
Eric Goplerud, Ph.D.
NORC at the University of Chicago
This report was prepared under contract between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and NORC at the University of Chicago. For additional information about the study, you may visit the DALTCP home page at http://aspe.hhs.gov/office_specific/daltcp.cfm or contact the ASPE Project Officer, Kirsten Beronio, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, SW, Washington, DC 20201. Her e-mail address is: Kirsten.Beronio@hhs.gov.
Acronyms
| ABA | applied behavioral analysis |
|---|---|
| ABD | adverse benefit determination |
| ASAM | American Society of Addiction Medicine |
| BLS | DOL Bureau of Labor Statistics |
| CBO | Congressional Budget Office |
| CHIP | Children's Health Insurance Program |
| CMS | HHS Centers for Medicare and Medicaid Services |
| DOL | U.S. Department of Labor |
| DRG | diagnosis-related group |
| E&M | evaluation and management |
| ECT | electroconvulsive therapy |
| EHB | essential health benefit |
| EOB | explanation of benefit |
| ER | emergency room |
| ERISA | Employee Retirement Income Security Act |
| FEHBP | Federal Employee Health Benefit Plan |
| GAO | U.S. Government Accountability Office (previously General Accounting Office) |
| HHS | U.S. Department of Health and Human Services |
| HRET | Health Research and Education Trust |
| IFR | Interim Final Rule |
| IOP | intensive outpatient program |
| IP INN MH | Inpatient In-Network Mental Health |
| IP INN SUD | Inpatient In-Network Substance Use Disorder |
| IP OON MH | Inpatient Out-of-Network Mental Health |
| IP OON SUD | Inpatient Out-of-Network Substance Use Disorder |
| KFF | Kaiser Family Foundation |
| MBHO | managed behavioral healthcare organization |
| MH | mental health |
| MHPAEA | Mental Health Parity and Addiction Equity Act |
| NAICS | North American Industry Classification System |
| NCS | National Compensation Survey |
| NQTL | non-quantitative treatment limitation |
| OOP | out-of-pocket |
| OP INN MH | Outpatient In-Network Mental Health |
| OP INN SUD | Outpatient In-Network Substance Use Disorder |
| OP OON MH | Outpatient Out-of-Network Mental Health |
| OP OON SUD | Outpatient Out-of-Network Substance Use Disorder |
| OP OV INN MH | Outpatient Office Visit In-Network Mental Health |
| OP OV INN SUD | Outpatient Office Visit In-Network Substance Use Disorder |
| OP OV OON MH | Outpatient Office Visit Out-of-Network Mental Health |
| OP OV OON SUD | Outpatient Office Visit Out-of-Network Substance Use Disorder |
| OP-Other INN MH | Outpatient-Other In-Network Mental Health |
| OP-Other INN SUD | Outpatient-Other In-Network Substance Use Disorder |
| OP-Other OON MH | Outpatient-Other Out-of-Network Mental Health |
| OP-Other OON SUD | Outpatient-Other Out-of-Network Substance Use Disorder |
| PBM | pharmacy benefits management |
| PCP | primary care physician |
| PDD | Plan Design Database |
| PHS Act | Public Health Service Act |
| PMPM | per member per month |
| PPACA | Patient Protection and Affordable Care Act |
| QTL | quantitative treatment limitation |
| RFI | Request for Information |
| RTF | residential treatment facility |
| Rx | prescription drug |
| SCP | specialty care physician |
| SMI | serious mental illness |
| SNF | skilled nursing facility |
| SPD | summary plan description |
| SUD | substance use disorder |
| UCR | usual, customary, and reasonable |
Introduction
The Paul Wellstone and Pete Domenici Mental Health Parity and Addiction Equity Act (MHPAEA) of 2008 was signed into law on October 3, 2008, and became effective for plan years beginning on or after October 3, 2009.6 For employers and group health insurance plans with more than 50 employees that offer coverage for mental illness and substance use disorders (SUDs), the law requires that coverage be no more restrictive than that for other medical and surgical procedures covered by the plan. MHPAEA does not require group health plans to cover mental health (MH) and SUD benefits, but when plans do cover these benefits, they must be covered at levels that are comparable to coverage levels for medical and surgical benefits offered by the plan. Specifically, MHPAEA renewed a preexisting requirement that employers and group health insurance plans eliminate more restrictive annual and lifetime dollar limits on MH coverage and MHPAEA added this requirement to SUD coverage as well. Furthermore, MHPAEA requires that employers and group health plans that provide both MH/SUD services and medical/surgical benefits ensure that:
The financial requirements applicable to such MH or SUD benefits are no more restrictive than the predominant financial requirements applied to substantially all medical and surgical benefits covered by the plan (or coverage), and there are no separate cost-sharing requirements that are applicable only to MH or SUD benefits.7
The treatment limitations applicable to such MH or SUD benefits are no more restrictive than the predominant treatment limitations applied to substantially all medical and surgical benefits covered by the plan (or coverage) and there are no separate treatment limitations that are applicable only to MH or SUD benefits.8
MHPAEA also includes requirements that group health plans make available information related to MH/SUD medical necessity criteria and reasons for any denials for MH/SUD services. If requested, medical necessity criteria must be provided to plan administrators (or offerors), potential participants, beneficiaries, and contracting providers. In addition, if requested, explanations of denials must be provided to participants or beneficiaries.9
After extensive public comment, the U.S. Department of Health and Human Services (HHS), the U.S. Department of Labor (DOL) and the Department of the Treasury released an Interim Final Rule (IFR)10 on February 2, 2010. The IFR provided guidance on the application of parity to financial, quantitative, and non-quantitative treatment limitations (NQTLs) and went into effect for plan years beginning on or after July 1, 2010. The IFR clarified several uncertainties:11
Deductibles and out-of-pocket limits. The IFR prohibited separately accumulating (separate but equal) financial requirements (e.g., deductibles) and quantitative treatment limitations (QTLs).
Separate coverage or benefits packages. Even though behavioral health benefits are sometimes carved out and administered by a separate insurer, each combination of plan offerings must have parity in behavioral health benefits when considered as a whole.
Financial requirements and quantitative treatment limitations (i.e., limits that can be expressed numerically as a dollar, a percentage, or number of visits or episodes). The compliance standard is that a particular type of financial requirement or QTLs (e.g., copays vs. coinsurance or limits on the number of outpatient visits) must apply to substantially all (i.e., at least two-thirds) of the medical/surgical benefits in a classification before it may be applied to MH/SUD benefits in that classification. If the requirement applies to at least two-thirds of all medical/surgical benefits in a classification, the permissible level of that financial requirement or treatment limit is set by determining the predominant level that applies to at least 50% of the medical/surgical benefits subject to that type of requirement or limit.
Non-quantitative treatment limitations (i.e., limits not expressed numerically that otherwise limit the scope or duration of benefits). NQTLs include but are not limited to medical management standards; prescription drug formulary designs; standards for provider admission to participate in a network; determination of usual, customary, and reasonable (UCR) amounts; requirements for using lower-cost therapies before a plan will cover more expensive therapies; and conditional benefits based on completion of a course of treatment. The IFR requires that any processes, strategies, evidentiary standards, or other factors used in applying an NQTL to MH or SUD benefits must be comparable to, and applied no more stringently than, the processes, strategies, evidentiary standards, or other factors used in applying the limitation to medical/surgical benefits, except to the extent that recognized clinically appropriate standards of care may permit a difference.
Classification of benefits. Six benefit classifications are specified in the IFR, with parity required for each: inpatient in-network, inpatient out-of-network; outpatient in-network; outpatient out-of-network; emergency care; and prescription drugs. On July 1, 2010, DOL released "safe harbor" guidance that allows for the creation of office visit and outpatient/other (non-office visit) sub-classes within the outpatient classifications of benefits.
Interaction with state insurance laws. MHPAEA does not supersede state parity law unless state law prevents the application of a MHPAEA requirement.
Availability of Plan Information. The IFR specifies that group plans governed by the Employee Retirement Income Security Act (ERISA) must follow the ERISA claims procedure regulations that provide, for example, that such reasons for claims denials must be provided automatically and free of charge. Other plans are encouraged to follow the ERISA requirements.
Application of the MHPAEA to Insurance and Health Plan Markets. Whether the MHPAEA applies to a particular insurance or health plan market depends both on whether the governing law applies its terms to the insurance market in question and on whether exemptions apply.12
ERISA-governed fully-insured group health benefit plans and ERISA-governed self-insured group health benefit plans. MHPAEA applies to all ERISA-governed group health plans and health insurance offered in connection with group health plans that offer coverage for both medical and surgical benefits and MH or substance abuse disorder benefits.13 MHPAEA also applies to group health plans and health insurance offered in connection with such plans in the non-ERISA market.14 Thus, MHPAEA applies to group health plans sponsored by private and public sector employers with more than 50 employees, including self-insured as well as fully-insured arrangements. MHPAEA also applies to health insurance issuers who sell coverage to employers with more than 50 employees. MHPAEA exempts small employers (i.e., employers having an average of 50 or fewer employees).15 Under the Patient Protection and Affordable Care Act (PPACA), the small employer exemption in the Public Health Service (PHS) Act is increased to 100 or fewer employees.16 DOL has determined that this upward revision in the PPACA of the size of small employer groups for PHS Act purposes does not affect ERISA-governed plans, whose small employer exemption remains at 50.17
State-regulated insurance products sold in the small group health or individual markets. HHS has proposed18 to incorporate the MHPAEA requirements into the essential health benefit (EHB) requirements for coverage of MH and SUD benefits under the PPACA.19 According to this interpretation, the MHPAEA compliance will be a required feature of all health insurance plans sold in the individual and small group markets starting in 2014.20
The state health insurance exchange market established under the PPACA. Because PPACA applies MHPAEA to all qualified health plans, health plans sold in state health insurance exchanges will be required to comply with federal parity requirements.
The Medicaid market, consisting of Medicaid fee-for-service, Medicaid managed care, Medicaid benchmark plans, and the separately administered Children's Health Insurance Program (CHIP) market. MHPAEA is incorporated by legislative reference into Medicaid, but only for certain forms of Medicaid coverage such as Medicaid Managed Care. MHPAEA also is incorporated by legislative reference into CHIP, although in states in which CHIP operates as a Medicaid expansion, the Medicaid expansion component of CHIP would be subject to Medicaid standards rather than to standards applicable to separately administered CHIP programs.21 MHPAEA also applies to Medicaid benchmark (a.k.a. alternative benefit plans) that will be offered by states that opt to extend Medicaid coverage to the low-income childless adult population as authorized by the PPACA.
The Medicare Market, including the fee-for-service market and the Medicare Advantage market. MHPAEA is not incorporated by reference into the Medicare statute. A limited provision aimed at removing Medicare's longstanding more restrictive treatment limitation for outpatient treatment of MH conditions was enacted into law by section 102 of the Medicare Improvements for Patients and Providers Act of 2008. This provision amended Medicare to phase out the law's historic outpatient MH treatment limitation over a 5-year period between 2010 and 2014.22 As the Centers for Medicare and Medicaid Services (CMS) notes in interpretive policies, this change means that beginning January 1, 2014, Medicare will pay 80% of the physician fee schedule for covered services and 80% of the encounter rate for covered treatments in federally qualified health centers and rural health clinics subject to their upper payment limit.23 With respect to the Medicare Advantage market, CMS interpretive regulations24 clarify that Medicare Advantage organizations offering special needs plans will be expected to comply with parity requirements. Whether the CMS definition of parity for Medicare Advantage Special Needs Plan purposes parallels that adopted in the IFR rule is not clear. MHPAEA does not apply to "stand alone" Medicare Advantage plans or Medicare fee-for-service plans.
Church plans. Because of their ERISA exemption, church plans are not affected by the MHPAEA's ERISA requirements. However, to the extent that an ERISA-exempt church purchases a product through a state health insurance exchange, or a state-regulated group insurance product governed by the PHS Act, the product would be subject to parity requirements, unless the church is otherwise exempt under state law.
Non-Federal Government health plans offered to state and local public employees. Non-Federal Government health plans are likewise ERISA-exempt, but their coverage would be subject to the MHPAEA's PHS Act provisions, whose scope reaches both the insurance market and non-Federal Government plans. At the same time, the law permits non-federally administered self-insured government health plans to opt out of these provisions.25
TriCare (the health program for uniformed service members, retirees, and their families) and the Federal Employee Health Benefit Plan (FEHBP). Although there is not a specific legislative requirement applying MHPAEA to the FEHBP program, these requirements do apply to the FEHBP through Executive Order and incorporation of these requirements into the purchasing and coverage standards issued by the Office of Personnel Management. MHPAEA does not generally apply to TriCare. The U.S. Department of Defense has not incorporated the MHPAEA's provisions into their purchasing and coverage standards.
Table 1 summarizes the applicability of the MHPAEA to 14 distinct insurance and health plan markets.
TABLE 1. Legal Application of the MHPAEA to 14 Distinct Public and Private Insurer/Employer-Sponsored Health Plan Markets
| Market | Yes/No |
|---|---|
| 1. ERISA-governed self-insured health benefit plans | Yes, MHPAEA and ERISA amendments apply; cost exemptions may apply, and size exemptions would apply in the case of small ERISA plans (fewer than 50 employees) that self-insure. |
| 2. ERISA-governed fully-insured health benefit plans | Yes, MHPAEA, PHS Act, and ERISA amendments apply; employer size and cost exemptions apply. |
| 3. State-regulated group and individual insurance markets | Yes, MHPAEA applies to health insurance issuers who sell coverage to employers with more than 50 employees and MHPAEA standards will extend to both the small group and individual markets through PPACA provisions and EHB requirements. |
| 4. Medicaid fee-for-service | No, CMS Medicaid standards apply. |
| 5. Medicaid managed care | Yes, CMS Medicaid managed care standards apply. |
| 6. Medicaid benchmark plans | Yes, CMS benchmark standards apply. |
| 7. Separately administered CHIP plans | Yes, MHPAEA standards apply. |
| 8. Medicare fee-for-service market | No, CMS Medicare standards apply. |
| 9. Medicare Advantage | No, CMS Medicare standards apply. |
| 10. State health insurance exchanges | Yes, MHPAEA standards apply. |
| 11. FEHBP | No, but FEHBP policies apply; FEHBP has explicitly adopted MHPAEA. |
| 12. TriCare | No, TriCare standards apply; MHPAEA not adopted. |
| 13. Church plans | No, churches are exempt from ERISA requirements, but PHS standards would apply to insured products unless churches have a state exemption. |
| 14. Non-federal public employee health benefit plans | Yes, covered by the MHPAEA's PHS Act provisions, but plan sponsors may opt out. |
MHPAEA Public Law 110-343.
See 75 Fed. Reg. 5410-5451 (February 2, 2010). See 45 C.F.R. §146.136(a) defining the scope of parity in relation to both qualitative and quantitative treatment limits.
Melek S. Implementing parity: Investing in behavioral health. Milliman Healthcare Reform Briefing Paper, May 20, 2010.
Rosenbaum SR, Goplerud EG, McDowell M, Jacobus-Kantor L, Melek S. Mental Health and Addiction Treatment Parity Across Public and Private Insurance Markets: An Analysis of Federal Laws. Presented to the Office of the Assistant Secretary of Planning and Evaluation, July 2012.
29 U.S.C. §1185a(a)(3).
42 U.S.C. §330(g)(2).
29 U.S.C. §1185a(c)(1).
42 U.S.C. §300gg-91(e)(4) as applied to MHPAEA by PPACA §1563(c)(4).
See U.S. Department of Labor, FAQs about Affordable Care Act Implementation Part V and Mental Health Parity Implementation, Q. 8. Available at: http://www.dol.gov/ebsa/faqs/faq-aca5.html. Accessed May 5, 2012.
Patient Protection and Affordable Care Act: Standards Related to Essential Health Benefits, Actuarial Value, and Accreditation; Proposed rule, 77 Fed. Reg. 70644-70677 (amending 45 CFR Parts 147, 155, and 156) (November 26, 2012).
42 U.S.C. §18022, added by PPACA §1302.
42 U.S.C. §300gg-6(a).
42 U.S.C. §1397cc(c)(6).
Social Security Act §1833(c)(1), 42 U.S.C. §1395l(c)(1).
CMS Manual System Pub. 100-02, Transmittal 114, Medicare Benefit Policy.
76 Fed. Reg. 54600, 54605 (September 1, 2011).
PHS Act §2722(a)(2), 42 U.S.C. §300gg-21(a)(2).
Brief Review of the Existing Literature
Necessity of Compliance Testing. The history of parity legislation shows that implementation of requirements in this area is not always straightforward and ensuring equitable treatment of MH and SUD treatment is often complicated. Experience with implementation of the Mental Health Parity Act of 199626 is a case in point. The 1996 Act mandated elimination of unequal annual and lifetime dollar limits on MH coverage in employer-sponsored and group health insurance plans. Compliance monitoring found that most health plans complied by eliminating dollar limits but increased restrictions on the number of hospital days or outpatient visits for MH services.27 Findings reported by the U.S. Government Accountability Office (GAO) are representative. Of 863 employer plans responding to its 1999 survey:
- 14% of employers had not complied with the law by 1999.28
- 51% reduced the number of outpatient visits covered.
- 36% reduced hospital days covered.
- 20% increased outpatient visit copayments.
- 18% increased the cap on enrollee out-of-pocket costs.29
Research studies focusing on implementation of previous parity requirements such as those applied to FEHBP can complement our other sources of information and enhance our understanding of the impact of MHPAEA.
FEHBP Parity. Monitoring of FEHBP parity implementation30, 31 revealed that all FEHBPs complied with parity, that no plan reported major problems implementing parity, and that no plan left the program to avoid implementing the policy. Plans enhanced their pre-parity MH/SUD benefits as required by the policy change (84% enhanced MH, 75% enhanced SUD benefits)32 and were more likely to carve-out the behavioral health benefit. Other expected changes (e.g., increased gate keeping at the primary care provider level, reduced provider networks, concurrent or retrospective review, use of disease management programs for MH/SUD care, and increased financial risk sharing) occurred infrequently.
Evaluations of FEHBP parity found no significant increase in total behavioral health spending. Nor did evaluations find an increased probability of any MH/SUD service utilization resulting from parity.33 In fact, the quantity of MH/SUD services patients received may have decreased slightly after parity was introduced. A recent study by Goldman and colleagues found that beneficiaries in plans that were subject to FEHBP parity demonstrated larger reductions in overall behavioral health visits, medication management visits, psychotherapy visits, and prescriptions for behavioral health medications (which the authors assume resulted from increased use of utilization management techniques by plans) following the introduction of parity than did a matched comparison group not subject to FEHBP parity.34 However, introduction of FEHBP parity was associated with a significant decrease in out-of-pocket spending for MH/SUD services.35, 36, 37
A separate study of the impact of parity on substance abuse treatment in FEHBP plans found that although the rate of out-of-pocket spending declined significantly for substance abuse treatment and more patients had new diagnoses of a SUD, there were no differences in rates of initiation and engagement in treatment under parity and total plan spending per user and average utilization of substance abuse services did not change.38
Researchers have examined the effects of FEHBP parity on specific populations, services, and diagnoses. A recent study examined utilization and costs for individuals having one of three diagnoses representing a continuum of condition severity: bipolar disorder, which was classified as both severe and chronic in nature; major depression, whose severity and chronicity vary considerably in the population; and adjustment disorder, which was classified as a less severe, non-chronic condition.39 Results suggested that, compared to a matched control group, enrollees having each of these conditions demonstrated no significant changes in utilization associated with medication management, inpatient days, or prescriptions following the implementation of parity. In the adjustment disorder group, there was a small, but statistically significant, reduction in psychotherapy utilization. Additional analyses revealed no changes in total behavioral health spending for individuals with bipolar disorder or major depression and small decreases in spending associated with individuals diagnosed with adjustment disorder.40 Out-of-pocket spending related to MH/SUD treatment decreased across all three diagnostic categories vs. the matched control group.
Another recent study of FEHBP parity attempted to identify specific subpopulations of beneficiaries who benefited most from the introduction of parity. Applying growth mixture modeling techniques to FEHBP data, Neelon and colleagues concluded that the effects of parity differed depending on an individual's pre-parity utilization patterns. Three distinct subgroups emerged: "low-spenders," (who had low levels of utilization of MH/SUD services in the pre-parity period) -- their utilization of MH/SUD services declined in the post-parity period; "moderate-spenders," (who had moderate pre-parity spending) -- their spending increased following the implementation of parity; and "high-users," (who had high MH/SUD spending during the pre-parity) -- their spending continued to be high in the post-parity period.41 Another study found that among enrollees who received MH treatment for a severe mental illness (e.g., schizophrenia, bipolar disorder, depression), the odds of using any MH/SUD services in subsequent years were more than 1.3 times greater than two matched control groups.42 The relative odds of using inpatient MH/SUD services in the parity group were 0.67 times that of the control groups, a decrease consistent with the hypothesis that managed care organizations might have guided patients toward more outpatient services in treating their severely ill enrollees. Prescription usage under parity appears to have increased. Individuals covered under FEHBP parity were 1.4 times more likely to fill any behavioral health prescription compared to their non-FEHBP counterparts. An analysis of the impact of FEHBP parity on rates of treatment for depression found no significant changes in rates of diagnosis of depression following introduction of parity and very little change in measures of the quality of care.43
Several additional evaluations of FEHBP parity have focused on the effects of the program on children and adolescents. Azrin and colleagues concluded that, following the introduction of FEHBP parity, children enrolled in the FEHBP program showed no significant increase in MH/SUD utilization compared to a matched control group.44 These findings are consistent with analyses of the impact of state parity laws that show no significant impact on access for children and adolescents.45 In evaluating only children and adolescents with high MH/SUD expenditures in the pre-parity period, a recent study concluded that compared to a matched control group, children enrolled in the FEHBP showed similar patterns of MH/SUD expenditures following the introduction of parity, but a statistically significant reduction (approximately $258 in 2011 dollars) in average out-of-pocket spending associated with MH/SUD services.46
In general, these studies of FEHBP parity found no significant increases in overall MH/SUD utilization rates, initiation or engagement rates, or total MH/SUD spending following the implementation of parity but significant decreases in out-of-pocket costs did result.
Vermont. Compliance monitoring of the MHPAEA can also be guided by the findings of studies examining the effects of state-level parity, such as Vermont.47 The Vermont Parity Act took effect January 1, 1998.48 The Vermont legislation mandated group health insurance to cover MH/SUD treatment equitably with other covered medical treatments (ERISA-governed self-insured plans are exempt from state parity legislation). An evaluation of the law's effects found an increased probability of an individual receiving any outpatient MH services and a decreased likelihood of an individual receiving any substance abuse services following the introduction of parity. The percentage of beneficiaries receiving outpatient MH services increased by a range of 6%-8%. The percentage of individuals receiving any substance abuse services decreased by a range of 16%-29%.49 Results also indicated that, in general, consumer cost-sharing for MH and substance abuse treatment services declined, from 27% to 16% of total costs, following the implementation of parity. The evaluation of the Vermont law's effects found little evidence that the introduction of parity resulted in employers dropping health coverage or switching to self-insured plans to avoid complying with the regulation. Only 0.3% of Vermont employers reported that they dropped health coverage for their employees primarily due to the parity law, and only 0.1% of employers reported that parity played a role in their decision to self-insure (to avoid complying with state law).50
Use of managed care techniques increased following Vermont's implementation of parity. Although one of the two major health plans already used managed care before the implementation of parity, the other health plan also shifted most of its members to a managed behavioral health care carve-out. In one plan, spending increased modestly by 19 cents per member per month (PMPM). Nonetheless, MH/SUD services accounted for only 2.5% of total spending in that plan after parity compared to 2.3% before parity. The other plan experienced a 9% decrease in spending for MH/SUD services following implementation of the state parity law. This decrease in spending was largely attributed to a decrease in SUD treatment service utilization.
Employers' knowledge of the parity law remained low, even after its implementation. A survey conducted 2 years after the implementation of parity suggested that approximately 50% of all fully-insured employers in Vermont had never heard of the parity law and that nearly three-fifths of all employers had little to no knowledge of the parity law.51 Small and medium-sized businesses were least likely to be familiar with the law, with approximately 70% of those employers having little to no knowledge of the law. Although the two major health plans in Vermont complied with the law on paper, lack of information, confusion, and mistakes by the state's largest plan generated complaints from beneficiaries and providers that led to changes in administration and consumer education in succeeding years.52
Oregon. Oregon's parity law, implemented January 1, 2007,53 mandated that group health insurance plans provide coverage for MH and substance abuse treatment services at the same level as other medical conditions. Results from Oregon are particularly informative for the current project in that the Oregon law, like the MHPAEA, went beyond the regulation of financial and QTLs and specified that plans cannot utilize unequal, NQTLs for MH and substance abuse treatment services compared to medical/surgical services. A recent analysis of the Oregon law suggested that each of the four plans studied made substantial changes to their MH and substance abuse treatment benefits following the implementation of parity. Each plan removed coverage limits related to inpatient and outpatient MH/SUD treatment services. After implementation of the NQTL provisions in the Oregon law, the use of management techniques stayed the same or decreased in the insurance plans studied. These changes were made without significant increases in total MH/SUD treatment spending. Importantly, the researchers found that these effects were achieved without the increased use of utilization management techniques.54 The authors also found no evidence of meaningful change in the rates of any behavioral health care service use.
In a separate analysis of only substance use spending, McConnell55 found that expenditures for alcohol treatment services increased significantly and spending on other drug abuse treatment services did not. The introduction of parity was associated with a small, but not statistically significant, increase in overall substance use treatment spending. In another study analyzing the impact of parity in Oregon on access to various behavioral health specialists, McConnell found that parity was associated with a slight increase (from 0.5% to 0.8%) in behavioral health treatment initiations with masters-level specialists, and relatively few changes for generalist physicians, psychiatrists, and psychologists. Patients were particularly sensitive to distance for non-physician specialists:56 the greater the distance between an individual and a non-physician specialist, the less likely that individual was to receive treatment. Following the introduction of parity, distance to the nearest psychiatrist, masters-level therapist, or psychologist tended to decrease.
California. California's Mental Health Parity Bill, which became effective on July 1, 2000, mandated that all group and individual health plans offer MH coverage as part of their overall health benefits and outlawed the use of MH treatment limitations and cost-sharing requirements that were more restrictive than those for physical health conditions.
The law required that health plans provide MH services to seriously mentally ill (SMI) adults and all children with serious emotional disturbances. Nine specific SMI diagnoses were included in the mandate: anorexia nervosa, bulimia nervosa, bipolar disorder, major depression, obsessive-compulsive disorder, panic disorder, pervasive developmental disorder/autism, schizophrenia, and schizoaffective disorder. SUDs were not covered by the California Parity Act. To assess health plan compliance with the Mental Health Parity Bill, the California Department of Mental Health undertook an intensive review of health plans that included an onsite survey, reviews of claims files, utilization review files, and internal management and performance reports. The report identified several areas of non-compliance. Six out of seven California plans that were subject to the legislation were incorrectly denying coverage for emergency room (ER) visits; five out of seven plans were failing to monitor whether beneficiaries had reasonable access to after-hours services; and five out of seven plans failed to include required information in claim denial letters.57
Trends in MH/SUD Spending and the Costs of Parity. An analysis by Mark and colleagues examined trends in behavioral health spending between 2001 and 2009 for a sample of over 100 large, self-insured employer plans. Results concluded that the average contribution of behavioral health care spending to total health care spending across each of the years examined was 0.3%, and only 2% of employers experienced a rate increase of more than 1% per year attributable to behavioral health costs.58
Given the small contribution of behavioral health care costs to overall health care costs, MHPAEA is expected to result in only very modest increases total health care expenditures. The Congressional Budget Office (CBO) estimated that MHPAEA itself would result in very modest cost increases, approximately 0.4%, in employer-sponsored group health care premiums and 0.2% in Medicaid payments to managed care plans.59 Recent analyses by Mark and colleagues utilizing MarketScan data are consistent with the CBO's estimate. Their analyses have suggested that an overwhelming majority of privately insured beneficiaries who utilized behavioral health care benefits in the pre-parity era did so at a rate that was far below pre-parity health care limits.60 Using econometric models to estimate the detailed effects of the MHPAEA on high-utilization beneficiaries who are likely to use its expanded coverage, these researchers estimated that the MHPAEA will likely increase total health care costs by 0.4%.
Early MHPAEA Compliance Analysis. In November 2011, GAO issued an early report on MHPAEA compliance in response to a statutory requirement.61 One hundred sixty-eight employers responded to a GAO survey asking detailed questions about changes in their behavioral health benefits between 2008 and 2010/2011 out of 707 employers who received the survey. Although the findings from this survey are not generalizable given the response rate of 24%, the survey did generate information on some questions regarding diagnoses covered not addressed in other studies. The vast majority of responding employers offered MH/SUD coverage in both 2008 and in 2010/2011, and most employers reported covering the same broad range of MH/SUD diagnoses in their current plan year as they also did in 2008. The remaining employers reported including more broad diagnoses.
In keeping with findings in other studies, employers responding to the GAO survey reported reducing their use of MH/SUD office visit and inpatient day limitations. In 2008, a significant percentage of these employers reported utilizing office visit limitations for SUDs. In 2010/2011, far fewer of these employers reported having such limitations. Likewise, in 2008, a significant percentage of employers reported utilizing limitations on inpatient days related to behavioral health conditions. By 2010/2011, the percentage of employers reporting using such limitations had dropped. The GAO did not assess NQTLs used by employers and health plans. While the results of the GAO survey should be interpreted with caution due to its small sample size and low response rate, the results from the survey suggest that employers were generally able to implement changes required by MHPAEA with little disruption to the insurance market.
P.L. 104-204.
Allen KG. Mental Health Parity Act: Employers' mental health benefits remain limited despite new federal standards. Testimony before the Committee on Health, Education, Labor and Pensions, U.S. Senate. Washington, DC: General Accounting Office, May 18, 2000. (Document no. GAO/T-HEHS-00-113.)
Burnam MA, Escarce JJ. Equity in managed care for mental disorders. Health Aff. 1999; 18:22-31.
Hennessy KD, Goldman HH. Full parity: Steps toward treatment equity for mental and addictive disorders. Health Aff. 2001; 20:58-67.
Allen KG. Mental Health Parity Act: Employers' mental health benefits remain limited despite new federal standards. Testimony before the Committee on Health, Education, Labor and Pensions, U.S. Senate. Washington, DC: General Accounting Office, May 18, 2000. (Document no. GAO/T-HEHS-00-113.)
Goldman HH, Frank RG, Burnam A et al. Behavioral health insurance parity for federal employees. N Engl J Med. 2006; 354:1378-1386.
Lichtenstein C et al. Evaluation of parity in the Federal Employees Health Benefits (FEHB) program: Final Report. Presented to the U.S. Department of Health and Human Services Administration, Office of the Assistant Secretary Planning and Evaluation, 2004. Available at: http://aspe.hhs.gov/daltcp/reports/parity.htm.
Goldman HH, Frank RG, Burnam MA et al. Behavioral health insurance parity for federal employees. N Engl J Med. 2006; 354:1378-1386.
Goldman HH, Barry CL, Normand ST, Azzone V, Busch AB, Huskamp HA. Economic grand rounds: The price is right? Changes in the quantity of services used and prices paid in response to parity. Psychiatr Serv. 2012; 63:107-109.
Goldman HH, Frank RG, Burnam MA et al. Behavioral health insurance parity for federal employees. N Engl J Med. 2006; 354:1378-1386.
Azrin ST, Huskamp HA, Azzone V, et al. Impact of full mental health and substance abuse parity for children in the Federal Employees Health Benefits Program. Pediatrics 2007; 119:452-459.
Azrin ST, Huskamp HA, Azzone V et al. Impact of full mental health and substance abuse parity for children in the Federal Employees Health Benefits Program. Pediatrics 2007; 119:452-459.
Azzone V, Frank R, Normand S, Burnam A. Effect of insurance parity on substance abuse treatment. Psychiatr Serv. 2011; 62:129-134.
Busch A, Yoon F, Barry C et al. The effects of parity on mental health and substance use disorder spending and utilization: Does diagnosis matter? Am J Psych. In press.
Busch A, Yoon F, Barry C et al. The effects of parity on mental health and substance use disorder spending and utilization: Does diagnosis matter? Am J Psych. In press.
Neelon B, O'Malley AJ, Normand ST. A Bayesian two-part latent class model for longitudinal medical expenditure data: Assessing the impact of mental health and substance abuse parity. Biometrics 2011; 67:280-289.
Yoon FB, Huskamp HA, Busch AB, Normand ST. Using multiple control groups and matching to address unobserved biases in comparative effectiveness research: An observational study on the effectiveness of mental health parity. Stat Biosci. 2011; 3:63-78.
Huskkamp HA. The impact of parity on major depression quality in the Federal Employees Health Benefit Program. Med Care 2006; 44:506-512.
Azrin ST et al. Impact of full mental health and substance abuse parity for children in the Federal Employees Health Benefits Program. Pediatrics 2007; 119:452-459.
Barry CL, Busch SH. Caring for children with mental disorders: Do state parity laws increase access to treatment. J Ment Health Policy Econ. 2008; 11:57-66.
Azrin ST et al. Impact of full mental health and substance abuse parity for children in the Federal Employees Health Benefits Program. Pediatrics 2007; 119(2):452-459.
Rosenbach M, Lake T, Young C et al. Effects of the Vermont Mental Health and Substance Abuse Parity Law. DHHS Pub. No. (SMA) 03-3822. Rockville, MD: Center for Mental Health Services, Substance Abuse and Mental Health Services Administration, 2003.
Vermont State Legislature. (2000) Section 4089, Mental Illness. Available at http://www.leg.state.vt.us/statutes/titles08/chap107.htm.
Rosenbach M, Lake T, Young C et al. Effects of the Vermont Mental Health and Substance Abuse Parity Law. DHHS Pub. No. (SMA) 03-3822. Rockville, MD: Center for Mental Health Services, Substance Abuse and Mental Health Services Administration, 2003.
