
This Issue Brief describes the extent to which Medicaid beneficiaries with schizophrenia and bipolar disorder in 22 states received evidence-based treatment using 2007 Medicaid claims data. This brief was prepared by Allison Barrett and Jonathan Brown of Mathematica Policy Research. Other members of the research team included Emily Caffery, Kerianne Hourihan, and Henry Ireys. A full report on the findings, which includes technical details on the methodology and further state-specific information, was released in February 2012 and is available from ASPE.
This brief was prepared under contract #HHSP23320095642WC between the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Office of Disability, Aging and Long-Term Care Policy and Mathematica Policy Research. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the ASPE Project Officer, John Drabek, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201, John.Drabek@hhs.gov.
Summary
As the single largest payer of mental health services, Medicaid can promote the delivery of evidence-based practices (EBPs) for individuals with serious and persistent mental illness (SPMI). This study used 2007 Medicaid Analytic eXtract (MAX) data from 22 states to examine the extent to which Medicaid beneficiaries with schizophrenia and bipolar disorder received evidence-based medications, psychosocial services, and physical health care. Although the vast majority of beneficiaries filled at least one prescription for an evidence-based medication, states varied widely in the proportion who maintained a continuous supply of medications and received recommended monitoring of medication levels. Beneficiaries living in states that required copayments or prior authorization for medications were less likely to fill prescriptions regularly. Across all study states, three-quarters of beneficiaries received at least one psychosocial service during the year, but it was difficult to discern from claims whether these services were evidence-based. Only 45 percent of beneficiaries with schizophrenia and 35 percent with bipolar disorder maintained a continuous supply of evidence-based medications and received at least one psychosocial service during the year. The findings suggest that there is much room for improvement in the delivery of evidence-based care for this costly and vulnerable population. This study also demonstrates that claims and encounter data can be used to measure EBP measures and identify populations to target for quality improvement.
Introduction
Medicaid provides critical access to physical and behavioral health care for beneficiaries with SPMIs. These individuals can live successfully in the community and avoid costly emergency and inpatient care with the assistance of EBPs, which include medications, psychosocial services, and physical health care. Because Medicaid pays for more mental health services than any other public or private payer in the nation, the program can influence the quality of care received by beneficiaries with SPMI by promoting providers use of EBPs through incentives and reimbursement policies.
Despite Medicaids importance in financing mental health care, few studies have systematically examined the extent to which beneficiaries with SPMI receive EBPs across states. As a result, policymakers, state mental health commissioners, providers, consumer groups, and other stakeholders lack important information on state variation in EBP receipt--information they could use to improve the quality of mental health care in their state. Such information can also shape quality improvement efforts by identifying factors that facilitate or impede the receipt of EBPs.
This issue brief presents findings from a study in which Medicaid claims data were used to investigate the receipt of EBPs in 22 states in 2007. The study focused on adult beneficiaries with schizophrenia and bipolar disorder, a segment of the SPMI population for whom there is a strong evidence base regarding treatment. The brief reports on the proportion of beneficiaries with schizophrenia and bipolar disorder who received EBPs in 2007, describes the state variation in the receipt of EBPs, and concludes with recommendations for policymakers, state Medicaid and mental health officials, and other stakeholders who are interested in increasing the receipt of EBPs by beneficiaries with SPMI.
How Many Medicaid Beneficiaries Receive EBPs?
In all states combined, 90 percent of beneficiaries--including 92 percent of those with schizophrenia and 87 percent with bipolar disorder--filled a prescription for an evidence-based medication at least once in 2007.1 However, continuous use of these medications was less common. Among beneficiaries who received any evidence-based medication, only 61 percent used it continuously.2 Beneficiaries with schizophrenia were more likely than those with bipolar disorder to use these medications continuously (64 percent compared with 54 percent).
Some medications for bipolar disorder should be regularly monitored through laboratory tests to ensure that the dose is appropriate and toxicity is avoided. In the study population, 66 percent of beneficiaries who filled a prescription for lithium received a blood level monitoring test during the year (Table 1). Rates of monitoring anticonvulsants were lower: only 54 percent of valproate users and 49 percent of carbamazepine users were monitored.
