
Colene Byrne, Ph.D.
Westat
Michelle Dougherty, MA, RHIA
AHIMA Foundation
This report was prepared under contract #HHSP23337004T between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and Westat. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/office_specific/daltcp.cfm or contact the ASPE Project Officer, Jennie Harvell, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. Her e-mail address is: Jennie.Harvell@hhs.gov.
The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
Acronyms
The following acronyms are mentioned in this report and/or appendices.
| AAA | Area Agency on Aging |
| ACA | Patient Protection and Affordable Care Act or Affordable Care Act |
| ACE | Angiotensin-Converting Enzyme |
| ACO | Accountable Care Organization |
| ACT | Advanced Care Transitions |
| ACTion | Appalachian Community Transitions |
| ADC | Adult Day Care |
| ADE | Adverse Drug Event |
| ADL | Activity of Daily Living |
| ADRC | Aging and Disability Resource Center |
| ADT | Admission, Discharge, and Transfer |
| AHA | American Hospital Association |
| AHIMA | American Health Information Management Association |
| AHRQ | HHS Agency for Healthcare Research and Quality |
| AIDS | Acquired Immune Deficiency Syndrome |
| ALF | Assisted Living Facility |
| AoA | HHS Administration on Aging |
| AOD | Answers on Demand |
| APN | Advanced Practice Nurse |
| ARB | Angiotensin Receptor Blocker |
| ARC | Aging Resource Center |
| ASPE | HHS Office of the Assistant Secretary for Planning and Evaluation |
| BCC | Bridge Care Coordinator |
| BHIX | Brooklyn Health Information Exchange |
| BMI | Body Mass Index |
| BOOST | Better Outcomes for Older Adults through Safe Transitions Project |
| BPCK | Brand Pack |
| BSL | Brookdale Senior Living |
| CAD | Coronary Artery Disease |
| CAH | Critical Access Hospital |
| CAHPS | Consumer Assessment of Healthcare Providers and Systems |
| CAST | Center for Aging Services Technology |
| CBO | Community-Based Organization |
| CCD | Continuity of Care Document |
| CCDA | Consolidated Clinical Data Architecture |
| CCHIT | Certification Commission for Health Information Technology |
| CCITI | Continuum of Care Improvement Through Information |
| CCRC | Continuing Care Retirement Community |
| CCT | Community Care Team |
| CCTP | Community-Based Care Transitions Program |
| CDA | Clinical Document Architecture |
| CDT | Current Dental Terminology |
| CEHRT | Certified Electronic Health Record Technology |
| CFO | Chief Financial Officer |
| CFR | Code of Federal Regulations |
| CHF | Congestive Heart Failure |
| CHIC | Community Health Information Collaborative |
| CHIDS | Center for Health Information and Decision Systems |
| cHIE | Clinical Health Information Exchange |
| CHIP | Children's Health Insurance Program |
| CIHIE | Central Illinois Health Information Exchange |
| CIO | Chief Information Officer |
| CMIO | Chief Medical Informatics Officer |
| CMIS | Client Management Information System |
| CMMI | CMS Center for Medicare and Medicaid Innovation |
| CMS | HHS Centers for Medicare and Medicaid Services |
| CMSA | Case Management Society of America |
| CNL | Clinical Nurse Leader |
| CoP | Community of Practice |
| COPD | Chronic Obstructive Pulmonary Disease |
| COR | Contract Office Representative |
| CORHIO | Colorado Regional Health Information Organization |
| CRISP | Maryland Chesapeake Regional Information System for Our Patients |
| CT | Computed Tomography |
| DAM | Domain Analysis Model |
| DETOG | Deep East Texas Council of Governments |
| DHIN | Delaware Health Information Network |
| DME | Durable Medical Equipment |
| DNR | Do Not Resuscitate |
| ECIN | Extended Care Information Network |
| ED | Emergency Department |
| EDPP | Enhanced Discharge Planning Program |
| EH | Eligible Hospital |
| EHR | Electronic Health Record |
| EMCC | Eastern Maine Community College |
| EMHC | Eastern Maine HomeCare |
| EMHS | Eastern Maine Health System |
| EMMC | Eastern Maine Medical Center |
| EMR | Electronic Medical Record |
| ENS | Encounter Notification Service |
| EP | Eligible Professional |
| esMD | Electronic Signature for Medical Document |
| FFS | Fee-For-Service |
| FIPS | Federally Information Processing Standards |
| FQHC | Federally Qualified Health Center |
| GPCK | Generic Pack |
| H&P | History and Physical |
| HCBS | Home and Community-Based Services |
| HCRR | Home Care Referral Registry |
| HCS | Health Commerce System |
| HEAL | Health Care Efficiency and Affordability Law |
| HF | Heart Failure |
| HHA | Home Health Agency |
| HHQI | Home Health Quality Improvement Initiative |
| HHS | U.S. Department of Health and Human Services |
| HIE | Health Information Exchange |
| HIEO | Health Information Exchange Organization |
| HIM | Health Information Management |
| HIMSS | Healthcare Information and Management Systems Society |
| HIN | HealthInfoNet |
| HIO | Health Information Organization |
| HIPAA | Health Insurance Portability and Accountability Act |
| HISP | Health Information Service Provider |
| HIT | Health Information Technology |
| HITECH | Health Information Technology for Economic and Clinical Health Act |
| HIV | Human Immunodeficiency Virus |
| HL7 | Health Level 7 |
| HMO | Health Maintenance Organization |
| HRS | Health Resource Solutions |
| HRSA | HHS Health Resources and Services Administration |
| HTN | Hypertension |
| IADL | Instrumental Activity of Daily Living |
| ICF | International Classification of Functioning |
| ICFMR | Intermediate Care Facility for Persons with Developmental Disabilities |
| ICPC | Integrating Care for Populations and Communities |
| ICU | Intensive Care Unit |
| IDN | Integrated Delivery Network |
| IDS | Integrated Delivery System |
| IHE | Integrating the Healthcare Environment |
| IHI | Institute for Healthcare Improvement |
| INTERACT | Interventions to Reduce Acute Care Transfers |
| IPA | Independent Physician Association |
| IRF | Inpatient Rehabilitation Facility |
| IRF-PAI | Inpatient Rehabilitation Facility-Patient Assessment Instrument |
| IS | Information Services |
| IT | Information Technology |
| ITCC | Illinois Transitional Care Consortium |
| IVD | Ischemic Vascular Disease |
| KHIN | Kansas Health Information Network |
| LAND | Massachusetts Local Adaptor for Network Distribution |
| LCC | Longitudinal Coordination of Care |
| LCSW | Licensed Clinical Social Worker |
| LIPIX | Long Island Patient Information Exchange |
| LTACH | Long-Term Acute Care Hospital |
| LTCH | Long-Term Care Hospital |
| LTPAC | Long-Term and Post-Acute Care |
