
U.S. Department of Health and Human Services
Nursing Home Selection: How Do Consumers Choose?
Volume I: Findings from Focus Groups of Consumers and Information Intermediaries
Lisa R. Shugarman and Julie A. Brown
RAND Corporation
December 2006
This report was prepared under contract #HHS-100-03-0023 between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and the RAND Corporation. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the ASPE Project Officer, Linda Bergofsky, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. Her e-mail addresses is: Linda.Bergofsky@hhs.gov.
The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
TABLE OF CONTENTS
I. INTRODUCTION
II. BACKGROUND AND CONCEPTUAL FRAMEWORK
A. Background
B. Conceptual Framework for Consumer Decision-Making
III. APPROACH AND METHODS
A. Summary of Focus Group Participation Characteristics
B. Themes Organized by Conceptual Framework
C. Themes that Fall Outside of Conceptual Framework
V. SUMMARY
VII. REFERENCES
APPENDICES
APPENDIX A: Focus Group Methods
APPENDIX B: Study Strengths and Limitations
APPENDIX C: Focus Group Protocols
APPENDIX D: Characteristics of Information Intermediaries
APPENDIX E: Characteristics of Consumers
APPENDIX F: Key Characteristics Informing Nursing Home Selection
EXECUTIVE SUMMARY
Introduction
More than a million elders enter a nursing facility each year, yet we know little about how consumers of skilled and long-term nursing care select the facility to which they or their loved ones will be admitted. Many members of the Baby Boomer generation are currently faced with long-term care (LTC) decisions for their parents, and those on the leading edge of the generation will soon be dealing with these issues themselves. The aging of the population points to consumers increasing need for useful and reliable information about their health and social care options, including nursing homes.
The purpose of this study, commissioned by the Office of the Assistant Secretary for Planning and Evaluation, Department of Health and Human Services, was to use qualitative methods to: (1) systematically review the existence and accessibility of Internet-based resources intended to support the decision to enter a nursing facility and select the appropriate facility for ones needs and preferences; (2) examine how consumers select a nursing home; (3) explore if and how existing information resources are used in the decision-making process; and (4) identify gaps in needed information resources.
Approach and Methods
This study was conducted in two parts. To identify and examine the accessibility of consumer information on nursing home selection, we conducted an Internet search for information resources on nursing home selection and examined the accessibility of the sites and the information they provided. We provided the findings from the web content review in Volume II of this report. To learn about the factors that influenced decisions about selecting a nursing home and the use of information resources, we conducted a series of focus groups among individuals who had experienced short-stays in nursing homes, individuals who had placed family members in LTC, and information intermediaries (hospital discharge planners and community-based case managers), whose role was to assist people in finding LTC for a family member. We present the findings from these focus groups here.
Focus groups were conducted in four states. The locations for these focus groups were Santa Monica, California; Des Moines, Iowa; Miami, Florida; and Arlington, Virginia. Six focus groups were conducted: two with former (Medicare-paid) short-stay nursing home residents, two with families of current nursing home residents, one with hospital discharge planners, and one with community-based case managers. The formulation of focus group questions was guided by a conceptual framework that assumes that the strategies consumers employ in choosing among facilities are expected to depend on many factors, including characteristics of the decision problem and the decision-maker, and the context in which the decision is made. The focus groups were conducted according to standard, well-defined methods designed to elicit participants views and experiences.
Findings from Consumer and Information Intermediary Focus Groups
The strategies consumers employ (e.g., how consumers actually come to a decision) in choosing among nursing facilities depend on many factors, including characteristics of the decision problem (e.g., number of choices and time available to make a decision), the decision-maker (e.g., knowledge level and approach to seeking information), and the social context in which the decision is made (e.g., short vs. long-stay and social norms around caring for older adults). These major types of factors can affect how readily one can access and process information designed to support the decision-making process. We organize the findings in this report around these three main factors.
The Decision Context
Timeframes: Consumers who participated in the focus groups, particularly those seeking short-stay placements, perceived that the timeframe for making decisions regarding nursing homes was too short, often only a day or two. Hospital discharge planners shared that the process of assisting patients with after-care planning begins within a day of admission, but that patients and their families often avoid facing these decisions until a day or two before discharge, possibly due to denial. The discharge planners did acknowledge that the short timeframes patients or their families had for these decisions was sometimes necessitated by a change in the patients condition over the course of the hospital stay.
Perception of Choice: Most consumers reported some choice of facilities, but some perceived their choices as narrow or constrained by factors such as managed care requirements or geographical location (specifically proximity to their residence, family, or referring physician).
Provision of Information: Information intermediaries support consumers throughout the nursing home selection process in a variety of ways. Most notably, participating discharge planners and community-based case managers mentioned that they provide a list of facilities to consumers to support them in the decision-making process. Information intermediaries also provide pamphlets, booklets, or magazines that include information about local LTC resources. Information intermediaries indicated that they are often unwilling to or may even be prohibited from making specific facility recommendations. This unwillingness or inability to share information may be a barrier to informed decision-making by the consumer. In some cases, discharge planners and case managers were unwilling to provide specific recommendations because they did not want to be subject to the anger or disappointment of patients/families who may be dissatisfied with the recommendation.
Personal Characteristics of the Decision-Makers
Knowledge Level: Consumers generally expressed a lack of knowledge about nursing homes, LTC, and technical quality issues. Often what they considered to be a high quality facility was one that looked nice, smelled nice, and had nice amenities, rather than one that provided good quality care. In general, consumers (residents as well as family members) were also unaware of the costs of LTC.
Information Gathering: Consumers in the focus groups reported using some of the resources provided by information intermediaries and supplemented what they received and used from the intermediaries with other sources of information they identified on their own. For short-stay residents, the list of facilities provided by the hospital discharge planner was generally the primary source of information. Both short-stay residents and families of LTC residents also relied heavily on prior personal experience and the experiences of friends and family to help establish a list of facilities to consider or to narrow down a pre-existing list to those worth considering. Visits to a small number of facilities were also a primary source of information used in decision-making. Written materials, other than lists generated by information intermediaries were generally not used. In addition, few consumers mentioned using the Internet and those who did, used it primarily to develop a list of local facilities for their consideration.
Perceived Utility of the Internet by Consumers: Hospitalized patients and their family members were generally unable to access the Internet in a timely fashion to help aid their selection of short-stay care. Few consumers participating in the focus groups were aware of the Medicare.gov site or Nursing Home Compare. Those who did use these Internet sites reported that they were difficult to navigate and lacked up-to-date or timely information items of importance in the nursing home selection process.
Role of Information Intermediaries: Short-stay residents reported relying heavily on hospital discharge planners for information on nursing homes in their area, usually by providing lists of facilities in the local area. In some cases, these professionals were their only resource. Few former residents or family members reported getting support or information from their or their loved ones physician but several indicated that they would have liked greater involvement from their physician in providing information. Some discharge planners also felt that the physician should play a greater role in the process of searching for and selecting a facility. One discharge planner stated that more active involvement by the physician in preparing the family for the nursing home stay might make the familys decision-making process easier.
Priorities for Nursing Home Selection: The single most frequently cited factor in the selection of a facility was location. This finding held for both skilled nursing stays and long-term custodial stays. While most were concerned with the facility being located close to the residents or familys home, some sought proximity to the hospital or to their referring physician. The second most common priority for nursing home care was that the facility staff took good care of the residents, information most often assessed by a visual inspection of a facility. Short-stay residents identified maintaining an existing relationship with a primary care physician as a priority in the selection of a facility, although this was not a priority for family members.
What Consumers Would Have Done Differently: In general, consumers expressed the belief that they had selected the best care option given the timeframe, information, and options available to support decision-making. A few consumers who articulated the desire to approach facility selection in a different manner wanted more information about specific facilities or options for care.
Social Context of Decision-Making
Social Pressures/Social Norms: In the case of placement of family members in LTC, a sense of stigma that care could not be provided in the familys residence was an important barrier to making a timely decision to place a loved one in a nursing facility. Often this barrier resulted in the decision being made under severe time pressures due to the emergent nature of the loved ones condition.
Effects of Differences in Type of Placement: Hospital patients always had the assistance of a discharge planner in preparing them for their discharge to a skilled nursing or rehabilitation facility. Former short-stay residents relied substantially on the lists provided by the discharge planner in helping them select a facility. Similar assistance was rarely available to families seeking a long-term custodial care facility for a loved one and who typically sought admission from the community rather than the hospital. Also, participants perceived that placements are easier to find when the placement is expected to be short-term and the patient is expected to return home.
Role of Culture or Language in Decision-Making: Consumers and information intermediaries identified culture, language, and ethnicity as factors influencing nursing home selection. In particular, they pointed out that information materials are seldom available in a range of languages. Participants also perceived the role culture can play in determining attitudinal norms toward the concept of LTC as a barrier to the selection process (both the process for deciding if placement is appropriate and the choice of a facility once the placement decision is made). Thus, facility support of a specific language and/or culture becomes the primary determinants in facility selection for some consumers.
Family Dynamics: The role of family members and the dynamics of family interaction during decision-making have a bearing on the social context in which selection occurs. Short-stay residents were unanimous in identifying the positive role or influence of family in decision-making, while families of current nursing home residents described experiences in which family dynamics supported or hindered decision-making.
Summary
Consumers generally do not avail themselves of the multitude of information resources available to them in the process of selecting a nursing facility. Even given the wide variety of information sources available either in print, by phone, or on the Internet, many of the focus group participants perceived that the information they needed or wanted was not available to them when they needed it. Several people mentioned the inability to find a particular type of information that is already available but about which they were not aware, such as facility inspection reports. Denial or lack of understanding about a loved ones condition and the circumstances around hospital discharge often resulted in little time to select a facility, making it difficult to seek out or use what formal information sources are available. In selecting a facility, consumers are most likely to rely on lists of facilities that provide general information such as location, supplemented by word of mouth and more easily observed characteristics of the facility that reflect a sense of quality of life. In contrast, consumers were less concerned with the clinical, more technical factors that influence quality of care.
Consumers based their selection of facility on information often not available on Internet-based resources. Most of the sites we reviewed as part of our content review did not include characteristics that were cited as important selection criteria for many consumers (e.g., information on costs and what activities were available in the facility). Both consumers and information intermediaries found that many of the available Internet resources, including Nursing Home Compare, were not user-friendly, and intermediaries were reluctant to recommend the sites to consumers. Most sites are not available in languages other than English, which some consumers and intermediaries cited as an important barrier to their use.
We propose at the end of this report a set of actionable items and areas for future research that may lead to information resources that better meet consumers needs and facilitate greater access to information resources for those seeking a nursing home.
I. INTRODUCTION
More than a million elders enter a nursing facility each year, yet little is known about how consumers of skilled and long-term nursing care select the facility to which they or their loved ones will be admitted. Many members of the Baby Boomer generation are currently faced with long-term care (LTC) decisions for their parents, and those on the leading edge of the generation will soon be dealing with these issues themselves. The aging of the population points to consumers increasing need for useful and reliable information about their health and social care options, including nursing homes. Numerous governmental and non-governmental agencies make information resources available to the public, presumably to support the decision-making process. While these resources are widely available through the Internet, by phone, and in print, little is known about whether consumers use them to support the decision-making process. Such information might help in selecting among LTC options and in distinguishing among different providers of those options. However, in the absence of careful evaluation, considerable skepticism exists about the ability of elders and their families to understand and translate that information into a decision, and about whether the available information is relevant to the decision-making process.
The purpose of this effort was to use qualitative methods to: (1) systematically review Internet-based resources (created by government and non-government entities and nationally relevant or state-specific) intended to inform the decision to enter a nursing facility and select the appropriate facility for ones needs and preferences; (2) examine how consumers select a nursing home; (3) explore if and how existing information resources are used in the decision-making process; and (4) identify gaps in needed information resources. We present the results of the focus group findings here. The findings from the Internet content review are presented in a separate volume (Shugarman and Garland 2006). Section II provides a discussion of the conceptual framework that organized the focus group questions and shapes the findings as well. Section III summarizes the methods we used and Section IV presents our focus group findings. We summarize our findings in Section V and then report a set of actionable items and areas for future research that may facilitate greater access to information resources for consumers seeking a nursing home in Section VI.
II. BACKGROUND AND CONCEPTUAL FRAMEWORK
A. Background
The Increasing Need for LTC. Demographic trends portend a major increase in demand for LTC. The American population is growing older: those ages 65 and over account for 12 percent of the total population now and will account for 20 percent by 2030, when the entire Baby Boom cohort -- that is, those born before 1960 -- will have entered old age. Today, persons over age 85 are the fastest growing segment of the aged population. Persons turning 65 today can expect an average of 5.3 years of dysfunction characterized by acute or chronic illnesses (Tennstedt 2001).
Nearly one-quarter (22.9 percent) of Americans aged 65 and over need some form of LTC. The most dependent of these may require institutional care. In 1999, about 1.6 million people received care in approximately 18,000 nursing facilities (Jones 2002). According to the National Nursing Home Survey, 43 out of every 1,000 individuals 65 and over resided in one of approximately 18,000 nursing facilities for at least part of 1999 (Federal Interagency Forum on Aging-Related Statistics 2004). This population has significant care needs. Approximately 48 percent of nursing home residents have dementia. Eighty-three percent are extremely impaired, needing help with three or more activities of daily living, such as bathing, eating, using a toilet, dressing, mobility, and transferring to a bed or a chair. Another 14 percent need help with at least one or two activities of daily living (Jones 2002).
Although a relatively small proportion of the population is in a nursing home at any given time, the proportion that will enter a nursing home at some point of their lives is high: an estimated 46 percent of individuals 65 and older (Spillman and Lubitz 2002). Improved health of the aged population has increased life expectancy and with that, increased the length of time that older adults may spend in a nursing facility (Laditka 1998).
Currently, federal and state governments are the largest single payer of nursing home care; the primary payer for over 73 percent of all nursing home discharges was either Medicare or Medicaid in 1998 (Jones 2002). Not surprisingly, numerous information sources have been developed by government agencies to assist consumers in selecting LTC providers. These include how-to guides for selecting a facility, facility locator databases/directories, miscellaneous educational efforts, lists of the types of LTC resources in a particular location (other than or in addition to nursing facilities), and information on quality (Castle and Lowe 2005). Most prominent are quality report cards. Quality information reports for nursing homes can range from the reporting of citations and health code violations to the reporting of quality indicators.
Initiatives to Help with Decisions. In November 2001, the U.S. Department of Health and Human Services implemented the Nursing Home Quality Initiative (NHQI). The NHQI is a broad-based initiative that includes the Centers for Medicare and Medicaid Services (CMSs) continuing regulatory and enforcement systems, new and improved consumer information, community-based nursing home quality improvement programs, and partnerships and collaborative efforts to promote awareness and support. As part of these efforts, CMS adopted a new set of nursing home quality measures, which included, for long-stay residents, the percentage of residents with urinary tract infections, pain, pressure sores, or physical restraints; and, for short-stay residents, the percentage with delirium, pain, and pressure sores.
