
U.S. Department of Health and Human Services
Report from the Working Group on Improving Public Policies and Programs Affecting Persons with Mental Retardation and Other Developmental Disabilities
Office of the Assistant Secretary for Planning and Evaluation
December 1988
toward independence, productivity, and integration into the community
PDF Version: http://aspe.hhs.gov/daltcp/reports/mrddwges.pdf (89 PDF pages)
This report was prepared under contract #500-96-0003 between the U.S. Department of Health and Human Services (HHS), Office of Social Services Policy (now Office of Disability, Aging and Long-Term Care Policy (DALTCP)). For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the office at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. The e-mail address is: webmaster.DALTCP@hhs.gov. The Project Officer was Margaret Porter.
The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
TABLE OF CONTENTS
- I. INTRODUCTION
- Background
- Purpose of the Report
- The Secretarys Mandate
- Organization of the Report
- II. POPULATION CHARACTERISTICS
- Developmental Disabilities Defined
- The Site of the Population
- III. THE SERVICE DELIVERY SYSTEM
- The Evolution of the MR/DD System
- Service Delivery Organization
- Types of Services and Service Settings
- The Research Case for Community Programs
- IV. THE FEDERAL ROLE
- Federal Legislation
- Overview of Federal Expenditures
- Federal MR/DD Service Programs
- Federal Income Maintenance
- Federal Leadership
- VI. POLICY ALTERNATIVES
- Comprehensive Reform of Federal Financing for MR/DD Services
- Selected Changes to Medicaid
- Congressional Initiatives
- APPENDICES
- APPENDIX A: Bibliography
- APPENDIX B: Research Findings
- LIST OF EXHIBITS
- EXHIBIT 1: SSI Eligibility Criteria
- EXHIBIT 2: Number of Persons with Mental Retardation and Congenital Anomalies Receiving Federally Administered SSI Payments: December 1986
- EXHIBIT 3: MR/DD Service Providers
- EXHIBIT 4: Agencies Involved in the Virginia MR/DD Service System
- EXHIBIT 5: MR/DD Living Arrangements and Services
- EXHIBIT 6: Total Federal MR/DD Spending by Program
- EXHIBIT 7: Distribution of Medicaid Waivers Expenditures for the Developmentally Disabled by Type of Service
WORKING GROUP MEMBERS
| WORKING GROUP | |
| Robert B. Helms, ChairAssistant Secretary for Planning and Evaluation | Arnold R. Tompkins, Co-ChairDeputy Assistant Secretary for Social Services Policy |
| Phillip HawkesActing Assistant Secretary Human Development Services | Ross AnthonyAssociate Administrator for Policy Development, HCFA |
| David RustAssociate Commissioner for Disability/SSA | Steven GrossmanDeputy Assistant Secretary for Health |
| Isabel DunstAssociate General Counsel | Kate OBeirneDeputy Assistant Secretary for Legislation |
| Anabel Smith Bowen, DirectorOffice of Intergovernmental Affairs | Richard TeskeDeputy Assistant Secretary for Public Affairs |
| Dennis WilliamsDeputy Assistant Secretary for Budget | Richard P. KusserowInspector General |
| TECHNICAL GROUP | |
| Mary Harahan, ChairOffice of Social Services Policy/ASPE | Peg Porter, Project CoordinatorOffice of Social Services Policy/ASPE |
| Health Care Financing Administration Wayne Smith Linda Hamm Tom Hoyer Alan Friedlob Penni St. Hilaire Judy Mohsberg | Social Services Administration Al Harrison Dale Anderson Jack Baumel |
| Office of the Secretary Bob Dublin/OGC Kathryn Zuckerman/ASMB Pat Woods/OIA Austin Kessler/ASPE Mike Fishman/ASPE | Office of Human Development Services Bob Stovenour Ron Conley George Bouthilet |
| Consultants Brian Burwell, Systemetrics Tecla Jaskulski K. Charlie Lakin, University of MN Rebecca Weader, Macro Systems Claude Whitehead | Public Health Service Bernard Arons/NIMH |
| ASPE Support Staff Bob Clark Paul Gayer Jewell Griffin Azalee Lattimore | |
I. INTRODUCTION
BACKGROUND
Prior to the 1960's, children and adults with mental retardation and other developmental disabilities either lived in large institutions or with their families. In general, people with severe disabilities were isolated from society and not a part of the public consciousness. Few received any services other than routine or custodial care regardless of where they lived.
The past two decades have witnessed extraordinary changes in our understanding of the needs and capabilities of people with disabilities, especially those with severe handicaps, and in the system of services available to them. Parents, other advocates and disabled people themselves have lobbied hard for services that actively promote individual development. Numerous lawsuits have been filed to secure the rights of people with disabilities. Many large public institutions have closed, and those that remain house a population half the size of what it was 20 years ago. Thousands of young people with developmental disabilities have moved through the public school system and are emerging with expectations for a meaningful adult life. A new system of services in the community is evolving including expanded educational programs, supports to families and new opportunities for employment.
A number of critics have questioned whether public policies, particularly Federal financing policies, have kept pace with the dramatic changes that have occurred in the field. The conclusion of this report is that the critics are largely right. The most significant Federal program specifically designed to finance services, the Intermediate Care Facilities for the Mentally Retarded (ICF/MR) program, is institution-based; to be eligible for services, individuals must be placed outside their homes and be in need of "active treatment" and 24 hour supervision. Three quarters of the persons served by this program are in large, (average size 155 beds) costly State mental retardation facilities which are segregated from the rest of society. These institutions frequently are unable to provide opportunities for independence, productivity and integration into the community, the Federal policy goals expressed in the Developmental Disabilities Act Amendments of 1984, and reaffirmed in 1987 amendments.
In contrast to the relatively generous Federal expenditures for institutions, Federal support for family care and community-based residential arrangements is limited. Responsibility for community services is fragmented across a widely divergent array of Federal, State and local programs. In many areas of the country, particularly in rural areas, community services, other than special education, are not readily available.
There is growing impetus to expand Federal financing of community-based services for people with developmental disabilities. Legislation to accomplish this goal has been introduced in the last two sessions of Congress, most recently in September 1987 when Senator Chafee introduced the Medicaid Home and Community Quality Services Act (S. 1673). This bill currently has 24 co-sponsors. Seventy-five members of the House are co-sponsors of a companion bill introduced by Congressman Florio. While there may be disagreement about the exact shape of needed reforms, there is a growing consensus that the time for change has arrived.
PURPOSE OF THE REPORT
This report analyzes the impact of current Federal policies and programs on the growth of community living arrangements and supportive services for people with mental retardation and other developmental disabilities. It supports the goals of the Developmental Disabilities Act and asks how Federal financing policy can be brought more in line with these goals in a fiscally responsible manner. It also analyzes the anticipated costs and effects of reforming Federal policies.
There are several points about the report that should be highlighted. First, it focuses on people with developmental disabilities who, with appropriate supports, can live successfully in family and community settings. Second, it uses a functional definition of developmental disability: severely handicapping conditions occurring prior to birth, in childhood, or in adolescence, and which limit functioning in several major life activities. A large proportion of this target population is mentally retarded; yet there are also people with cerebral palsy, spina bifida and other severe physical impairments who are not mentally retarded but need considerable support. Conversely, not all people with mental retardation and related conditions are significantly limited in their functioning. The important point in defining the population is to assess the extent to which a person's functioning is impaired and results in a need for assistance over an extended period, often a lifetime.
The third point is that the report does not directly address the circumstances and needs of people whose developmental disabilities result in severe medical problems. Many of these people may require constant care and medical supervision in specialized health care facilities. The analyses presented here assume that Federal financing should continue to permit reimbursement for medically related services to the extent they are needed. However, the report begins with the promise that the overwhelming majority of people with developmental disabilities does not require care that is predominantly medical in orientation and that Federal financing policy should reflect this.
Finally, during the course of this study we have gained a renewed appreciation for the limits of Federal policy in shaping the characteristics of the service delivery system. While Federal financing is extremely important, the initiative and preferences of State government, communities, service providers, and disabled people and their families also determine how public dollars are spent. Despite its significant influence, Federal reform cannot substitute for State and local initiative.
THE SECRETARYS MANDATE
The Department of Health and Human Services (HHS) transmitted a report to Congress in January 1986 on Policies for Improving Services for Mentally Retarded and Other Developmentally Disabled Persons under Title XIX of the Social Security Act called for in the 1984 Developmental Disabilities Act. As a follow-up to the report, the Secretary of HHS approved the establishment of a Departmental Working Group comprised of senior policy officials from the Health Care Financing Administration (HCFA), the Social Security Administration (SSA), the Office of Human Development Services (OHDS), the Public Health Services (PHS) and the office of the Secretary. The Assistant Secretary for Planning and Evaluation chaired the Working Group. The Working Group was instructed to analyze Federal policy barriers to community living and to develop cost-effective policy options to enhance the independence, community integration and productivity of persons with mental retardation and other developmental disabilities.
ORGANIZATION OF THE REPORT
The chapters which follow describe:
- the size and characteristics of the population with developmental disabilities;
- the organization of the services delivery system and the types of services provided;
- Federal financing policies;
- implications for policy development; and
- options for reform.
References and related research questions are included in the Appendices.
The Working Group has developed two major options for policy reform. The first proposes a significant departure from the Federal Government's existing approach to financing services for persons with developmental disabilities. It would replace Medicaid as the primary source of Federal financing by establishing an entirely new program targeted to developmentally disabled persons with severe impairments. The second option outlines incremental policy changes designed to promote improved support of community-based services to this population. In addition, two Congressional Medicaid reform initiatives are described and analyzed.
The Working Group expects this report to serve as a basis for reconsideration of the Federal financing role and hopes it will contribute to a more effective, equitable and efficient system of services and support for individuals with mental retardation and other developmental disabilities.
II. POPULATION CHARACTERISTICS
Chapter II defines developmental disabilities and uses various techniques to estimate the size of the developmentally disabled population.
DEVELOPMENTAL DISABILITIES DEFINED
The definition of developmental disabilities (DD) as outlined in the Developmental Disabilities Act has changed over the years. The original definition was categorical and utilized diagnostic categories (i.e. mental retardation, cerebral palsy and epilepsy, with autism added later). The 1978 legislation established a functional definition. It described persons with severe, chronic physical or mental impairments or a combination of physical and mental impairments, likely to continue indefinitely, who experience substantial functional limitations in three or more major life activities including self care, language, learning, mobility, self-direction, independent living and economic self-sufficiency.
The functional definition focuses on people whose disability occur red before birth or early in life and who are likely to need a range of services throughout their lives. While States are required to use the Federal DD definition for certain purposes, most State service systems focus on people with mental retardation.1 A majority of States operate mental retardation rather than developmental disability systems; some operate DD systems using the Federal or similar definitions; and a few operate dual systems. The lack of uniformity has contributed to the frequent interchange of the labels "mental retardation" and "developmental disabilities," for example, in studies of residential services.
There is a great deal of overlap among the categories associated with developmental disabilities. For example, Gollay identified more than three dozen health-related problems contributing to or causing developmental disabilities (Gollay, 1981). While many persons with developmental disabilities exhibit mental retardation, there is a high prevalence of multiple handicaps among the population.
THE SIZE OF THE POPULATION
It is difficult to estimate the size and characteristics of the population with developmental disabilities. First, there is no generally accepted standard for what constitutes a "substantial functional limitation" as there is for determining significantly sub-average intelligence in the assessment of mental retardation. Second, even if there were consensus, there are no national or State level surveys of this population.2
Most data bases categorize individuals by diagnosed major handicapping condition without measures of functioning level. This is true, for example, of State reports on handicapped children served in special education programs. These provide statistics on the basis of primary diagnosis, but do not report on the number of students meeting the Federal definition of developmental disability nor levels of severity within diagnostic categories. Reports on the 1984-85 school year note that the 4,363,031 handicapped children receiving services included 717,785 students with mental retardation; 71,780 students with multiple handicaps; and 69,118 students with other health impairments, for a total of 858,683 (U.S. Department of Education, 1987). This information, however, does not indicate limitations in functioning. Since many students with mental retardation are mildly retarded, the actual number of students receiving special education services who would meet the criteria for developmental disability is presumably much lower.
There is a wide variation in published estimates of the developmentally disabled population that is mentally retarded. These range from 35 percent (Gollay, 1981) to 90 percent (Lakin and Hill, 1985). The lower estimates are based on primary diagnosis while the higher estimates reflect use of the mental retardation/developmental disabilities (MR/DD) service system. For example, a New York State study of about 44,000 recipients of residential, developmental, habilitative and support services from both public and private MR/DD agencies found that less than 5 percent of clients had a diagnosis of autism, cerebral palsy or epilepsy without a concurrent diagnosis of mental retardation (Jacobson and Janicki, 1983). The California DD council reported similar findings. It estimated that 90 percent of the individuals receiving MR/DD services in that State are mentally retarded (California State Council on Developmental Disabilities, 1981).
Although the broad category of developmental disabilities includes people with a number of different impairments, there is evidence that the overwhelming majority of clients in State service systems are persons with mental retardation.
Estimating Techniques
Three methods are available to estimate the size of the developmentally disabled population. The first is based on the prevalence of various developmentally disabling conditions among the general population. The second method uses data on MR/DD beneficiaries in the Supplemental Security Income (SSI) and social security Disability Income (SSDI) programs. The third method synthesizes data on prevalence, SSI and SSDI beneficiaries, and participation in the MR/DD service system. Estimates based on these methods are discussed below.
Prevalence Estimates
The prevalence of categorical diagnoses commonly associated with developmental disability in the general population, as supported by numerous studies, is approximately as follows:
- mental retardation - 1 percent or 2,387,400 people; (mild mental retardation - .5 percent)
- cerebral-palsy - .35 percent or 83,559 people;
- epilepsy - .75 percent or 179,055 people; and
- autism - .05 percent or 11,937 people.
However, the mere presence of such conditions does not in itself reflect the degree of resulting limitations. For example, most epilepsy is reasonably well controlled by medication and would not result in "substantial functional limitation" (Lakin and Hill, 1985).
Population estimates based on functional criteria have produced estimates similar to those based on categorical criteria. One notable effort to study the prevalence of functional disabilities was that of Boggs and Henney (1981). Using data from the Bureau of the Census Survey of Income and Education (SIE), Boggs and Henney developed proxies for "substantive functional limitations" in each of the areas reflected in the Federal categorical definition of developmental disabilities. This process yielded a prevalence estimate of 1.6 percent, or approximately 3.8 million individuals based on current population figures. State Developmental Disability Planning councils use a variety of prevalence rates generally ranging from 1 to 2 percent. For example, the Minnesota council presents three estimates for planning purposes, ranging from a high rate of 2.4 percent to a low rate of I percent (Minnesota Developmental Disabilities Planning Council, 1987).
Prevalence data on mental retardation are much more available than data on other developmental disabilities. As noted above, there is now general consensus that mental retardation is found in approximately 1 percent of the population or 2.4 million individuals (Birch et al., 1970; Dingman and Tarjan, 1960; Farber, 1968; Lindberg, 1976; MacMillan, 1977; Mercy, 1973; Tarjan et al., 1973). Within the MR population prevalence rates have been differentiated for four levels of retardation (Abramowicz and Richardson, 1974; Lakin and Hill, 1985; Maloney and Ward, 1979; Stein and Susser, 1975):
| Mild mental retardation | 0.50 (1,193,700) |
| Moderate mental retardation | 0.34 (811,716) |
| Severe mental retardation | 0.12 (286,488) |
| Profound mental retardation | 0.04 (95,496) |
| Total | 1.00 (2,387,400) |
The population with mild mental retardation -- measured IQ's ranging from about 50 to 68 with deficits in adaptive behavior includes many individuals whose handicap is not severe enough to meet the functional criteria of developmental disability, especially in the absence of other handicapping conditions. Many people with mild retardation are identified as such only during their student years, when they participate in special education programs. Most of these people make acceptable adjustments to adulthood although they do remain vulnerable in times of economic and personal difficulty (Conley, 1985). Because many people move in and out of the mental retardation service system over their lifetimes, they may be designated as a transitory mentally retarded population.
In contrast, individuals with moderate, severe, or profound mental retardation -- measured IQ of 50 or below with concurrent deficits in adaptive behavior -- can be considered a stable mentally retarded population, characterized by a high likelihood of ongoing need for treatment and care due to the degree of their impairments. Persons identified as moderately, severely and profoundly retarded almost always retain the recognition as retarded and are usually provided formal and informal services from childhood and throughout their lives. The overwhelming majority would meet functional criteria for developmental disability. The prevalence of stable mental retardation has been estimated by a number of studies of specific catchment areas.3 It is estimated that .5 percent of the general population, or about 1.2 million persons, are mentally retarded at a level that will necessitate lifelong assistance.
A subgroup within the stable mentally retarded population, those experiencing severe and profound mental retardation with a measured IQ of 36 or below on a standardized intelligence scale, has been identified by the Working Group as individuals most in need of specialized assistance in order to reach their developmental potential. Based on accepted prevalence rates, this subgroup would include approximately 390,000 individuals. People affected at comparable levels of severity by other developmentally disabling conditions would increase the size of this subgroup to approximately 450,000 individuals, including 270,000 adults and 180,000 children (Lakin, 1987). Two important points to note about this population are
-
Nearly 1/3 of this subgroup lives in ICFs/MR, about 110,1000 or 76 percent of the 145,000 ICF/MR residents.
-
Most of the 180,000 children live at home with their families and receive the bulk of their services through the public education system.
The comprehensive reform proposal outlined at the conclusion of this report recommends that a limited entitlement to services be extended to this particularly vulnerable subgroup.
Social Security Data
Most developmentally disabled adults living in the community receive social Security benefits, usually through the Supplemental Security Income (SSI) program and/or the Social Security Disability Insurance (SSDI) program. Two diagnostic groups used in the disability determination process likely to include developmentally disabled persons are mental retardation and congenital anomalies. A limited number of people who might be considered developmentally disabled may also be counted in other diagnostic categories.
