
Web-based Information Exchange and Information Services Concept to Support the Exchange of Newborn Screening Information
Office of the Assistant Secretary for Planning and Evaluation U.S. Department of Health and Human Services
December 1, 2009
The views expressed in this report are solely those of the authors, and do not necessarily reflect the views of the Department of Health and Human Services.
This report is available on the Internet at:http://aspe.hhs.gov/sp/reports/2009/newbornscreenhit/index.shtml
Printer friendly version in PDF format (22 pages) [Free PDF reader  ]
]
ABSTRACT
State newborn screening (NBS) programs for heritable diseases and conditions provide vital health information that enables prevention and early detection of rare genetic conditions. Information management of the screening laboratory test orders and the reporting of laboratory is substantial challenge based on a variety of factors. Advances in health information technology have been advanced through recent work by the Department of Health and Human Services that may ultimately lead to improved program performance. This report assesses the applicability of a service oriented architecture approach to NBS data management to support broad needs in patient care, quality improvement, public health reporting, and clinical research.
Material contained in this publication is in the public domain and may be reproduced, fully or partially, without permission of the Federal Government. The courtesy of attribution is requested. The recommended citation follows:
- Office of Science and Data Policy, ASPE(2009) Web-based Information Exchange and Information Services Concept to Support the Exchange of Newborn Screening Information Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation.
Table of Contents
Rationale for the Newborn Screening Web-based Information Exchange Proposal
Newborn Screening Web-based Information Exchange Technical Overview
Key Stakeholders: Roles and Leadership
Scenario I: NBS Electronic Information Exchange Across State Jurisdictions
Expected Outcomes and Benefits of a Newborn Screening Web-based Information Exchange
Meaningful Use and Web-based Information Exchange Implementation
Community Partnership Opportunities
Risks and Mitigation Strategies
Comparison Examples of Health Systems in Other Countries: Sweden, Taiwan
Summary of Impact of Newborn Screening Interchange Implementation
Appendix: Detailed Overview of Information Exchanges - Current and Future State
Executive Summary
Management of newborn screening (NBS) laboratory test information represents a challenge for state public health laboratories, health departments, health departments, hospitals, and ambulatory care practices. The increasing use of integrated information management strategies for the rising number of screenable conditions and the complexity of their interpretation contributes to the need for electronic health information exchange of newborn screening data as an important test of tools and architecture in this convergence of individual patient care and public health.
This paper presents the rationale for designing and implementing a web-based information exchange intended to support the newborn screening information needs of a community using disparate and heterogeneous information systems with limited system interoperability. The proposed interchange will provide a conduit to facilitate newborn screening information exchange, allow assessment of program performance and improve quality of care.
The newborn screening web-based information exchange concept can improve child health outcomes, and develop a shared vision and establishes an action plan to move forward in a collaborative fashion.
The web-based information exchange will:
- Provide a First Step solution for standards-based interoperable newborn screening data exchange in form of a customizable, scalable assembly of software tools enabling a broad-range of inputs and outputs of data to ultimately enable a service-oriented architecture for newborn screening
- Build on and compliment existing state-based newborn screening and child health technologies
- Enable physicians to retrieve lab order sets and results
- Enable state newborn screening programs to implement and enforce quality measures based on data transparency
- Provide newborn screening information on demand and in response to queries
- Provide a transitional step on the path to a fully integrated state and national health information exchange network
The web-bases information exchange will not:
- Constrain individualized state-based approaches of newborn screening data representation to the clinical community
- Replace existing technologies used by state health departments and providers
The Challenge for Newborn Screening Information Exchange
The communication requirements for successful newborn screening and follow-up have created substantial challenges for state systems, especially with the increasing number and complexity of screening tests. Serious abnormal results need to be aggressively followed up by public health personnel. The resolution of indeterminate results or the completion of confirmatory testing, however, may lag for weeks because communication with the family or primary care provider is delayed. A physician seeing a newborn for the first time in the ambulatory care setting typically follows up on newborn screening results by calling the NBS laboratory. Alternatively, in some states, physicians have the option to check NBS results by accessing a secure web-site or having results faxed to them. A survey by Deposito et al. found that fewer than half of primary care physicians received notification of positive newborn screening results within 2 weeks and 4.5% never received results.1
This challenge represents a communication, connectivity, and coordination issue, which can be addressed through technological, organizational, and policy solutions.
