
U.S. Department of Health and Human Services
Risks of Entering Nursing Homes for Long and Short Stays
Korbin Liu, SC.D., Carol De Vita, Ph.D., Kenneth G. Manton, Ph.D. and Terri Coughlin, M.S.
Duke University
1988
PDF Version: http://aspe.hhs.gov/daltcp/reports/1988/nhlsstes.pdf (27 PDF pages)
This report was prepared under grant #87ASPE185A between the U.S. Department of Health and Human Services (HHS), Office of Social Services Policy (now known as the Office of Disability, Aging and Long-Term Care Policy (DALTCP)) and Duke University. For additional information about the study, you may visit the DALTCP home page at http://aspe.hhs.gov/daltcp/home.shtml or contact the office at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, SW, Washington, DC 20201. The e-mail address is: webmaster.DALTCP@hhs.gov. The DALTCP Project Officer was Robert Clark.
Support for this research was provided by the Travelers Companies Foundation and the Department of Health and Human Services.
Conclusions in this report are solely those of the authors and do not necessarily reflect the views of the Travelers Companies Foundation, the Department of Health and Human Services, The Urban institute, The Population Reference Bureau, or Duke University.
TABLE OF CONTENTS
- I. INTRODUCTION
- II. DATA SOURCE
- III. DESCRIPTIVE ANALYSIS
- LIST OF FIGURES AND TABLES
- FIGURE 1
- TABLE 1. Transitions Between 1982 Community Status and 1984 Status
- TABLE 2. Nursing Home Admissions by Socioeconomic and Functional Status
- TABLE 3. Nursing Home Length of Stay Distribution by Type of Nursing Home Patients
- TABLE 4. Logistic Regression of All Home Admissions
- TABLE 5. Logistic Regressions by Type of Nursing Home Patient
ABSTRACT
This paper describes research to estimate the rates of nursing home admissions and to identify the determinants of long and short stays in nursing homes. The research employed recently available data from the 1982 and 1984 National Long-Term Care Surveys. Hence, the results are both nationally representative and indicative of current nursing how use patterns by the disabled elderly population. The information presented has implications for public and private long-tem care policies.
I. INTRODUCTION
Nursing homes are used for different purposes ranging from short-term rehabilitative care for persons recovering from an acute illness to long-term care for persons with chronic disabilities that preclude their residency in the community. Because of the different reasons why people enter nursing homes, estimates of the risks of nursing home entry and the costs of nursing home care over time need to be made for patient subgroups. One useful categorization with implications for service use is that of long- and short-stay patients.
To date, the identification and measurement of long- versus short-stay nursing home episodes have been based primarily on surveys of persons already in nursing homes. Several studies of the 1977 National Nursing Home Survey described the admission characteristics and utilization patterns of nursing home patients after they were in institutions (Keeler et al., 1981; Liu and Manton, 1983, 1984). Generally, data have not been available to explore the risk of nursing home admission by reasons for nursing home use and circumstances preceding admission. With few exceptions (Hughes et al., 1987), studies of nursing home risks have also generally not distinguished between the various types of nursing home admissions.
That nursing homes are used by long and short stayers suggests that the determinants of institutionalization might be different for the two subgroups in the nursing home population. Moreover, because of the dramatic difference in their consumption of nursing home days, each group of patients bas different policy implications. For this reason, it is important to differentiate the characteristics of disabled older persons that predispose them to one or the other type of nursing home admission.
In this paper, we present information from the 1982 and 1984 National Long-Term Care Surveys (NLTCS) to describe the relationship between personal characteristics of older persons and their use of nursing homes. The aims of this analysis are to characterize the risks of nursing home use, distinguish between nursing home users who are long- and short-stay patients, and describe the relationship between nursing home use and functional and other personal status. In the following sections, we describe the 1982 and 1984 NLTCS and results from both descriptive and multivariate analyses.
II. DATA SOURCE
The 1982 National Long-Term Care Survey (NLTCS). The 1982 survey was a nationally representative survey of the Medicare population age 65 and older needing assistance with one or more Activities of Daily Living (ADL) or Instrumental Activities of Daily Living (IADL) on a long-term basis. A sample of 36,000 Medicare enrollees was drawn from the Health Care Financing Administration enrollee files and interviewed by telephone to identify those with assistance needs. Persons identified as requiring assistance with ADLs or IADLs for a period of three months or longer were interviewed personally in the second phase of the survey. Persons residing in institutions were excluded from the 1982 detailed interviews. No attempt was made to obtain information on deceased persons.
For all 36,000 sampled individuals, the screener document contained data on age, race, sex and birth date. For each of nine ADL and seven IADL items, the person was asked if he or she had problems performing that activity and the duration of the difficulty. If the individual responded that the actual or expected duration had been (or was expected to be) more than three months, the respondent was given the detailed interview.
The detailed portion of the long-term care survey was administered to all noninstitutionalized persons with chronic (90 days +) difficulty performing one or more ADL or IADL functions as indicated by the screener--6,393 persons qualified for interviews. Questions on functional status asked about the presence of 17 chronic medical conditions, and whether in the last 12 months any of 12 medical events had occurred (e.g., heart attack, stroke, broken hip, etc.). A series of detailed questions were asked regarding each function included in the ADL scale: eating, transferring, walking, dressing, bathing and toileting. Questions on health insurance involved coverage by Medicaid, CHAMPUS, other public assistance programs, or private health insurance.
Respondents were also asked a series of questions about stays in a nursing home or hospital, including admission dates and durations. Income questions addressed receipt of payments by any family member in the past month from various sources (e.g., Social Security or Railroad Retirement benefits, Supplementary Security Income, wages, salaries).
In the NLTCS, cognitive impairment could be measured in several ways. Some portion of the sample in 1982 was administered the Short Portable mental Status Questionnaire (SPMSQ), which is a clinical aide for identifying cognitive impairment (Pfeiffer, 1975). Other members of the sample had proxy respondents and were not administered the SPMSQ, but proxy respondents were asked if the sample person were "senile."
The 1984 NLTC Survey. The 1984 survey had both longitudinal and cross-sectional components. The survey was intended, in part, to provide insights into the factors contributing to or inhibiting change in functional and health status and institutionalization.