Rosenbach M, Lake T, Young C et al. Effects of the Vermont Mental Health and Substance Abuse Parity Law. DHHS Pub. No. (SMA) 03-3822. Rockville, MD: Center for Mental Health Services, Substance Abuse and Mental Health Services Administration, 2003.
ORS 743.556; OAR 830-053-1404, 1405, 1325, 1330; SB 1.
McConnell KJ, Gast SH, Ridgely MS et al. Behavioral health insurance parity: Does Oregon's experience presage the national experience with the Mental Health Parity and Addiction Equity Act? Am J Psychiatry. 2012; 169:31-38.
McConnell KJ, Ridgely MS, McCarty D. What Oregon's parity law can tell us about the federal Mental Health Parity and Addiction Equity Act and spending on substance abuse treatment services. Drug Alc Depend. 2012; 124:340-346.
McConnell KJ, Gast SH, McFarland BH. The effect of comprehensive behavioral health parity on choice of provider. Med Care. 2012; 50:527-533.
California Department of Managed Health Care. Mental Health Parity in California. Mental Health Parity Focused Survey Project: A Summary of Survey Findings and Observations. Available at: http://www.hmohelp.ca.gov/library/reports/med_survey/parity/sfor.pdf.
Mark TL, Vandivort-Warren R, Miller K. Mental health spending by private insurance: Implications for the Mental Health Parity and Addictions Equity Act. Psych Serv. 2012; 63(4):313-318.
Congressional Budget Office. Congressional Budget Office Cost Estimate: S558. March 20, 2007.http://www.cbo.gov/sites/default/files/private/cbofiles/ftpdocs/78xx/doc7894/s558.pdf.
Mark TL, Vandivort-Warren R, Miller K. Mental health spending by private insurance: Implications for the Mental Health Parity and Addictions Equity Act. Psych Serv. 2012; 63(4):313-318.
For its 2012 parity study, the GAO surveyed a stratified random sample of 707 small, medium, large, and very large employers about the MH/SUD covered in their health plans that covered the greatest number of lives for the most current plan year -- either 2011 or 2010 -- as well as for 2008. A total of 168 employers submitted usable survey responses, for a response rate of 24%. It may be difficult to generalize from this sample to the universe of employers and health plans subject to MHPAEA and the IFR.
Study Background and Purpose
Project Objective. NORC at the University of Chicago led a research team that included Milliman Inc., Aon Hewitt, Thomson Reuters/Truven Health Analytics, and George Washington University to perform an analysis of compliance with the MHPAEA and the IFR62among ERISA-governed employer-sponsored group health plans and health insurance coverage offered in connection with such group health plans. Our analysis includes information from a variety of existing and complementary data sources. Information on coverage provided by large health plans and insurers was provided by testing databases compiled by both Milliman Inc. and Aon Hewitt as well as data from Aon Hewitt's Plan Design Database (PDD) which contains more than 10,000 unique plan designs for more than 300 employer clients. Taken together, information from these sources was used to track health plan coverage in this market and estimate changes in coverage that apply to the 111 million covered lives that are included in this large employer market. Health plan offerings provided by midsized establishments was assessed using information from Summary Plan Descriptions (SPDs) of midsized establishments obtained from the DOL Bureau of Labor Statistics (BLS). Information from the BLS SPDs was used to track changes in health plan coverage that apply to approximately 39 million lives that are covered in the midsized market. Additional information on both markets was provided by published and unpublished data from national employer health benefits surveys conducted by the Kaiser Family Foundation and Health Research and Educational Trust (KFF/HRET)63 and Mercer.64 To assess plan responses to the MHPAEA's disclosure requirements, semi-structured interviews were conducted with a small number of health plan representatives who were responsible for their plans' compliance with MHPAEA.
Table 2 presents the study's key research questions and the data sources used to address each question.
TABLE 2. Key Research Questions and Data Source Used to Address Each Question
| Research Question | Data Sources |
|---|---|
| 1. What types of financial requirements (e.g., copays, coinsurance) do group health plans use for MH and SUD benefits, and are such requirements consistent with the new MHPAEA standards for calculating the predominant level that applies to substantially all medical and surgical benefits? |
|
| 2. What types of QTLs (e.g., day limits, visit limits) do group health plans use for MH and substance use conditions, and are such limitations consistent with the MHPAEA standards? |
|
| 3. What types of NQTLs are commonly used by plans and issuers for MH and/or substance abuse disorders and how do these compare to NQTLs in place for medical/surgical benefits? |
|
| 4. Are group health plans and insurers using separate deductibles for MH and/or SUD benefits? |
|
| 5. Have financial requirements and treatment limits on medical/surgical benefits become more restrictive in order to achieve parity (instead of requirements and limits for MH and substance use becoming less restrictive)? |
|
| 6. How many plans have eliminated MH and/or substance abuse treatment coverage altogether instead of complying with the MHPAEA? |
|
| 7. How have plans responded to the MHPAEA's requirements regarding the disclosure of medical necessity criteria and reasons for claim denials? |
|
See 75 Fed. Reg. 5410-5451 (February 2, 2010). See 45 C.F.R. §146.136(a) defining the scope of parity in relation to both qualitative and quantitative treatment limits.
KFF/HRET annually surveys a random, stratified sample of employers to assess year-to-year changes in health benefits. Employers are stratified by industry and employer size. For the most recently completed annual survey -- conducted from January 2010 to May 2010 and published in September 2010 -- 2,046 employers responded to the full survey, a 47% response rate.
Mercer surveys a stratified random sample of employers annually through mail questionnaires and telephone interviews. Mercer selects a random sample of private sector employers from a Dun & Bradstreet database, stratified into eight categories, and randomly selects public sector employers -- state, county, and local governments -- from the Census of Governments. A total of 2,833 employers responded to the 2010 survey. By using statistical weights, Mercer projected its results nationwide and for 4 geographic regions. The Mercer survey report contains information for large employers -- those having >500 employees -- and for categories of large employers with certain numbers of employees as well as information for small employers -- those having fewer than 500 employees. Mercer used the same methodology for its 2008 survey, which was published in 2009.
Overview of Key Data Sources and Methodologies
Milliman Compliance Testing Database. Information from Milliman's MHPAEA compliance testing database was used to evaluate 2010 plan design data for adherence to MHPAEA standards. This database includes detailed quantitative financial requirements and treatment limitations for post-parity, pre-IFR benefit levels for medical/surgical benefits and MH/SUD benefits. It also contains details regarding any NQTLs when they could be identified through SPDs.
Of approximately 1,500 plans available in the database, 124 were analyzed to obtain an unbiased and representative distribution of large group plans by geographic region and industry, including self-insured and fully-insured plans. To obtain sufficient information for testing, detailed plan documents and benefit descriptions were requested to identify any financial requirements or treatment limits by detailed service category. To test plan designs for adherence to the quantitative aspects of the legislation, we utilized Milliman's testing model that completes the "substantially all" and "predominant" tests described in the IFR for quantitative financial requirements and treatment limitations. The actuarial-based model relies on Milliman's Health Cost Guidelines for health plans or employers whose membership is not large enough to be statistically reliable, and it includes specific adjustments for variables that impact health care costs such as geographic area, provider contract arrangements, and degree of health care management. If the health plan's or employer's membership was large enough to be statistically reliable (typically more than 10,000 members), the compliance testing model was based on the health plan's or employer's claim costs, usually on a book-of-business basis.
If plan or group-specific costs were used, detailed health care cost data for the most recent complete plan year were requested from the health plan or offeror. Either total allowed dollars or allowed dollars on a PMPM basis were acceptable. Participating health plans and plan sponsors were provided with a template for the level of detail requested by service category, which align with the service categories in Milliman'sHealth Cost Guidelines. Approximately 50 different medical/surgical categories are included.
Quantitative testing was performed on an allowed claim dollar basis (before application of any financial requirements). After the testing model was set up with the costs by detailed health care service category, each medical/surgical service category is mapped into one of the six classifications as prescribed by the IFR, including the two outpatient sub-classifications. Detailed financial requirements and treatment limits by service category were then entered into the model and calculations were performed to determine which quantitative financial requirements (deductibles, coinsurance, copays, and so forth) and treatment limitations (calendar year limits, lifetime limits, other quantity limits, and so forth) meet the "substantially all" criteria required by the IFR. For those quantitative financial requirements and treatment limitations that met this test, the "predominant" level was identified. The results identified the benefit plan changes that are necessary in each benefit classification to be consistent with MHPAEA requirements. To confirm that the MH and SUD coverage was complete in all classifications, covered MH and SUDs were reviewed to determine if coverage is provided in all classifications where medical/surgical benefits are provided.
When a scope of service issue (such as the exclusion of residential treatment for substance use rehabilitation) was identified, it was discussed with the health plan or plan sponsor as being currently acceptable under the IFR, but potentially capable of becoming non-compliant if rules on required scope of services are enacted. In addition to the quantitative testing, detailed plan documents were reviewed to identify potential compliance problems with NQTLs. The IFR is less specific regarding where the line for non-compliance is drawn for NQTLs. Different interpretations exist among health plans and employers on what is allowable and compliant. Plan documents often contain details for some, but not all, NQTLs. Sometimes, information can be found on precertification requirements, step therapies, prescription drug formulary design, and conditioning benefits on the completion of a course of treatment. When this information is in the plan documents, we determined whether it appeared that the plan applied them in a "comparable" manner and in a manner "no more stringently" than those applied to medical/surgical benefits.
Aon Hewitt Compliance Testing Database. Aon Hewitt plan designs were reviewed to assess compliance with MHPAEA and the IFR standards. The plan design review and compliance testing was conducted in 2010, based on the plan designs each employer expected to implement in the 2011 plan year.
The Aon Hewitt testing database encompasses plan designs from more than 60 employers, ranging in size from 400 to more than 300,000 employees and representing 230 plan options. Each plan option represented a single combination of benefits (a combination of medical/surgical and MH/SUD benefits) that is available to an employer's participants. Plans whose adherence could not be assessed through a review of summary plan documents were subjected to detailed testing procedures. Of the 230 plan options reviewed, 140 required detailed testing to determine the benefit design that would apply to MH/SUD benefits. Plans that used identical coverage criteria for both MH/SUD and medical surgical services were considered to adhere to MHPAEA standards, and did not required detailed testing.
For most employer plans, the benefit type and level within the inpatient in-network and out-of-network, outpatient out-of-network, prescription drug, and emergency care classifications were consistent for both medical/surgical and MH/SUD and, as a result, demonstrated consistency with the parity regulations. For these benefit classifications, detailed testing was not required. Benefit design for the outpatient in-network classification, however, most frequently required detailed testing across employer programs. Within this classification, employer programs typically applied a variety of benefit types (copay or coinsurance) and benefit levels (primary care, specialty care, other). Detailed testing was required within this benefit classification to determine whether benefits met the "substantially all" and "predominant" requirements for MH/SUD services.
For each plan option requiring detailed testing, Aon Hewitt requested the employer's program administrator (vendor) to submit plan costs associated with each covered service category within the classification or sub-classification included in the testing process.
We first conducted the "substantially all" test for each plan option to determine which benefit type represents at least two-thirds of the plan costs in the benefit sub-classification. Plan cost data were grouped according to benefit type (e.g., copay, coinsurance, etc.) and were evaluated to determine the percentage of the total plan costs represented by each type. Once the benefit type representing "substantially all" was determined, we grouped the plan cost data associated with each benefit level (e.g., $15, $20, etc.) within that benefit type to determine the predominant benefit level in that sub-classification.
Aon Hewitt's Plan Design Database. Information obtained from Aon Hewitt's PDD included a review of 2009, 2010, and 2011 plan design data to determine how group health plan and employer-sponsored plan designs have evolved since federal parity was enacted in 2008. The information contained in the PDD allowed us to report on the plan designs that were in place before the implementation of federal parity in 2009 and evaluate how plan designs have changed since the implementation of the MHPAEA and the IFR. For most employers, the MHPAEA legislative requirements were implemented effective January 1, 2010. Further changes were made to employer plan designs effective January 1, 2011, to comply with the February 2010 IFR.
Information obtained from the database allows us to evaluate trends in how employer plan designs have changed since the implementation of the MHPAEA. The 2009 plan year serves as the baseline year, as the MHPAEA was not in effect until October 2009. Plan options in the 2010 plan year reflect plan designs that were in effect after the implementation of the MHPAEA. The plan options included in the 2011 plan year reflect plan designs that were in effect after the release of the IFR, which went into effect for most employers on January 1, 2011.
A total of 12,384 plan options, reflecting 252 employers, were included in the 2009, 2010, and 2011 plan design analysis. Of those options, 2,983 plan options (24.1%) were in the database in all three plan years. Not all plan options are reflected in the database all 3 years for a number of reasons, such as the option was terminated or the option was added in 2010 and 2011.
For many plan options, information on all fields included in this review was available. However, for some plan options certain information was unavailable, the information was unclear, or the information was potentially inaccurate. Therefore, the data for those plan options were excluded from our analyses. Therefore, although 12,384 plan options were included in the database, the actual number of plan options considered valid and used in the analysis for each comparison is much lower. We have reported the size of the sample included in each plan design analysis in Appendix C.
Summary Plan Description Data Provided by BLS. To supplement parity information from large employers that are heavily represented in the Aon Hewitt and Milliman databases, we analyzed a sample of 240 SPDs from midsized employers (establishments between 51 and 500 employees) collected by the BLS between 2008 and 2011 as part of the National Compensation Survey (NCS).65 Under ERISA, employers are required to provide their employees with SPDs of their health, pension, and welfare benefit plans. SPDs must include:
- Any cost-sharing provisions, including premiums, deductibles, coinsurance, and copayment amounts.
- Any annual or lifetime maximums or other limits on benefits.
- The extent to which preventive services are covered.
- Whether and under what circumstance existing and new drugs are covered.
- Whether, and under what circumstance, coverage is provided for medical tests, devices or procedures.
- Any provisions requiring preauthorization or utilization review as a condition of obtaining a benefit or service under the plan.
BLS requests that employers participating in the NCS submit full SPDs. However, many only provide summary tables of benefits, a more circumscribed description of benefits than the complete SPDs. BLS permitted NORC to abstract data from plan documents submitted by midsized employers between 2008 and 2011 to assess changes since the introduction of the MHPAEA and the IFR. The total sample size of abstracted documents was 240. One hundred sixty-seven covered the pre-parity era (plan years 2008-2009), and 73 covered the post-parity era (plan years 2010-2011). Not all documents included every data element of interest, but, when available, information related to the provision of quantitative limits (e.g., copays, coinsurance, and deductibles) was abstracted and analyzed. Observation level characteristics provided by BLS for each SPD was limited to principal industry. In order to increase the generalizability of the information obtained from the SPDs, analysis weights were constructed for each observation.66
To create the analysis weights, the sample was first divided into pre-parity observations (plan year 2008-2009; n = 167) and post-parity observations (plan years 2010-2011; n = 73) subsamples. Each subsample was treated as a separate sample with respect to weight construction. Within each subsample, the observations were assigned to one of seven industry categories based on the observation's North American Industry Classification System (NAICS) code.67
It should be noted that the utility of our analyses is limited by several factors. Many of the documents submitted to BLS were in fact not full SPDs, but brief tables of benefits that lacked many of the elements necessary to carefully track changes in financial requirements and treatment limitations. Our ability to construct weights to analyze the data that was abstracted was further limited by the lack of detailed establishment information available from the plan documents. Ideally, the weights would have been created using information including the number of workers at each establishment, detailed industry classification, and the physical location of the establishment. We were only provided information on basic industry categories. Therefore, we believe the weights as created, and applied in our analyses, are insufficient to remove all potential bias from the sample, and appropriate caution should be exercised when interpreting these results.
Employer Surveys. We reviewed the results of published national employer surveys from the KFF/HRET and Mercer. These surveys provided generalizable information on employers' coverage of MH/SUD. The 2010 KFF/HRET survey included 2,046 randomly selected public and private employers with more than three workers. The sample is randomly selected from a sample frame constructed by Survey Sampling Incorporated from Dun & Bradstreet's listing of public and private employers. KFF/HRET then stratifies the sample by industry and employer size. The 2010 Mercer Health Benefits Survey is also a random survey of employers identified from Dun & Bradstreet. The 2010 survey included 1,977 employers that offered health benefits. The survey uses sampling weights to calculate estimates both nationwide and for four geographic regions. The Mercer survey contains information for large employers (i.e., those with 500 or more employees), and for smaller employers (i.e., those with fewer than 500 employees).
Semi-structured Interviews with Health Plan Representatives. Lastly, we conducted detailed interviews with a non-generalizable sample of senior health plan officials who are responsible for seven major health insurers' compliance with the MHPAEA. The purpose of the interviews was to obtain specific information about plans' disclosure policies and practices required by the MHPAEA. Two behavioral health plan associations, the Association for Behavioral Health and Wellness and the National Behavioral Consortium recruited health plans to participate in the interviews.
Each of the seven individuals interviewed is a senior staff member responsible for leading the company's review of policies and procedures to bring the plan into compliance with MHPAEA and the IFR. The seven companies that participated collectively provide coverage for more than 100 million individuals and are among the largest health plans in the nation. Several of the plans exclusively provide behavioral health care services, and others provide behavioral health services within a larger health plan covering health, disability, and other benefits as well. Collectively, the companies operate in all 50 states, serving self-insured employers and employers purchasing fully-insured group health insurance products. Each interview elicited detailed information about:
- The use of medical necessity criteria for medical and MH/SUD services.
- The process for informing beneficiaries of reasons for claim denials for medicaland MH/SUD services and any changes in the processes for informing beneficiaries since implementation of the MHPAEA.
- The use of utilization management techniques formedical and MH/SUD services and any changes in the use of utilization management techniques.
- The management of out-of-network care.
- The presence of any unmet demand for residential and intensive outpatient substance abuse services since the implementation of the MHPAEA.
- The management of prescription medications, if the company is involved in this service.
Methodology for sample selection and technical specifications at http://www.bls.gov/ncs/ebs/smb_health.htm. The sample for the NCS is selected on the basis of a three-stage design. The first stage involved the selection of areas consisting of 152 metropolitan and non-metropolitan areas. In the second stage, the sample of establishments is drawn from a sampling frame comprised of state unemployment insurance reports within sampled areas. The third stage is a probability sample of occupations within a sampled establishment. BLS field economists visit sampled establishments or contact them by telephone to collect data for the survey. To reduce the reporting burden, field economists ask respondents to provide Summary Plan Provision documents for health and retirement plans. Approximately 3,300 establishments provide data for each annual NCS.
The analysis weights were calibrated to establishment and worker counts from the 2010 County Business Patterns created by the Department of Census. The end result is two sets of weights -- an establishment and a worker weight for pre-parity and an establishment and a worker weight for post-parity. The weight sums for the respective weights are identical between pre-parity and post-parity. Following describes the detailed process used to construct analysis weights.
Step 1: Calculate the proportion of observations within each subsample and industry such that:
rpi = npi Σinpi Where n = number of observations within subsample p and industry i.
Step 2: Calculate the share of establishments within each industry such that:
Ri = Ni ΣiNi Where N = the number of establishments from the 2010 County Business Patterns within industry i.
Step 3: Calculate the share of workers within each industry such that:
RWi = NWi ΣiNWi Where NW = the number of workers from the 2010 County Business Patterns within industry i.
Step 4: Calculate the final weights as the ratio of the share of establishments or workers within each industry and the proportion of observations within each subsample and industry such that:
Establishment Weight = Ri rpi Worker Weight = RWi rpi Where rpi = the proportion of observations within each subsample and industry, Ri = the share of establishments within each industry, and RWi = the share of workers within each industry.
The sum of both the establishment weight and the worker weight within each subsample equals the sample size within each subgroup. Each weight has a different impact on analyses. For example, the health care industry tends to have more workers as a share of the total workforce than establishments as a share of total establishments. Thus, the worker weight will grant health care observations more influence on an estimate than will the establishment weight. Comparisons of results obtained using both sets of weights demonstrated very minimal differences between the two sets of estimates. The estimates presented in this report were calculated using the establishment weights.
The industry categories are as follows: (1) Agriculture, Mining, Utilities, Construction, and Manufacturing (NAICS = 11, 21, 22, 23, 31, 32, 33); (2) Wholesale (NAICS = 42); (3) Retail (NAICS = 44, 45); (4) Transportation and Information (NAICS = 48, 49, 51); (5) Finance, Real Estate, Professional Services, and Management (NAICS = 52, 53, 54, 55, 56); (6) Health care (NAICS = 62); and (7) Education, Recreation, Food Service and Other (NAICS = 61, 71, 72, 81).
Study Results
Research Question #1: Health Plan and Employer Use of Financial Requirements
What types of financial requirements (e.g., copays, coinsurance) do group health plans use for MH and SUD benefits and are such requirements consistent with the new MHPAEA standards for calculating the predominant level that applies to substantially all medical and surgical benefits?
According to the IFR regulations, a plan must meet two testing requirements within each benefit classification in order to comply with parity financial requirements:
-
Substantially all. A requirement or limitation applies to substantially all if it applies to at least two-thirds of the benefits in that classification. If a type of requirement or limit does not apply to at least two-thirds of the medical/surgical benefits in a classification, then it cannot be applied to MH/SUD benefits in that classification.
-
Predominant. A requirement or limitation is considered predominant if it applies to at least one-half of the benefits in that classification.
Determination of "substantially all" and "predominant" is based on the dollar amount of all plan payments for medical/surgical benefits in the classification that are expected to be paid under the plan for the plan year. Plan design compliance must be assessed within the six benefit classifications specified by the regulations. Regulatory guidance defined two sub-classifications for outpatient services. The classifications and sub-classifications recognized by the regulations are:
- Inpatient in-network
- Inpatient out-of-network
- Outpatient in-network
- Office visits
- All other outpatient items and services
- Outpatient out-of-network
- Office visits
- All other outpatient items and services
- Emergency care
- Prescription drugs
Detailed testing was performed for each of these six classifications and two sub-classifications. Results for each of the six classifications are presented here, and results pertaining to the "office visit" and "other services" sub-classifications and the Safe Harbor provision can be found in Appendix A.
It should be noted that the testing models used in these analyses are based on Milliman's and Aon Hewitt's interpretation of provisions outlined in the IFR. The development of these models required Milliman and Aon Hewitt to make interpretations on issues that were not entirely settled by the IFR, or may be interpreted differently by regulators.
Results of the testing illustrate both the substantial changes that most plans have made since 2008 to comply with the MHPAEA's financial parity requirements and the specific areas where a small proportion of plans must still make changes to be consistent with MHPAEA standards. Milliman and Aon Hewitt data were analyzed using similar, though not identical, testing procedures. The two analyses provide glimpses into two successive time slices: The Milliman database included information on 2010 benefits, whereas the Aon Hewitt database included information on 2011 benefits. It should be noted that the IFR became effective for plan years beginning on or after July 1, 2010. Thus for calendar year plans, the IFR was not effective until January 1, 2011. Therefore, our 2010 testing results do not suggest that plans failing to meet the "substantially all" or "predominant" tests were non-compliant with MHPAEA requirements at the time, only that they were required to make additional changes in order to be consistent with MHPAEA standards going forward.
2010 Inpatient Financial Requirements
TABLE 3. Financial Requirements: Percentage of Plans in 2010 Requiring Changes to Inpatient Benefits to the Consistent With MHPAEA
| Deductible | Out-of-Pocket Maximum |
Copay | Coinsurance | |
|---|---|---|---|---|
| Inpatient in-network MH services | 6.7% | 8.7% | 6.7% | 7.5% |
| Inpatient out-of-network MH services | 1.0% | 7.8% | 0% | 5.8% |
| Inpatient in-network SUD Services | 6.7% | 8.4% | 6.7% | 7.6% |
| Inpatient out-of-network SUD services | 1.0% | 8.7% | 0% | 5.8% |
SOURCE: Milliman's Testing Data of 2010 plan designs.
Analyses of Milliman's data focused on identifying specific areas where a plan needed to make changes in its 2010 benefits to achieve consistency with MHPAEA. Analyses of Milliman's inpatient benefit designs found that overall, approximately 10% of plans offering inpatient MH/SUD benefits needed to make some changes to their 2010 inpatient financial requirements in order to be consistent with MHPEA standards. Table 3 presents the percentage of participating plans that appeared to offer benefits that were not consistent with MHPAEA's financial requirements (deductibles, out-of-pocket maximums, copays, and coinsurance). Relatively few plans needed to modify copays for inpatient in-network MH/SUD benefits, and no plans needed to make changes to their inpatient out-of-network MH or SUD benefits. Approximately one plan in 12 needed to change its member out-of-pocket maximums for inpatient MH and SUD to be equivalent to its medical/surgical inpatient maximums.
2010 Outpatient Financial Requirements
Analyses of Milliman's 2010 data suggest that substantially more plans required changes to their outpatient MH/SUD benefits than required changes to their inpatient benefits. More than one-quarter of plans were required to change deductible limits, one-third required changes to copays or coinsurance, and one-fifth needed to change out-of-pocket maximums. An almost identical pattern was found for in-network outpatient SUD treatment. A much smaller percentage of plans, less than 10%, needed to change out-of-network financial limitations. Table 4 presents the percentage of participating plans that were required to change outpatient financial requirements in order to be consistent with MHPAEA standards.
TABLE 4. Financial Requirements: Percentage of Plans in 2010 Requiring Changes to Outpatient Benefits to the Consistent With MHPAEA
| Deductible | Out-of-Pocket Maximum |
Copay | Coinsurance | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Outpatient in-network MH services | 26.7% | 21.7% | 33.3% | 34.2% | ||||||||||||||||||||
| Outpatient out-of-network MH services | 3.9% | 8.7% | 1.0% | 10.7% | ||||||||||||||||||||
| Outpatient in-network SUD services | 26.1% | 18.5% | 31.9% | 33.6% | ||||||||||||||||||||
| Outpatient out-of-network SUD services | 3.9% | 9.7% | 1.0% | 8.7% |
SOURCE: Milliman's Testing Data of 2010 plan designs.2010 Emergency Care and Prescription Drug Financial Requirements
Analyses of 2010 benefit designs suggest that the vast majority of plans offered emergency and prescription drug benefits that were consistent with MHPAEA's financial requirements. Table 5 presents the percentage of participating plans that needed to make changes in their emergency and prescription drug benefits in order to be consistent with MHPAEA's financial parity requirements. Fewer than 1% of plans needed any changes to their prescription drug benefits. But one-fifth needed to change coinsurance rates for behavioral health emergency care, and a smaller proportion needed to make changes in copay and deductible benefits.
TABLE 5. Financial Requirements: Percentage of Plans in 2010 Requiring Changes in ER and Prescription Drug Benefits to the Consistent With MHPAEA
| Deductible | Out-of-Pocket Maximum |
Copay | Coinsurance | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Emergency care -- MH/SUD | 5.6% | 0% | 7.2% | 19.2% | ||||||||||||||||||||
| Prescription drugs -- MH/SUD | 0% | 0% | 0% | 0% |
SOURCE: Milliman's Testing Data of 2010 plan designs.
2011 Inpatient Financial Requirements
Analyses of Aon Hewitt inpatient plan designs suggest that by 2011, the vast majority of health plans appeared to meet MHPAEA's financial requirements. As shown in Table 6, only a very small percentage of plans utilized inpatient financial requirements that did not comply with MHPAEA standards. None needed to modify copay or coinsurance levels, and less than 2% required modifications of their deductibles or out-of-pocket maximums.
Comparison of the 2010 Milliman data and the 2011 Aon Hewitt data indicates that most large employer plans met the inpatient financial parity standards by 2011. Small, but consistent improvements can be seen in each area tested.
TABLE 6. Financial Requirements: Percentage of Plans in 2011 Requiring Changes to Inpatient Benefits to the Consistent With MHPAEA
| Deductible | Out-of-Pocket Maximum |
Copay | Coinsurance | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Inpatient in-network MH services | 1.3% | 1.3% | 0% | 0% | ||||||||||||||||||||
| Inpatient out-of-network MH services | 1.3% | 1.3% | 0% | 0% | ||||||||||||||||||||
| Inpatient in-network SUD services | 1.3% | 1.3% | 0% | 0% | ||||||||||||||||||||
| Inpatient out-of-network SUD services | 1.3% | 1.3% | 0% | 0% |
SOURCE: Aon Hewitt Compliance Testing Database of 2011 plan designs.
2011 Outpatient Financial Requirements
Analyses of 2011 outpatient benefit designs suggest that nearly all large employer plans appeared to meet parity's financial requirements for deductibles, out-of-pocket maximums, and coinsurance requirements. However, nearly one-fifth had outpatient in-network copay requirements for MH and SUD that appeared not to conform to MHPAEA's financial parity requirements.
Comparison of the 2010 outpatient data to the 2011 data again suggests substantial improvement between the two periods. For example, the 2010 data indicated that more than one-third of plans had outpatient coinsurance requirements that appeared not to conform to MHPAEA standards. By 2011, that number had dropped to less than 4%. Likewise, more than 25% of 2010 plans were required to make changes to their outpatient in-network deductible benefits in order to be consistent with MHPAEA's standards. By 2011, the data suggested that less than 2% of plans still appeared to offer benefits that were not consistent with MHPAEA standards. However, adherence to MHPAEA standards was not universal. Although there was clearly improvement in the proportion of plans that appeared to conform to MHPAEA's outpatient in-network copay requirements, nearly one-fifth of 2011 plan designs continued to offer benefits that appeared not to conform to MHPAEA's financial requirements.
TABLE 7. Financial Requirements: Percentage of Plans in 2011 Requiring Changes to Outpatient Benefits to the Consistent With MHPAEA Standards
| Deductible | Out-of-Pocket Maximum |
Copay | Coinsurance | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Outpatient in-network MH services | 1.3% | 1.3% | 19.6% | 3.9% | ||||||||||||||||||||
| Outpatient out-of-network MH services | 1.3% | 1.3% | 0% | 0% | ||||||||||||||||||||
| Outpatient in-network SUD services | 1.3% | 1.3% | 19.6% | 3.9% | ||||||||||||||||||||
| Outpatient out-of-network SUD services | 1.3% | 1.3% | 0% | 0% |
SOURCE: Aon Hewitt Compliance Testing Database of 2011 plan designs.
2011 Emergency Care and Prescription Drug Financial Requirements
Analyses of 2011 benefit designs suggest that 100% of tested plans offered ER and prescription drug benefits that appeared to be consistent with MHPAEA's financial requirements.
TABLE 8. Financial Requirements: Percentage of Plans in 2011 Requiring Changes in ER and Prescription Drug Benefits to be Consistent With MHPAEA Standards
| Deductible | Out-of-Pocket Maximum |
Copay | Coinsurance | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Emergency care -- MH/SUD | 0% | 0% | 0% | 0% | ||||||||||||||||||||
| Prescription drugs -- MH/SUD | 0% | 0% | 0% | 0% |
SOURCE: Aon Hewitt Compliance Testing Database of 2011 plan designs.
Changes in Health Plans' Behavioral Health Financial Requirements, 2009-2011
Aon Hewitt's PDD was used to assess changes in group health plan and employer-sponsored plan designs between the 2009 and 2011. A total of 12,384 plan options, reflecting 252 employers, were included in the 2009, 2010, and 2011 plan design analysis.
It is important to note that data reported in this section do not indicate whether or not the plan design reported in the PDD is compliant with MHPAEA requirements. Rather, the information summarizes the data contained in the PDD within each plan year. Many factors influence the compliance status of each plan design, most notably, a review of the "substantially all" and "predominant" standards.
Inpatient Financial Requirements. Copay and coinsurance requirements for inpatient medical/surgical services were compared to those for inpatient MH/SUD services to determine if plans' behavioral health benefits were the same as, more restrictive, or less restrictive than medical/surgical services. Table 9 presents the percentage of plans in which the inpatient benefits were found to be more restrictive for MH/SUD than for medical/surgical benefits.
TABLE 9. Financial Requirements: Percentage of Plans With More Restrictive Inpatient MH/Substance Abuse Treatment Benefits Than Medical/Surgical Benefits, 2009-2011
| 2009 Percent of Plans | 2010 Percent of Plans | 2011 Percent of Plans | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Inpatient in-network MH services | 6.5% | 4.5% | 4.9% | ||||||||||||
| Inpatient out-of-network MH services | 9.4% | 6.5% | 5.6% | ||||||||||||
| Inpatient in-network SUD services | 6.4% | 5.3% | 4.0% | ||||||||||||
| Inpatient out-of-network SUD services | 11.1% | 5.8% | 3.8% |
SOURCE: Aon Hewitt's Plan Design Database (2009-2011).
These data suggest a slight decrease between 2009 and 2011 in the percentage of plans that applied more restrictive financial requirements for inpatient MH/SUD services than for medical/surgical inpatient services. By 2011, approximately one in 20 plans still had more restrictive financial requirements (higher copays or greater coinsurance rates) for inpatient MH and SUD treatment than for comparable medical/surgical inpatient treatment. Examples of the more restrictive benefit designs found in the analysis include:
-
MH/SUD services covered at 90% coinsurance after hospital copay vs. medical/surgical services covered at 100% coinsurance after hospital copay.
-
MH/SUD services covered at 90% coinsurance vs. medical/surgical services covered at 100%.
Outpatient Financial Requirements. Analysis of outpatient benefits compared copayment and coinsurance requirements for routine outpatient MH/SUD services and financial requirements for medical/surgical office visits to primary care physicians (PCPs) or to specialty care physicians (SCPs).
Table 10 presents the percentage of plans in which the outpatient benefits were found to be more restrictive for MH/SUD than for medical/surgical benefits.
TABLE 10. Financial Requirements: Percentage of Plans Using the Same Copay/Coinsurance for PCPs/SCPs and With More Restrictive Outpatient MH/Substance Abuse Treatment Benefits Than Medical/Surgical Benefits, 2009-2011
| 2009 Percent of Plans | 2010 Percent of Plans | 2011 Percent of Plans | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Outpatient in-network MH services | 12.9% | 5.3% | 2.0% | ||||||||||||
| Outpatient out-of-network MH services | 24.5% | 7.5% | 8.3% | ||||||||||||
| Outpatient in-network SUD Services | 24.0% | 20.8% | 1.3% | ||||||||||||
| Outpatient out-of-network SUD services | 22.3% | 6.8% | 7.4% |
SOURCE: Aon Hewitt's Plan Design Database (2009-2011).
