
Rachael E. Bennett, MA, Mark Tuttle, FACMI, Karis May, Jennie Harvell, Med, and Eric A. Coleman, MD, MPH
University of Colorado
Health Sciences Center
This report was prepared under contract #HHS-100-03-0028 between U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and the University of Colorado. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the ASPE Project Officer, Jennie Harvell, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. Her e-mail address is: Jennie.Harvell@hhs.gov.
The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
"
Executive Summary
STUDY OBJECTIVES
The study, entitled "Health Information Exchange in Post-Acute and Long-Term Care," was sponsored by the Office of the Assistant Secretary for Planning and Evaluation (ASPE), U.S. Department of Health and Human Services (HHS), and conducted from September 30, 2005 through October 15, 2007. The purpose of the study was fourfold: (1) describe the current status of the use of health information technology (HIT) in existing state-of-the-art health delivery systems (HDSs) and how health information is or is not exchanged with "unaffiliated"1 post-acute care (PAC) and long-term care (LTC) providers and other components of the health care delivery continuum (e.g., physician offices, laboratories, pharmacies, and hospitals) that use HIT; (2) identify the factors that support or deter the timely exchange of needed health information to and from unaffiliated PAC and LTC providers and other components of the health care delivery continuum that use HIT; (3) identify ways in which policy makers can encourage information exchange by HDSs that use HIT with unaffiliated PAC/LTC providers; and (4) summarize and organize information learned and describe the next steps that could be pursued to extend HIT into PAC/LTC.
The study was divided into three phases. The first phase included a review the literature. The second phase involved speaking with stakeholders and national experts in the area of health information exchange (HIE). The third phase built upon these first two phases by conducting four site visits with exemplar health systems to obtain more detailed information to address the stated study objectives. Based on national reputation and willingness to host a site visit, four "hub sites" were selected. The study team then identified both affiliated and unaffiliated providers (i.e., "spoke sites") in each of these geographic areas that received patient referrals from the hub sites. As the four hub sites were not selected at random, the findings and recommendations of this study are limited and may not be representative of all PAC and LTC settings in the United States.
WHY THIS RESEARCH IS IMPORTANT
There is increasing recognition in both the public and private sectors that significant improvements in health care quality, continuity of care, and efficiency of care may be realized through implementation of HIT. The ability to share health data between and among health care providers is critical to providing high-quality, cost-effective, informed health care. The ability of health providers to act on timely information improves workflow efficiencies and may save lives. A paper medical record does not allow for such efficiencies to be fully realized; yet at this time, the vast majority of PAC and LTC providers (and other health care settings, also) still use a paper medical record for the authoritative record.
In acknowledgement of the increasing importance of HIT implementation, a number of initiatives have followed the April 2004 Presidential Executive Order 13335. This Executive Order recognizes the need for the development and nationwide implementation of an interoperable HIT infrastructure and established the position of the National Coordinator for Health Information Technology (NCHIT) in the HHS to provide leadership for this effort. Shortly thereafter, the Office of the National Coordinator for HIT released a report, "The Decade of Health Information Technology: Delivering Consumer-Centric and Information-Rich Health Care" (Office for the NCHIT, 2004) that outlines a framework for realizing the goal that most Americans have an interoperable electronic health record (EHR) by 2014.
A previous study also conducted by the University of Colorado at Denver and Health Sciences Center (UCDHSC), entitled "Electronic Health Records in Post-Acute and Long-Term Care" found that health information shared across health settings (e.g., acute care hospitals, physician offices, nursing homes [NHs], home health agencies [HHAs], laboratories, and pharmacies) was inadequate to support high-quality patient care. When information was shared, it often was shared only with "affiliated"2 providers. The authors sought to understand if this trend had shifted in the three years since that study had concluded. This current study built upon those findings and posed additional questions: How is information shared across and between health care provider settings? Is information shared differently when shared with affiliated versus unaffiliated settings? Does involvement in a health information exchange network (HIEN) (e.g., a regional health information organization [RHIO]) make a difference in the types of or amount of data shared across health settings?
OBSERVATIONS
Four leading edge sites were chosen as "hub sites" for visitation based on the fact that each provider site: (a) was using a relatively robust electronic health information system; and (b) collaborated with a number of affiliated and unaffiliated PAC and/or LTC settings that treat their patients. Three of the four settings also were involved in some type of RHIO/HIEN.
The four hub sites were: Erickson Retirement Communities (Catonsville, Maryland), Montefiore Medical Center (Bronx, New York), Intermountain Health Care (IHC), specifically LDS Hospital (Salt Lake City, Utah), and the Regenstrief Institute/Indiana Health Information Exchange (IHIE) (Indianapolis, Indiana). Each hub site has earned the reputation for being a leader in promoting HIE, has strong ties to the community, strong local leadership, and an organizational and cultural commitment to enhancing quality of care and increasing efficiencies.
Each site visit was comprised of multiple components. On the first day, the site visit team visited a hub HDS (one was a continuous care retirement community (CCRC), two were acute care hospitals, and one was an academic health center). The second and third days of the site visits were spent visiting three or more LTC or PAC settings3 that receive referrals from the hub site. When possible the site visit team visited both affiliated (i.e., owned) and unaffiliated settings. In some cases, names of PAC/LTC settings were obtained from the hub site contact and in other cases the project team independently approached the PAC/LTC settings and requested their participation in the study.
Although there were geographic, socioeconomic, and organizational/structural differences at the four sites, a number of common themes emerged, which are highlighted below.
1. Limited Health Information Technology Adoption in PAC/LTC Settings
In general, the site visits revealed limited adoption of HIT in PAC and LTC settings. This finding is consistent with two studies on HIT adoption in PAC/LTC settings. A 2005 study by Kaushal and colleagues (Kaushal et al., 2005a; Kaushal et al., 2005b; Poon et al., 2006) estimated EHR adoption in 2005 for NHs to be 1% and less than 1% for HHAs. The authors projected that HIT adoption in five years will not increase much for either health sector (14% for NHs, and <1% for HHAs). The other study included a survey that was conducted by the American Health Care Association (AHCA) and the National Center for Assisted Living. Two of the key findings were: (1) paper continues to be the primary communication mechanism in NHs and assisted living facilities (ALFs); and (2) while respondents to this survey express that they are beginning to adopt more HIT, in three years, it is projected that these two settings will still be in the early stages of transitioning to HIT (American Health Care Association, 2006).
Because the project objectives included looking at state-of-the-art delivery systems, the majority of PAC/LTC sites visited were early adopters of HIT in some capacity. However, with a few exceptions, HIT use was generally limited, was not standards-based, and typically did not include data exchange capabilities. The visited PAC/LTC providers used information technology applications that met rudimentary regulatory requirements and billing needs, and were observed to be using HIT applications for some intra-facility functions. However, the use of HIT by PAC/LTC for HIE with other organizations (e.g., hospitals) was observed rarely. In some cases, there was no EHR used, nor were there future plans to implement HIT.
2. Poised for Interoperability
The Presidential Executive Order of August 2006 defines interoperability as "the ability to communicate and exchange data accurately, effectively, securely, and consistently with different information technology systems, software applications, and networks in various settings, and exchange data such that clinical or operational purpose and meaning of the data are preserved and unaltered" (Federal Register, 2006). At one hospital visited, a representative declared that health care enterprises in his region were "poised for interoperability." The same observation could be made at another hospital visited, and represented an important shift from only a few years earlier when interoperability was not of paramount concern. Although no site presented a schedule for achieving complete interoperability across all settings, each hospital had plans in place for some degree of data exchange outside of its enterprise. Moreover, each expressed some intent to include nearby LTC sites in those plans. The study team found that one of the biggest drivers for health data exchange was a desire to support "anytime/anywhere" access by physicians and other providers who practiced in multiple care settings. Care providers who had such access then wanted to be able to include information from the "remote" or referring system into the "local" or receiving system. Anytime/anywhere access often was supported by dial up connections, and, increasingly, by web interfaces. However, "electronic population" of the local or host system with information from a remote system was rare. Not surprisingly, once providers began having remote access in one care setting, they also wanted access in other care settings. However, staff at the various sites expressed various formidable challenges when they attempted to populate local or host electronic medical records (EMRs) with remote information.
The phrase "data exchange" was typically interpreted by the sites to mean the display of patient information on a local computer that originated from a computer at a remote, unaffiliated care site. Although it is implied that this involves a two-way data exchange method, more often than not, it was simply a one-way transaction.
Two clinical scenarios stood out for their ability to illustrate the demand for HIE and the inherent challenges: the transfer of patients from hospital to PAC or LTC settings, and the transfer of NH residents to the emergency department (ED). Care providers in NHs that receive patients from hospitals, and in EDs that receive patients from NHs want to know certain details about the patient's current status and medical history and they are willing to take the time to read this information on a computer screen if the information is current and trusted. The notion that, for example, the receiving provider's EHR would be able to represent information about the patient in a way that could feed into a decision support feature and influence the care plan was described as a goal by some sites, but not one that was expected to be achieved any time soon.
The three phases of this study helped inform a proposed framework for HIE that is illustrated in Table ES-1. One can think of these different kinds of data exchange arranged on a continuum or spectrum; at one end of the spectrum the phrase "data exchange" implies that computers can act as the informational equivalent of fax machines only; at the other end of the continuum, "data exchange" implies that information received by a computer can be used in the same way as information entered locally. An example of the latter would be an ability to import a medication list that had been reconciled in the hospital and represented in its EMR into an outpatient EMR that facilitated the local computer to analyze the synthesized list for drug-to-drug and drug-to-disease interactions.4
| TABLE ES-1: Levels of Health Information Exchange |
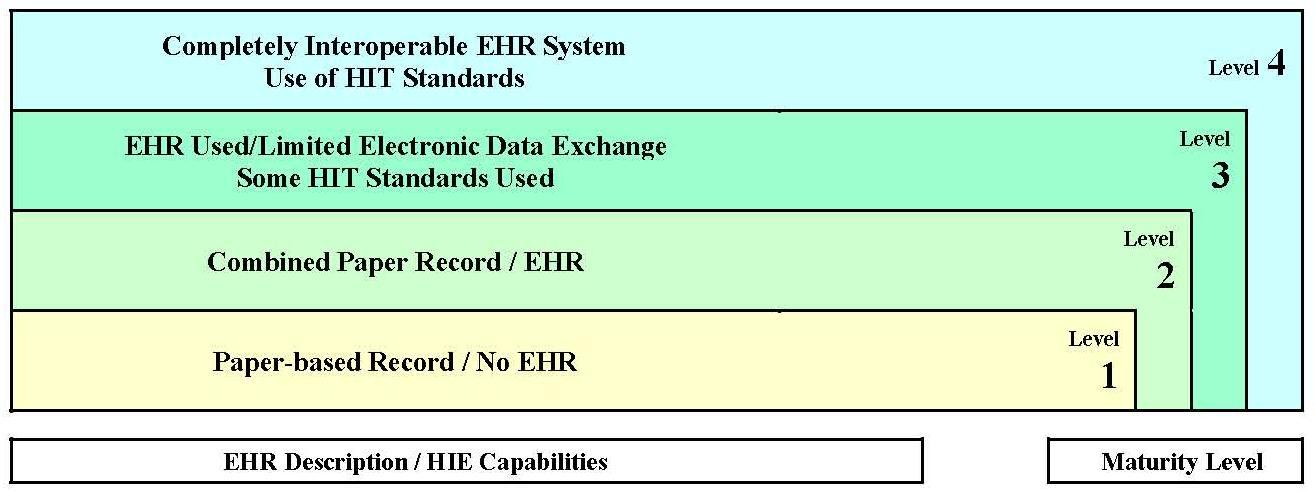 |
Table ES-2 expands upon the Table ES-1 framework by proposing specific features for each level to suggest a progression from less to more sophistication of HIE. This table was constructed based on the literature review as well as the study teams observations concerning HIE and use of EHRs across the sites selected for the study. Although none of the settings observed have reached Level 4 (i.e., completely interoperable EHR systems, using standards-based applications to share information with affiliated and non-affiliated providers), it is included as the purported future goal.
3. Data Exchange among Health Settings, Particularly Post-Acute and Long-Term Care
At every NH and HHA visited, the potential benefit from engaging in activities with external parties to support and increase HIE was observed. At Erickson, the local and national information technology staff are prepared to subsidize the implementation of HIE standards if such standards are available in the near future. In each of the other three visited locations, PAC and LTC enterprises are in a position to benefit from HIE efforts originating outside of their organizations. Although PAC and LTC sites are not leading HIE efforts and are not directly involved as collaborators; they will benefit nonetheless. As all PAC and LTC sites had some Internet connectivity and some local information technology systems (even if only to meet administrative data reporting requirements), the barriers to sending and receiving electronic patient information are lower than once observed. However, because the perceived and actual barriers to the simultaneous re-use of patient information remain high, driven by factors that include implementation and maintenance costs, mistrust of the data, a fear of litigation, and Health Insurance Portability and Accountability Act (HIPAA) and other privacy concerns, such interoperation is not yet in sight for any enterprise visited. Nevertheless, once human-readable electronic exchange is in place, the incentives for the automatic population of local systems from remote systems with computer-readable electronic health information will become more clear and measurable. For example, it will be easy to assess the amount of time, and therefore the cost, required to manually re-enter information in a local system that exists in electronic form elsewhere. In this sense, the fact that hospital is "poised for interoperability" will help expedite the incremental deployment of HIE at collaborating PAC and LTC sites.
a. Workflow. The four site visits reinforced the central role that workflow issues play in HIE. Information technology is a cross-cutting issue, an observation that permeated the site visit discussions at many levels. In general, relatively highly-paid professionals in hospitals, PAC, and LTC settings are expending a significant proportion of their time on clerical tasks rather than attending to patients' clinical needs. EHRs did not necessarily provide solutions to this inefficiency. Because of the lack of interoperable EHRs, it was common for sites to report that nurses and physicians read from a computer screen or print out a patient's health data from one electronic health application only to manually enter the information into another electronic health application (such as an EHR). Respondents described manually re-entering laboratory results received electronically into their own EHR system, because the two electronic systems did not have the capabilities of exchanging data. In most cases, the clinicians were not consciously aware of the amount of effort that was being expended. Rather, they had long accepted these tasks as inevitable.
Further probing revealed that manual data re-entry from one system or medium to another may add value in terms of improving quality and safety. For example, the process of printing the medication list from one electronic source and then manually entering into an EMR provided an opportunity for greater scrutiny than what would have been made had the medications been reviewed on a single computer screen. During these discussions, clinicians acknowledged that this manual re-entry activity was not simply a clerical process but rather something that provided an opportunity to cognitively assess whether the medications were in fact appropriate, whether any additional diagnostic testing was required, and whether the patient might be at risk for an adverse drug reaction. Alternatively, this process has the potential to introduce new errors due to transcribing errors (Brody, 2007). Thus, it remains to be determined how these vital tasks will be accomplished once more advanced (e.g., interoperable, standards-based) electronic solutions are forthcoming.
b. Majority of data sharing to and from PAC/LTC is done manually. Independent of the degree of EHR capability in place at the hub sites, the exchange of data between these hubs and affiliated and unaffiliated PAC/LTC settings is largely conducted manually (phone, fax, paper records that are mailed or accompanies the patient at the time of transfer). This information either is filed in a paper record and/or transcribed into the PAC/LTC setting's EHR. Phone, fax, and paper records continue to be used for patient referrals, discharge, and transfer documentation. Although some implementation efforts were underway, the study team did not witness any electronic transmission of data from PAC/LTC settings directly into the hospital's EHR systems.
| TABLE ES-2: Illustrative Examples of HIE Capabilities by Level | ||||||||
|---|---|---|---|---|---|---|---|---|
| Level 1 Paper-based Record/ No EHR | Level 2 Combined Paper Record/EHR | Level 3 EHR Used/Limited Electronic Data Exchange, Some HIT Standards Used | Level 4 Completely Interoperable EHR System, Use of HIT Standards | |||||
| HIE Methods |
|
|
|
| ||||
| Features/Attributes of Patient Health Information and Electronic HIE1 | No Electronic HIE (i.e., not electronic data) | No EHR | Some e-HIE | Limited use of EHR | Data exchange limited to certain systems | Access to data limited to user role/ discipline | EHR is primary record | Standards-based EHR system (i.e., EHR content is standardized) |
| May have software for AR/AP, scheduling | No Anytime/ Anywhere Access | May allow for images to be imported | Clinical information collected on paper & entered into EHR | Continued but limited use of paper record | Some use of standards (messaging &/or content) | Interoperable with internal & external systems | Record can be electronically exchanged/ is transportable | |
| Meets minimum regulatory requirements2 | Limited Anytime/ Anywhere Access | Decision support features & alerts used | Anytime/ Anywhere Access | Computer Empowered Interoperable System | Anytime/ Anywhere Access | |||
| Facilitators of HIE | Limited involved in HIE Network (e.g., admin/claims data) | Some clinical content exchanged within HIE Network | Greater amount clinical information exchanged/shared within HIE Network | |||||
| ||||||||
c. Importance of personal relationships in referrals. Although HIT can and will expedite referrals from one setting to the next; it was observed that today, personal relationships superseded any technological advancement in place. In other words, the "human element" is well engrained into the process of data exchange. One observation that crystallized this point was hearing that despite implementation and acceptance of an electronic mechanism to facilitate post-hospital patient placement in skilled nursing facilities (SNFs), discharge planners often finalized these arrangements outside of this mechanism telephonically with admission coordinators with whom they had a personal relationship. They trusted these people more willingly than an "anonymous" source of data.
d. Lack of standards used. Two primary observations regarding adoption of standards-based HIT solutions in PAC/LTC were observed. Firstly, among those PAC/LTC providers that had purchased and implemented an EHR system, the use of standards as a vetting criterion for vendor selection was not considered. Respondents clarified that standards development and adoption are still in the early stages, which is why most of the systems used by the visited PAC/LTC settings did not use standardized terminologies, messaging standards, or documents for the electronic recording and exchange of health information. They would like to see greater consensus on some of the standards work before they invest the resources necessary to adopt/convert their systems. The other observation is that many PAC/LTC settings visited were unaware of the extent of activity in the standards development community, and therefore did not see the potential value of having a standards-based EHR system to facilitate HIE across health settings.
In other cases, the lack of standards was not synonymous with a lack of sophistication in EHR adoption. In fact, national health care leaders including the Regenstrief Institute, IHC, and the Visiting Nurse Service (VNS) of New York were early adoptors of HIT applications that support clinical care, and as a result they developed their own "homegrown" systems prior to the emphasis on using national standards. When asked if they were planning on adopting balloted, Consolidated Health Informatics (CHI)-endorsed standards, representatives from these early adopters indicated that it was financially prohibitive to reconfigure their systems.
e. Lack of financial incentives for HIE. The site visits did not reveal any real or perceived financial incentives for adopting HIT that supports HIE with outside entities. The initial outlays for hardware and software remain prohibitive, training costs can be quite high, particularly considering the historically high staff turnover in PAC/LTC, and ongoing maintenance costs may be difficult to justify when the short-term return on investment is unclear. Furthermore, the benefits of HIE do not necessarily accrue to the institution that makes the investment in hardware/software, including the time to input and maintain the information. These costs and uncertainties regarding the return on investment will likely be particularly problematic for small, independent PAC/LTC settings. The business case for the referring organization that would need to make the HIT investment remains underdeveloped.
RECOMMENDED NEXT STEPS
A significant barrier to widespread electronic exchange of health information with PAC/LTC settings is that the majority of PAC/LTC providers and those health care organizations with which health information must be exchanged, have yet to implement EHR/HIT systems with the capacity to support interoperable HIE. It is not that leaders in those settings do not see the value in obtaining timely, accurate health data from a referring site (or providing it to other settings at discharge). It is possible that the functionality seems so far out of reach at this point, due to the lack of low-cost, reliable, well-supported hardware and software, and the lack of data available on the return on investment of adopting HIT, particularly in the PAC/LTC health sector. Thus, demonstration, dissemination, and education regarding the benefits of adopting an interoperable EHR system relative to the associated costs of not adopting these systems are imperative if providers and vendors are going to invest more heavily in EHRs for PAC and LTC.
The study team recommends that a thorough, targeted national survey of HIT adoption, use, and barriers to adoption in PAC/LTC should be conducted. There have been small-scale studies looking within a specific geographic region or market area (Continuing Care Leadership Coalition, 2006; Hudak & Sharkey, 2007), and the 2007 National Home and Hospice Care Survey includes, for the first time, questions on whether the responding HHA has an EMR, and if so, whether the HHA uses certain EMR functions or whether these functions are either not used or not available (personal communication with Jennie Harvell, ASPE Project Officer). Experts have convened and given their best impressions and projections for HIT readiness in all types of health sectors, including PAC and LTC (Kaushal et al., 2005a; Poon et al., 2006). However, to date, there has not been a scientifically-based, comprehensive survey on the specific types of HIT applications that are currently in use, or that are being considered for future implementation in NHs.
Continued development and adoption of standards-based work needs to take place. Recent developments are promising. For example, an important step forward is the recent letter from the Secretary of HHS to the National Committee on Vital and Health Statistics (NCVHS) that the CHI recommendations for HIT standards for the Functioning and Disability domains will be adopted for use in new federal health information systems and, to the extent possible, as existing health information systems are modified. Likewise, approval by Health Level Seven (HL7) and the Health Information Technology Standards Panel (HITSP) of the Continuity of Care Document (CCD) standard, a harmonized summary record standard is an important needed activity to facilitate interoperable data exchange across settings. These standards-based activities need to be built upon and expanded.
Related to the above point, PAC and LTC provider participation in standards development and encouragement of HIT adoption is paramount. The LTC provider and vendor communities were instrumental in the recent decision by the Certification Committee for Healthcare Information Technology (CCHIT) to include the certification of NH EHRs in its expanded scope of work. CCHIT certification can be a valuable asset for NH providers to reduce their risk when making costly HIT investments. Continued participation in standards development work is necessary to keep the LTC and PAC communities involved in the future directions that will evolve.
PAC and LTC settings' involvement in HIENs/RHIOs should be increased. Given the Federal Government's interest in moving the Nationwide Health Information Network (NHIN) to the next phase, it is clear that HIENs will be key players in that process. Education on the role that HIENs are playing in communities and encouragement of all setting types to get involved is important to ensuring their "voice" is heard in the design and development of HIE strategies.
Introduction
A. Overview: What is Unique about this Research
The Federal Government and many state administrations see the broad implementation of HIT as an important lever by which to improve health care quality and safety, and reduce costs. Implementing HIT will support the exchange of data as patients move between health care settings, and such exchange will measurably decrease errors, enable more timely and productive clinical decisions, and allow for a more comprehensive patient-centric longitudinal electronic record (Coleman, May, Bennett, Dorr, & Harvell, 2007). To this end, hospitals and ambulatory settings are implementing EHRs that are increasingly compliant with national standards. However, adoption of HIT solutions in NHs and HHAs has lagged behind hospitals and ambulatory care settings.
This project set out to identify what information is exchanged between hospitals, physician offices, and ancillary health providers (such as laboratories and pharmacies), and NHs and HHAs. The project also asked how and whether HIT is being used to facilitate HIE with and between NHs and HHA providers. These questions were posed to several early adopters that have implemented HIT to support the exchange of health information as patients change care settings. In particular, this effort focused on whether there were any differences in the types, content, or format of data that were shared with affiliated as opposed to unaffiliated care settings. Further, the project asked whether HIE strategies employed by leading HDSs could be replicated elsewhere and what lessons were learned as implementers developed their information technology solution(s). Specifically, the project team sought to understand what worked and what did not work as expected at the sites visited. More generally, the team wanted to identify what facilitated and impeded both electronic and non-electronic HIE.
Ultimately, the answers to these key questions can provide information to health care leaders and policy makers on: (1) the patient health information that needs to be exchanged with NHs and HHAs; and (2) the use of HIT to support HIE. This knowledge may help to inform a national strategy to promote more widespread interoperability towards the ultimate objective of improving the quality of health care in this country.
B. Project Objectives
The four goals of this project were to: (1) describe the current status of the use of HIT in state-of-the-art HDSs and how health information is or is not exchanged between "unaffiliated" PAC/LTC providers and other components of the health care delivery continuum (e.g., physician offices, laboratories, pharmacies, and hospitals) that use HIT; (2) identify the factors that support or deter the timely exchange of needed health information to and from unaffiliated PAC/LTC providers and other components of the health care delivery continuum that use HIT; (3) identify the policy levers that could be used to encourage information exchange by HDSs that use HIT with unaffiliated PAC/LTC providers; and (4) summarize and organize information learned and describe the next steps that could be pursued to extend electronic HIE (e-HIE) technologies into PAC/LTC.
All activities, which included a literature review, stakeholder interviews, site visits, and resultant case studies attempted to answer one or more of the following research questions:
-
In select health care delivery systems:
- What HIT is being used to support the: (1) creation, storage, and exchange of summaries of physician office visits and hospital stays; and (2) computerized provider order entry (CPOE) including medication ordering, and laboratory results reporting?
- What hardware and software are used to support these functions and how do they support these functions?
- To what extent does HIT use nationally-recognized (e.g., CHI-endorsed) HIT vocabulary and messaging standards to create and exchange health information within the HDS?
- What is the health system architecture that supports the creation, storage, and exchange of these summaries, orders, and reports of results?
-
What type of health information is needed for summary documents of hospital stays, physician office visits, medication orders, and laboratory tests?
-
Within selected health care delivery networks, what clinical information is exchanged as part of the summaries of physician office visits and hospital stays, physician orders, and reports of test results?
-
What health information is exchanged between health care providers and unaffiliated PAC/LTC settings and what are the mechanisms used to exchange information?
-
What factors do PAC/LTC providers and representatives from the selected health care delivery systems identify as supporting or creating barriers to the timely exchange (in any form; i.e., electronic, fax, paper, etc.) of physician and hospital summaries, physician orders, and results reporting between HDSs and PAC/LTC providers?
C. Navigating the Report
The audience for this report is broad and varied, including federal and state officials, PAC and LTC providers, standards development organizations (SDOs), and potentially payors, vendors and other stakeholders interested in HIT. As such, the report is written with the expectation that the reader may have little knowledge of the current state of HIT development and the corresponding policies put forth and planned. Section II explains the methods used to select and recruit the participating sites for the case studies. Section III presents our findings and results, separated into major areas focusing on clinical and organizational/management of HIE and technical issues. The purpose of this division is to make it easier for readers to separate out these related, but different observations and findings from the site visits. Section IV presents our interpretation of the findings, as well as a discussion of possible next steps.
Methods for Selection and Recruitment of Health Delivery Systems
For the purposes of this study, a "health delivery system" (HDS) was defined as an entity that includes a hospital with one or more affiliated or owned physician office practice(s), outpatient clinic(s), laboratories, and/or pharmacies. The goal was to identify up to ten candidate HDSs, from which four would be selected for site visits.
A. Criteria for Selecting the HDS and PAC/LTC Settings for Site Visits
The criteria used to select the HDSs was based on the type and scope of electronic health information creation, storage, and exchange believed to be implemented in the system; the anticipated level of effort required to gather data about the information exchange mechanisms at each system; and to the extent possible, how the HDS is representative of those around the country and/or provides an instructive contrast to the other sites selected.
More specifically, the following criteria were used to prioritize candidate sites. The HDS should: (1) have an electronic health information system that allows for the exchange of health information across two or more settings or providers (e.g., hospital and physician offices, laboratory, pharmacy, radiology), and preferably has documentation to explain the clinical/organizational and technical components and capabilities of the health information system; (2) refer patients to unaffiliated PAC and LTC settings (defined as SNFs, NHs, and HHAs) in the same general geographic location (unaffiliated, for the purposes of this screening was defined as not being owned by the HDS);5 (3) preferably have at least six months experience with the software application(s) that support information exchange; and (4) be amenable to a site visit by a three-person team of data collectors who would require access to a variety of staff (including clinicians, information technology specialists, and managers).
Although the criteria were established a priori, it was later recognized that provider arrangements often do not fall into neat categories of affiliated and unaffiliated. As noted above, in some cases, organizations may have a preferred provider relationship, although they are not officially affiliated. Rather, provider arrangements continue to evolve. For example, physicians with multiple affiliations have proven to be an impetus for data exchange across health settings. In fact, within many situations, physicians "follow" patients across settings muddying the waters as to what constitutes affiliated and unaffiliated relationships.
B. Inclusion of Site Involvement in a Regional Health Information Organization (RHIO) or Health Information Exchange Network (HIEN)
Because of the growing impact that RHIOs or HIENs are having in facilitating HIE, the criteria for selection also included sites with RHIO or HIEN involvement. The Healthcare Information and Management Systems Society (HIMSS) defines a RHIO as a group of organizations with a business stake in improving the quality, safety, and efficiency of (health) care delivery (Healthcare Informatics in collaboration with AHIMA and AMDIS, 2005). Because of the multiple issues (e.g., business, legal, legislative, technological, clinical, and cultural) involved in cross-organizational interoperable HIE, support for HIE organizations has become more attractive at both the state and federal levels. While grants are normally used for start-up and planning phases, recent surveys have indicated that additional funding sources for RHIO start-up and continuation is necessary (Healthcare Informatics in collaboration with AHIMA and AMDIS, 2005; HIMSS and the Center for Health Information and Decision Systems, 2006).
In response to this recognized need, federal programs have emphasized and increased the amount of funding for grants and demonstrations for RHIO and HIEN planning and implementation. Over 40 states are in some phase of planning, implementation, or have projects that are focused on HIE organizations (HIMSS and the Center for Health Information and Decision Systems, 2006).
As there are no "best practices" that a RHIO or HIEN can use to start itself, communities often have produced their own design, specific to their own needs, with funding or planned funding coming from a variety of sources, including hospitals; employers; physician groups; non-profit groups; insurers; local, state and Federal Government; user fees; financial incentives; and private investors. As such, involvement in collaboration with other area organizations was viewed as an important factor for inclusion in site selection.
C. Potential Site Visit Locations
The following list for potential site visits was created and reviewed by the project team and a group of leaders in the field of HIT identified by ASPE. Based on a review of the literature and recommendations from peers and grant-making organizations, 14 organizations were identified as being particularly innovative in the area of HIE. These sites did not ask to be considered, nor were they necessarily aware that their names had been put forth. Based on the criteria discussed above, the sites originally considered are listed in alphabetical order below:
- Allina Hospitals and Clinics, Minneapolis, Minnesota
- Deaconess Billings Clinic, Billings, Montana
- Erikson Retirement Communities, Maryland
- Indiana Health Information Exchange (IHIE), Indianapolis, Indiana
- Intermountain Health Care (IHC), Salt Lake City, Utah
- Kaiser Permanente, Oregon
- Maimonides Medical Center, Brooklyn, New York
- Mercy Medical Center, Rural Iowa Redesign of Care Delivery with EHR Functions, Mason City, Iowa
- Meridian Health, Jersey Shore University Medical Center, Jersey City, New Jersey
- Montefiore Medical Center, Bronx, New York
- Partners Healthcare System, Inc., Boston, Massachusetts
- PeaceHealth, Eugene, Oregon
- Rhode Island HIE Project, Providence, Rhode Island
- Taconic Independent Physicians Association, Hudson Valley, Albany, NY
D. Selected Sites
Preliminary information was gathered by the research team through web searches and interviews with informants at each site. The expectation was that the team would gather enough information to determine if each site met the majority of the selection criteria and if they would be amenable to a site visit. This information was then shared with the ASPE Project Officer and together the project team and the ASPE Project Officer prioritized the list of candidates. The final list of sites was selected in January 2006. The approach was to first select the host site, and then determine if the main referral recipients from this site included three or more (affiliated or unaffiliated) PAC or LTC settings. The exception to this approach was Erickson Retirement Communities. Erickson is a CCRC and provides the spectrum of health care to the elderly, with the exception of hospital and hospice care. Therefore, for this site visit, we asked Erickson to provide us with names of hospitals and any community PAC or LTC settings that may serve Erickson residents.
The following four host sites were selected for site visits based on the preliminary background information obtained. More in-depth information was obtained later in the project as the site visit details were confirmed, as well as during the site visit. Specifics can be found for each site visit in Appendices B through E, and are in the order in which the site visits were conducted.
Erickson Retirement Communities
(Site Visit Dates: July 12-14, 2006)
Erickson Retirement Communities, Catonsville, Maryland, owns and operates 13 CCRCs in the United States. Four of their communities are considered "mature campuses" aimed at providing "total care" for retired individuals. One of the mature sites, the Catonsville campus includes a medical center that acts much like a physician's office for Erickson residents, a Medicare-certified HHA, inpatient and outpatient rehabilitation services, a SNF, and an ALF (personal communication with Daniel Wilt, Vice President Information Technology, March 23, 2006). Erickson employs certain medical specialists (e.g., podiatry, dentistry) and allows other independent clinicians to treat patients on campus. However, it does not own or operate most specialty clinics and does not own or operate any acute care centers. Three additional CCRCs are under construction and Erickson plans to establish additional communities throughout the country. Because Erickson's information technology approach is highly centralized--all campuses' EHRs are run out of the central office in Maryland and accessed using high speed network connections--they believe that their per site information technology costs will be reduced as they implement EHRs in new locations.
Erickson uses one EHR (GE Centricity) at the medical center on campus, and another (HealthMEDX) for the SNF (Renaissance Gardens) and the HHA. One forward-thinking, patient-centric advancement made by the information technology team at Erickson is the development of an electronic chart summary, which is generated from their EMR and can be accessed via the web or at any of their facilities' workstations. The chart summary includes, but is not limited to, relevant current and historical clinical information such as advanced directives, medication lists, laboratory results, problem lists, and contact information for patients and caregivers. Care coordination is facilitated as physicians electronically access this information on or off campus and communicate pertinent data in a timely manner to the ED physician when a patient requires acute care. In November 2005, Erickson launched a website6 providing residents access to their medial records for no additional cost. This and other online health information services are discussed in greater detail in Section III.G below.
At the time of the site visit, Erickson was not involved in a HIE organization in their area/region, although it is their desire to do so. They have initiated preliminary discussions with providers in their region on this topic.
Unaffiliated HDSs and PAC/LTC sites: St. Agnes Hospital and Hospice, Johns Hopkins Home Health Agency.
Erickson PAC/LTC sites: Renaissance Gardens (SNF and LTC NH), Erickson's on-campus HHA.
Montefiore Medical Center
(Site Visit Dates: August 2-4, 2006)
Montefiore Medical Center (Montefiore) is an integrated HDS in Bronx, New York, providing a full range of services, including specialty care to Bronx residents as well as patients outside of this borough. Montefiore serves a medically underserved population, a large number of whom are young, minority, and poor (Greg Burke, Vice President of Planning, Montefiore Medical Center, presentation slides from November 2004). The Montefiore HDS includes an acute care hospital (Montefiore Medical Center), a large HHA, and contracts with a number of SNFs in the area. Montefiore uses IDX's LastWord in both the inpatient setting as well as for ambulatory care at 28 sites. LastWord contains data from every Montefiore encounter for 1.8 million patients; currently this includes laboratory test results, medications, and images, but does not include notes and consults. Some scanned information also is represented. E-prescribing has been in place for close to a year. Montefiore also is one of several acute care hospitals involved in the creation of the non-profit entity called the Bronx Regional Health Information Organization (BxRHIO). At the time of this report, the other collaborators in the BxRHIO include several hospitals, over 40 community-based primary care centers, one NH, two HHAs, payors, physician offices, and laboratories. A month prior to our August 2006 site visit, Montefiore was awarded $4.1 million from the New York Department of Health for seed money (called HEAL-NY) to commence a data exchange RHIO in the Bronx. The focus of the Bronx RHIO is to facilitate sharing of clinical data among providers with disparate systems and levels of sophistication in using EHR systems (personal communication with Greg Burke, Vice President of Planning, Montefiore Medical Center).
Unaffiliated PAC/LTC sites: Schervier Nursing Care Center (SNF), the VNS of New York (HHA), the Jewish Home and Hospital (SNF).
Affiliated PAC/LTC site: Montefiore Home Health Agency.
Intermountain Health Care
(Site Visit Dates: August 9-11, 2006)
IHC is a non-profit health care system that provides care to residents of Utah and Idaho. This institution is one of the pioneers in HIT, with a long history of excellence in the area of quality improvement. Homer Warner, MD; Stanley Huff, MD; and others at IHC were among the first users and developers of EHR systems. LDS Hospital, one of IHC's hospitals in Salt Lake City was visited. Intermountain provides over 60% of the acute care market in Salt Lake City and has more than 27,000 employees enterprise-wide. LDS Hospital alone has 4,700 employees. Intermountain employs 550 physicians and has another 3,000 affiliated physicians with limited (read-only) access privileges to the electronic health information system (HELP system). Intermountain also has 92 clinics. According to one source, 17,000 people can access (with varying levels of permission) the Clinical Data Repository that is part of the HELP2 system.7 LDS Hospital is a member of the Utah Health Information Network (UHIN), a community health information network that began in 1993. UHIN is a coalition of health care providers, payors, and state government with, initially, the common goal of reducing costs by standardizing the transmission of administrative data, particularly payment data. The network community sets the data standards, using recognized national standards (e.g., HL7 messaging and NCPDP standards), to which providers and payors voluntarily agree to adhere. The UHIN standards are then incorporated into the Utah state rule regarding payment of health care via the Insurance Commissioners Office (UHIN, 2007).
UHIN operates as a centralized secure network through which the majority of health care administrative transactions pass statewide. Nearly all Utah payers and providers are participating in this project. UHIN developed a tool (UHINT), which they provide free of charge to providers for use in submitting electronic claims. The tool is provided so that even the smallest sized provider can submit claims and electronically receive remittance advices.8 State officials indicate that the exchange of standardized electronic transactions has drastically reduced the amount of paper processing required for payors and has streamlined the payment of claims and remits, which has resulted in providers receiving payment more quickly. Under an Agency for Healthcare Research and Quality (AHRQ) grant, UHIN is pilot testing the electronic exchange of a limited set of administrative and clinical data (medication history, discharge summaries, history and physicals, and laboratory results with a small number of providers). This pilot involves the exchange of information form payer to hospital only, no PAC or LTC providers are in the pilot. The results of this pilot study are not yet available, but the UHIN developers note informally that health care providers involved in the UHIN are beginning to request and require these clinical and administrative data. For example, UHIN developers are noticing an increase in feature requests from users (e.g., setting a statewide standard for credentialing physicians, account reconciliation). Because of the adoption of emerging technologies such as messaging and web-based connectivity (in place of earlier less nimble, less scalable, and more expensive technologies), UHIN's ability to fulfill those requests is keeping pace (personal conversation with Jan Root, Standards Manager, UHIN.
Unaffiliated PAC/LTC sites: Christus St. Joseph Villa (SNF), Community Nursing Service (CNS) (HHA), Hillside Rehabilitation (SNF), and CareSource (HHA and Hospice).
Affiliated PAC/LTC sites: IHC does not own any PAC or LTC facilities.
Indiana Health Information Exchange
(Site Visit Dates: September 13-15, 2006)
The IHIE is a non-profit venture connecting a number of HDSs in Indiana. The IHIE, led by Dr. J. Marc Overhage, comprises over 48 hospitals and has approximately 3,000 physicians who access the network. With AHRQ funding and a variety of other sponsors including BioCrossroads,9 regional and local hospitals, and the Regenstrief Institute, the IHIE recently implemented a community-wide clinical messaging project to support e-HIE between physicians and hospitals. Each participating partner has access to a limited amount of patients' clinical results using a single IHIE-controlled electronic mailbox called Docs4Docs (discussed in detail in Section III.G.6 of this report).
The IHIE was a health care market member in one of the four consortia10 awarded a HHS contract in 2006 requiring the development of four prototypes for a NHIN architecture. All three health care market members within the Computer Science Corporation (CSC) consortia (IHIE, MA-SHARE [Massachusetts], and Mendocino HRE [California]) helped to develop, test, and demonstrate a prototype, based on common, open standards. Of particular interest for this project, required components for all four prototypes: (1) were designed to facilitate HIE using the Internet, not creating a new network; (2) allowed for communication to occur between many different types of EHR systems; and (3) allowed for different types of software and hardware that could be included in the system. As stipulated by HHS, the prototype architectures were submitted to HHS in January 2007 and on February 14, 2007, CSC announced their success with exchanging health information through their NHIN prototype. Health data were securely transferred between MA-SHARE, the IHIE, and the Mendocino Health Records Exchange, as well as local public health departments within those regions (CSC, 2007).
Unaffiliated PAC/LTC sites: Beverly Enterprises at Brookview (HHA), VNS of Central Indiana, Briarwood Rehabilitation, Kindred Long-Term Acute Care Hospital.
Affiliated sites: Lockefield Village Rehabilitation and Healthcare Center (SNF), Wishard Health Services (Hospital).