To conduct our analysis of the patterns of nursing home use between 1982 and 1984 by long- and short-stay patients, we focused on the sample of persons for whom information was available in both the 1982 and 1984 NLTCS. By 1984, most of these individuals were found either in the community or in nursing homes. A third possibility was that individuals in the 1982 sample died between 1982 and 1984.
Three types of survey instruments were used in addition to the screener and control card. A community questionnaire similar to the 1982 survey instrument was used for all functionally limited persons living in the community. This instrument was administered to community residents who were functionally disabled in 1982 and who continued to reside in the community in 1984.
A questionnaire to obtain information about deceased persons was unique to the 1984 study. This instrument had two sections: health care and personal information. The health care section elicited data on nursing home, convalescent home and hospital stays if that was where the patient died. Questions included the sources of payment for those stays. For patients who did not die in such institutions, the questionnaire asked about stays just prior to death. There were also questions about earlier periods of institutionalization. A specific question about hospice care was included. Finally, there were questions about others who provided care to the decedent, both paid and unpaid helpers. Personal information surveyed included marital status, race, ethnic origin and income.
A questionnaire for institutionalized persons included four sections: (1) cognitive functions, (2) ADL impairments, (3) payment sources at admission and at the time of survey, and (4) certified beds. As with the other questionnaires, there was an indicator for whether the sample person or a proxy answered the questions. Questions were asked about admission to nursing homes and periods of institutionalization prior to admission. There was also a question about hospital stays in the last 12 months. Finally, it was determined who paid for care, both at admission and on the date of the survey.
III. DESCRIPTIVE ANALYSIS
Transitions between 1982 and 1984. Table 1 presents the distributions of the 1982 sample by their 1984 residential status. About 72 percent of the community disabled persons in 1982 were still community residents in 1984. Only 7 percent were in nursing homes in 1984 while almost 21 percent died in the intervening two years. The mortality rate of this sample is consistent with estimates from other studies of this age group (Manton, 1987). The proportion of persons in nursing homes after two years (7.1%) is higher than that recorded from the Longitudinal Study on Aging (Kovar, 1988), but may be explained, in part, by the fact that the NLTCS sample consisted of disabled persons in 1982.
Table 1 also contains the 1984 residential status of subgroups of the 1982 community residents by their demographic and functional characteristics in 1982. As expected, the risk of being a nursing home resident increased with age, rising from 4 percent for those 65-74 to 12 percent for persons over age 85. Higher rates of nursing home use were found for females, whites, persons living alone, and those who were not married. Income was negatively related to nursing home use. Persons in the lowest income bracket had a risk of entering nursing homes more than double that of persons in the highest income bracket, i.e., 8.8 percent versus 3.6 percent. This relationship suggests that persons in the highest income groups had more resources to purchase home care which enabled them to remain in the community. Another explanation for this relationship is that higher income groups may have had a better overall health status than lower income groups.
Table 1 also presents distributions of the subgroups by disability status and select health conditions. The data indicate that nursing home residency is strongly related to a person's functional impairment level. A monotonic increase in use up to ADL 5-6 is observed. Persons with 5 to 6 ADL dependencies had a slightly lower use of nursing homes than persons with 3 to 4 ADLs, 9.8 percent versus 10.0 percent. Because of their severe disabilities, we might expect individuals with 5 to 6 ADLs to have had the highest rate of nursing home use. This ADL subgroup, however, also had high competing risks of mortality; that is, this subgroup may have had the highest use rate if many members had not died. Previous research using the NLTCS has shown that mortality risk during the 1982-84 period for the 1982 community sample was related directly to disability in 1982 (Manton, 1987). Health conditions that were found most strongly associated with being a nursing home resident were hip fracture and stroke. Persons with lung diseases had the lowest risk of being nursing home patients.
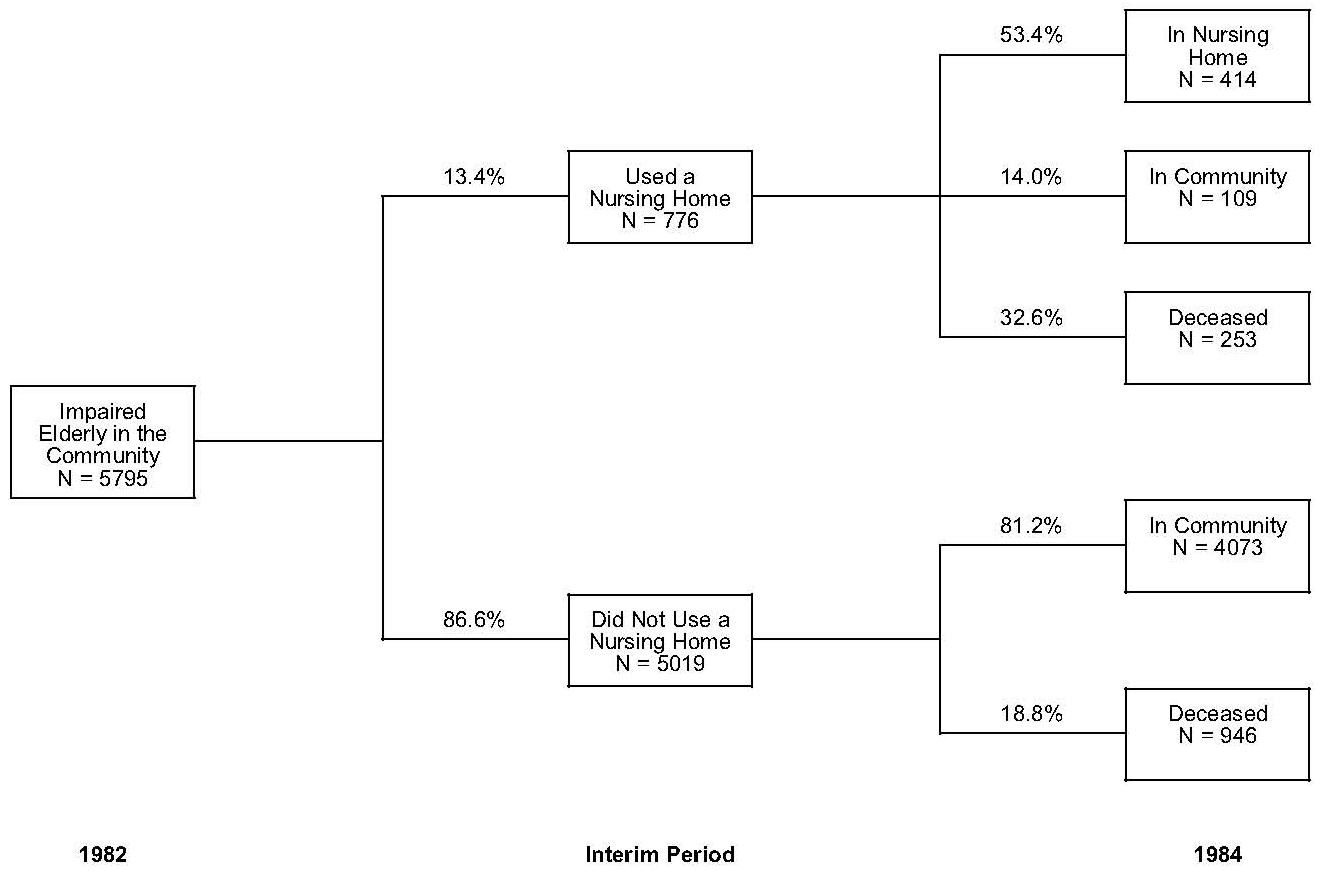
Risks of Nursing Home Admission. Although Table 1 presented the proportion of community residents who were found in nursing homes after two years, it does not fully represent the risk of using a nursing home at some time during the two-year interim. Some individuals, for example, could have entered a nursing home and died or returned to the community. A longitudinal assessment of nursing home admissions indicates far more use of long-term care facilities than is commonly reported in cross-sectional data. As Figure 1 illustrates, nearly twice as many study participants reported using a long-term care facility during the interim as were residents of one at the time of the 1984 survey. Slightly more than 13 percent of the 1982 sample, 776 persons, had experienced at least one nursing home episode during the study interim. of these, however, only 7 percent, 414 persons, were living in a nursing home in 1984. This comparison suggests that almost half of the nursing home admissions were for relatively short periods of tire.
