
Medicaid Substance Abuse Treatment Spending: Findings Report
Ellen Bouchery, Rick Harwood, Rosalie Malsberger, Emily Caffery, Jessica Nysenbaum, and Kerianne Hourihan
Mathematica Policy Research
September 28, 2012
This report was prepared under contract #HHSP23320095642WC between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and Mathematica Policy Research. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/office_specific/daltcp.cfm or contact the ASPE Project Officer, John Drabek, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. His e-mail address is: John.Drabek@hhs.gov.
The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
TABLE OF CONTENTS
- I. INTRODUCTION
- II. OVERVIEW OF DATA AND METHODS
- A. Identification of FFS SA Treatment Expenditures
- B. Imputation of Managed Care Expenditures
- C. Estimating Federal Share
- D. Methods for Projecting 2008 Estimates FY 2011
- III. SPENDING IN PREDOMINANTLY FEE-FOR-SERVICE STATES
- A. Description of Predominantly FFS States
- B. Medicaid FFS SA Treatment Spending
- C. Medicaid Enrollees in FFS States with an SA Diagnosis
- V. NATIONAL ESTIMATES OF MEDICAID SUBSTANCE ABUSE TREATMENT SPENDING
- A. CY 2008 SA Treatment Spending by State
- B. FY 2011 SA Treatment Spending by State
- VI. DISCUSSION
- A. Limitations of MAX Data and Study
- B. Comparison to Prior Estimates
- APPENDICES
- APPENDIX A: Study Methods
- APPENDIX B: Diagnosis Codes
- APPENDIX C: State Level Estimates, CY 2008
- APPENDIX D: State Level Projections, FY 2011
- APPENDIX E: State Variation in Substance Abuse Treatment Coverage, NASADAD Survey Results
- APPENDIX F: Mean Expenditures and Users Enrolled Month in Majority Fee-For-Service States
- LIST OF FIGURES
- FIGURE III.1: Specialty SA Treatment Clients per 1,000 Population, by State
- FIGURE III.2: Expenditures per Enrolled Month 12 or Other, by State
- FIGURE III.3: Distribution of Medicaid Core SA Expenditures, FFS States, by Demographic Group
- FIGURE III.4: Proportion of Core Medicaid SA Expenditures, FFS States, by Eligibility Group
- FIGURE III.5: Distribution of Prescribed Drug Expenditures
- FIGURE III.6: Distribution of Medicaid Enrollees in FFS States with an SA Diagnosis, by Source of Diagnosis
- FIGURE III.7: Distribution of Medicaid Enrollees in FFS States with an SA Diagnosis by Demographic Group
- FIGURE IV.1: Distribution of Medicaid FFS SA Expenditures in Managed Care States, by Demographic Group
- FIGURE IV.2: Proportion of Medicaid FFS SA Expenditures in Managed Care States, by Eligibility
- FIGURE V.1: Medicaid Expenditures for SA Treatment, CY 2008 by Type
- FIGURE V.2: Distribution of Expenditures 100% Attributable to SA, by Type
- LIST OF TABLES
- TABLE ES-1: Medicaid Substance Treatment Spending, CY 2008 and FY 2011
- TABLE ES-2: Medicaid Substance Treatment Users, CY 2008
- TABLE III.1: State Medicaid Delivery Systems
- TABLE III.2: SA and MH Services Coverage, by Delivery System
- TABLE III.3: Coverage of Optional Medicaid Groups, 2008
- TABLE III.4: Substance Abuse Treatment Coverage for Optional Services, by State
- TABLE III.5: Core SA Expenditures per Enrolled Month by State
- TABLE III.6: Core SA Expenditures per Enrolled Month for FFS States, by Demographic and Eligibility Group, Enrollees 12 or Older
- TABLE III.7: Distribution of SA Treatment Spending, by Service Type
- TABLE III.8: Distribution of SA Treatment Users, by Type of Service
- TABLE III.9: Expenditures on Non-Core SA Treatment Services, per Enrolled Month 12 or Older
- TABLE III.10: SA Treatment Expenditures as a Share of Overall Medicaid Spending
- TABLE III.11: Number of Enrollees in FFS States with an SA Diagnosis per 1,000 Enrolled Months, by Demographic and Eligibility Group, Enrollees 12 or Older
- TABLE III.12: Proportion of Enrollees with SA Diagnosis, by Type of Treatment Received, by State
- TABLE III.13: Proportion of Enrollees with SA Diagnosis, by Type of Treatment Received, by Demographic Group
- TABLE III.14: Proportion of Enrollees with SA Diagnosis Using ER and Inpatient Hospital, by State
- TABLE III.15: Proportion of Enrollees with SA Diagnosis Using ER and Inpatient Hospital, by Demographic Group
- TABLE III.16: Total Medicaid FFS Expenditures per FFS Enrolled Month Among Enrollees with an SA Diagnosis, by State and Demographic Group, Ages 12 or Older
- TABLE III.17: SA Service User FFS Expenditures as a Share of Mean FFS Expenditures per Enrolled Month for All Enrollees, by State and Demographic Group, Ages 12 or Older
- TABLE IV.1: Total Core SA Treatment FFS Expenditures, by Type of Service, Managed Care States
- TABLE IV.2: Distribution of Core SA Treatment FFS Expenditures, by Type of Service, Managed Care Services
- TABLE V.1: Medicaid Substance Treatment Users, CY 2008
- TABLE V.2: Projected Medicaid Substance Treatment Spending, FY 2011
- TABLE A.1: Mapping of NASADAD SA Service Categories to Study Categories
- TABLE A.2: State Medicaid Delivery Systems
- TABLE A.3: SA and MH Services Coverage, by Delivery System
- TABLE A.4: SA Treatment Supply Categories for the 18 FFS States
- TABLE B.1: Alcohol Abuse Diagnosis Codes
- TABLE B.2: Drug Abuse Diagnosis Codes
- TABLE B.3: MH Diagnosis Codes
- TABLE B.4: Prescription Drug Codes
- TABLE B.5: Classification of SA/MH Treatment Services by Type
- TABLE C.1a: Medicaid SA Treatment Users and Expenditures, CY 2008 Core SA Treatment Services
- TABLE C.1b: State and Federal Share of Medicaid SA Expenditures Core SA Treatment Services, CY 2008
- TABLE C.2a: Medicaid SA Treatment Users and Expenditures, CY 2008 Services Related to Fetal Drug or Alcohol Exposure and Poisoning
- TABLE C.2b: State and Federal Share of Medicaid SA Expenditures Services Related to Fetal Drug or Alcohol Exposure or Poisoning, CY 2008
- TABLE C.3a: Medicaid SA Treatment Users and Expenditures, CY 2008 Services for Other Medical Conditions 100% Attributable to Substance Abuse
- TABLE C.3b: State and Federal Share of Medicaid SA Expenditures, CY 2008 Services for Other Medical Conditions 100% Attributable to SA
- TABLE C.4a: Medicaid SA Treatment Users and Expenditures, CY 2008 MH Services with SA as a Secondary Diagnosis
- TABLE C.4b: State and Federal Share of Medicaid SA Expenditures, CY 2008 MH Services with SA as a Secondary Diagnosis
- TABLE C.5a: Medicaid SA Treatment Users and Expenditures, CY 2008 Non-MH Services with SA as a Secondary Diagnosis
- TABLE C.5b: State and Federal Share of Medicaid SA Expenditures, CY 2008 Non-MH Services with SA as a Secondary Diagnosis
- TABLE C.6: Unique Count of Medicaid Enrollees with a SA Diagnosis, CY 2008
- TABLE D.1: Projected Medicaid SA Treatment Expenditures, FY 2011 Core SA Treatment Services
- TABLE D.2: Projected Medicaid SA Treatment Expenditures, FY 2011 Services Related to Fetal Drug or Alcohol Exposure and Poisoning
- TABLE D.3: Projected Medicaid SA Treatment Expenditures, FY 2011 Services for Other Medical Conditions 100% Attributable to SA
- TABLE D.4: Projected Medicaid SA Treatment Expenditures, FY 2011 MH Services with SA as a Secondary Diagnosis
- TABLE D.5: Projected Medicaid SA Treatment Expenditures, FY 2011 Non-MH Services with SA as a Secondary Diagnosis
- TABLE E.1: State Medicaid Program Coverage of SA Services, NASADAD Survey Results
- TABLE E.2: Details of Coverage of MH and SA Services in HMOs and BHOs, by State
- TABLE F.1: Mean Expenditures and Users in Majority FFS State Core SA Treatment Services, Full-Benefit Enrollees
- TABLE F.2: Mean Expenditures and Users in Majority FFS State Core SA Treatment Services, Partial-Benefit and Dual Enrollees
- TABLE F.3: Mean Expenditures and Users in Majority FFS State Treatment Services Associated with Fetal Exposure to Alcohol or Drugs, Full-Benefit Enrollees
- TABLE F.4: Mean Expenditures and Users in Majority FFS State Treatment Services Associated with Fetal Exposure to Alcohol or Drugs, Partial-Benefit and Dual Eligibles
- TABLE F.5: Mean Expenditures and Users in Majority FFS State Treatment Services for Poisoning and Other Medical Conditions 100% Attributable to Alcohol or Drug, Full-Benefit Enrollees
- TABLE F.6: Mean Expenditures and Users in Majority FFS State Treatment Services for Poisoning and Other Medical Conditions 100% Attributable to Alcohol or Drug, Partial-Benefit Enrollees and Duals
- TABLE F.7: Mean Expenditures and Users in Majority FFS State MH Services with a Secondary SA Diagnosis, Full-Benefit Enrollees
- TABLE F.8: Mean Expenditures and Users in Majority FFS State MH Services with a Secondary SA Diagnosis, Partial-Benefit and Dual Enrollees
- TABLE F.9: Summary of Imputation for Enrollees with Coverage of SA Under Managed Care
ACRONYMS
| Acronyms | |
| ASAM | American Society of Addiction Medicine |
| BHO | behavioral health organization |
| BOE | basis-of-eligibility |
| CADA | Certified Alcohol and Drug Counselor |
| Cl | clinic |
| CMS | HHS Centers for Medicare and Medicaid Services |
| CY | calendar year |
| EDB | enrollment data base |
| EPSDT | early and periodic screening, diagnostic, and treatment |
| ER | emergency room |
| F-SHRP | Federal-State Health Reform Partnership |
| FFS | fee-for-service |
| FMAP | federal medical assistance percentage |
| FY | fiscal year |
| HCB | home and community-based waiver services |
| HCPCS | Healthcare Common Procedure Coding System |
| HHS | U.S. Department of Health and Human Services |
| HIO | health insuring organization |
| HMO | health maintenance organization |
| HOA | health opportunity account |
| Inp | general inpatient |
| IP | inpatient (MAX file) |
| LT | long-term care (MAX file) |
| M-CHIP | Medicaid expansion Children's Health Insurance Program |
| MAX | Medicaid Analytic eXtract |
| MCO | managed care organization |
| MFP | Money Follows the Person |
| MH | mental health |
| MMIS | Medicaid Management Information System |
| MnDHO | Minnesota Disability Health Options |
| MSHO | Minnesota Senior Health Options program |
| MSIS | Medicaid Statistical Information System |
| N-SSATS | National Survey of SA Treatment Services |
| NASADAD | National Association of State Alcohol and Drug Abuse Directors |
| NDC | National Drug Code |
| NHEA | National Health Expenditure Accounts |
| NSDUH | National Survey on Drug Use and Health |
| OT | other services (MAX file) |
| Outp | outpatient hospital |
| PASARR | Preadmission Screening and Annual Resident Review |
| PCCM | primary care case management |
| PHP | Pre-paid Health Plan |
| Phys | physician |
| PIHP | Pre-paid Inpatient Health Plan |
| PPO | preferred provider organization |
| Prac | other licensed practitioners |
| PRTF | psychiatric residential treatment facility |
| PS | person summary (MAX file) |
| QEx | QUEST Expanded |
| RBF | restricted-benefit flag |
| Rhb | rehabilitation |
| RX | prescription drug (MAX file) |
| S-CHIP | State Children's Health Insurance Program |
| SA | substance abuse |
| SAMHSA | HHS Substance Abuse and Mental Health Services Administration |
| SPCM | specialty physician case management |
| SSE | SAMHSA Spending Estimates |
| SSR&E | SAMHSA Survey of Revenue and Expenditures |
| SUD | substance use disorder |
| TCM | targeted case management |
| WMIP | Washington Medicaid Integration Program |
EXECUTIVE SUMMARY
This report presents the findings of a study conducted by Mathematica Policy Research to improve knowledge about the data on Medicaid substance abuse (SA) treatment available in the Medicaid Analytic eXtract (MAX), develop methods for using these data to estimate Medicaid SA treatment spending, and generate estimates of Medicaid SA treatment spending in calendar year (CY) 2008 and projections for fiscal year (FY) 2011.
The estimates in this study were developed based on MAX data. However, there are gaps in representation of the Medicaid population in MAX. The most significant gap is incomplete reporting of services provided to managedcare enrollees. In addition, data quality issues, reporting anomalies, and inconsistencies in reporting account for other data gaps. We addressed these gaps by imputing expenditures for the managed care enrollees and other populations for whom fee-for-service (FFS) claims data were not available.
This study produced two sets of findings. The first set focuses on a limited number of states for whom FFS SA treatment claims representing a majority of the Medicaid population in the state were available in MAX. The second set of findings reports national estimates of SA treatment expenditures for CY 2008 and projections to FY 2011. A summary of each of these sets of findings is presented here.
SA Spending in the FFS States
Across the 18 states with representative FFS data in MAX, spending on SA services accounted for less than 1 percent of total Medicaid spending. On average, these states spent $6.16 per Medicaid enrolled month 12 or older on medical services to treat a SA diagnosis. There was extreme variation across states in the average amount spent on SA treatment services, from less than $3 per enrolled month to over $26. This variation appears to be linked to differences between states in the supply of specialty SA treatment providers as well as to Medicaid program decisions regarding coverage of optional populations and optional benefits. States that have chosen to expand Medicaid coverage to optional adult populations, or to cover optional SA treatment services such as residential treatment programs and case management, tend to have higher average spending.
Despite mandatory coverage of SA treatment services for children through the early and periodic screening, diagnostic, and treatment benefit, across all 18 states, adolescents 12-17 represented only 18.1 percent of SA treatment expenditures, with males incurring twice the expenditures of females. Working age adults ages 18-64 represented 75.0 percent of SA treatment expenditures, with 38.9 percent of expenditures for females and 36.1 percent for males. Enrollees 65 or older represented 6.7 percent of expenditures, with males having more than double the expenditures of females.
About half of all SA spending in these states was for outpatient services, which were used by almost 90 percent of beneficiaries with a SA diagnosis. The next highest share of spending was 35.2 percent for inpatient hospital care. Prescribed drugs and residential treatment represented 5.4 percent and 7.5 percent, respectively.
Overall, 21.4 percent and 62.4 percent of enrollees with an SA diagnosis identified in CY 2008 MAX data used the emergency room with an SA-related or any diagnosis, respectively. Among the same group 33.6 percent had a SA-related inpatient hospital stay. Overall expenditures for enrollees with an identified SA diagnosis were 2.19 times higher than the average for Medicaid enrollees 12 or older.
National SA Spending Estimates
Medical expenditures to treat a SA disorder were 3.4 billion in CY 2008 (Table ES-1). These services were received by 1.1 million persons (Table ES-2) averaging 3,000 per service user per year. This spending amounted to slightly less than 1.0 percent of the total 334 billion spent on Medicaid, and provided care to about 1.9 percent of the 61 million persons covered by Medicaid.1 An estimated total of 2.0 billion--or 59 percent--of these expenditures were provided through FFS Medicaid, with the remaining 1.4 billion provided through Medicaid managed care plans. The Federal Government paid for 57 percent of these services.
| Type of SA Service | CY 2008 (in millions $) | FY 2011 (in millions $) | Annualized Percentage Growth Rate |
| Core SA Treatment Services | 3,367 | 3,952 | 6.0 |
| Fetal Drug or Alcohol Exposure and Poisoning | 87 | 98 | 4.6 |
| Other Medical Conditions 100% Attributable to SA | 257 | 292 | 4.8 |
| MH Services with SA as a Secondary Diagnosis | 1,432 | 1,586 | 3.8 |
| Non-MH Services with SA as a Secondary Diagnosis | 3,290 | 3,659 | 3.9 |
Spending is projected to have increased to 4.0 billion in federal FY 2011, just slightly slower than the increase in total Medicaid spending, which reflects the long-term correlation between SA treatment and total Medicaid spending.
| Type of SA Service | CY 2008 (in thousands) |
| Total Enrollees Identified with SA Related Claima | 1,717 |
| |
| Core SA Treatment Services | 1,138 |
| Fetal Drug or Alcohol Exposure | 35 |
| Poisoning Related to Drugs or Alcohol | 25 |
| Other Medical Conditions 100% Attributable to SA | 53 |
| MH Services with SA as a Secondary Diagnosis | 281 |
| Non-MH Services with SA as a Secondary Diagnosis | 575 |
Beyond the medical expenditures to treat SA disorders, this study estimated additional categories of costs solely or partially attributable to SA disorders. While these costs are not included in the national SA treatment expenditures, estimated by the Substance Abuse and Mental Health Services Administration (SAMHSA) and known as the SAMHSA Spending Estimates (SSE), such costs generally are included in cost-of-illness studies of drug and alcohol disorders. Costs solely due to drugs and alcohol include fetal exposure to alcohol and/or drugs (49 million, 35,000 persons); alcohol and/or drug poisoning (38 million, 25,000 persons); and other drug and/or alcohol-caused disorders (257 million, 53,000 persons). Much more extensive costs were caused partially by drug/alcohol disorders: mental health (MH) disorders with a co-morbid SA diagnosis (1.4 billion and 282,000 persons) and other health disorders with a co-morbid SA diagnosis (3.3 billion and 575,000 persons). Only a small fraction of these latter costs are due to drug/alcohol disorders, as these expenditures are related primarily to other conditions.
Discussion
The data quality behind these estimates is reasonably strong. SA treatment utilization data were available for 58 percent of Medicaid enrolled months. The data were missing primarily due to non-reporting of services for Medicaid managed care enrolled months. Utilization and expenditures for the 42 percent of enrolled months with missing data were imputed based either on data from the same state for FFS-insured beneficiaries or the average of data from 18 states with very complete reporting. Imputations were adjusted for age, gender, disability status, Medicare enrollment, and the availability/supply of SA treatment service in the state. Each of these factors was a strong and statistically significant predictor of per-capita utilization of and spending on SA treatment. The imputations represented 42 percent of the final estimates spending on medical treatment for SA disorders.
The estimate of Medicaid core SA treatment spending developed in this study for CY 2008 differs from the projected Medicaid SA treatment spending developed by SAMHSA in the SSE projections for 2004 to 2014.2 While no CY 2008 data point is displayed in the earlier SAMHSA study, it did project the 2006 level of Medicaid spending for SA treatment to be $4,279 million while this study indicates the spending as of 2008 to be $3,267 million. While the current study is limited because of the level of imputations, the SSE estimates were limited because data on unit prices and the "payer source" distribution for specialty SA treatment providers were unavailable to support development of the SSE after 1998--prior to the SAMHSA Survey of Revenue and Expenditures in 2009.
The core SA treatment estimates from this study parallel the estimates from the SSE including only services with a primary diagnosis of SA treatment. However, in this study we also examined spending on treatment for other medical conditions that are caused by SA. The addition of services with a primary diagnosis of fetal exposure, poisoning, and other medical conditions fully related to SA increased the estimate of expenditures for SA treatment by about 10 percent. In contrast to the SSE, this study also estimated spending on services with a secondary diagnosis of SA. We identified $1,433 million in expenditures for MH services with a secondary diagnosis of SA and $3,290 million in Medicaid expenditures for services with a non-MH primary diagnosis and a SA secondary diagnosis. Thus, overall slightly more than 1 percent of Medicaid spending was identified as primarily related to SA and an additional 1½ percent of total Medicaid spending was identified with a secondary SA diagnosis. Both the current study and the SSE exclude costs not directly related to treatment, such as costs stemming from lower productivity, missed workdays, and/or SA-related crimes.
I. INTRODUCTION
As federal and state substance abuse (SA) agencies work to establish priorities and coordinate their efforts, policymakers need reliable national and state estimates of Medicaid SA treatment spending and accurate methods for projecting Medicaid and Medicare SA spending. Spending estimates and projections are essential both for aligning funding with policy objectives and developing realistic budgets to support treatment and prevention. Given these needs, the Office of the Assistant Secretary for Planning and Evaluation in the U.S. Department of Health and Human Services ( HHS ) and the Office of National Drug Control Policy contracted with Mathematica Policy Research to conduct this study with the following purposes:
To improve knowledge about the data on Medicaid SA treatment available in the Medicaid Analytic eXtract (MAX).
To develop methods for using these data to estimate Medicaid SA treatment spending accurately and efficiently.
To generate estimates of Medicaid SA treatment spending in calendar year (CY) 2008 and projections for fiscal year (FY) 2011.
This report presents the findings of this study.3 In the next section, we provide a brief overview of the study data and methods. In Section III, we present SA treatment expenditure estimates for CY 2008 for states with predominant fee-for-service (FFS) coverage of SA. In Section IV, we review FFS spending estimates derived from MAX CY 2008 for the remaining states. The estimates in Section IV should be interpreted with caution, as they are not representative of all SA treatment spending in these states. A substantial portion of the SA treatment spending in these states is provided through pre-paid health plans and is not included in these estimates. Nevertheless, these estimates are reported to provide policymakers with information about FFS SA treatment spending in these states. Total FFS and managed care imputed expenditures are reported for all states and nationally in Section V. Section V also reports SA treatment spending projections nationally for federal FY 2011.
II. OVERVIEW OF DATA AND METHODS
In this chapter, we provide a brief overview of the data and methods for this study. A more complete description of the study methods is provided in Appendix A. The primary data sources are the MAX files for CY 2008. These data contain detailed information on Medicaid enrollment and the services received by Medicaid enrollees in each of the 50 states and the District of Columbia but do not reflect all services received by Medicaid beneficiaries. The most significant gap is incomplete reporting of services provided to managed care enrollees. In addition, data quality issues, reporting anomalies, and inconsistencies in reporting account for other data gaps. We address these gaps by imputing expenditures for the managed care enrollees and other populations for whom FFS claims data are not available. In the next section, we describe our approach to identifying and classifying services provided under FFS Medicaid. In Section II.B, we provide an overview of our approach to imputing expenditures for Medicaid enrollees with managed care coverage of SA or for whom FFS data are lacking in the MAX files.
A. Identification of FFS SA Treatment Expenditures
We used the CY 2008 MAX person summary (PS), inpatient (IP), other services (OT), long-term care (LT), and prescription drug (RX) MAX files to identify beneficiaries receiving SA services and their associated Medicaid expenditures. In these files, we identified FFS claims providing SA treatment in the following categories:
Core SA treatment services. This category includes claims for services with a primary diagnosis of an SA disorder. In Appendix Table B.1 and Table B.2, we display the diagnosis codes that we used to define treatments of alcohol and drug disorders, respectively. The third column of the tables identifies these services as "core." The diagnosis codes are consistent with those used by the Substance Abuse and Mental Health Services Administration (SAMHSA) in its estimates of National Expenditures for Mental Health Services and Substance Abuse Treatment, referred to as the SAMHSA Spending Estimates (SSE).4 Prescribed drugs for SA treatment are also included in this category. We identified prescribed drugs used to treat SA based on National Drug Codes. The codes used to identify SA treatment are listed in Appendix Table B.3.
Services related to fetal drug or alcohol exposure. This category includes services with a primary diagnosis of fetal drug or alcohol exposure. In Appendix Table B.1 and Table B.2, the services are identified as "fetus."
Services related to poisoning by drugs or alcohol. This category includes services with a primary diagnosis of poisoning related to drugs or alcohol. In Appendix Table B.1 and Table B.2, the services are identified as "poisoning."
Medical services for other conditions 100 percent attributable to SA. This category includes claims for other services with a primary diagnosis of a medical condition 100 percent attributable to SA. This category includes conditions such as alcoholic polyneuropathy and polyneuropathy due to drugs, as well as acute alcoholic hepatitis and alcoholic cardiomyopathy, gastritis, fatty liver, cirrhosis of the liver, and liver damage. In Appendix Table B.1 and Table B.2, the services are identified as "supplemental."5
Mental health (MH) services with a secondary diagnosis of SA disorders. This category includes services with a primary diagnosis of a mental disorder and a secondary diagnosis on the same claim from one of the first four groups above. We identified claims with a primary MH diagnosis based on the codes listed in Appendix Table B.3.
Other medical services with a secondary diagnosis of SA disorder. This category includes claims with primary diagnoses not identified as MH disorders but with a secondary diagnosis from the first four categories above.
All Medicaid enrollees with an FFS claim in any of the six categories above were labeled as SA treatment users in the results of this study. We used the Medicaid Statistical Information System (MSIS)-ID to identify enrollees who had multiple FFS claims. Based on the MSIS-ID, we created an unduplicated count of FFS SA treatment users. Within a state, Medicaid enrollees are assigned a single MSIS-ID. However, enrollees who receive treatment in more than one state would be assigned a different MSIS-ID in each state and thus would be counted once in each state. For each Medicaid enrollee identified as an SA treatment user, in addition to extracting SA treatment claims, we also extracted all claims with a primary diagnosis of an MH disorder and all claims for inpatient hospital and emergency room (ER) services. Additional information on Medicaid expenditures, eligibility, and demographic characteristics for SA treatment users was also obtained from each user's MAX PS file record.
B. Imputation of Managed Care Expenditures
Our method for estimating managed care SA treatment users and expenditures differed by state, depending on the extent to which state-specific information was available. We divided the states into three groups according to the level and type of available state-specific information. Some states may fall into two groups if they have high managed care penetration in some basis-of-eligibility (BOE) groups but not in others. The three groups of states follow:
Managed care states with usable encounter data. In these states, we imputed expenditures as the product of the number of service units provided in the state's managed care encounter data and the cost per service unit from its FFS data.
Other managed care states with less than 60 percent penetration in a given BOE group. In these states, we imputed expenditures as the product of the number of managed care enrolled months and expenditures per enrolled month by eligibility/demographic group from the state's FFS enrollees.
Other managed care states with 60 percent or greater penetration in a given BOE group and FFS states with substantial FFS data quality issues. In these states, we imputed expenditures as the product of the number of managed care enrolled months and expenditures per enrolled month by eligibility/demographic group from similar states' FFS enrollees.
Maine only reported prescribed drug claims in 2008. Thus, IP/LT/OT claims were not available for Maine in MAX 2008. Because claims data were not available for Maine, its expenditures were imputed in the same manner as a state with more than 60 percent managed care penetration. We considered using a prior year of data to estimate Maine's expenditures, but Maine also did not report IP/LT/OT claims in 2007. A detailed description of the imputation methods is provided in Appendix A.
C. Estimating Federal Share
We calculated the federal share of each state's SA treatment expenditures in 2008 based on its federal medical assistance percentage (FMAP). The Kaiser Family Foundation provides an FMAP time series from 2004 to 2011, with links to corresponding Federal Register notices.6
D. Methods for Projecting 2008 Estimates to FY 2011
We projected the FY 2008 estimates to FY 2011 based primarily on information reported by state Medicaid programs in CMS-64. The CMS-64 reports summarize annual Medicaid expenditures for each state. Information from the forms was available through FY 2011 for each state by service category.7 We used these data to project CY 2008 MAX data to FY 2011. SA treatment costs for each state and category of service (for example, inpatient, outpatient, prescription drugs) are projected to FY 2011 based on the annual change in overall Medicaid expenditures for the state among similar services between FY 2008 and FY 2011. Given that the rate of growth in SA treatment expenditures (as identified in the SSE) historically has fallen below that of general health care expenditures as identified in the Centers for Medicare and Medicaid Services (CMS) National Health Expenditure Accounts, we estimated the SA treatment spending trend as only 98 percent of the trend observed for overall Medicaid program spending in each category.
III. SPENDING IN PREDOMINANTLY FEE-FOR-SERVICE STATES
In this section, we focus on spending in the 18 states that had predominantly FFS coverage of SA treatment in CY 2008. Spending in the other 32 states and the District of Columbia is excluded from this discussion because FFS claims data were not available for a substantial share of the SA treatment services provided in the state, or because of data quality issues.
In the next section, we provide background on Medicaid eligibility guidelines and SA treatment coverage and reimbursement methods in these states. In Section III.B, we report our findings about SA treatment expenditures in these states. Finally, in Section III.C, we describe the Medicaid enrollees identified as SA treatment users in these states.
A. Description of Predominantly FFS States
In this section, we first describe how we selected these 18 states for this analysis. Then, we describe differences across these states in the individuals eligible for Medicaid and in Medicaid coverage of SA treatment services. We also describe differences in the supply of SA treatment services across these states.
1. Criteria for Inclusion
We selected the 18 states included in this section because they had predominantly FFS coverage of SA services and had limited data quality issues. Unfortunately, the CY 2008 MAX files did not include comprehensive encounter data for Medicaid enrollees in managed care programs. The 18 states with SA services and users described in this section thus are limited to those with FFS coverage of SA treatment; these FFS claims data in MAX are broadly representative of the SA treatment services provided to Medicaid enrollees in the state.
We used a two-stage process to identify states with predominantly FFS coverage of SA. First, we identified which states had Health Maintenance Organizations (HMOs), Managed Behavioral Health Organizations (BHOs), or both within their Medicaid program generally. We then looked at the program descriptions for the plans operating in the state to determine whether MH or SA treatment services were provided through the managed care plans operating in that state.
Table III.1 presents findings for the 50 states and the District of Columbia for the first stage of this analysis. We selected 11 of the 18 predominantly FFS states based on this first stage because they were identified as not using an HMO or BHO to provide services to their Medicaid population. In this analysis, we did not include two of the 13 states identified as FFS-only because of data quality issues. We identified Maine as an FFS-only state but excluded it from our analysis because it is missing a substantial amount of data, having been unable to report accurately on inpatient, long-term care, and other services in MAX 2008; only eligibility and prescription drug information were reported for the state. Alaska was also excluded because only 57 percent of its other services file claims had a primary diagnosis code, and SA services were identified for this analysis based on primary diagnosis.
| Managed Care | Count | States |
SOURCE: MAX 2008 Eligibility Anomaly Tables.
| ||
| FFS-Only | 13 | AK, AR, ID, LA, ME, MS, MT, NH, ND, OK, SD, VT, WY |
| State Has Only HMO | 18 | AL, CA, CT, DE, DC, IL, IN, KY, MD, MN, MO, NV, NJ, OH, RI, SC, VA, WV |
| State Has Both HMO & BHO | 18 | AZ, CO, FL, GA, HI, IA,a KS, MA, MI, NE, NM, NY, OR, PA, TN, TX, WA, WI |
| State Has Only BHO | 2 | NC, UT |
In the next stage, for each state using an HMO or BHO we assessed whether MH and/or SA services were covered by the managed care organization. We examined the 2008 National Summary of State Medicaid Managed Care Programs. This report provided qualitative information, including populations served, services covered, and quality improvement activities. The information in the report was not always sufficiently detailed to determine SA treatment coverage. In particular, if no information was reported about SA treatment coverage, we assumed that the organization providing MH services in the state also provided SA treatment. Table III.2 displays for each state whether MH and SA services were covered by an HMO, carved out of an HMO and covered through FFS or by a BHO, included under both an HMO and a BHO, or covered under a BHO if the state had no HMO.
| SA Coverage | Count | States |
SOURCE: 2008 National Summary of State Medicaid Managed Care Programs.
| ||
| SA services covered exclusively by HMO | 23 | AZ, DE, DC, FL, GA, HI, IL, IN, MD, MA, MI, MN, MO, NJ, NV, NY, OH, OR, RI, TN, TX, VA, WI |
| SA services carved out of HMO & provided through FFS | 2 | AL, KY |
| SA services carved out of HMO & provided through BHO | 7 | CO, CT, IA,a KS, NE, NM, PA |
| Both HMO & BHO cover SA services | 4 | CA, SC, WA, WV |
| BHO covers SA services (state does not have HMO) | 2 | NC, UT |
Following this review and an assessment of data quality, we added seven more states to the predominantly FFS states. With the exception of Alabama, all of these states have some managed care coverage of SA services, as identified here:
Illinois--Managed care program covered SA services, but a majority of enrollees were not enrolled in the comprehensive managed care plan. Only about 4 percent of enrolled months 12 and older were in the managed care plan.
Missouri--Managed care program covered SA services, but a majority of enrollees were not enrolled in the comprehensive managed care plan. About one-third of enrolled month 12 and older were in the managed care plan.
Alabama--Managed care program focused on maternity services and did not include SA treatment services.
Kentucky--Managed care program covered only medical detoxification services.
Connecticut--HMOs ceased providing services to Medicaid enrollees from December 2007 through July 2008, so there was no HMO enrollment during this period.
South Carolina--Managed care program covered SA services, but a majority of enrollees were not enrolled in the comprehensive managed care plan. Almost 20 percent of enrolled months 12 and older were in the managed care plan.
North Carolina--Pre-paid inpatient MH plan covered inpatient SA services in only five counties in the state.
In Illinois, Missouri, Connecticut, and South Carolina, the months during which an enrollee was covered under a managed care plan were excluded from our analysis. The estimates for Kentucky and North Carolina understated the SA treatment services provided, as the inpatient services provided through the managed care programs are not represented in the FFS claims data included in this analysis.
2. Medicaid Eligibility
To receive federal matching funds, state Medicaid programs must cover basic health services for all individuals in certain mandatory eligibility groups, including low-income children, pregnant women, infants born to Medicaid-eligible women, low-income families with children, SSI enrollees, and low-income Medicare enrollees. States may also elect to cover some optional groups in their Medicaid programs, including medically needy individuals, pregnant women and children with higher income levels, institutionalized individuals, or other groups authorized under waiver programs. Coverage of optional groups of individuals can have a significant impact on SA treatment expenditures. In particular, since children below age 12 have negligible SA treatment expenditures, expansions that shift the Medicaid population toward adults and groups such as childless adults may result in higher SA treatment expenditures in a given state relative to other states. Table III.3 summarizes coverage of optional groups in the 18 predominantly FFS states.
| State | Parent Expansion | Childless Adult Expansion | SSI Coverage (Institutionalized) | Medically Needy |
SOURCE: Eligibility Anomaly Tables, MAX 2008.
| ||||
| Alabama | X | |||
| Arkansas | Xa | X | X | |
| Connecticut | X | X | ||
| Idaho | X | |||
| Illinois | X | |||
| Kentucky | X | X | ||
| Louisiana | X | X | ||
| Mississippi | X | |||
| Missouri | ||||
| Montana | X | X | ||
| New Hampshire | X | X | ||
| North Carolina | X | |||
| North Dakota | X | |||
| Oklahoma | X | X | X | |
| South Carolina | X | |||
| South Dakota | X | |||
| Vermont | X | X | X | X |
| Wyoming | X | |||
Two types of SA treatment services must be covered in all states. Federal Medicaid guidelines require all states to cover medically necessary inpatient detoxification services. Also, all states are federally mandated to provide early and periodic screening, diagnostic, and treatment (EPSDT) services for individuals under 21 years of age. SA treatment needs identified as part of these screenings must be covered in all states. SA treatment services other than these two types of service are an optional category of Medicaid services that states may provide to Medicaid enrollees but are not mandated to provide. Thus, SA treatment coverage varies substantially across states, with some states offering almost no coverage and others offering a range of treatment services.
In November 2010, the National Association of State Alcohol and Drug Abuse Directors (NASADAD) produced a summary of SA services covered in each state, based on the Medicaid state plans and discussions with state Medicaid officials (47 states provided responses).8Table III.4 summarizes the findings of this survey for the 18 predominantly FFS states.
| State | ResidentialTreatment | IntensiveOutpatient/Partial Hospitalization | Methadone Treatment | Case Management | Outpatient Treatment | |
| Short-Term | Long-Term | |||||
| Alabama | No | No | Yes | Yes | No | Yes |
| Arkansas | No | No | No | No | No | No |
| Connecticut | Yes (only 21) | N/A | Yes | Yes | Yes | Yes |
| Idaho | No | No | Yes | No | Yes | Yes |
| Illinois | Yes | Yes | Yes | Yes | No | Yes |
| Kentucky | No | No | No | No | Yes | No |
| Louisiana | No | No | No | No | No | No |
| Mississippi | No | No | No | No | No | No |
| Missouri | No | No | Yes | Yes | Yes | Yes |
| Montana | Yes | Yes | Yes | No | Yes | Yes |
| New Hampshire | No | No | No | No | No | No |
| North Carolina | Yes | No | Yes | Yes | Yes | Yes |
| North Dakota | N/A | N/A | Yes | N/A | N/A | Yes |
| Oklahoma | Detox Only | No | N/A | No | Yes | Yes |
| South Carolina | Detox Only | No | Yes | No | Yes | Yes |
| South Dakota | Yes | No | Yes | No | No | Yes |
| Vermont | Yes | Yes | Yes | Yes | Yes | Yes |
| Wyoming | Yes | Yes | Yes | Yes | Yes | Yes |
According to this survey, Arkansas, Louisiana, Mississippi, and New Hampshire reported providing no SA treatment services beyond the mandatory coverage categories. Kentucky reported providing only case management services. All of the other states reported providing outpatient treatment. Nine of the states reported providing some residential treatment. Twelve reported providing partial hospitalization or intensive outpatient treatment. Seven reported providing methadone treatment, and ten reported providing case management.
4. Supply of Specialty SA Treatment Coverage
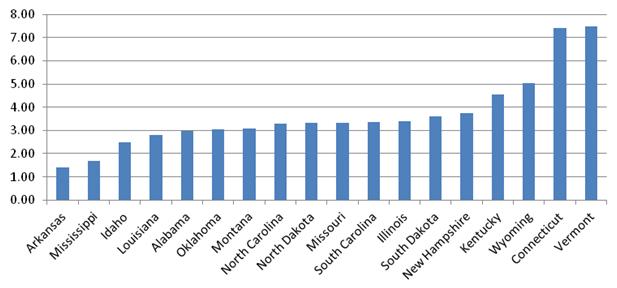
The availability of SA treatment services varied across the 18 predominantly FFS states. We measured this variation in service access based on the number of clients of all insurance types served in specialty SA treatment facilities in 2008 per 1,000 population. The number of clients served was identified in SAMHSA's National Survey of SA Treatment Services (N-SSATS). We divided these client counts by the total number of SA treatment clients in care on March 31, 2008 in all settings by the Census Bureau's estimate of state population.
Figure III.1 displays the number of specialty SA clients per 1000 population in each of the 18 FFS states. Connecticut and Vermont had much higher rates of treatment access relative to the other states. Kentucky and Wyoming also had rates above most states except Connecticut and Vermont. Arkansas and Mississippi had access rates below the average across the other states.
In the next section, we provide estimates of Medicaid SA treatment spending for these 18 states. The variation in these state characteristics should serve as a foundation for understanding these findings.
FIGURE III.1. Specialty SA Treatment Clients per 1,000 Population, by State
B. Medicaid FFS SA Treatment Spending
In this section, we present estimates of FFS SA treatment spending for the 18 states. Sections B.1 through B.3 describe expenditures for core SA treatment services only, using the definition used in the SSE. In Section B.1, we present estimates of these expenditures per enrolled month by state. In Section B.2, we disaggregate the estimates by eligibility and demographic group. In Section B.3, we then analyze the same set of SA treatment expenditures by setting of care. In Section B.4, we broaden the definition of SA treatment to look at categories of care not included in the SSE. Finally, in Section B.5, we analyze SA treatment expenditures as a share of overall Medicaid expenditures in the states.
1. Core SA Expenditures per Enrolled Month by State
Figure III.2 displays the overall average SA treatment expenditure per enrolled month among enrollees 12 or older in each of the 18 states. These estimates are developed by dividing the total amount of SA treatment expenditures by the total number of Medicaid enrolled months in the state for individuals 12 or older including enrolled months for both individuals who use SA-related services as well as those who do not use these services. The estimates reflect the variation in Medicaid eligibility, service coverage, and the supply of SA treatment services within the states. They may also reflect rates of treatment need among Medicaid enrollees.
