
Barbara A. Ormond, Kirsten J. Black, Jane Tilly and Seema Thomas
Urban Institute
"This report was prepared under contract #HHS-100-97-0010 between the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Office of Disability, Aging and Long-Term Care Policy and the Urban Institute. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the ASPE Project Officer, Gavin Kennedy, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. His e-mail address is: Gavin.Kennedy@hhs.gov.
ACKNOWLEDGMENTS
The authors thank members of the Technical Advisory Group for their contributions to this project:
James J. Callahan, Jr., Ph.D.
Professor and Director of the Policy Center on Aging
Brandeis UniversityMichael Hunt, Ph.D.
Professor and Chair of the Environments, Textiles and Design Department
University of WisconsinPenny Feldman, Ph.D.
Director, The Center for Home Care Policy and Research
Visiting Nurse Service of New YorkJon Pynoos, Ph.D.
National Resource and Policy Center on Supportive Housing and Home Modification
Andrus Gerontology Center
University of Southern CaliforniaFredda Vladeck
Project Director, Aging in Place Initiative
United Hospital Fund of New York
The authors also thank staff from the New York NORC-SPP, Deepdale Cares, and Lincoln Square Neighborhood Center for improving our understanding of NORC supportive services programs. Additionally, we thank staff from Baltimore's Senior Friendly Neighborhoods, Cleveland's Community Options Program, Pittsburgh's NORC Demonstration Program, Philadelphia's STAR NORC Program, and St. Louis' NORC Project for their contributions to the site visits.
INTRODUCTION
Policymakers are considerably interested in learning how best to encourage successful aging in place by supporting people at home and in the community. Health and social services to assist the elderly not only offer individuals the support they might need to maintain their independence in their own homes for as long as possible, but may also forestall early or unnecessary institutionalization in an acute or long-term care facility.1 In addition, surveys have consistently shown that older people want to remain in their own homes as long as possible.2
The population of those age 65 and over is expected to double over the next 30 years.3 Developing successful models to organize and deliver supportive services for this cohort will have important policy implications for the structure of long-term care services in light of the potential increased demand, the preference for services in the home, and the availability of public funding to pay for services for those most in need.
One possible delivery model involves establishing an integrated system of supportive services for residents of "naturally occurring retirement communities." A naturally occurring retirement community, or NORC, is a community with a large proportion of older people within a defined geographic area. It is distinguished from other areas that also have high concentrations of older residents, such as assisted living communities or continuing care retirement communities, in that it is "naturally occurring." In other words, the area was not designed specifically as a community for older people but rather has evolved in such a way that a large proportion of its residents are older. A service delivery model that targets NORCs may be able to meet the needs of a large group of older people in a community so more of them are able to maintain their independence and continue living at home. The concentrated population of older people in a NORC may allow economies of scale or scope in the organization and delivery of services.
Federal policymakers support the concept of NORCs as a potential focus for delivering long-term care services. As part of the Administration on Aging's (AoA) fiscal year 2001 appropriation, Congress earmarked over $3 million in grants for demonstration projects in five cities with NORCs. The five demonstration projects are organized around Jewish social services organizations that were already providing supportive services for the aging in Baltimore, Cleveland, Philadelphia, Pittsburgh, and Saint Louis. The grants promote, test, and develop site-specific service models that could, in turn, be used as possible frameworks for national models.
Because the NORC supportive services program model fits well with the federal policy shift away from institutional models of care and toward community-based and consumer-driven models, policymakers hope to learn important lessons about what does and does not work and why. Since the demonstration projects are organized and delivered by faith-based organizations, policymakers also hope to understand the perspective of stakeholders who play a key role in the current administration's faith-based and community-based initiatives. By examining existing programs providing support to NORC residents, policymakers can identify issues that might arise during program implementation. Studies of individual programs could also illuminate the broader policy implications using the NORC supportive services programs to organize community-based care for an aging population.
Here, we examine NORCs and NORC supportive services programs through a review of the literature, discussions with national experts on NORCs, and case studies of NORCs and their associated services programs in the five AoA demonstration sites. Following a brief background section, we describe our methods. We then present findings from the literature and our interviews with experts. Based on our review of the literature and refined through our discussions with the experts, we developed a NORCs conceptual model, which is presented in the fourth section. In the fifth section, we use the model to structure our exploration of the characteristics of the NORCs and NORC services programs in the five demonstration sites. Finally, we highlight policy issues related to aging in place that arise in NORC supportive services programs for consideration by stakeholders and policymakers at the federal, state, and local levels.
BACKGROUND
While many older people remain active throughout their lives, some may have deteriorating health that makes them unable to carry out daily activities.4 With increased impairment, older people may experience functional limitations that can manifest in increased difficulty performing instrumental activities of daily living (IADLs), including shopping, preparing meals, and managing medications.5 More serious limitations in activities of daily living (ADLs), such as eating, bathing, or dressing, can make independent living even more challenging without assistance.6 Cognitive impairment can affect a person's ability to carry out both IADLs and ADLs.7 Certain psychosocial factors, such as the death of a spouse, financial problems later in life, a decline in health or activity, and loneliness, may lead to social isolation and depression.8
As impairments and social isolation increase, so does an older person's need for assistance. A common course of action for people needing services has been to relocate, sometimes closer to family or friends, more often to residential facilities (such as continuing care retirement communities, nursing homes, assisted living facilities, and board and care homes) that are structured to provide assistance with numerous activities. Many people continue to live at home and receive help from family, friends, or neighbors. Others may attend adult day care or hire agency or individual workers to deliver the home health, personal care, and homemaker services they need. These options require individuals or their families to find, coordinate, manage, supply, or finance these services, sometimes with governmental assistance from Medicaid, the AoA, or state-sponsored programs. The assistance may be advisory, such as suggesting where to find needed services, or it may be financial, or both. These approaches are not necessarily mutually exclusive; people may use several as their circumstances change.
The NORC supportive services program concept embodies another approach that may successfully support older people and their families in the community. One articulation of the goal of NORC services programs is to provide services that are "flexible, responsive to needs and interests identified by the individual and, to a considerable extent, client-directed."9 NORC services programs help identify needed services and service providers, and coordinate service delivery. Some services may be publicly financed; others may be financed through philanthropic contributions and payments made by the individuals receiving the services.
One of the earliest models of a supportive services program was developed in 1986 in the Penn South Houses, a ten-building complex of cooperative apartments housing more than 6,000 residents in New York City. Based on resident input gathered through a survey, the Penn South Program for Seniors was created to provide both the well and frail elderly with opportunities to remain active and involved in the community, as well as to provide on-site health and social services to assist residents aging in place. The Penn South program served as a model for other programs in the city sponsored by the United Jewish Appeal-Federation of New York. Currently, 28 supportive services programs operate in NORCs in New York.
Supportive services programs for residents of NORCs can be similar to those offered in "purpose-built" communities for seniors. Accommodations made for seniors vary widely across different purpose-built housing, from accessibility considerations in the federal Department of Housing and Urban Development (HUD) Section 202 supportive housing for the elderly program,10 to a specified set of services available in a given assisted living facility,11 to the levels of assistance in continuing care retirement communities.12 These options do not have a standard program but vary by facility; residents may choose the level of service they want by the type of facility they choose and, often, by the level of services at an individual facility.
An important distinction between NORCs and purpose-built communities is how they were formed. NORCs are "naturally occurring," that is, they were not designed to serve as senior housing but developed over time as the community aged and changed. Many NORC residents chose to live in these communities before reaching age 65 and may not have considered the services available for seniors when they made that choice. In contrast, residents of purpose-built senior communities chose both the community and the level of available services when they chose the community. In purpose-built senior housing, both management and residents expect that some level of services or accommodation to the needs of seniors, if only in the physical layout of the structure, will be an integral part of the community. Often the level of available services is part of the contract governing the residences. In contrast, the need for services or improved accessibility in NORCs postdates the establishment of the community, so services must be integrated into the existing community structures. Further, because the residents of an NORC did not choose the community based on the level of available services, resident needs for services and preferences for service delivery are likely more heterogeneous. This heterogeneity presents a challenge for designing and implementing supportive services programs in NORCs.
METHODS
We base the findings presented in this report on information derived from three sources--a review of the literature, discussions with subject matter experts, and site visits to supportive services programs in NORCs in the five AoA demonstration sites. We first reviewed the published literature on NORCs and their associated services programs up to September 2003, focusing on how NORCs were defined, how they were formed and evolved, and the different types of services programs. Because the literature on services programs in NORCs was sparse, we also looked at studies on services linked with congregate housing that was "purpose-built" for seniors to broaden our understanding of services programs. An annotated bibliography of the literature we reviewed is provided in appendix 1.
Following our review of the literature, we held directed discussions with seven subject matter experts identified by the literature. Before the conversations, we sent each expert a discussion guide that included a review of the definitions of NORCs in the literature, information on the structure of their services programs, and questions designed to elicit the experts' opinions on these topics. In addition, we sent a draft of our conceptual model for comment and as a structure for observations on NORCs, their services programs, and the policies that might support them.
The discussion guide focused on the following research questions:
- What is a NORC?
- What factors affect the evolution of a NORC?
- What organizational structures are associated with services programs in NORCs?
- What services do NORC residents want or need?
- What services are typically available in NORC services programs?
- What factors affect resident participation in NORC services programs?
- How are NORC services program outcomes defined and measured?
- What are the principal funding sources for NORC services programs?
For each research question, the experts were asked to consider both the processes involved and the policies that might affect the processes. Finally, they were asked to consider the broader policy questions that might arise in researching the demonstration projects.
These research questions were also the basis for the discussion guide used for site visits to NORC services programs in Baltimore, Cleveland, Philadelphia, Pittsburgh, and St. Louis between May and September 2003. These five sites were the first recipients of AoA grant funding to start new NORC services programs or expand existing ones. The primary contact at each site received a copy of the discussion guide before our visit.
At each site, we talked with staff from the organizations running the NORC services programs and, when available, NORC residents. We held discussions with six people in Baltimore, seven in Cleveland, 16 in Philadelphia, 13 in Pittsburgh, and 18 in St. Louis. Because the Cleveland site turned over a significant proportion of its grant to subgrantees, the seven people we interviewed included four subgrantees, reached by phone. We sent a summary of the site visit findings to the primary staff at each site to correct any factual errors or omissions. After receiving their comments, we revised the reports. Copies of the revised site visit reports appear in appendix 2.
Our methodology has two notable limitations. First, although the literature we considered covers a wide range of NORCs and NORC services programs, and the subject matter experts we consulted have broad experience in these areas, the core of this report is based on our site visits to the five AoA grantee programs. As would be expected given the small number of programs, there is less variation across these NORCs and their programs than there is in the universe of NORCs and NORC supportive services programs. Where appropriate, we extend our discussion to consider the implications of the issues for NORCs and related programs not in our grantee sample. Such extrapolation, however, does not allow us to consider the issues for such NORCs as fully as we can consider them for the NORCs and NORC programs we actually visited. Second, owing to the nature of the AoA grants, the funded programs were not directed at clearly delineated program outcomes. Our study was also exploratory rather than evaluative. Therefore, our discussion of outcomes is not based on the reported progress toward the objective goals of the programs we visited. Rather, we focus on illuminating the contributions to the well-being of their participants that program staff attribute to program activities and the lessons that can be learned from these accomplishments.
FINDINGS FROM THE LITERATURE REVEIW AND EXPERT INTERVIEWS
What is a NORC?
Few studies of NORCs strictly define the concept of a NORC; most simply describe the demographic characteristics of the particular NORC under consideration. Those studies that define NORCs generally agree on what constitutes a NORC, but have competing criteria on the specifics. All researchers agree that a NORC is a geographic area that has a significant proportion of older people residing in a specific area or in housing that was not designed or planned with seniors in mind. They do not agree, however, on what constitutes a "significant proportion" or how old a person must be to be included in that proportion.
Michael Hunt wrote the seminal work on NORCs in 1990 based on his observations and studies of neighborhoods in Wisconsin.13 He defined NORCs as housing developments that are not planned or designed for older people where at least half of the residents are age 60 or older. He noted that NORCs could be found in apartment buildings or condominiums, neighborhoods, small towns, or rural areas.14
Other researchers define NORCs similarly but with differences in the age chosen as the cutoff for inclusion and the proportion of the community that must meet it. New York state legislation defines a NORC as an area where at least 50 percent of households have one member over 60 years old or where the housing complex contains over 2,500 residents who are elderly.15 In Atlanta, a local consortium targeting NORCs for comprehensive service delivery defines a NORC as a census block group with at least 25 percent of the population over age 65.16 The consortium further identifies census block groups with a high percentage of people age 75 and older and living alone as high-risk. Lyons and Magai define a NORC for the purposes of their study as a housing community where at least 65 percent of residents are age 50 years or older but do not explain their choice.17
Lanspery and Callahan, in their analysis of 1990 Census data, defined a NORC as a geographic area where at least 40 percent of the heads of households in a census block group with at least 200 households are age 65 and over.18 They chose 65 as the age cutoff rather than 60 as proposed by Hunt because this age offers a more conservative estimate of the number of NORCs, and because 65 is the age of eligibility for Medicare. In specifying a minimum number rather than a proportion of households, Lanspery and Callahan were focusing on the opportunities presented by NORCs for the provision of supportive services. Two hundred households represents the mid-range of what is generally considered large enough to support a full-time services coordinator in senior housing.
In the literature, the age at which a person is considered "older" ranges from 50 to 65 years old, and the definition of a "significant proportion" ranges from 40 to 65 percent. Subject matter experts we spoke with also disagreed on specifics. Some advocated 60 as the lower bound for who is considered older to provide consistency with the Older Americans Act. Others suggested that the cutoff should be related to the level of disability rather than a specific age.
About half the experts noted that density of the older population in the community is important, because of the economies of scale that can facilitate services provision. Others argued for the number of older people in a community as the key criterion. Most experts asserted that about half the population of a community must be older for it to be considered a NORC.
The distinction between the proportion of the population and the number of people who meet a particular criterion is important, since the proportion may contribute to defining a community's character. Lanspery and Callahan report that communities begin to feel the impact of an aging population when its share of the population exceeds about 26 percent, although density and geographic spread matter.19 The number of people meeting a criterion, however, has more bearing on how supportive services programs are implemented. In a densely settled urban area, the proportion of the population that meets the chosen age criterion may be below the chosen cutoff, and so not meet the definition of a NORC. But the number of older people may exceed a threshold that would allow for economies of scale in services provision.
It is noteworthy that some authors and experts define a NORC by referencing the idea of a supportive services program. There is, however, value in keeping the two concepts separate. A NORC is a community made up of people, some of whom may need services; a supportive services program may be an asset to such a community. Communities can have a significant proportion of older people without needing supportive services. Other communities may have residents needing services but not meet the definition of a NORC.
What Factors Affect the Development of a NORC?
The literature suggests several reasons NORCs develop. According to Hunt, NORCs evolve in three ways--"aged-left-behind," "aging in place," and "in-migration."20 The first two types of NORCs are similar in that both are populated chiefly by long-term residents--the first by residents who stayed in a community characterized by out-migration; the second by older residents who gradually became the dominant population in a stable community. The third type is distinguished by the proportion of older residents who are new to the community. In other articles, Hunt refers to this last type of NORC as "retirement destination."21
Marshall and Hunt focused on NORCs in rural areas and came up with different reasons.22 They used census data to classify rural NORCs by the factors that attract or retain older residents. Amenity NORCs attract younger, healthier, and more active retirees who typically move to escape urban lifestyles. Convenience NORCs often attract people from a nearby rural area, usually the older elderly, looking for greater availability of services and social opportunities. Bi-focal NORCs attract retirees seeking natural amenities who also want to be close to family and friends. Hunt also applied these distinctions in non-rural settings, noting that residents of the different types of NORCs generally have different characteristics, including age, health status, and income.23
Hunt describes many different circumstances that may lead to each type of NORCs. He considers the economic, social, and environmental conditions that affect the community itself and the options open to residents, both older and younger, given their available resources and abilities. According to Hunt, an aged-left-behind NORC may develop, for example, when an area has a significant economic decline. This type of community might be found in "rust-belt" areas where manufacturing jobs have declined. While younger residents may leave to find better economic opportunities, many older residents stay either because of emotional or economic ties to the area or lack of financial resources.
In contrast, an aging-in-place NORC typically has residents with a strong desire to remain in their communities and maintain ties to their social networks, which may include children and grandchildren, friends and neighbors, health providers, places of worship, and local businesses. Hunt notes that these communities may have residents with varying incomes.24 Some urban neighborhoods might be examples of this type of NORC, where the younger generation may have moved to the suburbs leaving the older generation in the family homes.
In-migration NORCs may develop when older people move to an area for the convenience or attractiveness of the community. For example, in-migrants may seek the companionship of others their age, proximity to shopping and services, a hospitable climate, availability of numerous activities, and a more leisurely life. These NORCs may be found in vacation or resort areas and may have first attracted seniors seasonally.
Hunt's research on apartment-based NORCs provides an example of the development of another type of NORC, which he calls an apartment-complex type.25 From his description, these NORCs appear to be a variant of the in-migration NORC. Hunt interviewed residents in three Madison, Wisconsin, apartment communities to learn what attracted older residents to the community. He found that older people often decided to move when the size and maintenance requirements of their homes became problematic--owing to the death of a spouse or the resident's poor health, for example. Residents reported that, once they decided to move, three main factors affected their choice of where to move. Location was identified as the chief initial attraction; residents often chose the site to be close to family or friends, shopping, and services. Management, particularly building maintenance, influenced the attractiveness of the apartment-complex, based on word of mouth and testimonials from residents. Finally, the design of the building can help eliminate potential barriers to independent living.
NORCs are not static; residents of all ages move in or out, resulting in an evolving demographic profile. In his study of apartment-complex type NORCs, Hunt examined the reasons older people leave the community.26 When asked if they planned to move, about 30 percent of the NORC residents in Hunt's survey said "maybe" and another 10 percent said "yes". Most respondents cited a need for more health care or lower rental costs. The importance of housing costs was confirmed in another survey of older people conducted in 2003 that found that 93 percent of older people surveyed wanted to remain in their homes for as long as possible but, of these, over a third were concerned about affordability.27 In Hunt's apartment-complex study, physical environment also played a role. Those who left the NORC reported they had left because of such barriers as stairs in the living unit or to the laundry room.28
Subject matter experts agreed that two major trends affect the evolution of NORCs--aging in place and migration of older people--and that people remain in their communities as they age or move into new communities for the reasons that Hunt noted in Wisconsin. Factors affecting migration include the community's affordability, accessibility, amenities, and proximity to family and friends. The experts speculated that there might also be a cultural component, based on such factors as religious, ethnic, or socioeconomic homogeneity.
The experts further agreed that the proportion of a community's population made up of older people could increase or decrease over time, so the community composition could change. Some communities can lose older people often for the same reasons that had originally attracted them, such as the changing affordability of housing or a change in building management that affects how management responds to the needs of older people. Some experts noted that NORCs might remain stable, sustaining themselves through in-migration, and cited the New York City NORCs as an example.
What Organizational Entities are Associated with Services Programs in NORCs?
NORC service programs may have their own organizational structure (e.g., lead agency plus service contractors), they may build on an organization within the NORC (e.g., a co-op board or residents' council), or both. If no organization exists within the NORC, the program may serve as the catalyst to establish one. If multiple organizations are involved, the roles they play and how well they work together can affect the implementation of the service program in the NORC.
Lanspery and Callahan point out a critical difference between NORC services programs and integrated service networks.29 In the latter, a set range of services is marketed to a membership group, while in the former, the emphasis is on giving discretion and control over the types of services included to the membership group. The authors find that having identifiable stakeholders with an interest in cooperation is an important factor in implementing services programs.
Yalowitz also emphasizes the importance of having a governance structure to determine program configuration and services, and of clearly spelling out the relationships and responsibilities within the governance structure.30 The experts we spoke with noted that a weak governance structure is often the result of the organizing entities, whether external or internal, not clearly defining the mission or purpose of the program.
The various types of organizations found in NORCs mirrors the various types of NORCs themselves. A suburban NORC may have no organizational entity of its own apart from the local government. On the other hand, an apartment-based NORC almost invariably has some form of building management and may also have resident councils or recreation committees. How a NORC is structured is an important factor in developing and managing a services program, since the structure can serve as a contact point for the services program within the community and a way to communicate with community residents.
Residents may have varying degrees of involvement with the internal NORC organization depending on whether it is self-generated, such as a condominium board, or comes from an outside agency, such as a community services agency. How successful NORC supportive services programs are may depend on whether service providers are able to establish strong relationships with the NORC organizational structure and its residents. Experts noted that struggles often arise between professionals and non-professionals who may not describe their work in the same terms. Experts stressed the importance of developing a common language among the members of the NORC partnership, including housing managers, social and health care workers, and residents.
The published literature sheds very little light on the internal organization of NORCs and the role it may play in supportive services programs. What discussion there is does not necessarily apply across all types of NORCs. For example, Lanspery and Callahan characterize NORCs as "closed" or "open" according to the relationship between the community's ownership and management.31 A closed NORC has one management entity; examples are individual owners or managers of apartment buildings or trailer parks. An open NORC shares management among two or more homeowners or management entities. This distinction is used to differentiate, for example, investor-owned apartment buildings from such living arrangements as co-op buildings, condominiums, or neighborhoods with single-family homes or row houses. Experts cited several examples of NORC supportive services programs that had been developed internally by active tenant associations or co-op boards, or where tenant associations and management had worked closely together on general resident issues.
The organization of the services programs also varies. Since NORC residents need assorted different services, services programs usually involve several agencies. Landsberg et al. note that having a key agency take the lead is important, and that problems within agencies and between agencies can interfere with service delivery.32 In a similar vein, Lanspery and Callahan find that the lead agency should be clearly defined and relatively autonomous. In the Penn South Cooperative, the board of directors of the cooperative contracts with an oversight agency to provide services.33
Subject matter experts agreed that the NORC's internal structure and the service program's organization could affect communication with residents and how responsive services programs are to residents' needs and preferences. Several experts emphasized that residents need to be involved in decisions and exercise some control in the organization and governance of the services program. They cautioned against service providers taking over to meet the needs of their own organization. In NORCs with co-op boards, building owners or managers, or condominium associations, a unit already exists that could act on behalf of residents and negotiate with service providers. In the absence of such structures (for example, as in most suburban neighborhoods), the service providers, by default, provide the organizational structure.
What Services do NORC Residents Want or Need?
According to experts, a NORC supportive services program encompasses supports, services, and activities organized to help meet identified needs and aspirations of residents and the NORC governing structure. However, they noted that it is possible for a supportive services program that provides many things to not meet residents' needs. Therefore, in addition to the range of services provided, a services program's ability to adapt to the changing needs and preferences of residents is critical to the program's success and longevity.
One concern the subject matter experts shared was that too often policymakers think of older people as a collection of deficits that need to be addressed. They felt that, ideally, the individual needs of older people would be examined in the broader context of supporting successful aging for the whole population. Not all older people need or want services, but some will. Supportive services programs, therefore, are just one possible component of a broader approach to meeting the needs of the population as it ages.
The published literature has few studies that focus on what older residents want or need. We found only one study of the service needs of NORC residents, and it emphasized services that should not be provided. In his survey of residents of three Wisconsin apartment-based NORCs, Hunt asked residents what should have been done to help residents who had moved away remain in the community. Most respondents felt that if residents needed more health care they should go somewhere else, and that nothing should have been done for them so they could stay in the community.34 The study does not give the reasons underlying these beliefs. This finding suggests that while residents may have service needs, they do not necessarily feel that it is the responsibility of building management or other community representatives to meet these needs.
For additional insights on service needs, we reviewed the published literature on public housing for seniors and found several relevant studies. Researchers at New Hampshire's Housing Finance Authority interviewed 503 residents in four pilot sites.35 Table 1 ranks the services that residents reported they most needed or were most useful, compared with the services they reported as most wanted or desired. (The study did not clarify the difference between "needed" and "wanted.") Where two entries appear in the same box, there was a tie in the ranking.
| TABLE 1 | ||
|---|---|---|
| Ranking | Most Needed | Most Wanted |
| 1 | Heavy household chores | Transportation |
| 2 | Shopping | Heavy household chores Service coordination |
| 3 | Service coordination | -- |
| 4 | Transportation | Personal emergency response system |
| 5 | Light household chores | Shopping |
| 6 | Personal emergency response system | Light household chores Meal preparation |
| 7 | Meal preparation | -- |
| 8 | Personal care | Personal care |
| SOURCE: Greenleaf, Lynn, Sheila Malynowski, New Hampshire Housing Finance Authority. Increasing Service Availability to Seniors in Housing: Final Report (Bedford, NH: New Hampshire Housing Finance Authority, 1993). | ||
In a second study, researchers interviewed residents of a public housing project in New York City where more than half of the heads of households were age 60 and over.36 The study, part of a demonstration project that provided community-based supportive services to older residents with one or more limitations in ADLs, found an unmet need for mental health services, as evidenced by older residents' social isolation and signs of depression. In response, the project hired a bereavement/mental health counselor. The study also found less need for emergency home care and home-delivered meals than project staff had expected. As a result, the staff shifted their emphasis to non-Medicaid covered services.
Hunt highlights the dilemma of meeting the needs of older residents without making the community (an apartment complex in this case) less attractive to younger residents.37 He identifies three approaches from the literature. Residents can leave when their needs exceed what is offered in the complex. Alternatively, the complex can expand services to meet the needs of residents as they age. Finally, in what Hunt terms the balanced model, the complex can expand services slightly and help residents meet their remaining needs by linking them with services in the broader community.
The subject matter experts did not agree on what NORC residents want or need. The experts noted that assessing residents' needs and preferences--through surveys or focus groups, for example--is important for program development and implementation. They also observed that what residents want will vary according to their level of frailty and may change abruptly when they are faced with a crisis. The services that residents might need from a new program will also depend on what services are available to them under other programs.
The lack of consensus on resident needs is not surprising given the many different types of NORCs and varying levels of need among the elderly. It seems likely that, in addition to the disparate needs and wants in any cross-section of older people, the range of services needed by NORC residents could vary depending on the type of NORC in question and its location. Residents who have aged in place will not need orientation to the community that might benefit in-migrants. Transportation might be a more critical need for suburban NORC residents than for residents of apartment-based NORCs in urban areas.
Several experts noted that property managers and residents frequently fear a supportive services program would make their residences look like nursing homes, with wheelchairs in the lobby or uniformed nurses in the building. For this reason, while some residents may favor establishing a services program in their building, others may resist in the interest of maintaining an age-integrated community. This feeling could limit the services that NORC residents say they want until they themselves need help with daily activities and medical care.
In addition, there are services that residents currently need and can readily identify, such as household repairs, as well as services they might need as they age that they might not have considered, such as help with ADLs. Determining the types of services NORC residents want or need and will use, while easier than it might be in the community at large, appears to be one of the most difficult tasks facing supportive services programs.
What Services are Typically Available in NORC Services Programs?
The 1997 report on the Naturally Occurring Retirement Community Supportive Services Program (NORC-SSP) from the New York City Department for the Aging is one of only a few published studies on service programs in NORCs that lists the categories of services provided.38 The categories are case management, emergency or general home care, meals, transportation, mental health and bereavement services, and informal supports. The NORC-SSP staff developed this complement of services by surveying residents about their needs.
Some information on available services can be gleaned from information on which services residents use. A survey of Penn South residents (no date provided) lists case management, information and referral, nursing services, classes and lectures, and health screenings as frequently used services.39 A survey of residents of Penn South and two other NORCs in 1996 found cultural events, exercise and dance classes, and health events among the most popular services.40 Such lists, however, do not represent a complete picture of services offered.
According to the subject matter experts, most NORC services programs provide transportation, housekeeping, and social activities or meals. These activities may be chosen because the lack of required licensed oversight makes them easier to provide. Casework and health care are often two core components of services programs, and program staff have found that health care education and preventive services such as blood pressure checks can be a good outreach technique for residents who may be more likely to get their blood pressure checked by a nurse than approach a social worker about health-related problems. Experts also noted that, in communities with no senior center or other such recreational organization, activities and recreation might become a central part of the program.
More literature is available on the range of services available in publicly funded housing for seniors, and these findings could apply to NORCs. The Service Coordinator Program (SCP), administered by HUD, is designed to meet the needs of older people and people with disabilities living in HUD-assisted housing. Under this program, service coordinators determine the needs of eligible residents, identify available community services including public programs for which residents might be eligible, link residents with needed services, monitor and evaluate service provision, and serve other functions as needed. An evaluation of the SCP found that transportation and housekeeping were the most frequently provided services.41 Other services included health screenings, exercise programs, and budget assistance.
A survey of HUD Section 202 housing residents found that services such as group dining, social work and counseling, and social and recreational activities were most likely to be provided by on-site staff.42 More personalized services, such as housekeeping, personal care, care management, medication management, and religious services, were usually provided by external agencies or contractors. Transportation and money management services were usually provided by family and friends.
Information from these studies shows that the most common services appear to be service coordination, transportation, group meals, and opportunities for socializing. Other health and personal care services appear less available. An agency may provide the services directly, it may facilitate delivery of services, or it may only provide residents with information and referral to service providers.
In general, these studies described the services offered or provided, not those that residents say they need. An agency may choose to offer those services residents have expressed an interest in, or that the agency knows from previous experience will be acceptable. It is also possible that an agency provides services it has provided in the past that it has found useful to the elderly, regardless of whether these services are the ones residents most need. In addition, the services needed may change over time. The literature did not discuss how agencies determine resident needs or if and how they adjust their offerings to resident preferences and changing needs.
What Factors Affect Resident Participation in NORC Services Programs?
Factors that could affect whether or how residents use NORC services programs include desirability of the services, resident knowledge of service availability, the price of the services to the resident, and location of the services. The desirability of services has been discussed in the two previous sections. Residents' knowledge about services is primarily a function of program communication with residents. We found no information about how the price of services affects resident participation. Two studies provide some insights regarding communication about and location of services.
In addition to these program characteristics, residents' demographic characteristics were seen to affect participation rates. Landsberg et al. report that users of supportive services in four NORCs in New York were more likely than non-users to be female, older than 85, and living alone compared to all older residents in the four surveyed NORCs.43
An evaluation of a services program in a New York NORC indicates that recruiting advisory committee and staff members from varied backgrounds facilitates reaching out to and working with minority populations in a NORC.44 The evaluation found that successful outreach efforts are varied, multilingual, and tailored to the cultural preferences of residents. Most clients who entered the program during the two-year demonstration had heard about it through the senior center or from a program flyer.
Physical accessibility affected participation in the Vladeck Cares program, a program designed for seniors living in Vladeck Houses, a large public housing complex in New York City. Analysis of client residence data showed that the closer residents' apartments were to the program office, the higher the residents' participation in programs. Participation rates also declined as resident age increased.45 An evaluation of the HUD SCP also cited accessibility as an important factor. The evaluators found that stairs represented a barrier to residents' access to services. They recommended that sites be accessible to older residents and located near where residents tend to congregate, such as mailboxes, dining rooms, or lounges.46
According to the literature, communication, location, and accessibility of offices and meeting space, and resident age are likely to affect the level of resident use of programs. The experts we spoke to concurred with these findings. In addition, several experts mentioned the role of volunteers, either resident volunteers or outside volunteers, as an important program feature. A well-developed volunteer program may help engage NORC residents in the planning and operation of program activities. Some NORCs have used volunteers from outside organizations, including college and high school students, adding an intergenerational component to services programs that residents find appealing.
How are the Outcomes of NORC Services Programs Defined and Measured?
The literature on outcomes associated with supportive services provision in NORCs is extremely thin, both conceptually and empirically. Researchers have identified the potential benefits of providing services in housing for older people, but we found no information on how to measure these benefits. The benefits were described broadly as helping residents remain independent, improving staff and resident morale, allowing managers more time to focus on managing the property, and lowering service costs for all parties.47 Yalowitz emphasizes the importance of including periodic "performance based evaluation" in program planning and evaluating programs for their contribution to the "continued independence of...seniors served by the program."48
Although we found no NORC-specific research on actual outcomes, findings from services programs linked with congregate housing could specify potential outcomes of NORC services programs. The studies of SCPs generally use qualitative methods, such as key informant interviews, case studies, and interviews with program participants. In a study of publicly funded housing for seniors in six developments in Connecticut, Sheehan reported that property managers believed resident service coordinators (RSCs) improved the quality of life for residents, reduced residents' risk of entering nursing homes, and contributed to savings from lower apartment turnover and vacancy rates as well as better upkeep of the apartments.49 The RSCs also freed property managers from trying to meet the support needs of elderly residents. Frail older people in the demonstration sites reported a large improvement in perceived health status as well as in functioning related to ADLs and IADLs between the pre-test and post-test interviews. There were no changes among frail elderly people in comparison sites. The majority of residents said that the RSCs had benefited them through providing emotional support, help with problems, and information and referral. Participation in social activities and housing satisfaction increased substantially for residents, regardless of their level of disability.
The available research on outcomes does not provide rigorous evidence of the effect of supportive services programs, but it points to areas for further research. It suggests that NORC services programs could improve residents' self-reported health status, mental and physical functioning, and quality of life. Changes in self-reported health status and quality of life are subjective and, although suggestive of an effect and relatively easy to measure, they are not a rigorous test of a program's effect. In contrast, changes in mental and physical functioning can be measured using standard screening tools and could provide a more objective measure. However, these screening tools would require a larger commitment of both time and funds to implement.
The subject matter experts believed there was insufficient evidence to characterize the outcomes of NORC services programs. They noted that while some programs are conducting research studies on resident satisfaction, service usage, and costs, most have not developed mechanisms to examine outcomes. The experts also noted that the lack of mechanisms to measure outcomes might reflect a lack of focus on quality assurance. Defining and measuring outcomes associated with NORC services programs is still a largely undeveloped field of inquiry.
What are the Principal Sources of Funding for NORC Services Programs?
Sustainable funding is a major challenge facing NORC supportive services programs, and there is little information available about how these programs raise money. We found only one source of information, and that study focused on programs in congregate housing rather than NORCs.50 In that study, Wilden and Redfoot found that funding sources variedy among the 17 subsidized housing projects examined. Programs often relied on an array of public and private funders. Among the 17 projects, 16 had funding from residents, nine from Medicaid, and six from private organizations. Others sources included federal, state, and county government funds.
The subject matter experts agreed that sustainable funding to support NORC services programs over the long term is a major concern. Programs must rely on several sources, including resident fees, fundraising by residents and the programs themselves, contributions by residents' families, and foundation and philanthropic contributions. In addition, some funding may be available indirectly from state entities, such as the Office of Mental Health, to support service programs in a wider area that may encompass the NORC.
Experts were unaware of any major state or federal funding for NORC supportive services programs other than the AoA grants and the money that New York State and the City of New York have devoted to programs throughout that state. Since 1998, New York has allocated approximately $1.2 million annually for supportive services programs. Except for public housing sites, state funds must be matched at the level of at least 25 percent of the total grant by the sponsoring agency. In 2000, New York City allocated $3.8 million to start 16 additional programs with funds matched at the level of at least one-sixth of the total grant by the sponsoring agency. The intention of these matching requirements is to communalize the funding in order to move away from a fee-for-service model and bring the housing entity into the program as a stakeholder and financial partner. Several experts felt that financing shared among federal, state, city, housing management, philanthropy, and residents would be ideal.
Funding implies that the organization or individual providing the funding finds value in the program. Therefore, the availability of sustained funding for NORC services programs might be one indicator of their perceived value, if only to the funders. Residents' willingness to pay a membership or activities fee might be a gauge of residents' valuation of the program, particularly of how well the program identifies and meets residents' needs. However, such fees risk discouraging participation by lower income groups. Developing and implementing outcome measures for programs would allow benefits to be quantified and might be instrumental in attracting sustained support from grantmakers or state or local governments.