Because the 1984 NLTCS elicited detailed information on nursing home use in the two years since the 1982 NLTCS, we were able to estimate the total incidence of nursing home admissions in this period, as well as to distinguish admissions that were long versus short stay. In this initial analysis we identified persons who entered nursing homes during the interval and who were no longer in nursing homes in 1984 as "short-stay" patients. Also included in this group of "short-stay" patients were persons who used a nursing home facility and died during the 1982-1984 interim. The assumption underlying this distinction is the observation that institutionalized persons captured in a cross-sectional sample (e.g. persons in nursing homes at the time of the 1984 survey) tended to have much longer lengths of stay on average than persons in an admission or discharge sample (Manton et al., 1984). For example, the median length of completed stays in the 1977 NNHS discharge sample was 75 days while the average length of stay in the 1977 NNHS current resident sample was 597 days (NCHS, 1979).
Table 2 presents the percent of persons who entered nursing homes at any time between 1982 and 1984 by socioeconomic and functional status in 1982. The column headed "All Users of Nursing Homes Between 1982 and 1984" refers to the 776 persons who experienced at least one nursing home episode during the period. Table 2 also presents the ratio of 1984 current residents to all users between 1982 and 1984. This measure was derived by dividing the number of 1984 current residents, as reflected by Table 1, by the numbers of all users between 1982 and 1984. On the basis of 1984 current residents representing long-stay patients, the higher the ratio the more likely a particular characteristic of a persons is associated with being a long-stay resident.
Similar to the cross-sectional data reported in Table 1, the longitudinal data in Table 2 show that the risk of nursing home use is strongly related to personal characteristics and disability level. A high rate of nursing home use was found for females, unmarried persons, and persons living alone. As expected, age was strongly related to nursing home use. About 23 percent of persons 85 and older entered a nursing home sometime during the two-year period between 1982 and 1984, while only 7 percent of persons aged 65 to 74 entered a nursing home during the same period. Also as expected, the risk of admission to nursing homes increased as functional status declined. only 8 percent of persons with IADLs, used nursing homes, whereas 19 percent of persons with ADL 5-6 entered nursing homes. Stroke and hip fracture were associated with a high risk of nursing home admission, while persons with lung disease had the lowest risk. These conditions were predictive of both any nursing home use and long-stay users. Only persons with incomes of $20,000 and more seem to have particularly low rates of nursing home use, approximately half of the rate of their counterparts with less than $20,000 of income.
We can use the ratio of 1984 residents to all users in the two-year period to identify characteristics of persons that are related to long versus short stays. By age, the ratio of residents to any users suggests that the "young-olds" who use nursing homes at all are likely to be long stayers, while older counterparts (i.e., 75+) are more likely to be short stayers. Being female, not married, and living alone are characteristics associated not only with higher risk of entering nursing homes, but also higher risks of being long-term stayers of nursing homes. No difference exists in the, ratio by race, although major differences were found in the use rates by race.
Persons who were more disabled tended to be associated with short stays. This is probably because their use of nursing homes was associated with postacute care. Higher proportions of long stayers in the IADL subgroup may have been due to problems such as cognitive impairments. Persons who entered nursing homes with a history of cancer in 1982 had the smallest proportion who were long stayers (40%), most likely because they were at high risk of dying by 1984.
The income pattern suggests the proportion of long-stay patients declines as income increases. This. might reflect higher income persons staying in the community longer because of a greater ability to purchase supplemental home-based care. Hence, their use of nursing homes might have been for the final stage of an episode of illness.
Long and Short Stayers in Nursing Homes. So far we have referred to the presence of long and short stayers among the persons who entered nursing homes between 1982 and 1984. We have also discussed the likelihood of being a long stayer if a person were found in a cross-sectional sample of nursing home patients. To address the issue of length of stay more directly, we derived the length-of-stay distributions of the nursing home users between 1982 and 1984 by the characteristics of their nursing home experience. Specifically, we derived lengths of stay for persons who (1) were in nursing homes in 1984 (the expected long stayers), (2) had entered nursing homes but had returned to the community by 1984, and (3) had entered nursing homes and were dead by 1984. These results, along with the distribution for all nursing home patients between 1982 and 1984, are presented in Table 3.
