
Abstract
The Affordable Care Act includes several provisions that are expected to significantly improve health outcomes for Latinos. New estimates from RAND suggest that 5.4 million Latinos who would otherwise be uninsured will gain coverage by 2016 through the expansion of Medicaid eligibility and the creation of Affordable Insurance Exchanges. Many other valuable benefits, including coverage for young adults and preventive services without cost-sharing, are already in effect and benefiting Latinos across the country.
Racial and ethnic disparities in health and health care in the United States are pervasive and well-documented. Racial and ethnic minorities still lag behind their non-Latino White counterparts across a range of health indicators, including life expectancy, prevalence of chronic diseases, and access to quality care.1,2 In addition, individuals from racial and ethnic minority groups represent about one-third of the nation’s population, but make up over half of the estimated 50 million Americans with no health insurance coverage.3 An estimated 30.7 percent of Latinos are uninsured, compared with 16.3 percent of all Americans.4
The Affordable Care Act includes several provisions that are expected to significantly improve health outcomes for Latinos.5 New estimates from RAND suggest that 5.4 million Latinos who would otherwise be uninsured will gain coverage by 2016 through the expansion of Medicaid eligibility and the creation of Affordable Insurance Exchanges. Many other valuable benefits, including coverage for young adults and preventive services without cost-sharing, are already in effect and benefiting Latinos across the country.
"
Expanded Insurance Coverage
Estimates from the RAND COMPARE microsimulation model suggest that 5.4 million Latinos who would otherwise be uninsured will gain coverage by 2016 under the Affordable Care Act.6 The Affordable Care Act expands Medicaid coverage to include Americans with family incomes at or below 133 percent of federal poverty guidelines (currently $30,657 for a family of four); the expansion includes adults without dependent children living at home, who have not previously been eligible in most states.7 Individuals with higher incomes (up to 400 percent of federal poverty guidelines, currently $92,200 for a family of four) will be eligible to purchase subsidized coverage from the new Affordable Insurance Exchanges.8
Young adults (ages 19-25) are already being covered under their parents’ employer-sponsored or individually purchased health insurance because of the Affordable Care Act.9 In the first nine months after this provision took effect (October 2010 to June 2011), the number of young adults in this age group with health insurance increased by 8.3 percent.10 An estimated 736,000 Latino young adults now have health insurance coverage because of this provision (Table 1).11
Preventive Health Services
Compared with other Americans, Latinos are less likely to receive preventive care and more likely to have chronic diseases such as diabetes, cancer, and HIV/AIDS.12,13 The Affordable Care Act helps to make prevention affordable and accessible by requiring most health insurance plans to cover prevention and wellness benefits with no cost-sharing.14 The services that these insurers are now required to cover with no cost-sharing include well-child visits, blood pressure and cholesterol screenings, Pap smears and mammograms for women, and flu shots for both children and adults. Pap smears are particularly important for Latino women, who contract cervical cancer at twice the rate of their non-Latino White counterparts.15 The law requires insurers to cover HIV screening without cost-sharing for individuals at high risk of infection. This is important for Hispanics/Latinos, who represent 20 percent of the total estimated number of HIV diagnoses among adults and adolescents.16 An estimated 6.1 million Latino Americans with private insurance currently have access to expanded preventive services with no cost-sharing because of the Affordable Care Act.17
The 3.9 million elderly and disabled Latinos who receive health coverage from Medicare also have access to an expanded list of preventive services with no cost-sharing under the Affordable Care Act. These benefits include an annual wellness visit with a personalized prevention plan, and access to such important screenings as colorectal cancer and obesity screening, bone mass measurement, and mammograms.18
The Affordable Care Act benefits Latinos in many other ways, including:
- Improving Chronic Disease Management. Racial and ethnic minorities often receive lower quality care and face more barriers in accessing care and chronic disease management than non-Latino Whites.19 Latinos report poorer quality of care and lower access to care than non-Latino Whites for approximately 60 percent of core quality measures and 83 percent of core access measures, including availability of cancer screenings and recommended treatments for diabetes.20,21 When chronic conditions are not properly managed, patients often acquire secondary conditions and experience poorer health outcomes. For example, Latinos with diabetes are more likely to incur kidney disease and foot amputations than their non-Latino White counterparts.22 The Affordable Care Act’s Innovation Center explores opportunities to invest in care innovations such as community health teams to improve the management of chronic disease.23 Such investments seek to improve care for Latinos suffering from chronic disease such as the estimated 4.3 million Latino adults with diabetes.24