Discussion
The literature on supportive services programs in NORCs is both thin and uneven. Much of it is purely descriptive, providing detailed pictures of individual programs, but lacking the consistency necessary for cross-site analysis. However, the literature we reviewed does provide a rich set of observations on which to base an analytical framework. Much of the literature focuses on NORCs based in multi-unit housing complexes, such as cooperatives, condominiums, and apartments, but recognizes the existence of other types, such as suburban or rural NORCs. The descriptions of supportive services programs provide examples of different organizational strategies and management that might foster the flexibility and responsiveness that program organizers argue is essential for success. The services available under the various programs are broadly similar, reflecting the core needs that characterize many aging populations as well as the diversity inherent in the age group. Finally, the paucity of information about outcomes points to an important area for program managers and policymakers to address.
Overall, the literature provides an understanding of the components that make up NORCs and the supportive services programs that seek to serve NORC residents. A common feature in the literature is a blurring of the line between the NORC itself, which is a community, and the NORC supportive services program, which serves that community. In the next section, we put the identified components of NORCs and their associated supportive services programs together to form a conceptual framework that clearly distinguishes between such communities and the programs that serve them, while emphasizing the dynamic nature of NORCs and the structure of their supportive services programs. We used this framework to explore the five AoA grantee programs and to point toward areas where policies might enhance the potential contributions of supportive services programs to successful aging in place.
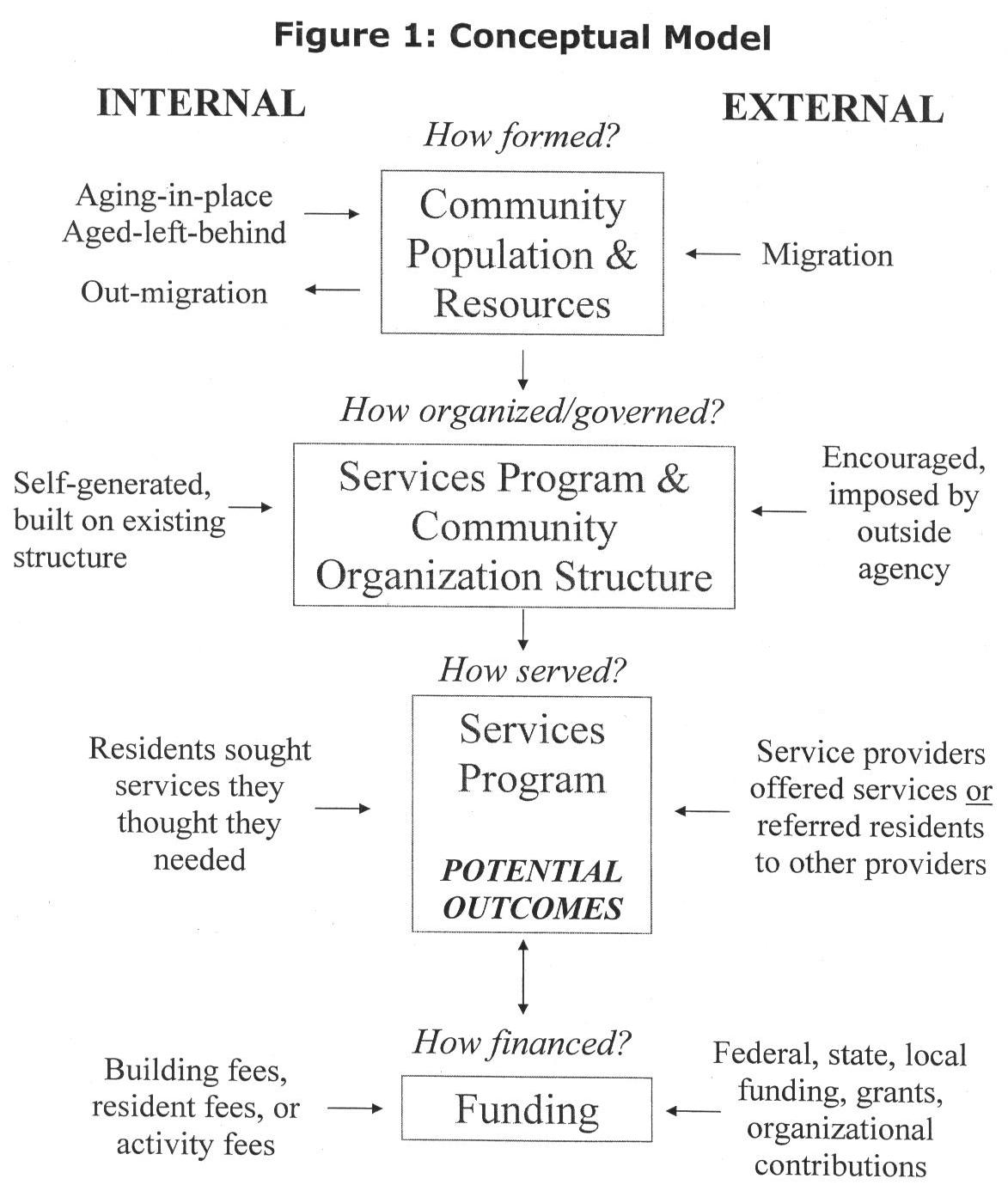
CONCEPTUAL MODEL
Our conceptual model of NORCs and NORC supportive services programs, shown in Figure 1, has four parts: the NORC and associated community resources, the organizational structure on which its services program depends, the services provided and outcomes potentially associated with these services, and funding. Each part is influenced by various forces that can be internal or external to the NORC. Although NORCs vary widely in their composition and functioning, each can be understood in reference to these features. We recognize that NORCs may be combinations of the types discussed here, rather than purely one type or another. In laying out the model, we present pure types. As we discuss later, the NORCs we visited generally represent mixed types.
Attributes of the NORC
A NORC is like any other community--it is constantly changing. NORCs grow or decline in response to two major forces affecting the proportion of older residents in the community: aging in place and migration, both in and out. How a NORC develops is likely reflected in both the composition of the NORC's population and the resources available in the community. These community characteristics, in turn, influence the types of programs that are may be needed or effective. For example, a NORC may develop primarily through an influx of older people who have chosen to move to the community; in such a community, new residents make up a greater proportion of total residents than in a community that has aged in place. An area that is attractive to in-migrants might have more community resources on which to build a program than an aged-left-behind NORC. In addition, by migrating, in-migration NORC residents have shown themselves open to change, and they might have greater financial resources that would enable them to pay for the services made available. In contrast, an aging in place community is formed internally; that is, it is made up of relatively long-term residents. Aged-left-behind residents may be more resistant to change and less able to contribute financially to getting what they need. They are, however, more likely to have deep knowledge of and strong ties to the community.
Services Programs and Community Organization
The organizational capacity and governance structures within communities that are demographically NORCs differ from community to community and are important factors in the development and operation of supportive services programs in these communities. The NORC organizational structure may exist before the services program or it may be established in response to the program. It may be instrumental in program development and operations or it may be more passive. Similarly, services programs might develop as the product of internal or external forces. An internally driven services program might be a response to the expressed needs of the residents. Alternatively, an existing community organization might recognize unmet needs of residents and approach building management for permission to provide activities or services, resulting in an externally driven program.
The origin and governance of the program can influence program operations. For example, an internally driven program is likely to have a lower need for outreach and communication than an externally driven program, at least initially.
Whatever its origin, a services program generally requires some structure that can serve, at the very least, as a point of contact between the program and community residents and, more expansively, as a way to explore residents' needs and preferences and measure program outcomes. The organizational structure can be internal to the community or external, or the responsibility can be shared. The structure is likely to influence how the program evolves; a predominantly externally operated program might be more influenced by the services the program organizers have historically offered in such settings, while an internally operated program might be more responsive to changing resident desires. Further, if the services program relies on an existing community structure, then the level of initial trust is likely to be higher than if the services program creates or imposes a new organization on the community.
Internal and external structures each have advantages and disadvantages. An internal structure might be better placed to identify resident needs, but might be hampered by cronyism or lack of professional insight. On the other hand, an external group might concentrate on the services it has historically offered rather than design new ones to meet the expressed needs of community residents. External groups may or may not seek the residents' input during program design. In practice, an organization may not be purely internal or external. The challenge is the same--to establish good communication between the residents and the program's organizers and service providers.
NORC Services Programs and Their Potential Outcomes
The potential outcomes of NORC services programs depend on what needs have been identified, what services are provided, and the level of resident participation in the program. The constellation of services and their scope can vary in their responsiveness to residents' preferences and needs. If the services match resident needs, then participation is likely high. If an internal NORC organization is seeking services from an outside agency or setting up its own services, services will likely be highly responsive to the expressed needs of residents, or at least those residents represented by the NORC organization. If an external agency is providing services, it may be more or less successful at gauging the preferences of residents and meeting their needs. How well residents' preferences are gauged, whether by the internal NORC organization or the external agency, will affect participation and, in turn, outcomes for residents. Because of the dynamic nature of NORCs, a services program's ability to respond to internal communication and to evolve to meet the needs and preferences of residents may be the most important factor in determining the long-term success of the program.
Services Program Funding Sources
One of the major challenges services programs report they face is generating sufficient funding to support their efforts. Funding sources can be internal or external to the NORC. Internal sources include NORC residents' contributions to the costs of services programs, for example, through payment of activity or membership fees. In addition, property owners or managers can contribute to program costs either financially or in kind. Residents are likely to contribute to the cost of programs if they find the services valuable. The level of expected contributions from the residents, however, must take into account their income and other demands on their resources. Similarly, owners or managers are more likely to contribute if they believe the program helps make the property more attractive to potential residents or if it reduces their operational or management costs. External funding can come from numerous sources including the agencies that operate services programs, grants from nonprofit charitable foundations, and federal, state, or local governments.
 |
CASE STUDY FINDINGS
We visited the five AoA grantee sites in Baltimore, Cleveland, Philadelphia, Pittsburgh, and St. Louis. Although the case study sites differ in their services provision and structures, certain issues and challenges are common to all sites. This section focuses on those commonalities, using the conceptual model as the framework for the discussion. A summary table comparing components of the conceptual model across the different sites appears in appendix 3.
Case Study Sites
Baltimore's Senior Friendly Neighborhoods (SFN) program is targeted to people age 62 and over and provides case management, information and referral services, preventive health screening, recreational activities, and transportation services. In addition to the AoA grant, SFN receives funding from a combination of foundation grants, the Jewish Community Federation, and membership fees.
Cleveland's Community Options Program uses its AoA grant money to provide technical assistance and support to four new sites across Ohio that are replicating the Community Options program in Cleveland. The original program has been in operation since 1995 and provides information, referral, and activities to NORC residents. It has substantial financial support from building management, a HUD grant, and resident fees.
Philadelphia's STAR NORC Program provides assessment, some preventive health services, case management, access to services, and opportunities to socialize. STAR NORC targets people who are isolated or who might have problems remaining at home. Funding comes from co-op building fees, foundation grants, and AoA.
Pittsburgh's NORC Demonstration Program develops individualized care plans for residents based on comprehensive in-home need assessments and providing information about and referrals to appropriate community services. In addition to its AoA grant, the program receives in-kind contributions from its organizing agencies.
The St. Louis site is using its AoA grant funding to develop a demographic profile of 1,351 older residents in a local NORC and to study the outcomes of seven pilot projects. These studies are designed to determine the service needs and preferences of older residents and to inform the design of a planned services program in the community.
NORCs and Community Resources
All the grantees define the communities they serve with reference to a specific geographic area or areas where a large share of the population is older. Some grantee sites cover a specific part of a city or neighborhood, such as Center City Philadelphia or Baltimore's Upper Park Heights. In contrast, the Pittsburgh program serves communities in a group of contiguous neighborhoods. In each study site, program representatives view the NORC as encompassing both the housing complexes and independent housing units where older residents reside, as well as the various resources available in the community. Most often, the grantees have established services programs for one or more specific housing complexes within the NORC, such as an apartment building or co-op. However, all sites except Philadelphia are also trying to establish programs to serve residents in neighborhoods with single-family homes.
The grantees have estimated the concentration of older people in their service areas, but most programs do not have an exact count of residents in the target age range. In St. Louis, where research on resident demographics was conducted before program implementation, staff cited 2000 Census data showing that 32 percent of the residents of its NORC, as defined by a census block, are age 65 or older. St. Louis program officials estimate that at least half the residents in the apartment buildings they serve are age 65 or older. Aside from St. Louis, the grantees have little firm demographic data about the communities or buildings they served.
In each community, local resources include community centers, houses of worship, health care providers, shopping centers, and some public transportation, although distance to and accessibility of these resources vary across the sites. In the Cleveland, Pittsburgh, and Philadelphia NORCs, some amenities are within walking distance of residents' apartment buildings or homes, but even short distances can present problems, particularly for older people with mobility impairments. In other sites, residents who can still drive have access to a broader range of services and amenities, but poor signage and residents' aversion to driving at night can limit accessibility and participation in some activities. Baltimore, Pittsburgh, and St. Louis have Jewish community centers and social services programs housed in or located close to the communities they serve. These facilities are open to residents of all faiths and are not frequented only by Jewish residents. In St. Louis, staff noted that making non-Jewish residents aware that services are open to all was a particular challenge.
Although resources in the community are an attraction for residents, respondents in all five sites identified physical layouts that present problems for older people as they become frail. Many apartment buildings have steps leading up to the entryway, and a few have automatic doors that close too quickly for people with mobility problems. Physical access barriers are more pronounced in row houses or single-family homes that have stairs without railings and bathrooms or laundry facilities that can be reached only by stairways. Neighborhoods with hilly landscapes or without sidewalks, particularly those neighborhoods farther from amenities such as shopping or entertainment, present additional obstacles for older people who can no longer drive or who would like to walk to their destinations. Similarly, neighborhoods with only sporadic public transportation present obstacles for those who are unable to walk to their destinations. Grantee staff identified inadequate transportation most often when asked about the challenges older people in their communities face.
According to grantee staff at all five sites, most older people have lived in their communities for decades, staying largely because of ties to friends and neighbors as well as connections with community resources like houses of worship, community centers, and health care providers. Staff also pointed to migration both into and out of the various communities. In some communities, such as Baltimore and Pittsburgh, out-migration has led to a growing though not dominant aged-left-behind population. In others, such as Philadelphia, older residents have moved in, frequently drawn by the amenities of city living. Most communities have a concentration of older Jewish residents.
Migration to the study communities includes immigrants from foreign countries. Staff in both Baltimore and Pittsburgh mentioned that an influx of older Russian immigrants in the late 1980s contributed to a change in the culture and languages of the community. In Pittsburgh, the small existing Russian community, itself the result of an earlier wave of migration, attracted these immigrants. In-migrants have also included retirees looking for smaller residences with lower maintenance requirements and easier access to amenities and necessities. In Philadelphia, some retirees migrated from suburban areas to the city to reduce their social isolation, and staff in St. Louis reported that older residents moved to the NORC to be closer to family, friends, and the Jewish community center.
The grantee sites provide good evidence of the dynamic nature of NORCs, and understanding these dynamics suggests steps that services programs can take to address resident needs. Each community has a core of long-term residents, and the amenities that bind those residents to the community attract other older people. The importance of a familiar culture in a foreign land in the case of the Russian immigrants or of centers for Jewish culture and community are part of the community resources for older people who are not of the majority culture. These cultural ties can focus outreach to new residents and ease the integration of newcomers into the community. The programs' use of Jewish community centers is an example. For other residents, the availability of living arrangements more in keeping with their needs and abilities attracted them to the communities. Outreach to residents without specific cultural ties or without existing ties to service organizations or houses of worship in the community may take more planning.
The grantee sites do not represent as wide a range of NORCs as depicted in the conceptual framework. Since most sites are characterized by continuing in-migration of older people, they seem to be places that remain attractive. There are, for example, no sites with a predominantly aged-left-behind population where the lack of amenities has driven all who can leave away. Nor are there the more dispersed communities that would be found in rural areas not adjacent to a large city or suburban communities. As will be discussed later, program staff in Baltimore, Pittsburgh, Cleveland, and St. Louis are considering expanding services to suburban neighborhoods with single-family homes. Supportive services programs in these communities will likely differ from those represented by the AoA grantees in the current study for several reasons, including lower population density, the lack of an internal organizational structure, scarcity of public transportation, and lower availability of health and social services resources.
Services Programs and Community Organization
In most grantee sites, community service agencies have taken the initiative in organizing services programs for NORC residents. Each grantee site is connected in some way to the local Jewish Federation, a fundraising umbrella organization for Jewish community services agencies. But services are not limited by religious affiliation. The grantees typically include a Jewish community center (JCC) and a Jewish social services agency that serves families, but other organizations, such as community housing organizations in Baltimore and St. Louis, are frequently involved. In each site, one agency has taken responsibility for forming a planning group to coordinate services.
In taking the lead in developing services programs, the agencies faced challenges that might not have arisen if the services programs had been internally driven. Some early challenges included securing the cooperation of building managers in program development and service delivery, gaining resident participation and support, and communicating with and getting to know the needs of the NORC residents. In many cases, the current program is an extension of the grantee's earlier activities in the community. In some sites, the residents' familiarity with the grantee agencies and some of the service providers has helped reduce program development challenges. For example, in Pittsburgh, many residents who participated in assessments also participated in JCC activities or frequently called ElderLink, an information and referral service that is a collaborative effort of the three sponsoring service agencies.
At two of the five grantee sites, program staff contacted building managers and owners to secure their cooperation in setting up services programs, with varying degrees of success. The attitudes of building managers and owners toward NORC services programs in the study sites could be either positive or negative, respondents reported. One group considered the services programs valuable because they help older tenants remain in place; older tenants are valued because they generally pay their rent on time, have long tenancy in their apartments, and are considerate neighbors. In contrast, other building managers or owners feared that their property would come to resemble a nursing home if services programs were provided to residents. In this group's view, older tenants limit the marketability of the building, keeping younger potential residents away. Building owner or management attitudes affect the implementation of the services programs over time. Management cooperation can range from sharing contact information on older building residents to facilitating program start-up to providing office space and other resources, as in Baltimore and Cleveland, making program implementation and management much easier.
A principal goal of the program's contact with the community organization is to establish a communication channel between the program and the residents. The service agencies have employed various communication methods with building residents, with the method depending in part on the level of cooperation of the building managers and the stage of the program. In the initial stages, identifying where in the community older residents live, introducing the program, and determining their interest in participating take priority. After program start-up, establishing a two-way communication between program staff and residents is critical, allowing staff to identify resident needs and residents to provide feedback on how well program activities are meeting those needs. Some building managers supply the ages, phone numbers, and locations of elderly residents, allowing agency staff to call residents or knock on their doors to introduce themselves and the program. Resource coordinators in Cleveland, for example, contact each new senior resident to introduce the program and inquire about resident's interests. Grantee staff generally consider face-to-face contact the most effective, albeit the most labor-intensive, method of introducing the program and fostering ongoing communication with residents. Other methods, such as articles in newsletters, flyers, and postings on bulletin boards, are considerably less expensive in terms of time, but are seen by program staff as less effective.
At most sites, program staff have either developed an internal entity that represents residents, as in Baltimore's SFN Advisory Council, or used an existing internal structure, such as Philadelphia's co-op boards. These internal structures provide a point of contact for staff to give residents information and hear their concerns. In St. Louis, program staff formed an external advisory committee made up of service providers, residents, religious organizations, and state representatives to help develop the services program and to serve as the vehicle for communication with residents. In Baltimore and Cleveland, the resident advisory councils developed by program staff are how residents become involved in and contribute to the program. In Pittsburgh, much of the organizational energy went into developing collaborative management arrangements among the three agencies running the services program; no organization internal to the community was used as a regular part of the services program.
Suburban areas present particular challenges to agencies trying to start services programs. Existing neighborhood organizational structures rarely represent the views of older residents, and no information about elderly households is readily available. Suburban decentralization also makes identifying a communal space for programs difficult. In Baltimore and Cleveland, program staff have tried to surmount these obstacles and start programs in suburban areas with row houses and single-family homes, but with little success. In neither city could staff find an easily accessible activity center, central space, or home to host neighborhood events, particularly one that was accessible for people with disabilities. Lack of transportation and inclement weather present other obstacles to organizing in dispersed neighborhoods that do not arise when all program participants reside in one building. Program staff have not given up on the idea of organizing in suburban neighborhoods, but are unsure how best to proceed.
The program in St. Louis is under development. The grantee decided to study various aspects of the community before initiating a program, using its grant funding to partner with researchers at Washington University in St. Louis's Center for Aging to conduct seven studies. Community service agencies will use the results to develop services programs. The center and the agencies intend to seek additional funding to track program outcomes and conduct longitudinal research to determine how residents and the community change over time.
The impetus for most of the services programs we studied came from an agency serving the NORC, rather than from the NORC residents themselves. The one exception was in Philadelphia, where residents of a cooperative contacted a community service agency to start a services program. The Philadelphia program is based in several cooperative apartment buildings and a condominium, each with a resident board. This type of housing may attract residents who have an interest in working together to address community needs. Alternatively, the experience of residents working together in co-op or condominium management may have engendered the more proactive stance. The program has strong support, as evidenced by the fact that each cooperative pays a building fee to participate in the program. The availability of social services has also attracted people to the buildings; three of the five buildings have waiting lists.
Program Services and Outcomes
The programs at the five sites show the various ways services programs can get started. In Baltimore and Cleveland, the programs grew naturally out of earlier community programs. Baltimore's program evolved from efforts to stabilize the neighborhood in the face of continuing out-migration; in Cleveland, the program staff is using AoA grant funds to replicate the existing program in four new communities in Ohio. In Philadelphia, residents learned about the services that social workers could provide and asked for one to work in their building. In contrast, in Pittsburgh, agencies sought to identify residents who needed the services they could provide. In St. Louis, program organizers are conducting research on which neighborhoods might need what services. At the time of our visit, the services program was still under development, so most of the discussion in this section will focus on the other four sites.
Most agencies began their services programs by implementing their own ideas about the programs residents would appreciate and use, generally based on their knowledge of the particular community or of similar communities, sometimes with input or feedback from residents. In the four grantee sites that have implemented programs, social workers or activity coordinators are the focal point for work with residents. These workers are generally based in the buildings and are responsible for contacting residents, organizing activities, assessing residents' needs, and referring residents to other professionals for additional services. The program staff use volunteers in these activities to varying degrees. In Philadelphia, for example, volunteers, both from within the community and from outside, are screened and matched with residents who need assistance. In Cleveland, resident volunteers help run the social activities.
These different development and implementation strategies rely on different mechanisms and have elicited different levels of resident input into program design. Nonetheless, the services offered are similar across the programs and vary more by the age of the residents and their levels of frailty than across sites. Transportation, reduction of physical barriers, opportunities to socialize, and opportunities to learn are common themes. In Cleveland and Baltimore, staff members report that activity preferences vary by building and over time within buildings. The younger members of the NORC population prefer activities such as trips outside the community and exercise programs such as yoga. The older residents prefer more sedentary activities that involve being entertained over those that require active participation. The staff have found that residents prefer a mix of activities, with interests that rotate among bingo games, current events discussions, and health lectures.
Despite the similarities in the service mix across the sites, there are some site-specific services and different approaches to service provision. In Baltimore, Cleveland, and Philadelphia, nurses deliver preventive health services such as blood pressure checks and presentations on health-related topics. In Philadelphia, the program arranges for chaplain services. In Cleveland, the program focuses on providing residents opportunities to socialize through activities organized by resource coordinators; the coordinators also provide service information and referral on request. In Pittsburgh, inter-agency care teams develop care plans for residents. Pittsburgh's program has the narrowest range of direct service provision, but the strongest emphasis on comprehensive individual resident assessment. When Pittsburgh staff found that program participants were not taking full advantage of the recommendations for services and activities, they realized that they sometimes needed to go beyond simply providing information and referral for services and actually help older people link up with the recommended services.
The grantees provide some services directly, but they address several categories of services only through referrals. If a person appears to need home health care or mental health services, program staff will refer the resident to a mental health professional or an appropriate agency. Some agencies affiliated with NORC programs offer these services, but residents must pay additional fees for them. Similarly, even within the services they provide, programs may limit the scope of their involvement. For example, meals are viewed as a social activity and not as part of a nutrition initiative. In some cases, residents themselves limit the types of services they are willing to accept from the program. For example, one program resource coordinator mentioned residents usually prefer to request assistance in relocating to an assisted living facility or nursing home from a family member.
All the grantees have had difficulty addressing the problem of resident mobility. Physical barriers within buildings have been eased in many cases but the solutions to broader barriers to mobility, such as environmental barriers between buildings and lack of suitable transportation options, do not appear easy to solve. Available paratransit at the sites can require long waits and advance reservations, which residents do not like. Although public transportation is available in all the grantee sites, it is not always accessible or efficient for residents with physical limitations. Baltimore's SFN program has created several services to address resident's transportation needs, including a shuttle bus that serves 16 buildings, subsidized vouchers for local taxi cab rides to medical appointments, and a weekly van service to shopping areas. The staff is also exploring the use of a sedan service, with drivers who can assist people into and out of the van, allowing residents with disabilities to get to medical appointments.
Residents' weaknesses or disabilities can create challenges for the conduct of program activities, particularly those that involve food service or transportation planned in advance. For example, staff reported that residents may sign up for activities and not remember having done so, or, if they do remember, they may feel ill or be otherwise unable to attend. Food may be wasted or transportation left unused.
The fact that resident preferences also change over time and by resident group presents a further challenge and reinforces the finding that ongoing feedback between residents and program staff is crucial. Grantees at several sites have set up mechanisms for internal feedback from residents. In Philadelphia, the co-op board solicits resident feedback and input on the program. The Baltimore program has hired senior residents to serve as on-site coordinators charged with seeking resident input and helping organize and publicize building events.
The grantee sites have very little information about program outcomes. While the overall goal of maintaining residents' ability to live independently is clear, gauging program impact is hampered by the lack of specified interim outcomes. St. Louis is attempting to address this problem in advance by incorporating the development of outcome measures into the program from the beginning. At some sites, staff members have tried to measure the outcomes of their programs by tracking resident participation in program activities and measuring resident satisfaction with the programs. Resident participation is one measure of program outcomes, since high participation probably indicates that the program is providing services that residents want or need. To meet the larger goal of helping residents stay independent, a services program should not only provide services that residents currently need but also publicize the availability of its services so residents will know where to turn when the need arises.
Running a NORC services program involves constant feedback from residents about what services they want and need, and trust is a key factor in getting residents to communicate their needs. Staff members note that residents are particularly sensitive to the notion that admitting their needs might be a prelude to being removed from their homes. Program staff report that it is easier to get people involved in social activities first and then build up residents' trust over time, suggesting that measuring sustained participation may be a good indicator of success. With increased trust, residents open up to staff about their more personal needs, such as a homemaker or home health services.
There is some evidence at the grantee sites that NORC residents, when faced with emergencies, may not have enough knowledge about community services to take advantage of them. Readily available information is particularly important for older people whose circumstances can change abruptly. As mentioned, staff in Pittsburgh found that the program participants who received referrals often did not follow up on them. They speculated that residents and their families might not make these arrangements unless faced with an emergency. Similarly, staff in St. Louis found that residents were unaware of many of the services available in their communities.
A potential measure of program outcomes is that residents view the program as a non-threatening source of services and information that they can turn to as their needs change. Unfortunately, it is unclear how to measure whether NORC services programs are evolving as a trusted information source. In the short run, participation rates may be a good proxy for progress toward this long-term goal.
It is difficult to gauge the effect of program activities on specific outcome measures. The programs at the study sites were in different stages of development when they received the AoA grant funding, so comparisons across sites are inappropriate. The grants were also not designed to support specific measurable goals, nor was funding directed toward research on the outcomes of program activities. Nonetheless, planned future research in some sites may illuminate how programs contribute to identified outcomes.
St. Louis has focused on getting primary data to establish a baseline and determine needs. Program organizers will then design a program to respond to those needs. Evaluation will be an ongoing part of the program. Staff expect commonalities across the St. Louis program sites and other NORCs, so their findings will be applicable to other NORCs. Because of the attention to both planning and outcomes, a follow-up visit to this site could yield useful information about mechanisms for measuring outcomes and the costs associated with this effort.
While evaluation and outcomes measurement are not components of the other sites we visited, outside researchers are conducting studies at two sites that may provide useful information on program outcomes. In Baltimore, the University of Maryland Baltimore College (UMBC) Center for Health Policy plans to follow service use of a random sample of SFN members and non-members over a year. This study will also include a process evaluation of SFN operations. In Cleveland, researchers at Case Western Reserve University will follow a group of 1,000 community-dwelling older people and compare their experiences to those of older people residing in buildings with Community Options. The study will look specifically at nursing home and home health use. Both studies are expected to be completed in 2004.
NORC Services Program Funding
Sustaining funding for the NORC services programs after the AoA grant funds run out is a challenge all sites will face. At the moment, most funding sources for the sites' programs are external to the NORC, including AoA, HUD, private foundations, and funding from the community service organizations themselves or their own fundraising efforts. The current AoA grants total $3.7 million across the sites, distributed as follows: Baltimore, $1 million; Cleveland, $987,000; Philadelphia, $200,000; Pittsburgh, $200,000; and St. Louis, $1.26 million. Each site provided matching funds at a ratio of $1 local dollar to $3 federal dollars.
External fundraising is in a very early stage in most grantee sites. Staff report approaching local foundations and governments as well as state governments. Initial reactions to these approaches have been positive, according to grantee staff, but no concrete plans for ongoing financial support have resulted to date.
Some programs have been able to attract internal funding in the form of residents' fees or activity costs (Baltimore and Cleveland) and building managers and co-op fees (Cleveland and Philadelphia). In Cleveland and Philadelphia, the ability to generate internal funding might reflect the fact that both programs have been around for some time and have built up credibility with the property managers and owners. Alternatively, the programs may have been able to remain in existence and become a trusted source of services because they have an internal source of funds. Cleveland's approach provides a good example of using external funding to attract internal funding that will sustain the program over the longer term. Cleveland's Community Options used a HUD grant to set up its initial program in 1995 and then approached building managers after one year of operation to request a contribution. The managers pay for supplies and the salaries of the resource coordinators and offer free office and activity room space because they view the program as a valuable resource for their tenants. Residents pay the cost of their activities themselves, suggesting that they too value the program. The five Cleveland subgrantee sites plan to follow this model after their first year of program operation.
DISCUSSION
Improving the ability of older people to remain in their homes for as long as possible is desirable for at least two reasons. Surveys have shown that staying at home is what older people want and that it is less expensive for most individuals than institutional care. As the baby boomers approach this phase of life, it will become even more important to find ways to achieve the dual goal of managing the cost of long-term care services while providing services in a desirable setting.
The NORC supportive services program is an intuitively appealing model to help more seniors age in place. As our review of the literature and visits to five, admittedly unrepresentative, sites has shown, there is little available evidence on either side as to whether that appeal is borne out in practice. The literature and the site visits have, however, yielded a great deal of information about useful practices in supportive services programs.
However clear the motivation for promoting supportive services to allow aging in place, the execution can be challenging, as the case studies presented here show. The needs of older people can and do differ widely across different groups, in different settings, and over time. Some older people do not need supportive services; others need a great deal. Over time, individuals may move either gradually or suddenly from no or low need to higher need. Identifying the physical, social, and emotional health needs of older people and designing programs to meet these needs requires constant attention to evolving circumstances and preferences.
Even if needs are identified and programs developed to meet them, the very frailties that supportive services programs are designed to counter often contribute to implementation challenges. Older people may be unaware of the extent or implications of their frailties, or outwardly deny them. Older people may fear that if the frailties are recognized they will be forced to move from their homes, making them reluctant to admit any need for help or accept services. Further, physical weakness, declining mental capacity, and daily fluctuations in health and energy levels can make even regular, eager participants not wholly reliable.
In discussing what constitutes a NORC, we included both the community's population and its resources. In that sense, once a supportive services program is established, it becomes part of the NORC. To understand the role of supportive services programs, it helps to think of them as just one of many community resources that can help successful aging in place. Our research here highlights many ways that supportive services programs can contribute to this goal. It also suggests some limitations that should be kept in mind as policies are developed.
Short-Term versus Long-Term Program Outcomes
Supportive services programs can be a vehicle for meeting either the immediate or anticipated needs of older community residents as they age. The short-term outcomes of these interventions are intuitively appealing--providing assistance with such immediate health and social needs as depression, isolation, or a particular health condition. A longer-term outcome of a good program will include developing trust between the residents and the program, so the program becomes a source residents can turn to when their needs change.
Broadly, a successful program must address community awareness by educating residents and their families about available services. Staff should not only have a range of services that they can tap for daily and ongoing needs and immediate crises, but should also be able to anticipate likely future needs based on experience. By meeting the current needs of residents reliably and with dignity, programs can establish themselves as places to go when new needs arise. Programs initiated by external organizations may have to first establish their legitimacy in the eyes of the community and, over time, earn the community's trust as a source for personal and health-related services.
In the programs we visited, we saw activities designed to further this longer term goal through the development of communication mechanisms between community residents and program staff. Staff members were able to assess resident needs without arousing their fear that assessment was a prelude to removal from the community. Staff also worked to maintain respect for residents' abilities and sensitivity to their ambivalence about recognizing or admitting their frailties. Programs sought by residents, as opposed to those initiated by service agencies, may have had an advantage in this area because residents had a greater sense of control over the program. As a result, the necessary relationship of trust may have been able to develop more quickly.
Communication and Program Evolution
The view of NORCs and their supportive services programs presented here is a dynamic one, recognizing that the composition of the community and the needs of residents are constantly changing. A services program must be designed to evolve with the community and the target population if it is to continue to meet their needs. Trust is central, as is open and effective communication. Supportive services programs need to design their communication strategies with the different populations of the community in mind. Two-way communication allows the program to learn about the residents' needs and preferences, and the community to learn what the program has to offer. Programs can use two-way communication to remain responsive as needs and interests change and as the community evolves through aging in place and migration into and out of the NORC.
Outcomes Measurement
Most programs used participation in sponsored activities as a measure of program outcomes. Participation is a valid, if limited, measure of short-term program accomplishments, but it may be a less informative gauge of the program's long-term contributions to successful aging in place. Tracking participation also does not provide information on residents who do not participate. Non-participants may represent a more isolated part of the community with greater needs who may need different services or activities.
Ideally, the development of outcome measures would be a part of program planning, as it is in St. Louis, and would be in place from the beginning. As with any program, available outcomes data could provide information to support funding decisions. Outcome data could also be used in program management to improve operations and effectiveness. In addition, strong outcome data on successful models could be used in considering program replicability.
Clearly, outcomes measurement greatly needs further research. Developing good outcomes measures begins with clearly stating the objectives that are expected to contribute to the overarching goal of promoting successful aging in place. Because of NORCs' inherent diversity, this step is not necessarily straightforward; different objectives are more or less important in different situations. Further, aging in place takes time, so both short and long-term objectives and outcomes measures are needed. Developing and testing mechanisms for outcome measurement are critical to understanding how NORC services programs contribute to successful aging in place. As such, they should be given greater weight in decisions about future projects and research. As outcomes measures become better defined, funders will have a clearer basis for decisions about supporting or expanding NORC supportive services programs.
Limitations of Supportive Services Programs
A supportive services program can be a valuable community resource for older people, but it cannot be expected to take on the full burden of meeting the changing needs of aging residents. For example, most programs we visited had identified physical and environmental hindrances to older residents' mobility and independence. Services programs can perform a useful service for the community by cataloguing such constraints, and solutions to some problems, such as individual apartment and home modifications, may logically fall within the purview of a services program. Other problems, such as better street signage to aid older drivers or paved sidewalks to facilitate pedestrian access, may be better addressed by public institutions within the larger community. Services programs can contribute to resolving such issues by educating the community about areas of particular concern to older residents, participating in coalitions of community stakeholders, and advocating on behalf of older residents. These programs can avoid spreading their resources too thin, however, by limiting their own projects to those that address issues within their scope of work or expertise.
Program Funding
Along with discussions about the appropriate role for supportive services programs must come a discussion about appropriate funding sources for such programs. The benefits of supportive services programs accrue first to individual recipients by allowing them to remain in their homes according to their preferences. Benefits also accrue to the larger community in fostering diversity across age groups within neighborhoods and allowing several generations to live in the same community. Benefits accrue to society when public costs associated with aging and declining health are lessened through the potential lower use of acute or institutional health care. The challenge, as with many supportive services programs, is finding the right private-public-philanthropic resource mix, and the right balance among individual, community, and societal obligations.
