
U.S. Department of Health and Human Services
Informal Caregiving: Compassion in Aging
June 1998
PDF Version (28 PDF pages)
AN INTRODUCTORY MESSAGE FROM:
Jeannette TakamuraAssistant Secretary for Aging
Bob Williams Deputy Assistant Secretary for Disability, Aging and Long-Term Care Policy Office of the Assistant Secretary for Planning and Evaluation
This booklet, developed by the U.S. Department of Health and Human Services (DHHS) is about informal caregiving--unpaid care given voluntarily to ill or disabled persons by their families and friends. Informal caregiving by families and friends is the backbone of America's long-term care system. According to recent surveys sponsored by DHHS, 52 million of our fellow Americans are informal caregivers. These caregivers provide help to individuals of all ages. They are the lifeline for aging parents. They provide loving care to spouses who can no longer care for themselves. With determination, and sometimes considerable sacrifice, they raise children with even the most severe disabilities at home. Increasingly, we see parents continuing to care for their sons and daughters with disabilities well into old age.
In our society, informal caregivers often go unnoticed except by those who depend on their care. The recipients of informal caregiving understand how important their caregivers' efforts are to their personal well-being. We would like the leaders of all segments of society--including policymakers, educators, the clergy and the media--to acknowledge and celebrate informal caregiving as one of the notable strengths of our Nation's families and communities. Nowhere are these strengths more evident than in the vital role that families and communities continue to play in providing informal care to family, friends, and neighbors who because of illness or disability need help with the routine activities of daily life.
Most of us think of "health care" as services provided by medical professionals (e.g., physicians and nurses) in hospitals, doctor's offices, and nursing homes. However, for individuals whose medical conditions or injuries have resulted in chronic illness or disability, the foundation of health care is access to help with daily living tasks, such as eating, bathing, leaving their homes to go to the doctor or the church. In most instances, this type of assistance can be provided by family members, friends, and neighbors because it involves helping others perform ordinary everyday activities.
In our view, we can draw two important lessons from the descriptive data presented in this booklet. The first lesson is that the contributions of informal caregivers are irreplaceable. We could not, as individuals or as a society, afford to pay the costs of replacing all informal caregivers with paid personnel. The second lesson is that we cannot take informal caregiving for granted. Providing informal care--particularly to an individual who requires a great deal of assistance on a daily basis--involves a substantial amount of time, dedication, and perseverance. Individuals who take on the role of "informal caregiver" will almost certainly be required to forfeit many hours of what might otherwise have been their leisure time. If employed, informal caregivers will likely face conflicts between their work and caregiving responsibilities. We also know that most informal caregivers gain personal satisfaction from helping family members, friends, and neighbors. Oftentimes this is what enables those who also experience considerable stress and burden to persevere.
In the years to come, it will become increasingly important to formulate policies that support and sustain informal caregiving. These policies must recognize that families and communities cannot always meet the needs of their ill and disabled members by themselves. Moreover, individual caregivers cannot be expected or required to do so much that their own health and well being is placed in jeopardy. A great deal of debate may need to go into determining what are reasonable expectations for informal caregivers and how much is "too much." In order to accommodate the needs of informal caregivers, society may also need to adjust expectations in other areas of life, such as in the workplace. Some "family-friendly" policies have been put in place, such as the 1993 Family and Medical Leave Act, but much more thought and effort needs to be given to developing additional ways of enabling--but also, when necessary, providing relief to--informal caregivers.
PART I: INFORMAL CAREGIVING TO FAMILY AND FRIENDS ACROSS THE LIFE COURSE INTRODUCTION
Individuals of all ages with disabilities depend on informal care provided by their families and friends to carry out many of the routine activities of daily life. Part I of this booklet presents information from the National Surveys of Families and Households. These surveys include data on the characteristics and extent of caregiving provided to all people with disabilities including young children, working age adults, and older people.
OVERVIEW
One in three Americans voluntarily provide unpaid informal care each year to one or more ill or disabled family members or friends.
- 52 million Americans (31 percent of the adult population age 20 to 75) provide "informal care" to a family member or friend who is ill or disabled. About 37 million of these caregivers provide help to family members and about 15 million provide help to friends.