- Increasing Access to Community Health Centers. Approximately 35 percent of patients served by community health centers in 2009 were Latino. The Affordable Care Act increases the funding available to the more than 1,100 community health centers—located in all fifty states, the District of Columbia, and Puerto Rico—to enable them to increase the number of patients they serve. Health centers have received funding to create new health center sites in medically underserved areas, to expand preventive and primary health care services, and to support major construction and renovation projects.25
- Diversifying the Health Care Workforce and Strengthening its Cultural Competency. The Affordable Care Act increases the racial and ethnic diversity of doctors, nurses, and other health care professionals. For example, the law has helped to nearly triple the number of clinicians in the National Health Service Corps, a network of primary care providers serving communities with significant medical, dental, or mental/behavioral health needs. 26 The Corps provides scholarships and loan repayment to medical students and primary care physicians, as well as other health professionals, in exchange for a commitment to serve in an underserved area. Latino physicians make up about 20.8 percent of the Corps, a percentage that greatly exceeds their 5.5 percent share of the national physician workforce.27 Other initiatives in the Affordable Care Act make it easier for people with disadvantaged backgrounds to become health care professionals and strengthen cultural competency training among health care providers.28 These initiatives will help providers to better address the needs of Latinos and other minorities and communicate more effectively with their patients.
- Addressing Health Disparities. The Affordable Care Act invests in data collection and research focused on disparities in health and health care to help us better understand the causes of healthcare disparities and develop effective programs to eliminate them.29 The law requires the Secretary of the U.S. Department of Health and Human Services (HHS) to establish data collection standards for race, ethnicity, sex, primary language, and disability status for inclusion in surveys conducted or sponsored by HHS. In 2011, HHS released ethnicity standards for data collection and has begun the process of upgrading data collection standards in the other areas. The ethnicity standards expand the response categories on HHS population surveys to Hispanic, Latino(a) or Spanish origin, include questions on specific origins (for example, Mexican, Puerto Rican, and Cuban), and will be asked of survey participants of all ages. This upgrade in data collection standards will help illuminate health disparities among this diverse ethnic group and gauge progress made towards eliminating these disparities.30 Leveraging the Affordable Care Act, HHS has also developed and is implementing the HHS Disparities Action Plan, the Department’s largest commitment to disparities elimination to date.31 The Affordable Care Act also invests in the Community Transformation Grant program to support states and communities by promoting healthy lifestyles (for example, tobacco-free living), especially among groups experiencing high rates of chronic disease such as Latinos. The program aims to improve health, reduce health disparities, and lower health care costs.32 The law promotes the National Center on Minority Health and Health Disparities at the National Institutes of Health (NIH) to Institute status, enabling it to access increased funding and to plan, coordinate, and evaluate disparity-related research within NIH.33 The law also creates a Patient-Centered Outcomes Research Institute which funds research that helps patients and their care providers make more informed treatment decisions, including the study of differences in healthcare outcomes among racial and ethnic minorities.34
- Puerto Rico. An estimated 23 percent of Puerto Rico residents are enrolled in Medicaid, but federal Medicaid funding for the Commonwealth, unlike that for the 50 states and the District of Columbia, is subject to a statutory cap. The Affordable Care Act provides additional funding to raise this cap and also increases the Federal Medical Assistance Percentage (FMAP) for Puerto Rico from 50 to 55 percent.35 The Affordable Care Act also allocates $925 million for subsidies to Puerto Rico residents who participate in the Commonwealth’s Affordable Insurance Exchange.36
Because of the Affordable Care Act, all Americans will have access to affordable health care coverage. For Latinos, the benefits are especially important. The law’s benefits will help reduce disparities in both health care and health outcomes through expanded insurance coverage and better access to high-quality health care services.
Table 1.
