
U.S. Department of Health and Human Services
Report on Health Information Exchange in Post-Acute and Long-Term Care
Eric A. Coleman, MD, MPH, Karis May, and Rachael E. Bennett, MAUniversity of Colorado, Denver and Health Sciences Center
David DorrOregon Health and Science University
Jennie HarvellU.S. Department of Health and Human Services
February 1, 2007
PDF Version (61 PDF pages)
This project summary was prepared under contract #HHS-100-03-0028 between the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Office of Disability, Aging and Long-Term Care Policy (DALTCP) and the University of Colorado. For additional information on this subject, you can visit the ASPE home page at http://aspe.hhs.gov or contact the ASPE Project Officer, Jennie Harvell, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201, Jennie.Harvell@hhs.gov.
The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
TABLE OF CONTENTS
- I. INTRODUCTION
- A. Previous Work Completed by the University of Colorado in Electronic Health Records
- B. Goals for this Research Project
- II. METHODS
- III. FINDINGS FROM THE LITERATURE SEARCH AND STAKEHOLDER INTERVIEWS
- A. Health Information Technology: A Growing Public and Private Policy Priority
- B. Other Standards Development Activities
- C. Efforts to Support Electronic Health Information Exchange
- D. Adoption of Health Information Technology: Other Select Efforts
- IV. HEALTH INFORMATION EXCHANGED AT TIMES OF TRANSITION
- A. Illustrative Case and Introduction
- B. Overview of Clinical Information Exchanged at Times of Transition
- V. IMPLICATIONS AND FUTURE CONSIDERATIONS
- A. Implications
- B. Areas of Further Study
- C. Next Steps
- D. In Closing
- APPENDIX A. LIST OF STAKEHOLDER CONTACTS
- LIST OF FIGURES AND TABLES
- FIGURE 1: Federal and Private Sector Process for Interoperability
- TABLE 1: Estimated HIT Adoption Rates
- TABLE 2: Continuity of Care Document (CCD) Recommended Data Domains
- TABLE 3: Uniform Patient Assessment for Post-Acute Care Proposed Data Domains
- TABLE 4: HMO Care Management Workgroup Recommended Data Domains
- TABLE 5: Veterans Affairs Geriatrics and Extended Care (GEC) Referral Data Domain Categories
- TABLE 6: Medicare CoPs Concerning Health Information Exchange at Times of Transfer
I. INTRODUCTION
Clinicians require accurate and timely data to provide high quality patient care (Institute of Medicine, 2001). Nowhere is this more important than at times of care transition, when patients are transferred from one health setting to another. Transfers among care settings are common. Twenty-three percent of hospitalized patients over the age of 65 are discharged to another institution, and 12% are discharged from hospital with skilled home care services (Agency for Healthcare Research & Quality HCUPnet, 1999). An estimated 19% of patients discharged from a hospital to a skilled nursing facility (SNF) are re-admitted to the hospital within 30 days (Kramer, Eilertsen, Lin & Hutt, 2000). One study tracked post-hospital transitions for 30 days in a large, nationally representative sample of Medicare beneficiaries. Transitions in this study were defined as transfers to or from an acute hospital, emergency department, skilled nursing or rehabilitation facility, or home with or without home healthcare. Overall, 46 unique care patterns were identified during this relatively brief time period (Coleman, Min, Chomiak & Kramer, 2004b).
As national awareness of medical errors and quality deficiencies that occur within particular care settings continues to rise (Institute of Medicine, 2000), expanding evidence points to similar problems that occur during care transitions. Significant lapses in information transfer threaten patient safety; each time a patient's medical record is re-created, it increases the chance for a medical error and subsequent harm to occur. Inadequate information transfer can potentially increase healthcare expenditures, largely due to recidivism back to high-intensity care settings. Further, re-creation of essential information is not only inefficient but also can increase costs due to redundant ordering of laboratory tests, diagnostic imaging, and procedures (Institute of Medicine, 2001; Coleman & Berenson, 2004; van Walraven, Seth & Laupacis, 2002b; van Walraven, Seth, Austin & Laupacis, 2002a; Coleman & Fox, 2004a).
Quantitative evidence increasingly indicates that patient safety is jeopardized during transitional care. Medication errors pose a significant threat to patients undergoing transitions (Forster, Murff, Peterson, Gandhi & Bates, 2003). Receiving care in multiple settings often means that patients obtain medications from different prescribers. Clinicians rarely have complete information to adequately monitor the entire regimen, much less intervene to reduce discrepancies, duplications, or errors. For example, Boockvar and colleagues studied the series of transfers from a long-term care (LTC) nursing home to a hospital and then back to the LTC nursing home. On average, residents experienced three medication changes that led to an adverse drug event 20% of the time (Boockvar et al., 2004). Qualitative studies consistently have shown that patients and their caregivers are unprepared for their role in the next care setting, do not understand essential steps in the management of their condition, and are unable to contact appropriate healthcare practitioners for guidance (Weaver, Perloff & Waters, 1998; vom Eigen, Walker, Edgman-Levitan, Cleary & Delbanco, 1999; Harrison & Verhoef, 2002; Coleman et al., 2002; Levine, 1998). Each of these types of problems conspire to increase rates of recidivism to high-intensity care settings when patients' care needs at lower-cost settings are not met (Beers, Sliwkowski & Brooks, 1992; Coleman et al., 2004b; Moore, Wisnevesky, Williams & McGinn, 2003; van Walraven et al., 2002a).
A. Previous Work Completed by the University of Colorado in Electronic Health Records
In October 2002, the University of Colorado Health Sciences Center was awarded a contract by the Office for the Assistant Secretary for Planning and Evaluation (ASPE) to examine and report on the status of electronic health records (EHRs) in post-acute care (PAC) and LTC. As part of the project, ten "early adoptors" of EHR systems were interviewed to learn more about what applications were being used in their health delivery system (HDS) and whether PAC and LTC settings were included in their current roll-out plans. Site visits also were conducted at four other leading HDSs that had some degree of connectivity to affiliated PAC/LTC settings. All four of the health systems visited included an urban referral medical center in a medium-sized city with outreach into rural areas and smaller communities and hospitals. These health systems owned most of the providers (e.g., hospital, nursing homes, home health agencies [HHAs]) and employed most of the physicians in their systems (Kramer et al., 2004).
The interviewed and/or visited sites were relatively advanced in terms of EHR adoption. In general, electronic exchange of health information between acute and/or ambulatory care and PAC/LTC was limited to settings that were owned by the HDS (Kramer, Bennett, Fish, Lampinen & Coleman, 2003). Electronic connectivity usually consisted of one-way communication (e.g., acute care to a SNF) and was circumscribed (e.g., read-only access by one or two employees, such as the director of nursing). In some cases, no electronic data exchange occurred between settings, although it was not necessarily merely a technological barrier that precluded this communication stream, but rather, was the result of other factors discussed below. Stakeholders in the PAC/LTC settings that received even limited electronic health information from other parts of the HDS perceived this type of exchange to be of significant value as a result of the implementation of an EHR by the HDS.
When probed about why PAC/LTC settings often were not included in the design and execution of the larger HDS's EHR roll-out, informants provided several reasons. Prioritization was placed on physician usage, both in the acute and ambulatory settings. Those interviewed about EHR system implementation firmly believed that if physicians "bought in" to EHR usage, other clinicians (e.g., nurses, therapists, social workers) and support and administrative staff would follow. The costs associated with EHR system adoption was a barrier and members of the delivery systems indicated that the PAC/LTC settings did not have the capital to initially purchase and support a robust, interoperable EHR system. Respondents from SNFs and HHAs indicated high staff turnover as another reason for limited EHR usage; training an ever-changing staff on the use of the EHR system was seen as a potential drain on their budget. Finally, a compelling business case had not been made for EHR adoption in many PAC/LTC settings. Thus, although interoperability between acute care and PAC/LTC settings was of potential value, this was not a high priority for many PAC/LTC settings.
B. Goals for this Research Project
ASPE undertook this current study to better understand: (1) the type of health information that needs to be exchanged; (2) the methods by which health information is exchanged; and (3) the factors that support or hinder timely health information exchange (HIE) including, but not limited to, electronic HIE. Building on the work previously described, this project is particularly focused on if information is exchanged and if so, the type of information that is exchanged and how it is exchanged between unaffiliated healthcare settings (i.e., the HDS does not own or operate the PAC/LTC setting). For example, how is information exchanged between an acute care setting and an unaffiliated SNF or HHA?
II. METHODS
This report is based on the most recent and current developments related to HIE in PAC and LTC. It builds upon the previous literature review conducted in the project that examined the status of EHRs in PAC and LTC and research on clinical information exchange needs at times of transition across the healthcare settings. Therefore, the literature reviewed for this project was a targeted search and was gathered from multiple and varied sources with the intention of obtaining only the most up-to-date material available.
The sources from which information was compiled included the OVID and Medline databases (available through the University of Colorado at Denver and Health Sciences Center, Denison Memorial Library), Internet searches, specific website searches, electronically-published periodicals, government reports, other relevant organizational information obtained and forwarded from the Task Order Manager (TOM), and stakeholder telephone interviews.
Searches of the OVID and Medline databases were made for peer-reviewed and nonpeer-reviewed publications within the last two years, using various key word and key word combinations (e.g., EHR, health information technology [HIT], Medicare, home health, nursing homes, or LTC). Titles and abstracts were reviewed and relevant articles were read, including mining each paper's reference list for any additional relevant work. Because the focus of the review required timely information combined with the delay often associated with publishing peer-reviewed journal articles, the selected searches resulted in limited peer-reviewed literature relevant to HIT and PAC/LTC. Significantly more literature was reviewed regarding HIT in general, and even more specifically, within hospital and ambulatory settings.
Internet searches were conducted using key terminology (e.g., interoperability, Regional Health Information Organizations [RHIO]) or key organizations (e.g., American Society for Testing and Materials [ASTM], Health Level 7 [HL7]) to narrow the requested information track. Also, because of the Federal Governments investment in this project, federal websites and links (e.g., U.S. Department of Health and Human Services [HHS], Agency for Healthcare Research and Quality [AHRQ], and Federal Register) were searched and regularly re-searched to keep abreast of current proceedings. Much of the historical information in this report was accessed from the government websites.
Several industry-related electronically-published periodicals and newsletters were subscribed to and/or accessed (e.g., Modern Healthcare's HITS [Health IT Strategist], and eHealth Initiative's EHI Smartbrief). The information gained from these sources was not always relevant to the project's focus, but rather gave an overview of the broader, more encompassing information technology and HIE topics.
Project-specific materials obtained by the TOM and forwarded to the project team also were used for background and preparation of this report. Meeting, seminar, and conversation summaries; conference presentations and handouts; and relevant links to organizational websites all were used to further the knowledge base for this project.
Approximately 20 stakeholder calls were conducted in February, March, and April 2006. The Project Director led each of the 30-60 minute calls, which also often included the TOM and/or the Principal Investigator. As an efficiency measure, calls frequently were scheduled with a group of people, although several were conducted with just one informant. Each individual (or group) was provided with a list of potential questions prior to the call; however, the conversations often covered other topics not provided beforehand. The open nature of these discussions ensured that the issues discussed were the most relevant and interesting topics specific to the stakeholder(s).
The types of representatives interviewed were specified in the contract, and in many cases, the TOM provided assistance in securing the interview. The complete list of stakeholders can be found in Appendix A. Stakeholders included representatives from HDSs, standards development organizations (SDOs), quality improvement organizations (QIOs), PAC/LTC associations, and various federal and state government agencies.
The following sections of this report are a synopsis as taken from the above-noted information sources. Topics included describe the growing HIT federal policy priority and its historical background, federal and private sector efforts to expand and support HIE, and current case models taken from stakeholder interviews.
III. FINDINGS FROM THE LITERATURE SEARCH AND STAKEHOLDER INTERVIEWS
The information gathered from the referenced collection of literature and Internet searches, telephone interviews, and background data were drawn upon for Section III and Section IV. The findings for this report are organized as follows:
Sections III.A, B, C, and D describe several initiatives underway in the public and private sectors to promote and support electronic HIE. Section IV describes the types of health information needed as patients transition to and from PAC/LTC and other healthcare settings, methods and requirements for HIE at times of transition, and the relationship of emerging electronic health exchange activities to the types of information that is required or other wise needed at times of transition.
A. Health Information Technology: A Growing Public and Private Policy Priority
There is increasing recognition in both the public and private sectors that significant improvements in healthcare quality, continuity of care, and efficiency of care may be realized through implementation of HIT solutions. This section describes several of the activities undertaken by the public and private sectors to support the development and implementation of interoperable HIT.
1. Executive Order Establishing the Office of the National Coordinator
Federal HIT activities took a major step forward on April 27, 2004 when President G.W. Bush signed Executive Order 13335 (Federal Register, 2004b). The Executive Order recognizes the need for the development and nationwide implementation of an interoperable HIT infrastructure and established the position of the National Coordinator for Health Information Technology in HHS to provide leadership for this effort. The Executive Order describes an interoperable health information infrastructure as one that:
- Ensures that appropriate information to guide medical decisions is available at the time and place of care;
- Improves healthcare quality, reduces medical errors, and advances the delivery of appropriate, evidence-based medical care;
- Reduces healthcare costs resulting from inefficiency, medical errors, inappropriate care, and incomplete information;
- Promotes a more effective marketplace, greater competition, and increased choice through the wider availability of accurate information on healthcare costs, quality, and outcomes;
- Improves the coordination of care and information among hospitals, laboratories, physician offices, and other ambulatory care providers through an effective infrastructure for the secure and authorized exchange of healthcare information; and
- Ensures that patients' individually identifiable health information is secure and protected.
The Executive Order requires the development of a strategic plan to support the development and implementation of the nationwide interoperable HIT infrastructure. The plan is required to address several issues:
- Advance the development, adoption, and implementation of healthcare information technology standards through public and private collaboration;
- Address privacy and security issues related to interoperable HIT; and
- Ensure that key issues affecting the adoption of HIT are addressed.