Before the passage of the MHPAEA, many employers and group health plans considered MH/SUD professionals to be specialists and applied coinsurance or copay requirements that were aligned with the financial requirements applied to SCPs. The MHPAEA requires that the test for financial parity compliance be based on a comparison of "substantially all" and "predominant" medical/surgical requirements and the IFR did not allow the separate classification of generalists and specialists in determining the predominant financial requirement or treatment limit that applies to substantially all medical/surgical benefits in a classification. A plan may still be able to impose the specialist level of a financial requirement or QTL if it is the predominant level that applies to substantially all medical/surgical benefits within a classification. Our analysis of the Aon Hewitt PDD compares plans' MH/SUD outpatient benefits with outpatient PCP and SCP services. Some plans apply the same copay or coinsurance to both PCPs and SCPs. Others apply different copays or coinsurance rates to PCP services and SCP services. Often the PCP copay or coinsurance is lower than that for SCP services (split copay/coinsurance). Table 10 and Table 11 present the percentage of plans using more restrictive outpatient MH/SUD services than medical/surgical services using both methods of handling financial requirements for PCPs and SCPs.
TABLE 11. Financial Requirements: Percentage of Plans Using Split Copay/Coinsurance for PCPs/SCPs that have More Restrictive Outpatient MH/Substance Abuse Treatment Benefits Than Medical/Surgical Benefits, 2009/2011
| 2009 Percent of Plans | 2010 Percent of Plans | 2011 Percent of Plans | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Outpatient in-network MH services | 28.2% | 8.6% | 4.9% | ||||||||||||
| Outpatient out-of-network MH services | 6.1% | 9.8% | 2.1% | ||||||||||||
| Outpatient in-network SUD services* | 25.8% | 10.9% | 10.6% |
SOURCE: Aon Hewitt's Plan Design Database (2009-2011).
* Results for outpatient out-of-network SUD services are not reported due to small sample size.
Plan Options With Same Copay/Coinsurance for PCPs/SCPs
Plans using the same copay/coinsurance structure for PCPs/SCPs rapidly reduced more restrictive financial requirements for outpatient MH/SUD following enactment of the MHPAEA. For example, these plans reduced disparities in copays and coinsurance for in-network MH services from 12.9% in 2009 to 2% in 2011. Unequal in-network SUD financial requirements declined from 24% in 2009 to 1.3% in 2011.
Plan Options With Split Copay/Coinsurance for PCPs/SCPs
Plans using split copay/coinsurance for PCPs/SCPS also rapidly reduced their use of more restrictive financial requirements following enactment of the MHPAEA. In 2009, one-quarter of plans used more restrictive benefit designs for in-network SUD services. By 2011, fewer than 11% used a more restrictive benefit design. And the decrease was even more dramatic for outpatient in-network MH services (from 28% to 9%) but for out-of-network MH the disparities increased in 2010 (from 6% to 9%) and then went down to 2%.
As seen in Table 12, in 2009, approximately one-third of plan options that had split copay/coinsurance designs aligned the outpatient MH benefit with their PCP benefit and one-third aligned the MH benefit with SCP. In 2010, a distinct change occurred in the benefit for MH services. Almost two-thirds of plan designs aligned the MH outpatient benefit with the SCP copay/coinsurance levels. In 2011, plans changed once again. More than half aligned the outpatient MH benefit with the PCP benefit.
TABLE 12. Financial Requirements: Percentage of Plans Using a Split Copay/Coinsurance Structure that Aligned Their Benefits with PCPs vs. SCPs, 2009-2011
| 2009 Percent of Plans | 2010 Percent of Plans | 2011 Percent of Plans | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mental Health | |||||||||||||||
| Outpatient MH benefit the same as PCP | 33.7% | 25.8% | 55.8% | ||||||||||||
| Outpatient MH benefit same as SCP | 32.0% | 61.2% | 25.2% | ||||||||||||
| Outpatient MH benefit is less restrictive than PCP | 6.2% | 4.3% | 14.1% | ||||||||||||
| Outpatient MH benefit more restrictive than SCP | 20.4% | 3.5% | 3.7% | ||||||||||||
| Outpatient MH benefit is more restrictive than PCP but less restrictive than SCP | 7.7% | 5.1% | 1.2% | ||||||||||||
| Substance Use Disorder | |||||||||||||||
| Outpatient SUD benefit the same as PCP | 54.8% | 55.0% | 52.6% | ||||||||||||
| Outpatient SUD benefit same as SCP | 15.1% | 13.2% | 39.7% | ||||||||||||
| Outpatient SUD benefit is less restrictive than PCP | 2.9% | 3.9% | 3.1% | ||||||||||||
| Outpatient SUD benefit more restrictive than SCP | 16.8% | 17.4% | 2.6% | ||||||||||||
| Outpatient SUD benefit is more restrictive than PCP but less restrictive than SCP | 10.4% | 10.4% | 1.9% | ||||||||||||
These changes suggest that employers and health plans were modifying benefits to comply with MHPAEA requirements as they understood them at the time. In 2010, after the enactment of MHPAEA, many employers aligned the outpatient MH benefit with the SCP level, suggesting that they interpreted the MHPAEA to mean that treating a MH provider as a specialist would comply with the legislation. The IFR clarified that compliance is instead governed by the "substantially all" and "predominant" criteria and the IFR did not allow the separate classification of generalists and specialists in determining the predominant financial requirement or treatment limit that applies to substantially all medical/surgical benefits. The 2011 benefit data suggest that employers and health plans once again reevaluated their designs and made adjustments, aligning outpatient MH copays and deductibles with their PCP benefits.
Results for SUD followed a slightly different pattern. As seen in Table 12, over half of the plan options using a split copay/coinsurance structure aligned their outpatient SUD benefits with the PCP benefit level in all 3 years (2009, 2010, and 2011). In 2009 and 2010, approximately 27% of plan options applied a benefit for outpatient SUD services that was either more restrictive than the SCP benefit level or in between the PCP and SCP benefit levels. This changed in 2011 when it appears that plans moved away from this approach and more plan options aligned outpatient SUD benefits with the SCP benefit level.
Midsized Employers. To investigate how plan designs used by midsized employers have changed since the implementation of MHPAEA, NORC conducted a separate analysis of financial requirements used by midsized employers. When available, information on copay, coinsurance, deductibles, and out-of-pocket maximums was abstracted from 240 SPDs collected between 2008 and 2011 by the BLS for the NCS.
TABLE 13. Financial Requirements: Percentage of Midsized Employers' Plans in Our Limited Sample That Appear to Provide More Restrictive MH/Substance Abuse Treatment Benefits Than Medical/Surgical Benefits: Pre and Post-Parity
| Pre-Parity (2008-2009) Percent of Plans (n = 167) |
Combined Post- Parity Sample (2010-2011) Percent of Plans (n = 73) |
|||||||
|---|---|---|---|---|---|---|---|---|
| Inpatient care: cost-sharing for in-network MH/SUD treatment higher than inpatient medical/surgical care | 10.2% | 0% | ||||||
| Inpatient care: cost-sharing for out-of-network MH/SUD treatment higher than inpatient medical/surgical care | 16.4% | 4.7% | ||||||
| Outpatient care: cost-sharing for in-network MH/SUD office visits higher than medical/surgical PCP visits | 51.5% | 41.3% | ||||||
| Outpatient care: cost-sharing for in-network MH/SUD office visits higher than medical/surgical specialist office visits | 23.7% | 8.5% | ||||||
| Outpatient care: cost-sharing for out-of-network MH/SUD treatment higher than outpatient medical/surgical treatment | 32.7% | 7.1% |
Table 13 presents the percentage of plans using more restrictive QTLs before and after the effective date of MHPAEA. As was the case with large employer plans, midsized plans appeared to be more likely to offer outpatient benefits that did not conform to MHPAEA's financial standards than inpatient benefits. Before the effective implementation date of the MHPAEA (2008-2009), more than 50% of midsized employers' plans in our sample used cost-sharing measures for outpatient MH/SUD office visits that were higher than those for medical/surgical PCP visits. In the post-parity sample (2010-2011), that percentage had decreased to a still-substantial 41% of midsized employers' plans. Likewise, nearly 24% of plans in the pre-parity sample had cost-sharing requirements for outpatient in-network behavioral health office visits that were higher than for SCP office visits. That percentage declined to 9% following implementation of MHPAEA. Before MHPAEA, in our sample, midsized employers' out-of-network MH/SUD outpatient benefits were more restrictive than medical/surgical outpatient benefits in approximately one-third of the plans. This rate decreased to 7% after implementation of MHPAEA.
Among midsized employers, inpatient MH/SUD coverage differs from the pattern observed for other cost-sharing requirements. Both before and after the implementation of parity, relatively few plans used more restrictive cost-sharing techniques. Only one plan in six applied more restrictive deductibles, out-of-pocket maximums, copay or coinsurance requirements for inpatient in-network MH/SUD than for medical/surgical inpatient care before parity, and even fewer plans used more restrictive inpatient MH/SUD requirements after the implementation of MHPAEA. This pattern is consistent with the findings for large employers in the Milliman and Aon Hewitt datasets.
TABLE 14. Financial Requirements: Results From the 2010 Mercer Survey
| Category | Sample Size | Decrease MH/SUD Copay or Coinsurance |
||||||
|---|---|---|---|---|---|---|---|---|
| Total | 1,433 | 3% | ||||||
| Employer Size | ||||||||
| Fewer than 500 employees | 332 | 3% | ||||||
| 500 or more employees | 1,101 | 8% | ||||||
| Industry | ||||||||
| Manufacturing | 228 | 9% | ||||||
| Wholesale/retail | 86 | 5% | ||||||
| Services | 261 | 6% | ||||||
| Trans./comm. | 59 | 5% | ||||||
| Health care | 180 | 13% | ||||||
| Finance | 86 | 10% | ||||||
| Government | 173 | 4% | ||||||
| Other | 28 | 6% | ||||||
| Region | ||||||||
| Northeast | 216 | 5% | ||||||
| Midwest | 334 | 7% | ||||||
| South | 359 | 10% | ||||||
| West | 192 | 10% | ||||||
SOURCE: 2010 Mercer Health Benefits Survey.
A closer examination of the pre and post-parity midsized employer data suggests that the proportion of plans using more restrictive financial limits on MH/SUD care declined each year following the effective date of parity. Even though the sample sizes are relatively small for each of the post-parity years and less reliable due to the small sizes, by 2011, the large majority of plans in this sample had eliminated unequal limits on MH/SUD. The table in Appendix D shows these year-to-year trends. Although the year-to-year results for midsized employers correspond to the decreases observed in large employers' health benefits, caution is warranted because only a small number of SPDs were available each year.
Employer Surveys. Employer use of different financial requirements for MH/SUD and medical surgical benefits following the implementation of MHPAEA is also assessed in Mercer's Health Benefits Survey. The 2010 survey asked employers to describe actions they had taken or planned to take to ensure that MH/SUD benefits are provided at the same level as medical/surgical benefits. Table 14 presents the results from 1,433 employers who responded to the survey. Results suggest that, overall, 3% of employers claim to have already decreased, or had plans to decrease MH/SUD copay or coinsurance levels to comply with the MHPAEA. Although these data provide some evidence of employer response to MHPAEA, they do not provide any evidence that employers who did not make adjustments to their QTLs were out of compliance with MHPAEA standards.
Research Question #2: Health Plan and Employer Use of Treatment Limitations
What types of QTLs (e.g., day limits, visit limits) do group health plans use for MH and SUD conditions, and do such limitations comply with the MHPAEA standards?
2010 Inpatient Quantitative Treatment Limits
Analyses of Milliman's 2010 data suggest that few plans used by large employers were required to make adjustments to their MH/SUD inpatient treatment limitations to be consistent with parity requirements. As shown in Table 15, almost one-fifth of plans (19.3%) covered fewer in-network inpatient days annually for SUD treatment and 16% covered fewer MH inpatient days than medical/surgical inpatient days. About one plan in 20 were required to remove dollar maximums for inpatient MH/SUD treatment.
TABLE 15. QTLs: Percentage of Plans in 2010 Requiring Changes to Inpatient Benefits to be Consistent with MHPAEA
| Day Limits | Dollar Maximum (Annual) |
|||||||
|---|---|---|---|---|---|---|---|---|
| Inpatient in-network MH services | 12.5% | 4.2% | ||||||
| Inpatient out-of-network MH services | 6.8% | 4.9% | ||||||
| Inpatient in-network SUD services | 19.3% | 6.7% | ||||||
| Inpatient out-of-network SUD services | 15.5% | 6.8% |
SOURCE: Milliman's Testing Database of 2010 plan designs.
2010 Outpatient Quantitative Treatment Limits
Outpatient MH/SUD visits were more frequently limited than were inpatient services. Table 16 shows that in 2010 half of the plans covered fewer in-network MH and SUD visits than they covered for medical/surgical outpatient treatment. Nearly two-thirds of the plans needed to modify visit limits for out-of-network outpatient substance use benefits and 14% need to change outpatient out-of-network MH visit limits.
TABLE 16. QTLs: Percentage of Plans in 2010 Requiring Changes to Outpatient Benefits to be Consistent with MHPAEA
| Visit Limits | Dollar Maximum (Annual) |
|||||||
|---|---|---|---|---|---|---|---|---|
| Outpatient in-network MH services | 50.0% | 0% | ||||||
| Outpatient out-of-network MH services | 13.6% | 0% | ||||||
| Outpatient in-network SUD services | 50.0% | 30.0% | ||||||
| Outpatient out-of-network SUD services | 63.6% | 9.1% |
SOURCE: Milliman's Testing Database of 2010 plan designs.
2010 Emergency Care and Prescription Drug Quantitative Treatment Limits
As presented in Table 17, none of the tested plans needed to change their behavioral health emergency care benefits or prescription benefits to comply with MHPAEA and the IFR.
TABLE 17. QTLs: Percentage of Plans in 2010 Requiring Changes to Emergency and Prescription Drug Benefits to be Consistent with MHPAEA
| Day Limits | Visit Limits | Quality Limits | Dollar Maximums (Annual) |
|||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Emergency care -- MH/SUD | N/A | 0% | N/A | 0% | ||||||||||||||||||||
| Prescriptions -- MH/SUD | N/A | N/A | 0% | 0% |
SOURCE: Milliman's Testing Database of 2010 plan designs.2011 Inpatient Quantitative Treatment Limits
Table 18 present the results of analyses examining consistency with MHPAEA's treatment limitation standards in 2011. By 2011, 100% of Aon Hewitt plans had removed unequal dollar limitations, and there was a significant reduction in the percentage of plans utilizing unequal day limits. These changes suggest substantial movement toward consistency with MHPAEA standards. Still, there was a minority of plans that continued to provide unequal benefits in 2011.
TABLE 18. QTLs: Percentage of Plans in 2011 Requiring Changes to Inpatient Benefits to be Consistent with MHPAEA Standards
| Day Limits | Dollar Maximum | |||||||
|---|---|---|---|---|---|---|---|---|
| Inpatient in-network MH services | 7.0% | 0% | ||||||
| Inpatient out-of-network MH services | 6.5% | 0% | ||||||
| Inpatient In-network SUD Services | 7.8% | 0% | ||||||
| Inpatient out-of-network SUD services | 7.0% | 0% |
SOURCE: Aon Hewitt's Testing Database of 2011 plan designs.2011 Emergency Care and Prescription Drug Quantitative Treatment Limits
As presented in Table 19, none of the plans analyzed needed to change their behavioral health emergency care benefits or prescription benefits to be consistent with MHPAEA and the IFR.
TABLE 19. QTLs: Percentage of Plans Requiring Changes to Emergency and Prescription Drug Benefits to be Consistent with MHPAEA Standards
| Day Limits | Visit Limits | Quality Limits | Dollar Maximums (Annual) |
|||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Emergency care -- MH/SUD | N/A | 0% | N/A | 0% | ||||||||||||||||||||
| Prescriptions -- MH/SUD | N/A | N/A | 0% | 0% |
SOURCE: Aon Hewitt's Testing Database of 2011 plan designs.
2011 Outpatient Quantitative Treatment Limits
Aon Hewitt's analysis of quantitative outpatient treatment limits in 2011 plans suggests substantial progress from the 2010 Milliman findings. As shown in Table 20, plans apparently made significant strides to improve their quantitative limits in their outpatient MH/SUD benefit designs. None of the plans failed to comply with parity in dollar limitations on outpatient MH/SUD benefits. There were also substantially fewer plans with unequal MH/SUD visit limitations. The percentage of 2011 plans with unequal outpatient SUD benefits ranged between 4% and 6%. These results contrast sharply with results from 2010, when more than 50% of plans tested needed to modify their more restrictive visit limits for outpatient SUD services.
TABLE 20. QTLs: Percentage of Plans Requiring Changes to Outpatient Benefits to Comply with MHPAEA
| Visit Limits | Dollar Limits | |||||||
|---|---|---|---|---|---|---|---|---|
| Outpatient in-network MH services | 6.1% | 0% | ||||||
| Outpatient out-of-network MH services | 4.3% | 0% | ||||||
| Outpatient in-network SUD services | 6.1% | 0% | ||||||
| Outpatient out-of-network SUD services | 4.3% | 0% |
SOURCE: Aon Hewitt's Testing Database of 2011 plan designs.
Changes in Health Plans' Behavioral Health Quantitative Treatment Limits 2009-2011
Inpatient Quantitative Treatment Limits
Aon Hewitt's PDD was used to assess changes in quantitative limits in plan designs between 2009 and 2011.As shown in Table 21 and Table 22, the data suggest that most plans that appeared not to conform to MHPAEA standards in 2009 modified their quantitative limits by 2011 to eliminate more restrictive MH/SUD quantitative limits. For example, in 2009, approximately 50% of the plans covered fewer MH and SUD inpatient in-network days annually than they covered for treatment of medical/surgical conditions. In 2010, that percentage dropped to 12% for MH services and 13.8% for SUD. By 2011, 7.5% of plans covered fewer MH inpatient in-network days and 8.5% covered fewer SUD inpatient days than they covered for medical/surgical conditions. Plans with more restrictive out-of-network inpatient MH day limits declined from more than 48% in 2009 to 10.5% in 2010 and 5.8% in 2011. More limited SUD out-of-network inpatient days were found in 40% of plans in 2009, decreasing to 7.6% in 2011. Similar declines were observed in lifetime MH and SUD inpatient day limitations. Although these declines are notable, one in 12 plans continued to impose annual in-network inpatient MH and SUD day limits that were more restrictive than medical/surgical benefits, and 4% had lifetime MH and SUD day limits that were more restrictive.
TABLE 21. QTLs: MH/SUD Inpatient In-Network Treatment Limitations That Were More Restrictive Than Medical/Surgical Treatment Limitations, 2009-2011
| 2009 Percent of Plans | 2010 Percent of Plans | 2011 Percent of Plans | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mental Health | |||||||||||||||
| Day limits (annual) | 54.0% | 12.0% | 7.5% | ||||||||||||
| Day limits (lifetime) | 13.0% | 5.4% | 4.0% | ||||||||||||
| Dollar limits (annual) | 0.5% | 0.2% | 0.2% | ||||||||||||
| Dollar limits (lifetime) | 0% | 0% | 0% | ||||||||||||
| Episode limits | 1.9% | 1.2% | 0.8% | ||||||||||||
| Substance Abuse | |||||||||||||||
| Day limits (annual) | 46.2% | 13.8% | 8.5% | ||||||||||||
| Day limits (lifetime) | 21.4% | 5.4% | 4.1% | ||||||||||||
| Dollar limits (annual) | 0.1% | 0.1% | 0.0% | ||||||||||||
| Dollar limits (lifetime) | 0% | 0% | 0% | ||||||||||||
| Episode limits | 2.5% | 1.1% | 0.4% | ||||||||||||
SOURCE: Aon Hewitt's Plan Design Database (2009-2011).
TABLE 22. QTLs: MH/SUD Inpatient Out-of-Network Treatment Limitations That Were More Restrictive Than Medical/Surgical Treatment Limitations, 2009-2011
| 2009 Percent of Plans | 2010 Percent of Plans | 2011 Percent of Plans | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mental Health | |||||||||||||||
| Day limits (annual) | 48.2% | 10.5% | 5.8% | ||||||||||||
| Day limits (lifetime) | 8.1% | 1.4% | 1.1% | ||||||||||||
| Dollar limits (annual) | 0.2% | 0.2% | 0.2% | ||||||||||||
| Dollar limits (lifetime) | 0% | 0% | 0% | ||||||||||||
| Confinement limits | 0.9% | 0.3% | 0.1% | ||||||||||||
| Substance Abuse | |||||||||||||||
| Day limits (annual) | 40.4% | 12.7% | 7.6% | ||||||||||||
| Day limits (lifetime) | 8.1% | 1.4% | 1.1% | ||||||||||||
| Dollar limits (annual) | 0.1% | 0.1% | 0.1% | ||||||||||||
| Dollar limits (lifetime) | 0% | 0% | 0% | ||||||||||||
| Confinement limits | 1.7% | 1.0% | 0.7% | ||||||||||||
SOURCE: Aon Hewitt's Plan Design Database (2009-2011).
Very few plans applied more restrictive annual and lifetime dollar limits or covered-episode limits on inpatient MH/SUD services than medical/surgical benefits in 2009. There were small declines in 2010 and 2011 in the proportion of plans that had more restrictive dollar or episode limits. The Mental Health Parity Act of 1996 prohibited unequal MH annual and lifetime dollar and covered episodes limits. Our analyses confirm that plans overwhelmingly complied for MH and for SUD, even though the latter conditions were not covered by the 1996 Act.
Outpatient Quantitative Treatment Limitations
As shown in Table 23 and Table 24, more restrictive MH/SUD quantitative outpatient treatment limits decreased sharply between 2009 and 2011. In 2009, more than half of the plans analyzed had more restrictive outpatient in and out-of-network MH and SUD visit and dollar limits than medical/surgical benefits. In 2010, unequal coverage dropped to approximately 11%, and by 2011, the proportion that appeared to offer benefits that were not consistent with MHPAEA standards was about 6%. Very few plan options (less than 1%) had more restrictive annual dollar limits for outpatient MH services than for medical/surgical care. But, consistently, SUD outpatient dollar limits were more likely to be lower than medical/surgical coverage. In 2009, nearly 10% of plans had more restrictive annual dollar limits on outpatient SUD. The percentage of plans with lower annual dollar limits for in-network outpatient SUD decreased to 1.5% in 2010 and to 1.0% in 2011. Similarly, the proportion of plans with lower annual dollar limits for out-of-network SUD outpatient treatment declined from 9.8% in 2009 to 2.9% in 2010 and 1.3% in 2011. The 1996 Mental Health Parity Act did not cover disparities in outpatient SUD dollar or treatment episode limits. Instead, these changes may suggest movement by plans to comply with provisions of the PPACA prohibiting lifetime dollar limits and phasing out annual dollar limits that became effective in 2010.
TABLE 23. QTLs: MH/SUD Outpatient In-Network Treatment Limitations That Were More Restrictive Than Medical/Surgical Treatment Limitations, 2009-2011
| 2009 Percent of Plans | 2010 Percent of Plans | 2011 Percent of Plans | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mental Health | |||||||||||||||
| Visit limitations | 56.1% | 11.1% | 6.5% | ||||||||||||
| Dollar limitations (annual) | 0.8% | 0.6% | 0.7% | ||||||||||||
| Substance Abuse | |||||||||||||||
| Visit limitations | 51.1% | 12.7% | 8.5% | ||||||||||||
| Dollar limitations (annual) | 9.4% | 1.5% | 1.0% | ||||||||||||
SOURCE: Aon Hewitt's Plan Design Database (2009-2011).
TABLE 24. QTLs: MH/SUD Outpatient Out-of-Network Treatment Limitations Were More Restrictive Than Medical/Surgical Treatment Limitations, 2009-2011
| 2009 Percent of Plans | 2010 Percent of Plans | 2011 Percent of Plans | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mental Health | |||||||||||||||
| Visit limitations | 59.6% | 11.0% | 6.4% | ||||||||||||
| Dollar limitations (annual) | 0.5% | 0.3% | 0.2% | ||||||||||||
| Substance Abuse | |||||||||||||||
| Visit limitations | 53.2% | 14.0% | 9.0% | ||||||||||||
| Dollar limitations (annual) | 9.8% | 2.9% | 1.3% | ||||||||||||
SOURCE: Aon Hewitt's Plan Design Database (2009-2011).
Quantitative Limits Among Midsized Employers. Information on day limitations and visit limitations were abstracted from SPDs provided by BLS. As shown in Table 25, in 2008, before MHPAEA implementation, 88% of midsized employers' plans in our limited sample had inpatient day limitations that were more restrictive for MH/SUD conditions than for medical/surgical conditions. Following the implementation of parity, the percentage dropped to 24%. As seen in Appendix D, in each year following parity there were fewer plans utilizing more restrictive day limits for inpatient MH/SUD care than medical/surgical care, so that by 2011, only 13% of plans in our sample still appeared to provide more restrictive MH/SUD day limitations. Likewise, before the implementation of parity, 84% of midsized plans in our sample used outpatient visits limitations that were more restrictive for MH/SUD than medical/surgical benefits. Following the implementation of parity, 26% of these plans provided more restrictive visit limitations for MH/SUD services than medical/surgical services. Again, the percentage of plans providing more restrictive MH/SUD services dropped each year following the implementation of MHPEA, so that by 2011, only 13% of plans in our sample provided outpatient visit limitations that were more restrictive for MH/SUD than medical/surgical services. Caution is warranted so as to not over-interpret the decline, as only a small number of SPDs were available for analysis for each of the post-parity years. Nevertheless, it appears that the pattern of decreasing percentages of plans serving midsized employers that had more restricted MH/SUD quantitative limits is consistent with the pattern observed among large employers' health benefits.
TABLE 25. Treatment Limitations: Percentage of Midsized Employers' Plans in Our Limited Sample That Appear to Include More Restrictive MH/Substance Abuse Treatment Limitations Than Medical/Surgical Limitations
| Pre-Parity (2008-2009) Percent of Plans (n = 167) |
Combined Post- Parity Sample (2010-2011) Percent of Plans (n = 73) |
|||||||
|---|---|---|---|---|---|---|---|---|
| Inpatient care: day limits for MH/SUD treatment higher than inpatient medical/surgical care | 73% | 17% | ||||||
| Outpatient care: visit limits for MH/SUD treatment higher than inpatient medical/surgical care | 79% | 18% |
SOURCE: Author's weighted analysis of data abstracted from SPDs provided by BLS.
Employer Surveys. The nationally representative employer health benefits surveys conducted by KFF/HRET and Mercer in 2010 provide additional perspectives on QTLs following the effective date of MHPAEA. In 2010, the KFF/HRET survey asked whether employers had eliminated limits in MH/SUD as a result of MHPAEA. Table 26 shows that one in five employers reported eliminating limits in coverage in response to MHPAEA. Employers with more than 1,000 workers, firms with self-insured plans, and firms in the transportation and communication industries were most likely to report removing limits on MH/SUD benefits. It cannot be determined from the KFF/HRET data, however, whether firms that did not report changing their benefits already had equitable benefits and did not need to make changes, or if they had inequitable benefits but did not take steps to change. The findings do indicate that a sizeable percentage of employers and health plans are making MHPAEA-related benefit adjustments.
TABLE 26. Percentage of Firms That Changed MH Benefits As a Result of MHPAEA by Firm and Worker Characteristics
| Eliminated Limits In Coverage | |||
|---|---|---|---|
| All Firms | 20.6% | ||
| Firm Size | |||
| 50-199 employees | 15.7%* | ||
| 200-999 employees | 24.1% | ||
| More than 1,000 employees | 50.3%* | ||
| Geography | |||
| Northeast | 14.6%* | ||
| Midwest | 27.1% | ||
| South | 24.6%* | ||
| West | 14.7% | ||
| Plan Funding | |||
| Underwritten by insurer | 14.2%* | ||
| Self-insured | 34.7% | ||
SOURCE: Estimates are from author analysis of data from 2010 Henry J. Kaiser Family Foundation/Health Research and Educational Trust 2010 Employer Health Benefits Survey public use file.
* Estimate is statistically different from reference group (P < 0.05). Reference groups were assigned as follows: firm size = 200-999 employees; region = South; plan funding = self-insured.
The 2010 Mercer Health Benefits Survey also asked employers whether they had made changes in benefit designs to meet parity requirements. More than seven in ten employers (74%) responded that no changes were necessary because their benefits already complied with MHPAEA. As shown in Table 27, of the 1,433 employers responding to the 2010 Mercer survey, 17% reported removing limitations in the number of office visits, inpatient days or dollar limits for MH/SUD benefits in response to MHPAEA requirements. Although the 2010 KFF/HRET and Mercer surveys differ somewhat in the proportion of respondents who report making quantitative changes in their MH/SUD benefits in response to MHPAEA, both reflect considerable activity among employers in response to MHPAEA.
TABLE 27. Employer Response to MHPAEA: Results From the 2010 Mercer Survey
| Sample Size | Remove Limits | |||||||
|---|---|---|---|---|---|---|---|---|
| Total | 1,433 | 17% | ||||||
| Firm Size | ||||||||
| Fewer than 500 employees | 332 | 15% | ||||||
| More than 500 employees | 1,101 | 35% | ||||||
| Region | ||||||||
| Northeast | 216 | 34% | ||||||
| Midwest | 334 | 42% | ||||||
| South | 359 | 32% | ||||||
| West | 192 | 32% | ||||||
SOURCE: 2010 Mercer Health Benefits Survey.
Research Question #3: Health Plan and Insurer Use of Non-Quantitative Treatment Limits
What types of NQTLs are commonly used by plans and issuers for MH and/or substance abuse disorders and how do these compare to NQTLs in place for medical/surgical benefits?
According to the MHPAEA regulations, NQTLs limit the scope or duration of benefits and can include, but are not limited to, plan provisions related to:
- Medical management.
- Prescription drug formularies.
- Provider admission to a network.
- Determination of UCR amounts.
- Step-therapy requirements.
- Conditioning benefits on completion of a course of treatment.
Any processes, strategies, evidentiary standards, or other factors used in applying the NQTL to MH/SUD benefits must be comparable to, and applied no more stringently than, the processes, strategies, evidentiary standards, or other factors applied to medical/surgical benefits. However, these requirements allow variations to the extent that recognized clinically appropriate standards of care may permit a difference. Assessing whether NQTLs that appear to be non-compliant are acceptable is difficult due to variations allowed by these requirements.
2010 NQTL Analysis
During Milliman's 2010 testing process of a nationally representative sample of 124 large employers' health plans, a number of NQTLs were identified that appeared to be non-consistent with MHPAEA standards. These NQTLs were identified through careful analysis of SPDs and other plan documentations and appeared to apply unequally to MH/SUD conditions when compared to medical/surgical conditions. However, no follow-up was completed with the plans in order to assess whether these variations were the result of differences in clinically appropriate standards of care. Therefore, the results of Milliman's NQTL analysis should be interpreted with caution as some of the identified NQTLs may be permissible as allowed by the IFR.
The analyses were conducted to determine changes that employers and health plans would need to take to make their 2010 plans consistent with IFR requirements for NQTLs for the 2011 plan year. As outlined in Table 28, almost 30% of plans used precertification procedures that were more stringent for MH/SUD services than for medical/surgical services.
TABLE 28. Percentage of 2010 Plans Utilizing NQTLs that Appeared to be Not Consistent With MHPAEA Standards if Continued into the 2011 Plan Year
| NQTL Description | Percent of Plans | ||
|---|---|---|---|
| MH/SUD precertification requirements were more stringent than for medical/surgical benefits. | 28.2% | ||
| Medical necessity was applied to MH/SUD benefits but not to medical/surgical benefits. | 8.2% | ||
| No MH/SUD benefits were provided outside the state of residence, but medical/surgical benefits were provided. | 0.9% | ||
| Pre-approval was required starting with the 13th outpatient MH/SUD office visit. | 1.8% | ||
| Out-of-network treatment was covered only if in-network treatment was unavailable. This applied only to MH/SUD benefits. | 0.9% | ||
| Plans imposed a probationary period only for substance abuse treatment. | 0.9% | ||
| Out-of-network eating disorder treatment was covered only if in-network services were unavailable; no such requirement applied to out-of-network medical/surgical benefits. | 0.9% |
SOURCE: Analysis of 2010 Milliman plan information.
Detailed 2010 NQTL Assessment
Aon Hewitt conducted detailed NQTL assessments in 2010 for 22 large national employers, each employing more than 1,000 workers. The analysis included the NQTL designs and practices of 17 national health vendors. The majority of these employers (72%) had 10,000 or more employees. The intensive NQTL review included a detailed assessment of how MH/SUD treatment is handled beyond plan design. The review encompassed precertification, concurrent and retrospective review, determination of reimbursement rates, and other medical management procedures to ensure that the processes in place for NQTLs are not more restrictive for MH/SUD than they are for medical/surgical treatment. Areas of potential concern identified by the NQTL testing frequently resulted in book-of-business benefit adjustments for these national vendors.
Each vendor that administered an employer's medical and MH/SUD benefit plans was requested to respond to an extensive questionnaire that collected details about the vendor's NQTL processes and procedures in place in 2010. The following NQTL areas were assessed:
- Precertification
- Procedures and services requiring precertification
- Responsibility for precertification (provider or member)
- Documentation required
- Medical necessity review conducted
- Guidelines used
- Concurrent Review
- Levels of care considered for review
- Source of guidelines
- Process
- Frequency of reviews
- Discharge Planning
- Process
- Frequency of reviews
- Follow-up after discharge
- Case Management
- Case identification process
- Case management process
- Retrospective Review
- Process
- Services included
- UCR Determination
- Data source
- Frequency of updates
- Percentile
- Reimbursement Rates
- Source
- Process
- Experimental and Investigational
- Definition
Each MH/SUD policy and procedure was compared with corresponding medical/surgical policies and procedures. Any procedures or requirements that could be considered to be more stringent for MH/SUD than medical/surgical were identified as potentially non-compliant with the MHPAEA regulations. Results of the assessment were communicated to the employer as well as to each vendor involved in the assessment process. Discussions were held between the employer and each vendor to review the findings and determine whether clinically appropriate differences in care explained the variance, and whether any actions were necessary to comply with MHPAEA regulations. Our initial review identified many areas that were deemed potentially non-compliant. However, after further investigation and follow-up documentation from the vendors, it was determined, in some instances, that the MH/SUD process was not more stringent than medical/surgical. Areas of concern, and proposed modifications are presented in Table 29.