E. Preparing for and Planning the Site Visits
A case study plan was developed and submitted to the ASPE Project Officer in June 2006, outlining the plan for how the site visits would be conducted (see Appendix A for the complete report).
The site visit team asked for assistance from each selected HDS in identifying which LTC/PAC agencies/facilities received their referrals, and also asked the HDS to provide contact information for these referral sites. The recommendations received from the host HDS were supplemented with additional PAC/LTC settings11 that were identified based on national reputation, ASPE Project Officer suggestion, and referral from industry associations (e.g., National Association for Home Care [NAHC], American Association of Homes and Services for the Aging [AAHSA], AHCA) and RHIOs.
Each of the four site visits consisted of multiple locations, which meant coordinating the review of four to five different providers at their separate locations. The site visit team visited an acute care hospital; three or more HHAs, NHs, or SNFs; and often another setting (e.g., a long-term acute care hospital or hospice). Coordination between the UCDHSC Project Director and leaders at each of the four respective sites was crucial for ensuring successful visits.
F. Development of Discussion Guide
To ensure that salient information was collected at each site while not constraining the site visit team to a single set of questions, discussion guides were purposely designed to be flexible and solicit open-ended responses. The site visit team used a variety of data collection methods to collect information. A "General Information about your Health Care Setting" form was submitted to all sites prior to the site visit. Using this form, we collected background information such as ownership, number of employees, EHR system used, etc. During the visits, site visit team members used in-person observation and formal and informal conversations, and questions and responses using the discussion guides created for this project. A set of the discussion guides and the general information form noted above can be found in the Case Study Plan in Appendix A.
G. Analysis of Focused Discovery Data Collection
Common themes and trends emerged as the data were collected and analyzed during the site visits. The site visit team sought to answer certain pre-determined questions at each site, and then observed and collected information on any actual (or potential) data exchange activities. The following narrative in Section III is a synopsis of these themes, which are largely a series of anecdotes. Specific details from each site visit can be found in Appendices B-E.
Results
The four site visits resulted in the findings illustrated in this section. Using all the data collected both prior to the four site visits and during each three-day visit, a compendium of findings for each site was created. Section A reviews the project objectives and background and Section B focuses on the clinical information exchange across the affiliated and non-affiliated PAC and LTC providers. Areas of HIE commonality are explored in Section C, Section D highlights solutions and future plans, and Section E discusses facilitators and barriers to HIE. The organizational and management issues related to HIT adoption are discussed in Section F, and Section G puts forth specific technological issues and observations made during the site visits.
A. Background
As noted in Section I, in addition to reporting on the current status of the use of HIT, one of the specific objectives of the visits was to identify the information needed at times of transition, determine how these data were (or were not) exchanged across care settings, and to identify barriers/facilitators to the exchange of data. Project objectives also included investigation of the method by which data are exchanged (electronically and not electronically) and the extent that data are exchanged between physician offices, laboratories, and pharmacies and PAC and LTC facilities.
The sites were not randomly selected, but rather were chosen based on criteria noted in Section II. The findings, therefore, are not necessarily representative for all settings, nor are the sites' HIT solutions replicable without taking into account the nuances of each site (e.g., size of the city, other competitors in the area, involvement of one or more "champions").
All four sites are located in medium to large metropolitan areas. Each site visit had a host or "hub" site and then three or more "spoke" sites. Three of the four host sites had an acute care hospital as the hub site, while the fourth (Erickson in Maryland) had a CCRC as the hub site. Three of the four had HIE organizations in various stages of development (Utah, Indiana, and New York). The fourth site (Maryland) had a well established albeit non-automated data exchange relationship with the local hospital. Thus, all four sites had processes in place that support information sharing across settings, including non-affiliated providers.
As suggested, health information can be exchanged across a variety of providers in a variety of ways. In an early attempt to delineate the different levels employed by different entities in sharing electronic health information, Walker and colleagues developed a four-level taxonomy describing the different stages of health care information exchange and interoperability (Walker et al., 2005). These levels are paraphrased below:
-
Level 1: Non-electronic data--no use of information technology to share information (examples: mail, telephone).
-
Level 2: Machine transportable data--transmission of non-standardized information using basic technology (e.g., fax or personal computer [PC]-based exchange of scanned documents, pictures, or portable document format [PDF] files). The information being exchanged cannot be electronically manipulated.
-
Level 3: Machine-organizable data--structured messages are used to transmit non-standardized data. This requires that the receiving computer "translate" data from the sending computer. This often results in imperfect translations and loss of meaning. Walker provides the following examples of this level of health information and interoperability: e-mail of free text, or PC-based exchange of files in incompatible/proprietary file formats, HL7 messages.
-
Level 4: Machine-interpretable data--exchange of structured messages that contain standardized and coded data.
Similarly, we observed the use of HIE applications and tools across many of these levels, including HIE that was completely paper-based, with the use of phone and fax to convey information to entities outside of the setting, to limited observations of standards-based, computer-readable, e-HIE that occurred using EHRs. Further, we found a wide range of HIE applications being used even within individual health care organizations. For example, during the site visits it was observed that organizations had both paper and e-HIE applications As a result, it was not possible to consistently apply the HIE and interoperability levels described by Walker et al. to describe the levels of HIE and interoperability within a single organization.
The following tables are heuristic guides to frame the site visit team's observations of HIE capabilities found as a result of the four site visits. Table 1 identifies four levels of HIE--where the first level reflects use of less sophisticated, earlier HIE applications (e.g., fax, telephone, mail) and the use of paper-based records, and the fourth level reflects completely interoperable HIE using standards-based EHRs.
| TABLE 1: Levels of Health Information Exchange |
|
Table 2 is illustrative with features described for each level to suggest a progression from less to more sophistication in terms of HIE. This table was constructed based on literature review as well as our observations concerning HIE and use of EHRs across the sites selected for this study. Although none of the settings observed have reached Level 4 (i.e., completely interoperable EHR systems, using standards-based applications to share information with affiliated and non-affiliated providers), it is included as the purported "future goal" for many of these settings. As will be described in more detail throughout this report, in general, we observed that:
-
Most HDSs (e.g., hospitals and physician offices) included in our site visits were at Levels 1, 2, and/or 3 for purposes of HIE, and were generally at Level 1 for purposes of HIE with PAC/LTC providers; and
-
Most PAC/LTC providers also were at Levels 1, 2, and/or 3. However, there were few instances in which PAC/LTC providers were observed to electronically exchange health information with hospitals, physicians, and other providers/clinicians, and there were a few instances in which the PAC/LTC providers were completely paper-based (Level 1).
-
Not unexpectedly, there may be variation within each Level as well so that, for example, a setting may be rather sophisticated in Level 3 for a function such as e-prescribing or laboratory result reporting, but in that same setting they may not have other electronic information sharing. So while they would be categorized as Level 3 using these criteria, they would be at the "low end" of it. Therefore, labeling an entire health setting at a particular level is not yet feasible, and this is why there are four areas of focus that are broken down by level later in the document. This report highlights our observations concerning the levels of HIE for the providers included in the site visits related to four clinical areas:
- transfer/discharge;
- communication with physicians/other clinicians;
- medication ordering/e-prescribing;
- laboratory/radiology ordering and results reporting.
| TABLE 2: Illustrative Examples of HIE Capabilities by Level | ||||||||
|---|---|---|---|---|---|---|---|---|
| Level 1 Paper-based Record/ No EHR | Level 2 Combined Paper Record/EHR | Level 3 EHR Used/Limited Electronic Data Exchange, Some HIT Standards Used | Level 4 Completely Interoperable EHR System, Use of HIT Standards | |||||
| HIE Methods |
|
|
|
| ||||
| Features/Attributes of Patient Health Information and Electronic HIE1 | No Electronic HIE (i.e., not electronic data) | No EHR | Some e-HIE | Limited use of EHR | Data exchange limited to certain systems | Access to data limited to user role/ discipline | EHR is primary record | Standards-based EHR system (i.e., EHR content is standardized) |
| May have software for AR/AP, scheduling | No Anytime/ Anywhere Access | May allow for images to be imported | Clinical information collected on paper & entered into EHR | Continued but limited use of paper record | Some use of standards (messaging &/or content) | Interoperable with internal & external systems | Record can be electronically exchanged/ is transportable | |
| Meets minimum regulatory requirements2 | Limited Anytime/ Anywhere Access | Decision support features & alerts used | Anytime/ Anywhere Access | Computer Empowered Interoperable System | Anytime/ Anywhere Access | |||
| Facilitators of HIE | Limited involved in HIE Network (e.g., admin/claims data) | Some clinical content exchanged within HIE Network | Greater amount clinical information exchanged/shared within HIE Network | |||||
| ||||||||
B. Exchange of Clinical Information
1. Introduction
HIE is an integral component of health care workflow and is important in the provision of quality care to patients. When the exchange of health information is performed well, care provision can achieve positive health outcomes. When information exchange is not performed well (e.g., it is untimely, inaccurate, or absent) potentially costly inefficiencies may occur or it may result in adverse events.
HIE across care settings is very complicated, regardless if the mechanism is electronic or manual. Such exchange involves multiple health settings with different information needs and with different levels of HIT adoption and technological sophistication. Ideally, information exchange should be two-way, with an opportunity for the receiving provider to ask clarifying questions or request supplemental information. However, often communication is a one-way transaction. Although information technology will not, nor should it replace face-to-face interactions, HIT can facilitate and augment information exchange. The goal of interoperable HIT has become a national priority in recent years. HIENs/RHIOs have been identified as important mechanisms in this regard and have experienced prolific growth. One of the requisite tasks for HIEN developers is to formalize who are the network partners and determine what information needs to be exchanged. Often, it seems that there has not been an explicit understanding and agreement about the range of partners that need to be involved in these networks, nor has there been a formal consensus building process for determining the content of information to be exchanged and when. A positive consequence of the push for HIT adoption has been the recognized need to formalize HIE relationships among information "trading partners." Therefore all entities that need information should be included as partners.
Understanding how HIT can be used to facilitate HIE requires a concomitant understanding of the influence of HIT on the daily workflow of health care professionals. In some cases, the workflow issues have been identified to be more challenging than technological issues. Discussions between HIE partners are beginning that further explore this interface and are focusing on questions such as: How can HIE be engineered such that it supports rather than detracts from health care professionals' patient care responsibilities? What information should be exchanged and when in the process of a daily routine should this occur? How can HIT facilitate this exchange?
With this recognition of the mutually dependent relationship between HIE and workflow, the following discussion provides a framework upon which the observations and key issues identified in subsequent sections can be interpreted.
2. What Are the Workflow/Communication Issues?
The four site visits reinforced the central roles that workflow and communication play in HIE and the importance of considering and planning for the desired workflow/communication issues to realize some of the efficiency gains that may be achieved though HIT implementation.
a. Workflow. Information technology is a cross-cutting issue, an observation that permeated the site visit discussions at many levels. In general, relatively highly-paid professionals in hospitals and PAC, and LTC settings are expending a significant proportion of their time on clerical tasks rather than attending to patients' clinical needs. Implementation of EHR solutions did not necessarily provide solutions to this inefficiency. It was common for sites to report that nurses and physicians read from a computer screen or print out a patient's health data from one electronic health application only to manually re-enter the information into another electronic health application (such as an EHR).
Physicians, nurses, and other representatives (admission coordinators, information technology professionals, etc.) from the study sites generally had not considered how the recipient of electronic information could re-use the information to streamline and make workflow processes more efficient. In most cases, the clinicians were not consciously aware of the amount of time and effort that was being expended on multiple tasks involving the re-entering of data that was otherwise electronically available. In many instances, representatives seemed to simply insert electronic documents into existing workflow processes and as a result perpetuating (unnecessarily) duplicative administrative tasks.
The lack of standardized HIT/HIE applications also contributed to inefficient practices. Because of the lack of interoperable EHRs, for example, respondents described manually re-entering laboratory results received electronically into their own EHR system, because the laboratory and receiving health care setting's EHR systems did not have the capabilities of exchanging this type of data electronically.
However, further probing revealed that the manual re-entry of data sometimes was considered to be of value. For example, the literature reports that manual re-entry of a medication list from one system or medium to another may add value in terms of quality and safety, while risking the introduction of new errors (e.g., transcribing the wrong dosage, misspelling the medication that is similar to another medication that treats something completely different or is contraindicated) (Brody, 2007). During site visit discussions, clinicians acknowledged that this manual re-entry activity was not simply a clerical process but rather something that provided an opportunity to cognitively assess whether the medications were in fact appropriate, whether any additional diagnostic testing was required, and whether the patient might be at risk for an adverse drug reaction. Occasionally, the notion of trust also would arise--clinicians seemed to place greater trust in information that had gone through the manual re-entry process. Thus it remains to be determined how these vital tasks will be accomplished once more advanced (e.g., interoperable) electronic solutions are forthcoming. The authors speculate that there always will be a need for "the human element" in reconciling information such as the medication list--information technology solutions will merely augment and assist them in these care processes.
In a typical workflow process, keeping track of when a particular task (e.g., obtaining physician's signature, orders) was completed so that the next person could do her/his job was reported as something on many people's "wish list" for what they would like their EHR to do for them. Current practice requires a great deal of time spent manually tracking tasks that could easily be automated in the EHR.
b. Importance of interpersonal relationships. The importance of interpersonal relationships among health care professionals cannot be overstated. The site visit team observed how established interpersonal relationships impacted HIE. Typically, patient information sharing occurred among hospital discharge planners and/or social workers, and NH and home health care agency intake coordinators. Interestingly, the importance of interpersonal communication was no less in care settings that had the capacity to share information electronically versus those that primarily shared information on paper. For example, despite the fact that several hospitals and NHs in New York and Utah have invested in a proprietary software program, Extended Care Information Network (ECIN), to facilitate more efficient referrals (described in further detail below), it is not uncommon for disposition discussions to precede the distribution of the ECIN information. Thus, although this technology was put in place to facilitate hospital referrals to SNFs/HHAs, informal, less technological approaches (e.g., face-to-face discussions, telephone, faxes) often were the primary mechanisms of data exchange, with HIT being a supplement to this data sharing activity. The perceived value of relationships that exists between these professionals was of more importance when compared to the technology. Our site visit team observed that intake coordinators in referred facilities often received the patient's information telephonically from their hospital colleagues in advance and had already accepted the patient by the time the patient's information is distributed in electronic transfer/discharge summaries, such as ECIN.
c. Other issues that impact communication between referring and receiving providers. Communication and information exchange between some of the observed health care settings was not hindered by a lack of technological solutions. For example, in Maryland, Erickson (a CCRC that provides all health care to their residents with the exception of acute care and hospice) and the local hospital (St. Agnes) have a very close working relationship and freely communicate. Erickson physicians are able to treat their patients should they be admitted to St. Agnes, and they have read-only access to the St. Agnes EHR, but still need to print out anything they would like to have in their Erickson health record. St. Agnes also allows an Erickson-employed nurse to work in the hospital to facilitate discharges back to one of the Erickson facilities (e.g., their SNF, Renaissance Gardens).
Clearly communication between these two entities is occurring, as is HIE, of which most at this point is still manual. Technology was not considered a hindrance; in fact, the leaders at St. Agnes commented that technology is a minor issue in solving the problem of e-HIE. Rather, issues such as who is responsible for protecting the privacy of data at the time of e-HIE and who is liable for the accuracy of the data were identified as the barriers to effective information exchange across health care settings, particularly unaffiliated settings. Further, it remains to be determined who should pay to populate the specific data fields that often are idiosyncratic to each referring/receiving provider. Transmitting data requested by the receiving provider likely will create additional costs (including personnel, programming, troubleshooting/maintenance, upgrades, etc.). The multiplicity of formats may be too burdensome and costly for some providers. For example, the development of an interface between St. Agnes and Erickson to facilitate data sharing was reported by Daniel Wilt (Senior Vice President of Erickson Information Technology Department) to initially cost approximately $50,000, which then would require maintenance and upgrades over time. This interface only benefits this one relationship between these two entities. Creating unique interfaces to support all referring and receiving sources may be unnecessarily costly and inefficient.
In fact, concern about the relatively high cost of an almost unlimited number of needed idiosyncratic interfaces gave rise to the emphasis in recent years concerning the need for HIT standards to support interoperable HIE. For example, it is anticipated that the use of: (i) the HL7 CCD implementation guide and the content standards referenced in that guide; and (ii) standards to support e-prescribing will allow the exchange and re-use of this information without the need for these costly interfaces. However, as described below, during out site visits we observed very limited use of HIT standards to support the electronic exchange of patient information.
d. Timeliness of the communication/information exchange. The element of time permeated through nearly every discussion that occurred during the four site visits. In particular, when hospital staff believe that a patient is ready for discharge and will require short-term placement in a NH or a referral for home health care, receiving providers must be in a position to quickly decide whether or not to accept the patient, often based on incomplete or even inaccurate information. NH staff at Jewish Home and Hospital Agency (JHHA) and Schervier (New York) both commented that information received from local hospitals often is incomplete, and varies depending on the person completing the discharge form at the hospital. As a result, the receiving facilities/agencies may make poorly informed, inaccurate decisions and may not be in a position to meet the patient's needs upon admission.
3. Health Information Exchange Across Care Settings: Hospitals, Post-Acute, and Long-Term Care
Older adults with acute and chronic health conditions often receive care in multiple, disparate settings by a number of care providers (e.g., primary care physician, one or more specialists) who may or may not share (complete) information. The transfer of timely and accurate information across settings and providers is critical to the execution of effective care transitions. Practitioners need an understanding of the patient's goals, baseline functional status, active medical and behavioral health problems, medication regimen, family or support resources, durable medical equipment needs, advanced directives, and ability for self-care (Coleman, 2002; Coleman, 2003; HMO Workgroup on Care Management, 2004). Without this information, service duplications may occur, important aspects of the care plan may be overlooked, and conflicting information may be conveyed to the patient and family caregivers. Incomplete information transfer can result in critical errors, such as the patient returning home without life-sustaining equipment (e.g., supplemental oxygen or equipment used to suction respiratory secretions). The absence of information about an older patient's baseline level of cognitive function may result in an acute decline in cognitive status being mistaken for chronic dementia. Furthermore, a lack of understanding of a patient's functional health status, including both physical and cognitive, may result in transfer to a care venue that does not meet her or his needs. Thus, improved HIE (manual or electronic) is a critical step toward reducing medical errors, improving quality, and increasing efficiencies for patients who receive care across settings.
This section focuses on HIE across affiliated and non-affiliated acute care hospitals, PAC, and LTC providers. Specifically, it examines information exchange between hospitals, physician offices, NHs, home health care agencies, and, in one setting, a CCRC. To frame this discussion, it is important to note that while there are similarities between how care is delivered in each of these settings, there also are key differences that potentially influence both the content and process of information exchange. Hospitals, PAC, and LTC settings treat patients with different needs, have different staffing ratios, different clinical information needs, different orientations and approaches to assessment and management, and face different regulatory and reimbursement requirements. These disparate requirements translate into different data needs. Further, providers' HIE often is guided by the need for compliance with existing policies and regulations, including required reporting for patient assessment instruments (PAIs) such as the MDS and OASIS, the Pre-Admission Screening and Annual Resident Review (PASARR),12 the New York State Patient Referral Instrument (PRI),13 and Medicare Conditions of Participation (CoPs).14
This section begins by describing the clinical domains that the literature identifies as needing to be exchanged and then compares these domains with what was observed on the four site visits, including what is not being exchanged. Next, promising new developments that could support improved HIE will be featured. Key aspects of clinical workflow issues then will be described, followed by comparing and contrasting how health information is exchanged among affiliated and unaffiliated providers. This section will conclude with observed facilitators and barriers to HIE, including e-HIE.
a. What is the content of information exchanged. Based on a review of published literature, summaries of large national conferences, and documents produced by professional societies; at present there is no consensus on the content and type of information exchange needed between hospitals, PAC, and LTC settings. Four distinct national efforts that have begun to address this question include:
-
The CCD (HL7 and ASTM, 2006).
-
The Uniform Patient Assessment for Post-Acute Care tool (CMS, 2006). The UCDHSC developed a concept paper for CMS that provided recommendations for developing a uniform assessment tool that would cut across all PAC settings. The Deficit Reduction Act of 2005 requires the demonstration of a comprehensive assessment at the time of hospital discharge to determine appropriate placement and the use of a use a standardized PAI across all PAC sites to measure functional status and other factors during the treatment and at discharge from each provider. CMS awarded a contract to RTI International to specify the elements of this tool (which has been named the Continuity Assessment Record and Evaluation (CARE) instrument) and perform a demonstration project.
-
The HMO Care Management Workgroup (HMO Workgroup on Care Management, 2004).
-
The Veterans Affairs Geriatrics and Extended Care (GEC) Referral Discharge Planning Tool (Department of Veterans Affairs, 2006).
Each of these efforts evolved separately. A comparison of the individual domains and classifications needed for information exchange from each of these efforts is shown in Table 3. While there are many similarities among the four efforts with respect to the selection and inclusion of key clinical domains, there are also a considerable number of differences observed as well. A detailed description of the first four efforts can be found on the ASPE website15 (Coleman, et al., 2007). One of the important differences between the CCD and the other activities listed above, is the HL7 CCD identifies not only the pertinent health care domains for which patient specific information may need to be exchanged at the end of an episode of care, but the CCD also specifies the HIE content and messaging standards that enable standardized electronic exchange of a CCD-compliant transfer/discharge document.
While there often was overlap in the clinical domains included in these HIE specification, there was considerable variation in the type of data within each of the domains. For example, each of the efforts identified a problem list and advance directives. However, the GEC (VA) tool does not list allergies and medications because the tool is designed to complement core information available in the VA EHR. The GEC (VA) tool and the Uniform Patient Assessment tool both are more strongly oriented toward PAC and LTC and as a result, have more items that reflect the types of care more typically addressed in these settings such as continence and skin integrity. Some care settings, such as EDs, desire a much smaller subset of core data items as they do not have the opportunity to review much data during the brief clinical encounter.
Within Medicare's regulatory framework, the CoPs include requirements concerning information exchange at the time of transfer for hospitals, NHs, and HHAs (CMS, 2001; Coleman et al., 2007; Hughes, 2003). Where explicitly identified in the CoPs, the required clinical domains at the time of transfer are comparable to those clinical domains specified in the four national efforts described in Table 3.
Responses from those interviewed revealed a high level of consistency in the content of information needed to support HIE at the time of transfer. For example, Wishard Hospital (Indiana) considers the discharge summary, insurance information, medication list, allergies, problem list, and advance directives among the core information needed at the time of transfer from an SNF or HHA to the hospital or vice versa. LDS Hospital in Utah assembled a similar list and added physical therapy (PT) notes. Erickson Retirement Community (Maryland CCRC) regards medications, allergies/intolerances, medical problem list, advance directives, clinical notes, radiology reports, laboratory results, and clinical notes as the highest priority clinical domains. When the JHHA, a New York NH, transfers a patient to hospital, an information packet is prepared that includes a medical summary of recent events completed by the physician, a handwritten medication list, immunization list, EKGs (if available), and recent laboratory tests. Staff at Schervier (New York NH) also send this same set of information with patients who are transferred to the ED or hospital and, in addition, complete an internally-developed standard transfer form that describes the reason for transfer.
| TABLE 3: Overlap of Clinical Domains and Clinical Information to be Exchanged Between Acute Care Hospitals, Post-Acute, and Long-Term Care Settings | ||||
|---|---|---|---|---|
| Key Clinical Information to be Exchanged | CCD (HL7, CDA) | Uniform Pt Assessment (CMS) | HMO Care Mgmt Workgroup | GEC (VA) |
| Purpose (i.e., transfer) | X | |||
| Payers | X | |||
| Advance directives | X | X | X | X |
| Support (persons/family)/Caregivers Information | X | X | X | |
| Functional status | X | X | X | |
| Cognitive | X | X | X | |
| Physical | X | X | ||
| ADLs/IADLS, baseline, current | X | X | X | |
| Problems, Prognosis | X | X | X | X |
| Family History | X | |||
| Social History | X | |||
| Allergies, Adverse Reactions, Alerts | X | X | X | |
| Medications | X | X | X | |
| Medical equipment | X | X | X | X |
| Suppliers | X | |||
| Immunizations | X | X | ||
| Vital signs | X | |||
| Results | X | |||
| Procedures | X | |||
| Encounters | X | |||
| Plan of Care | X | X | ||
| Health Care Providers, PCP | X | X | X | X |
| Goals of care | X | X | X | |
| Discharge instructions, disposition | X | X | ||
| Pain | X | |||
| Skin integrity | X | X | ||
| Sensory deficits | X | X | ||
| Dietary needs | X | X | ||
| Continence | X | X | ||
| Falls risk | X | |||
| Current services receiving in home | X | X | ||
| Capacity to perform self care, educational needs | X | X | X | |
| Ethnic/cultural considerations/language | X | X | X | X |
| Self-rated health status | X | |||
| Source of referral | X | |||
| Where does patient live, with whom | X | X | ||
| Homebound status | X | |||
| Additional information (environmental hazards) | X | |||
| Weight bearing | X | |||
| Referring to which program | X | X | ||
| Estimated duration of care | X | |||
| Skilled care services needed | X | |||
| Behaviors and symptoms | X | |||
In contrast to the states of Indiana, Utah, and Maryland, New York State regulations mandate the information that must be made available to the receiving care team prior to a patient's transfer. The sending institution (typically the hospital) must complete the PRI for all patients being referred for Part A covered SNF care, and New York nursing staff must be certified to complete the PRI. The PRI scores the patient on intensity of care with categories including physical and cognitive function, medications for the last seven days, recent laboratory results, x-rays, PT and occupational therapy (OT) notes, and wound care. In addition to supporting HIE, this tool facilitates an appropriate match between the patient care needs and the care setting.
b. What information is not being communicated/exchanged. Across all four of the site visits, the most common clinical content not routinely exchanged between the hospital and the PAC/LTC settings was the patients' current mental status and recently exhibited behavioral symptoms. NH staff at Lockefield Village (Indiana extended care facility associated with Wishard Hospital) commented that they rarely receive information about a patient's mental and behavioral status prior to transfer from the hospital. When information is provided, it often is incomplete or inaccurate. These frustrations were echoed by the JHHA and Schervier (New York SNFs/LTC facilities). Staff at both facilities recognized that current financial incentives to discharge patients from hospitals as quickly as is reasonably possible, are not always aligned with full disclosure by the referring hospital of a patient's status. Not only could this information delay a potential transfer or discharge from a hospital, disclosing such information may trigger PASARR screening and require further evaluation by mental health professionals. Consequently, hospitals may not share this information with potential receiving NHs.
While not included on any of the lists described above in Table 3 of clinical domains for which information exchange is needed, the second most cited type of clinical content that is not reliably transferred across settings is PT notes. Despite a relatively high level of integration, Erickson Retirement Communities staff (Maryland CCRC) noted that there is no existing mechanism to ensure that the clinical information charted by the physical therapist in Renaissance Gardens (their SNF) is transmitted to the physical therapist in home health care (which is on the same campus) to which the patient has been referred or discharged. Renaissance Gardens and the Erickson HHA both use the same EHR (HealthMEDX). Similarly, both JHHA and Schervier (New York NHs) identified PT notes as rarely included but nonetheless needed in the transfer information received from the referring hospital.
Patients' wound status was the third most commonly observed clinical data not reliably exchanged, but reported as needed. Briarwood (Indiana NH) staff commented that not having this information left them unprepared to meet a patient's needs, either because they did not have the on-site expertise to evaluate and treat the patient or because care required specialized equipment, dressings, or therapies that was not available in their facility upon admission. Had they known the extent of the patient's need prior to admission, they may not have accepted the patient knowing they did not have the on-site expertise.
Advance directives also were not consistently shared. Providers attributed part of the problem to the fact that these documents often "stand alone" from other health-related information and therefore are more likely to become separated from other transfer documents. Often, family caregivers were asked to provide a duplicate copy of the patient's advance directive, as providers noted that requesting the information from the transferring institution was often unproductive. Although regulatory requirements mandate that admitting facilities request an advance directive on all patients, the same requirements do not mandate what happens to the actual advance directive document and whether it becomes an integral part of the patient's record. Clinicians at the hospital and PAC/LTC sites visited often noted that advance directives are sometimes misplaced, misfiled, or mishandled by the receiving health setting. The importance of these documents for ensuring patient centered care cannot be overstated. Patients complete these documents to convey to health care professionals what type and duration of treatments that they believe to be either acceptable or unacceptable. The inaccessibility of these documents may result in undesired treatments being administered, desired treatments being withheld, or inexcusable violations of a patient's religious or cultural practices (Morrison, Olson, Mertz, & Meier, 1995).
With regard to medications, staff at JHHA and Schervier (New York NHs) were appreciative that they generally received the medication list and sometimes the Medication Administration Record (MAR) from the referring hospital. However, they expressed a desire to extend the time period that the hospital provides medication reporting to a full 14 days. This would facilitate more accurate completion of documentation required by the MDS (version 2.0 for NH resident assessment and care screening) and used in the calculation of Resource Utilization Groups-Version III (RUG-III) needed for payment. RUG-III categories and appropriate payment rates are based upon the level of nursing requirements, and residents with greater or specialized nursing requirements, therapies, and other conditions are reimbursed at a higher level. Receipt of timely and accurate information from transferring institutions is imperative for accurate assessment (CMS, 2007b).
Members of the site visit team uniformly heard that hospital and PAC settings would stop chronic care medications upon admission and inadvertently not restart them upon discharge. Often, if it were not for the patient or other family member's initiative, these chronic care medications would be forgotten with resulting potential for adverse effects.
Finally, information that describes the roles and contact information for family members was rarely shared across settings. Interestingly, this information was rarely identified during the site visits as key clinical content to be shared at the time of transfer, yet patients receiving home care rely on loved ones and other caregivers to a great extent.
In summary, considerable overlap was observed with regard to the type of health domains for which information was exchanged between the clinical categories addressed by the four national efforts described in Table 3 and the type of health information that was exchanged by providers in the sites that were visited. However, considerable variation in the specific type of data within each of the domains that was exchanged and sometimes reported as needed also was observed. Reasons for this variation include: (1) that the specific types of health information to be exchanged often reflect the idiosyncratic agreements between the sending and receiving providers; (2) providers within health delivery organizations/systems have not reached an agreement on the type of health information that is needed to be exchanged; and (3) regulations require the exchange of certain types of data; and in some cases, regulatory activity dictated the type of health information that must be exchanged. In addition, during the site visits two clinical categories were observed that had been mentioned in the previously described national efforts as not being the type of information routinely shared across care settings. The first was information that describes the roles and contact information for family caregivers, as they play an essential role in implementing the care plan. Secondly, the patient's physical, cognitive, and behavioral status were not routinely identified as a high priority clinical category by hospital, PAC, or LTC providers, despite the importance of this information in matching the patient's care needs to an appropriate PAC setting.
c. How and what information is exchanged with affiliated and unaffiliated health settings. Although it was anticipated that HIE between affiliated settings would be more complete, efficient, and likely be accomplished electronically, the site visits did not confirm these assumptions. In fact, HIE between affiliated settings was found not to be significantly different from HIE between unaffiliated settings. Generally, HIE was found not to be timely or complete regardless of affiliation between health care providers, and regardless of availability of electronic health information in the referring provider's health information system. What follows summarizes the findings for HIE between affiliated settings and unaffiliated settings, particularly at times of discharge and transfer to a new health entity.
In general, the site visits uncovered relatively few examples where HIE had been formally addressed by affiliated health settings. The receiving providers were rarely asked to articulate their needed clinical information or clinical content and their preferred mode of communication. Rather, the sending provider largely determined these parameters, and this is true regardless of the direction of the transfer. The exception to this is Erickson Retirement Communities; because their employees (e.g., physicians) functioned as both a "sender" and a "receiver" of health information (their physicians treated patients sent to St. Agnes hospital for acute care as well as at all phases of care on the Erickson campus), they were able to design and communicate the needed information.
C. Health Information Exchange Areas of Commonality
The four site visits afforded the opportunity to better understand approaches, and compare and contrast how HIE is (or is not) accomplished electronically or manually between both affiliated and unaffiliated health settings. The following discussion will focus on four areas of commonality addressed at each of the visited sites:
- Information exchange at times of discharge/transfer.
- Communication with physicians.
- Medication ordering/e-prescribing.
- Laboratory/radiology orders and results.
The illustrative Table 2 will be re-used in the following discussion to display the range of electronic functioning observed during the site visits for each of the focus areas noted above.
1. Information Exchange at Times of Transfer/Discharge
The single document designed to encapsulate a patient's hospital course, the hospital discharge summary, was frequently cited by the receiving care teams as not being available in a timely manner. Several sites confided that the receiving providers (i.e., acute care hospitals, specialists, and EDs) only want specific information, and receipt of "extraneous" information frustrates the sending providers' efforts to care for the patient. For example, PAC/LTC providers sending patients to the ED may include recent laboratory results, a current medication list provided by the NH or HHA, advanced directives, progress notes, and the like. Likewise, those interviewed from hospitals and EDs indicated that they often experienced "information overload," that is, the PAC/LTC settings provided too much detail at ED admission (i.e., information that the attending ED staff do not believe they need to care for the patient).
As Table 4 shows, despite the potential advantages that provider affiliation might suggest for e-HIE at times of transfer, little evidence for interoperability or auto-population of data fields (e.g., in transfer/discharge documents) was found. The site visits confirmed that when exchanging health information either between affiliated or unaffiliated providers, sending paper documents with the patient and/or facsimile transmissions remain the predominant communication approaches to support any type of HIE to and from physician offices, hospitals, PAC/LTC settings, pharmacies, and laboratories. The information sent was primarily in the form of handwritten summaries of electronically available information, supplemented by photocopies of pertinent information such as the MAR, recent laboratory results and diagnostic imaging results, or recent assessments. Medication information was more likely to be sent with the patient while laboratory data and hospital discharge summaries were more likely to be faxed at a later date. In some cases, paper and facsimile information transfer was supplemented by telephone communication. The examples below are illustrative and do not cover every observation found during the site visits.
Indiana -- When patients are transferred from Lockefield Village or Briarwood Health and Rehabilitation (two SNFs) following a Part A covered stay to home health care, communication with the receiving HHA is via phone or fax, or both (Level 1). However, the five participating hospitals involved in the IHIE Docs4Docs portal can remotely access information. Because this is a new technology, they first are starting with hospital discharge transcriptions and laboratory/radiology ordering and reports (not a complete discharge summary, but components of it). At the time of the site visit, medication ordering and monitoring (an integral part of a discharge summary for use at times of transition) were not accessible through the Docs4Docs portal, but the technology would allow for this capability--it is more the issue of when, which is why the authors rated the exchange of hospital discharge summaries as a Level 2/3 feature in Table 4.
The Wishard Hospital EHR can electronically produce a clinical summary for patients as they enter the ED that includes reason for visit, problem list, medications prescribed by affiliated doctors, recent dictations of affiliated physicians, recent laboratory results, recent radiology results, and immunizations. Advance directives are not part of the summary. For those patients who are not admitted to the hospital, there is an opportunity to update the ED summary and send this information with the patient back to the nursing facility at which the patient is placed. However, this is not done routinely (Level 2).
| TABLE 4: HIE Capabilities by Level With a Focus on Exchange of Information at Times of Discharge/Transfer | ||||||||
|---|---|---|---|---|---|---|---|---|
| Level 1 Paper-based Record/ No EHR | Level 2 Combined Paper Record/EHR | Level 3 EHR Used/Limited Electronic Data Exchange, Some HIT Standards Used | Level 4 Completely Interoperable EHR System, Use of HIT Standards | |||||
| HIE Methods |
|
|
|
| ||||
| Features/Attributes of Patient Health Information and Electronic HIE | No Electronic HIE (i.e., not electronic data) | No EHR | Some e-HIE | Limited use of EHR | Data exchange limited to certain systems | Access to data limited to user role/ discipline | EHR is primary record | Standards-based EHR system (i.e., EHR content is standardized) |
| May have software for AR/AP, scheduling | No Anytime/ Anywhere Access | May allow for images to be imported | Clinical information collected on paper & entered into EHR | Continued but limited use of paper record | Some use of standards (messaging &/or content) | Interoperable with internal & external systems | Record can be electronically exchanged/ is transportable | |
| Meets minimum regulatory requirements1 | Limited Anytime/ Anywhere Access | Decision support features & alerts used | Anytime/ Anywhere Access | Computer Empowered Interoperable System | Anytime/ Anywhere Access | |||
| Facilitators of HIE | Limited involved in HIE Network (e.g., admin/claims data) | Some clinical content exchanged within HIE Network | Greater amount clinical information exchanged/shared within HIE Network | |||||
| Discharge/ Transfer2 | Indiana | |||||||
| Maryland | ||||||||
| New York | ||||||||
| Utah | ||||||||
| ||||||||
Maryland -- Erickson Retirement Communities, a CCRC in Catonsville, Maryland, provides all PAC and LTC to their residents that live on campus, with the exception of hospice. Their campus also does not have an acute care hospital or specialists on staff, but their physicians treat their patients if they are transferred to St. Agnes (an unaffiliated hospital that receives the majority of Erickson residents who are hospitalized). Erickson sends an electronically-generated (i.e., auto-populated) transfer summary with all patients who are referred to the unaffiliated ED or acute care hospital, and also to any affiliated specialists. This summary is printed from the Erickson GE Centricity EHR and a paper copy accompanies the patient (Level 2). St. Agnes hospital's ED physicians provided input and feedback during the development of this transfer summary. Such input was considered an important factor to the utility of the transfer document.
New York -- Although the majority of HIE related to discharge/transfer was manual, exceptions also were noted. During the visit, the site visit team learned of the state-mandated PRI. Specifically, the State of New York requires hospitals to use the PRI when patients are transferred from a hospital to a NH or SNF. New York permits either electronic or manual exchange of the PRI form. The PRI and supplemental information are distributed electronically from Montefiore Medical Center (Bronx hospital) to local area NHs using ECIN, a software program that only requires the use of a web-enabled PC. Each provider needs to purchase and install the software and pay a monthly/annual fee for its use.16 ECIN is an Internet-based automated PRI that claims HL7 compliance. Use of the HL7v2.X standard supports the standardized messaging of the PRI form but the content of the PRI form is not standardized. This level of sophistication would be included in Level 3 of Table 4 above.
Awareness of ECIN capabilities (i.e., a software program that produces and electronically transmits hospital discharge information such as that found on the New York PRI form) seemed widespread among the four cities visited; however, no one at any site, including sites visited in New York, mentioned current or planned expansion of ECIN's use of HL7 messaging standards to support the exchange of additional clinical content such as demographic and clinical information. Instead, those who did use ECIN merely viewed the information on a web-display rather than importing this information and using it for other purposes. Information is sent by the referring institution to a list of NHs from a pick-list menu on line. As explained by NH staff in New York, when a referral arrives at the NH, an e-mail or pager alerts the staff. At this point, the receiving NH has the opportunity to e-mail back or call to ask questions and/or indicate its interest in accepting the patient. NHs without ECIN may receive the PRI via fax (Level 2).
According to Montefiore, ECIN helped reduce hospital length of stay (LOS) for NH-bound patients from ten to eight days. For Montefiore, some of the fields (mostly demographic and insurance) of the PRI can be auto-populated, while others (e.g., laboratory results, medications, and PT notes) are copied-and-pasted electronically from the Montefiore EHR (CIS). Representatives from Montefiore reported that prior to automation, the tool-based PRI completion process required 30-40 minutes to complete whereas after automation, it is completed in 10-15 minutes.
However, e-HIE is not necessarily maximally enabled even when a patient is transferred to an affiliated provider and both the sending and receiving providers have EHRs. For example, if a patient is admitted to Montefiore Medical Center (hospital) while actively receiving home health care, the Montefiore Home Health Agency (MHHA) coordinator based in the hospital will print a transfer summary from the MHHA EHR (which is a Misys product) and place a hard copy in the hospital record. This is particularly valuable as the ED and hospital staff do not have access to Misys and at present, there is no electronic interface between the Montefiore Medical Center EHR (CIS) and the MHHA EHR. MHHA staff have read-only access to the Montefiore Medical Center's EHR (CIS). This is a Level 2 capability. When a patient is discharged from Montefiore home health services, a discharge template in Misys is generated that is populated in part by Misys and in part completed by the nurse who manually types in remaining fields. This summary is sent to the attending outpatient physician in paper form that can then be scanned into the Montefiore Medical Center's EHR (also a Level 2 function).
In these examples, implementations of multiple non-standardized EHR products (the MHHA's use of Mysis, and the Montefiore Medical Center's use of CIS) while most likely decreasing staff time to complete discharge/transfer documents, have created a barrier to electronic exchange.