- Eight percent of these caregivers reported providing help over the last year to more than one care recipient.
| Adults 20-75 Providing Informal Care |
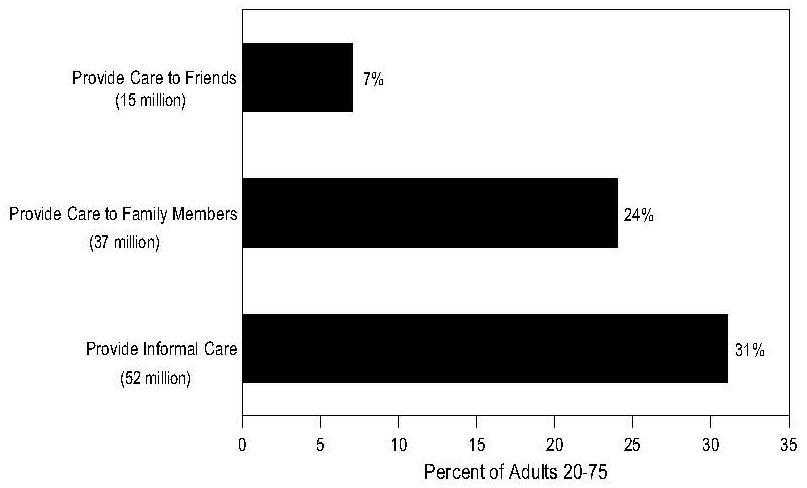 |
| SOURCE: National Survey of Families and Households |
People at all stages of life give and receive informal care.
- The most common informal caregiving relationship is that of an adult child assisting an elderly parent. Thirty eight percent of informal caregiving is provided by children to aging parents.
- Eleven percent of informal caregiving is provided by spouses, most often to their elderly wives or husbands.
- Seven percent of informal care is provided to significantly disabled children, most often to adult disabled children by middle-aged parents.
- Finally, about 20 percent of informal care is provided to other relatives such as grandparents, siblings, aunts, and uncles, and about 24 percent is provided to friends and neighbors.
| Recipients of Informal Care |
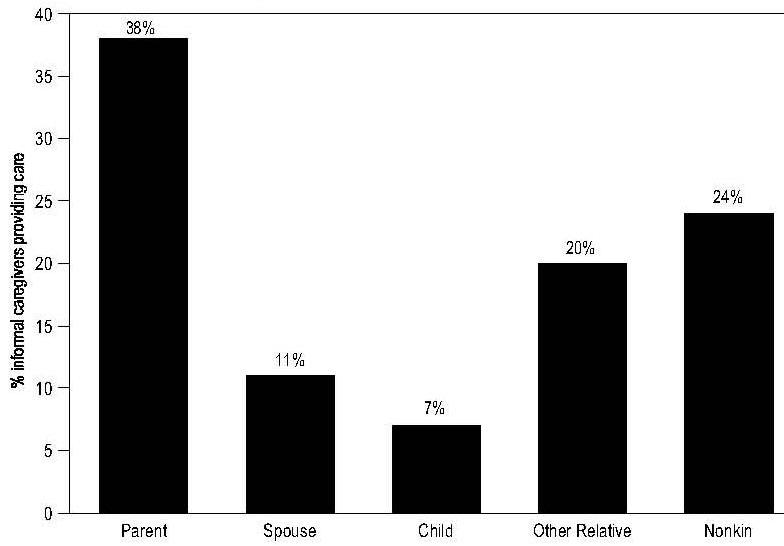 |
| SOURCE: National Survey of Families and Households |
One in five Americans are providing informal care to an ill or disabled family member at any point in time, reflecting the long-term nature of much informal care.
- Nearly 40 percent of individuals who reported providing informal care to an ill or disabled family member in the 1987 National Survey of Families and Households (NSFH) also reported providing informal care in the 1992 survey.
Caregiving responsibilities are assumed by adults of all ages but are most common in middle age.
- The average age of all informal caregivers is 43 years old. Spouses caring for their disabled husband or wife are somewhat older, with an average age of 55 years. Parents who care for an ill or disabled child have an average age of 46 years. The average age of those who assist other relatives is about 41/years.
- Adults in their forties and early fifties are twice as likely to provide informal care as adults in their twenties or seventies. Thirteen percent of Americans in their early twenties and 14 percent of adults aged 70 and older provide informal care, compared with 30 percent of Americans in the age group 40 to 54.
- Among Americans from their mid-twenties to their seventies, parents are the most frequent recipients of informal care. However, the likelihood of caring for an ill or disabled child is also greatest in middle age.
- Younger caregivers are more likely to care for other family members such as grandparents, aunts, and uncles. Caregiving to other relatives declines through middle age as other familial responsibilities take hold, but increases in the late fifties and early sixties. Over the age of 60, women frequently report providing care to a sibling.
Both men and women provide informal care. However, up to age 70, women are more likely to be caregivers and to provide more hours of care, to provide more care over longer periods, and to care for more than one person.
- Across all age groups, 27 percent of women as compared with 21 percent of men provide informal care over the course of a year.
- On average, women provide about 50 percent more hours of informal care per week to their care recipients than their male counterparts.
- Women are twice as likely as men to provide informal care to ill or disabled children. This is partly the result of traditional gender expectations for child care but also because of the increase in households headed by single mothers.
- Mothers also provide about three times more informal care to children with disabilities who do not live in the same household. However, fathers provide informal care over slightly longer periods--averaging about 19 weeks over the course of a year compared with 15 weeks for mothers.