In July 2004, the Office of the National Coordinator for Health Information Technology (ONCHIT) in HHS released a report, "The Decade of Health Information Technology: Delivering Consumer-Centric and Information-Rich Health Care" (Office for the National Coordinator for Health Information Technology, 2004). The report outlines a framework for realizing the goal that most Americans have an interoperable EHR by 2014. The report identifies four critical goals with three strategies to achieve each goal:
Goal 1: Inform clinical practice with use of EHRs. Strategy 1. "Incentivize" EHR adoption Strategy 2. Reduce risk of EHR investment Strategy 3. Promote EHR diffusion in rural and underserved areas
Goal 2: Interconnect clinicians so that they can exchange health information. Strategy 1. Foster regional collaborations Strategy 2. Develop a national health information network (NHIN) Strategy 3. Coordinate federal health information systems
Goal 3: Personalize care with consumer-based health records and better information for consumers. Strategy 1. Encourage use of Personal Health Records (PHRs) Strategy 2. Enhance informed consumer choice Strategy 3. Promote use of telehealth systems
Goal 4: Improve population health through advanced biosurveillance methods and streamlined collection of data for quality measurement and research. Strategy 1. Unify public health surveillance architectures Strategy 2. Streamline quality and health status monitoring Strategy 3. Accelerate research and dissemination of evidence
The first two goals and related strategies affect HIE between clinicians and providers. Activities that have been implemented that address these goals are described later in this report.
2. Information Gathering
After releasing the strategic framework, the ONCHIT released a request for information (RFI) on November 15, 2004 calling on all interested parties to answer 24 questions exploring the role of the Federal Government in facilitating the deployment of a NHIN (Federal Register, 2004a). ONCHIT received 512 responses to the RFI, including vendors, medical societies, healthcare providers, payors, and healthcare consumers (ONCHIT, 2005). The key themes that emerged from the responses indicated that the NHIN should be developed as a joint public/private effort, decentralized, and linked by standards. Respondents consistently indicated that the NHIN needed to address a variety of privacy and security issues. A summary report of the responses received from the RFI was released in June 2005 (ONCHIT, 2005).
Simultaneous with the RFI release, the ONCHIT convened the Secretary's Health Information Technology Leadership Panel, comprised of CEOs from nine major companies. Each CEO came from an industry outside healthcare (e.g., Federal Express, Wal-Mart, Procter and Gamble) that had been transformed by information technology. Three key imperatives were identified by the Leadership Panel:
- Widespread adoption of interoperable HIT should be a top priority for the United States healthcare system.
- The Federal Government should use its leverage as the nation's largest healthcare payor and provider to drive adoption of HIT.
- Private sector purchasers and healthcare organizations can and should collaborate alongside the Federal Government to drive adoption of HIT.
Additionally, the panel outlined these conclusions:
- Potential benefits of HIT far outweigh manageable costs.
- HIT needs a clear, broadly motivating vision and practical adoption strategy.
- The Federal Government should provide leadership, and industry will engage and follow.
- Lessons of adoption and success of information technology in other industries should inform and enhance adoption of HIT.
- Stakeholder incentives must be aligned to foster HIT adoption.
- Among its multiple stakeholders, the consumer -- including individual beneficiaries, patients, family members, and the public-at-large -- is essential in the adoption of HIT and realizing its benefits (The Lewin Group, 2005).
3. Establishing Public-Private Leadership
a. The American Health Information Community (AHIC): In September 2005, the Secretary of HHS formed the AHIC to help advance the goal that most Americans have EHRs within ten years. Membership of the AHIC is comprised of key public and private sector healthcare leaders. The AHIC is a federal advisory committee charged with providing input and recommendations to the Secretary of HHS on how to make health records digital and interoperable, while ensuring the privacy and security of these records.
To achieve this goal, the AHIC has focused on developing "uses cases" (i.e., applications of HIT that could produce a specific tangible value within a short period of time [e.g., 2-3 years]). The AHIC has identified "uses-cases" in the following areas: Biosurveillance; Consumer Empowerment; and Electronic Health Records.
The AHIC will be identifying additional uses cases, such as a use case for PHRs that would benefit from the deployment of interoperable HIT standards. The AHIC has been chartered for two years, with an option to renew for no more than five years, to be succeeded by a private sector health information community initiative to set additional standards, certify new HIT technology, and to provide governance for care transformation.
b. Health Information Technology Standards Panel (HITSP): As recognized in the Executive Order, an essential requirement for developing and implementing an interoperable nationwide health information infrastructure is healthcare information technology standards. While there are many standards for HIE, there also are variations and gaps in needed standards that limit widespread adoption of interoperable HIT. To support the development, adoption, and implementation of interoperable HIT standards, HHS awarded a contract to the American National Standards Institute (ANSI), a private sector non-profit organization that administers and coordinates the United States' voluntary standardization activities, to convene the HITSP. The HITSP convenes stakeholders from SDOs and others to develop, prototype, and evaluate a process for achieving interoperable HIT standards across healthcare software applications, particularly EHRs.
The initial work of the HITSP has focused on identifying the standards needed for software applications related to the three use cases prioritized by the AHIC (see discussion above). Specifically, the AHIC recommended that HITSP identify standards needed for:
- secure messaging between patients and clinicians (e.g., secure e-mail between patients and doctors);
- reporting laboratory results; and
- electronic patient registration information.
c. Certification Commission for Healthcare Information Technology (CCHIT): In September 2005, HHS awarded a three-year contract to the CCHIT to develop certification criteria and processes for HIT products. The CCHIT initially focused on criteria needed for physician office EHR products, and are now specifying criteria for inpatient hospital EHRs. The third year will focus on criteria development for the networks through which these products exchange information. The criteria specified by the CCHIT for physician office EHR products are divided into three categories:
- Functional requirements (i.e., minimum functional requirements for managing and documenting a patient encounter, including problem lists, allergies, medication lists and orders, patient's election of advance directives, laboratory results reporting, generating hard and electronic copies of summary reports, etc.).
- Interoperability (i.e., standards needed to exchange health information within and across healthcare settings).
- Security and reliability (i.e., standards needed to audit access to the patient's record, standards to ensure that information in an EHR is consistently displayed, etc.).
The criteria for physician office EHR products were developed by CCHIT through a series of public meetings at which comments were obtained regarding needed EHR certification criteria for ambulatory care EHRs. The CCHIT criteria overlap with the EHR System Functional Model and Standards developed by HL7 and the ambulatory care profile advanced by HL7 (see Section III.B.1 for more information on these criteria).
In May 2006, the AHIC unanimously approved the CCHIT: (1) functionality, and (2) security and reliability criteria for certification of ambulatory EHRs and recommended that the Secretary formally recognize these ambulatory care EHR certification criteria. To ensure interoperability, the AHIC also recommended that the CCHIT incorporate HITSP standards on an ongoing basis (HHS, 2006a).
In July 2006, CCHIT announced the certification of EHR products offered by 18 companies as meeting the criteria established by CCHIT. Another 11 EHR products were certified in October 2006. A listing of the certified products (by product name and by company name can be viewed on the CCHIT website (CCHIT, 2005).
The Secretary of HHS formally recognized the CCHIT ambulatory care EHR certification criteria in a July 2006 Federal Register notice (Federal Register, 2006). "CCHIT CertifiedSM product certification provides an objective set of criteria against which HIT products can be measured to enable purchasers to reliably make an investment in those products and to assure healthcare consumers that they can trust their healthcare information to be stored in those products" (CCHIT, 2006b). Certifying EHR products is one step toward minimizing the risk that healthcare providers encounter when making HIT investment decisions.
In November 2006, CCHIT issued a press release announcing that HHS authorized and funded CCHIT to expand its scope of work (SOW) for the certification of EHR products to include two to three medical specialties and specialized care settings during this next year. The press release notes that CCHIT will establish a "fair and objective process for prioritizing which specialties should be addressed first" and will take into account the: (i) amount of criteria development work required, (ii) readiness for the specialty/care setting to participate in development of EHR certification criteria, and (iii) potential positive impact certification could have on EHR adoption in the selected specialty/setting. The CCHIT anticipates discussing the readiness of additional healthcare settings and specialties for EHR certification standards during its January 2007 meeting.
4. Addressing Privacy and Security Issues
Timely access to complete and reusable health information is critical for improving quality, continuity, and efficiency of care. Ensuring appropriate disclosures of and providing adequate security for health information consistently have been identified as issues that must be addressed in the emerging national health information infrastructure. While the Health Insurance Portability and Accountability Act (HIPAA) established rules concerning healthcare privacy and security requirements for protected health information, many states and healthcare organizations have adopted policies that go beyond HIPAA. As a result, the variability in privacy and security policies poses challenges for electronic HIE.
To address these issues a contract was awarded to the Research Triangle Institute (RTI) to convene the Health Information Security and Privacy Collaboration (HISPC). In May 2006, 22 states and territories entered into subcontracts with RTI to address privacy and security policy questions affecting interoperable HIE. The subcontractors will examine variations in privacy and security practices that affect electronic HIE, and develop best practices and propose solutions to address identified challenges. The solutions that are identified via these subcontracts will provide a foundation for future work to facilitate HIE across states (ONCHIT & HHS, 2006).
5. Development of a National Health Information Network
In November 2005, HHS awarded contracts to four consortia to develop prototypes for a NHIN architecture that will allow for the secure exchange of healthcare information across the healthcare continuum. Each of the four consortia submitted functional requirements for a NHIN. To address the functional requirements needed for a nationwide health information network, the NHIN Forum was convened in June 2006, and was sponsored by multiple public and private entities (e.g., the ONC, the four consortia developing the NHIN prototypes, HITSP, CCHIT, and other key representatives of public and private HIT stakeholders).
Discussion at the forum focused on:
- the categories of "functional requirements" needed for a NHIN (e.g., security, data transmission and transformation, information location); and
- the components and requirements needed by the NHIN and the applications that will be participating in the exchange of health information.
In July 2006, the National Committee on Vital and Health Statistics (NCVHS) was asked to review and synthesize the results of the June 2006 NHIN Forum and by September 30, 2006, define a minimal, but inclusive, set of functional requirements needed for the initial definition of an NHIN and its possible architectural forms. Although these requirements will not make the actual architectural decisions per se, they should clearly designate common requirements as well as requirements that are specific to particular prototype architectures.
6. National HIT Infrastructure
Each of the public and private sector activities described above -- the AHIC, HITSP, CCHIT, HISPC, NHIN -- are critical components of the emerging National HIT infrastructure. The diagram in Figure 1, posted on the Federal Health Architecture (FHA) website (http://www.hhs.gov/fedhealtharch/fedpart.html), highlights the opportunities the Federal Government and the private sector will have in shaping and participating in the development and implementation of this infrastructure. The diagram reflects a process through which the Federal Government and private sector have input into a process that will result in interoperability between these two sectors.
7. The Federal Health Architecture and Standards
One stakeholder in the national HIT infrastructure is the FHA. The FHA emerged in March 2001, initially as one facet of the government's electronic government initiative, the Federal Enterprise Architecture. At that time, the FHA was a collaboration across federal agencies charged with creating "a consistent federal framework to facilitate communication and collaboration among all healthcare entities to improve citizen access to health-related information and high quality services" (HHS, 2006d).
| FIGURE 1: Federal and Private Sector Process for Interoperability |
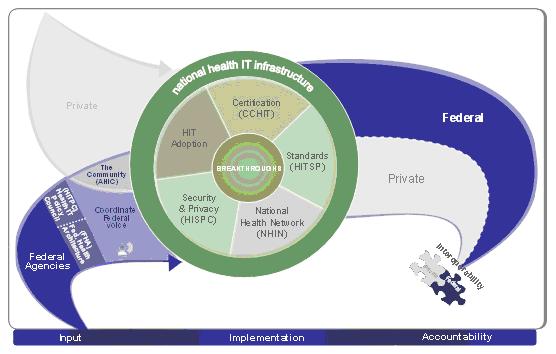 |
| SOURCE: U.S. Department of Health and Human Services, 2006d. |
In 2006, the scope of the FHA was redefined to support the President's vision of widespread adoption of interoperable EHRs by most Americans within ten years. Thus, the new focus of the FHA was expanded from interoperability across federal health agencies to supporting interoperability in both the public and private sectors.
One of the key activities of the FHA as originally implemented was the Consolidated Health Informatics (CHI) Initiative. The CHI Initiative was a collaborative effort that resulted in the adoption of several HIT interoperability standards (i.e., content and messaging standards) to be implemented by federal agencies to enable the exchange of electronic health information across the Federal Government. In 2005, HHS published a Federal Register notice stating that "[t]he portfolio of 20 adopted standards will be used by all federal agencies in implementing new, and to the extent possible modifying existing HIT systems, as well as related business processes" (Federal Register, 2005a).
The CHI Initiative is being disbanded, and will conclude with the production of reports on standards needed for the domain of patient assessments and disability content. On October 11, 2006 the NCVHS considered and endorsed the CHI recommended content and messaging standards for patient assessment and functioning and disability content (HHS NCVHS Subcommittee on Standards and Security, 2006; CHI, 2006). Implementation of these standards will support the development and use of interoperable HIT applications in PAC/LTC settings that are required to complete and submit electronic patient assessments.
It is expected that the HITSP will fill the role of identifying standards and implementation guides needed for specific use cases and other priority areas. HITSP is required to take into account CHI standards.
B. Other Standards Development Activities
HL7 is one of the most well known ANSI-approved SDOs in healthcare. It is a non-profit organization made up of volunteers in the healthcare industry, including healthcare providers, software vendors, payors, and government representatives who are interested in formulating standards for clinical and administrative health data. Currently, the most widely used HL7 standards are messaging standards that allow disparate healthcare applications to exchange sets of information with each other (Health Level Seven Inc., 2006a).
a. Electronic Health Record System Functional Model: The HL7 Electronic Health Record System (EHR-S) functional model (FM) is a different set of specifications than the traditional messaging standards approved by HL7. The EHR-S FM consists of three separate categories of functions that describe the myriad of functions possible in an EHR-S: (a) direct care functions, such as care management; (b) supportive functions, such as resource tracking and research, or report generation; and (c) information infrastructure. At the time of the writing of this report, this model is in draft standard trial use form and is awaiting final approval by HL7. This model represents a change from previous HL7 models by attempting to define functions, rather than technical or messaging components. The balloting timeframe for the EHR-S FM is anticipated to take place sometime in 2006, with ANSI-accreditation to follow.
HL7 workgroups have been formed to define the subset of EHR functional requirements needed in particular settings such as physician offices, hospitals, and nursing homes (Health Level Seven Inc., 2005). The specification of the subset of functions needed in particular settings is considered by HL7 to be a "profile." HL7 defines a profile as a "specification that uses the Functional Model to indicate which functions are required, desired, or implemented for certain EHR systems or healthcare delivery settings."
b. Long-Term Care Minimum Function Set Workgroup: The HL7 workgroup specifying the functional requirements for nursing homes is the Long-Term Care Minimum Function Set workgroup. The Long-Term Care Minimum Function Set workgroup is charged with creating conformance criteria for a LTC profile related to the direct care functions as described in the EHR-S functional model. EHR systems do not claim conformance to the HL7 EHR-S FM; rather, they conform to one or more profiles (defined by HL7 as a specification to indicate which functions are required, desired, or implemented for certain EHR systems or healthcare delivery settings). The LTC profile then, is a subset of the FM, which will define functions for a LTC EHR system pertinent in providing direct care to patients in nursing homes (Health Level Seven Inc., 2005). The completion of the LTC profile likely will not be completed until the end of 2006 (Stakeholder call with LTC Profile Group, February 3, 2006).