| LTSS | Long-Term Services and Supports |
| LVEF | Left Ventricular Ejection Fraction |
| LVSD | Left Ventricular Systolic Dysfunction |
| MAP | Measure Application Partnership |
| MAPCP | Multi-Payer Advanced Primary Care Practice |
| MAR | Medication Administration Record |
| MATCH | Medications at Transitions and Clinical Handoffs Toolkit |
| MD | Medical Doctor |
| MDS | Minimum Data Set |
| MeHI | Massachusetts e-Health Institute |
| MFP | Money Follows the Person |
| MLR | Minimum Loss Rate |
| MMIS | Medicaid Management Information System |
| MPFS | Medicare Physician Fee Schedule |
| MPI | Master Patient Index |
| MRI | Magnetic Resonance Imaging |
| MSA | Metropolitan Statistical Area |
| MSR | Minimum Savings Rate |
| MSW | Master of Social Work |
| MU | Meaningful Use |
| NAMCS | National Ambulatory Medical Care |
| NCPDP | National Council for the Prescription Drug Programs |
| NH | Nursing Home |
| NIST | National Institute of Standards and Technology |
| NP | Nurse Practitioner |
| NQF | National Quality Forum |
| NSRCF | National Survey of Residential Care Facility |
| NwHIN | Nationwide Health Information Network |
| NYCHHIP | New York Community Home Health Interoperability Project |
| OASIS | Outcome and Information Assessment Set |
| ONC | HHS Office of the National Coordinator for Health Information Technology |
| OT | Occupational Therapy |
| P4P | Pay For Performance |
| PAI | Patient Assessment Instrument |
| PCC | Point Click Care |
| PCMH | Patient-Centered Medical Home |
| PCP | Primary Care Physician or Primary Care Provider |
| PHIN | Public Health Information Network |
| PHQ | Patient Health Questionnaire |
| PHR | Personal Health Record |
| POC | Plan of Care |
| PPS | Prospective Payment System |
| PQRS | Physician Quality Reporting System |
| PSO | Patient Safety Organization |
| PT | Physical Therapy |
| QA | Quality Assurance |
| QI | Quality Improvement |
| QIO | Quality Improvement Organization |
| RACF | Residential Aged Care Facility |
| RARE | Reducing Avoidable Readmissions Effectively Campaign |
| REC | Regional Extension Center |
| RED | Re-Engineered Discharge Project |
| RHA | Illinois Rush Health and Aging |
| RHIO | Regional Health Information Organization |
| RIM | Reference Information Model |
| RN | Registered Nurse |
| RUMC | Rush University Medical Center |
| S&I | Standards and Interoperability |
| SARCOA | Southern Alabama Regional Council on Aging |
| SASH | Support and Services at Home |
| SBAR | Situation, Background, Assessment, and Recommendation |
| SBD | Semantic Brand Drug |
| SBDF | Semantic Brand Drug Form |
| SBDG | Semantic Brand Drug Group |
| SCD | Semantic Clinical Drug |
| SCDF | Semantic Clinical Drug Form |
| SCDG | Semantic Clinical Drug Group |
| SDM | Shared Decision-Making |
| SED | Severe Emotional Disturbance |
| SEE | Massachusetts Surrogate EHR Environment |
| SHA | Secure Hash Algorithm |
| SMI | Serious Mental Illness |
| SMRTNET | Secure Medical Records Transfer Network |
| SNF | Skilled Nursing Facility |
| STAAR | State Action on Avoidable Re-hospitalization Initiative |
| SWG | Sub-Workgroup |
| TARCOG | Top of Alabama Regional Council of Governments |
| TB | Tuberculosis |
| TCM | Transitional Care Management |
| UD | Unstructured Document |
| UHIN | Utah Health Information Network |
| UIC | University of Illinois at Chicago |
| URAC | Utilization Review Accreditation Committee |
| USDA | U.S. Department of Agriculture |
| UTF | Universal Transfer Form |
| VHIE | Vermont Health Information Exchange |
| VHR | Virtual Health Record |
| VLER | Virtual Lifetime Electronic Record |
| VNSNY | Visiting Nurse Service of New York |
| VPN | Virtual Provider Network |
Acknowledgments
Westat would like to acknowledge the contributions of Jennie Harvell, the Contract Officer's Representative from the Office of the Assistant Secretary for Planning and Evaluation who provided detailed edits and contributed to various sections of this report and informed the case studies.
Westat would also like to acknowledge the key informants who provided valuable information and insights on health information exchange to support long-term and post-acute care and long-term support services. We list those informants in this this report.
Finally, Westat is indebted to the many staff who helped organize and participated in the highly informative site visits, shared relevant materials, and who were also willing to respond to additional requests for information.
Abstract
In 2012 the U.S. Department of Health and Human Services (HHS) funded this project designed to expand the knowledge base related to the state of health information exchange (HIE) to support care for persons receiving long-term and post-acute care (LTPAC). The main tasks of the project included a targeted literature review, environmental scan, and key informant interviews to examine what is known about HIE to support transitions in care and shared care for persons receiving LTPAC. In-depth, on-site case studies were also conducted with three LTPAC providers engaged in different types of HIE to help understand the experiences of the providers and other participants involved in the HIE activity/intervention, the types of information exchanged, and the impact of these HIE activities. These tasks were guided by a framework developed for this study. This work was conducted by Westat, and sponsored by the Office of the Assistant Secretary for Planning and Evaluation (ASPE) under Task Order No. HHSP2337004T, Contract Number HHSP23320100026WI, for which Jennie Harvell served as the Project Officer.
Authors:
Colene Byrne, Ph.D., Westat
Michelle Dougherty, MA, RHIA, AHIMA Foundation
Other Contributors:
Heather McKenzie, MBA, RN
Benedicta-Osfo-Darko, MA, both Westat
Executive Summary
In 2012 the U.S. Department of Health and Human Services (HHS) funded this study to expand the knowledge base related to the state of health information exchange (HIE) to support care for persons receiving long-term and post-acute care (LTPAC) and long-term services and supports (LTSS). LTPAC providers play an important role in the United States health care system, providing care for elderly, frail, and disabled individuals, including persons who require ongoing treatment after an acute health episode. Over a third of all Medicare patients discharged from acute hospitals receive subsequent LTPAC services such as a skilled nursing facility (SNF) or home health services.1 As the United States population ages, the demand for health care services by Americans age 65 and older is expected to dramatically increase.