CMS is promoting consumers use of nursing home quality measures through an integrated communications campaign that includes the publication of facility-level quality measures on the Nursing Home Compare website (http://www.Medicare.gov) (CMS 2005), as well as advertisements and other outreach (information is also available by phone at 1-800-MEDICARE). The new quality information allows for comparisons across facilities and is designed to be used with other types of information, such as location and price, which may affect nursing home placement decisions. The main impetus for reporting quality comes from the expectation that publicizing quality performance will enable consumers to make informed choices and, thus, encourage nursing homes to compete on the basis of quality. The NHQI was implemented in six pilot states in April 2002 and nationally in November 2002.
With its focus on reporting comparative health outcomes data, the NHQI represents a sea change in quality improvement strategies in this sector. Although public reporting of quality information has been used in the acute care sector -- with mixed results -- for more than a decade, the strategy has not been used until recently in the long-term and post-acute care settings (Marshall, Shekelle et al. 2000).
Assessing the Impact of Decision Aids. Efforts to assess the impact of the NHQI have so far yielded mixed results. For example, an early analysis of the six state NHQI pilot found that, during the pilot, calls to 1-800-MEDICARE for nursing home information more than doubled, visits to the Medicare.gov site for nursing home quality information in the six pilot states increased tenfold, and users of the online quality information were highly satisfied (CMS 2002). However, anecdotal reports from nursing home providers suggest little consumer awareness of the site (Duff 2002; Johnson 2002; Thompson Corporation 2002). A separate report reflects this mixed picture -- generally positive in its comments about the six state pilot but characterizing the initial consumer response received by state LTC ombudsmen as almost nothing (Infeld 2003).
Despite the considerable effort of CMS and similar efforts by state agencies and non-governmental organizations to disseminate LTC information, little evidence exists about the actual day-to-day utility of these sites for consumers. A recent national survey conducted by the Kaiser Family Foundation suggests that nearly one-third of all respondents would not consult information from government agencies on the Internet in support of their decisions about nursing home care (Kaiser Family Foundation 2005). However, independent evaluation of the sister initiative to the NHQI, the Home Health Quality Initiative revealed some information about the utility of web-based provider information for selecting LTC providers. A test of a prototype Home Health Compare website for CMS found that both caregivers and health professionals responded positively to the prototype website and, more generally, to the notion of providing information on a wide range of quality measures, although the understanding and utility of the websites contents and format varied greatly (BearingPoint Inc. 2003). Nevertheless, consumer use of information resources may differ between those selecting among home health providers and those selecting among nursing home providers.
B. Conceptual Framework for Consumer Decision-Making
Much of our understanding of the effects of quality reporting on provider selection comes from acute care, particularly around the selection of health plans. One important assumption behind quality reporting is that consumers and large purchasers of care will value, understand, and develop the ability to use the information provided to select providers/plans. However, in the LTC sector, the federal and state governments are the primary payers (Levit, Smith et al. 2003), and the Federal Government is still in the early stages of designing reimbursement systems predicated on the basis of clinical performance and value. Thus, the utility of the quality information reported for selecting LTC providers is generally found at the consumer level and not the purchaser level.
This reliance on individual consumers makes understanding their decisions and the manner in which they access and process available information all the more important. Once again, consumer decision-making in acute care can give only incomplete insight into LTC decision-making. For example, RANDs work with CAHPS® has found that many consumers will consider plan performance information when it is available, but the empirical evidence is mixed about how they use it and its relative importance in their decision-making (Scanlon, Chernew et al. 1997; Marshall, Shekelle et al. 2000). With some exceptions (Mukamel and Mushlin 1998; Spranca, Kanouse et al. 2000; Chernew, Gowrisankaran et al. 2001; Scanlon, Chernew et al. 2002), studies have generally shown that publicly reported information has little effect on consumers choice of health plans, hospitals, or specialists, and that publicizing quality ratings has little effect on hospital occupancy rates, market share, or price. When making health plan choices, consumers seem to give a lower priority to considerations of quality and service than to the scope and generosity of coverage, provider choice, and premium costs (Sainfort and Booske 1996; Robinson and Brodie 1997; Tumlinson, Bottigheimer et al. 1997; Chernew and Scanlon 1998). However, the frequency of use and importance of plan performance information tends to increase as consumers are exposed to and learn how to interpret it (Sainfort and Booske 1996). It is not clear whether consumers might increase their use of such information when facing the potentially more long-range and more extended periods of service associated with LTC, in general, and nursing facility care, in particular.
Understanding how consumers make LTC decisions and which methods they apply in this decision-making process is necessary to understand whether and how they utilize available information resources and how to improve these resources. In our framework, the consumer is the person who makes the decision or who supports the decision-making process; this category includes the patients/residents themselves, spouses, children, or other informal caregivers. Health care professionals such as physicians, social workers, or hospital discharge planners are also consumers of such information; however, in this study, we refer to them as information intermediaries and focus on the patients, their families, and others as the consumers, as they are ultimately using the information they gather to make a placement decision.
The strategies consumers employ (e.g., how consumers actually come to a decision) in choosing among nursing facilities depend on many factors, including characteristics of the decision problem (e.g., number of choices, time available to make a decision, etc.), the decision-maker (e.g., knowledge level, etc.), and the context in which the decision is made (e.g., short vs. long-stay, social norms around caring for older adults, etc.). Figure 1 illustrates the three major classes of factors that influence the choice of decision strategy. These major types of factors can affect the availability, accessibility, processability, and perceived benefits of various decision strategies (Payne, Bettman et al. 1993, p.4). We used this framework to identify important variables in the decision-making process and assist the development of the focus group discussion guides in the current inquiry.
| FIGURE 1. Conceptual Framework for Decision-Making |
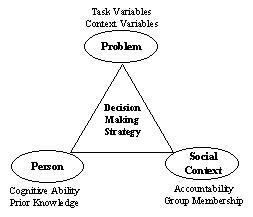 |
| SOURCE: Payne, Bettman, and Johnson (1993). |
Characteristics of the Decision Problem: The characteristics of the decision problem include the complexity of the task and context effects. Examples of increased task complexity include large numbers of alternatives to select from, many attributes to evaluate (e.g., quality items), a short timeframe in which to make a decision, and information that is not displayed in a manner that is easily accessible to the target audience. Many of the characteristics of the decision problem in selecting a facility are fixed; for example, the timeframe in which the decision is made is not necessarily fixed, but it is typically very short for most people. More than half of all nursing facility admissions come from the hospital (Jones 2002; Komisar 2002), and the nature of the discharge planning process from the hospital does not afford the consumer much time to make a decision about which provider to select. However, in some cases, the decision to move a loved one into a facility can be made over weeks or even months.
In order for consumers to select a decision-making strategy, they must first perceive they have a choice in the matter. Given that the choice of provider is generally limited to those who are located in close proximity to the consumers residence, we can assume that the number of alternatives available to a single individual is fixed. However, certain limiting factors, such as lack of bed availability in a facility located in the local area will curtail the ability of a consumer to make a decision.
Characteristics of the Person (decision-maker): Assuming that the supply of providers in the local area is sufficient and given that many of the characteristics of the decision problem are fixed, the characteristics of the decision-maker will likely have the strongest influence on the selection of decision strategy (Payne, Bettman et al. 1993). Consumers with prior experience in selecting a provider may have a much easier time in the process than those who are unfamiliar with the services that are available or the types of care appropriate for their loved ones. Additionally, the decision-making process can be very demanding if one does not have the cognitive capacity to understand the information presented. Time pressures can exacerbate these challenges. In such cases, consumers may simplify the decision process by choosing to ignore the quality information available and turn to other resources such as friends, family, or a provider to help them select a provider. Those who do choose to access the quality information might supplement that information with other resources as well, depending on how confident they feel in interpreting the information.
Characteristics of the Social Context: Finally, the social context in which the decision is made can influence the decision-making strategy selected. For example, a long-stay nursing facility admission may warrant a more considered decision strategy than one for a post-acute stay. The former is very often a permanent placement while the latter is more often temporary.
Given the ways in which nursing home information on the web has been designed and implemented, public and private entity priorities for this design will dictate in part how the information is used in the selection process. For example, given that the numbers of facilities available in a particular region are generally unchanging, the utility of the information will be affected by how it is displayed. High-level information can make the websites very accessible but may not provide enough information to make an accurate/appropriate decision. More detailed quality information might limit accessibility to some but have a large benefit for those who use it. The information must also be accessible at the time and place it is needed. Furthermore, consumers need to be receptive to the information, which may include having a perceived need for the information, knowing that the information is available, trusting its accuracy and objectivity, and viewing it as relevant to their unique health status or health care needs. A deficiency in any of these conditions is likely to diminish the influence of the nursing home resources (Internet or otherwise) on facility choice.
III. APPROACH AND METHODS
The primary task of this study was to learn how individuals faced with the need to select a nursing facility for themselves, a loved one, or a person in their professional care make that selection. Our interest was in identifying the factors considered and the processes used to make these decisions. To gather such information, we interviewed six small groups of individuals -- four groups comprising consumers (two groups of former nursing home residents and two groups of individuals who had selected or helped with the selection of nursing homes for a family member) and two groups comprising information intermediaries (one group each comprising hospital discharge planners and community-based case managers) -- in four selected states using the qualitative research technique of focus groups.
Qualitative research techniques in general, and focus groups in particular, are a common method used to explore topics, issues, or experiences that are not well-understood (Margan and Scannel 1998). Like all research techniques, focus group research is conducted using standard practices. The procedures we used to conduct our six focus groups are described in detail in Appendix A and briefly described below.
The focus groups were conducted using a standardized topic guide, which contained the issues or topics to be discussed in each focus group. These topics were designed to focus the group discussion on the factors that inform nursing home selection and the process and resources used by consumers and information intermediaries. To compare the information shared in each group, the topic guide contained a set of common topics for discussion in all groups (such as the information resources participants were aware of or consulted) as well as topics unique to each of the three populations (former residents, family members of residents, and information intermediaries). The topic guides for each group can be found in Appendix C.
IV. RESULTS AND FINDINGS
A. Summary of Focus Group Participant Characteristics
The two former resident focus groups included a total of 15 participants. The participants were predominantly female (66 percent), Medicare beneficiaries (66 percent), and White (66 percent), and had some college experience but not a four-year degree (53 percent). Another dominant characteristic of participants was that 93 percent of them had help in selecting their former nursing home. This help came from multiple sources. Reported helpers included spouse or family (40 percent of participants), information intermediaries (40 percent), friends (33 percent), and doctors (20 percent).
Seventeen family members of nursing home residents participated in the two family focus groups. Each of the family members had played a role in the selection of their loved ones nursing home (24 percent were solely responsible for facility selection). Family members reflected an even mix of gender (53 percent female, 47 percent male) and education (24 percent high school, 29 percent some college, 18 percent four-year college degree, 29 percent more than four-year degree), but were predominantly White (71 percent), and their family member in a nursing home was most likely to be a Medicare beneficiary (88 percent). About one-third of family members had a loved one in a nursing facility for which Medicare was the primary payor of the nursing home stay. The majority of nursing home stays were paid for by other sources including private pay. Another dominant characteristic was frequency of visits to their family member (76 percent visited one or more times per week). In addition, 76 percent of participants had help in selecting their family members nursing home. As with the former resident focus groups, help came from multiple sources. Reported helpers included spouse or family members (47 percent of participants), the nursing home resident him or herself (24 percent), information intermediaries (12 percent), doctors (6 percent) and pastors (6 percent).
The hospital-based discharge planner focus group had 11 participants. The discharge planners were female (100 percent), had five or more years of experience in their current position (82 percent), and were fairly split in the number of times per week they provided assistance with placement in a nursing home, rehab facility, or skilled nursing facility (SNF) (45 percent, ten or fewer times; 55 percent, 11 or more times).
The community-based case managers focus group included eight participants. As with discharge planners, the case managers were all female (100 percent). Participants were evenly divided by years of experience in their current position (50 percent up to five years, 50 percent five or more years). Participants provided assistance with placement in a nursing home, rehab facility, or SNF less often than discharge planners (63 percent, less than five times per week; 37 percent, 5-10 times per week).
We have provided a summary tabulation of the characteristics of focus group participants in Appendix D and Appendix E.
B. Themes Organized by Conceptual Framework
In the following sections we provide a summary of the key points regarding the decision-making approaches of consumers using the conceptual framework described previously as an organizational guide. In addition, we provide samples of some of the most relevant discussion to supplement our findings.
B.1. Task and Context (Decision Problem) Effects
B.1.a. Timeframe for Making Decision
Many consumer group participants described having had only one day or just a few days to select a facility. The short-stay residents typically reported having had one or two days to make a decision. One resident cited having had just a few hours to make a decision before being discharged. Discharge planners had a slightly different perspective on the timeframe in which a decision needed to be made. Whereas short-stay residents perceived they had a matter of hours to make a decision, most of the discharge planners described beginning the discharge planning process within 24 hours of hospital admission.
We do a screening from, on day one. So weve already established where the patient comes from, whats the situation, how sick -- and we anticipate [patient needs at discharge]. (Discharge Planner)
However, discharge planners expressed the belief that patients and their families spent much of the time during the hospital stay coming to terms with, the realization that they or their loved one might need LTC and trying to understand their options. Thus, for the family and patient, the shorter timeframe they reported for making a nursing home selection might reflect the time between notification of planned discharge date and actual discharge, rather than the total time they spent processing what was happening and exploring options prior to making a decision. Discharge planners also cited the vagaries of patients conditions and the discharge notification system as factors, which complicate the decision-making process and affect the time available for families and patients to make a decision. Physicians may make a decision to discharge the same day, giving the family little time to prepare. Although the discharge planner will sometimes try to keep the patient for at least one more night so the family can investigate their options and make a decision, insurance coverage might also dictate the time available to make the decision. One discharge planner shared that, in her experience, managed care plans tended to allow little time for decision-making: often just a few hours before discharge.
Among short-stay residents, only a small number reported having more than a couple days to make a decision.
I guess it was a week or so? They said, were going to move you to the rehab center or a nursing home. (Short-Stay Resident)
[We were given the weekend to make a decision.] We only had time to look at a couple of places. (Short-Stay Resident)
Some participants who had had elective surgeries reported having discussed in advance of their surgery with their physician the need for rehabilitation in a SNF following their hospital stay and having been provided with a list of facilities to consider prior to hospital admission. These pre-admission surgical orientations tended to occur several weeks to a month before the hospital stay, affording these patients much more time to consider their options.
The most significant differences in time available for making a decision were the result of the type of placement needed (e.g., skilled nursing/rehab vs. long-term/custodial). While both short-stay residents and discharge planners reported having no more than a few days to make a decision regarding placement following a hospital discharge, family members and community-based case managers seeking LTC cited longer timeframes to select a nursing facility; sometimes as much as several months or years elapsed before a decision was made.
We had probably I would say a couple of months. (Family Member)
About six months from the time my one aunt was put in the hospital and we knew the only place to put her was this [nursing facility]. She stayed in the hospital quite awhile. (Family Member)
During this time period, families would often explore their options while attempting to care for the loved one at home before concluding that a nursing home was needed. Once the decision was made to pursue a nursing home-level of care, family members usually spent between a few days and a month searching for the right facility for their loved one.
B.1.b. Perception of Choice
Most short-stay residents and informal caregivers recognized that they had a choice in their selection of nursing homes, although some described their choices in terms such as slim, or a few.
One focus group participant spoke of moving his mother from her home state to the home of a family member in another state due to the lack of reasonable facilities available near her home, until he finally moved her to a facility near his home.
