
This package--distributed at a national symposium held at the Wyndham Hotel, Washington, D.C. on May 23-25, 2004--was prepared by the Office of Disability, Aging and Long-Term Care Policy (DALTCP) with the U.S. Department of Health and Human Services (HHS) under Contract #HHS-100-03-0009 with the Lewin Group. For additional information, you may visit the DALTCP home page at http://aspe.hhs.gov then choose ASPE Office or contact the ASPE Project Officer, Andreas Frank, at HHS/ASPE/DALTCP, Room 424E, H.H Humphrey Building, 200 Independence Avenue, SW, Washington, DC 20201. His e-mail address is: Andreas.Frank@hhs.gov.
"Symposium Agenda
SUNDAY, MAY 23, 2004
5:30-7:30pm Welcome Reception
Hosted by John Hoff--Deputy Assistant Secretary for Disability, Aging and Long-Term Care Policy, Office of the Assistant Secretary for Planning and Evaluation, Department of Health and Human Services
MONDAY, MAY 24, 2004
7:30-8:00am Continental Breakfast
8:00-9:00am PLENARY ONE: "Welcome and Conference Overview"
8:00-8:20am Federal Sponsor Presentations
John Hoff--Deputy Assistant Secretary for Disability, Aging and Long-Term Care Policy, Office of the Assistant Secretary for Planning and Evaluation, Department of Health and Human Services
David E. Gray--Acting Assistant Secretary for Policy, Department of Labor
8:20-8:30am
Robyn Stone--Executive Director, Institute for the Future of Aging Services (Bio) (2003 Article) (October 2003 Paper) (May 2004 Paper) (Presentation)
Steven Dawson--President, Paraprofessional Healthcare Institute (Bio) (October 2003 Paper)
8:50-9:00am Audience Questions and Comments
9:00-10:15am PLENARY TWO: "Linking Staffing and Quality"
Robyn Stone--Executive Director, Institute for the Future of Aging Services (Bio) (2003 Article) (October 2003 Paper) (May 2004 Paper) (Presentation)
Overview and Introduction
Ted Benjamin--Professor, Department of Social Welfare, University of California Los Angeles (Bio) (Presentation)
“The Direct Care Workforce and the Quality of Care”
Larry Minnix--President, American Association of Homes and Services for the Aging (Bio)
“Quality Care, Healthy Cultures: Evidence of Success.”
Carol Raphael--CEO, Visiting Nurses Service of New York (VNSNY) (Bio)
"The Role of the Direct Care Worker and Quality Care”
Audience Questions and Comments
10:15-10:20am Instructions to Small Groups
Andreas Frank--Director, Division of Long-Term Care Policy, Department of Health and Human Services
Stephanie Swirsky--Office of the Assistant Secretary for Policy, Department of Labor
10:20-10:30am Break
10:30-11:45am Small Group Break Out Session 1
11:45am-1:30pm Luncheon Address
Introductory Remarks
Elaine E. Chao--Secretary, Department of Labor (invited)
Tommy G. Thompson--Secretary, Department of Health and Human Services (invited)
Keynote
Dirk Kempthorne--Governor, State of Idaho and Chair, National Governors Association (Bio)
“A Lifetime of Health and Dignity: Confronting Long-Term Care Challenges in America”
1:30-1:45pm Break
1:45-3:30pm PLENARY THREE: "Connecting Workforce Development Initiatives, Individual Economic Opportunity and Quality Care"
1:45-2:00pm Overview Presentation: “Recruiting and Retaining a Quality Paraprofessional Workforce: Building Collaboratives with the Workforce Investment System”
Mike Fishman--The Lewin Group (Bio) (May 21, 2004 Paper) (Presentation)
Burt Barnow--John Hopkins University (Bio) (May 21, 2004 Paper) (Presentation)
2:00-3:30pm Federal, State and Local Workforce Development Initiatives
Gay Gilbert--Employment and Training Administration, U.S. Department of Labor (Bio) (Presentation)
“Department of Labor’s High Growth Job Training Initiative”
Lloyd Schipper--Deputy Secretary, South Dakota Department of Labor (Bio) (Presentation)
“Good Samaritan Career Lattice Project”
Juan Manigault--CEO, Northern Indiana Workforce Investment Board (Bio) (Presentation)
“Healthcare Partnerships in Northern Indiana”
Charles Bodhi--Director of Employer Services, Regional Employment Board of Hampden County, Inc. (Presentation)
“Extended Career Ladders: A Local Workforce Development Perspective”
Audience Questions and Comments
3:30-3:45pm Break
3:45-5:15pm Small Group Break Out Session 2
5:15-6:15pm Break [Possible places to gather: Tower Lounge (Upper Mezzanine) or Federal Bar (Main Lobby Level)]
6:30-7:30pm Dinner and Presentation "HeartWork"
Introductory Remarks
Ms. Karen Kulp--President, Home Care Associates
Ms. Charlotte Hobson--Personal Care Attendant, HeartWork Performer
TUESDAY, MAY 25, 2004
8:00-9:00am Continental Breakfast [Free networking time for participants]
9:00-9:15am Presentation
Jean Moore--Center for Health Workforce Studies, SUNY School of Public Health (Bio) (Presentation)
“HRSA’s Study on Nursing Aides and Home Health Care Aides”
9:15-10:15am PLENARY FOUR: "The Impact of Workforce Improvement Initiatives on Workforce Recruitment and Retention"
Patsy Harris--Executive Director, Direct Care Alliance (Bio) (Presentation)
“The Direct Care Alliance”
Debra Lipson--Deputy Director of Better Jobs, Better Care, Institute for the Future of Aging Services (Bio) (May 2004 Paper) (Presentation)
“Better Jobs, Better Care”
Ruth Katz--Office of the Assistant Secretary for Planning and Evaluation, Department of Health and Human Services (Bio)
“Department of Health and Human Services Initiatives to Improve the Long-Term Care Workforce”
Audience Questions and Comments
10:15-10:30am Break
10:30am-12:10pm PLENARY FOUR: "The Impact of Workforce Improvement Initiatives on Workforce Recruitment and Retention" (continued)
Lauren Harris-Kojetin--Director of Research, Institute for the Future of Aging Services (Bio) (May 2004 Paper) (Presentation)
“Research Synthesis on Long-Term Care Workforce Recruitment and Retention Initiatives”
Vera Salter--Director, National Clearinghouse on the Direct Care Workforce, Paraprofessional Health Care Institute (Bio) (Presentation)
“National Clearinghouse on the Direct Care Workforce”
Michael Elsas--President, Cooperative Home Care Associates (Bio) (Presentation)
“The Impact of Workforce Initiatives on Recruitment, Training and Retention”
John Schnelle--Professor, School of Medicine, UCLA, and Director, Bourn Center for Gerontological Research (Bio) (Presentation)
"Nursing Home Workforce and Quality”
Audience Questions and Comments
12:10-12:30pm Break
12:30-2:30pm Working Lunch (in Break Out Rooms) and Break Out Session 3
2:30-2:45pm Break
2:45-3:45pm Concluding Session
4:00pm Adjourn
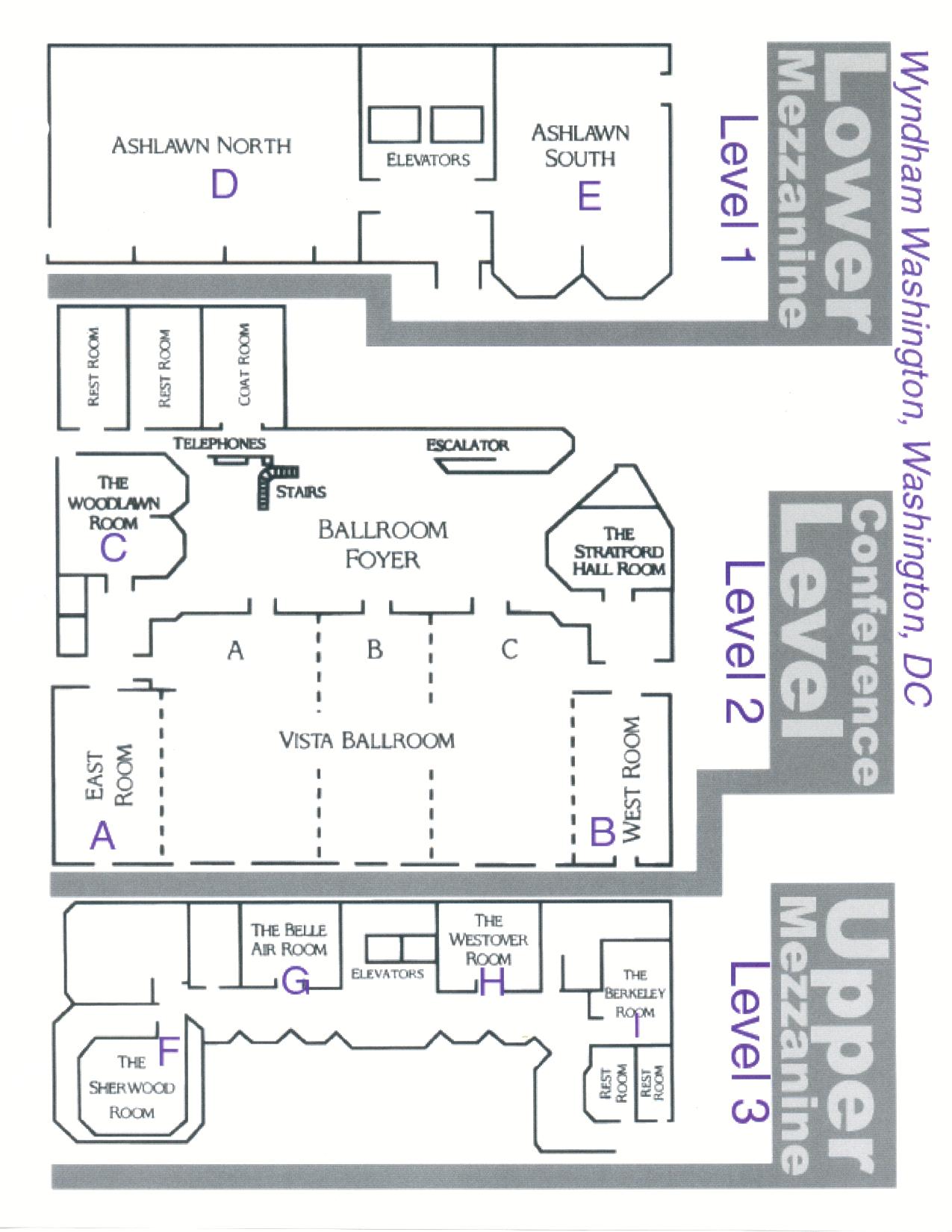
Hotel Orientation Map
 |
Participant List
Lisa Alecxih, M.P.A., Vice President, The Lewin Group, 3130 Fairview Park Drive, Suite 800, Falls Church, VA 22042, Phone: (703)269-5542, Fax: (703)269-5503, Email: lisa.alecxih@lewin.com
Zenobia Anderson, Certified Home Health Aide, Cooperative Health Care Associates, 349 East 149th Street, Fifth Floor, Bronx, NY 10451, Phone: (718)993-7104, Fax: (718)585-6852, Email: carin@paraprofessional.org
Dana Barbieri, U.S. Department of Labor, 200 Constitution Avenue, NW, Washington, DC 20210, Phone: (202)693-6151, Fax: (202)693-5960, Email: barbieri.dana@dol.gov
Burt Barnow, Ph.D., Associate Director for Research, Johns Hopkins University, Institute for Policy Studies, 3400 N. Charles Street, Baltimore, MD 21218, Phone: (410)516-5388, Fax: (410)516-8233, Email: barnow@jhu.edu (Bio) (May 21, 2004 Paper) (Presentation)
Cornelia Beck, Ph.D., R.N., F.A.A.N., University of Arkansas for Medical Sciences, 4301 W. Markham, Suite 808, Little Rock, AR 72205, Phone: (501)526-5750, Fax: (501)526-7560, Email: beckcornelia@uams.edu
Ted Benjamin, Ph.D., Professor, University of California, Los Angeles, School of Public Policy and Social Research, 3250 Public Policy Building, Los Angeles, CA 90095-1656, Phone: (310)206-6044, Fax: (310)206-7446, Email: tedbenj@ucla.edu (Bio) (Presentation)
Linda Bergofsky, M.S.W., Social Science Analyst, Office of Disability, Aging and Long-Term Care Policy, U.S. Department of Health and Human Services, 200 Independence Avenue, SW, Room 424E, H.H. Humphrey Building, Washington, DC 20201, Phone: (202)690-5741, Fax: (202)401-7733, Email: linda.bergofsky@hhs.gov
Brian Biles, M.D., Professor, George Washington University, 2021 K Street, Suite 800, Washington, DC 20006, Phone: (202)416-0066, Fax: (202)416-0075, Email: bbiles@gwu.edu
Christine Bishop, Ph.D., Professor, Schneider Institute for Health Policy, Brandeis University, 415 South Street, Mail Stop 035, Waltham, MA 02454-9110, Phone: (781)736-3942, Fax: (781)736-3905, Email: bishop@brandeis.edu
Carrie Blakeway, The Lewin Group, 3130 Fairview Park Drive, Suite 800, Falls Church, VA 22042, Phone: (703)269-5500, Fax: (703)269-5501, Email: carrie.blakeway@lewin.com
Carolyn Blanks, Vice President, Labor and Workforce Development, Massachusetts Extended Care Federation, 2310 Washington Street, Newton Lower Falls, MA 02462, Phone: (617)558-0202, Fax: (617)558-3546, Email: cblanks@mecf.org
Charles Bodhi, B.A., Regional Employment Board of Hampden County, Inc., 1441 Main Street, 1st Floor, Springfield, MA 01103, Phone: (413)755-1361, Fax: (413)755-1364, Email: bodhi@rebhc.org (Presentation)
John Booker, C.N.A., National Association for Direct Care Workers of Color, Inc., 2425 Poland Street, South Bend, Indiana 46619, Phone: (574)289-9326, Fax: (574)289-9326, Email: bookeru@aol.com
Robert Bowles, Ph.D., Labor Market Information Division, North Carolina ESC, P.O. Box 25903, Raleigh, NC 27611, Phone: (919)733-2936, Fax: (919)733-8662, Email: robert.bowles@ncmail.net
Diane Braunstein, Program Director, National Governors Association, 444 North Capitol Street, Suite 267, Washington, DC 20001-1512, Phone: (202)624-7854, Fax: (202)624-5313, Email: dbraunstein@nga.org
Dale Brown, B.A., Policy Advisor, Office of Disability Employment Policy, U.S. Department of Labor, 200 Constitution Avenue, NW, Room S1011, Washington, DC 20210, Phone: (202)693-7854, Fax: (202)693-4929, Email: brown-dale@dol.gov
Natasha Bryant, M.A., Institute for the Future of Aging Services, 2519 Connecticut Avenue, NW, Washington, DC 20008, Phone: (202)308-1214, Fax: (202)783-4266, Email: nbryant@aahsa.org
Robert Burke, Ph.D., Acting Chair, George Washington University, 2175 K Street, Suite 700 , Washington, DC 20037, Phone: (202)467-2288, Fax: (202)467-2289, Email: hsmreb@gwumc.edu
Anne Burns Johnson, M.P.H., President/CEO, California Association of Homes and Services for the Aging, 1315 I Street, Suite 100, Sacramento, CA 95814, Phone: (916)392-5111, Fax: (916)428-4250, Email: aburnsjohnson@aging.org
Donna Calame, J.D., Executive Director, San Francisco In-Home Supportive Services Public Authority, 939 Market Street, Suite 550, San Francisco, CA 94103, Phone: (415)243-4477, Fax: (415)243-4407, Email: dcalame@sfihsspa.org
Joy Calkin, Ph.D., M.Sc.N., D.Sc. (Hon), Professor Emerita, Joy D. Calkin Consulting, P.O. Box 264, 215 Victoria Street, Chester, Nova Scotia, Canada B0J 1J0, Phone: (902)275-2529, Fax: (902)275-5480, Email: j.calkin@ns.sympatico.ca
Denise Clark, Supervising Coordinator and Political Action Group Coordinator, Cooperative Health Care Associates, 349 East 149th Street, Fifth Floor, Bronx, NY 10451, Phone: (718)993-7104, Fax: (718)585-6852, Email: dclark@chcany.org
Elaine Cohen, M.S., R.N., Chief, Special Projects, Division of Nursing, Bureau of Health Professions, Health Resources and Services Administration, U.S. Department of Health and Human Services, 5600 Fishers Lane, Room 9-35, Rockville, MD 20857, Phone: (301)443-1405, Fax: (301)443-8586, Email: ecohen@hrsa.gov
Pearl Cunningham, Certified Home Health Aide, HomeCare Associates, 1315 Walnut Street, Philadelphia, PA 10451 , Phone: (267)238-3213, Email: kkulp@homecareassociatespa.com
LoriAnn Dancheck, Research Associate, Adult Communities Total Services Retirement-Life Communities, 375 Morris Road, West Point, PA 19486, Phone: (215)661-8330, Fax: (215)661-8320, Email: ldancheck@actslife.org
Steven Dawson, President, Paraprofessional Healthcare Institute, 349 East 149th Street, 10th Floor, Bronx, NY 10451, Phone: (718)402-7471, Fax: (718)585-6852, Email: steven@paraprofessional.org (Bio) (October 2003 Paper)
Angela Dayton, Employment and Training Administration, U.S. Department of Labor, 200 Constitution Avenue, NW, Suite N4641, Washington, DC 20210, Phone: (202)693-5969, Fax: (202)693-3890, Email: dayton.angela@dol.gov
Arlene deSilva, M.A., Chief Executive Officer, Council on Aging of Southwestern Ohio, 644 Linn Street, Suite 1100, Phone: (513)345-8611, Fax: (513)651-2534, Email: desilva@help4seniors.org
Angela Duran, M.P.P., Executive Director, Good Faith Fund, 2304 West 29th Avenue, Pine Bluff, AR 71603, Phone: (870)535-6233 ext.40, Fax: (870)535-0741, Email: aduran@goodfaithfund.org
Steven Edelstein, J.D., A.B., National Policy Director, Paraprofessional Healthcare Institute, 349 East 149th Street, 10th Floor, Bronx, NY 10451, Phone: (718)402-7766, Fax: (718)585-6852, Email: edelstein@paraprofessional.org
Eileen Elias, Deputy Director, U.S. Department of Health and Human Services, 200 Independence Avenue, SW, Room 637D, H.H. Humphrey Building, Washington, DC 20201, Phone: (202)205-1104, Fax: (202)260-3053, Email: eileen.elias@hhs.gov
Michael Elsas, President, Cooperative Health Care Associates, 349 East 149th Street, Fifth Floor, Bronx, NY 10451, Phone: (718)993-7104, Fax: (718)993-0971, Email: melsas@chcany.org (Bio) (Presentation)
Lenora Evans, C.N.A., Jewish Home and Hospital Lifecare System, c/o Andrea Reshen Bronx Division, 100 West Kingsbridge Road, Bronx, NY 10468, Phone: (718)410-1467, Fax: (718)410-1260, Email: areshen@jhha.org
Cheryl Feldman, M.S.W., Director, District 1199C Training and Upgrading Fund, 1319 Locust Street, Philadelphia, PA 19107, Phone: (215)735-5555, Fax: (215)735-7910, Email: cfeldman@1199ctraining.org
Thomas Finch, Ph.D., Consultant, Office of Disability, U.S. Department of Health and Human Services, 200 Independence Avenue, SW, Washington, DC 20201, Phone: (202)401-5844, Fax: (202)260-3053, Email: thomas.finch@hhs.gov
Diana Findley, Executive Director, Iowa CareGivers Association, 1117 Pleasant Street, Suite 221, Des Moines, IA 50309, Phone: (515)241-8697, Fax: (515)241-8587, Email: iowacga@aol.com
Michael Fishman, M.Pysc., M.P.A., Senior Vice President, The Lewin Group, 3130 Fairview Park Drive, Suite 800, Falls Church, VA 22042, Phone: (703)269-5655, Fax: (703)269-5503, Email: mike.fishman@lewin.com (Bio) (May 21, 2004 Paper) (Presentation)
Sandra Fitzler, B.S.N., Senior Director of Clinical Services, American Health Care Association, 1201 L Street, NW, Washington, DC 20005, Phone: (202)898-6307, Fax: (202)842-3860, Email: sfitzler@ahca.org
Brian Forschner, Ph.D., President, Mercy Senior Health and Housing, Mercy Health Partners, 2950 West Park Drive, Cincinnati, OH 45238, Phone: (513)347-8232, Fax: (513)451-3728, Email: beforschner@health-partners.org
Andreas Frank, Director, Division of Long-Term Care Policy, Office of Disability, Aging and Long-Term Care Policy, U.S. Department of Health and Human Services, 200 Independence Avenue, SW, Room 424E, H.H. Humphrey Building, Washington, DC 20201, Phone: (202)690-6443, Fax: (202)401-7733, Email: andreas.frank@hhs.gov
Elsie French, M.B.A., Managing Director, Adult Communities Total Services Retirement-Life Communities, 6901 SW 18th Street, Suite 301, Boca Raton, FL 33433, Phone: (561)362-8377, Fax: (561)416-1461, Email: efrench@actslife.org
Suellen Galbraith, M.S.W., Director of Government Relations, American Network of Community Options and Resources, 1101 King Street, Suite 380, Alexandria, VA 22314-2944, Phone: (703)535-7850, Fax: (703-535-7860, Email: sgalbraith@ancor.org
James Gardner, Ph.D., President/CEO, Council on Quality and Leadership, 100 West Road, Suite 406, Towson, MD 21204, Phone: (410)583-0060, Fax: (410)583-0063, Email: jfgardner@thecouncil.org
Denise Geolot, Ph.D., R.N., F.A.A.N., Director, Division of Nursing, Health Resources and Services Administration, U.S. Department of Health and Human Services, 5600 Fishers Lane, Room 9-35, Rockville, MD 20857, Phone: (301)443-5688, Fax: (301)443-8586, Email: dgeolot@hrsa.gov
Gay Gilbert, J.D., M.S.W., Director, Business Relation Group, Employment and Training Administration, U.S. Department of Labor, 200 Constitution Avenue, NW, Room N4643, Washington, DC 20210, Phone: (202)693-3892, Fax: (202)693-3890, Email: gilbert.gay@dol.gov (Bio) (Presentation)
Laura Ginsburg, M.A., Employment and Training Administration, U.S. Department of Labor, 200 Constitution Avenue, NW, Suite N4671, Washington, DC 20210, Phone: (202)693-2803, Fax: (202)693-2808, Email: ginsburg.laura@dol.gov
John Grace, M.Sc., President, Kansas Homes and Services for Aging, 217 SE 8th Street, Topeka, KS 66603, Phone: (785)233-7443, Fax: (785)233-9471, Email: jrgrace@kahsa.org
Leslie Grant, Ph.D., Professor, Department of Health Care Management, Carlson School of Management, University of Minnesota, 321 19th Avenue South, 3-150 CSOM, Minneapolis, MN 55455, Phone: (612)624-8844, Fax: (612)624-8804, Email: lgrant@CSOM.umn.edu
Jean Grochowski, M.B.A., B.S.M.E., MBA Fellow, Employment and Training Administration, Business Relations Group, U.S. Department of Labor, 200 Constitution Avenue, NW, Suite N4641, Washington, DC 20210, Phone: (202)693-3592, Fax: (202)693-3890, Email: grochowski.jean@dol.gov
George Gunn, Jr., M.S., Vice Chairman and CEO, Adult Communities Total Services Retirement-Life Communities, 375 Morris Road, West Point, PA 19486, Phone: (215)661-8330, Fax: (215)661-8320, Email: grgunnjr@actslife.org
Gayle Hamilton, MDRC, 16 East 34th Street, New York, NY 10516, Phone: (212)340-8665, Fax: (212)532-8511, Email: gayle.hamilton@mdrc.org
Brandy Danielle Harris, M.S., M.A., Institute for the Future of Aging Services, 4221 Waterford Lane, Trussville, AL 35173, Phone: (850)644-7927, Fax: (850)644-2304, Email: bdb4260@fsu.edu
Patsy Harris, Executive Director, Direct Care Alliance, 1054 31st Street NW, Suite 425, Washington, DC 20007, Phone: (202)338-1209 ext109, Fax: (202)337-6508, Email: patsy@directcarealliance.org (Bio) (Presentation)
Lauren Harris-Kojetin, Ph.D., M.A., Director of Research, Institute for the Future of Aging Service, 2519 Connecticut Avenue, NW, Washington, DC 20008, Phone: (202)508-9462, Fax: (202)738-4266, Email: lharris-kojetin@aahsa.org (Bio) (May 2004 Paper) (Presentation)
Conaway Haskins, M.R.P., Research Associate, Aspen Institute, 1 Dupont Circle, NW, Suite 700, Washington, DC 20036, Phone: (202)736-1495, Fax: (202)476-0790, Email: conaway.haskins@aspeninst.org
Tim Henderson, M.S.P.H., National Conference of State Legislatures, 444 North Capitol Street, NW, Suite 515, Washington, DC 20001, Phone: (202)624-3573, Fax: (202)737-1069, Email: tim.henderson@ncsl.org
Brenda Hipp, Manager, Butte One Stop Workforce Center, 2201 White Boulevard, Butte, MT 59701, Phone: (406)494-0300, Fax: (406)494-5481, Email: bhipp@state.mt.us
Charlotte Hobson, Residential Counselor, Heartwork Melinark, 248 Hampden Road, Upper Darby, PA 19082, Phone: (610)352-2401, Fax: (484)582-1269
Sabrina Horry, Certified Health Aide, Cooperative Health Care Associates, 349 East 149th Street, Fifth Floor, Bronx, NY 10451, Phone: (718)993-7104, Fax: (718)993-0971, Email: shorry@chcany.org
Roberta Jackson, Certified Home Health Aide, Cooperative Health Care Associates, 349 East 149th Street, Fifth Floor, Bronx, NY 10451, Phone: (718)993-7104, Fax: (718)993-0971, Email: rjackson@chcany.org
Clint Jones, Project Director, Foundation for Healthy Communities, 125 Airport Road, Concord, NH 03301, Phone: (603)225-0900, Fax: (603)225-4346, Email: cjones@healthynh.com
Ruta Kadonoff, M.H.S., Senior Policy Analyst, American Association of Homes and Services for the Aging, 2519 Connecticut Avenue, NW, Washington, DC 20008, Phone: (202)508-9450, Fax: (202)220-0044, Email: rkadonoff@aahsa.org
Carol Kapolka, Program Director, Extended Care Career Ladder Initiative, Commonwealth Corporation, 529 Main Street, Schrafft Center, Suite 110, Boston, MA 02129, Phone: (617)727-8158, Fax: (617)242-7660, Email: ckapolka@commcorp.org
Ruth Katz, Deputy to the Deputy Assistant Secretary, Office of Disability, Aging and Long-Term Care Policy, U.S. Department of Health and Human Services, 200 Independence Avenue, SW, Room 424E, H.H. Humphrey Building, Washington, DC 20201, Phone: (202)690-6443, Fax: (202)401-7733, Email: ruth.katz@hhs.gov (Bio)
Peter Kemper, Ph.D., Professor, Department of Health Policy and Administration, College of Health and Human Development, Pennsylvania State University, University Park, PA 16802, Phone: (814)863-2900, Fax: (814)863-2905, Email: pkemper@psu.edu
Kate King, M.P.A., Health Insurance Specialist, CMSO/DEHPG/DCSI, Centers for Medicare and Medicaid Services, 7500 Security Boulevard, Mail Stop S2-14-26, Baltimore, MD 21244-1850, Phone: (410)786-1283, Fax: (410)786-9004, Email: kking@cms.hhs.gov
Thomas Konrad, Ph.D., Senior Fellow, Cecil G. Sheps Center, National Cancer Institute on Aging, 725 Airport Road, CB 7590, Chapel Hill, NC 27599-7590, Phone: (919)966-2501, Fax: (919)966-3811, Email: bob_konrad@unc.edu
Karen Kulp, HomeCare Associates, 1315 Walnut Street, Suite 832, Philadelphia, PA 10451, Phone: (267)238-3213, Fax: (215)735-0644, Email: kkulp@homecareassociatespa.com
Alice LaGuerre, C.N.A., Peer Mentoring, Center for Nursing and Rehabilitation, 596 Prospect Place, Brooklyn, NY 11238, Phone: (718)636-1000, Fax: (718)585-6852, Email: carin@paraprofessional.org
Rebekah Lashman, M.B.A., Manager of Workforce Partnerships, Boston Private Industry Council, 2 Oliver Street, Boston, MA 02109, Phone: (617)488-1314, Fax: (617)423-1041, Email: Rebekah.Lashman@bostonpic.org
Charlene Liggins, M.P.H., M.P.A., Social Science Analyst, Office of Disability, Aging and Long-Term Care Policy, U.S. Department of Health and Human Services, 200 Independence Avenue, SW, Room 424E, H.H. Humphrey Building, Washington, DC 20201, Phone: (202)690-5765, Fax: (202)401-7733, Email: Charlene.Liggins@hhs.gov
David Lindeman, Ph.D., Director, Mather LifeWays, 1603 Orrington Avenue, Suite 1800, Evanston, IL 60201, Phone: (847)492-6810, Fax: (847)492-6789, Email: dlindeman@matherlifeways.com
Debra Lipson, M.H.S.A., Deputy Director, Better Jobs Better Care, American Association of Homes and Services for the Aging, 2519 Connecticut Avenue, NW, Washington, DC 20008, Phone: (202)508-1215, Fax: (202)783-4266, Email: dlipson@aahsa.org (Bio) (May 2004 Paper) (Presentation)
Pamela Loving, Career Alliance, Inc., 711 North Saginaw Street, Suite 300, Flint, MI 48503, Phone: (810)233-5974, Fax: (810)233-8652, Email: ploving@careeralliance.org
Juan Manigault, M.S.B.A., President and CEO, Northern Indiana Workforce Investment Board, 401 East Colfax Avenue, Suite 307, South Bend, IN 46617, Phone: (574)239-2380 ext. 212, Fax: (574)239-2386, Email: jam200@niwib.com (Bio) (Presentation)
Lorrene Maynard, C.N.A., Founder and Director, Virginia Association of Professional Nursing Assistants, Inc., P.O. Box 3732, Hampton, VA 23663, Phone: (757)595-1483, Fax: (757)886-0950, Email: professionalcna@aol.com
Sheila McConnell, U.S. Department of Labor, 200 Constitution Avenue, NW, Room S2312, Washington, DC 20210, Phone: (202)693-5903, Email: mcconnell.sheila@dol.gov
Diane Menio, M.S., Executive Director, Center for the Advocacy for the Rights and Interests of the Elderly, 100 North 17th Street, Suite 600, Philadelphia, PA 19103, Phone: (215)545-5728, Fax: (215)546-9963, Email: menio@carie.org
William Minnix, Jr., D.Min., D.Miv., American Association of Homes and Services for the Aging, 2519 Connecticut Avenue, NW, Washington, DC 20008, Phone: (202)508-9426, Fax: (202)220-0020, Email: lminnix@aahsa.org (Bio)
Jean Moore, M.S.N., Director, Center for Health Workforce Studies, School of Public Health, University of Albany, 1 University Place, Room B-334, Rensselaer, NY 12144, Phone: (518)402-0250, Fax: (518)402-0252, Email: jmm04@health.state.ny.us (Bio) (Presentation)
Jan Moxley, M.S., Office of Long Term Care, North Carolina Department of Health and Human Services, 2001Mail Service Center, Raleigh, NC 27699-2001, Phone: (919)715-0807, Fax: (919)715-1850, Email: jan_moxley@ncmail.net
Evvie Munley, B.S.W., Senior Policy Analyst, American Association of Homes and Services for the Aging, 2519 Connecticut Avenue, NW, Washington, DC 20008, Phone: (202)783-2242, Fax: (202)220-0044, Email: emunley@aahsa.org
Kerry Paige Nesseler, R.N., M.S., Captain, Health Resources and Services Administration, U.S. Department of Health and Human Services, 5600 Fishers Lane, Room 8-05, Rockville, MD 20857, Phone: (301)443-5794, Fax: (301)443-2111, Email: knesseler@hrsa.gov
Robert Newcomer, Ph.D., Professor, Personal Assistance Services Center, University of California, 3333 California Street, Suite 455, San Francisco, CA 94118, Phone: (415)476-1408, Fax: (415)476-6552, Email: rjn@itsa.ucsf.edu
Linda Noelker, Ph.D., Senior Vice President, Benjamin Rose, 850 Euclid Avenue, Suite 1100, Cleveland, OH 44114-3301, Phone: (216)373-1603, Fax: (216)621-3505, Email: lnoelker@benrose.org
Carol O’Shaughnessy, M.A., Specialist in Social Legislation, Congressional Research Service, 101 Independence Avenue, SE, Washington, DC 20540, Phone: (202)707-7329, Email: coshaughnessy@crs.loc.gov
Rose Padmore, Certified Home Health Aide, HomeCare Associates, 1315 Walnut Street, Philadelphia, PA 10451, Phone: (267)238-3213, Email: kkulp@homecareassociatespa.com
Timothy Palmer, M.S., Executive Director, Community of Vermont Elders, 79 River Street, P.O. Box 1276, Montpelier, VT 05602, Phone: (802)229-4731, Fax: (802)229-0156, Email: tim@vermontelders.org
Victoria Parker, D.B.A., Assistant Professor, Boston University, 200 Springs Road (152), Bedford, MA 01730, Phone: (781)275-7500 ext. 6054, Fax: (781)687-3106, Email: vaparker@bu.edu
Lori Porter, Co-founder and CEO, National Association of Geriatric Nursing Assistants, 2709 West 13th Street, Joplin, MO 64801, Phone: (417)623-6049, Fax: (417)623-2230, Email: lporter@nagna.org
D.E.B. Potter, M.S., Senior Survey Statistician, Co-Leader, Long Term Care Portfolio, Agency for Healthcare Research and Quality, 540 Gaither Road, Suite 500, Rockville, MD 20850, Phone: (301)427-1564, Fax: (301)427-1276, Email: dpotter@ahrp.gov
Peggy Powell, Director of Workforce Strategies, Paraprofessional Healthcare Institute, 349 East 149th Street, 10th Floor, Bronx, NY 10451, Phone: (718)402-7766, Fax: (718)585-6852, Email: peggy@paraprofessional.org
Jude Rabig, Director, Green House Project, 401 East 34th Street, N15K, New York, NY 10016, Phone: (212)217-0972, Fax: (866)209-6736, Email: greenhouseproject@rcn.com
Carol Raphael, M.P.A., President and CEO, Visiting Nurse Service of New York, 107 East 70th Street, New York, NY 10021, Phone: (212)609-1510, Fax: (212)794-6610, Email: craphael@vnsny.org (Bio)
Linda Redford, Ph.D., R.N., Director, Central Plains Geriatric Education Center, University of Kansas Medical Center, 3901 Rainbow Boulevard, Mail Stop 1005, Kansas City, KS 66160, Phone: (913)588-1636, Fax: (913)588-3179, Email: lredford@kumc.edu
Susan Reinhard, Ph.D., R.N., Center for State Health Policy, Rutgers University, 317 George Street, Suite 400, New Brunswick, NJ 08901, Phone: (732)932-3105 ext.230, Fax: (732)932-0069, Email: sreinhard@cshp.rutgers.edu
Robin Remsburg, Ph.D., A.P.R.N., B.C., Chief, Long-Term Care Statistics Branch, National Center for Health Statistics, Centers for Disease Control and Prevention, 3311 Toledo Road, Hyattsville, MD 20782, Phone: (301)458-4416, Fax: (301)458-4693, Email: rqr3@cdc.gov
Andrea Reshen, M.A., A.B.D., Director of Culture Change, Jewish Home and Hospital Lifecare System, 100 West Kingsbridge Road, Bronx, NY 10468, Phone: (718)410-1467, Fax: (718)410-1260, Email: areshen@jhha.org
Christine Rico, Vice President, Paraprofessional Healthcare Institute, 349 East 149th Street, 10th Floor, Bronx, NY 10451, Phone: (718)402-7446, Fax: (718)585-6852, Email: christine@paraprofessional.org
Carol Rodet, M.A., Home Care Association of New York State, 194 Washington Avenue, Albany, NY 12210, Phone: (518)426-8764, Fax: (518)426-8788, Email: croder@earthlink.net
Linda Rohrer, Deputy Director, Commonwealth Corporation, 529 Main Street, Schrafft Center, Suite 110, Boston, MA 02129, Phone: (617)727-8158, Fax: (617)242-7660, Email: lrohrer@commcorp.org
Emily Rosenoff, M.P.A., Office of Disability, Aging and Long-Term Care Policy, U.S. Department of Health and Human Services, 200 Independence Avenue, SW, Room 424E, H.H. Humphrey Building, Washington, DC 20201, Phone: (202)690-5740, Fax: (202)401-7733, Email: emily.rosenoff@hhs.gov
Vera Salter, Ph.D., Director, Paraprofessional Healthcare Institute, 349 East 149th Street, 10th Floor, Bronx, NY 10451, Phone: (718)402-7766, Fax: (718)585-6852, Email: Vera@paraprofessional.org (Bio) (Presentation)
Lila Sarante, Certified Home Health Aide, Cooperative Health Care Associates, 349 East 149th Street, Fifth Floor, Bronx, NY 10451, Phone: (718)993-7104, Email: lsarante@chcany.org
Dawn Savattone, M.S.W., Ombudsman Specialist, Area Agency on Aging, Region One, 1366 East Thomas Road, Suite 108, Phoenix, AZ 85014, Phone: (602)264-2255, Fax: (602)230-9132, Email: savattone@aaaphx.org
Lloyd Schipper, Deputy Secretary, South Dakota Department of Labor, 700 Governors Drive, Pierre, SD 57501, Phone: (605)773-3101, Fax: (605)773-4211, Email: lloyd.schipper@state.sd.us (Bio) (Presentation)
John Schnelle, Ph.D., Professor, University of California, Los Angeles, 7150 Tampa Avenue, Reseda, CA 91335-1656, Phone: (818)774-3234, Fax: (818)774-3346, Email: jschnell@ucla.edu (Bio) (Presentation)
Elizabeth Schultz, Director of Quality and Compliance, Providence Mount St. Vincent Pioneer Network, 4831 35th Avenue SW, Seattle, WA 98126-2799, Phone: (206)938-6033, Fax: (206)938-6249, Email: Elizabeth.Schultz@Providence.org
Gail Simms, P.C.A., H.H.A., Cooperative Home Care Associates, 1372 Washington Avenue, Apt. 18B, Bronx, NY 10456, Phone: (718)293-7812
Cynella Simon, C.N.A., Peer Mentoring, Center for Nursing and Rehabilitation, 596 Prospect Place, Brooklyn, NY 11238, Phone: (718)636-1000, Fax: (718)789-9212, Email: carin@paraprofessional.org
Navjeet Singh, Special Research Projects Director, Commonwealth Corporation, 529 Main Street, Schrafft Center, Suite 110, Boston, MA 02129, Phone: (617)727-8158, Fax: (617)242-7660, Email: nsingh@commcorp.org
Phyllis Snyder, M.A.T., M.C.P., Council for Adult and Experimental Learning, 1608 Walnut Street, Philadelphia, PA 19103, Phone: (215)731-7160, Fax: (215)731-0505, Email: psnyder@cael.org
Karen Soehner, Nursing Home Administrator, Avante at Ormond Beach Nursing and Rehabilitation Center, 170 North Kings Road, Ormond Beach, FL 32174, Phone: (386)677-7955, Fax: (386)676-9573, Email: ksoehner@bellsouth.net
William Spector, Ph.D., Senior Social Scientist, Agency for Healthcare Research and Quality, 540 Gaither Road, Rockville, MD 20850, Phone: (301)427-1446, Fax: (301)427-1430, Email: wspector@ahrp.gov
Melanie Starns, M.A.G., Program and Policy Analyst, Administration on Aging, U.S. Department of Health and Human Services, Washington, DC 20201, Phone: (202)357-3464, Fax: (202)357-3469, Email: melanie.starns@aoa.gov