Average expenditures for SA treatment per enrolled month in Vermont (25.98) were substantially higher than the average of 6.16 across the 18 states. Vermont had several Medicaid expansion programs targeting adults, including expansions targeting low-income parents and childless adults. Based on the NASADAD survey, Vermont covered a broad range of SA treatment services and, according to N-SSATS, Vermont's specialty SA treatment system served more clients per 1,000 population (7.5) than any of the other 18 states. Vermont is also unique in its more extensive use of prescribed drugs. Nineteen percent of Vermont's core SA treatment expenditures were for prescribed drugs in contrast to a 5 percent average across the 18 states. Connecticut had the second highest level of SA treatment expenditures per enrolled month (15.08). In contrast to Vermont, Connecticut provided coverage of SSI and medically needy populations, but did not have parent or childless adult expansions. However, like Vermont, the NASADAD survey indicated that Connecticut provided coverage for a broad range of treatment services and its specialty SA treatment system served a similar number of clients per population (7.4) as that in Vermont (7.5).
FIGURE III.2. Expenditures per Enrolled Month 12 or Older, by State
[highchart chart_id="93636" different_values="0"]
We estimated that five states (Arkansas, Louisiana, Alabama, Oklahoma, and Idaho) had SA treatment expenditures less than 3.00 per enrolled month. Based on the NASADAD survey Arkansas and Louisiana did not provide any SA services beyond the mandatory coverage categories. However, the NASADAD survey also indicated that Mississippi and New Hampshire did not provide coverage of SA treatment service beyond the mandatory services, but these states had substantially higher levels of treatment expenditures. Similar to Vermont, Oklahoma had a parent and childless adult expansion, but Oklahoma had more limited coverage of SA treatment services.
Table III.5 displays expenditures per enrolled month by state and demographic group. Males tend to have higher expenditure than females and older enrollees tend to have higher expenditures than enrollees 12-20. However, these patterns are not observed in all the states. For example, Illinois, Kentucky, Missouri, North Dakota and South Dakota had higher expenditures per enrolled month among males 12-20 relative to males 21-44. This pattern may result from coverage of SA through EPSDT programs in these states.
| State | Total | Male | Female | ||||
| 12 or Older | 12-20 | 21-44 | 45 or Older | 12-20 | 21-44 | 45 or Older | |
| Mean (18 States) | 6.16 | 6.19 | 10.84 | 11.52 | 2.81 | 7.25 | 3.22 |
| Alabama | 1.84 | 0.76 | 2.11 | 6.27 | 0.55 | 1.97 | 1.11 |
| Arkansas | 1.44 | 0.22 | 2.11 | 7.19 | 0.11 | 1.22 | 1.24 |
| Connecticut | 15.08 | 5.30 | 27.47 | 41.33 | 3.00 | 13.40 | 11.64 |
| Idaho | 2.80 | 0.61 | 3.49 | 9.49 | 0.53 | 3.91 | 2.61 |
| Illinois | 7.01 | 10.95 | 9.15 | 14.84 | 3.36 | 4.76 | 4.75 |
| Kentucky | 6.69 | 12.70 | 7.08 | 8.05 | 5.77 | 7.82 | 1.59 |
| Louisiana | 1.80 | 0.27 | 4.66 | 6.36 | 0.23 | 2.60 | 1.31 |
| Mississippi | 5.20 | 3.95 | 13.17 | 10.01 | 1.74 | 6.59 | 2.82 |
| Missouri | 10.80 | 23.27 | 16.68 | 10.87 | 10.72 | 13.12 | 3.71 |
| Montana | 10.93 | 8.01 | 7.74 | 27.65 | 5.13 | 12.13 | 7.29 |
| New Hampshire | 8.63 | 1.37 | 13.81 | 16.43 | 1.48 | 18.54 | 5.42 |
| North Carolina | 5.34 | 3.76 | 9.64 | 8.84 | 1.49 | 8.67 | 2.86 |
| North Dakota | 11.01 | 13.91 | 9.36 | 22.86 | 18.14 | 8.60 | 2.27 |
| Oklahoma | 2.49 | 1.75 | 3.92 | 7.22 | 0.64 | 3.13 | 1.70 |
| South Carolina | 4.58 | 6.41 | 4.91 | 3.43 | 3.58 | 9.00 | 1.32 |
| South Dakota | 9.03 | 21.95 | 0.80 | 0.80 | 20.27 | 1.50 | 0.12 |
| Vermont | 25.98 | 12.86 | 55.38 | 14.68 | 12.20 | 46.42 | 8.15 |
| Wyoming | 5.49 | 3.07 | 10.55 | 18.43 | 2.52 | 5.60 | 2.63 |
2. Core SA Expenditures by Demographic and Eligibility Group
In this section, we discuss the distribution of SA treatment expenditures across demographic and eligibility groups. Figure III.3 displays the distribution of SA treatment expenditures across age and gender group. Children less than 12 represented a negligible share of SA treatment spending. Adolescents 12-17 represented 18.1 percent, with males incurring twice the expenditures of females. Working age adults ages 18-64 represented 75.0 percent of SA treatment expenditures, with 38.9 percent of expenditures for females and 36.1 percent for males. Enrollees 65 or older represented 6.7 percent of expenditures, with males having more than double the expenditures of females.
FIGURE III.3. Core SA Expenditures per Enrolled Month by State
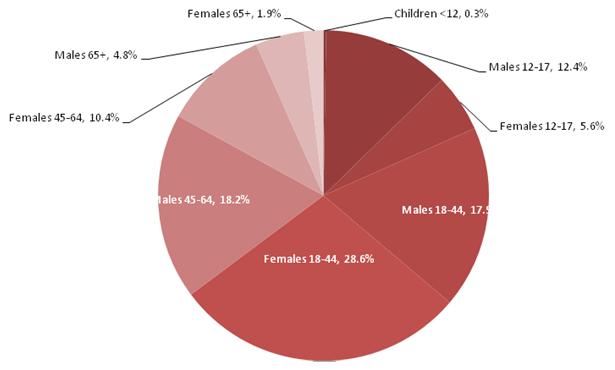
Figure III.4 displays the distribution of expenditures by eligibility group. Children 12-17 represented 18.1 percent of expenditures. Disabled and non-disabled adults have an almost equal share of expenditures (34.1 versus 32.4 percent). Enrollees dually eligible for Medicaid and Medicare represent 15.2 percent of expenditures. The difference in the share of expenditures across age and eligibility groups reflects different rates of Medicaid enrollment among these populations as well as different levels of SA treatment expenditures.
FIGURE III.4. Proportion of Core Medicaid SA Expenditures, FFS States, by Eligibility Groups
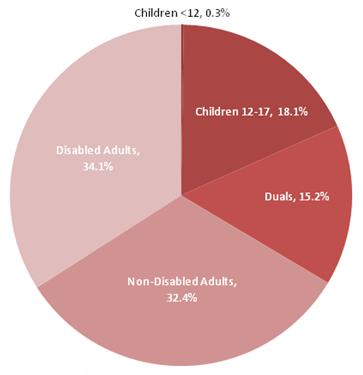
Table III.6 displays average SA treatment expenditures per enrolled month by demographic and eligibility group. Overall non-dual, disabled males age 35-44 (28.47) and 45-64 (26.60) with full Medicaid benefits tended to have the highest levels of expenditures. Females 12-17 (2.75), 18-20 (2.95), and 65 or older (0.96) tended have lower than average expenditures. Also, Medicare dual eligibles (3.27) and non-dual, disabled individuals with partial-benefits (2.71) tended to have lower than average expenditures.
We excluded from this analysis those Medicare dual eligibles who are eligible only for assistance with Medicare premium payments. For the remaining Medicare duals, Medicare is the first payer for SA services and Medicaid is a secondary payer, covering those services included in the state Medicaid benefit package not covered by Medicare. The expenditures represented are only those covered by Medicaid. In 2008, Medicare covered medically necessary inpatient treatment under Part A; however, inpatient stays were subject to deductibles and coinsurance, which would be covered by Medicaid. Under Part B, Medicare has a coinsurance rate of 50 percent for outpatient SA treatment; under Part D Medicare would have covered prescribed drugs for SA treatment. Given the substantial available coverage for SA under Medicare, Medicaid expenditures for duals are about 53 percent of the level estimated for enrollees who do not have Medicare coverage.
| All Groups 12 or Older | Non-Dual, Non-Disabled | Non-Dual, Disabled | Medicare Dual Eligibles | |||
| Full- Benefit | Partial- Benefit | Full- Benefit | Partial- Benefit | |||
| Mean (12 or Older) | 6.16 | 5.58 | 6.34 | 13.36 | 2.71 | 3.27 |
| Female | ||||||
| 12-17 | 2.75 | 2.69 | 3.59 | 2.07 | 1.64 | NA |
| 18-20 | 2.95 | 2.93 | 2.93 | 3.21 | 2.18 | 7.66 |
| 21-34 | 6.55 | 6.71 | 5.39 | 8.43 | 2.56 | 4.24 |
| 35-44 | 8.71 | 8.30 | 3.98 | 16.40 | 4.47 | 4.08 |
| 45-64 | 5.64 | 6.48 | 4.23 | 8.89 | 3.03 | 2.40 |
| 65 or Older | 0.96 | 1.56 | 1.74 | 4.22 | 0.12 | 0.91 |
| Male | ||||||
| 12-17 | 5.87 | 5.93 | 7.70 | 3.96 | 0.78 | NA |
| 18-20 | 7.46 | 7.58 | 13.84 | 4.61 | 2.45 | 5.36 |
| 21-34 | 9.09 | 10.77 | 23.31 | 9.43 | 2.18 | 4.43 |
| 35-44 | 12.88 | 9.16 | 10.60 | 28.47 | 4.02 | 5.37 |
| 45-64 | 14.49 | 6.47 | 7.22 | 26.60 | 5.64 | 6.38 |
| 65 or Older | 6.46 | 4.42 | 4.33 | 12.43 | 0.03 | 6.58 |
3. Distribution of Core SA Spending in FFS States by Service Type
Table III.7 reports the distribution of SA treatment spending by service type. Across the 18 states, 35.2 percent of expenditures were for inpatient hospital care, 51.9 percent was for outpatient care, 5.4 percent was for prescribed drugs, and the remaining 7.5 percent was for residential treatment. The expenditures for inpatient care may be somewhat understated for Kentucky and North Carolina, as Kentucky provided some medical detoxification services through a managed care plan and North Carolina had a pre-paid inpatient behavioral health plan in five counties.
The distribution of expenditures by service type varied substantially across the states. As noted in Section III.A.3, Alabama, Arkansas, Idaho, Kentucky, Louisiana, Mississippi, Missouri, and New Hampshire reported no coverage of residential SA treatment services under Medicaid. However, in Kentucky and Missouri, we identified some services that appear to be residential. These services are related to residential behavioral health and therapeutic foster care procedure codes. Vermont and South Dakota had the lowest share of inpatient expenditures (7.5 percent and 8.5 percent, respectively). Louisiana and Mississippi had the highest percentage of expenditures for inpatient care (80.7 percent and 75.6 percent, respectively). Prescribed drugs represented 19.2 percent of expenditures in Vermont, but represented 1 percent of expenditures in Louisiana and only 0.3 percent of expenditures in South Dakota. In North Carolina, New Hampshire, Missouri, and Connecticut, we found the highest share of expenditures devoted to outpatient care.
| State | Total | InpatientHospital | PrescribedDrug | ResidentialTreatment | OutpatientTreatment |
| NR = Not Reported. Cells representing fewer than 11 users are not reported to protect confidentiality. | |||||
| Expenditures | |||||
| Alabama | 8,309,625 | 4,733,159 | 686,260 | 0 | 2,890,206 |
| Arkansas | 4,960,347 | 3,305,162 | 165,897 | 0 | 1,489,288 |
| Connecticut | 53,443,687 | 14,235,623 | 2,276,104 | 3,580,303 | 33,351,657 |
| Idaho | 2,932,153 | 1,986,565 | 299,094 | 0 | 646,494 |
| Illinois | 107,452,301 | 46,765,187 | 2,907,050 | 1,207,071 | 56,572,993 |
| Kentucky | 35,384,118 | 14,140,912 | 3,907,976 | 1,641,780 | 15,693,450 |
| Louisiana | 11,681,116 | 9,431,405 | 120,271 | 0 | 2,129,440 |
| Mississippi | 20,132,385 | 15,226,817 | 753,521 | 0 | 4,152,047 |
| Missouri | 44,278,809 | 11,226,183 | 814,275 | 3,402,850 | 28,835,501 |
| Montana | 6,136,976 | 2,817,123 | 500,181 | 586,973 | 2,232,699 |
| New Hampshire | 7,066,142 | 1,655,401 | 686,548 | 0 | 4,724,193 |
| North Carolina | 47,771,308 | 8,554,328 | 1,970,798 | 2,637,339 | 34,608,843 |
| North Dakota | 4,280,975 | 1,197,730 | 104,204 | 606,873 | 2,372,168 |
| Oklahoma | 9,106,567 | 4,144,240 | 484,876 | 633,306 | 3,844,145 |
| South Carolina | 17,922,728 | 4,340,306 | 1,035,698 | 5,890,367 | 6,656,357 |
| South Dakota | 5,965,250 | 509,392 | 16,879 | 4,350,769 | 1,088,210 |
| Vermont | 30,132,534 | 2,262,989 | 5,781,915 | 6,914,864 | 15,172,766 |
| Wyoming | 1,977073 | 851,723 | 103,398 | NR | 1,021,952 |
| Total (18 states) | 418,934,094 | 147,384,245 | 22,614,945 | 31,452,495 | 217,482,409 |
| Percentage of SA Treatment Expenditures | |||||
| Alabama | 100.0 | 57.0 | 8.3 | 0.0 | 34.8 |
| Arkansas | 100.0 | 66.6 | 3.3 | 0.0 | 30.0 |
| Connecticut | 100.0 | 26.6 | 4.3 | 6.7 | 62.4 |
| Idaho | 100.0 | 67.8 | 10.2 | 0.0 | 22.0 |
| Illinois | 100.0 | 43.5 | 2.7 | 1.1 | 52.6 |
| Kentucky | 100.0 | 40.0 | 11.0 | 4.6 | 44.4 |
| Louisiana | 100.0 | 80.7 | 1.0 | 0.0 | 18.2 |
| Mississippi | 100.0 | 75.6 | 3.7 | 0.0 | 20.6 |
| Missouri | 100.0 | 25.4 | 1.8 | 7.7 | 65.1 |
| Montana | 100.0 | 45.9 | 8.2 | 9.6 | 36.4 |
| New Hampshire | 100.0 | 23.4 | 9.7 | 0.0 | 66.9 |
| North Carolina | 100.0 | 17.9 | 4.1 | 5.5 | 72.4 |
| North Dakota | 100.0 | 28.0 | 2.4 | 14.2 | 55.4 |
| Oklahoma | 100.0 | 45.5 | 5.3 | 7.0 | 42.2 |
| South Carolina | 100.0 | 24.2 | 5.8 | 32.9 | 37.1 |
| South Dakota | 100.0 | 8.5 | 0.3 | 72.9 | 18.2 |
| Vermont | 100.0 | 7.5 | 19.2 | 22.9 | 50.4 |
| Wyoming | 100.0 | 43.0 | 5.2 | NR | 51.6 |
| Overall (18 states) | 100.0 | 35.2 | 5.4 | 7.5 | 51.9 |
Table III.8 below identifies the number of individuals who used core SA treatment services according to each service type. Most SA treatment users received some outpatient care (89.9 percent) and 16.6 percent of users needed inpatient services. SA treatment users were much less likely to receive treatment in the form of prescribed drugs or residential services--only 9.8 percent and 4.3 percent, respectively. Vermont had a much higher rate of prescribed drug use (29.7 percent) and residential treatment use (16.9 percent) relative to the other states and also had a much lower rate of inpatient care use (6.3 percent).
| State | Total | Inpatient Hospital | Prescribed Drug | Residential Treatment | Outpatient Treatment |
| NR = Not Reported. Cells representing fewer than 11 users are not reported to protect confidentiality. | |||||
| Number of Users | |||||
| Alabama | 8,493 | 1,681 | 516 | 0 | 7,294 |
| Arkansas | 3,537 | 857 | 192 | 0 | 2,928 |
| Connecticut | 17,284 | 1,438 | 1,964 | 1,392 | 15,891 |
| Idaho | 1,841 | 293 | 323 | 0 | 1,559 |
| Illinois | 32,963 | 6,185 | 2,941 | 1,376 | 30,202 |
| Kentucky | 12,694 | 3,510 | 2,166 | 81 | 10,599 |
| Louisiana | 7,540 | 2,338 | 316 | 0 | 6,025 |
| Mississippi | 8,388 | 2,732 | 616 | 0 | 6,990 |
| Missouri | 17,163 | 2,486 | 1,431 | 1,241 | 15,729 |
| Montana | 2,692 | 399 | 315 | 86 | 2,502 |
| New Hampshire | 3,339 | 337 | 424 | 0 | 3,104 |
| North Carolina | 25,507 | 2,708 | 1,709 | 316 | 23,824 |
| North Dakota | 1,736 | 359 | 97 | 13 | 1,644 |
| Oklahoma | 6,366 | 997 | 553 | 63 | 5,578 |
| South Carolina | 9,995 | 1,177 | 566 | 793 | 9,300 |
| South Dakota | 1,398 | 97 | 50 | 482 | 1,117 |
| Vermont | 8,375 | 528 | 2,487 | 1,417 | 7,964 |
| Wyoming | 1,271 | 159 | 119 | NR | 1,183 |
| Total (18 states) | 170,582 | 28,281 | 16,785 | 7,260 | 153,433 |
| Percentage of All SA Treatment Users | |||||
| Alabama | 100.0 | 19.8 | 6.1 | 0.0 | 85.9 |
| Arkansas | 100.0 | 24.2 | 5.4 | 0.0 | 82.8 |
| Connecticut | 100.0 | 8.3 | 11.4 | 8.1 | 91.9 |
| Idaho | 100.0 | 15.9 | 17.5 | 0.0 | 84.7 |
| Illinois | 100.0 | 18.8 | 8.9 | 4.2 | 91.6 |
| Kentucky | 100.0 | 27.7 | 17.1 | 0.6 | 83.5 |
| Louisiana | 100.0 | 31.0 | 4.2 | 0.0 | 79.9 |
| Mississippi | 100.0 | 32.6 | 7.3 | 0.0 | 83.3 |
| Missouri | 100.0 | 14.5 | 8.3 | 7.2 | 91.6 |
| Montana | 100.0 | 14.8 | 11.7 | 3.2 | 92.9 |
| New Hampshire | 100.0 | 10.1 | 12.7 | 0.0 | 93.0 |
| North Carolina | 100.0 | 10.6 | 6.7 | 1.2 | 93.4 |
| North Dakota | 100.0 | 20.7 | 5.6 | 0.7 | 94.7 |
| Oklahoma | 100.0 | 15.7 | 8.7 | 1.0 | 87.6 |
| South Carolina | 100.0 | 11.8 | 5.7 | 7.9 | 93.0 |
| South Dakota | 100.0 | 6.9 | 3.6 | 34.5 | 79.9 |
| Vermont | 100.0 | 6.3 | 29.7 | 16.9 | 95.1 |
| Wyoming | 100.0 | 12.5 | 9.4 | NR | 93.1 |
| Overall (18 states) | 100.0 | 16.6 | 9.8 | 4.3 | 89.9 |
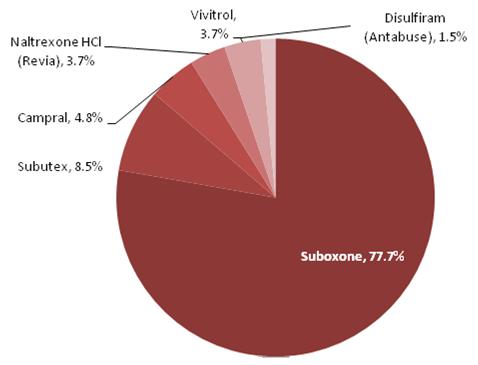
Figure III.5 displays the distribution of prescribed drug expenditures in the 18 FFS states. About three-quarters of expenditures (77.7 percent) were for Suboxone. Suboxone contains a combination of buprenorphine and naloxone. This drug is used to treat opiate addiction. The next highest share of expenditures is for Subutex with 8.5 percent. This is buprenorphine only and is used to treat narcotic addition. The third highest share of expenditures is for Campral at 4.8 percent. Campral is used to treat alcohol addiction. The share of prescribed drug users represented by Suboxone (57.6 percent) is lower than its share of expenditures. Campral has the next highest share of users (18.5 percent) followed by Naltrexone HCl (Revia) with 15.0 percent. Naltrexone HCl is used to treat narcotic or alcohol addiction.
FIGURE III.5. Distribution of Prescribed Drug Expenditures
4. Non-Core SA Treatment Spending
Our analysis in the previous sections focused on expenditures meeting the definition of SA treatment used in SAMHSA SA treatment spending estimates. In this section, we broaden that definition and look at other services that are SA related. Table III.9 displays these additional services in five categories. The first and second are expenditures related to fetal exposure to alcohol or drugs and poisoning from alcohol or drugs. Together, spending on these two categories is about 0.11 dollars per Medicaid enrolled month 12 or older. Other conditions fully attributable to alcohol include conditions such as alcoholic polyneuropathy and polyneuropathy due to drugs. This category also includes acute alcoholic hepatitis and alcoholic cardiomyopathy, gastritis, fatty liver, cirrhosis of the liver, and liver damage. These conditions on average add 0.64 dollars in expenditures per Medicaid enrolled month. The expenditures for fetal exposure, poisoning, and these other conditions are fully attributable to alcohol and drug use.
The expenditures reported in the final two columns of Table III.9 are related only partially to alcohol and drug use, as they are drawn from claims in which a primary diagnosis unrelated to alcohol or drugs was identified. Individuals with SA disorders may be co-morbidly diagnosed, and SA treatment programs increasingly treat both SA and MH diagnoses in tandem. In some states, it appears that reporting of a secondary SA diagnosis is more or less common. For example, expenditures for services with a primary MH diagnosis and a co-morbid SA diagnosis range from only 0.32 and 13.41 per enrolled month in Alabama and Wyoming, respectively. Differences in expenditures may be related to service coding, Medicaid program coverage, or differences in the treatment system across states. On average, 4.07 and 7.50 per enrolled month, respectively were spent on services with a non-MH primary diagnosis and a secondary SA diagnosis. The primary medical diagnoses included on the claims represented in this category often were medical diagnoses partially attributable to drug or alcohol use these included births with SA treatment, HIV, acute pancreatitis, pneumonia, and heptatic coma related to liver disease.
| State | Fetus | Poisoning | Other Conditions | MH Expenditures with Secondary SA Diagnosis | Non-MH Expenditures with Secondary SA Diagnosis |
| Total (18 states) | 0.02 | 0.09 | 0.64 | 4.07 | 7.50 |
| Alabama | 0.01 | 0.09 | 0.08 | 0.32 | 1.94 |
| Arkansas | 0.01 | 0.01 | 0.29 | 3.20 | 0.72 |
| Connecticut | 0.02 | 0.02 | 0.60 | 10.73 | 8.77 |
| Idaho | 0.03 | 0.03 | 0.70 | 3.54 | 7.68 |
| Illinois | 0.01 | 0.01 | 0.97 | 4.65 | 9.65 |
| Kentucky | 0.02 | 0.89 | 0.15 | 2.45 | 11.57 |
| Louisiana | 0.04 | 0.01 | 0.53 | 2.18 | 3.98 |
| Mississippi | 0.01 | 0.01 | 0.37 | 5.71 | 5.53 |
| Missouri | 0.00 | 0.04 | 0.89 | 6.68 | 4.02 |
| Montana | 0.06 | 0.04 | 1.68 | 6.31 | 11.01 |
| New Hampshire | 0.32 | 0.03 | 0.54 | 2.36 | 6.10 |
| North Carolina | 0.04 | 0.02 | 0.74 | 3.59 | 9.20 |
| North Dakota | 0.02 | 0.02 | 0.85 | 8.10 | 13.22 |
| Oklahoma | 0.02 | 0.02 | 0.78 | 4.28 | 8.23 |
| South Carolina | 0.01 | 0.01 | 0.61 | 1.37 | 11.09 |
| South Dakota | 0.03 | 0.02 | 1.04 | 4.72 | 6.87 |
| Vermont | 0.05 | 0.02 | 0.25 | 4.62 | 5.32 |
| Wyoming | 0.02 | 0.01 | 1.07 | 13.41 | 11.55 |
5. SA Treatment Spending as a Share of Overall Medicaid Spending
Table III.10 displays SA treatment expenditures as a share of overall Medicaid spending. Across all 18 states, core SA treatment expenditures accounted for 0.7 percent of Medicaid expenditures. If expenditures for fetal exposure, poisoning, and other medical conditions that are fully attributable to alcohol are added to the core SA treatment expenditures then this percentage increases slightly to 0.8 percent of Medicaid spending. SA spending as a share of overall Medicaid spending varies by state. Arkansas and Louisiana have the lowest share of Medicaid spending related to core SA services (0.1 percent and 0.2 percent, respectively). In Vermont core SA treatment spending represents 3.3 percent of overall Medicaid spending.
| State | Expenditures | Percent of OverallMedicaid FFS Expenditures | |||
| Total Medicaid FFS | Core SA Treatment | All Expenditures Fully Attributable to SA | Core SA Treatment | All Expenditures Fully Attributable to SA | |
| Total (18 states) | 57,489,360,593 | 418,937,734 | 473,832,741 | 0.7 | 0.8 |
| Alabama | 2,913,310,791 | 8,309,625 | 9,259,048 | 0.3 | 0.3 |
| Arkansas | 3,310,688,627 | 4,960,347 | 6,253,410 | 0.1 | 0.2 |
| Connecticut | 3,834,253,096 | 53,443,687 | 56,038,805 | 1.4 | 1.5 |
| Idaho | 1,230,169,201 | 2,932,153 | 3,812,654 | 0.2 | 0.3 |
| Illinois | 9,735,069,107 | 107,452,301 | 123,442,978 | 1.1 | 1.3 |
| Kentucky | 4,378,024,181 | 35,384,118 | 41,758,756 | 0.8 | 1.0 |
| Louisiana | 5,079,957,979 | 11,681,116 | 15,620,670 | 0.2 | 0.3 |
| Mississippi | 3,096,430,669 | 20,132,385 | 21,883,456 | 0.7 | 0.7 |
| Missouri | 4,282,354,451 | 44,278,809 | 48,188,389 | 1.0 | 1.1 |
| Montana | 657,488,444 | 6,136,976 | 7,176,917 | 0.9 | 1.1 |
| New Hampshire | 947,443,772 | 7,066,142 | 8,141,948 | 0.7 | 0.9 |
| North Carolina | 8,883,249,639 | 47,771,308 | 55,216,792 | 0.5 | 0.6 |
| North Dakota | 551,744,708 | 4,280,975 | 4,628,033 | 0.8 | 0.8 |
| Oklahoma | 3,279,858,237 | 9,106,567 | 12,120,378 | 0.3 | 0.4 |
| South Carolina | 3,208,396,386 | 17,922,728 | 20,532,386 | 0.6 | 0.6 |
| South Dakota | 668,219,313 | 5,965,250 | 6,714,524 | 0.9 | 1.0 |
| Vermont | 914,114,015 | 30,132,534 | 30,663,997 | 3.3 | 3.4 |
| Wyoming | 518,587,977 | 1,980,713 | 2,379,600 | 0.4 | 0.5 |
C. Medicaid Enrollees in FFS States with an SA Diagnosis
In this section, we describe the characteristics of Medicaid enrollees identified with a diagnosis of an SA disorder or SA-related diagnosis on a FFS Medicaid claim in CY 2008 in the 18 predominantly FFS states. In Section III.C.1, we describe the source of identification of these enrollees. In Section III.C.2, we discuss the distribution of treatment users by demographic and eligibility group. In Section III.C.3, we describe whether treatment was received for alcohol only, drug use only, or both, and whether treatment was received for an MH diagnosis. In Section III.C.4, we present statistics on ER and inpatient hospital use among SA treatment users. Finally, in Section III.C.5, we compare expenditures among SA treatment users and other Medicaid enrollees.
The analyses in this section used only the FFS claims data. For individuals who were enrolled in FFS Medicaid for part of the year and in a managed care plan for part of the year, we retained the FFS months and expenditures in this analysis. We assessed the impact of excluding these individuals and found it had a minor impact on the results, because the majority of enrollees in these 18 states have only FFS Medicaid. The most significant impact of this exclusion would have been on Connecticut where there was no managed care enrollment in the first half of the year, but where many Medicaid enrollees participated in managed care late in the year. We believe inclusion of the FFS experience of these enrollees provides an analysis population more representative of the full Medicaid population in Connecticut.
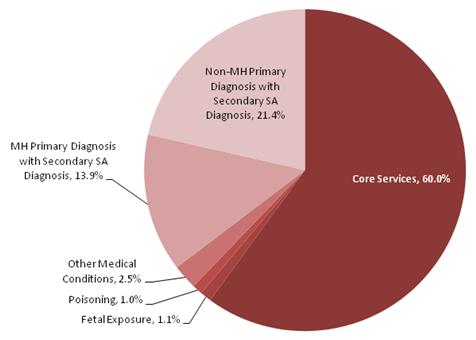
Figure III.6 shows the distribution of Medicaid enrollees with a SA diagnosis by source of identification. For individuals who had claims with more than one source, a hierarchy was used to assign one source in the following order: core, fetal exposure, poisoning, other medical conditions, MH primary with secondary SA diagnosis and non-MH with secondary SA diagnosis. The majority of Medicaid enrollees with a SA diagnosis (60.0 percent) were identified base a primary diagnosis of core SA treatment. Few enrollees were identified based on fetal exposure, poisoning, or another medical condition fully attributable to SA (1.1 percent, 1.0 percent and 2.5 percent, respectively). The remainder were identified based on a secondary diagnosis with 13.9 percent having a primary MH diagnosis and secondary SA diagnosis and 21.4 percent having a primary non-MH diagnosis and a secondary SA diagnosis.
FIGURE III.6. Distribution of Medicaid Enrollees in FFS States with an SA Diagnosis, by Source of Diagnosis
2. Demographic and Eligibility Characteristics
Figure III.7 displays the distribution of Medicaid enrollees with a SA treatment diagnosis by demographic group. Children less than 12 account for 3.8 percent of Medicaid enrollees with a SA treatment diagnosis. Individuals over 65 also represent a small share of enrollees with a SA diagnosis (4.5 percent). Adolescents 12-17 account for almost 10 percent of enrollees with a SA treatment diagnosis. Thus, the vast majority of enrollees with a SA diagnosis (81.7 percent) are working age adults 18-64. Females 18-44 (31.7 percent) represent more than double the share of females 45-64 (13.4 percent). In contrast, males 18-44 (18.6 percent) represent a similar share of enrollees with SA diagnosis as males 45-64 (18.0 percent).
FIGURE III.7. Distribution of Medicaid Enrollees in FFS States with an SA Diagnosis by Demographic Group
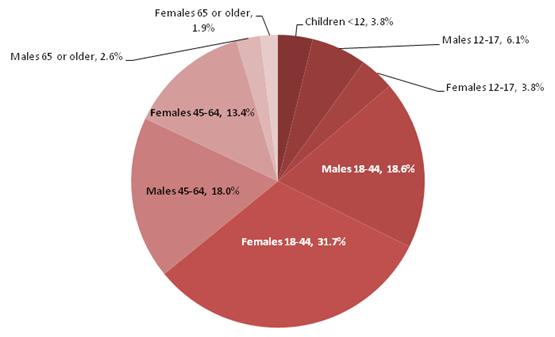
Table III.11 presents the number Medicaid enrollees with a SA diagnosis per 1,000 FFS enrolled months by eligibility and demographic group. In general non-disabled individuals tended to have a lower rate of SA diagnosis than disabled individuals in the same demographic group. Among males, partial-benefit enrollees tended to have higher rates of SA diagnosis, however, among females they had lower rates of diagnosis. By age group, the highest rates of diagnosis are among enrollees 18-44 with one exception. Males with a disability age 45-64 had higher diagnosis rates than their counterparts 18-44.
| Total FFS Enrolled Months | Non-Dual, Non-Disabled | Non-Dual, Disabled | Medicare Dual Eligibles | |||
| Full- Benefit | Partial- Benefit | Full- Benefit | Partial- Benefit | |||
| Total (18 States) | 67,584,197 | 1.34 | 1.14 | 2.17 | 1.15 | 2.44 |
| Female | ||||||
| 12-17 | 8,524,660 | 1.33 | 1.03 | 1.82 | 0.77 | NA |
| 18-20 | 3,313,437 | 2.86 | 1.96 | 4.00 | 1.95 | 3.85 |
| 21-34 | 10,162,599 | 5.10 | 3.12 | 7.49 | 2.66 | 5.40 |
| 35-44 | 4,916,023 | 5.45 | 3.17 | 10.90 | 6.23 | 5.40 |
| 45-64 | 7,691,548 | 4.51 | 3.10 | 7.09 | 4.91 | 3.45 |
| 65 or Older | 8,247,056 | 0.81 | 0.90 | 1.95 | 2.04 | 0.67 |
| Male | ||||||
| 12-17 | 8,810,212 | 2.07 | 1.53 | 2.31 | 1.07 | NA |
| 18-20 | 2,198,807 | 4.09 | 3.87 | 4.45 | 1.97 | 3.95 |
| 21-34 | 2,902,699 | 7.89 | 8.96 | 9.12 | 2.71 | 6.53 |
| 35-44 | 2,475,379 | 6.74 | 7.17 | 14.81 | 8.25 | 7.41 |
| 45-64 | 5,258,261 | 5.41 | 5.60 | 15.24 | 12.73 | 6.51 |
| 65 or Older | 3,083,516 | 2.24 | 2.95 | 6.54 | 8.39 | 2.44 |
Table III.12 shows the percentage of enrollees ages 12 or older with an SA diagnosis by the type of treatment received in the 18 predominantly FFS states by state. The enrollees are identified as having only alcohol-related claims, only drug-related claims, or both alcohol and drug-related claims. They also are identified (separately) as being treated for an MH condition.
| State | Count of Enrollees | Percentage of Enrollees | |||
| Alcohol Only | Drug Only | Alcohol & Drug | MH Condition Treated | ||
| Total (18 states) | 281,522 | 30.6 | 55.3 | 14.2 | 63.0 |
| Alabama | 13,709 | 31.0 | 60.4 | 8.6 | 53.7 |
| Arkansas | 7,784 | 34.4 | 58.9 | 6.7 | 70.5 |
| Connecticut | 23,445 | 24.7 | 57.5 | 17.8 | 61.6 |
| Idaho | 3,871 | 40.1 | 47.2 | 12.7 | 74.0 |
| Illinois | 51,502 | 31.7 | 52.5 | 15.8 | 57.5 |
| Kentucky | 21,915 | 24.0 | 65.0 | 11.0 | 69.6 |
| Louisiana | 17,386 | 30.6 | 57.0 | 12.4 | 60.3 |
| Mississippi | 14,051 | 34.7 | 49.3 | 16.0 | 67.8 |
| Missouri | 25,752 | 32.2 | 54.4 | 13.4 | 65.8 |
| Montana | 4,502 | 47.8 | 36.4 | 15.8 | 66.1 |
| New Hampshire | 4,643 | 28.5 | 62.3 | 9.2 | 69.7 |
| North Carolina | 45,941 | 28.5 | 56.6 | 14.9 | 65.2 |
| North Dakota | 2,725 | 45.1 | 28.0 | 26.9 | 71.9 |
| Oklahoma | 14,438 | 28.1 | 59.0 | 12.9 | 69.0 |
| South Carolina | 15,936 | 31.2 | 56.7 | 12.1 | 55.1 |
| South Dakota | 2,769 | 43.9 | 25.3 | 30.8 | 63.6 |
| Vermont | 9,242 | 29.6 | 53.3 | 17.1 | 58.6 |
| Wyoming | 1,911 | 46.3 | 41.8 | 12.0 | 61.7 |
Overall, 54.3 percent of the individuals identified with an SA diagnosis had only drug-related claims, 30.6 percent had only alcohol-related claims, and 14.2 percent had both types of claims. The percentage of enrollees by each type of treatment varied by state, but the percentage with only drug-related claims was near or above 50 percent, and higher than the percentages falling into the other two treatment categories, in 14 of the 18 states. Montana, Wyoming, and North and South Dakota had the highest share of enrollees with an SA diagnosis who received only treatment for alcohol-related conditions.
Overall, among the enrollees with an SA diagnosis, 63.0 percent had an MH-related claim. The percentage of enrollees with an SA diagnosis who also had an MH diagnosis ranged from 53.7 percent in Alabama to 74.0 percent in Idaho.
Table III.13 shows the percentage of enrollees ages 12 or older with an SA diagnosis by the type of treatment received by demographic group. Type of treatment was identified based on claim diagnosis codes in the first or later field. The diagnoses used to assign claims to alcohol, drugs, and MH are listed in Appendix B Table B.1, Table B.2 and Table B.3, respectively.
| Demographic Group | Count of Enrollees | Percentage of Enrollees | |||
| Alcohol Only | Drug Only | Alcohol & Drug | MH Condition Treated | ||
| Total (18 states) | 281,522 | 30.6 | 55.3 | 14.2 | 63.0 |
| Medicare Duals | |||||
| 12-64 | 48,084 | 36.1 | 50.4 | 13.5 | 71.2 |
| 65 or Older | 12,154 | 63.1 | 33.5 | 3.4 | 44.5 |
| Non-Disabled, Non-Dual | |||||
| 12-20 | 41,622 | 16.7 | 69.9 | 13.5 | 63.7 |
| 21-44 | 69,904 | 20.3 | 68.3 | 11.4 | 57.1 |
| 45 or Older | 9,050 | 43.0 | 44.7 | 12.4 | 47.6 |
| Disabled, Non-Dual | |||||
| 12-20 | 5,556 | 15.9 | 71.2 | 13.0 | 81.7 |
| 21-44 | 38,513 | 24.8 | 54.5 | 20.8 | 75.9 |
| 45 or Older | 56,639 | 45.1 | 38.0 | 17.0 | 58.4 |
Younger enrollees were more likely to receive treatment for drug use or abuse, while older enrollees were more likely to receive treatment for alcohol use or abuse. Relative to the other demographic groups, enrollees in the aged dual group had a much higher percentage (63.1 percent) of enrollees with only alcohol-related claims relative to the other groups and correspondingly lower percentages of enrollees with drug only (33.5 percent) and alcohol and drug-related claims (3.4 percent). In contrast, the disabled and non-disabled, non-dual groups ages 12-20 had the highest percentages (71.2 percent and 69.9 percent, respectively) of enrollees with only drug-related claims and the lowest percentage (15.9 percent and 16.7 percent, respectively) with only alcohol-related claims across all of the demographic groups. Not surprisingly, individuals with a disability, including Medicare dual eligibles ages 12-64 and non-duals with a disability, were more likely to have been treated for an MH condition relative to the average across all demographic groups.
4. Use of ER and Inpatient Hospital Services
Table III.14 shows the percentage of enrollees ages 12 or older with an SA diagnosis who used an ER or inpatient hospital. It also shows their expenditures for ER and inpatient hospital services per enrolled month. ER services were identified on IP and OT file records based on listing of a procedure code of 99281-99292 or a revenue center code of 450-459 or 981 on any claim. The place of service code equal ER was also used on OT service file claims.