Addressing the Newborn Screening Challenge: A Proposal
This proposal outlines the design and development of a demonstration project to provide electronic connectivity supporting rapid and reliable exchange and management of NBS information. To help states achieve such connectivity at minimum cost and in a short time-frame, we propose the development of a demonstration web-based information exchange in collaboration with a few states and/or integrated care organizations.
The aim of the newborn screening web-based information exchange is to facilitate data exchange between the birth center where the infant is first treated, the public health laboratory where the newborn screening test is performed and the primary care provider, counselors and specialists that participate in the long-term follow-up of the infant. The web-based information exchange should transmit the newborn screening lab test results using federally accepted standards and terminology to facilitate information exchange. Data from participants should be exchanged through the web-based information exchange and should be available for integration into the patients electronic health record (EHR) and personal health record (PHR).
From birth, infants and young children undergo an array of clinical and administrative services designed to give them an optimal start on a healthy life. Within the first 24 to 48 hours of life, each infant receives immunizations, undergoes dried blood spot screening for heritable disorders, undergoes auditory screening to detect congenital hearing loss, and is given a birth certificate. Additionally, the infant may be registered with the Social Security Administration, evaluated for eligibility in Medicaid or the Women, Infants, and Children (WIC) programs, and registered in a birth defects surveillance system.2,3
The following scenario describes the newborn screening test and provides a generic description of processes to exchange newborn screening information at the state level. The scenario begins with the birth, follows the laboratory testing of the blood spot sample, through confirmatory testing and follow-up care. This scenario does not encompass all approaches encountered within the states, but provides a general overview of information flows.
Shortly after birth, nursing staff and/or physicians perform the required collection of the newborn dried blood spot specimen (heel stick). Upon sample collection, the infants record and lab request is annotated with patient-specific information (diet, medications, antenatal history, etc.) and, sent via mail to the state public health laboratory. The infant is also screened for hearing loss using an electrophysiological measurement. In many states, the results of the hearing screen and other information are recorded on the same card that is sent to the newborn screening laboratory. In the laboratory, the patients test request is entered manually into a database and screening tests are performed according to panels adopted by a given state. Once verified, the screening test results are returned to the physician of record, usually associated with the birth hospital, and follow-up providers, if identified by the parents. Results are not provided to follow-up providers located out-of-state. Results may also be sent to state public health programs enabling results to be archived in state registries. If the screening test results yield an abnormal result requiring follow-up testing, the state newborn screening program is responsible for coordinating re-screens, diagnostic services and treatment.
Rationale for the Newborn Screening Web-based Information Exchange Proposal
In order for newborn screening programs to fulfill their patient-centric and population-based responsibilities, an integrated information service is needed. The system must be based on an extensible architectural model that is customizable and allows linking of centralized informatics infrastructures within a distributed organization, such as a newborn screening program.
Integration of state public health information systems in the United States is currently limited. There are a number of exceptions where integration has been achieved at a regional level in the form of the Health Resources and Services Administration (HRSA)-funded Newborn Screening Regional Collaboratives. However, most newborn screening systems consist of data silos that only meet the needs of a single program. While the national, state and professional communities of NBS are well-defined, the delivery of NBS services is complex; in particular, NBS care delivery faces challenges involving communication among very disparate elements of the health care system (hospitals, labs, physician practices and specialties, public health agencies, consumers), and over a patients lifetime. An effective electronic communication and coordination strategy in NBS would improve NBS-based care and serve as a model for:
- Broader use of health information storage and exchange for pediatric or lifelong care
- Communication among various elements of the health care system
- Communication across practice and specialty lines
- Integration of practice and public health information
A web-based NBS interchange capable of information exchange illustrates both the importance of NBS and the nature of e-communication opportunities in this area. Newborn screening is:
- An area of high public health importance
- Mandated by all 50 states including the District of Columbia and most territories
Intersecting public health newborn screening programs with primary care delivery systems to deliver state mandated screening is difficult. The interchange concept is an attempt to achieve better health outcomes in a timely manner, at decreased cost and improved efficiency. In addressing todays challenges before full information system integration and interoperability is achieved, development of an adoptable interchange using existing web infrastructure could obviate the need for state-by-state creation of NBS health information exchange systems or awaiting the advent of a national health information exchange system.
