
U.S. Department of Health and Human Services
Beyond Fair Hearings: How Five States Help Medicaid Managed Care Beneficiaries Resolve Disputes with Health Plans
Beth Stevens, Nancy Archibald and Leslie Foster
Mathematica Policy Research, Inc.
November 2001
http://aspe.hhs.gov/daltcp/reports/2001/fairhear.pdf (126 PDF pages)
This report was prepared under contract #HHS-100-97-0013 between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and the Mathematica Policy Research, Inc. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the ASPE Project Officer, Hunter McKay, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. His e-mail address is: Hunter.Mckay@hhs.gov.
The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
TABLE OF CONTENTS
A. Reasons for Greater Focus
B. The Evolving Policy Response
C. About This Study
D. Guide to the Rest of This Report
II. CHARACTERISTICS AND USE OF FAIR HEARING ADAPTATIONS
A. Ombudsman Programs
B. External Review Programs
C. Expedited Review Programs
D. Summary
III. OMBUDSMAN PROGRAMS
A. Introduction to the Programs
B. The Programs At Work
C. Variations in Program Characteristics
D. Accessibility of Ombudsman Programs
E. Stakeholders’ Expectations of Ombudsman Programs
F. The Impacts of Ombudsman Programs
G. Conclusions and Key Findings
A. Introduction to the Programs
B. The Programs At Work
C. Variations in Program Characteristics
D. Strengths and Weaknesses of External Review Programs
E. The Impact of External Review Programs
F. Conclusions and Key Findings
V. EXPEDITED REVIEW PROCEDURES
A. Expedited Review Procedures At Work
B. Variations in Expedited Review Program Structure
C. Accessibility of Expedited Review Procedures
D. Stakeholder Expectations
E. Impact of Expedited Review Procedures
F. Promising Components
A. Summary of State Initiatives and Adaptations
B. Conclusions
APPENDIX A. SITE VISIT REPORTS
Colorado Site Visit Report
Florida Site Visit Report
Minnesota Site Visit Report
New York Site Visit Report
Oregon Site Visit Report
LIST OF FIGURES
FIGURE I.1: Sequence of Events in the Use of a Fair Hearing to Resolve Medicaid Disputes Under Two Scenarios
FIGURE II.1: Distribution of Ombudsman Programs
FIGURE II.2: Distribution of External Review Programs
FIGURE II.3: Distribution of Expedited Fair Hearing Programs
FIGURE II.4: Distribution of Ombudsman, External Review and Expedited Fair Hearing Programs
FIGURE III.1: Example of State-Mandated In-Plan Appeal Procedures for Prospective Service Denials
FIGURE V.1: Comparison of Expedited Review Processes in Oregon and New York
LIST OF TABLES
TABLE ES-1: Adaptations by States Selected for Case Studies
TABLE I.1: Candidate and Selected States for Case Studies
TABLE III.1: Ombudsman Program Characteristics
TABLE V.1: Structural Characteristics of Expedited Review Programs in Oregon and New York
TABLE V.2: Comparison of Expedited Review Processes Using Best Practices Criteria
TABLE CO-1: Outreach Activities for the Managed Care Ombudsman Program
TABLE CO-2: Strengths and Weaknesses of Colorado’s Managed Care Ombudsman Program, as Identified by Site Visit Participants
TABLE CO-3: Outreach Activities for the Mental Health Ombudsman Program
TABLE CO-4: Strengths and Weaknesses of Colorado’s Mental Health Ombudsman Program, as Identified by Site Visit Participants
TABLE FL-1: Strengths and Weaknesses of the External Review Panel
TABLE MN-1: Outreach Activities for the Ombudsman/County Advocate Program
TABLE MN-2: Strengths and Weaknesses of Minnesota’s Ombudsman/County Advocate Program, as Identified by Site Visit Participants
TABLE NY-1: Outreach Activities for the External Appeals Program
TABLE NY-2: Strengths and Weaknesses of New York’s External Appeals Program
TABLE OR-1: OMAP Hearing Requests and Resolution of Cases
TABLE OR-2: Strengths and Weaknesses of Oregon’s Fair Hearing Process
TABLE OR-3: Strengths and Weaknesses of the OMAP Ombudsman Program
ACKNOWLEDGMENTS
This report could not have been prepared without the cooperation of the many people we met during our case study site visits in Colorado, Florida, Minnesota, New York, and Oregon. We are grateful to dozens of staff members in state and county health and insurance departments, administrative hearing offices, ombudsman programs, consumer and legal advocacy organizations, independent medical review agencies, and managed care organizations who spoke so thoughtfully with us about the Medicaid grievance and appeal procedures in their states. Any inaccuracies in our descriptions of their work are our own.
We appreciate the guidance and recommendations we received from several people as we selected states for case studies. In particular, we thank Brenda Jackson of the Centers for Medicare & Medicaid Services Region 7 Office, Jane Perkins of the National Health Law Program, Karen Pollitz of the Institute for Health Care Research and Policy at Georgetown University, Joanne Rawlings-Sekunda of the National Academy for State Health Policy, and Sara Rosenbaum of the Center for Health Policy Research at the George Washington University Medical Center.
Many people at Mathematica Policy Research, Inc. have also contributed to this project. An injury prevented Mia Cahill, the fourth member of our project team, from writing this final project report, but not from fully participating in other phases of the project. Jim Verdier provided helpful input based on his experience as a state Medicaid director, and Sue Felt-Lisk provided insightful comments on this and other project deliverables. We also thank William Garrett for producing this report, Walter Brower and Patricia Ciaccio for editing it, and Theresa Kim for programming of the graphics.
EXECUTIVE SUMMARY
Since the 1970s, federally mandated, state-administered “fair hearings” have been the primary mechanism with which Medicaid beneficiaries address disputes over Medicaid-covered health care services. More recently, the Federal Government has also required plan-level grievance and appeal procedures in all states that run Medicaid managed care programs.1 To address perceived shortcomings of fair hearings and in-plan procedures, many states have voluntarily introduced, in addition to these federally required activities, other mechanisms designed: (1) to be easy for beneficiaries to use, (2) to provide impartial review, and (3) to provide timely decisions.
BACKGROUND
This report presents the findings from a “Study of Medicaid Fair Hearing Adaptations,” which Mathematica Policy Research, Inc. (MPR) conducted for the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation (ASPE). The study was commissioned to assist ASPE in identifying, describing, and understanding innovative attempts by states to make Medicaid grievance and appeal procedures more effective, as well as more relevant to needs that have arisen as a result of broad-scale implementations of Medicaid managed care.
States’ increased focus on Medicaid grievance and appeal procedures stems from several factors. First, the nature of disputes that commonly arise under managed care is fundamentally different from that of fee-for-service disputes. While fee-for-service disputes typically involve retrospective denials of claims for services that have already been rendered, managed care disputes are more likely to arise over prospective denials of health care services (Perkins 2000; and Annas 1997). Second, because they are subject to restrictions--such as mandatory enrollment and lock-in provisions--Medicaid managed care beneficiaries are less free than fee-for-service consumers in their pursuit of health care services (Annas 1997). Third, Medicaid managed care beneficiaries may face greater physical, financial, and social disadvantages than their non-Medicaid counterparts. As a result, they may be less able to fend for themselves in disputes related to managed care (Rawlings-Sekunda 1999; and Molnar et al. 1996).
Given these circumstances, state governments have begun to recognize that alternative mechanisms may also be needed. The most important such mechanisms or adaptations are:
-
Ombudsman Programs, which provide guidance and advice as Medicaid managed care beneficiaries navigate fair hearings, in-plan procedures, and less formal dispute-resolution options.
-
External Review Programs, which make use of impartial, expert reviewers to evaluate and resolve disputes between managed care consumers and managed care organizations (MCOs).
-
Expedited Review Procedures, which give accelerated consideration to prospective denials of health care services that consumers and/or their providers believe to be urgently needed.
ABOUT THIS STUDY
MPR studied these three adaptations to provide federal and state policymakers with an understanding of state efforts to adapt federally required grievance and appeal procedures to the particular circumstances of their Medicaid managed care programs. We also sought to provide information about the design and operation of the three adaptations, and to identify the relative advantages and disadvantages of each.
We reviewed recent literature on fair hearings and state adaptations, and progressed to in-depth case studies of the adaptations as they work in five states. Our case study states--Colorado, Florida, Minnesota, New York, and Oregon--were selected, in part, because they run mandatory Medicaid managed care programs, use one or more of the adaptations but had not recently been the focus of similar research, and (in four states of five) enroll beneficiaries with disabilities or chronic illness into their Medicaid managed care programs. Table ES-1 identifies the adaptations we studied in each of five states.
| TABLE ES-1. Adaptations by States Selected for Case Studies | |
|---|---|
| Adaptation | Selected States |
| Ombudsman Programs | Minnesota, Colorado, and Oregon |
| External Review Programs | Florida, New York |
| Expedited Review Procedures | Oregon, New York |
THE ADAPTATIONS AT WORK
The adaptations in our study offer rich material to compare and contrast the decisions that states make regarding the design and operation of Medicaid grievance and appeal procedures that are not federally mandated. Nonetheless, it is difficult to say whether the adaptations in our study represent those in other states. No comprehensive inventory of all adaptations exists, no central authority encourages their implementation, they may be implemented with or without legislation, some exist more “on paper” than in practice, and they may be located almost anywhere in the configuration of state and local governments. As of this writing, our literature review and contact with selected states indicates that:
-
Roughly 31 states run ombudsman programs primarily for Medicaid managed care enrollees.
-
Thirty-nine states run external review programs, fewer than five of which are available to Medicaid beneficiaries.
-
Approximately 14 states operate state-level (as opposed to plan-level) expedited review procedures, including expedited fair hearings and expedited external reviews.
Key Findings About Ombudsman Programs
The ombudsman programs we studied in Minnesota, Colorado, and Oregon succeed in making it easier for Medicaid managed care beneficiaries to navigate complex grievance and appeal systems. However, because the states have committed only minimal resources to the programs, ombudsmen believe they are not nearly able to reach all the beneficiaries who may need their assistance. Though states regard them as the “eyes and ears” of their Medicaid managed care programs, the ombudsman programs in our study contribute to systemic quality assurance efforts to a very limited extent. Stakeholders credibly blame a lack of well-developed feedback mechanisms and resource constraints for this shortcoming.
Through our case studies, we identified four key determinants of the accessibility and effectiveness of ombudsman programs. The first is geography. In areas where an ombudsman program has a physical presence, the use of program services by beneficiaries appears to program staff to be higher. A second determinant is the use of effective outreach mechanisms. For example, putting information about an ombudsman program in MCO denial notices and on Medicaid identification cards--and not only in managed care enrollment materials--increases the likelihood that beneficiaries will see the information when they need it. Third, beneficiaries will use ombudsman programs only when they view them as being on their side or at least neutral with regard to their disputes with MCOs or the state. Neutrality, in turn, is partly dependent on whether the ombudsman is an independent actor, rather than a government employee. Finally, ombudsman programs are utilized when they achieve results, an impossibility if the program is not accepted by MCOs. MCOs cooperate with ombudsman programs when it is clear to them that: (1) the ombudsman program analyzes issues in an impartial manner, and (2) it understands the constraints and purposes of managed care.
Key Findings About External Review Programs
Unlike most states’ external review programs, those in Florida and New York are available to commercially insured managed care enrollees and Medicaid beneficiaries (whom other states exclude because of their access to fair hearings). The Florida and New York programs differ greatly in the types of disputes they adjudicate and the review formats they use. These differences have important implications for the Medicaid beneficiaries who must decide whether to use the programs, and for other states that may be interested in implementing external review programs themselves. Despite their differences, the Florida and New York programs are both viewed as impartial and fair by consumers, MCOs, and other stakeholders.
Making external review available to Medicaid beneficiaries expands their state-level dispute-resolution options beyond fair hearings. This expansion of options works to the advantage of a beneficiary who is informed about the tradeoffs between the two processes (such as whether the benefit in question will continue while a decision is pending, and the decision-maker’s area of expertise). Our studies in Florida and New York, however, suggest that Medicaid beneficiaries may not be well informed with regard to such tradeoffs, and may not even be aware of the external review option in the first place.
Key Findings About Expedited Review Procedures
Of the three types of adaptations we studied, expedited reviews are the most straightforward in their purpose and implementation. Oregon offers expedited reviews to Medicaid managed care beneficiaries in the form of foreshortened fair hearings, while New York offers expedited versions of fair hearings and external reviews. In both states, only very small percentages of hearings and/or external reviews are expedited. This may be a true reflection of the infrequency of disputes over urgent medical cases, but it probably also results from the way the states design and implement their expedited review policies. The accessibility of expedited review procedures depends largely on who has a say in deciding whether a case is urgent. Beneficiaries, attending physicians, fair hearings officials, and state medical directors all play a role in such decisions (depending on the state). Outreach activities that would publicize the existence of such review policies are minimal, which might explain their infrequent use. Finally, although they are seldom used, the expedited review procedures we studied do effectively reduce the length of the dispute-resolution process, typically from months to weeks, or even days.
CONCLUSIONS
As states design ombudsman programs, external review programs, and expedited review procedures, they make choices that affect the flexibility, accessibility, and impact of these adaptations to federally mandated grievance and appeal procedures. The most important choices pertain to: (1) whether the adaptation will be operated by a government agency or an independent organization under contract to the state; (2) the scope of disputes the adaptation is designed to address; and (3) where the state wishes to resolve most Medicaid managed care disputes--at the plan level, at the state level, or in less formal venues.
Programs based in state agencies offer expertise in Medicaid managed care regulations and experience with the policies of individual Medicaid MCOs, while independent organizations provide neutral ground for dispute-resolution, unshadowed by stakeholder interests. Broad definitions of the scope of eligible disputes give many beneficiaries a chance to press their interests but can overburden dispute-resolution systems with idiosyncratic issues, while narrow definitions of scope reduce access to the system and eliminate useful flexibility in policy and practice. Finally, an emphasis on resolving disputes at the level of state agencies can magnify and formalize disputes into entrenched conflicts, while an emphasis on resolution at the plan level creates a need for intensive state monitoring of in-plan grievance and appeal processes.
Promising Elements and Areas for Improvement
The states in our study made different decisions with regard to these tradeoffs, but their adaptations each reap important benefits for stakeholders:
-
They make grievance and appeals systems adaptable to a wide range of disputes, including those involving quality concerns and appealable access issues such as service denials, reductions, and terminations.
-
They ensure that Medicaid managed care beneficiaries have a “voice” in the managed care decisions that affect them personally.
-
They help improve ongoing quality assurance efforts.
In light of these benefits, it seems unfortunate that so few Medicaid beneficiaries use the programs we studied. Our case studies suggest that the low usage is due, in part, to shortcomings in the way the adaptations are implemented. In particular, we found that:
-
Not all states use the most effective outreach activities to promote their adaptations.
-
The procedures that some states use for accessing their programs can limit beneficiaries’ access to the adaptations and to fair hearings.
-
The adaptations lack some of the resources they need to be effective.
-
States do not take full advantage of the grievance and appeal data generated by the adaptations.
Acting in their traditional role as laboratories for social policy, the states in our study have fashioned several promising dispute-resolution alternatives within the Medicaid program. More fine-tuning of outreach activities could generate greater utilization of these new systems. Improvements in the collection, analysis, and dissemination of data on the numbers and types of disputes could lead to greater understanding of the trends in Medicaid managed care and provide information for better state management of the Medicaid program.
I. BACKGROUND AND OBJECTIVES
As more of the Medicaid population moves from fee-for-service health care coverage to managed care, traditional grievance and appeal procedures, through which beneficiaries can dispute their health plan’s decisions, may be becoming less effective.2 If these procedures do not work well, Medicaid managed care beneficiaries may be deprived of needed health care services, and state Medicaid agencies and managed care organizations (MCOs) may face undue administrative burdens and associated costs.
Since the 1970s, federally mandated, state-administered “fair hearings” have been the primary mechanism with which Medicaid beneficiaries can address disputes over health care services. Since the proliferation of Medicaid managed care, however, both the federal and state governments have begun to recognize that alternative mechanisms may be useful. As a result, the Federal Government now requires plan-level grievance procedures in all states that run Medicaid managed care programs. In addition, many states have introduced innovative grievance and appeal mechanisms to address what some stakeholders perceive as shortcomings of fair hearings and in-plan procedures. The new state mechanisms are designed: (1) to be easy for beneficiaries to use, (2) to provide timely decisions, and (3) to provide impartial review.
As Medicaid managed care continues to grow and states experiment with different managed care models, federal and state policymakers might benefit from understanding how these new state adaptations and initiatives work, and how they meet, or fail to meet, the needs of Medicaid managed care beneficiaries and other stakeholders. This report presents the findings of the “Study of Medicaid Fair Hearing Adaptations,” which Mathematica Policy Research, Inc. (MPR) conducted over the past year for the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation (ASPE). The goal of the study is to assist ASPE in identifying, describing, and understanding innovative attempts by states to make Medicaid grievance and appeal procedures more efficient and relevant to new needs and demands.
A. REASONS FOR GREATER FOCUS
Because MCOs operate under financial incentives to limit the quantity of health care services they provide, managed care procedures raise concerns about the possibility of inappropriate denials of service and increase the importance of consumer recourse. This emerging recognition of the important role of grievance and appeal procedures is evident in such policy initiatives as the patients’ rights bills passed by 45 states (National Conference of State Legislatures 2001) and by each chamber of the U.S. Congress.
In addition, all federal agencies that administer or manage health plans were given a Presidential directive in 1997 to adopt protections that would give all health care consumers the right to an independent system of external review for resolving differences with their health plans.3 The directive’s reference to the rights of all consumers raises questions about traditional Medicaid grievance procedures: Do Medicaid fair hearings meet the requirements of the directive? Do Medicaid beneficiaries enjoy the same or equal protections as other health care consumers? Several factors underlie these concerns, including: (1) the differing basis for disputes under managed care as compared to fee-for-service; (2) the rise of mandatory managed care participation and other Medicaid program restrictions; and (3) characteristics of the Medicaid managed care population.
1. A New Basis for Disputes
As more state Medicaid programs move from fee-for-service to managed care, disputes are less likely to involve retrospective denials of billing claims and more likely to involve prospective denials of health care services. As the nature of disputes has changed, the uses and consequences of state fair hearings have also fundamentally changed.
In fee-for-service programs, most state fair hearings determine whether Medicaid must reimburse a health care provider for services provided to a Medicaid beneficiary. In a typical scenario (see Figure I.1A), the Medicaid beneficiary receives services from a physician or other provider. The provider then submits a financial claim for those services to the state Medicaid agency. If the state denies the claim, the provider will likely bill the beneficiary. If the beneficiary disavows the bill, he or she may formally request a state fair hearing (Perkins et al. 1998a). States almost never hold Medicaid beneficiaries financially responsible for retroactively denied services.4 So although the beneficiary initiates the hearing request, it is the provider wishing to be paid and the Medicaid agency liable for paying who have the most at stake in the hearing.
By contrast, in managed care programs, the dispute-resolution process occurs almost in reverse of the fee-for-service sequence, leaving the beneficiary with the most to lose. In managed care settings, fair hearings determine not whether a provider is reimbursed for a particular service, but whether the Medicaid beneficiary receives that service in the first place (Perkins 2000; Annas 1997). In a typical scenario (Figure I.1B), MCOs are paid for their services to Medicaid beneficiaries on a prospective, flat-fee basis. When a beneficiary seeks care, the MCO, operating under financial incentives to limit services, may or may not approve or “preauthorize” it. If the care is denied, the beneficiary may request a state fair hearing, with hope that the denial be overturned. Thus, under managed care, fair hearing decisions are often tantamount to medical treatment decisions. The lengthy fair hearing process that may work in fee-for-service disputes may be too lengthy to meet needs under managed care. Under managed care, where the dispute-resolution process often precedes the provision of care, the need for timely grievance and appeal procedures is heightened.
| FIGURE I.1. Sequence of Events in the Use of a Fair Hearing to Resolve Medicaid Disputes Under Two Scenarios |
 |
2. Mandatory Enrollment and Other Consumer Restrictions
Compared to fee-for-service Medicaid beneficiaries, those in Medicaid managed care are less free in their pursuit of health care services (Annas 1997). There are three main reasons for this. First, because managed care enrollment is mandatory in many states,5 switching to fee-for-service insurance if a dispute arises is rarely an option for Medicaid beneficiaries. Second, many states have so-called lock-in policies that prohibit Medicaid beneficiaries from switching MCOs for a set period of time (often 12 months), as permitted under Section 1932(a)(4) of the Social Security Act (SSA) (Perkins and Olson 2000; Rodwin 2000). Third, all providers with whom an MCO contracts are subject to the same restrictions regarding covered services, so it would be futile for a beneficiary to switch providers in an effort to obtain the desired treatment (Rodwin 2000). In this situation, where Medicaid beneficiaries may face critical treatment decisions with no alternative options, access to impartial dispute-resolution is essential.
3. Characteristics of the Medicaid Managed Care Population
Compared to their counterparts in Medicare and commercial managed care plans, Medicaid managed care beneficiaries may face greater disadvantages when trying to resolve grievances. On average, Medicaid beneficiaries have greater health care needs, are less educated and less proficient in English, and have fewer financial resources (to pay either for uncovered medical treatment or for representation in a dispute) than the general population (Perkins 2000; Perkins et al. 1998b). Moreover, states are increasingly enrolling vulnerable members of their Medicaid populations--such as those with chronic illnesses or disabilities and those over age 65--into mandatory managed care programs. Such physical, financial, and social disadvantages are presumed to weaken Medicaid beneficiaries’ general ability to advocate for themselves in a managed care setting (Rawlings-Sekunda 1999; Molnar et al. 1996). They may suffer greater-than-average handicaps to navigating a grievance process, which may include multiple layers of in-plan and external proceedings (Bonnyman and Johnson 1998).6 Consequently, the availability of easy-to-use grievance and appeal procedures assumes great importance under Medicaid managed care.
B. THE EVOLVING POLICY RESPONSE
The resolution of consumer disputes under the Medicaid program is shaped by federal and state laws, including the U.S. Constitution, case law, acts contained in the U.S. Code and supporting regulations, and states’ contracts with Medicaid MCOs. Policies governing the resolution of Medicaid disputes date to 1970, with a landmark U.S. Supreme Court decision that established fair hearing rights for individuals facing the termination, reduction, or suspension of public benefits. Medicaid grievance policy then remained mostly unchanged for two decades, until states began introducing mandatory Medicaid managed care programs. Since then, policy activity around Medicaid grievance and appeal procedures has increased at the federal and state levels. In the following section of this report, we summarize this evolving policy response and its effect on the formal requirements for resolving disputes in state Medicaid programs.
1. Federal Policies
a. Constitutional Due Process Requirements
Whereas most consumer disputes are regulated under state contract law, consumer disputes under the Medicaid program and many other federal entitlement programs are regulated in part by the “due process” clause of the Fourteenth Amendment, which states that the government cannot “deprive any person of life, liberty, or property, without due process of law.” The interpretation of this constitutional law has been applied to Medicaid, and sets a legal standard to which state Medicaid programs must adhere.
In the landmark case of Goldberg v. Kelly 397 U.S. 254 (1970), the U.S. Supreme Court applied due process requirements to the withdrawal of public benefits. In this case, the New York City Department of Social Services intended to cut off welfare benefits to Kelly without notice, and without a hearing prior to the termination of the benefits. The Court reasoned that welfare benefits confer a “property” right and that their removal would cause Kelly to “suffer grievous loss.” Therefore, Kelly was entitled under the Constitution to due process. The defendant, the City of New York, argued that its interest in conserving fiscal and administrative resources outweighed the loss Kelly might suffer. The Court rejected this argument, holding that the rights of the individual have priority over state fiscal interests. In giving Kelly the right to a fair hearing, the Court set out key due process requirements. A beneficiary must have:
- Timely and adequate notice detailing the reasons for a proposed termination of benefits.
- The opportunity to take part in a pretermination evidentiary hearing.
- An opportunity to confront and cross-examine witnesses.
- An opportunity to present oral arguments and evidence before the decision-maker.
- An impartial decision-maker.
- A written decision.
While states may implement the Medicaid program differently, no state may deprive a person of his or her due process rights under the U.S. Constitution. In other words, while there are different state Medicaid programs, they all must adhere to constitutional law.
b. The Social Security Act (SSA) and Supporting Regulations
Two sections of the SSA address Medicaid grievance procedures. Together, they establish two tracks for dispute-resolution under Medicaid managed care. First, Section 1902(a)(3) addresses the fair hearing rights that have long been associated with traditional fee-for-service disputes.7 It says, “A state plan for medical assistance must…provide for granting an opportunity for a fair hearing before the State agency to any individual whose claim for medical assistance is denied or is not acted upon with reasonable promptness.” In turn, federal regulations that implement that section of the SSA specify that the hearing system must “meet the due process standards set forth in Goldberg v. Kelly.” Later, the Balanced Budget Act of 1997 led to the addition of Section 1932(a)(4) of the SSA, which requires the establishment of in-plan grievance procedures for any state operating a Medicaid managed care program.8 Federal regulations implementing this section of the act have yet to be finalized, which leaves states to be as prescriptive, or as lenient, as they see fit regarding the internal grievance procedures of Medicaid MCOs.
2. State Initiatives and Adaptations
Federal requirements for fair hearings and in-plan grievance procedures notwithstanding, some states have taken further steps to protect the rights of consumers, without neglecting their own interests or those of MCOs. Under Medicaid managed care, the interests of stakeholders are sometimes at odds with each other. Medicaid beneficiaries are interested in obtaining the most comprehensive and effective care for their health problems. Thus, they desire accessible, timely, and flexible grievance and appeal procedures that make it likely they can obtain that care. In contrast, Medicaid MCOs have interests in providing care as efficiently and effectively as possible within the financial limits imposed by their Medicaid contracts. As a result, MCOs are likely to favor grievance and appeal procedures that have clear principles and decision points and that consistently support their contracts with states. Finally, states desire grievance and appeal procedures that fit two different constraints. State Medicaid agencies want to protect the rights of beneficiaries and maintain the quality and effectiveness of the care they receive. At the same time, states must operate their Medicaid programs in a fiscally responsible manner; thus, they might not be able to fulfill every need of every beneficiary. States must also maintain good relations with the MCOs they need as participants in their Medicaid managed care programs. To do this, they must show that they understand and support managed care perspectives.
To balance these competing interests, to make existing grievance procedures more relevant to the types of disputes that arise in managed care, and to help Medicaid beneficiaries navigate a dispute-resolution system that already includes both fair hearings and in-plan procedures, many states have designed grievance and appeal mechanisms that adapt or complement those required in federal acts and regulations. The most important of such initiatives and adaptations are ombudsman programs, external review programs, and expedited review procedures, all of which may be implemented with or without legislation. These initiatives are described briefly below. (All three initiatives vary considerably across states, often in ways that influence their effectiveness. We identify and discuss key variables at length in later chapters.)
a. Ombudsman Programs
To help Medicaid managed care beneficiaries navigate existing grievance and appeal procedures (that is, fair hearings and in-plan processes), a number of states have set up ombudsman programs specifically for their Medicaid managed care populations. Ombudsman staff may be involved in all the possible phases of the grievance process. They often inform beneficiaries about appeal options, investigate disputes, advocate on behalf of beneficiaries, or act as an impartial mediator between a beneficiary and an MCO (Lee and Scott 1996; Perkins et al. 1998b; Horvath and Kaye 1996). Ombudsman programs may also perform more general functions, including educating beneficiaries about managed care and choosing an MCO, and collecting information to report on the status of Medicaid managed care in their state (Perkins et al. 1998b; Lee and Scott 1996).
b. External Review Programs
External (sometimes called “independent”) review programs make use of impartial, expert reviewers to evaluate and resolve disputes between managed care beneficiaries and MCOs when they deny, reduce, or discontinue covered medical services (Pollitz et al. 1998).9 Most states with external review programs limit their use to commercial managed care beneficiaries, excluding Medicaid beneficiaries on the basis of their access to fair hearings. In the few states where external review programs are available to Medicaid beneficiaries, the programs may be used in addition to fair hearings.
c. Expedited Review Procedures
Expedited review, which gives accelerated consideration to beneficiary appeals for urgently needed care, may occur in three settings: (1) internally within a Medicaid MCO; (2) within the fair hearing process; or (3) within a program of external review. Expedited reviews usually take between two and 14 days, considerably less time than the 30-90 day process for standard appeals. States use expedited review to address the time-dependent needs of managed care beneficiaries. As noted, managed care appeals typically involve prospective service denials. When the services in question are thought to be medically necessary and urgently needed, expedited review serves as a foreshortened version of existing procedures.
C. ABOUT THIS STUDY
1. Goals and Research Questions
In this report, we present and discuss findings from an in-depth study of three major initiatives--ombudsman programs, external review programs, and expedited review procedures--that states have taken to address the changing dispute-resolution needs of Medicaid managed care beneficiaries. The study serves three goals:
-
To provide federal policymakers with a greater understanding of the ways in which states have adapted or built upon federal requirements for fair hearings and in-plan grievance procedures to fit the circumstances of their Medicaid managed care programs.
-
To provide state policymakers with useful information about the design, implementation, and operation of the three types of state initiatives.
-
To provide all policymakers with an analysis of the advantages and disadvantages of each type of initiative.
To meet these goals, we addressed the following major questions:10
-
How do each of the state initiatives operate, both in themselves and in relation to fair hearings and in-plan grievance procedures?
-
How do Medicaid managed care beneficiaries learn about and choose among the array of grievance and appeal procedures available to them?
-
What do stakeholders identify as the strengths and weaknesses of the grievance and appeal procedures, particularly the newer initiatives, that are available to Medicaid managed care beneficiaries in their state?
2. Research Methods
a. Literature Review and Preliminary Data Collection
To build our understanding of grievance and appeal procedures under Medicaid managed care, we reviewed the literature on the Medicaid fair hearing process and the three state initiatives or adaptations of interest. Our review included searches of electronic databases of the published literature and a targeted Internet search of unpublished reports.11 The process of searching for and synthesizing relevant literature informed our understanding of the Medicaid grievance and appeal processes and helped us to identify states that would be suitable for case studies of the adaptations. Key findings of the literature review appear in Chapter II and serve as a frame for our analysis of the case study findings presented in Chapter III, Chapter IV, and Chapter V.
For further assistance in selecting states to study, we conducted interviews with four experts in the areas of Medicaid grievances and appeals, fair hearings law, and state Medicaid policy.12 In these interviews, we sought insights or other information about the states or the adaptations working in those states that would identify solid examples of each type and thus guide our selection.
b. Selection of Case Study States
MPR worked with ASPE to develop criteria for selecting case study states. To the extent practical, we considered states as candidates for further study if they: (1) run a mandatory Medicaid managed care program; (2) enroll into their Medicaid managed care program beneficiaries who have disabilities or chronic illnesses; (3) use one or more of the adaptations; and (4) were not included in a study of Medicaid due process procedures by Olson and Perkins (2000) (in order to avoid duplication of efforts).13 In addition, we considered whether the states’ adaptations were innovative (perhaps a best practice) and potentially replicable in other states. Finally, the state must have been mentioned as noteworthy by the literature or the interviewed experts. Table I.1 lists candidate states meeting these criteria and the states we selected.
| TABLE I.1. Candidate and Selected States for Case Studies | ||
|---|---|---|
| Adaptation | Candidate States | Selected States |
| Ombudsman Programs | Colorado, Florida, Minnesota, Oregon | Colorado, Minnesota, Oregona |
| External Review Programs | Florida, New York | Florida, New York |
| Expedited Review Programs | Florida, Maryland, Massachusetts, Oregon | Oregon, New Yorkb |
| ||
c. Case Studies
To develop an in-depth understanding of how each state initiative works, we conducted three-day visits in Colorado, Florida, Minnesota, Oregon, and New York. During these visits, we interviewed state Medicaid staff, fair hearings officials, representatives of consumer advocacy organizations, MCO staff, and--when relevant--independent external reviewers and ombudsmen.14 To facilitate the interviews, we developed protocols tailored for each category of interviewee in each state. The protocols allowed us to cover all our research questions in a systematic and consistent manner across the states, while building in the flexibility needed to address differences in the adaptations. The protocols contained open-ended questions that asked respondents to describe such things as the background context of the program and its genesis, the operational process of the adaptation, the volume of beneficiaries using the adaptation, beneficiaries’ interactions with the program, and the strengths and weaknesses of the adaptation.
d. Methods for Analyzing Case Study Data
After the site visits, we used the notes from our interviews to develop brief case study reports that described each site visit. These reports (supplied in Appendix A) contain an overview of the Medicaid managed care program in the state, a summary of the Medicaid complaints and appeals procedures in the state, a complete description of the adaptation in question, and a summary of our impressions. We used the information in the case studies as the basis for this analysis, in which we describe and compare the key characteristics of the adaptation in each state, focusing on the similarities of and differences between the two systems. We also examined whether differences were due to: (1) structural factors, such as the number of managed care plans, whether managed care was voluntary or mandatory, and the unique Medicaid rules of the state; or (2) idiosyncratic factors, such as the state’s political structure and the timing of the adaptation’s implementation.