Similar to the process established for ambulatory care EHRs and expected for hospital EHRs, CCHIT could consider the HL7 LTC Minimum Function Set for EHR functional and interoperability requirements should CCHIT ever establish EHR certification criteria for LTC EHRs.
2. ASTM Continuity of Care Record and HL7's Clinical Document Architecture/CCD
There are two, now related, standards development activities that are particularly pertinent to HIE. The Continuity of Care Record (CCR), developed by the ASTM, is a standard for compiling summary information for physicians to share with one another and is designed to provide a comprehensive clinical picture of a patient's current and relevant historical health status (Center for Health Information Technology, 2006; Stakeholder call with David Kibbe, February 17, 2006). According to the standard specifications, the CCR is "a core data set of the most relevant administrative, demographic, and clinical information facts about a patient's healthcare, covering one or more healthcare encounters" (ASTM International, 2006). The CCR is not a mini-medical record; rather it is a snapshot summary (a data set) of a medical record that is delivered from setting to setting, and could potentially be displayed in an EHR. It is anticipated that providers would be able to auto-populate the CCR with data elements from their EHR and then electronically send them. To date, ASTM has not specified whether certain clinical domains must be populated and whether certain data elements will be required for an acceptable CCR document (i.e., at what point does a partial update detract from the goal of information transfer).
HL7's Clinical Data Architecture (CDA), Release 2 (r2) was approved in June 2005 and is a document architecture standard designed to standardize how clinical documents are expressed. In other words, the structure and semantics of clinical documents are specified to facilitate HIE (Dolin et al., 2006). The CHI Initiative adopted, as an HIT standard, the CDA for text-based reports.
On November 2, 2005, HL7 announced that in collaboration with ASTM, they are developing an implementation guide to express the CCR data set in an HL7 Version 3 (V3) CDA, r2 document (Health Level Seven Inc., 2006b). This collaborative specification effort is referred to as the Continuity of Care Document (CCD) (Alschuler, 2006). The CCD will map CCR content into a CDA r2 representation, which will enable the exchange of human-readable (text) and/or coded transfer documents. The ability to send either coded or text documents has the potential to improve quality of care by making clinical information readily accessible to the clinician who has the option of reading the information while enabling computers to reuse the information for a variety of purposes (e.g., performing automated data extraction, facilitating the use of computerized decision support, implementing an adverse event alerting system).
The authors of the CCR and CCD have attempted to identify and represent categories of information important in care planning and care of patients as patients transition from setting/healthcare provider to another (e.g., discharge from acute care as well as from other settings). The structured representation of this information should help EHR vendors and HDSs better process information at times of care transition. HL7 and ASTM released a December 6, 2006 Informative Ballot for an HL7 Implementation Guide for the CCD to exchange standardized and text-based summary reports about a patient's health and functional status, and other pertinent data about a patient including advance directives, problems, family and social history, medications, immunizations, etc. The CCD Informative Ballot identifies the vocabulary sets (as approved the HL7 Vocabulary Committee) needed for some of the various clinical domains included in the CCD. The standards included in the CCD ballot include those standards recently endorsed by the CHI and NCVHS for patient assessments and functional and disability content. The HITSP has indicated that it will work "in the coming months to include a harmonized summary record (CCD) standard into interoperability specifications" and has indicated that it will likely endorse components of the CCD (e.g., demographics, medications and allergies) for the AHICs consideration (Office for the National Coordinator for Health Information Technology, 2006; Healthcare Information Technology Standards Panel, 2006).
Various groups have been examining the utility of various HIT exchange standards. One group is Integrating the Healthcare Enterprise (IHE), which is a consortium of vendors. They have been demonstrating the feasibility of integrating and transferring data from a wide variety of sources. IHE takes existing standards (e.g., CDA and HL7 v2 messages, DICOM, X12) and implementation guides (e.g., CCD) and creates profiles for how they can be put together with vendor applications to create an interoperable architecture. Using an analogy of the post office, the messaging standards are the envelope, the CDA is the letter inside the envelope, and the EHR systems are the senders and recipients. With this analogy in mind, the Patient Care Coordination group within IHE recently examined the CDA Care Record Summary (the precursor to the CCD) Implementation Guide and created a profile that demonstrated how different entities can send messages back and forth and move CDA around an exchange network into and out of EHR systems (Stakeholder interview, Liora Alschuler, April 10, 2006).
IHE also has held "Connectathons" for several years, inviting industry, providers, and others to find solutions to the barriers between electronic systems that limit the ability to transfer information and knowledge needed for optimal patient care. Sets of tasks are defined through use cases (such as sharing coded patient summary documents between institutions), the integration framework and actions needed to guarantee interoperability, and participants then are given the opportunity to demonstrate how they would make use of the framework, data standards, and other components to send information between systems. The example use cases involve within institution connectivity between different vendors (e.g., a radiology system to an EHR) as well as data sharing between institutions, such as discharge summaries or between specialists and primary care providers.
Until recently, little focus has been given to LTC/PAC, although the general frameworks and interoperability requirements for inter-institution information transfer are relevant to the needs of SNFs and HHAs (IHE, 2006). Currently, use cases that provide specific support for the unique communication requirements of aging services organizations are being advanced for IHE consideration. In particular, in October 2006, the Center for Aging Services Technologies (CAST) and the American Health Information Management Association (AHIMA) announced the formation of a workgroup to develop the requirements, recommendations, guidelines, and standards advocacy towards the adoption of an HL7 implementation guide for the CCD with support for functional status and wellness content. Their stated goals are to initiate work that will result in an HL7 approved implementation guide, progress standards related to functional status and wellness content, and complete formal interoperability demonstrations of vendor, provider and consumer uses (CAST, 2006).
3. National Council for Prescription Drug Program LTC e-prescribing
The National Council for Prescription Drug Programs, Inc. (NCPDP) is a non-profit ANSI-accredited standards organization with approximately 1,350 members (NCPDP, 2006b). The NCPDP workgroup 14 (WG14) currently is identifying fields that are pertinent to LTC and PAC to add to the NCPDP SCRIPT standard. The SCRIPT standard was developed to allow for the electronic transmission of prescription information between healthcare providers and pharmacies. The standard currently addresses the electronic exchange of new prescriptions, refills, prescription fill status notifications, and cancellation notifications (NCPDP, 2006a). As described in Section C.2, the NCPDP SCRIPT standard was adopted as one of the e-prescribing final rules required for electronic prescribing under the Medicare Part D drug benefit.
C. Efforts to Support Electronic Health Information Exchange
As mentioned above, the report prepared by the ONCHIT entitled, "The Decade of Health Information Technology: Delivering Consumer-Centric and Information-Rich Health Care" includes a goal to interconnect clinicians through the following strategies:
- fostering regional collaborations;
- developing a NHIN that develops and uses interoperable HIT standards; and
- coordinating the federal health information systems.
Much of the preceding discussion has described public and private efforts to develop a NHIN, including federal health information systems, using interoperable HIT standards. This section of the report describes some of the activities that have been undertaken by the public and private sectors to promote and support HIE.
1. Agency for Healthcare Research and Quality HIT Planning and Implementation Grants for State and Regional Health Information Exchange
The AHRQ has been a leader in supporting the goal of modernizing healthcare using information technology. To help in the dissemination of constantly changing knowledge regarding HIE, AHRQ created the National Resource Center for Health Information Technology and through this initiative, supports many wide ranging opportunities for HIE. Included are the AHRQ Transforming Healthcare Quality Through IT (THQIT) grants, which were created to help fund regional and local community planning, implementation, and demonstration grants to illustrate the value of HIT and exchange. At this time, AHRQ has awarded over 100 THQIT grants. Six State and Regional Demonstration (SRD) projects focused on establishing statewide HIE also have been funded. In October 2005, AHRQ awarded 16 grants (11 of which involved small, rural communities) in the amount of $22.3 million to implement HIT systems and improve the safety and quality of healthcare (AHRQ, 2006). In addition, in 2004, AHRQ made SRD awards totaling $34.7 million to Colorado, Indiana, Rhode Island, Tennessee, and Utah. These five-year SRD grants were awarded for development of statewide information technology networks that will facilitate data sharing and transfer among healthcare providers (including purchasers, payers, hospitals, and home health and nursing home providers). At the time of this writing, no findings are yet available on these efforts.
2. The Medicare Modernization Act (MMA) of 2003
The MMA included some provisions that support electronic HIE. These are described below.
a. e-Prescribing and the Prescription Drug Benefit Program: Beginning in January 2006, the MMA establishes an electronic prescribing program to support the Prescription Drug Benefit program. The MMA mandates the use of HIT standards for certain prescribing functions if a practitioner elects to engage in e-prescribing on behalf of Medicare beneficiaries. It also requires that drug plans participating in the new prescription benefit support electronic prescribing.
The Centers for Medicare and Medicaid Services (CMS) issued a final rule requiring the use of certain HIT standards for e-prescribing. As noted in the Final Rule for the Medicare Program; e-Prescribing and the Prescription Drug Program, 42 CHR Part 423, (Federal Register, 2005b), the e-prescribing program mandates specific standards for transactions, eligibility, communication between prescribers and drug plans, communication between dispensers and Part D sponsors, and formulary and benefit coverage. The adopted message format standards approved at this time are:
- NCPDP SCRIPT, version 5.0 from the NCPDP -- (the newer version 8.1 has been requested for use in lieu of version 5.0, using backward compatibility) -- for core functions and transactions between providers and dispensers;
- ANSI Accredited Standards Committee ASC X12N 270/271, Health Care Eligibility and Response Standard (004010X092A1) from the ANSI -- for eligibility and benefit inquiries, and responses between providers and Part D sponsors; and
- NCPDP Telecommunication Standards, v 5.1 (and equivalent Batch Standard, Version 1.1) from the NCPDP -- for eligibility and benefits (this is the HIPAA standard).
The final rule for e-prescribing exempts LTC settings because of their unique three-way prescribing process (facility-physician-pharmacy) and the uncertainty about the applicability of required standards for this type of HIE.
The final rule provides for the testing of additional standards through pilot studies funded by CMS and AHRQ. The standards to be evaluated in the pilots include those for information on formulary and benefits, patient instructions, prior authorization messages, and clinical drug terminology. The pilot studies were awarded in January 2006, with a Report to Congress due in April 2007, followed by the final rule for recommended additional standards scheduled for April 2008.
E-prescribing pilots were granted to Rand Corporation of California; Brigham and Women's Hospital of Boston; SureScripts; and Achieve Healthcare Technologies. The pilot study led by Achieve Healthcare Technologies, implemented in Eden Prairie, Minnesota is of particular interest to this study. This pilot is evaluating the use of e-prescribing standards for nursing homes (Benedictine Health Systems, Minnesota). It will test standards that augment an existing communication network between facilities, pharmacies, and physicians. As comparison sites, two LTC facilities will be included that will use the traditional, paper-based prescribing methods. The standards will be analyzed from the perspective of functionality, cost benefits, and improvements in patient safety and quality of care.
Electronic prescribing also can bring other changes in HIE to the home health and nursing home care settings. As mandated in the MMA of 2003, exceptions to the Stark Rule (CMS) and the anti-kickback statute (Office of the Inspector General) have been authorized. In August 2006, HHS published two final rules in the Federal Register providing limited exceptions to the Stark law and anti-kickback statutes. These changes now permit the sharing of: (1) information technology resources to support EHRs, easing the provision of information technology software and/or services to physicians and other healthcare entities; and (2) technology and services related to e-prescribing. Among the conditions noted is the requirement that software must be interoperable, in accordance with CCHIT. The above changes have increased the ability to advance HIE among all care providers by enabling smaller entities with financial limitations to become connected with hospitals, physicians, etc.
While the above regulation changes can facilitate interoperable HIE, the new e-prescribing program also has instigated problems that will need to be resolved. Many state laws take precedence over new e-prescribing regulations, such as New York State, which recently required that all prescriptions be written in triplicate, derailing the benefits that e-prescribing offers, including streamlining communication between physicians and pharmacies (Stakeholder call with Mark Callahan, New York Presbyterian, February 2006). Other issues that will need to be addressed within the scope of e-prescribing that affect the PAC/LTC environment include costs; different regulations, not only within states but for controlled substances; the federal Drug Regimen Review; and electronic signature standard requirements (Friedman, 2005).
b. Medicare Health Care Quality (MHCQ) Demonstration Program: The MMA of 2003 mandated several demonstration programs to improve and modernize the Medicare program. One of these demonstrations is Section 646 of the MMA, the MHCQ Demonstration Program. As stated by CMS, the objective of this major initiative is to improve quality while increasing efficiency through major, regional-level healthcare system redesign. As such, providers and communities have the opportunity to reform Medicare payment and redesign care delivery from the most basic to the highest level (CMS, 2006a).
Prior to the release of the Request for Proposals (RFP) in Spring 2005, CMS requested input and discussion from a variety of stakeholders and interested parties with regard to the overarching goals of the demonstration, and in September 2005, released RFP CMS-5017-N for submission of proposals with two separate solicitation phases (January 30, 2006, and September 29, 2006). From the submitted proposals, 8-12 healthcare organizations will be selected to participate in the five-year demonstration.
Within the context of the MMA, the goals of the Section 646 MHCQ demonstrations are to improve patient safety, enhance quality, increase efficiency, and reduce scientific uncertainty and medical variation that results in lower quality and higher costs (CMS, 2006b). To meet the above goals, CMS defined system redesign to include adoption and use of decision support tools, reform of payment methodologies, outcome measurements, and enhanced cultural competency in delivery of care. One component of system redesign should include adoption of and use of HIT within practice settings and clinical data exchange across and among practice settings within a community; in essence, a prototype national NHIN. To augment the across settings system exchange and encourage participation on a regional level, CMS identified specific groups that were eligible to compete in this demonstration award, including physician groups, integrated delivery systems, and/or organizations representing regional coalitions (which must include a full range of providers, including hospitals, clinics, HHAs, and SNFs). At the time of this report, these awards have not yet been announced.
D. Adoption of Health Information Technology: Other Select Efforts
Barriers to the adoption of electronic HIT, including concerns of funding, interoperability, security, and investment return are well documented. A recent survey published in Healthcare Financial Management Association reported that the primary reasons for slow adoption rates of interoperable information technology systems by physician practices and hospitals include the lack of funding, the lack of standards, engaging physicians to adopt new technology, and the lack of interoperability (Healthcare Financial Management Association, 2006). With the high start-up and on-going maintenance costs, limited standardized HIT products, uncertainty regarding the value of available products, and the absence of a strong business case for incurring such an expense, convincing these health providers to implement these systems remains a concern for these healthcare providers.
