8 | 3 | 3.8 | 0 | 0.0 |
| Patients who had previous admissions to psychiatric units during a single hospitalization | 2 | 0.4 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 1.3 | 0 | 0.0 | 1 | 1.1 |
| Patient unwillingness or inabilitya | 1 | 0.2 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 1 | 1.3 | 0 | 0.0 |
| Metabolic screening denominator after exclusions | 434 | 85.8 | 43 | 76.8 | 108 | 91.5 | 58 | 68.2 | 73 | 92.4 | 65 | 83.3 | 87 | 96.7 |
| Screening Measure | All IPS | Psychiatric Units | Freestanding Hospitals | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| IPF 1(private) | IPF 2(private) | IPF 3(private) | IPF 4(public) | IPF 5(public) | IPF 6(private) | |||||||||
| N | % | N | % | N | % | N | % | N | % | N | % | N | % | |
| SOURCE: Administrative data and medical records from 6 IPFs, corresponding to all discharges from October 1, 2013, to December 31, 2013. NOTE: Kappas are not presented due to small sample sizes and lack of variation between abstractors in some IPFs. | ||||||||||||||
| Metabolic | ||||||||||||||
| Exclusions | 57 | 98 | 10 | 100 | 10 | 90 | 10 | 100 | 7 | 100 | 9 | 100 | 11 | 100 |
| Numerator | 57 | 96 | 10 | 100 | 10 | 100 | 10 | 100 | 7 | 100 | 9 | 100 | 11 | 82 |
| Suicide | ||||||||||||||
| Exclusions | 58 | 98 | 10 | 100 | 10 | 90 | 10 | 100 | 7 | 100 | 10 | 100 | 11 | 100 |
| Numerator | 58 | 97 | 10 | 100 | 10 | 100 | 10 | 100 | 7 | 86 | 10 | 90 | 11 | 100 |
| Violence | ||||||||||||||
| Exclusions | 58 | 98 | 10 | 100 | 10 | 90 | 10 | 100 | 7 | 100 | 10 | 100 | 11 | 100 |
| Numerator | 58 | 93 | 10 | 100 | 10 | 100 | 10 | 100 | 7 | 43 | 10 | 100 | 11 | 100 |
| Substance use | ||||||||||||||
| Exclusions | 58 | 98 | 10 | 100 | 10 | 90 | 10 | 100 | 7 | 100 | 10 | 100 | 11 | 100 |
| Numerator | 58 | 97 | 10 | 100 | 10 | 100 | 10 | 100 | 7 | 71 | 10 | 100 | 11 | 100 |
APPENDIX E. SUMMARY OF STATE SELECTION PROCESS FOR FOLLOW-UP MEASURE ANALYSIS WITH MEDICAID CLAIMS
In Chapter VI, we present an analysis of dual eligible Medicare-Medicaid beneficiaries. To conduct this analysis, we merged Medicare and MAX data for dual eligible Medicare beneficiaries who visited IPFs in 2008 (the latest year for which MAX data were available at the beginning of this project). MAX data are created from eligibility and claims files submitted by states to CMS and then standardized into variables that can be used to create comparable measures of service use across states. These variables include information such as demographic characteristics (for example, race, ethnicity, gender, and age), diagnoses, and procedures performed for each beneficiary enrolled in Medicaid at any point during the year. A DUA with CMS governed our use of these MAX data.
We limited our analysis of MAX data to FFS claims because although MAX includes some encounters submitted by health maintenance organizations (HMOs) and managed behavioral healthcare organizations, Medicaid managed care encounter data do not undergo the data validation process applied to MAX FFS data, and are generally considered to be of lower quality.
Starting with all 50 states and the District of Columbia, we used a two-step process to select states that would be included in this analysis. We describe these steps below:
Step 1. As noted above, Medicaid managed care encounters are not reliably captured in MAX data. Thus, if a substantive proportion of dual eligible beneficiaries in a state are enrolled in Medicaid managed care, these analyses would underestimate their receipt of care. To avoid this potential bias, states with more than 25 percent of dual eligible beneficiaries enrolled in Medicaid managed care were excluded from the analyses during the first step of state selection. A total of 14 states were excluded in this first step: Arizona, Colorado, Hawaii, Iowa, Kansas, Maine, Minnesota, Montana, Oregon, Pennsylvania, Rhode Island, Tennessee, Utah, and Vermont.