D. GUIDE TO THE REST OF THIS REPORT
This report consists of six chapters, including this introduction. Chapter II summarizes the recent literature on the three state initiatives of interest, identifying the key variables and best practices associated with each. Chapter III, Chapter IV, and Chapter V present the findings of our in-depth examinations of ombudsman programs, external review programs, and expedited review procedures as they work in five states. In Chapter VI, we summarize our findings and draw conclusions about promising practices and areas for improvement.
II. CHARACTERISTICS AND USE OF FAIR HEARING ADAPTATIONS
In this chapter, we use information from the literature to sketch a picture of the characteristics of each of the three initiatives or adaptations and their popularity among states. Because no central authority encourages states to adopt these adaptations to fair hearing regulations, there are substantial variations in the way states have implemented them. Some states have been more successful than others in creating adaptations that are effective and efficient. Thus, we also use the literature to discuss theoretical best practices in the implementation of these adaptations. This discussion frames the analyses of the three adaptations explored in this study: ombudsman programs, external review programs, and expedited review procedures. These are explored in depth in Chapter III, Chapter IV, and Chapter V, respectively.
A. OMBUDSMAN PROGRAMS
1. Program Description
Judging from their recent proliferation in Medicaid managed care, ombudsman programs are an increasingly important mechanism that states make available to address beneficiaries’ disputes with managed care plans. While many states have developed ombudsman programs exclusively for their Medicaid managed care populations in recent years, such programs have long existed. They have been implemented by such federal agencies as the Social Security Administration and the Departments of Labor and Commerce. The Long-Term-Care Ombudsman Program, which states administer pursuant to the Federal Comprehensive Older Americans Act, has operated since the 1970s (Lee and Scott 1996).
An ombudsman program may facilitate all phases of the dispute-resolution process by: (1) informing beneficiaries of available appeal mechanisms; (2) investigating individual complaints; (3) advocating on behalf of beneficiaries in either informal or formal disputes; (4) acting as an impartial mediator between beneficiaries and health plans; and (5) issuing non-binding recommendations on dispute outcomes (Lee and Scott 1996; Perkins et al. 1998b; Horvath and Kaye 1996).15, 16 Not surprisingly, ombudsman programs vary considerably from state to state. For example, there are several ways ombudsman programs can come into being. They may be implemented through legislative or executive action, initiated by a Medicaid agency, or developed as part of a federal research and demonstration program (Perkins et al. 1998b; Horvath and Kaye 1996).17 Programs also vary by their territorial jurisdiction, with some programs operating on a statewide basis and others serving beneficiaries at the county level. (Perkins et al. 1998b). Sources of funding also vary. Most ombudsman programs are funded either by a state’s general revenues or through Medicaid, but they are supported increasingly by private foundations (Perkins et al. 1998b). In addition to the source of funding, states vary in terms of who operates the program, state Medicaid agencies or outside (third-party) entities. Finally, programs vary in their level of involvement in informal and formal external grievance processes (Fish-Parcham 2000; Horvath and Kaye 1996; Lee and Scott 1996; Perkins et al. 1998b; Rawlings-Sekunda 1999).
2. States with Ombudsman Programs
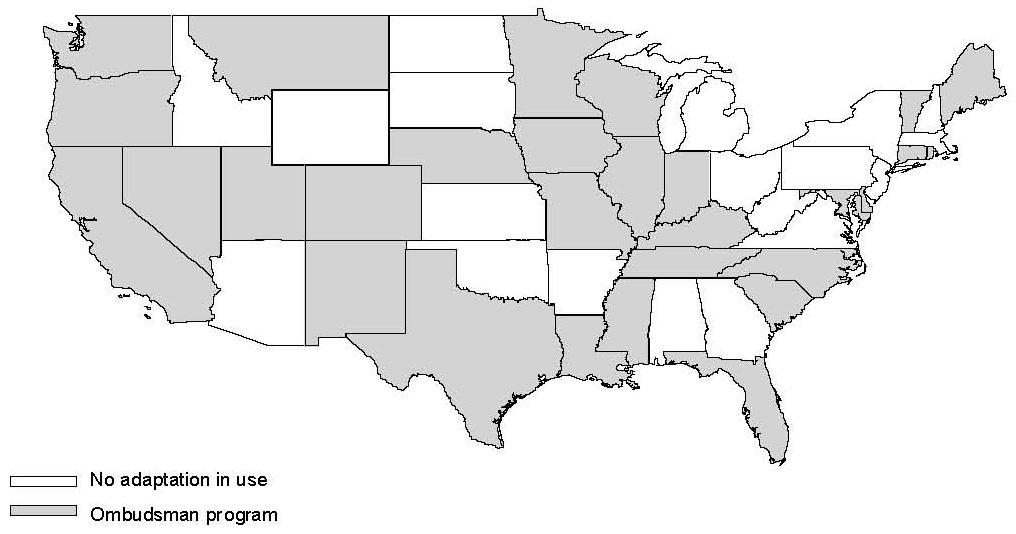
More and more states are requiring ombudsman programs through legislative or executive action. During the 1990s, the number of states with ombudsman programs increased dramatically. From 1994 to 1998, the number of states with ombudsman programs for their Medicaid managed care beneficiaries increased from five to 25, while the number with ombudsman programs for primary care case management beneficiaries increased from two to ten (Kaye and Pernice 1999). By 2001, eight additional states had begun ombudsman programs (Families USA 2001), bringing the total number of states with such programs to 31.
Although the numbers of ombudsman programs have climbed, some researchers contend that ombudsman programs are “the subject of much discussion” but are not widely used (Perkins et al. 1998b). Florida, for example, is noted in the literature for having model legislation that requires a statewide, independent ombudsman program (Families USA 1998a). As of our site visit in 2001, however, the program was being redesigned as a regional system and was operating in four districts on a small scale. It may be that, as in Florida, the programs of some states exist more on paper than they do in practice in a well-developed form. Figure II.1 shows states with a Medicaid managed care ombudsman program; however, it is unclear how many programs have actually been implemented or how frequently they are used, since there are few data on their operations.
3. Theoretical Best Practices
The recent literature focuses on three structural characteristics of ombudsman programs and evaluates their impact on program effectiveness. First, it favors ombudsman programs enacted through legislative or executive action, as opposed to those that “evolve” from enrollment broker programs, because high-level government support sends a message to health plans, state Medicaid agencies, and advocates about the importance of the ombudsman program. This makes them more effective grievance mechanisms (Perkins et al 1998b). Second, the literature also gives high marks to ombudsman programs serving Medicaid beneficiaries exclusively, because these programs have a presumed ability to meet the special needs of the Medicaid population more effectively as a result of their greater specialized expertise (Rodwin 2000; Perkins et al. 1998b; New York City Task Force 1997). However, the literature is ambivalent on the third issue, whether ombudsman programs are best run by Medicaid agencies or by independent, non-profit entities. While some advocates feel strongly that beneficiaries benefit most from impartial programs operated by non-profit organizations, others point out that programs based in state agencies have somewhat more clout and authority, and that they have access to resources and communication channels that independent programs do not (Families USA 1998a; New York City Task Force 1997; Rodwin 2000; Anderlik 1999).
| FIGURE II.1. Distribution of Ombudsman Programs |
 |
B. EXTERNAL REVIEW PROGRAMS
1. Program Description
External review programs use independent reviewers with medical or legal expertise to evaluate and resolve disputes between managed care beneficiaries and health plans when the plans deny, reduce, or discontinue covered medical services (Pollitz et al. 1998). These programs were originally designed for Medicare and commercial managed care beneficiaries, because such beneficiaries lack access to fair hearings as a means to resolve disputes with health plans. As a result, the literature provides more data on the use of external review programs in managed care in general, rather than in Medicaid managed care programs.
While external review programs vary from state to state, most follow the same basic processes.18 Notably, 12 out of the 13 states reviewed by Pollitz and colleagues (1998) do not grant consumers access to external review programs until they have exhausted in-plan grievance procedures. State regulatory agencies (such as Medicaid agencies or Insurance Departments) administer external review programs and, in most cases, contract with independent review organizations (IROs) to carry out the reviews. IROs, in turn, contract with practicing physicians or others, such as attorneys, to review cases in their area of expertise.
Within this basic framework, two main variations emerge in the context of Medicaid managed care. First, some states open their external review programs to both clinical and contractual issues, while others limit them to clinical issues or even to particular illnesses or treatment (Pollitz et al. 1998). Second, some states impose filing fees, filing deadlines, and minimum thresholds (dollar amounts) for the claim in dispute. This may further curtail Medicaid beneficiaries’ access to external reviews (Dallek and Pollitz 2000). These barriers are believed to prevent the filing of frivolous grievances and limit caseloads, but, as the research shows, so few consumers request external reviews that limiting caseloads hardly seems necessary (Dallek and Pollitz 2000).
2. States with External Review Programs
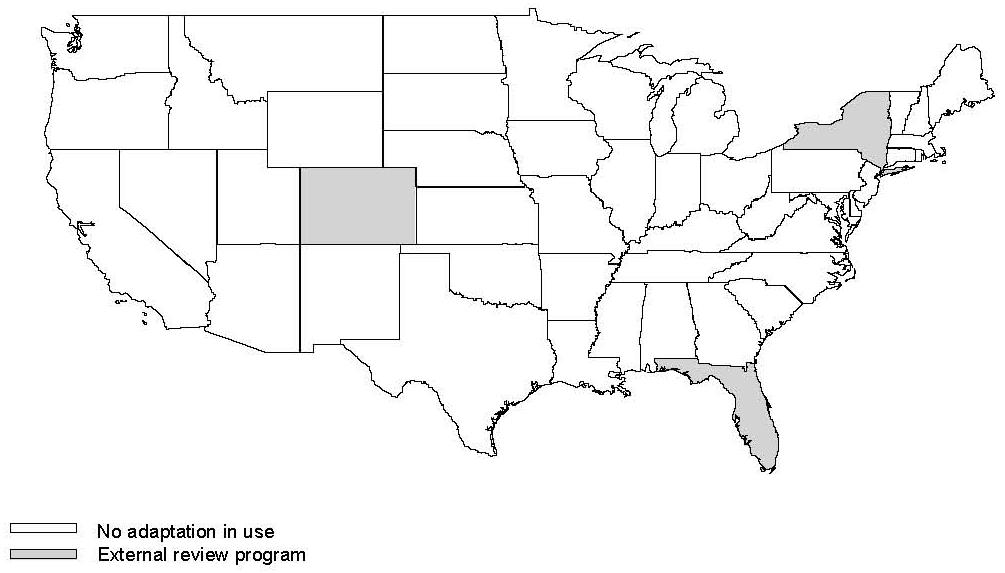
External review programs for commercially insured managed care enrollees have proliferated in recent years, but few have been made available to Medicaid managed care beneficiaries. As of 1998, 13 states had instituted commercial external review programs. Among the first were Michigan (1978), Florida (1985), and Pennsylvania (1991) (Pollitz et al. 1998). By 2001, 39 states required them (American Association of Health Plans 2001). While recent research has not focused on the availability of external review programs to Medicaid beneficiaries, we have learned in speaking to state officials that Florida (since 1985), New York (since 1999), and Colorado (since 2000) do make their programs available to Medicaid managed care beneficiaries (Figure II.2). We also learned that Michigan discontinued its external reviews for Medicaid beneficiaries in October 2000.
3. Theoretical Best Practices
According to the small body of available literature, managed care beneficiaries are best served by external review programs that: (1) allow review of a broad range of disputes; (2) do not restrict access by imposing claims thresholds, filing deadlines, or consumer charges; (3) are expeditious, and (4) provide regular feedback to health plans. More specifically, the literature unfavorably views external review programs that exclude coverage-related grievances or deal with them differently from the way they do medical grievances. This is because they create more complexity in the grievance system from the beneficiary’s perspective, and limit access to external review altogether for certain types of disputes (Pollitz et al. 1998; Dallek and Pollitz 2000). Likewise, programs that impose access barriers are seen as unnecessarily burdensome to consumers, especially since the volume of external reviews is small across all programs (Pollitz et al. 1998; Dallek and Pollitz 2000). Programs that are silent or ambiguous on time frames are considered less effective at ensuring that reviews occur within a reasonable time (Pollitz et al. 1998). Finally, health plans and consumers benefit when external review program data are shared with plans in ways that help them review their practices (American Association of Health Plans 2001). These best practice features are desirable for external review programs serving all types of managed care enrollees, including Medicaid beneficiaries.
| FIGURE II.2. Distribution of External Review Programs |
 |
C. EXPEDITED REVIEW PROGRAMS
1. Program Description
Expedited reviews programs give accelerated consideration to beneficiary disputes concerning the denial, termination, or reduction of emergency or urgent health care services. Such reviews can take place at three levels: (1) an internal appeal within a Medicaid health plan, (2) a fair hearing, or (3) an external appeal. Expedited review was created to address the special time-related circumstances of managed care and is an adjunct to standard health plan or state appeals processes, which often require 30-90 days for resolution of the beneficiary’s grievance.
As Olson and Perkins (2000) noted, the circumstances under which expedited reviews within health plans take place vary greatly by state. Many states use vague criteria such as “urgent or emergency conditions,” while others use more specific language to define eligible cases. Expedited review procedures can also vary in the time allowed for resolution of the beneficiary’s grievance. Because expedited reviews concern emergency or urgent care, these variations in the length of time needed to reach a decision can be critical to the well-being of the beneficiary. Time frames for conducting expedited reviews range from a few hours to as many as 14 days.
2. States with Expedited Review Procedures
Two sources describe state-level expedited review procedures. The first is an informal poll, conducted by the HCFA19 regional offices, that collected data on which states had an expedited fair hearing process (HCFA 2000). The survey indicated that 14 states had such processes. The second is a study by Olson and Perkins (2000), which, in contrast to the HCFA survey, identified by name only four states as having expedited review processes at the state level, and two of these, Arizona and Oregon, were not identified by the HCFA survey as having state-level expedited appeals processes.20 Expedited review procedures are often informal or integrated (as an option) into standard review procedures; as a result, they can be difficult to identify through surveys and literature reviews. In any case, a total of 16 states are identified as having state-level expedited review procedures by one source or the other.
| FIGURE II.3. Distribution of Expedited Fair Hearing Programs |
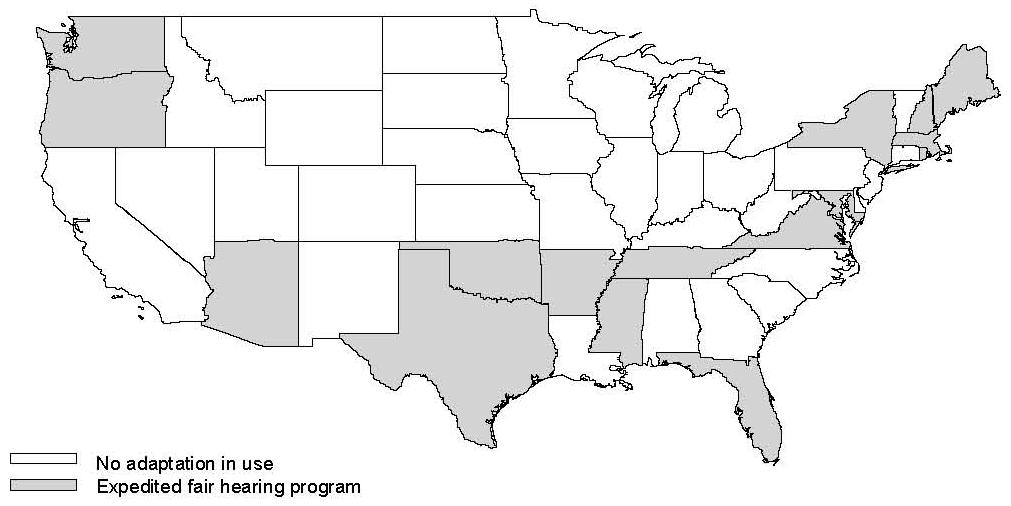 |
The literature provides a slightly more comprehensive view of state requirements for expedited reviews within Medicaid health plans. The number of states with such requirements has grown quickly in the last several years. A recent survey of state contract language identified 23 states requiring expedited review processes within the health plan before the matter reaches the state (Rosenbaum et al. 1999). Figure II.3 shows states state-level expedited review, but again we should note that although the literature has identified the existence of these programs, it is not clear how fully they have been implemented.21
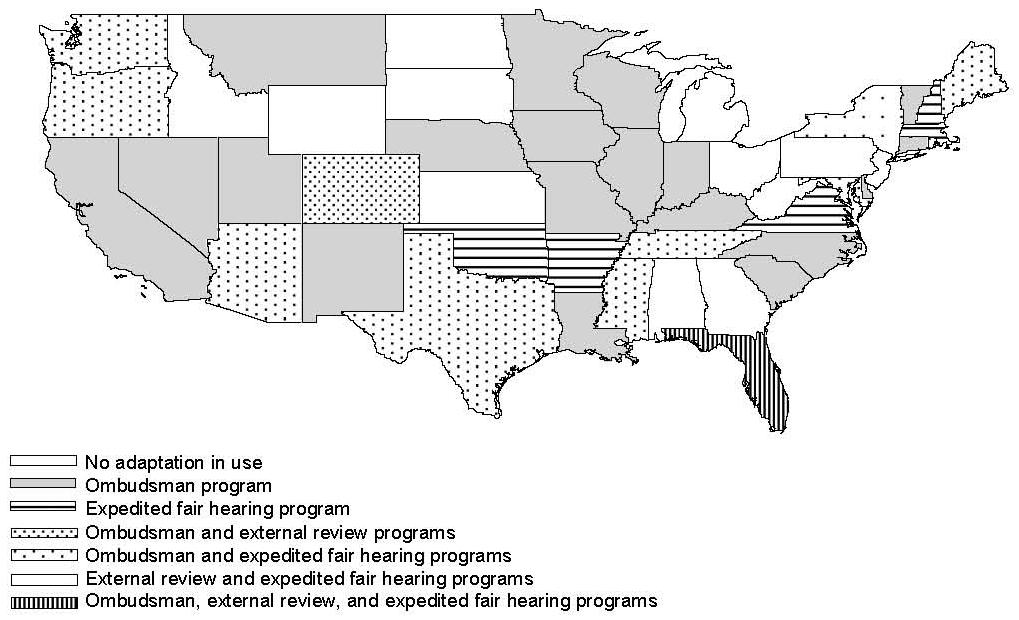
| FIGURE II.4. Distribution of Ombudsman, External Review and Expedited Fair Hearing Programs |
 |
3. Theoretical Best Practices
Perkins and Olson (1998) describe a theoretical best practice for state-level expedited review processes. Such a system would promote Medicaid beneficiaries’ right to due process, establish a standard of access to expedited review, and define a specific time frame for such review. A best practice process should meet four criteria. First, expedited review should be a formal process, even if it already occurs informally. A formal process is desirable, because it is more amenable to performance monitoring and quality improvement. Second, expedited reviews should be available when the beneficiary attests that services are urgently needed and that the failure to provide services promptly or to continue them may cause deterioration or impair improvement in the beneficiary’s medical condition. Third, a request for an expedited review should be filed with the state Medicaid agency, which notifies the health plan and requests medical records and documentation supporting the plan’s decision. This requirement prevents the health plan from potentially discouraging beneficiaries from filing for a hearing. Finally, the decision should be issued within two days of the request in order to reflect adequately the urgency of the patient’s situation.
D. SUMMARY
The use of fair hearing adaptations such as ombudsman programs, expedited review programs, and expedited review procedures is growing among states. However, there is considerable variation in the way states design and implement fair hearing adaptations. States also differ in the degree to which they promote access to these adaptations by Medicaid managed care beneficiaries. We will now explore each of these adaptations more thoroughly in Chapter III, Chapter IV, and Chapter V.
III. OMBUDSMAN PROGRAMS
While they share the same general goals, the Medicaid managed care ombudsman programs we studied--two in Minnesota, two in Colorado, and one in Oregon--differ from each other in numerous ways. They all help individual beneficiaries resolve disputes with MCOs and, to a limited extent, help states monitor their Medicaid managed care programs. Some have been doing so for 15 years, while others are quite new. Ombudsman programs vary in the scope of services they provide, the populations and areas they serve, and the types of data they collect and disseminate. The programs are also organized and funded differently. In this chapter, we describe what ombudsman programs do and how they do it; discuss the effects of the programs on various aspects of states’ grievance and appeal systems; and examine the expectations that various stakeholders bring to the programs. We conclude this chapter with a summary of key findings.
A. INTRODUCTION TO THE PROGRAMS
All the programs in our study were implemented at the same time as their respective states made significant commitments to mandatory Medicaid managed care. They came about, in large part, because consumer advocacy organizations--particularly those serving consumers with disabilities or chronic illnesses--insisted that their constituents not be enrolled in managed care unless they also had access to ombudsman programs that could help them address complaints and disputes with MCOs. The five programs in our study developed, therefore, through advocates’ efforts and numerous compromises among all stakeholders.
Since 1985, Minnesota has operated both a state Managed Care Ombudsman program and a County Advocate program. The Managed Care Ombudsman program is run by the state Medicaid agency, while the County Advocate program is composed of county staff who assist local Medicaid beneficiaries with managed care disputes in addition to performing other Medicaid functions. There is no formal relationship between the state ombudsman and the county advocates, but the ombudsman office does train county advocates in their grievance and appeal responsibilities.
Colorado also has two Medicaid managed care ombudsman programs, but their distinction is between general managed care and mental health services, rather than between levels of government. A general Medicaid Managed Care Ombudsman program was launched in 1998, followed by a Mental Health Ombuds program in 1999. Both programs are run by independent non-profit organizations under contract to the state. Colorado’s two ombudsman programs reflect the fact that Colorado’s Medicaid managed care program separates the administration and clinical care of physical and mental health services from each other.
Finally, Oregon’s current Medicaid managed care ombudsman program, known as the Consumer Advocate Services Unit, or CASU, was established in 1998 through the merger of two programs: (1) the state Medicaid agency’s general consumer hotline; and (2) an ombudsman program for Medicaid managed care beneficiaries who are elderly, blind, or disabled. Oregon’s Medicaid agency runs CASU.
B. THE PROGRAMS AT WORK
Ombudsman programs assist Medicaid beneficiaries with a range of disputes related to managed care. These include grievances over quality and “appealable” access issues such as service denials, reductions, and terminations. All such disputes may be resolved informally or through formal in-plan procedures; however, only denials, reductions, and terminations are eligible for fair hearings. Ombudsman program staff are involved in all or most of the Medicaid dispute-resolution processes offered in each state. In a typical case, a beneficiary with a complaint would contact the ombudsman program by using a toll-free telephone number or, less commonly, by writing a letter. The ombudsman would then assist the beneficiary by: (1) defining the problem and the desired outcome; (2) confirming that there is a case to pursue (that is, that the caller is enrolled in Medicaid managed care and seeks a covered service); (3) informing the beneficiary of all available grievance and appeal mechanisms, including fair hearings; (4) educating the beneficiary about his or her responsibilities as a complainant; (5) contacting and attempting to resolve the problem with the MCO’s member services department; (6) pursuing resolution with the MCO’s utilization review staff, if appropriate; and (7) if the complaint is unresolved, assisting the beneficiary in filing a formal grievance with the health plan, or the fair hearings office.
1. Informal Problem-Solving
The vast majority of disputes between beneficiaries and MCOs are resolved informally--without formal in-plan grievance and appeal procedures or a fair hearing. In keeping with that norm, most of an ombudsman’s involvement in disputes is also informal in nature. A typical complaint, one ombudsman program told us, may be settled in 5-10 phone calls between the program and the MCO or beneficiary.
Though the way to resolution may frequently be informal, it is always methodical. Ombudsman program staff, in both the older and the newer programs, described well-developed processes (such as the seven steps listed above) for assisting beneficiaries. They each rely on the techniques they find especially effective. For example, program staff in one state use three-way phone calls among the beneficiary, MCO, and ombudsman. Not only are many disputes resolved through such calls, but staff believe that they help beneficiaries learn how to conduct or participate in such conversations effectively. In another state, program staff rely on their familiarity with various health plans in order to contact directly the person with the authority to resolve the problem at hand. Depending on the plan and the problem, this person may be, for example, a customer service director or a treating clinician.
2. Formal In-Plan Procedures
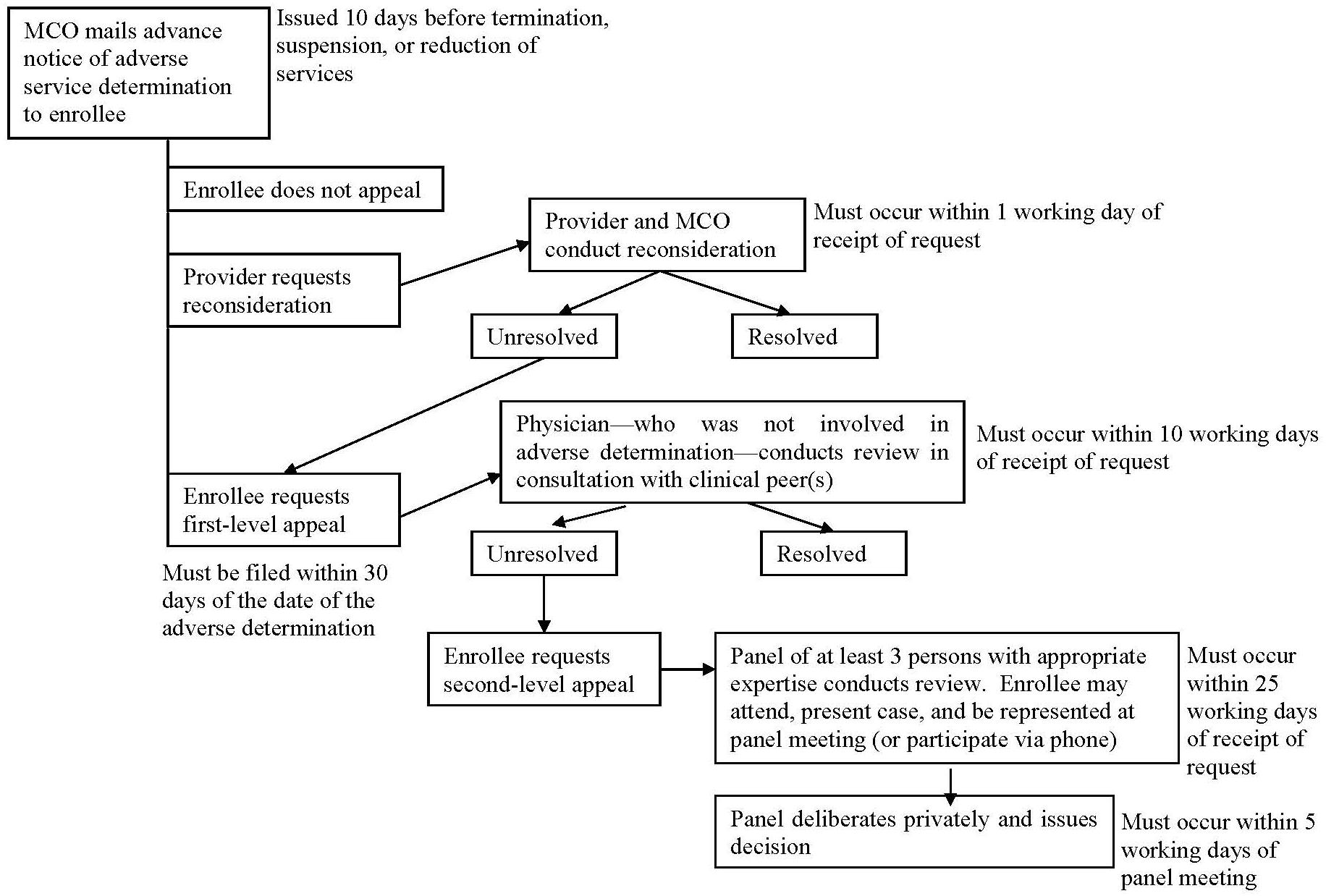
If informal techniques fail, ombudsman program staff may help beneficiaries with formal in-plan grievance and appeal procedures. Compared to informal negotiations, in-plan grievance and appeal procedures are laden with rules and deadlines, which apply to both beneficiaries and MCOs. Figure III.1 illustrates the in-plan procedures required by one of the states in our study, and notes some of the rules imposed on each party. The complexity of the process can create tension among the disputing parties and the ombudsman. For example, when helping a beneficiary register a complaint, an ombudsman may consider it good customer service to put the complaint in writing. However, written complaints, though useful as documentation, obligate MCOs to respond within state-mandated timelines. From one MCO’s perspective, timelines and other rules are at odds with “the way things work” inside an MCO. Thus, where the ombudsman sees an effective beneficiary advocate, the MCO sees a meddler--one who creates unnecessary work for MCO staff.
| FIGURE III.1. Example of State-Mandated In-Plan Appeal Procedures for Prospective Service Denials |
 |
3. State Fair Hearings
In any given period, some small percentage of Medicaid managed care beneficiaries in our study states request fair hearings, which tend to be the most complex appeal procedures available. Beneficiaries typically (but not necessarily) request hearings after other attempts at resolution have failed. The most common role that ombudsmen play in fair hearings is to help beneficiaries request and prepare for them. In Colorado and Minnesota, no legal barriers prevent ombudsman programs from directly representing beneficiaries in hearings, but they seldom do. In Oregon, the ombudsman program has a deliberately limited role in the fair hearing process. There, program staff explain the hearing process to beneficiaries and help them complete the state’s hearing request form, but once the beneficiary submits a request, the ombudsman’s involvement ends.
State laws in Colorado, Minnesota, and Oregon do not require Medicaid managed care beneficiaries to exhaust in-plan appeals procedures before they request fair hearings, but states generally encourage the use of in-plan resolutions to conserve resources and foster goodwill with MCOs. All the ombudsmen we interviewed noted that informing beneficiaries of fair hearing rights was one of their primary responsibilities. However, like the states that employ them, the ombudsmen view fair hearings as lengthy, cumbersome, perhaps needlessly adversarial processes to which they would rather not subject their clients. So they attempt an informal or plan-level resolution first, and request a hearing as a last resort. By contrast, legal advocates recommend that beneficiaries first request a hearing and then begin pursuing other channels. A hearing request, they say, lends clout to the beneficiary in the eyes of an MCO. In fact, available fair hearing data show that MCOs frequently reverse their decisions between the time a hearing is requested and the time it is scheduled to occur. Despite this evidence, we heard of no cases in which an ombudsman helped a beneficiary request a hearing and then began pursuing in-plan procedures.
Among stakeholders, the acceptability of an ombudsman’s direct involvement in state fair hearings seems to be related to how independent the ombudsman program is of the state. In Colorado, where both ombudsman programs are run by independent organizations, local legal advocates expect both the general Managed Care Ombudsman program (which is headed by a former trial attorney) and the Mental Health Ombuds program (which has no attorneys on staff) to represent enrollees directly in fair hearings. For their part, state officials seem comfortable with the idea of ombudsmen representing beneficiaries in hearings, as long as they first attempt other methods of dispute-resolution. By contrast, in Minnesota, which is home to a state-run Managed Care Ombudsman program and numerous County Advocates, state officials and legal advocates are more ambivalent about the appropriate role of ombudsmen in fair hearings. Because the ombudsman and county advocates are government employees, legal advocates do not support their playing a stronger representational role in hearings over government services. Among state officials and even some MCOs, however, there seems to be somewhat greater support for county advocates playing a direct representational role than there is for the ombudsman, perhaps because counties are “an arm’s length” from the state. Finally, in Oregon, where the CASU is housed within the Medicaid agency, it is assumed that CASU staff would not be credible beneficiary advocates in hearings involving the agency.