These concerns also are shared by HIE networks. From a 2005 survey of RHIO participants by Healthcare Informatics in collaboration with AHIMA and the Association of Medical Directors of Information Systems (AMDIS), 46% reported that funding is the largest challenge facing their organization and 33% reported that interoperability and standards development is the main challenge (Healthcare Informatics in collaboration with AHIMA and AMDIS, 2005). Recipients of AHRQ RHIO grants have been asked to develop business plans that will enable these organizations to be viable when their grant funding ceases. These grantees have identified potential alternative funding sources such as payments from hospitals, public health, laboratories, payors, and purchasers (see Section D.1 for more information on RHIOs).
While the AHIMA and AMDIS surveys discussed above were undertaken and targeted toward specific audiences (e.g., hospitals, physicians, industry executives, and other stakeholders), these same groups also are the leaders and beneficiaries of advancements in the health exchange technology. In currently operating RHIOs, hospitals make up the largest participants (88%), with clinics/group practices following at 74%, and LTC and PAC facility membership trailing at 20% (Healthcare Informatics in collaboration with AHIMA and AMDIS, 2005). As such, even though PAC/LTC are included in RHIO formations, the unique and specific needs and associated problems of PAC/LTC HIE go beyond the scope of these surveys. In fact, corresponding numbers for PAC/LTC settings are not available in the literature.
In one of the few studies that looked at EHR adoption in PAC/LTC, Kaushal and colleagues convened an expert panel in August 2005. Based on the experts opinions, this study: (i) characterized several HIT functions that would be needed in an interoperable nationwide health information infrastructure, and (ii) estimated current and projected HIT adoption rates for several healthcare provider types. The types of HIT functionalities that they considered that are relevant to this paper were billing/claims; eligibility processing; results reporting; EHRs (e.g., demographics, problem list, medication list, allergies, advance directives); and computerized physician order entry (Kaushal et al., 2005b; Kaushal et al., 2005a; Poon et al., 2006).
Using information gathered from healthcare providers in two market areas, the experts attempted to estimate current and future HIT adoption rates for physicians, hospitals, SNFs, HHAs, laboratories and pharmacies. Table 1 below presents these estimates for hospitals, physicians, SNFs, and HHAs.
| TABLE 1: Estimated HIT Adoption Rates | ||||||||
| Current Adoption Rates | Projected Adoption Rates in 5 Years | |||||||
| Hosp | MD | SNF | HHA | Hosp | MD | SNF | HHA | |
| Billing/claims | 84-92% | 78-90% | 77% | 73% | 99% | 99% | 99% | 99% |
| Eligibility processing | 18-24% | 10-19% | 17% | 16% | 58-65% | 53-64% | 54% | 56% |
| Results viewing | 53-68% | 23-35% | 8% | 6% | 69-83% | 51-69% | 29% | 29% |
| EHRs (e.g., demographics, problem list, medication list, allergies, advance directives) | 11-18% | 9-15% | 1% | --- | 29-41% | 25-38% | 14% | --- |
| Computerized provider order entry | 7-17% | 5-9% | 1% | --- | 37-54% | 21-32% | 14% | --- |
| SOURCE: Kaushal et al., 2005a. | ||||||||
While the Kaushal et al. findings are based on expert opinion rather than empirical research, other research (discussed below) also has reported findings that support differences in HIT adoption rates between hospital and physician practices and PAC/LTC settings. Until HIT/EHR adoption in PAC/LTC provider settings is increased, the promises of an interoperable nationwide health information infrastructure will not be realized.
A common explanation for low adoption rates is that PAC/LTC settings have inherently greater resource limitations as compared to inpatient and ambulatory settings because of their unique patient population, providers, payors, and business case. With many competing financial priorities necessary (e.g., staffing, maintenance), nursing homes and HHAs do not generally have the operating margins to develop or purchase EHR systems (American Medical Directors Association [AMDA], 2005; Gloth III, Coleman, Phillips & Zorowitz, 2005). However, as the United States population ages, more focus on these care settings will be imperative. An overwhelming majority of SNF care (82%) is provided to Medicare and Medicaid beneficiaries. Medicare also is the largest single purchaser of home care services in the United States with 41 million beneficiaries (CMS, 2003; CMS, 2004; Pettey, 2004). Other research has indicated that implementation of EHR systems would in theory reduce errors and duplicative procedures, and reduce approximately 30% of the annual Medicare spending (Fisher et al., 2003).
Many PAC/LTC settings have chosen not to implement an EHR system because a strong business case is lacking. Stakeholders mentioned that compared to acute and ambulatory settings, they receive a lower volume of patients, they have higher rates of staff turnover, and the implementation and ongoing costs for EHR maintenance are very expensive as is the corresponding staff training. Most importantly, the implementation of an EHR system could disrupt the existing workflow that has adapted to the use of paper as the means for exchanging data. As one stakeholder stated, "if it isn't broke, don't fix it."
However, in spite of these reasons why adopting technology to facilitate the exchange of health information is slow and challenging, it is notable that in the course of conducting the stakeholder interviews, several health settings and other related organizations stood out as having innovative strategies to facilitate information exchange. The following findings from the stakeholder interviews describe what steps some HDSs and other healthcare organizations are making to address the issue of HIE. When applicable, representatives of interviewed sites were given the opportunity to review and correct the information provided below.
1. Regional Health Information Organizations
The Healthcare Information and Management Systems Society (HIMSS) defines a RHIO as a group of organizations with a business stake in improving the quality, safety, and efficiency of (health) care delivery (Healthcare Informatics in collaboration with AHIMA and AMDIS, 2005). Because of the multiple issues (e.g., business, legal, legislative, technological, clinical, and cultural) involved in creating a cross-organizational interoperable health information network, the RHIO approach has become an attractive option at both the state and federal levels. Federal programs have emphasized and increased the amount of funding for grants and demonstrations for the planning and implementation of RHIOs. The ONCHIT indicates that the Federal Government has funded over 100 regional projects (http://www.os.dhhs.gov/healthhit/rhio.html, 2005). Over 40 states are in some phase of RHIO planning or implementation or have projects that are focused on a RHIO perspective (HIMSS and the Center for Health Information & Decision Systems, 2006). Surveys have indicated that although grants are normally used for start-up and planning phases, alternative funding sources for RHIO start-up and continuation is necessary (Healthcare Informatics in collaboration with AHIMA and AMDIS, 2005). As there are no best practice methods for RHIO start-up, communities have produced their own design, specific to their own needs, with funding and planned funding coming from a variety of sources, including hospitals, employers, physician groups, non-profit groups, insurers, local government, user fees, financial incentives, and public (e.g., AHRQ) and private investors. Stakeholder and business organizations have joined together to increase further acceptance on a federal and regional level, and the following programs were implemented in the past year to facilitate adoption of the regional organization approach:
- The HIMSS RHIO Federation was established in late 2005 for the purpose of collaboration and knowledge exchange among existing RHIOs and developing organizations.
- The HIT Dashboard, online in 2006, is a joint effort between HIMSS and the Center for Health Information and Decision Systems (CHIDS) at the Robert H. Smith School of Business, University of Maryland, that has collected, mapped, and updated project information on over 500 state, federal, and private HIT initiatives, including RHIOs (HIMSS and the CHIDS, 2006).
- eHealth Initiative released a Connecting Communities Toolkit in 2005 to help aid in the development, planning, and implementation stages for regional organizations. The toolkit was implemented as an ever-evolving information portal, with up-to-date information available on policies, governance, financing, technology, and resources. This toolkit was funded thru a Cooperative Agreement of the Health Resources Services Administration Office of the Advancement of Telehealth.
2. Quality Improvement Organizations (QIOs)
In March 2006, the American Health Quality Foundation (AHQF) released Quality Improvement Organizations and Health Information Exchange, a report discussing the current and future role of QIOs in the development of HIE. This report consists of: (1) input from an Advisory Panel that included QIO representatives, federal agencies, stakeholder groups, and industry experts; and (2) results from a national 2005 survey of QIOs. Findings from the report indicated that 42 of 53 QIOs were "substantially engaged in local HIE efforts, many in leadership roles." The report further broke down the types of involvement that QIOs are playing, ranging from liaising with physicians on issues related to HIE, to developing business plans for entire HIE networks. Results from the survey indicate that because QIOs are community-based and their primary goal is to improve healthcare quality, they are in an excellent position to further support HIE efforts (AHQF, 2006). HIE support also is evident through QIO work within the recently finalized CMS contracted 8th SOW, which includes a policy focus on physician and hospital adoption of HIE systems (e.g., EHRs, e-prescribing). Once again, however, there is little reference to HIT and PAC/LTC settings in this report.
3. AHIMA LTC Summit Report and Recommendations
The AHIMA is composed of over 50,000 members interested in facilitating and promoting the sharing of health information. In August 2005, AHIMA organized a "Summit on Health Information Technology and its Implications for Long-Term Care." More than 125 stakeholders from 14 organizations attended and participated in the summit. The result of their efforts is a list of 11 action steps to promote EHRs and other technology in LTC settings that should be taken over the next two years (AHIMA, 2005). Although all 11 recommendations are critical, three action steps are particularly pertinent to this project.
One salient recommendation is to "advocate for and adopt data content and messaging standards that support a unified language and promote interoperability across care settings." This recommendation highlights the need for interoperable data content and messaging standards for health and social status, cognitive ability, and functioning domains. The recommendation states that standardized assessments/data sets (for example, MDS and Outcome and Assessment Information Set [OASIS]) must incorporate HIT content and messaging standards. Any new data collection tools developed and mandated must also incorporate HIT content and messaging standards. Identifying the need for vocabulary and messaging standards for required patient assessments and functional status is a critical for encouraging the use of HIT in PAC/LTC settings. As noted earlier in this report, NCVHS endorsed in September 2006 the CHI content and exchange standards needed for functioning and disability content and patient/client assessments.
The second noteworthy recommendation is to "promote the design, development, and implementation of a standardized patient transfer/summary of care document to enhance the coordination of care across settings and reduce risk to the patient." Participants at the LTC Summit indicated that the value of a standardized transfer document in the provision of care cannot be understated. Patients are particularly vulnerable to errors at times of care transitions because of the various mechanisms that are currently used to transfer information. The HL7 CCD Implementation Guide balloted in December 2006, holds promise for the development of a standardized summary document. However, the likely HITSP endorsement of a subset of the CCD content will not include clinical content critically important for patients treated by PAC and LTC providers (e.g., advance directives, functional status, etc.). The impact of such a limited endorsement (e.g., on the specification of CCHIT criteria) is unknown. A more comprehensive discussion of the relevant content necessary in a transfer document is presented in Section IV.B.2 of this report.
The third recommendation that is particularly important for successfully advancing and implementing several of the recommendations that emerged from the LTC HIT Summit is [f]or the LTC community to engage in the national agenda, benefit from interoperability, and participate in HIEs, they must fully participate in standards activities" (AHIMA, 2005). Participation by members of the LTC community in the various SDOs that specify standards for EHRs and other HIT applications is essential if LTC providers wish to influence how interoperable HIT standards are developed. As noted through out this report, many standard setting activities do not include a focus on the content and messaging standards needed when treating chronically ill disabled and elderly persons who will receive a variety of services across numerous settings and providers. Establishing collaborations across stakeholders (i.e., various LTC provider types, vendors, physicians, nurses) could create opportunities for the perspectives of the LTC community to be considered when identifying and developing standards needed for interoperable HIT and EHR systems.
4. Indiana Health Information Exchange
The University of Indiana and the Regenstrief Institute have long been in the front in terms of adopting HIT to support clinicians and provide them with the information necessary to do their jobs. Building upon previous work led by Drs. Clem McDonald and Marc Overhage, the Indiana Health Information Exchange (IHIE) was established as a non-profit venture joined by a number of HDSs in Indiana. The is comprised of over 48 hospitals and has approximately 3,000 physicians who access the network (Stakeholder call with Marc Overhage on February 22, 2006). With AHRQ funding and a variety of other sponsors including BioCrossroads, regional and local hospitals, and the Regenstrief Institute, the recently implemented a community-wide clinical messaging project. Each participating partner has access to patients' clinical results using a single -controlled electronic mailbox (eHealth Initiative, 2006).
5. Utah Health Information Network
The Utah Health Information Network (UHIN) is a community health information network that began in 1993 (Stakeholder call with Jan Root on March 17, 2006). It is a coalition of healthcare providers, payors, and state government with the common goal of reducing costs by standardizing administrative data, particularly payment data. The network community sets the data standards that providers and payors voluntarily agree to adhere (Stakeholder call with Jan Root on March 17, 2006). The UHIN standards are then incorporated into the Utah state rule via the Insurance Commissioners Office.
UHIN operates as a centralized secure network through which the majority of healthcare transactions pass in the state. Nearly all payors and hospital providers are participating in this project. PAC and LTC providers recently began submitting Medicaid claims data through the UHIN, as it became mandatory in the state in the summer of 2006.
The UHIN developed a tool, which they provide free of charge to providers for use in electronically submitting claims. The tool is provided so that even the smallest provider can submit claims and electronically receive remittance advices. This has drastically reduced the amount of paper processing required for payors and has streamlined the payment of claims and remits, which has resulted in providers receiving payment more quickly. Under an AHRQ grant, they will use what they have learned standardizing the administrative data and pilot test the exchange of a limited set of clinical data (medication history, discharge summaries, history and physical, and laboratory results) with a small number of hospital providers, including an Intermountain Healthcare hospital, and one or two physician offices. This pilot began in August 2006.
6. Montefiore Medical Center
Montefiore Medical Center (Montefiore) is an integrated delivery system in Bronx, New York, providing a full range of services, including specialty care to both local and outside populations. It serves a medically underserved population, a large number of whom are young, minority, and poor (Burke, 2006). Montefiore owns a large HHA and contracts with a number of SNFs in the area. They are using information technology to support the use of clinical pathways and retrospective assessments of practice and outcomes to improve quality of care. Montefiore is one of several acute care hospitals involved in the formation of the non-profit entity called the Bronx RHIO. The other collaborators include other acute care hospitals, over 40 community-based primary care centers, two nursing homes, two HHAs, payors, physician offices, and laboratories. They recently received a grant from the New York Department of Health's initiative called HEAL-NY to start-up a data exchange RHIO in the Bronx. The focus of the Bronx RHIO is to facilitate the sharing of clinical data among providers with disparate systems and levels of sophistication in using EHR systems.
