
June 1, 2021
Link to Printer Friendly Version in PDF Format (66 PDF pages)
ABSTRACT: The COVID-19 pandemic has affected home care agencies--including home health agencies--and their staff in several important ways. Some of the challenges encountered were entirely new and resulted directly from the pandemic. In other cases, the pandemic worsened long-standing challenges in the industry. States and the federal government addressed some of these issues through changes to policies, regulations, and guidance. Home care agencies also responded with changes to their own policies and practices. The purpose of this study was to understand the challenges faced by home care (including home health) agencies due to the COVID-19 pandemic and the policies and practices put into place by the federal government, state governments, and home care agencies themselves to mitigate these challenges through a 50-state scan and interviews with stakeholders. This brief summarizes the overall findings of the study. The appendices summarize the findings from interviews with stakeholders, and summarize findings related to state and federal policy changes implemented due to COVID.
This report was prepared under contract #HHSP233201500039I between HHS's ASPE/BHDAP and RTI International. For additional information about this subject, you can visit the BHDAP home page at https://aspe.hhs.gov/bhdap or contact the ASPE Project Officers, at HHS/ASPE/BHDAP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201; Judith.Dey@hhs.gov, William.Haltermann@hhs.gov, Iara.Oliveira@hhs.gov, Marie.Squillace@hhs.gov.
DISCLAIMER: The opinions and views expressed in this report are those of the authors. They do not reflect the views of the Department of Health and Human Services, the contractor or any other funding organization. This report was completed and submitted on March 2, 2021.
TABLE OF CONTENTS
- Research Question 1
- Research Question 2
- Research Question 3
- Research Question 4
- Research Question 5
APPENDICES
- APPENDIX A. Interview Summary Report
- APPENDIX B. State and Federal Policy Tracker
LIST OF FIGURES
- FIGURE 1: State Policy Changes Related to Increased Medicaid Payment Rates to Home Care Agencies or Workers
- FIGURE 2: State Policy Changes Related to Employment Requirements and Qualifications for Home Care Workers
- FIGURE 3: State Policy Changes Allowing Payment to Family Caregivers
ACRONYMS
The following acronyms are mentioned in this report and appendices.
| ASPE | Office of the Assistant Secretary for Planning and Evaluation |
|---|---|
| CARES Act | Coronavirus Aid, Relief, and Economic Security Act |
| CDC | Centers for Disease Control and Prevention |
| CHC | Community HealthChoices |
| CMS | Centers for Medicare & Medicaid Services |
| COVID-19 | Novel Coronavirus 2019 |
| CPR | Cardiopulmonary Resuscitation |
| DCW | Direct Care Worker |
| FFCRA | Families First Coronavirus Relief Act |
| FTE | Full-Time Equivalent |
| GED | General Equivalency Diploma |
| HCBS | Home and Community-Based Services |
| HH | Home Health |
| HHA | Home Health Agency |
| IDD | Intellectual and Developmental Disability |
| KFF | Kaiser Family Foundation |
| LPN | Licensed Practical Nurse |
| LTC | Long-Term Care |
| MCO | Managed Care Organization |
| NASHP | National Academy for State Health Policy |
| OAA | Older Americans Act |
| OBRA | Omnibus Budget Reconciliation Act |
| OT | Occupational Therapist |
| PAS | Personal Assistance Services |
| PCS | Personal Care Service |
| PPE | Personal Protective Equipment |
| PPP | Paycheck Protection Program |
| PT | Physical Therapist |
| RN | Registered Nurse |
| RTI | RTI International |
| SLP | Speech-Language Pathologist |
| TB | Tuberculosis |
INTRODUCTION
The COVID-19 pandemic has affected home care agencies -- including home health agencies -- and their staff in several important ways. Some of the challenges encountered were entirely new and resulted directly from the pandemic. In other cases, the pandemic worsened long-standing challenges in the industry. States and the Federal Government addressed some of these issues through changes to policies, regulations, and guidance. Home care agencies also responded with changes to their own policies and practices.
|
KEY POINTS
|
BACKGROUND
In 2019, there were approximately 2.3 million home care workers in the United States.[1] Home care and home health agencies (HHAs) provide services and supports that help individuals remain safely in their homes. Home health refers to clinical services provided in the home, such as occupational therapy, physical therapy, and nursing, as well as personal care assistance services from aides that may supplement the necessary clinical care. These services are funded through both Medicare and Medicaid. There are about 12,000 Medicare-certified HHAs in the United States.[2]Home care, on the other hand, refers primarily to non-clinical services, such as personal care, supervision and companion care, meal preparation, and transportation. Home care is not paid for by Medicare and is optionally funded by state Medicaid plans or through private-pay. No data are available about the number of home care agencies in the United States.
|
For the purposes of this brief, we use the term "home care" to include workers and agencies in both home care and home health unless information is specific to one or the other. |
The COVID-19 pandemic is reshaping the provision of home care services and policy. Similar to nursing homes during the COVID-19 pandemic,[3] staffing shortages, increased risk of infection due to a lack of access to personal protective equipment (PPE), and inadequate training have all led to infection control concerns for home care agencies and their staff.[4] In addition, early reporting suggested consumers might abstain from care due to fear of infection, which would decrease agency census and impact their financial sustainability. Staff were leaving employment, recruiting new staff was difficult, and agencies had to scramble to secure supplies and develop new training and protocols.[5] More recent reports have highlighted how home care agencies have rebounded and are now viewed as an important means for reducing institutional care and preventing hospitalizations.[6] However, it remains unclear whether the industry is prepared for the volume of workers needed, both during and beyond the pandemic.
The purpose of this study was to understand the challenges faced by home care (including home health) agencies due to the COVID-19 pandemic and the policies and practices put into place by the Federal Government, state governments, and home care agencies themselves to mitigate these challenges. The five research questions shown below guided this work.
This study included a scan of federal and state policy changes enacted during the pandemic from March through December 2020, a scan of home care agency practices described in media reports, peer-reviewed literature, and grey literature focused on responses to workforce challenges encountered during the pandemic, and interviews with a variety of stakeholders. For the federal and state policy review, we identified federal and state stimulus packages, laws, regulations, policies, and practices designed to help home care agencies during the COVID-19 pandemic, with particular attention to policies that address workforce issues. To identify federal policies, we reviewed Centers for Medicare & Medicaid Services (CMS), Centers for Disease Control and Prevention (CDC), U.S. Department of Labor, and Coronavirus Aid, Relief, and Economic Security (CARES) Act guidance. To identify state policies, we reviewed three secondary sources that previously had documented state Medicaid policy changes that may affect home care agencies or their workforce[7, 8, 9] and scanned all state home care and HHA licensing websites for any COVID-19 specific guidance related to the workforce.
|
Research Questions
|
To understand how home care agencies have been addressing workforce challenges during the pandemic, we conducted a scan of media and industry reports, journal articles, and other grey literature. We considered results from March 2020 through December 2020. For the peer-reviewed literature, we used key search terms to identify relevant articles and reviewed abstracts to determine if the full text of the article should be reviewed. We used similar methods to identify and categorize information from the grey literature and media reports. The primary sources were Home Health Care News, Kaiser Family Foundation, LeadingAge, and PHI National, as well as ADvancing States' Home and Community Based Services Conference (December 2020).
After completing the scans, RTI conducted interviews with 25 key stakeholders across three categories -- home care and HHAs, advocacy groups representing these agencies or their workers, and government representatives at the state and federal level -- to learn more about challenges faced by home care agencies during the pandemic and policies and practices implemented as a result. We wanted to understand how stakeholders thought these policies have worked, what improvements could be made, and what policies and practices hold promise for the future.
FINDINGS
Like other long-term services and supports settings, the pandemic exacerbated existing workforce shortages faced by home care agencies. Because of differences in the definition of essential workers, several states have not recognized home care workers as part of this category. This has contributed to difficulties accessing some clients living in residential facilities, as well as difficulties obtaining PPE, testing for COVID-19, and accessing the vaccine. As a result, some workers have left the workforce due to fear of contracting the virus or infecting family members or clients, and others have been unable to maintain sufficient hours. It was more difficult for workers to maintain sufficient hours at the beginning of the pandemic when clients were refusing visits because they were fearful of allowing anyone into their homes and because fewer clients were being referred to home health when many states restricted elective surgeries.
Agencies have addressed these challenges by changing their policies and practices and by taking advantage of changes to federal and state policies and regulations. One policy change repeatedly noted as helpful to agencies was the authorization for non-physician practitioners, such as nurse practitioners or physician assistants, to certify clients for services. This has made it easier for agencies to take on new clients and saved staff time in having to seek out physicians. Many agencies have also taken advantage of increased telehealth opportunities, although agencies and advocates repeatedly noted that agencies cannot be reimbursed for services supplied via telehealth in most cases. Agencies also reported using new virtual means to hire, onboard, and train workers. Agencies reportedly took advantage of CARES Act funding, the Paycheck Protection Program (PPP), and the Families First Coronavirus Relief Act (FFCRA) to pay workers retainers, bonuses, and hazard pay, and to pay them for time spent sick or quarantining after exposure.
Despite this, home care and HHAs continue to face obstacles. Because their staff are not designated as essential workers, they have had limited access to vaccines in many states. Many stakeholders noted the continuing difficulties these workers face in terms of low wages, limited opportunities for career advancement and the need for better training. Some hoped that increased reliance on home care, in the wake of the pandemic, would result in positive changes to these long-standing issues.
RESEARCH QUESTION 1: What challenges do home care agencies face during the COVID-19 pandemic with regard to PPE, including stockpiling, supplies for staff, training, and infection control policies and procedures?
Workers not designated as essential. State definitions of essential workers differ, and some states have not recognized home care workers as part of this category. This has led to difficulties obtaining PPE, obtaining testing for COVID-19, accessing some clients living in residential facilities, and obtaining the vaccine. Stakeholders reported that it did not seem as though people understood how critical the home care field is to the wellbeing of their clients and said state governments were often classifying home care agencies as housekeeping services rather than health care entities.
|
"And so, we've kind of realized that our definition of what we are isn't necessarily the definition of the government. So, we've had to work a little extra hard to make sure that we are defined as essential... workers." --Home Care Agency |
Access to PPE. Acquiring PPE was a universal challenge reported among those interviewed. Respondents noted that it was difficult to access PPE during the first 3-6 months of the pandemic, but many said availability has since normalized. Typical vendor and supply chains were disrupted, it was difficult to identify legitimate suppliers, and surge pricing was rampant. Some respondents noted that even when they thought they had a good lead on securing PPE, orders would often be diverted to hospitals. Many reported that because home care agencies were not designated as "essential" they were not prioritized for receiving PPE.
Access to testing. As with accessing PPE, the fact that these agencies and staff were not designated as essential workers hindered access to COVID-19 testing for home care workers.
Access to the vaccine. At the time of our interviews in December 2020 and January 2021, access to COVID-19 vaccines was emerging as an issue for home care workers. As with access to PPE and testing, access to the vaccine was limited by the fact that home care workers have not been deemed essential.
Lack of guidance from government agencies. Home care agencies we interviewed noted there was a lack of direction and consistent information from federal and state government agencies. While they noted some helpful guidance from the CDC, they reported they were often left to fend for themselves to create infection control protocols and policies, including those related to testing for their employees. Government staff we spoke to agreed that there was a lack of communication, especially related to relaying information on staff and client exposure.
RESEARCH QUESTION 2: What challenges do home care agencies face during the COVID-19 pandemic with regard to their ability to maintain sufficient staffing levels and manage staff turnover?
Staffing shortages. Staffing in home care agencies was already problematic before the pandemic, and most respondents noted that staffing shortages have worsened. Many respondents reported that staff left their jobs due to fear of exposure to the virus. Some older workers and people with underlying conditions that made them more susceptible to hospitalization if exposed to COVID-19 chose to leave the field or retire.
The closure of schools and childcare centers placed another burden on the home care workforce. Although agencies and governments attempted to support staff by helping them find childcare or providing flexible schedules, many staff still needed to leave their employment to care for their families during this time. Other staff felt they needed to choose between protecting their families or working with clients who may have tested positive for COVID-19.
|
"But for home care agencies, especially personal care worker training, state training requirements vary by state and the infrastructure for training and what was needed at that time... it was just too scattered to really be effective." --Advocacy Group |
Difficulty recruiting staff. Despite there being an increase in unemployed workers who might be able to fill roles, interview participants reported it was harder than ever to find talent, in part because these jobs often have low wages and do not provide full-time employment or comprehensive benefits. COVID-19 added a very real threat to physical safety that potential employees have had a hard time overlooking. In addition, inconsistent training requirements made it more difficult to recruit staff from other health care sectors due to different training and certification requirements. A few stakeholders also noted their concern about the temporary relaxation of training requirements in many states and were uncertain whether staff hired under these conditions would eventually be required to complete the appropriate training.