Expanding Supportive Services Programs to Less Densely Settled Communities
Given the potential contribution of supportive services programs to successful aging in place, it would seem desirable to consider expanding such programs to all communities with older residents. However, some communities are better able to support or encourage such programs than others. All the programs we visited were in urban areas or suburban communities adjacent to urban areas, and the higher density of older residents (e.g., apartment buildings with large concentrations of older residents) appeared to ease many implementation problems. Programs that had attempted to serve residents of single-family houses in urban or suburban areas encountered greater difficulties. Further research is needed to adapt the supportive services program model to less densely settled communities, possibly in the form of pilot projects with associated research and evaluation components.
Understanding the evolution of NORCs and their supportive services programs can help public and private policymakers plan more livable, accessible communities; guide policy for these communities; and influence developer and urban planning by establishing guidelines for housing and community design. Because NORC residents represent many types of people, research on NORCs and their residents also highlights the lives of healthy, active seniors as a counterpoint to much of the current research, which often focuses on the mostly frail, homebound elderly. Expanding research on seniors living in the community will provide a broader picture of the various contributions seniors make in their communities as volunteers, community leaders, mentors, and teachers, and help demonstrate the ways intergenerational living enhances the community as a whole.
As the population ages, it will be important to understand how best to organize services to meet the needs of older residents who wish to remain in their homes and communities for as long as possible. Supportive services programs in NORCs will likely be an increasingly useful service arrangement that policymakers can support both to address the needs of the elderly living in a community and to anticipate the needs and future demands of an aging population. Our findings from the literature, discussions with experts, and case studies show the diverse approaches communities and services organizations have taken in forming and operating NORC supportive services programs, and how such programs can adapt to meet the various and changing needs and preferences of their target populations. The diversity highlights the fact that there is no one-size-fits-all NORC program model or approach. The challenge for the private sector and public policy seeking to foster supportive services programs in NORCs is to find a way to support the diverse program structures and the necessary flexibility while establishing clear guidelines for the similarly diverse range of program outcomes, all while keeping in mind the overall goal of successful aging in place.
NOTES
-
Gibson, Mary Jo, et al. Beyond 50.03: A Report to the Nation on Independent Living and Disability. Washington, DC: AARP, May 2004.
-
Bayer, Ada-Helen, and Leon Harper. Fixing to Stay: A National Survey on Housing and Home Modification Issues. Washington, DC: AARP, May 2000.
-
Administration on Aging. A Profile of Older Americans 2002. Accessed at http://www.aoa.gov/prof/statistics/profile/2.asp, August 2004.
-
National Institute of Mental Health. Breaking Ground, Breaking Through: The Strategic Plan for Mood Disorder Research of the National Institute of Mental Health. National Institute of Mental Health, U.S. Department of Health and Human Services, February 2003.
-
Vladeck, Fredda. A Good Place to Grow Old: New York's Model for NORC Supportive Service Programs. New York, NY: United Hospital Fund, 2004.
-
"Section 202 supportive housing for the elderly." Accessed at http://www.texashousing.org/txlihis/siterebuild/desc202/hudexplanation…, August 3, 2004.
-
National Center for Assisted Living. Assisted Living: Independence, Choice, and Dignity. Washington, DC: National Center for Assisted Living, 2001.
-
"Continuing Care Retirement Communities (CCRCs) and Lifecare." Accessed at http://www.seniorresource.com/hccrc.htm, August 3, 2004.
-
Hunt, Michael E., D. Arch, and Leonard Ross. "Naturally Occurring Retirement Communities: A Multiattribute Examination of Desirability Factors." The Gerontologist 30 (1990, 5): 667-74.
-
Marshall, Linda J., and Michael E. Hunt. "Rural Naturally Occurring Retirement Communities: A Community Assessment Procedure." Journal of Housing for the Elderly 13 (1999, 1-2): 19-34.
-
Yalowitz, Nat, and Karen Bassuk. An Intergenerational Community with Supportive Services, The NORC Model at Penn South Program for Seniors. Paper presented at the American Society on Aging, San Francisco, March 1998.
-
Lawler, Kathryn. Aging in Place, Coordinating Housing and Health Care Provision for America's Growing Elderly Population. Joint Center for Housing Studies of Harvard University and Neighborhood Reinvestment Corporation, October 2001.
-
Lyons, Beverly P., and Carol Magai. "Reducing Health Risks and Psychological Distress among Older Black Residents of Naturally Occurring Retirement Communities." Journal of Gerontological Social Work 35 (2001, 1): 53-69.
-
Lanspery, Susan C., and James J. Callahan. Naturally Occurring Retirement Communities: A report prepared for The Pew Charitable Trusts. Brandeis University, Waltham, October 3, 1994.
-
Hunt, Michael. "Naturally Occurring Retirement Communities." In Encyclopedia of American Cities and Suburbs. New York, NY: Garland Publishing, Inc., 1998, pp.517-18.
-
Hunt, Michael E. "Settings Conducive to the Provision of Long-Term Care." Journal of Architectural and Planning Research 18 (2001, 3): 223-33.
-
Marshall, Linda J., and Michael E. Hunt. "Rural Naturally Occurring Retirement Communities: A Community Assessment Procedure." Journal of Housing for the Elderly 13 (1999, 1-2): 19-34. Hunt, Michael E. "Settings Conducive to the Provision of Long-Term Care." Journal of Architectural and Planning Research 18 (2001, 3): 223-33.
-
Hunt, Michael E. "Settings Conducive to the Provision of Long-Term Care." Journal of Architectural and Planning Research 18 (2001, 3): 223-33.
-
Hunt, Michael. "Naturally Occurring Retirement Communities." In Encyclopedia of American Cities and Suburbs. New York, NY: Garland Publishing, Inc., 1998, pp.517-18.
-
Hunt, Michael E. "The Naturally Occurring Retirement Community." In Housing the Very Old, edited by Gloria M. Gutman and Norman K. Blackie. British Columbia, Canada: The Gerontology Research Center, Simon Fraser University, 1988, pp. 161-72. Hunt, Michael E., D. Arch, and Leonard Ross. "Naturally Occurring Retirement Communities: A Multiattribute Examination of Desirability Factors." The Gerontologist 30 (1990, 5): 667-74.
-
Hunt, Michael E. "The Naturally Occurring Retirement Community." In Housing the Very Old, edited by Gloria M. Gutman and Norman K. Blackie. British Columbia, Canada: The Gerontology Research Center, Simon Fraser University, 1988, pp. 161-72.
-
The AdvantAge Initiative. AdvantAge Initiative 2003 National Survey of Adults Aged 65 and Older. Center for Home Care Policy and Research, Visiting Nurse Service of New York. Personal communication from Penny Feldman and Elisabeth Simantov, March 2004.
-
Hunt, Michael E. "The Naturally Occurring Retirement Community." In Housing the Very Old, edited by Gloria M. Gutman and Norman K. Blackie. British Columbia, Canada: The Gerontology Research Center, Simon Fraser University, 1988, pp. 161-72.
-
Lanspery, Susan C., and James J. Callahan. Naturally Occurring Retirement Communities: A report prepared for The Pew Charitable Trusts. Brandeis University, Waltham, October 3, 1994.
-
Yalowitz, Nat. NORC Supportive Service Programs: The Need for Strong and Clear Governance. Paper presented at the Joint Conference of The National Conference on the Aging and the American Society on Aging, Denver. New York, NY: NORC Supportive Services Center, Inc., April 2002.
-
Lanspery, Susan C., and James J. Callahan. Naturally Occurring Retirement Communities: A report prepared for The Pew Charitable Trusts. Brandeis University, Waltham, October 3, 1994.
-
Landsberg, Gerald, Catharine MacLaren, and Harry Schwartz. The Accomplishments, Issues and Prospects of Supportive Service Programs in Naturally Occurring Retirement Communities. Prepared for the Fan Fox and Leslie R. Samuels Foundation. New York, NY: Ehrenkranz School of Social Work, New York University, September 2002.
-
Bassuk, Karen. "NORC Supportive Service Programs: Effective and Innovative Programs that Support Seniors Living in the Community." Care Management Journals 1 (1999, 2): 132-37.
-
Hunt, Michael E. "The Naturally Occurring Retirement Community." In Housing the Very Old, edited by Gloria M. Gutman and Norman K. Blackie. British Columbia, Canada: The Gerontology Research Center, Simon Fraser University, 1988, pp. 161-72.
-
Greenleaf, Lynn, Sheila Malynowski, and the New Hampshire Housing Finance Authority. Increasing Service Availability to Seniors in Housing: Final Report. Bedford, NH: New Hampshire Housing Finance Authority, 1993.
-
New York City Department for the Aging, and U.S. Administration on Aging. Support Services for the Frail Elderly Residents of Federally Assisted Housing: Final Report Findings and Recommendations. New York, NY: New York City Department for the Aging, 1997.
-
Hunt, Michael E. "Settings Conducive to the Provision of Long-Term Care." Journal of Architectural and Planning Research 18 (2001, 3): 223-33.
-
New York City Department for the Aging, and U.S. Administration on Aging. Support Services for the Frail Elderly Residents of Federally Assisted Housing: Final Report Findings and Recommendations. New York, NY: New York City Department for the Aging, 1997.
-
Landsberg, Gerald, Catharine MacLaren, and Harry Schwartz. The Accomplishments, Issues and Prospects of Supportive Service Programs in Naturally Occurring Retirement Communities. Prepared for the Fan Fox and Leslie R. Samuels Foundation. New York, NY: Ehrenkranz School of Social Work, New York University, September 2002.
-
KRA Corporation, and Office of Policy Development and Research, U.S. Department of Housing and Urban Development. Evaluation of the Service Coordinator Program. Washington, DC: U.S. Department of Housing and Urban Development, Office of Policy Development and Research, 1996.
-
Heumann, Leonard F., Karen Winter-Nelson, and James R. Anderson. The 1999 National Survey of Section 202 Elderly Housing. Washington, DC: Public Policy Institute, AARP, 2002.
-
Landsberg, Gerald, Catharine MacLaren, and Harry Schwartz. The Accomplishments, Issues and Prospects of Supportive Service Programs in Naturally Occurring Retirement Communities. Prepared for the Fan Fox and Leslie R. Samuels Foundation. New York, NY: Ehrenkranz School of Social Work, New York University, September 2002.
-
New York City Department for the Aging, and U.S. Administration on Aging. Support Services for the Frail Elderly Residents of Federally Assisted Housing: Final Report Findings and Recommendations. New York, NY: New York City Department for the Aging, 1997.
-
KRA Corporation, and Office of Policy Development and Research, U.S. Department of Housing and Urban Development. Evaluation of the Service Coordinator Program. Washington, DC: U.S. Department of Housing and Urban Development, Office of Policy Development and Research, 1996.
-
Lanspery, Susan. Clustering Services at Senior Housing Sites: A Technical Assistance Guide for the Aging Network. Los Angeles, CA: National Resource and Policy Center on Housing and Long-Term Care, University of Southern California, Andrus Gerontology Center, 1997.
-
Yalowitz, Nat. NORC Supportive Service Programs: The Need for Strong and Clear Governance. Paper presented at the Joint Conference of The National Conference on the Aging and the American Society on Aging, Denver. New York, NY: NORC Supportive Services Center, Inc., April 2002.
-
Sheehan, Nancy W. "Resident Services Coordinator Program: Bringing Service Coordination to Federally Assisted Senior Housing." Journal of Housing for the Elderly 13 (1999, 1-2): 35-49.
-
Wildon, Robert, and Donald L. Redfoot. Added Assisted Living Services to Subsidized Housing: Serving Frail Older Persons With Low Incomes. Washington, DC: Public Policy Institute, AARP, 2002.
APPENDIX 1. Annotated Review of the Literature on Housing with Services for Older People Who Age in Place
This annotated review focuses on research related to programs that bring community services into existing housing to foster aging in place and maximize older people's independence in the community. Examples of these programs include service programs in Naturally Occurring Retirement Communities (NORCs), support services in public housing, and "cluster care," where a group of home care agency workers serve clients who live in close proximity to one another. Research about facilities that were originally designed to provide long-term care, such as most assisted living facilities, continuing care retirement communities, and nursing facilities, are not part of the literature review. The annotated review also includes available descriptions of prominent NORCs.
The literature for NORCs is summarized first, followed by support services in public housing programs, cluster care, and assisted living programs that bring services to existing housing. In each section, articles are presented in reverse chronological order. When articles by the same author repeat information or concepts, the repetition is eliminated.
LITERATURE RELATED TO NATURALLY OCCURRING RETIREMENT COMMUNITIES (NORCs)
Yalowitz, Nat. NORC Supportive Service Programs: The Need for Strong and Clear Governance. For presentation at the Joint Conference of The National Conference on the Aging and the American Society on Aging, Denver, CO. New York, NY: NORC Supportive Services Center, Inc., April 2002.
There are over 35 NORC supportive services programs (NSSPs) in five states, all of which are community based and on site at the housing units they serve. These housing units have close relationships with many existing social and health service agencies that served the communities before the coming of the NSSPs.
The author uses the experience in these NSSPs to examine governance issues for service programs in NORCs. The author emphasizes the importance of a clear, strong, workable governance structure that is committed to the principle of supporting the continued independence of the seniors the program serves. There should be an organized body of people who will take responsibility for setting the policies of the program, be accountable for finances, and will clearly set out the mission of the program. Governance objectives should be spelled out in contract language between the NSSP and the service agencies. Performance-based evaluation should be part of the program. Care should be taken that the program design and implementation cater to the seniors involved and not to the staff of the agencies. Seniors should feel empowered and should feel ownership of the program. Staff training in these principles is critical. NORC programs should be concerned with the "continued building of the community in which they are organized as well as the broader community." The article gives several examples of problems that have arisen when these principles are not followed. The author endorses the position taken by New York and Maryland legislators that there be a strong presence of housing leaders and consumer input in the governance structure of NORCs.
The Jewish Home & Hospital Lifecare System. What We Do: Retirement Community Services (NORCs). http://www.jewishhome.org/script.asp?SubCatIS=41.
This web site describes the Community Services Division of The Jewish Home and Hospital. According to the web site, this division provides nursing consultation, health education, care management and social services to hundreds of frail elderly residing in naturally occurring retirement communities (NORCs) in New York City. The authors state that "the NORC model of providing health and social services to elders has been very successful in assisting senior citizens who wish to remain in their homes and 'age in place'."
Chicago Mutual Housing Network. Overview of NORC Programming. http://www.chicagomutual.org/level4/norc/norcprogramming.htm.
Chicago Mutual Housing Network is using the Penn South model in a pilot NORC program at two sites funded by the Department of Housing and Urban Development and NORC Supportive Services, Inc., in New York. The web site lists services provided by month for three months.
Landsberg, Gerald, Catharine MacLaren, and Harry Schwartz. The Accomplishments, Issues and Prospects of Supportive Service Programs in Naturally Occurring Retirement Communities. Prepared for the Fan Fox and Leslie R. Samuels Foundation. New York, NY: Ehrenkranz School of Social Work, New York University, September 2002.
In the introduction to the report, the authors define a NORC as "an apartment building, a housing development or a neighborhood with a large concentration of older adults" (p. 1). They note that more than twice as many people live in NORCs as in housing planned specifically for the elderly. Since NORCs are not planned specifically for the elderly, they often lack supportive services. Organized programs of supportive services have been in place since the mid-1980s for NORC residents, 35 in the country of which 28 are in New York City and two in upstate New York. The authors attribute the large number of programs developed in New York City and upstate New York between 1986 and 2001 to the availability of support and funding from the state and the city. Table 1 of the report (p. 9) gives a list of the programs, the date each was established, and the number of housing units in the NORC. Table 2 (p. 13) gives for each program the number of housing units and the number of elderly (total, minority, and disabled). Table 3 (p. 14) provides selected demographics for supportive services clients, 1995 and 2000.
This report provides a summary of the programs in New York and a brief history of how they emerged, including the development of state and city funding streams. The report reviews key factors that shaped the programs and identifies lessons learned, considers programs in other states, and discusses the development of supportive services and the educational activities undertaken by the project at New York University (NYU). The report also includes extensive bibliographies on NORCs and related topics, as well as appendices with statistical materials on program performance, authorizing legislation, and other information.
The New York supportive services program has four objectives: (1) to provide a range of flexible and integrated community-based services (health, social, and allied services), (2) to stress preventive care and services that will enable people to remain at home and live independently, (3) to give consumers and their caregivers an active role in the major decisions affecting their care, and (4) to use the number and density of older people in the NORCs to facilitate care and the delivery of services. Factors shaping the supportive services program include:
- Volunteer activities were the antecedents of the program; volunteer and intern activities remain important.
- Program planning is based on resident surveys, NORC board and management, perceptions, and agency experience; outreach to residents is through flyers, work of mouth, etc.
- Staffing issues (recruitment, retention, training, pay, case loads, shortage of geriatric social workers) affect the program.
- Program governance through the board allows resident input.
- The lead agency takes the major role in organizing and operating the program but partnerships with other agencies and linkages with other resources are important, and management of the NORC is important to keep the program running smoothly.
- Financing is from city and state governments, the board, residents, grants, and users.
According to the authors, the key lessons learned have been:
- The size and compactness of the NORC facilitates service delivery, enables outreach, and encourages social interaction and mutual support among residents.
- Diversity, responsiveness, and flexibility are important characteristics of the service program. Each program is different. Resident input is important.
- Staff relationships are important; changes to staff or services can be disruptive.
- Group services, volunteer activities, and opportunities for informal help all foster the social contacts important for healthy aging.
- Housing management can play a positive role in the program.
- Collaboration with other community resources makes a wider range of services available to residents.
Programs outside New York include Services To Apartment house Residents (STAR) in Philadelphia which serves high-rise cooperatives, the Community Options program in suburban Cleveland which serves residents of four privately owned rental complexes, the Assistance-In-Living program in Greenbelt, Maryland, which serves a mixture of apartments and houses, and programs in two clusters of moderate income cooperative apartments in Chicago. A new program, the AdvantAge Initiative operated by the Visiting Nurse Service of New York, uses surveys as a tool to identify "elder friendly" housing options. This program is operating on a pilot basis in 10 communities nationwide.
The report also includes case studies of seven open NORCs in New York that were done to assess the possibility of developing supportive services programs in such neighborhoods. The goal was to identify the problems of elderly residents of these communities and the services available to them and to identify the prerequisites for developing service programs for such communities. The authors identify eight general issues from these case studies:
- Demographic and cultural changes shape the need for and use of community-based services.
- Community institutions serve as conduits for information about programs and promote social cohesion as well as providing major services, such as hospital care.
- Housing patterns and deficiencies matter, as do public services and infrastructure such as transportation and public safety.
- Chronic illness and access issues are the major health problems identified.
- Other services needed are home care, mental health care, nursing, social service coordination, transportation, and home repair and maintenance.
- Problems within agencies and between agencies can interfere with service delivery.
- Resource gaps exist including funding for local services, gaps in health insurance for home care, and reluctance of seniors to tap their own assets for personal care.
The size of the NORC shapes the scope of the program. The authors assert that the minimum number of older residents necessary to sustain a program in a service area is 1,000 over the age of 75 and a total of 3,500 over the age of 65. Based on the case studies of open NORCs and on the evaluation of the service programs for closed NORCs, the authors developed a list of prerequisites for programs in communities with large numbers of elderly residents:
- A mix of housing densities and types.
- A basic network of health and social agencies.
- Inter-agency cooperation.
- Community institutions such as churches, associations, etc.
- A key agency to take the lead.
- Resources to sustain the program.
- A suitable space that is convenient, accessible, ample, reasonably priced, and comfortable.
- Community support.
The report provides some details from various reports done on NORCs. An evaluation of four NORCs between 1994 and 1998 by Landsberg and Rock of New York University compared users and non-users of supportive services; users are more likely to be women, older than 85, and living alone. A survey of Penn South households (no date provided) described proportions of clients who used services: 8 percent used social services such as case management, 7 percent used information and referral, 4 percent used nursing services, 24 percent attended classes, 20 percent attended health screenings, and 12 percent attended lectures. Of those who did not use services, 18 percent did not like the program, 17 percent go elsewhere for services, 16 percent were not aware of the services, 9 percent did not yet need the services, and 8 percent did not need the services at all. Satisfaction was generally good for services but varied by type of service. A 1996 survey at Penn South and two other NORCs found cultural events to be the most popular service, followed by exercise and dance classes, and health events. The report notes that residents tend to be selective in their use of services and that group services seem to be more popular than individual services.
Lyons, Beverly P., and Carol Magai. "Reducing Health Risks and Psychological Distress among Older Black Residents of Naturally Occurring Retirement Communities." Journal of Gerontological Social Work 35, no. 1 (2001): 53-69.
Overview
The purpose of this study was to determine if certain health and social interventions could reduce health risks or improve psychological well-being among older NORC residents. The authors defined a NORC as a housing community where at least 65 percent of residents are aged 50 years or older. The first hypothesis tested was that the experimental group would show improvements in health behavior as a result of the health intervention. The second hypothesis was that the experimental group would experience improvement in psychological well-being as a result of the social intervention. The authors expected that these improvements would continue after the end of the experiment.
Methodology
The study participants were 45 older black residents at two NORC sites located three blocks apart. The authors did not specify the minimum age for participation in the study or the location of the NORCs. Participants were drawn from attendees at a health education seminar; 19 participants were in the control group (group 2, n = 19), and 26 were in the treatment group for the eight-week study. The authors say that treatment and control groups were randomly assigned to the two buildings to prevent cross-contamination between the groups through "diffusion effects." The treatment was a program that residents attended once a week, with 45 minutes devoted to health education and the other 45 minutes devoted to facilitating socialization.
Data collection occurred from August 1999 through December 1999 in three waves--a baseline survey, a post-intervention survey at the end of the treatment, and third survey two months after the treatment ended. The third survey determined whether the treatment's effects were sustained. The researchers collected data from 24 of 26, and 17 of 19 participants in the treatment and the control groups, respectively.
Findings
The average age of participants was 79 years old and 89 percent were female. The authors report that the "median income range" for all participants was "$4,000-$6,999; the authors do not specify whether this is an annual figure. The first hypothesis regarding health behaviors was not supported. The treatment group had higher scores on good health behaviors than the control group for all three surveys, so the results cannot be attributed to the treatment. The second hypothesis related to psychological well-being was supported because the treatment group experienced an improvement in psychological well-being, and this improvement was sustained after the treatment ended.
Recommendations
Short-term psychoeducational interventions could improve the quality of life for older minority residents of NORCs. The implications for social work practice include the need for social workers to increased sensitivity to cultural differences, broaden the focus of their assessments of older black clients, and introduce inexpensive, innovative, and interesting interventions. However, future studies need to determine if individual, environmental, and behavior practices may prevent the onset of diseases among the black populations.
Study Limitations
The authors point out several limitations. Diffusion effects could have occurred because of close proximity of the two NORCs. The sample was small. Although study participants were representative of older blacks in New York City, this minority population may differ in other regions in the country, which may affect the generalizability of the study findings. A long-term intervention may have produced different outcomes. Finally, the health behavior measures were not widely used instruments with good psychometric properties.
Another limitation of the study is that participants came from people attending a health forum. These people might be more social by nature and inclined to participate in community life. Thus, it is not clear how programs similar to the one used in the treatment group might affect people who are more socially isolated.
Hunt, Michael E. "Settings Conducive to the Provision of Long-Term Care." Journal of Architectural and Planning Research 18, no. 3 (2001): 223-33.
Hunt notes the importance of a supportive social network to the well-being of older people and so asserts that environmental design should have as a goal the design of communities that are conducive to, or foster, such support networks so that people can age in place. He identifies three types of NORCs: (1) aged-left-behind localities, (2) aging-in-place localities, and (3) retirement destination localities. This article briefly describes the first two types but focuses on retirement destination localities.
Older people are attracted to retirement destination localities by a more convenient lifestyle or an amenity-oriented lifestyle. Those seeking convenience are usually the older elderly, often widowed women, looking for proximity to shopping, services, or companionship. Those seeking amenities are often the younger elderly, independent, married, and more affluent, looking for vacation or resort-type localities, or older migrants on a seasonal basis. Convenience-based NORCs are of particular interest to providers of long-term care. They show the importance of considering environmental design and social support together.
The author cites previous literature that identifies the characteristics of NORC residents, their reasons for moving to a NORC, both why they left their previous residence and what attracted them to the NORC, and their satisfaction with the NORC. He cites differences other studies found between younger and older NORC residents. He summarizes the factors that explain the attraction of apartment complexes that have become retirement destination NORCs: location, management, and design.
The NORC dilemma is how to meet the service needs of older residents without making the apartment complex less attractive to younger residents, in order to maintain the age-integration that is attractive to older NORC residents. Hunt cites three approaches identified in earlier literature. First, in the static approach, residents remain in the complex as long as their service needs do not exceed what the complex offers; when they do, they move to a more supportive environment. Second, the complex can expand services to meet the needs of residents as they age. The third approach, the balanced model, allows residents to add services for themselves but the complex expands the services it provides only to a limited degree or responds by linking residents in need with community-based services. Where the complex expands services to meet resident needs, it is likely to become known as retirement housing.
The author identifies two major lessons learned from retirement destination NORCs. First, a sense of community and the proximity of shopping combined with the availability of health care are key features of a retirement destination NORC. Second, an environment that is attractive to older people is also attractive to younger people; that is, a NORC is simply a good place to live. The possibility of social connections is a key attribute of retirement destination NORCs. Hunt links concepts from the New Urbanism, with its emphasis on fostering a sense of community, to NORCs.
Marshall, Linda J., and Michael E. Hunt. "Rural Naturally Occurring Retirement Communities: A Community Assessment Procedure." Journal of Housing for the Elderly 13, no. 1-2 (1999): 19-34.
Overview
The goals of the study were to develop a diagnostic tool that communities could use to determine what type of rural NORC exists in their localities and to determine which variables are associated with the various types of NORCs. In the introduction, the authors provide an overview of the benefits of NORCs to rural areas, with a particular focus on economic benefits.
Methodology
Based on previous research, the authors identified 62 villages or townships in 16 zip codes in rural Wisconsin with a "high percentage" of older residents (the authors did not specify the percentage). The authors then obtained Census data for these 62 communities. The authors classified these areas into three types of rural NORCs: amenity (17), bi-focal (36), or convenience (9). According to the authors, this classification was based, in part, on the characteristics of certain demographic groups likely to be attracted to specific areas. For example, the authors found that young, active retirees from urban environments were attracted to amenity NORCs. The bi-focal NORCs attracted retirees wanting both the natural amenities and the ability to live in close proximity to friends and family. In addition, local residents who were relocating from a rural area to a neighboring community were often more attracted to convenience NORCs. Using the variable, NORC type, a stepwise discriminate analysis was conducted on the variables available in the Census database.
Findings
Twelve out of a set of 27 Census variables showed significant results and were subsequently used in the authors' analyses. These variables included income variables (household income, retirement income, social security income), resident characteristics (percent over 50 years of age, percent with less than a ninth grade education, percent born in Wisconsin), housing characteristics (percent of housing units vacant), and resident employment characteristics (percent employed in forestry/agriculture, construction, transportation, retail sales, or entertainment).
Relative to the other two types of NORCs, amenity NORCs had higher vacancy rates and a smaller proportion of Wisconsin-born residents. Employment patterns also differed significantly with both convenience and bi-focal NORCs showing a higher percentage of forestry and agricultural workers than did amenity NORCs, amenity NORCs showing a higher percentage of construction workers compared to bi-focal NORCs, and bi-focal NORCs showing a higher percentage of transportation workers compared to amenity NORCs.
The authors identified four variables that distinguished among the three types of NORCs: percentage Wisconsin-born residents; percentage of transportation workers; percentage of retail or sales workers; and the percentage of residents age 21 and older with less than a ninth grade education. Using these four variables, the authors accurately classified 59.68 percent of the NORCs in their sample--100 percent of amenity NORCs, 36.1 percent of bi-focal NORCs, and 77.8 percent of convenience NORCs. Because the results for the bi-focal NORCs were poor, the authors eliminated the bi-focal NORCs from the analysis and repeated it. In this last analysis, the percentage of vacant housing, per capita retirement income, and the percentage of workers employed in the entertainment industry, were significant in discriminating between the amenity and the convenience NORCs.
Recommendations
The authors assert that they can accurately identify amenity and convenience NORCs using a small group of Census variables. However, they cannot identify bi-focal NORCs because people who seek out these NORCs likely differ from other retirees on the basis of "psychographic" rather than demographic variables such as those found in Census data.
Bassuk, Karen. "NORC Supportive Service Programs: Effective and Innovative Programs That Support Seniors Living in the Community." Care Management Journals 1, no. 2 (1999): 132-37.
Mutual Redevelopments Houses (more commonly known as Penn South Cooperative) was built in 1962 with union funds and tax breaks from New York City. Initially, Penn South was designed to be affordable housing for a working population in the Chelsea area of Manhattan. This complex of 10 buildings has over 6,200 residents living in more than 2,820 apartments. Seventy-five percent of current residents are age 60 or older. Most of these residents have aged in place; however, older people also have migrated into the community as supportive services became available.
The NORC has had supportive services since 1987, through the Penn South Program for Seniors (PSPS).1 The Board of Directors of the Penn South Cooperative forged a relationship with the United Jewish Appeal - Federation (UJA-F), which became the oversight agency for PSPS, and a source of funding for it.
PSPS programs included:
- Group activities, case management, home care coordination, and nonacute nursing.
- Organized volunteer activities and support groups.
- Adult day care.
- Social model day program for seniors with dementia.
- Case management.
- Program to help residents gain financial assistance.
- Legal guidance related to routine matters.
- Psychiatric care.
- Nursing and home care
- On-site location of a geriatric medical practice.
When PSPS was five years old, Penn South's Cooperative Board felt that, due to their financial commitment to the program, they should have more of a management role in PSPS. In reaction, the UJA-F helped transition with fiscal oversight and responsibility to Penn South Social Services, Inc., which the Board established for that purpose. The new nonprofit corporation continues to contract with outside agencies to provide services.
The author asserts that the NORC services program saved approximately $11 million in one year by preventing 460 hospital stays and 317 nursing home placements. It is not clear which program(s) saved money, nor is it clear how the number of prevented institutionalizations was calculated.
In 1997 through 1998, the case management team worked with 644 clients and families.2 Over 50 percent of these clients were age 85 years or older and almost 25 percent were over the age of 90. Furthermore, nearly 30 percent were never married; 79 percent live alone; 33 percent had no family or friends to provide assistance. In 1999, PSPS provided services for over 1,200 seniors and their families. The volunteer program had 149 senior citizen volunteers that donated over 8,000 hours of services, who saved $80,000. The total program budget was not provided.
Hunt, Michael. "Naturally Occurring Retirement Communities." In Encyclopedia of American Cities and Suburbs (517-18). New York: Garland Publishing, Inc, 1998.
Approximately 27 percent of Americans 55 years and older lived in NORCs (no date given). Only 5-7 percent lived in planned retirement communities. NORC design features, such as lack of elevators in multistory buildings, can prevent some residents from aging in place. The authors did not present information about their methods and analyses, which are largely described in other articles.
NORCs evolve in three ways--"aged-left-behind", "aging-in-place", and "in-migration." Residential managers find apartment NORCs ideal because older people tend to pay their rent consistently and there tends to be minimal damage to their apartments. Rural NORCs are appealing to their host communities because of the economic benefits they provide.
An aged-left-behind NORC develops when an area with an unpleasant environment experiences a significant economic decline. As a result, younger residents leave, while many older residents are unable to do so because of emotional or economic ties to the area, lack of financial resources, or the inability to move. Typically, older residents of these NORCs need medical, social, and personal services.
An aging-in-place NORC has residents who remain in their homes for many years and have a strong desire to remain in their communities. These communities can have residents with varying levels of income.
In-migration NORCs develop when older people move to an area for the convenience of its lifestyle. For example, residents may be seeking the companionship of others, proximity to shopping and services, a hospitable climate, availability of a range of activities, and a more leisurely life. Residents of some of these NORCs may live there on a seasonal basis.
Apartments and condominium complexes were consistently places of in-migration. Location, management, and design were the major factors that cause in-migration to certain housing complexes. Location mitigated the social isolation by improving proximity to friends and family. Management played a key role because referrals were important in older populations seeking hospitable environments.
Yalowitz, Nat, and Karen Bassuk. An Intergenerational Community with Supportive Services, The NORC Model at Penn South Program for Seniors. Presented at the American Society on Aging, San Francisco, March 1998.
In this article, the authors look at the definition of NORCs and their supportive services programs, the structure of the models developed, their financing, the clients served, and the need to see these programs as evolving entities with intergenerational issues. They emphasize the need for the models to remain flexible and to reflect the needs of the community they serve as well as the need for the community served to take major responsibility for the development of the program.
Penn South (officially the Mutual Redevelopment Houses, Inc.) is a 36-year-old, moderate/middle-income co-op in Manhattan. New York state legislation passed in 1994 established 10 NORC supportive services programs. Penn South developed into a NORC primarily through "aging-in" although there has also been some recomposition, immigration, and congregation as described in the literature. It is an example of a closed NORC.
The New York state legislation used as its criteria for a NORC that at least 50 percent of households have one member over 60 years of age or that the complex contain over 2,500 residents that are elderly. All of the New York state programs are constructed as private/public partnerships; each housing entity must match funds provided by the state. Financial participation gives the residents a feeling of having a stake in the program, which breaks down some of the barriers to accepting social services.
The Penn South Program for Seniors (PSPS) was started with funding and oversight through UJA-F and was the model for the legislation that was later passed. The Penn South model starts with the assumption of client participation. The program offers group activities, volunteer program, case management, home care coordination, and nonacute nursing care. Social activities include classes, holiday parties, and trips. Under the case management program, social workers work with the client and, where possible, the family to facilitate acquisition and management of services. Seventy-nine percent of clients live alone; 33 percent have no family or friends to help them. The nursing services program provides Medicare and non-Medicare reimbursable care that helps prevent hospitalization or nursing home placement.
Despite the success of the program, the authors assert that there is a need to evolve in order to meet any gaps in services, to strengthen the NORC multigenerational community, and to redefine NORCs in order to remain politically viable. Examples are given in each of these areas from programs and activities at Penn South. Many of the examples on meeting service gaps focus on how to get as many services as possible for as little money as possible. Strengthening the multigenerational aspect of the program is presented as a way to promote intergenerational activities, break down ageism, and help with the long-term survival of the program. Redefining NORCs from the original definition set out in the New York state legislation is also seen as a way to assure the long-term viability of the program by promoting its spread outside of urban areas.
The authors conclude with the observation by Bruce Vladeck, Health Care Financing Administration (HCFA), that NORCs are the future of long-term care. As cost effective and efficient ways to strengthen communities while delivering services, the authors assert that the NORC model deserves broader support in order to be replicated throughout the country.
New York City Dept. for the Aging, and United States Administration on Aging. Support Services for the Frail Elderly Residents of Federally Assisted Housing: Final Report Findings and Recommendations. New York, NY: New York City Department for the Aging, 1997.
Program Description
The demonstration project--Vladeck Cares Program for Seniors--was designed to (1) provide coordinated services to older people, with one or more limitations in activities of daily living (ADLs), who lived in Vladeck Houses, a large public housing complex and (2) to identify minority populations who needed but were not accessing services and recommend methods of outreach to these communities. Vladeck Cares was designed to meet the first goal by linking frail older people to needed services and entitlements through provision of case management and assistance, information and referral, transportation assistance, mental health counseling, arrangement of home care, and volunteer-provided support services. The project's second goal arose from the concern that attendees at the complex's Good Companions Senior Center were generally white and Jewish and did not live in the complex; this group did not reflect the demographic profile of the complex.
The New York City Department for the Aging, the New York City Housing Authority (which owns Vladeck Houses), and Henry Street Settlement house collaborated in funding and managing Vladeck Cares. Vladeck Houses is a public housing complex of 54, six-story buildings located on 14 acres in lower Manhattan. About half of the complex's 1,700 households were led by someone age 60 or older, totaling 1,008 people age 60 and older lived in the complex. About two-thirds of these older heads of household were female, 70 percent lived alone, and 63 percent had incomes below poverty. Only 20 percent of older residents are white, 53 percent are Latino, 17 percent Asian, and 11 percent black. Henry Street Settlement House, which is a long-standing social services provider, operated Vladeck Cares.
