
U.S. Department of Health and Human Services
Changing to Consumer-Directed Care: The Implementation of the Cash and Counseling Demonstration in Florida
Barbara Phillips and Barbara Schneider
Mathematica Policy Research, Inc.
July 2004
PDF Version (136 PDF pages)
This report was prepared under contract #HHS-100-95-0046 between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and the University of Maryland. For additional information about the study, you may visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the ASPE Project Officer, Pamela Doty, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, SW, Washington, DC 20201. Her e-mail address is: Pamela.Doty@hhs.gov.
The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
TABLE OF CONTENTS
I. INTRODUCTION
A. Background
B. Solicitation for the Cash and Counseling Demonstration
C. Design of the Evaluation
D. Guide to this Report
A. Florida's Goals
B. Advocates for Citizen Stakeholders
C. State Stakeholders
D. Organizational Stakeholders
E. Summary: Multiple Layers of Many Stakeholders
III. DESIGNING THE CONSUMER-DIRECTED CARE PROGRAM
A. Which Programs and Services to Cash Out?
B. Eligibility, Appropriateness, Outreach, and Enrollment
C. Consulting Services
D. The Monthly Budget
E. Purchasing Plan and Uses of the Monthly Budget
F. Fiscal Services
G. Poised for Implementation
IV. ORGANIZATION OF CONSULTING AND CONSULTANTS
A. Consulting Under DOEA
B. Consulting Under DDP/DCF
C. Consulting Under AS/DCF
D. Training Consultants
E. Monitoring of Consulting
F. Lessons About Organization of Consulting and Consultants
A. Selection Process and Host Agency
B. Responsibilities and Oversight
C. Payment and Costs
D. Quality of Fiscal Services
E. Lessons About Fiscal Services
A. Information Campaign
B. Initial Approach to Outreach
C. Enrollment Operations with Specialists
D. Assessment of Hiring Enrollment Specialists
E. Attractive and Unattractive Program Features
F. Lessons About Outreach and Enrollment
VII. CASH PLANNING AND MANAGEMENT
A. Developing the Purchasing Plan
B. Uses of Cash
C. Time to Receipt of Cash
D. Revisions of the Cash Plan
E. Lessons on Cash Planning and Management
VIII. REPRESENTATIVES
A. Selection of Representatives
B. Lessons About Representatives
IX. PREVENTING NEGLECT, EXPLOITATION, AND ABUSE
A. Preventing Neglect and Exploitation
B. Preventing Abuse of the Monthly Budget
C. Little Abuse and Little or No Exploitation or Neglect
D. Lessons About Monitoring
X. CROSS-CUTTING LESSONS THAT SET FLORIDA APART
A. Relying on Agencies Providing Traditional Services
B. Waiver Services for Children and Adults with Developmental Disabilities
C. Level of Consumer Responsibility
A. Extending Consumer Direction
B. Statewide Program of Consumer-Directed Care
LIST OF TABLES
TABLE III.1. Key Dates in Design and Early Operation of the CDC Project in Florida
LIST OF FIGURES
FIGURE III.1. Consumer Directed Care Demonstration: Geographic Implementation for Elders and Adults
ACKNOWLEDGMENTS
Many people contributed to this report. It is Floridas story, and we especially thank the Floridians who spoke to us, either in person or by telephone. They were very generous with their time and provided many insightful comments. Special thanks go to Tom Reimers and Lou Comer of the Department of Elder Affairs, who helped make the arrangements for our visit to Florida, and to Pamela Aveling of the Department of Children and Families, who made her staff available to us when she was unable to meet with us due to a death in her family and who later responded to remaining questions by telephone. We would also like to thank Kevin Mahoney of the Cash and Counseling Demonstration National Program Office and Pamela Doty of the Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services for their support for the reports in this series. Jennifer Schore, our colleague at Mathematica Policy Research, Inc., provided probing and very helpful comments on an earlier draft.
EXECUTIVE SUMMARY
Consumer direction seeks to give frail elders and people with disabilities more options and greater personal autonomy in determining how best to meet their care needs. Cash and Counseling is one model of consumer-directed home- and community-based services. Under the Cash and Counseling model, eligible people receive a monthly allowance. In turn, they assume responsibility for arranging and managing their care and must use the benefit to purchase goods or services to meet their needs for home- and community-based services--this includes hiring their own workers. Consumers may ask consultants for training on how to meet those responsibilities and may have a fiscal agent hold their allowance, manage payroll taxes, and disburse funds on their behalf.
The Robert Wood Johnson Foundation (RWJF) and the Office of the Assistant Secretary for Planning and Evaluation of the U.S. Department of Health and Human Services are sponsoring a demonstration and evaluation of Cash and Counseling. A National Program Office operates from the University of Maryland, Center on Aging and Boston College. The Centers for Medicare & Medicaid Services (CMS) provides technical assistance and waivers of certain federal Medicaid regulations. Mathematica Policy Research, Inc. (MPR) is evaluating the demonstration, which has been implemented in Arkansas, Florida, and New Jersey. The evaluation used a randomized design--half of the enrollees are assigned to a treatment group to receive the allowance, half to a control group to continue with traditional services.
This report describes the design and implementation of the Consumer-Directed Care Research Project (CDC), Floridas model of Cash and Counseling, and draws lessons from the states experience. The report is based primarily on in-person interviews conducted in January 2002, about 18 months after the project began enrolling beneficiaries. Interviews were conducted with Florida state officials, state employees at the regional level, CDC staff members, and staff members of organizations providing consulting and fiscal services under CDC. (Florida used the term consulting rather than counseling in its demonstration.)
The Consumer-Directed Care Project
Feeder Programs and Host Departments. Under Section 1115 demonstration authority, Florida chose to cash out home- and community-based services covered under its Medicaid 1915(c) waiver programs for children and adults with developmental disabilities, adults with physical disabilities, and elderly beneficiaries. The Developmental Disability Program (DDP) within the Department of Children and Families (DCF) was responsible for 1915(c) programs and for the CDC project for children and adults with developmental disabilities. The Office of Adult Services (AS), within DCF, had similar responsibilities for adults with physical disabilities, and the Department of Elder Affairs (DOEA) had similar responsibilities for elderly beneficiaries. DOEA was the official grantee and housed the central office for the CDC program. Each of these 1915(c) waiver programs covers a variety of goods and services. These goods and services range from personal care supplies, to personal assistance, to professional services (such as nursing and behavioral therapy).
Structure of Traditional Waiver Services. In Floridas waiver programs for children and adults with developmental disabilities, support coordinators help program participants manage their care (support coordination services were not cashed out). The support coordinators are employed by agencies (typically proprietary firms) or are independent contractors. Many support coordinators serve populous areas of the state, and consumers may choose a support coordinator with whom they are comfortable.
Similarly, in Floridas waiver programs for adults with physical disabilities and elderly beneficiaries, case managers help program participants manage their care (case management services also were not cashed out). In each county in Florida, a single agency--called a lead agency--provides case management services to all elderly participants in that county. The lead agencies typically are public agencies, and all lead agencies provide case management under contract to the local Area Agency on Aging (AAA). Each of the 11 AAAs in Florida is under contract to the state to procure and oversee Medicaid waiver services for elderly people living in its catchment area. Case management for adults with physical disabilities may be provided by state employees or case management agencies under contract to the state.
Eligibility for CDC. The only people eligible to enroll in CDC were beneficiaries receiving services under one of the Medicaid waiver programs being cashed out and living in the catchment area for the CDC project. For children with developmental disabilities, the catchment area consisted of the entire state. For adults with developmental disabilities, the catchment area consisted of the entire state, except for a few counties in the northern part of the state where another consumer-directed pilot program was already under way. For adults with physical disabilities and elderly beneficiaries, the catchment area consisted of 19 counties and included most of the states major metropolitan areas.
Waiver program participants who wished to enroll in CDC, but who were unable to manage their own services, were still eligible for CDC. Adults could name a family member or friend as a representative to act on their behalf. Representatives, invariably a parent or guardian, were mandated for children.
Outreach and Enrollment. Initially, Florida required agencies providing case management/support coordination services to conduct outreach for CDC. Case managers and support coordinators were required to inform waiver program participants of their eligibility for CDC, just as they were required to inform them of all programs for which they were eligible.
This approach to outreach and enrollment proved largely unsuccessful, however. Many case managers were skeptical about the value of consumer-directed care, and support coordinators were overwhelmed with work following a substantial expansion of funding for traditional waiver services for those with developmental disabilities.
Faced with lagging enrollment in CDC, Florida arranged for the state governor to send a CDC invitation letter to each waiver program participant. (Arkansas had also done this.) In addition, Florida hired temporary state staff as enrollment specialists to contact waiver program participants to describe CDC and to enroll those who were interested. After the state took these steps, enrollment surged. When enrollment for the evaluation sample ended (in July 2002), 1,004 children, 1,002 nonelderly adults, and 814 elderly beneficiaries had enrolled in CDC.
Determining the Amount of the Monthly Budget. Florida based the amount of the allowance (which it called the monthly budget) on the waiver recipients claims history or on his or her care plan or support plan (the latter term is used for those with developmental disabilities). The claims history methodology was not used for beneficiaries with developmental disabilities. For other beneficiaries, the care plan methodology was used if the beneficiary did not have a stable, recent claims history or the benefit amount based on the care plan was materially larger than that based on the claims history.
To try to ensure the budget neutrality of the CDC project, the amount of a monthly budget based on care/support plan hours was discounted to adjust for the fact that, on average, the cost of services received is less than the cost of services planned. Based on analyses of care plan and claims data for samples of beneficiaries, Florida set the discount rates at 89 percent for elderly beneficiaries, 83 percent for adults with physical disabilities, and 92 percent for children and adults with developmental disabilities.
About the time of our visit to Florida in January 2002, the average monthly budget (after discounting) in Florida was $975 for elderly adults and adults with physical disabilities and $1,825 for children and adults with developmental disabilities.
Purchasing Plan and Use of the Monthly Budget. Before consumers could receive the first payment, CDC required them to develop a plan for the purchase of goods and services. Plans could provide for the consumer to receive up to 20 percent of the monthly budget in cash (or more with special permission). (Later, the cash payment was limited to $250 a month.)
CDC consultants visited the consumers home to train the consumer on the permissible uses of the monthly budget and the development of the initial purchasing plan. Consumers were required to develop a revised purchasing plan if the amount of the monthly budget or the amount of any line item in the plan changed.
Consultants reviewed and approved all initial or revised purchasing plans, then submitted them to a state or district office for approval. Plans for consumers with developmental disabilities were reviewed and approved by the Medicaid specialist in the DDP district office for that region. The CDC project central office reviewed and approved the plans for adults with physical disabilities and elderly consumers.
Consumers used the monthly budget to purchase a wide variety of goods and services, just as CDC had intended. Many hired workers, most of whom were family members. Some hired a parent (for the demonstration, a waiver of Medicaid regulations permitted the hiring of a parent of a minor child or a spouse). A few representatives were hired as workers. Some consumers also purchased personal care supplies (such as diapers).
Monitoring. Florida required CDC consultants to visit consumers homes during the 2nd and 12th month after enrollment (and annually thereafter) to monitor the consumers condition. Consultants were also required to telephone consumers at least monthly.
Consulting Agencies. Florida asked agencies and independent contractors providing waiver program case management/support coordination to also provide consulting for beneficiaries who enrolled in CDC. The availability of funding was a major factor in this decision--state funds were already committed for the payment of these agencies and contractors. In addition, Florida believed that reliance on the existing networks would be beneficial to consumers for two reasons: (1) case managers and support coordinators were already knowledgeable about other programs and community resources, and (2) continuity of care could be enhanced by having a consumers case manager or support coordinator continue to work with that person as a CDC consultant.
In practice, however, only a few staff members at each agency provided CDC consulting (often only one or two even in large agencies). This approach was more efficient than having many staff members, each of whom provided consulting to only a few consumers. In addition, the shift in responsibilities under CDC from case manager/support coordinator to consumer was sometimes more difficult when the person who had been a case manager (or support coordinator) became the consultant.
CDC adopted different payment structures for consulting by support coordinators and consulting by case managers. A monthly rate per beneficiary was paid for support coordination/consulting; this rate was the same as that paid for traditional support coordination. In contrast, a flat sum was paid for each case management/consultant training visit to develop the purchasing plan (up to two visits), followed by an hourly rate for consulting services (payments at the hourly rate were capped).
Fiscal Services. Florida issued a solicitation to procure a single fiscal agent for CDC consumers across the state. After a lengthy delay, it contracted with a human services organization in another state on the eastern seaboard. This delay occurred after the initial consultant training sessions had already taken place, necessitating refresher training for consultants.
Florida required that CDC consumers purchase services from the fiscal agent. Those who wished to manage the monthly budget themselves had to demonstrate that they were capable of doing so and had to purchase a monthly review of their records and receipts from the fiscal agent. All other consumers were required to use the fiscal agent to cut checks and process payroll documents. For these consumers, the fiscal agents duties were to process employment forms, federal and state payroll taxes, and time sheets and vendor payments; disburse cash to consumers; and prepare monthly financial statements to consumers (with a copy to consultants).
Floridas approach to ensuring that expenditures conformed to the purchasing plan was to have consultants compare monthly financial statements to plans and retrain consumers if there were discrepancies. In addition, consumers had to retain receipts for the consultant to review for purchases made with cash from the monthly budget.
Most of the compensation for the fiscal agent was in the form of fees charged to consumers for the services they used. A consumer was charged about $5 per check cut, up to a maximum of $25 a month. Consumers who managed the monthly budget themselves were charged about $10 a month for fiscal agent review. Florida also paid the fiscal agent for some design tasks (such as design of the bookkeeping skills examination for consumers).
Lessons from the Consumer-Directed Care Project
Floridas experience provides many lessons about operating a consumer-directed program as an alternative to Medicaid home- and community based waivers. The state was willing to learn from its experience and try a different approach if problems arose. Here, we describe lessons pertaining to specific components of CDC, followed by lessons that cut across components and that are unique to Florida among the three Cash and Counseling states.
Outreach and Enrollment
- A consumer-directed program that cashes out traditional services needs the cooperation of the agencies providing those services; however, assigning these agencies responsibility for outreach and enrollment can be fraught with problems. Case management agencies often have their clients trust and can easily discourage enrollment if they are opposed to the concept of consumer direction. Even when that is not the case, agency staff members who are pressed by other responsibilities are unlikely to give priority to the time-consuming tasks of outreach and enrollment.
- If state agencies are responsible for outreach and enrollment, arranging for enrollment statistics to be reported to the highest levels of state government may be a useful way to get the attention of the responsible officials. When enrollment in CDC was lagging, DDP arranged for statistics on the outreach effort to be included in monthly reports reviewed by the governors office in assessing administrator performance. After that, enrollment improved.
- Providing information to advocacy groups can be a successful approach to generating interest in an allowance program. Florida has a tradition of strong advocacy for those with developmental disabilities, particularly through its Family Care Councils. Presentations to the councils generated considerable interest in Floridas allowance program.
- Because direct mailings to eligible beneficiaries are targeted, they are more efficient than outreach methods that blanket the community with information. Letters from the governor to recipients of Medicaid waiver services were particularly effective in generating enrollment in Floridas allowance program.
- Calculating the amount of the allowance before enrollment is important but can be time-consuming. Beneficiaries need to know the amount of the allowance to make an informed decision about enrollment. If the allowance is based on the claims history or the care/support plan, the amount must be calculated under each methodology.
- Hiring dedicated enrollment specialists may be the best approach to building a caseload relatively quickly. Unless agency staff are enthusiastic about consumer direction, hiring dedicated employees is preferable to paying agencies to have their staff conduct outreach and enrollment.
- A limited number of dedicated enrollment staff may successfully serve a wide geographic area. Dedicated enrollment staff can come into an area, contact all members of the eligible population there, and then move on. Floridas experience is that such enrollment specialists can be supervised from district offices or remotely by telephone, e-mail, and an Internet chat room.
- The explanation of the cash program provided to prospective enrollees should be as clear as possible. Although an allowance program can be difficult for consumers to understand, lack of clear explanation engenders confusion, which consultants must correct. Moreover, consumers might disenroll when the misunderstanding is corrected.
Consulting
- The same person can readily provide both consulting and case management (or support coordination) services. Case managers and support coordinators who were comfortable with the philosophy of consumer direction did not have difficulty providing case management or support coordination to waiver program participants and consulting to CDC consumers.
- Consultants require substantial training, followed shortly by practice. Florida limited its training session for consultants to one and a half days, and consultants generally felt that more time was needed. Knowledge gained in the initial training session was forgotten because consultants were not able to put it into practice quickly.
- Conference calls can provide updates and peer support to consultants working in far-flung agencies. Conference calls give consultants a means to learn tricks of the trade. Apart from cost, the only disadvantage of conference calls is that they may provide a forum for consultants to voice negative opinions that may adversely affect staff morale.
- Regional program supervisors can provide valuable support to frontline consulting staff. DDP Medicaid specialists reduced the burden on central CDC staff by supervising enrollment specialists and by reviewing and approving consumer purchasing plans. Some became so knowledgeable about CDC that they were able to offer technical assistance and support to consultants and consumers.
Purchasing Plans and Use of the Allowance
- Advance preparation can expedite the development of the purchasing plan. Some Florida consultants expedited the development of the purchasing plan. They did this, for example, by asking consumers to review the program manual and to begin, before the home visit, to think about their needs and what to purchase to meet those needs.
- A consumer manual is an important tool. It helps the consumer become familiar with program procedures and rules before the initial consultant training visit. It is also useful as a reference manual.
- Although working with a consumer on the initial purchasing plan can be time-consuming for consultants, a consumers need for help in completing the plan does not necessarily indicate inappropriateness for an allowance program. Florida learned that consumers and representatives were usually able to identify the goods and services to be included in an initial purchasing plan but that many needed help (for example, with arithmetic) to complete the plan. Of itself, the need for such help did not indicate that a consumer was inappropriate for CDC.
- Purchasing plans must be revised as consumer needs and plans change, and this requires a substantial amount of staff time. However, flexible plans can reduce the need for revision. Because the purchasing plan is critical to ensuring that the allowance is not abused, it must be revised to accommodate changes in consumer needs. Doing so requires a substantial amount of time from consultants and from other program staff who must approve revised plans. The need for revision can be reduced by listing the wage and hours for a position, earmarking a larger proportion for cash, and using an addendum to specify a change in the good or service for which funds are being saved.
- Consumers may be able to purchase goods for less than the Medicaid program does. By shopping for sale prices, Florida consumers were able to purchase goods such as personal care supplies from commercial establishments for less than the Florida Medicaid program paid vendors.
Representatives
- Consumers usually choose family or friends who were already helping them as representatives to assist in managing the benefit.
- All, or almost all, consumers with development disabilities will require a representative, and many elderly consumers will select a one. All minor children will require a representative.
- Naming representatives at enrollment may be advantageous. The consultant can begin to work with the representative on the purchasing plan before the initial home training visit, thereby reducing delay of the receipt of the allowance.
- Representatives are generally faithful to the best interests of consumers and try to take their wishes into account. While this was true for all consumers, Florida consultants reported that parents sometimes went to extraordinary lengths for their children.
- Special forms of monitoring are needed when a representative is also a worker, as this situation presents an inherent conflict of interest. Because representatives are responsible for supervising workers, allowing the same person to play both roles presents a conflict of interest. When such a situation could not readily be avoided, Florida asked someone identified by the consumers family to check on the consumers well-being, and the counselor telephoned that person as well as the representative. A similar approach might be beneficial when the representative is the coach of an adult with developmental disabilities living in a group home. Such a coach has a responsibility to the group home as well as to the consumer.
Fiscal Services
- A fiscal agent may need assistance with cash flow until it reaches a break-even caseload. The CDC project was a financial drain on the host organization for fiscal services, in part because of the slow buildup of the caseload.
- The quality of consumer services may suffer if the fiscal agent is under prolonged financial strain because its costs exceed its payments. The fiscal agent for CDC reduced its staff in response to the financial strain it faced, which adversely affected responsiveness to consumer requests and timely production of consumer financial statements.
- Timely, understandable, and detailed financial statements are important to consumers ability to manage the allowance, but a fiscal agent may have difficulty producing such statements. As in other Cash and Counseling states, the fiscal agent for CDC had difficulty producing monthly financial statements that were timely, easily understandable, and detailed. Consumers value statements that detail the date, amount, and payee of each debit from their accounts.
- Fiscal agents need procedures that minimize the use of postal services for time-critical deliveries. Examples of such procedures used in CDC are direct deposit of workers pay into bank accounts and submission of the first time sheet for a given worker by facsimile (with the original to follow by mail).
Monitoring to Prevent Neglect of Consumers and Abuse of the Allowance
Exploitation and neglect of consumers and abuse of the allowance were rare in the CDC project.
- Referral arrangements with organizations providing protective services may be beneficial. Florida developed formal arrangements for consultants to refer cases of potential neglect or exploitation to protective services so that expert assistance was available to consultants immediately.
- Telephone monitoring that involves only the representative is inadequate. The appropriate frequency for monitoring visits varies with the population served. If consumers can articulate their needs and concerns, a call to the consumer (as well as to the representative) is necessary to identify the rare cases of potential neglect or exploitation of the consumer. More frequent monitoring visits are likely required for consumers (such as those with developmental disabilities) who have difficulty articulating their needs and concerns.
- Relying on consultants to compare monthly financial statements to purchasing plans increases the need for communication between the consultant and the fiscal agent, which can be problematic. Having consultants compare expenditures to purchasing plans may be problematic, especially when consultants and fiscal staff are organizationally separate.
- Review of receipts is not critical to preventing abuse of funds held by the fiscal agent. CDC required review of receipts only for cash held by the consumer, and some consultants reported that they did not routinely review these receipts. Yet abuse of funds held by the fiscal agent was almost nonexistent.
Cross-Cutting Lessons Unique to Florida
Florida was the only one of the three Cash and Counseling programs to rely primarily on agencies providing traditional services to provide outreach, enrollment, and consulting under its cash program. It was the only one of the three to cash out services for children, services for beneficiaries with developmental disabilities, and services provided under a waiver rather than the state Medicaid plan. Arguably, Floridas program invested more responsibility in the consumer (or representative) than did the other two programs. Here, we draw cross-cutting lessons related to these unique features of Floridas allowance program.
- Many factors seem to affect the level of resistance of providers of traditional services to an allowance program. States interested in relying on agencies providing traditional services to implement an allowance program may be able to reduce their resistance. The factors that affect the level of resistance include agency monopoly position, competing demands on staff time, concerns about loss of agency revenue if consumers hire workers directly, adequacy of compensation for agency effort in outreach and consulting, concerns about agency liability for decisions that consumers make, and conflicting professional norms about responsibility for beneficiary welfare. Techniques to overcome these factors include avoiding reliance on agencies that have local monopolies on traditional services in favor of agencies that must compete, avoiding implementation of an allowance program when other demands on agency staff are high or when agencies are experiencing a reduction in revenue, ensuring agencies are fairly compensated, stressing that consumers (not agencies) are liable under a Cash and Counseling-like program, and demonstrating that some beneficiaries benefit dramatically from a cash program.
- States may be able to better able to secure the interest and support of organizations providing traditional services if they consult with these organizations early in the design of an allowance program. Florida regretted that the schedule for Cash and Counseling prevented early consultation with agencies providing traditional services.
- The Cash and Counseling model is very attractive to parents of children with developmental disabilities. As a percentage of those eligible, more children with developmental disabilities enrolled in a Cash and Counseling program than any other population. As of the end of intake for the evaluation, the percentages of the eligible elderly and adult populations enrolling in all three Cash and Counseling states were roughly 8 to 10 and 15 to 20 percent, respectively. The comparable percentage for children with developmental disabilities was roughly 25 percent.
- Paying parents to be workers is a sensitive issue, but parents rarely take unfair advantage of the situation. While the parents of minor children are legally responsible for their care, caring for a child with disabilities requires a tremendous amount of time and energy, which affects the time a parent can devote to other family members or to paid work. With the safeguards implemented in CDC (including special monitoring when the representative was also a worker), Floridas experience was that only very rarely did parents of minor children even appear to take unfair advantage of the opportunity to be paid.
- The evidence from Florida is that consumers and their representatives are able to manage some professional services, as well as personal care. Professional services (such as behavioral therapy and nursing) are covered under Floridas waiver programs and were cashed out. Thus, Florida consumers were implicitly given responsibility for making decisions about their need for professional services. This did not result in material neglect or exploitation of consumers.
I. INTRODUCTION
A. Background
1. A New Model of Medicaid Supportive Services
About 1.4 million people receive disability-related supportive services in their homes through state Medicaid plans or home- and community-based waiver services programs (Harrington and Kitchener 2003). Under state plans, services must be provided by licensed home care agencies and are largely restricted to human help with personal assistance and homemaking. The agencies recruit, train, schedule, and supervise the aides or attendants who assist beneficiaries. Under waiver programs, adult day care, assistive devices, and home modifications can be offered in addition to in-home aide services. However, coverage of these additional services is limited in many states, and a case manager, not the beneficiary, decides whether they are needed.
In contrast to these traditional service models, states are increasingly offering Medicaid beneficiaries and their families the opportunity to obtain personal assistance from individual providers (Velgouse and Dize 2000). This alternative is called consumer-directed care, as Medicaid beneficiaries who use individual providers assume the employers role of hiring, managing, and, possibly, terminating their workers (Eustis 2000). An expanded model of consumer direction would allow beneficiaries to manage not only their human assistance, but also other covered supportive services.
Cash and Counseling is an expanded model of consumer-directed supportive services. It provides a flexible monthly allowance (which Florida called a monthly budget) that consumers can use to hire their choice of workers, including family members, and to purchase other services and goods (as states permit). Cash and Counseling requires that consumers develop purchasing plans showing how they would use the monthly budget to meet their personal assistance needs. It also provides counseling and fiscal help to aid them in planning and managing their responsibilities. Consumers who are unable or unwilling to manage their care themselves may designate a representative, such as a family member, to help them or do it for them. These features make Cash and Counseling adaptable to consumers of all ages and with all types of impairments.
With funding from the Robert Wood Johnson Foundation (RWJF) and the Office of the Assistant Secretary for Planning and Evaluation (ASPE) of the U.S. Department of Health and Human Services, the Cash and Counseling Demonstration and Evaluation was implemented in three states--Arkansas, Florida, and New Jersey.1 The Centers for Medicare & Medicaid Services (CMS) was responsible for the waivers of federal Medicaid regulations required for the demonstration.2
Because their Medicaid programs and political environments differed considerably from each other, the demonstration states were not required to implement a standardized intervention. They did have to adhere to basic Cash and Counseling tenets as summarized above, however. The states resulting demonstration programs differed in their particulars, so each is being evaluated separately, by Mathematica Policy Research, Inc. (MPR).
2. Possible Advantages and Disadvantages of Cash and Counseling
When planning for the Cash and Counseling Demonstration began, its designers felt the monthly payment could give beneficiaries the power to purchase services that best fit their long-term care needs and individual values. Beneficiaries were expected to design individual service packages. As alternatives to disability-related supportive services, they could hire workers privately, make home modifications, purchase equipment and supplies, or purchase commercial services (Cameron 1995; and Kane 1996). Thus, they were in a better position to arrange for services at times that best met their needs. They could also hire their friends or relatives if they believed that doing so was in their best interest. Depending on the level of the monthly budget, the cost of traditional services, and the cost of alternative services, beneficiaries might also be able to purchase more hours of services than they received from the traditional program. These changes offered the potential to increase autonomy, address unmet needs better, and improve satisfaction--changes that might, in turn, result in improved functioning (Kane 1996).
In addition, at that time, reductions in public expenditures were viewed as possible because traditional case management services and administrative functions were being eliminated under Cash and Counseling, and beneficiaries took responsibility for managing their own services. If the cost of providing counseling was less than that of these traditional functions, savings would accrue. Savings might also accrue if the cost of the monthly payments was less than the cost of processing claims. Moreover, the consumer (not the state) was the employer of record under Cash and Counseling--a difference that could potentially reduce state costs (see, for example, Jackson 1994; Cameron 1995; Doty et al. 1996; and Flanagan 1994). Because the state was not the employer of record, it might avoid collective bargaining with attendant unions (and the costs of that bargaining). In addition, the likelihood of successful liability actions against the state (and costly settlements) might be reduced because it was not the employer of record.
At the time the Cash and Counseling Demonstration was being designed, states had little experience with cash programs. Therefore, public officials were concerned about possible abuse of the program. They feared that relatives or workers might neglect or exploit beneficiaries or that beneficiaries might not use their monthly budget for the intended purpose. Some public officials were also concerned that a monthly budget might create more demand for services (the so-called woodwork effect) and strain available resources.
There was concern that traditional providers of supportive services might object to Cash and Counseling because it might reduce their revenue and place them at a competitive disadvantage relative to privately hired workers. Traditional providers might also object that potential workers would not be adequately trained or supervised. Finally, because no collective bargaining entities existed to represent privately hired workers, organized labor might not support Cash and Counseling (Cameron and Lagoyda 1997).
B. Solicitation for the Cash and Counseling Demonstration
The central question RWJF and ASPE posed for the demonstration was: How does Cash and Counseling compare to traditional case-managed supportive services? States interested in participating in the demonstration were free to propose Medicaid personal assistance services (PAS) funded under the optional state plan benefit, Medicaid programs funded under home- and community-based waivers, or programs funded by state general revenues.3 These were the demonstration feeder programs (except that programs similar to Cash and Counseling were not eligible to be feeder programs).
RWJF and ASPE also stipulated an evaluation that employed a rigorous randomized design. Thus, people participating in the demonstration were to be assigned either to a treatment group (to receive the monthly budget) or to a control group (to continue under traditional PAS, home- and community-based waiver services, or a state-funded program). The effect of the requirement for a randomized design was to limit the demonstration to states with large PAS, waiver, or state-funded programs (or combinations of programs). Only in such states was it possible to obtain the sample sizes needed for the evaluation.