In 1985, new regulations were issued to establish eligibility for Social Security on the basis of a diagnosis of mental retardation or autism (Federal Register, August 28, 1985). These require that deficit(s) be first "manifested in the developmental period" (i.e., before age 22) with an upper IQ limit of 70, as well as other limitations depending on IQ level, as shown in Exhibit 1:
| EXHIBIT 1: SSI Eligibility Criteria |
| A. A mental incapacity evidenced by dependence upon others for personal needs (e.g., toileting, eating, dressing, or bathing) and inability to follow directions, such that the use of standardized measures of intellectual functioning is precluded; or |
| B. A valid verbal, performance, or full scale I.Q. of 59 or less; or |
C. A valid verbal, performance, or full scale I.Q. of 60 to 69 inclusive, or in the case of autism, gross deficits of social and communication skills, with two of the following:
|
| SOURCE: Federal Register, August 28, 1985. |
According to a one percent data sample developed by Social Security, an estimated 747,200 individuals (595,900 adults and 151,300 children) with mental retardation or congenital anomalies were receiving assistance through SSI as of December 1986 as shown in Exhibit 2. This includes persons in Medicaid-certified facilities. Another 522,300 adults in the same two diagnostic groups receive SSDI benefits, for a total of 1,269,500. After adjusting for individuals with dual benefits (203,000) the total unduplicated count of developmentally disabled persons receiving SSI and/or SSDI benefits in 1986 is 1,066,500.
A major limitation of Social Security data in estimating the size of the developmentally disabled population is that it does not include children under 18 who live with families in which the parents' income is too high to qualify for SSI. Also not included are an additional 75,000 ICF/MR residents and an unknown number of developmentally disabled people in nursing homes who do not receive SSI benefits.
| EXHIBIT 2: Number of Persons with Mental Retardation and Congenital Anomalies Receiving Federally Administered SSI Payments: December 1986 | |||
| Total | Adults | Children | |
| Blind and Disabled | 2,762,300 (100.0%) | 2,481,400 (100.0%) | 280,900 (100.0%) |
| With Mental Retardation | 677,700 (24.5%) | 555,400 (22.4%) | 122,300 (43.5%) |
| With Congenital Anomalies | 69,500 (2.5%) | 40,500 (1.6%) | 29,000 (10.3%) |
| Total with Developmental Disabilities | 747,200 (27.0%) | 595,900 (24.0%) | 151,300 (53.8%) |
| SOURCE: SSI one-percent sample file, Social Security Administration, Office of Research and Statistics. | |||
Using Social Security data to estimate service need is difficult since no information is provided on functional limitations other than work-related limitation. Nevertheless, it is important to note that these data are generally consistent with identified prevalence rates, in particular for mental retardation.
Synthesis and Summary
Although precise estimates of the total size of the target population are lacking, estimates of national prevalence rates and participation in income maintenance and service programs based on diagnoses highly related to developmental disabilities provide useful proxies. From these data we infer that nationwide there are about 800,000 adults with developmental disabilities who might be potential consumers of services targeted to the presence of developmental disabilities. We also estimate there are 400,000 children (birth through age 21) who are moderately to profoundly mentally retarded or who function at a similar level and who are likely to need long-term support, for a total of 1,200,000. Another 1,200,000 children might be considered eligible under a broad categorical definition of developmental disabilities including children and youth with less severe handicaps such as mild mental retardation or learning disabilities as well as children with autism and cerebral palsy but with no retardation.
Most of the estimated 1,600,000 children with developmental disabilities will not require extensive services beyond those provided through the education system. The estimated 400,000 children and adults with severe and profound mental retardation or other comparable functional limitations can be expected to require services throughout their lifetimes. The types of programs and services needed by these and other developmentally disabled people are described in the following chapter.
III. THE SERVICE DELIVERY SYSTEM
This chapter examines those forces which have changed the way services are delivered, how State service systems are organized, where developmentally disabled people live and how this affects their access to services. Finally, it summarizes some of the research which substantiates the advantages of community care.
THE EVOLUTION OF THE MR/DD SYSTEM
Twenty-five years ago it was common practice to place both children and adults with severe or profound mental retardation, as well as others with less severe developmental disabilities, in institutional settings (Lakin et al., 1986b). This out of home care was typically provided by State and local governments and by charitable organizations. Placements in institutional settings peaked in 1967. At that time, the average daily population of people in State mental retardation institutions was 194,650 (Lakin, 1979).
Since then the appropriateness of institutional care for all but those whose disabilities are associated with severe medical problems has been called into question. As a result, the average daily population in State mental retardation institutions had dropped to 100,190 by 1986 (White et al., 1987).
Several important social and philosophical concepts underlie this shift away from institutional care. The first of these is the normalization principle which contends that for both humane and habilitative reasons, people with developmental disabilities should live and function in ways that are as close as possible to those of the rest of society's. The second, the right to habilitation, argues against mere "warehousing" of people and supports opportunities for individualized training and personal growth. Closely related is the least restrictive alternative which emphasizes the promotion of optimum development through opportunities to participate in programs and living arrangements that enhance independence and integration. Deinstitutionalization has evolved as a social policy and as a reflection of these concepts. Parents and other advocates have effectively used these changing ideas in advocating for more family and community-based services, in promoting legislation and in taking legal action.
Litigation has been a significant force in shaping the service delivery system. Among the important legal cases is Wyatt vs. Stickney (1972) which established the right to treatment of an individual committed to an institution without a trial. In another important case, Romeo vs. Youngberg (1976), the Supreme Court found that involuntarily detained mentally retarded persons have the following constitutionally protected rights: reasonably safe conditions of confinement, freedom from unreasonable bodily restraints and minimally adequate training. A related case, Halderman vs. Pennhurst School and State Hospital (1977), resulted in court-ordered deinstitutionalization. The use of the courts to affect residential services has continued. At the present time, 30 States are operating under some form of consent decree from the courts covering residents in State-operated ICFs/MR (GAO, 1987a).
SERVICE DELIVERY ORGANIZATION
The MR/DD service system is comprised of a wide array of services and supports including income maintenance for basic subsistence (housing, clothing and food), health care, habilitation, education and training as well as a range of other services including advocacy, case management, transportation, counseling and social/ leisure services. Exhibit 3 illustrates a typical matrix of providers.
| EXHIBIT 3: MR/DD Service Providers | |||
| Service | Provider | Jurisdiction | Administration |
| Education | School | School district | School board |
| Medical services | Hospital | Health area | Board of directors |
| Transportation | Bus Company | Metropolitan | Transportation authority |
| Recreation | Town, City | Municipality | Town board, City council |
| Family support | MR/DD State Regional Office | Multi-county region | State agency |
| Case management | MH/MR Agency | County | County board of commissioners, agency board of directors |
| Housing and day services | Private agency | Indeterminate | Board of directors |
| Adapted from Castellani (1987): The Political Economy of Developmental Disabilities. | |||
The services provided to individuals with developmental disabilities are quite distinct from traditional long-term care with its heavy emphasis on custodial and nursing care. In contrast, the primary services considered essential to the MR/DD population in addition to food, shelter, and supervision, are habilitation, education, and vocational assistance.
State Roles
As illustrated in Exhibit 4, several different State agencies play key roles in the MR/DD system. However, the orientation and influence of these agencies on local service delivery varies dramatically from one State to another. In fact, the most dominant characteristic of the service delivery system is state variation -- in the amount of money spent per capita, in the types of services provided (particularly the extent to which institutions as opposed to community services are emphasized), in who is served and in how people get connected to services. For example, the State of Illinois places heavy emphasis on large public residential facilities, large private ICFs/MR, and nursing homes as the backbone of its MR/DD services system. Decision-making is centralized at the State level and there are no local service entities except in a few metropolitan areas.
In contrast, its neighbor Michigan has a system characterized by a high degree of decentralization with most community services administered by county level mental health authorities. The State Department of Mental Health plays a critical role in guiding the planning and implementation of community services policy. Since the late 19601s, Michigan has reduced the number of people in State-owned mental retardation facilities from 12,000 to 1,650.
| EXHIBIT 4: Agencies Involved in the Virginia MR/DD Service System |
|
| SOURCE: Jaskulski and Weader (1987) |
In fact, the proportion of residents in small vs. large MR/DD residential facilities varies significantly across the States. On June 30, 1986, the proportion of residents in facilities for 15 or fewer individuals averaged 41.3 percent nationally, but ranged from less than 20 percent in Illinois, Kansas, Mississippi, Oklahoma, and Virginia to more than 70 percent in Alaska, Maine, Montana, New Hampshire, and Vermont (Lakin et al., 19!87).
There is equally remarkable variation in State use of the ICF/MR program. For example, Minnesota relies heavily on the ICF/MR program to fund its network of small community residential programs while none of Nebraska's 174 MR/DD group homes is an ICF/ MR, although its one large State facility is. According to Lakin, as of June 1986 the proportion of residential placements in facilities certified as ICFs/MR ranged from a high of 92.7% it Louisiana to a low of 19.6% in West Virginia. In addition, 11 States had no small (15 person or less) ICFs/MR, while over two-thirds of the MR/DD facility residents in five States (Indiana, Louisiana, Minnesota, Rhode Island, and Vermont) were housed in small ICF/MR program to fund community living opportunities for persons with severe and profound mental retardation (Lakin et al., 1987). Finally, there are extreme variations across States in the annual per them costs of ICFs/MR which range from $12,061 per year to $87,141 per year.
A study carried out by Macro Systems for the office of the Assistant Secretary for Planning and Evaluation (ASPE) examined the determinants of State policy decisions with respect to MR/DD services. Findings suggest that the degree of emphasis States give to community-based service delivery results from a variety of related factors including:
- an historically strong commitment to human services generally and community-based services in particular;
- the presence of strong, well-organized advocacy groups; and
- a healthy State economy at the time that services expansion is considered (Jaskulski and Weader, 1987).
While Federal policy is important -- as witnessed by the heavy reliance of many States on the ICF/MR program -- it is not the dominant factor in State decision-making regarding MR/DD services. Faced with the same Federal policy options, States have made very different choices.
TYPES OF SERVICES AND SERVICE SETTINGS
Services for the MR/DD population can be categorized according to the degree of restrictiveness or independence associated with a person's living arrangement. Exhibit 5 illustrates the broad continuum of living arrangements available to the MR/DD populalation and the types of services typically available in those settings.
It is certainly true that where one lives does not always determine the types of service an individual can expect to receive. For example, some group home residents are competitively employed, while some children living with their natural families are still educated in separate "special" schools. However, there is enough association to warrant using living arrangements as a way of organizing a description of the MR/DD service system.
| EXHIBIT 5: MR/DD Living Arrangements and Services | ||||
| Living Arrangement | Daytime Habilitation/Vocational Services | Support Services | ||
| Children | Adults | |||
Most Restrictive | Nursing Homes | No Education | No Day Activity | Health-related Services |
| Public MI Hospitals | Homebound (tutoring in living unit) | Therapy Services | ||
| Public MR Institutions | School/Habilitation Program in Residential Institutions | Day Activity/Vocational Program in Residential Institution | Counseling and Behavioral Interventions | |
| Private Institutions/Residendial Schools | Day Program in Special Schools | Day Activity CenterWork Activity CenterSheltered WorkshopEmployment Training/EvaluationSupported WorkSubsidized Work | Specialized Services
Respite CareCase Management | |
| Group Homes | FT Special Class Regular School | |||
| Personal Care Homes | PT Regular Class (with tutoring, resource room) Assistance | |||
| Boarding & Care Homes | ||||
| Foster Care Homes | ||||
| Semi-independent Living (Adults) | ||||
Least Restrictive | Independent (Adults) Natural | Regular Classroom | Competitive Employment | Generic Community Services |
| Foster Family (Children) | ||||
| Adoptive | ||||
| SOURCE: Lakin, 1987. | ||||
Three basic types of living arrangements have been identified for purposes of this report:
-
Large facilities/institutions - 16 beds or more (average large ICF/MR is 155 beds); most services provided within the institution; many facilities in remote locations; nearly all certified as ICFs/MR. Nursing homes are another type of institution; almost all are certified as SNFs or ICFs.
-
Community facilities - less than 16 beds (average small ICF/MR is 8 beds), with most services provided off-site by a mix of public and private providers; most located in community neighborhoods; some certified as ICFs/MR (20 percent of ICF/MR residents are in small facilities).
-
Family settings - includes foster as well as natural and adoptive family homes and independent living for adults; virtually all services provided outside the home; ICF/MR support not available.
Large Institutions
Generally, large residential facilities represent the most restrictive form of living arrangement for disabled persons and remain the primary available residential service. In June, 1986, 147,314 people were residents of large institutions (Lakin et al., 1986). Typically, these large facilities are congregate care operations run by the States and located in rural areas. Many residents receive little more than custodial care, and few have access to programs and activities outside the institution.
Over the past decade, the census of State institutions has significantly decreased as a result of deinstitutionalization. Between June 1977 and June 1982, the number of people in large public facilities (16 or more residents) decreased 27,400, from 207,363 to 179,966 persons (Lakin, 1987). From June 1982 to June 1986, the average daily population of State mental retardation institutions (16 or more residents) decreased from 151,537 to 100,190 persons (White et al., 1987). Between 1977 and 1985, however, the number of profoundly retarded people in State institutions decreased only from 69,100 to 59,306 people (Lakin, 1987). Despite the overall decline in the size of large institutions, people with more severe impairments are less likely to have access to community residential settings.
Programming in large facilities varies. Many facilities, especially those in rural areas, provide most services on the grounds; residents of these facilities are often denied the opportunity to leave to attend school or to participate in community-based services or activities. While the Education for All Handicapped Children Act requires States to provide education services to school age residents of public and private facilities, investigations have shown that the children in State ICF/MR facilities have been particularly vulnerable to denial of their right to education (Lakin et al. 1982; Senate Subcommittee on the Handicapped, 1984).
Traditionally, adult residents of large facilities are likely to spend their days in social/recreational day activities and in gaining personal social skills (habilitation services). A limited number of persons in institutions are able to participate in sheltered workshops and work activity programs although most wage earnings have been insignificant (Whitehead, 1987a). Residents of large ICFs/MR typically have had access only to onsite day and vocational programs.
Nursing Homes
A significant number of developmentally disabled people also reside in nursing homes, most of which are Medicaid certified Intermediate Care Facilities (ICFs) or Skilled Nursing Facilities (SNFs). Nursing homes differ from ICFs/MR in that they are medically oriented and not specifically designed to meet the needs of developmentally disabled people.
An analysis of the 1977 National Nursing Home Survey indicated an estimated 44,000 mentally retarded residents in nursing homes. About 60 percent of the people with a diagnosis of mental retardation were less than 65 years of age (Lakin, 1986). The National Center for Health Statistics (NCHS) Inventory of Long-Term Care Places (1986) revealed 39,500 persons with mental retardation in nursing homes. More recently the Health Care Financing Administration estimated that there were 140,000 mentally retarded persons in SNFs and ICFs in 1985 (GAO, 1987a). In its review of nursing homes in three States, the General Accounting Office (GAO) found that the overwhelming majority of mentally retarded residents in need of active treatment were not receiving such services.
It is widely accepted that unless developmentally disabled people have medical needs which require specialized medical care, their placement in nursing homes is inappropriate. The Omnibus Budget Reconciliation Act of 1987 (P.L. 100-203) prohibits the admission of mentally retarded people to nursing facilities beginning January 1, 1989 unless the State MR/DD authority has determined that an individual requires nursing care because of a physical or mental condition. States will be required to develop pre-admission screening programs to determine whether nursing level care is required and, if so, whether the individual can benefit from active treatment. As of April 1, 1990, the case of each mentally retarded or other developmentally disabled nursing home resident will be reviewed to determine whether the placement is appropriate and active treatment is required. The law also mandates that those individuals who are inappropriately placed in nursing facilities and have lived there less than 30 months should be discharged and arrangements made for them to receive active treatment.
Community Residential Arrangements
Community living arrangements include group homes, supervised apartments and board and care homes. These vary according to the number of residents, the amount of care or protective oversight provided, and the functional level of the residents. Community residential alternatives are funded by a variety of sources, with increasing use of the ICF/1-M program. In 1982, there were about 1,202 ICF/MR certified group homes. By June 1986, the number of ICF/MR group homes had more than doubled to 2,672 housing about 27 percent of the estimated 77,800 group home residents (Lakin et al., 1987).
In group homes not certified as ICFs/MR, the Federal contribution generally includes SSI or SSDI payments (which pay for room and board), Medicaid or Medicare for medical care, and food stamps. State funds, both SSI supplements and general revenues, are also important funding sources. In some areas, county or other local funds are used as well.
Between 1982 and 1986, the number of small settings more than doubled and the number of residents increased by 60 percent. The University of Minnesota's June 1986 survey of mental retardation services identified 19,236 small'(15 or fewer residents) public and private group residences, including boarding and semi-independent living arrangements. These housed 90,174 people (Lakin et al., 1987).
While it is difficult to estimate the population of developmentally disabled people in specific types of community facilities, estimates can be made of the number of individuals in specially licensed care settings. For example, there are about 19,100 persons with mental retardation in-specialized foster care. According to data collected in 1982, there are also about 4,000 persons with mental retardation in specially licensed personal care homes and an unknown, but presumably large number, in personal care settings without mental retardation program licenses (Lakin et al., 1985).
In semi-independent living programs, clients typically reside in individual units or apartments, with supervisory staff in close proximity. These arrangements are sometimes used as training for independent or supported living but may also be long-term placements for persons who need monitoring for health, behavioral, or cognitive reasons. Supported independent living arrangements are even less restrictive. Clients live without on-site supervision although they usually receive supportive training, counseling and/or periodic supervision. Services provided to individuals include training or monitoring in independent living skills (e.g., cooking, shopping), and also may include home health/ homemaker types of services similar to those in semi-independent living programs. Supported independent living arrangements can function as a transition to more independent living.
Family Settings
The overwhelming majority of people with developmental disabilities live with their natural, adoptive or foster families. The number of children and youth (birth to 21 years) with mental retardation and other developmental disabilities in residential facilities has actually decreased in recent years, from over 110,000 in 1967 to 60,000 in 1982 (Lakin, et al 1985). The number has declined further with an estimated 48,000 children and youth in residential placements in 1986 (Lakin, 1987).