Overall, 21.4 percent and 62.4 percent of enrollees with an SA diagnosis used the ER with an SA-related or any diagnosis, respectively. Vermont and South Dakota had the lowest share of ER visits with a SA-related diagnosis (13.0 percent and 14.8 percent, respectively). Alabama, Arkansas, and Kentucky had the highest share of enrollees with a SA-related ER visit (about 26 percent). When ER claims with any diagnosis are considered, Vermont (55.4 percent) and South Dakota (52.7 percent) still have among the lowest shares, but Connecticut has the lowest share with 48.9 percent. The share of enrollees with a SA diagnosis using the ER was highest Arkansas with 87.1 percent.
| State | Count of Enrollees | Percentage Using | Expenditures per Enrolled Month (in $) | ||||
| ER with SA Diagnosis | ER with any Diagnosis | Inpatient Hospital | ER with SA Diagnosis | ER with any Diagnosis | Inpatient Hospital | ||
| Total (18 states) | 281,522 | 21.4 | 62.4 | 33.6 | 4.26 | 40.94 | 381.73 |
NOTES: Both full and partial-benefit enrollees are included in this table. All claims marked as ER services on the IP file are not included in the calculations of ER expenditures per enrolled month because these expenditures already are already included in the Inpatient hospital expenditures; ER service claims identified in the IP file make up 3.9% of total ER claims. | |||||||
| Alabama | 13,709 | 26.1 | 66.0 | 25.3 | 2.18 | 25.71 | 104.77 |
| Arkansas | 7,784 | 26.4 | 87.1 | 17.4 | 7.36 | 46.29 | 148.98 |
| Connecticut | 23,445 | 18.9 | 48.9 | 26.8 | 3.65 | 26.94 | 375.77 |
| Idaho | 3,871 | 20.1 | 57.0 | 38.9 | 2.32 | 22.92 | 396.21 |
| Illinois | 51,502 | 20.4 | 58.9 | 41.9 | 3.61 | 23.13 | 575.71 |
| Kentucky | 21,915 | 26.7 | 65.3 | 34.4 | 4.96 | 51.86 | 452.35 |
| Louisiana | 17,386 | 23.1 | 68.2 | 42.7 | 4.65 | 42.22 | 351.26 |
| Mississippi | 14,051 | 22.0 | 65.3 | 42.6 | 2.28 | 26.23 | 456.17 |
| Missouri | 25,752 | 19.8 | 59.6 | 28.2 | 8.52 | 74.95 | 293.31 |
| Montana | 4,502 | 22.3 | 60.4 | 35.1 | 2.47 | 20.47 | 311.45 |
| New Hampshire | 4,643 | 22.4 | 64.7 | 30.0 | 6.82 | 64.15 | 220.57 |
| North Carolina | 45,941 | 22.6 | 69.2 | 29.5 | 4.57 | 56.75 | 292.06 |
| North Dakota | 2,725 | 17.3 | 55.9 | 27.6 | 3.66 | 37.23 | 325.40 |
| Oklahoma | 14,438 | 19.9 | 63.6 | 43.1 | 2.14 | 37.06 | 450.61 |
| South Carolina | 15,936 | 18.1 | 58.2 | 33.9 | 4.47 | 52.82 | 475.39 |
| South Dakota | 2,769 | 14.8 | 52.7 | 33.0 | 1.55 | 31.51 | 334.89 |
| Vermont | 9,242 | 13.0 | 55.4 | 17.8 | 3.25 | 29.42 | 167.26 |
| Wyoming | 1,911 | 22.0 | 58.6 | 36.5 | 4.50 | 47.31 | 622.74 |
Turning to inpatient services, on average, 33.6 percent of enrollees with an SA diagnosis had a SA-related inpatient hospital stay. In Arkansas and Vermont only 17-18 percent of enrollees with an SA diagnosis used inpatient hospital services. In Illinois, Louisiana, Mississippi, and Oklahoma, more than 40 percent of enrollees with an SA diagnosis used inpatient care.
On average per enrolled month enrollees with a SA diagnosis used 4.26, 40.94 and 381.73 dollars in SA-related ER services, all ER services, and SA-related inpatient hospital services, respectively. ER expenditures per enrolled month for any type of diagnosis varied substantially across states: Montana had the lowest expenditures (20.47), and New Hampshire had the highest (64.15). SA treatment-related inpatient hospital expenditures per enrolled month were much higher than ER expenditures but also varied substantially across states: Alabama had the lowest expenditures (104.77), while Wyoming had the highest (622.74).
Table III.15 shows the percentage of enrollees with an SA diagnosis who used the ER or inpatient hospital by demographic group. Non-disabled enrollees 12-20 had a lower rate of both SA-related (16.8 percent) and any ER (51.0 percent) and inpatient hospital use (21.1 percent) relative to the average across all demographic groups. Aged duals and disabled, non-duals 45 or older had a higher rate of inpatient hospital use (45.3 percent and 47.6 percent) relative to the average across all demographic groups. In terms of expenditures Medicare duals had the lowest level of ER expenditures. Individuals with disability 21 and older had the highest ER expenditures and the highest inpatient hospital expenditures. The lowest inpatient hospital expenditures were for duals 12-64.
| State | Count of Enrollees | Percentage Using | Expenditures per Enrolled Month (in $) | ||||
| ER with SA Diagnosis | ER with any Diagnosis | Inpatient Hospital | ER with SA Diagnosis | ER with any Diagnosis | Inpatient Hospital | ||
| Total (18 states) | 281,522 | 21.4 | 62.4 | 33.6 | 4.26 | 40.94 | 381.73 |
| Medicare Duals | |||||||
| 12-64 | 48,084 | 22.0 | 66.5 | 28.0 | 1.70 | 15.56 | 125.25 |
| 65 or Older | 12,154 | 13.1 | 52.7 | 45.3 | 0.67 | 6.71 | 440.48 |
| Non-Disabled, Non-Dual | |||||||
| 12-20 | 41,622 | 16.8 | 51.0 | 21.1 | 2.62 | 22.10 | 261.04 |
| 21-44 | 69,904 | 17.2 | 58.5 | 27.1 | 3.37 | 42.88 | 183.78 |
| 45 or Older | 9,050 | 18.3 | 54.8 | 33.1 | 3.88 | 31.52 | 358.17 |
| Disabled, Non-Dual | |||||||
| 12-20 | 5,556 | 22.6 | 61.9 | 30.9 | 3.66 | 38.35 | 426.00 |
| 21-44 | 38,513 | 30.3 | 73.3 | 42.1 | 7.59 | 75.58 | 591.86 |
| 45 or Older | 56,639 | 25.4 | 68.2 | 47.6 | 7.21 | 59.55 | 742.44 |
Across all enrollees in the 18 FFS states represented in Table III.15, the three diagnoses with the highest total expenditures among ER claims were for alcoholic cirrhosis of the liver; schizoaffective disorder, unspecified; and acute pancreatitis. Taken together, these diagnoses represented 6.8 percent of total spending on ER visits for SA-related services. These were also the top three diagnoses for men (representing 7.9 percent of expenditures), while depressive disorder, not elsewhere classified, replaced acute pancreatitis for women (representing 6.0 percent of expenditures).
When disabled and non-disabled non-duals in the 18 FFS states were examined separately, the top three diagnoses by expenditure amount for non-dual disabled enrollees were alcoholic cirrhosis of the liver; unspecified schizoaffective disorder; and acute pancreatitis, which made up 7.8 percent of spending on ER services by this group. The top three diagnoses for non-dual, non-disabled enrollees were depressive disorder, not elsewhere classified; acute pancreatitis; and major depressive affective disorder, recurrent episode, severe, without mention of psychotic behavior, which made up 7.1 percent of spending by this group of enrollees on ER visits for SA-related services.
When examined separately for each of the 18 FFS states, alcoholic cirrhosis of the liver was among the top three codes in eight of the 18 states; acute pancreatitis was among the top three codes in six of the states; and unspecified schizoaffective disorder was among the top three codes in five of the states.
Across all enrollees in the 18 FFS states represented in Table III.15, the top three diagnoses representing inpatient hospital claims were for unspecified schizoaffective disorder; drug withdrawal; and alcoholic cirrhosis of the liver. Taken together, these diagnoses represented 9.6 percent of total spending on inpatient hospital stays for SA-related services. These were also the top three diagnoses for men (representing 10.2 percent of expenditures), while unspecified bipolar disorder replaced alcoholic cirrhosis of the liver for women (representing 9.5 percent of expenditures).
When examined separately for non-dual disabled versus non-disabled for each of the 18 FFS states, the top three diagnoses by expenditure amount for non-dual disabled enrollees were unspecified schizoaffective disorder; drug withdrawal; and alcoholic cirrhosis of the liver, which made up 11.8 percent of spending by this group of enrollees on inpatient hospital stays for SA-related services. The top three diagnoses for non-dual non-disabled enrollees were unspecified episodic mood disorder; unspecified bipolar disorder; and depressive disorder, not elsewhere classified, which made up 13.3 percent of spending by this group of enrollees on inpatient hospital stays for SA-related services.
| Total | Male | Female | |||||||
| 12-20 | 21-44 | 45-64 | 65 or Older | 12-20 | 21-44 | 45-64 | 65 or Older | ||
| Total (18 states) | 1,541 | 1,296 | 1,495 | 2,025 | 1,782 | 1,417 | 1,175 | 1,809 | 1,690 |
| Alabama | 805 | 704 | 659 | 757 | 1,395 | 1,016 | 626 | 776 | 1,362 |
| Arkansas | 1,455 | 1,562 | 1,436 | 1,596 | 2,186 | 1,445 | 1,155 | 1,428 | 2,104 |
| Connecticut | 1,663 | 904 | 1,549 | 2,193 | 2,806 | 1,153 | 1,116 | 2,008 | 2,807 |
| Idaho | 1,852 | 1,022 | 2,085 | 2,031 | 1,895 | 1,517 | 1,814 | 2,182 | 1,505 |
| Illinois | 1,823 | 1,155 | 1,944 | 2,903 | 2,300 | 1,377 | 1,101 | 2,299 | 2,358 |
| Kentucky | 1,647 | 1,905 | 1,346 | 2,107 | 2,050 | 1,714 | 1,260 | 2,132 | 1,951 |
| Louisiana | 1,339 | 627 | 1,437 | 1,867 | 1,284 | 740 | 1,096 | 1,701 | 1,123 |
| Mississippi | 1,296 | 1,469 | 1,117 | 1,420 | 1,596 | 1,705 | 1,069 | 1,332 | 1,320 |
| Missouri | 1,665 | 2,350 | 1,560 | 1,725 | 1,419 | 2,142 | 1,491 | 1,639 | 1,590 |
| Montana | 1,565 | 1,292 | 1,377 | 1,999 | 2,180 | 1,574 | 1,279 | 1,801 | 1,924 |
| New Hampshire | 1,327 | 1,677 | 1,203 | 1,727 | 2,436 | 1,470 | 987 | 1,441 | 2,206 |
| North Carolina | 1,519 | 1,448 | 1,542 | 1,880 | 1,341 | 1,305 | 1,231 | 1,811 | 1,391 |
| North Dakota | 1,508 | 965 | 1,396 | 2,253 | 2,470 | 1,384 | 1,078 | 2,122 | 2,677 |
| Oklahoma | 1,535 | 1,354 | 1,639 | 2,027 | 1,596 | 1,397 | 1,168 | 1,716 | 1,609 |
| South Carolina | 1,415 | 948 | 1,355 | 1,926 | 1,010 | 1,285 | 1,286 | 1,707 | 717 |
| South Dakota | 1,680 | 1,227 | 2,106 | 2,668 | 2,052 | 1,512 | 1,490 | 2,781 | 778 |
| Vermont | 1,175 | 1,498 | 850 | 1,214 | 1,853 | 1,752 | 1,135 | 1,384 | 2,485 |
| Wyoming | 2,097 | 1,713 | 2,210 | 2,713 | 3,145 | 2,252 | 1,593 | 2,705 | 2,197 |
When examined separately for each of the 18 FFS states, alcoholic cirrhosis of the liver, alcohol-induced persisting dementia, and unspecified episodic mood disorder were each among the top three codes for inpatient hospital services in seven of the 18 states. Unspecified schizoaffective disorder was among the top three codes in six of the 18 states.
5. Comparison of SA User and Non-SA Medicaid Expenditures
Table III.16 shows the total Medicaid FFS expenditures per FFS enrolled months for enrollees using SA services. Expenditures per FFS enrolled month averaged 1,541 across all SA users in the 18 FFS states. Expenditures were higher for individuals over age 45 relative to those 12-44. In the 12-20 age group, expenditures tended to be higher for females relative to males. This was true for 14 of the 18 states. In contrast, in the age 21-44 group, expenditures tended to be higher for males. This was true in 17 of the 18 states.
Table III.17 shows the expenditures per FFS enrolled months for SA users relative to expenditures per FFS enrolled months for all enrollees in the same demographic group. Overall expenditures for SA users were 2.19 times higher than the average enrollees. Across the states, SA treatment user expenditures ranged from 1.33 times higher than the average enrollee in New Hampshire to 3.42 times higher in Illinois. The difference between SA treatment user and average expenditures was most pronounced among individuals 12-20. Males 12-20 had expenditures 4.08 times higher than average, and females 12-20 had expenditures 4.81 times higher than average.
| Total | Male | Female | |||||||
| 12-20 | 21-44 | 45-64 | 65 or Older | 12-20 | 21-44 | 45-64 | 65 or Older | ||
| Total (18 states) | 2.19 | 4.08 | 1.64 | 1.63 | 1.57 | 4.81 | 2.17 | 1.78 | 1.43 |
| Alabama | 1.48 | 2.71 | 1.14 | 1.07 | 1.58 | 3.85 | 1.25 | 1.32 | 1.48 |
| Arkansas | 2.02 | 4.45 | 1.26 | 1.37 | 1.70 | 5.00 | 1.68 | 1.40 | 1.57 |
| Connecticut | 1.61 | 3.89 | 1.35 | 0.99 | 1.15 | 6.00 | 2.61 | 1.35 | 1.11 |
| Idaho | 2.01 | 2.53 | 1.37 | 1.36 | 1.31 | 4.21 | 1.81 | 1.51 | 0.97 |
| Illinois | 3.42 | 6.29 | 2.85 | 2.22 | 2.30 | 7.51 | 3.44 | 2.43 | 2.33 |
| Kentucky | 2.36 | 5.43 | 2.03 | 2.25 | 1.97 | 4.55 | 2.14 | 2.23 | 1.59 |
| Louisiana | 2.13 | 3.41 | 1.17 | 1.28 | 1.25 | 3.41 | 1.80 | 1.44 | 1.15 |
| Mississippi | 2.00 | 4.96 | 1.31 | 1.56 | 1.57 | 5.30 | 1.87 | 1.73 | 1.32 |
| Missouri | 1.69 | 3.94 | 1.40 | 1.39 | 1.28 | 4.67 | 1.83 | 1.44 | 1.30 |
| Montana | 1.63 | 2.20 | 1.76 | 1.65 | 1.26 | 3.00 | 1.82 | 1.51 | 1.00 |
| New Hampshire | 1.33 | 3.28 | 0.79 | 1.02 | 1.31 | 3.78 | 1.40 | 1.13 | 1.15 |
| North Carolina | 1.88 | 2.89 | 1.39 | 1.41 | 1.30 | 3.23 | 1.84 | 1.60 | 1.25 |
| North Dakota | 1.20 | 1.73 | 0.85 | 1.03 | 1.07 | 2.97 | 1.50 | 1.22 | 1.21 |
| Oklahoma | 2.17 | 3.96 | 1.58 | 1.56 | 1.55 | 4.58 | 1.71 | 1.57 | 1.40 |
| South Carolina | 2.10 | 2.78 | 1.52 | 1.78 | 1.20 | 3.67 | 2.01 | 1.94 | 0.85 |
| South Dakota | 2.03 | 2.60 | 1.82 | 1.91 | 1.44 | 3.85 | 2.11 | 2.29 | 0.56 |
| Vermont | 1.76 | 2.39 | 1.45 | 1.76 | 1.66 | 3.68 | 2.23 | 2.06 | 2.04 |
| Wyoming | 1.77 | 3.27 | 1.32 | 1.30 | 1.42 | 4.15 | 1.42 | 1.51 | 1.03 |
[highchart chart_id="93651" different_values="0"]
IV. FEE-FOR-SERVICE SPENDING IN MANAGED CARE STATES
In this section, we summarize FFS SA expenditures identified in MAX in those states that have predominantly managed care coverage of SA services or substantial reporting issues. Because these data are not representative of the full population of managed care enrollees or are derived from states with reporting anomalies, the results should be interpreted with caution. No results are reported for Maine because it is missing a substantial amount of data, having been unable to report accurately on inpatient, long-term care, and other services in MAX 2008; only eligibility and prescription drug information was reported for the state.
Figure IV.1 shows the distribution of Medicaid FFS SA expenditures in the 31 managed care states and the District of Columbia by demographic group. Males ages 45-64 and 18-44 constitute roughly half of the expenditures (27.9 percent and 24.0 percent, respectively). Females ages 65 and older and children under age 12 account for the smallest and second smallest percentage of all the demographic groups (1.6 percent and 2.5 percent, respectively).
FIGURE IV.1. Distribution of Medicaid FFS SA Expenditures in Managed Care States, by Demographic Group
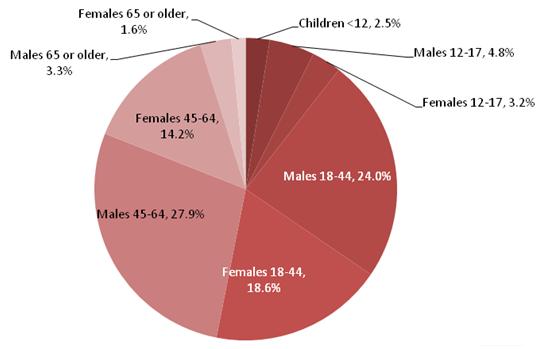
Figure IV.2 shows the distribution of Medicaid FFS SA expenditures in the managed care states by eligibility group. Disabled adults make up the highest percentage of expenditures (45.9 percent), while children under age 12 make up the smallest percentage (2.5 percent). Among those states with predominantly FFS coverage of SA treatment, adults with disability represented a share of expenditures similar to non-disabled adults. The increased share of FFS expenditures associated with individuals with disability in the managed care states likely results from their exclusion from managed care coverage. Expenditures for non-disabled adults are more likely to be covered under managed care and thus are not represented in these estimates.
FIGURE IV.2. Proportion of Medicaid FFS SA Expenditures in Managed Care States, by Eligibility Group
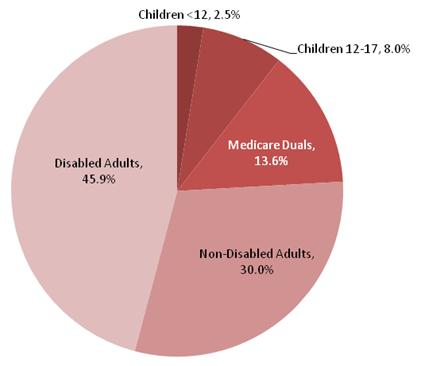
Table IV.1 shows the total core SA treatment FFS expenditures by type of service, state, and age 12 or older in the 32 managed care states. It also shows the percentage of non-duals 12 and older with at least one month of enrollment in a managed care plan that covers SA services. Although Alaska has no managed care enrollment, it was not included in the predominantly FFS service states because of concern that incomplete reporting of primary diagnosis would result in an underestimate of SA treatment services since primary diagnosis is used to identify SA treatment services.
Overall, 1.5 billion in FFS expenditures were identified in these states. This is almost four times the total expenditures identified in the predominantly FFS states. Several states make up a large share of the SA treatment expenditures reported. New York represents 49.4 percent of the FFS expenditures identified in managed care states, although about three-quarters of New York Medicaid enrollees are enrolled in comprehensive managed care, and program descriptions indicate that these plans cover both inpatient and outpatient SA treatment. California, Ohio, and Massachusetts also each represented a substantial share of expenditure, with 12.2 percent, 6.1 percent, and 4.9 percent of managed care states' FFS expenditures, respectively.
| Expenditures (thousands) | Percentage of Non-Duals12 & Older Enrolled in Managed Care | |||||
| TotalCore | Inpatient Hospital | Prescription Drug | Residential Treatment | Outpatient Treatment | ||
| Total (32 states) | 1,520,706 | 521,664 | 57,970 | 14,561 | 926,511 | 57.4 |
| NR = Not Reported. Cells representing fewer than 11 users are not reported to protect confidentiality. Expenditures related to these cells have been removed from column totals for the respective state. | ||||||
| Alaska | 6,687 | 1,523 | 432 | 165 | 4,568 | 0.0 |
| Arizona | 34,143 | 2,192 | 0 | 13 | 31,938 | 76.6 |
| California | 186,026 | 21,704 | 1,313 | 0 | 163,009 | 28.8 |
| Colorado | 14,939 | 8,681 | 542 | 0 | 5,716 | 93.7 |
| Delaware | 6,187 | 1,046 | 429 | 27 | 4,685 | 80.6 |
| District of Columbia | 5,644 | 2,560 | 522 | 0 | 2,562 | 67.4 |
| Florida | 27,034 | 12,950 | 528 | 25 | 13,531 | 41.2 |
| Georgia | 13,641 | 6,674 | 154 | NR | 6,813 | 67.4 |
| Hawaii | 4,447 | 724 | 143 | 1,380 | 2,200 | 86.8 |
| Indiana | 13,569 | 4,723 | 657 | 221 | 7,967 | 75.0 |
| Iowa | 3,127 | 2,188 | 321 | 0 | 619 | 70.9 |
| Kansas | 2,815 | 2,143 | 209 | 120 | 344 | 96.3 |
| Maryland | 13,391 | 5,808 | 244 | 0 | 7,339 | 80.0 |
| Massachusetts | 73,898 | 14,999 | 10,609 | 2,154 | 46,136 | 31.7 |
| Michigan | 7,863 | 5,535 | 1,137 | 0 | 1,191 | 73.2 |
| Minnesota | 38,095 | 18,249 | 626 | 429 | 18,791 | 67.0 |
| Nebraska | 15,568 | 11,692 | 113 | 786 | 2,977 | 90.0 |
| Nevada | 3,527 | 2,109 | 118 | 77 | 1,224 | 53.4 |
| New Jersey | 31,494 | 11,477 | 2,146 | 326 | 17,544 | 82.5 |
| New Mexico | 2,092 | 1,212 | 21 | 0 | 859 | 60.2 |
| New York | 751,205 | 312,526 | 16,704 | 0 | 421,974 | 76.7 |
| Ohio | 93,192 | 15,735 | 1,164 | 0 | 76,292 | 84.5 |
| Oregon | 8,697 | 2,409 | 127 | NR | 6,161 | 72.5 |
| Pennsylvania | 14,595 | 7,828 | 4,719 | NR | 2,048 | 90.8 |
| Rhode Island | 11,494 | 3,563 | 332 | 394 | 7,205 | 76.0 |
| Tennessee | 9,055 | 2,418 | 5,447 | 0 | 1,189 | 53.7 |
| Texas | 11,097 | 5,594 | 1,337 | 0 | 4,165 | 44.7 |
| Utah | 8,809 | 1,623 | 1,020 | NR | 6,166 | 0.0 |
| Virginia | 10,982 | 3,608 | 1,407 | 635 | 5,331 | 66.4 |
| Washington | 54,373 | 6,147 | 386 | 6,297 | 41,543 | 99.8 |
| West Virginia | 12,823 | 4,974 | 2,055 | 1,353 | 4,440 | 48.4 |
| Wisconsin | 30,183 | 17,051 | 3,007 | 143 | 9,982 | 60.4 |
Table IV.2 reports the distribution of FFS expenditures in managed care states by type of care. In the 18 predominantly FFS states, 35.2 percent of expenditures were for inpatient hospital care, 51.9 percent were for outpatient care, 5.4 percent were for prescribed drugs, and the remaining 7.5 percent were for residential treatment. For the managed care states, we found a greater share of expenditures for outpatient care (60.7 percent) and a similar percentage for inpatient care (34.0 percent). Residential treatment accounted for only 1.5 percent of expenditures, and prescribed drugs only 3.8 percent. New York's expenditures have a significant impact on this distribution, with no reported residential treatment expenditures, 2.2 percent for prescribed drugs, 41.6 percent for inpatient care, and 56.2 percent for outpatient care. Residential treatment makes up the smallest percentage across the four categories (inpatient hospital, prescription drug, residential treatment, and outpatient treatment) in 28 of the 32 states, with 11 of the 33 states spending zero dollars on residential treatment. We identified a very high share of outpatient treatment expenditures in Arizona, California and Ohio, with 93.5 percent, 87.6 percent, and 81.9 percent of FFS spending for outpatient care, respectively.
| State | Percentage of Core SA Treatment FFS Expenditures | Percentage of Non-Duals12 & Older Enrolled in Managed Care | |||
| Inpatient Hospital | Prescription Drug | Residential Treatment | Outpatient Treatment | ||
| Total (32 states) | 34.3 | 3.8 | 1.0 | 60.9 | 57.4 |
| Alaska | 22.8 | 6.5 | 2.5 | 68.3 | 0.0 |
| Arizona | 6.4 | 0.0 | 0.0 | 93.5 | 76.6 |
| California | 11.7 | 0.7 | 0.0 | 87.6 | 28.8 |
| Colorado | 58.1 | 3.6 | 0.0 | 38.3 | 93.7 |
| Delaware | 16.9 | 6.9 | 0.4 | 75.7 | 80.6 |
| District of Columbia | 45.4 | 9.2 | 0.0 | 45.4 | 67.4 |
| Florida | 47.9 | 2.0 | 0.1 | 50.1 | 41.2 |
| Georgia | 48.9 | 1.1 | 0.0 | 49.9 | 67.4 |
| Hawaii | 16.3 | 3.2 | 31.0 | 49.5 | 86.8 |
| Indiana | 34.8 | 4.8 | 1.6 | 58.7 | 75.0 |
| Iowa | 69.9 | 10.3 | 0.0 | 19.8 | 70.9 |
| Kansas | 76.1 | 7.4 | 4.3 | 12.2 | 96.3 |
| Maryland | 43.4 | 1.8 | 0.0 | 54.8 | 80.0 |
| Massachusetts | 20.3 | 14.4 | 2.9 | 62.4 | 31.7 |
| Michigan | 70.4 | 14.5 | 0.0 | 15.1 | 73.2 |
| Minnesota | 47.9 | 1.6 | 1.1 | 49.3 | 67.0 |
| Nebraska | 75.1 | 0.7 | 5.0 | 19.1 | 90.0 |
| Nevada | 59.8 | 3.3 | 2.2 | 34.7 | 53.4 |
| New Jersey | 36.4 | 6.8 | 1.0 | 55.7 | 82.5 |
| New Mexico | 57.9 | 1.0 | 0.0 | 41.1 | 60.2 |
| New York | 41.6 | 2.2 | 0.0 | 56.2 | 76.7 |
| Ohio | 16.9 | 1.2 | 0.0 | 81.9 | 84.5 |
| Oregon | 27.7 | 1.5 | 0.0 | 70.8 | 72.5 |
| Pennsylvania | 53.6 | 32.3 | 0.0 | 14.0 | 90.8 |
| Rhode Island | 31.0 | 2.9 | 3.4 | 62.7 | 76.0 |
| Tennessee | 26.7 | 60.2 | 0.0 | 13.1 | 53.7 |
| Texas | 50.4 | 12.1 | 0.0 | 37.5 | 44.7 |
| Utah | 18.4 | 11.6 | 0.0 | 70.0 | 0.0 |
| Virginia | 32.9 | 12.8 | 5.8 | 48.5 | 66.4 |
| Washington | 11.3 | 0.7 | 11.6 | 76.4 | 99.8 |
| West Virginia | 38.8 | 16.0 | 10.6 | 34.6 | 48.4 |
| Wisconsin | 56.5 | 10.0 | 0.5 | 33.1 | 60.4 |
V. NATIONAL ESTIMATES OF MEDICAID SUBSTANCE ABUSE TREATMENT SPENDING
In this section, we present our estimates of Medicaid SA-related expenditures. First, we present CY 2008 estimates of SA treatment spending. Second, we present projections to FY 2011.
A. CY 2008 SA Treatment Spending by State
In Appendix Tables C.1 through C.5, we present estimates of overall Medicaid SA expenditures for CY 2008. These estimates include FFS expenditures reported to MAX as well as imputed expenditure amounts for the managed care populations whose SA treatment expenditures cannot be identified in MAX. The tables array estimates for all 50 states and the District of Columbia for five types of SA-related services.
Appendix Table C.1: Core SA Treatment Services. The expenditures in this table pertain to core SA treatment services--that is, services with a primary diagnosis indicating treatment of an SA disorder. This set of expenditures is defined to parallel the set of services included in SSE.
Appendix Table C.2: Services Related to Fetal Exposure or Poisoning Related to Drugs or Alcohol. These services have either a primary diagnosis of fetal drug or alcohol exposure, noted in Appendix Table B.1 and Table B.2 as "fetus" or a primary diagnosis of poisoning related to drugs or alcohol, identified in Appendix Table B.1 and Table B.2 as "poisoning."
Appendix Table C.3: Services for Other Medical Conditions 100% Attributable to SA. This category includes claims for other services with a primary diagnosis of a medical condition 100 percent attributable to SA. In Appendix Table B.1 and Table B.2, the services comprise all other codes identified as "supplemental."
Appendix Table C.4: MH Services with a Secondary Diagnosis of SA Disorders (MH w/SA). This group comprises services with a primary diagnosis of a mental disorder and a secondary diagnosis on the same claim either from the core or one of the first three supplemental groups listed above. We identified claims with a primary MH diagnosis based on the codes in Appendix Table B.3.
Appendix Table C.5: Other Medical Services with a Secondary Diagnosis of SA Disorder (Non-MH w/SA). This group includes claims with primary diagnoses not identified as MH disorders that include a secondary diagnosis on the same claim either from the core or one of the first three supplemental groups listed above.
Overall, we estimate Medicaid core SA treatment spending in CY 2008 as 3.4 billion (Appendix Table C.1). The set of services defined as core SA treatment services is designed to parallel estimates of SA treatment spending reported in SAMHSA's spending estimate projections for 2004 through 2014.9 The SSE estimate for Medicaid spending on SA treatment in 2003 is $3,710 million with projection to 2006 of $4,279 million. The average annual growth rate projected for Medicaid SA treatment spending in the SSE is 5.8 percent for 2003 through 2014. Projecting the 2006 estimate forward based on this average projected growth rate would imply an estimate of Medicaid spending for CY 2008 of $4,790 million. The estimate from this study is approximately 30 percent below this prior estimate. Similar to the current study, the SAMHSA Survey of Revenue and Expenditures (SSR&E) estimates SA treatment expenditures in 2009 at a level below the SSE estimate for 2005. The SSR&E represents only specialty SA treatment providers, in contrast to the current study, which represents all providers. The specialty facility spending represented in the SSR&E is about half of all SA treatment spending represented in the SSE. The SSR&E estimate for 2009 for all payers is 94 percent of the SSE estimate for 2005. The SSR&E estimate of the Medicaid share of specialty SA treatment spending is 14 percent.10 This contrasts with the SSE estimate of the Medicaid payment share as 18 percent in 2006 increasing to 20 percent by 2014. The gap between the estimates from the SSR&E and the current study and SSE estimates may be attributable to limitations in the data available to support the SSE estimates at the time they were developed. In particular, comprehensive data on unit prices and the "payers source" distribution associated with specialty SA treatment expenditures were unavailable to support development of the SSE after 1998--prior to the SSR&E survey in 2009. Thus, a substantial portion of the SSE estimate of Medicaid SA treatment spending was imputed.
The SSE represents only those SA treatment expenditures to which we refer as core services. The SSE does not include the other five categories of SA treatment-related spending estimated in this study. The estimated expenditures for these categories are displayed in Figure V.1. Appendix Tables C.2 through C.5 display detailed estimates for these categories by state.
FIGURE V.1. Medicaid Expenditures for SA Treatment, CY 2008 by Type(in millions)
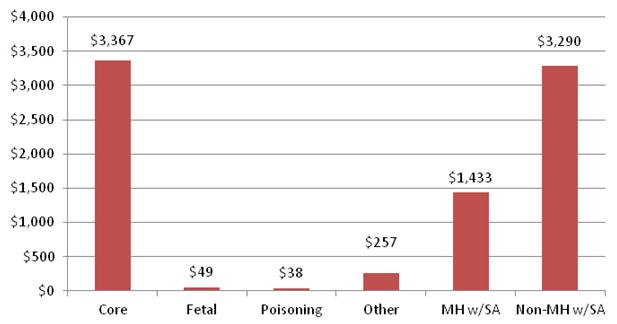
The expenditures in Appendix Tables C.1 through C.3 are 100 percent attributable to SA. As displayed in Figure V.2, among the costs 100 percent attributable to SA, 90.8 percent are related to core services. One percent is related to poisoning and another 1.3 percent to fetal exposure, with 6.9 percent related to other medical conditions fully attributable to SA.
FIGURE V.2. Distribution of Expenditures 100% Attributable to SA, by Type
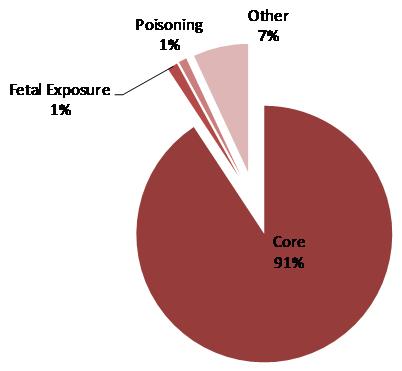
The expenditures in Appendix Table C.4 and Table C.5 are only partially related to SA. The $1.4 billion in expenditures reported in Appendix Table C.4 have a primary diagnosis of MH, and the $3.3 billion in expenditures reported in Appendix Table C.5 have a non-MH primary diagnosis.
Table V.1 below summarizes the number of Medicaid enrollees identified using SA treatment services in each category. Individuals using more than one category are counted in all service categories they used. Overall, we estimated 1.1 million Medicaid enrollees received core treatment services. Across the other categories of SA services analyzed approximately an additional 600,000 Medicaid enrollees were estimated to have a claim with a SA-related diagnosis.
| Type of SA Service | CY 2008 (in thousands) |
| Total Enrollees Identified with SA Related Claima | 1,717 |
| |
| Core SA Treatment Services | 1,138 |
| Fetal Drug or Alcohol Exposure | 35 |
| Poisoning Related to Drugs or Alcohol | 25 |
| Other Medical Conditions 100% Attributable to SA | 53 |
| MH Services with SA as a Secondary Diagnosis | 281 |
| Non-MH Services with SA as a Secondary Diagnosis | 575 |
B. FY 2011 SA Treatment Spending by State
We projected the CY 2008 estimates from Appendix C forward to FY 2011. In Appendix D, Tables D.1 through D.5, we present these projections. These tables include estimates for all 50 states and the District of Columbia for six types of SA-related services. Table V.2 below summarizes these projections.
| Type of SA Service | CY 2008 (in millions) | FY 2011 (in millions) | Annualized Percentage Growth Rate |
| Core SA Treatment Services | 3,367 | 3,952 | 6.0 |
| Fetal Drug or Alcohol Exposure and Poisoning | 87 | 98 | 4.6 |
| Other Medical Conditions 100% Attributable to SA | 257 | 292 | 4.8 |
| MH Services with SA as a Secondary Diagnosis | 1,432 | 1,586 | 3.8 |
| Non-MH Services with SA as a Secondary Diagnosis | 3,290 | 3,659 | 3.9 |
The projected trends vary by state and type of service. The estimated annual percentage growth rate across the service types ranges from 3.8 percent to 6.0 percent between CY 2008 and FY 2011. Based on the CMS-64 reports, overall total net Medicaid spending increased by 7.8 percent, 6.4 percent and 6.3 percent for the periods FY 2008-FY 2009, FY 2009-FY 2010, and FY 2010-FY 2011, respectively. Thus, the rate of increase for core SA treatment services was slightly lower than the overall rate of increase for Medicaid. Since our method entailed applying 98 percent of the Medicaid trend by service and state, increases below the overall Medicaid trend were likely. However, a rate of increase above that observed in the Medicaid program overall is possible, because states with higher rates of Medicaid spending increase tend to have a disproportionate share of SA treatment-related expenditures.
VI. DISCUSSION
Although MAX data have a number of limitations, MAX is a viable source for developing estimates of Medicaid SA treatment spending. In the first section below, we discuss the limitations of MAX data and of this study. We then discuss the programmatic implications of the study findings.
A. Limitations of MAX Data and Study
Despite gaps in and limitations to the data available from MAX for estimating Medicaid SA treatment expenditures, the MAX data provide information on SA treatment expenditures for the majority of Medicaid enrollees ages 12 and over who are eligible for SA treatment coverage. Overall, we imputed SA treatment expenditures for about 42 percent of Medicaid enrolled months. We based about 21 percent of the imputations on encounter data or own-state FFS population experience. We based the remaining 79 percent of the imputations on FFS states' experience. Overall 42 percent of the final estimate of core SA treatment spending was derived from the imputations.
A significant limitation to use of the experience of predominantly FFS states for imputation is the substantial variation in delivery systems and the differences in Medicaid eligibility and programmatic characteristics across states. Our method only partially compensates for these differences by developing estimates by demographic and eligibility groups and adjusting for differences in specialty SA treatment supply across states. The mean expenditures per enrolled month for beneficiaries ages 12 and over in each state generally correlate well with a state's classification as a low, medium, or high-supply state. However, in states with high managed care penetration, the correlation is a function of the imputation method; in other states, the relationship is based on the states' experiences as observed in MAX.
SA and MH treatment are provided through an array of services in various treatment settings. Coverage and delivery of these services vary substantially across states. We used the 2008 National Summary of State Medicaid Managed Care Programs to determine whether SA treatment services were covered under a capitated plan in 2008. However, this document does not detail the nuances of state and managed plan coverage. Our imputations do not capture the details of each state's coverage system and thus should be viewed as gross estimates of the approximate level of managed care spending in each state.
Another limitation of the imputation method relates to the lag in managed care enrollment. Typically, in managed care states, individuals new to Medicaid receive Medicaid coverage under FFS for an initial period as a function of retrospective eligibility and the time needed for an individual to choose and enroll in a managed care plan. The initial months typically involve higher average expenditures than those associated with managed care enrolled months, because an acute health care need often prompts enrollment in Medicaid and demand for medical services may be pent up. MAX does not identify retrospective months of eligibility or indicate the date an enrollee first became enrolled in Medicaid. Given these limitations of the MAX data, we did not make any related adjustments.
In addition to the lack of expenditure data for the population enrolled in managed care, MAX evidences some reporting anomalies and data quality issues for some states. The final column of Appendix Table F.9 summarizes issues related to these estimates for each of the 50 states and the District of Columbia. Maine's data have the most significant limitations because, with the exception of prescription drug claims, MAX does not include claims files. For other states, limitations are associated largely with the incompleteness of coding for primary diagnosis; our analysis relies on the primary diagnosis to identify SA treatment services. Twenty-one states have incomplete reporting of primary diagnosis in either the long-term care or other service files. However, incomplete reporting often affects only a small minority of claims and may result from claims types such as non-emergency transportation, on which a provider would not record an enrollee's diagnosis. Nonetheless, reporting anomalies and data quality issues bias our estimates downward.
B. Comparison to Prior Estimates
The estimate of Medicaid core SA treatment spending developed in this study for CY 2008 is substantially below the projections of Medicaid SA treatment spending developed by SAMHSA for 2004-2014 in the SSE. While the current study is limited because of the level of imputations, the SSE estimates were limited because data on unit prices and the "payer source" distribution for specialty SA treatment providers were unavailable to support development of the SSE after 1998--prior to the SSR&E survey in 2009. Thus, a substantial portion of the SSE estimates of Medicaid SA treatment spending were imputed. The SSE estimated Medicaid payments represented 18 percent of overall SA treatment payments in 2006 increasing to 20 percent by 2014. The findings from this study suggest that Medicaid likely represents a smaller share of overall SA treatment spending.
In addition to developing SA treatment spending estimates that parallel those in the SSE, this study also examined additional categories of medical treatment that are fully or partially related to SA. The addition of fetal exposure, poisoning, and other medical conditions fully related to SA increased the estimate of expenditures for SA treatment by about 10 percent. Also, we identified $1,433 million in expenditures for MH services with a secondary diagnosis of SA. This suggests only about 4 percent of Medicaid MH service expenditures had a secondary SA diagnosis.11 This percentage is low given the high rate of co-morbidity between MH and SA disorders. The low percentage of MH expenditures identified with a secondary SA diagnosis may be due to under-coding of secondary diagnoses. Finally, this study identified $3,290 million in Medicaid expenditures for services with a non-MH primary diagnosis and a SA secondary diagnosis. These expenditures represent almost 1 percent of overall Medicaid expenditures. Thus, overall slightly more than 1 percent of Medicaid spending was identified as primarily related to SA and an additional 1½ percent was identified with a secondary SA diagnosis.