7. New York Presbyterian Hospital
New York Presbyterian Hospital is one of the largest hospitals in the country and is the university hospital for the Cornell and Columbia Schools of Medicine. AHRQ funded the New York-Presbyterian Hospital/Weill Cornell Medical Center as an Integrated Delivery System Research Network (IDSRN) partner, one of nine IDSRN grant recipients. In collaboration with the Visiting Nursing Service of New York (VNSNY), New York Presbyterian developed an electronic home health plan of care, known as the e-485. CMS requires that a plan of care be developed and signed by a physician and be followed by the HHA staff. This plan of care needs to be updated every recertification period (currently 60 days). Historically, the 485 form was the plan of care, and although the form itself is no longer required by CMS, the development and updating of the plan of care is still mandated. Furthermore, although the form is not required by CMS, the information on the form is required for billing purposes, so most HHAs have elected to continue to use the form.
At present, New York Presbyterian is able to generate this form using data from their EHR system, print it out, and fax it to the VNSNY. The benefits of the electronic 485 are that it: (1) is legible; (2) provides a more complete order set; (3) facilitates the co-management of patient care between the physician and the HHA staff; (4) incorporates evidence-based order sets and prompts; and (5) involves the physician in developing the home health plan of care. The electronic 485 now is being used for multiple HHAs that receive referrals from New York Presbyterian/Weill Cornell. In November and December 2006, they pilot tested the electronic transmission of the care plan to a few HHA teams within the VNSNY via a web-based portal. The electronic transmission will allow for more interaction between the referring providers and the HHA, and will create a data-rich environment that allows for more active co-management of patients between physicians and HHA teams. This pilot was funded by a new AHRQ task order under the IDSRN contracting mechanism (Stakeholder call with Dr. Mark Callahan, February 16, 2006, and timeframe clarified by personal communication with Dr. Robert Rosati on January 4, 2007).
8. Erickson Retirement Communities
Erickson Retirement Communities, Catonsville, Maryland owns and operates 13 Continuing Care Retirement Communities (CCRCs) in the United States. Four of their communities are considered "mature campuses" and include a medical center, a certified HHA, inpatient and outpatient rehabilitation services, a SNF, and an assisted living facility (ALF) (Stakeholder interview, Daniel Wilt, March 23, 2006). Erickson does have some specialists on campus that are employed by Erickson and some that are not (e.g., podiatry and dentistry).
Erickson does not own or operate most specialty clinics and does not own or operate any acute care centers. Erickson has developed an electronic chart summary, which is generated out of their electronic medical record and can be accessed via the web or at any of their facilities' workstations. The chart summary includes relevant current and historical information such as advanced directives, medication lists, laboratory results, problem lists, contact information for patient and caregivers, etc. This chart enables electronic HIE between the physician and other Erickson providers who work in other health settings such as the HHA on the Erickson campus. Care coordination is facilitated as physicians can access this information on or off-campus and can then coordinate in a timely manner with the emergency department physician if a patient requires acute care. In November 2005, Erickson launched a website, https://myhealth.erickson.com, which is provided to their residents free of charge. Patients can have read-only access to their own medical record including the chart summary discussed above. Patients can download it to a USB (that Erickson provides free of charge) and take it with them (should they travel or be away for extended periods of time). Alternatively, patients can access this information via the web.
IV. HEALTH INFORMATION EXCHANGED AT TIMES OF TRANSITION
A. Illustrative Case and Introduction
Illustrative Case
A frail older person who lives alone in her apartment sustains a hip fracture. She is initially assessed by the paramedics and asked a series of questions about the circumstances surrounding her fall, in addition to her current medical problems, medications, and allergies. She is then evaluated in the emergency department by an intake coordinator who asks her about insurance coverage and next of kin, as well as a nurse and physician who repeat many of the same questions asked by the paramedics. The patient may or may not have any prior records that can be accessed by the emergency room staff and if she did have prior records, the staff may or may not have made the effort to review them. She then undergoes diagnostic imaging to confirm her fracture and is admitted to the inpatient orthopedic floor.
Upon arriving on the inpatient orthopedic floor, she undergoes a comprehensive nursing intake evaluation by a floor nurse and is seen by both the orthopedist and a hospital physician (hospitalist) who each undertake a different medical assessment in preparation for surgery. The patient also has contact with the anesthesiology service, and different nursing staff in the operating room and in the recovery center before returning to the orthopedic ward. The next day, she has contact with a physical therapist and occupational therapist, and a new floor nurse. Next she interacts with a discharge planner who arranges transfer to a SNF for her to continue with her rehabilitation. In transit, she has contact with two ambulance drivers.
Upon arrival at the SNF, she again undergoes an intake assessment by a nurse and an evaluation by either a physician, nurse practitioner, or physician's assistant. The SNF staff also will complete the required MDS assessment. In addition to meeting new SNF nurses, an SNF physical therapist, and an occupational therapist, the patient meets a new discharge planner who arranges for her to return to her apartment with skilled home care services.
Upon returning home, she undergoes a comprehensive assessment by a home care nurse that includes the required Outcome and Assessment Information Set (OASIS). She also is seen by a home care physical therapist, an occupational therapist, and may receive visits from a home health aide. Once home, she returns to her primary care physician and nursing team to provide ongoing continuity and coordination of her medical care.
At each of these transition points the patient is asked many of the same (or similar) demographic, insurance, and health-related questions.
This case illustrates the many transitions that occur for a fairly circumscribed and straightforward episode of care. For all of these transitions, a successful "hand-off" of health information between professionals in each setting is critical to achieving an optimal outcome. In many respects, this case has been oversimplified. For example, the patient did not develop any complications such as an infection or blood clot that would require transfer back to the hospital. The patient could have had dementia and therefore would have been unlikely to be able to provide accurate information regarding her medical history or her insurance. It also does not address the multiple medications that are likely to have been prescribed to this patient or the multiple medication changes that are likely to have occurred as the patient transitions from one setting of care to the next.
This scenario exemplifies why improved HIE is a critical step toward reducing medical errors, improving quality, and increasing efficiencies for patients who receive care across settings. HIT offers great potential to foster improved communication across these settings. However, to be effective, the technology needs to support and be integrated into workflow processes and be acceptable to practicing clinicians and patients.
The 2005 White House Conference on Aging recommended that the unique needs of older adults be identified and included in the development of a blueprint for a national health information system (White House Conference on Aging, 2005). Implementation of interoperable HIT would permit that, as Americans age, essential longitudinal health information be available to all healthcare providers across care settings. Interoperable HIE is particularly important to older adults with chronic illness in general and frail older adults in particular. As the case of the woman who suffers a hip fracture illustrates, this population often receives care in multiple, disparate settings. In addition, family caregivers play a significant role in executing the care plans and ensuring quality and safety before, during, and after care hand-offs. HIT could support the capture of patient and caregiver preferences and patient entered data. The AHIC has established a workgroup on Consumer Empowerment which has as its broad charge the need to promote wide spread adoption of a personal health record that is easy-to-use, portable, longitudinal, affordable, and consumer-centered (HHS, 2006c). Consumers use of PHRs is one strategy that would enable the exchange of longitudinal health information as patients transition from one healthcare provider to another. In addition, HIE between patients/caregivers and clinicians is another focus of another of the AHIC use cases (HHS, 2006b), confirming the importance of this information being included in an EHR.
However, as previously described, research has found HIT adoption rates are relatively low across healthcare settings. To date, most of the technological developments largely have occurred in hospitals and to a lesser extent in ambulatory settings. PAC and LTC settings face many of the same challenges as confronted by hospital and physician offices when considering HIT investments including: (i) concerns about how the market will change and whether the HIT/EHR products acquired today will continue to be functional as the market evolves; (ii) lack of understanding about HIT standards and uncertainty about which standards should be included in EHR/HIT products; and (iii) lack of standardized EHR/HIT products from which PAC and LTC providers may select. These uncertainties are believed to have contributed the low rates of more functional EHR/HIT solutions by PAC and longer care providers.
The supply of more robust and standardized EHR/HIT solutions have not as available to PAC settings, including HHAs and SNFs, and other LTC settings such as nursing homes and ALFs, to the same degree as has been the case for hospitals and physician offices (Kramer et al., 2004). Among the many possible reasons for this discrepancy is that care is delivered differently in acute and PAC/LTC settings. First, care in PAC and LTC settings is delivered primarily by certified nursing assistants (CNAs) and nurses, but also a more prominent role is played by a wide array of other healthcare professionals including dietary, social work, physical and occupational therapy, and recreational therapy. Thus, an EHR system must accommodate the needs of these professionals and paraprofessionals for gathering, synthesizing, and communicating information to support successful implementation of the overall care plan.
Discussion of interoperable EHR systems must acknowledge other key differences between care settings. Acute, post-acute, and LTC settings often have different staffing ratios, different clinical information needs, different orientations and approaches to assessment and management, and face different regulatory and reimbursement requirements. These disparate requirements translate into different data needs. For example, in PAC and LTC settings, healthcare professionals and paraprofessionals place greater emphasis on improving functional and cognitive status as patients in these settings generally have limitations in physical and/or cognitive functioning, assessments of these clinical domains are required by regulation, and payment for services in these settings is determined, in part, based on each patients physical and cognitive status.
PAC and LTC settings also face some unique challenges with respect to HIT implementation. As observed, in nursing homes, for example, CNAs deliver a large proportion of care. CNAs are characterized by a high degree of turnover, may speak English as a second language, and may have limited health and/or computer literacy (Hernandez-Medina, Eaton, Hurd & White, 2006; Stone & Wiener, 2001). Nonetheless, the information CNAs collect is very important to care planning and reflects many of the services delivered in nursing homes. Further, from a financial perspective, the typical operating margins in nursing homes are much lower than in hospitals and therefore may not support investment and maintenance of EHR systems (AHIMA, 2005; AMDA, 2005). Thus, while HIT could support data collection and exchange in PAC/LTC settings, the staff characteristics and turnover rates, and limited operating margins for facilities also may limit the ability to invest in HIT and support ongoing training costs.
B. Overview of Clinical Information Exchanged at Times of Transition
While HIT can support the collection and exchange of information collected by nurses, CNAs, and other staff in PAC/LTC settings (e.g., therapists, physicians), the level of detail typically captured at the point of care may not be the type of information needed at times of transitions (e.g., discharge or transfer from PAC/LTC settings to hospitals). As previously mentioned, members of the LTC community identified priority action steps needed to advance the use of HIT in LTC settings in the Roadmap for Health IT in Long-Term Care (AHIMA, 2005). One of the identified action steps was the need to design, develop, and implement a standardized patient transfer/summary of care document to enhance the coordination of care across settings and reduce risk to the patient. The Roadmap suggested starting with developing a standardized patient transfer/summary of care record or document, and integrating data format, content, definitions, and messaging to enable interoperable exchange of this information.
Based on a review of published literature, summaries of large national conferences, and documents produced by professional societies, at present there is no consensus on the specific content and type of information exchange needed between acute, post-acute, and LTC settings. Despite this lack of consensus, when data elements are proposed, most authors and organizations arrive at a very similar list of data elements that will be described herein. What is clear is that standardized core content needs to directly inform care delivery during the immediate time period at or around the time of transfer to facilitate the immediate provision of care by the receiving team (Coleman, Foley & Phillips, 2003; Coleman, 2003; Terrell et al., 2005). Too much information can be distracting to clinicians. Moreover, including a large number of data elements could create serious inefficiencies given that at each transfer point, these data may need to be reviewed and updated. Eventually, the process could buckle under its own weight.
Identifying and standardizing the needed core content of a transfer summary creates opportunities to support safe and efficient care transitions between settings, and could facilitate better decision making when it comes to matching patient care needs with the care setting.
1. Medium Used to Transmit Information
Each of the various mediums offers certain advantages and disadvantages. The sources consulted in preparing this report uniformly confirmed that sending paper documents with the patient and facsimile transmissions remain the two most frequently used communication approaches to support HIE to and from PAC/LTC settings. The information is predominantly handwritten, supplemented by photocopies of pertinent information such as the medication administration record, recent laboratory results and diagnostic imaging results, or recent assessments. Fax machine usage is nearly ubiquitous in most healthcare settings, which is a distinct advantage. However, it is possible for faxed pages to become misplaced or for the fax machine to fail and legibility of information continues to be an issue. While continued reliance on paper or fax transmission does not require the initial and ongoing costs associated with HIT implementation, continued reliance on paper and/or fax to exchange information at times of transition does not address the identified problems related to incomplete and/or untimely HIE. In addition, transmission of information in paper or fax form limits efficient reuse of information as patients transfer across settings. Because limited EHR adoption rates and limits on the ability of many existing HIT solutions to exchange and reuse content, healthcare systems that possess this technology often have to continue to utilize another medium to exchange information at the time of transfer. This may include printing a computer-generated summary to send with the patient or fax it to the next care setting.
Not all information exchange necessarily has to occur from provider to provider. There are distinct advantages to patients managing their own information during transfers (Coleman, 2003; Coleman, Parry, Chalmers & Min, 2006). There is a growing interest in exploring the feasibility of providing patients with up-to-date health information in an electronic format that they could convey from one provider to the next. Conceptually, the patient and caregiver would continue to function as a conduit through which clinicians in different settings would communicate key information, except now HIE would occur electronically. This could be accomplished using simple technology such as a Microsoft Word or Excel document contained in a binder, a CD-Rom, or a jump drive. A more advanced approach is to store the information in a shared care plan on a password-protected website. PeaceHealth, an integrated delivery system located in Alaska, Oregon, and Washington received an AHRQ grant to implement such an approach and the resultant PHR website can be viewed at https://www.sharedcareplan.org/Default.asp?Javascript=Yes. Erickson Retirement Communities, discussed in Section III.D.8, also provides their patients with access to a web-based summary document of their medical chart.
The transfer of timely and accurate information across settings is critical to the execution of effective care transitions. Practitioners need an understanding of the patient's goals, baseline functional status, active medical and behavioral health problems, medication regimen, family or support resources, durable medical equipment needs, and ability for self-care (HMO Workgroup on Care Management, 2004; Coleman, 2003; Coleman, 2002). Without this information, service duplications may occur, important aspects of the care plan may be overlooked, and conflicting information to the patient may be conveyed. Incomplete information transfer can result in critical errors, such as the patient returning home without life-sustaining equipment (e.g., supplemental oxygen or equipment used to suction respiratory secretions). The absence of information about an older patient's baseline level of cognitive function may result in an acute decline in cognitive status being mistaken for chronic dementia. Furthermore, a lack of understanding of a patient's functional health status, including both physical and cognitive, may result in transfer to a care venue that does not meet his or her needs.