States were expected to include elderly people whose functioning was impaired, as well as younger adults with disabilities, in the Cash and Counseling Demonstration. Younger adults with disabilities have long advocated for consumer-directed care. Adoption of a disability model for personal assistance for elderly people was being debated at the time the solicitation for the demonstration was issued, and there was policy interest in extending such care to elderly people whose functioning was impaired (see, for example, Simon-Rusinowitz and Hofland 1993; and Doty et al. 1996). The states could include children with disabilities if they wished.
The solicitation anticipated that states would seek waivers of the federal regulations restricting cash payments under the Medicaid program. To grant such waivers (as for demonstration waivers in general), CMS required that the cash program affect the federal budget no more than the PAS or home- and community-based waiver program being cashed out. That is, the cash program was required to be budget neutral. CMSs traditional approach to calculating budget neutrality involves comparing the monthly cost per recipient of the demonstration program and the traditional program over the life of the demonstration. Another of the terms and conditions for the demonstration waivers limited the potential impact of the demonstration on public costs by restricting the number of new entrants to the cash program. During the demonstration, the ratio of the number of new entrants to the number of current recipients entering the cash program was not to exceed the historical average for the traditional program.4
The demonstration solicitation required that the cash program cover a broad range of services (such as equipment and home modifications), in addition to personal assistance workers. Furthermore, the solicitation anticipated that legally liable relatives (that is, spouses and parents of minor children) might be hired as personal assistance workers and that states would have to seek a waiver of the federal restriction on such hiring.
Consistent with the Cash and Counseling model, the demonstration solicitation required that counseling and fiscal services be provided. These services were to help personal assistance recipients by giving them information and advice, teaching them skills, and providing support services, including help with payroll and bookkeeping activities. Demonstration states could decide what specific counseling services to offer.
In response to the solicitation for the Cash and Counseling Demonstration, 17 states submitted bids. Four states were selected: Arkansas, Florida, New Jersey, and New York. New York dropped out of the demonstration before beginning operations, because its local social service districts had little interest in participating.
This report on Florida is one of four describing the implementation of Cash and Counseling from the perspective of the state, Cash and Counseling program, and organizations participating in the demonstration.5 This report tells the story of the implementation of Floridas Cash and Counseling program, which it named the Consumer-Directed Care Research Project (CDC).6 Two reports tell the stories, respectively, of the implementation of the Cash and Counseling programs in Arkansas and New Jersey. The fourth report draws lessons from the experience of all three Cash and Counseling programs.
C. Design of the Evaluation
The MPR evaluation of the Cash and Counseling Demonstration has two goals. The first is to estimate the impacts of providing a monthly budget instead of disability-related supportive services. The second is to document and analyze the implementation of the Cash and Counseling model as it unfolded. These two goals are interrelated, as impacts can be interpreted and generalized only in light of how the Cash and Counseling model was implemented.7
1. Evaluation of Impacts
The evaluation will estimate impacts on consumers, caregivers, and costs to the public. It will also describe participation in the demonstration.
Cash and Counseling is expected to affect consumers use of, unmet need for, and satisfaction with supportive services. As a result, it may also affect their health and functioning. Because consumers purchase supportive services on their own, rather than relying solely on agencies, they are likely to have more control over who provides their services and how and when these services are delivered. Consumers may use different amounts or mixes of services than they would have received under traditional Medicaid programs. They may also use their funds to buy equipment that increases their independence. This greater flexibility should reduce consumers unmet need and improve their satisfaction with supportive services. In addition, if the quality of personal assistance improves, consumers functional independence and disability-related health may also improve. Although the cash program is expected to improve consumer outcomes, the evaluation will also assess whether any outcomes worsen.
Cash and Counseling could affect caregivers in several ways. If consumers hire attendants or use the monthly budget to purchase assistive equipment, family and friends who provided unpaid care to consumers before the consumers enrollment in the demonstration could face fewer demands on their time. If consumers mismanage their budgets, however, unpaid caregivers may need to provide more care than they did before. The evaluation will also investigate the experience of caregivers who are hired and paid under the demonstration. The working conditions, job satisfaction, and physical and emotional strain that paid caregivers experience will be measured and compared to that of agency workers providing care to control group members.
The evaluation will estimate Cash and Counselings effects on Medicaid costs for supportive services alone and for all costs paid by Medicaid and Medicare. Costs for personal assistance may increase or decrease, depending on the amount of the monthly budget (on average) and the number of months in which people receive the monthly budget, relative to traditional supportive services. Costs for other health care may also increase or decrease. For example, if consumers receiving the monthly budget are more likely to receive care when they need it, they may have fewer falls or pressure sores and, thus, have lower health care costs. On the other hand, if recipients of the monthly budget hire workers who are less well trained than agency workers, their health may suffer, resulting in higher health care costs.
The major sources of evaluation data for the impact analyses were (1) telephone surveys with demonstration participants and their caregivers, and (2) Medicare and Medicaid eligibility and claims data. People who agreed to participate in the demonstration had to complete a baseline telephone interview before they were randomly assigned to the treatment or control group. Six months later, MPR interviewed treatment group members about their early experiences with the program. Nine months after enrollment, MPR interviewed both treatment and control group members to collect information on their satisfaction, quality of care, quality of life, use of other formal and informal care, and health and functional status. Around the same time, unpaid caregivers identified at baseline were interviewed about the type and amount of care they provided, their relationship with the consumer, and their satisfaction with the paid care the consumer received. Samples of paid workers identified in the nine-month survey were also interviewed about earnings and benefits, job satisfaction, and problems encountered on the job. Medicaid and Medicare claims and eligibility data are being used to study the cost of supportive services, the use and cost of medical services, and the participation rate in the program being cashed out.
2. Process Analysis
Another component of the evaluation is examining program structure and implementation. This process analysis, of which this report is a part, has two objectives. First, it documents demonstration operations and the context in which the demonstration operated in each of the three states (Arkansas, Florida, and New Jersey) participating in the Cash and Counseling Demonstration. In doing so, it informs the quantitative analyses of impacts. Second, the process analysis develops lessons about designing and managing a Cash and Counseling program.
Specifically, this report seeks to address three major sets of questions:
- How did Florida structure its CDC program, and what led it to adopt this structure?
- How did Florida implement its program? Did it implement it according to its plans? If not, how and why did it depart from its plans?
- What lessons can we learn from the Florida experience about structuring and operating a Cash and Counseling program?
The process analysis is based mainly on three data sources. The primary one is in-person interviews conducted in January 2002 with staff of the state agencies responsible for the waiver programs to be cashed out and staff of the Cash and Counseling program in Florida. These staff members included:
- State officials of the Florida Department of Children and Families (DCF) and the Department of Elder Affairs (DOEA), the departments that participated in the CDC project while the evaluation was under way.
- State officials of the Department of Health, the department responsible for the Brain and Spinal Cord Injury program at the time of our visit.
- State-level CDC staff, including
- Program director, program manager, and other staff from DOEA
- Program director and other staff of the Developmental Disabilities Program in DCF
- Program director and program manager from the Office of Adult Services in DCF.
- Medicaid specialists for DOEA serving five different regions of the state (three of these specialists were interviewed by telephone) and Medicaid specialists at two district offices of DCF.
- Representative of Floridas Agency for Health Care Administration, the agency responsible for the Medicaid program in that state.
- Staff of the fiscal agent, including the executive director of the host organization and the program manager for CDC.
- The supervisor of enrollment for elderly beneficiaries.8
Staff of agencies providing consulting, including
- The director of the host organization and one or more consultants from four lead agencies serving elderly beneficiaries in different parts of the state. In addition, two consultants working in nearby rural counties participated in one of the interviews with a Medicaid specialist.
- The director of the host organization, one or more consultants from three support coordination agencies, and a support coordinator working as an independent contractor, in different parts of the state.
- The supervisor and a consultant providing consulting to adults with physical disabilities.
With the help of state CDC staff, we identified the agencies and independent contractors providing consulting. The agencies operate under different auspices (public, private nonprofit, and private for-profit) and are in different regions of the state. All were knowledgeable about CDC.
The second source of information for the process analysis is demonstration documents, such as demonstration operational protocols prepared for CMS, state quarterly reports required by the National Program Office, and forms and materials for consumers and consultants.
The third data source is information the authors obtained by participating in project meetings and telephone conference calls, which included project status reports and discussion of issues facing the Cash and Counseling states. The authors attended project meetings, which were held twice a year. One of the authors regularly participated in telephone conference calls held with state program staff weekly (later biweekly) throughout the demonstration.
A major strength of this process analysis is that it uses the reports of those directly involved in CDC. Many people were interviewed in person. The interviews were extensive and the interviewees extremely knowledgeable--at times, insightful. Their reports are certainly credible. Moreover, state CDC staff reported on the cash program in many telephone conference calls and meetings.
This strength is also a limitation, however, in that this report relies on the perceptions of those involved in the CDC project. To minimize the possibility of error based on misconception, we have, when possible, collected information on key topics from multiple perspectives.
Another project report will supplement this description of the implementation of CDC. It will combine the perspectives of program staff presented here with those of consumers and consultants and with descriptive data (such as fiscal agent data categorizing the actual uses of cash). When the quantitative analyses are complete, we will have better evidence about the validity of many of these perceptions. One of the strengths of this evaluation is having multiple data sources based on different methods.
D. Guide to this Report
This report contains 11 chapters. Chapter II describes the goals of the state and other key stakeholders. Chapter III describes the approach that Florida took to critical issues in designing its CDC project. Chapter IV explains how Florida arranged for organizations to provide consulting services and how consulting services were organized. Chapter V explains how Florida selected a fiscal agent and how the provision of fiscal services was organized, as well as describing the organization that the state chose. Chapter VI describes outreach and enrollment for CDC and how these tasks were organized. Chapter VII discusses the development and approval of cash management plans and the uses of cash. Chapter VIII details the selection and functioning of representatives named to manage the monthly budget on behalf of consumers. Chapter IX discusses monitoring and the lack of both abuse of the monthly budget and consumer neglect and exploitation. Chapter X considers whether the demonstration was implemented as planned, summarizes lessons about the components of the program discussed in Chapters IV through VIII, and describes the lessons of the Florida experience that cut across components of the program. Finally, Chapter XI looks at Floridas plans for the future and for an ongoing Cash and Counseling program.
II. GOALS AND STAKEHOLDERS
In applying for a Cash and Counseling Demonstration grant, Floridas goals were straightforward. Because several state departments and offices and various populations were involved in the demonstration, however, there were many diverse stakeholders.
A. Floridas Goals
When Florida applied for a Cash and Counseling Demonstration grant, a key goal was to promote the independence of its citizens. In discussing the states goals, a very senior official noted that Florida values self-direction and independence and cited the states implementation of charter schools and school voucher programs as embodying that value. He also noted that Cash and Counseling is consistent with disease management programs, because these programs teach people to manage their own care.
Florida believed that empowering consumers with choice and control of their services would allow them to tailor services to better meet their needs and encourage prudent use of resources. The state was concerned that the traditional waiver programs had a canned array of services, sometimes leading to ordering of services that consumers did not need. Florida believed that customized packages that consumers themselves created would better meet consumers needs. The state also believed that consumer control would encourage efficient use of resources. Consumers would have an incentive to be prudent buyers, and they could take advantage of competition among vendors to obtain the best available prices.
As Florida began to design the CDC project, another state goal was to assess the use of counseling services instead of the case management services provided to recipients of traditional waiver services. Because case management services are more intensive, Florida believed that counseling could be less costly.
The Cash and Counseling Demonstration offered an opportunity to test, and learn from, a consumer-directed model. One state official, noting that Florida has a higher percentage of elderly people than any other state in the country, stressed the importance of finding new and better alternatives to service provision with so much at stake. For example, the state, mindful of the fact that 1915(c) waiver services are provided instead of nursing home services, wanted to test whether CDC could reduce the level of nursing home use below that experienced with waiver services. The statement of a very senior state official, presented in Case Example II.1, reflects the focus on learning from the demonstration.
Florida did not view cost saving as a goal of the demonstration. The state believed, but was not sure, that CDC would be more efficient than traditional case management services. Moreover, Florida did not want anyone to be hurt by participating in the project.
Despite a problem with access to services in rural areas (such as the states Panhandle), Florida did not enter the Cash and Counseling Demonstration with the goal of improving access to services in rural and other hard-to-serve areas. Florida did not implement the demonstration for all populations and all counties in the state. If the project was successful, however, Florida recognized that it could be expanded to serve the entire state, including rural and other hard-to-serve areas.
B. Advocates for Citizen Stakeholders
Three types of citizens had a substantial stake in the CDC project: (1) elderly beneficiaries and their families, (2) adults with physical disabilities and their families, and (3) children and adults with developmental disabilities and their families. Only the last of these three groups had historically had strong advocates.
1. Elderly and Physically Disabled Adults
For the most part, advocacy organizations for the elderly did not become stakeholders in the CDC project. In many states, Area Agencies on Aging (AAAs) are advocates for the elderly. Although a limited number of AAA staff became strong advocates for the CDC program, AAAs generally do not act as advocates for the elderly in Florida. Rather, they act as an adjunct of state and local governments. They oversee the management of local services for the elderly, including Medicaid waiver services. They contract with agencies in the communities they serve to provide services to elderly beneficiaries, and they oversee the flow of state funds for these services.
Adults with physical disabilities did not have strong advocates who became stakeholders in CDC. An official with the Office of Adult Services (AS) indicated that Florida had no strong advocacy organizations for the conditions that caused the disabilities of most of the people her office served. Nor were organizations of adults with physical disabilities active advocates for consumer-directed programs in Florida. This situation was in strong contrast to that in Arkansas, where the actions of advocates for adults with physical disabilities had focused the attention of the state government on consumer-directed models of care (see Phillips and Schneider 2002). In contrast, the impetus in Florida to develop a consumer-directed model of services seemed to flow primarily from the state governments desire to make innovative changes to serve its citizens rather than from pressure from those citizens.
2. Children and Adults with Developmental Disabilities
The families of people with developmental disabilities have a strong history of advocacy in Florida. They are organized into local support groups and a statewide organization, called the Family Care Council. Case Example II.2 describes the functions of the Family Care Councils.
In addition, individual parents are politically active. Case Example II.3 presents the comments of one CDC official on the political activism of the families of people with developmental disabilities.
C. State Stakeholders
CDC had several state stakeholders, including the governor and legislature. It also had several departments and offices within the executive branch of government.
1. Governor and Legislature
CDC was designed and implemented under two Florida governors. Both were very supportive of the Cash and Counseling model and, later, of the CDC project. The model and project were popular in Florida, especially among parents of children with developmental disabilities, and both governors benefited politically from supporting a popular project.
Floridas legislature was not involved in CDC during its design or early implementation. However, the legislature was very supportive of programs offering consumers direction of their own care. The legislature approved state funding for Choice and Control, a project offering a monthly budget to adults with developmental disabilities in some counties in the northern part of the state that were not part of the catchment area for CDC (the choice of the CDC catchment area is discussed in Chapter III). The Florida legislature also funded the state match for a Medicaid waiver for beneficiaries with brain and spinal cord injuries that was later cashed out as part of the CDC project (see Chapter XI). Finally, in spring 2002, the legislature approved a bill authorizing the state to seek waivers from CMS to provide consumer-directed care in each of the states home- and community-based waiver programs (see Chapter XI).
2. Departments and Offices
Many departments and offices in Floridas state government were involved in its Cash and Counseling Demonstration. The official host state agency (and grant recipient) for CDC was the Florida Department of Elder Affairs (DOEA). Two units in the Florida Department of Children and Families (DCF) were also involved: (1) AS, and (2) the Developmental Services Program. Later, the Developmental Services Program was renamed the Developmental Disability Program (DDP), and we refer to it by that name throughout the rest of the report. Along with DOEA, DDP was a major player in the Cash and Counseling Demonstration, but AS was not. After introducing the other offices involved in the CDC project, we consider possible explanations for the limited participation of AS.
The initial design for CDC also called for participants from the Brain and Spinal Cord Injury Program (BSCIP), administered at that time by the Florida Department of Labor and Employment Security and later by the Florida Department of Health. Because the participation of BSCIP was delayed, beneficiaries participating in the BSCIP program were not included in the evaluation. Nonetheless, the steps necessary to enable them to participate are noteworthy and are described in Chapter XI.
a. Department of Elder Affairs
From the beginning, DOEA took the lead role in the Cash and Counseling Demonstration. A senior official there was responsible for drafting much of Floridas original proposal for a Cash and Counseling grant. The director of State and Community Services within DOEA, who himself had a disability, was very supportive and involved in strategic planning for the Cash and Counseling program at critical junctures. When we interviewed him, he explained that he appreciated the dignity value of the Cash and Counseling model, which he associated with having intimate personal care done by the person of your choice.
The CDC project office was housed in DOEA. Moreover, the staff of the project office was responsible for central functions for all of the populations involved in CDC (such as maintaining the database to track participants), as well as for the design and implementation of CDC for elderly beneficiaries.
Considerable turnover occurred within DOEA, however, and this adversely affected the Cash and Counseling Demonstration. During the demonstration, three secretaries left DOEA. The senior official who was the principal author of the Cash and Counseling grant and heavily involved early in the design phase was promoted to a senior post in DDP. While he continued to be involved in CDC (primarily for the DDP population), he was no longer directly responsible for the cash program. The former CDC project manager at DOEA succeeded him as director of CDC. Some months later, however, she resigned to take a position in the private sector. Another member of the CDC project staff was promoted to replace her but resigned after several months. Implementation was delayed while Florida sought a replacement.
Finally, a strong project manager and a strong director were hired. They arrived at a difficult juncture but tackled the problems CDC faced. One consultant we interviewed praised them as addressing problems right away and working hard to find a solution and then to implement it. Others involved with CDC credited this team, particularly the director of CDC, with rescuing the Cash and Counseling program in Florida.
b. Developmental Disabilities Program
The DDP program in DCF strongly supported the CDC demonstration. As noted earlier, an official in the department had been responsible for CDC in his former position within DOEA. DCF devoted substantial departmental resources to the CDC project. As the lead agency, DOEA received the grant for the CDC project. Given the diverse populations covered in Florida, however, the grant funds were not sufficient to staff the project. In response, DCF assigned four of its DDP staff (who were paid with state funds) to spend much or all of their time on the CDC project, putting their other responsibilities on the back burner. The four included a senior official who directed CDC for DDP.
c. Office of Adult Services
Floridas initial design for the CDC demonstration called for the participation of more than 400 adults with physical disabilities; however, fewer than 50 participated. Several factors seem to explain why AS was not fully engaged in the demonstration. The structure and reporting relationships of the state departments and units involved appear to have played an important role. AS was housed in DCF. However, because DOEA had once been responsible for the waiver for adults with physical disabilities that was being cashed out, AS activities for the CDC project were coordinated with those of DOEA (rather than DCF).9 Senior AS staff reported that they perceived their unit as an afterthought and the low man on the totem pole for DOEA attention. They cited as examples the fact that AS was not notified about some training sessions for consultants and that no dedicated staff were hired for outreach and enrollment of adults with physical disabilities, as was true both for the elderly and for children and adults with developmental disabilities.
The fact that AS is a small, understaffed office with few resources also helps explain the limited participation of adults with physical disabilities in CDC. The initial design for CDC called for the state to contract with nonprofit agencies to provide consulting services. AS staff supported this design, believing that it would reduce the caseloads of their case managers, which were already high. However, before implementation began, the state decided to work through the existing networks of agencies providing case management. Florida provides AS services out of district offices, and an AS district supervisor reported that he was advised that his office would be required to justify its position if it withdrew from CDC in response to this change in structure. This supervisor also said that he nevertheless had hoped that his district could benefit from CDC participation by using the payments it received for providing CDC counseling to help offset a deficit in its traditional waiver programs. Seeming to echo the statement that AS was treated as an afterthought, he also said that there had been confusion in developing a mechanism for the transfer of funds from one state office to another. At the time of our visit (when CDC had been operating for more than 18 months), he was not sure that his district had ever been compensated for the CDC consulting it had provided.
Because so few adults with physical disabilities participated in the CDC demonstration, we concentrated the resources for this analysis on the elderly and children and adults with developmental disabilities. Thus, this report does not include a detailed discussion of the operation of CDC for adults with physical disabilities.
3. Coordinating the Work of Multiple Offices and Departments
As work continued on designing the CDC demonstration, Florida expected to cash out the waiver services of participants in several Medicaid programs: one for elderly beneficiaries, one for adults with physical disabilities, and one for children and adults with developmental disabilities. In addition, Florida hoped to cash out services for beneficiaries with brain and spinal cord injuries. These programs were run by four offices--DOEA, AS/DCF, DDP/DCF, and BSCIP--in three departments of state government. It would be a major task to implement a common program despite differences in departmental procedures and coordinate the efforts of all these offices and departments.
In addition, Floridas Agency for Health Care Administration (AHCA) was a key stakeholder. As the states Medicaid agency, AHCA prepared the application for the demonstration Section 1115 waiver and submitted it to CMS. AHCA was also responsible for ensuring that the terms and conditions of the Section 1115 waiver were met, including the requirement that CDC be budget neutral (that is, cost no more per recipient per month than traditional waiver services) over the life of the five-year demonstration.
a. Interdepartmental Work Group
To coordinate the activities of the departments and offices involved in CDC, Florida established an interdepartmental work group, with representatives from DOEA, DDP/DCF, AS/DCF, BSCIP, and AHCA. The work group was actively involved in the design of the CDC project and continued to meet periodically throughout the demonstration.
b. Advantages and Disadvantages of Having Several Departments and Offices
Having several departments of state government participating in the CDC demonstration had both advantages and disadvantages. Senior state and project officials cited two major advantages of interdepartmental collaboration. First, because the populations served by the various waivers had many similarities, staff from different departments learned from one another. One senior official commented, I believe having the project integrated across all programs has been a strength. We have all learned from each other. Second, senior staff noted that having an umbrella organization at the top made the demonstration more efficient. For example, departments shared development costs and portions of the project data system.
On the other hand, project managers and staff responsible for day-to-day coordination across departments and offices were more likely to view interdepartmental collaboration as disadvantageous. While acknowledging the basic similarities in the populations, they also noted differences, such as greater need for behavioral and medical services among those with developmental disabilities than among the elderly. They also recalled their struggle to develop CDC project procedures that were consistent with the procedures of multiple departments and noted the increased complexity in CDC procedures that arose when consistency proved unworkable. Different procedures were adopted for important aspects of the project, such as the discount rate, consultant training, review of purchasing plans, and payment for consulting. One member of the CDC state staff summed it up as follows: CDC is a complex project with many details; it is hard to keep the procedures straight, and this is made more difficult by the differences between populations and departments. The standing joke was that the departments were joined at the top of the head. Finally, it is noteworthy that one office, AS/DCF, felt that its program and population were not well integrated into CDC.
At time of our visit early in 2002, Florida expected that the consumer-directed programs of the various offices and departments would be fully differentiated under the new ongoing state program. As of this writing, however, an integrated program is planned.
D. Organizational Stakeholders
The organizations providing traditional Medicaid services were stakeholders in the CDC project. No unions were stakeholders in the CDC project; home care workers in Florida are not unionized.
1. Area Agencies on Aging and Case Management Agencies
AAAs are mandated by the Older Americans Act. As noted earlier, DOEA contracts with Floridas AAAs for the provision of Medicaid waiver services to the elderly. Florida has 11 AAAs, and each serves a different region of the state. In each county, one AAA contracts with one lead agency to provide case management services to elderly Medicaid beneficiaries in that county. The lead agencies typically operated under public auspices (such as a county department of social services) and were responsible for all case management in the area they served. The lead agency could subcontract with other vendors to provide other Medicaid waiver services or supply these services directly, but the former was more common.
A case manager had several major responsibilities under the Medicaid waiver. The case manager assessed the consumers disabilities and prepared a care plan. He or she arranged for the provision of the services called for in the care plan. If problems arose with the service (such as the failure of an aide to come as scheduled), the consumer notified the case manager, who then contacted the vendor on behalf of the consumer.
a. Traditional Case Management Agency Concerns About CDC
The lead agencies and their case managers had several concerns about the Cash and Counseling model. First, they were concerned that funding for the lead agency would be cut. This fear was exacerbated because Florida was initially trying to carve out money for CDC activities at a given agency from funds earmarked for the home- and community-based waiver at that agency. The state seemed to be telling the lead agencies, Well take the money back and manage it for you. (Later, Florida took a different approach, arguing that the money followed the consumer but that the lead agencies still managed the funds.)
Lead agencies and case managers were also concerned that additional responsibilities were being thrust upon them with no additional compensation. Although outreach and enrollment (including looking up the information needed to calculate the amount of the monthly budget) for all prospective recipients was time-consuming, the state provided no increase in compensation for case managers or lead agencies to cover these costs.
Lead agencies and case managers were also worried that they could be held liable for poor outcomes arising from consumer decisions. One lead agency refused to participate in CDC due to concerns about its liability. It had recently settled a case in which it was sued when a known con artist had an accident when working as an aide.
Some case managers thought they might lose their jobs if there was no longer a need for case managers to assist the elderly, who would be directing their own care under CDC. Moreover, some tended to resist the philosophy of consumer direction, often seeing their value as diminished in a consumer-directed model of care.
While other case managers became enthusiastic about CDC, many genuinely believed that a cash program was not appropriate for most of their clients. (At the same time, they admitted that there were a few complainers they would prefer not to work with). Case managers were concerned that consumers would be exploited because they might hire a family member who would not do the work agreed upon. Case managers also were worried that consumers would be liable if a worker was hurt on the job and that consumers would not be able to bear this liability. (In Florida, workers compensation insurance is not required if an employer has no more than three employees.) A common view among case managers was, Elderly people cant do this. You guys in Tallahassee dont know anything.
b. Vendor Concerns About CDC
In contrast to the lead agencies themselves, vendors under contract to lead agencies were generally not opposed to CDC. Some vendors were concerned that they could lose revenue if consumers hired workers directly. However, they also realized that consumers could purchase services directly from vendors (as some did).
2. District Offices and Support Coordination Agencies and Contractors
Florida certifies professionals to provide support coordination for beneficiaries with developmental disabilities. Support coordinators are employed by agencies (typically proprietary firms), or they operate as independent contractors. Many support coordinators serve populous areas of the state, and consumers in those areas may choose a support coordinator with whom they are comfortable. Support coordinators develop care plans for their clients, arrange with other vendors to provide the services called for in the care plans, and monitor the provision of those services.
Initially, support coordination agencies and contractors seemed to ignore CDC. Just before CDC began, the state legislature appropriated additional funds for services to those with developmental disabilities, and the care plan of every recipient of waiver services had to be revised to incorporate the additional funding. For some months, support coordinators were overwhelmed with this responsibility and could not turn their attention promptly to CDC.
DDP/DCF employees working out of state district offices supervise the work of the support coordination agencies and contractors. District offices have a more active role in support coordination (for those with developmental disabilities) than do AAAs in case management (for elderly beneficiaries).
E. Summary: Multiple Layers of Many Stakeholders
As CDC began, Florida faced a complex situation with many stakeholders and the involvement of several levels of organizations. First, several state-level offices and departments were participating in CDC. They served populations with needs that were similar in many ways but different in others. Second, AAAs and state DDP staff in regional-level district offices each had some budgetary and managerial responsibilities for CDC, but their responsibilities differed. Third, a lead agency in each county provided case management to elderly beneficiaries. In contrast, in many areas of the state, several support coordinator agencies and independent contractors provided support coordination to those with developmental disabilities. Finally, vendors serving elderly beneficiaries operated under subcontracts to the lead agencies, while vendors serving beneficiaries with development disabilities operated independently of support coordination agencies and contractors.
III. DESIGNING THE CONSUMER-DIRECTED CARE PROGRAM
Decisions of the funders (RWJF and DHHS/ASPE) and federal law and regulations (including the terms and conditions of the demonstration waivers) set the basic parameters for the Cash and Counseling Demonstration. Within these parameters, Florida made the decisions that shaped the CDC program. These decisions were influenced by the experience of other consumer-directed programs and shaped by the work of the Cash and Counseling National Program Office. Many decisions were made jointly with other Cash and Counseling programs.
The Department of Elder Affairs (DOEA) and the Department of Children and Families (DCF) made program design decisions jointly, often working through the interdepartmental work group. The programs for elderly beneficiaries and beneficiaries with developmental disabilities were designed to be as similar as possible, consistent with the differing needs of the populations, the differences in the traditional programs serving them, and the differences in departmental procedures.
Most of Floridas decisions were made during the design phase of the Cash and Counseling Demonstration--that is, beginning in early 1997 (when RWJF provided the funding for Florida to design its program) through summer 1999 (when CMS completed a readiness review for all components of CDC except fiscal services). Enrollment was delayed until spring 2000, however, primarily due to difficulty in soliciting a fiscal agent and negotiating a contract with the agent. Table III.1 lists key dates for the design phase and first months of implementation of CDC.
The design decisions that Florida made involved all the major components of the Cash and Counseling model: eligibility and appropriateness, outreach and enrollment, services the monthly budget would cover, determination of the level of the cash benefit, and consulting and fiscal services.