In the United States, foster or family care programs specifically for people with mental retardation can be traced back to 1920 (Lakin, Bruininks, and Sigford, 1981); however, few of these programs survived the Great Depression. With efforts to depopulate State MR/DD institutions in the late 1960s, foster care regained popularity. In 1977, approximately 14,400 persons with mental retardation were in family care settings specifically licensed for people with mental retardation. By 1982, this number increased to 17,150, (Hill, B. et al., 1987). In 1986, States identified 19,000 persons in specialized foster care (Lakin et al., in preparation).
There are also many thousands of persons with developmental disabilities in generic foster care homes (i.e., homes not specifically licensed and/or contracted by States to provide services to persons with mental retardation). A comprehensive nationwide survey in 1980 identified approximately 23,000 children and youth in generic foster care who were considered mentally retarded (Office for Civil Rights, 1981). As of December 31, 1985, States reported 14,000 children (birth to 17 years) with mental retardation in generic foster care homes (Hill, B. et al., 1987).
State and local agencies increasingly offer programs providing training and support to families and other primary caregivers. Services for natural and foster families include respite care, special training in developmental service techniques and behavior management, support groups and counseling as well as information and referral services.
A 1984 survey of States indicated that all but Oklahoma had developed some form of supportive program for families of people with mental retardation although fewer than half of these were judged to be "extensive". About one-third of the States have developed family cash subsidy programs. These tend to be limited both in subsidy amount and in the number of participants, averaging about 115 clients statewide with a median subsidy of $250 per month and upper limits ranging from $115 to $500 (Agosta, Jennings and Bradley, 1985).
Other Services
There are several services that are not tied specifically to residential settings. These include education, day programs, vocational training and case management.
Educational Services
As a result of the Education for All Handicapped Children Act of 1975 (P.L. 94-142), children with mental retardation and other developmental disabilities are entitled to educational services through the local school district. Although a small number of children receive educational services at home, most go to school. Students may be in special classes all or part of the time. However, in more integrated school settings, disabled children have opportunities for interaction with their non-disabled peers.
Educational programs for teenagers and young adults may include vocational-training. When they leave school, they make the transition to employment or adult services, contingent on service availability.
Developmental/Vocational services
There are two general types of day habilitation programs for developmentally disabled adults: developmental (day activity/ work activity) programs and vocational (employment/employment training) programs. Day activity centers provide a range of skills training, including self-care, domestic, communication, social, recreational and prevocational activities. These services are used primarily by people with severe developmental disabilities and serve as an intermediate habilitation program for people who possess some vocational aptitude but whose productive capacity is considered less than 15 percent of that of a non-handicapped worker (Whitehead, 1987a).
The goal of vocational services is economic self-sufficiency, through training and employment in the most integrated work setting possible given an individual's ability. In the past, employment in sheltered workshops was the dominant form of vocational activity, including workshops where disabled workers perform tasks geared to their perceived abilities and pay is generally pro-rated to individual productivity. However, this type of employment is segregated and provides limited opportunity for interaction with non-disabled people. A more recent approach, supported employment, includes training and ongoing support at a regular work site, and interaction with co-workers. There is some evidence that supported work alternatives provide increased earning opportunity to disabled workers at comparable or lower overall program costs (Hill, M. et al., 1987a).
Although supported employment shows promise for economic independence for many persons with developmental disabilities, State reports indicate that lack of stable funding threatens its viability as a long-term vocational program option (Hill, M. et al., 1987; Jaskulski and Weader, 1987; Laski and Shultz, 1987; Whitehead, 1987a).
About 250,000 developmentally disabled adults live in family settings and participate in State-funded day and vocational training programs (Buckley and Bellamy, 1985). Additionally, most of the adults who live in smaller community-based residential facilities also participate in day treatment or vocational training programs outside their residence.
Case Management
Case management is increasingly viewed as a critical component in the MR/DD service system. The case manager's key function is to ensure the coordination of services in meeting the individual client's program goals. Case management is widely available in institutions, where services require monitoring and coordination even though they are provided within the facility. Case management in the community, while less available in many areas, may be more important than in institutional settings because community-based MR/DD services are dispersed and the role of the case manager is more complex.
It is not unusual for a person to have two or more service plans. For example, children receiving special education services have an Individualized Education Plan (IEP) while those individuals living in ICFs/MR must have an Individualized Program Plan (IPP). When a person becomes eligible for vocational rehabilitation services, an Individualized Written Rehabilitation Plan (IWRP) is developed. Ideally, these various service plans should be coordinated to ensure continuity and complementary activities.
The extent of case management and its organization varies across the States. Frequently case management is provided by a public or quasi-public entity. The role of case manager is that of a broker operating to balance competing interests, including those of service consumers, of service vendors, and of service purchasers. The effectiveness of the case manager is influenced by the relationship of case management to the various parties involved. For example, there may be a potential conflict of interest between a service provider's incentive to maximize revenues and a client's changing service needs. As a result, some argue that the only way case management can effectively focus on the client's interests is to be "independent" from both payers and providers.
THE RESEARCH CASE FOR COMMUNITY PROGRAMS
There is considerable research evidence that advances in adaptive behavior and independent living skills are associated with: 1) community living arrangements in small family-like settings and 2) learning experiences which provide opportunities for interaction with non-disabled people. For example, in one controlled study (Close, 1977), eight of 15 residents randomly selected from an institution were placed in a community residence with a supplemental vocational program. A one-year follow-up found that the experimental group made significantly greater gains in self-care and social interaction areas than their institutionalized peers. A similar study found that after four years, 18 severely retarded children from a large institution moved to "community" residential settings of 20 to 25 persons developed significantly better self-care and social skills than their matched peers who remained institutionalized (Kushlick, 1975). (See Appendix C.)
Two more recent studies of the effects of moving from an institution to community-based residence have supported these findings. As part of the Pennhurst longitudinal study, Conroy, Efthimiou, and Lemanowicz (1982) compared a group of 70 severely and profoundly retarded persons placed in community settings with a matched group of 70 who remained institutionalized. No significant differences existed between the groups at initial assessment, but at the end of two years the group who had moved to small community facilities (average of 3.2 residents each) showed significant increases in adaptive behavior skills, while the institution group's adaptive behavior remained essentially the same. More recently Rosen (1985) conducted a two year study of changes in adaptive behavior of two randomly selected groups of 58 institutional residents each; one group was placed in small community-based residential and vocational services while the other group remained in the institution. Although no statistical differences existed between the two groups at the outset, by the end of the two-year period clients placed in the community were statistically superior in adaptive behavior.
Although the studies cited above are only a few of those conducted and involve a small fraction of the residential care population, their findings are consistent and reflect important behavioral change clearly associated with movement from institutions to community-based living arrangements. More specifically, these studies demonstrate a consistent positive correlation between community integrated experience and the acquisition of adaptive behavior, particularly in the areas of self-care, social behavior, and communication.
Given the tendency for measures of adaptive behavior to reflect behaviors and skills that are part of daily community living, these findings should not be surprising. None the less, there is substantial empirical data to support the philosophical and social principles of continued depopulation of institutional settings and the expansion of family and community care.
Similar evidence of the effectiveness of community-based vocational training programs is available. A rapidly growing body of research shows people with severe handicaps, including many who in past decades would have been considered unlikely employment program clients, are succeeding in real work activities (Bellamy, Showers and Bourbeau, 1983; Brown et al., 1984; Gold, 1973; Hill, M. et al., 1987b; Katz, Goldberg and Shurka, 1977; Noble and Conley, 1987).
If policy is to seriously serve the goals outlined in the Developmental Disabilities Assistance and Bill of Rights Act -that is, "to enable (persons with developmental disabilities) to achieve their maximum potential through increased independence, productivity, and integration into the community" [Sec. 101(a)(5)) -- it must include efforts to promote community-based services. The relationship between Federal policy and the MR/DD service system is examined in Chapter IV.
IV. THE FEDERAL ROLE
The Federal Government influences the services and support av4iiable to people with mental retardation and other developmental disabilities in two principal ways: through financing policy and through leadership. This chapter examines how these roles are exercised, particularly their effect on the MR/DD services system and its clientele.
FEDERAL LEGISLATION
Prior to 1965, Federal support for the construction of mental retardation facilities, including State institutions and some community service centers, was provided through the Hill-Burton Hospital Construction Program. About $32 million was spent under this program on MR/DD projects during the period of 1958-1971 (Braddock, 1987). In 1963 the Mental Retardation Facilities and Community Mental Health Centers Act (P.L. 88-164) authorized the construction of research centers and community-based mental retardation facilities. A total of $155.7 million was expended under this Act between FY 1965 and FY 1971 (Braddock, 1987).
Federal involvement in financing MR/DD services in institutions expanded significantly with the enactment of the Medicaid program in 1965. This legislation allowed States to seek Federal financial participation (FFP) for mentally retarded "patients" in skilled nursing facilities (SNF). In 1967, a less expensive Intermediate Care Facility (ICF) benefit was authorized under Title XI of the Social Security Act. The ICF and SNF benefits were combined under Title XIX in 1971, and to this combination was added a little noticed, scarcely debated amendment which authorized an intermediate level of care specifically for persons with mental retardation, Intermediate Care Facilities for the Mentally Retarded (ICFs/MR).
The ICF/MR program has had a profound influence on the service delivery system. It provided Federal monies for upgrading the physical environment and quality of care in State institutions for the mentally retarded. It was the first open-ended funding source for services to mentally retarded persons. Its standards for active treatment and individualized habilitation plans have been major factors in the shift from custodial care to developmental programs in public institutions. It also permitted ICF/MR certification of small community-based facilities (15 beds or less). Forty-eight States and the District of Columbia participate in the ICF/MR program which is now the primary source of Federal financing for MR/DD services.
The Education for All Handicapped Children Act of 1975 (P.L. 94142) is another landmark piece of Federal legislation. This Act radically changed the relationship between Federal, State and local education agencies in providing special education. First, it guaranteed access to a free and appropriate education for all handicapped children and youth from 3-21 years old. Second, it developed numerous and demanding procedural standards for the delivery of special education. Third, it provided Federal funding directly for special education. Fourth, it created special incentives and assistance to stimulate State and local development of non-mandated services of importance (e.g., infant intervention). Finally, it supported research and demonstration activities directly related to the nature and quality of services provided under the Act.
P.L. 94-142 has greatly increased access to educational programs. For example, the total number of mentally retarded students receiving special education increased from 540,000 in 1966 (Mackie, 1969) to about 840,000 15 years later (U.S. Department of Education, 1984). In doing so it has had a dramatic effect on the number of children and youth with mental retardation in institutional care. Their numbers decreased from over 110,000 in 1967 to about 60,000 in 1982 and further declined to an estimated 44,000 in 1986 (Lakin et al., in preparation).
OVERVIEW OF FEDERAL EXPENDITURES
The previous chapter noted the dominant role of States in determining the mix of institutional and community services available to people with developmental disabilities. However, it is equally true that the Federal Government has assumed an instrumental role in financing services. Total Federal spending for MR/DD assistance programs in FY 1986 was about $8 billion (Braddock (1987). The distribution of these expenditures among Federal programs is illustrated in Exhibit 6. Federal expenditures represent about one-half of total public (Federal-State-local) spending for the MR/DD population (Braddock and Hemp, 1986).
The first thing to note about Federal financing is that over one-third of the Federal pie -- roughly $3 billion in FY 1986 -- is allocated specifically for residential services through the ICF/MR program. Three quarters of this $3 billion finances care in large State operated institutions. Prior to 1971, public institutions for the mentally retarded were supported exclusively by State revenues. By 1986, Federal payments accounted for almost one-half of all MR/DD institutional spending. This clearly represents a dramatic shift in financing from the States to the Federal Government.
The other large Federal expenditures are for income transfers, primarily the Supplemental Security Income Program (SSI) and the Social Security Disability Insurance Program (SSDI). SSI and SSDI benefits are used by disabled people living in the community for basic subsistence such as room and board. SSI expenditures were about $2 billion in 1986 with an additional $1 billion paid as SSDI benefits. The remaining Federal expenditures are spread across a large number of programs including special education grants, social services block grants, HUD 202/8 loan and rent subsidies, State vocational rehabilitation grants, Medicaid Home and Community-Based Care (HCB) Waivers and food stamps.
| EXHIBIT 6. Total Federal MR/DD Spending by Program(FY 1985 Total: $7.773 Billion) |
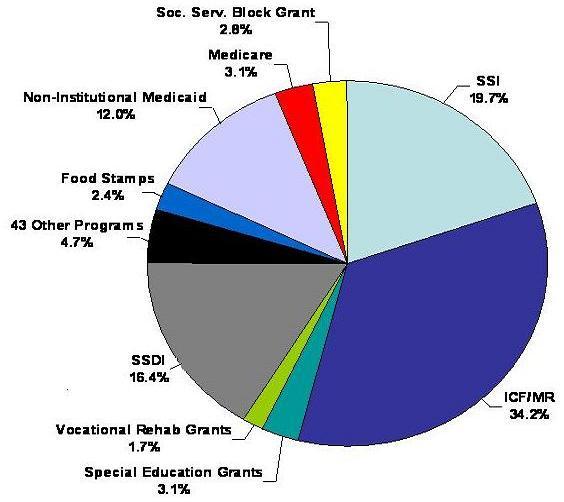 |
| SOURCE: Braddock, University of Chicago at Illinois, 1987. |
FEDERAL MR/DD SERVICE PROGRAMS
This section describes the specific Federal programs which provide services to the MR/DD population.
ICF/MR
Since its creation in 1971, the ICF/MR program has grown from approximately $200 million to $5.2 billion in 1986 (Burwell, 1987). To be certified as an ICF/MR, an institution must provide among other things, health or rehabilitative services to persons with mental retardation and related conditions who require 24 hour supervision. Services may be provided by the facility or through contracts with other providers. Every resident must have a written plan of care and be receiving "active treatment." While there are both large and small ICFs/MR, the overwhelming majority of ICF/MR residents (123,000 people or 85 percent) are in facilities with over 16 beds. The average size of these larger facilities is 155 beds (Lakin, 1987).
Medicaid eligibility for ICF/MR services includes categorical and financial criteria. ICF/MR recipients must first be determined categorically disabled according to SSI disability criteria. Their income and assets must also meet financial criteria established by each State Medicaid program. In actuality, however, virtually every person placed in an ICF/MR certified bed is eligible for Medicaid, and Medicaid pays for over 97 percent of the total cost of ICF/MR care (Burwell, et al., 1987). In addition, ICF/MR residents must be in need of active treatment with a diagnosis of mental retardation or "related conditions." Related conditions means a severe, chronic disability that meets all of the following conditions:
-
It is attributable to: cerebral palsy or epilepsy or any other condition, other than mental illness, found to be closely related to mental retardation because this condition results in impairment of general intellectual functioning or adaptive behavior similar to that of mentally retarded persons, and requires treatment of services similar to those required for these persons.
-
It is manifested before the person reaches age 22.
-
It is likely to continue indefinitely.
-
It results in substantial functional limitation in three or more of the following areas of major life activity: self-care, understanding and use of language, learning, mobility, self-direction, capacity for independent living.
SOURCE: 42CFRI Section 435.1009 (1986).
Several aspects of the ICF/MR program are particularly noteworthy:
-
ICF/MR expenditures of $5.2 billion (including the Federal and State shares) now constitute almost 13 percent of the total Medicaid budget.
-
Growth in the ICF/MR program alone accounts for the increased proportion of Medicaid spent for long-term care between 1975-1985.
-
Relatively few people participate; there were roughly 145,000 ICF/MR residents served in 1986 at an average annual cost of approximately $35,000 each.
-
ICF/MR expenditures overwhelmingly support care in large facilities of 16 or more beds; 87 percent of the expenditures in 1986 were for care in larger facilities and 75 percent were allocated to State operated institutions. The average annual reimbursement per person in State-operated facilities was $44,000.
-
The services paid for through the ICF/MR program are heavily influenced by the health and welfare orientation of the Medicaid program. As a result, there are gaps in client eligibility, (e.g., children living with parents who are not poor, young adults transitioning from the school system who do not need the level of care provided in ICFs/MR).
-
As noted in Chapter III, there is tremendous variation among States in their use of the ICF/MR program. As a result, Federal resources for persons with developmental disabilities are distributed unevenly across States. For example, five States (New York, Minnesota, Massachusetts, Rhode Island, and Louisiana), which account for 14 percent of the U.S. population, receive over 31 percent all Federal ICF/MR dollars. New York receives six Federal dollars per State resident for every one dollar received by Indiana, West Virginia, or Hawaii (Burwell, 1987).
-
The cost of ICF/MR care also varies significantly across States. In 1986, the average annual cost (reimbursement) per recipient ranged from $12,061 in West Virginia to $87,141 in Alaska. It is unclear the extent to which this variation reflects differences in the quality of care provided and/or differences in the actual cost of providing care., Some critics believe that reimbursement systems, particularly care provided in State-operated facilities, encourage the inefficient use of Federal resources for MR/DD services. It is frequently argued that excessive amounts of ICF/MR dollars are spent on administrative and other overhead costs, to the detriment of direct client services.
-
The most significant growth in the ICF/MR program is occurring in small facilities (under 15 beds), including the conversion of many non-certified group homes to ICFs/MR.
Home and Community Care Waivers
The most significant source of Federal funding for community services are the Medicaid Home and Community Care Waivers which allow Federal Financial Participation (FFP) for community services if the State demonstrates the "cost-effectiveness" of such services as substitutes for institutional care.
To be eligible for waiver services, clients must meet the functional (level of care) criteria established by each State for ICF/MR placements. Most developmentally disabled recipients of waiver services reside in small group homes which are not Medicaid certified. Client SSI income generally covers the cost of room and board while the waiver is used to finance the cost of residential program staff, day programs and transportation to and from the day program facility. As of June 30, 1986, approximately one-third of the 23,050 developmentally disabled waiver recipients were living with their natural families (Laudicina and Burwell, 1987). For these clients, the waiver usually pays for the cost of day program services and respite care. Exhibit 7 shows the distribution of waiver expenditures by type of service.