APPENDIX A. STUDY METHODS
The Medicaid Analytic eXtract (MAX) files for calendar year (CY) 2008 provide the foundation for this analysis. They contain detailed information on Medicaid enrollment and the services received by Medicaid enrollees in each of the 50 states and the District of Columbia, but do not reflect all services received by Medicaid beneficiaries. The most significant gap is incomplete reporting of services provided to managed care enrollees. Data quality issues, reporting anomalies, and inconsistencies in reporting account for other data gaps.
In this appendix, we first present an overview of state variation in coverage and delivery of substance abuse (SA) treatment services. In the second section, we describe the methods we used to develop estimates of SA treatment users and expenditures in states with fee-for-service (FFS) and managed care coverage of SA.
I. ASSESSMENT OF STATE VARIATION
In this section, we review variation by state in service coverage and delivery system for providing SA and mental health (MH) services and the quality and completeness of claims data available in MAX.
A. State Variation in SA Service Coverage
In November 2010, the National Association of State Alcohol and Drug Abuse Directors (NASADAD) produced a summary of SA services covered in each state, based on the Medicaid state plans and discussions with state Medicaid officials.12 We mapped the categories included in Table 2 of that document, Medicaid Program Coverage of Substance Abuse Services and the Service Categories in Which They Are Established, to the study categories as presented in Appendix Table A.1 below. The NASADAD study did not include a corresponding treatment category for institutional long-term care/specialty hospital care, and three of the outpatient treatment categories we considered for this study--outpatient treatment program, other counseling and therapy, and detoxification--mapped to a single NASADAD category for general outpatient treatment.
Appendix Table E.1 shows a subset of the results of NASADAD's survey of Medicaid SA treatment coverage, based on information provided by state officials (47 states, including the District of Columbia, provided responses) or from review of information on states' websites. Federal Medicaid guidelines require all states to cover certain benefits. Acute inpatient care is among these mandatory benefits and includes medically necessary inpatient detoxification services. Also included are early and periodic screening, diagnostic, and treatment (EPSDT) services for individuals under 21 years of age. SA treatment needs identified as part of these screenings must be covered in all states. Thus, services are provided by all states, even if not reported by them.
| NASADAD Category | Study Category |
SOURCE: NASADAD inquiry. NA = not available. | |
| Medically managed intensive inpatient treatment | Institutional care: acute inpatient care |
| NA | Institutional care: institutional long-term care/specialty hospital care |
| Short-term residential inpatient/long-term residential inpatient | Residential treatment |
| Intensive outpatient/partial hospitalization | Outpatient treatment: intensive treatment program |
| Outpatient treatment | Outpatient treatment: detoxification/counseling therapy/treatment program service |
| Early intervention/crisis | Outpatient treatment: other screening/intervention |
| Methadone treatment | Outpatient treatment: other medication management |
| Case management | Outpatient treatment: other case management |
Provision of other types of SA treatment services is optional under federal guidelines and thus varies substantially across the states. According to the information reported to NASADAD, eight states--Arkansas, Kentucky, Louisiana, Mississippi, Nevada, New Hampshire, Texas, and West Virginia--and the District of Columbia provide only these mandatory services or extremely limited coverage for SA treatment. In Arkansas, Mississippi, and the District of Columbia, SA treatment services are covered only for individuals with a co-occurring MH disorder. In Texas and Nevada, only methadone treatment services are generally available. Based on the NASADAD survey, all of the remaining 42 states (the 50 states less the eight mentioned above) provide outpatient treatment services. In addition, 34 provide methadone treatment, 33 provide intensive outpatient services and/or partial hospitalization, and 26 provide residential treatment.
B. Coverage of SA Services in Comprehensive Managed Care
This analysis used the person summary (PS), inpatient (IP), other services (OT), long-term care (LT), and prescription drug (RX) MAX files to identify beneficiaries receiving SA services and their associated Medicaid expenditures. Unfortunately, MAX data do not include all Medicaid-covered services. In particular, for services provided through managed care plans, MAX includes claims for capitation payments made by the states, but reporting of encounter data claims for these services is incomplete. Thus, in this section, we identify which states use health maintenance organizations (HMOs)/Health Insuring Organizations (HIOs), and behavioral health organizations (BHOs), and whether those providers are responsible for coverage of SA treatment services.
In Appendix Table A.2 below, we identify which states use primary FFS reimbursement and which use HMOs, BHOs, or both.
| Managed Care | Count | States |
SOURCE: MAX 2008 Eligibility Anomaly Tables.
| ||
| FFS Only | 13 | AK, AR, ID, LA, ME, MS, MT, NH, ND, OK, SD, VT, WY |
| State Has Only HMOs | 18 | AL, CA, CT, DE, DC, IL, IN, KY, MD, MN, MO, NV, NJ, OH, RI, SC, VA, WV |
| State Has Both HMOs & BHOs | 18 | AZ, CO, FL, GA, HI, IA,a KS, MA, MI, NE, NM, NY, OR, PA, TN, TX, WA, WI |
| State Has BHOs Only | 2 | NC, UT |
To assess which SA and MH services are covered by managed care organizations in each state with HMO or BHO programs, we examined the 2008 National Summary of State Medicaid Managed Care Programs. This report provides qualitative information, including populations served, services covered, and quality improvement activities. Data are collected by the Data and System Group at the Centers for Medicare and Medicaid Services (CMS) from state Medicaid agencies and CMS regional offices. The data presented are always current as of June 30 of the applicable year.
Using this report, we identified which state HMO and BHO programs listed MH and SA as included services. (They typically are not covered by other types of managed care organizations, such as long-term care plans, primary care case management programs, or disease management programs.) In cases in which the report noted that an HMO or BHO covers MH services but did not say whether it covers SA services, we assumed the delivery system or program responsible for providing the former is also responsible for providing the latter. For example, for a state in which MH services are carved out of an HMO, a BHO provides them, and the National Summary Report description of the programs did not mention SA, we assumed the BHO provides any SA services known to be covered by that state. For each state, Appendix Table E.2 displays whether MH and SA services are covered by an HMO, carved out of an HMO and covered through FFS or by a BHO, included under both an HMO and a BHO, or covered under a BHO if the state has no HMO. This information is summarized below in Table A.3.
MH and SA services are covered exclusively by an HMO in 23 of the 38 states with HMO and/or BHO programs (Table A.3). For nine states, MH and SA services are carved out of an HMO and covered either through FFS (Alabama and Kentucky) or under a BHO (Colorado, Connecticut, Kansas, Iowa, Nebraska, New Mexico, and Pennsylvania). For four states (California, South Carolina, Washington, and West Virginia), both an HMO and a BHO listed coverage for SA services. In North Carolina and Utah, the Medicaid program does not deliver services through an HMO. However, these states do have a BHO program. Appendix Table E.2 includes state-specific notes providing additional details about the managed care programs that cover these services.
| SA Coverage | Count | States |
SOURCE: 2008 National Summary of State Medicaid Managed Care Programs.
| ||
| SA Services Covered Exclusively By HMO | 23 | AZ, DE, DC, FL, GA, HI, IL, IN, MD, MA, MI, MN, MO, NJ, NV, NY, OH, OR, RI, TN, TX, VA, WI |
| SA Services Carved Out of HMO & Provided Through FFS | 2 | AL, KY |
| SA Services Carved Out of HMO & Provided Through BHO | 7 | CO, CT, IA,a KS, NE, NM, PA |
| Both HMO & BHO Cover SA Services | 4 | CA, SC, WA, WV |
| BHO Covers SA Services (state does not have HMO) | 2 | NC, UT |
Our analysis of which SA and MH benefits are covered under managed care plans feeds into our assessment of which states have data of suitable quality for analysis. Accordingly, among those states identified as having managed care coverage of SA, we conducted a preliminary assessment of which were likely to have complete encounter data of usable quality. We looked at states with at least 50 percent of enrollees in HMOs, as those with a high level of managed care enrollment are likely to devote more resources to and focus more on collecting accurate encounter data. We then looked at which of these states have HMO encounter data in MAX and made assessments based on knowledge gained by the project team from other work on MAX encounter data. Based on this analysis, we decided to assess the encounter data for SA services in Arizona, Indiana, Kansas, Maryland, New Mexico, Washington, and Virginia. We provide a description of this assessment in Section II.B below.
C. Data Quality Analysis
Information about state data quality was compiled from several sources. The Data Anomalies Report, produced by Mathematica's Medicaid Statistical Information System (MSIS) validation project, includes information on all known anomalies within the data, with clarification on the cause of each anomaly if it could be determined through research on the state in question. We also used the MAX 2008 Eligibility Anomaly Tables, Claims Anomaly Tables, and Cross-State Validation Tables.
Our analysis of each state's data was concerned with the following quality issues:
Known HMO or BHO reporting problems (Source: MSIS State Anomalies/ Issues).
Populations known to be missing (Source: MSIS State Anomalies/Issues).
Diagnosis code issues (Source: MSIS State Anomalies/Issues).
MSIS ID issues (Source: MSIS State Anomalies/Issues).
Inconsistencies between MAX and CMS June 2008 managed care data (Source: MAX 2008 Eligibility Anomaly Tables, Table 9).
Anomalies in the percentage of Medicaid Enrollment Data Base (EDB) dual eligibles not reported in MAX (Source: MAX 2008 Eligibility Anomaly Tables, Table 5).
Anomalies in the percentage of Records Missing Medicaid Eligibility Information (Source: MAX 2008 Eligibility Anomaly Tables, Table 1).
Restricted-Benefits Group 5 (other restricted benefits) issues (Source: MAX 2008 Eligibility Anomaly Tables, Table 8).
Restricted-Benefits Group A (Psychiatric Residential Treatment Facilities [PRTFs]) grant issues (Source: MAX 2008 Eligibility Anomaly Tables, Table 8).
Anomalies in the percentage of beneficiaries with private health insurance (Source: MAX 2008 Eligibility Anomaly Tables, Table 10).
Anomalies in the HMO/HIO ratio of capitation claims to person-month enrollment (Source: MAX 2008 Claims Anomaly Tables, PS Table 8).
Anomalies in the percentage of claims with primary diagnosis (Source: MAX 2008 Claims Anomaly Tables, IP Table 2, LT Table 2, and OT Table 2).
Anomalies in the average fees paid by Medicaid for key services: inpatient hospital, MH for the aged, inpatient psychiatric facility age 21, physician services, other practitioner services, outpatient services, clinic services, prescription drugs, psychiatric services, and other services (Source: MAX 2008 Claims Anomaly Tables, PS Tables 13-15).
Anomalies in the percentage of beneficiaries with reported managed care enrollment who have capitated payments (Source: State by State MAX 2008 Validation Tables, PS Table).
Our assessment, using the methodology described above, revealed some data quality limitations affecting this analysis. Some states are missing data in MAX 2008, and some with complete data have data quality issues. Maine is missing a substantial amount of data, having been unable to report accurately on inpatient, long-term care, and other services in MAX 2008; only eligibility and prescription drug information is included for the state. Massachusetts, Utah, and Wisconsin were not able to submit all of their claims by the deadline for MAX 2008 and are missing the final quarter of MSIS submissions typically included in MAX. For states with complete data, the most significant issue at this phase of analysis appears to be a high percentage (more than 40 percent) of missing primary diagnosis codes in the other services (OT) files for some states (Alaska, Massachusetts, New Mexico, and Oregon). The final column of Appendix Table E.2, Known Data Quality Issues, summarizes the most significant issues identified for each state.
II. ESTIMATION METHODS
In this section, we first describe the methods we used to develop estimates of SA treatment users and expenditures associated with SA treatment services for which FFS claims data are included in the MAX files. We then review the methods we used to estimate SA treatment users and expenditures associated with managed care enrollment or other gaps in the MAX data.
A. Development of Estimates for Enrollees and Services Represented in MAX Data
The Medicaid program covers several categories of enrollees that may vary both in their eligibility for coverage of SA treatment services and their treatment needs. As described below, we develop separate estimates for beneficiaries depending on their level of coverage, demographic characteristics and source of eligibility. Similarly, a range of treatment services is associated with SA. Some services primarily treat the SA disorder, and others may treat medical complications of SA or SA as a co-morbid condition. To address the range of SA treatment services, we divided SA treatment services into several categories.
1. Classification of Enrollees
We classified Medicaid enrollees into four groups: excluded, partial-benefit, near-full benefit, and full-benefit. After identifying those services and enrollees in MAX that are excluded from our analysis, we then discuss how the remaining enrollees are classified into groups.
a. Exclusions
Given that the goal of this analysis is to identify Medicaid SA treatment expenditures comprehensively, we excluded from the analysis file Medicaid enrolled months during which an enrollee was in a restricted-benefit population not covered for SA treatment services. These populations can be identified based on the MAX variables Restricted-Benefit Flag (RBF) and EDB Dual with the codes noted below. We also exclude State Children's Health Insurance Program (S-CHIP) enrollees and claims missing enrollment records because of incomplete data in MAX for these enrollees. These populations are the following:
S-CHIP only. The MAX files do not include claims for S-CHIP. Our estimates thus do not include the months in which beneficiaries are enrolled in S-CHIP only. However, given that claims for Medicaid expansion Children's Health Insurance Program (M-CHIP) enrollees are available in the MAX files, we include in our analysis the months of enrollment in M-CHIP.
Claims missing enrollment records. In the MAX file, 0.46 percent of claim expenditures cannot be linked to an enrollee and thus are excluded from our analysis.
RBF. Some groups of restricted-benefit enrollees are not eligible for SA treatment services, including enrollees receiving family planning benefits only (RBF = 6) and those receiving premium assistance only (RBF = W).
Medicare/Medicaid dual eligibles who are eligible only for payment of Medicare premiums (EDB Dual = 53, 55, 56, 57). These Medicaid enrollees are not eligible for coverage of any SA treatment service costs.
b. Classification of Enrollees by Level of Coverage
Several groups of Medicaid enrollees not eligible for full-coverage of SA treatment services are eligible for partial coverage. We divided the groups into those whose coverage per enrolled month is near that of the full-benefit package and those likely to have substantially lower coverage. In our analysis, the groups with near-full benefit coverage are combined with full-benefit enrollees. Individuals with partial coverage are addressed separately. The near-full benefit and partial-benefit groups are identified below. Enrollees identified as having partial-benefits in any month were assigned as partial-benefit enrollees for the full year. If the enrollee had no partial-benefit months, but had at least one month of near-full coverage they were assigned to near-full benefit for the whole year.
Near-full benefit enrollees:
Pregnancy-related coverage (RBF = 4). Individuals eligible for Medicaid based on pregnancy may receive comprehensive benefits during the pregnancy, including SA treatment.
Benchmark-equivalent benefits (RBF = 7). Even though individuals eligible for benchmark-equivalent benefits receive a different benefit package than that offered under the Medicaid state plan services, the services might include SA treatment. West Virginia and Idaho were the only states with substantial enrollment in the benchmark plan in 2008.
Health opportunity account (HOA) (RBF = B). The group of individuals with HOAs was new in MAX 2008. An HOA requires a particularly high deductible, and special HOAs are set up for Medicaid beneficiaries to help them manage out-of-pocket medical expenses. Our recent examination of the Medicaid expenditures of HOA enrollees in Indiana found the expenditures to be aligned with those of full-coverage beneficiaries; therefore, we recommend that HOA enrollees remain in the full or near-full benefit group rather than in the partial-benefit group.
PRTF (RBF = A). PRTFs are federally recognized facilities that provide psychiatric and medical services to individuals under age 21. Patients entering PRTFs must be certified by the state as meeting specific criteria for admission and additional criteria for continued stay. Such individuals receive an enhanced benefit for behavioral health and thus are part of the near-full benefit group.
Partial-benefit enrollees with FFS coverage of SA treatment:
Non-qualified aliens (RBF = 2). These individuals are eligible for Medicaid coverage of emergency services, some of which may be SA related.
EDB Dual eligibles (EDB Dual = 51, 52, 54, 58). Unlike the dual eligibles who receive premium assistance only and are excluded from the analysis, these duals are eligible for all Medicaid benefits. However, their Medicare insurance makes Medicaid a secondary payer, covering Medicare coinsurance and deductibles associated with SA treatment and SA treatment services not covered by Medicare.
Individuals with private insurance coverage (PVT INS CD = 2-4). Individuals with private insurance may not have comprehensive benefit packages. Medicaid may cover services related to SA treatment that are not covered by private insurance or coinsurance.
Other benefits (RBF = 5). Coverage varies by state.
Only prescription drug benefits (RBF = X, Y, or Z). Vermont and Wisconsin are the only states with significant programs in this category. Vermont provides drugs to low-income Medicare beneficiaries only. Wisconsin's SeniorCare waiver extends PharmPlus coverage to the elderly and does not cover premiums, pays smaller co-payments than Part D, and ensures no gaps in prescription drug coverage.
Money Follows the Person (MFP) (RBF = 8). This program helps Medicaid enrollees make the transition from an institution to the community by eliminating barriers and mechanisms in state law, state Medicaid plans, or state budgets that prevent or restrict the flexible use of Medicaid funds to enable eligible individuals to receive long-term care in the setting of their choice. The MAX data do not include services provided through grant funds under MFP.
Enrollees not excluded nor classified as partial or near-full are classified as full-benefit.
c. Demographic and Eligibility-Based Categories of Users
We grouped Medicaid enrollees into categories based on age, gender, and eligibility characteristics expected to have similar levels of need for SA treatment. For example, children younger than 12 were distinguished from those older than 12 because those younger than 12 rarely use SA treatment services. Individuals less than 21 were distinguished from those 21 and older because SA treatment services may be covered under the EPSDT program and those less than 21 are eligible for these benefits. We distinguished by gender because the National Survey on Drug Use and Health (NSDUH) indicates that males are more likely than females to have an SA or dependence disorder.13 Enrollees were assigned to categories based on their age as of January 1, 2008.
We also identified three eligibility-based groups: (1) individuals dually eligible for Medicare and Medicaid (Medicare dual eligibles); (2) individuals who are not dual eligibles and whose eligibility is not based on disability (non-dual, non-disabled); and (3) individuals who are not dual eligibles and whose eligibility is based on disability (non-dual, disabled). (We distinguished by whether an enrollee's eligibility is based on disability because we expected that there might be distinct patterns of SA treatment needs within groups. Specifically, the many individuals who qualify for disability based on MH disorders have a higher likelihood of an SA disorder than those who do not.) Enrollees were assigned to an eligibility category based on their eligibility status in their last month of Medicaid enrollment in the year.
2. Identification and Classification of Services
In this section, we discuss how we identified individuals with an SA diagnosis and categorized SA treatment services into groups. Our approach varied across the MAX data files. First, we outline our approach to three claims files: IP, LT, and OT files. We then discuss the approach used for the RX and the PS files.
a. Inpatient, Long-Term Care, and Other Claims Files
We identified several sets of SA-related services. If a service qualified for more than one category, we assigned it only to the first category listed. The service categories are the following:
Core SA treatment services. This category includes claims for services with a primary diagnosis of an SA disorder. In Appendix Table B.1 and Table B.2, we display the diagnosis codes we used to define treatments of alcohol and drug disorders, respectively. The third column of the tables identifies these services as "core." The diagnosis codes are consistent with those used by the Substance Abuse and Mental Health Services Administration (SAMHSA) in its estimates of National Expenditures for Mental Health Services and Substance Abuse Treatment, referred to as the SAMHSA Spending Estimates (SSE).14 As discussed below, prescribed drugs for SA treatment are also included in this category.
Services related to fetal drug or alcohol exposure. This category includes services with a primary diagnosis of fetal drug or alcohol exposure. In Appendix Table B.1 and Table B.2, the services are identified as "fetus."
Services related to poisoning by drugs or alcohol. This category includes services with a primary diagnosis of poisoning related to drugs or alcohol. In Appendix Table B.1 and Table B.2, the services are identified as "poisoning."
Medical services for other conditions 100 percent attributable to SA. This category includes claims for other services with a primary diagnosis of a medical condition 100 percent attributable to SA. In Appendix Table B.1 and Table B.2, the services are identified as supplemental conditions.15
MH services with a secondary diagnosis of SA disorders. This category includes services with a primary diagnosis of a mental disorder and a secondary diagnosis on the same claim from one of the first four groups above. We identified claims with a primary MH diagnosis based on the codes listed in Appendix Table B.3. Recognizing that the rate of co-morbidity between SA and MH disorders varies substantially by type of mental disorder, we divided mental disorders into several subgroups, as displayed in the table.
Other medical services with a secondary diagnosis of SA disorder. This category includes claims with primary diagnoses not identified as MH disorders but with a secondary diagnosis from the first four categories above.
For individuals with an identified SA diagnosis, our initial extraction of claims from the IP, LT, and OT claims files included all claims with a primary or secondary diagnosis of SA, as identified by the first four categories. In addition, we extracted all claims for individuals with an identified SA diagnosis with a primary diagnosis of an MH disorder regardless of whether the claims included a secondary SA diagnosis. We also extracted all claims for emergency room (ER) services for enrollees with an identified SA diagnosis.
b. Prescription Drug File
We used National Drug Codes (NDC) to identify SA-related prescriptions. In Appendix Table B.4, we present the SA-related codes. These services are categorized as core SA treatment services.
c. Person Summary File
We linked the MSIS-IDs of the Medicaid enrollees with identified SA diagnosis to the PS file to obtain additional information on eligibility and enrollment for these individuals. Also from the PS file, we obtained information on overall Medicaid expenditures by type of service for these individuals.
d. Classifying Services by Type
We classified SA treatment services into subgroups according to the following hierarchy:
Services included in the IP, LT, and RX files were classified as inpatient hospital, long-term care, and prescription drug, respectively.
Claims in the OT file with a procedure code included in Appendix Table B.5 were assigned to the category listed there.
Claims in the OT file that do not include a procedure code listed in Appendix Table B.5 were categorized according to the MAX type of service categories.
We identified the services included in Appendix Table B.5 according to the Substance Abuse HCPCS Code User's Guide: Unofficial Standard Definitions;16 Approved Healthcare Common Procedure Coding System (HCPCS) Codes and Modifiers Relating Substance Abuse Treatment, Mental Health, and Behavioral Health;17 and SAMHSA's list of Good and Modern Benefits: Procedure Codes and Titles. We excluded codes for services provided to populations at large rather than to individual beneficiaries. For example, we decided that code H0025, behavioral health prevention education service (delivery of services to a target population to affect knowledge, attitude, and/or behavior), was not relevant to the analysis. We examined the list of codes that states report under psychiatric services (type of service = 53) and, as appropriate, added state-specific codes to the classification scheme for each state.
In Section III.C.4, we identified enrollees with ER visits in the inpatient and other services files based on listing of a procedure code of 99281-99292 or a revenue center code of 450-459 or 981 on any claim. For other service file claims, we also used the place of service code equal to 23. ER expenditures were derived only from other service file claims, as the ER expenditures reported on inpatient claims are reported as inpatient expenditures.
B. Imputation of Expenditures for Enrollees and Services Not Represented in MAX Data
We identified 18 states in which accurate MAX data was available and SA treatment for all, or a substantial majority of beneficiaries, was covered by FFS Medicaid, so that expenditures can easily be classified and measured in FFS claims. However, the data to support development of estimates of expenditures on SA treatment services for the Medicaid population in: (1) states that cover such services under managed care plans; or (2) states that, for other reasons, lack FFS data on service use are substantially more limited. To allow flexibility in the set of services included in the national estimates for the population without FFS claims data, we produced aggregate estimates of total SA treatment users and expenditures by state for CY 2008 for the six alternative categories listed below. The services included in the categories are defined in Section II.A.
- Core SA treatment services;
- Services related to fetal drug or alcohol exposure;
- Services related to poisoning by drugs or alcohol;
- Medical services for other conditions 100 percent attributable to SA;
- MH services with a secondary diagnosis of SA disorder; and
- Other medical services with a secondary diagnosis of SA disorder.
Our method for estimating managed care SA treatment users and expenditures differed by state, depending on the extent to which state-specific information is available. We divided the states into three groups according to the level and type of available state-specific information. Some states fall into two groups if they have high managed care penetration in some basis-of-eligibility (BOE) groups but not in others. The three groups of states follow:
Managed care states with usable encounter data. In these states, we imputed expenditures as the product of the number of service units provided in the state's managed care encounter data and the cost per service unit from its FFS data.
Other managed care states with less than 60 percent penetration in a given BOE group. In these states, we imputed expenditures as the product of the number of managed care enrolled months and expenditures per enrolled month by eligibility/demographic group from the state's FFS enrollees.
Other managed care states with 60 percent or greater penetration in a given BOE group and FFS states with substantial FFS data quality issues. In these states, we imputed expenditures as the product of the number of managed care enrolled months and expenditures per enrolled month by eligibility/demographic group from similar states' FFS enrollees.
Appendix Table F.9 displays the imputation method used for each of the 50 states and the District of Columbia. We discuss our method for each group below.
1. Managed Care States with Usable Encounter Data
Since a comprehensive analysis of MAX encounter data has not been conducted, we assessed which states are likely to have complete encounter data of usable quality. This assessment looked at states with at least 50 percent of enrollees in HMOs. We then looked at which of these states have HMO encounter data in MAX and made assessments based on knowledge gained by the project team from other work on MAX encounter data. Based on this preliminary review, we decided to conduct a more comprehensive analysis of SA-specific encounter data in Arizona, Indiana, Kansas, Maryland, Virginia, Washington, and Wisconsin.
Our review of SA-specific encounter data began with an assessment of whether all types of SA treatment services provided under a state's FFS program are reported within the encounter data for its managed care program. We then assessed whether the encounter claims reported to MAX represent a reasonable level of service for the population covered. This assessment entailed estimating whether an imputation based on the managed care encounter data would result in an estimate of expenditures per enrolled month 12 and over within the range observed in majority FFS states with high quality data reporting in the same category of SA treatment supply. We refer to these FFS states with high quality reporting as the predominantly FFS states. Finally, for states with a level of reporting within a reasonable range, we reviewed whether encounter data are present for all health plans providing care to the Medicaid population in the states. We summarize our findings as follows:
In Arizona, encounters meeting the definition of a core SA treatment service based on primary diagnosis are included in the inpatient, long-term care, and other services files. Encounters from the other services file represent all service types provided under FFS Medicaid. The imputed estimate of expenditures per enrolled month 12 and older is $9.67--within the range of estimates for FFS medium-supply states. We reviewed the plan identification numbers observed and identified only one large general service managed care organization--Phoenix Health Plan, which did not report SA treatment encounters in the other services file. Expenditures for months enrolled in this plan were imputed based on FFS states experience.
In Indiana, encounters meeting the definition of a core SA treatment service based on primary diagnosis are included in the inpatient, long-term care, and other services files. The encounters in the other services file represent a range of services, including counseling/therapy, assessment/intervention/treatment planning, and medication management. However, imputed expenditures based on the encounter data are only $0.53 per enrolled month 12 and older, or 8 percent of the amount that otherwise would be imputed based on the number of enrolled months and observed expenditures in the Tier I and Tier II states. Based on this analysis, we found that the Indiana encounter data are not sufficiently complete for use.
In Kansas, encounters meeting the definition of a core SA treatment service based on primary diagnosis are included in the inpatient, long-term care, and other services files. Encounters from the other services file represent all service types provided under FFS Medicaid. The imputed estimate of expenditures per enrolled month 12 and older is $12.17. This amount is within the range of FFS medium-supply states. Plan identification numbers were not reported correctly, so we could not assess the completeness of reporting by plan.
In Maryland, encounters meeting the definition of a core SA treatment service based on primary diagnosis are included in the inpatient, long-term care, and other services files. However, the vast majority of claims identified in the other services file were classified as "other services: non-behavioral health." This implies that claims were not identified by the state as "type of service = 53 (behavioral health)," and the procedure codes on the claims do not appear in Appendix Table A.4. We did not continue with further analysis of Maryland's encounter data because the service classification did not parallel that of the FFS delivery system. Thus, substantial effort would be required to classify these services by type and find appropriate prices for each service category.
In Virginia, encounters meeting the definition of a core SA treatment service based on primary diagnosis are included in the inpatient, long-term care, and other services files. However, several SA treatment service types represented in the FFS claims data are not included in the encounter claims, including residential treatment, treatment program services, and community support/case management services. The imputed estimate of expenditures per enrolled month 12 and older is $0.73. This amount is below the range of the estimates represented in the FFS states with low-supply. Based on this analysis, we found that the Virginia encounter data are not sufficiently complete for use.
In Washington, encounters meeting the definition of core SA treatment services based on primary diagnosis are included in the inpatient and other services files. No SA treatment encounters were identified in the long-term care file. FFS SA treatment claims are included in this file. No residential treatment or treatment program service claims are included in the other services file; however, these service types are included in the FFS claims. The imputed estimate of expenditures per enrolled month 12 and older is $0.31. This amount is substantially below the range of the estimates represented in the FFS states with high-supply. Based on this analysis, we found that the Washington encounter data are not sufficiently complete for use.
In Wisconsin, encounters meeting the definition of core SA treatment services based on primary are included in both the inpatient, long-term care, and other services files. Encounter claims were identified in all SA treatment service types reported in the FFS claims for Wisconsin with the exception of residential care. In the NASADAD survey Wisconsin reported only providing limited inpatient residential treatment for detoxification. Since very few residential claims were identified in the FFS data and detoxification services can be provided in alternative care settings, the lack of residential treatment claims is possible with complete reporting. We classified Wisconsin as a low-supply state. The imputed estimate of SA expenditures based on the encounter data for Wisconsin is $2.66 per enrolled month 12 or older which is within the range of low-supply FFS states. We assessed the comprehensiveness of reporting by plan and found that there were numerous plan identification numbers for which capitation claims were reported, but for which encounter claims were not present. We could not determine whether these plans covered SA treatment services. Therefore we could not determine that the encounter data was sufficiently complete for use in our analysis, so we did not use the Wisconsin encounter data.
Thus, among the six states for which we reviewed the encounter data, we found that only Arizona and Kansas had sufficient quality encounter data for use in estimating SA treatment services. For these states, we estimated SA treatment expenditures under managed care for each eligibility group as a function of the following two components:
Units/claims of service by type of service (from managed care encounter data). We divided encounter utilization into the following types of service categories: inpatient hospital, institutional long-term care (including specialty psychiatric and SA treatment hospitals), residential, intensive outpatient, intensive treatment program, treatment program service, counseling/therapy, detoxification, medication management, and other services (including collateral, case management, school-based services, early intervention, and crisis). For each service type, we then summed the number of units of service or claims provided by eligibility group, based on the encounter data. For inpatient hospital, institutional long-term care, and residential treatment, the unit of service is a treatment day. For other service types, each claim is a unit of service.
Mean expenditure per unit or claim service by type (from FFS). In parallel to the classification of encounter claims by service type, we classified claims for services provided to FFS enrollees in the same state by type of service. We then estimated mean expenditure per unit (either treatment day or claim) for FFS enrollees.
We then multiplied the above components for each type of service and summed the results across service types to calculate the total SA treatment expenditures for the managed care population in these states for each eligibility/demographic group.
In addition to estimating total SA treatment expenditures, we estimated the number of SA treatment users. In those states with usable encounter data, we directly calculated the number of SA treatment users based on encounter claims data. Individuals with utilization represented in both encounter and FFS claims data were counted once as FFS users and again as managed care users.
In Arizona and Kansas, we used encounter data only to estimate expenditures related to core SA treatment services. To price each unit of service appropriately within each service type, each service category must include a homogeneous set of services. For core SA treatment services, we defined homogeneous categories of service as displayed in Appendix Table A.4. We did not use such an approach for the other categories of SA treatment (for example, costs related to other conditions 100 percent attributable to SA or non-MH services with a co-morbid SA diagnosis) because these categories include a variety of service types. We used the method described in Section II.B.3 to estimate expenditures for these other SA service categories for Arizona and Kansas.
2. Other Managed Care States with Less than 60 Percent Penetration
In states with managed care enrollment but a penetration rate of less than 60 percent, we estimated expenditures per enrolled month by eligibility/demographic category based on the state's FFS population for each type of SA treatment service. We then assumed that a state's managed care enrolled population with shared eligibility and demographic characteristics had the same expenditure level per enrolled month as the FFS population. We based the estimate on the following components:
Expenditure per enrolled month by SA treatment type and eligibility group (from FFS). The estimate of the mean expenditure per enrolled month by SA treatment type was based on the FFS experience of Medicaid enrollees in the given state by eligibility/demographic group.
Number of managed care enrolled months by eligibility group. The estimate of the number of months of enrollment in a capitated health plan covering SA treatment services was based on the eligibility/demographic group according to the MAX PS file data.
The above components were multiplied to calculate total SA treatment expenditures for the managed care population in each eligibility/demographic category with less than 60 percent managed care penetration.
Similarly, to estimate the number of SA treatment users, we estimated the mean number of users per enrolled month for each eligibility group in the areas of the state with FFS experience. We then multiplied the estimate by the number of managed care enrolled months in each eligibility group to estimate the number of SA treatment users in managed care in each eligibility group.
3. Other Managed Care States with Penetration 60 Percent or Greater
In contrast to the states in the previous two sections, for which usable encounter data or state-specific FFS experience is available, in states without usable encounter data and high managed care penetration, the small share of the population not enrolled in managed care is likely to exhibit expenditure levels distinct from those of managed care enrollees. Therefore, for such states, we imputed managed care enrollee expenditures using average expenditures from states with high shares of FFS enrollment and no significant data quality issues. We identified 18 states in which the majority of enrollees received SA treatment services through FFS and the state had no significant data quality issues. We refer to these states as the predominantly FFS states.
Using a linear regression model, we assessed the relationship of SA treatment expenditures per enrolled month in these states to several explanatory variables, including whether the enrollee lived in a metropolitan area; state wage indices for SA treatment professionals; indicators of the types of SA services that, according to the comments of a state Medicaid program representative responding to the NASADAD survey, the state provides to Medicaid enrollees;18 a Medicaid fee index;19 the supply of specialty SA treatment services per population; eligibility group (disabled and non-disabled); and age/gender. We found the largest differences in expenditures were explained by age/gender, eligibility group, and the supply of specialty SA treatment services provided per population in the state. In addition, the direction of the impact of these three sets of explanatory variables was robust to changes in specification. In contrast, the other explanatory variables produced a small impact on expenditures or did not consistently affect expenditures in the manner hypothesized. Therefore, we imputed expenditures to states with high managed care penetration using enrollee characteristics and the states' supply of SA treatment services only.
Measurement of the supply of specialty SA treatment services was based on the number of clients served in specialty SA treatment facilities in 2008, as identified in SAMHSA's National Survey of SA Treatment Services. We estimated the number of clients served per 1,000 population by dividing the total number of SA treatment clients in care on March 31, 2008 in all settings by the Census Bureau's estimate of state population. Based on the state-level estimate of clients served in a specialty SA treatment setting per population, we divided the 50 states and the District of Columbia into three categories. States with a supply above the 75th percentile (more than five clients per 1,000 population) were deemed "high"; those with a supply below the 25th percentile (fewer than three clients per 1,000 population) were deemed "low." Other states were deemed as "medium" supply. These categories capture a substantial portion of the variation in state Medicaid policy toward provision of SA treatment under Medicaid.
We used the supply categories to group the predominantly FFS states (Table A.4).
| Specialty SA Clients per 1,000 Population | Predominantly FFS States |
| Low -- Fewer than 3 | AL, ID, MS, AR, LA |
| Medium -- 3 to 5 | IL, KY, MO, MT, NH, NC, ND, OK, SD, SC |
| High -- More than 5 | CT, VT, WY |
Next, we grouped the Medicaid enrollees in states in the same supply category based on eligibility group and demographics. We then calculated the following components of the expenditure estimate:
Mean expenditure per enrolled month by SA treatment service type. SA treatment supply, and eligibility/demographic group (from FFS). We developed non-parametric estimates of average expenditures and users per enrolled month for each supply category for cells defined by age/gender/disability status.
Number of managed care enrolled months by eligibility/demographic group. We estimated the number of months of enrollment in a capitated health plan covering SA treatment services by eligibility/demographic group based on the MAX PS file data.
We multiplied the components to produce our estimate of the total SA treatment expenditures for the managed care population in each state by SA service type and eligibility/demographic group. We then summed the estimates for each eligibility/ demographic group to produce the total estimate of SA treatment spending by service type for the managed care population in the state reported in Appendix C.
To estimate the number of SA treatment users in a given managed care state, we similarly estimated the mean number of users per enrolled month for each SA treatment service type by eligibility/demographic group in the 18 FFS states in each service supply category. We then multiplied the number of managed care enrolled months in each eligibility/demographic group by the mean users per enrolled month in the eligibility/demographic group in the FFS states in the same SA service supply category. Next, we summed the products across the eligibility/demographic groups in the state to produce the estimate of managed care users.
In Appendix Tables F.1 through F.8, we report the estimated mean expenditures and users per enrolled month by eligibility/demographic group in the predominantly FFS states by level of SA treatment supply in the state. The SA treatment supply groups (Low, Medium, and High) are those reflected above in Table A.4. Table F.1 and Table F.2 contain this information for core SA treatment services. Tables F.3 through F.8 contain this information for non-core SA treatment categories. In addition to the columns for estimated mean expenditures and users per enrolled month, Tables F.3 through F.8 include additional columns for users labels "unduplicated." The averages in the unduplicated columns include only users who were not represented in a prior table. The averages from these columns were used to develop unduplicated counts of individuals using SA treatment services across all service types.
C. Estimating Federal Share
We calculated the federal share of each state's SA treatment expenditures in 2008 based on its federal medical assistance percentage (FMAP). The Kaiser Family Foundation provides an FMAP time series from 2004 to 2011, with links to corresponding Federal Register notices.20
III. METHODS FOR PROJECTING 2008 ESTIMATES TO FY 2011
We projected the fiscal year (FY) 2008 estimates to FY 2011 based primarily on information reported by state Medicaid programs in CMS-64. The CMS-64 reports summarize annual Medicaid expenditures for each state. Information from the forms is currently available through FY 2010 for each state by service category.21 We used the data to project CY 2008 MAX data to FY 2011. SA treatment costs for each state and category of service (for example, inpatient, outpatient, prescription drugs) were projected to FY 2011 based on the annual change in overall Medicaid expenditures for the state among similar services between FY 2008 and FY 2010. Given that the rate of growth in SA treatment expenditures (as identified in the SSE) historically has fallen below that of general health care expenditures, as identified in the CMS National Health Expenditure Accounts (NHEA), we estimated the SA treatment spending trend as only 98 percent of the trend observed for overall Medicaid program spending in each category.
We used the following steps to develop projections through FY 2011 by using CMS-64:
Step 1--Map service categories. We mapped the service types available in CMS-64 reports as closely as possible to the SA treatment categories developed from MAX data for 2008.
Step 2--Estimate overall Medicaid expenditure trends. We estimated the overall Medicaid expenditure trend for each state for each service category from FY 2008 through FY 2009 and from FY 2009 through FY 2011 based on the CMS-64 reports. In rare cases, where trends for a particular service category indicated more than a 35 percent increase or decrease, the service category-specific trend was replaced by the overall trend in state Medicaid spending.
Step 3--Adjust overall Medicaid general health expenditure trends for the historical difference in growth between SA treatment and general health care spending. Between 1986 and 2005, the estimated trend in Medicaid SA treatment spending based on the SSE was 98 percent of NHEA's estimated trend in Medicaid spending. Given that the rate of growth in SA treatment expenditures (as identified in the SSE) historically has fallen below that of general health care expenditures (as identified in the NHEA), we estimated the SA treatment spending trend as only 98 percent of the trend observed for overall Medicaid program spending in each category.
Step 4--Project the MAX 2008 estimates to FY 2011. With the 2008 MAX data representing a CY, we applied 9 months of each state's FY 2008 through FY 2009 trend and 24 months of the FY 2009 through FY 2010 trend, multiplying the growth rates by a factor of 0.98 to reflect the historically slower growth of SA treatment expenditures. We used 24 months of the FY 2009 through FY 2010 trend on the assumption that the trend in expenditures from FY 2010 to FY 2011 will be the same as the previous year's trend. The result is a set of estimates of FY 2011 expenditures for each state by service type.