A. Which Programs and Services to Cash Out?
The solicitation for the Cash and Counseling Demonstration permitted states to cash out either Medicaid state plan personal care services or Medicaid home- and community-based services. Cashing out state plan personal services was not an option in Florida, since personal care is not included in its state plan. The state offered Medicaid personal care services only under various home- and community-based services waivers, each of which served a different population.10 Florida had to decide which of its Medicaid waivers to cash out and whether to do so statewide or in only part of the state.
| TABLE III.1. Key Dates in Design and Early Operation of the CDC Project in Florida | |
| Datea | Event |
| February 1996 | Florida submitted a proposal to RWJF |
| January 1997 | Florida funded to design its program |
| October 1998 | CMS approves waiver for Cash and Counseling Demonstration |
| March 1999 | Finalists for fiscal agent chosen |
| May 1999 | First training session for consultants |
| June 1999 | First bids for fiscal agent dismissed due to flaw in the solicitation |
| June 1999 | Florida passes CMS readiness review for all components of CDC except fiscal services |
| December 1999 | Contract signed with the fiscal agent |
| January 2000 | CMS readiness review for fiscal services |
| March 2000 | Enrollment activities start in three counties |
| May 2000 | First random assignment |
| June 2000 | Enrollment begins in remaining counties |
| August 2000 | First monthly payments made |
| September 2000 | First population-specific training |
| October 2000 | First dedicated enrollment specialists hired |
| October 2000 | First letter from governor to recipients of waiver services |
| |
Each of Floridas Medicaid home- and community-based waivers covers a variety of goods and services, ranging from personal care supplies, to personal care, to professional services such as behavioral therapy and nursing. Florida also had to decide which of the services covered by a given waiver it was going to cash out.
1. Aged and Disabled Waivers
The Medicaid Aged and Disabled Waiver Program serves elderly beneficiaries (age 60 and older) and nonelderly adults with physical disabilities (younger than age 60) under two separate waivers.11 DOEA administers the Aged and Disabled Waiver Program for the elderly, and the Office of Adult Services (AS)/DCF administers the Aged and Disabled Waiver Program for nonelderly adults with physical disabilities. As work began on the design of the CDC demonstration, about 11,000 elderly beneficiaries and about 1,600 nonelderly adults were being served each year under the Aged and Disabled Waiver in the state of Florida.12
All of Floridas Medicaid waivers operate under Section 1915(c) of the federal Medicaid regulations, which requires that the recipients meet the states criteria for nursing home care (as determined by Floridas nursing home preadmission screening program). To be eligible for the Aged and Disabled Waiver Program, beneficiaries also have to meet functional eligibility criteria. Specifically, they have to meet at least one of the following criteria: (1) substantial impairment in at least one activity of daily living (ADL); (2) absence of regular or adequate assistance with ADLs; and (3) physical disability that placed the beneficiary at risk for abuse, neglect, or exploitation. Recipients of services under the Aged and Disabled Waiver receive annual functional assessments, and their care plans are reviewed semiannually (more often if events warrant--for example, if the beneficiarys condition deteriorates).
A variety of services are available under the Aged and Disabled Waiver Program. These include case management, homemaker services, personal assistance services, respite, adult day health care, environmental modifications, chore services, personal emergency response systems, consumable medical supplies, counseling, health risk management assessment, home-delivered meals, and caregiver training and support. The same services are available to both elderly and nonelderly beneficiaries under the Aged and Disabled Waiver Program.
Florida decided to cash out the Aged and Disabled Waiver Program in 19 counties. As Figure III.1 illustrates, these 19 counties cover the central and southern portions of the state, with the primary exception being the sparsely populated inland counties.13 Florida wanted a more compact catchment area for the CDC program than the entire state offered. At the same time, a populous catchment area was needed to meet the sample size targets for the evaluation. The 19-county area was relatively compact and included such major metropolitan areas as Fort Lauderdale, Miami, Palm Beach, Orlando, Sarasota, St. Petersburg, and Tampa.
Florida decided to cash out all the services under the Aged and Disabled Waiver, except for case management. The state decided that the funding that would have covered the cost of case management in the traditional program would be used to cover the cost of consultants under CDC and that the state would pay for consultant services directly. Case management agencies, support coordination agencies, and independent contractors would bill the Medicaid program for the CDC consulting services they provided.
| FIGURE III.1. Consumer Directed Care Demonstration: Geographic Implementation for Elders and Adults |
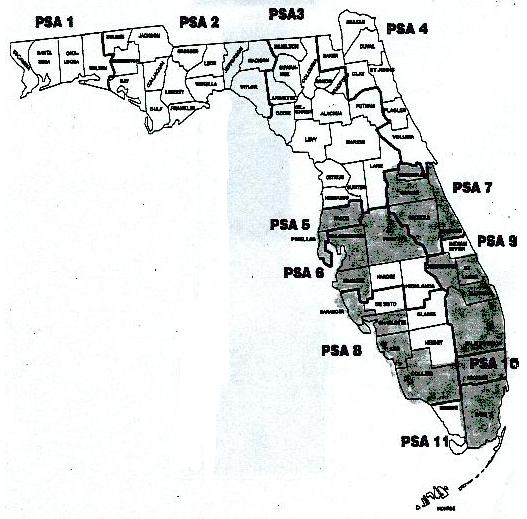 |
An alternative approach would have been for Florida to cash out case management services, and then require consumers to pay their consultants from their monthly budgets. One problem with this approach is that consumers may resent being required to pay for mandatory consulting services and may not wish to incur expense for voluntary consulting services even though they could benefit from them. In addition, Florida had decided to ask existing case management agencies to provide consulting to CDC participants. These agencies already invoiced the Medicaid program for the case management services they rendered. It would be much easier for a case management agency to invoice the state for CDC consulting services rendered by its employees than to invoice each consumer who chose to purchase consulting services with the monthly budget.
2. Developmental Services Waiver
The Medicaid Developmental Services Waiver Program serves children (3 to 17 years old) and adults with developmental disabilities (age 18 or older). The Developmental Disability Program (DDP)/DCF administers the waiver for both children and adults. As work began on the design of the demonstration, about 600 children were receiving services under this waiver. About another 3,300 children were enrolled in a state-funded program; Florida planned to channel participants in the state program into the Medicaid waiver program provided they met the waiver requirements. Overall, Florida estimated that about 3,000 children statewide met the waiver requirements. As work began on the design of the demonstration, about 7,500 adults were receiving services under the Developmental Services Waiver or were on the waiting list for this waiver. Shortly thereafter, the Florida legislature increased the funding for the state share of costs for the Developmental Services Waiver; the number of program slots was increased, and beneficiaries were moved off the waiting list.
To be eligible for the Developmental Services Waiver, children and adults must meet the criteria for Intermediate Care Facility/Developmental Disabilities (ICF/DD) care. These criteria include a diagnosis of autism, cerebral palsy, mental retardation, Prader-Willi syndrome, or spina bifida. In addition to having been diagnosed with one of these conditions, other impairments are required to be eligible for an ICF/DD level of care. To be eligible, a person has to have an intelligence quotient of 59 or less, an intelligence quotient between 60 and 69 with a secondary disabling condition, or three severe functional limitations in major life activities (self-care, understanding and use of language, learning, mobility, self-direction, or capacity for independent living). Both adults and children are assessed only once--when they enter the Developmental Services Waiver. Their support coordinators review their support plans annually (more often if events warrant).
Children receiving services under the Developmental Services Waiver live with their parents or legal guardians and attend public school programs. Adults live independently, with family, or in supported-living programs, such as those provided in group homes.
A variety of services are provided under the Developmental Services Waiver. These include support coordination, homemaker services, chore services, companion services, respite care, transportation, personal assistance, consumable medical supplies, adaptive equipment, environmental modifications, and training and therapy services (for example, speech, occupational, physical, and behavioral therapy). The same services are available to both children and adults with developmental disabilities.
To meet the evaluation target sample size for children (1,550), given a population of about 3,000 eligible children statewide, Florida decided to cash out the Developmental Services Waiver for children across the state.
Florida initially decided to cash out the developmental services waiver for adults only in the 19 counties in which the Aged and Disabled Waiver was being cashed out. Nonelderly adults with physical and developmental disabilities were to be combined in the evaluation analyses, and the population of nonelderly waiver recipients in the 19-county area was expected to be large enough to yield the target sample of nonelderly adults. Later, Florida expanded the CDC demonstration to serve adults with developmental disabilities in all counties in the state, except the counties in the northern portion of the state in which Choice and Control, a small, state-funded program, already offered a monthly budget instead of Medicaid waiver services. After enrollment for the Cash and Counseling Evaluation had been completed, Florida received approval from CMS to roll Choice and Control participants into CDC.
As for case management under the Aged and Disabled Waiver, Florida decided to cash out all the services under the Developmental Services Waiver except for support coordination. Funding that would have covered the cost of support coordination in the traditional program was used to cover the cost of consultants under CDC. Florida planned to ask support coordination agencies and independent support coordination contractors to provide CDC consulting. These agencies and independent contractors were to invoice the state directly. As for case management agencies, having these agencies and contractors invoice the state was much more straightforward than cashing out support coordination services and asking agencies and contractors to invoice individual consumers for CDC consulting services rendered.
By cashing out professional and clinical services such as speech therapy, behavioral therapy, and nursing under its Developmental Services Waiver, Florida was implicitly allowing consumers or their representatives, rather than medical professionals, to determine whether, and in what amount, these services were needed. This issue did not arise to the same extent in the Aged and Disabled Waiver, as most of the services covered under that waiver pertain to personal care. It did not arise in the other two Cash and Counseling states because both Arkansas and New Jersey cashed out only personal care services.
B. Eligibility, Appropriateness, Outreach, and Enrollment
Given the decision to cash out its Aged and Disabled Waiver and Developmental Services Waiver in all or part of the state, Florida needed to decide which, if any, Medicaid beneficiaries eligible for those waivers would be eligible for CDC. It also had to decide whether any of those eligible would be inappropriate for CDC (which could depend on whether they had appropriate people willing to serve as their representatives and manage the monthly budget on their behalf or help them do so). In addition, it had to decide how to identify those who were eligible but inappropriate so they could be excluded. Finally, because any new program in Florida must be presented to those who are eligible and who may be interested in enrolling, Florida had to decide how to present the CDC program to those who were eligible.
1. Eligibility
Florida decided that only service recipients under the Aged and Disabled Waiver and Developmental Services Waiver would be eligible to enroll in CDC. As work on the demonstration design began, there were Medicaid beneficiaries in state-funded programs who met the eligibility criteria for waiver services. Florida wanted to expand the use of Medicaid services for these individuals, thereby saving state funds for those who were not eligible for Medicaid services. However, rather than allowing these beneficiaries and others who were eligible for these waivers to move directly into CDC, Florida limited enrollment in CDC to those already receiving waiver services. It provided no way for those who were not already receiving waiver services to enroll directly in CDC, and it focused its outreach on waiver service recipients.
Floridas eligibility policy for CDC blunted the possibility of induced demand. Some beneficiaries might have enrolled in a waiver program, intending to move to the CDC program as soon as possible. However, prohibiting direct enrollment in the CDC program reduced the likelihood that demand for services would increase because beneficiaries who were not interested in traditional agency services found the CDC program attractive. While Florida could theoretically control induced demand by limiting the number of slots in its waiver programs, that approach left the state subject to political pressure to expand the number of program slots.14
2. Appropriateness
Florida decided against adopting a structured screening process to identify those appropriate for CDC (or who had appropriate representatives). This decision was consistent with Floridas goal of adopting an expansive policy in order to learn from the demonstration--CDC was an opportunity to learn for whom a program paying a monthly budget was most appropriate. In addition, this decision is a good example of the work of the National Program Office and the collaboration of the three Cash and Counseling states during the design phase of the demonstration. All three demonstration states were concerned about the feasibility of developing a valid process to screen for appropriateness. The National Program Office for Cash and Counseling formed a task force on screening. While deliberations on screening were under way, an attorney on Arkansass advisory council said that a structured process that denied participation might not be legally defensible. If the process was not legally defensible, and a consumer chose to contest exclusion from the program, a state might be held liable. In light of potential liability, and mindful that a structured screening process was inconsistent with the philosophy of consumer direction, all three demonstration states decided against implementing any structured formal screening criteria. Instead, as the other two states did in their Cash and Counseling demonstrations, Florida explained the rights and responsibilities of consumers and representatives under CDC to prospective participants and their families and allowed them to decide whether to try it. The state also decided that representatives were not to be paid for helping consumers manage the monthly budget.
3. Outreach and Enrollment
Floridas initial plan was to rely on the case management agencies (for the elderly) and the support coordination agencies and contractors (for those with developmental disabilities) to present the program to Medicaid waiver service recipients. Relying on existing agencies was an obvious approach to outreach. Florida already had a policy of presenting all new services and programs to all current recipients, so outreach for CDC would follow the established policy. Case managers and support coordinators would present the new program to waiver recipients when they saw their clients at their established monthly visits, just as they presented other new programs during these visits. The initial idea was to have the case managers and support coordinators give out brochures about CDC, with a tear-out postcard for consumers to send in if they wanted someone from CDC to call with more information. Later, Florida decided to have case managers and support coordinators trained as CDC consultants to complete the enrollment of the waiver service recipients interested in participating in the demonstration. Making these consultants responsible for enrollment had an added advantage in that they had ready access to beneficiaries care plans (as case managers for elderly beneficiaries) or support plans (as support coordinators for those with developmental disabilities). This access was advantageous because information from care/support plans would be needed to calculate the amount of the monthly budget for those interested in CDC. For reasons discussed in Chapter VI, however, this initial approach to outreach and enrollment was not successful, and Florida later hired temporary state employees to conduct outreach and enrollment for all populations of waiver service recipients.
C. Consulting Services
In designing CDC, Florida faced several major issues concerning consulting services. It had to decide what consulting services would be offered and how they would be organized and paid for.
1. Organization of Consulting Services
Florida decided to ask case managers to provide consulting for elderly and physically disabled adults who enrolled in CDC and to ask support coordinators to provide consulting for children and adults with developmental disabilities who enrolled in the program. The availability of funding was a major consideration in this decision. State funds were already committed for the payment of case management agencies, support coordination agencies, and contractors for the provision of services to Medicaid waiver service recipients. Diverting these funds to pay other entities to provide consulting under CDC would be a difficult political undertaking. Case Example III.1 presents the comments of one senior state official on this issue and shows the importance of funding in the decision to rely on existing networks to provide consulting services for CDC.
Florida also believed that reliance on the existing networks would be beneficial to consumers, for two reasons. First, case managers and support coordinators were already knowledgeable about Medicaid waiver services and community resources. CDC program staff wanted them to pass on their knowledge to consumers as they worked together to develop a purchasing plan. Second, reliance on the existing networks would allow for continuity. Initially, Florida anticipated that most consumers enrolled in CDC would have as a consultant the person who had served as their case manager or support coordinator. That person was already familiar with their situation, and presumably had the consumers trust. In addition, continuity of service would not be disrupted if the consumer decided to drop out of CDC and go back to the traditional waiver program.
The implication of providing continuity of service was that case managers and support coordinators would continue to provide traditional services to some clients at the same time that they provided CDC consulting to others. Thus, case managers and support coordinators would be providing CDC consulting part-time, and case management and support coordination agencies would have several staff members working with CDC consumers. For reasons explained in Chapter IV, this model of organization of consulting services was replaced by a model in which only one or two case managers (or support coordinators) per agency were responsible for CDC consulting.
2. Consulting Services
In designing the CDC project, Florida had to decide which aspects of consulting would be mandatory and which ones consumers might choose at their discretion.
a. Mandatory and Discretionary Consulting Services
Florida decided three aspects of consulting would be mandatory. First, all consumers were to receive consultant assistance with the development of the initial purchasing plan. This assistance was to include a home visit. Consultant review of the initial purchasing plan and all subsequent revisions to the purchasing plan were also mandatory. (We discuss procedures for review of purchasing plans in Section D.) Second, monthly monitoring telephone calls from the consultant to the consumer or representative and monitoring visits in the 2nd and 12th month after the consumers enrollment in CDC were also mandatory. Third, consultants were to monitor the receipts that consumers were required to retain for purchases made with cash received from the monthly budget. (We discuss the requirement for receipts further in Section F.1.)
To make consumers as independent as possible, Florida developed a consumer handbook (called the Consumer Notebook). Nonetheless, consultants were available to assist consumers by providing advice on recruiting and hiring and making suggestions about community programs and vendors. Consultants might also contact others (for example, the fiscal agent or the state CDC program office) on the consumers behalf. However, consumers were expected to take responsibility for most such contacts.
b. Reassessment and Care/Support Plan Review
Florida decided to make consultants responsible for reassessments and reviews of care plans (for elderly beneficiaries) and to make support coordinators responsible for reviews of support plans (for those with developmental disabilities). In the traditional waiver program, case managers and support coordinators are responsible for these tasks.
Differences in the reassessment and review procedures for CDC and the traditional program are of potential policy interest because such differences can lead to systematic increases in the care/support plan hours or services for cash recipients and thus increases in the cost of the cash program relative to that of the traditional program. Differences in reassessment and review procedures can arise if case managers or support coordinators in the traditional programs scale back care/support plan hours because a scarcity of funding or of labor limits the number of hours of direct services their agencies can supply. Such differences can also arise if consultants assume the role of advocates to a greater extent than do case managers or support coordinators in the traditional program.
Several factors, however, limited the potential for such differences in reassessment and review procedures in Florida. First, the same standard forms and procedures were used for reassessment and review for CDC consumers as for waiver recipients in the traditional programs. Second, CDC consultants continued to provide case management or support coordination services to other beneficiaries, increasing the likelihood that the reassessment and review procedures would be implemented in the same way for participants in both CDC and the traditional program. Third, if there was a difference in the extent to which consultants (on one hand) and case managers and support coordinators (on the other) acted as advocates, it seems likely that the difference would not favor CDC consumers. The central role of case managers and support coordinators is to assist beneficiaries; in contrast, the central role of CDC consultants is to train and advise consumers. Finally, case managers and support coordinators would rarely, if ever, have had a vested interest in the amount of direct services provided in the care plan. (Recall that few lead agencies provided direct services themselves and that no support coordination agencies did so.)
c. Other Services from Consulting Agencies
Florida did not require consulting agencies to provide CDC consumers with other services, such as worker registries, peer support, or back-up workers. Such requirements would have been difficult to implement. The CDC caseload was to be spread across many agencies and contractors, and none was likely to reach a CDC consulting caseload large enough to support the provision of special services for consumers.
3. Payment for Consulting Services
As noted earlier, reliance on the existing funding streams was a major factor underlying Floridas decision to ask the existing network of case management agencies, support coordination agencies, and contractors to provide CDC consulting. For those with developmental disabilities, the method and rate of payment for Medicaid waiver services was applied unchanged to CDC consulting services. At the time of our visit to Florida, support coordinator agencies and contractors were paid $148.39 a month under each program for each beneficiary on their caseloads. The monthly payment to consultants for those with developmental disabilities began as soon as they were assigned a CDC case.
For elderly consumers, the payment method differed for case management and CDC consulting. Florida paid agencies a separate, fixed payment for each consultant home visit made to teach the consumer how to develop the purchasing plan. The number of such visits was capped at two for each consumer; the payment for the first training visit was $125, and the payment for a subsequent training visit (if any) was $75. After the completion of the purchasing plan, case management agencies were paid an hourly rate for the provision of consulting services. This hourly rate was the same as the hourly rate the state paid that agency for case management services (these hourly rates were agency- specific). The quarterly average payment per consumer was capped at the historical average of quarterly payments per client for case management services at that agency.
D. The Monthly Budget
Florida had to decide how it would determine the value of the monthly budget. It also had to decide whether it would discount the monthly budget to take into account the fact that some portion of the goods and services in a traditional care/support plan are not delivered.
1. Determining the Value of the Monthly Budget
In cash programs, the level of the monthly budget may vary, depending on the consumers history of benefits in the traditional program or the consumers level of need (or a related concept, such as disability). There are two major problems with basing the level of the budget on the historical benefit level rather than on need. First, the beneficiarys condition or situation can change, perhaps dramatically--in such cases, the historical level of benefits may be inadequate. Second, those who have been enrolled in the traditional program for only a short time (or not at all) will not have a sufficient track record of historical benefits on which to base the amount of the budget.
Initially, Florida decided to base the amount of the monthly budget either on the beneficiarys waiver claims history or on his or her care/support plan for waiver services. Floridas preferred way to determine the amount of the monthly budget was to base it on claims history. When waiver claims expenditures were available for at least the past six months, Florida planned to calculate the monthly average of those expenditures. The only exception was to be when the beneficiarys condition or situation had changed recently; in that case, Florida planned to base the amount of the monthly budget on the waiver service care/support plan.
When implementation of CDC began, however, all consumers with developmental disabilities had experienced a recent change in their support plans due to the legislative increase in funding for this program. Floridas initial plan to use claims to determine the amount of the monthly budget was never implemented for those with developmental disabilities.
In addition, even if an elderly and physically disabled beneficiary had a stable claims history, in practice, the amount of the monthly budget was based on the care plan when that amount exceeded the average of the monthly waiver expenditures by more than $50. The amount of the benefit was determined both from claims and from care/support plans, to assess whether there had been a material change in the beneficiarys condition or situation. Usually, the cost of the care/support plan was readily available from an associated cost plan. If not, it was calculated based on the units of services in the care plan and the unit cost for the vendor specified in the care plan.
2. Discounting
When the amount of the monthly budget is to be based on care/support plans, a major issue that arises is the potential for differences between the value of the goods and services included in the plan and the value of the goods and services actually delivered.
The issue commonly arises for hours of service. The hours of service delivered usually do not exceed the number planned, since the care/support plan typically represents the maximum authorized. Rather, the number of hours of care received is often less than the hours planned, for several reasons. Agencies may plan for more care than they expect to provide so they can increase the amount, if necessary, without revising the care/support plan. More frequently, all planned hours of care may not be used because of unforeseen events. A client may be unexpectedly hospitalized and thus not be home when a therapist arrives. A homemaker may not appear for work when expected. An agency may be unable to find enough workers to provide the planned care. If a worker shortage is prolonged, an agency may reduce plan hours to lessen consumer expectations. CDC program staff believed that waiver services care/support plan hours were sometimes reduced for this reason, especially for beneficiaries living in rural areas of Florida.
Differences can also arise between the cost of goods planned and received. For example, a beneficiary might have a support plan calling for disposable medical supplies, such as diapers. If the beneficiary was hospitalized, and the hospital provided disposable medical supplies during the inpatient stay, that beneficiary might not purchase all the supplies in the plan.
When the average cost of the goods and services in the care/support plan exceeds the average cost of those actually received, a discount rate may be required to ensure budget neutrality. That is, in calculating the monthly budget, it may be necessary to discount the cost of the goods and services in the care/support plan to ensure that the cost of the cash program does not exceed the cost of the traditional program. As noted in Chapter I, such budget neutrality was a condition of the Cash and Counseling Demonstration waivers.
To assess the need for a discount rate, Florida collected information on care/support plan goods and services for historical samples of waiver clients. Separate samples were collected for (1) elderly recipients of Aged and Disabled Waiver services, (2) adults with physical disabilities who were recipients of Aged and Disabled Waiver services, and (3) children and adults who were recipients of Developmental Disability Waiver services. For each sample, the cost of the goods and services planned (at the relevant vendor-specific rates) was compared to actual expenditures for the period covered by the care/support plan as indicated by Medicaid claims. Florida determined that the cost of goods and services planned did exceed the cost of goods and services received and adopted discount rates of 89 percent for elderly beneficiaries, 83 percent for adults with physical disabilities, and 92 percent for children and adults with developmental disabilities.
About the time of our visit, the average monthly budget (after discounting) in Florida was $975 for elderly adults and adults with physical disabilities and $1,825 for children and adults with developmental disabilities.
E. Purchasing Plan and Uses of the Monthly Budget
The solicitation for the Cash and Counseling Demonstration did not envision that a state would provide unfettered cash, as in an income supplement program. However, it insisted that states permit the monthly budget to cover a range of goods and services that would help consumers function more independently. Two key issues that arose in designing the Cash and Counseling Demonstration were (1) how much flexibility would be permitted with respect to purchases, and (2) procedures for review of the purchasing plans.
1. Flexibility in Purchasing
Arguably, Florida gave the consumer more flexibility in purchasing than the other two Cash and Counseling states. First, Florida permitted consumers to receive a larger portion of the monthly budget in cash for purchases not amenable to invoicing (such as taxi fare or payment to a neighbor for lawn care), provided the purchases were specified in the purchasing plan. While Arkansas and New Jersey allowed consumers to receive up to 10 percent of the value of the monthly budget in cash for incidental expenses, Florida allowed them to receive up to 20 percent in cash (or more with special approval).15 Consumers could provide for the cash payments in their purchasing plans, or they could request an ad hoc cash payment from the fiscal agent up to two times a month.
Florida exercised the Cash and Counseling Demonstration waiver to allow legally liable relatives (spouses and parents of minors) to be hired as workers. Florida also allowed the same person to be both a (nonpaid) representative and a (paid) worker. Arkansas chose not to exercise the waiver on legally liable relatives, and relatively few married consumers enrolled in the Cash and Counseling program in New Jersey. Thus, Florida is the only Cash and Counseling state with substantial experience in paying legally liable relatives as workers. Florida is also the only one of the three states that allowed the same person to be both a representative and a worker.
In addition, CDC allowed consumers some discretion with respect to purchases covered by the plan, as long as the purchases related to the needs the plan identified. This procedure was intended to provide consumers with the flexibility to take advantage of sale prices for goods. For example, consumers were to be given flexibility to purchase extra amounts of diapers without preapproval if a store was offering them at a particularly good price. The other two Cash and Counseling states did not allow the consumer this type of flexibility.
2. Review of the Purchasing Plan
Approval of the purchasing plan is a critical step toward ensuring that the monthly budget will not be abused through the purchase of goods and services that are not permissible. Florida required all consumers to have an approved purchasing plan before receiving the monthly budget. Approval was also required for a formal revision of the purchasing plan.
Florida required that consultants review the purchasing plan, sign off on it, and forward it to the state CDC program office at DOEA (for elderly beneficiaries and adults with physical disabilities) or to the district office of DDP/DCF (for those with developmental disabilities) for review. Following approval by the CDC program office or the district office, a copy of the purchasing plan was sent to the fiscal agent so that the consumers account could be established or revised.
F. Fiscal Services
As for consulting services, Florida had to decide which fiscal services would be offered to CDC consumers and which would be mandatory. It also had to decide how these services would be organized and paid for.
1. Mandatory and Discretionary Fiscal Services
The solicitation for the Cash and Counseling Demonstration envisioned that consumers could choose to manage the monthly budget entirely on their own. In conjunction with Arkansas and New Jersey, Florida decided that consumers would be allowed to do so if they demonstrated that they could carry out the fiscal responsibilities of an employer. Both Florida and New Jersey required that consumers pass a skills examination prepared by the Cash and Counseling National Program Office to show they could manage these responsibilities. (Arkansas assessed consumer ability to manage the monthly budget but did not require an examination.)
Florida required that all recipients of the CDC monthly budget use some fiscal services. Consumers who did not choose to take (or did not pass) the skills examination had to use the fiscal agent to process payroll documents and cut checks. A consumer who passed the skills examination was required to obtain a monthly desk audit of his or her CDC account from the fiscal agent.
Florida also required consumers to retain receipts in two circumstances. First, consumers who managed the monthly budget entirely on their own had to retain receipts for review during the desk audit. Second, consumers who received part of their monthly budget in cash had to retain receipts for cash purchases.
2. Organization of Fiscal Services
A cash program may choose to combine consulting and fiscal services in the same host organization. Florida did not have that option, however, once it had decided that consulting was to be provided by the network of existing agencies and contractors that provided case management and support coordination. To keep the cost of fiscal services reasonable, a fiscal agent must serve many consumers. Moreover, the fiscal agent must have the technical expertise to act as an employers agent (for example, in filing payroll tax returns). Even if existing case management and support coordination agencies and independent contractors had been willing to take responsibility for fiscal services for the consumers to whom they provided consulting, the number of consumers each agency or contractor served was not large. Therefore, it would not have been efficient for each agency or contractor to acquire the specialized fiscal expertise that an employer agent needed. Mindful of the importance of economies of scale and expertise in the provision of fiscal services, Florida chose to have one organization provide fiscal services to all CDC consumers across the state.
3. Paying for Fiscal Services
Florida had to decide how to pay the fiscal agent, including whether consumers were to be charged directly for fiscal services. The major argument in favor of consumer charges is that they ensure that those who use the services bear the cost. The major argument against consumer charges is that they might discourage use of a service from which consumers could benefit.
Florida decided to have consumers charged service fees for the activities the fiscal agent performed for them. If the fiscal agent managed the monthly budget on their behalf, consumers were charged $5 per check cut, up to a maximum charge of $25 a month. Florida determined to set this cap because it was concerned that fiscal charges would eat too deeply into consumers monthly budgets. Consumers who managed the monthly budget themselves were each charged $10 a month for the fiscal agents desk audit of their account and records.
In addition to consumer charges, Florida paid the fiscal agent for some CDC design tasks. While these payments provided a source of start-up funds, the amounts were not large. Later, the state took responsibility for some tasks for which the fiscal agent was originally responsible.
G. Poised for Implementation
Working with the National Program Office, RWJF, DHHS/ASPE, and the other Cash and Counseling states, Florida completed the design of its CDC program by mid-1999, about two and a half years after it received funding to do so. The turnover of staff described in Chapter II had slowed the pace of design work in Florida. The state arranged for case management agencies, support coordination agencies, and contractors to provide CDC outreach, enrollment, and consulting. It also began to train consultants. More delay was in store, however. In June, the bids that had been received to provide fiscal services were dismissed when a flaw in the solicitation was uncovered. A new procurement effort was mounted for the fiscal agent. When a fiscal agent was finally selected, the contract negotiations were protracted, and the contract with the fiscal agent was not signed until December 1999. Florida persevered, however, and, in March 2000, CDC enrollment activities began in three counties. CMS gave approval for enrollment to begin in the rest of the state after a management information system was completed to prevent double billing of CDC and of traditional services. That system was completed, and enrollment began in the rest of the state in June 2000. Floridas Consumer-Directed Care Research Project was up and running. In the next several chapters, we describe its operation.
