
APPROACHES TO EARLY JAIL DIVERSION: COLLABORATIONS AND INNOVATIONS
Sue Pfefferle, Sarah Steverman, Elle Gault, Samantha Karon, and Holly Swan
Abt Associates
July 2019
Printer Friendly Version in PDF Format (91 PDF pages)
ABSTRACT
People with behavioral health conditions such as serious mental illness (SMI) and substance use disorders (SUDs), including opioid use disorder (OUD), are 3-6 times more likely than the general population to be represented in the criminal justice system. Even though the majority of incarcerated people with behavioral health diagnoses have not committed any violent crime, they may end up in jail as a consequence of both poverty and their behavioral health disorders. As a result without coordinated intervention, some people with behavioral health diagnoses risk cycling in and out of the mental health, substance use, and criminal justice systems. This cycling between systems, in and out of services, is both unconducive to recovery and costly to society.
Most research to date has been on interventions for people following arrest. These interventions include post-arrest diversion, drug and mental health courts, prison or jail treatment services, re-entry programs, and community supervision. With limited public resources and increasing numbers of people with behavioral health disorders entering criminal justice systems, jurisdictions have looked to develop alternatives to arrest and incarceration. The predominant conceptual framework for jail diversion and the interactions between community service providers and the criminal justice system is the Sequential Intercept Model (SIM). The SIM outlines the points, or intercepts, along the criminal justice continuum where there are potential interventions to divert people away from the criminal justice system.
This report was prepared under contract #HHSP233201600010I between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and Abt Associates. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/office-disability-aging-and-long-term-care-policy-daltcp or contact the ASPE Project Officers, Jhamirah Howard and Laurel Fuller, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201; Jhamirah.Howard@hhs.gov.
DISCLAIMER: The opinions and views expressed in this report are those of the authors. They do not reflect the views of the Department of Health and Human Services, the contractor or any other funding organization. This report was completed and submitted on November 9, 2018.
TABLE OF CONTENTS
1. INTRODUCTION
2. METHODS
2.1. Methods
2.2. Case Study Methods
3. FINDINGS
3.1. Environmental Scan Findings
3.2. Case Study Findings
4. DISCUSSION
4.1. Community Resources
4.2. Law Enforcement/Behavioral Health Collaboration
4.3. State and Local Policies and Legislation Regarding Jail Diversion
4.4. Assessment of Outcomes
4.5. Unspoken Assumptions and Knowledge Transfer
5. CONCLUSION
APPENDICES
- APPENDIX A: References
- APPENDIX B: Example Programs from the Environmental Scan
- APPENDIX C: Literature Search Terms
- APPENDIX D: Agency Web Search Terms
- APPENDIX E: Case Study Protocol
- APPENDIX F: Interview Guides
- APPENDIX G: Secondary Data Collection Form
- APPENDIX H: Case Study Summaries
LIST OF EXHIBITS
- EXHIBIT 1: SIM for Pre-Booking Jail Diversion
- EXHIBIT 2: Overview of Programs Examined through Case Studies
- EXHIBIT 3: Research Questions
- EXHIBIT 4: SMEs
- EXHIBIT 5: Jail Diversion Programs along the SIM
ACRONYMS
The following acronyms are mentioned in this report and/or appendices.
| AAOI | Arlington Massachusetts Opiate Outreach Initiative |
|---|---|
| ACT | Assertive Community Treatment |
| ASPE | HHS Office of the Assistant Secretary for Planning and Evaluation |
| BJA | DoJ Bureau of Justice Assistance |
| CEF | Community Endowment Fund |
| CHE | Community Health Endowment |
| CIT | Crisis Intervention Team |
| CMHS | SAMHSA Center for Mental Health Services |
| COD | Co-Occurring Disorder |
| COR | Contracting Office Representative |
| DART | Drug Abuse Response Team |
| DoJ | U.S. Department of Justice |
| FACT | Forensic Assertive Community Treatment |
| GPD | Gloucester Police Department |
| GSL | Good Samaritan Law |
| HHS | U.S. Department of Health and Human Services |
| HIPAA | Health Insurance Portability and Protection Act |
| HIV | Human Immunodeficiency Virus |
| HMIS | Homeless Management Information System |
| HOT | Homeless Outreach Team |
| JRI | BJA Justice Reinvestment Initiative |
| LA DOOR | Los Angeles Diversion Outreach and Opportunities for Recovery |
| LEAD | Law Enforcement Assisted Diversion |
| LPD | Lincoln Police Department |
| MAT | Medication-Assisted Treatment |
| MHA-NE | Mental Health America Nebraska |
| MHFA | Mental Health First Aid |
| MOA | Memorandum of Agreement |
| MOU | Memorandum of Understanding |
| NARCAN | Naloxone Hydrochloride Injection |
| OCHN | Oakland Community Health Network |
| OUD | Opioid Use Disorder |
| PAARI | Police Assisted Addiction and Recovery Initiative |
| PD | Police Department |
| PERT | Psychiatric Emergency Response Team |
| RCC | Resource and Crisis Center |
| REAL | Respond Empower Advocate Listen |
| SAMHSA | HHS Substance Abuse and Mental Health Services Administration |
| SIM | Sequential Intercept Model |
| SMART | Systemwide Mental Assessment Response Teams |
| SME | Subject Matter Expert |
| SMI | Serious Mental Illness |
| STEER | Stop, Triage, Engage, Educate, and Rehabilitate |
| SUD | Substance Use Disorder |
| TASC | Targeted Adult Services Cooperation |
| WRAP | Wellness Recovery Action Plan |
EXECUTIVE SUMMARY
Study Overview
People with behavioral health conditions such as serious mental illness (SMI) and substance use disorders (SUDs), including opioid use disorder (OUD), are 3-6 times more likely than the general population to be represented in the criminal justice system (National Association of Counties, 2016). Even though the majority of incarcerated people with behavioral health diagnoses have not committed any violent crime, they may end up in jail as a consequence of both poverty and their behavioral health disorders. As a result without coordinated intervention, some people with behavioral health diagnoses risk cycling in and out of the mental health, substance use, and criminal justice systems. This cycling between systems, in and out of services, is both unconducive to recovery and costly to society.
Most research to date has been on interventions for people following arrest. These interventions include post-arrest diversion, drug and mental health courts, prison or jail treatment services, re-entry programs, and community supervision. With limited public resources and increasing numbers of people with behavioral health disorders entering criminal justice systems, jurisdictions have looked to develop alternatives to arrest and incarceration. The predominant conceptual framework for jail diversion and the interactions between community service providers and the criminal justice system is the Sequential Intercept Model (SIM). The SIM outlines the points, or intercepts, along the criminal justice continuum where there are potential interventions to divert people away from the criminal justice system (Munetz & Griffin, 2006).
| Overarching Research Questions
|
The purpose of this study was fourfold:
-
Better understand state and local pre-booking jail diversion interventions for people with SMI, SUDs, and co-occurring disorders (CODs).
-
Investigate and contribute to the knowledge base on Intercept 0 of the SIM.
-
Assess how these interventions may inform broader federal policy, including new authorities in the 21st Century Cures Act, Medicaid, and the Administration's efforts to address the opioid epidemic.
-
Identify potential Intercept 0 and 1 programs for evaluation.
The current study examined pre-booking jail diversion services for people with SMI and SUD at Intercept 0; community behavioral health programs and at Intercept 1; law enforcement and emergency programs. (See Exhibit 1).
| EXHIBIT 1. SIM for Pre-Booking Jail Diversion |
|---|
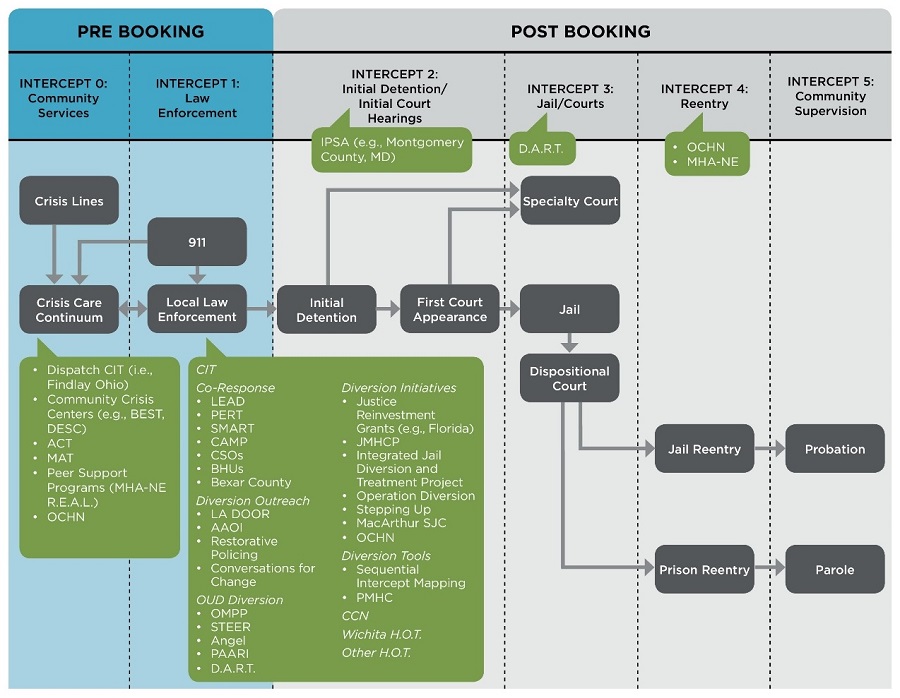 |
| Adapted from Munetz, M. R., & Griffin, P. A. (2006). Use of the Sequential Intercept Model as an approach to decriminalization of people with serious mental illness. Psychiatric Services, 57(4), 544-549. |
| ALT TEXT for EXHIBIT 1: Exhibit 1 demonstrates the Sequential Intercept Model (SIM) for pre-booking and post-booking jail diversion interventions. On the left side of the figure, two intercepts comprise pre-booking interventions; Intercept 0: Community Services and Intercept 1: Law Enforcement. On the right side of the figure, four intercepts comprise post-booking interventions: Intercept 2: Initial Detention/Initial Court Hearings; Intercept 3: Jails/Courts; Intercept 4: Reentry; and Intercept 5: Community Supervision.
|
Methodology
The study team first conducted an environmental scan to identify innovative pre-booking jail diversion programs and models from both the peer-reviewed and grey literature along with any other information identified from government and justice-related organization websites. In addition, the scan included telephone interviews with six subject matter experts (SMEs). From this research, the study team developed five case studies based on two-day site visits and extant data for five jail diversion programs.
These programs, identified through the environmental scan and additional web searches, were chosen to represent Intercept 0 and 1 programs that focus on SMI and/or SUDs including OUD. The programs studied were Mental Health America Nebraska (MHA-NE) Respond Empower Advocate Listen (REAL); the ANGEL Program, Gloucester, Massachusetts; the Oakland Community Health Network (OCHN), Oakland County, Michigan; Lucas County (Ohio) Drug Abuse Response Team (DART); and Wichita (Kansas) Homeless Outreach Team (HOT).
Findings
Most initiatives identified in the environmental scan are in the early stages and/or are just beginning their evaluations. Although a number of programs show promise, there were few rigorous evaluations of pre-booking jail diversion programs, and most evaluations examined program processes or implementation through descriptive studies.
One pre-booking jail diversion program that has been evaluated using a quasi-experimental design is Law Enforcement Assisted Diversion (LEAD). Participants in the LEAD program were more than twice as likely to be sheltered, more than 46% more likely to be employed, and 33% more likely to have an income through earned wages or benefits compared to people in the comparison group of individuals from non-LEAD neighborhoods (Collins, Lonczak, and Clifasefi, 2015a). LEAD participants were also 60% less likely to be arrested over the four years of the evaluation.
Exhibit 2 provides a brief overview of the five jail diversion programs visited to develop case studies.
The study team identified common critical factors impacting the jail diversion program models. All of the programs visited employed a community policing approach. Community policing involves collaboration with community members and organizations to develop practical systematic approaches to address the underlying conditions that impact public safety. As an example, all programs visited built on or developed community collaborations or advisory boards. Community policing is a philosophy of policing based on the idea that police can work closely with communities to address issues that can impact community safety (Schneider, Kimerer, Seaman, and Sweeny, 2003).
The majority of the case study programs were developed through cross-system collaboration and co-response type approaches. Such cross-system collaboration was the foundation of Crisis Intervention Teams. Novel collaborative approaches have emerged in response to the opioid crisis, such as community-led and police-led diversion outreach. Although jail diversion program services included interventions at Intercepts 0 and 1, they also included services across other SIM intercepts.
| EXHIBIT 2. Overview of Programs Examined through Case Studies | |
|---|---|
| Program | Overview |
| ANGEL Program | The ANGEL Program is a Gloucester (Massachusetts) Police Department (GPD) initiative and aims to help people with OUD access treatment. Anyone is able to come to GPD with drugs or drug equipment requesting help, and they are not charged with possession. The Watch Commander on duty directly refers them to detox or a treatment facility. The Care Advocate/Outreach Specialist, who is a person in recovery, assists the person in accessing follow-up care. |
| Drug Abuse Response Team (DART) | DART is the addiction resource unit of the Lucas County Sheriff's Office. DART officers respond to opioid overdoses, and offer assistance to the people by helping them enroll in substance use treatment, including detox. DART officers then follow people for 2 years, connecting them to treatment and advocating for them in the justice system. |
| Wichita PD Homeless Outreach Team (HOT) | HOT officers respond to 911 calls and direct referrals from the community to assist people experiencing homelessness to access behavioral health and housing resources. When a person faces charges for violating a public ordinance, HOT officers have the ability to address/remove charges retroactively if the person engages in services, or to request the person participate in mental health or drug court instead of entering the judicial system. |
| Oakland Community Health Network (OCHN) | OCHN is the county Medicaid behavioral health authority, which is required to work with law enforcement to divert people with mental health or substance use issues to the county crisis center. Officers are able to drop people at the crisis center 24/7, at which point they have access to all county behavioral health services. OCHN also offers outreach and training to the 43 law enforcement agencies in the county. |
| Mental Health America Nebraska (MHA-NE) Respond Empower Advocate Listen (REAL) | REAL is a peer-run pre-booking jail diversion program that provides free non-clinical services to people in mental health or substance use crisis. REAL collaborates with law enforcement to support people in the long term, and to provide Wellness Recovery Action Plan training to the Lincoln PD. Mental Health Association of Nebraska also operates 2 crisis respite houses, a housing program, an employment program, a residential program, and a 24/7 warm line. |
The case study findings also highlighted the importance of personal experience in understanding the needs of people with mental health and SUDs. Law enforcement officers often cited a personal connection to a person with SMI or OUD, or a personal/family connection of a leader in their agency, as the reason they began to explore options to increase pre-arrest jail diversion.
While MHA-NE REAL, Wichita HOT, and DART are considered distinct jail diversion programs, the ANGEL Program and OCHN's jail diversion activities are considered processes rather than distinct programs. (In the case of OCHN, the organization funds one staff person to serve as the jail diversion coordinator, but relies on law enforcement agency participation in a jail diversion process that OCHN has integrated into their crisis, intake, and treatment systems.) It has taken several years for these processes to become as effective as they are, but it can be argued that this approach has a lower threshold than establishing an entirely new program. That is, it is arguably most efficient to:
-
Establish, within existing law enforcement and behavioral health systems, processes that provide incentives for law enforcement officers to divert people in crisis to treatment.
-
Provide the infrastructure for behavioral health providers to work with law enforcement.
A consistent theme identified in the literature, SME interviews, and case studies was the need for novel approaches to strengthen community resources. The availability of accessible behavioral health services equipped to meet the needs of the people with mental health and substance use issues, and law enforcement officers who encounter them in the community are essential components of diversion practices. A robust array of community resources (Intercept 0) need to exist in order for law enforcement to divert people from the criminal justice system, and optimally to prevent future criminal justice involvement.
Future Considerations
The study found a variety of innovative and promising pre-booking jail diversion programs. Most programs were homegrown and developed by innovation entrepreneurs in response to local circumstances, such as a rash of opioid overdose deaths. As such, programs developed very context-specific solutions, often in collaboration with community stakeholders. The opioid epidemic requires an evolving response by both SUD treatment providers and police. The study found that a number of promising police-led diversion initiatives are springing up in response to the OUD crisis.
A key to pre-booking jail diversion, whether in response to opioid overdoses or to mental health issues, was shifting police culture toward community policing. Officers found their jobs were easier if they were not policing overdoses or behavior that could better be addressed by health professionals. However, behavioral health systems must have robust service arrays for law enforcement officers to divert people to. Neither law enforcement officers nor behavioral health providers felt that they could divert people from the criminal justice system alone without available services to which they can refer.
The study found that community collaborations coordination mechanisms are necessary to identify high-risk people--such as those who experience chronic homelessness--early, and divert them to appropriate services. In addition, the study found that community task forces and community meetings that foster collaboration among stakeholders create opportunities to provide preemptive and holistic services for high-risk people.
While a number of evaluations of pre-booking jail diversion programs have been undertaken, few pre-booking jail diversion programs have been rigorously studied. Such rigorous evaluation would assist law enforcement officials to choose the most effective approach for populations in their jurisdictions.
In conclusion, this study provides evidence that pre-booking jail diversion programs can intercept people with behavioral health conditions before they become enmeshed in the criminal justice system. Such programs are being implemented and replicated throughout the United States. Future studies can address both program effectiveness and local implementation, adaptations, and opportunities for program sustainability.
1. INTRODUCTION
Adults with serious mental illness (SMI), substance use disorders (SUDs), and co-occurring disorders (CODs) are greatly overrepresented in the criminal justice system when compared with the general population (Steadman, Osher, Robbins, Case, and Samuels, 2009; Council of State Governments Justice Center, 2017). Many of these individuals come into contact with the criminal justice system due to symptoms of mental illness or an SUD, and have not committed any violent crime (Knopf, 2013). Without appropriate intervention these people can cycle in and out of the mental health, substance use, and criminal justice systems, without receiving adequate treatment if any treatment at all (CMHS National GAINS Center, 2007).
Jails spend 2-3 times more money on adults with mental illnesses that require intervention compared to people without those needs. These places are neither cost-effective nor a humane solution for non-violent offenders with behavioral health disorders (Swanson et al., 2013). The current opioid epidemic has exacerbated this situation through jail overcrowding, an increase in jail suicide rates, and the need for SUD treatment in jails (Brown, Gassman, Hetzel, and Berger, 2013; Moser and Hensel, 2017; National Institute on Drug Abuse, 2017).
As the numbers of people entering courts and correctional institutions have swelled and public resources have dwindled, many jurisdictions are exploring diversion alternatives. One useful framework for conceptualizing jail diversion and the relationship between community service providers and the criminal justice system is the Sequential Intercept Model (SIM). The SIM outlines a series of points, or intercepts, along the criminal justice continuum where intervention could occur to divert people to community resources, and away from the criminal justice system (Munetz and Griffin, 2006).