Additionally, secondary benefits of increased interoperability, electronic storage and distribution of NBS data would also:
- Provide new resources for research
- Lay a foundation for use of genetic information in clinical care
- Expand consumer access to information
Newborn Screening Web-based Information Exchange — Technical Overview
Supporting Elements
Over the last several years significant progress has been made preparing for electronic information exchange based on standards and utilizing a health information exchange infrastructure.4,5 As a result, NBS is a strong candidate for activity in health information exchange prior to the development of a national health information exchange (HIE) system. The following resources are available to vendors for the development of EHR systems for newborn screening:
- NBS Use Case published December 31, 2008 and currently with the Healthcare Information Technology Standards Panel (HITSP) for Interoperability Specification development. Expected completion date is January 2010
- NBS Coding and Terminology Guide housed at National Library of Medicine at the National Institutes of Health: http://newbornscreeningcodes.nlm.nih.gov
- NBS Privacy and Security Guidance: http://healthit.hhs.gov/portal/server.pt/gateway/PTARGS_0_10779_868916_0_0_18/2009.05.13%20NBS%20Use%20Case%20Companion%20042409.pdf
- NBS Health Information Technology Implementation Committee (including Centers for Disease Control and Prevention (CDC), Health Resources and Services Administration (HRSA), National Institutes of Health (NIH), Agency for Healthcare Research and Quality (AHRQ), Administration for Children and Families (ACF), Indian Health Service (IHS), Substance Abuse and Mental Health Services Administration (SAMHSA).
- The following documents provide further details on the implementation strategies for information management of NBS laboratory orders and results reporting.
- Improving newborn screening laboratory test ordering and results reporting using health information exchange.6
- Enhancing the quality and efficiency of newborn screening programs through the use of health information technology.7
Key Stakeholders: Roles and Leadership
As in any effort for the electronic exchange of information, community-based leadership and support are critical for success. For newborn screening, the community of stakeholders includes the Department of Health and Human Services (HHS) and other federal agencies, state health officers, pediatric and other NBS professional organizations, infant health advocacy organizations, genetics organizations, and parents.
Figure 1 illustrates information flows using a web-based information exchange as a conduit between clinical care, testing laboratories, and public health facilities. This scenario does not account for the variations in process found in different states and instead represents a generic ideal.
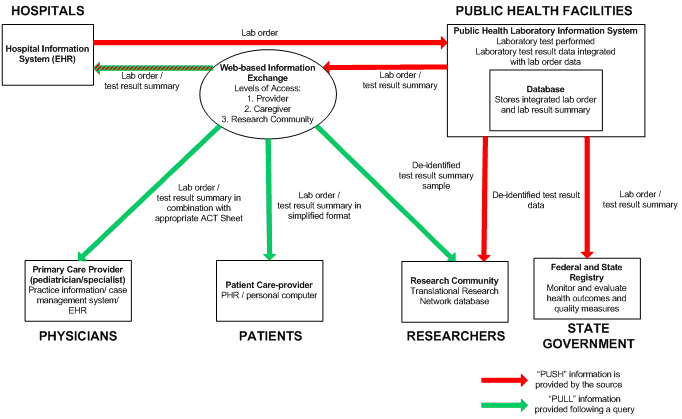
Figure 1: Newborn Screening Information Exchange using the Web-based information exchange
Shortly after the birth of an infant at a hospital and simultaneous with the creation of the infants hospital record in an electronic record system, an order set is generated for nursing and laboratory personnel of required newborn screening tests. Upon collection of a newborn dried blood spot specimen, the patients record and lab request is annotated with patient specific information (diet, medications, antenatal history, etc.) and transmitted electronically to the state public health laboratory. At the laboratory, the request is registered in the public health laboratory information system and the screening tests are performed. Once verified, test results are made available through the secure web-based information exchange which enables results to be accessed by appropriate entities, including the ordering provider (hospital), primary care provider (pediatrician identified by the parents), parent or guardian, and follow-up providers (specialists, nutritionists, counselor etc.). An optional functionality could be the provision of de-identified lab order and test result summaries by the public health laboratory to the approved members of the research community and federal and state registries, respectively.