Step 2. The completeness and reliability of MAX data varies across states. After excluding 14 states due to their relatively high proportion of dual eligible beneficiaries in Medicaid managed care (step 1), we excluded additional states that did not use provider Specialty codes in 2008 MAX data in a manner that could facilitate the identification of outpatient services provided by a mental health practitioner. States were excluded if they met any of the following three exclusion criteria: (1) the state did not use provider Specialty codes on any claims; (2) provider Specialty codes did not identify mental health practitioners; or (3) nearly all claims were missing provider Specialty codes.56 A total of 11 states were excluded in this second step: Alabama, District of Columbia, Georgia, Idaho, Kentucky, Mississippi, Nevada, Ohio, South Dakota, Washington, and Wyoming.
This two-step selection process resulted in a total of 26 states included in the analysis of dual eligible beneficiaries presented in Chapter VI, after excluding a total of 25 states (see Table E.1 for a full listing of included and excluded states).
| State | Step 1: Excluded Because More Than 25% of Dual Eligible Beneficiaries Enrolled in Medicaid Managed Care | Step 2: Excluded Due to Data Quality Concerns | Included in the Analysis | ||
|---|---|---|---|---|---|
| States do not Use Provider Specialty Codes | Provider Specialty Codesdo not Identify Mental Health Practitioners | A Substantial Portionof Claims are Missing Provider Specialty Codes | |||
| Alaska | X | ||||
| Alabama | X | ||||
| Arkansas | X | ||||
| Arizona | X | ||||
| California | X | ||||
| Colorado | X | ||||
| Connecticut | X | ||||
| District of Columbia | X | ||||
| Delaware | X | ||||
| Florida | X | ||||
| Georgia | X | ||||
| Hawaii | X | ||||
| Idaho | X | ||||
| Illinois | X | ||||
| Indiana | X | ||||
| Iowa | X | ||||
| Kansas | X | ||||
| Kentucky | X | ||||
| Louisiana | X | ||||
| Maine | X | ||||
| Massachusetts | X | ||||
| Maryland | X | ||||
| Michigan | X | ||||
| Minnesota | X | ||||
| Missouri | X | ||||
| Mississippi | X | ||||
| Montana | X | ||||
| North Carolina | X | ||||
| North Dakota | X | ||||
| Nebraska | X | ||||
| New Hampshire | X | ||||
| New Jersey | X | ||||
| New Mexico | X | ||||
| Nevada | X | ||||
| New York | X | ||||
| Ohio | X | ||||
| Oklahoma | X | ||||
| Oregon | X | ||||
| Pennsylvania | X | ||||
| Rhode Island | X | ||||
| South Carolina | X | ||||
| South Dakota | X | ||||
| Tennessee | X | ||||
| Texas | X | ||||
| Utah | X | ||||
| Vermont | X | ||||
| Virginia | X | ||||
| Washington | X | ||||
| Wisconsin | X | ||||
| West Virginia | X | ||||
| Wyoming | X | ||||
NOTES
-
These are the Hospital-Based Inpatient Psychiatric Services (HBIPS) measures 2-7, developed by The Joint Commission (TJC) and endorsed by the National Quality Forum.
-
Another TJC measure, Alcohol Use Screening (SUB-1) will be incorporated into the IPFQR in 2015, along with the follow-up measure presented in this report.
-
These are the Hospital-Based Inpatient Psychiatric Services (HBIPS) measures 2-7, developed by The Joint Commission (TJC) and endorsed by the National Quality Forum (NQF).
-
Another TJC measure, Alcohol Use Screening (SUB-1) will be incorporated into the IPFQR in FY 2015, along with the follow-up measure presented in this report.
-
These guidelines include the American Diabetes Association (ADA) and American Psychiatric Association (APA) Consensus Development Conference on Antipsychotic Drugs and Obesity and Diabetes (2004); the APA practice guideline on assessment and treatment of patients with schizophrenia (2002); the APA practice guideline on assessment and treatment of patients with bipolar disorder (2010); and the APA practice guideline on assessment and treatment of patients with major depressive disorder (2010).