Start-up Issues
The project advisory committee, composed of a diverse group of religious and service organizations, helped modify the project as needed, referred clients to the project, and helped recruit volunteers. The project developed Vladeck Cares: Policy and Program Guidelines at the beginning of the project and revised it after two years to accommodate what staff learned during the project implementation. The demonstration project found that the service coordinator and her staff did not have sufficient time to provide needed outreach and volunteer coordination or mental health services. Client intake screenings had revealed an unmet need for mental health services due to older residents' social isolation and signs of depression. Thus, the project hired two more staff; one was an outreach/volunteer coordinator and the other a bereavement/mental health counselor, both of whom reported to the service coordinator. The project also found less need for emergency home care and home delivered meals than originally thought so the project shifted emphasis to service coordination and non-Medicaid covered services. The program originally arranged for two vans to be available weekday afternoons for shopping and medical appointments, but found it more practical to arrange and provide carfare and escort services on demand.
Communication
Outreach methods to residents included print materials in English, Spanish, and Chinese, information fairs in building lobbies, articles in the housing site newsletter, and a survey distributed to all elderly Vladeck House residents. The survey appeared to be the most effective outreach method but ethnic groups varied in their responses to the other methods.
Participation
Each person contacting Vladeck Cares or the Good Companions Senior Center was offered information and referral about the project's potential benefits and entitlements. Clients potentially eligible for the program were interviewed using a client intake form and then assessed using a standard form if they appeared to be eligible for services. A professional assessment committee reviewed the project's screening and client assessment forms and made final determinations when eligibility was questionable.
Vladeck Cares projected it would have case management responsibility for up to 60 clients a year, but, by the end of the second year, project staff were serving 145 active cases. Staff conducted 1,100 office visits during the two-year demonstration project. The project recruited 14 volunteers and students to help with administrative tasks, telephone reassurance and friendly visiting for clients, assistance with instrumental activities of daily living (IADLs), and running small errands. Licensed nurses working toward their bachelor degrees did vital sign and medication monitoring, blood pressure screening, medication education, and nutrition counseling. Social work students did case management and counseling under the supervision of the service coordinator.
The program served a total of 145 clients with an average age of 75. Seventy-one percent of clients were Hispanic compared with 50 percent in the complex; Asian, white, and black populations were underrepresented in the program compared with their proportion of the elderly population in the complex. About 73 percent of clients lived alone. More than 8 in 10 self-referred to the Vladeck Cares after hearing about the program from the senior center, flyers, friends, or the survey, and 17 percent of clients heard about the program from agencies, including Good Companions Senior Center.
Evaluation/Data
The project set up a computerized client database for every client who entered the program. The first year's data indicated high penetration among the Latino senior population. Program staff felt at this point that a large number of older people were still underserved so they increased outreach to the underserved population. At the end of the grant period, 20 percent of Latino, 12 percent of African American, 11 percent of Asian, and 6 percent of white older people were enrolled in Vladeck Cares.
A survey of residents, conducted 18 months into the project, found that 71 percent of residents had not been aware of Vladeck Cares before it began outreach. Most who entered the program during the two-year grant period heard about it through the senior center or from a program flyer. Seventeen percent of clients were referred by an agency, primarily the senior center. The survey response rate was less than 20 percent. Analysis of client data showed that participation rates declined as residents lived further away from the program and as the age of residents increased.
Recommendations
The demonstration project had several recommendations for other NORC sites. Regarding cultural issues, the program must recruit advisory committee and staff members from varied backgrounds would facilitate reaching out to and working with the minority populations in a NORC. Outreach efforts should be varied and multilingual, as well as tailored to the cultural preferences of residents. The program must be flexible enough to evolve to meet the changing needs of residents and the changing environment within which the program works. The emphasis of a service program should be on coordinating and linking residents with existing community programs and services. The program offices should be as centrally located as possible when the older population lives in a geographically dispersed NORC and outreach should occur in the more remote locations. A computerized database is essential for reporting and analysis that promotes understanding of the NORC residents and their needs and for communication with funders. A resident survey should be conducted about six months after a project starts to give the program time to begin operations and work out implementation issues.
Nadeau, E.G., and David J. Thompson. "Senior Co-Op Housing: Focusing on Community, Health Care and Services." In Cooperation Works! How People Are Using Cooperative Action to Rebuild Communities and Revitalize the Economy, edited by Cooperative Development Services (77-94). Rochester, MN: Lone Oak Press, 1996.
Penn South is a co-operative with 2,820 units that provides a range of services. Penn South was built in the early 1960s by the International Ladies Garment Workers Union (ILGWU). The demographics changed significantly in the 1980s because many families left and the remaining residents aged in place. As they did, problems began occurring. For example, some residents needed help with financial management and others wandered without supervision.
In 1986, David Smith, board president of the Penn South co-op at the time, met with social service experts from the United Jewish Appeal - Federation (UJA-F) to discuss how to meet the needs of the aging population. Together they created the Penn South Program for Seniors (PSPS), which was a partnership between Self-help Community Services and the Jewish Home and Hospital for the Aged. Residents could access services by paying a $15 annual fee; fees were waived for those who could not afford it. PSPS now has over 700 members. There were approximately 12 paid staff and over 100 volunteers. The PSPS program had an annual budget of approximately $400,000 and received about $120,000 from UJA-F, and $100,000 from Penn South's board in 1996. The State Office of Aging, the City's Department of Aging, and foundations contributed the remaining amount.
The PSPS program has spurred the development of other programs in Coney Island, New York (Warbasse House), and the Lower East Side, New York (Co-op Village). The UJA-F created a consortium of agencies that provides a variety of services necessary for independent living. UJA-F and other co-op board organizations lobbied for the state legislation that appropriated $1 million in 1994 to assist 10 NORCs in New York. According to the authors, this was the first state funding made available to NORCs in the United States.
Hunt, Michael, John Merrill, and Carolyn Gilker. "Naturally Occurring Retirement Communities in Urban and Rural Settings." In Housing and the Aging Population: Options for the New Century, edited by W. Edward Folts (107-120). New York, NY: Garland, 1994.
The authors describe findings from their previous work on NORCs, most of which are described elsewhere in this annotated review. According to the authors, rural NORCs have a major, largely positive impact on the economy of local communities. In many rural areas, the older population's transfer payments, dividends, interest, and rent income are major contributions to the municipality's economic base.
According to the authors, the three main factors that affect the evolution of NORCs are location, management, and design, in order of importance. Location is the chief initial attraction of a NORC because residents are close to family or friends, shopping, and services. Management played a crucial role as well because the management's role in maintenance can spur word-of-mouth referrals. Finally, the design of a NORC was not necessarily an attraction, but could potentially be an impediment to independent living.
Lanspery, Susan C., and James J. Callahan. Naturally Occurring Retirement Communities: A report prepared for The Pew Charitable Trusts. Waltham, MA: Brandeis University, Heller School, Policy Center on Aging, October 3, 1994.
This article provides a summary of the literature on NORCs, discusses the NORCs program model, presents findings from analysis of 1990 Census data, and discusses and reframes recommendations.
The U.S. population is aging, with the share of the population over 65 expected to increase to 20 percent by 2025 from the current 12.5 percent. An AARP survey in 1992 showed that 86 percent of older Americans want to age in place, compared with 78 percent in 1986. NORCs are one of the major consequences of this trend. NORCs are defined in this report as housing developments or neighborhoods where at least half of the residents or heads of households are 60 years of age or older or where a large concentration of older people live.
Factors that have led to interest in programs focused on NORCs to facilitate the delivery of health and supportive services include (1) the potential for economies of scale, (2) the successes of similar programs linking senior housing and services, (3) the extensive number of NORCs nationwide, (4) the potential to help preserve communities, (5) the strong desire of older adults to age in place, and (6) the increasing support for helping people with disabilities to remain in the community rather than moving to institutions.
The definition of NORC has changed over time. Community informants report that the impact of an aging local population begins to be felt when their share of the population exceeds about 26 percent, although density and geographic spread make a difference. The authors conclude that it is preferable to specify a range of population and density when defining a NORC. They note that NORCs are "probably more varied than alike," varying by physical size, population size, population characteristics, and reason for existence among other things. They may come into existence by accumulation (older people left behind as more mobile segments of the population leave), recomposition (in which older people replace other residents who are leaving) and congregation (where population inflows are of all ages, but with greater numbers of older people). Recomposition and congregation NORCs in rural areas can be further characterized as amenity NORCs (which attract older people who are generally better off in most ways and are looking for the amenities of rural life), convenience NORCs (which attract local people generally moving from a rural area to a nearby rural community for the convenience it offers), and bi-focal NORCs with characteristics of both. NORCs can also be classified by management or ownership with a closed NORC having one management entity (e.g., an apartment complex or mobile home park) as compared with an open NORC that has multiple owners or management entities. Open NORCs may also consist of one or more closed NORCs.
The number of NORCs appears to be on the rise. The only data available are the 1990 Census data and the 1993 AARP survey. Demographically, NORC residents more closely resemble non-NORC members than people in retirement housing. The latter are more likely to be widowed and to have lived less long in their current residence or area. As compared with non-NORC residents, NORC residents are likely to be older, less likely to be employed, have slightly lower incomes, more likely to own their own homes outright, and have a slightly lower level of education.
Eighty-one percent of NORC residents say their neighborhood or building is a NORC because people have lived there a long time rather than because older people have moved in. They like living in the NORC because of common interests with their neighbors and the quiet atmosphere. Table 1 of the article gives comparative demographic information on NORC and non-NORC residents. NORC residents are more likely to rate highly the usefulness of current and proposed NORC services and these ratings are consistent across a range of services. (The study does not indicate whether the differences between the groups are statistically significant.)
The article discusses various types of NORCs and NORC-centered service programs. Minnesota has developed a block nurse program. UJA-Federation in New York has sponsored a comprehensive program of social, health, and individual services at the Penn South and other moderate-income cooperative housing units. In this program, resident needs are gauged through contact with residents in various ways, and the services are financed in part by the cooperative corporations themselves. Consumer-driven residence service programs (RSPs) have been started in New Jersey and Massachusetts with the goal of providing a single point of access to services. Other efforts have begun or are being considered in Boston, Philadelphia, Connecticut, and Washington, D.C., in NORC or NORC-like areas.
The growth of NORCs is not universally applauded. For example, housing policy in Minneapolis and Rochester appears to be designed to discourage the development of NORC-like situations. Planners fear that a predominance of older residents will result in negative votes on school funding issues, will require more expensive public services, and cause zoning problems.
After presenting this background on NORCs, the authors propose a model linking NORCs and services. The key elements of the proposed model are consumer participation, a focus on resource development and service coordination rather than case management, broad involvement of stakeholders from the beginning, and cost sharing. The model is derived from a model that has worked well in senior housing based on the assumption that density will allow economies of scale, collective activities, cooperation with local businesses, geographic-specific legislation, financing through membership fees, and development of a sense of community. The differences between this model and other models of senior services are presented in a chart (pp. 22-23). In particular, the NORC population is distinguished by being all of the elder population in a targeted geographic area rather than those eligible for specific programs such as private insurance or Medicare, and financing is drawn from numerous sources including insurance, government payments, block grants, and out-of-pocket payments.
The author then delineates important factors for developing and implementing NORC programs. Specifically, there should be a clearly identified lead entity. Other factors are listed that will facilitate development and implementation including a closed NORC, a homogeneous population, a service-rich area, consumer-oriented agencies, identifiable stakeholders with an interest in cooperation, urban-like concentration, strong neighborhood or consumer groups, higher consumer income, and a relatively autonomous lead entity.
The author uses 1990 Census data to identify NORCs using a definition of at least 40 percent of householders of age 65 or more in Census block groups or those with at least 200 householders over age 65. The age 65 is used as a cutoff rather than younger ages seen in some studies for three reasons: (1) age 65 is more conservative, (2) age 65 is more convenient statistically, and (3) age 65 is the age for Medicare eligibility. The choice of a minimum of 200 householders was made because it suggests some economies of scale; it is in the mid-range of what is generally considered large enough to support a full time services coordinator in senior housing. Using these definitions, the authors found that about 10 percent of all 1990 Census block groups qualify as NORCs, representing about 3.5 million households. These NORCs show great diversity in housing age, income, and functional limitations, but single elder residents predominate over married elder residents in all but one of the identified NORCs.
The authors point out a critical difference between NORCs and integrated service networks. In the latter, a set range of services is marketed to a membership group, while in the former, the emphasis is on giving discretion and control over the types of services included to the members of the group. Services are typically of a social services nature rather than traditional health services. The authors conclude that establishing a formal linkage between NORCs and health and supportive services will have considerable benefits. In appendices the authors provide a summary of their findings and highlights from their case study.
Hunt, Michael E., D. Arch, and Leonard Ross. "Naturally Occurring Retirement Communities: A Multiattribute Examination of Desirability Factors." The Gerontologist 30, no. 5 (1990): 667-74.
Overview
This study analyzed the factors critical to attracting older people to NORC apartment complexes. Apartment NORCs are unique because they have become the most widespread form of alternative housing for the elderly in the U.S, according to the authors. Previous research shows that the availability of desirable supportive neighborhood services are a major attraction for older people. Furthermore, safety and proximity to services and peers also attracts this population.
Methodology
The purpose of this study is to provide quantitative measures that describe the relative importance of certain apartment complex characteristics, as identified in a previous study, in attracting older residents to non-NORC apartments. Results from a preliminary survey of NORC residents identified three critical factors that explain the desirability of NORCs: location, management, and design. The current study looked at three NORC and two non-NORC apartment complex sites located in Madison, Wisconsin. The housing was intentionally selected to vary according to location, building type, age of the housing, and management company.
A subject sample from each apartment complex was drawn from either the apartment or city directory. Of those contacted, 64.7 percent agreed to a telephone interview, and 143 people were interviewed. In order to measure the relative importance of the three NORC attributes identified in the preliminary survey, a multi-attribute scaling procedure assigned weights to various apartment complex attributes that could affect decisions to move into the setting. These attributes were organized into a "tree" structure to compare the relative importance.
Findings
Location was the most important factor in attracting older residents to the apartment complex for both NORC and non-NORC elderly, with management and design relatively equal but less important. Location specifically included the distance to shopping/service facilities and proximity to friends, age peers, and family as well as neighborhood safety. Older NORC resident's valued social factors while older non-NORC residents placed more importance on distance factors. In terms of management, which includes factors such as upkeep and resident manager, both NORC and non-NORC residents valued upkeep more than the presence of a resident manager, and both found the design of the individual unit to be more important than the complex's design. Finally, the housing features that attracted older people were attractive to younger people as well.
Study Limitations
Some of the participants in the preliminary survey were in the final study as well. The authors did not think this posed a significant problem because the surveys occurred one year apart and used differing methodologies. It is not clear whether the authors randomly selected their pool of potential interviewees. Thus, the generalizability of these results is unclear.
Hunt, Michael E. "The Naturally Occurring Retirement Community." In Housing the Very Old, edited by Gloria M. Gutman and Norman K. Blackie (161-72). Burnaby, British Columbia, Canada: The Gerontology Research Center, Simon Fraser University, 1988.
Overview
This study focuses on how apartment complex-type NORCs evolve. According to the author, NORCs in apartment buildings are probably the most common form of alternative housing in North America and house more of the older population than do planned retirement communities. In Madison, Wisconsin, there are about three times as many NORCs as planned retirement communities.
Methodology
To learn more about how these communities evolve, three NORCs in Madison, Wisconsin, were studied. Interviews were conducted with a total of 72 residents, or approximately 25 percent of residents age 60 years and older. Interviews were also conducted with a representative from the management for each apartment complex. The four major categories of questions were designed to ascertain the demographic characteristics of the older population living in the NORC, reasons for attraction to the NORC, the quality of life in the NORC, and reasons for moving away from the NORC.
Findings
The following summarizes findings from interviews conducted with residents. The majority of residents interviewed for the study were widowed women living alone (80 percent). Approximately two-thirds were age 65 to 75 at the time of the interview. About a third said they moved to the NORC when they were under 60 years of age, while half moved to the apartment community between ages 60 and 75. About a third said they had lived in the NORC between 11 and 20 years, another 23 percent said they had lived in the NORC more than 21 years. Over three-quarters had moved to the NORC from the same part of town, with about half moving after selling homes they had lived in for a long period of time.
The most frequently cited reason for moving to a NORC was that the size and maintenance requirements of their former residence were becoming problematic. According to respondents, these problems were most frequently associated with death of a spouse or cohabitant and failing health. Respondents reported that they least liked the upkeep and isolation of their former residence, but most liked the privacy and location of their home near close friends and neighbors.
Consistent with their reasons for moving away from their former residence, respondents indicated they were attracted to the NORC mainly for two reasons, its location and that friends or relatives lived there. Older residents had heard of the NORC by word of mouth and personal referrals seemed to be the predominant form of advertising.
About half of respondents said they liked life in the NORC better than where they had lived before, with more than a third rating it about the same. The most common reasons for liking the NORC better were fewer stairs, less space, and management's ability to maintain the NORC. Almost half reported socializing with neighbors more often since moving to the NORC. Although some respondents mentioned that moving to a smaller apartment was difficult, most were willing to trade-off the disliked qualities of the apartment lifestyle for its location and freedom from maintenance responsibilities.
When asked if they planned to move away from the NORC about 30 percent of respondents said "maybe" and another 10 percent said "yes." Respondents said they would move either because of a need for more health care or to lower their rental costs. Respondents also said these reasons were the primary reasons most residents moved away from the NORC. However, those who moved away reported they had left because of barriers in the design of the NORC such as stairs in the living unit and laundry room. Nonetheless, most respondents felt that nothing should be done to provide assistance to help residents live independently in the NORC, and, if residents needed more health care then they should go somewhere else where care could be provided.
Conclusions
The author finds location, management, and design to be main factors in the initial attraction to a NORC. In terms of location, a NORC's proximity to shopping and service facilities as well as family and friends are key. Residents expect that NORC will be well maintained, thus building maintenance is important. The design of a NORC can also help eliminate potential barriers to independent living.
NORCs were also found to be desirable to housing managers. Resident managers reported that older residents were desirable tenants because of their stability, which is often cost-effective, dependability with rent payments, and lack of wear and tear on the apartment itself.
Study Limitations
It is not clear whether the survey sample was randomly selected, so the generalizability of findings is in doubt.
Hunt, Michael E., and Gail Gunter-Hunt. "Naturally Occurring Retirement Communities." Journal of Housing for the Elderly 3, no. 3/4 (1985): 3-21.
In this study, the authors examine the evolution of NORCs and compare them to a typology of planned retirement communities (RCs) and community-based housing. According to the authors, the supportive services available in neighborhoods are the main attraction for each living arrangement.
The authors define a NORC as "a housing development that is not planned or designed for older people, but which over time comes to house largely older people" and can range from an entire neighborhood to a single apartment building. NORCs differ from planned communities in several ways: (1) they are not specifically designed for older people, (2) they are age-integrated, (3) they are often single buildings or a small complex of buildings that house fewer than 500 people, (4) they are most often not marketed as retirement communities nor are they generally considered retirement communities by their residents, (5) they may provide few, if any, services to their residents, and (6) the residents are generally younger than residents of planned retirement communities. Given these differences, the authors propose that NORCs be added to the typology of retirement communities developed by University of Michigan researchers (M.E. Hunt et al., Retirement Communities: An American Original. New York: The Haworth Press, 1984).
Communities evolve into NORCs (that is, they become communities with at least 50 percent of their residents being 50 years old or older) either by aging in place (residents move in before they reach age 50 and stay until they are past that age) or by relocation (people older than 50 move into the community), or a combination of both. The authors use a case study of a NORC in Madison, WI, to demonstrate the process of becoming a NORC. The area has an array of readily accessible services (post office, medical care, banks, shops, restaurants, grocery store, and the like) and public transportation, as well as a range of housing options by type and cost. The services were present in the community before the older people settled there and may have contributed to the area's attractiveness. The apartments are well maintained and of adequate quality, and the physical environment is accessible. The large number of older people provides opportunities for companionship. Crime is low. The authors assert, "The evolutionary pattern of NORCs suggests that neighborhood and services are even more important than the housing unit itself". They note that planned retirement communities and NORCs have in common their proximity to neighborhood facilities and services.
Age heterogeneity is a major factor distinguishing planned retirement communities from NORCs. The authors state that, since people have different preferences regarding the age structure of their communities, NORCs provide an alternative to planned retirement communities. They stress the desirability of decentralizing services and planning multifamily housing around service centers; public transportation between decentralized service centers would increase access to services. Residents living in supportive neighborhoods may require fewer external services to remain independent.
Hunt, Michael, and Leonard Ross. Naturally Occurring Retirement Communities, The Invisible Housing Alternative. A brochure funded by the AARP Andrus Foundation, n.d.
In this brochure, a NORC is defined as a community that is not designed or planned for older people, but over time had attracted "a preponderance of residents 60 years of age." Three main factors are cited as determining the attractiveness of a NORC: location, management, and design. Location near a grocery store is particularly important. Good management, usually in the form of a resident manager, is important, as are well-maintained grounds and buildings. The design of the building, particularly the level of barriers to independence, is more often a reason that people move away rather than one that attracts them to the building. Many of the features that make a good NORC are also those that make housing desirable for all people. At the back of the brochure is a checklist of features to look for in "A NORC That's Right for You."
LITERATURE RELATED TO SUPPORT SERVICES IN PUBLIC HOUSING
Heumann, Leonard F., Ph.D., Karen Winter-Nelson, and James R. Anderson, Ph.D. The 1999 National Survey of Section 202 Elderly Housing. Public Policy Institute, AARP, Washington, DC (2002).
Overview
The Elderly Housing Program, commonly known by its section number, Section 202, is a federal program focused on constructing subsidized rental housing for older adults. In 1999, over 3,500 Section 202 facilities housed more than 300,000 older people. The 1999 National Survey of Section 202 housing is the third national survey of Section 202 sponsors and facility managers; previous surveys were conducted in 1983 and 1988. The survey continues to document changes in characteristics of the project, residents, consumer demand, offered services, management, and capital needs.
Methodology
The 1999 National Survey of Section 202 housing for older people involved a random sample of a third of existing projects and two different survey instruments, one for managers and another for sponsors. A total of 509 managers, (47 percent response rate), and 480 sponsors (44 percent response rate) participated in the survey. Because of the survey's focus on the effect of legislative and regulatory changes, analytic results compare project, resident, staffing, services, and financial characteristics over time. Facilities are categorized into five phases according to when they were built, these phases include: Moderate-Income Phase (1959-1974), Low-Income Phase (1974-1984), Cost-Containment or Very Low-Income Phase (1985-88), Transition Phase (1989-1994), and the Project Rental Assistance Contract (PRAC) Phase (1993-present).
Findings
The following is a summary of findings on staffing and management, service availability and usage in Section 202 elderly housing. Since authorization of professional service coordinators in 1990, more than a third of facilities (37.4 percent) in 1999 had professional service coordinators on staff. Another 43.8 percent of residents had access to community-based service coordination. Managers with service coordinators on staff report that service coordinators have increased the range of services (90.5 percent), increased the quality of services (78.3 percent), and allowed residents to stay independent longer (81.1 percent). There was a 17 percent increase in total staff hours per unit between 1988 and 1999, averaging 2.1 hours a week, while services hours increased 57 percent to an average of 1.1 hours per week. In the past decade, the number of part-time managers, working less than 30 hours per week has increased from 22 to 27 percent. This trend is concentrated mostly in small facilities.
Facilities that are more likely to provide supportive services to elderly residents tend to be older with large numbers of units, more residents over the age of 80, a higher percentage of frail residents, residents that pay for services, and large communal spaces for group services and activities. Section 202 projects reporting lower levels of full or partial congregate support (i.e., meals and housekeeping) were more likely to be developed between 1985 and the present. Higher levels of congregate support were reported from older projects developed between 1959 and 1985. Some projects (10.9 percent) extended services to nonresidents from the surrounding community.
Sources of funding differed by type of service. Resident funds were the primary source of income for group meals for 81.3 percent of moderate-income facilities and 57.9 percent in the other four phases. Medicaid was the most common source of income for personal care services in all phases, except for the moderate-income phase. For other services such as transportation or visiting nurse services resident funds were used by 63.8 percent of moderate-income facilities, and 42.8 percent of facilities in the other phases.
Services such as group dining, social work and counseling, and social and recreational activities were most likely to be provided by on-site staff. Personal care, housekeeping, care management, medication management, and religious services were most likely provided by external agencies or contractors, while transportation and money management are services most likely provided by family and friends. Support from family and friends remained unchanged across all Section 202 phases, suggesting that program changes or use of outside agencies had little effect on the use informal support networks.
Conclusions
Legislative and regulatory changes have improved the Section 202 program since 1988. For example, legislative changes in the early 1990s allowed facilities to hire service coordinators. Service coordinators have increased the range and quality of services as well as allowed residents to stay in their individual units longer. Residents in Section 202 housing are older and more likely to be frail than in previous surveys. In 1983 the average resident age was 72, compared with an average age of 75 in 1999. As residents continue to age in place, facilities are setting up congregate services or converting to assisted living to accommodate residents' needs. But, facilities built in the past decade are much smaller, on average, than those in previous years with fewer staff and services. It may be less economically efficient for these facilities to serve a smaller number of residents.
Recommendations
There are two important issues to examine in future research. The first is the need to address resident satisfaction and perceptions about the quality of federally subsidized housing and care. The second is to address quality of care issues in facilities providing support services, where currently there is no data about the adequacy or appropriateness of support services in elderly subsidized housing. It is also recommended that HUD improve its databases for the inventory of projects serving older people and people with disabilities, besides establishing a regular process for updating information in this survey.
Cox, Beth Madvin. "Linking Housing and Services for Low-Income Elderly: Lessons from 1994 Best Practice Award Winners." Journal of Housing for the Elderly 15, no. 1-2 (2001): 97-110.
Overview
This study identified the characteristics of HUD's Best Practice Award winners for subsidized multiunit housing facilities that offered supportive services program to older residents. Supportive housing was designed to provide services at a new site or pre-existing facility to an aging population, where the services increase as the population ages. Facility management typically developed supportive programs by providing direct services or securing community resources. Charitable organizations also provided supportive services to federally subsidized housing facilities.
Methodology
The author used data from 117 applications for the HUD 1994 Best Practice Award competition, and compared the 23 winners with the other 94. The purpose of this competition was to recognize and award HUD subsidized multiunit housing facilities.
Findings
The best practice sites had more access to supportive, clinical, and ancillary services, and astutely utilized community resources. The winners of the 1994 HUD Best Practice award provided linkages to a greater number of supportive services (p<0.0.1), and were more likely to provide on-site nursing services (p<0.01), mental health services (p<0.05), and security services (p<0.05). Winners used outside providers more often in the provision of service coordination (p<0.05), congregate meals (p<0.05), and mental health services (p<0.05).
Recommendations
These characteristics would be imperative in the continued development of comprehensive aging-in-place programs for older adults with low incomes. Winners were also more likely than non-winners to be located adjacent to community centers.
Ficke, Robert C., and Susan G. Berkowitz. Report to Congress: Evaluation of the Hope for Elderly Independence Demonstration Program and the New Congregate Housing Services Program. Washington, DC: U.S. Department of Housing and Urban Development, Office of Policy Development and Research, 2000.
Overview
This report presents the evaluation results from two Department of Housing and Urban Development (HUD) programs, the HOPE for Elderly Independence Demonstration program (HOPE IV) and the Congregate Housing Services Program (CHSP). Both programs combine housing assistance with case management and a range of supportive services for the frail, low-income elderly population. The purpose of evaluating these programs is to provide information and support in legislation, programs, and policies that address the housing and service needs of elderly individuals in federally assisted housing.
Background
Section 802(1) of the National Affordable Housing Act of 1990 mandated an evaluation of HOPE IV and the new CHSP. The objectives of the two evaluations were to provide a comprehensive description of each program, assess the effectiveness of the two programs in providing supportive services to frail elderly with the goal of maintaining their independence, and compare HOPE IV with the new CHSP. Although both programs provide similar services with the same goal, one major difference is that HOPE IV is tenant-based and CHSP is project-based. The HOPE IV program combines Section 8 rental vouchers with case management support services to enhance elderly residents' quality of life and prevent unnecessary institutionalization. These services are provided either in the tenants home or in other community locations. To be eligible for HOPE IV the person must have been at least 62 years of age, have income not exceeding 50 percent of the median for their area or be willing to move to a private rental unit that meets HUD's Section 8 standards, not participating in Section 8 or other housing assistance programs, and need assistance with personal care or home management activities.
The CHSP program provides a combination of housing and supportive services to low-income frail elderly or nonelderly with disabilities to encourage maximum resident independence, improve management's ability to assess service needs, and ensure delivery of needed services. Services are delivered in the resident's apartment or in the development's common areas (i.e., dining room, activity center). For eligibility to both HOPE IV and CHSP programs, HUD required that participants need assistance in three or more HUD defined ADLs: eating, bathing, dressing, grooming, and home management activities (e.g., housework, shopping, laundry).
Another difference between the two programs is in recruitment and participation. Participants for the HOPE IV program were recruited by grantees, but could not have been receiving HUD housing assistance before applying to the program. CHSP participants came from HUD-assisted congregate housing sites, many of them having lived in these communities for several years. One key feature of both programs was the establishment of a service coordinator position responsible for designing and implementing a system of case management and supportive services to their frail elderly residents.
Methodology
HUD awarded grants to 16 agencies or grantees for HOPE IV housing projects ranging from 25 to 150 residents during a five-year demonstration period. Grantees represented state-level agencies, county jurisdictions, and municipalities across the nation including states in the West (California, Colorado, Washington), Southwest (Arizona, Oklahoma, and Texas), Midwest (Iowa, Ohio), South (Kentucky), and East and Northeast (Maine, Massachusetts, New Hampshire, New Jersey, and Pennsylvania). Thirteen of the 16 grantees reported serving suburban, rural or small town communities.
Another 39 grants were awarded to fund CHSP projects in 45 developments with the number of participating residents in each development ranging from less than 10 to 100. These projects existed in various types of federally subsidized housing including Section 202, Public Housing Authorities (PHAs), Rural Housing Service, Section 236 and Section 8. Most of the CHSP developments were located in urban or metropolitan areas, only four were in nonmetropolitan areas. CHSP projects were concentrated geographically in the Midwest (12 developments) and Northeast (11 developments). West and Midwestern developments were located mainly in large metropolitan areas, while Northeastern developments were in moderately sized metropolitan areas, and Southern developments were mostly moderate-sized metropolitan areas to nonmetropolitan areas.
The service coordinator and professional assessment committee (PAC) were key parts of the HOPE IV and CHSP programs. The service coordinator's responsibilities included recruiting and formal case management, educating resident and staff, building a network of providers and service agencies, and linking participants to those providers and services. The PAC worked in conjunction with the service coordinator to determine eligibility, help develop the case plan for services, and monitor participants' condition.
Services provided to participants under HOPE IV and CHSP included: meals, housekeeping, grooming, dressing, maintaining personal hygiene, transportation, nonmedical supervision, wellness programs, preventive health screening, personal emergency response systems, and other supportive services approved by HUD. Grantees either provided services directly or through contract agencies or providers. HUD paid 40 percent of the program costs, the grantees paid an added 50 percent, and participants paid for the remaining 10 percent with a cap up to 20 percent of their income.
The report discusses program design, implementation, and operation. Subsequent chapters compare and contrast the demographic profile and functional health status of participants in each program. There is a discussion of the informal and formal assistance, social support, and service utilization of program participants and comparison of the effect of the two programs on measures of well-being and exit patterns (e.g., nursing home placement, mortality). Finally, the authors present conclusions, policy implications, and recommendations for how HUD and Congress might address the needs of the frail elderly in federally subsidized housing through housing and supportive services.
Findings
Program Implementation. Because of differences between CHSP and HOPE IV models, recruitment of HOPE IV participants took considerably longer than CHSP. Almost all HOPE IV grantees reported difficulty in recruiting and placing eligible applicants in subsidized rental housing, with 40 percent of applicants having to relocate to a qualifying apartment to receive the programs services. Public housing authorities had to make considerable changes to their Section 8 application and placement policies and procedures to accommodate the frail elderly in applying and finding subsidized housing as well as balance the implementation activities with supportive service requirements for participants. Because of the implementation requirements in the HOPE IV program, the role of the service coordinator developed differently from the CHSP program. Throughout the five-year demonstration period, HOPE IV service coordinators continued to work on efforts to recruit and retain participants, while CHSP service coordinators were able to focus on more case management activities. In follow-up surveys HOPE IV and CHSP participants reported they were satisfied with their service coordinators' help in providing information and linkages to services. HOPE IV participants stressed their role in finding housing and rental assistance, while CHSP participants focused on the personal and interactive relationship with the service coordinator.
Participant Characteristics. Most of the participants in the HOPE IV and CHSP programs were widowed, white females, living alone. Over half were 75 years of age or older, while the median age of CHSP participants was higher than HOPE IV (82 years versus 74 years). Half the HOPE IV participants changed residence within one year of enrollment, compared with 12 percent of CHSP residents, partly caused by the design differences of each program. All HOPE IV participants were new to HUD housing assistance, while CHSP participants were already living in HUD assisted congregate housing. In terms of ADL limitations, HOPE IV and CHSP participants were considerably frailer than the elderly population as a whole but less frail than people who receive, or are eligible, for institutional care. HOPE IV and CHSP participants report having many chronic health conditions. The most frequently reported chronic conditions were heart conditions, diabetes, arteriosclerosis, and stroke. A greater percentage of HOPE IV participants indicated they sought medical care because of falls during the past year compared with CHSP (22 percent HOPE IV, 12 percent CHSP), however a similar proportion (9 percent HOPE IV, 7 percent CHSP) reported they were hospitalized for more than one day due to a fall during that period. More than a third of participants in both programs reported that they had stayed overnight in a hospital over the past year, twice the rate of the elderly as a whole. But, a majority reported they had not been confined to a bed or chair during the month before the baseline interview.
Social Support and Service Utilization. HOPE IV and CHSP participants differed in their social support and interaction. HOPE IV respondents reported contact with family members in-person or on the phone at one or another extreme, either frequently (several times a week or more) or infrequently (less than once a month). More than a quarter (25 percent) of HOPE IV participants reported seeing their child more than three-times a week and 12 percent reported they saw their child every day, while 47 percent reported they saw a child less than once a month. The distribution of family contact with CHSP participants was much more even across categories. Participants in both programs reported similar levels of loneliness (20 percent HOPE IV, 21 percent CHSP). Not surprisingly, a greater proportion of CHSP participants compared with HOPE IV participants were receiving formal services before entering their program. However, the core services received by participants were similar across programs with almost four-fifths of participants in both groups reporting they received housekeeping services, slightly less than a half indicated they received transportation services, and about a third received personal care. Participants reported they were satisfied with both the program and the amount and types of services received.
Outcomes. A separate comparison group of frail elderly receiving Section 8 rental assistance but not enrolled in HOPE IV was part of the evaluation to determine what the level of services might be without the program. Both participant and comparison groups were interviewed at two points in time, during a baseline and follow-up survey two years apart. The evaluation found that HOPE IV participants received considerably more services than the comparison group, a disparity that continued to increase over time. At follow-up 32 percent of the comparison group reported receiving no services compared with 7 percent of the HOPE IV participants. HOPE IV service recipients scored higher on mental health measures (anxiety, depression, loss of behavioral/emotional control, and psychosocial well-being), social functioning, vitality, and other measures of social well-being. However, there was no statistical difference in the rate of nursing home placement, mortality, or exiting Section 8 housing between the HOPE IV participants and comparison group. Similarly there is no independent effect of receiving one specific individual CHSP service on continued participation in the CHSP program. Twenty-four months after the baseline study, half the residents were still in their respective programs. Nine percent had left the program but remained in their subsidized housing either because they were not eligible, were dissatisfied, or obtained services from some other source. More CHSP participants had moved into a nursing home compared with HOPE IV participants (25 versus 9 percent), possibly because of their higher median age. Another 14 percent of participants in both programs had died.