Certain antipsychotics that treat both schizophrenia and bipolar disorder can increase the risk for diabetes and cardiovascular disease. Less than half of all beneficiaries who filled a prescription for antipsychotics in 2007 were screened for metabolic side effects or cardiovascular disease: 43 were screened for cardiovascular disease through cholesterol testing, and 13 percent were screened for diabetes through glucose testing.3
| Proportion of Beneficiaries in Study Receiving EBP (%) | |
|---|---|
| SOURCE: Medicaid Analytic eXtract (MAX) data in 22 states.
| |
| Evidence-based medications | |
| Any evidence-based medication | 90.2 |
| Continuous use of evidence-based medication | 61.4 |
| Medication monitoring | |
| Blood test to monitor lithium levela,b | 66.2 |
| Blood test to monitor valproate levela,b | 53.8 |
| Blood test to monitor carbamazepine levela,b | 49.5 |
| Cholesterol test, among users of antipsychoticsb | 43.1 |
| Glucose test, among users of antipsychoticsb | 12.7 |
| Preventive physical health care | |
| Physical health exam or behavior counselingb | 12.8 |
| Physical health exam, behavior counseling, or cancer screeningb | 30.4 |
| Psychosocial services | |
| Any psychosocial service | 76.4 |
| Identifiable psychosocial EBPc | 59.0 |
In light of evidence that individuals with schizophrenia or bipolar disorder die one to two decades earlier than the general population, it is particularly important that they receive basic preventive health services.4 Premature death among this population is related to their increased prevalence of cardiovascular disease and diabetes brought on by illness-related or genetic risk factors, obesity, smoking or other unhealthy behaviors, and side effects of certain antipsychotic medications.5 While some research suggests that Medicaid beneficiaries are about as likely as those with private insurance to receive a preventive physical health exam, less than one quarter of adults in each group receive an annual exam.6 In addition, there is some limited evidence that older women with schizophrenia are one-quarter to one-third less likely than women without schizophrenia to receive guideline-concordant screenings for breast and cervical cancer.7
Despite the importance of basic preventive health services for this population, only 12 percent of beneficiaries with schizophrenia or bipolar disorder received a comprehensive physical examination or health counseling in 2007. Expanding the definition to include certain recommended cancer screenings increased the proportion of beneficiaries receiving basic preventive health services to 30 percent.8
Psychosocial services play an important role in helping beneficiaries with SPMI live successfully in the community and manage their symptoms and medication side effects. These services include a range of supports and therapies that vary considerably in their structure and duration. According to the literature, services considered to be psychosocial EBPs for schizophrenia and bipolar disorder include individual or group psychotherapy, cognitive behavioral therapy (CBT), family therapy or psychoeducation, Assertive Community Treatment (ACT), skills training, and supported employment.
Over three-quarters (76 percent) of beneficiaries had a claim for some type of psychosocial service in 2007.9 However, the exact nature of these services was sometimes unclear in the claims data. Some claims were identifiable as specific evidence-based treatments, but others were for nonspecific psychosocial services that may or may not be EBPs.10 Fifty-nine percent of beneficiaries had an identifiable claim for a psychosocial EBP during the year, typically for psychotherapy. Less than 5 percent of beneficiaries had an identifiable claim for ACT, family therapy, or skills training, and virtually no beneficiaries had an identifiable claim for CBT or supported employment. This may be in part a result of states using nonspecific billing codes for these services.
How Many Medicaid Beneficiaries Receive Most or All Recommended EBPs?
Although a substantial percentage of beneficiaries received at least one EBP, few received the full complement of evidence-based pharmacological and psychosocial services. Only 45 percent of beneficiaries with schizophrenia and 35 percent of beneficiaries with bipolar disorder received both a continuous supply of evidence-based medication and at least one psychosocial service in 2007 (Figure 1). Only 5 percent received these EBPs as well as laboratory monitoring of medication levels and screening for common physical complications.