Total Federal/State expenditures under the Home and Community-Based Care waiver for services to developmentally disabled people rose from $3 million in 1982 to about $200 million in 1986. It should be noted that the average cost to Medicaid per waiver recipient in 1986 was less than $9,000 per year, approximately one-fourth the average annual cost of $35,000 per ICF/MR program recipient in 1986 (Lakin, 1987).
| EXHIBIT 7. Distribution of Medicaid Waivers Expenditures for the Developmentally Disabled by Type of Service(N = 31 States) |
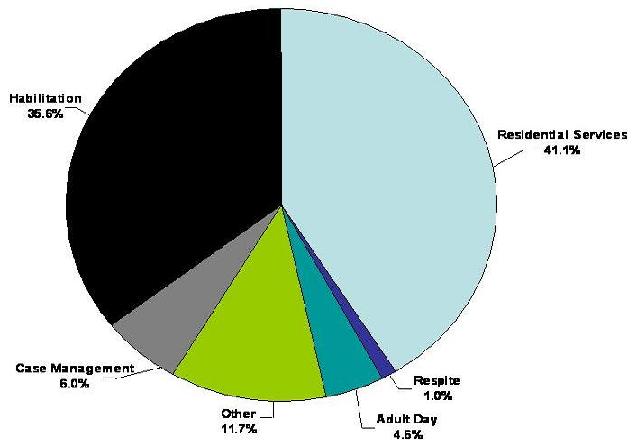 |
| SOURCE: Laudicina, S. and Burwell, B.: A Profile of Medicaid Home and Community-Based Care Waivers, 1985: Findings of a National Survey. Data are for FY 1985. |
Special Education and Vocational Education
Federal expenditures under the Education for all Handicapped Children Act P.L. 94-142 for State grants have now reached over $1 billion. According to the Department of Education, State grants represent approximately 8 to 9 percent of the per pupil costs of educating a handicapped child (Department of Education, 1987). The remaining costs are borne by State and local government.
The purpose of Special Education grants is to help States and schools to provide instruction and services tailored to the special needs of handicapped children.
Vocational Education, another source of Federal funds, provides vocational services for persons with developmental disabilities through school programs. Such programs frequently combine classroom instruction with on-site work experience. An estimated $25 million was spent in FY 1986 for vocational education services for people with developmental disabilities.
Vocational Rehabilitation
Vocational Rehabilitation (VR) is a federally funded, State operated program which assists persons with disabilities in entering or returning to employment. Under the Basic State Grant program, funds are provided to States on a formula basis for a variety of vocational rehabilitation services including counseling, training and job placement. Because people with developmental disabilities are often in need of sheltered or supported employment, in the past, many have been denied VR services. This has changed somewhat as a result of Federal funding for the development of supported employment.
The 1986 allocation for Vocational Rehabilitation services was $1.14 billion; the funding rate is 80 percent Federal, 20 percent State. In FY 1984, an estimated $125 million in Rehabilitation funds were expended to provide services to mentally retarded VR clients. Nearly 26,000 persons with mental retardation were rehabilitated, representing about 12 percent of the total VR caseload (Braddock, 1987a).
Other Service Programs
A variety of other Federal programs also are used to fund services in the community. For example, the Social Services Block Grant is a funding source for residential and MR/DD adult day programs in some States. Braddock et al. (1987) estimate Title XX expenditures for day programs at $101.8 million in 1986.
The Job Training Partnership Act (JTPA), administered by the Department of Labor, provides training and employment services to several special needs groups. However, its impact on the disabled population has been limited. Persons with all forms of disability completing the program in FY 1986 represented less than 10 percent of the total. Most developmentally disabled people would not be considered as JTPA candidates since eligibility is based on the capacity to earn hourly wages of at least $4.94, while the average starting hourly wage for MR/DD persons was $3.96 in 1985 (Kiernan, McGaughey, & Schalock, 1986). Total funding for JTPA in FY 1986 was nearly $1.8 billion; an estimated $23 million was spent for training and employment services for about 5,200 developmentally disabled people.
The primary Federally funded housing programs serving people with disabilities are Section 202, Section 106, and Section 8 programs. Section 202 provides direct Federal loans, for a maximum of 40 years, to assist private, non-profit corporations and consumer cooperatives in the development of new or substantially rehabilitated housing for elderly or handicapped individuals. By law, at least 10 percent of all Section 202 units must be reserved for use by handicapped people. Most proposals involving persons with developmental disabilities are for group homes (Larsen, 1987). The Section 106 program provides "seed money" to assist in Section 202 project planning. Section 8 assists persons with low income in obtaining housing through the use of rent subsidies. In March 1987, there were 390 Section 202 projects targeted to developmentally disabled people. These projects contained 5,204 units serving approximately 10,000 clients. Another 345 projects with 3,820 units were under development (Department of Housing and Urban Development, 1987). Some community services are financed by the Developmental Disabilities Act, primarily through the Basic State Grant program. States may use up to 65 percent of their allotment for special projects and services; however, funds are intended for project initiation and demonstration and are therefore not a source of long-term program support. The 1987 reauthorization of the Developmental Disabilities Act increased funding levels significantly to $62 million for Basic State Grants.
Health and Medical Care funding is provided by Medicaid, Medicare and programs administered by the Public Health Service. Most people who receive SSI are eligible for Medicaid services as outlined under the State Medicaid plan. Individuals not receiving SSI benefits may also qualify for Medicaid as "medically needy" if their medical expenses exceed their ability to pay. Most mentally retarded children in foster care placement are also covered by Medicaid. An estimated 660,000 developmentally disabled people are enrolled in the Medicaid program and comprise about 27 percent of the Medicaid disabled population. No definitive information is available about the level of Medicaid expenditures for acute care or other Medicaid services for this population beyond those provided under the ICF/MR program and the Home and Community-Based Waiver program. However, Burwell, in a study of Medicaid utilization among ICF/MR residents in three States, found these residents to be relatively low users of other Medicaid services. The exception was younger residents under 6 years who were relatively higher users of acute care (Burwell, 1987).
Developmentally disabled individuals who are SSDI beneficiaries are eligible for Medicare after a 24 month waiting period. Medicare has co-payment and deductible provisions; it does not require a means test as does Medicaid. However, Medicare benefits do not include long-term care.
Services for Children with Special Needs, funded under the Maternal and Child Health Block Grant, is another source of public monies. Braddock estimates that nearly $9.5 million was expended for services to developmentally disabled people in 1985 (Braddock, Hemp and Fujiura, 1986).
FEDERAL INCOME MAINTENANCE
Federal income maintenance programs are a significant source of cash benefits for people with disabilities living in the community.
The SSI Program
Title XVI of the Social Security Act, the Supplemental Security Income (SSI) program, authorizes a cash benefit for eligible disabled persons based on financial need. The program is centrally administered by the Social Security Administration, which supervises Disability Determination Units at the State level. These units determine eligibility based on disability for both the SSI and SSDI programs. To be eligible for SSI benefits, individuals must meet the following conditions:
- have little or no income or resources;
- be medically disabled as determined by the disability determination services (or by an appeals process entity such as administrative law judge) an the initial application, or during a continuing disability review; and
- initially not be working or working but earning less than the substantial gainful activity (SGA) level, currently $300 per month. Children below working age are considered eligible if their disability is of comparable severity to one that would preclude SGA in an adult.
Eligibility based on disability is defined in medical listings specific to the individual's primary diagnosis. For example, the medical listing for persons with mental retardation or autism requires that deficits in measured intelligence and/or functioning levels must be evident and have been initially exhibited prior to age 22.
The SSI program is presently the most important source of Federal assistance for people with mental retardation and related disabilities living in the community. Several aspects of financing and participation are important to note.
-
Federal SSI payments to persons with mental retardation were estimated to be over $2.0 billion in 1986 (Braddock, 1987).
-
The average payment to all disabled individuals was $250 per month, not including optional State supplements.
-
Recipients who earn income above a certain level lose $1 of their SSI benefit for every $2 earned; however, a number of exclusions are applied in determining earned income, and disability eligibility is maintained while the SSI recipient works.
-
The Federal Benefit Rate (FBR) for SSI recipients living in the household of another and receiving support is reduced by one-third. This primarily applies to developmentally disabled adults who live with their parents.
-
Persons institutionalized in Medicaid-certified facilities lose all SSI benefits except for a personal needs allowance of approximately $25.
-
All but two States elect to supplement SSI benefits for at least some beneficiaries; the monthly supplement ranges from $3.40 (Oregon) to $538.00 (Alaska), and does not necessarily cover all SSI beneficiaries.
-
According to the Social Security Administration there were about 747,200 persons with a primary diagnosis of mental retardation or congenital anomalies receiving SSI benefits in 1986. This represents approximately 27 percent of the SSI/disabled rolls.
The SSDI Program
Title II of the Social Security Act establishes an entitlement program for disabled workers and their dependents funded from the Disability Insurance Trust Fund, created by employer and employee contributions. Most developmentally disabled people who receive SSDI do so under the Adult Disabled Child benefit (ADC) which authorizes payments to surviving disabled children age IS or older of retired, deceased or disabled workers eligible for Social Security benefits. The average monthly benefit check for SSDI/ADC recipients is less than $150 a month. The Social Security Administration estimates that 522,300 people with mental retardation or congenital anomalies received SSDI/ADC benefits in 1986.
An SSDI provision with potential effect on people with severe disabilities is the requirement that workers in non-profit organizations be covered. This means that people with severe or profound retardation working in sheltered workshops and earning as little as $400 per quarter could qualify for disability insurance and be entitled to cash benefits, Medicare coverage and retirement income. The average monthly benefit, based on prior earnings, for disabled workers under SSDI was $466 per month in 1986.
Food Stamps
Since residents of small community living facilities became eligible for food stamp benefits in 1976, Federal expenditures for food stamps for people with developmental disabilities have risen to an estimated $200 million in FY 1986 (Braddock, 1987).
No estimates are available of numbers served; however, the average monthly food stamp benefit is about $45 per month per person.
FEDERAL LEADERSHIP
Federal leadership is evident in the promotion of quality in the ICF/MR program. Federal ICF/MR standards have been instrumental in upgrading the level of care in large public institutions. The recent "look behind" surveys successfully identified problem MR/DD providers, both public and private and required correction of identified deficiencies. Regardless of their concerns about possible loss of FFP, States have generally applauded Federal leadership in carrying out these reviews (Jaskulski and Weader, 1987). The revised Conditions of Participation for the ICF/MR program, provide further evidence of the Federal Government's commitment to improve the quality of residential care.
Perhaps the greatest manifestation of Federal leadership in this field is the Developmental Disabilities Act. Its significance is only marginally related to the amount of Federal dollars administered by its programs. The Developmental Disabilities Act goals -- independence, productivity and integration into the community -- establish the context for assessing Federal MR/DD policy and for formulating new directions.
V. WORKING GROUP FINDINGS
The previous chapters have described the size and characteristics of the Population with developmental disabilities; the organization of the service delivery system; and the Federal role in financing MR/DD services and support. In this chapter the conclusions of thick Working Group are presented. They are as follows:
-
The principal Federal financing program for the MR/DD population, the ICY/MR program, has not kept pace with changes in the field of developmental disabilities over the past twenty years.
-
While the ICF/MR program represents the largest Federal investment in services specifically for people with mental retardation and other developmental disabilities, almost 90 percent of its resources are allocated to services in large institutional settings.
-
This institutional care emphasis occurs despite the substantial body of research showing that significant advances in adaptive behavior and independent living skills of developmentally disabled people are strongly associated with:
- small family-like settings;
- community-based learning experiences that provide challenges and promote independence; and
- opportunities to interact with peers who are not disabled.
-
Research also shows that even severely disabled people can work productively and that people with substantial medical care needs can benefit from habilitation and community integration.
-
Most significantly, through litigation, advocacy and the! promotion of new legislation, parents, disabled people themselves and professionals have demonstrated their commitment to achieving family and community living for the great majority of the MR/DD population.
-
-
The most important Federal supports for the noninstitutionalized MR/DD population are the SBI and BSDI programs, neither of which is intended to pay for the full range of needed services.
-
SSI and SSDI are designed to provide basic subsistence, principally room and board.
-
The average SSI benefit and SSDI benefits for this population are $250 and $150 per month respectively. it is estimated that the average monthly cost for a young adult who needs habilitation and vocational services as well as a supervised residence is close to $1,900, based on 1982 cost estimates adjusted for inflation (Ashbaugh and Allard, 1984).
-
Nearly all States supplement SSI benefits; however, the average State supplement is only $51 per month. in some States, few SSI beneficiaries with developmental disabilities are eligible for the State supplement.
-
-
The lack of substantial Federal participation in the financing of community services is widely perceived as a barrier to independence, productivity and community integration for developmentally disabled individuals. It may also load, down the road, to a reinstitutionalization movement.
-
People with developmental disabilities who are placed out of their homes in an ICF/MR are assured services. In essence, they have an entitlement to care as long as they remain in a certified facility and meet ICF/MR eligibility criteria. Given the lack of community alternatives, it is not surprising that on average, an ICF/MR resident in a large public institution has spent 13 years in such a facility (Sigford et al., 1982).
-
People who live in a non-ICF/MR community residence or with their family have no such protection. They can either get some services, end up on waiting lists or do without altogether, depending on the service availability in their area and the commitment of their States to pay. Even people with the most severe impairments have no guaranteed access to services after they exit programs provided through the public school systems. A recent study of waiting lists includes reports of tens of thousands of persons with mental retardation waiting for community services across the various States (Association for Retarded Citizens/US, 1987).
-
Without a greater public commitment to community services, many of these young adults could end up losing most of the gains made through special education and, in the process, begin a new trend toward increased institutionalization.
-
-
Many features of the principal Federal funding source for KR/DD services -- the Medicaid program -- make it unattractive as the vehicle for Federal policy reform.
-
A basic issue in current financing policy is the large concentration of resources (ICFs/MR) devoted to the support of a relatively few people, primarily those in large public institutions. However, as this report tries to make clear, there is a much larger number of developmentally disabled people living in the community who could benefit from community services. Because of the open-ended nature of the Medicaid program, creating a community service benefit similar to the ICF/MR benefit would be prohibitively expensive. HCFA has estimated that. such an expansion could cost at least $700 million in additional Federal Medicaid costs in its first year. Other estimates are that expansion could add as much as $2.5 billion to Federal Medicaid costs (Burwell, 1987).
-
A second issue is Medicaid's welfare orientation. Medicaid was originally intended to provide Federal and State assistance to poor people. As a result, several sub-groups of the MR/DD population are generally excluded from receiving benefits. These groups include children who remain at home with parents whose income is above Medicaid eligibility levels and young adults making the transition from school to adult life.
-
A third issue is the health insurance orientation of Medicaid which imposes regulatory and administrative limitations on the nature of the services which can be covered. Most services needed by persons with developmental disabilities are not (and should not be) medical or even health related.
-
The reliance on Medicaid to pay for MR/DD services also creates widespread potential for administrative inefficiencies at the State level. State mental retardation agencies and State Medicaid agencies must coordinate eligibility, service coverage, provider licensing, payment system, and quality assurance policies to ensure Federal Financial Participation (FFP). Since State Medicaid Agencies and State Mental Retardation Agencies frequently operate under vastly different policy agendas, successful coordination is not always achieved.
-
Finally, the open-ended financing of the Medicaid program distorts policy decisions at the State level. States often emphasize maximizing FFP under Medicaid instead of developing a high quality MR/DD service system at a reasonable price.
-
-
Two central features of the Medicaid program, which are widely, viewed as strengths, make it difficult to create a new MR/DD program outside of Medicaid.
-
Advocacy groups and States believe that keeping MR/DD services within Medicaid will protect the entitlement aspects of the ICF/MR program and shield it from budget cuts.
-
Most interest groups strongly support the heavy involvement of the Federal Government in quality control that has been achieved in the Medicaid program and do not want to see this role diminished.
-
The Working Group recommends that these considerations be kept in mind in reviewing the policy options described in the final section of this report.
VI. POLICY ALTERNATIVES
This chapter outlines a range of policy alternatives for reforming MR/DD financing. The first two options were developed by an HHS Working Group. One would result in a comprehensive restructuring of Federal financing of services to persons with mental retardation and other developmental disabilities. The other Working Group option would make incremental changes to Medicaid. It should be noted that neither option developed by HHS staff has been endorsed by the Department nor by OMB. Two congressional initiatives are also presented. Each would expand Medicaid funding and eligibility to this population.
COMPREHENSIVE REFORM OF FEDERAL FINANCING FOR MR/DD SERVICES
Summary
The Working Group's first alternative would establish an entirely new Federal program for financing services to persons with mental retardation and other developmental disabilities. It would consolidate existing Medicaid funding for non-acute care services into a new program to be administered outside of Medicaid. The program would be budget neutral; aggregate Federal spending under the new program would equal actuarial projections of Medicaid spending for MR/DD services under current law, and would be capped. States would be allowed wide flexibility in the use of Federal funds for financing MR/DD services, but they could not exceed annual spending caps established for each State. The new program would retain an entitlement component by requiring States to provide a core set of supportive services to persons with severe developmental deficits. Persons with less severe disabilities would be eligible for, but not entitled to, Federally-financed services at the option of States.
How This Option Differs from Current Policy and Other Options Under Consideration
The comprehensive reform option is the most extreme departure from current policy in that it would move approximately $4.2 billion in Federal spending for MR/DD services under Medicaid (in FY 1990) into a new program. It would create a new financing mechanism specifically targeted to the service needs of persons with developmental disabilities. The proposal would also eliminate the current ICF/MR program, establish a cap on aggregate Federal spending, and gradually lead to a more even distribution of Federal resources for MR/DD services across the 50 States.
Administration, Eligibility, Services and Quality Assurance
A single Federal agency would implement and administer the new program. This agency would be responsible for State allocation formulae, payments to States, eligibility and service coverage requirements, and the development and enforcement of quality assurance standards. At the State level, a lead agency would be responsible for administering Federal funds. In all likelihood this would be the State Mental Retardation/Developmental Disabilities Services agency.
States would be required to enroll a mandatory population defined on the basis of functional level. The mandatory population would consist of persons with severe developmental deficits (more specifically defined in the full proposal). Persons who met these functional criteria would be entitled to a core set of services and protections regardless of income status, although cost sharing of parents and recipients would be required. States could also extend eligibility to persons with less severe disabilities at their option, but these persons would not be legally entitled to services under Federal law.
The core set of services and protections include case management, residential services, respite care and vocational/developmental services. Again, States could provide a broader package of services at their own option. The mandatory and optional eligibility and service coverage components of the program reflect the structure of the current Medicaid program. Access to acute care and other medical services would be available through Medicaid, Medicare, private health insurance, or other coverage mechanisms without change to existing laws.