-
This measure reported by TJC-accredited psychiatric inpatient hospitals. HBIPS-1 was endorsed by NQF in April 2014.
-
SUB stands for substance use. The two measures, recently recommended by Measure Applications Partnership for the IPFQR, SUB-1 and SUB-2, are part of a set of four linked measures related to alcohol and substance use developed for an acute care setting.
-
SUB-1 appeared on the Measures Under Consideration list published on December 1, 2012. Under the current schedule, facilities would be required to begin reporting SUB-1 in FY 2015.
-
Starting in 2014, SUB-1 required alcohol use screening within three days of admission, similar to HBIPS-1. However, in 2013 and in previous years, SUB-1 required screening prior to patient discharge.
-
Based on conversations with TJC staff, the rationale for requiring screening within three days of admission -- as opposed to within one or two days of admission -- is the lack of availability of qualified staff to complete screenings on weekends (particularly in small IPFs) as well as patients' possible reluctance to provide complete and accurate information immediately upon admission, particularly with respect to drug and alcohol use.
-
The suicide measure screening elements are cited in the following guidelines and screening tools: APA Guideline for Treatment of Patients with Major Depressive Disorder (2010), the Suicide Behaviors Questionnaire-revised (SBQ-R), Osman et al. (2001), Veterans Evidence-based Research, Dissemination, and Implementation Center (VERDICT), Suicide Assessment Five-Step Evaluation and Triage (SAFE-T), and Modified Simple Screening Instrument (MSSI). The substance use measure screening elements are cited in the following guidelines and screening tools: APA Guideline for the Treatment of Patients with Substance Use Disorders (2007), Alcohol Use Disorders Identification Test (AUDIT), the Global Appraisal of Individual Needs Short Screener (GAIN-SS), the Simple Screening Instrument for Substance Abuse (SSI-SA), and the Drug Abuse Screening Test (DAST-10). The violence measure screening elements are cited in the following guidelines and screening tools: the Violence Risk Screening-10 (V-RISK-10), the Broset Violence Checklist (BVC).
-
These tools include the AUDIT; the Alcohol Use Disorders Identification Test Consumption (AUDIT-C); Alcohol, Smoking and Substance Involvement Screening Test (ASSIST); Tolerance Worried Eye-opener Amnesia K/cut down (TWEAK); the Car, Relax, Alone, Forget, Friends, Trouble (CRAFFT); Michigan Alcohol Screening Test (MAST); and Geriatric Version-MAST (G-MAST), but may not include the Cut down, Annoyed, Guilty, and Eye-opener (CAGE). However, this list is not exhaustive.
-
Patient records were often the primary data source regarding whether patients were discharged on antipsychotics. However, most IPFs involved in testing migrated this information to their administrative data systems, primarily to report the quality measure HBIPS-4: Patients discharged on multiple antipsychotic medications.
-
Diabetes Screening for People with Schizophrenia or Bipolar Disorder who are Using Antipsychotic Medications (NQF #1932).
-
Some studies and consensus statements, including ADA-APA consensus statement, point to the higher risk of second-generation antipsychotic medications relative to first-generation medications. However, both medication types pose risks to metabolic functioning, particularly within 12 weeks of initiation of medication.
-
The ADA-APA guideline mandates that all four tests should be completed before or right after initiation of antipsychotic medications, and completed again at 12 weeks and/or 12 months after initiation.
-
Screening components could be completed over the course of multiple stays, as long as all components were completed in the 12 months prior to discharge.
-
IPF stays with a mental health diagnosis comprised 71 percent of all IPF discharges. As such, it was reasonable to limit the measure denominator to these stays, given that they comprised a majority of all fee-for-service (FFS) Medicare-paid stays. Non-mental health diagnoses included Alzheimer's (8 percent), psychosis (4 percent), senility (3 percent), and other diagnoses (14 percent).
-
Gaps in care are defined as variation in performance among IPFs or overall less than optimal performance.
-
One IPF received an additional $5,000 to offset their time providing additional assistance in the formative stages of designing chart-abstraction materials.
-
There was no abstractor turnover of during the course of testing, with the exception of one clinical resident who could not abstract all sampled charts and was assisted by another trained abstractor.