In many cases, particularly for the short-stay residents, their choices were presented to them in the form of a list of facilities from which they could select the facility to which they or their family member would be moved. Few consumers indicated they were given no choices.
In the case of one short-stay resident, the facility that was his first choice did not have a bed available when he needed to be placed, so he selected another. He stayed in this second facility for only a couple of days until a bed opened up in the first facility and he was able to move.
One short-stay resident, who had been in the same SNF on three separate occasions prior to her most recent stay, returned to the same facility for her fourth stay in part because she believed no other choices were available. She indicated that she wished she had known of other options, as she had become increasingly unhappy with this facility over her multiple stays, and during her last stay, reported that she received poor care. In this case, her decision was based on a perception that she had no other choices, rather than on prior knowledge.
I think I figured you took what you got. Once youve made the choice everything was supposed to be properly equipped and such. (Short-Stay Resident)
A family member echoed the perception that there were no choices for her as she was selecting a facility for her mother, citing time constraints as impeding the ability to have reasonable choices:
Sometimes you just dont have choices. Everything was so quick. We had to make all decisions by the time the hospital said she has to move on. (Family Member)
In another example, a family member who was making arrangements for two aging relatives in another state indicated that her choices were really limited by her aunts preferences. The rural town in which they resided had only one facility, and because they wished to remain in their home town, she viewed this facility as the only option.
However, lack of choice is not always regarded negatively. While the one participant who had stayed in the same facility four times expressed frustration at her perceived lack of choice, the participant who was seeking a placement for her aunts was quite comfortable with the ultimate placement, even given the lack of real choice in her situation.
B.1.c. What Information is Available (what do information intermediaries provide?)
Information intermediaries provide information to consumers in a variety of ways. Discharge planners and community-based case managers who participated in the focus groups most often mentioned that they provide a list of facilities to consumers to support them in the decision-making process. Sometimes this list is customized; other times, it is generic and contains information about all facilities within the local area. For patients in a managed care plan, the list is often abbreviated, only containing those facilities the discharge planner knows to be part of the members plan. Some participants mentioned receiving lists that were generated on a daily basis with information about which facilities are able to accept patients and which ones have suspended referrals or admissions, while others mentioned less frequent updates, as infrequent as once a year.
Most information intermediaries discussed the importance of education -- that simply providing a list was not sufficient.
it does take a lot of education and it takes a lot of discussion with the family, as well as, you know, with the patient. (Discharge Planner)
Several discharge planners discussed the use of a proprietary website (http://extendedcare.com) that they used to generate a list of facilities for their patients. This website is available on a membership basis and is paid for by the hospital. Patients and their families cannot access this site directly to search facilities. The discharge planner is able to enter the desired zip code or other geographic information and generate a list of facilities located in that area, which is shared with the patient. The advantage of this site is that the discharge planner can electronically communicate with facilities regarding bed availability and the ability to accept a patient. One case manager indicated that she refers to various directories, including one from the Alzheimers Association, another from Jewish Family Services, as well as others from local organizations, to identify facilities for referral. These directories are not available to the client.
Discharge planners and community-based case managers often refer to other websites as well. One case manager often used the California Nursing Home Search (http://www.calnhs.org) site to gather information for clients, or referred her clients to it directly, walking them through the use of the site. Another case manager referred clients to the Benefits Check Up website (http://www.benefitscheckup.org) sponsored by the National Council on Aging as a resource for identifying ways to provide care or become eligible for special programs. Patients and their families were rarely referred to Medicare.gov. One discharge planner indicated that she preferred to refer patients to the state website instead. When asked if she ever referred patients to Medicare.gov, the discharge planner responded:
occasionally, I do, but if its within the state that our hospitals located, I refer them to the Department of Inspections and Appeals website. (Discharge Planner)
A community-based case manager cited the lack of relevant information on the Medicare.gov site as the reason why she does not refer the site to clients:
One of the reasons we dont use the website is we find so many of the people who call us are very culturally specific and really are asking us for very specific information that is not dealt with on that website. (Community Case Manager)
Other materials provided by information intermediaries include pamphlets, booklets, or magazines that contain information about local LTC resources. The Lifestyles magazine was the most commonly mentioned resource. Other resources mentioned were a guidebook developed by a state Department of Aging, the Senior Home Guide, the Guide for Retirement Living, and Seniors Life. Some information intermediaries provided patients/clients with a paper checklist of what they should look for when they visit a facility, while others consult with clients to provide education regarding what to look for when making an inquiry or visit.
B.1.d. Barriers Imposed on Information Intermediaries
Discharge planners and case managers appear to be among some of the most knowledgeable individuals regarding the types of facilities in their area. However, these information intermediaries are often unwilling to make or may even be prohibited from making specific facility recommendations, whatever sources of information they may use or make available. This unwillingness or inability to share information may exacerbate the inherent problems that consumers and their families face in choosing a nursing home.
In some cases, discharge planners and case managers were unwilling to provide specific recommendations because they did not want to be subject to the anger or disappointment of patients/clients who were ultimately displeased with the recommended facility.
I never recommend. I will explain. I will say its closer to you, as far as location But I find I dont recommend, because sometimes it comes and bites you back (Discharge Planner)
Others believe that they are specifically prohibited from making recommendations:
We would never make those decisions for the client but We could get into lots of trouble We dont have the legal authority to do that. (Community Case Manager)
Private pay case managers perceive more flexibility in providing recommendations and some of them do so:
We will give our own humble opinions just because we have quite a bit of information for a lot of them. (Community Case Manager)
However, even the private pay case managers may shy away from providing recommendations for the same reasons stated by the hospital discharge planners, namely that they do not want to expose themselves to liability or blame if a client is unhappy with the recommendation.
B.2. Personal Characteristics
B.2.a. Knowledge Level
Knowledge about LTC: Consumers almost never understood the differences among the various types of LTC facilities. They often referred to all types of facilities as nursing homes, even though many of these facilities are intended specifically for rehabilitation following a hospital stay. Still, information intermediaries commented that consumers are becoming more knowledgeable about skilled nursing care:
in the past year -- many more consumers, families, are very informed and very aware of Medicare. Theyre very aware of the skilled nursing. They may not know about how all it works, and how their benefits work, but theyre usually requesting the skilled care. (Discharge Planner)
However, consumers of LTC (custodial care) appear less well-informed:
In terms of long-term [care] persons are really not very well informed of a multi-leveled facility, and they really dont understand the differences. Or they dont know what to look for. (Discharge Planner)
Knowledge about quality: Consumers generally do not understand the more technical concept of clinical quality. Often what they consider to be a high quality facility is one that appears clean and has amenities, rather than one that provides good quality care as evidenced by publicly reported quality measures or number of deficiencies. Sometimes they indicated using sensory information to ascertain quality -- most indicated that if they walked into a facility and it had a bad smell, they would walk out.
Most of them are not informed as to the medical care. They couldnt possibly. [They] walk in, and [they base] their decision on how clean, or how non-smelling [a facility is]. (Discharge Planner)
Other consumers also expressed concerns about the quality of the facility based on seeing residents sitting in wheelchairs in the hallways during a visit. Some expressed interest in knowing about staffing levels, a structural aspect of quality, but it was unclear if any of these consumers were aware of the optimal staffing ratio to evaluate that information. Short-stay residents who had first-hand experience with high staff-to-patient ratios in a facility were most likely to mention staffing as an issue.
[Families and patients with prior experience ask] well, whats the quality of care? Its usually, do they give good care? Are they going to treat my family member right? Do they have the right staff? (Discharge Planner)
Knowledge about cost/insurance: In general consumers (residents and family members) were unaware of the costs of LTC. Most of those who had insurance were familiar with what their insurance plan was and what it would cover. Still, one former resident insisted that Social Security had covered his skilled nursing stay, suggesting confusion exists over whom or what entities were responsible for covering his care. Equally important, residents were generally unconcerned about the costs, as they believed insurance would cover their stay. Even one former short-stay resident, who had no insurance, remained unaware of the costs of her stay subsequent to her discharge (her family took care of the costs of care).
Family members generally had no knowledge of the costs before they began the search process. Most were familiar with what insurance would cover, but given that most family members were in search of long-term, custodial care rather than skilled nursing care, insurance coverage was not relevant. Even prior experience helping to make LTC decisions for other family members did little to prepare them for their current situation. Many were overwhelmed by the costs and also uninformed about the ways to finance LTC.
[Cost is] a very major issue, because its not just finding a place. Its being able to afford it (Family Member)
I didnt know about the insurance, the LTC, Medicare, Medicaid, until I got involved with all this. Its awfully complicated (Family Member)
Interestingly, those who were better educated had few advantages over those with less education when it came to searching for and selecting a nursing home for their loved ones.
B.2.b. How do Consumers and Others Obtain Information?
As described above, information intermediaries have several resources available to them that they share with consumers to support the search for and selection of a nursing facility. The consumers in our focus groups used some of these resources and supplemented what they received and used from the intermediaries with other sources of information they identified on their own. For short-stay residents, the primary source of information was generally the list of facilities provided by the hospital discharge planner. Both short-stay residents and families also relied heavily on prior experience and the experiences of friends and family to help establish a list of facilities to consider or to narrow down a pre-existing list to those that would be worth considering.
Well, you talk to your friends too Theyre having relatives sick that have to go into these places so they tell you horror stories or good stories so that also helps you make a decision as to where you want to go. (Family Member)
Almost universally, visiting a small set of candidate facilities was an important part of the selection process. Short-stay residents were generally unable to visit facilities on their own, so family members visited the facilities and reported back to the resident what they learned and their impressions of each facility.
Well, [my children] visited every one in the area, and then came back and said, here is what we recommend. And thats where I went. (Short-Stay Resident)
Family members of long-stay residents also visited facilities, generally on their own. One family member, who was helping to place her aunts in a facility in another state, did not visit the facilities herself, but instead relied on family members in the local area to view the facility and report back to her what they learned.
A few focus group participants indicated that they used (or their family members used) the Internet to help gather information about nursing homes. Almost exclusively, the Internet was used to develop a list of facilities, rather than to gather quality or other information about facilities that were already under consideration. A few participants indicated that they consulted the Yellow Pages on the Internet to create a list of facilities; another mentioned using nursinghome.org.1
I went to the yellow pages in Miami. You can do that [on] the Internet. Then [I] typed in nursing homes and then it lists facilities. (Family Member)
Other ways that participants generated lists of candidate facilities included discussions with nursing home staff, administrators, and residents; advertisements (either ads in the newspaper or mailings); public information about pending lawsuits, and state reports.
B.2.c. Perceived Utility of the Internet, When Consulted and by Whom
One of the greatest challenges to using the Internet as an information source is accessibility at the time it is needed to support the decision-making process. In particular, hospital patients and their family members reported not being able to access the Internet in a timely fashion to help aid them in their selection. As discussed previously, information intermediaries often consult the Internet to help develop a list of facilities for their patients/clients, and one community-based case manager used a state-specific website to which she often referred her clients to do their own searches.
Few consumers participating in the focus groups were aware of the Medicare.gov site or Nursing Home Compare. None of the consumers mentioned using the Nursing Home Compare site, and when asked specifically if they had used the site, many consumers were not aware the site existed. Although information intermediaries were more familiar with the resource, some indicated reluctance to share this site with their patients or clients. Among the concerns were that the site is not considered up-to-date regarding the status of corrective actions stemming from prior surveys or the identification of new problems and thus can provide less-than-accurate information to consumers:
My experience with recommending the [Medicare] website is that its not always up-to-date, as far as, [the number of] deficiencies [for each facility]. (California Health Care Foundation) its not updated regularly, [facility management has] had time to correct what the deficiencies were. [Also, it] doesnt explain very clearly, what might be a staffing problem. (Discharge Planner)
Another indicated that the site was not user-friendly and for that reason, she was unwilling to direct patients and their families to the site:
[The Medicare website is] not very user-friendly Im thinking of families who [are] not able to manipulate a computer system. I mean, the website that I got into was not very user-friendly to me, but it took a while to [find what I needed] but I could finally get to the information I wanted. (Discharge Planner)
B.2.d. Role of Information Intermediaries (e.g., discharge planners, physicians, community-based case managers), When Contacted or Involved and by Whom
Short-stay residents reported relying on the hospital discharge planner to provide them with information and guidance regarding the search for and selection of a nursing facility. In some cases, the discharge planner was their only, or most important, resource. Some indicated that they would have liked the discharge planner to play a greater role in supporting the decision-making process, including giving recommendations. As discussed previously, discharge planners are reluctant to or, in some cases, prohibited from giving recommendations to patients regarding different facilities. Other consumers indicated that they would have liked their insurance plans to provide more guidance regarding nursing facilities. Few relied on their (or the family members) physician to provide information, and several indicated that they would have liked their physician to be more involved in the search and selection process. Physicians were sometimes characterized as out of touch or lacking sensitivity about the needs of their patients.
There are [Physicians] that some of our clients have who say, No, youre fine to go home and really dont know what the support system is at home or if theres any family, if the patient can afford a caregiver or how the patient is going to come in for follow-up care. (Community Case Manager)
Well, [often] the physicians will ask for the patient to be discharged that day, and the plans will have changed...a hundred degrees since the day before you try to advocate for the patient to at least give them the evening to send the patient out, so that the family can go look, but [often] its just a short time. (Discharge Planner)
One discharge planner stated that many patients and family members were reluctant to hear from her that they or their loved ones would need a nursing facility stay. She indicated that if the physician would take a larger role in preparing the patient and family, the decision-making process and transition might be easier:
Its kind of difficult for families [and] the patients -- not just families -- [to access] information about their loved ones care, or changes in communication with the physician, is kind of like they need to hear it from [the physician]. (Discharge Planner)
Family members seeking long-stay nursing home care had fewer, but more varied formal resources upon which to rely than those seeking short-stay care. Few had access to discharge planners, as their loved ones were generally not in a hospital at the time they needed to search for and select a facility. Family members most often consulted community-based case managers when their loved one was enrolled in a community-based program (e.g., publicly-funded [Medicaid or other state programs] home and community-based services), attended a senior center, or were already in a nursing facility and needed to relocate. Sometimes the clients paid for case management services. Several family members indicated that their family physician provided recommendations for nursing facilities. However, the most common resources family members relied upon in their search were informal sources such as family and friends, their own research on the Internet, and/or visits to the facilities for first-hand investigation.
B.2.e. Information Sources Used by Consumers
The decision-making process is often begun by the generation of a list of facilities for consideration. Often, as in the case of the former short-stay residents, the list is generated by a formal information intermediary (discharge planner). Although less common, the lists may also be generated by searches on the Internet or input from friends/family. This list is generally winnowed by de-selecting facilities that are not in the desired location (either near home/family or near the hospital). Word of mouth often then plays a significant role in further narrowing the list of candidate facilities. A discharge planner commented on the power of word of mouth:
I would say at first, everybody swears that they dont know what they want to do, and how theyre going to go about it. But as soon as I provide them with the list of places they all of a sudden know all kinds of reputations about all of the different types of places. (Discharge Planner)
The lists and word of mouth provide a starting point for selecting a facility. The final decision is often then made after visiting the facilities on the list.