In the case that the screening test results yield an abnormal result requiring follow-up testing, an alert is transmitted from the laboratory that notifies the individuals and organizations with actionable steps to confirmatory testing. Results presented to the primary care provider are reviewed with the parents and recorded electronically in the EHR where referral is generated for specialty consultation and diagnostic testing. The information about the results are transmitted to the referral center electronically and tracked using the web-based information exchange by the public health laboratory for verification of confirmatory testing results. Follow- up with the referral specialist and additional diagnostic tests are performed as required. The tests confirm an inherited disorder and the results are transmitted to the primary care practitioner, referral center, and state department of health via the web-based information exchange, where the screening test results are reconciled with the confirmatory tests. Added functionalities could include patient management information to provide nutritional support, registration for medical assistance for modified infant formulas, and medical and developmental follow-up (see appendix).
To achieve the information exchanges depicted above, the following is a candidate list of functionalities for a demonstration NBS web-based information exchange:
- Data interchange (including inpatient and outpatient settings)
- Remote data entry (i.e. demographics)
- Patient identity maintenance throughout exchanges and storage (including ability to accommodate changes in patients information over time)
- Integration of metabolic and clinical results (especially hearing)
- Ability to deliver both qualitative and quantitative results
- Integration of data exchanged through the interchange into EHRs and PHRs
- Secure results access (e.g. non-ordering physicians, public health agencies, consumers)
- Quality control capabilities (e.g. both near-term confirmation of testing orders, and broader public health quality overview)
- Standard coding and terminologies (e.g. for research purposes)
- Streamlining of administrative processes (with demonstrable reduction in manual operations)
- Support for information storage (e.g., in databases, registries)
- Support for or links to knowledge repositories (e.g., ACTion Sheets — for providers and consumers — including referral support)
- Security (including defined access requirements, audit log)
To illustrate how implementation of the newborn screening web-based information exchange would affect current workflow processes within the newborn screening system, a number of representative scenarios are presented below.
Scenario I: NBS Electronic Information Exchange Across State Jurisdictions
Challenge: initiating newborn screening via a paper-based lab order and receiving test results as a paper-based lab test summary as well as manual transfer of patient data into the hospital, physicians and patients EHR or PHR, respectively as well as the public health lab information management system (see appendix).
Stakeholders: hospital, public health lab, primary care physician, specialist and patient.
The following scenario represents an example of the multi-directional communication requirements involved in newborn screening and follow up across state borders, and how differences in privacy and security policies and newborn testing policies currently employed across states present a challenge that may be solved through electronic information exchange of newborn screening data via the web-based information exchange concept.
When considering electronic reporting of newborn screening results, the need for timely communication and sharing of screening results among appropriate clinicians and protections against inappropriate disclosure of screening results are important factors.
Jane and John live in Virginia and are expecting their first baby. Based on recommendations by their friends Jane and John have started looking at hospitals and associated ambulatory practices for pregnancy care and subsequent delivery. Jane and John decide that they really like a practice and hospital in Maryland as it seems to fit most within the criteria that are important to them. Nine months later, James is born and has his newborn screening and hearing test performed. The Maryland hospital orders the screening via electronic order followed by the physical blood spot card. The public health laboratory performs the test and returns the test result to the hospital in an electronic format. In addition, the Maryland public health lab makes the test results from the blood spot tests available through the newborn screening web-based information exchange. The lab also incorporates hearing screening test results into the interchange. This is important for Jane and John as they have chosen a pediatrician in Virginia to provide medical care for James. Once released from the hospital, Jane and John take James for his first appointment with the pediatrician. The pediatrician accesses the newborn screening results through the web-based information exchange in advance and reviews them before the office visit. All results for James were normal and no further follow-up was required.
Eighteen months later, James is suffering from sequential ear infections and his pediatrician recommends that Jane and John take him to a pediatric ear-nose and throat specialist located in the District of Columbia for further evaluation. Before the appointment the specialist retrieves the newborn screening test result report that also contained the hearing screening results from the newborn screening web-based information exchange to confirm that James had normal hearing screening results or had a second hearing screening test performed, if necessary. James indeed had normal hearing screening results, and upon examination, the specialist diagnoses a persistent bacterial infection of the ear and prescribes a more powerful antibiotic before recommending ear tubes for James.
Scenario II: Intra-State NBS Electronic Information Exchange with Limited or No Health Information Exchange Capabilities
Challenge: initiating newborn screening via a paper-based lab order and receiving test results in form of a paper-based lab test summary as well as manual transfer of patient data into the hospital, physicians and patients EHR or PHR, respectively as well as the public health lab information management system (see appendix).