IV. ORGANIZATION OF CONSULTING AND CONSULTANTS
As described in Chapter III, a variety of agencies, both public and private, and individuals provided consulting to the populations in Floridas CDC project. For each of these populations, Medicaid waiver specialists (housed at Area Agencies on Aging [AAAs] or at the district offices of the Department of Children and Families [DCF]) provided fiscal and administrative support to CDC consultants. Case managers (for the elderly and adults with physical disabilities) or support coordinators (for those with developmental disabilities) provided CDC consulting while continuing to perform traditional case management or support coordination services for other beneficiaries.
A. Consulting Under DOEA
AAAs and agencies providing traditional case management services were involved in the provision of consulting for elderly beneficiaries.
1. Role of the Area Agencies on Aging and Medicaid Waiver Specialists
As noted earlier, Florida contracts with AAAs in each region of the state to provide services, including Medicaid waiver services, to elderly beneficiaries. The AAAs provide regional fiscal and administrative oversight to the Department of Elder Affairs (DOEA) in administering waiver programs for elderly beneficiaries. The AAAs contract for services under state programs for the elderly or provide these services themselves.16 In addition, the AAAs house state employees, called Medicaid waiver specialists, who are responsible for several state programs.
In general, the duties of the Medicaid waiver specialists include:
- Fiscal administration, such as receiving state funds, preparing budgets for state programs in their region, and ensuring that state funds are transferred to the appropriate program accounts.
- Logistical support, such as maintaining a supply of forms and providing space for meetings of program staff.
- Community outreach, including provider education and fielding calls from members of the community interested in programs for the elderly.
- Technical assistance, such as responding to inquiries about project procedures.
- Quality assurance, including selection and review of a sample of case records to assess whether state-prescribed procedures are being followed and, occasionally, face-to-face interviews with beneficiaries (for example, if there is a suspicion of exploitation).
a. Fiscal Administration and Logistical Support for CDC
At the time of our visit, Medicaid waiver specialists had recently begun to receive regular reports from the state CDC project office listing elderly enrollees in CDC. The specialists used these reports to develop and monitor the budgets for CDC. For each elderly consumer enrolling in CDC, the Medicaid waiver specialist moved funds from the account for the traditional waiver program to the CDC account.
The Medicaid waiver specialists maintained supplies of CDC forms (for example, blank purchasing plans). The AAAs provided space for consultant training and for the offices of temporary enrollment staff hired by DOEA.
b. Community Outreach
The Medicaid waiver specialists with whom we spoke described different ways of giving the community information about CDC. One reported that she routinely gave a brief presentation about CDC at meetings of providers of waiver services (for example, agencies providing personal care services) that the local AAA convened every couple of months; she reported on the number of CDC enrollees or on an issue that had arisen in the project and its resolution. Because providers were interested in CDC, her presentations often generated debate. The providers were concerned about losing market share under CDC but were also aware that they might be able to market their services directly to consumers.
While the Medicaid waiver specialists were not responsible for supervising the CDC enrollment specialists, they did have some enrollment responsibilities. One Medicaid waiver specialist we spoke with said that she sent copies of the enrollment reports that she received from the central CDC office, which were arranged by county, to all the counties served by her AAA, so that the lead agencies with low CDC enrollment could see that other lead agencies were successfully enrolling beneficiaries. Another Medicaid waiver specialist reported that he had become more involved in CDC enrollment since the departure of the temporary enrollment staff and had begun to speak at length over the telephone to people from his community interested in the CDC project.
c. Technical Assistance
The Medicaid waiver specialists housed at the AAA also provided technical assistance to CDC consultants. Medicaid waiver specialists attended the same training sessions as consultants, so they could address routine questions. They also could relay problems that consultants had experienced to the state CDC project office. All Medicaid waiver specialists offered both types of assistance, although some were more involved than others in technical assistance.
The demand on the Medicaid waiver specialists for technical assistance lessened over time. As consultants became more familiar with CDC procedures, they had fewer questions. Moreover, as consultants developed relationships with staff in the state CDC project office, they began to call that office directly when they had a question about CDC procedures. In part, consultants may have turned to the state CDC office because they were not getting satisfactory answers to their questions from the Medicaid waiver specialist in their area. One consultant we spoke with reported that she directed her questions to the state CDC office because she had found communication with the Medicaid waiver specialist at the local AAA to be very hit and miss.
d. Quality Assurance
The Medicaid waiver specialists had a limited role in quality assurance for CDC for elderly beneficiaries. They were responsible for reviewing records for quality assurance for traditional waiver services, and some of the state-prescribed procedures for traditional services were relevant to CDC. To help ensure the quality of case management services, Medicaid waiver specialists review records for sampled beneficiaries, using a standard monitoring tool that collects information on whether the waiver services provided to that beneficiary conform to state-prescribed procedures. For each waiver program, DOEA selects a random sample of recipients for whom records are to be reviewed and transmits their identities to the appropriate Medicaid waiver specialist. DOEA did not select a CDC-specific sample of records for review, but CDC participants were included in the waiver population from which the sample was drawn. The state-prescribed review procedures call for the sampled beneficiarys record to be examined for documentation that (1) the beneficiary was eligible for waiver services, (2) the beneficiary had a current care plan, and (3) contact between beneficiaries and case managers (or consultants for CDC) occurred as frequently as required.17 Of specific concern to CDC, the quality assurance review also considered whether the CDC project had been described to waiver recipients as a new project for which they were eligible and in which they might be interested. (Florida requires that waiver recipients be reminded each time they are reassessed about the availability of the CDC project and all other waiver programs for which they are eligible.)
At the time of our visit, the state was developing other CDC-specific quality assurance procedures. One Medicaid waiver specialist we interviewed hoped the state would develop instructions to accompany the expected CDC-specific procedures. She felt that instructions were needed to reduce variation among Medicaid waiver specialists in the application of review procedures.
2. Participation of the Lead Agencies in CDC
Florida negotiated with the existing lead agencies already offering case management to arrange for these agencies to provide CDC consulting to elderly beneficiaries. In general, AAAs use a competitive bidding process to select lead agencies to offer case management, with the contract period lasting several years.18 Lead agencies usually are public or private nonprofit agencies, rather than proprietary agencies. A lead agency is the only organization in its county offering Medicaid waiver case management services.
The lead agencies we visited apparently differed in their desire to participate in CDC. One executive, noting that her agency served the largest population of elderly waiver recipients in that region of the state, commented, If there is a better way to serve them, we want to be a part of it. In contrast, executives of two other lead agencies that we visited were skeptical about the value of consumer-directed care for the elderly but felt they had little choice but to participate in CDC. One noted, We were told to do it by the AAA because we are the lead agency in the county. Another commented, As lead agency, we really did not have a choice about participating. The states attitude was, It has to work, or else.
While Florida was eager to secure the participation of the lead agencies in all 19 counties in the CDC catchment area for elderly beneficiaries, the perception that lead agencies had no choice but to participate is incorrect. One of the 19 lead agencies participated in only a token manner: by the time of our visit in January 2002, only a handful of beneficiaries in this county had enrolled in CDC. Another lead agency declined to participate. It had recently been sued over an apparently falsified claim for workers compensation and viewed CDC consultants as potentially liable for poor consumer outcomes or worker injuries, thereby opening the agency to further legal action. To try to secure this lead agencys participation in the cash project, senior CDC project staff met with officials of the agency to explain that consumers--not consultants and consulting agencies--were liable for any injuries to workers. Their efforts were to no avail, however: this lead agency continued to decline to participate in CDC.
As for the executives of lead agencies, we observed considerable variation in the level of enthusiasm for the CDC project among the case managers/consultants with whom we visited. One consultant, commenting about her difficulties helping consumers do the arithmetic necessary for their purchasing plans, seemed quite disheartened (her experience is discussed further in the next section). Other consultants viewed CDC as one of many programs for which they were responsible. Yet another was really sold on the cash project--she lauded the positive changes she had witnessed in consumers on her caseload.
3. Consultants for Elderly Beneficiaries
a. Who Are the Consultants?
The CDC consultants serving elderly beneficiaries were the employees of lead agencies for the counties. They were primarily professional social workers, although we did visit one agency in which the CDC consultant was a nurse with a background in patient education. Case managers at lead agencies were typically responsible for a number of programs in addition to the 1915(c) waiver and CDC projects.
b. What Makes a Good Consultant?
The state project staff and consultants we interviewed agreed that three factors are critical to being a good CDC consultant, particularly for one whose previous experience is in traditional case management. First, a good CDC consultant is open to a different service paradigm. One Florida official described the traditional paradigm as one in which the case managers know what is best for their clients. In contrast, CDC offers a paradigm in which consumers decide the best way to meet the needs arising from their disabilities, with the support and teaching of consultants. One Medicaid waiver specialist we interviewed stressed this point, commenting, Most case managers are really entrenched in the system. If CDC requires anything, it is thinking out of the box.
Second, a good CDC consultant has extensive knowledge of community resources. Consultants help consumers identify goods and services for which the consumer may be eligible at no cost or at reduced cost, as well as vendors that offer the goods and services that the consumer needs, ideally at favorable prices.
Third, a good CDC consultant knows CDC procedures well, especially those that consumers must follow. The procedures of any Cash and Counseling program are complex. They can be difficult for a consumer to understand, especially since the role and responsibilities of a participant in an allowance program differ substantially from those of a participant in a traditional waiver program. Consultants need to be well versed in CDC procedures so they can explain the procedures to consumers and can respond readily to consumer questions.
Helping consumers complete a purchasing plan is an important consultant responsibility and one that requires competency in arithmetic. However, CDC project staff did not believe that lack of such competency was a stumbling block for consultants. In fact, many case managers had to complete cost work sheets from other programs and were comfortable with that process. CDC project staff argued that those who were not comfortable with completing a purchasing plan could easily be taught to do so.
c. Working as a Consultant for the Elderly
Initially, Florida asked each lead agency to select one or two of the agencys best case managers and a supervisor to send to CDC training. The agencies we visited were responsive to this request, and they sent their old hands and trusted staff. (We discuss training in more detail in Section D.) Only a few CDC consultants were trained at each agency, however, in part because lead agencies objected to the expense that they incurred in sending their staff to training. Shortly after our visit, almost all the lead agencies had assigned all their CDC consumers to one or two consultants. In no lead agency did all case managers also provide CDC consulting.
Even with only a few CDC consultants per agency, the CDC caseload at an individual agency was seldom (if ever) large enough to require a full-time effort from a given consultant. Typically, those providing consulting to some beneficiaries continued to provide case management of waiver services to other beneficiaries. One consultant we spoke with indicated that she worked with beneficiaries receiving assisted-living services and adult protective services, as well as on CDC and the Aged and Disabled Waiver.
When consumers enrolled in CDC, they were transferred from their case managers to the CDC consultant, and the consultants did not seem to find this change difficult. A Medicaid waiver specialist explained that the roles of case manager and consultant were so different that the change in personnel was not an issue. Indeed, she argued that it was more difficult to be a CDC consultant for a beneficiary for whom one had once been a case manager, because that beneficiary was more likely to make requests for assistance that were properly made to a case manager but that went beyond the role of a consultant.
Some consultants, especially those in agencies with a single consultant, had only limited opportunities to interact with colleagues about CDC. For a number of months, the CDC project organized monthly conference calls (later, bimonthly and quarterly calls) in which state project staff and Medicaid waiver specialists responded to questions from consultants at lead agencies. Consultants reported that these conference calls were useful.
Florida did not set specific standards for supervision of CDC consultants. Some CDC consultants had supervisors who were knowledgeable about CDC procedures, and some did not. Some supervisors had attended the same training sessions as CDC consultants and were well versed in the CDC project. Others had not attended CDC training and had only limited knowledge of the CDC project. The latter situation seemed to arise in part from turnover of supervisory staff. One supervisor we spoke with had joined a lead agency after the initial CDC training; he was not sent to CDC training, because the agencys caseload of CDC consumers was so small that the investment of the supervisors time in CDC training did not seem warranted.
d. Being a Case Manager and a Consultant at the Same Time
In CDC, the responsibility for arranging and monitoring services shifts from the case manager, where it lies in the home- and community-based waiver program, to the consumer (or representative). The CDC consumer is responsible for initial arrangement of services and for routine scheduling. If a service is not satisfactory, it is the consumers responsibility to intervene. The consultant is responsible for supporting and teaching the consumer. Except for the tasks for which consulting was mandatory, CDC taught consultants not to intervene with a consumer unless the consumer (or a representative) asked for assistance. One interviewee described the CDC policy as stay clear.
The role of a consultant differs from that of a case manager in that the case manager arranges for services and acts as an advocate for a client if a problem arises with a service. While Florida case managers for the elderly do not schedule every instance of a service, they make the initial arrangements for a vendor to supply services. For example, a case manager would arrange for a particular transportation vendor to serve a given waiver client, but the client would telephone the transportation vendor to schedule a particular trip. In addition, the case manager intervenes on behalf of the client if a problem arises. For example, if a worker fails to report to a clients home, the case manager telephones the vendor employing the worker to resolve the situation.
Consultants reported that they did not find it difficult to switch hats. The potential difficulty of moving from the waiver program to CDC probably was reduced because case managers were used to working constantly with several programs at the same time. Some consultants reported that they simply reminded themselves that their goal as a consultant differed from their goal as a case manager. Case Example IV.1 presents the comments of four consultants on this issue.
The consultant is not the only one who must make a transition, however--the consumer also must do so. Some consumers found it difficult to adjust to the difference between having the hands-on assistance of a case manager and only the support and advice of a consultant. One consultant we spoke with reported that some consumers were concerned because they had not realized earlier that they would lose their social worker after joining CDC. She handled this situation by reminding them that, if they could not manage under CDC, they could go back to traditional waiver services. Consumer difficulty in adjusting to the role of the consultant occasionally created an awkward situation for consultants. One consultant reported that consumers sometimes became angry with her when she refused to do the kind of things that case managers do for their clients.
The same consultant also reported that some consumers needed her assistance, rather than her support and advice, to make the transition to planning and managing their own care. She noted that many elderly consumers stumbled over the arithmetic needed to complete the purchasing plan, even after she had visited them multiple times to train them in developing the plan. Since CDC would pay the agency for no more than two training visits, she resorted to doing the math for them on the second visit to prevent the consumer from dropping out of the cash project.19 When she related this experience during our visit to Florida, some of her coworkers at the agency were present. They stressed that CDC called for consultants to offer only support and advice, not hands-on assistance. The tension between the needs of consumers and the project philosophy appeared to be a source of discomfort for this consultant.
B. Consulting Under DDP/DCF
Several contiguous counties are grouped into districts across the state of Florida for regional administration of DCF programs. These district offices house DCF Medicaid waiver specialists for the Developmental Disability Program (DDP) and for the Office of Adult Services (AS) program, both of which have some administrative responsibilities for Medicaid waiver programs. These waiver programs include traditional support coordination for those with developmental disabilities, which is provided by proprietary agencies and independent contractors. They also include support coordination for adults with physical disabilities, which is provided by public agencies, as well as proprietary agencies and sole practitioners. Florida arranged for DDP support coordinators to provide CDC consulting to those with developmental disabilities and for AS support coordinators to provide CDC consulting to adults with physical disabilities.
1. DDP Medicaid Waiver Specialists in District Offices
The basic responsibilities of the DDP/DCF Medicaid waiver specialists were similar to those of the DOEA Medicaid waiver specialists (described in Section A). As for DOEA, the DDP Medicaid waiver specialists had similar responsibilities under CDC and under other state programs. Medicaid waiver specialists for DCF prepared budgets for CDC and made sure that funds were assigned to the CDC account as appropriate. They made space available for local training sessions for consultants. They interacted with providers and citizens within their communities--for example, they made presentations to local community providers and to advocates/support groups about CDC and fielded telephone calls from those interested in CDC. As part of the states ongoing quality assurance process, Medicaid waiver specialists for DDP reviewed records for sampled cases to make sure that state-prescribed procedures applicable to all waivers were followed.20 DDP Medicaid waiver specialists also provided technical assistance to consultants.
Beyond these basic responsibilities, DDP/DCF Medicaid waiver specialists had a much more extensive role in the CDC project than did the DOEA specialists. Their roles differed in two main ways. First, the DDP Medicaid waiver specialists had more responsibility for enrollment than did DOEA specialists. In addition to the fact that temporary enrollment specialists were housed in district offices, the DDP Medicaid waiver specialists were responsible for some enrollment tasks. Initially, they received the tear-out postcards left with recipients of waiver services for the developmentally disabled, and they received incoming calls from other interested parties. They referred calls from interested waiver recipients or their families to local support coordinators for followup. Later, when temporary enrollment specialists were hired, DDP Medicaid waiver specialists helped train them, and each Medicaid waiver specialist supervised the enrollment specialists in that district office. One of their supervisory tasks was to review the completed enrollment forms for completeness and accuracy before sending them to the state CDC project office.
Second, DDP Medicaid waiver specialists were responsible for reviewing consumer purchasing plans to determine whether they had been completed correctly and contained only permissible goods and services. (DOEA and AS Medicaid waiver specialists had no role in reviewing purchasing plans, which were reviewed at the state CDC office.) One DDP specialist reported that the purchasing plans were rarely correct when the consultants first submitted them, and those incorrect plans were returned to the consultants. Sometimes a plan went back and forth many times between the consultant and the Medicaid waiver specialist in the district office until it was correct.
At least some DDP Medicaid waiver specialists may have had difficulty completing their CDC responsibilities expeditiously on top of their other responsibilities. State project staff reported that district office review of purchasing plans sometimes created a bottleneck. When asked to recommend changes in the CDC project, one Medicaid waiver specialist suggested that someone be hired at the district office to be responsible for enrollment and review of purchasing plans. She complained that she currently had but one day a week to devote to these CDC tasks and noted, This could be a full-time job.
Some DDP Medicaid waiver specialists were more involved than others in the CDC project, and a few became expert in the CDC procedures. Consultants perceived the support of some Medicaid waiver specialists as extremely valuable. One DDP Medicaid waiver specialist had been a temporary enrollment specialist for CDC; her work was so impressive that she was later hired as a Medicaid waiver specialist for that district, with the CDC project as one of her responsibilities. After all the support coordination agencies in one county closed, another DDP Medicaid waiver specialist there became a temporary consultant until a new CDC consultant for that county could be identified and trained. This Medicaid waiver specialist also visited a consumers home to resolve an issue that had implications for the amount of the monthly budget. Before the state project office established a toll-free telephone line, one Medicaid waiver specialist gave the district office telephone number to beneficiaries and their parents so that they could call him if they had questions about the CDC project.
2. Working as a Consultant for Those with Developmental Disabilities
As indicated earlier, under Floridas waiver programs, the employees of proprietary firms and independent contractors provide support coordination to those with developmental disabilities. Many of these proprietary firms consist of a principal and a few employees and serve only a single geographic area. That is not always the case, however; we visited one support coordination firm with offices in two areas of the state. Support coordinators are professional social workers.
Senior DDP/DCF staff reported that their department values an opportunity for citizens with disabilities to choose among support coordinators. Unlike DOEA, DDP does not select a single lead agency per district to provide support coordination. Rather, multiple firms and practitioners within a geographic area can apply to the state for certification as a support coordinator. In one district we visited, there were several sole practitioners and three agencies (the largest of these agencies had five people on its staff) offering support coordination to the developmentally disabled.
Support coordination firms and sole practitioners decided for themselves whether to participate in CDC as consultants. Initially, the state predicted that most waiver beneficiaries would enroll in CDC. Some of the support coordinators we interviewed reported that they felt that they had little choice but to participate or risk losing revenue as their clients opted for CDC. As a result, many (more than 100) support coordinators were trained as CDC consultants. However, since fewer beneficiaries than initially predicted enrolled in CDC, some of those trained were not active CDC consultants at the time of our visit. Those providing CDC consulting to some beneficiaries typically continue to provide traditional support coordination to others. Often, an existing support coordination client would learn of CDC and ask his or her support coordinator to be his or her CDC consultant.
For the most part, consultants for those with developmental disabilities worked independently. However, they had some supervision and collaboration, and provision was made for backup. Two people we spoke with--the proprietor of a firm and the manager of an office of a larger firm--supervised the support coordinators, including their work as CDC consultants. They (and, sometimes, other colleagues in the firm) provided backup if a support coordinator/consultant was absent. Both these supervisors had been trained in CDC and had some CDC consumers on their own caseloads.
Independent contractors obviously did not have a formal supervisor in their organization. Some contractors relied heavily on district office staff for technical assistance regarding the CDC program; they may have done so to a greater extent than did consultants in firms who had supervisors and colleagues with whom they could discuss a CDC issue. Some sole practitioners arranged for backup by having another sole practitioner cover if they were unavailable. At least one district office had approved the practice of having sole practitioners cover for each other.
Like case manager/consultants, support coordinator/consultants reported that it was not difficult to switch hats between the traditional waiver program and CDC.
C. Consulting Under AS/DCF
Case managers for adults with physical disabilities also served as CDC consultants. The provision of case management services for adults with physical disabilities differs by county and district. In some counties, the lead agencies providing case management services to the elderly also serve adults with physical disabilities; in other counties, different agencies are under contract to provide these services. In some cases, AS/DCF case managers are state employees working out of the district office. We visited a district that had hired state employees in an effort to stretch its funds to serve as many of the people as possible who were on its waiting list for Medicaid waiver services. The district did this because it had found that hiring staff was appreciably less expensive than contracting with agencies. Another district in a very rural area assigned the task to a state employee, who was also responsible for implementing several other state programs.
D. Training Consultants
The goals of training for CDC consultants were to (1) make case managers and support coordinators comfortable with the concept of consumer direction, (2) reassure them that the consumer would not be hurt, and (3) teach CDC project procedures.
1. Description of Training
Training sessions for CDC consultants were short--one and a half days. Florida limited the length of the training sessions out of concern that agencies, uncomfortable about operating shorthanded, would be reluctant to send staff to anything longer. (CDC did not reimburse agencies for the cost of staff time to attend training.) Training on project procedures focused on helping the consumer develop the purchasing plan, although project staff also tried to summarize other procedures (for example, consultant interaction with the fiscal agent) so that consultants would at least have a nodding acquaintance with all facets of the CDC project. Even so, there was a tremendous amount of material to cover in a day and a half.
The initial materials and curriculum to train CDC consultants were developed by staff working out of the CDC project office housed in DOEA. Among the materials was the CDC handbook developed for consumers, which was used to train both consultants and consumers and which served as a reference manual for both groups. Initially, the same materials and curriculum were used both for the case managers and for the support coordinators. The materials were relevant to all three populations involved in the CDC project, and examples used in the training sessions were drawn from multiple populations.
Many consultants were trained during the initial sessions, which began in May 1999. However, the unforeseen delay in obtaining a fiscal agent kept Florida from enrolling beneficiaries in CDC until almost a year later. By that time, those consultants who attended the initial training sessions had forgotten what they had learned, especially since they had not been able to put their newly acquired knowledge into practice. To remedy this situation, staff from the CDC project office in DOEA provided refresher training for consultants when consumers finally began to enroll in spring and summer 2000.
2. Effectiveness of Training and Training Materials for Consultants
Both case managers and support coordinators complained that initial training was ineffective. Case Example IV.2 presents the comments of one support coordinator and of one case manager regarding the effectiveness of CDC consultant training.
A central problem with training was that there was too much material to cover in a day and a half. Trainers did not have time to provide detailed explanations. With no background in the CDC project, the trainees were unable to formulate meaningful questions. Trainees also struggled to learn the procedures that applied to the population that they were to assist, while disregarding those that applied only to other populations. Support coordinators found that examples involving elderly beneficiaries often were not pertinent to beneficiaries with developmental disabilities (similarly, case managers found that examples involving beneficiaries with developmental disabilities were not pertinent to elderly beneficiaries). The consultants reported that refresher training was an improvement, perhaps partly because they had acquired some background information during the initial training sessions. Nonetheless, they did not master the material until they learned it on the job.
Consultants made several suggestions for improving training. A major suggestion (which had already been implemented at the time of our visit) involved population-specific training to eliminate material that was irrelevant for the population of interest and focus on examples that were most pertinent to that population. In September 2000 (after CDC had been operating for several months), DDP staff took over training for consumers with developmental disabilities from project staff at DOEA and revamped the curriculum to make it population-specific. In addition, following an urgent petition from consultants for adults with physical disabilities, DOEA developed a discipline-specific training curriculum for that group. A related suggestion (which had not been implemented at the time of our visit) was to revise the consumer handbook (which, as noted, was used in consultant training) to make three manuals, each pertaining to a single population. Another suggestion was to revise the handbook to integrate the numerous revisions to procedures that were made in the first months of CDCs operation so that consultants would not have to review many addenda when a question arose.
The consultants we spoke with also said the training sessions needed to be longer. They suggested expanding the training to include additional material on other aspects of the consultants job besides the cash plan. For example, one suggested asking the fiscal agent to give a presentation at training so that consultants would better understand the projects fiscal procedures. Another suggested a training program similar to that the one the state provided for support coordination (see Case Example IV.3).
Consultants also recognized the importance of ongoing training and suggested that the CDC project give more emphasis to conference calls, noting that these calls allowed (1) state project staff to update consultants on changes in procedures, and (2) consultants to learn from one another. DCF had discontinued conference calls, partly because of the expense. DOEA project staff reported that the initial conference calls had been problematic, as many consultants used the calls to express negative views about the CDC project. DOEA continued the consultant conference calls, however. Eventually, as more consultants accepted the project, the discussions in these calls began to focus on procedures.
E. Monitoring of Consulting
As part of their general quality assurance procedures, AAA and district office specialists checked that waiver program staff were offering CDC to beneficiaries. As of our visit in winter 2002, however, no CDC-specific quality assurance plan was in effect.
Florida had submitted an initial quality assurance plan to CMS as part of the states operational protocol for the CDC project. This initial plan called for numerous visits by state staff to agencies offering consulting. It was later determined to be infeasible because it would have been so expensive to implement. Instead, the state CDC office developed a less extensive quality assurance process that relied largely on desk audits, with an agency visited only if the findings of its desk audit suggested that further investigation was necessary. At the time of our visit, the state was planning to implement the revised plan.
F.Lessons About Organization of Consulting and Consultants
-
Regional program supervisors can provide valuable support to frontline consulting staff.
Some DDP Medicaid waiver specialists were major assets in implementing CDC for that population. They reduced the burden on central CDC staff by supervising temporary enrollment specialists and by reviewing and approving consumer purchasing plans. In addition, some of them became so expert and involved in CDC that they were able to offer valuable technical assistance and support to consultants and consumers. The ability to offer technical assistance to consultants is especially important when consultants do not have coworkers or supervisors familiar with the program. The knowledge and involvement of DDP Medicaid waiver specialists also was important in providing back-up consulting services to consumers when no frontline consultants were available. Someone local who can visit the consumers home (if that seems advisable) is in a much better position to offer back-up consulting than a central office in a distant part of the state.
-
Because consulting under an allowance program is quite different from traditional case management and traditional support coordination, substantial training is required, followed shortly thereafter by an opportunity to practice.
Florida limited its training session for consultants to one and a half days, and consultants generally felt that amount time was inadequate. There was too much material to cover, especially since consultants came to training with no background on the CDC project. No one can be expected to master all the procedures of a new program based on a single training session. Moreover, knowledge will soon be forgotten if the consultant cannot put it into practice quickly. Therefore, states implementing allowance programs would be well advised to delay training of consultants until consumer enrollment in the program has been approved, even if waiting for consultants to be trained forces a delay in consumer enrollment.
-
It is not difficult for the same person to provide both consulting and case management (or support coordination) services, provided that person is comfortable with the philosophy of consumer direction.
Given the differences in the philosophies of the traditional services model and the Cash and Counseling model, some of those involved in the design of the CDC program were concerned that case managers and support coordinators would find it difficult to continue to provide traditional services at the same time that they served as CDC consultants. However, that was not the case. Case managers and support coordinators in Florida routinely assist participants in several different programs simultaneously. While many case managers and some support coordinators were not comfortable with the philosophy of consumer direction, those who were did not have difficulty providing case management or support coordination to some beneficiaries and traditional services to others. They were conscious of the differences in the programs and could readily switch from the role of case manager (or support coordinator) to the role of CDC consultant.
-
Conference calls for consultants can be a useful way to provide updates and peer support to consultants working in far-flung agencies.
Both DOEA and DDP used conference calls to provide updates about the CDC project and peer support to consultants at agencies across the state. These calls gave consultants a way to learn tricks of the trade that another consultant had developed. Several consultants we spoke with found the conference calls helpful. Apart from cost, the only disadvantage of the conference calls is that they may provide a forum for consultants to voice negative opinions about the program. Perhaps ground rules for the calls could ameliorate this problem.
V. FISCAL SERVICES
As Chapter III indicated, Florida decided to have a single entity provide fiscal services to all the populations the CDC project served throughout the state.
A. Selection Process and Host Agency
Florida used a competitive procurement process to select a fiscal agent. It selected a human services organization with experience providing similar fiscal services.
1. Procurement Process
The state employed a procurement process that used an Invitation to Negotiate, in which the state selected the top bidders and asked them to negotiate with the state on the provision of services. Competition was not restricted to entities in Florida.
Florida sought a fiscal agent that had a philosophy compatible with consumer direction and the expertise, staff, and other resources (for example, a toll-free telephone number, and the hardware and software needed to receive electronic funds transfer) necessary to implement the CDC project effectively. The state wanted an organization that believed in the importance of consumer empowerment and understood its own role as a supportive agent of the consumer. Furthermore, Florida sought an organization with the expertise and staffing to manage many consumer accounts and the capacity to add individual consumers to the fiscal systems as these consumers enrolled and completed purchasing plans. The state also sought an organization that could produce automated reports for each consumer, detailing how the cash benefit had been spent. In addition, it wanted an organization that could track accumulated cash for each consumer.
To help assess the ability of organizations to serve as the fiscal agent, Florida required that each bidder submit plans (including sample questions) for the skills examination that the fiscal agent was charged with developing for administration to consumers. The purpose of the examination was to assess whether consumers who wished to manage their monthly budgets themselves knew enough about payroll taxes and related payroll requirements to handle these tasks correctly.
