
Prepared by:
Stephanie S. Teleki, Melony e.s. Sorbero, Lee Hilborne, Susan Lovejoy, Lily Bradley, Ateev Mehrotra, Cheryl l. Damberg
RAND Corporation
This product is part of the RAND Health working paper series.
RAND working papers are intended to share researchers’ latest findings
and to solicit additional peer review.
Prepared for:
Office of the Assistant Secretary for Planning and Evaluation (ASPE)
U.S. Department of Health and Human Services (HHS)
This work was sponsored by ASPE and CMS under Task Order No. DHHSP2330000T under Contract No. 100-03-0019, for which Susan Bogasky served as the Project Officer.. The findings and conclusions of this report are those of the authors and do not necessarily represent the views of ASPE or HHS.
Acknowledgements
We gratefully acknowledge representatives of medical specialty societies and hospital associations who offered valuable information and insights about their experiences in developing performance measures and helping us to consider measures that may be applicable to the hospital outpatient setting. We thank Susan Bogasky, Project Officer, ASPE; Dr. Tom Valuck, Director, CMS Special Program Office for Value-Based Purchasing; and Dr. Julianne Howell, Project Coordinator Hospital VBP, CMS Special Program Office for Value-Based Purchasing for their review of this document and guidance on the project. We also appreciate the review of this document conducted by Drs. Allen Fremont and Steven Asch from RAND.
Preface
In response to a legislative mandate set forth in Section 109 (Title I) of the Tax Relief and Health Care Act of 2006 (PL 109-432) (TRHCA), which established new requirements for reporting quality data for services paid under the Outpatient Prospective Payment System (OPPS), the Centers for Medicare & Medicaid Services (CMS) is currently working to identify performance measures that can be used to evaluate care provided to Medicare beneficiaries in the hospital outpatient setting. This mandate was motivated by recognized deficits in quality of care across all settings of care and ongoing concerns about the growth in utilization of services and costs.
In September 2006, the Assistant Secretary for Planning and Evaluation (ASPE) within the U.S. Department of Health and Human Services (DHHS), in collaboration with CMS, contracted with the RAND Corporation to identify the key reasons for visits and costs in the hospital outpatient setting, to review existing performance measures to assess their applicability to conditions evaluated as well as services/procedures and drugs/biologicals provided in the hospital outpatient setting, and to begin to identify measurement gaps. This report presents the results of this review.
This work was sponsored by ASPE and CMS under Task Order No. DHHSP2330000T under Contract No. 100-03-0019, for which Susan Bogasky served as the Project Officer.
Executive Summary
Background
A variety of studies have documented substantial deficiencies in the quality of care delivered across the United States (Asch et al., 2006; Institute of Medicine [IOM], 2000, 2001, 2005; Schuster et al., 1998; Wenger et al., 2003). While there are no comparable studies of the quality of care delivered in the hospital outpatient setting, pervasive deficits across the health system suggest similar problems likely exist, particularly since a large fraction of care delivered in this setting is ambulatory care for acute and chronic conditions where deficits in quality have been amply demonstrated.
In addition to potential quality of care deficits in the hospital outpatient setting, the Centers for Medicare & Medicaid Services (CMS) has observed growth in the volume of services and costs for care delivered in this setting. In 2006, care provided to Medicare beneficiaries in the hospital outpatient setting accounted for 7 percent of total Medicare program spending (excluding beneficiary cost sharing) (MedPAC, 2007a), and overall spending nearly doubled between 1996 and 2006, reaching $31.6 billion (MedPAC, 2007b).
Under Section 109 of the Tax Relief and Health Care Act of 2006 (TRHCA)1, Congress established new requirements for hospitals serving Medicare beneficiaries to report outpatient quality data to secure their full annual update to the Outpatient Prospective Payment System (OPPS) fee schedule. This new program, the Hospital Outpatient Quality Data Reporting Program (HOP QDRP), will begin in January 2008. The HOP QDRP builds on other CMS initiatives that are measuring and making transparent quality information and beginning to use incentives to promote high-quality and cost-effective care — key steps identified in the Department of Health and Human Services (DHHS) Secretary’s “four cornerstones” for building a value-driven health care system (Leavitt, 2006).
A Scan of the Hospital Outpatient Landscape
The program requirements mandated under TRHCA have created a need for performance measures that CMS could use in the HOP QDRP. To assist CMS with the task of identifying both measurement opportunities and potential measures, the DHHS Assistant Secretary for Planning and Evaluation (ASPE) in partnership with CMS issued a contract to the RAND Corporation in September 2006 to conduct an initial assessment of the hospital outpatient measurement landscape. RAND was asked to determine the leading conditions treated and services/procedures provided in the outpatient setting as a function of both volume and costs, and to identify existing performance measures that may be applicable to care provided in this setting as well as measurement gaps. As part of the environmental scan, RAND:
- Conducted an analysis of 2005 Medicare facility data for services paid through the hospital Outpatient Prospective Payment System (OPPS) to determine the leading conditions and services/procedures;
- Scanned publicly available measures being used across a variety of settings to identify those that potentially apply to the care delivered in the hospital outpatient setting and to identify gaps, and
- Held discussions with medical specialty societies and hospital associations to determine whether they were aware of existing measures either being applied or that could be applied in the hospital outpatient setting, to learn about measure development work going on (to feed the measures pipeline), and to help identify measurement gaps.
For the purposes of our environmental scan, we defined the hospital outpatient setting as visits and/or services/procedures paid for under the Medicare OPPS. This care was further categorized for analyses and discussion in this report as either rendered in: (1) the ED, or (2) any other hospital-affiliated outpatient setting that is paid under OPPS (hereafter referred to as HOPS). We first classified services/procedures that obviously occur in the ED to the ED; all other services/procedures paid under the OPPS were classified as HOPS.
Key Findings
Analysis of Medicare OPPS Data
Based on our analysis of the Medicare OPPS facility data, in 2005 CMS was billed for 15,325,267 E&M encounters and 78,538,882 services/procedures in the HOPS. In the same year CMS was billed for 11,426,386 E&M encounters and 22,494,724 services/procedures in the ED. Overall, services/procedures represented a significant volume of the care provided in the hospital outpatient setting. More specifically, the top 20 most frequent services/procedures accounted for 58 percent of total services/procedures in the HOPS, and 94 percent of total services/procedures in the ED. Had 2007 payment rates been in effect in 2005, CMS would have paid $19.1 billion for services/procedures in the HOPS, and $1.7 billion for services/procedures in the ED2. The top 20 services/procedures, as a fraction of total costs based on application of 2007 payment rates, accounted for 44 percent of total dollars in the HOPS, and 83 percent of total dollars in the ED.
Of the conditions or services representing the greatest share of utilization and/or costs as a percentage of total use or spending, we find:
- General medical conditions are the most common reasons for visits in both the HOPS and ED.
- In the HOPS, general medical conditions (e.g., hypertension, aftercare for procedures, and specific and general symptoms like fever, dizziness) account for 35 percent of the care delivered, followed by oncology and neoplasia (13 percent); orthopedic conditions (10 percent) (e.g., back pain and arthritis); and endocrinology (7 percent) (e.g., diabetes).
- In the ED, general medical conditions (e.g., “symptoms,” injury like back sprains, lacerations) represented an even larger share of care delivered than in the HOPS (43 percent), followed by orthopedic conditions (17 percent).
- Ancillary services/ procedures, especially radiological, are the most common types of services/procedures provided in both the HOPS and ED settings.
- X-ray was found to be the most common service/procedure performed in both the HOPS and ED; however, it represents a larger proportion of the total in the ED (30 percent) as compared to the HOPS (12 percent).
- In the HOPS, other common services/procedures performed include Level III Pathology (5 percent) and electrocardiograms (4 percent).
- In the ED, electrocardiograms (16 percent) and Level II Drug Administration (9 percent) were found to be the most frequently performed services/procedures after X-ray.
- In the aggregate, many of the most common services/procedures also represent a substantial proportion of all costs in the hospital outpatient setting3. This finding is especially true of radiological services in both the HOPS and ED (X-ray, CT scans), and of X-ray in the ED (X-ray is one of the top two most frequent and most costly services provided in the ED). In the HOPS, the top two most costly services/procedures were cataract surgery (5 percent) and cardiac catheterization (5 percent), although neither of these procedures was found to be among the top 20 most frequently performed services/procedures in the HOPS. In the ED, the top two services/procedures as a function of total costs — CT scans (20 percent) and X-rays (17 percent) — accounted for 37 percent of total costs for services/procedures in the ED. Besides these areas, in the HOPS and ED, most single services/procedures were not found to account for a large proportion of total cost; however, services/procedures that account for even 1-2 percent of total spending in this setting represent significant spending.
- Imaging contrast material, blood products and cancer chemotherapy medications are among the most frequent drugs/biologicals used in both the HOPS and ED. In the ED, several thrombolytic agents are also among the most frequently used.
Scan of Existing Measures and Gaps
From our synthesis of information from the analysis of Medicare OPPS facility data, the scan of existing performance measures being applied in other settings, and discussions with medical specialty societies and hospital associations, we find:
Only a small number of measures specific for immediate application in the hospital outpatient setting currently exist or are in the pipeline. Ten measures comprise the initial hospital outpatient measure set to be used in HOP QDRP starting in January 2008; five pertain to care provided in the ED, and five assess performance related to diabetes, pneumonia, heart failure, and the use of antibiotics at time of surgery. Additionally, CMS has released 30 candidate measures for consideration that address a variety of conditions such as diabetes, fall risk, heart failure, depression, and stroke.
There is a large number of existing performance measures developed for use in other settings that are likely applicable to the care provided in the hospital outpatient setting. The scan of existing performance measures yielded approximately 700 measures that are publicly available and were developed for use in inpatient and ambulatory care settings, many of which are relevant to care delivered in the hospital outpatient setting. The majority of these publicly available, existing performance measures assess clinical effectiveness, primarily the underuse of services. Many are part of broad sets of ambulatory care measures (currently being applied at the physician, practice site, or medical group levels) that were developed by the American Medical Association’s Physician Consortium for Performance Improvement (PCPI), the National Committee for Quality Assurance (NCQA), the Assessing Care of Vulnerable Elders (ACOVE) project, and the Cancer Quality – ASSIST (Assessing Sympoms Side Effects and Indicators of Supportive Treatment) Project. A number of these measures assess performance related to key reasons for visits to the HOPS (e.g., acute myocardial infarction (AMI), coronary artery disease (CAD), congestive heart failure (CHF), diabetes); cancer (especially breast, gastrointestinal, and prostate); and mental health. Additionally, measures developed by medical specialty societies assess care for specific diseases/conditions treated by that specialty (e.g., chronic kidney disease, cancer, polyp surveillance). A few measures assess care provided for cataract extraction, indications for cardiac catheterization, and treatment for cardiac arrhythmias. Apart from clinical effectiveness, there are existing measures of patient experience (CAHPS Clinician & Group, and Hospital Surveys) and patient safety (e.g., culture of safety, medication safety) that may be applicable to the hospital outpatient setting, though modifications in the measures would likely be required to make them directly applicable. While, our review focused only on publicly available measures, there are propriety measures in existence that may be relevant for assessing care provided in the hospital outpatient setting (e.g., RAND’s Quality Assessment (QA) Tools to assess clinical effectiveness, Symmetry’s Episode Treatment Groups (ETGs) to assess relative resource utilization).
Important Gaps Exist in Hospital Outpatient Services Measurement Areas. Despite the large number of existing measures identified that assess clinical effectiveness, there is an absence of measures that examine the appropriateness of care or use of services/procedures, such as imaging which has seen dramatic growth in utilization. Other measurement gaps include: ED care (especially measures to assess care provided to patients who have not yet been definitively diagnosed-- a common situation in the ED); some types of cancer care (e.g., lung cancer); specialty care; follow-up care; coordination-of-care/transitions-in-care; transmission of test results; outcomes; and episodes of care. In light of the performance dimensions identified by the IOM, there is also an absence of well-tested and validated measures of efficiency, equity, and timeliness of care.
Overall, while deficits in measures exist for some performance dimensions, there are a substantial number of existing measures that could either be directly applied or readily adapted for use in the hospital outpatient setting, particularly those addressing acute and chronic care provided in the ambulatory care setting, thus providing a near-term source of candidate measures for the HOP QDRP.
Considerations in Performance Measurement for the Hospital Outpatient Setting
There are several issues that would be valuable to consider in identifying candidate measurement areas and developing performance measures for the hospital outpatient setting, including:
- The type of care and services delivered in the hospital outpatient setting is not homogenous across hospitals or populations served. Services/procedures delivered in the hospital outpatient setting vary hospital-to-hospital as a function of size, location, service mix, and populations served. Because hospitals will vary in their ability to report on various performance measures, it will be important to include some measures that all hospitals can report on to enable cross comparisons of performance and to enhance the ability of all hospitals to participate.
- The problem of small numbers. A key consideration in selecting any performance measure is whether a provider has a sufficient number of events to score in a stable and reliable way. It is important to consider the number of events that occur at the hospital- level for any given condition, service/procedure, or use of drugs/biologicals, to determine whether it is even feasible to measure performance and how many hospitals could be expected to produce scores. The fact that the small numbers problem is compounded when attempting to stratify performance scores by subgroups of patients, such as by race/ethnicity, socio-economic status, and/or gender, also merits consideration.
- Existing measures specifications may need to be modified prior to applying in hospital outpatient setting. Existing measures are being applied in other settings, where the data to populate the measure differ (i.e., the codes used to pull administrative data) and the process of delivering the care may differ. These differences will need to be carefully reviewed to determine whether and how adjustments to the measures specifications are required if they are to be applied to the hospital outpatient setting.
- Physician engagement will be critical. Much of the care delivered by facilities in the hospital outpatient setting is dependant on the actions of physicians, both those practicing in the hospital outpatient setting and those in the community who are ordering services delivered in the HOPS. Therefore, it is important to engage these physicians in measurement and accountability requirements and to coordinate measurement efforts so that the measures for which physicians are individually held accountable are aligned with hospital measures.
- Alignment with other measurement efforts will minimize reporting burden and strengthen their performance improvement signals to providers. Continuing to coordinate measurement efforts with key organizations such as the Hospital Quality Alliance (HQA), Ambulatory Quality Alliance (AQA), and the Joint Commission, as well as internally within CMS, to align measurement across settings of the health care system will be important to ensure that a consistent message is sent to all providers regardless of the setting(s) in which they provide care. This is a particularly critical undertaking given that the care delivered for a specific condition should not vary simply because of where a patient happens to present with that condition. To the extent possible, CMS could consider using the same measures to evaluate care in the hospital outpatient setting as are employed in other settings in which CMS tracks performance.
Next Steps for Consideration
Due to the limited resources for this project, the work completed here should be viewed as a preliminary assessment that requires follow-on work to fully flesh out how to apply existing performance measures in this setting and where the most important measurement gaps are for guiding the use of resources in the future.
As measurement efforts in the outpatient setting move forward, CMS could consider expanding on the work of this evaluation by:
- Conducting additional analyses of the OPPS data: Additional analyses using more detailed and complete OPPS data could refine the set of conditions, services/procedures, and drugs/biologicals that were identified in this study. This analysis could also include a broad set of clinical experts to help evaluate the care provided in the hospital outpatient setting to determine what the priorities should be for performance measurement and whether and how to group services and procedures for measurement. The analyses could address the limitations and suggested modifications noted in this study.
- Conducting a detailed mapping of measures to key areas of use and costs: Once more in-depth data analysis has occurred, a detailed mapping exercise between content areas and existing measures could determine measures that are ready to be used without modifications, and those that require modification and how they could be modified for use to assess performance at the hospital outpatient facility level. Once this work is completed, the candidate measures could be submitted to NQF for their review and endorsement.
- Determining where additional gaps exist and establish priorities for filling gaps: The information gathered from the in-depth data analyses and detailed measures mapping exercise could be used to identify gaps in measures. This review could consider the prioritization of conditions, services/procedures, and drugs/biologicals for determining future measures development work.
Glossary of Abbreviations
| Abbreviation | Definition |
|---|---|
| ACOVE | Assessing Care of Vulnerable Elders, a set of performance measures developed by RAND and UCLA |
| ACR | American College of Radiology |
| ABIM | American Board of Internal Medicine |
| ACC | American College of Cardiology |
| AGAI | American Gastroenterological Association Institute |
| AHRQ | Agency for Healthcare Research and Quality |
| AMA | American Medical Association |
| AMI | Acute myocardial infarction |
| APC | Ambulatory Payment Classification |
| APU | Annual payment update, and adjustment factor to CMS payment rates |
| AQA | Ambulatory Quality Alliance |
| ARBs | Angiostensin receptor blocker |
| ASC | Ambulatory surgical center |
| ASCO | American Society for Clinical Oncology |
| ASPE | Assistant Secretary for Planning and Evaluation |
| ASSIST | Assessing Symptoms Side Effects and Indicators of Supportive Treatment |
| CAD | Coronary artery disease |
| CAHPS | Consumer Assessment of Healthcare Providers and Systems, a suite of patient experience surveys |
| CHF | Congestive heart failure |
| CLFS | Clinical laboratory fee schedule |
| CLIA | Clinical laboratory improvement amendments |
| CMS | Centers for Medicare & Medicaid Services |
| CPT | Current Procedural Terminology |
| CT | Computed tomography scan |
| DRA | Deficit Reduction Act of 2005 |
| ED | Emergency department |
| E&M | Evaluation and management |
| EHR | Electronic health record |
| FY | Fiscal year |
| GERD | Gastroesophageal reflux disease |
| GI | Gastrointestinal |
| HCAHPS | Hospital Consumer Assessment of Healthcare Providers and Systems |
| HCPCS | Healthcare Common Procedure Coding System |
| DHHS | Department of Health and Human Services |
| HOPS | Hospital Outpatient Setting (distinct from the ED) |
| HQA | Hospital Quality Alliance |
| ICD-9 | International Classification of Disease Version 9 |
| ICSI | Institute for Clinical Systems Improvement |
| IOM | Institute of Medicine |
| IT | Information technology |
| LVSD | Left ventricular systolic dysfunction |
| MedPAC | Medicare Payment Advisory Commission |
| MQSA | Mammography Quality Standards Act |
| NCQA | National Committee for Quality Assurance |
| NCCN | National Cancer Care Network |
| NQF | National Quality Forum |
| OFMQ | Oklahoma Foundation for Medical Quality |
| OPPS | Outpatient Prospective Payment System |
| P4P | Pay for performance |
| P4R | Pay for reporting |
| PCI | Percutaneous coronary intervention |
| PCPI | Physician Consortium for Performance Improvement, AMA |
| PQRI | Physician Quality Reporting Initiative |
| PSI | Patient Safety Indicators, a set of patient safety measures developed by the Agency for Healthcare Research and Quality |
| QOPI | Quality Oncology Practice Initiative |
| RHQDAPU | Reporting Hospital Quality Data for Annual Payment Update, CMS’ quality reporting program for inpatient prospective payment hospitals |
| RUC | Relative Value Scale Update Committee |
| SCIP | Surgical Care Improvement Project |
| TRHCA | Tax Relief and Health Care Act of 2006 |
I. Introduction
Background
Deficits in Quality of Care
A variety of studies have documented substantial deficiencies in the quality of care delivered across the United States (Asch et al., 2006; Institute of Medicine [IOM], 2000, 2001, 2005; Schuster et al., 1998; Wenger et al., 2003). In a national examination of the quality of care delivered to adult patients, McGlynn and colleagues found that patients received on average only about 55 percent of recommended care and that adherence to clinically recommended care varied widely across medical conditions (McGlynn et al., 2003). Wenger and colleagues found similar results for vulnerable elders living in community settings, with worse performance for geriatric conditions (Wenger et al., 2003). While there are no similar studies of the quality of care delivered in the hospital outpatient setting, pervasive deficits across the health system suggest similar problems likely exist in this setting, particularly since a large fraction of care delivered in the hospital outpatient setting is ambulatory care for acute and chronic conditions.
The Growth in Expenditures for Hospital Outpatient Care
In 2006, care provided to Medicare beneficiaries in the hospital outpatient setting accounted for 7 percent of total Medicare program spending (excluding beneficiary cost sharing), ranking it fourth (along with skilled nursing) after care provided in the inpatient setting (29 percent), by physicians (15 percent), and in other fee-for-service settings (i.e., hospice, rural health clinics) (13 percent) (MedPAC, 2007a). Overall spending by the Medicare program and beneficiaries on hospital outpatient services (excluding clinical laboratory services) nearly doubled between 1996 and 2006, reaching $31.6 billion (Figure 1.1) (MedPAC, 2007b). The CMS Office of the Actuary projects continued growth in total spending, averaging 10.4 percent per year from 2003 to 2008 (MedPAC, 2007b). A prospective payment system for hospital outpatient services (Outpatient Prospective Payment System [OPPS]) was implemented in August 2000 and the services paid under it represent approximately 90 percent of spending on all hospital outpatient services.
Figure 1.1. Spending on All Hospital Outpatient Services, 1996-2006 (MedPAC 2007)
Notes: Spending amounts are for services covered by the Medicare OPPS and those paid on separate fee schedules (e.g., ambulance services or durable medical equipment) or those paid on a cost basis (e.g., organ acquisition or flu vaccines). They do not include payments for clinical laboratory services. * Estimate Source: CMS, Office of the Actuary.
According to a recent Medicare Payment Advisory Committee (MedPAC) report, spending increases are the result of both an increase in the volume of outpatient services and the mix of services4 (MedPAC, 2007c). Outpatient service volume grew rapidly from 2001, the first full year of prospective payment in the outpatient hospital setting, to 2005; however, the rate of increase slowed from 11.9 percent in 2002 to 3 percent in 2005 (Figure 1.2) (MedPAC, 2007c). Most of the growth in volume during this period was the result of an increase in the number of services per beneficiary. In addition to increases in the use of services per beneficiary, the complexity of services increased, further contributing to the escalation in costs.
Figure 1.2. Annual Growth in the Number of Medicare Outpatient Services (MedPAC 2007)
Note: Data are for hospitals covered under the Medicare OPPS. Source: (MedPAC, 2007),
hospital outpatient claims from CMS. These MedPAC analyses exclude separately paid drugs and pass-through devices.
A wide variety of care is provided in the hospital outpatient setting under OPPS, including evaluation and management (E&M) visits, services/procedures (such as diagnostic imaging and other tests), and the provision of drugs/biologicals. While procedures constituted only 18 percent of the volume of care, they represented 47 percent of the payments in 2005 (MedPAC, 2007b) (Table 1.1). Imaging constituted the second largest category based on volume (19 percent) and spending (23 percent) in 2005.
| Volume | % of total | Payments | % of total |
|---|---|---|---|
| Type of Service | Type of Service | ||
| Separately paid drugs/blood products | 29 | Procedures | 47 |
| Imaging | 19 | Imaging | 23 |
| Procedures | 18 | Evaluation and management | 14 |
| Evaluation and management | 16 | Separately paid drugs/blood products | 11 |
| Tests | 13 | Tests | 4 |
| Pass-through drugs | 4 | Pass-through drugs | 1 |
| Source: (MedPAC 2007b) | |||
The growth in the volume of and spending for hospital outpatient services highlights the importance of this care setting for Medicare beneficiaries. At present, there is no understanding of the quality of care delivered in this setting, and accountability for performance is only beginning to emerge through modifications to the Reporting Hospital Quality Data for Annual Payment Update Program (RHQDAPU Program). Given the likelihood for substantial deficits in care — both the under use and over use of services in this setting — important opportunities for quality improvement and potential cost reduction exist. The current absence of performance measurement and transparency in this setting hinders the ability to understand where deficits are occurring and how to adjust payment policies to drive improvements in care.
Federal Actions to Reform the System
On August 22, 2006, President Bush issued an Executive Order, “Promoting Quality and Efficient Health Care,” that requires the federal government to: (1) ensure that federal health care programs promote quality and efficient delivery of health care and (2) make readily useable information available to beneficiaries, enrollees, and providers (Bush, 2006). To support this mandate, DHHS Secretary Michael Leavitt embraced “four cornerstones” for building a value-driven health care system:
- Connecting the health system through the use of health information technology (HIT)
- Measuring and making transparent quality information
- Measuring and making transparent price information
- Using incentives to promote high-quality and cost-effective care (Leavitt, 2006).
Building on these four cornerstones, CMS has taken steps toward measuring and making quality information transparent to become a value-based purchaser of care. A key example is the CMS Reporting Hospital Quality Data for Annual Payment Update (RHQDAPU) Program, initially enacted under the Medicare Prescription Drug Improvement and Modernization Act of 2003 (MMA)5, and expanded through the Deficit Reduction Act (DRA) of 20056. The RHQDAPU Program provides differential payment updates in the Inpatient Prospective Payment System (IPPS) to hospitals based on whether they publicly report their performance on a defined set of inpatient care performance measures. As part of Section 109 of the Tax Relief and Health Care Act of 2006 (TRHCA)7, Congress established new requirements such that hospitals are required to report hospital outpatient quality data in order to secure the full annual payment update under the OPPS. The new program is referred to as the Hospital Outpatient Quality Data Reporting Program (HOP QDRP).
According to the Proposed OPPS Rule, effective January 2008, hospitals will be required to submit performance data on a set of 10 measures of care provided in the hospital outpatient setting (Table 1.2) to secure their full payment update in Calendar Year (CY) 2009 and each subsequent year;8 the Medicare annual OPPS fee schedule increase amount will be reduced by 2.0 percentage points for any "subsection (d) hospital" that does not submit required outpatient department quality data (CMS, 2007).9
| Measure | Source |
|---|---|
| Emergency Department Transfer: Aspirin at Arrival for AMI (acute myocardial infarction) | Oklahoma Foundation for Medical Quality (OFMQ) |
| Emergency Department Transfer: Median Time to Fibrinolysis for AMI | OFMQ |
| Emergency Department Transfer: Fibrinolytic Therapy Received Within 30 Minutes of Arrival | OFMQ |
| Emergency Department Transfer: Median Time to Electrocardiogram | OFMQ |
| Emergency Department Transfer: Median Time to Transfer for Primary PCI | OFMQ |
| Heart Failure: ACE or ARB Therapy for LVSD | American Medical Association Physician Consortium for Performance Improvement (AMA/PCPI) |
| Perioperative Care: Timing of Antibiotic Prophylaxis | AMA/PCPI |
| Perioperative Care: Selection of Prophylactic Antibiotic | AMA/PCPI |
| Empiric Antibiotic for Community Acquired Pneumonia | AMA/PCPI |
| Hemoglobin A1c Poor Control in Type 1 or 2 Diabetes Mellitus | National Committee for Quality Assurance (NCQA) |
Of the 10 measures, the five emergency department transfer measures were developed by the Oklahoma Foundation for Medical Quality (OFMQ), while the five other measures are physician-level measures for which existing measurement specifications have been revised by the OFMQ to address care provided in hospital outpatient settings. Anticipating the need for a broader range of measures to support this legislative mandate, CMS is seeking public comment on 30 additional measures of care provided in the hospital outpatient setting that are under consideration for reporting in future years (CMS, 2007) (see Appendix A).
Purpose of This Study
In September 2006, the DHHS Assistant Secretary for Planning and Evaluation (ASPE), in collaboration with CMS, issued a contract to the RAND Corporation to conduct a review of performance measures that might be applicable to care provided in the hospital outpatient setting. Specifically, RAND was tasked to conduct an environmental scan to:
- Determine the leading conditions treated and services/procedures provided in the outpatient setting as a function of volume and costs,
- Identify existing performance measures that may be applicable to care provided in this setting; and
- Identify measurement gaps.
The remainder of this report presents the findings of RAND’s environmental scan and is organized as follows:
- The framework and methods used in this study (Chapter 2);
- The results of an analysis of 2005 Medicare hospital outpatient data to determine key reasons for visits, as well as key services/procedures and drugs/biologicals provided in this setting, and of a scan of existing measures for those potentially relevant to hospital outpatient care (Chapter 3);
- A mapping of existing measures to the key reasons for visits, services/procedures, and drugs/biologicals relevant to the Medicare population, and discussion of gaps in existing measures (Chapter 4); and
- A summary of the key findings, including issues that need to be considered when developing measures for application in the hospital outpatient setting and a series of next steps for advancing CMS’ measures development work in the hospital outpatient setting (Chapter 5).