- The number of hours of informal care provided by men across the life course is relatively low--ranging from about five hours per week among men aged 60 to 64 to 11 hours per week among men in their late forties. The exception to this pattern is men in their late sixties who provide about 15 hours of help per week to their disabled wives.
- Nearly two-fifths of the women who reported providing informal care in 1987 also reported providing informal care in 1992--whereas only one-third of the men who were informal caregivers in 1987 also reported providing care in 1992.
Both black and white Americans are equally likely to provide informal care. However, black women are more likely to be caregivers than white women.
- Across the life course, black women are more likely to provide care to disabled relatives other than immediate family members than are white women. Additionally, the likelihood of parental caregiving to children with disabilities starts earlier in the life course for black women.
- White women are more likely to provide care to a disabled spouse, probably because of differences in marriage patterns between black and white women. White women are most likely to care for an ill or disabled child as young adults or in early middle age. Caregiving for a child is more prevalent in later middle age among black women. Six percent of black women in their fifties reported caring for an ill or disabled child.
- Parental caregiving for disabled children peaks for both blacks and whites in middle age. In addition, at similar ages, eight percent of black men provide care to an ill or disabled parent and 15 percent of white men provide such care.
Caregiving also varies by marital status.
- Married caregivers are most likely to be assisting their aging parents while never-married caregivers are more likely to be giving informal care to disabled relatives outside the immediate family. Widowed, divorced, and separated caregivers are more likely to provide care to friends and neighbors.
Caregivers generally tend to be as healthy--and sometimes healthier--as the general population or non-caregivers their age.
- Three-quarters of all caregivers report that they are in "excellent or good health," while about 18 percent report they are in "fair health," and only six percent report that they are in "poor health."
- Spouse caregivers are twice as likely to report being in "poor or fair" health than the caregivers of parents, children or other relatives. This can be explained by the older average age of spouse caregivers.
- Conversely, caregivers to other kin are more apt to report "good or excellent" health, probably because they are younger, on average, than other caregivers.
- Daughters providing care to their ill or disabled parents are more likely to report being in "good or excellent" health than the average population; however, sons who provide such care report being no more or less healthy than the average.
The majority of informal caregivers are also employed.
- Nearly 64 percent of all informal caregivers report being employed during the previous 12 months. About 65 percent of caregivers who provided care to more than one person over the last year also reported being employed.
- The percentage of employed women caregivers closely mirrors the average percent of non-caregiving women in the work force. Working women caregivers are only slightly more likely to be working part-time (i.e., less than 35 hours per week) than are employed women in general. In 1992, 31 percent of non-caregiving women worked part-time and 41 percent of caregiving women worked part-time.
- Male caregivers are as likely to be in the labor force as other men who do not provide informal care. For men, caregiving did not affect their likelihood of working part-time.
- Working women employed full-time generally provide as much care as women working part-time. On average, in 1992, full- and part-time employed women provided 11 and 12 hours, respectively, of informal care per week.
- Of "career caregivers" (those who reported providing informal care both in 1987 and 1992), nearly 65 percent were employed in both years. The majority (88 percent) of career caregivers worked 35 hours or more per week in 1992.
SUMMARY
Providing informal care to ill or disabled family and friends is a normative experience. Most Americans will be informal caregivers at some point during their lives, and many will provide informal care at various ages to multiple care recipients.
(DATA SOURCES: The statistics reported above are from the 1987 and 1992 National Surveys of Families and Households. These surveys were designed and conducted by the University of Wisconsin, Center for Demography and Ecology, Madison, Wisconsin (Principal Investigators: James Sweet and Larry Bumpass). Funding for the surveys was provided by the National Institute for Child Health and Human Development and the National Institute on Aging, U.S. Department of Health and Human Services. Data analyses were performed by Janice I. Farkas, Research Associate, Department of Sociology, Duke University, and Christine L. Himes, Senior Research Associate and Assistant Professor of Sociology, Center for Policy Research, Maxwell School, Syracuse University, under contract to the Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services.
PART II: IN-DEPTH FOCUS ON INFORMAL ELDERCARE
The most typical informal caregiving in the U.S. involves the provision of assistance to elderly persons who, because of chronic illness and/or disability, need help with everyday activities. The information in Part II of the booklet will takes a closer look at characteristics of caregiving for older people with functional disabilities.1 The information provided below is drawn from the National Long-Term Care Surveys. It is different from the information contained in Part I because it focused exclusively on elderly recipients of care and their primary caregivers.
OVERVIEW
Over seven million Americans provide 120 million hours of informal care to approximately 4.2 million functionally disabled elders each and every week. If the work of these caregivers had to be replaced by paid home care, the cost would run from $45 billion to $94 billion dollars a year.
- The majority of caregivers of disabled elders are assisting family members.
- The average number of informal caregivers per disabled elder is 1.7, and each caregiver provides an average of almost 20 hours of unpaid help each week.