Quality assurance standards would be client-based rather than facility or provider-based, with an emphasis on individualized assessment, treatment, and outcomes. All contracted providers, with the exception of client family members, would be required to be licensed by the State. States would have the option of contracting with independent accreditation and quality assurance agencies which met Federal standards.
Financing
Under the new MR/DD Services Program, States could claim Federal Financial Participation (FFP) for eligible expenditures up to a pre-determined ceiling, established in advance by the Department for each fiscal year. Federal/State matching rates would stay the same as those used in the Medicaid program.
The aggregate Federal ceiling for the first year of implementation would equal projected Federal expenditures for that year, based on the Medicaid Forecasting System, for ICF/MR, Medicaid waiver, and other non-acute care services for the MR/DD population. The ceiling would be adjusted downward to offset projected increases in Federal SSI benefits resulting from the elimination of the ICF/MR program.
After the first year of implementation, each State's ceiling would be indexed for State population growth and price increases, using the Average Wage Index for Social Security-Covered Employment. An additional adjustment would be made for States which currently spend less than the national mean (per capita) for MR/DD services. This adjustment is intended to gradually lead to the more equitable distribution of Federal resources for MR/DD services across States.
Elimination of the ICF/MR program will have a budgetary impact on the SSI program since under the new program current ICF/MR recipients will be entitled to receive full SSI benefits instead of a reduced personal needs allowance. The aggregate ceiling on FFP would be reduced by an amount equal to the aggregate increase in Federal SSI payments.
Advantages and Advantages of This Option
This option is intended to achieve the kinds of programmatic reforms that growing numbers of people in the field believe are needed in Federal MR/DD policy within a budget neutral framework. At the same time, States are guaranteed the same increases in Federal spending that are projected under current Medicaid law.
Incentives for families to place children in out-of-home residential settings would be eliminated; services would be available regardless of where a person chose to live. Services would be tailored to individual needs. Resources would be targeted to the most severely disabled and vulnerable population.
Increases in aggregate Federal spending would become more predictable in a fixed-budget program, and inequities in the allocation of Federal resources across States would be reduced.
Replacing Medicaid with a fixed-budget program as the primary funding source for MR/DD services is viewed by some as the major disadvantage of this proposal. Despite its eligibility and service coverage restrictions, and its inefficiencies, the open-ended financing aspect of Medicaid and its protection from Gramm-Rudman sequestrations remains attractive, particularly to State program administrators. The new program may also be criticized for not mandating expansions in community-based and family support services. The proposal rather assumes that the fiscal incentives built into the program will lead to expansions in community-based and family-support financing and delivery systems.
SELECTED CHANGES TO MEDICAID
Summary
The second option of the Working Group is to modify existing Medicaid program provisions, particularly the ICF/MR program, which limit opportunities for financing services in integrated, community-based settings. The intent of these proposals is to make the program more responsive to individual needs. Any or all changes could be implemented.
-
Limit ICF/MR Eligibility
This reform proposes four strategies to limit ICF/MR services to clients actually in need of active treatment:
- require State screening of prospective ICF/MR residents, using HCFA regulations (to be developed) based on degree of disability, functional status, and least restrictive alternatives
- require States to conduct ongoing reviews utilizing these criteria
- restrict new admissions to large ICFs/MR
- restrict ICF/MR admissions of children to small facilities.
The purpose of this reform is to clarify that the ICF/MR program is designed to serve only those developmentally disabled individuals who require active treatment in an intensive care setting.
-
Reform Reimbursement for Medicaid Services
This proposal would address inappropriate cost shifting to Federal financing, promote cost-effective care in community settings and reduce inequities among the States. Research is essential to develop reimbursement reforms in the ICF/MR and other Medicaid long-term care programs, in particular to gain understanding of the cost discrepancies between the States. This research should include:
- a comprehensive study of the cost of providing ICF/MR services in the States to provide a data base for precise and defensible payment reforms; and
- experimentation with prospective client-centered payment systems to reduce incentives for the use of high-cost options.
-
Improve Quality Assurance
Problems can occur because of the apparent conflict of interest when States survey and certify their own public facilities. Three options to address the conflict of interest issues are proposed:
-
Deemed status - States would give facilities the option to choose an approved private accrediting body to conduct certification surveys; the accreditation decision would thus be binding. Public facilities that chose not to use deemed status would be certified by HCFA rather than the State. This would require legislative change.
-
Federal survey and Certification of public facilities the Federal Government would be responsible, as the Institute of Medicine has recommended, for all Federally-financed long-term care facilities.
-
Increased Federal reviews - this option would retain the current quality assurance system but increase Federal "look behind" activities.
The first of these three options, deemed status, is recommended with HCFA certifying and possibly also surveying public facilities which do not use the deemed status option.
-
-
Ensure Parental Responsibility
Parents of children with developmental disabilities frequently do not contribute to the cost of publicly supported care, especially for Medicaid-funded services in an ICF/MR. A change in the Medicaid statute to require financially able parents to contribute to the cost of care for their minor children in an ICF/MR would reduce the incentive to institutionalize children, promote parental involvement, and provide additional funds for other Medicaid services. Federal cost sharing should also be considered for HCB waiver services.
-
Allow ICF/MR Residents to Retain Earnings
Supported employment and other advances in the MR/DD field have demonstrated that many ICF/MR residents have significant earnings potential. Under current regulations, however, only a small amount -- usually $25.00 per month -- may be retained by the resident for personal use, with the rest applied to the cost of care. This potential disincentive to gainful employment activity should be reduced by:
- permitting residents to retain earnings but requiring them to contribute toward their room and board at rates comparable to those in the community; and
- allowing employed residents to continue their eligibility for ICF/MR services, at least until such time as their earnings reach a level sufficiently adequate to support appropriate living arrangements outside an ICF/MR.
How This Option Differs from Current Policy and Other Options Under Consideration
The proposals discussed in this option are designed to modify elements of existing policy and represent an incremental approach to policy reform. Unlike the comprehensive reform proposal, they would maintain Medicaid as the primary funding source for MR/DD services. These incremental changes are far less sweeping than either the Working Group's reform proposal or the Congressional initiatives.
Advantages and Disadvantages of This Option
The changes proposed in this option would address some of the more troublesome features of-the current Medicaid ICF/MR program. These reforms could stimulate growth in small community-based ICFs/MR and help insure those individuals who are served are clearly in need of active treatment in an intensive service setting. Implementation of these changes could be viewed as an interim measure and would not necessarily inhibit the development of other proposals.
Since significant momentum has been building for reform of Federal financing of services to MR/DD people, these incremental changes are not likely to be favorably received, especially if it appears the Congress might enact major reform legislation.
CONGRESSIONAL INITIATIVES
Legislation was introduced during the 100th Congress which would have expanded Medicaid funding for home and community services to persons with mental retardation and other developmental disabilities. Two of the bills are discussed briefly here. Although neither piece of legislation was enacted, they will probably be reintroduced early in the next Congress.
Medicaid Home and Community Quality Services Act of 1987 (Chafee/Florio)
Summary
This bill was introduced by Senator Chafee; a House version of the bill was sponsored by Representative Florio. It would mandate that States provide an array of community and family support services to persons with developmental disabilities who are eligible for Medicaid. Persons with developmental disabilities are defined as those whose disability occurred prior to age 22. The age of onset limitation would gradually increase over time, to age 50, so that most persons whose disabilities were not developmental in nature would also eventually be entitled to these services. States also have the option to cover a broader array of supportive services, if they choose. Financial criteria for Medicaid eligibility would be liberalized for this population, also at State option. Funding for expanded community-based services for persons with developmental disabilities under Medicaid would be partially offset by a freeze on Federal matching funds for services provided in facilities with more than 15 beds. It is anticipated that this provision would provide a significant fiscal incentive for States to continue initiatives to deinstitutionalize clients from large State institutions to smaller, more integrated, residential settings.
Medicaid Quality Services to the Mentally Retarded Amendments of 1988 (Waxman)
Summary
This legislation, introduced by Representative Waxman, would allow States to provide community habilitation services to MR/DD persons as an option under the State Medicaid plan. It would also extend eligibility for community habilitation services to anyone who would be eligible for Medicaid if admitted to an institution (essentially waiving deeming of parental income for children under 18). It would reclassify ICFs/MR as "habilitative" facilities and establish detailed quality assurance standards for them. The legislation would essentially extend statutory authority to quality assurance-standards which are now in effect in regulatory form. Further, it would require States to ensure appropriate placement in habilitation facilities by conducting pre-admission screening and annual client reviews. The proposed legislation also includes detailed employee protection arrangements for employees affected by reduction plans for large facilities.
Now Those Initiatives Differ from Current Policy and Other Options
These initiatives differ from current policy in that they would considerably expand the availability of Federal Financial Participation for community-based services under Medicaid. They both also expand the population eligible for Medicaid-financed services at the option of States. These Congressional initiatives also differ from each other. The Chafee bill requires States provide community services while the Waxman bill only gives States the option of providing these services on a statewide basis. Another difference is their approach to Medicaid financing of large facilities. The Chafee bill would freeze Medicaid spending for large facilities at current levels while the Waxman bill prohibits payment limits for either community or institutional care.
The two bills also differ with respect to eligibility. The Waxman bill limits eligibility to persons whose disability initially occurred prior to age 22, and specifically excludes persons with a primary diagnosis of mental illness from eligibility for community habilitation services. The Chafee bill extends eligibility to all persons with disabilities with an age of onset prior to 22, and eventually increases the age of onset limitation to age 50. Overall, the Chafee bill is more proscriptive in mandating Medicaid changes for persons with developmental disabilities, while the Waxman bill allows financing and system changes to occur at the option of individual States.
Both Congressional initiatives retain Medicaid as the primary Federal funding source for MR/DD services while the HHS comprehensive reform proposal would remove funding of MR/DD services from Medicaid. The Working Group comprehensive reform proposal also establishes individual State funding ceilings and mandates a core set of services to the most severely impaired population.
Advantages and Disadvantages of the Congressional Initiatives
Both initiatives would expand access to home and community services for persons with developmental disabilities. The Chafee Bill gained a great deal of Congressional support with 47 co-sponsors in the Senate and 198 for its companion bill in the House.
The Chafee bill is most strongly supported by those who favor continued reduction in the use of large institutions as residential care settings. The Waxman bill is more neutral with regard to the preferred size of residential care facilities and provides increased protections for employees of large institutions. At the same time, the Waxman bill mandates increased Federal involvement in monitoring and enforcing quality assurance standards in Medicaid-certified facilities which serve persons with developmental disabilities.
Estimates of the cost of these legislative initiatives vary. The Congressional Budget office estimates only incremental costs for the Waxman Bill ($31 million in the second year of implementation). According to CBO, the Chafee bill would result in additional Medicaid costs of $30 million in the first year of implementation, but lead to net Federal savings of $765 million over the subsequent four years of implementation due to the freeze on spending for large-scale facilities. Initial analyses conducted by HCFA, however, estimate the Chafee bill would result in additional Federal Medicaid costs of $700 million in the first year of implementation with new Federal Costs Of $1.3 billion by the third year. Cost estimates of these two legislative proposals depend largely on assumptions about the degree to which States would move to expand the availability of Medicaid-financed community-based services for persons with developmental disabilities upon enactment of the legislation. It has been estimated by David Braddock, in his study of public MR/DD expenditures, that States now spend more than $2 billion dollars annually on community programs for persons with developmental disabilities. It seems reasonable to expect that a good proportion of these State expenditures would be shifted to Medicaid under either Congressional proposal.
Conclusion
All of these proposals all have a common goal: to expand access to home and community-based services for persons with mental retardation and other developmental disabilities. They represent, however, different approaches to policy reform. The Department's Working Group developed a major proposal to comprehensively reform the way in which the Federal government finances services for persons with developmental disabilities, and a second proposal which identifies selected changes to the Medicaid program. Both Congressional initiatives would significantly expand the availability of Federally-financed home and community-based services for the developmentally disabled, and promote other reforms in the service delivery system.
The policy debate will continue in the 101st Congress, in the new Administration, and among all persons concerned with Federal policy regarding persons with developmental disabilities. It is the purpose of this report to help inform these discussions.
APPENDIX A. BIBLIOGRAPHY
Abramowicz, H.K. and Richardson, S.A. (1975). Epidemiology of severe mental retardation in children: Community studies. American Journal of Mental Deficiency, 80(1)m 18-39.
Accreditation Council on Services for People with Developmental Disabilities (1987). Standards for services for people with developmental disabilities. Boston, MA: Author.
Adler, G., Burwell, B., Madigan, D., and Rymer, M. (1984). Short-evaluation of Medicaid: Selected issues. Report prepared for U.S. Department of Health and Human Services, Office of Assistant Secretary for Planning and Evaluation and Office of Research and Demonstrations, Health Care Financing Administration. Contract No. HHS-100-82-0038. Cambridge, MA: Urban Systems Research and Engineering, Inc.
Agosta, J., Jennings, D., and Bradley, V. (1985). Statewide family support programs: Nationwide survey results. In J. Agosta & V. Bradley (eds.), Family care for persons with developmental disabilities: A growing commitment. Boston MA: Human Services Research Institute.
Agosta, J., Bradley, V., Rugg, A., Spence, R. and Covert, S. (1985). Designing programs to support family care for persons with developmental disabilities: Concepts to practice. Boston, MA: Human Services Research Institute.
Allard, M.A. and Toff, G.E. (1980). Current and future development of Intermediate Care Facilities for the Mentally Retarded: A survey of state officials. Washington, DC: George Washington University, Intergovernmental Health Policy Project.
Ashbaugh, J. and Allard, M.A. (1984). Comparative analyses of the cost of residential, day and other programs within institutional and community settings. Boston MA: Human Services Research Institute.
Association for Retarded Citizens of the United States (1987a). A national status report on waiting lists of people with mental retardation for community services (draft). Arlington, TX: Author.
Association for Retarded Citizens of the United States (1987b). ARC facts: Introduction to mental retardation. Arlington, TX: Author.
Baroff, G.S. (1982). Predicting the prevalence of mental retardation in individual catchment areas. Mental Retardation, 20(3), 133-135.
Bellamy, G.T., Sowers, J., and Bourbeau, P. (1983). Work and work-related services: Post-school options for students with severe handicaps. In M.E. Snell (ed.), Systematic instruction for the moderately and severely handicapped (2nd ed.). Columbus, OH: Charles E. Merrill.
Berkowitz, M. and Hill, M.A. (eds.) (1986). Disability and the labor market: Economic problems, policies, and programs. ILR Press.
Birch, H.G., Richardson, S.A., Baird, D., Horobin, G., and Illsley, R. (1970). Mental abnormality in the community: A clinical and epidemiological study. Baltimore, MD: Williams and Wilkins.
Boggs, E.M. (1987). Toward timely corrections of mental retardation/developmental disabilities policy. In Commentaries on Braddock et al., American Jouranl of Mental Deficiency, 29(2), 138-139.
Boggs, E. and Henney, R.L. (1979). A numerical and functional description of the developmentally disabled population in the United States: By major life activities as defined in the Developmental Disabilities Assistance and Bill of Rights Act as amended in PL 95-602. Philadelphia, PA: EMC Institute.
Braddock, D. (1987a). Federal policy toward mental retardation and developmental disabilities. Baltimore, MD: Paul Brookes Publishing.
Braddock, D. (1987b). On values, determinants of spending, and civil rights: Response to commentaries on Braddock et al. America Journal of Mental Deficiency, 92(2), 144-150.
Braddock, D. (1985). Federal spending for mental retardation and developmental disabilities. Public Policy Monograph Series, No. 7. Chicago, IL: Institute for the Study of Developmental Disabilities, University of Illinois at Chicago.
Braddock, D. and Fujiura, G. (1987). State government financial effort in mental retardation. American Journal of Mental Deficiency, 20(5).
Braddock, D. and Hemp, R. (1986). Governmental spending for mental retardation and developmental disabilities, 1977-1984. Hospital and Community Psychiatry, 37(7), 702-707.
Braddock, D., Hemp. R., and Fujiura, G. (1987). National study of public spending for mental retardation and developmental disabilities. American Journal of Mental Deficiency, 92(2), 121-133.
Braddock, D., Hemp, R., and Fujiura, G. (1986). Public expenditures for mental retardation and developmental disabilities in the United States: State profiles (2nd ed.). Chicago, IL: Institute for the Study of Developmental Disabilities, University of Illinois at Chicago.
Braddock, D., Hemp, R., and Howes, R. (1987). Financing community services in the United States: Results of a nationwide study. Mental Retardation, 25, 21-30.
Braddock, D., Hemp, R., and Howes, R. (1984). Public expenditures for mental retardation and developmental disabilities in the United States: State profiles (2nd ed.). Chicago: Institute for the Study of Developmental Disabilities, University of Illinois at Chicago.
Bradley, V.J., Conroy, J.W., Ashbaugh, J.W., and Walbridge, R.H. (1983). Pennhurst longitudinal study 1979 to 1983: Fourth year summary. Boston, MA: Human Services Research Institute.
Bruininks, R.H., Meyers, C.E., Sigford, B.B., and Lakin, K.C. (eds.). (1981). Deinstitutionalization and community adjustment of mentally retarded people. Washington, DC: American Association on Mental Deficiency.
Buckley, J. and Bellamy, G. (1985). National survey of day and vocational programs for adults with severe disabilities: A 1984 profile. Unpublished paper.
Burwell, B. (1987a). ICF/MR program trends: 1975 to 1985. In Rymer, M. and Burwell, B. Medicaid eligibility: Analysis of trends and special population groups. Medicaid program evaluation (Working paper 5.6). Baltimore, MD: Department of Health and Human Services, Health Care Financing Administration, Office of Research and Demonstrations, February 1987.
Burwell, B. (1987b). Working papers. Boston, MA: SysteMetrics/McGraw-Hill.
Burwell, B., Clauser, S., Hall, M., and Simon J. (1987). Medicaid recipients in intermediate care facilities for the mentally retarded. Health Care Financing Review 8(3), 1-12.
Castellani, P. (1987). The political economy of developmental disabilities. Baltimore, MD: Paul Brookes Publishing.
Close, D.W. (1977). Community living for severely and profoundly retarded adults: A group home study. Educational and Training of the Mentally Retarded, 12(3), 256-262.