Conclusions
The HOPE IV and CHSP service coordinators played a key role by providing case management services to participants, educating PHA staff and building managers, and linking community agencies with each other and the low-income elderly population in federally assisted housing. Linking federal, state, and community-based programs on aging was a key factor in the programs success. According to service coordinators, information sharing among grantees on the stages of initial development across programs would have provided them with the ability to build on existing conceptual designs and avoided duplication of models. Shared information on client assessment instruments and procedures for selecting participants would have also been useful. The evaluation showed a high level of frailty and unmet need for services among current HUD housing residents, patterns that are likely to exist in other communities. Long waiting lists for congregate housing and limited availability of Section 8 rental vouchers leaves barriers to expansion of HUD's housing assistance programs for the frail elderly. Although the evaluation demonstrated high satisfaction among participants, turnover was also high between the two-year baseline and follow-up period suggesting that increasing levels of frailty even with supportive services may preclude elderly residents from participation. Finally, the HOPE IV and CHSP program models are complementary and respond to different population needs, with the tenant-based approach responding to those frail elderly living in scattered-site housing that meet HUD housing quality standards and the project based-approach to those living in subsidized congregate housing. The authors also note that the HOPE IV and CHSP models are similar to and correspond with the Medicaid waiver and assisted living programs professionals are using in the development of alternative long-term care policies.
Recommendations
The following are recommendations for action from the lessons learned from the evaluations of HOPE IV and CHSP. These recommendations include, in the absence of funding, expanding the congregate service coordinator's role to support tenant-based HUD programs. This would create some central organization for the recruitment, placement, and arrangement of supportive services to frail elderly tenants. To facilitate this expanded role for the service coordinator, HUD could encourage formal links with other federal, state, and community-based programs that provide these services. Also, Congress and HUD can encourage the dissemination and utilization of the evaluation results and information about the specific design, implementation, and operation of these programs through HUD's Office of Policy Development and Research, national conferences, and publication of journal articles. Congress and HUD should also provide incentives for pubic housing authorities to set aside vouchers for the frail elderly or offer additional vouchers to meet demand for Section 8 and congregate housing. This effort might encourage public housing authorities to set up supportive services or offer additional money to service coordinators as incentives to congregate housing sponsors who include supportive services. It is recommended that HUD continue monitoring HOPE IV and CHSP grantees after the program ends to determine how successful grantees were in continuing the program using alternative resources. Further promotion of the adoption of the HOPE IV and CHSP models by Congress and HUD would help toward the increasing demand for housing assistance and supportive services programs. Finally, HUD policies must ensure that a range of housing assistance options, both tenant-based and project-based, exists for the frail elderly.
Schafer, Robert. Housing America's Seniors. Cambridge, MA: Joint Center for Housing Studies of Harvard University, 2000.
Overview
This study examined the housing choices of the elderly population and the public policy challenges innate to housing for the elderly.
Methodology
This study analyzed a recent survey conducted by AARP in Understanding Senior Housing, (1996) as well as the 1993 AHEAD survey, the 1995 American Housing Survey, the 1997 American Housing Survey, and the 1997 Current Population Survey
Findings
About 80 percent of older people prefer to remain in their own homes, and this percentage increases with age, with almost all people age 85 and over preferring to remain in their homes. However, 39 percent of American changed residences after they reach the age of 60, with most moves being local. Typically, about one percent of the elderly moved across a state boundary, and even these moves were within the same metropolitan region.
In 1993, three-fourths of the nation's population age 70 and over lived in conventional housing, whereas 5 percent of this group live in supported housing (i.e., where "seniors receive assistance from outside the home from a nonfamily member or an organization"). Seniors who chose supported housing normally had difficulties with activities of daily living, but continued to have good cognitive ability. Younger, married seniors preferred conventional housing, particularly those with children in the home or nearby. Three percent of those age 70 and older in 1993 lived in the most expensive living arrangement--assisted communities (i.e., "age-restricted communities that provide some assistance"; this category includes assisted living communities and continuing care retirement communities). The housing choices were influenced by age, need for assistance, and availability of children. Assisted communities without income limitations resulted in out-of-pocket costs for the average resident of $1,461 monthly. Then the order was shared housing ($442), conventional housing ($351), and supported housing ($328). These figures do not include the cost of purchased support services.
Seniors frequently need environmental modifications to accommodate their disabilities, but only 20 percent of conventional housing have bathroom grab bars; only five to eight percent of such housing has call devices, railings, and ramps.
Study Limitations
The differences in the definitions of assisted communities and supported housing are not distinct. The 1993 data probably does not reflect the major shift to assisted living facilities and other group housing that has occurred during the last decade.
Sheehan, Nancy W. "Resident Services Coordinator Program: Bringing Service Coordination to Federally Assisted Senior Housing." Journal of Housing for the Elderly 13, no. 1-2 (1999): 35-49.
Overview
The author reviewed the role of service coordinators in six state-assisted housing developments for the elderly by analyzing a two-year federally funded, on-site program in Connecticut called the Resident Services Coordinator Program.
Methodology
The evaluation included: key informant interviews with property managers, resident services coordinators (RSCs), and management company representatives; case studies of elderly residents at risk of entering a nursing facility; RSCs' weekly activity logs; and, pre-test and post-test interviews with elderly residents in the six demonstration sites and random samples of residents living in two other senior housing sites, which were included for comparison purposes. Post-test interviews were conducted eight months after the program began at each site.
Findings
The typical resident was white, female, and living alone. About half of those residents in the demonstration sites characterized their health status as fair or poor, compared with less than 40 percent in the comparison sites. Levels of disability also differed among the six sites.
The RSCs expressed concerns about being able to maintain the confidentiality of communications with residents with respect to the on-site property managers who wanted to know about residents' needs and circumstances. Working relationships between RSCs and property managers could be somewhat problematic; part of the issue was that RSCs believed that they needed on-going supervision from someone who had the training necessary for supervision.
Property managers believed that the RSCs improved the quality of life for residents, reduced residents' risk of entering nursing homes, and resulted in savings due to lower apartment turnover, and vacancy rates as well as better upkeep of the apartments. RSCs also freed property managers from trying to meet the support needs of elderly residents.
Frail older people in the demonstration sites reported significant improvement in perceived health status in comparison to their peers as well as functioning related to activities of daily living and instrumental activities of daily living between the pre-test and post-test interviews. There were no changes among frail elderly people in the comparison sites.
The majority of residents said that the RSCs had benefited them through providing emotional support, help with problems, and information and referral. As a result, participation in social activities and housing satisfaction had increased significantly for residents, regardless of their level of disability.
Study Limitations
The authors state that key informants might have been reluctant to criticize a program that benefited them and responses might have changed if interviews had been conducted later in the life of the programs. Since the authors could not match residents from the demonstration and comparison sites, the conclusions that can be drawn from comparing these results are limited. Finally, one third of residents who received help from the RSCs did not participate in the pre-test interviews.
Park, Jungwee, and Jean Burritt Robertson. "Mental Health Needs and Supportive Services for Elderly and Disabled Residents." Journal of Housing for the Elderly 13, no. 1-2 (1999): 79-91.
Overview
This study examined the effects of the provision of supportive services on the mental health and quality of life of older adults, including those with mental disabilities, living in 12 housing developments for older people and people with disabilities.
Methodology
The authors interviewed 205 residents of 12 housing projects in Rhode Island, who were interviewed at baseline and six months after they began receiving chore, homemaker, and personal care services. Of these residents, 44 reported that they had or were "known to have" mental health conditions. The majority of services that residents received fell into the chore and homemaker categories.
During both interviews residents completed an assessment designed to measure their cognitive and affective functioning as well as their psychosocial well-being. The assessment was drawn from items in several recognized assessment tools, such as the Mini Mental Health Status Exam.
Findings
At baseline, there were significant differences related to cognitive and affective functioning, but not psychosocial well-being, between the full sample and the 44 residents with reported mental health conditions. Six months after support services began, there were no significant differences in any of the three areas of functioning between the entire sample and the subset of 44. The authors conclude that the provision of supportive services to residents with mental illness led to increases in their cognitive, affective and psycho-social scores, and that such services may be more important for those with mental illness than for those without.
Recommendations
The authors speculate that reminders to take medications may have contributed to improvements in the functioning of the 44 with reported mental health conditions. The authors also contend that the program was less expensive than personal care programs in congregate housing settings.
Study Limitations
The subset of 44 people may well have had mental health conditions but the authors did not supply information on diagnosis or the level of cognitive impairment. And, the cost savings estimates are not methodologically sound.
Howe, Judith L. "Linkage House: A Case Study Highlighting the Challenges and Opportunities in Linking Housing and Programs for Older Adults." Care Management Journals 1, no. 2 (1999): 138-45.
Program Description
The Mount Sinai Medical Center, New York City and three community-based organizations sponsored supportive services programs in the Linkage House, a 70-unit building with low-income residents, using a capital grant under HUD 202 program. The Linkage House program fostered an environment of communal living and the formation of support networks, while enabling a resident to maintain his/her privacy. The model for the Linkage House program was dynamic, thus enabling it to adapt to the changing needs of its residents. In 1991, the Department of Geriatrics and Adult Development at Mount Sinai Medical Center commissioned New York Community Trust to do a feasibility study of the program. By 1992, Mount Sinai began to include leaders from the East Harlem community in development of the Linkage House program. According to the author, it was difficult to achieve successful aging in place, primarily because there was separate housing and health & social service funding streams. However, health programs, including health education and on-site medical care, were critical to the Linkage House success.
Participation
The continuum of care covers a broad range from services for healthy adults to those with chronic or acute health conditions that need more assistance. The Linkage House model included a full-time, bilingual social worker with graduate level education to provide care and service coordination for the residents. Furthermore, the residents must be at least 62 years of age and meet federal income guidelines. For example, a single person household cannot have more than $17,100 in annual income from all sources, and a two-person household cannot have more than $19,600. Furthermore, potential residents must be either homeless, have poor housing, have difficulty paying the rent, or documentation of elder abuse.
Barriers
According to the authors, there was difficulty in securing funding for the program at the Linkage House because the HUD Section 202 program provided support only for construction costs, operation, and rent subsidies.
Environment
Other elements of the program included building design. The building was designed to create space for examination and consultation rooms for the health programs. Additional space was created for furnished common areas and meetings places for tenants. Five one-bedroom apartments were grouped around each common area to promote socialization.
Long-Term Viability
According to the author, securing funding and the hiring of an on-site social services coordinator were critical to the program's success.
Lanspery, Susan. Service Coordination in Senior Housing: Roles, Problems, and Strategies: A Guide for Aging Network and Other Professionals. Los Angeles, CA: National Resource and Policy Center on Housing and Long Term Care, University of Southern California, Andrus Gerontology Center, 1997.
Overview
This guide reviewed the role of service coordinators in state-assisted housing developments for older people, the challenges they faced, and alternatives they could use to address these challenges. Many housing developments have added service coordination to manage daily activities in housing developments to improve the quality of life and minimize early institutionalization.
Methodology
The methods were not described in the guide.
Findings
The guide asserts that the five most common functions service coordinators perform are: advocacy with community agencies for services, mediating disputes among residents, advocacy with housing management for supportive services, assisting resident organizations, and assisting residents with financial management. The challenges they faced were lack of funding, unresponsive agencies, "turf" issues, varying syntax, minimal monitoring, and fragmentation with the supportive services delivery system.
Recommendations
Two major factors influenced success, namely the level of involvement of residents in meaningful ways and the nature of the collaboration among the entities involved in the housing development. According to the author, the service coordinators could develop new services, establish an interagency group, promote volunteer programs, and possibly work with agencies to find new sources of funding to combat the challenges they face.
Study Limitations
Since this is a practice guide, there is no emphasis on research methods. However, the lack of information on methods makes it difficult to judge the guide's conclusions.
Schulman, Abbott. "Service Coordination: Program Development and Initial Findings." Journal of Long-Term Home Health Care 15, no. 2 (1996): 5-12.
Overview
The study's purpose is to describe the development and one-year evaluation of a service coordination program designed to help older people and people with disabilities experience an improved quality of life and to minimize institutionalization.
Methodology
Service coordinators served residents of 20 Section 202/8 housing projects in 12 states and Puerto Rico. The 20 Service Coordinator programs were implemented during the first 10 months of 1993. The service coordinator had four major functions: (1) to identify the needs of residents, (2) to arrange for supportive services to cover residents' needs, (3) to monitor the quality of those services, and (4) to reassess the residents' needs. Assessment of residents' needs has varied by program. The needs driven assessments used the medical model, where the service coordinator made an evaluation prior to determining what services were needed, where the resident had little input. The consumer driven model did not have an assessment, and the service coordinator marketed the services available, and then allowed the residents to choose what services they want to purchase.
The author selected 25 randomly chosen residents who had used service coordination from each of the 20 properties, totaling 500 individuals. The residents were then asked to complete a survey of 12 true-false statements about their perspectives on the Service Coordinator program in their projects. The service coordinator distributed the survey and asked residents to complete it at their leisure. About 458 people responded, 120 of whom were men and 338 were women, but not all respondents answered all questions.
Findings
Due to the cost of the services offered by the service coordinator, and fear of possible rent increases or evictions from their apartment, many residents were afraid of approaching the service coordinator. About 75 percent of male and 72 percent of female respondents believed that the service coordinator involved their families in their care. While over 98 percent of both male and female respondents saw the service coordinator as being available when needed, 15 percent and 11 percent, respectively, thought the service coordinator was too busy to see them when they desired. About 90 percent of the respondents had used the service coordinator to help them avoid loneliness. Over 93 percent in both populations believed that they benefited from the service coordinator's support.
Recommendations
The author believed this survey showed the importance of a service coordinator's role and made some assertions regarding such things as delayed institutionalization that were not supported by the research conducted.
KRA Corporation, and Office of Policy Development and Research, U.S. Department of Housing and Urban Development. Evaluation of the Service Coordinator Program. Washington, DC: U.S. Department of Housing and Urban Development, Office of Policy Development and Research, 1996.
Overview
The Housing and Community Development Act Amendments of 1992 authorized HUD to administer the Service Coordinator Program (SCP). The program is designed to meet the needs of people with disabilities living in HUD-assisted housing by directly funding service coordinators who are to coordinate provision of supportive services for this group. Service coordinators (SCs) determine the needs of eligible residents, identify available community services, link residents with needed services, monitor and evaluate services used, and carry out other functions as needed; coordinators are prohibited from direct service provision. Projects eligible for SCP are Section 202, Section 8, Section 221(d), and Section 236 projects; Section 811 projects are not eligible. The goals of the study were to describe the Service Coordinator Program and the residents served, assess resident satisfaction with programs, as well as to identify implementation problems and recommendations for improvement in the programs.
Methodology
The reported data came from two sources: (1) information from application forms from 645 programs that received HUD funding. These data were only used to describe programs and residents; and (2) site visits to 18 SCP projects during 1995. Site visits involved interviews with service coordinators and HUD project managers, as well as resident focus groups. The 18 sites were selected to represent the variation in characteristics of HUD projects, service coordinator type, and geographic location of programs sites. However, the sample cannot be considered nationally representative.
Findings
Of the 645 projects that received funding, about one-third had 100 or more units, one-third had 50-99 units, and one-third had fewer than 50 units. The projects were located in all but three states. In 99 percent of the projects, at least one-quarter of residents had disabilities. Similarly, in 17 of the 18 case study sites, 25 percent or more of residents had disabilities. The majority of residents at all sites were elderly, at least two-thirds of all but one site's residents were female, 11 projects were majority white and two projects majority black. Thirteen projects had part-time service coordinators, 11 coordinators worked at more than one SCP, and three projects contracted with other agencies for coordinators. Most coordinators had bachelor degrees and relevant prior work experience. All but one coordinator had received some type of training.
Service coordinators in the 18 sites worked with autonomy but coordinated with project directors when planning activities. More than half the coordinators had contacts with 90 percent or more of the project residents and case loads ranged from 7 to 112 residents, which represented between 10 and 96 percent of residents. Coordinators' outreach to residents consisted of print materials and presentations at resident meetings. Coordinators in the 18 sites arranged for services to come into the project; transportation and housekeeping were the most frequently provided services. Other services included health screenings, exercise programs, and budget assistance. Service coordinators sometimes provided services themselves despite the HUD prohibition against doing so; services included transport to medical appointments and housekeeping chores. Half of coordinators said that more transportation was needed at their sites; other needed services included housekeeping, financial counseling, errand services, and eye and dental services.
Residents in the 18 sites reported that SCP linked them to services and that the coordinator was someone to confide in about their problems and made them aware of how to access available services. The 18 sites did not report serious obstacles to program implementation, but seven sites reported inadequate office space primarily due to lack of privacy, and one site required residents to climb stairs to access the office.
Recommendations
Sites recommended improvements to the SCP program including: ensuring that the SCP office is accessible and that SCs do not share office space with project staff so that SC conversations with residents can be confidential. Additionally, the SC office should be located where residents tend to congregate such as mailboxes, the dining room, lounges, or community rooms. SCs also believed that they should be able to provide some services themselves where services are not readily available, including transportation in rural areas and social activities planning, and that HUD could fund these activities through the SCP. SCs would welcome HUD identification of training opportunities in rural areas and HUD development of materials such as assessment and service tracking and monitoring forms. SCs also made recommendations for changes to the annual reporting form.
Study Limitations
The 18 case study sites cannot be considered representative of the 645 sites in existence at the time of the study.
Nachison, Jerold S. "The Housing Programs of the Department of Housing and Urban Development: Description and Issues." In Housing and the Aging Population: Options for the New Century, edited by W. Edward Folts (83-104). New York, NY: Garland, 1994.
Program Description
The Congregate Housing Services Program (CHSP) provides grants to various public housing programs to enable them to purchase supportive services for their residents who are aging in place. The federal Department of Housing and Urban Development (HUD) provides up to 40 percent of funding for services, the users of services pay 10 percent of the cost of services, and funding must be raised from other third parties to cover 50 percent of the cost of services. Funding is available in Section 8 and Section 236 HUD housing projects for the older population, Farmers Home Administration projects; states, Indian tribes and local governments also can seek this funding. Projects must accept food stamps as full or partial payment for meals, and a service coordinator must provide case management and service coordination to program participants.
National Eldercare Institute on Housing and Supportive Services, and U.S. Administration on Aging. Linking Housing and Services: Six Case Studies. Los Angeles, CA: National Eldercare Institute on Housing and Supportive Services, Andrus Gerontology Center, University of Southern California, 1994.
After consultation with key informants, the authors chose six study sites that represent a range of approaches to linking housing with services. This paper provides descriptive information about six program sites, focusing on how they "operationalize" the housing and supportive services linkage and address challenges unique to each services program. It then offers advice for replication of similar program types.
The Housing Authority of St. Paul, Ravoux and Valley Hi-Rises, in St. Paul, Minnesota, is a HUD CHSP and the first national program linking housing and services. The program's staff credit its success to several key skills the CHSP Supervisor demonstrates, such as flexibility, creativity, knowledge of community services, and good organizational skills. Other factors that have contributed to the program's long-term success are community education and involvement and resident support. The program faces several challenges including long-term funding viability and a changing resident population that includes a frailer elderly population, a growing younger disabled population, and a more culturally diverse resident profile.
The Southern California Presbyterian Homes, Los Angeles, California, is a Section 202 federal housing site with a "circuit rider" approach to community service coordination. The program staff links frail residents with available community services. The only program cost is staff salaries, which are currently funded by HUD. The paper identifies limitations to this model as service gaps or lack of service providers, which can restrict resident's choices, and the lack of ability to monitor the quality of care provided.
The State of Maryland, Office on Aging, Multi-Family Senior Assisted Housing (SAH) Program operates in several public and private senior facilities. The SAH program provides a package of services that allows frail elderly residents to remain in their own homes, potentially avoiding any Medicaid costs that would incur due to premature institutionalization. Payment for services is on a sliding scale. The SAH program has faced several challenges, including residents' resistance to having to pay for services, the meals component of the service package is somewhat inflexible, maintaining high enrollment across the state has been difficult, and limited funding has been a problem. Additionally, there is still an independent living "mind set" that is difficult to overcome with housing managers and some of the more independent residents.
The Silsbee Tower's Supportive Services Program in Senior Housing in Lynn, Massachusetts, is a large national program linking housing with supportive services that began as a national demonstration funded by the Robert Woods Johnson Foundation (RWJF). The program is now privately funded, although it takes pubic support when available, and is currently being replicated through the national No Place Like Home program, also funded by RWJF. According to the authors, the program has been successful because of its close connection to the Area Agency on Aging (AAA), ongoing communication with residents through surveys and meetings, and the service coordinator's ability to balance different stakeholder agendas, including the building manager, residents, and AAA.
The Area Agency on Aging Senior Home Care Services, Inc. in Gloucester, Massachusetts, allows the agency to take advantage of economies of scale in offering alternatives to nursing home placement by providing supportive services to residents of senior housing. The program's success has been attributed to good communication and willingness to collaborate, good planning and management, and willingness to learn from other programs that link housing and services. Obstacles include lack of funding and flexibility, "turf issues" that may lead to service duplication, and an emphasis on process rather than outcomes.
One key component of the On Lok program in San Francisco, California, is the On Lok House, a HUD Section 202 building, which has demonstrated that very frail elderly can live in their own apartments with health and supportive services provided by a capitated managed care program based on an adult day care model. While the program does not provide skilled nursing care, the program has found it difficult to distinguish itself from a nursing home. Staff also face the challenge of determining when a resident is too frail to live independently at On Lok House.
Nenno, Mary K. "Public Housing: A Pioneer in Housing Low-Income Older Adults." In Housing and the Aging Population: Options for the New Century, edited by W. Edward Folts (61-81). New York, NY: Garland, 1994.
Program Description
This article provides a brief history of public housing programs and policies for low-income elderly in the United States. Starting with the development of programs initiated in the 1930s that spurred the Housing Act of 1956, which first recognized the elderly as a distinct population needing public housing assistance. Then, the Housing and Urban Development Act of 1970 authorized the use of about 10 percent of all public housing development for the elderly, displaced, and handicapped. The next major development occurred in 1978: the Congregate Housing Services Program, which was a demonstration program for 33 public housing agencies and 30 HUD Section 202 nonprofit housing sponsors. Subsequently, the National Affordable Housing Act of 1990 restructured the Congregate Housing Services Program and expanded its coverage. As the elderly public housing program continued to mature, a medley of structure types evolved.
Participation
By 1989, over 1.4 million households headed by an elderly person lived in federally subsidized housing. A subset of 517,000 resided in public housing, which comprised 38 percent of national public housing occupancy. By the late 1970s and early 1980s, the proportion of public housing occupied by elderly households leveled off at about 45 percent.
Evaluation/Data
Congress directed HUD to carry out a CHSP evaluation, which was designed as a four-year evaluation involving three types of evaluation: process, performance, and impact. The CHSP evaluation denoted missed success and was devoid of positive outcome during the first 14 months.
Long-Term Viability
According to the author, there are four areas that need considerable attention for public housing to remain a viable housing option. First, many of the public housing developments are over 30 years of age and need significant renovation. Second, many of the elderly developments have not designed or made accommodations for community space and other types of support services. Third, support services are only available on an ad-hoc basis. In the future, long-term and integrated resources must be made available. Finally, the author suggests that new housing policy must emerge to resolve issues of grouping the elderly with handicapped people. Ultimately, public housing will need to develop and hone an integrated system of support services, and provide adequate information about the various types of housing in all areas of the country.
King, Nancy Koury, Janet Hofmann, Ohio Department of Aging, and the U.S. Administration on Aging. Supportive Services in Federally Assisted Housing for the Elderly. Columbus, OH: Ohio Department of Aging, 1993.
Overview
This report discusses findings from several evaluation components of the Ohio Department of Aging's (ODA) Supportive Services in Federally Assisted Housing for the Elderly Project, a two-year grant program awarded by the U.S. Administration on Aging. The project's purpose was to develop a model to promote supportive services to the elderly in federally assisted housing by linking community-based services to public housing, thus allowing elderly residents greater access to support services. Specific program objectives include improving housing managers' ability to work with elderly tenants, linking housing providers with local assessment and delivery systems, developing programs that encourage volunteerism and integration of the facility into the local community, and managing current resource needs with available funding while advocating for future funding. Project activities were designed to address the development, implementation, and evaluation of the program's objectives. These activities included development of a working agreement between the ODA and other state agencies, a survey of Ohio's public housing managers, and a problem indicator resource tool for housing managers. Other activities included development and implementation of a training program and resource manual for housing managers, and improvement of a computer database program for Ohio's Area Agencies on Aging (AAAs) to use in maintaining directories of elderly housing facilities.
Methodology
Public housing facilities in two pilot sites, Portsmouth, a rural area in southern Ohio, and Cleveland, an urban area in northeastern Ohio, were selected for program implementation. Both pilot sites developed and facilitated a coalition of organizations concerned with older adults in public housing. Coalition members collaborated to plan new services for the elderly tenants. The manager training and resource manual was revised. The housing manager-training program, a two day Train the Trainer course, was implemented in each of Ohio's 12 planning and service areas (PSAs).
Evaluations of the new programs for elderly residents at pilot sites were conducted. The pilot site evaluations contained two components: (1) results of each site's needs assessment survey, and (2) a qualitative evaluation of each site's activities. A sample of residents age 60 and older in the Miles Elmarge public housing facility in Cleveland were surveyed in-person to determine their characteristics and service preferences, 67 of the 139 residents living in Miles Elmarge were interviewed. In Portsmouth, Ohio, 95 older adults were interviewed in their apartments.
Findings
The following summarizes findings from a survey of housing managers in pilot site facilities, evaluations of the housing manager training program, resource manual and train the trainer program, and evaluations of the pilot site activities. According to findings from the housing managers' survey few housing facilities offered services other than housing, about a quarter (24 percent) had social or recreational activities, 10 percent offered congregate meals, 5 percent housekeeping, and 2 percent transportation. Managers perceived that medical and or physical health problems were the main functional or health difficulty, and transportation the major service requested by residents age 62 and older. Managers indicated they spend an average of 15.7 hours per week of staff time on personal, family, or health problems associated with residents. The majority of managers (88 percent) referred residents to social services agencies. However, more than half of managers (60 percent) report that residents' capabilities are assessed when problems arise.
Managers stated their biggest challenges were meeting the needs of residents aging in place, developing services for residents, and understanding mental health issues. This need for assistance was indicated by awareness of senior services such as homemaker services and meals on wheels, but lack of referrals to these services. Also there was limited awareness of Ohio's PASSPORT program, a statewide Medicaid waiver program for in-home community services for older adults, a potential benefit to managers and residents. Housing managers also expressed a desire for more information about dealing with the challenges of elderly residents.
Post-program evaluation results of the housing manager training program indicated that housing managers viewed both the training program and housing resource manual as useful, relevant, and effective. Housing managers improved their knowledge about aging related issues, and confidence in their ability to identify residents at risk, address problems, develop policies and procedures for action, and work with the appropriate service agencies in the aging services network. Overall, participants in the train the trainer program were satisfied with each components of the course.
Cleveland Pilot Site. The majority of residents were female (66 percent), African-American (98 percent), living alone (68 percent), and either active (10 percent) or interested (50 percent) in volunteering. Slightly more than a third (37 percent) reported health problems that limited their functional ability, and 60 percent rated their health as "fair." The majority of respondents (82 percent) indicated they could turn to relatives for help. Respondents were frequently unaware of many support services such as legal services, companionship visiting, personal care services, mental health counseling, exercise and adult education classes, and information and referral services. The most desirable services for respondents were transportation, homemaker, personal care, meals, and social clubs.
The program augmented many of the services Cleveland residents identified as desirable such as transportation, adult education, social activities, meals, information and referral, and nursing services. Other services such as homemaker and home health aide were identified but not strengthened other than increasing housing managers' awareness of resident service needs. The community coalition met monthly to address service access to the elderly in public housing and played an instrumental role in improving communication between the aging services network and housing community. The coalition has committed itself to continue efforts toward meeting the needs of elderly in pubic housing. At the request of housing managers, the Cleveland pilot site went beyond the ODA's housing manager training program and implemented a series of workshops on dealing with mental health issues. The coalition will continue to meet beyond the grant period, plan future training programs for housing managers, and retain many services such as educational opportunities, transportation, food distribution, and health promotion programs.
Portsmouth Pilot Site. Transportation, cleaning, shopping, and laundry were the activities respondents reported having most difficulty with. Transportation services (36 percent), house keeping (27 percent), the senior center (21 percent), and home delivered meals (18 percent) were other supportive services for which respondents indicated high usage. Although the survey did not ask residents about preferences for supportive services, respondents were asked about their interest in a variety of activities. Respondents most frequently requested music and wellness programs.
Besides the ODA's housing manager training program, a first aid and CPR class was conducted and the aging sensitivity training program became available to all Portsmouth Metropolitan Housing Authority (PMHA) employees. The coalition helped in overseeing the needs assessment, developing welcome baskets for new tenets, conducting a health fair, working with the senior center to improve transportation, assist the tenant council, and oversee resident programs. With added community resources and continued involvement from the coalition, welcome baskets, social activities, and first aid/CPR classes will continue along with blood pressure screening and blood sugar checks for residents and scheduled visits from a mobile mammography unit.
Conclusions
The Ohio Department of Aging's public housing manager survey was useful in understanding the needs of both public housing managers and tenants. Managers felt more knowledgeable and confident in dealing with issues involving their elderly tenants. AAAs were able to customize training programs to individual communities and provide networking opportunities for training participants and key stakeholders in the community. Involving the management of the local housing authority in planning and implementation of the training program was instrumental in gaining participation among housing managers.
Both pilot sites were able to successfully recruit a broad based group of local support services including social services, health service providers, housing groups, and community leaders. These coalitions were able to target attention on specific problems facing the elderly in federally assisted housing in their communities and find creative solutions. These community coalitions will continue to collaborate with residents of public housing and their communities to target needed services and programs to the elderly resident population.
Recommendations
For those considering development of similar or related projects, the authors recommend that AAAs develop a more complete understanding of the housing authority structure and role of housing manager. Future research and training should emphasize mental health issues, the role of the housing manager, and integration of the young person with mental health conditions into senior housing. Furthermore, the project should strengthen efforts to form broad-based community coalitions that include residents, community leaders, besides social service providers. There is also a need to address barriers in public housing's design and environment that may prevent elderly residents from living independently, and nonaging social problems that impact the elderly in public housing.
Lynn Greenleaf, Sheila Malynowski, and the New Hampshire Housing Finance Authority. Increasing Service Availability to Seniors in Housing: Final Report. Bedford, NH: New Hampshire Housing Finance Authority, 1993.
Overview
This report describes an Administration on Aging (AoA) grant project directed by the New Hampshire Housing Finance Authority (NHHFA). The project expanded the NHHFA's model of supportive services programs, originally developed for seniors living in privately owned, subsidized housing (Section 8 housing), to seniors living in public housing. The primary purpose of the program was to establish closer linkages between the network of state and local services for seniors and those older adults living in federally subsidized housing to prolong their ability to live independently in the community. Objectives of the study included allowing seniors to determine which services they wanted and providing increased service delivery to seniors in public housing for those identified services.
Methodology
The NHHFA chose six public housing authorities in New Hampshire as pilot sites to develop supportive service programs. Each housing authority was responsible for designing and implementing supportive services programs to best meet the needs of their residents with the goal of financial self-sufficiency over the long-term. Services included transportation, meal preparation, light and heavy housework, and personal care. Service coordinators also helped residents apply for eligible entitlement benefits. Pilot sites implemented community-building programs that included social and recreational activities, and informational programs for elderly residents. The NHHFA provided technical assistance and oversight.
The NHHFA also developed and implemented a pilot statewide, telephone network between the housing and service provider network called Senior Care Connections (SCC). For an annual subscription fee, the service provided housing managers with a master's level social worker to help housing providers find and help residents access services.
Findings
Senior Care Connections, the pilot statewide, telephone network, faced several implementation challenges. Faced with lower participation than expected, focus group discussions were conducted with housing managers to determine the participation barriers and identify potential candidates for the program. Feedback from the focus groups identified management agents who are the best candidates for the program. These management agents are typically interested in supportive services, unable to hire a service coordinator, or have a service coordinator that requested social work support. Barriers to participation that were identified include a complex's financial constraints, a service coordinator with extensive experience or a background in support services, and managers who believed they could handle things on their own. Because of low demand, the program was cut by 50 percent for the second year of the grant and marketing efforts were enhanced. Face-to-face meetings with managers were determined to be the best marketing strategy during the program's second year.
Senior Care Connections enrolled 11 management companies representing 786 senior housing units in over 20 complexes. This represented about 25 percent of the potential market share. The program handled a total of sixty-one service requests and 46 follow-up contacts over the two-year grant program. The majority of requests involved assistance with mental health issues, followed by assistance with medical problems, and suspected abuse or self neglect. A follow-up program evaluation survey was developed and completed. The survey found that managers believed they were supported by the service, that the service relieved stress, enhanced their skills and abilities, and prevented resident situations from worsening.
The project helped 731 residents at the six pilot sites in getting services such as light and heavy household chores, shopping, transportation, meals, and personal care. The following table shows the number of residents who received assistance by service type.
| Support Services | Number of Residents Receiving Assistance |
|---|---|
| Light/heavy household chores | 141 |
| Transportation | 246 |
| Meals | 59 |
| Personal care | 41 |
| Managing finances or filling out forms | 152 |
| Reassurance calls/visits | 248 |
| Total | 887* |
| NOTE: Some residents received more than one service. | |
Interviews were conducted with 503 residents by NHHFA staff in four of the six public housing authorities chosen as pilot sites to determine residents' demographics and service needs. Laconia and Somersworth Housing Authorities opted to use preexisting information on support services programs rather than a survey to form the basis for designing their program expansion. Respondents to the resident market/needs assessment survey were overwhelmingly female (80 percent), single (85 percent), and living alone (84 percent). About half of respondents (47 percent) were 75 years of age and older. About half of respondents said they had lived in their complex six or more years, 10 percent had lived there more than 15 years, indicating the "aging in place" phenomenon. Most of the respondents had low incomes with 68 percent having gross annual incomes of $7,500 or less. Respondents rated their health favorably compared with others their age with 77 percent reporting excellent or good health. But, 27 percent reported putting off needed health care in the past year, with the most frequently reported reason being lack of financial resources followed by lack of transportation. It is important not to generalize from the resident market/needs assessment survey because the surveys were not from a random sample of resident.
The number of reported residents receiving services varied by complex, as did the number of reported residents in need of such services. The following table shows the ranking of services residents reported most needed compared with services reported most wanted. Except for shopping and transportation, what residents needed ranked closely with what they most wanted.
| Ranking | Most Needed | Most Wanted |
|---|---|---|
| 1 | Heavy household chores | Transportation |
| 2 | Shopping | Heavy household chores Service coordination |
| 3 | Service coordination | -- |
| 4 | Transportation | Personal emergency response system |
| 5 | Light household chores | Shopping |
| 6 | Personal emergency response system | Light household chores Meal preparation |
| 7 | Meal preparation | -- |
| 8 | Personal care | Personal care |
Long-Term Viability
According to the authors, the supportive services pilot programs in senior public housing were successful, however, they do not state how the program's success was measured. Housing managers and residents benefited from the programs developed. The supportive services programs not only improved the quality of life for many seniors but allowed seniors to remain in their homes. All the supportive services programs developed under the AoA grant continued beyond the end of the grant, however, the funding came from a number of sources and future funding is uncertain. Education at the federal level is needed to ensure that supportive services programs in senior housing are valued and that funds are appropriated to HUD for inclusion of the program as part of a housing complex's regular operating expenses.
The Senior Care Connections telephone consultation service provided support to managers and service coordinators in need of social work services. Education of management agents about the benefits of a social worker led to increased participation in the SCC program during the second year of the grant. Although the SCC program had difficulty becoming financially self-sufficient, the program is continuing on past the end of the grant with slight increases in the enrollment fee and funding support by the parent organization, the Crotched Mountain Foundation. The service might be more successful in areas with larger markets of management agents for subsidized senior housing. Combining the SCC program with other services requiring social work staff might improve the program's financial situation.