II. Analytic Framework and Methods
In this section, we present the approach we used to conduct this study. Figure 2.1 shows the organizing framework for our work. The environmental scan involved two main steps: (1) identification of the leading conditions treated and services/procedures provided in the outpatient setting (on the basis of cost and volume), and (2) identification of existing measures that may be applicable to outpatient care. In carrying out these steps, we conducted:
- An analysis of 2005 Medicare hospital outpatient data to determine conditions, services/procedures, and drugs/biologicals addressed in this setting,
- A scan for existing, publicly available measures potentially applicable to the hospital outpatient setting, and
- A series of semi-structured telephone discussions with representatives of medical specialty societies and hospital associations, informed by the analyses described in #1 and #2 above.
The methods for each of the data collection activities are described below. Having completed these data collection activities, we then synthesized the results to provide an initial assessment of which existing measures may reasonably apply to care provided in the hospital outpatient setting, and to identify gaps in those measures. This synthesis was used to inform our recommendations regarding next steps for advancing CMS’ measures development work in the hospital outpatient setting.
Due to the limited resources for this project, the work completed here should be viewed as a preliminary assessment which requires follow-on work to fully flesh out how to apply existing performance measures in this setting and where the most important measurement gaps are for guiding the use of resources in the future.
Figure 2.1. Framework Used in this Study
An environmental scan that takes the determing key conditions and procedures in the oupatient setting, and the determining measures that may be applicable to outpatient care; synthesizes the results, and identifies gaps; and recommends options for addressing the gaps.
Defining the Hospital Outpatient Setting
The hospital outpatient setting can be an elusive concept to define and the care provided in this setting is not homogenous across hospitals. While hospitals typically consider the Emergency Department (ED) to be part of the hospital outpatient setting, there is no standard classification of other care and services/procedures as “hospital outpatient.” The classification of a service as HOPS reflects the structure and organization of the local health system as well as the location where the service is provided, as opposed to the nature of the service itself. For example, facility charges for a hospital-based physician performing a colonoscopy in a hospital-based outpatient clinic would be billed under the OPPS. Meanwhile, another physician practicing in the same market, but not in the hospital-based outpatient department, and who is performing the same service/procedure may bill for practice expenses using the rates established as part of the Physician Fee Schedule.
For the purposes of our environmental scan, we defined the hospital outpatient setting as visits and/or services/procedures paid for under the Medicare OPPS. This care was further categorized for analyses and discussion in this report as either rendered in: (1) the ED, or (2) any other hospital-affiliated outpatient setting that is paid under OPPS (hereafter referred to as HOPS). We first classified services/procedures that obviously occur in the ED to the ED; all other services/procedures paid under the OPPS were classified as HOPS.
Methods
Analysis of Medicare Hospital Outpatient Data
RAND analyzed 2005 Medicare facility data for services paid through the hospital OPPS. The data file contained summary data aggregated to the diagnosis-service category level. This level of detail provides sufficient information to understand, in the aggregate, the types of services Medicare beneficiaries receive, but lacks specificity to describe individual patient encounters or episodes of care. CMS provided two data files, which included the diagnosis for an encounter,10 as well as visits aggregated to the Ambulatory Payment Classification (APC)11 level or the Healthcare Common Procedure Coding System (HCPCS) level. Each file contained code descriptions (APC, HCPCS, International Classification of Disease Version 9 or “ICD-9”), the total frequency, the APC paid in 2005, the 2007 payment rate for either the APC or HCPCS (total, and by diagnosis), and a CMS status indicator describing the type of service.
These data were analyzed to determine the following:
- The most common reasons (diagnoses) for visits (E&M services),
- The most frequent services/procedures provided,
- The services/procedures representing the largest costs within this setting,12 and
- The most frequent drugs and biologicals provided in this setting.
E&M visits were identified using the status indicator V (i.e., the status indicator associated with APC codes that indicate clinic or emergency department visits). Services/ procedures were identified with the status indicators S, T or X (i.e., the status indicators associated with APC codes that indicate significant services/procedures and ancillary services). Drugs and biologicals were identified using status indicators G (pass through drugs and biologicals), H (pass through devices, radiopharmaceuticals, brachytherapy), or K (non-pass through drugs and biologicals)13. The analyses did not include laboratory services14 or durable medical equipment (DME),15 which are not paid under OPPS.16
The total cost associated with the provision of each service/procedure was calculated by multiplying the frequency of the service/procedure by the 2007 APC payment for that service/procedure to obtain total Medicare costs. In our analyses, we applied 2007 payment rates to the 2005 utilization data; therefore, the estimates of 2007 spending based on these calculations assume that the volume and distribution of visits and services/procedures did not substantially change over the two year period.
Under Medicare OPPS rules, multiple APCs may be reported on a single claim when patients receive multiple, separately billable services. For example, a patient visiting the HOPS may be billed for a clinic visit (an E&M-related service), a chest x-ray, and an electrocardiogram during the same encounter. Because the files we used for these analyses did not have patient- or encounter-specific data, we were unable to explicitly link visit data (i.e., APCs with status indicator V) with significant services/procedures (i.e., APCs with status indicator S, T or X). Therefore, we cannot describe the spectrum of individual services a Medicare beneficiary receives during a single visit (e.g., we could not identify at the patient level, multiple services/procedures as part of the same encounter, or patients with E&M services/procedures during the same encounter).
For each common or costly APC representing services/procedures, clinical experts at RAND identified the specialties that most frequently bill for these professional services based on data from the American Medical Association’s (AMA) 2005 Relative Value Scale Update Committee (RUC) database. This database indicates the specialties that commonly bill for individual services/procedures at the HCPCS (Current Procedural Terminology [CPT]) level. In making the determination, RAND examined the providing specialties for any HCPCS code that accounted for at least five percent of the claims within an individual APC in 2005. This assignment was done to assist in the identification of measures potentially relevant to common services delivered in the hospital outpatient setting.
To facilitate examination of diagnoses associated with visits and services/procedures, RAND researchers grouped common diagnoses. Individual diagnoses were aggregated into diagnostic groups by two physicians using headers in the ICD-9-CM codebook as a guide.17 Diagnoses were also grouped by organ or body systems. The main driver for grouping diagnoses was to ensure that the most common diagnoses that have multiple diagnosis codes at the four-digit level (e.g., diabetes, hypertension) were aggregated, thereby allowing our analyses to accurately reflect their collective frequency and costs.18
We examined E&M visits separately from services/procedures to assist us in our efforts to identify performance measures, as E&M visits mimic the type of preventive, acute and chronic care provided in the ambulatory setting for which a large number of measures currently exist. Additionally, all data analyses were performed separately for the ED and the HOPS, given the distinct types of care provided by these two departments.
Scan of Existing Measures
The second component of the environmental scan was a search for existing performance measures. Between January and June 2007, RAND searched for existing, publicly available measures of any type (e.g., process, outcome) that might be appropriate to assess care provided in the hospital outpatient setting. We reviewed the websites of organizations known to produce, list, and/or approve outpatient/ambulatory care measures, including the following organizations:
- NCQA,
- AQA Alliance (formerly known as the Ambulatory Quality Alliance),
- CMS,
- American Medical Association Physician Consortium for Performance Improvement (AMA/PCPI),
- Agency for Healthcare Research and Quality (AHRQ) National Measures Clearinghouse,
- Institute for Clinical Systems Improvement (ICSI),
- RAND,
- National Quality Forum (NQF), and
- Websites of medical specialty societies.
Finally, Google searches were performed using the following terms: hospital outpatient performance, hospital outpatient performance measures, health care quality measures, health care performance measurement, and physician performance measurement. Measures identified in the search were categorized by their application to particular diseases and/or conditions.
Discussions with Medical Specialty Societies and Hospital Associations
Between April and June 2007, RAND held telephone discussions with nine medical specialty societies and four hospital associations to determine whether these organizations had existing measures, measures in the pipeline, or knew about measures being developed by other organizations that could be used to assess performance in the hospital outpatient setting as well as potential challenges associated with performance measurement in this setting. To focus the conversation with medical specialty societies, RAND provided each discussant with background information on the most frequent conditions and services that members of the given specialty provide to Medicare patients in the outpatient setting. RAND also provided discussants with background information on measures identified through its web searches that might be applicable to the care delivered by the given specialty in the hospital outpatient setting. Appendix B contains the list of the organizations with which RAND held discussions.
Synthesis of Findings from Environmental Scan
We mapped the clinical measures identified through our measures scan to the most common diagnoses and conditions treated, services/procedures, and drugs/biologicals provided in the HOPS, as identified in the data analysis described above. In the mappings of measures to diagnoses and conditions, we used subcategories of the diagnostic groupings to better match reasons for visits to topics relevant to metric development. For example, within endocrinology, we separately identified the common diagnoses of diabetes and thyroid disease – clinical conditions with sufficient specificity that measures could be matched to these diagnoses.
In conducting our work, we note several limitations which CMS could consider addressing in subsequent work to develop performance measures in the outpatient hospital setting:
- We elected to focus on the HOPS (as opposed to the ED) for this measures mapping exercise because the majority of existing measures correspond to conditions and diagnoses that most commonly occur in the HOPS, rather than the ED. We acknowledge that some conditions and services/procedures occur more frequently in the ED setting; therefore a separate synthesis focusing on mapping measures to the care provided in the ED merits consideration for future analyses.
- The mapping of measures to common diagnoses and clinical conditions focused on encounters that involved only E&M care for acute and chronic conditions.
We recognize that other encounters are specifically for a service/procedure (e.g., mammography), and many encounters involve both E&M care and services/procedure(s). Given that multiple APCs are frequently submitted for an encounter, future analyses examining data at the patient encounter level would provide a better understanding of services provided at that level.
We then combined the results from the mapping exercise described above with the findings from our discussions to identify measurement gaps. Gaps refer to clinical areas or other domains of care where care was delivered but few or no measures exist or areas flagged by discussants as having a lack of existing measures. The gap analysis was organized by the six IOM aims viewed as important in the provision of high-quality care (IOM, 2001). This gap analysis considered both the HOPS and the ED.
III. Findings from the Environmental Scan
In the discussion that follows, we summarize the results from our analysis of 2005 Medicare facility data for services paid through the hospital OPPS. The analyses were conducted to determine the most common reasons for visits in this setting, the most frequent and the most costly services/procedures rendered, as well as the drugs and biologicals that represented the largest share of costs in this setting. This analysis is a first step in determining which conditions and services/procedures might be suitable for measurement, given that they represent high volume or high costs to the Medicare program. We then present the results of our scan of existing measures, identifying those that could potentially be applied to the care delivered in the hospital outpatient setting. The discussion draws upon findings from our discussions with medical specialty societies and hospital associations.
Findings from Analysis of Medicare Data
Overall Finding
As noted previously, we examined E&M visits separately from services/procedures to assist us in identifying measures that are relevant to each category, given that different types of measures apply. Additionally, all data analyses were performed separately for the ED and the HOPS, given the distinct type of care provided in these two settings.
Based on our analysis of the 2005 Medicare OPPS facility data, CMS was billed for 15,325,267 E&M encounters and 78,538,882 services/procedures in the HOPS. In the same year CMS was billed for 11,426,386 E&M encounters and 22,494,724 services/procedures in the ED. Thus, in 2005, services/procedures represented a significant volume of the care provided in the hospital outpatient setting. More specifically, the top 20 most frequent services/procedures accounted for 58 percent of total services/procedures in the HOPS, and 94 percent of total services/procedures in the ED.
In terms of cost, had 2007 payment rates been applied in 2005, CMS would have paid $19.1 billion for services/procedures in the HOPS, and $1.7 billion for services/procedures in the ED.19 The top 20 services/procedures as a fraction of total costs would have accounted for 44 percent of total dollars in the HOPS, and 83 percent of total dollars in the ED. In both the HOPS and ED, a relatively small share of the services/procedures represented a significant proportion of costs — especially in the ED.
| Hospital Outpatient Setting | Emergency Department | |
|---|---|---|
| Evaluation and Management (E&M) Visits21 | ||
| Total E&M Visits | 15,325,267 | 11,426,386 |
| Total Cost of E&M Visits | $1,000,166,031 | $1,774,375,562 |
| Services/Procedures | ||
| Total Services/Procedures | 78,538,882 | 22,494,724 |
| Top 20 Services/Procedures by Volume | 45,806,040 | 21,227,715 |
| Top 20 Percent of Total Volume | 58% | 94% |
| Total Service/Procedure Expenditures | $19,055,431,864 | $1,709,238,878 |
| Top 20 Services/Procedures by Expenditure | $8,420,413,916 | $1,424,886,799 |
| Top 20 Percent of Total Expenditure | 44% | 83% |
Common Reasons for Visits in the Hospital Outpatient Setting and Emergency Department
Figures 3.1 and 3.2 and Table 3.1 highlight the common reasons for E&M visits to the HOPS and ED. The clinical categories in Figures 3.1 and 3.2 represent 100 percent of the primary diagnoses associated with visits to the HOPS and ED, respectively, and are organized alphabetically. Table 3.1 provides additional information for the clinical categories that represent at least five percent of either HOPS or ED visits. Within these clinical categories, Table 3.1 presents more detailed diagnostic groups that account for at least 0.5 percent or more of the total diagnoses. The diagnostic groups are listed in order of the HOPS percentage of total diagnoses. Therefore, the sum of the percentages for diagnostic groups within a clinical category will not equal the percentage for the category. Appendix C presents more detailed information (i.e., for all of the clinical categories).
Figure 3.1. HOPS Visits by Clinical Category, 2005
Figure 3.2. ED Visits by Clinical Category, 2005
The analysis reveals that in 2005 the key reasons for HOPS (i.e., non-ED) hospital outpatient visits tended to be similar to the major reasons for visits in the physician office setting (see Figure 3.1 and Table 3.1). General medical conditions (35.2 percent) constitute the largest proportion of HOPS visits by Medicare patients and address common chronic conditions, such as hypertension (7.4 percent), aftercare for procedures (6.4 percent), and specific and general symptoms (e.g., fever, dizziness) for which an underlying etiology is sought (4.6 percent). Oncology and neoplasia conditions were the next most frequent reasons for visits (13.1 percent), followed by orthopedic conditions (10.4 percent), particularly diagnoses such as back pain and arthritis. Endocrinology conditions, such as diabetes, were the fourth most common clinical category, representing 7.0 percent of HOPS visits. These findings are similar to those of the 2004 National Ambulatory Medical Care Survey in which the top diagnoses in physician offices for individuals ages 65 and older were: (1) malignant neoplasm, (2) essential hypertension, (3) diabetes mellitus, (4) arthroplasties and related disorders, and (5) heart disease, excluding ischemic (Hing et al, 2006).
Our analysis also reveals that in 2005 general medical conditions (43.4 percent) were the key reasons for ED visits (see Figure 3.2 and Table 3.1). The most common reason for such visits was found to be “symptoms” (20.4 percent), generally for unanticipated acute care where patients either present with: (1) new onset of symptoms, from which a differential diagnosis is created and a plan developed to determine the etiology of the presenting findings; or (2) a new or worsening diagnosis for which acute intervention is sought. Injury, either orthopedic (e.g., back pain, sprains, fractures) or of a more general nature (e.g., laceration), constituted the next most common reason for ED encounters within the general medical category (6.15 percent). Given the nature of ED practice, patients’ reasons for seeking emergency care overlap nearly every clinical discipline.
|
HOPS
|
ED
|
|||||
|---|---|---|---|---|---|---|
| Total Encounters |
15,325,267*
|
11,426,386*
|
||||
| Clinical Category |
Diagnostic Group
|
Diagnostic Group
|
||||
| Medicine-General | 35.21% | 43.40% | ||||
| Hypertension | 7.42% | Symptoms | 20.35% | |||
| Aftercare, specific procedures | 6.40% | Injury | 6.15% | |||
| Symptoms | 4.48% | COPD and related | 3.49% | |||
| Metabolic/nutrition | 2.37% | Acute respiratory infection | 2.78% | |||
| Health system encounter | 2.18% | Metabolic/nutrition | 1.47% | |||
| COPD and related | 1.99% | Complications | 1.41% | |||
| Venous disease | 1.97% | Hypertension | 1.39% | |||
| General exam | 1.49% | Infectious and parasitic disease | 1.23% | |||
| Acute respiratory infection | 1.34% | Aftercare, specific procedures | 1.08% | |||
| Complications | 1.04% | Venous disease | 0.72% | |||
| Arterial disease | 0.83% | Poisonings | 0.55% | |||
| Upper respiratory tract | 0.56% | Toxic effects-external causes | 0.50% | |||
| Medicine-Oncology/Neoplasia | 13.10% | 0.88% | ||||
| Cancer | 9.17% | Hematology | 0.58% | |||
| Hematology | 2.35% | |||||
| Neoplasm-uncertain behavior | 0.54% | |||||
| Orthopedics | 10.39% | 16.61% | ||||
| Back disorders | 3.92% | Back disorders | 3.94% | |||
| Arthropathies | 1.95% | Sprains and strains | 3.63% | |||
| Rheumatism | 1.73% | Fracture | 2.75% | |||
| Other joint disorders | 1.31% | Rheumatism | 2.59% | |||
| Osteopathies, chondropathies | 0.90% | Other joint disorders | 2.02% | |||
| Arthropathies | 0.70% | |||||
| *Totals represent all encounters associated with an E&M claim in 2005 | ||||||
|
HOPS
|
ED
|
|||||
|---|---|---|---|---|---|---|
| Total Encounters |
15,325,267*
|
11,426,386*
|
||||
| Clinical Category |
Diagnostic Group
|
Diagnostic Group
|
||||
| Medicine-Endocrinology | 7.03% | 1.62% | ||||
| Endocrine, metabolic | 6.98% | Endocrine, metabolic | 1.62% | |||
| Medicine-Cardiology | 6.68% | 3.45% | ||||
| Conduction/dysrhythmias | 2.48% | Conduction/dysrhythmias | 1.28% | |||
| Ischemic heart | 1.82% | Heart failure | 0.86% | |||
| Heart failure | 1.33% | Symptoms | 0.62% | |||
| Ischemic heart | 0.60% | |||||
| Dermatology | 6.65% | 4.21% | ||||
| Other skin diseases | 4.39% | Skin infections | 1.93% | |||
| Skin infections | 0.81% | Symptoms | 1.09% | |||
| Inflammatory skin conditions | 0.75% | Other skin diseases | 0.63% | |||
| Symptoms | 0.60% | Inflammatory skin conditions | 0.56% | |||
| Medicine-GI | 2.37% | 6.26% | ||||
| Upper GI | 0.62% | Symptoms | 1.78% | |||
| Upper GI | 1.17% | |||||
| Functional digestive | 0.93% | |||||
| Inflammatory bowel | 0.84% | |||||
| Urology | 2.12% | 5.32% | ||||
| Symptoms | 0.61% | Urinary tract infection | 2.40% | |||
| Urinary tract infection | 0.53% | Symptoms | 1.20% | |||
| Notes: *Totals represent all encounters associated with an E&M claim in 2005. Table note: The percentages associated with each diagnosis within a clinical category may not sum to the percentage for the clinical category given that we only list diagnoses at 0.5 percent or higher. |
||||||
Most Commonly Provided Services/Procedures and Associated Diagnoses in the Hospital Outpatient Setting and Emergency Department
Tables 3.2 and 3.3 highlight the 20 most common classes of services/procedures, grouped by APC, and their associated diagnoses in the HOPS and ED setting, respectively, based upon the analysis of 2005 Medicare data. For each of the APCs presented in the table, the five most common primary diagnosis groups associated with the APC are presented. In some cases, findings cluster into fewer than five key diagnostic categories, so fewer than five are listed. Additionally, Tables 3.2 and 3.3 present the physician specialty most likely to provide the given service/procedure, as distinguished from the ordering specialty (i.e., the physician requesting the service/procedure, but not actually providing it).
The most frequent services/procedures in the HOPS were ancillary services/procedures commonly used to diagnose and treat many different clinical symptoms and conditions. These include radiology services (e.g., x-rays, computed tomography (CT) scans, ultrasound), surgical pathology (i.e., Level III pathology, commonly used by pathologists and dermatologists), electrocardiograms, and drug administration. Most primary services/procedures (e.g., cataract extraction, angiography, arthroscopic surgery), while frequent, do not rise to the top of the OPPS services/procedures because they are dwarfed by the volume of ancillary services. The most common HOPS service/procedure (X-ray) accounted for 12 percent of the total services/procedures examined; and every other service/procedure listed in the top 20 for the HOPS accounted for five percent or less, each, of the total.
As in the HOPS, the most frequent services/procedures in the ED were ancillary services/procedures, especially radiology services. In the ED, the top few services/procedures account for a larger proportion than in the HOPS and the proportion represented by other services/procedures diminishes quickly thereafter. For example, the top two most common services/procedures in the ED -- X-rays and electrocardiograms-- accounted for approximately 30 percent and 16 percent, respectively, of the services/procedures included in these analyses; the remaining top 20 each accounted for nine percent or less of the total of services/procedures included in these analyses.
The total number of any one or a group of related services/procedures may have important implications when considering performance measures. While the overall volume of services/procedures is high — for example, in the 2005 Medicare data, there were over 78 million services/procedures performed in the HOPS and 22 million in the ED — as data are parsed at the hospital level to examine specific conditions or services/procedures, the sample size may be too small at the level of an individual hospital to be able to produce stable estimates of performance.
| Rank | Frequency | Percent of Total | APC | APC Description | Most Common Clinical Categories Within APC | Specialty Providing Service |
|---|---|---|---|---|---|---|
| 1 | 9,526,216 | 12.13% | 260 | Level I Plain Film Except Teeth | Medicine-General, Orthopedics, Medicine-Oncology/Neoplasia, Medicine-Cardiology, Urology | Radiology, Facility |
| 2 | 3,934,292 | 5.01% | 343 | Level III Pathology | Medicine-GI, Medicine-Oncology/Neoplasia, Medicine-General, Dermatology, Surgery-General | Pathology, Dermatology |
| 3 | 3,049,223 | 3.88% | 99 | Electrocardiograms | Medicine-General, Medicine-Cardiology, Orthopedics, Medicine-Oncology/Neoplasia, Surgery-General | Internal Medicine, Cardiology |
| 4 | 2,984,113 | 3.80% | 301 | Level II Radiation Therapy | Medicine-Oncology/Neoplasia, Medicine-General | Radiation Oncology |
| 5 | 2,873,862 | 3.66% | 283 | Computerized Axial Tomography with Contrast Material | Medicine-General, Medicine-Oncology/Neoplasia, Medicine-GI, Orthopedics, Urology | Radiology, Facility |
| 6 | 2,797,689 | 3.56% | 437 | Level II Drug Administration | Medicine-Oncology/Neoplasia, Medicine-General, Medicine-Cardiology, Orthopedics, Medicine-Infectious Disease | Facility |
| 7 | 2,303,689 | 2.93% | 95 | Cardiac Rehabilitation | Medicine-General, Medicine-Cardiology | Cardiology |
| 8 | 2,091,415 | 2.66% | 266 | Level II Diagnostic and Screening Ultrasound | Medicine-General, Orthopedics, Urology, Gynecology, Medicine-GI | Urology, Radiology |
| 9 | 1,831,696 | 2.33% | 409 | Red Blood Cell Tests | Medicine-Oncology/Neoplasia, Medicine-General, Orthopedics, Medicine-Cardiology, Medicine-GI | Laboratory |
| Rank | Frequency | Percent of Total | APC | APC Description | Most Common Clinical Categories Within APC | Specialty Providing Service |
|---|---|---|---|---|---|---|
| 10 | 1,765,455 | 2.25% | 440 | Level V Drug Administration | Medicine-Oncology/Neoplasia, Medicine-General, Medicine-Cardiology, Orthopedics, Dermatology | Facility |
| 11 | 1,622,281 | 2.07% | 697 | Level I Echocardiogram Except Transesophageal | Medicine-Cardiology, Medicine-General, | Cardiology, Internal Medicine |
| 12 | 1,467,273 | 1.87% | 143 | Lower GI Endoscopy | Medicine-GI, Medicine-General, Medicine-Oncology/Neoplasia | Gastroenterology, General Surgery, Internal Medicine |
| 13 | 1,377,463 | 1.75% | 433 | Level II Pathology | Medicine-Oncology/Neoplasia, Medicine-GI, Medicine-General, Urology, Surgery-General | Pathology |
| Laboratory | ||||||
| 14 | 1,351,504 | 1.72% | 304 | Level I Therapeutic Radiation Treatment Preparation | Medicine-Oncology/Neoplasia, Medicine-General | Radiation Oncology |
| 15 | 1,217,589 | 1.55% | 368 | Level II Pulmonary Tests | Medicine-General | Family Practice, Internal Medicine |
| 16 | 1,200,061 | 1.53% | 438 | Level III Drug Administration | Medicine-Oncology/Neoplasia, Medicine-General, Medicine-Cardiology, Orthopedics, Medicine-GI | Facility |
| 17 | 1,175,648 | 1.50% | 325 | Group Psychotherapy | Psychiatry | Psychiatry |
| 18 | 1,160,024 | 1.48% | 332 | Computerized Axial Tomography and Computerized Angiography without Contrast | Medicine-General, Medicine-Oncology/Neoplasia, Orthopedics, Urology, Neurology | Radiology, Facility |
| 19 | 1,058,882 | 1.35% | 267 | Level III Diagnostic and Screening Ultrasound | Medicine-General, Neurology, Medicine-Cardiology, Orthopedics, Dermatology | Cardiology, Vascular Surgery |
| 20 | 1,017,665 | 1.30% | 399 | Nuclear Medicine Add-on Imaging | Medicine-General, Medicine-Cardiology | Radiology, Cardiology |
| Rank | Frequency | Percent of Total | APC | APC Description | Most Common Clinical Categories Within APC | Specialty Providing Service |
|---|---|---|---|---|---|---|
| 1 | 6,638,015 | 29.51% | 0260 | Level I Plain Film Except Teeth | Medicine-General, Orthopedics, Medicine-Cardiology, Medicine-GI, Surgery-General | Radiology, Facility |
| 2 | 3,595,431 | 15.98% | 0099 | Electrocardiograms | Medicine-General, Medicine-Cardiology, Medicine-GI, Orthopedics, Neurology | Internal Medicine, Cardiology |
| 3 | 1,984,224 | 8.82% | 0437 | Level II Drug Administration | Medicine-General, Orthopedics, Surgery-General, Head and Neck, Medicine-GI | Facility |
| 4 | 1,913,623 | 8.51% | 0438 | Level III Drug Administration | Medicine-General, Medicine-GI, Orthopedics, Medicine-Cardiology, Urology | Facility |
| 5 | 1,834,962 | 8.16% | 0332 | Computerized Axial Tomography and Computerized Angiography without Contrast | Medicine-General, Head and Neck, Urology, Orthopedics, Neurology | Radiology, Facility |
| 6 | 1,223,868 | 5.44% | 0440 | Level V Drug Administration | Medicine-General, Medicine-GI, Urology, Orthopedics, Medicine-Cardiology | Facility |
| 7 | 756,543 | 3.36% | 0077 | Level I Pulmonary Treatment | Medicine-General | Family Practice, Internal Medicine |
| 8 | 587,764 | 2.61% | 0261 | Level II Plain Film Except Teeth Including Bone Density Measurement | Medicine-General, Orthopedics, Medicine-GI, Urology, Head and Neck | Radiology, Facility |
| 9 | 507,923 | 2.26% | 0283 | Computerized Axial Tomography with Contrast Material | Medicine-General, Medicine-GI, Orthopedics, Urology, Surgery-General | Radiology, Facility |
| 10 | 382,798 | 1.70% | 0024 | Level I Skin Repair | Head and Neck, Surgery-General, Medicine-General, Orthopedics | Dermatology |
| Rank | Frequency | Percent of Total | APC | APC Description | Most Common Clinical Categories Within APC | Specialty Providing Service |
|---|---|---|---|---|---|---|
| 11 | 306,538 | 1.36% | 266 | Level II Diagnostic and Screening Ultrasound | Medicine-General, Orthopedics, Dermatology, Medicine-GI, Urology | Urology, Radiology, Surgery |
| 12 | 274,110 | 1.22% | 409 | Red Blood Cell Tests | Medicine-General, Medicine-GI, Medicine-Oncology/Neoplasia, Orthopedics, Urology | Laboratory |
| 13 | 270,657 | 1.20% | 58 | Level I Strapping and Cast Application | Orthopedics | Emergency Medicine, Podiatry |
| 14 | 248,571 | 1.11% | 340 | Minor Ancillary Procedures | Urology, Medicine-General, Medicine-GI, Orthopedics, Head and Neck | Urology, Ophthalmology |
| 15 | 154,572 | 0.69% | 697 | Level I Echocardiogram Except Transesophageal | Medicine-General, Medicine-Cardiology, Neurology | Cardiology |
| 16 | 143,991 | 0.64% | 282 | Miscellaneous Computerized Axial Tomography | Medicine-General, Orthopedics, Head and Neck | Radiology, Facility |
| 17 | 124,793 | 0.55% | 345 | Level I Transfusion Laboratory Procedures | Medicine-General, Medicine-GI, Medicine-Oncology/Neoplasia | Laboratory |
| 18 | 111,433 | 0.50% | 267 | Level III Diagnostic and Screening Ultrasound | Medicine-General, Orthopedics, Neurology, Dermatology, Medicine-Cardiology | Cardiology, Vascular Surgery, Radiology |
| 19 | 87,602 | 0.39% | 269 | Level II Echocardiogram Except Transesophageal | Medicine-General, Medicine-Cardiology, Neurology, Orthopedics, Medicine-GI | Cardiology |
| 20 | 80,297 | 0.36% | 399 | Nuclear Medicine Add-on Imaging | Medicine-General, Medicine-Cardiology | Radiology, Cardiology |
Services/Procedures and Associated Diagnoses Representing the Largest Share of Costs in the Hospital Outpatient Setting and Emergency Department
Tables 3.4 and 3.5 highlight the 20 costliest services/procedures in the HOPS and ED, respectively, as well as the associated diagnoses based upon analysis of 2005 Medicare data with 2007 APC payment rates applied.25 These data show that, had 2007 payment rates been in force in 2005, many of the most common services/procedures also would have accounted for a substantial share of total costs, although there are some changes in distribution given the relative weight of the more costly services. For example, while Level I plain films (APC 0260) and Level III Pathology (APC 0343) are the first and second most frequent APCs billed in the HOPS, APC 0260 ranks only sixth in cost and APC 0343 is not among the top 20 most costly services/procedures. Similarly, neither cataract surgery (APC 0246) nor cardiac catheterization (APC 0080), the two services/procedures accounting for the greatest share of payments for HOPS services, are among the 20 most frequent services/procedures provided in the HOPS. In the ED, CT scans were found to be the costliest (vs. X-rays which were most frequent). No single service/procedure accounted for a large proportion of the total cost; however, given the magnitude of the costs involved, even one to two percent of total costs remains significant.