Robyn Stone, Dr.P.H., Executive Director, American Association of Homes and Services for the Aging, 2519 Connecticut Avenue, NW, Washington, DC 20008, Phone: (202)508-1206, Fax: (202)783-4266, Email: rstone@aahsa.org (Bio) (2003 Article) (October 2003 Paper) (May 2004 Paper) (Presentation)
Julie Stone-Axelrad, M.P.A., Analyst in Social Legislation, Congressional Research Service, 101 Independence Avenue, SE, Washington, DC 20540, Phone: (202)707-1386, Fax: (202)707-3097, Email: jstone@crs.loc.gov
Rick Surpin, President, Independence Care System, 257 Park Avenue South, New York, NY 10010, Phone: (212)584-2500, Fax: (212)584-2555, Email: surpin@icsny.org
Stephanie Swirsky, Policy Analyst, Office of Policy, U.S. Department of Labor, 200 Constitution Avenue, NW, Room S2312, Washington, DC 20210, Phone: (202)693-5909, Fax: (202)693-5960, Email: swirsky.stephanie@dol.gov
Marianne Taylor, M.A., Human Services Research Institute, 2336 Massachusetts Avenue, Cambridge, MA 02140, Phone: (617)876-0426, Fax: (617)492-7401, Email: taylor@hsri.org
Anna Thompson, M.Ed., Coordinator of Special Projects, Atlanta Regional Workforce Board, 40 Courtland Street NE, Atlanta, GA 20202, Phone: (404)463-3331, Fax: (404)463-3310, Email: athompson@atlantaregional.com
Julie Trocchio, R.N., Senior Director, Continuing Care Ministries, Catholic Health Association, 1875 Eye Street, Suite 1000, Washington, DC 20006, Phone: (202)721-6320, Fax: (202)296-4024, Email: jtrocchio@chausa.org
Jean Tuller, M.P.A., Executive Director, Oregon Technical Assistance Corporation, 3886 Beverly Avenue, NE, Suite I-21, Salem, OR 97305, Phone: (503)364-9943, Fax: (503)364-1939, Email: jtuller@otac.org
Hollis Turnham, J.D., Michigan Policy Director, Paraprofessional Healthcare Institute, 5013 Applewood Drive, Lansing, MI 48917, Phone: (517)327-0331, Fax: (517)327-0331, Email: hturnham@aol.com
Paula Vereen, H.H.A., C.N.A., Cooperative Home Care, 623-5 Courtland Avenue, Apt 4C, Bronx, NY 10451, Phone: (718)402-0893, Email: dclark@chcany.org
Amanda Wallace, Senior Program Specialist, National Network of Sector Partners, 2201 Broadway, Suite 815, Oakland, CA 94612, Phone: (510)251-2600, Fax: (510)251-0600, Email: amy@nedlc.org
Julie Ward, Director of Employment and Transportation Policy, The Arc and UCP Public Policy Collaboration, 1660 L Street, Suite 700, Washington, DC 20036, Phone: (202)973-7146, Fax: (202)776-0414, Email: jward@ucp.org
Joan Weiss, Ph.D., R.N., C.R.N.P., Chief, Allied, Geriatrics and Rural Health Branch, Bureau of Health Professions, Health Resources and Services Administration, U.S. Department of Health and Human Services, 5600 Fishers Lane, Room 8-103, Rockville, MD 20857, Phone: (301)443-0430, Fax: (301)443-0162, Email: jweiss@hrsa.gov
Paul Wing, D.Engin., Deputy Director, Center for Health Workforce Studies, School of Public Health, University of Albany, 1 University Place, Room B-334, Rensselaer, NY 12144, Phone: (518)402-0250, Fax: (518)402-0252, Email: pow01@health.state.ny.us
Dan Wood, M.H.S.A., AVP, HCR-Manorcare, 333 North Summitt Street, Toledo, OH 43699-0086, Phone: (419)252-5715, Fax: (419)252-5510, Email: dwood@hcr-manorcare.com
Bernadette Wright, Ph.D, Policy Research Analyst, American Association of Retired Persons, 601 E Street, NW, Washington, DC 20049, Phone: (202)434-6291, Fax: (202)434-6402, Email: bwright@aarp.org
Wendy Yallowitz, M.S.W., Program Associate, Robert Wood Johnson Foundation, Route 1 and College Road East, Princeton, NJ 08543, Phone: (609)627-7553, Fax: (609)419-8332, Email: wyallow@rwjf.org
Lee Zacharias, The Zacharias Group, 441 North Pownal Road, New Gloucester, ME 04260, Phone: (207)926-5767, Fax: (207)926-5763, Email: Leezach1@aol.com
Michael Zelley, Disability Network, 3600 South Dort Highway, Suite 54, Flint, MI 48507, Phone: (810)742-1800, Fax: (810)742-2400, Email: mikezelley@aol.com
Sharon Zeruld, M.H.S.A., Senior Manager, The Lewin Group, 3130 Fairview Park Drive, Suite 800, Falls Church, VA 22042, Phone: (703)269-5967, Fax: (703)269-5503, Email: sharon.zeruld@lewin.com
Thomas Zwicker, Sapient, LLC, W210N11170, Mountbrooke Drive, Germantown, WI 53022, Phone: (414)477-9223, Fax: (262)532-0115, Email: Tzwicker@wi.rr.com
Speaker Biographies
Burt S. Barnow (May 21, 2004 Paper) (Presentation)
An economist with over 25 years of experience in the fields of labor economics, program evaluation, and applied econometrics. In his current position, Dr. Barnow teaches graduate and undergraduate courses in public policy and economics, conducts research for federal and state governments, and supervises research activities at the Institute for Policy Studies at Johns Hopkins University. Dr. Barnow currently serves as Vice Chair of the National Academy of Sciences Committee on the Information Technology Workforce, Chair of the Governor’s Workforce Investment Board Performance Measurement Committee, and Chair of the National Association of Schools of Public Affairs and Administration Research Committee. In addition, Dr. Barnow has served as an expert witness and consultant for many attorneys in the Washington, D.C. area and throughout the nation. Prior to joining the Institute for Policy Studies at Johns Hopkins University in August 1992, he was a Vice President of Lewin-ICF for 8 years and worked for nearly 9 years in the U.S. Department of Labor.
A.E. Benjamin (aka Ted) (Presentation)
At the University of California-Los Angeles, he is Professor and Chair in the Department of Social Welfare, School of Public Policy and Social Research. He has a joint PhD from the University of Michigan in political science and social work, and his interests involve long-term services for people with chronic conditions, particularly comparative access, service design and quality issues. He has done research across various populations with chronic health conditions in order to assess approaches to unifying rather than segmenting public policy responses to common service needs across groups. This research has involved the elderly, younger adults with disabilities, people with HIV disease, and children with special health needs. His current work addresses the impact of consumer-direction for people needing supportive services as well as a range of entry-level work force issues. This research has been supported by the U.S. Department of Health and Human Services, the Robert Wood Johnson Foundation, and the State of California. He is the author of numerous articles and book chapters and co-author (with Bob Newcomer) of an edited volume titled Indicators of Chronic Health Conditions.
Steven L. Dawson (October 2003 Paper)
President of the Paraprofessional Healthcare Institute, and has worked with PHI since its inception 12 years ago. PHI is a national health care employment, training and policy nonprofit, based in the South Bronx, New York. PHI, http://www.paraprofessional.org, is the nonprofit affiliate of the worker-owned, 800-employee Cooperative Home Care Associates. In early 2001, PHI launched the National Clearinghouse on the Direct Care Workforce, http://www.directcareclearinghouse.org the nation’s primary information center for direct-care staffing policy and practice initiatives.
Steven chairs Independence Care System, a project of PHI and New York’s first Medicaid-funded chronic care demonstration program for adults living in their homes with disabilities. He is also the author of several publications on low-wage and health care employment issues, including Jobs and the Urban Poor (co-authored with Peggy Clark of the Aspen Institute), Direct-Care Health Workers: The Unnecessary Crisis in Long-Term Care (co-authored with Rick Surpin of Independence Care System), and Long-Term Care Financing and the Long-Term Care Workforce Crisis: Causes and Solutions (published by the Citizens For Long Term Care).
Michael Elsas (Presentation)
President of Cooperative Home Care Associates, a licensed home health care agency located in the South Bronx. With just over 750 paraprofessional workers and an administrative staff of 50, Cooperative Home Care Associates has been nationally recognized for its unique worker centered philosophy which links quality jobs to quality home care services. Prior to joining Cooperative Home Care Associates in 2000, Mr. Elsas was the Chief Operating Officer of the Visiting Nurse Association of Hudson Valley. From community liaison to President, Mr. Elsas has over 30 years of experience in the home care industry. His professional affiliations include the Home Care Association of New York State, trustee of the 1199 SEIU Home Health Aide Benefit Fund, Catholic Charities and the Medical Society of New York. Mr. Elsas received a Bachelor of Arts degree from the C.W. Post Center of Long Island University.
Michael E. Fishman (May 21, 2004 Paper) (Presentation)
A Senior Vice President and Director of the Applied Economics Practice at The Lewin Group. Since joining The Lewin Group, Mr. Fishman has developed a practice related to welfare reform, employment and training, child support enforcement and the broad range of human service programs with which he has worked throughout his career. He has directed numerous projects for the Office of the Assistant Secretary for Planning and Evaluation (ASPE) and the Administration for Children and Families (ACF) in DHHS, the Social Security Administration, the Department of Labor, and other agencies. He has also testified before House Subcommittees on the results of his studies.
Prior to joining The Lewin Group, Mr. Fishman was the Director of the Office of Analysis and Evaluation in the Department of Agriculture’s Office of Food and Nutrition Service (FNS), and the Director of the Office of Income Security Policy in the ASPE. He has expertise in numerous areas of human services policy and has led project management initiatives in the areas of program research and evaluation, policy analysis, program development, and strategic planning. Mr. Fishman received his Masters in Public Administration from the University of Southern California, Washington Public Affairs Center in 1989 and a Masters in Organizational Psychology from Antioch College in 1977.
Gay M. Gilbert (Presentation)
Named Director of the Business Relations Group in March 2003, a special office formed by Assistant Secretary for the Employment and Training Administration, Emily Stover DeRocco, that is leading ETA efforts to more effectively engage business in the public workforce system. She has been with the U.S. Department of Labor since November 2000 and formerly served as Chief of the U.S. Employment Service and America’s Labor Market Information System (ALMIS).
Prior to coming to USDOL, Gay worked with the Ohio Bureau of Employment Services for over ten years, the last seven of which she served as Deputy Administrator overseeing core workforce development programs. She led Ohio’s implementation of their one-stop systems as well as the initial implementation of the Workforce Investment Act. Prior to her tenure in workforce development Gay served as Assistant City Attorney for the City of Columbus, Ohio in the area of public employment law and eight years with the West Virginia Department of Human Services. Her education includes: Bachelor of Arts, Michigan State University; Master of Social Work, West Virginia University; and Juris Doctor, Ohio State University.
Patsy Harris (Presentation)
Executive Director of the Direct Care Alliance (DCA), a national coalition of long-term care consumers, direct-care workers, and concerned health care providers working for broad-based reforms, within both public policy and industry practice, to ensure a stable, valued, and well-trained direct-care workforce. As the organization's first executive director, she is working to grow the membership of the DCA and to attain the financial support the alliance will need to become its own 501(c)3 nonprofit organization separate from PHI. Patsy has over 12 years of experience in management, health care consulting, and programming and has participated in economic and workforce development initiatives in the Austin, Texas area. She graduated from Sam Houston State University with a BA in government and business and completed her MPA at Southwest Texas State University.
Ruth E. Katz
Deputy to the Deputy Assistant Secretary for the Office of Disability, Aging and Long-Term Care Policy, in the Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services. She oversees a range of policy and research activities related to disability and aging. With over 25 years of experience with disability and long-term care issues, these include: managed care and other health and long-term care delivery systems--financing, structure and quality; home and community-based services; nursing home and post-acute care financing and quality; Medicare, Medicaid and private insurance policy related to people with disabilities and chronic conditions; alternative residential systems; and health information technology as it relates to post acute and long-term care.
Dirk Kempthorne, Governor of Idaho
He was born in San Diego, California, and attended the University of Idaho, earning a bachelor's degree in political science in 1975. Kempthorne was elected mayor of Boise, Idaho, in 1984 and served for seven years. He was elected to the U.S. Senate in November 1992. His first bill, legislation to end unfunded federal mandates on state and local governments, became Senate Bill 1 in the 104th Congress. It was signed into law on March 22, 1995, at a Rose Garden ceremony. Kempthorne authored the new Safe Drinking Water Act in 1996, which provided clean, safe, and affordable drinking water without federal restrictions. He was a member of the Environment and Public Works Committee, which produced a highway bill to dramatically increase the amount of federal funds coming to the states for road, bridge, and infrastructure repair. He chaired the Drinking Water, Fisheries, and Wildlife Subcommittee; served on the Armed Services Committee, chairing the Military Personnel Subcommittee; and served on the Small Business Committee. The Idaho Jaycees selected him as Outstanding Young Idahoan in 1988, and he has earned the Distinguished Service Medal, the top civilian honor from the Idaho National Guard. Kempthorne is past president of the Council of State Governments, past chair of the Western Governors' Association, and a member of the Executive Committee of the Republican Governors Association. Governor Kempthorne is chairman of the National Governors Association.
Lauren Harris-Kojetin (May 2004 Paper) (Presentation)
Director of Research at the Institute for the Future of Aging Services. She directs and coordinates the Institute’s research agenda. Dr. Harris-Kojetin has 15 years experience in applied research with an emphasis on: health care quality, access, and education for older adults and program evaluation. She leads and contributes to projects to: improve the quality and stability of the long-term care workforce; improve the quality of services provided to elders; educate consumers about quality in health care and aging services; and, promote healthy behaviors in older adults through education, programming, and environmental design. Her methodological expertise includes case studies, surveys, key informant interviews, usability testing, statistical analysis, experimental and quasi-experimental design, and focus groups and interviews with elders and persons with disabilities. She has directed numerous federal research studies for the Agency for Healthcare Research and Quality, the Centers for Medicare and Medicaid Services, and the Assistant Secretary for Planning and Evaluation on topics such as health plan quality, survey design, health education and decision making for older adults, Medicare education, and using research to help develop a quality long-term care workforce. Dr. Harris-Kojetin has published frequently on measuring and communicating health care quality for older adults. She has a PhD and MA in Public Policy from Rutgers University.
Debra J. Lipson (May 2004 Paper) (Presentation)
She has over 20 years experience as a health policy analyst, program administrator and community organizer, at the local, state, national and international level. Currently, she is Deputy Director of the Better Jobs Better Care Program at the Institute for the Future of Aging Services, based at the American Association of Homes and Services for the Aging in Washington DC. Better Jobs Better Care is a $15 million research and demonstration program funded by the Robert Wood Johnson Foundation and The Atlantic Philanthropies, which tests and studies effective ways to strengthen the long-term care workforce. She directs the grant selection and management process, develops communications strategies and products, and oversees and provides technical assistance to grantees.
Prior to her current position, Ms. Lipson worked at the World Health Organization in Geneva Switzerland, where she analyzed the implications for national health policies of international development programs and global and regional trade agreements. She has served as Associate Director of the Alpha Center, a health policy organization in Washington DC, where she specialized in policy studies related to Medicaid, state programs to cover the uninsured, and maternal and child health, and worked in several other Washington-based state health policy organizations. At the local level, she helped to create a long-term care case management program in San Francisco, and adolescent health promotion programs in Detroit. Ms. Lipson is widely published in health professional journals. She has a Masters in Health Services Administration from the University of Michigan, School of Public Health.
Juan A. Manigault (Presentation)
President and Chief Executive Officer of the Northern Indiana Workforce Investment Board, Inc. This business-led Board is the regional agency responsible for managing the demand and supply-side of the region’s labor market. He is a graduate of the University of Notre Dame with a B.A. in English and received his M.S.B.A. from Indiana University Northwest.
Mr. Manigault’s career includes experience in the private, public and non-profit sectors. His areas of expertise include leadership development, strategic planning, technology utilization, collaboration and visioning. He is recognized as a leader in Indiana having served as a member of the Indiana Human Resource Investment Council, Indiana School-to-Work Advisory Council, Governor’s Commission on Workforce Preparation, Indiana Career Education Advisory Council, and the Governor’s Task Force on Economic Development. He is currently a member of the Board of Directors of Teachers Credit Union, the Country’s 54th largest Credit Union, Ray Bird Ministries, Business Development Corporation and the Indiana Adult Literacy Coalition.
Larry Minnix
President and CEO of the American Association of Homes and Services for the Aging (AAHSA), a position he has held since 2001. AAHSA represents several thousand not-for-profit aging services organizations. Dr. Minnix received his undergraduate and graduate degrees from Emory University. He has been in mental health and aging services fields for over 35 years. He was associated with the Wesley Woods Center of Emory University for 28 years, where he started as an administrative intern in 1972 and rose to the position of CEO, a position he held for 10 years until he joined AAHSA. Wesley Woods is a comprehensive aging services organization, with acute, outpatient, outreach, housing, and nursing home car within the academic context of Emory University. He is a frequent speaker on long term care, quality, ethics, and policy. He has served on numerous commissions and boards.
Jean Moore (Presentation)
Director of the New York Center for Health Workforce Studies at the School of Public Health at SUNY Albany. Ms. Moore has worked at the Center for four years and has served as principal project staff for health workforce studies that focus on the supply, demand, use, and education of health personnel, particularly the nursing workforce. She has also conducted studies of the availability of health care services in areas that may qualify for shortage designation.
Prior to joining the Center, Ms. Moore spent more than fifteen years at the New York State Department of Health where she was responsible for overseeing more than $100 million dollars per year in health workforce education and training funds.
Ms. Moore is currently completing a Masters of Public Health at the SUNY Albany School of Public Health. She holds two masters degrees from Russell Sage College, one in nursing education and one in psychiatric nursing as a clinical specialty. She received her bachelors in nursing from the SUNY College at Plattsburgh.
Carol Raphael
President and Chief Executive Officer of the Visiting Nurse Service (VNS) of New York, the country’s largest voluntary home health care organization with a budget of $867 million, and 10,400 employees. The organization provides a wide range of acute, rehabilitative and long-term care services to 25,400 patients daily. It operates a managed long-term care plan for dually eligibles and the Center for Home Care Policy and Research which studies the management, cost quality, and outcomes of home- and community-based services.
Previously, Ms. Raphael held positions as Director of Operations Management at Mt. Sinai Medical Center and Executive Deputy Commissioner of the Human Resources Administration in charge of the Medicaid and Public Assistance programs in New York City. Ms. Raphael is a member of MedPAC, the commission that advises Congress on Medicare payments and policies. She serves on several Robert Wood Johnson Foundation advisory committees and New York State panels including the Medicaid Reform Task Force, and the New York State Hospital Review and Planning Council, for which she chairs the Fiscal Policy Committee. She is on the Boards of Lifetime Healthcare Companies, Future Health Corporation, The Greater New York Hospital Association, the Continuing Care Leadership Coalition, the American Foundation for the Blind, Pace University and a fellow of the New York Academy of Medicine. She was a member of the Pfizer Hispanic Advisory Board and the Kaiser Permanente Planning Group and an Issues Expert at the White House Conference on Aging. She was a recipient of the Harvard Kennedy School of Government Alumni Achievement Award and the YWCA’s Academy of Women Achievers awards. Ms. Raphael was a Visiting Fellow at the King’s Fund in the United Kingdom. She has authored papers and presentations on post-acute, long-term care and end-of-life care and co-edited the book “Home Based Care for A New Century.” She has an M.P.A. from Harvard University’s Kennedy School of Government and completed its Senior Executive Program.
Vera K. Salter (Presentation)
Director of the National Clearinghouse on the Direct Care Workforce at the Paraprofessional Healthcare Institute (PHI). The National Clearinghouse brings together policy- and practice-related resources from around the country and makes them available to providers, consumers, workers, researches, and policy-makers who are concerned with the growing labor crisis in long-term care. PHI is committed to improving the quality of jobs for paraprofessional health care workers through demonstration projects, policy analysis, education and advocacy.
Prior to joining PHI, she was co-owner of a national planning and marketing firm that consulted with clients across the continuum of health and long-term care services.
She has also served as Vice-President with a multi-institutional healthcare system for over ten years, and has held a number of health planning and research positions.
Dr. Salter holds a Ph.D. in Sociology from the University of Pittsburgh, with a concentration in health services research. She has Master's degree in Social Administration from the University of Essex, and a Bachelor's degree in Economics from the University of Sussex, both in the United Kingdom. She has also served as a visiting Senior Research Associate at the Health Policy Institute at the University of Pittsburgh and has held an adjunct faculty position at Carnegie Mellon University's Heinz School.
Lloyd Schipper (Presentation)
He is Deputy Secretary of the South Dakota Department of Labor. A twenty-three year veteran of this department, he has served in several leadership roles throughout his career. Like most small-state administrators he wears numerous hats, but perhaps his most challenging task is to oversee the activities of South Dakota’s statewide system of sixteen “Career Centers.” These Centers are the primary delivery system for employment and training programs designed to meet the needs of job seekers and employers alike. South Dakota can be considered a rural state with a population of 755,000 people spread over an area of 77,000 square miles.
John Schnelle (Presentation)
Professor of Medicine and Director of the UCLA/Jewish Home/Borun Center for Gerontological Research. He has over 30 years of experience implementing interventions in nursing homes to improve urinary and fecal incontinence, weight loss, and mobility decline. This work is reflected in 175 publications. His efforts to translate these interventions into nursing home practice have led to the identification of system-wide barriers to change that are directly related to issues concerning the nursing home workforce.
Robyn I. Stone (2003 Article) (October 2003 Paper) (May 2004 Paper) (Presentation)
She is a noted researcher and internationally recognized authority on health care and aging policy. In June 1999, she joined the American Association of Homes and Services for the Aging to establish and oversee the Institute for the Future of Aging Services. She is the Institute’s executive director.
Dr. Stone has held senior research and policy positions in both the U.S. government and the private sector. She was a political appointee in the Clinton Administration, serving in the U.S. Department of Health and Human Services as Deputy Assistant Secretary for Disability, Aging and Long-term Care Policy from 1993 through 1996 and as Assistant Secretary for Aging in 1997. In the 1980s and early 1990s, she was a senior researcher at the National Center for Health Services Research and at Project HOPE’s Center for Health Affairs. Dr. Stone has been on the staff of two important national task forces, the 1989 Bipartisan Commission on Comprehensive Health Care (the Pepper Commission) and the 1993 Clinton Administration Task Force on Health Care Reform.
Dr. Stone is a distinguished speaker and has been published widely in the areas of long-term care policy and quality, chronic care for the disabled, workforce development and family caregiving. Her doctorate in public health is from the University of California, Berkeley.
Acronyms For HHS-DOL "Pathway to the Future" Symposium
| ADL AJB ASP ASPE |
Activity of Daily Living
(such as bathing, eating, dressing, toileting) America’s Job Bank Assistant Secretary for Policy, DOL Assistant Secretary for Planning and Evaluation, HHS |
| BLS BRG |
Bureau of Labor Statistics,
DOL Business Relations Group (part of DOL’s Employment and Training Administration) |
| CMS CNA |
Centers for Medicare and
Medicaid Services, HHS Certified Nursing Assistant |
| DCW DOL DON |
Direct Care Worker
Department of Labor Director of Nursing |
| ETA | Employment and Training Administration, DOL |
| HCBS HHA HHS HRSA |
Home and Community Based
Service Home Health Aides Department of Health and Human Services Health Resources and Services Administration, HHS |
| IADL IFAS IOM |
Instrumental Activity of
Daily Living (such as money management, housework, meal prep)
Institute for the Future of Aging Services Institute of Medicine |
| LPN LTC LVN |
Licensed Practical Nurse
Long-Term Care Licensed Vocational Nurse |
| ODEP | Office of Disability Employment Policy, DOL |
| PAS PHI |
Personal Assistance Service
Paraprofessional Healthcare Institute |
| RN | Registered Nurse |
| SNF | Skilled Nursing Facility |
| TA TANF TO |
Technical Assistance
Temporary Aide to Needy Families Turnover |
| WIA WIB |
Workforce Investment Act of
1988 Workforce Investment Board |
Related Links
Additional papers written for the Office of the Assistant Secretary for Planning and Evaluation in conjunction with this conference include:
-
Raynor, Charissa R.: Federal Workforce Development Programs: A New Opportunity for Recruiting and Retaining Direct Care Workers in the Long-Term Care Field (August 2003). [http://aspe.hhs.gov/daltcp/reports/fedwfdp.htm]
-
Pathway to the Future: How Workforce Development and Quality Jobs Can Promote Quality Care--Symposium Summary (July 2004). [http://aspe.hhs.gov/daltcp/reports/04cfpksum.htm]
-
Harris-Kojetin, Lauren, Debra Lipson, Jean Fielding, Kristen Kiefer and Robyn I. Stone: Recent Findings on Frontline Long-Term Care Workers: A Research Synthesis 1999-2003 (May 2004). [http://aspe.hhs.gov/daltcp/reports/insight.htm]
-
Fishman, Michael E., Burt Barnow, Asaph Glosser and Karen Gardiner: Recruiting and Retaining a Quality Paraprofessional Long-Term Care Workforce: Building Collaboratives with the Nation's Workforce Investment System (May 21, 2004). [http://aspe.hhs.gov/daltcp/reports/natwis.htm]
Background Materials
Below are a list of background material provided at the National Symposium. Found will be the abstract, introduction, executive summary and/or full report (and a link to another site) depending on the Internet availability or release approval. At the end of each "handout" is information about where the full report can be obtained.Nursing Aides, Home Health Aides, and Related Health Care Occupations - National and Local Workforce Shortages and Associated Data Needs Executive Summary (1)
National Center for Health Workforce Analyses, Bureau of Health Professions, Health Resources and Services Administration
February 2004
Preface
Nursing aides and home health aides are two of the major occupations responsible for providing patient care of a paraprofessional nature to chronically ill, disabled, and elderly persons in nursing homes and other institutional or community-based settings as well as at home. The challenges faced by long-term care facilities in recruiting and retaining these workers have been increasing in recent years, resulting reduced services for many Americans.
Recognizing the importance of this segment of the health workforce in meeting the care needs of an increasing percentage of the population, the National Center for Health Workforce Analysis (NCHWA) in the Health Resources and Services Administration's (HRSA) Bureau of Health Professions (BHPr) has commissioned and directed this study. The study concludes that informed workforce planning is needed to document the extent of existing shortages in these occupations and thereby assist states and institutions in addressing them, as well as to assess the impact of present and future initiatives to balance supply and demand.