Stakeholders: hospital, public health lab, primary care physician and specialist.
The process for newborn screening in an upper plains state currently consists of a paper-based system involving the birth hospital, public health laboratory, primary care physician, specialist, and state health department who exchange information using primarily mail, fax, or telephone.
In an attempt to improve continuity of care, provide complete information to physicians and patient caregivers as well as the state health department, and implement a cost-effective solution to electronic information exchange before in the absence of a fully implemented and integrated health information exchange (HIE), the upper plains state took the approach of using the newborn screening web-based information exchange. The upper plains state considers the web-based information exchange a temporary solution that allows standards-based information exchange to allow time for building and extending states the health information exchange network.
The public health laboratory decided to host the newborn screening web-based information exchange as it is the main conduit for the newborn screening information exchange process. In an attempt to streamline processes even further the lab customized the web-based information exchange through the addition of an electronic scanner allowing the direct electronic upload of information supplied on the paper Guthrie cards into the lab information management system.
Some larger hospitals provided an automatic upload link between the hospital electronic health (EHR) system and the newborn screening web-based information exchange. Similarly, some larger pediatric practices were able to achieve the same for their EHR systems to enable the download of information accessed via the newborn screening web-based information exchange directly into the patients record.
Based on these pre-requisites, the electronic information exchange process starts with the birth hospital collecting a patients blood spot sample and either submitting an electronic lab order via the web-based information exchange directly followed by the Guthrie card, or simply sending the Guthrie card, thereby providing the lab test order in paper format. Independent of the method of lab order entry, the blood spot samples must be physically sent to the public health lab. The initial electronic lab order however, also indicates to the laboratory that a sample has been sent, allowing the lab to anticipate work-load and employ a flexible staffing arrangement based on work-flow.
In cases where the lab order arrives at the lab on a Guthrie card, the card is scanned in and the patients information associated with the blood sample is captured in the lab information management system. Subsequently the lab tests are performed and the results added to the initial lab order to provide a consolidated lab test report summary containing the patients demographic, relevant medical data as well as the newborn screening lab results. The consolidated lab test report summary is made available to pediatricians, specialists and the hospital through the newborn screening web-based information exchange. This access is used to confirm completion of newborn screening testing, initiate pediatric care and arrange for follow-up care with counselors and specialists based on the result of the newborn screening test result.
Scenario III: NBS Electronic Information Exchange by a Large Health System Incorporating a Number of Providers Using Different EHR Systems
Challenge: incorporating patient data from multiple practices within a health system to conduct performance analysis based on quality measures, standards of care, cost etc. (see appendix).
Stakeholders: health system administration, including chief information officer and quality officials, care providers.
Large health systems face challenges incorporating the patient records provided by a number of providers using different EHR systems that may or may not be interoperable. Health systems are forced to manually enter and consolidate patient data from a variety of sources. In addition, health systems interested in performing comparative analysis need to harmonize the incoming data and must ensure that data is complete and current. The stakeholders involved are primary care physicians, specialists, hospitals, public health labs and staff at the health system responsible for patient data capture and analysis.
A health system with a large number of individual practices utilizes the newborn screening web-based information exchange in order to compile newborn screening lab test summaries across different primary care and specialty practices and EHR systems used within these practices. As in scenario I, the web-based information exchange allows primary care physicians to access patients newborn screening lab test summaries and integrate them into the patients EHR.
The large health system uses the newborn screening interchange to integrate patient data including newborn screening test report summaries from different provider EHR systems into the patients health plan record:
Use of the web-based information exchange allows the health system to compile newborn screening test result summaries from a large number of provider practices ensuring that complete data sets for newborn screening test results have been received from the public health lab for each patient and that the appropriate follow-up has been initiated in cases of abnormal results. Based on the data received health plan personnel can conduct performance evaluations across the provider practices assessing timeliness and the implementation of quality care measures relevant to newborn screening.
Bench-marking provider practices should lead to measurable financial and operational improvements but first and foremost to improved quality of patient care. Effective benchmarking relies on the analysis of complete, comparable and current data sets. By implementing the newborn screening web-based information exchange, the health system receives complete and current patient data in a standardized format allows for comparisons to determine best practices within the area of newborn screening.