Coalition on Human Needs (1986). Block grants: Beyond the rhetoric. An assessment of the last four years. Washington, DC: Author.
Congressional Research Services (1986). Services for persons with mental retardation and developmental disabilities: Background information and discussion of issues. Washington, DC: Author.
Congressional Research Service (1984). Legislative history, trends, and adequacy of the Supplemental Security Income program: A ten year overview. An information paper prepared for the Special Committee on Aging, United States Senate. Washington, DC: Author.
Conley, R.W. (1985). Impact of federal programs on the employability of mentally retarded persons. In K.C. Lakin and R.H. Bruininks (eds.), Strategies for achieving community integration of developmentally disabled citizens. Baltimore, MD: Paul Brookes Publishing.
Conley, R.W. (1973). The economics of mental retardation. Baltimore, MD: John Hopkins University Press.
Conroy, J.R. (1985). Medical needs of institutionalized mentally retarded persons: Perception of families and staff members. American Journal on Mental Deficiency, 89(5), 510-514.
Conroy, J.W. and Bradley, V.S. (1985). The Pennhurst longitudinal study: A report of five years of research and analysis. Philadelphia, PA: Temple University Developmental Disabilities Center. [http://aspe.hhs.gov/daltcp/reports/5yrpenn.htm]
Conroy, J., Efthimiou, J., and Lemanowicz, J. (1982). A matched comparison of developmental growth of institutionalized and deinstitutionalized mentally retarded clients. American Journal of Mental Deficiency, 86, 581-587.
Dingman, H.F., and Tarjan, G. (1960). Mental retardation and the normal distribution curve. American Journal on Mental Deficiency, 64(6), 991-994.
Farber, B. (1968). Mental retardation: Its social context and social consequencies. Boston, MA: Houghton Mifflin Co.
Gettings, R.M. (1980). Utilization of federal/state medical assistance programs on behalf of mentally retarded persons: A discussion of relevant federal policy issues. Alexandria, VA: National Association of State Mental Retardation Program Directors.
Gettings, R. and Katz, R. (1987). Supported employment: Federal policies and State activities related to integrated work opportunities for persons with developmental disabilities. Alexandria, VA: National Association of State Mental Retardation Program Directors.
Gettings, R.M., and Mitchell, D. (1980). Trends in capital expenditures for mental retardation facilities: A state-by-state survey. Washington, DC: National Association of State Mental Retardation Program Directors.
Gold, M. (1973). Research on the vocational habilitation of the retarded. In N.R. Ellis (ed.), International review of research in mental retardation (Vol. 6). New York, NY: Academic Press.
Gold, M. (1972). Stimulus factors in skill training of the retarded on a complex assembly task: Acquisition, transfer, and retention. American Journal of Mental Deficiency, 76, 517-526.
Gollay, E. (1981). Summary report on the implications of modifying the definition of developmental disabilities. Contract No. HEW-105-78-5003. Santa Fe, NM: Gollay and Associates.
Gollay, E. (1980). Operational definition of developmental disabilities. Columbia, MD: Morgan Management Systems.
Gollay, E., Freedman, R., Wyngaarden, M., and Kurtz, N.R. (1978). Coming back: The community experiences of deinstitutionalized mentally retarded people. Cambridge, MA: Abt Books.
Griss, B. (1985). Report on health care coverage for working-aged persons with physical disabilities: A key to reducing disincentives to work. Madison, WI: Wisconsin Department of Health and Social Services, Division of Community Services.
Haber, L. (1987). State disability prevalence rates: An ecological analysis of social and economic influences on disability. Prepared under Mary Switzer Research Fellowship, National Institute on Disability and Rehabilitation Research.
Halderman v. Pennhurst, 46 F. Supp. 1295 (E.D. Pa. 1977); affd. 612 F.2d 84 (3rd Cir. 1979); revd in part 451 U.S. 1 (1981); affd 673 F.2d 645 (3rd Cir. 1982), cert granted 100 S. Ct. 3046.
Hamilton, B.B., Betts, H.D., Ruth, G.J., Gillette, H.E., Green, G.M., Garrity, S.D., and Libman, A.S. (1978). A study of the medical and allied health services delivery system for substantially handicapped disabled adults. Chicago, IL: Northwestern University, Rehabilitation Institute of Chicago.
Hauber, F., Bruininks, R., Hill, B., Lakin, K.C., and White, C. (1984). National census of residential facilities: Fiscal year 1982. Minneapolis, MN: University of Minnesota, Department of Educational Psychology.
Heal, L.W. (1987). Institutions cost more than community services. In Commentaries on Braddock et al., American Journal of Mental Deficiency, 92(2), 136-138.
Hemming, H., Lavender, T., and Phil, R. (1981). Quality of life of mentally retarded adults transferred from large institutions to new small units. American Journal of Mental Deficiency, 86(2), 157-169.
Henney, R.L. (1980). The impact of the amendment of the definition of developmentally disabled on the DD program in FY 79 and FY 80. Washington, DC: Institution for Comprehensive Planning.
Hill, B.K., Bruininks, R.H., and Lakin, K.C. (1983). Physical and behavioral characteristics of mentally retarded people in residential facilities. Health and Social Work, 8(2), 85-95.
Hill, B.K., and Lakin, K.C. (1986). Classification of residential facilities for mentally retarded people. Mental Retardation, 24, 107-115.
Hill, B.K., Lakin K.C., and Bruininks, R.H. (1984). Trends in residential services for mentally retarded people, 1977-1982. The Journal of the Association for Persons with Severe Handicaps, 9(4), 243-250.
Hill, B.K., Lakin, K.C., Novak, A.R., and White, C.C. (1987). Foster care for children and adults with handicaps: Child welfare and adult social services (Report No. 23). Minneapolis, MN: University of Minnesota, Department of Educational Psychology. [http://aspe.hhs.gov/daltcp/reports/fosteres.htm]
Hill, B.K., Lakin, K.C., Sigford, B.B., Hauber, F.A., and Bruininks, R.H. (1982). Programs and services for mentally retarded people in residential facilities. Minneapolis, MN: University of Minnesota, Department of Educational Psychology.
Hill, M., Hill, J., Wehman, P., Revell, G., Dickerson, A., and Noble, J. (1987a). Supported employment: An interagency funding model for persons with severe disabilities. Journal of Rehabilitation, 53(3), 13-22.
Hill, M., Wehman, P., Krezel, J., Banks, P., and Metzler, H. (1987b). Employment outcomes for people with moderate and severe disabilities: An eight-year longitudinal analysis of supported competitive employment. Journal of the Association for Persons with Severe Handicaps, 12(3), 182-189.
Holman, J.G., and Bruininks, R.H. (1985). Assessing and training adaptive behaviors. In K.C. Lakin and R.H. Bruininks (eds.), Strategies for achieving community integration of developmentally disabled citizens. Baltimore, MD: Paul H. Brookes.
Human Services Research Institute (1985). Summary of data on handicapped children and youth. Boston, MA: Author.
Jacobson, J.W., and Janicki, M.P. Observed prevalence of multiple developmental disabilities. Mental Retardation, 21(3), 87-94.
Janicki, M., Mayeda, T., Epple, W. (1983). Availability of group homes for persons with mental retardation in the United States. Mental Retardation, 21(2), 45-51.
Jaskulski, T. and Weader, R. (1987). Analysis of federal and state policies affecting services to mentally retarded and other developmentally disabled persons. Prepared for the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Contract No. HHS-100-84-0035. Washington, DC: Macro Systems, Inc. [http://aspe.hhs.gov/daltcp/reports/stapersp.htm]
Jones, P., Conroy, J., Feinstein, C., and Lemanowicz, J. (1982). A matched comparison study of cost-effectiveness: Institutionalized and deinstitutionalized clients. Philadelphia, PA: Temple University, Developmental Disabilities Center.
Kiernan, W., McGaughey, M., and Schalock, R. (1986). Employment survey for adults with developmental disabilities. Boston, MA: Developmental Evaluation Clinic, Childrens Hospital.
Kierman, W.E. and Stark, J.A. (eds.) (1986). Pathways to employment for adults with developmental disabilities. Baltimore, MD: Paul H. Brooks.
Kotler, M., Wright, G., Jaskulski, T., and Kreisberg, I. (1985). Synthesis of cost studies on the long term care of health impaired elderly and other disabled persons. Washington, DC: Macro systems, Inc. [http://aspe.hhs.gov/daltcp/reports/syncost1.htm]
Kushlick, A. (1975). Epidemiology and evaluation of services for the mentally handicapped. In M.J. Begab and S.A. Richardson (eds.), The mentally retarded and society: A social sciences perspective. Baltimore, MD: University Park Press.
Lakin, K.C. (1987). Working papers.
Lakin, K.C. (1979). Demographic studies of residential facilities for the mentally retarded: An historical review of methodologies and findings. Minneapolis, MN: University of Minnesota, Department of Psychoeducational Studies.
Lakin, K.C., and Bruininks, R.H. (1985). Strategies for community integration of developmentally disabled citizens. Baltimore, MD: Paul H. Brookes.
Lakin, K.C., Bruininks, R.H., and Sigford, B.B. (1981). Early perspectives on community adjustment of mentally retarded people. In R.H. Bruininks, C.E. Meyers, B.B. Sigford, and K.C. Lakin (eds.). Deinstitutionalization and community adjustment of mentally retarded people. Washington, DC: American Association on Mental Deficiency.
Lakin, K.C., and Hill, B.K. (1985). The target population. In K.C. Lakin, B.K., Hill, R.H. Bruininks (eds.). An analysis of Medicaids Intermediate Care Facility for the Mentally Retarded (ICF-MR) program. Minneapolis, MN: University of Minnesota, Department of Educational Psychology.
Lakin, K.C., Hill, B.K., and Bruininks, R.H. (eds.). (1985). An analysis of Medicaids Intermediate Care for the Mentally Retarded (ICF-MR) Program. Minneapolis, MN: University of Minnesota, Department of Educational Pyschology.
Lakin, K.C., Hill, B.K., Bruininks, R.H., Hauber, F.A., and White, C.C. (1985). Status and recent change in residential services for mentally retarded people. In K.C. Lakin, B.K. Hill, and R.H. Bruininks (eds.). An analysis of Medicaids Intermediate Care for the Mentally Retarded (ICF-MR) program. Minneapolis, MN: University of Minnesota, Department of Educational Psychology.
Lakin, K.C., Hill, B.K., Bruininks, R.H., White, C.C., and McGuire, S.P. (in preparation). Sourcebook on long-term care for persons with developmental disabilities. (2nd ed.). Minneapolis, MN: University of Minnesota, Department of Educational Psychology.
Lakin, K.C., Hill, B.K., Hauber, F.A., and Bruininks, R.H. (1982). Changes in age at first admission to residential care of mentally retarded people. Mental Retardation, 20(5), 216-219.
Lakin, K.C., Hill, B.K., Street, H., and Bruininks, R.H. (1986). Persons with mental retardation in state-operated residential facilities: Years ending June 30, 1984 and 1985 with longitudinal trends from 1950-1985. Minneapolis: University of Minnesota, Department of Educational Psychology.
Lakin, K.C., Hill, B.K., White, C.C., and Wright, E.A. (1987). Medicaids Intermediate Care Facility for the Mentally Retarded (ICF-MR) program: An update. (Report #25). Minneapolis, MN: University of Minnesota, Department of Educational Psychology.
Landesman-Dwyer, S., Sackett, G.P., and Kleinman, J.S. (1980). Relationship of size to resident and staff behavior in small community residences. American Journal of Mental Deficiency, 85, 6-17.
Landesman-Dwyer, S., Stein, J.G., and Sackett, G.P. (1976). Group homes for the mentally retarded: An ecological and behavioral study. Olympia, WA: State Department of Social and Health Services.
Larsen, L. (1987). National housing plan for persons with severe disabilities. Project No. DU1000741416, U.S. Department of Housing and Urban Development. Baltimore, MD: Johns Hopkins University School of Continuing Studies.
Laudecina, S. and Burwell B. (1987). A profile of Medicaid home and community-based care waivers, 1985: Findings of a national survey. Baltimore, MD: Health Care Financing Administration, Office of Research, August 1986.
Lindberg, D. (1976). Prevalence of developmental disabilities in West Virginia. Elkins, WV: Davis and Elkins College.
Lubitz, J., and Pine, P. (1986). Health care use by Medicares disabled enrollees. Health Care Financing Review, (7) 4.
Luckey, R.E., and Neman, R. (1976). Practices in estimating mental retardation prevalence. Mental Retardation, 14(1), 16-18.
Mackie, R. (1969). Special education in the United States: Statistics 1948-1966. New York, NY: Teachers College Press.
Medicaid Home and Community Quality Services Act of 1987. Congressional Record, September 10, 1987, S11956-S11971.
Mercer, J. (1973). The myth of the 3% prevalence. In R.K. Eyman, C.E. Meyers, and G. Tarjan (eds.), Sociobehavioral studies in mental retardation. Washington, DC: American Association on Mental Deficiency.
Minnesota Governors Planning Council on Developmental Disabilities (1987). A new way of thinking. St. Paul, MN: State Planning Agency.
Moon, S., Goodall, P., and Wehman, P. (eds.) (1986). Critical issues related to supported employment. Richmond, VA: Rehabilitation Research and Training Center, Virginia Commonwealth University.
National Association of State Directors of Special Education (1986). Severely handicapped youth exiting public education: Issues and concerns. Washington, DC: Author.
National Association of State Mental Retardation Program Directors (1987). Community service systems: Accepting the challenge of proactive management. Report of annual meeting. Washington, DC: Author.
National Council on the Handicapped (1986). Toward independence: An assessment of Federal laws and programs affecting persons with disabilities. Report to the President and the Congress. Washington, DC: Author.
National Governors Association, Center for Policy Research (1984). State reimbursement policies for privately operated intermediate care facilities for the mentally retarded: 1984. Washington, DC: Author.
National Institute of Child Health and Human Development (1986). An evaluation and assessment of the state of the science: Mental retardation and developmental disabilities. Washington, DC: Public Health Service, National Institutes of Health.
National Study Group on State Medicaid Strategies (1983). Restructuring Medicaid: An agenda for change. Washington, DC: Center for the Study of Social Policy.
Nirje, F. (1976). The normalization principle. In R.B. Kugel and A. Shearer (eds.), Changing patterns in residential services for the mentally retarded (rev. ed.). Washington, DC: U.S. Government Printing Office.
Noble, J. and Conley, R. (1987). Accumulating evidence on the benefits and costs of supported and transitional employment for persons with severe disabilities. Journal of the Association for Persons with Severe Handicaps, 12(3), 163-174.
Office for Civil Rights, Department of Health and Human Services (1981). 1980 children and youth referral survey: Public welfare and social services agencies (3 volumes). Washington, DC: Author.
Office of the Inspector General (1984). A program inspection on the transition of developmentally disabled young adults from school to adult services. Washington, DC: U.S. Department of Health and Human Services.
Perlman, L., and Austin, G. (1986). The transition to work and independence for youth with disabilities. A report of the Tenth Mary Switzer Memorial Seminar. Alexandria, VA: National Rehabilitation Association.
Romeo v Youngberg, 102 S. Ct. 2452 (1982).
Rosen, D.B. (1985). Differences in adaptive behavior of institutionalized and deinstitutionalized mentally retarded adults. Ann Arbor, MI: University Microfilms International (No. 85-08,127).
Rusch, F. (ed.) (1986). Competitive employment: Issues and strategies. Baltimore, MD: Paul Brookes Publishing.
Rymer, M., Burwell, B., Madigan, D., and Adler G. (1984). Short-term evaluation of Medicaid: Selected issues. Cambridge, MA: Urban Systems Research and Engineering, Inc.
Schalock, R.L., and Harper, R.S. (1981). A systems approach to community living skills development. In R.H. Bruininks, C.E. Meyers, B.B. Sigford, and K.C. Lakin (eds.), Deinstitutionalization and community adjustment of mentally retarded people. Washington, DC: American Association on Mental Deficiency.
Senate Subcommittee on the Handicapped (1984). Services for mentally retarded persons. Senate Hearing 98-1045.
Sigford, B.B., Bruininks, R.H., Lakin, K.C., Hill, B.K., and Heal, L.W. (1982). Resident release patterns in a national sample of public residential facilities. American Journal on Mental Deficiency, 87(2), 130-140.
Social Security Administration (1987a). A summary guide to Social Security and Supplemental Security Income work incentives for the disabled and blind. SSA Pub. No. 64-030. Baltimore, MD: Office of Disability.
Social Security Administration (1987b). Model presentation: SSI and work (1987 revision). Baltimore, MD: Author.
Social Security Administration (1987c). Section 1619 quarterly statistical report. Baltimore, MD: Office of Supplemental Security Income.
Social Security Administration (1987d). Number and percentage distribution of blind and disabled persons receiving federally administered SSI payments by reason for eligibility, age, and diagnostic group, December 1986. Baltimore, MD: Office of Supplemental Security Income, Division of Program Management and Analysis.
Social Security Administration (1987e). Social Security Bulletin, 50(3), March 1987.
Social Security Administration (1987f). Social Security Bulletin, 50(5), May 1987.
Social Security Administration (1987g). Social Security Bulletin, 50(6). June 1987.
Social Security Administration (1987h). Status of administration of state supplementation, Medicaid decisions, and interim assistance programs as of July 1987. Baltimore, MD: Office of Supplemental Security.
Social Security Administration (1986a). Disability evaluation under Social Security. SSA Pub. No. 05-10089. Baltimore, MD: Author.
Social Security Administration (1986b). The Supplemental Security Income program for the aged, blind, and disabled: Characteristics of state assistance programs for SSI recipients. U.S. Department of Health and Human Services. SSA Publication 17-002.
Social Security Administration (1984). Social Security handbook. U. S. Department of Health and Human Services.
State Council on Developmental Disabilities (1981). Informational report: Who is being served by the Regional Centers? Sacramento, CA: Author.
Stein, Z. and Susser, M. (1975). Public health and mental retardation: New power and new problems. In M.J. Begab and S.A. Richardson (eds.), The mentally retarded and society: A social science perspective. Baltimore, MD: University Park Press.