| Rank | Total Cost | Percent of Total | APC | APC Description | Most Common Clinical Categories Within APC | Specialty Providing Service |
|---|---|---|---|---|---|---|
| 1 | $998,098,614 | 5.24% | 246 | Cataract Procedures with IOL Insert | Ophthalmology | Ophthalmology |
| 2 | $893,140,496 | 4.69% | 80 | Diagnostic Cardiac Catheterization | Medicine-Cardiology, Medicine-General | Cardiology |
| 3 | $790,845,474 | 4.15% | 143 | Lower GI Endoscopy | Medicine-GI, Medicine-General, Medicine-Oncology/Neoplasia, Surgery-General | Gastroenterology, General Surgery, Internal Medicine |
| 4 | $721,166,930 | 3.78% | 283 | Computerized Axial Tomography with Contrast Material | Medicine-General, Medicine-Oncology/Neoplasia, Medicine-GI, Orthopedics, Urology | Radiology, Facility |
| 5 | $460,378,894 | 2.42% | 141 | Level I Upper GI Procedures | Medicine-GI, Medicine-General, Medicine-Oncology/Neoplasia, Surgery-General | Gastroenterology |
| 6 | $415,343,018 | 2.18% | 260 | Level I Plain Film Except Teeth | Medicine-General, Orthopedics, Medicine-Oncology/Neoplasia, Medicine-Cardiology, Urology | Radiology, Facility |
| 7 | $408,942,846 | 2.15% | 301 | Level II Radiation Therapy | Medicine-Oncology/Neoplasia, Medicine-General | Radiation Oncology |
| 8 | $371,722,046 | 1.95% | 280 | Level III Angiography and Venography | Medicine-General, Neurology, Medicine-Cardiology | Cardiology, Facility |
| 9 | $347,637,485 | 1.82% | 107 | Insertion of Cardioverter-Defibrillator | Medicine-General, Medicine-Cardiology | Cardiology |
| 10 | $345,378,970 | 1.81% | 336 | Magnetic Resonance Imaging and Magnetic Resonance Angiography without Contrast | Orthopedics, Medicine-General, Neurology, Medicine-Oncology/Neoplasia, Neurology/Neurosurgery | Radiology, Facility |
| Rank | Total Cost | Percent of Total | APC | APC Description | Most Common Clinical Categories Within APC | Specialty Providing Service |
|---|---|---|---|---|---|---|
| 11 | $305,728,764 | 1.60% | 207 | Level III Nerve Injections | Orthopedics | Anesthesia, Pain Management |
| 12 | $304,144,743 | 1.60% | 337 | MRI and Magnetic Resonance Angiography without Contrast Material followed | Medicine-General, Orthopedics, Neurology, Medicine-Oncology/Neoplasia, Ophthalmology | Radiology, Facility |
| 13 | $283,460,736 | 1.49% | 131 | Level II Laparoscopy | Surgery-General | Surgery-General, OB/GYN |
| 14 | $282,675,723 | 1.48% | 81 | Non-Coronary Angioplasty or Atherectomy | Medicine-General, Medicine-Nephrology, Medicine-Cardiology | Radiology, Nephrology |
| 15 | $282,329,852 | 1.48% | 154 | Hernia/Hydrocele Procedures | Surgery-General | Surgery-General |
| 16 | $272,367,293 | 1.43% | 41 | Level I Arthroscopy | Orthopedics | Orthopedics, Hand Surgery |
| 17 | $256,608,392 | 1.35% | 412 | IMRT Treatment Delivery | Medicine-Oncology/Neoplasia, Medicine-General | Radiation Oncology |
| 18 | $238,689,974 | 1.25% | 108 | Insertion/Replacement/Repair of Cardioverter-Defibrillator Leads | Medicine-Cardiology, Medicine-General | Cardiology |
| 19 | $221,360,707 | 1.16% | 377 | Level III Cardiac Imaging | Medicine-Cardiology, Medicine-General | Cardiology |
| 20 | $220,392,959 | 1.16% | 332 | Computerized Axial Tomography and Computerized Angiography without Contrast | Medicine-General, Medicine-Oncology/Neoplasia, Orthopedics, Urology, Neurology | Radiology, Facility |
| Rank | Total Payment | Percent of Total | APC | APC Description | Most Common Clinical Categories Within APC | Specialty Providing Service |
|---|---|---|---|---|---|---|
| 1 | $348,624,430 | 20.40% | 332 | Computerized Axial Tomography and Computerized Angiography without Contrast | Medicine-General, Head and Neck, Urology, Orthopedics, Neurology | Radiology, Facility |
| 2 | $289,417,454 | 16.93% | 260 | Level I Plain Film Except Teeth | Medicine-General, Orthopedics, Medicine-Cardiology, Medicine-GI, Surgery-General | Radiology, Facility |
| 3 | $136,094,122 | 7.96% | 440 | Level V Drug Administration | Medicine-General, Medicine-GI, Urology, Orthopedics, Medicine-Cardiology | Radiology, Facility |
| 4 | $127,458,198 | 7.46% | 283 | Computerized Axial Tomography with Contrast Material | Medicine-General, Medicine-GI, Orthopedics, Urology, Surgery-General | Radiology, Facility |
| 5 | $93,423,075 | 5.47% | 438 | Level III Drug Administration | Medicine-General, Medicine-GI, Orthopedics, Medicine-Cardiology, Urology | Facility |
| 6 | $83,737,588 | 4.90% | 99 | Electrocardiograms | Medicine-General, Medicine-Cardiology, Medicine-GI, Orthopedics, Neurology | Internal Medicine, Cardiology |
| 7 | $48,117,432 | 2.82% | 437 | Level II Drug Administration | Medicine-General, Orthopedics, Surgery-General, Head and Neck, Medicine-GI | Facility |
| 8 | $44,164,587 | 2.58% | 261 | Level II Plain Film Except Teeth Including Bone Density Measurement | Medicine-General, Orthopedics, Surgery-General, Head and Neck, Medicine-GI | Radiology, Facility |
| 9 | $34,926,490 | 2.04% | 24 | Level I Skin Repair | Head and Neck, Surgery-General, Medicine-General | Dermatology |
| 10 | $31,091,509 | 1.82% | 80 | Diagnostic Cardiac Catheterization | Medicine-Cardiology, Medicine-General | Cardiology |
| Rank | Total Payment | Percent of Total | APC | APC Description | Most Common Clinical Categories Within APC | Specialty Providing Service |
|---|---|---|---|---|---|---|
| 11 | $29,406,190 | 1.72% | 266 | Level II Diagnostic and Screening Ultrasound | Medicine-General, Orthopedics, Dermatology, Medicine-GI, Urology | Urology, Radiology |
| 12 | $19,823,305 | 1.16% | 333 | Computerized Axial Tomography and Computerized Angiography without Contrast | Medicine-General, Medicine-GI, Urology, Orthopedics, Surgery-General | Radiology, Facility |
| 13 | $19,371,442 | 1.13% | 662 | Computerized Tomography Angiography | Medicine-General, Orthopedics, Medicine-Cardiology, Neurology, Medicine-GI | Radiology, Facility |
| 14 | $17,646,836 | 1.03% | 58 | Level I Strapping and Cast Application | Orthopedics, Medicine-General | Emergency Medicine, Podiatry |
| 15 | $17,331,919 | 1.01% | 377 | Level III Cardiac Imaging | Medicine-General, Medicine-Cardiology | Cardiology |
| 16 | $17,313,659 | 1.01% | 269 | Level II Echocardiogram Except Transesophageal | Medicine-General, Medicine-Cardiology, Neurology, Orthopedics, Medicine-GI | Cardiology |
| 17 | $17,241,882 | 1.01% | 336 | Magnetic Resonance Imaging and Magnetic Resonance Angiography without Contrast | Medicine-General, Orthopedics, Neurology, Head and Neck, Dermatology | Radiology, Facility |
| 18 | $16,854,241 | 0.99% | 267 | Level III Diagnostic and Screening Ultrasound | Medicine-General, Orthopedics, Neurology, Dermatology, Medicine-Cardiology | Cardiology, Vascular Surgery |
| 19 | $16,440,588 | 0.96% | 141 | Level I Upper GI Procedures | Medicine-General, Medicine-GI | Gastroenterology |
| 20 | $16,401,852 | 0.96% | 77 | Level I Pulmonary Treatment | Medicine-General | Family Practice, Internal Medicine |
Most Frequent Used Drugs and Biologicals in the Hospital Outpatient Setting and Emergency Department
Table 3.6 shows the 50 most frequent, separately billed drugs and biologicals associated with services in the HOPS and ED.28 In both the HOPS and ED, imaging contrast material, blood products and medications associated with cancer chemotherapy are among the most frequently used. In the ED, several thrombolytic agents are also frequently used. These findings derive from the data provided by CMS and have not been aggregated by drug or drug class. Additional analyses of drugs and biologicals would inform opportunities for measure development.
|
HOPS
|
Emergency Department
|
||||
|---|---|---|---|---|---|
| APC | APC definition | Volume | APC | APC definition | Volume |
| 4646 | Contrast 300-399 MGs iodine | 951,639 | 768 | Ondansetron hcl injection | 180,380 |
| 733 | Non esrd epoetin alpha inj | 610,121 | 4646 | Contrast 300-399 MGs iodine | 124,136 |
| 768 | Ondansetron hcl injection | 486,806 | 750 | Dolasetron mesylate | 27,611 |
| 1600 | Tc99m sestamibi | 359,301 | 1600 | Tc99m sestamibi | 26,186 |
| 954 | RBC leukocytes reduced | 309,368 | 954 | RBC leukocytes reduced | 21,140 |
| 734 | Darbepoetin alfa, non esrd | 303,060 | 705 | Tc99m tetrofosmin | 17,722 |
| 9027 | Supp- paramagnetic contr mat | 209,894 | 9223 | Inj adenosine, tx dx | 17,236 |
| 705 | Tc99m tetrofosmin | 203,824 | 7028 | Fosphenytoin, 50 mg | 10,410 |
| 1775 | FDG, per dose (4-40 mCi/ml) | 146,799 | 1603 | TL201 thallium | 10,313 |
| 750 | Dolasetron mesylate | 137,086 | 4644 | Contrast 100-199 MGs iodine | 9,483 |
| 4645 | Contrast 200-299 MGs iodine | 130,186 | 733 | Non esrd epoetin alpha inj | 9,161 |
| 764 | Granisetron HCl injection | 125,375 | 764 | Granisetron HCl injection | 8,755 |
| 1603 | TL201 thallium | 121,426 | 9042 | Glucagon hydrochloride/1 MG | 8,395 |
| 9223 | Inj adenosine, tx dx | 119,916 | 4645 | Contrast 200-299 MGs iodine | 7,956 |
| 9115 | Zoledronic acid | 104,174 | 9027 | Supp- paramagnetic contr mat | 7,716 |
| 9114 | Nesiritide | 89,536 | 959 | Red blood cells unit | 6,989 |
| 811 | Carboplatin injection | 87,670 | 1670 | Tetanus immune globulin inj | 6,938 |
| 4644 | Contrast 100-199 MGs iodine | 83,853 | 9508 | Plasma 1 donor frz w/in 8 hr | 5,790 |
| 863 | Paclitaxel injection | 82,377 | 3033 | Technetium tc-99m pentetate | 5,539 |
| 959 | Red blood cells unit | 81,503 | 1607 | Eptifibatide injection | 3,564 |
| 828 | Gemcitabine HCl | 72,729 | 379 | Injection adenosine 6 MG | 3,289 |
| 728 | Filgrastim 300 mcg injection | 67,612 | 935 | Clonidine hydrochloride | 3,265 |
| 9119 | Injection, pegfilgrastim 6mg | 67,361 | 9139 | Rabies vaccine, im | 3,173 |
| 7043 | Infliximab injection | 65,192 | 917 | Adenosine injection | 3,086 |
| 765 | Granisetron HCl 1 mg oral | 64,247 | 734 | Darbepoetin alfa, non esrd | 2,081 |
|
HOPS |
Emergency Department |
||||
|---|---|---|---|---|---|
|
APC |
APC definition |
Volume |
APC |
APC definition |
Volume |
| 4646 | Contrast 300-399 MGs iodine |
951,639 |
0768 | Ondansetron hcl injection |
180,380 |
| 0733 | Non esrd epoetin alpha inj |
610,121 |
4646 | Contrast 300-399 MGs iodine |
124,136 |
| 0768 | Ondansetron hcl injection |
486,806 |
0750 | Dolasetron mesylate |
27,611 |
| 1600 | Tc99m sestamibi |
359,301 |
1600 | Tc99m sestamibi |
26,186 |
| 0954 | RBC leukocytes reduced |
309,368 |
0954 | RBC leukocytes reduced |
21,140 |
| 0734 | Darbepoetin alfa, non esrd |
303,060 |
0705 | Tc99m tetrofosmin |
17,722 |
| 9027 | Supp- paramagnetic contr mat |
209,894 |
9223 | Inj adenosine, tx dx |
17,236 |
| 0705 | Tc99m tetrofosmin |
203,824 |
7028 | Fosphenytoin, 50 mg |
10,410 |
| 1775 | FDG, per dose (4-40 mCi/ml) |
146,799 |
1603 | TL201 thallium |
10,313 |
| 0750 | Dolasetron mesylate |
137,086 |
4644 | Contrast 100-199 MGs iodine |
9,483 |
| 4645 | Contrast 200-299 MGs iodine |
130,186 |
0733 | Non esrd epoetin alpha inj |
9,161 |
| 0764 | Granisetron HCl injection |
125,375 |
0764 | Granisetron HCl injection |
8,755 |
| 1603 | TL201 thallium |
121,426 |
9042 | Glucagon hydrochloride/1 MG |
8,395 |
| 9223 | Inj adenosine, tx dx |
119,916 |
4645 | Contrast 200-299 MGs iodine |
7,956 |
| 9115 | Zoledronic acid |
104,174 |
9027 | Supp- paramagnetic contr mat |
7,716 |
| 9114 | Nesiritide |
89,536 |
0959 | Red blood cells unit |
6,989 |
| 0811 | Carboplatin injection |
87,670 |
1670 | Tetanus immune globulin inj |
6,938 |
| 4644 | Contrast 100-199 MGs iodine |
83,853 |
9508 | Plasma 1 donor frz w/in 8 hr |
5,790 |
| 0863 | Paclitaxel injection |
82,377 |
3033 | Technetium tc-99m pentetate |
5,539 |
| 0959 | Red blood cells unit |
81,503 |
1607 | Eptifibatide injection |
3,564 |
| 0828 | Gemcitabine HCl |
72,729 |
0379 | Injection adenosine 6 MG |
3,289 |
| 0728 | Filgrastim 300 mcg injection |
67,612 |
0935 | Clonidine hydrochloride |
3,265 |
| 9119 | Injection, pegfilgrastim 6mg |
67,361 |
9139 | Rabies vaccine, im |
3,173 |
| 7043 | Infliximab injection |
65,192 |
0917 | Adenosine injection |
3,086 |
| 0765 | Granisetron HCl 1 mg oral |
64,247 |
0734 | Darbepoetin alfa, non esrd |
2,081 |
|
HOPS |
Emergency Department |
||||
|---|---|---|---|---|---|
|
APC |
APC definition |
Volume |
APC |
APC definition |
Volume |
| 7049 | Filgrastim 480 mcg injection |
60,354 |
9112 | Inj perflutren lip micros,ml |
1,926 |
| 0849 | Rituximab cancer treatment |
59,390 |
7048 | Alteplase recombinant |
1,762 |
| 9210 | Palonosetron HCl |
55,903 |
3030 | Sumatriptan succinate / 6 MG |
1,695 |
|
0823 |
Docetaxel |
54,261 |
0769 |
Ondansetron HCl 8mg oral |
1,571 |
|
0869 |
IVIG lyophil 1g |
44,227 |
9501 |
Platelet pheres leukoreduced |
1,557 |
|
9042 |
Glucagon hydrochloride/1 MG |
42,442 |
9114 |
Nesiritide |
1,459 |
|
9046 |
Iron sucrose injection |
40,848 |
7049 |
Filgrastim 480 mcg injection |
1,424 |
|
0769 |
Ondansetron HCl 8mg oral |
38,847 |
0728 |
Filgrastim 300 mcg injection |
1,202 |
|
9501 |
Platelet pheres leukoreduced |
38,257 |
9015 |
Mycophenolate mofetil oral |
1,172 |
|
0730 |
Pamidronate disodium /30 MG |
36,150 |
0891 |
Tacrolimus oral per 1 MG |
1,167 |
|
9148 |
I123 iodide cap, dx |
35,333 |
9002 |
Tenecteplase injection |
1,112 |
|
7316 |
Sodium hyaluronate injection |
35,074 |
9202 |
Inj octafluoropropane mic,ml |
1,001 |
|
0969 |
RBC leukoreduced irradiated |
34,997 |
9005 |
Reteplase injection |
965 |
|
9214 |
Bevacizumab injection |
33,170 |
0965 |
Albumin (human), 25%, 50ml |
891 |
|
1613 |
Trastuzumab |
32,886 |
9133 |
Rabies ig, im/sc |
883 |
|
0830 |
Irinotecan injection |
32,192 |
0969 |
RBC leukoreduced irradiated |
877 |
|
0917 |
Adenosine injection |
31,416 |
9124 |
Daptomycin injection |
683 |
|
9205 |
Oxaliplatin |
30,843 |
9026 |
High dose contrast MRI |
664 |
|
9124 |
Daptomycin injection |
29,519 |
9044 |
Ibutilide fumarate injection |
639 |
|
0871 |
IVIG non-lyophil 1g |
28,313 |
0811 |
Carboplatin injection |
558 |
|
3048 |
Doxorubic hcl 10 MG vl chemo |
26,629 |
9155 |
Technetium tc99mlabeledrbcs |
528 |
|
7000 |
Amifostine |
25,682 |
0888 |
Cyclosporine oral 100 mg |
505 |
|
9218 |
Injection, Azacitidine |
25,349 |
9025 |
Rubidium-Rb-82 |
485 |
|
1622 |
Technetium tc99m mertiatide |
24,340 |
9046 |
Iron sucrose injection |
474 |
|
9207 |
Bortezomib injection |
24,216 |
1019 |
Plate pheres leukoredu irrad |
473 |
Findings from the Scan of Existing Measures and Discussions
Below we summarize the findings from our scan of existing, publicly available performance measures and discussions with representatives of medical specialty societies and hospital associations. Our review identified nearly 600 measures that may be potentially relevant to application in the hospital outpatient setting. It should be noted that there are propriety measures in existence that may be relevant for assessing care provided in the hospital outpatient setting (e.g., RAND’s Quality Assessment (QA) Tools to assess clinical effectiveness; Symmetry’s Episode Treatment Groups (ETGs) to assess efficiency); however, our review focused only on publicly available measures.
Existing Measures
Our review of publicly available performance measures revealed that there are few clinical performance measures that are being used to assess care provided at the hospital outpatient facility level. The exception is five ED measures recently developed by the OFMQ, which address the timing of care for acute myocardial infarction (AMI). Discussants were not aware of other hospital outpatient measures in use or available for use.
The majority of measures that are potentially applicable to the hospital outpatient setting address a broad array of diseases/conditions that are reimbursed under the OPPS (see Appendix D for the complete list of measures). However, the vast majority of these measures were designed to be used or are currently being used to evaluate care provided by individual physicians or medical groups, not hospital facilities; as a consequence, the existing measures may require modification of the specifications prior to their application within the hospital outpatient setting.
Regarding existing physician performance measures, the largest and broadest sets of measures have been developed by the AMA’s PCPI, the NCQA, the Assessing Care for Vulnerable Elders (ACOVE) project and the Assessing Symptoms Side Effects and Indicators of Supportive Treatment (ASSIST) project. A description of the measurement development activities of each of these groups appears in Appendix E. In addition, other organizations--such as the Renal Physicians Association, American Society of Clinical Oncologists (ASCO), and the American Gastroenterological Association Institute (AGAI)--have developed clinical performance indicators to assess care for specific diseases/conditions treated by that specialty (e.g., chronic kidney disease, cancer, polyp surveillance), some of which may be pertinent to care delivered in the hospital outpatient setting. For example, ASCO’s Quality Oncology Practice Initiative (QOPITM) has developed practice-level, cancer-specific measures that may be suitable for application in the hospital outpatient setting.
The list of candidate measures also includes a majority of the measures included in the CMS Physician Quality Reporting Initiative (PQRI). These physician measures derive primarily from the AMA’s PCPI, NCQA, and the National Cancer Care Network (NCCN).29 Of the 74 measures currently included in the program, 63 apply to Medicare enrollees in the ambulatory setting and the remaining apply to inpatient care or children.
Table 3.7 summarizes the clinical areas addressed by measures potentially relevant to the hospital outpatient setting and emergency department. We have included measures from the Consumer Assessment of Health Providers and Systems (CAHPS) family of surveys. 30
Of the over 700 measures identified, the vast majority are clinical process measures.
- Approximately 10 percent (75 of 718) measure patient outcomes; these are in the areas of diabetes and chronic kidney disease control; depression treatment outcomes; complications from colonoscopy, cataract surgery and MRI; and outcomes of prostate cancer treatment.
- The only structural measures identified apply to prostate cancer treatment and include the number of patients a physician has treated, availability of psychological counseling for patients, board certification of urologists and radiologists, and the availability of outcome information for patients treated by an institution.
- There are seven measures that address resource use for low back pain, cardiovascular conditions, uncomplicated hypertension, asthma, COPD and deep vein thrombosis.
- The CAHPS family of surveys provides the largest source of potentially relevant patient experience measures. Specifically, many of the ambulatory questions from the CAHPS Clinician & Group Survey apply to the hospital outpatient setting fairly readily; some inpatient-related questions from the CAHPS Hospital Survey (HCAHPS) are also relevant to the hospital outpatient context. For the majority of measures we identified, detailed specifications are in the public domain and are available on the websites of the measure developers.
| Clinical Area | Key Conditions/ Procedures Addressed by Measures |
|---|---|
| Prevention and Screening | Breast Cancer, Colorectal Cancer, Cervical Cancer, Tobacco Use, Vaccination, Medication Use, Problem Drinking, Obesity, Osteoporosis, Fall Risk, Depression, Vision, Hearing, Sleep Disorders |
| Allergies/Sinus | Sinusitis, Rhinitis |
| Ambulatory Surgery | Preoperative Assessment, Antibiotic Timing, Antibiotic Selection, Venous Thromboembolism Prophylaxis |
| Behavioral Health | Depression, Bi-polar Disorder, Alcohol/Drug Dependence, Dementia |
| Bone and Joint Conditions | Osteoporosis, Osteoarthritis, Rheumatoid Arthritis, Low Back Pain, Ankle Sprain, Physical Therapy for Hip/ Knee/ Lumbar/ Shoulder |
| Cancer | Blood, Breast, Colorectal, Head and Neck, Lung, Prostate, General (including symptom control) |
| Cardiovascular Conditions | Acute Myocardial Infarction (AMI), Coronary Artery Disease (CAD), Heart Failure (HF), Venous Thromboembolism (VTE) |
| Dermatological Conditions | Melanoma, Pressure Ulcers |
| Diabetes | HbA1c, Blood Pressure, Cholesterol, Eye Exam, Foot Exam, Smoking, Depression, Aspirin Use |
| Eye Disease/Vision | Diabetic Retinopathy, Cataracts, Glaucoma, Macular Degeneration |
| Gastrointestinal Disorders | Gastroesophageal Reflux Disease (GERD) |
| Hearing Loss | Testing, Referral, Rehabilitation |
| Hepatitis C | Testing, Antiviral Therapy, Vaccination, Alcohol Use, Contraception Use |
| HIV/AIDS | ARV Management, Self Management, Health Maintenance, Case Management |
| Hypertension | Blood Pressure, Patient Education, Plan of Care, Renal Function, Alcohol Intake, NSAID Reduction, Resource Use |
| Medication Use (Vulnerable Elders) | Patient Education, Drugs to be Avoided |
| MRI | Complications |
| Neurological Disorders | Migraine, Stroke, Sleep Disorders |
| Renal Disease | Chronic Kidney Disease |
| Respiratory Illness/Asthma | Chronic Obstructive Pulmonary Disease (COPD), Asthma, Acute Bronchitis, Viral Upper Respiratory Disease, Pharyngitis |
| Under-nutrition | Weight Measurement, Vitamin D, Co-Morbid Conditions |
| Urological Conditions | Urinary Incontinence, Urinary Tract Infections (UTI), Benign Prostatic Hyperplasia (BPH) |
| Other Clinical | Emergency Department Discharge, Radiology Reporting, Pain Management, End of Life Care, Continuity and Coordination of Care, Falls and Mobility |
| Patient Experience | HCAHPS, C-G Ambulatory CAHPS |
Measures in the Development Pipeline
Our discussions with representatives of medical specialty societies and hospital associations yielded information about other measures currently under development. According to the representatives with whom we spoke, CMS’s pressing need to respond to the legislative mandate set forth in the TRHCA of 2006 has significantly increased interest in and resources devoted to the development of hospital outpatient performance measures, both within CMS and more broadly.