LITERATURE RELATED TO CLUSTER CARE
Lanspery, Susan. Clustering Services at Senior Housing Sites: A Technical Assistance Guide for the Aging Network. Los Angeles, CA: National Resource and Policy Center on Housing and Long Term Care, University of Southern California, Andrus Gerontology Center, 1997.
Housing is a vital element in long-term care, however its priority is often minimized. Often senior housing residents only receive shelter assistance, but lack services. Finally, residents in assisted housing are often older, more isolated, less well off, and frailer than other seniors in other settings. Service clustering is a strategy to minimize costs by taking advantage of economies of scale; clustering involves consolidating the fragmented services of many clients. Many programs, such as HUD's Congregate Housing Services Program, the RWJ Supportive Services in Senior Housing, and No Place Like Home, have combined housing and services. The benefits of service clustering can include: more people receiving assistance, residents finding more support, housing sponsors having better staff and resident morale, managers focusing more on managing the property, and all parties benefiting from lower costs. Typical activities included congregate meals, care management and crisis management, planning and advocacy, and participating in inter-organizational groups or task forces.
Service coordinators in public housing primarily assist residents in finding needed services; coordinators also provide information and advocacy, and organize activities. Some see this coordination as unnecessarily duplicating aging network activities. Technically, the service coordinators should complement the aging network's coordination efforts. Some aging network staff assume that housing managers are ready to evict residents who need assistance, while network staff see themselves as advocates for older people. Some aging network staff believed that older people who live in senior housing have more support than older people who do not. To ensure long-term viability of service clustering the following factors are important: the extent to which the program promotes aging in place, how the program coordinates services, the development of new services, the extent of environmental modifications, and how much resident input would be used.
The factors that need to be examined in promoting aging in place are: supply and demand for services in the community, laws and regulations that restrict a program's ability to provide services, what services residents may use, characteristics of the physical setting of the housing, and the applicable financing streams for housing and services. Aging networks, as expected, had limited budgets.
The guide provides examples of service clustering. The New Jersey Congregate Housing Services Program provided supportive services to eligible frail, low-income residents of subsidized housing. In Massachusetts, the Managed Care in Housing and Group Adult Foster Care programs targeted low-income older people, primarily residents of multiunit housing, who were at high risk of losing their independence. The Massachusetts programs incorporated a clustering approach to service delivery and provided a range of services. The New York State Office for the Aging established the Resident Advisor Program, which helps assisted housing developments in hiring service coordinators.
Feldman, Penny H., Eric Latimer, and Harriet Davidson. "Medicaid-Funded Home Care for the Frail Elderly and Disabled: Evaluation the Cost Savings and Outcomes of a Service Delivery Reform." Health Services Research 31, no. 4 (1996): 489-505.
Overview
This article evaluates New York City's Cluster Care demonstration, a model where one home care agency serves a number of Medicaid beneficiaries with disabilities living in the same senior housing site. Cluster care was tested as an alternative to the City's one-on-one attendant care system (i.e., traditional care). The differences between cluster care and traditional care were: (1) under cluster care, a single agency provided services at one site, rather than multiple agencies delivering services in one site as in traditional care; (2) teams of workers served people whose apartments were close to one another under cluster care, rather than one aide serving one client at a time under traditional care; and (3) in cluster care, clients' service schedules were based on the tasks that clients needed accomplished compared with attendants delivering services in blocks of four, eight, or 12 hours under the traditional care system. The demonstration was designed to test cluster care's potential to reduce costs by reorganizing delivery of traditional agency home care services. The evaluation addressed cost issues as well as client well-being, which was measured by functional status, mortality, depression, and satisfaction with services.
Methodology
The experimental group consisted of Medicaid beneficiaries who lived in seven senior housing sites with an on-site social worker or a senior center. Clients were not included in cluster care if their physical health condition made it unsafe for them to be alone, if they could not provide access to their apartments, or if they were psychotic. The control group was Medicaid clients receiving traditional care at four other senior housing sites. The study design involved comparing 229 clients at seven cluster care demonstration sites to 175 clients at four comparison sites. Medicaid clients in the experimental and control groups were interviewed in-person before and 16 months after the demonstration began. Home care agency and Medicaid records were used for the cost analysis and agency records were accessed to determine what happened to clients who were not available for follow-up at 16 months.
Measured variables included clients' average hours of home care used and the average cost of their home care per week in the 36 weeks preceding the intervention; post-intervention hours of care per week and home health costs per quarter; mortality; functional status using a scale of 10 ADLs and IADLs; a depression scale; a client satisfaction scale; severity of illness based on the number of classes of drugs that a client used, and the client need trajectory (the rate of change in the clients' use of hours of home care prior to the intervention).
Findings
On average, clients at cluster care sites used six fewer hours of care a week or 300 fewer hours a year than traditional clients. The reduction in hours was a result of reductions in hours of care for clients with higher functional needs at baseline. Clients in cluster care and traditional care sites with four or fewer limitations used about the same number of hours of care per week on average. Those with five to 10 limitations in cluster care sites used 7 fewer hours per week or 350 hours fewer per year than their counterparts in traditional care.
The lower hours of care in the cluster care sites resulted in cost savings. Controlling for differences in client characteristics, those in cluster care cost on average $720 less per quarter or $2900 less per year than clients in the traditional sites. Savings were achieved largely among those with 5 to 10 limitations in daily activities. The cluster care clients with this level of disability cost, on average, $4600 less per year than similar clients in traditional care. There were no significant differences in mortality, functioning, or depression between the experimental and control groups. However, when measuring functional differences, those with four or fewer limitations in cluster care sites had better functioning at follow-up than those at traditional sites and those with five to 10 limitations at baseline in cluster care fared worse than people with same level of disability in traditional sites. Client satisfaction at cluster care sites was lower than at traditional sites.
Study Limitations
The authors do not say whether they attempted to match the experimental and control groups on demographic or functional characteristics. There were significant differences between the two groups that were controlled for in the multivariate regression analysis.
LITERATURE RELATED TO ASSISTED LIVING
Wilden, Robert, and Donald L. Redfoot. Added Assisted Living Services To Subsidized Housing: Serving Frail Older Persons With Low Incomes. Washington, DC: Public Policy Institute, AARP, 2002.
Overview
The purpose of this study is two-fold, the first being an examination of research on the potential demand for assisted living services in federally subsidized housing and the ability to provide such services, and the second, a discussion of findings from case studies of subsidized housing projects that have developed assisted living services.
Methodology
This study first examines the existing research on the issues related to assisted living services among older residents in subsidized housing, including a summary of the research on supportive services provided in subsidized housing, specifically the service coordinator program and the federal Congregate Housing Services Program (CHSP). The second approach uses a case study method to examine policy and management issues. Interviews were conducted with 17 sponsors of subsidized housing for the elderly in nine states. Sponsors were chosen in states that provide Medicaid funding for assisted living services, such as New Jersey and North Carolina, and states that do not provide such funding, such as Connecticut. Other states, such as Maryland and New Hampshire, were chosen because of their substantial experience with state or federal Congregate Housing Services Programs. In-person interviews with sponsors in seven states (CT, KY, MD, NJ, NH, NC, and VA) were conducted between October 1999 and January 2000. Six interviews with sponsors were conducted by telephone or mail. Sponsors were mailed a project interview schedule before the interviews to obtain relevant data. The annotated review reports only the case study findings as the findings from the literature are covered in other sections of this review.
Findings
The findings from the case studies of 17 projects that provide assisted living services to the elderly cover financial issues, service delivery issues, state efforts and housing types, management, and other issues. Funding sources vary among subsidized housing sponsors, and are often an array of public and private sources. Among the 17 projects, 16 have funding from residents, nine from Medicaid, and six have private funding. Other funding includes other federal, state, and county sources. Funding limitations often result in low staff pay and high staff turnover.
Most projects have assisted living residents scattered throughout the building rather than concentrated in one location. Sponsors for grouping assisted living residents in one location argue that clustering creates economies of scale and saves staff time. Others feel that assisted living residents should not feel stigmatized or isolated from other residents, allowing residents to obtain services without having to move. All of the 11 sponsors visited on-site have managed to incorporate assisted living services while retaining a residential environment. Although most sponsors contract out some of their assisted living services, some owners find that providing services directly can save money. Other owners feel they lack the necessary skills to administer such programs and contracting out services may provide some liability protection. Most sponsors provide individual "a la carte" services rather than bundled services. Sponsors who provide "a la carte" services feel this allows residents to maintain decision-making power and focus on their individual needs. Other sponsors find it easier to structure a system of bundled services, however, those tend to be the larger projects that provide services directly through project staff. Section 202 policy changes have prevented newer housing projects built in the 1980s from establishing mandatory meals, thus, these projects and smaller sponsors, who often lack a commercial kitchen or central dining room, and have more difficulty developing meals programs for assisted living residents
Conclusions
Findings from case studies show that assisted living services can be successfully integrated with subsidized housing for seniors with funding, training, and coordination of housing and service staff major obstacles for implementation. States that have funded such services have also played a key role in development of assisted living services in subsidized housing. But, state efforts to regulate and monitor specific assisted living services will become more common as they begin to address the issue of developing way to monitor and enforce quality. Further research is needed to develop models and strategies for continued expansion and improved quality of assisted living services in subsidized housing for elderly.
LITERATURE RELATED TO GENERAL HOUSING AND POLICY
Robert, Stephanie A. "Community Context and Aging, Future Research Issues." Research on Aging 24, no. 6, (2002): 579-99.
This article was written as the introduction to a special volume of Research on Aging addressing "Community Context in Aging Research." It provides an overview of the issue of community context and a brief summary of the four articles on the topic in the volume. It begins with a review of definitions of community. Community can be defined by the physical space in which people live, by political boundaries, or other physically delineated spaces; or it can be defined by social rather than physical boundaries such as shared interests, identity, or interactions. The community context is crucial in life-course and aging research because of the need to consider the spatial distribution of the aging population and the implications that this distribution has for meeting the needs of the aging population. In addition, community can be the repository for social capital and social inequalities that may require response through services.
Different communities may attract different types of older adults with different needs and different capacities for contribution to the community. Some communities made up predominately of older adults were formed primarily through the in-migration of older adults and others primarily by the out-migration of younger adults, which may have implications for the characteristics of the older adult population. Furthermore, although racial and ethnic diversity of communities is increasing, segregation is still the norm, which may affect individual well-being.
The problems that communities face may depend on the community context. Specifically, some areas may be looking at the best way to attract healthy and wealthy older adults while others may be struggling to determine how to best meet the needs of the population they already have. The rate of growth of the community may determine the rate of growth in the need for services. The devolution of responsibility from the Federal Government to the states and from the states to local communities means that communities must balance services across age groups and service groups. There is a great diversity in the ability of communities, both within states and across states, to accept publicly funded services at home rather than in nursing homes.
There is growing popular and scientific interest in the role of community in individual well-being. For example, there is interest in how income inequality within the community affects individuals in the community even when they are not poor, or in whether older individuals are seen as resources for the community or drains on community resources.
The availability of survey data has had the effect of focusing attention on the individual outside of the community context. The four articles summarized in this article all extend research to the effects of the community on the individual. Cotter, Hermser, and Vanneman discuss the contribution of the structure of the labor market on employment patterns. Specifically, they consider whether metropolitan areas with higher demand for female labor lead to narrower gender variation in employment rates, if the shifts made to accommodate female labor market participation makes workplaces more amenable to older female workers and differences in individual and community expectations of women's roles. Extensions to this research might include looking at whether "gendered labor markets" are associated with quality of life in retirement, particularly for women.
Kim and Lauderdale look at the determinants of living arrangements of older adults with a particular focus on the Korean-American immigrant community. They find that differences in living arrangements in metropolitan areas are partly explained by co-location of Korean ethnic businesses and subsidized housing. They conclude that government-subsidized housing provides Korean-American older adults, who on average have lower incomes, the opportunity for independent living. They suggest that the acceptability of services may vary by cultural preferences.
Lee and Robert look at the role of race differences in the community context in explaining health disparities at older ages. They show that older black adults tend to live in socially and economically disadvantaged communities compared with non-black older adults of similar income and education and that the observed health differences are only partly explained by individual socioeconomic status.
Lawrence and Schigelone look at community coping responses to the stressors of aging in a continuing care retirement community. They describe communal responses to problems such as the institution of a buddy system to check up on community members and provide social support.
Finally, this introductory article proposes the research approach of trying to look at old problems in new ways and also to look at new problems in new ways. The author asserts that the four articles in this volume show that community characteristics provide additional information useful for explaining individual level outcomes.
Lawler, Kathryn. Aging in Place, Coordinating Housing and Health Care Provision for America's Growing Elderly Population. Joint Center for Housing Studies of Harvard University and Neighborhood Reinvestment Corporation, 2001.
In this paper, Lawler discusses the relationship between health and housing and their roles in addressing the needs of a growing elderly population. The author argues that the bureaucratic separation of services and the lack of coordination between health and housing combine to deter seniors from successfully aging in place. She advocates a customized care model of service delivery, that is, one that can be tailored to the needs of the individual, rather than the current production model of service delivery that can lead to either "overcare" or "undercare." The author asserts that aging in place allows individuals to maintain their social support network, can limit the negative effects of relocation and transitions, and may lead to cost savings by minimizing the provision of inappropriate care. She cites results from a survey conducted in 2000 by AARP suggesting that the majority of seniors wish to remain in their current residence for as long as possible. However, the current system of public subsidy for housing and health care services presents structural barriers that prevent the coordination of these services for those in need. These barriers include separate federal funding sources, separate administrative jurisdictions (state vs. locality), and separate regulatory standards (medical vs. construction and development). Additionally, the eligibility criteria for health care and housing services differ and often conflict with each other.
Using information from a series of 60 interviews the author conducted with senior service providers across the nation between June and August of 2001, the author identifies four key elements consistently present in most successful aging-in-place programs: a choice of health care and housing options; flexibility in the range of services offered; the ability to maintain mixed generation communities; the ability to provide ongoing assessments of health-service needs in order to identify the appropriate level of services and make any adjustments. She also identifies challenges to developing and maintaining an aging-in-place program, which include: differences between rural and urban settings; lack of understanding of the elderly community's perceptions of alternative residential care settings; the physical deterioration of housing stock; and different skill sets of housing and service providers. She notes that the different skill sets may also create opportunities for partnership.
Several opportunities exist for the coordination of health and housing services at the federal, state, and local levels, in particular, aligning HHS and HUD programs and funding streams toward one another. Programs that HHS and HUD have initiated in the last few years that the author feels should be continued and expanded include the HUD Service Coordinator Grant, the HUD Assisted Living Conversion Program, and the HHS-sponsored PACE Program. Alternatively, a program that pulls funding from both federal health and housing streams could be developed in one agency. The 1999 Supreme Court-issued Olmstead v L.C. ruling, which requires states to develop an Olmstead Plan that redirects services from institutional settings to community-based alternatives, presents states with an opportunity to address housing and health-service needs within the long-term care delivery system.
Numerous opportunities already exist for better coordinating the health and housing needs of seniors. Community development corporations and community-based nonprofits can play a large role in identifying housing and health service needs of elderly residents in the community. Naturally Occurring Retirement Communities (NORCs) offer models for service delivery based on the concept that a neighborhood or apartment building with a high density of seniors aging-in-place affords the opportunity to bring services to seniors instead of transporting or relocating seniors to the services or to alternative residential settings. Community-based organizations can serve elderly residents aging-in-place by offering paraprofessional support services that are often less costly than the services of licensed medical or housing professionals. These organizations are also helpful in facilitating the organization of long-range community planning efforts and development issues that address the needs of elderly residents aging-in-place. Furthermore, community efforts to encourage and support aging-in-place can be linked with goals to build community stability or revitalize neighborhoods by focusing on rehabilitating the housing stock, encouraging diverse resident demographics, and promoting home ownership since most seniors own the homes they live in.
The author summarizes findings from case studies of three different projects that offer ways state and local governments can combine health and housing services for seniors. The first case study focused on Atlanta, Georgia, and used GIS technology to locate communities with a high density of seniors, communities with seniors at risk, and communities with diverse age structures. The location of health services and housing services were also mapped. This information was designed to assist government officials in planning services to meet the needs of a growing elderly population.
The second case study focused on the Penn South NORC, a cooperative housing arrangement of 2,820 units and 6,200 residents. In 1985, more than 75 percent of Penn South's resident population was 60 years old or older. At that time, Penn South's board organized to develop services programs to forestall nursing home placement and encourage the elderly to remain in their own homes. The cooperative organized various social and health-related community organizations to provide care coordination, group recreation, cultural and artistic programs, home-care coordination and non-acute nursing care, volunteer opportunities, and preventive health and education services among other programs.
The third case study focused on Florida's Elder Community Program, which offers communities within the state of Florida the opportunity to assess their own facilities, services, housing stock and recreational activities. The program was a grassroots effort with the state providing the framework and assessment tools and residents doing the work, thereby affording residents the opportunity to design their own programs and plan changes to create more Elder Friendly Communities. This program offered communities the flexibility to decide how much or how little to spend to improve transportation, recreation, and housing. Currently 23 communities are participating in the program, and one grocery chain has become an elder friendly business.
National Investment Center for the Seniors Housing and Care Industries. NIC National Survey of Adult Children: How They Influence Their Parents' Housing and Care Decisions. Annapolis, MD: National Investment Center for the Seniors Housing and Care Industries, 2000.
Overview
The goal of this study was to ascertain the roles, knowledge, and decisions that influence adult children who may have responsibility for their parents' housing and care.
Methodology
The study employed a telephone survey of approximately 1,500 adult children between the ages of 45 to 64. Two-thirds of this population had a parent who did not currently need supportive care. However, 14 percent were responsible for a parent who had received professional care services within the past two years at home. About 7 percent had a relative residing in an "assisted living" community. Finally, 3.5 percent had a relative residing in an "independent living" community.
Findings
Many adult children were uninformed about independent living and assisted living options. Only 40 percent were familiar with independent living and 27 percent with respite care services. Many adult children found the terminology about senior housing and care to be confusing and irregular. Despite the fact that 73 percent of the respondents stated that their older relative has less than $25,000 annual household income, 77 percent of adult children had not discussed the costs of seniors housing with that relative. Physicians' recommendations were most often used for decisions about home health care services. Furthermore, the authors believed that seniors housing and care providers needed to educate other professionals about the benefits they offer. Finally, adult children provided financial support for senior housing and care services.
Recommendations
The authors suggested a massive campaign to educate consumers about their options, as well as changing the perception of financial affordability.
Pynoos, Jon, and Phoebe S. Liebeg. Housing Frail Elders: International Policies, Perspectives, and Prospects. Baltimore, MD: Johns Hopkins University Press, 1995.
Overview
The authors of this study analyzed past and current housing program policies for frail elders in industrialized societies, and compare them to the United States.
Several efforts over the past two decades have tried to improve integration of services into government-assisted housing for the elderly. For example, Congress in 1978 created the Congregate Housing Services Program (CHSP) to provide service coordinators and a variety of services to older tenants in public and Section 202 housing. While the program began in 63 sites, controversy existed over whether HUD's should be responsible for payment of services. Additionally, an evaluation of the CHSP created further disagreement; OMB argued that CHSP did not save money, and the money would have been better spent on nursing-home care. However, Congress insisted the CHSP program continue, but because of budget constraints and lack of enthusiasm for support among the Reagan and Bush administrators, it was limited to the same number of participants at the same sites. The second phase of the CHPS involved more restrictive targeting.
Findings
The experience of the CHSP demonstrates how political and bureaucratic influences can make it difficult to create a strong housing and services relationship. The authors cite three major structural changes that prompted the transition of the United States toward a system of residentially based long-term care. First, private markets and consumer preferences favored residential care. Second, state governments had limited resources, yet growing demands for services as a result of federal mandates. Finally, budget implications had a major impact on current efforts to reform federal housing and long-term care policy.
AARP. "Understanding Senior Housing for the 1990s, An American Association of Retired Persons Survey of Consumer Preferences, Concerns, and Needs." Washington, DC: AARP, 1990.
Overview
This study reports results of an AARP housing study on emerging housing trends for older adults. Notable findings include the preference for aging in place is more prevalent in the current survey (1989) than in 1986 (86 versus 78 percent), there is more receptivity to age-segregated housing (40 versus 32 percent), more awareness among older people of the need for help around the house (65 versus 40 percent), and more anticipation of the need for help in the future (55 versus 33 percent). Over half of respondents reported that they have done little or no planning for their future housing needs, especially among those over 75 years of age, with lower incomes, and those not currently married. As a result, the most vulnerable older people are those who have done the least planning for the future and are most susceptible to being forced out of their homes because of a crisis.
Methodology
The survey updates a 1986 AARP national survey. The sample included 1,500 adults age 55 and older interviewed by telephone in 1989 about (1) current housing arrangements, (2) community preferences, (3) preferences for housing options and related services, (4) household activities, (5) housing costs, (6) safety and security concerns, and (7) planning for future housing needs. Results were analyzed by gender, age (55-64, 65-75, and 75 and over), income, marital status, race, home ownership, health limitations (no limitations, some limitations, or a great deal of limitations), mobility (moved within the past five years or not), planning (planned a lot or a moderate amount for future housing needs, or planned a little or none) and community type. Community type consisted of the following categories: retirement housing or buildings planned for older adults, communities or buildings where the majority of residents are 60 and older (NORC), and communities in which the majority are under 60 (non-NORC). The questionnaire is provided as an appendix to the report.
Findings
With respect to community type, 5 percent lived in a retirement community or building and 27 percent live in a NORC. Of those in a NORC, 80 percent said the older people had lived there a long time rather than having moved in recently. Most residents of NORCs or retirement communities like living in communities with a majority of older residents; only 11 and 7 percent of residents of retirement communities and NORCs, respectively, would prefer a better mix of ages. Social activities were mentioned by 10 percent of those living in communities composed predominately of older people as a positive attribute of their living situation; those in retirement buildings or communities were twice as likely as those in NORCs to mention this (20 versus 9 percent).
With respect to housing option preferences, 32 percent of older Americans are considering moving to an apartment that provides meals, housekeeping, transportation, and social activities, and 17 percent are considering moving in with a family member. Those limited by health were the most likely to be interested in board and care homes and were more likely to be interested in age-segregated housing.
With respect to help with household activities, both heavy and light household chore help was the most frequent help used (23 to 30 percent, depending on the chore), followed by light housekeeping (9 percent) and grocery shopping (9 percent). These percentages more than double when older adults talk about expected future assistance needed. In addition, 14 and 11 percent expect to need help with cooking and personal grooming, respectively, in the future.
More than 8 in 10 older people do not want to leave their current home. Those living in NORCs are more likely to want to stay. Over one-fifth expect to move but only 13 percent say they want to move. Most would like to live in a neighborhood with people of all ages but in a household of people of the same age. Residents of NORCs were less likely than residents in retirement communities or buildings to have moved in the past five years (23 versus 53 percent).
Conclusions
In conclusion, the report states that those who least want to leave their homes are those who are most vulnerable and who may lack a support system, presenting a challenge to policy makers that want to help these individuals remain at home and to providers of services for such people.
Newman, Sandra, and Raymond J. Struyk. "Housing and Supportive Services: Federal Policy for the Frail Elderly and Chronically Mentally Ill." In Building Foundations: Housing and Federal Policy, edited by Denise DuPasquale (435-64). Philadelphia, PA: University of Pennsylvania Press, 1990.
Overview
There was not a strong market response to the dearth of housing for the frail elderly and chronically mentally ill because typically these households have lower incomes, and developers lack the experience needed to meet the needs of these groups. These populations have a high demand for supportive services and could require environmental features to enable independent living. The largest disparity between the two groups was that characteristics of care varied and the median age drastically differed.3 Coupled with differences in informal support, this fostered different living environments to sustain independent living.
Approximately, 9 percent of the elderly needed assistance in physical activities due to the chronic health problems. Most of this requires help with toileting and getting in and out of bed or a chair. In 1985, about 400,000 people in elderly headed households were at risk of being institutionalized. The author anticipated that the number of households headed by an elderly person would remain stable until the baby boom generation reaches retirement in the early part of the 21st century, where it would then increase drastically. Institutionalization could be averted if people received varying levels and types of nonmedical supportive services where they lived. However, obtaining this help was difficult and expensive. The primary challenge was to create a cost-effective program that still provided valuable services. The author reviewed various housing programs created by the government.
Housing with Support Services
There were three types of housing with support services. The first type consisted of projects designed for use by physically impaired people. The second type provided support services to people living in government-subsidized housing. The third type was the small Congregate Housing Services Program, which is used to delay the need for institutional placement of its residents. Several states have launched congregate housing programs, which were "mixed income" and primarily financed by state housing bonds and insured under the FHA 221 (d)(4) program. Since 1980, the number of additional households assisted each year had dropped notably, and the composition of the funded units has been shifted from constructing homes to rent supplements or housing vouchers. Moreover, funds were being appropriated only for the elderly and handicapped by the Section 202 program.
Housing in Relation to Long-Term Care Policy
Housing and long-term care policies were technically not linked because the United States had no articulated long-term care policy. The current legislation through two clauses enabled the expansion of community-based services. First, it could occur through the "creative use of coverage options in the state Medicaid plans." Second, another possibility was through the Section 2176 "waiver program."4 Furthermore according to the authors, community-based programs have not been able to effectively prove that they minimize costs because many experimental programs have not been able to define the appropriate target population. The targeting issue would need to be a grave concern in designing new housing initiatives.
Future Policies
Housing-based options were packages of assistance that combine supportive services with a housing-based solution, such as the CHSP. A long-term care based option was where housing assistance was added as necessary to community-based long-term care assistance.
Housing-Based Options
CHSP. In 1985, the monthly cost of supportive services received by CHSP participants was about $340.5 The authors then derived the approximate cost of the housing services and housing subsidies and concluded that total rent was $430 per month and federal outlays were $274 per month. Therefore, the full cost of services was $770 and the subsidy component was $614 per month.6
Intermediate Care Facilities. The authors claimed this costs approximately $45 per day, or $1,350 per month, where residents received assistance through Medicaid and paid all their income except $35 per month for this care. The authors then estimated the monthly cost of Medicaid to the government to be $890.
Targeting and State Interest in Congregate Housing
Two major considerations arose about congregate housing as a substitute for nursing homes care. The first concern was how to determine the appropriate margin of error in selecting low-income tenants for congregate facilities, such that congregate care would not cost more for each person who has not entered the nursing home. Secondly, the interest of the states in congregate housing programs was crucial because the cost sharing varied and could foster a strong interest on the part of the states to forestall or delay institutionalization. According to the authors, if congregate housing services could demonstrate effectiveness in reducing institutionalization, then states should be more willing to share in the cost of a federal congregate housing program.
LTC-Based Options
Life Care at Home (LCAH) and Social/Health Maintenance Organizations (S/HMO) were new long-term care insurance and service delivery models primarily for middle-income households. LCAH combined financial and health security of a CCRC with the freedom and independence of living at home. LCAH pooled the risk of its enrollees and enabled more individuals to participate it. This was currently done in Philadelphia. The S/HMO relied heavily on HMOs as the service provider, where the provider assumed responsibility for a full range of services
Conclusions
Congregate housing according to the authors was considered to be the most promising housing-based approach. However, the complexity and types of support services offered must be studied and altered continuously to continue program effectiveness. States should have a genuine interest in creating a joint federal-state congregate housing program, since congregate programs could possibly reduce overall long-term care costs by minimizing entry into nursing homes and reliance on Medicaid. In addition, the authors suggested that a stronger working relationship was needed to evolve between HUD and HHS to improve cost savings and services.
NOTES
-
West Side between 14th and 34th Street; Contact: Adeena Horowitz, 212-243-3670.
-
Penn South's group activities had about 900 members (Bassuk, p. 134).
-
The median age of a sample of CMI at NIMH's Community Support Program was 42 years of age.
-
States could apply to HCFA, now CMS, for permission to substitute such services for institution-based services.
-
This includes costs directly paid for by the program and matching services provided by the housing facility.
-
This was based on two assumptions: (1) the income of the elderly receiving this assistance was the same as that of all elderly receiving housing assistance; (2) the cost in public housing and Section 202 projects was the same as the average outlays under the entire Section 8 program.
APPENDIX 2. NORC Site Visit Summaries
SUMMARY OF THE SITE VISIT TO SENIOR FRIENDLY NEIGHBORHOODS
Baltimore, Maryland
June 5, 2003
The following information was derived from discussions with six staff from The Associated Jewish Community Federation of Baltimore (hereafter The Associated) and four organizations that operate under the umbrella of The Associated. They are Comprehensive Housing Assistance, Inc. (CHAI), Jewish Family Services (JFS), the Jewish Community Center (JCC), and the Myerberg Senior Center (MSC). These organizations run the Northwest Baltimore NORC services program called Senior Friendly Neighborhoods (SFN) that grew out of the earlier Senior Friendly Apartments (SFA) program. The Agency on Aging (AoA) grant enabled the organizations to subsume SFA into SFN by serving new apartment buildings and planning to expand into adjacent neighborhoods of row houses and single-family homes. Two members of the SFN resident advisory council to the NORC service program also participated in the discussion.
Description of the NORC and Its Residents
SFN serves the community of Upper Park Heights, located in Northwest Baltimore. The community is largely Jewish, but about 25 percent of its residents are black and a small minority are Hispanic. A subset of the older Jewish residents are Russian immigrants who came in the late 1980s. Most of the community's older residents have aged in place, living in the same homes or apartments for 30 years or more. Services are provided to residents regardless of religion affiliation or ethnicity, and SFN staff could not supply data on the percentages or total numbers of people in each demographic category.
In the late 1980s, Jewish community leaders decided to try to stabilize the community because they feared that the "Northwest flight" of people leaving Baltimore, which has been underway for about 50 years, would eventually change the community's profile. Under this stabilization initiative, The Associated and its affiliated agencies helped families buy homes and helped older people remain in their homes. In addition, they provided a range of programs such as volunteer days and sponsored community associations for Jewish people in the neighborhood.
Upper Park Heights is home to a number of agencies that are part of The Associated--the Jewish Community Center, the Myerberg Senior Center, and Baltimore Hebrew University. There are numerous synagogues, two large churches, and a public library. The community has grocery stores, shopping areas, and two activity hubs--the senior center, which operates with Baltimore City and private funding, and the JCC. The community has public bus transportation, and a senior shuttle, which holds up to 20 passengers, is accessible to people with disabilities. The shuttle has 36 stops and runs a continuous loop, five days a week.
Upper Park Heights is bordered by several major thoroughfares and has market-rate apartments, subsidized apartments, Section 8 apartment buildings, garden style apartments, row houses, and single-family homes. Each apartment building has a different character. The buildings with predominantly American-born residents have older physical plants, and the residents are frailer than those in the buildings with a high proportion of Russian immigrant residents. The latter group is younger in age, with fewer disabilities. Some of the smaller buildings do not have community spaces for programs and meetings, and the older buildings have accessibility problems such as stairs and curbs in front of building entrances.
The typical row house or semidetached home in the community is at least 30 years old, with street parking, stairs leading to the entrances, and steep interior stairs that do not have double banisters. Many homes do not have air conditioning and their exterior paint and lawns are in poor condition. The homes typically have only one bathroom, located on the second floor and lacking such aids as grab bars. Laundry facilities are located in the basement, which generally has stairs without railings. The layout of the homes presents problems related to accessibility, cleanliness, and risk of falls, and similar problems. For over 10 years, CHAI has provided home assessments and modifications to help people with low incomes remain in their homes.
SFN currently provides services in 13 buildings in Upper Park Heights and plans to expand services to the neighborhoods with row houses and single-family homes. Eight buildings originally received services under SFA; the remaining five buildings were added with the creation of SFN. Two of the 13 buildings were built using Section 8 funds from the federal Department of Housing and Urban Development (HUD). The buildings that SFN serves range in size from 45 to 190 apartments. The latest building to become part of SFN was the Milbrook building in 2002. The Milbrook building has 705 garden apartments, 450 of which have a resident who is age 62 or older. Most of these residents are Russian immigrants.
NORC Building Management and Communication with Residents
All of the new SFN buildings are either market-rate or HUD-subsidized buildings. Building management companies operate these buildings, with at least a part-time building manager on site in each building. Two of the apartment buildings have resident councils, floor captains, and phone trees, all of which were in place before the SFN program started. SFN has hired residents in two buildings as on-site coordinators; their jobs involve seeking input from residents, informing residents about activities, and coordinating these activities. SFN is hiring residents to determine if this is a cost-effective model for organizing and delivering programs.
NORC Service Organizations
The four organizations that run SFN have different roles. CHAI's mission is to stabilize the communities for Jewish residents and their neighbors in Northwest Baltimore, primarily through housing and neighborhood services. CHAI received the AoA grant and coordinates SFN and its outreach to residents and businesses in the NORC. CHAI has a Board of Directors and a Senior Citizens Committee. CHAI sought the participation of JFS, JCC, and the Myerberg Senior Center as it began developing SFN.
Jewish Family Services (JFS) offers a wide variety of social services to Jewish people of all ages. JFS supervises the SFN caseworkers, nurse, and volunteers. The Jewish Community Center and the Myerberg Senior Center serve as activity hubs for SFN. The senior center receives funding from the Baltimore City Commission on Aging and Retirement Education, the Jewish Community Federation of Baltimore, and the Center's own fundraising activities. Since these agencies are part of The Associated, their working relationships have evolved without formal screenings, competitions, or contractual relationships.
CHAI developed SFN with limited formal input from older people, but has since established a SFN Advisory Council, which began operations in February 2003, to facilitate resident involvement and empowerment. CHAI staff asked residents who were involved in SFN programs to volunteer to serve on the Council to provide advice about SFN's operations. Staff are now turning over the chair function to the Council members and the precise function of the council is under development. Every NORC building has a quarterly SFN forum where residents can ask questions as well as share concerns and ideas.
Evolution of the NORC Service Program
CHAI staff found out about the concept of NORC service programs through their work with older people (age 62 and older) in the community. They sought and received a small grant ($20,000) from the local Morris Goldman Foundation in 1996 to begin providing services in apartment buildings as part of their efforts to stabilize the community and enable older people to age in place. The new program, Senior Friendly Apartments, paid for two JFS case workers to work in the apartment buildings and provide information and referrals, brief assessments, and, where needed, case management. SFA also made arrangements with the local Sinai Hospital to provide some health education programming.
In 1998, JFS decided to assign caseworkers to specific buildings so that residents would get to know them and so the workers' travel time would decrease. JFS also asked for and received donated community space from the buildings in which the caseworkers operated. CHAI used the NORC AoA grant to create SFN in 2002 by incorporating the original eight SFA buildings and an additional five buildings chosen based on staff's experience in the community and pre-established relationships with building owners and managers.
When CHAI received the AoA grant, it held open community meetings in the eight SFA buildings to explain how the grant would affect SFA and to talk about plans for SFN. Some older residents expressed concern about changes to their existing services and were initially confused about them. For the additional five buildings, CHAI initiated contacts with residents and housing management in the targeted buildings to explain the program and assess their interest in participating.
CHAI's outreach to the row houses and single-family homes in the neighborhood surrounding the apartment buildings is based on the concept of "warm houses"; individual residents would open their homes to community programs and activities, which would become community spaces like those in the apartment buildings. The "warm house" concept has been challenging to implement, but SFN plans to continue organizing in this community.
Services Available to NORC Residents
SFN services are targeted to people age 62 and over who live in the Upper Park Heights and the new Milbrook building. SFN services include case management, information and referral services, preventive health screening, recreational activities, and transportation, all designed to keep people independent in the community for as long as possible. Apartment residents must become members of SFN to receive services; membership requires a short application and a $15 annual membership fee. SFN currently has 149 members. "Case aides," who are JFS-contracted employees, assess a member's physical and psychosocial needs in the member's apartment or another private location, provide information and referral to needed services, and help residents obtain such services as Meals on Wheels, home care, and others. SFN does not provide hands-on assistance with daily activities; however, staff refer residents to agencies that can provide these services. Case aides will also follow up with members who have received a referral, if the resident has further need of assistance. NORC residents can tap into additional services from JFS, including counseling, advocacy, home care services, outpatient mental health care, geriatric services, volunteer services, and limited financial assistance.