The focus of this study was as follows:
-
Synthesize evidence-based practices regarding HIE interventions and activities to support transitions in care and shared care by multiple members of the care team.
-
Describe these HIE interventions and activities including electronic HIE.
-
Characterize the HIE interventions, activities, LTPAC and LTSS providers, and external entities who are engaged in HIE to support care coordination and transitions of care, guided by a framework developed for this study.
-
Identify factors that enable or create barriers to implementing these HIE interventions/activities.
-
Describe the availability of process, outcome, and cost measures and metrics to assess the impact of identified HIE interventions.
Methodological Approach
The study was guided by several research questions described in the report. The study methods included a targeted literature review, environmental scan, and key informant interviews to examine what is known about HIE to support transitions in care and shared care for persons receiving LTPAC. In-depth, on-site case studies were also conducted with providers in three communities engaged in different types of HIE involving LTPAC/LTSS providers to help understand the experiences of the providers and other participants involved in the HIE activity/intervention, types of information exchanged, and impact of these HIE activities.
Study Framework
Two frameworks were adapted for this study to describe and characterize HIE interventions. The information exchange could be electronic or through other means (e.g., telephone, fax, paper). Key dimensions of the care coordination framework are care functions and mechanisms that support care transitions, shared care, and administrative functions; the staff; the organizational affiliations of organizations exchanging information (e.g., staff within or between organizations); and HIE between these organizations and their patients, family members or caregivers. A health information technology (HIT) organizational framework was adapted to this study to capture and describe the important dimensions of the HIE, including applicable HIT systems that may support HIE; data exchanged; and data interoperability and use of standards for technology-enabled HIE. The frameworks also captured other important characteristics such as environmental facets including policy drivers and financial incentives for HIE, users and uses of the information, workflow around HIE, and any outcomes associated with HIE.
Key Findings
Benefits of HIE for Care Coordination to Support Persons Receiving LTPAC/LTSS
LTPAC providers often admit and care for patients with incomplete information about their medical status. The literature review and environmental scan produced evidence that sharing and communicating information supports care coordination, particularly during transitions of care, and can reduce medication errors and other adverse events associated with preventable hospitalizations. Many interventions and tools to reduce preventable hospitalizations, including readmissions, incorporate best and promising practices that include the exchange of key information at the time of transitions and shared care.
Much of the evidence on the benefits of HIE on care coordination is anecdotal and based on qualitative information. However, a few HIE interventions that involved exchange with LTPAC providers reported positive, quantitative (although not peer-reviewed and published) impacts of HIE including reduced rates of hospital admissions/readmissions, avoided transfers to emergency departments, and improved physician followup after hospital discharge. Other benefits reported as a result of implementing the interventions included more comprehensive and useful information for care planning and timely services delivery post-discharge, ensuring that important care and services that can prevent rehospitalization are provided soon after discharge. Study informants also reported that having access to information through HIE allowed them to better assess whether patients are suitable for their LTPAC services, plan for patient care before admission, better assess functional and cognitive status and risks (e.g., fall risk), and avoid unnecessary and duplicative tests and procedures.
Barriers to HIE Participation by LTPAC/LTSS
Barriers to adoption and use of HIT by LTPAC have been widely reported. This report discusses some of the more pervasive barriers including costs and limited resources for LTPAC providers to adopt and use HIT, certified electronic health record technology (CEHRT), and interoperable HIE. There is a general lack of awareness of HIE standards and interoperable HIE solutions and their value by LTPAC providers. Current standards in LTPAC electronic health record (EHR) solutions are generally outdated and do not support efficient interoperable HIE and information reuse. Even with available standards, LTPAC providers must often develop costly customized interfaces to participate in HIE. Other barriers and challenges are the differences in clinical processes and information needs between LTPAC/LTSS and other health care providers, which impacts agreement on and availability of key HIE information; a lack of LTPAC provider organizational commitment and capacity to acquire, implement, and use HIT including HIE; and high LTPAC staff turnover rates. In addition, privacy and security policies and requirements, while important to ensure secure HIE, pose barriers to LTPAC use of HIE. Some states' HIE policies restrict disclosure of protected health information for primary uses such as treatment only, which prevents LTPAC providers from accessing needed information before a treatment relationship has been established (e.g., for preadmission planning).
Drivers Accelerating HIE by LTPAC/LTSS
This study identifies and describes several payment policies and programs that support HIE with and by LTPAC/LTSS providers. These initiatives are discussed in this report and summarized below and include: HIT/EHR grant programs, health care service and payment reform models, the EHR Incentive Programs, EHR certification programs, and HIT standards that support HIE.
HIT and HIE Adoption Support
Despite the demonstrated benefits of HIE, the use of EHR technology by LTPAC providers, including interoperable technology, appears to be lagging behind other sectors. LTPAC providers are not eligible for the Medicare and Medicaid EHR Incentive Programs and have lower rates of technology use in comparison to inpatient and ambulatory care settings. However, there has been some funding available to help LTPAC providers implement HIT such as EHRs and participate in electronic HIE. These include Office of the National Coordinator for Health Information Technology (ONC) grant funds to LTPAC providers and their affiliated health care delivery systems through the Challenge grants and Beacon Community grants, and the ONC State HIE Initiative, through which some states are providing assistance to to engage LTPAC providers in HIE. In addition, in three states the Medicare Quality Improvement Organizations are supporting LTPAC use of HIT to support medication management and care coordination in transitions of care, and advancing HIE. Most of the LTPAC providers identified as actively exchanging health information were recipients of these additional funds and other supports such as training, software, Internet access, and interfaces to an HIE organization (HIEO).
Health Care Payment Reforms and Service Delivery Models
Funding and programmatic initiatives and incentives such as those funded and authorized under the Patient Protection and Affordable Care Act (Affordable Care Act) promote and highlight the importance of care coordination around transitions and shared care. These incentives and initiatives include new federal, state, and private health care payment and delivery models such as Accountable Care Organizations and Patient-Centered Medical Homes, and other initiatives such as the Balancing Incentive Programs targeting LTSS providers and various programs implemented through the Administration for Community Living. Some of these initiatives are designed to reduce LTPAC transfers to hospitals, including readmissions. Many of the LTPAC HIE interventions identified in this study were participating in these initiatives. For example, the HHS Centers for Medicare and Medicaid Services (CMS) Innovations Models include the Community-based Care Transitions Program, which tests models for improving care transitions from the hospital to other settings and reducing readmissions for high-risk Medicare beneficiaries. The CCTP requires participation by community-based organizations such as LTSS. Some of the State Innovations Models also focus on care coordination and target LTPAC, and permit funding for the acquisition and use of HIT by these providers.