Benchmarking can benefit a healthcare organization most when it strives to determine best actual practices, not just lowest overall costs. Benchmarking that focuses on best practices can provide managers with an impetus for change based on ideas and practices that have been proven successful elsewhere. Clinicians are more likely to be persuaded to change their practices if they see how they can put such data to practical use to emulate best practice.
Expected Outcomes and Benefits of a Newborn Screening Web-based Information Exchange Value and Impact at the Federal Level
The newborn screening web-based information exchange is a tool to assess NBS program performance in order to improve the quality of care. This would support the mission of the federal coordination group that represents the interests of all the federal agencies involved in newborn screening and child health. Successful implementation of the NBS web-based information exchange would also provide a demonstration case and provide the tipping point for primary care providers to adopt standards and systems.
Value and Impact at the State Level
In recent years many states have made great strides to improve and expand the number of metabolic disorders screened for through more readily affordable and accessible tandem mass spectrometry screening. However, in addition to the technical component of performing the laboratory test, a more effective screening process also requires effective and efficient data sharing to notify parties of a normal result or initiate follow-up for infants identified with an abnormal screening result.
Overall, the implementation of a NBS web-based information exchange would result in the following benefits:
Benefits to Patients and Parents:
- Improved coordination of care for newborns and young children
- Improved child safety (adverse event avoidance)
- Availability of complete newborn screening information
- Portability of patient record
- Reduced loss to follow-up
Benefits to Primary Care Providers:
- Actionable information for primary care providers, public health and specialists
- Reduced time and effort entering data manually
- Improved timely and appropriate data sharing to support follow-up care and treatment. This includes reduced frequency of rescreening based on data omission as a result of manual data transfer from NBS filter paper into public health laboratory data systems.8
- Cost savings though the elimination of unnecessary duplication of records and charts
Benefits to State Health Department / Public Health Laboratory:
- Preserve the systems that healthcare professionals already use
- Reduced cost of specimen processing due to more effective recording and reporting. In 2002 the average cost across states was $18 per specimen. 8
- Connect local systems into regional network
- Provide a centralized data exchange
- Reduced cost and deployment time compared to fully integrated HIE
Meaningful Use and Web-based Information Exchange Implementation
The purpose of health information technology in a pediatric setting is to improve health promotion and early detection, prevention and timely intervention for childhood disorders. As outlined by the Office of the National Coordinator of Health Information Technology within the Department of Health and Human Services, the American Recovery and Reinvestment Act (ARRA)/Health Information Technology for Economic and Clinical Health (HITECH) is not about technology, but instead, it is about improving outcomes through the application and use of technology.9 The newborn screening web-based information exchange concept presents a real-life example of a meaningful use application since it is the use of technology to improve outcomes through increased efficiency, timeliness, and availability of comprehensive patient data.
Furthermore, the NBS web-based information exchange concept is a short-term strategy to address medical care and public health needs by providing a tool supporting the medical home concept described by Hinman et al. as primary health care that is accessible, continuous, comprehensive, family-centered, coordinated, comprehensive, continuous, compassionate and culturally effective.2 Large-scale integration of child health information systems is a long-term process.2,3 To ensure quality and continuity of care prior to the maturity of these large scale systems, small applications are necessary to bridge the gap as well as eventually connect to a statewide or nationwide health information exchange.
Proposed Timeline for Development and Deployment
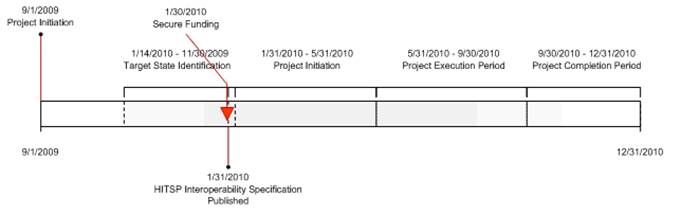
Figure 2: Proposed timeline for newborn screening web-based information exchange development
Community Partnership Opportunities
Central to a project of this nature is a community-centric, community-led effort to provide input into the development, implementation and use of information exchange. The demonstration web-based information exchange presents an opportunity for states, organizations and stakeholders to provide a setting in which to demonstrate the utility and benefits of implementing a system to facilitate the exchange of health information surrounding newborn screening. Not incorporated in this plan at its earliest stage are detailed strategies for public-private partnerships, community engagement and challenge opportunities that are viewed as essential to the projects success. The federal governments role is as a catalyst while effector organizations include many, such as healthcare delivery organizations, consumer advocacy groups, professional societies and health plans to name but a few.