In June 2007, CMS awarded a contract to the OFMQ to develop a preliminary set of hospital outpatient clinical performance measures for inclusion in the proposed rule released August 2, 2007 (CMS, 2007). CMS tasked the OFMQ with writing specifications for 10 existing measures to make them applicable to the hospital outpatient setting. The measures include:
- Three PQRI measures addressing diabetes, pneumonia, and heart failure,
- Two Surgical Care Improvement Project (SCIP)31 measures addressing use of antibiotics at the time of surgery, and
- Five ED measures addressing AMI care for patients transferred from one ED to another hospital for admission
Additionally, CMS is seeking public comment on a list of 30 measures under consideration in the hospital outpatient setting These measures address a wide variety of conditions relevant to the Medicare population, including:
- Diabetes,
- Fall risk,
- Depression,
- Stroke,
- Acute myocardial infarction,
- Medication safety,
- Asthma,
- Osteoporosis,
- Pneumonia,
- Cancer screening and treatment,
- Emergency department care for chest pain, syncope and pneumonia,
- Glaucoma,
- Macular degeneration,
- Urinary incontinence, and
- Advance care planning.
Many of these measures are being used as part of the PQRI for physician measurement. To use these measures in the hospital outpatient setting will require adjustments to the technical specifications to ensure they can be operationalized from the HOPS and ED data sources.
Besides measures that CMS is developing, medical specialty societies and hospital associations said that the next most significant source of clinical performance measures in the pipeline for use in the hospital outpatient setting are existing physician performance measures. These measures provide a valuable foundation on which to build a set of hospital outpatient measures because of the breadth of clinical conditions covered and the credible process used to develop these measures. Discussants noted that the PCPI is an ongoing initiative that will continue to generate new clinical performance measures addressing a variety of conditions, many of which could apply to care delivered in the outpatient hospital setting.
Existing hospital inpatient measures are another potential source applicable to the hospital outpatient setting, according to some discussants. This is because some of the care and many of the services/procedures formerly performed in the inpatient setting are now occurring in the outpatient setting. However, another discussant cautioned that, at least for surgery, there are a limited number of inpatient measures that would apply to outpatient surgery. This is because many of the inpatient measures apply to antibiotic use and venous Thromboembolism prophylaxis which are not used in many outpatient surgeries. A few discussants also noted that existing clinical practice guidelines might serve as a potential pipeline for hospital outpatient measures, but these discussants cautioned that much work is required to translate such guidelines into detailed measure specifications.
Other measurement development efforts mentioned by discussants that are on the near-term horizon and are directly applicable to the hospital outpatient setting include:
- The American College of Radiology (ACR) is developing facility-level measures for outpatient care. These are safety measures that relate to minimizing radiation exposure to individual patients, equipment use, use of contrast material, and screening patients for allergies and the potential for renal impairment. In considering these measures, the developers found that they were difficult to attribute to any one physician and determined that they are more appropriate for facility-level measurement.
- The Ambulatory Surgery Center (ASC) Quality Collaboration32 has submitted eight facility-level measures to the NQF. These measures were reviewed in June 2007, and NQF has recommended five for public review and comment. The measures cover patient burns, antibiotic timing, hospital transfer/admission, patient falls, and wrong site/side/patient/procedure/implant.
- The NQF issued a “call for measures” in June 2007 to identify measures that address the quality of hospital-based ED care with particular emphasis on clinical quality, coordination, and efficiency. Initially, the NQF will focus on ED transfers only, but plans to address other aspects of hospital-based ED care (e.g., patient wait times, overcrowding) later in the year.
- The American College of Cardiology (ACC) and the American Heart Association currently have measures under development for atrial fibrillation, primary prevention of cardiovascular disease, and peripheral arterial disease.
The medical specialty societies and hospital associations underscored that when they prioritize measures for development, they tend to assess the following factors: high volume, high cost/ resource allocation, high variation, high risk, the amount of evidence, and the interest of constituents. Almost all remarked that clinical performance measures are their highest priority at present; however, several noted their interest in coordination of care measures.
Measures that Are Lacking
Discussants noted that measures are missing in several key areas:
- ED care: According to discussants, it is critically important to have a robust set of ED measures not only because of the significant role the ED plays in clinical care (“Everything is seen in the ED, one way or another”), but also because the ED is a clearly identifiable part of the hospital outpatient setting (“Everyone can actually agree that the ED is part of the hospital outpatient setting, whereas other areas are more murky and/or variable”). In the context of the ED, there are two main circumstances for which there are a need for measures: (1) the management of patients with a definitive diagnosis, and (2) the management of patients who present with certain signs and symptoms, but for whom a definitive diagnosis has not yet been established. Regarding the former, the small set of ED-specific measures developed by the OFMQ is a good start, according to discussants. Additionally, measures developed for the non-ED, ambulatory setting may be applicable, given use of the ED for routine care by some patients. Regarding the management of patients in the absence of a definitive diagnosis, however, more measures are needed. Additionally, some discussants noted a particular need for ED-specific mental health measures, given that a substantial number of patients may come to the ED for a physical ailment, but may also have mental health issues requiring evaluation and treatment.
- Cancer: Discussants noted that there are many measures evaluating breast and colorectal cancer care, but significantly fewer, if any at all, for other important cancer diagnoses, such as lung cancer.
- Specialty care: Discussants said that few measures are available that address conditions requiring specialty care.
- Follow-up care: Discussants pointed out a need for measures that track the provision of follow-up care. However, they noted that the science is not robust in many areas related to such care (e.g., appropriate follow-up care after procedures, ED visits, and hospitalizations).
- Coordination-of-care/transitions-in-care: According to discussants, measures are lacking that bridge transitions from inpatient to outpatient settings and also among different outpatient settings (e.g., ED to ambulatory care).
- Transmission of imaging results: Discussants commented that, for the hospital outpatient setting in particular, facilities in which radiological imaging is conducted should be held responsible for reporting imaging results to the appropriate providers to ensure timely and well-informed care. Measures are needed that track this transmission.
- Outcomes: Many discussants highlighted interest in tracking outcomes in the hospital outpatient setting, but recognized the challenge created by the fact that multiple factors influence outcomes.
- Episodes of care: Discussants said that measures are lacking to track entire episodes of care, regardless of setting, rather than “pieces of care” that are delivered in different settings.
- Efficiency: Discussants noted that there is significant and growing interest in efficiency measures across the health care system. However, to date, there are still not many measures that have been developed, tested, and validated. Discussants pointed out that both the NQF and the AQA have assembled workgroups to address this gap.
- Patient-centered care: Discussants underscored the importance of patient-centered care and pointed to the CAHPS Hospital, and Clinician & Group Surveys, developed with support from AHRQ, as an excellent source of measures. However, these CAHPS measures are not sufficient, according to those to whom we spoke. In particular, discussants said there should also be measures to assess the reporting of test results conducted in the hospital outpatient setting to patients. Additionally, there is a need for measures related to providing understandable explanations to patients, per at least one discussant who emphasized that institutions should be held responsible for engaging patients “on their level” when providing instructions/education about care and medication use.
- Patient safety: Discussants noted that existing patient safety measures are being applied primarily in the inpatient hospital setting and they were not aware of safety measures specific to the hospital outpatient setting. However, a number of the existing patient safety measures such as hand washing, medication safety, and a culture of safety are applicable to the care delivered in the hospital outpatient setting and could be adapted for use in this setting.
- Timeliness: The ED measures developed by the OFMQ address the timing of AMI care in the ED setting, but discussants said more measures are needed that address other diagnoses and other hospital outpatient settings.
Finally, across a variety of types and topics of measures, discussants pointed out the lack of distinction in existing measures between providers ordering a procedure/service, and those delivering care. They said that more attention should be paid to this distinction during the development of measures so that the most appropriate providers are evaluated and held accountable.
IV. Synthesis of Existing Measures and Identification of Gaps. Synthesis of Existing Measures and Identification of Gaps
In this chapter, we draw from our analysis of 2005 Medicare data, scan of publicly available existing measures, and discussions with medical specialty societies and hospital associations to synthesize the reach of existing measures and identify the gaps in potential measures for the HOPS and ED. We also describe several data collection challenges associated with the development of measures for the hospital outpatient setting.
Equity
Although there is widespread awareness of health disparities by population subgroups, our review did not identify any specific measures of equity. However, many existing measures could be applied and the results stratified by various sub-populations to determine where disparities are occurring and to focus attention on closing these gaps provided subgroup identifiers are in the data. The IOM has identified equity as a priority area for measure development (IOM, 2005), and the Robert Wood Johnson Foundation has issued a call for proposals in an effort to improve the understanding of how to measure equity and its role in promoting quality. Additionally, the National Academy of Social Insurance has made recommendation to CMS of ways in which it could strengthen its capacity to assess and address disparities (Vladeck et al, 2006).
Mapping of Clinical Measures
Figure 4.1 provides an overview of our mapping of existing measures to HOPS and ED encounter data. Encounters were grouped into three categories in our analyses: visits, drugs/biologicals, and services/procedures. For each category, we considered the types of activities that typically occur during the encounters. We then used this assessment to determine which measures are relevant to each type of encounter for the mapping exercise. We performed this measures mapping exercise to determine the clinical conditions and services for which measures currently exist and those for which there is a deficit.
When we examined reasons for visits, we found that appropriate measures and services would include additional E&M services (i.e., visits), such as referral to other doctors and specialists; medications appropriate to findings from the examination; or a request for an appropriate service/procedure, such as colonoscopy or referral to a dermatologist to remove a pigmented mole. For example, existing measures specify that an overweight patient should have this issue addressed annually, and geriatric patients should be screened annually for cognitive and functional impairment. Measures exist to assess whether patients presenting with community-acquired pneumonia receive empiric antibiotic therapy, a situation where a visit prompts prescription of a medication. Visits may also result in referral for a service/procedure such as colonoscopy, mammography, or a laboratory test (such as creatinine for patients receiving cisplatin).
Figure 4.1. Mapping of Reasons for Visits to Existing Clinical Measures
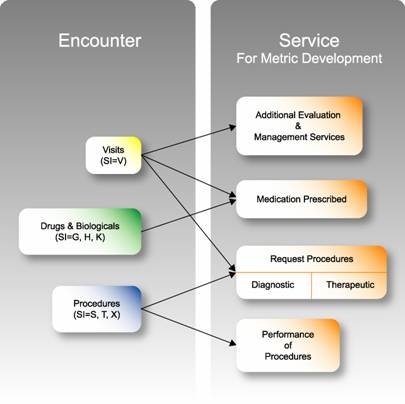
Some encounters occur wherein patients only receive drugs or biologicals, such as interferon for Hepatitis C or Trastuzumab administration for HER2/Neu positive patients. There are some existing measures that address the appropriate use of medications and biologics, and these may be appropriate to care delivered in the outpatient hospital setting. A careful review of existing measures against the care provided in the outpatient hospital setting would be a key next step, to see if the measures are applicable and how their specifications may need to be adapted to be operationalized using hospital outpatient data sources. Given the large number and type of drugs and biologicals used, it is likely that there are substantial measure gaps related to the appropriate use of drugs and biologicals in treating Medicare beneficiaries.
Finally, with respect to the services/procedures we examined, we found two points of interest: (1) the appropriateness of ordering of the service/procedure, such as a measure specifying the clinical situations under which a patient in the ED should undergo an MRI; and (2) the quality of the provision of the service/procedure by the performing specialist, such as a measure addressing the documentation of pre-surgical axial length in cataract patients, or a measure assessing the communication of colonoscopy results to the primary care physician.
Syntheses of Measures
Synthesis of Measures Relating to Reasons for Visits
Table 4.1 presents the key diagnostic categories that we identified as the reasons for visits (based on V codes) to the HOPS by Medicare beneficiaries in 2005, and the corresponding counts of publicly available measures that pertain to these diagnoses. A more thorough review of the measures would be required to fully consider their applicability and how they might need to be modified for use in the hospital outpatient setting.
As Table 4.1 illustrates, there are many existing ambulatory measures designed to assess physician performance that address many of the key reasons for visits to the HOPS. For example, there are a substantial number of cardiology measures for ischemic heart conditions (AMI and coronary artery disease [CAD]) and congestive heart failure (CHF). Likewise, there are a fair number of measures that address diabetes, general medicine screening, respiratory conditions (such as COPD/asthma and pneumonia), and cancer (especially breast, gastrointestinal (GI), and prostate). There are also a significant number of mental health measures.
| Category |
HOPS
|
|
|---|---|---|
| Diagnostic Category | Number of Related Measures | |
| Dermatology | Ulcer | 9 |
| Infection | 1 | |
| Inflammation | 0 | |
| Wounds | 0 | |
| Benign Lesions | 0 | |
| Gynecology | Breast | Mammogram-1 |
| Pelvic | Cervical Cancer Screen-3 | |
| Head and Neck | Ear | Hearing Loss-6 |
| Esophagus | 0 | |
| Hematology34 | Anemia | Chronic Kidney Disease-3 Medication Use-1 |
| Red cell | 0 | |
| Platelets | 0 | |
| Medicine-Cardiology | Conduction/dysrhythmias | 3 |
| Ischemic heart | AMI/ACS-15 Coronary Artery Disease-14 | |
| Valvular disease | 0 | |
| Heart failure | 17 | |
| Medicine-Endocrinology | Diabetes | 15 |
| Thyroid | 0 | |
| Gout | 0 | |
| Medicine — General | Hypertension | 16 |
| Hyperlipidemia | 3 | |
| Nutrition/Metabolism |
Undernutrition- 5 |
|
| Category |
HOPS
|
|
|---|---|---|
| Diagnostic Category | Number of Related Measures | |
| Medicine — General (cont) | Drug monitoring | 12 |
| Screening | 52 | |
| Vaccination | 6 | |
| General Symptoms35 | 0 | |
| Follow up related to previous care | 0 | |
| Rheumatology | Osteoporosis-8 Rheumatoid Arthritis-1 | |
| Urinary | Incontinence-12 Urinary Tract Infection-2 Benign Prostatic Hyperplasia-12 | |
| Venous system | 6 | |
| Medicine-GI | Abdominal symptoms, pain | 0 |
| Hepatitis, cirrhosis | Hepatitis C-9 | |
| Gastroenteritis | 0 | |
| Diverticulitis | 0 | |
| Medicine-Infectious Disease | HIV | 4 |
| Herpes | 0 | |
| Medicine — Oncology/Neoplasia36 | Chemotherapy | 34 |
| Radiotherapy | 24 | |
| Leukemia/Lymphoma | 5 | |
| Breast | 31 | |
| Respiratory | 1 | |
| GI | 22 | |
| Gynecology | 0 | |
| Skin | 3 | |
| Urology (prostate) | 18 | |
| Head and Neck | 1 | |
| Medicine-Respiratory | Sinusitis | 2 |
| Bronchitis | 1 | |
| Pneumonia | 12 | |
| Upper respiratory infection, cough | 3 | |
| COPD/Asthma/Emphysema | COPD-13 Asthma-17 | |
| Category |
HOPS
|
|
|---|---|---|
| Diagnostic Category | Number of Related Measures | |
| Neurology | Parkinson’s disease | 0 |
| Alzheimer’s disease | Dementia-14 | |
| Cerebrovascular | 17 | |
| Seizures | 0 | |
| Multiple Sclerosis | 0 | |
| Peripheral nerve disorders | 0 | |
| Ophthalmology | Glaucoma | 2 |
| Cataract | 28 | |
| Retinal Disorders | 2 | |
| Orthopedics | Spinal conditions | 3 |
| Joint pain/Arthritis | 16 | |
| Osteomyelitis | 0 | |
| Physical therapy, orthopedic aftercare | 6 | |
| Limb pain | 0 | |
| Abnormal radiologic finding | 0 | |
| Psychiatry | Depression | 30 |
| Psychoses | Bi-Polar-5 | |
| Dementia-14 | Neuroses | 0 |
| Surgery-Genera37 | Follow-up care | 0 |
| Preoperative services | 5 | |
| Vascular conditions | 5 | |
| Complications | 0 | |
| Urology | Kidney | Chronic Kidney Disease-33 |
| Prostate | Benign Prostatic Hyperplasia-12 | |
| Symptoms38 | 0 | |
| Bladder | Urinary Tract Infection-2 Incontinence-12 | |
Synthesis of Measures Relating to Services/Procedures
Our synthesis of existing measures and the most frequent and costly services/procedures (based on S codes) performed in the HOPS revealed that there are a few publicly available existing measures to address these services/procedures. Topics addressed by existing measures include cataract extraction, indications for cardiac catheterization, colonoscopy, MRI complications, and treatment for cardiac arrhythmias. However, there are many services/procedures for which there are no existing measures. In addition, existing measures that focus on diagnostic and therapeutic services/procedures are concerned primarily with whether or not the service/procedure was provided, not the quality with which it was performed. For example, performance measures on Papanicolaou [Pap] smear relate to the physician obtaining the smear, not the screening of the smear by the cytotechnologist and cytopathologist; mammography measures relate to the frequency and indications for the procedure rather than the whether appropriate and adequate views were obtained or the completeness of the radiologists assessment of the mammography. Identifying the providing specialty is especially of interest given that quality of patient care is optimized when the requesting and providing specialties work together; frequently the providing specialty knows best how to obtain the optimal results from the services provided.
Some specialty organizations have developed measures to provide guidance to physicians from other specialties who order their services. For example, the AGAI, which represents gastroenterologists, worked with the PCPI and NCQA to develop physician-level measures for colorectal cancer screening and GERD that are applicable to primary care physicians also.
The above discussion should not be taken to mean that expectations for the quality with which services are delivered, which are relevant to performing specialties, do not exist for some conditions. For example, radiologists and radiology facilities offering mammography services must comply with the Mammography Quality Standards Act (MQSA) of 1992. Additionally, pathologists, other laboratory professionals, and clinical laboratories must comply with the Clinical Laboratory Improvement Amendments (CLIA) regulations, including Section 493.855(a) that relates to cytology proficiency testing (CLIA 88). Furthermore, the AMA’S PCPI has developed physician-level measures for surgery related to the timing of antibiotic administration and venous thromboembolism prophylaxis. Some of these measures are applicable to outpatient surgeries.
Synthesis of Measures Relating to Drugs and Biologicals
Few measures were identified that address the use or dosing of drugs and biologicals (based on G, H, and K codes) that are paid separately under OPPS. The vast majority of identified measures address the use of cancer chemotherapy. The identification or development of measures that specifically focus on high-volume drugs and biologics that represent the most significant expense to the Medicare program, such as blood products and contrast material used for imaging for the OPPS and thrombolytic agents in the ED, would be valuable.
Identification of Gaps in Measures
In conducting our gap analysis, we considered how the measures identified in our review relate to the six aims identified by the IOM (2001) as being critical to ensuring a high-quality health care system: (1) effectiveness, (2) efficiency, (3) equity, (4) patient-centeredness, (5) safety, and, (6) timeliness.
Effectiveness
While we found many measures of clinical effectiveness, our analysis also revealed a number of key gaps in existing measures:
- ED Care: With the exception of the ED measures being developed by the OFMQ, there are no existing measures to evaluate care at the ED facility level. However, as noted previously, the NQF released a call for ED transfer measures in June 2007 and has plans to address other ED issues in the coming year, so some measures for this setting are likely to be forthcoming in the near future.
- Cancer: While measures exist that address breast and colorectal cancer care, they are lacking for many other cancer diagnoses (e.g., lung cancer).
- Specialty care: While hospital outpatient clinics tend to focus on specialty care, we found that most existing measures address diagnoses that impact primary, not specialty care. The PCPI is working to fill some of these gaps.
- Follow-up care: Measures are lacking to assess appropriate follow-up care after services/procedures, ED visits, and hospitalizations. As discussants noted, measure development is challenging, given that the science related to follow-up care in many areas is not robust.
- Coordination-of-care/Transitions-in-care: There is a lack of measures that bridge transitions from inpatient to outpatient settings and also among different outpatient settings (e.g., ED to ambulatory care). Kaiser Permanente has developed some measures; however, given Kaiser’s unique closed-model health system, implementation of them in other types of health systems may differ. The American Board of Internal Medicine (ABIM), with grant support from AHRQ, has led a consortium of specialty societies and other stakeholders in developing a set of principles and standards for improving transitions across locations of care. It is anticipated that these principles will serve as the basis of measure development by the PCPI. Additionally, NQF’s recent call for ED transfer measures will likely generate some transitions in care measures for this setting.
- Transmission of Test Results: Measures are lacking that assess the timely and accurate transmission of test results, such as from radiological imaging or laboratory tests or from provider to provider within in the hospital outpatient setting as well as to providers in other care settings.
- Outcomes: The overwhelming majority of measures assessing clinical effectiveness that we identified are clinical process measures. Given the increasing interest in the tracking outcomes (the “bottom line” of health care, in the words of some discussants), there is a need to develop outcome measures. Such development will require further strides in risk adjustment methodologies, given the multiple factors that can influence outcomes.
- Episodes of care: The overwhelming majority of measures assessing clinical effectiveness that we identified track components of care in isolation, rather than taking into account care delivered for a specific condition or clinical event across different health care settings. As such, there is a need for evidence-based measures that assess the clinical care provided for the entirety of an episode of care, regardless of setting or level within the health care system. The AQA/Hospital Quality Alliance (HQA) Steering Committee has convened an Efficiency/Episodes of Care Work Group to address this need.
Efficiency
Discussants stressed the existence of a significant and growing interest in efficiency measures. At this time, existing efficiency measures reflect measures of relative resource utilization and have not taken into account differences in quality by resource use. Existing efficiency measures have been applied primarily by private sector health plans looking for opportunities for cost savings to reduce the growth in health care trend. Information derived from application of these tools typically has been provided to physicians, integrated health systems, and hospitals as part of internal improvement efforts; the tools are only in their early stages of being validated for use in public reporting and pay for performance.
Discussants noted that both the NQF and the AQA have assembled workgroups to identify and endorse measures of efficiency. The AQA has also proposed a starter set of cost-of-care measures pertaining to seven conditions (diabetes, AMI, CHF and CAD, asthma, depression, and low back pain), but measures have not yet been developed and would need to be linked to quality-of-care measures to assess efficiency (rather than cost alone). The AQA/HQA Steering Committee has convened an Efficiency/Episodes of Care Work Group to develop a comprehensive approach to efficiency measurement, which includes an examination of the overall system, medical group, practice site and individual physicians, and that takes into account episodes of care as well as primary responsibilities for the care provided (AQA, 2007).
Patient-Centeredness
Although the CAHPS Hospital, and Clinician & Group Surveys provide a strong source of measures that could be used to evaluate patient-centeredness in the hospital outpatient setting, patient experience measures are lacking that address the provision of clinical care, such as the reporting of specific test results. At present there are also no measures that assess whether or how institutions address health literacy39 and health numeracy.40
Safety
A large number of existing patient safety measures apply primarily to care provided in the inpatient setting (e.g., Leapfrog’s Safety Leaps, AHRQ’s Patients Safety Indicators (PSIs), and the SCIP measures). However, a number of these safety measures that apply more universally — such as a culture of safety, hand washing and other infection control measures, and medication verification — would be appropriate for application in the hospital outpatient setting.
Timeliness
Measures are lacking to assess the turnaround times for the provision of care and for diagnostic tests being performed. As discussants noted, the OFMQ has developed ED measures that assess the timing of AMI care; more measures are needed that address the timing of care related to other diagnoses in the ED, as well as in the HOPS.
Challenges in Performance Measurement
In addition to identifying the need for additional measures, our synthesis and gap analysis underscored several challenges related to the operational aspects of measurement from the vantage point of the hospital, including:
- Sample Size: Although the 2005 dataset used in our analyses contains many millions of claims, the number of visits and services/procedures that occur in any given hospital outpatient setting for a specific condition may be small. As measures are developed, it will be important to examine the data to assess whether there are adequate patient volumes at the hospital-level to ensure stable estimates of HOPS or ED performance. Additionally, the fact that additional sample size would be required to stratify data by such factors as race/ethnicity, socio-economic status, and/or gender to assess equity of care also merits consideration.
- Lack of Provider Engagement: Most physicians are not employed directly by hospitals, making it difficult for hospitals to force adherence to hospital protocols – in either the inpatient or outpatient setting. Discussants encouraged gain-sharing as a means to encourage joint accountability for physicians and hospitals. As one said, “In order to get traction, everyone (i.e., hospitals and physicians) has to have something at risk.” Appropriately and fairly assigning accountability for specific actions is another important way to engage providers; however, it is not always clear how to do so. For example, some patients have several physicians, raising the question of who should be held responsible in such situations.
- Lack of Staff: Although the HOPS and ED may be able to draw staff from their associated hospitals (which generally have quality departments with analysts experienced in data abstraction), hospital outpatient settings have not traditionally been staffed or budgeted to provide the medical record abstraction and analytic services needed for performance measurement activities.
- Lack of Adequate Detail in Existing Claims Data to Support Quality Measurement: Because claims data are generated for billing and not quality of care purposes, data elements needed for quality of care assessment are often lacking, particularly those data required for risk adjustment.
- E&M codes broadly address the level of service provided, but do not capture specific service details and organ systems addressed. For example, it would not be possible, using standard claims data, to ascertain whether a patient’s blood pressure was taken as part of an office visit
- Claims data also do not include specific laboratory, radiographic, or clinical values, so it is not possible to use claims data to score quality of care measures that require these data elements. For example, laboratory data indicating the need for altered diabetic therapy would be dependent on the HbA1c level. Claims data will reflect only that an HbA1c was ordered, not whether the result was such that action should be undertaken. Similarly, knowing that a hematocrit was performed is insufficient to determine whether a patient met criteria for receipt of erythropoietin. Capturing medication prescribing information related to specific conditions is notably difficult, although increasingly data may start to become available with the Medicare Prescription Drug benefit.
- While the date of a service is captured, the actual timing of the care provided is often not evident from claims data; thus, it could not support measures that examine timing in hours, such as many measures addressing AMI care.
Development of new CPT Category II performance measurement codes as well as Medicare G codes (HCPCS level II codes) is underway, which, if used, will shed more light on the care provided during visits. In the meantime, however, this information is often not available given that it is beyond what is currently required for claims submission. Claims submissions forms may require modification to collect the necessary data elements to produce a performance measure, if administrative data sources will be used to construct measures.
Although some discussants expressed hope that electronic health records (EHRs) will be able to provide easily retrievable data, they underscored that the implementation of EHR systems ready for use in clinical performance measurement is still “a long way off.” In the near term, implementation of measures will likely entail manual chart abstraction or changes in billing codes. Registries were mentioned as a potential source of data for performance measures by representatives of at least two organizations. They indicated they were placing a higher priority on registries, as opposed to developing specific performance measures. One group believes that utilizing registries is a more effective way to improve health care quality. Both groups encouraged CMS to do more to develop and encourage national registries in a broad spectrum of clinical areas. It should be noted that TRHCA requires that, as part of rulemaking for 2008 measures, CMS address a mechanism for providing data on quality measures through an appropriate medical registry. As such, CMS is currently exploring the possibility of drawing on existing databases and registries maintained by a variety of organizations (e.g., medical professional societies, medical boards, medical group management organizations), with the goal of decreasing the burden of quality reporting for all involved while increasing the quality and usefulness of the data (Kuhn, 2007).
V. Conclusions
The passage of the Tax Relief and Health Care Act of 2006 (TRHCA), which requires hospitals serving Medicare beneficiaries to report hospital outpatient quality data to secure their full Outpatient Prospective Payment System (OPPS) fee schedule update, has precipitated a need to identify performance measures applicable to the hospital outpatient setting. RAND’s environmental scan provides a preliminary assessment of the measures landscape in the context of care provided in the hospital outpatient setting, by determining the leading conditions treated and services/procedures provided in the hospital outpatient setting and by identifying existing and potentially relevant performance measures as well as gaps in measures. Below we highlight the key findings and describe next steps the Centers for Medicare and Medicaid Services (CMS) could consider as it works to develop its performance measurement agenda for this setting.