HITECH EHR Incentive Programs
The Health Information Technology for Economic and Clinical Health (HITECH) Act, enacted as part of the American Recovery and Reinvestment Act of 2009, advances the adoption and "meaningful use" (MU) of CEHRT including the interoperable exchange of health information.a This legislation was the foundation of the EHR Incentive Programs for eligible professionals, eligible hospitals, and critical access hospitals; the development of criteria for what constitutes the MU of EHRs; and the specification of EHR certification criteria and standards that must be integrated into CEHRT used by eligible providers in the EHR Incentive Programs.
To receive EHR incentive payments, hospitals and physicians must use CEHRT. As EHR adoption and interoperability requirements continue to advance in the acute care and ambulatory care sectors, it will be increasingly important for LTPAC providers to adopt technology solutions that have the capability of exchanging standardized clinical data with care partners such as hospitals, primary care practitioners, reference laboratories (labs), and pharmacies. Adopting CEHRT, particularly systems that meet ONC defined certification requirements for exchanging clinical care summaries at transitions of care, is one important step towards supporting care coordination through more efficient HIE.
Beyond implementing certified EHRs, the EHR Incentive Programs encourage providers to use their EHRs in ways that positively impact the care of their patients. Thus, HIE is a key focus in MU Stage 2 and beyond, and the Stage 2 criteria place an emphasis on HIE between providers to improve care coordination for patients. One of the core objectives in Stage 2 of the EHR Incentive Programs requires eligible providers who transition or refer a patient to another setting or provider provide a summary of care record for more than half of these transitions of care and referrals. Additionally, MU Stage 2 includes other new requirements for the electronic exchange of summary of care documents. Stage 3 MU requirements are expected to include new requirements to support the interoperable exchange of additional content at times of transitions and referrals.
HIT and HIE Standards and Certification
This report describes several initiatives around the development of standards to support the exchange of information to support care coordination on behalf of persons receiving LTPAC/LTSS. It also describes activities to advance EHR certification for technology needed by LTPAC providers. These efforts support the HIT infrastructure for HIE by advancing standards for documents, content, data elements, and privacy and security requirements. One of the central findings from this study is that the adoption of electronic HIE by LTPAC providers is just beginning, and interoperable exchange appears to be non-existent.
Available standards for key HIE requirements that are applicable to LTPAC providers and patients are identified in this report (Appendix L). Standards will be required beginning in 2014 as part of Stage 2 of the EHR Incentive Programs. Standards are currently available to support the secure exchange of summaries of care, care plans, functional/cognitive status, medication reconciliation, laboratory test orders and results. However, these standards are not yet widely adopted.
Characterization of LTPAC/LTSS HIE Interventions to Support Care Coordination
Over 25 HIE interventions that engage LTPAC and/or LTSS in HIE to support care coordination were identified in 22 states. Almost all of these interventions include electronic HIE. Most of these initiatives are through state HIE initiatives, and LTPAC/LTSS participation is through a state or community HIEO. The care coordination and HIT frameworks were applied to characterize, describe, and better understand how HIE is used by LTPAC/LTSS providers for transitions, referrals in care, shared care, and other purposes.
HIE to Support Care Transitions
All of the identified interventions use some form of HIE to support care transitions. Key functions or use cases for HIE include preadmission assessments and referrals to LTPAC, discharges and transfers from hospitals to LTPAC, and transfers from LTPAC to acute care or home and community-based services or LTSS. The types of information required to support transitions are complex and varied, and electronic HIE is typically supplemented with other means of exchange such as fax, paper, and telephone. In addition, some hospitals provide LTPAC provider access to the hospital EHR system which allows HIE.
The most common type of electronic HIE to support care coordination was found to be point-to-point HIE during transitions from an LTPAC/LTSS provider (e.g., SNF) to a hospital or from a hospital to an LTPAC/LTSS provider, where information is electronically exchanged through secure messaging directly between providers. A less frequent type of electronic HIE is LTPAC staff querying and retrieving patient information from a HIEO repository that contains information from an exchange partner (e.g., hospital). HIE is often triggered by specific use cases and alerts, such as a change in patient or resident status that may result in a transfer to a hospital. This study also identified interventions and tools that included an HIE component to support transitions between LTPAC and hospitals. These interventions included electronic/non-electronic (e.g., telephone, fax, paper) methods of exchange.
An important gap in data at times of care transitions is the lack of current medication information to support medication reconciliation. For example, reconciling pre-hospitalization medications with post-hospital medications to determine the ongoing medication regime is difficult because complete medication history data are usually not available at transitions. Furthermore, HIEOs may be the primary source of a majority, but not all, prescription history data. Other identified gaps in information that, if addressed, could improve care transitions is the lack of information from LTSS and community-based providers such as the patient's home care environment, current and previous use of support services, and receipt of durable medical equipment, homemaker, and other services.
HIE to Support Shared Care
Although use of HIE to support shared care is less frequent than in the case of transitions in care, there is an increasing focus on shared care and coordination of care across multidisciplinary health care teams and across provider settings for ongoing care. Shared care creates significant HIE opportunities for a variety of health care providers to support the assessment of ongoing needs and goals; develop and update the patient's care plan; monitor and respond to changes in the patient's status; and medication reconciliation and management.
Opportunities to Expand Health Information Exchange to Support Long-Term and Post-Acute Care and Long-Term Services and Supports
A number of opportunities emerged from this study to advance the efficient use of HIE to support care coordination for persons receiving LTPAC. These opportunities are discussed in the report, and include the following areas:
-
Exploring opportunities in the policy and service delivery environments to advance HIE, particularly in new health care delivery models.
-
Supporting multiple methods of electronic information exchange by LTPAC/LTSS, particularly as HIT standards mature.
-
Identifying the information that LTPAC/LTSS can provide to HIEOs to support care coordination such as assessment data (e.g., cognitive, functional), medication administration records, care plans, and flow sheets.
-
Specifying EHR certification criteria for LTPAC providers that align with the EHR and HIE requirements for other providers (e.g., physicians/hospitals).
-
Establishing policies that encourage greater use of CEHRT by LTPAC to support HIE with other providers.