This project was designed to assist the U.S. Department of Health and Human Services (HHS) Office of the Assistant Secretary for Planning and Evaluation (ASPE) to better understand pre-booking--Intercepts 0 and 1--jail diversion programs and approaches for people with SMI, SUD, and COD. Specifically, this project focuses on jail diversion for adults with SMI, SUD, and/or COD at Intercepts 0 and 1 on the SIM. The research questions addressed by the study are shown below (See Exhibit 3).
| EXHIBIT 3. Research Questions |
|---|
|
2. METHODS
2.1. Environmental Scan Methods
The environmental scan included a review of the scientific literature on pre-booking jail diversion programs, a scan of gray literature, and interviews with subject matter experts (SMEs) on jail diversion programs and approaches.
The study team searched EBSCO Host, PsycINFO, and PubMed to identify the peer-reviewed literature. The team identified 66 articles from over 956 returned results for pre-arrest jail diversion programs. They also searched websites of government agencies and non-governmental organizations, scanning for relevant unpublished literature, white papers, and research briefs.
Reports, publications, press releases, blog posts, and conference proceedings were identified through a search of official websites of the following agencies and organizations: HHS, Substance Abuse and Mental Health Services Administration (SAMHSA), U.S. Department of Veterans Affairs, ASPE, U.S. Department of Justice (DoJ) Office of Justice Programs, Bureau of Justice Assistance (BJA), National Association of Drug Court Professionals, Pretrial Justice Institute University Pretrial Library, National Adult Protective Services Association, National Institute of Justice Crime Solutions Clearinghouse, Justice Reinvestment Initiative (JRI), and National Association of Counties.
The team used a similar process to determine the relevance of both peer-reviewed and gray literature. They entered search terms into the website's search function and reviewed the results for relevance. In cases where a website did not contain a search function, a study team member reviewed publications posted to the website's resource page. The abstract or executive summary of a report or white paper, if one existed, was reviewed for titles determined to be relevant. A total of 172 documents were identified through this process. The articles, reports, and papers were further reviewed to determine applicability for inclusion in the environmental scan.
2.1.1. Discussion with Experts
Interviews with SMEs augmented information collected during the environmental scan. SMEs were identified in collaboration with the Contracting Office Representative (COR), based on their area of expertise (Exhibit 4). During the interviews, SMEs were asked to identify pre-booking jail diversion programs, with a particular emphasis on innovative or novel programs, and to identify any agencies that might be appropriate and receptive to participating in the case studies for this project. They were also asked to discuss key issues that needed to be considered related to implementation of jail diversion programs.
| EXHIBIT 4. SMEs | ||
|---|---|---|
| Name | Title | Affiliation |
| Dan Abreu, MS, CRC, LMHC | Senior Project Associate | Policy Research Associates |
| Ron Manderscheid, PhD | Executive Director | National Association of County Behavioral Health and Developmental Disability Directors |
| Mark Munetz, MD | Principal Investigator | Promoting Jail Diversion Alternatives for People with Mental Health Disorders, Criminal Justice Coordinating Center of Excellence, Northeast Ohio Medical University |
| Fred Osher, MD | Director of Health Systems and Services Policy | Council of State Governments Justice Center |
| Debra Pinals, MD | Medical Director, Behavioral Health and Forensic Programs | Michigan Department of Health and Human Services |
| Ruth Simera, MEd, LSW | Director | Criminal Justice Coordinating Center of Excellence, Northeast Ohio Medical University |
2.2. Case Study Methods
We identified ten sites for possible inclusion in the case study sample through the environmental scan, discussion with experts, and web searches. All of the proposed sites were Intercept 0 or 1 pre-booking diversion programs. In consultation with the COR, we identified five priority sites based on intercept, diversity of geographic location, population served, and availability of evaluation data. Two of those sites declined to participate, and the COR identified two additional sites from the original ten proposed sites. The final five sites chosen were Lucas County's Drug Abuse Response Team (DART) program in Ohio; Mental Health America Nebraska's (MHA-NE's) Respond Empower Advocate Listen (REAL) program in Lincoln, Nebraska; Wichita Homeless Outreach Team (HOT) in Kansas; Oakland Community Health Network (OCHN) in Michigan; and Gloucester's ANGEL Program in Massachusetts.
Each site visit was a two-day visit with two Abt staff members, who interviewed program staff, partners, and service users. Several site visitor teams were invited to go on ride-alongs with police officers, and visited different locations of programs.
3. FINDINGS
This section outlines the findings of both the environmental scan and case studies of pre-booking jail diversion programs.
3.1. Environmental Scan Findings
The programs reviewed in the environmental scan covered a wide range of Intercept 0 and 1 programs, from community behavioral health programs and police/behavioral health collaborations, to police-led diversion efforts. Overall, the study team found that there was a great deal of variation in pre-booking jail diversion programs in the United States (See Appendix B). Many programs are slight variations of each other, with local variation differences in implementation of any given model. Most police-initiated initiatives were local in nature, although some, such as a Crisis Intervention Team (CIT) and Law Enforcement Assisted Diversion (LEAD) have been replicated across the nation. Despite program variation and local differences in implementation, there are a number of common threads, including:
-
Mental health and SUD and opioid use disorder (OUD) training for law enforcement officers.
-
Collaboration between police, behavioral health providers, and other community providers such as housing and vocational service providers:
-
High-risk task forces and other cross-system coordination meetings; and
-
Data sharing to identify high-risk populations.
-
-
Team based approaches, such as police and behavioral health co-response teams and multi-disciplinary behavioral health teams including use of peer providers.
Behavioral health based pre-booking jail diversion programs and models (Intercept 0) have long addressed those individuals at the highest risk of repeated hospitalizations and arrest. Assertive Community Treatment (ACT), developed in the 1970s (Weisbrod, Test, and Stein, 1980), is focused on providing intensive community-based services to individuals at risk of re-hospitalization and/or homelessness. As the model has evolved, Forensic Assertive Community Treatment (FACT) programs have been developed to focus specifically on individuals at risk of involvement in the criminal justice systems (Lamberti, Weisman, and Faden, 2004).
CIT is the most widely implemented and researched pre-booking jail diversion model. Most co-responder models (Intercept 1) include CIT or enhanced CIT training for officers in addition to pairing officers with behavioral health clinicians for response to behavioral health emergencies. Education on mental health, SUDs, specifically OUD and use of naloxone to reduce overdoses was also central to many pre-booking jail diversion models. Behavioral health training curricula varied amongst the investigated programs.
Jurisdictions funded their programs through a variety of mechanisms and grants. Sustainability for some programs was not assured due to the time-limited nature of grants. With the exception of many Intercept 0 programs such as ACT and FACT teams, and LEAD, few of the models have been rigorously evaluated.
One special consideration for program models focused on OUD is the presence of state Good Samaritan Laws (GSLs) that can provide legal protection from lowlevel drug charges and/or parole violation for overdose victims and bystanders who call 911 as a critical tool in law enforcement's ability to help people with substance use issues. As of 2017, 41 states have passed GSLs, although the legal protections vary by state. GSLs generally provide immunity from arrest, charge, and/or prosecution for: possession of controlled substance and/or paraphernalia; protective or restraining order violation; pretrial, probation, or parole violations; and other controlled substance crimes (Latimore and Bergstein, 2017).
Naloxone is widely administered by first responders and in hospital settings, but there is controversy regarding whether laypersons should be permitted to administer Naloxone in opioid overdose cases. In 2001, New Mexico became the first state to enact a GSL in which a layperson is allowed to administer Naloxone to a person experiencing an opioid overdose. Since 2001, many other states have enacted GSLs, but only five states (Illinois, Massachusetts, New Mexico, New York, and Washington) allow prescribing of naloxone to third parties as part of those GSLs (Hewlett and Wermeling, 2013).
In conclusion, findings from the environmental scan showed a number of established and emerging pre-booking jail diversion programs, many of which were local adaptations of established programs. It also uncovered the need for rigorous evaluation of at least the components of Intercept 1 pre-booking jail diversion programs and peer-run pre-booking diversion programs.
3.2. Case Study Findings
Case studies were completed on five jail diversion programs. The site visits focused on a range of pre-booking jail diversion models that are Intercept 0 or Intercept 1 along the SIM. This section briefly describes the site visit program models and highlights some of the unique characteristics of the programs identified through the environmental scan and case studies. Case studies included the following programs: the ANGEL Program, Gloucester, Massachusetts; DART, Lucas County, Ohio; Wichita Police Department HOT, Wichita, Kansas; OCHN, Oakland County, Michigan; and MHA-NE REAL.
The ANGEL Program is a Gloucester Police Department (GPD) initiative and aims to help people with OUD access treatment. Anyone is able to come to GPD with drugs or drug equipment requesting help, and they are not charged with possession. The Watch Commander on duty directly refers them to detox or a treatment facility. The Care Advocate/Outreach Specialist, who is a person in recovery, assists the person in accessing follow-up care.
| ANGEL Program |
|---|
| Location: Gloucester, Massachusetts |
| Intercepts: 1 |
| Diversion Type: Law enforcement diversion |
| Target Population: People with OUD |
| Description: The GPD launched the ANGEL Program in June 2015 as an amnesty program for people with OUD. Any person who enters the GPD and requests help with opioid use is immediately screened into the ANGEL program. People who possess drugs or drug equipment when requesting help are not charged with possession. Originally, after individuals arrived at the GPD, the Watch Commander on duty would contact a volunteer "Angel" to sit with the person while a clinician identified a detox bed, which took several hours. After realizing that police were able to access beds faster than clinicians, the program discontinued using clinicians and "Angels." Currently, the Watch Commander on duty directly refers a person to a detox or treatment facility. If the individual signs a release of information form, the police supervisor or Care Advocate/Outreach Specialist, a person in recovery, from the PAARI assists the person in accessing longer-term treatment. |
| Partnerships: The Gloucester High Risk Task Force, which has participants from all the treatment, housing, and social service providers in the city, is one key facilitator of strong interagency and provider relationships. The police chief and mayor also attend the task force. Other partners include the Grace Center, day drop-in social service center, Action Housing; SUD treatment providers, and other social service providers. The PAARI Care Advocate/Outreach Specialist is the liaison with community providers, and sends out a daily list of available treatment beds. He also works to connect people to recovery services, and provides reintegration assistance once people have completed treatment. |
| Structure: All Sergeants and Lieutenants in the department can be the assigned as "Watch Commander" for the shift. When someone enters the GPD requesting help, the officer the person first has contact with immediately notifies the Watch Commander. The Watch Commander then finds a local detox facility to connect the person, provides transportation, and assists that person into services. At any point a person may choose to decline those services and leave. Massachusetts law provides for involuntary commitment to inpatient SUD treatment services. When police become aware of an overdose in the community, within a few days, a police officer, the PAARI Care Advocate/Outreach Specialist, and, if available, a behavioral health clinician, will visit the person and provide information on local resources, treatment options, and additional community support. They also leave the person or family member with NARCAN. |
| Financing: Police positions funded through PD, PAARI Care Advocate/Outreach specialist funded through private foundation. |
| Data on Outcomes: A process evaluation found that in the first 12 months, from June 2015 through May 2016, 376 unique individuals came to the GPD for the ANGEL Program a total of 429 times. Of those individuals available for referral to treatment, 94.5% were offered placement in treatment facilities. Separately, the Care Advocate/Outreach Specialist reported 583 client interactions in October 2016-July 2018, serving about 259 unique individuals. |
DART is the addiction resource unit of the Lucas County Sheriff's Office. DART officers respond to opioid overdoses, and offer assistance to individuals by helping them enroll in substance use treatment, including detox. DART officers then follow people for two years, connecting them to treatment and advocating for them in the justice system.
| Drug Abuse Response Team (DART) |
|---|
| Location: Lucas County, Ohio |
| Intercepts: 1, 3 |
| Diversion Type: Law enforcement diversion |
| Target Population: Adults with SUD, specifically OUD |
| Description: DART is the addiction resource unit of the Lucas County Sheriff's Office, comprising officers designated to respond to opiate overdose calls. DART officers respond to every overdose case in Lucas County, and have responded to over 3,000 overdose cases from the team initiation in 2014 to date. After arriving on the scene, the DART officer offers immediate assistance enrolling the person in substance use treatment, including transportation to detox. If the person accepts the offer, that person becomes that officer's case. DART aims to make contact with people who have overdosed within 20 minutes of receiving the dispatch call. After initial contact, officers are responsible for linking clients to services in the community and following them for a 2-year period to monitor progress, foster connections, and serve as their advocate in the law enforcement system. The unit also conducts outreach activities with the public, and forms networks among service agencies and local stakeholders, such as businesses, schools, and civic organizations. In addition to pre-booking diversion, DART includes a jail intervention component, and partners with a local treatment provider to provide Vivitrol shots to clients prior to discharge; officers will also pick up clients from jail and transport them directly totreatment. |
| Partnerships: OUD inpatient and outpatient treatment providers, recovery programs, housing providers, Lucas County Jail, Toledo public schools, local businesses, state and local agencies such as the mental health board, and the Ohio Attorney General. |
| Structure: DART has 9 full-time officers and 2 full-time Community Advocate/Outreach Officers. The unit is overseen by a police Sergeant, who reports to the police Captain and the Sheriff. DART is notified of overdose cases through the county's centralized dispatch system, and also receives referrals from hospitals, from courts, and through word of mouth: people can contact DART directly to connect with an officer and get linked to treatment. Officer caseloads are about 55 cases per officer. There are 2 overlapping regular shifts (7am-10pm), and 1 officer is always on call outside of regular hours. Officers also have a strong rapport with court system staff and can serve as advocates for clients who are facing minor charges. Compliance with treatment and a good standing with DART can lead to minor charges being dropped. Officers spend about 50% of their time in the office, 40% on the street, and 10% in court. |
| Financing: DART was originally funded by a grant from the state's Attorney General; it is now a 501(c)(3) charitable organization supported through a combination of grants, fundraising, and donations. |
| Data on Outcomes: Although the unit has not undergone an official evaluation, it does track the number of client contacts, along with the number of linkages made to treatment providers, per case. DART measures success in terms of number of clients linked to treatment, and reports an average linkage rate of 80%. |
Wichita HOT officers respond to 911 calls and direct referrals from the community to assist people experiencing homelessness to access behavioral health and housing resources. When a person faces charges for violating a public ordinance, HOT officers have the ability to withdraw charges retroactively if the person engages in services, or request the person participate in mental health or drug court instead of the judicial system.
| Wichita Police Department Homeless Outreach Team (HOT) |
|---|
| Location: Wichita, Kansas |
| Intercepts: 1 |
| Diversion Type: Law enforcement diversion |
| Target Population: Individuals experiencing homelessness |
| Description: HOT is a community policing program with the mission to divert people experiencing homelessness from jail by linking them to behavioral health and housing resources. HOT officers are connected to people experiencing homelessness in 2 ways: through 911 calls and direct referrals from the community. HOT officers respond, assess the situation, and offer assistance. HOT partners with numerous behavioral health and housing agencies to refer people they encounter to trusted service providers. HOT serves as a conduit between community members and advocates, responding to the concerns of business owners and civilians while also protecting the civil rights of people experiencing homelessness. In situations where a person is violating a public ordinance, he or she may face charges, though HOT officers have the ability to drop minor charges retroactively if people agree to engage in services via a standard petition to the prosecutor. Officers may also request that a judge send a person through mental health court or drug court instead of the judicial system. HOT also conducts education and outreach activities with fellow agencies and the public to address misinformation about policies and misguided attempts to help people experiencing homelessness. |
| Partnerships: Wichita Housing Authority (Housing First, case management services); shelters, e.g., Union Rescue (immediate and short-term housing); and COMCARE (CIT training for officers, behavioral health services, case management, MAT); HOT is a part of the Continuum of Care. |
| Structure: HOT is currently composed of 2 CIT trained police officers. After receiving a call, the officer arrives on the scene and introduces him or herself to the person, with the primary aim of building rapport and connecting that person to necessary resources. If the person accepts the officer's offer of linkage to services, the officer will offer transport to the service agency, or people may choose to transport themselves. Services are provided by local behavioral health and housing agency partners. If the person declines services, the officer leaves the scene. Officers enter data on every person contacted in their internal database, which is merged with the HMIS system, allowing HOT to track referrals and outcomes. HOT obtains signature release from people at first contact to permit them to collect data and share it with partner agencies. |
| Financing: HOT officer salaries are funded through the city government, while HOT program components are privately funded through charitable contributions. |
| Data on Outcomes: HOT has not been externally evaluated. HOT's internal database shows that in 2011, officers made contact with over 12,500 people experiencing homelessness and helped place 932 people in housing. |
OCHN is the county Medicaid behavioral health authority, which is required to work with law enforcement to divert people with mental health or substance use issues to the county crisis center. Officers are able to drop people at the crisis center 24/7, at which point they have access to all county behavioral health services. OCHN also offers outreach and training to the 43 law enforcement agencies in the county.
| Oakland Community Health Network (OCHN) |
|---|
| Location: Oakland County, Michigan |
| Intercepts: 0, 1, 4 |
| Diversion Type: Law enforcement diversion |
| Target Population: People with SMI, SUD, or COD |
| Description: OCHN is the private non-profit behavioral health authority in Oakland County, Michigan, that oversees the county's jail diversion process in collaboration with PDs and service providers. OCHN established the jail diversion process in in 2000 with the aim of changing responses by law enforcement to people with mental health or substance use issues such that these issues are not criminalized. OCHN facilitates the jail diversion process through the Jail Diversion Coordinator, who works to empower officers to divert to services rather than press charges, and ensures that the county provider network, especially the crisis center, is equipped to provide services to people whom law enforcement has diverted. OCHN's RCC is the primary diversion resource for police. The RCC is the only comprehensive crisis center in Michigan, providing services for both mental health and substance use crises. Services include a 24/7 helpline, mobile crisis teams, a 24/7 emergency drop off door for police, crisis beds (up to 24-hour hold), a detox facility staffed by peer-recovery specialists, and an inpatient residential (up to 2-week) recovery program. |
| Partnerships: PDs, Oakland County Sheriff's Office, OCHN mental health and substance use treatment providers (Common Ground, Easter Seals). |
| Structure: The Jail Diversion Coordinator is a full-time OCHN employee who conducts frequent and continuous outreach to the 43 PDs in the county, trains officers on the diversion process, and works with OCHN leadership to ensure law enforcement personnel have easy access to OCHN's diversion resources. OCHN is required to work with law enforcement as part of its Medicaid contract with the state, and in turn has contract requirements with its providers to facilitate law enforcement/behavioral health collaboration. The state requires PDs to sign coordination agreements with OCHN; to date only 14/43 PDs have signed agreements. |
| Financing: The Jail Diversion Coordinator position is considered key staff and funded through OCHN general funds. Additional support staff are funded through grants as they are available. Crisis and treatment services are funded through Medicaid dollars as part of the OCHN provider network. |
| Data on Outcomes: Michigan State University is conducting an evaluation of the state Diversion Task Force, which includes Oakland County's efforts. The Jail Diversion Coordinator tracks the number of diversions through a log at Common Ground. He also tracks other diversions that are reported to him, but there are many diversions that occur as a result of officer training that he is unable to count. |
The Mental Health Association of Nebraska's REAL program is a peer-run pre-booking jail diversion program that provides free non-clinical services to people in mental health or substance use crisis. REAL collaborates with law enforcement to support people in the long term, and provides Wellness Recovery Action Plan (WRAP) training to the Lincoln Police Department (LPD). Mental Health Association of Nebraska also operates two crisis respite houses, a housing program, an employment program, a residential program, and a 24/7 warm line.