[Networks, friends give] you a starting point. I had a couple of starting points and when I walked into them is when the vibes came out and your visual goes into it, your nose goes into it. (Family Member)
As this family member stated above, it is often the individuals intuition, gut feeling, vibe from the facility, or common sense that are the factors that play into the decision. Visitors to the facility often take their cues from sensory information such as the sniff test in the facility, whether or not they see residents sitting in the hallways, how residents are dressed, and cleanliness of the facility.
A striking difference was observed between short-stay and long-stay nursing facility consumers in terms of the information sources used, but these differences were generally limited to the approach used to generate a list of facilities for consideration. Above, we described the information sources consumers often accessed during their search. Generally, the families of hospital patients, sometimes with input from patients, made their decision based solely on the list provided by the discharge planner, supplemented by word of mouth and information gathered through visits to selected facilities. Given the time constraints they are under to make a decision, rarely do they perceive that they have the time or the ability to access the Internet to gather additional information. As mentioned previously, few family members feel they are able to access the Internet in the time they have and often spend that time talking to friends or family and visiting the facilities instead. In contrast, fewer family members of LTC residents (as opposed to short-stay skilled care residents) had information intermediaries to rely on to identify candidate facilities. These family members still generated a list of facilities but their lists often were derived from prior experiences, recommendations from friends or family (word of mouth), their own Internet searches, and, although less common, advertisements. However, the process of narrowing the list down to the selected facility was very similar to the approach taken by patients and families in search of skilled nursing care.
B.2.f. Priorities for Nursing Home Selection
Consumers were asked to identify the key or priority characteristics that informed the selection of a specific skilled nursing or LTC facility. Information intermediaries were asked to provide their perception of the characteristics that consumers identify as key or priority. In the text below, we provide a summary of the most common priorities overall.
Our analysis of the focus group transcripts showed that the single most frequently cited factor in the selection of a facility was location. This finding held for both skilled nursing stays and long-term custodial stays. While most were concerned with the facility being located close to the residents or familys home, some wanted the facility to be in close proximity to the hospital, in case they needed to be readmitted.
The second most common priority for nursing home care was that the facility staff took good care of the residents. This information was most often assessed by a visual inspection of a facility, as described above. Additional factors that played into the decision included the following:
- The facility staff speaking the language of the resident (either a foreign language, if relevant, or English: some family members indicated the importance of staff speaking English well).
- The perceived cleanliness of the facility.
- The newness/age of the facility.
- The existence or availability of social activities (games, music, etc.) appropriate to the consumers age.
- The affordability of the facility.
- The safety of the neighborhood or the presence of a locked ward to keep residents from wandering.
- The availability of a private room for the resident.
- The facilitys affiliation with a religious order or the availability of religious services.
- The residents physician having privileges in the facility.
Appendix F provides a summary of the priorities for nursing facility selection, distinguishing those stated by former short-term residents, family members, and information intermediaries. Family members and information intermediaries both listed proximity to family or home as the most important characteristics used in selecting a facility. Recommendations from family, friends, and physicians or other providers were also commonly cited as factors playing into the selection of a facility. Although information intermediaries perceived that consumers placed a very high priority on the cost of the facility as they made their decision, cost was not mentioned routinely as a concern for the former short-stay residents (most of whom had some insurance coverage), nor did family members rank cost as highly as other factors. Former residents and information intermediaries placed a much higher priority than did family members on the appearance or the newness of the facility in the selection process, although it was mentioned by a few family members as being important. Overall, former residents, family members, and information intermediaries appeared to identify many similar issues that factor into the decision-making process, although the priorities they placed on these factors differed.
Role of bed availability in decision-making. Rarely did bed availability play into decision-making. Two former short-stay residents did indicate that because their first choice facility was not available when they needed the bed, they had to be placed in another facility until a bed became available. A family member said that the facility she chose for her mother did not have a room available on the day they made their selection, so they had to wait until one became available. Her mother resided with her in the community until the bed became available.
Tradeoffs between cost and location. Few focus group participants explicitly made a trade-off between cost and location. However, one family member was comfortable with spending more in order to have his mother nearby:
Well, the cost, you look at it as [youll] spend a little bit more if its closer to your house. Youll spend a little more if you feel comfortable with the nurses and aides already. (Family Member)
B.2.g. Managed Care Influence
Several focus group participants in the short-stay resident groups who were enrolled in managed care plans mentioned that the contracts their plans had with a select number of facilities simplified their selection process. Given the limited choices, one participant simply chose the facility closest to his home; no other factors played into his decision. While fewer choices may simplify the decision-making process, health maintenance organization (HMO) enrollment may raise other problems that might be important to consider. One discharge planner raised the issue that managed care patients and their families are frustrated because they are not always able to go to the facility they prefer. Further complicating the decision process, hospital stays may be shorter for managed care enrollees. Whereas the discharge planner may be able to work with the physician to extend the hospital stay of a non-managed care patient to enable the family to select a facility and prepare for the move, that flexibility is not always possible for managed care patients.
With an HMO, again, its always been difficult [for] the family, because they only have hours to work on it. (Discharge Planner)
B.2.h. Continuity of Physician and Hospital Care
Maintaining an existing physician relationship was not identified as a priority in the decision-making process in our consumer focus groups; however, some patients and family members did want to know if their physician had privileges at the facility they went to, or selected a facility that was close to a hospital, rather than close to home. Several factors may contribute to the lack of priority assigned to continuity of care. First, in most cases, the family members were seeking LTC and as a result focused more on amenities related to quality of life (such as the physical environment) than whether an existing physician relationship could be more readily maintained at one facility than another. Second, when residents are being moved from another state, county, or city to a facility that is suited to their needs or close to family, the option of continuity is not an issue. Third, while some family members did consider the hospitals a facility routinely uses when hospital treatment is needed, the goal or priority in selecting the facility was to identify one affiliated with a hospital viewed as providing quality care, rather than a hospital with which their loved one had a treatment history.
I always ask what hospital does the rescue take you to. And my choice is [hospital name] or [hospital name]. Those are the two choices I want, so thats where I have my mom. (Family Member)
Because it just was so bad, you have no control of where theyre taken But with the hospital they took them to [it] used to be called The Toilet Hospital. (Family Member)
Continuity appears to be of greater concern to short-stay residents than to those seeking LTC. For example, one short-stay resident reported that she selected a facility to minimize travel time from the hospital (or back to the hospital in the event of a complication or emergency). In addition, the importance of continuity in the selection process was mentioned by several of the information intermediaries in the discharge planner focus group.
Theyll make trade-offs against being near a family member so that they can be near the doctor and hospital. (Discharge Planner)
If they can keep them in the same area in which they live, so that they can be close to the hospital (Discharge Planner)
If the doctor also goes to the [facility] because they like staying with the same doctor... (Discharge Planner)
B.2.i. Psychology of Decision-Making
The decision-making process is sometimes challenged by the patient or familys denial of the need for nursing facility care. While most discharge planners indicated that the hospital initiates after-care planning shortly after the patient is admitted to the hospital, the families that participated in our groups did not always accept the need for a nursing facility until shortly before discharge. While some of this initial lack of acceptance is certainly due to changes in the patients condition during the hospital stay, often that is not the case; rather, the discharge planner indicates to the family from the outset that the plan is to discharge the patient to a SNF. However, family members may believe that they can care for their loved one at home; some even try but soon realize they are unable to provide the level of care the patient needs. Consequently, the decision to place an individual in a facility becomes emergent, reducing the time available to search for and select a facility.
[Family are] trying to figure out if theres any other options available, or [waiting to see] if they just wait long enough, that the diagnosis will change (Discharge Planner)
B.2.j. How Consumers Would Approach Selection in the Future
When asked specifically what they would do differently to select a nursing home, given the benefit of having gone through the process at least once, most consumers felt they had made the best choice they could.
In my case, I can't find anything better. (Family Member)
I dont think I would have made any other choice -- a different choice -- if I had more time. (Short-Stay Resident)
Some consumers expressed their dissatisfaction with the facility they were in but could not articulate a plan for doing things differently in the future:
I wouldnt refer to where I was, or go back to the same place again. Thats all I know. (Short-Stay Resident)
Others expressed a desire to have had more information, either about their care options or the specific facilities available, but did not have clear plans for obtaining the information:
I guess I didnt know other skilled centers existed, or other hospitals had skilled centers of their own, or there were other places you could go, so I would check into that, and definitely go with, to a different place... (Short-Stay Resident)
B.3. Social Context
B.3.a. Social Pressures/Social Norms
A common theme heard throughout each of the focus groups, particularly the family and information intermediary groups, was that nursing homes are the last resort. With this mindset, many try other options to provide the care their loved one needs before moving the person to a facility. One family member moved his mother three times across three states to get her the care she needed in a community setting with family. Ultimately, he was not successful in meeting her needs in the community and had to make arrangements to move her into a facility. For many family members, there was a certain amount of stigma attached to putting a family member in a nursing facility. Some expressed the feeling that in some ways, it is a sign of failure on the familys part if they have to place a loved one in a facility. This stigma may contribute to delays in beginning the search for and selecting a facility for a loved one:
Nursing homes are very taboo. It shows a failure of the family unit, not taking care of the elderly. (Family Member)
[Family members want to keep patient in the] hospital as long as possible, because the hospital -- its better. Its nicer. In the hospital, its not as bad, for someone. So wheres the mom? Oh, shes in the hospital. Wheres your mom? Shes in the nursing home. So that plays a lot in them stalling. (Discharge Planner)
Many family members who were uncomfortable making the decision to place their family member in a facility stated that they would have preferred the decision be taken out of their hands, so that they would not feel so guilty. One family member said:
I think a lot of people dont want to make the decision so they dont want to be responsible for it, so that way they can gripe about it. Its much easier to say its your decision but then I can fault you for it. (Family Member)
A community-based case manager discussed how family guilt shapes her role in working with families. The case manager shared that she spends a good portion of her time working with the family on the guilt issues before a facility is selected.
The one other thing that no ones really mentioned, though, is the guilt factor that families have when they have to place somebody in the nursing home. You know, I made this promise never I promised never to do it. Now were doing it. So a lot of the work has to do with, you know, relieving that guilt. (Community Case Manager)
B.3.b. Type of Placement
Short-stay residents experienced decision-making and decision support in a different context than individuals seeking a long-term placement for a family member. Hospitals have an institutional structure that assures the patient and/or patients family will come in contact with an information intermediary in the form of a discharge planner or social worker. The hospital environment and the more typical need for post-acute care or rehabilitation services shape the nature of the interaction between patients and information intermediaries. For patients and family, the presence of a discharge planner assures a minimum level of information and assistance in identifying facilities.
Intermediaries reported that it is easier to engage a patient in a discussion of care options if the patient believes he or she will eventually return home. Some intermediaries also reported that it is easier to find beds for patients in need of post-acute or skilled nursing care than for patients in need of long-term, custodial care, implying that payor source influences availability:
One thing I did want to mention that is kind of overlooked in the placement of custodial versus skilled nursing is the payment. Because you tend to have more availability for skilled nursing thats covered by Medicare. (Discharge Planner)
For families seeking long-term or custodial care for a family member who currently resides at home, there is no mechanism to promote or assure contact with community-based information intermediaries. None of the participants in our family groups mentioned interaction with community-based case managers, although several mentioned hospital social workers and discharge planners. Families seeking to place a loved one who has been residing at home could choose to seek out and identify case management resources for which they are eligible or for which there is no cost, such as social workers or case managers at local multi-purpose senior centers. However, participants in the consumer groups did not identify private or paid case managers as a resource. As a result, decision-making for individuals seeking long-term or custodial care was often made without the assistance of any information intermediary.
B.3.c. Cultural Issues
Culture, language, and ethnicity are factors that affect the context in which consumers make decisions about nursing home care. These factors can represent barriers to information access for individuals with limited English proficiency, or these factors can drive choice when cultural and/or language issues are top priorities in decision-making. Cultural issues were identified by participants in the groups conducted with families of nursing home residents and in the groups conducted with information intermediaries. Participants in the groups conducted with short-stay residents did not mention culture or language in discussing their use of information, priorities for decision-making, or identification of gaps in the available information.
According to focus group participants, culture and language can affect consumers access to information on care options and facilities, as most information is presented in English. Even when material is also available in Spanish, it does not meet the needs of individuals whose primary language is not English or Spanish:
The information that we have, we only have in two languages. And we serve a diverse population. Its the information itself. It needs to be in more than just two languages because we serve more than people that speak one or two languages. (Community Case Manager)
Culture can also act as a barrier to access in that some families and information intermediaries reported that they must overcome cultural stigma associated with placing a loved one in residential care.
[In the] Cuban [culture] you dont ever put your family members in a home ever because they always take care of them. That was not an option. (Family Member)
We have a very large Hispanic community here, which is not mentally prepared to place their loved ones in a nursing home. (Discharge Planner)
Language and cultural needs can promote access to a specific facility or type of facility when used to drive the selection process.
I found for most ethnicities above everything else, the food, the language (Community Case Manager)
I decided that I wanted her to be, to feel comfortable, [to] have somebody in the room, somebody who speaks Spanish, even though sometimes she doesnt want to speak Spanish (Family Member)
B.3.d. Family Dynamics
The interaction among family members is another factor or force in decision-making in that it shapes the environment or context in which decision-making occurs. Participants in the focus groups conducted with short-stay residents were unanimous in identifying the positive role or influence of family in decision-making. For these consumers, family either had sole or partial responsibility for the selection of a specific facility, or acted as a sounding board for former residents as they made their selection.
Participants in the groups conducted with families of current long-stay nursing home residents communicated a different perspective on the role family played in decision-making. Some participants reported that an extended network of family members shared responsibility for facility selection. Other participants reported that they were placed in a leadership role for decision-making because they were their loved ones only family, other relatives lived too far away, or other relatives failed to act or made decisions that were not best for the loved one.
I have an aunt that lives north of here in Florida. And her two sons are in New York so Ive inherited most of their burden being local. (Family Member)
I had carte blanche by other family members to move forward because I took the responsibility, no one else would, but I did have to, want to include everybody every step of the way, including my mother, who in the beginning knew where she was headed. (Family Member)
C. Themes that Fall Outside of Conceptual Framework
C.1. Perceived Gaps in Information
Many of the focus group participants reported that the information they needed or wanted was not available to them when they needed it. Several people mentioned the inability to find a particular type of information that is already available but about which they were not aware, such as the results of the most recent state survey. For example, one family member discussed the desire to have had a resource that would allow comparison of one facility to another.
Theres no governmental standard you can go to and say this is choice of A, B, C, D. Youre comparing apples to oranges everywhere you go and you cannot trust anybody and rely on anybody and theres nobody you can turn to who will give you a black and white answer. There just isnt there. I can go to Consumer Reports and find out more about a bicycle than I can about a nursing home. (Family Member)
Another family member wanted to see a consumer rating, like the Good Housekeeping seal:
Why can't they rate them like the hotel chains, five star, four star. Why is it so complicated? (Family Member)
Some wanted more readily accessible information about regulations (either state or federal) related to staffing, background checks on or qualifications of staff, and lawsuits settled or pending. These types of information are generally not included in the publicly available consumer resources. Another participant wanted a report card on facilities. Others simply wanted to have someone sit down with them and take the time to explain what they needed to know to make a decision.
C.2. Focus Group Participant Ideas for Improving Information Resources/Selection Process
The ideas generated by focus group participants for improving access to information needed for decision-making fall into three main categories: (1) information access and dissemination; (2) information content; and (3) consumer understanding and comprehension.