FIGURE 1. Receipt of Multiple EBPs by Medicaid Beneficiaries with Schizophrenia and Bipolar Disorder, 2007
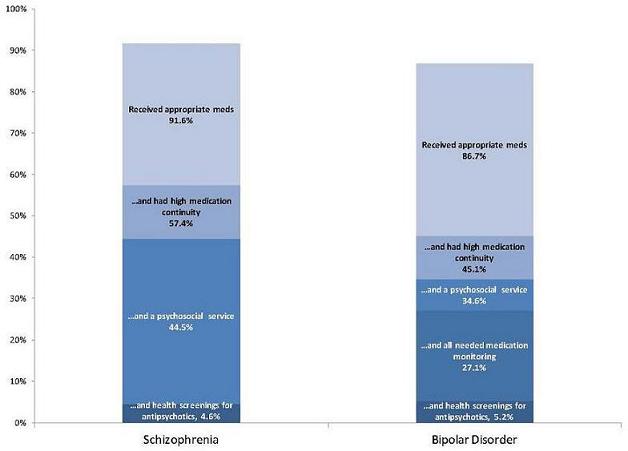
SOURCE: Medicaid Analytic eXtract (MAX) data in 22 states.
NOTES: Psychosocial services include any ambulatory mental health visit for a reason other than screening, assessment, or medication administration or management. Medication monitoring was only measured among users of lithium, valproate, or carbamazepine, and health screenings for antipsychotics was only measured among users of antipsychotics. Data from Maryland was excluded from the measures of medication monitoring and health screenings due to missing encounter data for physical health services.
Does the Receipt of EBPs Vary Across States?
In all 22 study states, the rate of using at least one evidence-based medication was consistently high (above 80 percent), while the rate of receiving preventive physical health services was consistently low (below 40 percent). However, the rates of continuous medication use, medication monitoring, and psychosocial services varied greatly from one state to the next. This may reflect differences in the demographics of the Medicaid population, in the structure or orientation of service systems, or in Medicaid policies and practices that could limit access to some EBPs.
The proportion of beneficiaries with schizophrenia or bipolar disorder who continuously used an evidence-based medication throughout 2007 ranged from a low of 45 percent in the District of Columbia to more than 81 percent in North Dakota. This variation was not driven by differences in the likelihood of being prescribed an evidence-based medication (Figure 2): in every state, more than 80 percent of beneficiaries filled at least one prescription for an appropriate medication. Rather, the variation resulted from the fact that beneficiaries in states with low rates of medication continuity were more likely to refill these prescriptions sporadically or not at all.
Underlying differences in the characteristics of Medicaid enrollees explain some state variation in medication continuity. While the proportion of beneficiaries who were female or older varied between states, this variation had little effect on medication continuity rates. However, many of the states with the lowest rates of medication continuity had a higher-than-average proportion of African-American beneficiaries, who are less likely to use medications continuously. After adjusting the medication continuity rates to account for these differences in race and ethnicity,11 some states such as Louisiana and Maryland had rates close to the overall average. Other states such as the District of Columbia, Georgia, and Mississippi remained significantly below average. Even after adjusting rates to account for race and ethnicity, states with below average rates of medication continuity remained below average, indicating that differences in medication continuity are not fully explained by demographic differences between states.
Some Medicaid policies were associated with the likelihood that beneficiaries used medication continuously. Controlling for demographic characteristics and enrollment in a health maintenance organization (HMO), beneficiaries with schizophrenia living in states that required $2 or $3 copayments for preferred or generic drugs were significantly less likely to use antipsychotics continuously compared with beneficiaries living in states that did not require a copayment.12 For example, a beneficiary living in a state with no medication copayments who had a 70 percent probability of using antipsychotics continuously given his age, race, and co-occurring conditions, would have only a 63 percent likelihood of continuously using antipsychotics if he lived in a state that was otherwise similar but required medication copayments of $3. Living in a state that required prior authorization for antipsychotics was also inversely associated with the likelihood of using antipsychotics continuously.