-
Medicare Part B provides limited coverage of outpatient mental health services. In contrast, depending on the state, Medicaid covers long-term support services and community-based mental health care.
-
Although the variables in MAX are standardized to create comparable measures of service use across states, the data on beneficiaries enrolled in managed care is often incomplete; this is because data submitted by MCOs do not undergo the same review as data submitted for FFS beneficiaries.
-
States with more than 25 percent of dual eligible beneficiaries enrolled in Medicaid managed care included Arizona, Colorado, Hawaii, Iowa, Kansas, Maine, Minnesota, Montana, Oregon, Pennsylvania, Rhode Island, Tennessee, Utah, and Vermont. States with data completeness issues included Alabama, District of Columbia, Georgia, Idaho, Kentucky, Mississippi, Nevada, Ohio, South Dakota, Washington, and Wyoming.
-
Notably, there is heterogeneity in Medicaid data in states' use of CPT/HCPCS codes as well as provider codes. Because options 1 and 2 rely on these codes, using Medicaid claims alone would likely underestimate the receipt of follow-up care in states that do not use these codes in a manner that is consistent with Medicare claims.
-
This analysis used a fixed population of Medicare beneficiaries to ensure that measured differences in performance were the result of supplementing Medicare claims with Medicaid claims.
-
This IPF supplied only one month of discharge data because one month's data were sufficient to meet the minimum chart-abstraction requirement of 120 patient records.
-
Longer lengths of stay among freestanding hospitals (compared to psychiatric units) likely reflects these facilities' functions and patient populations. In general, freestanding hospitals serve patients with chronic mental health conditions who are admitted for an extended period of time, whereas psychiatric units have a larger proportion of patients who require short-term stabilization.
-
Documented full completion of theSAFE-T constituted a full assessment, as it covered all five screening elements.
-
Documented full completion of the V-RISK-10 constituted a full assessment, as it contained both required screening elements.
-
Documented full completion of the AUDIT was equivalent to completing the first three elements for alcohol use (but not substance use).
-
It should be noted that one psychiatric ward with relatively low performance (IPF 1) effectively lowers average performance on the new measures across the six IPFs. If this IPF's data were excluded from the calculation, performance on the new measures would be approximately 2-8 percentage points lower than performance on relevant HBIPS-1 components.
-
The three-day version of the measures required alternate exclusions: notably, patients with stays of fewer than three days were excluded from the measures.
-
Slightly more than 1 percent of sampled patients received a partial lipid panel, which did not count toward the measure numerator.
-
For all admission screening measures the highest performance was among the group missing a primary diagnosis. However, we excluded this category from the analysis because it is relatively small (approximately 3 percent of the denominator).
-
One IPF reported that it routinely gathers information on suicide and violence risk from patients but that some of its records fail to reflect information provided by patients on these screening elements.
-
Five TEP members expressed an opinion on this topic.
-
Other TEP members did not articulate a preference for one time frame over another during the meeting.
-
Medicare claims are available within a few months of service receipt, whereas finalized Medicaid claims generally have a multiyear time lag (depending on the state).
-
The HEDIS FUH measure uses health plan records to determine whether a provider is a mental health practitioner. We use provider taxonomy and Specialty codes in Medicare and Medicaid claims to make this determination. Specifically, we use providers' NPI numbers to determine their exact Taxonomy code and specialty. Based on consultation with stakeholders, the team expanded the list of eligible providers to include psychiatric nurses and physician assistants with a psychiatric specialty.
-
These diagnosis codes are used in the HEDIS FUH measure to determine the denominator of individuals hospitalized for mental illness. In adapting and testing the FUH measure for IPFs, we use these same diagnosis codes to calculate the numerator for options 2 and 3.
-
This is slightly less IPFs than the 1,703 IPFs that had at least one FFS Medicare-paid stay in 2008. A total of 34 IPFs in the sample dropped out of the non-dual analysis because all of their FFS Medicare-paid stays pertained to dual beneficiaries.
-
The IQR is the difference between the values at the 25th and 75th percentiles of a distribution. A larger IQR indicates greater variation in performance. Measures with a low IQR (for example, less than 10 percentage points) may be less useful for comparing entities.
-
Exclusions are defined using the 30-day follow-up period, but exclusions are applied uniformly across the seven-day and 30-day versions of the measure.