Enhanced information access and dissemination were more likely to be identified as means of improving or easing the process of nursing home selection by consumers than by information intermediaries. Specific enhancements identified by consumers included improving information on where and how to find an information intermediary, more ready access to an information intermediary who can recommend for or against specific facilities, better access to an intermediary who is trusted (such as a physician or hospital social worker/discharge planner), and having information available in a range of locations (such as doctors offices, public libraries). Both consumers and intermediaries mentioned that information should be available on paper as well as the Internet, as the web is not readily accessible to all consumers or intermediaries when they need it to support time-critical decision-making.
It should be public record. Accessible by either the Internet or the others, as [participant] mentioned, go to the library. But it should be public information, easily accessed. (Family Member)
In terms of improving the content of information, consumers and intermediaries had similar recommendations, which included using terminology or language that is clear and easy to understand and providing information in several languages to serve the broad range of consumers with limited English proficiency.
In addition, consumers and intermediaries recommended providing information, testimonials, or referrals from individuals with direct experience with a facility (either from their own stay or that of a loved one). In addition, consumers also recommended providing facility-specific assessments from professionals or experts (such as physicians or social workers who have visited the facility).
Information intermediaries (hospital discharge planners and community-based case managers) identified consumer knowledge as an area that could contribute to improving information and the selection process. Intermediaries suggest that campaigns or efforts to educate the public about LTC in general (such as public service announcements, seminars at churches or other community locations) would reduce some of the burden that consumers face in the selection of a nursing home or other care facility.
I think if we had our younger generation better educated -- if there were something put out that explained what a skilled nursing level of care is. What custodial care is. What part of that is covered by Medicare or Medicaid. (Discharge Planner)
V. SUMMARY
The findings from these focus groups echo the findings of other qualitative and quantitative research on the factors associated with the search for and selection of a nursing facility (Maloney, Finn et al. 1996; Rodgers 1997; Shemwell and Yavas 1997; Lawrence, Moser et al. 1998; Kellett 1999; Lundh, Sandberg et al. 2000; Ryan and Scullion 2000; Castle 2003; Edwards, Courtney et al. 2003). Older adults and their family or other health care agents do not generally avail themselves of the large quantities of quality information and information resources in the process of selecting a facility. In order to begin the search for a nursing facility, one must first recognize that there is a need for that level of care. Denial of or lack of understanding about the needs of a loved one may result in delays in beginning the search process. Few plan well in advance of an emergent need and most have only a day or two to select a facility.
While those being discharged from the hospital to a SNF generally had less actual time to make a decision, even family members considering a nursing home for a loved one on a long-term basis often waited until the need became emergent, thus curtailing any opportunities to make a more considered facility selection. Given these constraints on the decision-making process, patients and their families are likely to rely upon lists of facilities (when available), more obvious physical and sensory characteristics of the facilities, and word of mouth, and be more concerned with the location of the facility than with the technical aspects of the clinical quality of care provided.
Information resources did not always provide useful information for consumers. Some information that consumers desired was missing or inconsistent across information resources such as quality of life information. Also, consumers perceived that resources were limiting due to information being presented only in English when other languages were needed or because consumers found the websites difficult to navigate.
Few focus group participants accessed the Internet for information. For a variety of reasons, discharge planners were reluctant to provide information from Medicare.gov or even to recommend it to their patients. Short-stay residents and their families did not typically have access to the Internet at the time when a decision was needed. Thus, even if they had obtained positive information from the Internet about a particular facility, they would have been unlikely to follow up in the short time available. Although family members seeking long-stay facilities were more likely to include the Internet as one of their information sources during their search process, none reported using Nursing Home Compare.
VI. SUMMARY OF FINDINGS
Below, we review some of the major findings from the website content review (Shugarman and Garland 2006) and the focus groups.
Finding: In the web content review reported in a companion volume of this report (Shugarman and Garland 2006), we found that the reading level of most of the sites was at the college-level, which is far higher than the average reading level of the public (Kirsch, Jungeblut et al. 1993; National Center for Education Statistics 2003) and which makes these sites potentially impossible for most to access and understand. Several focus group participants mentioned their desire to have information in plain and simple language.
Not only was reading level a challenge, but many consumers and information intermediaries cited the lack of information in languages other than English as a challenge in communicating with consumers. Only about one-quarter of the sites we reviewed had information available in a language other than English, and in most cases, the only other language in which the information was available was Spanish. Particularly in the focus group locations that had great cultural diversity, language of information resources was cited as a primary concern to consumers.
Finding: The PEW Internet and American Life Project (Fox 2005) found that 26 percent of Americans age 65 and older are online using the Internet for email and other purposes, compared to 67 percent of Americans age 50-64. Other studies, which focus on use of the Internet for activities other than email, have found lower rates of Internet use -- 8 percent for Americans age 65 and older, and 29 percent of Americans age 50-64 (Harris Interactive 2005). These studies indicate that older adults use of the Internet is dominated by email, and as a result this population, the largest LTC consumer group, may not be web-savvy. For example, websites that require the viewer to scroll down a page to find the information they need may not be entirely intuitive to someone who is not already comfortable navigating the Internet. As discussed in the companion web content review report, not all websites are appropriately labeled, include working web links, or can be viewed with larger font sizes or be resized for those with visual impairments. All of these only serve as barriers to the use of LTC information resources on the Internet in supporting the decision-making process.
Finding: Consumers are often in search of big picture information about facilities such as where they are located -- information that could easily be found on the Internet. At the same time, consumers are in need of specific details about facilities that are not currently available through most Internet information resources, including information on quality of life issues such as activities available in the facility, languages spoken, whether food can be provided to meet residents dietary or cultural needs, the physical appearance and cleanliness of the facility, how it smells, and how the facility cares for residents (e.g., do residents sitting in the hallways and are they dressed appropriately).
Consumers are also concerned about how current is the information available on the Internet. Family members and former short-stay residents reported dismissing the information that they felt was not up-to-date such as information on deficiencies, and information intermediaries would often not refer their patients/clients to resources they felt were not up-to-date. Although bed availability was not a prominent issue among consumers and discharge planners generally had up-to-date information from the facilities, a few consumers mentioned waiting additional days or weeks to get a bed in their facility of choice or going into a second choice facility because a bed was not available in their first choice.
Finally, consumers indicated a desire for a report card or grading system that could summarize the performance and quality of a nursing facility in a succinct way. A Consumer Reports style report card or star ratings might help to facilitate the selection of candidate facilities by presenting information in an easily understood format, similar to that used in other industries to rate or grade services. For example, the California Nursing Home Search website (http://www.calnhs.org) presents three-star ratings for each facility in several domains including staffing, quality of facility, quality of care, and finances and cost. This site also facilitates the comparison of these ratings across multiple facilities to quickly identify the best facility based on the consumers preferences.
Finding: Consumers place location of the facility at the top of their list of important considerations in selecting a facility. Other factors were stated as important but not all were included in existing information resources. These factors include cost, availability of special services (e.g., dementia care, rehabilitation, etc.), and various quality of life measures as discussed above. If offered at all, most information resources only allow the consumer to select candidate facilities to review more carefully based on state, county, or zip code. Other facility characteristics might play a more prominent role in selecting the facility if the consumer could include those priorities in the search process.
There are examples of very sophisticated filters such as this for a variety of consumer product companies. For example, the website for Office Depot (http://www.officedepot.com) allows the consumer to select the general consumer product he/she is most interested in and then select further refinements on the product selection (e.g., by price, brand, or other features of the product). After each selection, the consumer can see the pool of candidate products reduce from a large number to smaller numbers as he/she narrows the criteria. This approach could also prove a useful model for nursing home information resources. As the consumer selects additional criteria important to his/her facility selection, he/she would be able to see how many facilities are available in the local area that meet those criteria. If there are no facilities in the area that fulfill all those criteria, he/she could then establish priorities among the criteria and select a facility that meets the majority of their needs.
The California Nursing Home Search website (http://www.calnhs.org) provides a filtering mechanism that may serve as an example for the design of other Internet resources. This website includes the ability to filter out facilities based on selected criteria including facility type (e.g., free-standing or hospital-based), payment options (e.g., the facility accepts Medi-Cal or Medicare), type of care (e.g., skilled, intermediate, or psychiatric care), and specialized services (e.g., rehabilitation or Alzheimers services).
Finding: Consumers expressed an interest in having a mechanism by which they could share their own experiences with a facility or review others experiences. By making consumers part of the process, they can speak directly on issues they find important in the selection process. Focus group participants cited examples of websites in other service industries (e.g., the hotel industry) that allow the consumer to rate his/her experience with that service and provide detail about their ratings.
Finding: We learned from focus group participants that discharge planners and community-based case managers are seen as the only professional information resource to which consumers have access during their search for and selection of a nursing facility. According to consumers in our focus groups, physicians rarely provided support to the decision-making process, and yet, they are often the most intimately involved in the patients care and are usually the ones who make the initial recommendation or referral to LTC. Physicians may be in an ideal position to provide support during the decision-making process. Furthermore, information intermediaries identified the physician as the most appropriate provider to prepare the patient and his/her family for the possible need for a nursing home.
Finding: There is a wealth of community resources that have the potential to support the decision-making process of consumers in search of a nursing facility. These resources include the national and local aging networks, which include Area Agencies on Aging, Aging and Disability Resource Centers, caregiving networks, and might also include LTC ombudsman programs. When asked, focus group participants indicated not knowing about or not using many of these community resources. Other non-traditional resources that could provide support include religious institutions, community centers, and libraries. Some of the consumers in the focus groups mentioned the library in particular as a potentially important location in which to place information about the nursing home selection process and be able to access the Internet as well. Each of these resources is an example of an entity that regularly provides support to the local community on a wide variety of issues.
Finding: Consumers who participated in the focus groups, particularly those seeking short-stay placements, perceived that the timeframe for making decisions regarding nursing homes was too short, often only a day or two. As a result of the short timeframe, most consumers do not have sufficient time to do a thoughtful search and thus rely on simple lists of facilities and/or informal sources of information to support the decision-making process. No widespread mechanism exists to inform consumers of the different types of resources that are available. Additionally, information intermediaries, often the most knowledgeable resources with whom consumers will have contact are not always willing or able to give guidance about specific facilities. As cited in a recent report by the California Health Care Foundation on LTC reform in California (California Health Care Foundation 2006), there is a serious disconnect between medical and social services. Discharge planners are burdened by heavy caseloads and do not have the time or incentive to work with the patient to identify the discharge location that best matches the patients needs. Little coordination between the hospital and community resources means that patients and their families often have only the discharge planner to rely on as an information source.
Finding: The Internet may not always be accessible at the time the selection of a nursing facility is needed. Information resources have little utility if they are not accessible when needed. In particular, as we learned from the focus group participants, the time constraints placed upon them and the fact that many consumers search for a facility while they or their loved one are in a hospital bed makes accessing the Internet to inform the decision-making process a challenge.
Finding: We learned that family members were often unprepared to tackle the challenge of identifying the best nursing facility for their loved one. Several made comments during the focus groups that, as a result of the process of placing their mother, father, aunt, uncle or other loved one, they are beginning to think about and prepare for their own future potential need for LTC. Those who have not already had the experience of placing a family member in a facility are rarely prepared for the emotional and financial challenges that are often associated with this activity.
Finding: Most of the participants in our consumer focus groups were not aware of the wealth of existing resources that promote a comparison of nursing home facilities. In particular, Medicare resources (i.e., 1-800-Medicare and Medicare.gov) were not being consistently accessed. Individuals who require a nursing home admission following a hospital stay are guaranteed access to a discharge planner or hospital social worker who can act as an information resource. For individuals seeking placement in a facility directly from home or the community, no similar mechanism exists to promote access to information. In addition, when Medicare is not the primary payor for the nursing facility stay, consumers may not perceive that it is still a useful resource in their search for and selection of a facility. Also, family members who are not currently Medicare beneficiaries but are in a decision-making role may not believe that they can access those resources to support their decision.
VII. REFERENCES
Agency for Healthcare Research and Quality (2000). Expenses and Sources of Payment for Nursing Home Residents, 1996, MEPS Research Findings Report No. 13. Rockville, MD: AHRQ (AHRQ Pub. No. 01-00010).
BearingPoint Inc. (2003). Consumer Testing of the Home Health Compare Website Prototype. McLean, VA: CMS (Contract No. 500-01-0002).
California Health Care Foundation (2006). Long Term Care Reform: Ten Years After Little Hoover. Retrieved December 18, 2006, from http://www.chcf.org/documents/hospitals/LTCLittleHoover.pdf.
Castle, N.G. (2003). Searching for and selecting a nursing facility. Med Care Res Rev 60(2): 223-47; discussion 248-52.
Castle, N.G. and T.J. Lowe (2005). Report cards and nursing homes. Gerontologist 45(1): 48-67.
Centers for Medicare and Medicaid Services (2002). Report on Evaluation Activities for the Nursing Home Quality Initiative Pilot. Baltimore, MD: CMS.
Centers for Medicare and Medicaid Services (2005). Nursing Home Compare. Retrieved August 12, 2005, from http://www.medicare.gov/NHCompare/Home.asp.
Chernew, M., G. Gowrisankaran and D.P. Scanlon (2001). Learning and the Value of Information: The Case of Health Plan Report Cards. Cambridge, MA: NBER.
Chernew, M. and D.P. Scanlon (1998). Health plan report cards and insurance choice. Inquiry 35(1): 9-22.
Decker, F.H. (2005). Nursing Homes, 1977-99: What Has Changed, What Has Not? Hyattsville, MD: National Center for Health Statistics.
Duff, S. (2002). Questionable quality initiative. Nursing homes frustrated with CMS measures. Mod Healthc 32(20): 20-1.
Edwards, H., M. Courtney and L. Spencer (2003). Consumer expectations of residential aged care: Reflections on the literature. Int J Nurs Pract 9(2): 70-7.
Federal Interagency Forum on Aging-Related Statistics (2004). Older Americans 2004: Key Indicators of Well-Being. Washington, DC: U.S. Government Printing Office.
Harris Interactive (2005). The Harris Poll #40, May 12, 2005. Retrieved November 27, 2006, from http://www.harrisinteractive.com/harris_poll/index.asp?PID=569.
Infeld, D. (2003). Nursing Home Quality Initiative: Evaluation of the Relationship Between Long-Term Care Ombudsman Programs (LTCOPs) and Quality Improvement Organizations (QIOs). Retrieved June 15, 2004, from http://www.ltcombudsman.org//uploads/NHQIFinalReport.pdf.
Johnson, C.K. (2002). Project aims to improve quality. Spokane Spokesman Review (August 2, 2002).
Jones, A. (2002). The National Nursing Home Survey: 1999 summary. Vital Health Stat 13 152: 1-116.
Kaiser Family Foundation (2005). May/June 2005 Health Poll Report Survey. Washington, DC: Kaiser Family Foundation.
Kellet, U.M. (1999). Transition in care: Family carers experience of nursing home placement. J Adv Nurs 29(6): 1474-81.
Kirsch, I., A. Jungeblut, L. Jenkins and A. Kolstad (1993). Adult Literacy in America. Washington, DC: National Center for Education Statistics.
Komisar, H.L. (2002). Rolling back Medicare home health. Health Care Financ Rev 24(2): 33-55.