FIGURE 2. Gap Between Proportion of Medicaid Beneficiaries with Continuous Use and Any Use of Evidence-Based Medications, by State
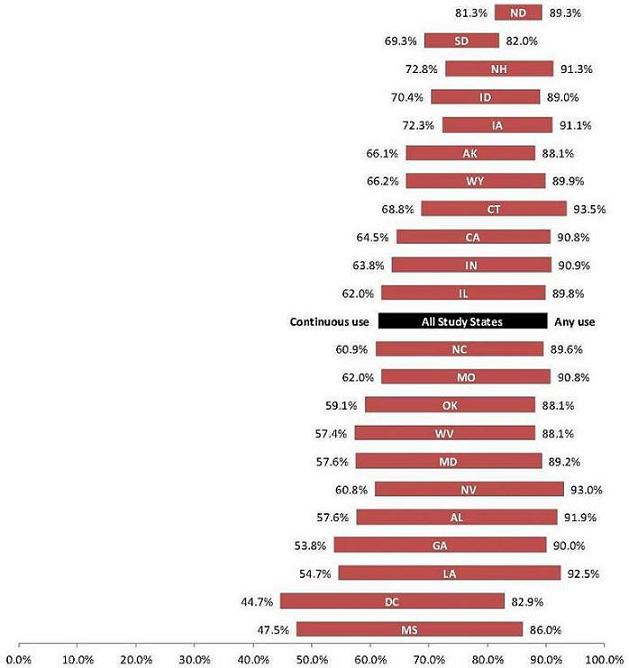
SOURCE: Medicaid Analytic eXtract (MAX) data in 22 states.
NOTES: Any use of appropriate medications includes antipsychotics for schizophrenia and antipsychotics, lithium, valproate, carbamazepine, or lamotrigine for bipolar disorder. Continuous use of appropriate medications is defined as a medication possession ratio of 0.8 or higher.
Beneficiaries with bipolar disorder living in states that required prior authorization for one or more class of mental health drugs (antipsychotics, antidepressants, or anticonvulsants) were less likely to use evidence-based medications continuously, although this finding was only marginally statistically significant. Each additional prior authorization requirement was associated with a lower likelihood that a beneficiary would continuously use an evidence-based medication.
Since it was difficult to measure all state policies that may affect medication continuity, these results must be interpreted with caution. It is possible that higher copayment amounts and prior authorization policies are associated with other unmeasured policies or state characteristics that influence the likelihood of a beneficiary continuously using medication. Further analysis is needed to understand how the complex interaction of Medicaid policies and service system characteristics affect the likelihood that beneficiaries maintain continuous access to evidence-based medications.
There was a two to three-fold difference between states with the lowest and highest rates of medication monitoring for lithium and evidence-based anticonvulsants (carbamazepine and valproate). In states with the lowest rates, only one-fifth to one-third of medication users had their medication levels monitored in 2007, depending on the medication (Table 2). In most states, 65-80 percent of lithium users were monitored, as were 45-65 percent of valproate users, and 40-60 percent of carbamazepine users.
| State | Percent of Anticonvulsant UsersReceiving Medication Monitoring | Percent of Antipsychotic UsersReceiving Side Effect Screening | |||
|---|---|---|---|---|---|
| Lithium Users | Valproate Users | Carbamazepine Users | Cholesterol Screening | Glucose Screening | |
| SOURCE: MAX data, calendar year 2007 NOTE: Data from Maryland is not displayed, as very low rates of medication monitoring and health screenings may be a result of missing laboratory encounter data for HMO enrollees. Rates are not displayed when fewer than ten beneficiaries used the medication in 2007. | |||||
| AK | 45.0 | 35.3 | n.r. | 33.5 | 8.6 |
| AL | 67.5 | 58.9 | 52.4 | 43.6 | 15.8 |
| CA | 64.6 | 52.6 | 50.4 | 52.4 | 13.3 |
| CT | 79.3 | 60.6 | 47.6 | 40.1 | 29.7 |
| DC | 35.1 | 30.8 | 30.8 | 44.7 | 5.6 |
| GA | 71.8 | 59.3 | 48.2 | 9.1 | 5.7 |
| ID | 75.5 | 52.6 | 41.9 | 47.2 | 9.0 |
| IL | 47.2 | 37.0 | 41.0 | 24.2 | 9.6 |
| IN | 69.5 | 66.1 | 52.6 | 47.3 | 18.5 |
| IA | 77.2 | 66.0 | 32.1 | 41.1 | 20.2 |
| LA | 78.0 | 64.0 | 66.0 | 47.0 | 12.8 |
| MD | n.r. | n.r. | n.r. | n.r. | n.r. |
| MS | 69.2 | 59.2 | 50.0 | 39.2 | 11.8 |
| MO | 64.3 | 54.6 | 44.4 | 43.0 | 9.8 |
| NC | 74.6 | 64.8 | 61.7 | 52.4 | 11.1 |
| ND | 50.0 | 83.3 | n.r. | 60.0 | 22.4 |
| NH | 91.2 | 75.4 | 46.7 | 58.6 | 22.5 |
| NV | 47.5 | 49.5 | 43.5 | 42.9 | 8.9 |
| OK | 64.7 | 49.0 | 55.6 | 39.0 | 12.9 |
| SD | 69.2 | 47.4 | n.r. | 45.2 | 25.2 |
| WV | 73.1 | 63.4 | 57.9 | 49.8 | 13.0 |
| WY | 71.4 | 58.3 | n.r. | 33.5 | 4.8 |
There was a six-fold difference between states with the highest and lowest rates of cardiovascular and glucose screening for antipsychotic users. Except for a few states with low rates, 40-60 percent of beneficiaries who used antipsychotic medications were screened for cardiovascular disease with a cholesterol test in 2007. Rates of glucose screening among these beneficiaries were much lower, ranging from 5 percent to 30 percent depending on the state.