As stated earlier, there is no consensus as to what comprises the core clinical information that practitioners require as patients transition from setting to setting. However, there are several efforts underway that will attempt to describe the content that is needed as patients transition across healthcare settings. With support from the John A. Hartford Foundation, the Society for Hospital Medicine (SHM) has undertaken a consensus effort to create a model for Idealized Hospital Discharge Planning. This effort emphasizes the importance of creating a discharge summary that is explicitly focused on the receiving healthcare team rather than a historical document that is created to satisfy the requirements of the medical records department (Halasyamani et al., 2007). Within its Transforming Care at the Bedside initiative, the Institute for Healthcare Improvement has launched a transition out of the hospital initiative that includes an emphasis on information transfer to the next care setting (Institute for Health Care Improvement, 2006b).
In addition, a review of different national efforts that have attempted to define important clinical content needed at times of transition is potentially instructive for describing the types of information needed to be exchanged. Included among these efforts is the HL7/ASTM CCD work. The CCD not only describes the type of information needed for clinical summary documents (using the domains identified by the CCR), but also specifies in an implementation guide, being balloted by HL7, the structure and semantics of clinical documents for the purpose of [electronic] exchange (Health Level Seven and ASTM, 2006). The CCD and three other efforts that specify the types of information needed at times of transition are highlighted herein:
- Table 2: Continuity Care Document (CCD) (Health Level Seven, Inc. and ASTM, 2006);
- Table 3: Uniform Patient Assessment for Post-Acute Care tool proposed by the University of Colorado at Denver Health Sciences Center to CMS (CMS, 2006c);
- Table 4: The HMO Care Management Workgroup (which is comprised of medical and nursing operations leaders from many of the nation's exemplar Medicare Advantage programs (HMO Workgroup on Care Management, 2004); and
- Table 5: The Veterans Affairs Geriatrics and Extended Care (GEC) Referral Discharge Planning Tool (Department of Veterans Affairs, 2006).
The type of clinical information specified in each of these efforts is presented in Tables 2-5. Generally, the intent of these efforts is to help the receiving care team quickly develop an understanding of an individual patient from the standpoint of functional status (pre-morbid as well as present status), the immediate care needs that require attention, an accurate and up-to-date medication list, self-care ability and family support, and insurance coverage. Although there are some differences between these four efforts, what is most instructive is the observed high degree of overlap among the identified domains. The overlapping domains of clinical information may be instructive to the LTC Community, SDOs, and others as they consider the type of clinical content that needs to be exchanged and continue to advance the standards needed for the exchange of patient transfer/summary documents.
| TABLE 2: Continuity of Care Document Recommended Data Domains | |
| Payers Advance Directives Support (persons/family) Functional Status Problems Family History Social History Alerts Medications | Medical Equipment Immunizations Vital Signs Results Procedures Encounters Plan of Care Healthcare Providers |
| SOURCE: HL7 Implementation Guide: CDA Release 2 -- Continuity of Care Document, 2nd Informative Ballot, December 6, 2006. | |
| TABLE 3: Uniform Patient Assessment for Post-Acute Care Proposed Data Domains |
|
| SOURCE: Centers for Medicare and Medicaid Services, 2006c. |
| TABLE 4: HMO Care Management Workgroup Recommended Data Domains | |||
| Domains | Information Required | Short-Term Goals* | Long-Term Goals* |
| Functional Status |
| ||
| Medical Status |
| ||
| Self-Care Ability |
| ||
| Social Support |
| ||
| Disposition |
| ||
| Communication |
| ||
| Advance Directives |
| ||
| Durable Medical Equipment (DME) |
| ||
| Coverage/Benefits |
| ||
| SOURCE: HMO Workgroup on Care Management, 2004. * Goals take into account the patients values and preferences. ** ADLs = Activities of Daily Living; IADLs = Instrumental Activities of Daily Living. | |||
| TABLE 5: Veterans Affairs Geriatrics and Extended Care Referral Data Domain Categories | |
| 1. Source of referral. 2. With whom does the patient live/Where does the patient live. 3. Primary caregiver information. 4. Language. 5. Homebound status. 6. Instrumental activities of daily living. 7. Services in the home. 8. Additional information. 9. Skilled care. 10. Basic activities of daily living. 11. Continence. | 12. Skin. 13. Patient behaviors and symptoms. 14. Cognitive status. 15. Prognosis. 16. Weight bearing. 17. Diet. 18. What equipment does the patient need. 19. What supplies does the patient need. 20. Goals of care. 21. Referring to which program. 22. Estimated duration of care. |
| SOURCE: Department of Veterans Affairs, 2006. | |
The CCHIT Certification Functional Criteria for Ambulatory EHR Products includes requirements related to an EHR systems capacity to produce reports, including a requirement to produce hard or electronic copies of summary information (such as hospital discharge summaries (CCHIT, 2006c). The CCHIT final interoperability criteria for Ambulatory EHR products recognizes the need to exchange clinical documentation to "refer or transfer clinical care of patient" and indicates that the work HL7/ASTM CCD is conducting may address this need. The CCHIT placed consideration of this standard on its Roadmap for May 2007 (CCHIT, 2006d).
The 2007 CCHIT roadmap for interoperability criteria for Ambulatory EHR Products identifies several criteria for which the HL7/ASTM CCD will be considered, including the ability to send a medical summary when referring or transferring the clinical care of patients, the receipt of medical summaries and importing them into the EHR for consultations or for transfer, the ability to send summary data to PHRs, and the receipt of data from PHRs for import into EHRs (respectively, item numbers IA-5.7, IA-5.8, IA-5.9, and IA-5.10). CCHIT anticipates specifying EHR interoperability certification criteria for these functions in 2008 (CCHIT, 2006a).
The proposed CCHIT Functional Certification Criteria for Inpatient EHR Products includes criteria for managing, documenting, and tracking referrals between care providers or healthcare organizations (whether internal or external to the referring organization), and supporting the creation of health service reports at the end of an episode of care (including, but not limited to, discharge summaries), (respectively, criteria #IF-2.11.1 and #IF-2.14.1) (CCHIT, 2006e). CCHIT anticipates specifying these (and other) functional requirements for inpatient EHRs in 2008.
The CCHIT roadmap for inpatient EHR criteria indicates the need to include interoperability criteria for exchanging clinical documents such as hospital discharge summaries. The criteria to be considered include sending and receiving medical summary documents to referral settings or transferring the clinical care of patient to other clinicians. The CCHIT will consider HL7 CDAr2 and HL7/ASTM CCD as possible exchange standards (http://www.cchit.org/work/inpatient+criteria.htm).
As noted above, in November 2006, CCHIT announced an expansion of its certification efforts to include additional medical specialties and healthcare settings. At this time, it is unknown which settings will be selected.
3. Preference by Provider and Practitioner Type
There is not an extensive literature that documents providers' and practitioners' preferred methods of cross-setting communication. What is known suggests moderate variation. For example, more recent graduation from training is associated with higher levels of comfort with using EHR systems to exchange health information (Healthcare Financial Management Association, 2006). In some practice settings, physicians, nurse practitioners, and physician assistants are given privileges to remotely access clinical information from EHRs based in hospital or ambulatory settings. Under these circumstances, clinicians can care for patients in remote locations (e.g., nursing homes, in patients homes) by using HIT to access and exchange health information at these locations. However, it should be noted that case studies and stakeholder informants indicate PAC and LTC health professionals (e.g., nurses, CNAs, physical and occupational therapists) are not usually granted this same access (Kramer et al., 2004).
Electronic communication offers greater efficiency and less need to re-create information. However, it also has the potential to propagate inaccurate information more widely (i.e., garbage in, garbage out), making it particularly important that the information is verified and updated in a timely manner as needed. In the current environment where most healthcare providers are not HIT-enabled, there are advantages to paper communication. For example, if an ambulance that is in transport between a nursing home and a particular hospital is diverted to a different hospital, the paper information may be the only information available to health professionals in the receiving hospital.
Despite the opportunity to access health information electronically, some physicians prefer to continue to receive discharge/transfer information via fax. In a survey of rural physicians completed by the University of Nebraska, the majority of physicians explained that the daily workflow in their offices already was established for receiving information via fax and that to use the hospital's EHR system would disrupt this flow and create additional work for office staff (Xu, 2004).
4. Volume, Frequency, and Timing of Clinical Information Exchange
There is a growing literature exploring information transfer at the time of hospital discharge. Studies by van Walraven and colleagues have documented not only failures in information transfer, they also have documented that the transferred information frequently is incomplete and even inaccurate (van Walraven et al., 2002a; van Walraven et al., 2002b). Leaders from the AMDA have shown that SNFs do not receive legible transfer information from the hospital approximately 28% of the time (Coleman et al., 2003).
A nursing home in Galveston, Texas gathered input from its local emergency department as to what information was pertinent and what information was irrelevant to send with the patient. Through its consensus process, the essential data elements were identified. These included medical history, current medications, chief complaint, change from baseline, resuscitation status, family member name and contact information, and a contact number if more information. A form was designed to ensure that this information could fit on a single page. By achieving "buy-in," the facilities were able to agree on a standard transfer document (Davis, Brumfield, Smith, Tyler & Nitschman, 2005).
Timely information transfer can financially benefit both the hospital and the PAC/LTC setting. Under the Diagnostic Related Group payment system, the hospital has the financial incentive to transfer the patient as soon as s/he is stable. Under the nursing home Resource Utilization Groups III (RUGs III) reimbursement system, the nursing facility receives a daily payment rate that is based, in part, on the patients medical problems and co-morbid conditions. To determine whether a facility can meet a patient's care needs under the prevailing daily rate, timely communication of a patient's PAC needs from the hospital can facilitate a more timely and appropriate transfer. Ensuring that the SNF has comprehensive information on a patients current needs and plan of care can facilitate appropriate classification under the RUGS III system. Thus, within this context, more timely information transfer may enable hospitals to more efficiently discharge patients into SNFs in which the appropriateness of a particular patients placement is prospectively determined.
5. Available Information
In general, practitioners have little time to gather, review, and incorporate clinical information into a new care plan in the new care setting. Thus, whether in paper or electronic form, the content needs to be found easily and flow in an intuitive way (e.g., medication information should be contiguous with medication allergy information). Providing too much information or requiring searching and clicking on too many data fields may ultimately be counterproductive.
The Institute for Healthcare Improvement and the SHM have advanced specific recommendations concerning the type of medication information that should be exchanged at times of transition. They have recommended that not only should medications be reconciled prior to transfer, but that every medication should be identified in one of the following categories: (1) new medication; (2) continued medication, new instructions; (3) continued medication, same instructions as before; and (4) discontinued medication. In addition, both generic and brand names of medications should be listed and every medication also should include its indication for use (Institute for Health Care Improvement, 2006a).
Unaffiliated providers have the opportunity to delineate the timing and types of information transferred during their contract negotiations (Coleman et al., 2004a; HMO Workgroup on Care Management, 2004). For example, a healthcare system can require that the SNFs and HHAs with which they contract contribute to or update the patient's problem list, allergies, medications, advance directives, and recent diagnostic tests while patients are under their care. In this instance, a payor can mandate that contract providers adopt protocols for HIE at the time of transfer as a condition to receive payment.
6. Regulatory and Organizational Requirements
Within Medicare's regulatory framework, the Conditions of Participation (CoPs) explicitly include requirements concerning information exchange at the time of transfer for hospitals, HHAs, clinics, rehabilitation agencies, and public health agencies (Table 6). The Joint Commission and Accreditation of Healthcare Organization has deemed status from CMS to provide oversight for these CoPs (Hughes, 2003). Health information transfer for nursing homes is largely governed by state regulations not the CoPs.
Notably absent from each of the preceding requirements are any requirements clearly specifying the timing of the exchange of the required discharge/transfer documents.
The Emergency Medical Treatment and Labor Act requires hospitals with emergency departments to provide a medical screening examination to any individual who comes to the emergency department and requests such an examination, and prohibits hospitals with emergency departments from refusing to examine or treat individuals with an emergency medical condition. If a decision is made to transfer the patient to another hospital, the sending hospital is required to send all pertinent records to the receiving hospital.
The HIPAA allows the exchange of patients' health information for purposes of treatment, payment, and healthcare operations without patient authorization. However, misinterpretations of HIPAA regulations are common (Coleman et al., 2003). Clinicians may be apprehensive to share information for fear of violating HIPAA laws and facing accompanying penalties. In addition, States may establish privacy protections that exceed those established by HIPAA and organizations may have established different business practices to comply with federal and/or state privacy requirements. Thus, the complexity and variation in privacy requirements have created challenges to HIE.
| TABLE 6: Medicare CoPs Concerning Health Information Exchange at Times of Transfer |
| HOSPITAL The hospital must transfer or refer patients, along with necessary medical information, to appropriate facilities, agencies, or outpatient services, as needed, for follow-up or ancillary care (42 CFR 482.43). |
| HOME HEALTH AGENCY A written summary report for each patient is sent to the attending physician at least every 60 days (42 CFR 484.14). If a patient is transferred to another health facility, a copy of the record or abstract is sent with the patient. The record contains copies of summary reports sent to the attending physician and a discharge summary. The HHA must inform the attending physician of the availability of a discharge summary. The discharge summary must be sent to the attending physician upon request and must include the patients medical and health status at discharge (42 CFR 484.48). An assessment (including use of OASIS) is required upon discharge (42 CFR 484.55(d)(3)). |
CLINICS, REHABILITATION AGENCIES, AND PUTLIC HEALTH AGENCIES All patients must be referred to the facility by a physician who provides the following information to the facility before treatment is initiated (42 CFR 485.58):
The following are obtained by the organization before or at the time of initiation of treatment (42 CFR 485.711 Subpart H):
|
| SOURCE: National Archives and Record Administration-Code of Federal Regulations, 2004a; National Archives and Record Administration-Code of Federal Regulations, 2004b; Federal Register, 2001; Hughes, 2003. |
V. IMPLICATIONS AND FUTURE CONSIDERATIONS
To summarize the prior sections of this report, the need for complete, legible, accurate and timely information at time of transitions is critical to ensuring patient safety and high quality patient care. Lack of access to a patient's most recent clinical information further contributes to rising healthcare costs as it often leads to duplicative testing or patient referrals to higher intensity care settings for unnecessary or redundant evaluations. Yet despite requirements outlined in the Medicare CoPs, HIE among acute, PAC, and LTC providers currently has been found to be lacking both in terms of the timing and content of the exchange. The purpose of this final section is to discuss the implications of the findings from the literature review, stakeholder calls, and what is understood about the current state of play with respect to HIE. This section will conclude with a look ahead to this projects planned site visits that will explore HIE in greater depth in four exemplar HDSs/organizations/regions across the country.