Transportation issues. Several agencies also noted that transportation presented a challenge for their employees. Staff felt unsafe using public transportation, and clients were uncomfortable having people in their homes if they had been on public transportation. A lack of safe, reliable transportation has made it difficult to maintain sufficient staffing during the pandemic.
Reduced census. Finally, shifting client loads also caused staffing challenges during the pandemic. When the pandemic began, people were afraid to have others outside of their immediate family unit in their homes for fear of exposure. Many clients who did not have life-threatening needs, such as those primarily using home care for meal preparation or housekeeping, canceled services. Others had family members working from home who could take on the additional care. Some clients at first refused services and then later only wanted to let nurses into their homes, not therapists or aides, to reduce the number of people coming in. Respondents also noted that agencies did not get as many post-acute referrals as elective surgeries were cancelled. This led to an initial decline in demand for home health and home care services and resulted in cuts to staff hours. However, many respondents reported that their client load had mostly returned to normal by the time of our interviews in December 2020 and January 2021.
RESEARCH QUESTION 3: What new federal and state assistance, policies, and practices have been implemented to address challenges in home care and home health agencies as a result of the COVID-19 pandemic? How effective did states and providers perceive them to be?
Increased payment rates. Some states used funds from the CARES Act or other state funding to provide increased Medicaid payment rates to home care agencies. Some of these funds were intended to help agencies purchase PPE and other needed supplies. Our policy scan found that 21 states provided these types of payment rate increases (Figure 1). Some states intended these funds to help agencies provide workers with add-on pay, hazard pay, and retainer payments. Federal and state officials described hazard pay and retainer payments as primarily used for staff who were put at risk for contracting COVID-19 during work or if they had to quarantine after exposure. Our policy scan found that 19 states utilized hazard pay or add-on payments for workers and 27 states implemented retainer payments (Figure 1).
| Figure 1. State Policy Changes Related to Increase Medicaid Payment Rates to Home Care Agencies or Workers |
|---|
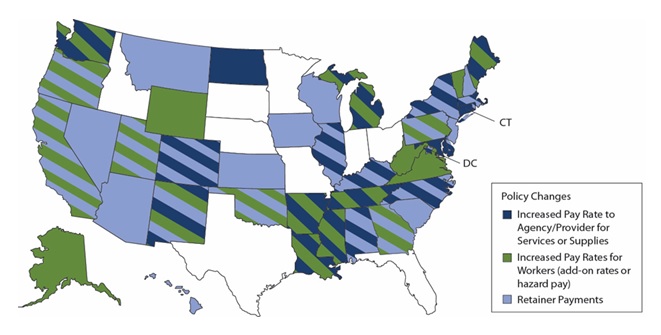 |
| NOTES: This figure was created from multiple secondary sources. The timeframe of the review was limited to March 1, 2020, through December 18, 2020. Some states used federal disaster funding outside of temporary changes to their Medicaid policy. This figure does not account for those uses of disaster relief funding. |
Disaster relief funding. Advocates and providers highlighted the federal assistance provided by the disaster relief funding that went directly to agencies, such as through the PPP and the FFCRA, enabling them to pay workers bonuses, pay for childcare, and provide paid leave when needed. Several advocates representing large numbers of agencies noted some challenges to providers accessing these funds, including a wariness of some providers to use the funds because of shifting federal and state guidelines and lack of provider relief fund access for private-pay only agencies and larger agencies (i.e., >500 employees). As one advocate explained, "those dollars were very slow to flow"; some agencies had yet to receive their funds from the second distribution of relief funds by the time of our interviews.
|
"The provider relief and the Paycheck Protection Program has allowed agencies to do things like pay for childcare, pay for transportation, pay for various kinds of leave, give bonuses... Some of these resources have been used to augment some of our providers who actually are providing wrap around services for, particularly, the front line. And those wrap arounds include help with transportation, help with daycare, health with food insecurity, which is a big issue for the frontline workforce. --Advocacy Group |
Electronic communications. The expanded use of telehealth and other electronic communications to protect both workers and clients was an important paradigm shift. Specifically, the CARES Act encouraged the use of telehealth by HHAs; however, advocates and agencies commented that although agencies were using telehealth more frequently, they were unable to be reimbursed for it through Medicare. CMS clarified in the March 26, 2020 Interim Final Rule that it could not reimburse home health providers for these services due to a statutory provision that prohibited visits made via telecommunications technology from being considered as equivalent to in-person visits. Reportedly, there was also wide variability among states in how they adopted telehealth for home care providers. Collecting electronic signatures and verbal consent allowed for less contact between staff and clients and assisted with reducing administrative burden.
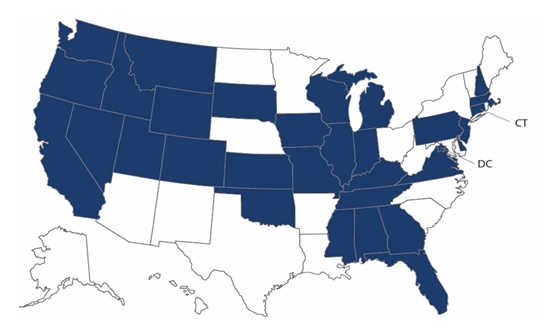
Changes to staff training, qualifications, or duties. The ability to train staff virtually or delay certain pre-employment requirements also were regarded as important changes during the pandemic. Our policy scan found that 32 states made changes to pre-employment requirements to ease entry into the field or retain workers who were due for training or updates to other employment qualifications (Figure 2).
| Figure 2. State Policy Changes Related to Employment Requirements and Qualifications for Home Care Workers |
|---|
 |
Ordering of services by non-physician practitioners. Many different stakeholders felt that the federal policy change allowing non-physician practitioners to order home health and home care services was key. This change allows nurse practitioners or physicians assistants to certify clients for services and has made it easier for agencies to take on new clients. Agencies and advocates reported that this contributed to an increase in the number of clients, reversing the losses that had occurred early in the pandemic due to fear on the part of existing clients and a decline in referrals for post-acute care after the dramatic decrease in elective surgeries. This helped agencies maintain consistent staff hours and reduced staff time following up with physicians. One state official commented that due to the success of this policy change, it may continue beyond the COVID-19 pandemic.
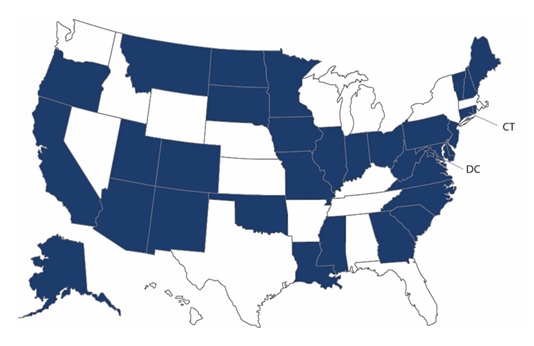
Paying family caregivers. Our policy scan found that 34 states changed policies allowing payment (or increased payments) to family caregivers. Paying family caregivers to provide the care that home care workers would have otherwise been providing helped reduce the demand for these workers at a time when staff recruitment and retention were particularly difficult.
| Figure 3. State Policy Changes Allowing Payment (or Increased Payments) to Family Caregivers |
|---|
 |
RESEARCH QUESTION 4: What new policies and practices have home care agencies implemented to address challenges resulting from the COVID-19 pandemic?
Infection control practices. Agencies focused heavily on infection control and access to PPE to try to maintain some level of in-person care. Agencies reported following CDC guidelines such as wearing masks and hand washing, and a few established their own medical advisory councils to help inform and develop infection control procedures more specific to COVID-19 and the home care client population. Agencies also reported developing their own procedures with regard to COVID-19 testing. Some providers required their staff to be tested regularly, and agencies implemented processes to monitor any positive tests and ensure that their staff would be able to safely quarantine.
Shifting to new virtual processes. We found that home care agencies moved many services and processes to a virtual format. All agencies we spoke with reported adding telehealth services in order to continue to provide care and monitor clients remotely. These services ranged from providing medication reminders over the phone to conducting physical therapy sessions over video applications, such as Zoom or Facetime. Most agencies we spoke with said this was primarily done telephonically and did not involve adding telehealth infrastructure. Many agencies also reported developing tools, such as Apps, to screen their staff and their clients on a regular basis and monitor COVID-19 exposure, symptoms, or any high-risk travel. Agencies also used technology to communicate with and support family caregivers when agency staff were not able to go into the client's home.
|
"... I firmly believe that we're able to add a significant value through telehealth and remote patient monitoring… with the monitoring that we have. Ours also has the capacity for instructional videos and reminders for medication." --Home Care Agency |
Flexible staffing and scheduling. We found that agencies used flexible staffing arrangements -- such as having staff play multiple roles -- to offset staffing reductions. Agencies also allowed flexible scheduling to help staff accommodate for things like childcare needs or second jobs.
Increased communication. According to agency and advocacy group representatives we spoke with, communication between agencies and their staff has become increasingly important throughout the pandemic, to ensure that the staff are kept up-to-date on infection control policies and for the staff to inform leadership of any challenges they were facing on the ground. A few providers started monthly "town hall" meetings with agency leadership and staff. Informal education was also an important initiative for providers as they communicated with staff and shared resources on a variety of topics, such as the epidemiology of the virus, proper hand washing techniques, and the safety of the vaccines.
Other types of support. According to interviews and our media scan, some agencies provided mental health services for their staff, and even helped to provide basic everyday needs like groceries, transportation, and childcare. Many respondents agreed that the career ladder for home care workers needs to improve in order to retain this workforce, and some agencies were able to create internal opportunities for promotions or planned to collaborate with local nursing schools to create programs for their staff to continue their nursing education.
RESEARCH QUESTION 5: Which policies hold promise for meeting projected needs for home care in the future? Where are there still gaps?
According to stakeholders, there are far more policy gaps than those that hold promise. This is not surprising, considering many of the challenges existed for this workforce prior to the pandemic. All stakeholder groups agreed that the most successful policy was the one permitting non-physician practitioners to order home care and home health services. This boosted client census after it had dropped considerably, and freed agencies from having to chase down physicians when they were busy with pandemic-related responsibilities. Because it was ultimately up to the states to adopt this policy change, there was variability in how this policy was implemented across states.
Most stakeholders noted the following ongoing challenges that could be addressed to improve the situation for home care workers during the pandemic and into the future:
-
Ensuring that home care workers are designated as essential workers, and providing them with priority access to PPE, testing, and vaccines.
-
Improving the wages of workers, especially aides, personal care workers, and direct service providers, to improve retention.
-
Improving career opportunities for workers through better training and career ladders. Some stakeholders suggested standardizing training and other requirements across states to make these more portable.
-
Providing government reimbursement to HHAs for certain telehealth services.
Many stakeholders stated they hoped a bright spot from the pandemic would be increased availability of home and community-based services and increased appreciation of home care workers for the essential role they play in keeping clients safe in their homes and communities.
APPENDIX A. INTERVIEW SUMMARY REPORT
Summary of Findings
Like other long-term services and supports industries, home care and home health agencies faced workforce shortages prior to the pandemic that were exacerbated when the pandemic began. Because of differences in the definition of essential workers, some states have not recognized home care and home health workers as part of this category. This has led to difficulties obtaining personal protective equipment (PPE), obtaining testing for the virus, accessing some clients living in residential facilities, and more recently, obtaining the vaccine. As a result, some workers have left the workforce due to fear of contracting the virus or infecting family members or clients, and others have been unable to maintain sufficient hours. It was more difficult for workers to maintain sufficient hours at the beginning of the pandemic, when clients were refusing visits because they were fearful of allowing anyone into their homes, and because fewer clients were being referred to home health when many states restricted elective surgeries.
Agencies addressed these challenges through changes to their own policies and practices as well as by taking advantage of changes to federal and state policies and regulations. One policy change repeatedly noted as helpful to agencies was the authorization for non-physician practitioners, such as nurse practitioners or physician assistants, to certify clients for services. This has made it easier for agencies to take on new clients and saved staff time in having to seek out physicians. Many agencies also took advantage of increased telehealth opportunities, although it was repeatedly noted by agencies and advocates that agencies cannot be paid for services supplied via telehealth in most cases. Agencies also reported using virtual means to hire, onboard and train workers. Agencies reportedly took advantage of Coronavirus Aid, Relief, and Economic Security (CARES) Act funding, the Paycheck Protection Program (PPP), and the Families First Coronavirus Relief Act (FFCRA) to pay workers retainers, bonuses and hazard pay and pay them for time spent sick or quarantining after exposure.