The first column indicates that approximately 20 percent of the nursing home patients were found in each of the length-of-stay categories: The length of stay patterns are distinctly different, however, when each of the subsets are examined. Among the expected long stayers, the persons still in nursing homes in 1984, 34 percent had been institutionalized for over one year, whereas only 22 percent had been in nursing homes for less than 3 months. It should be noted that the lengths of stay of persons in this group are incomplete because we were only able to measure the duration between admission to the date of the 1984 survey. Since all of the persons in this category were still nursing home patients, their eventual length of stay could be considerably longer than that measured in the 1984 survey. Hence, even persons in the less-than-three-months category could have eventual lengths of stay that would allow them to be classified as long-term nursing home patients.
In contrast to the long stayers, persons who entered nursing homes and returned to the community, and those who died, had dramatically different length-of-stay distributions. Among the short stayers who returned to the community, over two-thirds were in nursing homes for less than 3 months, with 10 percent staying for more than 6 months. Among the short stayers who died by 1984, only 27 percent stayed for more than 6 months. Hence, the length-of-stay patterns of the long and short stayers are inversely related.
The results in Table 3 suggest that our strategy for disaggregating long- and short-stay patients is reasonable. Although we found persons with longer than 6 month stays in both the short-stay groups, the proportions were relatively small. We also found partial lengths of stay that were short among persons in the long-stay group. Since in 1984 only incomplete duration could be recorded for this group, it is likely that few persons would ultimately be short stayers. Future research could refine the estimate of whether persons were long or short stays by considering such characteristics as Admission diagnoses and ADL at admission.
IV. MULTIVARIATE ANALYSIS OF NURSING HOME ADMISSIONS
In the prior sections we examined the relationships between personal characteristics of disabled individuals living in the community in 1982 and various outcomes in the intervening two years, including the rate at which they entered nursing homes. The tables presented the univariate distribution by characteristics. In this section, we examine the direction and magnitude of impact of multiple variables on the risks of nursing home admissions.
We employed logistic regression analyses to determine the effects of the factors examined above along with additional characteristics. Because we expect that the characteristics predicting long-stay patients are likely to be different than those predicting short-stay patients, we developed separate models. Hence, this section presents results of analyses of three categories of nursing home patients: (1) all nursing home users between 1982 and 1984; (2) persons who were in nursing homes at the time of the survey in 1984, the long stayers; and (3) persons who were admitted to nursing homes between 1982 and 1984 but either returned to the community or had died by the tire of the survey in 1984. We combined the community and dead groups to increase the size of the short-stay group.
The dependent variable in this analysis, nursing home admission, is qualitative. In other words, it is binary with individuals either entering or not entering nursing homes. Because of the binary dependent variable, we used a multimonial logit model (Nerlove and Press., 1973). The results of this analysis are presented in terms of risk odds ratio (RM) which expresses the risk of nursing home admission for persons with a particular characteristic relative to those without the characteristic.
The variables that we used to predict nursing home admission were socio-demographic characteristics, medical conditions, ADL limitations cognitive impairment status, income, formal and informal community-based care, and prior nursing home use. All of the characteristics were based on responses to the 1982 NLTCS. For categorical independent variables, one level of the variable was omitted. Coefficients for the included variables can be interpreted as deviations in the logit from the omitted group.
-
Medical conditions. Nine categories of medical conditions were created from the 1982 NLTCS. Some of the source variables from the survey were combined to create the categories. For example, bronchitis, emphysema and asthma were combined into the lung disease category.
-
ADL limitations. Four categories of ADL were created: (1) only Instrumenntal Activities of Daily Living (IADL); (2) one or two ADLs; (3) Three or four ADLs, and (4) Five or six ADLs. In the regression analyses, the IADL category was omitted.
-
Cognitive status. Five categories of cognitive status were created. Sample persons with proxy respondents were divided into two groups those indicated by their proxies to be senile and those who were not senile according to the proxies. The remaining sample persons were grouped according to their SPMSQ scores (Pfeiffer, 1975); mild to no impairment, moderately impaired and severely impaired. In the regression analyses, the category representing mildly or not impaired according to SPMSQ scores was omitted.
-
Socio-demographic characteristics. Age, sex, race, marital status, living arrangements, home ownership, and metropolitan residency were included in the analyses. The age category for persons 65-74 was omitted from the regression analyses.
-
Income. Sample persons and spouse income was grouped into 5 broad categories ranging from less than $4,000 to more than $20,000 per year in 1982. The income category $4-7,000 was omitted from the regression analyses. In addition, Medicaid status in 1982 was included as a separate variable.
-
Community-based care. Volume of community care was operationalized by recording total episodes of care per week by all helpers; normally this measure reflected the volume of assistance from more than one person. Four groups were created ranging from no helper days to 15+ helper days per week. The category 1-5 helper days per week was omitted from the regression analysis. As an approximation of the financial burden of community-based care, we also developed a measure of paid care as a percent of income. Categories of this measure ranged from zero percent to 25+ percent. The category representing zero out-of-pocket payments was omitted from the regression analyses.
-
Prior nursing home use. A nursing home stay prior to the 1982 survey was included to determine if individuals who had been reported to enter nursing homes had a higher risk of reentering nursing homes than persons who had never been institutionalized.
All Users of Nursing Homes. Table 4 presents the results of the logistic regression analysis for all nursing home stays between 1982 and 1984. The first column presents the sample means for each of the characteristics that were used to predict nursing home admission. Since we used the same characteristics for each model, these means apply to subsequent models as well. The second column in Table 4 presents the coefficients for each of the variables and their level of statistical significance. The third column presents the relative odds ratio.
Among the medical conditions, arthritis and lung disease were found to have a negative and statistically significant effect on nursing home admissions, whereas cancer and neurological diseases increased the risk of nursing home admission. The relative odds ratio indicates, for example, that a person with cancer in 1982 had 1.42 times the odds of entering nursing homes as a person who did not have cancer (ROR = 1.42), all other characteristics in the table being equal. In contrast, persons with lung diseases had lower odds of entering nursing homes than persons who did not have lung disease (ROR = .70)
Higher levels of activities of daily living were also associated with risk of entering nursing homes. In comparison to persons with only IADL level disabilities, persons dependent in ADLs had higher risks of entering nursing homes. Although the ADL 5-6 group appeared to have a slightly lower risk than the ADL 3-4 group, this might be explained by the high risk of mortality in the former. Because of the competing risk of mortality, the observed risk of entering nursing homes was likely to be lower than would be expected in the absence of mortality.