C. VARIATIONS IN PROGRAM CHARACTERISTICS
In this section, we describe the basic structural features of the five ombudsman programs in our study: whom they serve, the resources states use to offer these services, and where the ombudsman is located within the state’s health care system and governmental structure. These characteristics are summarized in Table III.1.
| TABLE III.1. Ombudsman Program Characteristics | |||||
|---|---|---|---|---|---|
| Program | Target Population | Area Served | Legal Authorization | Organizational Placement | Revenue Source |
| MINNESOTA | |||||
| State Managed Care Ombudsman | All Medicaid managed care beneficiaries, plus enrollees of other state-subsidized managed care programs | State | State law | State Medicaid agency | General Medicaid funds, annual budget basis |
| County Advocates | All Medicaid managed care beneficiaries | Counties that participate in Medicaid managed care | State law | County agencies | General Medicaid funds, per-beneficiary basis |
| COLORADO | |||||
| Managed Care Ombudsman | All Medicaid managed care beneficiaries | State | State fiscal note | Independent non-profit agency under state contract | General Medicaid funds, annual budget basis |
| Mental Health Ombudsman | Medicaid managed care beneficiaries who consumer mental health services | State | State contracts | Independent non-profit agency under state contract | General Medicaid funds, as a proportion of state’s payment to prepaid mental health plans |
| OREGON | |||||
| Consumer Advocate Services Unit | Adult Medicaid managed care enrollees | State | State law | State Medicaid agency | General Medicaid funds from three state agencies, annual budget and per-beneficiary basis |
| SOURCE: Interviews conducted in spring 2001 with state Medicaid managed care officials and ombudsman program staff. | |||||
1. Target Populations
The ombudsman programs in Minnesota, Colorado, and Oregon serve different subsets of Medicaid beneficiaries. With the exception of Minnesota’s County Advocate system, all the programs offer statewide service. Three serve all Medicaid managed care beneficiaries in their state or county, one serves adult Medicaid beneficiaries (including those receiving fee-for-service care), and one serves Medicaid managed care beneficiaries who use mental health services.
Specifically, in Minnesota, the Managed Care Ombudsman serves all mandatory Medicaid managed care beneficiaries in the state.22 The County Advocate program, as its name suggests, serves beneficiaries in counties that participate in the state Medicaid managed care program. In Colorado, the general Managed Care Ombudsman program serves all Medicaid managed care beneficiaries in the state (outside its Medicaid contract, the same organization also serves commercially insured and Medicare managed care beneficiaries). Colorado’s Mental Health Ombuds program also offers statewide services, but it targets those members of the Medicaid managed care population who are also consumers of mental health care services. In Oregon, CASU serves all adult Medicaid beneficiaries (children are served by a separate telephone hotline).
2. Organizational Placement and Legal Authorization
States’ decisions about the organizational placement of ombudsman programs have interesting consequences. Beneficiaries, MCOs, and advocacy organizations have different perceptions and reactions based on whether the ombudsman staff are perceived as state employees or as independent actors. As noted earlier, both Minnesota programs operate within governmental units (either state or county agencies). In contrast, both Colorado programs are operated by independent non-profit organizations under contract to state agencies. Oregon’s ombudsman program is situated with the state Medicaid agency.
The ombudsman programs we studied are authorized in different ways and, as a result, vary in their flexibility and capacity to adjust to constantly changing Medicaid regulations and budgets. Of the five ombudsman programs we studied, three were established by state law as part of Section 1115 waiver demonstrations; one was established through a state fiscal note; and one is authorized through contracts between the state and participating MCOs. Those established through state legislation (for example, through waiver demonstrations) or fiscal notes seem to have greater permanency, though they may be less adaptable to changing conditions. By contrast, contractually authorized programs can be adjusted each contract term.
3. Resources
Medicaid managed care ombudsman programs are not vast operations. No more than six people operate each of the programs in our study, even for statewide Medicaid populations averaging 285,000. Typically, a small number of staff perform ombudsman functions and receive administrative and clerical support from one additional staff member. The programs all receive general Medicaid revenues, including federal matching funds. Operating budgets were not readily available for most programs, but state officials and program staff described them as tight. In Minnesota, the state Medicaid agency funds the County Advocate system on a per-beneficiary basis (one full-time equivalent per 25,000 Medicaid managed care beneficiaries in the county), while the state-level ombudsman program has its budget set by the Medicaid agency according to overall agency priorities. In Colorado, the Department of Mental Health Services funds the Mental Health Ombuds program by earmarking some proportion of its payments to plans (not to exceed one-quarter of 1 percent) for the program. The general Managed Care Ombudsman is funded through an annual fiscal set-aside. In Oregon, CASU receives funding from the three state agencies whose constituents it serves (one such agency funds CASU on a per-beneficiary basis).
To supplement their paid staffs, the independent non-profit organizations that run Colorado’s managed care ombudsman programs recruit volunteers to perform clerical tasks and outreach activities. While reliance on volunteers has some inherent pitfalls (such as lack of accountability), volunteers do help tight budgets go further. In this regard, ombudsman programs run by non-profit organizations may have an advantage over those run by government agencies.
D. ACCESSIBILITY OF OMBUDSMAN PROGRAMS
Theoretically, ombudsman program staff can serve as important allies for Medicaid beneficiaries in obtaining medical services that beneficiaries believe are critical. The programs are ostensibly easy to access--beneficiaries avail themselves of services by dialing a toll-free telephone number from anywhere in the state. In practice, however, program accessibility is affected by a number of factors, including geographic proximity, outreach and educational activities, and the location of the program within the Medicaid managed care system.
1. The Effects of Geographic Proximity on Accessibility
Accessibility is governed largely by geography. Whether ombudsman program staff are located in the state capital or are dispersed in satellite offices affects a program’s ability to reach beneficiaries in all parts of a state, particularly those in rural areas. For example, Colorado’s Mental Health Ombuds program has offices in four areas of the state. In areas where the program has a physical presence, program staff have noticed that the use of services is higher than it is where the program does not have a physical presence (even in relation to the size of the areas’ Medicaid populations). They have concluded not that consumers experience more problems with MCOs in the areas where the program has an office, but that the very presence of an office results in greater use of program services. In contrast, Colorado’s general Managed Care Ombudsman program, whose annual budget would not accommodate satellite offices, concedes that it rarely serves beneficiaries outside the Denver area. In Minnesota, even though the state Managed Care Ombudsman has only one office, in St. Paul, the state generates access to ombudsman services through its decentralized County Advocate system. Of the programs in our study that operate from a single location, only Oregon’s CASU believes it reaches the entire state equally well. CASU attributes this to the fact that county human services offices are well acquainted with the program and refer beneficiaries to it.
2. The Effects of Outreach and Education on Accessibility
Accessibility is also affected by efforts to educate Medicaid beneficiaries that they have the right to dispute an MCO’s decisions and that they can call on the assistance of an ombudsman. Beneficiary awareness is fueled by several types of educational or outreach activities. Each ombudsman program makes an effort to acquaint Medicaid beneficiaries with their services. Ombudsman programs produce and distribute a variety of printed materials that describe their services, and most participate in community events and other speaking engagements. Program staff cited speaking at community events as their most effective outreach activity. One program, however, deliberately limits its public speaking engagements lest it create a demand for services it could not meet. State (and county) agencies, MCOs, and advocacy organizations also promote the ombudsman programs in their states. Some do so voluntarily; others do so at the state’s behest. Government agencies promote their ombudsman programs in Medicaid managed care welcome materials and periodic mass mailings. Oregon prints contact information for CASU on beneficiaries’ Medicaid cards, a practice it cites as a particularly effective promotional tool. Neither Colorado nor Minnesota makes use of this tool, but some Minnesota counties print special wallet-sized cards with contact information for county advocates. In addition, all the states require Medicaid MCOs to promote the ombudsman programs through their member handbooks and other materials, such as statements of beneficiary rights and responsibilities. Minnesota also requires MCOs to include contact information for the state ombudsman in their denial notices to beneficiaries. This was also cited as a particularly effective practice.
In the few states we studied, it seems that advocacy organizations may be somewhat more likely to promote and refer clients to ombudsman programs that are run by independent non-profit organizations (Colorado) than by government agencies (Minnesota and Oregon). However, consumer advocates in Oregon do readily refer certain types of problems (Medicaid billing disputes) to CASU, which they say is especially adept at handling them.
3. The Effects of Organizational Placement on Accessibility
Finally, whether an ombudsman program is perceived as independent of government (that is, the state Medicaid agency) affects accessibility. According to many stakeholders we interviewed, beneficiaries often fear they will lose their Medicaid benefits if they complain about them to government agencies. Thus, if beneficiaries think of ombudsman program staff as government employees, they may trust them less. Not surprisingly, stakeholders generally spoke less of beneficiaries’ fear and distrust with respect to ombudsman programs run by independent non-profit organizations than those run by government agencies. In addition, Colorado’s Mental Health Ombuds program employs several self-identified mental health care consumers, which it believes engenders trust among beneficiaries who use the program.
E. STAKEHOLDERS’ EXPECTATIONS OF OMBUDSMAN PROGRAMS
Ombudsman programs work within a complex environment of stakeholders with differing interests and expectations. As ombudsman program staff help Medicaid managed care beneficiaries resolve disputes with MCOs, they may adopt approaches that fit the interests of one party over another. For example, they may act as a neutral mediator between the beneficiary and the MCO or as an advocate for the beneficiary. Even though ombudsman programs theoretically and rhetorically have the choice between serving as a neutral mediator among the parties or as a champion of the beneficiary, none of the states in our study expect their ombudsmen to act as neutral mediators. In Colorado, where the programs are run by independent non-profit organizations under contract to the state, the state contracting agencies presume program staff will advocate for beneficiaries. In reality, the programs’ executive directors say they lean toward advocacy, but know they must at times tread gingerly, lest they alienate MCOs to the point where MCOs will not work with them to resolve disputes. In Minnesota, the state expects the Managed Care Ombudsman program to be “in the beneficiary’s court but not confrontational,” while County Advocates are presumed to lean even closer to advocacy.
Despite a tendency toward advocacy, all program staff described themselves as impartial fact-gatherers as they investigate the circumstances of a dispute. In addition, they use several criteria to determine whether to take the complaint to any in-plan or fair hearing process. These include:
- Whether the Medicaid managed care program covers the desired service.
- Whether obtaining the desired service is in the best interest of a particular beneficiary.
- Whether a solution can be found within a managed care framework.
As one ombudsman explained, “We’re very aware of the need to balance competing interests. We know the constraints of the Medicaid budget and the costs of health care. It is not our job to help consumers at the expense of everyone else in the system.”
While striking such a balance may seldom be easy, the task can be especially difficult when the ombudsman has strong ties to more than one interest. As noted earlier, Minnesota’s county advocates are also human services workers, who may screen people for Medicaid eligibility and help them enroll in an MCO. In one instance of these dual roles conflicting, a county advocate was helping a beneficiary request an expedited fair hearing when she learned that the urgency of his request stemmed from the fact that he had recently become employed and so was about to become ineligible for Medicaid benefits. In another attempt to strike a balance among competing interests, Minnesota has changed the reporting relationship between the executive director of the state ombudsman program and the Medicaid managed care office, so that the executive director no longer reports to the person who directly oversees the state’s contracts with MCOs. This step was taken to avoid conflicts of interest, but it also seems to have resulted in an ombudsman program more willing to advocate for beneficiaries rather than merely negotiate with MCOs.
For their part, MCOs have mixed experiences when they interact with ombudsman programs. No MCOs think of the ombudsmen in their states as neutral mediators, and none would initiate contact with an ombudsman to discuss a dispute. However, one MCO said it has worked cooperatively with an ombudsman program outside the arena of disputes. For example, the ombudsman gave a training seminar about consumer-directed advocacy to the MCO’s advisory boards, and the MCO helped the ombudsman program translate outreach materials into Spanish. When MCOs do interact with ombudsman programs over disputes, they appreciate it when ombudsmen listen to their side of the story, and they are frustrated when ombudsmen appear to ignore managed care principles or take an adversarial stance. Such favorable and unfavorable perceptions exist in all the states we studied, without a consistent relationship to such program characteristics as whether the ombudsman program is run by the Medicaid agency or by a non-profit organization.
F. THE IMPACTS OF OMBUDSMAN PROGRAMS
1. Impact on the Number of Complaints Resolved
Very small percentages of Medicaid managed care beneficiaries use the ombudsman programs in most of the states studied (which is not to say that these thinly staffed programs are not busy helping those who do).
Colorado is home to approximately 254,000 Medicaid managed care beneficiaries (CMS 2000). Its general Managed Care Ombudsman program has investigated and resolved disputes for about 20 Medicaid managed care beneficiaries per month since operations began in June 1998. This translates into an annual rate of about 9.6 users per 10,000 beneficiaries. In the first three years of operation, the ombudsman program filed fair hearing requests on behalf of two beneficiaries. (Both disputes were mediated before the hearing date.) Colorado’s Mental Health Ombuds program assisted about 18 beneficiaries a month in its first year of operation. Between the program’s inception in July 1999 and our visit in March 2001, program staff were involved in two fair hearings. In both cases, the aggrieved beneficiary took his or her dispute to the ombudsman program. The program then asked legal advocates to represent the beneficiary at hearing, but program staff provided testimony about the case.
Approximately 291,000 Medicaid managed care beneficiaries reside in Minnesota (CMS 2000). The state Managed Care Ombudsman program, now in its 16th year of operation, receives approximately 500 calls a month from managed care enrollees with inquiries or complaints.23 In 2000, beneficiaries in Minnesota’s Medicaid managed care program and two other state-subsidized managed care programs for low-income residents requested 204 fair hearings, excluding hearings related to administrative matters. On average, state ombudsman staff are involved in less than 5 percent of the requested hearings, about half of which actually take place (the others are resolved beforehand). In one of Minnesota’s larger counties, two staff performing full-time county advocate functions receive a combined total of about 400 inquiries or complaint-related calls a month from Medicaid managed care beneficiaries in that county. One advocate was involved in five fair hearings in 2000, but none in the first half of 2001.
Finally, the two ombudsmen at Oregon’s CASU serve an adult Medicaid population of roughly 212,000. Each ombudsman handles between 30 and 50 active cases at any time. A single ombudsman might make 60 phone calls per day, usually on behalf of about five clients. In addition to the more complex cases ombudsmen handle, CASU’s telephone hotline staff answer and log about 19,000 inquiries or complaint-related calls a month. As noted, CASU ombudsmen are not involved in fair hearings except to tell beneficiaries how to request them. In 2000, Oregon’s Medicaid managed care beneficiaries requested 415 fair hearings, about one-third of which took place.
2. Impact on the Use of Fair Hearings
Stakeholders in the three study states were of mixed opinion about whether ombudsman programs result in greater or lesser use of state fair hearings. Ombudsman programs may increase the use of hearings by encouraging beneficiaries not to abandon disputes when they otherwise might have. As a result, larger proportions of complaints may eventually lead to fair hearings. By the same token, ombudsman programs may decrease the likelihood of fair hearings by successfully resolving disputes early, through informal approaches and mediation.
The hope and promise of ombudsman programs is that they make existing grievance and appeal procedures easier for Medicaid managed care beneficiaries to use. For the individual beneficiaries they serve, the programs we studied are achieving this objective quite successfully. That success, however, has consequences for grievance systems in their entirety. In addition to providing direct services to beneficiaries (for example, by interacting with MCOs on their behalf), ombudsman programs generally try to teach and empower beneficiaries to resolve disputes on their own. Such consumer-directed skills are undeniably beneficial to consumers. As one ombudsman noted, “People with chronic illnesses have to be comfortable with self-advocacy,” or they will likely have unmet needs under managed care. On the other hand, as the consumer-directed approach increases beneficiary willingness and capacity to utilize the grievance and appeal system, it inevitably puts greater demands on MCOs and states to address complaints. Moreover, ombudsman programs seem to be making grievance and appeal procedures easier to use by seeking informal or “low-level” resolutions, to the exclusion of formal in-plan appeals and state fair hearings. As we have seen, state officials and MCOs prefer informal approaches, and ombudsmen like them because they subject individual beneficiaries to less stress. However, the downside of relying on informal solutions is that, unlike fair hearings, they rarely contribute to systemic change.
3. Impact on States’ Ability to Monitor Medicaid Managed Care Programs
Grievance and appeal data help states monitor the successes and failures of their Medicaid managed care programs. The states in our study require (often as a condition of their federal Medicaid waivers) that MCOs collect and submit internal grievance and appeal data, but they also think of their ombudsman programs as the “eyes and ears” of their managed care programs. We found that ombudsman programs do act in this capacity, but whether because of resource constraints or lack of formal feedback mechanisms, they do so more successfully on an individual, rather than a systemic, level.
The ombudsman programs in our study collect data as they assist beneficiaries. The programs all maintain computerized case logs and, as they handle incoming telephone calls, they capture information about the caller’s demographic characteristics along with the details of the complaint. Later, program staff update the logs with outcome data. The data that programs collect while serving beneficiaries is used mostly for internal tracking purposes and is reported to state (or county) agencies that administer Medicaid managed care programs. In addition, Colorado’s Mental Health Ombuds program publishes an annual report of its activities, and in Minnesota, some county advocates meet quarterly with the MCOs in their county to provide them with informal feedback about the cases they have handled.
However, states have not progressed toward using information collected through their ombudsman programs for more broad-based quality assurance monitoring, such as states might use in contract renewal decisions. Moreover, states are not using their ombudsman programs to detect whether some MCOs breach requirements to notify beneficiaries of adverse service determinations and their attendant appeal rights. The ombudsman program in one of our study states is, by law, a repository for copies of the denial notices that MCOs send to beneficiaries and the formal written complaints the MCOs receive from beneficiaries. Unfortunately, the ombudsman program lacks the resources to do anything other than file these documents. As a result, individual MCOs feel they give information to the ombudsman program without getting any in return, and the state does not get information that might identify weak points in the grievance and appeal system.
G. CONCLUSIONS AND KEY FINDINGS
Though they were once the “passive purchasers” of fee-for-service care, states operating Medicaid managed care programs assume a level of responsibility for the accessibility and quality of beneficiaries’ health care that reaches beyond “systemic quality assurance functions…all the way to the individual beneficiary” (Bonnyman and Johnson 1998). Indeed, we found that what ombudsman programs do best is to help states meet their obligations to individuals: the programs make it easier for Medicaid managed care beneficiaries to navigate complex grievance and appeal systems. However, because states have committed only minimal resources to these programs, ombudsmen believe they are not nearly able to reach all the beneficiaries that may need their assistance. Also because of resource constraints or a lack of well-developed feedback mechanisms, ombudsman programs help states monitor their Medicaid managed care programs only to a very limited extent.
Those beneficiaries who do access ombudsman programs receive assistance from knowledgeable, dedicated, and well-connected professionals. Moreover, the ombudsman programs we studied are flexible: beneficiaries may request their assistance at any stage of most, if not all, procedures; and much of an ombudsman’s work is aimed at avoiding the hardening of stakeholders’ positions. Despite such flexibility and the range of dispute-resolution techniques they employ, ombudsman programs have no authority to determine the outcome of disputes. They can advise and negotiate, but they cannot reverse MCO decisions or enforce the resolutions they help bring about.
When designing ombudsman programs for Medicaid managed care beneficiaries, states make numerous decisions that have lasting consequences for the accessibility and effectiveness of those programs. Perhaps the most important determinants of accessibility and effectiveness are: (1) the program’s geographic proximity to beneficiaries; (2) the use of outreach activities that inform beneficiaries of a program’s existence when they are most likely to use it; (3) the degree of trust beneficiaries have in the program; and (4) the acceptability of the program among MCOs. With respect to such factors, we found the following considerations to be especially important:
-
Geographic proximity can be achieved by composing a program of a headquarters and satellite offices, or by running a system of decentralized programs. Beneficiaries may enjoy the privacy that comes with a decentralized system, but states would benefit from the systemwide perspective afforded by the former model.
-
Beneficiaries are more likely to contact ombudsman programs when they need help if contact information is printed on documents that beneficiaries consult frequently (such as Medicaid identification cards) or in times of trouble (such as MCOs’ denial notices).
-
Ombudsman programs that are run by independent non-profit organizations seem “safer” to beneficiaries who may believe that complaining will result in the loss of Medicaid benefits. On the other hand, programs run by government agencies may seem more authoritative to MCOs, and staff at such programs are likely to have better access to the people and information that lead to resolutions.
-
Establishing a special ombudsman program for consumers of mental health care services engenders beneficiary trust, but may also fragment the grievance and appeal system.
-
States help make ombudsman programs more acceptable to MCOs by upholding expectations that program staff gather facts impartially and screen cases against basic eligibility criteria before taking them on. In addition, acceptability is fostered when ombudsmen and MCOs work together proactively--not merely when individual disputes arise.
IV. EXTERNAL REVIEW PROGRAMS
External review programs for Medicaid managed care beneficiaries are rare, existing only in a handful of states. Those operating in Florida and New York offer rich material for comparison. While they are alike in their unique status of being available to Medicaid managed care enrollees, they differ in most other aspects of their designs. The programs of both states are administered by state agencies that use reviewers with medical or legal expertise to evaluate and resolve medical service disputes between managed care enrollees and MCOs, but they differ greatly in their scope, popularity, and approach to data collection and analysis.
A. INTRODUCTION TO THE PROGRAMS
The external review programs in Florida and New York were created by state legislatures in efforts to allay consumer concerns over managed care. The pioneer external review program was the Statewide Provider and Subscriber Assistance Panel (or simply the Panel), first formed by the Florida Department of Insurance in 1985, in response to the early and rapid development of managed care plans in Florida. Since 1993, the state Agency for Health Care Administration (AHCA) has been authorized to operate the program through its Division of Managed Care and Health Quality.24 AHCA also houses the state Medicaid division. In 1998, the responsibilities and the budget of the Panel were expanded to its current scope, which includes not only disputes over medical necessity issues, but contractual disputes as well. This expansion occurred after the state decided to emphasize strong external review rather than implement proposed legislation that would have allowed patients to sue their health plans in courts of law.
New York’s External Appeals Program is authorized by the New York External Appeal Law of 1998 and was launched in July 1999. The legislation followed on that of another important consumer-protection law, the Managed Care Reform Act of 1996, which required MCOs to establish in-plan grievance and appeal procedures. Both pieces of legislation were supported by high-level state officials and consumer advocacy groups.25 The external review program is jointly administered by the New York State Department of Health (DOH) and the State Insurance Department (SID), but independent state-certified external review agents conduct the actual reviews through contractual arrangements.
B. THE PROGRAMS AT WORK
1. The Process from the Beneficiary’s Perspective
For beneficiaries in New York and Florida, the external review process begins in much the same way--with a written request for review and permission to release medical records. In New York, a beneficiary who has completed one level of in-plan appeal procedures has 45 days from receipt of the MCO’s adverse determination of the first-level appeal to request an external review. To do so, the beneficiary must submit some form of written request to the Insurance Department. Typically, beneficiaries use the Department’s preprinted applications, which MCOs are required to mail to beneficiaries with adverse determinations of appeals. A beneficiary who requests an expedited review (discussed in detail in Chapter V) or a review over investigational or experimental treatment must also obtain and submit a physician’s written attestation as to the urgency or, in experimental cases, the superiority of the requested treatment.
Florida’s application process is similar to New York’s, but it may be less complicated in that beneficiaries need only fill out an application, which their MCOs send along with final adverse determinations (or which they can obtain from the state Medicaid agency upon request). Florida beneficiaries do not need to obtain any physician or provider cooperation to request a hearing, as New York appellants do in some instances. Most important, however, Florida’s procedures are more complicated than New York’s in that Florida beneficiaries cannot apply to the Panel until they have completed their health plan’s entire internal grievance process. This requirement can be a source of confusion for Medicaid beneficiaries.
Florida and New York employ different forms of external review; this leads to very different experiences for Medicaid beneficiaries who use the programs. In New York, reviews are conducted “on paper.” Once a beneficiary files a request, he or she plays a passive role in the ensuing process. At most, staff from the Insurance Department or external review agency may request additional information from the beneficiary. Then, about one month later, the beneficiary will receive a decision in the mail.
In Florida, beneficiaries continue to play an active role in the dispute after they file a review request. This is because external reviews are conducted as informal hearings, with the disputing parties, any representatives they may bring, and an eight or nine-member decision-making panel all present at the hearing. The hearings are held either in person in Tallahassee, where AHCA is located, or via videoconference at video facilities near the beneficiary’s hometown. Independent reviewers are generally brought in to the hearing and give their testimony by telephone. At the hearing, each party is allowed 15 minutes to present its case, and each is allowed a rebuttal. Cross-examination is not permitted, but each party responds to questions from the Panel. MCOs may send a variety of representatives to the hearing, including medical directors, grievance coordinators, and underwriters. Beneficiaries can bring attorneys or physicians, but usually represent themselves. Attorneys are rarely present at the hearings, because the Panel discourages formality. About two weeks after the hearing, the beneficiary will receive the Panel’s decision in the mail.
In both New York and Florida, Medicaid beneficiaries use external review programs at no cost. In New York, MCOs bear the costs of individual reviews.26 MCOs may charge non-Medicaid appellants up to $50 per review, but that fee is returned to the appellant if the MCO’s decision is ultimately reversed. In Florida, the Panel incurs the cost of the reviews it performs. Funds come out of the general AHCA budget.
2. Behind the Scenes of External Review
Most of the steps in New York’s external review process are invisible to the beneficiary. When Insurance Department staff receive requests for external reviews, they screen them for eligibility and completeness. (They must screen standard requests within five business days and expedited requests within 24 hours). If a request is complete and eligible for the program, staff randomly assign it to one of three state-certified external review agents. (During the program’s first two years, there were two such agents, Island Peer Review Organization and Medical Care Management Corporation. Both agents are established health care review organizations that serve public and private clients.) The external review agent prepares a complete case file, assigns the case to physician reviewer(s), and renders a final determination. Reviews of medical necessity are conducted by one physician reviewer, while reviews of investigational or experimental treatment are conducted by an odd-numbered panel of reviewers (usually three). The external review agent issues a final determination to the disputing parties. The determinations are binding, and leave no forum for appeal other than suing the state.
In comparison to New York’s program, less in Florida is invisible to the beneficiary. When the Panel receives a request for an external review, they request medical records and other pertinent information from the MCO, obtain an independent review by an external consulting physician specialist (if relevant), and prepare the case for a hearing. Then, as described above, the hearing occurs, and within 15 days the Panel makes a decision. Both parties have ten days to disagree with the written decision, which is then finalized within another ten days. MCOs have 30 days to comply with the decision, and Panel staff follow up with beneficiaries to find out whether they have done so. While the Panel itself cannot enforce compliance, the state AHCA can. MCOs may appeal the Panel’s decision to another state agency (the Department of Administrative Hearings); beneficiaries would have to apply to the Department of Children and Family Services (DCFS) for a fair hearing, or sue the state.
3. Relationship Between External Reviews and Fair Hearings
Unlike their commercially insured counterparts, Medicaid managed care beneficiaries in Florida and New York have access to external reviews and fair hearings. Both states have rules about whether the two processes can be invoked simultaneously or in a specific sequence. In both states, however, fair hearing decisions trump external review determinations.
In New York, Medicaid managed care beneficiaries may request a fair hearing and apply for an external review at the same time. Alternatively, beneficiaries who complete the external review process first but lose may then go on to request a fair hearing (assuming they would still meet the 60-day filing deadline). On the other hand, beneficiaries who complete the fair hearing process first but lose would not be eligible for external review. Although these rules exist, so far state officials know of no instances of a beneficiary using both processes.
In Florida, beneficiaries must make an initial choice between a fair hearing and an external review. Those who at first choose external reviews have the prerogative to change their minds, withdraw their request, and request a fair hearing at any time (including during the in-plan review). Those who at first choose fair hearings, however, are given no such leeway to change their minds and request external reviews. In other words, once a request for a fair hearing is filed, an external review will not proceed. Florida state officials and advocates also could not recall an instance where beneficiaries who filed for external review went on to a fair hearing.
C. VARIATIONS IN PROGRAM CHARACTERISTICS
1. Target Populations
The external review programs in Florida and New York were designed principally for commercially insured managed care enrollees but are, as noted, also available to Medicaid managed care beneficiaries. In both states, all program procedures are the same for commercial and Medicaid consumers (although, as mentioned, Medicaid beneficiaries technically have an additional option in their right to a fair hearing, and their review fees are waived).
2. Disputes Eligible for Review
Florida’s external review program addresses the full range of contractual issues (such as disputes over excluded benefits, out-of-network referrals, and contract interpretations) and clinical issues (such as disputes over medical necessity determinations, experimental treatment, and service non-authorizations). In contrast to Florida’s all-encompassing program, New York’s program addresses only coverage denials based on MCO determinations that the requested services are not medically necessary or are investigational or experimental. Contractual issues are not eligible for the New York program.
States encounter potential disadvantages no matter what eligibility criteria they set. Florida’s inclusion of disputes over contractual issues (and, in particular, cases involving clearly excluded benefits) means that the Panel’s workload is inflated by cases that have few grounds for consideration, because the Panel does not have authority to change the terms of contracts. For example, a consumer who seeks 53 covered psychotherapy sessions when his insurance contract explicitly covers only 52 sessions may bring his case before the Panel, but he will almost certainly lose. By contrast, New York’s more exclusionary approach to eligibility requires program administrators (rather than physician reviewers) to distinguish between contractual and clinical issues, even when distinctions may not be clear. For example, an MCO may deny a surgical procedure on the basis that it is cosmetic--and therefore not a contractually covered benefit--though a beneficiary requested it on medical necessity grounds. If the program administrator determines that a case hinges on contractual issues, a review is not conducted, and the beneficiary is thus on technical grounds denied the right to appeal. In short, either approach to dispute eligibility generates some problem.
3. Staffing and Other Resources
External review programs can be resource-intensive. They require staff to receive and process applications, organize the collection of evidence, select and supervise the external reviewers (whether organizational or individual), process the eventual decision, and monitor MCO compliance. New York’s initial external appeal legislation required the Health and Insurance Departments to implement an external review program, but it did not give them a budget to do so. In the first year of program operations, neither department hired additional staff to implement the program, but instead expanded the responsibilities of existing staff. Attorneys in the Insurance Department’s Health and Consumer Services bureaus, and staff in the Health Department’s Office of Managed Care, certify and oversee external review agents and monitor MCOs’ compliance. Day-to-day program operations, such as screening external review requests for completeness and eligibility, randomly assigning cases to an external review agent, and operating the toll-free external appeals hotline, are handled by Insurance Department staff. In the first year of operations, six staff members performed these responsibilities. Because the volume of requests was much higher than anticipated, the department requested, and received, funding for a few additional staff members for the program’s second year.
Florida has several categories of personnel involved in its external review program. The Panel itself consists of eight or nine members, seven of which are state employees (from both the Department of Insurance and AHCA), who sit on the Panel in addition to their other duties. (The other panel members are a physician and a consumer advocate, both members of the public appointed by the Governor.) Eight office staff perform the day-to-day operations of collecting evidence, scheduling, and notification. Up until 1998, the Panel had almost no support staff, and the backlog of cases was quite large. In the 1998-1999 fiscal year, it took the Panel 219 days, on average, to close a case. In 1998, the Governor and the legislature became aware of the problems, and funding and staff were increased. The backlogs and decision times have decreased accordingly; by the 2000-2001 fiscal year, cases were closed in about 65 days.
4. Organizational Placement
In general, the organizational placement of external review programs has few implications for operations or outcomes, because the key component of the external review is the use of independent experts who have no connection to the government. However, organizational placement is relevant to Medicaid managed care beneficiaries in one important way: in the built-in overlap between external review and fair hearings, which are set up as alternatives to each other. Florida has a bifurcated structure for the administration of Medicaid managed care appeals. The external review Panel is operated by AHCA, which is responsible for Medicaid managed care operations and policy, but fair hearings are administered by DCFS, the agency that operates the Temporary Assistance for Needy Families program. The result is that state officials have gaps in their knowledge concerning parts of the complaints and appeals process. AHCA officials have little understanding of the fair hearings process, while the DCFS officials in charge of fair hearing know little about the Panel. Beneficiaries are not advised on the advantages or disadvantages of either option, nor are processes coordinated, so that if a beneficiary wanted to go from one to the other, they could use the same files.
New York, which has located its external review program within the Departments of Health and Insurance, does not have such a problem. The DOH sets Medicaid fair hearing policy (although actual hearings are performed by a separate state unit) and is involved in making external review policy.
D. STRENGTHS AND WEAKNESSES OF EXTERNAL REVIEW PROGRAMS
1. Accessibility to Medicaid Managed Care Beneficiaries
The accessibility of external review programs (or any grievance procedure) depends first on whether beneficiaries are aware of the program, and second on whether the program is easy to use. It is an irony of the New York program that it may be easier for Medicaid beneficiaries to use than it is visible to them in the first place. While New York’s state agencies and MCOs do promote the external review program, some of their efforts would be unlikely to reach Medicaid beneficiaries, and none are geared specifically toward them. For example, the Insurance and Health Departments make impressive use of their Web sites to provide consumers with information about the program. However, compared to other consumers, Medicaid beneficiaries are probably less likely to have access to the Web. For their part, whenever they issue final adverse determinations, MCOs (in addition to describing the external review program in their member handbooks) are supposed to provide beneficiaries with copies of the state’s external review application (a nine-page document) and notice of their fair hearing rights. This is undoubtedly a well-intentioned practice--it attempts to inform beneficiaries of their grievance options at the very moment they are likely act on them. However, such a large amount of information may be so off-putting that some beneficiaries, especially those with low literacy skills, will not attempt or even be able to read it.27
Ironically, for those beneficiaries who happen to become aware of New York’s program, the state does make it easy to use. For example, the Insurance Department actually treats any document sent to a designated post office box as a request for a review, and staff follows up with the beneficiary to request additional information needed to complete an application. The agency also operates a toll-free telephone hotline to answer consumers’ questions and help them fill out applications. As noted earlier, the beneficiary’s job is largely done once the application is complete, so New York seems to be providing the type of assistance Medicaid beneficiaries need to access external reviews.