The only bid from within Florida was disqualified, but the state received several satisfactory out-of-state bids in response to its solicitation for a fiscal agent. Florida considered the bids of the three organizations chosen as finalists to be very competitive. Florida was impressed with the organization it chose to be the fiscal agent and with its personnel. This organization had experience providing services to another state similar to those it would provide under CDC. In addition, its plan for the skills examination and the illustrative questions were much better thought out than those of the other finalists.
As discussed later, the payment methodology for fiscal services subsequently proved to be inadequate to cover the costs of the fiscal agent, particularly when its caseload was small. However, there was no evidence during the solicitation process that the winning bid was a low ball. The bid from a nationally known employer services agent was close to that of the organization chosen.
2. Host Organization and Accounting Services Subsidiary
The successful bidder for the position of fiscal agent was a wholly owned subsidiary of a nonprofit human services organization that provides training, employment services, and other services to people who have disabilities and other disadvantages and who are experiencing barriers to employment. Among the services the host organization provides are day habilitation, a sheltered workshop/vocational day program, and supported employment. Through these and other programs, the host organization had extensive experience working with people with developmental and physical disabilities. The host organization emphasizes working with each individual on goals designed to increase the persons level of independence, an emphasis that is consistent with the philosophy of consumer direction. The members of senior management of the host organization were highly supportive of consumer-directed programs and believed such programs to be the wave of the future. One executive we interviewed stressed, We believe in the idea. The subsidiary specialized in providing accounting services for personal attendants.
The chief financial officer (CFO) of the host organization was responsible for the work of the subsidiary and, thus, for the CDC project. The CFO operated from the headquarters of the host organization in Maryland, while the subsidiary operated in a city in Virginia about 40 miles from the headquarters office. A full-time manager oversaw the operations of the subsidiary.
B. Responsibilities and Oversight
The contract between the state and Florida laid out the duties of the fiscal agent. It also provided for state oversight.
1. Responsibilities of the Fiscal Agent
As laid out in its contract with Florida, the fiscal agent was to provide a standard service package for consumers. Under this package, the duties of the fiscal agent included:
- Receiving Medicaid funds on behalf of consumers.
- Preparing and distributing a start-up kit that included information on contacting the fiscal agent and the forms necessary for a consumer to designate one.
- Preparing and distributing employment forms packets, including multiple copies of the time sheet for employee use and federal and state forms such as the Immigration and Naturalization Service I-9 form, Internal Revenue Service W-4, and Florida New Hire Reporting Form.
- Managing federal and state employment taxes, preparing filings, and distributing funds, net of employment taxes.
- Processing time sheets and payments to independent contractors and home care agencies and disbursement of cash to consumers.
- Reconciling consumer accounts monthly and mailing statements to each consumer, with a copy to the consumers consultant.
In addition to the standard package, the fiscal agent was required to offer additional services (called a la carte services), available to consumers upon their request. These included out-of-cycle consumer reports of account expenditures and balances and out-of-cycle payroll checks.
The fiscal agent had different duties for consumers who themselves assumed responsibility for payroll and tax functions and check writing. First, as mentioned earlier, the fiscal agent was responsible for developing a skills examination to determine whether consumers were sufficiently knowledgeable to assume responsibility for managing the monthly budget. The fiscal agent also checked the completed examination for those consumers who chose to take it. (The National Program Office paid for the development of a guidebook to train consumers on payroll and tax functions and check writing; the fiscal agent had no responsibility for training them.) Consumers who assumed responsibility for managing the monthly budget themselves had to establish a dedicated bank account for the CDC funds (with which personal funds were not to be co-mingled). Each month, the fiscal agent was responsible for depositing the amount of the monthly budget into this dedicated account. Consumers were required to forward documentation on expenditures from the dedicated account each month to the fiscal agent. The purpose of this desk audit was to identify errors and noncompliance with legal requirements for employers. In addition, the fiscal agent had to enter information on the consumers expenditures into its tracking system for reporting to the state on expenditures under CDC.
Beyond these specific duties, the contract between the fiscal agent and the state of Florida envisioned that the fiscal agent would provide strong support to consumers. This was seen as requiring communication with consumers, responsiveness to their needs, and flexibility in dealing with them. The preface for the contract described a need for excess capacity on the part of the fiscal agent to make possible (1) the establishment of ongoing relationships with consumers (to facilitate the identification of anomalies and the correction of deficiencies in a cooperative learning atmosphere), and (2) allowances for consumers who might not appreciate the importance of timeliness.
2. Standards
The contract between Florida and the fiscal agent imposed some operating standards on the agent. The agent was required to have one account manager and one account clerk for every 250 consumers on cash (except that a team of one manager and one clerk was allowed to serve up to 350 consumers on a temporary basis to allow time to add and train additional staff). For every 10 teams, the fiscal agent was required to hire an account specialist to provide troubleshooting, problem resolution, and oversight. The contract set a standard of 100 percent accuracy for processing payrolls, writing checks to independent contractors and home care agencies, and preparing state and federal taxes. If the fiscal agent failed to process a payroll check by the deadline (for a time sheet that had been submitted on time), the agent was required to discount the consumers fee to the fiscal agent for the next payroll check by 10 percent. Similarly, the contract specified that all tax documents were to be filed within the legally required deadlines. In addition, the contract required that the toll-free telephone line be answered during all business hours. Finally, Florida expected the fiscal agent to notify a consumers consultant if the account was being spent down too quickly, if payment was being made to obviously inappropriate providers, or if the consumer requested cash more than twice a month or an amount of cash in excess of 20 percent of the amount of the monthly budget.
3. Oversight
Florida provided for extensive oversight of the fiscal agent. This included quarterly reports to the state on fiscal operations and conference calls with senior CDC project staff, as well as regular discussions with other CDC project staff about day-to-day issues, regular visits by senior state staff, compliance visits by an independent auditor, and visits by a contractor hired by the National Program Office. Among the information collected in the quarterly report are the number of consumers served (with the standard service package and with desk review); monthly budget amounts (current and cumulative); purchases, overall and by type of purchase; remaining balances; and the number of items returned by the U.S. Postal Service. The visits by the contractor the National Program Office hired included review of the status of the plant, equipment, and information systems and other technology; staffing; compliance with state and federal requirements; and operational issues, such as development of policies and procedures.
A senior executive of the host organization said that this oversight was reasonable and adequate to assess performance, adding that the most important aspects of the fiscal agents work were timely and accurate performance of fiscal tasks.
C. Payment and Costs
As described in Chapter III, Florida decided that consumers would be charged for the services of the fiscal agent. Indeed, consumer fees were the major source of payment to the agent. Florida paid the fiscal agent for design tasks, such as development of the skills examination (these payments totaled about $50,000) but did not supplement the fees paid by consumers for fiscal services.
1. Consumer Fee Schedule
For providing the standard package of services, the fiscal agent was allowed to charge the consumer a fee of $4.99 per worker time sheet processed or check generated in the first year of the project, up to a cap of $25 per consumer per month. The payment per time sheet or check increased by 2 percent in each successive project year; however, the cap remained $25. For out-of-cycle reports of account balances and out-of-cycle payroll checks, consumers incurred additional charges (of $4.99 and $9.99 respectively), but there were no additional consumer fees for direct deposit of worker pay or for withholding of additional income tax.
The fee for the standard package of services did not apply to consumers who assumed responsibilities for payroll and tax functions and check writing. The fiscal agent charged each such consumer $9.99 a month for transmitting the monthly budget and for reviewing the consumers records.
2. Costs
Over time, it became clear that providing fiscal services for the CDC project was a financial drain on the host organization. First, the fiscal agent received no payment (apart from those for design tasks) until the consumer had completed the purchasing plan and had begun to receive the monthly budget. Yet, for each consumer, it incurred start-up costs (such as establishing a consumers account and processing employment forms).
Second, the monthly cost per consumer far exceeded the maximum fee of $25 a month. The fiscal agent had expected to be able to keep its costs under the cap. However, costs were higher than expected because the CDC project was more labor intensive than the fiscal agent had anticipated when preparing its cost proposal. The average consumer hired more workers than expected and purchased a broader variety of services. This forced the fiscal agent to process more worker time sheets (including cutting more payroll checks and processing more payroll taxes) and to write more checks to other vendors. Many consumers had more than five payroll or check-writing tasks each month (each with a potential fee of about $5). Yet the fiscal agent could charge each consumer no more than $25 a month. In addition, the costs of some tasks were more than anticipated. For example, the fiscal agent was required to process direct-deposit transactions using each individual banks software, as well as its own internal software. That processing required additional staff time, which offset the reduction in mailing costs gained through direct deposit.21 Overall, the fiscal agent estimated that its costs would be $40 per consumer per month with a caseload of 3,000 consumers--far more than the monthly maximum fee of $25. However, even $40 per consumer per month was roughly half the cost incurred by the fiscal agent in New Jersey, which had similar (but not identical) tasks.22
Third, the fiscal agent was unable to realize economies of scale due to slow caseload buildup, which also increased its costs. The CDC caseload grew very slowly, and the buildup of caseload for the fiscal agent lagged behind that for the program as a whole. For example, as of the end of calendar year 2000, more than 80 beneficiaries had been enrolled in the CDC treatment group, but only 9 of them were on cash.
The fiscal agent and its host organization persevered despite the financial drain they faced. Florida took over responsibility for some fiscal tasks to reduce the financial strain. The state began to assign consumers an identification number as part of the states CDC identification code. It assumed responsibility for copying employment form packets and mailing them to consumers assigned to the CDC treatment group. CDC project staff also developed instructions for completing the forms in the employment packet, which reduced questions coming into the fiscal agent from consumers. Also as part of its effort to reduce the number of questions the fiscal agent received from consumers, the state tried to clarify what had been a gray area--the responsibilities of the fiscal agent vis-à-vis those of consultants. It provided consumers with additional guidelines about the tasks for which consultants and the fiscal agent were responsible, while stressing the requirement for consumers to shoulder their own responsibilities under CDC. Moreover, the state entered into negotiations with the fiscal agent to amend its contract. At the time of our visit, these negotiations were ongoing.
D. Quality of Fiscal Services
The fiscal agent handled many tasks very well. A senior state program staff member reported that the state felt pretty good about the fiscal agents processing of payroll and tax documents. The contractor the National Program Office hired to audit all the state programs fiscal agents reported that the Florida fiscal agent had accurately managed federal tax processes (despite having to switch to a different form following a revision in IRS procedure) and had correctly refunded over collection of federal employment taxes (in Arkansas, such refunding had not been handled correctly). There were few problems with the accuracy of checks or with timely payment of vendors (other than payment to workers, as discussed below).
Nonetheless, there was considerable dissatisfaction with fiscal services with respect to three issues: (1) timeliness of payment of workers, (2) consumer financial statements, and (3) consumer service.
1. Timeliness of Worker Payment
Payroll processing normally required at least three weeks. After a pay period ended, the consumer had a week to submit the time sheet. In late 2001, after terrorist attacks involving mailing of anthrax-laden letters, the mail from Florida to Virginia could take a week or more. (Earlier, the fiscal agent had checked the time for mail delivery between Florida and Virginia and found that it required three to four days.) After receipt of the time sheets, the fiscal agent had a week in which to cut the paychecks.
Additional steps had to be completed before the first payroll check could be cut for a given worker. After the CDC project was notified that a worker had been recruited, a week would be required for shipping of the employment packet. After the fiscal agent received the completed employment forms, it would take a week to process those forms. The first paycheck could be delayed if these tasks were not completed before the worker took up his or her responsibilities.
Consumers and workers complained about the lag in workers receipt of their first paycheck. Some workers were strapped for funds until their first paycheck arrived. Others complained that the program was some kind of scam when they did not receive their initial pay as expected.
While the fiscal agent had only marginal ability to control the factors leading to delay in receipt of paychecks, it introduced practices to reduce such delay. It would cut checks out of cycle and send them by courier if the consumer was desperate (although it would not continue to send checks by courier if the workers time sheet was repeatedly not submitted on schedule). For a time, consumers were allowed to submit time sheets by fax as long as they immediately submitted a signed original time sheet; however, this practice was discontinued after the number of faxes became unmanageable. Shortly before our visit in winter 2002, the fiscal agent had instituted direct deposit to speed payment of workers.
2. Consumer Financial Statements
State program staff, Medicaid specialists, and consultants we spoke with voiced their concern about the failure of the fiscal agent to produce understandable, regular, monthly financial statements for consumers. (A similar problem arose in the other Cash and Counseling states, especially in New Jersey.) Case Example V.1 presents the comments of one consultant on this issue. Without understandable, regular statements, consumers could not readily monitor the payments made by the fiscal agent from their accounts or track their balances. Moreover, consultants (who were to receive copies of the statements) could not monitor consumer spending to ensure that consumers had not overspent their monthly budgets.
The fiscal agent did not produce consumer financial statements for three months in spring 2001 and for another three months in the fall and early winter of that year. The root cause of the difficulty in the spring was the financial crisis that the fiscal agent faced because its costs exceeded its payment. In response to this crisis, the fiscal agent reduced it staff, including eliminating the position of the person responsible for producing the monthly financial reports. The difficulty in the fall and early winter of 2001 occurred when it was necessary to revise the program that produced the monthly financial statement after the fiscal agent changed accounting software. When we visited in January 2002, a monthly financial report was again being produced. (We consider consumer financial statements further in Chapter IX.)
3. Consumer Service
There were complaints about the quality of the consumer services the fiscal agent provided. Lack of responsiveness to consumer and consultant requests was a common complaint. For example, one consultant reported that a consumer had wanted to take the skills examination and called the fiscal agent three times to request a copy. Finally, the consumer was told that the examination was being sent overnight; however, it arrived two weeks later. In addition, while some members of the staff of the fiscal agent were described as kind, others were reportedly rude to consumers or consultants. One consultant reported having seen a fellow consultant yelled at by a member of the fiscal agents staff.
Part of the explanation for poor consumer support seems to be that the staff of the fiscal agent was overwhelmed. The position of project manager for CDC fiscal services was vacant, and other staff had been let go in response to the financial crisis. Then, after a slow buildup of caseload for many months, enrollment came on like gangbusters following the mailing of the governors letter to recipients of developmental disability waiver services and their parents. As enrollment surged, the remaining staff of the fiscal agent was overwhelmed. Yet the financial drain on the host organization continued, which caused it to refuse to allow overtime for the fiscal agents remaining staff.
Senior state staff thought that lack of leadership and lack of training for the accounting staff on how to handle difficult consumers contributed to poor consumer service. At the same time, the state was not sure whether the complaints originated with a vocal minority or represented widespread dissatisfaction. At the time of our visit in winter 2002, the state was preparing to conduct a postcard survey of CDC consumers about satisfaction with support from the fiscal agent.
Fundamentally, the fiscal agent seems to have been unable to meet the expectations of others regarding consumer service, certainly not with its reduced staff. The agent had done much to set up these expectations by emphasizing, in the proposal, the type of consumer service that would be provided. Given the financial crisis, the agent could not meet these expectations when caseload finally began to build--and very quickly.
E. Lessons About Fiscal Services
Floridas experience suggests several lessons about the provision of fiscal services.
-
Time for mailing materials can contribute to lag in payment. Fiscal agents need procedures that minimize the use of postal services for time-critical deliveries.
After terrorist attacks slowed postal service, the time required for mail delivery became a serious problem for some sensitive fiscal tasks, particularly the delivery of a workers first paycheck. Adopting certain procedures can reduce mailing time. For example, direct deposit of workers pay eliminates the need for checks to be mailed. In addition, consumers might be allowed to submit time sheets by fax (with a signed original to follow by mail). To reduce the burden on the staff of the fiscal agent, submission by fax might be allowed only for the first paycheck for a given worker. In the future, automated systems may make it possible for consumers to submit time sheet information by telephone or through the Internet.
-
Fiscal agents may have difficulty in producing timely, understandable financial statements regarding consumer accounts.
The CDC project had been operating for many months before the fiscal agent was able to supply consumers with timely, easily understandable monthly financial statements. (New Jerseys fiscal agent also had difficulty initially with the routine provision of clear financial statements for consumers.) Part of the problem stemmed from the financial difficulties that Floridas fiscal agent faced. Part stemmed from changes in accounting software: the software that the fiscal agent used did not readily accommodate the production of consumer financial statements.
-
While the fiscal agent must be prepared to support consumers, it is important to avoid the creation of expectations that cannot be fulfilled. At the same time, the payments to the fiscal agent must be sufficient to allow it to employ the staff necessary to support consumers.
The fiscal agent in Florida was a subsidiary of a human services organization that had a mission of helping people with disabilities achieve independence. It understood the population that CDC serves and intended to serve that population well. The fiscal agent had helped to raise expectations about the quality of consumer service it would provide by focusing on consumer service in its proposal. However, due in part to financial difficulties, the agent was not able to deliver, which in turn affected its credibility with consumers and consultants. While consumer service is critical, it is important to consider the level of service that can realistically be delivered given the payment to the fiscal agent.
-
A fiscal agents costs will likely exceed payment when caseload is small, and organizations that provide fiscal services may need assistance with cash flow until they reach break-even caseload.
The CDC project was a financial drain on the host organization for fiscal services, partly as a result of the slow buildup of caseload. A senior executive of that organization reported that the subsidiary serving as the CDC fiscal agent would have had to go out of business before it reached break-even caseload had it not been able to draw on the resources of a host organization that was financially stable and committed to the concept of consumer-directed care. Despite differences in payment methodology and program structure, the fiscal agents in Arkansas and in New Jersey had similar difficulties with cash flow when caseloads were small. Their collective experience suggests that fiscal agents need assistance with cash flow in the early months of program like Cash and Counseling.
-
The Florida experience suggests that $40 per consumer per month is a rock bottom payment that might be sufficient to cover the costs of a fiscal agent only when caseload is very large and only when others are responsible for many tasks necessary for the provision of fiscal services.
Apart from some design tasks, the payment to the fiscal agent in Florida consisted of fees from consumers for processing payroll and writing checks. Mindful of the needs of consumers and the limited monthly budgets that some of them would received under CDC, Florida capped the consumer fee at $25 a month, no matter how many workers the consumer employed or how many checks to other vendors the consumer requested. However, the costs of the fiscal agent under the CDC project far exceeded the fees it earned, and consumer support suffered as a result. The fiscal agent estimated that the break-even fee would be $40 per consumer per month when the caseload reached 3,000 cash recipients, and that was after the state took over responsibility for several tasks to relieve the fiscal agent of the costs. Thus, the Florida experience suggests that $40 per consumer per month is a rock bottom price that could cover costs only after the caseload was very large and only when others handled many tasks necessary for fiscal services.
VI. OUTREACH AND ENROLLMENT
Generating enrollment in CDC was a particularly demanding task, because the demonstration was the subject of a rigorous evaluation. A large caseload was needed to yield the evaluation sample necessary to engender confidence in detecting any program impacts. Moreover, this caseload had to be generated quickly. The demonstration waiver had been approved for a five-year period, but about half this time had elapsed before CDC was ready to begin operations. With one readiness issue still unresolved, CMS allowed CDC to begin enrollment in three counties in the Tampa/St. Petersburg area in March 2000. Enrollment began in the rest of the state two months later, in June 2000.
In this chapter, we describe the operation of outreach under the CDC project, the enrollment process, and the features of CDC that potential participants found most attractive or unattractive. We then draw lessons about designing effective outreach and enrollment procedures.
A. Information Campaign
Almost all the outreach efforts focused on those with disabilities or their parents, supplemented by some outreach to educate service providers about the CDC project. Most outreach was through letters from the governor to Medicaid waiver clients, targeting those eligible to enroll in CDC. Under CDC, there was little outreach to the general public.
Before CDC began to operate, the Developmental Disability Program (DDP) started an information campaign directed primarily toward people with developmental disabilities and their parents. As described in Chapter II, the families of people with developmental disabilities are politically active advocates in Florida. Perhaps with that in mind, one DDP staff member described an objective of the community information campaign as follows: The more you keep people in the sunshine, the easier it will be to implement the program.
Presentations by state project and district staff kept advocacy organizations, such as Family Care Councils, informed of the progress of the CDC project. The presentations to the Family Care Councils did engender interest in enrolling in the CDC project when it began to operate. Furthermore, DDP district office staff made presentations about CDC to local providers of services to people with developmental disabilities.
Some presentations were also made to providers of services to the elderly and to groups of elderly people. As indicated in Chapter IV, Department of Elder Affairs (DOEA) Medicaid specialists made presentations about CDC to providers of services to the elderly (for example, the Lighthouse for the Blind) to keep them apprised of the projects status. In general, the specialists did not make presentations to advocacy organizations for the elderly. As described in Chapter II, elderly people and their families are must less politically active in Florida than those with developmental disabilities and their families. After dedicated enrollment staff were hired, their DOEA supervisor made presentations about CDC at senior centers and spoke at some conferences.
CDC project staff deliberately avoided using newspaper articles to educate the general community about the project. As CDC began operations in the Tampa/St. Petersburg area, local newspapers there did publish a few articles. However, the articles contained errors and omissions that led people not eligible for CDC to telephone the project for more information. For example, one newspaper article only mentioned the need for Medicaid eligibility--it failed to mention that only recipients of Medicaid home- and community-based waiver services were eligible for CDC. The small staff in the state CDC project office struggled to respond to telephone calls from Medicaid beneficiaries who were not receiving waiver services and thus were not eligible for CDC. After this incident, and mindful of a similar one in Arkansas, Florida downplayed newspaper articles as a means of community education.
However, articles about the CDC project were included in both DOEA and Department of Children and Families (DCF) departmental newsletters. CDC project staff had more control over newsletter articles than newspaper articles, and the departmental newsletters were distributed primarily to departmental staff and beneficiaries receiving departmental services.
In another attempt to avoid generating inquiries from those who were ineligible, CDC made little use of public service announcements. The only major exception was announcements on a Spanish-language radio station serving the Miami area. To reach the Spanish-speaking community, DOEA used this station to make announcements about the CDC project in South Florida.
B. Initial Approach to Outreach
As Chapter III indicated, Floridas initial approach to outreach relied on staff members of traditional agencies to offer the CDC project to individual beneficiaries. However, that approach stalled (as we describe later), and both DDP and DOEA hired temporary state employees as dedicated enrollment staff.
1. Initial Approach
Floridas initial plan called for case managers and support coordinators to mention CDC during their regular visits to beneficiaries and leave a brochure with a tear-out postcard to be returned if the beneficiary (or the parents of a minor beneficiary) was interested in participating in CDC. This plan followed Floridas general practice of acquainting waiver clients with all programs for which they were eligible. For DDP, the tear-out postcards were returned to the Medicaid specialist in the appropriate district office, who notified that beneficiarys support coordinator/consultant of the need to follow up with the beneficiary or his or her parents and set a deadline for doing so. (One support coordinator/consultant complained that the Medicaid specialist had no right to impose a deadline on this task.) For DOEA, the postcards were returned to the lead agency serving the county in which the beneficiary lived. In turn, the lead agency arranged for a CDC consultant to visit the beneficiary to explain the project.
2. Problems with the Initial Approach
When left to the traditional agencies, enrollment stalled both for the elderly and for people with developmental disabilities.
a. Population with Developmental Disabilities
Not only were DDP support coordinators/consultants skeptical about the value of the CDC project, they initially also were overwhelmed with other responsibilities. To comply with a court ruling (Doe vs. Chiles 1998), the Florida legislature had recently greatly increased the funding for the DDP waiver program. Beneficiaries were moved off the waiting list, and support coordinators had to assess them and prepare their support plans. Support coordinators were also required to review the support plans for all current participants in the DDP program to determine if needs were being met and increase services if they were not. At the same time, the DDP program was losing support coordinators to more profitable employment. One support coordinator we spoke with about enrollment summarized the situation as follows: Honestly, I did not have time. Nor did support coordinators receive additional pay for following up with people who expressed interest in CDC.
DDP tried to get its district offices to focus on the lagging enrollment for the CDC project. DDP staff held conference calls with district staff and arranged for statistics on the outreach effort in each district to be included in a monthly situation report to the governors office. These reports got the attention of district administrators, whose evaluations were tied to them. Several administrators were taken aback, as they had not been paying attention to outreach and enrollment in CDC. However, this effort was not enough to increase the pace of enrollment such that evaluation targets were met.
Mindful that a letter from the governor had succeeded in boosting enrollment in the Arkansas Cash and Counseling program, DDP next arranged a direct mailing of such a letter (in English and Spanish) to all waiver clients with developmental disabilities. (Several months later, DOEA and DCF/Office of Adult Services (AS) arranged for a similar letter from the governor to all recipients of waiver services who were elderly and physically disabled.) Response to this letter initially overwhelmed the state DDP staff working on CDC.
Moreover, support coordinators/consultants could not respond quickly to those who expressed interest in the CDC project. When the governors letter was mailed, 12,000 beneficiaries were receiving waiver services for the developmentally disabled. Given their other responsibilities, it was not feasible for the support coordinators/consultants to visit all interested beneficiaries in a timely manner. Usually, they were unable to see a beneficiary before their next regular monthly support coordination visit.
b. Elderly Population
For reasons explained in Chapter II, many case managers resisted the concept of consumer-directed care. In addition, they felt that they were being asked to sell the project, which they found distasteful. One member of the state CDC project staff reported that some case managers were not so subtly sabotaging enrollment in the CDC project. For example, they might tell an elderly beneficiary, You need me. Even after Florida began direct mailings of a letter from the governor to recipients of waiver services, case managers could easily discourage elderly beneficiaries from participating in CDC. (We further discuss the letters from the governor later in this chapter.) The first thing that many elderly waiver clients would do after receiving a letter about CDC was call their case managers and ask for advice about whether to enroll. As one state project staff member remarked, If the case managers were not at least neutral, the cash program did not have a chance.
Some case managers conscientiously did their duty by the CDC project, and a few were enthusiastic. One case manager/consultant reported that, after other case managers left the CDC brochure, she had personally telephoned every single waiver participant her lead agency served about their interest in the project. If they were interested, she followed up, explaining the project in a down-to-earth way. She described her efforts as a tremendous amount of work. Nonetheless, she found that few beneficiaries were interested. Case Example VI.1 lists some reasons beneficiaries reported for lack of interest, as documented in the notes of this case manager/consultant.
- Im happy the way things are.
- I am being well taken care of.
- I cant get along without a case manager.
- It is too much for a 96-year-old to undertake.
- I have enough to worry about as it is.
When it was clear that only a few elderly waiver clients were enrolling in CDC and that many case managers opposed the project, senior CDC project staff and senior state officials met frequently with executive staff of the lead agencies and with professional organizations representing case managers. CDC project staff and senior state officials wanted to use the meetings to make the case managers comfortable with the concept of consumer direction, but they were largely unsuccessful in doing so.
3. Decision to Hire Dedicated Enrollment Specialists
After the CDC project had been operating for about six months, it was clear that making case managers and support coordinators responsible for consumer outreach was not working. The Cash and Counseling National Program Office arranged for selected consultants to participate in focus groups to discuss CDC enrollment. The comments of the focus group participants helped Florida identify factors that were impeding enrollment and helped inform the subsequent decision to hire dedicated enrollment staff.
Beginning late in 2000 and continuing into 2001, both DOEA and DDP hired temporary state employees (outside civil service) as enrollment specialists. The decision to hire enrollment specialists followed a national Cash and Counseling meeting, which a senior DOEA official recently made responsible for CDC for elderly beneficiaries had attended. He listened to reports from the Arkansas and New Jersey programs about their dedicated enrollment staff and decided that Florida had to hire dedicated outreach workers to enroll the elderly population. DDP concurred, deciding that hiring dedicated staff would make it easier to enroll people with developmental disabilities.
To pay the enrollment staff, Florida used RWJF funds and, later, state funds. Some RWJF funds were received when New York dropped out of the Cash and Counseling demonstration and funds remaining in its RWJF grant were divided between Arkansas, Florida, and New Jersey. These funds were used to hire enrollment specialists for the population with developmental disabilities. Later, RWJF provided additional funds for hiring enrollment specialists for Floridas elderly population. The RWJF funds were supplemented with state funds.
C. Enrollment Operations with Specialists
About 20 dedicated enrollment specialists were hired for temporary positions split about equally between DDP and DOEA, with the latter also responsible for enrolling physically disabled beneficiaries. The first such specialists were hired in fall 2000. By the time of our visit to Florida in early 2002, no DDP enrollment specialists remained on the payroll. Only a single full-time DOEA enrollment specialist remained on the payroll at that time (for the Miami area); two were still working part-time for DOEA in other parts of the state. The total cost to hire the temporary enrollment staff was about $350,000.
Some of the enrollment specialists who were hired were very dedicated and enthusiastic; they believed in the concept of the CDC project. One applicant for the position (a retired funeral director) believed so strongly in CDC that he remarked, If you dont hire me, Ill do it for free. It would be great to have this for the elderly. (He was hired.) At least one DDP enrollment specialist was a parent of a child with developmental disabilities.
Dedicated enrollment specialists for DOEA worked from home or out of Area Agencies on Aging (AAA) offices. A DOEA enrollment specialist would visit a lead agency, contact all its waiver clients, then move on to another lead agency.
Enrollment specialists for DDP worked out of the DDP district offices. Each enrollment specialist enrolled waiver clients residing in his or her assigned district and responded to inquiries coming into the district office through the tear-out postcard or by telephone.
When an enrollment specialist was not present, the CDC consultants (for both elderly beneficiaries and people with developmental disabilities) were responsible for following up with waiver clients interested in the project, just as before the enrollment specialists were hired.
In addition, some enrollment specialists, especially those for DCF, became so knowledgeable about the program that consultants would contact them with questions.