The presence of cognitive impairments increased the likelihood of entering nursing homes. Persons who were judged senile by proxies and those rated as moderately impaired based on SPMSQ scores had more than two times the risk of entering nursing homes as those persons who were mildly or not cognitively impaired according to their SPMSQ scores. The higher risk of entering nursing homes for those persons judged "not senile" by a proxy was probably due to unmeasured health or functional problems that demanded that a proxy respond to the survey.
Advanced age is a significant predictor of nursing home use. Persons 75-84 had almost twice the likelihood of entering nursing homes as persons aged 65-74 (i.e., ROR = 1.99). Persons aged 85 and over had an even higher risk than 65-74 year olds--almost two and one-half to one (ROR = 2.48). Being white was also associated with a higher likelihood of entering nursing homes. Living alone increased the risk of entering nursing homes by 55 percent.
Income was not related to the risk of nursing home admission except for those with incomes greater than $20,000 per year. Persons with this level of income had a lower risk (ROR = .58) of entering nursing homes than persons with incomes between $4-7,000. Moreover, Medicaid status did not predict nursing home admission risks.
No significant differences in risk of entering nursing homes was found for different levels of community-based care received in 1982. Percent of income used for paid home-based care did, however, seem to make a difference. In comparison to persons who spent nothing, persons spending 1-10 percent (ROR = 1.27) and persons spending 11-25 percent (ROR = 1.86) had higher risks of nursing home entry. Although persons who spent more than 25 percent of their income also had a positive coefficient, this result was not statistically significant. Finally, prior nursing home use was strongly related to readmission to nursing homes. Persons who had been nursing home patients had twice the risk of those who had not.
Differences Between Long and Short Stayers. In this section, we compare the determinants of long- and short-stay patients of nursing homes. Table 5 presents the results of two separate regression analyses. The first two columns contain the coefficients and relative odds ratios for long-stay patients (i.e., persons institutionalized in 1984), and the third and fourth columns contain similar information for persons admitted between 1982 and 1984 but were not in nursing homes at the tire of the 1984 survey, the short stayers. In the following, we focus on the relative odds ratios for variables that are statistically significant for either or both of the regressions.
Among the conditions, persons with neurological diseases had 1.28 times the odds of entering nursing homes for extended durations as those without neurological disease. On the other hand, cancer increased the likelihood that persons entered for short stays. These results are consistent with the natural history of the two diseases and the likely reasons why persons with such conditions use nursing homes. Neurological diseases, such as Parkinson's, tend to be characterized by relatively long periods of severe functional disabilities requiring continuous supervision. For many families, the caregiving burdens associated with managing a family member with Parkinson's would be too much to bear at home, so a prolonged stay in a nursing home is likely. On the other hand, persons entering nursing homes because of cancer have a strong likelihood of being placed there for terminal care associated with the final segment of an episode of illness.
ADL status was positively associated with nursing home admission for both long- and short-stay patients. For long-stay patients the ADL 3-4 category had a ROR of 1.60 indicating a high risk for this group relative to persons with only IADL problems. For short-stay patients, all three ADL groups had higher relative odds of entering nursing homes than the omitted IADL group. The competing risk of mortality may be responsible, in part, for the ADL 5-6 group not exhibiting the highest level of long-stay nursing home use. It appears that competing mortality risks may have caused the relative odds ratios for those with 5-6 ADLs from being the highest for the short-stay patients as well.
All four cognitive impairment categories had significantly higher risks of long-term nursing home stays in comparison to persons with no cognitive impairments. The moderately impaired SPMSQ group had two and one-half times and the severely impaired SPMSQ group had four times the risk of the cognitively intact persons. Persons judged senile by proxies had a ROR of 2.75. The positive ROR of persons judged not senile by proxies probably represented unmeasured health or functional problems predisposing the individuals to long stays in nursing homes. In contrast to the importance of cognitive impairment in increasing the risks of nursing home admissions for long stays, this factor did not appear to affect short stays. Only the proxy judged senility status had a significant coefficient, indicating a 45 percent increase in the likelihood of entering nursing homes for a short stay.
Increasing age was significantly associated with increasing risks of both long and short stays in nursing homes. Based on the ROR scores, it appears that age is a stronger predictor for short stays. Surprisingly, sex was not predictive of the risks of either long or short nursing home stays when all other factors were held constant. Being white increased the risks of both long and short stays in nursing homes. As might be expected, persons living alone had higher risks of long stays in nursing homes, but not short ones. Owning one's own home reduced the risk of long stays in nursing homes, and had no effect an short-stay risks. As with all nursing home admissions, only those with greater than $20,000 income had significantly lower risks of a long stay. This category had a ROR = .53. Income had no effects on short-stay risks. Medicaid status had no effects on either long- or short-stay risks.
Persons with no community-based caregiver days had a slightly lower risk of entering nursing homes for long stays than the omitted category of persons with 1-5 days of helpers. This result suggests that persons using no community-based care were probably healthier than persons who did use services in terms of some unmeasured health factor. The significant RORs for persons with out-of-pocket expenditures suggest an association between use of paid care and long-stay nursing home risks. The interpretation of this association, however, is difficult. It is likely that out-of-pocket payments represent unmeasured health problems that would predispose individuals to entering nursing homes. It is possible that paid care is an inadequate substitute for informal caregiving requirements; that is, persons had sufficient resources to purchase some amount of formal care, but could not afford the volume or type of care that would be available from spouse and other family members. It is also possible that high out-of-pocket expenditures created a situation where insufficient finances stimulated decisions to enter nursing homes possibly as Medicaid patients. All of these reasons appear to be plausible, but we do not have the information to determine the effect of each.
Prior nursing home use increased the risk of entering nursing homes for long stays by two-to-one (ROR = 2.08) and the risks of entering nursing homes for a short stay by 50 percent. It is unknown whether the nursing home use that we observed between 1982 and 1984, either long or short, was for the same condition as the stay before 1982. Nonetheless, it is likely that a person's health status, as reflected by a prior nursing home stay, was vulnerable to a future nursing home admission.