Florida also reaches out to beneficiaries, both when they enroll (when beneficiaries are told of the Panel in their membership materials) and when they are sent their final adverse determinations. Both of these efforts are as effective in Florida as they are in New York. However, Florida also uses a third outreach strategy, which involves MCOs’ unresolved complaint data. Every quarter, the state sends a letter to all managed care clients who have an unresolved grievance and notifies them of their right to use the Panel process. State officials find that 50 percent of the cases filed with the Panel are in response to these advisory letters.
When beneficiaries begin to use the Panel, they find it easy to deal with. Panel staff collect all pertinent information from providers instead of leaving the task to the beneficiary. The hearings are held at videoconferencing facilities near beneficiaries’ homes, so they do not have to travel far to present their case; and finally, the hearing is informal, with the opposing sides each presenting their story to the Panel rather than debating one another.
2. Impartiality
Generally speaking, external review programs exist to provide managed care consumers with impartial reviews of MCO decisions. New York’s program succeeds in this regard, as evidenced by the following:
-
It makes use of physician reviewers who do not have material or professional interests in the outcome of the cases they review.
-
Reviewers apply medical necessity standards that are imposed by statute. MCOs’ definitions of medical necessity are taken into account, but they are not determinative.
-
Stakeholders--including MCOs and consumer organizations--perceive the program as impartial and fair to both parties. They trust it.
In addition, several stakeholders cited the results of the program as evidence of its impartiality. In the first year of operations, the program yielded 331 decisions in favor of consumers and 328 in favor of MCOs.
The Florida external review program also makes use of physician (and other professional) experts who do not have a material interest in the outcome of the case. It too applies medical necessity standards that are independent of MCO definitions, relying instead on physician experts’ personal knowledge of and experience with clinical research. In other ways, however, the program is less clearly impartial. Several panel members reported that they try to decide cases in favor of the beneficiary. Despite this propensity, program data indicate that the Panel finds for the MCOs in at least half of all cases. Moreover, Florida MCOs are generally content with the Panel process itself. Several said they appreciated the Panel’s decisions because the decisions identified flaws or ambiguities in their contract language. The plans regard this as useful feedback that subsequently helps them rework their contracts with the state.
E. THE IMPACT OF EXTERNAL REVIEW PROGRAMS
1. Impact on the Resolution of Medicaid Managed Care Disputes
While national data from the American Association of Health Plans (2001) show that the use of state external review programs by commercial managed care enrollees is low--about 0.7 reviews for every 10,000 enrollees--use of the programs by Medicaid managed care beneficiaries in Florida or New York is even lower. In the first year of program operations in New York, nine external review decisions were rendered for Medicaid beneficiaries. This translates into an annual rate of 0.1 appeals per 10,000 beneficiaries.28 By contrast, the appeal rate among New York’s commercial enrollees was 1.7 appeals per 10,000 enrollees in 2000, which made it the busiest external review program in the nation (American Association of Health Plans 2001). In a recent six-month period, Florida’s external review panel heard 140 commercial cases and six Medicaid cases, equal to annual appeal rates of about 0.8 for commercial enrollees and 0.2 for Medicaid beneficiaries.29
Like their commercial counterparts, Medicaid beneficiaries who do use external review programs have about a 50 percent chance of a resolution in their favor. Florida’s Panel found in favor of appellants in 45 percent of the cases it heard in a recent fiscal year. Similarly, in the program’s first year, reviewers in New York reversed half of MCOs’ decisions (and upheld half).
2. Usefulness in Monitoring Medicaid Managed Care Programs
By collecting and analyzing data from their external review programs, states have a useful tool with which to monitor consumer complaints that are not resolved at the plan level. Both New York and Florida have data collection procedures that help them analyze trends in their managed care systems.
The New York state employees who administer the External Appeals Program do a thorough job of collecting, synthesizing, and disseminating program data--most of which pertain to commercial enrollees, who use the program more than their counterparts in Medicaid. State law requires MCOs and state-certified external appeal agents to report annually to the state health commissioner the number of external appeals requested by enrollees, as well as the outcomes. The commissioner, in turn, must report such information to the Governor and the legislature. In fact, program staff surpass the law’s requirements. After a year of program operations, staff produced an annual report that, among other things, presents data on appeal results by agent, by health plan, and by type of denial. It also reports the cost of appeals and the reasons that requests for appeals are rejected, and it discusses problems encountered and solutions developed in that first year. The annual report is available on the Internet http://www.ins.state.ny.us/acrobat/extapp.pdf. Plan-level external review data are also included in the New York Consumer Guide to Health Insurers.
The Florida Panel also collects data from the Panel’s operations for use in monitoring the managed care system and combines them with quarterly data on unresolved complaints from each MCO. These data are used in two ways: (1) in the annual state report card (available at http://www.fdhc.state.fl.us/mchq/managedhealthcare), which provides information on the cost, content, and quality of care provided by managed care plans in the state; and (2) by AHCA officials, as one of the criteria in the annual deliberations over the renewal of Medicaid contracts with managed care plans.
3. Impact on the Use of Fair Hearings
As noted earlier, few, if any, Medicaid managed care beneficiaries pursue both fair hearings and external reviews, even though their cases may be eligible for both. This raises questions about whether external review programs draw cases away from fair hearing caseloads and, if so, whether this is good for beneficiaries. Our visits to New York and Florida suggest that beneficiaries make important tradeoffs when they choose one procedure over another (whether or not they are aware of them), but that there is no clearly “better” choice other than perhaps in individual cases.
In Florida, the separation of fair hearings and external review into two separate agencies has meant that the two systems operate completely independently of each other. Neither agency refers beneficiaries to the other. It is likely, therefore, that few beneficiaries make a choice between the two options; rather, the beneficiary follows the procedure that he or she happens to hear about. Few Medicaid beneficiaries use either system. As noted, only six of the 146 cases the Panel heard in the first half of 2001 pertained to Medicaid managed care cases; only ten of the hundreds of fair hearings were for Medicaid managed care.30 No matter the choice, there are advantages and disadvantages. The fair hearings process does not require the completion of the in-plan grievance procedures (while the external review panel does); the fair hearings process provides due process protections, such as prior notification and cross-examination, that the Panel does not. On the other hand, the Panel’s deliberations are more informal, and they are more focused on the specific policies of individual MCOs, because members of the Panel also work in the state Office of Managed Care.
In New York, as in Florida, few Medicaid beneficiaries use either fair hearings or external reviews in a given year. However, in the two years in which they have had the option, New York Medicaid managed care beneficiaries with disputes over clinical issues have been as likely to request fair hearings as external reviews. Between summer 1999 and spring 2001, 70 beneficiaries requested fair hearings and 67 requested external reviews. Under both procedures, about 30 percent of beneficiaries pursue the process to its completion, where they are equally likely to get resolutions in their favor (about half do). As in Florida, New York stakeholders note important differences between external appeals and fair hearings. Unlike the external appeals program, the fair hearings process: (1) does not require completion of any in-plan appeals; (2) allows for the continuation of Medicaid benefits while a decision is pending; (3) encompasses clinical and some contractual issues; and (4) may be requested orally. Stakeholders view these features of fair hearings as advantageous to Medicaid enrollees. The relative advantages and disadvantages of other differences are less clear. For example, administrative law judges (ALJs) knowledgeable about Medicaid policies decide fair hearings, while practicing medical experts (who may not have knowledge of Medicaid) make determinations on external appeals. Finally, New York beneficiaries choosing between a fair hearing and an external review have an additional consideration that Florida beneficiaries do not: in New York, beneficiaries may participate in person in fair hearings, but not in external appeals. In-person participation may be an advantage for some, but a disadvantage or even a deterrent for others.
F. CONCLUSIONS AND KEY FINDINGS
The external review programs in Florida and New York are noteworthy for their differences and their similarities. Florida’s program is the country’s oldest, but consumers use it at a rate below the national average of 0.7 appeal per 10,000 managed care enrollees. It entertains all manner of managed care disputes and brings disputing parties together in an informal hearing before a panel of eight or nine reviewers from different areas of expertise. By contrast, New York’s program is the country’s busiest, although it is only two years old. The program is limited to disputes over medical necessity determinations and experimental or investigational treatments. It makes use entirely of “paper” reviews conducted by (at most) three physicians, rather than in-person panel hearings. Despite these differences, the two programs yield similar outcomes. Both find in favor of MCOs in about half of all cases and in favor of consumers in the other half. More important, consumers and MCOs view the programs as impartial and fair. In addition, of course, the two programs are alike in their availability to Medicaid managed care beneficiaries--a feature not found in most states’ programs.
Differences in the states’ program designs raise important considerations, both for Medicaid beneficiaries in Florida and New York who must decide whether to use the programs and for other states who may interested in implementing external review programs. Among the most important considerations are:
-
Deciding what types of disputes will be eligible for the program. If the scope is broad, like Florida’s, more consumers will be able to use the program. On the other hand, time and resources will occasionally be spent on cases that are not truly arguable--such as cases over contractually excluded benefits. If the program’s scope excludes such contractual issues, however, program administrators will have to prejudge the eligibility of some cases that are not clearly contractual or clinical.
-
Deciding whether to conduct reviews on paper or as informal panel hearings. From the state’s point of view, panel hearings are more logistically challenging than paper reviews. From the appellant’s perspective, however, panel hearings offer an opportunity to verbalize, and perhaps humanize, one’s case. By contrast, appellants play a more passive role in paper reviews than they do in panel hearings, which may be preferable to appellants who find in-person reviews intimidating.
From the perspective of Medicaid managed care beneficiaries, it is instructive to compare external review programs not only with each other, but also with fair hearing processes. Making external review programs available to Medicaid beneficiaries expands their state-level dispute-resolution options beyond fair hearings. Assuming both procedures are impartial and well administered, this expansion of options works to the beneficiary’s advantage if:
- Beneficiaries are aware of the relative tradeoffs of each process, including:
- Whether the benefit in question will continue while a decision is pending,
- What requirements exist for completing in-plan procedures,
- The reviewers’ areas of professional expertise,
-
The review format in use (that is, in person or on paper).
-
State program administrators are knowledgeable of both processes and share their knowledge with beneficiaries.
Conversely, the availability of both external reviews and fair hearings would work to the beneficiary’s disadvantage if the beneficiary “chooses” one out of ignorance of the other, is steered to one or the other according to the interests of an MCO or the state, or is so confused or overwhelmed by the choice that he or she pursues neither. Our studies in Florida and New York suggest that Medicaid managed care beneficiaries may not be well informed with regard to the choice between external review and fair hearings. Neither state makes especial efforts to educate beneficiaries about their choices, and some state staff themselves lack thorough knowledge about both procedures. Nonetheless, in New York, as many Medicaid managed care beneficiaries with clinical disputes have chosen fair hearings as have chosen external reviews in the two years in which they have had the option. This suggests, as does Florida’s experience, that the states’ general outreach efforts are effectively reaching at least some Medicaid beneficiaries.
V. EXPEDITED REVIEW PROCEDURES
Of the three fair hearings adaptations we studied, expedited reviews are the most straightforward in their purpose and implementation. They are used to adjudicate appeals of denials, terminations, or reductions in service that are critical to the patient’s life or health. Expedited reviews accelerate the time frame of the adjudication process to address medically urgent cases that cannot wait for the decisions of standard (and usually lengthy) reviews.
This chapter describes and compares the expedited review procedures used in Oregon and New York. Oregon provides Medicaid managed care beneficiaries access to expedited fair hearings. In contrast, New York offers three channels for expedited review: (1) in-plan appeals, (2) fair hearings, and (3) external reviews. While we will focus on the similarities of and the differences between the two states’ expedited fair hearings processes, we will also provide some details on New York’s expedited in-plan appeals and external review processes for comparison.
As would be expected with states that lie on opposite ends of the country yet deal with the same health care system, the expedited review procedures of Oregon and New York have some similarities and some differences. They are similar in the criteria they use to determine whether a case is eligible for expedited review, the amount of enrollee outreach they perform, the data they generate, and the degree to which beneficiaries use the process. On the other hand, they differ on the levels of review they offer, the location of decision-makers and reviewers, and the outcomes of their review processes.
The biggest difference between Oregon and New York is not a characteristic of their expedited review programs, but of their Medicaid programs in general. This general difference is critical to how their expedited fair hearings programs operate. In Oregon’s Medicaid managed care program, the Oregon Health Plan (OHP), coverage for specific services is determined by a list that ranks more than 700 diagnosis/treatment pairs from most to least treatable and cost-effective. The state legislature determines, and the federal CMS approves, where the line for coverage is drawn. Treatments that fall below the line are not covered. OHP currently covers services numbered one through 574. An exception to this is if a beneficiary has a condition above the line that is being exacerbated by the presence of a comorbid condition below the line and coverage of the below-the-line service will improve the above-the-line condition. As we will describe in later sections of this chapter, Oregon’s use of this list influences its fair hearings (and expedited fair hearings) program in important ways. We begin our comparison of Oregon and New York by examining the structural characteristics of their expedited review programs.
A. EXPEDITED REVIEW PROCEDURES AT WORK
In Oregon, the only type of expedited review procedures available to Medicaid managed care beneficiaries are expedited fair hearings, which were introduced in 1994 at the start of the OHP.31, 32 A case meets the criterion for expedited review when there is an immediate or serious threat to the enrollee’s life or health. As an example, a fair hearings official described an expedited hearing request from a beneficiary who wished to receive transplant surgery in an out-of-state hospital. Oregon’s expedited fair hearing process is used infrequently. The number of expedited fair hearings has not been tracked separately from standard fair hearings, but state officials estimate that there have been three expedited fair hearings in the past three years.
In comparison to Oregon, the expedited review process in New York is quite complex. As noted above, New York offers Medicaid managed care beneficiaries access to expedited review through three channels: (1) in-plan appeals, (2) fair hearings, and (3) external reviews.33 The criterion for determining if a case is eligible for expedited review is the same for each channel--a delay would pose a serious or imminent threat to the enrollee’s health. (A fair hearings official cited as an example the case of a beneficiary who had been denied chemotherapy.) As in Oregon, New York does not report data on expedited reviews separately from those of standard reviews. State officials estimate that since the start of the programs in 1999 there have been one or two expedited fair hearings and perhaps one expedited Medicaid external review.
In Oregon, the expedited fair hearing process begins when a beneficiary completes an Administrative Hearing Request form and checks the box indicating a request for an expedited hearing (the conditions under which an expedited hearing is available are listed on the back of the form).34 The form is forwarded to the medical director of the Office of Medical Assistance Programs (OMAP), which administers the OHP. The medical director has 48 hours to gather relevant documentation and medical records and decide whether or not to grant the expedited review request. Although no beneficiary has ever disputed a denial of a request for an expedited hearing, the medical director’s decision can be appealed to the director of OMAP. If an expedited review request is granted, a hearing is scheduled within five days. The case is heard by a hearing officer from the Department of Employment, who must reach a decision within 14 days.35Figure V.1 illustrates Oregon’s expedited fair hearing process.
| FIGURE V.1. Comparison of Expedited Review Processes in Oregon and New York |
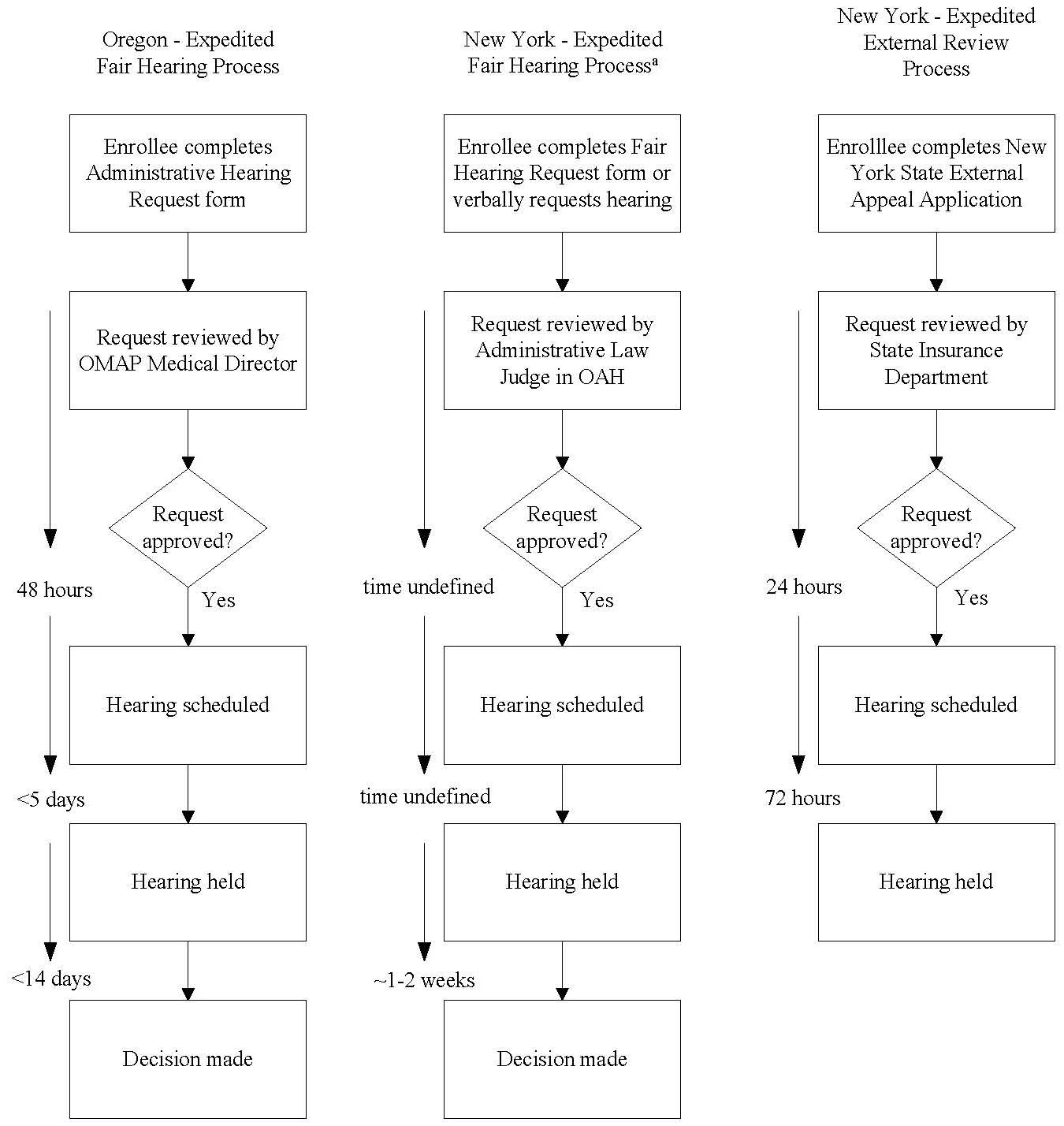 |
|
Medicaid managed care beneficiaries in New York can either seek an expedited in-plan appeal or go directly to an expedited fair hearing. If they choose an in-plan appeal, health plans are required to examine the case and notify beneficiaries of their findings within two business days after receipt of the necessary documents. Alternatively, beneficiaries can request an expedited fair hearing either by calling New York’s Office of Administrative Hearings (OAH) or by submitting a completed fair hearing request form. The form does not indicate that an expedited hearing is available; instead, the enrollee must describe the reason for requesting the hearing and indicate a “time frame.” The omission from the form of a direct reference to the possibility of expedited review is due to the fact that the Operational Protocols governing New York’s Medicaid program explicitly direct OAH to grant priority scheduling to all clinical cases whether or not the beneficiary requests it. The OAH expedites all hearing requests to the extent volume permits and, if the enrollee’s case involves an urgent need for medical services or supplies, they will give it priority scheduling.36 A fair hearings official indicated that priority hearings are usually held within two weeks of the request. An ALJ reviews requests for priority scheduling and decides whether or not to grant the request based on his or her own opinion of the urgency of the situation, without the input of a physician or other medical expert.37Figure V.1 illustrates New York’s expedited fair hearings process.
Medicaid managed care beneficiaries in New York also have the option of an expedited external review, which operates as a condensed version of the standard external review described in Chapter IV. To qualify for this option, beneficiaries must have completed one level of in-plan appeal (either expedited or standard). Beneficiaries who have already had a fair hearing are not eligible for external review, because a fair hearing decision will always preempt a decision made through external review. In the external review process, the beneficiary completes a special request application that includes a section on requesting an expedited review. In addition, the beneficiary’s attending physician must complete an Attestation for External Appeal, which justifies the medical necessity of the expedited review. The SID reviews expedited external appeals requests and must decide within 24 hours, based on the physician’s attestation, whether or not to grant the request. If the request is complete and eligible for external review, it is randomly assigned to an external appeal agency. An independent physician, assigned by the external review agency, must reach a decision on the case within 72 hours. Figure V.1 illustrates New York’s expedited external review process.
The expedited review option a beneficiary chooses may depend on the nature of the case. External review decisions are made by a physician, but fair hearing decisions are made by an ALJ or hearing officer. Thus, a beneficiary with strong clinical grounds for appeal may prefer an external review. Alternatively, because they are entitled to continuing benefits, beneficiaries who are already receiving the service in question may prefer a fair hearing. New York State does not provide beneficiaries with any written materials that describe the differences between an expedited fair hearing and an expedited external review.
B. VARIATIONS IN EXPEDITED REVIEW PROGRAM STRUCTURE
We examined the expedited review programs in Oregon and New York to identify the ways in which the programs are structured: the types of beneficiaries who are eligible to use the process, the types of cases targeted, program location within state government, and program staffing and financial resources. Table V.1 compares the expedited fair hearings processes in Oregon and New York and then examines New York’s expedited external review program.
The expedited fair hearing processes in Oregon and New York are similar in terms of the types of Medicaid beneficiaries eligible to use the process (both managed care and fee-for-service) and the types of cases eligible for expedited review (denials, terminations, or reductions in medically necessary care).38 New York’s expedited external review process is slightly different; it is open only to Medicaid managed care beneficiaries with cases regarding denials of medically necessary care or denials of investigational or experimental treatments.39
| TABLE V.1. Structural Characteristics of Expedited Review Programs in Oregon and New York | |||
|---|---|---|---|
| Structural Characteristic | Oregon Expedited Fair Hearings | New York Expedited Fair Hearings | New York Expedited External Review |
| Eligible Beneficiaries | Managed care and fee-for-service | Managed care and fee-for-service | Managed care |
| Target Cases | Denials, terminations, or reductions in medically necessary services | Denials, terminations, or reductions in medically necessary services | Denials, terminations, or reductions in medically necessary services or denials of investigational or experimental treatments |
| Organizational Location of Program | |||
| Administration/oversight | Office of Medical Assistance Programs, Department of Human Services | Office of Administrative Hearings, Department of Family Assistance | State Insurance Department/Department of Health |
| Adjudication of cases | Department of Employment | Office of Administrative Hearings, Department of Family Assistance | Independent Review Organizations (IROs) |
| Staffing | |||
| Administration | 4 administrative staff | 100+ administrative staff | 6+ administrative staff |
| Adjudication | 12 hearing officers | 100+ administrative law judges and hearing officers | Reviewers under contract to IROs |
Fair hearings programs reside in different locations within Oregon’s and New York’s state agency structure. In Oregon, OMAP administers both Medicaid fair hearings and the state’s Medicaid program, including its managed care component, OHP. New York, in contrast, administers fair hearings outside the Medicaid agency. In both states, the administration of fair hearings includes gathering evidence and documentation, scheduling hearings, and communicating with beneficiaries and health plans. Also in both states, the ALJs and hearing officers who preside over the hearings and render decisions are located in agencies that centralize all hearings for state programs. These “hearings” agencies have no specific expertise in Medicaid (or even health). Both states weighed the economies of scale that accrue from having a centralized hearing agency and the advantages of greater knowledge of Medicaid regulations held by Medicaid agencies, and both have tended to favor the centralized approach. We have no evidence that the lack of expertise in health or Medicaid on the part of the adjudicators affects the determinations.
Precise quantification of the resources needed to run an expedited review program is difficult. In terms of financial resources (that is, program budgets), Oregon and New York do not distinguish between funds for expedited fair hearings and funds for standard fair hearings. New York’s expedited external review program is funded by the same mechanism that funds standard external reviews described in Chapter IV. Staffing resources needed for an expedited review program are only slightly less difficult to quantify. In Oregon, four staff members in the OMAP medical director’s office handle all Medicaid fair hearings, not just expedited ones. In New York, it is much more difficult to identify those staff responsible for Medicaid fair hearings, because all fair hearings (not just Medicaid-related cases) are administered in one office. Thus, neither funding nor staffing levels of Oregon and New York can be compared. However, given the very small number of expedited reviews in both states, such reviews, as a subset of standard reviews, probably consume little staff time or other financial resources.
C. ACCESSIBILITY OF EXPEDITED REVIEW PROCEDURES
Expedited review processes hold promise as a safety valve mechanism that can help managed care systems adjust appeals of denials or terminations of services to the urgencies of a critical medical case. Yet how easy is it for Medicaid beneficiaries to receive an expedited review? Ostensibly, requesting an expedited review is simple: just check-off a box or fill in a “time frame.” In practice, promotional (or educational) outreach activities, as well as the complexities of obtaining the requisite documentation, affect access.
1. Effects of Outreach and Program Structure on Accessibility
Accessibility is dependent on the awareness of beneficiaries that they have the right to a quick decision in their appeal of a denial, termination, or reduction of some critical medical service. This awareness, in turn, depends upon the quality and quantity of education and outreach activities conducted by the state, health plans, and advocacy organizations.
Both Oregon and New York require that information about the right to an expedited fair hearing, and the circumstances under which one can be granted, be included in each notice of action that a Medicaid managed care plan issues. This information is also required in member handbooks and welcome packets. However, fair hearings officials in New York told us that health plans frequently issue notices of action that do not contain this information. Similarly, several advocates in Oregon said that health plans will often deny a service without issuing a written notice of action. Thus, this key point of enrollee education may lack information on expedited review.
Beyond these “required” educational activities, in neither state did we hear of additional outreach activities that provide information on expedited fair hearings, such as special mailings, speakers at community meetings, or public service announcements in the media. This is true of activities conducted by the states, health plans, and advocacy organizations. In Oregon, one advocacy organization said that, while they do give community presentations regarding fair hearings rights, they do not specifically mention expedited fair hearings.
In addition to beneficiary awareness, accessibility is also dependent on the structure of an expedited review program. Beneficiary access may be limited by barriers such as the lack of an explicit statement that expedited review is available, and New York’s fair hearing request form indeed creates such a barrier. Similarly, New York’s requirement (for external review) that the beneficiary’s physician attest to the medical urgency of the case creates another barrier.
D. STAKEHOLDER EXPECTATIONS
Because these programs are seldom used, stakeholders in New York and Oregon had few comments regarding expedited review processes. In New York, fair hearings officials seemed satisfied with the process. Perhaps with so few beneficiaries seeking this option, any problems the system does have surface only infrequently. Similarly, health plans and advocates have had very little experience with expedited fair hearings and were not able to cite any particular strengths or weaknesses of the program. However, staff of New York’s external review program felt that it was often very difficult for them to complete expedited reviews within the prescribed 72 hours. Although the program handles very few expedited Medicaid cases, there have been enough expedited commercial cases for the staff to gain some experience with the process. External review agency staff reported that compliance with the 72-hour time frame was most difficult on weekends and holidays, when it was more difficult to obtain necessary documentation and access to staffing resources. Insurance department staff now have developed administrative procedures to ensure access to physician expertise over the weekend.
In Oregon, state officials believed that the expedited review process was successful in offering a quick resolution to beneficiaries’ urgent appeals. As in New York, health plans and advocates did not cite any strengths or weaknesses of the expedited fair hearing program. Although health plans and advocates did not voice either positive or negative opinions of the expedited fair hearing process, we can theorize about their interests. For example, health plans may dislike expedited fair hearings because the process forces them to produce medical records and other internal documentation quickly. Advocates may try to discourage beneficiaries from seeking an expedited hearing because they may get continuing benefits for a longer period of time if they choose a standard hearing. Alternatively, advocates may like expedited review because it serves the urgent medical needs of beneficiaries better than standard review. In addition, we hypothesize that, in Oregon, the use of the prioritized list of covered services and the extreme difficulty of reversing a plan’s denial of a “below-the-line” service may discourage advocates from suggesting the option of expedited review to their clients.
E. IMPACT OF EXPEDITED REVIEW PROCEDURES
1. Number of Complaints Resolved
Very few Medicaid managed care beneficiaries, in either state we studied, use the expedited review process. Oregon does not track requests for expedited fair hearings separately from those for standard fair hearings, but state officials estimate that less than 10 percent of the 415 fair hearing requests received in 2000 were for expedited reviews.40 On average, only one request for an expedited fair hearing is granted each year. Thus, in Oregon almost 98 percent of expedited fair hearing requests are denied.
Like Oregon, New York does not track requests for expedited fair hearings separately from those for standard fair hearings, but fair hearings officials estimate that one or two of the 44 Medicaid managed care hearings requests between August 1999 and May 2001 were for priority scheduling (that is, expedited review). The officials said that they have always been able to accommodate beneficiary requests for priority scheduling. Thus, although the number of requests for priority scheduling is low, their approval rate is high. This is in direct contrast to Oregon, which, as mentioned earlier, has a very low approval rate for expedited fair hearing requests. The reasons for this difference are not clear. Oregon’s high denial rate may be due to beneficiaries’ requests for services that are not covered on the prioritized list. Alternatively, Oregon’s OMAP medical director may require a higher burden of proof of medical urgency than do the ALJs approving requests for expedited fair hearings in New York.
As noted in Chapter IV, New York’s external review program also is infrequently used by Medicaid managed care beneficiaries. Of 569 decisions by the state external review program, only nine concerned Medicaid beneficiaries. Furthermore, only 43 of the 659 reviews were expedited. We can infer from these statistics that there is approximately one expedited external review for Medicaid managed care per year.
2. Outcome of Disputes in Expedited Review
The outcomes of expedited review cases are not tracked separately from those of standard reviews in either Oregon or New York. However, the outcomes of expedited reviews are probably similar to those of standard reviews in terms of the proportion of decisions “for” and “against” beneficiaries. In Oregon, more than 95 percent of all fair hearing decisions are in favor of the health plan. In New York, 28 percent of fair hearing decisions are in favor of the health plan, compared with 50 percent of external review decisions. We can hypothesize that the difference between the states in the percentage of decisions in favor of health plans is due to Oregon’s use of the prioritized list for covered services. Beneficiaries have little hope of having their denials overturned if the service they have requested is not “above the line.”
3. Use of Expedited Review Procedures to Monitor Utilization Review Decisions
The number of appeals of denials, terminations, and reductions of service based on urgent medical need is a measure of the appropriateness and flexibility of the utilization review decisions made by health plans. Feedback to health plans on the numbers and types of expedited hearing requests could be useful in their quality improvement processes. Such data could be used to guide states in developing and refining the contractual requirements to which they hold health plans.
It appears that neither Oregon nor New York takes as full advantage of the potential of expedited review data as they might. As we noted, neither state has tracked expedited fair hearing requests or decisions separately from standard reviews. New York does track expedited external review cases, but this data is not published separately, perhaps because there are so few cases. In New York, they do some tracking of fair hearings data in general for reports required by litigation or regulation, such as the timeliness of fair hearings decisions or health plan compliance with them. For Oregon’s fair hearings, the OMAP medical director’s office tracks data on an ad hoc basis and reports trends to state Medicaid officials.
F. PROMISING COMPONENTS
This chapter has described the similarities and differences in the structural characteristics of the expedited review programs in New York and Oregon. As a means of summarizing this discussion, we will return to the criteria in Perkins and Olson (1998) for a best practices expedited review program, described in Chapter II. Table V.2 lists these criteria and assesses the performance of New York’s and Oregon’s expedited fair hearing processes and New York’s expedited external review process.
| TABLE V.2. Comparison of Expedited Review Processes Using Best Practices Criteria | |||
|---|---|---|---|
| Best Practices Criterion | Oregon Expedited Fair Hearings | New York Expedited Fair Hearings | New York Expedited External Review |
| Formal process | Yes | Yes | Yes |
| Expedited review available when enrollee attests service is urgently needed and failure to provide may cause deterioration or delay improvement | Yes, but criteria strictly applied | Yes, criteria leniently applied | No, physician must attest to medical necessity |
| Request filed with state Medicaid agency that then notifies health plan | Yes | Yes | Yes |
| Decision issued within two days of request | No, may be as many as 21 days | No, 1-2 weeks | No, may be as many as four days.a |
| |||
States that wish to improve their grievance and appeal systems, or reap as many potential benefits from their ongoing expedited review procedures as possible, might consider the following findings:
-
Multiple types of expedited review--in-plan appeals, fair hearings, and external review--provide beneficiaries with greater flexibility to choose the type of review with which they are most comfortable, yet they increase the complexity of the system.