Utah -- All health settings visited in Utah (including LDS Hospital, two NHs and two HHAs) are at Level 1 or 2 as it relates to discharge/transfer. When patients are discharged from Brookview (NH) to an HHA, information is printed from their EHR or photocopied from the chart and mailed or faxed to the receiving provider setting. At CNS, another HHA in Utah, intake care coordinators manually re-enter information received from the hospital into its EHR (HomeSys) because information received from the hospital is not standardized and does not interoperate with the CNS EHR. Intake coordinators at Hillside Rehabilitation, a NH, scan (digitize) paper-based hospital information as they receive it and upload the digital representations into its EHR (Blue Step).
At LDS Hospital, the discharging physician routinely dictates the complete discharge summary after the patient is discharged. The lag between when the patient is discharged and the dictation is complete varies depending on the physician and ranges from one day to three weeks. The dictated hospital discharge summary is transmitted by fax or mail to the receiving NH/HHA. For example, when admitting a new patient, CareSource, a HHA in Utah, requests a history and physical, demographic sheet, medication list, and current progress notes. On average, they receive this information 75% of the time (in a paper format and it may require up to three follow-up phone calls to obtain (Level 1). This observation confirms an earlier observation about the incentives for e-HIE; whatever the incentives, they do not operate uniformly across patients and across providers. For example, the incentives for a SNF administrator to move toward e-HIE with a hospital may be that she/he would get timely and accurate information at the time of discharge. For the hospital, the incentive to adopt HIE strategies with a local SNF may be to have the capacity to discharge their patients more quickly and therefore save money and free up a bed for a new patient.
With respect to transfers in the reverse direction (e.g., NH to hospital), the site visits revealed a modest improvement when it came to the completeness and timeliness of HIE. For example, when patients are urgently transferred to the hospital, the staff member in charge of medical records at Brookview NH helps to create a handwritten form that includes a current medication list, recent laboratory results, insurance status, skin status, code status, physician name and contact, and facility contact information. Many of these clinical domains are gathered from the NH's EHR but are handwritten onto the form (this would fall between Levels 1 and 2). The template for this form was not the result of a discussion between Brookview and the receiving hospital.
2. Communication with Physicians and other Clinicians
It is worth repeating that electronic access to an EHR is sometimes limited to certain physicians and other clinicians (e.g., nurse practitioners, physician assistants, nurses, therapists, social workers). As such, Table 5 shows that some sites have fairly sophisticated modes of communication, including electronic means, while others rely solely on phone and/or fax.
Indiana -- As previously mentioned, IHIE has launched the Docs4Docs physician portal. Participating physicians (no other clinicians such as nurses, therapists, or social workers had access at the time of the site visit) and five Indianapolis hospitals can obtain a limited set of information (laboratory and radiology results and discharge descriptions on patients treated by any of the participating hospitals and/or physician practices). Each physician has a unique identifier within the portal, and is able to look at these results for any of their patients being treated at any of the participating health settings. However, currently there are no NHs or HHAs that are part of the IHIE. So access to any health data obtained while patients are being treated in these settings is limited to the ordering physician. Thus, although the range of use puts Indiana at a Level 3 in Table 5 for this function, the electronic capability documented is limited to certain physicians and hospitals.
At Wishard hospital, a computer terminal has been set up in Lockefield Village (an extended care facility that offers both Part A SNF coverage and LTC, and is physically located on the Wishard campus). To some extent, Wishard hospital and Lockefield access the same EHR (at least for Medicare Part A SNF patients), but the amount of data stored in the EHR is limited for Lockefield Village residents. Specifically, some of the daily physician and nurse charting for the Medicare Part A SNF patients at Lockefield Village is entered into the Wishard EHR, but physical therapists only enter their discharge summary into the Wishard EHR (Level 2). Other documentation gathered and entered by the physical therapists for patients in Lockefield Village (e.g., therapy notes) are stored in a paper record maintained by Lockefield. For their LTC residents (i.e., non-Medicare Part A), no physician and nurse charting is entered or stored in the Wishard EHR. Rather, all medical record information on behalf of all non-Part A covered nursing facility residents at Lockefield Village is paper (Level 1).
| TABLE 5: HIE Capabilities by Level Regarding Communication with Physicians and Other Clinicians | ||||||||
|---|---|---|---|---|---|---|---|---|
| Level 1 Paper-based Record/ No EHR | Level 2 Combined Paper Record/EHR | Level 3 EHR Used/Limited Electronic Data Exchange, Some HIT Standards Used | Level 4 Completely Interoperable EHR System, Use of HIT Standards | |||||
| HIE Methods |
|
|
|
| ||||
| Features/Attributes of Patient Health Information and Electronic HIE | No Electronic HIE (i.e., not electronic data) | No EHR | Some e-HIE | Limited use of EHR | Data exchange limited to certain systems | Access to data limited to user role/ discipline | EHR is primary record | Standards-based EHR system (i.e., EHR content is standardized) |
| May have software for AR/AP, scheduling | No Anytime/ Anywhere Access | May allow for images to be imported | Clinical information collected on paper & entered into EHR | Continued but limited use of paper record | Some use of standards (messaging &/or content) | Interoperable with internal & external systems | Record can be electronically exchanged/ is transportable | |
| Meets minimum regulatory requirements1 | Limited Anytime/ Anywhere Access | Decision support features & alerts used | Anytime/ Anywhere Access | Computer Empowered Interoperable System | Anytime/ Anywhere Access | |||
| Facilitators of HIE | Limited involved in HIE Network (e.g., admin/claims data) | Some clinical content exchanged within HIE Network | Greater amount clinical information exchanged/shared within HIE Network | |||||
| Communication with Physician/ Clinician2 | Indiana | |||||||
| Maryland | ||||||||
| New York | ||||||||
| Utah | ||||||||
| ||||||||
Maryland -- As described before, Erickson provides care for residents who are independent and may require occasional check ups, PAC SNF care, long-term NH care, and home health services. Their outpatient clinic uses GE Centricity and their SNF/NH (Renaissance Gardens) and home health services use HealthMEDX. The physicians have access to both EHR systems while on campus. Nursing and other clinical staff working at the SNF/NH or HHA only have read/write access to HealthMEDX and, based on role of the staff person, may or may not have read-only access to the outpatient clinic's EHR (GE Centricity). Specifically, Erickson NH and home care nurses and administrators have read-only access to outpatient physician notes, medication list, and recent laboratory tests from the outpatient clinic's EHR (GE Centricity), which is the same permissions offered to the St. Agnes ED physicians and nurses (Level 2). When an Erickson resident is seen by an Erickson physician in St. Agnes, they have read-only access to the St. Agnes EHR and can print information and bring it back to Erickson where it becomes part of the medical record. (It is manually entered into the EHR of the location that the resident is placed in once they return to the Erickson campus. Erickson physicians also can remotely access the St. Agnes hospital EHR, again with read-only privileges (Level 2).
New York -- Through a recently awarded New York State HEAL NY grant, the VNS of New York is developing a portal for physicians to access health information of VNS patients with a common data presentation. The goal is to improve communication between home care and physicians to reduce re-hospitalizations, complications, and duplication of tests. Portal information will go directly into the physician's EHR as the VNS of New York medical record. At the time of the visit, the VNS of New York was piloting the web portal with seven regional physician practices that all use GE Centricity/Logician EHR (Level 2/3).
The VNS of New York also is participating in a pilot project with Weil Cornell Medical School to develop an electronic CMS 485 (e-485) form, which is the plan of care for home care services. Although the actual use of the e-485 form is no longer required by CMS, CMS does require that the HHA collect and document all of the information found on the form, so many HHAs continue to use the form out of convenience. The project expectation is that using the form will improve communication between the referring hospital, the VNS, and patients' primary care physicians; patient care; and reimbursement processes (Level 3). The hospital physician would begin the process of writing electronic orders on the e-485 at the time of hospital discharge. The outpatient physician would then be asked to sign the original e-485 and any subsequent additions electronically. The original and subsequent e-485 are transmitted to the VNS. This software comes with a timer that can count the number of minutes the start of care clinician spent on home health plan of care oversight to facilitate documentation for billing. Pilot testing conducted in four physician practices has revealed that use of the e-485 led to enhanced data completion. For example, the physical function section went from 28% complete to 94% complete and the mental status section went from 6% complete to 100% complete.
Utah -- In Utah, the NHs and HHAs visited corresponded with outpatient physicians via phone and fax (Level 1). There is no electronic transfer of information with unaffiliated physicians.
3. Medication Ordering/Electronic Prescribing
There is an expanding evidence base that documents serious medication quality and safety problems are occurring during care transfers (Coleman & Berenson, 2004; Forster, Murff, Peterson, Gandhi, & Bates, 2003; Moore, McGinn, & Halm, 2007). Older persons who receive care across multiple settings often are prescribed medications from different physicians who may or may not have knowledge of the complete medication list. The Joint Commission and the Institute for Health Care Improvement have recognized the scope of this problem and have provided national leadership to providers to support their efforts in counteracting medication problems through reconciliation at each point of transfer.17 Just as the systematic ordering, tracking, reconciling, and administration of medication are crucial to ensuring that quality and safety, so is the exchange of this information across providers and across settings. Thus, the four site visits explicitly addressed HIE with respect to medications and is shown in Table 6.
| TABLE 6: HIE Capabilities by Level Regarding Medication Ordering/E-prescribing | ||||||||
|---|---|---|---|---|---|---|---|---|
| Level 1 Paper-based Record/ No EHR | Level 2 Combined Paper Record/EHR | Level 3 EHR Used/Limited Electronic Data Exchange, Some HIT Standards Used | Level 4 Completely Interoperable EHR System, Use of HIT Standards | |||||
| HIE Methods |
|
|
|
| ||||
| Features/Attributes of Patient Health Information and Electronic HIE | No Electronic HIE (i.e., not electronic data) | No EHR | Some e-HIE | Limited use of EHR | Data exchange limited to certain systems | Access to data limited to user role/ discipline | EHR is primary record | Standards-based EHR system (i.e., EHR content is standardized) |
| May have software for AR/AP, scheduling | No Anytime/ Anywhere Access | May allow for images to be imported | Clinical information collected on paper & entered into EHR | Continued but limited use of paper record | Some use of standards (messaging &/or content) | Interoperable with internal & external systems | Record can be electronically exchanged/ is transportable | |
| Meets minimum regulatory requirements1 | Limited Anytime/ Anywhere Access | Decision support features & alerts used | Anytime/ Anywhere Access | Computer Empowered Interoperable System | Anytime/ Anywhere Access | |||
| Facilitators of HIE | Limited involved in HIE Network (e.g., admin/claims data) | Some clinical content exchanged within HIE Network | Greater amount clinical information exchanged/shared within HIE Network | |||||
| Medication Ordering/ E-prescribing2 | Indiana | |||||||
| Maryland | ||||||||
| New York | ||||||||
| Utah | ||||||||
| ||||||||
Observations on medication ordering and/or electronic prescribing, particularly at the NHs and HHAs visited, indicate that with few exceptions, care settings are at Level 1 or 2. In general, NHs worked primarily with their own LTC pharmacy. Physicians did not send electronic medication orders but rather faxed medications orders to the NH. Staff at these NHs then faxed the order to the LTC pharmacy and manually entered the order into their EHR (if they had an EHR). For those NHs with a more robust EHR (e.g., Erickson Retirement Communities in Maryland), the re-entry of medication information into an e-MAR application was possible.
With respect to home health care patients, physicians prescribed medications directly to the patient who was responsible to have them filled. HHAs do not have an equivalent electronic MAR, but rather are accountable for documenting what the patient reports she/he is taking. This reconciliation in the home is done at the start of care, usually by a start of care nurse or therapist. Of the HHAs visited, most reconciled this medication list on paper and kept it in a paper chart. The list also may have been entered into the EHR either at the point of care (e.g., the VNS of New York has laptops that clinicians use in the home and collect/enter health data during the home visit) or at the end of the day by either the clinician who collected the information or by a clerk at the agency.
Other observations obtained during the site visit related to e-prescribing and medication ordering are discussed by state below, including sites' future plans. (Note, as future plans have not yet been implemented, they are not reflected as an electronic capability in Table 6.)
Indiana -- The site visitors were informed by the host site (IHIE) that the state was close to finalizing a statewide mandate for e-prescribing, but at the time of the visits, this was not required and not widely used. John Pipas, the CEO of the VNS of Central Indiana (HHA), confirmed that the VNS's communication with pharmacies was by fax but that this would change once mandated statewide e prescribing was initiated (date to be determined). In a follow-up communication in July 2007 with Michael Weiner, MD (host at the University of Indiana/Regenstrief), Dr. Weiner mentioned that Wishard Health Services (the hospital visited as part of the Indiana site visit) did move to uniform e-prescribing in early 2007 even though the state has not yet mandated it.
Brookview (NH) uses a single pharmacy that is part of a national chain, Pharmerica. All communications with this pharmacy are via fax.
Maryland -- Erickson Retirement Communities uses Omnicare/Neighborhood Pharmacy (which has a branch located on its campus). Approximately 80% of independent residents and close to 100% of residents receiving PAC and LTC use this pharmacy. All data from Omnicare are sent to Erickson via fax or phone and are manually re-entered into either CareMEDX for Renaissance Gardens (the NH/SNF) or home health patients, or GE Centricity (for the on-campus outpatient clinic). Erickson is developing a pilot e-prescribing program between the physicians who treat residents of the RG facility and Omnicare/Neighborhood Pharmacy, but at the time of the site visit, this pilot study had not been launched.
New York -- The hospital and NHs visited all have a single in-house pharmacy that is used.
Utah -- The skilled NHs visited in Utah also use fax and phone to communicate with their single unaffiliated pharmacy (Level 1).
4. Laboratory/Radiology Ordering and Results
HIE on behalf of patients receiving PAC/LTC services who also require radiology or clinical laboratory services generally were observed to be manual (Level 1), see Table 7. As above, innovative or future plans are highlighted in the discussion below.
| TABLE 7: HIE Capabilities by Level Regarding Laboratory/Radiology Orders and Results | ||||||||
|---|---|---|---|---|---|---|---|---|
| Level 1 Paper-based Record/ No EHR | Level 2 Combined Paper Record/EHR | Level 3 EHR Used/Limited Electronic Data Exchange, Some HIT Standards Used | Level 4 Completely Interoperable EHR System, Use of HIT Standards | |||||
| HIE Methods |
|
|
|
| ||||
| Features/Attributes of Patient Health Information and Electronic HIE | No Electronic HIE (i.e., not electronic data) | No EHR | Some e-HIE | Limited use of EHR | Data exchange limited to certain systems | Access to data limited to user role/ discipline | EHR is primary record | Standards-based EHR system (i.e., EHR content is standardized) |
| May have software for AR/AP, scheduling | No Anytime/ Anywhere Access | May allow for images to be imported | Clinical information collected on paper & entered into EHR | Continued but limited use of paper record | Some use of standards (messaging &/or content) | Interoperable with internal & external systems | Record can be electronically exchanged/ is transportable | |
| Meets minimum regulatory requirements1 | Limited Anytime/ Anywhere Access | Decision support features & alerts used | Anytime/ Anywhere Access | Computer Empowered Interoperable System | Anytime/ Anywhere Access | |||
| Facilitators of HIE | Limited involved in HIE Network (e.g., admin/claims data) | Some clinical content exchanged within HIE Network | Greater amount clinical information exchanged/shared within HIE Network | |||||
| Lab/Radiology Ordering and Reporting2 | Indiana | |||||||
| Maryland | ||||||||
| New York | ||||||||
| Utah | ||||||||
| ||||||||
Indiana -- The Docs4Docs portal, as previously described has the capacity for participating physicians and hospitals to electronically access laboratory results. It is limited, however, because patients seen at local area PAC or LTC settings that have laboratory or radiology orders/results will not be included. Furthermore, the IHIE's future plans include having laboratory and ambulatory imaging sites included in the network.
Brookview (NH) contracts with a single laboratory and all laboratory orders and results are provided via fax and are filed in a paper record. These results also are entered into their EHR, VistaKeane.
Maryland -- Erickson uses Quest Laboratories and Mobile X Radiology. Data from these two providers are sent to Erickson via fax or phone and in most cases, laboratory and radiology data are manually re-entered into either CareMEDX for Renaissance Gardens (the NH/SNF) or home health patients, or GE Centricity (for the on-campus outpatient clinic) (Level 2). Quest Laboratories are used by the outpatient clinic, home care, SNF and the LTC facility (referred to as the Residents Gardens or RG). As noted earlier in this report, Erickson is developing a pilot e-prescribing program between the physicians who treat residents of the RG facility and Omnicare/Neighborhood Pharmacy.
New York -- Montefiore Medical Center (hospital) has a single clinical laboratory. The JHHA (SNF/NH) and the MHHA also use the hospital's laboratory. JHHA staff have read-only access to laboratory results and must maintain paper copies of the Montefiore laboratory results as part of the JHHA record systems. All MHHA laboratory results go to the Montefiore Medical Center's clinical laboratory. One result of this centralization is that ordering staff physicians or their agents (e.g., physician assistant or nurse practitioner) have electronic access to results in a timely manner if they initiate that access by querying the EHR for the results. In other words, they are not sent a reminder that results are available, but nonetheless, they have access to the results.
Schervier (New York NH) uses a single laboratory, Lawrence Laboratory. Clinicians (e.g., therapists, nurses, social workers) at the Schervier NH may initiate view-only computer access to the laboratory results from Lawrence Laboratory. They are then printed out and stored in the paper record at Schervier.
Utah -- All sites visited in Utah are at Level 1 or 2; that is, all laboratory and radiology information exchange among the sites visited is by phone, fax, or paper accompanying the patient.
LDS Hospital has a robust EHR that has the capability to electronically share information, but when asked why this was not done with any local NHs or HHAs, informants remarked that their information technology department was faced with more pressing priorities that needed their attention.
Interestingly, although St. Joseph's Villa (Utah NH) uses IHC's laboratory, the IHC laboratory sends laboratory results via fax or phone (in the case of urgent results). Nursing staff at St. Joseph's Villa then send results to the attending physician via the physician's hand-held Blackberry®, and a paper copy of results are maintained as part of the patient record.
Hillside Rehabilitation Center, another NH in Utah, uses Schrieber Laboratory. Physician orders for and results from laboratory services are faxed (urgent results are phoned); and do not populate the EHR (BlueStep). However, Hillside has made a financial investment in a single pharmacy and can electronically send (order) medication information that auto-populates the pharmacist's queue.
CNS, an HHA in Utah, uses multiple laboratories with the specific selection largely governed by insurance or geography. Physician orders for laboratory and radiology services are not received electronically by CNS. These results are sent via fax, with critical values conveyed via phone. CNS maintains paper copies of laboratory and radiology orders and results and also manually enters orders and results into their EHR. The other HHA visited in Utah, CareSource, communicated only with outside parties (e.g., laboratories, pharmacies, physicians, hospitals) via fax or phone.
D. Solutions and Future Plans for e-HIE and HIT Implementation
Few PAC/LTC settings expressed short or long-term plans to either: (1) implement an EHR system if they did not already have something in place; or (2) augment or replace their existing medical record system with something that was standards-based, interoperable, and/or more robust. Likewise, only a few settings (discussed below) had knowledge about the work being planned and conducted with SDOs such as HL7, NCPDP, CCD/CCR,18 and other standards-related activities (e.g., CHI and HITSP). None of the PAC/LTC settings, with the exception of the VNS of New York and to a lesser extent Erickson Retirement Communities, had representation in any of the SDO workgroups. However, the sites that we visited were more involved and active in participating in local, regional, and especially the national NH and home health organizations. Such professional associations (e.g., AHCA, NAHC, AAHSA) are becoming more connected with SDO activities and it is expected that their involvement will expand in years to come.
Several solutions for advancing e-HIE were observed during the site visits.
1. Portals
a. Patient/family caregiver portals. One possible answer to improving HIE between providers and settings, particularly PAC and LTC settings, is to enlist the participation of the patient and family caregivers. Erickson Retirement Community (Maryland CCRC) is developing a resident portal into its EHR (GE Centricity), which includes read-only access to medications, laboratory results, appointments, and problem lists. Once operational, patients can selectively share access to this information with unaffiliated providers. For example, the patient may be out of town and require care from a local ED. The patient could provide the ED staff with the access information to view key clinical information through the portal. Because the patient controls who is allowed to view the data, privacy protections are promoted.
b. Provider portals. Physicians are another potential target for innovative HIE solutions. As mentioned previously through a New York State HEAL NY award, the VNS of NY is developing a web portal for primary care physicians with a common data presentation. The MHHA (New York) also is piloting a web portal project with physicians in its service area with similar intent.
As previously discussed, the IHIE is developing a portal, called Docs4Docs, that will provide physicians and other clinicians with access to admission and discharge transcriptions, laboratory results, radiology, EKGs, and pathology reports across care settings. Using a web-based platform, physicians will be able to access this information from their outpatient offices, from the hospital or NH, or even from their private residence. The portal is supported by five of the large hospitals in the Indianapolis metropolitan area. At present, medication lists are not yet available via the portal. As implementation of this portal is fairly new, information is incomplete. At present, the hospitals do not yet collect all encounter information for all patients. The hospitals collect most of the inpatient encounter information from their own EHR and some information from outpatient or off-site encounters (i.e., one of the other hospitals that feed into the Docs4Docs). While the stated IHIE vision is to facilitate physician access to needed patient information regardless of location of the information, enabling physician access to patient information in NHs is not actively being pursued because at this time the IHIE does not include any representatives from PAC or LTC.
2. Disaster Preparedness
Hurricane Katrina increased awareness for the importance of having timely availability of health information during a natural or man-made disaster. One provider in the four cities included in this study addressed this concern. Hillside Rehabilitation, a NH in Utah, has developed a contingency plan to make available their patients' electronic health information in the event of an emergency. In partnership with its software vendor, BlueStep, Hillside patients' health information could be made available to health care providers in different parts of the country via a secure website.
E. What Are the Facilitators and Barriers to Health Information Exchange?
1. Facilitators
a. Timely Communication. Timely information transfer can financially benefit both the hospital and the PAC/LTC provider. For all Medicare-certified SNFs, the reimbursement for Part A Medicare patients (i.e., the daily payment rate) is based, in part, on the patient's medical problems and co-morbid conditions. To determine whether a facility can meet a patient's care needs under the prevailing rate, timely communication of a patient's PAC needs from the hospital can facilitate a more efficient and clinically appropriate transfer. Ensuring that the receiving provider has comprehensive information on a patient's current needs and plan of care can facilitate appropriate classification under the Medicare payment system. Under the diagnosis-related group payment mechanism, hospitals have an incentive to discharge patients as quickly as possible. To the extent that timely communication translates into a reduced LOS, hospitals stand to benefit financially.
It is worth noting that the four site visits were conducted in geographic regions that have a relatively small penetration of Medicare Advantage (managed Medicare) providers. Thus, the site visit team did not have the opportunity to explore the influence of a health plan on HIE. In other regions of the country, a health plan can require that contracted NHs and HHAs contribute to or update the patient's problem list, allergies, medications, advance directives, and recent diagnostic tests while patients are under their care (Coleman, 2002; Coleman, 2003; HMO Workgroup on Care Management, 2004).
b. Interpersonal Relationships as a Facilitator to HIE. As previously mentioned, good, cross-organization interpersonal relationships are important to ensuring that health information is exchanged and the value of interpersonal relationships in facilitating HIE persists even when HIT solutions are being implemented by the health care providers involved in the information exchange. Clinicians who practice in multiple settings can facilitate timely and accurate HIE across care settings. For example, at Erickson Retirement Communities (Maryland), the primary care physicians follow their patients when they are hospitalized at St. Agnes hospital. This creates opportunities for the physicians to gather more complete information while managing the patient across either care setting. The physicians are responsible for medication reconciliation across sites of care. In addition, Erickson employs a care coordinator who also follows Erickson patients while being treated in St. Agnes hospital, arranges their discharge back to Erickson, and where appropriate, initiates services such as Part A Medicare skilled nursing care. The coordinator collects pertinent information prior to hospital discharge, including the treatment course and discharge information, and faxes it/hand-delivers it to the appropriate clinician at Erickson. Evidence of the importance of this coordinator was a response to many site team questions regarding information exchange--"Our coordinator handles that."
Similarly, a physician practice employed by Montefiore Medical Center (New York hospital) continues to follow discharged patients who require skilled care in selected NHs. Having physician groups employed by the provider creates the opportunity to develop more standardized protocols to patient care, including clinical pathways and expectations for information exchange. MHHA has staff liaisons in Montefiore Medical Center who facilitate home health care referrals. Along with the VNS of New York, MHHA has coordinators who visit two or three of the larger NHs to attend weekly patient reviews and help facilitate referrals from Part A skilled nursing to home care. At Wishard Hospital (Indiana), the VNS of Central Indiana has a staff liaison who is granted limited access to the hospital EHR. The liaison begins the process of entering hospital data into a laptop that provides access to the home health EHR (Misys), and then this information is shared electronically with the home health nurse assigned to the case.
c. Patient Identifiers. Use of HIT to appropriately exchange accurate patient information is facilitated by the ability to identify the patient who is the subject of the exchange, sources of needed information, and the providers and other persons who are the intended recipients of the information. Montefiore Medical Center (New York hospital) recently mandated the use of a single patient identifier to track patients in their electronic health information system. An important advantage of this approach, particularly in an area such as the Bronx that tends to serve the patient from cradle to grave, is that historical data stored in the Montefiore system are more easily accessible. A single patient identifier also helps ensure that the care team is treating the correct patient, particularly when the patients' first and last names are the same or similar. Prior to the single patient identifier, Montefiore used algorithms to develop possible matches, requiring more time for the clinician to verify they were reviewing the chart of the patient currently being treated. The ability to require the use of a single patient identifier and have all participants agree to this is another example of how the establishment and nurturing of interpersonal relationships has helped establish trust and a willingness to be a part of a HIEN.
2. Barriers
a. Lack of interoperability. Once health care partners agree upon the need to exchange information, perhaps the greatest barrier to e-HIE witnessed during the site visits was a lack of interoperability between EHRs and other health information systems. The lack of interoperable health information systems was a leading contributor to the inefficient practice of manually re-entering data, which was observed at all sites. This was observed whether the two EHR systems were owned by the same institution or owned by separate institutions. For example, Erickson (Maryland CCRC) has invested in two EHR systems, GE Centricity and CareMEDX. GE Centricity functions as the primary record for residents in independent living who see physicians in the on-campus clinic, while CareMEDX functions as the primary record for patients in home health care, Part A SNF, and LTC. Erickson staff manually transfer information between its two electronic systems (as well as between paper and electronic systems). At the time of EHR selection, Erickson was not able to identify a single EHR solution that could address the care needs of the various types of patients treated throughout the campus. Erickson staff noted that because of this, they were forced to purchase two separate systems and plan to pay additional costs to build interfaces to allow the two systems to be interoperable (i.e., allow for electronic exchange and re-use of content). If a viable HIT product that met their needs had been available, they would have readily opted for a single EHR solution.
Similarly, despite common ownership, Montefiore Medical Center's EHR (CIS) and MHHA's EHR (Misys) do not interoperate (i.e., do not: (i) electronically exchange or (ii) re-use content). When a laboratory result appears in CIS, the result has to be manually entered into Misys. Medications also are copied-and-pasted from one screen in CIS to another in Misys. When a home health care patient is admitted to the hospital, there are no fields in CIS that can identify that this patient is actively receiving home health care services. MHHA staff commented that having this information in the ED might influence the decision as to whether the patient should be admitted or could be managed in the home with the HHA's support. Still, in general, providers were pleased that current, reliable information was available electronically "somewhere," even if it required them to copy and paste it into their EHR or local system--an observation that proved common during the site visits.
b. Lack of access to existing systems. A related barrier to HIE identified during all four of the site visits concerned a lack of access to existing EHR systems. In general, the sending institution did not extend user privileges to clinicians in the receiving institution to view, much less edit or add content to their EHR system. In rare instances, physicians, nurse practitioners, and physician assistants practicing in the NH are given privileges to remotely access clinical information in EHRs in either the hospital or ambulatory settings. Under these circumstances, clinicians can care for patients in NHs or in patients' homes with the benefit of the information available from these sources. However, it should be noted that other PAC and LTC health professionals (e.g., nurses, CNAs, physical and occupational therapists) are not usually granted this same access. For example, in Utah, staff in two NHs (St. Joseph's Villa and Hillside Rehabilitation) do not have access to the LDS Hospital HELP2 EHR.
c. Health Insurance Portability and Accountability Act (HIPAA). The site visits confirmed that whether real or perceived, the implementation of HIPAA poses a barrier to information sharing across care settings in general or granting access to information contained in EHRs in particular. HIPAA allows the exchange of patients' health information for purposes of treatment, payment, and health care operations without patient authorization. However, misinterpretations of these HIPAA regulations were common. Clinicians were reluctant to share information or grant access to EHRs for fear of violating HIPAA laws and facing accompanying penalties. The site visitors were unable to determine the degree to which HIPAA concerns masked deeper concerns about competitiveness and liability that information sharing might elicit.
d. The referral process. Finally, the site visits highlighted the fact that in general, NHs and HHAs are dependent upon hospital for referrals. Within this context, NHs/HHAs expressed a reluctance to confront the hospital when the hospital did not supply necessary information at the time of transfer for fear that the hospital would choose to refer patients elsewhere. These providers acknowledged that a more objective third party might be needed to afford oversight of the referral process to ensure that NH referrals are not at risk should they speak up as to what they need from the discharging acute care hospital.
F. Organizational/Management Issues
1. Organizational Structure
Of the PAC and LTC settings visited, there was a fairly even distribution of agencies/facilities that were part of a larger regional or national chain (e.g., Golden Gate National Senior Care [formerly Beverly Living Centers]) and those that were smaller, privately-held. Similarly, some were hospital-based, while others were freestanding. The majority of SNFs and HHAs visited were non-profit.
In general, there was a higher level of HIT adoption in PAC/LTC settings that were owned by other health settings, including being owned by a local hospital; or being part of a local, regional, or national chain. In addition, it was observed that HHAs that were one of the nation's visiting nurse associations also had higher rates of HIT adoption than other HHAs. Agencies/facilities in these categories tended to have purchased, at a minimum, software allowing them to electronically submit claims and remittances, and administrative data to payers (e.g., OASIS, MDS data). This is in contrast to using free software made available by the CMS, such as HAVEN or RAVEN, which tends to be adopted by smaller providers (not visited as part of this study).
The PAC/LTC settings that were involved with other health entities also tended to have additional reporting capabilities built into their system, including accounts payable/receivable, staff scheduling, clinically-relevant alerts (e.g., drug-to-drug interactions, drug-to-food interactions), quality monitoring reports, and in some cases, trending capabilities. These facilities may have had a paper chart, but much of the chart consisted of computer-generated information that was subsequently printed out and placed in the chart.
On the other hand, the group of PAC/LTC settings that were smaller and/or independent tended to have less information technology capabilities and relied fairly exclusively on a paper record/chart. Much of the record was handwritten, and little automation was in place (again, with the exception of meeting regulatory requirements such as OASIS or MDS reporting). The information technology in use was typically to support administrative tasks; the medical record was seen as a separate document altogether.
2. Organizational Impetus to Adopt HIT
As previously described, when selecting the sites, the "hub" delivery system had sophisticated HIT in place, and in some cases, showcased later in the report, some of the PAC/LTC settings did as well. That said, a great deal of variation in HIT adoption by the visited PAC/LTC settings was observed. The majority of NHs/HHAs visited collected information on paper and entered clinical and administrative data (i.e., MDS/OASIS and claims data) into a software specifically designed for those purposes. If additional HIT applications were available, they were add-on modules provided by niche software. Thus, HIE was generally observed to be a traditional process not facilitated through the use of HIT even when the providers had an electronic health information system in place.
When asked what the criteria were for selecting a software vendor and/or software application, costs and ongoing maintenance fees were the most commonly cited. Related training costs also were usually mentioned as a concern. With some notable exceptions (the VNS of New York and Erickson Retirement Communities), interoperability with other settings was not mentioned as a vendor or product selection criterion, and was not necessarily perceived as a necessary or even a desired attribute to an EHR system.
There are multiple reasons that may explain why NHs and HHAs have not made significant investments in and use of more robust EHR systems. In general, both setting types operate with very small margins, and are financially constrained even more now that the Prospective Payment System is in place (CMS, 2007a; National Bureau of Economic Research, 2007).
On more than one occasion the site visitors heard, "if the Federal Government would build and mandate 'it,' then the PAC and LTC market would find a way to make it work." Informants cited the fact that once OASIS/MDS reporting was required to be submitted electronically, NHs and HHAs acquired the necessary equipment to meet that requirement.
HHAs and NHs have a very high rate of staff turnover, averaging close to 50% per year (AHCA, 2003; Seavey, 2004). The costs of implementing an EHR system are high, but the ongoing maintenance and training costs are additional substantial costs that may represent an ongoing additional barrier to adoption. Concerns about the affordability of EHR systems continue to be expressed by NHs despite some anecdotal evidence that some NHs have been able to recover their HIT investment cost through more accurate Medicare SNF claims.
Part of the presumed "cost" is the risk associated with EHR deployments in that they may "fail." This concern was expressed by many of the smaller NHs/HHAs visited. The JHHA (New York SNF) lived this reality--they implemented an EHR system in their SNF only to have to abandon it several years later because it did not meet their needs. The Administrator of the JHHA commented that they are committed to implementing HIT and are currently vetting new software options. This is described in more detail in Appendix C. The decision by the CCHIT to specify certification criteria for NH EHRs could help to minimize NH provider risk in making HIT investment decisions.
At several sites (Briarwood in Indianapolis, St. Joseph's Villa and CareSource in Utah), leaders in the PAC/LTC settings were unfamiliar with the private and public initiatives related to EHR adoption and work being done by RHIOs in their own communities. It was observed that although innovators in these communities are involved in implementing and expanding data exchange efforts, the PAC/LTC settings have either not been invited to participate in the planning or are choosing not to become involved.
As is true with all care settings attempting to implement an EHR system, the disruption of current processes and workflow are great, and the long-term benefits and rewards associated with the adoption of an interoperable EHR system are not always tangible or even imaginable, especially to those expected to use the system. As is the case for other health care settings, NH and HHA providers need "champions," persons who can lead the HIT implementation within their organizations. This person needs to be able to lead by implementing and embracing the changes, understand HIT, and take into account workflow issues inherent in the organization. The champion needs to be able to understand and articulate to others how HIT implementation can alter workflow to increase efficiency and improve care quality.
In some cases, making an EHR investment was not even being considered by key decision-makers' of the organizations that we visited. What is most important to PAC/LTC administrators and staff is the ability to receive legible, timely, complete, and accurate data from the referring health setting. The particular medium used for this information transmission (e.g., phone, fax, hard copy, electronic) was of secondary concern, as was any concern about the cost, time, effort, and opportunity for error involved in re-entering available information stored electronically "somewhere else." Furthermore, several administrators indicated that hospitals (including EDs) and physician offices often are not interested in much of the data collected at SNFs and HHAs. What information is shared often is not trusted, valued, or read by the receiving entity. As previously described, sometimes the information that is being exchanged is not what the receiving organization describes as needed. In addition, liability and fear of litigation were mentioned as reasons why physicians at the receiving hospital or ambulatory setting are skeptical of the information received from PAC/LTC settings, thereby resulting in duplicate testing and procedures to ensure the data they are acting upon are reliable.
The authors note that the literature concerning the organizational benefits of adopting an EHR system, such as worker productivity gains, optimization of billing processes, and other efficiencies is limited and those few studies that report the impact of HIT implementation in hospitals or physician offices have mixed (i.e., positive and negative) results (Booz Allen Hamilton, 2006; Poissant, Pereira, Tamblyn, & Kawasumi, 2005; Sidorov, 2006). Poissant and colleagues conducted a systematic review of the literature on the impact of physician and nurse documentation time in hospital and ambulatory care settings that recently implemented an EHR system. They reviewed findings from studies that used methodologies such as randomized control trials, self-report/survey, as well as time and motion studies. Poissant et al. concluded that increased or decreased documentation times for both nurses and physicians were dependent upon many variables, including the type of computerized system used (i.e., bedside terminals, desktops, PDAs), the length of time since EHR implementation, and the information being documented (e.g., admissions, CPOE functions, etc.). In general, nurses were more likely than physicians to gain time efficiencies by using a computer system to document patient information. However, for separate select tasks, nurse documentation time increased, while physician documentation time decreased.
G. Specifics Regarding Technology Observed During Site Visits
As described in previous sections, the site visit team observed that while in some instances computers enabled remote access to health information there was no "clinical data interoperation," that is, we did not observe any instance of semantic interoperability that would enable computer-to-computer data exchange and re-use of clinical content between non-affiliated sites. No site reached Level 4 in Table 2 for HIE for any of the four clinical areas that were examined during the course of this study. As previously mentioned, there also were no instances where information was exchanged using both agreed upon messaging and content HIT standards.
To frame our specific observations regarding interoperation (or lack thereof), firm definitions of the relevant concepts in this report are outlined below, because use of these concepts in current health care discussions is so highly variable.
1. Health Information Exchange (HIE)
As described throughout this report, HIE applies to any mode of transmission of HIE--voice, paper, fax, or digital--about a given patient. The broader definition of HIE (rather than considering only electronic (i.e., digital) exchange) for several reasons is used. Not only were instances observed where patients' health information was exchanged using more traditional (voice, paper and fax) methods and in some case standardized (but not semantically interoperable) e-HIE, but it also was observed that HIE was often a hybrid of the more traditional and digital methods. There were instances when the information exchanged resided in a computer on one or both ends of the exchange, but the actual exchange of data was done via phone or fax. For example, site visitors heard a description of a discharge planner viewing her computer screen while talking on the phone to an admitting planner typing things into her computer during an initial conversation regarding placement of a patient. More frequently, it was explained, the person receiving the voice (usually telephonic) information will be taking handwritten notes, and later these notes are transcribed into the local computing system.
Representatives from the selected sites provided the following reasons for not more fully utilizing their HIE capacity.
2. Interoperation and Interoperability
Over the last few years, several efforts have been aimed at developing a universal (beyond health care) definition of interoperation and interoperability. (In this report, the terms will be considered synonymous.) The Presidential Executive Order of August 2006 (E.O. 13410) defines interoperability as "the ability to communicate and exchange data accurately, effectively, securely, and consistently with different information technology systems, software applications, and networks in various settings, and exchange data such that clinical or operational purpose and meaning of the data are preserved and unaltered.19 The ability to exchange data and retain the meaning of such data across different HIT systems and software applications requires the use of agreed up HIT messaging and content standards.
As noted, a variety of methods of HIE were observed during our site visits and in the rare case that HIE was automated such exchange was not standardized. HIE that is automated, but not standards-based, is by definition ad hoc though from a local point of view it is no less useful. For example, the occasional pre-population of records in one system from information in another system, as was observed at Montefiore Medical Center (New York), was always seen as desirable in the few places it was observed, and it was desired in many contexts where it did not yet exist (e.g., as was reported by Erickson). Only rarely did automated (i.e., electronic) data exchange make use of HL7 Version 2 (HL7v2) messaging standards, although intra-enterprise use of such messaging was observed (e.g., at LDS Hospital in Utah where HL7v2 is used extensively). Some sites planned to make use of HL7v2 messages as the basis for inter-enterprise interoperation. No where was it observed that the use of "semantic" standards, wherein information in one computer was transmitted to a computer in a different care enterprise in a way that the meaning, for the sending computer, was retained in the receiving computer. For example, one can imagine an electronic representation of a discharge medication list from a hospital being "understood" by a computer at a PAC site (in the same way that a local medication list would be understood, and, say, checked for drug interactions), but we did not observe such "exchange by meaning." Instead, universally, we saw manual (i.e., human) "medication reconciliation" at receiving sites.
While the site visit team believes that the observed lack of deployment of data, terminology, and messaging standards may result for deep reasons not yet fully understood, the following hypotheses based on the sites visited are offered. First, knowledge of such standards is limited at the sites visited; there is little awareness of messaging standards and no unilateral mention of terminology standards. Further, there seems to be little motivation to acquire this knowledge. The simplest explanation for this first hypothesis is that "anywhere, anytime" access of patient information that follows the patient is a multi-enterprise, multi-disciplinary objective that all stakeholders can understand, and therefore imagine. The idea that computer-empowerment of one computer by another should be part of such access is just not something that the visited sites tended to think of first, and this is in spite of the burden manual re-entry imposes. Second, at sites where inter-enterprise interoperation based on standard messaging is contemplated, the information technology staff are focused on acquiring the resources required for the translation of the patient information, which might be only a summary, into HL7v2 and the translation of the resulting HL7v2 message back into something the receiving computer can (at least) display. Often the business case for paying for the resources necessary to translate patient information in a standardized way is not yet well articulated and the required resources are not always easy to procure. Third, the notion that terms (e.g., the names of diagnoses, laboratory tests, medications, procedures and the like and their meanings (are to be shared across enterprise boundaries seems to cause concerns and sometimes anxiety among some providers. Often these concerns focus on the fact that terms are used differently at different but neighboring enterprises (i.e., the same term may mean something different or different terms are used to name the same meanings). Shared, local use of language may support local care and providers cannot imagine using standardized terms while retaining the way they are used to doing things. A more sophisticated view of the potential use of standard language is that the latter will (locally) reduce the quality of care.