- Each disabled elder receives an average of 29 hours of help from informal caregivers each week.
| Average Weekly Hours of Eldercare |
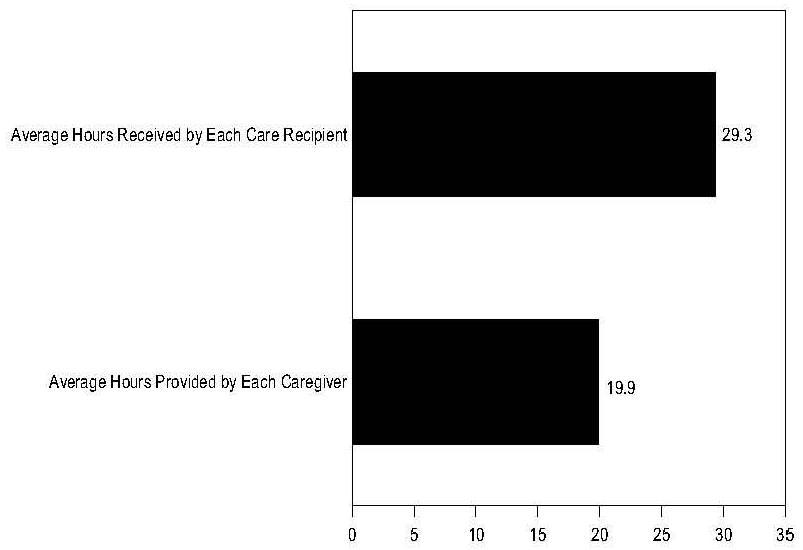 |
| SOURCE: 1994 National Long-Term Care Survey |
Most older people with functional disabilities live in the community rather than in nursing homes.
- Less than one-quarter of the elderly with functional disabilities--about 1.4 million people--live in nursing homes at any point in time, while 4.2 million live in their own homes and communities.
- Research suggests that informal care plays a significant role in preventing or delaying the need of a disabled elder to go into a nursing home. In fact, 1.6 million elders with severe long-term disabilities (defined as having three or more ADL dependencies or severe cognitive impairment) are able to live in the community in their own or relatives' homes. There are 1.4 million elders who live in nursing homes.
A PORTRAIT OF ELDERS LIVING IN THE COMMUNITY IN NEED OF LONG-TERM CARE
Of the 31.4 million Americans aged 65 and older living in the community, about 4.4 million (14 percent) have long-term functional disabilities. These disabled elders require on-going help from others for an extended period (three or more months) to perform one or more ADL or IADL tasks.
- About 2.3 million elders need help with one or more ADL tasks such as eating, bathing, or dressing.
- About 2.2 million elders need help with only IADL tasks, such as cooking, shopping or going outside of their house.
- Almost one million elders are severely cognitively impaired because they have Alzheimer's disease or another form of dementia.
| Percent of Older Persons with Long-Term Functional Disabilities |
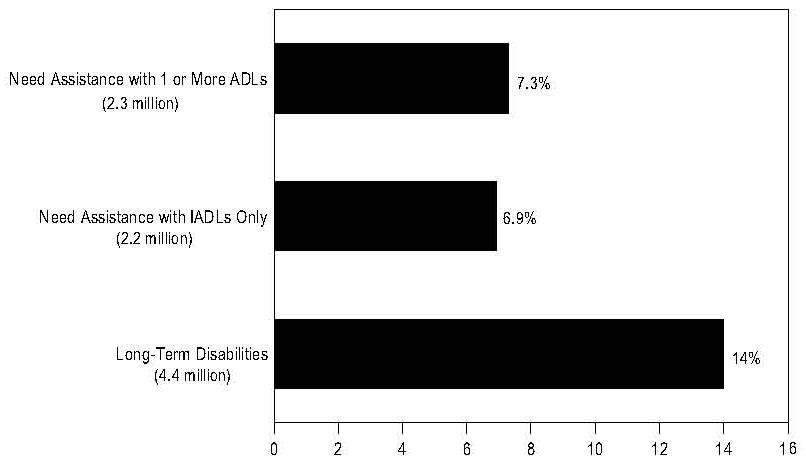 |
| SOURCE: 1994 National Long-Term Care Survey |
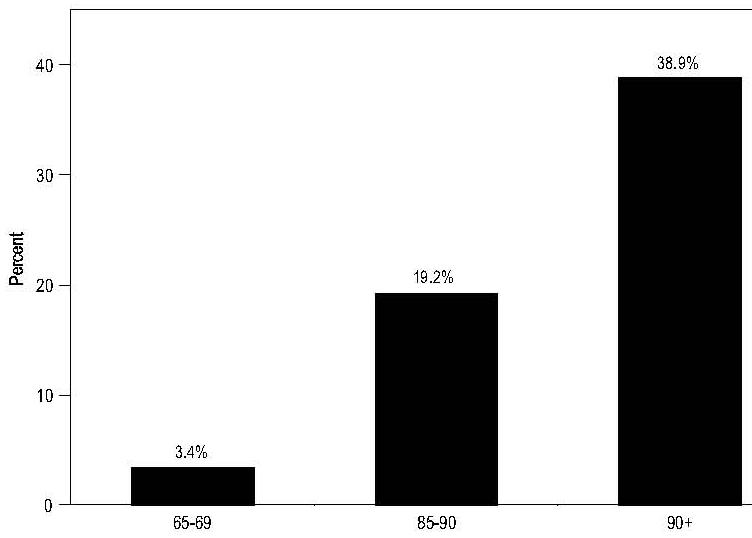
Functional disability increases at older age and is more common among elderly women than men.