Key Benefits of the Affordable Care Act for Latinos
Figure 1:
More than Five Million Latinos Will Gain Coverage Under the Affordable Care Act
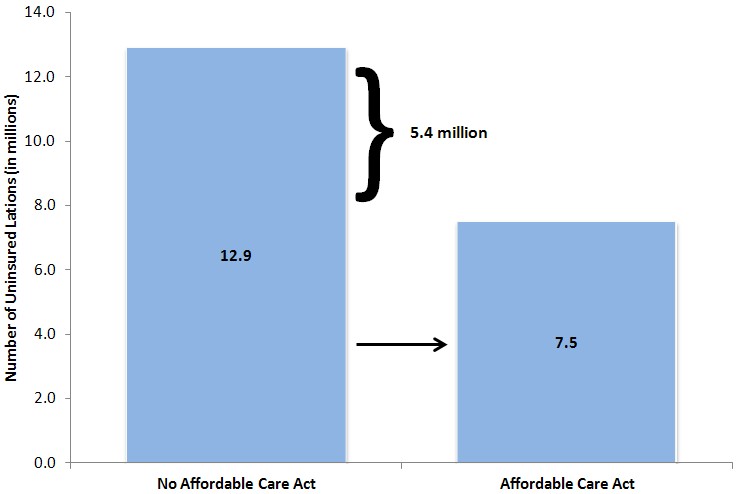
Source: RAND COMPARE microsimulation model.
Note: Estimates shown are for 2016 coverage of individuals ages 0-64 identifying themselves as Spanish, Hispanic, or Latino.
Endnotes
1 “Health disparities: A case for closing the gap.” Office of Health Reform, Department of Health and Human Services, 2009. (Accessed at http://www.healthreform.gov/reports/healthdisparities/).
2 Russell, L. M. (2011). “Reducing disparities in life expectancy: What factors matter?” The Institute of Medicine. (Accessed at http://www.iom.edu/~/media/Files/Activity%20Files/SelectPops/HealthDisparities/2011-FEB-24/Commissioned%20Paper%20by%20Lesley%20Russell.pdf).
3 “Overview of the Uninsured in the United States: A Summary of the 2011 Current Population Survey.” Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services, 2011. (Accessed at http://aspe.hhs.gov/health/reports/2011/CPSHealthIns2011/ib.shtml).
4 Carmen DeNavas-Walt, Bernadette D. Proctor, and Jessica C. Smith, U.S. Census Bureau, Current Population Reports, P60-239, Income, Poverty, and Health Insurance Coverage in the United States: 2010, U.S. Government Printing Office, Washington, DC, 2011. P. 26. (Accessed at http://www.census.gov/prod/2011pubs/p60-239.pdf).
5 Patient Protection and Affordable Care Act (Public Law 111-148) and Health Care and Education Reconciliation Act of 2010 (Public Law 111-152).
6 Estimates provided to the Office of the Assistant Secretary for Planning and Evaluation under contract no. HHSP23320095649WC. Information on the RAND COMPARE model is available at http://www.rand.org/health/projects/compare.html.
7 Section 2001. Section 2002 provides for an income disregard of 5 percent of Federal Poverty Guidelines, raising the effective income limit to 138 percent ($31,809 for a family of four).
8 Section 1401.
9 Section 1001.
10 Benjamin D. Sommers and Karyn Schwartz, “2.5 million young adults gain health insurance due to the Affordable Care Act.” Office of the Assistant Secretary for Planning and Evaluation, Department of Health and Human Services, 2011. (Accessed at http://aspe.hhs.gov/health/reports/2011/YoungAdultsACA/ib.shtml). The estimate is based on data from the June 2011 National Health Interview Survey (NHIS).
11 “New Report Shows Affordable Care Act Has Expanded Insurance Coverage Among Young Adults of All Races and Ethnicities.” Office of the Assistant Secretary for Planning and Evaluation, Department of Health and Human Services, 2011. (Accessed at http://aspe.hhs.gov/health/reports/2012/YoungAdultsbyGroup/ib.shtml).
12 “Health disparities: A case for closing the gap.” Office of Health Reform, Department of Health and Human Services, 2009. (Accessed at http://www.healthreform.gov/reports/healthdisparities/).
13 National Diabetes Information Clearinghouse (NDIC), “Racial and Ethnic Differences in Diagnosed Diabetes” (Accessed at http://diabetes.niddk.nih.gov/dm/pubs/statistics/#Racial, February 2, 2012).
14 Section 1001. Information on the preventive services that are covered is available at http://www.healthcare.gov/news/factsheets/2010/07/preventive-services-list.html. Certain plans designated as “grandfathered” are not subject to this provision.
15 “Health disparities: A case for closing the gap.” Office of Health Reform, Department of Health and Human Services, 2009. (Accessed at http://www.healthreform.gov/reports/healthdisparities/).
16 CDC Slide Set: HIV Surveillance by Race/ Ethnicity through 2010 (March 2012). (Accessed at http://www.cdc.gov/hiv/topics/surveillance/resources/slides/race-ethnicity/slides/2010-HIV-RaceEthnicitySlides.pdf).