The multivariate analysis of nursing home admissions presented in this section confirmed and clarified the results of the univariate analyses presented earlier. The determinants of "any nursing home use" have been found in other studies (Cohen, et al., 1986; Branch and Jette, 1982). Few studies, however, have distinguished long from short nursing home stays, so the results of this disaggregation of types of nursing home patients provide new insights. The specific factors that predict long-stay, in contrast to short-stay, nursing home patients appear to be intuitively and clinically reasonable.
V. SUMMARY AND DISCUSSION
The two objectives of the research reported were to estimate the rates of nursing home admissions and to identify the determinants of nursing home admissions. This information is important for the development of financing options for long-term care such as private insurance. In conjunction with length-of-stay information, risks of admission provide the necessary data to estimate the potential costs of specific policies. At the present time, only partial information is available from area studies or nationally representative studies with old data. This study was developed to provide information on nursing home admissions based an the recently available 1982 and 1984 National Long-Term Care Surveys. Hence, the results are both nationally representative and indicative of current nursing home utilization patterns by the disabled elderly population.
We found that 13 percent of the functionally impaired elderly living in the community in 1982 entered nursing homes in the following two years. We estimate, however, that only about 50 percent of the nursing home admissions were for long-term care, with the remainder being short-term convalescent or terminal care. For the consideration of long term care policies, the distinction between long and short stays appears to be critical, since the short-stay patients are unlikely to be in nursing homes long enough to incur private insurance benefits, although they would likely be Medicare SNF patients.
Results from the analyses were consistent, for the most part, with prior research. Higher nursing home use was found for older persons, females, whites, and persons living alone. Health status was also related to nursing home use in the expected directions. Higher ADL levels and specific conditions such as cancer were related to higher rates of nursing home use. Cognitive impairment was also strongly related to use of nursing homes, with the highest rates being observed for those with the most severe impairments based on the SPMSQ or on the judgment of proxy respondents. Income was negatively related to nursing home use, with particularly low rates being observed for persons with more than $20,000 per year. Finally, persons with prior nursing home use had considerably higher use rates than those who had not been institutionalized in the past.
To distinguish long from short stayers in nursing homes in this study, we defined long stayers to be those persons who were found in nursing homes at the time of the 1984 NLTCS. Prior research has shown that the "stock" of nursing home patients captured in a point-in-time survey tend to have dramatically longer stays than persons who are admitted and discharged during a short interval of time. To validate the definition that we employed, we measured the lengths of stay of persons who were institutionalized and those who had been admitted and discharged between 1982 and 1984. This comparison showed that even the incomplete lengths of stay of the institutionalized group were dramatically longer than the completed stays of the persons who were admitted and discharged.
We conducted analyses to determine the factors that were associated with risk of short- and long-stay patients separately. Some of the characteristics of disabled elderly persons predicted both long and short stays, while others were significantly associated with one type of stay but not with the other. For example, although age was positively associated with the risk of both long and short stays, living alone was associated with higher risks only for long-stay patients. The medical conditions also showed contrasting patterns for long- and short-stay patients. Persons with neurological impairments had higher risks of entering nursing homes for long stays, whereas cancer patients had higher risks of short stays.
Since the long stayers are the subgroup of nursing home patients who would be likely to use most of the nursing home days, information on this group would be the most valuable new information for the consideration of public and private long term care policies. In addition to the examples noted above, we found that private expenses for home-based care was associated with higher odds of entering nursing homes. We also found that persons with some community care had higher risks of entering nursing homes than those with no care, although the member of helper days, among persons with some help, did not appear to differentiate risks of nursing home admissions.
Although this research has produced new findings from a recent survey of disabled elderly persons, additional analyses with this and other data sources would further our understanding of nursing home risks. For example, we used individual conditions as potential predictors of nursing home use. Because of the clinical complexity of older persons, a strategy that reflects the multiple chronic conditions of given persons might provide more significant results than were found. In addition, improved results might be obtained if competing risks of nursing home admission and mortality could be taken into consideration.
In conclusion, information on the factors determining nursing home use presented above were intended to guide the development of public and private long-term care policies. Perhaps most important, this project distinguished between long- and short-stay nursing home users. Because of the dramatic difference in their consumption of nursing hone days, each group of nursing home patients has different policy implications. For this reason, it is important to differentiate the characteristics of disabled older persons that predispose them to one or the other type of nursing home admission.
REFERENCES
Branch, L.G. and Jette, A.M. 1982. "A Prospective Study of Long-Term Care Institutionalization Among the Aged." AJPH 72 (December):1373-1379.
Cohen, M.A., Tell, E.G., and Wallack, S.S. 1986. "Client-Related Risk Factors of Nursing Home Entry Among Elderly Adults." Journal of Gerontology 41(6):785-792.
Hughes, S.L., Manheim, L.M., Edelman, P.L. and Conrad, K.I. 1987. "The Impact of Long-Term Home Care on Hospital and Nursing Home Use and Cost." Health Services Research 22:19-47.
Keeler, E.B., Kane, R.L., and Soloman, D.H. 1981. "Short- and Long-Term Residents of Nursing Homes." Medical Care 19:363.
Kovar, M.G. 1988. "Aging in the Eighties, People Living Alone--Two Years Later." Advance data, No.149. DHHS Pub.No. (PHS)88-1250. Public Health Service, Hyattsville, MD.
Liu, K. and Manton, K.G. 1984. "The Characteristics and Utilization Pattern of an Admission Cohort of Nursing Home Patients (II)." The Gerontologist 24:71-76.
_____. 1983. "The Characteristics and Utilization Pattern of an Admission Cohort of Nursing Home Patients." The Gerontologist 23:92-98.
Manton, K.G. 1987. "Gender Differences in the Linkages Between Functioning, Disability, and Mortality." Presented at the NIA Conference on Gender and Longevity, Bethesda, MD, September 17-18.
Manton, K.G., Woodbury, M.A., and Liu, K. 1984. "Life Table Methods for Assessing the Dynamics of U.S. Nursing Home Utilization: 1976-1977." J. of Gerontology 39, 1:79-87.
National Center for Health Statistics. 1979. "The National Nursing Home Survey: 1977 Summary for the United States." Vital and Health Statistics, Series 13, Number 43.