A small number (10) of hospital outpatient measures comprise the initial measure set to be used in the Hospital Outpatient Quality Data Reporting Program (HOP QDRP), and CMS has another 30 candidate measures that it has put forth for public comment. Our review found that there are approximately 700 publicly available, existing inpatient and ambulatory care measures that may be potentially applicable to the types of conditions treated and services/procedures provided in the hospital outpatient setting. While the vast majority of existing measures assess clinical effectiveness, primarily underuse of services, there are a few measures that address other care domains identified in the 2001 Institute of Medicine (IOM) Crossing the Quality Chasm report as critical to enhancing system performance, such as patient experience with care and patient safety. Among the next steps that CMS could consider are to: (1) conduct a more detailed mapping of existing measures to specific areas of care provided in the hospital outpatient setting, and (2) for those measures that are directly relevant, adapt the technical specifications for this setting of care, which may provide a near-term source of additional candidate measures for the HOP QDRP. Broadening the use of existing measures also will help to align measurement and accountability across various Medicare settings.
Although the many existing measures that RAND identified hold the promise of applicability to the hospital outpatient setting, there are gaps. Some examples include measures of cancer care (e.g., lung cancer); specialty care; follow-up care; coordination-of-care/transitions-in-care; transmission of test results; outcomes; episodes of care; and measures of high-volume/high-cost drugs/biologicals (e.g., blood products; thrombolytic agents). In the use of various services/procedures, such as imaging, there is an absence of measures that address appropriate use — which is a critical issue given that services/procedures are a key driver of the cost growth within the hospital outpatient setting. To the extent that CMS also wishes to address the various domains highlighted in the 2001 IOM report, there are also gaps in available measures of efficiency, equity, and timeliness of care.
Study Limitations and Considerations for Future Analysis and Measurement Development
This study constitutes an initial assessment of the hospital outpatient measurement landscape. We identify several limitations that could be addressed by additional analytic work to flesh out the best opportunities for performance measurement in the hospital outpatient setting:
- The analytic files made available contained service-line information rather than information aggregated at the level of an encounter or an episode of care. As such, we were not able to describe the spectrum of individual services a Medicare beneficiary receives during a single visit. The data used in this analysis only permitted us to examine separate pieces of encounters without being able to account for the full set of services provided to a patient during an encounter, for example a patient with diabetes. Subsequent analyses conducted using encounter-level data, or possibly even the level of an episode, would provide a more complete picture of the quality of care Medicare beneficiaries receive for a given condition.
- The analysis of International Classification of Disease Version 9 (ICD-9-CM) diagnostic and procedure codes was restricted to the first four digits. Analyses conducted at the level of the fifth digit could assist, in some cases, in further elucidating distinctions that may not have been apparent based on our more aggregated analyses. These distinctions may have important implications for measures development for some diagnoses and services/procedures that are specified in greater detail than was examined in our analyses. For example, the fifth digit of diabetes codes (250.xx) is used to distinguish between both type I and type II diabetes, and whether the diabetes is controlled (i.e., whether the current treatment regimen keeps the blood sugar level of a patient within acceptable levels) or uncontrolled.41
- The analysis compared reasons for visits to the Hospital Outpatient Setting (HOPS) to existing measures. For the measures mapping segment of our analysis, we focused on the HOPS because the majority of existing measures correspond to conditions and diagnoses that most commonly occur in the HOPS, rather than the ED. We acknowledge that some conditions and services/procedures occur more frequently in the ED setting. Therefore, a separate synthesis that focuses on mapping measures to the care provided in the ED, in order to capture encounters in the ED that are distinct from the HOPS and do not result in an acute admission, merits consideration for future analyses.
- The groupings used to classify reasons for visits were informed by the judgment of two clinicians and not an interdisciplinary panel of physicians and measurement experts. RAND developed diagnosis groupings to ensure that the most common diagnoses that have multiple diagnosis codes at the four-digit level were aggregated, thereby accurately reflecting their collective frequency and costs. While these groupings were established by two RAND physicians-researchers, it may be useful to convene a larger, interdisciplinary group to revisit them to ensure they have clinical face validity.
- The analysis examined only the five most common diagnoses within an Ambulatory Payment Classification (APC) code. While this level of analysis provides a useful overview, a more detailed examination of APCs may shed light on additional issues related to services/procedures than were captured in our review.
- The findings regarding drugs/biologicals were not aggregated by drug or drug class. For our analyses, we had information only for drugs paid via APCs and we had incomplete information even for those drugs with APC payments. Because of the data incompleteness, we did not go the next step and aggregate drugs/biologicals by particular drugs or drug classes, as our estimates would have been inaccurate. Future analyses could examine a complete set of drug/biologics information and consider opportunities for measure development.
- The analysis did not consider changes in cost over time. To better understand the key drivers of cost growth in the Medicare hospital outpatient setting, future analyses could include an analysis of changes in costs over time by various conditions, services/procedures, and drugs/biologicals.
- The analysis did not assess the density of services/procedures or conditions within each hospital that bills under OPPS, to determine whether there are likely to be a sufficient number of scoreable events. In addition to these limitations, we identified a number of issues that could be taken into account during the measures development process. These include the following:
- Care and services delivered in the hospital outpatient setting are not homogenous across hospitals or populations served. The types of services/procedures delivered in the hospital outpatient setting vary hospital to hospital, making it challenging to develop a set of hospital outpatient measures that can be applied to all institutions because of differences in service mix and patient populations. As one discussant noted, outpatient care is “a hodgepodge of ambulatory and inpatient-like care.” Consequently, CMS may wish to consider having a stable of measures, and hospitals would be required to submit data on all measures applicable to their service mix and patient population. The variations will create unevenness in the burden of data collection and reporting across institutions.
- Some existing ambulatory care measures may need to be modified for use in the hospital outpatient setting. The majority of existing clinical effectiveness measures has been developed to assess ambulatory care (applied at the physician level), and many of them likely could be directly applied with minimal changes to ensure the administrative codes or other data sources used to populate the measure are correct. Existing measures should be carefully reviewed by measurement and clinical content experts to determine whether and how adjustments to the measures specifications are required in order for them to be applied to the hospital outpatient setting.
- To assess appropriate use of services/procedures, it is necessary to distinguish between the provider ordering a service and the one delivering it. Most ambulatory care measures do not explicitly distinguish the fact that the physician ordering a service (e.g., an ED physician ordering an MRI) may differ from the one providing it (e.g., the radiologist reading the MRI results). This is often true for services provided by consulting physicians (e.g., radiologists, pathologists, cardiologists), and is of significant interest given the frequent use and cost of such services. Our analysis found that radiological imaging services were among the top 20 most common and most costly for both the HOPS and ED — underscoring the need to have measures that assess appropriate ordering of these services by providers. Measures that take this issue into account could assist CMS in better understanding the drivers of use, and in assessing whether that use is appropriate.
Next Steps for Consideration
Due to the limited resources for this project, the work completed here should be viewed as a preliminary assessment that requires follow-on work to fully flesh out how to apply existing performance measures in this setting and where the most important measurement gaps are for guiding the use of resources in the future.
As measurement efforts in the outpatient setting move forward, CMS could consider expanding on the work of this evaluation by
- Conducting additional analyses of the OPPS data: Additional analyses using more detailed and complete OPPS data could refine the set of conditions, services/procedures, and drugs/biologicals that were identified in this study. This analysis could also include a broad set of clinical experts to help evaluate the care provided in the hospital outpatient setting to determine what the priorities should be for performance measurement and whether and how to group services and procedures for measurement. The analyses could address the limitations and suggested modifications noted in this study.
- Conducting a detailed mapping of measures to key areas of use and costs: Once more in-depth data analysis has occurred, a detailed mapping exercise between content areas and existing measures could determine measures that are ready to be used without modifications, and those that require modification and how they could be modified for use to assess performance at the hospital outpatient facility level. Once this work is completed, the candidate measures could be submitted to NQF for their review and endorsement.
- Determining where additional gaps exist and establish priorities for filling gaps: The information gathered from the in-depth data analyses and detailed measures mapping exercise could be used to identify gaps in measures. This review could consider the prioritization of conditions, services/procedures, and drugs/biologicals for determining future measures development work.
Appendix A: Additional Measures Under Consideration for Inclusion in Hospital Outpatient Quality Data Reporting Program (HOP QRDP)
| Number | Measure | Source |
|---|---|---|
| 1 | Type 1 or 2 Diabetes Mellitus: Low Density Lipoprotein Control | NCQA |
| 2 | Type 1 or 2 Diabetes Mellitus: High Blood Pressure Control | NCQA |
| 3 | Screening for Fall Risk | AMA/PCPI |
| 4 | New Episode of Major Depression: Antidepressant Medication During Acute Phase | NCQA |
| 5 | Stroke and Stroke Rehabilitation: CT or MRI Reports | AMA/PCPI |
| 6 | Stroke and Stroke Rehabilitation: Carotid Imaging Reports | AMA/PCPI |
| 7 | Osteoporosis: Communication with the Physician Managing Ongoing Care Post Fracture | AMA/PCPI |
| 8 | Osteoporosis: Screening or Therapy for Women Aged 65 and Older | AMA/PCPI |
| 9 | Osteoporosis: Management Following Fracture | AMA/PCPI |
| 10 | Osteoporosis: Pharmacologic Therapy | AMA/PCPI |
| 11 | Medication Reconciliation | AMA/PCPI |
| 12 | Community Acquired Pneumonia: Assessment of Mental Status | AMA/PCPI |
| 13 | Community Acquired Pneumonia: Vital Signs Recorded and Reviewed | AMA/PCPI |
| 14 | Breast Cancer: Post-Breast Conserving Surgery Irradiation | NCCN/ASCO |
| 15 | Breast Cancer: Adjuvant Chemotherapy | NCCN/ASCO |
| 16 | Breast Cancer: Adjuvant Hormonal Therapy | NCCN/ASCO |
| 17 | Breast Cancer: Needle Biopsy Diagnosis | AMA/PCPI |
| 18 | ECG for Diagnosis of Non-Traumatic Chest Pain | AMA/PCPI |
| 19 | ECG for Diagnosis of Syncope | AMA/PCPI |
| 20 | Primary Open Angle Glaucoma: Optic Nerve Evaluation | AMA/PCPI |
| 21 | Age-Related Macular Degeneration: Dilated Macular Examination | AMA/PCPI |
| 22 | Age-Related Macular Degeneration: Antioxident Supplement | AMA/PCPI |
| 23 | Diabetic Retinopathy: Documentation of Presence or Absence of Macular Edema and Level of Severity of Retinopathy | AMA/PCPI |
| 24 | Diabetic Retinopathy: Communication with Physician Providing Ongoing Diabetes Care | AMA/PCPI |
| 25 | Colonoscopy for Polyp Surveillance: Description of Polyp Characteristics | AGAI |
| 26 | Advance Care Plan | AMA/PCPI |
| 27 | Urinary Incontinence: Assessment Of Presence in Women Aged 65 and Older | AMA/PCPI |
| 28 | Urinary Incontinence: Characterization of UI in Women Aged 65 Years and Older | AMA/PCPI |
| 29 | Urinary Incontinence: Plan of Care for Women Aged 65 Years and Older | AMA/PCPI |
| 30 | Asthma: Pharmacologic Therapy | AMA/PCPI |
Appendix B: List of Organizations Included in Environmental Scan Discussions
Medical Specialty Societies
American College of Surgeons
American Society of Clinical Oncology
American Academy of Orthopaedic Surgeons
American Academy of Ophthalmology
American College of Emergency Physicians
American Gastroenterological Association
American College of Cardiology
American College of Radiology
American College of Physicians
Hospital Associations
American Hospital Association*
Federation of American Hospitals*
American Association of Medical Colleges*
University Health System Consortium
* These organizations are also lead members of the Hospital Quality Alliance (HQA)
Appendix C: Diagnoses Associated with Visits to the Hospital Outpatient Setting and Emergency Departments by Medicare Beneficiaries, 2005
In the following table, the key clinical categories listed are organized alphabetically and represent 100 percent of the primary diagnoses associated with Evaluation & Management (E&M) visits in the Hospital Outpatient Setting and Emergency Departments. Within each clinical category, we present more detailed diagnostic groups that account for at least 0.5 percent or more of the total diagnoses. Therefore, the sum of the percentages for diagnostics groups within a clinical category will not equal the percentage for the category.
|
Hospital Outpatient Setting
|
Emergency Department
|
|||||
|---|---|---|---|---|---|---|
| Total Encounters |
15,325,267
|
11,426,386
|
||||
| Percent Included In list |
100%
|
100%
|
||||
| Clinical Category |
Diagnostic Groups
|
Diagnostic Groups
|
||||
| Cardiothoracic Surgery | 0.01% | 0.01% | ||||
| Dentistry | 0.10% | 0.59% | ||||
| Dermatology | 6.65% | 4.21% | ||||
| Other skin diseases | 4.39% | Skin infections | 1.93% | |||
| Skin infections | 0.81% | Symptoms | 1.09% | |||
| Inflammatory skin conditions | 0.75% | Other skin diseases | 0.63% | |||
| Symptoms | 0.60% | Inflammatory skin conditions | 0.56% | |||
| Dysmorphology-Genetics | 0.15% | 0.02% | ||||
| Gynecology | 0.79% | 0.47% | ||||
| Head and Neck | 1.09% | 3.97% | ||||
| Ear and mastoid | 0.85% | Laceration/open wound | 1.92% | |||
| Ear and mastoid | 1.00% | |||||
| Injury | 0.67% | |||||
| Medicine-Cardiology | 6.68% | 3.45% | ||||
| Conduction/dysrhythmias | 2.48% | Conduction/dysrhythmias | 1.28% | |||
| Ischemic heart | 1.82% | Heart failure | 0.86% | |||
| Heart failure | 1.33% | Symptoms | 0.62% | |||
| Ischemic heart | 0.60% | |||||
| Medicine-Endocrinology | 7.03% | 1.62% | ||||
|
Hospital Outpatient Setting
|
Emergency Department
|
|||||
|---|---|---|---|---|---|---|
| Total Encounters |
15,325,267
|
11,426,386
|
||||
| Percent Included In list |
100%
|
100%
|
||||
| Clinical Category |
Diagnostic Groups
|
Diagnostic Groups
|
||||
| Endocrine, metabolic | 6.98% | Endocrine, metabolic | 1.62% | |||
| Medicine-General | 35.21% | 43.40% | ||||
| Hypertension | 7.42% | Symptoms | 20.35% | |||
| Aftercare, specific procedures | 6.40% | Injury | 6.15% | |||
| Symptoms | 4.48% | COPD and related | 3.49% | |||
| Endocrine, metabolic | 2.37% | Acute respiratory infection | 2.78% | |||
| Health system encounter | 2.18% | Endocrine, metabolic | 1.47% | |||
| COPD and related | 1.99% | Complications | 1.41% | |||
| Venous disease | 1.97% | Hypertension | 1.39% | |||
| General exam | 1.49% | Infectious and parasitic disease | 1.23% | |||
| Acute respiratory infection | 1.34% | Aftercare, specific procedures | 1.08% | |||
| Complications | 1.04% | Venous disease | 0.72% | |||
| Arterial disease | 0.83% | Poisonings | 0.55% | |||
| Upper respiratory tract | 0.56% | Toxic effects-external causes | 0.50% | |||
| Medicine-GI | 2.37% | 6.26% | ||||
| Upper GI | 0.62% | Symptoms | 1.78% | |||
| Upper GI | 1.17% | |||||
| Functional digestive | 0.93% | |||||
| Inflammatory bowel | 0.84% | |||||
| Medicine-Infectious Disease | 2.25% | 1.27% | ||||
| Infectious and parasitic disease | 1.84% | Infectious and parasitic disease | 1.21% | |||
| Medicine-Nephrology | 0.92% | 0.37% | ||||
| Chronic renal failure | 0.58% | |||||
| Medicine-Oncology/Neoplasia | 13.10% | 0.88% | ||||
| Cancer | 9.17% | Hematology | 0.58% | |||
| Hematology | 2.35% | |||||
| Neoplasm-uncertain behavior | 0.54% | |||||
| Neurology | 2.82% | 2.45% | ||||
| Cerebrovascular | 0.64% | Migraine | 0.87% | |||
| Hereditary/degenerative | 0.75% | Cerebrovascular | 0.76% | |||
| Peripheral nerve disorders | 0.57% | |||||
| Neurology/Neurosurgery | 0.13% | 0.37% | ||||
| Obstetrics | 0.13% | 0.08% | ||||
| Ophthalmology | 4.18% | 0.83% | ||||
| Glaucoma | 1.14% | |||||
| Cataract | 0.95% | |||||
| Retinal disorders | 0.76% | |||||
| Orthopedics | 10.39% | 16.61% | ||||
| Back disorders | 3.92% | Back disorders | 3.94% | |||
| Arthropathies | 1.95% | Sprains and strains | 3.63% | |||
| Rheumatism | 1.73% | Fracture | 2.75% | |||
| Other joint disorders | 1.31% | Rheumatism | 2.59% | |||
| Osteopathies, chondropathies | 0.90% | Other joint disorders | 2.02% | |||
| Arthropathies | 0.70% | |||||
| Psychiatry | 1.49% | 3.59% | ||||
| Psychoses | 0.75% | Neuroses | 2.11% | |||
| Neuroses | 0.70% | Psychoses | 1.47% | |||
| Surgery-General | 1.73% | 2.49% | ||||
| Laceration/open wound | 1.10% | Laceration/open wound | 2.49% | |||
| Trauma | 0.17% | 0.68% | ||||
| Urology | 2.12% | 5.32% | ||||
| Symptoms | 0.61% | Urinary tract infection | 2.40% | |||
| Urinary tract infection | 0.53% | Symptoms | 1.20% | |||
| Calculus | 0.52% | |||||
Table notes: The percentages associated with each diagnosis within a clinical category may not sum to the percentage for the clinical category given that we only list diagnoses at 0.5 percent or higher.
The data presented in Table 3 do not account for all hospital outpatient setting claims, as some hospital outpatient setting services may be entirely procedural and, therefore, not accompanied by a separately identifiable E&M code.
Appendix D: Measures Potentially Relevant to the Hospital Outpatient Setting and Emergency Department
| Measure | Specialties | Source of Measure | Included in PQRI as of 6/1/07 |
|---|---|---|---|
| Prevention/Screening: | |||
| Breast Cancer Screening*+ | PC¹, OB/GYN | CMS/NCQA, AMA/PCPI, ICSI, ACOVE² | |
| Colorectal Cancer Screening*+ | PC, Gastroenterology | NCQA, AMA/PCPI, ICSI, ACOVE | |
| Colonoscopy: Procedure Complication Rate | Gastroenterology | Accreditation Assoc for Ambulatory Health Care (AAAHC) | |
| Colonoscopy: Patient Understanding of Procedure | Gastroenterology | AAAHC | |
| Colonoscopy-Polyp Surveillance: Cecal Intubation Documentation | Gastroenterology | American Gastroenterological Assoc Institute (AGAI) | |
| Colonoscopy-Polyp Surveillance: Rate of Cecal Intubation | Gastroenterology | AGAI | |
| Colonoscopy-Polyp Surveillance: Preparation Adequacy Documentation | Gastroenterology | AGAI | |
| Colonoscopy-Polyp Surveillance: Rate of Preparation Adequacy | Gastroenterology | AGAI | |
| Colonoscopy-Polyp Surveillance: Description of Polyp Characteristics | Gastroenterology | AGAI | |
| Colonoscopy-Polyp Surveillance: Assessment of Polyp Removal | Gastroenterology | AGAI | |
| Colonoscopy-Polyp Surveillance: Pathology Results Present and Reviewed | Gastroenterology, Pathology | AGAI | |
| Colonoscopy-Polyp Surveillance: Appropriateness of Follow-up Interval Recommended | Gastroenterology | AGAI | |
| Colonoscopy-Polyp Surveillance: Communication of Results and Follow-up Interval to PCP | Gastroenterology | AGAI | |
| Colonoscopy-Polyp Surveillance: Communication of Results and Follow-up Interval to Referral Source | Gastroenterology | AGAI | |
| Colonoscopy-Polyp Surveillance: Communication of Results and Follow-up Interval to the Patient | Gastroenterology | AGAI | |
| Colonoscopy: Abdominal Pain Within 30 Days | Gastroenterology | Wynn et al | |
| Colonoscopy: Hemorrhage Within 30 Days | Gastroenterology | Wynn et al | |
| Colonoscopy: Chest Pain Within 30 Days | Gastroenterology | Wynn et al | |
| Colonoscopy: Dyspnea Within 30 Days | Gastroenterology | Wynn et al | |
| Colonoscopy: Small Bowel Obstruction Within 30 Days | Gastroenterology | Wynn et al | |
| Colonoscopy: Arrythmia Within 30 Days | Gastroenterology | Wynn et al | |
| Colonoscopy: Vasovagal Reactions Within 30 Days | Gastroenterology | Wynn et al | |
| Colonoscopy: Sepsis and Other Infections Within 30 Days | Gastroenterology | Wynn et al | |
| Colonoscopy: Abdominal Distention Within 30 Days | Gastroenterology | Wynn et al | |
| Colonoscopy: Other Complications Within 30 Days | Gastroenterology | Wynn et al | |
| Colonoscopy: Hypotension Within 30 Days | Gastroenterology | Wynn et al | |
| Colonoscopy: Perforation Within 30 Days | Gastroenterology | Wynn et al | |
| Colonoscopy: Splenic Rupture Within 30 Days | Gastroenterology | Wynn et al | |
| Colonoscopy: Altered Mental Status Within 30 Days | Gastroenterology | Wynn et al | |
| Colonoscopy: Endocarditis Within 30 Days | Gastroenterology | Wynn et al | |
| Colonoscopy: Hypoxia Within 30 Days | Gastroenterology | Wynn et al | |
| Colonoscopy: Hypertension Within 30 Days | Gastroenterology | Wynn et al | |
| Colonoscopy: Death Within 1 Week | Gastroenterology | Wynn et al | |
| Cervical Cancer Screening*+ | PC, OB/GYN | NCQA, ICSI, ACOVE | |
| Avoid Pap Smear After Hysterectomy | PC, OB/GYN | ACOVE | |
| Follow up of Abnormal Pap Smear | PC, OB/GYN | ICSI, RAND | |
| Tobacco Use Assessment and Cessation*+ | PC, OB/GYN | AMA/PCPI, ICSI, ACOVE | |
| Smoking Cessation-Medical Assistance*+ | PC, OB/GYN, Specialists | NCQA, ACOVE | |
| Influenza Vaccination (50-64)*+ | PC | NCQA, AMA/PCPI, ICSI, | |
| Influenza Vaccination (65+)* | PC | CMS/NCQA, AMA/PCPI, ICSI, ACOVE | |
| Pneumonia Vaccination*+ | PC | NCQA, AMA/PCPI, ICSI, Resolution Health, ACOVE | |
| Tetanus-Diphtheria Booster | PC | ACOVE | |
| Drugs to be Avoided in the Elderly* | PC | NCQA, ACOVE | |
| Potentially Harmful Drug-Disease Interactions in the Elderly | PC | NCQA, ACOVE | |
| Annual Monitoring for Patients on Persistent Medications*+ | PC | NCQA, ACOVE | |
| Medication Reconciliation for Elderly (Care Coordination)+ | PC | AMA/PCPI, ACOVE | X |
| Documentation of Allergies and Adverse Reactions in Outpatient Medical Record* | PC | CMS/SCRIPT | X |
| Documentation of Medication List in the Outpatient Record* | PC | CMS/SCRIPT, ACOVE | |
| Advance Care Planning for Elderly+ | PC | AMA/PCPI, ACOVE | X |
| Screening for Fall Risk*+ | PC | AMA/PCPI, ACOVE | X |
| Screen for Problem Drinking | PC | AMA/PCPI, ACOVE | |
| Counseling for Problem Drinking | PC | ACOVE | |
| Counseling on Physical Activity in Older Adults* | PC | NCQA, ACOVE | |
| Obesity: BMI Documentation* | PC | NYC-DHMH, ACOVE | |
| Prevention and Management of Obesity | PC | ICSI, ACOVE | |
| Depression Screening for Older Adults | PC | ACOVE | |
| Osteoporosis Screening for Women (65+)* | PC, Orthopedics, Rheumatology, Endocrinology | NCQA, AMA/PCPI, ICSI, ACOVE | X |
| Osteoporosis Screening for Men with Risk Factors | PC | ACOVE | |
| Screening for Persistent Pain | PC | ACOVE | |
| Hormone Replacement Therapy: Risks and Benefits | PC, OB/GYN | ACOVE | |
| Screening for Elder Abuse | PC | ACOVE | |
| Comprehensive Geriatrics Assessment | PC | ACOVE | |
| Comprehensive Eye Exam | PC, Ophthalmology | ACOVE | |
| Cognitive and Functional Screening | PC | ACOVE | |
| Annual Evaluation for Changes in Memory, Function | PC | ACOVE | |
| Annual Evaluation of Hearing Status | PC | ACOVE | |
| Annual Screening for Sleep Disorders | PC | ACOVE | |
| Allergies/Sinus: | |||
| Rhinitis: Prophylactic Medication | PC, Immunology, ENT, Pulmonology | ICSI | |
| Acute Sinusitis: Sinus X-Ray After Initial Visit | PC, Immunology, ENT, Pulmonology | ICSI | |
| Acute Sinusitis: First Line Antibiotic When an Antibiotic is Prescribed | PC, Immunology, ENT, Pulmonology | ICSI | |
| Ambulatory Surgery: | |||
| Patients Having a Preoperative Health Assessment and Any Adjunctive Evaluation Prior to Scheduled Procedure | All Surgery, PC, Anesthesiology | ICSI, ACOVE | |