| Mental Health America Nebraska (MHA-NE) Respond Empower Advocate Listen (REAL) |
|---|
| Location: Lincoln, Nebraska |
| Intercepts: 0, 4 |
| Diversion Type: Peer specialists and peer-run respites |
| Target Population: People with SMI, SUD, or COD |
| Description: REAL is a peer-run pre-booking jail diversion program that provides free, voluntary, and non-clinical services to people in crisis, whether due to mental illness or SUDs. REAL collaborates with law enforcement, who embrace a community policing philosophy that involves a long-term relationship with the people they have referred to the program. Police also serve as a conduit to a range of community resources including housing, food, transportation, and legal assistance. People are often referred by police, but as community awareness of the REAL program has grown, family members, neighbors, friends, and landlords also make referrals. The REAL program operates 2 crisis respite houses and a 24/7 warm line, and provides WRAP training to the LPD. MHA-NE also has a housing and employment program through which people in the REAL program are linked to community resources, and a prison re-entry program that operates a 21-bed community residential facility. |
| Partnerships: LPD, national and state housing investment authorities, local behavioral health service provider, CEF. |
| Structure: Following a mental health or substance use-related encounter, a police officer can refer the person to the REAL program, which then deploys 1 of 38 peer-support specialists within 24 hours to contact and offer assistance. If the person decides to participate, peers collaborate with him or her to establish a plan for working together to support recovery. In the months after the referral, peer specialists update the referring officer about the person's status, and collaborate to develop additional plans, if needed. The police officer does not just "drop off" the person, but works with REAL to help access resources and establish long-term plans. Collaboration between the LPD and MHA-NE also takes place through quarterly meetings to improve cooperation, enhance outreach, and develop plans for high users of police services. MHA-NE also provides behavioral health training to police. |
| Financing: REAL is entirely grant funded. The original grant was provided by the CHE. The Nebraska Department of Correctional Services, the city of Lincoln, and SAMHSA all provide grants to support the program. REAL does not bill Medicaid, because the definition of "peer services" excludes MHA-NE, because MHA-NE does not have an on-site clinician. |
| Data on Outcomes: MHA-NE is not conducting a formal evaluation of the REAL program. An analysis of police data found that, compared to people who were not referred to the program, referred people were 33% less likely to be taken into emergency protective custody (2 years after initiating REAL services), and 44% less likely to be taken into emergency protective custody (3 years after initiating REAL services). These findings may be biased due to lack of a formal comparison group of people who were not referred for services. |
3.2.1. Jail Diversion Programs and Processes
While MHA-NE REAL, Wichita HOT, and DART are considered distinct jail diversion programs, the ANGEL Program and OCHN's jail diversion activities are considered processes rather than distinct programs. (In the case of OCHN, the organization funds one staff person to serve as the jail diversion coordinator, but relies on law enforcement agency participation in a jail diversion process that OCHN has integrated into their crisis, intake, and treatment systems.) It has taken several years for these processes to become as effective as they are, but it can be argued that this approach has a lower threshold than establishing an entirely new program. That is, it is arguably most efficient to:
-
Establish, within existing law enforcement and behavioral health systems, processes that provide incentives for law enforcement officers to divert people in crisis to treatment.
-
Provide the infrastructure for behavioral health providers to work with law enforcement.
3.2.2. Access to Community Resources
In Oakland County, Michigan, the county behavioral health system has designed its crisis services and intake and assessment processes to be responsive to law enforcement's needs. OCHN's crisis center's policy is that even if they are full and do not have the capacity to take an additional person, they never turn away a person experiencing a mental health or substance use crisis who is brought in by a law enforcement officer. Services offered at the crisis center include detoxification, buprenorphine induction, and sub-acute level mental health crisis stabilization. Law enforcement credits the reliability of the crisis system and their ability to access a 24-hour crisis line for assistance as essential to their ability to get people help and avoid arrest.
Another critical aspect of some programs' success was the law enforcement officers' ability to easily access the services. If a crisis center or behavioral health provider is too far away, an officer will be less likely to take the time to bring a person there. The Oakland County Jail Diversion program has had difficulty engaging law enforcement agencies in their county that are further away from the crisis center. They find that it is impractical for law enforcement officers to drive more than 45 minutes to drop a person at the crisis center.
The success of jail diversion programs is highly dependent on community factors, and those factors vary from jurisdiction to jurisdiction. In Oakland County, one such community factor that had a large impact on the success of the program was related to the lack of resources of the Aurora Hills Police Department. Aurora Hills is a large town in Oakland County and a key partner with OCHN; law enforcement and behavioral health staff team up often to provide trainings to other law enforcement agencies in the county. A key factor in their high use of the jail diversion process is their lack of a jail. Aurora Hills Police Department does not have any holding cells, so if they need to arrest someone, they have to take the person to the county jail, which is further away. This disincentive to arrest people has helped promote a community policing approach, and has led officers to avoid arrest unless absolutely necessary and rely on the jail diversion process to help people access help.
3.2.3. Community Collaborations
Some programs visited began with the formation of a local task force to understand the issue and determine solutions. These local task forces may have been formed as a result of state requirements, local policies (e.g., county ordinance), or community stakeholder concern. In Oakland County, the jail diversion program began as a task force led by the current jail diversion coordinator, and brought together behavioral health providers and many of the 43 local law enforcement agencies in the county. Michigan also has a current statewide task force on jail diversion that has provided some support to Oakland County and the other counties in Michigan, including funding a statewide evaluation.
In Gloucester, Massachusetts, community providers and partners created the High-Risk Task Force to identify ways to connect high-risk people in the community to treatment and other services. The task force was instrumental in the development of the ANGEL Program, and remains an essential forum for relationship-building between providers and law enforcement. Representatives from all community providers are task force members.
3.2.4. Critical Factors Impacting Service Models
We found common critical factors impacting the jail diversion program models emerging from the case studies.
-
For law enforcement, a common critical feature is a community policing philosophy in the department. Community policing is a philosophy of policing based on the idea that police can work closely with communities to address issues that can impact community safety (Schneider, Kimerer, Seaman, and Sweeny, 2003).
-
For behavioral health, the availability of accessible behavioral health services equipped to meet the needs of the people with mental health and substance use issues, and law enforcement officers who encounter them in the community, is the models' critical element.
The law enforcement agencies leading or participating in jail diversion programs have commonalities, and perhaps the most prominent one is their commitment to community policing. With that focus on community policing, law enforcement officers engage with their community through attempting to identify people with behavioral health problems early and help them access treatment, and avoiding arrest for non-violent offenders when possible. A major factor is their leaders' support of the community policing philosophy, and the result is that culture and practice are dictated from the top. Community policing may look somewhat different based on the jurisdiction; Wichita's HOT take a much more proactive approach to community outreach than do other law enforcement agencies in the study.
The case study findings also highlighted the importance of personal experience in understanding the needs of people with mental health and SUDs. Law enforcement officers often cited a personal connection to a person with SMI or OUD, or a personal/family connection of a leader in their agency, as the reason they began to explore options to increase pre-arrest jail diversion.
We did not observe major differences in the law enforcement practices among the sites visited in terms of common community policing philosophy and practices. Greater variability was found in the behavioral health services available in the community and therefore what services people could be used for diversion.
As the opioid crisis continues to plague communities across the country, the availability of services to treat people with OUD is a critical factor in the success of some of the jail diversion programs visited. For instance, the ANGEL Program's target population--people with SUD, and particularly OUD--has led to the Care Advocate/Outreach Specialist spending time each morning creating and disseminating lists to GPD and other area police departments with available open detox, clinical support services beds, and medication-assisted treatment (MAT) openings.
Jail diversion program staff identified champions, often within both the behavioral health and law enforcement communities, who were instrumental in the establishment of their programs as well as their success. Among case study sites, both law enforcement leaders and behavioral health organization leadership have championed the need for program establishment and funding. Unfortunately, a tragic event such as opioid overdose deaths of high-profile citizens, as is the case in Gloucester, Massachusetts, or a fatal police shooting, which all law enforcement officers fear, can be the impetus for beginning to plan for a jail diversion program.
4. DISCUSSION
The study found a variety of pre-booking jail diversion models and approaches for people with SMI and SUDs, including OUD. Although jail diversion program services included interventions at Intercepts 0 and 1, they also included services across other SIM intercepts, as shown in Exhibit 5. While the study was originally designed to examine both state-level and local-level jail diversion models, we found only one statewide approach to jail diversion.
| EXHIBIT 5. Jail Diversion Programs along the SIM |
|---|
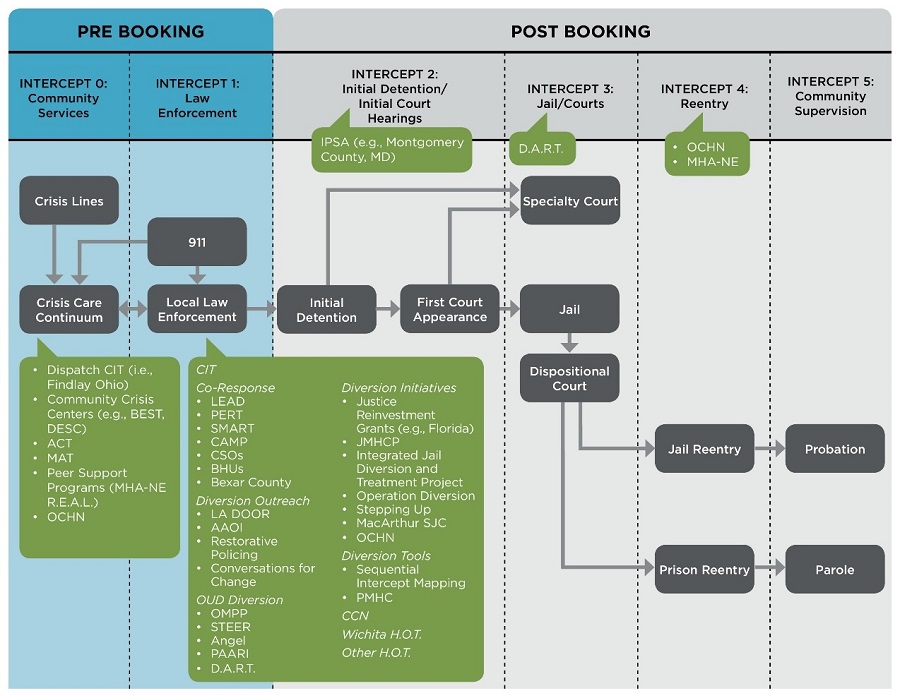 |
| ALT TEXT for EXHIBIT 5: Exhibit 5 demonstrates the pre- and post-booking jail diversion programs and interventions along the equential Intercept Model (SIM). On the left side of the figure, two intercepts comprise pre-booking interventions; Intercept 0: Community Services and Intercept 1: Law Enforcement. On the right side of the figure, four intercepts comprise post-booking interventions: Intercept 2: Initial Detention/Initial Court Hearings; Intercept 3: Jails/Courts; Intercept 4: Reentry; and Intercept 5: Community Supervision.
|
4.1. Community Resources
A consistent theme identified in the literature and the SME interviews was the need for novel approaches to strengthen community resources. Providers and police cannot divert people from the justice system if there is nothing to divert them to. A robust array of community resources (Intercept 0) need to exist in order for law enforcement to divert people from the criminal just systems, and optimally, to prevent further criminal justice involvement.
The majority of the programs studied in the case studies were developed through cross-system collaboration and co-response type approaches. Such cross-system collaboration was the foundation of CITs. Novel approaches have also emerged in response to the opioid crisis, such as community and police-led diversion outreach.
A major factor in the success of jail diversion programs is the availability of behavioral health services in the community. As has consistently been found with successful jail diversion programs, having a robust mental health and substance use treatment system, especially behavioral health providers able to provide crisis response, is essential.
Many programs reviewed in the environmental scan and case studies relied on the use of peers both for outreach to the community and to help in crisis, treatment, and recovery settings. MHA-NE's REAL program is entirely peer run. OCHN's process relies on peers in all aspects of the behavioral health treatment system, at the crisis center, in residential treatment, and in outpatient services. Staff at each site that used peers noted that they enhance engagement in services and are an invaluable part of the team.
The environmental scan and case studies revealed that investment and resources are a common facilitator of implementation and sustainability of jail diversion programs. Case study and environmental scan findings showed that while there is often a policymaker, community member, or task force that serves as a catalyst for the development of a program, community support and investment in the project grows over time, as law enforcement, community members, behavioral health providers, families, and the target population see its benefits.
4.2. Law Enforcement/Behavioral Health Collaboration
For each model reviewed in the environmental scan and every program included in the case studies, partnerships between law enforcement and behavioral health were crucial to their success. Most partnerships served multiple purposes and had multiple aims. For instance, several programs had law enforcement and behavioral health providers working together in the community to offer direct support to people and families. Other program models relied on law enforcement's ability to help a person access services, and although a behavioral health provider did not ride along or come to behavioral health-related calls with the officers, these providers were available virtually for consultation or in a crisis setting for the officer to refer the person to appropriate services.
Generally, it was found that a program was initiated and led by either a law enforcement agency or a behavioral health provider organization. Although partnerships are crucial for program success, models reviewed in the environmental scan and the case studies had a lead organization that was either law enforcement or behavioral health and partnered with the other sector. One agency had to have ownership and oversight over the program and its funding. While one agency was the lead, the level of coordination with their complementary partner varied between programs. Some programs had formal agreements such as memoranda of understanding (MOUs), memoranda of agreement (MOAs), or formal contracts/subcontracts that outlined the working relationship between the two or more organizations, while others were informal and relied on relationships and experience of working together over time.
Different models also have varying levels of law enforcement-behavioral health communication following a diversion. Some programs, like MHA-NE's REAL, have the behavioral health staff continue to update and involve law enforcement as they work with the person to stay in recovery. Other programs, like OCHN, provide updates to law enforcement if they ask for it. As the OCHN process has evolved and OCHN has gained increased trust from law enforcement, officers rarely follow up with the jail diversion coordinator or behavioral health staff related to a particular person. Although it was not immediate, law enforcement officers grew to believe that if they diverted a person to behavioral health treatment rather than arresting the person, the providers would act in good faith by engaging the person in treatment and doing their best to help the person get well and avoid such encounters with law enforcement in the future.
In addition to addressing the needs of people in their community with mental health and substance use needs, law enforcement and behavioral health providers often collaborated on trainings. Having law enforcement and behavioral health co-facilitators adds credibility to the training, bringing the perspective of someone who is in the community and encountering difficult situations, as well as behavioral health expertise.
Other community stakeholders were found to be key to jail diversion program success. Housing and other social services were often critical partners, as most people at risk for justice involvement and in need of behavioral health treatment also had other housing and social needs. Having both formal and informal partnerships can ease the programs' ability to access open housing spots or other social services available in the community.
The case studies yielded several anecdotes from law enforcement and jail diversion program staff who have had local businesses offer formal and informal support to the program after determining it is working to reduce loitering and other problematic behaviors and situations. In many cases, this began with the businesses calling the program for assistance rather than calling police. At times, business leaders saw the benefit of this and joined task forces or other coalitions to offer support to the initiative.
4.3. State and Local Policies and Legislation Regarding Jail Diversion
The environmental scan and case studies found several policies that have been implemented to promote the implementation of jail diversion programs and/or support the sustainability of jail diversion programs and processes.
There have been examples of state and local policymakers passing legislation to promote jail diversion programs and processes. In some cases, legislation requires specific trainings on program components. Other policies have more broadly supported jail diversion in the community, including requirements for law enforcement and/or behavioral health agencies to develop task forces to identify issues and propose policies and programs to reduce justice system involvement for people with mental health and SUD.
| Department Jail Diversion Policy: Aurora Hills Police Department "Responding to Persons Affected by Mental Illness or in Crisis," (General Order #3.10). This policy is based on an International Association of Chiefs of Police model policy and provides guidance to officers when they are "responding to or encountering situations involving persons displaying behaviors consistent with mental illness or crisis." The policy includes ways to recognize a person is in crisis and respond to the individual, and options for referring individuals to mental health professionals. The policy also outlines the jail diversion process, including eligible and ineligible offenses, jail diversion procedures, behavioral health crisis center contact information, and diversion follow-up procedures. |
At times, state and local policies or task force recommendations can result in unfunded mandates to implement law enforcement and/or behavioral health system changes. Identifying ways to address the requirements at minimal cost and/or identify additional funding sources is a challenge. However, when state or local mandates are accompanied by funding support, this can be the impetus to address issues that law enforcement, behavioral health, and other community stakeholders have identified.
Law enforcement agencies leading or partnering with jail diversion programs reported several policies that support officers' ability to engage with and divert people with mental health or substance use issues and partner with behavioral health agencies.
| Naloxone Policies Many PDs, including Aurora Hills PD (General Order #3.13), have implemented a Naloxone Policy to establish guidelines for administering naloxone to prevent fatal opioid overdoses. As the opioid crisis continues to impact communities across the country, many law enforcement officers are trained and authorized to carry and administer naloxone. |
The majority of case study sites noted that while the GSL policy is critical for engaging people with SUDs, the policy is not enough to encourage people to seek help through law enforcement and jail diversion programs. The policy must be accompanied by public awareness initiatives to educate the community and earn trust so people will come forward to seek help for themselves or a loved one without fear of arrest.
4.3.1. Challenges to Sustainability
Identifying sustainable financing for jail diversion programs was a critical issue for each of the case study sites. Programs varied in their start-up financing and impetus. They also received financing with or without a policy mandate to address the issue of preventing people with mental health and substance use issues from becoming involved in the justice system. For some sites, the funding was not something they sought out, but was a result of a state task force or decision-making by a policymaker outside their system (e.g., local funding provided to a police department for jail diversion activities). For other programs, the leadership of the law enforcement agency or behavioral health provider organization recognized the need for a jail diversion program or process and identified a funding source to support its development and implementation. In some cases, sites identified a main source of financing such as federal grants and local tax dollars with additional funding from foundations and local businesses.
Several of the sites have a law enforcement training component to their model. Three sites provide CIT Training. OCHN also provides Mental Health First Aid (MHFA) for Public Safety to officers in their county. These trainings require time investment for the trainers to prepare and conduct the trainings, and additional monetary resources for the required materials, and there is also a cost to the law enforcement agency for pulling officers out of the community to attend trainings. The environmental scan and case studies revealed that police departments have difficulty funding overtime to cover shifts needed to cover trainings, which is even more burdensome for small police departments.
Although many assume financing for law enforcement trainings is an up-front cost that lessens significantly after initial rounds of training, sites reported that being able to cover the costs of trainings, in terms of both time and materials for the trainers and officer time for attendance, remain a significant challenge. Law enforcement officers reported the following reasons for needing ongoing trainings. First, a single training on skills and strategies for working with populations with SMI and/or SUD is not enough. Refresher trainings are needed to enable officers to hone their skills and stay up to date with best practices. Jail diversion processes and community resources are constantly evolving and changing, and law enforcement need to be up to date on the jail diversion resources in their community. In addition, many law enforcement agencies undergo significant turnover. New officers need to be oriented to community policing, de-escalation, and diversion strategies as well as the behavioral health resources in their community.