APPENDIX B. DIAGNOSIS CODES
| ICD-9-CM | Description | Category of Service |
| 291 | Alcoholic psychoses | Core |
| 2910 | Delirium tremens | Core |
| 2911 | Alcohol amnestic syndrome | Core |
| 2912 | Alcoholic dementia NEC | Core |
| 2913 | Alcohol hallucinosis | Core |
| 2914 | Pathologic alcohol intoxication | Core |
| 2915 | Alcoholic jealousy | Core |
| 2918 | Alcoholic psychosis NEC | Core |
| 2919 | Alcoholic psychosis NOS | Core |
| 303 | Alcohol dependence syndrome | Core |
| 3030 | Acute alcohol intoxication | Core |
| 3039 | Alcohol dependency NEC/NOS | Core |
| 3050 | Alcohol abuse | Core |
| 9800 | Toxic effects of ethyl alcohol | Poisoning |
| 9801 | Toxic effects of methyl alcohol | Poisoning |
| E8600 | Accidental poisoning by alcoholic beverages | Poisoning |
| E8601 | Accidental poisoning by ethyl alcohol | Poisoning |
| E8602 | Accidental poisoning by methyl alcohol | Poisoning |
| E8609 | Accidental poisoning by unspecified alcohol | Poisoning |
| 7903 | Excessive blood level of alcohol | Poisoning |
| 3575 | Alcoholic polyneuropathy | Supplemental |
| 4255 | Alcoholic cardiomyopathy | Supplemental |
| 5353 | Alcoholic gastritis | Supplemental |
| 5710 | Alcoholic fatty liver | Supplemental |
| 5711 | Acute alcoholic hepatitis | Supplemental |
| 5712 | Alcoholic cirrhosis of liver | Supplemental |
| 5713 | Alcoholic liver damage, unspecified | Supplemental |
| 6554 | Suspected damage to fetus from alcohol addiction | Fetus |
| 76071 | Fetal alcohol syndrome | Fetus |
| ICD-9-CM | Description | Category of Service |
| 292 | Drug psychoses | Core |
| 2920 | Drug withdrawal syndrome | Core |
| 2921 | Drug paranoid/hallucinosis | Core |
| 2922 | Pathologic drug intoxication | Core |
| 2928 | Other drug mental disease | Core |
| 2929 | Drug mental disorder NOS | Core |
| 304 | Drug dependence | Core |
| 3040 | Opioid type dependence | Core |
| 3041 | Barbiturate dependence | Core |
| 3042 | Cocaine dependence | Core |
| 3043 | Cannabis dependence | Core |
| 3044 | Amphetamine dependence | Core |
| 3045 | Hallucinogen dependence | Core |
| 3046 | Drug dependence NEC | Core |
| 3047 | Opioid/other drug dependence | Core |
| 3048 | Combinations of drug dependence NEC | Core |
| 3049 | Drug dependence NOS | Core |
| 305 | Nondependent drug abuse | Core |
| 3052 | Cannabis abuse | Core |
| 3053 | Hallucinogen abuse | Core |
| 3054 | Barbiturate abuse | Core |
| 3055 | Opioid abuse | Core |
| 3056 | Cocaine abuse | Core |
| 3057 | Amphetamine abuse | Core |
| 3058 | Antidepressant abuse | Core |
| 3059 | Drug abuse NEC/NOS | Core |
| 6483 | Drug dependence in pregnancy | Fetus |
| 357.6 | Polyneuropathy due to drugs | Supplemental |
| 6555 | Suspected damage to fetus from drugs | Fetus |
| 76072 | Fetus affected by narcotics | Fetus |
| 76073 | Fetus affected by hallucinogenic agents | Fetus |
| 76075 | Fetus affected by cocaine | Fetus |
| 7795 | Drug withdrawal symptoms in newborns | Fetus |
| 965 | Poisoning related to narcotics | Poisoning |
| 967 | Poisoning by sedatives and hypnotics | Poisoning |
| 968 | Poisoning by central nervous system muscle tone depressants | Poisoning |
| 969 | Poisoning by psychotropic agents | Poisoning |
| 970 | Poisoning by central nervous system stimulants | Poisoning |
| E850-E858 | Accidental poisoning by drugs, medicaments, and biologicals | Poisoning |
| E863 | Accidental poisoning by agricultural and horticultural chemical & pharmaceutical preparations other than plant food & fertilizer | Poisoning |
| E950.0-E950.6 | Suicide & self-inflicted injury by drugs or medicinal substances | Poisoning |
| ICD-9-CM | Description | Analytical Classification |
| 295 | Schizophrenic disorders | Schizophrenia |
| 2950 | Simple schizophrenia | Schizophrenia |
| 2951 | Hebephrenia | Schizophrenia |
| 2952 | Catatonic schizophrenia | Schizophrenia |
| 2953 | Paranoid schizophrenia | Schizophrenia |
| 2954 | Acute schizophrenic episode | Schizophrenia |
| 2955 | Latent schizophrenia | Schizophrenia |
| 2956 | Residual schizophrenia | Schizophrenia |
| 2957 | Schizoaffective type | Schizophrenia |
| 2958 | Schizophrenia NEC | Schizophrenia |
| 2959 | Schizophrenia NOS | Schizophrenia |
| 296 | Affective psychoses | Other affective disorder |
| 2960 | Manic disorder, single episode | Bipolar I |
| 2961 | Manic disorder, recurrent episode | Bipolar I |
| 2962x (x = 3 or 4) | Depressive psychosis, single episode, severe | Major depression, severe |
| 2962x (x ne 3 or 4) | Depressive psychosis, single episode, non-severe | Major depression, non-severe |
| 2963x (x = 3 or 4) | Depressive psychosis, recurrent episode, severe | Major depression, severe |
| 2963x (x ne 3 or 4) | Depressive psychosis, recurrent episode, non-severe | Major depression, non-severe |
| 2964 | Bipolar affective, manic | Bipolar I |
| 2965 | Bipolar affective, depressive | Bipolar I |
| 2966 | Bipolar affective, mixed | Bipolar I |
| 2967 | Bipolar affective NOS | Bipolar I |
| 2968 | Manic-depressive NEC/NOS | Other or unspecified bipolar |
| 2969 | Affective psychoses NEC/NOS | Other affective disorder |
| 297 | Paranoid states | Delusional disorder |
| 2970 | Paranoid state, simple | Delusional disorder |
| 2971 | Paranoia | Delusional disorder |
| 2972 | Paraphrenia | Delusional disorder |
| 2973 | Shared paranoid disorder | Delusional disorder |
| 2978 | Paranoid states NEC | Delusional disorder |
| 2979 | Paranoid state NOS | Delusional disorder |
| 298 | Other nonorganic psychoses | Other MH diagnosis |
| 2980 | Reactive depressive psychosis | Other MH diagnosis |
| 2981 | Excitative-type psychosis | Other MH diagnosis |
| 2982 | Reactive confusion | Other MH diagnosis |
| 2983 | Acute paranoid reaction | Other MH diagnosis |
| 2984 | Psychogenic paranoid psychosis | Other MH diagnosis |
| 2988 | Reactive psychosis NEC/NOS | Other MH diagnosis |
| 2989 | Psychosis NOS | Other MH diagnosis |
| 299 | Psychoses of childhood | Other MH diagnosis |
| 2990 | Infantile autism | Other MH diagnosis |
| 2991 | Disintegrative psychosis | Other MH diagnosis |
| 2998 | Early childhood psychoses NEC | Other MH diagnosis |
| 2999 | Early childhood psychosis NOS | Other MH diagnosis |
| 300 | Neurotic disorders | Anxiety disorder |
| 3000 | Anxiety states | Anxiety disorder |
| 3001 | Hysteria | Anxiety disorder |
| 3002 | Phobic disorders | Anxiety disorder |
| 3003 | Obsessive-compulsive disorder | Anxiety disorder |
| 3004 | Neurotic depression | Anxiety disorder |
| 3005 | Neurasthenia | Anxiety disorder |
| 3006 | Depersonalization syndrome | Anxiety disorder |
| 3007 | Hypochondriasis | Anxiety disorder |
| 3008 | Neurotic disorders NEC | Anxiety disorder |
| 3009 | Neurotic disorder NOS | Anxiety disorder |
| 301 | Personality disorders | Other personality disorder |
| 3010 | Paranoid personality | Other personality disorder |
| 3011 | Affective personality | Other personality disorder |
| 3012 | Schizoid personality | Other personality disorder |
| 3013 | Explosive personality | Other personality disorder |
| 3014 | Compulsive personality | Other personality disorder |
| 3015 | Histrionic personality | Other personality disorder |
| 3016 | Dependent personality | Other personality disorder |
| 3017 | Antisocial personality | Antisocial personality disorder |
| 3018 | Other personality disorder | Other personality disorder |
| 3019 | Personality disorder NOS | Other personality disorder |
| 302 | Sexual disorders | Other MH diagnosis |
| 3020 | Egodystonic homosexuality | Other MH diagnosis |
| 3021 | Zoophilia | Other MH diagnosis |
| 3022 | Pedophilia | Other MH diagnosis |
| 3023 | Transvestism | Other MH diagnosis |
| 3024 | Exhibitionism | Other MH diagnosis |
| 3025 | Transsexualism | Other MH diagnosis |
| 3026 | Psychosexual identity disorder | Other MH diagnosis |
| 3027 | Psychosexual dysfunction | Other MH diagnosis |
| 3028 | Psychosexual disorder NEC | Other MH diagnosis |
| 3029 | Psychosexual disorder NOS | Other MH diagnosis |
| 306 | Psychophysiologic disease | Other MH diagnosis |
| 3060 | Psychogenic musculoskeletal disease | Other MH diagnosis |
| 3061 | Psychogenic respiratory disease | Other MH diagnosis |
| 3062 | Psychogenic cardiovascular disease | Other MH diagnosis |
| 3063 | Psychogenic skin disease | Other MH diagnosis |
| 3064 | Psychogenic GI disease | Other MH diagnosis |
| 3065 | Psychogenic GU disease | Other MH diagnosis |
| 3066 | Psychogenic endocrine disease | Other MH diagnosis |
| 3067 | Psychogenic sensory disease | Other MH diagnosis |
| 3068 | Psychogenic disorder NEC | Other MH diagnosis |
| 3069 | Psychogenic disorder NOS | Other MH diagnosis |
| 307 | Special symptom NEC | Other MH diagnosis |
| 3070 | Stammering and stuttering | Other MH diagnosis |
| 3071 | Anorexia nervosa | Other MH diagnosis |
| 3072 | Tics | Other MH diagnosis |
| 3073 | Stereotyped movements | Other MH diagnosis |
| 3074 | Nonorganic sleep disorder | Other MH diagnosis |
| 3075 | Eating disorders NEC/NOS | Other MH diagnosis |
| 3076 | Enuresis | Other MH diagnosis |
| 3077 | Encopresis | Other MH diagnosis |
| 3078 | Psychalgia | Other MH diagnosis |
| 3079 | Special symptom NEC/NOS | Other MH diagnosis |
| 308 | Acute reaction to stress | Acute reaction to stress |
| 3080 | Stress reaction, emotional | Acute reaction to stress |
| 3081 | Stress reaction, fugue | Acute reaction to stress |
| 3082 | Stress reaction, psychomotor | Acute reaction to stress |
| 3083 | Acute stress reaction NEC | Acute reaction to stress |
| 3084 | Stress reaction, mixed disorder | Acute reaction to stress |
| 3089 | Acute stress reaction NOS | Acute reaction to stress |
| 309 | Adjustment reaction | Adjustment reaction |
| 3090 | Brief depressive reaction | Adjustment reaction |
| 3091 | Prolonged depressive reaction | Adjustment reaction |
| 3092 | Adjustment reaction/other emotion | Adjustment reaction |
| 3093 | Adjustment reaction--conduct disorder | Adjustment reaction |
| 3094 | Adjustment reaction--emotion/conduct | Adjustment reaction |
| 3098 | Other adjustment reaction | Adjustment reaction |
| 3099 | Adjustment reaction NOS | Adjustment reaction |
| 310 | Non-psychotic brain syndrome | Other MH diagnosis |
| 3100 | Frontal lobe syndrome | Other MH diagnosis |
| 3101 | Organic personality syndrome | Other MH diagnosis |
| 3102 | Postconcussion syndrome | Other MH diagnosis |
| 3108 | Non-psychotic brain syndrome NEC | Other MH diagnosis |
| 3109 | Non-psychotic brain syndrome NOS | Other MH diagnosis |
| 311 | Depressive disorder NEC | Other depressive disorder |
| 312 | Conduct disturbance NEC | Conduct disorder |
| 3120 | Unsocialized aggression | Conduct disorder |
| 3121 | Unsocialized, unaggressive | Conduct disorder |
| 3122 | Socialized conduct disorder | Conduct disorder |
| 3123 | Impulse control disorder NEC | Conduct disorder |
| 3124 | Mixed disturbance conduct/emotion | Conduct disorder |
| 3128 | Other conduct disturbance | Conduct disorder |
| 3129 | Conduct disturbance NOS | Conduct disorder |
| 313 | Emotional disorder child/adolescent | Other MH diagnosis |
| 3130 | Overanxious disorder | Other MH diagnosis |
| 3131 | Misery and unhappiness disorder | Other MH diagnosis |
| 3132 | Sensitivity and withdrawal | Other MH diagnosis |
| 3133 | Relationship problems | Other MH diagnosis |
| 3138 | Other emotional disturbance, child | Other MH diagnosis |
| 3139 | Emotional disturbance, child, NOS | Other MH diagnosis |
| 314 | Hyperkinetic syndrome | Other MH diagnosis |
| 3140 | Attention deficit disorder | Other MH diagnosis |
| 3141 | Hyperkinetic with developmental delay | Other MH diagnosis |
| 3142 | Hyperkinetic conduct disorder | Other MH diagnosis |
| 3148 | Other hyperkinetic syndrome | Other MH diagnosis |
| 3149 | Hyperkinetic syndrome NOS | Other MH diagnosis |
| 6484 | Mental disorders in pregnancy | Other MH diagnosis |
| V402 | Mental problems NEC | MH V-code |
| V403 | Behavioral problems NEC | MH V-code |
| V409 | Mental/behavior problems NOS | MH V-code |
| V61 | Other family circumstances | MH V-code |
| V610 | Family disruption | MH V-code |
| V611 | Marital problems | MH V-code |
| V612 | Parentchild problems | MH V-code |
| V613 | Problem with aged parent | MH V-code |
| V614 | Health problem in family | MH V-code |
| V615 | Multi-parity | MH V-code |
| V616 | Illegitimate pregnancy | MH V-code |
| V617 | Unwanted pregnancy NEC | MH V-code |
| V618 | Family circumstances NEC | MH V-code |
| V619 | Family circumstance NOS | MH V-code |
| V663 | Mental disorder convalescence | MH V-code |
| V673 | Psychiatric followup | MH V-code |
| V701 | Psychiatric exam--authority required | MH V-code |
| V702 | General psychiatric exam NEC | MH V-code |
| V710 | Observation for mental conditions | MH V-code |
| E950.7-E950.9, E951-E959 | Suicide & self-inflicted injury by cause other than drugs or medicinal substances | Suicide & self-inflicted injury |
| ne = not equal. | ||
| Drug Name | NDC Code | |
SOURCE: Food and Drug Administration's NDC data base, Drugs.com, and rxlist.com. NOTE: NDCs are for the listed drug and any generic equivalent. | ||
| Alcoholism Medications | ||
| Campral | 0456-3330 | |
| Naltrexone HCl (Revia) | 51285-275, 0555-0902, 52152-105, 185-39, 406-1170, 16590-897, 16729-81, 47335-326, 60793-430, 60793-431, 60793-433, 60793-434, 60793-435, 60793-437 | |
| Vivitrol | 63459-300, 65757-300, 65757-301 | |
| Disulfiram (Antabuse) | 51285-523, 51285-524, 64980-171, 64980-172, 65473-706 | |
| Opiate and Heroin Addition Medications | ||
| Subutex | 12496-1310, 12496-1278 | |
| Suboxone | 12496-1202, 12496-1208, 54868-5707, 54868-5750, 63629-4028, 63629-4034 | |
| Vivitrol | 65757-300, 65757-301 | |
| Naltrexone HCl (Revia) | See above | |
| Nalmefene Hydrochloride (Revex) | 10019-315, 10019-311, 11098-311 | |
| Other Drug Abuse Medications | ||
| Naloxone Hydrochloride (Narcan) | 63481-365, 63481-368, 63481-359, 0409-1212, 0409-1215, 0409-1219, 63481-358, 63481-3771, 52584-469, 52584-782, 16590-556, 63739-463, 54868-2062,54868-6259, 60429-570, 68387-531, 548-1469, 548-3369, 43063-142, 43386-680, 52584-212, 52584-215, 409-1782 | |
| Types of SA Treatment Services | SA-Specific Codes | Other Behavioral Health Codesa | Other Types of Identifiers |
NA = not available.
| |||
| ER care | NA | NA | OT file claim with place of service code = 23 |
| Inpatient care | H0008, H0009 | ||
| Residential treatment | H0010, H0011 | H0017, H0018, H0019, S5145, S5146, T2048 | |
| Intensive treatment program | H0015, S9475, H2036, | S9480, S9485, H0035, T2034 | |
| Treatment program service | H2035, S0201 | H2012 | |
| Individual/ group psychotherapy | 90804, 90805, 90807, 90808, 90809, 90810, 90811, 90812, 90813, 90814, 90815, 90816, 90817, 90818, 90819, 90821, 90822, 90823, 90824, 90826, 90827, 90828, 90829, 90875, 90876, 90846, 90847, 90849, 90853, 90857, G0410, G0411 | ||
| Other assessment/ screening/ intervention/ evaluation/ prevention/ treatment planning | H0001, H0003, H0022, H0028, H0049, H0050, H0007, H0048, H0026, G0396, G0397, T1007, 99408 | H0030, H2011, S9484, 90801, S9083, H0002, H1011, 96150, 96151, 90802, H0031, T1001, H1000, 90889, 90801, 90885, 96101, 96102, 96103, 96100, 96125, 99456, S9446, H1003, H0023, H0032, 00100, G8405 G8404, 96115, 96116, 96117, T2010, T2011, T1023, 96105, 96111, 96110, 96125 | |
| Other medication management | H0020, J0592, J1230, J3490, J2315, J8499, S0109 | 90862, H0034, H2010, H0033, M0064, T1502 | |
| Other counseling/ therapy | H0005, T1006 | H0004, 90806, 90845, 90870, 90871, 90880, 96152, 99510, H2032, G0176, 96153, 96154, 96155 | |
| Other case management or community supports | H0006, T1007, T1012, T1009 | T1016, T1017, H0037, H2015, H2016, H2021, G0177, S5110, H5111, T1027, H2014, H2017, H2018, H2027, H0025, H2023, H2024, H2025, H2026, H2019, H2020, S0280, S0281, 90882, H0039, H0040, T1024, H1004, H0036, H2022, S9482, H2033 H0038, T2040, T2041, G0409 | |
| Detoxification | H0012, H0013, H0014 | ||
| Housing (including halfway house) | H2034 | H0043, H0044 | |
| Other | H0016, H0047, T1010, T1011, T1013, T2025, H2037 | 90899 | |
APPENDIX C. STATE LEVEL ESTIMATES, CY 2008
| State | SA Treatment Users | Total Expenditures (in $ thousands) | ||||||||
| Total | FFS Medicaid | % FFS | Medicaid ManagedCare | % Managed Care | Total | FFS Medicaid | % FFS | Medicaid ManagedCare | % Managed Care | |
| Total | 1,138,247 | 721,898 | 63 | 416,349 | 37 | 3,366,952 | 1,993,990 | 59 | 1,372,962 | 41 |
| Alabama | 8,493 | 8,493 | 100 | 0 | 0 | 8,310 | 8,310 | 100 | 0 | 0 |
| Alaska | 3,175 | 3,175 | 100 | 0 | 0 | 6,757 | 6,757 | 100 | 0 | 0 |
| Arizona | 23,162 | 3,505 | 15 | 19,657 | 85 | 142,853 | 34,522 | 24 | 108,331 | 76 |
| Arkansas | 3,537 | 3,537 | 100 | 0 | 0 | 4,960 | 4,960 | 100 | 0 | 0 |
| California | 134,099 | 78,395 | 58 | 55,704 | 42 | 316,631 | 186,448 | 59 | 130,183 | 41 |
| Colorado | 21,432 | 7,307 | 34 | 14,125 | 66 | 60,183 | 14,981 | 25 | 45,202 | 75 |
| Connecticut | 17,916 | 17,284 | 96 | 632 | 4 | 54,980 | 53,444 | 97 | 1,537 | 3 |
| Delaware | 4,186 | 1,726 | 41 | 2,460 | 59 | 11,438 | 6,188 | 54 | 5,251 | 46 |
| District of Columbia | 5,206 | 2,524 | 48 | 2,682 | 52 | 12,910 | 5,648 | 44 | 7,262 | 56 |
| Florida | 29,334 | 19,390 | 66 | 9,944 | 34 | 40,969 | 27,198 | 66 | 13,772 | 34 |
| Georgia | 14,561 | 9,664 | 66 | 4,897 | 34 | 20,896 | 13,661 | 65 | 7,235 | 35 |
| Hawaii | 5,261 | 2,920 | 56 | 2,341 | 44 | 8,344 | 4,452 | 53 | 3,892 | 47 |
| Idaho | 1,841 | 1,841 | 100 | 0 | 0 | 2,932 | 2,932 | 100 | 0 | 0 |
| Illinois | 34,142 | 32,963 | 97 | 1,179 | 3 | 111,204 | 107,452 | 97 | 3,751 | 3 |
| Indiana | 18,501 | 10,389 | 56 | 8,112 | 44 | 33,133 | 13,613 | 41 | 19,520 | 59 |
| Iowa | 5,860 | 2,819 | 48 | 3,041 | 52 | 9,983 | 3,135 | 31 | 6,848 | 69 |
| Kansas | 5,665 | 2,255 | 40 | 3,410 | 60 | 16,960 | 2,823 | 17 | 14,137 | 83 |
| Kentucky | 12,889 | 12,694 | 98 | 195 | 2 | 36,953 | 35,384 | 96 | 1,569 | 4 |
| Louisiana | 7,540 | 7,540 | 100 | 0 | 0 | 11,681 | 11,681 | 100 | 0 | 0 |
| Maine | 12,966 | 12,966 | 100 | 0 | 0 | 50,581 | 50,581 | 100 | 0 | 0 |
| Maryland | 22,766 | 5,759 | 25 | 17,007 | 75 | 67,462 | 13,535 | 20 | 53,928 | 80 |
| Massachusetts | 49,135 | 36,482 | 74 | 12,653 | 26 | 99,141 | 74,133 | 75 | 25,009 | 25 |
| Michigan | 32,558 | 9,836 | 30 | 22,722 | 70 | 65,736 | 7,908 | 12 | 57,828 | 88 |
| Minnesota | 16,732 | 10,731 | 64 | 6,001 | 36 | 53,818 | 38,119 | 71 | 15,699 | 29 |
| Mississippi | 8,388 | 8,388 | 100 | 0 | 0 | 20,132 | 20,132 | 100 | 0 | 0 |
| Missouri | 26,469 | 17,163 | 65 | 9,306 | 35 | 76,198 | 44,279 | 58 | 31,919 | 42 |
| Montana | 2,692 | 2,692 | 100 | 0 | 0 | 6,137 | 6,137 | 100 | 0 | 0 |
| Nebraska | 5,497 | 4,349 | 79 | 1,148 | 21 | 17,951 | 15,681 | 87 | 2,270 | 13 |
| Nevada | 3,408 | 1,770 | 52 | 1,638 | 48 | 8,267 | 3,539 | 43 | 4,728 | 57 |
| New Hampshire | 3,339 | 3,339 | 100 | 0 | 0 | 7,066 | 7,066 | 100 | 0 | 0 |
| New Jersey | 28,208 | 14,324 | 51 | 13,884 | 49 | 73,139 | 31,604 | 43 | 41,535 | 57 |
| New Mexico | 10,245 | 1,876 | 18 | 8,369 | 82 | 28,712 | 2,093 | 7 | 26,618 | 93 |
| New York | 246,207 | 162,521 | 66 | 83,686 | 34 | 1,137,298 | 751,323 | 66 | 385,975 | 34 |
| North Carolina | 25,568 | 25,507 | 100 | 61 | 0 | 47,974 | 47,771 | 100 | 203 | 0 |
| North Dakota | 1,736 | 1,736 | 100 | 0 | 0 | 4,281 | 4,281 | 100 | 0 | 0 |
| Ohio | 75,981 | 41,230 | 54 | 34,751 | 46 | 183,778 | 93,399 | 51 | 90,380 | 49 |
| Oklahoma | 6,366 | 6,366 | 100 | 0 | 0 | 9,107 | 9,107 | 100 | 0 | 0 |
| Oregon | 5,653 | 5,625 | 100 | 28 | 0 | 40,556 | 8,703 | 21 | 31,853 | 79 |
| Pennsylvania | 47,470 | 17,662 | 37 | 29,808 | 63 | 103,010 | 14,639 | 14 | 88,371 | 86 |
| Rhode Island | 7,209 | 4,272 | 59 | 2,937 | 41 | 20,105 | 11,497 | 57 | 8,608 | 43 |
| South Carolina | 12,353 | 9,995 | 81 | 2,358 | 19 | 22,775 | 17,923 | 79 | 4,852 | 21 |
| South Dakota | 1,398 | 1,398 | 100 | 0 | 0 | 5,965 | 5,965 | 100 | 0 | 0 |
| Tennessee | 9,930 | 6,673 | 67 | 3,257 | 33 | 15,729 | 9,081 | 58 | 6,648 | 42 |
| Texas | 17,077 | 12,159 | 71 | 4,918 | 29 | 22,307 | 11,180 | 50 | 11,127 | 50 |
| Utah | 4,506 | 4,506 | 100 | 0 | 0 | 8,838 | 8,838 | 100 | 0 | 0 |
| Vermont | 8,375 | 8,375 | 100 | 0 | 0 | 30,133 | 30,133 | 100 | 0 | 0 |
| Virginia | 9,329 | 5,285 | 57 | 4,044 | 43 | 18,529 | 11,008 | 59 | 7,521 | 41 |
| Washington | 50,986 | 29,753 | 58 | 21,233 | 42 | 143,779 | 55,719 | 39 | 88,060 | 61 |
| West Virginia | 10,925 | 7,051 | 65 | 3,874 | 35 | 23,897 | 12,842 | 54 | 11,055 | 46 |
| Wisconsin | 16,704 | 12,417 | 74 | 4,287 | 26 | 40,492 | 30,206 | 75 | 10,286 | 25 |
| Wyoming | 1,271 | 1,271 | 100 | 0 | 0 | 1,981 | 1,981 | 100 | 0 | 0 |
| State | Total Expenditures (in $ thousands) | % Attributable to State | % Attributable to Federal | |
| Total State | Total Federal | |||
| Total | 1,454,920 | 1,912,032 | 43 | 57 |
| Alabama | 2,503 | 5,806 | 30 | 70 |
| Alaska | 3,106 | 3,651 | 46 | 54 |
| Arizona | 45,138 | 97,715 | 32 | 68 |
| Arkansas | 1,265 | 3,695 | 26 | 74 |
| California | 149,141 | 167,490 | 47 | 53 |
| Colorado | 28,771 | 31,413 | 48 | 52 |
| Connecticut | 26,090 | 28,891 | 47 | 53 |
| Delaware | 5,428 | 6,010 | 47 | 53 |
| District of Columbia | 3,625 | 9,285 | 28 | 72 |
| Florida | 16,579 | 24,390 | 40 | 60 |
| Georgia | 7,171 | 13,726 | 34 | 66 |
| Hawaii | 3,429 | 4,915 | 41 | 59 |
| Idaho | 821 | 2,111 | 28 | 72 |
| Illinois | 52,688 | 58,515 | 47 | 53 |
| Indiana | 11,489 | 21,644 | 35 | 65 |
| Iowa | 3,644 | 6,339 | 36 | 64 |
| Kansas | 6,590 | 10,370 | 39 | 61 |
| Kentucky | 10,426 | 26,527 | 28 | 72 |
| Louisiana | 2,996 | 8,685 | 26 | 74 |
| Maine | 17,409 | 33,172 | 34 | 66 |
| Maryland | 32,250 | 35,212 | 48 | 52 |
| Massachusetts | 47,394 | 51,747 | 48 | 52 |
| Michigan | 25,657 | 40,079 | 39 | 61 |
| Minnesota | 25,538 | 28,280 | 47 | 53 |
| Mississippi | 4,404 | 15,728 | 22 | 78 |
| Missouri | 26,955 | 49,243 | 35 | 65 |
| Montana | 1,812 | 4,325 | 30 | 70 |
| Nebraska | 7,189 | 10,761 | 40 | 60 |
| Nevada | 3,682 | 4,585 | 45 | 55 |
| New Hampshire | 3,424 | 3,643 | 48 | 52 |
| New Jersey | 34,964 | 38,175 | 48 | 52 |
| New Mexico | 7,870 | 20,842 | 27 | 73 |
| New York | 543,685 | 593,613 | 48 | 52 |
| North Carolina | 16,107 | 31,867 | 34 | 66 |
| North Dakota | 1,485 | 2,795 | 35 | 65 |
| Ohio | 67,713 | 116,065 | 37 | 63 |
| Oklahoma | 2,818 | 6,289 | 31 | 69 |
| Oregon | 14,787 | 25,769 | 36 | 64 |
| Pennsylvania | 44,992 | 58,018 | 44 | 56 |
| Rhode Island | 8,976 | 11,129 | 45 | 55 |
| South Carolina | 6,382 | 16,393 | 28 | 72 |
| South Dakota | 2,254 | 3,711 | 38 | 62 |
| Tennessee | 5,333 | 10,396 | 34 | 66 |
| Texas | 8,345 | 13,961 | 37 | 63 |
| Utah | 2,370 | 6,468 | 27 | 73 |
| Vermont | 11,691 | 18,441 | 39 | 61 |
| Virginia | 8,858 | 9,671 | 48 | 52 |
| Washington | 66,577 | 77,202 | 46 | 54 |
| West Virginia | 5,783 | 18,114 | 24 | 76 |
| Wisconsin | 16,355 | 24,137 | 40 | 60 |
| Wyoming | 960 | 1,021 | 48 | 52 |
| State | SA Treatment Users | Total Expenditures (in $ thousands) | ||||||||
| Total | FFS Medicaid | % FFS | Medicaid ManagedCare | % Managed Care | Total | FFS Medicaid | % FFS | Medicaid ManagedCare | % Managed Care | |
| Total | 62,663 | 32,293 | 52 | 30,370 | 48 | 86,757 | 50,931 | 59 | 35,826 | 41 |
| Alabama | 1,668 | 1,668 | 100 | 0 | 0 | 585 | 585 | 100 | 0 | 0 |
| Alaska | 335 | 335 | 100 | 0 | 0 | 805 | 805 | 100 | 0 | 0 |
| Arizona | 1,802 | 291 | 16 | 1,511 | 84 | 1,838 | 436 | 24 | 1,402 | 76 |
| Arkansas | 343 | 343 | 100 | 0 | 0 | 285 | 285 | 100 | 0 | 0 |
| California | 6,606 | 2,414 | 37 | 4,192 | 63 | 5,200 | 1,707 | 33 | 3,493 | 67 |
| Colorado | 1,210 | 425 | 35 | 785 | 65 | 1,833 | 844 | 46 | 989 | 54 |
| Connecticut | 282 | 259 | 92 | 23 | 8 | 527 | 473 | 90 | 54 | 10 |
| Delaware | 254 | 64 | 25 | 190 | 75 | 206 | 40 | 20 | 165 | 80 |
| District of Columbia | 286 | 31 | 11 | 255 | 89 | 309 | 106 | 34 | 203 | 66 |
| Florida | 5,911 | 3,988 | 67 | 1,923 | 33 | 13,489 | 9,251 | 69 | 4,238 | 31 |
| Georgia | 1,682 | 645 | 38 | 1,037 | 62 | 1,230 | 397 | 32 | 833 | 68 |
| Hawaii | 251 | 40 | 16 | 211 | 84 | 189 | 8 | 4 | 182 | 96 |
| Idaho | 155 | 155 | 100 | 0 | 0 | 148 | 148 | 100 | 0 | 0 |
| Illinois | 1,780 | 1,673 | 94 | 107 | 6 | 1,249 | 1,183 | 95 | 66 | 5 |
| Indiana | 1,397 | 498 | 36 | 899 | 64 | 1,269 | 492 | 39 | 777 | 61 |
| Iowa | 652 | 290 | 44 | 362 | 56 | 664 | 328 | 49 | 336 | 51 |
| Kansas | 402 | 83 | 21 | 319 | 79 | 496 | 175 | 35 | 321 | 65 |
| Kentucky | 2,639 | 2,639 | 100 | 0 | 0 | 5,601 | 5,601 | 100 | 0 | 0 |
| Louisiana | 803 | 803 | 100 | 0 | 0 | 494 | 494 | 100 | 0 | 0 |
| Maine | 464 | 464 | 100 | 0 | 0 | 550 | 550 | 100 | 0 | 0 |
| Maryland | 1,266 | 307 | 24 | 959 | 76 | 2,401 | 1,248 | 52 | 1,153 | 48 |
| Massachusetts | 2,295 | 1,008 | 44 | 1,287 | 56 | 4,983 | 1,876 | 38 | 3,106 | 62 |
| Michigan | 2,309 | 764 | 33 | 1,545 | 67 | 1,731 | 409 | 24 | 1,321 | 76 |
| Minnesota | 1,563 | 999 | 64 | 564 | 36 | 9,504 | 8,931 | 94 | 573 | 6 |
| Mississippi | 561 | 561 | 100 | 0 | 0 | 313 | 313 | 100 | 0 | 0 |
| Missouri | 574 | 289 | 50 | 285 | 50 | 340 | 212 | 62 | 128 | 38 |
| Montana | 152 | 152 | 100 | 0 | 0 | 96 | 96 | 100 | 0 | 0 |
| Nebraska | 313 | 113 | 36 | 200 | 64 | 266 | 80 | 30 | 186 | 70 |
| Nevada | 413 | 220 | 53 | 193 | 47 | 457 | 201 | 44 | 256 | 56 |
| New Hampshire | 172 | 172 | 100 | 0 | 0 | 635 | 635 | 100 | 0 | 0 |
| New Jersey | 1,482 | 673 | 45 | 809 | 55 | 2,862 | 1,629 | 57 | 1,233 | 43 |
| New Mexico | 682 | 178 | 26 | 504 | 74 | 1,000 | 413 | 41 | 588 | 59 |
| New York | 4,867 | 1,160 | 24 | 3,707 | 76 | 6,464 | 1,446 | 22 | 5,018 | 78 |
| North Carolina | 1,612 | 1,612 | 100 | 0 | 0 | 896 | 896 | 100 | 0 | 0 |
| North Dakota | 23 | 23 | 100 | 0 | 0 | 16 | 16 | 100 | 0 | 0 |
| Ohio | 2,481 | 676 | 27 | 1,805 | 73 | 2,890 | 1,157 | 40 | 1,733 | 60 |
| Oklahoma | 362 | 362 | 100 | 0 | 0 | 176 | 176 | 100 | 0 | 0 |
| Oregon | 576 | 116 | 20 | 460 | 80 | 755 | 101 | 13 | 654 | 87 |
| Pennsylvania | 2,628 | 527 | 20 | 2,101 | 80 | 3,114 | 1,010 | 32 | 2,104 | 68 |
| Rhode Island | 293 | 94 | 32 | 199 | 68 | 295 | 65 | 22 | 230 | 78 |
| South Carolina | 350 | 265 | 76 | 85 | 24 | 272 | 211 | 78 | 61 | 22 |
| South Dakota | 112 | 112 | 100 | 0 | 0 | 64 | 64 | 100 | 0 | 0 |
| Tennessee | 1,265 | 802 | 63 | 463 | 37 | 1,508 | 898 | 60 | 611 | 40 |
| Texas | 1,474 | 857 | 58 | 617 | 42 | 2,053 | 1,091 | 53 | 962 | 47 |
| Utah | 118 | 118 | 100 | 0 | 0 | 296 | 296 | 100 | 0 | 0 |
| Vermont | 360 | 360 | 100 | 0 | 0 | 246 | 246 | 100 | 0 | 0 |
| Virginia | 1,784 | 991 | 56 | 793 | 44 | 1,121 | 560 | 50 | 561 | 50 |
| Washington | 1,882 | 656 | 35 | 1,226 | 65 | 2,112 | 476 | 23 | 1,636 | 77 |
| West Virginia | 388 | 189 | 49 | 199 | 51 | 248 | 114 | 46 | 134 | 54 |
| Wisconsin | 1,346 | 791 | 59 | 555 | 41 | 2,659 | 2,140 | 80 | 519 | 20 |
| Wyoming | 38 | 38 | 100 | 0 | 0 | 16 | 16 | 100 | 0 | 0 |
| State | Total Expenditures (in $ thousands) | % Attributable to State | % Attributable to Federal | |
| Total State | Total Federal | |||
| Total | 36,001 | 50,726 | 42 | 58 |
| Alabama | 176 | 409 | 30 | 70 |
| Alaska | 370 | 435 | 46 | 54 |
| Arizona | 581 | 1,257 | 32 | 68 |
| Arkansas | 73 | 213 | 26 | 74 |
| California | 2,449 | 2,751 | 47 | 53 |
| Colorado | 876 | 957 | 48 | 52 |
| Connecticut | 250 | 277 | 47 | 53 |
| Delaware | 98 | 108 | 47 | 53 |
| District of Columbia | 87 | 222 | 28 | 72 |
| Florida | 5,459 | 8,030 | 40 | 60 |
| Georgia | 422 | 808 | 34 | 66 |
| Hawaii | 78 | 111 | 41 | 59 |
| Idaho | 41 | 106 | 28 | 72 |
| Illinois | 592 | 657 | 47 | 53 |
| Indiana | 440 | 829 | 35 | 65 |
| Iowa | 242 | 422 | 36 | 64 |
| Kansas | 193 | 303 | 39 | 61 |
| Kentucky | 1,580 | 4,021 | 28 | 72 |
| Louisiana | 127 | 367 | 26 | 74 |
| Maine | 189 | 360 | 34 | 66 |
| Maryland | 1,148 | 1,253 | 48 | 52 |
| Massachusetts | 2,382 | 2,601 | 48 | 52 |
| Michigan | 675 | 1,055 | 39 | 61 |
| Minnesota | 4,510 | 4,994 | 47 | 53 |
| Mississippi | 69 | 245 | 22 | 78 |
| Missouri | 120 | 220 | 35 | 65 |
| Montana | 28 | 68 | 30 | 70 |
| Nebraska | 107 | 159 | 40 | 60 |
| Nevada | 204 | 254 | 45 | 55 |
| New Hampshire | 308 | 327 | 48 | 52 |
| New Jersey | 1,368 | 1,494 | 48 | 52 |
| New Mexico | 274 | 726 | 27 | 73 |
| New York | 3,090 | 3,374 | 48 | 52 |
| North Carolina | 301 | 595 | 34 | 66 |
| North Dakota | 6 | 11 | 35 | 65 |
| Ohio | 1,065 | 1,825 | 37 | 63 |
| Oklahoma | 54 | 122 | 31 | 69 |
| Oregon | 275 | 480 | 36 | 64 |
| Pennsylvania | 1,360 | 1,754 | 44 | 56 |
| Rhode Island | 132 | 163 | 45 | 55 |
| South Carolina | 76 | 196 | 28 | 72 |
| South Dakota | 24 | 40 | 38 | 62 |
| Tennessee | 511 | 997 | 34 | 66 |
| Texas | 768 | 1,285 | 37 | 63 |
| Utah | 80 | 217 | 27 | 73 |
| Vermont | 96 | 151 | 39 | 61 |
| Virginia | 536 | 585 | 48 | 52 |
| Washington | 978 | 1,134 | 46 | 54 |
| West Virginia | 60 | 188 | 24 | 76 |
| Wisconsin | 1,074 | 1,585 | 40 | 60 |
| Wyoming | 8 | 8 | 48 | 52 |
| State | SA Treatment Users | Total Expenditures (in $ thousands) | ||||||||