-
Current methods of beneficiary education do not appear to have heightened awareness of the availability of expedited fair hearings and expedited external review.
-
A simple check-box on the hearing request form appears to heighten beneficiary awareness of the option for expedited review.
-
States have the option of requiring beneficiaries to provide the attestation of their physician regarding the medical urgency of the case (which perhaps creates access barriers) or of allowing beneficiaries access to expedited appeals based on the beneficiary’s own sense of urgency (which perhaps creates a larger administrative burden for the state).
The expedited review programs in New York and Oregon have some shortcomings, but they contain useful elements that could be adopted by other states in the design of their own expedited review procedures.
VI. SUMMARY AND CONCLUSIONS
As Medicaid managed care programs proliferate and mature, the need for effective and efficient grievance and appeal procedures has intensified. In fee-for-service settings, grievance and appeal procedures--namely, fair hearings--determine whether an insurer must reimburse a provider for services already rendered. Under managed care, however, grievance and appeal procedures often determine whether services will be provided in the first place. This changing nature of disputes, coupled with common Medicaid consumer restrictions (such as mandatory enrollment and lock-in provisions) and concerns about Medicaid beneficiaries’ ability to advocate for themselves, has led some states to develop innovative programs or procedures to complement traditional fair hearings and in-plan procedures.
A. SUMMARY OF STATE INITIATIVES AND ADAPTATIONS
This report has described the operations and implications of three major adaptations to fair hearings--ombudsman programs, external review programs, and expedited review procedures--as they exist in five states (Colorado, Minnesota, Florida, Oregon, and New York). By implementing such programs and procedures, these states seek to protect beneficiaries’ grievance and appeal rights without neglecting their own interests or those of the MCOs with whom they contract.
1. Program Objectives
Acknowledging that many Medicaid beneficiaries need expert assistance in voicing complaints and navigating grievance and appeal systems, Colorado, Minnesota, and Oregon have established ombudsman programs to provide such assistance. Recognizing that some MCO decisions (such as whether treatment is medically necessary, whether it is preferable to another treatment, or whether it should be provided in a specialized facility) warrant review by independent experts, Florida and New York avail Medicaid managed care beneficiaries of external review programs in addition to fair hearings. Finally, realizing that some service denials can have dramatic consequences for patients with serious medical conditions, Oregon and New York have established expedited review procedures (including expedited fair hearings and expedited external reviews) to provide timely review of decisions regarding urgent medical treatment.
2. Tradeoffs Related to Program Design
In constructing the programs and procedures mentioned above, states face a set of choices that have implications for the flexibility, accessibility, and impact of these adaptations. One choice states face is a tradeoff between locating the adaptation within state government and placing it with an organization under contract to the state. Colorado, for example, provides ombudsman services to Medicaid managed care beneficiaries through contracts with two independent non-profit organizations. Likewise, New York certifies independent medical review organizations to render external appeal decisions through their contracts with independent physician reviewers. In contrast, Minnesota operates its ombudsman programs through state and county agencies, and Florida uses state employees (supplemented by individual medical consultants) to adjudicate external review disputes. States like Colorado and New York assert that their contractual arrangements assure Medicaid managed care beneficiaries that deliberations and decisions about their health care are conducted by people who are not beholden to the state. States like Minnesota and Florida, on the other hand, emphasize that beneficiaries are well-served by the insider knowledge and access of their agency run programs.
A second choice the states make in constructing their grievance and appeal systems is between situating hearings (including state fair hearings and external hearings) within the state Medicaid agency itself and placing them in a separate state agency that holds hearings for all state programs. New York and Oregon send their expedited (and standard) fair hearings to a centralized state agency, arguing that this choice has the advantages of economies of scale and generalized expertise in dispute-resolution. Florida, in contrast, uses state Medicaid personnel to staff their external review panel, arguing that extensive knowledge of Medicaid regulations and the Medicaid plans themselves improves the quality of the decisions of the panel.
A third tradeoff stems from the scope of disputes that state adaptations are designed to address. For example, Colorado has established an ombudsman program especially for disputes over prepaid mental health services. This choice reflects a philosophy that mental health care issues are so different from physical health issues that they require a separate ombudsman program. Proponents of more inclusive ombudsman programs argue, conversely, that mental and physical health are intertwined and should be treated together. Similar issues of dispute eligibility arise in external review programs. Florida’s all-inclusive program promotes accessibility yet also attracts contractual exclusion of coverage disputes that have no meaningful basis for consideration under the program. New York’s program, on the other hand, is closed to all but clinical issues. This restriction requires program administrators to distinguish between contractual and clinical issues, even when such distinctions are not clear.
Finally, states face a choice as to where they attempt to channel the bulk of their Medicaid managed care disputes. With the exception of Florida, none of the states in our study require beneficiaries to exhaust in-plan procedures before requesting fair hearings. Nonetheless, all of them encourage beneficiaries to attempt informal and in-plan resolutions first, and save formal state processes, like external reviews and fair hearings, for last. In-plan resolutions generally require fewer resources of states and MCOs and may generate less stress for beneficiaries. However, state decisions to emphasize in-plan processes tend to mean (at least in our study states) that states develop detailed regulations regarding those processes. Florida’s regulations, to give one example, explicitly specify the time periods to which MCOs must adhere during dispute processes and the types of employees that must be involved in them.
B. CONCLUSIONS
1. Promising Elements
The ombudsman programs, external review programs, and expedited review procedures that have resulted from these choices each address important needs and reap benefits for stakeholders. These benefits (not all of which are borne out by each adaptation) can be seen in the increased capacity of Medicaid managed care programs to identify, process, and ultimately resolve Medicaid managed care disputes. More specifically, the adaptations:
-
Make grievance and appeal systems adaptable to a wide range of disputes, including those involving quality concerns and appealable access issues such as service denials, reductions, and terminations.
-
Ensure that Medicaid managed care beneficiaries have a “voice” in the managed care decisions that affect them personally.
-
Provide a choice of dispute-resolution processes (in some states).
-
Increase the use of independent clinical expertise to guide decisions.
-
Provide feedback processes for learning that have the potential to improve the system.
-
Build the legitimacy of Medicaid dispute-resolution processes by increasing beneficiary trust in the system (in some states).
By implementing one or more of the adaptations in this study, states ensure that grievance and appeal procedures appropriately address the unique circumstances of individual disputes. Expedited review procedures allow disputes involving emergency or critical treatments to be resolved in an appropriate time frame, shortening the process from months to weeks or even days. In some states, disputes involving decisions over medical necessity can now be resolved using the expertise of independent physicians, while disputes involving customer service can be resolved with the assistance of an ombudsman. Similarly, the establishment of these adaptations has created alternative channels or mechanisms that beneficiaries can use to resolve disputes. In all states, beneficiaries have a bit more choice between fair hearings and one or two of the other mechanisms, which allows them to tailor the dispute-resolution process to their style and capacity.
In a variety of ways, the adaptations help amplify the voices of individual beneficiaries as they seek health services in a managed care setting. Ombudsman program staff (and even some members of some external review panels) in particular champion the interests of individual beneficiaries. Program staff help beneficiaries define and articulate their complaints, discuss the issues with MCO staff, and file formal grievances and appeals. All these activities advance the beneficiary’s interests in ways that many beneficiaries themselves cannot. The role of independent expertise has also grown larger in grievance and appeal processes, as expedited and external review programs rely on the clinical and/or legal expertise of independent consultants in addition to the beneficiary’s medical records (which carry great weight in many fair hearings). These independent experts can refine the analysis of the situation at hand, identify alternative solutions or compromises, or lend legitimacy to MCOs’ original medical decisions.
The adaptations discussed in this report have developed alongside continuous quality improvement, which emphasizes MCO learning through feedback. As a result, these adaptations often mandate the collection of data on the number and nature of unresolved conflicts between MCOs and beneficiaries, and feed this information back to MCOs in the hope of improving their operations. This feedback can take the form of official report cards on health plan activity (as in Florida and New York) or of informal meetings between ombudsman and health plans (as in Minnesota and Colorado). These feedback processes, moreover, have the potential to alter the system, since they offer both state Medicaid agencies and MCOs opportunities to learn from the disputes and adjust their regulations, contracts, and practices to avoid future conflicts.
Finally, the development of these adaptations, with their capacity to offer advocacy, independent expertise, and flexibility, increases the legitimacy of the overall grievance and appeal system. State officials, MCO representatives, and advocates generally agreed that beneficiaries trust the Medicaid managed care system more with these adaptations in place.
2. Areas for Improvement
Perhaps the most striking finding of our study is that very few Medicaid managed care beneficiaries actually use fair hearings or the three types of adaptations upon which we focused. In a typical year, less than 1 percent of beneficiaries request standard or expedited fair hearings or external reviews.41 Somewhat larger percentages of beneficiaries access ombudsman programs, mostly because the programs handle simple inquiries in addition to full-fledged grievances and appeals. Without directly interviewing beneficiaries about their knowledge of and need for grievance and appeal procedures, it is impossible to explain fully such low levels of use. However, our interviews with representatives of state agencies, advocacy organizations, and MCOs suggest that the low use is due, in part, to shortcomings in the way the adaptations are implemented. In particular, we found that:
-
Not all states use the most effective outreach activities to promote their adaptations.
-
Some state procedures for accessing grievance and appeal systems limit beneficiaries’ access to the adaptations and to fair hearings.
-
The adaptations lack some of the resources they need to be effective.
-
States do not take full advantage of the grievance and appeal data generated by the adaptations.
According to stakeholders we interviewed, effective outreach activities are those that: (1) are likely to be remembered; or (2) give beneficiaries grievance and appeal information when they are most likely to use it. Presentations at community events, such as health fairs, are an example of the former. Medicaid identification cards and MCO denial notices that include information on how to contact state grievance and appeal programs are an example of the latter. Unfortunately, not all the states in our study use such outreach activities. States more commonly include grievance and appeal information in state enrollment materials and MCO member handbooks, even though they concede that beneficiaries rarely consult these materials.
Those beneficiaries who do become aware of their grievance and appeal options may encounter a complex set of procedures and choices. Some states require beneficiaries to put complaints or review requests in writing--a potential obstacle to anyone with below-average education and literacy skills. States may also require beneficiaries to obtain attestations from physicians in order to access certain types of review--an obstacle to anyone without easy access to transportation, a telephone, or a fax machine, or without the perseverance to follow up with busy physicians. In addition, states may require beneficiaries to pursue resolutions in specific sequences. However, the more steps a beneficiary must take, the greater the chance of a misstep, such as a lost document or missed deadline. States do attempt to alleviate some of these burdens (for example, by helping beneficiaries complete forms and by operating toll-free customer assistance lines), but important barriers remain. Ironically, the adaptations’ very existence also creates a potential barrier to their use. In other words, the more grievance and appeal options one has, the harder it may be to choose among them. Though ombudsman program staff help beneficiaries weigh the pros and cons of each option, beneficiaries are generally not given much guidance in this regard. Thus, the choice between various in-plan procedures, fair hearings, external reviews, and expedited versions of standard procedures may well be daunting.
A third shortcoming is an overall lack of resources to operate the grievance and appeal systems at effective levels. One of the reasons given for minimal outreach campaigns is a desire to restrict outreach lest it generate demand that the grievance and appeal program could not meet because of a lack of staff. Limited funding also is given as an explanation for the lack of geographic proximity of ombudsman program offices, as well as for the lack of systematic data collection and monitoring of both the in-plan and the state run grievance and appeal procedures.
Finally, the adaptations fail to take full advantage of the information they obtain through the operation of their programs. Theoretically, data on the number and types of disputes beneficiaries have with MCOs can be a useful indicator of the customer relations policies of MCOs. State Medicaid agencies could use this information in contracting with and regulating Medicaid MCOs. With the exception of Florida and New York, however, few state programs we studied kept systematic data on their grievance and appeal systems. Only Florida actively uses the information in contract negotiations with MCOs.
3. Recommendations
Our study has identified several simple actions that states could take to strengthen their grievance and appeal systems, including fair hearing procedures and state-level adaptations. Some of our recommendations are easy to implement, including: (1) printing the grievance and appeal program telephone number on each Medicaid card for easy reference; (2) maintaining a well-staffed hotline to field inquiries and generate written applications for beneficiaries to sign; (3) using graphic design techniques to include simple check-off boxes on complaint forms and requests for reviews; (4) listing state agency and/or ombudsman program phone numbers on denial notices and other complaint-related correspondence; and (5) using videoconferencing facilities for hearings so that state employees and independent consultants can hold hearings without expensive travel around their state.
Other actions to strengthen grievance and appeal systems may be more challenging to undertake. Outreach activities that spread awareness of grievance and appeal options would be productive and inexpensive, but they would likely generate greater utilization by beneficiaries, which would in turn generate higher costs for the state. Improvements in tracking Medicaid managed care complaints would also be useful, because better data could help develop greater insight into trends in the overall Medicaid system. However, current state-level economic conditions may not permit many states to make the additional investment of staff and computer resources that such actions would require. This is particularly true in states with dramatically increasing Medicaid expenditures.
In summary, the five states in this study have embarked on creative experiments to generate innovations in how disputes between Medicaid beneficiaries and MCOs are resolved. Acting in their traditional role as laboratories for social policy, states have fashioned some interesting alternatives. More fine-tuning of the outreach and monitoring activities that could generate a greater use of these new systems could yield important benefits for all stakeholders.
REFERENCES
American Association of Health Plans. “Independent Medical Review of Health Plan Coverage Decisions: A Framework for Excellence.” Washington, DC: American Association of Health Plans, April 2001.
Anderlik, Mary R. “Ombudsman Programs for Managed Care.” Health Law Perspectives, an on-line collection of articles collected by the Health Law & Policy Institute of the University of Houston. Available at [http://www.law.uh.edu/healthlawperspectives/Managed/990620/Ombuds.html]. Posted June 29, 1999. Accessed November 27, 2000.
Annas, George. “Patients’ Rights in Managed Care: Exit, Voice, and Choice.” New England Journal of Medicine, vol. 337, no. 3, July 17, 1997, pp. 210-215.
Bonnyman, Gordon, and Michele Johnson. “Inadequate Grievance Protections in Public Managed Care Programs.” Tennessee Law Review, winter 1998, pp. 360-387. Available at [http://www.tnjustice.org/Spanish/Links/lawrev.html]. Accessed November 27, 2000.
Centers for Medicare & Medicaid Services. “Medicaid Managed Care Enrollment Report, June 2000.” Available at [http://www.hcfa.gov/medicaid/omc2000.htm]. Accessed September 27, 2001.
Dallek, Geraldine, and Karen Pollitz. “External Review of Health Plan Decisions: An Update.” Menlo Park, CA: Henry J. Kaiser Family Foundation, May 2000.
Families USA Foundation. “Consumer Health Assistance Programs: Report on a National Survey.” Washington, DC: Families USA, June 2001.
Families USA Foundation. “Hit and Miss: State Managed Care Laws.” Washington, DC: Families USA, July 1998a.
Families USA Foundation. “The Best from the States II: The Text of Key HMO Consumer Protection Provisions.” Washington, DC: Families USA, October 1998b.
Fish-Parcham, Cheryl. “A Guide to Monitoring Medicaid Managed Care.” Washington, DC: Families USA, 2000. Available at [http://www.familiesusa.org/pubs/medmocre.html]. Accessed November 27, 2000.
Foster, Leslie, Nancy Archibald, Mia Cahill, and Beth Stevens. “Medicaid Fair Hearing Adaptations: A Literature Review.” Princeton, NJ: Mathematica Policy Research, Inc., June 2001.
Health Care Financing Administration. “Short Survey on State Fair Hearings.” Draft compilation of results as conveyed in personal communication to Hunter McKay from Brenda Jackson, March 30, 2000.
Horvath, Jane, and Neva Kaye. “Snapshot of Medicaid Managed Care Ombudsman and Grievance Procedures.” Portland, ME: National Academy for State Health Policy, November 1996.
Kaye, Neva, and Cynthia Pernice. Medicaid Managed Care: A Guide for States. Fourth edition. Edited by Helen Pelletier. Portland, ME: National Academy for State Health Policy, March 1999.
Kirsch, Irwin, et al. A First Look at the Findings of the National Adult Literacy Survey. Washington, DC: National Center for Education Statistics, 1993.
Lee, Peter V., and Carol Scott. “Managed Care Ombudsman Programs: New Approaches to Assist Consumers and Improve the Health Care System.” Los Angeles, CA: Center for Health Care Rights, December 1996.
Molnar, Christine, Denise Soffel, and Wendy Brandes. “Knowledge Gap: What Consumers Know--And What They Don’t--About Managed Care.” New York, NY: Community Service Society of New York, December 1996.
National Conference of State Legislatures. “Fact Sheet: Comprehensive Consumer Rights Bills.” National Conference of State Legislatures, Health Policy Tracking Service, July 23, 2001. Available at [http://www.hpts.org/info/info.nsf]. Accessed September 30, 2001.
New York City Task Force on Medicaid Managed Care Ombudsprogram Committee. “How to Make Managed Care in New York Consumer-Friendly; Ombudsprogram Feasibility Study.” New York: New York City Task Force on Medicaid Managed Care, 1997. Available at [http://www.legal-aid.org/ombuds.html]. Accessed November 21, 2000.
Olson, Kristi, and Jane Perkins. “Medicaid Managed Care and Due Process: The Law, Its Implementation, and Recommendations.” Princeton, NJ: Center for Health Care Strategies, May 2000.
Perkins, Jane. “Resolving Complaints in Medicaid Managed Care: The ‘Brutal Need’ for Consumer Protection.” Washington, DC: National Health Law Program, 2000. Available at [http://www.nls.org/conf/nidrgrie.htm]. Accessed November 21, 2000.
Perkins, Jane, and Kristi Olson. “Medicaid Managed Care and Due Process.” Princeton, NJ: Center for Health Care Strategies, November 2000.
Perkins, Jane, Kristi Olson, and Lourdes Rivera. “Ombudsprograms and Member Advocates: Consumer-Oriented Approaches to Problem Solving in Medicaid Managed Care.” Washington, DC: National Health Law Program, September 1998b.
Perkins, Jane, Lourdes Rivera, and Cheryl Fish-Parcham. “A Guide to Complaints, Grievances, and Hearings Under Medicaid Managed Care.” Washington, DC: Families USA, January 1998a.
Pollitz, Karen, Geraldine Dallek, and Nicole Tapay. “External Review of Health Plan Decisions: An Overview of Key Program Features in the States and Medicare.” Menlo Park, CA: The Henry J. Kaiser Family Foundation, November 1998.
Rawlings-Sekunda, Joanne. “Addressing Complaints and Grievances in Medicaid Managed Care.” Portland, ME: National Academy for State Health Policy, January 1999.
Rodwin, Marc. “Promoting Accountable Managed Health Care: The Potential Role for Consumer Voice.” Bloomington, IN: Indiana University, September 2000.
Rosenbaum, Sara, Colleen Sonosky, Karen Shaw, and Marcie Zakheim. “Negotiating the New Health System: A Nationwide Study of Medicaid Managed Care Contracts” (third edition), Volume 2. Washington, DC: George Washington University Medical Center, Center for Health Services Research and Policy, 1999.
The White House. “Remarks by the President at Consumer Bill of Rights and Responsibilities Ceremony.” Washington, DC: The White House, Office of the Press Secretary, November 20, 1997. Available at [http://www.hcqualitycommission.gov/press/potusbor.html]. Accessed September 28, 2001.
APPENDIX A: SITE VISIT REPORTS
COLORADO SITE VISIT REPORT
This report summarizes Mathematica Policy Research, Inc.’s (MPR’s) site visit to learn about Colorado’s general and mental health ombudsman programs for Medicaid managed care enrollees.42 As we study other states, we expect some of the facts and themes discussed here (or captured in our site visit notes) to take on greater importance and others to recede. We will synthesize findings from all states in the final project report.
A. OVERVIEW OF MEDICAID MANAGED CARE IN COLORADO
Colorado introduced voluntary managed care for Medicaid enrollees in 1992. Two years later, the state began transferring Medicaid enrollees from fee-for-service care to managed care plans, but allowed them to opt out of managed care if they preferred fee-for-service. Mandatory managed care began in 1997, when Colorado passed a law requiring the enrollment of 75 percent of all Medicaid beneficiaries in managed care by July 1, 2000. As of June 30, 2000, a full 90 percent of the state’s 281,764 Medicaid enrollees were enrolled in managed care plans (Centers for Medicare & Medicaid Services (CMS) 2001).
Colorado uses two managed care models for primary care services and one model for mental health services. Primary care is provided either through prepaid managed care organizations (MCOs) or a Primary Care Physician Program (PCPP). Upon enrolling in Medicaid, beneficiaries choose to join an MCO or the PCPP for primary health care services. (The state assigns those who do not choose one or the other to an MCO.) For mental health services, all Medicaid enrollees are automatically assigned to the Mental Health Assessment and Services Agency (MHASA) that serves their county of residence. MHASAs are prepaid MCOs.
Colorado’s Medicaid program is administered by the Department of Health Care Policy and Financing (HCPF), Office of Medical Assistance. HCPF also administers the Colorado Medicaid Mental Health Capitation Program but has delegated many of that program’s functions to the Colorado Department of Human Services (DHS), Office of Mental Health Services (MHS). The administrative and clinical separation of primary health services and mental health services is reflected in Colorado’s decision to implement two managed care ombudsman programs--one for general services, the other for mental health services.
B. SUMMARY OF COMPLAINTS AND APPEALS PROCEDURES
In-plan and state-level complaints and appeals procedures are briefly described below.
1. In-Plan Procedures
The state’s Medicaid managed care contracts stipulate the notification and complaint resolution procedures that MCOs must follow when they intend to terminate, suspend, or reduce a member’s Medicaid-covered services (known as issuing an “adverse service determination”). To contest an adverse service determination, an enrollee may request--orally or in writing--a first-level appeal. During a first-level appeal, a physician not involved in the original adverse decision reviews the decision in consultation with one or more clinical peers. An enrollee who is not satisfied with the outcome of a first-level appeal may request a second-level appeal. In second-level appeals, a panel of at least three people with appropriate expertise reviews the complaint. The enrollee may attend the panel meeting (in person or by telephone), present his or her case, or be represented at the meeting by any individual of his or her choice.43 Medicaid beneficiaries’ use of first and second-level appeals is low. For example, one MCO reported that 32 (0.2 percent) of its 18,000 Medicaid enrollees requested first-level appeals in 2000. Only one requested a second-level review.44
MCOs are also required (by their Medicaid contracts) to establish written procedures for the expedited review of adverse service determinations. Expedited reviews must be available when the time frames for standard reviews would seriously jeopardize the life or health of the enrollee, jeopardize the enrollee’s ability to regain maximum function, or, for enrollees with disabilities, limit the enrollee’s existing ability to live independently.
2. State-Level Procedures
Enrollees who desire state-level review of an MCO’s adverse service determination may request a fair hearing through the Colorado Department of Administration, Division of Administrative Hearings (DAH). Enrollees are not required to exhaust in-plan complaint procedures before requesting a fair hearing, but the state encourages them to do so.
DAH administers the hearing and notifies the enrollee of his or her right to state assistance in preparing a case. After the hearing, the presiding administrative law judge (ALJ) issues an initial decision and forwards it to HCPF’s Office of Appeals. The Office of Appeals then forwards that decision to the disputing parties. After the parties have had an opportunity to file exceptions to the initial decision, the Office of Appeals issues a final agency decision. As a final appeal, parties may request a judicial review of the final agency decision.45
An important difference between MCO and state-level procedures is that MCOs must adhere to specific time frames during each phase of the complaint process, while no time frames exist for the state. According to legal advocates we interviewed, the state routinely takes between six and nine months to issue initial decisions. During state-level appeals, all Medicaid benefits affected by an adverse service determination continue in full force until a final agency decision is reached.
3. Informal Processes
By all accounts, formal appeals are rarely used; most complaints are resolved informally. At the MCO level, informal resolutions may occur when enrollees call their MCO’s customer service department or Office of Consumer and Family Affairs. There are also informal ways for enrollees to involve the state in complaint resolution. For example, HCPF’s Customer Service Unit operates a telephone hotline to assist consumers with queries or complaints, although this unit often refers callers back to their MCOs or, in more complex cases, to the managed care ombudsman. In addition, some consumers access the state through HCPF’s managed care contract managers, who have a reputation (among a variety of stakeholders) for being accessible and helpful. MHS also reported that enrollees can come to them directly with complaints, and they assist enrollees as much as possible.
C. MANAGED CARE OMBUDSMAN
1. Program Background
Colorado’s managed care ombudsman program began operating in June 1998. Its existence and state funding are mandated in a fiscal note that accompanied Colorado’s major Medicaid managed care legislation, Senate Bill 5.46 The ombudsman program was born of compromise between the state, which was eager to pass Senate Bill 5, and advocates for consumers with disabilities, who wield considerable power in Colorado and who wanted an ombudsman program. Independent legal advocates helped draft legislation acceptable to both groups.
The managed care ombudsman program is funded with general Medicaid revenues. Although stakeholders unanimously say the program’s annual funding of $100,000 is insufficient, they believe it is secure; removing it from the state budget would be tantamount to a legislative amendment. HCPF’s Customer Service Unit administers the managed care ombudsman program through a contract with an independent non-profit organization. Colorado’s decision to provide ombudsman services through a contractual arrangement was based on stakeholders’ common desire for an ombudsman who is independent of the state and MCOs. By some accounts, the decision to have the ombudsman’s contract overseen by HCPF’s Customer Service Unit, rather than its Division of Managed Care (which oversees the state’s contracts with MCOs), was meant to further such independence. By another account, workload issues drove the decision.
The Patient Advocacy Coalition (PAC) holds the current ombudsman contract.47 PAC’s guiding philosophy is that, when ill, people who have problems with their health care providers or insurers should be able to resolve those problems without litigation. Moreover, PAC seeks to preserve relationships between patients and their health care providers and insurers. PAC serves all types of managed care enrollees, but only its services to Medicaid beneficiaries are covered by its contract with HCPF.
2. Ombudsman’s Involvement in Plan-Level Complaints
As noted earlier, most enrollees’ complaints are resolved informally; thus, most of the ombudsman’s involvement in resolving plan-level complaints is also informal. A typical complaint may be settled in 5-10 telephone calls between the ombudsman and the MCO or enrollee.
The managed care ombudsman handles about 20 complaints from Medicaid managed care enrollees per month. Most of these involve quality of care, experimental therapies, or inadequate transportation to care. Relatively few involve denials of benefits, a fact that the ombudsman attributes to Colorado’s rich Medicaid benefits package.
Stakeholders disagree on whether the ombudsman’s role in in-plan complaint processes is to be an advocate for the aggrieved enrollee or a more neutral mediator between disputing parties. The consumer and legal advocates we interviewed expect the ombudsman to be a staunch, pro-enrollee advocate. They are disappointed that the current ombudsman seems unwilling to aggressively oppose the state or MCOs. By contrast, the ombudsman herself described her role as that of a negotiator who “leans toward” advocacy. She finds Colorado’s Medicaid MCOs to be cooperative and primarily concerned with their members’ well-being. An MCO we spoke with described the ombudsman as an advocate who has enrollees’ trust but is “willing to listen to [the MCO’s] side.”
3. Ombudsman’s Involvement in State-Level Appeals
Since the introduction of the Medicaid managed care ombudsman in 1998, no Medicaid managed care cases have reached a fair hearing. The ombudsman has filed requests for hearings for two clients, but both cases were settled before the hearing. This dearth of cases limits discussion of the ombudsman’s role in state-level appeals. It also raises questions about whether the volume of state-level appeals should be higher and, if so, whether the ombudsman should act to increase case volume.
No legal barrier exists to the ombudsman’s full involvement in fair hearings. By Colorado law, an enrollee may be represented or assisted in a fair hearing by anyone he or she chooses. Moreover, legal advocates involved in drafting Senate Bill 5 say they intended for the ombudsman to be actively involved in fair hearings. In practice, the current ombudsman (who is a lawyer) has shown little enthusiasm for fair hearings. She intimates that, on the two occasions when she helped clients file requests for fair hearings, she did so as a last resort.
Not surprisingly, the ombudsman and independent legal advocates also disagree over whether the ombudsman ought to initiate more fair hearings. Legal advocates favor fair hearings and emphasize their potential benefits. For example, they say fair hearings are more likely than informal or in-plan processes to bring about systemic change in Colorado’s Medicaid managed care system. In addition, individual enrollees who request a fair hearing may enjoy more “clout” with MCOs even as they pursue in-plan resolution. In contrast, the ombudsman emphasized the more negative aspects of fair hearings, including increased stress on enrollees and strain on provider-patient relationships.
Because so few Medicaid managed care enrollees have requested fair hearings, it is difficult to characterize the nature of the ombudsman’s interaction in relation to the enrollee and the state. However, we did learn that the state seems to view the ombudsman as an enrollee advocate, rather than as a neutral mediator between parties. For this reason, HCPF’s Office of Appeals, which reviews the initial decisions of ALJs in fair hearings, refrains from discussing cases with the ombudsman.
In contrast, the ombudsman frequently works informally with the state. For example, HCPF’s Customer Service Unit refers cases to the managed care ombudsman when they involve complex issues, when understanding the differences between MCOs is important, or when the state cannot resolve the complaint fairly easily (for example, by making a few telephone calls). The ombudsman also interacts with HCPF’s plan managers, who, as noted earlier, are increasingly involved in informal complaint resolution. The ombudsman and the state personnel with whom she interacts speak highly of each other.
4. Outreach and Enrollee Awareness
The state, Medicaid MCOs, advocates, and the ombudsman’s office all help promote the managed care ombudsman program, either voluntarily or at the state’s behest. Table CO-1 summarizes the outreach activities of each stakeholder.
Stakeholders agree that Medicaid managed enrollees seem more aware than commercial enrollees of the ombudsman program. It is unclear, however, whether awareness is any higher among Medicaid enrollees with disabilities (the ombudsman says most of her Medicaid clients do have disabilities) than it is among those who do not have disabilities (an advocate for consumers with disabilities says the ombudsman’s outreach activities are geared toward mainstream enrollees). By all accounts, awareness levels decrease outside the Denver area.
| TABLE CO-1. Outreach Activities for the Managed Care Ombudsman Program | |
|---|---|
| Stakeholder | Outreach Activities |
| State Agency (HCPF) | Lists ombudsman’s contact information in its “Medicaid Client’s Guide to Filing Complaints” pamphlet and on enrollee’s Medicaid cards (as of second half of 2001). Describes ombudsman’s responsibilities in its Medicaid managed care regulations, which are posted on HCPF’s Web site. |
| Ombudsman Program | Maintains a Web site. Prints and distributes promotional brochures and posters. Participates in events attended by Medicaid managed care enrollees and community representatives. |
| Managed Care Organizations | Must include information about the ombudsman program in member handbooks. Some include additional information in welcome packets for new enrollees. |
| Consumer and Legal Advocates | Display promotional posters and brochures. |
5. Serving Enrollees with Disabling or Chronic Conditions
Colorado’s regulations governing in-plan complaint procedures are the same for Medicaid managed care enrollees with and without disabling or chronic conditions. State officials we interviewed stressed, however, that the regulations were developed with disabled/chronically ill enrollees in mind. More specifically, consumer advocates insisted that expedited reviews be available not only in cases of medical emergency, but whenever the termination or reduction of Medicaid benefits would hamper an enrollee’s ability to live independently.