-
Leveraging of existing standards to support HIE; developing and testing HIT standards that can be easily used and deployed to support interoperability and HIE by LTPAC providers.
-
Defining key HIE use case and modifying the workflow to support electronic HIE.
-
Increasing resources for the acquisition and use of HIE technology for LTPAC/LTSS providers.
-
Improving communication across all providers, HIEOs, and state and federal programs, of the value proposition of including LTPAC/LTSS providers in HIE activities including supporting administrative processes.
-
Addressing privacy and consent issues that hinder LTPAC/LTSS engagement in HIE activities.
-
Exploring the feasibility, benefits and limits of making available electronic pharmacy data (including from long-term care pharmacies) to support medication reconciliation.
1. Introduction
Long-Term and Post-Acute Care (LTPAC) providers play an important role in the United States health care system providing care for elderly, frail, and disabled individuals, including persons who require ongoing treatment after an acute health episode. Over a third of all Medicare patients discharged from acute hospitals receive subsequent LTPAC services such as skilled nursing or home health services.1 Health information exchange (HIE) involving LTPAC providers is expected to play a significant role in improving and achieving health policy goals, such as those in the Patient Protection and Affordable Care Act (Affordable Care Act), related to care coordination and reducing avoidable hospital readmissions.2 Currently, there is limited information on the use of HIE interventions/activities to support care coordination by LTPAC providers.
To fill this information gap, the Office of the Assistant Secretary for Planning and Evaluation (ASPE) contracted with Westat to conduct a literature review, environmental scan, interviews with key informants, and in-depth, on-site case studies with three providers engaged in HIE to support care coordination for persons receiving LTPAC/Long-Term Services and Supports (LTSS). This report summarizes the findings with a focus on:
-
Synthesizing evidence-based practices regarding HIE interventions and activities to support transitions in care and shared care by multiple members of the care team.
-
Describing these HIE interventions and activities including electronic HIE.
-
Characterizing the HIE interventions, activities, LTPAC/LTSS providers and external entities that are engaged in HIE to support care coordination and transitions of care, guided by a framework developed for this study.
-
Identifying factors that enable HIE or create barriers to implementing these HIE interventions/activities.
-
Describing the availability of process, outcome, and cost measures and metrics to assess the impact of the HIE interventions identified.
This report provides information to help advance the use of HIE for policymakers charged with improving quality and efficiencies across the health care continuum and LTPAC providers who seek to improve the quality and continuity of care, and participate in the changing delivery system.
1. Accountable Care Organizations (ACOs). See http://www.acofp.org/Practice_Management/ACO/Medical_Home/, accessed March 2013.
2. Encyclopedia of Nursing and Allied Health, ©2002 Gale Cengage.All Rights Reserved. Full copyright.
1.1. Long-Term Services and Supports, and Long-Term and Post-Acute Care
In the United States health care system, there are a wide array of institutional and home and community-based providers that deliver specialized care to elderly, frail, or disabled persons and to individuals who require ongoing treatment or care, often following an acute health episode. There is no single agreed upon definition that encompasses this wide array of services. Recently, the concept of "Long-Term Services and Supports" has emerged as a way to describe certain institutional and community-based services such as nursing homes/skilled nursing facilities (SNFs), care management, adult day care, home-delivered meals, transportation providers, and other services.3, 4 LTPAC is another concept that has been used to describe services such as nursing homes/SNFs, long-term care hospitals (LTCHs), inpatient rehabilitation facilities, and home health agency (HHA) providers.1 For the purposes of this report, both concepts are used.
LTPAC and LTSS providers deliver services to people with functional and/or cognitive limitations and/or chronic illnesses who may need assistance to perform routine daily activities such as bathing, dressing, preparing meals, and administering medications; and may require medical and skilled nursing care.3
Given the diverse range of institutional and community-based LTPAC/LTSS, for the purposes of this report persons who receive LTPAC/LTSS will described as "patients," "residents," or "clients," depending on the setting, and these terms may be used interchangeably. A glossary with definitions of these and other key terms used in this report is included in Appendix M.
1. Accountable Care Organizations (ACOs). See http://www.acofp.org/Practice_Management/ACO/Medical_Home/, accessed March 2013.
3. Continuity of Care Document. See http://en.wikipedia.org/wiki/Continuity_of_Care_Document
4. Dolin, RH, L Alschuler, C Beebe, PVBiron, SL Boyer, D Essin, and JE Mattison. (2001). The HL7 clinical document architecture.Journal of the American Medical Informatics Association, 8(6): 552-569. The National Alliance for Health Information Technology. Available at: U.S. Department of Health and Human Services. Report to the Office of the National Coordinator for Health Information Technology on Defining Key Health Information Technology Terms. http://healthit.hhs.gov/defining_key_hit_terms, accessed June 4, 2012.
1.2. Health Information Exchange
Electronic HIE is defined as the electronic movement of health-related information among organizations using national standards.5 The use of standards to support electronic HIE is often referred to "interoperable" HIE. HIE moves clinical information among disparate health care information systems while maintaining the integrity of the information during the exchange. Formal organizations providing HIE services are known as HIE organizations (HIEOs), Health information organizations (HIOs), or health information service providers (HISPs). HIE initiatives and activities in the United States may include participation of state, regional, and community (including private or enterprise) HIEOs or HIOs, statewide state-designated entities, health care delivery organizations, non-governmental organizations or policy/advocacy groups, academic institutions, technology vendors, public health departments, and state governments.6 HIE also occurs without the services provided by formal HIEOs, HIOs, or HISPs, such as HIE between the same electronic health record (EHR) users across non-affiliated providers, HIE between a hospital and affiliated independent physician practices, and through point-to-point exchange between non-affiliated partners (e.g., hospital to community-based SNF). The expanding reach of HIE initiatives has begun to attract and integrate new stakeholder entities such as behavioral health, home and community-based services (HCBS), aging services, other LTSS, and LTPAC providers.
For the purposes of this study and report, ASPE and the investigators considered various forms of exchange of health information, including electronically-enabled interoperable HIE, as well as more traditional forms such as paper-based approaches, fax, and telephone. Thus, the literature review and environmental scan, which examined the evidence around the exchange of information at times of transition and shared care, was not limited to electronically-enabled interoperable exchange.