Despite this, home care and home health agencies continue to face obstacles. Their workers have not been recognized as essential workers and this has resulted in limited access to vaccines in many states. Many stakeholders noted the continuing difficulties these workers face in terms of low wages, limited opportunities for career advancement and the need for better training. Some hoped that increased reliance on home care and home health in the wake of the pandemic would result in positive changes to these long-standing issues.
Background
The COVID-19 pandemic is potentially reshaping the provision of health services and health policy in the United States. Specifically, the effect of COVID-19 on those working in home care and home health agencies is of concern because of the potential impact on staffing shortages and a growing need for services. Home care and home health agencies both provide services and supports that help individuals remain safely in their homes. Home health refers to clinical services provided in the home, such as occupational therapy, physical therapy, and nursing as well as non-skilled services such as personal care assistance from aides that may supplement the necessary clinical care. These services are funded through both Medicare and Medicaid. Home care, on the other hand, refers primarily to non-clinical services, such as supervision and companion care, meal preparation, and transportation. Home care is not paid for by Medicare and is optionally funded by state Medicaid plans.
Similar to nursing homes during the COVID-19 pandemic, staffing shortages, increased risk of infection due to a lack of access to PPE, and inadequate training have all led to infection control concerns for home care agencies and their staff (Rowe, et al., 2020; Sterling, et al., 2020). In addition, early reporting suggested consumers might abstain from care due to fear of infection, thus exacerbating the industry-wide impacts (Span, 2020). But recent reports have highlighted how home care and home health agencies have rebounded and are now viewed as an important sector of care for reducing institutional care and preventing hospitalizations (Flynn, Morley, & Bentley, 2020). Questions remain if the industry is prepared for the volume of workers needed, both during and beyond the pandemic.
To help ASPE better understand the landscape of policy factors affecting home care and home health agencies and their workforce, staff at RTI conducted stakeholder interviews to address five key policy research questions:
-
What challenges do home care/health agencies face during the COVID-19 pandemic with regard to PPE, including stockpiling, supplies for staff, training, and infection control policies and procedures?
-
What challenges do home care/health agencies face during the COVID-19 pandemic with regard to their ability to maintain sufficient staffing levels and manage staff turnover?
-
What new federal and state assistance, policies, and practices have been implemented to address challenges in home care/health agencies as a result of the COVID-19 pandemic? How effective did states and providers perceive them to be?
-
What new policies and practices have home care/health agencies implemented to address challenges resulting from the COVID-19 pandemic?
-
Which policies hold promise for meeting projected needs for home care in the future? Where are there still gaps?
Methods
RTI conducted interviews with 25 key stakeholders across three categories: home care and home health agencies, advocacy groups representing these agencies or their workers, and government representatives at the state and federal level. Interviews were conducted with individuals identified in collaboration with ASPE and also based on findings from two environmental scans previously completed, one that focused on state and federal policy changes implemented to address challenges faced in home care and home health during the pandemic and a second focused on home care/health agency policy and practice changes implemented during the pandemic.
The purpose of the interviews was to learn more about challenges faced by home care and home health agencies during the pandemic and what policies and practices have been implemented as a result. We sought to learn how stakeholders think these policies have worked, as well as what improvements can be made and what policies and practices are promising for the future. Interview protocols for each stakeholder type were drafted by RTI and reviewed by ASPE to ensure all topics of interest were covered.
Prospective interviewees were contacted by email using a recruitment email template approved by ASPE. Non-responders were contacted each week for a total of four contacts. Interviews were recorded and transcribed using the TEMI transcription service.[11] Transcripts were cleaned and analyzed by the same RTI staff member who conducted the interview. Key passages in each transcript were highlighted and these highlighted passages were summarized into key themes.
Findings by Research Question
1. What challenges do home care/health agencies face during the COVID-19 pandemic with regards to PPE, including stockpiling, supplies for staff, training, and infection control policies and procedures?
Acquiring PPE was a universal challenge among those interviewed. Respondents noted that it was difficult to access PPE at the beginning of the pandemic, but many said availability has since normalized. They described the experience of purchasing PPE as "harrowing" and "like the Wild West." This was particularly true of smaller agencies that lacked pre-existing relationships with suppliers or the purchasing power to order very large quantities of PPE. Typical vendor and supply chains were disrupted, and fraud and surge pricing were rampant at the beginning of the pandemic. Some respondents noted that even when they thought they had a good lead on securing PPE, orders would often be diverted to hospitals. Many reported that because home care and home health agencies were not categorized as "essential" at the beginning of the pandemic, they were not prioritized for receiving PPE.
Higher than normal burn rates exacerbated the issue of acquiring PPE. Many agencies began mandating more PPE usage than they normally would. For example, staff have been required to wear both a mask and gloves at all visits during the pandemic, but they may have only worn gloves on a regular basis before the pandemic began. The fear surrounding infection at the beginning of the pandemic also may have led staff to request and use more PPE.
Similar challenges were mentioned in accessing testing for home care and home health workers. One respondent described his experience of driving from pharmacy to pharmacy hoping to put a credit card on file so that he could send his staff there to get tested if necessary. As with accessing PPE, the fact that these agencies and staff were not designated as essential workers made testing availability much harder to navigate. Respondents reported that it did not seem as though people understood how critical the home care field is to the wellbeing of their clients and said state governments were classifying home care as housekeeping services rather than health care entities.
There was quite a bit of variability in how often testing was provided to staff. Not all settings provided testing for home care staff on a regular basis. Although facilities, including senior housing and other congregate living settings, may have been required to screen their own staff, those facilities were reportedly resistant to testing agency staff. This impacted access to clients and placed burden on the home care agency. Agencies reported they do not have the power to mandate testing -- or more recently, vaccination -- for their staff without the backing of the appropriate government agency. This means that even within similar settings, testing requirements differed. One home care agency reported that because it uses a franchise model, it was up to franchise owners to decide how often they would test their staff. Some provided testing only when staff were showing symptoms or had an expected exposure; others tested staff randomly regardless of symptoms or exposure. Although some staff initially pushed back against testing, interview respondents reported that more staff are now very willing to be tested on a regular basis. This may have been due to improved education and communication about testing.
Home care/health agencies noted there was a lack of direction and consistent information from federal and state government agencies. Employers attempted to use Centers for Disease Control and Prevention (CDC) guidance to update their infection control procedures but found the changing recommendations difficult to relay to their staff. Home care agencies reported they were left to fend for themselves to update infection control protocols and policies. Some turned to advocacy groups they are members of to support this process. Some state government staff agreed that there was a lack of communication, especially related to relaying information on staff and client exposure. Others noted that although the lack of information was challenging, trying to correct the misinformation about COVID-19 their staff were getting from social media and other sources was even more difficult.
Home care and home health agencies stated that they are doing what they can to protect staff, but they noted that much of the work ultimately requires sustained, face-to-face encounters, which increases the likelihood of virus transmission. Some of the strategies used to mitigate risk came with their own challenges. For example, one agency reported needing to add a respirator program to their scope of work to keep their staff and clients safe. They reported that program required the agency staff to learn those skills, create new protocols, and implement the program during an already demanding situation. Another way agencies tried to keep staff safe was by moving many aspects of training to a virtual platform. However, that transition required people to learn a new technology and create new resources. Even once the training was transferred to a virtual platform, it was difficult for people to demonstrate that they had acquired the skills they need when they were not in-person. The need to mitigate the risks that COVID-19 presented put additional pressure on agencies that were already feeling a lot of strain and uncertainty.
2. What challenges do home care/health agencies face during the COVID-19 pandemic with regard to their ability to maintain sufficient staffing levels and manage staff turnover?
Staffing in home care and home health agencies was already precarious pre-pandemic, but most respondents noted that staffing shortages have worsened during the pandemic. Despite there being an increase in unemployed workers who might be able to fill roles, providers felt it was harder than ever to find talent. Even before the pandemic, agencies struggled to retain workers, especially aides, personal care workers, and direct service providers. These jobs often have low wages and do not provide full-time employment or comprehensive benefits. Several interview respondents mentioned that workers do not go into this field for the paycheck, but because they have a "caring gene." However, COVID-19 added a very real threat to physical safety that potential employees have had a hard time overlooking. Because of this, COVID-19 has made it more difficult than ever to recruit new staff.
Many respondents reported that staff left their jobs due to fear of exposure to the virus. This was especially true early in the pandemic when there were many unknowns about COVID-19 transmission. Some staff were uncomfortable or unable to provide in-person services, and although many agencies attempted to provide other work opportunities to staff that would limit exposure, such as limiting them to clients who only required telemonitoring or allowing them to perform non-patient care duties in the office, this was not always possible. Some older workers or people with underlying conditions that made them more susceptible to hospitalization if exposed to COVID-19 chose to leave the field or retire. When staff did become infected, they had to quarantine. Some respondents noted that because testing was so hard to acquire, they were forced to quarantine staff even if they had a suspected exposure with no symptoms. Infection control measures like quarantine, although necessary, were a huge challenge to employers trying to maintain their workforce. In addition to physical health concerns, respondents also mentioned the mental health toll that the pandemic had on direct care workers and how that led to staff turnover.
Interview respondents also reported that because they would not have an opportunity to provide in-person training to new hires, they wanted to hire staff who had previous experience. However, respondents noted that they found it difficult to recruit workers from other health care settings into home care. They also noted that it is difficult for staff to move from one setting to another, or from one state to another, due to different training and certification requirements.
The closure of schools and childcare centers placed a huge burden on the home care/ home health workforce. Although agencies and governments attempted to support staff by helping them find childcare or providing flexible schedules, many staff still needed to leave their employment to care for their families during this time. Other staff felt they needed to choose between protecting their families or working with clients who had tested positive for COVID-19. Some state government and agency respondents also noted that they suspected that increased unemployment payments provided an incentive for people not to work because direct care workers made more money taking unemployment than they would have if they continued in their positions. However, other research shows that this was likely not the case (Altonji et al., 2020).
Several respondents also noted that transportation presented a challenge for their employees. Staff felt unsafe using public transportation, and clients were uncomfortable having people in their homes if they had been on public transportation. A lack of safe, reliable transportation has made it difficult to maintain sufficient staffing during the pandemic.
Finally, shifting client loads also caused staffing challenges during the pandemic. When the pandemic began, people were afraid to have others outside of their immediate family unit in their homes for fear of exposure. Many clients who did not have life-threatening needs, such as those primarily using home care for meal preparation or housekeeping, canceled services. Others had family members working from home who could take on the additional care. Some clients at first refused services and then later only wanted to let nurses into their homes, not therapists or aides, to reduce the number of people coming in. Respondents also noted that agencies did not get as many post-acute referrals as elective surgeries were cancelled. This led to an initial decline in demand for home care and home health services and resulted in cuts to staff hours. However, many respondents reported that their client load had mostly returned to normal by the time of our interviews in January 2021.
3. What new federal and state assistance, policies, and practices have been implemented to address challenges in home care and home health agencies as a result of the COVID-19 pandemic? How effective did states and providers perceive them to be?
In response to the pandemic, new federal and state policies and guidance were created to assist with the continued delivery of home and community-based services (HCBS), including both home care and home health. Our interviews found that these policies were imperative during a time when face-to-face services were threatened because of the highly contagious nature of COVID-19. Some policies were more successful than others, according to stakeholders. Advocates and large organizations with agencies across states commented that state-specific policies varied widely and were difficult to manage and roll out training for in some cases.
Many different stakeholders felt that the federal policy change allowing non-physician practitioners to order home care and home health services was key. This change allows nurse practitioners or physicians assistants to certify clients for services and has made it easier for agencies to take on new clients. Agencies and advocates reported that this change increased the number of clients after many had been lost due to fear on the part of existing clients and decreasing referrals for post-acute care after the dramatic decrease in elective surgeries. This helped agencies maintain consistent staff hours and reduced staff time following up with physicians. One state official commented that due to the success of this policy change, it may continue beyond the COVID-19 pandemic.