The only way to overcome the challenges implicit in these hypotheses may be to gain experience with terminology standards while simultaneously reducing the technical and financial barriers impeding their deployment and use. It may be for instance that actual use is not nearly as difficult as it is imagined to be.
The lack of agreed upon HIT standards needed by PAC and LTC providers was observed to be a particular challenge. At the time of the site visits, while the NCVHS had endorsed the CHI Patient Assessment and Disability standards,20 the Secretary of HHS had not yet endorsed the use of these standards. PAC/LTC providers are understandably reluctant to demand/request standards-based EHR systems of the PAC/LTC vendors when such standards are not recognized. However, the endorsement by the Secretary in August 2007 of these standards and his approval that these standards be used by federal agencies in implementing new and to the extent possible in modifying existing health information systems should help address providers' uncertainty about which standards should be included in their EHR applications. The commitment by CMS to include CHI standards in the development of the new patient assessment CARE instrument also could help mitigate provider concerns.
Similarly, the recently balloted and approved HL7 CCD standard (i.e., that supports the standardized exchange of human-readable and/or coded documents, such as transfer/discharge documents) and endorsement by the HIT Standards Panel (HITSP) of the CCD as an exchange standard should help reduce provider's uncertainties about the exchange standard that software should support. Further, the expected endorsement of this standard by the American Health Information Community (AHIC) should work to further reduce providers' risks in this area. The CCD could be something that any vendor can understand and any of the vendor's customers can imagine using. This standard specifies a way of exchanging information about a patient so that the receiver can use standard software to display, process, and store that information.
Further, the decision by the CCHIT to specify the certification criteria for NH EHRs by 2009 and develop a roadmap by which future certification criteria will be adopted should assist both NH providers and HIT vendors in anticipating and planning for needed EHR functionality. The CCHIT NH EHR certification criteria likely will include use of the "Patient Assessment and Disability Standards" endorsed through CHI and the HL7 CCD information exchange standard endorsed by HITSP.
While it is unrealistic to assume that the adoption of the CHI Patient Assessment and Disability standards and the HL7 CCD HIE standard will change anything quickly, formalization and use of these standards could promote realistic planning and resource allocation on the part of vendors and providers alike. Providers in communities that were visited could plan to implement these standards in some incremental way as soon as resources could be allocated. For example, Erickson and St. Agnes Hospital (Maryland) could ask their vendors to implement the CCD standard so as to support HIE for patients treated at these two health settings. The fact that implementation of the standard may be a resource-intensive and burdensome undertaking for the vendors could potentially be ameliorated in proportion to the vendor's market share.
3. World Wide Web
The most powerful example of information technology use today is the World Wide Web. Its use is pervasive and so successful in many arenas such as retail commerce and banking that health care providers (and to a lesser extent patients) are beginning to have expectations for their health care experience that rival these other interactions.21 When care providers are asked what they want from HIT, they often express their wishes in web-based analogies; which for the purposes of this paper has been reduced to personalized "anytime/anywhere" access. However, health care providers (and patients) also want other attributes that come to mind when they think of this immediate access, namely autonomous, maintenance-free, low-cost, system and vendor-independent communication. However, while the web often is used as the model against which other frameworks are compared, the site visitors observed only one new and one planned use of web-based technology. Significantly, they both involved new technology investments. As part of the IHIE, Docs4Docs is deploying remote web-based physician access to local patient encounter information. At Hillside Rehabilitation Center (Utah NH), their ongoing deployment of the BlueStep EHR will take advantage of web-accessible backup for the patient information they accumulate. One important use of this backup will be for "disaster-recovery" (i.e., by having the patients' data off-site, in the event of a disaster, care providers will have intact medical records from which to provide care). Another explanation why only two sites showcased their use of the web may be that the web is pervasive enough to be an assumed tool. Therefore, some sites may be planning use of the web for data exchange but did not make mention of it, and in other circumstances those interviewed may not have been aware that their system makes use of the web.
4. Communication Gaps Across Organizations
One of the biggest challenges observed during this study was the lack of awareness of HIE-related opportunities going on outside the doors of each enterprise. These challenges presented themselves as both technological and organizational issues. As HHS Secretary Leavitt observes, "All health care is local."22 As most organizational energy in most provider enterprises is allocated to existing problems within their own organization, the idea that answers, or, more likely, partial solutions may exist "out there" is only rarely considered. For example, the site visit team observed many instances where organizations unilaterally decided on what information a receiving care provider needed in the event of a patient transfer, without any discussion between the two organizations about the type of information that both organizations actually needed to provide care for transferred patients. Similarly local, unilateral attempts at local HIT solutions often are pursued without any awareness/understanding of the efforts of others in the health care community to address the same or similar problems. Instead, providers tend to look outside their organization for solutions (if they are considered at all) when the solution become overwhelming in size and complexity and only then do enterprises look to partner with nearby providers or otherwise enlarge their search for solutions. Because of this, substantive progress, however partial, in one place is often completely unknown even to nearby providers. Conversely, because trust among the parties exchanging data about a given patient is a major requirement for collective action, and it generally was observed that e-HIE only occurred among regional providers who know one another well or have an agreement with one another to be able to cooperate and share solutions. This happens in spite of the fact that some providers (e.g., Erickson) are committed as a matter of organizational objective to sharing their experiences with other providers. The simple exercise of the site visit team asking the various settings how data are (or are not) transferred illuminated the wide communication gap. Presumably, communication about the fact that HIE is possible needs to precede planning for HIE, as it is hard to implement HIE solutions without thinking what problems one would like to solve.
5. Health Information Exchange Network (HIEN) Involvement
Three of the four site visits were in communities with some type of RHIO/HIEN. One was a fairly established regional network (IHIE), one was established within a state (UHIN), and one was a newly-formed RHIO (Bronx RHIO). The ability for these networks to exchange information was idiosyncratic to the location visited. The UHIN largely exists because of state-regulated requirements regarding claims submission and credentialing of physicians. The IHIE was established over time and spearheaded by a few forward-thinking physicians and informaticists. It was through Drs. McDonald and Overhage's good will and perseverance that the IHIE was able to get initial buy-in with the participating hospitals and physicians. The Bronx RHIO is just getting started, and has been heavily funded by both the state (NY HEAL money) and the Federal Government.
6. Site-Specific Technology
In the remainder of this section, each site will be reviewed against a number of emerging criteria for interoperation readiness, or lack thereof. For more details, see appendices corresponding to each site visit.
a. Erickson Retirement Communities: Hardware and Software. Erickson's main HIT priority has been the Erickson-wide (one or more facilities in each of ten states)23 rollout of GE Centricity functionality for "100% of Erickson physicians."24 While this functionality does not yet include CPOE, it does include web-based "anytime/anywhere" access for physicians. Currently, this deployment does not make use of CHI standards except as are required for reimbursement. However, internal standards are sufficient to create comparable data within the Erickson enterprise and these are being used to predict the incidence of falls, and they will be used to track the efficacy of interventions that attempt to prevent falls. Interestingly, given Erickson's commitment to an internal ethic of "enter once, read many times" (aimed at avoiding the re-entry of internal data already in an Erickson computer), it was surprising that no plans were described to exchange data between Centricity and CareMEDX, the primary record for patients in home health care, Part A SNF, and LTC.25 More predictably, as with most providers, neither system interoperates with external laboratories or pharmacies, although health care providers often are content to have the information they need available even if it is on two computer screens. Still, the fact that Centricity is deployed nationally by Erickson is a singular accomplishment, one from which significant benefits are already accruing. For instance, Erickson's information technology philosophy and systems seemed to contribute significantly to employee satisfaction and a trend toward staff retention.
At the time of the site visit, Erickson discussed its readiness to adopt HL7 messaging standards. They have initiated discussions with St. Agnes hospital (their primary, unaffiliated acute care hospital in Maryland) to deploy a custom data exchange solution with their two EHR systems. The site visit occurred before the CCD standard was an approved and widely available standard.
Summary: Erickson uses a national EHR that supports web-based access. This EHR does not interoperate with non-affiliated sites, although Erickson would like it to interoperate with their preferred local hospital as soon as possible, nor does it interoperate with the Erickson EHR product used by the Erickson PAC and LTC providers. They do not use HIT standards except as are required for reimbursement. Centricity makes use of Oracle to store patient information. Because of organizational priorities and experience and the relatively contemporary, highly scalable implementation of Centricity, Erickson is positioned to productively leverage any relevant national standard (e.g., a standard for patient data exchange). Erickson will probably be able to send and receive data using any emerging national exchange standard before many of the unaffiliated providers in the 16 communities in which Erickson is located are ready to receive or send health data.
b. Montefiore Medical Center: Hardware and Software. Montefiore uses LastWord as the hospital EHR, the exports from which periodically refresh a Sybase data repository. The Sybase supports general querying and aggregation of patient data, functions not available in the LastWord system. Montefiore is the anchor provider in the recently-funded Bronx RHIO. The RHIO will include other hospitals (e.g., the Bronx VA), some ambulatory care sites, and one PAC/rehabilitation/LTC nursing facility (JHHA). Other PAC/LTC sites may join soon, as will local laboratories and pharmacies. Data exchange in the RHIO will depend on a common computer-represented patient summary (which, at the time of the site visit was called a virtual patient object [VPO]). The latter will make use of dbMotion technology to manage secure access, among other things.26 A basic premise of the RHIO is that patient data remain stored at its source and only the patient summaries, in the form of a VPO, are transmitted to requesting providers. Although the Bronx RHIO is committed to the use of relevant standards, the developers have not yet finalized the list of standards they will incorporate. For example, they are not yet considering the use of the CCD. However, the VPO, dbMotion technology, and the Montefiore patient data repository, should allow for incorporation of any emerging national patient data exchange standard.
The VNS of New York exchanges patient data with Montefiore and other Bronx providers using traditional fax and phone methods. However, the VNS of New York has projects underway in which they are exchanging information--computer-to-computer--with physician office EHRs and with Cornell Weil Medical Center (discussed in Appendix C). The VNS of New York's long-standing innovative use of information technology enables it to leverage that technology as part of attempts to exchange data with other providers. The VNS of New York has achieved sufficient intra-enterprise interoperation so that it is now focusing its development efforts on data exchange with non-affiliated providers.
Summary: No non-affiliated interoperability was observed and no use of HIT standards was observed except those used for reimbursement. Montefiore Medical Center, the VNS of New York, and some Bronx RHIO sites are self-reportedly "poised for interoperability." The now-funded Bronx RHIO is well positioned to leverage any emerging national patient data exchange standards. Not coincidentally, the VNS of New York has several HIE pilots underway with non-Bronx providers. (see Appendix C for a discussion of the VNS pilot projects).
c. LDS Hospital: Hardware and Software. LDS Hospital continues to evolve its EHR, which today consists of a heterogeneous mix of internally-developed and commercial-off-the-shelf (COTS) components. The distinguishing features of the IHC system (including LDS Hospital) include a longitudinal data repository that is accumulating both inpatient and outpatient information on the IHC population, and an ongoing effort to make all the components interoperate internally using HL7v2 messaging. An IHC goal is to use its recent partnership with GE Healthcare to move all components, including the data repository, to COTS status. IHC has pioneered the use of HL7 messaging and the use of LOINC, a CHI standard, for use within its own enterprise in these intra-enterprise messages. Other uses of CHI standards are those required for reimbursement. LDS Hospital and almost all other providers in Utah make use of the UHIN for accelerated in-state billing and reimbursement. LDS Hospital will be participating in a pilot project aimed at use of the UHIN to communicate limited clinical information to and from other Utah health settings. No further details, such as whether there will be a UHIN Master Patient Index were provided to the site visit team.
All PAC/LTC sites visited in Utah had some HIT in place. One site, Hillside Rehabilitation Center, is installing a relatively advanced EHR system developed by BlueStep, which is entirely web-based and hosted remotely. Features include a focus on workflow management and web-accessible disaster-recovery backup. For further background information, see Appendix D.
Summary: Interoperability with unaffiliated sites was not observed, however all sites made use of the UHIN for claims submission, which is significant in and of itself. No use of CHI standards was observed, except for LDS Hospital's extensive use of HL7 messaging and LOINC for laboratory test result reporting. However, all sites could be poised to exchange clinical information with one another by building on their current use of the UHIN for financial transactions. Predictably, the first types of electronic clinical data exchange through UHIN will likely be laboratory results and medication ordering, which have standardized codes already used for payment.
d. Indiana Health Information Exchange/Indiana University: Hardware and Software. The Indiana University's EHR (Indiana Network for Patient Care) is a locally developed, deployed, and maintained system that is a pioneer system in the development and evaluation of physician order entry and decision support and the creation and use of longitudinal patient records (Overhage, Suico, & McDonald, 2001). Today, it makes use of commodity hardware to run legacy (MUMPS and Windows) software. More significantly, this system was one factor that enables the retrieval of previous encounter information from different hospitals by local EDs. This retrieval does not pre-populate the local system today, but pre-population is one planned feature of the Indianapolis-wide Docs4Docs system. This feature supports web-based physician access to available patient encounter information stored in the EHRs of Indianapolis hospitals by collecting this information in a regional data repository. An example provided during the site visit described a patient seen in one ED for chest pain who proved to have had a recent negative cardio-vascular work-up at another hospital. The patient was later discovered to have a pulmonary embolism and a second, costly cardio-vascular work-up was avoided because the ED physicians could see the (negative) results of the cardio-vascular work-up. Currently, this repository does not feature a uniform patient summary. The IHIE is an expanding umbrella that leverages these and other planned data exchange projects including the data to be collected from state-mandated e-prescribing. Thus, the goal of being able to retrieve all available information about a patient is being approached incrementally. The IHIE is open to all settings that would like to participate, and generally project leaders assist with the inclusion of each site. At the time of this report, the only members of the IHIE are local hospitals and physicians.
Summary: Non-affiliated, human-readable HIE exists on a systematic basis between Indianapolis EDs and selected local hospitals, including Wishard Hospital, which was visited by the site visitors. Indianapolis-wide physician access to available (i.e., data that are collected and stored for other reasons) patient encounter information is supported by the web-based Docs4Docs system, and plans are in place for historical information on the patient to also be entered into the participating providers' EHRs. CHI standards were not being used (other than those required for reimbursement) with the notable exception of the widespread use of LOINC to normalize laboratory report data and for widespread use of HL7v2 messages. The Beverly Healthcare Nursing Home at Brookview made use of relatively advanced national (Beverly) proprietary HIT that does not use HIT (e.g., CHI) standards. At present there are no plans for Beverly to join the emerging IHIE. The VNS of Indiana supports its home care nurses and other clinicians with a laptop-accessible EHR, which also does not use HIT (e.g., CHI) standards. The full site visit report can be found in Appendix E.
Summary and Suggested Next Steps
As described throughout this report, HIE across care settings has been observed to be costly, complicated, and challenging, as it, involves:
- exchange of the full spectrum of health information (e.g., summaries to transfer care from one setting to another, exchange of medication and other orders, reporting of results, etc.);
- exchange of health information between multiple parties, including across a number of unaffiliated clinicians, providers, and organizations;
- use of a variety of information exchange mechanisms (e.g., face-to-face, telephone, fax, or the use of computers) within and across organizations, often employing more than one modality for a given "exchange;" and
- varied e-HIE capacities within and across organizations (e.g., the ability to generate and/or receive any type of electronic health information [including standardized health information]).
During the site visits, in some instances HIE challenges stemmed from the technological inability to efficiently exchange electronic information (e.g., lack of software, including the lack of software that uses HIT standards). However, much of the complexity and variability in HIE appeared to be rooted in the different priorities various health care organizations placed on the exchange (by any method) of certain types of health information.
This section of the report summarizes findings identified through the site visits, literature review (see interim report entitled "Report on Health Information Exchange in Post-Acute and Long-Term Care"27), and other more recently available information related to HIE on behalf of persons receiving PAC and LTC, focusing particularly on the use of e-HIE. The report concludes with a discussion of activities that are or could be considered to accelerate the implementation of e-HIE on behalf of persons receiving PAC and LTC.
A. Health Information Exchange by Any Means
Several factors were identified as facilitating or creating barriers to the timely exchange of health information by any means, including non-e-HIE, needed to care for persons receiving care from PAC and LTC providers. As observed during the site visits, many stakeholders indicated that, at present, the key for securing timely information exchange were strong, cross-organizational interpersonal relationships. Such relationships were identified as essential for supporting timely and needed HIE regardless of the method(s) by which health information is exchanged (e.g., manually, by fax, or using HIT). At all sites it was observed that the relationships built between staff at institutions (e.g., hospital discharge planner and admission coordinator at a NH, liaisons from HHA/NH working in hospitals prior to discharge) were of paramount importance. Not only did these relationships tend to ensure that referrals were made more efficiently and the information shared was more complete (i.e., these relationships seemed to help reinforce accountability for information transfer), but also it seemed to increase job satisfaction. The site visitors observed that even to the extent e-HIE was used, personal relationships were not completely supplanted by technology, and it is likely that as HIT implementation becomes more widespread, this observation will persist.
Other factors that were identified through the site visits and a review of the literature as facilitating HIE included:
-
Medicare payment policies that some believe have created indirect incentives for HIE (e.g., capitated, episode-based prospective payment methods) and other policies that include direct incentives for the timely exchange of health information across organizations (e.g., pay-for-performance incentives).
-
Medicare requirements to use e-prescribing standards to support electronic medication ordering.
-
State requirements for the exchange of health information as patients transition across settings of care (e.g., requirements in the state of New York to use the PRI).
-
Cross-organizational use of software products that enable the standardized electronic exchange across settings of patient discharge information (e.g., use of ECIN to exchange the PRI in New York).
-
Anticipated revisions to the Joint Commission (previously known as JCAHO) hospital requirements that will focus, in part, on ensuring safe and effective hand-offs as patients transition out of hospitals to other settings of care.
Several factors that were identified as creating barriers to HIE included:
-
The perception (whether well-informed or not) that implementation of and concerns about being out of compliance with HIPAA creates barriers to HIE across health care settings.
-
The belief held by many PAC/LTC providers that they are effectively unable to request more complete/accurate health information from referring hospitals given the dependence of PAC/LTC providers on hospitals as a primary source of referrals.
-
Lack of awareness of the availability of HIT standards that, if implemented, could support e-HIE and health information re-use.
-
Failure to use HIT products that support standardized exchange of health information and information re-use.
B. Implementation of HIT including e-HIE
This report described several factors that contributed to the limited use of e-HIE to support the exchange of information needed for PAC and LTC patients including:
-
The limited use of electronic health information exchange (e-HIE) products. The limited use of such products was attributed to the: (a) cost of products; (b) lack of requirements to use such products; (c) questions about the relative costs and benefits of HIT and HIE applications; (d) lack of provider awareness of the need for and availability of HIT standards; and (e) a failure to consider how HIT and HIE applications could be used to enhance workflow in PAC and LTC settings (e.g., how service delivery could be made more efficient through the re-use of electronic health information received through e-HIE).
-
Hospitals and HIE organizations sometimes had not given clinicians in PAC and LTC settings access (such as view-only access) to patient data in hospital EHRs for those patients who were to be discharged from hospitals and admitted by the PAC/LTC providers.
-
HIE organizations often did not involve PAC and LTC providers in the formation of these exchange partnerships.
-
PAC and LTC providers sometimes choose not to participate in discussions with HIE organizations.
C. Interoperable HIT
As mentioned above and described throughout this report and the literature review, the lack of HIT standards particularly for: (i) PAC and LTC providers; and (ii) e-HIE often have been identified as barriers to more timely exchange of needed, interoperable health information. However, over the last few years, there have been several significant advances related to the identification, endorsement, and/or use of HIT standards that will, if implemented, support interoperable HIE, including HIE on behalf of PAC and LTC patients, including the:
-
The endorsement by the Secretary of HHS in August 2007 of the CHI Disability and Patient Assessment standards and commitment that these standards will be used by federal agencies in implementing new and to the extent feasible in modifying existing health information systems. These standards:
- Have been and will continue to be applied to the NH MDS;
- Will be applied to the home health OASIS instrument; and
- Will be applied to the CARE assessment instrument (previously known as the "PAC-PAI") and will be used by CMS in the Medicare Post-Acute Care Payment Reform demonstration required in Section 5008 of the Deficit Reduction Act.
-
Approval by HL7 of the CCD implementation guide for the standardized exchange of clinical documents (e.g., discharge and transfer documents).
-
Approval by the HITSP of the CCD as the standard for certain types of HIE.
-
Projected use of the CCD standard by the CCHIT as the standard to support the exchange of documents by certified physician office and hospital EHRs.
-
Announcement by CCHIT of its intent to specify certification criteria for NH EHRs. Such criteria are expected to include specifications concerning the functionality of certified EHRs and the interoperability standards that certified EHRs must support. For example, certification criteria are expected to include the need for EHRs to support standardized assessments and standardized exchange of patient summaries.
-
Use of the CCD standard and/or CHI Patient Assessment standards in upcoming private sector HIE demonstrations that will include PAC and LTC providers.
-
Findings from the AHRQ/CMS e-prescribing pilots that found that standardized e-prescribing (including in NHs) created efficiencies gains and quality improvements.
-
CMS regulations requiring the use of certain standards to support e-prescribing under Medicare Part D (however, it is important to note that at present NHs are excluded from the requirement to use these standards).
-
Approval in September 2007 by ANSI of the e-prescribing standard needed to support e-prescribing in NHs (i.e., NCPDP SCRIPT v10.1).
-
Approval by the AHIC of the need for a use case that will focus on HIE at the time of referrals and transfers in care. This use case should be developed in 2007 and submitted to the HITSP in early 2008 for the identification of the specific standards needed to support the exchange.
The endorsement of CHI standards for patient assessments, the application of these standards to the NH MDS and expected application to the home health OASIS; approval by HL7 of the CCD implementation guide and the use of this standard by CCHIT; specification by CMS of e-prescribing standards and the approval by ANSI of the e-prescribing standards needed to support e-prescribing in NHs will enable providers to request and HIT vendors to develop products that support: (i) standardized assessments; and (ii) the exchange of certain types of information needed on behalf of patients treated by PAC and LTC providers.
The specification of NH EHR certification criteria by CCHIT is expected to level the playing field between HIT vendors and providers, enabling providers to have greater confidence in the functionality and standards included in the HIT products they purchase, and creating a roadmap that vendors can use for the development of increasingly standardized EHR products.
The application of the CHI Patient Assessment standards to the NH MDS and planned application to the home health OASIS; use of these standards by CMS in the demonstration of the CARE instrument; expected use of the patient assessment and information exchange standards in private sector demonstrations to be conducted by CAST and Integrating the Healthcare Enterprise, and the anticipated specification of HITSP standards for an AHIC use case on referrals and transfers of care will provide guidance to the vendor and provider communities about how these standards can be applied to support standardized HIT products and interoperable HIE to support the care needed by PAC and LTC patients.
D. Accelerating the Implementation of e-HIE
Despite the identification and endorsement of several important HIT standards, including standards to support HIE, and the expected use of these standards in public and private sector demonstrations, e-HIE by health care providers, including PAC and LTC providers, is quite limited, and the use of interoperable HIT and e-HIE is even less common. The following describes several activities that could be considered to accelerate implementation of standardized e-HIE on behalf of patients treated by PAC and LTC providers.
The identification and specification of additional HIT standards is needed in certain areas including:
-
Specification by the AHIC of a transfer of care use case that involves the exchange of information on behalf of patients being treated in PAC and LTC settings would enable this type of exchange to be included in and focused on as part of the national HIT agenda, and would likely result in a nationally-recognized endorsement (i.e., by the HITSP and AHIC) of the HIT standards needed to support this type of exchange. Members of the PAC and LTC communities are working on developing a use case focusing on admission and/or discharge from PAC/LTC that could be considered by AHIC and if approved, the HITSP would identify the standards needed to support this type of HIE.
-
Specification of an implementation guide that would provide guidance to the PAC and LTC vendor communities as to how to integrate the CHI-endorsed patient assessment and HL7 CCD HIE standards into their software products.
-
Implementation of the NCPDP SCRIPT v10.1 standard in CMS e-prescribing regulations will enable NH providers and vendors to knowledgably invest in standardized e-prescribing products.
However, as observed during the site visits, implementation of HIT in general, much less the implementation of interoperable HIT and e-HIE remains a huge gap. Unaffiliated PAC and LTC providers were less likely to have implemented HIT than their counterparts that are part of chain organizations and/or are affiliated with integrated delivery systems. The anticipated public and private sector demonstrations of the use of the CHI-Patient Assessment standards and the HL7 CCD standard to exchange needed patient summary/discharge information as patients transition across settings of care are expected to demonstrate the use of and increase awareness of how standardized applications can support HIE. These demonstration efforts may wish to consider the feasibility of including unaffiliated PAC and LTC providers in the demonstration efforts.
Identification by the HITSP and endorsement by AHIC of HIE standards needed to support referrals and transfers in care, and the likely identification by CCHIT of the CHI-Patient Assessment and HL7 CCD standards as criteria for certified NH EHRs also will support implementation standardized e-HIE.
A dominant theme to emerge from the third annual LTC-HIT Summit in June 2007 was the need to accelerate and support the implementation of standardized HIT in PAC and LTC. Recommendations that were discussed during the 2007 LTC Summit included:
-
Request the Secretary of HHS to provide assistance to PAC and LTC providers in implementing HIT (including, for example, using standards for e-prescribing in LTC and federally-required patient assessments).
-
Engage state agencies (including Medicaid programs and the National Governors' Association) to support the implementation of interoperable HIT in LTC.
-
Educate providers regarding interoperable HIT (e.g., its uses, known and expected benefits, costs, etc.).
-
Further analyze and disseminate information on the costs and benefits of HIT implementation on behalf of PAC and LTC patients, including information on who incurs these costs and who reaps the benefits.
-
Reduce the risks PAC and LTC providers encounter in the acquisition of HIT products.
-
Identify and share information among PAC and LTC providers on how the use of HIT can change and enhance workflow.
Several actions are being undertaken to address many of these recommendations including:
-
The recent endorsement by the Secretary of HHS of the use of the CHI-Patient Assessment standards in federal health care programs.
-
Research being sponsored by ASPE to:
- examine the costs and benefits of HIT implementation, including e-HIE, on behalf of patients receiving PAC and LTC;
- support an infrastructure building effort that will:
- further apply CHI-endorsed standards to the MDS and OASIS;
- specify the HIE infrastructure for standardized patient assessments and patient summaries (respectively using the CDA and CCD standards); and
- examine intellectual property issues associated with federally-required assessments (i.e., the MDS, OASIS, and Inpatient Rehabilitation Facility PAI); and
- design a survey of NH EHR adoption and use.
-
The work being led by the private sector LTC community, and supported by ASPE, to specify the functions and standards needed in NH EHR products. The product of this work will be considered by CCHIT in specifying the certification criteria for EHRs used in NHs.
-
The anticipated private sector demonstrations of interoperable HIE involving PAC and LTC providers.
Additional consideration is needed to develop and implement a widespread education and outreach strategy to educate PAC and LTC providers and other stakeholders on a variety of HIT issues to increase awareness and use of interoperable HIT. Such an educational campaign could also share information about how workflow can be made more efficient through the implementation of various HIT applications. Educational and outreach efforts also should include discussions with other health care provider types (e.g., hospitals, physicians, HDSs), HIE organizations, and other stakeholders about the need to include PAC and LTC providers in HIE efforts.
References
American Health Care Association (2003). Results of the 2002 AHCA Survey of Nursing Staff Vacancy and Turnover in Nursing Homes. http://www.ahca.org/research/rpt_vts2002_final.pdf [On-line].
American Health Care Association (2006). A Snap-Shot of the Use of Health Information Technology in Long Term Care. http://www.amda.com/news/othernews/2007/ahca_hit_longtermcarewhitepage1206.pdf [On-line].
Booz Allen Hamilton (2006). Evaluation Design of the Business Case of Health Technology in Long-Term Care: Final Report. Washington, DC: Office of Disability, Aging and Long-Term Care Policy, ASPE, HHS. http://aspe.hhs.gov/daltcp/reports/2006/BCfinal.htm [On-line].
Brody, J. (2007). Personal Health; To Protect Against Drug Errors, Ask Questions. http://www.nytimes.com/2007/01/02/health/02brody.html?ei=5088&en=e96599a5fa428c85&ex=1325394000&partner=rssnyt&emc=rss&pagewanted=print [On-line].
Centers for Medicare & Medicaid Services (2001). Conditions of participation: Discharge planning. Federal Register, Section 482.43, 503-504.
Centers for Medicare & Medicaid Services (2006). Uniform Patient Assessment for Post-Acute Care -- Final Report. http://www.cms.hhs.gov/QualityInitiativesGenInfo/Downloads/QualityPACFu… [On-line].
Centers for Medicare & Medicaid Services (2007a). Press Release: Details for Long-Term Care Hospital Prospective Payment System Proposed Rule for Rate Year 2007. http://www.cms.hhs.gov/apps/media/press/release.asp?Counter=1757 [On-line].
Centers for Medicare & Medicaid Services (2007b). Revised Long-Term Care Facility Resident Assessment Instrument User's Manual, Version 2.0. http://www.cms.hhs.gov/NursingHomeQualityInits/downloads/MDS20Update200… [On-line].
Coleman, E.A. (2002). Aspen Transitional Care Conference Proceedings. http://www.uchsc.edu/hcpr/documents/AspenTransitionProceedings.pdf, Accessed November 17, 2003.
Coleman, E.A. (2003). Falling through the cracks: Challenges and opportunities for improving transitional care for persons with continuous complex care needs. J Am Geriatr Soc, 51, 549-555.
Coleman, E.A. & Berenson, R.A. (2004). Lost in transition: Challenges and opportunities for improving the quality of transitional care. Annals of Internal Medicine, 141, 533-536.
Coleman, E.A., May, K., Bennett, R.E., Dorr, D., & Harvell, J. (2007). Report on Health Information Exchange in Post-Acute and Long-Term Care. http://aspe.hhs.gov/daltcp/reports/2007/HIErpt.htm [On-line].
Computer Sciences Corporation (2007). CSC and Connecting for Health Team Successfully Demonstrate Nationwide Health Information Network Prototype. http://www.csc.com/newsandevents/news/8468.shtml [On-line].
Consolidated Health Informatics (2006). Standards Adoption Recommendation -- Functioning and Disability. http://www.ncvhs.hhs.gov/061011p2b.pdf [On-line].
Continuing Care Leadership Coalition (2006). Health Information Technology in Long Term Care Survey Findings 2006. New York, NY.
Department of Veterans Affairs (2006). VA Geriatrics and Extended Care (GEC) Referral. http://www1.va.gov/geriatricsshg/docs/vha-10-0415-fill.pdf [On-line].
Federal Register (2006). Executive Order 13410: Promoting Quality and Efficient Health Care in Federal Government Administered or Sponsored Health Care Programs --August 28, 2006. Volume 71, Number 166, 51087-51091.
Forster, A., Murff, H., Peterson, J., Gandhi, T., & Bates, D. (2003). The incidence and severity of adverse events affecting patients after discharge from the hospital. Annals of Internal Medicine, 138, 161-167.
Healthcare Informatics in collaboration with AHIMA & AMDIS (2005). Mapping a changing healthcare landscape: Results of a Regional Health Information Organization Survey. http://www.ahima.org/hitweek/Mapping_Survey.pdf [On-line].
Healthcare Information & Management Systems Society & the Center for Health Information & Decision Systems (2006). HIT Dashboard. http://www.hitdashboard.com [On-line].
HMO Workgroup on Care Management (2004). One patient, many places: Managing health care transitions. Washington, DC: AAHP-HIAA Foundation.
Hudak, S. & Sharkey, S. (2007). Health Information Technology: Are Long Term Care Providers Ready? Oakland, CA: California HealthCare Foundation.
Hughes, G. (2003). Transfer of Patient Health Information Across the Continuum (Updated). AHIMA Practice Brief, Practice Guidelines for Managing Health Information, 64S-64Z.
Kaushal, R., Bates, D.W., Poon, E.G., Jha, A.K., Blumenthal, D., & the Harvard Interfaculty Program for Health Systems Improvement NHIN Working Group (2005a). Functional Gaps In Attaining A National Health Information Network. Health Affairs, 24, 1281-1289.
Kaushal, R., Blumenthal, D., Poon, E.G., Jha, A.K., Franz, C., Middleton, B., et al. (2005b). The Costs of a National Health Information Network. Annals of Internal Medicine, 143, 165-173.
Moore, C., McGinn, T., & Halm, E. (2007). Tying Up Loose Ends: Discharging Patients With Unresolved Medical Issues. Archives of Internal Medicine, 167, 1305-1311.
Morrison, R.S., Olson, E., Mertz, K.R., & Meier, D.E. (1995). The inaccessibility of advance directives on transfer from ambulatory to acute care settings [see comment]. JAMA 274(6):478-82.
National Bureau of Economic Research (2007). Prospective Payment System (PPS) Data. http://www.nber.org/data/pps.html [On-line].
National Committee on Vital and Health Statistics (2006). Letter to the Honorable Michael O Leavitt, Secretary, HHS. http://www.ncvhs.hhs.gov/061128lt.pdf [On-line].
Office for the National Coordinator for Health Information Technology (2004). The decade of health information technology: Delivering consumer-centric and information-rich health care. Washington DC.
Overhage, J.M., Suico, J., & McDonald, C.J. (2001). Electronic Laboratory Reporting: Barriers, Solutions and Findings. Journal of Public Health Management & Practice, 7, 60.
Poissant, L., Pereira, J., Tamblyn, R., & Kawasumi, Y. (2005). The Impact of Electronic Health Records on Time Efficiency of Physicians and Nurses: A Systematic Review. Journal of the American Medical Informatics Association, 12, 505-516.
Poon, E., Jha, A., Christino, M., Honour, M., Fernandopulle, R., Middleton, B., et al. (2006). Assessing the level of healthcare information technology adoption in the United States: a snapshot. BMC Medical Informatics and Decision Making, 6, 1.
Seavey, D. (2004). The cost of frontline turnover in long-term care. Washington, DC: Better Jobs Better Care, Institute for the Future of Aging Services.
Sidorov, J. (2006). It Ain't Necessarily So: The Electronic Health Record And The Unlikely Prospect Of Reducing Health Care Costs. Health Affairs, 25, 1079-1085.
Utah Health Information Network (2007). http://www.uhin.com/ [On-line].
Walker, J., Pan, E., Johnston, D., Adler-Milstein, J., Bates, D.W., & Middleton, B. (2005). The Value of Health Care Information Exchange and Interoperability. http://content.healthaffairs.org/cgi/reprint/hlthaff.w5.10v1 [On-line].
Acronyms
| AAHSA | American Association of Homes and Services for the Aging |
|---|---|
| ACE | Acute Care for Elders |
| AHCA | American Health Care Association |
| AHIC | American Health Information Community |
| AHRQ | HHS Agency for Healthcare Research and Quality |
| ALF | assisted living facility |
| ASP | application service provider |
| ASPE | HHS Office of the Assistant Secretary for Planning and Evaluation |
| BxRHIO | Bronx Regional Health Information Organization |
| CARE | Continuity Assessment Record and Evaluation [instrument] |
| CCD | continuity of care document |
| CCHIT | Certification Committee for Healthcare Information Technology |
| CCR | continuity of care record |
| CCRC | continuous care retirement community |
| CDR | Clinical Data Repository |
| CHI | consolidated health informatics |
| CICS | Customer Information Control System |
| CIS | clinical information system |
| CMS | HHS Centers for Medicare and Medicaid Services |
| CNS | Community Nursing Service |
| CoPs | Conditions of Participation |
| COTS | commercial-off-the-shelf |
| CPOE | computerized provider order entry |
| CSC | Computer Science Corporation |
| C-II | Schedule 2 Controlled Substances |
| DME | disposable medical equipment |
| ECIN | Extended Care Information Network |
| ED | emergency department |
| EHIT | Emerging Health Information Technologies |
| EHR | electronic health record |
| EMR | electronic medical record |
| e-HIE | electronic health information exchange |
| FFS | fee-for-service |
| FTE | full-time employee |
| GEC | VA Geriatrics and Extended Care |
| HCPR | University of Colorado Division of Health Care Policy and Research |
| HDS | health delivery system |
| HHA | home health agency |
| HHS | US Department of Health and Human Services |
| HIE | health information exchange |
| HIEN | Health Information Exchange Network |
| HIMSS | Healthcare Information and Management Systems Society |
| HIPAA | Health Insurance Portability and Accountability Act |
| HIT | health information technology |
| HITSP | Health Information Technology Standards Panel |
| HL7 | Health Level Seven |
| H&P | history and physical |
| IHC | Intermountain Health Care |
| IHIE | Indiana Health Information Exchange |
| INPC | Indianapolis Network for Patient Care |
| IU | Indiana University |
| JHHA | Jewish Home and Hospital Agency |
| JHHLS | Jewish Home and Hospital Lifecare System |
| LAN | local area network |
| LOS | length of stay |
| LTAC | long-term acute care |
| LTC | long-term care |
| MAR | medication administration record |
| MDS | minimum data set |
| MHHA | Montefiore Home Health Agency |
| MLTC | managed long-term care |
| NAHC | National Association for Home Care |
| NCHIT | National Coordinator for Health Information Technology |
| NCVHS | National Committee on Vital and Health Statistics |
| NH | nursing home |
| NHIN | National Health Information Network |
| NYDoH | New York Department of Health |
| OASIS | Outcome and Assessment Information Set |
| OT | occupational therapy |
| PAC | post-acute care |
| PAI | patient assessment instrument |
| PAL | PTXT application language |
| PASARR | Pre-Admission Screening and Annual Resident Review |
| PC | personal computer |
| PCP | primary care physician primary care provider |
| PCRS | Patient Care Record System |
| portable document file | |
| POC | point-of-care |
| POLST | physician orders for life sustaining treatment |
| PRI | Patient Referral Instrument Patient Review Instrument |
| PT | physical therapist physical therapy |
| RHIO | regional health information organization |
| RN | registered nurse |
| RUG-III | resource utilization groups-Version III |
| SDO | standards development organization |
| SNCC | Schervier Nursing Care Center |
| SNF | skilled nursing facility |
| TAL | tandem application language |
| TOM | Task Order Monitor |
| UCDHSC | University of Colorado at Denver and Health Sciences Center |
| UHIN | Utah Health Information Network |
| UHINT | Utah Health Information Network tool |
| VNS | Visiting Nurse Service |
| VNSNY | Visiting Nurse Service of New York |
| VSP | vertical service provider |
Notes
-
Unaffiliated, for the purposes of this study was defined as not being owned by the hub site.
-
Affiliated, for the purposes of this study, refers to settings that are owned by the hub site.
-
In the case of Erickson Retirement Communities, the protocol was turned on its head. That is, because the Erickson campus included a skilled nursing facility and a home health agency, the referral sites were places that served the needs of Erickson residents that could not be met on the campus (i.e., acute care and hospice services). Johns Hopkins Home Health also was visited, as they receive a few referrals from Erickson per year, based on the patients request.
-
In general this is not possible today because different sites use different, usually proprietary, lists of drug names.
-
Although this definition was used for initial screening of candidate sites, the site visits did include a few settings that had some type of relationship with one another. For example, the Visiting Nurse Service, Inc. (VNS) of Central Indiana has gone through a vetting process at some of the local hospitals and after meeting the hospitals criteria, have established a preferred provider status with these referral sources. So although they are not owned or affiliated in a legal sense, this relationship does directly influence their referral stream. Similarly, at Erickson (Maryland CCRC), St. Agnes Hospital receives close to 100% of acute care referrals, although strictly speaking they are unaffiliated.
-
Website: http://intermountainhealthcare.org/xp/public/documents/institute/facult….
-
A remittance advice or remit is an electronic notice received by the provider or biller after Medicare has processed a claim and gives an explanation for the payment.
-
BioCrossroads is an entity that provides money and support to both existing and new life sciences businesses, expanding collaboration and partnerships among Indianas life science institutions, expanding science education, and building awareness and marketing Indianas life sciences industry. See http://www.biocrossroads.com for more information.
-
The four consortia are IBM, Accenture, Northrup Grumman, and CSC.