| Capacity to Consent to Surgery | All Surgery, PC | ACOVE | |
| Preoperative Discussion | All Surgery | ACOVE | |
| Preoperative Diabetes Evaluation | All Surgery, PC | ACOVE | |
| Preoperative Delirium Assessment | All Surgery, PC | ACOVE | |
| Timing of Prophylactic Antibiotic-Ordering Physician+ | General, Orthopedic, Colorectal, Hand, Plastic, Thoracic, Vascular | AMA/PCPI | X |
| Timing of Prophylactic Antibiotic-Administering Physician+ | Anesthesiology, All Surgery | AMA/PCPI | X |
| Antibiotic Selection+ | General, Orthopedic, Colorectal, Hand, Plastic, Thoracic, Vascular | AMA/PCPI | X |
| Antibiotic Discontinuation within 24 Hours+ | General, Orthopedic, Colorectal, Hand, Plastic, Thoracic, Vascular | AMA/PCPI | X |
| Venous Thromboembolism Prophylaxis*+ | General, Orthopedic, Colorectal, Hand, Plastic, Thoracic, Vascular | AMA/PCPI | X |
| Selection of IV Antibiotic Administration | All Surgery | CMS | |
| Behavioral Health: | |||
| Follow-up After Hospitalization for Mental Illness | Psychiatry, PC | NCQA, ICSI, ACOVE | |
| Major Depressive Disorder: Diagnostic Evaluation* | Psychiatry | AMA/PCPI, ACOVE | |
| Major Depressive Disorder: Suicide Risk Assessment* | Psychiatry, PC | AMA/PCPI, ACOVE | |
| New Episode of Depression: Evaluate for Co-Morbid Conditions | Psychiatry, PC | ACOVE | |
| New Episode of Depression: Optimal Practitioner Contacts for Medication Management* | Psychiatry, PC | NCQA | |
| Depression: Acute Phase Treatment*+ | Psychiatry, PC | NCQA | X |
| Depression: Continuation Phase Treatment*+ | Psychiatry, PC | NCQA, AMA/PCPI | |
| Depression: Severity Classification | Psychiatry | AMA/PCPI | |
| Depression Treatment: Psychotherapy, Medication Management, and/or ECT | Psychiatry, PC | AMA/PCPI, ACOVE | |
| Depression: Antidepressant Choice | Psychiatry, PC | ACOVE | |
| Depression: Psychotic Depression Treatment | Psychiatry | ACOVE | |
| Depression: ECG for Tricyclic Use | Psychiatry, PC | ACOVE | |
| Depression: Interactions with MAOI | Psychiatry, PC | ACOVE | |
| Depression: Follow-up- Response and Medication Side Effects Documented | Psychiatry, PC | ACOVE | |
| Depression: Follow-up — Suicide Risk | Psychiatry, PC | ACOVE | |
| Depression: Follow-up 6 Weeks-No Symptom Response | Psychiatry, PC | ACOVE | |
| Depression: Follow-up 12 Weeks-Partial Response | Psychiatry, PC | ACOVE | |
| Depression: Continuing Therapy | Psychiatry, PC | ACOVE | |
| Depression: Maintenance Therapy | Psychiatry, PC | ACOVE | |
| Depression: Patients who Attain a 5 Point or Greater Reduction in Patient Health Questionnaire (PHQ) Score Within 6 Months After Their New Episode PHQ | Psychiatry, PC | Heath Resources and Services Administration (HRSA) | |
| Depression: Documented PHQ Reassessment Between 4-8 Weeks After New Episode PHQ | Psychiatry, PC | HRSA | |
| Depression: Follow up 1-3 Weeks After New Episode PHQ | Psychiatry, PC | HRSA | |
| Depression: Antidepressant and/or Psychotherapy Within 1 Month of Last New Episode PHQ. | Psychiatry, PC | HRSA | |
| Depression: 50% or Greater Reduction in PHQ 4 Months or Longer After Last New Episode PHQ | Psychiatry, PC | HRSA | |
| Depression: PHQ Score < 5, 4 Months or Longer After Last New Episode PHQ | Psychiatry, PC | HRSA | |
| Depression: Patients With a Diagnosis of Minor Depression, Depression NOS, or Adjustment Disorder Who Are Not on an Antidepressant | Psychiatry, PC | HRSA | |
| Depression: Diagnosis of Depression and a PHQ Score Within Last 6 Months | Psychiatry, PC | HRSA | |
| Depression: Patients Reporting an Improvement in Function | Psychiatry, PC | HRSA | |
| Depression: Documented Self-Management Goals Set Within Last 12 Months | Psychiatry, PC | HRSA | |
| Depression: Patients With a Diagnosis of Major Depression or Dysthymia Taking an Antidepressant | Psychiatry, PC | HRSA | |
| Depression: Patients With a Diagnosis of Major Depression or Dysthymia Who Have Been on an Antidepressant for At Least 6 Mos | Psychiatry, PC | HRSA | |
| Bipolar Disorder and Major Depression: Assessment for Manic or Hypomanic Behaviors* | Psychiatry | STABLE Project | |
| Bipolar Disorder and Major Depression: Appraisal for Alcohol or Chemical Substance Abuse* | Psychiatry | STABLE Project | |
| Bipolar Disorder: Appraisal for Risk of Suicide* | Psychiatry | STABLE Project | |
| Bipolar Disorder: Level of Function Evaluation* | Psychiatry | STABLE Project | |
| Bipolar Disorder: Assessment for Diabetes* | Psychiatry, PC | STABLE Project | |
| Initiation and Engagement of Alcohol and Other Drug Dependence Treatment* | Psychiatry, PC | NCQA | |
| Dementia: Cognitive Evaluation | PC, Neurology | ACOVE | |
| Dementia: Medication Review | PC, Neurology | ACOVE | |
| Dementia: Medication Changes | PC, Neurology | ACOVE | |
| Dementia: Neurologic Examination | PC, Neurology | ACOVE | |
| Dementia: Laboratory Testing | PC, Neurology | ACOVE | |
| Dementia: HIV Testing | PC, Neurology | ACOVE | |
| Dementia: Depression Screening | PC, Psychiatry, Neurology | ACOVE | |
| Dementia: Alzheimer’s, Vascular Dementia, Lewy Body Dementia- Medication Discussion | PC, Neurology | ACOVE | |
| Dementia: Moderate Vascular or Mixed Dementia- Stroke Prophylaxis | PC, Neurology | ACOVE | |
| Dementia: Caregiver Support and Patient Safety | PC, Neurology | ACOVE | |
| Dementia: Behavioral/Psychological Symptoms | PC, Psychiatry | ACOVE | |
| Dementia: Behavioral Interventions and Pharmacotherapy | Psychiatry, Neurology | ACOVE | |
| Dementia: Antipsychotic Risk/Benefit Discussion | Psychiatry, Neurology | ACOVE | |
| Dementia: Driving | PC, Psychiatry, Neurology | ACOVE | |
| Bone and Joint Conditions: | |||
| Osteoporosis Management in Women Who Had a Fracture* | PC, Orthopedics, Rheumatology, Endocrinology | NCQA,AMA/PCPI, ACOVE | X |
| Osteoporosis: Communication with Physician Managing* Care Post Fracture | Ortho, Rheumatology, Endocrinology, | AMA/PCPI | X |
| Osteoporosis: Pharmacologic Therapy-Female* | PC, OB/Gyn, Orthopedics, Rheumatology, Endocrinology | AMA/PCPI, ACOVE | X |
| Osteoporosis Pharmacologic Therapy for Males | PC, Orthopedics, Rheumatology, Endocrinology | ACOVE | |
| Osteoporosis: Testosterone for Males | PC, Orthopedics, Rheumatology, Endocrinology | ACOVE | |
| Osteoporosis: Counseling for Vitamin D, Calcium Intake, Exercise | PC, Orthopedics, Rheumatology, Endocrinology | AMA/PCPI, ACOVE | X |
| Osteoporosis: DXA Measurement for Glucocorticosteroids and Other Secondary Causes | PC, Orthopedics, Rheumatology, Endocrinology | AMA/PCPI | |
| Osteoporosis: Prophylaxis for Steroids | PC, Orthopedics, Rheumatology, Endocrinology | ACOVE | |
| Osteoarthritis: Functional and Pain Assessment* | PC, Orthopedics, Rheumatology | AMA/PCPI, ACOVE | |
| Osteoarthritis: Physical Examination of the Involved Joint | PC, Orthopedics, Rheumatology | AMA/PCPI | |
| Osteoarthritis: Assessment for OTC Medications* | PC, Orthopedics, Rheumatology | AMA/PCPI, ACOVE | |
| Osteoarthritis: Anti-inflammatory/Analgesic Therapy | PC, Orthopedics, Rheumatology | AMA/PCPI | |
| Osteoarthritis: NSAID Risk Assessment | PC, Orthopedics, Rheumatology | AMA/PCPI | |
| Osteoarthritis: Gastrointestinal Prophylaxis | PC, Orthopedics, Rheumatology | AMA/PCPI | |
| Osteoarthritis: Therapeutic Exercise for the Involved Joint | PC, Orthopedics, Rheumatology | AMA/PCPI, ICSI, ACOVE | |
| Osteoarthritis: Patient Education | PC, Orthopedics, Rheumatology | Arthritis Foundation | |
| Osteoarthritis: Radiograph For Worsening Condition | PC, Orthopedics, Rheumatology | Arthritis Foundation | |
| Osteoarthritis: Referral to Orthopedic Surgeon | PC, Rheumatology | Arthritis Foundation, ACOVE | |
| Osteoarthritis: Advised to Lose Weight | PC, Orthopedics, Rheumatology | Arthritis Foundation | |
| Osteoarthritis: Referred to Weight Loss Program | PC, Orthopedics, Rheumatology | Arthritis Foundation | |
| Osteoarthritis: Ambulatory Assistive Devices | PC, Orthopedics, Rheumatology | Arthritis Foundation, ACOVE | |
| Osteoarthritis: Non-Ambulatory Assistive Devices | PC, Orthopedics, Rheumatology | Arthritis Foundation, ACOVE | |
| Degenerative Joint Disease (DJD) of the Knee: X-Rays Including a Standing View of the Knee | PC, Orthopedics, Rheumatology | ICSI | |
| DJD of the Knee: Documented Education on Protecting the Joint, Exercise, Pain Relief, Healthy Habits | PC, Orthopedics, Rheumatology | ICSI | |
| Use of Imaging Studies for Low Back Pain* | PC, Orthopedics, Radiology | NCQA, ICSI | |
| Relative Resource Use for Acute Low Back Pain | PC, Orthopedics, Rheumatology Radiology | NCQA | |
| Arthritis: Disease Modifying Anti-Rheumatic Drug Therapy in Rheumatoid Arthritis* | Rheumatology | NCQA | |
| Ankle Sprain: X-Rays Within 3 Days of Initial Injury | PC | ICSI | |
| Ankle Sprain: Documentation of Patient Education | PC | ICSI | |
| Change in Foot/Ankle Functional Status | PT | Focus on Treatment Outcomes (FOTO) | |
| Change in Hip Functional Status | PT | FOTO | |
| Change in Knee Functional Status | PT | FOTO | |
| Change in Lumbar Functional Status | PT | FOTO | |
| Change in Physical Functional Status | PT | FOTO | |
| Change in Shoulder Functional Status | PT | FOTO | |
| Cancer-Blood: | |||
| Myelodyplastic Syndrome (MDS): Cytogenetic Testing on Bone Marrow+ | Hematology, Oncology | AMA/PCPI | X |
| MDS: Iron Stores Prior to Erythropoietin Therapy+ | Hematology, Oncology | AMA/PCPI | X |
| Multiple Myloma: Treatment with Biophosphonates+ | Hematology, Oncology | AMA/PCPI | X |
| Chronic Lymphocytic Leukemia: Baseline Flow Cytometry+ | Hematology, Oncology | AMA/PCPI | X |
| Non Hodgkin’s Lymphoma (Aggressive): White Blood Cell Colony Stimulating Factors for Patients >60 Undergoing Chemotherapy | Hematology, Oncology | ASSIST | |
| Cancer-Breast: | |||
| Diagnosis: Average Number of Days Between Breast Abnormality and Biopsy | PC, OB-GYN, Radiology, Oncology | ICSI | |
| Diagnosis: Class 4-5 Abnormal Mammograms Followed by a Biopsy Within 14 Days | PC, OB/GYN, Oncology | ICSI | |
| Patients with Stage 0, I, II or III Breast Cancer With Documentation of Discussion of Clinical Trials | Oncology | ICSI | |
| Hormonal Therapy for Stage IC-III , ER/PR Positive Breast Cancer *+ | Oncology | National Cancer Care Network/American Society of Clinical Oncology (NCCN/ASCO), ACOVE | X |
| Radiation Therapy for Invasive Breast Cancer Patients Who Have Undergone Breast Conserving Therapy* + | Oncology, Radiation Oncology | NCCN/ASCO, ACOVE | X |
| Patients < 70 with Stage II-III Breast Cancer Receiving Adjuvant Chemo within 120 Days After Diagnosis* | Oncology | NCCN/ASCO | |
| Trastuzumab Administration for Her2Neu Positive Patients | Oncology | NCCN/ASCO | |
| Biphosphonates for Patients with Bone Metastases | Oncology | NCCN/ASCO, ACOVE | |
| Creatinine Assessed for Patients Receiving Biphosphonates | Oncology | NCCN/ASCO | |
| Resection Pathology Report Includes the pT Category and Histologic Grade | Pathology | AMA/PCPI | |
| Breast Cancer Diagnosis: History-Physical and Psychosocial Performance Status | Surgery, Oncology | ACOVE | |
| Breast Cancer Diagnosis: History-Co-morbid Illnesses | Surgery, Oncology | ACOVE | |
| Breast Cancer Diagnosis: Discussion of Options | Surgery, Oncology | ACOVE | |
| Breast Cancer Diagnosis: Surgical Documentation | Surgery | ACOVE | |
| Breast Cancer Diagnosis: Estrogen Receptor Status Documented | Surgery, Pathology | ACOVE | |
| Breast Cancer Diagnosis: HER-2/neu Receptor Status Documented | Surgery, Pathology | ACOVE | |
| Breast Cancer Diagnosis: HER-2/neu Receptor Status Confirmed | Surgery, Pathology | ACOVE | |
| Breast Cancer Diagnosis: Bone Evaluation | Oncology | ACOVE | |
| Breast Cancer Diagnosis: Surgical Care- Axillary Staging | Surgery | ACOVE | |
| Breast Cancer Diagnosis: Surgical Care-Lobular Carcinoma In-Situ | Surgery | ACOVE | |
| Breast Cancer Diagnosis: Surgical Care-DCIS | Surgery | ACOVE | |
| Breast Cancer Diagnosis: Surgical Care-Mastectomy, Breast Reconstruction | Surgery | ACOVE | |
| Breast Cancer Diagnosis: Radiation Therapy-Lumpectomy | Oncology, Radiation Oncology | ACOVE | |
| Breast Cancer Diagnosis: Radiation Therapy-Mastectomy | Oncology, Radiation Oncology | ACOVE | |
| Breast Cancer Diagnosis: Adjuvant Chemotherapy | Oncology | ACOVE | |
| Breast Cancer Diagnosis: Adjuvant Chemotherapy and Trastuzumab | Oncology | ACOVE | |
| Breast Cancer Diagnosis: Treatment-Limited Surveillance | Oncology | ACOVE | |
| Breast Cancer Diagnosis: Metastatic Disease-Endocrine Therapy | Oncology | ACOVE | |
| Breast Cancer Diagnosis: Metastatic Disease-Chemotherapy Offered | Oncology | ACOVE | |
| Breast Cancer Diagnosis: Metastatic Disease-Trastuzumab Offered | Oncology | ACOVE | |
| Nausea and Vomiting-3-Drug Regimen Post Chemotherapy of Moderate Acute and Delayed Emetic Risk | Oncology | ASSIST | |
| Cancer-Colorectal: | |||
| Post Operative Adjuvant Chemo Within 9 Months After Diagnosis of Stage II-III Rectal Cancer | Oncology, Surgery/Colorectal Surgery | NCCN/ASCO | |
| Pelvic Radiation Therapy Before or After Surgery for Stage II-III Rectal Cancer | Oncology, Surgery/Colorectal Surgery | NCCN/ASCO | |
| Chemotherapy for Stage III Colon Cancer Patients w/in 4 mos *+ | Oncology, Surgery/Colorectal Surgery | NCCN/ASCO, ACOVE | X |
| Carcinoembryonic Antigen (CEA) Assessed for Colon and Rectal Cancers | Oncology, Surgery/Colorectal Surgery | ASCO, ACOVE | |
| Chemotherapy Recommended Appropriately for Colon and Rectal Cancers | Oncology, Surgery/Colorectal Surgery | ASCO | |
| Colorectal Cancer Pathology Reporting: pT Category and pN Category with Histologic Grade | Pathology | AMA/PCPI | |
| History-Physical and Psychosocial Status | Surgery/Colorectal Surgery | ACOVE | |
| History-Co-Morbid Illness | Surgery/Colorectal Surgery | ACOVE | |
| Staging Evaluation-CT scan | Surgery/Colorectal Surgery | ACOVE | |
| Staging Evaluation-Ultrasound, MRI or CT | Surgery/Colorectal Surgery | ACOVE | |
| Colon Examination Prior to Surgery | Surgery/Colorectal Surgery | ACOVE | |
| Colon Exam After Surgery | Surgery/Colorectal Surgery | ACOVE | |
| Discussion of Options | Surgery/Colorectal Surgery, Oncology | ACOVE | |
| Discussion of Surgical Findings | Surgery/Colorectal Surgery, Oncology | ACOVE | |
| Non-Surgical Treatment Plan | Surgery/Colorectal Surgery, Oncology | ACOVE | |
| Preoperative Exam | Surgery/Colorectal Surgery | ACOVE | |
| Preoperative Ostomy Sitting | Surgery/Colorectal Surgery | ACOVE | |
| Adjuvant Therapy: Preoperative Neoadjuvant Chemotherapy and/or Radiation | Oncology, Radiation Oncology | ACOVE | |
| Post-Operative Surveillance: History and Physical Exam | Surgery/Colorectal Surgery, PC, Oncology | ACOVE | |
| Post-Operative Surveillance: CEA Level | Oncology, PC | ACOVE | |
| Post-Operative Surveillance: Colonoscopy | Oncology, PC | ACOVE | |
| Post-Operative Surveillance: Evaluate Rising CEA | Oncology, PC | ACOVE | |
| Cancer-Head and Neck: | |||
| Mucositis: Midline Radiation Blocks and Three Dimensional Treatments for Patients Undergoing Radiation | Radiation Oncology | ASSIST | |
| Cancer-Lung: | |||
| Dyspnea: Symptom Management or Treatment | Oncology | ASSIST | |
| Cancer-Prostate: | |||
| Number of Patients a Physician Has Treated | Urology, Oncology | Litwin et al | |
| Availability of Radiation Oncology Facilities and Psychological Counseling for Patients | Urology, Oncology, Radiation Oncology | Litwin et al | |
| Board Certification of Urologist and Radiation Oncologists | Urology, Oncology, Radiation Oncology | Litwin et al | |
| Information About Outcomes for Patients Treated by an Institution | Urology, Oncology, Radiation Oncology | Litwin et al | |
| Assess Stage of Disease Before Treatment Begins | Urology, Oncology, Radiation Oncology | Litwin et al | |
| Document Pre-Treatment Urinary, Sexual and Bowel Function | Urology, Oncology, Radiation Oncology | Litwin et al | |
| Assess Family History of Prostate Cancer | Urology, Oncology, Radiation Oncology | Litwin et al | |
| Give Treatment Choices, Opportunity for Consultation, Description of Risk | Urology, Oncology, Radiation Oncology | Litwin et al | |
| Management of Pathology Specimens | Pathology | Litwin et al | |
| Use of Computerized Tomography to Plan Treatment | Oncology, Radiation Oncology | Litwin et al | |
| Immobilizing Patient During Treatment | Oncology, Radiation Oncology | Litwin et al | |
| Delivering Recommended Doses of Radiation | Oncology, Radiation Oncology | Litwin et al | |
| Follow-up After Treatment | Oncology, Urology, Radiation Oncology | Litwin et al | |
| Communicating with PCP | Urology, Oncology, Radiation Oncology | Litwin et al | |
| Treatment Failure Detected by Biochemical Tests | Urology, Oncology, Radiation Oncology | Litwin et al | |
| Hospitalization or Medical or Surgical Treatment for Serious Complications | Urology, Oncology, Radiation Oncology | Litwin et al | |
| Patients’ Assessment of Urinary, Sexual and Bowel Functioning After Treatment | Urology, Oncology, Radiation Oncology | Litwin et al | |
| Patient’s Satisfaction with Treatment Choice, Continence, and Potency | Urology, Oncology, Radiation Oncology | Litwin et al | |
| Cancer-General: | |||
| Pathology Report in the Chart | Oncology | ASCO | |
| Staging Documented | Oncology | ASCO | |
| Clinical Trials Assessment | Oncology | ASCO | |
| Pain Assessment on First Visit | Oncology | ASCO, ACOVE, ASSIST | |
| Treatment of Severe Pain | Oncology | ACOVE, ASSIST | |
| Effectiveness of Pain Medication Assessed After Prescription | Oncology | ASCO, ASSIST | |
| Documented Plan for Chemotherapy+ | Oncology | ASCO | X |
| Flow Sheet for Chemotherapy | Oncology | ASCO | |
| Consent for Chemotherapy in Chart | Oncology | ASCO | |
| Creatinine Assessed For Patients Receiving Cisplatin | Oncology | ASCO | |
| Chemotherapy-Related Documentation and Patient Discussions | Oncology | ASCO, ASSIST | |
| Smoking Cessation | Oncology | ASCO | |
| Monthly Patient Evaluation | Oncology | ASCO | |
| Administration of Entiemetic Medications | Oncology | ASCO, ASSIST | |
| Erythroid Growth Factor Administration | Oncology | ASCO | |
| Comfortable Dying* | Oncology, PC, Palliative Care | National Hospice and Palliative Care Org (NHPCO) | |
| Family Evaluation of Hospice Care * | Hospice Provider, Palliative Care | NHPCO | |
| ER Visits in Last 30 Days of Life | Oncology, PC | Dana Farber Cancer Institute (DFCI) | |
| Hospitalizations in the Last 30 Days of Life* | Oncology, PC | DFCI | |
| ICU Admission in the Last 30 Days of Life* | Oncology, PC | DFCI | |
| Not Admitted to Hospice* | Oncology, PC | DFCI | |
| Admitted to Hospice for < 3 Days * | Oncology, PC | DFCI | |
| Death in an Acute Care Setting* | Oncology, PC | DFCI | |
| Pain: Assess Likely Etiology | Oncology, PC | ASSIST | |
| Pain: Assessment of Functional Impairment | Oncology, PC | ASSIST | |
| Pain: Education if Starting Pharmacologic Treatment | Oncology, PC | ASSIST | |
| Pain: Long-Acting and Short Acting Opioids | Oncology, PC | ASSIST | |
| Pain: Bowel Regimen if Chronic Opioid Treatment | Oncology, PC | ASSIST | |
| Pain: Dose of Opioids Across Care Settings | Oncology, PC | ASSIST | |
| Pain: Change in Pain Regimen for Severe or Worsening Pain | Oncology, PC | ASSIST | |
| Pain: Changes in Regimen Assessed at Next Visit | Oncology, PC | ASSIST | |
| Pain: Single Fraction Radiation For Bone Metastasis | Oncology, PC | ASSIST | |
| Pain: Steroids for Spinal Cord Compression | Oncology, PC | ASSIST | |
| Pain: MRI for New Neurological Symptoms or Potential Spinal Chord Compression | Oncology, PC | ASSIST | |
| Pain: Radiotherapy or Surgical Decompression Within 24 Hours for Confirmed Spinal Chord Compression | Oncology, PC | ASSIST | |
| Pain: Follow-up Neurologic Symptoms After Treatment for Spinal Chord Compression | Oncology, PC | ASSIST | |
| Depression: Screen Within One Month of Diagnosis | Oncology, PC | ASSIST | |
| Depression: Screen for Newly Diagnosed Patients Undergoing Chemotherapy or Radiotherapy | Oncology, PC | ASSIST | |
| Depression: Treatment Plan | Oncology, PC | ASSIST | |
| Depression: Response to Therapy Documented Within 6 Weeks | Oncology, PC | ASSIST | |
| Depression: Assess if Expression of Desire for Hastened Death | Oncology, PC | ASSIST | |
| Nausea and Vomiting: Assess at Every Visit if Chemotherapy or Advanced Cancer Affection Gastrointestinal Tract or Abdomen | Oncology, PC | ASSIST | |
| Nausea and Vomiting: 3-Drug Regimen Prior to Chemotherapy With High Acute Emetic Risk | Oncology, PC | ASSIST | |
| Nausea and Vomiting: 2-Drug Regimen Post Chemotherapy With a High Delayed Emetic Risk | Oncology, PC | ASSIST | |
| Nausea and Vomiting: 2-Drug Regimen Prior to Chemotherapy With a Moderate Acute Emetic Risk | Oncology, PC | ASSIST | |
| Nausea and Vomiting: 5-HT3 Receptor Antagonist or Dexamethasone Post Chemotherapy With a Moderate Delayed Emetic Risk | Oncology, PC | ASSIST | |
| Nausea and Vomiting: Post-Chemotherapy Communication Plan for High to Moderately Emetic Chemotherapy Regimen | Oncology, PC | ASSIST | |
| Nausea and Vomiting: Assess for Underlying Causes if no Chemotherapy or Radiation | Oncology, PC | ASSIST | |
| Nausea and Vomiting: Evaluate Treatment With Antiemetic Medication Before or on Next Visit | Oncology, PC | ASSIST | |
| Fatigue: Assessment of Fatigue if Undergoing Chemotherapy | Oncology, PC | ASSIST | |
| Fatigue: Assessment of Fatigue if New Diagnosis of Advanced Cancer | Oncology, PC | ASSIST | |
| Fatigue: Assessment for Insomnia or Depression if New Fatigue | Oncology, PC | ASSIST | |
| Fatigue: Assessment For Response to Treatment | Oncology, PC | ASSIST | |
| Anemia: Assess Presence or Absence of Anemia-Related Symptoms for Hemoglobin < 10g/dl | Oncology, PC | ASSIST | |
| Anemia: Transfusion Offered for Severe Symptomatic Anemia | Oncology, PC | ASSIST | |
| Anemia: ESP Treatment Discontinued if no Significant Hematological Response | Oncology, PC | ASSIST | |
| Fatigue/Anemia: Assessment for Presence of Anorexia or Dysphagia For Cancers Affecting the Oropharynx or Gastrointestinal Tract or Advanced Cancers | Oncology, PC | ASSIST | |
| Fatigue/Anemia: Evaluation For New Anorexia for Constipation, Nausea or Vomiting, Oral Discomfort, Depression or Dysphagia | Oncology, PC | ASSIST | |
| Fatigue/Anemia: Nutritional Counseling When Treatment Affects Nutritional Intake | Oncology, PC | ASSIST | |
| Fatigue/Anemia: Treatment of Underlying Cause of Anorexia | Oncology, PC | ASSIST | |
| Fatigue/Anemia: Assessment of Treatment for Anorexia | Oncology, PC | ASSIST | |
| Fatigue/Anemia: Assessment Prior to Treatment with Enteral or Parenteral Nutrition | Oncology, PC | ASSIST | |
| Dyspnea: Document Cause of New or Worsening Dyspnea | Oncology, PC | ASSIST | |
| Dyspnea: Symptomatic Management or Treatment | Oncology, PC | ASSIST | |
| Dyspnea: Opioids For Advanced Cancer When Non-Opiod Medications Not Effective | Oncology, PC | ASSIST | |
| Dyspnea: Thoracentesis if Malignant Pleural Effusion | Oncology, PC | ASSIST | |
| Dyspnea: Repeat Assessment of Dyspnea if Thoracentesis | Oncology, PC | ASSIST | |
| Dyspnea: Pleurodesis or Drainage Procedure if Reaccumulation and Dyspnea After Thoracentesis | Oncology, PC | ASSIST | |
| Mucositis: Oral Care Protocols Established Prior to Treatment | Oncology, PC | ASSIST | |
| Mucositis: Prophylactic Use of Palifermin For High Dose Chemotherapy or Total Body Irradiation Followed by Stem Cell Transplantation | Oncology, PC | ASSIST | |
| Mucositis: Documentation of Severity During Cytotoxic Treatments | Oncology, PC | ASSIST | |
| Mucositis: Evaluate Presence or Absence of Pain | Oncology, PC | ASSIST | |
| Mucositis: Analgesic For Pain Secondary to Treatment-Related Mucositis | Oncology, PC | ASSIST | |
| Mucositis: Nutritional Assessment Prior to Treatment | Oncology, PC | ASSIST | |
| Mucositis: Re-evaluate Mild to Moderate Mucositis Within 1 Week | Oncology, PC | ASSIST | |
| Mucositis: Re-evaluate Severe Mucositis Within 1-3 days | Oncology, PC | ASSIST | |
| Diarrhea: Assess History and Symptoms if Chemotherapy | Oncology, PC | ASSIST | |
| Diarrhea: Antidiarrheal Agent on or Before Chemotherapy if High Risk of Chemotherapy Inducement | Oncology, PC | ASSIST | |
| Diarrhea: Post-Chemotherapy Communication Plan if High Risk of Chemotherapy Inducement | Oncology, PC | ASSIST | |
| Delirium: Antipsychotic for Terminal Restlessness for Patients with Advanced Cancer | Oncology, PC | ASSIST | |
| Insomnia: Assessment for Depression or Pain | Oncology, PC | ASSIST | |
| Neutropenia: Evaluation for Patients on Chemotherapy with Fever | Oncology, PC | ASSIST | |
| Skin Rash: Education for Patients Undergoing Radiation Treatment | Oncology, PC | ASSIST | |
| Skin Rash: Treatment for Radiation-Induced Dermatitis | Oncology, PC | ASSIST | |
| Skin Rash: Evaluate if Treatment with Agents that Block Epidermal Growth Factor | Oncology, PC | ASSIST | |
| Care Planning, Advanced Cancer: Discussion of Prognosis and Advance Care Planning for Patients with Newly Discovered Advanced Cancer | Oncology, PC | ASSIST | |
| Care Planning, Advanced Cancer: Documentation of Advance Directive or Surrogate Decision Maker for Advanced Cancer | Oncology, PC | ASSIST | |
| Care Planning, Advanced Cancer: Documentation of Assessment of Pain, Spiritual Concerns, Caregiver Burdens, Financial Concerns | Oncology, PC | ASSIST | |
| Care Planning, Advanced Cancer: Referral for Palliative Care | Oncology, PC | ASSIST | |
| Care Planning, Advanced Cancer: Discussion of Prognosis and Planning for Patients with Central Nervous System Metastases | Oncology, PC | ASSIST | |