1. Training
The DOEA enrollment specialists were trained by the CDC consultant who had been hired by the CDC project to supervise them (see below). She developed a presentation about the CDC project, with an accompanying flip chart, in both Spanish and English. The supervisor trained the enrollment specialists to be realistic in describing the responsibilities that consumers take on under the CDC project. She also trained them to notice the surroundings in the home to identify things that might be important to the waiver recipient (such as family pictures) and to describe how CDC might enhance those aspects of their lives. Similarly, the DDP enrollment specialists were trained by state DDP staff, with the participation of the Medicaid specialists in the DCF district offices.
In addition, both the DOEA and the DDP enrollment specialists attended a training session run by a social marketing firm hired by the Cash and Counseling National Project Office. Important topics included how, when presenting the CDC project, to address any fears consumers might have. The training session was highly regarded, and the enrollment specialists seemed to perceive it as an enjoyable experience. The DOEA supervisor for outreach and enrollment described it as a lot of fun.
2. Supervision
As described in Chapter IV, the Medicaid specialists in the district offices supervised the DDP enrollment specialists, who worked out of the same district offices. The supervisory duties of the Medicaid specialists included ensuring that enrollment forms were complete and accurate before they were submitted to the state CDC project office.
Rather than rely on the Medicaid specialists housed in AAAs, DOEA hired a case manager/consultant enthusiastic about CDC to supervise enrollment specialists. She took a leave of absence from her job as a case manager/consultant, reviewed the applications that the state project office had received for the position of enrollment specialist, and selected individuals from among the applicants. She then supervised them, and her duties included reviewing enrollment forms for completeness and accuracy.
The techniques the DOEA supervisor used to supervise far-flung enrollment specialists are of particular interest. She sometimes visited them; for example, she initially traveled to each of the lead agencies with an enrollment specialist to introduce that specialist to the agency staff. However, she supervised mainly through telephone calls and e-mail, talking to the DOEA enrollment specialists daily and e-mailing them several times a day. If DOEA enrollment specialists had questions while in a beneficiarys home, they called their supervisor from there. At the end of each day, all the enrollment specialists filed electronic reports on their work that day, from which the supervisor compiled a weekly report to DOEA. Case Example VI.2 describes her use of electronic media to supervise the enrollment specialists. She also randomly called consumers to check that data entered on the enrollment forms were accurate.
3. Calculating Amount of Monthly Budget Before Enrollment Presentation
Enrollment staff worked with lead agency staff (often with case manager/consultants) to calculate the amount of the monthly budget if a beneficiary were to enroll and be assigned to the treatment group. Without this information, the beneficiary could not make an informed choice about participation. Calculating the amount of the monthly budget required access to the beneficiarys records. State regulations restricted access to these records to protect the privacy of beneficiaries.
Determining the amount of the monthly budget was more time-consuming in Florida than in the other Cash and Counseling states. First, each of the other two states cashed out a single service with a single statewide rate. In contrast, Florida cashed out all of the services in the beneficiarys care plan (except case management/support coordination) and many care/support plans included several services. These services were provided by numerous vendors paid at different rates. Care/support plans generally included the total value of the plan; however, when that information was missing, computing the amount of the cash benefit could require looking up the rates paid to specific vendors of several services. Staff at one AAA reported that it used 20 different providers for a single service, all of which could have different rates.
The second reason that calculating the amount of the monthly budget could be more time-consuming in Florida than in the other two Cash and Counseling states was that, for elderly consumers, Florida used either the claims history or the care/support plan to determine the amount of the monthly budget, while the other two states relied exclusively on the former. Each lead agency received a report from state DOEA staff with information on the amount of the monthly budget based on claims history. Lead agency staff then obtained the amount based on the care plan and compared that to the amount based on the claims history. The procedure was that the amount of the monthly budget would be based on claims history, unless the amount of the monthly budget based on the care plan exceeded the amount based on claims history by $50 or more. (The claims history amount should not have exceeded the care plan amount, as the care plan represented the maximum amount of approved service.)
4. Scheduling Visits
After the enrollment specialists had an estimate of the value of the CDC monthly budget, they telephoned waiver recipients to schedule visits to describe CDC. For efficiency, visits to the clients home were scheduled by zip code. DOEA enrollment specialists were generally expected to conduct four to five enrollment visits a day. The DDP specialists sometimes held meetings of several families with members with developmental disabilities. This option was generally not open to the DOEA enrollment specialists, as it was difficult for the elderly population to travel. To avoid overzealous selling of CDC, neither the DOEA nor the DDP enrollment specialists had a quota for the number of clients enrolling in CDC.
During the enrollment visit, the specialist described the CDC project and responded to questions from beneficiaries and their families. DOEA enrollment specialists often used a flip chart indicating key project features. The video that had been produced with funds from the National Program Office for the Cash and Counseling Demonstration saw little use. The DOEA supervisor did not favor using it, because the people shown in the video were not like the people we go to see. While elderly people were shown on the video, they were obviously not Floridians and did not appear representative of the typical elderly Medicaid wavier recipient there.
If the beneficiary (or the parents of a recipient who was a minor) decided to enroll in CDC before the enrollment specialist left the home, the specialist would prepare the enrollment and consent forms and ask the beneficiary (or a parent) to sign them. If the beneficiary (or parent) was not ready to make a decision at that time, the specialist left the forms and asked that they be signed and returned by mail if a decision was made to participate. The specialist would call back in 30 days if he or she had not received the forms or had not heard from the beneficiary (or parent).
Enrollment specialists returned the completed enrollment and consent forms to the lead agency (for elderly beneficiaries) or to the DDP district office (for those with developmental disabilities). DOEA enrollment forms were sent to the beneficiarys case manager for traditional waiver services, who completed a portion of the form. Both the enrollment and the consent forms then were forwarded to the central CDC office. The Medicaid specialist in the district office reviewed the DDP forms for completeness before they were sent to the DDP program office and then on to the central CDC office.
D. Assessment of Hiring Enrollment Specialists
CDC project staff members and consultants reached different conclusions about the value of hiring enrollment specialists.
1. From the State Perspective
State CDC project staff members were convinced that dedicated enrollment specialists were critical to generating enrollment in the cash program. The pace of enrollment increased only after the specialists were hired. The specialists were enthusiastic and not distracted by other responsibilities.
For DDP, the governors letter had boosted enrollment so much that state staff were worried about having enough trained consultants to serve new consumers. Less than a year after the first DDP enrollment specialists were hired, the evaluation target sample size was reached for children (all of whom were developmentally disabled). A few months later, the target sample size was reached for nonelderly adults (nearly all of whom were developmentally disabled). Florida continued to enroll waiver recipients after these targets were reached, but enrollment slowed again as the temporary enrollment specialist positions were phased out. A slowing was to be expected, since the enrollment specialists already had contacted nearly all the waiver recipients in the state to ascertain their interest.
2. From the Consultant Perspective
During our visit to Florida, both case manager/consultants and support coordinator/consultants gave the enrollment specialists mixed reviews. Some complimented an enrollment specialist they had worked with. For example, one noted, He did a good job. Give him a name and he would be there the next day. On the other hand, some consultants complained that CDC enrollees often did not understand the cash project because an enrollment specialist had not explained it thoroughly and correctly. In such cases, the job of the consultant was more difficult, at best. At worst, the beneficiary would drop out of CDC. One consultant suggested that the enrollment specialists might not have had enough time to present the CDC project during the home visit, as their schedule was very tight. However, several consultants judged that the enrollment staff deliberately misrepresented what could be purchased with the monthly budget to influence beneficiaries to enroll in CDC. One consultant reported that the number of such misunderstandings had declined since the enrollment specialists left, and she was again responsible for explaining CDC to waiver recipients who expressed interest. Case Example VI.3 presents the complaints of one consultant about the enrollment specialists who worked in her lead agency.
District office and state CDC staff were mindful that beneficiaries might simply have heard what they wanted to hear, and that some might have tried to manipulate project rules (for example, saying, I was told I could buy shoes). Therefore, they investigated complaints that enrollment specialists were misrepresenting what could be purchased with the monthly budget. The DOEA enrollment supervisor reported at least one case in which an enrollment specialist had indicated that the beneficiary could purchase a television with the monthly budget, thus misrepresenting the covered goods and services. To counter this tendency, the DOEA supervisor reported stressing that outreach workers describe the projects features realistically: Dont sell the project. If you really believe in it, then you dont have to sell it.
Other consultants we spoke with complained about enrollment specialists approaching developmentally disabled adults in assisted-living facilities. These consultants argued that such consumers might be worse off under the CDC project than under traditional waiver services. The charge for the assisted-living facility--their major expense--is the same whether they are on CDC or the traditional waiver. Because of the discounting of care plan hours, however, the beneficiary on the CDC project will get less money with which to pay the facility charge.
Still other consultants indicated that the enrollment specialists would have been valuable had they been available when the CDC project first began to operate in their communities. Some reported being insulted that enrollment specialists were sent to re-do the work they had sincerely attempted. These consultants felt the enrollment specialists were too much, too late.
E. Attractive and Unattractive Program Features
During our visit to Florida, we asked consultants and state project staff about the features of CDC that consumers found attractive and those they found unattractive.
1. Attractive Features
Being able to hire relatives was cited as one of the most attractive features of CDC, both for elderly beneficiaries and for those with developmental disabilities. The relatives hired were sometimes the parents themselves. That was not always the case, however, as Case Example VI.4 shows.
Having flexible and expeditious service was cited as another attractive feature of CDC, according to consultants and state project staff. Consumers could purchase a service that they valued (provided it was related to their disability), even if it was not covered in the traditional program. An example of a valued, but uncovered, service is after-school habilitation at home. Reportedly, consumers also found it attractive to be able to ask the workers they hired with their CDC monthly budget to complete tasks that agency aides do not do. Because of concerns about liability, agency aides are not allowed to transport consumers or accompany them on trips from home. In contrast, CDC allowed consumers to go out with their worker (for example, to go shopping). Being able to get out was a source of great satisfaction to many consumers and a very attractive feature of the CDC project. In addition, agency aides do not do windows, but consumers can ask the workers hired with their CDC monthly budget to take care of such chores. Fundamentally, consumers are empowered to insist that workers do the tasks they were hired to do. One consultant told of a man who complained that the agency sent an aide with a knack for doing nothing. With CDC, he could fire a worker who did not complete assigned tasks.
Even if a service is covered under the traditional program, consumers reportedly value CDC because it has much less red tape. One consultant commented that consumers were pleased that they did not need three approvals from Medicaid to make a purchase.
CDC consultants and other project staff also cited continuity of care and dependable service as features of CDC that consumers found attractive. They noted that, because agency aides turn over frequently, the consumer repeatedly must become accustomed to an unfamiliar person. Doing so can be particularly difficult for people with developmental disabilities. In addition, consumers could hire someone they knew was dependable--they did not have to put up with aides who did not come as scheduled.
2. Unattractive Features
Consultants and other CDC project staff reported that CDC had three unattractive features: (1) random assignment, (2) paperwork, and (3) project rules and limits. Random assignment was a requirement of the evaluation and would not be a part of an ongoing program of consumer-directed care, but the other two would be features of an ongoing Cash and Counseling program.
Consumers reportedly found paperwork to be the most unattractive feature. The initial paperwork to enroll in the project and the packet of employment forms were particularly unattractive.
Some consumers had little experience with paperwork. Sixty percent of the elderly enrollees in CDC were widows. Few had ever been a manager or employer; indeed, most had never been employed outside the home. Many may never even have kept a checkbook; their husbands had always assumed that responsibility. Paperwork was also a problem for those who had little or no formal education or were functionally illiterate, such as some migrant farmworkers. One family of migrant workers who declined to participate in CDC explained, This is for educated people.
Consultants tried to prepare consumers for the paperwork, and CDC kept working to simplify it. One consultant reported telling consumers, You are going to get a big, white envelope full of paper. Dont get scared. Call me. To simplify the paperwork, CDC staff developed an illustrative employment packet in which the items that the consumer (or worker) needed to complete were highlighted. The state printed the illustrative packet at considerable expense (a result of the need to print the highlighting in color over other material) and distributed it to those assigned to the treatment group.
Consultants and other CDC project staff reported that some consumers found the project rules and limits unattractive. Many elderly consumers were reluctant to give up the services of their case managers, as required under CDC. Some consumers found the rules irksome. One consultant quoted a consumer who asked, Why cant you just give me the money?
F. Lessons about Outreach and Enrollment
Floridas experience offers several lessons about outreach and enrollment.
-
A consumer-directed program that cashes out traditional services needs the cooperation of the agencies providing those services. However, assigning these agencies responsibility for outreach and enrollment can be fraught with problems.
The cooperation of agencies providing traditional services is needed to implement a program such as Cash and Counseling. Case management agencies often have their clients (especially elderly clients) trust. If such agencies and their staff are resistant to a Cash and Counseling program, they can easily discourage consumers from enrolling. In addition, information from agency care plans often is the basis for determining the amount of the monthly budget.
Floridas initial approach of implementing outreach and enrollment through its existing networks for case management and support coordination was largely unsuccessful. Case managers and support coordinators were pressed by other responsibilities and were sometimes opposed to consumer-directed care, so few gave priority to the time-consuming tasks of outreach and enrollment. Even case managers and support coordinators who were not opposed to the concept of consumer direction found that they simply had no time for CDC outreach and enrollment.
-
Providing information to advocacy groups can be a successful approach to generating interest in a cash allowance program.
Florida has a tradition of strong advocacy for those with developmental disabilities, particularly through the Family Care Councils, which were established by the state legislature to advise DCF. Through presentations to the councils, DDP staff generated considerable interest in the CDC project. Many months elapsed between the time of the first presentations to the Family Care Councils and the time the contract was signed for the fiscal agent. Consequently, the interest the initial presentations generated was not immediately translated into enrollment. Nonetheless, the presentations piqued the interest of families of those with developmental disabilities.
-
The amount of the allowance needs to be calculated for everyone who is seriously considering enrolling in a cash program. More effort is required if the amount based on the care plan is to be compared to the amount based on claims history.
To make an informed decision about participation in a cash program, beneficiaries need at least a good estimate of the amount of the allowance. Therefore, it is necessary to calculate what the amount of the allowance would be for everyone who is seriously considering enrollment.
The time required to calculate the allowance (monthly budget) was greater in Florida than in the other Cash and Counseling states, for two reasons. First, numerous services (each of which could have a unit cost that varied by vendor) had to be taken into account in Florida, but only a single service with one or two unit costs had to be taken into account in Arkansas and New Jersey. Second, Florida based the amount of the monthly budget for elderly consumers on either the claims history or the care plan, depending on which was amount was greater. Obviously, it was necessary for Florida to calculate the amount of the monthly budget under each method and compare them. When the effort required to calculate the allowance is substantial, states should consider that time when estimating the time and resources that will be required for outreach and enrollment.
-
If state agencies are to be responsible for outreach and enrollment, but their efforts are not satisfactory, arranging for statistics on the outreach effort to be reported to the highest levels of state government may get the attention of the responsible officials.
When enrollment in CDC was lagging, DDP arranged for statistics on the outreach effort in each district to be included in a monthly situation report to the governors office. The CDC project then got the attention of district administrators, as their evaluations were tied to the situation reports, and enrollment improved.
-
Hiring employees through traditional agencies is problematic, because they may not be enthusiastic about the concept of a cash allowance. Hiring dedicated employees may be the best approach to staffing when trying to build a caseload quickly.
Belief in the concept of a cash allowance is an important component of successful outreach and enrollment. Consequently, unless agencies and their staff are enthusiastic about a cash program, it seems preferable for the cash program to hire enrollment staff rather than paying agencies to do so. Some burden on agency staff may still remain (for example, if enrollment staff are not permitted to review client files to calculate the amount of the allowance), and compensation for their time seems appropriate.
To produce enrollment to meet the evaluation sample-size targets (as well as to build caseloads sufficient for viable programs), Florida hired temporary state employees whose time was dedicated to outreach and enrollment. The pace of enrollment surged after their employment and direct mailing of a letter about the CDC project from the governor to waiver clients.
If the cash program is to hire staff to be responsible for outreach and enrollment, they should be in place when operations begin. By hiring enrollment specialists only after agency enrollment had failed, CDC antagonized some staff members of traditional agencies who had done their best to implement the program. It also confused some consumers who had already been approached and declined to participate.
-
Because direct mailings to eligible beneficiaries are targeted, they are more efficient than outreach methods that blanket the community with information. Letters from the state governor are particularly effective in generating enrollment.
Florida largely eschewed blanket outreach methods such as newspaper articles and public service announcements. Having observed the experience of the Arkansas Cash and Counseling program (in which blanket outreach methods generated an overwhelming number of inquiries from ineligible people), Florida was already wary of such methods. This feeling was confirmed when CDC staff were overwhelmed with inquires from ineligible people following some early newspaper articles on CDC that omitted key information about eligibility.
Even with limited initial support from providers and professionals, a cash program can nevertheless generate substantial enrollment by going around those people and communicating directly with consumers who find the cash program attractive. When coupled with enrollment staff to follow up with interested clients and families, both DDP and DOEA found a letter to the governor to eligible beneficiaries to be effective in generating enrollment in CDC.
-
The effect of direct methods (such as a letter) on generating enrollment depends on the ability of the eligible population to influence the traditional system.
If direct outreach methods are to succeed, consumers must be willing and able to demand enrollment. The letter from Floridas governor was particularly effective for the population with developmental disabilities, whose families had a strong tradition of advocacy and political activity. Once sold on CDC, the families of those with developmental disabilities demanded the project of their support coordinators, who were then faced with offering CDC consulting or losing business to another support coordinator who did offer consulting. In contrast, elderly beneficiaries were likely to ask their case managers opinion about the CDC project after receiving the governors letter. If discouraged by their case manager, most elderly clients did not demand CDC. Even if they had, they would not have been able to take their business elsewhere, since only one lead agency served each community.
-
Dedicated enrollment staff may successfully serve a wide geographic area.
Only a few weeks or months are required to contact all the existing population of waiver services recipients in a given region. One approach to organizing the work of dedicated enrollment staff is to have them come into an area, contact all members of the eligible population in that area, then move on. Florida found that this approach worked. The enrollment specialists can be supervised by staff in district offices (if such exist) or remotely by telephone, e-mail, and via the Internet. Part-time enrollment specialists might be retained in more populous areas to contact new recipients of waiver services.
-
Enrollment staff should not have a quota for the number of clients they are expected to enroll in the cash program.
If enrollment staff are expected to enroll a certain number of waiver recipients in a given period, they may misrepresent the cash program to meet their quota. Quotas for the number of home visits to be made to explain the program do not have the same incentive, however, and can promote efficiency.
Misrepresentation of the cash program by enrollment staff must be avoided if consultants are to maintain their faith in an allowance program. Consultants may be discouraged if they have to frequently re-explain program rules and observe consumers dropping out when their misunderstandings are corrected.
VII. CASH PLANNING AND MANAGEMENT
Consumers received a letter telling them that they had been assigned to the treatment group. The letter also notified consumers to expect a telephone call from the CDC project. While the letters were being prepared and mailed, CDC staff notified the lead agency (for elderly beneficiaries) or the district office (for those with developmental disabilities) of that consumers assignment to the treatment group to receive the monthly budget.
A. Developing the Purchasing Plan
A consultant trained consumers on the development of the purchasing plan.
1. Consultant Selection
The procedure to select a consultant differed for elderly consumers and for those with developmental disabilities. For elderly consumers, the lead agency assigned the case to a consultant. Since, at most lead agencies, one or two consultants handled the entire CDC caseload, the assignment process was straightforward. After a consultant was assigned to a case, it was that consultants responsibility to contact the consumer to schedule a training visit at the consumers home.
In contrast, consumers with developmental disabilities (or their parents) could select their CDC consultant (just as they could select their support coordinator in the traditional waiver program). When a beneficiary with development disabilities was assigned to the treatment group, the Medicaid specialist in the district office called that person (or his or her representative) and described the options for selecting a CDC consultant. The consumer could choose to work with his or her current support coordinator if that person was trained (or willing to be trained) as a CDC consultant, or the consumer might choose to work with another staff member of the same agency who had been trained as a consultant. Alternately, the consumer could review brochures from other agencies and individuals offering CDC consulting in the area where the consumer lived and select from among those consultants.
2. Consumer Training
Florida devoted substantial resources to developing a notebook for consumers, and the state expected consumers to make good use of it. During home training visits, a key task for consultants was to teach consumers about program rules and procedures and how to use the consumer notebook as a program reference document.
a. Consumer Notebook--the Blue Book
The central CDC office mailed consumers the consumer notebook after they were randomized to the treatment group. Consumers were to keep the notebook throughout the project. The notebook, written in simple language, was intended to be both an aid in training consumers on the management of the monthly budget and a reference manual. Among other topics, the consumer notebook described the CDC project and the roles of the consumer or representative, consultant, and fiscal agent. It also contained guidance on how to decide what goods or services to purchase with the monthly budget and how to recruit a worker. Perhaps the more important function of the consumer notebook was to serve as a reference manual to which consumers could refer for information on CDC rules and procedures. The notebook also contained blank copies of forms that consumers in CDC would need.
Consultants we spoke with said that they asked consumers and their representatives to read the notebook before the consultant arrived for the first training visit. Usually, the representatives had read most of the notebook by the time the consultant arrived; however, only a minority of consumers had done so. Consultants also encouraged consumers to use the notebook as a reference manual. One consultant reported that, when a consumer asked a question, he would respond, Lets look at the book. Where do you think the answer to that could be? Some parts of the notebook were relevant only to consumers with developmental disabilities, other parts only to elderly consumers. One consultant reported that some representatives added tabs to identify the parts of the manual that were applicable in their situation.
b. Explaining the Program Again
In addition to teaching consumers and representatives how to use the consumer notebook, consultants explained the CDC project again as necessary during the initial home training visit. If the consumer (or representative) had already studied the consumer notebook, the consultant might need to answer only a few questions. However, consultants reported that many consumers had serious misunderstandings about the program. As described in Chapter VI, some were misunderstandings about what types of purchases were permissible.
Other common misunderstandings concerned case manager (or support coordinator) services and the role of the CDC consultant. Some consumers mistakenly believed that they would still have a case manager or support coordinator after they began to receive the monthly budget. One consultant commented, I tell them, Once the budget starts I will no longer arrange your services. I am not the one you call if your aide does not show. You are your own social worker. Other consumers mistakenly thought that the consultants role was to render the kind of assistance that case managers (or support coordinators) render. In the words of one consultant, Consumers have the mind-set, You have to do this for me. I have to tell them thats not so in CDC. Consultants reported that, after these misunderstandings were cleared up, some consumers chose to go back to traditional waiver services. For example, one consultant noted that a consumer who had expected the consultant to recruit and hire workers dropped out of CDC after being informed that was not the consultants responsibility.
c. Developing the Purchasing Plan
Beginning at the initial training visit, the consultant helped the consumer develop the purchasing plan. One consultant we spoke with said that she telephoned consumers or representatives) before the initial training visit to prompt them to review the notebook and begin to think about the purchasing plan. Case Example VII.1 describes this approach in her own words.
Other consultants reported adopting different approaches to developing the purchasing plan when the consumer (or representative) was not familiar with the contents of the notebook. Some consultants would read through the notebook with the consumer or representative during the initial visit. Then they would tell the consumer or representative to develop a purchasing plan and to call them when it was complete. Others consultants would walk the consumer (and/or representative) through the development of the purchasing plan at the initial training visit.
The time required for the development of the purchasing plan varied, but the process could be time-consuming and difficult. Consultants reported that some purchasing plans could be developed in an hour. In such cases, consultants might begin to review the documents in the employment packet during the initial training visit so that the consumer could proceed with the paperwork to hire a worker. However, three to four hours were required to develop some other purchasing plans. One consultant commented, You sit with a parent for four hours. It is exhausting. How much can one person absorb? Some consultants divided the training into more manageable segments. For example, they might focus on the purchasing plan during the initial visit and schedule a supplemental training visit (after the plan had been submitted for approval) to discuss the documents in the employment packet.
One difficulty in developing the purchasing plan was reaching agreement between the consumer and family on the wage rate to be paid a worker (who was often a family member). Another difficulty was the arithmetic computations to determine the cost of the purchasing plan. Case Example VII.2 presents the approaches of two consultants to dealing with the arithmetic computations. One consultant presented examples to help the consumer or representative do the arithmetic, with little success. The other consultant simply worked through the arithmetic with the consumer or representative present.
Elderly consumers and their representatives, as well as consumers with developmental disabilities and their representatives, found developing the purchasing plan difficult. Consumers with business backgrounds needed the least assistance. One consultant (whose CDC caseload was made up entirely of children with developmental disabilities) reported that, in her experience, the only representatives who did not need help with the purchasing plan were an accountant and someone who owned a business.
3. Approved Purchases and Review of the Purchasing Plan
At the end of the planning process, the formal purchasing plan form was completed. All purchasing plans were subject to review (even if all services were clearly within the program guidelines). For elderly consumers, purchasing plans were sent to the state CDC office for review and approval. For consumers with developmental disabilities, the district office for that area reviewed and approved purchasing plans; the state CDC office did not review them.
The consumer notebook described the types of purchases that consumers could make with the monthly budget. It stated, The most basic rule is that everything you buy must be related to your long-term care needs or your needs for community supports. The notebook also gave examples of the types of good and services that were permissible, such as help with personal care and household chores, companionship services, home repair and maintenance, nonmedical transportation, independent living supports or coaching, supported employment and job coaching, and adaptive equipment. It also listed examples of prohibited purchases--these included gifts, loans, rent or mortgage payments, clothing, groceries, and entertainment.
The consultants we interviewed described the coverage rules for the monthly budget as generally clear. One issue that had needed clarification was whether the expense of transportation for an activity such a concert was an entertainment expense. A memorandum was issued as a supplement to the consumer notebook indicating that the expense of such transportation was permissible because it allowed the consumer to take part in social activities.
Some consultants complained that procedures for interacting with the fiscal agent with respect to purchases were not clear. One described a case in which the purchasing plan included saving for a wheelchair. Because the wheelchair was listed in the purchasing plan, the consultant was frustrated that the fiscal agent asked for a letter from the consultant indicating that the wheelchair purchase was acceptable before it would pay for it from the funds that the consumer had saved.
Some requests for purchases were not approved. Examples include requests for (1) the cost of heating a swimming pool for therapy, which was denied on the grounds that other family members used the pool; (2) educational software, which was denied on the grounds that it was entertainment; and (3) a cell phone for a caregiver, which was denied on the grounds that it would not benefit the consumer.
B. Uses of Cash
Consultants reported that consumers used the monthly budget to purchase a broad array of goods and services, just as CDC had intended. Many consumers hired workers. Most of the workers hired were family members who were already familiar with the consumers needs and preferences. In some cases, a parent became the worker. In others, consultants reported suggesting hiring neighbors or a current aide. Case Example VII.3 describes one case in which a consumer hired a neighbor.
Many consumers purchased supplies (such as diapers) with the monthly budget. Consumers often shopped for sales on supplies at retail establishments. Consultants reported that consumers could reap considerable savings relative to the amount that Medicaid would have paid its vendors for the same supplies.
Some consumers used the cash benefit to purchase services not otherwise available. One example is residential habilitation services to teach living skills, such as instrumental activities of daily living. (Habilitation services are usually not covered by the Florida Medicaid program, except in a group home.) Another such example is the use of the monthly budget to purchase dental services locally when no dentist in the consumers community would accept Medicaid assignment. By using the monthly budget to pay for the services of a local dentist, the family was relieved of the burden of transporting the consumer to another area for dental care.
Some purchases made with the monthly budget made a tremendous difference in the lives of consumers and their families. Case Example VII.4 gives several examples.
C. Time to Receipt of Cash
According to interview data collected for an early cohort of about 230 treatment group members, a substantial minority of adult consumers--particularly, elderly consumers--still had not begun to receive the monthly budget nine months after assignment to the treatment group.23 This was true for 45 percent of those older than age 65 and for 26 percent of nonelderly adult consumers (most of whom have developmental disabilities). In addition, 17 percent of children assigned to the treatment group had not begun to receive the monthly budget nine months later. Data compiled by DOEA as of February 2002 also show long delays in the receipt of the monthly budget among elderly consumers. Of the 662 elderly consumers assigned to the treatment group as of that month, 149 had disenrolled from CDC, and 70 percent of the rest had been enrolled more than 90 days but were not receiving the monthly budget.
1. Factors Leading to Delay
Consultants reported that several factors affected the length of time it took for consumers to receive the monthly budget. Some of these factors were beyond the control of the CDC project, because they pertained to the consumers condition or situation or the workers requirements or situation. In some cases, pain interfered with the consumers ability to think through issues. In others, the consumer became seriously ill and entered a hospital. In still other cases, the consumer lost an informal caregiver, and care plans had to be reconsidered. As noted earlier, completion of the purchasing plan might be delayed due a dispute over the wages a family member was to receive as a worker. A worker might not be able to start right away--perhaps he or she had to give notice at another job or arrange for child care.
Procedural issues, over which CDC had at least some control, also led to delay in receipt of the monthly budget. If a consumer did not receive the consumer notebook promptly, this could delay the initial training visit and the development of the purchasing plan. There were sometimes delays in the approval of purchasing plans by some district offices (for plans of consumers with developmental disabilities) and by the state CDC office (for other consumers). To avoid delay at this step, consultants would sometimes call the state or district office in advance to see if a proposed expenditure was acceptable. Delays also occurred because a monthly budget could start only at the beginning of a month. All materials had to be completed and submitted before the 20th of one month for the monthly budget to begin as of the first of the following month. Case Example VII.5 presents one consultants description of the steps in the process leading to receipt of the monthly budget.
The number of people involved in the CDC project also made communication more difficult, which likely increased the time to receipt of the monthly budget. One consultant for the elderly commented, Now it is us, the client, the representative, the state, and the fiscal agent. Theyve added extra steps, and the coordination is frustrating.