-
As stated before, in the case of the site visit to Erickson Retirement Communities, the authors asked for referrals to an acute care hospital and any other PAC or LTC settings that may treat the Erickson residents.
-
See, for example, http://dhfs.wisconsin.gov/forms1/DDES/dde2191.doc.
-
Website: http://aspe.hhs.gov/daltcp/reports/2007/HIErpt.htm.
-
Websites: http://www.jointcommission.org/SentinelEvents/SentinelEventAlert/sea_35…; http://www.ihi.org/IHI/Topics/PatientSafety/MedicationSystems/Tools/Medication+Reconciliation+Review.htm.
-
On November 2, 2005, HL7 announced that in collaboration with ASTM, they are developing an implementation guide to express the CCR data set in an HL7 Version 3 (v3) CDA, r2 document. The CCR is snapshot summary of a medical record that is delivered from setting to setting, and could potentially be displayed in an EHR. This collaborative specification effort is referred to as the CCD. HL7 approved and the HITSP has endorsed the CCD. The CCD will map CCR content into a CDA r2 representation, which will enable the exchange of human-readable (text) and/or coded transfer documents.
-
Website: http://www.whitehouse.gov/news/releases/2006/08/20060822-2.html.
-
As the then Secretary of HHS, Tommy Thompson, often observed, If Lands End can remember my shirt size, why cant my doctors office remember my phone number and other demographic informatiom?
-
Website: http://www.hhs.gov/news/press/2007pres/20070103.html.
-
Website: http://www.ericksoncommunities.com/wellness/centricity.asp.
-
Dan Cobb, CareMEDX Chief Technology Officer, and prominent contributor to professional and standards organizations, accompanied us on relevant portions of the Erickson site visit.
-
Website: http://aspe.hhs.gov/daltcp/reports/2007/HIErpt.htm.
Appendices
APPENDIX A: Draft Case Study Plan
CHAPTER 1: INTRODUCTION
Having learned a great deal from reviewing recent literature and from speaking with experts in the area of health information exchange (Task 5), the Division of Health Care Policy and Research (HCPR) team is well positioned to conduct on-site case studies at four health delivery systems and affiliated and non-affiliated post-acute and/or long-term care settings. The purpose of this deliverable is to outline the plan for these case studies (Task 7), during which we will address the following overarching research questions:
- What information is needed at times of transfer from acute care hospitals to post-acute or long-term care?
- How is this information exchanged and how is health information technology used (or not used) to support this exchange with affiliated and unaffiliated health settings?
- What factors support (or create barriers to) timely information exchange?
- What policies would facilitate information exchange (including electronic information exchange)?
The original contract called for HCPR to adopt the use cases from the Federal Health Architecture Electronic Health Record work group as the basis for the data collection materials. Upon review of these use cases, the Task Order Manager (TOM), Principal Investigator, and Project Director concurred that they were not suitable to meet the needs of this project. As such, different clinical scenarios were established by the HCPR team, in collaboration with the TOM.
To address the four overarching research questions above, open-ended discussion guides and scenarios will be developed for the four site visits (draft versions of the questions that will make up the guides and scenarios can be found in Attachment A). The HCPR Research Team recognized that the guides needed to be sufficiently flexible and open-ended in order to capture the uniqueness of each systems' and PAC/LTC providers' information exchange processes. The guides and scenarios were designed to maintain a balance between the amount of clinical and technical information gathered at the site visits. Because so few skilled nursing facilities and home health agencies have adopted electronic health record systems (Kaushal et al., 2005), it is anticipated that there may be limited technical information at some sites. It also is possible that the unaffiliated PAC/LTC providers may predominantly rely on paper-based communication and this may result in a shift in focus toward a more clinically oriented discussion. Regardless, it will be important to understand what data are and are not exchanged through whatever medium is used.
The HCPR team will use various approaches to obtain the needed information. For example, at the selected health delivery systems and PAC/LTC providers, the HCPR site visit team will conduct discussions with different individuals (e.g., clinical, administrative, health information technology [HIT] staff); observe the use of HIT by the selected health care delivery system for the creation, storage, and/or exchange of information needed by PAC/LTC providers; and run through various scenarios these settings are likely to encounter, determining how the data exchange would be handled given these circumstances.
Each site visit will essentially be comprised of two site visits--one to the health delivery system and an affiliated PAC/LTC setting, and the other to three unaffiliated PAC/LTC providers in the area. This design has increased the complexity of scheduling and conducting the visits at all health settings. Time management while on site will be crucial for the success of the visit and the guides are developed to ensure that all requisite information will be successfully obtained. To this end, the two-part site visits will attempt to obtain as much information from the health delivery systems regarding their health information systems prior to the visit. These information systems also may be discussed during the site visit, but the HCPR team will be cautious that these discussions do not detract from the main purpose of the site visits or consume a disproportionate amount of time. The site visit team will attempt to strike a balance between the amount of time devoted to gathering information about the health care delivery system and the unaffiliated PAC/LTC sites. When pressed for time, the latter focus will receive higher priority.
CHAPTER 2: SAMPLING POTENTIAL SITES
INTRODUCTION
Four health delivery systems have been selected for participation as case study sites. Within these systems, three unaffiliated post-acute or long-term care settings have been identified. In this chapter, we describe the criteria used for site screening and selection, and the process through which we recruited the final four sites.
CRITERIA FOR SITE SELECTION
Identification of Candidate Health Delivery Systems
For the purposes of this study, a health delivery system initially was defined as an entity that included a hospital with one or more affiliated or owned physician office practice(s), outpatient clinic(s), laboratories, and/or pharmacies. After an interview with Erickson Continuous Care Retirement Communities (CCRC), some of which include a medical center, a certified home health agency, inpatient and outpatient rehabilitation services, a skilled nursing facility, and an assisted living facility, it was decided to broaden the definition to include this type of health delivery system.
Suggestions from the Agency for Healthcare Research and Quality (AHRQ) and the ASPE TOM, and the site's national reputation of HIT readiness informed the development of our list. We initially identified 14 candidate health delivery systems and prioritized them according to the following broad criteria:
- The type and scope of electronic health information creation, storage, and exchange believed to be implemented in the system.
- The anticipated level of effort required to gather data about the information exchange mechanisms at each system.
- To the extent possible, how the health delivery system is representative of those around the country and/or provides an instructive contrast to the other sites selected.
The following were specific criteria used to further prioritize candidate sites:
- An electronic health information system that allows for the exchange of health information across two or more settings (e.g., acute care hospital and physician offices, laboratory, pharmacy, radiology, discharge information), and preferably documentation to explain the components and capabilities of the health information system.
- Unaffiliated post-acute and long-term care settings (defined as skilled nursing facilities, nursing homes, and home health agencies) in the same general geographic location. (Unaffiliated, for the purposes of this project, is defined as not being owned by the health delivery system, however, the health delivery system is a referral source).
- Preferably, at least six months experience with the software application(s) that support information exchange.
- Amenable to a site visit by a three-person team of data collectors with access to a variety of staff (including clinicians, information technology specialists, and managers).
- If possible, at least one of the four sites would be located in a rural area.
PRIORITIZED LIST OF POTENTIAL SITES
Table A.1 shows the prioritized list of sites using the criteria noted above. Although attempts were made to contact representatives from the majority of these institutions, in some cases that was not possible. In other cases, we spoke with individuals who may not have had the organization's long view; that is, we did not always get to speak with the leaders at the organization. Finally, the places that we vetted did not have the opportunity to review the accuracy of the information provided in this document, including Table A.1 below.
| TABLE A.1: Potential Site Visit List | |||||
|---|---|---|---|---|---|
| Health Delivery System and Location | Exchange Across 2+ Settings? | Has Unaffiliated PAC/LTC? | 6 m. + Experience with Software? | Amenable to Site Visit? | Rural Area? |
| Intermountain Health Care, Salt Lake City, Utah | Yes | Yes | Yes | Yes | No |
| Maimonides, Brooklyn, New York | Yes | Yes | In transition to new software? | Not asked | No |
| Mercy Medical Center, Rural Iowa Redesign of Care Delivery with EHR Functions, Mason City, Iowa | Yes | Yes | Some sites yes, some are in process of rollout | No | Yes |
| Meridian Health, Jersey Shore University Medical Center, Jersey City, New Jersey | Yes | Yes | Yes | Not asked | No |
| Montefiore Medical Center, Bronx, New York | Yes | Yes | Yes | Yes | No |
| Indiana Health Information Exchange, Indianapolis, Indiana | Yes | Yes | Yes | Yes | No |
| Erickson Continuous Care Retirement Communities, Catonsville, Maryland | Yes | Yes | Yes | Yes | No |
| Taconic Independent Physicians Association, as part of the Taconic Health Information Network & Community (THINC), Fishkill, New York | Yes | Unknown | Yes | Not asked | No |
| Allina Hospitals and Clinics, Minneapolis, Minnesota | Yes | Yes | Yes | Not asked | No |
| Rhode Island HIE project, Providence, Rhode Island | Unknown | Unknown | Unknown | Not asked | Rural/Urban |
| Deaconess Billings Clinic, Billings, Montana | Yes | Yes | Yes | Not asked | Yes |
| Kaiser Permanente, Oregon | Yes | Yes | Yes | Not asked | No |
| Partners Healthcare System, Inc., Boston, Massachusetts | Yes | Yes | Yes | Not asked | No |
| PeaceHealth, Eugene, Oregon | Yes | Yes | Yes | Not asked | No |
SCREENING/RECRUITMENT PROCESS
A screening/recruitment process was used to determine if a site met the selection criteria, could devote sufficient resources for a site visit, and would provide access to key information and operational processes. The process included the following steps:
- Creation of a site call list.
- Initiation of a calling process to identify an initial contact person to assist in screening the site for more detail about the system.
- When a site met the selection criteria, negotiations were begun by the Project Director to determine the feasibility of participation in a site visit. Information was supplied as needed to support receiving approval for a site visit. The goals were to establish what site visit information needed to be sent and to whom; establish a timeline for a decision by the site; and determine what, if any, limitations would be imposed by the site. The project abstract that discussed the overarching research questions and project goals was provided (see Attachment B). As appropriate and as requested, additional information was provided to the sites to maintain interest.
- Discussions were held to work through various conditions required by the site to receive site visit approval. The ability to obtain key organizational information (e.g., strategic plans, implementation timelines/progress reports, system measures for return on investment, quality improvement measures, error tracking, internal surveys) was assessed. The ability to interact with the site's operations (e.g., conduct staff interviews, review computer systems, learn hardware/software specifications) also was assessed. Any special conditions/restrictions applicable to each site were noted. Evaluation of conditions may have led to a site being eliminated at various points in the screening process.
- Once the decision to participate was confirmed, the original contact designated a site visit liaison and the Project Director worked with her/him to verify the visit dates and finalize details such as specific meetings, meeting locations, contact information, site visit locations, timing, limitations, etc. In addition, further detailed information will be collected prior to the site visit about the overall health system and contact names/titles for each of the different types of care settings on the schedule.
SELECTED SITES
Erickson Continuous Care Retirement Communities
(Site Visit Dates: July 12-14, 2006)
Erickson Retirement Communities, Catonsville, Maryland, owns and operates 13 Continuing Care Retirement Communities (CCRCs) in the United States. Four of their communities are considered "mature campuses" and include a medical center, a certified home health agency, inpatient and outpatient rehabilitation services, a skilled nursing facility, and an assisted living facility (personal communication with Daniel Wilt, March 23, 2006). Erickson does have some specialists on campus who are employed by Erickson and some that are not (e.g., podiatry, dentistry), however, they do not own or operate most specialty clinics and do not own or operate any acute care centers. Erickson has developed a chart summary, which is generated out of their electronic medical record and can be accessed via the web or at any of their facilities' workstations. The chart summary includes relevant current and historical information such as advanced directives, medication lists, laboratory results, problem lists, contact information for patient and caregivers, etc. Care coordination is facilitated as physicians can access this information on or off-campus and then can coordinate in a timely manner with the emergency department physician if a patient requires acute care. In November 2005, Erickson launched a website (https://myhealth.erickson.com), which is provided to their residents free of charge. Patients have read-only access to their own medical record including the chart summary discussed above and can download it to a USB memory stick (provided by Erickson free of charge) and take it with them (should they travel or be away for extended periods of time). Alternatively, patients can access this information via the web.
Unaffiliated PAC/LTC sites: St. Agnes hospital, St. Agnes hospice, Johns Hopkins Home Health Agency.
Montefiore
(Site Visit Dates: August 2-4, 2006)
Montefiore is an integrated delivery system in Bronx, New York, providing a full range of services, including specialty care to both local and outside populations. It serves a medically underserved population, a large number of whom are young, minority, and poor (Greg Burke presentation slides from November 2004). Montefiore owns a large home health agency and contracts with a number of skilled nursing facilities in the area. They are using information technology to support the use of clinical pathways and retrospective assessments of practice and outcomes to improve quality of care (Source: Greg Burke presentation slides from November 2004). Montefiore is one of several acute care hospitals involved in the creation of the non-profit entity called the Bronx Regional Health Information Organization (RHIO). The other collaborators include additional acute care hospitals, over 40 community-based primary care centers, two nursing homes, two home health agencies, payors, physician offices, and laboratories. They recently were awarded $4.1 million from the New York Department of Health (NYDoH) for seed money (called HEAL-NY) to start up a data exchange RHIO in the Bronx. The focus of the Bronx RHIO is to facilitate sharing of clinical data among providers with disparate systems and levels of sophistication in using EHR systems (personal communication with Greg Burke).
Unaffiliated PAC/LTC sites: Schervier Nursing Care Center, the VNS of New York, the Jewish Home and Hospital.
Intermountain Healthcare
(Site Visit Dates: August 9-11, 2006)
Intermountain Healthcare is a non-profit health care system that provides care to residents of Utah and Idaho. This institution is one of the pioneers in health information technology, with a long history of excellence in the area of quality improvement. Stanley Huff and others at Intermountain were among the first users and developers of electronic health record systems. Intermountain Healthcare is a member of the Utah Health Information Network (UHIN), a community health information network that began in 1993. UHIN is a coalition of health care providers, payors, and state government with the common goal of reducing costs by standardizing administrative data, particularly payment data. The network community sets the data standards that providers and payors voluntarily agree to adhere. The UHIN standards are then incorporated into the Utah state rule via the Insurance Commissioners Office and are required for provider payment.
UHIN operates as a centralized secure network through which the majority of health care transactions pass in the state. Nearly all payors and providers are participating in this project. UHIN developed a tool (UHINT), which they provide free of charge to providers for use in electronically submitting claims. The tool is provided so that even the smallest provider can submit claims and electronically receive remittance advices. This has drastically reduced the amount of paper processing required for payors and has streamlined the payment of claims and remits, which has resulted in providers receiving payment more quickly. Under an AHRQ grant, they will use what they have learned standardizing the administrative data and pilot test the exchange of a limited set of clinical data (medication history, discharge summaries, history and physical, and laboratory results) with a small number of providers. This pilot is scheduled to occur in the summer of 2006.
Unaffiliated PAC/LTC sites: Christus St. Joseph Villa (not confirmed as of June 23), Community Nursing Service, Mission Health Services, CareSource (not confirmed as of June 23).
Indiana Health Information Exchange
(Site Visit Dates: September 13-15, 2006)
The Indiana Health Information Exchange (IHIE) is a non-profit venture connecting a number of health delivery systems in Indiana and led by Dr. Marc Overhage. The IHIE comprises over 48 hospitals and has approximately 3,000 physicians who access the network. With AHRQ funding and a variety of other sponsors including BioCrossroads, regional and local hospitals, and the Regenstrief Institute, the IHIE recently implemented a community-wide clinical messaging project. Each participating partner has access to patients' clinical results using a single IHIE-controlled electronic mailbox.
In November 2005, the HHS announced the award of contracts totaling $18.6 million to four consortia to develop a prototype for a Nationwide Health Information Network (NHIN) architecture. IHIE, MA-SHARE (Massachusetts), and Mendocino HRE (California) are involved in the Connecting for Health consortium that will launch a prototype of an electronic national health information exchange based on common, open standards. Components of these prototypes that are particularly interesting for this project are: (1) the prototypes will be designed to facilitate HIE using the Internet, not creating a new network; (2) they will allow for communication to occur between many different types of EHR systems; and (3) they will allow for different types of software and hardware that can be included in the system.
Unaffiliated PAC/LTC sites: Beverly Healthcare at Brookview, the VNS of Central Indiana, TLC Management (not confirmed as of June 23).
CHAPTER 3: CONDUCTING THE SITE VISITS
INTRODUCTION
This chapter provides more detail on how it is envisioned the site visits will be conducted. To minimize burden on any host site, HCPR staff will be as flexible as possible in terms of setting up interviews with key individuals at each site. In some cases, those individuals with whom a member of the HCPR team should speak may be unavailable during the visit. In these cases, phone calls (either before of after the site visit) will be set up to attempt to collect the salient information over the telephone.
Overall case study objectives, the site visit participants, the protocols for conducting the visits, and a description of the logistics for setting up the visits are included below. See Attachment A for a copy of the scenarios and proposed questions that will be or already have been distributed prior to the site visit.
CASE STUDY/SITE VISIT OBJECTIVES
Three overarching topic areas inform the manner in which the site visits will be conducted:
- Pertinent clinical data that are and are not exchanged at times of transfer from acute care hospitals to post-acute or long-term care. For example, how does the acute care hospital determine key elements of a SNF resident's history upon admission? What information is deemed important? How is this information recorded and transmitted? How are data shared with outside pharmacies? How are medication lists reconciled? How are patient-specific idiosyncrasies communicated to others at different health settings?
- Organizational, cultural, technological, and policy levers or barriers that exist (or do not exist) that allow (or hinder) information exchange with other health care settings. For example, what are/were the barriers to implementing and maintaining the electronic health information system? How did the health delivery system overcome these barriers? What types of resistance from staff, if any, was encountered? What is preventing more information from being shared across settings (electronically or otherwise)? What changes in the health delivery system occurred as a result of implementing the EHR system? How did the health institution cover the financial costs of EHR system implementation? Is there a solid business case for PAC/LTC settings to adopt an EHR system? What is the role of the patient and family in the preparation of the care plan?
- Mechanisms that are used to exchange data across settings. For example, are there settings where true electronic interoperability exists? What are the technological barriers to achieving interoperability? Are settings using standards-based EHR systems?
SITE VISIT TEAM COMPOSITION
Site visits are anticipated to require three days on site, and one day following each site visit to summarize in writing the site visit findings. The site visit team will include Dr. Eric Coleman and Rachael Bennett from the University of Colorado, both with clinical expertise, particularly in acute hospitals, PAC, and LTC services. The Contractor has subcontracted with Mark Tuttle, from Apelon, Inc., to be the HIT expert of the site visit team. Dr. Coleman, Ms. Bennett, and Mr. Tuttle will conduct all four site visits. Jennie Harvell, the ASPE Task Order Manager, has indicated she will attend two site visits, Montefiore and Erickson CCRC.
RESPONDENTS AT EACH HEALTH SETTING
A list of key "types" of individuals that should be interviewed and/or observed during the course of the site visit has been identified. Table A.2 provides illustrative examples of the variety of people with whom the HCPR team may wish to speak, but should not be considered a comprehensive list. Each health setting will have its own unique set of personnel and each setting at each site visit will have a schedule tailored to their unique circumstances.
| TABLE A.2: Illustrative Categories of Individuals to be Interviewed/Observed During Site Visit | |||
|---|---|---|---|
| Management | Information Technology | Clinicians | Other |
| Director of Nursing/Administrator of Facility Medical Director Business Office Compliance Officer/Regulatory Staff | Chief Information Officer Information System Administrator Staff that implemented the EHR system Staff that provide technical assistance to the EHR system users | Physician(s) Supervising RN Therapist(s) (if appropriate for setting) Nursing staff (RN, LPN, as appropriate) Pharmacist (if appropriate for setting) Other clinical staff (nursing aide, if appropriate for setting) | Data entry staff (if appropriate) Medical records (paper) |
OBSERVATION AND INTERVIEW PROTOCOLS
The site visit protocols will be conducted using multiple types of data collection including interview, observation, and various sample clinical scenarios. In addition, general information about the health system will be collected from the administrator and/or system administrator prior to the site visit.
Participating sites are fairly complex health systems. With regard to visits to Intermountain HealthCare, Montefiore, and Indiana Health Information Exchange, the schedule is to visit an acute care hospital and one affiliated skilled nursing facility or home health agency the first day. The second and third days will be spent visiting unaffiliated SNFs/NHs and/or HHAs. At Erickson, the first day will be spent at the Charlestown Campus (in Catonsville, Maryland) where the HCPR team will visit the medical center, as well as the on-campus SNF and HHA. The second day will be spent visiting the local acute care hospital, St. Agnes, which provides acute care services to Erickson residents, as well as the St. Agnes hospice. On the third day, the HCPR team will visit Johns Hopkins HHA, as they receive some referrals from Erickson.
At each care setting, three types of staff will be interviewed: clinicians, information technology, and business office/managers. In some cases, we will have large group discussions and in other cases, we will break off and have the expertise of each HCPR site visit team member speak with someone one-on-one.
SITE VISIT SET UP
At the time of the writing of this report, all four site visits have been confirmed. There were a number of challenges faced when the prioritized sites were contacted. The first challenge was getting the health delivery system to commit to a site visit. One of the preferred sites initially agreed to a site visit and then tacitly refused by neglecting to respond to any further correspondence. Of the four sites ultimately selected, two of the four required an amount of persuasion before agreement.
A second challenge was identifying a date when key individuals would be available in both the health delivery system and the unaffiliated PAC/LTC providers. The schedules of these key individuals are not within the control of the Contractor and every effort was made to identify a time that maximized participation.
A third and related challenge is the time of year in which the site visits are scheduled, which is July-September 2006, a time when many health delivery system and PAC/LTC staff are on vacation.
A fourth challenge was non-responsiveness on the part of the site liaison. Although the initial assignment of a liaison at each health delivery system went smoothly, follow-up communication with each HDS liaison has proved to be problematic. Furthermore, a liaison not only is needed at each health delivery system, but also at each of the PAC/LTC settings visited (three per site visit). Because the PAC/LTC settings are not affiliated with the health delivery system, the staff at some of the unaffiliated PAC/LTC settings has been less responsive to our request for a site visit than we had hoped. We interpret their reluctance to respond as likely the result of not fully understanding the short time commitment we were asking of their institution.
HCPR Site Visit Coordinator
The Project Director will be responsible for facilitating and preparing for each site visit (e.g., working with the host liaison to schedule interviews prior to our arrival, setting the schedule, knowing how to maneuver around the city to get to the next appointment, keeping us on schedule, and collecting the appropriate information at each setting). Once the site visit schedule has been approved and dates have been scheduled, the Project Director will continue with the following preparations:
- Work with the HDS site liaison in setting up all meetings with those we would like to interview and/or observe. This includes identifying names and contact information of the people attached to each "type" of respondent that we would like to interview/observe and determining the physical location of each person. To the extent feasible, interviews will be set up prior to the arrival of the HCPR team. If possible, biographies of those we will interview will be made available to the HCPR team prior to the visit.
- Identify, contact, and schedule the site visits with three unaffiliated skilled nursing facilities, nursing homes, and/or home health agencies that receive a number of referrals from the health delivery system.
- Work with the site liaison in setting up meeting rooms for the entrance and exit briefings, as well as for interviews.
- Identify any potential scheduling conflicts (e.g., scheduled vacations) with the help of the site liaison that may preclude any of these individuals from being able to participate in an interview. Determine, with the liaison, appropriate designees, or replacements.
- Provide background information on the site to HCPR team members who will be visiting the site.
- Facilitate the entrance and exit briefings.
- Collect documentation, reports, etc., from the site during the visit and include as part of the site visit report.
- Consolidate the HCPR site visit team's individually prepared site visit reports into one document after the site visit.
Distributing Information to the Site Prior to the Arrival of the HCPR Team
HCPR will develop and disseminate a packet of materials to the appropriate individual (e.g., the administrator, Director of Nursing) prior to the site visit for confirmation and completion. The following are some potential items that may be included in the packet:
- An introductory cover letter to the administrator.
- A partially-completed discussion guide regarding the overall health system and each individual care setting that make up the health system. Examples of the types of data to be collected include size, ownership, volume of patients seen, and contact information of the administrator. Most of this information already has been collected in order to appropriately set up the visit, but there are some items that we are unable to ascertain by telephone. Ideally, this document will be reviewed, revised, and returned to us prior to the site visit.
- A loosely constructed agenda for the site visit.
- A project overview document outlining the goals and objectives of the project and the case studies in particular (see Attachment C for the two versions--one for the host health delivery system and one for the post-acute/long-term care sites).
- A list (including biographic sketches) of the three individuals that comprise the HCPR site visit team.
- The name of the site liaison with whom HCPR's site visit coordinator has been working.
Designation of Site Liaison
One person at each site will be designated as the site liaison and this person will be requested to take on the following responsibilities:
- Assist the Project Director in scheduling interviews with appropriate individuals at the HDS as well as at each of the three unaffiliated PAC/LTC settings. This will include providing us with all necessary contact information for each of these individuals.
- Provide documents that include background information on the health setting.
- Reserve a meeting space for the entrance and exit briefings, and any other interviews, if necessary.
- Attend and help facilitate the entrance and exit briefings.
Travel Arrangements
Once the site is selected, dates will be confirmed with HCPR and site participants. A HCPR staff member will set up the travel and lodging arrangements for the travelers, including a rental car, as appropriate for off-site travel.
Duration of Site Visits
The goal will be to conduct the site visits as expeditiously as possible to minimize the burden on the host sites. We estimate that each site visit can be completed in two and a half to three days. Appointments at each health care setting will be set up prior to our arrival and will require each site visitor to conduct up to four interviews each day, along with observing various staff conduct their routine tasks.
The following assumptions were made regarding the schedule and duration of a site visit:
- With the exception of Erickson CCRC, day one will be spent with the acute care health delivery system and one affiliated PAC/LTC setting. On days two and three, no more than three unaffiliated PAC/LTC settings will be visited. The Erickson site visit will be different, as the campus has a medical center, a SNF, and an HHA. The "unaffiliated" settings will be an acute care hospital, one unaffiliated hospice, and one unaffiliated home health agency.
- Each member of the HCPR team may want to speak with a number of people at each care setting. In some cases, there may be two or three HCPR personnel involved in an interview with one or more contacts at the health setting.
- The entrance and exit briefings should last no more than 45 minutes. The liaison will determine who should attend these briefings.
- If there are key individuals with whom the HCPR team is unable to contact while on site, information will be gathered from these individuals after the completion of the site visits.
Summary of Findings
Each of the HCPR site visitors is responsible for writing a site visit report, following a standard format (to be created). They also are responsible for participating in a phone call with the TOM within one week of the site visit to discuss key findings. The Project Director is responsible for preparing a one-page report to be used in conjunction with this debriefing phone call.
To ensure the accuracy of the report, we will ask a designated person at each visited health setting if s/he would be willing to review the site visit report summary for accuracy. Findings from the site visits will be included in the draft final report, due mid-November 2006.
REFERENCES
Kaushal, R., Blumenthal, D., Poon, E.G., Jah, A.K., Franz, C., Middleton, B., Glaser, J., Kuperman, G., Christino, M., Fernandopulle, R., Newhouse, J.P., Bates, D.W. (2005). The costs of a national health information network. Annals of Internal Medicine, 143(3):165-73.
ATTACHMENT A. DRAFT DATA COLLECTION AND DISCUSSION GUIDES, CLINICAL SCENARIOS
This first table would be converted into a data collection form we would send to all sites (acute care hospital and PAC/LTC settings) prior to the visit.
| General Information about Health Care Setting |
|---|
| Area served (urban, rural, both) |
| Year established |
| Ownership (gov't, for-profit, nonprofit) |
| Number of full-time employees |
| Number of nursing homes--owned |
| Number of nursing homes--affiliated |
| Number of home health agencies--owned |
| Number of home health agencies--affiliated |
| Physician practices--owned |
| Physician practices--affiliated |
| Do you have an inpatient pharmacy (yes/no) |
| Does SNF use a dedicated pharmacy or does it contract with large/retail pharmacies or multiple pharmacies? |
| Number of Pharmacies--outpatient |
| Do you have an in-house laboratory? |
| How many outside laboratories are used? |
| Do you have an in-house radiology department? |
| How many outside radiology centers/MR centers do you work with? |
| Number of affiliated physician practices |
| Main software vendor |
| Are your physicians affiliated with your HDS or are they independent? |
| Clinical EHR system differentiate from appointment or billing (yes/no) |
| Short-term (6 months?) HIE future plans |
| Long-term HIE future plans |
The following tables represent potential questions in various areas that we anticipate we will ask. Once we receive approval from the TOM, we will convert these questions into data collection guides.
| Health information exchange: | ||||
|---|---|---|---|---|
| Electronic Exchg | Manually (fax [F], hardcopy [HC], or phone [P]) | Standards-based? (yes/no) | What is exchanged, comments | |
| HDS and pharmacy inpatient or community? | ||||
| HDS and laboratory inpatient or community? | ||||
| HDS and radiology inpatient or community? | ||||
| HDS and physician practice | ||||
| HDS and SNF 1 | ||||
| HDS and SNF 2 | ||||
| HDS and HHA 1 | ||||
| HDS and HHA 2 | ||||
| Other HDS (hospitals, clinics) | ||||
| HDS and unaffiliated HHAs/SNFs | ||||
| Other: | ||||
| SNF and pharmacy (dedicated or contracted) | ||||
| SNF and laboratory (dedicated or contracted) | ||||
| SNF and radiology (dedicated or contracted) | ||||
| SNF and physician practice | ||||
| SNF and HDS(s) | ||||
| SNF and ED | ||||
| Other PAC/LTC settings | ||||
| Other: | ||||
| HHA and pharmacy (dedicated or contracted) | ||||
| HHA and laboratory (dedicated or contracted) | ||||
| HHA and radiology (dedicated or contracted) | ||||
| HHA and physician practice | ||||
| HHA and HDS(s) | ||||
| HHA and ED | ||||
| Other PAC/LTC settings | ||||
| Other: | ||||
| Acute Care Hospitals & Medical Centers/Clinics |
|---|
| What information is necessary to exchange at time of transfer from acute care hospitals to PAC/LTC? |
| focus on physician referrals, consultation reports, meds, lab work |
| Caregivers & coordination of care (including family) |
| What information actually is exchanged? |
| focus on physician referrals, consultation reports, meds, lab work |
| Caregivers & coordination of care (including family) |
| What medium (phone, fax, paper, electronic, a combination of all) is used to exchange information? |
| Who has access to and uses the information? |
| How is this information accessed? |
| Do all clinicians (physician, nurse, social worker, therapist, and nutritionist) have the same access to the information? Probe: between disciplines vs. within disciplines. |
| How is information communicated to the different clinicians (physicians, nurse, social workers, therapists, nutritionists, etc.)? Probe: between disciplines vs. within disciplines. |
| Do unaffiliated providers (e.g., PAC providers) have the same access to health information as affiliated providers? If not, how does access differ between affiliated and unaffiliated providers? |
| When is health information exchanged to PAC/LTC facilities? Is there a delay and if so, how long? |
| Is time-sensitive information exchanged in a timely manner with PAC/LTC? (Define what we mean by time-sensitive, then ask if this information is transmitted specially or separately, then what percentage of the time is the info transferred in a timely manner (e.g., by the time the patient arrives at your health setting) |
| Has this changed with the use of electronic health information exchange (e-HIE)? |
| What information is not being communicated/exchanged at time of transfer from acute care hospitals to PAC/LTC? |
| What are the plans for the future in terms of HIE including when/how/where HIE will become automated/become more automated? |
| What are the workflow/communication issues (positive and negative) with having (1) automated or (2) non-automated HIE? |
| What are the facilitators/barriers to (1) automated and (2) non-automated HIE? |
| Who were/are the advocates/champions for embracing e-HIE in your HDS (if applicable)? What did these champions have in common across all the sites? Did you use push or pull strategies (or both)? |
| How did the champions get others to embrace the concept that HIE was valuable? What points were most compelling? |
| Does your EHR system use CHI-endorsed content and messaging standards, and do these standards support electronic HIE? If so, which standards are used and how do these support HIE? |
| Who is responsible for ensuring data are up to date upon the patients arrival? |
| Who reconciles the information from the previous health care setting with the current care setting? (e.g., medications)? How long does this take on average? |
| What policies would promote information exchange (including electronic information exchange)? |
| Are the policies HDS? State? Federal? Accreditation? |
| Skilled Nursing Facilities--Home Health Agencies |
|---|
| Define the clinically relevant information at times of transition into and out the facility/agency? |
| How is information exchanged with (i.e., to and from) the hospital (acute care)? Probe: What % of the time does this happen? |
| How is information exchanged with (i.e., to and from) physicians (both in and outside of your health care setting)? |
| How is information exchanged with (i.e., to and from) pharmacies (inside and outside)? |
| How is information exchanged with (i.e. to and from) laboratories (inside and outside)? |
| How is information exchanged with (i.e., to and from) other PAC/LTC providers? |
| What data are exchanged with acute care? |
| What data are not exchanged with acute care? |
| What data are exchanged with physicians? |
| What data are not exchanged with physicians? |
| What data are exchanged with pharmacies? |
| What data are not exchanged with pharmacies? |
| What data are exchanged with laboratories? |
| What data are not exchanged with laboratories? |
| What data are exchanged with other PAC/LTC? |
| What data are not exchanged with other PAC/LTC? |
| Is the flow of info different if you are working with a provider that is not affiliated? How is it different? |
| Have you invested in an EHR system/applications? |
| If so, what functionalities are supported by the EHR system/applications? |
| To what extent and how are these applications adhering to CHI-endorsed standards for content and format? |
| Does the EHR-S support HIE? If so, w/ whom and how? |
| If you haven't already done so, what are your future plans in terms of adopting an EHR system? What criteria are you using to select one? |
| Are standards considered when implementing EHR systems or choosing vendors? If so which standards? |
| What kind of staff turnover do you experience? How difficult is it to get new staff trained on the EHR system (if applicable)? What other issues does staff turnover greatly affect? |
| How technologically savvy are the NHs/HHAs we visited? (opinion of site visit team member) |
| What policies would promote information exchange (including electronic information exchange)? Probe for things such as the greatest technological challenges (financial, integration of services, network security, electronic signature/ensuring person is who s/he says she is, others) |
| What are the facilitators/barriers to (1) automated and (2) non-automated HIE? |
| Technological--Electronic exchange of information |
|---|
| Interoperable internal information exchange |
| Interoperable information exchange with external parties |
| What can be exchanged |
| CHI-endorsed |
| Messaging standards |
| What EHR system, vendor, etc. |
| What hardware |
| What software |
| e-prescribing capabilities |
| Description of each EHR system |
| Architecture of EHR systems at PAC/LTC (if applicable) |
| How are the data stored? Shared? Accessed? Transmitted? Accepted at other setting? Entered? Etc. |
| How are you addressing any interoperability issues using standards-based EHR systems? Also includes (1) within each HDS, and (2) in terms of the broader context, including how HIE happens with unaffiliated providers (including e-HIE). |
| How does electronic health information exchange (E-HIE) vary between affiliated and unaffiliated providers within a single HDS? |
| How does e-HIE vary when exchanging to outside entities? To what extent could the e-HIE mechanisms being used with each HDS easily support e-HIE across HDS? If so how? If not, why not? |
| What are the facilitators/barriers to (1) automated and (2) non-automated HIE Probe for things such as the greatest technological challenges (financial, integration of services, network security, electronic signature/ensuring person is who s/he says she is, others) |
| Short-term plans (0-6 months) |
| Long-term plans |
| Organizational Issues/Business/Managerial |
|---|
| Have you articulated a business case for electronic HIE in PAC/LTC? |
| How was this business case developed? Probe: We are after clinical data that needs to be exchanged as well as billing data or MDS |
| When EHR system was implemented, was the adoption of a product that had CHI-endorsed standards a high, medium or low priority? |
| How did you choose your vendor(s) and which vendor did you choose? |
| When considering an EHR system, was interoperability with other systems a high, medium, or low priority? Please explain. |
| Approximately, what percentage of your overall annual budget is allocated to health information technology (HIT)? |
| Are any of your staff involved in SDOs? If yes, which ones? |
| How has staff turnover affected the training on the use of the EHR system? |
| Number of specific/dedicated information technology staff |
| Are any portions of the HIT outsourced? If so, what? |
| Is this part of a large chain or is it a freestanding health care setting? |
| Are they using CHI-endorsed and other HIT content and messaging standards? If so, which ones are they using? Messaging? Vocabulary? Direct care FM? |
| Is the organizational culture open to the idea of exchanging information to "outside entities" or is it more of a closed system? |
| What are the facilitators/barriers to (1) automated and (2) non-automated HIE? Probe for things such as the greatest technological challenges (financial, integration of services, network security, electronic signature/ensuring person is who s/he says she is, others) |
| Short-term plans (0-6 months) |
| Long-term plans Probe for top three information technology priorities. Examples might be creating a data warehouse, developing better network security, joining/expanding a RHIO or other data exchange group, reducing medical errors/increasing patient safety, upgrading existing clinical systems, implementing/choosing/vetting and EHR system, adopting technology-driven devices such as handheld PDAs for data collection or "smart pens" or whatever. |
Draft Clinical Scenario
Script: We believe that illustrative cases are one of the more effective and efficient ways of learning more about how you exchange information with health care clinicians in other settings.
For the purpose of this exercise, we have selected an 82-year-old woman. The key elements of her history include that she:
|
Now, lets say this patient suffers a fall while bathing and is taken to the acute care hospital where her hip fracture is diagnosed and repaired without complications. Please help us understand how health information exchange either does or does not occur in response to each of the following questions.
We will begin by focusing on the acute care hospital:
- Please describe how the acute care hospital determines the above key elements of her history.
- Is it obtained electronically? If so, from what source? What is the time frame?
- Is it obtained non-electronically? If so, from what source? What is the time frame?
- Is it obtained directly from the patient/family member through an intake process?
- Where is information regarding the role of the patients family caregiver recorded?
- Who is responsible for medication reconciliation upon admission and again on transfer from your facility?
- On admission, her lisinopril is stopped in preparation for her surgery. Who is responsible for re-starting this medication after surgery or communicating this change to the next [post-hospital] care team prior to her discharge/transfer?
- On admission, the patient shares with the intake nurse that she has an intense fear of needles and that she strongly prefers that staff use a butterfly needle rather than a straight needle. Who is responsible for recording this information and where would it be recorded? How might this information be shared with the next care team?
- On post-operative day #1, she is given diphenhydramine [Benadryl] for sleep and develops acute altered mental status. Where would this new information be recorded? How might this information be shared with the next care team?
- Which member of the care team oversees the administration of anticoagulation? Which member of the care team is responsible for communicating this information to the next care team [SNF or home health agency or primary care physician]?
- On post-operative day #1, she begins physical therapy but her session is aborted due to poor control of her pain. On post-operative day #2, working with her therapist, it is determined that pre-treating her with vicodin 20 minutes prior to therapy was effective in controlling her pain. Who is responsible for recording this information and where would it be recorded? How might this information be shared with the next care team? Is there an opportunity for communication between the hospital physical therapist and the skilled nursing facility therapist?
- Who is responsible to determining the circumstances surrounding the patients fall? Who is in a position to intervene so that this patient does not return home only to suffer another fall and fracture?
- Who is responsible for ensuring that this patient who most likely suffers from osteoporosis is started on protective therapy including calcium, vitamin D and possibly Fosamax or Actonel?
- Is there a mechanism in place for how to communicate the following information to the next care team?
- Last bowel movement.
- Skin integrity/prevalence of pressure ulcers.
- On post-operative day #2, she is transferred to a skilled nursing facility. After she leaves, her serum potassium lab result comes back low at 3.0. How might this information be shared with the next care team?
Next, we will focus on the transfer from the acute care hospital to the skilled nursing facility
- Please describe how the SNF determines the key elements of her history.
- Is it obtained electronically? If so from what source? What is the time frame?
- Is it obtained non-electronically? If so from what source? What is the time frame?
- Is it obtained directly from the patient/family member through an intake process?
- A few more specific questions:
- How would you become aware that this patient requires glasses to read and the support of hearing aid?
- How would you become aware that this patient has mild cognitive impairment? Where would this information be recorded? If this information is determined from the MDS, how would this information be reflected in the standard medical record?
- Where is information regarding the role of the patients family caregiver recorded?
- Who is responsible for medication reconciliation upon admission and again on transfer from your facility? How is the indication for the medication determined? Do you explicitly identify:
- New medications?
- Medications to be stopped?
- Medications to be continued at the same dose?
- Medications to be continued but at a different dose?