Due to these high costs of trainings, the OCHN jail diversion coordinator often found law enforcement agencies were reluctant to provide comprehensive trainings to their officers. In order to introduce the county's jail diversion process and provide resources to the officers in those departments, he made himself available for short meetings and trainings during other scheduled trainings and shift changeover meetings. In these short 10-minute to 15-minute presentations the jail diversion coordinator has been able to forge relationships with law enforcement agencies in the county and provide information about OCHN's jail diversion process. Although not as effective as 8-hour or 40-hour meetings, these presentations have at times led police department leaders to determine that they should invest time and funds for more extensive trainings.
4.4. Assessment of Outcomes
The environmental scan and case studies found that while there is increasing awareness among law enforcement and behavioral health stakeholders that jail diversion programs and processes must be a priority, there is little in the way of evaluation results identifying what works. None of the case study sites were conducting an evaluation of their programs. A main barrier to evaluation was difficulty identifying funding. Without exception, the programs operated on limited funding, and any resources sites identified were used for training and programming. Programs were unlikely to finance evaluations when they were having difficulty keeping their staff employed.
Law enforcement agencies have access to encounter data, and behavioral health providers generally have access to claims data. Several of the programs, including DART, REAL's law enforcement partner, the LPD, HOT, and the ANGEL Program track their client encounters. However, having the ability to analyze those data is a challenge without funding. Despite inadequate funding for evaluation, some case study sites were able to analyze their data and provide noteworthy findings, which suggests additional analyses might be informative.
Additionally, sometimes the behavioral health program staff are able to track descriptive data for people participating in the program/process. The ANGEL Program Care Advocate/Outreach Specialist tracks client interactions. Likewise, the OCHN jail diversion coordinator, with the help of the Crisis Center's intake process, tracks the number of people who receive formal diversions (i.e., a law enforcement officer brings a person to the crisis center). However, OCHN staff and their partner law enforcement agency, Aurora Hills Police Department, reported that there are many other informal diversions in the community, where a person who might otherwise be ticketed or arrested is encouraged to seek treatment and provided resources without the jail diversion coordinator being aware and tracking the encounter.
Both law enforcement and behavioral health program staff identified difficulty in obtaining data that demonstrate the full picture about a particular person. For instance, Oakland County, Michigan has 43 separate law enforcement agencies, and some participate in the jail diversion program and track those data, while others do not. Without access to data from all 43 agencies, it is difficult to know for certain what justice involvement a person may have had. Likewise, behavioral health providers may not know whether a person accessed treatment outside their current system. So although a person did not engage in treatment through the jail diversion partner, the person might have received treatment elsewhere at the urging of law enforcement or another community member with support of the jail diversion program.
4.5. Unspoken Assumptions and Knowledge Transfer
One theme identified in the environmental scan and case studies is the chasm many law enforcement agencies and behavioral health provider organizations have to bridge to make their programs and partnerships work. There are often differences in incentives, knowledge, and culture that need to be bridged to create an effective jail diversion program, and this takes a lot of training, trial, and leadership. Police department leadership that valued community policing was noted as key to an agency considering establishment of a jail diversion program or partnering with a behavioral health provider organization already addressing jail diversion.
Law enforcement officers spoke about the difficulty they have with determining how to deal with people in crisis, and for many law enforcement agencies, a significant number of their encounters are related to mental illness or substance use. Aurora Hills Police Department in Oakland County, Michigan reported that of the 35,000 calls they received in 2017, 10% involved mental illness. The frequency of behavioral health-related calls has been exacerbated in many jurisdictions by the increased frequency with which law enforcement officers encounter people experiencing an opioid overdose. Law enforcement officers reported that repeated encounters with this population were a challenge because they come from a public safety rather than behavioral health perspective. Their feelings of inadequacy in how to help people and frustration with continually encountering the same people who are non-violent and clearly need behavioral health treatment was the impetus for pursuing the development of the jail diversion program. They recognized that partnering with behavioral health partners to assist with getting these people help would make their jobs easier.
The case study findings also highlighted the importance of personal experience in understanding the needs of people with mental health and SUDs. Law enforcement officers often cited a personal connection to a person with SMI or OUD, or a personal/family connection of a leader in their agency, as the reason they began to explore options to increase pre-arrest jail diversion.
A main challenge law enforcement and behavioral health providers faced is the difficulty in reaching people and engaging them in treatment. The case studies revealed several strategies jail diversion program staff have implemented to reduce barriers between law enforcement officers and people with mental health and substance use needs, as well as barriers to client engagement for behavioral health providers. In Wichita, the HOT officers use pickup trucks rather than police cruisers in their outreach work. They find it is less intimidating to their target population, which helps promote engagement. The HOT program also has a direct line that patches calls to the HOT officer's cell phone. Rather than calling 911, which many community members are reticent to do, this direct line allows people in crisis, family members, or other bystanders to contact trusted officers directly. Additionally, HOT officers carry supplies that people experiencing homelessness might need, such as toiletries, as a way of engaging the person and demonstrating value to the target population.
In Oakland County, Michigan, the crisis center, sobering unit, and residential treatment facilities run by OCHN partners have purposely been designed to be as non-clinical as possible. OCHN staff want these settings to be welcoming and home-like to make clients want to stay in the treatment. As a method of increasing engagement, MHA-NE's REAL program relies entirely on peer-support specialists and provides non-clinical care, relying on lived experience to assist people with maintaining recovery.
5. CONCLUSION
Most initiatives are at the early stages and/or are just beginning any form of evaluation. Although a number of programs show promise, evidence of effectiveness is still lacking. Most evaluations examined program processes or implementation through descriptive studies. Some jail diversion programs, such as the Crisis Response Center in Bexar County, Texas, were evaluated solely on cost savings. The LEAD program was evaluated using a quasi-experimental design.
Potential barriers to continued jail diversion through the REAL program include the changing state-level regulations related to peer-support programs; potential withdrawal of funding, especially if there is a visible community "failure" that receives negative publicity; the management of stakeholder expectations; and the lack of understanding of peer services by, and strained relationship with, many behavioral health service providers in the community.
The environmental scan and the case studies both found that a key factor in the success of a jail diversion program was the partnerships stakeholders were able to establish. The most obvious of these partnerships were between law enforcement and behavioral health providers, but the involvement of other community stakeholders and organizations was also critical to their success. Finally, the study found a critical need for the availability of community behavioral health resources, which are essential to divert people with SMI, OUD, and other SUDs from the criminal justice system.
6. FUTURE CONSIDERATIONS
The current study found a variety of innovative and promising pre-booking jail diversion programs. Most programs were homegrown and developed by innovation entrepreneurs in response to local circumstances, such as a rash of opioid overdose deaths. As such, programs developed very context-specific jail diversion solutions, often co-created in collaboration with community stakeholders. In specific, the unfolding opioid epidemic required an evolving response by both SUD treatment providers and police. The study found that a number of very promising police-led diversion initiatives are springing up around OUDs.
Key to pre-booking jail diversion, whether in response to opioid overdoses or mental health issues, was shifting police culture by departments moving toward community policing.
Officers found their jobs were easier if they were not policing overdoses, or behavior that could better be addressed by health professionals. However, behavioral health systems must have robust service options for law enforcement officers to use. Neither law enforcement officers nor behavioral health providers can divert people from the criminal justice system alone.
Community collaborations, such as high-risk tasks forces, and other coordination mechanisms are necessary to quickly identify people at high risk for SMI and SUD, such as people who experience chronic homelessness, and divert them to appropriate services. Community task forces and community meetings that foster collaboration among stakeholders allow preemptive and holistic services for high-risk people.
While a number of preliminary or formative evaluations of pre-booking jail diversion programs have been undertaken, few pre-booking jail diversion programs have been rigorously studied. Such evaluations, using randomized controlled trials or strong quasi-experimental designs, would assist law enforcement officials to choose the most effective approach for their jurisdictions.
In conclusion, the current study provides evidence that pre-booking jail diversion programs can intercept people with behavioral health conditions before they become enmeshed in the criminal justice system. Such programs are being implemented and replicated throughout the United States. Future studies can address both program effectiveness and local implementation; adaptations; and opportunities for program sustainability.
APPENDIX A. REFERENCES
Appel, P.W., Tsemberis, S., Joseph, H., Stefancic, A., & Lambert-Wacey, D. (2012). Housing First for severely mentally ill homeless methadone patients. Journal of Addictive Diseases, 31(3), 270-277.
Bart, G. (2012). Maintenance medication for opiate addiction: The foundation of recovery. Journal of Addictive Diseases, 31(3), 207-25.
Bond, G.R., Drake, R.E., Mueser, K.T., & Latimer, E. (2001). Assertive community treatment for people with severe mental illness. Disease Management and Health Outcomes, 9(3), 141-159.
Brown, R., Gassman, M., Hetzel, S., & Berger, L. (2013). Community-based treatment for opioid dependent offenders: A pilot study. American Journal on Addictions, 22(5), 500-502.
California Board of State and Community Corrections. (2017). Board Awards $103m in Prop 47 funds to innovative rehabilitative programs. Retrieved from http://www.bscc.ca.gov/news.php?id=125 on January 25, 2018.
Californians for Safety and Justice. (2015). Breaking the cycle of low-level crime: Public safety innovations during an era of change. Retrieved from https://university.pretrial.org/HigherLogic/System/DownloadDocumentFile… on January 25, 2018.
Center for Mental Health Services, National GAINS Center. (2007). Ten years of learnings on jail diversion from the CMHS National GAINS Center. Delmar, NY: CMHS National GAINS Center.
Center for Substance Abuse Treatment. (2005). Medication-assisted treatment for opioid addiction in opioid treatment programs. Treatment Improvement Protocol (TIP) Series 43. HHS Publication No. (SMH) 12-4214. Rockville, MD: Substance Abuse and Mental Health Services Administration.
Clark, A.K., Wilder, C.M., & Winstanley, E.L. (2014). A systematic review of community opioid overdose prevention and naloxone distribution programs. Journal of Addiction Medicine, 8(3), 153-163.
Clifasefi, S.L., Lonczak, H.S., & Collins, S.E. (2016). LEAD program evaluation: The impact of LEAD on housing, employment and income/benefits. Seattle, WA: University of Washington Harm Reduction Research and Treatment Center.
Coldwell, C.M., & Bender, W.S. (2007). The effectiveness of assertive community treatment for homeless populations with severe mental illness: A meta-analysis. American Journal of Psychiatry, 164(3), 393-399.
Collins, S.E., Lonczak, H.S., & Clifasefi, S.L. (2015a). LEAD program evaluation: Criminal justice and legal system utilization and associated costs. Seattle, WA: University of Washington Harm Reduction Research and Treatment Center.
Collins, S.E., Lonczak, H.S., & Clifasefi, S.L. (2015b). LEAD program evaluation: Recidivism report. Seattle, WA: University of Washington Harm Reduction Research and Treatment Center.
Compton, M.T., Bahora, M., Watson, A.C., & Oliva, J.R. (2008). A comprehensive review of extant research on Crisis Intervention Team (CIT) programs. Journal of the American Academy of Psychiatry and the Law, 36(1), 47-55.
Council of State Governments Justice Center. (2017). Stepping Up Initiative. Retrieved from https://csgjusticecenter.org/mental-health/county-improvement-project/stepping-up/ on January 25, 2018.
Currier, G.W., Fisher, S.G., & Caine, E.D. (2010). Mobile crisis team intervention to enhance linkage of discharged suicidal emergency department patients to outpatient psychiatric services: A randomized controlled trial. Academic Emergency Medicine, 17(1), 36-43.
Cusack, K.J., Morrissey, J.P., Cuddeback, G.S., Prins, A., & Williams, D.M. (2010). Criminal justice involvement, behavioral health service use, and costs of forensic assertive community treatment: A randomized trial. Community Mental Health Journal, 46(4), 356-63.
Davidson, C., Neighbors, C., Hall, G., Hogue, A., Cho, R., Kutner, B., & Morgenstern, J. (2014). Association of Housing First implementation and key outcomes among homeless persons with problematic substance use. Psychiatric Services, 65(11), 1318-1324.
Davidson, L., Bellamy, C., Guy, K., & Miller, R. (2012). Peer support among persons with severe mental illnesses: A review of evidence and experience. World Psychiatry, 11(2), 123-128.
Hewlett, L., & Wermeling, D.P. (2013). Survey of naloxone legal status in opioid overdose prevention and treatment. Journal of Opioid Management, 9(5), 369-377.
Illinois Criminal Justice Information Authority. (2017). Rethinking law enforcement's role on drugs: Community drug intervention and diversion efforts. Chicago, IL: Illinois Criminal Justice Information Authority.
Irving, C.B., Adams, C.E., & Rice, K. (2006). Crisis intervention for people with severe mental illnesses. Cochrane Database of Systematic Reviews, 4. Retrieved from https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD001087.pub3/media/CDSR/CD001087/rel0003/CD001087/CD001087_abstract.pdf on November 7, 2018.
Knopf, A. (2013). Jail diversion for mentally ill makes sense, but lacks funds. Retrieved from https://www.behavioral.net/article/jail-diversion-mentally-ill-makes-sense-lacks-funds on October 16, 2018.
Lamberti, J.S., & Weisman, R.L. (2004). Persons with severe mental disorders in the criminal justice system: Challenges and opportunities. Psychiatric Quarterly, 75(2), 151164.
Lamberti, J.S., Weisman, R., & Faden, D.I. (2004). Forensic assertive community treatment: Preventing incarceration of adults with severe mental illness. Psychiatric Services, 55(11), 1285-1293.
Latimore, A.D., & Bergstein, R.S. (2017). "Caught with a body" yet protected by law? Calling 911 for opioid overdose in the context of the Good Samaritan Law. International Journal of Drug Policy, 50, 82-89.
Lewis, B. (2017). Arlington Outreach Initiative treats overdoses, increases community trust. TECHBeat. Retrieved from https://www.justnet.org/InteractiveTechBeat/eTECHBEAT/eTechbeat_Apr_2017/content/pdf/eTechbeat_Apr_2017.pdf on November 2, 2018.
Morrissey, J.P., & Louison, A. (2014). Forensic assertive community treatment: Updating the evidence. Rockville, MD: SAMHSA GAINS Center for Behavioral Health and Justice Transformation.
Munetz, M.R., & Griffin, P.A. (2006). Use of the Sequential Intercept Model as an approach to decriminalization of people with serious mental illness. Psychiatric Services, 57(4), 544-549.
National Association of Counties (NACO). (2016). Stepping Up: a national initiative to reduce the number of people with mental illnesses in jail. Retrieved from http://www.naco.org/sites/default/files/New_Stepping%20Up_FINAL.pdf on October 8, 2017.
National Institute on Drug Abuse. (2017). Treatment of opioid use disorder in the criminal justice system. Rockville, MD: National Institute on Drug Abuse.
Police Executive Research Forum. (2016). Building successful partnerships between law enforcement and public health agencies to address opioid use. COPS Office Emerging Issues Forum. Washington, DC: Office of Community Oriented Policing Services.
Repper, J., & Carter, T. (2011). A review of the literature on peer support in mental health services. Journal of Mental Health, 20(4), 392-411.
Schneider, A., Kimerer, C., Seaman, S., and Sweeny, J. (2003). Community policing in action! A practitioner's eye view of organizational change. Retrieved from https://ric-zai-inc.com/Publications/cops-c001-pub.pdf on October 16, 2018.
Sedlack, A. (2017). Behavioral health unit: Case study at the Portland Police Department. Thinking Matters, 94.
Sells, D., Davidson, L., Jewell, C., Falzer, P., & Rowe, M. (2006). The treatment relationship in peer-based and regular case management for clients with severe mental illness. Psychiatric Services, 57(8), 1179-1184.
Steadman, H.J., Deane, M.W., Borum, R., & Morrissey, J.P. (2000). Comparing outcomes of major models of police responses to mental health emergencies. Psychiatric Services, 51(5), 645-649.
Steadman, H.J., Osher, F.C., Robbins, P.C., Case, B., & Samuels, S. (2009). Prevalence of serious mental illness among jail inmates. Psychiatric Services, 60(6), 761-765.
Substance Abuse and Mental Health Services Administration. Strategic Prevention Framework. Retrieved from https://www.samhsa.gov/spf on August 8, 2018.
Swanson, J.W., Frisman, L.K., Robertson, A.G., Lin, H., Trestman, R.L., Shelton, D.A., Parr, K., Rodis, E., Buchanan, A., & Swartz, M.S. (2013). Costs of criminal justice involvement among persons with serious mental illness in Connecticut. Psychiatric Services, 64(7), 630-637.
Tsembris, S., & Henwood, B. (2013). Housing First: Homelessness, recovery and community integration. In V. Vandiver (Ed.), Best practices in community mental health: A pocket guide. Chicago, IL: Lyceum Books, Inc.
Weisbrod, B.A., Test, M.A., and Stein, L.I. (1980). Alternative to mental hospital treatment II: Economic benefit-cost analysis. Archives of General Psychiatry, 37(4), 400-405.