During our visit to Florida in early 2002, consultants reported that competing demands on their time sometimes resulted in delay in completing the purchasing plan for elderly consumers. Consultants for those with developmental disabilities did not seem to be so sorely pressed (the demand on the time of support coordinators that had arisen early in CDC had abated). One consultant for elderly consumers commented, My other work fell behind when I was working with consumers. My biggest problem is finding time to work with them.
Differences in caseload size may partly explain the apparent difference in the demands on case managers and support coordinators. State regulations permit case managers a maximum caseload of 80 elderly clients. For support coordinators, the maximum caseload is 38 clients with developmental disabilities.
The philosophy with which the CDC project began also seems to have increased time to the receipt of the monthly budget, particularly for consumers who enrolled early in the project. The initial view of many in the CDC project apparently was that consumers who could not complete the purchasing plan themselves (or who did not have a representative who could do so) did not belong in CDC. As long as a consultant abided by this philosophy, time to the monthly budget was increased because many consumers and representatives could readily decide what goods and services to purchase but struggled with completing the plan (particularly, the arithmetic) and needed multiple training visits to complete it. Other consumers simply dropped out of the program before ever getting the monthly budget because they could not complete the plan themselves.
With experience, many consultants and the CDC project learned that most consumers needed more help completing the purchasing plan but could largely manage on their own thereafter. Case Example VII.6 presents two consultants views on this issue. Consultants who were strong supporters of CDC were among those who reported that most consumers needed substantial help with the purchasing plan.
At the time of our visit, not all consultants fully understood or accepted this change. At one agency we visited, a consultant who described doing arithmetic when consumers were unable to do so themselves was reminded by other staff members that she was not supposed to do the work for the consumer.
One consultant we spoke with reported that consumers became more independent over time. Case Example VII.7 presents that consultants views on the ability of elderly consumers.
2. State Efforts to Reduce Delay
As in any experimental program, issues arose for which a procedure had not been anticipated. Some consultants reaction to this was that the state was making it up as they went along. Others recognized that problems were inevitable but felt that state CDC staff addressed issues right away when they arose.
In addition to the revision in program philosophy already described, the state took several concrete steps to reduce the delay to the receipt of the monthly budget. As described in Chapter VI, the state prepared detailed instructions on the completion of employment forms and sample forms that highlighted the material the consumer or worker was to enter. In addition, at the time of our visit to Florida in early 2002, the state CDC project was sending a letter to each consumer who was not on cash 90 days after his or her enrollment to see if he or she needed assistance to get on the monthly budget. Members of the state CDC staff also were telephoning consultants about these consumers to see if they could help the consultant expedite the completion of the purchasing plan.
D. Revisions to the Cash Plan
Changes in the purchasing plan are required as consumer needs and plans change. CDC procedures required a formal revision of the purchasing plan if any line item or the amount devoted to any line item was to change. The consultant had to review the revised plan. Next, it was sent to the state CDC office (for elderly consumers) or district office (for those with developmental disabilities) for approval. Finally, the fiscal agent had to revise the consumers account to conform to the revised purchasing plan.
1. Limited Experience with Formal Revision
Consultants we spoke with said they had little experience so far with revisions to purchasing plans. At the time of our visit, most consultants had only a few consumers on the monthly budget, and most of these consumers had been on the monthly budget only for a short period. The consultants reported that few consumers on the monthly budget had experienced changes in their needs or plans that necessitated a revision to the purchasing plan.
State CDC staff had a different perspective, however--they said that consumers were making changes in their care arrangements but that consultants were not on top of these changes. Consequently, the purchasing plans were not being revised when that was appropriate.
2. Writing Flexible Plans
Florida tried to write flexible initial purchasing plans to minimize the need for formal revision. Florida most likely learned some approaches to flexibility from the experience of the other states in the Cash and Counseling Demonstration. For example, as in Arkansas and New Jersey, DOEA did not require that the purchasing plan identify the worker by name. Rather, the plan might specify only the number of hours and the wage rate. This made it unnecessary to revise the purchasing plan if the worker was replaced but the hours and wage rate did not change. Of course, the new worker would still have to complete employment forms. (DDP, however, did require that workers be listed in the plan by name.)
As described in Chapter III, Florida allowed consumers whose monthly budget was managed by the fiscal agent to receive 20 percent (or more with special approval) of the monthly budget as cash for purposes specified in the plan when an invoicing process would not work. (The name of the vendor and an invoice were required for purchases not made with the cash portion of the monthly budget.) Floridas intent in allowing more of the monthly budget to be provided in cash was to enhance consumer ability to purchase items at sale prices. For example, the purchasing plan might specify that the cash was to be used to purchase diapers, leaving the consumer free to purchase them at whatever store had the best price that month.
DDP adopted another approach to reducing the need for revision of purchasing plans for children and adults with developmental disabilities. (DOEA did not use this approach). In the other two Cash and Counseling states, a revision of the plan was required to indicate a change in the good or service for which the consumer was saving. Thus, a change was required when the consumer had saved enough to purchase one good or service and now wanted to begin to save for another purchase. If none of the amounts involved changed, Florida allowed an addendum to the purchasing plan in such a situation, rather than a formal revision to the plan. The addendum was a letter or memorandum from the consultant to the fiscal agent authorizing the use of savings to purchase a good or service not specified in the purchasing plan.
E. Lessons on Cash Planning and Management
Floridas experience provides several lessons on development of the purchasing plan and management of the monthly budget.
-
Advance preparation can expedite the development of the purchasing plan.
CDC allowed for several training visits to help the consumer develop the purchasing plan. Some consultants, however, expedited the development of the purchasing plan by asking consumers to begin to think, before the visit, about their needs and what goods and services they might purchase to meet their needs.
-
A consumer manual is an important tool, which is useful in familiarizing the consumer with program procedures and rules before the initial consultant training visit and as a reference manual. The manual should be population-specific.
Although some consumers and representatives will not review a manual before the initial home training visit, sending a manual in advance is still useful. Many consumers and representatives will begin to familiarize themselves with program rules, and some will study them thoroughly. Moreover, a manual becomes an important consumer reference book.
If a cash program serves different populations, and if the procedures and rules differ for these populations, separate manuals should be provided for each population. Doing this can make the manual for each population as understandable and easy to use as possible.
-
Working with a consumer on the initial purchasing plan can be time-consuming for counselors. However, a consumers need for assistance in developing the initial purchasing plan does not indicate inappropriateness for Cash and Counseling.
Some consumers and representatives need substantial assistance from consultants in completing initial purchasing plans. Some need help understanding the program procedures and rules and documents that must be completed (including employment documents, such as W-4 forms). For other consumers and representatives, the arithmetic necessary to compute the cost of the plan is a stumbling block (although aids such as charts giving taxes at each wage rate are helpful). In Florida, some consumers were functionally illiterate in arithmetic.
When Florida began to implement the CDC project, it adhered to the philosophy that consumers were not appropriate for the cash program if they or their representatives could not complete the purchasing plans after training from the consultant. With experience, however, consultants and CDC project staff learned to distinguish between the steps in developing the purchasing plan. Many consumers can identify what goods and services they would like to purchase but have difficulty calculating the price of these goods and services and, thus, are unable to complete the purchasing plan. Difficulty in completing the purchasing plan does not of itself indicate that a consumer is not appropriate for Cash and Counseling. Those who struggle with completing the plan can usually manage their own day-to-day care once the plan has been implemented.
-
Purchasing plans must be revised as consumer needs and plans change, and revision of the purchasing plan requires a substantial amount of time from program staff. However, flexible plans can reduce the need for revision, and paperwork can be expedited.
The purchasing plan is critical to ensuring that the allowance is not abused; therefore, the plan must be revised to accommodate changes in consumer needs and plans. This process requires a substantial amount of program staff time. In Florida, consultants reviewed the revised plans, central or district office program staff approved the revised plans, and fiscal staff had to revise their records.
The need for revised plans can be reduced--while still guarding against abuses of the allowance--by writing more flexible purchasing plans. CDC did this by (1) listing the wage and hours for a position, rather than naming a specific person; (2) earmarking a larger proportion of the allowance for cash; and (3) allowing addenda to purchasing plans to specify a change in the good or service for which funds are being saved (provided that the amount being saved does not change).
-
Consumers may be able to purchase goods on sale for less than the Medicaid program purchases them from vendors.
By shopping for sale prices, consumers in CDC were able to purchase personal care supplies, such as diapers, from commercial establishments for less than Florida purchased these supplies from vendors through the Medicaid program.
VIII. REPRESENTATIVES
As described in Chapter III, CDC consumers could name a representative to help manage the monthly budget. Minor children were required to have a representative, and consultants reported that almost all, adults with developmental disabilities, and most elderly consumers, named representatives.
A. Selection of Representatives
1. When Are Representatives Selected?
In general, representatives were identified during the enrollment visit for the CDC demonstration. A representative was named on the application form for the cash program, which the consumer signed. CDC decided to name representatives at enrollment partly in response to the evaluators request that representatives be named before random assignment.
Usually, the need for a representative was obvious at enrollment. Minors need representatives because they cannot enter into legally binding agreements, and adults who have severe developmental disabilities or have Alzheimers disease or other dementia generally are not able to manage the monthly budget themselves. In addition, consultants reported that they usually suggested a representative to consumers who had difficulty seeing and thus difficulty reading worker time sheets, consumer financial statements, and other project documents. Not all consumers who had difficulty seeing named a representative, however; one consumer who was legally blind insisted on managing the monthly budget without a representative. The consultants we spoke with felt that the consumers who had representatives did in fact need them.
2. Who Are the Representatives?
The choice of representative usually was obvious because it stemmed directly from the consumers current relationships. Usually, representatives were family members who were already helping the consumer with personal care or household tasks. Many elderly consumers named their daughters as representatives. Not surprisingly, the representative of a minor child was almost always a parent. In a few cases, a child was not in the care of his or her parents, and the representative was a legal guardian (such as a grandparent). Adults with developmental disabilities who were living with their families usually selected a parent as representative.
Naming a representative for adults with development disabilities who were not living at home was not always straightforward. Even if a consumer had relatives willing to take on this role, the consumer might not want a family member as a representative. The friends of adults with developmental disabilities often had disabilities as well and were unable to take on the responsibilities of a representative. While their number was not large, some consumers who had developmental disabilities and lived in group homes wanted to name their coach at the group home as their representative. (The coach is a member of the staff of the agency that runs the home.) Florida determined that it was appropriate for a coach to serve as a CDC representative, and coaches were told that it was their responsibility to serve if a CDC consumer named them. A consultant we spoke with, however, reported that, in her experience, coaches did not want to serve as representatives. The interest of the coachs employer was for the consumer to continue to purchase the same amount of group home services. However, a CDC consumer might wish to drop some group home services to free some funds for other purchases. In that case, being a representative could create a conflict of interest for a group home coach.
3. What Happens When Representatives Are Also Workers?
The person named as representative could also be a worker. Florida was aware of the potential conflict of interest inherent in the same person being a representative and a worker. This conflict arises because representatives sign worker time sheets and often serve as workers supervisors. From its inception, CDC tried to minimize the number of situations in which the representative and worker were the same person. However, some consumers had few relatives or friends who could share the responsibilities of representative and worker. An example is a case in which the representative/worker was a single parent with a child with developmental disabilities.
CDC staff reported that a few of these worker/representatives took advantage of the opportunity to pay themselves a good salary for numerous tasks (see the discussion in Chapter IX). That was by no means always true, however. For example, a sister of an elderly woman who was both her representative and her worker refused to pay herself more than $5 an hour. Other representatives (such as the mother of a child with developmental disabilities) refused any payment at all for the many hours of care that she provided her child.
After operations began, CDC staff learned that Florida law probably did not allow people to sign their own time sheets, as would normally occur when a representative was also a worker. In response, CDC adopted an approach based on the concept of circles of support, in which multiple relatives and friend support a person with disabilities. An advocate for the consumer from the circle of support would monitor the case, including validating that the worker/representative had performed the services agreed upon. The consultant telephoned the advocate and the representative/worker each month.
B. Lessons About Representatives
Floridas CDC program offers several lessons about representatives.
-
All, or almost all, consumers with development disabilities will need a representative to help them manage the benefit. Many elderly consumers will name a representative; the percentage doing so may vary with the level of disability of the consumers and the amount of assistance available from consultants.
Obviously, minors will require a representative, regardless of the nature of their disability. Floridas experience in CDC also suggests that all, or almost all, adults with developmental disabilities will name a representative and that many elderly consumers will do so.
Based on the qualitative data available for this analysis, it is impossible to definitively compare the percentages of elderly consumers who named representatives in the three Cash and Counseling states. However, it appears that the percentage may be higher in Florida than in Arkansas. The Florida consultants we interviewed reported very few elderly consumers who did not have representatives.24 In contrast, slightly more than half of elderly consumers in Arkansas did not name a representative at enrollment (Schore and Phillips 2004).25
Assuming that the percentage of elderly consumers naming a representative is higher in Florida than in Arkansas, what factors might explain the difference? Two major factors seem possible. First, to be eligible for CDC (as for traditional 1915(c) home- and community-based waiver services), all consumers in Florida had to qualify for a nursing home level of care. That was not the case in Arkansas, where state plan personal care services, rather than waiver services, were cashed out. Second, the program philosophy seems to have differed in Arkansas and Florida--at least initially. Arkansas consultants did not assume that consumers had to complete the purchasing plan themselves to be appropriate for the program. Such an assumption may have led Florida consultants to suggest representatives in situations where Arkansas consultants might have simply helped the consumer themselves.
-
The selection of representatives is an extension of existing relationships.
In Florida, as in the other two Cash and Counseling programs, the selection of representatives is an extension of existing relationships. In Arkansas, Florida, and New Jersey, most of those named as representatives were family members or friends who were already helping the consumer.
-
Naming representatives at enrollment may be advantageous.
Naming representatives at enrollment may be advantageous for the consumer, because doing so tends to expedite the development of the purchasing plan. If a representative has already been named, a consultant can begin to work with that person on the development of the purchasing plan before the initial home training visit.
However, enrollment procedures should ensure that potential representatives seriously consider the responsibilities involved before agreeing to serve. If the decision is not well considered, the representative can later withdraw. In that case, the consumer may be forced to withdraw from the cash program if he or she cannot identify another representative.
-
Representatives are generally faithful to the best interest of the consumer and try to take their wishes into account. Parents do a particularly good job of representing their childrens interests.
CDC consultants we spoke with reported that nearly all representatives properly served the interests of the consumers they were helping and that representatives generally tried to take the consumers wishes into account. For example, one consultant for elderly consumers noted that representatives might ask the consumer, Do you understand? What do you think you need?
Consultants reported that the CDC program seemed to work particularly well for children. Parents (or guardians) have their childrens best interests at heart and try to take their wishes into account, sometimes going to extraordinary lengths for their child. Case Example VIII.1 describes one such parent/representative through the eyes of her childs consultant.
Case Example VIII.1: A Representative Serves Her Childs InterestsI have one mother who is so excited about the ability to save and get things for her child that she has been energized to have fund-raisers. For example, she has Krispy Kreme days at her office to raise money to buy the special type of lift that would be best for her child but that Medicaid will not cover. Because of CDC, she is supported and celebrated as a mother.One notable exception was reported to the general rule that parent/representatives serve the best interests of their child. Sometimes it is hard for a parent to let go of an adult child. One consultant told of a mother of a [60-year-old consumer] with developmental disabilities. The mother did not want her son to move out of her home, noting, She had been a parent for more than 50 years.
-
Special forms of monitoring can be used when a representative is also a worker, as this situation presents an inherent conflict of interest.
Because representatives supervise workers, allowing the same person to play both roles presents a conflict of interest. With special monitoring, Florida allowed the same person to be both representative and worker, thereby permitting a parent to serve in both roles for the child. To monitor cases where the same person was both, the state asked someone the consumers family identified to check on the consumers well-being, and the counselor telephoned that person and the representative.
Florida also allowed one parent to be a worker and the other the representative. While one could argue that this situation also presented an inherent conflict of interest, since the childs parents would usually be husband and wife, Florida did not ask a third party to check on the consumers well-being in such cases. No instances of exploitation or abuse attributable to this situation were identified.
A conflict of interest situation may also arise for adults with developmental disabilities who are living in group homes. They sometimes named group home coaches as representatives, but doing so may create a conflict of interest for the coaches, who also must represent the interests of the agency running the group home. An approach similar to the one that Florida adopted when the representative was also the worker might be an appropriate way to monitor such situations.
IX. PREVENTING NEGLECT, EXPLOITATION, AND ABUSE
The possibility that consumers could be neglected or exploited or that the monthly budget could be abused was a major concern of all involved in the CDC project, as it was for all the Cash and Counseling Demonstration programs. Policymakers wanted to ensure that vulnerable consumers were not harmed and that public funds were not squandered. There had been fraud and abuse in Floridas traditional Medicaid waiver program, and the state legislature expected that proper controls would be in place to prevent similar occurrences in CDC. In addition, case managers and support coordinators particularly wanted to ensure that workers did not take advantage of consumers by failing to perform agreed-upon tasks.
Even so, everyone directly involved in the Cash and Counseling Demonstration realized that extensive control and close oversight were inconsistent with the philosophy of consumer direction. Consumers must be free to make choices and manage on their own, even if others view some of their decisions as misguided.
At the time of our visit early in 2002, there had been only a few isolated cases of abuse of the monthly budget and only one case of possible neglect or exploitation of a cash recipient in CDC. We describe these cases in this chapter. First, however, we consider the methods CDC adopted to prevent abuse of the monthly budget and neglect or exploitation of consumers.
A. Preventing Neglect and Exploitation
Under CDC, consultants monitored for neglect or exploitation of consumers by their representatives or workers.
1. Procedures for Contact Between Consultants and Consumers
CDC required that consultants contact consumers (or representatives) monthly by telephone and visit the consumers home 2 and 12 months after enrollment and annually thereafter. Consultants could also visit, unannounced, at any time (this is not true of all Florida Medicaid programs). In addition, consultants were responsible for conducting reassessment visits at least annually to determine whether the consumers condition or situation had changed and thus whether a revised care/support plan was needed. The date of the annual reassessment visit was unrelated to the date of the annual monitoring visit for CDC. Thus, these two visits would not generally coincide.
One purpose of the consultant monitoring calls and visits was to check on how the consumer was doing. (The other purpose, as described in Section B, was to conduct a financial review.) CDC did not develop a structured interview or checklist for the monitoring calls and visits. Instead, consultants were expected to use their knowledge of the particular case (including information gained in prior telephone calls and visits) to frame questions pertinent to possible neglect or exploitation in that case. For example, if a consultant knew that a consumer had hired a brother who had a criminal record, the consultant was expected to ask the consumer how that brother was working out as a caregiver.
2. Contacts Between Consultants and Consumers in Practice
Most consultants we interviewed reported routinely making monthly monitoring calls. However, two consultants were not doing so at the time of our visit. One of them reported that, after the monthly budget started, she waited for the consumer to call her, since (in her view) this practice was consistent with CDCs philosophy to leave the consumer alone. The other consultant reported that she did not make the monthly monitoring calls because, without the monthly consumer financial statement, there was nothing to discuss (at the time of our visit, the fiscal agent had not prepared consumer financial statements for several months). Apparently, this consultant focused only on financial monitoring, not recognizing the need to check on the consumers condition and situation.
At the time of our visit to Florida, few consumers had been enrolled in CDC for a year. Therefore, few consultants had conducted the annual monitoring visit. Some consultants we spoke with said they were confused about the purpose of this annual visit and how it related to the annual reassessment visit (see Case Example IX.1).
Consultants developed different practices for monitoring calls and visits. Some said they established close working relationships with consumers: Sometimes they call me, and sometimes I call them. They also get e-mails from me, and I follow up by telephone. Another consultant reported listening for subtle clues during the monthly monitoring calls, such as hesitation in responding to a question, and probing for more information if something seemed to be amiss. Yet another consultant reported that she made unannounced visits if something seemed amiss during the monthly telephone monitoring call and that she found such visits useful in identifying issues that needed her attention.
Two consultants (one working with elderly beneficiaries and one with children and adults with developmental disabilities) said they thought telephone calls to representatives were insufficient to ensure that consumers were not being neglected or exploited. These two consultants also visited the consumer periodically. One sought out the developmentally disabled children on her CDC caseload when she visited schools for monitoring visits with her traditional clients. To assess a childs well-being, she spoke with the child briefly and looked for a change in appearance, such as a weight change. Case Example IX.2 presents her comments on the value of the school as a source of information.
B. Preventing Abuse of the Monthly Budget
The CDC project used three methods to prevent abuse of the monthly budget. First, consultants had to review the consumers monthly financial statement with the consumer (or representative) during the monthly call or visit. Second, consumers were to maintain a record of purchases with funds that the consumer had received in cash (usually, funds for incidental expenses) and retain receipts for these purchases. Third, in most cases, the fiscal agent was to pay only for purchases specifically listed in the purchasing plan.
1. Consumer Monthly Financial Statements
Floridas contract with the fiscal agent called for it to prepare a monthly financial statement for each consumer receiving the monthly budget, with a copy sent to the consultant.
CDC procedures anticipated that consultant review of consumer financial statements would be important in preventing abuse of the monthly budget, and consultant training stressed the importance of this review. As discussed in Chapter III, CDC allowed consumers some discretion to vary their purchases, provided the purchases addressed needs that the plan identified. To allow for this, the fiscal agent did not initially adopt a policy of paying only for the purchases listed in the plan and only in the amounts listed (as in the other two Cash and Counseling programs).
Rather than requiring strict adherence to the purchasing plan, CDC relied on consultant review of financial statements to ensure that discretionary purchases addressed needs that the plan identified and to pinpoint overspending. If purchases were inappropriate, the consultant was responsible for reteaching the consumer about permissible services. If overspending occurred, the consultant was responsible for reminding consumers of the importance of tracking their own expenditures to avoid future overspending. In either case, the consultant was to notify the fiscal agent so that arrangements could be made to reimburse the project from future monthly budget payments as appropriate.
To ensure that expenditures (apart from payments to the consumer in cash) were exactly as specified in the purchasing plan, the consultant needed to see detailed monthly statements. For example, knowing the total of wages given for all workers (as reported on the initial consumer financial statements for CDC) would not permit the consultant to determine whether each worker had as many hours as specified and at the specified wage rate.
The monthly consumer financial statements also informed consumers how the funds in their accounts had been spent and told them their account balances (as of the end of the period covered by the statement). Without these statements, it was difficult for consumers to track their account balances themselves. For example, suppose a worker did not work the hours called for in the purchasing plan. As a result, the consumer would have unplanned savings. Without a financial statement, the consumer would be unlikely to know the exact amount saved, after taking into account deductions for payroll taxes. Without knowing the exact amount of savings, the consumer could not complete a revised purchasing plan to specify a use for the savings.
2. Difficulties with Consumer Financial Statements
The fiscal agent had several difficulties with monthly consumer financial statements. First, there were periods when the fiscal agent was unable to produce the monthly consumer financial statements (see discussion in Chapter V). Second, the initial monthly statements were not detailed enough and were difficult to understand. The fiscal agent revised the format of the statement. However, the consultants we interviewed reported that, after the first set of revisions, the statement was still not detailed enough to determine whether a purchasing plan was being followed to the letter. Shortly after our visit in early 2002, the fiscal agent began to send out more detailed monthly statements to consumers. The fiscal agent reported that it had tried to learn the needs of consumers and consultants through discussions with them and had designed the revised statement to meet those needs. The revised statement resembles a check register in that it has the name of the party to whom the check was made out, as well as the amount.
The final problem with consumer financial statements was the difficulty the fiscal agent had maintaining an up-to-date list of each consumers consultant and contact information for that consultant. This difficulty arose from the large number of consultants (especially for beneficiaries with developmental disabilities) and from consultant turnover. Lack of an up-to-date list obviously hampered timely mailing of copies of consumer financial statements to consultants.
3. Review of Receipts
As indicated earlier, CDC required consumers to retain receipts for purchases made with cash, which consultants were to monitor. The CDC consultants we spoke with reported that many consumers were retaining records and receipts for purchases made with cash, as required. Most, but not all, of these consultants reported reviewing receipts, but they had different approaches to doing so. One reported asking consumers (or representatives) to mail her copies of their receipts, which she discussed with them during their monthly telephone calls. Another reported that she told consumers and representatives to be sure to save the receipts, as she might make an unannounced visit at any time and ask to review the receipts during that visit. Two consultants we interviewed were not reviewing receipts. One reported that she asked consumers on her caseload to retain receipts for cash purchases, even though CDC did not require consumers to retain receipts. (Her understanding was that consumers were only required to maintain a record of cash purchases.) The other consultant reported that she was told not to monitor receipts unless she suspected fraud.
The fiscal agent reviewed the financial records of the small number of consumers who were managing the monthly budget without the fiscal agents help. There is no evidence that any of these consumers attempted to abuse the monthly budget.
4. Checks Against the Purchasing Plan
Initially, CDC does not seem to have provided the fiscal agent with clear guidance on payment for a purchase not specifically listed in the purchasing plan. As described earlier, CDCs initial policy was to allow consumers some flexibility, as long as the purchase was consistent with the plan. Staff of the fiscal agent that we interviewed reported receiving conflicting instructions on how closely payments were to adhere to the plan. They reported that CDC project staff sometimes told them to only follow the purchasing plan and other times to be a little more flexible. (Staff of the fiscal agent said they had requested written guidance from the state regarding payment in such cases but had not received it by the time of our visit.)26
The staff of the fiscal agent were concerned that paying for purchases not specifically listed in the plan might cause problems. Even if paying for a purchase that was not listed in the plan did not result in a negative account balance, the fiscal agent might not be able to pay a later invoice for a purchase specified in the plan because payment of the second invoice would result in a negative balance. This situation would be particularly problematic if the second invoice was a workers time sheet.
To avoid this potential problem, the fiscal agent began to require written authorization from a consultant before paying an invoice for a good or service not specified in the purchasing plan. In effect, without a formal revision to the plan, it required addenda to the purchasing plan.
C. Little Abuse and Little or No Exploitation or Neglect
Under CDC, there was little abuse of the monthly budget and only one case of possible exploitation or neglect of the consumer. The CDC project identified and addressed all these cases. None resulted in negative publicity for the project.
1. Little Abuse of the Monthly Budget
The CDC project staff and consultants we interviewed reported two clear cases of material abuse of the monthly budget. In the first case, an amount exceeding the monthly budget amount was paid out after a consumer submitted a signed time sheet for more hours than the purchasing plan called for. The fiscal agent issued a check to the worker on the grounds that it was bound by state law to pay the worker if a time sheet had been signed (regardless of the amount in the consumers account) and promptly notified the CDC project of its action. There were several cases of overpayment stemming from payment for additional worker hours. However, all but one of these cases proved upon investigation by Florida to be instances of honest errors in which consumers did not understand that overtime would be charged at time and a half. Only one case appeared to be a deliberate abuse of the monthly budget. Florida recouped all the overpayments in these cases.
The second case of abuse of the monthly budget involved a woman who had agreed to be a worker for a family member but who hired an illegal immigrant to do the work in her stead. Although the consumer in this case was receiving the agreed-upon care and that care was satisfactory, it was not the intent of the CDC project to allow those who had agreed to be workers to hire substitutes for themselves, legal or otherwise.27
In a few cases in which families paid themselves from the monthly budget, the consultants we interviewed regarded this as double dipping and bordering on abuse. These cases may not have involved violation of CDC project rules but, rather, behavior the consultants felt was unseemly. Case Example IX.3 presents a consultants description of one such case.
2. A Single Case of Neglect
By the time of our visit early in 2002, only one case that might have been exploitation or neglect of a consumer had occurred. In this case, stimulating after-school activities had not been arranged for a child with developmental disabilities. The consultant intervened to arrange for enrichment activities and increased the level of monitoring of the case to ensure that the childs future care was satisfactory. Senior state staff felt that the consultant handled the case well. CDC project staff, concerned about cases such as this one, arranged for consultants to refer cases of possible neglect or exploitation to protective services.
3. No Exploitation of Workers Reported
Under a consumer-directed program, exploitation of workers is a potential problem. It does not seem to have been a serious problem in CDC, however. Consultants reported only two cases in response to our question on this topic. It is not clear that either case was exploitation, although they do seem to involve insensitive or arbitrary behavior on the part of the consumer as employer. In one case, a personal care worker was reportedly asked to act as a baby-sitter for a sibling of the consumer. In the other, a consumer reportedly terminated the employment of a worker who earlier had been providing unpaid care on the grounds that the care was not satisfactory. The consumer instead hired a friend who had not been helping earlier.
D. Lessons About Monitoring
We can draw several lessons about monitoring from Floridas experience.
-
The appropriate frequency for monitoring visits varies with the population served. Monitoring that involves only the representative is inadequate; consultants need to interact with the consumer and, perhaps, with others.
Cash and Counseling programs must try to balance the need for monitoring to prevent exploitation and neglect of the consumer with the philosophy of consumer-directed care and the public expense involved in monitoring.
Only one case of possible neglect or exploitation of the consumer had been identified in CDC by the time of our visit in early 2002. This is not necessarily evidence that an annual visit is sufficient for routine monitoring, for three major reasons. First, few consumers had been in CDC for a year at the time of our visit; thus, consultants and project staff had not had much opportunity to observe what occurred when monitoring visits were many months apart. Second, some consultants reported routinely visiting consumers frequently (for example, monthly or every other month). Third, most CDC project staff we spoke with said they believed annual visits were insufficient for routine monitoring.
The appropriate frequency of routine monitoring visits most likely depends on the population served. One consultant serving elderly beneficiaries suggested that semiannual visits would be enough for most consumers. In contrast, a consultant whose clients included children with developmental disabilities arranged to visit them monthly because she felt monthly visits were necessary to assess the well-being of these children.
Some CDC consultants reported that one could not assess the well-being of the consumer based on discussion with the representative alone. (Consultants in the Arkansas Cash and Counseling program routinely telephoned both the representative and the consumer.) Although most consultants believed that most representatives were faithful to the best interests of the consumer, some consultants believed that they were unlikely to uncover the rare case in which that was not true by speaking only to the representative.