Krueger, R.A. (1998). Analyzing and Reporting Focus Group Results. Thousand Oaks, CA: SAGE Publications.
Laditka, S.B. (1998). Modeling lifetime nursing home use under assumptions of better health. J Gerontol B Psychol Sci Soc Sci 53(4): S177-87.
Lawrence, F.C., E.B. Moser, A.D. Prawitz and M.W. Collier (1998). Helpfulness of information sources in the selection of a nursing home. Psychol Rep 83(3 Pt 2): 1217-8.
Levit, K., C. Smith, C. Cowan, H. Lazenby, A. Sensenig and A. Catlin (2003). Trends in U.S. health care spending, 2001. Health Aff (Millwood) 22(1): 154-64.
Lundh, U., J. Sandberg and M. Nolan (2000). I dont have any other choice: Spouses experiences of placing a partner in a care home for older people in Sweden. J Adv Nurs 32(5): 1178-86.
Maloney, S.K., J. Finn, D.L. Bloom and J. Andresen (1996). Personal decisionmaking styles and long-term care choices. Health Care Financ Rev 18(1): 141-55.
Marshall, M.N., P.G. Shekelle, S. Leatherman and R.H. Brook (2000). The public release of performance data: What do we expect to gain? A review of the evidence. JAMA 283(14): 1866-74.
Morgan, D.L. and A.U. Scannel (1998). Planning Focus Groups. Thousand Oaks, CA: Sage.
Mukamel, D.B. and A.I. Mushlin (1998). Quality of care information makes a difference: An analysis of market share and price changes after publication of the New York State Cardiac Surgery Mortality Reports. Med Care 36(7): 945-54.
National Center for Education Statistics (2003). National Assessment of Adult Literacy (NAAL): Key Findings. Retrieved October 23, 2006, from http://nces.ed.gov/NAAL/index.asp?file=KeyFindings/Demographics/Overall.asp&PageId=16.
Payne, J.W., J.R. Bettman and E.J. Johnson (1993). The Adaptive Decision Maker. Cambridge: Cambridge University Press.
Robinson, S. and M. Brodie (1997). Understanding the quality challenge for health consumers: the Kaiser/AHCPR Survey. Jt Comm J Qual Improv 23(5): 239-44.
Rodgers, B.L. (1997). Family members experiences with the nursing home placement of an older adult. Appl Nurs Res 10(2): 57-63.
Ryan, A.A. and H.F. Scullion (2000). Nursing home placement: An exploration of the experiences of family centers. J Adv Nurs 32(5): 1187-95.
Sainfort, F. and B.C. Booske (1996). Role of information in consumer selection of health plans. Health Care Financ Rev 18(1): 31-54.
Scanlon, D.P., M. Chernew and J.R. Lave (1997). Consumer health plan choice: Current knowledge and future directions. Annu Rev Public Health 18: 507-28.
Scanlon, D.P., M. Chernew, C. McLaughlin and G. Solon (2002). The impact of health plan report cards on managed care enrollment. J Health Econ 21(1): 19-41.
Shemwell, D.J. and U. Yavas (1997). Congregate care facility selection: A conjoint approach. Health Mark Q 14(4): 109-20.
Shugarman, L.R. and R. Garland (2006). Nursing Home Selection: How Do Consumers Choose? Volume II: Findings from the Website Content Review. Santa Monica, CA: RAND Corporation (WR-457/2-ASPE). [Available at http://aspe.hhs.gov/daltcp/reports/2006/chooseII.htm]
Spillman, B.C. and J. Lubitz (2002). New estimates of lifetime nursing home use: Have patterns of use changed? Med Care 40(10): 965-75.
Spranca, M., D.E. Kanouse, M. Elliott, P.F. Short, D.O. Farley and R.D. Hays (2000). Do consumer reports of health plan quality affect health plan selection? Health Serv Res 35(5 Pt 1): 933-47.
Tennstedt, S. (2001). Family Caregiving in an Aging Society. Retrieved July 17, 2002, from http://www.aoa.gov/caregivers/FamCare.html.
Thompson Corporation (2002). Quality initiative set for October, concerns linger. Nursing Home Regulations Manual (September).
Tumlinson, A., H. Bottigheimer, P. Mahoney, E.M. Stone and A. Hendricks (1997). Choosing a health plan: What information will consumers use? Health Aff (Millwood) 16(3): 229-38.
APPENDIX A. FOCUS GROUP METHODS
In this document we describe the methods used to conduct focus groups with consumers and information intermediaries on the search for and selection of a nursing facility either for themselves, a family member, or a client. The goal of this research was to conduct focus groups with consumers of nursing home care (former residents and family members of current nursing home residents) and information intermediaries who are often resources for consumers (defined as hospital discharge planners and community-based case managers). We planned for six focus groups: two with former residents, two with family members of current residents, and two with information intermediaries. As an initial step we had to identify the states in which we would conduct the focus groups
State Selection Process
As part of the Website Content Review report, we selected six states for the review of state-specific website content: California, Iowa, Ohio, Florida, Maryland, and Virginia.
-
Perceived depth of Internet resources: We grouped states based on perceived availability of LTC information on the Internet. To develop hypotheses about states in these groups, we interviewed experts in nursing home care, including the Office of the Assistant Secretary for Planning and Evaluation (ASPE) and CMS staff, considered the literature describing other reviews of relevant LTC websites and reviewed the Nursing Home Compare links to state resources. We then proceeded to identify states that were considered resource rich or resource poor with regard to LTC information on the Internet (which may not be consonant with the availability of non-Internet resources).
-
Feasibility for follow-up focus groups: We sought to identify states with a sufficient number of facilities located within a reasonable distance of the location where we might hold a focus group (generally a larger metropolitan area of the state), with a local area that is in close proximity to a RAND facility for conducting the focus groups, and where RAND has a prior relationship with the state or a local area within the state and/or familiarity with providers/LTC users in the state. In addition, at least one state needed to be in close proximity to Washington, DC in order to allow ASPE to observe a focus group. To that end, we included Maryland and Virginia to reflect the greater Washington, DC metropolitan area.
-
State demography: We attempted to identify states that had a large number of potential or actual LTC users (i.e., percent of population age 65 and older), substantial racial diversity, and a good mix of highly urbanized or rural locations within the state (where we might conduct the focus groups). We used Census data to evaluate the states and locations for site visits by these characteristics.
Based on practical considerations, we elected to conduct the focus groups in only four of the six states. The focus group locations were Santa Monica, California; Des Moines, Iowa; Miami, Florida; and Arlington, Virginia. In California, we selected RANDs Santa Monica headquarters, which is readily accessible to individuals from metropolitan Los Angeles. In Iowa, we selected the state capital, Des Moines, due to prior experience conducting focus groups in the area. In Florida, we selected Miami based on the demographics of the area and due to prior experience conducting focus groups in the area. The Virginia site was selected to promote participation by individuals from Maryland, Virginia, and the District of Columbia and to facilitate attendance by ASPE. Before finalizing the locations, we reviewed the Nursing Home Compare website to assess the number of nursing homes within 25 miles of each location as a means of determining the richness of the potential pool of participants for groups conducted with former residents or with families of current nursing home residents.
Participant Recruitment and Eligibility Screening
We allocated our six focus groups across our four locations in the following way:
- California: one group with community-based case managers.
- Iowa: one group with former nursing home residents.
- Florida: two groups with families of nursing home residents.
- Virginia: one group with former nursing home residents.
Our sixth group, conducted with hospital-based discharge planners, was conducted by telephone, to allow the participation of discharge planners from all of the states in which we conducted focus groups. The RAND staff moderating this focus group were in Santa Monica and ASPE participated from Washington, DC.
The first step in recruitment was to define the eligibility criteria for each of the planned focus groups. Starting with the former resident population, we made an initial decision to limit the groups to individuals who had had a short-term stay paid for by Medicare (referred to as short-stay residents in the rest of this report). The rationale for this decision was two fold. First, Medicare is the payor for a growing proportion of nursing home stays, paying for 39 percent of all nursing home discharges and 19 percent of all nursing home expenditures (Agency for Healthcare Research and Quality 2000; Decker 2005). Second, short-stay residents account for 95 percent of all nursing home discharges, making this population a large audience for information on nursing homes (Decker 2005) as well as providing a sufficient pool of potential recruits. Thus, a Medicare-paid short-stay was our primary inclusion criterion. We operationalized short-stay as a stay lasting less than three months. In terms of exclusion criteria, we elected to exclude individuals who had worked in a nursing home in the prior five years. We also excluded individuals who had ever worked for a market research company. This last exclusion is applied to most focus group work conducted by RAND, as we prefer to limit participation to individuals who do not have significant experience in the conduct of focus group research.
We engaged a professional focus group vendor for the recruitment and screening of all participants for the focus groups composed of former residents. In our experience, recruitment by vendor is the most efficient and cost effective way to recruit participants, as most vendors maintain databases of individuals who have volunteered to be contacted about a range of topics. In addition, most vendors have on-going community relationships or networks they can draw upon to expand the pool of candidates for a specific project.
For the focus groups composed of families of nursing home residents, we made an initial decision to limit the groups to individuals related to a current resident of a nursing home. Our rationale was that including individuals whose family member no longer resided in a facility could result in the inclusion of individuals whose family member was deceased, and that such participants might suffer emotional distress in talking about and remembering the nursing home selection experience. We decided to focus on individuals whose family member had been admitted in the prior 12 months, as, in our experience, this limitation yields a pool of individuals with sufficiently fresh recall of the process of selecting a facility. As with the short-stay resident groups, we excluded individuals who had worked in a nursing home in the prior five years and individuals who had ever worked for a market research company. As with the resident groups, we engaged a professional focus group vendor in the recruitment and screening of all participants in the family focus groups.
For the groups composed of hospital-based discharge planners, we focused on individuals with at least one year of experience as a discharge planner. We focused on discharge planners who had given assistance to individuals or families in need of post-acute care, skilled nursing care, or LTC in the prior 12 months, as our goal was to identify individuals with sufficient experience to contribute to the discussion. As with resident and family groups, we excluded individuals who had worked in a nursing home in the prior five years and individuals who had ever worked for a market research company. We engaged professional focus group vendors in California, Iowa, Florida, and Virginia to recruit discharge planners from a mix of hospital types: non-profit and for-profit facilities, facilities with and without a religious affiliation, and facilities with and without an attached or affiliated nursing home.
For the focus groups composed of community-based case managers, we used similar inclusion and exclusion criteria. We focused on individuals with at least one year of experience as a community-based case manager and who had given assistance to individuals or families in need of post-acute care, skilled nursing care, or LTC in the prior 12 months. As with all the other groups, we excluded individuals who had worked in a nursing home in the prior five years and individuals who had ever worked for a market research company. Recruitment for this group was conducted by members of the RAND team rather than a vendor. We felt that defining the concept of a community-based case manager was sufficiently complex that we wanted to have direct control of the recruitment task. We used the Internet to generate a list of multi-purpose senior centers and community organizations within ten miles of RAND that provided case management services. Such services are provided without cost to consumers. We supplemented this list by talking with key informants familiar with the case management community in Los Angeles. The key informants helped us to identify private pay case managers (case managers who provide services on a fee basis). This process allowed us to recruit participants who reflected the range of settings in which community-based service are provided.
Development of Topic Guides
We worked collaboratively with ASPE to develop the topic guides used to conduct the focus groups. We began the process with a review of the research questions identified in the original proposal and project work plan. Additional topics were identified based on the findings from the web content review, discussion with the Task Order Monitor, and our prior focus group work in the area of consumer experience with nursing home care. Our goal was to develop similar guides for all of the focus groups to assure that we covered similar topics with consumers and information intermediaries and to promote analysis of the information we collected. The final topic guides can be found in Appendix C.
Analytic Approach
We analyzed the data from the focus groups using a transcript-based approach. According to Krueger (1998), a transcript-based analysis is one of the more rigorous methods for analyzing focus group data. We began with a transcript of each focus group, produced by a professional transcription vendor. The transcripts were used in two ways. First, the transcripts were reviewed to identify all text associated with key themes, that is, the topics of the research questions the focus groups were convened to answer. Our key themes included participant knowledge of nursing home care, how consumers obtained information, what information sources consumers used, and what priorities drove the selection of a nursing home. All participant comments and moderator summation related to the key themes were grouped and reviewed to identify the sub-themes and views expressed by group participants. Second, the transcripts were reviewed to identify additional themes relevant to the focus of this research. Such secondary themes include familiarity with Medicare.gov and Nursing Home Compare, the importance of the physical characteristics of a facility (such as the smell), and how consumers would use their experience in the event of a future nursing home admission. All participant comments and moderator summation related to the secondary themes were grouped and reviewed to identify the views and experiences expressed by group participants. The transcripts were used in conjunction with a participant seating guide from each group, moderator and note-taker notes, and a debriefing completed after each group.
Because of our use of systematic methods we are confident that the findings we have generated are an accurate reflection of the opinions, attitudes and experiences expressed by the focus group participants.
APPENDIX B. STUDY STRENGTHS AND LIMITATIONS
Role of Qualitative Methods as a Research Tool
For decades, focus groups have been used as a research tool in academic research, product marketing, evaluation research, and quality improvement. They are especially useful as an exploratory tool to learn more about an issue or topic that is not well-understood. They can also provide insight into the background or context that motivates or influences behavior -- in this case selection of a nursing home.
Limitations of Qualitative Research
Although the objective of a focus group is to elicit a rich understanding of attitudes, beliefs and experience, the focus group is not a tool to measure or predict attitudes or behavior. Thus the limitations of qualitative research in general and this project in particular are that it provides a framework for understanding the perceptions and experiences of consumers and information intermediaries on the issue of nursing home selection but it does not provide a body of data from which statistical inference can be made. These data simply provide the user with an understanding of the context in which nursing home decision-making occurs and the factors that may shape the context. In many instances, such data can complement, clarify or amplify quantitative data.
Strength of Our Focus Group Findings
The strength of the data and findings from this focus group effort lie in the systematic methods that were used to collect the data, analyze the data and report the findings.
Data collection: These focus groups were conducted by professional moderators, using a standardized topic guide, in a manner consistent with the best practices of the survey research community and the literature on focus group method. During the focus group discussions, the moderators were consistent in asking participants to explain their views or comments, if the meaning was not explicit. Each groups discussion was recorded so that a transcript could be generated for analysis. Client participation was encouraged so that the process would be transparent to ASPE.
Data analysis: The same tools were used to analyze the data from each focus group. These tools included a transcript produced by a professional transcription service, a seating guide from the focus group, moderator and note-taker notes taken during the focus group, and post-group debriefing on the main themes expressed by group participants. Two individuals systematically reviewed the transcript to identify the key points and findings.
Reporting of findings: During the focus groups, the moderators would summarize or report the main themes back to the group participants for verification. Following each group, the moderators debriefed to review the themes that emerged as dominant or key in each group. The themes come directly from a review of the transcripts, in which we examined patterns of experience or attitudes across groups as well as within groups.
By following best practice and systematic methods, we are confident that the findings we have generated are an accurate reflection of the opinions, attitudes and experiences expressed by the focus group participants.