| Total | FFS Medicaid | % FFS | Medicaid ManagedCare | % Managed Care | Total | FFS Medicaid | % FFS | Medicaid ManagedCare | % Managed Care | |
| Total | 53,041 | 37,313 | 70 | 15,728 | 30 | 256,600 | 176,414 | 69 | 80,186 | 31 |
| Alabama | 397 | 397 | 100 | 0 | 0 | 364 | 364 | 100 | 0 | 0 |
| Alaska | 154 | 154 | 100 | 0 | 0 | 585 | 585 | 100 | 0 | 0 |
| Arizona | 1,060 | 241 | 23 | 819 | 77 | 4,205 | 1,144 | 27 | 3,060 | 73 |
| Arkansas | 351 | 351 | 100 | 0 | 0 | 1,008 | 1,008 | 100 | 0 | 0 |
| California | 7,767 | 5,660 | 73 | 2,107 | 27 | 36,306 | 27,973 | 77 | 8,333 | 23 |
| Colorado | 882 | 517 | 59 | 365 | 41 | 3,986 | 2,443 | 61 | 1,543 | 39 |
| Connecticut | 514 | 512 | 100 | 2 | 0 | 2,133 | 2,122 | 99 | 11 | 1 |
| Delaware | 167 | 81 | 49 | 86 | 51 | 834 | 493 | 59 | 341 | 41 |
| District of Columbia | 194 | 144 | 74 | 50 | 26 | 1,463 | 1,366 | 93 | 97 | 7 |
| Florida | 1,921 | 1,386 | 72 | 535 | 28 | 5,497 | 3,888 | 71 | 1,609 | 29 |
| Georgia | 1,117 | 1,008 | 90 | 109 | 10 | 4,763 | 4,468 | 94 | 295 | 6 |
| Hawaii | 212 | 136 | 64 | 76 | 36 | 411 | 155 | 38 | 255 | 62 |
| Idaho | 175 | 175 | 100 | 0 | 0 | 655 | 655 | 100 | 0 | 0 |
| Illinois | 2,140 | 2,118 | 99 | 22 | 1 | 14,858 | 14,807 | 100 | 51 | 0 |
| Indiana | 836 | 704 | 84 | 132 | 16 | 3,511 | 3,070 | 87 | 441 | 13 |
| Iowa | 497 | 316 | 64 | 181 | 36 | 2,182 | 1,180 | 54 | 1,002 | 46 |
| Kansas | 495 | 319 | 64 | 176 | 36 | 3,228 | 2,278 | 71 | 950 | 29 |
| Kentucky | 529 | 529 | 100 | 0 | 0 | 773 | 773 | 100 | 0 | 0 |
| Louisiana | 653 | 653 | 100 | 0 | 0 | 3,445 | 3,445 | 100 | 0 | 0 |
| Maine | 284 | 284 | 100 | 0 | 0 | 1,552 | 1,552 | 100 | 0 | 0 |
| Maryland | 935 | 505 | 54 | 430 | 46 | 5,810 | 3,553 | 61 | 2,257 | 39 |
| Massachusetts | 2,062 | 1,740 | 84 | 322 | 16 | 7,715 | 6,409 | 83 | 1,306 | 17 |
| Michigan | 1,736 | 722 | 42 | 1,014 | 58 | 9,133 | 3,906 | 43 | 5,227 | 57 |
| Minnesota | 891 | 753 | 85 | 138 | 15 | 5,126 | 4,430 | 86 | 696 | 14 |
| Mississippi | 417 | 417 | 100 | 0 | 0 | 1,438 | 1,438 | 100 | 0 | 0 |
| Missouri | 1,137 | 1,098 | 97 | 39 | 3 | 3,751 | 3,698 | 99 | 53 | 1 |
| Montana | 246 | 246 | 100 | 0 | 0 | 943 | 943 | 100 | 0 | 0 |
| Nebraska | 257 | 182 | 71 | 75 | 29 | 1,311 | 890 | 68 | 421 | 32 |
| Nevada | 197 | 182 | 92 | 15 | 8 | 1,196 | 1,154 | 96 | 42 | 4 |
| New Hampshire | 144 | 144 | 100 | 0 | 0 | 441 | 441 | 100 | 0 | 0 |
| New Jersey | 933 | 463 | 50 | 470 | 50 | 4,762 | 2,364 | 50 | 2,398 | 50 |
| New Mexico | 516 | 323 | 63 | 193 | 37 | 2,260 | 1,300 | 58 | 960 | 42 |
| New York | 4,948 | 3,082 | 62 | 1,866 | 38 | 34,660 | 20,007 | 58 | 14,653 | 42 |
| North Carolina | 1,936 | 1,936 | 100 | 0 | 0 | 6,550 | 6,550 | 100 | 0 | 0 |
| North Dakota | 78 | 78 | 100 | 0 | 0 | 331 | 331 | 100 | 0 | 0 |
| Ohio | 2,867 | 1,321 | 46 | 1,546 | 54 | 13,455 | 5,553 | 41 | 7,902 | 59 |
| Oklahoma | 577 | 577 | 100 | 0 | 0 | 2,838 | 2,838 | 100 | 0 | 0 |
| Oregon | 502 | 295 | 59 | 207 | 41 | 2,639 | 1,380 | 52 | 1,259 | 48 |
| Pennsylvania | 2,467 | 757 | 31 | 1,710 | 69 | 13,574 | 4,025 | 30 | 9,550 | 70 |
| Rhode Island | 187 | 152 | 81 | 35 | 19 | 1,297 | 1,169 | 90 | 128 | 10 |
| South Carolina | 619 | 539 | 87 | 80 | 13 | 2,834 | 2,398 | 85 | 435 | 15 |
| South Dakota | 120 | 120 | 100 | 0 | 0 | 685 | 685 | 100 | 0 | 0 |
| Tennessee | 720 | 513 | 71 | 207 | 29 | 3,241 | 2,225 | 69 | 1,016 | 31 |
| Texas | 3,872 | 2,310 | 60 | 1,562 | 40 | 20,144 | 11,811 | 59 | 8,333 | 41 |
| Utah | 155 | 155 | 100 | 0 | 0 | 988 | 988 | 100 | 0 | 0 |
| Vermont | 163 | 163 | 100 | 0 | 0 | 285 | 285 | 100 | 0 | 0 |
| Virginia | 887 | 514 | 58 | 373 | 42 | 2,717 | 1,425 | 52 | 1,292 | 48 |
| Washington | 1,809 | 1,172 | 65 | 637 | 35 | 7,490 | 3,790 | 51 | 3,699 | 49 |
| West Virginia | 475 | 455 | 96 | 20 | 4 | 1,573 | 1,534 | 98 | 38 | 2 |
| Wisconsin | 760 | 631 | 83 | 129 | 17 | 5,272 | 4,741 | 90 | 532 | 10 |
| Wyoming | 83 | 83 | 100 | 0 | 0 | 382 | 382 | 100 | 0 | 0 |
| State | Total Expenditures (in $ thousands) | % Attributable to State | % Attributable to Federal | |
| Total State | Total Federal | |||
| Total | 107,209 | 149,390 | 42 | 58 |
| Alabama | 110 | 255 | 30 | 70 |
| Alaska | 269 | 316 | 46 | 54 |
| Arizona | 1,329 | 2,876 | 32 | 68 |
| Arkansas | 257 | 751 | 26 | 74 |
| California | 17,101 | 19,205 | 47 | 53 |
| Colorado | 1,905 | 2,080 | 48 | 52 |
| Connecticut | 1,012 | 1,121 | 47 | 53 |
| Delaware | 396 | 438 | 47 | 53 |
| District of Columbia | 411 | 1,052 | 28 | 72 |
| Florida | 2,225 | 3,273 | 40 | 60 |
| Georgia | 1,634 | 3,128 | 34 | 66 |
| Hawaii | 169 | 242 | 41 | 59 |
| Idaho | 183 | 471 | 28 | 72 |
| Illinois | 7,040 | 7,818 | 47 | 53 |
| Indiana | 1,217 | 2,293 | 35 | 65 |
| Iowa | 797 | 1,386 | 36 | 64 |
| Kansas | 1,254 | 1,974 | 39 | 61 |
| Kentucky | 218 | 555 | 28 | 72 |
| Louisiana | 884 | 2,562 | 26 | 74 |
| Maine | 534 | 1,018 | 34 | 66 |
| Maryland | 2,777 | 3,033 | 48 | 52 |
| Massachusetts | 3,688 | 4,027 | 48 | 52 |
| Michigan | 3,564 | 5,568 | 39 | 61 |
| Minnesota | 2,433 | 2,694 | 47 | 53 |
| Mississippi | 315 | 1,123 | 22 | 78 |
| Missouri | 1,327 | 2,424 | 35 | 65 |
| Montana | 279 | 665 | 30 | 70 |
| Nebraska | 525 | 786 | 40 | 60 |
| Nevada | 533 | 663 | 45 | 55 |
| New Hampshire | 214 | 227 | 48 | 52 |
| New Jersey | 2,277 | 2,486 | 48 | 52 |
| New Mexico | 619 | 1,640 | 27 | 73 |
| New York | 16,569 | 18,091 | 48 | 52 |
| North Carolina | 2,199 | 4,351 | 34 | 66 |
| North Dakota | 115 | 216 | 35 | 65 |
| Ohio | 4,957 | 8,497 | 37 | 63 |
| Oklahoma | 878 | 1,960 | 31 | 69 |
| Oregon | 962 | 1,677 | 36 | 64 |
| Pennsylvania | 5,929 | 7,645 | 44 | 56 |
| Rhode Island | 579 | 718 | 45 | 55 |
| South Carolina | 794 | 2,040 | 28 | 72 |
| South Dakota | 259 | 426 | 38 | 62 |
| Tennessee | 1,099 | 2,142 | 34 | 66 |
| Texas | 7,536 | 12,608 | 37 | 63 |
| Utah | 265 | 723 | 27 | 73 |
| Vermont | 111 | 175 | 39 | 61 |
| Virginia | 1,299 | 1,418 | 48 | 52 |
| Washington | 3,468 | 4,022 | 46 | 54 |
| West Virginia | 381 | 1,192 | 24 | 76 |
| Wisconsin | 2,130 | 3,143 | 40 | 60 |
| Wyoming | 185 | 197 | 48 | 52 |
| State | SA Treatment Users | Total Expenditures (in $ thousands) | ||||||||
| Total | FFS Medicaid | % FFS | Medicaid ManagedCare | % Managed Care | Total | FFS Medicaid | % FFS | Medicaid ManagedCare | % Managed Care | |
| Total | 280,727 | 168,219 | 60 | 113,862 | 40 | 1,432,738 | 769,500 | 54 | 663,238 | 46 |
| Alabama | 1,282 | 1,282 | 100 | 0 | 0 | 1,403 | 1,403 | 100 | 0 | 0 |
| Alaska | 1,215 | 1,215 | 100 | 0 | 0 | 5,968 | 5,968 | 100 | 0 | 0 |
| Arizona | 6,438 | 636 | 10 | 5,802 | 90 | 20,131 | 1,540 | 8 | 18,591 | 92 |
| Arkansas | 2,449 | 2,449 | 100 | 0 | 0 | 10,774 | 10,774 | 100 | 0 | 0 |
| California | 22,621 | 8,661 | 38 | 13,960 | 62 | 59,739 | 17,635 | 30 | 42,104 | 70 |
| Colorado | 6,305 | 1,330 | 21 | 5,116 | 79 | 38,600 | 4,301 | 11 | 34,299 | 89 |
| Connecticut | 7,080 | 6,911 | 98 | 169 | 2 | 37,388 | 36,750 | 98 | 638 | 2 |
| Delaware | 868 | 173 | 20 | 695 | 80 | 3,174 | 802 | 25 | 2,372 | 75 |
| District of Columbia | 1,907 | 1,042 | 55 | 865 | 45 | 15,197 | 12,050 | 79 | 3,147 | 21 |
| Florida | 4,241 | 2,891 | 68 | 1,350 | 32 | 13,647 | 8,800 | 64 | 4,846 | 36 |
| Georgia | 5,330 | 3,481 | 65 | 1,849 | 35 | 13,186 | 7,815 | 59 | 5,371 | 41 |
| Hawaii | 1,736 | 974 | 56 | 762 | 44 | 3,177 | 1,382 | 43 | 1,795 | 57 |
| Idaho | 914 | 914 | 100 | 0 | 0 | 3,467 | 3,467 | 100 | 0 | 0 |
| Illinois | 11,010 | 10,698 | 97 | 312 | 3 | 68,590 | 67,171 | 98 | 1,420 | 2 |
| Indiana | 8,756 | 6,364 | 73 | 2,392 | 27 | 34,063 | 25,538 | 75 | 8,525 | 25 |
| Iowa | 2,240 | 1,014 | 45 | 1,226 | 55 | 7,924 | 2,610 | 33 | 5,314 | 67 |
| Kansas | 2,620 | 1,410 | 54 | 1,210 | 46 | 10,951 | 4,734 | 43 | 6,217 | 57 |
| Kentucky | 4,281 | 4,281 | 100 | 0 | 0 | 12,396 | 12,396 | 100 | 0 | 0 |
| Louisiana | 5,360 | 5,360 | 100 | 0 | 0 | 13,978 | 13,978 | 100 | 0 | 0 |
| Maine | 3,282 | 3,574 | 100 | 0 | 0 | 28,433 | 28,433 | 100 | 0 | 0 |
| Maryland | 10,526 | 4,937 | 47 | 5,733 | 54 | 78,805 | 32,632 | 41 | 46,173 | 59 |
| Massachusetts | 8,983 | 7,045 | 78 | 1,938 | 22 | 32,250 | 25,216 | 78 | 7,034 | 22 |
| Michigan | 9,578 | 2,438 | 25 | 7,140 | 75 | 35,224 | 3,718 | 11 | 31,506 | 89 |
| Minnesota | 10,040 | 8,374 | 83 | 1,666 | 17 | 43,649 | 37,010 | 85 | 6,640 | 15 |
| Mississippi | 3,911 | 3,911 | 100 | 0 | 0 | 21,564 | 21,564 | 100 | 0 | 0 |
| Missouri | 8,188 | 6,383 | 78 | 1,805 | 22 | 34,112 | 24,834 | 73 | 9,278 | 27 |
| Montana | 1,007 | 1,007 | 100 | 0 | 0 | 3,555 | 3,555 | 100 | 0 | 0 |
| Nebraska | 1,421 | 932 | 66 | 489 | 34 | 6,440 | 4,199 | 65 | 2,241 | 35 |
| Nevada | 1,145 | 795 | 69 | 350 | 31 | 7,552 | 5,471 | 72 | 2,080 | 28 |
| New Hampshire | 670 | 670 | 100 | 0 | 0 | 1,743 | 1,743 | 100 | 0 | 0 |
| New Jersey | 9,555 | 4,792 | 50 | 4,763 | 50 | 56,323 | 27,109 | 48 | 29,215 | 52 |
| New Mexico | 3,437 | 799 | 23 | 3,199 | 80 | 21,575 | 426 | 2 | 21,149 | 98 |
| New York | 28,730 | 14,347 | 50 | 14,383 | 50 | 320,268 | 162,248 | 51 | 158,020 | 49 |
| North Carolina | 11,636 | 11,636 | 100 | 0 | 0 | 30,592 | 30,592 | 100 | 0 | 0 |
| North Dakota | 942 | 942 | 100 | 0 | 0 | 3,160 | 3,160 | 100 | 0 | 0 |
| Ohio | 13,456 | 5,692 | 42 | 7,764 | 58 | 45,657 | 15,888 | 35 | 29,769 | 65 |
| Oklahoma | 3,653 | 3,653 | 100 | 0 | 0 | 15,341 | 15,341 | 100 | 0 | 0 |
| Oregon | 3,355 | 849 | 25 | 2,573 | 75 | 25,735 | 2,241 | 9 | 23,493 | 91 |
| Pennsylvania | 14,097 | 3,265 | 23 | 10,832 | 77 | 63,588 | 7,836 | 12 | 55,753 | 88 |
| Rhode Island | 2,124 | 1,509 | 71 | 615 | 29 | 10,231 | 6,681 | 65 | 3,550 | 35 |
| South Carolina | 2,547 | 2,033 | 80 | 514 | 20 | 6,388 | 4,890 | 77 | 1,498 | 23 |
| South Dakota | 658 | 658 | 100 | 0 | 0 | 3,025 | 3,025 | 100 | 0 | 0 |
| Tennessee | 1,804 | 1,342 | 74 | 462 | 26 | 2,554 | 805 | 32 | 1,749 | 68 |
| Texas | 5,063 | 3,199 | 63 | 1,864 | 37 | 27,081 | 15,521 | 57 | 11,560 | 43 |
| Utah | 432 | 432 | 100 | 0 | 0 | 463 | 463 | 100 | 0 | 0 |
| Vermont | 652 | 652 | 100 | 0 | 0 | 5,123 | 5,123 | 100 | 0 | 0 |
| Virginia | 3,783 | 2,011 | 53 | 1,772 | 47 | 13,299 | 7,453 | 56 | 5,846 | 44 |
| Washington | 8,636 | 1,977 | 23 | 6,808 | 77 | 74,249 | 7,320 | 10 | 66,928 | 90 |
| West Virginia | 4,743 | 2,860 | 60 | 1,883 | 40 | 21,981 | 11,272 | 51 | 10,709 | 49 |
| Wisconsin | 5,742 | 4,141 | 72 | 1,601 | 28 | 14,204 | 9,794 | 69 | 4,410 | 31 |
| Wyoming | 278 | 278 | 100 | 0 | 0 | 4,823 | 4,823 | 100 | 0 | 0 |
| State | Total Expenditures (in $ thousands) | % Attributable to State | % Attributable to Federal | |
| Total State | Total Federal | |||
| Total | 605,980 | 826,758 | 42 | 58 |
| Alabama | 423 | 980 | 30 | 70 |
| Alaska | 2,743 | 3,224 | 46 | 54 |
| Arizona | 6,361 | 13,770 | 32 | 68 |
| Arkansas | 2,748 | 8,025 | 26 | 74 |
| California | 28,138 | 31,600 | 47 | 53 |
| Colorado | 18,453 | 20,147 | 48 | 52 |
| Connecticut | 17,742 | 19,647 | 47 | 53 |
| Delaware | 1,506 | 1,668 | 47 | 53 |
| District of Columbia | 4,267 | 10,930 | 28 | 72 |
| Florida | 5,522 | 8,124 | 40 | 60 |
| Georgia | 4,525 | 8,661 | 34 | 66 |
| Hawaii | 1,306 | 1,872 | 41 | 59 |
| Idaho | 971 | 2,496 | 28 | 72 |
| Illinois | 32,498 | 36,092 | 47 | 53 |
| Indiana | 11,811 | 22,252 | 35 | 65 |
| Iowa | 2,892 | 5,032 | 36 | 64 |
| Kansas | 4,255 | 6,696 | 39 | 61 |
| Kentucky | 3,498 | 8,899 | 28 | 72 |
| Louisiana | 3,585 | 10,393 | 26 | 74 |
| Maine | 9,786 | 18,647 | 34 | 66 |
| Maryland | 37,673 | 41,132 | 48 | 52 |
| Massachusetts | 15,417 | 16,833 | 48 | 52 |
| Michigan | 13,748 | 21,476 | 39 | 61 |
| Minnesota | 20,713 | 22,937 | 47 | 53 |
| Mississippi | 4,718 | 16,847 | 22 | 78 |
| Missouri | 12,067 | 22,045 | 35 | 65 |
| Montana | 1,050 | 2,505 | 30 | 70 |
| Nebraska | 2,579 | 3,861 | 40 | 60 |
| Nevada | 3,363 | 4,188 | 45 | 55 |
| New Hampshire | 844 | 898 | 48 | 52 |
| New Jersey | 26,925 | 29,398 | 48 | 52 |
| New Mexico | 5,914 | 15,661 | 27 | 73 |
| New York | 153,104 | 167,164 | 48 | 52 |
| North Carolina | 10,271 | 20,321 | 34 | 66 |
| North Dakota | 1,096 | 2,063 | 35 | 65 |
| Ohio | 16,822 | 28,835 | 37 | 63 |
| Oklahoma | 4,747 | 10,595 | 31 | 69 |
| Oregon | 9,383 | 16,352 | 36 | 64 |
| Pennsylvania | 27,774 | 35,814 | 44 | 56 |
| Rhode Island | 4,567 | 5,663 | 45 | 55 |
| South Carolina | 1,790 | 4,598 | 28 | 72 |
| South Dakota | 1,143 | 1,882 | 38 | 62 |
| Tennessee | 866 | 1,688 | 34 | 66 |
| Texas | 10,132 | 16,949 | 37 | 63 |
| Utah | 124 | 339 | 27 | 73 |
| Vermont | 1,988 | 3,135 | 39 | 61 |
| Virginia | 6,358 | 6,942 | 48 | 52 |
| Washington | 34,381 | 39,868 | 46 | 54 |
| West Virginia | 5,319 | 16,662 | 24 | 76 |
| Wisconsin | 5,737 | 8,459 | 40 | 60 |
| Wyoming | 2,337 | 2,486 | 48 | 52 |
| State | SA Treatment Users | Total Expenditures (in $ thousands) | ||||||||
| Total | FFS Medicaid | % FFS | Medicaid ManagedCare | % Managed Care | Total | FFS Medicaid | % FFS | Medicaid ManagedCare | % Managed Care | |
| Total | 574,557 | 363,421 | 63 | 211,136 | 37 | 3,290,465 | 2,079,862 | 63 | 1,210,603 | 37 |
| Alabama | 6,340 | 6,340 | 100 | 0 | 0 | 8,952 | 8,952 | 100 | 0 | 0 |
| Alaska | 1,618 | 1,618 | 100 | 0 | 0 | 2,917 | 2,917 | 100 | 0 | 0 |
| Arizona | 14,562 | 2,596 | 18 | 11,966 | 82 | 65,647 | 16,495 | 25 | 49,152 | 75 |
| Arkansas | 3,758 | 3,758 | 100 | 0 | 0 | 3,149 | 3,149 | 100 | 0 | 0 |
| California | 56,202 | 27,749 | 49 | 28,453 | 51 | 119,312 | 34,677 | 29 | 84,634 | 71 |
| Colorado | 10,893 | 5,870 | 54 | 5,023 | 46 | 49,677 | 26,626 | 54 | 23,051 | 46 |
| Connecticut | 6,141 | 6,033 | 98 | 108 | 2 | 36,986 | 36,184 | 98 | 802 | 2 |
| Delaware | 2,015 | 633 | 31 | 1,382 | 69 | 12,612 | 6,886 | 55 | 5,726 | 45 |
| District of Columbia | 4,260 | 2,545 | 60 | 1,715 | 40 | 48,960 | 45,781 | 94 | 3,179 | 6 |
| Florida | 26,206 | 19,035 | 73 | 7,171 | 27 | 171,389 | 118,812 | 69 | 52,577 | 31 |
| Georgia | 15,891 | 11,039 | 69 | 4,852 | 31 | 83,603 | 65,265 | 78 | 18,338 | 22 |
| Hawaii | 3,024 | 1,525 | 50 | 1,499 | 50 | 12,419 | 7,030 | 57 | 5,388 | 43 |
| Idaho | 1,545 | 1,545 | 100 | 0 | 0 | 7,544 | 7,544 | 100 | 0 | 0 |
| Illinois | 22,064 | 21,530 | 98 | 534 | 2 | 169,715 | 167,340 | 99 | 2,374 | 1 |
| Indiana | 10,669 | 6,468 | 61 | 4,201 | 39 | 50,043 | 35,674 | 71 | 14,369 | 29 |
| Iowa | 6,712 | 3,866 | 58 | 2,846 | 42 | 29,244 | 14,520 | 50 | 14,724 | 50 |
| Kansas | 5,408 | 3,020 | 56 | 2,388 | 44 | 34,231 | 20,819 | 61 | 13,412 | 39 |
| Kentucky | 10,727 | 10,727 | 100 | 0 | 0 | 67,966 | 67,966 | 100 | 0 | 0 |
| Louisiana | 8,983 | 8,983 | 100 | 0 | 0 | 28,907 | 28,907 | 100 | 0 | 0 |
| Maine | 3,954 | 3,954 | 100 | 0 | 0 | 20,862 | 20,862 | 100 | 0 | 0 |
| Maryland | 11,885 | 6,078 | 51 | 5,807 | 49 | 75,712 | 44,889 | 59 | 30,823 | 41 |
| Massachusetts | 17,860 | 12,724 | 71 | 5,136 | 29 | 114,745 | 80,284 | 70 | 34,461 | 30 |
| Michigan | 21,863 | 8,483 | 39 | 13,380 | 61 | 110,940 | 42,324 | 38 | 68,616 | 62 |
| Minnesota | 11,350 | 8,301 | 73 | 3,049 | 27 | 52,948 | 39,615 | 75 | 13,333 | 25 |
| Mississippi | 6,559 | 6,559 | 100 | 0 | 0 | 23,771 | 23,771 | 100 | 0 | 0 |
| Missouri | 9,785 | 7,781 | 80 | 2,004 | 20 | 25,229 | 19,980 | 79 | 5,248 | 21 |
| Montana | 2,037 | 2,037 | 100 | 0 | 0 | 6,869 | 6,869 | 100 | 0 | 0 |
| Nebraska | 3,122 | 1,834 | 59 | 1,288 | 41 | 17,414 | 10,204 | 59 | 7,211 | 41 |
| Nevada | 2,611 | 2,013 | 77 | 598 | 23 | 14,102 | 11,931 | 85 | 2,171 | 15 |
| New Hampshire | 1,732 | 1,732 | 100 | 0 | 0 | 5,838 | 5,838 | 100 | 0 | 0 |
| New Jersey | 11,361 | 5,039 | 44 | 6,322 | 56 | 73,270 | 32,176 | 44 | 41,094 | 56 |
| New Mexico | 5,365 | 2,562 | 48 | 2,803 | 52 | 23,924 | 9,915 | 41 | 14,009 | 59 |
| New York | 59,280 | 32,680 | 55 | 26,600 | 45 | 684,441 | 402,880 | 59 | 281,561 | 41 |
| North Carolina | 20,856 | 20,856 | 100 | 0 | 0 | 89,067 | 89,067 | 100 | 0 | 0 |
| North Dakota | 985 | 985 | 100 | 0 | 0 | 5,363 | 5,363 | 100 | 0 | 0 |
| Ohio | 31,145 | 13,437 | 43 | 17,708 | 57 | 168,405 | 67,255 | 40 | 101,150 | 60 |
| Oklahoma | 8,412 | 8,412 | 100 | 0 | 0 | 33,142 | 33,142 | 100 | 0 | 0 |
| Oregon | 4,864 | 2,185 | 45 | 2,679 | 55 | 27,881 | 10,597 | 38 | 17,284 | 62 |
| Pennsylvania | 29,915 | 9,774 | 33 | 20,141 | 67 | 179,308 | 58,521 | 33 | 120,787 | 67 |
| Rhode Island | 2,395 | 1,477 | 62 | 918 | 38 | 5,560 | 2,339 | 42 | 3,221 | 58 |
| South Carolina | 8,188 | 6,855 | 84 | 1,333 | 16 | 56,063 | 46,513 | 83 | 9,550 | 17 |
| South Dakota | 1,252 | 1,252 | 100 | 0 | 0 | 4,951 | 4,951 | 100 | 0 | 0 |
| Tennessee | 14,054 | 9,503 | 68 | 4,551 | 32 | 35,391 | 22,265 | 63 | 13,126 | 37 |
| Texas | 18,626 | 11,545 | 62 | 7,081 | 38 | 151,566 | 88,191 | 58 | 63,374 | 42 |
| Utah | 1,965 | 1,965 | 100 | 0 | 0 | 8,899 | 8,899 | 100 | 0 | 0 |
| Vermont | 1,656 | 1,656 | 100 | 0 | 0 | 7,257 | 7,257 | 100 | 0 | 0 |
| Virginia | 11,853 | 6,889 | 58 | 4,964 | 42 | 75,429 | 42,186 | 56 | 33,243 | 44 |
| Washington | 15,421 | 7,840 | 51 | 7,581 | 49 | 114,977 | 68,475 | 60 | 46,502 | 40 |
| West Virginia | 6,373 | 4,708 | 74 | 1,665 | 26 | 18,674 | 15,545 | 83 | 3,129 | 17 |
| Wisconsin | 10,114 | 6,724 | 66 | 3,390 | 34 | 50,824 | 37,842 | 74 | 12,983 | 26 |
| Wyoming | 701 | 701 | 100 | 0 | 0 | 4,369 | 4,369 | 100 | 0 | 0 |
| State | Total Expenditures (in $ thousands) | % Attributable to State | % Attributable to Federal | |
| Total State | Total Federal | |||
| Total | 1,367,057 | 1,923,408 | 42 | 58 |
| Alabama | 2,697 | 6,255 | 30 | 70 |
| Alaska | 1,341 | 1,576 | 46 | 54 |
| Arizona | 20,743 | 44,904 | 32 | 68 |
| Arkansas | 803 | 2,346 | 26 | 74 |
| California | 56,199 | 63,113 | 47 | 53 |
| Colorado | 23,748 | 25,929 | 48 | 52 |
| Connecticut | 17,551 | 19,435 | 47 | 53 |
| Delaware | 5,985 | 6,627 | 47 | 53 |
| District of Columbia | 13,748 | 35,212 | 28 | 72 |
| Florida | 69,357 | 102,032 | 40 | 60 |
| Georgia | 28,688 | 54,914 | 34 | 66 |
| Hawaii | 5,103 | 7,316 | 41 | 59 |
| Idaho | 2,113 | 5,431 | 28 | 72 |
| Illinois | 80,411 | 89,304 | 47 | 53 |
| Indiana | 17,352 | 32,691 | 35 | 65 |
| Iowa | 10,673 | 18,571 | 36 | 64 |
| Kansas | 13,301 | 20,930 | 39 | 61 |
| Kentucky | 19,177 | 48,789 | 28 | 72 |
| Louisiana | 7,413 | 21,494 | 26 | 74 |
| Maine | 7,180 | 13,682 | 34 | 66 |
| Maryland | 36,194 | 39,518 | 48 | 52 |
| Massachusetts | 54,854 | 59,891 | 48 | 52 |
| Michigan | 43,300 | 67,640 | 39 | 61 |
| Minnesota | 25,125 | 27,823 | 47 | 53 |
| Mississippi | 5,200 | 18,570 | 22 | 78 |
| Missouri | 8,925 | 16,304 | 35 | 65 |
| Montana | 2,029 | 4,841 | 30 | 70 |
| Nebraska | 6,974 | 10,440 | 40 | 60 |
| Nevada | 6,281 | 7,821 | 45 | 55 |
| New Hampshire | 2,828 | 3,009 | 48 | 52 |
| New Jersey | 35,027 | 38,243 | 48 | 52 |
| New Mexico | 6,558 | 17,367 | 27 | 73 |
| New York | 327,197 | 357,244 | 48 | 52 |
| North Carolina | 29,904 | 59,163 | 34 | 66 |
| North Dakota | 1,861 | 3,502 | 35 | 65 |
| Ohio | 62,049 | 106,356 | 37 | 63 |
| Oklahoma | 10,254 | 22,888 | 31 | 69 |
| Oregon | 10,165 | 17,716 | 36 | 64 |
| Pennsylvania | 78,317 | 100,991 | 44 | 56 |
| Rhode Island | 2,482 | 3,078 | 45 | 55 |
| South Carolina | 15,709 | 40,354 | 28 | 72 |
| South Dakota | 1,871 | 3,080 | 38 | 62 |
| Tennessee | 11,999 | 23,392 | 34 | 66 |
| Texas | 56,705 | 94,861 | 37 | 63 |
| Utah | 2,387 | 6,512 | 27 | 73 |
| Vermont | 2,816 | 4,441 | 39 | 61 |
| Virginia | 36,059 | 39,370 | 48 | 52 |
| Washington | 53,240 | 61,737 | 46 | 54 |
| West Virginia | 4,519 | 14,155 | 24 | 76 |
| Wisconsin | 20,528 | 30,296 | 40 | 60 |
| Wyoming | 2,117 | 2,252 | 48 | 52 |
| State | Total | Source of Identification | |||||
| Core SA Treatment Service | Fetus Affected by Alcoholor Drug | Poisoning or Toxic Effects of Alcoholor Drugs | Other Medical Conditions Attributable to SA | MH Primary Diagnosis with SecondarySA Diagnosis | Non-MH Primary Diagnosis with SecondarySA Diagnosis | ||
| Total | 1,716,795 | 1,138,247 | 31,357 | 18,487 | 37,573 | 159,778 | 331,353 |
| NR = Not Reported. Cells representing fewer than 11 users are not reported to protect confidentiality. These users are excluded from the column totals for the respective state. | |||||||
| Alabama | 14,938 | 8,493 | 198 | 1,321 | 303 | 674 | 3,949 |
| Alaska | 5,047 | 3,175 | 272 | 18 | 104 | 700 | 778 |
| Arizona | 37,233 | 23,162 | 943 | 534 | 723 | 3,579 | 8,292 |
| Arkansas | 8,572 | 3,537 | 248 | 71 | 280 | 1,962 | 2,474 |
| California | 189,267 | 134,099 | 3,562 | 1,802 | 5,859 | 13,106 | 30,839 |
| Colorado | 32,609 | 21,432 | 710 | 247 | 623 | 3,128 | 6,469 |
| Connecticut | 24,527 | 17,916 | 170 | 17 | 312 | 3,577 | 2,535 |
| Delaware | 6,191 | 4,186 | 135 | 62 | 124 | 484 | 1,200 |
| District of Columbia | 8,640 | 5,206 | 94 | 59 | 125 | 1,003 | 2,153 |
| Florida | 57,232 | 29,334 | 1,340 | 3,303 | 1,541 | 2,716 | 18,998 |
| Georgia | 30,600 | 14,561 | 1,058 | 431 | 880 | 3,064 | 10,174 |
| Hawaii | 8,340 | 5,261 | 100 | 111 | 148 | 984 | 1,736 |
| Idaho | 3,702 | 1,841 | 119 | 26 | 140 | 603 | 973 |
| Illinois | 54,612 | 34,142 | 890 | 571 | 1,546 | 5,529 | 11,934 |
| Indiana | 32,975 | 18,501 | 867 | 319 | 580 | 6,266 | 6,442 |
| Iowa | 12,710 | 5,860 | 397 | 165 | 374 | 1,488 | 4,426 |
| Kansas | 11,584 | 5,665 | 214 | 121 | 362 | 1,766 | 3,465 |
| Kentucky | 23,330 | 12,889 | 341 | 1,779 | 342 | 2,550 | 5,429 |
| Louisiana | 18,020 | 7,540 | 686 | 25 | 504 | 3,761 | 5,504 |
| Maine | 17,183 | 12,966 | 171 | 146 | 199 | 1,509 | 2,192 |
| Maryland | 37,827 | 22,766 | 688 | 316 | 689 | 6,538 | 6,830 |
| Massachusetts | 63,425 | 49,135 | 1,468 | 86 | 1,156 | 4,381 | 7,199 |
| Michigan | 53,626 | 32,558 | 1,255 | 629 | 1,188 | 5,471 | 12,525 |
| Minnesota | 30,087 | 16,732 | 1,151 | 210 | 518 | 6,017 | 5,459 |
| Mississippi | 14,969 | 8,388 | 156 | 324 | 269 | 2,249 | 3,583 |
| Missouri | 37,641 | 26,469 | 287 | 98 | 726 | 4,798 | 5,263 |
| Montana | 4,712 | 2,692 | 102 | 16 | 153 | 604 | 1,145 |
| Nebraska | 8,772 | 5,497 | 187 | 87 | 184 | 871 | 1,946 |
| Nevada | 6,426 | 3,408 | 315 | 50 | 143 | 768 | 1,742 |
| New Hampshire | 4,802 | 3,339 | 136 | NR | 83 | 365 | 879 |
| New Jersey | 41,136 | 28,208 | 887 | 306 | 682 | 5,352 | 5,701 |
| New Mexico | 16,257 | 10,245 | 386 | 165 | 388 | 1,824 | 3,249 |
| New York | 296,061 | 246,207 | 2,140 | 1,123 | 2,961 | 13,846 | 29,784 |
| North Carolina | 47,626 | 25,568 | 1,250 | 63 | 1,329 | 7,042 | 12,374 |
| North Dakota | 2,808 | 1,736 | 11 | NR | 35 | 492 | 534 |
| Ohio | 105,134 | 75,981 | 1,333 | 631 | 2,020 | 7,558 | 17,611 |
| Oklahoma | 15,749 | 6,366 | 273 | 46 | 433 | 2,645 | 5,986 |
| Oregon | 10,948 | 5,653 | 319 | 134 | 343 | 1,695 | 2,804 |
| Pennsylvania | 77,463 | 47,470 | 1,344 | 750 | 1,725 | 8,243 | 17,931 |
| Rhode Island | 9,633 | 7,209 | 154 | 59 | 104 | 1,050 | 1,057 |
| South Carolina | 19,769 | 12,353 | 232 | 24 | 462 | 1,425 | 5,273 |
| South Dakota | 2,931 | 1,398 | 88 | 12 | 106 | 479 | 848 |
| Tennessee | 22,914 | 9,930 | 870 | 143 | 600 | 1,163 | 10,208 |
| Texas | 39,607 | 17,077 | 1,224 | 93 | 3,325 | 3,527 | 14,361 |
| Utah | 6,124 | 4,506 | 57 | 27 | 103 | 239 | 1,192 |
| Vermont | 9,526 | 8,375 | 231 | NR | 95 | 212 | 613 |
| Virginia | 21,448 | 9,329 | 598 | 914 | 640 | 2,389 | 7,578 |
| Washington | 65,731 | 50,986 | 998 | 402 | 1,195 | 3,958 | 8,192 |
| West Virginia | 17,149 | 10,925 | 212 | 51 | 298 | 2,469 | 3,194 |
| Wisconsin | 27,210 | 16,704 | 460 | 581 | 485 | 3,367 | 5,613 |
| Wyoming | 1,954 | 1,271 | 22 | NR | 59 | 190 | 412 |
APPENDIX D. STATE LEVEL PROJECTIONS, FY 2011
| State | Expenditures (in $ thousands) | % Attributable to State | % Attributable to Federal | ||
| Total | State | Federal | |||
| Total | 3,951,517 | 1,533,874 | 2,417,643 | 39 | 61 |
| Alabama | 10,635 | 2,792 | 7,843 | 26 | 74 |
| Alaska | 9,112 | 3,879 | 5,233 | 43 | 57 |
| Arizona | 161,075 | 45,866 | 115,209 | 28 | 72 |
| Arkansas | 5,848 | 1,356 | 4,492 | 23 | 77 |
| California | 419,497 | 181,181 | 238,316 | 43 | 57 |
| Colorado | 73,146 | 31,592 | 41,555 | 43 | 57 |
| Connecticut | 92,543 | 39,969 | 52,574 | 43 | 57 |
| Delaware | 13,563 | 5,468 | 8,095 | 40 | 60 |
| District of Columbia | 16,424 | 4,092 | 12,332 | 25 | 75 |
| Florida | 50,238 | 18,735 | 31,503 | 37 | 63 |
| Georgia | 22,092 | 6,447 | 15,645 | 29 | 71 |
| Hawaii | 9,204 | 3,537 | 5,667 | 38 | 62 |
| Idaho | 3,402 | 860 | 2,542 | 25 | 75 |
| Illinois | 113,731 | 48,822 | 64,909 | 43 | 57 |
| Indiana | 32,318 | 9,080 | 23,238 | 28 | 72 |
| Iowa | 10,809 | 3,442 | 7,367 | 32 | 68 |
| Kansas | 19,383 | 6,763 | 12,620 | 35 | 65 |
| Kentucky | 39,941 | 9,408 | 30,533 | 24 | 76 |
| Louisiana | 11,367 | 2,827 | 8,540 | 25 | 75 |
| Maine | 55,107 | 16,416 | 38,691 | 30 | 70 |
| Maryland | 86,835 | 37,504 | 49,331 | 43 | 57 |
| Massachusetts | 107,899 | 46,602 | 61,297 | 43 | 57 |
| Michigan | 82,430 | 23,707 | 58,723 | 29 | 71 |
| Minnesota | 61,250 | 26,454 | 34,796 | 43 | 57 |
| Mississippi | 21,941 | 4,291 | 17,650 | 20 | 80 |
| Missouri | 73,865 | 22,335 | 51,530 | 30 | 70 |
| Montana | 7,579 | 2,023 | 5,556 | 27 | 73 |
| Nebraska | 16,073 | 5,749 | 10,325 | 36 | 64 |
| Nevada | 11,117 | 4,562 | 6,555 | 41 | 59 |
| New Hampshire | 7,443 | 3,215 | 4,228 | 43 | 57 |
| New Jersey | 85,771 | 37,044 | 48,726 | 43 | 57 |
| New Mexico | 36,014 | 8,669 | 27,345 | 24 | 76 |
| New York | 1,331,535 | 575,090 | 756,445 | 43 | 57 |
| North Carolina | 52,954 | 15,606 | 37,349 | 29 | 71 |
| North Dakota | 4,306 | 1,484 | 2,823 | 34 | 66 |
| Ohio | 203,518 | 62,439 | 141,079 | 31 | 69 |
| Oklahoma | 11,043 | 3,104 | 7,939 | 28 | 72 |
| Oregon | 60,165 | 18,920 | 41,245 | 31 | 69 |
| Pennsylvania | 127,838 | 48,626 | 79,211 | 38 | 62 |
| Rhode Island | 27,916 | 11,300 | 16,616 | 40 | 60 |
| South Carolina | 20,426 | 5,044 | 15,382 | 25 | 75 |
| South Dakota | 6,257 | 2,064 | 4,193 | 33 | 67 |
| Tennessee | 17,477 | 5,017 | 12,460 | 29 | 71 |
| Texas | 29,501 | 9,895 | 19,607 | 34 | 66 |
| Utah | 7,856 | 1,848 | 6,009 | 24 | 76 |
| Vermont | 21,806 | 7,576 | 14,231 | 35 | 65 |
| Virginia | 21,695 | 9,370 | 12,325 | 43 | 57 |
| Washington | 166,909 | 70,402 | 96,507 | 42 | 58 |
| West Virginia | 26,857 | 5,717 | 21,140 | 21 | 79 |
| Wisconsin | 43,947 | 14,886 | 29,061 | 34 | 66 |
| Wyoming | 1,859 | 803 | 1,056 | 43 | 57 |
| State | Expenditures (in $ thousands) | % Attributable to State | % Attributable to Federal | ||
| Total | State | Federal | |||
| Total | 98,236 | 36,496 | 61,740 | 37 | 63 |
| Alabama | 637 | 167 | 470 | 26 | 74 |
| Alaska | 1,050 | 447 | 603 | 43 | 57 |
| Arizona | 1,999 | 569 | 1,430 | 28 | 72 |
| Arkansas | 325 | 75 | 249 | 23 | 77 |
| California | 6,790 | 2,933 | 3,858 | 43 | 57 |
| Colorado | 2,313 | 999 | 1,314 | 43 | 57 |
| Connecticut | 613 | 265 | 348 | 43 | 57 |
| Delaware | 239 | 96 | 142 | 40 | 60 |
| District of Columbia | 421 | 105 | 316 | 25 | 75 |
| Florida | 15,658 | 5,839 | 9,819 | 37 | 63 |
| Georgia | 1,275 | 372 | 903 | 29 | 71 |
| Hawaii | 222 | 85 | 137 | 38 | 62 |
| Idaho | 175 | 44 | 131 | 25 | 75 |
| Illinois | 1,275 | 547 | 728 | 43 | 57 |
| Indiana | 1,296 | 364 | 932 | 28 | 72 |
| Iowa | 739 | 235 | 503 | 32 | 68 |
| Kansas | 548 | 191 | 357 | 35 | 65 |
| Kentucky | 6,142 | 1,447 | 4,696 | 24 | 76 |
| Louisiana | 493 | 123 | 371 | 25 | 75 |
| Maine | 531 | 158 | 373 | 30 | 70 |
| Maryland | 2,849 | 1,231 | 1,619 | 43 | 57 |
| Massachusetts | 5,516 | 2,383 | 3,134 | 43 | 57 |
| Michigan | 1,970 | 567 | 1,403 | 29 | 71 |
| Minnesota | 10,591 | 4,574 | 6,017 | 43 | 57 |
| Mississippi | 340 | 67 | 274 | 20 | 80 |
| Missouri | 358 | 108 | 250 | 30 | 70 |
| Montana | 109 | 29 | 80 | 27 | 73 |
| Nebraska | 263 | 94 | 169 | 36 | 64 |
| Nevada | 506 | 208 | 299 | 41 | 59 |
| New Hampshire | 641 | 277 | 364 | 43 | 57 |
| New Jersey | 3,014 | 1,302 | 1,712 | 43 | 57 |
| New Mexico | 1,015 | 244 | 771 | 24 | 76 |
| New York | 6,749 | 2,915 | 3,834 | 43 | 57 |
| North Carolina | 875 | 258 | 617 | 29 | 71 |
| North Dakota | 20 | 7 | 13 | 34 | 66 |
| Ohio | 3,347 | 1,027 | 2,320 | 31 | 69 |
| Oklahoma | 190 | 53 | 136 | 28 | 72 |
| Oregon | 949 | 298 | 651 | 31 | 69 |
| Pennsylvania | 3,642 | 1,385 | 2,257 | 38 | 62 |
| Rhode Island | 320 | 129 | 190 | 40 | 60 |
| South Carolina | 294 | 73 | 221 | 25 | 75 |
| South Dakota | 68 | 22 | 46 | 33 | 67 |
| Tennessee | 1,580 | 454 | 1,126 | 29 | 71 |
| Texas | 2,496 | 837 | 1,659 | 34 | 66 |
| Utah | 319 | 75 | 244 | 24 | 76 |
| Vermont | 269 | 93 | 175 | 35 | 65 |
| Virginia | 1,343 | 580 | 763 | 43 | 57 |
| Washington | 2,307 | 973 | 1,334 | 42 | 58 |
| West Virginia | 278 | 59 | 218 | 21 | 79 |
| Wisconsin | 3,258 | 1,104 | 2,155 | 34 | 66 |
| Wyoming | 17 | 7 | 9 | 43 | 57 |
| State | Expenditures (in $ thousands) | % Attributable to State | % Attributable to Federal | ||
| Total | State | Federal | |||
| Total | 291,703 | 108,750 | 182,953 | 37 | 63 |
| Alabama | 397 | 104 | 293 | 26 | 74 |
| Alaska | 764 | 325 | 439 | 43 | 57 |
| Arizona | 4,573 | 1,302 | 3,271 | 28 | 72 |
| Arkansas | 1,146 | 266 | 880 | 23 | 77 |
| California | 47,412 | 20,477 | 26,934 | 43 | 57 |
| Colorado | 5,030 | 2,173 | 2,858 | 43 | 57 |
| Connecticut | 2,481 | 1,072 | 1,410 | 43 | 57 |
| Delaware | 968 | 390 | 578 | 40 | 60 |