A. Implications
HIE is still predominantly conducted with paper documents that are transferred with patients and/or communicated via facsimile. To date, implementation of electronic health information systems has been more prevalent in hospitals and ambulatory care clinics compared with PAC and LTC settings (Kaushal et al., 2005a; Grossmank & Reed, 2006). Further, the percentage of HIT/EHR products deployed in PAC and LTC settings that support HIE is suspected to be low. To date, in contrast to hospital and physician office settings, no EHR certification criteria (including EHR functional and interoperability criteria) have been specified for PAC and LTC settings. These differences have and will undoubtedly influence the extent to which electronic HIE can be accomplished across settings. In addition, while the HL7/ASTM Implementation Guide for the CCD holds considerable promise for an exchange standard for summary documents, this standard is only currently being balloted. The goal of widespread interoperability only can be met if the respective care settings implement HIT/EHR solutions and, if standards exist and are adopted across healthcare settings, for the standardized HIE of information needed at times of transfer/discharge/referral.
As discussed earlier in this report, PAC and LTC settings face unique challenges with respect to adopting emerging HIT, particularly among smaller providers. In general, these health settings operate with much lower profit margins, experience higher staff turnover, and receive referrals and information from a broad array of healthcare providers. If implementation of standardized HIT in PAC/LTC facilities continues to lag behind hospitals and ambulatory clinics, this will limit the ability to realize the promises of a nationwide interoperable health information infrastructure including limiting the realization of needed quality and safety improvements, and cost reductions. Stakeholders and industry experts have attempted to speak to this concern and are aware of the ramifications of lower rates of implementation by these providers (Kaushal et al., 2005a).
In addition to specifying standards for HIT/EHR applications used in PAC and LTC settings, closing the gap of HIT implementation will require that industry leaders articulate a compelling business case for PAC and LTC settings to adopt standardized, electronic HIT to support HIE. To date, however, there is a dearth of information on the costs and benefits of HIT implementation in the literature, including the costs and benefits that are incurred when HIT/EHRs are implemented in caring for patients in PAC and LTC settings. Yet relatively straightforward elements to support the business case are apparent. For example, one important leverage point might include the potential of electronic HIE to facilitate more efficient referrals that could potentially financially benefit both the sending and receiving providers. Just as small physician offices have questioned whether adoption of an EHR system will ultimately impact their practice, PAC and LTC providers are seeking information about the costs and benefits of HIT implementation, including how these products will address their business needs (e.g., facilitating the production and exchange of information at times of transition) and how to minimize their risks of making unsound HIT/EHR investment decisions.
Several public and private sector activities may provide much of the foundation for advancing standardized HIT/EHR implementations in PAC and LTC settings. The CHI/NCVHS-endorsed standards for patient assessments and functional and disability content establishes standards by which the content of federally-required patient assessments may be standardized and exchanged. ASPE is funding research examining the costs and benefits of HIT/EHR acquisition and use in PAC and LTC settings. Some of this work includes the development of a taxonomy of HIT applications that are used or could be used in PAC and LTC, as well as a plan to identify the cost and benefits metrics that could be used to evaluate HIT applications. This study requires case studies of PAC and LTC settings to begin gathering HIT cost/benefit information and the development of a quantitative data analysis plan to understand more completely the costs and benefits.
While research has found that most nursing homes and HHAs have implemented HIT solutions for administrative functions, members of the LTC provider community have conducted preliminary surveys and data collection efforts to explore the implementation of more robust HIT/EHR applications. In addition, involvement of the LTC community in standards development activities has contributed to the advancement of HIT standards needed in this sector. For example, the LTC community is working to specify a LTC EHR Profile using the HL7 EHR-System Functional Model. In addition, participation by LTC representatives in the development of the HL7/ASTM CCD implementation guide (presently being balloted) has contributed to the inclusion in that guide of the patient assessment standards recently endorsed by NCVHS-CHI. The LTC EHR Profile and successful balloting of the CCD implementation guide could be considered by the CCHIT as it evaluates which settings it will include in its expanded SOW to specify EHR certification criteria. Finally, the CAST and AHIMA efforts to demonstrate interoperable exchange of a summary document including wellness and functional status information using the HL7/ASTM CCD standard is important to demonstrate the exchange of this content to and heighten the awareness of the vendor, provider, and consumer communities of how this standard can be used for this type of exchange.
Implementation of e-prescribing by the Medicare Part D drug benefit may further help drive improvements in HIE. Implementation of this program required the identification of e-prescribing standards that have now been required for use by the Medicare program. Implementation of the Medicare e-prescribing program and the related pilots required under the MMA may stimulate PAC and LTC providers, attending physicians, and affiliated pharmacies to identify how to implement standardized e-prescribing in SNFs/nursing homes. As the LTC community and SDOs (such as the NCPDP LTC workgroup) work to identify e-prescribing standards that are particularly pertinent to LTC providers, it will be especially important to explore how nursing home contract pharmacies can support electronic medication orders on behalf of institutionalized patients not just during static times when patients are receiving care in the facility, but also during more dynamic times during transfers to higher or lower intensity care settings. This type of HIE is critical to comprehensive medication reconciliation, an essential function needed to avoid and potentially reduce medication errors. Standards are needed for HIT/EHR applications that are used in caring for PAC and LTC patients that include requirements for electronic medication reconciliation.
B. Areas of Further Study
The work of the public and private sector entities is still evolving. While several critical HIT infrastructure issues have been addressed to support the standardized exchange of health information at times of transition, many of these solutions have yet to be implemented and key gaps that remain.
Additional work is needed to identify and implement standards/criteria for more robust EHR/HIT applications needed for patients with PAC and LTC needs. For example, as described, medication reconciliation is an important function, particularly with respect to PAC and LTC patients. Nursing home patients receive on average 6-7 prescribed medications per day. As these patients are transferred to and from hospitals, medication changes are common due to clinical conditions, admission assessments, and hospital formulary requirements, etc. (Boockvar et al., 2004). Medication reconciliation is very time consuming, accountability for who performs reconciliation is unclear, and this task is rarely performed electronically. The AHRQ/CMS e-prescribing pilot being conducted in nursing homes will identify several standards needed for medication ordering in nursing homes. Medication reconciliation is a critical function that likely could be supported and enhanced with a standardized HIT solution.
Findings from the literature and stakeholder interviews suggest that the exact clinical content needed at the time of transition varies based on the status of the patient and the types of health settings involved in providing his/her care. In addition, although providers can negotiate the timing and type of information to be exchanged with the healthcare organizations with which they do business, the health information that is actually exchanged is often lacking in terms of its timeliness, completeness, and/or accuracy. Future studies may want to ask clinicians/specific care settings what they believe is the desired content needed at time of transition and explore barriers to timely, complete, and accurate HIE.
In addition, it will be important to ensure that the data elements that are particularly relevant for older and more complex patients and are needed to be exchanged at times of transition can be represented in the CCD standard for electronic HIE for summary documents. Needed data for this population includes, for example, a prominent place to feature the role, strengths and limitations of family caregivers, as well as the patients baseline and current physical and cognitive functional status. Inclusion in the ballot of standards to represent functional status content and assessments is one critical component of information that needs to be exchanged on behalf of this population. The CAST/AHIMA demonstration of the use of the CCD standard will be an important step for demonstrating the utility of this standard.
Finally, the dearth of peer-reviewed literature on studies related to EHR and HIT adoption in PAC and LTC studies is telling. To make informed decisions about how to increase and enhance HIT adoption rates, there is a need for empirical evidence on the current status of EHR/HIT adoption in these settings, as well as trending for future adoption.
C. Next Steps
The next step in this project is to conduct four site visits to locations that have implemented or have planned HIE strategies. Each site visit will be comprised of a visit to a host site such as an acute care hospital, CCRC, or HIE entity, and three or more unaffiliated PAC/LTC settings. The purpose of the site visits is to: (1) gather information from clinicians about what health information they want/need at times of care transitions; (2) determine how information is shared across both affiliated and unaffiliated settings; and (3) identify the facilitators and barriers to the exchange of health information across these settings.
These site visits will enhance our understanding about HIE on behalf of patients who receive PAC and LTC services, including the barriers to more timely and complete health information (in both electronic and paper form) and what collaborative solutions may have emerged to address some of these barriers. Some of these locally derived solutions may be generalizable to other healthcare communities nationwide. These site visits also will offer the opportunity to explore additional important areas that are not well described in the literature. For example, one area of interest will be how clinicians workflow patterns are affected by the introduction of emerging technologies.
D. In Closing
Greater understanding of the factors that contribute to the current state of HIE (both electronically and non-electronically) across acute, PAC and LTC settings is important for identifying opportunities for improvement. Drawing from the lessons in the literature and the insights of national leaders and stakeholders, this report has attempted to elucidate many of these contributing factors and begins to suggest promising areas for further exploration. With a growing number of groups representing both the private and public sectors beginning to consider the unique needs of patients in need of PAC and LTC services in the development and implementation of electronic HIE standards, the opportunity for significant advancement in the field has become possible.
REFERENCES
Agency for Healthcare Research & Quality (2006). AHRQ and Health Information Technology. http://healthit.ahrq.gov/portal/server.pt?open=512&objID=562&&PageID=5663&mode=2&in_hi_userid=3882&cached=tru.
Agency for Healthcare Research & Quality HCUPnet (1999). Outcomes by Patient and Hospital Characteristics for all Discharges. http://hcup.ahrq.gov/HCUPnet.asp (last accessed June 29, 2004).
Alschuler, L. (2006). Continuity of Care Document. Power Point slide presentation for HIMSS, February 2006.
American Health Information Management Association (2005). A Road Map for Health IT in Long Term Care. http://www.ahima.org/infocenter/whitepapers/ltc.asp.
American Health Quality Foundation (2006). Quality Improvement Organizations and Health Information Exchange. http://www.ahqa.org/pub/uploads/QIO_HIE_Final_Report_March_6_2006.pdf.
American Medical Directors Association (2005). White Paper Response to Questions Posed by the Long Term Health Care Summit, August 22-23, 2005.
ASTM International (2006). Document Summary. Active Standard: E2369-05 Standard Specification for Continuity of Care Record (CCR). http://www.astm.org/cgi-bin/SoftCart.exe/DATABASE.CART/REDLINE_PAGES/E23....
Beers, M., Sliwkowski, J., & Brooks, J. (1992). Compliance with medication orders among the elderly after hospital discharge. Hosp Formul, 27, 720-724.
Boockvar, K., Fishman, E., Kyriacou, C.K., Monias, A., Gavi, S., & Cortes, T. (2004). Adverse events due to discontinuations in drug use and dose changes in patients transferred between acute and long-term care facilities. Arch Intern Med, 164, 545-550.
Burke, G. (2006). A RHIO for the Bronx: Overview of the Approach, Impact and Organization of the Effort. Power Point presentation.
Center for Aging Services Technologies (2006). Development of a Continuity of Care Document with Functional Status and Wellness Content. Continuity of Care Document Task Group Meeting, November 10, 2006.
Center for Health Information Technology (2006). Essential Similarities and Differences Between the HL7 CDA/CRS and ASTM CCR. http://www.centerforhit.org/PreBuilt/chit_ccrhl7.pdf.
Centers for Medicare & Medicaid Services (2006a). Medicare Demonstration to find ways to improve quality of health care. Press Release. http://www.cms.hhs.gov/apps/media/press/release.asp?Counter=1549.
Centers for Medicare & Medicaid Services (2006b). Medicare Program: Solicitation for Proposals for the Medicare Health Care Quality Demonstration Programs. No. CMS-5017-N. http://www.cms.hhs.gov/DemoProjectsEvalRpts/downloads/MMA646_Solicitatio....
Centers for Medicare & Medicaid Services (2006c). Uniform Patient Assessment for Post-Acute Care -- Final Report. http://www.cms.hhs.gov/QualityInitiativesGenInfo/Downloads/QualityPACFul....
Centers for Medicare & Medicaid Services (2003). Medicare enrollment -- All beneficiaries as of July 2003. http://www.cms.hhs.gov/MedicareEnRpts/Downloads/03All.pdf.
Centers for Medicare & Medicaid Services (2004). CMS Financial Data. http://www.cms.hhs.gov/CapMarketUpdates/downloads/2004walletcard.pdf.
Certification Commission for Healthcare Information Technology (2005). CCHIT Certified Ambulatory Electronic Health Record HER Products by Product. http://www.cchit.org/certified/2006/CCHIT+certified+products+by+Product.htm.
Certification Commission for Healthcare Information Technology (2006a). 2007 Interoperability Criteria and Roadmap Ambulatory EHRs. November 28, 2006. http://www.cchit.org/files/Ambulatory_Domain/INTEROPERABILITY_Ambulatory....
Certification Commission for Healthcare Information Technology (2006b). Certification Handbook. Ambulatory HER Products 2006, Version 1.2. http://www.cchit.org/files/ambulatory%20domain/final%20certification%20H....
Certification Commission for Healthcare Information Technology (2006c). Final Criteria: Functionality for 2006 Certification of Ambulatory EHRs -- Effective May 1, 2006. http://www.cchit.org/files/Ambulatory%20Domain/Final%20Criteria%20-%20FU....
Certification Commission for Healthcare Information Technology (2006d). Final Criteria: Interoperability for 2006 Certification of Ambulatory EHRs -- Effective May 1, 2006. http://www.cchit.org/files/Ambulatory%20Domain/Final%20Criteria%20-%20IN....
Certification Commission for Healthcare Information Technology (2006e). Proposed Functionality for 2007 Certification of Inpatient EHRs and Roadmap for Public Comment. September 25, 2006. http://www.cchit.org/files/Inpatient_Domain/Functionality_-_Inpatient_-_....
Coleman, E.A. (2002). Aspen Transitional Care Conference Proceedings. http://www.uchsc.edu/hcpr/documents/AspenTransitionProceedings.pdf (accessed November 17, 2003).
Coleman, E.A. (2003). Falling through the cracks: Challenges and opportunities for improving transitional care for persons with continuous complex care needs. J Am Geriatr Soc, 51, 549-555.
Coleman, E.A. & Berenson R.A. (2004). Lost in transition: Challenges and opportunities for improving the quality of transitional care. Annals of Internal Medicine, 141, 533-536.
Coleman, E.A., Eilertsen, T.B., Smith, J.D., Frank, J., Thiare, J.N., Ward, A. et al. (2002). Development and testing of a measure designed to assess the quality of care transitions. J Integrated Care, Volume 2. http://www.ijic.org.
Colemand, E.A., Foley, C. & Phillips, C. (2003). Falling through the cracks: Practical strategies for reducing adverse events among older patients transferring between sites of care. Annals of Long Term Care, 11, 33-36.
Coleman, E.A. & Fox, P.D. (2004a). One patient, many places: Managing health care transitions, Part I: Introduction, accountability, information for patients in transition. Ann Long-Term Care, 12, 25-32.