In every state, less than one-third of beneficiaries with schizophrenia or bipolar disorder received a comprehensive health examination or preventive health counseling. In three states, less than 5 percent of beneficiaries received one of these basic physical health services. Even when certain cancer screenings (mammograms, colonoscopies, and Pap smears) were included, only 25-40 percent of beneficiaries with SPMI in a given state received a preventive physical health service in 2007.
The proportion of beneficiaries who received any psychosocial services in 2007 varied from 46 percent to 88 percent (Figure 3). Less than half received any psychosocial service in North Dakota and Connecticut, while in 12 other states, more than three-quarters of beneficiaries received some type of psychosocial service. Differences in state billing codes for psychosocial services prevent comparison of the receipt of specific evidence-based psychosocial services across states.
FIGURE 3. Proportion of Beneficiaries with Schizophrenia or Bipolar Disorder who Received Any Psychosocial Service, by State, 2007
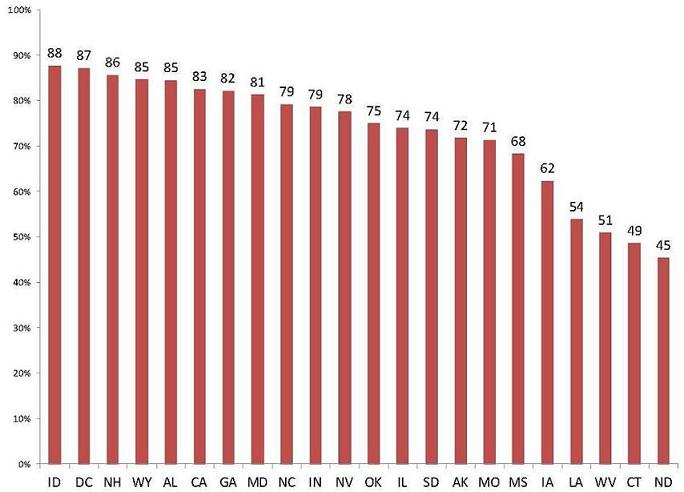
SOURCE: Medicaid Analytic eXtract (MAX) data in 22 states.
The proportion of beneficiaries who received multiple EBPs also varied widely (Table 3): nearly twice as many beneficiaries with schizophrenia and bipolar disorder were continuously using an evidence-based medication in the state with the highest rate compared to the lowest rate (72 percent versus 35 percent). Similarly, the proportion of beneficiaries continuously using an evidence-based medication and receiving at least one psychosocial service ranged from 24 percent to 55 percent of beneficiaries. However, the proportion of beneficiaries who received these services plus medication monitoring or screening for common physical side effects was uniformly low: no more than 15 percent of beneficiaries in any state.
| State | Received an Appropriate Medication | and had High Medication Continuity | and Received at Least One Psychosocial Service | and Received Medication Level Monitoringa | and Received Screening for Medication Side Effectsb |
|---|---|---|---|---|---|
| SOURCE: MAX data, calendar year 2007 NOTES: Data on medication monitoring and health screenings is not displayed for Maryland, as very low rates of medication monitoring and health screenings may be a result of missing laboratory encounter data for HMO enrollees.