Nerlove, M. and Press, S. 1973. "Univariate and Multivariate Log-Linear and Logistic Models." Manuscript R-1306-EDA/NIA. Santa Monica, California: Rand Corporation.
Pfeiffer, E. 1975. "A Short Portable Mental Status Questionnaire for the Assessment of Organic Brain Deficit in Elderly Patients." Journal of the American Geriatrics Society 22(10):433-444.
| TABLE 1. Transitions Between 1982 Community Status and 1984 Status | |||
| 1982 Status | Community | Nursing Home | Deceased |
| All Cases (N=5795) | 72.2% | 7.1% | 20.7% |
| Age: | |||
| 65-74 | 80.8 | 4.1 | 15.1 |
| 75-84 | 69.5 | 8.1 | 22.4 |
| 85+ | 59.2 | 11.7 | 29.1 |
| Male | 68.3 | 5.2 | 26.6 |
| Female | 74.3 | 8.2 | 17.4 |
| White | 71.9 | 7.7 | 20.4 |
| Nonwhite | 73.9 | 3.6 | 22.5 |
| Married | 74.4 | 4.4 | 21.2 |
| Not married | 70.4 | 9.2 | 20.3 |
| Lives alone | 72.6 | 10.3 | 17.1 |
| Lives with others | 72.0 | 5.7 | 22.3 |
| Income Status: | |||
| Under $4,000 | 72.2 | 8.8 | 19.0 |
| $4,000 - 6,999 | 70.6 | 8.0 | 21.4 |
| $7,000 - 9,999 | 70.9 | 7.1 | 22.0 |
| $10,000 - 19,999 | 73.5 | 6.0 | 20.5 |
| $20,000 or more | 76.9 | 3.6 | 19.4 |
| Disability Status: | |||
| IADL only | 81.7 | 4.6 | 13.7 |
| ADL 1-2 | 72.4 | 7.5 | 20.0 |
| ADL 3-4 | 66.7 | 10.0 | 23.3 |
| ADL 5-6 | 54.1 | 9.8 | 36.1 |
| Health Conditions: | |||
| Arthritis | 74.9 | 7.0 | 18.2 |
| Neurological | 70.2 | 8.3 | 21.5 |
| Diabetes | 70.6 | 5.0 | 24.4 |
| Cancer | 48.2 | 6.5 | 45.3 |
| Arteriosclerosis | 65.7 | 8.5 | 25.9 |
| Cardiovascular | 72.1 | 6.8 | 21.2 |
| Stroke | 54.1 | 11.1 | 34.9 |
| Lung | 72.4 | 4.3 | 23.3 |
| Hip Fracture | 65.7 | 14.2 | 20.2 |
| TABLE 2. Nursing Home Admissions by Socioeconomic and Functional Status | ||
| 1982 Status | All Users of Nursing HomesBetween 1982 and 1984 | 1984 Institutionalized asPercent of All Users |
| All Cases (N=5795) | 13.4% | 53% |
| Age: | ||
| 65-74 | 6.9 | 59 |
| 75-84 | 15.8 | 51 |
| 85+ | 22.5 | 52 |
| Male | 11.2 | 46 |
| Female | 14.6 | 56 |
| White | 14.4 | 53 |
| Nonwhite | 6.9 | 52 |
| Married | 9.5 | 46 |
| Not married | 16.4 | 56 |
| Lives alone | 17.4 | 59 |
| Lives with others | 11.6 | 49 |
| Income Status: | ||
| Under $4,000 | 14.5 | 61 |
| $4,000 - 6,999 | 14.6 | 55 |
| $7,000 - 9,999 | 13.7 | 52 |
| $10,000 - 19,999 | 12.5 | 48 |
| $20,000 or more | 7.3 | 49 |
| Disability Status: | ||
| IADL only | 8.0 | 58 |
| ADL 1-2 | 13.9 | 54 |
| ADL 3-4 | 19.8 | 51 |
| ADL 5-6 | 19.2 | 51 |
| Health Conditions: | ||
| Arthritis | 12.6 | 56 |
| Neurological | 15.4 | 54 |
| Diabetes | 11.9 | 42 |
| Cancer | 16.4 | 40 |
| Arteriosclerosis | 16.0 | 54 |
| Cardiovascular | 13.2 | 52 |
| Stroke | 20.6 | 54 |
| Lung | 9.8 | 44 |
| Hip Fracture | 23.1 | 62 |
| TABLE 3. Nursing Home Length of Stay Distribution by Type of Nursing Home Patients | ||||
| Duration | All Nursing Home Users Between 1982 & 1984 | Persons in Nursing Homes in 1984a | Entered Nursing Homes & Returned to Community by 1984 | Entered Nursing Homes and Died |
| 1 month | 19.2 | 7.6 | 35.5 | 32.9 |
| 1-3 months | 20.3 | 14.8 | 33.6 | 23.2 |
| 3-6 months | 20.0 | 21.8 | 19.6 | 16.5 |
| 6-12 months | 17.1 | 21.8 | 9.3 | 12.8 |
| >1 year | 23.4 | 34.3 | 2.0 | 14.6 |
| ||||
| TABLE 4. Logistic Regression of All Home Admission | |||
| Mean | Coefficients | ROR | |
| Medical Condition | |||
| Arthritis | 0.73 | -0.22* | 0.80 |
| Neurological | 0.33 | 0.22* | 1.25 |
| Diabetes | 0.16 | -0.06 | |
| Cancer | 0.06 | 0.35* | 1.42 |
| Arteriosclerosis | 0.32 | 0.00 | |
| Cardiovascular | 0.77 | -0.05 | |
| Stroke | 0.07 | 0.16 | |
| Lung | 0.26 | -0.35* | 0.70 |
| Hip Fracture | 0.02 | 0.13 | |
| Disability Status | |||
| ADL 1-2 | 0.33 | 0.37* | 1.45 |
| ADL 3-4 | 0.14 | 0.79* | 2.20 |
| ADL 5-6 | 0.16 | 0.60* | 1.82 |
| Cognitive Status | |||
| Not Senile (proxy) | 0.21 | 0.33* | 1.39 |
| Senile (proxy) | 0.09 | 0.82* | 2.27 |
| Severely Impaired | 0.01 | 1.05 | |
| Moderately Impaired | 0.03 | 0.81* | 2.25 |
| Age 75-84 | 0.40 | 0.69* | 1.99 |