The comprehensive assessment presented in this report was based on a review of eight key Federal datasets, certified nursing aide registries in 45 states, and fieldwork in four states (California, Illinois, New York, and Wyoming). The fieldwork included interviews and focus groups with long-term care providers and State officials to assess both their current data collection activities and the data needed for future program and policy development. The project was guided by an expert advisory panel and interviews with leaders in the long-term care field. These efforts, along with a review of the literature, resulted in (a) confirmation that there exists a widespread shortage of long-term care paraprofessionals and (b) affirmation that the shortage is likely to be far more severe in the future. The report concludes with a series of suggested strategies for improving data collection relating to these occupations, building on existing datasets and data collection activities.
Executive Summary
Introduction
This report focuses on nursing aides and home health aides, two of the major occupations responsible for providing patient care of a paraprofessional nature to chronically ill, disabled, and elderly persons in nursing homes and other institutional or community-based settings as well as at home. Faced with an aging population and a material shift of patient care to non-hospital venues, the Nation is experiencing an unprecedented demand for individuals with the training and experience needed to provide such care. There is a high turnover rate associated with these occupations, the result of a variety of factors relating to job satisfaction, such as low pay, lack of a career ladder, and occasional less than ideal treatment by supervisors. As a consequence, the supply of these individuals, while continuing to grow, has been slipping relative to demand, a situation likely to continue well into the future.
Because of the importance of this segment of the health workforce in meeting the care needs of an increasing percentage of the population, the National Center for Health Workforce Analysis (NCHWA) in the Health Resources and Services Administration's (HRSA) Bureau of Health Professions (BHPr) has commissioned and directed this study. The study concludes that informed workforce planning is needed to document the extent of existing shortages in these occupations and thereby assist states and institutions in addressing them, as well as to assess the impact of present and future initiatives to balance supply and demand. Current data systems were found to be limited in their ability to assist in such planning efforts. They do not, for the most part, accurately estimate the supply of individuals working in these occupations, including their numbers, locations, characteristics, and qualifications.
The comprehensive assessment presented in this report was based on a review of eight key Federal datasets, certified nursing aide registries in 45 states, and fieldwork in four states (California, Illinois, New York, and Wyoming). The fieldwork included interviews and focus groups with long-term care providers and State officials to assess both their current data collection activities and the data needed for future program and policy development. The project was guided by an expert advisory panel and interviews with leaders in the long-term care field. These efforts, along with a review of the literature, resulted in (a) confirmation that there exists a widespread shortage of long-term care paraprofessionals and (b) affirmation that the shortage is likely to be far more severe in the future. The report concludes with a series of suggested strategies for improving data collection relating to these occupations, building on existing datasets and data collection activities.
Nature of the Problem
Across the United States, there is growing concern about current and projected shortages of frontline, direct care workers who provide care and services to the elderly, chronically ill, and disabled. National studies cite annual turnover rates in nursing homes ranging from 45 to 105 percent (Stone, 2001). In 1999, Ohio's nursing assistant turnover rate ranged from 88 to 137 percent while in Florida, only 53 percent of the state's certified nursing aides (CNAs) were working in a health-related field one year after certification. Long-term care provider organizations have either reduced services due to shortages of permanent staff or, alternatively, hired temporary replacement staff at significantly higher hourly rates (Forschner et al., 2001). In areas where levels of service have been reduced, elderly or chronically ill persons deprived of access to care must either remain in more restrictive, more costly environments (notwithstanding the Supreme Court Olmstead decision affirming the right of nursing-home-eligible people to live in the "least restrictive" setting) or seek care from family or friends. Both quality of care and quality of life suffer as people are denied services, or services are provided by persons less qualified or experienced.
Over the next several decades, as population aging and advances in medicine increase the number of persons living with chronic medical conditions, the need for long-term care workers will continue to grow. The Bureau of Labor Statistics (BLS) projects that between 2000 and 2010, an additional 1.2 million nursing aides, home health aides, and persons in similar occupations will be needed to (a) cover the projected growth in long-term care positions and (b) replace departing workers. This rapid increase in demand--over half the year 2000 supply--can be expected, for similar reasons, to continue well beyond 2010. The pool, however, from which such workers have traditionally been drawn--largely women between 25 and 50 without post-secondary education--continues to shrink. It is questionable, therefore, whether the Nation will have an adequate supply of workers in these occupations to meet the expected increase in demand.
Nursing aides and home health aides provide much of the care in long-term care settings, both in nursing homes and in the community. Policymakers and the health care community have sought to understand the problems in maintaining an adequate supply of such healthcare workers. While some studies have led to an improved understanding of these occupations and the causes of the shortages, they have tended to rely on case studies, focus groups, and data that are incomplete. The lack of system-wide data has weakened efforts to understand the scope of the problem and to develop programs and policies that could address it.
Characteristics of Long-Term Care in the United States
Recipients. Long-term care recipients in the United States numbered about 12.1 million in 1995 (Kaiser Commission on Medicaid and the Uninsured, 1999). A diverse population with a wide age range and variety of service needs, the common element linking these individuals is their need for assistance with activities of daily living (ADL). Most received services at home or in community-based settings such as adult day care facilities, although about 12 percent (1.5 million) were cared for in nursing homes or other institutional residential facilities (ibid.).
As shown in Table ES-1, persons 65 or older constituted slightly over half (6.4 million) of the estimated 12.1 million long-term care recipients in 1995. Within that group, 1.3 million (20 percent) received care in nursing homes; the rest were cared for at home or in community settings. Of those receiving care at home or in the community, about two-thirds relied exclusively on unpaid caregivers, i.e., family and friends (Stone, 2001).
| Age Group | Setting in Which Care Was Received | All Settings Combined | |
|---|---|---|---|
| Nursing Home | Home or Community | ||
| SOURCE: Kaiser Commission on Medicaid and the Uninsured, 1999 | |||
| 65 or Older | 1.3 million | 5.1 million | 6.4 million |
| Under 65 | 0.2 million | 5.5 million | 5.7 million |
| All Ages | 1.5 million | 10.6 million | 12.1 million |
The dichotomy between nursing home and community-based care is even more pronounced for persons under 65. Of the nation's long-term care recipients below the age of 65, well over 95 percent--all but about 0.2 million--received care at home or in community settings. Of these, roughly three-fourths relied exclusively on family and friends for care. Long-term care recipients below the age of 65 include persons with mental retardation and serious mental illness, as well as adults living with AIDS or other chronic disorders and children with developmental disabilities.
Providers. The three major categories in the latest (1998) Standard Occupational Classification (SOC) system whose members provide long-term care of a paraprofessional nature are as follows:
| The three major categories in the latest (1998) Standard Occupational Classification (SOC) system whose members provide long-term care of a paraprofessional nature | |
|---|---|
| Nursing aides, orderlies, and attendants (SOC 31-1012) | Provide basic patient care under the direction of nursing staff. Perform attendants duties such as feeding, bathing, dressing, grooming, moving patients or changing linens. |
| Home health aides (SOC 31-1011) | Provide routine personal health care such as bathing, dressing, or grooming, to elderly, convalescent, or disabled persons at patient's home or residential care facilities. |
| Personal and home care aides (SOC 39-9021) | Assist elderly or disabled adults with daily living activities at person's home or daytime non-residential facilities. Duties may include keeping house and preparing meals. May also provide meals and perform supervised activities at non-residential care facilities. |
The number of individuals employed in these categories, based on year 2000 BLS data, are as follows:
| The number of individuals employed in these categories, based on year 2000 BLS data | |
|---|---|
| Total | 2,206,300 |
| Nursing aides, orderlies, and attendants | 1,262,000 |
| Home health aides | 577,700 |
| Personal and home care aides | 366,600 |
Table ES-2 shows their percentage distribution by industry group in which employed.
| Occupational Category | Industry Group | ||||
|---|---|---|---|---|---|
| Home Health Care | Nursing and Personal Care | Residential Care | Other | Total | |
| SOURCE: BLS Occupational Employment Survey | |||||
| Home Health Aides | 32.9% | 5.4% | 22.3% | 39.4% | 100% |
| Nursing Aides, Orderlies, and Attendants | 2.7% | 51.9% | 4.5% | 40.9% | 100% |
| Personal and Home Care Aides | 30.8% | 3.5% | 24.1% | 41.6% | 100% |
Approximately 60 percent of the workers in each occupational category are seen to be employed in the three industry groups most clearly associated with the delivery of long-term care (home health care, nursing and personal care, residential care). In addition, a significant portion of those in industries classified as "Other" may also be assumed to have been engaged in the delivery of long-term care. For example:
- A substantial percentage of nursing aides, orderlies, and attendants in industries classified as "Other" work in specialty hospitals that provide long-term care for the chronically ill or rehabilitation/restorative/ adjustive services to physically challenged or disabled persons.
- One of every five home health aides in industry groups classified as "Other", as well as one of every ten nursing aides, orderlies, and attendants in that category, work for Personnel Supply Services, i.e., temporary agencies. When employed in that capacity, they too may provide long-term direct care.
There also exists a substantial "gray market" of individuals hired directly by individuals and families, who do not show up as employed in either BLS or other government data systems. One national study found that 29 percent of workers providing assistance to the Medicare population in the home were self-employed (Leon and Franco, 1998a).
Workers in the described occupational categories earn relatively meager wages. In 2000, the median wage for each of these categories was less than $9 an hour, an annualized salary of less than $19,000 for a full work-year of 2,080 hours (BLS, National Occupational and Wage Estimates for 2000). Many of these individuals work only part-time. Long-term care paraprofessionals are reported to work only about 30 hours a week on average, reducing their annualized earnings to well below $15,000. A high percentage (28 percent) live in poverty, and are more likely than other workers to rely on public benefits to supplement their wages (Himmelstein et al., 1996). Among single-parent nursing home and home health aides, 30 to 35 percent receive food stamps (General Accounting Office, 2001). Many also rely on publicly funded health care.
Data from the BLS Current Population Survey (CPS) March Supplement indicate that over 90 percent of the two specific occupations "nursing home aide" and "home care aide" are female, with the vast majority falling between the ages of 25 and 54. A significant percentage of these individuals (12 to 23 percent) are foreign-born, of whom only about a third are naturalized. Contrary perhaps to public perception, a substantial proportion (28 to 35 percent) reported at least some college education.
Provider Organizations. Organizations that draw upon long-term care paraprofessionals to provide needed services include:
- Nursing facilities
- Intermediate care facilities for the mentally retarded
- Residential facilities for adults or aged
- Residential facilities for non-aged
- Adult day care centers
- Home health agencies (certified or licensed)
- Hospice organizations (certified or licensed)
There were approximately 120,000 such organizations in the United States in 1998 (Harrington et al., 1999), of which roughly 43 percent (51,200) were residential facilities for adults or the aged and another 20 percent (23,300) were home health care agencies. Nursing facilities accounted for 15 percent (17,500) and residential facilities for the non-aged for 11 percent (13,300).
In addition to these types of organizations, there are a growing number of alternative organizational and service configurations as consumers and providers seek to expand the options for both health services and housing arrangements for the elderly and chronically ill. Many states have developed Home and Community Based Services (HCBS) options, with a sharp increase in assisted living arrangements and options. In addition, many states are promoting approaches to giving individuals more control over the selection of caregivers under programs generally referred to as "consumer-directed care".
Shortage Issues
Factors affecting supply. The high turnover and vacancy rates associated with these occupations are consistently found to be the result of job dissatisfaction stemming from the following:
- Jobs are physically and emotionally demanding. Many nursing home injuries consist of back problems resulting from lifting or transferring residents, a high rate of injury corroborated by data from the BLS Survey of Occupational Injuries and Illnesses (BLS, 1999). Patient load in many nursing homes is excessive; the consequent pressure to "speed up" results in increased job stress (Wilner, 1994; Foner, 1994; Diamond, 1992).
- Wages and benefits are generally not competitive with other available jobs (Case et al., 2002; Himmelstein et al., 1996).
- Jobs are often not well designed or supervised (Kopiec, 2000), with few or no opportunities for advancement. Workers perceive a general lack of respect from management.
Factors affecting demand. Factors responsible for the increased demand for long-term care include:
- Aging of the population as baby boomers advance to the ranks of the elderly.
- Technological advances that extend the lives of those with chronic ailments.
- The greater availability of services in less restrictive, less costly community settings.
Population aging, in and of itself, might present less of a problem if the supply of care providers were growing at approximately the same rate. Unfortunately, it is not. It is growing at a significantly lower rate--not only are providers leaving the field for reasons of job dissatisfaction but the pool from which such providers have typically been drawn in the past has been dwindling compared to the growth in demand due to aging. In 2000, there were 1.74 females between the ages of 25 and 54 for every person 65 and older; by 2030, that ratio is projected to drop to 0.92 (calculations based on Census Bureau National Population Projections). Since women provide the majority of both paid and family-provided long-term care, this "care gap" will increase. Families unable to care for their loved ones by themselves will find, when they turn to the formal system for assistance, relatively fewer paid staff available.
Data Issues
Need for Data. Data that are clear, comprehensive, current, and correct are needed in the case of long-term care paraprofessionals, as they are for any other health occupation. Such data are a valuable tool for meeting the following purposes:
- Workforce planning. Providing planners and managers at all levels, especially State and local, with accurate, timely data to help them plan and effectively manage health care delivery.
- Policy formulation. Informing the process by which public policies and programs that could influence workforce supply and demand are generated, e.g., setting reimbursement policies and rates for Medicare and Medicaid, establishing licensure and regulation policies as well as policies involving employee benefits, upward mobility, etc.
- Patient safety. Promoting patient safety by ensuring that individual workers are properly trained and have no record of inappropriate activities.
- Quality improvement. Monitoring the performance of facilities and provider organizations for dissemination to patients and their families.
- Program evaluation. Monitoring and assessing program performance over time and identifying best practices.
- Informing the marketplace. Supplying education and training organizations, health providers, and the public with useful information to serve their individual needs.
Relevant Data Sources. As noted earlier, the data systems reviewed in this study, although helpful in many respects, were limited in their ability to present an accurate and timely picture of nursing aides, home health care aides, and related occupations in the United States. The datasets reviewed included six maintained by the Bureau of Labor Statistics, one on nursing homes maintained by the DHHS Centers for Medicare and Medicaid Services (CMS), one maintained by the Bureau of the Census, and 45 certified nursing aide (CNA) registries maintained at the State level. A brief summary of these datasets follows:
Bureau of Labor Statistics. The six BLS datasets cover six separate aspects of the Bureau's data collection activities:
- Occupational Employment Statistics (OES). A mail survey of 400,000 establishments per year, resulting in a total sample of 1.2 million establishments over three years.
- Current Population Survey (CPS). A monthly survey of 50 to 60 thousand households, conducted on behalf of BLS by the Bureau of the Census (personal and/or telephone interview).
- CPS March Supplement. A somewhat more detailed version of the CPS, conducted once a year on a slightly larger sample.
- National Compensation Survey (NCS). An annual compilation of data on earnings, benefits, and work hours, based on visits to some 36,000 establishments.
- Employment Projections. Projected labor force trends based on analysis of OES and CPS survey results.
- Survey of Occupational Injuries and Illnesses. An annual survey of 250,000 private sector organizations with at least eleven employees to obtain data relevant to occupational safety.
Centers for Medicare and Medicaid Services. The CMS dataset, labeled Online Survey Certification and Registration or OSCAR, consists of staffing data and associated facility characteristics for approximately 17,000 CMS-certified nursing homes. The data are self-reported and updated once a year as part of the CMS annual recertification process.
Bureau of the Census. The decennial Census collects limited data on the occupation of residents of the United States. These data, updated every 10 years, provide estimates of the numbers of persons employed in different occupations by Census tract. The data are tabulated by place of residence rather than employment.
State CNA Registries. Registries of this nature, mandated by the Omnibus Budget Reconciliation Act of 1987, are maintained by every State and the District of Columbia. Used for background checks and other relevant purposes, they contain information on certified, licensed, or registered nursing aides working in skilled nursing facilities (SNFs), although some states have gone beyond the legislative mandate to include other direct care paraprofessionals. Of the 45 State registries reviewed, nine include home health aides as well.
Data Limitations. The limitations presented by these data sources, in terms of meeting the purposes of this study, fall into three categories: data exclusions, inconsistency of definitions, and categorizations that are in some cases excessively broad.
Data exclusions. Important data exclusions are as follows:
- State CNA registries. As noted above, State CNA registries are required by legislation to cover nursing aides only; only a small percentage--less than a fourth--include health aides or other occupational categories as well. Moreover, these systems were designed--and in most cases are being used--to track eligibility (completion of mandatory training) rather than employment. While most State registries include some information of a demographic nature, about a fourth do not. Since most registries do not track the actual employment of eligible CNAs, they do not generally provide information on work setting or location.
- Online Survey Certification and Registration (OSCAR). OSCAR covers staff in nursing homes only. Nursing aides, LPNs, and RNs are the only professions/occupations for which separate tabulations are available.
- BLS Occupational Employment Statistics (OES). OES data, while disaggregated to the State and metropolitan area level as well as to industry group, provide no detail on demographic characteristics, work conditions, or setting in which services are delivered. Also, the numbers do not include self-employed or unpaid family providers of care.
- BLS Current Population Survey (CPS) March Supplement. Since the CPS March Supplement contains no State variable, the employment numbers cannot be disaggregated to the State level.
Inconsistency of definitions. Occupational and industry classifications used have differed by dataset and varied over time. However, as announced in the Federal Register Notice of September 30, 1999, all Federal agencies that collect occupational data are now required to use the 1998 Standard Occupational Classification, the largest revision to the SOC in two decades. In addition, all State and local government agencies, as well as private sector organizations, that gather occupational data are strongly encouraged to use the 1998 SOC. In the words of the announcement, "This national system ... provides a common language for categorizing occupations in the field of work."
While the Federal government has attempted to standardize classifications through the SOC, inconsistencies among state-reported data remain; this includes differing definitions of workers and different methods used to quantify the number of workers.
Excessively broad categorizations. The occupational category "nursing aides, orderlies, and attendants", retained in the 1998 SOC, includes three separate occupations, each with its own set of demographic characteristics, work settings, and job responsibilities. Similar problems exist with respect to the classification of industries: some industry codes contain work settings irrelevant to the provision of direct care, e.g., medical laboratories, youth services, crisis centers, food banks, etc.
Making Workforce Data More Useful
The limitations noted above apply not only to the present study but also to future attempts to achieve a comprehensive assessment of the long-term care paraprofessional workforce at national, state, and local levels. To assure the accurate, comprehensive, timely data needed to support workforce planning in this area and offset possible future shortages, the following options are identified:
Upgrade and augment existing CNA registries. Possible options in this area include:
- Expanding the occupational categories included in the registries beyond nursing aides to include home health aides and personal care aides, with agreed-upon definitions.
- Expanding the recorded data elements to include demographic characteristics, educational background, and current job status, among others.
- Maintaining data timeliness and accuracy by requesting employers to submit annual lists of individuals currently employed, including hours worked and other non-sensitive information.
Adopt and implement state-level workforce data collection systems for nursing aides, home health aides, and related health care occupations. Such systems, using standard definitions and terminology, would permit useful totals and subtotals to be collected from facilities and agencies, to be shared and compared across states. A proposed data collection instrument of this form is shown in Appendix B of this report.
Involve long-term care provider organizations and professional associations in data collection efforts. Such groups would be a valuable source of information. Organizations that collect and maintain informative workforce data report fewer recruitment and retention problems than their relatively data less counterparts.
Endnotes
1. The full paper is available online at http://bhpr.hrsa.gov/healthworkforce/reports/nursinghomeaid/nursinghome.htm.
The Future Supply of Long-Term Care Workers in Relation to the Aging Baby Boom Generation: Report to Congress Executive Summary (1)
Department of Health and Human Services and Department of Labor
May 14, 2003
Preface
In the FY 2002 Senate Appropriations Subcommittee for Labor-HHS Education and the Conference Committee Report for the FY 2002 Labor-HHS Appropriation, Congress requested that the Secretaries of Health and Human Services and Labor identify the causes of the "shortage" of frontline workers (registered and licensed practical nurses, certified nurse aides and other direct care workers) in long-term care settings such as nursing homes, assisted living and home health care. The Subcommittee and Committee requested that the Department of Labor (DOL) and Department of Health and Human Services (HHS) make comprehensive recommendations to the respective Committees to address the increasing demand of an aging baby boomer generation.
This report is a product of collaboration between HHS and DOL in response to the requests from the U.S. Congress. Staff at these Departments worked collaboratively to share information and data pertaining to direct care workers in long-term care settings and to develop a joint set of recommendations for the future. The results of those efforts are presented in this unified Report to Congress. In addition, HHS and DOL included information from the following activities:
- HHS's recent meetings with state and local policy makers, long-term care providers, direct care workers, researchers, and labor economists on recruitment and retention of direct care workers in long-term care. Topics included: (1) extrinsic rewards and incentives (such as wage and fringe benefits), (2) workplace culture (organizational structures, social factors, physical settings, environmental modifications and technology), and (3) expanding labor pools of direct care workers.
- Survey data from both Departments on the supply of and demand for direct care workers in long-term care settings, including DOL's industry and occupational employment data from its Occupational Outlook Program and HHS data on the direct care workforce from the National Nursing Survey and the National Home and Hospice Care Study. New projections were developed for some occupational groups.
- Research and practice literature related to the shortage of long-term care workers, including information from surveys of direct care workers, and a review of state-sponsored efforts and provider surveys.
Executive Summary
One of the challenges facing the U.S. in the 21st Century will be to ensure that individuals throughout their life will have the supports they need and will be treated with dignity. For the growing population of the elderly and people with disabilities, ensuring the adequacy and availability of direct care workers is key to meeting this ideal. As this report shows, the aging "baby boomer generation" will be the most significant factor increasing the demand for long-term care services over the next half century. The number of individuals using either nursing facilities, alternative residential care, or home care services is expected to increase from 15 million in 2000 to 27 million in 2050. Most of this increase will be driven by the growth in the number of elderly in need of such care, which is expected to double from approximately 8 million in 2000 to 19 million in 2050.2
In 2000, approximately 1.9 million direct care workers (defined in this report as including registered nurses (RNs), licensed practical and vocational nurses, nurse aides (NAs), home health and personal care workers) provided care to 15 million Americans in long-term care settings (defined in this report as including nursing and personal care facilities, residential care facilities, and home health care services).3 The Bureau of Labor Statistics (BLS) estimates that by 2010, direct care worker jobs in long-term care settings should grow by about 800,000 jobs, or roughly 45 percent.4 Paraprofessional long-term care employment will account for 8 percent of the estimated increase in the nation's jobs for workers in occupations generally requiring only short-term on-the-job training.
According to estimates developed by HHS's Office of the Assistant Secretary for Planning and Evaluation (ASPE), after 2010, the demand for direct care workers in long-term care settings becomes even greater as the baby boomers reach age 85, beginning in 2030. ASPE estimates project the demand for direct care workers to grow to approximately 5.7-6.6 million workers5 in 2050, an increase in the current demand for workers of between 3.8 million and 4.6 million (200 percent and 242 percent respectively). This increase in demand will be occurring at a time when the supply of workers who have traditionally filled these jobs is expected to increase only slightly.
These projections indicate that it is critical to retain existing long-term care workers and attract new ones. Since many industries will be competing for the supply of workers, pay and working conditions will play a key role in attracting new workers and consequently influencing the supply of long-term care services. Providing adequate levels of high quality, compassionate care will require sustained effort by many actors. While the Federal Government has an important role to play, much of what needs to be done will require action on the part of current and new employers who will expand and alter the market itself and shape new solutions. Other solutions will inevitably be crafted by state and local governments, health care providers and industry associations, education and training institutions, workforce investment systems, faith-based organizations, and workers themselves.
Recommendations
HHS and DOL identified a comprehensive set of recommendations to address potential imbalances between the future demand for and supply of direct care workers in long-term care settings. The recommendations are geared to address key issues relating to:
- Finding new sources of workers;
- The initial and continuing education of workers;
- Compensation, benefits, and career advancement; and
- Working conditions and job satisfaction.
The recommendations include:
National Dialogue With Employers: Engage employers and employees as well as medical professionals and state and local government, in a dialogue on issues relating to improved pay, benefits, career ladders, and working conditions in long-term care.
Outreach to Faith and Community-Based Organizations: Explore with faith and community-based organizations their potential roles in addressing shortages in labor imbalances through strengthening relationships with the workforce investment system, and in recruiting volunteers for respite care for family members, "back-up" services, and home-based support.
Enhanced Use of Technology: Explore use of new technology in recruitment, education and training, recordkeeping and patient care. Expand and work with industry to market CareCareers.net.
State and Local Initiatives: Encourage and support state and local efforts, involving both the private and public sectors to explore use of business partnerships with individual employers or consortiums of employers, training providers and public agencies.
Enhanced Training and Education: Support multiple initiatives including implementation of the newly passed Nurse Reinvestment Act, expanding efforts to leverage private sector funds similar to DOL's Partnerships for Jobs, encouraging states to expand training slots for nurses and paraprofessionals, promoting registered apprenticeship training programs to paraprofessional occupations, and others.
New Sources for Workers: Seek ways to broaden the supply of frontline long-term care workers by reaching out to older workers, former Temporary Assistance for Needy Families (TANF) recipients, military personnel transitioning to civilian life, individuals with recent experience providing care to family members, dislocated workers from other industries and young people.
Support for Informal Caregivers: Continue efforts to support informal caregivers, such as through tax incentives and grants to state and local organizations (e.g., the Administration on Aging's (AoA) National Family Caregiver Support Program), provide information and referral resources, and explore the effectiveness of respite care demonstrations.
Regulatory Changes: Explore areas for potential federal and state regulatory changes, which could include enhanced information sharing and policy coordination among states, and possible federal requirements on patient recordkeeping.
Worker Safety: Continue to support worker safety education and outreach to employers, such as through DOL's National Emphasis Program, and through enhanced safety training within schools of nursing and within the paraprofessional training curriculum.
Research Efforts: Continue to support research and evaluation activities on such subjects as wages, benefits, worker characteristics, and workplace cultures.
Endnotes
- The full paper is available online at http://aspe.hhs.gov/daltcp/reports/ltcwork.htm.
- Elderly Long-Term Care Projections, prepared by the Lewin Group for ASPE, draft July 15, 2002.
- Estimates developed by the ASPE Office of Disability, Aging and Long-Term Care Policy, using data from the 1994 National Health Interview Survey, and 2001 Census population projection. For the institutionalized population: 1998 Residential Information Systems Project, 1996 Medical Expenditure Panel Survey.
- Bureau of Labor Statistics, National Employment Matrix, 2000-2010.
- This estimate varies due to different assumptions of the growth rate of home health care. See discussion associated with Table 7 for a more in depth explanation.
Results of the 2003 National Survey of State Initiatives on the Long-Term Care Direct-Care Workforce (1)
Paraprofessional Healthcare Institute and North Carolina Department of Health and Human Services
March 2004
Background Information
The Paraprofessional Healthcare Institute (PHI) and the North Carolina Department of Health and Human Services (NCDHHS) have once again collaborated to survey states about direct-care workforce issues. The 2003 survey updates and expands upon information collected from states in prior surveys to examine public policy actions taken by states to strengthen the direct-care workforce. Specifically, the purpose of this survey was to:
- Obtain an updated assessment from states as to whether directcare worker vacancies are currently a serious workforce issue;
- Determine whether state budget constraints during 2003 had any effect on planned or existing direct-care worker initiatives, and/or whether the direct-care workforce was affected by Medicaid program changes;
- Identify new direct-care workforce public policy actions taken by states since the June 2002 survey;
- Determine the degree to which states are, or are considering, tying reimbursement to outcomes associated with direct-care workforce and/or quality of care initiatives;
- Compile additional information from states that use a uniform methodology to track turnover rates of direct-care workers in one or more long-term care settings regarding data tracking methods used, data trends, etc.; and
- Update individual state charts of known public policy actions taken since the first survey conducted in 1999.
Methodology
This is the fourth national survey on the direct-care workforce developed by PHI and NCDHHS. Surveys were sent to all state Medicaid agencies and state Units on Aging in September 2003; some surveys were redirected to a more appropriate state entity for completion. Completed surveys were received between October and December 2003; clarification was sought as needed. Responses were received from 44 states, representing an 88% response rate.
A summary of results from the 2003 survey is available in Table 1 and detailed comments are described in Table 2. A snapshot of each state’s existing or enacted direct-care worker initiatives is presented in individual charts in Appendix A, reflecting information collected from this and prior national surveys conducted by PHI and NCDHHS. New information provided from the 2003 survey is reflected in bold type.
Data Caveat: All analyses and percentages reported are based on the 44 states responding to this survey.
National Statistics on the Direct-Care Workforce
Employment Growth:
Many states continued to indicate that high rates of vacancies exist among direct-care workers occupations. This is not surprising given the growth in demand nationally for direct-care workers as projected by the US Bureau of Labor. Between 2002 and 2012, the Bureau of Labor projects employment growth of direct-care workers to more than double (33.8%) the projected growth in overall employment nationally (14.8%).
Wage Rates:
The national average of median hourly wages for the three major categories of direct-care workers (nurse aides, orderlies, and attendants; home health aides; and personal and home care aides) has increased from $7.97 in 1999 to $8.70 in 2002. This represents a 9.15% increase over the four-year period for an average annual increase of 2.28%. Wage rates for direct-care workers in 2002 are presented below:
| National Wage Data for Direct-Care Workers, 2002 | |
|---|---|
| Median Hourly Wage | |
| See Table 3 for state unemployment data from 2001 to 2003. Also included in Table 3 are average median hourly wages, by state, across direct-care worker categories from 1999 to 2002. | |
| Nurse Aides, Orderlies, and Attendants | $9.59 |
| Home Health Aides | $8.70 |
| Personal and Home Care Aides | $7.81 |
| Average median wage across 3 categories | $8.70 |
National Economic Outlook
During calendar year 2003 the national unemployment rate peaked at 6.3% in June and dropped to 5.7% by December. When examining individual state unemployment rates, however, twelve states had unemployment rates at, or in excess of, 6.0% in November 2003. Of these, three states (Alaska, Michigan, and Oregon) had unemployment rates of 7.0% or higher.
Information collected during the 2003 survey continued to show that, generally, vacancies of direct-care workers continued to be a serious workforce issue for most states. This trend has continued since the first survey conducted in 1999 and in subsequent surveys conducted during both strong and declining economic periods. It is worth noting that the severity of direct-care worker vacancy rates did diminish for some states: in 2003, 79% of the 44 states responding to the survey indicated that high vacancy rates continue, compared to 88% of states in 1999 and 86% of states in 2002. Thus, the recent high unemployment rates may have contributed to improved vacancy rates in some states. It will be interesting to observe whether those workers who were attracted to enter (or re-enter) direct care during the recession because of limited job opportunities, remain in the field once the overall job market significantly improves.
However, responses received from states re-affirm that the economy is not the primary factor impacting serious vacancies of direct-care workers. Repeating trends found in previous surveys, both the state with the highest unemployment rate as of November 2003 (Alaska at 7.5%) and the state with the lowest unemployment rate (North Dakota at 3.2%) reported serious direct-care workforce vacancies.
In spite of the unemployment rate and continued slow job growth during 2003, there were clear signs an economic recovery was underway. Indications that state economies were improving were welcome news for states, which have struggled to balance their budgets over the past several years. A November 12, 2003 article in USA Today reported that state and local spending increases were annualized at 1% for the two consecutive quarters ending September 2003.2 This growth rate represented the smallest growth spending during back-to-back quarters reported since 1952. In contrast, the good news for states during this same period was that revenue collection was picking up, increasing to a 9.2% annualized rate during these same two quarters. However, much of these increases was reportedly due to increased federal payments to states, a significant portion of which was one-time money to offset Medicaid costs, and increased tax collections.
The December 2003 Fiscal Survey of States published by the National Governors Association and the National Association of State Budget Officers confirmed that while the economy was improving, states continued to have difficulty balancing their budgets during State Fiscal Year 2003.3 Medicaid is a major expense for states, and the report indicates that every state has taken at least one step to control Medicaid costs during State Fiscal Years 2002-2004. The report listed the following key actions:
- All 50 states either reduced or froze payments to provider organizations;
- All 50 states took steps to control prescription drug costs;
- 35 states reduced benefits;
- 34 states took steps resulting in reduced or restricted eligibility for services; and
- 32 states increased co-payments required by consumers.
Some of these actions have had a direct impact on direct-care workforce issues. Detailed Medicaid policy actions taken by states during the 2003 fiscal year are described in Section D below.
Endnotes
- The full paper is available online at http://www.directcareclearinghouse.org/download/2003_Nat_Survey_State_Initiatives.pdf.
- Cauchon, D. "States Getting Budgets Under Control." USA Today. November 12, 2003.
- National Governors Association and the National Association of State Budget Officers. Fiscal Survey of States. Washington, DC. December 2003.