TABLE 29. NQTLs: Areas of Concern and Modifications Made to Ensure Consistency With the MHPAEA and the IFR
| NQTL Category |
Process/Procedure | Potential Concern | Outcome | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Medical management | Outpatient precertification | Precertification required for all outpatient MH/SUD services. Precertification not required for all outpatient medical/surgical services. |
Precertification requirement removed for all outpatient services, but maintained for services requiring greater oversight and supported by recognized clinically appropriate standards of care (e.g., psychiatric testing, electroconvulsive therapy [ECT], etc.) | ||||||||||||
| Outpatient medical necessity review | All outpatient MH/SUD counseling services authorized for 8-12 visits (varied by vendor); after 8th or 12th visit, clinical/medical necessity review conducted. Similar procedure not in place for outpatient medical/surgical services |
Some vendors extended the threshold for conducting medical necessity review on outpatient MH/SUD counseling services to allow for review of cases that represent outliers (e.g., 20 visits). | |||||||||||||
| Concurrent review | Concurrent review conducted for MH/SUD cases include a medical necessity review as well as a review for adherence to benefit provisions. Concurrent review conducted for medical/surgical cases includes a review for adherence to benefit provisions; no medical necessity reviews. |
Concurrent review conducted for MH/SUD cases will include only a review for adherence to benefit provisions; no medical necessity reviews. | |||||||||||||
| Retrospective review | Retrospective review process for MH/SUD included a review for medical necessity, as well as a review for adherence to benefit provisions. Retrospective review process for medical/surgical included a review for adherence to benefit provisions and only when no prior notification was provided. |
MH/SUD retrospective review will include a review for adherence to benefit provisions only when no prior notification was provided. No medical necessity review will be conducted. | |||||||||||||
| Inpatient medical necessity review | All inpatient MH/SUD cases require precertification, with a medical necessity review conducted during the precertification process. For medical/surgical inpatient cases, members notify the vendor; no medical necessity review is conducted. |
Notification process implemented for MH/SUD (eliminated medical necessity review requirement). Medical necessity reviews conducted only for cases considered to be outliers based on diagnosis, high-cost and complex cases, and provider outliers. |
|||||||||||||
| Provider network management | Reimbursement rates | MH/SUD provider reimbursement rates were determined based on vendor's internal set of data. Medical/surgical provider reimbursement rates were determined using an external database. |
MH/SUD provider reimbursement rates were modified to reflect a similar process and data source as medical/surgical provider reimbursement rates. | ||||||||||||
| UCR percentile | Percentile used to determine reimbursement rates for MH/SUD services was set at the 50th percentile. Medical/surgical services were reimbursed at the 80th percentile. |
Reimbursement percentile rate modified to the 80th percentile for MH/SUD services. | |||||||||||||
| Network admission criteria | Site visits required for some MH/SUD network providers but not for medical network providers. | Requirement maintained, as the requirement is essential to ensuring quality and safety of MH/SUD network providers; site visits conducted at facilities and programs that are not accredited. | |||||||||||||
| Prescription drugs | Smoking cessation drug requirements | Member is required to participate in a smoking disease management program in order to receive coverage for smoking cessation medication. Similar requirement not in place for any other drug or drug class. |
Program revised to eliminate the requirement that members participate in a smoking disease management program in order to receive coverage for smoking cessation medication. | ||||||||||||
| Smoking cessation drug limits | Smoking cessation drugs limited to 12 or 24 weeks per year, depending on brand; similar limits not imposed on other drugs or drug classes. | Limitation removed for smoking cessation drugs. |
SOURCE: Analysis of Aon Hewitt plan information and plan/vendor questionnaire.
Results from Employer Surveys. The 2010 KFF/HRET survey provides additional information on employer use of utilization management techniques in response to MHPAEA. Table 30 presents results from this question, based on employer weights. Results suggest that, overall, 4.9% of employers reported increasing their use of utilization management techniques in response to MHPAEA. Very large employers (1,000 or more employees) were significantly more likely to report an increased reliance on utilization management techniques (8.5%) than were midsized employers. Employers in the South (9.8%) were also more likely to report increasing their use of utilization management than were employers in the Northeast (2.3%) and Midwest (3.0%). Employers in the health care and retail industries were least likely to report an increased use of utilization management techniques, and self-insured employers (9%) were significantly more likely to report increased use of utilization management than their fully-insured counterparts (3.1%).
TABLE 30. Percentage of Firms that Changed Utilization Management as a Result of the MHPAEA by Firm and Worker Characteristics: Results from KFF/HRET
| Increased Utilization Management of MH Benefits |
|||
|---|---|---|---|
| All Firms | 4.9% | ||
| Firm Size | |||
| 50-199 employees | 4.6% | ||
| 200-999 employees | 4.6% | ||
| 1,000 or more employees | 8.5%* | ||
| Plan Funding | |||
| Underwritten by insurer | 3.1%* | ||
| Self-insured | 9.0% | ||
SOURCE: Estimates are from author analysis of data from 2010 Henry J. Kaiser Family Foundation/Health Research and Educational Trust 2010 Employer Health Benefits Survey public use file.
* Estimate is statistically different from reference group (P < 0.05).
This issue is also addressed in the 2010 Mercer Survey, which asked responding employers to describe planned or implemented changes made to their health benefits in response to the MHPAEA. Of the 1,433 participating employers, approximately 8% of employers reported adding or adjusting their use of utilization management techniques in response to MHPAEA.
Research Question #4: Health Plan and Insurer Use of Separate Deductibles
Are group health plans and insurers using separate deductibles for MH and/or SUD benefits?
Very few health plans continued to use separate deductibles after MHPAEA was enacted. Milliman's analysis of 2010 benefit designs found that only 3.2% of health plans had separate deductibles for MH/SUD benefits in which MH/SUD out-of-pocket costs did not accumulate toward a single deductible combined with medical/surgical benefits. Aon Hewitt's analysis of 2011 plan designs found only 1.3% of plans had separate deductibles for MH/SUD.
Among the midsized employers' plans analyzed by NORC from the BLS sample, none of the SPDs indicated a separate deductible for MH/SUD in the years before parity implementation (2008-2009), and fewer than 3% used separate deductibles in the post-parity period (2010-2011).
Research Question #5: Health Plan and Insurer Restriction of Medical/Surgical Benefits Following the Implementation of MHPAEA
Have financial requirements and treatment limits on medical/surgical benefits become more restrictive in order to achieve parity (instead of requirements and limits for MH/SUD becoming less restrictive)?
Analyses of the Aon Hewitt and Milliman testing databases identified no evidence of any plan that had increased medical/surgical financial requirements or treatment limits in order to achieve parity.
Research Question #6: Health Plan and Insurer Elimination of MH and Substance Abuse Services Following the Implementation of the MHPAEA
How many plans have eliminated MH and/or SUD treatment coverage altogether instead of complying with the MHPAEA?
Analyses of Milliman's database suggest that participating plans did not respond to MHPAEA and the IFR's parity requirements by eliminating MH/SUD benefits. No plans in Milliman's database failed to offer any MH/SUD benefits during 2009-2011.
Results from Aon Hewitt's yearly Request for Information (RFI) provide further evidence that plans have continued to offer MH/SUD benefits following the introduction of the MHPAEA and the IFR. In their 2011 Annual RFI, Aon Hewitt requested behavioral health care organizations to respond to several questions regarding the impact of the MHPAEA. Responses to the MHPAEA questions were received from seven national behavioral health care organizations, representing all major carve-in and carve-out vendors. Vendor responses indicated that very few employers reported eliminating MH or SUD coverage following the implementation of the MHPAEA. In 2010, 57% of responding vendors reported that no employers had eliminated coverage, and 43% of vendors reported that 1% of employers had eliminated coverage. In 2011, 43% of responding vendors reported that no employers had limited coverage, and 57% reported that 1% had eliminated coverage.
Information obtained from BLS data provides further evidence that the vast majority of midsized employers' plans did not eliminate MH coverage following the implementation of MHPAEA. Results of analyses comparing benefits outlined in a pre-parity (2008-2009) sample of SPDs suggest that 100% of analyzed plans provided MH/SUD benefits. In the post-parity (2010-2011) sample, 97.2% of plans provided MH/SUD benefits.
Additional confirmation can be found in results from the 2010 KFF/HRET and 2010 Mercer surveys. Results from both surveys suggest that very few employers reported dropping coverage of MH/SUD benefits. Based on employer weights, Table 31 presents results from the KFF/HRET survey. Approximately 1.6% of firms reported dropping MH/SUD benefits.
TABLE 31. Percentage of Firms That Reported Eliminating MH Benefits as a Result of MHPAEA: Results from the 2010 KFF/HRET Survey
| Dropped MH Coverage | |||
|---|---|---|---|
| All Firms | 1.6% | ||
| Geography | |||
| Northeast | 0.0% | ||
| Midwest | 0.3% | ||
| South | 0.5% | ||
| West | 5.1% | ||
SOURCE: Estimates represent author analysis of data from 2010 Henry J. Kaiser Family Foundation/Health Research and Educational Trust 2010 Employer Health Benefits Survey public use file.
Overall, approximately 2% of employers responding to Mercer's 2010 survey claimed to have dropped or to be planning to drop MH/SUD benefits in response to the implementation of the MHPAEA. Employers were also asked to report whether they had increased the number of excluded MH/SUD conditions. Overall, less than 1% of employers reported increasing the number of exclusions covered under their insurance benefits in response to MHPAEA.
In 2010, Mercer reported that 18% of employers offered no coverage for autism spectrum disorders. In the 2011 report, 22% offered no autism spectrum coverage. Whether this increase represents a change in employer's actual coverage rates or is an artifact of the survey, it is notable that about one of five employers offered no coverage for autism screening, medication management or other treatments. In both years, approximately two-thirds of employers reported covering diagnostic services for autism, and more than half covered medications, inpatient and outpatient treatments.
The 2011 GAO report68 on MHPAEA provides additional context on how employers utilized condition exclusions before and after the implementation of parity (Table 32). GAO elicited responses from 168 employers that detailed treatment exclusions utilized in 2008 and 2010/2011. Although response rates were low (168 responses from 707 employers initially surveyed), the GAO results suggest that employers' use of condition limitations has decreased since the introduction of parity. For example, in 2008, eight out of 81 responding plans reported excluding treatment for smoking cessation/tobacco dependence. In 2010/2011, only two out of 96 responding plans reported that exclusion. Likewise, in 2008, nine plans reported excluding treatment for learning disorders, but by 2010, that number had decreased to five.
TABLE 32. Excluded MH/SUD Conditions and Diagnoses: Results From the GAO Survey
| Excluded Diagnosis/Condition | 2008 (n = 81) | 2010/2011 (n = 96) | ||||||
|---|---|---|---|---|---|---|---|---|
| Alcoholism | 2 | 3 | ||||||
| Attention deficit disorder | 2 | 0 | ||||||
| Autism | 4 | 2 | ||||||
| Conduct/impulse disorders | 2 | 3 | ||||||
| Developmental Disorders/disabilities/delays | 10 | 6 | ||||||
| Learning disorders | 9 | 5 | ||||||
| Mental retardation | 7 | 3 | ||||||
| Organic mental disorders | 7 | 3 | ||||||
| Sexual dysfunction/deviancy | 9 | 2 | ||||||
| Smoking cessation/tobacco dependence | 8 | 2 |
68. Government Accountability Office (GAO). Mental Health and Substance Use: Treatment Exclusions in Employers' Health Insurance Coverage. GAO-12-761R. Available at: http://www.gao.gov/assets/600/591261.pdf.
Research Question #7: Health Plan Response to the MHPAEA's Disclosure Requirements
How have plans responded to the MHPAEA's requirements regarding the disclosure of medical necessity criteria and reasons for claim denials?
To assess plan response to MHPAEA's disclosure requirements, NORC and its research partners conducted a series of semi-structured interviews with a small number of representatives from health plans and MBHOs. Although the number of individuals interviewed was small, representatives from the seven companies that participated collectively provide coverage for more than 100 million covered lives and are among the largest health plans in the nation. Figure 1 outlines the process for contacting respondents. Potential respondents received an initial e-mail from Truven Health Analytics that explained the purpose of the study, listed several topics of interest, and requested a 30-minute telephone call. Seven of the 11 companies contacted responded affirmatively, and a semi-structured interview was conducted with each. Notes were taken during every call, and each participant had the opportunity to review and provide feedback on a draft version of the notes before they were finalized. Six of the seven companies provided feedback on the notes.
Results
The results are organized by interview topic. Additional detail appears in Appendix E. Identifying personal or corporate names have been excluded from the results, and the order of responses varies across topics -- measures taken to assure the anonymity of participants' responses.
FIGURE 1. Process for Contacting and Interviewing Companies
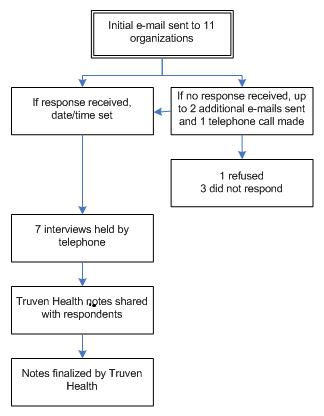
Medical Necessity Criteria
Most respondents (four MBHOs) reported that the content of medical necessity criteria have not changed as a result of the parity law. Two sets of criteria that are commonly used for behavioral health services are McKesson's InterQual criteria and the American Society of Addiction Medicine (ASAM) criteria. Some companies have developed their own criteria through consultation with experts and a regular review and improvement process. One company that had developed its own, proprietary medical necessity criteria expressed concern regarding copyright infringements because the PPACA requires companies to share the criteria with members. Some states have developed their own set of criteria that their public plans must use, or they specify criteria that must be used, such as those of ASAM.
Although the MHPAEA has not affected the scientific content of the necessity criteria, the application of the criteria has sometimes changed. According to a representative of one MHBO, in the late 1990s and early 2000s, health plans had moved away from medical necessity criteria for medical care, but by 2008 the plans had begun to increase their use again. Following the MHPAEA, health plans served by this MHBO had to decrease use of medical necessity criteria for behavioral health services in order to match similar medical services. Since then, the use of medical necessity criteria has grown at equal levels for behavioral and medical services. The other MHBOs interviewed did not report a similar circumstance in the plans they work with, however, so the extent of this phenomenon is unclear.
Another MBHO explained that, due to the parity law, medical necessity criteria are not used to manage the utilization of behavioral health services when utilization management techniques are not used for other medical services within the same plan.
Respondents reported that individual members may receive a copy of the medical necessity criteria upon request. One company also stated that it makes its medical necessity criteria publicly available on its website.
Informing About Claim Denials
Companies interviewed stated that the PPACA, not the MHPAEA, has been driving changes in procedures for claim denials. The PPACA, DOL rules, and state law dictate the content and timing of the letters, and these rulings applied to both behavioral health and other medical services.
If a claim is denied, a letter is sent to the member and to the provider or facility. The letter explains the reason for the denial and may also cite the medical necessity criteria used for the decision. Denials made in advance of treatment are delivered in adverse benefit determination (ABD) letters. Denials of reimbursement for services rendered come in explanation of benefits (EOB) statements.
Utilization Management Techniques
Respondents reported that among NQTLs, particularly for outpatient services, utilization management has changed the most since implementation of the parity law. Prior authorization had not traditionally been used for medical services except for non-routine outpatient services such as ambulatory surgery. As a result of MHPAEA, five MBHOs interviewed stated that they have moved away from using prior authorization for outpatient services, except for unusual services such as ECT.
In its place, four respondents reported having moved to a process of managing individuals who use significantly more MH or SUD services than is "normal" and "expected." They reported that the process is similar to the management of medical services such as physical therapy, radiology, or skilled nursing. For example, if a company identifies an individual who has received 20 sessions of therapy when the average length of treatment is 6-8 sessions, the company will start to manage the case more closely through reviews and reauthorization for future outpatient services. One company noted, however, that, with the implementation of the parity law, it has seen an increase in the average length of treatment and a larger percentage of individuals are receiving more than eight therapy sessions.
Three respondents also reported that they have focused more on managing the quality of treatment. For example, one company identifies enrollees who are not receiving treatment according to best practice clinical guidelines. In these situations, the company works with the providers to better understand why the best practice guidelines have not been followed. If the provider is not willing to provide treatment for the patient more consistent with the guidelines, he or she will not be reauthorized for coverage of additional treatments. Another company uses the reauthorization process to ask providers whether they collaborate with family members and other medical providers in treatment.
Another company reported that rather than managing claims for individuals, it has reduced its administrative burden by managing providers and facilities. Among providers that serve a substantial number of its enrollees, the company examines the average length of treatment for its enrollees. If the provider meets a specific standard, reauthorization over the course of its enrollees' treatment is not required. If the provider does not meet the standard or has patients with extremely long lengths of treatment, and the provider does not change, the provider may be moved to a lower tier and stop receiving referrals from the company. For inpatient care, this company has established a similar program in which concurrent review is waived for facilities that maintain a certain standard of care. If these practices are only used with MH/SUD services, this may suggest a potential area of NQTL non-compliance.
Respondents report that utilization management techniques for inpatient services generally have remained the same after the implementation of parity. Because health plans often require preauthorization for medical and surgical inpatient services, preauthorization is still frequently required for non-emergent inpatient behavioral health services. Respondents reported that a significant difference between inpatient medical and behavioral health services is the incentive to increase length of stay. Most medical services are paid based on the diagnosis-related group (DRG) assigned, regardless of the length of stay, whereas behavioral health services are typically paid on a per-diem basis. This means that longer stays result in greater revenue for treating hospitals. To manage length of stay, most MBHOs carry out concurrent reviews, monitoring the need for additional inpatient services every few days. The respondents reported that this follows a similar pattern of utilization management for medical services that are not paid on the DRG system.
One company found that prior authorization was not as common for inpatient medical services as for behavioral health services. As a result, it slightly decreased the use of prior authorization but increased the use of retrospective authorization, which is authorization for reimbursement after a service is performed. Retrospective review is also commonly used for out-of-network services, where other types of utilization management are challenging to employ.
Managing Out-of-Network Care
Respondents reported different methods for managing out-of-network services. One MBHO noted that commercial plans that covered out-of-network behavioral health services did not manage those services before the parity law. Since the implementation of the MHPAEA, however, more commercial accounts have covered out-of-network behavioral health services in order to establish parity with medical and surgical benefits. That MBHO has also observed that many more of the commercial plans want to manage their out-of-network services, with retrospective review being the most common method to do so.
Another MBHO that uses retrospective review to manage out-of-network care mentioned that providers do not like the uncertainty of reimbursement that comes with retrospective reviews. The company has compensated for this by working with the providers to change treatment patterns prospectively. This company also remarked that most plans' strategy is to have lower copayments and cost-sharing for in-network care, thereby producing a financial incentive to use in-network care. Some companies interviewed do not manage out-of-network services.
Demand for Residential or Intensive Outpatient Substance Abuse Services
Four of the companies interviewed reported that they have not observed a significant increase in the overall frequency of residential or intensive outpatient services for substance use treatment. In some benefit designs, plans do not cover residential substance use treatment. In other designs, there have been changes in how these services are used. For example, one company has noted more individuals using out-of-network residential services. Another has seen an increase in the average length of treatment and the average number of visits for structured substance use intensive outpatient services per week. One company reported experiencing an increase in the number of beneficiaries seeking residential SUD treatment. The two companies reporting increased substance use treatment utilization reported that states in which they work had recently expanded the scope of required benefits to include residential treatment or intensive outpatient services, and that increased demand appeared to be associated with increases in the number of licensed residential treatment facilities (RTFs) in specific geographic areas that they cover.
Plans report eliminating quantitative day limitations for residential treatment because of the parity law. Residential treatment is often classified as an inpatient service. Since most plans do not limit the number of days of medical inpatient services, substance use residential days cannot be limited. Some MBHOs reported considering comparing residential treatment to skilled nursing facilities (SNFs), which usually have day limitations. However, the parity law does not include a SNF category among the six categories of services specified in the IFR for comparing behavioral health and physical health services. As a result, plans cannot make a SNF to residential substance use treatment comparison. One company mentioned that the removal of day limitations has not resulted in a significant change in use or costs because many health plans did not limit total days before implementation of the parity law.
One MBHO reported that some plans considered excluding residential substance use treatment completely following passage of MHPAEA. The company reported that, from a legal perspective, residential care could have been eliminated as long as other inpatient behavioral health services were covered. However, the MBHO determined that residential treatment is a part of a continuum of care, and that residential treatment could prevent the need for more acute (and expensive) inpatient care.
Establishing parity for intermediate substance use treatments, such as intensive outpatient programs (IOPs), has been more challenging for plans than decisions about covering residential treatment. IOPs could be classified as either an inpatient or an outpatient service. If intermediate care is classified as an outpatient service, the challenge to the plan is in making the copayments comparable to those of medical services. Intensive outpatient treatment requires 3-5 visits per week, for example, so using a standard medical copayment could result in large out-of-pocket expenses. One company recommended to employers and health plans that it contracts with that patients either make a single copayment for an entire course of intermediate treatment or be liable for much smaller copays per visit.
Quantitative day limitations have also been removed for intermediate services. One company noted that, even with the removal of these limitations, the length of IOPs has not increased significantly. It has, however, allowed for individuals who have a relapse after finishing the program to go through the program again.
Management of Prescriptions
Only one of the MBHOs interviewed manages prescription medications for beneficiaries with behavioral health conditions, and even the one plan that does manage prescription medications does so only for certain public insurance plans in states that specify formularies. Most health plans manage prescriptions through a pharmacy benefits management (PBM) vendor. In some cases, the companies interviewed knew that the health plans with which they work had found that formulary tiers were no more restrictive of psychiatric drugs than of other medical drugs.
Additional Comments About Parity
Four respondents reported that they had seen increased use of behavioral health services after the parity law was implemented. One reported that this increase was less than what was expected. Another observed that increased utilization and cost of behavioral health services have now begun to plateau as new management techniques have taken effect. One company observed that states have been so preoccupied with health care reform that parity requirements, regulations and enforcement have been ignored. If the parity law had been in effect a few years prior to enactment of PPACA, oversight by state insurance commissioners and the speed of parity implementation within the state-regulated environment would likely have been very different.
Before the parity law, many health plans had deductibles and lifetime spending maximums that applied solely to behavioral health benefits, entirely separate from copayments and coinsurance for medical benefits. MHPAEA requires that health plans use a unified set of financial and QTLs that accumulate spending for both behavioral and physical health benefits. These are called shared accumulators. One MBHO expressed concern that this has increased the administrative burden of collaborating with health plans to determine whether the maximums have been met. Working with small commercial plans to establish the shared accumulators for each enrollee has been especially challenging.
A few respondents reported that providers have become more aware of the implications of the parity law in recent years. In some cases, plan representatives believe that providers have tried to take advantage of parity to justify new or more extensive treatments. For example, some psychiatrists argue that their services should be reimbursed at the same level as obstetrician/gynecologists or other primary medical care and medical specialists, using the general evaluation and management (E&M) procedure code. As a result, one MBHO reported seeing an increase in psychiatrists using E&M codes to bill for services. Another MBHO observed that the removal of QTLs has coincided with increases among some providers in treating individual patients more than once weekly. This company has advised its providers that open-access to care does not eliminate the need to monitor quality of care and that treatment goals and progress are still necessary for continued payment of claims.
One company raised the challenges it experiences in trying to determine if and how to cover treatments for autism. The plan representative reported an absence of consensus on whether autism should be categorized as a behavioral health condition, a birth defect, or a medical condition. Treatments for autism may be very expensive and lengthy and lack scientific evidence of clinical effectiveness. States have been active in regulating insurance coverage for autism. Many states with mandates have annual dollar limits on the services covered. To limit plans' exposure to very high autism treatment expenses and avoid conflict with the MHPAEA requirements, some states designate autism as a medical condition or a birth defect. This designation permits coverage limitations. New Jersey is the only state that precludes a dollar limit for any plan that covers autism if the plan is subject to federal parity; plans not subject to federal parity may enforce a benefit limit.
Some respondents report that they still have questions about parity, including issues such as:
- Whether it is necessary to harmonize MBHO and medical contracts with facilities and providers.
- Whether parity applies to network access.
- How to reconcile different payment strategies for medical and behavioral health inpatient services.
- How parity applies to the reimbursement of providers.
Summary of Interview Results
Health plans and their subcontracted MBHOs have made significant changes to their management of behavioral health services in response to the MHPAEA. Companies have moved away from managing the initiation of outpatient treatment by preauthorization and now focus on managing treatment patterns. They target management of individuals receiving more services than what is "expected" or "normal". Another strategy used is to focus on managing providers, using providers' distribution of patients' lengths of treatment to identify outliers. Plans are using claims data to determine if providers are frequently providing care that is not consistent with best practice guidelines. Plans work with the providers to change practice patterns, and if changes are not observed, to move the providers out-of-network.
Preauthorization and concurrent reviews remain respondents' most common methods for managing inpatient behavioral health services. MBHOs continue to require preauthorization because this is comparable to medical/surgical inpatient service procedures. Concurrent review for behavioral health services is also used in a comparable way to medical and surgical inpatient services that are not paid through the DRG system.
Some health plans now cover more out-of-network behavioral health services in order to maintain parity with other medical services. Parity has also affected some of the treatment patterns of residential treatment or intensive outpatient services. Most respondents found that increased out-of-network benefits and coverage of substance use IOP and residential care have not led to significantly increased utilization by beneficiaries.
MBHOs are rarely responsible for pharmacy benefits. More intensive study of the practices of PBMs and general health plans is needed to determine whether behavioral health pharmacy benefits and formulary practices conform to parity requirements.
Summary of Findings
Taken as a whole, analyses presented in this report show that employers and health plans have made substantial changes to their plan designs in order to comply with MHPAEA and the IFR. Our sources indicate that by 2011, most ERISA-governed group health plans and health insurance offered in connection with group health plans removed most financial requirements that did not meet MHPAEA standards. Nearly all eliminated the use of separate deductibles for MH/SUD treatment and medical/surgical treatment. The number of plans that apply unequal inpatient day limits, outpatient visit limits or other QTLs for MH/SUD dropped substantially.
Although we document substantial changes since the enactment of MHPAEA, a substantial minority of large employers and health plans still offer some benefits that appear to be inconsistent with MHPAEA and the IFR. Data from 2011 suggests that one out of five large employers required higher copays for in-network outpatient MH/SUD services than for equivalent medical/surgical treatments. Coinsurance rates were still higher for in-network outpatient MH/SUD services than for medical/surgical services in 4% of large employers' plans.
Likewise, preliminary analyses of our limited sample of midsized employer SPDs suggests that in 2010-2011, a substantial minority of the health plans offered by businesses with between 51 and 500 employees required greater cost-sharing for in-network outpatient MH/SUD office visits than for equivalent PCP office visits.
Although the percentage of plans providing benefits that appeared not to conform to MHPAEA's other quantitative limits was much lower in our sample of plans for 2011 compared to 2010, a minority of plans in 2011, between 7% and 9%, still covered fewer MH and SUD inpatient days annually and fewer MH and SUD outpatient visits annually than they covered for medical/surgical conditions.
Assessing compliance with NQTLs is difficult from document review and self-report from employers and plans. We assessed NQTLs through a detailed review of plan documents and responses from an extensive questionnaire administered to plans' MH/SUD and medical/surgical vendors. Our analyses uncovered numerous areas of concern which warrant more intensive investigation. For example, in 2010, nearly three in ten plans used more stringent precertification and utilization management controls for MH/SUD than for medical/surgical conditions. Network management processes were inconsistent, with different standards and processes for including MH/SUD providers in plans' network than were used for medical/surgical providers. MH/SUD provider reimbursement rates were sometimes found to be set at a lower percentage of prevailing community rates than comparable medical/surgical rates. Rates were sometimes determined by the plan based on its internal data, but set medical/surgical reimbursement rates from external, multi-payer databases. Although we were able to identify some areas of non-compliant NQTLs, it is likely that our reliance on these limited sources of information drawn primarily from large employers' health plans resulted in a significant under-identification of non-complaint NQTLs. A careful, in-depth and longitudinal compliance monitoring of plans' NQTL policies and practices would be likely to turn up correctable problems that our analysis could not detect. The California Department of Mental Health's processes for monitoring plans' compliance with California's Mental Health Parity Act included onsite surveys, reviews of claims files, utilization review files, and internal management and performance reports. California was able to detect patterns in practice that could not be identified from the kind of reviews undertaken in the current report: plans incorrectly denying coverage for ER visits; plans were failing to monitor whether beneficiaries had reasonable access to after-hours services; and plans failed to include required information in claim denial letters.69
Some concerns about the impact of MHPAEA were not borne out in our analyses. A very small proportion of employers, between 1% and 2%, dropped or plan to drop coverage for MH or SUD, or for specific MH/SUD diagnoses as a result of MHPAEA. No employers reduced medical/surgical benefits to comply with parity. A very small percentage excluded specific conditions, and most of those were for learning disabilities, developmental delays, and court-ordered services. We did not detect any movement to exclude residential or intensive outpatient services.
Whether the changes that we observed in employers' and health plans' benefit designs constitute compliance with MHPAEA will have to be tested over time in actual practice. Parity should result in greater access to care, improved quality of services, and better outcomes for people with mental illnesses and SUDs.
Limitations. Although it is reasonable to assume that many of the changes we have documented were made in reaction to the implementation of the MHPAEA, it is important also to recognize that other legislative and employer-specific initiatives may have influenced plan design changes that occurred during this time period. Therefore, caution should be used when interpreting these changes as solely attributable to MHPAEA and the IFR.
It is also important to note that many of the comparisons made in this report rely on data obtained from two distinct data sources: the Aon Hewitt database and the Milliman database. Although the general characteristics of employers included in these two databases are similar, there is insufficient information on employers included in each sample to conclude that they are statistically comparable. Therefore, some of the observed differences between these two datasets may be attributable to inherent differences between the two samples, rather than to changes attributable to the implementation of MHPAEA.
In addition, there are significant limitations associated with our analyses of the BLS dataset. One notable limitation is the lack of detailed establishment information provided with the data. The most important characteristic needed to describe differences in establishments is the number of workers at the establishment. Of secondary importance are the industry classification and the physical location of the establishment. We were only provided information on basic industry categories. Therefore, we believe the weights as created, and applied in our analyses, are insufficient to remove all potential bias from the sample.
Our BLS analyses are also limited by the small number of health plans included in each subsample and the amount of information that could be obtained from each SPD. In some cases, plan information was limited to data obtained from a one-page table of benefits, making abstraction of some data points problematic, and further reducing our sample sizes. Because the number of plans included in each subsample is relatively small, it is only possible to detect relatively large changes between the pre-parity and post-parity samples with any certainty. Therefore, caution should be exercised when interpreting the results of these analyses.
Finally, the results of our health plan/vendor interviews should be interpreted with appropriate caution. Participating respondents represent only a small convenience sample of MBHOs. Although they include some of the largest firms in the field, they represent only a fraction of all MBHOs in the United States. Because the MBHOs work with many health plans, the responses tended toward commonalities; they will not reflect the experiences of every patient or plan associated with these MBHOs. Finally, we made no attempt to verify the information provided by respondents. Their comments should be viewed as the informed opinions of employees.
69. California Department of Managed Health Care. Mental Health Parity in California. Mental Health Parity Focused Survey Project: A Summary of Survey Findings and Observations. Available at: http://www.hmohelp.ca.gov/library/reports/med_survey/parity/sfor.pdf.
Appendixes
Appendix A. Detailed Compliance Testing Results: Milliman Database (2010)
There were no plans in the Milliman sample that did not offer any MH/SUD benefits during 2009-2011.
The percentage of plans with separate deductibles and/or out-of-pocket (OOP) maximums for MH/SUD in their 2010 benefit designs is as follows:
3.2% of plans had separate deductibles for MH/SUD benefits. That is, MH/SUD member OOP costs did not accumulate towards a single deductible combined with their medical/surgical benefits.
7.2% of plans had separate OOP maximums for MH/SUD and medical/surgical benefits.
3.2% of plans had separate deductibles and separate OOP maximums for MH/SUD benefits and medical/surgical benefits.
These separate MH/SUD deductibles and OOP maximums were removed such that the post-parity benefits had integrated deductibles and OOP maximums for MH/SUD and medical/surgical benefits.
We were not able to identify any plan that increased medical/surgical financial requirements or eliminated certain coverage for MH/SUD disorders to achieve parity.
The following sections present the testing results in tables that summarize the percentage of plans and the specific changes that had to be made to become parity compliant. There are tables for each classification of MH/SUD benefits as defined by the IFR (Inpatient In-Network, Inpatient Out-of-Network, Outpatient In-Network, Outpatient Out-of-Network, Emergency Care, and Prescription Drug (Rx). Results also report when the outpatient benefits safe harbor was used to separately test Outpatient Office Visits from Outpatient-Other benefits.
Nearly all the tables have the identical format. The first column displays the type of quantitative financial requirement or treatment limitation applicable to the benefit classification in question. The subsequent columns summarize the percentage of plans where each type of financial requirement was unchanged, added, converted to a different type of cost-sharing, increased, decreased, or modified in other ways.
"No Change" shows the percentage of plans where no changes were required to become compliant with MHPAEA.
"Added" indicates the percentage of plans that did not have a certain type of financial requirement when one was allowed by MHPAEA, and had the option of adding one.
"Converted" indicates the percentage of plans that had to change the type of member cost-sharing. Typically, plans had to either switch from a dollar copay to the use of the deductible with coinsurance and OOP maximum structure, or vice versa.