APPENDIX B. EXAMPLE PROGRAMS FROM THE ENVIRONMENTAL SCAN
| Programs | Features | Example of Evaluations |
|---|---|---|
| Intercept 0 | ||
| ACT and FACT | A wide range of intensive clinical and recovery supports targeted at preventing hospitalizations, homelessness, and criminal justice involvement. | Numerous studies:
|
| MAT | Behavioral therapy with 1 of the 3 approved medications for OUD: methadone, buprenorphine, or naltrexone. |
|
| Community Crisis Programs such as Emergency Service Programs, Downtown Emergency Service Center Crisis Solutions Center, etc. | Mobile crisis outreach, assessment, and connection to treatment, detoxification and/or buprenorphine induction, stabilization services, and brief counseling. | Randomized trial:
Cochrane systematic review:
|
| Peer-Support Programs | Peer-run respites and peer bridging from hospitals to community supports. Forensic peer-recovery specialists work across all intercepts, including Intercept 0, providing referrals, linkages to services, and a number of supports (Croft & Isvan, 2015; Los Angeles County Department of Mental Health, 2015; Izquierdo, 2018; Segal, 2014). | Descriptive study:
Review:
Randomized trial of peer based case management versus usual case management:
|
| Housing First | Housing provided without the pre-condition of being "clean and sober." Intensive supports, including case management and clinical services are provided and/or coordinated along with permanent supportive housing. Relapse in and of itself does not automatically lead to the loss of housing. |
|
| Intercept 1 | ||
| CIT | First-responder/law enforcement-based diversion model used in over 40 states. Training for law enforcement officers in crisis intervention and de-escalation techniques for use when responding to behavioral health crises. Includes collaboration with behavioral health professionals and individuals with lived experience of behavioral health conditions. CIT is a core component of many co-responder models. | Descriptive study only:
|
| LEAD | Diversion intervention targeted at low-level drug and non-violent offenders (Beckett, 2014) with training police to identify signs of behavioral health conditions and to refer eligible individuals to case management and other supportive services. | Quasi-experimental study:
Within subjects design for employment outcomes:
Single case study:
|
| Psychiatric Emergency Response Team (PERT) | Co-responder jail diversion model with teams staffed by a licensed mental health clinician and a PERT-trained law enforcement officer. Police receive 80 hours of training on assessing people with mental illness and identifying resources for referral. Police officers and mental health professionals trained in PERT respond together to calls involving people with SMI, and work together to de-escalate mental health emergencies and redirect people to mental health services instead of hospitals or jails (Hartford et al., 2006). | Single case study:
|
| Systemwide Mental Assessment Response Teams (SMART) and
Case Assessment Management Program | Since 1993, as a co-responder model, the SMART strategy has deployed teams that comprise a specially trained officer and a mental health clinician. Developed in 2005, the Case Assessment Management Program uses a crisis response team focused on people who are high users of emergency services and at risk for violent encounters with first responders (Californians for Safety & Justice, 2015). | Single case study:
|
| Community Services Officers and Behavioral Health Unit | Community Service Officers in Birmingham Alabama's Police Team accompany officers who are responding to mental health emergencies. They provide crisis intervention and follow up with individuals if needed. Replicated in Portland Oregon with three police/behavioral health provider response teams and enhanced CIT training (City of Portland, Oregon, n.d.). | Descriptive study only:
|
| Portland Maine Behavioral Health Response Program. | Behavioral health clinician and police officer co-responder teams with use of enhanced CIT. Staffed with a full-time behavioral health coordinator, a full-time crisis counselor from a local mobile crisis team, counseling interns, and CIT trained officers. | Single case study:
|
| Prescription Drug Diversion: Opioid Misuse Prevention Program | Prescriber and dispenser education on opioid prescribing and misuse; Prescription Drug Monitoring Program awareness and enrollment; media campaigns about sharing, storing, and disposal of prescription medications; youth education regarding the risks and harms of opioid misuse; public awareness of naloxone and the GSL; drug take-back events and drop boxes; dissemination of locked storage boxes for parents and senior citizens; use of Screening, Brief Intervention, and Referral to Treatment; and training for law enforcement and first responders on referring users to treatment (Maryland Department of Health, n.d.). The program is based on SAMHSA's Strategic Prevention Framework (https://www.samhsa.gov/spf). | Not yet evaluated |
| Los Angeles Diversion Outreach and Opportunities for Recovery (LA DOOR) | Pre-booking, health-focused drug intervention program implemented by the Los Angeles City Attorney's Office and cross-sectoral partners (California Board of State & Community Corrections, 2017) implemented in 5 areas in Los Angeles that have a high density of misdemeanors and homeless encampments. Program components include: multi-disciplinary social service (clinician, peer-support staff, nurse) outreach teams that provide direct services and connect individuals to SUD treatment, mental health services, and wraparound services prior criminal justice involvement; a 24/7 hotline officers can call after making a misdemeanor drug-related arrest, triggering peer navigator intervention to divert from booking to services; continuous community engagement through an LA DOOR advisory committee. | Evaluation is in process |
| Stop, Triage, Engage, Educate, and Rehabilitate (STEER) | Police-led diversion program that diverts individuals in need of SUD treatment, including those who have experience drug overdose (Addiction Policy Forum, 2017a; Center for Health & Justice at TASC, 2017). Services include connection to SUD treatment, coordination of services, and peer-support services. Coordination between police, other emergency responders and behavioral health providers and training on SUDs, including OUD is included in the model. Police officers are also trained to conduct evidence-based screening in the field, using the STEER Deflection Screening Tool (Addiction Policy Forum, 2017a).The program has been replicated in a number of other jurisdictions in addition to Montgomery County Maryland. | Evaluation underway:
|
| PAARI: Arlington Massachusetts Opiate Outreach Initiative (AAOI) | Police-led community outreach initiative that uses information gathered during criminal investigations, community policing, and 911 dispatches and contact arising from criminal investigation, in which information on clients of known drug distributors gathered during a criminal investigation is shared with the program to identify people who use heroin, and proactively offer them linkage to treatment (Arlington PD, 2015). Referrals are sent to the AAOI Coordinator, a social worker embedded in the Arlington PD (Police Executive Research Forum, 2016). The AAOI Coordinator provides outreach to individuals to offer support in entering treatment and co-facilitates the Arlington Community Training Support program, a series of community meetings aimed at reducing stigma and increasing community support for people with OUD and their families. The group is co-facilitated by community partners, including social workers, health professionals, and clinicians. Topics covered in meetings include naloxone training and distribution, referrals to outpatient and inpatient programs; with direct access to mental health and substance use professionals who attend the meeting. | Descriptive report:
Use of Naloxone:
|
| Restorative Policing | Model developed by the Santa Barbara PD in response to high rates of arrest and incarceration among the city's homeless population (Californians for Safety & Justice, 2015). A team of 2 police officers make daily contact with the city's homeless population to identify people in need of mental health and/or SUD treatment, housing, and employment services. They facilitate transportation and linkage to these services (City of Santa Barbara, 2013). The model includes a team of community liaison officers, who work to deter local crime by communicating with local business owners, and a Restorative Court (Californians for Safety & Justice, 2015), a joint effort between the Santa Barbara PD, court system, health care system, and social service agencies that processes cases for homeless people and can dismiss cases for people who comply with SUD or mental health treatment requirements (City of Santa Barbara, 2013). Staff from the Restorative Court regularly engage with individuals who experience homelessness in the community. | Single case study:
|
| Conversations for Change | Model developed in Dayton, Ohio, as a discussion-based community outreach initiative jointly led by the Dayton PD and East End Community Services (East End), a local non-profit organization, in response to rising opioid-related fatalities in the community (Police Executive Research Forum, 2016). Together, the Dayton PD and East End host meetings to inform the community about addiction, treatment, and support services for people with SUD. The meetings target people experiencing SUD or people involved in prostitution. The Dayton PD and East End work with local service agencies and news media to raise awareness about Conversations for Change events. Meeting participants have the choice to engage in one-on-one conversations with a counselor trained in Motivational Interviewing to discuss their treatment options. The meetings feature presentations by nurses on the science of addiction, training and distribution of naloxone kits, and in-person access to treatment providers who offer a range of treatment services, from abstinence-based treatment to MAT. | Descriptive study:
|
APPENDIX C. LITERATURE SEARCH TERMS
| Database | Search String | Results Returned |
|---|---|---|
| EBSCO Host | AB (program OR practice OR "evidence based" OR model OR policy) AND AB ("mental health" OR "mental illness" OR "behavioral health" OR addiction OR "substance abuse") AND AB ("jail diversion" OR "pre-booking" OR arrest OR "pretrial detention" OR "crisis intervention" OR booking OR arraignment) | 320 |
| EBSCO Host | AB (program OR practice OR "evidence based" OR model OR policy) AND AB ("opioid" OR "opioid abuse" OR "opioid dependence") AND AB ("jail diversion" OR "pre-booking" OR arrest OR "pretrial detention" OR "crisis intervention" OR booking OR arraignment) | 80 |
| PsycINFO | AB (program OR practice OR "evidence based" OR model OR policy) AND AB ("mental health" OR "mental illness" OR "behavioral health" OR addiction OR "substance abuse") AND AB ("jail diversion" OR "pre-booking" OR arrest OR "pretrial detention" OR "crisis intervention" OR booking OR arraignment) | 287 |
| PsycINFO | AB (program OR practice OR "evidence based" OR model OR policy) AND AB ("opioid") AND AB ("jail diversion" OR "pre-booking" OR arrest OR "pretrial detention" OR "crisis intervention" OR booking OR arraignment) | 8 |
| PubMed | AB (program OR practice OR "evidence based" OR model OR policy) AND AB ("mental health" OR "mental illness" OR "behavioral health" OR addiction OR "substance abuse") AND AB ("jail diversion" OR "pre-booking" OR arrest OR "pretrial detention" OR "crisis intervention" OR booking OR arraignment) | 219 |
| PubMed | AB (program OR practice OR "evidence based" OR model OR policy) AND AB ("opioid" OR "opioid abuse" OR "opioid dependence") AND AB ("jail diversion" OR "pre-booking" OR arrest OR "pretrial detention" OR "crisis intervention" OR booking OR arraignment) | 42 |
APPENDIX D. AGENCY WEB SEARCH TERMS
| Agency/Organization | Search Terms | Results Returned |
|---|---|---|
| HHS | Jail diversion program | 33 |
| SAMHSA | Diversion; jail diversion program | 10 |
| Veterans Affairs | "Jail diversion" | 13 |
| ASPE | "Jail diversion" | 11 |
| Office of Justice Programs | "Jail diversion" | 10 |
| BJA | Diversion | 9 |
| National Association of Drug Court Professionals | Scan of publications page | 5 |
| Pretrial Justice Institute University Pretrial Library | Diversion program | 25 |
| National Adult Protective Services Association | Scan of diversion page | 5 |
| National Institute of Justice Crime Solutions Clearinghouse | Diversion; pre-booking diversion | 26 |
| JRI | Diversion | 1 |
| National Association of Counties | Scan of Stepping Up Initiative resources page | 24 |
APPENDIX E. CASE STUDY PROTOCOL
Case Study Overview
The purpose of the case studies is to develop a more comprehensive, in-depth understanding of the critical factors related to the implementation and effectiveness of jail diversion programs. Information gathered through this effort will be used to develop an "on the ground" understanding of the successful models being used. More specificity will also be obtained on data and outcomes measures being used to assess effectiveness, and on policies at the state level that affect local implementation initiatives. Abt Associates will conduct five in-person (two staff/two days) site visits to collect data for the case studies. The Abt team will conduct interviews with key staff and stakeholders, review program materials, and develop a two-page summary for each visit. Abt will collaborate with program staff to set a date and develop an agenda for the visit. A virtual meeting will be held prior to the site visit to request relevant materials and review the draft site visit agenda.
The goals and activities of the case studies are described below. Case study interview guides and other materials are included in the appendices.
Goals
-
Understand the design and implementation of the program.
-
Understand challenges and achievements to date.
-
Obtain secondary data and program materials including aggregate data, reports, presentations, as well as program procedures, and information on organizational structures and policies used to implement each program.
Activities
-
Conduct interviews with key staff members, program partners and stakeholders for each project.
-
Tour program facilities and observe program activities whenever possible.
-
Collect extant data on:
-
Evaluation designs, if any.
-
Performance measures.
-
Outcomes.
-
Local contextual data, including crime rates, local poverty rates, behavioral health resources, and other economic indicators.
-
-
Collect information on:
-
Program components.
-
Target populations.
-
Collaborative relationships.
-
Data sharing procedures, if any.
-
Implementation successes and challenges.
-
Information on policy facilitators, barriers, funding, and budget impact.
-
-
Develop summary reports.
Research Questions
-
What [pre-booking] strategies are used by state and local agencies to divert individuals with SMI, SUD and CODs from incarceration? To what extent have these strategies been demonstrated to reduce recidivism, increase access to treatment, and improve outcomes for individuals in the program? If programs have not been evaluated how does the program define and monitor success?
-
What policy and programmatic barriers have these states/localities encountered in implementing [pre-booking] diversion programs? Which were overcome and how? How does the involvement of stakeholders, at the time programs are proposed and implemented, influence the design of the program?
-
What program impacts have been measured and with what degree of confidence? What data have been used to measure impacts?
-
What lessons and insights from existing state/local efforts are available to inform the implementation of new federal policy regarding diversion efforts, as reflected in the 21st Century Cures Act, ongoing Medicaid policy, efforts to address homelessness, and other national efforts including the Administration's priority to combat the opioid epidemic?
-
What is the availability of treatment and support (e.g., housing, employment, peers) services for adults with SMI and/or SUD?
-
What is the form of collaboration between the criminal justice and behavioral health systems (e.g., MOA, planning, training, funding, data exchange)?
-
What are specific issues and differences as related to policies and funding for jail diversion for persons with SMI versus persons with SUD?
-
What are specific issues and differences as related to models, policies and funding for jail diversion for persons using opioids?
Secondary Data Collection
Abt will collect secondary data before, during, and after the in-person site visits. Prior to the site visits for the case studies, the Task 4 Lead will request that sites share any evaluation designs, logic models, reports, conference presentations, issue briefs, and peer-reviewed articles, via e-mail prior to the interviews. The interview guides also contain probes on evaluation design, data availability and exchange, process measures, outcome measures, cost-effectiveness measures, and any evaluation findings. The lead interviewer may also probe whether the jail diversion Program Director or manager can share any aggregate data MOU, data sharing agreements, protocols, or procedures with the Abt team. The Abt team will collect physical copies of specified materials sources during the site visit, when possible. Collection of extant data will be tracked using a secondary data collection tracking tool (See Appendix D). A study team member will request that a program representative send any additional materials via e-mail following the site visit. A secure file transfer protocol is available for use in transferring materials and aggregate data, should the jail diversion program staff prefer. If Abt has not received the requested data within two weeks of the site visit, the site visit lead will send a second request to the site contact by e-mail, and follow up by phone if necessary.
Analysis Plan
The analysis plan is built on our understanding of the policy significance and focus of the research questions to build the knowledge and evidentiary base for developing future policy and program implementation strategies, including taking effective jail diversion strategies to scale. As feasible, analysis will begin with a classification of jail diversion program types and logic models used for each evaluation; and continue with a variability assessment to assess common methods, measures and outcomes used for each model. Study reviews will follow a set protocol for assessing the rigor of each study, and findings by outcome for each jail diversion model.
The Abt team will conduct qualitative analyses in order to identify common themes related to program start-up, funding, collaborations, as well as implementation successes and challenges. Client outcomes, such as reduction in arrest rates, connection to services, etc. will be summarized whenever possible. If any programs use common designs, outcomes, and measures for their jail diversion program model, the Abt team, in consultation with the COR may conduct some kind of cross-program analyses.
The Abt team will develop a two-page summary for each visit. Draft versions will be shared with each program to validate information contained in the summary. Each summary will be structured to answer the research questions.
APPENDIX F. INTERVIEW GUIDES
Lead Agency
Behavioral Health Agency
Interviewee
-
Very briefly, what is your role in the [Name of Jail Diversion Program]?
-
How long have you worked in the program?
-
-
Please provide a one minute overview of [Name of Jail Diversion Program].
COMMUNITY CHARACTERISTICS (RQ 5)
-
Please tell us about the community your program serves.
Probes
-
What geographic area does [Name of Jail Diversion Program] program cover?
-
What aspects of the community support good behavioral health? Interfere with behavioral health?
-
How do communities of color (if any) and law enforcement interact?
-
-
What treatment services are available in your community, including mental health, SUD, medical, insurance, and other services and supports? Please describe them.
-
What are the service gaps?
-
How many MAT providers are in the community?
Probes
-
How long do people have to wait to access SUD services?
-
How easy is it for individuals with OUD to access MAT?
-
How are SUD services funded in your state? In your community?
-
What recovery residences and transitional housing services are available in your community?
-
How far do people have to travel to reach care?
-
What other services and supports are difficult to access in your community?
-
What other services and supports are easy to access in your community?
-
-
PROGRAM ORIGIN (RQ 6)
-
Please tell us about the history of [Name of Jail Diversion Program].
-
Was there a problem identified that needed to be solved?
Probes
-
How did community leaders and the business community define the problem?
-
How did police define the problem?
-
How did behavioral health providers define the problem?
-
Who, if anyone, championed the program?
-
-
How did you go about creating a common understanding of the need for jail diversion?
Probes
-
What issues/cultural conflicts still remain?
-
Were law enforcement officers amenable to changing the way they interacted with people with behavioral health conditions?
-
Were law enforcement officers amenable to working with behavioral health providers?
-
What were their attitudes toward mental illness?
-
Illicit drug use and dependence?
-
People who experience homelessness?
-
-
What were behavioral health providers' attitudes toward working with police/sheriffs?
-
Who was instrumental in starting [Name of Jail Diversion Program]?
-
How was [Name of Jail Diversion Program] initially funded? Has this changed over time?
-
IMPLEMENTATION FACTORS (RQ 2, 6, 7, 8)
-
How was [Name of Jail Diversion Program] developed?
Probes (If not addressed in origin discussion.)
-
Who were the organizational champions? Who were the community champions?
-
Who took the lead in planning?
-
-
How did you identify the model for implementation? How did you select the evidence-based practice(s)?
Probes
-
Was there discussion about the particular Intercept? If so, which one and what was discussed? [In other words, was there discussion about where on the continuum (from law enforcement involvement prevention to re-entry/recidivism prevention) to intervene?]
-
Who was involved in identifying the model for implementation? Were organizational partners, community partners, funders, or other stakeholders involved? How were they involved and at what level of effort?
-
Who was involved in identifying the evidence-based practice(s) you are using? Were organizational partners, community partners, funders, or other stakeholders involved? How were they involved?
-
-
What organizational resources were identified as being needed to implement the program? What organizational resources were added?
Probes
-
Staff
-
Resources/financing
-
IT/Data Systems
-
Training
-
Partnerships
-
Building/physical locations
-
-
What community resources were identified as being needed? What community resources were added?
-
What barriers or challenges did you encounter in the planning process? How did you overcome them?
-
What training did [Jail Diversion Program Name] staff and partners receive prior to program implementation?
-
What barriers did you encounter during implementation of your program?
-
How did you overcome them?
-
PROGRAM COMPONENTS (RQ 1, 2, 5)
-
What is the target population for your program? [Ask only if not addressed above].
-
What major life challenges are encountered by the population you serve?
Probe
-
SMI, OUD, COD, poverty, HIV, other SUD, homelessness, language barrier?
-
-
-
What services does [Jail Diversion Program Name] provide?
-
Where are services provided?
Probe
-
How do you determine what services are provided where?
-
-
Which services are provided by the lead agency and which services are provided by partners?
-
What are the eligibility criteria for program participation?
-
-
What gaps in services have you identified that still remain? How are you working, if at all, to address the identified gaps?
-
What is the staffing configuration for [Name of Jail Diversion Program]?
-
How many full-time equivalents work in the program?
Probes
-
How many police officers are on the team?
-
How many behavioral health providers are on the team?
-
How do behavioral health staff/officers share the work of the program?
-
-
Where are staff primarily located/co-located? Do you feel you have the correct staffing mix?
Probes
-
Who would you add?
-
What expertise or capabilities would you add to your program if you could?
-
-
Do forensic peer-support staff work in your program? If yes, please tell me about their role(s).
Probes
-
How do they work with other team members?
-
With people being served?
-
-
CRIMINAL JUSTICE/BEHAVIORAL HEALTH COLLABORATION (RQ 6)
-
What is the relationship criminal justice and behavioral health agencies have in your community. What coalitions and advisory bodies do behavioral health providers and law enforcement participate in? Please describe.
Probes
-
What is your role on these entities?
-
Who else belongs to these groups? (Advocates, peers, health care organizations, hospitals? What is their role?
-
-
Who are your program partners?
-
How would you describe the level of collaboration you have with them?
-
What are keys to a successful working relationship with each of your partners?
-
What challenges have you faced in working with your partners?
Probe
-
How did you work to overcome those challenges?
-
-
-
How do you cultivate your community partnerships? What is your process for meeting and updating one another?