Federal Workforce Development Programs: A New Opportunity for Recruiting and Retaining Direct Care Workers in the Long-Term Care Field (1)
Charissa R. Raynor
August 2003
Introduction and Purpose
Across the country, long-term care providers are facing a shortage of qualified and committed direct care workers--those certified nursing assistants (CNAs), home health aides and personal care workers who provide hands-on care to millions of older adults and individuals with physical disabilities. Vacancy rates in excess of 10 percent and turnover rates in excess of 100 percent are not unusual.2
Over the next 10 years, the country will need an estimated 874,000 additional direct care workers to meet growing demand.3 At the same time, the supply of workers traditionally relied upon to fill these positions--middle-age women--will fall by about half by 2030.4 To address this emerging "care gap," providers, policy-makers and consumers are likely to consider a broad range of strategies: improving wages and benefits of direct care workers, tapping new worker pools, strengthening the skills that new workers bring at job entry and providing more relevant and useful continuing education and training. A key strategy in this mix will be a focus on workforce development--providing workers with the knowledge and skills they need to perform their jobs.
The purpose of this report is to describe five federal workforce development programs and how some long-term care agencies and service providers use them to improve the recruitment and retention of direct care workers. The five programs are:
- The Workforce Investment Act;
- The Perkins Act;
- Temporary Assistance for Needy Families;
- Job Corps; and
- National Registered Apprenticeships.
Endnotes
- The full paper is available online at http://aspe.hhs.gov/daltcp/reports/fedwfdp.htm.
- Stone, R.I. and Wiener, J.M. (2001). Who will care for us? Addressing the long-term care workforce crisis. Washington, DC: The Urban Institute and the American Association of Homes and Services for the Aging. [Can be accessed at http://aspe.hhs.gov/daltcp/reports/ltcwf.htm.]
- Hecker, D.E. (2001). Employment outlook: 2000-2010. Occupational employment projections to 2010. Monthly Labor Review, 57-84.
- Scanlon, W.J. (2001, May 17). Nursing workforce: Recruitment and retention of nurses and nurse aides is a growing concern. Testimony before the Committee on Health, Education, Labor and Pensions, U.S. Senate (GAO-01-750T). U.S. General Accounting Office. Retrieved July 1, 2002 from http://frwebgate.access.gpo.gov/cgi-bin/useftp.cgi?Ipaddress=162.140.64.21&filename=d01750t.pdf@director=/diskb/wais/data/gpo. In 2000, there were 16.1 traditional caregivers per person aged 85 and older. By 2030 it is estimated that there will only be 8.5 traditional caregivers per person aged 85 and older. Traditional caregivers are women between 25 and 54 years of age.
Health Care Industry: Identifying and Addressing Workforce Challenges Executive Summary (1)
Alexander, Wegner, & Associates
February 2004
Preface
The following is a report prepared by Alexander, Wegner, & Associates for the U.S. Department of Labor, Employment and Training Administration’s Business Relations Group. This report details what the U.S. Department of Labor, Employment and Training Administration (DOL ETA) has learned from employers, employees, educators, workforce professionals, and researchers about health care workforce challenges and solutions. It provides the basis for developing strategic partnerships that include industry, education, and the public workforce system.
At the federal level alone the public workforce system invests over $15 billion each year providing employment and training services to people who need them. ETA is always looking for more effective and efficient ways to use these resources. The Initiative, of which this report is a part, is directed toward forging these partnerships and making these improvements.
To address workforce needs in health care and other industries, ETA created the Business Relations Group. Recognizing that workforce development is part of economic development, the Business Relations Group’s focus is on the education, employment, and economic development partnerships that are needed to fuel our nation’s economy. ETA’s goal is to prepare the workforce system to better serve the needs of business, and to connect businesses with the workforce system through targeted initiatives.
Based on ETA’s review of major areas of job growth, the health care industry was selected as one of 12 industries for the High Growth Job Training Initiative.
The reality of the situation allows employers the opportunity to reach out and offer jobs in health care that are enticing to potential job seekers. Health care occupations are attractive because they are located across the nation, provide a professional work environment, and are portable. The health care industry needs greater diversity among its workforce, and therefore may be attractive to new labor pools. There is an increased building of career ladders and lattices that are available to workers so they can shape their careers.
Meeting the short-term needs and the projections for the coming decade is only part of the challenge. The long-term care sector alone will see an increase of 5.7 to 6.6 million direct-care workers by the year 2050.2 Even the most optimistic hopes for increased technological solutions or improvements in the health of Americans will not prevent this increased need for direct care workers.
ETA heard from employers, and others associated with health care, of some of their actions to identify challenges and implement effective workforce strategies. ETA heard of the pressures they experience to do much more, to do it quickly, and to do it in a way that is sustainable over a long period of time. Health care leaders are committed to dealing with major workforce issues. However, the challenges they face are far too complex for any one institution or sector to solve alone. It has never been more important for ETA to build partnerships between employers, employees, educators, workforce professionals and government.
The Employment and Training Administration and the public workforce system will now move to partner with industry and education institutions to act on solutions from this report that highlight innovative ways that the workforce system can be a catalyst for meeting the health care industry’s workforce needs.
To those who gave generously of their time, effort and other resources for this initial work -- thank you for your thoughtful contributions. To those reading about this initiative for the first time -- ETA looks forward to your contributions to building a responsive and sustainable health care workforce system throughout the country.
As ETA heard from different industries, it found several workforce challenges that are common throughout different sectors. ETA will look to partner to address these workforce problems across industries. Solutions will be categorized under the following categories: pipeline, competency models, post-secondary and alternative training, new labor pools, retention, transitioning/declining industries, and small businesses.
Executive Summary
A top priority for the Department of Labor’s (DOL) Employment and Training Administration (ETA) is serving America’s workers through effectively meeting the workforce needs of business. The High Growth Job Training Initiative of ETA and its Business Relations Group recognizes that workforce development is not separate from economic development but an integral part of it.
The health care industry was selected as one focus within the High Growth Job Training Initiative. Health Services comprised 5.8 percent ($589.9 billion) of Gross Domestic Product in 2001.3 In 2002, the total employment in health services was 11,529,000.4 The Labor Department’s Bureau of Labor Statistics projects that the industry will add 3.5 million new jobs, or 16 percent of all wage and salary employment, between 2002 and 2012. Nine out of the twenty fastest growing occupations will be in health care.5
Significant workforce supply and demand gaps currently exist across the U.S. that affect acute care, long-term care and primary care health care provider sectors. These gaps are even more significant across all three sectors in rural America.
This report provides the results of information gathering from key health care informants regarding workforce issues as reported by the ‘demand’ side of the workforce. The provider or owner/operator associations employing the greatest numbers of health care workers are the primary employer informants. Parallel to meetings and interviews with employers, relevant workforce reports and information were sought from the DOL Bureau of Labor Statistics, the Department of Health and Human Services Health Resources and Services Administration, health care workforce researchers, reports of provider associations, educators, public and private workforce professionals -- including Workforce Investment Boards, and the contacts suggested in interviews with members of these sources.
The initial analysis of the information generated concluded with a clustering of the workforce issues or challenges by topic and by sector within the health care industry:
- Pipeline Challenges/Issues: Recruitment and Retention
- Increasing available labor pool
- Increasing diversity and seeking workers from non-traditional labor pools
- Reducing turnover
- Skill Development Challenge/Issues
- Entry-level worker preparation
- Incumbent worker training
- Need for targeted and specialized areas of skills
- Capacity of Education and Training Providers Challenges/Issues
- Lack of academic and clinical instructors
- Lack of facilities and resources
- Lack of alignment between employer requirements and curricula, and specialized skills areas
- Sustainable Workforce: Leadership, Policy, and Infrastructure Challenges/Issues
- Need for sustainable and adaptive workforce partnerships at national, state and local levels
- Opportunities to leverage funding and other resources
- Planning tools (data, projections, and information systems that are useful in projections of demand at the single facility and local levels)
- Policy issues including those of regulation
The majority of the workforce issues reported are the same or similar across primary, long-term care and acute care sectors. For example, all types of provider groups report that the current number one problem in occupational vacancies is for registered nurses. There are, however, some identifiable differences among the provider sectors. For example, long-term care providers identify a serious concern regarding the current and projected supply/demand gap of senior managers, while neither acute nor primary care providers share the same degree of concern. The acute care providers’ vacancies include a significant number of direct care workers, medical diagnostic and treatment technologists and support workers. The rural health vacancies across a wide spectrum of occupations are of continuing concern and made more problematic with the current vacancy rates nationally.
A second step in information gathering and analysis was performed prior to and during the course of three Workforce Development Industry Forums held in October 2003. The 126 forum participants were selected from a pool developed through nominations from owner/operator associations, the National Association of State Workforce Agencies, the National Association of Workforce Boards, the American Association of Community Colleges, and other workforce leaders from whom project staff had previously sought information. Some of the participants represented health care workforce projects currently funded by the Employment and Training Administration. Participants were asked to complete a validation tool containing challenges gathered in Phase I and invited to suggest additional issues. In addition, at the forums they were presented with an overview of the challenges and issues and asked for additional input. No changes in the challenges were made.
Participants in the forums were assigned to one of four groups. They clarified challenges or issues, generated 1001 solutions, and ranked the solutions by a voting procedure. For the 83 highest-ranked solutions, small teams worked to develop a matrix that includes the challenge, the solution, critical attributes for a successful solution, key stakeholders, resources required, policy barriers at the local, state and national or federal level, and any other needed clarifications.
The highest-ranked solutions include recommendations in the following areas:
- Issue: Pipeline: Recruitment and Retention
- Solution: Creating and expanding youth-focused programs to better inform young people about health care careers and encourage them to consider health care occupations.
- Issue: Pipeline: Recruitment and Retention
- Solution: Ensuring that public workforce programs provide adequate preparation of entry-level workers in the basic knowledge required to enter many health care occupations, adequate social and financial supports during the training period, opportunities for work placement, and support during the transition to the workplace so these workers can succeed and be retained in the health care industry.
- Issue: Pipeline: Recruitment and Retention
- Solution: Marketing health care career opportunities to youth, potential worker pools that do not traditionally enter the health care industry, dislocated workers, immigrant communities, older workers, and traditional worker pools.
- Issues: Pipeline: Recruitment and Retention and Skill Development
- Solution 1: Attracting and retaining workers through significant improvement of the “culture” of the health care workplace by implementing shared governance, incumbent worker training, career ladders, access to education and training opportunities, and other attributes identified by employees, researchers, and from exemplary continuous improvement programs.
- Solution 2: Providing management training and credentialing in long-term care, consistent with this type of workplace improvement.
- Solution 1: Attracting and retaining workers through significant improvement of the “culture” of the health care workplace by implementing shared governance, incumbent worker training, career ladders, access to education and training opportunities, and other attributes identified by employees, researchers, and from exemplary continuous improvement programs.
- Issue: Skill Development
- Solution: Designing health care occupation curricula that provide the basic knowledge and skills needed for effective entry to practice in the high-growth areas of employment in primary care, long-term care and acute care sectors. Develop curricula so that there is a fit between programs for advancing the careers of health care workers (often provided through the workplace) and the requirements of the educational institutions.
- Issue: Skill Development
- Solution: Examining the state credentialing requirements with the goal of expanding less traditional paths to meeting occupational requirements, such as career ladders, apprenticeships and other workforce development strategies. Creating “cross walks” from practice to educational programs and credentialing requirements based on nationally developed measurement of worker skills.
- Issue: Capacity of Education and Training Providers
- Solution: Addressing the capacity problems (i.e., lack of faculty, resources, etc.) in many community colleges and other post-secondary education and training organizations where barriers to applicants exist and where there are inadequate numbers of qualified applicants for actual or projected demand for some health service occupations. Capacity is affected by lack of faculty and other resources.
- Issue: Sustainability: Leadership, Policy, and Infrastructure
- Solution: Partnering among a wide range of stakeholders in the health care workforce in order to project changes in workforce demand at the local/regional, state and national levels and to generate long term, efficient, and sustainable approaches to those changes.
- Issue: Sustainability: Leadership, Policy, and Infrastructure
- Solution: Developing methods for projection of medium-term occupational needs that can be used by a health care entity, such as a hospital or home care agency, as a basis for internal planning and for planning with partners in education, workforce development and other health care workforce stakeholders.
The Department of Labor Employment and Training Administration’s Business Relations Group reviewed the solutions generated during the Workforce Development Industry Forums. The purpose of the review was to:
- Identify for referral those solutions that are both the responsibility of other entities and not in the domain of the Department of Labor;
- Identify solutions that are jointly in the domain of the Department of Labor and another federal department;
- Identify solutions where the Department of Labor or the public workforce system already have program commitments; and,
- Identify solutions within the Department of Labor’s domain that if implemented effectively and widely will have a significant impact on managing the present and future workforce challenges of the health care industry. The latter group of solutions was examined by asking the question: “How can the Employment and Training Administration best use its resources and influence to have a positive impact on the challenges identified by the health care industry?” The solutions selected for initial action are ones that can be adapted to many settings, that are built on partnerships among stakeholders, that provide other opportunities to leverage resources (including funding), and that are relevant to the basic problem of adapting the workforce to changing industry needs.
The solutions anticipated to have the clearest impact include the following program areas:
- Youth-related programs developed and implemented by partnerships that include schools, health care employers, post-secondary programs for health occupations, and public workforce system entities.
- Programs focused on non-traditional and traditional pools for health care entry-level workers that both broaden approaches to preparation programs and enhance career mobility in health care and related industries. Competency models for these programs should be developed through a partnership of educators, employers, and workforce professionals.
- Initiatives that meet the needs for academic and clinical faculty in high-demand health care education programs and that are designed to adapt to changing levels of workforce demand.
- Programs that deal with the community college and other educational organizations’ insufficient capacity through innovative partnerships and other approaches. These capacity issues include the need for appropriate clinical practice opportunities, funding for students, diagnostic and treatment equipment, and laboratory support.
- Improvement of health care workplaces by interventions such as management training, incumbent worker training, career mobility programs, accessible education and training opportunities, and reducing staff fluctuations through workforce projections.
- Effective initiatives to build a sustainable national infrastructure with local, state, and national elements tasked with continuous balancing of workforce demand and supply within the health care industry.
The majority of the solutions identified by forum participants are not sector specific. However, many solutions can be adapted to the particular needs of a sector or a community.
National, State and Local Partnerships for Implementing Workforce Solutions
Dealing with workforce challenges in the health care industry requires collaboration at the national, state and local levels, and between these levels. Executive and Workforce Development Industry Forum participants recommend a national, systemic approach that aligns the workforce resources available with the challenges facing the health care industry today and well into the future. This direction is consistent with the thinking behind the High Growth Job Training Initiative.
A central role of the Employment and Training Administration is that of identifying and communicating effective workforce solutions that can be replicated to respond to national challenges such as management training or youth-related recruitment programs. A second aspect of that role is the funding of pilot programs, by ETA alone or in partnerships, that are most effective in dealing with some aspect of workforce challenges, and that are replicable by other entities. At the national level, providers and others also identify the need for a national warehouse of sound and effective workforce interventions with a search engine that makes it possible for a local Workforce Investment Board, a human resources manager, or others to identify solutions that have worked elsewhere.
The actions of state governments and state-level entities are pivotal to any national workforce effort. State government decisions direct how some federal funding is used to support some workforce programs. For example, the Workforce Investment Act provides funding to states, and through the states to local Workforce Investment Boards and workforce-related programs. These funds and others, such as Temporary Assistance to Needy Families and Medicaid, are used to provide training, support, and placement for many occupations including those in health care. It is at the state level that policy and funding decisions are made about higher education, licensing and regulation. Medicaid programs that directly affect employment conditions and delivery of care, worker training, collection of information for programs and policy development, and other initiatives that directly influence the implementation, are among many of the solutions recommended in the Executive Forums and Workforce Development Industry Forums. A sustainable, adaptive and effective workforce strategy in health care requires strong public and private partnerships in every state. Without these partnerships ETA cannot respond adequately to current problems or prevent future ones.
Local partnerships, including Workforce Investment Boards, employers, employees, educators and other community members, are needed to implement workforce solutions closest to health care delivery sites, and to potential labor pools. Through such partnerships, both the workforce demand and supply sides can identify the needs in their own communities. Partners can use their state and national networks to find solutions to better manage their particular challenges.
Endnotes
- The full paper is available online at http://www.doleta.gov/BRG/pdf/pdf3.pdf.
- U.S. Department of Labor. Bureau of Labor Statistics. July 2002. Projected Growth Rates by Industry (Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation).
- U.S. Department of Commerce. Bureau of Economic Analysis. November 2002. Gross Domestic Product by Industry for 2001.
- U.S. Department of Labor. Bureau of Labor Statistics. February 2004. Monthly Labor Review.
- Ibid.
President’s High Growth Job Training Initiative: Health Care Industry (1)
Employment and Training Administration, U.S. Department of Labor
The New Americans in Nursing Program, a $1.4 million grant to Florida International University’s School of Nursing, retrains unemployed or underemployed foreign-educated physicians to become registered nurses. ($60,150 in leveraged funds)
Efficacy of Tutoring to Reduce Health Care Occupation Bottleneck, a $224,088 grant to Capital IDEA, Austin, Texas, fills the health care pipeline by offering tutoring to students who fail a key course required for graduation in a nursing or allied health occupation. (over $700,000 in leveraged funds)
Oregon Governor’s Healthcare Workforce Initiative is a $300,000 grant to the State of Oregon to enhance the capacity of educational institutions to provide health care clinical requirements by funding seven Sim Man® real-time interactive human patient simulators. This technology will be used by faculty and over the state’s broadband Internet network. ($450,000 in leveraged funds)
Grow Our Own, a $4 million grant to the Rio Grande Valley Health Training Alliance for the region surrounding McCallum, Texas, will enroll students in Post-Licensures Specialty Training, create a Skills Workforce Academy, and develop a comprehensive Faculty Sharing Program. ($4.5 million in leveraged funds)
Specialty Nurse Training is a $4 million grant to a partnership between the Hospital Corporation of America (HCA) and Broward Community College in Ft. Lauderdale, Fla., and Austin Community College in Austin Tex. To address the nursing shortage, the Florida program will create a distance learning model; the Texas fellowship program will create an intensive, hands-on, accelerated learning setting similar to a medical residency program. Both programs provide approaches that produce quicker results than traditional on-the-job training. (over $6 million in leveraged funds)
The Hospice and Palliative Care Certificate Program, a $516,154 grant to Excelsior College, Albany, N.Y., will develop curriculum and deliver an online hospice and palliative care certificate program that can be accessed from any location.
Johns Hopkins Health System’s Incumbent Worker Career Acceleration Program, a $3 million grant to the Johns Hopkins Health System, Baltimore, Maryland, provides a continuum of solutions for incumbent workers to move up the health career ladder starting at entry-level. ($3.9 million in leveraged funds)
Healthcare Career Lattice: A Model for Enhanced Learning, a nearly $1.9 million grant to Evangelical Lutheran Good Samaritan Society (ELGSS), addresses the need to attract more youth and other alternative labor pools into health care occupations, including non-nursing occupations. The project, which will operate in North Dakota, South Dakota and Minnesota, will also build the capacity of education providers. ($1,204,000 in leveraged funds)
The Maryland Healthcare Workforce Initiative is a $1.5 million grant to the State of Maryland and the Governor’s Workforce Investment Board. The grant provides strategies, including scholarships, to enhance the skill levels of nurses along the career ladder and to back fill the gaps left by nurses transitioning into teaching. ($700,000 in leveraged funds)
Developing Partnerships and Initiatives to Resolve Long-Term Care Workforce Challenges, a $113,296 grant to the American Health Care Association Foundation, will provide a practical “How To” or “Cookbook” for nursing home managers and administrators combating the nursing shortage in long-term care. The information can be used to spearhead the formation of partnerships across the country.
Recruitment and Retention of Direct-Care Workers, a nearly $1 million grant to the Paraprofessional Healthcare Institute, will focus on multiple workforce challenges related to recruitment and retention of direct care workers in the long-term care industry. The project, operating in New York, North Carolina and Pennsylvania, will demonstrate problem-solving training curriculum and publish a series of guidebooks and teaching manuals in both English and Spanish on effective paraprofessional workforce development practices. ($999,902 in leveraged funds)
Three-Year, Hospital-Based Degree Nursing At a Rural Community Hospital is a $200,000 grant to the Berger Health System in Circleville, Ohio. To increase the number of trained nurses, Berger Health System will provide instructors, space for training, and clinical experiences; Ohio University will supply curriculum and faculty for a three-year, university-based Associate Degree nursing program. ($405,939 in leveraged funds)
Pueblo Project HEALTH, a $715,402 grant to Pueblo Community College, Colorado, will assist counties designated as Health Professional Shortage Areas and Medically Underserved Areas. The program delivers training to rural areas through traditional classroom instruction, distance learning, and mobile clinical experiences.
The Contextualized Literacy Pre-LPN Program is a $192,500 grant to 1199 SEIU League Grant Corporation, New York. The grant will help entry-level health care workers, out of school for a long period of time, to enter LPN training by providing literacy and pre-LPN classes. ($100,000 in leveraged funds)
Rural Health Care Job Training Pilot Economic Recovery Demonstration Project is a $1.2 million grant to Columbia Gorge Community College, Oregon. The grant will implement a health care career ladder program with multiple entry points to enable individuals, at any place in their career, to enter or move ahead in the health care field. ($870,982 in leveraged funds)
Healthcare Services Business Connection is a $762,659 grant to the Tacoma-Pierce County Workforce Development Council in the State of Washington. Ten regional health care organizations are partnering with the public workforce system to develop of Western Washington Invasive Cardiovascular Technologist Program, a Healthcare Educator Network, and strategies to reach out to minority populations and youth. ($751,000 in leveraged funds)
Project H.E.A.L.T.H., a $1.5 million grant to the North Carolina Department of Commerce, is designed to help transition North Carolina workers in declining industries into health care jobs experiencing shortages. ($170,504 in leveraged funds)
Meeting America’s Healthcare Employment Needs: The Job Corps/Community College Solution is a $1.5 million grant to Management and Training Corporation. The grant will link Job Corps health care training with advanced training in community colleges leading to certification for health care occupations. It also provides easy access for Hispanic youth to take advantage of English courses and become part of a high-demand bilingual workforce.
Endnotes
1. This information is available online at http://www.doleta.gov.
President’s High Growth Job Training Initiative: Health Care Industry Demonstration Grants (1)
Employment and Training Administration, U.S. Department of Labor
Local Solutions with National Applications to Address Health Care Industry Labor Shortages
U.S. Secretary of Labor Elaine L. Chao is pleased to announce a series of investments totaling more than $24 million to counter health care labor shortages. For the past nine months, the U.S. Department of Labor has taken part in forums with health care industry leaders, educators, and the public workforce system.
DOL has sought to understand and implement industry-identified strategies to confront critical workforce shortages. It has listened at sessions conducted by associations representing thousands of health care institutions, and considered viewpoints expressed in-person by over 300 health care leaders. Solutions that have been adopted as a result of eight forums will act as national models through the President’s High Growth Job Training Initiative.
This set of solutions cuts across the national labor needs of the health care industry in acute care, long term care, allied health care professions, as well as the unique challenges facing rural areas. It focuses on specific as well as the broader range of challenges in the health care arena, including:
- expanding the pipeline of youth entering the health care profession;
- identifying alternative labor pools such as immigrants, veterans, and older workers that can be tapped and trained;
- developing alternative training strategies for educating and training health care professionals, such as apprenticeship, distance learning, and accelerated training;
- developing tools and curriculum for enhancing the skills of health care professionals for nationwide distribution;
- enhancing the capacity of educational institutions through increased numbers of qualified faculty and new models for clinical training;
- developing strategies to retain and help current health care workers move into higher level positions in shortage areas;
- helping workers in declining industries build on existing skills and train for health care professions.
Overall, grants totaling more than $24 million are being funded across the nation. They are intended to provide genuine solutions, leadership, and models for partnerships that can be replicated in different parts of the country. The U.S. Department of Labor anticipates offering additional grants in a competitive process later this year.
Specialty Nurse Training
Grant amount: $4,000,000 Total (Florida: $2,000,000; Texas: $2,000,000)
Leveraged amount: $6,076,930
- Florida: $4,303,350 in cash from HCA and 149,580 in-kind from Broward Community College
- Texas: $1,624,000 in-kind from St. David’s HealthCare Partnership
Grantee: Hospital Corporation of American (HCA)
Key partners: Broward County Community College, Ft. Lauderdale, FL; Austin County Community College, Austin, TX; St David’s HealthCare Partnership, Austin, TX
Grant activities will take place in South Florida and Austin, Texas
Challenge
A shortage of critical care nurses threatens the nation's health care system. In addition, without sufficient patient contact, inexperienced graduate nurses cannot fill openings in critical care areas quickly enough. Unless innovative solutions are developed, this lack of experienced nurses will continue to adversely affect health care services in the U. S.
Addressing the Challenge
With its $4,000,000 grant from ETA, this Specialty Nurse Training pilot program will implement two approaches to address the lack of experienced nurses and set standards that can be replicated across the country. The Florida program will create a distance learning model, and the Texas fellowship program will create an intensive, hands-on, accelerated learning setting similar to a medical residency. Both programs furnish the specialized training nurses need to perform at higher levels more quickly than traditional approaches.
Projected Outcomes
Florida: At least 100 students will enter the critical care core program during the grant's first year. In their second year, these students will specialize in either critical care or the emergency department. Meanwhile, another 100 students will enroll in the critical care core program. When their clinical rotations end, students will be able to provide care on their own. Texas: Eighty candidates will complete a year in the Nursing Apprenticeship/Fellowship program, qualifying them to work in specialty areas such as intensive care units, emergency departments, and surgical services.
Sustainable Impact
This grant's partners are committed to these activities beyond the grant period. A new, self-supporting Specialty Training Institute that will offer courses and technical expertise nationally will assure the sustainability of the program. Grant funds will offset start-up costs associated with curriculum development for both programs.
Grow Our Own
Grant amount: $4,000,000
Leveraged amount: $1,620,000 cash and $2,837,200 in-kind from participating hospitals.
Grantee: Rio Grande Valley Allied Health Training Alliance -- Weslaco, Texas
Key partners: 10 hospitals, five educational institutions, four counties, two workforce development boards, and one faith-based community organization.
Grant activities will take place in Cameron, Hidalgo, Starr, and Willacy Counties, Texas.
Challenge
Multiple barriers contribute to the severe nursing and allied health professionals shortages occurring in rural border communities. If these barriers are not addressed, the skills shortage will worsen, jeopardizing health care services in these communities.
Addressing the Challenge
With its $4,000,000 grant, the Rio Grande Valley Allied Health Training Alliance will assist area businesses and community leaders to develop, attract, and retain homegrown talent. Key objectives include enrolling students in Post-Licensures Specialty Training, creating a Skills Workforce Academy for Nursing and Allied Health candidates, retaining them through tuition assistance, and developing a High School Concurrent Enrollment Program and comprehensive Faculty Sharing Program while drawing from Alliance hospitals' supply of Masters of Science in Nursing.
Projected Outcomes
Grow Our Own will: a) Enroll 135 participants in Post Licensure Specialties with a completion rate of 95 percent; b) Prepare 70 students annually in academies; c) Write curricula and learning objectives so that 90 high school juniors and seniors have the annual opportunity to take college classes d) Expand comprehensive case management services to 360 participants with retention rates for all students reaching 90 percent; e) Utilize online coursework by Fall 2005 as part of the Faculty Sharing Program for one allied health specialty; and f) Develop an online, regional scheduling system in 2004 for coordinating 400 students' clinical rotations in Fall 2005.
Sustainable Impact
The members that comprise the Alliance are well positioned to ensure the sustainability of this project beyond the cessation of federal funds.
A System for Upgrading Incumbent Health Care Workers into High-Skill Jobs
Grant amount: $3,000,000
Leveraged amount: $3,900,000 in-kind from Johns Hopkins Health System
Grantee: Johns Hopkins Health System
Key partners: Baltimore City Community College; Community College of Baltimore County
Grant activities will take place in Baltimore, Maryland
Challenge
There is an immediate, severe shortage of skilled health care workers, and a wide range of evidence exists that the demand for these workers will increase while the number of individuals enrolled in accredited programs to receive training for the most critical skills is decreasing. If unaddressed, this problem will continue to threaten the availability and quality of health care in the United States.
Addressing the Challenge
Under its $3,000,000 grant from ETA, Johns Hopkins Health System will develop and execute an Incumbent Worker Career Acceleration Program, which will be comprised of five components: (1) An initiative for addressing retention and growth of at-risk workers; (2) A GED and diploma preparation program; (3) An initiative for retraining of employees in declining jobs for emerging jobs; (4) A high-potential worker assessment and skills training program; and (5) An initiative to upgrade training of incumbent workers into critical skills shortage positions.
Projected Outcomes
Johns Hopkins projects an 80% success rate in employment retention for 100-150 employees participating in the Retention and Growth of At-Risk Workers initiative. It also expects to achieve a 70% retention rate among 50 incumbent workers receiving a GED or diploma through this initiative. In addition, of those 70% at least 50% are expected to go on to further skills training and higher-skilled positions. 75 of Johns Hopkins' workers will be assessed, counseled, and provided skills-based training for emerging new jobs. High-Potential Worker Assessment will result in an estimated 200- plus workers entering either remedial education or various skills-based training programs leading to the staffing of more critical skilled positions.
Sustainable Impact
Johns Hopkins is strongly committed to share all initiatives of its Incumbent Worker Career Acceleration Program with the health care industry and the public workforce system.
A Model for Enhanced Learning
Grant amount: $1,877,517
Leveraged amount: $910,000 in cash and $294,000 in-kind from Evangelical Lutheran Good Samaritan Society (ELGSS)
Grantee: The Evangelical Lutheran Good Samaritan Society, Sioux Falls, South Dakota
Key partners: In South Dakota: Lake Area Technical Institute, Watertown; South Dakota State University, Brookings; University of South Dakota, Vermillion; Sioux Valley Hospitals and Health System, Sioux Falls; pullUin software/South Dakota Health Technology Innovations Inc., Vermillion. In Nebraska: Bellevue University, Bellevue.
Grant activities will unfold through the use of distance learning technology. Mentoring will be delivered at 25 sites mostly in Minnesota, North Dakota, and South Dakota.
Challenge
Recruitment and retention of health care professionals is especially challenging in rural communities where educational opportunities are limited. Without more access to education, the health care industry's labor pool will keep shrinking.
Addressing the Challenge
With its $1,877,517 grant, ELGSS will recruit from high schools and non-traditional labor pools such as displaced workers, and collaborate with Sioux Valley Hospitals and Health System to raise public awareness of health care career opportunities. To increase retention, ELGSS will start a Mentor project for entry-level workers and develop Management Certificate training. To build the capacity of education and training providers, ELGSS will deliver online nursing programs up through the Master's degree level. Training will be offered in employees' own ELGSS long-term care facilities -- 50% of which are located in Minnesota, South Dakota, North Dakota, Iowa, and Nebraska -- through an innovative blend of distance learning, mentoring, and clinical experience in health care sites near the employees' homes.
Projected Outcomes
ELGSS will implement an apprenticeship model program for Management Certificate Training with DOL and Bellevue University. ELGSS also will partner with Lake Area Technical Institute to develop and deliver an online LPN program, as well as with South Dakota State University to deliver online BSN and MSN programs, with an emphasis on geriatrics. Each part of the overall project is replicable for use throughout the nation's health care industry.
Sustainable Impact
ELGSS has made a strong commitment sustain this project. Tuition and fees generated by education providers involved in this initiative will sustain their established history of producing qualified nurses.
Maryland Healthcare Workforce Initiative
Grant amount: $1,500,000
Leveraged amount: $700,000 from State of Maryland Employer Matching Fund
Grantee: State of Maryland
Key partners: To be determined during grant activities
Grant locations: Statewide
Challenge
There are two major challenges facing the health care industry: (1) lack of nurses and allied health professionals; and (2) lack of qualified academic and clinical health care faculty. The lack of faculty is preventing the admission of applicants into nursing and allied health programs which ultimately affects the number of qualified nurses and allied health professionals available for employment. If these two challenges are unaddressed, this worker shortage will have severe and damaging impacts upon the availability and quality of health care services in the United States.
Addressing the Challenge
Under its $1,500,000 grant from ETA, the Maryland Governor's Workforce Investment Board (GWIB) will address the faculty capacity problem by implementing a scholarship program for nurses who pursue credentials to teach nursing and allied healthcare professions. The GWIB will also implement a scholarship program for Licensed Practical Nurses (LPNs) and other incumbent workers that are seeking their Registered Nurse (RN) credentials to backfill the RNs that pursue their Master's Degree. Additionally, an Incumbent Worker Training strategy will be implemented to assist health care employers to upgrade the skills of existing workers.
Projected Outcomes
The "Teaching for the Health of It" scholarship program will provide 40 one-time only scholarships in the amount of $10,000 each for nurses pursuing teaching credentials. The other scholarship program will provide 40 one-time only scholarships in the amount of $10,000 for LPNs and other incumbent workers who are seeking their RN credentials. Partnerships between employers and the community college system will be created to provide allied health care training for incumbent workers.
Sustainable Impact
The GWIB has established a Governor's Healthcare Workforce Steering Committee that consists of members from industry, economic development, employment services, and education to develop and implement collaborative solutions. Currently the health care industry in Maryland spends over $11,140,000 to educate, attract, and retain health care workers because of the faculty shortfall. The GWIBs and the Maryland Healthcare Workforce Steering Committee are committed partners for continuing and sharing the model throughout the nation.
Project H.E.A.L.T.H.
Grant amount: $1,500,000
Leveraged amount: $170,504 in-kind contributions from most key partners listed below
Grantee: North Carolina Department of Commerce, Commission on Workforce Development -- Raleigh
Key partners: NC Hospital Association, NC Community College System, University of North Carolina System, NC Department of Health and Human Services, NC Area Health Education Centers, JobLink Career Center system, and local Workforce Development Boards
Grant activities will take place in the western, eastern, and piedmont regions.