- How would the knowledge that this patient has an intense fear of needles and that she strongly prefers that staff use a butterfly needle rather than a straight needle be transmitted from the hospital [where she revealed this] to the skilled nursing facility? Who is responsible for recording this information and where would it be recorded? How might this information be shared with the next care team?
- How would the knowledge that this patient had an adverse reaction to diphenhydramine [Benadryl] be recorded? How might this information be shared with the next care team?
- How do you determine what the patient is to receive with regards to anticoagulation? How do you communicate this information to the next care team [home health agency or primary care physician]?
- Is there an opportunity for communication between the hospital physical therapist and the SNF physical therapist? Is there an opportunity for communication between the skilled nursing physical therapist and an outpatient [home health agency or outpatient clinic] therapist? If yes to either question, how does the communication take place? E-mail? Phone? Fax?
- Who is responsible for recording information on pain status and where would it be recorded? How might this information be shared with the next care team?
- Who is responsible to determining the circumstances surrounding the patients fall? Who is in a position to intervene so that this patient does not return home only to suffer another fall and fracture?
- Who is responsible for ensuring that this patient who most likely suffers from osteoporosis is started on protective therapy including calcium, vitamin D and possibly Fosamax or Actonel?
- Is there a mechanism in place for how to communicate the results of an abnormal lab value that was drawn in the hospital but was not reported until after the patient was transferred to the SNF?
Next, we will focus on the transfer from the skilled nursing facility to emergency department [ED] located in the same acute care hospital from which she was recently released. Lets say that the patient develops a swollen leg and becomes short of breath. The concern is that she may have suffered a deep venous thrombosis and possibly a pulmonary embolus despite being on an anticoagulant.
- How are the recent acute developments conveyed to the nurse and physician in the emergency department?
- Please describe how the ED determines the key elements of her history.
- Is it obtained electronically? If so, from what source? What is the time frame?
- Is it obtained non-electronically? If so, from what source? What is the time frame?
- Is it obtained directly from the patient/family member through an intake process?
- Is it obtained from records from the patients prior hospital stay?
- Where is information regarding the role of the patients family caregiver recorded?
- How would the knowledge that this patient has an intense fear of needles and that she strongly prefers that staff use a butterfly needle rather than a straight needle be transmitted from the SNF to the ED? Who is responsible for recording this information and where would it be recorded? How might this information be shared with the next care team?
- How would the knowledge that this patient had an adverse reaction to diphenhydramine [Benadryl] be recorded? How might this information be shared with the next care team?
- <Maybe add more here or just focus on the immediate care problem. We could also explore what the transfer back to SNF might look like with her new regimen designed to treat her pulmonary embolism>
Next, we will focus on the transfer from SNF to the home health agency
- Please describe how the home health agency determines the key elements of her history.
- Is it obtained electronically? If so, from what source? What is the time frame?
- Is it obtained non-electronically? If so, from what source? What is the time frame?
- Is it obtained directly from the patient/family member through an intake process?
- A few more specific questions:
- How would you become aware that this patient requires glasses to read and the support of hearing aid?
- How would you become aware that this patient has mild cognitive impairment? Where would this information be recorded?
- Where is information regarding the role of the patients family caregiver recorded?
- Who is responsible for medication reconciliation upon admission and again on transfer from your facility? How is the indication for the medication determined? Do you explicitly identify:
- New medications?
- Medications to be stopped?
- Medications to be continued at the same dose?
- Medications to be continued but at a different dose?
- How would the knowledge that this patient has an intense fear of needles and that she strongly prefers that staff use a butterfly needle rather than a straight needle be transmitted from the SNF to the home health agency? Who is responsible for recording this information and where would it be recorded? How might this information be shared with the next care team?
- How would the knowledge that this patient had an adverse reaction to diphenhydramine [Benadryl] be recorded? How might this information be shared with the next care team?
- How do you determine what the patient is to receive with regards to anticoagulation? How do you communicate this information to the next care team [primary care physician]?
- Is there an opportunity for communication between the skilled nursing physical therapist and an outpatient [home health agency or outpatient clinic] therapist?
- Who is responsible for recording information on pain status and where would it be recorded? How might this information be shared with the next care team?
- Who is responsible to determining the circumstances surrounding the patients fall? Who is in a position to intervene so that this patient does not return home only to suffer another fall and fracture?
- Who is responsible for ensuring that this patient who most likely suffers from osteoporosis is started on protective therapy including calcium, vitamin D and possibly Fosamax or Actonel?
- Is there a mechanism in place for how to communicate the results of an abnormal lab value that was drawn in the skilled nursing but was not reported until after the patient was transferred to home?
ATTACHMENT B. PROJECT ABSTRACT/OVERVIEW
Awareness and support for the need of interoperable, standardized electronic health records (EHRs) have greatly increased. To date, these efforts have largely focused on hospitals and ambulatory settings. Post-acute care (PAC) and long-term care (LTC) settings have unique needs for health information exchange (HIE). This project will examine how HIE is occurring between health delivery systems and unaffiliated PAC/LTC settings and the factors that promote or hinder this exchange. These research questions will be addressed:
- What HIT is being used to support the creation, storage, and exchange of: summaries of physician office visits and hospital stays, CPOE, and laboratory results reporting?
- What type of health information is needed for summary documents of hospital stays, physician office visits, medication orders, and laboratory tests?
- What clinical information is exchanged as part of the summaries of physician office visits and hospital stays, physician orders, and results reports?
- What health information is exchanged between health care providers and unaffiliated PAC/LTC settings and what are the mechanisms used to exchange information?
- What factors do PAC/LTC providers and representatives from the selected health care delivery systems identify as supporting or creating barriers to the timely exchange of physician and hospital summaries, physician orders, and results reporting?
Project activities will include a literature search and discussions with stakeholders involved in the development of EHR architecture and standards. Based on the information learned, a plan will be developed for conducting site visits, modifying previously developed tools to gather information. In the Summer of 2006, four site visits will be conducted. Progress presentations to the Office of the Assistant Secretary for Planning and Evaluation will be made in months 7 and 15 of the project. The information gathered through all the sources will be summarized and presented in the final report, which will identify policies that could promote information exchange and propose next steps on to how to support information exchange with PAC/LTC settings.
ATTACHMENT C. SITE VISIT OBJECTIVES AND EXPECTATIONS
AT HOST HEALTH DELIVERY SYSTEM
We are pleased that your organization has agreed to participate in our study of health information exchange (HIE) in post-acute and long-term care. This project is examining how HIE is occurring between health delivery systems and unaffiliated post-acute and/or long-term care settings and the factors that promote or hinder this exchange. A better understanding will allow us to make informed recommendations to the Department of Health and Human Services about what needs to be done to facilitate more exchange with these often overlooked health care settings.
This document provides you with the objectives we would like to accomplish during the site visits as well as our expectations of you as a host sites. Our research team at the University of Colorado at Denver and Health Sciences Center (UCDHSC) is excited to visit your health setting; we will make every effort to minimize the burden placed on your staff and be as unobtrusive as possible. We also hope that members of your organization find the visit rewarding and stimulating.
Although our site visit will be three days, we plan to conduct the visit at your organization in one day. During the course of the site visit we plan to visit an acute care hospital and an affiliated home health agency (HHA) or skilled nursing facility (SNF) and three unaffiliated HHAs or SNFs.
Following is a summary of your organization's responsibilities as a participant in this research study:
- Identification of an individual who can act as a host site liaison. Once a site visit has been scheduled, we would like to work with one individual from your organization to set up the visit (we are calling this person a site liaison). This person will provide background information on the health setting, including what post-acute and long-term care settings are included in the overall health system. S/he will work with Ms. Rachael Bennett in setting up interviews with key personnel prior to the site visit and arranging meeting rooms for the interviews.
- Completion of data collection form on your health system. Ms. Bennett or Ms. Karis May will contact the host site liaison to gather preliminary data and prepare for the site visit. We plan on sending you a form at least one week prior to the site visit for you to complete. The completed form can be given to Ms. Bennett during the site visit, or e-mailed/faxed back to us prior to the visit.
- Participation in interviews. Once we have identified the key personnel to be interviewed, the site visit liaison will ensure that they are available to participate in an interview during the time frame we have established. We may request to interview key people by phone if they are unavailable while we are on site.
- Allow site visitors to observe your health setting's employees conduct their routine tasks. We will attempt to be as unobtrusive as possible while we observe how the health setting staff interacts with and uses the electronic health record system and other mediums of exchanging health information.
- Review of site visit summary report. Once our team members have completed their site visit reports, they will be synthesized into one report. We will distribute this report to the appropriate contact at your site for an accuracy check and the augmentation of any areas in which we need more information.
- Communication of any difficulties or issues to any member of the site visit team. We expect that any issues or problems related to the site visit will be brought to the attention of the UCDHSC team.
All information gathered at each health care setting through this research will be held in the strictest confidence. No patient-level information will be collected or accessed. Only provider-level information will be provided in any study publications.
AT HOST POST-ACUTE/LONG-TERM CARE SETTING
We are pleased that your organization has agreed to participate in our study of health information exchange (HIE) in post-acute and long-term care. This project is examining how HIE is occurring between health delivery systems and unaffiliated post-acute and/or long-term care settings and the factors that promote or hinder this exchange. A better understanding will allow us to make informed recommendations to the Department of Health and Human Services about what needs to be done to facilitate more exchange with these often overlooked health care settings.
This document provides you with the objectives we would like to accomplish during the site visits as well as our expectations of you as a host sites. Our research team at the University of Colorado at Denver and Health Sciences Center (UCDHSC) is excited to visit your health setting; we will make every effort to minimize the burden placed on your staff and be as unobtrusive as possible. We also hope that members of your organization find the visit rewarding and stimulating.
Although our site visit will be three days, we plan to conduct the visit at your organization in one-half day (no more than three or so hours). During the course of the site visit we plan to visit an acute care hospital and an affiliated home health agency (HHA) or skilled nursing facility (SNF) and three unaffiliated HHAs or SNFs.
Following is a summary of your organization's responsibilities as a participant in this research study:
- Identification of an individual who can act as a host site liaison. Once a site visit has been scheduled, we would like to work with one individual from your organization to set up the visit (we are calling this person a site liaison). This person will provide background information on the health setting, including what post-acute and long-term care settings are included in the overall health system. S/he will work with Ms. Rachael Bennett in setting up interviews with key personnel prior to the site visit and arranging meeting rooms for the interviews.
- Completion of data collection form on your health system. Ms. Bennett or Ms. Karis May will contact the host site liaison to gather preliminary data and prepare for the site visit. We plan on sending you a form at least one week prior to the site visit for you to complete. The completed form can be given to Ms. Bennett during the site visit, or e-mailed/faxed back to us prior to the visit.
- Participation in interviews. Once we have identified the key personnel to be interviewed, the site visit liaison will ensure that they are available to participate in an interview during the time frame we have established. We may request to interview key people by phone if they are unavailable while we are on site.
- Allow site visitors to observe your health setting's employees conduct their routine tasks. We will attempt to be as unobtrusive as possible while we observe how the health setting staff interacts with and uses the electronic health record system and other mediums of exchanging health information.
- Review of site visit summary report. Once our team members have completed their site visit reports, they will be synthesized into one report. We will distribute this report to the appropriate contact at your site for an accuracy check and the augmentation of any areas in which we need more information.
- Communication of any difficulties or issues to any member of the site visit team. We expect that any issues or problems related to the site visit will be brought to the attention of the UCDHSC team.
All information gathered at each health care setting through this research will be held in the strictest confidence. No patient-level information will be collected or accessed. Only provider-level information will be provided in any study publications.
APPENDIX B: Site Visit Report--Erickson Retirement Communities, Catonsville, Maryland
Health Settings visited: Erickson Retirement Communities (including the medical center, Renaissance Gardens [skilled nursing facility], home health agency, and administrative center), St. Agnes Hospital, and the Johns Hopkins Home Care Group.
I. OVERVIEW OF THE LOCATION/CITY AND VISITED HEALTH SETTINGS
Erickson Retirement Communities is a non-profit, continuous care retirement community (CCRC), founded and led by an articulate visionary named John Erickson. This Chairman and CEO enthusiastically believes that both health care providers and patients need timely, non-redundant, anytime/anywhere access to patient health data. He is especially focused on removing the remaining impediments to achieving what he regards as seamless care, and he keeps informed about how healthcare and other community services are provided by observing and visiting the various buildings on the campus. His ambitious, forward-thinking approach is shared by other leaders within the organization, including Matt Narrett, MD, the Chief Medical Officer, and our host, Daniel Wilt, Vice President of Information Technology and Security Officer.
Originally, the Erickson model was designed to serve lower to middle income residents who owned their own homes and had a pension. A substantial deposit is required to reserve space or become a resident; this deposit is returned to heirs upon death of the resident. In addition, residents pay a fee based on the level of service (and care) they receive. More recently, the Erickson market has broadened socio-economically because of the quality and competitiveness of their care provision in this market.
The Charlestown campus--former home of a religious order on spacious grounds overlooking suburban Baltimore--is Erickson's flagship location and national headquarters. Currently it has 2,300 residents, five physicians, three nurse practitioners, and 1.4 FTE in mental health. The Erickson community is highly integrated and largely self-contained--the main exception being that residents who need acute care or hospice services are sent to nearby non-Erickson health delivery settings. The average Erickson resident's tenure is 12 years. They implemented Erickson Advantage (a CMS Medicare Advantage demonstration) about three months prior to the site visit, and enjoy a 7% penetration; the other 93% of residents are fee-for-service.
Erickson has an on-campus outpatient pharmacy that serves approximately 80% of the residents and their skilled nursing facility, Renaissance Gardens, uses them exclusively.
As observed, the Erickson campus does not provide hospice care nor does it have an acute care hospital. The majority of residents that need acute care go to St. Agnes Hospital, a few miles from the Charlestown campus. The Johns Hopkins Home Care Group receives a few referrals per month from Erickson.
Ericksons EHR (GE Centricity) serves all sites, currently in 13 states and expanding to 16 states in the near future. A single installation of the GE Centricity EHR, managed from the Charlestown Campus, serves all Erickson sites, nationally. Administrative and billing (reimbursement) functions appear to be paperless. The Centricity problem list makes use of the ICD-9-CM codes used for reporting and billing. Incremental deployment of additional Centricity clinical functions is physician satisfaction driven; for the moment, this means that computer-based provider order entry (CPOE) is not deployed, although it is being piloted. At present, the Erickson system does not interoperate with non-Erickson systems when Erickson patients receive care at nearby emergency departments, although Erickson-associated physicians are allowed read/write remote access. At present, this access is supported through dial-up connection; web-based access is being contemplated but is not yet scheduled. Some internal nursing and home care information is kept using HealthMEDXs product CareMEDX, which also produces MDS and OASIS submissions.
St. Agnes is a teaching hospital with the third busiest Emergency Department (ED) in the State of Maryland. They began looking at information technology strategies nearly a decade ago, before electronic health records were widely marketed and deployed by software vendors in the hospital market space. This planning led them to purchase and deploy a Meditech hospital EHR. They have a volunteer medical staff and hospitalists on service. Usually, Erickson doctors take care of Erickson patients while they are at St. Agnes.
St. Agnes information technology staff built their first portal to allow Erickson physicians access to St. Agnes data in the Meditech system in 1999. Erickson and St. Agnes have been discussing building a local, custom peer-to-peer interface to allow for the exchange of data between Meditech and Centricity, but the costs and risks associated with the project are a barrier to completing this effort. Part of the technical challenge facing such an effort is the fact that the Meditech (hospital) EHR is care episode-based and the Centricity (outpatient-centric) system is organized longitudinally.
Because Erickson Retirement Communities are able to provide most post-acute and long-term care services (with the exception of hospice), they rarely make referrals to outside providers. Johns Hopkins Home Care Group receives only a few referrals annually from Erickson, which is why they were included in this study. Johns Hopkins makes use of the McKesson Horizon health information system. See Table B.1 at the end of this appendix for a comprehensive compilation of the information requested from and supplied by each site, prior to their scheduled site visit.
II. SPECIFICS ON CLINICAL DATA SHARING
1. What data are shared? What data should be shared but arent?
Access to information regarding medications, laboratory results, and clinical notes has been identified as the highest priority data at Erickson. Additional data discussed include allergies/intolerances, advance directives, medical problem list, and radiology reports. As part of a falls reduction program, a patients fall-risk status is being explored, using data currently collected. Interventions are being planned based on conclusions drawn from this analysis.
The one area noted where information should be shared but is not is the transfer of clinical information from the physical therapist in the SNF to the physical therapist in home health care.
2. How are the data shared?
Data sharing is accomplished through a combination of strategies. Erickson sends an electronically generated paper transfer summary with all patients who are referred off campus (e.g., acute care hospital, specialist, emergency department [ED]). This summary is printed from the Erickson GE Centricity system and accompanies the patient. St. Agnes ED physicians provided input during the development of this summary document. In spite of the fact that information from one computer system was being re-entered in another system, care providers seemed pleased with the paper reports, especially given their relative currency, completeness, and readability. This paper transfer of information may be an advantageous differentiator for Erickson relative to other sources of ED admissions. However, one reason this exchange works as smoothly as it does is the presence of Erickson associated physicians on both ends of the transfer.
The St. Agnes ED and Erickson home care nurses and administrators have read-only access to GE Centricity. Erickson physicians have read-only access to the St. Agnes health information system and also can remotely access it. They also will print out information from St. Agnes when they are on-site and bring it back to Erickson, where the hardcopy is kept.
St. Agnes ED physicians call the Erickson physician prior to sending the patient back to Erickson. For ED and hospital visits that do not result in Part A SNF admission at Erickson, the Erickson physician is responsible for updating the medications and the problem list in GE Centricity.
3. Timeliness and completeness of the data.
Timeliness, non-redundancy, and anytime/anywhere access have been established as a high priority by Erickson CEO John Erickson and have been a primary driver for innovation. It is believed, and internal evidence supports this, that better health information technology will improve customer satisfaction and safety, and ultimately favorably influence the bottom line. Within Erickson, care and the information about care received, appears to be relatively seamless.
4. Specifics about medications, laboratories, and radiology.
Quest Diagnostics, Mobile X radiology, and Omnicare/Neighborhood Pharmacy (located on the Erickson campus) are the three primary vendors. Quest Diagnostics is used by the outpatient clinic, home care, and the Renaissance Gardens (their SNF and assisted living facility [ALF]). Eighty percent of the independent residents and 100% of LTC residents use Omnicare/Neighborhood Pharmacy on campus, which creates opportunities for collaboration. For example, a pilot program is under development between the Renaissance Gardens at Erickson and the Omnicare campus pharmacy to initiate an e-prescribing program. Currently, prescribing is done on paper or by fax.
Laboratory, radiology, and medication data are re-entered manually into either or both of CareMEDX or Centricity. One side effect of this re-entry process is a sense of information trust and ownership for those doing the data entry.
5. Areas under development (e.g., CPOE, decision-making tools).
Meditechs Provider Order Entry function is being piloted at St. Agnes. However, because St. Agnes does not employ their physicians and thereby cannot mandate its use, use is voluntary for the time being. CPOE is being explored at Erickson but was not in full operation at the time of the site visit.
St. Agnes and Erickson are exploring the bilateral development of a peer-to-peer HL7-based link that would support limited clinical information exchange (primarily discharge summary and medication lists) between these two settings. Both Erickson and St. Agnes would rather have their respective EHR vendors implement appropriate national data exchange standards, so that patient information could be exchanged automatically between the two systems, but they are concerned that this will take too long. Instead, they are contemplating investing in a custom bilateral exchange mechanism. One anticipated impediment to either a standard or custom exchange mechanism is the differences in the Centricity and Meditech data models. Centricity, as would be appropriate for an ambulatory care practice, supports a longitudinal patient-centric data model. Meditech, as is the tradition for inpatient care, supports an encounter-based model--that is, patient information is archived once that patient is discharged after an acute care episode.
6. Barriers to clinical data exchange.
At present, the Erickson (Centricity+CareMEDX) and St. Agnes (Meditech) systems do not interoperate and the amount of effort invested to re-enter information already represented in one system into the other is enough to warrant the exploration of a bilateral solution. However, perhaps because each system is relatively high function, neither Erickson nor St. Agnes staff view the lack of interoperation as something to complain about. Instead, the fact that each system has current, accurate, and relatively complete information is seen as a positive feature of the care environment.
The clinical documentation and notes for the SNF are electronic, but the majority of ancillary information such as laboratory and radiology reports are paper. The medications and nurse practitioner notes are in GE Centricity but are not available outside of the SNF/LTC. In general, all of the Renaissance Gardens information is electronically available to Erickson business lines, but is not electronically available to unaffiliated providers such as acute care hospitals.
Erickson utilizes relatively highly trained clinical professionals to transfer information manually across electronic systems as well as between paper and electronic systems. The time devoted to the clerical rather than clinical portion of this task was not perceived as onerous, nor was the possibility of transcription errors a concern.
7. Facilitators to clinical data exchange.
Erickson is unusual in that the primary care provider (PCP) or an associate physician from the same practice follows each Erickson patient when he or she is hospitalized. This creates opportunities for the attending physician to gather more complete information, sometimes using remote access while managing the patient across the various levels of care. Put differently, continuity of care is supported primarily by physicians and less so by the technology in place.
In addition, Erickson has a full-time care coordinator who follows Erickson patients at St. Agnes and arranges their discharge back to Erickson as well as all services including Part A SNF and home health care. This coordinator collects pertinent information, including the hospital course of treatment and the discharge summary, and faxes it back to the Erickson PCP, HHA, or SNF. Just as having physician continuity across care sites improves continuity of care, the care coordinator provides a channel and safety net for critical information as it moves across levels of care. One practical result of the care coordinator position is more timely coordination of information and resources, so that everything is ready when a patient is transferred, an example of integrated management of workflow and information transfer.
When specialists see Erickson residents (including when on campus), the dictated notes are not entered into GE Centricity but rather are faxed back to Erickson. An outpatient nurse has been hired to read the referral letters and use her clinical judgment to ascertain action items and new diagnoses and then transcribes this information into GE Centricity.
Erickson has developed an electronic chart summary, which is generated out of their electronic medical record and can be remotely accessed via the web or at any of their facilities' workstations. The chart summary includes relevant current and historical information such as advanced directives, medication lists, laboratory results, problem lists, contact information for patient and care providers, etc. This chart enables health information exchange between the physician and other providers in all of the health settings available to Erickson residents. Care coordination is facilitated as physicians can access this information on or off-campus and can then coordinate in a timely manner with the emergency department physician if a patient requires acute care.
In November 2005, Erickson launched a website, http://myhealth.erickson.com, which is provided to their residents free of charge. Patients can have read-only access to their own medical record including the chart summary discussed above. Patients can download it to a personal USB device (that Erickson provides free of charge) and take it with them (should they travel or be away for extended periods of time). Alternatively, patients can access this information via the web. Ideally, an ED physician or specialist could access this information via the portal upon obtaining the residents permission.
III. TECHNOLOGY
1. Hardware and software.
Erickson deploys a single copy of GE Centricity managed centrally from their Baltimore site. They also make use of a single copy of CareMEDX system for documenting home care, rehabilitation, and SNF care. St. Agnes Hospital, which provides acute care services for Erickson Charlestown patients, deploys a Meditech inpatient EHR.
2. Description of EHR system at Erickson, Johns Hopkins HHA, and St. Agnes.
Use of CHI standards is incidental only, if their use is required for other means such as reimbursement. No integration of different systems was observed. Inter-system information transfer is done manually, usually from paper generated by the originating system, or through mind-ware supported by remote access.
The EHR system at Johns Hopkins Home Care Group currently does not interoperate with any outside entities, including Johns Hopkins Hospital. Except for the aforementioned plans for a potential link between Erickson and St. Agnes, there are no immediate plans at Erickson, Johns Hopkins, or St. Agnes to modify or expand upon their existing EHR systems to promote the exchange of health information with either affiliated or unaffiliated health care settings.
3. Data storage, sharing, and access.
At each of the visited health settings, the data entry observed was manual, typically from paper copies of the information. Usually the paper copies were computer-generated. Within these limitations, health information technology usage seemed high-function, widely accepted, and relied upon. In-house access seemed readily available; remote access was available to select personnel, usually through dial-up connections. Gaps in this information umbrella were filled by transferring paper copies of records from one location to another.
4. Interoperability using standards-based EHR systems or other HIT solutions for HIE.
Ad hoc interoperation is being contemplated, though such custom interoperation may take advantage of a local version of HL7v2 messages. Other standards are not part of the planning process except as they are required for other reasons.
There is no electronic exchange of data between unaffiliated providers. At Erickson, because care provision on campus includes the medical clinic, skilled nursing, rehab, and home health, and the same physician follows the patient through all modalities of care, the data collected at each health setting are accessible to the physician. However, specialists submit reports in writing, and communication with pharmacies is via paper prescriptions or faxes. Physicians may use remote access to gain information about a patient that resides in a non-local system.
5. Health Information Exchange with outside entities.
Both Erickson Charlestown and St. Agnes would like to make use of standards-based data exchange between their two systems if appropriate standards existed and if those standards were implemented by their respective vendors. Because both sites are contemplating custom interoperation, presumably they would be willing to expend some funds to achieve standard interoperation in its place. However, a representative from St. Agnes noted that they did not want to take the financial hit of being an early adopter, but rather, were willing to wait until the dust settles and standards were more widely adopted before committing future resources into any type of HIE mechanisms. Erickson believes interoperation with St. Agnes, whether standard or bilateral, is a current priority, although no decision has been made regarding development of a link between the two systems.
IV. ORGANIZATIONAL ISSUES
1. Business case for PAC/LTC.
No formal business case was described; however, there is sufficient business interest to consider developing a custom exchange with St. Agnes. Erickson has the long-range vision of what adopting technology can do for their care provision as well as their bottom line, and although they have sought partners in the community to discuss interoperability, they have faced apathy or indifference from potential collaborators. No future plans to include other settings in an electronic HIE network were described.
2. Adoption of EHR systems.
Erickson, St. Agnes, and Johns Hopkins Home Care Group did not consider CHI-endorsed standards when selecting their EHR system(s) largely because they made these decisions years ago before standards had been put into place. Johns Hopkins Home Care Group uses McKessons Horizon, St. Agnes hospital uses Meditech, and Erickson uses GE Centricity (Medical Offices) and HealthMEDX (home health and SNF/NH).
Interoperability with outside entities was not a driving force in the selection of software vendors. In addition to functions supported, price of initial roll out and ongoing maintenance were the most frequently noted high priority criteria. Other criteria mentioned included access to technical support, ease of use for end user, meeting regulatory requirements (e.g., OASIS, MDS reporting or billing). The tradeoffs implicit in the incremental rollout of the next EHR function (e.g., CPOE), are being weighed carefully.
Unlike other regional care contexts, there is not a push from St. Agnes hospital's ED physicians (main referral source) to have electronic data readily available. Relatively speaking, it is working the way it is now.
3. Staffing.
Unlike many other long-term and post-acute care settings, Erickson has a very stable workforce, with an 82% retention rate. This consistency has benefited Erickson as a whole because the training and re-training of staff is kept to a minimum. Existing electronic patient information systems at Erickson seem to be well regarded by Erickson Staff. Johns Hopkins Home Care Group and St. Agnes experience a relatively high turnover rate, typical in the home health and hospital sectors, respectively.
With regard to training, representatives from the Erickson and St. Agnes information technology departments indicated that compared to the nurses, aides were more receptive to using technology (e.g., PDAs, laptops). The ability to have a mouse and click option and/or touch screen kiosks made the aides' workflow much easier. With the nurses, there had to be some computer competency training (e.g., how to enter notes into the record). At Johns Hopkins Home Care Group, the nurses and therapists are computer-literate and receptive to using technology to streamline their workflow; anytime/anywhere access is seen as a major productivity enhancer.
No one from St. Agnes or Johns Hopkins Home Care Group currently is or has been involved in standards development organizations (SDOs). Erickson information technology personnel participate in professional and standards organizations, but not as a central priority.
V. CONCLUSION/FINAL THOUGHTS
Erickson is a very high functioning retirement enterprise. They would readily make use of interoperation with pharmacies, laboratories, and other levels of care if standards and Commercial-Off-The-Shelf (COTS) products supported it. Their workforce seems very happy with the completeness of information in the Erickson EHR and with its anytime/anywhere accessibility. Erickson is an example of an enterprise that is ahead of the National Health Information Network (NHIN) exchange standard development. Further, if such standards are not created and deployed soon, Erickson (at Charlestown) may expend resources on the development of a custom exchange capability with its acute care provider.
| TABLE B.1: General Information Supplied by Visited Sites* | |||
|---|---|---|---|
| Name of Health System | Erickson Retirement Communities | St. Agnes Hospital | Johns Hopkins Home Care Group |
| Location | Catonsville, MD | Baltimore, MD | Baltimore, MD |
| Relationship to Host Site | Host site | Main referral for acute care | Referral recipient |
| Year established | 1983 | 1876 | >10 |
| Area served (urban, rural, both) | Urban | Urban and Rural | Both, mostly urban |
| Ownership | Non-profit, privately held, CCRC | Non-profit, hospital-based | Non-profit, freestanding |
| No. full-time employees | 11,000 | 2,200 | 450 for all lines of business; specifically for home health ~100 |
| No. of Nursing Homes (owned, affiliated) | 8 owned | 0 owned | 0 owned |
| No. of Home Health Agencies (owned, affiliated) | 13 owned | 1 owned | 1 owned |
| No. of Physician Practices (owned, affiliated) | 13 owned | 12 owned | 0 owned |
| Are physicians affiliated with health delivery system or are they independent? | Affiliated | Both | n/a |
| Inpatient pharmacy? | We have a pharmacy in the communities that is not affiliated | Yes | No |
| Does SNF use dedicated pharmacy or contract with large/retail, or multiple pharmacies? | We use an institutional pharmacy, OmniCare | n/a | n/a |
| No. of Pharmacies--outpatient | Two outpatient pharmacies on campus | 1 | 4 |
| In-house laboratory? | No | Yes | No |
| How many outside laboratories? | One, Quest | 2 | Many, based on pts insurance |
| In-house radiology department? | No | Yes | No |
| How many outside radiology centers/MR centers do you work with? | Refer to local centers | 1 | n/a |
| Electronic Health Record (EHR) system--scheduling, billing, or claims? | Yes. Medical Manager for the Medical Center & Keane for all other care | Yes | Limited |
| Clinical Electronic Health Record (EHR) system? | Yes. GE Centricity POE EMR 2005 for the Medical Center & HealthMEDX CareMEDX for our SNF, ALF, Home Health, & Rehab | Yes | Yes |
| Primary software vendor for electronic health information system (if applicable) | GE Centricity POE EMR 2005 and HealthMEDX CareMEDX | Meditech | Horizon/McKesson |
| Short-term (6 months?) HIE* future plans | We are focused on getting a few local hospitals and specialists integrated with our electronic medical records through HIEs | RHIO development with Erickson | Electronic referral |
| Long-term HIE* future plans | We are focused on getting all local hospitals and specialists integrated with our electronic medical records through HIEs | RHIO development with Erickson | On-line physician order/referral process with signature of forms |
| Miscellaneous notes | JHHCG include home care, infusion, home medical equipment, respiratory services, and outpatient pharmacies. | ||
| * Information in this table was collected from a General Information About Health Care Setting form sent to all sites prior to the scheduled site visit. | |||
APPENDIX C: Site Visit Report--Montefiore Medical Center, Bronx, New York
Health Settings visited: Montefiore Medical Center, Montefiore Home Health Agency (MHHA), the Visiting Nurse Service of New York (VNSNY), the Jewish Home and Hospital Agency (JHHA), and Schervier Nursing Care Center (Schervier).
I. OVERVIEW OF THE LOCATION/CITY AND VISITED HEALTH SETTINGS
New York State, and especially New York City and surrounding counties, have a relatively long history of collaboration in health information technology; this is one reason NY leads all other states in public health functionality and public health information technology and is among the leaders in the use of in-patient health information technology (HIT).
The majority of the site visit was located in the Bronx, a densely populated urban area with circumscribed geography. The Bronx patient demographics are characterized as young, poor, minority, disease burdened, and underinsured. For these and other reasons, Bronx residents tend to receive healthcare in the Bronx as opposed to the other New York boroughs and Montefiore is self-defined as the preferred acute care and primary care provider by the community, and the only Bronx academic medical center. Increased awareness of fragmented, multi-institutional,1 and multi-level care and a long-standing sense of medical community have helped promote collaborative participation in the newly-funded Bronx regional health information organization (RHIO). One informant matter of factly stated that "geography is destiny," meaning that the Bronx is six miles by six miles and this geographic reality is one explanation for why there is a greater proclivity for collaboration with other health settings in the Bronx. Another informant observed, capitated care led the way, meaning that capitated care provided clearer incentives for information sharing and use of HIT to support that sharing. Included in the population examined as part of Bronx RHIO planning were 27,000 Medicare lives.
Despite this advantage, of the high concentration of nursing homes located in the Bronx (53), only one (the Jewish Home and Hospital Agency [JHHA]) has so far agreed to be involved in the Bronx RHIO, which is moving from a planning and study phase to a deployment phase now that it has received $4.1 million in HEAL NY funding. Not coincidentally, the Bronx has an excess of nursing home (NH) beds, at present. The Schervier Nursing Care Center (Schervier) was initially involved in the Bronx RHIO, but the Administrator determined that they were not ready, at present, to fulfill the technological requirements for participation so they dropped out. For an unknown reason, another large skilled nursing facility (SNF) in the area also dropped out of the RHIO, despite being involved in the planning stage discussions. Studies done prior to RHIO planning included attention to NH admissions, opportunities for hospital to NH-care coordination, avoidable hospital readmissions, and the distribution of hospital to long-term care transfers (49% of transfers to post-acute care from Montefiore Medical Center during the study period were to five NHs). Since the initiation of the Bronx RHIO, another four nursing homes have expressed interest in joining as institutional members.
Currently, the fact that the myriad of health care enterprises in the Bronx can communicate--person-to-person--at multiple organizational levels has not translated into electronic communication--or even person-to-computer communication. However, there seems to be some expectation that settings receiving patients should have remote access to patient information from where the patients came from, but at present, such hand-offs of electronic information are the exception rather than the norm.
The Bronx RHIO has a number of committees involved in various aspects of its design and implementation management. One committee is focusing on clinical issues and is in the process of defining an initial core data set of "normalized" information about individual patients that would be ready to be exchanged with all RHIO participants and be available at the point of care. Another part of the RHIO process links patient identifiers. The creation of a standardized patient transfer form for use in the Bronx and in the larger area covered by the VNSNY was discussed at several visited sites. Representatives at each site expressed interest in and some level of readiness for this transfer dataset to be finalized.
See Table C.1 at the end of this appendix for a comprehensive compilation of the information requested from and supplied by each site, prior to their scheduled site visit.
II. SPECIFICS ON CLINICAL DATA SHARING
1. What data are shared? What data should be shared but are not shared?
New York State requires that hospitals complete the Patient Review Instrument (PRI) for all patients being referred for Medicare Part A SNF care. This document scores the patient on the intensity of care required.2 Its domains include physical and cognitive function, medications (last seven days), recent laboratory tests, x-rays, physical therapy (PT) and occupational therapy (OT) notes, and wound care. Ideally, this tool would help facilitate an appropriate match between patient care needs and care settings. Nursing staff must be certified on how to complete the PRI.3
More generally, the two nursing homes (NHs) we visited, JHHA and Schervier, made concrete suggestions for how Montefiore Medical Center could improve hospital to post-acute care information transfer. These suggestions included more frequent PT notes and especially greater documentation of mental status alteration and psychiatric/behavioral symptoms. NHs also would like the look-back period for medication reporting to extend to a full 14 days prior to NH admittance to help support completion of IV medication use required by the RUGs, thereby ensuring they are adequately reimbursed for more expensive services.
When a patient leaves JHHA (to go back to the hospital or discharged home), a discharge packet is prepared that includes a medical summary of recent events completed by the physician, a handwritten medication list, immunizations (to conform to current hospital quality initiatives), EKG, and laboratory tests.
When NH staff at Schervier transfer a patient to an emergency department (ED) or hospital, they attach a paper-based Schervier-standard patient summary including a transfer form (which describes the reason for transfer), physician transfer sheets, laboratory results, x-rays, and ECG.
The VNSNY has pilot projects underway that will implement data sharing with selected physician offices and, separately, with Weill Cornell Medical Center. The Montefiore HHA (MHHA) has a pilot project in place to share information with physicians via a web portal. (See Section III.2 for more details.)
2. How are the data shared?
The Patient Review Instrument (PRI) and supplemental information are distributed from Montefiore Medical Center to local area NHs via Extended Care Information Network (ECIN),4 which is a web-accessible application designed to facilitate the discharge process. ECIN is an Internet-based automated PRI that is HL7 compliant. Nursing homes pay $300/month to subscribe and, at present, 30 Bronx NHs make use of ECIN. Patient information is sent to a list of NHs selected from an on-line pick-list. When a referral arrives at a selected NH, an e-mail or page alerts the staff. The receiving NH then has the opportunity to e-mail back or call to ask questions and/or indicate its interest in accepting the patient. NHs without ECIN access may receive the PRI via fax. According to informants at Montefiore, their use of ECIN has helped reduce hospital length of stay (LOS) for nursing home bound patients from ten to eight days--in a context where a half-day reduction in LOS would pay for incremental use of information technology.
At Montefiore, PRI fields such as demographics and insurance can be auto-populated using information from other information systems, while other fields such as laboratories, medications, and physical therapy notes can be completed by copying and pasting from data fields in the Montefiore EHR. Prior to automation (auto-population), tool-supported creation of the PRI required 30-40 minutes to complete, whereas after automated pre-population and manual copying and pasting, it reportedly is completed in 10-15 minutes.
The MHHA uses MISYS for documentation and charting. If a patient is admitted to Montefiore Medical Center while actively receiving home health care, the home care coordinator based in the hospital can print a summary from MISYS and place that summary in the hospital paper record. Aside from this, emergency department (ED) and hospital nurses and physicians do not have access to MISYS. At present, the only way that MISYS and the Montefiore EHR (IDX LastWord) interoperate is via e-mail. MHHA has a field dedicated to capture the patients Montefiore Medical Record Number. All documentation that is generated to the physician (e.g., orders, discharge summary, admission notice) will include the Medical Record Number to make patient identification for documentation for the medical record seamless. MHHA has a process in place that auto-e-mails the physician when her or his patient is admitted to home care. The e-mail contains contact information of the team caring for the patient as well as the date the patient was admitted. In general, e-mail appears to be used increasingly often for fulfillment of non-time-critical information needs, much as voice mail is still used today. MHHA staff have read-only access to Montefiore Medical Centers clinical information system (CIS). Montefiore representatives also commented that the JHHA physicians have limited read-only access to CIS, and these physicians would like to expand their access. For example, informants at JHHA indicated that care providers cannot always get access to laboratory results or radiology images in Montefiores CIS and they cannot access the medication list, although this access has been requested for several years.
When a patient is discharged from home health services, a discharge template in MISYS is used that is populated in part by MISYS and in part completed by a nurse who manually types in the remaining fields. The information typed into the EHR could be blood sugar ranges if the patient is a diabetic, wound status if the patient is being seen by the wound care team, or care providers at home. This type of information is patient-specific and is not captured via check boxes. The resulting summary is then sent to the attending physician via email.
The VNSNY pilots are implementing back population of EHRs at selected physician offices; this data transfer will make use of a web portal and HL7 messaging. The application being developed in collaboration with Weill Cornell Medical Center is web-based. The MISYS Physician Portal also is web-based and MHHA recently received a grant to modify the portal to allow the physician to access telehealth reports.
3. Timeliness and completeness of the data.
NH staff at JHHA and Schervier both commented that despite the fact that nursing staff require special certification to complete the PRI, the data contained within the PRI can be of inconsistent quality and is often incomplete. The information available from ECIN is similarly variable.
JHHA reports that the hospital discharge summary arrives with the patient (rather than prior to nursing home admission) and occasionally is misplaced or lost during this transition.
Schervier staff create their own paper medical record using some of the data received from the hospital. Staff commented that they would like to receive a discharge summary ahead of time but it frequently arrives with the patient, which reduces their ability to prepare to meet the patients needs upon arrival. They also mentioned that the PRI does not always adequately describe the patient. For example, NHs are particularly interested in the mental and psychiatric status of referred patients. The discharge summary from Montefiore often is illegible, as it is a carbon copy, and the Schervier informants mentioned that about 80% of the time, the primary care physician information is not included in the discharge packet.
The VNSNY tries to re-synchronize all patient information between care provider tablet and laptop computers and backend databases at least once every 24 hours. MHHA care providers (e.g., nurses, social workers, therapists) are required to synchronize their laptops once every 24 hours. MHHA recently deployed 50+ broadband wireless cards allowing staff to connect to the office while in the field.