| |||||
| AK | 88.1 | 57.4 | 44.6 | 41.1 | 3.7 |
| AL | 91.9 | 51.9 | 46.5 | 44.8 | 7.7 |
| CA | 90.8 | 57.3 | 47.2 | 45.3 | 6.2 |
| CT | 93.5 | 63.3 | 31.5 | 30.5 | 6.0 |
| DC | 82.9 | 35.4 | 32.6 | 31.0 | 1.4 |
| GA | 90.0 | 46.7 | 39.2 | 38.0 | 0.9 |
| IA | 91.1 | 65.1 | 40.9 | 39.2 | 8.6 |
| ID | 89.0 | 61.1 | 55.1 | 52.1 | 5.8 |
| IL | 89.8 | 54.2 | 39.8 | 37.0 | 2.0 |
| IN | 90.9 | 56.3 | 45.0 | 42.9 | 8.3 |
| LA | 92.5 | 48.7 | 28.0 | 27.1 | 4.5 |
| MD | 89.2 | 49.8 | 41.9 | n.r. | n.r. |
| MO | 90.8 | 54.6 | 39.1 | 35.9 | 4.7 |
| MS | 86.0 | 39.5 | 27.7 | 27.1 | 3.0 |
| NC | 89.6 | 53.0 | 42.3 | 40.8 | 5.3 |
| ND | 89.3 | 71.8 | 31.6 | 30.6 | 8.6 |
| NH | 91.3 | 64.7 | 54.6 | 53.5 | 12.4 |
| NV | 93.0 | 56.1 | 45.7 | 43.0 | 5.7 |
| OK | 88.1 | 50.6 | 38.7 | 36.6 | 4.8 |
| SD | 82.0 | 55.9 | 45.6 | 44.1 | 13.5 |
| WV | 88.1 | 48.9 | 24.4 | 22.6 | 4.2 |
| WY | 89.9 | 58.6 | 49.8 | 46.7 | 2.2 |
How Can States Improve the Receipt of EBPs?
The findings underscore the need to improve the receipt of EBPs among Medicaid beneficiaries with SPMI. These beneficiaries make up a relatively small proportion of each states Medicaid population, but have complex and costly needs: total Medicaid spending on the population in this study averaged $26,119 per year, compared with $5,337 for the Medicaid population as a whole.13 While the study found that most beneficiaries with schizophrenia or bipolar disorder received an evidence-based medication in 2007, in many states the continuous use of those medications was poor. Many beneficiaries taking antipsychotics, lithium, and anticonvulsants did not receive recommended monitoring of medication levels and side effects. In some states, nearly half of all beneficiaries did not receive any psychosocial service. Few beneficiaries received basic preventive physical health services.
Medicaid agencies, state mental health agencies, state and federal policymakers, and other stakeholders may wish to consider the following opportunities to improve the quality of care for Medicaid beneficiaries with SPMI:
-
Foster further efforts to integrate mental health, physical health, and substance abuse services for Medicaid beneficiaries with SPMI. All adults should receive preventive physical health services, but those with SPMI in particular need regular health screenings because of the potential for medication side effects. Some Medicaid agencies are taking steps to improve the delivery of physical health services to beneficiaries with SPMI by removing restrictions on same day billing for mental health and physical health services and by creating billing codes specifically to support integrated physical behavioral health care.14 Other Medicaid agencies have adopted Health and Behavior Assessment and Intervention (HBAI) codes, which provide a mechanism to bill for services that address the psychological, emotional, behavioral, and cognitive factors that affect physical health.15 At the same time, some Medicaid agencies and managed care organizations have developed promising strategies for coordinating and integrating physical and behavioral health care.16 The Center for Integrated Health Solutions17 and the Integrated Care Resource Center18 can provide Medicaid programs and mental health systems technical assistance with integrating physical and behavioral health care. Resources to help states and providers better integrate services and deliver EBPs such as integrated treatment for co-occurring substance use disorders, ACT, supported employment, and family psychoeducation are available through the EBP Tool Kit from the Substance Abuse and Mental Health Services Administration (SAMHSA).
-
Improve the delivery of evidence-based psychosocial services. In some states, 25-50 percent of beneficiaries did not receive any psychosocial services; in other states, the majority of beneficiaries received these services, but the degree to which they were consistent with EBPs is unclear. There were few or no claims for certain psychosocial EBPs in many states, including ACT, CBT, family therapy, skills training, and supported employment, but this may reflect nonspecific mental health billing codes. States may want to examine the extent to which the psychosocial services being reimbursed are consistent with the latest EBPs. States may also want to find ways not only to motivate providers to deliver EBPs, but also to maintain fidelity to proven models through provider certification or other mechanisms. Finally, there may be a need for some states to either adopt national CPT and Healthcare Common Procedure Coding System (HCPCS) codes or develop their own billing codes for psychosocial EPBs to facilitate the accurate tracking and monitoring of these services.