To help agencies maintain staffing, new policies allowed for increased rates, hazard pay, and retainer payments. Federal and state officials primarily described changes in Medicaid rates that allowed for the provision of both hazard pay and retainer pay to staff who were put at risk for contracting COVID-19 during work or if they had to quarantine after exposure. Two state officials commented that pay adjustments had been successful among some home care providers, but that some agencies were resistant. Agency concerns included fear of not being able to extend the benefit beyond the pandemic and union pushback. Advocates stated that some rate increases went directly to agencies and did not make it to the workers themselves. Advocates and providers highlighted the assistance provided by the disaster relief funding (e.g., CARES Act, PPP, and the FFCRA) that enabled them to pay workers bonuses, pay for childcare, and provide leave when needed. Several advocates representing large numbers of agencies, noted some challenges to providers accessing these funds including a weariness of some providers to use the funds because of shifting federal and state guidelines, lack of provider relief fund access for private-pay only agencies and larger agencies (i.e., >500 employees). And, as one advocate explained, "those dollars were very slow to flow" adding that some agencies had yet to receive their funds from the second distribution of relief funds by the time of our interviews.
State officials and agencies commented that unemployment benefits may have been a barrier to maintaining adequate staffing but understood why workers would choose unemployment over risking their or their family's health.
Multiple respondents also described the expanded use of telehealth and other electronic communications to protect both workers and clients as an important paradigm shift. Federal officials clarified this was not a change in federal policy and that providers could use telehealth previous to the pandemic but that it was dependent on state adoption. Advocates and agencies commented that although agencies were using telehealth more frequently, they were unable to be reimbursed for it. Reportedly, there was also wide variability among states in how they adopted telehealth for home health or home care providers. One state official noted that having more telehealth was beneficial, but that the expansion to telephonic delivery of services was just as important because most of her state was rural, with limited Wi-Fi access, and because many clients did not have the means to purchase or own a tablet or computer.
Other newly introduced electronic innovations benefited workers specifically. Collecting electronic signatures and verbal consent allowed for less contact between staff and clients and assisted with reducing administrative burden. Most respondents commented that changes such as allowing for electronic signatures and verbal consent were small but important. The ability to train staff virtually or delay certain pre-employment requirements were also regarded as important changes during the pandemic.
The expansion of payments to family caregivers is an additional flexibility that states took advantage of during the pandemic. According to one federal official, many more states have exercised this option during the pandemic. All respondents commented that this method of expanding the paid caregiver pool helped to stabilize the growing need for home care and home health workers during the pandemic.
4. What new policies and practices have home care/health agencies implemented to address challenges resulting from the COVID-19 pandemic?
Agencies focused heavily on infection control and access to PPE to try and maintain some level of in-person care. Most agencies reported following CDC guidelines on infection control, and a few also reportedly established their own medical advisory councils to help inform and develop COVID-19 infection control procedures. This similarly applied to COVID-19 testing. As testing became more widely available, some providers required their staff to be tested regularly. The testing was either provided by the agency themselves, or by long-term care institutions or other organizations with which the agency had a relationship. All agencies we interviewed implemented processes to monitor any positive tests and ensure that their staff would be able to safely quarantine for the required 14 days.
At the beginning of the pandemic, home care/health agencies we interviewed moved as many services and processes as possible to a virtual format. All agencies we spoke with reported making improvements to their telehealth services in order to continue to provide care and monitor clients remotely. Some providers did not feel comfortable labeling these changes formally as "telehealth" since many of these services were provided over the phone, rather than using telehealth technology. These services ranged from providing medication reminders over the phone to conducting physical therapy sessions over video applications, such as Zoom or Facetime. However, some of the agencies that we interviewed did report eventually purchasing and utilizing more formal types of telehealth, such as remote patient monitoring devices. Many agencies also reported developing tools such as Apps to screen their staff and their clients on a regular basis and monitor COVID-19 exposure, symptoms, or any high-risk travel. Many of their clients were also being cared for by family caregivers, and so providers used technology to communicate and support family caregivers when agency staff was not able to go into the client's home.
Communication between providers and their staff became increasingly important throughout the pandemic to ensure that the staff were kept up to date on infection control policies and for the staff to inform leadership of any challenges they were facing on the ground. A few providers started having monthly "town hall" meetings with agency leadership and staff. Education was also an important initiative for providers as they developed and shared resources with their staff on a variety of topics such as the epidemiology of the virus, proper hand washing techniques, and the safety of the vaccine. Many agencies reported updating their training requirements to reinforce their staff's training around infection control.
As previously noted, the pandemic also amplified the many staffing challenges that the home care and home health workforce had already been facing. Providers used creative staffing arrangements -- such as having staff play multiple roles -- to offset staffing reductions. For example, one provider described the expansion of their Employee Health Division, which involved promoting some of their nurses who were knowledgeable about infection control practices to become employee health nurses who monitor the health of the agency's staff. This allowed them to be a medium for communication between the staff who were going into the homes and the agency leadership team. It also allowed them to monitor exposure to the virus amongst their staff.
Agencies also allowed flexible scheduling to help staff accommodate for things like childcare needs or second jobs, provided mental health services for their staff, and even helped to provide basic everyday needs like groceries. Many respondents agreed that the career ladder for home care/health workers needed to improve in order to retain this workforce, and some agencies were able to create internal opportunities for promotions or planned to collaborate with local nursing schools to create programs for their staff to continue their nursing education.
5. Which policies hold promise for meeting projected needs for home care in the future? Where are there still gaps?
There are far more policy gaps than those that hold promise, according to stakeholders. This is not surprising, considering many of the challenges existed for this workforce prior to the pandemic. The most successful policy noted by all types of stakeholders was the ordering of home care and home health services by non-physician practitioners. This boosted client census after it had dropped considerably and freed agencies from having to chase down physicians when they were busy with pandemic-related responsibilities. Because it was ultimately up to the states to adopt this policy change there was variability in how this policy was implemented across states.
From the perspective of many stakeholders, the primary remaining challenge is getting home care workers recognized as essential workers, which would allow them easier access to PPE, testing, and vaccines. The variation between states in how an "essential worker" was defined has likely added to this lack of understanding both in and across states. Some states license home care agencies, and some do not. Others have different levels of care with and without licensure requirements. There is also variation in the nomenclature used to describes these agencies across states (e.g., home care agency, basic home care agency, comprehensive home care agency). Staff training requirements can also vary by state, and the naming conventions used to describe home care agency workers (e.g., caregivers, personal care assistants, personal care aides) also vary across states.
Stakeholders also commented on the promise of continued remote delivery of staff training and some client services. However, as previously noted, telehealth reimbursement for health care services remains a challenge in most cases for home care and home health agencies.
Dissemination of guidance about the vaccine was limited-to-nonexistent, according to providers and advocates. Some state officials recognized this as a continued challenge and noted that they can only refer provider vaccine questions, for example, to their state's health department.
The supply of workers was described as an ongoing challenge. Several advocates and agencies commented that increased Medicaid rates could assist with ensuring adequate pay for workers. One agency commented that the rate should increase to meet $15 minimum wage expectations. A few state officials and advocates commented on the need to provide standardized worker training and other requirements across states and to align training expectations with new career pathways that would justify increased salaries and better benefits. Beyond pay, other recommendations for worker provisions included assistance to pay for childcare or transportation.
Finally, many respondents also commented on the need to ensure access to HCBS to beneficiaries and clients during and beyond the pandemic and discussed the potential expansion of telehealth or remote delivery of services as a continued option. Some advocates expressed concern that pandemic flexibilities would end, and that provider burden would increase as a result.
Discussion
Workforce shortages that have long existed in the home care and home health industries were exacerbated by the COVID-19 pandemic. Difficulties obtaining PPE caused some workers to leave employment due to fear of becoming ill. Similarly, because some clients feared the virus, they discontinued or reduced their visits, causing some workers to lose hours. Agencies utilized a variety of policy and practice changes (some resulting from changes to state and federal policies, regulations, or guidance) to recruit and train staff. For example, some states temporarily increased payment rates for services, allowing agencies to pay workers retainers, bonuses, or hazard pay. Some used this funding to cover workers' childcare or transportation costs, or even to purchase necessities, such as groceries. In some cases, agencies were able to pay staff for time they were sick with the virus or were quarantined due to exposure.
Telehealth and other forms of virtual and telephonic communications have been used to improve communication with clients, their family caregivers, and staff. Video conferencing has been used to interview potential staff, onboard new staff, and provide training to staff. Similarly, electronic means have been used to obtain signatures, complete check-ins with clients, monitor staff and client symptoms and possible exposure, and increase communications between teams of staff. However, a challenge repeatedly noted by stakeholders was the inability of agencies to be reimbursed for telehealth services.
The policy change most frequently cited as helpful during the pandemic was the change allowing non-physician practitioners to certify for services. Other notable changes were the funds available through the CARES Act, PPP and FFCRA.
Most stakeholders noted the following ongoing challenges that should be addressed to improve the situation for home care and home health workers during the pandemic and into the future:
-
Ensuring that home care and home health workers are recognized as essential workers, providing them with priority access to PPE, testing and now the vaccines.
-
Improving the wages of workers, especially aides, personal care workers, and direct service providers, so that they can support themselves and their families through these jobs. This will also decease the proportion of workers who must work more than one job, which may increase transmission rates (Chen, Chevalier & Long, 2021). Some stakeholders thought this would likely require increased state Medicaid reimbursement rates for agencies.
-
Improving career opportunities for workers through better training and career ladders. Some stakeholders suggested standardizing training and other requirements across states to make these more portable.
-
Medicare reimbursement for HHAs for certain telehealth services during public health emergencies.
-
Allowing non-physician practitioners to continue certifying for services after the pandemic is over.
Many stakeholders stated they hoped a bright spot from the pandemic would be increased availability of HCBS and increased appreciation of home care and home health workers for the essential role they play in keeping clients in their homes and communities. For this to happen, long-standing issues facing this workforce will likely need to be addressed.
References
Altonji, J., Contractor, Z., Finamor, L., Haygood, R., Lindenlaub, I., Meghir, C., O'Dea, C., Scott, D., Wang, L., & Washington, E. (2020). Employment Effects of Unemployment Insurance Generosity During the Pandemic. Retrieved from https://tobin.yale.edu/sites/default/files/files/C-19%20Articles/CARES-UI_identification_vF(1).pdf.
Chen, M.K., Chevalier, J.A., & Long, E.F. (2021). Nursing home staff networks and COVID-19. Proceedings of the National Academy of Sciences, 118(1).
Flynn, H., Morley, M., & Bentley, F. (2020). Hospital Discharges to Home Health Rebounding, but SNF Volumes Lag. Avalere Health. Retrieved from: https://avalere.com/press-releases/hospital-discharges-to-home-health-rebound-while-snf-volumes-lag.
Rowe, T., Patel, M., O'Connor, R., McMackin, S., Hoak, V., & Lindquist, L. (2020). COVID-19 Exposures and Infection Control Among Home Care Agencies. Archives of Gerontology & Geriatrics, Advance online. Retrieved from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7390796/.
Span, P. (2020). Navigating Home Care During the Pandemic. New York Times, p. 3.
Sterling, M.R., Tseng, E., Poon, A., Cho, J., Avgar, A.C., Kern, L.M., Ankuda, C.K., & Dell, N. (2020). Experiences of Home Health Care Workers in New York City During the Coronavirus Disease 2019 Pandemic: A Qualitative Analysis. JAMA Internal Medicine.
APPENDIX B. STATE AND FEDERAL POLICY TRACKER
Summary
The COVID-19 pandemic has affected home care agencies -- including home health agencies -- and their staff in several important ways. Some of the challenges encountered were entirely new and resulted directly from the pandemic. In other cases, the pandemic worsened long-standing challenges in the industry. States and the federal government addressed some of these issues through changes to policies, regulations, and guidance. Home care agencies also responded with changes to their own policies and practices. The purpose of this study was to understand the challenges faced by home care (including home health) agencies due to the COVID-19 pandemic and the policies and practices put into place by the federal government, state governments, and home care agencies themselves to mitigate these challenges through a 50-state scan and interviews with stakeholders. This tracker summarizes findings related to state and federal policy changes implemented due to COVID.
Methods
Scan Methods:
We reviewed secondary and some primary sources describing Medicare and Medicaid Policy changes that may affect home care and home health agencies and their workers during the COVID-19 pandemic. The review covers March 2020 through mid-December 2020.
Federal Scan: Home Health Agencies and Workers
-
We reviewed Centers for Medicare & Medicaid Services (CMS), CDC, Department of Labor, and Cares Act guidance for Home Health Agencies.
-
We categorized the information into 6 columns including the following categories: Modify Worker Benefits; Modify Qualifications, Duties, Training or Supervision; Testing of Clients or Workers, Telehealth or virtual expansion, Infection Control Practices, and CARES Act Guidance.