Tarjan, G., Wright, S.W., Eyman, R.K., and Keran, C.W. (1973). National history of mental retardation: Some aspects of epidemiology. American Journal of Mental Retardation, 77(4), 369-379.
Taylor Institute (1987). Evaluation and service identification project for developmentally disabled residents of intermediate care and skilled nursing facilities. Report for Illinois Department of Public Aid and the Governors Planning Council on Developmental Disabilities. Chicago, IL: Author.
Toff, G.E. (1982). Current and future developments of Intermediate Care Facilities for the Mentally Retarded: An update. Washington, DC: George Washington University, Intergovernmental Health Policy Project.
Turnbull, H.R. (1987). Policy research needs to be connected. In Commentaries on Braddock et al., American Journal of Mental Deficiency, 92(2), 138-139.
U.S. Department of Education (1987). To assure the free and appropriate education of all handicapped children. Ninth annual report to Congress on the implementation of the Education of the Handicapped Act. Vol. 1. Washington, DC: Author.
U.S. Department of Education (1986). To assure the free and appropriate public education of all handicapped children. Eighth Annual Report to Congress on the Implementation of the Handicapped Act. Vol. 1. Washington, DC: Author.
U.S. Department of Education (1984). Digest of data on persons with disabilities. Washington, DC: National Institute on Handicapped Research, Office of Special Education and Rehabilitative Services.
U.S. Department of Education (1980). Summary of existing legislation relating to the handicapped. Washington, DC: Office of Special Education and Rehabilitative Services, Office for Handicapped Individuals. Publication E-80-22014.
U.S. Department of Health and Human Services (1986a). Report to the Congress on policies for improving services for mentally retarded and other developmentally disabled persons under Title XIX of the Social Security Act. Washington, DC: Office of the Assistant Secretary for Planning and Evaluation.
U.S. Department of Health and Human Services (1986b). Summary of information: Social Services Block Grant pre-expenditure reports for Fiscal Year 1985. Washington, DC: Office of Human Development Services.
U.S. Department of Health and Human Services (1981). Financing community-based care for mentally retarded persons. Prepared for Office of Management and Budget. Washington, DC: Author.
U.S. General Accounting Office (1987a). Medicaid: Addressing the needs of mentally retarded nursing home residents. Report to the Secretary of Health and Human Services by the Comptroller General. GAO/HRD-87-77.
U.S. General Accounting Office (1987b). Social Security: State vocational rehabilitation agencies reimbursement for the disabled. Briefing report to the chairman, Subcommittee on Ways and Means, House of Representatives. GAO/HRD-87-36BR.
U.S. General Accounting Office (1977). Returning the mentally disabled to the community: Government needs to do more. Report to the Congress by the Comptroller General. HRD-76-152A. Washington, DC: Author.
Wehman, P. and Hill, J. (eds.) (1985). Competitive employment for persons with mental retardation: From research to practice. Richmond, VA: Rehabilitation Research and Training Center, Virginia Commonwealth University.
Weicker, L. (1987). It is time to reform Medicaid. In Commentaries on Braddock et al., American Journal of Mental Deficiency, 92(2), 139-140.
White, C.C., Lakin, K.C., Hill, B.K., Wright, E.A., and Bruininks, R.H. (1987). Persons with mental retardation in state-operated residential facilities: Year ending June 30, 1986 with longitudinal trends from 1950 to 1986 (Report No. 24). Minneapolis, MN: University of Minnesota, Department of Educational Psychology.
Whitehead, C. (1987a). Strategies for expanding employment options and opportunities for persons with developmental disabilities. Report to Ohio Developmental Disabilities Planning Council. Columbus, OH: Author.
Whitehead, C. (1987b). Supported employment: Challenge and opportunity for sheltered workshops. Journal of Rehabilitation, 53(3), 23-30.
Whitehead, C., and Rhodes, S. (1985). Guidelines for evaluating, reviewing, and enhancing employment-related services for people with developmental disabilities. Washington, DC: National Association of Developmental Disabilities Councils.
Wieck, C.A., and Bruininks, R.H. (1980). The cost of public and community residential care for mentally retarded people in the United States. Minneapolis, MN: University of Minnesota, Department of Educational Psychology.
Wolfensberger, W. (1987). Values in the funding of social services. In Commentaries on Braddock et al., American Journal of Mental Deficiency, 92(2), 141-143.
Wyatt v Stickney, 344 F. Supp. 387 (M.D. Ala. 1972) affd sub nom. Wyatt v. Aderhold, 503 F.2d 1305 (5th Cir. 1974).
APPENDIX B. RESEARCH FINDINGS
| Re: | Developmental change associated with community placement |
| Title: | Differences in adaptive behavior of institutionalized and deinstitutionalized mentally retarded adults |
| Authors: | D.B. Rosen |
| Published: | Ann Arbor, MI: University Microfilms International (#DA8508127) |
| Date: | 1985 |
| Method: | Two year longitudinal study of randomly selected experimental and control groups each with 58 adult subjects each sampled from residents of Arkansas Childrens Colony at Booneville. Experimental group received community based residential and vocational services from an existing human services agency. Control group continued to receive residential and habilitation services in the state institution. Pre-test/post-test measures were gathered on three instruments, two adaptive behavior scales (Becoming Independent and Street Survival Skills Questionnaire) and an intelligence test (Stanford Binet). Complete pre-test and post-test data were obtained on 56 subjects in each group (i.e., 112 subjects altogether). |
| Summary of Findings: | While there were no statistical differences between experimental and control groups at the time of selection, statistically significant differences were found to favor the experimental group in overall adaptive behavior as well as for each subscale (domain) of the Street Survival Skills Questionnaire at the end of two years. No significant differences were found in the assessed I.Q. of experimental or control group members either at pre-test or post-test. Subsequent analyses showed that the differences between groups in adaptive behavior gains could not be accounted for by differences between the groups at either pre-test or post-test in a range of variables including I.Q., age, sex, or years institutionalized prior to the study. |
| Re: | Developmental change associated with community placement |
| Title: | Effects of Deinstitutionalization on Adaptive Behavior of Mentally Retarded Adults |
| Authors: | Joel Kleinberg and Betsy Galligan |
| Published: | American Journal of Mental Deficiency |
| Date: | 1983 (Vol. 88, No. 1, 21-27) |
| Method: | Twenty mentally retarded adults (18-75 years; IQ = 10-51) were moved from a developmental center to 3 community centers for a period of one year. Client functioning was measured at 0, 4, 8, and 12 months using the Adaptive Behavior Scale (ABS) and the Minnesota Developmental Planning System; in the areas of Language Development, Domestic Activity, Antisocial Behavior, Social Interaction, Grooming, Responsibility, Recreation, and Vocational functioning. |
| Summary of Findings: | Data were analyzed using repeated measures analysis of variance with client IQ (20 or below and above 20) as a grouping factor. The results based on the ABS, antisocial behavior decreased over time with clients with higher IQs. Increases in Language Development and Responsibility were seen across time for participants. With the Minnesota Scales, Social Interaction and Domestic Behavior showed an increase. No consistent changes were seen in Recreation, Grooming, and Vocational functioning scores. The study does not incorporate a control group. |
| Re: | Developmental change associated with community placement |
| Title: | Assessment of Progress of Institutionalized and Deinstitutionalized Retarded Adults: A Matched-Control Comparison |
| Authors: | Stephen R. Schroeder and Carol Hanes |
| Published: | Mental Retardation |
| Date: | April 1978 |
| Method: | Pre- and posttest scores on the Progress Assessment Chart (PAC) of 19 deinstitutionalized persons placed in group homes and an equal number of randomly selected matched control counterparts who remained institutionalized. The domains assessed were self-help, communication, socialization, and occupation over a period of one year. Repeated measures analysis of variance with sex and experimental vs. controls was performed on the pretest scores. |
| Summary of Findings: | Greater general gains in self-help, communication, and socialization skills were seen in the experimental group, with the greatest gains noted in the area of communication. Rank order correlations performed for each group between PAC gain scores, pretest scores, CA, MA, and length of institutionalization (for the experimental group only), showed a positive relationship existed between mental age and PAC pretest scores and a negative relationship between PAC gain scores and length of institutionalization. |
| Re: | Developmental change associated with community placement |
| Title: | Adaptive Behavior Changes of Group Home Residents |
| Authors: | David Hanes and Marilyn Moen |
| Published: | Mental Retardation |
| Date: | August, 1976. |
| Method: | Forty six adult group home residents with mental retardation were rated on the Adaptive Behavior Scale Part I over a period of one year. The ABS assesses 27 domain and subdomain areas concerning developmental skills covering a wide range of behavior. A students t-test used for comparing the residents rating in 1974-1975. A two-tailed t-test for correlated samples was computed on each of the domain and sub-domain areas on the ABS. |
| Summary of Findings: | Significant improvements/gains were found in the area of independent functioning. In the domains of language development and socialization, significant differences in a positive direction were noted for the group. No differences were found in the domains or subdomains of physical development, responsibility, and economic activity. |
| Re: | Development change associated with community placement |
| Title: | A Matched Comparison of the Developmental Growth of Institutionalized and Deinstitutionalized Mentally Retarded Clients |
| Authors: | James Conroy, Joelle Efthimiou, & James Lemanowicz |
| Published: | American Journal of Mental Deficiency |
| Date: | May, 1982 |
| Method: | Seventy deinstitutionalized subjects were matched for gender, level of retardation, CA + 5 years, years institutionalized, prerelocation Personal Self Sufficiency Score + 4 points and IQ with an equal number of institutionalized controls. The Behavior Development Survey, which is a short research version of the ABS, was used to measure client functioning in the areas of adaptive and maladaptive functioning. A quasi-experimental, pre-post nonequivalent control group design with subjects matched on pretest scores and other variables. The subjects functioning was measured at Time 1 and Time 2 over two years. |
| Summary of Findings: | The 70 clients who were placed in community settings were functioning as a higher level of adaptive behavior at Time 2 than their institutionalized peers. Clients with ambulation difficulties, and those who came from the most institutionalized cottages as measured by the Resident Management Scale gained more when relocated to community settings. Older clients gained more in adaptive behavior than did younger clients. No significant changes were noted in the problem behavior of either group. |
| Re: | Developmental change associated with community placement |
| Title: | Community Living for Severely and Profoundly Retarded Adults: A Group Home Study. |
| Authors: | Daniel W. Close |
| Published: | Education and Training of the Mentally Retarded |
| Date: | October, 1977. |
| Method: | The study investigated effectiveness of habilitation factors, such as acquisition of self-care sills and performance of social skills, associated with the postinstitutional community placement of adults classified as severely and profoundly mentally retarded. Eight members of this group were randomly selected for placement in a community vocational program and group home, while the remaining seven continued to receive treatment at a state institution for a period of one year. The people selected for community placement were phased into the group home in groups of 4. The training procedures were designed to remediate skill deficiencies in self care areas and social performance; data were collected by means of the Developmental Record, and the Community Living Observational System for observational information. |
| Summary of Findings: | Mean rater reliability on the specific skills observed for the 6 month period was .94. Posttest values for eating, toileting, and hygiene indicated significant differences favoring the experimental group. Differences in the area of social behavior also favored the experimental groups (both in social interaction and lower levels of self-stimulation). |
| Re: | Nutritional status change associated with placement in community setting |
| Title: | From Institution to Foster Care: Impact on Nutritional Status. |
| Authors: | Ninfa S. Springer |
| Published: | American Journal of Mental Deficiency |
| Date: | 1987, Vol. 91(4). |
| Method: | Subjects were eighty two persons who transferred from a large regional institution to foster-care homes in a county in Michigan--most of whom were either severely or profoundly retarded. Their medical records were screened to identify those at nutritional risk. Comprehensive nutritional assessment was conducted every year from 1982-1984. Results of the assessment were incorporated in the Individual Program Plan along with reports from the clinical team. Data collected were statistically analyzed and these included height, weight, and other bodily changes. |
| Summary of Findings: | Most of the clients diets were determined to be generally adequate as compared to the RDA. Majority of the children were short for their age. Findings indicated that 43 of 47 of the clients demonstrated positive changes in height, weight, dietary adequacy, and/or biochemical indices. Results of nutrition assessment demonstrated that most of the clients who were at high nutritional risk generally thrived in foster care despite the more formalized nutritional services associated with the large ICF-MR institution from which they were transferred. |
| Re: | Developmental change associated with community placement in family care or group homes |
| Title: | Comparison of Family Care and Group Homes as Alternatives to Institutions. |
| Authors: | Barry Willer and James Intagliata |
| Published: | American Journal of Mental Deficiency |
| Date: | May, 1982 |
| Method: | Three and eighty eight mentally retarded adults (mean age=46) from 5 institutions in N.Y. state who were place in family care (N=229) and group homes (N=109) were studied. Five aspects of community adjustment self care skills, adaptive behavior, community living skills, social support, and community access were evaluated to determine effective levels of behavioral adaptation. The Devereaux Behavior Rating Scale, apart from the questionnaires mailed to the clients principal care provider, was used as a second measure of adaptive behavior. |
| Summary of Findings: | No significant difference was seen in the amount of improvement in self care skills regardless of placement or level of retardation. In the domain of community living skills, mildly and moderately retarded individuals tended to have more progress than severely or profoundly retarded individuals and residents of group homes showed more progress than persons in family care settings. Significant improvement in adaptive behavior was observed with individuals placed in family care homes; this was supported by results of the Devereux Behavior Rating Scale. In the domains of social support and community access, no significant differences were observed between group placements. Overall, the results indicated substantial improvement in residents adaptive and maladaptive behavior following placement from an institution to a community placement, but that mildly and moderately retarded individuals tended to have more reported progress than did severely/profoundly retarded individuals. There was no control group for this study so it can not be argued with evidence that these changes might not otherwise have occurred. |
| Re: | I.Q. change associated with placement in community settings |
| Title: | Changes in Levels of Mental Retardation: A Comparison of Institutional and Community Populations. |
| Authors: | Kenneth D. Keith and L. Rene Ferdinand |
| Published: | TASH Journal |
| Date: | Spring, 1984. |
| Method: | The programs studied were the Community Based Mental Retardation Services (CBMR) of Nebraska. In all, 198 persons served by the CBMR and 146 by the institution with varying degrees of mental retardation formed the sample. Individuals in the community received vocational services and generic community services within small residential settings. Institution residents received residential services in dormitory type buildings along with other services available at the institution. Comparisons between initial mental retardation classification and current classification using AAMD criteria were done in 4 ways. |
| Summary of Findings: | Persons in the community tended to increase more in functioning level than did those who received services from an institution when using AAMD criteria. The groups subjected to statistical analysis were the moderately and severely retarded groups--the mildly and profoundly retarded subgroups were not subjected to analysis on account of sample size. The persons at the institution showed a greater decrease in functioning level. Regression to the mean effects may have affected the findings. |
| Re: | Development change associated with placement in smaller units within institutional settings |
| Title: | Quality of Life of Mentally Retarded Adults Transferred from Large Institutions to New Small Units. |
| Authors: | Heather Hemming, Tony Lavender, and Roisin Rill. |
| Published: | American Journal of Mental Deficiency |
| Date: | 1981, Vol. 86(2) |
| Method: | The study was designed to assess changes in quality of life for residents transferred from large traditional institutions to new small units within the general confines of the larger institution. The instruments used were King and Raynes Scale of Management Practices (indicator of quality of care), Butler and Bjaanes criteria for therapeutic institutions, and the ABS to assess changes in adaptive behavior. An own-control, pre- and post-condition design and matched-pairs design were used with 51 severely mentally retarded adults (experimental=38, control=33) for a period of 2 years. |
| Summary of Findings: | A significant decrease in institution-oriented practices of both the large and new small institutions was seen during the research period. Frequency and quality of interactions increased greatly in the small units; participation in normal or near normal activities tended to decrease for the more able residents. Significant ABS increases in Language Development were confined to higher ability residents in the first year only; both higher and lower ability residents attained their peak improvement 9 months after transfer. Higher ability residents (IQs 40-50) maintained their improvements 2 years after transfer if they lived in restricted environments. Total maladaptive behavior increased between transfer and 4 months after transfer, with the lower ability residents accounting for the increase. The general instability of developmental gains by persons moved to the new units when compared with those remaining in the traditional institution provides no support for the practice of building group homes on the grounds of larger institutions (as New York has been doing recently). |
| Re: | Developmental change associated with placement in smaller units within institutional settings |
| Title: | Institutional Reform and Adaptive Functioning of Mentally Retarded Persons: A Field Experiment |
| Authors: | Ann E. MacEachron |
| Published: | American Journal of Mental Deficiency |
| Date: | 1983, Vol. 88(1) |
| Method: | The study consisted of one year treatment for 289 randomly assigned mentally retarded residents of 29 buildings in a large institution. Fifteen units were new units designed to be more normalized; 14 units were part of the traditional institution. The experimental year represented the one year period from the day the cottages opened and all the clients entered it to a year later. The average IQ of subjects with treatment group being significantly higher (26 versus 21 for controls) was 23, the average age was 32 years. There were a total of 160 members in the experimental group and 129 in the control group. Three behavioral measures of the physical environment, several measures of social normalization, two measures of resident programming, and the ABS for a measure of adaptive behavior were used. |
| Summary of Findings: | Measures of physical design and features social conditions of the new cottages indicated that they were more normalized than the institution units. Residents of the new units had significantly greater gains in adaptive behavior over the year. |
| Re: | Developmental change associated with ICF-MR certification of institutions |
| Title: | Increase in Adaptive Behavior Level After Residence in an Intermediate Care Facility for Mentally Retarded Persons (ICF-MR). |
| Authors: | Sandra Johnson Witt |
| Published: | Mental Retardation |
| Date: | April, 1981. |
| Method: | Fifty-seven male and 38 female mentally retarded residents of a Florida State ICF-MR were studied longitudinally from before certification to 10 months after certification. Changes in their behavior were also compared to a matched control group consisting of 31 residents randomly selected from a non-ICF-MR state institution unit. Subjects ranging in age from 14-46 years with a mean length of institutionalization of 18.3 years were included in the study. The Vineland Social Maturity Scale was used annually as the measure of behavioral maturity and an intellectual evaluation using the Stanford-Binet Intelligence Scale was conducted. |
| Summary of Findings: | There was a trend indicating an increase in the VSMS scores for the 95 subjects, both prior and subsequent to certification of the residential units as ICF-MR units. However, the rate of change accelerated significantly under certification. The match control group continued the rate of developmental progress established over the three previous years during the 10-month experimental period. The group with adaptive level scores under 3 years of age showed maximum gains in the areas of self help after the ICF-MR program was initiated. Similar gains were seen in the areas of socialization (peer interaction) and occupation. For those in the experimental groups with adaptation scores above 3.0 years, significant gains were in the areas of communication and socialization. In general this suggests that the kinds of changes produced in institutions by the ICF-MR program may be ones that lead to increased developmental progress of residents over expected levels of progress prior to certification, but the one published account of this nature is probably insufficient for such a general conclusion in that it involves only 2 residential units. |