- Among individuals aged 65-69, only 3.4 percent have an on-going need for help with an ADL activity. Among those aged 85 to 90, this percentage rises to a little over 19 percent, and by age 90 almost 40 percent of elders are limited in their ability to perform ADL activities.
- Long-term functional disability is also more common among older women than older men. For example, in the 65 to 69 age group only about 2.5 percent of men have an ADL limitation while four percent of women do. Among elders age 90 or older, only about one-quarter of men need help to perform an ADL task while over 44 percent of women need such assistance.
| ADL Disability by Age |
 |
| SOURCE: 1994 National Long-Term Care Survey |
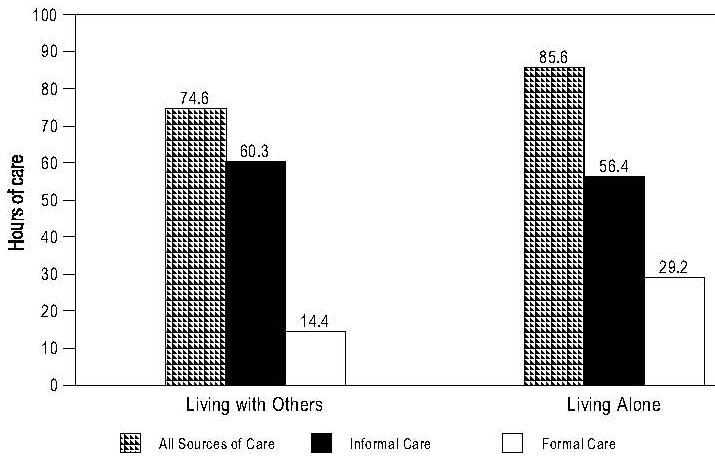
Informal care is the main source of help for the majority of disabled elders living in the community.
- The majority of elders with functional disabilities continue to reside in the community rather than in nursing homes, even at higher levels of disability.
- The overwhelming majority (about 96 percent) receive at least some assistance from informal caregivers, and about two-thirds rely exclusively on informal caregiving.
- As disability increases, elders receive more and more informal care. Eighty-six percent of elders at greatest risk of nursing home placement (those with three or more ADL disabilities) live with others and receive about 60 hours of informal care per week, supplemented by a little over 14 hours of assistance from paid helpers.
- The small proportion (four percent) of disabled elders who live alone and experience high levels of disability receive more paid care (56 hours per week) than informal care (about 29 hours per week).
| Care Received by Elders At Risk for Nursing Home Placementby Living Arrangement |
 |
| SOURCE: 1994 National Long-Term Care Survey |
THE ROLE OF FORMAL PAID HOME CARE
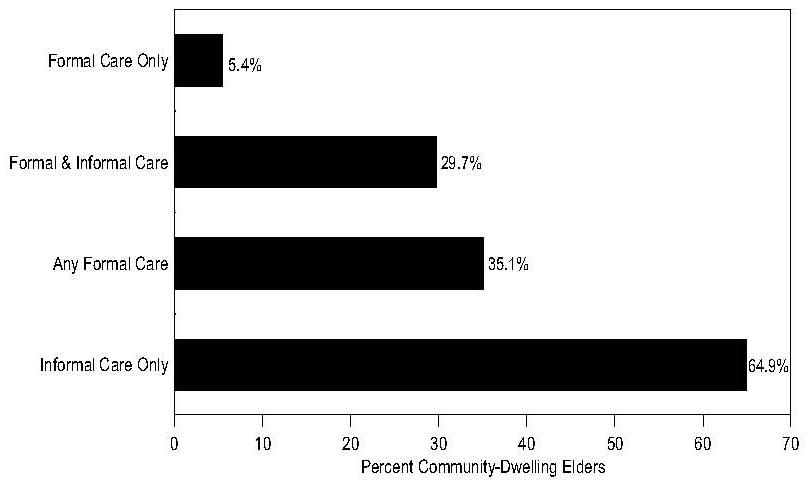
Formal paid home care is the exception, not the rule, for the great majority of functionally disabled elders.
- Slightly over one-third (35.1 percent) of disabled elders with long term care needs use any formal home care--and only 5.4 percent rely entirely on paid helpers.