In addition to case aides, JFS contracts with one nurse and resident activity coordinators in each SFN apartment building. The nurse conducts preventive health screening activities such as blood pressure checks. She can also assess a resident's health care needs and, based on her findings, refer individuals to appropriate health care providers. Due to funding limitations and liability concerns, the nurse cannot provide most health care services. The activity coordinators in each building help find out what services residents want, publicize activities, and help organize them.
Residents would rather attend group activities, which might include a health care component, than seek out services individually. The types of activities that are popular include "Eating Together," which is a meals program funded by the Baltimore Commission on Aging, discussions of current events, and book clubs. Residents want to be entertained, but at minimal cost. Also, the types of programs that appeal to the younger-old Russian immigrants involve activities such as yoga. Residents who are in the oldest age groups would rather go to events where they can sit and observe.
JFS coordinates a broad range of volunteer activities under SFN in which residents may either offer or receive help. For example, some residents volunteer in schools, while others request friendly visitors. Some volunteers drive people to appointments or do minor home repairs. Other groups of residents have become involved in group programs such as a writing program where they become pen pals with 3rd grade students. JFS recruits and screens volunteers and coordinates their efforts.
In 1998, CHAI surveyed neighborhood residents about their transportation needs and designed several services to help meet the identified needs. After receipt of the federal grant, SFN began operating a shuttle bus that serves about 16 buildings, not all of which are part of SFN. Residents must make reservations a day in advance of their trips. SFN also sells residents subsidized vouchers for local taxi-cab rides to be used for medical appointments up to twice a week. Residents pay only one-third of the usual cost of a taxi. In July 2003, SFN will explore providing an accessible sedan service to enable residents with disabilities to go to their medical appointments; drivers would be able to help people into the van and to and from their medical appointments. Also in July, SFN will provide a van to shopping areas every Monday. SFN staff suggested that a vehicle purchase might be a more economical option than the numerous hired vehicles but the AoA grant rules prevent purchase of automobiles in demonstration projects.
NORC Service Program's Communication Methods
The primary methods that CHAI and its partners use to communicate with SFN members include flyers, telephone calls, monthly newsletters in two languages, posters, word of mouth, and mass mailings. Staff were not sure which communication methods work best.
Case aides, who are assigned to particular buildings, send out flyers or put up posters to introduce themselves and to advertise their drop-in hours. Some case aides go door to door to introduce themselves. Case aides also try to speak with building management about tenants who seem to be having problems remaining independent.
SFN also has an outreach worker whose job is to work with building managers and to identify people who need services. The outreach worker began working in November 2002. Staff believed that they should dedicate one staff person to marketing activities to develop a strong publicity plan and improve their effectiveness.
NORC Service Program Challenges
SFN has faced the related challenges of engaging the interest of both NORC residents and building managers in its programs. Turnout for programs varies by building, with low cost or free activities drawing the most attendees. According to SFN staff, almost anyone will come out for a party, so parties tend to be some of the most well attended activities. Reaching isolated residents is a challenge; staff must rely on other residents to seek isolated residents out. How well this works is not known.
One group that has resisted the SFN program is condominium associations. Over the last six years, four different buildings have turned SFN down, primarily because the associations do not want to be viewed as nursing homes or to receive what some view as charity. Some older people do not want to "spend time with old people." When apartment building managers were resistant at the beginning of the program, staff turned to building owners whom they knew through their work in the larger community. Some of these owners encouraged building management to try out the program.
Outreach into the neighborhoods composed of row houses and single-family homes has been particularly difficult. SFN has not been able to identify any appropriate "warm houses" to date. Homes in the NORC neighborhood are generally not accessible for people with disabilities; lack of transportation presents another obstacle. CHAI staff have tried to identify these houses through mass mailings in the neighborhood and by contacting neighborhood associations. Neither method has produced any volunteers willing to serve as "warm houses." Despite the difficulties, SFN plans to continue its search for appropriate sites.
NORC Service Program Quality Assurance and Outcomes
SFN has a number of quality monitoring methods. SFN staff collect information on the number of people attending each program and on the people using the case aide service. Members provide data on their age and service preferences, but no data are collected on ethnicity. Periodically, SFN volunteers call members to ask for feedback on activities or services. SFN also holds quarterly open forums to hear from residents about the program.
JFS social workers supervise the case aides through weekly meetings. In addition, all staff participate in team meetings to discuss their work and any relevant administrative matters. The aides can present resident problems or needs for services in the weekly peer group meetings. JFS also conducts a formal utilization review that involves review of clients' clinical records.
Beginning in June 2003, The University of Maryland Baltimore College (UMBC) Center for Health Policy will conduct a survey of a random sample of 100 SFN members and 80 nonmembers from the group of 507 NORC residents who have used SFN services. These users will be followed until June 2004. UMBC will also conduct a process evaluation of SFN's operations. The study results will be used to seek ongoing funding from local foundations and other sources.
NORC Service Program's Funding Sources
The program's funding comes from a combination of The Associated: Jewish Community Federation of Baltimore, local foundations, and Baltimore County funding. Funding for the first program, SFA, came primarily from The Associated; total funding was $187,309 for the first seven buildings, which was split between CHAI, JFS, and JCC five years ago when the program first started. Funding for services in Milbrook comes from a variety of sources: $25,000 from Baltimore County, $125,000 from the Weinberg Foundation, and free use of an apartment valued at $7,000. The AoA grant money is split between the original three agencies and the Myerberg Senior Center; funding is about $1 million over 14 months--$180,000 to the JCC, $200,000 to JFS, $100,000 to CHAI for staff, and the balance for the Senior Center. Baltimore County, The Associated, and the Weinberg Foundation provide the remaining matching money.
Funding is a significant challenge for the NORC because residents only bear a small share of the cost through their annual $15 fee. SFN is considering instituting user charges but has not yet imposed them. State and federal funding, apart from the AoA grant, are currently not available.
Recommendations
SFN staff and NORC residents made a number of recommendations regarding development of service programs. Before beginning, there should be a market assessment of who needs or wants what types of services in the target geographic area and an assessment of existing community resources--public and private sector. In particular, relationships with businesses can bring additional resources to the NORC service program.
Outreach is a critical component of the service program. A door-to-door marketing scheme is important because sometimes residents do not come out of their homes. Word-of-mouth referral also makes a big difference. The cooperation of building management is important so that when new residents move in they hear about available services.
Interviewees disagreed about the organizational foundation and structure of service programs. Some believe that a community development agency should take the lead in developing the program. Others believe that several agencies should collaborate to develop services. All staff acknowledged that having one central agency handle the administrative infrastructure helps keep intra-agency coordination informal and provides economies because the central agency in Baltimore--The Associated--carries required insurance, takes care of information technology services, employee benefits, capital repair, and central planning for the system.
SFN staff agreed that access to community space in buildings and neighborhoods was key to residents socializing together. Nine of the 13 apartment building owners provide such space, which promotes residents' participation in programs.
SFN staff agreed that careful consideration of the staffing for the case management function is critical. The original grant funded three master's level social workers. It has proved very difficult to recruit social workers at this level, despite much effort. SFN ended up hiring people with bachelor's degrees in social work. All staff need to be trained to actively help people, rather than just react to crises. Thus, all staff need training on appropriate assessment so that the NORC services program does not follow a traditional reactive model.
SUMMARY OF THE SITE VISIT TO UNITED JEWISH FEDERATION OF CLEVELAND'S COMMUNITY OPTIONS PROGRAM AND A DISCUSSION WITH THREE OF ITS SUBGRANTEE SITES
The Jewish Community Federation of Cleveland began its Community Options program in 1995 using a grant from the federal Department of Housing and Urban Development (HUD). When the AoA grant money became available in 2001, Community Options officials proposed to use the money to determine whether its NORC services program was replicable in other sites in Ohio. Program staff successfully marketed the model and provided AoA grant money and technical assistance to four new sites--Canton, Cincinnati, Columbus, and a new site in Cleveland. These sites will be referred to as subgrantees--the term that Community Options staff use.
This site visit summary describes the original Community Options program in Cleveland as well as developments in three of the subgrantee sites--Canton, Cincinnati, and Columbus--that participated in this study. The following information comes from discussions with two staff people from Community Options and five staff from the three subgrantees. The subgrantees were in the early stages of developing their programs in the summer of 2003.
Description of the NORC and Its Residents
The Original Program
Community Options. The original Community Options program operates in five private apartment buildings where resident incomes range from lower- to upper-middle class. The buildings within which Community Options operates are located east of the Cuyahoga River in Cleveland. Although the Jewish Community Federation of Cleveland received the AoA grant and most Jews in Cleveland live in the east, the buildings that Community Options serves are not predominantly Jewish and Community Options programs are open to anyone who resides in the buildings they serve.
There are two distinct groups of older residents in these buildings. The longer-term residents are typically widows who sold their homes upon retirement and moved to the apartments with their husbands, who have since died. More recent residents are people who chose to hold on to their homes as long as possible, and have relocated to apartments during their eighth decade rather than their sixth. These apartments are attractive to residents because they are within walking distance of synagogues, shopping, and bus lines.
Community Options first began operations in two buildings managed by separate landlords. A year later, both landlords requested that the program be expanded to another building for a total of four buildings. The program added a fifth building in 2002. In two of the buildings, initially 70 to 75 percent of the residents were age 60 and over. Over the past eight years, as younger families have moved into the apartment buildings, this percentage has dropped to about 50 percent. In another building, there is a rising proportion of older African Americans. Few immigrants live in any of the five buildings, and in only one are the residents predominantly Jewish.
The five buildings in the program are each six- to seven-story high rises, located on a major thoroughfare. Although all have elevators, they also have steps leading to the entrances so that wheelchair accessibility is an issue. In contrast, the subgrantee sites operate in various types of buildings and neighborhoods.
The Subgrantee Sites
Canton. The Canton Program--Community Connections--serves three apartment buildings in an urban, primarily residential, area. The three buildings are not on the same campus but are less than a block apart. One landlord owns all of the buildings, each of which has about 100 residents, about half of whom are age 65 and older and aging in place. Two of the buildings have old physical plants with concomitant accessibility problems akin to those in the buildings that Community Options serves. The third building is newer, with few older people and, unlike the older buildings, has no common areas. The Area Agency on Aging in Canton, which is receiving the AoA funds from Community Options, chose these three buildings because they were close to one another and staff knew that the buildings had substantial numbers of older people.
Cincinnati. Jewish Family Services operates its NORC services program in two locations in a suburban area of Cincinnati. The first is a combination of town homes and "mini-rises" consisting of four three-story buildings where 80 to 90 percent of residents are age 60 and over. Because of steps and curbs, accessibility is an issue. Together, the four buildings contain 144 private rental units. The second location is a more traditional high rise with 100 units where 90 to 95 percent of residents are over age 60. Both locations have common areas. The residents are predominantly white middle to upper-middle class with few minorities. The agency targeted these locations because they have clients in the buildings, but NORC program services are not limited to Jewish residents.
Columbus. Wexner-Heritage Village, a Jewish, nonprofit provider of health, housing, social, and spiritual services, including a CCRC, an SNF, community services, as well as housing for older people and people with developmental disabilities, sponsors the Connections program. The program operates in four sites representing a range of populations and building types. One building is a mid-rise, private rental apartment with upper-income residents, most of whom are age 65 and older. The building's entry presents no barriers to access but the bathrooms are small. The second location is a combination of town homes and apartments on a large campus owned by the same landlord that owns the first building. Access is good but there are no common areas. The third has two buildings with garden-style apartments that are private rental units. The fourth is a public housing complex that covers 50 acres and has a diverse population. The complex has been plagued with frequent management turnover and episodes of violence.
NORC Building Management and Communication with Residents
Community Options has generally had enthusiastic support from the buildings' management, who have supplied the names and addresses of older residents. The building owners have contributed funding to the on-site program costs because their residents value Community Options programs and thus may be more likely to remain in the buildings and tell others about the value of living in them. In addition, Community Options helps management by providing certain support services to residents.
Program staff's early experience with management at the subgrantee sites runs the gamut from tepid to supportive. Staff report that at some locations landlords view the NORC service programs as a "value added" that helps keep tenants happy and encourages others to move in. At other sites, landlords cite privacy and liability concerns in refusing to give information about their residents to program staff. Landlords at the subgrantee sites have not yet been approached for financial contributions because program staff want to demonstrate the value of their programs to landlords before asking for support.
NORC Service Organizations
Community Options, the original NORC services program, is an independent program sponsored by the Jewish Community Federation of Cleveland. The program began in 1995 under a $2 million dollar special purpose grant from HUD. In 1995 or 1996, The Federation convened a committee made up of volunteers of all ages to oversee the program; most of the members still do. A consultant, Susan Lanspery, then at Brandeis University, helped the committee determine the program design. The proposed design was based on a community organizing, consumer-directed model, largely because The Federation typically uses a community organizing approach in its work. The three subgrantees for which we have information, although they are largely adopting the Community Options model, have not yet formed advisory or oversight committees, although they are considering doing so.
Evolution of the NORC Service Program
The goal of the Community Options program is to allow people to stay in their homes by providing them with access to social activities and by helping them access community services, such as transportation and home help, through information and referral. The program's staff use the community organizing model, which involves empowering people by talking with them about their needs and issues without any preconceived ideas. Then, with the assistance of community residents, the program organizes the desired services. The program is never static because residents' needs and desires change over time as the community changes. The residents feel a sense of ownership of the program because it is based on their expressed needs. As program staff began using this model, they observed that many older adults in Greater Cleveland felt marginalized. The program was designed, in part, to help counter these feelings by involving residents in program design.
The Federation decided to develop Community Options in apartment buildings that housed a large number of older people. Staff visited likely buildings during the day to observe whether large numbers of older people lived there. Of the 12 possible sites they identified, two had owners who were open to the program. They began operations in these two buildings--Huntington Green and Sherri Park--in August 1997, after building managers agreed to try the program for a year.
Although the owners were enthusiastic, their building managers were concerned that the buildings might be viewed over time as senior housing, thus decreasing their attractiveness to other age groups. These fears were not realized; since Community Options began offering services in 1997, the ratio of older to younger people has remained relatively stable in the buildings they serve.
Currently, the program operates in five buildings; it employs four resource coordinators, one of whom is responsible for activities in two buildings. The coordinators are in the buildings about 20 hours a week, organizing and running activities as well as communicating with residents. In addition to the director, Community Options has an administrative assistant and an assistant director in the main office. The assistant director works full-time managing the program and the office staff who spend 12 to 14 hours a week keeping provider referral lists accurate.
With the availability of new funding under the AoA grant in 2001, Community Options addressed the possibility of replicating its successful program in other sites. It is in the planning stages of expanding its own program into the western part of Cleveland. In looking for the subgrantee sites, program staff canvassed likely nonprofit organizations in several areas of Ohio to determine if any were interested in using the AoA grant funds to replicate Community Options in their locales. The sponsoring organization at the new sites needed to be a large nonprofit and had to be willing to match one-third of the money it obtained from the grant. Community Options found that few organizations wanted to receive a large amount of money that had to be spent in one year and had matching requirements. Thus, Community Options staff undertook a major education effort as it recruited the subgrantee sites.
Eventually, the Community Options staff identified four organizations that met the requirements and were interested in the program. The Canton and Western Reserve AAA saw the NORC services program as a natural outgrowth of its mission to serve older people and help them remain independent in their homes and communities. The Cincinnati Jewish Family Services had already been doing case management for older clients and saw this opportunity as a logical next step in service provision. The executive director at Wexner-Heritage Village in Columbus had previously worked in Pittsburgh and was familiar with NORC service program there and had a great deal of interest in helping people age in place.
Services Available to NORC Residents
Community Options and its subgrantee sites focus on organizing socialization opportunities for building residents and on making referrals to community providers when residents need additional services to help them remain independent at home. The program usually refers residents to up to three different agencies for any given service, while trying not to show a preference. The agencies come from a provider database that the program maintains, which has information on services and prices. The types of referrals that residents request most include transportation, homemaker services, and beauticians.
The types of activities that residents want vary by building. For example, some buildings' residents like playing Bingo while others prefer book reviews. The range of activities currently includes senior exercise classes, current events discussions, luncheons, and monthly blood pressure checks. The activities vary over time in response to residents' expressed preferences. Transportation is a large and ongoing problem for residents because many older people cannot drive and public transportation in Cleveland is not well developed.
Most health-related activities are preventive in nature and include such things as speakers on pharmaceutical issues, a podiatric clinic, and safety lectures. Building management and tenants will not allow medical staff, such as a nurse, on site because they want to avoid having the building appear to be a nursing facility. Most activities take place in the apartment buildings' party rooms. Those living in the buildings with the party rooms tend to participate more frequently than those who live further away.
Attendance at activities varies. For lunches, one of the most popular activities, Community Options sites typically have between 30 to 50 residents in attendance. Most activities require a reservation because resource coordinators need to know how much food or other supplies will be needed. Different people attend different events; for example, those who come to luncheons are not always the ones who go to other events. The variety of events offered by the program attracts residents of different incomes and ages.
Community Options also has a role for volunteers. Residents volunteer their services at activities, particularly for entertainment purposes. Resident volunteers distribute newsletters, set up events, take money, and make phone calls, among other activities. Residents either offer to serve as volunteers or, in some cases, the resource coordinator asks the more active participants to serve as volunteers.
The three subgrantee sites were beginning to implement their programs in the Summer of 2003. Like Community Options, their programs focus on socialization activities and information and referral. Two of the new sites are considering whether to help residents link up to service providers by contacting the provider on behalf of the resident and helping to ensure that residents obtain services they say they need. The final decision on this matter will be made as the subgrantee sites gain experience with their residents' needs.
NORC Service Program's Communication Methods
Community Options has several methods of communicating with residents of the buildings they serve. Staff held resident focus groups and surveyed the older residents of their first two buildings to determine what they wanted. In 2003, an intern conducted a new resident survey in these buildings to determine how resident interests had changed. The results are still being analyzed.
Resource coordinators also engage in outreach when they begin a program in a building and as new, older residents move in. When the program opens at a new site, management sends a letter to the residents introducing the program and gives a list of older people to the resource coordinators who then knock on all doors to introduce the program and find out what residents want. Based on the results of the outreach, the coordinator develops a profile of the building and its residents' preferences, which then goes to residents for their feedback. Coordinators also track attendance at activities to determine whether to continue a particular activity in a building.
Resource coordinators hold office hours in each of Community Options' buildings, Tuesday through Thursday. The office is located in the activities room in two buildings and is located near the mailboxes in the other three. The coordinator produces a quarterly newsletter and puts flyers in elevators, laundry rooms, mailrooms, and on bulletin boards. In addition, the coordinator and volunteers place personal phone calls to residents they have not seen in a while.
One resource coordinator we spoke with believes that communication with residents could be better because management does not always notify the coordinator when new older people move into the building. As a result, the outreach to new residents may be delayed.
The new sites also rely on door-to-door outreach to communicate with residents. In addition, two of the subgrantee sites have surveyed residents to determine their needs and preferences regarding activities. Preliminary results of these activities indicate that residents' value outside trips, socialization, and transportation. This last service appears to be a big unmet need among older people at all locations.
NORC Service Program Challenges
The challenges that the NORC service programs face have some common aspects but vary somewhat from site to site. Younger old people tend not to participate in programs because they are busy doing other things, such as volunteering in the community. In addition, some residents find it difficult to remember whether they have signed up for an activity that requires payment of a fee or pre-registration. Or, residents may remember their commitments but not feel up to fulfilling them on a given day. The resource coordinator has started to address these issues by having volunteers make telephone calls to remind residents and sending out electronic voice mail messages to senior residents regarding programs.
Community Options tried to set up a program in a suburban neighborhood on the east side of Cleveland, but had to withdraw because it could not get the funding to sustain that site. In addition, the suburban neighborhood presents obstacles to organizing, such as inclement weather and transportation that had not been encountered in the programs that were established in apartment buildings. Staff could not find a central activity center or office space that was easily accessible, and without a building manager who was familiar with building residents, they had to knock on every door in a neighborhood to locate the older residents. From this experience, one of the key lessons learned is to organize in partnership with a parish, synagogue, or other established institution in the target neighborhood.
In the subgrantee sites, staff found that transportation between separate buildings is difficult even when the buildings are in close proximity to one another. In addition, some building managers have unrealistic expectations about the program's ability to deal with tenant problems, such as cleaning the apartments of messy tenants. Some landlords are unwilling to release tenants' ages, citing confidentiality concerns, or the information they offer is inaccurate. One new site found that the management resisted door-to-door outreach in one location even though this task is part of the program's contract with building management. Staff have had to rely on other methods of communication, such as flyers and general word of mouth.
NORC Service Program Quality Assurance and Outcomes
Community Options has well-developed feedback mechanisms for quality assurance and measurement of outcomes that the new programs are adapting to their needs. The program has a master database that enables resident coordinators to call all residents for whom they have made referrals to determine if the resident was satisfied with the provider they chose. Resident satisfaction is then entered in the database. When Community Options staff note a pattern of dissatisfaction among consumers with regard to a certain provider, that provider will be removed from the computerized referral list.
The database also enables coordinators to track clients' interest and participation in activities. The database shows that about 86 percent of seniors in the five Community Options buildings have had contact with resident coordinators beyond door-to-door outreach or have participated in activities. Seventy-nine percent of residents have attended activities more than once over the past six years. The most frequently requested service referral is transportation, followed by housecleaning. The new sites are in various stages of planning to adopt the same approach to data collection that Community Options uses.
The AoA grant has allowed the Community Options program to participate in a research project that Dr. Eva Kahana at Case Western Reserve University is leading. The study will follow a group of 1,000 community-dwelling older people in Cleveland and compare their experiences to those of older people residing in buildings with Community Options and two of the new subgrantee sites. The outcomes that will be tested include nursing home and home health use. The report will be available in 2004.
NORC Service Program's Funding Sources
Community Options is unique in that it has substantial financial support from building management. When program staff approached the management at its first buildings, they asked for and received free office space and free use of the party room for each site. Using its $2 million HUD grant, the program initially paid for the telephone and resource coordinators' salaries. After the first year, the Community Options Oversight Committee proposed asking the building management to contribute financially. Because of positive feedback management had received from residents, they were willing to pay for on-site costs such as the coordinators' salary and benefits, office and party room space, and other programmatic costs such as paper and copying. Community Options covers its overhead costs at the main office through use of the HUD grant. Residents pay the costs of the activities, which range from 25 cents for coffee to $23 to $50 for transportation to various events.
Because the initial HUD grant was a spend down grant with no time limit, Community Options has not had to seek other funding. But now that the HUD grant is running out, the program is approaching foundations and like organizations. Initial reactions have been positive.
Like Community Options, the new sites initially asked for and received office and activity room space from landlords and plan to approach them in the second year for support with the costs associated with the resource coordinators and communications.
Lessons Learned
The form a grant takes can affect program implementation. Too much money to spend during a short time can cause implementation problems because organizations have insufficient time to plan.
The type of relationship the resource coordinator establishes with building residents enables trust to develop; having an accessible office on site facilitates this process. It is also important to avoid giving residents the perception that they are being assessed because they associate assessment with entry into an assisted living or nursing facility. Trusting relationships with resource coordinators often lead to requests for referrals for housekeeping, transportation, or other services that are more personal in nature.
SUMMARY OF THE SITE VISIT TO JEWISH FAMILY AND CHILDREN'S SERVICES OF GREATER PHILADELPHIA
The following information was derived from discussions with 16 people on May 5, 2003--ten employees of the Jewish Family and Children's Services (JFCS), two JFCS contractors, and three residents and one building manager at a NORC building located in the Center City section of Philadelphia.
Description of the NORC
The NORC encompasses four cooperative apartment buildings (co-ops) and one condominium in the Center City section of Philadelphia. Four were constructed using federal Department of Housing and Urban Development funds--2101 Walnut Street, Penn Center House, Kennedy House, and Rittenhouse Plaza. The fifth building is The Philadelphian, built with private financing.
The buildings are all high-rises with apartments ranging in size from studios to two-bedroom units. The apartments are not considered accessible housing for people with disabilities. Although the buildings have elevators, which help foster accessibility, public areas of the buildings visited have features that pose difficulties for some older residents. For example, residents have slipped and fallen due to problems with the automatic doors; building management responded by adjusting the doors to close more slowly. Of the five buildings, three have few, if any, chairs in the lobby, and one has expressly forbidden people to sit in the lobby to avoid having the building "seem like a nursing home."
The building managers annually inspect residents' apartments to find and eliminate safety hazards and to ensure that equipment is functioning properly. Every year these inspections uncover some unsafe situations. The building management works with residents to eliminate the problems and brings in social workers from Jewish Family and Children's Services, if needed, to help facilitate the process. Problems that remain unsolved can lead to eviction. Starting eviction proceedings is seen as a last resort for both compassionate and legal reasons. First, people may deny that they need help, even if they need substantial assistance with daily activities, or they may be reluctant to leave their homes. Second, although people can be evicted if they are deemed incompetent, legal protections against being declared incompetent can be very difficult to overcome.
Some financial issues related to the NORC buildings have proved burdensome or divisive for the residents and might cause some to leave their apartments. A person moving into the building we visited would have to pay about $65,000 in 2003 for a one-bedroom apartment plus a nonrefundable "buy-in fee" that ranges from $17,000 to $25,000. In addition, the monthly "carrying charge," which ranges from $350 to $750, is becoming difficult for some residents to meet. Property taxes are increasing as well, with some residents facing a doubling of their tax burden following the city's reassessment of most of Center City Philadelphia properties in 2002. Some residents would like the ability to sell their apartments on the open market and, thus, turn the co-op into a condominium, an issue that has become divisive. At present, the co-op's by-laws prohibit such sales, a restriction that can only be lifted by a vote of two-thirds of the residents.
NORC Residents
According to JFCS staff, at least 75 percent of residents in the five apartment buildings are age 65 or older, and those who have lived in the buildings the longest came in the 1970s. The typical resident is white and, while the population includes a substantial number of Jewish residents, the resident population is diverse, including blacks, Protestants, and Catholics. Residents tend to be well educated; they are retired teachers, social workers, and others who are committed to the concept of co-op living. Residents come from all economic strata, although most have incomes at or below 200 percent of the federal poverty level. The few younger residents have an average annual household income of about $75,000. Precise demographic data about NORC residents are not available.
Most residents have aged in place, but some in-migration has occurred for several reasons. Retirees have sold homes in the suburbs and moved to these Center City buildings because costs are relatively low compared to other city residences. The neighborhood is attractive; people can walk to their health care providers, use public transit, and take advantage of educational and cultural opportunities close to their homes. Temple University and the University of Pennsylvania are located nearby, as are museums and restaurants. People have also moved to the five buildings because of what they have heard about the availability of social services. Three of the five buildings have waiting lists. For example, the building we visited has 800 people on its waiting list, some of whom have been on it for 17 years.
NORC Building Management and Communication with Residents
Four of the five buildings have elected co-op boards, and each has at least a part-time building manager. The co-op we visited has two floor captains for each floor, elected annually or biannually. One of the buildings is a condominium governed by a condominium association.
The co-op board in the building we visited hears from its residents formally and informally. Residents are comfortable voicing their opinions to board members both during and outside of board meetings. Formal feedback comes from residents when they leave the building and fill out the requisite questionnaire, or when the family of a deceased resident does so. Residents also have monthly House Council meetings to discuss issues of concern to residents. Part of each meeting is open to all residents, while the rest of the meeting is limited to discussion among the floor representatives. Upon request, the board appoints one or more of its members to attend House Council meetings.
NORC Service Organization
The founding organizations that merged to form Jewish Family & Children Services of Greater Philadelphia (JFCS) began offering services in Philadelphia as early as 1855. Although its name and mission have evolved since then, JFCS has always focused on serving as a social safety net for people of all ages and creeds. The agency currently has 300 employees in 10 offices, offering a variety of social services for all ages. The organization's total budget for 2003 is $16 million. During fiscal year 2002, JFCS served about 40,000 unduplicated clients. (The term client includes the person being served directly and his or her family.)
Since 1953, JFCS has provided elderly services that focus on keeping people in the community in the least restrictive setting possible. JFCS has several departments involved in serving the older population.
- Core Services for Older Persons provides subsidized services, such as assessment, care management, support services and counseling, in residents' homes or in the program's offices. The program serves community-dwelling, homebound older people throughout Philadelphia and its adjoining counties.
- The City Line Aging Support Program (CLASP) provides outreach and service coordination to frail, isolated elderly in the City-Line/Wynnefield Heights area, which has a high density of very poor people age 65 and over.
- Senior Horizons is a private-pay geriatric care-management program. This unsubsidized program helps generate income to support the subsidized programs.
- Boarding Home Outreach Project serves residents in 18 boarding homes that house deinstitutionalized people with mental health conditions. The program employs a nurse who provides health education, advocacy, and organizes wellness groups, as well as a chaplain who performs nonsectarian services on the Sabbath and holidays. All age groups are served.
- Critical Needs provides emergency financial assistance for people of all ages in economic need.
Evolution of the NORC Service Program
JFCS's work with the five Center City apartment buildings began in the early 1990s when the retired Dean of Temple University's undergraduate School of Social Work approached a JFCS employee to ask for help with a conference. The employee helped arrange for speakers at a conference on Medicare and Medicaid for residents of the four co-ops. About 1,000 people attended the free event in 1992.
Following the success of the conference, its organizer approached the agency employee about the need for a social worker at one of the buildings to help residents find and secure the services they needed to remain at home. Despite strong resistance by a vocal minority of residents in this building who did not want the building to resemble a nursing facility, JFCS created the original Services to Apartment Residents (STAR) program in 1993. Under this program, a social worker visited each building to help residents arrange for services with JFCS and other community providers and to place people who could not live on their own into group residential settings such as nursing homes and assisted living facilities.
Other service programs have been tried in the buildings. For example, in 1994, a board member at the one of the buildings arranged for a local hospital to have a nurse visit periodically. The hospital participated in the hope that making a nurse available would increase its admissions. When it became clear that admissions were not affected and the board member supporting the nurse's activities went off the board, the hospital dropped out of the program.
In 2002, JFCS obtained the AoA grant to expand the STAR program, starting in August 2002. Under the expanded program, which was renamed STAR NORC, the social workers spend one half-day a week in each of the five buildings. The primary benefit of the expansion has been the evolution of the program from a reactive one, where workers only dealt with people who needed a service, to a more proactive one, under which a nurse, group educator, and chaplain provide group services. Grant funding also permitted an increase in the number of social workers from one to three; this increase enabled the workers to reach out to residents who previously did not seek services.
Services Available to NORC Residents
The goal of the STAR NORC program is to keep older people living independently in the community in the least restrictive environment for as long as possible. The program targets people who are isolated or who might have problems remaining at home. JFCS has not created any formal eligibility criteria for services.
The JFCS social workers are the key actors in the STAR NORC program. A social worker spends four to six hours a week in each building coordinating services for residents, formally interviewing residents who have requested or been identified as needing services, and seeing residents by appointment or drop-in. When not on site, the social workers arrange for services for the residents, speak with families, work with the manager and board of the building, and recruit for the various group events provided by STAR NORC staff. These staff--the geriatric nurse practitioner, the chaplain, and the community educator--tell the social worker about residents they believe may need help. All of the professionals make initial contacts with residents through the programs that they conduct in the five buildings. In addition, when the social worker finds that a resident has a particular need, he or she will arrange for the appropriate professional to help the resident. Building management will also alert the social worker when they know of a resident who may need assistance.
The staff who conduct group meetings and see individual residents work under contract with JFCS. A geriatric nurse practitioner spends four hours each week in each of the five buildings visiting residents or holding "drop-in" hours for residents; this time also includes a monthly program on a health topic, such as "questions to ask your doctor." The nurse practitioner also provides preventive health services such as blood pressure screenings and advice about medications. The nurse sees individual clients in their apartments to discuss their health problems, take medical histories, assess residents' physical and mental functioning, and review medications. After obtaining the resident's permission, the nurse may contact his or her primary care physician about any problems in communication. The nurse currently works with 43 people, all of whom were referred by a social worker. A community educator facilitates group socialization opportunities once a month in each building; most of the participants are women in their late 80s or early 90s who cannot get out of the building without great difficulty. A geriatric psychiatrist is on call through JFCS to provide services to residents, if needed. All of the group activities are delivered in the apartment buildings, and the individual services are delivered in residents' apartments or the social workers' office in the building. Residents do not pay for their STAR NORC services because the program does not want to discourage participation. In the future, the program will explore some method of co-payment such as a membership fee for those wanting to attend group meetings.
In addition to the services provided directly by the program staff, the social workers offer information and referrals for services provided by outside agencies, including JFCS. JFCS services include in-home assessments and care plans, case management, home care, shopping, individual or family therapy, guidance on alternative living arrangements, support groups, outreach to Jewish Holocaust survivors, respite care, meals, and transportation. When residents receive homecare or chore services, they pay between 25 and 30 percent of the cost of the services; other services are offered at market rates. JFCS also provides spiritual counseling through its chaplain, who is an intern at the agency. Although the intern is training to be a rabbi, the counseling is nondenominational and he refers people to practitioners of other faiths upon request. The chaplain offers one program a month in each building.
Transportation is one of the most frequently requested services. The local transportation system for seniors is viewed as extremely unreliable, and residents avoid using it rather than risk being stranded somewhere for long periods of time. Residents generally have to rely on the subway, taxis, and buses. The STAR NORC program has begun to develop paratransit (i.e., public transit for people with disabilities) and other pooling options to address the transportation problem. In addition, STAR NORC issues transportation vouchers for taxis, and volunteers sometimes provide transportation. In spite of these initiatives, transportation remains a problem that STAR NORC staff feel has been only partially addressed.
JFCS makes extensive use of volunteers to help provide some of its services to NORC residents. All volunteers undergo a criminal background check and receive a training manual. The social worker fills out a volunteer request form based on discussions with residents about their need for services and tries to match a volunteer with the resident. The volunteer who agrees to provide services sends in a confirmation form and files monthly reports that describe the services rendered to the resident.
JFCS had about 40,000 unduplicated clients for all of its services in fiscal year 2002;1 this count includes clients of all ages and residents of the five STAR NORC buildings as well as those in JFCS's other services areas. During the same period, the original STAR program had 102 clients and provided information and referral services to 224 clients. In the first 10 months of the expanded program (August 2002 through May 2003), STAR NORC had 325 clients and 506 instances of information and referral services.
JFCS supplied the following demographic data on their STAR NORC clients from September 1, 2002 through April 28, 2003: 17 percent were age 90 or older, 49 percent were age 81 to 90, and 24 percent were age 71 to 80. Sixteen percent of clients were divorced, 12 percent were married, 17 percent had never married, and the remainder were widowed.
Program participation varies across activities. The chaplain had a total of 116 people attend the eight programs he conducted in two buildings over eight months. Maximum attendance at a program was 15. Several programs have brought in six to eight participants and one had no attendees.2 In a four-month period, the nurse held 13 group meetings attended by a total of 104 people. In addition, she averages 43 individual visits per month. Group meetings address such topics as Heart Health, Questions to Ask Your Doctor, Memory and Aging, Recipes for Healthy Living, Blood Pressure Screening, and Test Your Stress Level. A group specialist has been holding psychoeducational discussion groups for six months in all buildings on a biweekly basis. Attendance averages 11 people per session.
NORC Service Program's Communication Methods
The STAR NORC program uses many communication methods with residents of the five buildings. Written materials include newsletters, flyers, brochures, and monthly advertising in building newsletters. Buildings have in-house television stations that announce STAR NORC activities. The program also maintains contact with the residents it serves via telephone and makes available telephone numbers where other residents can obtain general information about available services. The geriatric nurse practitioner's monthly health screening provides a means of communicating with residents individually.
Program staff have found that flexibility and persistence are important in communicating with residents. For example, the health educator placed flyers throughout the buildings and met informally with residents to announce program activities. She found that flyers are effective but not sufficient because not everybody responds to them. So, she made calls to key residents who helped spread the word to other residents prior to the scheduled program.