17 Benjamin D. Sommers and Lee Wilson, “Fifty-four million additional Americans are receiving preventive services without cost-sharing.” Office of the Assistant Secretary for Planning and Evaluation, Department of Health and Human Services, 2011. (Accessed at http://aspe.hhs.gov/health/reports/2012/PreventiveServices/ib.shtml).
18 The Medicare preventive services provisions are in Section 4104. Medicare enrollment data computed from 2009 Medicare Current Beneficiary Survey. The complete list of benefits covered with no cost-sharing is available in “The Affordable Care Act: Strengthening Medicare in 2011,” U.S. Department of Health and Human Services (Accessed at http://www.cms.gov/apps/files/MedicareReport2011.pdf).
19 “HHS action plan to reduce racial and ethnic health disparities.” U.S. Department of Health and Human Services, 2011. (Accessed at http://minorityhealth.hhs.gov/npa/files/Plans/HHS/HHS_Plan_complete.pdf).
20 Agency for Healthcare Research and Quality, “Disparities in health care quality among racial and ethnic minorities: Selected findings from the 2010 national healthcare quality and disparities reports.” (Accessed at http://www.ahrq.gov/qual/nhqrdr10/nhqrdrminority10.pdf).
21 Agency for Healthcare Research and Quality, “2008 National Healthcare Disparities Report,” (Accessed at http://www.ahrq.gov/qual/nhdr10/Chap10.htm#racial).
22 “Health disparities: A case for closing the gap.” Office of Health Reform, U.S. Department of Health and Human Services, 2009. (Accessed at http://www.healthreform.gov/reports/healthdisparities/).
23 Innovation Center, Health Care Innovation Challenge Funding Opportunity Number: CMS-1C1-12-001, CFDA: 93.610, (Accessed at http://www.innovations.cms.gov/Files/x/Health-Care-Innovation-Challenge-Funding-Opportunity-Announcement.pdf).
24 We computed this estimate by multiplying the 30.8 million Hispanics age 20 and above in the March 2011 Current Population Survey Annual Social and Economic Supplement (CPS-ASEC), for Calendar Year 2010, by the 14.0 percent prevalence rate for 2005 in Mead, H., Cartwright-Smith, L., Jones, K., Ramos, C., Siegel, B., Woods, K. (2008). “Racial and ethnic disparities in U.S. healthcare: A chartbook.” The Commonwealth Fund. (Accessed at http://www.commonwealthfund.org/usr_doc/Mead_racialethnicdisparities_chartbook_1111.pdf).
25 “The Affordable Care Act helps Latinos.” The White House, 2012. (Accessed at http://www.whitehouse.gov/sites/default/files/private/docs/the_aca_helps_latinos_fact_sheet_0.pdf).
26 Relevant sections include 5207, 10503, and 10908.
27 National Health Service Corps numbers from the Department of Health and Human Services, Health Resources and Services Administration, Bureau of Clinician Recruitment and Service, March 30, 2012; physician workforce estimates from Association of American Medical Colleges, Diversity in the Physician Workforce: Facts & Figures 2010 (accessed at http://www.brynmawr.edu/healthpro/documents/AAMC_DiversityPhysicianWorkforce.pdf),
28 For example, Section 5402 provides for loan repayments and educational assistance for health care professionals with disadvantaged backgrounds, and provision of training in cultural competency is a priority criterion for support and development of primary care training programs under Section 5301.
29 Sections 4302, 6301, 10334.
30 More information on HHS ethnicity standards is available on:
http://aspe.hhs.gov/datacncl/standards/ACA/4302/index.shtml.
http://www.minorityhealth.hhs.gov/templates/browse.aspx?lvl=2&lvlid=208.
31 More information on the HHS Disparities Action Plan can be accessed at http://minorityhealth.hhs.gov/npa/templates/content.aspx?lvl=1&lvlid=33&ID=285.
32 More information on the Community Transformation Grant program can be accessed at http://www.cdc.gov/communitytransformation/.
33 Section 10334.
34 Section 6301.
35 HHS Office of Intergovernmental Affairs, Medicaid in the Territories—Current Law Including those in Health Reform, February 22, 2011. (Accessed at http://www.doi.gov/oia/Firstpginfo/igiaPDF/14.Medicaid_in_the_Territories-HHS.pdf.) These changes are in Section 2005.
36 Section 1323.