Challenge
Since the mid-90's, North Carolina's health care industry has experienced severe shortages of registered nurses and direct care workers due to the aging of nurses and nursing educators. Meanwhile, the state has been devastated by worker dislocation.
Addressing the Challenge
With its $1,500,000 grant, Project H.E.A.L.T.H.: Helping Employers and Labor Transition to Health Care will address North Carolina's critical nursing and direct care worker shortages. It targets the state's large and diverse labor pool of dislocated workers, and will test and expand innovative approaches to worker education, training, and employment in the nursing and direct care workforce sectors. In this model, H.E.A.L.T.H. will work to enhance health career development and employability of dislocated workers and provide the needed support for an education and training institution for nursing.
Projected Outcomes
Up to 450 displaced workers are projected to enroll in Human Resource Development Plus pilot sites that support other initiatives addressing direct care shortages. Additional outcomes include 300 workers expected to enroll in further training, 200 placed in jobs -- of which 120 will be direct care workers. Thirty-three individuals will be placed in degree programs to increase the availability of instructors and applicants for health care programs.
Sustainable Impact
An advisory team drawn from hospitals, the long-term care industry, and key Project H.E.A.L.T.H. partners will build the foundation for sustainability. Project H.E.A.L.T.H. will provide innovative models that can be replicated throughout North Carolina and the nation.
Meeting America’s Health Care Employment Needs: The Job Corps/Community College Solution
Grant amount: $1,500,000
Grantee: Management & Training Corporation, Centerville, Utah
Key partners: In Illinois: City Colleges of Chicago and the Metropolitan Chicago Healthcare Council; In Ohio: Cincinnati State Technical and Community College and Sinclair Community College; In Pennsylvania: Luzerne County Community College and Lehigh/Carbon County Community College
Grant activities will take place at the Paul Simon Chicago Job Corps Center, the Cincinnati Job Corps Center, the Dayton Job Corps Center, and the Keystone Job Corps Center in Drums, Pa.
Challenge
The health care industry faces three key problems: a shortage of qualified health care employees, a lack of bilingual employees, and available, yet untrained out-of-school youth.
Addressing the Challenge
Management & Training Corporation will unite the efforts of Job Corps Centers with community colleges to address the health care workforce challenges in Illinois, Ohio, and Pennsylvania. Job Corps students finished with their vocational training in basic health will be recruited to pursue advanced training and certification at the community college. Additionally, this project provides instruction, assessment, career development, academic training, and support services. It also provides easy access for Hispanic youth to take advantage of English courses, and become part of a high-demand bilingual workforce.
Projected Outcomes
Management & Training Corporation's projects will affect four Job Corps Centers and 125 students, who will ultimately be employed in health care.
Sustainable Impact
Management & Training Corporation, Job Corps Centers, and participating community colleges will provide a firm foundation for sustainability once federal funding has been expended. The model will be documented so that it can be replicated in Job Corps Centers across the nation.
New Americans in Nursing Program
Grant amount: $1,421,639
Leveraged amount: $500,000 in cash from the Hospital Corporation of America (HCA) and 60,150 in-kind from Florida International University (FIU)
Grantee: Florida International University School of Nursing
Key partners: Hospital Corporation of America, Nashville, TN
Grant activities will take place in Miami-Dade County and Tallahassee, Florida
Challenge
Nurse shortages left unaddressed will have severe and damaging impacts upon the availability and quality of health care services in the United States.
Addressing the Challenge
With its $1,421,639 grant, the New Americans in Nursing Program will address the challenges by retraining unemployed or underemployed foreign-educated physicians to become registered nurses.
Projected Outcomes
One hundred nursing students with prior clinical knowledge and experience will graduate during the grant period. Under this grant, FIU also will test distance education through the use of interactive television, with 70 students in Miami and 30 in Tallahassee. The grantee will also share data on the program's effectiveness as a retraining model for other areas of the country.
Sustainable Impact
FIU's School of Nursing, through its strong track record of attracting financial support, will ensure the sustainability of this project. FIU will evaluate this program's impact and effectiveness for foreign physician students and the overall nursing workforce. Because of the large applicant pool of foreign-educated physicians and the worsening nursing shortage, there will be lasting interest from various hospital and corporate entities to support the continuation of this program.
Rural Healthcare Job Training and Economic Recovery Program in the Columbia River Gorge
Grant amount: $1,250,000
Leveraged amount: $542,501 from four local hospitals, four long-term care facilities, foundations, and Columbia Gorge Community College; $328,481 in-kind from health care businesses and Columbia Gorge Community College
Grantee: Columbia Gorge Community College, The Dalles, Oregon
Key partners: Eight area hospitals and health care providers, Region 9 Workforce Investment Board and its One-Stop Career Centers, K-12 school districts, Oregon Health and Science University, and city and county governments
Grant activities will take place in Gilliam, Hood River, Sherman, Wasco, and Wheeler Counties in Oregon; Klickitat and Skamania Counties in Washington.
Challenge
Economic downturns have left high numbers of displaced workers requiring education and retraining to transition into health care positions. Without programs, the health care industry will not be able to draw from this non-traditional labor pool to fill vacancies.
Addressing the Challenge
With its $1,250,000 grant, Columbia Gorge Community College and its partners will create a Health Occupations Career Ladder Nursing Program to train 200 new workers. CGCC will expand its offerings and opportunities for an Associate Degree in Nursing and a distance learning option for a Bachelor Degree of Nursing Program.
Projected Outcomes
Trainees will emerge from the Health Occupations Program with the skills, licenses, and experience needed for health care employment. Of the 200 trainees who enter the Career Ladder, 85 percent will pass licensing exams, and 85 percent will achieve employment at their target career level within the grant period. Further, 90 percent of incumbent workers will receive pay raises as a result of their additional credentials. Forty nurses of 200 total trainees will have the opportunity to earn a BSN through Columbia Gorge's dual admission agreement with Oregon Health and Science University.
Sustainable Impact
Besides the matching funds already supplied, regional businesses have committed financial support to the program for at least one year after the grant. Also, the Healthcare Demonstration Project grant will be replaced with Oregon State Reimbursement Funds at the end of the grant period.
Recruitment and Retention of Direct-Care Workers
Grant amount: $999,902
Leveraged amount: $999,902 cash from the Charles Stewart Mott Foundation and The Atlantic Philanthropies
Grantee: Paraprofessional Healthcare Institute, Bronx, New York
Key partners: Lehman College of New York; North Carolina Foundation for Advanced Health Programs; Workforce Investment Board of Lancaster County, Pennsylvania; local community colleges and workforce investment boards
Grant activities will take place in New York City, in and around Lancaster County, Pennsylvania, and at sites to be determined in North Carolina.
Challenge
The long-term care industry's shortage of direct-care workers is particularly acute in home-based care. Long-term care providers realize that they must transform standard practices regarding recruitment, training, supervision, and support in order to effectively attract and retain new workers as paraprofessionals.
Addressing the Challenge
With its $999,902 grant, the Paraprofessional Healthcare Institute will provide a range of technical assistance, training initiatives, and materials for the long-term care workforce. Emphasis will be placed on Hispanic caregivers and supporting the nation's Workforce Investment Boards and community colleges in recruiting and training.
Projected Outcomes
The Paraprofessional Healthcare Institute will: (1) develop a recruitment and apprenticeship career-lattice model; (2) create a coaching approach for front-line supervisors, with a curriculum designed for employer-based community colleges; (3) demonstrate a problem solving training curriculum, in partnership with Lancaster's Workforce Investment Board; (4) publish a series of guidebooks, curricula, and teaching manuals -- written in English and Spanish -- on effective paraprofessional workforce development practices; (5) create strategic relations with faith-based health systems capable of bringing about nationwide change.
Sustainable Impact
Well-established partnerships of The Paraprofessional Health Institute, The Charles Stewart Mott Foundation, and The Atlantic Philanthropies along with local community colleges and Workforce Investment Boards will provide a firm foundation for replicating the model throughout the nation after the federal funds have been expended.
Healthcare Services Business Connection
Grant amount: $762,659
Leveraged amount: $200,000 in cash and $500,000 in-kind contributions from multiple partners
Grantee: Tacoma-Pierce County Workforce Development Council
Key partners: More than 20 organizations ranging from health providers to universities, community colleges, and workforce boards
Grant activities will take place in Pierce County, Washington.
Challenge
Serious health care workforce shortages exist throughout the United States. Without a multi-pronged, regional approach, gaps in the health care workforce will not be filled.
Addressing the Challenge
With its $762,659 grant, the Tacoma/Pierce County Workforce Development Council will implement four distinct projects to improve and expand the pool of qualified professionals in high-demand health care jobs. The first project confronts a clear need to train invasive cardiovascular technologists; the second targets current health care workers through a Comprehensive Career Coaching Program; the third seeks to establish connections through a Healthcare Educator Network; and the fourth project incorporates multiple strategies to reach out to minorities and youth.
Projected Outcomes
Tacoma/Pierce County Workforce Development Council will (a) admit 15 students to the Invasive Cardiovascular Technologist Program; (b) develop and launch the Healthcare Educator Network website; (c) translate Healthcare Occupations Workshop materials into Spanish, Korean, and Russian; (d) increase the Medical Rotation Program participants by eight; (e) start a Health Summer Camp for youth; (f) increase minority youth participation in job shadow and volunteer programs by 10 percent.
Sustainable Impact
At least 10 regional health care organizations will commit to ongoing funding of the Invasive Cardiovascular Technologist Program. At least 10 organizations, including regional colleges, universities, and the Washington State Nursing Association, will be approached for resources for the Healthcare Educator Network beyond the grant period. The partners involved in the Targeted Populations Outreach Program -- community colleges, the local workforce system, and health care providers -- already have a strong history of collaboration and will continue to work together after the grant ends.
Pueblo Project Health
Grant amount: $715,402
Leveraged amount: $595,062 from grantee and state and local governments
Grantee: Pueblo Community College, Pueblo, Colorado
Key partners: Pueblo Work Link (One-Stop Career Center), Trinidad State Junior College, Parkview Episcopal Medical Center
Grant activities will take place in Colorado's Pueblo, Costilla, Conejos, and Alamosa Counties.
Challenge
A shortage of medical personnel in rural Colorado, communities is compounded by two key challenges. First, many rural communities have Emergency Medical Services comprised of volunteer personnel, who often leave to pursue paid employment elsewhere. In addition, there are no training programs in rural Colorado to prepare health care practitioners.
Addressing the Challenge
With its $715,402 grant, Pueblo Project HEALTH addresses this shortage by bringing training opportunities to outlying areas, and helps volunteer medical personnel secure paid employment. Pueblo Project HEALTH combines the Emergency Medical and Respiratory Care positions into one hybrid curriculum, and administers their training through traditional classroom instruction, distance learning technology, and mobile clinical experiences. Graduates will be able to secure employment in Respiratory Care and serve as volunteer Emergency Medical Technicians. This project will assist counties that have been designated as Health Professional Shortage Areas and Medically Underserved Areas, and will target minority/disadvantaged individuals.
Projected Outcomes
The hybrid curriculum will prepare individuals for both the Intermediate Emergency Medical Technician and the Respiratory Care Practitioner positions. The number of minority/disadvantaged individuals enrolled in the program will increase significantly during the second and third years of the project.
Sustainable Impact
Pueblo Project HEALTH will result in an innovative curriculum that can be used by community colleges throughout the state. Further, local WIA funds can continue to be a source of funding after ETA demonstration funds expire. Third, Pueblo Project HEALTH is committed to expanding the program throughout the state using the community college system.
Hospice and Palliative Care Certificate
Grant amount: $516,154
Leveraged amount: $80,556 in-kind from Excelsior College
Grantee: Excelsior College, Albany, New York
Key partners: Fourteen hospices in New York state, along with one each in Montana, North Carolina, Rhode Island, South Carolina, and Texas
Grant activities will take place at locations determined immediately following implementation. Local hospices will be identified in Montana, New York, North Carolina, Rhode Island, South Carolina, and Texas.
Challenge
Many hospices and their associations have reported that the shortage of nurses is having a significant impact on access to hospice services, and that hospices have had to deny services to eligible patients because they do not have adequate staff to provide nursing care. Without immediate solutions to the hospice nurse shortage, dying patients and their families will increasingly face abandonment by the health care delivery system.
Addressing the Challenge
With its $516,154 grant, Excelsior College will develop a Hospice and Palliative Care Online Certificate Program (HPCC) that includes a period of practical experience and training supervised by an expert or specialist. In doing so, HPCC will directly address two major national health care workforce needs: (1) expanding the number of registered nurses (RNs) working in the health care field; and (2) creating a stable, highly skilled RN workforce for hospices throughout the nation.
Projected Outcomes
Excelsior College will operate HPCC for 16 months as a pilot program in Montana, New York State, North Carolina, Rhode Island, South Carolina and Texas. The program will serve 60 interns and approximately 30 preceptor supervisors affecting the quality of care of over 15,000 patients from 19 hospice partners.
Sustainable Impact
Excelsior College has over 30 years of experience in developing educational programs for working adults. While other organizations have educational materials for hospice and palliative care, none are online and easily accessible. By the 17th month, the HPCC program will be offered nationally and will be self-sufficient.
Oregon Governor’s Healthcare Workforce Initiative
Grant amount: $300,000
Leveraged amount: $200,000 in cash and $250,000 in-kind from the State's Employer Workforce Training Fund
Grantee: Governor's Healthcare Workforce Initiative, Salem, Oregon
Key partners: In Portland: Oregon Consortium for Nursing Education (OCNE); Oregon Center for Nursing; Northwest Health Foundation. In Tualatin: Oregon Health Career Center; Community College Healthcare Action Plan.
Grant activities will take place statewide.
Challenge
Overcoming nursing shortages requires that the education system devise ways to supply clinical facilities and faculty. Otherwise, the education system will be unable to fill the pipeline with qualified nurses.
Addressing the Challenge
With its $300,000 grant, the Oregon Governor's Healthcare Workforce Initiative will purchase seven SimMan,® real-time interactive human patient simulators made by Laerdal Medical Corporation. The simulation technology will be integrated into health care curricula for use by well-prepared and networked faculty, available over the state's broadband Internet network, and affordable for all education and service groups in the state.
Projected Outcomes
The Governor's Healthcare Workforce Initiative will report on the use of simulators to ensure that they: (a) Increase the capacity of educational programs; (b) Increase access to simulation-based education; (c) Increase simulation technology expertise statewide; and (d) Prove satisfactory as a quality educational tool.
Sustainable Impact
Firm commitments from community colleges, universities, high schools and health care organizations will help to ensure this project's long-term sustainability. This project's major stake-holding partners have each demonstrated their continuing efforts to meet the demand for a qualified health care workforce.
Efficacy of Tutoring to Reduce Health Care Occupation Bottleneck
Grant amount: $224,088
Leveraged amount: $456,091 in cash contributions from public and private sources.
Grantee: Capital IDEA, Austin, Texas
Key partners: In Austin: Austin Community College; Seaton Healthcare Network; St. David's Healthcare Partnership; Austin Heart; Worksource-Greater Austin Area Workforce Development Board; In San Marcos: Central Texas Medical Center.
Grant activities will take place in Central Texas.
Challenge
A Department of Labor-funded research project in Central Texas found that candidates for health care occupations had a very high failure rate in a key prerequisite course, Anatomy and Physiology I (A&P I). About one-third of students interested in health care careers were eliminated by A&P I. Taking A&P I multiple times delays admission for approximately one-quarter of the students.
Addressing the Challenge
With its $224,088 grant, Capital IDEA will test a strategy that starts tutoring the first week of classes in order to: (a) Increase the success rate of students, thereby reducing the extra expense of tuition, counseling, child care, and time associated with students repeating the course; (b) Accelerate graduations; and (c) Increase the success rate of disadvantaged students. Rather than take remedial action after students fall behind, the tutoring will raise their chances of enrolling in a nursing or allied health occupation.
Projected Outcomes
The Capital IDEA project will increase the percentage of students achieving a C or better in A&P I from 50 percent to at least 70 percent. Students achieving a B or better will rise from a baseline of 25 percent to at least 45 percent. Removing this bottleneck will then enable students and lower-skill hospital employees to advance to the career training courses much more quickly, thus addressing recruitment and retention issues of health care employees.
Sustainable Impact
Capital IDEA is a joint effort of Austin Interfaith and leaders in the business community, including the area's two largest hospital systems. Along with Austin Community College and local Workforce Investment Boards, a firm foundation for continuing the model will be in place after federal funds have been expended.
Telelink Consortium Network
Grant amount: $215,600
Leveraged amount: $196,000 in cash and in-kind contributions from key partners listed below.
Grantee: Telelink Consortium Network, Ashland, Wisconsin
Key partners: Burnett Medical Center, Grantsburg; Flambeau Hospital, Park Falls; Memorial Health Center, Medford; Memorial Medical Center, Ashland; Northwest Wisconsin Workforce Investment Board, Ashland
Grant activities will take place in Northwest Wisconsin.
Challenge
Small, rural health care providers often do not have the resources to implement the continuous training and skills-upgrading programs necessary to keep employees.
Addressing the Challenge
With its $215,600 grant, the Telelink Consortium Network (TLC) will establish ongoing, collaborative relationships among rural health care providers in Northwest Wisconsin and the One-Stop Career Center system. TLC will pool financial, material, and human resources of small, remote hospitals and clinics for the purposes of increasing the supply and retention of health care professionals.
Projected Outcomes
TLC's efforts will concentrate on delivering higher skills training using appropriate, cost effective, web-based means. Training topics will include continuing professional development, managerial subjects, and skills upgrading in such areas as sonograms, Xrays, CAT scans, and MRIs -- all of which have a significant impact on worker retention. Under the project, 300 incumbent workers will complete at least one professional development/skills upgrading module, and a 15 percent larger pool of candidates interested in training for higher skilled health care occupations will be created.
Sustainable Impact
Four of the region's largest hospitals form the core of the TLC Network, and have agreed to take responsibility for the sustainability of this project. A combination of TLC Network membership fees and access fees will be the specific method for achieving self-sustainability.
Three-Year, Hospital-Based Nursing Degree at a Rural Community Hospital
Grant amount: $200,000
Leveraged amount: $405,939 cash and in-kind contributions from Berger Health System
Grantee: Berger Health System, Circleville, Ohio
Key partners: Ohio University
Grant activities will take place in Pickaway County and adjacent counties and small cities in Ohio.
Challenge
The acute care sector in rural areas experiences nursing shortages due to up-front costs for education and books, lack of role models, and a lack of knowledge of career opportunities. Hence, rural citizens often do not take advantage of the opportunity to attain the professional goal of becoming a registered nurse. There is also a lack of capacity at the local university to educate all qualified nursing school applicants.
Addressing the Challenge
With its $200,000 grant, the Berger Health System and Ohio University will meet the needs of the rural community hospital by holding all classes and clinical rotations at the Berger Hospital facilities for the three-year, university-based Associate Degree nursing program. Berger Health System agreed to sponsor one instructor, provide space, and accept students into clinical rotations. Ohio University agreed to supply the curriculum, faculty, and degrees.
Projected Outcomes
The Berger Health System and Ohio University will educate 30 incumbent employees and non-traditional students to become registered nurses in a community hospital versus a university setting. They also will document their progress and results so that the program can serve as a framework for other rural communities and hospitals.
Sustainable Impact
The project provides new and innovative ways to meet educational and workforce needs in rural regions. Due to the strong partnerships of the Berger Health System, Ohio University, and the local community, the project will serve as a model and be able to be repeated throughout the nation.
The Contextualized Literacy Pre-Lpn Program
Grant amount: $192,500
Leveraged amount: At least $100,000 in matching funds from Service Employees International Union's Training and Upgrading Fund (TUF)
Grantee: 1199 SEIU League Grant Corporation -- New York City
Key partners: NYC Department of Education; the Consortium for Worker Education
Grant activities will take place in New York City, Nassau, and Westchester Counties.
Challenge
Shortages of nursing and affiliated health care workers will have severe impacts upon the availability and quality of services if they are not addressed. One strategy for addressing the need for Licensed Practical Nurses (LPNs) calls for low-level health care workers to complete LPN training programs and secure employment. However, the challenge of the work-family balance, as well as other issues, make it difficult for workers who are new to academic environments to perform well on training programs' entrance exams.
Addressing the Challenge
SEIU's TUF will expand its Contextualized Literacy Pre-LPN Program, which combines literacy and job training in preparation for LPN programs. This pre-LPN program has been designed for low-level health-care workers who have been out of school for a long period of time and have had difficulty passing entrance exams. TUF will provide 10 classes and train instructors, enabling New York City area health care workers to enter LPN programs and find employment.
Projected Outcomes
Pre-LPN classes will prepare 250 students to pass entrance exams and enroll in LPN programs. 90 percent of the 250 participants will complete the pre-LPN program and advance to LPN programs within six months. The number of students in pre-LPN classes that successfully complete the LPN program will increase by 80 percent over last year.
Sustainable Impact
The Contextualized Literacy Pre-LPN Program will have a sustained impact on the LPN shortage because additional instructors will increase the TUF's training capacity. In addition, the pre-LPN program will have a sustained impact because the TUF has demonstrated its commitment to the program, providing at least $100,000 in matching funds to expand the program. Finally, the program will serve as a replicable model for other entities, with recommendations and best practices disseminated through papers and conferences.
Developing Partnerships and Initiatives to Resolve Long-Term Care Workforce Challenges
Grant amount: $113,296
Leveraged amount: $7,615 from the American Health Care Association
Grantee: National Foundation for the Advancement of Elder and Disabled Care in America (part of the American Health Care Association) -- Washington, D.C.
Key partners: George Washington University's Center for Health Services Research and Policy and Wertlieb Educational Institute for Long Term Care Management.
Grant activities will take place at locations determined through research proposed as part of this grant.
Challenge
Adequate staffing of facilities is essential for providing quality nursing home care. Without an infrastructure for this high-growth sector, nursing homes are challenged in building their workforce.
Addressing the Challenge
With its $113,296 grant, the American Health Care Association will develop an infrastructure of "Best Practice" models that can be expanded, evaluated, replicated, and transported to other areas of the country.
A major objective of this effort includes the development of a practical "How To" or "Cookbook" to build partnerships for combating the nursing shortage in long-term care. Another major objective calls on long-term care providers to develop ways to effectively team up with the public workforce system and take actions that will make the profession an attractive employer.
Projected Outcomes
The American Health Care Association will develop the infrastructure of "Best Practice" models for long-term care facilities along with a "How To" book of best practices, and partner with the public workforce system to make the long-term care sector an attractive employment option.
Sustainable Impact
The American Health Care Association (AHCA) and the National Commission on the Nursing Workforce for Long-Term Care have the foundation to communicate and implement the "Best Practice" models identified by the project.
Endnotes
1. This information is available online at http://www.doleta.gov/BRG/IndProf/HCEIA.cfm.
Keeping America in Business: Advancing Workers, Businesses, and Economic Growth (1)
102nd American Assembly, Columbia University
February 2003
Preface
On February 6, 2003, seventy-fi ve men and women representing business, labor, academia, government, workforce intermediaries, academia, nonprofit organizations and the media gathered at Arden House in Harriman, New York, for the 102nd American Assembly entitled “Achieving Worker Success and Business Prosperity: The New Role for Workforce Intermediaries.” For three days, participants examined policies, approaches and actions that need to be taken to assure that workers have access to economic opportunity and to assure that employers have access to the skilled workforce required for them to be globally competitive.
This project was directed by Robert Giloth, director, The Annie E. Casey Foundation; John Colborn, deputy director, Economic Development Unit, The Ford Foundation; and Betsy Biemann, associate director, Working Communities, The Rockefeller Foundation. The project was also ably assisted by a steering committee of distinguished leaders from around the country, whose names and affi liations are listed in the appendix to this report.
Background papers were prepared for participants under the editorial supervision of Robert Giloth and will appear as chapters in a book tentatively entitled Workforce Intermediaries for the 21st Century, to be published by Temple University Press in fall 2003. The chapters are listed on the inside back cover.
During the Assembly, participants heard formal addresses by David Ellwood, Lucius N. Littauer Professor of Political Science, John F. Kennedy School of Government, Harvard University; and Jeremy Nowak, president/CEO, The Reinvestment Fund. Richard M. McGahey, managing vice president, Abt Associates, Inc., moderated a panel of Timothy M. Barnicle, co-director, Workforce Development Program, National Center on Education and the Economy; Steve Crawford, director, Employment and Social Services Policy Studies, National Governors Association; and Jackie Edens, Commissioner, Mayor’s Office of Workforce Development, Chicago. Mr. Giloth also moderated an introductory panel that included Cynthia E. Marano, director, National Network of Sector Partners, National Economic Development and Law Center; Marlene Seltzer, president, Jobs for the Future; and Julie Strawn, senior policy analyst, Center for Law and Social Policy.
Following their discussions, participants issued this report on February 9, 2003. It contains both their findings and recommendations.
The text of this report is available on both The American Assembly’s website (http://www.americanassembly.com) and the project’s webpage (http://www.opportunitiesatwork.org), which also contains links to many of the organizations involved in this project.
We gratefully acknowledge the support of The Annie E. Casey Foundation, The Ford Foundation, The Rockefeller Foundation, The John D. and Catherine T. MacArthur Foundation, and the Open Society Institute, Baltimore.
The American Assembly takes no positions on any subjects presented here for public discussion. In addition, it should be noted that participants took part in this meeting as individuals and spoke for themselves rather than for their affiliated organizations and institutions.
We would like to express special appreciation for the fi ne work of the discussion leaders, rapporteurs and advisors in helping to prepare the final draft of this report: Daniel Berry, Paul Brophy, Terri Feeley, Lisa Kaplan Gordon, Ed Hatcher, Cynthia Marano, Richard McGahey, Julie Strawn, and Orson Watson.
David H. Mortimer
The American Assembly
Foreword
Over the past decade, a set of workforce development policies and strategies has emerged to meet the needs of both businesses and low-wage, low skilled workers. In some cases, the results have been nothing less than remarkable: employers are finding a well-trained competitive workforce while at the same time workers are being placed in jobs that can sustain their families.
The opportunity exists to spread this workforce intermediary approach, as this Assembly has named it, to a wider array of existing institutions in order to achieve greater impact. Achieving this impact will not be easy. Employers and job training providers simply adopting “promising workforce practices” won’t get the job done.
The challenge ahead is about transforming workforce development practices in a variety of institutional settings, such as community colleges, workforce boards, labor unions, employer associations, and community organizations. It is about creating and sustaining entrepreneurial organizations that have the commitment and capacity for innovation and to build partnerships, learn, change directions, and relentlessly pursue results.
Transforming workforce development practices, however, will only occur if there is top-level leadership committed to this agenda. Public and private workforce development resources must lay the groundwork to support the pursuit and achievement of substantial results.
The report of this American Assembly provides hope and, most importantly, direction for a broad spectrum of workforce practitioners, business organizations, and advocates who are ready to take on this challenge. Given the current and impending workforce crises that threaten the future of America’s families and businesses, the time is right.
We are proud to have supported and participated in this important civic dialogue. But this is just the beginning. We look forward to working in collaboration with our workforce development colleagues to advance this critical agenda in the months and years to come.
Betsy Biemann
John Colborn
Robert Giloth
Co-directors
The 102nd American Assembly
At the close of their discussions, the participants in the 102nd American Assembly on “Achieving Worker Success and Business Prosperity: The New Role for Workforce Intermediaries,” at Arden House, Harriman, New York, February 6-9, 2003 reviewed as a group the following statement. The statement represents general agreement; however, no one was asked to sign it. Furthermore, it should be understood that not everyone agreed with all of it.
Introduction
As the 21st century begins, the prosperity of the United States depends increasingly on the strength of its workforce. The world is becoming one economy, and nations that fully utilize their workers are more likely to thrive than those that do not.
There is a crisis emerging in America: workforce. The future worker shortage in the United States, the lack of worker skills, the increasing wage gaps, the disjointed public programs, and the absence of business participation all contribute to the crisis. But most importantly, it is the failure of our nation to recognize and respond to these challenges that presents the greatest risk.
Over the past twenty years, a dramatic increase in the size and skill of America’s labor force has driven its economic growth. Baby boomers were in their prime employment years, and large numbers of women entered the labor force. New workers emerged far more educated than those they replaced. The number of college-educated workers more than doubled.
These trends have ended. More than one third of the nation’s current workforce lack the basic skills needed to succeed in today’s labor market. During the next twenty years, the American workforce is expected to grow by only half of its earlier pace: there will be no growth of native-born workers in their prime working years; the percentage of the labor force composed of four-year college graduates is predicted to stagnate over the next two decades; the number of workers with two-year degrees and skill certificates will fall far short of the economy’s needs.
These labor force trends are exacerbated by globalizing competition and accelerating technological requirements in both domestic and export sectors. Taken together, these trends will lead to severe consequences for the vibrancy of the American economy and businesses. Problems on the horizon include:
- Unfilled jobs and productivity;
- Skill shortages;
- A decrease in regional economic competitiveness for some of the nation’s cities and rural communities;
- A loss of jobs to overseas workers.
However, these problems can create opportunities to better involve overlooked labor market pools in the United States.
A strong economy depends on labor force growth and increased productivity. But if the nation’s labor force does not grow, then we must find ways to increase the productivity of all American workers to meet the demands of future jobs.
Today, U.S. tax dollars support workforce development through a fragmented and under-funded patchwork system. In many communities, employers indicate that the workforce development system does not meet their needs and their engagement in workforce development programs has been superficial; publicly funded workforce programs have been constrained by funding that follows individual personal eligibility and political boundaries rather than regional economies; and systems improvements have proved elusive. As a result, employers still struggle to find workers who can help their businesses succeed, and workers still struggle to find and keep jobs that can sustain their families.
A new strategy -- what this Assembly calls a “workforce intermediary” strategy -- seeks to help workers advance, help businesses fi ll critical job shortages, and, ultimately, change systems to bolster regional and national economic development. This approach does not require creating a new category of organization or overhauling public systems but it does require the transformation of existing policies and programs so that they are more adaptable to the local labor markets. It challenges existing organizations and systems to redefine whom they serve and how they do business through the forging of new partnerships and building the capacity to do so.
Workforce intermediary approaches are practiced by a variety of organizations -- including community colleges, federally mandated Workforce Investment Boards (WIBs), state and local government agencies, unions, employer organizations, community development corporations, community development financial institutions, faith-based organizations, and community-based organizations. Groups using workforce intermediary approaches have these goals:
- To bring workers into the American mainstream. Success for these organizations means that workers are employed in jobs that offer the promise of financial stability.
- To increase business efficiency and productivity. They are equally concerned with serving employers’ needs and helping businesses become increasingly productive. They realize that business and worker success are interdependent.
- To enhance regional competitiveness. These groups understand that the health of regional economies affects the ability to advance workers and strengthen business.
This intermediary approach is results-driven, entrepreneurial and flexible, trusted by employers and workers, and collaborative.
A Promising Start
More and more organizations in places as diverse as Wiscasset, Maine and San Francisco are showing encouraging results by using workforce intermediary approaches to help workers and business. But what exactly are these practices?
This approach arose in response to some of the limitations of the present workforce system. The current system is characterized by single customer focus on job applicants; a lack of knowledge of employers and their needs; a focus on limited employability training and initial placement and little post-placement retention and advancement services; and the fragmentation of the workforce community and its funding streams.
The “workforce intermediary” approach has several common characteristics. At their core, workforce intermediaries:
- Pursue a “dual customer approach” by serving businesses looking for qualified workers, and by serving job-seekers and workers looking to advance their careers;
- Organize multiple partners and funding streams around common goals, bringing together businesses, labor unions, educational institutions, social service agencies, and other providers to design and implement programs and policies to improve labor market outcomes;
- Provide or broker labor market services that go beyond recruitment and referral by understanding the special needs -- and gaining the trust -- of firms and industries;
- Reduce turnover and increase economic mobility for workers by assuring continued support and opportunities to upgrade skills;
- Achieve results with innovative approaches and solutions to workforce problems;
- Improve outcomes for firms and their workers by catalyzing improvements in public systems and business employment practices.
Business organizations, labor supported programs, nonprofit community organizations, the public workforce investment system, and community colleges all can pursue workforce intermediary strategies. The number of such efforts has risen from a handful in the early 1990s to several hundred today. Although they approach their tasks in different ways, successful intermediary organizations bring together key partners and functions to advance careers for all workers -- recognizing the special needs of low-skilled, low-wage workers -- increase business productivity, and improve regional competitiveness. (For descriptions of groups that perform workforce intermediary functions, go to http://www.opportunitiesatwork.org.)
Results
“There aren’t too many programs for people like me who have worked all their lives and never had a chance to move up… You need training in this world to survive and stride forward, and this program gives people that chance. I see a career path that’s open to many new things” -- Worker
“We have found that partnerships allow us to save money on a cost-per-hire basis. Our partners are actually pre-screening candidates for us and pre-training them.” -- Employer
The workforce intermediary approach promises to improve the economic well being of job seekers, workers, and their families. Outcomes, where they have been measured, are positive especially when compared to the impacts of other more traditional workforce development activities.