- The use of paid home care is much greater among elders with moderate to severe levels of disability (that is, those requiring assistance with one or more ADL task). Roughly half of the most severely disabled elders (those who are considered at high risk of nursing home placement because they have three or more ADLs) use some paid home care.
| Use of Informal and Formal Care by Community-Dwelling Elders with Chronic Disabilities |
 |
| SOURCE: 1994 National Long-Term Care Survey |
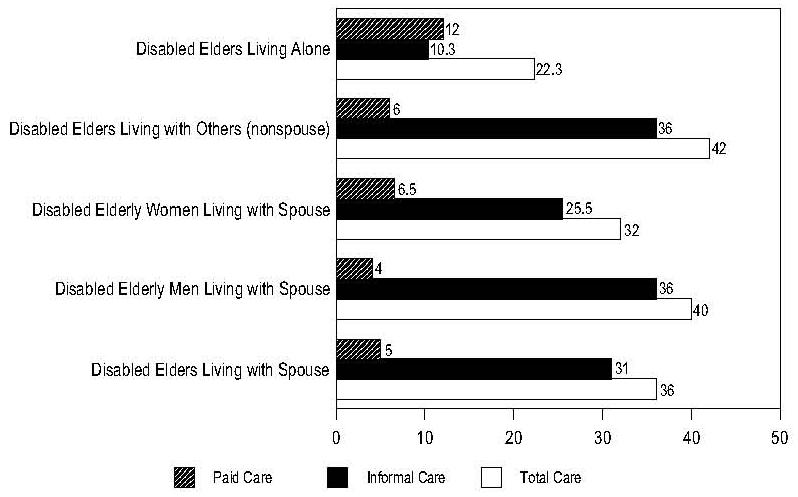
- Disabled elders who live with their spouses are least likely to rely on formal help, receiving on average about five hours of assistance from paid caregivers each week in comparison to the 36 hours of help they receive each week from informal caregivers. Disabled elderly men cared for by their wives use the least amount of paid care, averaging about four hours a week from formal home care providers in comparison to about 40 hours received informally.
- On the other hand, disabled elderly women who live with their husbands receive somewhat less informal help (about 32 hours per week) from their husbands and more help from paid caregivers (about 6.5 hours per week).
- The use of paid home care, although it still constitutes a relatively small proportion of all home care, has been slowly increasing from the early 1980s to the mid-1990s. In 1982, only 25 percent of elders with long-term care needs used any formal home care. By 1992, over 35 percent used paid care.
On average, disabled elders who live alone are less severely disabled than those who live with others. Even though disabled elders who live alone receive fewer total weekly hours of assistance from all sources, they receive more hours of paid help per week than those who live with others.
- Disabled elders who live with other relatives or with friends receive an average of 42 hours of care per week, of which 6 hours are from paid helpers.
- Disabled elders who live alone receive an average of 22 hours of care, of which 12 hours are from paid helpers.
| Hours of Assistance Received Per Week By Type of Assistance, Care Recipient, and Living Arrangement |
 |
| SOURCE: 1994 National Long-Term Care Survey |
WHO PAYS FOR HOME CARE?
- Almost half of disabled elders who use formal home care pay for it themselves or their families pay for it out of pocket.
- Medicare is the most common third party payer. In 1994, slightly under one-third (31 percent) of disabled elders with long-term care needs used Medicare home health services at some point during the year. To qualify for Medicare home health coverage, beneficiaries must require skilled nursing or therapy services.
- Other payers include Medicaid, the Social Services Block Grant, Title III of the Older Americans Act, and the Veterans' Administration. Private long-term care insurance currently finances only very small amounts of home care--but may develop into a more significant funding source over the next twenty years.
In sum: Because the care that severely disabled elders require is very labor intensive, the evidence strongly suggests that most elders with three or more ADL disabilities are able to avoid nursing home admission and continue residing in the community because they do not live alone and are able to obtain most of the help they require on an unpaid basis, from family, friends, and neighbors.
PRIMARY INFORMAL CAREGIVER CHARACTERISTICS
Experts on eldercare typically refer to the person who regularly provides the most assistance as the "primary" informal caregiver. Most disabled elders have a primary informal caregiver who provides the bulk of their care and obtains and coordinates additional help from other paid and unpaid "secondary" caregivers.
- Almost three-quarters of primary informal caregivers are women.
- The average age of primary caregivers is over 60 years old. Half are 65 or older, and slightly over one-third are between the ages of 45 and 64.
- Over two-thirds (68 percent) of primary caregivers live in the same household with the disabled elders for whom they provide care, and a majority of primary caregivers are spouses (40 percent) or adult children (36 percent). The prevalence of spouse caregiving is higher among elders with moderate to severe levels of disability.
In sum: Disabled elders rely primarily on their spouses if they have spouses healthy enough to provide assistance. Adult (mostly middle-aged) children are the next most frequent source of informal eldercare--and constitute the main source of assistance for disabled elders who are widowed. Other relatives and friends are most often secondary helpers, stepping into the role of primary caregiver only when spouses or adult children are not available.