5. What is Consolidated CDA? See http://www.hl7standards.com/blog/2012/03/22/consolidated-cda/, accessed March 2013.
6. NwHIN Direct page. See http://www.nhindirect.org/.
1.3. Care Coordination During Care Transitions and Shared Care
Care coordination is the deliberate organization of patient care activities to facilitate the appropriate delivery of health care services. It involves activities to promote, improve, and assess integration and consistency of care across primary care physicians, specialists, acute and LTSS/LTPAC services, patients and care providers, including methods to manage care throughout an episode and during transitions.7 Examples of care coordination activities include supporting individuals during transitions (e.g., the movement of a patient from one setting of care to another), and arranging for the timely delivery of needed services. Transitions coordination may involve discharge planning, setting up post-discharge followup appointments with primary care and specialty providers, coordinating medication and other therapy services post-discharge, in addition to arranging for other supports such as medical equipment that may be needed in the home. Care coordination is also important for assessing patient needs and goals, creating a plan of care (POC), monitoring, following up, responding to changes in the patient, and linking patients to community resources. These coordination activities require sharing of patient health and other information to ensure continuity of care and services needed for the recovery, rehabilitation, and health maintenance of the patient.
The Agency for Healthcare Research and Quality (AHRQ), in its Care Coordination Measures Atlas, proposed a definition and framework for integrated care. Integrated care is viewed as multidimensional construct rather than one-dimensional organizational activities, and is defined as "patient care that is coordinated across professionals, facilities, and support systems; continuous over time and between visits; tailored to the patient's needs and preferences, and based on shared responsibility between the patient and caregivers for optimizing health."8 Relevant constructs from the AHRQ framework that informed this study are the need to coordinate care across teams, between teams, and with community resources; shared responsibility with patients and caregivers; and continuous familiarity with the patient over time.9
Shared care and decision-making10 can be facilitated by care coordination, communication, and HIE among all care organizations providing care and support to the patient. Shared care, also referred to as "shared management of care" refers to patient and health care providers (e.g., physicians and LTPAC/LTSS providers) working together as a team, which may also include family members, friends, or lay caregivers designated by the patient, guided by the preferences and expectations of the patient. Shared decision-making is a collaborative process that allows patients and their providers to make health care decisions together, taking into account the best scientific evidence available, as well as the patient's values and preferences.11
Poorly coordinated care transitions, especially those from hospitals, and other care hand-offs, are associated with hospital readmissions, emergency department (ED) visits, medication errors, adverse drug events (ADEs), and other negative outcomes, which greatly affect the cost of care.12, 13, 14, 15, 16, 17, 18 The high rates of hospital readmissions of Medicare beneficiaries within 30 days of discharge in general (20%)19and for those beneficiaries discharged to SNFs (almost 25%) have been widely reported.13, 19, 20, 21 Approximately half of all hospital-related medication errors, and 20% of all ADEs, have been attributed to poor communication during transitions of care, and these can result in hospital readmissions.22 Communication breakdowns are the root cause of approximately 80% of sentinel eventsb reported to the Joint Commission.23 When care transitions are enhanced through care coordination activities such as expedited patient information flow, these activities can reduce duplication of care services and costs of care, resolve conflicting care plans,13, 18 and prevent medical errors.24 Many care transition models, programs, initiatives (see Appendix A), and best practices emphasize the importance of timely communication and information exchange between transferring and receiving providers.14, 25, 26
-
LTPAC Health IT Collaborative. A roadmap for health IT in long term and post-acute care, 2010-2012. Available athttp://library.ahima.org/xpedio/groups/public/documents/ahima/bok1_047579.pdf. Accessed July 25, 2013.
-
McDonald K, Schultz E, Albin L, et al. Care coordination measures atlas version 3. Rockville, MD: Prepared by Stanford University under Subcontract to Battelle on Contract No. 290-04-0020 for the AHRQ; 2010. AHRQ Publication No. 11-0023-EF.
-
Singer SJ, Burgers J, Friedberg M, et al. Defining and measuring integrated patient care: Promoting the next frontier in health care delivery. Medical Care Research and Review; 2011; 68(1):112-127.
-
Office of the National Coordinator for Health Information Technology policy framework RFTOP. Solicitation No 12-233-SOL-00615; 2012.
-
Informed Medical Decisions Foundation. What is shared decision making? Available at http://informedmedicaldecisions.org/what-is-shared-decision-making/. Accessed January 12, 2013.
-
Gruneir A, Bronskill S, Bell C, et al. Recent health care transitions and emergency department use by chronic long-term care residents: A population-based cohort study. J Am Med Dir Assoc; 2012; 13(3): 202-206.
-
Mor V, Intrator O, Feng Z, et al. The revolving door of rehospitalization from skilled nursing facilities. Health Aff; 2010; 29(1): 57-64.
-
Naylor MD, Kurtzman ET, Pauly MV. Transitions of elders between long-term care and hospitals. Pol. Polit. Nurs. Pract.; 2009; 10(3): 187-194.
-
Boling PA. Care transitions and home health care. Clin in Geriatr Med; 2009; 25(1): 135-148.
-
Bayley KB, Savitz LA, Rodriguez G, et al. Barriers associated with medication information handoffs. In: Henriksen K, Battles JB, Marks ES, et al., editors. Advances in Patient Safety: From Research to Implementation. Rockville, MD; 2005.
-
Chhabra PT, Rattinger GB, Dutcher SK, et al. Medication reconciliation during the transition to and from long-term care settings: A systemic review. Res Soc Admin Pharm; 2012; 8(1): 60.
-
Forster AJ, Murff HJ, Peterson JF, et al. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med; 2003; 138(3): 161-167.
-
Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med; 2009; 360(14): 1418-1428.
-
Thorpe KE. The Medicare advantage experience: Lessons for reform to original Medicare. Atlanta, GA: Emory University Rollins School of Public Health; 2012.
-
Clancy CM. Commentary: Reducing hospital readmissions: Aligning financial and quality incentives. Am J Med Qual; 2012; 27(5): 441-443.
-
Barnsteiner JH. Medication reconciliation: Transfer of medication information across settings-keeping it free from error. J Infus Nurs; 2005; 28(2 Suppl): 31-36.
-
Sentinel events statistics for 2011. Jt Comm Perspect; 2012; 32(5): 5.
-
Office of the National Coordinator for Health Information Technology. Getting to impact: Harnessing health information technology to support improved care coordination. In State HIE Bright Spots Synthesis: Care Coordination Part 1. Washington, DC: ONC; 2012. Available at http://statehieresources.org/wp-content/uploads/2013/01/Bright-Spots-Synthesis_Care-Coordination-Part-1_Final_010913.pdf.
-
Murray LM, Laditka SB. Care Transitions by older adults from nursing homes to hospitals: Implications for long-term care practice, geriatrics education, and research. J Am Med Dir Assoc; 2010; 11(4): 231-238.