6. Strengths and Weaknesses of the Managed Care Ombudsman Program
Stakeholders identified numerous strengths and weaknesses of the managed care ombudsman program, sometimes directly contradicting each other. Table CO-2 summarizes the strengths and weaknesses, with attributions to the type of stakeholder (ombudsman, state official, advocate, or MCO) who identified them.
| TABLE CO-2. Strengths and Weaknesses of Colorado’s Managed Care Ombudsman Program, as Identified by Site Visit Participants | |
|---|---|
| Strengths | Weaknesses |
| The ombudsman program is independent of the state. (State, Ombudsman) The ombudsman is willing to consider the MCO’s position in a dispute. (Ombudsman, MCO) The ombudsman is a strong policy analyst. (Advocate) The ombudsman’s law degree is a tremendous asset. (State) The ombudsman understands all sectors (Medicaid, Medicare, and commercial) of the managed care market and their relation of each other. (Ombudsman) The ombudsman is familiar with the differences between MCOs. (State) The ombudsman program collects complaint data useful to the state and consumers. (Ombudsman, State, Advocate) The organization that won the ombudsman contract had existing relationships with Medicaid MCOs. (Ombudsman) Consumers trust the ombudsman. (State, Ombudsman, MCO) | The ombudsman program is not independent of the state because it is state-funded. (Advocate) The ombudsman attempts to see both sides of every case. (Advocate) The ombudsman has political aspirations, so is unwilling to offend health plans and insurers. (Advocate) The ombudsman is not a “real” enrollee advocate. (Advocate) The ombudsman program targets only a narrow set of issues--those involving managed care--and excludes others that arise under Medicaid, such as long-term care. (Advocate) The ombudsman does not know the “intricacies” of the MCOs. (MCO) The program is underfunded. (Ombudsman, Advocates) |
| SOURCE: Interviews with state officials and employees, the managed care ombudsman, representatives of Medicaid MCOs, and consumer and legal advocates. The type of stakeholder who identified each strength or weakness is listed in parentheses. | |
7. Changes Recommended by Stakeholders
In addition to asking stakeholders about their perceived strengths and weaknesses of the managed care ombudsman program, we asked them what changes they would make to the program if they were given the chance. The following changes were recommended:
- State Officials Recommend:
- Producing promotional and educational materials in languages other than English.
-
Increasing outreach and services to rural areas of Colorado.
- Consumer and Legal Advocates Recommend:
- Codifying program rules through statute, rather than through regulations.
- Allowing the ombudsman to litigate against MCOs for breach of contract.
- Expanding the scope of the ombudsman program beyond managed care issues.
- Funding the ombudsman program through an agency other than the Medicaid agency to increase the ombudsman’s independence.
- Separating funding and monitoring functions (HCPF now handles both).
-
Emphasizing customer service over consumer empowerment.
- The Ombudsman Recommends:
- Increasing program funds to support satellite offices throughout the state.
-
Combining the managed care ombudsman program with the mental health ombudsman program.
The MCOs we interviewed said they had too little interaction with the managed care ombudsman program to recommend changes.
D. MENTAL HEALTH OMBUDSMAN
1. Program Background
Although it has been operating for only two years, Colorado’s mental health ombudsman program has a long history. Consumers and advocates introduced the idea for the program in 1995, when Colorado began transferring Medicaid enrollees from fee-for-service to managed care. In 1997, as Colorado debated Senate Bill 5 and mandatory managed care loomed large, the MHS “got serious” about designing and implementing an ombudsman program that would: (1) help consumers navigate the mental health system and advocate for themselves; and (2) operate independently of MHS and the MHASAs. Both MHS and consumers/advocates were involved in designing the program. Securing funding for the mental health ombudsman program, the first hurdle in the design process, was handled primarily by MHS. Initially, MHS sought funding for the program from the Colorado Division of Insurance (DOI) so that the program would be sufficiently independent of MHS. MHS abandoned this option, however, upon learning that it would have to steer a request for DOI funding through the state legislature’s budget process, an 18-month endeavor. As an alternative, MHS decided to fund the ombudsman program through its contracts with MHASAs. In other words, some proportion (one-quarter of 1 percent at most) of the state’s payments to MHASAs would be earmarked for the mental health ombudsman program. MHS continues to view this funding mechanism--which currently yields about $325,000 a year for the ombudsman--as an acceptable compromise between independence and ease of implementation.
After program funding was secured, an eight-person team of consumers, family members, and advocates designed the other aspects of the program. By all accounts, this phase of the design process was contentious. A powerful consumer run advocacy organization, Consumer-Centered Services of Colorado (CCSC), proposed incorporating the ombudsman program under its 501(c)(3) status. MHS and the MHASAs supported such a plan, but many family members, wary of the burden involved in running an ombudsman program, opposed it. In addition, the state disagreed with consumers over whether the program should provide legal services. The state was in favor of allowing the ombudsman to litigate against MHASAs, but consumers resisted adopting an adversarial approach. (Interestingly, the MHASAs were largely silent on the points of contention described above. Their main concern was that the ombudsman program not be a new complaint procedure, but that it help enrollees navigate existing procedures.)
In the end, the mental health ombudsman program was incorporated under CCSC’s authority, without a legal services component.48 A former mental health counselor was hired as the executive director of the program in spring 1999. Today, the mental health ombudsman program includes offices in Denver (two full-time ombudsmen plus support staff), the Western Slope region of the state (one full-time ombudsman plus volunteer support), and Pueblo (one full-time ombudsman as of July 2001). The hiring of a part-time ombudsman for the Sterling/Fort Collins area is planned for later this year. Many of the programs professional and volunteer staff are consumers of mental health services (the executive director is not).
2. Ombudsmans Involvement in Plan-Level Complaints
As with the managed care ombudsman, the mental health ombudsman’s involvement in plan-level complaints is usually informal. Most complaints involve access to medication or residential treatment, and a substantial proportion involve doctor-patient relationships. In a typical case, the ombudsman: (1) helps the enrollee articulate his or her problem and the desired outcome; and (2) informs the enrollee of his or her rights and of the complaint procedures that might resolve the problem. The enrollee then decides whether to self-advocate or be assisted by the ombudsman.
When the ombudsman does assist, he attempts to negotiate a resolution with the MHASA by interacting directly with the staff member or treating clinician with the authority to resolve the problem. In other words, the ombudsman may bypass the MHASA’s usual complaint procedures if another route seems faster or more effective. A typical complaint would be resolved through a series of meetings (usually between the ombudsman and the enrollee) and telephone contacts (usually between the ombudsman and the MHASA). If needed, the ombudsman also reviews medical records or consult the enrollee’s family members.
When informal processes do not lead to resolution, the ombudsman helps enrollees pursue formal in-plan appeals. The ombudsman and MHASAs disagree, however, on the usefulness of formal appeals and whether their tenor is needlessly adversarial. When helping an enrollee with a formal appeal, the ombudsman considers it good customer service to put the complaint in writing. In addition to their usefulness as documentation, written appeals obligate MHASAs to respond within state-mandated timelines. From the MHASAs’ perspective, timelines and other procedural rules are at odds with “the way things work” inside MHASAs and are “too complicated” for enrollees to understand. Thus, where the ombudsman sees himself as an effective enrollee advocate, the MHASA may see an overbearing intermeddler--one who creates more work for the MHASA.
3. Ombudsmans Involvement in State-Level Appeals
Since the inception of the mental health ombudsman program, the ombudsman has been involved in two fair hearings. In both cases, the aggrieved enrollee took his or her complaint to the ombudsman. The ombudsman then asked legal advocates to represent the enrollee, making himself available to provide testimony about the cases. MHS, legal advocates, and the ombudsman interpret this set of facts differently. MHS, which discourages enrollees from using fair hearings except as a last resort (because they are too formal and intimidating), says two appeals in two years is about right. In contrast, legal advocates and the ombudsman would prefer to see more fair hearings because of their potential (relative to informal complaints) to bring about systemic change. However, while the ombudsman and legal advocates agree on the merits of fair hearings, they disagree on the ombudsman’s role in such appeals. As noted earlier, legal advocates have always expected both ombudsmen to represent enrollees in fair hearings. However, the mental health ombudsman seems more comfortable playing an assistive role.
4. Outreach and Enrollee Awareness
As with the managed care ombudsman program, the mental health ombudsman program is promoted by the state, MHASAs, advocates, and the ombudsman’s office. Table CO-3 summarizes the outreach activities of each stakeholder.
MHS believes enrollees are well aware of the existence of the mental health ombudsman program. They cited two reasons: (1) the program’s executive director was already familiar, as a mental health counselor, to stakeholders; and (2) the program reaches people through its satellite offices.49 A consumer advocate suggested that having mental health care consumers on staff is in itself an effective form of outreach because their presence puts enrollees at ease about seeking assistance.
| TABLE CO-3. Outreach Activities for the Mental Health Ombudsman Program | |
|---|---|
| Stakeholder | Outreach Activities |
| State Agency (MHS) | Requires MHASAs to promote the program in member handbooks. |
| Ombudsman Program | Prints and distributes brochures and posters (in English and Spanish). Makes presentations at community and consumer events. Uses volunteers as outreach coordinators and “local conduits.” Upon opening for business, paid for an advertisement in a newsletter produced by the Colorado Cross-Disability Coalition. |
| Managed Care Organizations (MHASAs) | Must include information about the ombudsman program in member handbooks. Some include additional information in welcome packets for new enrollees and provide verbal notification. |
| Consumer and Legal Advocates | Display promotional posters and brochures. |
5. Strengths and Weaknesses of the Managed Care Ombudsman Program
Table CO-4 summarizes the strengths and weaknesses of the mental health ombudsman program identified by stakeholders. As with the managed care ombudsman program, stakeholders’ responses were sometimes contradictory.
| TABLE CO-4. Strengths and Weaknesses of Colorado’s Mental Health Ombudsman Program, as Identified by Site Visit Participants | |
|---|---|
| Strengths | Weaknesses |
| The program has strong support from most stakeholders. (State) The mental health ombudsman helps health plans improve their services to customers; the ombudsman interacts cooperatively with health plans, not only when problems arise. (MCO) Mental health plans are represented on the program’s board of directors.a (MCO) The program gives consumers a non-bureaucratic approach to resolving their problems. (State) Consumers view the ombudsman as independent of the state and of the mental health plans, which they tend to mistrust. (State, MCO) The ombudsman reaches people throughout the state and raises their expectations about the services they are entitled to. (State) The program provides a formal way for the state and MCOs to get a perspective on how Medicaid managed care is working. (MCO) The program makes consumer rights more visible. (MCO) The program hires consumers to do professional jobs, which has an empowering effect. (MCO) The program has improved the self-empowerment movement in Colorado while also providing tangible services to people who need them. (Ombudsman) | Most mental health plans are not buying into the idea of having a partnership with the ombudsman; the ombudsman must do a better job of forging such relationships. (MCO) Some mental health plans find the ombudsman program to legalistic and threatening. (State) Mental health plans are represented on the program’s board of directors.a (Advocate) Having Medicaid revenues as the source of the program’s funding weakens its independence from the state. (MCO) The mental health ombudsman program is not providing enough services in rural parts of Colorado, a primarily rural state. (MCO) The ombudsman automatically assumes the consumer is right, without having all the information about a case. (State, MCO) The ombudsman has a narrow perspective of the mental health system and of the way plans in local services areas operate. (MCO) |
SOURCE: Interviews with state officials and employees, the executive director of the mental health ombudsman program, representatives of mental health MCO, and consumer and legal advocates. The type of stakeholder who identified each strength or weakness is listed in parentheses.
| |
6. Recommended Changes
We asked stakeholders what changes they would make to the program if they were given the chance. The following changes were recommended:
- State Officials and Employees Recommend:
- Strengthening relationships between the ombudsman and the MHASAs, at the initiative of the ombudsman.
-
They would not recommend other changes until the program has been evaluated by an independent contractor.
- Consumer and Legal Advocates Recommend:
- More emphasis on training staff to resolve clients problems, less on empowerment and self-advocacy.
-
More frequent use of fair hearings.
- MHASAs Recommend:
-
Increasing the diversity of program staff, with a focus on representing the Native American, Latino, and Pacific Islander communities.
-
- The Ombudsman Recommends:
- Giving the ombudsman a stronger official mandate so that he or she would have greater authority in the eyes of MHASAs.
- Making it easier for the ombudsman to access MHASAs medical records when they are relevant to a case.
-
Exploring the possibility of funding the program with non-Medicaid revenues.
E. SUMMARY
The story of Colorado’s managed care ombudsman programs includes several striking elements. First, it seems unlikely that either program would exist today but for the efforts and influence of consumer advocacy organizations, particularly those serving people with disabilities. Those interviewed agreed that health care consumers held particularly strong positions in Medicaid policy issues in Colorado. Second, although ombudsmen in general may exist to lend a neutral perspective to or play a mediating role in disputes, Colorado’s two managed care ombudsmen are clearly perceived as enrollee advocates (although to varying degrees, depending on the stakeholder). That said, the two ombudsmen approach their work with Medicaid enrollees in distinct ways. The managed care ombudsman favors direct service delivery, doing what needs to be done to resolve a problem as quickly as possible. In comparison, the mental health ombudsman program is geared more toward empowerment and self-advocacy. (Although the ombudsman himself says he strives to strike the right balance between direct service and empowerment, the program is clearly a product of Colorado’s consumer-centered movement.) Finally, the low volume of fair hearings involving Medicaid managed care enrollees is striking. Of the possible explanations that emerged during interviews, perhaps the most convincing is that the state, the health plans, and the ombudsmen encourage informal, rather than formal, complaint resolution almost exclusively. As many interviewees remarked, informal resolutions have the advantages of being expedient, non-adversarial, and preferred by enrollees; however, they are also unlikely to lead to large-scale changes in Medicaid managed care, should such changes be warranted.
FLORIDA SITE VISIT REPORT
This report summarizes the site visit undertaken by a team from MPR to learn about Florida’s external review program for its Medicaid managed care enrollees.50 As we study other states, we expect some of the facts and themes discussed here to take on greater importance and others to recede. We will synthesize findings from all states in the final project report.
A. OVERVIEW OF MEDICAID MANAGED CARE IN FLORIDA
Florida first implemented its Medicaid program in 1970. Managed care has been part of the state’s Medicaid program since the late 1970s and became mandatory for most categories of beneficiaries in 1996.51 The program is administered by the Agency for Health Care Administration (AHCA) through its Division of Medicaid. Eligibility for the program is actually determined by another state agency, the Department of Children and Families, which also administers the Medicaid Fair Hearings program. Florida currently has 1.3 million Medicaid beneficiaries. Medicaid managed care in Florida is made up of two types of managed care: (1) health maintenance organizations (HMOs); and (2) a primary care case management (PCCM) system called MediPass. As of 1998, 450,000 of the 1.3 million beneficiaries were enrolled in a Medicaid HMO and 700,000 in MediPass. Starting on July 1, 1998, beneficiaries who had not chosen one of the two managed care options were automatically enrolled in the HMO option. This was to be done until parity between HMOs and MediPass was achieved. After that, beneficiaries are to be randomly assigned to one of the two while keeping equal numbers in each option. As of our visit in 2001, this parity had not yet been achieved.
B. SUMMARY OF COMPLAINTS AND APPEALS PROCEDURES
1. In-Plan Procedures for Complaints and Appeals
The contract between the state of Florida and private managed care plans includes a requirement for in-plan grievance (complaint and appeals) procedures. Each plan is required to refer all beneficiaries dissatisfied with the plan to a grievance coordinator for appropriate followup. The plan is required to resolve a formal grievance (a written complaint) within 60 days.52 All plans must have a grievance process that has enough staff support to meet all deadlines and must also include plan representatives who have the authority to resolve problems. When medical issues are in dispute, the grievance process must include at least one physician in addition to the beneficiary’s own primary care physician. Notice of the right to file a complaint must be given to the beneficiary in the member handbook. The beneficiary retains the right to pursue a complaint to a Medicaid fair hearing at any time, in addition to pursuing the plan’s grievance procedure. In practice, however, the state often holds the fair hearings requests until the issues are considered “ripe” for resolution, and the internal grievance procedures have been used.
Most plans have several levels of appeal within their own appeals process (although the contract with the state does not require this). The procedures vary across the plans.53 Most have an initial appeal of the complaint or grievance to the local medical director. If the case is not resolved at this point, the grievance goes to either an independent consultant or a panel of independent physicians for review. After this step, the beneficiary can appeal to a committee at the plan’s board level. Most plans do not permit beneficiaries to be represented by attorneys in their in-plan processes. Some plans have internal timelines for appeals; in general, they appear to give themselves 30 days to resolve grievances.
If the plan is unable to resolve the grievance to the beneficiary’s satisfaction, and the beneficiary has not filed for a fair hearing, the plan must then notify the beneficiary that he or she has the right to appeal to the state Medicaid agency (AHCA) and its Statewide Provider and Subscriber Assistance Panel (hereafter referred to as the Panel). Written notice of this right does not have to be given to the beneficiary until the in-plan grievance process has been completed.
2. State-Level Complaints and Appeals Procedures
Florida has a bifurcated structure for the administration of complaints and appeals in Medicaid. The external reviews grievance and appeals system (the Panel) is operated by AHCA, which is responsible for Medicaid managed care operations and policy. Fair hearings, on the other hand, are undertaken by the Department of Children and Family Services (DCFS), the agency that operates the Temporary Assistance for Needy Families (TANF) program in Florida. This structure results in state officials having a gap in their knowledge of all parts of the complaints and appeals process. AHCA officials have little understanding of the fair hearings process, while the DCFS officials in charge of fair hearings know nothing about the Panel. First, we describe the fair hearings system overseen by DCFS; we then describe the external review process overseen by AHCA.
The use of fair hearings by Medicaid managed care beneficiaries is minimal. The fair hearings officials at DCFS estimated that only ten out of hundreds of cases that they heard in the past year were from Medicaid managed care beneficiaries. DCFS holds fair hearings for Medicaid managed care beneficiaries under a memorandum of understanding with AHCA. Only a small percentage of their fair hearings are for AHCA. The majority of cases that they hear are appeals for denial of eligibility for the Medicaid and TANF programs.
The process for fair hearings begins with a denial of benefits from the managed care plan. At this point, the beneficiary receives a notice that he or she may appeal the decision. According to the fair hearings official interviewed, however, the language in the denial letter is ambiguous. Beneficiaries do not necessarily know whether to file an appeal with the external review panel or with DCFS for a fair hearing.54 Once the subscriber writes a letter to DCFS (the subscriber has 90 days to do this), the fair hearings file is set up. DCFS notifies AHCA and sets up a review process. Beneficiaries are entitled to bring a lawyer to the fair hearing, but few do so. Unlike the external review panel process (described in the next section), fair hearings allow for procedural rights such as discovery and cross-examination. Similarly, unlike under the external review panel, the decisions are made according to state Medicaid rules; internal rules of the managed care plan are not considered. There is no appeal after the fair hearing, but unsatisfied parties can go to court to appeal.
C. THE EXTERNAL REVIEW PANEL
1. Program Background
Medicaid beneficiaries who are not satisfied with the results of their health plan’s efforts to resolve their complaint can appeal to the state external review panel, the Statewide Provider and Subscriber Assistance Panel (the Panel), instead of, or in addition to, filing a request for a fair hearing. This panel hears complaints from both commercial managed care and Medicaid managed care enrollees. It was formed in 1985 by the Department of Insurance and has included Medicaid enrollees from the beginning. The Panel was moved to its current location in the Division of Managed Care and Health Quality within the AHCA in 1993. It is funded by a combination of general revenue and specific Medicaid program funding.
2. Program Structure and Operations
The Panel is made up of eight to nine members. The governor appoints two of them--a consumer advocate and a physician (currently a state employee). Three are employees of AHCA--one each from the Division of Managed Care and Health Quality, the Division of Medicaid, and the Department of Health Performance Improvement. Three are alternates from the Department of Insurance, all of whom are specialists in contracts. Additional (independent) physicians with expertise relevant to the case are brought in if the case involves a medical necessity issue.55 The Panel is designed to cover several areas of expertise: legal, medical, and regulatory. Eight staff members support the work of the Panel. When asked why the Panel was not independent of the state Medicaid agency, respondents pointed out that, in 1985, no one thought to have a panel external to the state--it was not considered as an option. They mentioned that there has been discussion about changing the Panel to be an independent board but that this was not on an immediate agenda.
The Panel has several objectives:
- To monitor the HMO grievance process.
- To provide a forum for hearing beneficiary unresolved grievances against their HMOs.
- To hear and resolve grievances as quickly as possible.
- To reduce the numbers of grievances entering the legal system.
The process the Panel oversees is straightforward. Using a form sent to them by their health plan (included in the letter reporting the final decision of the in-plan grievance process), or after a phone request to the state agency for the form, beneficiaries submit a completed authorization releasing medical records and all identifying information. The HMO then submits its grievance file, including the medical records and the contract. Panel staff review the documents, obtain an independent review by an external consulting physician specialist (if relevant), and prepare the case for a panel hearing. The hearing takes place either in Tallahassee or by videoconference.56 Attorneys may be present. Most often, however, if one is present, it is from the managed care plan. Few beneficiaries are represented by an attorney. The Panel prefers an informal process and does not encourage the use of attorneys. The managed care plans send a variety of representatives, depending on the issues of the case. These can include the medical director, a grievance coordinator, or an underwriter. Each party is allowed 15 minutes to present its side of the case, and both are allowed a rebuttal at the end of the presentations. There are no specific rules of evidence. Recommendations are based on findings of fact.
The Panel must make a decision within 15 days of the hearing. Both parties have ten days to disagree with the written decision; after another ten days, it is finalized. The HMOs have 30 days to comply with the written decision. Panel staff check with the beneficiary to see if the decision has been implemented. When all these deadlines are added up, the Panel must resolve the issue within 120 days of receiving the complaint. In practice, an issue usually is resolved within 60 days.
The Panel itself does not have the power of enforcement. It makes its recommendation to AHCA, which enforces the decision. If the HMOs disagree with the Panel’s decision, they can appeal to the state Department of Administrative Hearings. Beneficiaries must either go on to a fair hearing or go to court.
The Panel will not hear a complaint until the in-plan appeal process has been exhausted. When beneficiaries contact state officials, they encourage the beneficiary to work with the plan. Prior to the Governor J. Bush Administration, the AHCA hotline was manned by nurses who worked with a beneficiary and the HMO to work out the problem and thus to resolve the grievance before it turned into a formal complaint. The current administration takes a more hands-off approach. The approach, we were told, is one of a regulatory agency, not an investigating agency. Nor does the Panel hear the complaints of beneficiaries who have filed for a fair hearing. The state has determined that the fair hearing process has legal precedence over the state’s own appeal processes. Technically, if the Panel denies the case of a beneficiary, he or she can then file for a fair hearing. However, none of the state officials or legal advocates had heard of a beneficiary doing so.
Issues heard by the Panel in fiscal year 1999-2000 include those dealing with excluded benefit (27 percent), out-of-network (20 percent), medical necessity (19 percent), formulary (9 percent), contract interpretation (7 percent), experimental treatment (1 percent), non-authorization for service (1 percent), and other (16 percent). In fiscal year 2000-2001, the Panel received 249 cases and heard 116 of them. According to state data, 45 percent of the cases are found in favor of the subscriber.57 Few of the cases heard by the Panel are Medicaid cases--most Medicaid appeals in Florida go to fair hearings. Of the 146 cases heard by the Panel as of April 2001, only six were Medicaid managed care complaints. Two of the panel members told us that they try to find in favor of the beneficiary, but this is not always possible. Two of the three managed care plans interviewed also believe that the Panel does try to find for the beneficiary if at all possible. The remaining health plan and one advocate believe that the Panel favors the managed care plans. The number of cases coming before the Panel is declining. Panel staff attribute this to their pressure on the managed care plans to run an effective internal grievance process.58
The Panel also has another function--monitoring the grievance processes of the MCOs. AHCA requires a quarterly report from each managed care plan that reports on the numbers of unresolved grievances. These quarterly reports are used in two ways. First, they are used in the annual state report card that provides information on the cost, content, and quality of care provided by managed care plans in the state. Second, the data on internal grievances and their resolution are used as one of the criteria in the annual deliberations over the renewal of Medicaid contracts with managed care plans.
3. Outreach and Beneficiary Awareness
Medicaid beneficiaries are notified about the existence of the Panel and their rights to use its services in the membership handbook distributed by the managed care plans when they enroll. They are also formally advised about their right to appeal to the Panel after the in-plan grievance process has concluded and they are given their final denial letter.59 Finally, every quarter, as the state receives the data from health plans on the number of unresolved grievances, it sends a letter to all managed care clients with an unresolved grievance, notifying them of their right to use the Panel process. State officials find that 50 percent of the cases filed with the Panel come in response to these advisory letters.
State officials and advocates assert that most Medicaid beneficiaries do not appear to absorb the information in these notices, as most beneficiaries do not seem aware of the Panel. Several mentioned that commercial enrollees in managed care use the Panel to a much greater extent than Medicaid beneficiaries, although there is no reason to assume that the systems are any different in the conditions that might generate complaints. The managed care plans, in contrast, believe that beneficiaries have adequate opportunities to find out about the Panel.
Advocates assert that the current outreach activities (the notices in the handbooks and denial letters) are insufficient. They argue that a notification process based on printed materials is a problem with a beneficiary population that has a low level of literacy. AHCA officials are aware of the dearth of outreach information, and they are currently preparing a brochure to explain the Panel. Their plans for distributing it, however, are still to be determined. State officials are worried that improved outreach will overwhelm the Panel with requests for assistance that it cannot handle with current resources.
4. Serving Beneficiaries with Disabling or Chronic Conditions
Florida’s regulations governing complaint procedures are the same for disabled Medicare managed care beneficiaries as for able-bodied beneficiaries. State officials, however, stressed that the videoconferencing arrangements were friendly to those who had physical limitations.
5. Strengths and Weaknesses of the External Review Program
Stakeholders identified several strengths and weaknesses of the external review program in Florida. Table FL-1 summarizes their comments, with attributions to the type of stakeholder who identified them.
| TABLE FL-1. Strengths and Weaknesses of the External Review Panel | |
|---|---|
| Strengths | Weaknesses |
| The Panel gives beneficiaries an unbiased opinion. (State Officials) Having the Panel sponsored by the state helps state officials think about the regulatory issues. (State Officials) The Panel helps control the disputes between MCOs and physicians about what treatment is necessary. (MCO) The Panel helps us make better contracts; when we dispute an issue in a contract, we try to rewrite it to remove the ambiguity. (MCO) The Panel’s existence gives the HMO an incentive to reach a resolution. Unless you have a strong case, you won’t win at the panel. (MCO) Since the Panel is on public record, HMOs have incentive to resolve disputes earlier to avoid bad publicity. (MCO) Panel members know managed care issues, while fair hearings examiners do not. (Advocate) | The Panel cannot be too hard on MCOs because they do not want to lose them from the Medicaid program. (State Officials, Advocates) HMOs are slow and not motivated to provide data to the Panel within the deadlines. (State Officials, Advocates) The Panel cannot exclude any cases, even if the case is an obvious contract exclusion. This overloads the Panel. (State Officials) The Panel could be politicized because the Governor appoints some Panel members. (MCO) Panel members not sufficiently trained to understand the larger health care context beyond the individual case. (MCO) The Panel looks at technicalities in order to find for the beneficiary. (MCO) The HMO can stall the process by prolonging the in-plan grievance process. They do not meet their own deadlines. (Advocates) There is insufficient outreach to educate beneficiaries about the Panel. (State Officials, Advocates) The Panel does not operate with sufficient regard to due process issues. (Advocates) |
6. Changes Recommended by Stakeholders
In additional to asking stakeholders about the strengths and weaknesses they perceive about the external review panel, we asked them what changes they would make to the panel if given the chance. The following changes were recommended:
- State Officials recommend:
- Increasing outreach services to beneficiaries (although they worry about the impact of increased demand on their available resources).
-
More clearly specifying the types of cases that can be heard by the Panel, to eliminate the cases dealing with straightforward contract exclusions.
- MCOs recommend:
- Providing more training to Panel members to help them understand the MCO reasoning process.
-
Looking at the potential for politicization of the Panel.
- Consumer Advocates recommend:
- Providing much more beneficiary education about both the in-plan and external review panel process.
- Improving the monitoring of the in-plan grievance process to eliminate plan practices that discourage complaints and grievances from being made formally.
- Tightening the deadlines for submission of information by HMOs.
-
Holding hearings on the district level to avoid videoconferencing.
D. SUMMARY
The external review program for Florida’s Medicare managed care beneficiaries has several interesting elements. First, as one of the earliest external review programs in the country, Florida’s system has the advantages of long-term operation. Over the past years of operation, the Panel has developed a data system to collect information on the complaints and appeals process that is, by now, more detailed and reliable than those of other states. The procedures to obtain and integrate the expertise of independent medical reviewers have matured into an efficient and accepted system. Second, the Panel has support from most of the stakeholders in the system. The governor and the managed care industry have grown comfortable with its deliberations. Advocates have only minor problems with the deliberations of the Panel itself (mostly in terms of its lack of outreach) but reserve their harshest criticisms for the failure of the Panel to adequately monitor or limit the internal grievance systems of the health plans.
The program is distinctive in two ways. First, the separation of responsibility for the external review panel and fair hearings into two state agencies has resulted in a breakdown in the effective administration of the complaints of Medicaid managed care beneficiaries. State officials do not know how the other system works or whether some types of cases are better resolved by one mechanism than another. Advocates report that beneficiaries are confused about which system to use (or whether there even are different systems). Second, the decision to limit external review to those cases that have already completed the health plan’s own review process has placed great importance on the quality and timeliness of the in-plan grievance systems. The Panel requires managed care plans to submit data quarterly on the number, type, and age of the grievances filed by their members that they are adjudicating as in-plan grievances. According to Panel staff, there are few resources or staff to enforce the required time limits, however, and this gives plans that do not have a commitment to responding effectively to grievances and appeals substantial leeway for abuse.
MINNESOTA SITE VISIT REPORT
This report summarizes MPR’s site visit to learn about Minnesota’s ombudsman/county advocate program for Medicaid managed care enrollees.60 As we study other states, we expect some of the facts and themes discussed here (or captured in our site visit notes) to take on greater importance and others to recede. We will synthesize findings from all states in the final project report.
A. OVERVIEW OF MEDICAID MANAGED CARE IN MINNESOTA
Minnesota has mandated the managed care enrollment of Medicaid recipients (except for blind and disabled SSI recipients) in selected counties since 1985, when it established its Prepaid Medical Assistance Program (PMAP). PMAP is federally authorized under a Section 1115 waiver. The state DHS administers PMAP, as well as Minnesota’s other state-subsidized health care programs. Sixty-two percent of Minnesota’s 465,898 Medicaid recipients were enrolled in PMAP as of June 30, 2000 (CMS Web site 2001). Depending on where they reside, they may receive care from any of eight MCOs. Upon enrollment, PMAP participants are subject to a 12-month lock-in period during which they cannot change MCOs. Minnesota does not operate a PCCM program.
B. SUMMARY OF COMPLAINTS AND APPEALS PROCEDURES
1. In-Plan Procedures
The Minnesota DHS prescribes the appeal and complaint procedures to which PMAP MCOs must adhere. MCOs are required to have informal and formal procedures for resolving enrollee complaints, and they must send enrollees written notification when they intend to deny, terminate, or reduce services (this is known as issuing a “DTR”). Informal complaints are those the enrollee makes in person or by telephone. Formal complaints are those the enrollee or an authorized representative submits in writing. MCOs must respond to informal complaints within ten days and formal complaints within 30 days. In addition, MCOs must send copies of all DTRs and formal complaints to the managed care ombudsman. MCOs’ DTRs and written responses to formal complaints must include information on how to request a state-level appeal and the telephone number of the ombudsman’s office.
2. State-Level Procedures
Minnesota has two types of fair hearings, which the state calls “appeals.” The first type--administrative appeals--pertain to issues of mandatory PMAP participation and enrollment. The second type--service appeals--pertain to health care services that have been denied, reduced, or terminated. This report focuses on service appeals, which are resolved through hearings administered by DHS’s Appeals Unit. (Administrative appeals are not relevant to our study of fair hearing adaptations because they do not address disputes between enrollees and their MCOs.)
To file a service appeal/hearing request, an enrollee must complete and sign an Appeal Form and an Authorization to Release Medical Information within 30 days of receiving an adverse determination from a health plan.61 However, to have services continue pending a hearing decision, the enrollee must request a hearing within ten days of receiving an adverse determination. Enrollees are not required to exhaust plan-level complaint procedures before requesting a state hearing. They may designate someone to represent them during their hearing; however, fewer than 10 percent are represented by attorneys.
After a hearing has been requested, the case is assigned to any of 12 hearing referees throughout the state.62 Pre-hearing conferences are not routinely used. Although hearings have traditionally been held in county social services offices, they are increasingly conducted by telephone. Following the hearing, the referee prepares an opinion (recommendation) and submits it to the chief appeals referee, in St. Paul. The chief referee reviews the opinion, seeks any clarifying information, and then issues a final decision.63 An enrollee who is not satisfied with the chief referee’s decision may request an agency reconsideration. The next, and final, recourse is district court.
C. OMBUDSMAN/COUNTY ADVOCATE PROGRAM
1. Program Background
By 1985, state-run ombudsman offices and the use of county-level agencies to provide services both had historical precedent in Minnesota. Not surprisingly, the state chose to make complaint and appeals assistance available to PMAP enrollees at the state and county levels through its ombudsman/county advocate program. The state operates the Managed Care Ombudsman program, located in the Health Care Administration section of the Purchasing and Service Delivery division of the Medicaid agency (all of which are under the DHS umbrella). The program consists of four ombudsmen (and two support staff) who serve enrollees from one office in St. Paul. In addition, every county that participates in PMAP must have a staff member (or full-time equivalent) available to help enrollees with complaints and appeals. These staff members are known as county advocates, and they typically work in county human services departments. In addition to coordinating complaints and appeals, county advocates perform PMAP enrollment functions. Minnesota currently has 85 county advocates in 57 PMAP counties. There is no formal, or reporting, relationship between the ombudsman and the county advocates (the county advocates ultimately report to the county board). In recent years, however, the ombudsman office has held semiannual seminars to train county advocates in their appeal and complaint responsibilities.