4. Specifics about medications, laboratories, and radiology.
The Montefiore EHR integrates access to a medication list (Montefiore has a single in-patient pharmacy), lab results (if done by the Montefiore laboratory), and imaging reports. At present, none of these data elements are represented using national standards; when the relevant decisions were made there was no reason to use these standards. However, to better support re-use of such data elements by RHIO participants, such standards are an objective for the Bronx RHIO.
All MHHA laboratory results go to the Montefiore Medical Centers clinical lab, thereby enabling timely access to results by ordering staff physicians.
JHHA has an in-house pharmacy and uses a single lab. JHHA staff have read-only access to a patients laboratory results performed at Montefiore Medical Center prior to transfer as well as radiology reports, but they do not have access to medication data.
Schervier uses one outside pharmacy, Shore Pharmacy, and a single lab, Lawrence Laboratory. The nursing unit has view-only computer access to the laboratory results from Lawrence Lab.
5. Areas under development (e.g., CPOE, decision-making tools).
Through a New York State HEAL NY award, the VNSNY is developing a portal for physicians with a common data presentation. The goal is to improve communication and specifically to reduce complications, duplication, and need for re-hospitalization. Portal information will include data elements that the VNSNY routinely collects, including hospital discharge summaries, radiology/lab/ECG reports, name of PCP, names of family caregivers, advance directives (whether or not on file), and wound images. The information will go directly into the electronic health record (EHR), which the physicians office is using as well as the VNSNY medical record. Currently, the VNSNY is piloting the web portal with seven regional physician practices that all use GE Centricity/Logician EHR. (Contemporary software features of the Logician EHR system reduce the difficulty of implementing this back-population, relative to other EHRs.) The VNSNY already is observing an anticipated change in their relationship with MDs using the portal--the MDs are new users with new requirements. While the current goal of this effort is to (greatly) improve access to information about patients common to the MDs and the VNSNY, this access could support use of standards in the future.
The VNSNY also is participating in a pilot project with Weill Cornell Medical Center to develop an electronic CMS 485 form where the doctor could begin to write orders on the 485 at the time of discharge.5 The physician can sign the original 485 and any subsequent additions electronically. This advancement also would allow them to map data elements to the Continuity of Care Record (CCR). One advantage for physicians is that this feature includes a timer that can count minutes spent on home care oversight to facilitate documentation for billing. The electronic 485 has led to enhanced data completion. For example, the physical function section went from 28% complete to 94% complete and mental status went from 6% complete to 100% complete in a pilot study of four physician practices.
The VNSNY also is piloting a home monitoring project. In January 2007, they will be able to take results from the telehealth devices in the home and incorporate these data into the current database. They then would be able to trend these data with other data their clinicians have collected to get a more complete, accurate picture of the home care patients health status.
MHHA currently has a home monitoring project in place with Cardiocom. MISYS has partnered with Cardiocom to build a bi-directional HL7 interface that will allow information to flow seamlessly from the devices to the MHHA EHR.
JHHA is developing a database to establish a unique identifier that will be the basis for sharing information among all JHHA programs and services. Not coincidentally, this identifier will make it easier for JHHA to share patient information through the Bronx RHIO.
6. Barriers to clinical data exchange.
Montefiore Medical Centers EHR (CIS) and the MHHAs record system (MISYS) do not interoperate. For example, when a laboratory result appears in the CIS, the result must be entered manually into MISYS. Medications also are transferred manually from one screen in CIS to another in MISYS. HHA staff acknowledges the potential for transcription errors.
Representatives from the VNSNY indicated that communication streams that currently exist with Montefiore Medical Center are potentially subject to errors. For example, Montefiore liaisons have to fax the referral form to VNS headquarters and those data are then re-entered into the VNS electronic health record.
Challenges noted by Schervier staff are completeness of the information from the referring hospital (not necessarily just Montefiore Medical Center, but any referring hospital) and inaccuracy of the data that is sent, thereby reducing trustworthiness of the information. For example, descriptions of ongoing expensive medications or treatments (e.g., IVs, blood transfusions, chemotherapy) often do not accompany the patient and the SNF is forced to scour the information available to them to determine if the patient is on medications that will affect their RUG payments.
The biggest current barrier to clinical data exchange among the sites visited is a lack of electronic communication between existing information systems; not surprisingly, this is a major motivation behind planning for the Bronx RHIO. The next barrier will be the need to transform local electronic health information into the uniform patient summary required by the RHIO. After that, the biggest challenge will be the need to back-populate local health information with that available from the RHIO (e.g., to enable better local decision support through a more complete medication list, laboratory results, and problem list).
7. Facilitators to clinical data exchange.
As described above, the main facilitator to future electronic clinical data exchange is a regional organizational history of inter-enterprise (care provider-to-care provider) communication and inter-enterprise patient care. Beyond this, Montefiore Medical Center and MHHA plan to use a single patient identifier to track patients in their electronic health information system so that historical data in the Montefiore system are accessible and they can ensure that the patient they are treating is the correct patient. Among other benefits, this single identifier increases the utility of the Montefiore data warehouse. Because most Montefiore patients continue to receive care at Montefiore health settings for as long as they live in the Bronx, this creates an opportunity for a rich, life-long patient health record.
Montefiore Medical Center staff physicians (hospitalists) care for hospitalized nursing home patients. A different group of Montefiore staff physicians care for nursing homes patients in the nursing home (SNFists). Having organized physician groups employed by the regional provider creates an opportunity to develop more standardized protocols for patient care, including clinical protocols and higher expectations for information exchange.
MHHA has on-site care coordinators/liaisons in the Montefiore Medical Center to facilitate hospital-to-HHA referrals. It also has coordinators who visit two or three of the larger SNFs to help facilitate referrals from SNF to home care.
Another example of existing manual clinical data exchange across enterprises is weekly visits by HHA liaisons from Montefiore Medical Center and the VNSNY to JHHA to review and coordinate potential referrals. By being on site, these liaisons are able to collect and communicate needed clinical information to their respective employer (the VNSNY or JHHA) on soon-to-be discharged patients.
State-of-the-art information technology used by the VNSNY will be make it relatively easy to exchange patient data going forward with HIT systems at referring sites and with many EHRs used by primary care MDs who follow the patients during and after care by the VNSNY.
A fundamental facilitator of anticipated information exchange is the general computer literacy of regional care providers and their growing expectation that anytime/anywhere access to patient information should be supported.
III. TECHNOLOGY
1. Hardware and software descriptions of the main health delivery system and the affiliated PAC/LTC settings.
Back in 1995, after a year-long search, including visits to United States academic medical centers with EHRs, Montefiore Medical Center selected IDXs LastWord EHR based on its ability to function in an integrated delivery system, and because it was perceived as user-friendly for physicians. Deployed initially as an in-patient EHR, LastWord was deployed for ambulatory care at 28 sites in 1996-1997. LastWord contains data from every Montefiore encounter for 1.8 million patients; currently this includes laboratory test results, medications, and images, but does not include notes and consults. Some scanned information also is represented. E-prescribing has been in place for close to a year. Currently, about 9,000 NH patients/year use Montefiores hospitals for inpatient care. Greg Burke, Vice President of Planning mentioned a recent study of Medicare claims data performed by Milliman that indicated that in the Bronx, two-thirds of the NH patients who die, die as hospital inpatients, and that about one-third of the Medicare-enrolled NH population die per year. As with several other deployed EHRs, LastWord was originally implemented in MUMPS. (IDX was purchased by General Electric in June 2006). Montefiores deployment of LastWord makes use of the proprietary physician-friendly problem-list vocabulary developed by James Campbell, MD. One feature of this list is the accompanying repertoire of links to SNOMED-CT. Primary care physicians own this problem list, and, at present, ED physicians do not have the authorization to update it. Because LastWord is not designed for population analysis and other aggregative data tasks, Montefiore Medical Center makes use of an adjacent Sybase data warehouse. The warehouse accumulates query-able patient information exported regularly from LastWord. The warehouse environment supports a growing repertoire of analytic reports, some of which were used as part of RHIO planning. Current RHIO plans call for use of a dBMotion product to extract the RHIO-standard information from EHRs and other patient information systems used by RHIO participants. One side of each dBMotion instance does the local extraction and the other side makes the patient information available in standard form to external RHIO users.
MHHA uses MISYS Homecare software for their EHR. Field clinicians can instantly access health care plans, patient demographics, medications, and other clinical information to improve quality of care. OASIS data collection is integrated into the patient health assessment. Assessments captured on laptops at the point of care are remotely synchronized to the EHR in minutes. Field staff is required to synchronize their laptops a minimum of once every 24 hours.
Fourteen years, ago the VNSNY began developing its own patient record system that continues to evolve to this day and currently supports more than 2,000 care providers. One reason that the VNSNY developed custom software is that there was so little available when they started. Currently, their system makes use of a three-tier architecture--an outer tier of software residing on care providers tablet computers and laptops, a middle tier of management and system applications and asynchronous communication support, and an inner tier of DB2 relational databases. The point-of-care (POC) component is written in Microsoft Visual Basic with a supporting Microsoft client Data Engine SQL database. Office-based management and analytic tasks are conducted either by using mainframe IBM Customer Information Control System (CICS) COBOL applications or web-based Java applications. Data are synchronized between the POC and host DB2 databases using internally-developed store and forward processing via an intermediary RISC-based processor. Thus, each morning each home health clinician has access to her or his caseload for the day. During the day, case workers record information on tablet computers. While unique, the VNSNYs EHR system has been built whenever possible using commercial-off-the-shelf (COTS) systems and tools, such as SQL Server and Visual Basic. The VNSNYs advanced information technology position was achieved at the cost of some less successful efforts along the way (e.g., premature attempts to get tablet computers deployed). However, their ability to contemplate participation in multiple RHIOs and to experiment with connections to physician practices is evidence of the soundness of their investment in scalable designs and components. They are in an increasingly better position to learn more about the appropriate use of information technology in home care settings. One important source of experiential learning is their current management of content and software updates; for example, formulary updates are pushed (sent) to the care provider laptops--the outer layer of the three tiered architecture--on demand, and twice annually these laptops are brought to headquarters for major updates to software and geriatric decision support. The latter generates a problem for each medication and therapy, and constellations of problems make explicit potential connections between congestive heart failure and depression. Currently, e-mail is not considered secure enough to use in home care provider communications involving patient information. Incrementally, the VNSNY system involves workflow management (e.g., management of lab tests, beginning with physicians currently phoning in orders, and ending with faxing the result to the physician). In between, the laboratories have access to the relevant work-lists and dispatching of phlebotomists. The VNSNY has a grant to implement the receipt of laboratory tests in HL7 messages containing LOINC codes.
MHHA decided against developing their own software product and instead purchased their EHR from MISYS Healthcare, a recognized leader in the homecare field. By partnering with MISYS, MHHA can utilize their clinical and process knowledge with their software expertise to build an efficient EHR that meets every one of their needs and can be used by other home care agencies across the county. MHHA is Premier Partner with MISYS, which allows them access to developers and other business partners. MHHA has used this status to request custom functions for streamlining the admissions process.
More recently, JHHA has been exploring different EHR alternatives but currently uses only component systems such as the QS1 Pharmacy System.6 Also used are the 3M Home Care program, and a scheduling and billing system--where indications accompany orders. The MISYS (formerly Per Se) Patient1 system was deployed during a recent trial but the expense of adapting the propriety database outweighed any other benefits of that system and the trial was terminated. The currently deployed ADT system stores a problem list with ICD coding and it can be used to generate a face sheet. The Lintech Comet system is used to complete and submit MDS, develop associated care planning, and support some order entry.7 OASIS submissions are handled using OCS.8 JHHA is networked, mainly for administrative purposes, with other affiliated sites in Manhattan and the Bronx, including community services and a primary care site. Another site supports redundant data that will be used for data disaster recovery.
Schervier uses American Health Care management software at present, and looks forward to the day when they will have a more robust EHR. They estimate that a satisfactory EHR will cost more than $750,000/year. The American Health Care software is specialized for long-term care and includes an MDS-reporting application. Their current extra-enterprise communication makes use of faxes and remote access for laboratory test results and they do not yet have computers available on care units.
2. Architecture of EHR system at main HDS.
a. Are they using CHI-endorsed and other HIT content and messaging standards? If so, which ones are they using? Messaging? Vocabulary? Direct care FM?
Current use of formerly CHI-endorsed and, prospectively Health Information Technology Standards Panel (HITSP)9 endorsed standards, such as ICD-9-CM and CPT, is incidental and not because of any perceived benefit of use of these standards, other than that they are required for regulatory or reimbursement reasons; again, decisions to use particular terminologies were made some time ago, before CHI existed. HL7 messaging is part of RHIO planning and HL7 capabilities (e.g., as part of ECIN) came up in discussion, but no use of HL7 messaging was observed. No site contemplated use of RxNorm for medication lists, and all sites made use of one or more proprietary formularies, such as First Databank or Micromedex.
Montefiore Medical Center created their lab codes before LOINC was available. They have been evaluating LOINC adoption along with the other RHIO participants and face the same challenge as other United States care enterprises in that they have homegrown coding systems, especially for lab tests.
b. Description of each EHR system and HIT solution(s) to support HIE
Each site visited had some deployed patient-care information technology. However, the only mode of HIE observed besides faxing and phoning was occasional remote access, usually by physicians. All sites have planned HIT enhancements; some of these are specifically focused on anticipated RHIO involvement, and others are unilateral.
All HIE observed was manual; sometimes this manual access was electronically remote, enabling users to create data in one system while viewing it in another. Usually, this step was described as taking ownership of the data (e.g., the patients medication list). Included in taking ownership is medication reconciliation.
3. Architecture of EHR systems at PAC/LTC (if applicable) and HIT solution(s) to support HIE.
All architectures observed were based on a central computer access through real-time networks, except in the case of the VNSNY, which used episodic (e.g., daily) network connections to tablet or laptop computers for resynchronization. As described above, Montefiore makes use of a Sybase warehouse that supports non-real-time access to patient information exported from LastWord. Web-based, anytime/anywhere connections were not observed at any site, although support for such applications was being contemplated as part of the Bronx RHIO and VNSNY pilots. Lack of any current deployment of HIE is a major reason behind the selection of dBMotion as a RHIO-common interface for Bronx RHIO members. dBMotion supports secure, virtual patient records.10 dBMotion is an architectural solution that supports a uniform interface to uniform extractions from each native system at each RHIO site. The dBMotion solution does not commit users to any particular HL7, CHI, or HITSP standard, instead it allows the RHIO to support an elective, collective repertoire of standards in the virtual patient record. This repertoire has yet to be defined. One reason for this delay is that each site would then be required to translate local information into RHIO-standard information. Currently, the degree to which dBMotion will support such translations has yet to be determined.
4. How are the data stored? Shared? Accessed? Transmitted? Accepted at other setting? Entered? Etc.
All sites observed store patient data in proprietary formats and databases in commercial applications, except for Montefiore, MHHA, and the VNSNY. The proprietary nature of how the data are stored was one reason why JHHA stopped deployment of a COTS EHR. The latter sites have information technology staff sufficient to support some storage and access via standard SQL. Montefiore Medical Center maintains a data warehouse of historical patient records accessible using (Sybase) SQL and this warehouse is updated regularly by exporting information from LastWord, the Montefiore EHR. The VNSNY uses backend (DB2) and laptop (Microsoft) client databases accessible using IBM and Microsoft SQL. Except for the JHHA use of read-only CIS terminals to access clinical information in Montefiores system and the VNSNY physician office pilots, we observed no extra-enterprise data sharing other than by paper, faxes, phone calls, and limited dial-up access.
Although the VNSNY certainly has the information technology expertise and capital to build interfaces with either ECIN or e-discharge, they have opted not to invest in this effort. As the largest home health agency in the county, they have a 25,000 patient load at any one time and are the home health agency many opt to refer to with "difficult patients.
As observed earlier in this report, all sites reported re-entering patient information manually that came from a computer somewhere else. Each site saw this as taking ownership of the data.
5. How are you tackling any interoperability issues using standards-based EHR systems or other HIT solutions for health information exchange?
Although JHHA expressed interest in improving the bilateral exchange of data with care enterprises such as Montefiore, no site except the VNSNY described plans for bilateral interoperation. As previously mentioned, the VNSNY has pilots underway to exchange information with physician practices, and plans in place to interoperate with regional medical centers such as Weill Cornell. All sites visited anticipated being part of the Bronx RHIO either right away, or, in the case of Schervier, when facilities and funding permitted. The RHIO plans include anticipated potential use of a variety of standards, but no specifics are yet available.
6. How does electronic health information exchange (e-HIE) vary between affiliated and unaffiliated providers within a single HDS?
Of the sites visited, only the MHHA had a strong affiliation with another visited site, Montefiore Medical Center. This affiliation smoothed referrals, most referrals are from our (Montefiore) system, but these referrals did not include HIE. Instead, the MHHA employed 18 nursing FTEs to workup each patient prior to field care. Access variation is usually organizationally mediated; that is, affiliation determines who may have remote access to patient information from the sending care site.
Montefiore Medical Center plans to exchange summary information with Bronx RHIO members. Today, the only extra-enterprise data sharing of consequence, besides selective dial-up access, takes place through the PRI and ECIN.
JHHA is not affiliated with other care providers except through common training programs, such as with Mt. Sinai.
Schervier is part of the Bon Secours Health System, which is comprised of acute and non-acute care facilities but not affiliated with any New York City health care providers.
7. How does e-HIE vary when exchanging to outside entities?
Montefiore Medical Centers information technology subsidiary, Emerging Health Information Technologies (EHIT), provides HIE services under contractual relationships to a number of other hospitals, including Bronx-Lebanon Hospital Center in the Bronx. EHIT also is the technology provider to the Bronx RHIO. It does not currently support e-HIE services with PAC/LTC beyond its organization, except for its use of ECIN.
MHHA does not support e-HIE beyond its organization except for its use of ECIN and planned participation in the Bronx RHIO.
JHHA does not support e-HIE beyond its organization, though it looks forward to participating in the Bronx RHIO.
Schervier does not support e-HIE beyond its organization, and has temporarily withdrawn from the Bronx RHIO. Schervier plans to purchase an EHR, but there is no schedule yet for doing so.
All sites found the current manual (fax, phone, or paper) bilateral exchanges of information inadequate and problematic, although some pairs of enterprises reported better paper exchanges than with other pairs. All sites found their use of ECIN an improvement over the way things were before it was available, but no site believes ECIN will be adequate indefinitely.
The VNSNY's future plans already have been extensively discussed in this report (see Section II.5).
IV. ORGANIZATIONAL ISSUES
1. Organizational Activities Supporting Electronic HIE.
Montefiore Medical Center has invested significant resources in the development of the business case for implementing and promoting electronic HIE across its extensive delivery system and within the region, as is evidenced by their leadership in promoting the Bronx RHIO, and being a key player in the grant writing process that led to the HEAL-NY award to form this RHIO.
JHHA and Schervier (the two NHs we visited) are both large, well-established skilled nursing facilities who have weighed the pros and cons of implementing an EHR, including one that has interoperable features with other health settings. Both SNFs are committed to providing quality care and are not averse to using technology to support or improve their care provision. That said, neither SNF has been particularly impressed with the software options available to SNFs in the current market. JHHA, for example, invested in an EHR, including all of the start-up hardware, software, and training costs, only to jettison it several years later when the leadership realized that the software capabilities were not as promised, and ultimately, it was not able to meet their organizational needs. At this time, JHHA currently is vetting other software options and is hoping to implement one in the next year.
Although Schervier was initially involved in the formation of the Bronx RHIO, the director declined to participate when commitments were being requested because she said they were not ready. They continue to collect most of their data on paper and enter the data into niche software--American Health Care Software--that does not interoperate with other systems.
The VNSNY, on the other hand, has a very sophisticated, well-funded information technology department that is involved in or planning a number of internally and externally funded standards-based initiatives to encourage and facilitate electronic HIE. These planned activities are discussed in detail in Section II.5 above. The bulk of their EHR system is homegrown and was built up over more than a decade of development, as they were and continue to be an early adopter of information technology.
2. Adoption of EHR systems.
None of the settings we visited necessarily selected their vendor(s) based on criteria such as use of CHI-endorsed standards or ability to interoperate with other systems.
Some health settings were early adopters of EHR systems (e.g., Montefiore, JHHA, VNSNY) and CHI-endorsed standards were not in place at the time they were selecting software. Montefiore Medical Center selected their EHR system in the mid-1990s, well before standards were being used in the development of EHR systems. The VNSNY found the home health software options wanting and opted to build their own EHR system.
As previously mentioned, Montefiore Medical Center and JHHA are heavily involved in the formation and implementation of the Bronx RHIO, having devoted significant resources to obtain the funding and persuading other participants to join. They are committed to and involved in efforts supporting interoperability among systems, albeit in the early stages. Montefiore has representation on some of the standards development organizations (SDOs). For example, the chief radiologist sits on the IHE standards board, others are involved with e-health Initiative, and others are involved in SDOs that focus on the financial/billing side of healthcare. The VNSNY has a very active, energetic, vocal information technology group, led by Tom Check, and they are educated on and involved in a number of SDOs.
In contrast, Schervier Nursing Care Center, which uses niche software (American Health), did not consider use of standards or interoperability when selecting this software vendor. Schervier is just one SNF in the Bon Secours New York Health System and the Bon Secours corporate office determined which software best met the organizations needs.
In general, most SNF clinicians and administrators we visited in New York (and elsewhere) have very modest, reasonable goals with respect to data exchange. They are most interested in having complete, accurate, legible, and timely data, regardless of the format. That is, a legible printout from a computer that is received prior to patient admission and contains complete accurate information would be considered a big win. Interestingly, all sites reported wanting more complete information, while admitting that there was an implied risk to getting too much information, because they would be liable for providing care in that context. Thus, receiving electronic data that are both machine and human readable, as opposed to just human readable, is not necessarily their immediate goal, or even a consideration in the near term.
Bronx RHIO participants are committed to a relatively advanced form of patient information exchange, through which providers in or affiliated with participating organizations will be able to access locally-generated electronic information--a specified core data set that abstracts what that site knows about the patients local encounters. The encounter might be a laboratory test result or it might be a visit to the local VA facility. For a given patient, at a given site, these distributed data sets form a series of virtual longitudinal patient records. A care provider at another site can retrieve and display a consolidated view of clinical information from all participating organizations as a message to be viewed locally. Further, in principle, each core data set has normalized data elements, potentially using standard terminology; therefore, in principle, a unified medication list could be created, for instance. While details remain to be determined and no testing has yet taken place, evidence of the extent of prior and current collaboration is the energy and planning that have gone into the RHIO proposal and plans.
V. CONCLUSION/FINAL THOUGHTS
The Bronx and Manhattan sites visited represent a significant opportunity for HIE. Currently, information about thousands of patients flows between care sites as part of relatively mature manual--fax, phone, and paper--processes. Thus, the collaborations necessary to support HIE exist or can be created, and there appear to be few competitive barriers to interoperation. That said, these enterprises face the myriad technical choices and tradeoffs required to start electronic information flowing between non-affiliated care enterprises using non-common HIT. However, over the last few decades, New York State and the New York Metropolitan area have demonstrated an ability to successfully undertake large health care projects, many involving the use of HIT, and this has created an expectation that they will succeed in deploying a useful, sustainable RHIO.
| TABLE C.1: General Information Supplied by Visited Sites* | |||||
|---|---|---|---|---|---|
| Name of Health System | Montefiore Medical Center | Montefiore Home Health Agency (MHHA) | Visiting Nurse Service of New York (VNSNY) | Jewish Home and Hospital Bronx Division** | Bon Secours New York Health System (Schervier Nursing Care Center) |
| Location | Bronx, NY | Bronx, NY | New York, NY | Bronx, NY | Riverdale, NY |
| Year established | 1882 | 1947 | 1893 | 1950 | 1938 SNCC 1983 Home Care |
| Area served (urban, rural, both) | Urban | Urban | Urban, suburban | Urban | Urban--SNCC Both--Home Care |
| Ownership | Non-profit | Non-profit | Non-profit | Non-profit | Non-profit, freestanding |
| No. full-time employees | 10,000 | 266 | Approx. 11,700 | Approx. 1,000 in Bronx Division | 450 |
| No. of Nursing Homes (owned, affiliated) | 0 owned 30 Affiliated | 0--we have liaisons on site at 3 NHs | n/a | 3 owned | 1 owned |
| No. of Home Health Agencies (owned, affiliated) | 1 owned | 1 owned | 1 owned | 1 owned | 1 owned |
| No. of Physician Practices (owned, affiliated) | 21 Primary Care (owned) | 1 owned | 1 owned | ||
| Are physicians affiliated with health delivery system or are they independent? | Both 1,000 FT faculty 1,000 voluntary | MHHA receives referrals from physicians who are employees of the health system and from physicians who have their own practices. | There are some MDs on staff in Hospice, our managed care plan, etc., but they are staff within programs. VNS obtains referrals from many MD practices and hospitals. They are independent and have only a referral relationship with VNSNY. | They are employees of JHHLS. | Independent |
| Inpatient pharmacy? | Yes | No | No | Yes--in-house pharmacy | No |
| Does SNF use dedicated pharmacy or contract with large/retail, or multiple pharmacies? | n/a | No | VNSNY does not own a skilled nursing facility. | See above. | Dedicated pharmacy |
| No. of Pharmacies--outpatient | 8 | 0 | 0 | 0 | 0 |
| In-house laboratory? | Yes | No | No | No | No |
| How many outside laboratories? | 4 major ones | 3, but we primarily use the vendor that links to CIS. | 3 | Mt. Sinai Hospital | 1 |
| In-house radiology department? | Yes | No | No | No | No |
| How many outside radiology centers/MR centers do you work with? | 4 major ones | n/a | n/a | Health Trac, Montefiore hospital | 1 |
| Percentage of overall budget dedicated to IT? | <5% | 2.2% of the home care budget is dedicated to IT. | |||
| Electronic Health Record (EHR) system--scheduling, billing, or claims? | Yes | EHR, Scheduling and billing is handled by MISYS. MISYS Healthcare Systems is one of the top HIT companies in North America, develops and supports reliable, easy-to-use software and services of exceptional quality that enable physicians and caregivers to more easily manage the complexities of health care. MISYSs clinical products incorporate web-based technologies and are designed from the ground up to share patient data across all medical care settings. The Homecare system can exchange data with hospitals and other systems. | Billing: The CHHA uses an internally developed billing system. Third-party software is used for hospice, the Medicaid Managed LTC (MLTC) plan, and a pediatric program. Third-Party Administrator is used for the new Medicare Advantage plan. Claims: For the MLTC plan, claims are done via internally developed systems but will shift to third-party software. | Site provided additional information in a separate document. | AHC is used for billing. |
| Clinical Electronic Health Record (EHR) system? | CareCast | MHHA uses MISYS Homecare software for our EHR. Clinicians in the field can instantly access health care plans, patient demographics, medications, and other clinical information to improve quality of care. OASIS collection is integrated into the patient health assessment. Assessments made on laptops at the point of care are remotely synchronized to our EHR in minutes. Field staff is required to sync their laptops a minimum of once every 24 hours. | VNSNY has developed an integrated EHR called the Patient Care Record System (PCRS), an accessible system via pen tablets by over 2,000 nursing and therapy staff. | Site provided additional information in a separate document. | No |
| Primary software vendor for electronic health information system (if applicable) | GE (IDX)--CareCast | MHHA utilizes MISYS for our EHR. The software was externally developed and is one of the top three home care software packages in use today. The software is housed on a MS SQL Server. | The system is internally developed and supported. PCRS uses three-tier system architecture. The mobile component is written in MS VB 6 with a supporting MSDE/SQL database. Office-based functions are done by either using mainframe CICS/COBOL systems or on web-based Java applications. Data is synchronized between the mobile and host databases using internally developed store and forward processing via an intermediary RISC-based processor. | Site provided additional information in a separate document. | American Health Care |
| Short-term (6 months?) HIE* future plans | Many | MHHA projects included the expansion of our Web-based Physician Portal for orders. Implementing an interface between our Telehealth devices and MISYS to incorporate the data into our EHR. Developing an interface between MISYS and the hospitals EHR. Implemented auto-email to notify physicians when their patients are admitted to home care. | Planning for mobile-intake, MD web-based portal, RHIOs, and PCRS expansion to other clinical units, etc. | Participating in Bronx RHIO. We are developing a database to establish a unique identifier that will be the basis for sharing information within all JHHLS programs and services. | |
| Long-term HIE* future plans | Integrated expanded EMR spanning ambulatory, home health, and inpatient care, supported by online decision support. | MHHA will focus to ensure that 100% of all patient documentation will be captured in our EHR. MHHA will operationalize the HL7 interface to import information from referral sources automatically into MISYS. | Implementation of mobile-intake, MD web-based portal, RHIOs, and PCRS expansion to other clinical units, etc. | Electronic Medical Record | |
| * Information in this table was collected from a General Information About Health Care Setting form sent to all sites prior to the scheduled site visit. ** A division of the Jewish Home and Hospital Lifecare System. | |||||
APPENDIX D: Site Visit Report--Intermountain Health Care, Salt Lake City, Utah
Health Settings visited: LDS Hospital (an Intermountain Health Care hospital), Christus St. Joseph's Villa, the Community Nursing Service (CNS), Hillside Rehabilitation Center, and CareSource Home Health and Hospice.
I. OVERVIEW OF THE LOCATION/CITY AND VISITED HEALTH SETTINGS
Intermountain Health Care is a not-for-profit health care enterprise that has over 60% of the acute care hospital market in Salt Lake City. Intermountain Health Care has more than 27,000 employees enterprise-wide, with approximately 4,700 at LDS Hospital, the hospital visited by the site visit team. Intermountain employs 550 physicians and has another 3,000 affiliated physicians with limited (read-only) access privileges to the enterprise electronic health information system (HELP system). The hospital employs hospitalists. Intermountain also has 92 clinics. According to one source, 17,000 people can access (with varying levels of permission) their Clinical Data Repository (CDR) that is part of the HELP2 system.11 HELP2 is the next generation of their CDR, and spans inpatient and outpatient settings, but it is not yet comprehensive in terms of clinical content. HELP2 is a single enterprise-wide longitudinal electronic health record (EHR) system that spans both inpatient and outpatient settings. The HELP2 database receives data from a heterogeneous collection of ancillary systems that communicate with the HELP2 database via HL7 interfaces. Currently, HELP2 houses over 2,000,000 patient records. Intermountain Health Care has a health plan division called Select Health, however, 35-40% of hospital admissions are traditional Medicare fee-for-service (FFS).
LDS Hospital and other Intermountain-owned hospitals have a decades-old tradition of ground breaking in-house development of information technology, and, more recently, they have entered into an alliance agreement with General Electric Healthcare to develop a next generation EHR system. The goal is to eventually run the enterprise using commercial-off-the-shelf (COTS) software. They have been and continue to be leading proponents and users of standard messaging.
Christus St. Josephs Villa (St. Josephs) is a non-profit skilled nursing facility (SNF) that receives the majority of their referrals from LDS Hospital, as well as two other local hospitals (Cottonwood and Altaview). St. Joseph's has 48 Medicare beds. They have a house physician who sees the majority of residents and a Medical Director who works at several SNFs in the community. None of St. Josephs staff, including the Medical Director, may access (even on a read-only basis) the Intermountain HELP system. They have begun a conversion to the Meditech EHR, starting first with billing, admissions, medications and treatment sheets, and MDS reporting. The decision to use Meditech at all St. Josephs sites was made at the corporate office based in Texas. St. Josephs Corporate is a healthcare enterprise that mainly focuses on hospitals, and has only three SNFs, of which St. Joseph's Villa is one.
Community Nursing Service (CNS) is a visiting nurse service. They receive about 45-50 referrals from LDS Hospital per year, and about the same from another area facility, Cottonwood Hospital. They have used Infosys/Homesys for four years. This software supports intake, staff scheduling, OASIS reporting, billing, and has a payroll interface. They indicated they are just beginning to roll out some of the clinical modules available with this software vendor.
Hillside Rehabilitation Center (Hillside) is a non-profit SNF and long-term care (LTC) nursing home with 120 beds, 82 of which are used. Their owner and administrator, Warren Walker, has a history of embracing technology focused on improving their processes, increasing staff satisfaction by reducing their workload, and promoting quality care. They are currently implementing an EHR developed by Utah-based Bluestep;12 it is being built on a core web application and the EHR is being designed for use in LTC environments. Thus, in contrast to Application Service Providers (ASPs), who provide web-accessible horizontal (generic) applications, Bluestep is a Vertical Service Provider (VSP); they have adapted their general purpose tools and applications to the specific needs of long-term care providers. Hillside has participated in the adaptation. A strength of the Bluestep LTC solution is its approach to the management of care workflow, including the management of tracking and acquisition of patient information such as a laboratory test result.
CareSource Home Health and Hospice is a home health agency (HHA) and in-patient hospice, the only in-patient hospice in Utah. They use McKessons Horizon and have modified it for use in both their home care program as well as in their hospice.
See Table D.1 at the end of this appendix for a comprehensive compilation of the information requested from and supplied by each site, prior to their scheduled site visit.
II. SPECIFICS ON CLINICAL DATA SHARING
1. What data are shared? What should data should be shared but arent?
LDS Hospital discharge planners noted that most SNFs desire the same information on patients about to be discharged from the hospital, but in need of post-acute or long-term care. These requirements include: demographics, history and physical (H&P), therapy notes, and medication list. They report that the most patients have completed a Physician Orders for Life Sustaining Treatment (POLST)13 and that this follows the patient. Hospital staff report that many nursing homes transferring a patient to the hospital send the POLST. (Under Utah regulation, a POLST is optional, but if it exists, the POLST should follow the patient during a transfer of care.)
St. Josephs reports that patients received from Intermountain-owned hospitals come with a demographic sheet, H&P, consultant reports, medications used in the past 72 hours, labs, radiology, and therapy notes. However, St. Joseph Villa informants report that they rarely receive a POLST from an Intermountain-owned hospital, or from any of their other referring hospitals.
CNS estimates that approximately 5% of patients are admitted to home care with a completed POLST from the hospital.
When admitting a new patient, CareSource requests a H&P, the demographic sheet, medication list, and current progress notes. On average, they receive this information 75% of the time and it requires (on average) three follow-up phone calls. Physical therapy notes and prior Disposable Medical Equipment (DME) authorizations seem to be the most problematic data elements to obtain.
When Hillside residents are admitted from a hospital, they request and generally receive a face sheet, H&P, nursing notes, therapy notes, and a medication list. Hillside reports that they need to call the referring hospital ward clerk to get information on IV medication use, chemotherapy use, and ventilator use.
St. Josephs states that upon discharge to home, the nursing staff prepares a paper transfer packet to include a demographic sheet, H&P, therapy notes, wound care and a medication list. Upon transfer to the acute care hospital, nursing staff prepare the above information and add the POLST, recent labs and the MAR.
2. How are the data shared?
Electronic information exchange between unaffiliated levels of care was not observed during the site visit. All information transfer between the sites visited is by phone, fax, or paper accompanying the patient. Only rarely did post-acute care enterprises receive what they believed was sufficient information from the hospital on the first try; on average several phone calls were required to retrieve necessary information from paper or electronic records at the originating site. One exception was Cottonwood Hospital, another Intermountain Health Care enterprise; apparently, Cottonwood sends a complete printout of the patients hospital EHR.
In some cases, the information is transmitted via a phone call with the hospital discharge planner who manually abstracts the desired data elements from both the paper and electronic charts.
CNS intake care coordinators enter information received from the hospital into HomeSys.
Hillside intake coordinators scan hospital information and upload into their Bluestep system.
St. Josephs is beginning to enter patient information received into their newly-deployed Meditech system.
3. Timeliness and completeness of the data.
At LDS Hospital, the discharging physician dictates the complete discharge summary after the patient in discharged. The lag between when the patient is discharged and the dictation is complete varies depending on the physician and ranges from one day to three weeks. As observed, this means that the LDS Hospital discharge planner is the source of patient information provided to NHs until this summary is available. That said, LDS personnel have access to all current information.
4. Specifics about medications, labs, and radiology.
LDS Hospital has its own laboratory, radiology, and pharmacy services, and these services are supported by a mixture of locally developed and COTS applications that use a combination of local and national standards. LOINC codes are used for laboratory results and First Databank is used for medications.
St. Joseph's uses Intermountains laboratory, and the lab results are communicated via fax or phone (in the case of urgent results). Nursing staff then re-enter and send results to the medical director via her Blackberry®. St. Joseph's uses a single pharmacy (not Intermountains pharmacy) and generally gets admission medication 4-6 hours after arrival.
CNS uses multiple labs, largely governed by insurance or geography.
CareSource works with a single pharmacy and communicates via fax or phone.
Hillside uses Schrieber lab and results are faxed (urgent results are called). Results do not populate Blue Step, that is, they will be (are) entered manually. Hillside has made a financial investment in a single pharmacy and can electronically send medication information. This information auto-populates the pharmacists queue. However, scheduled C-II (Schedule 2 Controlled Substances) medications require a paper prescription in the State of Utah.
5. Areas under development (e.g., CPOE, decision-making tools).
LDS Hospital continues to improve the integration and interoperation of its many in-house software applications.
CNS is developing a physician portal that will allow physicians to sign orders electronically and modify the care plan.
Hillside is implementing decision support tools for nurses and CNAs within the framework of the BlueStep EHR. (Bluestep claims knowledge management as a feature of their core technology.)
6. Barriers to clinical data exchange.
At present, LDS Hospital physician progress notes are all in the paper chart. Intermountain does not allow home care or SNF coordinators into the hospital unless invited. Thus, they are not able to collect information on site.
St. Joseph's staff and Hillsides staff do not have access to the Intermountain electronic health record.
CNS identifies their biggest information barrier to clinical data exchange is identifying the patients' primary care physician in the community.
Current SNF information exchange goals were almost always expressed in the form of the desire for the completeness of a paper record from the hospital. Some sites acknowledged that a complete record might be too much, or introduce accountability and liability concerns, but on balance all sites wanted more information that was commonly available.
7. Facilitators to clinical data exchange.
Placement decisions for Intermountain patients requiring post-acute care seems to be done almost exclusively by personal relationships--in the form of voice-to-voice communications between hospital discharge planners and the post-acute care intake coordinators. These personal relationships have taken years to develop and are the backbone of the referral process. One example of when such placements are over-ridden is a family request for geographic proximity. These personal relationships also support information exchange--from acute-care hospitals and emergency departments to post-acute care--both prior to and after a NH accepts the post-acute patient. At present, the two processes--placement and conveyance of patient information--are conjoined.
In sharp contrast to the personal relationships supporting post-acute care placement, the Utah Health Information Network (UHIN) is a community health information network that began in 1993. It is a coalition of health care providers, payors, and state government with, initially, the common goal of reducing costs by standardizing the transmission of administrative data, particularly payment data. The network community sets the data standards to which providers and payors voluntarily agree to adhere. The UHIN standards are then incorporated into the Utah state rule via the Insurance Commissioners Office. UHIN operates as a centralized secure network through which the majority of administrative health care transactions pass in the state. Nearly all payers and providers are participating in this project. UHIN developed a tool (UHINT), which they provide free of charge to providers for use in submitting electronic claims. The tool is provided so that even the smallest provider can submit claims and electronically receive remittance advices. The exchange of standardized electronic transactions has drastically reduced the amount of paper processing required for payers and has streamlined the payment of claims and remits, which has resulted in providers receiving payment more quickly. Under an Agency for Healthcare Research and Quality (AHRQ) grant, UHIN is pilot testing the exchange of a limited set of clinical data (medication history from payer to hospital), discharge summaries, history and physical, and laboratory results) with a small number of providers. The results of this pilot study are not yet available, but developers note evidence of demand for this service.
UHIN developers also are noticing an acceleration of development and feature requests given current software best practices--such as messaging and web-based connectivity. This is in contrast to formerly used object-based standards. Evolution of the UHIN is now more rapid, and more responsive to evolving user requests.
III. TECHNOLOGY
1. Hardward and software descriptions of the main health delivery system and the PAC/LTC settings.
The HELP2 system at LDS Hospital is a single large longitudinal EHR that integrates data across all care settings. It receives data from a heterogeneous collection of ancillary systems via HL7 Version 2 messaging that is standard across the enterprise. The HELP2 system was initially deployed in the outpatient environment but is now seeing widespread use within Intermountain hospitals. HELP2 desktops need support only a web browser with adequate computing power.14 HELP, (the first version of the system), is implemented on Tandem hardware, using the Tandem Application Language (TAL) programming language and PTXT Application Language (PAL), and uses the proprietary Tandem file system (Enscribe). The HELP system is still the primary system used in all Intermountain hospitals. Thus, HELP2 is intended as a complete replacement for the HELP system, but the transition from HELP to HELP2 enterprise wide will be a very long process.