-
LaMantia MA, Scheunemann LP, Viera AJ, et al. Interventions to improve transitional care between nursing homes and hospitals: A systemic review. J Am Geriatr Soc; 2010; 58(4): 777-782.
b. A sentinel event is an unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof.
2. Methodological Approach
2.3. Literature Review
A targeted literature review was conducted using peer-reviewed scientific and academic articles and the gray literature. Sources included trade journals, reports from the public and private sectors, and other identified material relevant to HIT and HIE in LTPAC/LTSS settings, and interventions to reduce hospital readmissions and medication errors in this population. Care coordination and care transitions literature were also reviewed to identify effective models of care and the role of information sharing and exchange. Sources for published articles were PubMed, Google Scholar, and the International Medical Informatics Association Inventory of HIT Evaluation Studies and Systematic Reviews (http://evaldb.umit.at). The inclusion criteria included studies based in the United States from 2007 and later. References from the most relevant articles were also reviewed to identify any important published articles that were not identified from the targeted search.d
d. Search terms included "Health Information Exchange" and other terms including, but not limited to: "Care Coordination," "Care Transitions," "Long-Term Care," "Long-Term and Post-Acute Care," "Nursing Home," "Post-Acute Care," "Home Health," "Long-Term Support Services," "Hospice," "Care Transitions," "Hospital Readmissions," "Medication Management," "Medication Reconciliation," "Outcomes," and "Measures."
2.4. Environmental Scan
The environmental scan sources used for this study were widespread (see Appendix C for a complete description of sources used). In brief, the environmental scan included web sites of HIEOs and participating health care systems with participating LTPAC/LTSS providers (e.g., ONC sponsored Challenge and Beacon community grantees); materials provided by key informants and expert project advisors; information including reports on initiatives to promote the adoption of HIT to facilitate electronic HIE;28 state, federal, and other web sites of initiatives and programs that support care coordination and transitions such as the Standards and Interoperability (S&I) framework; and information on CMS programs, rules, and funding initiatives that support new models of care and that include LTPAC/LTSS care. All literature review and environmental scan sources are cited and listed in the bibliography, and were used to summarize key findings.
28. Office of the National Coordinator for Health Information Technology. Update on the adoption of health information technology and related efforts to facilitate the electronic use and exchange of health information. Washington, DC: Office of the National Coordinator for Health Information Technology; 2013.
2.1. Research Questions
The following research questions guided the work during the literature review, environmental scan, and interviews with key informants:
-
What HIE interventions and activities are being implemented/advanced to support transitions in care and shared care involving persons who receive LTPAC/LTSS services?
-
What is the evidence base for these HIE interventions?
-
How does the use of health information technology (HIT) support these HIE interventions?
-
What factors are enablers or create barriers for needed HIE on behalf of persons who receive LTPAC/LTSS services?
-
What is a framework that can be used to synthesize and describe the HIE care models, interventions/activities, and barriers/enablers to support transitions in care and instances of shared care on behalf of person who receive LTPAC/LTSS services?
-
Who are the LTPAC/LTSS providers engaged in HIE for transitions in care and shared care? What interventions are they implementing, and what are the key characteristics of these providers and the communities within which they are located?
-
What information do LTPAC/LTSS providers have that other providers want for care planning, coordination, and transitioning? Functional status? Cognitive status? Medications? More medically-oriented information such as medications, diagnoses, allergies? Other information? (This question is agnostic as to whether HIT is used for HIE.)
-
What is the state of electronic exchange for LTPAC/LTSS providers as it relates to assessments, care plans, and other documents to support transitions in care?
- How do the following impact the feasibility of adoption and type of HIE by LTPAC/LTSS providers?
- Workforce preparation and support;
- Payer mix;
- Payer and other financial incentives;
- Availability of HIT such as EHRs, interoperable standards-based information exchange, and/or summary of care records;
- Type of information available to be exchanged; and
- Exchange between non-affiliated exchange partners.
-
What, if any, federal and state requirements create competing policies and/or priorities that may inhibit HIE?
-
What public (e.g., Centers for Medicare and Medicaid Services [CMS]) payer incentives exist for HIE, and what, if any, other payer incentives support HIE in LTPAC/LTSS settings for projects identified in the conduct of this work?
-
What is the payer mix related to each case study site and its impact on their HIE?
-
How are LTPAC/LTSS being paid for and how does payment impact HIE including facilitators and barriers?
-
What programs are developing and/or expanding that include an HIE component involving LTPAC/LTSS providers including Affordable Care Act and U.S. Department of Health and Human Services (HHS) initiatives (e.g., through CMS and the Office of the National Coordinator for Health Information Technology [ONC])?
2.2. Framework to Characterize Health Information Exchange for Persons Receiving Long-Term and Post-Acute Care/Long-Term Services and Supports
This study developed a framework to describe key care coordination constructs and functions, and selected HIE activities. Two frameworks were used and adapted to describe and characterize HIE models, interventions, and activities, as well as facilitators and barriers. These frameworks were used to guide and structure the literature review, environmental scan, site visits, and the resulting study findings. One framework was largely based on the HIT organizational framework developed by Westat researchers27 that identifies five major, interrelated facets (aspect of a particular feature, similar to a dimension) that provide a structure to organize and capture information on the implementation and use of HIT such as HIE. The framework in Rippen et al. (2013) was supplemented with the framework used by AHRQ for care coordination functions or mechanisms as discussed earlier8 (e.g., support care transitions and care planning), and was used to help characterize the care coordination processes and purpose of information exchange (e.g., to reduce rehospitalizations, coordinate post-discharge support services, improve medication safety). This study framework also uses the concept of care coordination constructs (coordinate between and across teams, providers, and family and caregivers).9 The care coordination functions and constructs were modified for this study to capture and characterize how HIE supports care transitions and shared care for persons receiving LTPAC care services.
The care coordination functions/mechanisms used for this study are: (1) to support care transitions or hand-offs (e.g., medication reconciliation, referrals); (2) to support shared care (e.g., assessment, monitor, develop POC); and (3) to support other functions such as public health reporting, quality reporting, and legibility determination. The care integration mechanisms used to describe HIE for this study are: (1) across members of the care team within affiliated organization; (2) between staff in an organization and other non-affiliated care providers including community services; and (3) between staff in an organization and patient/family members. Table 2-1 presents these care coordination constructs and functions, and examples of key HIE activities.