Probes
-
Do you have formal coalitions? Please describe. [If not answered above.]
-
Do you contribute to their work in other ways, e.g., present at events they host, serve on their board of directors.
-
-
What Memorandum of Agreement (MOA) or Memorandum of Understanding (MOU) are in place between law enforcement and behavioral health organizations?
-
Do you have MOAs or MOUs with other organizations?
Probes
-
For housing, case management, transportation?
-
Other services?
-
-
Please describe if and how they facilitate/allow the agencies to work together on this program or other programs in the community.
-
-
What data sharing agreements do you have?
-
What data are shared?
-
How are the data used to inform programmatic decisions?
Probes
-
Do you use it for hot spotting?
-
Service expansion?
-
-
-
How do you and your partner community behavioral health/criminal justice agency collaborate on training?
POLICY FACTORS/FACILITATORS/BARRIERS (RQ 2, 4)
-
Did organizational policies have an impact on your ability to implement the program? If yes, please describe.
Probes
-
Did implementation of the program require amending any organizational policies? If yes, please describe which policies and the process for changing them.
-
What organizational policies support implementation of [Name of Program]?
-
What organizational policies get in the way of [Name of Program] implementation?
-
-
Did local policies have an impact on program implementation? If yes, please describe.
Probes
-
Were they health, behavioral health, or criminal justice-related?
-
Describe local policies that facilitated implementation.
-
What local policies were a hindrance or barrier to implementation?
-
Did implementation of the program require amending any local government policies? If yes, please describe which policies and the process for change.
-
What local policies continue to serve as facilitators or barriers to program implementation and success?
-
-
Were there any champions for the program or the population at the local level that impacted your ability to implement the program? How did they impact the process (e.g., championing policy change)?
-
What state policies affected local implementation of the program? Please describe.
Probes
-
Were any state policies amended to facilitate the implementation of the program? If yes, please describe which policies and the process for change.
-
What state policies that continue to serve as a facilitator to program implementation and success?
-
What state policies continue to serve as a barrier to program implementation and success?
-
-
Were there any champions for the program or the population at the state level that impacted your ability to implement the program? How did they impact the process (e.g., championing policy change)?
FUNDING AND BUDGET IMPACT (RQ 7)
-
What resources were available to start the process of planning for the program?
Probes
-
Wheredid those resources come from?
-
Were there any in-kind resources in the form of staff time?
-
-
What funding sources were used to implement the program?
Probes
-
What is the source of these funds--grants (BJA, SAMHSA, other) state general funds, local tax dollars, etc.?
-
-
If implementation funding was a grant, start-up funds, etc. that is/was time limited, what approaches are you using/have you used to sustain program funding?
Probes
-
What is the source of potential/current sustainability funds--behavioral health, law enforcement, etc.?
-
What funding sources to support this work, if any, are you planning to explore?
-
-
How are cost offsets considered in discussions of ongoing financing of this program (or other jail diversion programs), if at all?
-
Do you currently have a funded evaluation? If so, please describe funding for the evaluation.
EVALUATING EFFECTIVENESS (RQ 1, 3)
-
Are you evaluating your program? If so, please describe.
Probes
-
Do you currently have a funded evaluation? If so, please describe funding for the evaluation. [If this was not answered above]
-
If not, how are you evaluating the effectiveness of [Jail Diversion Program]? What resources are you using? [e.g., in house staff, already established data systems, interns]
-
-
Who was involved in developing the evaluation design?
Probes
-
Were organizational partners, community partners, funders, or other stakeholders involved?
-
If so, what was their role? How were they identified/selected?
-
-
Given the chance, is there anything you would do differently?
-
How do you use evaluation findings to support your program?
Probes
-
To support quality improvement?
-
Justify funding?
-
To demonstrate cost offsets to obtain additional financing?
-
-
Do you have a logic model you can share?
-
What inputs and process measures you are tracking for your process evaluation, if any?
-
How do you obtain/collect those data?
-
-
What individual-level outcome measures are you using in your outcome evaluation?
-
How do you obtain/collect those data?
-
-
What challenges have you encountered in collecting/obtaining the data?
-
What other individual outcomes do you wish you hope to assess in the evaluation?
-
-
What population-level outcome measures are you using in your evaluation?
-
How do you obtain/collect those data?
-
-
What challenges have you encountered in collecting/obtaining the data?
-
What other population-level outcomes do you wish you hope to assess in the evaluation?
-
-
What cost-effectiveness or cost-offset measures are used in your evaluation? Please describe.
-
What are the evaluation findings (if any) to date?
-
What reports/papers can you share? (If not already shared)
-
Other data you can share?
-
WHAT WORKS
-
What have been the project successes to date? Please describe.
Probes
-
What do you attribute that success to?
-
-
What factors do you think were most impactful in successful implementation?
-
What factors do you think were most impactful in sustaining the program (if the program has been sustained past implementation)?
-
What have been the project challenges to date? How have you tried to address them?
Probes
-
For challenges or barriers that have not been overcome, if any, how do you think they are hindering implementation of your program?
-
How are they affecting the population you serve?
-
-
What lessons learned have your learned that you could share with other communities that might want to implement a similar jail diversion program?
-
What federal policies are barriers to program success?
-
What suggestions would you provide to federal policymakers to help address those issues?
-
-
What insights can you share that might help the Federal Government address the opioid epidemic?
-
What suggestions would you provide to state policymakers to help address the opioid epidemic?
-
What policies are needed to support implementation of pre-booking jail diversion programs?
-
Where do you see [Name of Jail Diversion Program] in 1, 5, or 10 years?
Probes
-
Do you plan to sustain it? Expand it?
-
Do you think the need will remain or will your program be a success and not be needed in the future? Please describe.
-
-
Is there anything else about the project that you would like to share with us?
Lead Agency
Criminal Justice Agency
Interviewee
-
Very briefly, what is your role in the [Name of Jail Diversion Program]?
-
How long have you worked in the program?
-
-
Please provide a one minute overview of [Name of Jail Diversion Program].
COMMUNITY CHARACTERISTICS (RQ 5)
-
What geographic area does [Name of Jail Diversion Program] program cover?
-
Please tell us something about the community/county.
-
What are the most pressing issues currently facing law enforcement in your community/county?
Probes
-
How do communities of color (if any) and law enforcement interact?
-
-
From your point of view, how well do behavioral health treatment services work?
-
What do you see as the service gaps?
-
How often do you bring someone to the emergency department for a mental health assessment or detox, only to have the person return to the community without services?
-
PROGRAM ORIGIN (RQ 6)
-
Please tell us about the history of [Name of Jail Diversion Program].
-
Was there a problem identified that needed to be solved?
Probes
-
How did community leaders and the business community define the problem?
-
How did police define the problem?
-
How did behavioral health providers define the problem?
-
Who, if anyone, championed the program?
-
-
How did you go about creating a common understanding of the need for jail diversion?
Probes
-
What issues/cultural conflicts still remain?
-
What cultural hurdles got in the way of law enforcement officers changing the way they interacted with people with behavioral health conditions?
-
What attitudes did law enforcement officers have about behavioral health providers prior to [Jail Diversion Program Name] implementation?
-
What were their attitudes toward mental illness?
-
Illicit drug use and dependence?
-
People who experience homelessness?
-
-
What were behavioral health providers' attitudes toward working with police/sheriffs?
-
Who was instrumental in starting [Name of Jail Diversion Program]?
-
How was [Name of Jail Diversion Program] initially funded? Has this changed over time?
-
IMPLEMENTATION FACTORS (RQ 2, 6, 7, 8)
-
How was [Jail Diversion Program Name] developed?
Probes (If not addressed in origin discussion.)
-
Who were the organizational champions? Who were the community champions?
-
Who took the lead in planning?
-
-
How did you identify the model for implementation? How did you select the evidence-based practice(s)?
Probes
-
Was there discussion about the particular Intercept? If so, which one and what was discussed? [In other words, was there discussion about where on the continuum (from law enforcement involvement prevention to re-entry/recidivism prevention) to intervene?]
-
Who was involved in identifying the model for implementation? Were organizational partners, community partners, funders, or other stakeholders involved? How were they involved and at what level of effort?
-
Who was involved in identifying the evidence-based practice(s) you are using? Were organizational partners, community partners, funders, or other stakeholders involved? How were they involved?
-
-
What organizational resources were identified as being needed? What organizational resources were added?
Probes
-
Staff
-
Resources/financing
-
IT/Data Systems
-
Training
-
Partnerships
-
Building/physical locations
-
-
What community resources were identified as being needed? What community resources were added?
-
What barriers or challenges did you encounter in the planning process? How did you overcome them?
-
What training did [Agency Name] and program partners received during the implementation process?
-
What barriers did you encounter during implementation of your program? How did you overcome them?
PROGRAM COMPONENTS (RQ 1, 2, 5)
-
How does [Jail Diversion Program Name] operate?
-
Where does it operate?
Probes
-
Headquarters, satellite stations, partner organizations, community locations?
-
-
Who is eligible to enter the program?
-
-
What types of staff work in the program? (Police officers, behavioral health staff, peers, clerical staff, evaluators?)
Probes
-
Staff
-
Resources/financing
-
How many behavioral health staff are on the team?
-
Where are staff primarily located/co-located?
-
What expertise or capabilities would you add to your program if you could?
-
Do forensic peer-support staff work in your program? If yes, please tell me about their role(s).
Probes
-
How do they work with other team members?
-
With people being served?
-
-
BEHAVIORAL HEALTH COLLABORATION (RQ 6)
-
What is the relationship between law enforcement, courts, and behavioral health agencies in your community?
-
What coalitions and advisory bodies do behavioral health providers and law enforcement both participate in? Please describe.
Probes
-
Who else belongs to these groups? (Advocates, peers, health care organizations, hospitals? What is their role?
-
-
-
What agencies/programs partner with [Name of program]?
-
What are keys to a successful working relationship with each of your partners?
-
What challenges have you faced in working with your partners?
-
-
How do you cultivate community partnerships?
-
What is your process for meeting and updating one another?
Probes
-
Do you have formal coalitions? Please describe. [If not answered above.]
-
Do you contribute to their work in other ways, e.g., present at events they host, serve on their board of directors.
-
-
-
What Memorandum of Agreement (MOA) or Memorandum of Understanding (MOU) exist between law enforcement and behavioral health organizations?
-
Do you have MOAs or MOAs with other organizations?
Probes
-
For housing and case management?
-
Other services
-
-
How do these MOAs/MOUs help the agencies to work together on this program or other programs in the community?
-
-
What data sharing agreements, if any, do you have? With whom?
-
What data are shared?
-
How are the data used to inform programmatic decisions? Hot spotting?
-
-
How do you and your partner community behavioral health/criminal justice agency collaborate on training?
-
How is your program funded?
Probe
-
Does your program braid or blend funding from state general funds, Medicaid, SAMHSA grants, BJA grants, other federal funds? Please describe.
-
POLICY FACTORS/FACILITATORS/BARRIERS (RQ 2, 4)
-
Did implementation of the program require amending any policies related to dealing with people who have mental health and/or substance use? If yes, please describe which policies and the process for changing them.
-
What state policies, if any, affected local implementation of the program?
Probes
-
What state policies, if any, were amended to facilitate the implementation of the program?
-
(If applicable) Who, if anyone, championed changes in state policy?
-
FUNDING AND BUDGET IMPACT (RQ 7)
-
What resources were available to start the process of planning for the program?
Probes
-
Where did those resources come from?
-
Were any in-kind resources in the form of behavioral health staff time?
-
-
What funding sources were used to implement the program?
Probe
-
What is the source of these funds--grants (BJA, SAMHSA, state general funds local tax dollars)?
-
-
If implementation was funded by a grant, have you been able to identify a sustainable financing model for the program? Please describe.
Probes
-
What is the source of potential/current sustainability funds--federal, state, local, etc.?
-
What funding sources might support this work that you are planning to explore? Please describe.
-
-
What cost savings, to other parts of the system, can be used to fund the project? If so, please describe. Are cost offsets considered in discussions of ongoing financing of this program (or other jail diversion programs)?
EVALUATING EFFECTIVENESS (RQ 1, 3)
-
Do you currently have a funded evaluation?
-
If so, please describe funding for the evaluation.
-
If not, how are you evaluating the effectiveness of [Jail Diversion Program]?
-
-
Who was involved in developing the evaluation design?
Probes
-
Were organizational partners, community partners, funders, or other stakeholders involved?
-
What was their role?
-
How were they identified/selected?
-
-
Given the chance, is there anything you would do differently?
-
How do you use evaluation findings to support your program?
Probes
-
To support quality improvement?
-
Justify funding?
-
To demonstrate cost offsets to obtain additional financing?
-
-
Do you have a logic model you can share?
-
What inputs and process measures are you tracking for your process evaluation, if any?
Probes
-
How do you obtain/collect those data?
-
-
What individual-level outcome measures you using in your outcome evaluation?
Probes
-
How do you obtain/collect those data?
-
-
What challenges have you encountered in collecting/obtaining the data?
-
What other individual outcomes do you wish you hope to assess in the evaluation?
-
-
What population-level outcome measures you using in your evaluation?
-
How do you obtain/collect those data?
-
-
What challenges have you encountered in collecting/obtaining the data?
-
What other population-level outcomes do you wish you hope to assess in the evaluation?
-
-
What cost-effectiveness or cost-offset measures are used in your evaluation? Please describe.
-
What are the evaluation findings (if any) to date?
-
What reports/papers can you share? (if not already shared)
-
bOther data you can share?
-
WHAT WORKS
-
What have been the project successes to date? Please describe.
Probes
-
What do you attribute that success to?
-
-
What factors do you think were most impactful in successful implementation?
-
What factors do you think were most impactful in sustaining the program (if the program has been sustained past implementation)?
-
What have been the project challenges to date?
Probes
-
How have you tried to address them?
-
For challenges or barriers that have not been overcome, if any, how do you think they are hindering implementation of your program?
-
How are they affecting the population you serve?
-
-
What lessons learned have you learned that you could share with other communities that might want to implement a similar jail diversion program?
-
What federal policies are barriers to program success?
-
What suggestions would you provide to federal policymakers to help address those issues?
-
-
What insights can you share that might help the Federal Government address the opioid epidemic?
-
What suggestions would you provide to state policymakers to help address the opioid epidemic?
-
What policies are needed to support implementation of pre-booking jail diversion programs?
-
Where do you see [Name of Jail Diversion Program] in 1, 5, or 10 years?
-
Do you plan to sustain it? Expand it?
-
Do you think the need will remain or will your program be a success and not be needed in the future? Please describe.
-
-
Is there anything else about the project that you would like to share with us?
Partner Agency
Behavioral Health Agency
GENERAL QUESTIONS
-
Briefly, what is your role in the [AGENCY], how did you become involved in [Name of Jail Diversion Program].
-
Can you provide an overview of [Name of Agency]? Who at [Name of Agency] works with [Name of Jail Diversion Program] and in what capacity?
COMMUNITY CHARACTERISTICS
-
Please tell us about the community served by [Name of Jail Diversion Program]?
-
What aspects of the community support good behavioral health? Interfere with behavioral health?
-
How do communities of color (if any) and law enforcement interact?
-
What substance use and mental health treatment services are available in your community?
-
What is the relationship between criminal justice and behavioral health agencies in your community?
-
Besides the lead agency, what other community partners do you work with to address the criminal justice, behavioral health, diversion, etc. needs of the community?
PROGRAM COMPONENTS
-
Who from your agency works on [Name of Jail Diversion Program]?
-
Do you use volunteers? If yes, please describe?
-
Do you use forensic peer-support specialists? Please describe.
-
What is the level of collaboration with the [Name of Lead Agency or Police Department]?
-
(If there is more than one partner agency participating in the project) How do you collaborate with other program partners (not the lead agency)?
-
What are keys to a successful working relationship with each of your partners?
-
What challenges have you faced in working with your partners?
-
IMPLEMENTATION FACTORS
-
What role did [Name of Agency] play in the program origin, planning, and implementation of this program? Please describe in detail.
-
What organizational resources did [Name of Agency] bring to the implementation process?
-
What local policies, if any serve as barriers to program implementation or success?
-
What state policies, if any serve as barriers to program implementation or success?
-
What local policies, if any, helped the implementation and/or sustainability of the program?
-
What state policies, if any, facilitated the implementation and/or sustainability of the program?
-
What training have [Name of Agency] staff received through [Jail Diversion Program Name]?
-
Which trainings were most useful?
-
What other trainings would help your staff implement [Jail Diversion Program Name]?
-
What are the barriers to the training needed for your staff to implement [Jail Diversion Program Name]?
-
EVALUATING EFFECTIVENESS
-
What is your role, if any, in the program's evaluation?
-
How do you make use of data from the evaluation?
-
Who receives data reports? (Staff, peers, community, law enforcement?)
-
How are decisions about program implementation/funding/etc. informed by the evaluation data?
-
What improvements would you make to the evaluation, if any?
-
-
What aggregate data can you share?
-
What reports/papers can you share?
WHAT WORKS
-
What have been the project successes to date? Please describe.
Probes
-
What do you attribute that success to?
-
-
What factors do you think were most impactful in successful implementation?
-
What factors do you think were most impactful in sustaining the program (if the program has been sustained past implementation)?
-
What have been the project challenges to date?
Probes
-
How have you tried to address them?
-
For challenges or barriers that have not been overcome, if any, how do you think they are hindering implementation of your program?
-
How are they affecting the population you serve?
-
-
What lessons learned have your learned that you could share with other communities that might want to implement a similar jail diversion program?
-
What federal policies are barriers to program success?
-
What suggestions would you provide to federal policymakers to help address those issues?
-
-
What insights can you share that might help the Federal Government address the opioid epidemic?
-
What suggestions would you provide to state policymakers to help address those issues?
-
-
What policies are needed to support implementation of intercept pre-booking diversion programs?
-
Where do you see [Name of Jail Diversion Program] in 1, 5, or 10 years?
Probes
-
Do you plan to sustain it? Expand it?
-
Do you think the need will remain or will your program be a success and not be needed in the future? Please describe.
-
-
Is there anything else about the project that you would like to share with us?
Partner Agency
Law Enforcement Agency
GENERAL QUESTIONS
-
Briefly, what is your role in the [Department Name]? How did you become involved in the program?
-
Please provide a general overview of your department. What [Department Name] officers or team works with the [Name of Jail Diversion Program]? In what capacity? For what level of effort?
COMMUNITY CHARACTERISTICS
-
Tell us about the community/county covered by your department.
-
What are the major challenges that the community is currently facing.
-
What is relationship between criminal justice and behavioral health agencies in this community?
Probes
-
How has the relationship changed over time?
-
What is working well?
-
What are some of the challenges?
-
Who are the key players?
-
PROGRAM COMPONENTS
-
What is the department's role in [Name of Jail Diversion Program]?
-
How does [Department Name] partner with [Name of Lead Agency] to implement [Name of Jail Diversion Program].
-
Do you make use of volunteers? If so, how?
-
How would you describe the level of collaboration with [Name of Agency]?
-
(If there is more than one partner agency participating in the project) How do you collaborate with other program partners (not the lead agency)?