EMPLOYMENT AND CAREGIVING
- While the great majority of primary informal caregivers are not employed because they are beyond retirement age, almost one-third (31 percent) do work. About two-thirds of those who are employed work full-time (35 or more hours per week). Employed primary caregivers work an average of about 40 hours per week.
- Employed caregivers personally provide fewer weekly hours of assistance than non-employed caregivers but they still make a substantial weekly time commitment to informal caregiving (18 hours per week, on average).
- Employed primary caregivers are less likely than nonemployed primary caregivers to be sole caregivers; they are able to maintain their primary caregiving role even to elders with high levels of disability (three to five ADLs) by obtaining supplemental assistance from other family members, paid caregivers, or a combination of help from both these sources.
- Even with supplemental help, employed primary caregivers contribute personally between 32 and 39 hours per week of informal care to their disabled elders with three, four, or five ADL dependencies.
CAREGIVING--THE GREAT BALANCING ACT
Caregiving can create some conflict for caregivers who have to balance work and caregiving responsibilities or who have health problems of their own.
- Primary caregivers of disabled elders are typically in late middle-age or even older, and as a result, a significant minority have health problems of their own. About one-third (31 percent) describe their own health as "fair to poor."
- Two-thirds of working caregivers report experiencing conflicts between work and caregiving that caused them to rearrange their work schedules, work fewer hours than they otherwise would have, or take an unpaid leave of absence from work.
- Although most employed caregivers work full-time (35 or more hours per week), a significant minority of employed women who are primary caregivers cut back their hours of work in order to provide eldercare. Close to half of part-time employed female primary caregivers report working less because of eldercare responsibilities. A smaller percentage of full-time employed female primary caregivers (16 percent) say that caregiving causes them to work fewer hours than they otherwise would.
- Nevertheless, the great majority of caregivers believe that their caregiving experience is rewarding to them.
SUMMARY
Most disabled elders with long-term disabilities rely primarily on informal care, predominantly from family members, to provide them with the functional assistance they require. When elders are severely disabled, it is most often the availability of informal care from relatives and friends, who provide substantial hours of assistance on a weekly basis, that makes it possible for them to avoid nursing home placement.
(DATA SOURCES: The statistics reported in Part II on informal eldercare in the community are from the 1982 and 1994 National Long-Term Care Surveys and the Informal Caregiver Supplement to the 1989 National Long-Term Care Survey. These surveys have been designed and conducted by the Duke University Center for Demographic Studies (Principal Investigator: Kenneth G. Manton). Funding for these surveys was provided by agencies of the U.S. Department of Health and Human Services, principally the National Institute on Aging. Data analyses were carried out by Pamela Doty, of the Office of the Assistant Secretary for Planning and Evaluation (OASPE), U.S. DHHS, and Mary Elizabeth Jackson, of the MEDSTAT Group, Cambridge, MA., under contract to OASPE.)
PART III: ADDITIONAL SOURCES OF INFORMATION ABOUT CAREGIVING AND ASSISTANCE AVAILABLE TO INFORMAL CAREGIVERS
THE ELDERCARE LOCATOR
1-800-677-1116
The Locator provides information about community assistance for seniors in communities across the United States. The toll-free number is a public service sponsored by the U.S. Administration on Aging. An informative brochure describing the Eldercare Locator service is available free by contacting:
The National Aging Information Center 330 Independence Avenue, S.W. Washington, D.C. 20201 (202) 619-7501
U.S. ADMINISTRATION ON AGING
The Administration on Aging (AOA) is the focal point for services to seniors in the U.S. Department of Health and Human Services. Through a nationwide network of State and Area Agencies on Aging and Tribal Organizations, AoA plans, develops, and supports comprehensive in-home and community services including information and referral services, job and volunteer opportunities, senior center and day care center programs, transportation, a nationwide congregate and home delivered meals program, and homemaker and home health aide services in addition to legal services, nursing home ombudsmen services, and counseling programs to assist seniors if they are abused, neglected, or exploited.
330 Independence Avenue, SW Washington, DC 20201 (202) 619-0724 Internet: http://www.aoa.dhhs.gov/elderpage.html
OFFICE OF DISABILITY, AGING, AND LONG-TERM CARE POLICY, ASPE, HHS
The Office of Disability, Aging, and Long-Term Care Policy, under the Assistant Secretary for Planning and Evaluation, conducts policy research on informal caregiving for the U.S. Department of Health and Human Services. For a list of recent research publications on informal caregiving, contact:
DALTCP/ASPE/DHHS Room 424E, H.H. Humphrey Building 200 Independence Avenue, SW Washington, DC 20201 (202) 690-6443 E-mail: daltcp2@oaspe.dhhs.gov Internet: http://aspe.hhs.gov/_/office_specific/daltcp.cfm
NATIONAL INSTITUTE ON AGING
The National Institute on Aging conducts biomedical and social and behavior research on aging. The Public Information Office at the National Institute on Aging produces science-based educational materials on a wide range of topics related to health and aging. Topics cover specific diseases and health conditions, treatments, and research. The materials are for use by the general public, patients and family members, health professionals, voluntary and community organizations, and the media.