The ombudsman and the county advocates operate under the authorizing legislation that established PMAP. DHS funds both the ombudsman and the county advocates. The amount of funding it provides to the ombudsman office is set according to the agency’s budgetary priorities. State officials explained that funding for the program is secure, but it has not increased with the growing PMAP population. In contrast, DHS funds the county advocate program on a per-enrollee basis. It funds one full-time equivalent per 25,000 PMAP enrollees in the county.
2. Involvement of the Ombudsman and County Advocates in Plan-Level Complaints
Both the ombudsman and the county advocates help enrollees with plan-level complaints and appeals. From the enrollee’s perspective, there seem to be few, if any, differences in the complaint resolution services provided by the ombudsman versus the county advocates. (Each does perform some distinct complaint-related functions, however. For example, as noted earlier, the ombudsman receives and files copies of MCOs’ DTRs and formal complaints.) Because enrollees are not instructed or encouraged to call one over the other, enrollees generally seek assistance with whom they are most comfortable. Stakeholders we interviewed said that most enrollees seek assistance from county advocates.64 Available data seem to confirm this observation. In one large county, two advocates receive a combined total of about 20 calls a day from PMAP enrollees in that county. In contrast, the ombudsman program receives approximately 25 calls a day from callers throughout the state.65
In a typical plan-level case, a county advocate (or an ombudsman) helps an enrollee by: (1) defining the problem and the desired outcome; (2) confirming that there is a case to pursue (that is, the complainant is enrolled in PMAP and seeks a PMAP-covered service); (3) contacting and attempting to resolve the problem with the MCO’s member services department; (4) pursuing resolution with a utilization management nurse, if necessary; (5) filing a formal plan-level and/or state-level appeal, if necessary; and (6) educating the enrollee about his or her responsibilities as a complainant. Both the ombudsman and the county advocate we interviewed cited the value of three-way telephone calls (among the enrollee, MCO, and ombudsman/advocate). Many disputes are resolved during such calls, and the enrollee learns how to effectively conduct or participate in such conversations. Notably, contact between MCOs and county advocates is frequent enough that some MCOs have staff whose principal responsibility is to interact with county advocates. Others provide the county advocates with a list of designated in-plan contacts.
According to the stakeholders we interviewed, Minnesota’s county advocates function as pro-enrollee supporters, rather than as neutral mediators. One MCO complained that some advocates, especially those in rural counties, either do not understand or disregard managed care principles when they are helping an enrollee pursue a complaint. For its part, the state ombudsman office is mostly seen as a facilitative party. Compared to the county advocates, the ombudsman was more often described as a negotiator than someone who takes sides.
3. Involvement of the Ombudsman and County Advocates in State-Level Appeals
Between 1998 and 2000, enrollees in Minnesota’s state-subsidized managed care programs (including PMAP, MinnesotaCare, and a third program for low-income adults without dependents) requested 793 state hearings. Ninety percent of the requests pertained to medical or dental services and supplies, the rest to administrative matters. Stakeholders estimated that about half of all hearing requests are withdrawn before a hearing occurs, either because the enrollee abandons the case or because the MCO reverses its decision.
The most common role the ombudsman and county advocates play in hearings is to help enrollees request and prepare for them. Although no legal barriers prevent the ombudsman or the county advocates from representing enrollees during hearings, they seldom do. Over the years, the ombudsman, who estimates that she participates in less than 5 percent of hearings, has altered her approach to disputes. She had served exclusively as a neutral mediator, but she has become increasingly comfortable in an advocate’s role. A county advocate we interviewed, who participated in five hearings in 2000 and none in the first half of 2001, finds that increasingly more cases get resolved before a hearing occurs. Thus, her involvement or lack of involvement in hearings has more to do with solving problems in the most practical manner than with her perception of herself as a mediator or advocate.
As noted earlier, state law requires PMAP MCOs to forward copies of DTRs and formal complaints to the ombudsman office. At the time of our site visit, the ombudsman office neither analyzed the data contained in such documents nor performed any other related activities (such as monitoring outcomes). Although the office recognizes the potential usefulness of such activities, it lacks the human (and, until recently, technological) resources to undertake them.
The legal advocates with whom we spoke would encourage the ombudsman and the county advocates to refer more clients to them for legal representation in the state hearing process. Their emphasis is on referrals only; because the ombudsman and county advocates are government employees, legal advocates do not seem to support their playing a stronger representational role in hearings on government services. Legal advocates spoke of the ombudsman as a customer service provider who is able to solve some problems. In comparison, they commented that some county advocates too often refer enrollees back to their plan’s member services department, rather than taking on the case themselves.
4. Outreach and Enrollee Awareness
The state, MCOs, and the counties all help promote the managed care ombudsman/county advocate program, either voluntarily or at the state’s behest. Table MN-1 summarizes the outreach activities of each stakeholder. The legal advocates with whom we spoke do not perform outreach activities that would promote the program.
| TABLE MN-1. Outreach Activities for the Ombudsman/County Advocate Program | |
|---|---|
| Stakeholder | Outreach Activities |
| State Agency (DHS) | Describes complaint and appeals procedures, lists ombudsman’s telephone number, and mentions county advocates in a “Notice of Rights and Responsibilities” brochure provided with other enrollment materials and sent to PMAP enrollees twice a year. |
| Ombudsman Office | Contributes to the activities described above. |
| County Advocates | Distribute enrollment materials developed by state. Other outreach activities vary by county. May print and distribute wallet cards with important telephone numbers and attend community events. |
| Managed Care Organizations | Must mention the ombudsman’s office in members’ certificates of coverage and handbooks. Must describe state-level appeal rights and the ombudsman’s office in denial notices. Instruct enrollees to inform county advocates of change of address, change in dependents, etc. |
5. Strengths and Weaknesses of the Ombudsman/County Advocate Program
Stakeholders identified many strengths and weaknesses of the ombudsman/county advocate program. Table MN-2 summarizes the strengths and weaknesses, with attributions to the type of stakeholder (ombudsman, county advocate, state official, legal advocate, or MCO) who identified them.
| TABLE MN-2. Strengths and Weaknesses of Minnesota’s Ombudsman/County Advocate Program, as Identified by Site Visit Participants | |
|---|---|
| Strengths | Weaknesses |
| OMBUDSMAN PROGRAM | |
| Ombudsman is knowledgeable about state systems and has access to eligibility data. (State, Ombudsman) The ombudsman program serves as an early warning system for plan-level problems. (State) The ombudsman program has a strong, qualified staff. (Ombudsman) The ombudsman program has clout with MCOs because it is state-operated. (Ombudsman) The ombudsman program realizes that it should do a better job of collecting and analyzing data. (Legal Advocacy Organization) Funding for the ombudsman program is secure. (Legal Advocacy Organization) The ombudsman program performs a valuable customer service function. (State, MCO) Relationships between the ombudsman and the MCOs are good and not adversarial. (Ombudsman, MCO) The ombudsman is flexible, acting as an advocate or mediator as circumstances require. (State) The ombudsman does a good job training county advocates. (Ombudsman, County Advocate) The ombudsman effectively guides enrollees through the fair hearings system. (State) | The ombudsman is not a real advocate because the program is not independent of the state. (Legal Advocacy Organization) The ombudsman program needs a larger staff. (Ombudsman) The ombudsman program should measure client satisfaction with program services. (Ombudsman) The ombudsman collects data but does not use it or make it available for others to analyze. (MCOs, Legal Advocacy Organization) The ombudsman and county advocates should educate PMAP enrollees about using managed care effectively. (Legal Advocacy Organization, MCO) |
| COUNTY ADVOCATE PROGRAM | |
| County advocates have a good understanding of Medicaid and managed care (MCO) Having a decentralized system makes the appeals mechanism more geographically and emotionally accessible to enrollees. (State) There is little turnover among county advocates. (County Advocate, MCO) | Some county advocates do not understand managed care. (MCOs) Semiannual training of county advocates by the ombudsman does not provide enough contact between those entities. (MCO) County advocates often have many responsibilities other than helping enrollees with complaints and appeals. (Legal Advocacy Organization, State) As a decentralized system, the county advocates program dissipates the effects of dispute-resolution, leaving it at the individual level. (Legal Advocacy Organization) |
| SOURCE: Interviews with state officials and employees, the managed care ombudsman, a county advocate, representatives of Medicaid MCOs, and consumer and legal advocates. The type of stakeholder who identified each strength or weakness is listed in parentheses. | |
6. Changes Recommended by Stakeholders
In addition to asking stakeholders about the perceived strengths and weaknesses of the ombudsman/county advocate program, we asked them what changes they would make to the program if they were given the chance. The following changes were recommended:
- State Officials (other than the ombudsman) Recommend:
- A more proactive, less reactive, ombudsman program.
- More effective data collection and analysis by the ombudsman program.
-
Creating clearer lines of authority and responsibility for some county advocates, to lessen conflicts that can arise when one employee is involved in both advocacy issues and eligibility determinations.
- Consumer and Legal Advocates Recommend:
- Providing federal funding for the ombudsman (in all states).
- Establishing full-time regional (rather than county-level) advocates who report to the state ombudsman.
-
Establishing an ombudsman program that conducts policy-level work, rather than one that provides assistance to individuals.
- The Ombudsman Recommends:
- Performing more community outreach activities (assuming program staff would increase to meet new levels of demand).
-
Separating the ombudsman office from the state so that it would have more influence, access to the legislature, and more credibility with MCOs and independent advocacy organizations.
- MCOs Recommend:
- Having the ombudsman report to a higher level of management within DHS.
- Putting the data collected by the ombudsman to use.
- Increased funding for the ombudsman program.
- Building consistent, ongoing opportunities for dialogue between MCOs and the ombudsman, whether or not there is a specific problem to address.
- More frequent training seminars for county advocates.
- Creating a reporting relationship from the county advocates to the ombudsman.
- Not having county advocates perform enrollment functions and complaint resolution functions.
-
Some MCOs even recommend eliminating the ombudsman program because having state and county-level advocates confuses enrollees.
D. SUMMARY
Several aspects of Minnesota’s ombudsman/county advocate program are noteworthy. First, the program is well established in that it: (1) has operated for 15 years; and (2) uses the state’s long-standing traditions of state-run ombudsman programs and county-level service provision. Second, PMAP enrollees use the services provided by the ombudsman and the county advocates, which seems to be a result of effective outreach among a variety of stakeholders. Third, most PMAP disputes are resolved at the MCO level rather than at the state level; thus, the ombudsman and the county advocates devote most of their time to MCO-level disputes. Fourth, county advocates see themselves, and are seen by others, as pro-enrollee advocates rather than mediators. The ombudsman is seen as somewhat more facilitative and less adversarial. Finally, neither the ombudsman nor the county advocates are seen as independent actors in PMAP disputes. Their insider status has benefits, such as access to enrollee data, and drawbacks, such as a lack of credibility among advocacy organizations.
NEW YORK SITE VISIT REPORT
This report summarizes MPR’s site visit to learn about New York’s external appeals program, which is available to both commercial and Medicaid managed care enrollees.66 As we analyze our findings from other states, we expect some of the facts and themes discussed here to take on greater importance and others to recede. We will synthesize findings from all states in the final project report.
A. OVERVIEW OF MEDICAID MANAGED CARE IN NEW YORK
Medicaid managed care in New York dates back to 1991, when 43 of the state’s 58 counties introduced voluntary managed care programs. In 1997, New York began implementing statewide mandatory managed care through the Partnership Plan, a federally authorized Section 1115 waiver demonstration.
When fully implemented, the Partnership Plan will encompass most of New York’s non-elderly, non-institutionalized Medicaid beneficiaries, including blind and disabled SSI recipients. Most beneficiaries are (or will be) enrolled in MCOs, and are subject to one-year lock-in periods after selecting a plan. For the time being, Medicaid beneficiaries who are HIV-positive or who have serious and persistent mental illness are exempt from mandatory managed care participation, although they may participate voluntarily. Eventually, the state plans to mandate the enrollment of such individuals in Special Needs Plans, which are conceived of as capitated health plans with intensive case management components. The Partnership Plan waiver is being implemented on a county basis. As of September 2000, it had been implemented in 14 counties. As of April 2001, the Medicaid managed care penetration rate among mandatory populations across all 58 counties was 33 percent. Penetration in upstate counties (42 percent) was substantially higher than in New York City counties (28 percent).
The Office of Managed Care in the New York State Department of Health (DOH) is responsible for the overall design, implementation, and oversight of the Partnership Plan. The Office of Medicaid Management in DOH is responsible for fair hearings policy, eligibility policy, and claims processing. Counties are responsible for eligibility determinations, enrollment functions, contracting with MCOs, and some MCO monitoring activities. The New York State Department of Family Assistance conducts fair hearings for all public assistance programs through its Office of Administrative Hearings (OAH).
B. IN-PLAN COMPLAINT PROCEDURES AND STATE FAIR HEARINGS
In addition to the external appeals program, New York’s newest complaint mechanism, Medicaid managed care enrollees have access to the internal complaints and appeals procedures of MCOs and to state fair hearings. In this section of this report, we briefly describe in-plan procedures and state fair hearings. In the remaining sections, we focus more intently on the external appeals program.
1. In-Plan Procedures
DOH has developed standard guidelines for the notification and complaint resolution procedures that Partnership Plan MCOs must follow when they intend to terminate, suspend, or reduce ongoing treatment or when they deny a request for Medicaid-covered services. More generally, MCOs must also describe internal procedures and state fair hearings policy in their enrollee handbooks.
State guidelines refer to two levels of in-plan disputes--complaints and appeals.67 Complaints are the enrollee’s first expression of dissatisfaction. They may be filed at any time, orally or in writing. MCOs are required to log complaints, acknowledge their receipt, and respond to them in writing (within 48 hours for medically urgent cases, 30 days for non-urgent referrals and coverage issues, and 45 days in all other instances). When responding to a complaint, the MCO must include written notification of the enrollee’s right to appeal internally, to request a state fair hearing, and to complain to the state less formally (such as through a telephone hotline). The enrollee may pursue any or all of these avenues. An enrollee who pursues an in-plan appeal must do so in writing within 60 days of receiving the MCO’s initial complaint response. The MCO then has two or 30 days (depending on whether the appeal is expedited) to respond to the appeal. For both complaints and appeals, the MCO’s clinical reviewers or medical director determine when to use expedited time frames.
Both of the MCOs we interviewed use the same internal complaint and appeals procedures for their commercial and Medicaid enrollees. Compared to their commercial counterparts, however, Medicaid enrollees in both MCOs are less likely to file complaints and appeals. Asked for possible explanations, the MCOs noted that Medicaid offers a richer benefits package than do most commercial insurers, perhaps giving the average Medicaid beneficiary less reason to complain. One MCO further hypothesized that Medicaid enrollees are often reluctant to complain because they fear that their Medicaid and other public benefits may be at risk.
2. State Fair Hearings
As noted, MCOs must notify Medicaid enrollees of their fair hearing rights when responding to enrollees’ complaints. MCOs must also send notification when they intend to terminate, suspend, or reduce an ongoing course of treatment in defiance of a physician’s order or when they deny a physician’s request for Medicaid-covered services.
To request a fair hearing, an enrollee must call, write, or send a copy of a denial notice to OAH in the Department of Family Assistance within 60 days of receiving a denial notice. If the dispute involves a termination, suspension, or reduction of treatment, the disputed benefits will continue as long as the enrollee requests a hearing before the intended action is taken. Continuation is automatic unless the enrollee requests otherwise.
OAH intake staff sort hearing requests from Medicaid beneficiaries by whether they involve: (1) Medicaid eligibility or managed care enrollment issues; or (2) clinical managed care issues. Requests involving clinical issues are immediately brought to the attention of an ALJ, who decides whether the case is eligible for priority scheduling. Eligible cases include those that involve a termination, reduction, or suspension of services. According to OAH, cases given priority scheduling are heard within a few days, and decisions are issued not more than one day later.
If New York may be said to have an expedited fair hearing program, then the priority scheduling process is that program. The process seems to consist almost entirely of ALJs screening hearing requests and scheduling apparently urgent cases for hearings within a few days’ time. “If we think it’s important, we get right to it,” said one judge. For their part, enrollees are welcome to request priority hearings, if they happen to know such hearings exist. OAH does not publicize their availability, nor does it provide enrollees with hearing request forms (which some other states use to allow enrollees to request expedited hearings).
Priority scheduling aside, OAH generally schedules fair hearings for within 3-4 weeks of the date they are requested. Hearings are conducted by state hearing officers, who must be lawyers. To remain neutral until the time of the hearing, hearing officers do not participate in pre-hearing conferences with either party. Most hearings are conducted in person, and evidence is introduced at the hearing, not shared with the parties beforehand. If the enrollee is homebound, he or she may send a representative to the hearing or request a telephone format. OAH estimates that fewer than 5 percent of all complainants--and an even smaller percentage of Medicaid complainants--have legal representation during their hearings. When the complainant is without legal representation, it is the responsibility of the hearing officer to help the complainant present the facts and develop a complete record of the case. MCOs sometimes send attorneys or physicians to fair hearings; however, MCOs are just as likely to waive their rights to appear as they are to attend the hearing.
After the hearing, the hearing officer has one day to write his or her decision and forward it to a supervising ALJ. For efficiency and consistency, hearing officers use preformatted electronic templates to prepare their decisions. ALJs review the decisions, ask clarifying questions, and issue a final agency decision to all parties within two days of the hearing. If the complainant is dissatisfied with the final decision, OAH will conduct an informal reconsideration of the case, another procedure it does not publicize. The official recourse for an enrollee who is still dissatisfied after the informal reconsideration is to file a lawsuit.
OAH handles a high volume of hearings and requests for hearings, only a tiny fraction of which involve Medicaid managed care issues. In an average year, the office receives 180,000 requests for hearings from all programs and holds 80,000 hearings. In contrast, between August 1999 and May 2001, a 22-month period, the office received 44 hearing requests involving clinical Medicaid managed care issues.68 Of those, 14 cases went to a hearing. OAH and MCOs both feared a glut of fair hearings at the advent of mandatory managed care, but none transpired. An ALJ suggested that few Medicaid managed care enrollees request hearings because they believe that in-plan resolutions are faster. New York, like other states, encourages (but does not require) enrollees to pursue in-plan resolution before requesting a hearing.
C. EXTERNAL APPEALS PROGRAM
1. Program Background
New York’s external appeals program is designed to enable managed care enrollees to obtain independent medical review of MCO decisions involving medical necessity determinations or investigational or experimental treatment. The program was launched in July 1999, a time when consumer-protection issues were high on the public agenda in New York. The program and its supporting legislation grew out of the state’s Managed Care Reform Act of 1996, which, among other things, required MCOs to establish internal complaints and appeals procedures. Although designed principally for commercially insured managed care enrollees, the external appeals program is also available to Medicaid managed care and Child Health Plus enrollees.
When New York’s external appeals program was in its planning phase, it was strongly supported by consumer advocates, well publicized by the governor’s office, and opposed by MCOs. Two years later, the program is largely viewed as a success, even among MCOs. The only stakeholders who seem to be paying little attention to the program and its effect on Medicaid managed care enrollees are legal advocates for the poor, whose focus remains fixed on fair hearings.
2. Program Structure and Design
The external appeals program is jointly administered by DOH and the State Insurance Department (SID). The two agencies were equally involved in implementing the program legislation and developing supporting regulations. Today, SID is responsible for day-to-day program operations, while DOH is primarily involved in evaluating and overseeing external review agents. State-certified external review agents conduct the actual medical reviews through contractual arrangements with practicing physicians.
To be eligible for an external appeal, a case must involve a medical necessity determination or investigational or experimental treatment. Contractual issues are not eligible for external appeal. In addition, enrollees are required to complete one in-plan appeal before requesting an external review. Medicaid enrollees may request an external review before or at the same time as they request a fair hearing. However, if a fair hearing decision has already been rendered, the case will be ineligible for external review. Having completed one in-plan appeal, the aggrieved enrollee has 45 days from receipt of the MCO’s adverse determination to request an external appeal. To do so, the enrollee may submit a completed external appeal application (MCOs must provide blank copies of the application when they issue adverse determinations of in-plan appeals) or another form of written request to SID.
SID staff screen applications and other requests for eligibility and completeness. They must screen standard requests within five business days and expedited requests within 24 hours. (Expedited requests are those accompanied by a physician’s attestation that a delay would pose a serious or imminent threat to the complainant’s health.) If a request is complete and eligible for the program, SID randomly assigns it to one of three state-certified external review agents. (During the program’s first two years, there were two such agents, both established health care review organizations serving public and private clients.)
The external review agent is responsible for preparing a complete case file, assigning the case to a physician reviewer, and rendering a final determination. Agents are given 30 days to complete this process for standard appeals (plus five business days when additional information is needed) and three days for expedited appeals. Reviews of medical necessity determinations are conducted by one physician reviewer, while reviews of investigational or experimental treatment are conducted by an odd-numbered panel of reviewers. Appeals are conducted entirely on paper--neither of the disputing parties appears before, or talks to, the physician reviewers.
The external review agent issues a final determination to the disputing parties. Their decisions are binding, leaving no forum for appeal other than court. For each review they conduct, external review agents are paid by the MCO in question. (The fees charged by external review agents are approved by SID and DOH for two-year periods. In the first year of program operation, MCOs paid about $674 per review.) MCOs, in turn, may charge commercial enrollees up to $50 for each review if the MCO decision is upheld. Such fees are waived for Medicaid and Child Health Plus enrollees.
3. The First Two Years of Operation
By the time of our site visit, two years after the program was launched, stakeholders spoke uniformly about many aspects of the program. The following messages came through repeatedly in our interviews:
-
The program is attracting many more applications than anyone anticipated, based on other states experiences. In the first year of operation, SID processed 1,400 external appeals requests, and external review agents rendered 659 determinations. (Of the remaining 741 cases, 421 were rejected as ineligible and the 320 others were at some other phase of the process when SID produced its snapshot of the status of cases.)
-
Few Medicaid managed care enrollees use the program. Of the 659 decisions rendered in the first year of operation, nine cases (1.4 percent) pertained to Medicaid.
-
Stakeholders, including MCOs, view the process as fair to both parties. Many stakeholders cited the reviewers determinations--50 percent in favor of MCOs, 50 percent in favor of enrollees--as evidence of fairness.
-
Expedited appeals are problematic for SID, the external review agents, and physician reviewers. First, many requests for expedited appeals do not seem to warrant priority handling, even though they include the required physician attestation. Second, the three-day turnaround time required of external review agents is often difficult to meet, particularly when weekend days are involved or certain types of specialists are needed as reviewers. Unfortunately, it seems that neither of these problems can be remedied without legislative changes.
In addition, some stakeholders noted important differences between external appeals and fair hearings. Unlike the external appeals program, the fair hearings process: (1) does not require completion of any in-plan appeals; (2) allows for the continuation of Medicaid benefits while a decision is pending; (3) encompasses clinical and some contractual issues; and (4) may be requested orally. Stakeholders view these features of fair hearings as advantageous to Medicaid enrollees. The relative advantages and disadvantages of other differences are less clear. For example, ALJs knowledgeable about Medicaid policies decide fair hearings, while practicing medical experts (who may not have knowledge of Medicaid) make external appeals determinations. In addition, enrollees may participate in person in fair hearings, but not in external appeals. Participation may be an advantage for some, but not for others.
4. Outreach and Enrollee Awareness
State officials described many types of initial and ongoing outreach activities in connection with the external appeals program, but none that specifically target Medicaid managed care enrollees. Moreover, officials say awareness of the program is high among commercial managed care enrollees but not among enrollees who receive Medicaid benefits. DOH staff explained that the program has not targeted Medicaid enrollees because they already seem so comfortable with the fair hearings process. Nonetheless, the same officials conceded that the state could “do a better job” of promoting the program to the Medicaid population.
Table NY-1 summarizes the outreach activities undertaken by the state, MCOs, and advocacy organizations. As noted above and in the table, the law requires MCOs to provide external appeal applications to enrollees when they issue final adverse determinations of in-plan appeals. Stakeholders uniformly attribute the high level of program use to the fact that enrollees receive applications at the very moment they are most likely to use them. However, consumer and legal advocates noted that the length and complexity of the application may deter enrollees with poor literacy skills. The application for a standard appeal of a medical necessity determination is four pages long. An additional five pages are required for expedited appeals and appeals involving experimental therapy.
| TABLE NY-1. Outreach Activities for the External Appeals Program | |
|---|---|
| Stakeholder | Outreach Activities |
| State Agencies (SID and DOH) | Conduct informational presentations to MCOs, hospital associations, medical societies, and consumer organizations; provide program information and applications on their Web sites; publish annual program reports (also posted on agency Web sites); maintain a dedicated hotline to help consumers request appeals and navigate the process. |
| MCOs | Provide enrollees with copies of the external appeal application whenever they issue adverse determinations of in-plan appeals. |
| Consumer Advocacy Organizations | Some provide enrollees with sample or fill-in-the-blank grievance and appeals letters. |
| Legal Advocacy Organizations | None (most outreach activities are related to fair hearings). |
| External Review Agents | None. |
5. Accommodations for Enrollees with Special Needs
While New York’s external appeals program does not offer explicit accommodations to enrollees with special needs, some aspects of the program may be beneficial to such individuals. For example, SID operates a toll-free telephone hotline to help callers fill out program applications and answer other questions. (The application is available in English only. However, in response to pressure from advocacy organizations, the state did have it specially edited to a lower language level.) In addition, some beneficiaries who are homebound, or who may be intimidated by appearing at a hearing, may prefer the paper review format of the external appeals program.
6. Strengths and Weaknesses of the New York External Appeals Program
Stakeholders spoke of program strengths in mostly broad terms--for example, by praising the program for overall fairness and objectivity. In contrast, they cited weaknesses that are specific and procedural, amounting to relatively minor flaws in an otherwise effective program. Table NY-2 summarizes both types of characteristics, with attributions to the type of stakeholders (state official, MCO, advocate, or external review agent) who identified them.
| TABLE NY-2. Strengths and Weaknesses of New York’s External Appeals Program, as Identified by Site Visit Participants | |
|---|---|
| Strengths | Weaknesses |
| The program gives consumers the feeling that they have been heard. (MCO, External Review Agent) The program takes some of the pressure off MCOs in making important medical decisions by themselves, while giving them an opportunity to show enrollees that their decisions are sound. (MCO, External Review Agent) The program provides objectivity because of a clinical review by qualified experts who have no financial stake in the outcome. (MCO, External Review Agent, Consumer Advocate) The program helps assuage the public’s fear of HMOs. It does so by assuring enrollees that they will have access to an objective review of HMO decisions should they need one. (MCO) The program provides an outlet for bringing about resolution without litigation. (External Review Agent) The program works well for enrollees with complaints about clinical issues. (Legal Advocate) The program has led MCOs to think more carefully about their medical necessity determinations. (Consumer Advocate, MCO) The external appeals program leads to resolutions more quickly than does the fair hearings process. (MCO) | Some providers attempt to use the program to collect claims retrospectively, an unintended use of the program. (MCO, State Officials) The state does not consistently enforce the requirement of two pieces of supporting literature from providers in the case of experimental therapies. (MCO) The deadlines that apply to the external review agent are often difficult to meet because of the need to collect additional documentation. Deadlines in expedited cases are especially difficult if cases arise on weekend days or require a panel of reviewers. (External Review Agent) The program’s eligibility criteria are too narrow; contractual issues should also be eligible. (Advocate) The program application is too complex for the majority of Medicaid enrollees. (Advocate) |
| SOURCE: The type of stakeholder who identified each strength or weakness is listed in parentheses. | |
7. Changes Recommended by Stakeholders
In addition to asking stakeholders about the strengths and weaknesses they perceived in the external appeals program, we asked them what changes they would make to the program if they were given the chance. The following changes were recommended:
- State Officials Recommend:
- Giving more attention to the states staffing needs in administering the program.
- Creating a separate appeals process for hospitals and other providers to resolve fee disputes.
-
Changing the time frames for expedited appeals from three days to three business days.
- MCOs Recommend:
-
Eliminating fair hearings and using external appeals entirely.
-
- External Review Agents Recommend:
-
Having the state screen requests for expedited review to ensure that they really are medically urgent cases.
-
- Advocates Recommend:69
- Expanding the program to address a greater array of cases, including contractual issues and out-of-network referrals.
- Simplifying the program application and other information provided to consumers.
- Accepting oral requests to use the program in addition to written requests.
- Accepting attestations about the need for experimental therapies from non-physician providers, such as social workers.
-
Adhering to statutory definitions of disabling conditions in cases of experimental therapy (program administrators are said to use another definition).
D. SUMMARY
After two years of operation, New York’s external appeals program appears to be meeting its primary objective: it provides a substantial number of commercial managed care enrollees with an independent review of MCOs’ medical necessity determinations and some other clinical decisions. Some stakeholders, however, say the program could do more. For example, although the program is available to Medicaid managed care enrollees, it is neither highly visible to nor used by them. At the same time, stakeholders argue against the external appeals program because it lacks some important features of the fair hearings process, including continuation of benefits. For the most part, stakeholders we interviewed fell into three categories with regard to Medicaid enrollees’ use of the external appeals program. First, some (including legal advocates who may have invested a lot of their own time and money in improving the fair hearings process) strongly favor fair hearings over external appeals. Second, some (including MCOs) strongly favor external appeals over fair hearings. Finally, however, the largest category consists of those who would suggest ways to make the external appeals program easier for those Medicaid enrollees who do use it, but who would not necessarily push for more widespread program use among this population.
OREGON SITE VISIT REPORT
This report summarizes MPR’s site visit to Oregon to learn about its expedited fair hearing process and ombudsman program, both of which are made available to Medicaid managed care enrollees.70 As we study other states, we expect some of the facts and themes discussed here (or captured in our site visit notes) to take on greater importance and others to recede. We will synthesize findings from all states in the final project report.
Expedited hearings, unlike the other fair hearing adaptations we have studied (ombudsman programs and external review), are really just a special type of fair hearing and not a completely new process or program. Therefore, to describe expedited hearings, we must first describe the fair hearing process. Our report begins with a description of Medicaid managed care in Oregon. Next, we describe the complaints and appeals processes available to enrollees within health plans and at the state level (the fair hearing process). We then discuss the expedited fair hearing process. Because expedited hearings share so many features with the standard fair hearing process, we discuss such issues as program strengths and weaknesses and recommended changes for the overall fair hearing process. After describing the expedited hearing process, we discuss Oregon’s ombudsman program. A final section summarizes our impression of both the expedited hearing process and the ombudsman program.
A. OVERVIEW OF MEDICAID MANAGED CARE IN OREGON
Oregon’s Medicaid managed care program, known as the Oregon Health Plan (OHP), began its first phase of enrollment in February 1994. During Phase I, OHP enrollment was mandatory for Medicaid recipients who were also recipients of Aid to Families with Dependent Children (now TANF), children under age 6, or pregnant women with incomes less than 133 percent of the federal poverty level. In Phase II, which began in January 1995, enrollment became mandatory for all other Medicaid recipients, including the elderly, SSI recipients (that is, the blind or disabled), and foster children. During Phase II, OHP expanded its coverage to include mental health and chemical dependency services. OHP is now mandatory for all Medicaid beneficiaries except American Indians and Alaska Natives.
As of June 2001, Oregon had 407,456 Medicaid beneficiaries: 58 percent are enrolled in fully capitated health plans, 4 percent are in PCCM, and 38 percent receive fee-for-service Medicaid. OHP offers 15 fully capitated health plans, ten mental health plans, and seven dental care plans. No health plans are available in five of Oregon’s 36 counties, so enrollees must enroll in PCCM or remain in fee-for-service Medicaid. In addition, several health plans have left OHP or restricted the number of patients they are willing to enroll. Thus, the percentage of enrollees in fully capitated health plans decreased from 70 percent in 1995 to 58 percent in 2001. Oregon’s Medicaid program is administered by the Office of Medical Assistance Programs (OMAP) in the DHS.
In OHP, coverage for specific services is determined by a prioritized list. The list ranks more than 700 diagnosis/treatment pairs in order, from most to least treatable and cost-effective. The state legislature determines, and CMS (formerly the Health Care Financing Administration) approves, where the line for coverage is drawn. Treatments that fall below the line are not covered. OHP currently covers services numbered 1 through 574. An exception to this is if a beneficiary has a condition above the line that is being exacerbated by the presence of a comorbid condition below the line, and coverage of the below-the-line service will improve the above-the-line condition.