-
What issues are you trying to address with your partners?
-
What are keys to a successful working relationship with each of your partners?
-
What challenges have you faced in working with your partners?
-
-
Besides the [Name of Agency], what other community partners do you work with to address the needs of the community? Please describe those partnerships.
IMPLEMENTATION FACTORS
-
What role did [Department Name] play in the program origin, planning, and implementation of this program? Please describe in detail.
-
What resources did your department bring to the implementation process?
-
What local policies, if any, serve as barriers to program implementation or success?
-
What state policies, if any, serve as barriers to program implementation or success?
-
What local policies, if any, helped the implementation and/or sustainability of the program?
-
What state policies, if any, facilitated the implementation and/or sustainability of the program?
-
What training did your officers receive related to [Name of Jail Diversion Program]?
-
What trainings that have been especially useful?
-
What additional training would be useful?
-
What barriers to needed training, if any, have you all faced?
-
EVALUATING EFFECTIVENESS
-
What is your role in the [Name of Jail Diversion Program] evaluation?
-
What data sharing agreements, if any, do you have with the [Name of Jail Diversion Program]?
-
-
What aggregate data, if any, you can share? Reports?
WHAT WORKS
-
What have been the project successes to date? Please describe.
Probes
-
What do you attribute that success to?
-
-
What factors do you think were most impactful in successful implementation?
-
What factors do you think were most impactful in sustaining the program (if the program has been sustained past implementation)?
-
What have been the project challenges to date?
Probes
-
How have you tried to address them?
-
For challenges or barriers that have not been overcome, if any, how do you think they are hindering implementation of your program?
-
How are they affecting the population you serve?
-
-
What lessons learned have your learned that you could share with other communities that might want to implement a similar jail diversion program?
-
What federal policies are barriers to program success?
-
What suggestions would you provide to federal policymakers to help address those issues?
-
-
What insights can you share that might help the Federal Government address the opioid epidemic?
-
What suggestions would you provide to state policymakers to help address the opioid epidemic?
-
-
What policies are needed to support implementation of pre-booking jail diversion programs?
-
Where do you see [Name of Jail Diversion Program] in 1, 5, or 10 years?
Probes
-
Do you plan to sustain it? Expand it?
-
Do you think the need will remain or will your program be a success and not be needed in the future? Please describe.
-
-
Is there anything else about the project that you would like to share with us?
Site Visit Protocol--Discussion Guide Service Users
Thank you for taking the time to speak with us today. My name is _____ and this is my colleague________. We're doing a project for the U.S. Department of Health and Human Services, Assistance Secretary of Planning and Evaluation to help understand how jail diversion programs work. We are having discussions with you, program staff, partners, and others to help us better understand what makes these programs a success and what things need to be improved to better serve people with behavioral health diagnoses.
We would like to discuss your thoughts on services that can divert people from jail into appropriate services and supports. During our discussion, we ask that you not share your personal stories, but rather, think in general about what services and supports or are needed to people with behavioral health diagnoses out of jail. We are not recording this discussion nor will we use your name without permission.
Your participation in this interview is completely voluntary. We encourage you to answer these questions honestly and thoroughly, however, you do not have to answer any questions you are not comfortable with.
ACCESS TO SERVICES
-
Are acceptable mental health services available in your community?
-
What are the barriers to accessing the mental health services in your community?
-
Are acceptable SUD treatment programs available in your community?
-
What are the barriers to accessing the substance abuse treatment programs in your community?
-
Are there accessible peer-support groups or other programs where people with mental health diagnoses or SUD can get support from others who are going through the same thing?
-
Is there affordable housing in your area?
-
Are there programs in the community that help people find affordable housing?
-
Are there services that are needed in your community that do not exist? Please describe.
-
Is health insurance or lack thereof a barrier to receiving services in your community? Please describe.
LAW ENFORCEMENT
-
What do you think about how the police interact with people with substance use or mental health conditions in your community?
-
How do law enforcement and behavior health service providers work together in [Name of Jail Diversion Program]?
-
How would you like to see interactions change between police and people with behavioral health diagnoses?
CONCLUSION
-
If you were to design this program, what would you include?
Probes
-
What would you change?
-
What could be improved?
-
-
Is there anything else you'd like to share about [Name of Jail Diversion Program]?
APPENDIX G: SECONDARY DATA COLLECTION FORM
| Site Name: | |
| Intercept | |
| _____Intercept 0 | _____Intercept 1 |
| Program Model | |
| Community Services Models | Law Enforcement Models |
| _____Assertive Community Treatment (ACT) | _____Crisis Intervention Team (CIT) |
| _____Medication-Assisted Treatment (MAT) | _____Expanded Crisis Intervention Training |
| _____Crisis Center | _____Law-Enforcement Assisted Diversion (LEAD) |
| _____Mobile Crisis Team | _____Psychiatric Emergency Response Team (PERT) |
| _____Housing First | _____Other Co-Response Model
|
| _____Peer Specialist | _____Other: ________________________________ |
| _____Peer-Run Respite | |
| _____Other: ________________________________ | |
| Partner Agencies | |
| Agency Name | Agency Type |
| Persons Interviewed | ||
| Name | Title | Agency |
| Secondary Data Collected | |
| Data Type | Description |
| _____Logic Model | |
| _____Evaluation Plan | |
| _____Conference Presentation | |
| _____Issue/Research Brief | |
| _____Evaluation/Outcome Report | |
| _____Peer-Reviewed Paper | |
| _____Memorandum of Understanding | |
| _____Data Sharing Agreement | |
| _____Protocol | |
| _____Procedure | |
| _____Data Table | |
| _____Poverty Rate | |
| _____Crime Rate | |
| Population Density | |
| _____Percent Minority Poplation | |
| _____Mental Health Beds Per 1000 | |
| _____Medicaid Expansion State (Y/N) | |
| _____Other | |
| _____Other | |
| _____Other | |
| _____Other | |
| _____Other | |
| _____Other | |
| _____Other | |
| _____Other | |
| _____Other | |
APPENDIX H. CASE STUDY SUMMARIES
Name of Site: Lucas County Drug Abuse Response Team (DART)
Date of Site Visit: June 27-28, 2018
Abt Site Visitors: Holly Swan & Samantha Karon
Program Overview: DART is a unit within the Lucas County Sheriff's Office--an office that embraces a community policing approach. The unit comprises select police officers who are designated to respond to calls regarding adults who have had an opiate overdose in Lucas County. The mission of DART is to link people who have experienced or are experiencing an opiate overdose to treatment services, primarily ensuring transition from emergency rooms/hospitals to detox beds and inpatient treatment facilities. DART responds to every overdose case in Lucas County, and has responded to over 3,000 overdose cases to date. DART aims to make contact with people who have overdosed within 20 minutes of receiving the dispatch call, as immediate response is critical to diverting people to treatment and away from environments where they are likely to overdose again. After making initial contact, officers are responsible for linking clients to services in the community and following them for a two-year period to monitor progress, foster connections, and serve as their advocate in the law enforcement system. Officers wear plain clothes and drive unmarked cars in an effort to reduce the distrust many of their clients feel towards police officers and distance themselves from the stigma against law enforcement held by both their clients and service agencies. As one officer put it, "DART is like "social work on steroids"--the "steroids" referring to the officers' law enforcement capacity. Although not a service-provider in the clinical sense, DART provides a touch point to the system at a critical time for intervention with adults with OUD (immediately after an overdose).
Program Components: DART is notified of overdose cases through the county's centralized dispatch system, which routes calls to 911, EMS, the fire department, the police department, and the Sheriff's office. DART also receives referrals from hospitals, courts, and through word of mouth: people can contact DART directly to connect with an officer and get linked to treatment. After arriving on the scene, the DART officer offers immediate assistance enrolling the person in substance use treatment, including transportation to detox. If the person accepts the offer, that person becomes that officer's case. Officer caseloads are about 55 cases per officer. Officers monitor cases using a software system specially developed for the unit. Officers log notes from initial and ongoing communication with their clients in the system. Officers are able to access one another's notes and collaborate with one another on case management. Families also play a significant role in the case management process; officers communicate directly with families and information is shared bi-directionally. There are two overlapping regular shifts (7am-10pm), and one officer is always on call outside of regular hours. Officers spend about 50% of their time in the office, 40% on the street, and 10% in court.
The unit includes two Community Advocate/Outreach Officers whose role is to conduct outreach activities with the public and form networks among service agencies and local stakeholders, such as businesses, schools, and civic organizations. Officers also have a strong rapport with the court system and can serve as advocates for their clients who are facing minor charges; compliance to a treatment plan and a good standing with DART can lead to minor charges being dropped. Finally, in addition to pre-booking diversion, DART includes a jail intervention component and partners with a local treatment provider to provide Vivitrol shots to clients prior to discharge; officers will also pick up clients from jail and transport them directly to treatment.
Staffing: There are nine full-time officers in DART: six deputies, an officer from the Toledo Police Department, an officer from the Mercy Health Police Department, and a Children's Services officer. Numerous part time officers from various departments throughout the county also participate in DART. There are also two full-time Community Advocate/Outreach Officers, who are social workers/counselors responsible for conducting outreach (one of the counselors has been granted arresting powers by the Sheriff). The unit is overseen by a police sergeant, who reports to the police captain and the Sheriff.
Population of Focus: Adults in Lucas County with an opiate addiction, and their families.
Program Partners: DART is built on a strong community presence and partnerships with the community are critical for its success. Partners for the main goal of an initial linkage include: hospitals; local treatment centers, particularly inpatient treatment centers with detox beds; and jails. Partners for outreach, case follow-up, and education include the Toledo Public Schools, hospitals, jail, recovery housing, local businesses, state and local agencies (e.g., mental health board), and politicians (e.g., Attorney General).
Program Evaluation: Although the unit has not undergone an official evaluation, they do track the number of client contacts, and the number of linkages made to treatment providers, per case. DART measures success in terms of number of clients linked to treatment, and reports an average linkage rate of 80%. Aggregate data has not yet been provided. Among the unit and the Sheriff's office more broadly, success also comprises the harder-to-measure outcomes of crimes prevented and lives saved.
Policy: DART was originally funded by a grant from the state's Attorney General; it is now a 501(c)(3) charitable organization supported through a combination of grants, fundraising and donations. There is some DART funding allocated and protected by the county commissioner and county mental health board. DART does not have an MAT policy, but does partner with a local treatment provider to provide Vivitrol to clients prior to discharge from jail.
Implementation: Some challenges to implementing DART are: (1) finding funding; (2) HIPAA restrictions; (3) overcoming stigma of addiction (in general, and heroin use in particular) by the community and service providers, police/law enforcement by the community, and "soft policing" (referring to helping people with an addiction, rather than incarcerating them) by other law enforcement colleagues; (4) finding resources in the community (e.g., number of detox beds); and (5) lack of recovery housing (16 detox beds in the county when DART was established, 139 today, which still is far fewer than needed). Despite these challenges, DART has succeeded at obtaining bi-directional buy-in (i.e., grassroots at the community level and also at the top among local and state officials) and establishing trusting relationships between officers and the community, doctors, and judges. Factors that have contributed to this success include relentless outreach with the target population (DART officers are at the bedside for every overdose--it might take repeated contact to get the person to engage, but DART ensures an officer will be there at every overdose occurrence; DART officers engage with their cases for two years) and the community (breaking down stigma; providing education; uniting the community around a common platform, i.e., the opiate epidemic, particularly in Lucas County); and consistency in mission and practice which breaks down stigma and promotes trust (e.g., "we are not here to arrest your client/patient/son, we are here to help them").
----- ----- ----- ----- -----
Name of Site: Mental Health Association of Nebraska (MHA-NE): Respond Empower Advocate Listen (REAL)
Date of Site Visit: June 27-28, 2018
Abt Site Visitors: Vijay Ganju and Elle Gault
Program Overview: REAL has evolved over the last 8 years from a fledgling e-mail referral service to a pre-booking jail diversion program in Lincoln, Nebraska with multiple community partners, strong credibility, and broad community support. There are several unique aspects to the program: (1) the entire program is peer-run and operated; (2) that services are free, voluntary and non-clinical; (3) collaborations with law enforcement and other service providers have become community partnerships; and (4) the perceived success of the program has resulted in community "ownership," as reflected in statements made during the site visit made by police chiefs, hospital and prison administrators, local foundation staff, media personnel, state senators, program staff, and people who have or who are using the program.
Program Components: Following a mental health/substance use encounter, a police officer can refer the person to the REAL program, which then deploys a peer specialist within 24 hours to contact and offer assistance. If the person decides to participate, peers collaborate with him/her to establish a plan for working together to support recovery. In the months after the referral, peer specialists update the referring officer about the person's status and collaborate to develop additional plans, if needed. The police officer does not just "drop off" the person but works with REAL to help access resources and establish long-term plans.
The REAL program also operates two crisis respite houses and a 24/7 warm line, and provides WRAP training to the LPD. MHA-NE also has a housing and employment program through which persons in the REAL program are linked to community resources. Besides the REAL program, MHA-NE also operates a prison re-entry program, a major component of which is a 21-bed community residential facility.
Staffing: REAL has 38 peer specialists on staff.
Population of Focus: The population of focus is people in crisis, whether it is due to mental illness or SUDs. Individuals are often referred by police, but as community awareness of the REAL program has grown, family members, neighbors, friends, and landlords also make referrals. Lincoln has not experienced the opioid crisis in a significant way so this has not been a focus for the REAL program.
Program Partners: The LPD has been a critical part of the REAL program. The department supports the program by making referrals and providing funding. A major aspect of this collaboration is also the "community policing" philosophy the LPD has embraced, which involves a long-term relationship with the people they have referred to the program. Police also act as a conduit to a range of community resources including housing, food, transportation, and legal assistance. Collaboration between LPD and MHA-NE also takes place through quarterly meetings to improve cooperation, enhance outreach, and develop plans for high users of police services. MHA-NE also provides behavioral health training to police.
While MHA-NE has its own housing and employment specialists, REAL peer specialists work closely with national and state housing investment authorities. The National Investment Finance Authority collaborated with MHA-NE on their respite housing program. REAL peer specialists work with Targeted Adult Services Cooperation (TASC), a local behavioral health service provider that collaborates with MHA-NE peers to assist clients entering more formal behavioral health treatment. The Community Endowment Fund (CEF) is the original funder of the REAL program. The CEF collaborates with and funds many MHA-NE programs, as well as advocates for the programs with local and state stakeholders and funders. MHA-NE rents offices from Nebraska's Region V HHS offices and this co-location also facilitates collaboration with federal HHS staff.
Program Evaluation: MHA-NE is not conducting a formal evaluation of the REAL program. HHS Region V, police, and self-report client survey data are available for a program evaluation, but MHA-NE does not currently have a method to analyze the data. Hospital data are not available due to HIPAA restrictions, but efforts are in place to access this information. To date, data have been used for the disposition of person cases rather than evaluation of the program. There is potential for an evaluation if funding is identified.
LPD Officer Luke Bonkiewicz used internal police resources and data to conduct an analysis of 775 people referred to the program from its inception in 2011 to 2013 and a comparison group of people who were not referred to the program. The study, which resulted in two published papers, found that referred people were 33% less likely to be taken into emergency protective custody two years after initiating REAL services as compared to non-referred people and 44% less likely to be taken into emergency protective custody as compared to non-referred people three years after initiating REAL services. It was noted that the program required 12-24 months of involvement before benefits of the program were seen.
Anecdotally, the program staff, police, and service users report numerous "success" stories in terms of reduced police contact and improved health, social, and vocational outcomes that have led to increased credibility of and trust in the program. Many of the REAL staff are living proof of the transition from multiple incarcerations to a community life as taxpayers with a job, housing, and family.
Funding: The REAL program is funded entirely through grants. The original grant was provided by the Community Health Endowment (CHE). The Nebraska Department of Correctional Services, the city of Lincoln, and SAMHSA all provide grants to support the program. A critical aspect of initial funding was the willingness of CHE to risk supporting an unproven program. LPD advocates for continued and increased funding of REAL Community and consumer volunteers also make significant contributions to the program. REAL does not bill Medicaid because the definition of "peer services" excludes MHA-NE as they do not have an on-site clinician.
Implementation: The commitment, collaboration, and stability of the leadership of MHA-NE and LPD are critical success factors. The peer specialists' commitment to their community and mission has resulted in a culture that is both outcome-based and consistent. Police repeatedly stated that peers "say what they're going to do and then go and do it." Potential barriers to continued jail diversion through the REAL program are the changing state-level regulations related to peer-support programs; potential withdrawal of funding, especially if there is a visible community "failure" that receives negative publicity; the management of stakeholder expectations; and the lack of understanding of peer services by and strained relationship with many behavioral health service providers in the community.
While many components of the REAL program are transferable to other programs, the key components of REAL program success are the leadership and community collaboration that have evolved over time. The provision of peer specialists support, and buy-in from community stakeholders, has led to an intersectional approach to address housing, employment, and social outcomes. Time to "allow" the program to work has also been key to success. State Senators are very interested in replicating REAL across Nebraska but the program cannot be easily transplanted because REAL has built its capacity and success on the specific characteristics and supports available in the local community. Programs building on the REAL model will need to tailor and adapt program components to fit their communities.
----- ----- ----- ----- -----
Name of Site: Wichita Police Department Homeless Outreach Team (HOT)
Date of Site Visit: July 10-11, 2018
Abt Site Visitors: Brandy Wyant & Samantha Karon
Program Overview: The Wichita Police Department Homeless Outreach Team (HOT) is a community policing program with the mission to divert people experiencing homelessness from jail by linking them to behavioral health and housing resources. HOT officers are connected to people experiencing homelessness in two ways: through 911 calls and direct referrals from the community. HOT officers respond, assess the situation, and offer assistance. HOT partners with numerous behavioral health and housing agencies to refer people they encounter to trusted service providers. HOT serves as a conduit between community members and advocates, responding to the concerns of business owners and civilians while also protecting the civil rights of people experiencing homelessness. All officers have received CIT training and are willing to take on case management and housing referral work.
The Wichita HOT program was established in 2011 and modeled after the pilot HOT program implemented in Colorado Springs, Colorado, in 2009, which has been recognized by the U.S. Interagency Council on Homelessness and the DoJ as a best practice. The Wichita HOT program was founded in response to data indicating that increasing arrest rates are not associated with decreasing levels of chronic homelessness. From 2009 to 2011, Wichita saw a 65% increase in homelessness, though arrest rates did not decrease over the same time period. HOT serves as a non-traditional approach to law enforcement in that HOT officers aim to issue tickets and make arrests only as a last resort.[1]
Program Components: The HOT team utilizes an app called RingCentral Phone to allow calls to a direct line to be patched through to each HOT officer's cell phone. The direct line mitigates the hesitation some community members feel about calling the police regarding people who are without housing. After receiving a call, the officer arrives on the scene and introduces themselves to the person on the street, with the primary aim of building rapport and connecting that person to necessary resources. If the person accepts the officer's offer to link them to services, the officer will offer transport to the service agency, or the person may choose to transport themselves. Services are provided by local behavioral health and housing agency partners. If the person declines services, the officer leaves the scene and notes the person's decision in the HOT database. In situations where a person is violating a public ordinance, he or she may face charges, though HOT officers have the ability to drop minor charges retroactively if people agree to engage in services via a standard petition to the prosecutor. Officers may also request that a judge send a person through mental health court or drug court instead of the judicial system.