| District of Columbia | 1,993 | 497 | 1,496 | 25 | 75 |
| Florida | 6,382 | 2,380 | 4,002 | 37 | 63 |
| Georgia | 4,937 | 1,441 | 3,496 | 29 | 71 |
| Hawaii | 483 | 185 | 297 | 38 | 62 |
| Idaho | 776 | 196 | 580 | 25 | 75 |
| Illinois | 15,166 | 6,511 | 8,656 | 43 | 57 |
| Indiana | 3,586 | 1,008 | 2,579 | 28 | 72 |
| Iowa | 2,428 | 773 | 1,655 | 32 | 68 |
| Kansas | 3,568 | 1,245 | 2,323 | 35 | 65 |
| Kentucky | 848 | 200 | 648 | 24 | 76 |
| Louisiana | 3,439 | 855 | 2,584 | 25 | 75 |
| Maine | 1,499 | 447 | 1,053 | 30 | 70 |
| Maryland | 6,895 | 2,978 | 3,917 | 43 | 57 |
| Massachusetts | 8,541 | 3,689 | 4,852 | 43 | 57 |
| Michigan | 10,397 | 2,990 | 7,407 | 29 | 71 |
| Minnesota | 5,713 | 2,467 | 3,245 | 43 | 57 |
| Mississippi | 1,560 | 305 | 1,255 | 20 | 80 |
| Missouri | 3,957 | 1,197 | 2,761 | 30 | 70 |
| Montana | 1,069 | 285 | 783 | 27 | 73 |
| Nebraska | 1,296 | 464 | 833 | 36 | 64 |
| Nevada | 1,325 | 544 | 781 | 41 | 59 |
| New Hampshire | 445 | 192 | 253 | 43 | 57 |
| New Jersey | 5,015 | 2,166 | 2,849 | 43 | 57 |
| New Mexico | 2,293 | 552 | 1,741 | 24 | 76 |
| New York | 36,190 | 15,631 | 20,560 | 43 | 57 |
| North Carolina | 6,400 | 1,886 | 4,514 | 29 | 71 |
| North Dakota | 406 | 140 | 266 | 34 | 66 |
| Ohio | 15,584 | 4,781 | 10,803 | 31 | 69 |
| Oklahoma | 3,056 | 859 | 2,197 | 28 | 72 |
| Oregon | 3,317 | 1,043 | 2,274 | 31 | 69 |
| Pennsylvania | 15,875 | 6,039 | 9,837 | 38 | 62 |
| Rhode Island | 1,407 | 569 | 837 | 40 | 60 |
| South Carolina | 3,056 | 755 | 2,301 | 25 | 75 |
| South Dakota | 727 | 240 | 487 | 33 | 67 |
| Tennessee | 3,394 | 974 | 2,420 | 29 | 71 |
| Texas | 24,491 | 8,214 | 16,277 | 34 | 66 |
| Utah | 1,063 | 250 | 813 | 24 | 76 |
| Vermont | 311 | 108 | 203 | 35 | 65 |
| Virginia | 3,254 | 1,405 | 1,849 | 43 | 57 |
| Washington | 8,183 | 3,452 | 4,731 | 42 | 58 |
| West Virginia | 1,762 | 375 | 1,387 | 21 | 79 |
| Wisconsin | 6,461 | 2,189 | 4,273 | 34 | 66 |
| Wyoming | 385 | 166 | 219 | 43 | 57 |
| State | Expenditures (in $ thousands) | % Attributable to State | % Attributable to Federal | ||
| Total | State | Federal | |||
| Total | 1,586,344 | 598,637 | 987,707 | 38 | 62 |
| Alabama | 1,528 | 401 | 1,127 | 26 | 74 |
| Alaska | 7,787 | 3,315 | 4,472 | 43 | 57 |
| Arizona | 21,894 | 6,234 | 15,659 | 28 | 72 |
| Arkansas | 12,252 | 2,841 | 9,411 | 23 | 77 |
| California | 78,013 | 33,694 | 44,319 | 43 | 57 |
| Colorado | 48,716 | 21,040 | 27,675 | 43 | 57 |
| Connecticut | 43,503 | 18,789 | 24,714 | 43 | 57 |
| Delaware | 3,684 | 1,485 | 2,199 | 40 | 60 |
| District of Columbia | 20,697 | 5,157 | 15,540 | 25 | 75 |
| Florida | 15,841 | 5,908 | 9,934 | 37 | 63 |
| Georgia | 13,669 | 3,989 | 9,680 | 29 | 71 |
| Hawaii | 3,735 | 1,435 | 2,300 | 38 | 62 |
| Idaho | 4,108 | 1,039 | 3,069 | 25 | 75 |
| Illinois | 70,014 | 30,055 | 39,959 | 43 | 57 |
| Indiana | 34,794 | 9,775 | 25,018 | 28 | 72 |
| Iowa | 8,815 | 2,807 | 6,008 | 32 | 68 |
| Kansas | 12,105 | 4,224 | 7,882 | 35 | 65 |
| Kentucky | 13,594 | 3,202 | 10,392 | 24 | 76 |
| Louisiana | 13,951 | 3,470 | 10,481 | 25 | 75 |
| Maine | 27,464 | 8,182 | 19,283 | 30 | 70 |
| Maryland | 93,516 | 40,389 | 53,126 | 43 | 57 |
| Massachusetts | 35,704 | 15,421 | 20,284 | 43 | 57 |
| Michigan | 40,099 | 11,533 | 28,567 | 29 | 71 |
| Minnesota | 48,642 | 21,008 | 27,633 | 43 | 57 |
| Mississippi | 23,396 | 4,576 | 18,821 | 20 | 80 |
| Missouri | 35,988 | 10,882 | 25,106 | 30 | 70 |
| Montana | 4,026 | 1,074 | 2,952 | 27 | 73 |
| Nebraska | 6,367 | 2,277 | 4,090 | 36 | 64 |
| Nevada | 8,364 | 3,432 | 4,932 | 41 | 59 |
| New Hampshire | 1,760 | 760 | 1,000 | 43 | 57 |
| New Jersey | 59,312 | 25,617 | 33,695 | 43 | 57 |
| New Mexico | 21,889 | 5,269 | 16,620 | 24 | 76 |
| New York | 334,403 | 144,429 | 189,974 | 43 | 57 |
| North Carolina | 29,894 | 8,810 | 21,084 | 29 | 71 |
| North Dakota | 3,880 | 1,337 | 2,543 | 34 | 66 |
| Ohio | 52,883 | 16,224 | 36,658 | 31 | 69 |
| Oklahoma | 16,519 | 4,643 | 11,877 | 28 | 72 |
| Oregon | 32,342 | 10,171 | 22,171 | 31 | 69 |
| Pennsylvania | 74,367 | 28,287 | 46,080 | 38 | 62 |
| Rhode Island | 11,097 | 4,492 | 6,605 | 40 | 60 |
| South Carolina | 6,887 | 1,701 | 5,187 | 25 | 75 |
| South Dakota | 3,210 | 1,059 | 2,151 | 33 | 67 |
| Tennessee | 2,675 | 768 | 1,907 | 29 | 71 |
| Texas | 32,925 | 11,043 | 21,882 | 34 | 66 |
| Utah | 498 | 117 | 381 | 24 | 76 |
| Vermont | 5,590 | 1,942 | 3,648 | 35 | 65 |
| Virginia | 15,931 | 6,880 | 9,050 | 43 | 57 |
| Washington | 81,123 | 34,218 | 46,905 | 42 | 58 |
| West Virginia | 24,629 | 5,242 | 19,386 | 21 | 79 |
| Wisconsin | 17,405 | 5,895 | 11,509 | 34 | 66 |
| Wyoming | 4,859 | 2,099 | 2,760 | 43 | 57 |
| State | Expenditures (in $ thousands) | % Attributable to State | % Attributable to Federal | ||
| Total | State | Federal | |||
| Total | 3,659,241 | 1,349,365 | 2,309,876 | 37 | 63 |
| Alabama | 9,752 | 2,560 | 7,192 | 26 | 74 |
| Alaska | 3,807 | 1,621 | 2,186 | 43 | 57 |
| Arizona | 71,397 | 20,330 | 51,067 | 28 | 72 |
| Arkansas | 3,581 | 831 | 2,751 | 23 | 77 |
| California | 155,809 | 67,294 | 88,515 | 43 | 57 |
| Colorado | 62,696 | 27,078 | 35,617 | 43 | 57 |
| Connecticut | 43,035 | 18,587 | 24,448 | 43 | 57 |
| Delaware | 14,638 | 5,901 | 8,737 | 40 | 60 |
| District of Columbia | 66,679 | 16,613 | 50,066 | 25 | 75 |
| Florida | 198,955 | 74,195 | 124,760 | 37 | 63 |
| Georgia | 86,666 | 25,291 | 61,375 | 29 | 71 |
| Hawaii | 14,598 | 5,610 | 8,989 | 38 | 62 |
| Idaho | 8,936 | 2,260 | 6,676 | 25 | 75 |
| Illinois | 173,238 | 74,367 | 98,871 | 43 | 57 |
| Indiana | 51,116 | 14,361 | 36,755 | 28 | 72 |
| Iowa | 32,533 | 10,360 | 22,173 | 32 | 68 |
| Kansas | 37,841 | 13,203 | 24,638 | 35 | 65 |
| Kentucky | 74,532 | 17,556 | 56,976 | 24 | 76 |
| Louisiana | 28,853 | 7,177 | 21,677 | 25 | 75 |
| Maine | 20,151 | 6,003 | 14,148 | 30 | 70 |
| Maryland | 89,845 | 38,804 | 51,041 | 43 | 57 |
| Massachusetts | 127,036 | 54,867 | 72,169 | 43 | 57 |
| Michigan | 126,295 | 36,323 | 89,973 | 29 | 71 |
| Minnesota | 59,004 | 25,484 | 33,520 | 43 | 57 |
| Mississippi | 25,790 | 5,044 | 20,746 | 20 | 80 |
| Missouri | 26,617 | 8,048 | 18,568 | 30 | 70 |
| Montana | 7,780 | 2,076 | 5,704 | 27 | 73 |
| Nebraska | 17,217 | 6,158 | 11,059 | 36 | 64 |
| Nevada | 15,619 | 6,409 | 9,210 | 41 | 59 |
| New Hampshire | 5,894 | 2,546 | 3,348 | 43 | 57 |
| New Jersey | 77,158 | 33,325 | 43,834 | 43 | 57 |
| New Mexico | 24,272 | 5,843 | 18,429 | 24 | 76 |
| New York | 714,649 | 308,657 | 405,992 | 43 | 57 |
| North Carolina | 87,035 | 25,649 | 61,386 | 29 | 71 |
| North Dakota | 6,585 | 2,268 | 4,316 | 34 | 66 |
| Ohio | 195,056 | 59,843 | 135,213 | 31 | 69 |
| Oklahoma | 35,687 | 10,030 | 25,657 | 28 | 72 |
| Oregon | 35,039 | 11,019 | 24,020 | 31 | 69 |
| Pennsylvania | 209,702 | 79,765 | 129,937 | 38 | 62 |
| Rhode Island | 6,031 | 2,441 | 3,590 | 40 | 60 |
| South Carolina | 60,448 | 14,926 | 45,522 | 25 | 75 |
| South Dakota | 5,254 | 1,733 | 3,521 | 33 | 67 |
| Tennessee | 37,071 | 10,642 | 26,429 | 29 | 71 |
| Texas | 184,274 | 61,806 | 122,469 | 34 | 66 |
| Utah | 9,574 | 2,252 | 7,323 | 24 | 76 |
| Vermont | 7,918 | 2,751 | 5,167 | 35 | 65 |
| Virginia | 90,353 | 39,023 | 51,329 | 43 | 57 |
| Washington | 125,621 | 52,987 | 72,634 | 42 | 58 |
| West Virginia | 20,923 | 4,453 | 16,470 | 21 | 79 |
| Wisconsin | 62,276 | 21,094 | 41,181 | 34 | 66 |
| Wyoming | 4,402 | 1,901 | 2,501 | 43 | 57 |
APPENDIX E. STATE VARIATION IN SUBSTANCE ABUSE TREATMENT COVERAGE, NASADAD SURVEY RESULTS
| Study Category | Institutional Care: Acute Inpatient Care | Residential Treatment | Outpatient Treatment: Intensive Treatment Program | Outpatient Treatment: Other Screening/Intervention | Outpatient Treatment: Other Medication Management | Outpatient Treatment: Other Case Management | Outpatient Treatment: Detoxification; Other Counseling/ Therapy; Treatment Program Service | ||
| NASADAD Category | Medically Managed Intensive Inpatient Treatment | Short-Term Residential/ Inpatient | Long-Term Residential/ Inpatient | Intensive Outpatient/ Partial Hospitalization | Early Intervention | Crisis | Methadone Treatment | Case Management | Outpatient Treatment |
SOURCE: NASADAD Inquiry. State Medicaid and S-CHIP Coverage of Substance Abuse Services. Washington, DC. November 2010. NOTES: Inp = General Inpatient; Phys = Physician; Outp = Outpatient hospital, FQHC, and RHC; 21 = Psychiatric Facility Services for Children Under age 21; Prac = Other Licensed Practitioners, Rhb = Rehabilitation; Cl = Clinic; TCM = Targeted Case Management; HCB = Home and Community-Based Waiver Services; Under Waiver; Other; MH = mental health; SA = substance abuse.
| |||||||||
| Alabama | No | No | No | Rhb | No | Rhb | Rhb | No | Rhb |
| Alaska | Yes | Yes | N/A | N/A | Yes | N/A | Yes | N/A | Yes |
| Arizona | Under waiver | Under waiver (room & board not reimbursed) | Inp; 21; Inp-Detox Only; EPSDT1 | Under waiver | Under waiver | Under waiver | Under waiver | Under waiver | Under waiver |
| Arkansas1 | No | No | No | No | N/A | No | No | No | No |
| California | N/A | Inp; EPSDT | Inp; EPSDT | Rhb; Cl; EPSDT | No | Rhb; Cl; EPSDT | Cl | TCM; Rhb; Cl; EPSDT2 | Rhb; Cl; EPSDT |
| Colorado | No | 21; Inp-Detox Only | 21 | No | No | No | Phys; Cl; EPSDT | TCM; Cl; EPSDT; Prac | Phys; Rhb; Cl; 21; EPSDT; Prac; TCM |
| Connecticut | Yes | Yes-for children 21 | N/A | Yes | N/A | Yes | Yes | Yes | Yes |
| Delaware3 | No | Inp; Inp-Detox Only | 21 | Outp; Rhb; EPSDT; Under waiver | EPSDT; Phys | Outp; EPSDT | Rhb; Cl | Rhb; Provided by Div. Substance Abuse & Mental Health & Children Mental Health | Outp; Phys; Rhb; Cl; EPSDT; Prac; Under waiver |
| District of Columbia1 | No | No | No | No | N/A | No | No | No | No |
| Florida | N/A | 21; EPDST+ | No | Outp; Rhb; EPSDT; Cl; HCB; Prac; Phys | No | Cl | Phys; Rhb; Under waiver | TCM; Rhb; Cl | Phys; Rhb; Cl; EPSDT; Prac; TCM |
| Georgia | No | Yes | 21 | Rhb | No | Rhb | Rhb | No | Rhb |
| Hawaii | N/A | Yes | No | N/A | Rhb | N/A | N/A | N/A | Yes |
| Idaho | Inp | No | No | Rhb; Cl; Prac; Phys | No | No | No | Rhb; Cl | Phys; Rhb; Cl; Prac |
| Illinois | Yes | Yes | Yes | Cl | No | No | Rhb4 | No | Cl |
| Indiana | 21 | No | No | Outp; Rhb; Cl; Prac | No | Outp | Phys; Cl | No | Outp; Rhb; Cl; Prac |
| Iowa | Yes | Yes | Yes | Yes | Yes | Yes | Yes5 | Yes6 | Yes |
| Kansas | Inp | Under waiver | Yes | Rhb | No | Rhb | Rhb | Rhb | Rhb |
| Kentucky7 | No | No | No | No | No | No | No | TCM; Cl | No |
| Louisiana | No | No | No | No | No | No | No | No | No |
| Maine | N/A | No | No | Yes | N/A | N/A | N/A | N/A | Yes |
| Maryland | No | 21 | 21 | Yes | Yes | Yes | Yes | No | Yes |
| Massachusetts | Yes | No | No | Pregnant women only | Yes | Yes | Yes | Yes | Yes |
| Michigan | No | Inp | Inp | Cl; under waiver | Cl; Under waiver | No | Cl; Under waiver | No | Cl; Under waiver |
| Minnesota | Yes | Yes | N/A | Yes | N/A | N/A | Yes | Yes | Yes |
| Mississippi1 | No | No | No | No | No | No | No | No+ | No |
| Missouri | No | No | No | Rhb | No | No | Rhb | Rhb | Rhb |
| Montana | No | Rhb | Rhb | Rhb; Cl; Prac; Phys | Phys | No | No | TCM | Phys; Rhb; Cl; Prac; TCM |
| Nebraska | Inp; Under waiver | 21; Inp- Detox Only; EPDST; Under waiver+ | 21; EPSDT | Outp; Rhb; EPSDT; Cl; HCB; Prac; Phys; Under waiver | No | No | Phys; Rhb; Cl; Prac | TCM; Cl; EPSDT; Prac | Outp; Phys; Rhb; Cl; 21; EPSDT; Prac; Under waiver |
| Nevada8 | 21 | No | No | No | EPSDT | No | Yes | No | No |
| New Hampshire | No | No | No | No | No | No | No | No | No |
| New Jersey | Yes | No | No | Yes | Yes | Yes | Yes | Yes | Cl |
| New Mexico | Yes | Yes | Yes | Yes | N/A | N/A | N/A | N/A | Yes |
| New York | No | Inp; 21+ | No | Outp; Cl | In emergency department only | Outp; Cl | Phys; Cl | No | Outp; Cl |
| North Carolina | Inp | Medically monitored community residential treatment & non-medical community residential treatment-licensed facility | No | Outp; Rhb; Cl; Other-licensed facility | Rhb; Phys; Cl | Rhb; Cl; Mobile Crisis Management, Detox services, facility- based crisis services | Yes | Rhb | Phys; Rhb; Cl; Prac |
| North Dakota | Yes | N/A | N/A | Yes | N/A | Yes | N/A | N/A | Yes |
| Ohio | No | No | No | Rhb | No | Rhb | Rhb | Rhb+ | Rhb |
| Oklahoma | No | Inp-Detox Only9 | No | N/A | Yes | Outp; Rhb | No | TCM; Outp; Cl | Outp; Phys; Rhb; Cl; 21; EPSDT; Prac; TCM |
| Oregon10 | Yes | Yes | Yes | Outp; Rhb; EPSDT; Cl; HCB; Prac; Phys; Under waiver | EPSDT, Rhb; Cl; Phys; Under waiver | Yes | Must be a state- approved opiate treatment program | Yes | Outp; Phys; Rhb; Cl; 21; EPSDT; Prac; TCM; Under waiver |
| Pennsylvania | Inp; Under waiver | Yes | Yes | No | No | No | Under waiver | Under waiver | Cl; TCM |
| Rhode Island | Yes | Yes (no room & board) | No | Yes | N/A | Yes | Yes | Yes | Yes |
| South Carolina | Yes | Inp; Inp- Detox Only | Inp; Inp- Detox Only | Outp; Rhb | No | Outp; Rhb; TCM | No | TCM; Outp; Rhb | Outp; Phys; Rhb; Cl; 21; TCM |
| South Dakota | Yes | Yes | No | Yes | No | Yes | No | No | Yes |
| Tennessee | Yes | Yes | Yes (for 21 & SPMI) | Yes | N/A | Yes | Yes | Yes | Yes |
| Texas | No | No | No | EPSDT | No | No | Phys; Under waiver | No | EPSDT11 |
| Utah12 | No | N/A | N/A | N/A | N/A | N/A | N/A | N/A | Yes |
| Vermont | No | Under waiver; State plan | Other-State plan | Rhb; Under waiver | No | No | Rhb; Under waiver; State plan | TCM; Rhb; Under waiver; State plan | Rhb; Cl; Prac; TCM; Under waiver; State plan |
| Virginia | For pregnant women only | Inp; 21; EPDST | Inp; 21; EPSDT | Rhb; EPSDT; Cl; Prac; Phys | EPSDT, Rhb; Phys; Cl; Other- psychiatric services; MH clinic | Licensed SA outpatient program | Phys; Cl; Prac; Other- Opioid Treatment Services | Rhb; Qualified SA case manager not required to be part of an organizational unit that provides only case management | Phys; Cl; Prac; Other- Opioid Treatment Services |
| Washington13 | No | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes |
| West Virginia | N/A | N/A | N/A | N/A | N/A | N/A | No | Yes | No |
| Wisconsin | Inp | Inp; Inp-Detox Only (room & board not reimbursed) | No | Outp; Rhb; EPSDT; Cl; Prac; Phys | Cl; Phys; Other-ERs, hospitals, prenatal care coordination agencies, crisis intervention agencies | County-based agencies | Cl | TCM; CL; Other-County-based providers | Cl |
| Wyoming | Inp | Inp; Inp-Detox Only | Inp | Rhb | Rhb; Cl; Phys | No | Phys; Cl | TCM; EPSDT; Under waiver | Phys; Cl |
| State Has HMO/HIO | State Carves SA Out of HMOs/HIOs | State Includes SA Services in HMOs/HIOs | Notes on Managed Care Coverage of SA Services | Source of Managed Care Coverage Information | Known Data Quality Issues | |
| Alabama (AL) | X | X | Alabama has a maternity care Prepaid Inpatient Health Plan (PIHP) managed care program that is paid using capitation. This program does not include behavioral health services. | 2008 National Summary of State Medicaid Managed Care Programs -- page 1 | No significant issues. | |
| Alaska (AK) | NA | NA | NA | NA | 62.9% of enrollees indicated to have private health insurance coverage. Only 56.7% of claims in the OT file have a primary diagnosis code. | |
| Arizona (AZ) | X | X | State carves MH & SA services from the HMO, yet also has a BHO. | 2008 National Summary of State Medicaid Managed Care Programs -- page 205 | No significant issues. | |
| Arkansas (AR) | NA | NA | NA | NA | IP claims have a maximum of 2 DX codes only. 2.1% of records have no eligibility information. Identification of private insurance coverage is unreliable. | |
| California (CA) | X | X | X | CA has a statewide FFS MH plan covering specialty MH services for all that meet medical necessity criteria, but county MH departments have the first right of refusal to serve as the MH plan. The Partnership Health Plan of CA HIO & the Sacramento Geographic managed care organization (MCO) include inpatient/outpatient MH. The San Diego Geographic MCO, the AIDS Healthcare MCO, & the Prepaid Health Plan (PHP) Program MCO include outpatient MH. The Senior Care Action Network MCO includes inpatient MH/substance use disorder (SUD) & outpatient MH. The Caloptima HIO, the Central Coast Alliance for Health HIO, the Health Plan of San Mateo MCO, the Santa Barbara San Luis Obispo Regional Health Authority HIO, & the Two-Plan Model Program MCO carve out MH services. | 2008 National Summary of State Medicaid Managed Care Programs -- pages 11, 16, 24, 29, 31, 36, 41, 359, 365, 370, 506, 514, & 520 | IP claims only have a maximum of 2 DX codes & LT claims only 1. |
| Colorado (CO) | X | X | State carves out MH service from MCO. Has an MH PIHP that does not specifically mention SA services but includes a fairly comprehensive list of MH services. | 2008 National Summary of State Medicaid Managed Care Programs -- pages 42, 527 | No significant issues. | |
| Connecticut (CT) | X | X | CT's Husky A has an MH ASO that covers SUD services. | 2008 National Summary of State Medicaid Managed Care Programs -- page 49 | CT's HMOs ceased providing services to Medicaid enrollees from December 2007 through July 2008, so there was no HMO enrollment during this period. | |
| Delaware (DE) | X | X | DE's Diamond State Health Plan MCOs cover SA services. | 2008 National Summary of State Medicaid Managed Care Programs -- page 218 | No significant issues. | |
| District of Columbia (DC) | X | X | DC Medicaid Managed Care Program (comprehensive benefits, risk-based capitation) includes services for inpatient MH & SA & outpatient MH (does not mention outpatient SA). | 2008 National Summary of State Medicaid Managed Care Programs -- page 375 | In the LT file, only 9.3% of claims have a primary DX code. | |
| Florida (FL) | X | X | FL has 2 MCOs: Managed Health Care MCO includes inpatient MH/SUD & MH targeted case management, & Florida Medicaid Reform MCO includes community MH services, inpatient/outpatient MH/SUD services, & outpatient MH. The state also has an MH PIHP, a Statewide Inpatient Psychiatric Program, & a Shared Savings Model that covers community MH. | 2008 National Summary of State Medicaid Managed Care Programs -- pages 57, 61, 63, 72, 225 | In the LT file, only 32% of claims have a primary DX code; in the OT file only 78.3% do. Correctable mismatch between claim & eligibility file MSIS-IDs. LT & Medical--Only PIHPs reported in CMS data but not MAX. | |
| Georgia (GA) | X | X | GA has an MCO that covers inpatient/outpatient MH/SUD services. The state also has a BHO, which became FFS in 2007. Preadmission Screening & Annual Resident Review (PASARR) program ceased operating as a MH PIHP on September 30, 2007. Effective October 1, 2007, this program uses only 1915(b)(4) authority solely for FFS reimbursement arrangement. | 2008 National Summary of State Medicaid Managed Care Programs -- pages 73, 384 | In the OT file, only 94.8% of claims have primary diagnosis codes. Individuals in a MH PIHP 1915b waiver program were incorrectly assigned to primary care case management (PCCM) instead of PHP. This error is correctable. | |
| Hawaii (HI) | X | X | HI QUEST Expanded (QEx) MCO & MH/SUD PIHP cover all MH & SUD services (risk-based capitation). If enrollee is in both, it is unclear who pays for SA services. | 2008 National Summary of State Medicaid Managed Care Programs -- page 234 | 3.3% of records missing eligibility information. In the OT file, only 75.2% of claims have a primary diagnosis code. | |
| Idaho (ID) | NA | NA | NA | NA | No significant issues. | |
| Illinois (IL) | X | X | IL's Voluntary Managed Care includes inpatient/outpatient MH & SUDs through the MCO. | 2008 National Summary of State Medicaid Managed Care Programs -- page 538 | No significant issues. | |
| Indiana (IN) | X | X | Under Hoosier Healthwise, all MH & SA services are covered through the MCO. Under HIP, inpatient SA is covered, but there is no mention of MH services or outpatient SA. | 2008 National Summary of State Medicaid Managed Care Programs -- pages 77 & 243 | No significant issues. | |
| Iowa (IA) | X | X | All services are through the BHO; none provided through the HMO. By February 2005, only 1 HMO was left in the state. As of February 2009, enrollment in this HMO ended. | 2008 National Summary of State Medicaid Managed Care Programs -- page 393 | In the LT file, only 88% of claims have a primary diagnosis code. Only 96.6% of managed care enrollees have capitation payments reported. | |
| Kansas (KS) | X | X | MCO does not cover MH/SUD services. State has SUD PIHP & MH PAHP. | 2008 National Summary of State Medicaid Managed Care Programs -- pages 402 & 620 | BHP-ASO (Administrative Services Only) benefit, which covers only administrative costs of coordinating MH benefits, not benefits themselves, is not recorded in Claims or Eligibility data. | |
| Kentucky (KY) | X | X | KY Health Care Partnership Program MCO does not cover MH or SUD services, with the exception of inpatient medical detoxification. | 2008 National Summary of State Medicaid Managed Care Programs -- page 248 | Private health insurance reporting unreliable before October 2008. | |
| Louisiana (LA) | NA | NA | NA | NA | Private health insurance reporting may be unreliable in 2008. In the LT file, only 86.9% of claims have primary DX code. | |
| Maine (ME) | NA | NA | NA | NA | ME was unable to report accurately its IP/LT/OT claims, as it did not have a fully functional MMIS. The MAX 2008 files contain only the RX & eligibility information. | |
| Maryland (MD) | X | X | MD's HealthChoice MCO includes coverage for inpatient/outpatient SUDs. | 2008 National Summary of State Medicaid Managed Care Programs -- page 255 | In the LT file, only 63.7% of claims have primary DX code. Only 88.1% of managed care enrollees have capitation claims. | |
| Massachusetts (MA) | X | X | MA's Mass Health covers services under 'MH/SUD PIHP -- Risk-based Capitation,' (this is their BHO) & 'MCO (Comprehensive Benefits) -- Risk-based Capitation.' If enrollee is in both, it is unclear who pays for services. | 2008 National Summary of State Medicaid Managed Care Programs -- pages 262264 | MAX 2008 contains only claims adjudicated through Q2 FY 2009. In the LT file, only 7.9% of claims have a primary diagnosis code; in the OT file, only 44.6% do. A high percentage (24.7%) of MA enrollees have private health insurance. Only 94.4% of managed care enrollees have capitation payments. | |
| Michigan (MI) | X | X | MI's Comprehensive Health Plan includes outpatient MH services under the MCO. MI's Specialty PIHPs (the BHO) include SA services. It appears the BHO pays for SA services, but if enrollee is in both, it is unclear who pays for MH services. | 2008 National Summary of State Medicaid Managed Care Programs -- pages 87, 629 | In the OT file, only 79.5% of claims have primary diagnosis codes. Only 95% of managed care enrollees have capitation claims. | |
| Minnesota (MN) | X | X | MN's Consolidated Chemical Dependency Treatment Fund includes SA inpatient & outpatient services under the County Case Manager program paid FFS. MN's Prepaid Medical Assistance Program--1115(a), MinnesotaCare Program For Families & Children, MN Prepaid Medical Assistance Program--1932(a), MN Disability Health Options (MnDHO), MN Senior Health Options Program (MSHO), Special Needs Basic Care, & MN Senior Care/MN Senior Care Plus all include services for inpatient/outpatient SA. | 2008 National Summary of State Medicaid Managed Care Programs -- pages 93, 273, 279, 417, 543, 548, 553, 634 | Through September 2008, some aliens eligible only for emergency services may have been reported to RBF 5. MN moved these individuals to RBF 2 in October 2008. | |
| Mississippi (MS) | NA | NA | NA | NA | No significant issues. | |
| Missouri (MO) | X | X | MO's HealthNet Managed Care program includes MH/SA services. | 2008 National Summary of State Medicaid Managed Care Programs -- page 96 | No significant issues. | |
| Montana (MT) | NA | NA | NA | NA | Some individuals in UEGs 11-12, 22, 34-35, 42, 44, & 48 may have been incorrectly assigned RBF 5. | |
| Nebraska (NE) | X | X | NE Health Connection Combined Waiver Program--1915(b) includes adult SA treatment & inpatient & outpatient MH services under the Specialty Physician Case Management (SPCM) Program. The MCOs under this program do not cover MH/SA services. | 2008 National Summary of State Medicaid Managed Care Programs -- page 108 | No significant issues. | |
| Nevada (NV) | X | NV's Mandatory Health Maintenance Program includes inpatient/outpatient MH services under the MCO. SA is not mentioned. | 2008 National Summary of State Medicaid Managed Care Programs -- page 428 | No significant issues. | ||
| New Hampshire (NH) | NA | NA | NA | NA | In the OT file, only 79.3% of claims have primary diagnosis code. DMP plan not reported in MAX data. | |
| New Jersey (NJ) | X | X | NJ FamilyCare--1915(b) & NJ FamilyCare --1932(a) include inpatient/outpatient SA services under the MCOs. | 2008 National Summary of State Medicaid Managed Care Programs -- pages 116 & 437 | No significant issues. | |
| New Mexico (NM) | X | X | NEW MEXICO SALUD! Includes services under the MH PIHP, a BHO for MH services. SA services are not mentioned specifically. | 2008 National Summary of State Medicaid Managed Care Programs -- page 124 | In the OT file, only 54.7% of claims have primary diagnosis codes. | |
| New York (NY) | X | X | NY's Federal-State Health Reform Partnership (F-SHRP), F-SHRP--Medicaid Advantage, Partnership Plan--Family Health Plus (both MCO & PPO), & Partnership Plan Medicaid Managed Care Program include inpatient/outpatient substance misuse services under the MCOs. | 2008 National Summary of State Medicaid Managed Care Programs -- pages 284, 292, 296, 298, 301 | Only 92.2% of managed care enrollees had capitation claims. | |
| North Carolina (NC) | X | X | NC's Piedmont Cardinal Health Plan, a BHO, covers MH & SUD services. This plan operates in only 5 counties in the state. | NA | No significant issues. | |
| North Dakota (ND) | NA | NA | NA | NA | No significant issues. | |
| Ohio (OH) | X | X | Ohio's full-risk managed care program includes both inpatient & outpatient SA services. | 2008 National Summary of State Medicaid Managed Care Programs -- page 453 | In the LT file, only 88% of claims have a primary diagnosis code; | |
| Oklahoma (OK) | NA | NA | NA | NA | In the LT file, only 89.3% of claims have a primary diagnosis code; some of the diagnosis codes may have an extra 0 or 2 because this field is not edited by the state. | |
| Oregon (OR) | X | X | OR MH/SUD PIHP is the state's BHO & includes SA services. OR also has an MCO program that includes SA services. It is unclear who would pay for services if enrollee is in both BHO & HMO. | 2008 National Summary of State Medicaid Managed Care Programs -- pages 317 & 320 | In the OT file, only 50.6% of claims have a primary diagnosis code. | |
| Pennsylvania (PA) | X | X | PA has a BHO that appears to cover all SA services. The HealthChoices MCO program does not cover these services. | 2008 National Summary of State Medicaid Managed Care Programs -- page 143 | In the OT file, only 79.9% of claims have primary diagnosis codes. The diagnosis code on some EPSDT screens is "EPSDT." | |
| Rhode Island (RI) | X | X | RI's Rite Care program includes inpatient & outpatient SA services. Also, RI's Rhody Health Partners program includes inpatient & outpatient SA services. | 2008 National Summary of State Medicaid Managed Care Programs -- page 329 | Private insurance enrollment information is not reliable. | |
| South Carolina (SC) | X | X | X | SC's HMO program includes alcohol & drug screening & physical exams through the Department of Alcohol & Drug Abuse Services; however, no mention of inpatient/outpatient SA services. SC also has a Medically Fragile managed care program, which excludes these services. Palmetto Physician Connections Offers a special MH & SA program. The other HMOs do not offer this program. | 2008 National Summary of State Medicaid Managed Care Programs -- page 591 | In the LT file, only 4.3% of claims have a primary diagnosis code; in the OT file, 70.4% do. |
| South Dakota (SD) | NA | NA | NA | NA | In the LT file, only 2.7% of claims have primary diagnosis code. Only 96.2% of managed care enrollees have capitation payments. | |
| Tennessee (TN) | X | X | TN's MH/SUD PIHP is the state's BHO & includes SA services. However, the state's MCOs in the TennCare program also include inpatient & outpatient services. It is unclear if an enrollee is enrolled in both plans, which covers SA services. | 2008 National Summary of State Medicaid Managed Care Programs -- pages 335 & 337 | No significant issues. | |