State Scan: Home Care Agencies and Workers
-
We identified and used three secondary scan sources that had previously documented the state Medicaid policy changes that may affect home care and home health agencies, their workforce, and clients (we did not focus on the latter).
-
ATI Advisory: Federal and State Policy Waivers: COVID-19, updated as of August 24, 2020. Source: https://atiadvisory.com/wp-content/uploads/2020/08/COVID-19-Policy-Summary_August-24.pdf.
-
National Academy for State Health Policy (NASHP): States Use of Appendix K and Emergency Waivers to Support Home- and Community-Based Services in Responses to COVID-19, updated December 18, 2020. Source: https://www.nashp.org/states-use-appendix-k-waivers-to-support-home-and-community-based-services-in-response-to-covid-19/.
-
Kaiser Family Foundation (KFF) article: Medicaid Emergency Authority Tracker: Approved State Actions to Address COVID-19 updated December 21, 2020. Source: https://www.kff.org/coronavirus-covid-19/issue-brief/medicaid-emergency-authority-tracker-approved-state-actions-to-address-covid-19/.
-
The ATI Advisory and NASHP scans were our primary sources; the KFF scan was used last to confirm findings and add details.
-
-
-
We scanned all state home care and home health agency licensing websites for any COVID-19 specific guidance for the workforce.
-
We categorized the information into 10 columns including the following categories: Increased Pay, Hazard Pay or Change in Benefits; Increased Pay Rate to Agency/Provider for Services or Supplies; Retainer Payments; Operations Guidance or Funding Available; Expand/Modify Delivered Services; Modify Qualifications, Duties, Training or Supervision; Informal/Family Caregivers: Expanded Payment and Benefits; Testing of Clients; Telehealth/Telephonic; Infection Control Practices.
-
We summarized or combined details from multiple sources.
-
-
We added some additional details to the amounts of increased payment rates that applied to home care workers by reviewing the NASHP scan a second time, only for states where we previously had found information, and then reviewed the state's 1915(c) Appendix K documentation; we only included new information if specific details on pay increases were found.
Terminology and Definitions
| Terms | Definitions |
|---|---|
| Direct Care Worker (DCW) | This terminology is often used to describe any staff providing direct services to a patient or client. It can include many terms used to describe home health and home care workers including home health aides, chore assistants, direct services staff, nursing staff (RNs and LPNs), for example. |
| Hazard Pay | Add-on pay for performing additional hazardous duty or work involving physical hardship (source: https://www.brookings.edu/research/the-covid-19-hazard-continues-but-the-hazard-pay-does-not-why-americas-frontline-workers-need-a-raise/#:~:text=Hazard%20pay%20is%20additional%20pay,deadly%20risks%20of%20COVID%2D19). For this scan hazard pay includes taking care of COVID-19 positive or presumptively positive patients. |
| Home and Community-Based Services (HCBS) | HCBS provide opportunities for Medicaid beneficiaries to receive services in their own home or community rather than institutions or other isolated settings (source: https://www.medicaid.gov/medicaid/home-community-based-services/index.html). |
| Home Health Agency (HHA) | These agencies provide Medicare, Medicaid, and private-pay medical services in the home such as nursing or therapy. |
| Home Care Agency | These agencies provide Medicaid covered and private-pay non-medical care in the home such as assisting with activities of daily living including bathing, dressing, and meal preparation. Some states refer to these as HHAs. |
| Retainer Payments | Payments to certain habilitation and personal care providers intended to maintain capacity during the emergency. Unlike interim payments, which are made before services are provided and subsequently reconciled so that providers are paid only for services actually rendered, retainer payments allow providers to continue to bill and be paid for certain services that are authorized in person-centered service plans to enable providers to maintain capacity when circumstances prevent enrollees from actually receiving those services (source: https://www.kff.org/coronavirus-covid-19/issue-brief/options-to-support-medicaid-providers-in-response-to-covid-19/). |
| CARES Act | The Coronavirus Aid, Relief, and Economic Security (CARES) Act and the Coronavirus Response and Relief Supplemental Appropriations Act of 2021 provide fast and direct economic assistance for American workers, families, and small businesses, and preserve jobs for American industries (source: https://home.treasury.gov/policy-issues/cares). |
| Column Headers | Explanations |
|---|---|
| Table 1a Information | |
| Home Care Agency: Increased Pay Rate to Agency/Provider or for Services or Supplies | Policy, regulation or guidance changes that increase payment rates to agencies or certain kinds of providers for services rendered or supplies, such as personal protective equipment (PPE). |
| In-home Workers: Increased Pay, Hazard Pay or Change in Benefits | Policy, regulation or guidance changes providing pay increases, hazard pay or other benefits to certain workers. |
| In-home Workers: Retainer Payments | Policy, regulation or guidance changes providing retainer payments to certain workers. |
| Home Care Agency: Operations Guidance or Funding Available | Policy, regulation or guidance changes affecting home care agency operations or funding. |
| In-home Workers: Expand/Modify Delivered Services | Policy, regulation or guidance changes expanding or modifying the types of services that certain workers can provide or that can be provided through certain programs. |
| Table 1b Information | |
| In-home Workers: Modify Qualifications, Duties, Training or Supervision | Policy, regulation or guidance changes modifying the qualifications required of certain workers, the duties certain workers may perform, or the training or supervision required of certain workers. |
| Informal/Family Caregivers: Expanded Payment and Benefits | Policy, regulation or guidance changes that provide increased (or new) payments or benefits to family or other informal caregivers. |
| Testing of Clients | Policy, regulation or guidance changes related to testing clients for COVID-19. |
| Telehealth/Telephonic | Policy, regulation or guidance changes affecting the use of telehealth or other telecommunications with clients. |
| Infection Control Practices | Policy, regulation or guidance changes affecting the infection control practices used by home care or HHAs. |
State Policy Scan
| TABLE 1a. State Medicaid and Other Guidance That May Affect Home Care/Health Agency Staff During the COVID-19 Pandemic | |||||
|---|---|---|---|---|---|
| State | Home Care Agency: Increased Pay Rate to Agency/Provider or for Services or Supplies | In-home Workers: Increased Pay, Hazard Pay or Change in Benefits | In-home Workers: Retainer Payments | Home Care Agency: Operations Guidance or Funding Available | In-home Workers: Expand/Modify Delivered Services |
| Alabama |
Increases payment rates for personal care, homemaker, respite services by 10% and case mgmt. rate by 5.5% to cover additional staffing and PPE supplies.1,2 |
Retainer payments are provided for certain waiver staff for up to 90 days (3-30 day increments).1,2 |
|||
| Alaska |
Increased payment rate for chore services ($6.87/15 minute units) provided in the home.3 |
||||
| Arizona |
Retainer payments are provided for certain waiver staff.1,2 |
Adds electronic service delivery method for case management; PCS only requiring verbal cueing; and in-home habilitation.2 Certain HCBS can be delivered during an acute-care hospital or short-term institutional stay.2 |
|||
| Arkansas |
Increased payment rate for certain waiver services.2 |
Base supplemental rate increase or COVID-19 add-on payment available to attendance care staff.1,2 Each direct worker will only be able to claim payment in one category. Tiered payments are $125.00 for working 0-19 hours per week, $250.00 for working 20-39 hours per week, $500.00 for working 40+ hours per week, and $500.00 for working a regularly planned split shift schedule that overlap weeks that equal or exceed 150 hours per month without overtime.5 |
|||
| California |
Supplemental COVID-19 sick leave included in In-Home Supportive Services provider rate, up to 80 hours.1 Allows supplemental paid sick leave, up to 80 hours, to all non-food sector employees.6 |
Retainer payments are provided for certain waiver staff for up to 30 days.2 |
Allows certain services (e.g., OT/PT/SLP) to be provided in the home.1 |
||
| Colorado |
Increased rate, 8.2% for specified services including personal care.2 |
Retainer payments are provided for certain waiver staff for up to 30 days.2 |
State staff are postponing agency certification and license reviews case-by-case until end of state of emergency.2 |
Waives certain consumer-directed attendant support services requirements.2 |
|
| Connecticut |
Time and a half for companion and PCS to cover staffing shortages.1 |
Removes 6 hour per week limit for HCBS homemaker services.1 Expands coverage to add option of additional agency-based staff (i.e., Personal Care Attendants).1 |
|||
| Delaware |
Increased payment rate for certain waiver services.1 MCOs may be required to increase fee schedules for certain service providers.2 |
MCOs may be required to make retainer payments for certain waiver staff.2,7 |
HHAs can apply for CARES Act relief funds.8 |
||
| District of Columbia |
Increased payment rates to HHAs for specific services including increasing direct care staff pay and overtime.1,2 |
Retainer payments are provided for certain waiver staff.1,2 |
|||
| Florida | Expanded scope of services for waiver providers (e.g., allowing OAA providers to provide adult companion and LTC PCS).1
Temporarily adds live-in caregiver services, but spouses/legal guardians cannot provide services.2 Adds medication administration and medication management when direct service worker is qualified as RN/LPN.2 Exceed service limits to maintain the health and safety of recipients diagnosed with COVID-19 or when it is necessary to maintain a recipient safely in their home (home health, etc.).9 |
||||
| Georgia |
Increased payment rate for home-based hourly LPNs.2 |
Retainer payments are provided for certain waiver staff, for up to 90 days (3-30 day increments.1,2 |
Allows certain service limits to be exceeded (e.g., community living supports and community access).1 Certain HCBS can be delivered during an acute care hospital or other institutional stay.2 |
||
| Hawaii | Retainer payments are provided for certain waiver staff.1,2
|
Temporarily suspends specified limits on number of hours of HCBS or budget for personal assistance Level I, personal assistance Level I and II, and private duty nursing. Expands settings for Personal Assistance Level II, Level II, and private duty nursing; settings can include relatives' homes, hotels, cruise ships, or other settings in certain circumstances related to the pandemic.1
|
|||
| Idaho | |||||
| Illinois |
Increased payment for certain waiver services (staffing, monitoring, cleaning, and PPE).2 |
Retainer payments are provided for certain waiver staff up to 90 days (3-30 day increments).1,2 |
Certain HCBS can be provided in acute care hospitals.2 |
||
| Indiana |
Certain HCBS can be provided in acute care hospitals or institutional settings.1 |
||||
| Iowa |
Retainer payments are provided for certain waiver staff.1,2 |
Allows direct care providers to move into member's homes; lifts existing limitation on 5 person homes to allow providers to consolidate members into homes.1,2 Certain HCBS can be provided in acute care hospitals.2 |
|||
| Kansas |
Retainer payments are provided for certain waiver staff, up to 90 days (3-30 day increments).2 |
||||
| Kentucky |
Allows flexibility to increase rates by geographic location.1,2 |
Retainer payments are provided for certain waiver staff.1,2 |
Service limitations increased for some personal care/personal assistance wavier and companion services.2 |
||
| Louisiana |
Flexibility to increase payment rates for some waiver services and providers.1,2 |
Hazard premium pay of $3.16 per hour ($0.79 per total hour) provided to direct service workers providing PAS only when caring for COVID-19 positive, presumptively positive or quarantining individuals. The $0.79 per quarter hour includes a $0.50 wage increase for the direct service worker and $.29 for overhead costs for the home care agency. The average wage increase is approximately 22%.1,2 |
Participants can receive PAS while living in the home of a service provider unrelated by blood/marriage; service can be provided in another state without prior written approval.2 |
||
| Maine |
Increased payment rate for workforce rate increases and overtime pay.1 |
Increased payment rates for attendant care services, PCS, skilled nursing visit, RN visit, and LPN visit when providing services to COVID-19 positive individuals.2 |
Increases limit on a range of services including available personal care hours and care coordination. Removes budget allocation limits and individual caps on services to accommodate temporary service increases.2 Certain HCBS can be provided in acute care hospitals.2 |
||
| Maryland |
Increase of up to 50% for certain service rates including, Personal Supports and Supported Living, when providing services to COVID-19 positive individuals.1,14 |
Expands certain services including shared supports hours, meaningful day services, environmental modifications, individual support services, adult life planning, and other services.1 Allows for out of state provision in surrounding states.1 |
|||
| Massachusetts |