| Re: | Developmental change associated with community placement |
| Title: | Evaluation of Adaptive Behavior: Institutional vs. Community Placement and Treatment for the Mentally Retarded |
| Authors: | Michael L. DAmico, Marta A. Hannah, John A. Milhouse, and Arlene K. Froleich |
| Published: | National Clearinghouse of Rehabilitation Materials, Oklahoma State University |
| Date: | March, 1978 |
| Method: | The Camelot Behavioral Checklist was used to compared overall client progress in one institutional and one community based program. The study sought to identify components of each program which produced higher client progress. Thirteen male subjects (Experimental group 1=4; Experimental group 2=2; Control=7) were matched for age, sex, IQ, anomalies (hearing, vision, speech, ambulation), and self help. The Checklist was administered prior to being placed in the community or state institution. They were retested once every 6 months for a year. The first experimental group was moved to a training program and sheltered workshop. The second experimental group stayed on in the institution for 6 mos. and then moved to a group for a year. The 3 x 3 analysis of variance (group x trial) provided significant evidence that both experimental groups (community-based program and later placements) attained greater gains in performance over the control on total as well as 8 of the 10 subscale scores. |
| Summary of Findings: | While all groups performed on a comparable level at baseline, the total effects of the community based program on client progress became evident over time. After participating in the community program and placement, both experimental groups showed higher gains in independent self-help items than the control. Both experimental groups performed better on the physical development subscale. Accessibility of resources, consistent modeling, and program quality were hypothesized as factors responsible for higher performance by experimental groups. The community program, when applied in a natural setting, affected greater change in adaptive behavior when compared to a similar program in an institutional setting. |
| Re: | |
| Title: | Trends in Maladaptive Behavior of Mentally Retarded Persons Placed in Community and Institutional Settings |
| Authors: | R.K. Eyman, S.A. Borthwick, and C. Miller |
| Published: | American Journal of Mental Deficiency |
| Date: | 1981 |
| Method: | The purpose of the study was to examine changes in maladaptive behavior of persons with mental retardation placed in community vs. institutional settings over a 3 year period, controlling for preplacement maladaptive behavior. 214 clients were placed in a state institution while 212 clients resided in various community placements. They were matched for age (ave. age = 12.4), ambulation, and degree of retardation. A shortened version of Part Two of the Adaptive Behavior Scale was given at the time of the intake and then after 2 years. Eleven items of problem behavior were selected for the analysis based on their adequacy in interrater reliability and representativeness of the subdomains that comprise Personal and Social Maladaptation subscales. |
| Summary of Findings: | The results appear to indicate that whatever maladaptive behavior was present during the time of placement, was likely to persist, regardless of the clients age group, level of retardation, or residence (the independent variables). Institutionalized residents displayed more maladaptive behavior than did community residents before placement and two years after placement. Within the community based group, the individuals who were profoundly retarded had the highest degrees of adaptive behavior; this group, however, was the least deviant in the institution. The individuals who were relatively higher functioning had the most maladaptive behavior. The older individuals displayed greater deviance than the younger clients. Community facilities in this study included everything from family care to nursing homes. To the extent (unknown) from this study that the most severely impaired individuals were in those nursing homes, it is probably difficult to differentiate between community and institutional treatment. |
| Re: | |
| Title: | Quantity and Quality of Participation in Community Environments by Mentally Retarded Adults |
| Authors: | John M. Crapps, John Langone, and Sharon Swain |
| Published: | Education and Training of the Mentally Retarded |
| Date: | June 1985 |
| Method: | Fifteen mentally retarded adults (11 men, 4 women) living in group homes and intermediate care facilities, all of whom participated in the same sheltered work activity setting within the community, were the focus of the study. Data were gathered in 3 segments: The first and final segments consisted of direct observation of subject participation in community environments. The middle segment consisted of an interview with each subject concerning participation in community environments. Independent rater reliability for the observation data was 100%. Each subject was observed for a total of 52 hours. |
| Summary of Findings: | Subjects spent a majority of their time in their homes apart from time spent in sheltered employment. Actual participation was observed in community environments was less than that reported by the subjects. None of the subjects was observed using public transportation. Most of the time, subjects were accompanied by supervisors thus displaying more passive than active integration. Even though subjects reported that they hardly needed help, they rarely went anywhere independently. Regardless of living arrangements, women in particular spent little time participating in community environments. |
| Re: | |
| Title: | A Matched Sample Investigation of Nonadaptive Behavior of Severely Handicapped Adults Across Four Living Situations |
| Authors: | Cheryl A. Scanlon, Joel R. Arick, and David A. Krug |
| Published: | American Journal of Mental Deficiency |
| Date: | 1982 (Vol. 86, No. 5) |
| Method: | The purpose of this study was to determine whether specific types of nonadaptive behavior differentiate among severely handicapped residents living in state institutions, private institutions, group homes, and parents homes. Thirty six sets of matched severely handicapped subjects (4 subjects per set) were selected form a total population of 519 subjects. They were rated on the Autism Behavior Checklist--by their caretakers and/or parents. Subjects were matched for CA, sex, and language age. Adequate intrarater, interrater, and split-half reliability have been demonstrated with the Checklist. |
| Summary of Findings: | The state institutional population had significantly higher total nonadaptive behavior score than did all other residential categories. No significant total nonadaptive behavior score differences were found between any combination of private institution, group home, and parents home. In the area of behavior management problems and current job placements of these adults, 50% of the state institution population were rated as having the former and 52.8% had no job placement. The behavior in the aggressive, impulsive, and object dependency problem areas appear to reflect the most severe types of problem behavior. |
| Re: | Relationship of size to behavior of residents/staff in community facilities (6-20 residents) |
| Title: | Relationship of Size to Resident and Staff Behavior in Small Community Residences |
| Authors: | Sharon Landesman-Dwyer, Gene P. Sackett, and Jody Stein Kleinman |
| Published: | American Journal of Mental Deficiency |
| Date: | 1980 (Vol. 85, No. 1) |
| Method: | 419 staff members and residents of 43 group homes (of 6-20 residents) representing heterogenous groups and spanning various geographic locations, age, sex, and functional levels were sampled. Each subject was observed on one day during the week form early morning until late night; 15 categories of behavior being recorded; once every 15 minutes. Interobserver reliability for each category was 88% or higher. |
| Summary of Findings: | Eating and organized activities decline slightly with increasing group home size; general social and unobservable behavior increased with home size. Residents spent 41% of their time being inactive as compared to 11% by the staff. Staff members spent more time periods interacting with visitors and other people than did residents. Resident spent one fourth of their observed time interacting with other residents. Greatest amount of peer interaction was seen in medium size homes (9-17 people) and least in small homes (6-8 people). Best friend relations were seen in large homes. Residents interactions with staff members did not vary as a function of home size but time spent in peer interaction did. Four activity categories that did not show a main effect of home size were: teaching, supervising, problem solving, and negative social behavior; which occurred less than .5% of the observed times. Multiple-regression analyses performed to determine whether certain characteristics of the home were associated with the observed differences in behavior indicated low intercorrelations between variables except the associations between group home size and the average age of residents. Larger homes (18-20 residents) primarily served adult residents. |
| Re: | Developmental changes following an institution training program |
| Title: | A Follow-up of Severely and Profoundly Mentally Retarded Children After Short-Term Institutionalization |
| Authors: | Normal R. Ellis, George E. Bostick, Sheila A. Moore, and Janine J. Taylor |
| Published: | American Journal on Mental Deficiency |
| Date: | February 1981 |
| Method: | 100 children with severe and profound mental retardation were admitted to a public residential facility for the purposes of providing self-help skill training for 6-12 months and then returning them home. 50% of the children had no language skills, the remaining 50% had mixed language skills. Reanalysis of the clinical records, training, and progress reports, staff interviews was done and these data were converted to scores on four scales of the AAMDs ABS. Home visits, interviews with parents of each child, and an administration of the ABS during the home visit were conducted. The interviewer later rated various aspects of the family-SES, educational levels of the parents, etc. |
| Summary of Findings: | Early intent of the parents regarding institutionalization influenced the long-term care plan despite the training program. Fewer of the children whose parents supported home care returned to institutions after the program (4% to 37.5%). The training program made home adjustment easier for parents who supported home care. Those who preferred long-term institutionalization also noted the progress wrought by the training program, but also admitted experiencing a relief from the burden of child care. Slight gains were seen in the areas on the ABS through training. Slight improvements in maladaptive behavior were seen after deinstitutionalization. Reinstitutionalized children exhibited lower skill levels than children who receive home care; they also showed a decline in skill levels (language development and self care) upon returning to the institution. Gains in toileting, dining, and social skills are negligible. Both groups of children showed an increase in maladaptive behavior; the increase was not statistically greater for either group. |
| Re: | Personal/facility affecting adaptive behavior |
| Title: | Predicting Adaptive Functioning of Mentally Retarded Persons in Community Settings |
| Authors: | John T. Hull and Joy C. Thompson |
| Published: | American Journal of Mental Deficiency |
| Date: | 1980 (Vol. 85, No. 3, 253-261) |
| Method: | The study examined the extent to which individual, residential, and community characteristics were related to the functioning of persons with mental retardation in a variety of residential facilities. 369 retarded persons from 144 special residential facilities in Manitoba formed the sample. The Adaptive Functioning Index (AFI) was used to collect adaptive behavior data in the domains of Personal Routines, Community Awareness, and Social Maturity. A modified version of the ABS was also used. Other information regarding age, sex, IQ, length and number of times institutionalized, characteristics of residences, staff attitudes, physical disabilities of residents, etc. was collected. Four regression analyses, one for each of the individual domains of the AFI and for the total score were done. |
| Summary of Findings: | Clients residing in urban facilities with access to effective transportation systems had better skills; indicating that the nature of the community is an important factor. Individual characteristics of each resident such as inappropriate aggression, etc. were found to influence behavior and adaptation. The appropriateness of staff-resident interactions was a strong contributory factor to social maturity, and successful functioning in the community. Those placed in smaller communities tended to demonstrate slightly more social maturity on the AFI than residents placed in large communities. While community awareness was more a function of intellectual capacity than Personal Routines, the contribution of environmental normalization variables to the latter was higher. Other individual factors such as age, behavioral problems, and the extent to which residents were satisfied with their current residence were significantly related to various aspects of adaptive functioning. |
| Re: | Differential effects of various community placements |
| Title: | Residential Placement and Adaptation of Severely and Profoundly Retarded Individuals |
| Authors: | Sharon Landesman-Dwyer and Frederica MacL. Sulzbacher |
| Published: | AAMD (Monograph #4), Deinstitutionalization and Community Adjustment of Mentally Retarded Persons. |
| Date: | 1981 |
| Method: | In 1975 and 1976, the authors conducted a statewide survey of 6,952 individuals with developmental disabilities placed in 479 group residential facilities and 1,357 individual homes. Data from an ethological study of 20 group homes and another study of 210 retarded individuals who returned to institutions after unsuccessful community placements in Washington state are also presented. Data related to demographic and diagnostic characteristics, current functional and behavioral abilities, and medical and nursing needs were collected. The population was severely and profoundly mentally retarded as defined by the AAMD Manual on Terminology and Classification, 1973. |
| Summary of Findings: | Despite the large decline in institutionalizations and growth in community-based alternatives, most SMR/PMR individuals continue to live in large state institutions. Community residences, as a majority, tended to have a medical orientation, large size, and lack of privacy. Those SMR/PMR persons who were returned to institutions did so because of behavior problems. Those clients in the community generally tended to have a higher average of self-help, communication, and social skills and fewer medical and behavioral problems. The returnees to state institutions did not differ with regard to SMR/PMR categories, only with regard to age. Twice as many males returned than females. The majority of returnees had been placed in nursing homes which had little or no experience with residents who were mentally retarded. Two most frequently cited reasons for returning to the institution were inflicting physical harm on others and destroying objects. Indicates that community success for persons with severe and profound retarded is largely affected by the appropriateness of the placement and that nursing home placement is a significant predictor of reinstitutionalization. |
| Re: | |
| Title: | Relationship between Community Environments and Resident Changes in Adaptive Behavior: A Path Model |
| Authors: | Richard K. Eyman, Gail Carter Demaine, and Tzuen-Jen Lei |
| Published: | American Journal of Mental Deficiency |
| Date: | 1979 (Vol. 83, No. 4) |
| Method: | 245 DD individuals, residents of 87 family care homes and 11 board-and-care homes formed the sample. Program Analysis of Service Systems (PASS-3) had been administered between 1976 and 1977 by trained raters; the PASS-3 is an evaluation done by teams of trained raters who arrive at final scores which represent a consensus of opinion on each of the 50 items. The purpose of the study was to characterize what type of resident appeared to benefit from a normalized environment. All subjects were rated on the ABS as well. |
| Summary of Findings: | Older and mildly retarded individuals improved far more than did younger or more severely retarded residents. The path analysis provides an estimate of the strength of the relationship between the resident characteristics, PASS facility ratings, and change in adaptive behavior defined in the path model. Significant correlations were found between all of the independent variables (age, IQ, initial adaptive behavior domain scores and PASS-3 factor scores) in one set and 3 measures of improvement in adaptive behavior in the other set. One the Personal Self-Sufficiency factor, age level of retardation, and the initial score in this domain were highly related to average annual gain on this domain. Residents with higher IQs shoed more positive change than residents with lower IQs regardless of age. Age was not related to positive change in Domain 2: Community Self-Sufficiency was independent of IQ. Age, IQ, and initial score, however, were all significantly related to improvement on Personal-Social Responsibility; with older, less retarded residents and those with lower initial scores demonstrating most improvement. |
| Re: | |
| Title: | Community Living for Severely and Profoundly Retarded Persons |
| Authors: | E.J. Silver, W.P. Silverman, and R.A. Lubin |
| Published: | Perspectives and Progress in Mental Retardation Volume I - Social, Psychological, and Educational Aspects |
| Date: | 1984 |
| Method: (Investigation I) | Two investigations were conducted. The first investigation included 115 profoundly mentally retarded and physically disabled residents of a DD specialty hospital, 102 residents of 14 ICF/DD programs and 10 persons living in family care homes. Adaptive behavior was assessed using the Minnesota Developmental Programming System (MDPS)--Abbreviated Form, while the MDPS Alternate Form C was used with low-functioning persons. Information on resident health status and medical services received was obtained using the Health Status Indictor (HIS). |
| Summary of Findings: | The hospital residents had greater frequencies of physical and developmental disabilities, were more likely to be nonambulatory, exhibit expressive/receptive language skills, and to be totally dependent on others for basic self care than residents of community programs. |
| Method: (Investigation II) | The second investigation looked at whether community programs for profoundly disabled persons provided residential environments that were as normalized as those provided by ICF/DD programs and community residents (CR) serving less disabled persons. A comparison group consistent of 49 facilities randomly selected from 499 ICF/DD and CR programs functioning in New York was found. Environments within community programs were evaluated using an abbreviated version of the Program Analysis of Service Systems (PASS), the Characteristics of the Treatment Environment/Mental Retardation (CTE Scale) and Developmental Disabilities Community Home Survey Activity Subscale; and the Group Home Management Schedule (GHMS). Data were collected over a one year period. |
| Summary of Findings: | No group differences were found on environmental ratings for 2 instruments - the PASS and the CTE activity scale. It appears that severely and profoundly disabled and less disabled persons were provided with similar opportunities to engage in social and recreational activities. The GHMS scores indicated that management activities in community programs for profoundly disabled persons were found to be more facility oriented than were activities in programs for less disabled persons. |
| Re: | |
| Title: | Characteristics and Adaptive Behaviors of New Yorks Group Home Occupants |
| Authors: | J.W. Jacobson, E. Sersen, and A.A. Schwartz |
| Published: | Perspectives and Progress in Mental Retardation Volume I - Social. Psychological, and Educational Aspects |
| Date: | 1984 |
| Method: | Longitudinal data on the adaptive functioning of 1,027 persons with varying degrees of mental retardation were collected through the New York Developmental Disabilities Information System. This instrument includes an abbreviated version of the Minnesota Developmental Programming System Behavior Scales (MDPS-AF). A stepwise multiple regression was performed for each MDPS-AF domain with final domain score as the dependent variable and age, intellectual level, and Time 1 and Time 2 as the independent variables. The investigation was conducted for 12 months. |
| Summary of Findings: | Older persons scored higher than younger persons with similar skills at both times and scored higher at Time 2. Adults with severe/profound MR scored higher at Time 2, persons with mild/moderate MR scored higher than those with severe/profound MR at both times. All clients scored higher at Time 2. Pearson product-moment correlation coefficients calculated between change scores and baseline scale scores for each MDPS-AF domain were universally negative: higher initial domain scores were associated with small change scores. A positive association was found between intellectual level and final scores, indicating that persons with lower adaptive scores may show the most change and change was more pronounced among persons with mild/moderate retardation. |
NOTES
-
The DD definition must be used to develop State DD plans, in other activities supported by Basic State Grants, as well as in Federally-funded DD protection and advocacy systems and research programs.
-
There was a State household survey to determine the prevalence of developmental disabilities in West Virginia in the mid-1970's (Lindberg, 1976); however, this survey was based on the diagnostic or "categorical" definition of developmental disabilities (i.e., mental retardation, cerebral palsy, epilepsy or autism) and not the functional definition since adopted.
-
As reviewed by Abramowicz and Richardson (1974) and Stein and Susser (1975), average prevalence rates for moderate to profound mental retardation were .46 percent and .4 percent respectively. Given contemporary influences on these historical rates, Lakin and Hill (1985) suggest a prevalence rate of .5 percent may be reasonably expected today.