"Removed" indicates the percentage of plans that had to completely remove the financial requirement (and were not allowed to convert it to a different form of cost-sharing).
"Increased" indicates the percentage of plans that were charging a lower cost-sharing (or OOP maximum) than was allowed by MHPAEA, and had the option of increasing it.
"Decreased" indicates the percentage of plans that were charging a higher cost-sharing (or OOP maximum) than was allowed by MHPAEA, and were required to reduce it.
"Exception" indications the percentage of plans that had to make changes that are not adequately described by any of the other options in the table.
Please note that in several of the tables that describe cost-sharing changes (sub-section "a"), the percentages across rows may not sum to 100%. For example, in section 4a, the percentage of plans that did not have to make any changes to their deductible is 93.3% (second column). The percentage of plans that had to make a change to their deductible was 5.7% (sum of the next six columns). These two percentages sum to only 99.0%. The reason for this is that 1.0% of the plans had copays which had to be converted to a deductible/coinsurance structure. This conversion was counted under the "Converted" column of the copay line. To avoid double counting, they did not include these plans anywhere in the "Deductible" row, resulting in total percentages below 100%.
Inpatient MH benefits.
Copay/coinsurance/deductible/OOP maximum levels (quantitative financial requirements).
The table below shows summarized results of compliance testing of the Inpatient In-Network Mental Health (IP INN MH) benefits.
Percent of Plans Covering IP INN MH Services: 96.0% Cost-Sharing No Change Added Converted Removed Increased Decreased Exception Deductible1,2 93.3% 3.3% 0.0% 0.8% 0.0% 0.8% 0.8% OOP max1 91.7% 7.5% 0.0% 0.0% 0.0% 0.0% 0.0% Copay1 93.3% 2.5% 0.8% 0.8% 0.0% 1.7% 0.0% Coinsurance1 92.5% 0.0% 0.8% 0.0% 0.0% 5.8% 0.0% - Note that some percentages do not add up to 100%. The difference is due to plans where deductible, coinsurance, and OOP max were added to replace a copay or vice versa. These conversions are recorded under the row that represents the original cost-sharing.
- Indicated exceptions include plans where a partial hospital benefit deductible was removed but could be replaced by a per admit deductible with coinsurance up to OOP max.
Over 90% of the plans that provided IP INN MH benefits did not have to make any changes to their financial requirements to comply with MHPAEA and the IFR.
About 7.5% of the plans were required to accumulate the member OOP payments for these benefits towards the same OOP maximum that was applicable to medical/surgical benefits.
Nearly 6% of the plans were required to reduce their coinsurance on this benefit to be parity compliant.
The table below shows summarized results of the compliance testing of the Inpatient Out-of-Network Mental Health (IP OON MH) benefits.
Percent of Plans Covering IP OON MH Services: 82.4% Cost-Sharing No Change Added Converted Removed Increased Decreased Exception Deductible1 99.0% 0.0% 0.0% 0.0% 0.0% 0.0% 1.0% OOP max 92.2% 7.8% 0.0% 0.0% 0.0% 0.0% 0.0% Copay 100.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% Coinsurance 94.2% 0.0% 0.0% 0.0% 0.0% 5.8% 0.0% - Indicated exceptions include plans where a partial hospital benefit deductible was removed but could be replaced by a per admit deductible with coinsurance up to OOP max.
Over 90% of the plans that provided IP OON MH benefits did not have to make any changes to their cost-sharing to comply with MHPAEA and the IFR.
About 8% of the plans were required to accumulate the member out-of-payments for these benefits towards the same OOP maximum that was applicable to corresponding medical/surgical benefits.
Nearly 6% of the plans were required to reduce their coinsurance on this benefit to be parity compliant.
Quantitative treatment limitations.
The following table summarizes the percentage of plans that had to remove various QTLs placed on their IP INN MH benefits.
Service/Dollar Limitations Plans (%) Percent of plans where day limits were removed 12.5% Percent of plans where visit limits were removed N/A Percent of plans where quantity limits were removed 0.0% Percent of plans where dollar limits were removed 4.2% The most common IP INN MH treatment limitation removed was the day limit in a calendar year on inpatient stays (12.5% of the plans).
Other changes that certain plans had to make to their IP INN MH benefits to become parity compliant are listed below.
Exceptions Plans (%) Day limits were removed for Inpatient In-Network RTF services only 0.8% The following table summarizes the percentage of plans that had to remove various QTLs placed on their IN OON MH benefits.
Service/Dollar Limitations Plans (%) Percent of plans where day limits were removed 6.8% Percent of plans where visit limits were removed N/A Percent of plans where quantity limits were removed 0.0% Percent of plans where dollar limits were removed 4.9% The most common IP OON MH treatment limitation removed was the day limits in a calendar year on inpatient stays (6.8% of the plans).
Other changes that certain plans had to make to their IP OON MH benefits to become parity compliant are listed below.
Exceptions Plans (%) Plans where day limits were removed for Inpatient Out-of-Network RTFs only 1.9% Plans where out-of-network benefits were previously not covered, but were recommended they be added to comply with the cover one, cover all classification requirement 2.9% For precertification requirements and penalties for lack of precertification, please see section 13.
Inpatient SUD benefits.
Copay/coinsurance/deductible/OOP maximum levels (quantitative financial requirements).
The table below shows summarized results of the compliance testing of the Inpatient In-Network Substance Use Disorder (IP INN SUD) benefits.
Percent of Plans Covering IP INN SUD Services: 95.2% Cost-Sharing No Change Added Converted Removed Increased Decreased Exception Deductible1,2 93.3% 3.4% 0.0% 0.8% 0.0% 0.8% 0.8% OOP max1 91.6% 7.6% 0.0% 0.0% 0.0% 0.0% 0.0% Copay1 93.3% 2.5% 0.8% 0.8% 0.0% 1.7% 0.0% Coinsurance1 92.4% 0.0% 0.8% 0.0% 0.0% 5.9% 0.0% - Note that some percentages do not add up to 100%. The difference is due to plans where deductible, coinsurance, and OOP max were added to replace a copay or vice versa. These conversions are recorded under the line that represents the original cost-sharing.
- Indicated exceptions include plans where a partial hospital benefit deductible was removed but could be replaced by a per admit deductible with coinsurance up to OOP max.
Over 90% of the plans that provided Inpatient IP INN SUD benefits did not have to make any changes to their financial requirements to comply with MHPAEA and the IFR.
About 7.6% of the plans were required to accumulate the member OOP payments for these benefits towards the same OOP maximum that was applicable to medical/surgical benefits.
Nearly 6% of the plans were required to reduce their coinsurance on this benefit to be parity compliant.
The table below shows summarized results of the compliance testing of the Inpatient Out-of-Network Substance Use Disorder (IP OON SUD) benefits.
Percent of Plans Covering IP OON SUD Services: 82.4% Cost-Sharing No Change Added Converted Removed Increased Decreased Exception Deductible1,2 99.0% 0.0% 0.0% 0.0% 0.0% 0.0% 1.0% OOP max1 91.3% 8.7% 0.0% 0.0% 0.0% 0.0% 0.0% Copay1 100.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% Coinsurance1 94.2% 0.0% 0.0% 0.0% 0.0% 5.8% 0.0% - Indicated exceptions include plans where a partial hospital benefit deductible was removed but could be replaced by a per admit deductible with coinsurance up to OOP max.
Over 90% of the plans that provided IP OON SUD benefits did not have to make any changes to their financial requirements to comply with MHPAEA and the IFR.
About 8.7% of the plans were required to accumulate the member OOP payments for these benefits towards the same OOP maximum that was applicable to medical/surgical benefits.
Nearly 6% of the plans were required to reduce their coinsurance on this benefit to be parity complaint.
Quantitative treatment limitations.
The following table summarizes the percentage of plans that had to remove various QTLs placed on their IP INN SUD benefits.
Service/Dollar Limitations Plans (%) Percent of plans where day limits were removed 19.3% Percent of plans where visit limits were removed N/A Percent of plans where quantity limits were removed 0.0% Percent of plans where dollar limits were removed 6.7% The most common IP INN SUD treatment limitation removed was the day limit in a calendar year on inpatient stays (19.3% of plans).
Other changes that certain plans had to make to their IP INN SUD benefits to become parity compliant are listed below.
Exceptions Plans (%) Day limits were removed for Inpatient In-Network RTFs only 0.8% Inpatient Detoxification Days are covered but Inpatient Rehabilitation Days are not covered1 2.5% - This is a scope of services issue which plans could ignore if they so choose
The following table summarizes the percentage of plans that had to remove various QTLs placed on their IN OON SUD benefits.
Service/Dollar Limitations Plans (%) Percent of plans where day limits were removed 15.5% Percent of plans where visit limits were removed N/A Percent of plans where quantity limits were removed 0.0% Percent of plans where dollar limits were removed 6.8% The most common out IP OON SUD treatment limitation removed was the day limits in a calendar year on inpatient stays (15.5% of plans).
Other changes that certain plans had to make to their IP OON SUD benefits to become parity compliant are listed below.
Exceptions Plans (%) Plans where day limits were removed for Inpatient Out-of-Network RTFs 1.9% Plans where IN OON SUD benefits were previously not covered but should be under the cover one, cover all classification requirements 2.9% Inpatient Detoxification Days are covered but Inpatient Rehabilitation Days are not covered1 2.9% - This is a scope of services issue which plans could ignore if they so choose
For precertification requirements and penalties for lack of precertification, please see section 13.
About 8% of the plans were tested without making use of the safe harbor provision provided by the IFR. The remaining plans were tested using the safe harbor provision. The safe harbor has implications for how many benefit classifications can be created for parity compliance testing purposes. Prior to the safe harbor provision, there was only one outpatient classification for in-network benefits and a separate one for out-of-network benefits. The safe harbor allows splitting of the outpatient classifications into office visits and outpatient-other sub-classifications. Sections 6 and 7 present the compliance testing results for plans that were tested without the safe harbor. Sections 8 through 11 present the results for plans tested with the safe harbor. Sections 8 and 9 show the results for the Outpatient Office Visit benefit sub-classification, while sections 10 and 11 show the results for the Outpatient Other sub-classification.
Outpatient MH benefits.
Copay/coinsurance/deductible/OOP maximum levels (quantitative financial requirements).
The table below shows summarized results of the compliance testing of the Outpatient In-Network Mental Health (OP INN MH) benefits.
Percent of Plans covering OP INN MH Services -- Tested Without Safe Harbor: 8.0% Cost-Sharing No Change Added Converted Removed Increased Decreased Exception Deductible 100.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% OOP max 70.0% 30.0% 0.0% 0.0% 0.0% 0.0% 0.0% Copay 100.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% Coinsurance 100.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% Only 8% of all plans provided OP INN MH benefits and were tested without making use of the safe harbor provision. Most of them were compliant with MHPAEA and the IFR; 30% of these plans required only one notable change to become compliant -- these plans were required to subject the OP INN MH benefits to the predominant medical/surgical OOP maximum.
The table below shows summarized results of the compliance testing of the Outpatient Out-of-Network Mental Health (OP OON MH) benefits.
Percent of Plans Covering OP OON MH Services -- Tested Without Safe Harbor: 17.6% Cost-Sharing No Change Added Converted Removed Increased Decreased Exception Deductible 100.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% OOP max 90.9% 9.1% 0.0% 0.0% 0.0% 0.0% 0.0% Copay 100.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% Coinsurance 90.9% 0.0% 0.0% 0.0% 0.0% 9.1% 0.0% Only about 18% of all plans provided OP OON MH benefits and were tested without making use of the safe harbor. Nearly all of them were compliant. The only notable changes that needed to be made to a few of the plans to become compliant was subjecting the OP OON MH benefits to the predominant medical/surgical OOP maximum, and reducing the coinsurance applicable to these services to the predominant medical/surgical coinsurance level.
Quantitative treatment limitations.
The following table summarizes the percentage of plans tested without the Outpatient safe harbor that had to remove various QTLs placed on their OP INN MH benefits.
Service/Dollar Limitations Plans (%) Percent of plans where day limits were removed N/A Percent of plans where visit limits were removed 50.0% Percent of plans where quantity limits were removed 0.0% Percent of plans where dollar limits were removed 0.0% The most common OP INN MH treatment limitation removed was the calendar year visit limits on outpatient professional visits (50% of the plans tested without safe harbor).
The following table summarizes the percentage of plans tested without the Outpatient safe harbor that had to remove various QTLs placed on their OP OON MH benefits.
Service/Dollar Limitations Plans (%) Percent of plans where day limits were removed N/A Percent of plans where visit limits were removed 13.6% Percent of plans where quantity limits were removed 0.0% Percent of plans where dollar limits were removed 0.0% The most common OP OON MH treatment limitation removed was the calendar year visit limits on outpatient professional visits (13.6% of the plans tested without safe harbor).
Other changes that certain plans tested without the Outpatient safe harbor had to make to their OP OON MH benefits to become parity compliant are listed below.
Exceptions Plans (%) Plans where OP OON MH benefits were previously not covered but were recommended be covered under the cover one, cover all classification requirement 13.6% For precertification requirements and penalties for lack of precertification, please see section 13.
Outpatient SUD.
Copay/coinsurance/deductible/OOP maximum levels (quantitative financial requirements).
The table below shows summarized results of the compliance testing of the Outpatient In-Network Substance Use Disorder (OP INN SUD) benefits.
Percent of Plans Covering OP INN SUD Services -- Tested Without Safe Harbor: 8.0% Cost-Sharing No Change Added Converted Removed Increased Decreased Exception Deductible 100.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% OOP max 70.0% 30.0% 0.0% 0.0% 0.0% 0.0% 0.0% Copay 100.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% Coinsurance 100.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% Only 8% of all plans provided OP INN SUD benefits and were tested without making use of the safe harbor. Most of them were compliant. The only notable change that was needed to become compliant was subjecting the OP INN SUD benefits to the predominant medical/surgical OOP maximum; 30% of these plans needed this change.
The table below shows summarized results of the compliance testing of the Outpatient Out-of-Network Substance Use Disorder (OP OON SUD) benefits. Approximately 18% of the plans provided this benefit.
Percent of Plans Covering OP OON SUD Services and Were Tested Without Safe Harbor: 17.6% Cost-Sharing No Change Added Converted Removed Increased Decreased Exception Deductible 100.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% OOP max 90.9% 9.1% 0.0% 0.0% 0.0% 0.0% 0.0% Copay 100.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% Coinsurance 90.9% 0.0% 0.0% 0.0% 0.0% 9.1% 0.0% Only 18% of all plans offered OP OON SUD benefits and were tested without making use of the safe harbor. Nearly all of them were compliant. The only notable changes that were needed to become compliant was subjecting the OP OON SUD benefits to the predominant medical/surgical OOP maximum, and reducing the coinsurance applicable to these services to the predominant medical/surgical coinsurance level.
Quantitative treatment limitations.
The following table summarizes the percentage of plans tested without the safe harbor that had to remove various QTLs placed on their OP INN SUD benefits.
Service/Dollar Limitations Plans (%) Percent of plans where day limits were removed N/A Percent of plans where visit limits were removed 50.0% Percent of plans where quantity limits were removed 0.0% Percent of plans where dollar limits were removed 30.0% The calendar year professional visit limits for OP INN SUD benefits were removed from 50% of the plans, and calendar year dollar limits were removed for these services from 30% of the plans.
The following table summarizes the percentage of plans tested without the safe harbor that had to remove various QTLs placed on their OP OON SUD benefits.
Service/Dollar Limitations Plans (%) Percent of plans where day limits were removed N/A Percent of plans where visit limits were removed 63.6% Percent of plans where quantity limits were removed 0.0% Percent of plans where dollar limits were removed 9.1% The most common treatment limitation removed was the calendar year professional visit limits on OP OON SUD visits (64% of the plans). Calendar year dollar limits were removed in 9% of the plans.
Other changes that certain plans had to make to their OP OON SUD benefits to become parity compliant are listed below.
Exceptions Plans (%) Plans where OP OON SUD benefits were previously not covered but plans were advised to cover it under the cover one, cover all requirement 13.6% For precertification requirements and penalties for lack of precertification, please see section 13.
Outpatient office visits for MH disorders.
Copay/coinsurance/deductible/OOP maximum levels (quantitative financial requirements).
The table below shows summarized results of the compliance testing of the Outpatient Office Visit In-Network Mental Health (OP OV INN MH) benefits.
Percent of Plans Covering OP OV INN MH Benefits -- Tested with Safe Harbor: 88.0% Cost-Sharing No Change Added Converted Removed Increased Decreased Exception Deductible1 94.5% 0.9% 0.0% 3.6% 0.0% 0.0% 0.0% OOP max1 99.1% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% Copay1,2,3 76.4% 0.0% 0.9% 2.7% 0.0% 6.4% 6.4% Coinsurance1,4 89.1% 0.0% 7.3% 0.9% 0.0% 0.9% 0.9% - Note that some percentages do not add up to 100%. The difference is due to plans where deductible, coinsurance, and OOP max were added to replace a copay or vice versa. These conversions are recorded under the line that represents the original cost-sharing.
- Indicated exceptions include plans that reduced OP OV INN MH copays only for specialist visits.
- Indicated exceptions include plans where plans were advised they could increase the OP OV INN MH copay to the specialist level.
- Indicated exceptions include plans were advised to change coinsurance to copay for "other services in physician office".
Over 75% of the plans that provided OP OV INN MH benefits did not have to make any changes to their financial requirements to comply with MHPAEA and the IFR.
About 6% of the plans were required to reduce their OP OV INN MH copays.
Over 7% of the plans were required to convert their coinsurance to copays for this benefit category.
The table below shows summarized results of the compliance testing of the Outpatient Office Visit Out-of-Network Mental Health (OP OV OON MH) benefits.
Percent of Plans Covering OP OV OON MH Benefits -- Tested with Safe Harbor: 64.8% Cost-Sharing No Change Added Converted Removed Increased Decreased Exception Deductible 100.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% OOP max 91.4% 8.6% 0.0% 0.0% 0.0% 0.0% 0.0% Copay 98.8% 0.0% 0.0% 0.0% 0.0% 1.2% 0.0% Coinsurance 92.6% 0.0% 0.0% 0.0% 0.0% 7.4% 0.0% Over 90% of the plans that provided OP OV OON MH benefits did not have to make any changes to their financial requirements to comply with MHPAEA and the IFR.
About 9% were required to accumulate the member OOP payments for these OP OV OON MH benefits towards the same OOP maximum that was applicable to medical/surgical benefits.
Over 7% of plans were required to reduce their coinsurance that was application to this benefit category.
Quantitative treatment limitations.
The following table summarizes the percentage of plans that were tested with the safe harbor that had to remove various QTLs placed on their OP OV INN MH benefits.
Service/Dollar Limitations Plans (%) Percent of plans where day limits were removed N/A Percent of plans where visit limits were removed 11.8% Percent of plans where quantity limits were removed 0.0% Percent of plans where dollar limits were removed 4.5% The most common treatment limitation removed was the calendar year professional visit limits on OP OV INN MH benefits (12% of plans). Nearly 5% of these plans had to remove calendar year dollar limits for these benefits.
The following table summarizes the percentage of plans that were tested with the safe harbor that had to remove various QTLs placed on their OP OV OON MH benefits.
Service/Dollar Limitations Plans (%) Percent of plans where day limits were removed N/A Percent of plans where visit limits were removed 14.8% Percent of plans where quantity limits were removed 0.0% Percent of plans where dollar limits were removed 6.2% The most common treatment limitation removed was the calendar year professional visit limits on OP OV OON MH benefits (15% of plans). Nearly 6% of the plans had to remove calendar year dollar limits.
Other changes that certain plans had to make to their OP OV OON MH benefits to become parity compliant are listed below.
Exceptions Plans (%) Plans where OP OV OON MH benefits were previously not covered but were recommended be covered under the cover one, cover all classification requirement 3.7% For precertification requirements and penalties for lack of precertification, please see section 13.
Outpatient office visits for SUD.
Copay/coinsurance/deductible/OOP maximum levels.
The table below shows summarized results of the compliance testing of the Outpatient Office Visit In-Network Substance Use Disorder (OP OV INN SUD) benefits. Approximately 87% of the plans provided this benefit.
Percent of Plans Covering OP OV INN SUD Benefits -- Tested with Safe Harbor: 87.2% Cost-Sharing No Change Added Converted Removed Increased Decreased Exception Deductible1 91.7% 0.9% 0.0% 6.4% 0.0% 0.0% 0.0% OOP max1 99.1% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% Copay1,2,3 77.1% 0.0% 0.9% 0.9% 0.0% 5.5% 7.3% Coinsurance1,4 87.2% 0.0% 8.3% 2.8% 0.0% 0.9% 0.0% - Note that some percentages do not add up to 100%. The difference is due to plans where deductible, coinsurance, and OOP max were added to replace a copay or vice versa. These conversions are recorded under the line that represents the original cost-sharing.
- Indicated exceptions include plans that reduced copays only for specialist visits.
- Indicated exceptions include plans where plans were advised they could increase office visit copay to the specialist level.
- Indicated exceptions include plans where plans were advised to change coinsurance to copay for "other services in physician office".
Over 75% of the plans that provided OP OV INN SUD benefits did not have to make any changes to their financial requirements to comply with MHPAEA and the IFR.
About 6% of the plans were required to remove calendar year deductibles from this benefit category.
About 5.5% of the plans were required to reduce their copays for these benefits. An additional 7% of the plans could increase their OP OV INN SUD copays on specialist services without violating parity, or were required to change from coinsurance to copays for any physician services other than regular outpatient office visits.
Over 8% of the plans were required to convert their coinsurance to copays for these benefits.
The table below shows summarized results of the compliance testing of the Outpatient Office Visit Out-of-Network Substance Use Disorder (OP OV OON SUD) benefits. Approximately 65% of the plans provided this benefit.
Percent of Plans Covering OP OV OON SUD Benefits -- Tested with Safe Harbor: 64.8% Cost-Sharing No Change Added Converted Removed Increased Decreased Exception Deductible 98.8% 0.0% 0.0% 1.2% 0.0% 0.0% 0.0% OOP max 90.1% 9.9% 0.0% 0.0% 0.0% 0.0% 0.0% Copay 98.8% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% Coinsurance 93.8% 0.0% 1.2% 0.0% 0.0% 4.9% 0.0% Over 90% of the plans that provided OP OV OON SUD benefits did not have to make any changes to their financial requirements to comply with MHPAEA and the IFR.
About 10% were required to accumulate the member OOP payments for these benefits towards the same OOP maximum that was applicable to medical/surgical benefits.
Nearly 5% of the plans were required to reduce their coinsurance percentage that was application to this benefit category.
Quantitative treatment limitations.
The following table summarizes the percentage of plans tested with the safe harbor that had to remove various QTLs placed on their OP OV INN SUD benefits.
Service/Dollar Limitations Plans (%) Percent of plans where day limits were removed N/A Percent of plans where visit limits were removed 20.2% Percent of plans where quantity limits were removed 0.0% Percent of plans where dollar limits were removed 4.6% The most common in-network treatment limitation removed was the visit limits on OP OV INN SUD benefits (20% of plans). Nearly 5% of these plans had to remove calendar year dollar limits for these benefits.
The following table summarizes the percentage of plans tested with the safe harbor that had to remove various QTLs placed on their OP OV OON SUD benefits.
Service/Dollar Limitations Plans (%) Percent of plans where day limits were removed N/A Percent of plans where visit limits were removed 14.8% Percent of plans where quantity limits were removed 0.0% Percent of plans where dollar limits were removed 6.2% The most common out-of-network treatment limitation removed was the visit limits on OP OV OON SUD benefits (15% of plans). Nearly 6% of these plans had to remove calendar year dollar limits for these benefits.
Other changes that certain plans had to make to their OP OV OON SUD benefits to become parity compliant are listed below.
Exceptions Plans (%) Plans where OP OV OON SUD benefits were previously not covered but were recommended be covered under the cover one, cover all requirement 3.7% For precertification requirements and penalties for lack of precertification, please see section 13.
Outpatient other benefits for MH disorders.
Copay/coinsurance/deductible/OOP maximum levels.
The table below shows summarized results of the compliance testing of Outpatient-Other In-Network Mental Health (OP-Other INN MH) benefits.
Percent of Plans Covering OP-Other INN MH Services -- Tested with Safe Harbor: 88.0% Cost-Sharing No Change Added Converted Removed Increased Decreased Exception Deductible1 74.5% 2.7% 0.0% 8.2% 0.0% 0.0% 0.0% OOP max1 79.1% 3.6% 0.0% 0.0% 0.0% 0.0% 0.0% Copay 73.6% 0.0% 17.3% 7.3% 0.0% 1.8% 0.0% Coinsurance1 68.2% 0.0% 0.0% 10.0% 0.0% 4.5% 0.0% - Note that some percentages do not add up to 100%. The difference is due to plans where deductible, coinsurance, and OOP max were added to replace copays or vice versa. These conversions are recorded under the line that represents the original cost-sharing.
Nearly 70% of the plans that provided OP-Other INN MH benefits did not have to make any changes to their cost-sharing to comply with MHPAEA and the IFR.
Over 17% of the plans were required to convert their copays to coinsurance for this benefit category, and over 7% had to remove copays completely
10% of the plans were required to remove the coinsurance completely on this benefit, while another 4.5% of the plans were required to reduce the coinsurance level.
The table below shows summarized results of the compliance testing of OP-Other Out-of-Network Mental Health (OP-Other OON MH) benefits.
Percent of Plans Covering OP-Other OON MH Services -- Tested with Safe Harbor: 64.8% Cost-Sharing No Change Added Converted Removed Increased Decreased Exception Deductible1 95.1% 0.0% 0.0% 3.7% 0.0% 0.0% 0.0% OOP max 91.4% 8.6% 0.0% 0.0% 0.0% 0.0% 0.0% Copay 98.8% 0.0% 1.2% 0.0% 0.0% 0.0% 0.0% Coinsurance1 88.9% 0.0% 0.0% 1.2% 0.0% 8.6% 0.0% - Note that some percentages do not add up to 100%. The difference is due to plans where deductible, coinsurance, and OOP max were added to replace copays or vice versa. These conversions are recorded under the line that represents the original cost-sharing.
Over 90% of the plans that provided OP-Other OON MH benefits did not have to make any changes to their cost-sharing to comply with MHPAEA and the IFR.
Nearly 9% were required to accumulate the member payments for these benefits towards the same OOP maximum that was applicable to medical/surgical benefits.
Nearly 9% of the plans were required to reduce their coinsurance that was application to this benefit category.
Quantitative treatment limitations.
The following table summarizes the percentage of plans tested with the safe harbor that had to remove various QTLs placed on their OP-Other INN MH benefits.
Service/Dollar Limitations Plans (%) Percent of plans where day limits were removed N/A Percent of plans where visit limits were removed 8.2% Percent of plans where quantity limits were removed 0.0% Percent of plans where dollar limits were removed 4.5% The most common treatment limitation removed was the visit limits on OP-Other INN MH benefits (8% of plans). Nearly 5% of the plans had to remove dollar limits.
The following table summarizes the percentage of plans tested with the safe harbor that had to remove various QTLs placed on their OP-Other Out-of-Network Mental Health benefits.
Service/Dollar Limitations Plans (%) Percent of plans where day limits were removed N/A Percent of plans where visit limits were removed 9.9% Percent of plans where quantity limits were removed 0.0% Percent of plans where dollar limits were removed 6.2% The most common treatment limitation removed was the visit limits on OP-Other OON MH benefits (10% of plans). Nearly 6% of the plans had to remove dollar limits.
Other changes that certain plans had to make to their OP-Other OON MH benefits to become parity compliant are listed below.
Exceptions Plans (%) Plans where OP-Other OON MH Disorder benefits were previously not covered but were recommended be covered under the cover one, cover all requirement 3.7% For precertification requirements and penalties for lack of precertification, please see section 13.
Outpatient other benefits for SUD.
Copay/coinsurance/deductible/OOP maximum levels.
The table below shows summarized results of the compliance testing of the Outpatient-Other In-Network Substance Use Disorder (OP-Other INN SUD) benefits.
Percent of Plans Covering Op-Other INN SUD Services -- Tested with Safe Harbor: 87.2% Cost-Sharing No Change Added Converted Removed Increased Decreased Exception Deductible1 78.0% 2.8% 0.0% 8.3% 0.0% 0.0% 0.0% OOP max1 82.6% 3.7% 0.0% 0.0% 0.0% 0.0% 0.0% Copay 77.1% 0.0% 13.8% 7.3% 0.0% 1.8% 0.0% Coinsurance1 70.6% 0.0% 0.0% 8.3% 0.0% 7.3% 0.0% - Note that some percentages do not add up to 100%. The difference is due to plans where deductible, coinsurance, and OOP max were added to replace a copay or vice versa. These conversions are recorded under the line that represents the original cost-sharing.
Over 70% of the plans that provided OP-Other INN SUD benefits did not have to make any changes to their cost-sharing to comply with MHPAEA and the IFR.
About 8% of the plans were required to remove deductibles from this benefit category, while 3% of the plans were not subjecting these benefits to a deductible but could do so without violating parity.
Nearly 14% of the plans were required to convert their copays to coinsurance, and another 7% had to completely remove copays from this benefit.
About 7% of the plans were required to reduce their coinsurance, while another 8% had to completely remove coinsurance from this benefit.
The table below shows summarized results of the compliance testing of the Outpatient-Other Out-of-Network Substance Use Disorder (OP-Other OON SUD) benefits.
Percent of Plans Covering OP-Other OON SUD Services -- Tested with Safe Harbor: 64.8% Cost-Sharing No Change Added Converted Removed Increased Decreased Exception Deductible 96.3% 0.0% 0.0% 3.7% 0.0% 0.0% 0.0% OOP max 90.1% 9.9% 0.0% 0.0% 0.0% 0.0% 0.0% Copay 100.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% Coinsurance 92.6% 0.0% 0.0% 1.2% 0.0% 6.2% 0.0% Over 90% of the plans that provided OP-Other OON SUD benefits did not have to make any changes to their cost-sharing to comply with MHPAEA and the IFR.
About 4% of the plans were required to remove deductibles from OP-Other OON SUD benefits.
Nearly 10% were required to accumulate the member payments for these benefits towards the same OOP maximum that was applicable to the corresponding medical/surgical benefits; over 6% of the plans were required to reduce their coinsurance that was applied to this benefit category.
Quantitative treatment limitations.
The following table summarizes the percentage of plans that were tested with the safe harbor that had to remove various QTLs placed on their OP-Other INN SUD benefits.
Service/Dollar Limitations Plans (%) Percent of plans where day limits were removed N/A Percent of plans where visit limits were removed 16.5% Percent of plans where quantity limits were removed 0.0% Percent of plans where dollar limits were removed 4.6% The most common in-network treatment limitation removed was the visit limits on OP-Other INN SUD benefits (17% of plans). Nearly 5% of the plans had to remove dollar limits on OP-Other INN SUD benefits.
The following table summarizes the percentage of plans that were tested with the safe harbor that had to remove various QTLs placed on their Outpatient-Other Out-of-Network Substance Use Disorder benefits.
Service/Dollar Limitations Plans (%) Percent of plans where day limits were removed N/A Percent of plans where visit limits were removed 9.9% Percent of plans where quantity limits were removed 0.0% Percent of plans where dollar limits were removed 6.2% The most common treatment limitation removed was the visit limits on OP-Other OON SUD benefits (10% of plans). Nearly 6% of the plans had to remove dollar limits on OP-Other OON SUD benefits.
Other changes that certain plans had to make to their OP-Other OON SUD benefits to become parity compliant are listed below.
Exceptions Plans (%) Plans where OP-Other OONSUD benefits were previously not covered but were recommended be covered under the cover one, cover all requirement 3.7% For precertification requirements and penalties for lack of precertification, please see section 13.
Emergency Care, including true emergency and non-emergent care provided in ERs -- MH and SUD benefits.
Copay/coinsurance/deductible/OOP maximum levels.
The table below shows summarized results of the compliance testing of ER MH/SUD benefits. 100% of the plans provided this benefit.
Percent of Plans Covering ER MH/SUD Services: 100.0% Cost-Sharing No Change Added Converted Removed Increased Decreased Exception Deductible1 94.4% 2.4% 0.0% 1.6% 0.0% 0.0% 1.6% OOP max 100.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% Copay1 92.8% 2.4% 0.0% 0.0% 0.0% 0.0% 1.6% Coinsurance1,2 80.8% 0.0% 3.2% 1.6% 0.0% 1.6% 12.8% - Indicated exceptions include plans where cost-sharing was reduced for ambulance only.
- Indicated exceptions include plans were only professional services cost-sharing was reduced.
Over 80% of the plans that provided ER MH/SUD benefits did not have to make any changes to their cost-sharing to comply with MHPAEA and the IFR.
Over 2% of the plans could subject their ER MH/SUD benefits to a deductible without violating parity but were previously not doing so, while another 2% were required to remove deductibles altogether from these benefits.
Over 2% of the plans could apply a copay to these benefits without violating parity but were previously not doing so.
Over 3% of the plans were required to convert their coinsurance to copays, another 1.6% had to completely remove the coinsurance, and another 1.6% had to reduce the coinsurance levels applicable to this benefit. 13% of the plans were required to reduce their coinsurance on professional services only.
Quantitative treatment limitations.
The following table summarizes the percentage of plans that had to remove various QTLs placed on their ER MH/SUD benefits.
Service/Dollar Limitations Plans (%) Percent of plans where visit limits were removed 0.0% Percent of plans where (annual) dollar limits were removed 0.0% As shown above, no treatment limits applied to the ER MH/SUD benefits.
Certain plans were non-compliant with MHPAEA and the IFR in ways other than those described above.
Exceptions Plans (%) Percent of plans where non-emergency use of ER had different cost-sharing than for true emergencies 10.4% Percent of plans where out-of-network ER cost-sharing had to be changed to be the same as in-network ER cost-sharing 28.0% Percent of plans where members were required to pay the amount above the allowed charge for out-of-network behavioral health emergency services in a non-parity compliant way 0.8%
Rx -- MH and SUD benefits.
Copay/coinsurance/deductible/OOP maximum levels.
The table below shows summarized results of the compliance testing of MH/SUD Rx benefits; 99% of the plans provided this benefit.