If the consumer is able to articulate his or her needs and concerns, a monitoring call to the consumer (as well as to the representative) seems sufficient to identify cases in which consultant followup is needed. Frequent, routine visits are not necessary. On the other hand, to assess the well-being of consumers who are not able to articulate their needs and concerns, consultants need to visit the consumer frequently (at least every two or three months) or to speak to external parties (such as school authorities) or members of a circle of support who can observe the consumer.
-
Referral arrangements with organizations providing protective services may be beneficial.
While there was very little evidence of consumer neglect or exploitation in CDC, project staff did develop formal arrangements for consultants to refer cases of potential neglect or exploitation to protective services. Such arrangements may enable consultants to get expert help quickly, so prompt action can be taken to help consumers who might be vulnerable.
-
Monthly financial statements are important to consumers ability to manage their allowance and obviously necessary if consultants are to compare monthly financial statements to purchasing plans to prevent abuse of the allowance.
According to the consultants we interviewed, consumers were more dissatisfied with the lack of timely, understandable financial statements than with any other aspect of the CDC project. Without access to timely, understandable financial statements, consumers cannot identify errors in payment on the part of the fiscal agent. Moreover, they are unlikely to know the balance in their accounts as unplanned savings accumulate (such as when a worker does not come as scheduled). To prepare a formal revision to the purchasing plan, the consumer and consultant need to know the exact balance in the account.
Consultants also need detailed financial statements to determine whether expenditures are consistent with purchasing plans. Financial statements that report expenditures for a given type of expenditure are not adequate for this purpose. For example, if the statement gives only the total wages paid to all workers, the consultant cannot determine if the hours and wage rates listed in the purchasing plan were being honored.
-
Relying on consultants to compare monthly financial statements to purchasing plans increases the need for communication between the consultant and the fiscal agent, which can be problematic.
If procedures call for consultants to compare monthly financial statements to purchasing plans to prevent abuse of the monthly budget, the fiscal agent must routinely supply consultants with copies of consumers financial statements. This process was seriously deficient in CDC--the fiscal agent had great difficulty producing statements and getting them to consultants quickly. Especially when consultants and fiscal staff are in separate organizations, having consultants compare expenditures to purchasing plans may be a problem.
-
Review of receipts is not critical to preventing major instances of abuse of the allowance.
CDC required review of receipts only for cash held by the consumer, not for funds managed by the fiscal agent. In almost all cases, the cash was limited to 20 percent of the allowance. Moreover, some consultants reported that they did not routinely review receipts for incidental expenses. The fact that abuse of the allowance was almost nonexistent--despite the limited review of receipts--indicates that such review is not critical to preventing abuse of funds managed by the fiscal agent.
-
Some consumers need training in employer responsibilities.
The experience of the CDC project suggests that consumers need training in the responsibilities of an employer. Some of this training is straightforward. For example, if consumers are to be allowed discretion to increase the hours of one worker to substitute for a worker who cannot work as scheduled, consumers need to understand their states law regarding payment of overtime hours. Without understanding this, a consumer might believe that increasing the hours of one worker, one for one, to substitute for another earning the same hourly wage is an even trade that has no cost implications. Under CDC, consumer accounts were overdrawn in a few cases because the consumer did not understand that the employee would be paid time and a half for overtime hours.
Some consumers also need training in the appropriate treatment of employees. Consumers need to understand that maintaining a good employer-employee relationship requires that the employer act in a responsible way and not impose on that relationship by asking personal favors of the employee, who may not feel that he or she can refuse. As mentioned earlier, a consultant reported a case where a worker was asked to baby-sit for another family member in a situation that took unfair advantage of the worker (at least, in the consultants judgment). Another CDC consultant reported a case where she felt a consumer had exploited a worker by arbitrarily terminating the worker in favor of hiring a friend.
-
Cash and Counseling programs may want to adopt a policy that workers are required to perform the agreed-upon tasks themselves.
Under CDC, one worker hired an illegal immigrant to perform the tasks that she had been hired to do. Cash and Counseling programs may want to adopt a policy prohibiting a worker from contracting out caregiving tasks that he or she had agreed to do and to educate consumers, representatives, and consultants about this policy. Such situations seem most likely to arise when the representative can also be the worker.
-
Monitoring does not appear to have an adverse effect on the relationship between a consultant and consumer.
One concern that is sometimes expressed about Cash and Counseling programs is that monitoring will set up an adversarial relationship between the consultant and the consumer, leading to a diminution of trust between the two. However, that does not seem to have been a serious issue in CDC. Only one consultant we spoke with raised that as a concern, and even that consultant did not report that monitoring had adverse consequences. This consultant simply may have been personally uncomfortable with the monitoring role.
X. CROSS-CUTTING LESSONS THAT SET FLORIDA APART
Floridas experience with the Cash and Counseling model provides many valuable lessons. In earlier chapters describing the implementation of the CDC project in Florida, we have presented lessons specific to the various components of the model. In this chapter, we present lessons that cut across components and focus on aspects of the Florida project that differed from those of the Cash and Counseling Demonstrations in Arkansas and New Jersey. These aspects are (1) extent of reliance on agencies providing traditional services, (2) cashing out of waiver services for children and adults with developmental disabilities, and (3) level of consumer responsibility.
A. Relying on Agencies Providing Traditional Services
Florida was the only one of the three Cash and Counseling states to rely primarily on agencies providing traditional services to provide outreach, enrollment, and consulting under its cash program.
-
Many factors seem to affect the level of resistance of providers of traditional services to an allowance program. They include competing demands from other programs, monopoly position, concerns about agency revenue, adequacy of compensation for agencies under the allowance program, concerns about liability, and conflicting professional norms. States interested in relying on agencies providing traditional services may be able to reduce this resistance.
CDC initially relied on providers of traditional services for outreach and enrollment. This approach was largely unsuccessful, however, and CDC adopted an approach that relied much less on providers of traditional services. CDC began direct mailings to members of the eligible population and hired temporary state employees to be responsible for outreach and enrollment for most Medicaid waiver recipients. This approach to outreach and enrollment generated a demand for the cash program among consumers with developmental disabilities and their families, many of whom were politically active. The waiver for those with developmental disabilities allowed them to choose their support coordinator. Faced with the demand for the cash program, many support coordinators began to offer CDC consulting rather than lose clients and revenues to others who offered it. Florida enrolled a large number of children and adults with developmental disabilities in a relatively short time. Moreover, many of those assigned to the treatment group completed their purchasing plans and began to receive the monthly budget in a reasonable period of time. CDC was successfully implemented for beneficiaries with developmental disabilities, especially children.
CDCs reliance on direct mailing and temporary outreach and enrollment staff was much less successful with elderly beneficiaries than with those with developmental disabilities. Elderly Medicaid beneficiaries are not politically active in Florida, especially compared to the families of those with developmental disabilities. Many elderly beneficiaries sought the advice of their case manager before deciding whether to enroll in the cash program, making it easy for case managers who were resistant to CDC to discourage enrollment. Moreover, case management agencies held local monopolies on the provision of Medicaid waiver services. Thus, an elderly beneficiary who wanted to enroll in the cash program could not take his business elsewhere. In CDC, much consultant effort is required early in the process. Case management agencies did not give high priority to CDC consulting. In addition, case managers already were responsible for several programs and were carrying substantial caseloads. Competing demands often took priority over helping an elderly consumer develop a purchasing plan, leading to long delays in receipt of the monthly budget.
States interested in a program like Cash and Counseling should carefully examine the characteristics of the existing system to assess resistance before relying on providers of traditional services to implement an allowance program. Several factors seem to affect the level of resistance from the existing system.
First, the demands of an existing caseload tend to decrease the likelihood of successfully implementing the cash program. States may want to avoid relying on providers of traditional services to implement a cash program when other major programs are beginning or other demands are high.
Second, inadequate compensation for the staff time required to implement a cash program increases resistance. States should realistically assess the time involved and adequately compensate consultants and the organizations employing them for time and other resources, including time for outreach and enrollment, devoted to a program like Cash and Counseling.
Third, local monopolies tend to decrease the likelihood of successful implementation because they decrease responsiveness to beneficiary demand for any new program, including a cash program. States may want take particular care in implementing a cash program through an existing network of providers that is resistant and that holds a local monopoly over the service being cashed out.
Fourth, concern about loss of business and revenue tends to increase resistance among providers of traditional services. These concerns are likely to be greater among providers that render hands-on services than among those that render only case management or support coordination. The Florida experience suggests that traditional case managers and support coordinators may find employment as consultants (assuming that they are comfortable with the philosophy of consumer direction). However, few consumers hired their agency aide as a worker; in all three Cash and Counseling programs, most consumers hired relatives and friends. States interested in a cash program may want to avoid implementing that program through traditional agencies if those agencies provide hands-on services or if the state is experiencing a reduction in the population served (perhaps as a result of budget shortfalls). In that situation, providers will already be concerned about future business and revenue. The language used to describe funding changes also may increase agency resistance. Instead of presenting funding for traditional agencies as reduced in favor of funding for a cash program, states may want to stress to traditional agencies that funding follows the consumer from traditional services to a cash program.
Fifth, the providers of traditional services likely will be more resistant to programs that appear to fail to validate the professional norms of their discipline. An allowance program may threaten norms involving protection and nurture of vulnerable populations. States may be able to reduce resistance by demonstrating that some beneficiaries benefit dramatically from a cash program and by appealing to client advocacy--another professional norm.
Finally, a concern that consultants and consulting agencies will be held responsible for consumer outcomes increases resistance. States may want to stress that this is not how a program like Cash and Counseling works. In such a program, consumers assume liability for their own decisions--regardless of the outcomes of those decisions. The consultant is responsible only for following project procedures.
-
States may be better able to secure the interest and support of organizations providing traditional services if they consult these organizations early in the design of an allowance program.
Due to the tight schedule imposed by solicitation for grants to states to design a Cash and Counseling Demonstration, Florida did not consult agencies providing traditional services before it submitted its application. Senior officials in Florida regretted this. In designing the Choice and Control project for adults with developmental disabilities, Florida consulted agencies providing traditional services and families of those with developmental disabilities.
B. Waiver Services for Children and Adults with Developmental Disabilities
Floridas CDC program was the only one of the three Cash and Counseling programs to cash out services for children, services for beneficiaries with developmental disabilities, and services provided under a waiver rather than the state Medicaid plan.
-
Parents of children with developmental disabilities find the Cash and Counseling model very attractive.
As a percentage of those eligible, more children with developmental disabilities enrolled in a Cash and Counseling program than any other population. As enrollment for the evaluation of the Cash and Counseling Demonstration ended, the number of elderly enrollees in Florida and in the other two states represented about 8 to 10 percent of the number of elderly Medicaid waiver or state plan personal care recipients in the year before the demonstration.28 The number of nonelderly adults represented about 15 to 20 percent of the number of people eligible before the demonstration. In Florida, about 15 percent enrolled, and most of these were adults with developmental disabilities. The number of children with developmental disabilities who had enrolled when enrollment for the evaluation ended was about 25 percent of the number who were eligible in the year before the demonstration.
-
Paying parents to be workers is a sensitive issue, but parents rarely take unfair advantage of the situation.
Paying parents to care for their children is both a legal issue and a social one. On the one hand, caring for a child with disabilities requires a tremendous amount of time and energy, which affects the time a parent can devote to other family members and paid work. On the other hand, the parents of minor children are legally responsible for their care. (A waiver of Medicaid regulations was required to allow parents to be paid as workers for their children in CDC.) Moreover, the law against paying parents of minors reflects traditional social norms. Some CDC consultants and district Medicaid specialists expressed misgivings about the appropriateness of paying people to do something they should be doing anyway.
However, only very rarely did parents of minor children participating in CDC even appear to take unfair advantage of the opportunity to be paid. Although CDC consultants reported a few cases of entrepreneur parents who were apparently trying to make the most of the opportunity to be paid, these cases are rare, and even they do not represent clear abuse of the monthly budget under CDC rules. In addition, CDC consultants reported cases in which parents refused to be paid for the many hours they devoted to the care of their child.
-
To provide for situations with inherent conflicts of interest, special forms of monitoring may be needed in cash programs for minor beneficiaries and for beneficiaries with developmental disabilities living in group homes.
Situations with inherent conflicts of interest arose in CDC that did not arise in the Cash and Counseling programs in the other two states. Only Florida allowed the same person to be both a representative and a worker. The state did so primarily to avoid precluding a parent from serving in both roles for their child. Because representatives are responsible for supervising workers, allowing the same person to play both roles creates a conflict of interest (and may violate state law). A similar, but perhaps less acute, conflict of interest is created when one parent is the worker and the other is the representative, since the childs parents would usually be husband and wife.29
Another conflict of interest that arose in Florida involved naming group home coaches as representatives for adults with developmental disabilities. To free some funds for other purchases, consumers might wish to purchase fewer services from the group home. In that case, a coach would be put in a conflict-of-interest situation because the coach also has a responsibility to represent the interests of his or her employer, the agency running the group home. While group home coaches were required to act as representatives if named by a CDC consumer, some were apparently uncomfortable with that role.
Aware of the inherent conflict of interest involving worker/representatives, CDC tried to avoid naming a person who was a worker as the representative. However, in a few situations, no good alternative was available (for example, in the case of a single parent of a developmentally disabled child). CDC developed a special monitoring procedure for cases in which the same person was a worker and the representative. Drawing on the concept of a circle of support, Florida asked a third party trusted by the consumers family to check on the consumers well-being, and the consultant telephoned that person monthly, as well as telephoning the representative. The concept of a circle of support might also be useful in alleviating conflict of interest for group home coaches who are also representatives.
C. Level of Consumer Responsibility
Arguably, Floridas CDC project gave the consumer (or representative) more responsibility than did the other two Cash and Counseling programs. Three aspects of CDC that gave consumers (or representatives) increased responsibility are particularly noteworthy. First, Florida cashed out professional services if these were included in the care/support plan, thus implicitly allowing consumers to assess their need for such services. Second, it devoted considerable effort to developing consumer-training materials. Finally, it allowed addenda to purchasing plans to revise the designation of the good or service for which the consumer was saving.
-
A consumer manual is useful in training consumers. However, a manual is not a substitute for consultant help in developing the purchasing plan.
Floridas experience was that the consumer notebook was useful in the initial training sessions and as a reference manual. Many representatives and some consumers prepared for the initial visit with a consultant by reviewing the handbook as they had been asked to do. However, most consumers needed consultant assistance to complete the first purchasing plan.
-
The evidence from Florida is that consumers and their representatives can manage some professional services, as well as personal care.
Professional services (such as behavioral therapy and nursing) are covered under Floridas waiver programs and were cashed out. Thus, Florida consumers were implicitly given responsibility for making decisions about their need for professional services. Allowing consumers to decide about their need for professional services, as well as their need for personal care services, did not result in material neglect or exploitation of consumers. Only one case of possible neglect or exploitation occurred during the first 18 months of CDCs operation.
-
Consumers who have accumulated some savings from the allowance can be permitted to make purchases not specifically listed in the purchasing plan, while still preventing abuse of the allowance. Consultants can authorize such purchases as addenda to plans.
Allowing consumers the discretion to purchase a good or service not specifically listed in the purchasing plan has a potential problem in that a consumer might attempt to spend more than the amount of the allowance in a given month. Even if sufficient funds were available to pay an invoice for a purchase that was not specified in the purchasing plan, sufficient funds might not be available to pay for a subsequent purchase that was specified in the purchasing plan. Such a situation would be particularly problematic if the second purchase involved payment of a workers wages.
One way to prevent such situations is to strictly enforce a requirement that the fiscal agent pays only for goods and services specified in the purchasing plan and only in the amounts specified in the plan. However, formal revision of the purchasing plan takes a long time. In addition, as a practical matter, delay in revising the plan stifles consumer discretion and ability to take advantage of sale prices.
For CDC, DDP developed a procedure that allowed consumers some discretion without a formal revision of the purchasing plan. The fiscal agent would pay an invoice for a purchase not specified in the purchasing plan if it had written authorization from the consumers consultant. In effect, that authorization was an addendum to the purchasing plan. The consultant should not authorize such expenditure unless the consumer had savings from which to pay for the purchase. (If the consumer did not have sufficient savings, a formal revision of the purchasing plan was in order.) Thus, in practice, consumer discretion in CDC was available to consumers who had accumulated some savings in their accounts. This process made it possible for such consumers to take advantage of sale prices.
Increasing the percentage of the allowance that may be provided as cash (from 10 percent in Arkansas and New Jersey to 20 percent in Florida) also allows consumers discretion to take advantage of sale prices. However, it is difficult to ensure that cash is used for permissible purposes, as that requires review of receipts.
Arkansas developed a process that (in some circumstances) may allow consumers enough discretion to take advantage of sale prices. Consultants may orally approve changes in the purchasing plan, with a formal revision following by mail or the next time the consultant visits the consumer. However, oral revisions would be less straightforward when someone other than the consultant is responsible for comparing invoices to the purchasing plan before approving them for payment. If someone else is responsible, that person must be notified of the change in the plan, and the process becomes similar to that of adding an addendum to the purchasing plan as developed in Floridas CDC project.
XI. TOWARD AN ONGOING PROGRAM
While the Cash and Counseling Demonstration was under way, Florida implemented two other consumer-directed programs--one for another population and one for a part of the state that the CDC project did not serve. Based on its experience with these programs and with the Cash and Counseling Demonstration, Florida is working to implement a version of CDC as an ongoing program.
A. Extending Consumer Direction
While CDC was being planned and implemented, Florida developed and implemented a statewide program for adults with traumatic brain and spinal cord injuries and a program in a northern part of the state (that CDC did not serve) for adults with developmental disabilities.
1. Brain and Spinal Cord Injury Program
As planning for CDC began, the Florida Department of Labor was operating the Brain and Spinal Cord Injury Program (BSCIP) with funds from a trust fund established by the state. (Later, the Department of Health assumed responsibility for BSCIP.) At that time, BSCIP was providing comprehensive post-acute services to those with brain and spinal cord injuries to help reintegrate them into the community. In addition, Florida was planning a new program to respond to the need of these people for long-term home- and community-based services that were not covered under the Medicaid state plan and to provide long-term services to help people living in skilled nursing facilities to return to the community. To secure federal funding, Florida planned to operate the new program under a Medicaid 1915(c) home- and community-based waiver, with state trust fund monies used as the state match for the waiver. The waiver was approved in 1999, and Florida planned to allow the recipients of the new waiver services to enroll in the CDC demonstration. However, the new program had not been fully implemented by the time that the CDC began to operate in the spring of 2000, in part due to difficulty in developing a discount rate that would ensure budget neutrality but that was not so steep as to make participation unattractive. Due to this delay in implementation, beneficiaries with brain and spinal cord injuries were not included in the evaluation of the Cash and Counseling Demonstration. In 2001, the first consumers with brain and spinal cord injuries began to enroll in CDC.
2. Choice and Control
As described in Chapter III, CDC was not initially available to adults with developmental disabilities who lived in some areas of the state. After CDC began, Florida developed the Choice and Control pilot project with state funds in 14 largely rural counties in three districts in the northern part of the state that did not have CDC. Later, in March 2001, CDC expanded to cover adults with developmental disabilities living in all counties in the state except those in which Choice and Control was being offered.
Florida had been unable to spend much time getting input from families and traditional providers on the design of the CDC program. Senior state staff viewed that as a major failing in the development of CDC. In contrast, Florida spent much time and effort working with families and providers as it developed Choice and Control. In addition, Florida wanted to assess the value of an allowance program in rural areas, which typically have shortages of traditional services.
Choice and Control was a small program (only about 150 participants). Because it was funded with state monies, both those receiving home- and community-based waiver services and those who were not receiving these services could participate in Choice and Control (provided they were adults with developmental disabilities).
As in CDC, the goal of the Choice and Control pilot project was to enable consumers to remain as independent as possible in the community. The projects features were similar to those of CDC in that consumers managed the dollars allocated for their care and were able to purchase services from a variety of sources, including family members.
The downturn in the economy and the resulting shortfall in state funding led Florida to seek a Medicaid waiver for Choice and Control. The waiver was delayed, and consumers participating in Choice and Control were forced to return to the traditional program, to the considerable disappointment of many of them. Eventually, CMS approved a waiver that allowed Florida to roll the Choice and Control pilot project into CDC. This occurred after the target sample size for the evaluation had been reached and evaluation enrollment had been closed.
B. Statewide Program of Consumer-Directed Care
During our visit to Florida early in 2002, the state legislature was holding hearings on bills to provide consumer-directed care on an ongoing basis. The following summer, the state legislature passed the Florida Consumer-Directed Care Act. This act directs Floridas Agency for Health Care Administration (AHCA), Department of Elder Affairs, Department of Children and Families, and Department of Health to develop consumer-directed programs and to seek Medicaid waivers for these programs. The act envisions a program similar to CDC and to Choice and Control. As the Medicaid agency, AHCA was selected to lead the effort.
Cost was the major issue in the legislature when it was considering this act. Choice and Control had been more expensive than traditional waiver services. A study done for the state had determined that Choice and Control costs were about a quarter higher than those for recipients of traditional services. Senior state officials attributed this increase in cost to the relative unavailability of traditional services in rural areas and to beneficiary satisfaction with Choice and Control.
After the passage of the Florida Consumer-Directed Care Act, the state began developing a waiver application based on the Independence Plus templates developed by CMS for 1915(c) and 1115 demonstration waivers for consumer-directed programs. In developing the Independence Plus templates, CMS drew heavily on the experiences of the three Cash and Counseling programs in Arkansas, Florida, and New Jersey.
REFERENCES
Cameron, Kathleen. Cash and Counseling: A Model for Empowerment and Choice for Long-Term Care. Perspectives on Aging, July-September 1995, pp. 22-25.
Cameron, Kathleen, and Robert Lagoyda. Cash and Counseling Technical Analysis #1: The Counseling Component, Draft. Washington, DC: Center on Consumer-Directed Services at the National Council on Aging and University of Maryland, Center on Aging, February 1997.
Doty, Pamela, Judith Kasper, and Simi Litvak. Consumer-Directed Models of Personal Care: Lessons from Medicaid. Milbank Quarterly, vol. 74, no. 3, 1996, pp. 337-409. [Available online at http://aspe.hhs.gov/daltcp/reports/lessons.htm]
Eustis, Nancy. Consumer-Directed Long-Term Care Services: Evolving Perspectives and Alliances. Generations, vol. 20, no. 3, fall 2000, pp. 10-15.
Flanagan, Susan. Payment, Employment-Related Tax, Legal Liability, and Quality Assurance Issues Related to In-Home Care Programs That Use Consumer-Directed Attendants. Cambridge, MA: SysteMetrics, March 1994.
Harrington, Charlene, and Martin Kitchener. Medicaid Long-Term Care: Changes, Innovation, and Cost Containment. San Francisco, CA: University of California, San Francisco, July 2003. Available at http://www.ncsl.org/programs/health/harrington. Accessed March 18, 2004.
Jackson, Mary. Rationing Case Management: Six Case Studies. Cambridge, MA: MEDSTAT Group, November 1994. [Available online at http://aspe.hhs.gov/daltcp/reports/rationes.htm]
Kane, Rosalie. Lets Just Send Cash for Long-Term Care: Conceptual Underpinning for a Cash and Counseling Demonstration. Paper presented at the Annual Meeting of the Cash and Counseling Demonstration, Washington, DC, October 1996.
Kitchner, Martin, and Charlene Harrington. Medicaid 1915(c) Home and Community Based Waivers: Program Data: 1992-1999. San Francisco: University of California, San Francisco, August 2001.
LeBlanc, Allen, Christine Tonner, and Charlene Harrington. State Medicaid Programs Offering Personal Care Services. Health Care Financing Review, vol. 22, no. 4, summer 2001, pp.155-173.
Phillips, Barbara, and Barbara Schneider. Moving to IndependentChoices: Implementation of the Cash and Counseling Demonstration in Arkansas. Princeton, NJ: Mathematica Policy Research, Inc., May 2002. [Available online at http://aspe.hhs.gov/daltcp/reports/movingic.htm]
Phillips, Barbara, Kevin Mahoney, Lori Simon-Rusinowitz, Jennifer Schore, Sandra Barrett, William Ditto, Tom Reimers, and Pamela Doty. Lessons from the Implementation of Cash and Counseling in Arkansas, Florida, and New Jersey. Mathematica Policy Research, Inc., June 2003. [Available online at http://aspe.hhs.gov/daltcp/reports/cclesson.htm]
Schore, Jennifer, and Barbara Phillips. Consumer and Counselor Experiences in the Arkansas IndependentChoices Program. Princeton, NJ: Mathematica Policy Research, Inc., January 2004. [Available online at http://aspe.hhs.gov/daltcp/reports/arkexp.htm]
Simon-Rusinowitz, L., and B. Hofland. Adopting a Disability Approach to Home Care Services for Older Adults. Gerontologist, vol. 33, no. 2, 1993, pp. 159-167.
Velgouse, Linda, and Virginia Dize. A Review of State Initiatives in Consumer-Directed Long-Term Care. Generations, vol. 24, no. 3, fall 2000, pp. 28-33.
NOTES
-
For simplicity, we refer to a single Cash and Counseling Demonstration. Because each state was expected to design its own demonstration (within the constraints laid down by the funders and federal regulations, including waiver terms and conditions), the program was originally referred to as the Cash and Counseling Demonstrations. However, because a single National Program Office provided oversight and guidance to all the states and a single evaluation contractor was selected, references to a single demonstration eventually supplanted references to multiple demonstrations.
-
At that time, CMS was called the Health Care Financing Administration (HCFA).
-
The Medicaid PAS benefit covers personal assistance services only; as a state plan service, it must be made available to all eligible Medicaid beneficiaries statewide who apply. In contrast, home- and community-based waivers may cover a variety of goods (for example, personal care supplies) and services (for example, chore services and behavioral therapy). Waiver services can be restricted to particular groups (for example, medically fragile children), and the number of slots in waiver programs can be capped.
-
Only those who were currently receiving waiver services were eligible for Floridas Cash and Counseling program. As a result, this term and condition had no effect on the Florida program.
-
Three other reports, one for each state, integrate the information from state and program perspectives reported in this series with information from the perspective of consumers and consultants.
-
Later, the word research was generally dropped from the programs name, so we follow that usage in the rest of the report.
-
In addition, the University of Maryland, Baltimore County, is conducting a qualitative study of triads consisting of consumers, their caregivers, and their consultants.
-
We did not interview any enrollment staff for beneficiaries with developmental disabilities because enrollment was over by the time of our visit, and none of these staff members were available.
-
Until 1991, AS and DOEA were part of the same department.
-
In addition to personal care under waiver services, Florida offered personal care services as part of its Early and Periodic Screening, Diagnosis, and Treatment (EPSDT) program. Federal regulations for EPSDT stipulate that states must provide regular, periodic examinations for eligible children and any necessary services pursuant to the examinations. Personal care was occasionally provided under the provision of the EPSDT program.
-
As they reached age 60, adults were transferred from the program administered by AS/DCF to the program administered by DOEA.
-
Florida provided the statistics reported in this section on numbers of beneficiaries served. The numbers are for state fiscal year 1996-1997.
-
In alphabetical order, the 19 counties are Brevard, Broward, Charlotte, Collier, Dade, Hillsborough, Lee, Manatee, Martin, Okeechobee, Orange, Osceola, Palm Beach, Pasco, Pinellas, Polk, St. Lucie, Sarasota, and Seminole.
-
Arkansas and New Jersey could not control induced demand by limiting slots. Federal regulations permit waiver services to be provided to only a limited number of beneficiaries. In contrast, a state plan service must be provided to all beneficiaries who are eligible for that service across the state.
-
Routine cash payments were later limited to $250 per month.
-
There is no evidence that AAAs that directly provided services to beneficiaries were less likely to cooperate with CDC. As of February 2002, 6 of the 10 counties with the largest proportions of the eligible population enrolled in CDC were counties in which the lead agency provided direct services.
-
A quarterly visit is required for an elderly recipient of waiver services unless the case manager waives the visits on the grounds that it is unnecessary.
-
Alternately, a contract may be awarded on a sole-source basis. In one of the 19 counties in the CDC catchment area for the elderly, the local county government had been appointed lead agency on a sole-source basis.
-
While the payment structure provided for separate payment for up to two training visits, additional consultant time for training would be paid for at the regular case management hourly rate.
-
Shortly before our visit, DCF hired a contractor to conduct these record reviews; Medicaid waiver specialists housed at AAAs continued to conduct quality assurance reviews of records for elderly beneficiaries.
-
After our visit, the fiscal agent was required to complete a separate state unemployment tax form for each worker, rather than filing in the aggregate, and this also increased its costs.
-
As the Cash and Counseling demonstration ended, the going rate for fiscal services was reportedly $60 or more per consumer per month.
-
"Memorandum Describing Responses for an Early Cohort of Florida Treatment Group Members. Princeton, New Jersey: Mathematica Policy Research, Inc., April 17, 2002.
-
Precise information on the percentage of CDC consumers naming representatives at enrollment was collected on the evaluations enrollment forms and will be presented in a later report.
-
That information is not available for New Jersey, where representatives were not named until the first home visit by a consultant.
-
This guidance was provided in May 2002.
-
This case was reported to us during our visit. We reported it to senior project staff, who promptly investigated.
-
In Florida, people who had been on waiting lists for Medicaid waiver services were also eligible and are included in the population as described here. (See Phillips et al. 2003.)
-
Logically, this situation could arise when an adult child of a beneficiary was a representative (say, a son) and the spouse of that child was a worker (say, a daughter-in-law). However, none of the rare incidents of abuse of the allowance or exploitation of the consumer in any of the Cash and Counseling states were associated with a conflict of interest involving a married couple, one of whom was the representative and one of whom was a worker.