| Care Planning, Advanced Cancer: Planning Should Occur Prior to Beginning a New Chemotherapy Regimen | Oncology, PC | ASSIST | |
| Care Planning, Advanced Cancer: Document Goals of Care Before Interventions (New Hemodialysis, Pacemaker or ICD Placement, Major Surgery, Gastric Tube Placement) | Oncology, PC | ASSIST | |
| Information: Diagnosis Communicated with a Translator if the Patient Speaks a Primary Language that the Physician Does Not Speak Fluently | Oncology, PC | ASSIST | |
| Cardiovascular: | |||
| Electrocardiogram for Syncope*+ | Emergency, Cardiology, Neurology | AMA/PCPI | X |
| AMI: Electrocardiogram for Non-Traumatic Chest Pain*+ (physician) | Emergency | AMA/PCPI | X |
| AMI/ACS: Aspirin at Arrival*+ (physician) | Emergency | AMA/PCPI, ACOVE | X |
| AMI: Aspirin at Arrival (ED) | Emergency | OK QIO | |
| AMI/ACS: Beta Blocker at Arrival | Emergency | ICSI, ACOVE | X |
| AMI: Fibrinolytic/Thrombolytic Therapy Ordered+ | Emergency, Cardiology | AMA/PCPI, ICSI, ACOVE | |
| AMI: Median Time to Fibrinolysis (ED) | Emergency, Cardiology | OK QIO | |
| AMI: Fibrinolytic Therapy Received Within 30 Minutes (ED) | Emergency, Cardiology | OK QIO | |
| AMI: Median Time to ECG (ED) | Emergency, Cardiology | OK QIO | |
| AMI: Median Time to Transfer to Another Facility (ED) | Emergency, Cardiology | OK QIO | |
| AMI: Care Coordination for PCI for AMI (communication with cardiology within 10 minutes of ECG)+ | Cardiology, Emergency | AMA/PCPI | |
| AMI: LVF Assessment (within 7 days of discharge) | Cardiology | ACOVE | |
| AMI: Depression Screening | Cardiology, PC | ACOVE | |
| MI or CABG: Cardiac Rehabilitation | Cardiology | ACOVE | |
| ACS: Non-Invasive Stress Testing (within 2 weeks of discharge) | Cardiology, PC | ACOVE | |
| ACS/Chest Pain: IV Access, Oxygen, Nitroglycerin, Morphine, Aspirin | Emergency | ICSI | |
| CAD: Antiplatelet Therapy*+ | Cardiology, PC | AMA/PCPI, ICSI, ACOVE | X |
| CAD: Drug Therapy for Lowering Cholesterol*+ | Cardiology, PC | AMA/PCPI | |
| CAD: Beta Blocker Therapy-Post MI*+ | Cardiology, PC | NCQA, AMA/PCPI, ACOVE | X |
| CAD: Persistent Beta Blocker Treatment After Heart Attack*+ | Cardiology, PC | NCQA, ACOVE | |
| CAD: Blood Pressure Management* | Cardiology, PC | NCQA, AMA/PCPI | |
| CAD: Percentage of Members who Have Optimally Managed Modifiable Risk Factors* | Cardiology, PC | Health Partners | |
| CAD/IVD: Lipid Profile and LDL Control* | Cardiology, PC | NCQA, AMA/PCPI. ICSI, ACOVE | |
| CAD: Drug Therapy for LDL-Cholesterol* | Cardiology, PC | AMA/PCPI | |
| CAD: Symptom and Activity Assessment* | Cardiology, PC | AMA/PCPI | |
| CAD: ACEI/ARB Therapy* | Cardiology, PC | AMA/PCPI, ACOVE | |
| CAD: Smoking Cessation | Cardiology, PC | AMA/PCPI, ACOVE | |
| CAD: Screen for Diabetes | Cardiology, PC | AMA/PCPI | |
| CAD: Estrogen/Progesterone Counseling | Cardiology, PC | ACOVE | |
| IVD: Use of Aspirin or other Antithrombotic | Cardiology, PC | NCQA, ACOVE | |
| HF: History | Cardiology, PC | ACOVE | |
| HF: ACEI/ARB Therapy*+ | Cardiology, PC | AMA/PCPI, ICSI, ACOVE | X |
| HF: LVF Assessment*+ | Cardiology, PC | AMA/PCPI, ICSI, ACOVE | |
| HF: Diagnostic Testing | Cardiology, PC | ACOVE | |
| HF: Weight Measurement* | Cardiology, PC | AMA/PCPI | |
| HF: Blood Pressure Measurement | Cardiology, PC | AMA/PCPI | |
| HF: Exam-New Diagnosis (Weight, BP, Lung Exam, Cardiac, Abdominal, Lower Extremity) | Cardiology, PC | ACOVE | |
| HF: Patient Education* | Cardiology, PC | AMA/PCPI, ACOVE | |
| HF: Beta Blocker Therapy*+ | Cardiology, PC | AMA/PCPI, ACOVE | X |
| HF: Warfarin Therapy for Patients with Atrial Fibrillation*+ | Cardiology, PC | AMA/PCPI , ICSI | |
| HF: Assessment of Clinical Symptoms of Volume Overload (Excess)* | Cardiology, PC | AMA/PCPI | |
| HF: Assessment of Activity Level* | Cardiology, PC | AMA/PCPI | |
| HF: Laboratory Tests | Cardiology, PC | AMA/PCPI | |
| HF: Calcium Channel Blocker Use | Cardiology, PC | ACOVE | |
| HF: Antiarrhythmic Use | Cardiology, PC | ACOVE | |
| HF: Digoxin Toxicity | Cardiology, PC | ACOVE | |
| HF: Outpatient Visit (Weight, BP, Heart Rate, Assessment of Volume Overload) | Cardiology, PC | ACOVE | |
| VTE: Patients Receiving a Baseline Platelet Count Before Starting Heparin | Cardiology, Hematology, PC | ICSI | |
| VTE: Leg Duplex Ultrasound With Depression | Cardiology, Hematology, PC | ICSI | |
| VTE: Patients Who Meet the Criteria for LMWH and for Whom LMWH is Used | Cardiology, Hematology, PC | ICSI | |
| VTE: Assessed for Graded Compression Stockings | Hematology, PC | ICSI | |
| VTE: Patients with a High Clinical Pretest Probability for PE Who Received LMWH During Evaluation | Hematology, PC, Pulmonology | ICSI | |
| VTE: Patients with DVT Treated in an Outpatient Setting | Hematology, PC | ICSI | |
| Relative Resource Use for People with Cardiovascular Conditions | PC, Cardiology | NCQA | |
| Dermatological Conditions: | |||
| Melanoma: Patient History+ | Dermatology | AMA/PCPI | X |
| Melanoma: Complete Physical Skin Exam+ | Dermatology | AMA/PCPI | X |
| Melanoma: Counseling on Self-Exam+ | Dermatology, PC | AMA/PCPI | X |
| Pressure Ulcers: Prevention Intervention-Pressure Reduction | PC | ACOVE | |
| Pressure Ulcers: Prevention Intervention- Nutritional Assessment | PC | ACOVE | |
| Pressure Ulcers: Assessment of Wound Characteristics | PC | ACOVE | |
| Pressure Ulcers: Pain Assessment and Treatment | PC | ACOVE | |
| Pressure Ulcers: Management-Debridement | PC | ACOVE | |
| Pressure Ulcers: Management-Wound Cleansing | PC | ACOVE | |
| Pressure Ulcers: Management-Topical Dressing | PC | ACOVE | |
| Pressure Ulcers: Management-Infection | PC, Emergency | ACOVE | |
| Pressure Ulcers: Management-Reassess Post Treatment | PC, Geriatrics | ACOVE | |
| Diabetes: | |||
| A1C Screen*+ | PC, Endocrinology | NCQA, AMA/PCPI, ICSI, ACOVE | |
| A1C Control*+ | PC, Endocrinology | NCQA, AMA/PCPI, ICSI, ACOVE | X |
| Blood Pressure Control*+ | PC, Endocrinology | NCQA, AMA/PCPI, ICSI, ACOVE | X |
| Lipid Screen*+ | PC, Endocrinology | NCQA, AMA/PCPI, ICSI, ACOVE | |
| LDL Cholesterol Control*+ | PC, Endocrinology | NCQA, AMA/PCPI, ICSI, ACOVE | X |
| Eye Exam*+ | PC, Endocrinology, Ophthalmology | NCQA, AMA/PCPI, ICSI, ACOVE | |
| Urine Protein Screening* | PC, Endocrinology | NCQA, AMA/PCPI, ICSI, ACOVE | |
| ACE Inhibitor or ARB for Proteinuria | PC, Endocrinology | ACOVE | |
| Foot Exam* | PC, Endocrinology, Podiatry | NCQA, AMA/PCPI, ICSI, ACOVE | |
| Smoking Status | PC, Endocrinology | NCQA, AMA/PCPI, ICSI | |
| Smoking Cessation | PC, Endocrinology | NCQA, AMA/PCPI, ICSI | |
| Aspirin Use | PC, Endocrinology | AMA/PCPI, ICSI, ACOVE | |
| Optimally Managed Modifiable Cardiovascular Risk Factors (A1C, LDL, Blood Pressure, Aspirin Use, Non-Tobacco Use) | PC, Endocrinology | Health Partners | |
| Screen for Depression | PC, Endocrinology | ICSI | |
| Relative Resource Use for People with Diabetes | PC, Endocrinology | NCQA | |
| Eye Disease/Vision: | |||
| Diabetic Retinopathy: Documentation of Presence or Absence of Macular Edema* | Ophthalmology | AMA/PCPI, ACOVE | X |
| Diabetic Retinopathy: Communication with the Physician Managing Ongoing Patient Care*+ | Ophthalmology | AMA/PCPI | X |
| Cataracts: Assessment of Visual Functional Status+ | Ophthalmology | AMA/PCPI, ACOVE | X |
| Cataracts: Documentation of Pre-surgical Axial Length+ | Ophthalmology | AMA/PCPI | X |
| Cataracts: Pre-surgical Dilated Fundus Evaluation+ | Ophthalmology | AMA/PCPI | X |
| Cataracts: Extraction Offered | Ophthalmology | ACOVE | |
| Cataracts: Follow-up Exam After Extraction | Ophthalmology | ACOVE | |
| Cataract Surgery: Other Complications | Ophthalmology | Wynn et al | |
| Cataract Surgery: Stroke Within 30 Days | Ophthalmology | Wynn et al | |
| Cataract Surgery: Retained Nuclear Fragment Within 30 Days | Ophthalmology | Wynn et al | |
| Cataract Surgery: Myocardial Infarction Within 30 Days | Ophthalmology | Wynn et al | |
| Cataract Surgery: Nausea and Vomiting Within 30 Days | Ophthalmology | Wynn et al | |
| Cataract Surgery: Secondary Glaucoma Within 30 Days | Ophthalmology | Wynn et al | |
| Cataract Surgery: Arrythmia Within 30 Days | Ophthalmology | Wynn et al | |
| Cataract Surgery: Endophtalmitis Within 30 Days | Ophthalmology | Wynn et al | |
| Cataract Surgery: Dislocated Ocular Lens Within 30 Days | Ophthalmology | Wynn et al | |
| Cataract Surgery: Cataract Fragments in the Eye Within 30 Days | Ophthalmology | Wynn et al | |
| Cataract Surgery: Iris Prolapse Within 30 Days | Ophthalmology | Wynn et al | |
| Cataract Surgery: Hypotension Within 30 Days | Ophthalmology | Wynn et al | |
| Cataract Surgery: Retinal Detachment Within 30 Days | Ophthalmology | Wynn et al | |
| Cataract Surgery: Persistent Corneal Edema Within 30 Days | Ophthalmology | Wynn et al | |
| Cataract Surgery: Vitreous Loss Within 30 Days | Ophthalmology | Wynn et al | |
| Cataract Surgery: Persistent Iridocyclitis | Ophthalmology | Wynn et al | |
| Cataract Surgery: Respiratory Failure From Surgery Within 30 Days | Ophthalmology | Wynn et al | |
| Cataract Surgery: Hyphema Within 30 Days | Ophthalmology | Wynn et al | |
| Cataract Surgery: Persistent Cystoid Macular Edema Within 30 Days | Ophthalmology | Wynn et al | |
| Cataract Surgery: Aspiration Pneumonia Within 30 Days | Ophthalmology | Wynn et al | |
| Cataract Surgery: Ocular Hypertension Within 30 Days | Ophthalmology | Wynn et al | |
| Cataract Surgery: Retinal Break Within 30 Days | Ophthalmology | Wynn et al | |
| Cataract Surgery: Hypertension Within 30 Days | Ophthalmology | Wynn et al | |
| Glaucoma Screening in Older Adults | Ophthalmology | NCQA, ACOVE | |
| Primary Open Angle Glaucoma: Optic Nerve Evaluation*+ | Ophthalmology | AMA/PCPI | X |
| Dilated Macular Examination (50+)*+ | Ophthalmology | AMA/PCPI, ACOVE | X |
| Antioxidant Supplement for Age-Related Macular Degeneration+ | Ophthalmology | AMA/PCPI | X |
| Vision: Urgent Signs and Symptoms | PC, Ophthalmology | ACOVE | |
| Vision: Chronic Signs and Symptoms | PC, Ophthalmology | ACOVE | |
| Vision: Corrective Lenses | Ophthalmology | ACOVE | |
| Gastro-intestinal Disorders: | |||
| GERD: Assessment for Alarm Symptoms+ | Gastroenterology, PC | AMA/PCPI | X |
| GERD: Chronic Medication Therapy+ | Gastroenterology, PC | AMA/PCPI | |
| GERD: Upper Endoscopy for Patients with Alarm Symptoms+ | Gastroenterology, PC | AMA/PCPI | X |
| GERD: Biopsy for Barrett’s Esophagus+ | Gastroenterology | AMA/PCPI | X |
| GERD: Barium Swallow Appropriateness+ | Gastroenterology | AMA/PCPI | X |
| Hearing Loss: | |||
| Annual Evaluation of Hearing Status | PC | ACOVE | |
| Formal Audiologic Evaluation (referral to Otolaryngologist/Audiologist) | PC | ACOVE | |
| Hearing Rehabilitation | Otolaryngology | ACOVE | |
| Conductive Hearing Loss (referral) | PC | ACOVE | |
| Cochlear Implantation | Otolaryngology | ACOVE | |
| Assistive Listening Device | PC, Otolaryngology | ACOVE | |
| Hepatitis C: | |||
| Testing for Chronic Hepatitis C | Gastroenterology, Infectious Disease, PC | AMA/PCPI | |
| Initial HCV RNA Testing | Gastroenterology, Infectious Disease, PC | AMA/PCPI | |
| HCV Genotype Testing Prior to Therapy | Gastroenterology, Infectious Disease, PC | AMA/PCPI | |
| Consideration of Antiviral Therapy | Gastroenterology, Infectious Disease, PC | AMA/PCPI | |
| Combination Antiviral Therapy | Gastroenterology, Infectious Disease, PC | AMA/PCPI | |
| HCV RAN Testing at Week 12 of Therapy | Gastroenterology, Infectious Disease, PC | AMA/PCPI | |
| Hepatitis A and B Vaccination | Gastroenterology, Infectious Disease, PC | AMA/PCPI | |
| Counseling Regarding Use of Alcohol | Gastroenterology, Infectious Disease, PC | AMA/PCPI | |
| Counseling Regarding Use of Contraception | Gastroenterology, Infectious Disease, PC | AMA/PCPI | |
| HIV/AIDS: | |||
| ARV Management | Infectious Disease | HRSA | |
| Adherence Self Management | Infectious Disease | HRSA | |
| Health Maintenance | Infectious Disease | HRSA | |
| Case Management | Infectious Disease | HRSA | |
| Hypertension: | |||
| Evaluation of New Hypertension-Cardiovascular Risk | PC, Cardiology | ACOVE | |
| Renal Function Check | PC, Cardiology | ACOVE | |
| Alcohol Intake Check | PC, Cardiology | ACOVE | |
| NSAID Reduction | PC, Cardiology | ACOVE | |
| Discussion of Goal Blood Pressure | PC, Cardiology | ACOVE | |
| Improving Persistent Hypertension | PC, Cardiology | ACOVE | |
| Addressing Uncontrolled HTN | PC, Cardiology | ACOVE | |
| Immediate Care for Severe HTN | PC, Cardiology | ACOVE | |
| Orthostatic Hypotension Check | PC, Cardiology | ACOVE | |
| Beta Blocker for Hypertension and Ischemic Heart Disease | PC, Cardiology | ACOVE | |
| ACEI or ARB for Co-morbid Vascular Disease | PC, Cardiology | ACOVE | |
| Blood Pressure Measurement* | PC, Cardiology | AMA/PCPI | |
| Blood Pressure Control* | PC, Cardiology | CMS/NCQA, ICSI, ACOVE | |
| Patient Education | PC, Cardiology | ICSI, ACOVE | |
| Documented Plan of Care* | PC, Cardiology | AMA/PCPI, ACOVE | |
| Relative Resource Use for Uncomplicated Hypertension | PC, Cardiology | NCQA | |
| MRI (Head, Neck and Brain) | |||
| Dizziness Within 30 Days | Radiology | Wynn et al | |
| Headache Within 30 Days | Radiology | Wynn et al | |
| Chest Pain Within 30 Days | Radiology | Wynn et al | |
| Seizure Within 30 Days | Radiology | Wynn et al | |
| Syncope Within 30 Days | Radiology | Wynn et al | |
| Dyspnea Within 30 Days | Radiology | Wynn et al | |
| Paresthesia Within 30 Days | Radiology | Wynn et al | |
| Bradycardia Within 30 Days | Radiology | Wynn et al | |
| Hypotension Within 30 Days | Radiology | Wynn et al | |
| Altered Mental Status Within 30 Days | Radiology | Wynn et al | |
| Rash Within 30 Days | Radiology | Wynn et al | |
| Tachycardia Within 30 Days | Radiology | Wynn et al | |
| Other Complications Within 30 Days | Radiology | Wynn et al | |
| Anaphylaxis/Anaphylactoid Reaction Within 30 Days | Radiology | Wynn et al | |
| Hypertension Within 30 Days | Radiology | Wynn et al | |
| Death Within 1 Week | Radiology | Wynn et al | |
| Medication Use (Vulnerable Elders): | |||
| Medication Use: Clearly Defined Indication | PC, All Clinical Specialties | ACOVE | |
| Medication Use: Patient Education | PC, All Clinical Specialties | ACOVE | |
| Medication Use: Response to Therapy Documentation | PC, All Clinical Specialties | ACOVE | |
| Medication Use: Warfarin Education | PC, Cardiology | ACOVE | |
| Medication Use: Monitoring Warfarin | PC, Cardiology | ACOVE | |
| Medication Use: Lab Monitoring for ACEI | PC, Cardiology | ACOVE | |
| Medication Use: Lab Monitoring for Loop Diuretic | PC | ACOVE | |
| Medication Use: Avoid Propoxyphene | PC | ACOVE | |
| Medication Use: Taper Benzodiazepines | PC, Psychiatry | ACOVE | |
| Medication Use: Avoid Strong Anticholinergics | PC | ACOVE | |
| Medication Use: Avoid Barbituates | PC | ACOVE | |
| Medication Use: Avoid Medperidine | PC | ACOVE | |
| Medication Use: Limit Ketorolac | PC | ACOVE | |
| Medication Use: Limit Muscle Relaxants | PC | ACOVE | |
| Medication Use: Avoid Ticlopidine | PC | ACOVE | |
| Medication Use: Iron Dosing for Anemia | PC | ACOVE | |
| Medication Use: Antipsychotic Drug Response | PC, Psychiatry | ACOVE | |
| Medication Use: Acetaminophen | PC | ACOVE | |
| Medication Use: NSAIDs – Gastrointestinal Bleeding Risks | PC, Orthopedics | ACOVE | |
| Medication Use: Daily Aspirin-Gastrointestinal Bleeding Risks | PC, Cardiology | ACOVE | |
| Medication Use: NSAIDs-Misoprostol | PC, Cardiology | ACOVE | |
| Medication Use: Aspirin-Misoprostol | PC, Cardiology | ACOVE | |
| Neurological Disorders: | |||
| Migraine: Documented Education | PC, Neurology | ICSI | |
| Migraine: Treatment Plans | PC, Neurology | ICSI | |
| Stroke: Carotid Artery Imaging Ordered | Emergency, Neurology, PC | ACOVE | |
| Stroke: Carotid Imaging Reports: Reference to Measurement of Distal Internal Carotid Diameter*+ | Radiology | AMA/PCPI | X |
| Stroke: CT or MRI Reports: Includes Documentation of the Presence or Absence of Hemorrhage and Mass Lesion and Acute Infarction*+ | Radiology | AMA/PCPI | X |
| Stroke: t-PA Considered*+ | Neurology, Emergency | AMA/PCPI | X |
| Stroke: Administration of Heparin (overuse) | Neurology | AMA/PCPI | |
| Stroke: Carotid Endarterectomy | Neurology, Vascular Surgery | ACOVE | |
| Stroke Risk: Anticoagulate Atrial Fibrillation | Neurology, Cardiology, PC | ACOVE | |
| Stroke Risk: Anticoagulate for Atrial Fibrillation-INR Goal | Neurology, Cardiology, PC | ACOVE | |
| Stroke Risk: Atrial Fibrillation- Antiplatelet Therapy | Neurology, Cardiology, PC | ACOVE | |
| Stroke: Ischemic Stroke Prophylaxis | Neurology, PC | ACOVE | |
| Stroke: LDL Cholesterol | Neurology, PC | ACOVE | |
| Stroke: Smoking Status | Neurology, PC | ACOVE | |
| Stroke: Smoking Cessation | Neurology, PC | ACOVE | |
| Stroke: Exercise Prescription | Neurology, PC | ACOVE | |
| Stroke: Alcohol Misuse | Neurology, PC | ACOVE | |
| Stroke: Hormone Replacement Therapy | Neurology, PC | ACOVE | |
| Stroke: Patient Education | Neurology, PC | ACOVE | |
| Sleep Disorders: Sleep History | PC | ACOVE | |
| Sleep Disorders: Sleep Hygiene Discussion | PC | ACOVE | |
| Sleep Disorders: Sleep Study Referral | PC | ACOVE | |
| Sleep Disorders: Discussion of Treatment Options | PC | ACOVE | |
| Sleep Disorders: Nocturnal Limb Movements-Referral | PC | ACOVE | |
| Sleep Disorders: Avoid Antihistamines | PC | ACOVE | |
| Sleep Disorders: Discontinue Antihistamines | PC | ACOVE | |
| Sleep Disorders: Taper Chronic Benzodiazepines | PC | ACOVE | |
| Sleep Disorders: Treat Pain Disturbing Sleep | PC | ACOVE | |
| Pneumonia: | |||
| Chest X-Ray for CAP | Emergency, PC | AMA/PCPI, ICSI | |
| Assessment of Co-Morbid Conditions | Emergency, PC | AMA/PCPI | |
| Vital Signs for CAP* | Emergency, PC | AMA/PCPI | X |
| Assessment of Oxygen Saturation for CAP* | Emergency, PC | AMA/PCPI | X |
| Assessment of Mental Status for CAP* | Emergency, PC | AMA/PCPI | X |
| Assessment of Hydration Status | Emergency, PC | AMA/PCPI | |
| Blood Culture Prior to Antibiotic | Emergency, PC | AMA/PCPI | |
| Empiric Antibiotic for CAP | Emergency, PC | AMA/PCPI | X |
| Smoking Assessment/Intervention | PC | AMA/PCPI | |
| Influenza Immunization Status | PC | AMA/PCPI | |
| Pneumococcus Immunization Status | PC | AMA/PCPI | |
| Follow-up Care for Pneumonia | PC | AMA/PCPI | |
| Renal Disease: | |||
| Advanced Chronic Kidney Disease (CKD): Patients on a Phosphate Binder with iPTH Measured w/in Last 3 Months | Nephrology, PC | Renal Physician Association (RPA) | |
| CKD: ACE Inhibitors or ARBs | Nephrology, PC | RPA | |
| CKD: Lipid Lowering Treatment | Nephrology, PC | RPA | |
| CKD: Elemental Calcium | Nephrology | RPA | |
| CKD: Vitamin D2 | Nephrology | RPA | |
| CKD: Calcitriol, Alfacalcidol, or Vitamin D analogues | Nephrology | RPA | |
| CKD: Referrals to Vocational Rehabilitation Center | Nephrology | RPA | |
| CKD: Screen for Dyslipidemia Within 1 Year | Nephrology | RPA | |
| CKD: Erythropoietin or Analogue | Nephrology | RPA | |
| CKD: Erythropoietin Analogue to a Hemoglobin of 12 g/dL in Women and 13 g/dL in Men | Nephrology | RPA | |
| CKD: Patients Who are Anemic, Iron Deficient and on Iron Therapy | Nephrology | RPA | |
| CKD: Patients Referred for a Transplant Evaluation | Nephrology | RPA | |
| CKD: Patients With 25 (OH) Vitamin D Levels Measured | Nephrology | ||
| CKD: Anemia Work-Up | Nephrology | RPA | |
| CKD: Patients with Antihypertensive Therapy Intensified | Nephrology | RPA | |
| CKD: Blood Pressure Checked at Every Erythropoietin or Analogue Dose | Nephrology | RPA | |
| CKD: Blood Pressure Checked at Least Once Within Last 3 Months | Nephrology | RPA | |
| CKD: Patients with Blood Pressure < 130/80mmHg and are Receiving Erythropoietin or Analogue | Nephrology | RPA | |
| CKD: Patients with Blood Pressure < 130/80 mmHg on Index Date | Nephrology | RPA | |
| CKD: Counseling for Increased Physical Activity | Nephrology | RPA | |
| CKD: Discussion of Renal Replacement Therapy Modalities | Nephrology | RPA | |
| CKD: Education Provided | Nephrology | RPA | |
| CKD: Hemoglobin Measured at Least Every 3 Months | Nephrology | RPA | |
| CKD: Patients with iPTH > 100pg/mL and/or Phosphorous > 4.5 mg/dL and are Prescribed a Low Phosphorous Diet for 1 Month | Nephrology | RPA | |
| CKD: Patients with iPTH > 100 pg/mL | Nephrology | RPA | |
| CKD: Measurement of Body Weight and Serum Albumin Within the Last 3 Months | Nephrology | RPA | |
| CKD: Patients with 1 Measurement of iPTH | Nephrology | RPA | |
| CKD: Patients with Phosphorous > than 4.5 mg.dL After a Low Phosphorous Diet for 1 Month, Now on a Phosphate Binder | Nephrology | RPA | |
| CKD: Patients with Phosphorous > 4.5 mg/dL | Nephrology | RPA | |
| CKD: Qualified Nutritional Counseling | Nephrology | RPA | |
| CKD: Patients with Serum Bicarbonate > 22 MMOL/L | Nephrology | RPA | |
| CKD: Patients with Serum Bicarbonate Measured Within the Last 3 Months | Nephrology | RPA | |
| CKD: Patients with Serum Calcium and Phosphorus Measured Within the Last 3 months | Nephrology | RPA | |
| Respiratory Illness/Asthma: | |||
| COPD: Spirometry Results Documented* | Pulmonology, PC | AMA/PCPI, ACOVE | X |
| COPD: Annual Assessment | Pulmonology, PC | AMA/PCPI | |
| COPD: Inhaled Bronchodilator* | Pulmonology, PC | AMA/PCPI, ACOVE | X |
| COPD: Long-Acting Bronchodilator | Pulmonology, PC | AMA/PCPI, ACOVE | |
| COPD: Inhaler Device Training | Pulmonology, PC | AMA/PCPI, ACOVE | |
| COPD: Inhaled Corticosteroids | Pulmonology, PC | AMA/PCPI, | |
| COPD: Smoking Assessment/Cessation | Pulmonology, PC | AMA/PCPI,ACOVE | |
| COPD: Assessment of Oxygen Saturation* | Pulmonology, PC | AMA/PCPI, ACOVE | |
| COPD: Long Term Oxygen Therapy | Pulmonology, PC | AMA/PCPI, ACOVE | |
| COPD: Pulmonary Rehabilitation | Pulmonology, PC | AMA/PCPI | |
| COPD: Influenza Immunization | Pulmonology, PC | AMA/PCPI | |
| COPD: Pneumococcus Immunization | Pulmonology, PC | AMA/PCPI | |
| Asthma Assessment*+ | Pulmonology, Immunology, PC | AMA/PCPI | X |
| Asthma: Appropriate Medications*+ | Pulmonology, ImmunologyPC | NCQA, ICSI | |
| Asthma: Pharmacologic Therapy*+ | Pulmonology, Immunology, PC | AMA/PCPI | X |
| Asthma: Spirometry Evaluation | Pulmonology, Immunology, PC | ICSI | |
| Asthma: Bronchodilator Therapy | Pulmonology, Immunology, PC | AMA/PCPI | |
| Asthma: Patient Education Documented | Pulmonology, Immunology, PC | ICSI | |
| Asthma: Management Plan* | Pulmonology, Immunology, PC | IPRO (NY QIO) | |
| Asthma: Average Number of Lost Work Days in Past 30 Days | Pulmonology, Immunology, PC | HRSA | |
| Asthma: Average Number of Symptom Free Days in the Previous 2 weeks | Pulmonology, Immunology, PC | HRSA | |
| Asthma: Influenza Immunization | Pulmonology, Immunology, PC | HRSA | |
| Asthma: Patients Who Have Had a Visit to the ED in the Past Year | Pulmonology, Immunology, PC | HRSA | |
| Asthma: Depression Screening | Pulmonology, Immunology, PC | HRSA | |
| Asthma: Patients with Reported Exposure to Environmental Tobacco Smoke at Last Visit | Pulmonology, Immunology, PC | HRSA | |
| Asthma: Patients with a Severity Assessment at the Last Visit | Pulmonology, Immunology, PC | HRSA | |
| Asthma: Patients with Documented Self Management Goals | Pulmonology, Immunology, PC | HRSA | |
| Asthma: Anti-inflammatory Medication | Pulmonology, Immunology, PC | HRSA | |
| Relative Resource Use for People with Asthma | Pulmonology, Immunology, PC | NCQA | |
| Relative Resource Use for People with COPD | Pulmonology, Immunology, PC | NCQA | |
| Acute Bronchitis: Inappropriate Antibiotic Treatment* | PC, Emergency | NCQA | |
| Viral Upper Respiratory Infection: Patient Education | PC, Emergency | ICSI | |
| Viral Upper Respiratory Infection: Appropriate Antibiotic Use | PC, Emergency | ICSI | |
| Viral Upper Respiratory Infection: Inappropriate Office Visit | PC, Emergency | ICSI | |
| Pharyngitis: Appropriate Testing | PC, Emergency | ICSI | X |
| Undernutrition: | |||
| Weight Measurement | PC | ACOVE | |
| Vitamin D | PC | ACOVE | |
| Document Weight Loss | PC | ACOVE | |
| Evaluate Weight Loss | PC | ACOVE | |
| Evaluate Co-Morbid Conditions | PC | ACOVE | |
| Urological Conditions: | |||
| Discussing Urinary Incontinence* | PC | NCQA, ACOVE | |
| Receiving Urinary Incontinence Treatment* | PC, Urology | NCQA, ACOVE | |
| Assessment of Presence of Urinary Incontinence (Women 65+)*+ | PC, OB/GYN, Urology | AMA/PCPI, ACOVE | X |
| Incontinence: History | PC, Urology | ACOVE | |
| Incontinence: Urine Evaluation | PC, Urology | ACOVE | |
| Incontinence: Post-Void Residual | PC, Urology | ACOVE | |
| Incontinence: Behavioral Therapy Assessment | PC, Urology | AMA/PCPI, ACOVE | |
| Incontinence: Characterization of UI (Women 65+)*+ | PC, OB/GYN, Urology | AMA/PCPI, ACOVE | X |
| Incontinence: Plan of Care for UI (Women 65+)*+ | PC, OB/GYN,Urology | AMA/PCPI, ACOVE | X |
| Incontinence: Assess Response to Treatment | PC, OB/GYN, Urology | ACOVE | |
| Incontinence: Preoperative Urodynamic Testing | Urology, OB/GYN | ACOVE | |
| Incontinence: Chronic Urethral Catheter | Urology | ACOVE | |
| UTI: Urine Culture Performed | PC | ICSI, ACOVE | |
| UTI: Recommended Short Course Therapy | PC | ACOVE | |
| BPH: History | PC, Urology | ACOVE | |
| BPH: Exam | PC, Urology | ACOVE | |
| BPH: Urine Evaluation | PC, Urology | ACOVE | |
| BPH: Post-Void Residual | PC, Urology | ACOVE | |
| BPH: Urologic Trauma (referral to urologist) | PC | ACOVE | |
| BPH: Hematuria-Urinalysis | PC | ACOVE | |
| BPH: Hematuria-Testing and Referral | PC, Geriatrics, Urology | ACOVE | |
| BPH: PSA Testing | PC, Geriatrics, Urology | ACOVE | |
| BPH: Referral Indications | PC, Geriatrics | ACOVE | |