| Texas (TX) | X | X | TX has an MH/SUD PIHP, its BHO, known as NorthSTAR. However, this BHO is reimbursed with a combination of FFS & risk-based capitation (mostly FFS). It is unclear what services are included in the capitation payment. TX also has risk-based MCOs, (the STAR, STARHealth, & STAR+PLUS programs) that include inpatient & outpatient SA services. State has a disease management program, TX Medicaid enhanced program, which does not include SA. This program is not coded as HMO in data. | 2008 National Summary of State Medicaid Managed Care Programs -- pages 157, 163, 601, & 649 | In the LT file, only 89.9% of claims have a primary diagnosis code; in the OT file, only 66.2% do. TX submits a few HMO capitation claims with a type of claim of FFS, instead of capitation. These are premium payments for private health insurance (OT). 2.5% of claims are missing eligibility information. Only 95.2% of managed care enrollees have capitation claims. | |
| Utah (UT) | NA | NA | UT's Prepaid Mental Health Program covers MH services. There is no discussion of SA. | NA | MAX 2008 contains only claims adjudicated through Q1 FY 2009. 3.9% of claims are missing eligibility, & these are primarily capitation claims. In the OT file, only 78.8% of claims have primary diagnosis code. 3.9% of claims are missing eligibility information, & these are primarily capitation claims. | |
| Vermont (VT) | NA | NA | NA | NA | No significant issues | |
| Virginia (VA) | X | X | VA's Medallian MCO program includes inpatient MH & outpatient SA services. | 2008 National Summary of State Medicaid Managed Care Programs -- page 189 | From Q2 2007 to Q3 2008, 7,000-11,000 HMO enrollees were reported with 0-filled plan IDs. The state indicated that these people were not actually enrolled in HMOs. Only 94.7% of managed care enrollees have capitation payments. | |
| Washington (WA) | X | X | X | WA has a BHO known as the Integrated Mental Health Services program -- it is not clear whether this program covers SA services, as they are not mentioned specifically. WA also has MCOs in the WA Medicaid Integration Program (WMIP) that cover inpatient & outpatient SA services. It is not clear who covers SA costs when individuals are enrolled in both. MCOs in the Healthy Options program do not cover SA services. | 2008 National Summary of State Medicaid Managed Care Programs -- pages 194 & 482 | In the LT, file only 19.9% of claims have a primary diagnosis code; in the OT file, only 71.3% do. |
| West Virginia (WV) | X | X | X | WV's Mountain Health Choices covers inpatient MH & outpatient MH. There is no mention of SA. WV's Mountain Health Trust MCOs do not cover any MH or SA services. | 2008 National Summary of State Medicaid Managed Care Programs -- pages 198 & 703. | DX codes are missing on most LT claims. |
| Wisconsin (WI) | X | X | WI MCOs in the BadgerCare Plus, Medicaid SSI Managed Care, & WI Partnership programs include inpatient & outpatient SA services. The state also has a BHO in the Children Come First & Wraparound Milwaukee programs that provides SA services. If individuals are enrolled in both the BHO & MCO, it is unclear who covers their SA services. In addition, WI has a long-term care PIHP program (1915(b)(c) waiver) that is risk-based & includes outpatient SA services. | 2008 National Summary of State Medicaid Managed Care Programs -- pages 487, 493, 498, 606, 610, 655 | WI was unable to report all of its claims by the prescribed deadline. The MAX 2008 files contain only claims adjudicated through Q3 FY 2009. RBF assignments became unreliable starting in October, when WI implemented a new MMIS, causing some enrollees to be mapped to incorrect RBF assignments. Only 97.4% of managed care enrollees have capitation claims. | |
| Wyoming (WY) | NA | NA | NA | NA | No significant issues. |
APPENDIX F. MEAN EXPENDITURES AND USERS PER ENROLLED MONTH IN MAJORITY FEE-FOR-SERVICE STATES
| Eligibility/ Demographic Group | Expenditures per Month | Users per 1,000 Months | ||||
| Low | Medium | High | Low | Medium | High | |
| Children 12 | 0.02 | 0.03 | 0.03 | 0.04 | 0.03 | 0.04 |
| Non-Disabled | ||||||
| 12-17, Female | 0.46 | 4.00 | 2.51 | 0.38 | 1.13 | 1.10 |
| 12-17, Male | 0.80 | 9.00 | 4.14 | 0.67 | 2.14 | 1.89 |
| 18-20, Female | 0.63 | 3.36 | 10.46 | 0.86 | 1.93 | 3.84 |
| 18-20, Male | 0.99 | 10.04 | 15.72 | 1.24 | 3.41 | 7.44 |
| 21-34, Female | 2.82 | 6.65 | 18.11 | 2.07 | 3.64 | 5.98 |
| 21-34, Male | 6.34 | 6.49 | 33.83 | 3.99 | 5.04 | 11.66 |
| 35-44, Female | 3.98 | 8.06 | 15.22 | 2.77 | 3.90 | 5.40 |
| 35-44, Male | 8.31 | 6.23 | 22.98 | 4.70 | 4.27 | 8.52 |
| 45-64, Female | 4.74 | 5.76 | 11.37 | 2.73 | 2.98 | 4.08 |
| 45-64, Male | 5.62 | 4.38 | 14.47 | 3.81 | 2.99 | 5.64 |
| 65 or Older, Female | 3.31 | 1.15 | 1.12 | 0.47 | 0.35 | 0.57 |
| 65 or Older, Male | 2.84 | 4.27 | 9.35 | 0.68 | 0.95 | 2.62 |
| Disabled | ||||||
| 12-17, Female | 0.91 | 3.06 | 3.72 | 0.66 | 1.13 | 2.67 |
| 12-17, Male | 1.81 | 5.83 | 3.82 | 1.18 | 1.91 | 3.12 |
| 18-20, Female | 1.90 | 3.51 | 16.71 | 1.46 | 2.17 | 7.34 |
| 18-20, Male | 2.44 | 5.63 | 16.65 | 1.88 | 2.87 | 8.08 |
| 21-34, Female | 4.40 | 9.12 | 32.46 | 3.11 | 4.79 | 11.49 |
| 21-34, Male | 5.68 | 9.46 | 40.18 | 3.36 | 5.49 | 14.36 |
| 35-44, Female | 7.17 | 18.30 | 60.08 | 4.25 | 7.11 | 19.73 |
| 35-44, Male | 12.13 | 31.30 | 94.53 | 5.91 | 9.11 | 23.89 |
| 45-64, Female | 3.95 | 9.34 | 36.77 | 2.73 | 3.99 | 10.45 |
| 45-64, Male | 13.61 | 26.72 | 108.67 | 5.68 | 8.31 | 22.72 |
| 65 or Older, Female | 4.50 | 3.76 | 11.03 | 1.07 | 0.69 | 1.70 |
| 65 or Older, Male | 7.91 | 14.35 | 3.36 | 2.24 | 2.99 | 4.51 |
| Eligibility/ Demographic Group | Expenditures per Month | Users per 1,000 Months | ||||
| Low | Medium | High | Low | Medium | High | |
| Children 12 | 0.00 | 0.00 | 0.00 | 0.02 | 0.02 | 0.02 |
| Non-Disabled | ||||||
| 12-17, Female | 0.27 | 4.74 | 1.67 | 0.24 | 0.86 | 0.73 |
| 12-17, Male | 0.26 | 10.21 | 3.54 | 0.31 | 1.56 | 1.19 |
| 18-20, Female | 0.18 | 3.02 | 7.41 | 0.46 | 1.20 | 2.59 |
| 18-20, Male | 0.55 | 16.76 | 14.09 | 0.67 | 3.10 | 5.13 |
| 21-34, Female | 1.14 | 2.72 | 28.56 | 0.98 | 1.60 | 5.81 |
| 21-34, Male | 6.19 | 2.94 | 71.93 | 5.14 | 2.79 | 18.41 |
| 35-44, Female | 2.77 | 2.14 | 13.14 | 1.36 | 1.67 | 3.55 |
| 35-44, Male | 7.03 | 2.93 | 32.40 | 4.86 | 2.77 | 11.90 |
| 45-64, Female | 5.48 | 1.59 | 9.31 | 0.89 | 1.40 | 3.08 |
| 45-64, Male | 1.52 | 1.63 | 16.52 | 1.50 | 1.43 | 7.08 |
| 65 or Older, Female | 0.33 | 1.37 | 9.93 | 1.00 | 0.54 | 0.42 |
| 65 or Older, Male | 0.54 | 5.73 | 0.76 | 1.18 | 1.94 | 0.67 |
| Disabled | ||||||
| 12-17, Female | 0.01 | 0.01 | 0.14 | 0.11 | 0.04 | 0.52 |
| 12-17, Male | 0.01 | 0.01 | 0.00 | 0.05 | 0.08 | 0.00 |
| 18-20, Female | 0.10 | 2.71 | 0.40 | 0.31 | 0.63 | 1.56 |
| 18-20, Male | 0.12 | 1.23 | 0.56 | 0.47 | 0.95 | 0.32 |
| 21-34, Female | 0.20 | 2.25 | 14.64 | 0.41 | 0.87 | 4.52 |
| 21-34, Male | 0.25 | 3.67 | 1.28 | 0.65 | 1.32 | 1.99 |
| 35-44, Female | 0.86 | 1.84 | 15.94 | 0.63 | 1.47 | 4.44 |
| 35-44, Male | 0.99 | 1.70 | 11.23 | 0.64 | 1.32 | 3.45 |
| 45-64, Female | 0.94 | 3.23 | 38.26 | 1.19 | 2.55 | 12.82 |
| 45-64, Male | 2.39 | 4.02 | 11.84 | 1.30 | 2.68 | 6.17 |
| 65 or Older, Female | 2.74 | 1.64 | 21.65 | 1.17 | 1.45 | 5.11 |
| 65 or Older, Male | 3.27 | 5.89 | 12.37 | 2.09 | 3.58 | 7.51 |
| Duals | ||||||
| Less than 18 | 0.06 | 0.06 | 0.06 | 0.73 | 0.73 | 0.73 |
| 18-34, Female | 0.81 | 4.23 | 17.70 | 0.80 | 3.25 | 7.84 |
| 18-34, Male | 1.22 | 4.35 | 16.76 | 1.20 | 3.69 | 9.20 |
| 35-44, Female | 2.77 | 4.14 | 15.13 | 1.36 | 3.08 | 7.91 |
| 35-44, Male | 7.03 | 5.18 | 20.50 | 4.86 | 4.03 | 9.71 |
| 45-64, Female | 5.48 | 2.24 | 10.44 | 0.89 | 1.68 | 4.94 |
| 45-64, Male | 1.52 | 5.16 | 23.23 | 1.50 | 3.25 | 8.35 |
| 65 or Older, Female | 0.33 | 0.78 | 3.12 | 1.00 | 0.22 | 0.46 |
| 65 or Older, Male | 0.54 | 5.37 | 21.32 | 1.18 | 0.99 | 2.05 |
| Eligibility/ Demographic Group | Expenditures per Month | Users per 1,000 Months -- Unduplicated | Users per 1,000 Months -- All | ||||||
| Low | Medium | High | Low | Medium | High | Low | Medium | High | |
| Full-Benefit Enrollees | |||||||||
| 1 year old | 0.39 | 0.98 | 3.04 | 0.30 | 0.48 | 1.28 | 0.33 | 0.52 | 1.41 |
| Children, 1-11 | 0.02 | 0.02 | 0.04 | 0.01 | 0.02 | 0.04 | 0.01 | 0.02 | 0.04 |
| Women of Childbearing Age, 18-44 | 0.08 | 0.06 | 0.06 | 0.20 | 0.20 | 0.08 | 0.22 | 0.25 | 0.21 |
| All Others | 0.00 | 0.01 | 0.01 | 0.01 | 0.01 | 0.00 | 0.01 | 0.01 | 0.01 |
| Eligibility/ Demographic Group | Expenditures per Month | Users per 1,000 Months -- Unduplicated | Users per 1,000 Months -- All |
| Partial-Benefit Enrollees | |||
| 1 year old | 0.71 | 0.11 | 0.13 |
| Children, 1-11 | 0.01 | 0.01 | 0.01 |
| Women of Childbearing Age, 18-44 | 0.03 | 0.11 | 0.13 |
| All Others | 0.01 | 0.01 | 0.01 |
| Dual Eligibles | |||
| Women of Childbearing Age, 18-44 | 0.04 | 0.08 | 0.10 |
| All Others | 0.01 | 0.00 | 0.00 |
| Eligibility/ Demographic Group | Expenditures per Month | Users per 1,000 Months -- Unduplicated | Users per 1,000 Months -- All |
| Poisoning Related to Drugs or Alcohol | |||
| 18 | 0.02 | 0.04 | 0.04 |
| 18 or Older | 0.16 | 0.06 | 0.10 |
| Other Medical Conditions 100% Attributable to Drugs or Alcohol | |||
| 21 | 0.00 | 0.00 | 0.00 |
| Non-Dual, Non-Disabled | |||
| 21-34, Female | 0.04 | 0.02 | 0.03 |
| 21-34, Male | 0.17 | 0.06 | 0.08 |
| 35-44, Female | 0.31 | 0.06 | 0.09 |
| 35-44, Male | 0.84 | 0.13 | 0.21 |
| 45-64, Female | 0.51 | 0.12 | 0.17 |
| 45-64, Male | 1.19 | 0.26 | 0.37 |
| 65 or Older, Female | 0.01 | 0.05 | 0.07 |
| 65 or Older, Male | 0.98 | 0.19 | 0.23 |
| Non-Dual, Disabled | |||
| 21-34, Female | 0.49 | 0.04 | 0.08 |
| 21-34, Male | 0.74 | 0.07 | 0.14 |
| 35-44, Female | 2.41 | 0.22 | 0.39 |
| 35-44, Male | 6.03 | 0.49 | 0.83 |
| 45-64, Female | 2.42 | 0.35 | 0.49 |
| 45-64, Male | 8.40 | 1.03 | 1.55 |
| 65 or Older, Female | 0.42 | 0.17 | 0.20 |
| 65 or Older, Male | 5.56 | 0.57 | 0.66 |
| Eligibility/ Demographic Group | Expenditures per Month | Users per 1,000 Months -- Unduplicated | Users per 1,000 Months -- All |
| Poisoning Related to Drugs or Alcohol | |||
| Non-Dual | |||
| 18 | 0.00 | 0.01 | 0.02 |
| 18 or Older | 0.03 | 0.02 | 0.03 |
| Dual | |||
| 18 | 0.00 | 0.00 | 0.00 |
| 18-64 | 0.06 | 0.05 | 0.06 |
| 65 or Older | 0.03 | 0.02 | 0.02 |
| Other Medical Conditions 100% Attributable to Drugs or Alcohol | |||
| 21 | 0.00 | 0.00 | 0.00 |
| Non-Dual, Non-Disabled | |||
| 21-34, Female | 0.05 | 0.02 | 0.02 |
| 21-34, Male | 1.37 | 0.05 | 0.09 |
| 35-44, Female | 0.15 | 0.05 | 0.07 |
| 35-44, Male | 0.50 | 0.11 | 0.19 |
| 45-64, Female | 0.50 | 0.09 | 0.12 |
| 45-64, Male | 0.66 | 0.24 | 0.33 |
| 65 or Older, Female | 0.10 | 0.17 | 0.19 |
| 65 or Older, Male | 1.12 | 0.56 | 0.72 |
| Non-Dual, Disabled | |||
| 21-34, Female | 0.06 | 0.03 | 0.03 |
| 21-34, Male | 0.04 | 0.02 | 0.02 |
| 35-44, Female | 1.11 | 0.12 | 0.17 |
| 35-44, Male | 1.82 | 0.47 | 0.67 |
| 45-64, Female | 1.20 | 0.21 | 0.26 |
| 45-64, Male | 7.61 | 1.08 | 1.47 |
| 65 or Older, Female | 0.01 | 0.07 | 0.07 |
| 65 or Older, Male | 0.04 | 0.04 | 0.04 |
| Duals | |||
| 21-64, Female | 0.19 | 0.10 | 0.13 |
| 21-64, Male | 0.47 | 0.23 | 0.32 |
| 65 or Older, Female | 0.12 | 0.03 | 0.03 |
| 65 or Older, Male | 0.42 | 0.14 | 0.18 |
| Eligibility/ Demographic Group | Expenditures per Month | Users per 1,000 Months -- Unduplicated | Users per 1,000 Months -- All | ||||||
| Low | Medium | High | Low | Medium | High | Low | Medium | High | |
| |||||||||
| Children 12a | 0.02 | 0.02 | 0.02 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 |
| Non-Dual, Non-Disabled | |||||||||
| 12-20, Female | 1.08 | 2.86 | 6.58 | 0.17 | 0.33 | 0.44 | 0.23 | 0.52 | 0.64 |
| 12-20, Male | 1.58 | 3.37 | 6.10 | 0.23 | 0.38 | 0.47 | 0.32 | 0.62 | 0.71 |
| 21-44, Female | 1.98 | 1.76 | 3.47 | 0.55 | 0.48 | 0.62 | 0.89 | 0.93 | 1.20 |
| 21-44, Male | 3.02 | 1.77 | 4.18 | 0.81 | 0.56 | 0.52 | 1.58 | 1.03 | 1.16 |
| 45-64, Female | 2.13 | 1.37 | 2.23 | 0.57 | 0.33 | 0.49 | 0.99 | 0.65 | 0.91 |
| 45-64, Male | 0.53 | 0.89 | 3.08 | 0.47 | 0.29 | 0.30 | 0.93 | 0.54 | 0.65 |
| 65 or Older, Female | 0.01 | 0.38 | 2.00 | 0.04 | 0.05 | 0.18 | 0.04 | 0.06 | 0.21 |
| 65 or Older, Male | 0.00 | 1.54 | 5.03 | 0.03 | 0.09 | 0.15 | 0.06 | 0.18 | 0.31 |
| Non-Dual, Disabled | |||||||||
| 12-20, Female | 3.16 | 6.26 | 54.03 | 0.37 | 0.76 | 1.39 | 0.53 | 1.13 | 2.69 |
| 12-20, Male | 4.63 | 7.31 | 15.70 | 0.51 | 0.80 | 0.91 | 0.74 | 1.19 | 1.34 |
| 21-44, Female | 8.67 | 14.88 | 64.17 | 1.41 | 1.69 | 2.64 | 2.29 | 3.17 | 7.55 |
| 21-44, Male | 16.2 1 | 27.10 | 99.82 | 2.20 | 2.27 | 3.70 | 3.28 | 4.35 | 9.29 |
| 45-64, Female | 4.71 | 7.15 | 32.00 | 0.82 | 0.90 | 1.94 | 1.29 | 1.63 | 4.54 |
| 45-64, Male | 9.76 | 17.05 | 49.83 | 1.17 | 1.35 | 2.55 | 1.99 | 2.90 | 7.13 |
| 65 or Older, Female | 4.54 | 0.23 | 19.80 | 0.05 | 0.08 | 0.00 | 0.10 | 0.08 | 0.85 |
| 65 or Older, Male | 1.31 | 1.64 | 2.21 | 0.24 | 0.29 | 0.00 | 0.24 | 0.41 | 1.13 |
| Eligibility/ Demographic Group | Expenditures per Month | Users per 1,000 Months -- Unduplicated | Users per 1,000 Months -- All | ||||||
| Low | Medium | High | Low | Medium | High | Low | Medium | High | |
| |||||||||
| Children 12a | 0.02 | 0.02 | 0.02 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 | 0.01 |
| Non-Dual, Non-Disabled | |||||||||
| 12-20 | 0.45 | 1.88 | 5.54 | 0.12 | 0.25 | 0.29 | 0.14 | 0.37 | 0.40 |
| 21-44 | 1.02 | 0.67 | 4.13 | 0.37 | 0.29 | 0.20 | 0.61 | 0.48 | 0.66 |
| 45-64 | 2.32 | 0.55 | 2.41 | 0.49 | 0.17 | 0.12 | 0.73 | 0.36 | 0.34 |
| 65 or Older | 0.07 | 0.64 | 5.00 | 0.00 | 0.14 | 0.26 | 0.13 | 0.21 | 0.26 |
| Non-Dual, Disabled | |||||||||
| 12-20 | 1.82 | 3.11 | 7.55 | 0.24 | 0.36 | 0.19 | 0.33 | 0.50 | 0.48 |
| 21-44 | 1.18 | 4.40 | 12.47 | 0.36 | 0.58 | 0.56 | 0.53 | 0.89 | 1.21 |
| 45-64 | 0.93 | 1.78 | 6.82 | 0.28 | 0.49 | 0.12 | 0.44 | 0.81 | 0.70 |
| 65 or Older | 0.00 | 0.00 | 0.00 | 0.00 | 0.02 | 0.00 | 0.00 | 0.02 | 0.00 |
| Duals | |||||||||
| 12-20 | 3.04 | 33.18 | 52.76 | 0.78 | 1.16 | 1.93 | 0.91 | 2.39 | 2.89 |
| 21-44 | 4.80 | 3.84 | 16.07 | 1.41 | 1.48 | 2.58 | 2.03 | 2.16 | 4.88 |
| 45-64 | 2.05 | 2.00 | 10.42 | 0.71 | 0.79 | 1.83 | 1.02 | 1.14 | 3.24 |
| 65 or Older | 0.23 | 0.29 | 1.34 | 0.05 | 0.06 | 0.14 | 0.08 | 0.09 | 0.21 |
| State | Basis for Imputation | Number of Enrolled Months, 12+ | % of Months with Expenditures Imputed | % of Months Imputed Based on FFS States | Core Expenditures per Enrolled Month, 12+ | Specialty SA Treatment Supply Category | Notes |
| Total | 329,928,722 | 42.4 | 33.4 | 10.20 | |||
| Alabama (AL) | No managed care SA coverage | 4,508,429 | 0.0 | 0.0 | 1.84 | Low | |
| Alaska (AK) | No managed care SA coverage | 659,931 | 0.0 | 0.0 | 10.24 | Medium | Only 57% of OT file claims have primary diagnosis code |
| Arizona (AZ) | Encounter data for full-benefit core SA services, AZ FFS experience for all others | 8,892,311 | 75.1 | 9.5 | 16.06 | Medium | |
| Arkansas (AR) | No managed care SA coverage | 3,419,417 | 0.0 | 0.0 | 1.45 | Low | |
| California (CA) | CA FFS experience for disabled & partial-benefit/Tier I & Tier II state experience for adults & children | 48,737,825 | 41.3 | 33.0 | 6.50 | Medium | Institutional long-term care claims have only one diagnosis code. Not able to load one of 50 other service file claim CDs. |
| Colorado (CO) | Tier I & Tier II state experience | 2,770,430 | 92.2 | 92.2 | 21.72 | High | BHO is assumed to cover SA services although these services are not specifically mention in the program summary |
| Connecticut (CT) | CT FFS experience for full-benefit/Tier I & Tier II state for duals & partial-benefit | 3,696,547 | 4.7 | 0.5 | 14.82 | High | |
| Delaware (DE) | Tier I & Tier II state experience | 1,151,093 | 66.6 | 66.6 | 9.94 | Medium | |
| District of Columbia (DC) | DC FFS experience for disabled/Tier I & Tier II state experience for all others | 1,203,121 | 53.3 | 51.2 | 10.73 | High | Only 9% of claims in the institutional long-term care file have a primary diagnosis |
| Florida (FL) | FL FFS experience for adult, children & disabled/ Tier I & Tier II state experience for duals & partial-benefit. | 15,267,255 | 28.2 | 3.0 | 2.68 | Low | Only 32% of institutional long-term care & 78% of other services file claims have a primary diagnosis code. |
| Georgia (GA) | GA FFS experience for disabled/Tier I & Tier II state experience for all others | 8,008,475 | 41.9 | 41.4 | 2.61 | Low | |
| Hawaii (HI) | HI FFS experience for disabled/Tier I & Tier II state experience for all others | 1,575,353 | 65.7 | 65.0 | 5.30 | Low | Only 75% of OT file claims have primary diagnosis. |
| Idaho (ID) | No managed care SA coverage | 1,046,461 | 0.0 | 0.0 | 2.29 | Low | |
| Illinois (IL) | IL FFS experience full-benefit non-duals/Tier I & Tier II experience for all others | 15,996,529 | 4.4 | 0.2 | 6.95 | Medium | |
| Indiana (IN) | IN FFS experience for disabled/Tier I & Tier II state experience for all others | 5,948,452 | 50.9 | 49.1 | 5.57 | Medium | |
| Iowa (IA) | Tier I & Tier II state experience | 2,726,468 | 71.6 | 71.6 | 3.66 | Low | Only 88% of institutional long-term care claims have a primary diagnosis code. |
| Kansas (KS) | Encounter data for core SA services full-benefit enrollees & Tier I & Tier II expenditures for other services | 1,735,951 | 83.3 | 28.2 | 9.77 | Medium | Expenditures associated with care coordination for BHO are not included in claims data. |
| Kentucky (KY) | No managed care SA coverage | 5,255,303 | 0.0 | 0.0 | 7.03 | Medium | |
| Louisiana (LA) | No managed care SA coverage | 6,447,109 | 0.0 | 0.0 | 1.81 | Low | Only 87% of institutional long-term care claims have a primary diagnosis code. |
| Maine (ME) | Tier I & Tier II state experience | 2,702,131 | 100.0 | 100.0 | 18.57 | High | MAX does not include inpatient hospital, institutional long-term care or other service claims for ME. |
| Maryland (MD) | Tier I & Tier II state experience | 4,704,518 | 66.8 | 66.8 | 14.34 | High | Only 64% of institutional long-term care claims have a primary diagnosis code. |
| Massachusetts (MA) | MA FFS experience full-benefit/Tier I & Tier II state experience duals & partial-benefit | 9,846,726 | 29.0 | 0.0 | 10.07 | High | Only 8% of institutional long-term care claims & 45% of other service file claims have a primary diagnosis code. |
| Michigan (MI) | Tier I & Tier II state experience | 12,003,858 | 49.9 | 49.9 | 5.48 | Medium | Only 80% of other service file claims have a primary diagnosis code. |
| Minnesota (MN) | MN FFS experience for disabled/Tier I & Tier II state experience for all other | 4,614,974 | 57.6 | 56.9 | 11.66 | Medium | |
| Mississippi (MS) | No managed care SA coverage | 3,848,621 | 0.0 | 0.0 | 5.23 | Low | |
| Missouri (MO) | MO FFS experience full-benefit/Tier I & Tier II state experience duals & partial-benefit. | 5,949,243 | 33.6 | 2.4 | 12.81 | Medium | |
| Montana (MT) | No managed care SA coverage | 560,597 | 0.0 | 0.0 | 10.95 | Medium | |
| Nebraska (NE) | Tier I & Tier II state experience | 1,269,547 | 76.4 | 76.4 | 14.14 | Low | |
| Nevada (NV) | NV FFS experience for disabled/Tier I & Tier II state experience for adults & children | 1,213,271 | 34.4 | 34.4 | 6.59 | High | |
| New Hampshire (NH) | No managed care SA coverage | 816,263 | 0.0 | 0.0 | 8.66 | Medium | |
| New Jersey (NJ) | NJ FFS experience for disabled/Tier I & Tier II state experience for all others | 6,784,507 | 60.6 | 53.1 | 10.78 | Medium | |
| New Mexico (NM) | Tier I & Tier II state experience | 2,979,072 | 53.7 | 53.7 | 9.64 | High | |
| New York (NY) | NY FFS experience for disabled/Tier I & Tier II state experience for all others | 35,887,261 | 60.6 | 55.2 | 31.69 | High | |
| North Carolina (NC) | No managed care SA coverage | 8,900,845 | 0.0 | 0.0 | 5.37 | Medium | |
| North Dakota (ND) | No managed care SA coverage | 388,689 | 0.0 | 0.0 | 11.01 | Medium | |
| Ohio (OH) | OH FFS experience for disabled/Tier I & Tier II state experience for all others | 13,214,717 | 62.0 | 53.6 | 13.91 | Medium | Only 88% of institutional long-term care claims have a primary diagnosis code. |
| Oklahoma (OK) | No managed care SA coverage | 3,648,815 | 0.0 | 0.0 | 2.50 | Medium | Only 89% of institutional long-term care claims have a primary diagnosis code. |
| Oregon (OR) | Tier I & Tier II state experience | 2,905,508 | 63.4 | 63.4 | 13.96 | High | Only 51% of other service file claims have a primary diagnosis code. |
| Pennsylvania (PA) | Tier I & Tier II state experience | 13,873,346 | 89.4 | 89.4 | 7.43 | Medium | Only 80% of other service file claims have a primary diagnosis code. |
| Rhode Island (RI) | RI FFS experience for disabled/Tier I & Tier II state experience for all others | 1,410,457 | 51.5 | 49.8 | 14.25 | High | |
| South Carolina (SC) | SC FFS Experience full-benefit/Tier I & Tier II state for all others | 4,725,345 | 18.8 | 1.5 | 4.82 | Medium | Only 4% of institutional long-term care claims & 70% of other service file claims have a primary diagnosis code. |
| South Dakota (SD) | No managed care SA coverage | 658,947 | 0.0 | 0.0 | 9.05 | Medium | Only 3% of institutional long-term care claims have a primary diagnosis code. |
| Tennessee (TN) | TN FFS experience | 9,815,245 | 32.3 | 32.3 | 1.60 | Low | |
| Texas (TX) | TX FFS Experience | 15,329,081 | 41.4 | 12.7 | 1.46 | Low | 90% of institutional long-term care claims & 66% of other service file claims have a primary diagnosis code. |
| Utah (UT) | No managed care SA coverage | 1,305,163 | 0.0 | 0.0 | 6.77 | Medium | SA is carved-out of MH managed care program, but may miss co-morbid services. Only 79% of other service file claims have a primary diagnosis code. MAX 2008 contains only claims adjudicated through Q1 FY 2009, thus expenditures may be incomplete. |
| Vermont (VT) | No managed care SA coverage | 1,159,336 | 0.0 | 0.0 | 25.99 | High | |
| Virginia (VA) | VA FFS experience for disabled/Tier I &Tier II state experience for all others | 5,052,885 | 45.5 | 45.5 | 3.67 | Low | |
| Washington (WA) | Tier I & Tier II state experience | 5,909,882 | 100.0 | 100.0 | 24.33 | High | State-specific data for the disabled population was not used because expenditures for this population were substantially higher costs per enrolled month than averages for Tier I & Tier II high-supply states. Only 20% of institutional long-term care claims & 71% of other service file claims have a primary diagnosis code. |
| West Virginia (WV) | WV FFS experience for full-benefit/Tier I & Tier II state for duals & partial-benefit. | 2,461,378 | 19.2 | 2.2 | 9.31 | Medium | Diagnosis codes are missing on most institutional long-term care claims. |
| Wisconsin (WI) | WI FFS experience for disabled/Tier I & Tier II state experience for all others. | 6,565,021 | 41.1 | 41.0 | 6.17 | Low | MAX 2008 contains only claims adjudicated through Q3 FY 2009, thus expenditures may be incomplete. |
| Wyoming (WY) | No managed care SA coverage | 358,612 | 0.0 | 0.0 | 5.52 | High |
NOTES
Total Medicaid expenditures and enrollment are based on federal FY 2008 as reported by the Centers for Medicare and Medicaid Services at http://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-State/By-State.html.
Levit, K.R., C.A. Kassed, R.M. Coffey, T.L. Mark, D.R. McKusick, E. King, R. Vandivort, J. Buck, K. Ryan, and E. Stranges. Projections of National Expenditures for Mental Health Services and Substance Abuse Treatment, 2004-2014. SAMHSA Publication No. SMA 08-4326. Rockville, MD: SAMHSA, 2008.
Technical issues related to this study are discussed in a separate report: Developing Medicare and Medicaid Substance Abuse Treatment Spending Estimates. Available at http://aspe.hhs.gov/daltcp/reports/2012/MSATest.shtml.
Levit, K.R., C.A. Kassed, R.M. Coffey, T.L. Mark, D.R. McKusick, E. King, R. Vandivort, J. Buck, K. Ryan, and E. Stranges. Projections of National Expenditures for Mental Health Services and Substance Abuse Treatment, 2004-2014. SAMHSA Publication No. SMA 08-4326. Rockville , MD: SAMHSA, 2008.
Bouchery, E.E., H.J. Harwood, J.J. Sacks, C.J. Simon, and R.D. Brewer. "Economic Costs of Excessive Alcohol Consumption in the United States, 2006." American Journal of Preventive Medicine, November 2011; Harwood, H., D. Fountain, and G. Livermore. The Economic Costs of Alcohol and Drug Abuse in the United States, 1992. National Institute on Drug Abuse Publication Number 98-4327. Rockville, MD: National Institutes of Health, 1998.
Available at http://www.statehealthfacts.org/comparetable.jsp?ind=184&cat=4. Accessed July 29, 2012.
Available at https://www.cms.gov/Research-Statistics-Data-and-Systems/Computer-Data-and-Systems/MedicaidBudgetExpendSystem/CMS-64-Quarterly-Expense-Report.html. Accessed on July 30, 2012.
National Association of State Alcohol and Drug Abuse Directors. NASADAD Inquiry--State Medicaid and SCHIP Coverage of Substance Abuse Services. Washington, DC: NASADAD, November 2010.
Levit, K.R. et al. Projections of National Expenditures for Mental Health Services and Substance Abuse Treatment, 2004-2014. SAMHSA Publication No. SMA 08-4326. Rockville, MD: SAMHSA, 2008.
Salvucci, S., E. Bouchery, J. Ingels, E. Grau, H. Harwood, Y. Zheng, and C. Ye.SAMHSA Survey of Revenue and Expenditures: Data on Specialty Substance Abuse and Mental Health Treatment Facilities: Final Report. Mathematica Report to SAMHSA, submitted September 1, 2011.
According to the SSE, the Medicaid program spent approximately $29,059 million on MH treatment in 2006. Using the SSE average annual projected growth rate from 2003 to 2014 (6.9 percent), we estimate spending in CY 2008 as $33,207 million.
National Association of State Alcohol and Drug Abuse Directors. NASADAD Inquiry--State Medicaid and SCHIP Coverage of Substance Abuse Services. Washington, DC: NASADAD, November 2010.
Substance Abuse and Mental Health Services Administration. Results from the 2008 National Survey on Drug Use and Health: National Findings. NSDUH Series H-36, HHS Publication No. SMA 09-4434. Rockville, MD: SAMHSA, 2009, chapter 7. Available at http://oas.samhsa.gov/NSDUH/2k8NSDUH/2k8results.cfm#7.3. Accessed July 27, 2012.
Levit, K.R., C.A. Kassed, R.M. Coffey, T.L. Mark, D.R. McKusick, E. King, R. Vandivort, J. Buck, K. Ryan, and E. Stranges. Projections of National Expenditures for Mental Health Services and Substance Abuse Treatment, 2004-2014. SAMHSA Publication No. SMA 08-4326. Rockville, MD :SAMHSA, 2008.
Bouchery, E.E., H.J. Harwood, J.J. Sacks, C.J. Simon, and R.D. Brewer. "Economic Costs of Excessive Alcohol Consumption in the United States, 2006."American Journal of Preventive Medicine, vol. 41, no. 5, November 2011, pp. 516-524; Harwood, H., D. Fountain, and G. Livermore. The Economic Costs of Alcohol and Drug Abuse in the United States, 1992. National Institute on Drug Abuse Publication Number 98-4327. Rockville, MD : National Institutes of Health, 1998.
National Association of State Alcohol and Drug Abuse Directors. Substance Abuse HCPCS Code User's Guide: Unofficial Standard Definitions. Washington, DC: NASADAD, 2007.
National Association of State Alcohol and Drug Abuse Directors. Approved HCPCS Codes and Modifiers Relating to Substance Abuse Treatment, Mental Health, and Behavioral Health. Washington, DC: NASADAD, 2003.
National Association of State Alcohol and Drug Abuse Directors. NASADAD Inquiry--State Medicaid and SCHIP Coverage of Substance Abuse Services. Washington, DC: NASADAD, November 2010.
Zuckerman, Stephen, Aimee Williams, and Karen Stockley. "Medicaid Physician Fees Grew By More Than 15 Percent From 2003 to 2008, Narrowing Gap With Medicare Physician Payment Rates." Health Affairs, April 2009. Available at http://www.kff.org/medicaid/kcmu042809oth.cfm. Accessed July 27, 2012.
Available at http://www.statehealthfacts.org/comparetable.jsp?ind=184&cat=4. Accessed July 27, 2012.
Available at https://www.cms.gov/Research-Statistics-Data-and-Systems/Computer-Data-and-Systems/MedicaidBudgetExpendSystem/CMS-64-Quarterly-Expense-Report.html. Accessed July 26, 2012.
OTHER REPORTS AVAILABLE
- Developing Medicare and Medicaid Substance Abuse Treatment Spending Estimates
- Full HTML Version http://aspe.hhs.gov/daltcp/reports/2012/MSATest.shtml
- Full PDF Version http://aspe.hhs.gov/daltcp/reports/2012/MSATest.pdf
- Medicaid Substance Abuse Treatment Spending: Findings Report
- Executive Summary http://aspe.hhs.gov/daltcp/reports/2012/MSATspendes.shtml
- Full HTML Version http://aspe.hhs.gov/daltcp/reports/2012/MSATspend.shtml
- Full PDF Version http://aspe.hhs.gov/daltcp/reports/2012/MSATspend.pdf
To obtain a printed copy of this report, send the full report title and your mailing information to:
U.S. Department of Health and Human ServicesOffice of Disability, Aging and Long-Term Care PolicyRoom 424E, H.H. Humphrey Building200 Independence Avenue, S.W.Washington, D.C. 20201FAX: 202-401-7733Email: webmaster.DALTCP@hhs.gov
RETURN TO:
Office of Disability, Aging and Long-Term Care Policy (DALTCP) Home [http://aspe.hhs.gov/office_specific/daltcp.cfm]Assistant Secretary for Planning and Evaluation (ASPE) Home [http://aspe.hhs.gov]U.S. Department of Health and Human Services (HHS) Home [http://www.hhs.gov]
Last Updated: 06/18/2013