NORC Service Program Challenges
JFCS has faced sporadic resident resistance to STAR services. When JFCS originally presented the STAR program to the boards in the five buildings, they encountered resistance from some residents who did not want their buildings "turned into nursing homes" through the provision of services. Certain accommodations have been made to assuage these residents' concerns. For example, the nurse who conducts programs and visits residents wears street clothes. Residents also resist using mental health services; some program staff speculate that residents do not want the stigma attached to the use of such services. JFCS has even faced resistance from building management when it has offered to hold seminars, provide one-on-one counseling, or do group work when traumatic events, such as a suicide, occur in a building. Building managers turned down every free offer except for services offered after the 9/11 attacks. JFCS has dealt with this resistance by using health screenings and other programs in which professionals interact with residents to identify residents who may need services and to make discreet referrals to the geriatric psychiatrist, social workers, and other professionals.
There are some major problems in the physical environment of the five buildings. Some residents need home modifications such as grab bars in showers to be able to stay safely in their homes. Perhaps the biggest environmental issue is the lack of acceptable transportation options. For example, paratransit services are unpopular because they require making an appointment. Residents also feel that they waste a considerable amount of time because they have to travel long distances and must wait to be picked up when going home. Getting people to doctors' offices is one of the most challenging issues because people have to commit to appointment times and then may get delayed due to transportation problems. Staff have not yet identified an acceptable and affordable solution to this problem.
NORC Service Program Quality Assurance and Outcomes
The STAR NORC program has no formal outcome measures yet, but informal feedback from residents is available from resident interactions with various program staff. In addition, when the social worker closes a case, he or she gives the client a satisfaction form to fill out that provides an indication of both the outcome and quality of the interaction. Social workers may also interview clients or the clients' families.
According to the building manager we interviewed, some residents have been able to remain in their homes rather than going into an assisted living facility because of the availability of program services. STAR NORC also relieves the burden that the building manager would have, were he or she to broker services for residents. For example, when the manager notes that a resident has become reclusive, he or she can refer the problem to JFCS. Residents often benefit from contact by the program since, in some cases, the residents have not realized how much help they needed.
NORC Service Program's Funding Sources
The JFCS funding for the STAR NORC program comes from building fees that range from $5,000 to $7,500 a year per building; grants from foundations, such as The Pew Charitable Trusts, and The Connelly, Tuttleman, and Clayman Foundations; and from resident payments. The foundation grants for older people amounted to $2 million in 2003. Buildings pay $25,000 (about 13 percent) toward the STAR NORC budget. At present, state programs have no role in funding STAR NORC programs. However, in July 2003, STAR NORC staff met with the Pennsylvania Secretary of Aging who expressed great interest in this program and has offered to make available some state funds. Although JFCS is considering pursuing Medicaid funding, the potential may be limited because many residents with low incomes have financial resources that exceed Medicaid's eligibility standard.
Recommendations
Our discussants had two main recommendations. First, they noted that it is important that any NORC service program seek and receive buy-in from most residents before beginning services. Second, program organizers should make sure that events are properly marketed so that attendance is high. Specifically, the elderly population is not likely to attend events that present aging in any negative way.
SUMMARY OF THE SITE VISIT TO UNITED JEWISH FEDERATION OF PITTSBURGH'S NORC PROJECT
The following information comes from discussions with 13 staff from the three agencies that operate the Pittsburgh NORC Demonstration Program under the auspices of The United Jewish Federation of Pittsburgh. The three agencies that jointly run the program are Jewish Family and Children's Services of Pittsburgh (JFCS), the Jewish Association on Aging (JAA), and the Jewish Community Center of Greater Pittsburgh (JCC).
In 2002, the three agencies jointly applied for and received a grant from the Administration on Aging (AoA) for $197,400. The AoA grant enabled the three agencies to set up a new, joint program designed to help older people remain in their own homes through development of individualized care plans based on a comprehensive, in-home assessment of need and provision of information about and referrals to appropriate community services. In certain emergency situations or in cases where a client demonstrated difficulty in seeking services on their own, program staff assisted clients in connecting to services. Using the second round of grant funding they received in federal fiscal year 2003, program staff plan to help connect more clients to services. This site visit focused on activities in the first year of funding under the AoA grant.
Description of the NORC and Its Residents
The NORC program serves adults age 60 and older living in the following contiguous Pittsburgh neighborhoods: Squirrel Hill North and South, Point Breeze, Regent Square, Swisshelm Park, Oakland, and Greenfield. As of July 31, 2003, the program had 60 clients.
According to the 2000 Census, Squirrel Hill South has the highest number of elderly men living alone at about 267 and the second highest number of elderly women living alone at 657 compared with all other Pittsburgh neighborhoods. About one-third of the elderly population living alone in Squirrel Hill and its adjacent neighborhoods has a low income, defined as less than 200 percent of the federal poverty level (FPL). Squirrel Hill also has the highest number of older Soviet Union immigrants in the Pittsburgh area. This population came to the area in the 1980s and is generally among the younger members of the elderly population. The neighborhood has also attracted Asians during the 1990s who were drawn to the universities and medical service opportunities in the area. The black population represents about 10 percent of the neighborhood's residents and is generally under age 65. With the exception of recent immigrants, most of the elderly population in Squirrel Hill has aged in place.
Squirrel Hill has been considered a Jewish neighborhood for the past 60 to 70 years. The Jewish community organizations in Pittsburgh are headquartered primarily in the southern part of Squirrel Hill in close proximity to one another. This area includes much of the lower income population; however, these organizations serve the entire neighborhood.
According to the 2002 Pittsburgh Jewish Community study, one-fifth of Jewish households in Greater Pittsburgh report needing assistance with an elderly relative, with one in ten reporting it was very difficult to get assistance. While use of social service organizations such as JCC, JFCS, and JAA among survey respondents in the Jewish community ranged between 5 and 26 percent, an overwhelming majority of users would use them again or recommend them to someone else (74 to 91 percent).
Squirrel Hill's physical environment creates barriers to independent living for the older population. The community has apartments, semi-detached housing, and detached homes that are often located on hills, have poor sidewalks, and require residents to mount many stairs to get to their homes. Not all apartment buildings have elevators. Since there is very little new housing, residents would have to renovate their homes to improve accessibility, and many cannot afford to do so. So accessibility remains a concern for these older people.
The neighborhood has four universities that partner with local agencies to run community programs such as JAA's Council Arts Program, which is a collaboration between JAA and Generations Together, a component of the University of Pittsburgh's Center for Social and Urban Research. The program brings older people at JAA's adult day services, assisted living, and other community sites together with high school students and resource artists to paint, quilt, write stories, and play music. The universities also have libraries, a music hall, lectures, and other cultural activities that help anchor the community. In neighborhoods adjacent to Squirrel Hill, there are "first rate" medical institutions, including hospitals and mental health services.
The neighborhood is self-contained in that people who are still mobile can get to shopping centers and have most of their needs met within a few blocks of their homes. Transportation from Squirrel Hill to the universities and downtown Pittsburgh is convenient but older people who have difficulties with mobility face problems getting transportation to doctors' appointments, shopping, etc. because getting to and then on and off the buses is difficult. There is a public transportation system called ACCESS, which is accessible but requires people to make arrangements and purchase tickets in advance. People also must spend a great deal of time waiting to be picked up and dropped off at their homes.
NORC Building Management and Communication with Residents
The NORC demonstration program does not have any formal links to particular apartment buildings in the community. Rather, it endeavors to serve the entire community. It communicates with community residents through a mailed monthly calendar; articles in the Jewish Chronicle (the weekly community newspaper); distribution of the NORC program brochure; regular, ongoing marketing efforts of the three partner agencies; and community education programs. For program clients--those seniors who have had a thorough needs assessment and who have been provided with a care plan listing contact information for appropriate community resources--contact is maintained via follow-up calls every two weeks and subsequent quarterly follow-up calls.
NORC Service Organizations
The United Jewish Federation of Pittsburgh contacted JAA, JCC, and JFCS about the opportunity to obtain the AoA grant. JAA takes the lead in coordinating the three agencies' NORC activities and its traditional service area is home and community services. JCC has its roots in the Jane Addams Settlement House, which served immigrants to the Pittsburgh area beginning over 100 years ago. Since World War II, the JCC has operated in Squirrel Hill, adding a branch in the southern suburbs of Pittsburgh in the late 1990s. JFCS provides a wide range of services for people of all ages and served 30,000 people in 2002. The JFCS is an accredited social services agency, which also provides services to people of all ages. The agency's $3 million annual budget comes from government, fees for services, foundations, contributions, donations, and the United Way. JAA began operations in 1993 and is the most recent entrant to Jewish community services. It consolidated the kosher home-delivered meals program, which had been operated by JFCS, with its adult day services program and added new programs, such as Sivitz Jewish Hospice. In addition to coordinating the NORC demonstration project, JAA operates residential and rehabilitation facilities and an information-and-referral phone service called ElderLink. Elderlink is a collaborative effort of the three service agencies. Residents can contact the NORC Demonstration Project by dialing the number for ElderLink.
The three agencies crafted a memorandum of understanding under which they operate the NORC program. They collaborated on developing and training the care teams (see below). The care plans the teams developed link clients to existing community resources and also help identify any gaps in service. These gaps are brought to the attention of the interagency NORC workgroup for problem-solving discussion and action planning. The program also links clients and caregivers, as appropriate, to support groups facilitated by the agencies.
The three agencies share responsibility for working with Unicentric, Inc., to design, develop, and continually refine the software used for the project's web-based information system. The system serves as the communications center, data warehouse, care plan preparation method, and project management center. JCC has the lead daily contact with Unicentric, Inc., working with the firm to coordinate the training of work group members in use of the information system. JAA has chief responsibility for preparing and distributing a monthly calendar that informs clients and families of NORC-related programs, educational events, and support group meetings.
Evolution of the NORC Service Program
Prior to development of the NORC Demonstration Program, JAA had a program called "Neighbors." Neighbors started in 1995 providing services in three large apartment complexes with at least 50 percent of the apartments occupied by at least one older person. Services include wellness, education, social services and activities, and monitoring of clients' physical conditions.
The three agencies noted the difficulty that some older people were having remaining independent in their homes. So they created the NORC Demonstration Program with the goal of helping people remain independent in their homes. They targeted people age 60 or older, establishing two interdisciplinary "care teams" each composed of one member from each agency to inform older people about available community services. The teams each have at least one clinical social worker. After the care team assesses the client's needs and available support network, they provide information to the client about services and programs that are available to help them meet these needs.
The NORC project was designed, in its early stages, to take advantage of the partner agencies' knowledge and experience to link clients to existing community services such as JAA's home and community services, JFCS's geriatric social work assessment and care management services, and JAA's senior adult programs. In the program's second year, activities will be expanded to include serving additional clients, following up on existing clients, and helping them to secure services.
Since the three agencies had rarely worked together in the past, they used part of the federal grant to fund an equine training program designed to promote group collaboration and team building. To meet the challenge of bringing staff together from three different agencies with different cultures, histories, and operating procedures, throughout the project's first year, project coordinators from the three agencies met regularly to continue working on and strengthening interagency collaboration. This collaboration is crucial to the project's success. These discussions will continue for the duration of the project.
Services Available to NORC Residents
The NORC Demonstration Program began sending three person care management teams to visit clients in their homes on December 1, 2002. Since that time, 60 clients have received home visits (as of June 26, 2003) with comprehensive assessments of their health, wellness, psychosocial skills, and mental attitude. The care team obtains assessment information during the home visit from the client, personal observations, a home check, and from family members or caregivers, when available. The team meets within one week after the assessment to develop a care plan for the client. The care plan specifies the community services that could benefit the client, including those provided by the three agencies, and provides contact information for the client to use to obtain services. A care management team member follows up with each client two weeks after the client receives the care plan and then quarterly thereafter to determine whether clients have contacted available community services.
There is a proposal under review for a new van service to overcome problems identified (and mentioned above) in getting less mobile clients, and community seniors generally, to doctors' appointments, shopping, to programs, etc. The review is being coordinated by the United Jewish Federation of Greater Pittsburgh, with major input from JAA, JFCS, and JCC.
NORC Service Program's Communication Methods
The program faced two communication challenges--interagency communications and communication with the community at large. The three collaborating agencies worked together to redesign and consolidate the agencies' existing assessment forms into one assessment tool that all could use. Although the project teams meet monthly, staff are located in different agencies and therefore need a way to communicate easily about clients. The agencies tackled this problem by hiring Unicentric, Inc., as noted above, to set up a virtual office and create uniform electronic formats for the redesigned assessment tools, ensuring that client's charts were accessible to all.
To recruit clients from the community, the program publishes articles in newsletters and calendars with information about the program and distributes these materials to social service agencies, doctors' offices, and other organizations. Clients have come to the program upon referral from these and other professionals. The program also held two public forums at different sites, including the JCC. Apartment building managers have also referred residents to the program and allowed the program to leave brochures in their buildings. Although the program does not have any special links to specific apartment buildings, it is currently exploring ways of developing such connections.
Despite these communication efforts, most of the program's initial clients were already connected to one of the three agencies in some way. Some participated in Neighbors, some were repeat callers to ElderLink, some were identified by JFCS geriatric social workers and other staff, and others participated in JCC activities.
NORC Service Program Challenges
The program has faced two major challenges, one internal and one related to program activities. The equine team building exercise, online communication, and, especially, regular meetings among the three agency project coordinators helped overcome the internal challenge of coordinating the activities of the three agencies. The activities-related challenge was that many clients failed to secure the community services that the care plan outlined. Barriers clients face in securing services include lack of an informal support system to facilitate connections, dementia, lack of money to pay for services (when payment is required), and an unwillingness to admit that they need help. The program is seeking to address this challenge through increased follow-up with clients.
NORC Service Program Quality Assurance and Outcomes
The only quality assurance activity is informal, positive feedback from clients. The program is considering implementing a client satisfaction survey during the second grant year to provide more consistent feedback.
NORC Service Program's Funding Sources
Funding sources for the program are the AoA grant and in-kind contributions from the three agencies. The project's total funding for 2002 through 2003 was $328,271 ($197,400 federal, the remainder in-kind). The program has been granted $250,000 in U.S. Administration on Aging funds for 2003 through 2004, with a total project cost of $334,342.
Future Plans and Recommendations
The Pittsburgh NORC Demonstration Project has already determined that it will maintain follow-up contact with the 2003-2004 clients to ensure that they are actually connecting with the services recommended in their care plans. The project also plans three community-oriented informational programs that will target families of elderly individuals and one program for social service agencies interested in what the demonstration project has accomplished and learned. Partnership opportunities with these agencies will also be explored.
NORC staff said that service programs cannot simply supply information to clients about available programs; staff must help clients access those programs. Unless there is a crisis, clients and families do not always recognize the benefits to be gained from participating in the service programs identified for them and so may not take action. And sometimes the family and the client have different agendas. For example, the family may want elderly clients to move into protected settings, while the elderly might prefer to remain in their home. NORC programs might well consider developing information programs for family members to bridge this gap.
SUMMARY OF THE SITE VISIT TO THE NORC PROJECT
The following information is based on discussions with the following 20 people on September 9, 2003: the NORC Coordinator, two advisory committee members, one staff person each from Jewish Family & Children's Service (JFCS), Jewish Community Center (JCC), and Covenant/CHAI Senior Housing, four NORC residents, and 10 research team members from the Washington University in St. Louis Center for Aging.
Description of the NORC and Its Residents
The Jewish Federation of St. Louis, which received the AoA grant, is taking a different approach than the other four AoA grantees in that St. Louis is studying the community and several types of programs in depth before designing its NORC service program. The Center for Aging at Washington University in St. Louis is partnering with the grantee to conduct the research.
Grantee staff define a NORC as an unplanned (naturally occurring) building, complex, neighborhood, or community housing in which there is a disproportionate number of individuals age 65 and older. These communities develop when residents age in place or people relocate to the community after age 50.
Using 2000 census data, research staff determined that "census tract 2150.02 and part of census tract 2153.01," which cover approximately one square mile in the western end of St. Louis, contained a large proportion of older people. Staff studied this area because it is adjacent to JCC, JFCS, and the publicly funded senior congregate housing site (Covenant House/CHAI), which has been in existence since the early 1970s for retirees and low-income older adults. The site has on-site services and programs for residents such as meals and activities.
The NORC community evolved, in part, through white and Jewish migration west to avoid integration in St. Louis City and the old neighborhoods of University City during the 1970s. Younger white families moved to Creve Coeur, which was a rapidly expanding area of new homes, schools, and small businesses. Jews migrated to the area to be closer to the JCC and a growing Jewish community. From 1961 to 1981, the number of Jewish households in the area increased by 25 percent. At present, the percentage of the population that is Jewish is declining (for unknown reasons).
The people who moved to Creve Coeur have aged in place. They have been joined by some older people who have moved to the neighborhood to be close to family, friends, or the JCC. Most Covenant/CHAI congregate housing applicants come from the community's condominiums and apartments and are people who report feeling isolated due to the "lack of community feeling" in the private residences.
The Creve Coeur neighborhood's private residences are not accessible to older adults who are frail or have mobility problems. The largely garden-style apartments have several stories and no elevators. These apartment complexes typically are 30 years old and were not built to be accessible in that they lack such things as walk-in showers, grab bars, or levers for faucets. The hilly neighborhood has few sidewalks, which makes walking to service providers and stores difficult, and limited public transportation. The neighborhood's ranch style houses have one step into the house, sometimes steep driveways, and laundry facilities typically located in basements that are difficult for older residents to access. The carpeting in homes may hinder residents' mobility, especially for those who use assistive devices.
Residents who can still drive have access to a broader range of services and activities. The neighborhood has the JCC, JFCS, two churches, a grocery store, a kosher restaurant, a gas station, a restaurant area with a movie theater, and a gym. Service providers and restaurants are at opposite ends of the neighborhood. However, signage in the area is poor and many residents are less comfortable driving at night, which can limit participation in certain activities.
NORC Residents
The Center for Aging used Census 2000 data to develop a profile of the NORC and its older residents. A total of 4,370 people live in the NORC community. Eighty-two percent of NORC residents are Caucasian, 7 percent African American, and 6 percent Asian. Grantee staff say that the neighborhood experienced an influx of Russian immigrants in the early 1970s and late 1980s. Comparable percentages for St. Louis County as a whole are 77 percent Caucasian, 19 percent African American, and 2 percent Asian. About 11 percent of the population has incomes at or below the federal poverty level, compared to 5.3 percent of St. Louis County.
Thirty-one percent (of the 1,337 NORC residents) are age 65 or older. Sixty-nine percent of this older population is age 75 or older, a large number of whom live in the congregate housing site, where the mean age is 79. The majority of older people are women living alone. Twenty percent of people age 65 or older report having a disability. Among this 20 percent, the most frequently reported disabilities are physical problems (44 percent), difficulty going outside alone (25 percent), sensory disabilities (17 percent), mental disabilities (8 percent), and self-care problems (7 percent) (individuals could report more than one disability).
NORC Building Management and Communication with Residents
The NORC has several privately owned apartment complexes and condominiums, as well as a publicly funded congregate senior housing complex. These complexes are receptive to programs for older people to varying degrees. Each private complex has a management company or a condominium association board. Most of these entities have been reluctant to assist their older residents, according to grantee staff. Apartment managers are reported to be uninterested in home modifications, likely because of the cost. Condominium boards have also resisted making modifications, perhaps because they would rather have older people move out than make a safe or comfortable environment for them. One exception is an apartment complex managed by an Ohio-based company that, until recently, sponsored programs for all residents, particularly those who are older. For example, the complex established an after-school program in which older residents tutor children. The complex has also sponsored bagel breakfasts. These programs are being cut back and it is not clear why. Covenant/CHAI has a number of programs for its residents and has a tenant council that meets every other month to advise on program planning and other issues of concern to residents.
NORC Service Organization Structure
The two partner agencies--JCC and JFCS--offer mental health, limited transportation, recreation, socialization, nutrition, adult day services, and homemaker assistance. JCC administers the adult day care and cafeteria-style nutrition programs, which are open to the community and located in the Covenant/CHAI house. The nutrition program is the most successful program in terms of use; it provides a congregate meal five days a week to approximately 200 residents.
The Covenant/CHAI house offers limited programming, which includes one social worker for each of the three buildings. These staff used to limit their activities to such things as helping residents fill out food stamp applications, but now staff refer residents to service providers, such as housekeeping services. The staff also make arrangements for services such as podiatric care, nutrition, employment counseling, home health services, and blood pressure checks. Although these services are open to the community, those taking advantage of them are generally building residents.
Evolution of the NORC Service Program
Grantee staff believe that doing primary research on the service needs of the NORC community is the best way to determine which types of NORC service programs would be most responsive to community need. The goals of the new programs will be to stabilize the neighborhood, improve property values, contribute to the economic vitality of the business community, and offer cost efficiencies in service delivery. Staff contacted the Center for Aging and asked them to conduct the research because the Center offered a multidisciplinary approach to studying older adults.
NORC Service Program's Communication Methods
An external advisory committee was developed with representatives from service providers, churches and temples, resident complexes, state representatives, and lay leaders to provide input into the development of the service program. The committee had met once as of September 2003. The goal is to have the advisory committee be the vehicle of communication with NORC residents. In addition, the advisory committee has plans to publish a quarterly newsletter about the NORC service program as it develops.
Studies Related to Services Program Development for the NORC
The Center for Aging screened 494 NORC residents out of a total population of 1,337 people age 65 and over to determine their suitability for participation in one or more of seven studies. People were eligible to participate in the studies if they were age 65 or older, lived in the NORC, and did not have dementia.
Researchers said they did not have sufficient time because of grant funding deadlines to select a random sample of NORC residents, so they recruited volunteers from the community. Participants were recruited using a variety of methods, including visiting people in their homes, direct mail, and word of mouth; staff considered this last method to be the most effective way to recruit participants. Staff held a "kickoff breakfast" in September 2002, which approximately 200 NORC residents attended. Then staff made presentations at places older people in the community were likely to frequent, such as churches and shopping centers. Research staff did some limited mail recruiting from Covenant House, and also included Covenant House residents if they volunteered.
Recruiting took longer than researchers had anticipated because multiple contacts were necessary to assure older adults that no one was going to invade their privacy. Many potential participants were reluctant to join the study or too busy. Others did not understand why staff were talking about offering programs when no program yet existed.
The volunteers completed an initial telephone screening interview, which lasted 10 to 15 minutes. The researchers could not say how many of the people screened had dementia. People that completed the interview were demographically similar to NORC residents.
Of the 494 study participants,
- 72 percent lived in privately owned or rented condominiums, apartments, or houses;
- 69 percent were female and 59 percent of all participants lived alone;
- 33 percent did not drive;
- 14 percent still worked;
- 36 percent volunteered; and
- 17 percent were family caregivers.
On average, they had 13.5 years of education and were 79.3 years old.
Analysis of the data has not yet been completed, but early results indicate that older residents need transportation, knowledge of available community resources, home delivered meals/meal preparation, in-home care, and access to health care. Next steps for the researchers are to complete the data analysis and finish the seven studies that are in various stages of development.
The seven studies include the following:
-
Needs assessment. Of the 494 participants, 320 will participate in a one-to-two hour interview to gain information on residents' personal characteristics, social support networks, self-rated health, well-being and life satisfaction, social and religious activities, current service use and unmet needs, and perceptions of the neighborhood. The interview relies largely on standardized measures, such as a depression scale and an activity checklist. Trained graduate student interviewers conduct the interviews.
-
Community Connections. Eleven participants were recruited for an eight-week wellness program. Researchers first conducted focus groups with 48 participants who expressed interest in this type of program during the telephone screening. The focus groups were designed to elicit information on the residents' sense of health and wellness, concerns, enablers, barriers to engaging in everyday activities, and level of interest in a new wellness program. Focus group participants expressed the desire to feel more connected with the community and to be more aware of available supports and resources. Their concerns about the future focused on finances, driving, where to get support, and feeling alone, and they expressed interest in a course to address these needs. Transportation was also an area of expressed concern.
The course that evolved from these focus groups is called "Community Connections for Successful Aging." The 11 participants were recruited from the focus groups. Researchers had to call far more than 11 people during recruitment because many focus group participants were too busy for the class. Three of the 11 original program participants withdrew for health reasons.
Based on results from questionnaires that program participants filled out before and after the class, participants achieved their personal goals for the class and increased perceived knowledge, self-confidence, and the frequency of healthy behaviors. A few of the participants agreed to be peer leaders for future courses.
-
Home modification. Researchers selected a convenience sample of 80 residents who received an assessment of their homes to determine the modifications necessary to improve safety and/or mobility. Then, residents received any recommended home modifications that they agreed to have free of charge. Residents were chosen based on their responses during the needs assessment. For example, if respondents expressed a fear of falling, they were considered for inclusion in the study. The project was designed to determine the outcomes of the home modifications with respect to residents' quality of life. A follow-up visit will be conducted with all 80 recipients three months after the modifications and the associated training are completed. Researchers will be assessing residents' satisfaction with and confidence in navigating their home environments. The barriers that assessors most frequently encountered included unsafe showers or bathtubs, dim lighting, low or soft chairs, items out of reach, steps at home or entry way, long distances to carry items, and opening jars (jar design). The most frequently employed solutions were grab bars in showers, recessed lighting and lamps, hydraulic seat boosters, reachers for high and low items, ramps, rolling carts for carrying items, and jar openers requiring minimal hand strength or grip.
-
Cognitive mapping. This study had 26 participants who left their home at least three times a week to participate. Participants gave demographic and other information to researchers who conducted "cognitive mapping interviews" in which participants drew diagrams of places they visited during a three-day period. The study found that older people
- tend to use the facilities and resources within the community and "stay within their zip code,"
- try to avoid night activities,
- find construction zones confusing,
- find some street signs difficult to read,
- change doctors and other service providers so routes are accessible,
- use landmarks to guide them in their travels, and
- are frustrated with current transportation options or do not want to rely on family and friends for transportation.
The researchers have concluded that features of the environment that influence the choices older adults make about where they go include lighting, signage, store size, staff friendliness, accessibility, financial incentives, and proximity of services. In addition, NORC residents need transportation options for evening events and cultural and social activities that are both flexible and inexpensive. Municipalities need to be aware of the importance of signage, construction zone planning, and landmarks.
-
Service provider survey. Ninety-nine service providers, including local Area Agencies on Aging (AAAs) , health care agencies, transportation providers, and counseling providers, received mail surveys to determine their perceptions of gaps in services and the needs of the NORC's older population. Twenty-seven percent of the surveys were completed; these were used as the basis for the data analysis.
-
Family Education/Communication. This project is designed to help NORC residents and their adult children make decisions about service needs and preferences before a crisis occurs. The sample consists of 30 older residents who are single and have at least two of their adult children living in the St. Louis area. Methods included a mail survey and an interview with residents to gather information that was not captured in the needs assessment. Participating families received an in-home educational session with parents and their children that utilized an individualized workbook consisting of responses from each family member's surveys. The session also focused on the families' communication skills and decision making processes. Researchers follow up with assessments one month after the educational sessions to see how family relationships changed. This study is not yet complete.
-
Informal Support Systems. The purpose of this project is to identify and describe the types of informal and formal support networks that exist among NORC residents. The researchers conducted field observations, informal interviews with 35 key informants, and five focus groups. The interviewees were those who answered, "Yes" to the question "Do you help your neighbor or friends?" on the needs assessment.
Preliminary findings are that residents moved to the NORC to be close to services, close to family and friends, to find security, and to find housing adapted for older adults (e.g., buildings with elevators, ranch-style houses). Characteristics of people who provide informal support include "do gooders," people with special talents, immediate neighbors, and kinship groups. The types of support these people provide include transportation, picking up groceries, carrying heavy loads, picking up newspapers or mail, sharing information, helping in emergencies, and watching out for very frail people. There are limits to how much help people will provide with transportation because some feel overwhelmed by the volume of requests they receive. Some people expressed reluctance to give help in emergencies because of fear of liability in the case of accidents. People watch out for their frail neighbors but expressed the thought that those who are frail should move to another environment because they might harm themselves or others. The kinds of help that people will not provide include transportation for frail people and help with personal care needs. Finally, people are reluctant to help those who are not congenial.
NORC Service Program's Communication Methods
An external advisory committee was developed with representatives from service providers, churches and temples, resident complexes, state representatives, and lay leaders to advise on the development of the service program. The committee had met once as of September 2003. The goal is to have the advisory committee be the vehicle of communication with NORC residents. In addition, the advisory committee plans to publish a quarterly newsletter for NORC residents about the NORC service program.
NORC Service Program Challenges
Although staff have not yet developed the service program for the NORC, they anticipate some challenges. One is NORC residents' lack of awareness that JCC and JFCS serve people who are not Jewish. In addition, it will be challenging to serve people in single-family homes because of the difficulties in finding an activities center in such neighborhoods. Another issue is that staff believe that residents do not want to hear about services until they need them, nor do they want to live in an area where residents are perceived as needy. Finally, it is hard to recruit Asian NORC residents because of language barriers and the fact that Asian elders often take care of their grandchildren and stay within their own communities.
NORC Service Program's Funding Sources
The AoA grant amounted to $1.26 million. Approximately $500,000 is being used to fund the research that the Center for Aging is conducting. In the future, The Jewish Federation hopes to provide administrative funding for the project sufficient to cover one staff person and mailing and printing costs. The original 17-month grant award has been approved for a 12-month, no-cost extension. The conclusion of the grant is now December 31, 2004. Future funding sources will be determined as the service program develops.
Recommendations
No recommendations were provided at the time of the site visit.
NOTES
-
One client can refer to one person or may include a family, so the impact may be greater than the number indicates. JFCS may be understating the impact on the community.
-
Maurice Harris, Report on NORC Building Programs, April 2003.
APPENDIX 3. Comparison of the Conceptual Model by NORC Sites
| COMPARISON OF THE CONCEPTUAL MODEL BY NORC SITES | |||||
|---|---|---|---|---|---|
| Baltimore's Senior Friendly Neighborhoods (SFN) | Cleveland's Community Options Program | Philadelphia's STAR NORC Program | Pittsburgh's NORC Demonstration Program | St. Louis's NORC Project | |
| NORC Definition | Residents 62 and older living in Baltimore's Upper Park Heights neighborhood and the Milbrook building. Services provided in 13 buildings with plans to expand to neighborhoods with row houses and single family homes. | NORC program exists in 5 private apartment buildings east of the Cuyahoga River in Cleveland. | NORC is comprised of 4 cooperative buildings and 1 condominium located in the Center City section of Philadelphia. | Adults 60 and older living in Squirrel Hill, Point Breeze, Regent Square, Swisshelm Park, Oakland, and Greenfield neighborhoods. | Used Census data to determine specific census tracts covering approximately 1 square mile in Creve Coeur, St. Louis, that contains a large proportion of older people and is the site of several Jewish community services. |
| Community Resources | JCC, Myerberg Senior Center, Baltimore Hebrew University, synagogues and churches public library, shopping areas, public bus transportation, and a senior shuttle. | Apartments are within walking distance of synagogues, shopping, and bus lines. | Within walking distance of health care providers, access to public transportation, close proximity to Temple University and the University of Pennsylvania, museums, and restaurants. | Social service organizations such as the JCC, JFCS, and JAA, 4 universities, libraries, a music hall, hospitals and mental health services, and public transportation. | Service organizations such as JCC, JFCS, and a publicly funded senior congregate housing site (Covenant House/ CHAI), churches, grocery store, kosher restaurant, gas station, restaurant area with movie theater and gym. |
| NORC Formation | |||||
| - Internal | Most residents have aged in place, living in their homes or apartments within the community for over 30 years. | Long-term residents have aged in place, mostly widows. | Most residents have aged in place. | Most of the elderly have aged in place. | Most have aged in place. |
| - External | Some older Russian immigrants who settled in the area in late 1980s. | In migration of elderly residents in their 70s and 80s. | Some in-migration of retirees moving from the suburbs into the city. | In-migration of Soviet immigrant population in 1980s who are generally among the young elderly. | Some older persons have moved to the neighborhood to be close to family, friends, or the JCC. |
| Organizational Structure | |||||
| - Internal | SNF program developed an Advisory Council of resident member volunteers to facilitate resident involvement and empowerment. | Resident advisory councils per building. | Residents approached JFCS about need for a social worker in 1 building. In response, JFCS developed the STAR program. | Advisory committee of residents, members of community organizations, and state representatives to assist in development of NORC service program. Goal to have committee be the vehicle for communication with NORC residents. | |
| - External | Coordinated by 4 Jewish community service organizations. Nurse and resident activities coordinator organize activities and events in NORC buildings. | Began by Jewish Community Federation of Cleveland. A volunteer committee oversees the program. Resource coordinators organize activities and provide referrals to service providers. | JFCS expanded the STAR program into STAR NORC. Social workers are key actors in program along with a nurse, community educator, and chaplain. | Operated by three organizations under the United Jewish Federation. Three-member care teams comprised of one staff member from each sponsoring organization. | Jewish Federation of St. Louis partnered with the Center for Aging at Washington University in St. Louis to conduct research on service program options and the community before designing its NORC service program. |
| Service Program | |||||
| - Internal | Program has hired residents in buildings as on-site coordinators who seek input from residents, and help to publicize and organize activities. Two apartment buildings continue to have residence councils, floor captains, and phone trees that existed prior to SFN program. | Outreach by resource coordinators to determine what seniors want from the program. Resident volunteers help publicize and organize events. | Co-op board or condominium association hears from residents. Residents have monthly House Council meetings, part of which is open to all residents and the rest limited to floor representatives. | Conducting primary research to determine which NORC service programs will be most responsive to the elderly communities' needs. | |
| - External | Case aides, nurse, and resident activity coordinator provide range of services including case management, information and referral to services, preventative health, recreational activities, and transportation. | Social events, preventative health, and referrals to providers. | Services social workers can arrange include in-home assessments and care plans, case management, home care, shopping, individual or family therapy, guidance on alternative living arrangements, support groups, outreach to Holocaust survivors, respite care, and spiritual counseling. | Interdisciplinary care teams develop care plans based on in-home assessments. Provide information and referrals to community services. | |
| Funding | |||||
| - Internal | Small share of program's costs paid by resident member's annual $15 fee. | Financial support from building management includes office space, use of party room, salary and benefits of resource coordinator, and program costs such as paper and copying. Residents pay for costs of activities. | JFCS funding for the STAR NORC program comes from building fees ranging between $5,000 and $7,500 a year per building. Additional resident payments. | ||
| - External | Combination of funding from the AoA grant, the Jewish Community Association of Baltimore, local foundations, and Baltimore County funding. | HUD spend down grant covers overhead costs of main office. AoA grant used to replicate Community Options program in 4 other Ohio sites. | JFCS used AoA grant money to expand the STAR program into STAR NORC. Addition funding includes grants from the Pew Charitable Trusts, and the Connelly, Tuttleman, and Clayman foundations. | AoA grant and in-kind contributions from the 3 coordinating agencies. | AoA grant used to fund research conducted by the Center for Aging at Washington University in St. Louis. Also received grant funding from State of Missouri and uses matching funds from sponsoring organizations. |
| Outcomes | Collect information on the number of people attending programs and using the case aide service. Future plans include a survey of members and nonmembers with service users followed for 1 year and a process evaluation of the program's operations. | Master database tracks participation in activities and houses a computerized referral list of providers. Database automatically alerts resource coordinators to follow up with residents referred to services. Staff remove service providers with a noted pattern of dissatisfaction from list. AoA grant money used to participate in Case Western Reserve University research project that will compare community-dwelling older people in Cleveland with residents in Community Options buildings. | No formal outcome measures, but informal feedback has been obtained by program staff and from interviews with clients' families. Client fills out satisfaction form when a social worker closes a case. | Program contracted with Unicentric, Inc., to create a virtual office with electronic formats and a client database that could be accessed by care teams and program staff who do not share a common office. No formal outcome measures, but informal feedback from clients has been positive. Program is considering implementation of a client satisfaction survey during the second grant year. | No formal outcome measures developed at this time. |