APPENDIX C. FOCUS GROUP PROTOCOLS
Document: Focus Group Topic Guide -- Groups 1 and 2 Flesch-Kincaid Grade Level: 7.5
Topic Guide for Focus Group Discussion with Short-Stay Nursing Home Residents
I. Introduction (5 minutes)
Hello! My name is (insert) and I work at RAND, a non-profit research center in Santa Monica, California. Joining me today is (insert) we are part of a research team that is trying to learn how people who need a short-term stay in a nursing home go about finding and selecting the right nursing home for their needs. [Introduce any observers.] Everyone here has gone through that experience, and we really appreciate your willingness to share your experience with us today. Lets make it clear, however, that we are not just idly curious. We are involved in a broader research project to understand the kinds of information people use when choosing a nursing home. Our research is supported by the U.S. Department of Health and Human Services.
As you know, we are audio taping this focus group. The purpose of taping is to make sure we have a complete and accurate record of what happens in the group. Only members of the research team at RAND, and a small number of researchers at the agency that oversees the work, will listen to the tapes. When we write up a report of what we learn, we will use the tapes to pull together the full range of ideas and opinions expressed by people in the focus groups. Once the report is finalized, RAND and our federal sponsor will destroy the tapes. The report will include quotes from what different people say in the group. I want to assure you that no persons name will appear in the report, and we will not include any information that would let a reader identify the person. We are taking all possible measures to protect your confidentiality and privacy.
For example, note that your name tags have only your first name, again to protect your confidentiality. Please use only your own and others first names during the group. Here are some other ground rules for our discussion:
- There are no right or wrong answers -- everyones opinion has value to us.
- If you dont want to answer a particular question or discuss a particular topic, just say so -- you dont have to answer or discuss anything you dont want to.
- We want to hear from as many of you as possible, so please give your colleagues opportunities to participate. It is best if only one person speaks at a time.
- Especially because we are taping, please speak up, and also refrain from side conversations.
- We do have a limited time, and several issues to discuss. Please dont be offended if I ever have to step in on a discussion to refocus us and move us ahead.
- We are not planning a formal break, so feel free to get up to get refreshments, etc. whenever you like.
- Point out restroom location.
- Ask participants to turn off cell phones.
- Remind participants that theyll receive thank you payments at the conclusion of the group.
Any questions? Lets get going then.
II. Warm Up (10 minutes)
Go around the room and ask each person how long their (most recent) nursing home stay was, and to share as much as they are comfortable about the reason for the stay. During the warm up probe each participant to find out what terms participants use to describe the place they were in.
III. Knowledge and Awareness of Long-Term Care (25 minutes)
Id like to talk about how much you knew about nursing homes before you were admitted to a nursing home.
-
How much did you know about nursing homes before your most recent nursing home stay? Probe on how much they knew about SNFs; how much they knew about the cost; and how to find the best facility available. What did they know about the range of short-term care facilities available (post-acute rehab facilities, SNFs)?
-
Before you knew you would need to have a nursing home stay, had you ever talked with your family or friends about nursing home care? Probe on who, when, why, and what the result of that discussion was, including whether they made any initial attempts to look at their options.
-
What were your biggest concerns about which nursing home you would stay in? Why? Probes on availability, location, cost, aspects of quality or service of greatest concern (were they concerned about having a private room, better meals, or a phone in their room), knowing other people who had received care there. Probe on if they had concerns about how long they would stay or how it would be decided that they could return home. PROBE: At any point, did you think you would never come home?
IV. Information Sources and Decision Support (45 minutes)
I want to ask you about decision-making and what kind of information is helpful in choosing a nursing home. I realize that you each have unique situations. Some of you may have only had a few hours or days to decide which nursing home you would go to. Others may have known weeks in advance that a nursing home would be needed. Lets talk about how much time you had...Ask each participant to share how much time elapsed between when they learned a nursing home stay would be needed and the start of the nursing home stay. Goal is to learn how much lead time participants had in which to seek information and select a facility. Probe to learn when they knew they needed a nursing home; who told them and how they told them.
-
Before you were admitted to the nursing home did you or your family look for information about facilities to consider? Probe on the extent to which they thought they had real options and why or why not; whether they asked for help and whom they asked; how they went about figuring out which nursing home was right for them; where they looked for information; whether anyone provided them with help or information.
-
How did you decide which nursing home you would stay in? Probe on whether they visited facilities; whether other family members visited facilities; whether they sought out additional information on their options; if yes what kind of information and whether it was at all helpful; did they have enough time to make a decision. Critical probe: Were you able to figure out if one facility was better for you than another? (How could you tell there would be a difference?)
-
Who helped you to decide which nursing home you would stay in? Probe on the role of the former resident, family, friends; ask about role of physicians or other health care professionals (ask specifically about whether they sought or got assistance from family doctor, hospital discharge planner, social worker, case manager); ask if they called Medicares toll free line (1-800-Medicare) or visited Medicares website; Probe on who was really helpful and supportive and who might actually have made things more difficult.
-
Thinking about all the information or help you got in deciding on a nursing home how did you decide which information to focus on? Probe to learn how they prioritized the information they received (i.e., what sources of information are more important and which are less important?); how they determined if information could be trusted; how they prioritized input from providers or family who assisted with or participated in decision-making. PROBE: What source of information was the most helpful to you? (Why?) PROBE: Did you get any information that you didnt use? (Why?) PROBE: Did you get any information that so hard to understand that you couldnt use it? (What kind of information? What made it hard to understand?)
-
How confident were you in your decision about which nursing home to stay in? Probe for confidence in their decision, concerns they had after the fact, and whether their concerns were justified.
-
Was there any information you wished you had but could not get? Probe for the types of information they wanted but did not have available.
V. Future Decision-making (20 minutes)
What if you needed to stay in a nursing home again in the future? Would you do anything differently? Has anyone done more research on care facilities? (What kind of facilities did you research? Did you research facilities that provide the same level of care you had before? )
-
What information would you want to help you to make a choice? Probe on whats the most important thing that someone who is looking for nursing home care should know (and why); probe on what is the least important (and why); make sure we understand where that information comes from (Federal Government or other source).
-
Who would you go to for advice or help in making a choice? Probe on role of family, friends, providers, others.
-
Would you do anything differently if you were looking for a nursing home for someone else? Do participants have a different perspective when the choice of for someone else?
-
Do government agencies have a role in providing information to help you compare nursing homes? Probe on role of local, state, Federal Government. Goal is to generate a clear allocation of tasks or role for the agencies participants identify as having a role. PROBE: Based on your experience, how can government agencies be more effective in providing information? Goal is to elicit specific feedback on how agencies can be more effective, what did they do vs. what should they do.
VI. Wrap-up and Closing (10 minutes)
Weve talked a lot this morning about your experience choosing a nursing home and the kind of information that was and wasnt helpful. Is there anything about choosing a nursing home or looking for information to help you compare nursing homes that we have not talked about that you think is important to share?
These last couple of hours have been so valuable to us. We really appreciate it that you have been willing to take the time to share your experience and opinions. We hope it will make it easier for people like yourselves to deal with this kind of situation in the future. Thanks!
Elapsed time estimated at 115 minutes.
Document: Focus Group Topic Guide -- Groups 3 and 6 Flesch-Kincaid Grade Level: 8.1
Topic Guide for Focus Group Discussion with Family Members of Nursing Home Residents
I. Introduction (5 minutes)
Hello! My name is (insert) and I work at RAND, a non-profit research center in Santa Monica, California. Joining me today is (insert) we are part of a research team that is trying to learn how people who have to place a loved one in a nursing home go about finding and selecting the right nursing home for their needs, their own and that of their loved one. [Introduce any observers.] Everyone here has gone through that difficult experience, and we really appreciate your willingness to share your thoughts with us today. Lets make it clear, however, that we are not just idly curious. We are involved in a broader research project to understand the kinds of information people use when choosing a nursing home. Our research is supported by the U.S. Department of Health and Human Services.
As you know, we are audio taping this focus group. The purpose of taping is to make sure we have a complete and accurate record of what happens in the group. Only members of the research team at RAND, and a small number of researchers at the agency that oversees the work, will listen to the tapes. When we write up a report of what we learn, we will use the tapes to pull together the full range of ideas and opinions expressed by people in the focus groups. Once the report is finalized, RAND and our federal sponsor will destroy the tapes. The report will include quotes from what different people say in the group. I want to assure you that no persons name will appear in the report, and we will not include any information that would let a reader identify the person. We are taking all possible measures to protect your confidentiality and privacy.
For example, note that your name tags have only your first name, again to protect your confidentiality. Please use only your own and others first names during the group. In addition, when you talk about your loved one, please use only their first name, or a term like Mom, since we really want to protect their privacy as well. Here are some other ground rules for our discussion:
- There are no right or wrong answers -- everyones opinion has value to us.
- If you dont want to answer a particular question or discuss a particular topic, just say so -- you dont have to answer or discuss anything you dont want to.
- We want to hear from as many of you as possible, so please give your colleagues opportunities to participate. It is best if only one person speaks at a time.
- Especially because we are taping, please speak up, and also refrain from side conversations.
- We do have a limited time, and several issues to discuss. Please dont be offended if I ever have to step in on a discussion to refocus us and move us ahead.
- We are not planning a formal break, so feel free to get up to get refreshments, etc. whenever you like.
- Point out restroom location.
- Ask participants to turn off cell phones.
- Remind participants that theyll receive thank you payments at the conclusion of the group.
Any questions? Lets get going then.
II. Warm Up (10 minutes)
Go around the room and ask each person to tell us the following: how they are related to their family member who is in a nursing home and how long that family member has been in his/her (current) nursing home.
III. Knowledge and Awareness of Long-Term Care (25 minutes)
Id like to talk about how much you knew about nursing homes before your family member was admitted to a nursing home.
-
How much did you know about nursing homes before your family member was admitted to a nursing home? Probe on how much they knew about nursing homes; how much they knew about the cost; and how to find the best facility available. What did they know about the range of care facilities available (nursing home, post-acute rehab facilities, SNFs, board and care, assisted living). How did they know a nursing home was what they needed?
-
Before you knew your family member would need to have a nursing home stay, had anyone in your family ever talked about the possibility? Probe on who initiated the conversation, when, who participated (did they include the family member or not?) what prompted it, and what the result of that discussion was, including whether they made any initial attempts to look at their options (how far in advance did these attempts occur? Over what period of time?)
-
What were your biggest concerns about which nursing home your family member would stay in? Why? Probes on availability, location, cost, quality dimensions of greatest concern, knowing other people who had received care there.
IV. Information Sources and Decision Support (45 minutes)
I want to ask you about decision-making and what kind of information is helpful in choosing a nursing home. I realize that you each have unique situations. Some of you may have only had a few hours or days to decide which nursing home your family member would go to. Others may have known weeks or months in advance that a nursing home would be needed. Lets talk about how much time you had...Ask each participant to share how much time elapsed between when they learned a nursing home stay would be needed and the start of the nursing home stay. Goal is to learn how much lead time participants had in which to seek information and select a facility. Probe to learn when they knew they needed a nursing home; who told them and how they told them.
-
In the amount of time that you had before your family member was admitted to the nursing home, did you look for information about facilities to consider? Probe on the extent to which they thought they had a choice of facilities and why or why not (was that choice real?); whether they asked for help and whom they asked; how they went about figuring out which nursing home was right for their family; where they looked for information; whether anyone provided them with help or information.
-
How did you decide which nursing home your family member would stay in? Probe on whether they visited facilities; whether other family members visited facilities; what role their family member played in decision-making; whether they sought out additional information on their options; if yes what kind of information and whether it was at all helpful; did they have enough time to make a decision. Probe to find out if anyone moved to a different facility after an initial placement (why?). Critical probe: Were you able to figure out if one facility was better for your family member than another? (How could you tell there would be a difference?)
-
Who helped to decide which nursing home your family member would stay in? Probe on the role of the resident, friends, other family members; ask about role of physicians or other health care professionals (ask specifically about whether they sought or got assistance from family doctor, hospital discharge planner, social worker, case manager); ask if they called Medicares toll free line or visited Medicares website; Probe on who was really helpful and supportive and who might actually have made things more difficult.
-
Thinking about all the information or help you got in deciding on a nursing home how did you decide which information to focus on? Probe to learn how they prioritized the information they received (i.e., what sources of information are more important and which are less important?); how they determined if information could be trusted; how they prioritized input from providers or family or resident who assisted with or participated in decision-making. PROBE: What source of information was the most helpful to you? (Why?) PROBE: Did you get any information that you didnt use? (Why? Probe to find out of they got any information they couldnt understand.) PROBE: Did you feel like the information you got was accurate or up-to-date? (How could you tell?)
-
How confident were you in your decision about which nursing home your family member should stay in? Probe for confidence in their decision, concerns they had after the fact, and whether their concerns were justified.
-
Was there any information you wished you had but could not find? Probe for the types of information they wanted but did not have available.
V. Future Decision-making (20 minutes)
What if your family member needed to change nursing homes or needed another nursing home stay in the future. Would you do anything differently?
-
What information would you want to help you to make a choice? Probe on whats the most important thing that someone who is looking for nursing home care should know (and why); probe on what is the least important (and why); make sure we understand where that information comes from (federal government or other source).
-
Who would you go to for advice or help in making a choice? Probe on role of resident, family, friends, providers, others.
-
Do government agencies have a role in providing information to help you compare nursing homes? Probe on role of local, state, Federal Government. Goal is to generate a clear allocation of tasks or role for the agencies participants identify as having a role. PROBE: Based on your experience, how can government agencies be more effective in providing information? Goal is to elicit specific feedback on how agencies can be more effective, what did they do vs. what should they do.
VI. Wrap-up and Closing (10 minutes)
Weve talked a lot this morning about your experience choosing a nursing home and the kind of information that was and wasnt helpful. Is there anything about choosing a nursing home or looking for information to help you compare nursing homes that we have not talked about that you think is important to share?
These last couple of hours have been so valuable to us. We really appreciate it that you have been willing to take the time to share your experience and opinions. We hope it will make it easier for people like yourselves to deal with this kind of situation in the future. Thanks!
Elapsed time estimated at 115 minutes.
Document: Focus Group Topic Guide -- Group 4 Flesch-Kincaid Grade Level: 9.2
Topic Guide for Focus Group Discussion with Hospital Discharge Planners
I. Introduction (5 minutes)
Hello. My name is (insert) and I work at RAND, a non-profit research center in Santa Monica, California. Joining me today is (insert) we are part of a research team that is trying to learn how people who have to place a loved one in a nursing home go about finding and selecting the right nursing home for their needs, their own and that of their loved one. [Introduce any observers.] Weve talked with consumers to get their perspective and now we are talking with you to understand your role as an information resource. We are involved in a broader research project to understand the kinds of information people use when choosing a nursing home. Our research is supported by the U.S. Department of Health and Human Services.
As you know, we are audio taping this focus group. The purpose of taping is to make sure we have a complete and accurate record of what happens in the group. Only members of the research team at RAND, and a small number of researchers at the agency that oversees the work, will listen to the tapes. When we write up a report of what we learn, we will use the tapes to pull together the full range of ideas and opinions expressed by people in the focus groups. Once the report is finalized, RAND and our federal sponsor will destroy the tapes. The report will include quotes from what different people say in the group. I want to assure you that no persons name will appear in the report, and we will not include any information that would let a reader identify the person. We are taking all possible measures to protect your confidentiality and privacy.