Public Information Office National Institute on Aging Building 31, Room 5C27 31 Center Drive, MSC 2292 Bethesda, MD 20892-2292. (301) 496-1752 E-mail: niainfo@access.digex.net Internet: http://www.nih.gov/nia/
THE RESOURCE DIRECTORY FOR OLDER PEOPLE
The Resource Director for Older People is available on the AoA website (http://www.aoa.dhhs.gov) and is also available in hard copy. It is intended to serve a wide audience including older people and their families, health and legal professionals, social service providers, librarians, researchers, and others with an interest in the field of aging. The directory contains contact information for organizations which provide information and other resources on matters relevant to the needs of older persons. The directory is a joint project of the Administration on Aging and the National Institute on Aging.
A hard copy of the Directory is available for $11.00 from:
Superintendent of Documents P.O. Box 371954 Pittsburgh, PA 15250-7954 Publication Number - 0106200145-6 (202) 512-1800
THE NATIONAL RESPITE LOCATOR SERVICE
1-800-773-5433
The National Respite Locator Service helps parents, caregivers, and professionals caring for children with disabilities, those with chronic or terminal illness, or children at risk for neglect and abuse to find respite services in their state and local area. This service is funded by the U.S. Department of Health and Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Children's Bureau under contract with the North Carolina Department of Human Resources, Division of Mental Health/Developmental Disabilities/Substance Abuse Services, Child and Family Services Branch of Mental Health Programs, Raleigh, North Carolina.
ARCH National Resource Center Chapel Hill Training-Outreach Project 800 Eastowne Drive, Suite 105 Chapel Hill, NC 27514 1-800-773-5433 Internet: http://www.chtop.com/locator.htm
NATIONAL FAMILY CAREGIVERS ASSOCIATION
1-900-896-3650
The National Family Caregivers Association, a caregiver membership organization, provides services in the areas of information and education, support and validation, public awareness and advocacy for caregivers.
10605 Concord St., Suite 501 Kensington, MD 20895-2504 1-800-896-3650 E-mail: info@nfcacares.org Internet: http://www.nfcacares.org/home/html
NATIONAL ALLIANCE FOR CAREGIVING
The National Alliance for Caregiving, a partnership of several aging organizations, conducts research, develops national projects, and works to increase public awareness of the issues of family caregiving for older Americans.
4720 Montgomery Lane, Suite 642 Bethesda, MD 20814 (301) 718-8444
FAMILY VOICES
Family Voices is a national advocacy organization and clearinghouse for information and education concerning the health care of children with special health needs. Family Voices has a volunteer coordinator in every State, 10 regional coordinators, and a small staff working in several locations around the country. Families share their expertise and experiences with State and national policymakers, the media, health professionals, and other families.
Family Voices National Office P.O. Box 769 Algodones, New Mexico 87001 (505) 867-2368 E-mail: famvoi@usa.net Internet: http://www.familyvoices.org
THE ARC (FORMERLY THE ASSOCIATION FOR RETARDED CITIZENS)
The Arc, a national organization on mental retardation, works to secure for all people with mental retardation the opportunity to choose and realize their goals of where and how they learn, live, work, and play. Through its national, State, and local offices, the Arc provides education, research, advocacy, and the support of families, friends, and community.
The Arc of the United States 500 East Border Street, Suite 300 Arlington, Texas 76010 (817) 261-6003 E-mail: arc@metronet.com. Internet: http://www.thearc.org
NATIONAL ASSOCIATIONS
For information and assistance resources for persons with particular diseases and conditions, the national associations, e.g., the Alzheimer's Disease and Related Disorders Association, the American Cancer Society, the American Diabetes Association, United Cerebral Palsy Associations, etc., provide a great deal of information and guides to supportive services. Many of the associations also have local offices.
For Additional Information Contact:
Pamela Doty Senior Policy Analyst Office of Disability, Aging, and Long-Term Care Policy Office of the Assistant Secretary for Planning and Evaluation U.S. Department of Health & Human Services 200 Independence Avenue, S.W. Washington, D.C. 20201 Telephone: (202) 690-6172 E-Mail: pdoty@osaspe.dhhs.gov
NOTES
-
Functional disability is defined as an inability to perform, without human and/or mechanical assistance, one or more of six basic Activities of Daily Living (ADLs) including bathing, dressing, moving around indoors, transferring from bed to chair, using the toilet, or eating, and/or one or more of nine Instrumental Activities of Daily Living (IADLs) including light housekeeping, meal preparation, grocery shopping, laundry, taking medications, managing money, telephoning, outdoor mobility, and transportation.