Percent of Plans Covering MH/SUD Rx: 99.2% Cost-Sharing No Change Added Converted Removed Increased Decreased Exception Deductible 100.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% OOP max 100.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% Copay 100.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% Coinsurance 100.0% 0.0% 0.0% 0.0% 0.0% 0.0% 0.0% 100% of the plans that provided MH/SUD Rx benefits did not have to make any changes to their cost-sharing to comply with MHPAEA and the IFR.
Quantitative treatment limitations.
The following table summarizes the percentage of plans that had to remove various QTLs placed on their MH/SUD Rx benefits.
Service/Dollar Limitations Plans (%) Percent of plans where quantity limits were removed 0.0% Percent of plans where dollar limits were removed 0.0% As shown above, no limits applied to the MH/SUD Rx benefits.
Certain plans were non-compliant with MHPAEA and the IFR in ways other than those described above.
Exceptions Plans (%) Percent of plans with different cost-sharing for preferred vs. non-preferred pharmacies. Plans were advised to consult with legal counsel. 18.5% Percent of plans where only 3 smoking cessation drugs are covered. 2.4% Percent of plans that had a supply limit on smoking cessation drugs/supplies. 21.0% The IFR does not specify that having different Rx cost-sharing for preferred vs. non-preferred pharmacies is compliant. Therefore, a strict interpretation of only having a single Rx benefit classification implies that this cost-sharing structure for MH and SUD drugs would be non-compliant.
However, Milliman did receive additional informal guidance on this manner that this strict interpretation was not the intent of the sponsoring Departments. The IFR states that "if a plan or issuer applies different levels of financial requirements to different tiers of Rx benefits based on reasonable factors (determined in accordance with the NQTL rules) and without regard to whether a drug is generally prescribed for medical/surgical benefits or MH/SUD benefits, then the plan or issuer satisfies the substantially all/predominant test". Here, if the differences in financial requirements are considered to be based on reasonable factors (discounts for preferred pharmacies), then the tests are satisfied. Therefore, the 18.5% of plans who are reported to be in violation of parity in the table above would not be out of compliance. Hopefully, additional formal guidance will be provided on this issue.
Non-quantitative treatment limitations.
The following table describes the NQTLs that were found in various plans in the Milliman database. These limitations appear to be non-compliant with MHPAEA and the IFR.
NQTL Description % of Plans MH/SUD precertification requirements were more stringent than for medical/surgical benefits. 28.2% Pre-approval was required starting with the 13th OP OV MH visit. 1.8% The external/expedited fees charged to appeal a service denial for treatment of a mental condition were higher than for medical/surgical conditions. 4.5% No MH/SUD benefits were provided outside the state of residence but medical/surgical benefits were. 0.9% Some smoking cessation benefits were covered in one or more benefit classifications but not in all benefit classifications that covered medical/surgical benefits. 12.7% Medical necessity was applied to MH/SUD benefits but not to medical/surgical benefits. 8.2% Out-of-network treatment was covered only if in-network treatment was unavailable. This applied only to MH/SUD benefits. 0.9% Plans imposed a probationary period only for substance abuse treatment. 0.9% Smoking cessation drugs were only covered on a mail-order basis. 0.9% Out-of-network eating disorder treatment was covered only if in-network services were unavailable; no such requirement applied to OON medical/surgical benefits. 0.9% Plans did not include smoking cessation for dependent children. 2.7% In addition to the NQTLs listed above, other plan design features which have not been previously mentioned which plans should consider regarding MHPAEA compliance. These changes include removal of QTLs that are not mentioned in the sections above.
Other Treatment Limitations % of Plans Plans placed limits on professional counseling for tobacco use/smoking 24.5% Plans placed a benefit limit on early intervention services which includes psychological counseling. 0.9% Plans imposed a dollar penalty for not getting pre-approval for inpatient MH/SUD admissions, and no such penalty applied to inpatient medical/surgical benefits. 0.9% Inpatient SUD services are covered but limited to detoxification. No change was recommended to plan design because this situation is currently allowed under the "scope of services" provision in MHPAEA. 2.7%
Appendix B. Detailed Compliance Testing Results: 2011 Plan Year
The Paul Wellstone and Pete Domenici MHPAEA of 2008 (MHPAEA) was enacted on October 3, 2008. Interim final regulations were posted in the Federal Register on February 2, 2010, and clarifying guidance was released on July 1, 2010. The MHPAEA prohibits group health plans providing MH/SUD benefits from imposing more restrictive financial requirements or treatment limitations than those provided for medical/surgical benefits. A distinction is made between QTLs (such as day limits, visit limits, etc.) and NQTLs, such as medical management and formulary design.
In 2010, Aon Hewitt worked with a number of clients to provide guidance on the legislation requirements and to evaluate benefit design and program provisions to assess compliance. A summary of the results of the plan design compliance testing and the NQTL compliance review provided in this report.
Annual Behavioral Health Request for Information Results
Background
Each year, Aon Hewitt requests behavioral health care organizations to respond to a RFI that collects information regarding their administrative, operational, and clinical capabilities. In their 2011 Annual RFI, behavioral health care organizations were asked to respond to several questions regarding the impact of MHPAEA. Responses to the MHPAEA questions were received by seven national behavioral health care organizations, representing all of the major carve-in and carve-out vendors. Vendor responses are summarized below:
| RFI Questions | Vendor Response |
|---|---|
| Percent of employers* that eliminated MH/SUD coverage. | 2010: 57% of vendors reported no employers eliminated MH/SUD coverage; 43% of vendors reported 1%. 2011: 43% of vendors reported no employers eliminated MH/SUD coverage; 57% of vendors reported 1%. |
| Percent of employers* that moved from carve-out to carve-in MH/SUD administration due to federal parity. | 18% (range by vendor from 0% to 80%). |
| Percent of employers* who were required to cover outpatient MH/SUD at 100% due to compliance testing. | 2.1% (range by vendor from 0% to 10%). |
| Percent of employers* required to cover outpatient MH/SUD at the PCP copay level due to compliance testing. | 85% (range by vendor from 29% to 100%). |
| Percent of employers* required to cover outpatient MH/SUD at the specialist copay level due to compliance testing | 15% (range by vendor from 0% to 100%) |
* Within the vendor's book-of-business.
Plan Design Compliance Testing Results
Background
According to the regulations, a plan must meet two testing requirements within each benefit classification in order to comply with parity requirements:
Substantially all: A requirement or limitation applies to substantially all if it applies to at least two-thirds of the benefits in that classification. If a benefit type does not apply to at least two-thirds of the medical/surgical benefits in a classification then it cannot be applied to MH/SUD benefits in that classification.
Predominant: A requirement or limitation is considered predominant if it applies to at least one-half of the benefits in that classification.
Determination of substantially all and predominant is based upon the dollar amount of all plan payments for medical/surgical benefits in the classification expected to be paid under the plan for the plan year.
Plan design compliance must be assessed within the six benefit classifications specified by the regulations. Regulatory guidance also clarified the ability to review compliance in two sub-classifications for outpatient services. The classifications and sub-classifications recognized by the regulations are listed below:
- Inpatient In-Network
- Inpatient Out-of-Network
- Outpatient In-Network
- Office Visits
- All Other Outpatient Items and Services
- Outpatient Out-of-Network
- Office Visits
- All Other Outpatient Items and Services
- Emergency Care
- Rx
Overview
In order to assess compliance with the MHPAEA regulations, plan designs were analyzed to determine the compliant design for MH/SUD benefits. The plan design review and compliance testing were conducted in 2010 and were based on the plan designs each employer expected to implement in the 2011 plan year.
The plan design review encompassed over 60 employers, ranging in size from 400 to over 300,000 employees and representing 230 plan options. Each plan option represented a single combination of benefits (a combination of medical/surgical and MH/SUD benefits) that is available to employer participants. Of the 230 plan options reviewed, 140 plan options required compliance testing to determine the benefit design that would apply to MH/SUD benefits.
For most employer plans, the benefit type and level within the inpatient in-network and out-of-network, outpatient out-of-network, Rx, and emergency care classifications were consistent for both medical/surgical and MH/SUD and, as a result, demonstrated compliance with the parity regulations. For these benefit classifications, detailed compliance testing was not required.
Benefit design for the outpatient in-network classification, however, required compliance testing most frequently across employer programs. Within this classification, employer programs typically applied a variety of benefit types (copay or coinsurance) and benefit levels (primary care, specialty care, other). Compliance testing was required within this benefit classification to determine the benefit that met the substantially all and predominant requirements for MH/SUD services.
In addition to the compliance testing that was conducted employer plan designs were reviewed to ensure other aspects of the MHPAEA regulations were compliant, such as the elimination of QTLs (e.g., day and visit limitations, dollar maximums, etc.). In our review, we noted several plan options that applied QTLs to MH/SUD benefits and recommended these limitations be removed in order to comply with MHPAEA. It is our understanding that these plan design provisions were eliminated. A summary of the plan provisions that required removal of the quantitative limitations is provided below:
| QTLs | Number (%*) of Plan Options | Examples |
|---|---|---|
| Inpatient day limitations for MH/SUD | 18 (7.8%) |
|
| Outpatient day limitations for MH/SUD | 14 (6.1%) |
|
| Separate deductible and OOP maximum for MH/SUD | 3 (1.3%) | N/A |
| Penalty for not precertifying care (similar requirement not in place for medical/surgical) | Outpatient: 10 (4.3%) IOP/PHP: 3 (1.3%) |
|
| Annual dollar maximum for smoking cessation Rx (similar requirement not in place for other drugs or drug classes) | 6 (2.6%) |
|
| Supply limits for smoking cessation Rx (similar requirement not in place for other drugs or drug classes) | 4 (1.7%) |
|
* Percent of total plan options reviewed (230).
Testing Process
For each plan option requiring compliance testing, the employer's program administrator (vendor) was asked to submit plan costs associated with each covered service category within the classification or sub-classification included in the testing process.
We first conducted the substantially all test for each plan option to determine which benefit type represents at least two-thirds of the plan costs in the benefit sub-classification. Plan cost data was grouped according to benefit type (e.g., copay, coinsurance, etc.) and evaluated to determine the percentage of the total plan costs represented by each type.
Once the benefit type representing substantially all was determined, we then grouped the plan cost data associated with each benefit level (e.g., $15, $20, etc.) within that benefit type to determine the predominant benefit level in that sub-classification.
The benefit type and level determined to represent substantially all and predominant within the sub-classification is the benefit that can be applied to MH/SUD services in the same benefit sub-classification. This benefit represented the most restrictive benefit permitted within the sub-classification.
Results of the compliance testing process were documented and communicated to the employer for review by their internal legal counsel. It is our understanding that any plan design changes that were identified as a result of the testing process were implemented by the employer in 2011.
Compliance Testing Findings
Results of the compliance testing conducted by Aon Hewitt in 2010 are summarized below:
A total of 140 plan options were tested.
- Testing for all 140 plan options was conducted in the outpatient in-network office visit sub-classification.
Benefit designs for the 140 plan options that were tested included a variety of benefit types:
- 98 plan options (70%) applied copays to all outpatient services.
- 77% applied split copays for PCPs and SCPs where higher copays are applied for SCP office visits than for PCP office visits (e.g., $40 copay for SCPs and $20 copay for PCPs). Of those applying split copays, 71% (53 plan options) applied the SCP copay level to outpatient MH/SUD services. The remaining 22 plan options applied the PCP copay level to outpatient MH/SUD services.
- 23% applied the same copay for both medical/surgical and MH/SUD services.
- 35 plan options (25%) applied coinsurance to all outpatient services.
- Seven plan options (5%) applied a mix of copay and coinsurance to outpatient services.
- 98 plan options (70%) applied copays to all outpatient services.
Of the 140 plan options tested, only 33% required benefit changes (benefit type and/or benefit level) in order to comply with MHPAEA regulations. An additional 6% (eight plan options) made benefit design changes that were not required, but maintained compliance.
Testing results for the 98 plan options that apply copays to all outpatient services determined that the PCP benefit level was predominant for 76 plan options (78%), requiring that the MH/SUD benefit level be no more than the PCP benefit level. For 21 plan options (21%), testing results determined that the SCP benefit level was predominant. And, for one plan option (1%), the results showed that neither copay nor coinsurance could be applied to MH/SUD outpatient benefits.
- For plan options where the SCP copay is applied to MH/SUD outpatient benefits (53 plan options), the compliance testing results determined that the PCP level was predominant for 36 plan options (68%) and the SCP level was predominant for 17 plan options (32%).
- For the 36 plan options where the testing results determined PCP to be predominant, the employers modified the MH/SUD outpatient copay from the SCP level to the PCP level.
- For the 17 plan options where the testing results determined SCP to be predominant, 25% (four plan options) moved to the PCP level to reflect best practices and maintain consistency across benefit options, while the remainder maintained the benefit at the SCP level.
- For the plan options where the PCP copay is applied to MH/SUD outpatient benefits (45 plan options), the compliance testing results determined that the PCP level was predominant for 40 plan options (89%), the SCP level was predominant for four plan options (9%), and neither copay nor coinsurance could be applied to MH/SUD outpatient benefits for one plan option (2%).
- For the 40 plan options where the testing results determined PCP to be predominant, employers maintained the PCP copay level for outpatient MH/SUD benefits.
- For the four plan options where the testing results determined SCP to be predominant, employers increased the copay for MH/SUD outpatient benefits from the PCP benefit level to the SCP benefit level.
- For plan options where the SCP copay is applied to MH/SUD outpatient benefits (53 plan options), the compliance testing results determined that the PCP level was predominant for 36 plan options (68%) and the SCP level was predominant for 17 plan options (32%).
Testing results for the 35 plan options that apply coinsurance to all outpatient services determined the following:
- Four plan options (11%) were required to apply a less restrictive coinsurance level for MH/SUD outpatient benefits.
- 31 plan options (89%) were compliant at the current coinsurance level and were not required to modify the outpatient MH/SUD benefit.
Testing results for the seven plan options that applied a mix of copays and coinsurance to outpatient services determined that the majority (72%) were required to apply a copay to MH/SUD outpatient benefits at a less restrictive level than what was currently in place. The remaining two plan options (28%) were not required to make a benefit change to comply.
Non-Quantitative Treatment Limitation Assessment Results
Background
According to the regulations, NQTLs limit the scope or duration of benefits and can include, but are not limited to, plan provisions related to:
- Medical management,
- Rx formulary,
- Provider admission in a network,
- Determination of UCR amounts,
- Step-therapy requirements, and
- Conditioning benefits on completion of a course of treatment.
Any processes, strategies, evidentiary standards, or other factors used in applying the NQTL to MH/SUD benefits must be comparable to, and applied no more stringently than, the processes, strategies, evidentiary standards, or other factors applied to medical/surgical benefits. However, these requirements allow variations to the extent that recognized clinically appropriate standards of care may permit a difference.
Overview
In order to assess compliance with the MHPAEA regulations, NQTLs processes in place for MH/SUD and medical/surgical benefits were evaluated. NQTL assessments were conducted for self-insured programs when requested by an employer. In 2010, NQTL assessments were completed for 22 different employers, representing 17 different medical and MH/SUD vendors. All employers were national employers with at least 1,000 employees. The majority of employers (72%) for whom NQTL assessments completed were large employers with 10,000 or more employees.
When the MHPAEA regulations were released, many health plans and behavioral health care organizations assured employers that they would conduct an analysis of their program procedures and, if identified, would implement the necessary changes to ensure compliance with MHPAEA regulations. As NQTL analyses were completed for only 22 employers, we can only assume that most employers relied on the health plans and behavioral health care organizations to conduct the NQTL analysis and make any necessary changes to comply with the regulations.
Employers participating in the analysis review did so for a number of reasons, including:
Recognized that the employer is ultimately responsible for plan compliance due to the self-insured status of the plan and wanted to engage with an objective third party to conduct the analysis; and/or
Required written documentation of the assessment process, results, and outcomes.
In the process of conducting the analyses, we evaluated medical/surgical and MH/SUD procedures in place for most of the major medical and behavioral health care organizations in the country. As we communicated our findings to these organizations, issues identified as potential areas of non-compliance could be addressed and our recommendations could be applied across the vendors' book-of-business. As a result, it is likely that the analyses conducted for the 22 employers helped to shape the vendor response to and compliance with the regulations.
Assessment Process
Each vendor that administered an employer's medical and MH/SUD benefit plans was requested to respond to an extensive questionnaire that collected details about the vendor's NQTL processes and procedures in place in 2010. Information was collected on both medical/surgical and MH/SUD procedures. Any differences between the vendor's standard procedures and employer-specific procedures were noted. We also requested each employer's Rx vendor to respond to specific questions regarding NQTLs related to medical and MH/SUD Rx benefits.
Once the questionnaire was completed, we reviewed vendor responses and conducted a detailed comparison of the processes and procedures that were in place for medical/surgical and for MH/SUD. The following areas were reviewed:
- Precertification
- Procedures and services requiring precertification
- Responsibility for precertification (provider or member)
- Documentation required
- Medical necessity review conducted
- Guidelines used
- Concurrent Review
- Levels of care considered for review
- Source of guidelines
- Process
- Frequency of reviews
- Discharge Planning
- Process
- Frequency of reviews
- Follow-up after discharge
- Case Management
- Case identification process
- Case management process
- Retrospective Review
- Process
- Services included
- UCR Determination
- Data source
- Frequency of updates
- Percentile
- Provider Network Admission
- Credentialing process and requirements
- Timing to complete credentialing process
- Ongoing monitoring
- Re-credentialing frequency
- Performance Networks
- Specialties included
- Criteria
- Network model
- Reimbursement Rates
- Source
- Process
- Experimental and Investigational
- Definition
Each process and procedure was compared to determine which, if any, were more stringent for MH/SUD than they were for medical/surgical. Any procedures or requirements that could be considered to be more stringent for MH/SUD than medical/surgical were identified as potentially non-compliant with the MHPAEA regulations.
Results of the assessment were communicated to the employer as well as to each vendor involved in the assessment process. Discussions were held between the employer and each vendor to review the findings and determine the appropriate and necessary actions to comply with MHPAEA regulations.
Areas of Potential Non-Compliance
Our initial review identified many areas that were deemed potentially non-compliant. However, after further investigation and follow-up documentation from the vendors, it was determined, in some instances, that the MH/SUD process was not more stringent than medical/surgical.
Additional issues that were identified as potential for non-compliance required modification in order to meet MHPAEA regulation requirements. Modifications to NQTL provisions occurred more frequently when the employer used a carve-out vendor to administer the MH/SUD benefit (i.e., MH/SUD benefit was administered by a specialty behavioral health care organization and not the same vendor as medical/surgical).
The non-compliance issues identified through the NQTL Assessment are listed below along with the outcome as reported by the vendor and/or employer:
| NQTL Category | Process/ Procedure | Potential Non-Compliance Issue | Outcome |
|---|---|---|---|
| Medical Management | Outpatient Precertification | Precertification required for all outpatient MH/SUD services. Precertification is not required for all outpatient medical/surgical services. | Precertification requirement removed for all outpatient services, but was maintained for services requiring greater oversight and supported by recognized clinically appropriate standards of care (e.g., psychiatric testing, ECT, etc.). |
| Outpatient Medical Necessity Review | All outpatient MH/SUD counseling services are authorized for up to 8-12 visits (varied by vendor). After the 8th or 12th visit, a clinical/medical necessity review is conducted. Similar procedure not in place for outpatient medical/surgical services. | Some vendors extended the threshold for conducting medical necessity review on outpatient MH/SUD counseling services to allow for review of cases that represent outliers (e.g., 20 visits). | |
| Concurrent Review | Concurrent review conducted for all MH/SUD conditions and levels of care, including inpatient, intermediate (i.e., partial hospitalization, intensive outpatient), and outpatient. Concurrent review was conducted only for inpatient medical/surgical cases. | Vendor revised procedures to include only inpatient MH/SUD in concurrent review process to align with medical/surgical process. | |
| Concurrent Review | Concurrent review conducted for MH/SUD cases includes a medical necessity review as well as a review for adherence to benefit provisions. Concurrent review conducted for medical/surgical cases includes a review for adherence to benefit provisions; no medical necessity reviews. | Concurrent review conducted for MH/SUD cases will include only a review for adherence to benefit provisions; no medical necessity reviews. | |
| Retrospective Review | Retrospective review process for MH/SUD included a review for medical necessity, as well as a review for adherence to benefit provisions. Retrospective review process for medical/surgical included a review for adherence to benefit provisions and only when no prior notification was provided. | MH/SUD retrospective review will include a review for adherence to benefit provisions only when no prior notification was provided. No medical necessity review will be conducted. | |
| Inpatient Medical Necessity Review | All inpatient MH/SUD cases require precertification and a medical necessity review is conducted during the precertification process. For medical/surgical inpatient cases, members notify the vendor; no medical necessity review is conducted. | Notification process implemented for MH/SUD (eliminated medical necessity review requirement). Medical necessity reviews conducted only for cases considered to be outliers based on diagnosis, high-cost and complex cases, and provider outliers. | |
| Provider Network Management | Network Admission Criteria | Specific number of years of experience (e.g., 3 years of experience) required for MH/SUD network providers. Years of experience not required for medical/surgical network providers. | Years of experience requirement eliminated for MH/SUD network providers. |
| Network Admission Criteria | Site visits required for some MH/SUD network providers. Site visits not required for medical network providers. | Requirement maintained, as the requirement is essential to ensuring quality and safety of MH/SUD network providers; site visits conducted at facilities and programs that are not accredited. | |
| Reimbursement Rates | MH/SUD provider reimbursement rates were determined based upon vendor's internal set of data. Medical/surgical provider reimbursement rates were determined using an external database. | MH/SUD provider reimbursement rates were modified to reflect a similar process and data source as medical/surgical provider reimbursement rates. | |
| UCR Percentile | Percentile used to determine reimbursement rates for MH/SUD services was set at the 50th percentile. Medical/surgical services were reimbursed at the 80th percentile. | Reimbursement percentile rate modified to the 80th percentile for MH/SUD services. | |
| Rx | Smoking Cessation Drug Requirements | Member is required to participate in a smoking disease management program in order to receive coverage for smoking cessation medication. Similar requirement not in place for any other drug or drug class. | Program revised to eliminate the requirement that members participate in a smoking disease management program in order to receive coverage for smoking cessation medication. |
| Smoking Cessation Drug Limits | Smoking cessation drugs limited to 12 or 24 weeks per year depending on brand. Similar limits not imposed on other drugs or drug classes. | Limitation removed for smoking cessation drugs. |
Appendix C. Detailed Plan Design Database Results (2009-2011)
Plan Design Database Overview
Aon Hewitt's PDD contains data on 252 employers and 12,384 plan designs. The majority of employers in the database are large national employers (over 10,000 employees). However, the PDD does contain employers that represent small and midsize organizations. The following provides an overview of the employers and plan design options included in the database.
Employer Size
The database consists of employers ranging in size from fewer than 1,000 to over 250,000. The distribution by employer size is reported in the table below.
| Range | Percent of Employers | Number of Employers |
|---|---|---|
| 1 to 1,000 | 4.8% | 12 |
| 1,001 to 5,000 | 20.2% | 51 |
| 5,001 to 10,000 | 19.8% | 50 |
| 10,001 to 20,000 | 17.9% | 45 |
| 20,001 to 50,000 | 15.5% | 39 |
| 50,001 to 100,000 | 6.0% | 15 |
| 100,001 to 250,000 | 3.2% | 8 |
| Over 250,000 | 0.4% | 1 |
| Unavailable | 12.3% | 31 |
| 100% | 252 |
Employer Industry
The employers included in this analysis represent a broad array of industries.
| Industry | Percent of Employers | Number of Employers |
|---|---|---|
| Chemicals | 1.6% | 4 |
| Consumer Products | 6.8% | 17 |
| Energy Production/Transmission | 2.0% | 5 |
| Entertainment & Hospitality | 6.4% | 16 |
| Financial | 10.7% | 27 |
| Government/Education | 7.1% | 18 |
| Health Care | 4.4% | 11 |
| Insurance | 6.4% | 16 |
| Manufacturing | 11.9% | 30 |
| Pharmaceuticals | 2.4% | 6 |
| Printing & Publishing | 2.0% | 5 |
| Professional Services | 2.0% | 5 |
| Retail | 6.0% | 15 |
| Technology | 8.7% | 22 |
| Telecommunications | 2.8% | 7 |
| Transportation | 3.6% | 9 |
| Utilities (Gas & Electric) | 3.2% | 8 |
| Unknown | 12.3% | 31 |
| 100.0% | 252 |
Plan Options
A total of 12,384 plan options were included in our review for each plan year. The actual number of plan options included in the review of each plan design field varies and reflects only the plan options that reported credible data. The number of plan options included in each plan design field review is reported for each comparative analysis.
Plan Type
Plan design data used for this analysis reflected several different types of plans. The types of plans and percent of options with each type is summarized below.
| Plan Type | Percent of Plan Options | Number of Plan Options |
|---|---|---|
| Consumer Directed Plan (CDP) | 2.5% | 305 |
| Exclusive Provider Organization (EPO) | 2.0% | 251 |
| Health Maintenance Organization (HMO) | 31.4% | 3,894 |
| Indemnity | 9.6% | 1,184 |
| Point-of-Service (POS) | 5.9% | 734 |
| Preferred Provider Organization (PPO) | 36.2% | 4,483 |
| Passive Preferred Provider Organization (PPP) | 0.2% | 24 |
| Not Available | 12.2% | 1,509 |
| 100.0% | 12,384 |
Plan Funding
A large portion of plan options included in this analysis are self-insured (i.e., the employer pays an administrative fee to a health plan to administer the benefit and pay claims; the employer is responsible for funding claim payments). The percent of plan options that reflect fully-insured and self-insured funding arrangements is summarized below.
| Plan Type | Percent of Plan Options | Number of Plan Options |
|---|---|---|
| Fully-Insured | 26.7% | 3,312 |
| Self-Insured | 43.0% | 5,319 |
| Not Available | 30.3% | 3,753 |
| 100.0% | 12,384 |
Summary Observations
The plan design data reviewed in this analysis suggests a significant degree of change in the benefits applied to MH/SUD services after the implementation of MHPAEA. Although some of the changes may have been implemented due to other legislative or employer-specific initiatives, we have observed some notable changes in plan designs between 2009 and 2011. Some of the key trends identified in the data analysis are described below:
Benefits for inpatient MH/SUD services have remained relatively stable from 2009 to 2011.
- The vast majority of plan options applied the same benefit design for both inpatient medical/surgical and MH/SUD services in 2009 and the percentage remained relatively stable in 2010 and 2011.
For plan options where the same copay/coinsurance was applied to PCP and SCP office visits, we noted no significant change in the level of copay/coinsurance applied to outpatient MH/SUD services from 2009 to 2011.
For plan options that apply a different copay/coinsurance level for PCP and SCP, data showed a movement in the distribution of plan options which aligned the MH/SUD outpatient benefit with PCP and SCP office visit benefits.
- In 2009, percentage of plan options were equally distributed among those that aligned the outpatient MH benefit with the PCP copay/coinsurance, aligned with the SCP copay/coinsurance, and in between the PCP and SCP copay/coinsurance level. However, in 2011, over half the plan options reported that the outpatient MH benefit was aligned with the PCP benefit level.
The percentage of plan options that applied quantitative limits (annual day limits and annual visit limits) decreased dramatically from 2009 to 2011.
- In 2009, approximately half of the plan options reported applying day limits on in-network inpatient MH and SUD benefits. In 2011, the percent of plan designs with annual day limits for in-network inpatient MH services decreased to 7.54% for MH and 8.51% for SUD.
- In 2009, more than half of the plan options reported applying visit limitations on in-network and out-of-network outpatient MH and SUD benefits. In 2011, the percent of options with visit limits on in-network outpatient MH and SUD benefits dropped to 6.49% for MH and 8.51% for SUD.
Detailed plan design analysis results are reported below.
Inpatient MH/SUD
Inpatient Benefit Design
Our analysis reviewed the benefit design in effect in each plan year for inpatient medical/surgical and MH/SUD services. We compared the benefits applied to inpatient medical/surgical with those for MH/SUD services to determine if the benefit in place for MH/SUD services is the same as, more restrictive, or less restrictive than medical/surgical services.
For purposes of this analysis, we evaluated only the copay and/or coinsurance levels applied for each plan option. This analysis did not consider day, dollar, or confinement limitations. The analysis on quantitative limitations is reported separately. Results are reported in three categories:
Inpatient benefit is the same for MH/SUD and medical/surgical: This category includes all plan options where the copay and/or coinsurance level for MH/SUD and medical/surgical are the same.
- Example: Inpatient MH/SUD services are covered at 80% coinsurance after the deductible and inpatient medical/surgical services are covered at 80% coinsurance after the deductible.
Inpatient benefit is more restrictive for MH/SUD than for medical/surgical: This category includes all plan options where the plan applies a more restrictive benefit for MH/SUD than for medical/surgical.
- Example #1: Inpatient MH/SUD services are covered at 50% coinsurance after deductible and inpatient medical/surgical services are covered at 80% coinsurance after deductible.
- Example #2: Inpatient MH/SUD services are subject to a $250 copay, then are covered at 80% coinsurance and medical/surgical services are covered at 80% coinsurance.
Inpatient benefit is less restrictive for MH/SUD than for medical/surgical: This category includes all plan options where the plan applies a less restrictive benefit for MH/SUD than for medical/surgical services.
- Example: MH/SUD services are covered at 80% coinsurance and medical/surgical services are subject to a $100 copay, then are covered at 80% coinsurance.
Observations
For both in-network and out-of-network inpatient benefit designs in all 3 years of this analysis, the vast majority of plan options apply the same benefit design for both medical/surgical and MH/SUD benefits. The data suggests a slight increase in the percent of plans that aligned the inpatient MH/SUD benefit design with the medical/surgical inpatient benefit design from 2009 to 2010 and a decrease in the percent of plan options that applied a more restrictive benefit design for MH/SUD than for medical/surgical. However, the distribution among plans that apply a more restrictive, less restrictive or the same benefit design as medical/surgical stayed relatively stable in all 3 years.
There are a number of plan options that report having a less restrictive MH benefit for inpatient MH services than for medical/surgical services, for example, 11.75% in 2011. Some examples of less restrictive MH benefit designs are listed below:
Example #1: MH/SUD services covered at 80% coinsurance (no deductible); medical/surgical services covered at 80% coinsurance after the deductible.
Example #2: MH/SUD services covered at 100% after deductible; medical/surgical services covered at 80% coinsurance after deductible.
Example #3: MH/SUD services covered at 90% coinsurance; medical/surgical services covered at 80% coinsurance.
Of note is the percentage of plan options where the MH and SUD benefit designs are more restrictive than the medical/surgical inpatient benefit design. Although we cannot confirm these designs are non-compliant with federal parity requirements, they do raise concern. We have provided some examples of the more restrictive benefit design for inpatient MH and SUD as recorded in the PDD below:
Example #1: MH/SUD services covered at 90% coinsurance after hospital copay; medical/surgical services covered at 100% coinsurance after hospital copay.
Example #2: MH/SUD services covered at 90% coinsurance; medical/surgical services covered at 100%.
Example #3: MH/SUD services covered at 80% coinsurance; medical/surgical services covered at 90% coinsurance.
| In-Network Benefit Design | Percent of Plan Options | Number of Plan Options | ||||
|---|---|---|---|---|---|---|
| 2009 | 2010 | 2011 | 2009 | 2010 | 2011 | |
| Mental Health | ||||||
| Inpatient benefit is the same for MH and medical/surgical | 79.6% | 82.8% | 83.3% | 4,329 | 3,862 | 3,871 |
| Inpatient benefit is more restrictive for MH than for medical/surgical | 6.5% | 4.5% | 4.9% | 353 | 210 | 228 |
| Inpatient benefit is less restrictive for MH than for medical/surgical | 13.9% | 12.7% | 11.8% | 758 | 594 | 546 |
| Total | 100.00% | 100.00% | 100.00% | 5,440 | 4,665 | 4,645 |
| Substance Use Disorders | ||||||
| Inpatient benefit is the same for SUD and medical/surgical | 77.2% | 79.4% | 82.5% | 3,548 | 3,154 | 3,249 |
| Inpatient benefit is more restrictive for SUD than for medical/surgical | 6.4% | 5.3% | 4.0% | 292 | 211 | 159 |
| Inpatient benefit is less restrictive for SUD than for medical/surgical | 16.5% | 15.3% | 13.5% | 758 | 606 | 532 |
| Total | 100.0% | 100.0% | 100.0% | 4,598 | 3,971 | 3,940 |
| Out-Network Benefit Design | Percent of Plan Options | Number of Plan Options | ||||
|---|---|---|---|---|---|---|
| 2009 | 2010 | 2011 | 2009 | 2010 | 2011 | |
| Mental Health | ||||||
| Inpatient benefit is the same for MH and medical/surgical | 80.5% | 77.6% | 79.1% | 1,376 | 1,354 | 1,544 |
| Inpatient benefit is more restrictive for MH than for medical/surgical | 9.4% | 6.5% | 5.6% | 160 | 113 | 110 |
| Inpatient benefit is less restrictive for MH than for medical/surgical | 10.1% | 15.9% | 15.3% | 173 | 278 | 298 |
| Total | 100.00% | 100.00% | 100.00% | 1,709 | 1,745 | 1,952 |
| Substance Use Disorders | ||||||
| Inpatient benefit is the same for SUD and medical/surgical | 76.7% | 75.0% | 79.8% | 1,164 | 1,133 | 1,359 |
| Inpatient benefit is more restrictive for SUD than for medical/surgical | 11.1% | 5.8% | 3.8% | 168 | 88 | 64 |
| Inpatient benefit is less restrictive for SUD than for medical/surgical | 12.3% | 19.2% | 16.4% | 186 | 290 | 280 |
| Total | 100.00% | 100.00% | 100.00% | 1,518 | 1,511 | 1,703 |
Inpatient Quantitative Limitations
As MHPAEA legislation prohibits group health plans providing coverage for medical/surgical and MH/SUD benefits from imposing more restrictive financial requirements or treatment limitations for MH/SUD than those provided for medical/surgical benefits, our analysis included a review of the plan options that applied quantitative limits, including day, dollar, or confinement limitations, to inpatient MH/SUD services.