2. Architecture of EHR system at main HDS.
a. Are they using CHI-endorsed and other HIT content and messaging standards? If so, which ones are they using? Messaging? Vocabulary? Direct care FM?
Perhaps to a greater degree than in any comparable large acute care hospital, internal inter-system communication is done using internally standard HL7 Version 2 messages. LDS Hospital and other Intermountain enterprises have pioneered such use, and incremental economies of scale were claimed for recent integration efforts. In contrast to most acute care medical centers where standards adoption is incidental to other considerations, LDS Hospital has adopted standards both because they are standards and because of perceived benefit.
Not unexpectedly, other than LOINC and HIPAA required terminologies CHI standards were not visible. For example, there was no visible use of SNOMED.
b. Description of each EHR system and HIT solution(s) to support HIE.
Currently, LDS Hospital has a rich and heterogeneous mixture of internally developed and COTS systems centered around core systems developed internally or in partnership with 3M. As of this writing, Intermountain has expanded the scope of its partnership with GE to further develop HELP2 capabilities.15
St. Josephs, CNS, and CareSource run their locally-deployed, proprietary applications on mini-computers, accessible from Local Area Networks (LAN) and dial-up lines. Hillside is making use of the web-based (remotely hosted) Bluestep product. CareSource uses McKesson Horizon, and they indicated that although they have not necessarily taken advantage of this fact, McKesson does have the flexibility to have custom programming done at a cost. McKessons future plans include going platform independent, much like todays web browsers. It was unclear whether or not CareSource would immediately be taking advantage of these innovations when they become available.
c. If they have used "best of breed" how are these different software integrated?
Integration at LDS Hospital is via locally standard HL7 Version 2 messages using locally developed content standards, except for LOINC, some HIPAA standards, and occasional use of proprietary content solutions such as drug knowledge base (First Databank).
At Hillside, Bluestep achieves functional integration by implementing all functions using Bluestep core components and tools; thus, at present the Hillside system does not interoperate with other systems--though, because of its use of software best practices there is no reason why it could not easily do so in the future.
UHIN is achieving integration through the incremental deployment of state-wide data standards, that local systems program to. At present, these standards are largely Utah-specific, but work is underway on the deployment of content standards. One example appears in a Utah State Rule16 that describes use of national standards for claims-related transactions as an objective.
2. Architecture of EHR systems at PAC/LTC (if applicable) and HIT solution(s) to support HIE.
As described above, heterogeneous components inter-operate within LDS using internally standard HL7 Version 2 messages. Many components make use of a central patient data repository (another component) in addition to or instead of their own component-specific databases.
Hillside makes use of the Bluesteps Vertical Service Provider (VSP) architecture, a variation on the web-based Application Services Provider (ASP).
3. How are the data stored? Shared? Accessed? Transmitted? Accepted at other setting? Entered? Etc.
The main LDS (current) patient record store is a proprietary database developed jointly by 3M and Intermountain. Archival (older) patient information is still stored in the LDS-developed HELP system.
At present, this information is not shared electronically outside LDS. Instead, the relevant information is transferred either voice-to-voice by the discharge planner, via fax, or paper copies accompanying the patient.
4. How are you tackling any interoperability issues using standards-based EHR systems or other HIT solutions for health information exchange?
Interoperation at LDS is currently aimed at integrating all information technology components used in LDS in-patient and outpatient care. Once intra-LDS integration is achieved, UHIN involvement will be one path by which both LDS, specifically, and Intermountain, in general, interoperate with other Utah healthcare enterprises including SNFs.
5. How does electronic health information exchange (e-HIE) vary between affiliated and unaffiliated providers within a single HDS?
Among LDS-affiliated providers, there is one method of interoperation--HL7v2-based messaging; currently the only non-affiliated interoperation is through the UHIN.
Other sites visited did not interoperate with non-affiliated sites.
6. How does e-HIE vary when exchanging to outside entities?
Exchange using the UHIN is currently limited to administrative transactions; as described above, limited clinical exchange is being piloted.
At Hillside, the Bluestep system being deployed will make it possible, technically, to develop bilateral interoperation (e.g., to get lab results), and to communicate with the UHIN.
The applications employed at the other sites--St. Josephs, CNS, and CareSource--are not designed with interoperation in mind; thus, exchange of information with the UHIN will become more difficult as the scope of doing so increases--from administrative data to clinical data.
IV. ORGANIZATIONAL ISSUES
1. Business Case for PAC/LTC.
With the exception of LDS Hospital, the settings visited were unaware of the UHIN, and its efforts to support and facilitate health information exchange. The exception to this is at Hillside where they did recognize that Medicaid claims now were solely done electronically, but were unaware that they were transmitted through the UHIN. Stan Huff is a consultant on the AHRQ-funded UHIN pilot, but no one else, including LDS Hospital staff, was aware that the UHIN project was in progress.
None of the post-acute or long-term care settings visited had any immediate or future plans to implement HIT to improve and/or facilitate HIE. Although LDS Hospital has the technical infrastructure in place to share data with other settings, when asked about sharing data with community PAC/LTC settings, Stan Huffs response was standards are not widely used with outside entities because no one has made it a priority [the business case for LDS Hospital] is population driven. There is a limited amount of money to devote to EHR systems, and we use scarce HIT resources where they will have the greatest benefit for the largest number of patients. PAC/LTC is not the highest priority because they have few medical events or patient visits when compared to outpatient facilities or the acute care hospitals. Stan Huff went on to say that most SNFs/NHs do not have the IT expertise to accept electronic data, and they are only a small piece of the pie. The individual institutions are not large enough to support IT staff that can deal with electronic data exchange.
2. Adoption of EHR systems.
LDS Hospital developed its own EHR system unilaterally and later in collaboration with their software vendor 3M. They used their own vocabularies and when standards became available they used them opportunistically; however, when they first implemented the HELP system when few if any standards were available.
For all the post-acute and long-term care settings visited, vendor selection was not based on if they used standards or if they had an interoperable EHR system. With the exception of LDS Hospital and Hillside, none of these settings is involved in standard development organizations; none are they members of the UHIN.
V. CONCLUSION/FINAL THOUGHTS
LDS Hospital has a long history of groundbreaking HIT development. More recently, their technical leadership has included an intra-enterprise commitment to use messaging--currently their implementation of the HL7v2 standard--for all inter-component communication.
Perhaps inspired by this example and by the early use of the internet in Utah, former Governor, now HHS Secretary, Michael Leavitt, led the creation of a state-wide network to support state services and educational institutions--Kindergarten through grade 12 as well as post-secondary institutions. This popular and highly successful effort raised consciousness around the state and may have laid the ground work for the collaboration necessary to launch the now successful RHIO (Utah Health Information Network [UHIN]), and the fact that it includes erstwhile (network) "competitors."
Medicaid reimbursement is incrementally moving to the UHIN, as we saw at Hillside Rehabilitation that is now using UHIN to submit their Medicaid claims, as six months ago, Medicaid suspended their use of bulletin boards to submit the claims.
The RHIO is already clearly a success today--as measured by use and demand for services--although post-acute and LTC use does not seem to be a current priority, excepting use for Medicaid reimbursement. Initial drivers are: (1) patient eligibility; (2) provider credentialing and enrollment with payers; and (3) reimbursement. They have started a pilot on the exchange of clinical data, but it began in late summer, so it is too early to discuss findings. While serving the specific needs of post-acute and long-term care may not be a current RHIO priority, these care settings may derive significant benefit from general (planned) RHIO activities such as the uniform reporting of lab tests and e-prescribing.
Finally, while all sites wish they had a patient-centric longitudinal record, there is little if any movement to meet that goal. There is awareness of the possibility and potential of patient-accessible/writable health records, especially if they were UHIN accessible but the site visitors did not know of any plans, either short-term or long-term to facilitate this concept.
| TABLE D.1: General Information Supplied by Visited Sites* | |||||
|---|---|---|---|---|---|
| Name of Health System | Intermountain Health Care, LDS Hospital | Community Nursing Services | Christus St. Josephs Villa | Hillside Rehabilitation Center | CareSource Home Health and Hospice |
| Location | Salt Lake City, UT | Midvale, UT | Salt Lake City, UT | Salt Lake City, UT | Salt Lake City, UT |
| Year established | 1975 | 1925 | 1947 | 1970 | 1997 |
| Area served (urban, rural, both) | Intermountain--both LDS Hospital--urban, major referral center, established in 1905 | Urban and rural | Urban | Urban | Urban |
| Ownership | Non-profit | Non-profit | Non-profit | Non-profit | For profit, privately held, freestanding |
| No. full-time employees | Intermountain has 27,000 total employees LDS Hospital has 4,700 | 161 full-time (plus 195 part-time) | 75 | 66 | |
| No. of Nursing Homes (owned, affiliated) | 0 owned | 0 | 1 owned | 0 owned 3 affiliated | 0 |
| No. of Home Health Agencies (owned, affiliated) | 1 owned | 1 owned | 0 | 0 owned 0 affiliated | 1 owned |
| No. of Physician Practices (owned, affiliated) | 96 owned | 0 | 0 | 0 owned 0 affiliated | 1 owned |
| Are physicians affiliated with health delivery system or are they independent? | Affiliated, employed, and independent | n/a | Independent | n/a | Affiliated |
| Inpatient pharmacy? | Yes | n/a | No | No | No |
| Does SNF use dedicated pharmacy or contract with large/retail, or multiple pharmacies? | n/a | n/a | Dedicated | Dedicated | Dedicated |
| No. of Pharmacies--outpatient | Intermountain has 19 LDS Hospital has 1 | Home infusion only | 1 | 0 | 0 |
| In-house laboratory? | Yes | n/a | No | No | No |
| How many outside laboratories? | 3 | 1 | 1-2 | 2 | |
| In-house radiology department? | Yes | n/a | No | No | No |
| How many outside radiology centers/MR centers do you work with? | 0 | n/a | 1 | 3 | 0 |
| Percentage of overall budget dedicated to IT? | |||||
| Electronic Health Record (EHR) system--scheduling, billing, or claims? | Yes | Yes | Yes | Yes | Yes |
| Clinical Electronic Health Record (EHR) system? | Yes | No | No (in process of development) | Yes | Yes |
| Primary software vendor for electronic health information system (if applicable) | In-house developed | Infosys/ Homesys | Meditech | American Data | McKesson and Resource Systems |
| Short-term (6 months?) HIE* future plans | Discuss at interview | In process of implementing clinical software | Developing Meditech for clinical records | New system | |
| Long-term HIE* future plans | Discuss at interview | Maintain | |||
| * Information in this table was collected from a General Information About Health Care Setting form sent to all sites prior to the scheduled site visit. | |||||
APPENDIX E: Site Visit Report--Indiana Health Information Exchange, Indianapolis, Indiana
Health Settings visited: Indiana Health Exchange (IHIE), Regenstrief Institute, Indiana University (IU) School of Medicine, Wishard Health Services, Lockefield Village Rehabilitation and Healthcare Center, the Visiting Nurse Service (VNS) of Central Indiana, Kindred Long-Term Acute Care Hospital, Beverly Enterprises at Brookview, and Briarwood Rehabilitation.
I. OVERVIEW OF THE LOCATION/CITY AND VISITED HEALTH SETTINGS
Indiana Health Information Exchange/Regenstrief/Indiana University School of Medicine. Indianapolis, Indiana has several major hospital systems including the Indiana University hospitals, St. Vincent, St. Francis, Community Health, and Westview. The five Indiana University hospitals are Wishard Hospital (part of Wishard Health Services, the county-managed system that serves vulnerable populations of Marion County, Indiana), the Roudebush VA Medical Center, Riley Children's Hospital, Methodist Hospital, and the Indiana University Hospital. The latter three are owned by Clarian Health Partners.
Our primary host for the site visit was Dr. Michael Weiner, MD, MPH, Associate Professor of Medicine, IU School of Medicine, Scientist at Regenstrief Institute, and Center Scientist at the IU Center for Aging Research. Many of the other individuals we spoke with the first day are dually appointed as faculty at the University as well as research scientists at the Center for Aging Research or Regenstrief Institute.
Dr. Weiner is leading a new program at Indiana University called Gero-Informatics (defined as the application of medical informatics to geriatrics care). The mission of this program is to advance research, clinical care, and education related to gero-informatics.
Under the leadership of Clement McDonald, MD, Indiana University deployed an early (1973) electronic medical record system (the Regenstrief Medical Record System), evolutionary descendents of which are still in use today. Again with leadership from Dr. McDonald and with assistance from J. Marc Overhage, MD, PhD, success with the medical record system led to the formation of the Indianapolis Network for Patient Care (INPC), which permits emergency department (ED) physicians at all major Indianapolis hospitals to retrieve patient information stored at one of the other hospitals. A simple example of the utility of this arrangement was a recent patient being seen in an Indianapolis hospital ED for chest pain. Because the ED physicians could retrieve patient history information and see that the patient recently had a cardiovascular workup at a regional hospital a few months before, as well as read the results that showed the workup had at that time ruled out cardiovascular disease, they were able to diagnose a pulmonary embolism more quickly and at less cost and risk to the patient. While there are many factors that led to the current success of the INPC, regional ED physicians were the primary drivers and early users of this health information exchange and are credited with both pushing the concept of health information exchange within the Indianapolis community of health care settings and with being the early adopters who participated in its development.
Steven R. Counsell, MD, Director of IU Geriatrics, described current plans to build on the elements of regional "informational continuity of care" achieved to date; specifically, his goal is to build and maintain an increasingly complete, up-to-date, longitudinal patient-centric record. An early sub-goal is to exchange data with local primary care physicians, pharmacies, and laboratories. Dr. Counsell and his colleagues are positioned to formulate and pursue these ambitious goals because of the decades of effort in collaborative processes and infrastructure invested by Drs. Clement McDonald, Marc Overhage, and regional co-workers, and also by early adopters and users. Development of the INPC has demonstrated to the regional health care community that an incremental approach to a patient-centric record is both possible and the best way to proceed.
Because of these and other past successes, the physicians presently leading the Indiana Health Information Exchange are overwhelmed with opportunity relative to other regional care sites; their challenge and opportunity--per Dr. McDonalds legacy17--is to identify real, solvable health information technology (HIT) problems, and then solve them. An example of the application of this method is Regenstriefs early focus on the processing of laboratory test results. Their development paradigm enables them not to worry about the big picture, nor about painting themselves into a corner--as, for instance, they have done by continuing to use an unsupported version of the Microsoft OS for some of their order entry interfaces. (For skilled users, however, these interfaces are very high function--making use of fast keystroke-based commands.) Instead, they can invest their finite resources working on what they perceive to be the next most useful system function, learn from that effort, and go on to the next problem that is both important and solvable.
Part of Regenstriefs repertoire of lessons learned is that they have sufficient accumulated experience processing data feeds, such as laboratory data, from other hospitals that they prefer to take the remote data "as is" and deal with things like undetected duplicate patient records later. This is a tradeoff that few others are in a position to make. Because of their hard-won experience and their associated investment in tool development, they have lowered the bar for the next hospital, medical practice, or other source of encounter data to join the Network. That is, they take the data stream from whatever system the next care setting has in place and then they develop the software transformations and mappings required to integrate that data into the IHIE. Again, they can do this easily and productively because of the economies of scale resulting from decades of experience and tool investment. The alternative--requiring that each hospital or other care setting develop its own transformations and mappings into some abstract data model--is so expensive and fraught with delays and risk that few regions have succeeded in achieving clinical data exchange using this approach. An important, but little appreciated feature of the IHIE approach, is that the integration team is focused only on the next data stream; it is not burdened, yet, with the necessity of solving the problem for rest of the region, the state of Indiana, the Midwest, or the nation. By focusing on the next data stream, they do not take on problems that are too large, and they can benefit--learn--from each step completed. Another little appreciated feature of the IHIE paradigm is that collaborative organizational energies can be focused on data issues--sharing, re-use, security, and the like--and not on technical details, which participants typically defer to the McDonald-Overhage Regenstrief leadership.
The deliberate focus on data as opposed to software has led Regenstrief to invest in the representation of transferred text-based information using formatted ASCII and to avoid using scanned images or unformatted text, wherever possible. This means that laboratory test result names can make use of the LOINC standard and, potentially, lab test results from different sites can be compared and aggregated.18 It also means that the IHIE may someday be able to interoperate by meaning using medication and problem list data. That is, patients may one day have a unified medication list. For instance, the daily dose of acetaminophen in combination drugs can be computed with a resulting unified problem list, showing both chronic and acute diagnoses. Thus, even if the goal and benefit today is uniform human readability of exchanged clinical data, IHIE is in a position to explore use of other computer-empowering terminology standards such as RxNorm (medications) and SNOMED (problem list) in the future.
IHIE is in the early stages of implementing a portal called Docs4Docs19 that provides access across care providers to admission and discharge transcriptions, laboratories, radiology, EKGs, and pathology. At present, medications are not included. Physicians see Docs4Docs as a "glorified mail service," giving them web-based (anywhere, anytime) access to health care transaction reports. It is supported by the large hospitals in the Indianapolis metro area. There are a few places currently using this technology, including Kindred Long-Term Acute Care (LTAC) Hospital.
The Docs4Docs portal is very new, and potentially revolutionary. Those in charge do not feel pressure yet to open it up to patients, as Kaiser Permanente health care has accomplished, but they will feel this pressure soon. Right now, Docs4Docs is, as the name suggests, very physician centric. The portal leverages the experience and good will that has been generated by long-standing regional ED physician collaboration and interoperation among the five hospitals currently participating in the Network portal. One novel aspect of the portal is that physicians manage--create and maintain--their own patient links. This approach overcomes the challenges of physicians having multiple affiliations (and thus multiple identifiers) and it allows physicians to track down encounter records for the same patient that the master patient index has failed to link.
Kindred Long-Term Acute Care Hospital. The purpose of our visit to Kindred was to see a demonstration of the IHIEs Docs4Docs portal. This LTAC site receives patients from all surrounding hospitals, including Wishard. Their average length of stay (LOS) is 25 days, with an average census of 30 patients. The demonstration emphasized the utility of Docs4Docs--instead of rummaging through a paper-based in-box, or (less likely) a not always up-to-date paper chart, physicians can find the lab (or other encounter) result they want and display it. Optionally, the result can be displayed in the context of all recent encounters. The fact that the portal made these results accessible from any Web browser and displayable along with past results over time is viewed as a powerful feature; again, the principle early benefit of the portal is that a physician can retrieve recent results (from subscribing hospitals) for any patient (known to the system) from any web browser, and display them, aggregated in a graph, if appropriate. We were told that demand to have feeds available from the portal exceeded current personnel resources, and that the project--funded initially by grants--was modestly cash-flow positive from hospital subscription fees.
Wishard Health Services and Lockefield Village Rehabilitation and Healthcare Center. Wishard Health Services provides a spectrum of health care for older persons, including sub-acute care, extended/long-term care, outpatient/ambulatory care, and house calls for seniors, under one umbrella, the Acute Care for Elders (ACE) unit. It is a county-managed system staffed by university faculty and surrounded by other hospital chains, including Clarian (which also is part of the IU campus). By its mission, but to some extent also by patients choice, Wishards patient population is largely low-income. Their payor mix is 35.7% uninsured, 27.3% Medicaid, 22.5% Medicare (mainly FFS), 9.7% commercial, and 4.8% other. Wishard Hospital has an ACE Unit and an SNF (Lockefield Village), which also was visited by the team. The electronic Regenstrief Medical Record System was first developed in the Wishard system, and Wishard is unsurprisingly a participant in the IHIE. Wishard will complete deployment of mandatory e-prescribing processes for its physicians in January 2007.
Beverly Enterprises at Brookview is a nursing home with a Part A SNF, a dementia unit, and long-term care services. It is one of hundreds of facilities that are part of the national Beverly chain. The LOS for Part A patients is 37 days and occupancy is usually in the mid-90%. The IHIE was in communication with a Beverly Corporate representative concerning potential participation in the IHIE until that representative left Beverly during a recent reorganization. At the time of the writing of this report, there is no action being taken by either the IHIE or by Beverly Brookview to join the Network. However, Beverly Brookview has reported renewed interest in participating in the IHIE.
Beverly Brookview uses an EHR called VistaKeane that is used throughout all corporate facilities and maintained by corporate headquarters in Fort Smith, Arkansas. Floor staff entries--created by entering data on touch screens located outside of patient rooms--are monitored closely by supervisors within the facility as well as within the corporate office. The corporate office keeps a tight rein on each of the facilities. Beverly Brookviews copiers and fax machine have digital scanning capabilities and are able to create, receive, and transmit digital documents for representation in a corporate document repository (Documentum).
Reportedly, Beverly corporate information technology can and does deploy enhancements to their information technology systems nationally if they are of sufficient importance.
VNS Healthcare System of Central Indiana is the largest HHA in Indiana. Established in 1913, it has 212 full-time employees. The VNS is the preferred provider for seven hospitals (i.e., there is a formal affiliation with these hospitals). At Wishard, they have a clinical liaison in the hospital who has access to the hospitals EHR. The liaison also can access information for referrals that come from the ambulatory clinic and begin the process of populating the home health agencys electronic record using a laptop.
The VNS recently upgraded to the MISYS system, previously having used McKesson. They are exploring a physician portal but this is not imminently available. They are heavily invested in telehealth (currently with 101 units) and plan to have 200 Honeywell units in operation by the end of 2007.
When asked about the IHIE, John Pipas, the CEO was familiar with the HIEs activities in general, but to date, they have not been asked to participate, nor have they indicated to the IHIE group that they are interested in participating but would consider options if offered.
Briarwood Rehabilitation is a for-profit, long-term care facility with a Part A SNF. They have 113 skilled beds and an average LOS of 60-90 days. They use MDI for their MDS reporting and claims submission and do not have any future plans to implement an interoperable EHR system.
See Table E.1 at the end of this appendix for a comprehensive compilation of the information requested from and supplied by each site, prior to their scheduled site visit.
II. SPECIFICS ON CLINICAL DATA SHARING
1. What data are shared? What data should be shared but aren't?
Wishard Hospital considers the discharge summary, insurance information, medication list, allergies, problem list, and advance directives among the core information needed at time of transfer.
SNF staff at Lockefield Village comment that they rarely receive information about a patient's mental status and behavior prior to transfer. When it is provided, it is sometimes incomplete.
The most common information that Beverly Brookview does not always receive from referring hospitals including Wishard is the discharge summary (again because it may be dictated later by the attending physician). Beverly Brookview has a full-time recruiter who visits acute care facilities to obtain patient information regarding potential Beverly Brookview patients. The information obtained is passed to an RN in charge of Brookview admission (or denial of admission).
When an urgent problem requires that a patient be transferred to a hospital, the Beverly Brookview person in charge of medical records helps to complete a handwritten form that includes a current medication list, recent laboratory results, insurance status, skin status, code status, physician name and contact, and facility contact. Many of these data elements are gathered from the Beverly Brookview computer but are handwritten onto the form. Beverly Brookview's patient records are reviewed once every 24 hours by remote care providers who can contact Beverly Brookview care providers if something in the record signals a potential problem.
Briarwood commented that the two data elements found to be missing with the highest frequency from referring hospitals are wound status and behavioral status.
2. How are the data shared?
The Wishard Hospital EHR can produce an abstract/clinical summary for patients as they enter an ED. The summary includes the reason for visit, a problem list, medications prescribed (that may or may not match what medications actually are taken), recent dictations available, recent laboratory results, recent radiology results, and immunizations. Advance directives are not part of the summary. An unusual feature of the system is a means by which the ED can update the ED summary and then send it with the patient back to the facility, but updating happens only infrequently.
At Wishards Lockefield Village extended-care facility, the EHR is available to retrieve data and also has integrated provider order entry in part of the facility, which is physically located on the Wishard campus, adjacent and connected to Wishard Hospital. Physicians, physical therapists (PTs), and nurses (RNs) can access information from the hospital prior to transfer and during transfer as needs arise. Some of the MD and RN charting is in the EHR but physical therapists only enter the final note/discharge summary. On Lockefield Village floors without provider order entry, SNF medications are not managed via the EHR. Lockefield Village also provides long-term care, but most of the charting is paper-based and separate from the EHR.
When patients leave the Part A SNF at Lockefield Village, communication with the receiving HHA is via phone and fax. This is an example of the lack of informational continuity of care that the Regenstrief gero-informaticians would like to overcome. Beverly Brookview made a related observation indicating, for example, that patients sent to the emergency department with potential internal bleeding sometimes were returned with the bleeding stopped but without information on what was done during the stay in the emergency room.
Extended Care Information Network (ECIN) is used by some of the referring hospitals, but referrals are largely made based on personal relationships between discharge planners and intake coordinators.
At Briarwood, a paper "standard transfer summary" is prepared when patients are transferred to the ED and a verbal report is called into the ED. This summary includes the reason for transfer, demographics, problem list, medications, allergies, and recent laboratory results.
When patients are discharged from Beverly Brookview to home health, information is printed from their EHR or photocopied from the chart.
The VNS does not share data contained in their MISYS with Wishard Health Services or any other hospital.
3. Timeliness and completeness of the data.
In general, the SNFs and HHA visited indicated that the Indianapolis area hospitals provide relatively complete data at the time of discharge. The exceptions to this would be that behavioral issues, wound assessments, and the other locations in which the patient/resident were recently treated often are missing. For home care, the Primary Care Physician (PCP) information often is not there, making it more time-consuming for the home health agency to locate and interact with the patients primary physician.
The staff at the VNS also mentioned that the discharge summary is faxed to them--if it is coming from the medical side of the hospital it generally has good documentation; if it is coming from the surgical side, the documentation is often incomplete. Their biggest issue, however, is that the discharge summary often is not available at the time of discharge (e.g., the physician having not yet dictated her/his orders).
As observed on other site visits, securing information about potential patients on a timely basis is a high priority task, the successful completion of which often depends on long-standing personal relationships between acute care and long-term care personnel.
4. Specifics about medications, labs, and radiology.
The IHIE Docs4Docs portal provides access across care sites to discharge transcriptions, laboratory results, and radiology. At present, medications have not been configured. The portal is supported financially by the large hospitals in the Indianapolis metro area. Kindred LTAC has access to the IHIE Docs4Docs portal and recently has begun to use it.
For Wishard Hospital patients, 80% of outpatient medications are dispensed from the Wishard-based pharmacies.
Beverly Brookview uses a single pharmacy, Pharmerica, (a national chain). Communications with the pharmacy are via fax. They also contract with a single laboratory, DCL Laboratories. The initial order is faxed, but staff can dial in to get results. The lab results also are provided via fax, but the results are not entered into VistaKeane.
At Briarwood, laboratory tests are ordered via fax and results are received via fax. Pharmacy orders are faxed.
At the VNS, communication with pharmacies is currently by fax; however, this will change once e-prescribing is initiated. Lab results are obtained via fax and placed in a paper chart.
5. Areas under development (e.g., CPOE, decision-making tools).
Beginning January 2, 2007, all prescribing will be electronic in the State of Indiana.
The VNS is exploring a physician portal but this is not imminently available.
The IHIE is working with the Centers for Medicare and Medicaid Services (CMS) to import Medicare claims data (encounters, tests, procedures) that could support multiple efforts including performance measurement reporting. Reportedly, this also would include MDS, OASIS, and Part D data.
Doc4Docs will increase its coverage of regional health care encounter records. Currently, most information comes from the five initial participating hospitals. Aside from the fact that they help provide financial support, their pre-processing (homogenization) of the data makes it easier for Doc4Docs to perform its processing. However, gradually Docs4Docs will start collecting the information from the original source (e.g., a laboratory, instead of from the hospital that ordered the lab test, or from a pharmacy instead of the enterprise that ordered the medication). The portal has regional completeness as a goal for both laboratory results and medications.
6. Barriers to clinical data exchange.
The primary barriers to clinical data exchange identified were the general lack of access to another providers existing electronic health record system, as all sites had some access to the Internet and all sites had at least some level of electronic record keeping. As all sites can support web-access, even if only by (rarely) dial-up, Docs 4 Docs should help reduce this barrier.
The post-acute and long-term care providers were largely unaware of the IHIE initiatives and activities. They have not been invited to join, nor have they initiated joining, largely because of the lack of knowledge that this exchange exists.
7. Facilitators to clinical data exchange.
Referrals from Briarwood to home health often involve an on-site evaluation by the home health liaison who is permitted to collect information concurrently.
At Wishard Hospital, the VNS has a clinical liaison who has access to the EHR. The liaison begins the process of populating the MISYS record using a laptop.
Beverly Brookview has a highly developed manual, paper, and fax-based patient recruiting and admission process supported by two full-time employees (FTEs).
The IHIE is starting to facilitate data exchange, at least with the five major hospitals in the Indianapolis area. These hospitals collect and refine information from a variety of other sources, such as clinical laboratories.
The VNS care providers, often deployed from home, use laptops to upload patient encounter information and to download visit assignments. Currently, care providers tend not to make use of laptops when they are with patients.
All sites make use of HIT to at least some degree, all sites are connected to the Internet (though not all have high-speed connections), and all sites make use today of phone, fax, and paper-based access to remote information.
III. TECHNOLOGY
1. Hardware and software descriptions of the main health delivery system and the affiliated PAC/LTC settings.
The IU (Regenstrief) EHR makes use of commodity servers that run a dialect of MUMPS; order entry via these servers is accessible through hospital Local Area Networks (LANs) by early generation (commodity) PCs running a now obsolete version of Microsoft Windows, or increasingly via Windows-based Citrix sessions for remote deployment and management. Data retrieval via EHR can be accomplished via the older text-based interface or by the web, using common web browsers with a Secure Sockets Layer or Virtual Private Network.
Docs4Docs makes use of a server-based data repository of data loaded from the EHRs of five hospitals; this server is accessible through web-based browsers.
2. Architecture of EHR system at main HDS.
a. Are the sites visited using CHI-endorsed and other HIT content and messaging standards? If so, which ones are they using? Messaging? Vocabulary? Direct care FM?
Except for the use of LOINC in the Indiana Network for Patient Care (INPC), use of CHI-endorsed standards is incidental at all sites (i.e., such standards are used only for regulatory or reimbursement reasons).
b. Description of each EHR system and HIT solution(s) to support HIE.
As described, IU makes use of a legacy, locally developed, MUMPS-based EHR. Beverly Brookview uses VistaKeane; the VNS uses MISYS; and for the present, Briarwood is content to continue to make use of largely paper-based processes.
INPC supports emergency department results retrieval from the EHRs at five hospitals to the emergency departments at the five hospitals; feedback of encounter or summary information from the emergency departments to the relevant remote EHR is not generally implemented.
Docs4Docs permits hospital-associated physicians to retrieve results residing in the EHRs of the five participating hospitals. Often these physicians are associated with more than one hospital or care site.
The nursing homes visited do not yet participate in either the INPC or Docs4Docs, though they might wish to if they had the opportunity.
c. If the sites visited have used "best of breed," how are these different software integrated?
The INPC and Docs4Docs process streams of data from hospital EHRs; sometimes these streams contain HL7v2 messages. No other inter-site integration was observed.
3. Architecture of EHR systems at PAC/LTC (if applicable) and HIT solution(s) to support HIE.
Both INPC and Docs4Docs make use of a central data repository. INPC is accessible from emergency department terminals. Docs4Docs supports web-based access.
4. How are the data stored? Shared? Accessed? Transmitted? Accepted at other setting? Entered?
All data are stored in MUMPS file systems (in the case of IU) or in the proprietary databases of the EHR or other record keeping applications for the other sites. Data from INPC and Docs4Docs make use of evolving messaging and web technologies specifically selected by Docs4Docs developers to be the best near-term solution. While the Docs4Docs application will be a very powerful demonstration of the utility of anytime, anywhere, access, it is not being designed to be a national solution; instead, continued local success and growth is its objective.
5. How are the sites visited tackling any interoperability issues using standards-based EHR systems or other HIT solutions for health information exchange?
Both the INPC20 and IHIE21 make use of HL7v2 messages and LOINC. The remaining aspects of these interoperation solutions make use of pragmatically determined, local best practices.
6. How does electronic health information exchange (e-HIE) vary between affiliated and unaffiliated providers within a single HDS?
The IU and Wishard use a single integrated EHR system. The five major hospitals in Indianapolis participate in the INPC and the IHIE. At present, neither the INPC nor the IHIE are available to NHs.
7. How does e-HIE vary when exchanging to outside entities?
Outside entities must, at present, obtain information from IU and other IHIE hospitals through the traditional methods--fax, paper, and telephone.
IV. ORGANIZATIONAL ISSUES
1. Adoption of EHR systems and Electronic Health Information Exchange with PAC/LTC.
Regenstrief Institute and IU were trailblazers with regard to developing their EHR system, the RMRS (Regenstrief Medical Record System). They established the INPC, which is the cornerstone of the IHIE model for data exchange. The EHR and INPC systems were established well before CHI-standards were selected.
The business case for the IHIE is relatively simple. Physicians and other clinicians value having access to previous encounters because it allows them to provide better care and because it will reduce costs by minimizing the duplication of tests and procedures, and it will enable physicians to determine more accurate diagnoses because they will have a more complete picture of the patients recent medical history.
Today, it is not a major goal for the IHIE to get an EHR into physician offices or post-acute/long-term care settings. The IHIE has plenty of work to do with the current and planned participants in the network, and although our impression is that they would welcome involvement by the PAC/LTC community, they are not going to actively recruit them into the HIE at this time.
For Beverly Enterprises, their EHR system was selected by the corporate office and all 300 facilities are required to use it. Likewise, any interfaces with other systems at the local level (e.g., Indianapolis), would first need to be approved and paid for by the corporate office. The Administrator did note that in vetting the software companies, use of standards was a criterion, which is one reason they selected VistaKeane. However, interoperability with other systems does not appear to be a current feature, or an immediate concern for Beverly Enterprises.
The VNS enjoys the status of being the largest home health agency in the area and is the preferred provider for many feeder hospitals. Interoperable EHR systems have not been a consideration to date, nor does it appear to be a near-future goal for John Pipas and his staff at the VNS.
Briarwood expressed no future plans to improve upon their current MDI software. Interoperability and the exchange of electronic data between their LTC facility and other health settings is not a priority at this time. They would be very happy to receive complete, legible, timely information via fax or phone.
2. Standards Development Organizations
With the exception of faculty and staff at IU, the Regenstrief Institute, and the IHIE, no other group reported being involved in any standards development organizations (SDOs).
V. CONCLUSION/FINAL THOUGHTS
The Indianapolis INPC and IHIE form the leading RHIO in the United States, a lead that may only increase once the IHIE obtains medication information and primary care encounter reports. The coverage of the IHIE appears to be scalable to the region and should achieve this coverage within a few years--at least for area physicians. A critical requirement for the success of the INPC, and later for the IHIE, was the trust originally cultivated by Dr. McDonald that information from one hospital would not be misused by another (e.g., competitive uses). Once this trust was established, the remaining problems were technical, and therefore solvable.
The Regenstrief software and system development paradigm has enabled the timely creation of incremental utility sufficient to produce and sustain Indianapolis current pre-eminent position. When combined with the use of commodity hardware, powerful systems can be built quickly and inexpensively. Were such systems built using current CHI-endorsed standards, they would be a replicable model for RHIOs throughout the country. Regardless, the INPC and IHIE are a model that can raise consciousness nationally regarding what can be accomplished given the organization will and resources to do so.
Finally, a rising tide carries all boats. While the INPC and IHIE are not aimed at nursing homes and/or home care, their success should help these enterprises. The latter are already making local use of HIT and were appropriate standards in place, the cost of connecting to the INPC and IHIE would be modest.
| TABLE E.1: General Information Supplied by Visited Sites* | |||||||
|---|---|---|---|---|---|---|---|
| Name of Health System | Indiana Health Info. Exchange/ Regenstrief Institute | Wishard Health Services | Lockefield Village (Wishard-owned SNF) | Kindred Long-Term Acute Care Hospital | VNS Healthcare System | Beverly Healthcare Brookview | Briarwood Health and Rehab. Center |
| Location | Indianapolis, IN | Indianapolis, IN | Indianapolis, IN | Indianapolis, IN | Indianapolis, IN | Indianapolis, IN | Indianapolis, IN |
| Relationship to Host Site | Host Site | Host Site | Application Demo Site | ||||
| Year established | IHIE Feb 2004 Regenstreif about 35 years ago | 1992 | 1913 | 1967 | 1998 | ||
| Area served (urban, rural, both) | Both | Both | Urban and rural 30 counties | Urban | Urban | ||
| Ownership | Non-profit | Corporately owned | Non-profit, freestanding | For profit, privately held | For profit | ||
| No. full-time employees | 16 IHIE | 113 | 212 FTE | 89 FTE | |||
| No. of Nursing Homes (owned, affiliated) | 0 | 0 owned 7 affiliated | 0 owned 0 affiliated | 0 owned 0 affiliated | 0 owned 14 affiliated | ||
| No. of Home Health Agencies (owned, affiliated) | 0 | 0 | 1 owned 7 preferred providers affiliated | 1 owned 0 affiliated | 0 owned 1 affiliated | ||
| No. of Physician Practices (owned, affiliated) | 0 | 0 | 0 owned 0 affiliated | 0 owned 0 affiliated | 0 owned 0 affiliated | ||
| Are physicians affiliated with health delivery system or are they independent? | n/a | Practicing physicians are with Indiana University | Independent | Independent | Independent | ||
| Inpatient pharmacy? | 0 | Yes | No | No | No | ||
| Does SNF use dedicated pharmacy or contract with large/retail, or multiple pharmacies? | n/a | Unknown | Hospice program contracts with one pharmacy | 1--Pharmerica Pharmacy | Dedicated | ||
| No. of Pharmacies--outpatient | 0 | 0 | 1 | 0 | 0 | ||
| In-house laboratory? | 0 | Yes | No | No | No | ||
| How many outside laboratories? | n/a | Unknown | Minimum of 20 outside labs | 1--DCL Laboratories | 1 | ||
| In-house radiology department? | n/a | Yes | 0 | No | No | ||
| How many outside radiology centers/MR centers do you work with? | 1 or 2 | 1 | 8-12 centers | 1--Mid-West Radiology | 1 | ||
| Percentage of overall budget dedicated to IT? | Not answered | Unknown | 5% | ||||
| Electronic Health Record (EHR) system--scheduling, billing, or claims? | Working towards that throughout the community--many of these services are in place at Regenstrief/ Wishard | 0 | Yes | Yes, EDS | Yes--billing/ claims submission for MDS purposes only | ||
| Clinical Electronic Health Record (EHR) system? | See above | In-house system | Yes | Yes | MDI--for MDS reporting only | ||
| Primary software vendor for electronic health information system (if applicable) | Developed internally | Internal | MISYS Telehealth Honeywell HomMed | VistaKeane | MDI--for MDS purposes only | ||
| Short-term (6 months?) HIE* future plans | Continue expansion of clinical messaging | Continue utilizing current internal system and available community resources | Having an internal EMR set up and interfaced with disease management and telehealth programs. Looking for potential web access by physicians, patients, and families to the telehealth program. | No | No formal plans | ||
| Long-term HIE* future plans | Same as above with further development of clinical quality initiative | Not established | To have web access portal for patient information to be reviewed by physicians | No | No formal plans | ||
| * Information in this table was collected from a General Information About Health Care Setting form sent to all sites prior to the scheduled site visit. | |||||||
NOTES
-
9,000 Bronx residents were admitted to two or more hospitals in 2004, accounting for 30,000 admissions.
-
Website: http://www.health.state.ny.us/funding/rfp/0608071010/questions_and_answ….
-
Website: http://www.qs1.com/qs1home.nsf/Web+Pages/RxCare+Plus?OpenDocument.
-
Website: http://www.ansi.org/standards_activities/standards_boards_panels/hisb/hitsp.aspx?menuid=3.
-
Website: http://www.hospitalmanagement.net/contractors/it/dbmotion/dbmotion3.html.
-
Website: http://intermountainhealthcare.org/xp/public/documents/institute/facult….
-
Website: http://intermountainhealthcare.org/xp/public/physician/help2/learnmore/….
-
Website: http://egems.gehealthcare.com/proom/internet/NewsandEvents.jsp?release_….
-
Website: http://www.rules.utah.gov/publicat/code_rtf/r590-164.rtf.
-
Dr. McDonald has just recently been named the Director of the Lister Hill Center at the National Library of Medicine.
-
As reported by Dr. Overhage, an aggregation of data from different emergency rooms was use to detect a recent outbreak of gastro-intestinal illness caused by food-born bacteria.
-
Website: http://www.regenstrief.org/medinformatics/i3/clinical-care/docs4docs.
-
Website: http://www.tkgnet.com/conference/summer2005/presentations/Clem_McDonald.pdf.