-
This rule is largely in place to protect patient privacy.
-
The last quarter of 2008, from October 1 to December 31, could not be included in this analysis because claims data from January 2009 would have been required to calculate follow-up rates for December 2008.
-
This analysis used a fixed population of Medicare beneficiaries to ensure that measured differences in performance were the result of supplementing Medicare claims with Medicaid claims.
-
Staff's reported lack of access to patient files appears to reflect administrative procedures that block access to patient records following discharge. In at least one IPF, these procedures appear to be designed to protect patient privacy following their stay.
-
Additional statistics on these IPFs are available in Table IV.2.
-
Based on 2008 Medicare data, we found that dually eligible beneficiaries accounted for 59 percent of IPF stays paid by FFS Medicare. A recent MedPac report had similar findings: MedPac (2012). A Data Book: Health Care Spending and the Medicare Program, Section 6. http://www.medpac.gov/chapters/Jun12DataBookSec6.pdf.
-
IPFs were only able to report the primary payer for hospital stays. Because IPFs were not able to systematically report patients' full insurance coverage, Medicare and Medicaid dual eligible status was not directly measurable using information provided by the IPFs. As a result, we apply the basic assumption that approximately half of FFS Medicare beneficiaries that used IPFs were dually eligible, based on findings from our claims analysis.
-
TJC is the steward for these measures. For more information, visit http://www.jointcommission.org/hospital-based_inpatient_psychiatric_services/.
-
Consistent with the HEDIS FUH measure, the IPF follow-up measure's denominator is composed of patients with a principal mental health diagnosis. This includes patients with diagnoses of schizophrenia, bipolar disorder, and depression, but excludes patients with diagnoses of substance use disorders, Alzheimer's, and dementia.
-
As many as 63 percent of FFS Medicare stays may involve dual beneficiaries, on average; however, we use a 50 percent estimate for the sake of simplicity. As such, claims-based measure sample sizes presented below can be interpreted as the maximum potential sample size under a claims-based approach that uses only FFS Medicare beneficiaries as the denominator.
-
However, Medicare beneficiaries could still obtain mental health services outside of Medicare reimbursement, such as from community mental health centers or physicians that do not accept Medicare. These follow-up services would not be captured in a claims-based measure.
-
The primary concern with MAX data was that a lack of uniform practitioner codes would underestimate IPF performance on the measure using numerator option 1, which defines follow-up care as a procedure (as specified by a CPT/HCPCS code) performed by a mental health practitioner (as specified by a practitioner Specialty code). For this reason, our data quality checks focused on identifying instances in which a lack of information on the practitioner specialty would result in an underestimation of follow-up care under option 1.
DEVELOPMENT AND TESTING OF BEHAVIORAL HEALTH QUALITY MEASURES
This report was prepared under contract #HHSP2332010016WI between HHS's ASPE/DALTCP and Mathematica Policy Research. Additional funding provided by the HHS Centers for Medicare and Medicaid Services. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/office_specific/daltcp.cfm or contact the ASPE Project Officer, D.E.B. Potter, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. Her e-mail address is: D.E.B.Potter@hhs.gov.
Reports Available
Development of Quality Measures for Inpatient Psychiatric Facilities: Final Report
Executive Summary http://aspe.hhs.gov/daltcp/reports/2015/IPFes.cfm
Full HTML Version http://aspe.hhs.gov/daltcp/reports/2015/IPF.cfm
Full PDF Version http://aspe.hhs.gov/daltcp/reports/2015/IPF.pdf
Strategies for Measuring the Quality of Psychotherapy: A White Paper to Inform Measure Development and Implementation
Executive Summary http://aspe.hhs.gov/daltcp/reports/2014/QualPsyes.cfm
Full HTML Version http://aspe.hhs.gov/daltcp/reports/2014/QualPsy.cfm
Full PDF Version http://aspe.hhs.gov/daltcp/reports/2014/QualPsy.pdf
U.S. Department of Health and Human ServicesOffice of Disability, Aging and Long-Term Care PolicyRoom 424E, H.H. Humphrey Building200 Independence Avenue, S.W.Washington, D.C. 20201FAX: 202-401-7733Email: webmaster.DALTCP@hhs.gov