Risks and Mitigation Strategies
- Variability in State Screening Programs. Mandated newborn screening programs exhibit a high degree of heterogeneity among the states. The newborn screening web-based information exchange would be able to accommodate the variability in state requirements, capabilities and current infrastructure.
- Integrating Processes. This would involve system modifications/interfaces and process changes at each laboratory where NBS is performed, and at each hospital where newborn blood is collected. This will involve a significant amount of system implementation, process redesign, and training work at each facility.
- Project Partnership. Identification of a state for implementation of the demonstration web-interchange has not been addressed. Consultation with the vendor community may aid in this process.
Comparison Examples of Health Systems in Other Countries: Sweden, Taiwan
The vision for the NBS web-based information exchange concept is to utilize the emerging standards for newborn screening information exchange to provide a cost-effective, timely service for the exchange of NBS lab orders as well as result reporting in addition to holding great potential for bringing the newborn screening community, healthcare providers, patients and public health officials closer together. A recent study performed in Sweden was designed to explore pediatric practitioners attitudes towards the introduction of a local Web-based information exchange for providing young type 1 diabetes patients with interactive pedagogic devices, social networking tools, and locally produced self-care and treatment information. The study sought to analyze the opportunities and barriers related to the introduction of such systems into clinical practice. In a survey as part of the study, participants in the diabetes web-based information exchange project reported that the interchange concept helped reduce data entry time, increased and improved communication with patients and as such resulted in a sense of community. In this particular case, some participants of the study suggested that the interchange functionality could be extended beyond clinics and even offered to help in the future development process of the interchange.10
The NBS web-based information exchange concept is not intended to replace existing infrastructure or communication channels but rather add in a meaningful way to improve and extend data sharing and patient — provider communication capabilities. In Taiwan the original standalone architecture, having various heterogeneous systems operating individually, was restructured into a Service-Oriented Architecture (SOA) resulting in a distributed platform for further integration and enhancement of sample collections, testing, diagnoses, evaluations, treatments or follow-up services, screening database management, as well as collaboration and communication among health care providers. In addition the newborn screening SOA supports decision support and improves screening accuracy across Taiwan neonatal systems.11
Summary and Conclusion
The benefits of electronic exchange and storage of newborn screening information are virtually self-evident. Many of the most significant challenges in the newborn screening area involve the management, exchange and longer-term availability of patient information. The professional community surrounding newborn screening is aware of the potential offered by health information technology to address the challenges it faces, and the community is prepared to embrace workable and affordable moves toward e-based solutions. A foundation of use case development, coding harmonization and other work has been carried out in recent years with participation throughout this community.
At the same time, development of systems of health information exchange can be daunting in its complexity and cost. For newborn screening, these challenges are exacerbated by the heterogeneity of screening programs from state to state. Further the development of a national system of health information exchange which might be applied for newborn screening is not expected in the near term.
Development of a prototype web-based information exchange tool is proposed in order to deliver a health information exchange solution in the newborn screening area that 1) can be developed rapidly at low cost, 2) would be adoptable by states, regions or integrated health systems to be customized to their own needs, and 3) would serve customers throughout each state in a technology-neutral fashion that would accommodate any standards-based platform. The interchange would support the full spectrum of newborn screening information needs:
- Test ordering
- Inclusion or addition of patient data
- Secure and rapid results delivery to specified recipients
- Secure results availability upon authorized request for professionals and consumers
- Support for follow-up testing and follow-up results reporting
- Transfer of standards-based information to EHRs and PHRs
- Results archiving
- Public health reporting
- Capacity to make de-identified data available for research purposes.
In the longer run, an interchange solution might be supplanted by a broader health information exchange solution. In the shorter run, however, it has the potential to provide a rapid and affordable solution to significant challenges in the newborn screening area, and its implementation would both improve health outcomes and provide important experience in the implementation of a health information exchange mechanism. We propose development of the interchange tool, in collaboration with the newborn screening community, using the IT resources of existing health information exchange architecture such as the Nationwide Health Information Network (NHIN), Public Health Information Network (PHIN) and the cancer Biomedical Informatics Grid (caBIG). Consideration should be given to a demonstration program in which a number of states, regions or integrated health care systems would adopt and utilize the interchange. Such an interchange project would help fulfill an important element of the Congressional mandate for federal HIT efforts which calls for particular attention to the needs of infants and children.