Early research indicates that businesses reap economic benefits from partnering with workforce intermediary organizations. These benefits include:
- Access to new sources of job applicants;
- Reduced recruitment costs;
- Higher retention rates compared to traditional hires;
- Increased productivity;
- Tax credit savings;
- An enhanced reputation within the community;
By attending to business concerns and increasing productivity, workforce intermediary organizations also bolster regional competitiveness. For example, in New York City, the Garment Industry Development Corporation introduced production changes that enabled area firms to increase profits while maintaining decent wages and benefit packages.
What Types of Organizations Use Intermediary Approaches?
More than 200 organizations in thirty-nine states responded to a recent survey that described their use of workforce intermediary approaches. Most organizations participating in the survey are just a few years old, but two-thirds of them each serve more than 500 job seekers and workers annually.
While workforce intermediary organizations take many forms, not every education, training, or economic development entity plays this role. Efforts that are single-purpose in character -- attend to one particular activity or attend to the needs of a single employer -- do not meet the workforce intermediary definition. The power of the workforce intermediary approach is its multifaceted nature, and its potential impact goes beyond the sum of its component parts.
Indeed, many public workforce development agencies -- including local Workforce Investment Boards (WIBs), economic development agencies and community colleges-act as workforce intermediaries. More often, however, workforce intermediary efforts work to complement these public systems by expanding their reach through new partnerships and adding depth in industry sectors.
Consistent with the mission of the public workforce development systems, workforce intermediary efforts seek to:
- Expand economic opportunity for workers and job-seekers and enhance the competitiveness of firms and regions by identifying the needs of a variety of stakeholders;
- Invite firms, civic institutions and leaders to address these needs;
- Integrate services and funding streams in ways that enhance effectiveness;
- Leverage new resources;
- Engage in systematic and rigorous assessment of outcomes.
A Call To Action
A workforce intermediary strategy seeks to help workers advance, businesses fi ll critical job shortages, and ultimately boost regional and national economic growth and productivity. Such ambitious goals require a “high impact” strategy, one that results in quality services to a greater share of workers and employers and meaningful changes to local and regional labor markets. The challenge is to get beyond what one Assembly participant called “pockets of unreplicable greatness” to a wider scale.
This strategy is an important response to the larger workforce crisis confronting this nation.
The severity of the impending workforce crisis requires nothing less than a major transformation in how the workforce system and workforce organizations go about their business. This change will require that intermediary functions and practices should be widely adopted by thousands of existing organizations -- Workforce Investment Boards, community colleges, employer associations, labor programs, community development venture capital funds and community-based organizations. New partnerships between these groups can increase effectiveness in serving employers.
To accomplish this transformation, the system will require:
- An understanding that workforce development is as much an economic policy as a social policy;
- New policies that increase the accountability and impact of programs;
- Decisions by funders to create incentives for the use of dual-customer approaches;
- A venture capital orientation on the part of funders, rewarding adaptive capacity and good results over sustained periods;
- Increasing research that demonstrates what works;
- Timely data on local labor markets for mapping labor supply and demand and career opportunities, and identifying job training opportunities and gaps and evaluating the effectiveness of workforce policies and investments;
- Leadership across employer associations, labor groups, community organizations, and community colleges with entrepreneurial vision and the skills to manage these “double bottom line” endeavors, and
- Cross-sector sharing of information and most effective practices that advance workers in the American mainstream, increase business productivity, and enhance regional competitiveness.
Implementing the workforce intermediary approach is itself a challenge. For example, finding common ground between business and worker/jobseeker interests is a challenge. At times, these two perspectives have been assumed to be in opposition. However, finding the intersection between these two is essential in order to ensure business productivity, worker advancement, and regional competitiveness in the new skills economy. In addition, intermediary organizations operate in a fragmented policy and institutional environment and must often negotiate new roles and relationships while sidestepping destructive turf battles. This requires trust, credibility, and influence -- as well as careful diplomacy.
Further, the intermediary approach often faces all the challenges of an emerging business venture. Financial instability, limited resources, strained leadership, and the risks of taking success to scale must be successfully managed.
Many organizations have struggled with the constantly changing landscape of public workforce funding. Public funds have been cut and strict eligibility requirements, short-term timelines, and disparate performance measures have negatively affected outcomes. In general, some level of funding has been available for recruiting and training, but limited funding has been available to help businesses retain new workers and to help workers advance to higher quality jobs. In addition, there is no dedicated public funding for research and planning efforts that bring together stakeholders within specific industries to implement long-term strategies that address changing skill standards and related business needs. More and smarter funding is needed.
Workforce intermediary organizations and employer partners need flexible capital to create innovations in the public or private sector. Several states have created bond financing tools and investment tax strategies to support efforts of intermediary organizations to meet skill shortage demands and wage advancement goals. Other intermediary organizations have created blended financing strategies that include public funding and revenue-generating businesses. Based on the experience of these intermediary organizations, flexible financing options are needed to expand the impact of these strategies as well as support their efforts to increase capacity.
In addition to financial challenges, a variety of environmental forces constrain the emerging workforce intermediary efforts. A sometimes rigid policy environment and long-standing practices limit the acceptance of this new approach. Furthermore, slow decision making, inappropriate outcome measures, and cumbersome rules impede the attainment of positive outcomes for workers, firms, and regions.
Recommendations
The crisis facing America’s labor market is not widely recognized. This American Assembly recommends the following:
Raise the Nation’s Awareness
Faced with the immediate threats-of international tensions and economic recession-it is easy for the nation to overlook future workforce conditions that threaten the health of our economy. This American Assembly calls on America’s civic, education, labor, and business leaders to understand and address this looming crisis, which threatens the nation’s prosperity and democratic future.
This Assembly thinks it is especially important for private business to play a leading role in this effort. For more than thirty years, a variety of efforts have attempted to increase support for traditional workforce development activities. Those efforts have experienced, at best, mixed success, in part because the business sector did not perceive that the system met its needs for trained and productive workers and small and medium-sized firms were not organized and supported to participate effectively in the system. If there is one lesson that successful workforce intermediary efforts have taught us, it is that business sector involvement is critical to success. This has been demonstrated by Project QUEST in San Antonio and elsewhere, and will prove true for any national effort to address these issues.
Business leaders, who create jobs, must be actively and immediately approached, invited and tasked to become key actors in local, state, and national consciousness-raising efforts. This effort could take the form of a national commission, a business-led summit, a major public awareness and media campaign, or any and all of these. This Assembly thinks these issues should be immediately debated and made part of the public policy agenda.
At the same time, given the realities of competing pressures that make it hard for this issue to be heard, this Assembly also recommends the following steps.
Develop an Effective Workforce Intermediary Policy for Business, Workers, and Regions
The current disjointed policy environment creates a multi-faceted problem, including funding streams that are not aligned, and have difficulty achieving meaningful results. Concerns have been expressed from many fronts, including businesses, community-based organizations, educational institutions, unions, and government agencies.
Addressing this workforce development problem will require:
- Broadening the focus of public workforce development to provide both job applicants and incumbent workers with the skills training needed for competitiveness and career advancement in a technologically driven, globalizing economy. This requires flexibility, meaningful incentives and resources for companies, industries, labor, and business organizations to foster and engage in training, growth, and productivity.
- Incentives aimed at encouraging business investment to hiring, training, and advancing low-wage workers need to be simple to receive, administer, and address the needs of employers and workers. For example, in Maryland, the state legislature appropriated $2 million for worker advancement training at a coalition of hospitals and other employers, leading to significant wage increases and promotions. In Philadelphia, Pennsylvania, contributions from sixty-one employers, belonging to a Taft-Hartley labor management trust fund under the leadership of the District 1199C Training and Upgrading Fund, matched $3 million in federal funds to prepare 1,500 incumbent, dislocated, and new workers for careers in high-skilled nursing and allied health.
- Supporting industry-specific workforce development strategies, which engage the self-interest of key stakeholders within a particular industry that help to organize a complex web of public and private resources into effective workforce development programs.
- Creating strategic economic development initiatives in states, regions, and localities that fully integrate workforce and economic development. Several states have led the way by developing such plans and integrating funding streams to support them.
- Redesigning educational financing and regulations to support workforce development. Much of the available student aid and state support for post-secondary education does not address the demands of both workers and firms. Because community colleges and other post-secondary education institutions are critical parts of the workforce development system, this needs to change. Policy makers should consider the promising results from Individual Development Accounts and the Lifelong Learning Account demonstration, and important proposals to expand Pell grant eligibility, adult education supports, and other student aid programs, especially for less than half-time students. Community colleges and other post-secondary institutions are critical parts of solving this problem because of the pending need for technical skills, certificates, and portable credentials.
- Maintaining and enhancing adequate work supports that enable workers to succeed and business to increase retention. Child care, transportation, health care, the Earned Income Tax Credit, and food stamps are essential to ensuring that no one who works should be in poverty and that workers can succeed and progress on the job. These supports should also be accessible and available for time spent in training.
- Aligning the performance measures required by diverse funding streams to get real accountability while supporting career advancement goals. Although a great deal of work must be done to get the measures right, this Assembly commends current efforts to establish consistent outcome measures for diverse federal programs. Congress and the Administration should continue with this effort, making sure that their work reflects the real needs of business and workers. For example, many intermediaries, businesses, state and local officials, and others report ongoing difficulties and confusion around conflicting standards among the Workforce Investment Act (WIA), and other publicly funded workforce development programs (e.g. TANF, Perkins). These should be remedied in upcoming reauthorizations. Outcome measures in Temporary Assistance for Needy Families (TANF) must be revised to reward employment and advancement outcomes rather than just caseload reduction.
- Developing new ways to capture the effects of workforce interventions on businesses, workers, and labor markets. While the current workforce system stresses the importance of actual customer focus, current measures do not adequately capture the benefits that accrue to employers by participating in this system. Several new efforts are under way by the Aspen Institute, National Governors Association, and others to develop and test new demand-side measures that begin to address this problem.
Promoting Smarter Financing
Although coordinating existing public and private funding will help make progress towards growing the workforce intermediary approach, coordination alone is not enough. There is a need for more resources to help intermediary organizations meet the pressing demands of businesses, especially small businesses and workers. Even the most exemplary organizations, which juggle multiple funding streams and provide high performing services to businesses and workers, face a daily struggle to finance their work. Because of limited resources, public agencies also face impossible choices between supporting required core activities, and intermediary approaches like strategic planning and employer engagement that would strengthen their work and the critical need for training.
Federal, state, business, and philanthropic dollars all need to be expanded, and new types of financing mechanisms should be developed. Specifically, this Assembly recommends the following financing improvements:
- Expand and target federal, state, business, and philanthropic resources for necessary intermediary functions, such as labor market information, research and development, convening of stakeholders, and business services. New resources should be identified to support investments in intermediary functions -- including business services -- that will lead to better outcomes in the broad range of existing workforce funding streams. This includes ensuring that the WIA and TANF are flexible funding streams that allow local actors to design programs that meet local needs. Policy makers should support a proposal to provide new resources for Business Linkage Grants and other employer services in TANF.
- Develop ways to create long-term capital flows by leveraging relevant employer investments, such as contributions to Taft-Hartley funds and/or tuition reimbursement; existing tax credits; social venture funds and other financial innovations. The relevance and applicability for workforce development of a tax credit strategy, such as the Low Income Housing Tax Credit model, should be studied. Financing is an important topic for foundations, and their support of Living Cities, formerly National Community Development, is a model that could be adapted.
- Connect permanent sources of public financing, such as infrastructure spending, to workforce development. For example, in several communities, port authorities provide stable investment in workforce development and career advancement tied to their infrastructure spending. Likewise, bond financing for the Pennsylvania Convention Center in Philadelphia has generated a resource that supported training in the hospitality industry.
- Implement major comprehensive federal, state, and private sector demonstrations of the workforce intermediaries approach. This Assembly endorses recent efforts by the Department of Labor to create Regional Skills Alliances, help workforce boards and other workforce intermediaries begin industry-specific workforce development projects, assist health care employers address worker shortages, and expand the role of employer associations in providing intermediary services through the Workforce Innovation Networks (WINs) project. These types of demonstrations should be continued and expanded, and include partners from the philanthropic community, as WINs has since its inception.
Build Capacity
Organizations that successfully carry out these strategies conduct a dizzying range of activities to achieve their mission. They coordinate or provide training, work closely with employers, study their local and sectoral economies and labor markets, and link workers with support services like childcare. They do this in an environment where they must constantly seek funds from a variety of sources, each of which has its own demands for accountability and reporting. These demands would challenge the most sophisticated organization. Achieving higher impact, both for the specific organizations and for the system as a whole, will require investments in capacity building, like the following:
- Invest in the adaptive capacity of organizations to learn, function, and innovate, developing the ability to effectively serve both workers and businesses. The Annie E. Casey Foundation’s Jobs Initiative and the Aspen Institute’s Sectoral Employment Development Learning Project (SEDLP) are good examples of building the long-term capacity of workforce organizations to use outcome data to shape their work.
- Develop technical assistance capacity to help organizations in fostering intermediary functions. Public/Private Ventures’ Working Ventures program, a training series for workforce development professionals, has shown both the value of and the unmet demand for this type of service.
- Help develop the entrepreneurial skills and competencies of workforce development professionals, not only in meeting the needs of their customers, but also in running their organizations. National centers in higher education, vocational education, and community development have contributed to the professionalization of those fields, and a similar effort is needed in workforce development.
- Build the field by linking leading intermediaries into regional and national networks to foster innovation, provide peer learning, and develop a clearinghouse for innovative practice. Good examples include such efforts as the National Network of Sector Partners, which has created learning forums and a peer technical assistance fund for sector programs around the country, and the AFL-CIO’s Working for America Institute, which has successfully stimulated new labor/management partnerships and expanded existing partnerships to serve the interests of low-wage workers and businesses. These networks should distill and disseminate the lessons learned from decades of the nation’s investment in the military addressing training and career advancement needs of highly diverse populations.
- Build marketing and communications capacity of the organizations. Leaders and staff need to learn to speak the language of business and frame organization-appropriate messages that counter negative employer perceptions and therefore stimulate interest in partnerships.
Build a Constituency for Action
Although it is critical for the nation’s future economic success, workforce development has not been a national priority. In part, this is because of competition for public funds and attention, but also because of a perception of poor training results and little understanding or knowledge of the emerging successes. Paradoxically, the broad tasks of advancing workers, increasing business productivity, and enhancing regional competitiveness span so many institutions and stakeholders that they inhibit the necessary attention and public support. As the nation strives to build a more effective workforce development system, the workforce intermediary strategy can serve as an effective way to simplify the system for both business and workers, and foster their long-term advancement. Part of the strategy for achieving this success is building a broad constituency for action. Building that constituency requires:
- Engaging business as a driving force in support of this effort;
- Building new coalitions and alliances across traditional dividing lines, especially in states and regions. In Massachusetts, the Direct Care Worker Initiative, led by the Paraprofessional Healthcare Institute, brought together employers, business, consumers, unions, and the workforce training community to advocate for enhanced wages and upgraded training for health care workers. These types of alliances will need to be expanded to have the high impact that is necessary;
- Engaging political leadership at all levels. The issues raised in this report merit attention from such organizations as the National Governors’ Association, the U.S. Conference of Mayors, the National Association of Counties, and others to inform political leaders at all levels about what workforce intermediaries can do;
- Expanding the voice of the workforce development community. At the local, state, and national levels, the Workforce Alliance is providing valuable leadership in increasing the presence of the workforce development community in policy and legislative discussions;
- Emphasizing workforce development as an essential element of economic policy at the federal, state, and local government levels. This includes forging new alliances that integrate workforce development goals with those of economic development organizations, including the Council on Competitiveness, the Economic Development Administration, the International Economic Development Council, and the National Congress on Community and Economic Development, and the Community Development Venture Capital Alliance.
- Expanding relationships with higher education organizations to create support for these workforce development initiatives. It is critical that groups such as the American Association for Community Colleges and other members of the American Council on Education, as well as the League for Innovation, engage their members in activities that transform post-secondary education in support of the nation’s workforce system.
- Mobilizing a broader spectrum of foundations. Regional, local, and national foundations that have invested in workforce development should continue their leadership and seek to engage other funders in support of this agenda. One promising start is an emerging group of sixty local and national foundations with an interest in workforce development that have come together under the auspices of the Neighborhood Funders Group. Another is the local funding collaboratives emerging in Baltimore, New York City, and Boston.
- Strengthening local constituencies. In the Southwest, community organizations affiliated with the Industrial Areas Foundation not only pioneered one of the early pilots, but then built six more workforce intermediaries in multiple states. These and similar efforts should be supported.
- Researching and documenting the nature and extent of current investments as well as the return on those investments to employers, workers, and the community. Expanded support for rigorous research that links outcomes with intermediary practices and documents the return on investment to employers, workers, and the community is needed. This research is essential for addressing misperceptions for documenting cases and context in which training works, and for justifying further public and private investment in these strategies.
Conclusion
This report builds upon twenty years of innovation, practice, and research in workforce development. It calls America to action and challenges the nation to use the workforce intermediary approach as a strategy to solve the nation’s workforce crisis. There is a great deal at stake. Without aggressive action to expand the labor force in ways that increase productivity for employers, the nation’s long-term economic health will be challenged. Workforce intermediary approaches can make a major contribution to meeting this national need.
Endnotes
1. The full paper is available online at http://www.americanassembly.org/wfi/KeepingAmericaInBusiness.pdf.
Recent Findings on Frontline Long-Term Care Workers: A Research Synthesis 1999-2003 (1)
Lauren Harris-Kojetin, Debra Lipson, Jean Fielding, Kristen Kiefer and Robyn I. Stone
May 2004
Introduction
The purpose of the synthesis paper is to review, summarize, and discuss the significance of available research findings on the frontline long-term care (LTC) workforce since 1999, in both home and community-based and nursing home settings. This paper builds on the review article by Stone (2001) that reviewed the seminal practice and policy research related to recruitment and retention of frontline workers in LTC. Writing in 2001, Stone noted the lack of empirical research and, in particular, of evaluations to determine the effectiveness of programs and polices intended to recruit and retain LTC direct care workers.
This paper provides an updated review of the status of empirical findings, focusing on what has been learned between 1999 and 2003. The primary goal is to learn what initiatives have worked to reduce LTC direct care workforce recruitment and retention problems. A secondary goal is to provide empirically-based insights on the factors that contribute to recruitment and retention problems. This paper is intended to help policymakers, providers, worker and consumer groups, and researchers create a framework for future evidence-based policy, practice, and applied research initiatives to address LTC direct care workforce shortages.
Background
The paraprofessional LTC workforce -- over 2.4 million nursing aides, orderlies, and attendants, home health aides, and personal and home care aides (USBLS, 2004a) -- forms the core of the formal LTC system.2 Direct care workers serve as the eyes and ears of the formal LTC system and provide most of the care in this system. Even with relatively high unemployment rates, LTC providers and state agencies responsible for LTC services are reporting unprecedented vacancies and turnover rates among direct care workers, ranging from 45 percent to over 100 percent annually for nursing homes. Most states consider direct care worker recruitment and retention major issues (NCDFS, 1999; PHI and NCDHHS, 2004).
Significant societal factors are converging that will likely result in a 21st Century LTC direct care workforce crisis, or “care gap,” in the US. These dynamics include an unprecedented increase in the elderly population and those with chronic medical conditions, a decrease in the traditional pool of women available to provide formal care, fewer adult children available to provide care, and a potential increase in the need for paid care for elderly parents of dual-income and single-parent households. Policymakers and providers need to know what workforce initiatives have been shown to work to address the direct care workforce shortage.
Previously reported research (discussed in Stone, 2001 and Stone and Wiener, 2001) highlights a variety of factors associated with LTC direct care workforce recruitment and retention problems. These factors include but are not limited to: inadequate training; poor public image of the LTC direct care workforce; low pay; insufficient benefits; inadequate job orientation and lack of mentoring; little or no opportunities for continuing education and development within the position; poor supervision; emotionally and physically hard work; workplace stress and burnout; personal life stressors, such as problems with housing, child care, and transportation; lack of respect from residents’ families; and, short staffing. In the past several years, states, providers, and worker groups have developed, implemented and, in some cases, evaluated a variety of initiatives to address these challenges. This paper gives an overview of the most recent evidence base on both problems and possible solutions, to inform future investment choices and initiatives.
Methodology
We review both published reports and articles, unpublished conference presentations and working papers reporting results of research and evaluations on recruiting, retaining, and sustaining a quality frontline workforce in nursing homes, home care, and assisted living facilities. The review updates research findings reported in a seminal piece by Stone (2001) to better understand the problems facing the frontline LTC workforce and to identify effective solutions to chronic shortages, high turnover, and training needs. Studies on the relationship between LTC staffing levels and quality of care were not included, as they are beyond the scope of this paper; however, studies that examine links between staffing levels and worker satisfaction or turnover rates are included in this review.
Research and evaluation reports and articles completed or initiated between 1999 and 2003 were identified using Internet searches, personal communication with researchers, and database searches (e.g., PubMed). Search terms used when conducting web site and database searches included: LTC workforce, recruiting, labor force, nurse aides, job tenure, employment practices, work environment, aging services personnel, paraprofessional personnel, and intervention strategies. While published articles in peer-reviewed journals generally were preferred, unpublished reports and interim progress reports were included if based on sound research methods. We include studies that use qualitative and/or quantitative methods. Initiatives that were at an early stage of development in the Stone (2001) article were investigated to determine if the research or evaluation was now complete. We also obtained relevant working papers and presentations at professional conferences (e.g., American Society on Aging, Gerontological Society of America) and made personal communications.
The studies abstracted and analyzed for this report fall into two main categories: (1) empirical research (i.e., results of surveys and qualitative studies) on direct care workers that describe their working conditions or further elucidate the causes of turnover; and (2) evaluations of the implementation and impact of public and private initiatives designed to improve the recruitment and retention of direct care workers (e.g., wage and/or benefit enhancements, new training programs, and revised certification requirements).
Section IV reviews studies on characteristics of direct care workers and the wages and health insurance benefits available. Section V synthesizes research on factors contributing to high turnover and chronic shortages. Section VI summarizes findings from evaluations of interventions designed to improve recruitment and retention of direct care workers. Section VII discusses the implications of these recent findings for public policies and provider practices that seek to expand and stabilize the labor pool of direct care workers, and for future research intended to support these initiatives.
Endnotes
- The full paper is available online at http://aspe.hhs.gov/daltcp/reports/insight.htm.
- In this report we use the terms paraprofessional workers, direct care workers, and frontline workers interchangeably to refer to nurse aides or assistants, personal care aides or assistants, home health aides, home care aides and others who provide paid hands-on assistance with bathing, eating, dressing and other activities of daily living for persons with disabilities.
Recruiting and Retaining a Quality Paraprofessional Long-Term Care Workforce: Building Collaboratives with the Nation’s Workforce Investment System (1)
Michael E. Fishman, Burt Barnow, Asaph Glosser and Karen Gardiner
May 21, 2004
Introduction
This paper sets the stage for an ongoing conversation between representatives of the long-term care sector and the workforce investment system. The long-term care sector provides care to chronically ill, disabled, and elderly persons in a variety of care settings such as individual homes, residential care, nursing homes, and other institutional settings. Long-term care consists of an array of services and supports for persons with functional limitations whose needs range from limited personal assistance to total care. The workforce investment system supports both employers and workers by providing -- at the local level -- labor market information, job placement services, and training.
This conversation is critically important for our nation. In 1995, there were approximately 12.1 million long-term care recipients in the United States (Kaiser Foundation, 1999.) As the baby boom generation ages and technological advances extend life, these numbers will grow rapidly in the coming decades. The elderly population in the United States is expected to increase by over 130 percent between 2000 and 2050 (ASPE, 2003). Much of the formal care for these populations is provided by paraprofessional workers: certified nurse assistants (CNAs), home health aides, and personal and home care aides. For a variety of reasons described later in this paper, there is a growing shortage of these workers.
In addition to the care needs of our nation’s elderly and disabled population, there is an economic imperative to support the viability of long-term care services. Spending on institutional and home care for adults -- including Medicare, Medicaid, private long-term care insurance, family resources, and other payers -- is expected to more than double between 2000 and 2025, from $98 billion to $208 billion. By 2050, spending is projected to reach $380 billion (ASPE/Lewin, 2001). The majority of long-term care is provided by unpaid, informal caregivers. Often, formal long-term care services support the care provided by informal caregivers -- typically adult children -- enabling some informal caregivers to enter paid work. Exploring the costs of informal caregiving to employers, MetLife (1997) found that the cost to business through lost productivity as a result of informal caregiving is over $11 billion per year. In short, developing a long-term care paraprofessional workforce is an economic development issue for communities and individuals. The workforce investment system is well-positioned, through its network of One-Stop Career Centers, to serve as a valuable resource for both long-term care providers and workers.
This paper provides the fundamental context of both the long-term care sector and the workforce investment system in order to build understanding among members of each system. It is not intended to be comprehensive but to provide enough information to stimulate dialogue. Section II briefly describes the characteristics of the long-term care paraprofessional workforce. Section III outlines the growth in the long-term care sector. Section IV discusses workforce shortages from an economic perspective and why they exist in the long-term care sector. Section V describes the response of the long-term care sector to the shortage of paraprofessionals. Section VI describes the Workforce Investment Act (WIA) and the role of the workforce system. Section VII provides some examples of workforce investment initiatives in the long-term care sector. Finally, Section VIII presents some opportunities for collaboration.
Endnotes
1. The full paper is available online at http://aspe.hhs.gov/daltcp/reports/natwis.htm.
Why Workforce Development Should Be Part of the Long-Term Care Quality Debate (1)
Robyn I. Stone, DrPH, Steven L. Dawson and Mary Harahan
October 2003
Introduction
Since the Nursing Home Reform Act of 1987, public policy makers, consumers and providers have expressed growing interest in the quality of long-term care in nursing homes and other long-term care settings. The Nursing Home Reform Act, known as “OBRA 87,” transformed federal oversight of nursing home quality from its traditional emphasis on structure and process indicators to a focus on maintaining and improving resident outcomes. Since the passage of that landmark federal legislation, consumers, providers, regulators, insurers, and researchers have continuously struggled with how to define measure, assess and ensure long-term care quality.
The purpose of this paper is to introduce a largely overlooked feature of the long-term care system -- direct-care workers -- into the long term care quality debate. For the typical nursing home resident, direct-care staff -- not nurses or doctors -- provide eight out of every ten hours of the care they receive (McDonald, 1994). For home care clients, every hour of non-skilled nursing service is provided by paraprofessional workers. Our thesis is that the quality of long-term care -- the recipients’ clinical and functional outcomes and quality of life -- is significantly influenced by the attributes these workers bring to their caregiving jobs, the education and training they receive, and the quality of their jobs. The attitudes, values, skills and knowledge of these workers, how they are compensated and rewarded, and the way their jobs are organized and managed, all have a role to play in determining long-term care quality. Workforce development activities designed to increase the capacity of these individuals to participate effectively in long-term care settings should be integrated into all ongoing and new long-term care quality improvement and quality assurance initiatives.
The paper addresses the following topics:
- The scope of federal quality initiatives to date;
- Why workforce development should be considered an important dimension of long-term care quality;
- The key policy and practice constraints that impede linking workforce development issues and long-term care quality;
- Examples of quality improvement initiatives that have incorporated workforce development activities; and,
- Applied research activities to examine the link between workforce development and long-term care quality.
Endnotes
1. The full paper is available online at http://www.futureofaging.org/PublicationFiles/LTC%20Quality%20Debate%20Paper.pdf.
Selecting a Model or Choosing Your Own Culture (1)
Robyn I. Stone
Journal of Social Work in Long-Term Care, Volume 2, Issue 3/4, 2003
Summary
In this article the author reviews the practical issues related to implementing culture change in nursing homes. The merits of model replications are discussed and the barriers to creating and sustaining culture change in nursing homes are highlighted. This is followed by a description of the various dimensions of culture that must be changed including the approach to clinical training and practice, the nature of management and job design, the approach to caring, and the characteristics of the residential environment. The article then identifies the major elements required to maximize the potential for nursing homes to create and sustain cultural change.
Endnotes
- The full paper is available online at http://www.haworthpress.com/store/Research.asp.
Speaker Presentations
Plenary Two: Linking Staffing And Quality
Linking Workforce Development to Long-Term Care Quality
Robyn I. Stone, Dr.P.H.
American Association of Homes and Services for the Aging
WORKFORCE FACTORS INFLUENCING LTC QUALITY
- Attributes the workers bring to the job
- Education and training
- Quality of the job
- Compensation and other benefits
- Job design
- Organizational and management culture
CASE FOR LINKING WORKFORCE DEVELOPMENT AND LTC QUALITY
- Workforce issues generally afterthought in quality debate
- New interest in workforce/quality links
- 2001 IOM Nursing Home Quality Report
- CMS Staffing Quality Study
- Provider-initiated Quality First
- Central importance of human interaction in LTC
- Caregiver/care recipient relationships
- Supervisor/direct care worker relationships
- Peer relationships
BARRIERS TO INTEGRATING WORKFORCE DEVELOPMENT INTO LTC QUALITY ASSESSMENT AND IMPROVEMENT
- Providers lack motivation to invest in workforce
- Race and class barriers
- Hidden nature of consumer/worker relationship
- Workers lack a strong voice
- Regulatory system does not address workforce issues
- Models of successful workforce development are limited
QUALITY IN AGING SERVICES
- Quality of services/care outcomes
- Quality of “caring”/quality of life
- Quality for whom
- Residents, home care consumers
- Families
- Staff
HEALTH DIMENSION OF QUALITY
- Medical/clinical
- Technical aspects of care
- Quality indicators capture clinical processes and outcomes
- MDS
- OASIS
SOCIAL DIMENSION OF QUALITY
- Quality of the physical environment
- Quality of the social supports
- Relationship between care recipients and caregivers
- Measures more sensitive to the needs and preferences
- Life satisfaction
- Satisfaction with interactions
- Sense of autonomy/control
QUALITY OF WORKLIFE
- Key to quality of care and life in aging services
- Focus on staff, particularly direct care workforce
- Interaction between care recipient and caregiver from staff perspective
INTEGRATED MODEL IS REQUIRED
- Good quality aging services combine a focus on both the clinical and social/environment
- Also focuses on work environment and quality outcomes for caregivers
- Clinical and social aspects are intertwined
- Requires organizations that have management structure and philosophy conducive to promoting quality of care and life.
- Appropriate for all settings from independent living to skilled nursing facilities
CULTURE CHANGE IN LTC TO IMPROVE QUALITY
- Focus on where people live and work
- Culture change is comprehensive -- not just one intervention
- Focus on empowering staff and residents/clients
ORGANIZATION-LEVEL INTERVENTIONS
- Flattening management hierarchy
- Creating resident-centered environment
- Mentoring and coaching rather than supervising
- Creating meaningful, rewarding training experiences for all staff
- Focus on intra-staff communication and staff/resident relationships
- Fostering and enhancing community
FUTURE OF CULTURE CHANGE
- Can we move beyond the pioneers?
- What is just rhetorical and what is real?
- Need for evidence-based research
- What works?
- Who benefits?
- What are the costs?
- Building culture change into the Quality Debate
- Making culture change the norm rather than the exception
Home Care: Does a Better Workforce = Better Care?
A.E. Benjamin, Ph.D.
University of California, Los Angeles
THE BROAD CHALLENGE(S)
- Expanding demand.
- Worker shortages.
- Worker turnover.
- Worker quality.
- Policy indifference.
- Hidden nature of home care work.
HOME HEALTH CARE
- Stronger arguments, growing data.
- Outcomes data (OASIS, etc.).
- Structure, process (causal links?).
PERSONAL ASSISTANCE SERVICES
- Passionate arguments, little data.
- Defining outcomes
- Improvement vs. maintenance vs. slowing decline.
- Measuring outcomes.
- Specifying causal chains
- The worker connection.
NEW DEVELOPMENTS -- NEW CHALLENGES
- Client/consumer as employer.
- Cash/discretionary spending.
- Family and friends as workers.
- Public authorities as C-W link.
ASPE STUDY IN CALIFORNIA
- 1994-98.
- Service outcomes.
- Clients (1,095) and workers (618) in IHSS.
- Two home care models:
- Agency-based.
- Consumer-directed.
SETTING: IN-HOME SUPPORTIVE SERVICES PROGRAMS (IHSS)
- Medicaid state plan PAS.
- 200,000+ recipients.
- Up to 283 hours/month.
- Consumer-directed and agency models.
CASH & COUNSELING DEMONSTRATION AND EVALUATION
- 1996-2003.
- Cash (flexible monthly allowance).
- Counseling (supportive services).
- C. flexibility to hire and purchase.
- Setting: Medicaid in Arkansas, Florida, New Jersey.
- Design: Randomized assignment to cash vs. usual Medicaid PAS.
WHAT DO CONSUMERS (CLIENTS) REPORT?
- UCLA
- More satisfaction.
- Better quality of life.
- No differences: Unmet needs, safety concerns.
- More client empowerment.
- Less worker turnover.
- Fewer language problems.
- Cash & Counseling
- Very good worker performance.
- Capable and reliable.
- Less disrespectful.
- Less worker theft.
- Fewer unmet needs.
- Fewer indicators of low-quality care.
- More QOL satisfaction.
POSSIBLE EXPLANATIONS OF BETTER OUTCOMES
- Matching.
- Familiarity.
- Responsiveness.
- Interpersonal relationships.
- Targeted, informal training.
FUNCTIONS OF PUBLIC AUTHORITIES IN CALIFORNIA
- Bargaining agent.
- Training resource.
- Registry.
- Background screening.