Coleman, E.A., Min, S., Chomiak, A. & Kramer, A.M. (2004b). Post-hospital care transitions: Patterns, complications, and risk identification. Health Serv Res, 39, 1449-1465.
Coleman, E.A., Parry, C., Chalmers, S., & Min, S. (2006). The care transitions intervention: Results of a randomized controlled trial. Archives of Internal Medicine, 166, 1882-1828.
Consolidated Health Informatics (2006). Standards Adoption Recommendation -- Functioning and Disability. http://www.ncvhs.hhs.gov/061011p2b.pdf.
Davis, M.N., Brumfield, V.C., Smith, S.T., Tyler, S., & Nitschman, J. (2005). A one-page nursing home to emergency room transfer form: What a difference it can make during an emergency! Annals of Long-Term Care, 13, 34-38.
Department of Health & Human Services National Committee on Vital & Health Statistics Subcommittee on Standards & Security (2006). Transcript of the October 11, 2006 NCVHS Subcommittee on Standards and Security Hearing. http://www.ncvhs.hhs.gov/061011tr.htm.
Department of Veterans Affairs (2006). VA Geriatrics and Extended Care (GEC) Referral. http://www1.va.gov/geriatricsshg/docs/vha-10-0415-fill.pdf.
Dolin, R., Alschuler, L., Boyer, S., Beebe, C., Behlen, F., Biron, P. et al. (2006). HL7 Clinical Document Architecture, Release 2. Journal of the American Medical Informatics Association, 13, 30-39.
eHealth Initiative (2006). CCBH Awardee: Indiana Health Information Exchange. http://ccbh.ehealthinitiative.org/awardee_.mspx.
Federal Register (2001). Rules and Regulations. Volume 66, Number 117, 32778.
Federal Register (2004a). Development and Adoption of a National Health Information Network. Volume 69, Number 219, 65599-65601.
Federal Register (2004b). Executive Order 13335: Incentives for the Use of Health Information Technology and Establishing the Position of the National Health Information Technology Coordinator. Volume 69, No. 81, 24059.
Federal Register (2005a). Consolidated Health Informatics (CHI) Initiative; Health Care and Vocabulary Standards for Use in Federal Health Information Technology Systems. Volume 70, No. 246, 76287-76288.
Federal Register (2005b). Medicare Program; E-Prescribing and the Prescription Drug Program; Final Rule. Volume 70, Number 214, 67567-67595.
Federal Register (2006). Notice of availability: Secretarial recognition of certain Certification Commission for Healthcare Information Technology (CCHIT) functionality, interoperability, security and reliability criteria for ambulatory electronic health records. Volume 71, Number 150, 44295-44296.
Fisher, E., Wennberg, D., Stukel, T., Gottlieb, D., Lucas, F. & Pinder, E. (2003). The Implications of Regional Variations in Medicare Spending. Part 2: Health Outcomes and Satisfaction with Care. Annals of Internal Medicine, 138, 288-298.
Forster, A., Murff, H., Peterson, J., Gandhi, T. & Bates, D. (2003). The incidence and severity of adverse events affecting patients after discharge from the hospital. Annals of Internal Medicine, 138, 161-167.
Friedman, M. (2005). E-Prescribing and the Medicare Prescription Drug Program, Office of E-Health Standards and Services Power Point slide presentation, presented November 17, 2005.
Gloth III, F.M., Coleman, E.A., Phillips, S.L. & Zorowitz, R.A. (2005). Using electronic health records to improve care: Will "high tech" allow a return to "high touch" medicine? J Am Med Dir Assoc, 6, 270-275.
Grossmank, J. & Reed, M. (2006). Most Medicare Outpatient Visits are to Physicians with Limited Clinical Information Technology. Center for Studying Health System Change. http://hschange.org/CONTENT/759/.
Halasyamani, L., Kripalani, S., Coleman, E., Schnipper, J., van Walraven C, Torcson, P. et al. (2007). Transition of care for hospitalized elderly -- the development of a discharge checklist for hospitalists. Journal of Hospital Medicine, in press.
Harrison, A. & Verhoef, M. (2002). Understanding coordination of care from the consumer's perspective in a regional health system. Health Serv Res, 37, 1031-1054.
Health Level Seven Inc. and ASTM (2006). HL7 Implementation Guide: CDA Release 2-Continuity of Care Document (CCD). http://www.hl7.org/documentcenter/ballots/2007JAN/downloads/CDAR2_IMPL_CCD_I2_2007JAN.zip.
Health Level Seven Inc. (2005). HL7 EHR TC, Committee Level Ballot on the EHR-S Functional Model: Conformance Clause.
Health Level Seven Inc. (2006a). http://www.hl7.org/.
Health Level Seven Inc. (2006b). HL7 to develop Continuity of Care Record Clinical Document Architecture Implementation Guide. http://www.hl7.org/documentcenter/public/pressreleases/20051102.pdf.
Healthcare Financial Management Association (2006). Overcoming barriers to electronic health record adoption. Washington, DC: HFMA.
Healthcare Informatics in collaboration with AHIMA and AMDIS (2005). Mapping a changing healthcare landscape: Results of a Regional Health Information Organization Survey.
Healthcare Information and Management Systems and Society and the Center for Health Information and Decision Systems (2006). HIT Dashboard. http://www.hitdashboard.com.
Healthcare Information Technology Standards Panel (2006). Document Number: HITSP 06 N 135. http://publicaa.ansi.org/sites/apdl/Documents/Standards%20Activities/Healthcare%20Informatics%20Technology%20Standards%20Panel/HITSP%20Numbered%20Documents/HITSP%2006%20N%20135%20-%20HITSP%20Letter%20Supporting%20CCD%20(Approved).doc.
Hernandez-Medina, E., Eaton, S., Hurd, D., & White, A. (2006). Training Programs for Certified Nursing Assistants (Rep. No. 2006-08). Washington, DC: AARP Public Policy Institute.
HMO Workgroup on Care Management (2004). One patient, many places: Managing health care transitions. Washington, DC: AAHP-HIAA Foundation.
Hughes, G. (2003). Transfer of Patient Health Information Across the Continuum (Updated). AHIMA Practice Brief, Practice Guidelines for Managing Health Information, 64S-64Z.
Integrating the Healthcare Enterprise (2006). IHE North America Connectathon 2006 Results. http://www.ihe.net/Connectathon/connectathon_results.cfm.
Institute for Health Care Improvement (2006a). Medication Reconciliation Across the Continuum -- Improvement Report. http://www.ihi.org/IHI/Topics/PatientSafety/MedicationSystems/ImprovementStories/MedicationReconciliationAcrosstheContinuum.htm.
Institute for Health Care Improvement (2006b). Transforming Care at the Bedside. http://www.ihi.org/IHI/Programs/TransformingCareAtTheBedside/Transformin....
Institute of Medicine (2000). To Err Is Human: Building A Safer Health System. Washington, DC: National Academy Press.
Institute of Medicine (2001). Crossing the quality chasm: A new health system for the 21st century. Washington, DC: National Academy Press.
Kaushal, R., Bates, D. W., Poon, E. G., Jha, A. K., Blumenthal, D. & the Harvard Interfaculty Program for Health Systems Improvement NHIN Working Group (2005a). Functional gaps in attaining a national health information network. Health Affairs, 24, 1281-1289.
Kaushal, R., Blumenthal, D., Poon, E. G., Jha, A. K., Franz, C., Middleton, B. et al. (2005b). The costs of a national health information network. Annals of Internal Medicine, 143, 165-173.
Kramer, A., Bennett, R., Fish, R., Lin, C., Floersch, N., Conway, K. et al. (2004). Case Studies of Electronic Health Records in Post-Acute and Long-Term Care. Denver, CO: University of Colorado Health Sciences Center.
Kramer, A., Bennett, R., Fish, R., Lampinen, L. & Coleman, E. (2003). Summary of status of electronic health records in post-acute and long-term care. Denver, CO: University of Colorado Health Sciences Center.
Kramer, A., Eilertsen, T., Lin, M., & Hutt, E. (2000). Effects of nurse staffing on hospital transfer quality measures for new admissions. In Appropriateness of minimum nurse staffing ratios for nursing homes (pp. 9.1-9.22). Baltimore, MD: Health Care Financing Administration.
Levine, C. (1998). Rough crossings: Family caregivers odysseys through the health care system. New York, NY: United Hospital Fund of New York.
Moore, C., Wisnevesky, J., Williams, S. & McGinn, T. (2003). Medical errors related to discontinuity of care from an inpatient to an outpatient setting. J Gen Intern Med, 18, 646-651.
National Archives and Record Administration -- Code of Federal Regulations (2004a). Chapter IV -- Health Care Financing Administration, Department of Health and Human Services Part 482 -- Conditions of Participation for Hospitals. http://www.access.gpo.gov/nara/cfr/waisidx_00/42cfr482_00.html.
National Archives and Record Administration -- Code of Federal Regulations (2004b). Chapter IV -- Health Care Financing Administration, Department of Health and Human Services Part 484 -- Home Health Services. http://www.access.gpo.gov/nara/cfr/waisidx_00/42cfr484_00.html.
National Council for Prescription Drug Programs (2006a). Basic Guide to Standards. http://www.ncpdp.org/PDF/Basic_guide_to_standards.pdf.
National Council for Prescription Drug Programs (2006b). NCPDP Active Task Groups. http://www.ncpdp.org/pdf/Task_groups_list_2006-01.pdf.
Office for the National Coordinator for Health Information Technology (2004). The decade of health information technology: Delivering consumer-centric and information-rich health care. Washington, DC.
Office for the National Coordinator for Health Information Technology (2006). American Health Information Technology (The Community) October 31, 2006 Meeting Details. http://www.hhs.gov/healthit/m20061031.html.
Office of the National Coordinator for Health Information Technology (2005). Summary of Nationwide Health Information Network (NHIN) Request for Information (RFI) Responses. Washington, DC.
Office of the National Coordinator for Health Information Technology & Department of Health and Human Services (2006). State Subcontracting Information. http://www.hhs.gov/healthit/subcontinfo.html.
Pettey, S.M. (2004). Government promotes application of information technology to health care. Caring for the Ages, 5, 6-8.
Poon, E., Jha, A., Christino, M., Honour, M., Fernandopulle, R., Middleton, B. et al. (2006). Assessing the level of healthcare information technology adoption in the United States: A snapshot. BMC Medical Informatics and Decision Making, 6, 1.
Stone, R.I. & Wiener, J.M. (2001). Who Will Care for Us? Addressing the Long-Term Care Workforce Crisis. http://aspe.hhs.gov/daltcp/reports/ltcwf.htm.
Terrell, K. M., Brizendine, E. J., Bean, W. F., Giles, B. K., Davidson, J. R., Evers, S. et al. (2005). An extended care facility-to-emergency department transfer form improves communication [see comment]. Academic Emergency Medicine, 12, 114-118.
The Lewin Group (2005). Health Information Technology Leadership Panel: Final Report. Washington, DC: US Department of Health and Human Services.
U.S. Department of Health and Human Services (2006a). American Health Information Community Approves First Set of Recommendations. News Release. http://www.hhs.gov/news/press/2006pres/20060517a.html.
U.S. Department of Health and Human Services (2006b). American Health Information Community Workgroups. http://www.hhs.gov/healthit/ahic/workgroups.html.
U.S. Department of Health and Human Services (2006c). American Health Information Community Workgroups: Consumer Enpowerment Workgroup. http://www.hhs.gov/healthit/ahic/ce_main.html.
U.S. Department of Health and Human Services (2006d). Federal Health Architecture (FHA). http://www.hhs.gov/fedhealtharch/index.html.
van Walraven, C., Seth, R., Austin, P.C. & Laupacis, A. (2002a). Effect of discharge summary availability during post-discharge visits on hospital readmission. J Gen Intern Med, 17, 186-192.
van Walraven, C., Seth, R. & Laupacis, A. (2002b). Dissemination of discharge summaries. Not reaching follow-up physicians. Canadian Family Physician, 48, 737-742.
vom Eigen, K., Walker, J., Edgman-Levitan, S., Cleary, P., & Delbanco, T. (1999). Carepartner experiences with hospital care. Med Care, 37, 33-38.
Weaver, F. M., Perloff, L., & Waters, T. (1998). Patients' and caregivers' transition from hospital to home: needs and recommendations. Home Health Care Serv Q, 17, 27-48.
White House Conference on Aging (2005). Report to the President and the Congress, The Booming Dynamics of Aging: From Awareness to Action, December 11-14, 2005.
Xu, L. (2004). Factors associated with information technology use by rural and urban physician practices.
APPENDIX A. LIST OF STAKEHOLDER CONTACTS
| Stakeholder Category | Organization | Name(s) |
| FHA EHRWG | VA | Linda Fischetti |
| FHA EHRWG | MITRE Corp. | Erik Phelps |
| ASTM, Standard on Continuity of Care Record | Center for Health Information Technology, American Academy of Family Physicians | David Kibbe |
| CCD/CCR (SDO) | Kaiser Permanente | Bob Dolin |
| CCD/CCR (SDO) | HL7 and private consulting | Liora Alschuler |
| NCPDP (SDO) | Achieve Technologies | Mike Bordelon |
| SDO | CAST EHWR Task Force | Peter Kress |
| HL7 EHR Technical Committee and Interoperability Subcommittee (SDO) | HL7 and private consulting | Gary Dickinson Patricia Gibbons Jean Stanford |
| HL7's LTC Profile committee (as an SDO) | AHIMA | Michelle Dougherty, RHIA, CHP |
| HDS that extends into PAC/LTC | Meridian Health | Rebecca Weber Bob Radvanski |
| HDS that extends into PAC/LTC | Montefiore Medical Center | Gregory C. Burke |
| HDS that extends into PAC/LTC | New York Presbyterian | Mark Callahan, MD |
| HDS that extends into PAC/LTC | VNS of New York | Penny Feldman, PhD Chris Murtaugh, PhD Bob Rosati, PhD |
| HDS that extends into PAC/LTC | Regenstrief and the University of Indiana | J. Marc Overhage, MD, PhD |
| PAC/LTC HDS | Erickson Retirement Community | Daniel Wilt |
| Medicare and Medicaid officials knowledgeable about the need for information exchange in PAC/LTC | Centers for Medicare & Medicaid | Nancy Delew Mary Pratt |
| Public sector initiatives that support HIE | AHRQ National Resource Center for HIT | Dan Gaylin (NORC) Jon White (AHRQ) |
| QIO/public sector initiative that supports HIE | American Health Quality Association (AHQA) | Dave Adler |
| RHIO | Utah Health Information Network (UHIN) | Jan Root, PhD |
| Rural HDS | Trinity Health | Donald Crandall, MD |