| BPH: Treatment-If AUA SI Score < 7 and Symptoms not Bothersome, No Medication or Surgery | PC, Geriatrics, Urology | ACOVE | |
| BPH: Treatment- If AUA SI score > 7, With Moderate to Severe Symptoms, Discuss Treatment Options | PC, Geriatrics, Urology | ACOVE | |
| BPH: Preoperative Urine Evaluation | PC, Geriatrics, Urology | ACOVE | |
| Other Clinical: | |||
| Radiology: Timeliness of Verifying Reports | Radiology | Veteran’s Health Admin | |
| ED Patients who Left Against Medical Advice or Without Being Seen | Emergency | CMS | |
| Patient Received Discharge Instructions on Discharge from the ED | Emergency | CMS | |
| Pain Management: Education for Persistent Pain | PC | ACOVE | |
| Pain Management: Preventing Constipation with Opioids | PC | ACOVE, ASSIST | |
| Reassessing Pain Control with Opioids | PC | ACOVE, ASSIST | |
| End of Life Care: Comprehensive Assessment | PC, Palliative, All Clinical Specialties | ACOVE | |
| End of Life Care: Goals of Care Surrogate Discussion | PC, Palliative, All Clinical Specialties | ACOVE | |
| End of Life Care: Advance Directive Continuity | PC, Palliative, All Clinical Specialties | ACOVE, ASSIST | |
| End of Life Care: Follow Treatment Preferences | PC, Palliative, All Clinical Specialties | ACOVE | |
| End of Life Care: Gastrostomy – Tube Placement | PC, Palliative, All Clinical Specialties | ACOVE | |
| End of Life Care: Dyspnea Assessment | PC, All Clinical Specialties | ACOVE | |
| End of Life Care: Treatment of Dyspnea | PC, All Clinical Specialties | ACOVE | |
| End of Life Care: Plan for Management of Emergent Dyspnea | PC, All Clinical Specialties | ACOVE | |
| End of Life Care: Document Dyspnea Care | PC, All Clinical Specialties | ACOVE | |
| End of Life Care: Plan for Management of Emergent Pain | PC, All Clinical Specialties | ACOVE | |
| End of Life Care: Document Presence or Absence of Pain | PC, All Clinical Specialties | ACOVE | |
| End of Life Care: Plan for Management of Emergent Obstruction | PC, All Clinical Specialties | ACOVE | |
| End of Life Care: Caregiver Stress Assessed | PC, All Clinical Specialties | ACOVE | |
| End of Life Care: Spouse/Significant Other Assessed for Depression or Suicidality | PC, All Clinical Specialties | ACOVE | |
| Continuity and Coordination of Care: Identify Source of Care | PC, All Clinical Specialties | ACOVE | |
| Continuity and Coordination of Care: Medication Continuity-Follow-up Visit | PC, All Clinical Specialties | ACOVE | |
| Continuity and Coordination of Care: Medication Continuity-> 2 Physicians | PC, All Clinical Specialties | ACOVE | |
| Continuity and Coordination of Care: Consultation Continuity | PC, All Clinical Specialties | ACOVE | |
| Continuity and Coordination of Care: Test Continuity | PC, All Clinical Specialties | ACOVE | |
| Continuity and Coordination of Care: Prevention Reminders | PC | ACOVE | |
| Continuity and Coordination of Care: Communication with PCP Following ED Visit | Emergency | ACOVE | |
| Continuity and Coordination of Care: Post-Hospitalization Medications | PC, All Clinical Specialties | ACOVE | |
| Continuity and Coordination of Care: Post-Hospitalization Tests | PC, All Clinical Specialties | ACOVE | |
| Continuity and Coordination of Care: Post-Hospitalization Appointments | PC, All Clinical Specialties | ACOVE | |
| Continuity and Coordination of Care: Outside Medical Records | PC | ACOVE | |
| Continuity and Coordination of Care: Interpreter | PC, All Specialties | ACOVE | |
| Fall Risk Management* | PC | NCQA, ACOVE | X |
| Falls and Mobility Problems: Fall History | PC | ACOVE | |
| Falls and Mobility Problems: Fall Exam-Orthostatic Vital Signs | PC | ACOVE | |
| Falls and Mobility Problems: Fall-Exam-Eye Exam | PC | ACOVE | |
| Falls and Mobility Problems: Gait, Balance and Strength Evaluation | PC, Orthopedics | ACOVE | |
| Falls and Mobility Problems: Cognitive Evaluation | PC | ACOVE | |
| Falls and Mobility Problems: Home Hazard Evaluation | PC | ACOVE | |
| Falls and Mobility Problems: Benzodiazepine Discontinuation | PC | ACOVE | |
| Falls and Mobility Problems: Assistive Device for Balance Disorder | PC | ACOVE | |
| Falls and Mobility Problems: Assistive Device Review | PC | ACOVE | |
| Falls and Mobility Problems: Exercise Program | PC | ACOVE | |
| Patient Experience: | |||
| Hospital CAHPS (selected questions) | PC, All Specialties | AHRQ | |
| Clinical-Group Ambulatory CAHPS | PC, All Specialties | AHRQ |
PC Indicates Primary Care, including Geriatrics.
ACOVE (Assessing Care of Vulnerable Elders) measures are applicable to community-dwelling individuals age 65 and older at increased risk of functional decline and death over a two-year period.
This table includes measures that are publicly available. RAND’s review did not include proprietary measures.
Appendix E: Description of Primary Developers of Candidate Measures
AMA/PCPI is a consortium convened by the AMA and comprised of over 100 national medical specialty and state medical societies, the Council of Medical Specialty Societies, the American Board of Medical Specialties and its member-boards, experts in methodology and data collection, the Agency for Healthcare Research and Quality (AHRQ, and CMS. Its mission is to enhance the quality of care through the development, testing, and maintenance of evidence-based performance measures; it accomplishes this mission through cross-specialty workgroups that translate evidence-based guidelines into measures. Through these work groups, the Consortium had developed 184 physician-level performance measures for 27 different conditions, as of June 1, 2007. Some of the conditions addressed early in the effort include asthma, chronic stable coronary artery disease, heart failure and hypertension, while more recent measures addresses emergency services, gastroesophageal reflux disease (GERD), melanoma, stroke, and other conditions for which fewer measures have been available. The majority of these measures are candidate hospital outpatient measures. Those that are not relevant assess care not covered by the OPPS (e.g., hospital inpatient-only services, dialysis) or relate to non-Medicare populations (e.g., children, pregnant women). The AMA/PCPI measures are routinely submitted to the National Quality Forum (NQF), a voluntary consensus standard-setting organization established to standardize health care quality measurement and reporting, As of June 1, 2007, 48 of the measures submitted by the AMA/PCPI that are potentially relevant to the HOPS had been approved, however, 29 of these received a “time limited” endorsement. This designation is for measures that satisfy all NQF criteria but have not yet been field tested. Once the field testing has been completed and the measures have been demonstrated to produce valid and reliable results, NQF will give them full endorsement.
NCQA develops quality standards and performance measures through a consensus process that includes large employers, policymakers, physicians, patients and health plans. Each year the organization releases a set of measures known as the Health Plan Employer Data and Information Set (HEDIS) that includes measures of underuse, overuse, value, process and outcome. Measures are developed utilizing available evidence and expert consensus. The 2007 HEDIS measures are intended to be used to compare the quality of care provided by managed care organizations, preferred provider organizations, or physician practices, but many address care that may also be provided in the hospital outpatient setting. HEDIS measures are publicly reported by the NCQA following one year of testing for feasibility, reliability and validity. Additionally, the majority of HEDIS measures that may be relevant to the hospital outpatient setting have been approved by the NQF.
The ACOVE project is a collaboration between the RAND Corporation, a nonprofit research organization, and Pfizer Inc. to develop quality indicators for medical care provided to vulnerable elders, defined as community dwelling individuals age 65 and older at increased risk of functional decline over a two year period. The first set was created in 1999 and has been updated twice in order to stay abreast of the current medical literature and to create a more comprehensive set. The ACOVE-3 Quality Indicator Measurement Set, is comprised of 392 quality indicators measuring processes of care for 26 conditions. For each condition, a content expert assembled a candidate list of indicators based on a review of the literature, guidelines, and existing measures. The evidence underpinning each quality indicator is presented in a series of peer-reviewed monographs (ACOVE investigators, in press). The indicators were then reviewed and rated by two multidisciplinary panels of clinical experts. Most of these indicators are intended to measure care at the level of the health system, health plan, or medical group, and may apply to the hospital outpatient setting; a small number are not relevant to the hospital outpatient setting due to their focus on inpatient or nursing home care. A subset of these indicators (less than 20) has been submitted to the NQF for approval. The original set of 236 indicators (ACOVE-1) was tested using vulnerable elder data from two senior managed care plans, and then used in an intervention by two additional medical groups. Some of these indicators that can be measured using administrative data have been applied to a sample of “dual eligible” (i.e., Medicare/Medicaid) patients in California. While many components have been implemented, the complete ACOVE-3 set has not been tested.
The ASSIST project, led by RAND Corporation, developed a comprehensive set of quality indicators addressing symptoms and symptomatic complications, treatment-related toxicities, and information and care planning needs for adults living with cancer. The indicators were intended to apply to major clinical sites where cancer patients seek care including general practice and oncology settings. They were selected through a multi step process starting with the development of a list of topics ranked by prevalence, likely impact on patient and family quality of life, existing literature and the strength of medical evidence. Through an iterative process of team discussion, revision and advisory board input, the five member research team drafted a set of indicators after reviewing relevant clinical trials, guidelines and quality indicators and soliciting expert opinion from national clinical leaders. Nine panelists representing multidisciplinary disciplines including medicine, nursing, and social work; geographic diversity; academic and community settings; oncology and other specialties including palliative medicine; and general internal medicine rated the indicators on validity and feasibility. A total of 92 of 133 (69 percent) proposed indicators were judged valid and feasible by the panel. The indicators were developed for group practice and may be applied to health plans or systems of care.
References
ACOVE Investigators. The ACOVE-3 Quality Measurement Set for Vulnerable Elders. Journal of the American Geriatrics Society. In press.
AQA. Defining Cost of Care Measures. Draft working paper accessed online at http://www.aqaalliance.org/may30meeting/PerformanceMeasurement/Defining… on July 2007.
Asch SM, Kerr EA, Kersey J, Adams JL, Setodji CM, Mali S, and McGlynn EA. (2006) Who Is at Greatest Risk for Receiving Poor-Quality Health Care? New England Journal of Medicine 354(11):1147 – 1156.
Bush, President George W. (2006) Executive Order: Promoting Quality and Efficient Health Care in Federal Government Administered or Sponsored Health Care Programs. Washington, DC: Office of the Press Secretary.
Centers for Medicare & Medicaid Services (CMS). (2007) Regulation No. CMS-1392-P. Proposed Changes to the Hospital Outpatient Prospective Payment System and CY 2008 Payment Rates. Accessed online at http://www.cms.hhs.gov/HospitalOutpatientPPS/HORD/itemdetail.asp?filter… on July 2007.
Hing E., Cherry DK, and Woodwell DA. (2006) National Ambulatory Medical Care Survey: 2004 Summary. CDC’s Advance Data from Vital and Health Statistics of the National Center for Health Statistics No. 374.
Institute of Medicine. (2000) To Err Is Human: Building a Safer Health System. Kohn LT, Corrigan JM, Donaldson MS (eds.). Washington, DC: National Academy Press.
Institute of Medicine. (2001) Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy of Sciences.
Institute of Medicine. (2005) Performance Measurement: Accelerating Improvement. Washington, DC: National Academy of Sciences.
Kuhn H, Acting Deputy Administrator Center for Medicare & Medicaid Services. (May 10, 2007) Testimony before the House Ways and Means Subcommittee on Health. Hearing on Physician Quality and Efficiency. Available at http://www.cms.hhs.gov/apps/media/press/testimony.asp?Counter=2181&intN…
Leavitt MO. (2006) Better Care, Lower Cost: Prescription for a Value-Driven Health System. Washington, DC: Department of Health and Human Services, Office of the Secretary.
Litwin MS, Steingberg M, Malin J, Naitoh J, McGuigan KA, Steinfeld R, Adams J, and Brook RH. (2000)Prostate Cancer Patient Outcomes and Choice of Providers; Development of an Infrastructure for Quality Assessment. Santa Monica, CA: RAND Corporation, MR-122 7-BF.
Lorenz KA, Dy SM, Naeim A, et al. (2007) Quality Measures for Supportive Cancer Care: The Cancer Quality ASSIST (Assessing Symptoms Side Effects and Indicators or Supportive Treatment) Project. Paper in submission.
McGlynn EA, Asch SM, Adams J, Kersey J, Hicks J, DeChristofaro A, and Kerr EA. (2003) The Quality of Health Care Delivered to Adults in the United States. New England Journal of Medicine 348(26):2635 – 2645.
MedPAC. (2007a) “Section 1, National Health Care Spending and Medicare Spending,” in A Data Book: Healthcare Spending and the Medicare Program. Washington, DC: MedPAC.
MedPAC. (2007b) “Section 8, Ambulatory Care: Physicians, Hospital Outpatient Services, Ambulatory Surgical Centers and Imaging Services,” in A Data Book: Healthcare Spending and the Medicare Program. Washington, DC: MedPAC.
MedPAC. (2007c) Report to the Congress: Medicare Payment Policy. Washington, DC: MedPAC.
Schuster MA, McGlynn EA, and Brook RH. (1998) How Good Is the Quality of Health Care in the United States? Milbank Quarterly 76(4):517 – 563.
Vladeck BC, Van de Water PN, and Eichner J (eds.). (2006) Strengthening Medicare’s Role in Reducing Racial and Ethnic Health Disparities. Washington, DC: National Academy of Social Insurance.
Wenger NS, Solomon DH, Roth CP, MacLean CH, Saliba D, et al. (2003) The Quality of Medical Care Provided to Vulnerable Community-Dwelling Older Patients. Annals of Internal Medicine 139(9):740 – 747.
Wynn BO, Sloss EM, Fung C, Shugarman LR, Ashwood JS, and Asch SM. (2004) Services Provided in Multiple Ambulatory Settings: A Comparison of Selected Procedures. A study conducted by RAND Health for the Medicare Payment Advisory Commission. Accessed online at http://www.medpac.gov/publications/contractor_reports/Oct04_ASC_Rpt(Con…
Footnotes
1.Public Law 109-432, See Section 1833(t) of the Social Security Act. (December 20, 2006).
2.The data file that RAND obtained from CMS for analysis contained 2005 utilization data and 2007 payment rates. Thus all financial analyses contained in this report apply 2007 payment rates against 2005 utilization experience, and as such cannot be directly mapped to the actual spending numbers that occurred in 2005 using the 2005 payment rates.
3.RAND applied 2007 payment rates to the 2005 frequency data to produce estimates of spending by types of services/procedures. The estimates shown do not reflect true spending that occurred in 2005 as a function of applying 2005 payment rates, so cannot be directly mapped to final spending figures for care provided in the hospital outpatient setting.
4.The service mix index is calculated as the sum of the relative weights of all OPPS services divided by the volume of all services. The concept is similar to the case mix index for inpatient services.
5.Public Law 108-173, December 8, 2003.
6.Section 5001(a), Public Law 109-171, February 8, 2006.
7.Public Law 109-432, See Section 1833(t) of the Social Security Act. (December 20, 2006).
8.The Final OPPS Rule is scheduled to be released November 1, 2007.
9.A subsection d hospital is one located in one of the fifty States or the District of Columbia other than the following: a psychiatric hospital; a rehabilitation hospital; a hospital whose inpatients are predominantly individuals under 18 years of age; a hospital which has lengthy average inpatient lengths of stay (e.g. greater than 25 days); a cancer center
10.International Classification of Disease Version 9.0, Clinical Modification. CMS provided RAND with ICD-9-CM codes aggregated to the fourth of five possible digits. RAND and CMS agreed that this level of detail would provide sufficient specificity in most cases without overwhelming the analysis with the granularity of the five digit level.
11.APCs are categories of outpatient services that are clustered based on similar resources use as well as clinical similarities. OPPS pays a set amount for each APC. The services within each APC are represented by HCPCS codes, which refers to the Healthcare Common Procedure Coding System, a standardized coding system for describing the specific items and services provided in the delivery of health care. These codes are used by Medicare, Medicaid, and other health insurance programs to process claims. The American Medical Association’s (AMA) Current Procedural Terminology (CPT) codes are part of the HCPCS.
12.Based on the analytic file that RAND obtained from CMS, which contained 2005 utilization data and 2007 payment rates, RAND’s spending estimates provided in the tables in this report apply 2007 payment rates to the 2005 utilization data.
13.Not all drugs administered in the HOPS are separately billed under OPPS; drugs under $50 are bundled with the infusion APCs and HCPCS codes. Our analyses of the most costly drugs do not include those drugs that are not separately billed under OPPS.
14.With the exception of transfusion medicine and anatomic pathology, laboratory services are paid under Medicare by the Clinical Laboratory Fee Schedule (CLFS), irrespective of the venue in which they are provided.
15.DME is billed to a separate fee schedule which was not included in the data RAND analyzed.
16.Analyses also did not include APCs with a status indicator of “P”-partial hospitalization or “Q” packaged services subject to separate payment under OPPS, which are both very low frequency services and do not contribute significantly to either the volume or cost of services provided under OPPS.
A list with the groupings of ICD-9-CM utilized for the analyses is available upon request.
17.A list with the groupings of ICD-9-CM utilized for the analyses is available upon request.
18.The subjective classification of diagnoses determines which diagnoses are identified as most frequent. Other approaches to the classification may alter the specific diagnoses that rise to the top.
19.RAND applied 2007 APC payment rates to the 2005 utilization data. The estimates of spending by category assume that the volume and distribution of visits and services/procedures did not substantially change over the two-year period. Note: the estimates shown cannot be mapped to actual 2005 spending figures which are based on 2005 APC payment rates
20.The visit and services/procedure volumes presented in Table 3.1 reflect 2005 data, the most current frequency data that were made available to RAND. RAND applied the 2007 APC payment rates to the 2005 frequency data based on the data obtained from CMS; thus spending estimates shown in this report will not map to final published spending for 2005 based on 2005 payment rates. Drugs/biologicals are excluded from this table because RAND did not have access to complete payment data for these services. Also hospital outpatient expenses not covered under OPPS (e.g., clinical laboratory services) are also not included in this tally.
21.E&M visits were identified using the status indicator V (i.e., the status indicator associated with APC codes that indicate clinic or emergency department visits). Services/procedures were identified with the status indicators S, T or X (i.e., the status indicators associated with APC codes that indicate significant procedures and ancillary services).
22.The data presented in Table 3.1 do not account for all hospital outpatient setting claims, as some hospital outpatient setting services may be entirely procedural and, therefore, not accompanied by a separately identifiable E&M code.
23.Table 3.2 was constructed using 2005 Medicare facility data for services paid through the hospital outpatient prospective payment system (OPPS). Emergency department data were analyzed separately (Table 3.3) from data reflecting care provided in the HOPS. Given the focus on tests and procedures rather than clinic visits, analyses were restricted to APCs with a Status Indicator of S, T or X. The most common diagnoses codes were identified for each of the most frequent APCs. A clinical expert identified the related specialty for the APCs.
24.Table 3.3 was constructed using 2005 Medicare facility data for services paid through the hospital outpatient prospective payment system (OPPS). HOPS data were analyzed separately (Table 3.2) from data reflecting care provided in the ED. Given the focus on tests and procedures rather than clinic visits, analyses were restricted to APCs with a Status Indicator of S, T or X. The most common diagnoses codes were identified for each of the most frequent APCs. A clinical expert identified the related specialty for the APCs.
25.As noted previously, the data file provided to RAND by CMS contained 2007 payment data and 2005 utilization data. The estimates shown here do not reflect actual spending in 2005 as 2005 payment data were not available in the analysis file, thus the estimates provided here cannot be mapped directly to final actual spending in 2005 for Hospital Outpatient Setting care.
26.The expenditure data presented in Table 3.4 reflect APC payment rates for 2007. Based on the data supplied to RAND by CMS, we applied the 2007 payment rates to the 2005 utilization data to provide estimates of spending by type of services. Note: the estimates shown in Table 3.4 cannot be mapped to actual 2005 spending figures which are based on 2005 payment rates.
27.The expenditure data presented in Table 3.5 reflects APC payment rates for 2007. Based on the data supplied to RAND by CMS, we applied the 2007 payment rates to the 2005 utilization data to provide estimates of spending by type of services. Note: the estimates shown in Table 3.4 cannot be mapped to actual 2005 spending figures which are based on 2005 payment rates.
28.Only drugs and biologicals exceeding $50 are separately billable; less-expensive drugs are incorporated into the drug infusion OPPS payments. Consequently this list only represents a subset of the entire spectrum of these treatments that patients receive
29.The NCCN is a not-for-profit alliance of 21 cancer centers that develops evidence-based treatment guidelines for most cancers. The organization has collaborated with ASCO and the Commission on Cancer in the development of cancer measures.
30.The CAHPS Clinician and Group Survey asks patients about their experiences with physicians and their staff in primary and specialty care settings; the Hospital CAHPS survey addresses patient experiences in the inpatient setting.
31.The SCIP is a national quality partnership of organizations working to improving surgical care by significantly reducing surgical complications. The group is focused on four target areas including infection, adverse cardiac events, deep vein thrombosis, and post operative pneumonia.
32.The ASC Quality Collaboration is an 18 member private-public collaboration with representation from CMS, the Joint Commission, the Federated Ambulatory Surgery Association, the American College of Surgeons and others.
33.This table reflects measures that are publicly available.
34.Some hematology diagnoses are also relevant to the oncology/neoplasia subcategory. Anemia includes anemia of chronic disease and other unspecified anemias. Polycythemia vera is the most common red cell condition and unspecified thrombocytopenia is the most frequent platelet condition.
35.General symptoms include presenting complaints that usually have a broad differential diagnosis such as malaise, fever, sleep disturbances, dizziness, headache, swelling, and myalgia.
36.Some measures are included in more than one category such as chemotherapy measures (included in counts for chemotherapy and breast) and radiotherapy (included in radiotherapy, breast and urology).
37.All surgical oncology is included in the oncology/neoplasia category.
38.Includes urinary frequency, retention, incontinence.
39.Health literacy is defined in Healthy People 2010 as: "The degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions".
40.Health numeracy is defined as: The degree to which individuals have the capacity to access, process, interpret, communicate, and act on numerical, quantitative, graphical, biostatistical, and probabilistic health information needed to make effective health decisions.
41.For diabetes codes, fifth digits having the following values are translated as follows: 0 = type II or unspecified, not stated as uncontrolled; 1=type I, not stated as uncontrolled; 2=type II or unspecified, uncontrolled; and 3=type I, uncontrolled.