- Quality of care monitoring.
PUBLIC AUTHORITIES AND QUALITY OF CARE?
- Documenting quality issues.
- Enhancing C-W matching.
- Improving C-specific trainign.
- Addressing interpersonal problems.
- Marketing to improve responsiveness.
CONCLUSIONS
- Workforce and service quality are related.
- Relationships are complex.
- Expanding choice may be key to enhancing quality.
- Stronger ties between PAs and WIBs may be productive.
| Who are the Workers? | |
|---|---|
| UCLA | Cash & Counseling (Arkansas) |
| Middle-aged women | Most females age 40-64 |
| Same race/ethnicity | Same race |
| Family (50%) and friends (25%) | Family and friends (90%) |
| Half: previous care | Most: previous care |
| 1/3 live with consumer | 1/4 live with consumer |
| What Do Workers Do? | |
|---|---|
| UCLA | Cash & Counseling |
| Serve one consumer | Serve one consumer |
| More unpaid hours | More unpaid hours |
| More flexible scheduling | More non-business |
Perform wider range of tasks
|
Variety of tasks
|
| Wages, Benefits, Working Conditions | |
|---|---|
| UCLA | Cash & Counseling |
| Lower wages | Lower wages |
| Almost no benefits | Almost no benefits |
| Little formal training | Little formal training |
| No professional supervision | No professional supervision |
| Half have another job | Typically part time |
| How Do Workers Assess their Work Lives? | |
|---|---|
| UCLA | Cash & Counseling -- More satisfied with... |
| Well-prepared | Job preparation |
| Well-informed about C’s conditions | Information about C’s condition |
| Satisfied with supervision | Feedback on performance |
| Able to get needed information | Compensation |
| Working conditions | |
 |
Plenary Three: Connecting Workforce Development Initiatives, Individual Economic Opportunity And Quality Care
Recruiting and Retaining a Quality Paraprofessional Workforce: Building Collaboratives with the Workforce Investment System
Michael Fishman, M.Pysc., M.P.A., The Lewin Group
Burt Barnow, Ph.D., Johns Hopkins University
MOTIVATION FOR PAPER
- Shortage of long-term care paraprofessional workers exists
- Increasing the supply of these workers can benefit the community and the workers
- Long-term care sector is large and growing rapidly
- Increased collaboration between long-term care sector and workforce investment can solve labor shortage problems and benefit both systems
PRESENTATION STRUCTURE
- Describe briefly:
- Long-term care paraprofessional workforce
- Growth in long-term care sector
- Reasons for workforce shortages
- Overview of the workforce investment system
- Long-term care sector response to shortages
- Examples of workforce investment initiatives
- Opportunities for collaboration
CHARACTERISTICS OF LONG-TERM CARE PARAPROFESSIONAL WORKFORCE
- Currently over 2.5 million employed in variety of roles and settings
- More likely than overall workforce to be:
- Female
- African-American
- Less educated
- Unmarried parents
- Poor
- Uninsured
- Wages are low compared to other short-term training occupations
- Lowest for home health aides and personal and home care aides
- Better benefits if:
- Employed full time
- Work in hospital or nursing home
- Many work part-time
GROWTH IN LONG-TERM CARE SECTOR
- Need for long-term care predicted to increase 110 percent between 2000 and 2050
- From 13 million to 27 million individuals
- Bureau of Labor Statistics (DOL) predicts large increase in paraprofessional occupations between 2002 and 2012
- 48 percent for home health aides
- 40 percent for personal and home care aides
- 25 percent for nursing assistants
- Outpaces predicted increase for all short-term training occupations (14%)
- Growth in demand for paraprofessional workers compounded by high turnover rates
WORKFORCE SHORTAGES
- What is a shortage?
- A sustained market disequilibrium between supply and demand
- Studies indicate a current shortage in long-term care paraprofessional occupations
- Employers in long-term care sector often lack flexibility to address shortages due to government and third party reimbursement rates
OVERVIEW OF THE WORKFORCE INVESTMENT SYSTEM
- 1998 Workforce Investment Act created more demand-driven workforce investment system
- Workforce Investment Board (WIB), comprised of business leaders and other stakeholders, plays major role in determining local services
- One-Stop Career Centers provide three levels of services: core, intensive, and training
- Core services are available to all, but if funds are limited intensive services and training reserved for low-income customers
TRAINING UNDER WIA
- Most training is done through individual training accounts (ITAs) that are like vouchers
- State and local WIBs restrict training to high-demand occupations
- Only training programs with good records for placement and wages can receive WIA funds
- Performance measures for all WIA programs hold programs accountable for employment, earnings, retention, credentials, and (soon) costs
LONG-TERM CARE INDUSTRY’S RESPONSE TO SHORTAGES
- A number of factors contribute to recruitment and retention problems
- Low wages
- Poor working conditions
- Lack of upward mobility
- Part-time work with irregular hours
- Approaches for dealing with shortages include:
- Improving wages and benefits
- Creating advancement opportunities
- Improving the workplace environment
- Developing new worker pools
EXAMPLES OF WORKFORCE INVESTMENT INITIATIVES WITH LTC
- Delaware County Employment Intervention Project
- California Caregiver Training Institute
- Cleveland Achieve
- Mennonite Village
- Tucson Direct Caregiver Association
OPPORTUNITIES FOR COLLABORATION
- Workforce investment can work with long-term care employers:
- Conduct outreach to employers; ask them to list openings with state and local WIA programs
- Encourage employers to participate on WIBs and committees
- Develop sectoral strategies, customized training, and on-the-job training (OJT)
- Long-term care employers can:
- List openings with state and local WIA programs
- Participate on state and local WIBs
- Participate in development and offering of sectoral programs, customized training, and OJT
- Make jobs more attractive to workforce investment and job seekers by improving pay and retention
CONTACT THE AUTHORS
- Mike Fishman, Senior Vice President, The Lewin Group, (703)269-5655, mike.fishman@lewin.com
- Burt Barnow, Associate Director for Research, Institute for Policy Studies, Johns Hopkins University, (410)516-5388, barnow@jhu.edu
Linking Employment, Education, and Economic Development
Gay Gilbert, J.D., M.S.W.
Employment and Training Administration
PRESIDENT’S HIGH GROWTH JOB TRAINING INITIATIVE CONCEPT
Building America’s skilled workforce to provide paths to career enhancing opportunities in high-growth industries and occupations
INITIATIVE PROCESS
- Information Gathering
- Environmental scan
- Five Executive Forums
- American Health Care Association
- American Association of Homes and Services for the Aging
- Analysis and Planning
- Workforce Solutions Forums
- 126 participants
- 1,001 solutions
- 84 priority solutions
- Workforce Solutions Forums
- Implementation
- Demonstration projects
- 22 health care models
- Demonstration projects
FOUR MAIN CATEGORIES OF WORKFORCE CHALLENGES
- Pipeline: Recruitment and Retention
- Skill Development
- Capacity of Education and Training Providers
- Sustainability: Infrastructure, Leadership and Policy
DOL ETA LONG-TERM CARE FUNDED MODELS
- Healthcare Career Lattice: A Model for Enhanced Learning
- Developing Partnerships and Initiatives to Resolve Long-Term Care Workforce Challenges
- Recruitment and Retention of Direct-Care Workers
- Council for Adult and Experiential Learning (CAEL) CNA Apprenticeship Program
- Excelsior College’s Hospice Palliative Care Certificate Program
DOL ETA HEALTH CARE MODELS
13 of the remaining 17 models will impact the pipeline of health care workers that could potentially work within the long-term care sector
NEXT STEPS
ETA will continue to explore more innovative projects throughout the year by launching a competitive grant opportunity for the health care industry. This competitive process will allow ETA to fund more new and innovative national models that address the industry’s identified workforce challenges.
HOW TO FIND THE BUSINESS RELATIONS GROUP
Gay Gilbert, Director
Business Relations Group
U.S. Department of Labor
Employment and Training Administration
businessrelations@dol.gov
(202)693-3949
www.doleta.gov
www.careervoyages.gov
Good Samaritan Career Lattice Project
Lloyd Schipper
South Dakota Department of Labor
EVANGELICAL LUTHERAN GOOD SAMARITAN SOCIETY
- Nation’s largest private non-profit long-term care organization
- 240 facilities–25 states--24,000 staff--28,000 residents
- Began in 1923
- Mission
SOUTH DAKOTA DEPARTMENT OF LABOR
- 16 Career Centers (see Figure 1)
- “One Stop” service for Business and Job Seekers
- Our role
NEED
- The Baby Boomer effect
- Average wage of CNA in SD is $9.03
- SD ranks 7th in % of population 65+ and 3rd in % of population 85+
PROJECT GOALS
- Develop a career lattice offering options for career growth and development
- Improve the image of CNA positions
- Develop enhanced performance standards to improve quality of care
- Decrease CNA turnover rate
- Improve customer satisfaction
PROJECT STRATEGIES
- Career “lattice” approach
- Apprenticeship and Mentors
- Distance Learning
CNA LATTICE
| Certified Nurse Assistant (CNA) Competency Based Model Good Samaritan Society |
|||
| The following examples reflect a performance-based competency driven Nurse Assistant apprenticeship program. | |||
| Occupation | Term Hours | Classroom Hours | Completion/ Certificate |
|---|---|---|---|
| CNA I (Level 1) |
300-600 | 34 | Certificate of Training |
| CNA, Advanced (Level 2) |
300-600 | 72 | Certificate of Advanced Training |
| Upon completion of CNA I and CNA, Advanced, an apprentice must select a specialty area to complete their apprenticeship. His/Her Certificate of Completion of Apprenticeship will reflect the specialty area in which they have “Specialized.” | |||
| CNA, Geriatric Specialty (Level 3) |
1,000-1,370 | 88 | Certificate of Specialization Geriatric |
| CNA, Restorative Specialty (Level 3) |
1,000-1,300 | 80 | Certificate of Specialization Restorative |
| CNA, Dementia Specialty (Level 3) |
825-1,125 | 72 | Certificate of Specialization Dementia |
| CNA, Mentor Specialty (Level 3) |
600-925 | 68 | Certificate of Proficiency Mentor |
PARTNERS
- USDOL Bureau of Apprenticeship and Training
- CAEL
- Post Secondary Education (USD, SDSU, and LATI)
- South Dakota Career Centers
- Local Good Samaritan Centers
OUTCOME MEASUREMENTS
- CNA Turnover
- CNA Vacancies
- Quality Indicators/Measures
- Occupancy Rates
- Community Perceptions
- Customer Satisfaction
- Staff
- Resident and family
FUTURE PLANS
- High Growth Initiative Grant
- Walk before you run
- Thank you
 |
OLDER POPULATION COMPARISON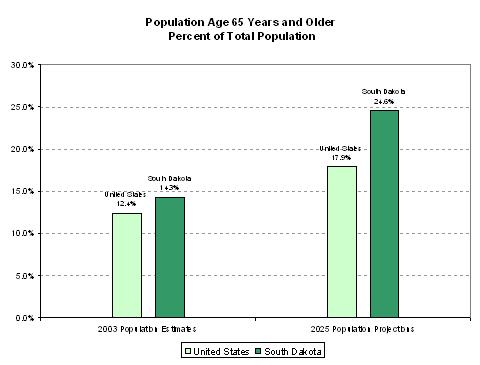 |
Healthcare Partnerships in Northern Indiana
Juan Manigault, M.S.B.A.
Northern Indiana Workforce Investment Board
PRESENTATION OVERVIEW
- Workforce Investment Board
- Workforce Issues
- Healthcare Career Ladder Project
- Healthcare Coalition Project
- Summary
REGIONAL OVERVIEW
- Four county region, which includes Elkhart, Kosciusko, Marshall and St. Joseph Counties in north central Indiana with a population of 576,780. Growing Hispanic population throughout region at 6.79% of total population.
- Educational center with 13 colleges and universities including the University of Notre Dame, Indiana University South Bend and Ivy Tech State College.
- Regional healthcare center with over 2,000 healthcare providers from four major hospital systems to direct care providers. Includes 22 long-term health care providers.
- Diverse mix of industry including: health services, transportation, pharmaceuticals, recreational vehicles/manufactured housing, orthopaedic instrumentation, food services and financial services.
BOARD OVERVIEW
- The federal Workforce Investment Act, requires the establishment of local workforce investment boards, organized around local labor market areas. There are approximately 650 workforce boards in the country.
- The Northern Indiana Workforce Investment Board is comprised of 50 members with a business majority, plus education, organized labor, government, community-organizations and economic development entities.
- Appointed by Local Elected Officials and certified by the Governor.
- $5+ million direct budget from federal, state, local sources and fees.
- Indirectly impacts a minimum regional budget of over $15 million from partner organizations through policy and oversight.
BOARD FUNCTIONS
- Assist in the development and growth of the regional economy through strategic planning initiatives, labor market information and convening partnerships that support economic growth through a rained and adaptable workforce.
- Support the development of the incumbent workforce by developing employer-driven strategies that support ongoing training and development.
- Support the development of the emerging (new entrants) workforce by strengthening their academic, career and life skills.
- Develop systems that support economic growth and workforce development.
VISION STATEMENT
To improve the quality of life, raise the standard of living, and enhance the productivity and competitiveness of the region.
MISSION STATEMENT
To define needs, identify resources, and broker relationships that impact regional economic sustainability, business growth and the education and training of a quality workforce.
MACRO-LEVEL WORKFORCE ISSUES
- The Workforce is changing
- Baby boomers approaching retirement
- Labor force shortages critical in non-professional and technical positions
- Skill and Knowledge requirements are changing
- Increasing need for computer literacy, communication skills, decision-making and problem solving skills
- Youth are inadequately prepared for participation in the workforce
- Youth aspirations aren’t consistent with economy and educational performance
- Graduation rates are too low in urban school districts
MACRO-LEVEL NURSING ISSUES
- RN employment has fallen by 2.4% from 1996 to 2000 in Indiana.
- Increasing number of RN’s are 50 years of age or older.
- The average age of long-term care nurses is over 50 years.
- 15% of RN, 13.2% of LPN and 8.5% of QMA positions are vacant in Indiana. Percentages much higher in the long-term healthcare arena.
- The expansion of career opportunities for young people, and particularly women, has reduced the number of individuals pursuing nursing careers since 1983.
- The average age of nurse educators is beginning to exceed age 50.
HEALTHCARE CAREER LADDER PROJECT PROCESS
- Identify healthcare occupations in demand
- Conduct county focus groups with healthcare providers
- Conduct one-to-one interviews with primary healthcare providers
- Identify common skill sets (WorkKeys) needed for entry level positions
- Determine specific occupations for career ladder development
- Identify and recruit career ladder employer partners
- Identify healthcare training programs
- Conduct focus group with employer partners, education/training providers and One-Stop partners
- Identify barriers in meeting employer need
- Identify strategies for eliminating training barriers
- Develop an employer driven matrix of career opportunities linked to entry level positions that will demonstrate advancement possibilities throughout the employer partner network.
- Nurses
- Therapists
- Technicians
- Develop matrix of healthcare scholarships, One-Stop training opportunities, on-the-job training and/or employer-paid training opportunities for career ladder advancement.
- Employer educational advancement programs
- State training grants
- WorkOne career scholarships
- On-the-job training opportunities
- Post-secondary scholarships
- Engage WIB Youth Council in development of plan to communicate healthcare needs, skill requirements and training opportunities to the emerging workforce.
HEALTHCARE COALITION PROJECT
- Regional Skill Alliances, involving 3 or more employers, are encouraged by the Indiana Department of Workforce Development to support common skills training.
- Workforce Investment Boards are responsible for forming these Alliances, and may apply for up to $200,000 in training grants to support training activities of participating companies. 10% is reserved for administration with the balance reserved for training costs only.
- Requirements include employer match, which may involve training on company time, and a recognized credential.
- Grants are for one year with the possibility of a no-cost one year extension.
- Initial meeting included representatives from the Workforce Board, Indiana Health Care Association, Ivy Tech State College, and the Indiana Department of Workforce Development.
- Basic elements for the training program were agreed to and included:
- Apply for three $200,000 grants for St. Joseph County, Elkhart County, and Kosciusko/Marshall Counties.
- Stagger implementation to coincide with semester enrollment opportunities.
- Workforce Board will write grants, serve as grant recipient and intermediary, and file all reports.
- Training program will incorporate elements of the Workforce Board career ladder approach for nursing occupations
- Indiana Health Care Association will coordinate activities with member institutions in each county, including an initial orientation meeting.
- Ivy Tech State College and Indiana University South Bend will serve as the primary training institutions for the program.
- Project Guidelines:
- All participating individuals are incumbent workers at participating long-term health providers.
- Training program allows dietary, maintenance, and janitorial workers with the basic skills and aptitudes to apply for the program at the CNA/QMA, LPN or ASN level.
- Existing nurses may apply to pursue the appropriate LPN to ASN, ASN to BSN, or BSN to MSN program.
- Companies will allow for training on company and use wages and fringe benefits as an allowable match, plus pay for books and travel expenses.
- Upon successful completion and the awarding of the appropriate credential, individuals will be promoted and receive increases in pay.
- Training Outcomes:
- 15 certified as QMAs, which includes CNA designation
- 19 certified as LPNs
- 12 receive the ASN degree and are eligible to take the state exam to become RNS
- 2 receive the BSN degree
- 2 receive the MSN degree
- Total grant of $208,000, plus matching funds of $211,000.
- Program begins with the summer semester.
- Next Steps
- Submit grant application for 2nd County in June for implementation in August.
- Submit grant application for remaining counties in November for implementation in January.
SUMMARY
- Workforce Boards can:
- Develop partnerships
- Convene partnership meetings
- Develop strategic approaches
- Seek resources
- Manage grant relationships
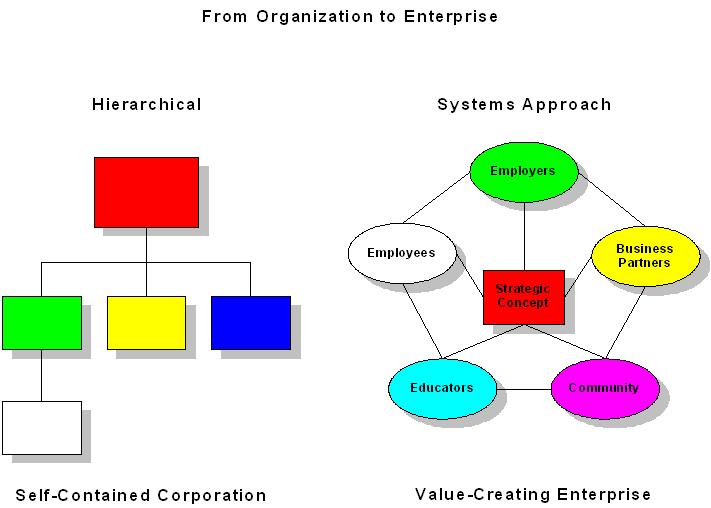 From The Northbound Train, Karl Albrecht |
Extended Care Career Ladder Initiative (ECCLI)
Charles Bodhi, B.A.
Regional Employment Board of Hampden County, Inc.
HISTORICAL PERSPECTIVE ON ECCLI
- ECCLI - part of the broader Nursing Home Quality Initiative.
- Originally thought of as a career ladder for CNA’s.
- Stakeholders worked in partnership to discuss issues in long-term care (LTC) industry.
INTENT OF ECCLI LEGISLATION
- Improve quality of care.
- Promote skills development.
- Improve employee retention.
- Create and institutionalize career ladders and other workplace practices that support and develop workers.
ECCLI NUMBERS TO DATE
- 81 sites have participated in ECCLI.
- Over 4,000 entry-level workers have participated in at least one ECCLI training.
- Over 700 managers have attended some type of leadership training.
NEW ROUNDS OF FUNDING
- Projects beginning April 2004.
- 30 awards being given over 3 rounds of funding.
- Collaboration and partnership across the rounds of funding encouraged.
- 27 additional long-term care facilities involved.
ECCLI EVALUATION
- Baseline Evaluation Report.
- Interim Evaluation Report.
- Report to the ECCLI Statewide Advisory Board
- Preliminary results from several exploratory analysis:
- ECCLI participation
- Participant outcome
- Patient outcome
- Employer/facility outcome data
- Preliminary results from several exploratory analysis:
- Study the impact ECCLI has had on quality of patient care evaluation: phase one
- Contract with Hebrew Centre for the Aged
- MDS data application
- Quantitative analysis
- What effect has ECCLI had on quality of patient care?
- Possible qualitative analysis in near future.
TECHNICAL ASSISTANCE
- Workforce Investment Boards involved in performance management of Round 4 projects.
- Operational.
- Organizational/culture change.
- Eden Alternative
- Tom Zwicker
- Individual assistance, by site
| ECCLI Advisory Board Members Include Representatives from the Following Organizations | |
|---|---|
| Massachusetts Extended Care Federation | Massachusetts Workforce Board Association |
| Massachusetts AFL-CIO | Massachusetts Department of Transitional Assistance |
| Paraprofessional Healthcare Institution | Massachusetts Department of Education |
| Home and Health Care Association | Department of Public Health |
| Department of Labor and Workforce Development | Executive Office of Health and Human Service |
| Massachusetts Community Colleges | Jamaica Plain Neighborhood Development Corporation |
| Massachusetts Council for Home Care Aides | Representation from Senator Mark Montigny’s Office |
| Massachusetts Aging | |
Plenary Four: The Impact Of Workforce Improvement Initiatives On Workforce Recruitment And Retention
The Impact of Workforce Improvement Initiatives on Workforce Recruitment and Retention
Patsy Harris
Direct Care Alliance
INTRODUCTION
- Collaborative Partnerships (Kinds of...)
- Why Partner
- Potential Workforce Goals or Desired Outcomes of Collaborative Partnerships
- Workforce Improvement Initiatives Case Study Examples
COLLABORATIVE PARTNERSHIPS (KINDS OF...)
- Multi-Stakeholder coalitions (workers, consumers, community-based organizations and employers).
- Sectorial Initiatives (employers, industry leaders, local community colleges).
- Worker Associations (primarily direct care workers).
WHY PARTNER...
- Recognize the power of partnering with leaders/representatives within the social and economic systems that impact not only the recruitment and retention efforts, but understand how these efforts are connected with the overall well-being of the communities in which they exist and operate.
- Intervene and connect low-income workers to better jobs.
- Make and impact policy and practice changes in low-paying industries to increase livable wage and access to benefit opportunities.
- Appreciate the importance of involving employers and industry leaders in the strategic design and mission of the workforce improvement initiatives.
POTENTIAL GOALS OR DESIRED OUTCOMES FOR COLLABORATIVE PARTNERSHIPS IN LONG-TERM CARE
- Improve wages through a concerted federal earned income tax credit campaign targeting this workforce.
- Secure more hours of employment.
- Access to training, where to find it, costs, content, job placement and certification, etc.
- Access to health care coverage for in-home workers.
- Identify new approach to supervision that emphasizes problem solving, communication and critical thinking such as “coaching.”
- Connect workers to existing supports for housing, health care, transportation and childcare.
MULTI-STAKEHOLDER PARTNERSHIPS EXAMPLE
- Direct Care Alliance: A national coalition of workers, consumers and employers working together to build a stable and valued direct care workforce.
- Core Principles: To shape both public policy and industry practice toward
- Improving the quality of jobs for the direct care staff (nursing home aides, home health aides and personal care attendants), recognizing these workers as the cornerstones of god care and thereby...
- Improving the quality of care for consumers, in particular the elderly, the chronically ill and people living with disabilities.
- Contact information www.directcarealliance.org or email patsy@directcarealliance.org.
SECTORIAL PARTNERSHIPS EXAMPLE
- Project QUEST, Inc.
- An innovative job training program in San Antonio with a mission to demonstrate the social and economic benefits that can be achieved through investments in long-term training for those who otherwise would not have the opportunity.
- Project QUEST defines the skills required to succeed in targeted, hard-to-fill occupations and then recruits, trains, and develops adults so that they are qualified and ready to fill employers’ needs for skilled workers.
- Contact
- Jobs For The Future (Boston, MA)
- A non-profit research, consulting and advocacy organization working to strengthen our society by creating educational and economic opportunities for those who need it most.
- JFF works to:
- Understand the challenges and barriers that keep people from participating full in the economy;
- Accelerate the adoption of what’s new, what’s needed, and what works in helping youth and adults acquire the skills that employers require; and
- Influence the policies that drive our nation’s educational and training systems to improve economic opportunities for those who need it most.
- Contact information www.jff.org or info@jff.org.
WORKER ASSOCIATION PARTNERSHIP EXAMPLE
Worker Associations: Are coalitions developed primarily to assist and empower direct care workers with building support for quality work and quality jobs.
Core Principles for Worker Associations have included: worker empowerment; forming coalitions to build employer support; create opportunities for workers to network; and to promote respect for the worker and the consumer.
Some Worker Associations include: Iowa Caregivers Association, Virginia Association Professional Nursing Assistants, Career Nurse Assistants Programs, Inc., National Association of Geriatric Nursing Assistants.
Pathways to Better Care: Investing in the Long-Term Care Workforce
Debra J. Lipson, M.H.S.A.
American Association of Homes and Services for the Aging
OVERVIEW
- Better Jobs Better Care (BJBC) Goals and Premises
- BJBC Demonstration Projects
- Policy/practice themes and initial experiences
- National Study of Demonstration Projects
- BJBC Applied Research Projects
BETTER JOBS BETTER CARE (BJBC) GOAL
- Support changes in long-term care policy and provider practice that:
- Help to reduce high vacancy and turnover rates among direct care staff across the spectrum of long-term care settings.
- Improve workforce quality.
KEY PREMISES OF BJBC
- Coalitions of providers, consumers and workers are key to making sustained changes.
- Public policies and workplace practices should support and reinforce each other.
- More/better research needed to document the effectiveness of public policies and workplace practices.
BJBC PROGRAM STRUCTURE
- Co-funded by The Robert Wood Johnson Foundatino and The Atlantic Philanthropies.
- National Program Office -- Institute for the Future of Aging Services, providing program direction and technical assistance.
- Technical Assistance partner -- Paraprofessional Healthcare Institute.
- 2 grant programs:
- Demonstration grants.
- Applied Research and Evaluation grants.
BJBC DEMONSTRATION GRANTS
- 5 Demonstration grants:
- Up to $1.4 million over 3½ years awarded to coalitions in five states
- Multi-stakeholder coalitions including:
- Long-term care providers, workers and consumers, working with state and local agencies, workforce development agencies, educational institutions, etc.
BJBC STATE COALITIONS AND LEAD AGENCIES
- Iowa -- Iowa Caregivers Association
- North Carolina -- North Carolina Foundation for Advanced Health Programs
- Oregon -- Oregon Technical Assistance Corporation
- Pennsylvania -- Center for Advocacy for the Rights and Interests of the Elderly
- Vermont -- Community of Vermont Elders
BJBC STATE COALITION POLICY INITIATIVES
- Efforts to link payment, or rewards, to positive workforce development practices and outcomes
- Wage/benefit enhancements and/or wage parity across long-term care provider types.
- DCW Training:
- State recognition of additional DCW skills.
- Universal core curriculum for all types of DCWs.
- Increased access to advanced training.
BJBC STATE COALITION WORKPLACE PRACTICE IMPROVEMENTS
- Organization culture change to empower and value DCWs.
- Peer mentoring, supervisor training programs.
- Promoting/valuing cultural diversity in the workforce.
- Development of innovative curricula and training methods.
SYNERGY BETWEEN POLICY AND PRACTICE INITIATIVES
- State licensing designation and “quality awards” for better DCW workforce inputs/outcomes reinforces provider investment in training.
- State recognition of additional training and skills gives incentives to DCWs to advance or stay in the field, which are reinforced by pay increases and public training subsidies.
BJBC NATIONAL DEMONSTRATION STUDY
- Penn State University -- Kemper/Brannon
- Document and analyze grantee activities, successes and challenges.
- Assess impact of policy and practice changes on provider organizations, quality of DCW jobs and worker perceptions of quality of care.
- Management Information System, PSU Survey Research Center
- Consistent web-based system to track employee retention, turnover, changes in working conditions in all providers participating in BJBC demonstration activities.
BJBC APPLIED RESEARCH AND EVALUATION GRANTS
- 8 Applied Research and Evaluation Grants awarded
- Up to $500,000 each over 2 years to university and non-profit research institutes.
- Designed to generate practical, empirical knowledge about the strategies and practices that work best to attract and retain a high-quality direct care workforce.
- Impact of wage/benefit enhancements.
- Potential to expand labor pool by recruiting family/friends, older workers.
- Organizational and management practices.
- Cultural competency.
- Training needs of CNAs/HHAs.
PUBLIC/PROVIDER/POLICYMAKER EDUCATION AND AWARENESS
- Dissemination of project findings, results and policy implications
- Website
- Newsletter -- Insights -- and Issue Briefs
- Professional conferences
- Policy seminars in Washington, DC
- Media briefings, interviews, etc.
FOR MORE INFORMATION
- Visit the BJBC website:
- http://www.bjbc.org
- See project profiles and descriptions under each type of grant program
- Download newsletters, issue briefs, etc.
- Contact us or join our mailing list:
- bjbc@aahsa.org
- 202-508-1216
 |
Workforce Improvement Initiatives to Improve Workforce Retention: What is the Evidence Base?
Lauren Harris-Kojetin, Ph.D., M.A.
Institute for the Future of Aging Services
PRESENTATION OVERVIEW
- IFAS
- Why evaluate?
- What has been evaluated recently?
- What works and should be invested in?
- What additional investments are needed to promote long-term care (LTC) direct care workforce improvements that are evidence-based?
INSTITUTE FOR THE FUTURE OF AGING SERVICES (IFAS)
- Independent policy research center within the American Association of Homes and Services for the Aging (AAHSA).
- Conduct research...
- to improve the quality of aging services
- to support a quality, stable LTC workforce
- through partnerships with AAHSA members and other organizations.
- Disseminate findings and evidence-based practice models to AAHSA members and others.
WHY EVALUATE?
- Need to know what works and what does not:
- Where should limited resources go?
- Do they really work?
- Which works best?
- Was there a change in outcomes of interest?
- Did the change in outcomes occur because of the initiative or because of something else?
- How sustainable and replicable are practices?
RECENT INSIGHTS ABOUT FRONTLINE LONG-TERM CARE WORKERS: A RESEARCH SYNTHESIS 1999-2003
- Authors:
- Lauren Harris-Kojetin, PhD
- Debra Lipson, MHSA
- Jean Fielding, MGS
- Kristen Kiefer, MPP
- Robyn I. Stone, DrPH
- Funded by ASPE, DHHS
A NOTE ON TERMINOLOGY
- Paraprofessional workers
- Direct care workers
- Frontline workers
- Nurse aides or Nursing assistants
- Personal care aides or assistants
- Home health aides
- Home care aides
- Others who provide hands-on assistance with bathing, eating, dressing, and other activities of daily living for persons with disabilities (focus on elderly)
TYPES OF INITIATIVES EVALUATED 1999-2003
- Alternative labor pools
- Career ladders
- Culture change
- Enhanced staff-family communication
- Multi-faceted initiatives
- Peer mentoring
- Self-managed work teams (SMWTs, in process)
- Wage enhancement
- Fifteen interventions reviewed in research synthesis
- Two have not (yet) had outcome evaluation
- Two did not measure actual turnover or retention
- Eight showed non-significant, negative, or inconclusive results or did not use robust quasi-experimental design
- Three showed significant positive results using a pre-post comparison group design with retention and/or turnover
WHAT INITIATIVES WORK?
- Pre-post comparison group design
 retention and/or
retention and/or  turnover of direct care
turnover of direct care- Peer mentoring
- Growing Strong Roots
- Multi-faceted initiative
- WIN A STEP UP -- education and payment incentive
- Culture change
- Wellspring -- quality improvement and organizational change process
GROWING STRONG ROOTS
- Trained, experienced certified nursing assistants (CNAs) matched with new CNAs.
- Training
- 6-hour project coordinator orientation and manual
- 6-hour mentor training, manual, and newsletter
- guide to orienting mentors’ supervisors/gaining facility support
- booster training
- Mentoring active 8 weeks.
- Salary increase for mentor.
GROWING STRONG ROOTS EVALUATION RESULTS
- Pre-post comparison group design.
- Twelve nursing homes (six treatment, six comparison) in New York state.
- Data collected immediately prior to implementation and 3 months after implementation.
- Statistically significant improvement in retention among those mentored
- 18 point increase in average retention rate while increase not significant among comparison group.
WIN A STEP UP
- Education and incentive program.
- Ten modules on clinical skills, interpersonal skills, and communication.
- Nurse aides (NAs) get $70 per completed module.
- Facilities must agree to commit staff time and give either retention bonus ($75) or wage increase (>$0.25/hour) 3 months after completion of modules.
- NAs who complete >7 modules and stay at facility >3 months after training get matching $75 bonus from WIN A STEP UP.
WIN A STEP UP EVALUATION RESULTS
- Pilot.
- Pre-post comparison group design.
- Four nursing homes, one home health agency, one adult care home in North Carolina.
- Data collected immediately prior to implementation and several months after implementation.
- Annual turnover rates significantly lower (15%) for NAs in the program compared to those in the matched comparison group (32%).
- Program active in 37 North Carolina nursing homes as of April 2004, with plans to involve 55 nursing homes by July 2005.
WELLSPRING INNOVATIVE SOLUTIONS
- Alliance super structure.
- Clinical training modules.
- Shared advanced practice nurse.