In addition to linking people to local resources, HOT operates Finding A Way Home, a program that provides people experiencing homelessness with bus tickets to reunite them with people from their personal networks who are able to house them. After verifying with the family or friend that this person will be stably housed, the HOT Team will purchase that person a bus ticket using funds from private donations. Participation in the program is optional.
HOT conducts education and outreach activities with fellow agencies and the public to address misinformation about policies and misguided attempts to help people experiencing homelessness.
Staffing: HOT is currently comprised of two police officers. A third officer has been hired to join the team in the near future, but per the HOT model, the Team should be staffed by four officers so that the officers can work in pairs. HOT officer salaries are funded through the city government while HOT program components are privately funded through charitable contributions. HOT is supervised by one Sergeant, who also supervises all the Wichita Police Department community policing programs.
Population of Focus: All people experiencing homelessness in the city of Wichita, Kansas.
Program Partners: HOT partners with housing and behavioral health providers to connect people experiencing homelessness to services, including: the Wichita Housing Authority (Housing First, case management services); shelters, e.g., Union Rescue (immediate and short term housing); and COMCARE (CIT training for officers, behavioral health services, case management, MAT).
HOT has a data sharing agreement with HUD's Homeless Management Information System (HMIS), COMCARE, and the U.S. Department of Veterans Affairs. HOT is a part of the Continuum of Care, and officers attend regular meetings with these partners. Officers also have a strong relationship with the Wichita City Council.
Program Evaluation: HOT has not been evaluated by an external evaluator. Officers enter data on every person contacted in their internal database, which is merged with the HMIS system, allowing HOT to track referrals and outcomes. HOT obtains signature release from people at first contact to permit them to collect data and share it with partner agencies. Since 2011, HOT has made contact with over 12,500 people experiencing homelessness and helped place 932 people in housing.
Policy: HOT monitors court cases involving homeless policy and updates local policies in accordance to judicial rulings. For example, HOT worked with the city government to change Wichita's encampment ordinance in response to Supreme Court rulings on encampments. In Wichita, only HOT officers can enforce encampment policy; people must have shelter to go to in order to be required to vacate, and people must be given notice of 48 hours to vacate. HOT has not made any arrests under the encampment ordinance since the program was started.
Implementation Challenges: There is a lack of housing slots for women as well as a gap in case management and access to services for uninsured or underinsured residents. The program also faces public misinformation about policies affecting people experiencing homelessness, such as the panhandling restrictions and camping ordinances. While those policies are often perceived as unjust, they are the least restrictive possible while still maintaining constitutional rights.[2]
----- ----- ----- ----- -----
Name of Site: Oakland Community Health Network (OCHN)
Date of Site Visit: July 23-24, 2018
Abt Site Visitors: Sarah Steverman & Samantha Karon
Program Overview: The OCHN is the private non-profit behavioral health authority in Oakland County, Michigan which oversees the county's jail diversion process, in collaboration with police departments and service providers. OCHN established the jail diversion process in in 2000 with the aim of decriminalizing responses to people with mental health or substance use issues by law enforcement. OCHN facilitates the jail diversion process through the jail diversion coordinator, who works to empower officers to divert to services rather than press charges, and ensures that the county provider network, especially the crisis center, is equipped to provide services to people who have been diverted by law enforcement. The jail diversion coordinator conducts frequent and continuous outreach to the 43 police departments in the county, raising awareness of the jail diversion process and letting officers know he is a resource to them. OCHN also provides training to police departments in MHFA for Public Safety and provides CIT training as a joint effort with the Sherriff's Office, Oakland County Jail, and police departments.
Program/Process Components: OCHN facilitates the jail diversion process in Oakland County via the jail diversion coordinator, a full-time OCHN position. The jail diversion coordinator trains officers on the diversion process and works with OCHN leadership to ensure law enforcement have easy access to OCHN's diversion resources, namely the Resource and Crisis Center (RCC). The process includes the following steps:
-
Police officers determine the person's immediate needs. For medical attention they can transport to the nearest emergency department. If a person is a potential danger to self or others, or simply need an assessment and to be linked to treatment, the officer can bring the person to Common Ground, located at the RCC. For non-emergency treatment, the officer can contact OCHN's Access department, which receives and responds to all non-emergency calls.
-
Police officers determine the type of diversion. Law enforcement can divert people from jail by formal or informal means. Formal diversions occur when an officer transports a person to Common Ground, OCHN's crisis provider. An informal diversion occurs when an officer directs the person to other community resources, such as the emergency department or OCHN's Access (intake) number, rather than arresting them.
-
Police officers drop off at Common Ground. Common Ground has an emergency door for law enforcement to expedite the drop off for police officers. Even if Common Ground is full and does not have any available beds, their policy is to accept people brought by police officers to ensure law enforcement can count on the crisis center as a resource.
Police generally consider a case closed once a person is dropped off at a participating provider. They trust OCHN and its contracted providers to appropriately engage the person in treatment. The jail diversion coordinator spends approximately 20% of his time working on person cases, and is authorized to view all client information in the OCHN system, but he must obtain a signed release from the person in order to share information with police.
OCHN's RCC is the only comprehensive crisis center in Michigan, and provides services for both mental health and substance use crises. Common Ground represents approximately 80% of the RCC. Common Ground services include:
-
24/7 Helpline--receives 80,000 calls/IMs/texts per year.
-
Mobile crisis team--10am-10pm unit, consisting of a social worker and peer.
-
Oakland Assessment and Crisis Intervention Service--receives drop offs from police department via the 24 hour emergency drop off door and has nine adult beds and two child beds, where people can be held up to 24 hours.
-
Sober Support Unit--ten beds staffed by peer-recovery support specialists and paramedics; people can enter via Rides for Recovery (Sherriff's office program), police drop off via Oakland Assessment and Crisis Intervention Service, or self/family referral.
-
Crisis Residential Unit--up to two-week residential program with 16 beds for people who need additional inpatient recovery; focused on psychosocial therapies (art, music, groups).
Access, also located at RCC, is the centralized entry point to OCHN funded services. It includes telephone screening and referral to specialists within OCHN, provides warm handoffs to the crisis helpline, and can do in-person OCHN enrollment in the Sober Support Unit.
Staffing: The jail diversion coordinator is considered key staff and funded through OCHN general funds. Additional support staff are funded through grants as they are available. Crisis and treatment services are funded through Medicaid dollars as part of the OCHN provider network.
Population of Focus: The jail diversion process targets people who could be charged with non-violent misdemeanors or who are in situations that may lead to some criminal behavior. Due to cuts in general funds, OCHN's providers only serve Medicaid-eligible people, although the crisis center accepts any person from law enforcement, regardless of insurance status.
Program Partners: OCHN's partners include the 43 police departments in the county. Police departments have varying levels of engagement with the jail diversion process. The Auburn Hills Police Department is a major partner, jointly providing MHFA and CIT training. The Oakland County Sheriff's Office operates Rides for Recovery and partners with OCHN on CIT Trainings. OCHN mental health and substance use treatment providers make up the treatment network for people who have been diverted from arrest. The primary OCHN provider partner in jail diversion efforts is Common Ground, providing crisis services. Easter Seals, an OCHN mental health provider, provides community treatment as well as in-jail services and assists with re-entry for people returning to the community from jail.
Program Evaluation: Michigan State University is conducting an evaluation of the state Diversion Task Force, which includes Oakland County's efforts. The jail diversion coordinator tracks the number of diversions through a log at Common Ground. He also tracks other diversions that are reported to him but there are many diversions that occur as a result of officer training that he is unable to count.
Policy: OCHN is required to work with law enforcement as part of their Medicaid contract with the state, and in turn have contract requirements with their providers to facilitate law enforcement/behavioral health collaboration. Other policies that have facilitated jail diversion in Oakland County include:
-
State requirements starting in 2016 for coordination agreements between OCHN and police department s within Oakland County. All police departments are required to sign, but to date only 14/43 have signed agreements.
-
A Statewide Diversion Task Force has provided a platform and some grants for implementing jail diversion.
-
A GSL that ensures that no charges are made for minor drug possession, reducing barriers to calling 9-1-1 in cases of crisis or overdose.
-
The County Board of Commissioners signed on to the Stepping Up Initiative, a national effort to reduce the number of people with mental illnesses in jails.
-
The jail diversion coordinator was previously employed by an OCHN provider, Easter Seals, but is now an OCHN employee, which allows him to monitor cases across the OCHN system and report to law enforcement with proper releases, if requested. (Police follow-up with diversion cases has reduced dramatically as they have increased confidence in the process.)
Auburn Hills Police Department also has additional policies in place to promote jail diversion:
-
A formal jail diversion policy (effective 2015) and NARCAN policy (effective 2016).
-
Engagement in the International Association of Chiefs of Police's One Mind Campaign, requiring training and procedures to ensure successful interactions between police and people affected by mental illness.
-
They recently signed on to Hope Not Handcuffs, a non-profit initiative that runs ANGEL programs in police departments in Michigan.
-
Lack of a jail means Auburn Hills officers can only hold people by bringing them to the county jail, which they are reluctant to do for non-violent misdemeanors and is a key factor facilitating diversion rather than arrest.
Implementation Challenges: Several issues were identified as challenges to widespread implementation of jail diversion processes. First, much of the state requirements for collaboration between behavioral health and police departments have been unfunded. The Jail Diversion Coordinator is funded by OCHN general funds, but this is the only OCHN position supporting the jail diversion process that receives such funding; all other support positions are subject to grant cycle instability. There are challenges to the service system, including behavioral health workforce shortages; lack of engagement of hospitals in the jail diversion process, so there is no coordination with OCHN or police after a person is dropped at the emergency department; and lack of affordable housing. Additionally OCHN and their partners noted that antiquated licensure requirements have been a barrier to obtaining proper licenses for specialized crisis units. The crisis center requirement to hold a person for less than 24 hours is often not enough time to identify an appropriate treatment plan. Medicaid coverage suspension for incarcerated people (a 30 day lag between jail discharge and coverage returning) can lead to a gap in contact with reentering citizens who might have been engaged in treatment. Law enforcement is challenged by funds, time, and availability of CIT and MHFA training. Police departments have recently hired many new officers to replace retiring veteran personnel. Training up so many new officers in jail diversion procedures has been challenging. Finally, the jail diversion coordinator has had varying success engaging police departments across the county in jail diversion activities because of some police department leadership's view on behavioral health and community policing, competing priorities for training time and funds, and proximity to Common Ground.
----- ----- ----- ----- -----
Name of Site: ANGEL Program
Date of Site Visit: August 6-7, 2018
Abt Site Visitors: Sue Pfefferle & Elle Gault
Program Overview: The ANGEL Program was launched by the GPD in June 2015 in response to three fatal overdoses by high-profile people in the community. Originally, the program launched as an amnesty program for those with OUD to safely turn in their drugs or equipment and to then be connected to behavioral health services. People rarely turned in drugs, but did use the program to access help. Once a person arrived at the police department, the Watch Commander on duty would contact a volunteer "Angel" to sit with the person while a clinician identified a detox bed, which took several hours. After about six months, the officers involved in the program realized that they were able to access beds faster than the clinician so they discontinued using clinicians and "Angels." Currently, the Watch Commander on duty directly refers a person to a detox or treatment facility. If the person signs a release of information form, the police supervisor or Care Advocate/Outreach Specialist from the Police Assisted Addiction and Recovery Initiative (PAARI) assists the person in accessing longer term treatment.
PAARI was founded alongside the ANGEL Program to encourage police departments across the country to adopt and implement pre-arrest jail diversion programs focused on helping people with OUD access treatment. PAARI's premise is that OUD is a chronic illness. Since 2015, over 143 police departments nationwide have joined PAARI on its mission to reduce the impact of SUDs on communities.
In the early 2000's, preceding the inception of the ANGEL Program, now Chief John McCarthy and community partners created the High Risk Task Force for Gloucester community stakeholders to come together and discuss how to connect high-risk people in the community to treatment and other services. The task force is an essential forum for relationship-building between providers and strategizing ways to meet the needs of Gloucester residents at the highest risk. Meetings take place monthly, alternating bi-monthly between didactic presentations on relevant topics (e.g., harm reduction, MAT and case conferences on specific people who have provided consent to have their situation discussed. All community providers are task force members. The Chief of Police and Lieutenant in charge of the ANGEL Program also attend.
Program Components: There are three components to the ANGEL Program:
-
Police referral for treatment. Any person who enters the GPD and is requesting help with their opioid use is immediately screened into the ANGEL program. If such a person who has requested help with their addiction has drugs or drug equipment while requesting help, they are not charged for possession. All officers having contact with people entering the GPD for help with their addiction are professional, compassionate, and understanding. The officer immediately notifies the Watch Commander (i.e., the Sargent or Lieutenant on duty) that a person is requesting help with their addiction. That prompts the Watch Commander to find a local detox facility to connect the person, provide a taxi or transportation, and assist that person into services. At any point a person may choose to decline those services and leave.
-
Chapter 123, Section 35 commitment to treatment. Massachusetts law provides for involuntary commitment to inpatient SUD treatment services. This is often a coordinated effort in collaboration with members of the High Risk Task Force to successfully document a person's substance misuse problems and to secure and execute a warrant to check that person into an inpatient facility.
-
Overdose outreach. When an overdose occurs in the Gloucester community and the police are called to the scene or made aware, the police follow-up with that person or their family. Within a few days, a Gloucester police officer, the PAARI Care Advocate and Outreach Specialist, and, if available, the part-time mental health clinician co-responder who is an employee of Lahey Behavioral Health will visit the person and provide information on local resources, treatment options, and additional community support. They also leave the person or family member with NARCAN.
Staffing: The GPD is a 58-person unit with 43 uniformed officers, seven Sergeants, seven Lieutenants, and the Chief of Police. All Sergeants and Lieutenants in the department can be the assigned as "Watch Commander" for the shift.
Population of Focus: Individuals with SUD, specifically opioids. Community stakeholders identified that the population of people with OUD has changed. Community providers previously saw an older population who were without housing who had chronic illness and OUD, but as the opioid epidemic has worsened in Gloucester, younger people ages 18-22 are most frequently impacted by the epidemic. Some of these young adults are casual users who do not realize that the "Demerol" or other drug they are taking is actually Fentanyl.
Program Partners: The ANGEL Program has many partners in the Gloucester community who contribute to the program's success. Relationships between treatment providers were identified as crucial to the success of the program. The Gloucester High Risk Task Force is one key facilitator of strong interagency and provider relationships. The other factor is the strong sense of community in Gloucester, which has a proud history of fishing and interdependence between community members. The mayor is also extremely supportive of the ANGEL program.
The Grace Center is a local facility that provides two meals a day, as well as space and programming for people in need in the area. They have four staff-members, including a full-time social worker who provides information on local services available in Gloucester. Action runs a local homeless shelter and provides additional housing options to those in need in Gloucester. There is also a private sober housing provider in the city. PAARI funds a Care Advocate/Outreach Specialist located in Gloucester to assist the police department with overdose outreach and engagement follow-up. The Care Advocate/Outreach Specialist works to connect people to recovery services, and provides reintegration assistance once people have completed treatment. Each morning he creates and disseminates a list that includes the available open detox and Clinical Support Services beds and MAT openings in the area to the GPD, other police departments, ANGEL partners, and other local community service providers. He also provides NARCAN and NARCAN education to community members, library staff, family members, and fishing captains. The Grace Center uses this list each day to connect people to detox services when necessary. One Stop is a local HIV and Hepatitis C harm reduction project that provides free NARCAN, risk reduction education, and syringe services. Lahey Behavioral Health Services has supported the ANGEL program by funding a co-located part-time mental health clinician through an IMPACT program grant focused on mental health diversion and providing transportation through another grant. Open Door is the local food pantry that supplies food to the Grace Center and offers free meals to low income Gloucester residents. All of the ANGEL program partners are a part of the High Risk Task Force.
Program Evaluation: The Boston Medical Center and the Boston University School of Public Health conducted a process evaluation of the first year of the ANGEL Program. They found that in the first 12 months, from June 2015 through May 2016, 376 unique people came to the police department for the ANGEL Program a total of 429 times. Of those people available for referral to treatment, 94.5% were offered placement in treatment facilities. The program sometimes cannot offer placement due to insurance coverage issues, people not being Massachusetts residents, or when there are no available treatment facilities at the time of the referral. While the police track their referrals, they do not conduct follow-up with people once they enter treatment.
The Care Advocate/Outreach Specialist tracks his own client interactions. He reports 583 client interactions from October 2016-July 2018, serving about 259 unique people. Additional people are served through Grace House, where he provides outreach. The Grace House clinician refers people for OUD detox and treatment on her own, with support from the Care Advocate/Outreach Specialist as needed.
Policy: The only funds needed to operate the ANGEL Program are staff labor, which is included in the GPD budget, funds to transport people to treatment, and the Care Advocate/Outreach Specialist position, which is funded by the Lutz Foundation. Lahey Behavioral Health Services has a crisis transportation grant that covers taxis to detox until September, 2018. Staff hope that the grant can be renewed. In addition, the GPD receive "scholarships" from secondary and long-term treatment centers to send people referred from the ANGEL program into OUD rehabilitation. These were referred to as "Golden Tickets" and used sparingly. The GPD has sent people to facilities on Cape Cod, Florida, California, and Hawaii because these facilities offer free long term treatment.
Implementation: The ANGEL Program started the first program of its kind in the nation without adequate planning. The excessive promotion of the program nationwide before its launch and lack of preparation created stress on the department for the first six months of implementation. The GPD and local treatment services were at first overwhelmed with an influx of people hoping to participate, from as far away as California. Waiting for "Angels" and clinicians to arrive at the police department before referring a person to services slowed down the treatment referral process. Once the police department removed the "Angel" and clinician component of the program, they found they were able to shorten the time it took to connect a person directly to services by about two-thirds. The adaptation of the program to the needs of the Gloucester community was critical in establishing a more successful program. The success of the Gloucester ANGEL program can also be contributed to the changing attitudes and culture of police officers in the department. The emphasis from department leadership for officers to be compassionate to those effected by substance use and misuse helped spur a cultural change within the department, and the community.
GPD leadership suggested that other departments looking to start a similar program begin with establishing relationships with partners, implementing an unadvertised pilot program, tailoring the program to their own community needs and resources, and collecting data before advertising the program to policymakers and the public.
NOTES
-
Traditionally, officers commonly issued tickets for "public nuisance" offenses like blocking the flow of traffic while panhandling or public urination. Tickets generally go unpaid because the individual cannot afford to pay it, leading to an arrest. Once released from jail, the individual soon engages in similar behaviors, repeating the cycle of ticket, arrest, and incarceration. To prevent this cycle, HOT officers rarely issue tickets or make arrests.
-
For example, individuals may panhandle as long as they do not block traffic. Additionally, officers cannot remove a camp without an identified alternative place for the individual to go. Because Wichita has a dearth of shelter beds for women, most women who are camping will not have their camps removed due to a lack of an alternative shelter.