B. SUMMARY OF COMPLAINTS AND APPEALS PROCEDURES
1. In-Plan Procedures
OMAP’s contracts with MCOs describe the internal complaints and appeals processes the MCOs must have in place. MCOs are required to have formal processes for registering and resolving enrollee complaints and grievances. MCOs must log all complaints, accept either oral or written complaints, and resolve complaints within five working days.71 No distinction is made between formal and informal complaints. Medicaid managed care enrollees have access to one level of internal plan appeal (commercial enrollees have two levels of appeal).
MCOs must send enrollees a written Notice of Action for any decision to deny, terminate, or reduce services. OMAP does not require a standard notice format, but it must approve the notice format. Notices must state the date of the notice and date the action will be taken, member’s and requesting physician’s name, service requested, reason the action will be taken, and notification of the right to complain to the plan and to request a fair hearing. OMAP’s Notice of Hearing Rights form must be included with the Notice of Action. The enrollee can request a continuation of the service in question if he or she requests a fair hearing before the effective date of the Notice of Action and requests that services be continued (by checking a box on the hearing request form). If the hearing is resolved against the enrollee, the enrollee can be held liable for the cost of the services. However, none of the interviewees we spoke with indicated that this rule had ever been enforced.72
2. State-Level Procedures
State-level appeals are handled through the fair hearing process, known in Oregon as an administrative hearing. Fair hearings may pertain to eligibility, enrollment, or coverage issues and are administered by the Hearings Unit in the OMAP medical director’s office. Hearings are heard by hearing officers from a central hearings panel in Oregon’s Employment Department.
The central administrative hearings panel was created in 1999 by Oregon House Bill 2525. Before that, OMAP hearings were heard only by hearing officers from OMAP. The rationale for this change was the concern that claimants were being denied a fair hearing by having their cases heard by hearing officers from the same agency whose decision was being contested. The central hearings panel serves seven agencies/departments, including OMAP. Agencies retain decision-making authority by requesting a proposed order from the hearing officer, then issuing the final order themselves. Thus, if a hearing officer issues a proposed decision in favor of an enrollee, OMAP may reject this decision and find for the plan. The OMAP officials we spoke with indicated that they sometimes issue their own final decisions because they feel that many hearing officials on the central panel do not understand OMAP regulations well enough to render an appropriate decision on a case.
To file a hearing request, an enrollee or his or her representative must complete an Administrative Hearing Request form. Enrollees must request a hearing within 45 days of the date of the Notice of Action. Enrollees are not required to exhaust the plan-level complaint process before requesting an administrative hearing. Enrollees may bring a representative (family member, friend, physician, attorney, or other advocate) to their hearing. Only a small percentage of enrollees are represented by an attorney.
Although the hearing officers are from the Employment Department, the Hearings Unit in the OMAP medical director’s office actually processes and schedules hearing requests. Once OMAP receives a hearing request, a hearings representative from the OMAP Hearings Unit has 30 days to request the enrollee’s medical record and any other information gathered by the MCO and to schedule the hearing. Most hearings are conducted by telephone and recorded. Following the hearing, the hearing officer prepares a decision and submits it to OMAP. Decisions must be issued within 90 days of the hearing. An enrollee who is not satisfied with the decision may file suit in district court.
OMAP encourages the use of pre-hearing conferences as a way to educate enrollees about OHP and the hearing process. OMAP tries to resolve the enrollee’s problem in the pre-hearing conference and avoid a formal hearing. The advocates we spoke with discourage their clients from participating in pre-hearing conferences because they feel that OMAP uses the pre-hearing conference to get enrollees to drop their claim rather than to attempt to resolve the issue. OMAP also has other more informal discussions with enrollees prior to a hearing. The advocates felt that these informal discussions were more beneficial than pre-hearing conferences because OMAP uses them to identify and resolve the enrollees’ problems.
C. EXPEDITED FAIR HEARING PROCESS
1. Program Background
No legislative action or court ruling required OMAP to make expedited fair hearings available to enrollees. Instead it appears that expedited hearings have always been available if an enrollee stated that his or her situation was an emergency and OMAP agreed that there was good cause to expedite the hearing process. In 1999, OMAP added a check box to the Administrative Hearing Request form for enrollees to request an expedited hearing.73 This change was made to address the concern of Legal Aid attorneys that their clients were not aware of the expedited hearing option.
Expedited hearings are available if the enrollee’s medical condition is an “immediate, serious threat” to the enrollee’s “life or health.” One state official remarked that these criteria are vague, but that they are suitable for OMAP’s purposes. The enrollee or the enrollee’s representative completing the Administrative Hearing Request form must describe the urgency of the enrollee’s condition. There is no typical case for which an expedited hearing is granted. However, OMAP cited a recent case in which an expedited hearing was granted for an enrollee who had been denied transplant surgery.
The primary difference between an expedited hearing and a standard hearing is the time frame under which the process is completed. The enrollee uses the same Administrative Hearing Request form to request either an expedited or a standard hearing. If the enrollee requests an expedited hearing, the OMAP medical director has 48 hours to gather the relevant documentation and medical records and decide whether an expedited review can be granted.74 If the request for an expedited hearing is granted, a hearing is scheduled within five days, and the decision on the hearing must be reached within 14 days. Enrollees who have had an expedited hearing and who wish to appeal the decision of the hearing officer have a right to take their case to district court, as in standard appeals.
2. Volume of Expedited and Standard Fair Hearings
There are very few expedited fair hearings in Oregon. OMAP does not track requests for expedited reviews separately from standard fair hearings, but it estimates that requests for expedited hearings are less than 10 percent of all hearings requested. Requests for expedited hearings are granted infrequently, averaging about one per year. None of the advocate groups we spoke with had ever assisted a client with an expedited hearing. Neither of the two MCOs we spoke with has had a dispute go to an expedited hearing, although each said that it had two members request an expedited hearing in the past year (neither was granted).
In 2000, OMAP received more than 400 hearing requests (Table OR-1). The number of hearing requests has been increasing steadily. OMAP attributes this increase to enrollees becoming more aware of their ability to complain and appeal rather than to any specific changes in OHP operations. Of all the hearing requests OMAP receives, approximately one-third are dropped by the claimant, one-third are resolved when the health plan agrees to reverse its position, and one-third go on to a hearing. Of those cases that go on to a hearing, more than 95 percent are decided in favor of the health plan/OMAP. OMAP officials stated that most cases were found in favor of the plan because enrollees did not understand how OHP works and whether their appeal was legitimately “hearable.” Many cases are related to services below the line on the list of prioritized services. These cases are not hearable unless the enrollee can present sufficient evidence that he or she has a comorbidity requiring a service ranked below the cutoff line on the priority list.
| TABLE OR-1. OMAP Hearing Requests and Resolution of Cases | ||
|---|---|---|
| 1/1/2000-12/31/2000 | 1/1/2001-3/31/2001 | |
| Hearing Requests Received | 415 | 100 |
| Resolution:a | ||
| Hearing held | 152 | 36 |
| Claimant withdrew request | 139 | 27 |
| MCO/OMAP changed actionb | 125 | 34 |
| ||
3. Outreach and Awareness
There are few outreach activities that educate OHP enrollees about their appeal rights. The enrollee’s right to a fair hearing, and specifically an expedited hearing, is described in the welcome packet issued by OMAP to new members, the plans’ member handbooks, and the Notice of Action issued by plans for denials, terminations, or reductions in service. OMAP currently does not do any outreach activities to increase enrollees’ awareness of their right to a fair hearing or an expedited fair hearing. When OHP began, however, Oregon received money from the Federal Government to educate enrollees and potential enrollees about a variety of issues, including the right to appeal. This outreach took place in 1994 and 1995 and included presentations at community centers, schools, and libraries, as well as in newspaper articles and television and radio public service announcements. Outreach targeted minority groups and was done in several languages. This outreach ceased when the federal money ran out, however, and OMAP does not have plans to conduct additional outreach activities. Advocate groups conduct limited outreach activities around the fair hearing process, mostly through newsletters. The advocates do not perform any outreach that specifically focuses on expedited hearings.
State officials, advocates, and health plans had mixed opinions as to whether enrollees understood their appeal rights. Some felt that enrollees understood the process and increasingly exercised their right to a hearing, and others thought that enrollees had a poor understanding of their right to appeal and how to access the appeal process.
4. Serving Enrollees with Chronic or Disabling Conditions
Enrollees with chronic or disabling conditions may request modifications to the hearing process if their condition would prevent full participation. For example, a hearing-impaired enrollee could request an in-person hearing rather than one conducted by telephone. The advocates with whom we spoke agreed that they often had to repeatedly and forcefully request accommodation for their disabled clients and that OMAP was not forthcoming with offers of assistance. No modifications are made to the expedited hearing process for enrollees with chronic or disabling conditions.
5. Strengths and Weaknesses of the Fair Hearing Process
Because the volume of expedited hearings is so low and because the expedited hearing process is so similar to the standard hearing process, stakeholders had few specific opinions of the strengths or weaknesses of the expedited hearing process. Instead, we asked stakeholders to identify strengths and weaknesses of the fair hearing process in general. Table OR-2 summarizes their comments, with attributions to the type of stakeholder (State Official, Advocate, or MCO) giving the comment.
| TABLE OR-2. Strengths and Weaknesses of Oregon’s Fair Hearing Process | |
|---|---|
| Strengths | Weaknesses |
| Hearings increase enrollee trust in health plans, serving as a “second-opinion” to validate plan decisions. (MCO) Hearings educate enrollees about the system and make them feel more empowered. (Advocate, State Official) Hearing officers are seen as neutral parties who give the enrollees every opportunity to be heard. (Advocate, State Official) Expedited hearings give the state the flexibility to meet emergency needs. (State Official) | Representatives cannot adequately prepare a case because evidence is not available until a day or two before the hearing. (Advocate) Hearings are administratively burdensome and costly for health plans. (MCO, State Official) Many disputes go to a hearing that do not belong there. (State Official) Enrollees who appear before a hearing without legal representation do not fare as well as those who do. (Advocate) Many hearing officers are not familiar with OMAP regulations and do not function effectively. (Advocate) |
| SOURCE: Interviews with state officials, representatives of Medicaid MCOs, and consumer and legal advocates. | |
6. Changes Recommended by Stakeholders
In addition to asking stakeholders about the strengths and weaknesses of the fair hearing process, we asked them what changes they would make to the process if they were given the chance. They recommended the following changes:
- State Officials Recommend:
- There should be greater consistency in the decisions of the hearing officers.
- More disputes should be resolved before they get to the hearing stage.
- The hearings unit should include staff with investigational skills.
-
There should be a claims threshold (dollar amount of claim) over which a hearing request should be required to pass.
- Consumer and Legal Advocates Recommend:
- Hearing officers should be more independent; OMAP should not have the ability to reject the hearing officers’ decisions.
-
All enrollees going to a hearing should be given legal representation.
- MCOs Recommend:
-
Hearings should not be allowed for services that are specifically excluded from Medicaid coverage.
-
D. OMBUDSMAN PROGRAM
1. Program Background
Oregon has two ombudsman programs within DHS. The first is located in the DHS director’s office and has advocacy and investigative powers for the entire department. When the DHS ombudsman program receives a call from an OHP enrollee, it refers the caller to the second ombudsman program, which is located in OMAP.75
The OMAP ombudsman program was created in 1994 (at the start of OHP) to advocate for OHP enrollees and investigate complaints. The same authorizing legislation that expanded OHP to include the elderly and SSI recipients also required that these special needs populations have someone to whom they could bring their complaints. In October 1998, the OMAP ombudsman program was renamed the Consumer Advocate Services Unit (CASU). The ombudsman staff feel that the name change from “ombudsman” to “client advocate” signified a shift in the approach of the unit from retroactive investigation to prospective advocacy. Because CASU is the primary ombudsman program for Medicaid managed care enrollees, the rest of this section refers to CASU as the “ombudsman program.”
When the ombudsman program was created, there was some discussion of making the program external to OMAP. However, OMAP decided to keep the program in house because it would give the ombudsman better access to policymakers and administrators. Originally, the advocates had wanted an external ombudsman, but now they are satisfied with they way the program is working. OMAP also made a conscious decision to have one ombudsman program for both medical and mental health services. They believe this approach is consistent with their mission of serving the “whole” person.
The ombudsman program has six staff members: two ombudsmen, three people answering the telephones, and one clerical person. These six staff members handle more than 3,000 calls per month. The program receives funding from three agencies in DHS: OMAP, Adult and Family Services, and Senior and Disabled Services (SDS). The funding from SDS is based on the number of enrollees in managed care.
2. Ombudsmans Involvement in Plan-Level Complaints and Appeals
The ombudsman has a small role in plan-level complaints and appeals. When the ombudsman’s office receives calls from enrollees, they often direct callers back to their health plans to try to get the plan to address the enrollee’s problem. However, the ombudsman will actively call plans and physicians to try to resolve issues if it appears that the plan is not addressing the enrollee’s complaint adequately. The ombudsman staff said they do not often recommend that enrollees request an in-plan appeal because they feel that few of these appeals are resolved in favor of the enrollee. The ombudsman’s office does not help the enrollee complete an in-plan appeal request, nor do they hold conference calls with the plan and the enrollee to try to resolve the enrollee’s problems.
3. Ombudsmans Involvement in State-Level Appeals
The ombudsman’s role in the fair hearing process is limited. The ombudsman staff explained that, to avoid the appearance of a conflict of interest, they are not involved in state-level appeals. They feel that they would not be seen as a credible advocates for enrollees in disputes involving their own agency.
The ombudsman will explain the hearing process to enrollees and help them complete the Administrative Hearing Request form. Once the enrollee submits a hearing request, the ombudsman’s involvement stops. The ombudsman does not represent enrollees at hearings or pre-hearing conferences. When an enrollee requests a hearing, the OMAP hearing representative requests data from the ombudsman’s information system regarding any contacts the ombudsman may have had with the enrollee. The information in the contact log can be used as evidence at the hearing. For example, the log may include enrollees’ description of their complaint or explain the circumstances surrounding their request.
4. Outreach and Enrollee Awareness
OMAP markets its ombudsman program by including the ombudsman’s telephone number in the welcome packet sent at the time of enrollment and on the Medicaid cards that OMAP mails to enrollees every month. OMAP does not conduct any other outreach or marketing activities for the ombudsman program. For example, the ombudsman’s telephone number is not included on the Notice of Action sent out by the health plans. Despite this limited marketing and outreach, the ombudsman believes that enrollee awareness of the program is high, as demonstrated by the high volume of calls their office receives each month.
5. Serving Enrollees with Disabling or Chronic Conditions
The ombudsman program does not offer any special services to enrollees with chronic or disabling conditions. While the ombudsman program was created to serve as a resource for seniors and disabled people, the ombudsman staff said they have found over time that seniors and disabled people are very knowledgeable about the health care system and capable of doing their own advocacy. However, the ombudsman staff felt that the low-income enrollees need the most help navigating the system, and this population actually needs the ombudsman program’s services more.
Although the ombudsman does not provide specific services for enrollees with chronic or disabling conditions, OMAP requires that health plans provide an Exceptional Needs Care Coordinator (ENCC) for all enrolled SSI recipients. The ombudsman interacts frequently with the health plans’ ENCCs on behalf of these enrollees. For example, if an enrollee receiving ENCC services requests a fair hearing, the ombudsman may hold a roundtable discussion with the enrollee, ENCC, caseworker, and physician (not the OMAP hearing representative) to identify issues needing attention. The ombudsman indicated that these discussions are often held for enrollees with challenging behavioral health problems.
6. Strengths and Weaknesses of the Ombudsman Program
We asked stakeholders to identify strengths and weaknesses of the ombudsman program. Table OR-3 summarizes their comments, with attributions to the type of stakeholder (State Official, Advocate, MCO) giving the comment. Although the majority of stakeholders had positive comments about the ombudsman program, almost all felt that the office was too small and could not adequately handle the volume of calls it received.
| TABLE OR-3. Strengths and Weaknesses of the OMAP Ombudsman Program | |
|---|---|
| Strengths | Weaknesses |
| The ombudsman staff are knowledgeable, good at resolving communication and billing issues, and good at diffusing tense situations. (Advocate, State Official) The ombudsman staff are enrollee-oriented, but they hear both sides of the issue. (Advocate) The ombudsman program is effective in getting issues resolved. (Advocate, MCO) The ombudsman staff have a good relationship with both the MCOs and the rest of OMAP. (State Official) The ombudsman staff are effective in changing policy; they have been successful in making changes to the prioritized list. (State Official) The ombudsman program meets the needs of a culturally diverse community. (State Official) | The ombudsman program does not have enough funding. (Advocate, State Official) The ombudsman program does not have enough staff. (Advocate, State Official) Enrollees have a difficult time getting through on the telephone because the program is so understaffed. (Advocate) The ombudsman staff do not seem to have any power to get information out of the Mental Health Services Division (but neither does anyone else). (Advocate) The role of the ombudsman program is not well defined. It is not clear that they help anyone. (MCO) |
| SOURCE: Interviews with state officials, representatives of Medicaid MCOs, and consumer and legal advocates. | |
7. Changes Recommended by Stakeholders
In addition to asking stakeholders about the strengths and weaknesses of the ombudsman program, we asked them what changes they would make to the program if they were given the chance. They recommended the following changes:
- State Officials Recommend:
- Staff with a clinical or case management background should be added.
-
A better relationship with Mental Health Services Division should be developed.
- Consumer and Legal Advocates Recommend:
- The staff size should be quadrupled.
-
The ombudsman should have more clout with the MCOs.
- MCOs Recommend:
-
The ombudsman should refer enrollees to community resources that will provide services not covered by OHP either free or at a reduced fee.
-
E. SUMMARY
Oregon’s expedited fair hearing process is seldom used, making it difficult to gauge its effectiveness. Except for agency staff in the Hearings Unit, stakeholders had so little experience with the expedited hearing process that they could provide only the most basic information about it. Although about 50 requests for expedited hearings are received per year, an average of only one request is granted. The reason for the low number of expedited hearings is not clear. The conditions under which an expedited hearing is available are vague, and all requests for expedited hearings are decided by one person—the OMAP medical director. Enrollees may have a poor understanding of their chances for obtaining an expedited hearing and may be requesting expedited hearings for issues that are not critical or for services not covered on the prioritized list. Alternatively, enrollees could be making appropriate requests, but the criteria may be applied narrowly. Because requests for expedited hearings are not logged or tracked, no data are available to resolve this question.
Given the volume of expedited hearing requests and actual hearings held, the process OMAP uses to approve or deny requests and schedule and hold expedited hearings appears adequate. However, it is not clear how well this process would transfer to a state with a larger enrollee population and therefore a larger number of expedited hearing requests and expedited hearings. Oregon’s use of the prioritized list of covered services affects the types of appeals that go to both standard and expedited hearings; therefore, Oregon’s expedited hearing process may not be adaptable to states with different criteria for granting expedited review or larger Medicaid managed care populations.
In contrast to the expedited hearing process, Oregon’s ombudsman program is both frequently used and well regarded as effective in resolving enrollee problems. The ombudsman program has defined its role as the enrollees’ advocate and established communication links within the state and with MCOs and providers.
NOTES
-
See section 1932(a)(4) of the Social Security Act and, analogously, 42 U.S.C. 1396(u)(2).
-
The percentage of Medicaid beneficiaries enrolled in managed care plans increased from 40 percent in 1996 to 56 percent in 2000 (Centers for Medicare & Medicaid Services (CMS) 2000).
-
This directive was issued by President Clinton during a Consumer Bill of Rights and Responsibilities Ceremony on November 20, 1997 (White House 1997).
-
Information about beneficiaries’ retroactive financial responsibilities was provided by former Indiana Medicaid Director James Verdier (personal communication by telephone, December 2000).
-
As of 1998, Medicaid managed care enrollment was mandatory in 37 states (Kaye and Pernice 1999). Moreover, a growing number of states (23 as of 1998) mandate the managed care enrollment not only of welfare and poverty-related Medicaid beneficiaries, but of at least some disabled and chronically ill beneficiaries as well (Kaye and Pernice 1999).
-
Research has shown that, at least in the mid-1990s, Medicaid beneficiaries were poorly informed about grievance procedures. In one study, few beneficiaries said they would know how to “register their dissatisfaction” with their MCO or the state Medicaid agency (Molnar et al. 1996).
-
Section 1902(a)(3) of the SSA is analogous to 42 U.S.C. 1396(a).
-
Section 1932(a)(4) of the SSA is analogous to 42 U.S.C. 1396(u)(2).
-
The term “external review” is sometimes applied to the resolution of many types of managed care problems, including those related to MCOs’ marketing behavior and states’ eligibility determinations. In this report, however, we use the term to describe a formal process for resolving disputes over medical and/or contractual issues.
-
The original proposal for the study included an additional question about how state initiatives have changed since they were first implemented. As our research proceeded, however, it became clear that, because most of the initiatives were implemented quite recently, they had not undergone significant changes.
-
Foster et al. (2001) contains a complete description of the literature review methodology.
-
The interviews were with Jane Perkins of the National Health Law Program, Inc.; Brenda Jackson of the CMS Region 7 Office; Joanne Rawlings-Sekunda of the National Academy for State Health Policy; and Sara Rosenbaum of the Center for Health Policy Research at George Washington University Medical Center.
-
In the end, we did choose one state--Minnesota--for further study even though its Medicaid managed care program excludes beneficiaries who are blind or disabled.
-
Some key interviewees were not available at the time of our site visits. We conducted telephone interviews with these people either immediately before or immediately after the site visit, using the appropriate interview protocol.
-
Ombudsman programs are different from so-called member advocates. Unlike ombudsmen, member advocates are employed by health plans and thus lack the independence of ombudsmen.
-
Ombudsman programs also perform general functions, including educating beneficiaries about managed care and choosing a health plan, and aggregating information to report on the status of Medicaid managed care in their state (Perkins et al. 1998b; Lee and Scott 1996).
-
Although some states, such as Delaware, have developed ombudsman programs as part of their applications for Section 1115 waivers, such programs are not a condition of receiving waiver approval from the Health Care Financing Administration (HCFA).
-
This discussion applies only to external review programs for commercial and Medicaid managed care beneficiaries. Medicare, a federal program, administers its own external review programs for Medicare managed care beneficiaries; it does not vary by state.
-
Now CMS.
-
The HCFA survey indicates that these two states did not respond to the question.
-
We did not find any description in the literature of states that make an expedited external review process available to their Medicaid managed care beneficiaries. However, during our inquiries, we found that New York State makes such a process available.
-
The Managed Care Ombudsman also serves beneficiaries of two other state-subsidized managed care programs for low-income adults and families.
-
Callers include Medicaid managed care beneficiaries as well as beneficiaries in two state-subsidized managed care programs for low-income residents.
-
Florida Statutes 408-7056.
-
Within a year of its launch, New York’s program became the busiest in the nation in terms of the number of requests it received from prospective appellants and the number of decisions it rendered (American Association of Health Plans 2001). At least part of the program’s popularity seems to be due to the support and publicity it has received from high-level officials, including Governor George Pataki.
-
The fees paid by MCOs are set by external review agents and approved by state for two-year periods. In the first year of the program, MCOs paid about $674 per review.
-
Researchers estimate that up to 40 percent of the American adult population have low levels of functional literacy (Kirsch 1993).
-
The number of New York Medicaid beneficiaries enrolled in MCOs was 659,205 as of June 30, 2000 (CMS 2000).
-
In Florida, 496,609 Medicaid beneficiaries and 3,679,935 commercially insured people were enrolled in fiscal year 2000 (Florida Department of Insurance 2001).
-
The Fair Hearings Office in DCFS does not yet distinguish managed care cases from their fee-for-service cases in their database. Therefore, this figure is an estimate.
-
Health plans serving Medicaid populations are not under contractual obligation to the state to provide an expedited in-plan review process and have not chosen to offer expedited review on their own, perhaps because of added cost or administrative complexity.
-
In Oregon, the right to an expedited hearing is guaranteed by law (OAR 410-141-0265).
-
New York has granted expedited in-plan appeals and fair hearings since the start of mandatory Medicaid managed care enrollment in 1999. Their external review program (and its expedited component) also began in 1999. Requirements for expedited review were part of the original authorizing legislation for the external review program.
-
The addition of the check box is a relatively recent change. In 1999, the state added the check box at the request of advocates who felt that beneficiaries were not sufficiently aware of the possibility of an expedited hearing.
-
In Oregon, a pool of 12 hearing officers preside over administrative hearings dealing with a range issues from Medicaid fair hearings to land use and water rights. The hearing officers have no particular background in either Medicaid regulations or medicine. During the hearing, health plans use their own experts--either nurses or physicians--to provide the clinical background and rationale for their decision to deny services. Beneficiaries can, but very rarely do, have their own physicians present during the hearing.
-
Fair hearing officials stated that they have never been unable to provide expedited review because of volume constraints.
-
In contrast to Oregon, requests for priority scheduling of a fair hearing are seldom, if ever, denied in New York.
-
Physicians said expedited fair hearings generally are not needed by fee-for-service Medicaid beneficiaries because their care is not subject to utilization review procedures as in managed care. In fee-for-service, the Medicaid agency may refuse payment for services already rendered. These disputes would not qualify for expedited review because there would be no danger to the life or health of the beneficiary.
-
Note that in New York state, the scope of cases eligible for external review is more narrow than for fair hearings in that denials based on contractual issues are not eligible (for example, a beneficiary denied treatment because they wanted an out-of-state provider).
-
Following MPR’s site visit in June 2001, the OMAP medical director’s office began to track the number of requests for expedited fair hearings and whether or not the request was granted.
-
As we have previously noted, however, states have rarely kept records that separate Medicaid managed care beneficiaries from non-Medicaid, or non-managed care, beneficiaries. Thus this figure is based on estimates made by respondents.
-
We conducted the site visit in Denver, Colorado, from March 27 through March 29, 2001. The visit consisted of in-person interviews with state officials, ombudsmen, representatives of managed care organizations, and consumer and legal advocates. For scheduling purposes, we also conducted three telephone interviews from our offices in Princeton, New Jersey.
-
The appeals processes for commercial and Medicaid managed care enrollees are much the same. Two important differences are that: (1) MCOs are given more time (20 days) to conduct commercial reviews than Medicaid reviews (ten days); and (2) MCOs set their own policies about accepting oral or written requests for commercial appeals but must accept either type of request from Medicaid enrollees. A third difference had existed: Medicaid enrollees--unlike their commercial counterparts--did not have access to independent external reviews. As of June 2000, however, external review has also been available to Medicaid enrollees.
-
The plan’s commercial enrollees filed complaints at similar levels: of 165,000 commercial enrollees, 380 (0.2 percent) requested first-level appeals.
-
Judicial reviews are held in State District Courts.
-
Senate Bill 5 required the state to contract with a Medicaid managed care enrollment broker. During the ensuing budget process, the state decided to award two contracts--one to an enrollment broker and another to a managed care ombudsman. Thus, the managed care ombudsman program is not mandated in state legislation, per se, but it is designated to receive state funding through a fiscal note.
-
The contract was meant to be awarded through a competitive process; however, only PAC bid on the contract. That contract expires this year and will be rebid.
-
CCSC sought to minimize its involvement in the ombudsman program soon after it began operating. The program now operates under its own 501(c)(3) status.
-
Similarly, the program’s first annual report includes the observation that the “physical presence of [program] staff has a direct correlation to the utilization of services.”
-
We conducted the site visit in Tallahassee, Florida, from April 25 through April 27, 2001. The visit consisted of in-person interviews with state officials, representatives of MCOs, consumers, and legal advocates. We also conducted telephone interviews of Medicaid managed care plans in Tampa and Gainesville during the site visit, and did a telephone interview with a consumer who had used the external review process in the weeks after the visit.
-
Exceptions include pregnant women, institutionalized people, Supplemental Security Income (SSI) beneficiaries who belong to a Medicare HMO, children with special needs, and people in residential placements for substance abuse treatment.
-
Plans are permitted to extend the time period to 90 days if they need to obtain medical records or other information from sources outside the state, and they must notify the beneficiary if this is the case. The amount of time spent on resolution is important because all reimbursement stops when there is a denial by the plan. Reimbursement can only resume when either the plan or the state resolves the grievance in the beneficiary’s favor.
-
In Florida, HMOs distinguish between “complaints,” which are issues stated by telephone, and “grievances,” which are issues filed in writing.
-
At this point, beneficiaries can file for either procedure. The sequences are complicated, however. The beneficiary can file for external review, then change his or her mind and subsequently file for a fair hearing. The beneficiary cannot do the reverse, however. The external review process cannot proceed after a request for a fair hearing is filed.
-
Consulting specialists are paid $100 per hour. This averages about $300 per case. The Panel pays the cost of these reviews.
-
Videoconferencing costs $50 per hour. Court reporters, also present, receive $25 per case.
-
These data are for all cases (commercial managed care and Medicaid managed care grievances). The Panel did not begin to count Medicaid cases separately until August 2000.
-
State officials also believe that the declining numbers may be due to their success in working through their extensive backlog.
-
This applies to both Medicaid beneficiaries and commercial enrollees.
-
We conducted the site visit in Minneapolis/St. Paul, Minnesota, from May 21 through May 23, 2001. The visit consisted of in-person interviews with state officials, the ombudsman, a county advocate, representatives of MCOs, and consumer and legal advocates. For scheduling purposes, we also conducted one telephone interview from our office in Princeton, New Jersey.
-
While enrollees are supposed to complete hearings request forms, the appeals unit accepts any form of written objection as sufficient to invoke the hearing process.
-
Of the 12 hearings referees, nine are lawyers and three are social workers. All new referees must be lawyers.
-
The chief appeals referee rarely reverses recommendations. He may do so, however, if he provides justification.
-
As several stakeholders observed, most enrollees feel more comfortable approaching county advocates for assistance because the enrollees are familiar with county offices. Other enrollees contact the ombudsman for the same reason--they feel anonymous talking to a state-level employee and are more comfortable talking to the ombudsman.
-
However, the ombudsman receives calls from PMAP enrollees and MinnesotaCare enrollees (MinnesotaCare is a state-subsidized managed care program for low-income residents), while county advocates serve PMAP enrollees only. While our comparison of daily call volume is imperfect, it suggests that the volume of calls from PMAP enrollees to county advocates is higher than the volume of calls to the ombudsman.
-
We conducted site visits in Albany, New York, on June 26 and 27, 2001, and in New York City on July 17, 2001. The visits consisted of in-person interviews with state officials, representatives of MCOs, consumer and legal advocates, and external review agents. We conducted telephone interviews with individuals in Lake Success, Rochester, and Woodstock.
-
In reporting to the state, MCOs classify all enrollee disputes as complaints or appeals. For their own purposes, however, MCOs may use more complex classification systems. For example, the MCOs we interviewed used classifications such as concerns, inquiries, and grievances in addition to complaints and appeals.
-
Most Medicaid-related hearings pertain to enrollment, not to managed care. However, even they are a small proportion of hearings overall. Between August 1999 and May 2001, Medicaid enrollment issues yielded 2,336 hearing requests and 601 actual hearings.
-
In addition to the recommendations listed here, advocates made numerous recommendations regarding New York’s fair hearing process.
-
We conducted a site visit to Salem, Oregon, and Portland, Oregon from June 20 through June 22, 2001. The visit consisted of in-person interviews with state Medicaid officials, an ombudsman, representatives of MCOs, and consumer and legal advocates. To accommodate the schedules of some interviewees, we conducted two telephone interviews from our office in Princeton, New Jersey, in the week following the site visit.
-
MCOs may request an extension, in which case they are given 30 days to resolve the complaint.
-
The back of the Administrative Hearing Request form states, “If your benefits stay the same and the hearing is not in your favor, you must pay back the amount you were not entitled to.” The advocates we spoke with felt that this statement was a deterrent to enrollees’ requesting a continuation of benefits.
-
The reverse side of the form explains the circumstances under which an expedited hearing can be granted.
-
Although no enrollee has ever disputed a denial of a request for an expedited hearing, enrollees could appeal the medical director’s decision to the director of OMAP.
-
The DHS ombudsman and the OMAP ombudsman programs share a common computer information system that logs calls and tracks resolution of enrollee problems.
To obtain a printed copy of this report, send the full report title and your mailing information to:
U.S. Department of Health and Human Services
Office of Disability, Aging and Long-Term Care Policy
Room 424E, H.H. Humphrey Building
200 Independence Avenue, S.W.
Washington, D.C. 20201
FAX: 202-401-7733
Email: webmaster.DALTCP@hhs.gov
RETURN TO:
Office of Disability, Aging and Long-Term Care Policy (DALTCP) Home [http://aspe.hhs.gov/_/office_specific/daltcp.cfm]
Assistant Secretary for Planning and Evaluation (ASPE) Home [http://aspe.hhs.gov]
U.S. Department of Health and Human Services (HHS) Home [http://www.hhs.gov]
Last Updated: 02/22/2013