- Nursing coordinator to link components at facility level.
- Care resource teams.
- Systematic collection and use of outcome data.
- Non-hierarchical management philosophy.
WELLSPRING EVALUATION RESULTS -- RETENTION
- Wellspring facilities fared better than other Wisconsin facilities on retention:
- CNA’s: Wellspring retention increased by 6 percent, other homes decreased by 6 percent.
WELLSPRING EVALUATION RESULTS -- TURNOVER
- Wellspring facilities fared better than other Wisconsin homes on turnover.
- RN’s: Wellspring exhibited 6 percent lower turnover rates post implementation, while other homes saw a 7 percent increase.
- LPN and CNA turnover rates increased for both Wellspring and other homes, but increase was smaller for Wellspring.
GAPS-STRENGTHEN EVIDENCE BASE
- Evaluate existing models.
- Distinguish relative role of different model elements in outcomes.
- Develop and test new interventions.
- Strengthen evaluation designs.
- Measure longer-term effects.
- Measure variation within facilities (units, shifts).
- Measure actual behavioral outcomes.
- Measure outcomes consistently.
- Use of a comparison group.
- Determine transferability of evidence-based models across settings.
GAPS-PROMOTE EVIDENCE BASE
- Disseminate evidence-based practices for replication more broadly.
- Provide technical assistance to providers to implement and sustain new models.
- Give on-going feedback to providers.
- Determine how to replicate effective interventions beyond the initial demonstration (inform technical assistance).
- Assess extent to which replicated models are really being implemented.
- Determine how to sustain interventions.
- “Incentivize” the use of evidence-based models.
The National Clearinghouse on the Direct Care Workforce
Vera Salter, Ph.D.
Paraprofessional Haelthcare Institute
A NATIONAL RESOURCE CENTER
- Collect and analyze information about the direct-care workforce.
- Identify knowledge gaps.
- Distribute information to multiple stakeholders.
- Connect people with common interests.
- Respond to requests from users.
RESOURCES
- Library of publications and other resources:
- National reports on the workforce crisis.
- Surveys of state initiatives.
- Curricula and “how to” materials.
- Worker voices.
- “Best practice” database.
- State resource section.
- Up to 15,000 visits per month.
- Quality Jobs/Quality Care e-newsletter with over 1,200 subscribers.
PRACTICE PROFILE DATABASE
- Collaboration between IFAS and PHI, funded by Health and Human Services (ASPE and CMS).
- Objectives:
- To identify what has worked to improve worker recruitment and retention.
- Promote cross-learning between innovators.
- Looking for programs that are in place and have shown results.
- Make examples available in a web database.
INFORMATION COLLECTION
- Conversations with experts around the country seeking recommendations.
- Calls for help at conferences and through newsletters.
- Interviews with providers about what they have done.
- Collection of related written material.
EXAMPLES OF FINDINGS
- Screening and recruitment.
- Entry-level training.
- Peer support and mentoring.
- Career advancement.
- Management and supervisory training.
- Comprehensive interventions.
- Wages, benefits and worker support.
RECRUITMENT AND ENTRY-LEVEL TRAINING
Many innovative models that used workforce funds:
- George G. Glenner School of Dementia Care in San Diego.
- Co-operative Home Care Associates in the Bronx, New York (CHCA).
- The Shirley Ware Education Center (SEIU).
- Hope for Health Care in Richmond, Virginia.
- LEAP in Cleveland, Ohio trains people with disabilities.
- Direct CareGiver Association (Arizona).
MENTORING AND CAREER ADVANCEMENT
- WIN A STEP UP -- North Carolina.
- Iowa CareGivers Association: “For those who mentor.”
- Luther Manor Nursing Home in Iowa -- facility mentoring program.
- St. Peter Villa in Memphis -- career ladder.
MANAGEMENT AND SUPERVISORY TRAINING
- Mather Lifeways LEAP (IL).
- Co-operative Home Care Associates (CHCA): Coaching Supervision (NY).
- Resthaven Christian Services: Director of CNA position (IL).
- Vinfen: Seld Managed Teams (MA).
COMPREHENSIVE INTERVENTIONS
- Apple Health Care (CT, MA, RI).
- Co-operative Home Care Associates (NY).
- Leelanau Memorial Health Center (MI).
- Mercy Franciscan Health Systems.
- Ararat Nursing (CA).
- Wellspring Innovative Solutions (WI).
WAGES, BENEFITS AND SUPPORTS
- San Francisco IHSS Public Authority.
- Bon Secours wage parity initiative.
- Cooperative Care Waushara Wisconsin.
- Nazareth home wage enhancement program.
- Kahl home employee assistance program.
TO ACCESS THE CLEARINGHOUSE
QUALITY JOBS/QUALITY CARE
Quality Jobs/Quality Care is a free e-mail newsletter that covers issues concerning direct-care workers in long-term care. It’s published twice a month by the National Clearinghouse on the Direct Care Workforce (www.directcareclearinghouse.org), which provides reliable, up-to-date information related to the direct-care workforce nationwide. The Clearinghouse is a project of the Paraprofessional Healthcare Institute (www.paraprofessional.org).
The Impact of Workforce Initiatives on Recruitment, Training, and Retention
Michael Elsas
Cooperative Health Care Associates
OVERVIEW
- CHCA’s Philosophy.
- CHCA’s Model for Recuritment, Training, and Retention.
- Outcomes.
THE PHILOSOPHY
- To create high-quality jobs for home care workers by offering enhanced training, a supportive work environment, and opportunities for personal and professional growth.
- To improve the quality of care delivered to the chronically ill, elderly and disabled by creating a stable workforce.
THE MODEL
- CHCA’s model for recruitment, training, and retention encompasses five elements:
- Targeted recruitment.
- Enhanced entry-level training.
- Supportive services.
- Opportunities for advancement.
- Wage and benefit enhancements.
TARGETED RECRUITMENT
- Assessment and Selection
- 35% of those who interview are enrolled in the training program.
- 80% complete the program and are hired by CHCA.
- Recruitment Partnerships
- CHCA has built strategic relationships with human service organizations.
ENHANCED TRAINING
- Adult Learner Centered Training.
- Communication and problem solving.
- Three Months of “On the Job” training.
SUPPORT SERVICES
- Employment Counseling.
- Peer Mentor Program.
- “Coaching As Supervision”
PERSONAL AND PROFESSIONAL GROWTH
- Worker Participation
- Worker Council.
- Regional Meetings.
- Leadership Development.
- Policy Action Group.
OPPORTUNITIES FOR ADVANCEMENT
- Senior Aide.
- Peer Mentor.
- Associate Instructor.
- Administrative Staff.
WAGES AND BENEFITS
- Higher Base Wages.
- Wage Differentials.
- Guaranteed Hours Program.
- Benefits
- Health insurance.
- 401K.
- Paid vacation and sick leave.
- Annual dividends for worker owners.
OUTCOMES
- For individuals hired between July 2002 and June 2003:
- 84% were employed for at least 90 days.
- 64% achieved their 365 day employment milestone.
- Overall Paraprofessional turnover rate between July 2002 and June 2003 was 23.3%.
Nursing Home Workforce and Quality
John Schnelle, Ph.D.
University of California, Los Angeles
MAJOR POINTS
- Staffing numbers are related to quality.
- Staffing low in most homes.
- Training and management interventions will have limited effectiveness.
- National reports on the workforce crisis.
- Counter-productive if they imply unrealistic work expectations.
- What should staffing levels be?
STAFFING REQUIREMENTS
- Kramer: 4.1 nurse + aide hours.
- Expert consensus: 4.5 total hours.
- IOM recommendation: 4.1 total hours.
- Simulation: 2.8-3.1 aide hours (CMS study).
IF PROJECTIONS CORRECT
- THEN, Staffing above 4.1.
- Better process implementation related to outcomes.
FIELD TEST EVALUATION
- Directly measured care process implementation in:
- Homes in upper decile staffing vs. all others.
STUDY SAMPLE
- N=34 homes.
- Lower 90th vs. upper 10th percentile.
- Total staff hours = 3.1 vs. 4.5.
- Aide hours = 2.3 vs. 2.9.
- Aide report = 9.8 vs. 7.6 ratio.
QUALITY ASSESSMENT
Seven Standardized Measurement Protocols
STAFFING CONCLUSIONS
Different on 13 out of 16 care processes implemented by aides (Schnelle et al, Health Serv Res J 2004).
NO OR MARGINAL DIFFERENCE
- Social interaction during meals.
- Repositioning at night.
- Reported walking assists [low across all homes].
- Licensed nurse/physician driven indicators.
WHAT ARE THE SOLUTIONS?
- Objective analysis of staff requirements to meet regulations.
- Staffing projections (unit level).
- Staff at required levels or reduce care expectations.
- Will increasing staff to required levels be enough?
SECOND STEP
- Accurate and timely information about care delivery.
- Training and management.
- Job design.
- Environmental design.
ACCURATE AND USABLE INFORMATION
- Point of service documentation technology.
- Auditing controls.
- Electronic medical record.
TRAINING AND MANAGEMENT MODEL
- Brief.
- Ongoing.
- Focused on realistic work conditions (see accurate information and staffing requirement slides).
- Quality monitoring between sessions.
- Meaningful incentives.
JEWISH HOME NUTRITION PROGRAM
Training and Management Model
- 5-minute weekly sessions.
- Focused on specific objectives (talk to resident before assistance).
- Illustrated with video (real residents and aides).
- Quality monitoring between sessions.
- Feedback/Discussion.
- Incentive (employee involvement).
CONCLUSIONS
- Workforce related to quality.
- We should know more about staffing issues than we do.
- First step: Realistic evaluation of staffing requirements.
| Out of Bed/Engagement | ||
|---|---|---|
| Low Staffing N = 432 Residents |
High Staffing N = 125 Residents |
|
| % observations out of bed | 54 | 74 |
| % observations engaged | 45 | 52 |
| SOURCE: Bates-Jensen et al., JAGS (in press). | ||
| Feeding Assistance | |||
|---|---|---|---|
| Low N = 217 |
High N = 72 |
Chart | |
| % residents require assistance and receive >5 minutes | 57% | 80% | 100% |
| SOURCE: Simmons et al., JAGS 2003. | |||
| Incontinence | ||
|---|---|---|
| Low N = 102 |
High N = 31 |
|
| Number of toileting assists reported (MDS recall 2+) | 1.8 | 2.8 |
| SOURCE: Schnelle et al., Medical Care 2003. | ||
Other Presentations
Long-term Care Paraprofessionals: National and Local Workforce Shortages and Data Needs (1)
Jean Moore, M.S.N.
University of Albany
THE CENTER FOR HEALTH WORKFORCE STUDIES AT THE UNIVERSITY AT ALBANY
- Conducts studies of the supply, demand, use and education of the health workforce.
- Committed to collecting and analyzing data to understand workforce dynamics and trends.
- Goal to inform public policies, the health and education sectors and the public.
- One of six regional centers with a cooperative agreement with HRSA/Bureau of Health Professions.
OVERVIEW OF PRESENTATION
- Background on the health workforce.
- Implications of the aging of America on the health care system and its workers.
- Long-term care paraprofessionals: what we know and what we don’t know.
- Next steps.
CURRENT HEALTH WORKFORCE ISSUES
- Health worker shortages.
- The squeeze--few new dollars and the high cost of more workers--limit response options.
- Concerns with medical errors and quality.
- Worker and management dissatisfaction.
- Frustration with paperwork and regulation.
- Racial and ethnic imbalances in professions.
- Lack of systematic data on supply and demand for health workers.
FACTORS CONTRIBUTING TO HEALTH WORKFORCE SHORTAGES
- Short-term Factors:
- Competition for workers and the economy.
- Growing demand.
- Increased intensity and complexity of services.
- Educational system cycles and response lags.
- Long-Term Factors:
- Changing racial/ethnic mix in the US.
- Expanded career choices for women.
- The economy and public expectations.
- Increases in credential requirements.
- The aging of America: increase in demand.
- The aging of America: decrease in supply of workers.
A STUDY OF THE IMPACT OF AGING ON THE HEALTH WORKFORCE IN THE US
Recently completed study funded by HRSA
- Aging: Demographics, Models of Care, Family Caregivers, Technology, Reimbursement
- Profile of the Current Workforce:
- Over 20 health professions.
- Services to the elderly.
- Training, education, credentials related to aging.
- Supply trends/demand projects and gap.
- Profession-specific issues.
THE GROWING ELDERLY POPULATION WILL HAVE A SMALL POOL OF POTENTIAL FAMILY CAREGIVERS
- Compared to the current elderly, the growing cohort of aging Americans:
- Have had fewer children than their parents.
- Are more likely to be divorced.
- Are more likely to live alone as they enter old age.
IMPACT ON HEALTH SERVICES DELIVERY SYSTEM
- The elderly consumer more health care services than younger age groups.
- The elderly have different health care needs than younger age groups.
- The elderly will have a greater range of health care models to choose from than in the past.
- Access to care will be a greater issue for the elderly.
IMPACT OF THE AGING OF AMERICA ON THE HEALTH WORKFORCE
- Many health professions and occupations do not offer formal credentials focused on the needs of the elderly.
- When such a credential is offered, the number of workers with the credential is typically very small.
- A majority of health care workers in most settings deal with substantial numbers of elderly people whether or not they are specialists.
- Demand for health care professionals to serve the elderly will be affected by:
- Medicare reimbursement policies.
- New technologies.
- New models of care.
- Changes in profession-specific scope of practice focused on the needs of the elderly.
LONG-TERM CARE PARAPROFESSIONALS: NATIONAL AND LOCAL WORKFORCE SHORTAGES AND ASSOCATED DATA NEEDS
- Study funded by HRSA’s Bureau of Health Professions.
- Objectives of study:
- Review existing sources of data for states.
- Compile latest data.
- Identify strengths and weaknesses of sources.
- Suggest ways to improve the data.
- Full report is posted to HRSA’s website: http://bhpr.hrsa.gov/healthworkforce/reports/nursingandhomeaide.htm.
WHAT IS THE PROBLEM?
- Shortages of front-line workers serving the elderly, the chronically ill and the disabled.
- Service reductions due to shortages.
- Use of temporary workers at higher hourly rates.
- Shortages impact both quality of care and quality of life.
- Between 2000 and 2010, more than 1.2 million long-term care workers will be needed to fill new jobs and to replace those leaving the field.
WORKFORCE SHORTAGE ISSUES
- Supply
- Demanding work.
- Jobs often not well designed or supervised.
- Low pay.
- Lack of career ladders.
- Demand
- Aging of population.
- More types of providers.
- New technologies.
NEED FOR BETTER DATA
- Workforce planning.
- Policy formulation.
- Patient safety.
- Quality improvement.
- Program evaluation.
- Consumer information
APPROXIMATELY 120,000 ORGANIZATIONS USED LONG-TERM CARE PARAPROFESSIONALS IN 1998
- Long-Term Care Providers include:
- Nursing homes.
- Intermediate care facilities for the mentally retarded.
- Residential facilities for adults or aged.
- Residential facilities for non-aged.
- Adult day care centers.
- Home health agencies (certified or licensed).
- Hospice organizations (certified or licensed).
- Assisted living facilities.
NINE SOURCES OF DATA
- Bureau of Labor Statistics (BLS)
- Occupational and Employment Statistics (OES).
- Current Population Survey (CPS).
- CPS March Supplement.
- National Compensation Survey (NCS).
- Employment Projections.
- Survey of Occupational Injuries and Illnesses.
- OSCAR (CMS system).
- Decennical Census.
- State CNA registries.
LIMITATIONS OF THE DATA
- Data exclusions
- Lack of detail about states or counties.
- Incomplete coverage of facilities and/or occupations.
- Inconsistencies in definitions.
- Excessively broad categories.
- Self-reported and unaudited.
- Delays in availability.
OPTIONS FOR THE FUTURE
- Upgrade CNA registries
- Cover other providers in addition to nursing homes.
- Add variables relevant to workforce planning
- Demographics
- Workload
- Add other workers.
- Coordinate with background checks.
- Require annual workforce snapshots on a single day.
- Encourage compatible state-level systems
- Facilitate sharing.
- Provide bases for comparisons.
- Involve provider associations
- They have additional information.
- More and better data is positively correlated with better outcomes.
IN CONCLUSION
- Informed workforce planning is needed to:
- Better understand current shortages.
- Assess impact of present and future initiatives to balance supply and demand.
- Current data systems were limited in their ability to assist in such planning efforts.
- Better data on both providers and workers are needed by planners and policy makers.
| Impact of the Aging of America on the Health Workforce | |||
|---|---|---|---|
| Median Age | 1989 | 1999 | Change 1989-1999 |
| Dentists | 40.7 | 44.0 | + 3.3 |
| Dietitians | 38.3 | 40.0 | + 1.7 |
| Health records technologists | 35.3 | 40.3 | + 5.0 |
| Radiologic technicians | 34.3 | 38.0 | + 3.7 |
| Registered nurses | 37.3 | 42.7 | + 5.4 |
| Respiratory therapists | 32.3 | 38.0 | + 5.7 |
| Social workers | 38.7 | 40.3 | + 1.7 |
| Speech therapists | 35.7 | 40.7 | + 5.0 |
| Pharmacists | 36.7 | 41.3 | + 4.6 |
| Total civilian labor force | 35.7 | 38.7 | + 3.0 |
| SOURCE: Bureau of Labor Statistics, Current Population Survey - Annual Demographic Supplement, 1988-2000. NOTES: Figures presented are averages of three years’ data. Civilian labor force only. |
|||
| Recipients of LTC in the U.S., 1995 | |||
|---|---|---|---|
| Age Group | Setting of Service | All Settings Combined |
|
| Nursing Home | Home or Community | ||
| 65 or Older | 1.3 million | 5.1 million | 6.4 million |
| Under 65 | 0.2 million | 5.5 million | 5.7 million |
| All Ages | 1.5 million | 10.6 million | 12.1 million |
| SOURCE: Kaiser Commission, 1999. | |||
| Workers by Industry Group in 2000 | |||||
|---|---|---|---|---|---|
| Occupational Category | Industry Group | ||||
| Home Health Care |
Nursing and Personal Care |
Residential Care |
Other | Total | |
| Home Health Aides | 32.9% | 5.4% | 22.3% | 39.4% | 100% |
| Nursing Aides, Orderlies, and Attendants | 2.7% | 51.9% | 4.5% | 40.9% | 100% |
| Personal and Home Care Aides | 30.8% | 3.5% | 24.1% | 41.6% | 100% |
| SOURCE: BLS Occupational Employment Survey. | |||||
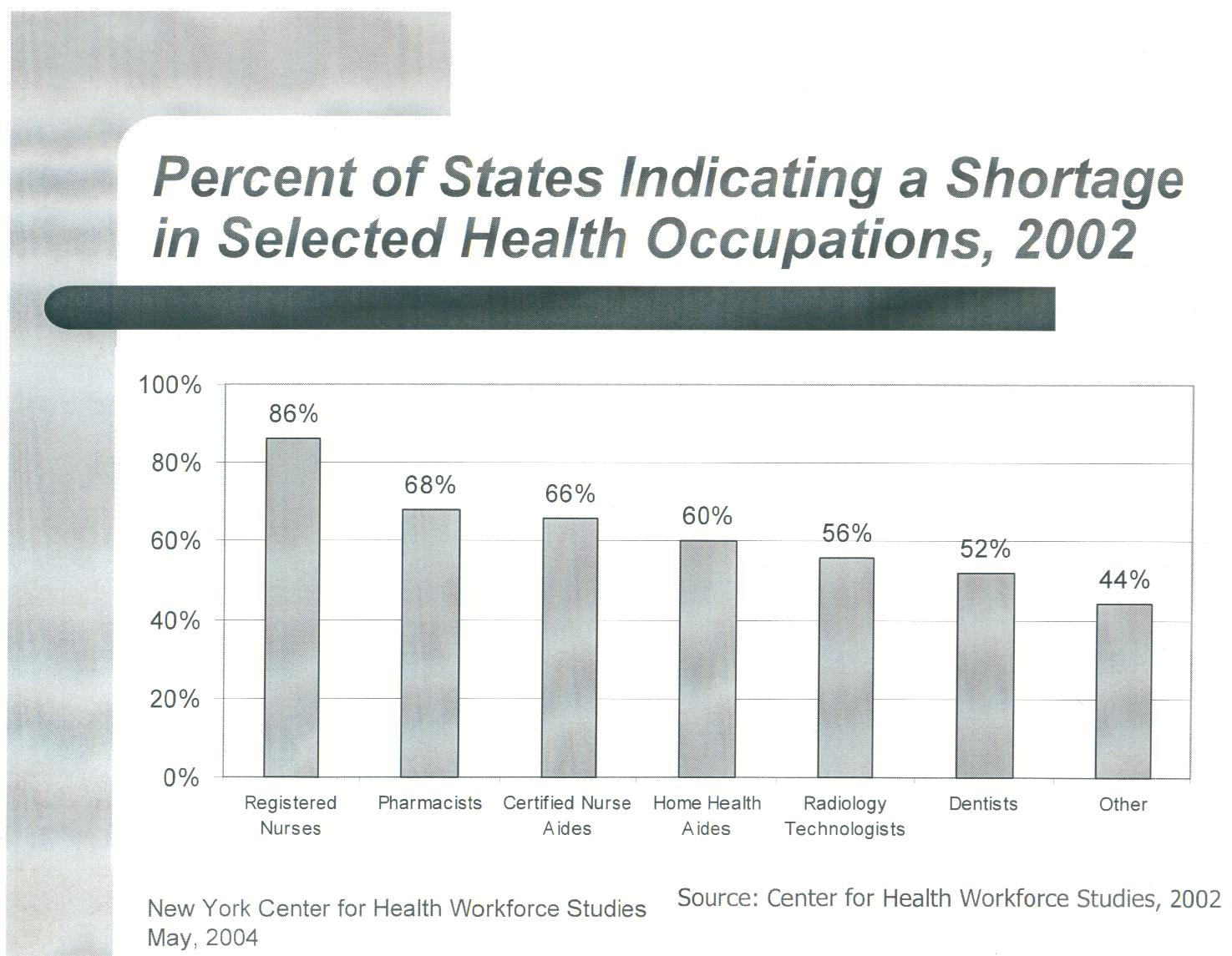 |
 |
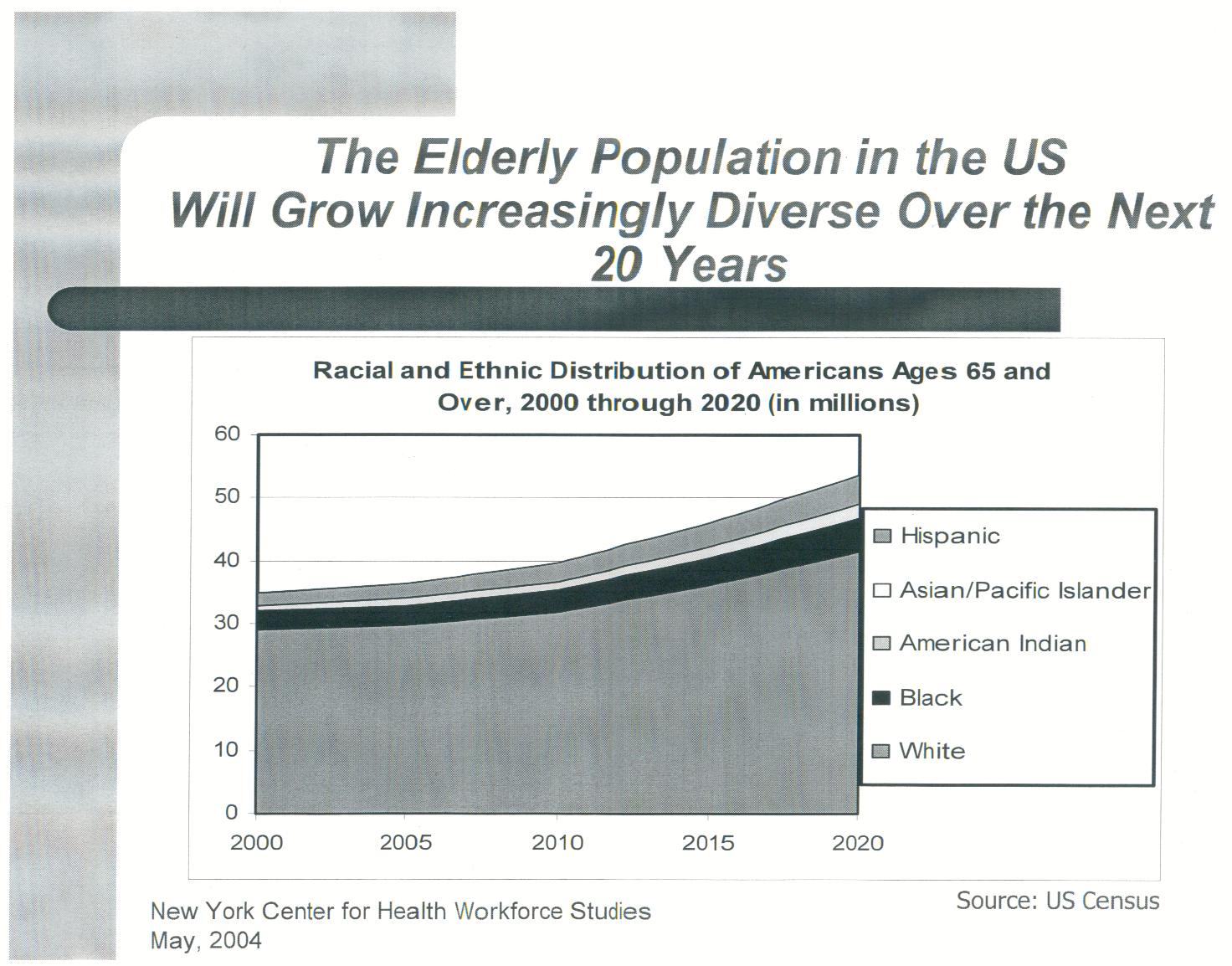 |
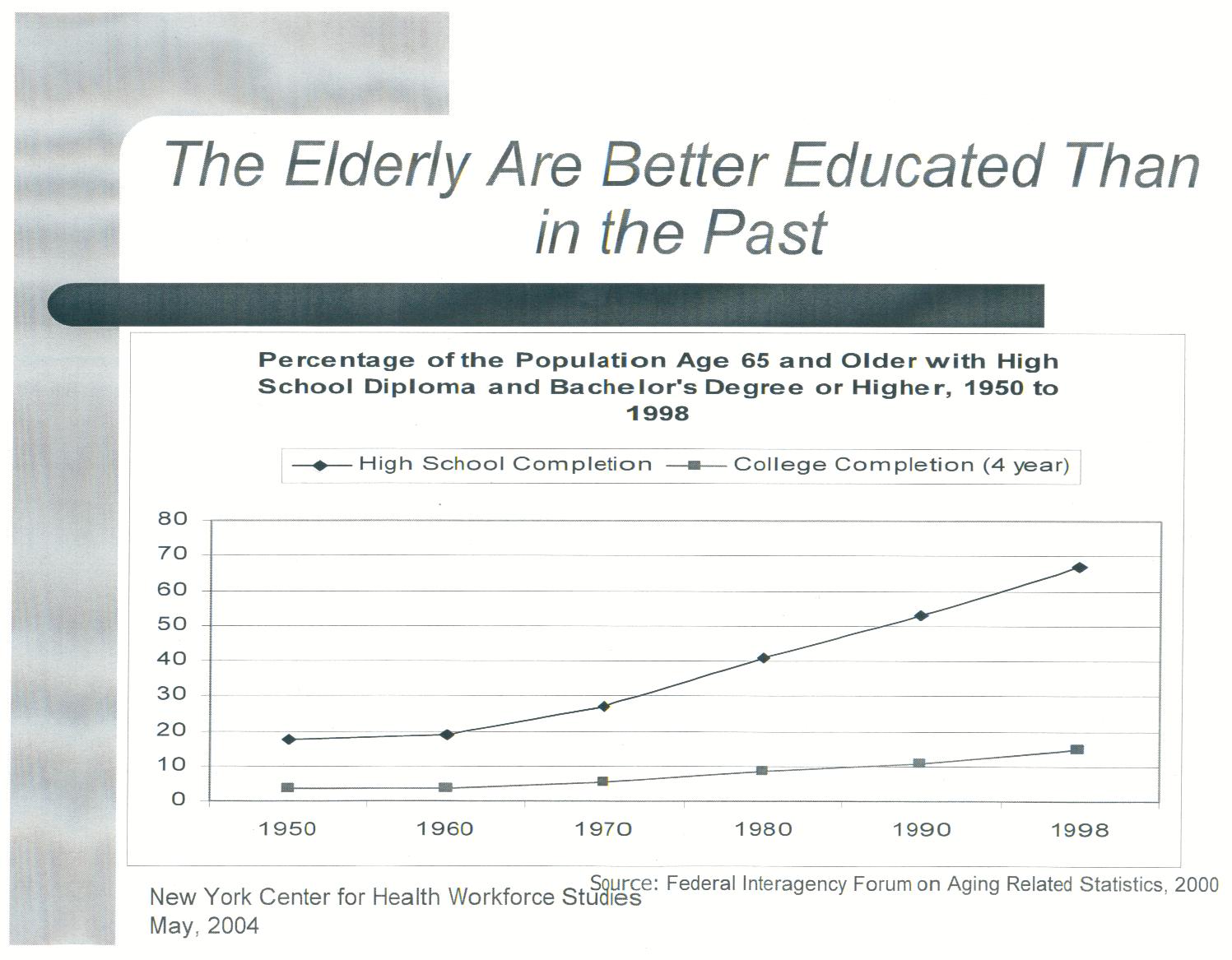 |
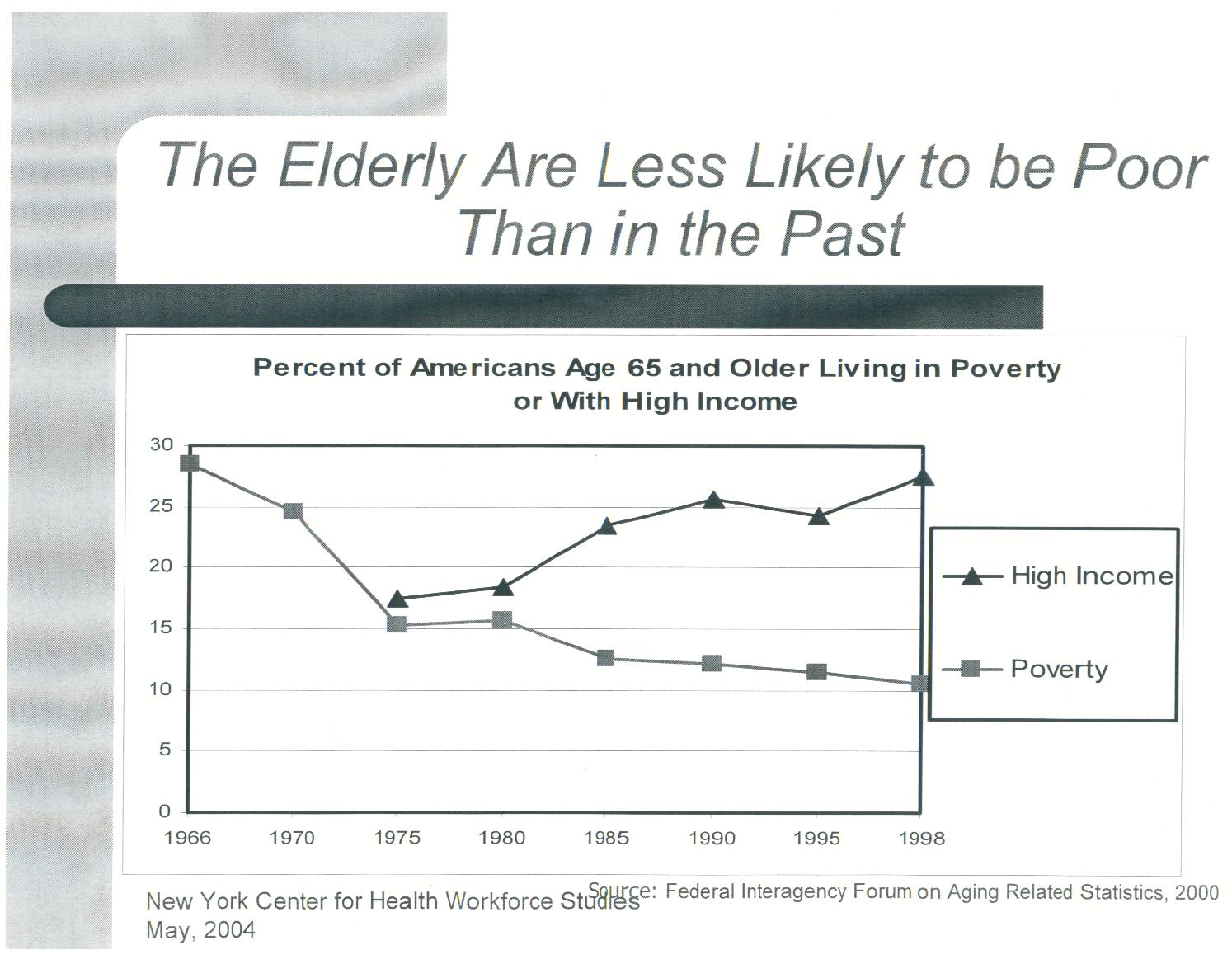 |
|