| Age 85+ | 0.19 | 0.91* | 2.48 |
| Female | 0.64 | 0.01 | |
| White | 0.87 | 0.82* | 2.27 |
| Married | 0.43 | -0.19 | |
| Lives Alone | 0.31 | 0.44* | 1.55 |
| Owns Home | 0.63 | -0.11 | |
| Lives in Metro Area | 0.66 | 0.08 | |
| Income | |||
| Under $4,000 | 0.18 | -0.11 | |
| $7,000-9,999 | 0.20 | -0.11 | |
| $10,000-19,999 | 0.32 | 0.06 | |
| $20,000 or more | 0.04 | -0.54* | 0.58 |
| No Helper Days | 0.24 | -0.17 | |
| 6-14 Helper Days | 0.52 | -0.07 | |
| 15+ Paid Helper Days | 0.05 | -0.10 | |
| Percent Out-of-Pocket | |||
| 1-10 | 0.07 | 0.24** | 1.27 |
| 11-25 | 0.02 | 0.62* | 1.86 |
| 25+ | 0.02 | 0.32 | |
| Prior NH Use | 0.07 | 0.70* | 2.01 |
| Medicaid in 1982 | 0.24 | -0.00 | |
| * Significant at 0.05** Significant at 0.06-0.10 | |||
| TABLE 5. Logistic Regressions by Type of Nursing Home Patient | ||||
| Long-StayCoefficients | ROR | Short-StayCoefficients | ROR | |
| Medical Condition | ||||
| Arthritis | -0.02 | -0.39* | 0.67 | |
| Neurological | 0.25* | 1.28 | 0.14 | |
| Diabetes | -0.33* | 0.72 | 0.18 | |
| Cancer | 0.01 | 0.56* | 1.75 | |
| Arteriosclerosis | 0.03 | -0.04 | ||
| Cardiovascular | -0.23 | 0.17 | ||
| Stroke | 0.21 | 0.08 | ||
| Lung | -0.57* | 0.57 | -0.07 | |
| Hip Fracture | 0.28 | -0.08 | ||
| Disability Status | ||||
| ADL 1-2 | 0.22 | 0.50* | 1.65 | |
| ADL 3-4 | 0.47* | 1.60 | 1.00* | 2.72 |
| ADL 5-6 | 0.29 | 0.86* | 2.36 | |
| Cognitive Status | ||||
| Not Senile (proxy) | 0.44* | 1.55 | 0.14 | |
| Senile (proxy) | 1.01* | 2.75 | 0.37* | 1.45 |
| Severely Impaired | 1.40* | 4.06 | -0.12 | |
| Moderately Impaired | 0.90* | 2.46 | 0.51 | |
| Age 75-84 | 0.37* | 1.45 | 0.96* | 2.61 |
| Age 85+ | 0.45* | 1.57 | 1.26* | 3.53 |
| Female | 0.14 | -0.10 | ||
| White | 0.89* | 2.44 | 0.61* | 1.84 |
| Married | -0.13 | -0.25 | ||
| Lives Alone | 0.63* | 1.88 | 0.11 | |
| Owns Home | -0.23* | 0.79 | 0.05 | |
| Lives in Metro Area | 0.10 | 0.04* | 1.04 | |
| Income | ||||
| Under $4,000 | 0.03 | -0.26 | ||
| $7,000-9,999 | -0.19 | 0.01 | ||
| $10,000-19,999 | -0.12 | 0.22 | ||
| $20,000 or more | 0.63** | 0.53 | -0.37 | |
| No Helper Days | -0.29** | 0.75 | -0.03 | |
| 6-14 Helper Days | 0.03 | -0.15 | ||
| 15+ Paid Helper Days | 0.25 | -0.48 | ||
| Percent Out-of-Pocket | ||||
| 1-10 | 0.33** | 1.39 | 0.09 | |
| 11-25 | -0.09 | 0.97* | 2.64 | |
| 25+ | 0.72* | 2.05 | -0.44 | |
| Prior NH Use | 0.73* | 2.08 | 0.41* | 1.51 |
| Medicaid in 1982 | -0.05 | 0.06 | ||
| * Significant at 0.05** Significant at 0.06-0.10 | ||||
| FIGURE 1 |
 |
CHARACTERISTICS OF THE ELDERLY LONG-TERM CARE POPULATION AND ITS SERVICE USE REPORTS AVAILABLE
- Epidemiological, Demographic and Social Correlates of Disability among the Elderly
- HTML http://aspe.hhs.gov/daltcp/reports/1988/epdemes.htm
- PDF http://aspe.hhs.gov/daltcp/reports/1988/epdemes.pdf
- Recent Changes in Service Use Patterns of Disabled Medicare Beneficiaries
- HTML http://aspe.hhs.gov/daltcp/reports/1990/recentes.htm
- PDF http://aspe.hhs.gov/daltcp/reports/1990/recentes.pdf
- Risks of Entering Nursing Homes for Long and Short Stays
- HTML http://aspe.hhs.gov/daltcp/reports/1988/nhlsstes.htm
- PDF http://aspe.hhs.gov/daltcp/reports/1988/nhlsstes.pdf
- The Effect of Nursing Home Use on Medicaid Eligibility
- HTML http://aspe.hhs.gov/daltcp/reports/1989/nhumedes.htm
- PDF http://aspe.hhs.gov/daltcp/reports/1989/nhumedes.pdf
To obtain a printed copy of this report, send the full report title and your mailing information to:
U.S. Department of Health and Human ServicesOffice of Disability, Aging and Long-Term Care PolicyRoom 424E, H.H. Humphrey Building200 Independence Avenue, S.W.Washington, D.C. 20201FAX: 202-401-7733Email: webmaster.DALTCP@hhs.gov
RETURN TO:
Office of Disability, Aging and Long-Term Care Policy (DALTCP) Home [http://aspe.hhs.gov/_/office_specific/daltcp.cfm]Assistant Secretary for Planning and Evaluation (ASPE) Home [http://aspe.hhs.gov]U.S. Department of Health and Human Services Home [http://www.hhs.gov]