Increased payment rate for certain HH staff and services including home health aides, supportive home care aides, personal care, homemaking, companion, etc.) when providing services to COVID-19 positive individuals. Payment rates for these services may be increased up to an additional 50% of the maximum rate for each service.2,15 |
Retainer payments are provided for certain waiver staff.1,2
|
Allows for exceeding the 84 hr./week limit on in-home, non-residential services.2 Certain HCBS can be provided during an acute care hospital or institutional settings stay. Services include: personal care; adult companion/companion; behavioral supports and consultation; expanded habilitation, education.2 |
||
| Michigan |
Flexibility allowed for paying higher rates for certain waiver services and staff.2 |
Permanent rate increase for Home Help caregivers who earn less than $9.90/hr.16 |
|||
| Minnesota |
Suspend all new applications and in-progress applications for temporary home care licenses.17 Extend existing temporary home care licenses as needed to allow for an initial full survey for providers who have submitted a notice of providing services.17 |
||||
| Mississippi |
Increased payment rate for certain waiver services and staff.2 |
Increased service fee of up to 25% (increased to 30% in a later waiver update) for PCS.2 |
Allows qualified provider agencies to also provide PCS.2 |
||
| Missouri |
Allows providers to deliver any necessary PCS even if not listed in plan of care and if not previously approved by the state.1,2 Certain HCBS can be provided in hospitals.2 |
||||
| Montana |
Retainer payments are provided for certain waiver staff.2 |
Temporarily waives prior authorization limits and increases the amount and/or duration of certain services, including companion, PAS, non-medical transportation.2 Certain HCBS can be provided in an acute care hospital, critical access hospital, nursing facility or swing bed.2 |
|||
| Nebraska | |||||
| Nevada |
Retainer payments are provided for certain waiver staff.18 |
||||
| New Hampshire |
Retainer payments are provided for certain waiver staff.1,2 |
Certain HCBS may be delivered during an acute care hospital stay.2 |
|||
| New Jersey |
Retainer payments are provided for certain waiver staff, if no other reimbursable services are being delivered.2 |
Certain HCBS may be delivered during an acute care hospital stay.2 |
|||
| New Mexico |
Increased payment rates for certain waiver services and staff.1,2 |
Increased payment rates 23% monthly, or $581.94/month, for case management staff services.1,2 |
Retainer payments are provided for certain waiver staff.1,2 Retainer payment only if client impacted by COVID-19 (hospitalized or quarantined).1,2 |
Certain HCBS may be delivered during an acute care hospital or short-term institutional stay.2 |
|
| New York |
Increased payment rates to certain providers and certain settings.1 |
Retainer payments are provided for some waiver staff, for up to 90 days (3-30 day increments).1,2 Retainer Payments are available when client utilization drops to 80% of the avg. monthly rate.1,2 |
The provider will not lay off staff and will maintain wages at existing levels.2 |
||
| North Carolina |
Increased payment rate HH providers and OT staff.1 Uniformly increase Medicaid rates by 5% for all programs or services.1 |
Retainer payments are provided for some waiver staff, up to 90 days (3-30 day increments).1,2 Retainer payment only if client impacted by COVID-19 (hospitalized or quarantined).2 |
In-home care and PAS are not required to be used on a monthly basis or to follow the service plan.1,2 Some services may be provided in any necessary setting, including out of state.2 Certain HCBS may be delivered during an acute care hospital or short-term institutional stay.2 |
||
| North Dakota |
Increased payments for certain waiver services and staff.2 |
||||
| Ohio |
Suspends limits on HH services per day and week.1 |
||||
| Oklahoma |
COVID-19 "add-on" retroactive rate for serving COVID-19 positive individuals; rate cannot exceed 20% of providers current rate.2 |
Retainer payments are provided for certain waiver staff.1,2 Retainer payments for PCS (excluding respite) members not to exceed 7 days of authorized services.2 |
Temporarily allows personal care assistants to perform the duties of advanced supportive/restorative assistants.2 Certain HCBS may be provided in an acute care hospital.2 |
||
| Oregon |
Increased payment rate for direct nursing services to the highest currently approved rate of $15.50/quarter-hour to help maintain nursing pool capacity.2 |
Retainer payments are provided for certain waiver services.1 Retainer payments will be provided when attendance and utilization for the service drops below 75% of the monthly average.1,2 |
Temporarily allows staff who are not classified as case managers to provide case management services unless the service includes a level of care evaluation or re-evaluation.2 |
||
| Pennsylvania |
Hazard pay provided for HH staff. CARES Act grant funds can be used for hazard pay for direct, full-time and part-time employees earning less than $20/hour, excluding fringe benefits and overtime for the 10-week period from August 16, 2020 through October 24, 2020. Employers applied for up to $1,200 per eligible FTE employee, up to 500 eligible FTE employees per location.22 |
Retainer payments are provided for some waiver staff.1,2 |
Staffing shortage guidance: The home care agency should evaluate capacity to meet participant's service needs in the event staffing is impacted by the COVID-19 pandemic. If sick, the DCW should not be working and the home care agency is responsible to find a replacement for the DCW. If the agency is unable to find a replacement they should notify the CHC MCO or OBRA waiver service coordinator and assist in implementing the participant's emergency back-up plan.22 The Department expects that each agency's has an Emergency Preparedness Plan including provisions for: staff shortages that may include contracts/agreements with other home care/home health care/hospices or staffing agencies. Agencies should review, assess and prioritize their patients/consumers based on the complexity and frequency of their care needs. Modifications of assignments based on care needs and frequency should be made from most complex to simpler personal care tasks. Notifications and explanations related to changes need to be made with patient/consumer/ responsible party.23 Additionally, agencies need to ensure that participant/consumer files include emergency back-up supports that are identified and are current. For those patients/consumers utilizing services in CHC or the OBRA Waiver program, agencies must collaborate with the designated MCO or Service Coordinator and ensure back-up supports are identified.23 For participants enrolled in certain waiver programs, agencies should work with MCOs and Service Coordinators on service prioritization of participants and to support agency efforts to identify appropriate resource allocation.23 |
Allows for supportive living services and staffing ratios to be exceeded service limits.1 A HHA may extend its geographic service areas beyond adjoining, surrounding counties. An agency that extends its service delivery areas must ensure that it provides adequate supervision and monitoring of care to its consumers.23 Onsite RN requirements for HHAs are temporarily suspended.22 |
|
| Rhode Island |
Increased payment rates for certain services.2 |
Retainer payments are provided for some waiver staff, up to 90 days (3-30 day increments).2 Retainer payments can continue when clients remain hospitalized or quarantined after the emergency ends.2 |
For certain services (community-based day habilitation) allows exceeding service limites.2 Removed staffing ratio requirements.2 |
||
| South Carolina |
Retainer payments are provided for certain providers, for up to 90 days.2 |
||||
| South Dakota |
Allows other practitioners in lieu of approved providers.2 |
||||
| Tennessee |
Increases payment rates for certain waiver services.2 |
Hazard pay, $5.00/hr., provided for some staff serving COVID-19 positive individuals.2, 24 Overtime pay and PPE for certain providers covered by COVID-19 "add-on" rate.2 A 30% increase for attendant care services to allow for more competitive rates. |
Allows flexibility for licensed providers to provide services in alternative settings.2 Certain HCBS may be delivered during an acute care hospital or short-term institutional stays.2 |
||
| Texas | |||||
| Utah |
Hazard pay for direct care services when providing care to COVID-19 positive individuals; allows up to an additional 50% of the maximum rate. Case management may be eligible for enhanced reimbursement without in-person contact.1,2 |
Retainer payments are provided for certain waiver staff, up to 90 days (3-30 day increments).2 Retainer payments may be provided when providers have experienced significant decline in service utilization; allows for reimbursement to providers up to 100% of average monthly pre-COVID costs.2 |
Certain HCBS may be delivered during an acute care hospital or short-term institutional stay.2 |
||
| Vermont |
One-time hazard pay available to HHA staff. HHA eligible include those providing physical, speech, respiratory, or OT. An employer shall only be permitted to receive a grant to provide hazard pay to its employees for therapy services provided on behalf of the HHA. Agencies, not individuals must apply. Lump sum grant awards in the amount of 1,200 or 2,000 per employee are availabe.25 |
||||
| Virginia |
One-time, hazard pay lump sum (up to $1,500) available to HH aides.26 HH aides will have a permanent raise increase of 7%.26 |
||||
| Washington |
Increased payment rate for certain waiver services and providers.1,2 |
Add-on COVID-19 rate for certain essential services, but must not exceed 25% of providers current rate.2 |
Increases the amount and duration of waiver services as necessary on a case-by-case basis.2 Allow case management entities to be HCBS direct service providers.4 |
||
| West Virginia |
Increased payment rate for personal attendance service from 17/hr. to 18/hr. to $18 to incentivize and improve recruitment and retention of personal attendant service workers.2 |
Can exceed service limits for personal attendant services and direct care services if the primary care provider becomes unavailable.1,2 Certain HCBS may be delivered during an acute care hospital stay.2 |
|||
| Wisconsin |
Retainer payments are provided for some waiver staff, cannot exceed 30 days.2 |
HHA guidance for staff who work in multiple settings, including staff assignments. Home care providers should schedule or assign staff appropriately to ensure they do not place individuals in the location where participants are receiving services at risk for COVID-19. Staff who work in multiple locations should be encouraged to tell providers if they have had exposure to other settings with recognized COVID-19 cases.27 Providers should have a contingency plan for continuing participant care if a large proportion of staff become sick.27 |
Allows for temporarily providing HCBS waiver services in out-of-state settings.2 Certain HCBS may be delivered during an acute care hospital or short-term institutional stay.2 |
||
| Wyoming |
Increased payment rate for certain staff; reimbursement rates by 15% for HH aides and skilled nursing care.2
Temporarily increases the wage cap for wages paid to individuals employed under the participant-directed service option, from 13.5%, from $12/hr. to $13.62/hr., to allow participants/designated employers of record the ability to offer employees temporary hazard/retention pay.2 |
Certain HCBS may be delivered during an acute care hospital or short-term institutional stay.2 |
|||
State Policy Scan Footnotes
-
ATI Advisory: Federal and State Policy Waivers: COVID-19, updated as of August 24, 2020. Source: https://atiadvisory.com/wp-content/uploads/2020/08/COVID-19-Policy-Summary_August-24.pdf.
-
See National Academy for State Health Policy (NASHP): States Use Appendix K and Emergency Waivers to Support Home- and Community-Based Services in Responses to COVID-19, updated December 18, 2020. Source: https://www.nashp.org/states-use-appendix-k-waivers-to-support-home-and-community-based-services-in-response-to-covid-19/.
-
See https://www.medicaid.gov/state-resource-center/downloads/ak-combined-appendix-k-appvl.pdf.
-
See KFF article: Medicaid Emergency Authority Tracker: Approved State Actions to Address COVID-19 updated December 21, 2020. Source: https://www.kff.org/coronavirus-covid-19/issue-brief/medicaid-emergency-authority-tracker-approved-state-actions-to-address-covid-19/.
-
See https://www.medicaid.gov/state-resource-center/downloads/ar-combined-appendix-k-appvl.pdf.
-
See https://www.dir.ca.gov/dlse/Comparison-COVID-19-Paid-Leave.html.
-
See https://www.medicaid.gov/medicaid/section-1115-demonstrations/downloads/de-dshp-appendix-k-appvl.pdf.
-
See https://dch.georgia.gov/announcement/2020-03-25/important-notice-fingerprint-background-checks.
-
See https://dhs.iowa.gov/sites/default/files/DHS_COVID19_Home_Visitation-Guidance.pdf?120220202101.
-
See https://chfs.ky.gov/cv19/HomeHealthClinicalDefinitions.pdf.
-
See https://www.medicaid.gov/state-resource-center/downloads/md-combined-appendix-k-appvl.pdf.
-
See https://www.medicaid.gov/state-resource-center/downloads/ma-combined-appendix-k-appvl.pdf.
-
See https://www.michigan.gov/documents/mdhhs/L_20-26_689145_7.pdf.
-
See https://www.health.state.mn.us/facilities/regulation/homecare/docs/licensingwaiver.pdf.
-
See https://www.medicaid.gov/state-resource-center/downloads/nv-combined-appendix-k-appvl.pdf.
-
See https://www.dhhs.nh.gov/dcbcs/documents/dltss-covid19-guidance-2.pdf.
-
See https://www.health.ny.gov/health_care/medicaid/covid19/docs/2020-03-14_guide_chha_lthhc.pdf.
-
See https://www.tn.gov/content/dam/tn/tenncare/documents/CHOICESAndECFCHOICESCOVIDRelatedPayments.pdf.