Summary of Impact of Newborn Screening Interchange Implementation
Test ordering
Present Filter paper is physically submitted. Web-based Interchange As filter paper is submitted, the submission is recorded on the interchange system and a permanent record is initiated.
Inclusion or addition of patient data
Present Data may be included with filter paper, but is not easily amended.Web-based Interchange Significant patient data may be added at any time.
Results delivery and availability
Present Results are delivered in one-off fashion (largely by fax or mail), generally to clinicians only. There is no easily accessed subsequent availability. Web-based Interchange Results are delivered and made permanently available to authorized recipients. Patients/families can access information, without time limitation.
Support for follow-up testing and reporting
Present Relies on clinician or family initiative, without other systemic support. Web-based Interchange Web-based information sources accessible on a central interchange assist clinicians and families in carrying out follow-up, and permanent interchange record provides supports and tracking.
Transfer standards-based information to EHRs and PHRs
Present No present support for embedding in e-records. Web-based Interchange NBS results are EHR/PHR-ready.
Results archiving
Present No reliable system. Web-based Interchange Permanent secure availability of NBS reports for authorized persons, supporting longitudinal health care delivery regarding NBS-discovered conditions
Public health reporting and availability for research purposes
Present Public health reporting required, but supported only by paper-based systems. Web-based Interchange E-availability for rapid availability and interoperability of data.
References
- Desposito F, Lloyd-Puryear MA, Tonniges TF, Rhein F, Mann M. Survey of pediatrician practices in retrieving statewide authorized newborn screening results. Pediatrics (2001);108(2):E22
- Hinman AR, Eichwald J, Linzer D, Saarlas KN. Integrating child health information systems. Am J Public Health (2005); 95: 1923-1927.
- Ross DA, Hinman AR, Saarlas KN, Lloyd-Puryear M, and Downs, SJ. The near-term future for child health information systems. J Public Health Management and Practice (2004); S99-104.
- Glaser J, Henley DE, Downing G. Advancing personalized health care through health information technology: an update from the American Health Information Communitys Personalized Health Care Workgroup. JAMIA (2008); Vol. 15(4): 391 396.
- Brinner KA, Downing GJ. Advancing patient-centered pediatric care through health information exchange: update from the American Health Information Communitys Personalized Health Care Workgroup. Pediatrics (2008); Vol. 123 Suppl. Jan 2009: S122 S124.
- Downs SM, van Dyck PC, Rinaldo P, McDonald C, Howell RR, Zuckerman A, Downing G. Improving newborn screening laboratory test ordering and result reporting using health information exchange. J Am Med Inform Assoc 2010;17:13-18.
- Downing GJ, Zuckerman, AE, Coon C, Lloyd-Puryear, M. Enhancing the quality and efficiency of newborn screening programs through the use of health information technology. Seminars in Perinatology (in press).
- PriceWaterhouse Coopers. Newborn Screening Programs: An Overview of Cost and Financing. New York, NY: PriceWaterhouseCoopers; 2002. Available at: www.marchofdimes.com/files/Final_PWC_NBS_Report2.pdf. Accessed September 9, 2009.
- Blumenthal D. Stimulating the Adoption of Health Information Technology. New England Journal of Medicine (2009); 360(15): 1477 1479.
- Nordqvist C, Hanberger L, Timpka T, Nordfeldt S. Health professionals attitudes towards using a Web 2.0 portal for child and adolescent diabetes care: qualitative study. J Med Internet Res (2009); Vol. 11(2): e12
- Hsieh SH, Hsieh SL, Chien YH, Weng YC, Hsu KP, Chen CH, Tu CH, Wang Z, Lai F. Newborn Screening Healthcare Information System Based on Service-Oriented Architecture. J Med Syst (2009); DOI: 10.1007/s10916-009-9265-x
Appendix: Detailed Overview of Information Exchanges Current and Future State
| Perspective | Current State | Future State |
| Hospital |
|
|
| Newborn Screening Lab |
|
|
| Primary Care Provider |
|
|
| Specialist |
|
|
| State Health Registry |
|
|
| Patient/Family |
|
|
| Research Community |
|
|