-
Consider whether certain Medicaid policies and practices impede care. As states refine their Medicaid benefit packages in light of continuing budget pressures and federal health care reform, they may want to consider eliminating policies that might impede the receipt of EBPs. Although this study could not measure every factor associated with the receipt of EBPs, the findings indicate that in states with higher copayments and more stringent prior authorization requirements, the rate of continuous medication use was lower. It is not clear from the data available for this study whether lower rates of medication continuity are caused by these policies. However, given that low rates of medication continuity are associated with relapse and costly hospitalizations among individuals with SPMI,19 states may consider exempting these beneficiaries or certain medications from policiesthat limit the circumstances under which a treatment is eligible for reimbursement. In addition, states may wish to closely consider the potential harms to this population of other restrictive medication policies, such as fail-first policies and medication quantity or refill limits.
-
Use claims and enrollment data to monitor quality of care. State and federal agencies should continue to monitor the quality of care for Medicaid beneficiaries with SPMI. The National Behavioral Health Quality Framework, developed by SAMHSA, establishes priorities for improving the accessibility, quality, and outcomes of behavioral health services. Medicaid claims data are valuable not only in tracking progress toward the goals of the quality framework, but also in determining whether certain subgroups of beneficiaries receive inadequate care. States could use claims data to track such differences and take steps to address them. Nonetheless, the completeness and reliability of Medicaid claims data varies by state. Those that do not have the billing codes to track certain services, particularly psychosocial EBPs, may need to enhance their data to make it sufficient for monitoring the receipt of services.
Too few Medicaid beneficiaries with SPMI receive the medications, psychosocial services, and physical health care needed to support their ability to live independently, maintain employment, and prevent a relapse. For Medicaid programs and state mental health agencies, the findings from this study can be a starting point for a closer look at the factors within their state that are associated with the receipt of EBPs. For federal and state policymakers, the findings can serve as a baseline from which they can assess progress towards the broader use of EBPs.
Study Methodology
This issue brief is based on analysis of MAX enrollment and claims files from 2007. The study population includes all adult Medicaid beneficiaries (aged 18-64) who qualified for full benefits on the basis of disability, were continuously enrolled for at least 10 months, and had at least one inpatient or two outpatient diagnoses of bipolar disorder or schizophrenia. Medicaid beneficiaries who were also enrolled in Medicare or private insurance were excluded from the study. In total, the study population included 143,710 beneficiaries in 22 states (Alaska, Alabama, California, Connecticut, District of Columbia, Georgia, Iowa, Idaho, Illinois, Indiana, Louisiana, Maryland, Missouri, Mississippi, North Carolina, North Dakota, New Hampshire, Nevada, Oklahoma, South Dakota, West Virginia, and Wyoming). Other states were not included in the study due to missing or incomplete claims or encounter data for physical or mental health services, as often occurs in states with high rates of managed care enrollment. Further details on the study methodology, including EBP measure specifications, are available in the full report.
Notes
-
Any antipsychotic was considered an evidence-based medication for schizophrenia. Antipsychotics, lithium, and three anticonvulsants (valproate, carbamazepine, and lamotrigine) were considered evidence-based medications for bipolar disorder.
-
Continuous use is defined as a medication possession ratio of 0.8 or higher, which occurs when a beneficiary refills a prescription often enough to have the medication on-hand for at least 80 percent of the days following their first prescription fill. With claims data, actual medication use cannot be observed but rather is inferred from the pattern of prescription fills and refills.
-
Maryland was excluded from the measures of cardiovascular and diabetes screening, and of lithium and anticonvulsant monitoring, because relevant managed care encounter data may have been missing from the 2007 MAX data.
-
Laursen, T.M. (2011). Life Expectancy Among Persons with Schizophrenia or Bipolar Affective Disorder. Schizophrenia Research, vol., 131, pp. 101-104.