The limitations included in this analysis are described below:
Inpatient day limitations are typically plan provisions that limit the number of inpatient days covered under the plan and can be annual or lifetime limits.
- Example: Inpatient MH/SUD services covered up to 20 days per year.
Inpatient dollar limitations are plan provisions that limit the amount the plan will pay for inpatient MH/SUD services and is typically an annual or lifetime limit.
- Example: Inpatient MH/SUD services covered up to $10,000 per year and/or $20,000 lifetime.
Inpatient confinement limitations reflect plan provisions that establish limits regarding each MH/SUD confinement.
- Example: Inpatient MH/SUD services are limited to one confinement per lifetime.
Observations
The data suggests that most plan options reflected in the PDD have made modifications from 2009 to 2011 to eliminate quantitative limitations on inpatient MH/SUD benefits and are offering the MH/SUD benefits in parity with medical/surgical.
The plan design data shows a drastic reduction in the percent of plan options that applied annual or lifetime day limits to inpatient MH/SUD benefits. For example, in 2009, approximately half of the plan options reported applying annual day limits on in-network inpatient MH and SUD benefits. In 2010, the percent of plan designs that apply annual day limits for in-network inpatient MH services decreased to 12.01% for MH and 13.84% for SUD. A similar trend was observed in out-of-network benefit designs. No significant change was noted in limits in 2011.
Few plan options reported applying annual and lifetime dollar and confinement limitations on inpatient MH/SUD services in 2009. These statistics stayed relatively stable in 2010 and 2011 with no significant change in the percent of plans with dollar or confinement limitations. Although the majority of plan options do not apply these types of quantitative limits to inpatient MH/SUD services, the data does show some options with quantitative limits that are more restrictive for MH/SUD than for medical/surgical.
Quantitative limitations on MH/SUD benefits that are more restrictive than medical/surgical could potentially be non-compliant with MHPAEA requirements. However, we were not able to assess the compliance status of those plans that report such limits on inpatient MH/SUD services.
| In-Network Limitations | Percent of Plan Options | Number of Plan Options | ||||
|---|---|---|---|---|---|---|
| 2009 | 2010 | 2011 | 2009 | 2010 | 2011 | |
| Mental Health | ||||||
| Day limitations (annual) | ||||||
| Day limits are more restrictive for MH than medical/surgical | 54.0% | 12.0% | 7.5% | 3,337 | 635 | 393 |
| Day limits are less restrictive for MH than for medical/surgical | 0.1% | 0.1% | 0.1% | 8 | 7 | 5 |
| Day limits are the same for MH and medical/surgical (no limits in place) | 45.9% | 87.9% | 92.4% | 2,839 | 4,647 | 4,814 |
| Total | 100.0% | 100.0% | 100.0% | 6,184 | 5,289 | 5,213 |
| Day limitations (lifetime) | ||||||
| Day limits are more restrictive for MH than medical/surgical | 13.0% | 5.4% | 4.0% | 803 | 283 | 210 |
| Day limits are less restrictive for MH than for medical/surgical | 0.0% | 0.0% | 0.0% | 1 | 2 | 1 |
| Day limits are the same for MH and medical/surgical (no limits in place) | 87.0% | 94.6% | 96.0% | 5,380 | 5,004 | 5,002 |
| Total | 100.0% | 100.0% | 100.0% | 6,184 | 5,289 | 5,213 |
| Dollar limitations (annual) | ||||||
| Dollar limits are more restrictive for MH than medical/surgical | 0.5% | 0.2% | 0.2% | 29 | 9 | 10 |
| Dollar limits are less restrictive for MH than for medical/surgical | 0.0% | 0.0% | 0.0% | 1 | 1 | 0 |
| Dollar limits are the same for MH and medical/surgical (no limits in place) | 99.5% | 99.8% | 99.8% | 6,154 | 5,279 | 5,203 |
| Total | 100.0% | 100.0% | 100.0% | 6,184 | 5,289 | 5,213 |
| Dollar limitations (lifetime) | ||||||
| Dollar limits are more restrictive for MH than medical/surgical | 0.0% | 0.0% | 0.0% | 0 | 0 | 0 |
| Dollar limits are less restrictive for MH than for medical/surgical | 0.3% | 0.1% | 0.1% | 16 | 6 | 5 |
| Dollar limits are the same for MH or medical/surgical (no limits in place) | 99.5% | 99.6% | 99.7% | 6,155 | 5,270 | 5,195 |
| Total | 100.0% | 100.0% | 100.0% | 6,171 | 5,276 | 5,200 |
| Confinement limitations | ||||||
| Confinement limits are more restrictive for MH than medical/surgical | 1.9% | 1.2% | 0.8% | 116 | 64 | 43 |
| Confinement limits are less restrictive for MH than for medical/surgical | 0.3% | 0.3% | 0.3% | 21 | 17 | 17 |
| Confinement limits are the same for MH or medical/surgical (no limits in place) | 97.8% | 98.5% | 98.8% | 6,045 | 5,208 | 5,151 |
| Total | 100.0% | 100.0% | 100.0% | 6,184 | 5,289 | 5,213 |
| Substance Use Disorders | ||||||
| Day limitations (annual) | ||||||
| Day limits are more restrictive for SUD than medical/surgical | 46.2% | 13.8% | 8.5% | 2,562 | 656 | 395 |
| Day limits are less restrictive for SUD than for medical/surgical | 0.2% | 0.7% | 0.2% | 12 | 32 | 10 |
| Day limits are the same for SUD and medical/surgical (no limits in place) | 53.6% | 85.5% | 91.3% | 2,975 | 4,053 | 4,236 |
| Total | 100.0% | 100.0% | 100.0% | 5,549 | 4,741 | 4,641 |
| Day limitations (lifetime) | ||||||
| Day limits are more restrictive for SUD than medical/surgical | 21.4% | 5.4% | 4.1% | 1,187 | 285 | 212 |
| Day limits are less restrictive for SUD than for medical/surgical | 0.1% | 0.1% | 0.1% | 3 | 5 | 5 |
| Day limits are the same for SUD and medical/surgical (no limits in place) | 78.5% | 94.5% | 95.8% | 4,356 | 4,999 | 4,996 |
| Total | 100.0% | 100.0% | 100.0% | 5,546 | 5,289 | 5,213 |
| Dollar limitations (annual) | ||||||
| Dollar limits are more restrictive for SUD than medical/surgical | 0.1% | 0.1% | 0.0% | 3 | 3 | 2 |
| Dollar limits are less restrictive for SUD than for medical/surgical | 0.0% | 0.0% | 0.0% | 0 | 0 | 0 |
| Dollar limits are the same for SUD and medical/surgical (no limits in place) | 99.9% | 99.9% | 99.9% | 5,539 | 4,727 | 4,628 |
| Total | 100.0% | 100.0% | 100.0% | 5,542 | 4,730 | 4,630 |
| Dollar limitations (lifetime) | ||||||
| Dollar limits are more restrictive for SUD than medical/surgical | 0.0% | 0.0% | 0.0% | 0 | 0 | 0 |
| Dollar limits are less restrictive for SUD than for medical/surgical | 5.3% | 0.8% | 0.7% | 293 | 37 | 31 |
| Dollar limits are the same for SUD and medical/surgical (no limits in place) | 94.7% | 99.2% | 99.3% | 5,258 | 4,704 | 4,608 |
| Total | 100.0% | 100.0% | 100.0% | 5,551 | 4,741 | 4,639 |
| Confinement limitations | ||||||
| Confinement limits are more restrictive for SUD than medical/surgical | 2.5% | 1.1% | 0.4% | 141 | 50 | 19 |
| Confinement limits are less restrictive for SUD than for medical/surgical | 1.2% | 1.0% | 0.9% | 64 | 47 | 42 |
| Confinement limits are the same for SUD or medical/surgical (no limits in place) | 96.3% | 98.0% | 99.0% | 5,346 | 4,645 | 4,580 |
| Total | 100.0% | 100.0% | 100.0% | 5,551 | 4,742 | 4,641 |
| Out-Network Limitations | Percent of Plan Options | Number of Plan Options | ||||
|---|---|---|---|---|---|---|
| 2009 | 2010 | 2011 | 2009 | 2010 | 2011 | |
| Mental Health | ||||||
| Day limitations (annual) | ||||||
| Day limits are more restrictive for MH than medical/surgical | 48.2% | 10.5% | 5.8% | 1,252 | 249 | 146 |
| Day limits are less restrictive for MH than for medical/surgical | 0.5% | 0.5% | 0.2% | 14 | 11 | 4 |
| Day limits are the same for MH or medical/surgical (no limits in place) | 51.3% | 89.0% | 94.1% | 1,331 | 2,110 | 2,388 |
| Total | 100.0% | 100.0% | 100.0% | 2,597 | 2,370 | 2,538 |
| Day limitations (lifetime) | ||||||
| Day limits are more restrictive for MH than medical/surgical | 8.1% | 1.4% | 1.1% | 210 | 33 | 28 |
| Day limits are less restrictive for MH than for medical/surgical | 0.0% | 0.0% | 0.0% | 0 | 0 | 0 |
| Day limits are the same for MH and medical/surgical (no limits in place) | 91.9% | 98.6% | 98.9% | 2,387 | 2,337 | 2,510 |
| Total | 100.0% | 100.0% | 100.0% | 2,597 | 2,370 | 2,538 |
| Dollar limitations (annual) | ||||||
| Dollar limits are more restrictive for MH than medical/surgical | 0.2% | 0.2% | 0.2% | 4 | 4 | 5 |
| Dollar limits are less restrictive for MH than for medical/surgical | 0.0% | 0.0% | 0.1% | 1 | 0 | 3 |
| Dollar limits are the same for MH or medical/surgical (no limits in place) | 99.8% | 99.8% | 99.7% | 2,592 | 2,366 | 2,530 |
| Total | 100.0% | 100.0% | 100.0% | 2,597 | 2,370 | 2,538 |
| Dollar limitations (lifetime) | ||||||
| Dollar limits are more restrictive for MH than medical/surgical | 0.0% | 0.0% | 0.0% | 0 | 0 | 0 |
| Dollar limits are less restrictive for MH than for medical/surgical | 0.1% | 0.0% | 0.0% | 3 | 0 | 1 |
| Dollar limits are the same for MH or medical/surgical (no limits in place) | 99.6% | 99.7% | 99.7% | 2,587 | 2,363 | 2,530 |
| Total | 100.0% | 100.0% | 100.0% | 2,590 | 2,363 | 2,531 |
| Confinement limitations | ||||||
| Confinement limits are more restrictive for MH than medical/surgical | 0.9% | 0.3% | 0.1% | 24 | 7 | 3 |
| Confinement limits are less restrictive for MH than for medical/surgical | 0.0% | 0.0% | 0.4% | 0 | 0 | 11 |
| Confinement limits are the same for MH or medical/surgical (no limits in place) | 99.1% | 99.7% | 99.9% | 2,573 | 2,363 | 2,535 |
| Total | 100.0% | 100.0% | 100.0% | 2,597 | 2,370 | 2,538 |
| Substance Use Disorders | ||||||
| Day limitations (annual) | ||||||
| Day limits are more restrictive for SUD than medical/surgical | 40.4% | 12.7% | 7.6% | 924 | 266 | 174 |
| Day limits are less restrictive for SUD than for medical/surgical | 0.5% | 0.6% | 0.3% | 12 | 12 | 6 |
| Day limits are the same for SUD or medical/surgical (no limits in place) | 59.0% | 86.8% | 92.1% | 1,349 | 1,824 | 2,099 |
| Total | 100.0% | 100.0% | 100.0% | 2,285 | 2,102 | 2,279 |
| Day limitations (lifetime) | ||||||
| Day limits are more restrictive for SUD than medical/surgical | 8.1% | 1.4% | 1.1% | 210 | 33 | 28 |
| Day limits are less restrictive for SUD than for medical/surgical | 0.0% | 0.0% | 0.0% | 0 | 0 | 0 |
| Day limits are the same for SUD or medical/surgical (no limits in place) | 91.9% | 98.6% | 98.9% | 2,387 | 2,337 | 2,510 |
| Total | 100.0% | 100.0% | 100.0% | 2,597 | 2,370 | 2,538 |
| Dollar limitations (annual) | ||||||
| Dollar limits are more restrictive for SUD than medical/surgical | 0.1% | 0.1% | 0.1% | 3 | 3 | 2 |
| Dollar limits are less restrictive for SUD than for medical/surgical | 0.0% | 0.0% | 0.0% | 0 | 0 | 0 |
| Dollar limits are the same for SUD or medical/surgical (no limits in place) | 99.9% | 99.9% | 99.9% | 2,275 | 2,092 | 2,270 |
| Total | 100.0% | 100.0% | 100.0% | 2,278 | 2,095 | 2,272 |
| Dollar limitations (lifetime) | ||||||
| Dollar limits are more restrictive for SUD than medical/surgical | 0.0% | 0.0% | 0.0% | 0 | 0 | 0 |
| Dollar limits are less restrictive for SUD than for medical/surgical | 7.3% | 1.1% | 0.8% | 166 | 22 | 18 |
| Dollar limits are the same for SUD and medical/surgical (no limits in place) | 92.7% | 99.0% | 99.2% | 2,119 | 2,080 | 2,261 |
| Total | 100.0% | 100.0% | 100.0% | 2,285 | 2,102 | 2,279 |
| Confinement limitations | ||||||
| Confinement limits are more restrictive for SUD than medical/surgical | 1.7% | 1.1% | 0.7% | 39 | 22 | 16 |
| Confinement limits are less restrictive for SUD than for medical/surgical | 0.0% | 0.0% | 0.0% | 0 | 0 | 0 |
| Confinement limits are the same for SUD and medical/surgical (no limits in place) | 98.3% | 99.0% | 99.3% | 2,246 | 2,080 | 2,263 |
| Total | 100.0% | 100.0% | 100.0% | 2,285 | 2,102 | 2,279 |
Outpatient MH/SUD
Outpatient Benefit Design
Our analysis reviewed the benefit design in effect in each plan year for outpatient medical/surgical and MH/SUD services. Specifically, our review focused on routine outpatient MH/SUD services compared to the benefit design for medical/surgical office visits for PCP and SCP services.
We recognize that there may be other outpatient services that may fall into the outpatient office visit classification. However, our review is focused on comparing routine outpatient MH/SUD services to medical/surgical office visits, as we felt this comparison to be most relevant to the assessment of how MHPAEA has impacted employer plan designs since implementation. Office visit services for medical/surgical services are the closest in terms of scope to typical outpatient MH/SUD visits, and PCP and SCP office visit benefits are often the point of comparison when determining how outpatient MH/SUD benefits are handled relative to medical/surgical.
Historically, many employers have considered MH/SUD professionals to be specialists and therefore applied a coinsurance or copay that was in alignment with the benefit for SCPs. With MHPAEA, there is recognition that the parity compliant benefit for outpatient MH/SUD services should be determined based on an evaluation of substantially all and predominant. As such, aligning the MH/SUD outpatient benefit to the SCP benefit may or may not be compliant, depending upon the outcome of compliance testing. As we do not have access to employer compliance testing results for the employers represented in the PDD, our analysis focuses on the benefits that are documented on the PDD and the comparison between benefits for routine MH/SUD outpatient services and PCP and SCP office visit services. We are unable to assess the compliance status of the plan options included in this analysis.
The results of our analysis show how outpatient MH/SUD benefits compare to the benefits for PCP and SCP office visit services. This comparison did not consider visit or dollar limits, as these plan provisions were evaluated separately.
Some plan options apply the same level of copay or coinsurance to both PCPs and SCPs. Other plan options apply differing copays or coinsurance for PCPs and SCPs, where the PCP copay or coinsurance is often lower than the SCP copay or coinsurance (referred to as Split Copay/Coinsurance Plans). So that the analysis is clear and results are not skewed, we are reporting the results for each group of plan designs separately.
Comparative results are reported as described below:
Plan Options with Same Copay/Coinsurance for PCPs/SCPs
Outpatient MH/SUD benefit is the same as PCP/SCP: This category includes all plan options where the MH/SUD benefit and the benefit for PCPs and SCPs are the same.
- Example #1: MH/SUD benefit is 80% after deductible; PCP and SCP benefit is 80% after deductible.
- Example #2: MH/SUD benefit is $30 copay; PCP and SCP benefit is $30 copay.
Outpatient MH/SUD benefit is more restrictive than PCP/SCP.
- Example #1: MH/SUD benefit is 50% after deductible; PCP and SCP benefit is 80% after deductible.
- Example #2: MH/SUD benefit is $50 copay; PCP and SCP benefit is $30 copay.
Outpatient MH/SUD benefit is less restrictive than PCP/SCP.
- Example #1: MH/SUD benefit is 90% after deductible; PCP and SCP benefit is 80% after deductible.
- Example #2: MH/SUD benefit is $20 copay; PCP and SCP benefit is $30 copay.
Plan Options with Split Copay/Coinsurance for PCPs/SCPs (copay/coinsurance varies for PCPs and SCPs)
Outpatient MH/SUD benefit is the same as PCP: This category includes all plan options where the outpatient MH/SUD benefit and the PCP benefit are the same.
- Example #1: MH/SUD copay is $20; PCP copay is $20.
- Example #2: MH/SUD coinsurance is 80%; PCP coinsurance is 80%.
Outpatient MH/SUD benefit is the same as SCP: This category includes all plan options where the outpatient MH/SUD benefit and the SCP benefit are the same.
- Example #1: MH/SUD copay is $40; SCP copay is $40.
- Example #2: MH/SUD coinsurance is 70%; SCP coinsurance is 70%.
Outpatient MH/SUD benefit is less restrictive than PCP: This category includes all plan options where the MH/SUD benefit is less restrictive than the PCP benefit.
- Example #1: MH/SUD copay is $10; PCP copay is $20.
- Example #2: MH/SUD coinsurance is 90%; PCP coinsurance is 80%.
Outpatient MH/SUD benefit is more restrictive than SCP: This category includes all plan options where the MH/SUD benefit is more restrictive than the SCP benefit.
- Example #1: MH/SUD copay is $50; SCP copay is $40.
- Example #2: MH/SUD coinsurance is 60%; SCP coinsurance is 70%.
Outpatient MH/SUD benefit is more restrictive than PCP but less restrictive than SCP: This category includes all plan options where the MH/SUD benefit falls between the PCP and SCP benefit level.
- Example #1: MH/SUD copay is $25; PCP copay is $20; SCP copay is $30.
- Example #2: MH/SUD coinsurance is 75%; PCP coinsurance is 80%; SCP coinsurance is 70%.
Observations
Plan Options with Same Copay/Coinsurance for PCPs/SCPs
The vast majority of plan options in each plan year utilized the same copay/coinsurance for in-network outpatient MH as the PCP/SCP benefit. However, the data shows a decrease in the percent of plan options with a MH benefit design that is more restrictive than the PCP/SCP benefit level. For example, in 2009, 12.87% of plan options applied a more restrictive in-network benefit for MH than for PCP/SCP services. This percentage decreased to 1.99% in 2011. A similar trend was observed for outpatient SUD and out-of-network MH and SUD benefits.
Plan Options with Split Copay/Coinsurance for PCPs/SCPs
In 2009, approximately one-third of plan options aligned the outpatient MH benefit with PCP, one-third with SCP, and one-third more or less restrictive than PCP or SCP. In 2010, a distinct change occurred in the benefit for MH services. Almost two-thirds of plan options aligned the MH outpatient benefit with the SCP copay level. In 2011, plan designs changed once again. Over half of plan options reported that the outpatient MH benefit aligned with the PCP benefit.
The changes observed across plan options suggest that employers responded to the parity legislation. In 2010, after the enactment of MHPAEA, many employers aligned the outpatient MH benefit with the SCP level, suggesting that employers made the interpretation that treating a MH provider as a specialist would be compliant under the legislation. The interim final regulations were released in early 2010 (implemented in 2011 for most plans) and clarified that design compliance is governed by a review of the benefit design that represents substantially all and predominant. Plan design information reported for 2011 suggests employers evaluated plan designs once again and made adjustments to comply with the interim final regulations. As a result, more plan options were adjusted to align the outpatient MH benefit design with the PCP benefit level.
The plan design data shows that over half of the plan options aligned the outpatient SUD benefit with the PCP benefit level in all 3 years (2009, 2010, and 2011). In 2009 and 2010, approximately 27% of plan options applied a benefit for outpatient SUD services that was either more restrictive than the SCP benefit level or in between the PCP and SCP benefit level. This changed in 2011 when we observed movement away from this approach and more plan options aligned the outpatient SUD benefit with the SCP benefit level.
| In-Network Benefit Design | Percent of Plan Options | Number of Plan Options | ||||
|---|---|---|---|---|---|---|
| 2009 | 2010 | 2011 | 2009 | 2010 | 2011 | |
| Mental Health | ||||||
| Plan Options With Same Copay/Coinsurance for PCPs/SCPs | ||||||
| Outpatient MH benefit is the same as PCP/SCP | 84.9% | 89.8% | 93.9% | 2,059 | 2,451 | 2,357 |
| Outpatient MH benefit is more restrictive than PCP/SCP | 12.9% | 5.3% | 2.0% | 312 | 144 | 50 |
| Outpatient MH benefit is less restrictive than PCP/SCP | 2.2% | 5.0% | 4.0% | 54 | 135 | 102 |
| Total | 100.0% | 100.0% | 100.0% | 2,425 | 2,730 | 2,509 |
| Plan Options with Split Copay/Coinsurance for PCPs/SCPs | ||||||
| Outpatient MH benefit is the same as PCP | 33.7% | 25.8% | 55.8% | 778 | 424 | 1,093 |
| Outpatient MH benefit is the same as SCP | 32.0% | 61.2% | 25.2% | 739 | 1,005 | 494 |
| Outpatient MH benefit is less restrictive than PCP | 6.2% | 4.3% | 14.1% | 144 | 71 | 277 |
| Outpatient MH benefit is more restrictive than SCP | 20.4% | 3.5% | 3.7% | 472 | 58 | 73 |
| Outpatient MH benefit is more restrictive than PCP but less restrictive than SCP | 7.7% | 5.1% | 1.2% | 179 | 83 | 23 |
| Total | 100.0% | 100.0% | 100.0% | 2,312 | 1,641 | 1,960 |
| Substance Use Disorder | ||||||
| Plan Options With Same Copay/Coinsurance for PCPs/SCPs | ||||||
| Outpatient SUD benefit is the same as PCP/SCP | 73.8% | 76.1% | 97.6% | 535 | 325 | 2,007 |
| Outpatient SUD benefit is more restrictive than PCP/SCP | 24.3% | 20.8% | 1.3% | 176 | 89 | 26 |
| Outpatient SUD benefit is less restrictive than PCP/SCP | 1.9% | 3.0% | 1.2% | 14 | 13 | 24 |
| Total | 100.0% | 100.0% | 100.0% | 725 | 427 | 2,057 |
| Plan Options with Split Copay/Coinsurance for PCPs/SCPs | ||||||
| Outpatient SUD benefit is the same as PCP | 54.8% | 55.0% | 52.6% | 897 | 631 | 657 |
| Outpatient SUD benefit is the same as SCP | 15.1% | 13.3% | 39.7% | 248 | 152 | 496 |
| Outpatient SUD benefit is less restrictive than PCP | 2.9% | 3.9% | 3.1% | 48 | 45 | 39 |
| Outpatient SUD benefit is more restrictive than SCP | 16.8% | 17.4% | 2.6% | 275 | 200 | 32 |
| Outpatient SUD benefit is more restrictive than PCP but less restrictive than SCP | 10.4% | 10.4% | 1.9% | 170 | 119 | 24 |
| Total | 100.0% | 100.0% | 100.0% | 1,638 | 1,147 | 1,248 |
| Mental Health | ||||||
| Plan Options With Same Copay/Coinsurance for PCPs/SCPs | ||||||
| Outpatient MH benefit is the same as PCP/SCP | 72.0% | 88.2% | 89.3% | 1,304 | 1,518 | 1,713 |
| Outpatient MH benefit is more restrictive than PCP/SCP | 24.5% | 7.5% | 8.3% | 444 | 129 | 160 |
| Outpatient MH benefit is less restrictive than PCP/SCP | 3.4% | 4.4% | 2.4% | 62 | 75 | 46 |
| Total | 100.0% | 100.0% | 100.0% | 1,810 | 1,722 | 1,919 |
| Plan Options with Split Copay/Coinsurance for PCPs/SCPs | ||||||
| Outpatient MH benefit is the same as PCP | 20.7% | 48.8% | 37.5% | 17 | 20 | 18 |
| Outpatient MH benefit is the same as SCP | 70.7% | 39.0% | 27.1% | 58 | 16 | 13 |
| Outpatient MH benefit is less restrictive than PCP | 2.4% | 2.4% | 33.3% | 2 | 1 | 16 |
| Outpatient MH benefit is more restrictive than SCP | 4.9% | 7.3% | 2.1% | 4 | 3 | 1 |
| Outpatient MH benefit is more restrictive than PCP but less restrictive than SCP | 1.2% | 2.4% | 0.0% | 1 | 1 | 0 |
| Total | 100.0% | 100.0% | 100.0% | 82 | 41 | 48 |
| Substance Use Disorder | ||||||
| Plan Options With Same Copay/Coinsurance for PCPs/SCPs | ||||||
| Outpatient SUD benefit is the same as PCP/SCP | 74.2% | 89.1% | 89.4% | 1,161 | 1,332 | 1,527 |
| Outpatient SUD benefit is more restrictive than PCP/SCP | 22.3% | 6.8% | 7.4% | 349 | 101 | 126 |
| Outpatient SUD benefit is less restrictive than PCP/SCP | 3.5% | 4.2% | 3.2% | 55 | 62 | 55 |
| Total | 100.0% | 100.0% | 100.0% | 1,565 | 1,495 | 1,708 |
| Plan Options with Split Copay/Coinsurance for PCPs/SCPs | ||||||
| Outpatient SUD benefit is the same as PCP | Data set too small to report credible results | |||||
| Outpatient SUD benefit is the same as SCP | ||||||
| Outpatient SUD benefit is less restrictive than PCP | ||||||
| Outpatient SUD benefit is more restrictive than SCP | ||||||
| Outpatient SUD benefit is more restrictive than PCP but less restrictive than SCP | ||||||
Outpatient Quantitative Limitations
As MHPAEA legislation prohibits group health plans providing coverage for medical/surgical and MH/SUD benefits from imposing more restrictive financial requirements or treatment limitations for MH/SUD than those provided for medical/surgical benefits, our analysis included a review of the plan options that applied some type of visit or dollar limitation to outpatient MH/SUD services.
The limitations included in this analysis are described below:
Outpatient visit limitations are typically plan provisions that limit the number of outpatient visits covered under the plan and can be annual or lifetime limits.
- Example #1: Outpatient MH/SUD services covered up to 30 visits per year.
- Example #2: Outpatient MH/SUD services covered up to 100 visits lifetime.
Outpatient dollar limitations are plan provisions that limit the amount the plan will pay for outpatient MH/SUD services and is typically an annual or lifetime limit.
- Example: Outpatient MH/SUD services covered up to $5,000 per year and/or $10,000 lifetime.
Observations
Similar to the results reflected for inpatient MH/SUD benefits, outpatient data shows a decrease in the percent of plan options with visit and dollar limits for outpatient MH/SUD benefits from 2009 to 2011 and the majority of plan options are offering the MH/SUD benefit in parity with medical/surgical.
The plan design data reported shows a drastic reduction in the percent of plan options that apply visit limitations to outpatient MH and SUD services. In 2009, more than half of the plan options reported applying visit limitations on in-network and out-of-network MH and SUD benefits. In 2010, the percent of plan options that apply visit limitations for in-network and out-of-network MH and SUD benefits decreased to approximately 11% and was further reduced to approximately 6% in 2011.
Few plan options (less than 0.1%) reported applying annual dollar limitations on outpatient MH services, while almost 10% of plan options applied annual dollar limitations to outpatient SUD services in 2009. The percentage of plan options with annual dollar limitations on outpatient MH services remained relatively stable, while the percent of plan options with annual dollar limitations on outpatient SUD services decreased from 2009 to 2010. No significant changes were noted in 2011.
Although the majority of plan options do not apply visit or dollar limitations to outpatient MH and SUD services, in 2011, several plan options continue to report that these limits are in place. Examples of the types of limits in place in 2011 are noted below:
- Outpatient MH/SUD services covered up to 20 visits per year.
- Outpatient MH/SUD services covered up to 60 visits lifetime.
- Outpatient MH/SUD services covered up to $2,000 per year and/or $5,000 lifetime.
Limitations on MH/SUD benefits that are more restrictive than medical/surgical could potentially be non-compliant with MHPAEA requirements. However we were not able to assess the compliance status of those plans that report quantitative limits on outpatient MH/SUD services.
| In-Network Limitations | Percent of Plan Options | Number of Plan Options | ||||
|---|---|---|---|---|---|---|
| 2009 | 2010 | 2011 | 2009 | 2010 | 2011 | |
| Mental Health | ||||||
| Visit Limitations | ||||||
| Visit limitations apply to MH services | 56.1% | 11.1% | 6.5% | 3,649 | 617 | 359 |
| No MH visit limitations | 43.9% | 88.9% | 93.5% | 2,854 | 4,939 | 5,173 |
| Total | 100.0% | 100.0% | 100.0% | 6,503 | 5,556 | 5,532 |
| Dollar Limitations (Annual) | ||||||
| Dollar limitations apply to MH services (annual) | 0.8% | 0.6% | 0.7% | 52 | 32 | 38 |
| No MH dollar limitations | 99.2% | 99.4% | 99.3% | 6,451 | 5,524 | 5,494 |
| Total | 100.0% | 100.0% | 100.0% | 6,503 | 5,556 | 5,532 |
| Substance Use Disorders | ||||||
| Visit limitations apply to SUD services | ||||||
| Visit limitations apply to SUD services | 51.1% | 12.7% | 8.5% | 3,038 | 639 | 417 |
| No SUD visit limitations | 48.9% | 87.3% | 91.5% | 2,907 | 4,378 | 4,482 |
| Total | 100.0% | 100.0% | 100.0% | 5,945 | 5,017 | 4,899 |
| Dollar limitations (Annual) | ||||||
| Dollar limitations apply to SUD services (annual) | 9.4% | 1.5% | 1.0% | 561 | 73 | 51 |
| No SUD dollar limitations | 90.6% | 98.5% | 99.0% | 5,384 | 4,944 | 4,848 |
| Total | 100.0% | 100.0% | 100.0% | 5,945 | 5,017 | 4,899 |
| Out-Network Limitations | Percent of Plan Options | Number of Plan Options | ||||
|---|---|---|---|---|---|---|
| 2009 | 2010 | 2011 | 2009 | 2010 | 2011 | |
| Mental Health | ||||||
| Visit Limitations | ||||||
| Visit limitations apply to MH services | 59.6% | 11.0% | 6.4% | 1,672 | 281 | 171 |
| No MH visit limitations | 40.4% | 89.0% | 93.6% | 1,135 | 2,279 | 2,512 |
| Total | 100.0% | 100.0% | 100.0% | 2,807 | 2,560 | 2,683 |
| Dollar Limitations (Annual) | ||||||
| Dollar limitations apply to MH services (annual) | 0.5% | 0.3% | 0.2% | 14 | 7 | 6 |
| No MH dollar limitations | 99.5% | 99.7% | 99.8% | 2,793 | 2,553 | 2,677 |
| Total | 100.0% | 100.0% | 100.0% | 2,807 | 2,560 | 2,683 |
| Substance Use Disorders | ||||||
| Visit limitations apply to SUD services | ||||||
| Visit limitations apply to SUD services | 53.2% | 14.0% | 9.0% | 1,339 | 320 | 216 |
| No SUD visit limitations | 46.8% | 86.0% | 91.0% | 1,178 | 1,959 | 2,179 |
| Total | 100.0% | 100.0% | 100.0% | 2,517 | 2,279 | 2,395 |
| Dollar limitations (Annual) | ||||||
| Dollar limitations apply to SUD services (annual) | 9.8% | 2.9% | 1.3% | 246 | 65 | 31 |
| No SUD dollar limitations | 90.2% | 97.2% | 98.7% | 2,271 | 2,214 | 2,364 |
| Total | 100.0% | 100.0% | 100.0% | 2,517 | 2,279 | 2,395 |
Considerations
Some of the results contained in this report suggest that some employer plan designs may not be compliant with MHPAEA. For example, the copay or coinsurance for MH/SUD is more restrictive than medical/surgical or the plan reports quantitative limits in effect for MH and SUD benefits. Although some plan options may not seem to align with MHPAEA compliance requirements, it is important to consider the following:
Employer reviewed their plan design based on the substantially all and predominant tests and the benefit reported in the PDD is compliant with parity requirements.
Some plan designs could reflect plan options offered to union groups and have not yet been updated to reflect MHPAEA requirements. For collective bargaining agreements ratified before the date of enactment of the MHPAEA, MHPAEA applies to plan years beginning after the later of July 1, 2010 or the date that the last collective bargaining agreement terminates.
We assume all data (except those data points that have been excluded from the analysis) to be accurate. It is possible that some data fields may not have been updated by the employer.