-
See https://dcist.com/story/20/10/15/virginia-hazard-pay-home-health-workers-covid/.
| TABLE 1b. State Medicaid and Other Guidance That May Affect Home Care/Health Agency Staff During the COVID-19 Pandemic | |||||
|---|---|---|---|---|---|
| State | In-home Workers: Modify Qualifications, Duties, Training or Supervision | Informal/Family Caregivers: Expanded Payment and Benefits | Testing of Clients | Telehealth/ Telephonic | Infection Control Practices |
| Alabama |
For existing providers, the state will suspend follow-up verifications of provider qualifications that come due during the pandemic.2 Temporarily allows initial training for new employees to be performed via other means, such as telephone or webinars.2 |
Allows for virtual or telephonic service planning and delivery of HCBS.1,2 |
Rate increases for some services to cover cost of PPE supplies.1 Requires providers to submit incident reports for participants who test positive for COVID-19, and disclose exposure of participant to other participants and/or staff.2 |
||
| Alaska |
Permits payment to family caregivers to provide certain waiver services.1,2,4 |
Allows for virtual or telephonic service planning and delivery of HCBS.1,2 |
Delays HH face-to-face encounters for up to 12 months after the service starts.4 |
||
| Arizona |
Increases billable family provided services for certain waiver services.1,2 |
Allows for virtual or telephonic service planning and delivery of HCBS.1,2 |
Delays HH face-to-face encounters for up to 12 months after the service starts.4 |
||
| Arkansas |
Allows for virtual or telephonic service planning and delivery of HCBS.1,2 |
||||
| California |
Allows waiver PCS providers to provide PCS to individuals receiving services through the state plan.1 Temporarily allows flexibilities in providing services across specified programs when other provider unavailable. Modifies provider type to include use of certified nurse assistants along with currently authorized HCBS waiver nurse providers and HHAs.2 |
Permits payment to family caregivers to provide certain waiver services.1,2 |
Covers COVID-related testing through Emergency Medicaid.4 |
Allows for virtual or telephonic service planning and delivery of HCBS.1,2 |
|
| Colorado |
HHAs providing state plan services can temporarily provide certain skilled and unskilled services outside enrolled specialties, including in-home supportive services, and personal care.1,2 Includes flexibility to suspend staff training requirements for specified services, with online/telehealth options.2 Temporarily waives requirement for health care professionals to be licensed in-state if they have equivalent out-of-state licensing.2 |
Permits payment to family caregivers to provide certain waiver services.1,2 Waives family caregiver age requirement (18 to 16, case-by-base).1,2 Waives training requirements for new family caregiver.1,2 |
Covers COVID-related testing through Emergency Medicaid.4 |
Allows for virtual or telephonic service planning and delivery of HCBS.1,2
|
|
| Connecticut |
Allows substitution of lower level staff in service plan when necessary in order to maximize available staff resources.1,2 |
Permits payment to family caregivers to provide certain waiver services.1,2 |
Covers COVID-related testing through Emergency Medicaid.4 |
Allows for virtual or telephonic service planning and delivery of HCBS.1,2 Provides payment parity for virtual or telephonic service delivery.1,2 |
Delays HH face-to-face encounters for up to 12 months after the service starts.4 |
| Delaware |
Allows flexible staffing ratios.1 |
Permits payment to family caregivers to provide certain waiver services.1 |
Covers COVID-related testing through Emergency Medicaid.4 |
Allows for virtual or telephonic service planning and delivery of HCBS.1,2 Provides payment parity for virtual or telephonic service delivery.1,2 |
|
| District of Columbia |
Expands which HCBS approved providers can render IDD companion services.1 Temporarily extends CPR/First Aid training and certification deadlines for certified workers whose certification expired.2 |
Permits payment to family caregivers to provide certain waiver services.1 |
Allows for virtual or telephonic service planning and delivery of HCBS.1,2 Lifts cap on proportion of services that may be provided via telehealth.1,2 |
||
| Florida |
Allows certain HCBS providers (qualified employees of adult day health centers, independent RNs, LPNs, community care for the elderly providers, nurse registry staff, OAA service providers, employees of health care service pools, and employees of Centers for Independent Living) to render additional LTC services when there are workforce shortages.1,2,10 |
All services required to test or treat for COVID-19 are covered under Medicaid.10 |
Allows for virtual or telephonic service planning and delivery of HCBS.1,2 Waive certain electronic visit verification requirements for HH services.9 |
||
| Georgia |
Temporarily removes or modifies training requirements for direct service staff, allows trainings electronically/ telephonically.2 Extends the grace period for fingerprint criminal background checks.11 |
Permits payment to family caregivers to provide certain waiver services.1,2,4 Includes caregivers living in other states.1 |
Allows for virtual or telephonic service planning and delivery of HCBS.1,2 |
||
| Hawaii |
Allows for electronic service planning and delivery of HCBS.2 |
||||
| Idaho |
Allows newly hired direct care staff to provide services prior to completing a submitted background check under specific conditions.2 |
Allows for virtual or telephonic service planning and delivery of HCBS.2 |
|||
| Illinois |
Temporarily suspends certain educational requirements (GED/high school diploma) for home care aides; allows delays in collecting fingerprints for criminal background checks.2 For the remainder of calendar year 2020 and through January 26, 2021, a minimum of 6 hours of in-service training is mandatory for home care aides.2 |
Permits payment to family caregivers to provide certain waiver services.2 | Covers COVID-related testing through Emergency Medicaid.4 | Allows for virtual or telephonic service planning and delivery of HCBS.1,2
|
|
| Indiana |
Temporarily modifies Division of Aging and state administrative requirements for attendant care, HCBS assistance (homemaker), and integrated health care coordination.2 |
Permits payment to family caregivers to provide certain waiver services.2 |
Allows for virtual or telephonic service planning and delivery of HCBS.1 |
Participant screened for COVID-19 prior to any home-based visited by a provider.2 |
|
| Iowa |
Allows case management entities to provide direct services when no other staff are avaiable.1 |
Permits payment to family caregivers to provide certain waiver services.2,4 |
Allows for virtual or telephonic service planning and delivery of HCBS.1 |
Participant screened for COVID-19 prior to any home-based visit by a provider.12 |
|
| Kansas |
Allows case management entities to provide direct care services, when no other staff are available.4 |
Training requirements waived during pandemic.2 |
Cost-sharing waived for COVID-19 testing.1 |
Allows for virtual or telephonic service planning and delivery of HCBS.1 |
|
| Kentucky |
Required training/qualifications for non-skilled direct service providers can be delayed to allow employees to begin immediately.2 Certain providers (personal assistance, attendant care, home and community supports, community living supports, and companion providers) can qualify as direct workers while their background check and pre-employment screenings are still pending.2 |
Allows for virtual or telephonic service planning and delivery of HCBS.1 |
Governor ordered ban on all non-urgent home health practices.13 |
||
| Louisiana |
Permits payment to family caregivers to provide certain waiver services.1,2 |
Allows for virtual or telephonic service planning and delivery of HCBS.1 |
Delays HH face-to-face encounters for up to 12 months after the service starts.4 |
||
| Maine |
Permits payment to family caregivers to provide certain services.1 Training requirements waived during pandemic.2 |
Covers COVID-related testing through Emergency Medicaid.4 |
Allows for virtual or telephonic service planning and delivery of HCBS.1 |
Rate increases to cover cost of PPE supplies.1 |
|
| Maryland |
Permits payment to family caregivers to provide certain waiver services.4 Training requirements waived during pandemic.1 |
Cost-sharing waived for COVID-19 testing.1 |
Allows for virtual or telephonic service planning and delivery of HCBS.1 |
||
| Massachusetts |
Expands professional and occupational licenses, certifications, and registrations of licensed health care and other registered professionals in good standing extending licensure that would otherwise expire.1,2 Extensions apply to a range of specified services, including personal care and home health aide.2 Suspends requirements for providers to obtain national background checks including fingerprinting before beginning work.2 |
Cost-sharing waived for COVID-19 testing.1 Covers COVID-related testing through Emergency Medicaid.4 |
Allows for virtual or telephonic service planning and delivery of HCBS.1 |
Rate increases to cover cost of PPE supplies and training for PPE use.1 |
|
| Michigan |
Temporarily modifies certain provider training requirements for community living supports.2 Relaxed provider qualifications during the state of emergency for HCBS waivers.2 |
Covers COVID-related testing through Emergency Medicaid.1,4 |
Allows for virtual or telephonic service planning and delivery of HCBS.1 |
||
| Minnesota |
Permits payment to family caregivers to provide certain waiver services.2,4 |
Covers COVID-related testing through Emergency Medicaid.4 |
Allows for virtual or telephonic service planning and delivery of HCBS.1 |
State is waiving timelines for survey requirements to reduce administrative requirements for home care facilities, allowing them to focus their limited time and resources on PPE and infection control training.17 |
|
| Mississippi |
Allows flexibility for expiring state-issued ID, training, background checks, and other pre-employment requirements.2 |
Permits payment to family caregivers to provide certain waiver services.1,2 |
Cost-sharing waived for COVID-19 testing.1 |
Allows for virtual or telephonic service planning and delivery of HCBS.1,2 |
Coverage of additional medical supplies, equipment and appliances over and above those in the state plan.2 |
| Missouri |
Suspends training requirements for personal care and advanced personal care aides.1,2 Allows authorized nurse visits to be performed by graduate nurses.1 |
Permits payment to family caregivers to provide certain waiver services.1,2 |
Cost-sharing waived for COVID-19 testing.1 |
Allows for electronic service planning and delivery of HCBS.1 |
Delays HH face-to-face encounters for up to 12 months after the service starts.4 |
| Montana |
Temporarily suspends training requirements for PCS.2 |
Permits payment to family caregivers to provide certain waiver services.1,4 |
Allows for electronic service planning and delivery of HCBS.1 |
Requires incident reports for participants who test positive for, display symptoms of, or are exposed to COVID-19.2 |
|
| Nebraska |
Cost-sharing waived for COVID-19 testing.1 |
Allows for virtual or telephonic service planning and delivery of HCBS in HH setting.1 |
|||
| Nevada |
Waives certain licensure and background checks for providers.1 Waives requirement to be licensed with the state licensure office for homemaker services, respite, and chore services.2 |
Allows for virtual or telephonic service planning and delivery of HCBS.1,2 |
Allows cleaning companies with Nevada business licenses to perform chore services if needed to sanitize home after COVID-19 exposure.2 |
||
| New Hampshire |
Allows flexible staffing ratios.1 Waives certain provider (re)enrollment requirements.1 |
Permits payment to family caregivers to provide certain waiver services.4 |
Allows for electronic service planning and delivery of HCBS.1 |
Delays HH face-to-face encounters for up to 12 months after the service starts.4 DCWs prioritized for testing.19 |
|
| New Jersey |
For managed long-term services and supports, allows individuals with specified alternative professional qualifications to provide personal care assistance services.2 |
Permits payment to family caregivers to provide certain services.2,4 |
Allows for virtual or telephonic service planning and delivery of HCBS.2 |
||
| New Mexico |
Permits payment to family caregivers to provide certain waiver services.1,2,4 |
Allows for virtual or telephonic service planning and delivery of HCBS.1,2 |
|||
| New York |
Covers COVID-related testing through Emergency Medicaid.4 |
Allows for virtual or telephonic service planning and delivery of HCBS.2 |
Rate increases to cover cost of PPE supplies.1 Delays HH face-to-face encounters for up to 12 months after the service starts.4 Staff screening required. Staff showing symptoms of illness must not be permitted to remain at work or visit patients and must not return to work until completely recovered.20 |
||
| North Carolina |
Permits payment to family caregivers to provide certain waiver services.1,2 |
Cost-sharing waived for COVID-19 testing.1 |
Allows for virtual or telephonic service planning and delivery of HCBS.1,2 Provides payment parity for electronic service delivery.1,2 |
Coverage of additional medical supplies, equipment and appliances over and above those in the state plan and training for PPE.1,2 Delays HH face-to-face encounters for up to 12 months after the service starts.4 |
|
| North Dakota |
Increases payment to family caregivers to provide certain waiver services.2,4 |