For example, note that we used first names only during the conference roll call, again to protect your confidentiality. Please use only your own and others first names during the group. Here are some other ground rules for our discussion:
- There are no right or wrong answers -- everyones opinion has value to us.
- If you dont want to answer a particular question or discuss a particular topic, just say so -- you dont have to answer or discuss anything you dont want to.
- We want to hear from as many of you as possible, so please give your colleagues opportunities to participate. It is best if only one person speaks at a time.
- Especially because we are taping, please speak up, and also refrain from side conversations.
- We do have a limited time, and several issues to discuss. Please dont be offended if I ever have to step in on a discussion to refocus us and move us ahead.
- For telephonic group: review any instructions related to conference call.
- For telephonic group: remind participants that theyll receive thank you payments via federal express within two business days.
Any questions? Lets get going then.
II. Warm Up (10 minutes)
Ask each participant to tell us the following: how long have you been a (discharge planner/community-based social worker)? Probe each participant in turn to ask how many times/how often did you provide support to someone who needed nursing home care in the last year?
III. Consumer Knowledge of Nursing Home Care (20 minutes)
Id like to start with your impressions of how much the clients you meet with know about nursing homes when they first meet with you.
-
First off, is there such a thing as a typical client? Probe to find out if clients are primarily family members, patients themselves or some combination. Who do you generally speak with first? The patient him/herself? Family member? Or do you meet with both initially (if available)?
-
How knowledgeable is the average consumer or (patient/clients/family) you work with? Do (patients/families) demonstrate any knowledge of the range of care facilities available (nursing home, post-acute rehab facilities, SNFs, board and care, assisted living)? How do the families you counsel know a nursing home is what they need?
-
What types of questions do you hear most often from the (patients/families) you work with? Probe on whether (patients/families) ask questions about the cost, about services, about amenities, about how to compare or evaluate facilities.
IV. Disseminating Information to Consumers (30 minutes)
-
What information do you (or your facility) currently provide for (patients/families) who need to arrange for nursing home care? Probe on content and specifics of the material they distribute; is this something they or their facility have created? Probe to determine the media or formats in which information is available (paper, web, video, in-person tours of facilities). Probe to find out if any of the following are resources the use or provide to (patients/clients/families):
- Medicare.gov?
- Internet sites other than Medicare.gov (which ones?)
- Print materials created by local/national organizations (e.g., Area Agencies on Aging, AARP, national/state nursing home association).
- Information from local nursing facilities, etc.
-
Probe to determine if they use standard materials for everyone or create personalized resources depending on the patient/client and their needs. How does the supply of facilities in your area affect the information you provide? PROBE: Are there any rules or regulations that limit the type of information you can provide? PROBE: Do you use Medicares nursing home compare website? Probe on how they use it, why they use it. If they dont use it, probe to find out why not.
-
How much time do you spend on average with each (patient/family)? Does this take place in one meeting or do you have several meetings with the (patients/families) prior to their making a decision about nursing home care?
V. Consumer Priorities and Decision Support (45 minutes)
-
How do you think (patients/families) use the information you provide? Is the information they get from you their only source of information or are they using it in conjunction with other material?
-
How much time do the (patients/families) you work with generally have to make a decision? How do you think that impacts their decision-making process? Probe on what factors might affect the (patients/families) ability to make use of the time available.
-
What is your impression of the criteria (patients/families) use to select a nursing home? Probe to find out if there are any common themes or if each (patient/family) is unique.
-
How do you think families prioritize selection criteria? What is most important to them? Probe to find out if/how the time available to make a decision impacts this process.
-
What role do you play in assisting (patients/families) to make a choice? Probe to find out if their role is limited to disseminating information or if they assist (patients/families) in using the information or evaluating individual facilities. PROBE: Are there any rules or regulations that limit your role as decision support? Probe to find out if their role is limited by any issues related to supply (such as the number or type of facilities in the area, availability of a bed when needed).
-
Does your role get easier with time and experience, or does each (patient/family) present a unique set of needs and priorities?
-
Do you think there are any gaps in the information system? By that I mean do you find yourself in need of information that doesnt exist? If yes, probe to find out what information they think is missing and what organization or agency they think is responsible for this information.
-
What strategies should be used to disseminate information such as comparative information about different facilities?
-
Do government agencies have a role in providing information to help families compare nursing homes? Probe on role of local, state, Federal Government. Goal is to generate a clear allocation of tasks or role for the agencies that participants identify as having a role. PROBE: Based on your experience, how can government agencies be more effective in providing information? Goal is to elicit specific feedback on how agencies can be more effective, what did they do vs. what should they do.
VI. Wrap-up and Closing (10 minutes)
Weve talked a lot this morning about your experience working with families who need to find a nursing home. Is there anything about working with these families or providing information to help them compare nursing homes that we have not talked about that you think is important to share?
This discussion has been so valuable to us. We really appreciate it that you have been willing to take the time to share your experience and opinions. Thanks!
Elapsed time estimated at 120 minutes.
Document: Focus Group Topic Guide -- Group 5 Flesch-Kincaid Grade Level: 9.1
Topic Guide for Focus Group Discussion with Community-Based Case Managers
I. Introduction (5 minutes)
Hello. My name is (insert) and I work at RAND, a non-profit research center in Santa Monica, California. Joining me today is (insert) we are part of a research team that is trying to learn how people who have to place a loved one in a nursing home go about finding and selecting the right nursing home for them. (Introduce any participants from ASPE.) Weve talked with consumers to get their perspective and now we are talking with you to understand your role as an information resource. We are involved in a broader research project to understand the kinds of information people use when choosing a nursing home. Our research is supported by the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation.
As you know, we are audio taping this focus group. The purpose of taping is to make sure we have a complete and accurate record of what happens in the group. Only members of the research team at RAND, and a small number of researchers at the agency that oversees the work, will listen to the tapes. When we write up a report of what we learn, we will use the tapes to pull together the full range of ideas and opinions expressed by people in the focus groups. Once the report is finalized, RAND and our federal sponsor will destroy the tapes. The report will include quotes from what different people say in the group. I want to assure you that no persons name will appear in the report, and we will not include any information that would let a reader identify the person. We are taking all possible measures to protect your confidentiality and privacy.
For example, note that we used first names only during the conference roll call, again to protect your confidentiality. Please use only your own and others first names during the group. Here are some other ground rules for our discussion:
- There are no right or wrong answers -- everyones opinion has value to us.
- If you dont want to answer a particular question or discuss a particular topic, just say so -- you dont have to answer or discuss anything you dont want to.
- We want to hear from as many of you as possible, so please give your colleagues opportunities to participate.
- Especially because we are taping, please speak up, and also refrain from side conversations.
- We do have a limited time, and several issues to discuss. Please dont be offended if I ever have to step in on a discussion to refocus us and move us ahead.
- Remind participants that theyll receive thank you payments at the end of the group.
Any questions? Lets get going then.
II. Warm Up (10 minutes)
Ask each participant to tell us the following: how long have you been a community-based case manager? Probe each participant in turn to ask how many times in a typical week do you provide support to someone who needs nursing home care?
III. Consumer Knowledge of Nursing Home Care (20 minutes)
Id like to start with your impressions of how much the clients and families you meet with know about nursing homes when they first meet with you.
-
First off, is there such a thing as a typical client? Probe to find out if planner works primarily with clients themselves, primarily with family members, or some combination. Who do you generally speak with first? The client him/herself? Family member? Or do you meet with both initially (if available)?
-
How knowledgeable about LTC (in general) and nursing home care (in particular) is the average client (or family) you work with? Do clients and families demonstrate any knowledge of the range of care facilities available (nursing home, post-acute rehab facilities, SNFs, board and care, assisted living)? How do the families you counsel know a nursing home is what they need?
-
What information are people looking for when they come to you for assistance? What types of questions do you hear most often from the clients and families you work with? What terms do they use to describe their needs? Probe on whether clients and families ask questions about the staffing, about cost, about services/programs, about amenities, quality measures or deficiencies, about how to compare or evaluate facilities.
IV. Disseminating Information to Consumers (30 minutes)
-
What information do you (or your facility) currently provide for clients and families who need to arrange for nursing home care? Probe on content and specifics of the material they distribute; is this something they or their organization have created? Probe to determine the media or formats in which information is available (paper, web, video, in-person tours of facilities). Probe to find out if any of the following are resources the use or provide to clients and families:
- Medicare.gov (Ask specifically about Nursing Home Compare).
- Other government sources, such as Guide to Choosing a Nursing Home, Administration on Aging, Area Agencies on Aging, or the state survey and certification agency.
- Internet sites other than Medicare or the Federal Government (which ones?).
- Print materials create by local/national organizations (e.g., AARP, national/state nursing home association).
- Information from local nursing facilities, etc.
-
How often do you visit facilities in your area? (To what extent do you share your impressions from those visits with clients and families?)
-
Probe to determine if they use standard materials for everyone or create customized resources depending on the client and their needs. (IF CUSTOMIZED: In what ways do you customize or tailor materials?) How does the supply of facilities in your area affect the information you provide? PROBE: Are there any rules or regulations that limit the type of information you can provide? PROBE: Do you use Medicares nursing home compare website? Probe on how they use it, why they use it. If they dont use it, probe to find out why not. In particular, do they identify gaps between the type of information that is on Nursing Home Compare and the type of information clients/clients/families need?
-
Walk me through the process you got to when you respond to requests for assistance. Typically, how much time do you have to work with? Probe to determine if 1 day, 1 hour, or everything in between.
V. Consumer Priorities and Decision Support (45 minutes)
-
In your experience how do clients and families use the information you provide? Is the information they get from you their only source of information or are they using it in conjunction with other material? (What other material?)
-
How do you think the time available for decision-making impacts the decision-making process? Probe on what factors might affect the (clients/familys) ability to make use of the time available, try and get a sense of a typical timeline for decision-making.
-
If a client is unable to communicate his/her preferences or needs, who speaks for that client? What if that client has no family?
-
What is your impression of the criteria clients and families use to select a nursing home? Probe to find out if there are any common themes or if each (client/family) is unique.
-
How do you think families prioritize selection criteria? What is most important to them? Probe to find out if/how the time available to make a decision impacts this process.
-
What role do you play in assisting clients and families to make a choice? Probe to find out if their role is limited to disseminating information or if they assist clients and families in using the information or evaluating individual facilities. PROBE: We talked earlier about rules or regulations that limit the type of information you can provide. Are there any rules or regulations that limit your role as decision support? Probe to find out if their role is limited by any issues related to supply (such as the number or type of facilities in the area, availability of a bed when needed).
-
Do you think there are any gaps in the information available to help people choose a nursing home that best meets their needs? By that I mean do you find yourself in need of information that doesnt exist? If yes, probe to find out what information they think is missing and what organization or agency they think is responsible for this information.
-
What strategies could be used to disseminate information such as comparative information about different facilities?
-
Do government agencies have a role in providing information to help families find and compare nursing homes? Probe on role of local, state, Federal Government. Goal is to generate a clear allocation of tasks or role for the agencies that participants identify as having a role. PROBE: Based on your experience, how can government agencies be more helpful in providing information? Goal is to elicit specific feedback on how agencies can be more effective, what did they do vs. what should they do.
VI. Wrap-up and Closing (10 minutes)
Weve talked a lot this morning about your experience working with families who need to find a nursing home. Is there anything about working with these families or providing information to help them compare nursing homes that we have not talked about that you think is important to share?
This discussion has been so valuable to us. We really appreciate it that you have been willing to take the time to share your experience and opinions. Thanks!
Elapsed time estimated at 120 minutes.
APPENDIX D. CHARACTERISTICS OF INFORMATION INTERMEDIARIES
| Characteristics | Hospital Discharge Planners | Community-Based Case Managers |
| Number of Participants | 11 | 8 |
| Gender | Female = 11 | Female = 8 |
| Job Title | Case Manager = 1 Nurse Case Manager = 2 Discharge Planner = 4 Discharge Planner/Case Manager = 1 Medical Social Worker = 3 | Community-Based Case Manager = 2 Community-Based Case Manager Supervisor = 1 Care Management Supervisor = 1 Geriatric Care Manager = 2 Senior & Social Services Specialist = 1 Social Worker = 1 |
| Years of Experience | 1 year = 0 1-3 years = 0 3-5 years = 2 5-10 years = 5 >10 years = 4 | 1 year = 1 1-3 years = 1 3-5 years = 2 5-10 years = 1 >10 years = 3 |
| Number of Times per Week Provide Assistance with Facility Placement | 5 times = 1 5-10 times = 4 11-15 times = 2 >15 times = 4 | 5 times = 5 5-10 times = 3 11-15 times = 0 >15 times = 0 |
APPENDIX E. CHARACTERISTICS OF CONSUMERS
| Characteristics | Short-Stay Residents | Family Members |
| Gender | Male = 5Female = 10 | Male = 8Female = 9 |
| Age | 64 or younger = 565 to 74 = 775 to 84 = 285 or older = 1 | 25 to 34 = 235 to 44 = 445 to 54 = 555 to 64 = 465 to 74 = 2 |
| Education | Diploma or GED = 3Some College = 8 4-Year Degree = 2More than 4-Year Degree = 2 | Diploma or GED = 4Some College = 54-Year Degree = 3More than 4-Year Degree = 5 |
| Ethnicity | Hispanic or Latino = 1Not Hispanic or Latino = 14 | Hispanic or Latino = 4Not Hispanic or Latino = 13 |
| Race | White = 10Black or African-American = 4Asian = 0Other = 1 (Hispanic) | White = 12Black or African-American = 4Asian = 1Other = 0 |
| Marital Status | Married = 9Live w/Partner = 0Widowed = 3Separated = 0Divorced = 1Never Married = 2 | Married = 9Live w/Partner = 2Widowed = 0Separated = 1Divorced = 3Never Married = 2 |
| Number of Nursing Homes Considered | One = 4Two = 2Three = 5Four or More = 3No Data = 1 | One = 3Two = 3Three = 5Four or More = 0No Data = 0 |
| Who Took Part in Choosing a Nursing Home | Spouse = 4Child/Children = 6Other Family = 3Friend = 5Doctor = 3Nurse/Social Worker/Discharge Planner = 6Case Worker = 0 | Loved One = 4Loved Ones Spouse = 2Loved Ones Doctor = 1Nurse/Social Worker/Discharge Planner = 2Participants Spouse = 1Other Family = 8Pastor = 1Alone = 4 |
| Rating of Nursing Home | Mean = 6.4Range = 0,10 | Mean = 5.9Range = 2,10 |
| Sources of Information on Health Issues | Doctor/Pharmacist/Other Prof. = 14Newspapers/Magazines = 1Television/Radio =0Internet = 1Family/Friends = 7Other = 1No Data = 1 | Doctor/Pharmacist/Other Prof. = 14Newspapers/Magazines = 5Television/Radio =3Internet = 6Family/Friends = 15Other = 3 |
APPENDIX F. KEY CHARACTERISTICS INFORMING NURSING HOME SELECTION
| Short-Stay Residents | Family Members of Residents | Information Intermediaries |
|
|
|
| NOTE: The top ten characteristics are listed in order of frequency with which they were mentioned during the focus groups. Additional characteristics, which were mentioned less often, are listed below in bulleted form. | ||
NOTES
-
This URL links to the Illinois Council on Long Term Care. It appears that the participant may not have clearly recalled the site viewed but nevertheless had identified a site that was useful in her search.