Appendix D. Detailed Analysis of Year-by-year Changes in Cost-sharing by Midsized Employers, 2009-2011
| Pre-Parity (2008) Percent of Plans (n = 86) | Post-Parity (2009 Only) Percent of Plans (n = 78) | Post-Parity (2010 Only) Percent of Plans (n = 40) | Post-Parity (2011 Only) Percent of Plans (n = 36) | |
|---|---|---|---|---|
| Cost-Sharing | ||||
| Inpatient care: cost-sharing for in-network MH/SUD treatment higher than inpatient medical/surgical care | 9% | 12% | 0% | 0% |
| Inpatient care: cost-sharing for out-of-network MH/SUD treatment higher than inpatient medical/surgical care | 16% | 89% | 10% | 6% |
| Outpatient care: cost-sharing for in-network MH/SUD office visits higher than medical/surgical PCP visits | 56% | 40% | 28% | 32% |
| Outpatient care: cost-sharing for in-network MH/SUD office visits higher than medical/surgical specialist office visits | 29% | 15% | 9% | 8% |
| Outpatient care: cost-sharing for out-of-network MH/SUD treatment higher than outpatient medical/surgical treatment | 30% | 25% | 13% | 0% |
| Treatment Limitations | ||||
| Inpatient: day limitations for MH/SUD treatment more restrictive than medical/surgical care | 84% | 64% | 22% | 13% |
| Outpatient: visit limitations for MH/SUD treatment more restrictive than for medical/surgical care | 81% | 75% | 23% | 13% |
| SOURCE: Author's analysis of SPDs of midsized employers. NOTE: Detailed information on employer size was unavailable from BLS. Instead, establishment size was used to identify midsized employers (establishment sizes of 51-500). NOTE: Analyses should be interpreted with caution due to small sample sizes. | ||||
Appendix E. Detailed Interview Responses by Topic
The responses from the seven participating companies are listed below. These responses have been de-identified, and within each section they are randomly sorted and given the name of Company A, B, C, D, E, F, or G.
Medical Necessity Criteria
Company A uses McKesson's InterQual criteria for all behavioral health services. Many behavioral health facilities use these criteria internally, which allows for better coordination with Company A. InterQual criteria are updated regularly. The updates are added to Company A's electronic system for review of claims and requests for services. The system enables Company A's staff to explain a denial to providers over the telephone. Upon request, Company A will send the InterQual criteria on paper to a provider or member.
In some cases, Company A has developed criteria of its own. For example, within the area of residential treatment programs Company A has decided that it will not cover wilderness residential programs.
Nearly all of the various health plans with which Company B works use medical necessity criteria for behavioral health services. Some health plans had moved away from medical necessity criteria for medical care in the late 1990s and early 2000s, but in 2008-2009 the plans started moving back to using them. After passage of MHPAEA, the utilization of medical necessity criteria for behavioral health plans dropped to the point that it equaled the use of such criteria in medical plans. Having achieved that equilibrium, any future changes in medical necessity criteria will affect behavioral health and medical benefits equally.
Company C uses its own medical necessity criteria that were developed in combination with other available criteria and expert opinion. Company C uses McKesson InterQual criteria for a couple of accounts. For the public sector, it uses state-specific criteria. It uses ASAM criteria for substance abuse services. Company C's criteria are updated each year.
The PPACA has had a greater effect on medical necessity criteria than the MHPAEA, because the PPACA requires that health plans provide the criteria to their members. There is some worry about copyright restrictions on sharing this information.
There are several sets of medical necessity criteria. In general, Company D uses guidelines from McKesson InterQual for specialized psychiatric treatment and MH services. It also generally uses ASAM criteria for the substance abuse services. States may require a specific set of medical necessity criteria for certain services, such as community-based services. One state with which Company D works is an exception to the norm of using InterQual and ASAM criteria, in that it requires the use of its own internally created medical necessity criteria. Sister health plans also use McKesson InterQual as well Milliman Care Guidelines. None of these practices have changed because of the parity law.
Company E has home-grown medical necessity criteria that are updated yearly. Each year they give the professional community the opportunity to comment on them. In 2010, Company E redesigned their medical necessity criteria. Before 2010 the criteria were calledlevel of care guidelines. The parity law has not changed Company E's medical necessity criteria, but it has changed the circumstance in which the criteria are applied. For example, if an account does not provide utilization management services for medical inpatients, then Company E is unable to provide utilization management services for behavioral health at this level of care.
Medical necessity criteria are shared with individuals upon request. They are also made available to the public on Company E's website.
Under health plan contracts, Company F is obligated to use the medical necessity criteria specific to the member's health plan. Some health plans use McKesson's InterQual criteria, whereas others have developed their own. If a health plan lacks medical necessity criteria for behavioral health, Company F may use its own. Medical necessity criteria have not changed with the implementation of the parity law.
Company G develops behavioral health medical necessity criteria in a manner similar to that used by health plans to develop criteria for medical/surgical criteria. Company G likewise reviews new technologies on a similar schedule and with similar criteria. This has not changed since the parity law (MHPAEA) went into effect. Some of Company G's senior clinical leaders were with full service health plans previously, so the organization had already adopted clinical practices aligned with those of medical care.
Company G has developed its own medical necessity criteria that incorporates feedback from outside consultants (e.g., physicians, psychologists), and these criteria are reviewed and updated annually. Some states, however, require Company G to use the ASAM criteria or medical necessity criteria that were created by the state.
Informing About Claim Denials
Company A's patients are notified of claim denials through EOB statements and adverse determination letters. DOL rules and state law dictate the content and timing of the letters. The letters state the reason(s) for denial. The letters were affected by PPACA but not by MHPAEA. The rules apply equally to behavioral health services and medical services.
Denial rates have always been low; less than 1% of outpatient claims were denied even before MHPAEA. Denying care does not manage a person's treatment. The goal is to shape treatment rather than deny it.
If the claim is denied, Company B sends a letter explaining the reason for denial to the provider and to the member. The process has not changed since implementation of the parity law.
There are two major types of claim denials: administrative denials (e.g., a denial for a service that is not covered or that is not filed in time) and a medical necessity denial.
Company C has not seen changes in the claim denial process since the implementation of the parity law. What is influencing this process is the PPACA, which is changing the regulations on what is contained in the EOBs and denial letters, how quickly the company must respond, and the beneficiary's options in such a situation.
It is standard protocol to give the patient a written letter of denial.
If a provider submits a claim and the claim is denied then Company D will send a written notice to the provider as well as the member receiving treatment. If the claim is submitted by the member directly, and the claim is denied, then the denial would be communicated just to the member. These denials would take place after a claim is submitted. Denials can be sent in advance of services being rendered where an authorization requirement applies and the request is submitted for authorization in advance of the services. If the request is urgent and comes prior to the service, the explanation of will be verbal followed by a letter. If it occurs after the service has been offered, notification happens through an EOB form. Parity has not changed this process.
If a claim or treatment request has been denied, a notice in writing is provided to the practitioner with a copy to the member. The content of the letters and timeline for when they are distributed are dictated by the states in which Company E operates. There is some variance on the required response timeline based on level of care and whether the treatment is life threatening or urgent. In general, the letters must contain both a reason for denial and the criteria that were used for deciding that the treatment request was denied.
Separately, seven of Company E's markets require distribution of an EOB be sent to both the practitioners and members once the claim for services rendered to the member is adjudicated. Company E also started a process to help identify fraud; it sends EOBs to a random sample of members to see if the members call back to confirm that the treatment did not take place. In addition, Company E routinely calls individuals to discuss claims that it suspects are fraudulent as a means of confirming whether the services billed were actually provided.
Company F is delegated by some plans to carry out the denial process. It provides letters to members and providers. First level appeals always go through the health plan. Clinical denials also have to go through the medical director for his or her review. Once the medical director has reviewed the denial and agreed that it should take place, the process switches to helping the member understand the right to appeal. Company F shares with their members how the claims denial process works. Company F also assists with complaints and grievances.
Parity has not changed the claims denial process. The PPACA has had a greater effect on this process because it has required changes in the language of the denial letters and the timeframe for appeals of the denials.
An ABD letter is sent out immediately once a benefit denial is issued when a treatment request does not meet medical necessity criteria. EOBs are sent out when a claim has been submitted. If the request for services was not authorized due to a Medical necessity denial, this will be documented on the EOB as a reason for non-payment. The timeframe and language of these letters are determined primarily by DOL regulations established in 2000. Further changes to this process may come from the PPACA regulations. For Company G, no changes have occurred to this process as a result of the MHPAEA, as all the requirements in MHPAEA were already met by adopting the DOL standards.
Utilization Management Techniques
For Company A, medical management depends on the plan with which it is working.
The definition of prior authorization varies. In some cases it is merely notification for the sake of patient registration. In other cases it involves free determination of clinical necessity. Retrospective review occurs when prior review was not possible. Outlier managementis when plans start to manage after the 20thsession of outpatient counseling because at that point the patient becomes an outlier from the norm (the norm is only about eight sessions). Concurrent review is often used for behavioral health services, but it is rarely used for medical outpatient care. Examples of outpatient medical care that would have concurrent review include physical therapy, speech therapy, occupational therapy, home health services, and skilled nursing services.
Company A has seen that most behavioral health plans apply some form of concurrent review, particularly for inpatient services and in some form for outpatient services. Since MHPAEA, Company A has had to look closely at what happens on the medical side. Inpatient medical services are managed and paid quite differently from behavioral health services. Typical medical inpatient stays are paid via DRGs, so payment does not depend on length of stay. With behavioral health services, however, there is much broader variability and DRG methods are not used. Based on a subjective determination of necessity, a decision will be made about allowable length of stays. Company A has had to study medical processes and try to align with behavioral health processes and services. Company A is moving in the direction of retrospective review to meet parity. Retrospective review occurs after treatment is completed but before the provider is reimbursed. Company A sees a downside -- less certainty for patient and provider about funding. Prior authorization does not exist as often on the medical side, so Company A has moved away from it for behavioral health services. They stated that this "seems perverse" but they do not see an option.
For outpatient medical care the situation is even worse, because very few routine outpatient services require prior authorization. With routine behavioral health services they now typically cannot require preauthorization for outpatient care because it is not used for medical services. This was removed because of MHPAEA. Only non-routine outpatient, specialized services require preauthorization, such as ECT and psychological testing. This is similar to non-routine outpatient medical services such as ambulatory surgery.
Before parity, there was a single standard within each carrier, mostly, for prior authorization. The parity law requires that behavioral health match the particular medical plan to which the patient belongs. Thus, rules about prior authorization will vary by patient within the same carrier if two patients belong to different plans with different rules for prior authorization of medical care. This adds complexity to administration for the providers.
Previous to the parity law health plans often wanted to precertify all behavioral health outpatient services. In response to MHPAEA, there is no requirement for precertification for outpatient in Company B. Physicians and other medication prescribers are never required to precertify and are not subjected to any review concurrently. For other behavioral health professionals who provide psychotherapy services, there are periodic quality checks, designed to insure that medications are being used when indicated, and communication with other professionals and family members are maintained. Company B periodically requests this quality information from professionals to identify enrollees that are not receiving treatment according to best practice clinical guidelines.
As a provider seeks recertification for treating a patient, he or she must fill out a form and report on some quality indicators. For example, if the patient is an adolescent then the provider will need to report whether they are working with the parents of the patient. The provider must give an explanation if he or she has not done this. Similarly, if an individual has anorexia the provider may be asked if he or she has coordinated with the patient's medical provider. Company B works with the providers to established coordinated care for patients. In the contract that network physicians sign there is a clause that states that they will cooperate with Company B on issues of quality. If a provider does not cooperate, for example with coordinating with other providers that treat the same patient, then the provider may not be reauthorized to provide services for the patient. If this happens, Company B will attempt to contact the member to arrange further care.
Prior to the parity law, Company B spent much time managing the initiation of treatment for its enrollees. This is no longer the case. Some treatments, however, are still managed from the very beginning. For example, applied behavioral analysis (ABA) is managed closely from the beginning, as the state mandates intensive treatment (up to 40 treatment hours each week) to be approved in blocks of 6-12 months. Health plans manage speech therapy and physical therapy for those with autism, but Company B manages ABA. Before starting ABA, Company B verifies that the member has autism, that the member has been evaluated appropriately for the functional disabilities related to autism, and that the treatment the member is seeking falls within ABA guidelines that are usually set by the state. The mandates from the states usually specify whether autism should be is considered a behavioral health or medical condition.
Since most accounts manage medical inpatient care, Company B also manages behavioral health inpatient care for those plans. In one large plan, Company B does not manage inpatient behavioral health because the plan does not manage inpatient medical services. For this account Company B still conducts quality reviews of the inpatient services; however, it does not do any other utilization review (e.g., concurrent review). Parity has had no other major effects on utilization management of inpatient services.
Company C uses the standard non-qualitative treatment limitations (NQTLs) of prior authorization, concurrent and retrospective review, and case management. States generally set the quantitative limits but do not impose requirements for prior authorization and the use of other NQTLs. These have not changed since the parity law was enacted.
Company C worked with Milliman to conduct a review of several markets and to examine how parity regulations from the CMS might change its work. Milliman determined that Company B met the parity test with regard to NQTLs across two sample markets.
The largest changes stemming from the parity law have been in management of outpatient services. Since implementation of the law, Company D has developed an open-access registration model for outpatient services. Company D assists members with access and referral to services. For example, if an individual calls before receiving a service, Company D will check the person's eligibility and may conduct clinical triage. However, Company D no longer engages in utilization management for routine services. It manages a few psychological outpatient services, but they are not routine or typical.
In place of utilization management for outpatient services, since 2010 Company D has focused on operational review and quality management. It looks for claims that fall outside of normal practice: outliers, multiple visits per week, and other potential patterns of fraud, waste, or abuse. For example, if an individual is receiving treatment for longer than normal given his or her diagnosis, Company D will contact the provider. If the care falls outside of good clinical practice or does not meet medical necessity criteria and the provider continues to offer the treatment, Company D will prospectively deny claims from that provider for treatment of the individual. Because Company D tries to speak with the provider first, there have been relatively few cases where it has prospectively denied claims.
For outpatient care, Company D has replaced most preauthorization with quality management. Before the parity law was implemented, an extensive amount of time was spent reviewing requests for outpatient treatment. Now, almost all time is spent on intensive follow-up reviews of the process and quality of services being provided.
Company D does not conduct concurrent review or retrospective review for routine outpatient services. Concurrent review refers to the practice of checking whether medical necessity criteria continue to be met as the member receives a service. For inpatient services, a concurrent review typically takes place every 2-3 days; for outpatient services it will take place every eight sessions or every 15-20 sessions, depending on the plan. Retrospective review is also conducted. With both concurrent and retrospective review, the claim is paid only if it passes the review. Under quality management, however, Company D will pay a claim as long as the services are covered under the member's benefit package. The review process can be performed even after a claim has been processed. If an outlier is identified, Company D tries to resolve it prospectively with the provider so that treatment will not continue if deemed inappropriate.
Company D requires preauthorization for inpatient services but not for emergency department services. For inpatient care it conducts utilization review of several kinds, including preauthorization, concurrent reviews, and some retrospective reviews. Company D may conduct a peer reviewif an individual does not appear to be making progress with treatment based on information gathered during a concurrent review. In this case, the medical director of Company D speaks with the attending physician about the patient. Peer review has reduced the number of denials because Company D is able to get more complete information about the individual. This process has not changed with implementation of the parity law.
Prior to the parity law there were varying session limits for different types of treatment. These limits were eliminated in response to the parity law, and use of these services has increased slightly since then. Company E anticipated this result. To offset the cost of more encounters, Company E began to manage practice patterns rather than the treatment of individual members. In the earlier system, a provider obtained authorization prior to starting treatment and reauthorization after every 8-10 sessions. Among providers that serve enough of its members, Company E now looks only at the average length of treatment for its members. If the average meets a certain standard, Company E takes a hands-off approach -- eliminating the requirement for reauthorization. If providers do not meet the standard or have patients with extremely long lengths of treatment, Company E may move these providers to a lower tier within their network. Providers in the lower tier do not receive referrals from Company E.
In conjunction with parity, but not necessarily as a result of it, Company E has also established a similar program with facilities. Facilities that meet certain standards -- such as no member complaints and good member follow-up -- still need prior authorization, but they are exempt from concurrent review. This incentivizes facilities to have good outcomes and to partner with Company E.
Company E has reduced its use of authorization and concurrent review through this process, leaving it similar to its associated medical plans. Although Company E has seen a slight increase in utilization because of the parity law, it has been able to reduce costs associated with authorizations through this new approach.
The impact of MHPAEA on care management practices has varied by plan. Company F is moving away from requiring precertification (preauthorization) for all outpatient procedures. Company F instead tries to steer these services toward outlier management. Precertification may be retained for certain disorders or procedures, such as ECT for major depression. Company F has proprietary algorithms for identifying outliers. The program involves outreach calls, primarily to the provider, in an attempt to shape the treatment. If treatment is not progressing appropriately, a utilization management program may be implemented on case-by-case basis to ensure medical necessity; this would happen at around 20 sessions of treatment. (Note that the average outpatient case resolves during 6-8 sessions.) Similarly, health plans with which Company F works typically manage outliers rather than require precertification for medical services that are reoccurring and may continue for long periods (e.g., physical therapy, radiology, or skilled nursing). The health plans also manage some of these services with visit limits, but this is not an option that Company F can utilize because of parity.
Under-utilization can also be a problem because it increases the likelihood of an inpatient stay. For example, if an individual with a severe mental illness like schizophrenia is receiving outpatient visits but no medication management, Company F may call their provider to encourage use of medications.
Precertification is typically required for both behavioral health and medical non-emergent inpatient care. Other care management techniques include concurrent and retrospective reviews. Concurrent review is used only for inpatient care. Retrospective review mostly applies to inpatient care and to out-of-network outpatient care. Inpatient behavioral health providers have an incentive to keep patients longer because they are paid a per-diem rate. These types of reviews are less needed for medical stays because the DRG payment system does not offer more money for an extra day of stay. In most plans, inpatient behavioral health services and inpatient medical services -- at least those not reimbursed through DRGs -- are reviewed with the same frequency through a concurrent review process. DRGs cover most but not all medical/surgical conditions.
For Company G, the parity law has changed how they use preauthorization, concurrent review, and retroactive review.
Before the law almost everything required preauthorization, but parity has stripped behavioral health plans from preauthorization. There are still some services that require preauthorization, but these are generally more specialized services.
For the medical side there has been no change in preauthorization. A challenge is with mental or behavioral disorders that require both physical and behavioral health treatment (e.g., anorexia). The medical field can do more preauthorization and utilization management if needed, but the behavioral health organizations are responsible for these individuals and are limited by the parity law to do more utilization management.
Company G now uses an outlier process where the preauthorization begins after a certain number of visits. Parity allows for clinical exceptions where there is a clinically appropriate reason to try a different treatment.
Company G stated that one challenge with parity is that it does not require behavioral health services to be covered. At times behavioral health services may be excluded for other add-ons. Parity is now a big part of plan design and in considering how plans will incorporate utilization management.
Managing Out-of-Network Care
Company A does not manage out-of-network benefits. If it needed a provider outside of its network, it would negotiate a single-case agreement to purchase the necessary services for the member.
Management of out-of-network care has changed with the implementation of parity. Prior to the law, Company B had several commercial accounts that offered out-of-network options that were not managed. With the implementation of parity, more commercial accounts have needed to offer more out-of-network care to be comparable to physical health benefits. Many more commercial accounts are now managing their out-of-network accounts. Company B uses processes for managing out-of-network care that are similar to those used for in-network care, such as notification, concurrent review, and retrospective review. Retrospective review is most frequently used for out-of-network care. No level of care now requires prior authorization, so Company B instead uses notification.
For Company C certain types of out-of-network providers are problematic, such as wilderness programs and resort-like substance abuse treatment facilities. There is little incentive for these out-of-network providers to cooperate, and they often do not cooperate with retrospective review. Prior to parity, many plans limited behavioral health services to credentialed in-network facilities.
Company D is obligated to meet minimum network access standards, meaning that at least a certain percentage of patients using behavioral health services through Medicaid must use contracted (par) providers. The percentage threshold varies by market. Some states set a threshold and require monitoring of claims received from non-par providers. Company D tries to redirect members to access par providers. In some cases it establishes single-case agreements with a non-par provider, essentially making it a par provider for the sake of one plan member.
Enrollees may access non-par providers directly and may self-refer to care. However, once the provider conducts an initial assessment, the patient would need authorization by Company D to be reimbursed for any further services. Single-case agreements are established if they promote continuity of care. For example, if a new member has been working with a non-par provider, Company D will establish a single-case agreement to maintain continuity of care. Prior authorization is required if an individual seeks treatment outside of the state where he or she has public health insurance.
Company D conducts an ongoing analysis of the need to expand provider options for its members.
Company E was not asked about managing out-of-network services.
Previous to parity, Company F had day limits on out-of-network services. These limits have now been removed. The strategy of most plans is to provide incentives for individuals to receive in-network rather than out-of-network care. They do this by having lower copayments and cost-sharing for in-network care.
With regard to non-quantitative services, health plans have had to move away from prior authorization for out-of-network care. As a result more retrospective review is used instead of prior authorization. This has been a challenge for providers because they want prior authorization to ensure that they will be paid for the services they provide.
Company F conducts a targeted retrospective review of claims for out-of-network services. They examine practice patterns of providers. For example, they may look to see if a certain diagnosis was needed before a treatment was provided to an individual. If Company F finds a procedure that is not acceptable, it typically works with the provider to change things prospectively rather than retrospectively.
There has been more change for outpatient rather than inpatient NQTLs for out-of-network care because of the removal of prior authorization for outpatient services. Many behavioral health inpatient services still maintain prior authorization, because this is comparable to the procedures for physical health services.
The same utilization management techniques for in-network services are used for out-of-network services. The difference is that some contracts do not cover out-of-network benefits. In these cases Company G will inform the provider if he or she calls in with a treatment request.
There may have been a slight increase in the use of out-of-network services; however, Company G did not have any statistics to share.
Demand for Residential or Intensive Outpatient Substance Abuse Care
Company A has not seen an increase in utilization or demand for residential services. With the establishment of parity, customers actually wanted to exclude residential care. They asked Company A if they were mandated to include it or not, and Company A informed them that from a legal perspective they could exclude it if they were including other inpatient services. However, Company A explained to them that it would not be cost effective to exclude residential care. Company A explained that by excluding residential services the customers would be removing part of a continuum of care, and some individuals might need that specific level of care to prevent them from multiple acute inpatient visits that over time cost more than residential services. Company A explained to their customers that it would be unwise to exclude residential services. Customers did some analyses and came to the same conclusion.
Parity has impacted the day limitations with residential services. Residential services were categorized as inpatient services that do not have any day limits. Some customers wanted to compare residential services to SNFs, because SNFs have day limits; however, they could make this comparison based on the parity law because a SNF is not one of the six categories of services that are the basis for comparison between MH and physical health services. Customers needed to classify these services as inpatient services.
Intensive outpatient (IOP) care is slightly different from residential care. It is an intermediate level of care; some customers classified IOP care as an inpatient service and others classified it as an outpatient service. Customers are responsible for disclosing how they are categorizing IOP care so that parity between mental and physical health services can be established.
Company A has not seen an increase in demand or utilization with IOP. For those that treat IOP as an inpatient service, the day limits are excluded. It is a greater struggle to meet the parity requirements when IOP is classified as an outpatient service, because IOP is not a standard outpatient therapy. For example, it is unclear how to establish parity with copayments for IOP programs because individuals will be attending the program 3-5 days per week. It would be costly to patients if they were required to pay a $25 copayment for these visits. Company A's recommendation has been that individuals should be required to pay a copayment for the course of treatment or, if copayment is paid by the visit, the individuals should be required to pay a smaller copayment (e.g., $5 per visit).
There has possibly been a modest increase in the length of stay or number of days these services are provided; however, Company A did not know at the time of the interview how much these figures have changed, if at all.
Company B was not asked about residential treatment and IOPs.
Company C has had no significant increase in the request for residential treatment services.
Especially for out-of-network care, but also to some extent for in-network residential care, individuals making calls to check the coverage of a residential service speak with a clinician to ensure that the client meets medical necessity criteria and the residential service of interest is covered under the member's benefit package. This is to avoid the problem of parents sending their youths to an outdoor leadership residential program (e.g., Outward Bound), and then calling the company and finding out that the residential service is not covered.
Company C has not seen an increase in the utilization of structured outpatient services for substance abuse. It has, however, seen an expansion in the length of treatment. Previously clinicians were seeing individuals 3 days per week, but now they are seeing them 5-7 days per week. Previously structured outpatient programs lasted a total of 10-12 days, but now they are lasting 20-25 days. This increase has persisted even with reviews to ensure that the enrollees meet medical necessity criteria.
Some states have recently expanded the scope of their benefit package to include more behavioral health services. One of Company D's markets recently added substance abuse services, such as intensive outpatient services, to its benefit package in order to more fully comply with the parity law. Another market expanded its CHIP benefits to include more behavioral health services.
Other than the states that have recently started to cover intensive outpatient services and other behavioral health services, Company D has not seen any significant change in the demand for or utilization of residential and intensive outpatient services among public insurance plans.
Company E has seen an increase in the number of 21-26 year olds being admitted to chemical dependency programs. This is due to the PPACA regulation that allows young adults up to the age of 26 to be covered under their parents' insurance plans.
There has not been a significant change in the utilization of residential treatment services. Most plans that Company E works with do not cover residential services. Some plans have tried to compare RTFs to SNFs; however, SNFs are not one of the six areas of coverage defined by HHS. Coverage of residential treatment services has not changed with the implementation of the parity law.
Most plans cover IOP services and did so even before the parity law. Company E has not noticed more people using IOP services. Even with the removal of QTLs the length of IOP programs has not increased significantly to this time. It has, however, allowed for individuals who have a relapse after finishing the program to go through the program again.
An FEHBP that Company E works with is currently experimenting with not managing partial hospitalization and IOPs. In the next couple of years the health plan will evaluate this experimental program.
With Company F, the utilization of residential treatment and intensive outpatient services has not changed since MHPAEA went into effect; however, now more patients seek to use out-of-network facilities. The day limitations for residential treatment have not changed significantly, because even before the implementation of the parity law most plans did not set day limitations for residential treatment.
Recently, Company G has seen more requests for residential treatment. In particular, more individuals are requesting to initiate treatment at the residential level. Company G noted that there have been more licensed and available residential facilities in the state where it works in recent years. The length of stay has not changed notably.
Company G has also seen growth in partial hospitalization IOP services in recent years. In the public sector IOP services are commonly considered outpatient services, whereas in the commercial sector they are frequently classified as inpatient services. IOP is often billed as a daily facility charge or a bundled payment. IOP services are an important part of the treatment continuum, especially for those with chemical dependency.
Management of Prescriptions
Company A does not manage prescriptions for commercial accounts; however, it does manage prescriptions for some public accounts. Nothing has changed in Company A's management of prescriptions for public accounts because public Medicaid accounts do not yet fall under the parity law.
Company B does not manage prescriptions.
Company C does not manage prescriptions. Its associated health plans contract with a pharmacy benefit manager. The manager administers the contract, pays pharmacy claims, establishes networks, and manages prior authorizations. Company C directs providers to the manager when they have issues about access to pharmacies or use of specific drugs.
The states establish formularies for publicly funded plans. If a state has not established a formulary, the health plan will establish a formulary to use.
The health plans with which Company C works have examined the parity of the pharmacy benefits it manages. It found that step-therapy-- covering a medication only after one or more alternatives have been tried without success -- was applied consistently across all drug categories. The health plans also found parity in the pharmacy benefits for psychiatric drugs relative to other drugs.
Company D does not manage prescriptions and has not tried to ensure parity in medication coverage. That task would fall to any PBM firm hired by the plan. Most behavioral health medications are prescribed by primary care providers, who are not within the behavioral health carve-out; thus, Company D would not be well placed to manage their prescribing. Moreover, there might be little gain from managing behavioral health medications -- most health plans cover them in the belief that they are less expensive than counseling.
Company E is not involved with prescription management in any way.
Company F does not typically manage Rx. The responsibility to manage Rx usually remains with the manager for the plan. In the case where Company F is an internal client to a health plan, it has been able to talk with the manager and ensure that the formulary and tiers do not discriminate or are not more restrictive for psychiatric drugs. As a carve-out vendor, Company F provides information to their customers regarding not discriminating in formularies; however, they cannot do more than this.
Before parity, there was a movement to try to limit psychiatric drugs prescribed by primary care providers. With the advent of parity, there is no way to legally enforce these limitations; thus, the movement has ended.
Company G was not asked about managing prescriptions.
Additional Comments About Parity
The overall utilization of services has not increased as significantly as Company A was expecting with the implementation of the parity law.
States dictate the benefit package and limitations of services for public insurance plans. Company B has no say in establishing or changing the benefits it is responsible to cover under public programs.
Company B has noticed that states have been so preoccupied with health reform that parity has not been as emphasized. If the parity law had been established a few years earlier, the results and speed of change would have likely been very different.
With one exception, states are not asking Company B if they meet parity requirements. States appear to be preoccupied with lowering the cost of their share of Medicaid programs and addressing health reform. Rather than ask about parity, states are interested in innovative and more effective ways to manage care and reduce costs.
In one state, Company B is working to improve the managed care system by providing behavioral health homes to those with serious mental illness (SMI). This is different than the normal health homes in that the primary line of service is related to behavioral health and the secondary line of service is related to physical health.
Company C has seen an increase in cost of care for behavioral health services. It is unclear if this increase in cost has come from the changes in benefit design (e.g., cost-sharing and copayments), or the limitations on what utilization management techniques can be used.
As a result of the parity law, psychiatrists can be reimbursed at the same rate as an obstetrics and gynecology physician for using an E&M code. Company C has seen an increase in the use of E&M codes for psychiatric services, possibly because psychiatrists can be reimbursed at a slightly higher rate by using these codes. This has caused some complaints by health plan providers.
A challenge working with health plans, especially the smaller commercial plans, is in keeping up to date on the shared accumulators, members' deductibles and lifetime maximums. Prior to the parity law, Company D had lifetime maximums that applied solely to behavioral health benefits. Now, Company D must use a unified set of maximums, called shared accumulators, in conjunction with members' medical health plans. This has increased the administrative burden of determining whether a claim should be denied based on exceeding a limit.
Company D works with McKesson continually to improve the InterQual criteria. Clinical areas on which they have collaborated include residential services, psychological testing, and ABA for people with autism, among others.
Company D conducts internal reviews to ensure compliance with parity regulations. They are evaluated externally by state agencies such as a state's Department of Managed Care.
Company E has seen an increase in the length of stay and in the number of admissions. There has also been an increasing number of outpatient visits. Most people are receiving fewer than eight sessions of outpatient therapy, and the distribution of the length of treatment is getting wider. In general, Company E noticed that it takes longer for the outpatient community to make benefit changes than the inpatient community.
It is a challenge to figure out what the regulations mean. Many providers disagree on the various interpretations of the law.
Parity still does not cover everyone. It does not apply to small groups and individual policies. Some providers have misunderstood parity, thinking that it gives everyone unlimited behavioral health services. This is not the case.
There are a small number of plans that decided to drop all behavioral health services because of the parity regulations. Other plans have experimented with excluding certain diagnoses from the diseases they cover.
Company E has had ample discussion on NQTLs, yet some questions still remain. It is unclear whether it is necessary to totally harmonize MBHO and medical contracts with facilities and providers. Some advocates have also suggested that parity has not yet been established between the level of network access within the field of behavioral health and the level of network access within the rest of the medical field. Company E uses the exact same standards for access to facilities, professionals, and other programs that the medical part of the health plan uses. This strategy should insure similar access to behavioral health and medical professionals. It is also unclear how to reconcile different payment strategies for inpatient services, where payment is based on DRGs for medical services and per-diem rates for behavioral health services. Even though the parity law was designed to establish parity across behavioral health and medical insurance benefits, providers have also tried to use the law to establish parity in how much they are reimbursed, which did not appear to be the original intent of the law.
Company F has seen an overall increase in the utilization of behavioral health services in the last few years, although the level has begun to plateau. In addition to changes in limitations and management of behavioral health services, more plans in Company F's state where Company F works started to cover substance abuse services because of the parity law.
The PPACA has also caused increases in the utilization of behavioral health care. By eliminating preexisting condition clauses and extending coverage to more adolescents and young adults, it has increased demand for all services. Use of certain services has risen dramatically, such as treatment for chemical dependence among adolescents and young adults.
Company F has not received any complaints that the behavioral health services it offers are not comparable to the physical health benefits of its members. They do receive requests from members regarding the behavioral health medical necessity criteria.
There appears to be more advocacy regarding parity within the last 6 months than during the whole year after the parity law was passed. A small minority of providers has begun to see members multiple times per week with no clear treatment plan or goals. This pattern of practice was more frequent prior to care management. Company F advises providers that open-access to care does not eliminate the need to monitor its quality. Treatment goals and progress are still required for continued payment.
Self-funded employer plans have multiple medical vendors, some of which are not forthcoming with information to allow parity analysis. Some of those vendors also have their own behavioral health business line and may be attempting to steer the customer to their own services. In cases where information has not been shared, Company G assumes a typical benefit package when helping the self-funded plan to ensure that the parity regulations are met.
"Apples-to-apples" comparisons between behavioral health and medical services are sometimes difficult. For example, there is no medical/surgical equivalent to intensive outpatient services or partial hospitalization.
Autism presents special difficulties for several reasons. There is no agreement on whether to treat it as a behavioral health condition, a birth defect, or a typical medical condition. It has no analogs in medical care, making parity comparisons difficult.
States have been active in regulating insurance coverage for autism. Most states with mandates have annual dollar limits. In order to avoid contravening MHPAEA, some of the states designate autism as a medical condition or a birth defect. Others seem to have paid no attention to MHPHEA at all, and it is unclear if MHPAEA was contemplated. Most of the states have the autism applied behavior analysis mandates as standalone mandates. Notably, these rules do assign autism to the same category as SMI or biologically based mental illness; instead, they issue a standalone mandate. Dollar caps, when they exist, are relatively high (e.g., $36,000, $50,000, $70,000). The laws passed are usually based on the Autism Speaks model. New Jersey is the only state that precludes a dollar limit for any plan that covers autism treatment if the plan is subject to federal parity; for plans not subject to federal parity, the plans may enforce the dollar cap.
Soon after the regulations implementing MHPAEA were released, Company G worked with customer plans to check their compliance with the law. This process took many hours of work for each customer. Now, a few years later, the issue of parity rarely surfaces except with respect to autism.
The parity analyses were not conducted for each plan that Company G works with. A single large customer can have more than 300 separate plans (certificates). Analyzing parity for each one was not possible. The typical approach was to use the customer's largest or most typical plan. The result would apply broadly, because most plans from a particular customer had similar characteristics.