-
Fleischhacker, W.W., M. Cetkovich-Bakmas, M. De Hert, C.H., Hennekens et al., (2008). Comorbid Somatic Illnesses in Patients with Severe Mental Disorders: Clinical, Policy, and Research Challenges. Journal of Clinical Psychiatry, vol. 69, no. 4, pp. 514-519.
-
Mehrotra, A., A.M. Zaslavsky, J. Z. Ayanian. (2007). Preventive Health Examinations and Preventive Gynecological Examinations in the United States. Archives of Internal Medicine, vol. 167, no. 17, pp. 1876-1883.
-
Lindamer, L.A., D.C. Buse, L. Auslander, J. Unutzer, S.J. Bartels, and D.B. Jeste. (2003). A Comparison of Gynecological Variables and Services Use Among Older Women With and Without Schizophrenia. Psychiatric Services, vol. 54, no. 6, pp. 902-904.
-
Recommended cancer screenings include tests for cervical cancer, breast cancer, and colorectal cancer.
-
Psychosocial services include any ambulatory mental health visits for a reason other than screening, assessment, and medication administration or management. These services include psychosocial EBPs as well as other treatment.
-
It is difficult to identify evidence-based psychosocial services in Medicaid claims because many state Medicaid programs have developed unique billing codes which are often nonspecific. For example, one state may use a billing code that provides reimbursement specifically for ACT, while another state may use a billing code for community support services to reimburse ACT. In addition, psychosocial EBPs may be billed and paid as part of a larger bundled mental health service. For example, in some states, a beneficiary could receive CBT during as part of a set of services billed as a partial hospitalization visit.
-
Medication continuity rates were adjusted using direct standardization to account to differences in the race and ethnicity of beneficiaries in each state. These adjusted rates use the observed rates of high medication continuity for each racial or ethnic group in the state, but apply the rates to a population with the same demographic composition as the entire study population in all 22 states. The adjusted rate reflects the medication continuity rate the state would have been expected to have if its beneficiaries had more closely resembled the entire study population.
-
The states Medicaid medication policies and practices, including prior authorization, copayment requirements, medication quantity and refill limits come from the National Pharmaceutical Council (2008). Pharmaceutical Benefits Under State Medical Assistance Programs, 2007. The full regression models are presented in the final report, available from ASPE.
-
Beneficiaries enrolled in managed care were excluded from the calculation of average Medicaid costs for the study population, as data on payments made to managed care programs is incomplete. The average per beneficiary spending for all states is for fiscal year 2008 from Kaiser State Health Facts, available at http://statehealthfacts.org/comparemaptable.jsp?ind=183&cat=4.
-
Available at http://www.integration.samhsa.gov/financing/billing-tools.
-
Available at http://www.integration.samhsa.gov/financing/Maine_Health_code.pdf.
-
Available A., Verdier, J., & Au. M. (2011). State options for integrating physical and behavioral health care. Integrated Care Resource Center. Available: http://www.integratedcareresourcecenter.com/pdfs/ICRC_BH_Briefing_document_1006.pdf.
-
Available at http://www.thenationalcouncil.org/cs/center_for_integrated_health_solutions.
-
West et al. (2010). Medicaid medication access problems and increased psychiatric hospital and emergency care. General Hospital Psychiatry, 32(6), 1-10.
Evidence-Based Practices for Medicaid Beneficiaries with Schizophrenia and Bipolar Disorder
Executive Summary http://aspe.hhs.gov/daltcp/reports/2012/ebpsbdes.shtml
Full HTML Version http://aspe.hhs.gov/daltcp/reports/2012/ebpsbd.shtml
Full PDF Version http://aspe.hhs.gov/daltcp/reports/2012/ebpsbdes.pdf
Evidence-Based Treatment for Schizophrenia and Bipolar Disorder in State Medicaid Programs: Issue Brief
Full HTML Version http://aspe.hhs.gov/daltcp/reports/2012/sbpdIB.shtml
Full PDF Version http://aspe.hhs.gov/daltcp/reports/2012/sbpdIB.pdf
To obtain a printed copy of this report, send the full report title and your mailing information to:
U.S. Department of Health and Human ServicesOffice of Disability, Aging and Long-Term Care PolicyRoom 424E, H.H. Humphrey Building200 Independence Avenue, S.W.Washington, D.C. 20201FAX: 202-401-7733Email: webmaster.DALTCP@hhs.gov