Allows for virtual or telephonic service planning and delivery of HCBS.1 |
|||
| Ohio |
Permits payment to family caregivers to provide certain waiver services.1,2 |
Allows for virtual or telephonic service planning and delivery of HCBS.1 |
Participant screened for COVID-19 prior to any home-based visited by a provider.21 |
||
| Oklahoma |
Relaxes provider (re)enrollment requirements.1 Temporarily modifies annual provider qualifications by extending current verification. Waives fingerprint criminal background checks. Removes requirement for advanced in-home training, allows online training.2 |
Permits payment to family caregivers to provide certain waiver services.1,2 |
Cost-sharing waived for COVID-19 testing.1 |
Allows for virtual or telephonic service planning and delivery of HCBS.1,2 |
|
| Oregon |
Expands providers permitted to render certain services.1 |
Permits payment to family caregivers to provide certain waiver services.2,4 |
Covers COVID-related testing through Emergency Medicaid.4 |
Allows for virtual or telephonic service planning and delivery of HCBS.1,2 |
Delays HH face-to-face encounters for up to 12 months after the service starts.4 |
| Pennsylvania |
Modifies provider qualifications to allow more flexibility in reassigning staff to provide PAS.2 Face-to-face interviews with applicants for employment are temporarily suspended.23 TB test requirements suspended.23 |
Permits payment to family caregivers to provide certain waiver services.1,2,4 |
Cost-sharing waived for COVID-19 testing.1 Covers COVID-related testing through Emergency Medicaid.4 |
Allows for virtual or telephonic service planning and delivery of HCBS.1,2 |
|
| Rhode Island |
Permits payment to family caregivers to provide certain waiver services.2 |
Allows for virtual or telephonic service planning and delivery of HCBS.1,2 |
|||
| South Carolina |
Permits payment to family caregivers to provide certain waiver services.2 |
Allows for virtual or telephonic service planning and delivery of HCBS.1,2 |
Requires case managers to submit incident reports for participants who test positive for COVID-19.2 Delays HH face-to-face encounters for up to 12 months after the service starts.4 |
||
| South Dakota |
Flexible provider enrollment/recertification for HCBS waivers.1 Modifies provider standards for direct service workers to qualify as direct workers while background check and pre-employment screenings are pending.2 |
Permits payment to family caregivers to provide certain waiver services.1,2 |
Cost-sharing waived for COVID-19 testing.1 |
Allows for virtual or telephonic service planning and delivery of HCBS.1,2 |
|
| Tennessee |
Eases provider (re)enrollment processes.1 |
Allows for virtual or telephonic service planning and delivery of HCBS.1,2 |
Rate increases to cover cost of PPE supplies.2 |
||
| Texas |
Allows for virtual or telephonic service planning and delivery of HCBS.4 |
||||
| Utah |
Suspends provider licensing (including background checks/fingerprinting) or certification for up to 1 year. Training may also be conducted via online/ telephone/electronic means. Allows for a 90-day window post-expiration of training.2 |
Permits payment to family caregivers to provide certain waiver services.1,2 |
Allows for virtual or telephonic service planning and delivery of HCBS.1,2 |
Coverage of PPE provided by operating agency.2 Delays HH face-to-face encounters for up to 12 months after the service starts.4 |
|
| Vermont |
Permits payment to family caregivers to provide certain waiver services.2,4 |
Allows for virtual or telephonic service planning and delivery of HCBS.2 |
|||
| Virginia |
Allows personal care and respite, and companion aides hired by an agency to provide services prior to receiving the required 40 hours of training; they must receive this training within 90 days of starting care.2 Suspends many other provider qualifications. Allows online/telephonic training.1,2 |
Permits payment to family caregivers to provide certain waiver services.1 |
Allows for virtual or telephonic service planning and delivery of HCBS.1,2 |
||
| Washington |
Waives the timing of training, certification, and recertification for including home care agencies.2 Flexibility to modify who is responsible for (re)assessments and (re)assessment timing.1 |
Covers COVID-related testing through Emergency Medicaid.4 |
Allows for electronic service planning and delivery of HCBS.1,2 |
Delays HH face-to-face encounters for up to 12 months after the service starts.4 |
|
| West Virginia |
Permits payment to family caregivers to provide certain waiver services; when formal caregiver is unavailable.1,2 |
Allows for virtual or telephonic service planning and delivery of HCBS.1,2 |
|||
| Wisconsin |
Suspends requirements to complete initial and required periodic credentialing of providers.2,4 |
Allows for virtual or telephonic service planning and delivery of HCBS.2 |
Participant screened for COVID-19 prior to any home-based visit by a provider.27 Staff screened for COVID-19 before conducting direct care.27 |
||
| Wyoming |
Modifies provider (case management, home health aide, personal support services) qualifications to suspend certain background and recertification requirements.1,2 |
Allows for virtual or telephonic service planning and delivery of HCBS.1,2 |
|||
State Policy Scan Footnotes
-
ATI Advisory: Federal and State Policy Waivers: COVID-19, updated as of August 24, 2020. Source: https://atiadvisory.com/wp-content/uploads/2020/08/COVID-19-Policy-Summary_August-24.pdf.
-
See National Academy for State Health Policy (NASHP): States Use Appendix K and Emergency Waivers to Support Home- and Community-Based Services in Responses to COVID-19, updated December 18, 2020. Source: https://www.nashp.org/states-use-appendix-k-waivers-to-support-home-and-community-based-services-in-response-to-covid-19/.
-
See https://www.medicaid.gov/state-resource-center/downloads/ak-combined-appendix-k-appvl.pdf.
-
See KFF article: Medicaid Emergency Authority Tracker: Approved State Actions to Address COVID-19 updated December 21, 2020. Source: https://www.kff.org/coronavirus-covid-19/issue-brief/medicaid-emergency-authority-tracker-approved-state-actions-to-address-covid-19/.
-
See https://www.medicaid.gov/state-resource-center/downloads/ar-combined-appendix-k-appvl.pdf.
-
See https://www.dir.ca.gov/dlse/Comparison-COVID-19-Paid-Leave.html.
-
See https://www.medicaid.gov/medicaid/section-1115-demonstrations/downloads/de-dshp-appendix-k-appvl.pdf.
-
See https://dch.georgia.gov/announcement/2020-03-25/important-notice-fingerprint-background-checks.
-
See https://dhs.iowa.gov/sites/default/files/DHS_COVID19_Home_Visitation-Guidance.pdf?120220202101.
-
See https://chfs.ky.gov/cv19/HomeHealthClinicalDefinitions.pdf.
-
See https://www.medicaid.gov/state-resource-center/downloads/md-combined-appendix-k-appvl.pdf.
-
See https://www.medicaid.gov/state-resource-center/downloads/ma-combined-appendix-k-appvl.pdf.
-
See https://www.michigan.gov/documents/mdhhs/L_20-26_689145_7.pdf.
-
See https://www.health.state.mn.us/facilities/regulation/homecare/docs/licensingwaiver.pdf.
-
See https://www.medicaid.gov/state-resource-center/downloads/nv-combined-appendix-k-appvl.pdf.
-
See https://www.dhhs.nh.gov/dcbcs/documents/dltss-covid19-guidance-2.pdf.
-
See https://www.health.ny.gov/health_care/medicaid/covid19/docs/2020-03-14_guide_chha_lthhc.pdf.
-
See https://www.tn.gov/content/dam/tn/tenncare/documents/CHOICESAndECFCHOICESCOVIDRelatedPayments.pdf.
-
See https://dcist.com/story/20/10/15/virginia-hazard-pay-home-health-workers-covid/.
Federal Policy Scan
| Federal Policy Changes that Affect Home Health Agencies (HHAs) | |||||
|---|---|---|---|---|---|
| Modify Worker Benefits | Modify Qualifications, Duties, Training or Supervision | Testing of Clients or Workers | Telehealth or Virtual Expansion | Infection Control Practices | CARES Act Guidance |
|
FFCRA will reimburse private employers that have fewer than 500 employees with tax credits for the cost of providing employees with paid leave taken for specified reasons related to COVID-19. The legislation will ensure that workers are not forced to choose between their paychecks and the public health measures needed to combat the virus, while at the same time reimbursing businesses.1 |
CMS waived certain screening requirements, postponed all revalidation actions, and expedited any pending or new applications from providers.2 CMS waived the HHA requirement for a RN to make an annual onsite supervisory visit for each aide and conduct on onsite visit every 2 weeks.2 CMS modified the requirement that aides receive 12 hours of in-service training in a 12 month period.2 CMS waived the requirements that rehabilitation skilled professionals may only perform the initial and comprehensive assessment when only therapy services are ordered. This temporary blanket modification allows any rehabilitation professional (OT, PT, or SLP) to perform the initial and comprehensive assessment for all patients receiving therapy services as part of the plan of care, to the extent permitted under state law.2 |
Health care providers undergoing testing should receive clear information on: the purpose of the test, the reliability of the test and any limitations associated with the test, who will pay for the test and how the test will be performed, how to interpret results and any next steps related to the results, who will receive the results, how the results may be used, any consequences for declining testing.3 |
HHAs can provide more services to beneficiaries using telecommunications technology within the 30-day period of care, so long as it's part of the patient's plan of care and does not replace needed in- person visits as ordered on the plan of care. We acknowledge that the use of such technology may result in changes to the frequency or types of in-persons visits outlined on existing or new plans of care. Telecommunications technology can include, for example: remote patient monitoring; telephone calls (audio only and TTY); and 2-way audio-video technology that allows for real-time interaction between the clinician and patient. However, only in-person visits can be reported on the home health claim.2 The required face-to-face encounter for home health can be conducted via telehealth (i.e., 2- way audio-video telecommunications technology that allows for real-time interaction between the physician/allowed practitioner and the patient).2 |
CMS narrowed the scope of the QAPI program to concentrate on infection control issues, while retaining the requirement that remaining activities should continue to focus on adverse events.2 |
Encouraging Use of Telecommunications Systems for Home Health Services Furnished During the Emergency Period. Encourages the use of telehealth technology, including remote patient monitoring, for home health services that are consistent with the patient's plan of care (CARES Act Section 3707).2 |
Federal Policy Scan Footnotes
-
Source: https://www.cms.gov/files/document/covid-home-health-agencies.pdf.
-
Source: https://www.cdc.gov/coronavirus/2019-ncov/hcp/testing-healthcare-personnel.html.
ENDNOTES
-
PHI National. (2019). US Home Care Workers: Key Facts. Retrieved from https://phinational.org/resource/u-s-home-care-workers-key-facts-2019/.
-
See https://www.cdc.gov/nchs/data/series/sr_03/sr03_43-508.pdf.
-
See https://aspe.hhs.gov/sites/default/files/private/pdf/264156/COVIDNH.pdf.
-
Rowe, T., Patel, M., O'Connor, R., McMackin, S., Hoak, V., & Lindquist, L. (2020, November-December). COVID-19 Exposures and Infection Control Among Home Care Agencies. Archives of Gerontology and Geriatrics, Advance online. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7390796/.
-
Span, P. (2020, June 6). Navigating Home Care During the Pandemic. New York Times, p. 3.
-
Flynn, H., Morley, M., & Bentley, F. (2020, September 28). Hospital Discharges to Home Health Rebounding, but SNF Volumes Lag. Retrieved from https://avalere.com/press-releases/hospital-discharges-to-home-health-rebound-while-snf-volumes-lag.
-
ATI Advisory. (2020). Federal and State Policy Waivers: COVID-19. Retrieved from https://atiadvisory.com/wp-content/uploads/2020/08/COVID-19-Policy-Summary_August-24.pdf.
-
National Academy for State Health Policy (NASHP). (2020). States Use Appendix K and Emergency Waivers to Support Home- and Community-Based Services in Responses to COVID-19. Retrieved from https://www.nashp.org/states-use-appendix-k-waivers-to-support-home-and-community-based-services-in-response-to-covid-19/.
-
Kaiser Family Foundation. (2020). Medicaid Emergency Authority Tracker: Approved State Actions to Address COVID-19. Retrieved from https://www.kff.org/coronavirus-covid-19/issue-brief/medicaid-emergency-authority-tracker-approved-state-actions-to-address-covid-19/.
RELATED PAPERS
COVID-19 Intensifies Home Care Workforce Challenges
https://aspe.hhs.gov/covid-home-care-workforce-challenges
COVID-19 Intensifies Home Care Workforce Challenges: Agency Perspectives Issue Brief
https://aspe.hhs.gov/covid-home-care-agency-perspectives
COVID-19 Intensifies Home Care Workforce Challenges: Policy Perspectives Issue Brief
https://aspe.hhs.gov/covid-home-care-policy-perspectives
HHS OFFICE OF THE ASSISTANT SECRETARY FOR PLANNING AND EVALUATION
SUGGESTED CITATION
Tyler, D., Hunter, M., Mulmule, N., & Porter, K. COVID-19 Intensifies Home Care Workforce Challenges. Washington, DC: Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services. June 1, 2021.
COPYRIGHT INFORMATION
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
___________________________________
Subscribe to ASPE mailing list to receive email updates on new publications: aspe.hhs.gov/join-mailing-list
For general questions or general information about ASPE: aspe.hhs.gov/about