TABLE 2-1. Care Coordination Constructs and Functions Based on Study Framework, With Selected Examples Describing HIE
| Care Coordination Constructs -- HIE Across/Between | |||
|---|---|---|---|
| Across members of the care team within affiliated organization | Between staff in an organization and other non-affiliated care providers including community services | Between staff in an organization and patient/family members | |
| Care Coordination Functions Supported by HIE: | |||
| Support Transitions in Care | |||
| Referral/Assessment | Preadmission assessment process: gathers information to evaluate the patient for appropriateness of admission and to obtain clinical, demographic and financial information for communication with care team | ||
| Transfer/Discharge | LTPAC/LTSS to Acute Care | ||
| SNF charge nurse sends admission/discharge/ transfer (ADT) form via secure e-mail to hospital ED intake manager | |||
| Acute Care to LTPAC/LTSS | |||
| Hospital case manager notifies affiliated primary care physician via e-referral software of patient transfer to LTPAC/LTSS | Hospital sends home health nurse wound care notes, ostomy notes, social worker notes, physical therapy (PT), occupational therapy (OT), via e-referral software used by both settings. This information is automatically integrated into the HHA EHR, and populates some fields, including demographics. Notes have to be printed and scanned into HER. LTPAC/LTSS (e.g., skilled nursing) intake manager queries and access HIE virtual data repository of hospital data prior to admission |
||
| LTPAC/LTSS to Subsequent Placement | |||
| Followup Post Transfer/Discharge | Hospital case manager follows up by secure e-mail with affiliated primary care physician to ensure patient has scheduled followup appointment | Patient/family/ caregiver portal access to HIE data in virtual data repository | |
| Support Shared Care | |||
| Assess Needs and Goals | Aging Services receives information about patient living alone at home from hospital case manager in electronic formats, fax, and hard-copy | ||
| Create and Maintain Plan of Care | HHA receives notification of patient admission to hospital from HIE, initiate services planning for return to home | ||
| Monitor, Followup, and Respond to Change | Primary care physician receives notification of patient admission to hospital from HIE, monitors and plans for discharge | ||
| Support Other Administrative Functions | |||
| Quality and Public Health Reporting | LTPAC provider sends e-mail via Direct to local public health agency of reportable infectious disease | ||
| Payment authorization and eligibility determination | LTPAC providers submit required documentation for Medicaid authorization via HIE to state Medicaid agency | ||
HIE approaches, interventions, and tools can be implemented through many processes and mechanisms, which are related to and vary with respect to the other facets including the participants, organizations, setting, technology, and contextual factors. Five facets based on the HIT framework were used to describe and characterize the HIE interventions and frame the study findings:
-
HIE Technology captures elements relevant to HIT applications that enable electronic HIE. Key information captured includes the technology functionality, purpose of design, performance, and how technology facilitates the exchange of information.
-
HIE Data captures the characteristics of the data being exchanged.c
-
HIE Use and Workflow characterizes the use and users of the electronic or HIT-enabled HIE information, within and across exchange partners. For this study, this facet was expanded to also include manual, non-electronic, traditional means of exchanging information. It focuses on the workflow involved in exchanging information, the workflow insertion points for the HIE, and who has access to the information within and across the organization.
-
HIE Environment addresses the environmental and contextual factors including the settings exchanging information, their affiliations, and facilitators and barriers such as organizational support for care coordination, resources, and local factors.
-
HIE Outcomes describes outcomes from HIE to support care coordination, including care coordination measures, health care utilization such as hospitalizations, and patient safety and care quality measures such as medication-related errors, and adverse events.
These facets were originally conceptualized to characterize and understand HIT implementations, but, with the exception of the technology facet, for purposes of this study were applied to all forms of HIE, electronic and other forms. Appendix B provides the HIT frameworks, care coordination constructs and the HIT facets, with examples that are relevant to LTPAC/LTSS.
8. McDonald K, Schultz E, Albin L, et al. Care coordination measures atlas version 3. Rockville, MD: Prepared by Stanford University under Subcontract to Battelle on Contract No. 290-04-0020 for the AHRQ; 2010. AHRQ Publication No. 11-0023-EF.
9. Singer SJ, Burgers J, Friedberg M, et al. Defining and measuring integrated patient care: Promoting the next frontier in health care delivery. Medical Care Research and Review; 2011; 68(1):112-127.
27. Rippen HE, Pan EC, Russell C, et al. Organizational framework for health information technology. Int J Med Inf; 2013; 82(4): e1-e13.
c. According to the Rippen framework, data and interoperability are a sub-category under the Technology facet. For purposes of this study the data sub-category was treated as another facet and describes the characteristics of all data exchanged, electronic and other forms.
2.5. Key Informant Interviews
Westat conducted seven key informant interviews with persons who provided perspectives on the state of HIE in LTPAC/LTSS settings. The key informants interviewed are shown in Table 2-2. Information from the interviews, primarily descriptions of HIE interventions and activities, was summarized and incorporated throughout this report.
TABLE 2-2. Key Informants and Their Organizations
| Key Informant and Title | Organization | HIE Organization (HIEO) | Initiatives/ Programs |
|---|---|---|---|
| Dr. Larry Garber, Medical Director for Informatics | Reliant Health & Challenge Grant PI | Massachusetts SAFE Health | Challenge Grant |
| Lisa Harvey, Director of Care Continuum | Eastern Maine Health System, Eastern Maine HomeCare | Maine HealthInfoNet | Beacon Community, ACO |
| Barbara Gorenflo, Assistant Administrator | Beechwood Continuing Care | Western New York, HealtheNet | Beacon Community |
| Matt Cairns, Vice President* | Yeaman & Associates, & Challenge Grant Lead | Oklahoma SMRTNET | Challenge Grant |
| Rodolfo Alvarez del Castillo. MD* | Director LTC, Physician Advisor, Yeaman & Associates | Oklahoma SMRTNET | Challenge Grant |
| Larry Wolf, HIT Strategist | Kindred Healthcare | A few HIEOs in selected Kindred care markets (e.g., Indiana HIE) | N/A |
| Scott Ranson, Chief Information Officer | Brookdale Senior Living | No HIEO | CMS Innovations Grant, INTERACT program** |
| Seth Vilensky, Administrative Director | The Cleveland Clinic | Currently exchange through EPIC HIE with other EPIC users, plan to join Clinisys, Ohio's statewide HIEO | N/A |
* Two representatives from Secure Medical Records Transfer Network (SMRTNET) were interviewed to better assess the HIE technology, data and standards (M. Cairns), as well as the provider perspective, enablers, barriers, and workflow to support care transitions (Dr. Alvarez del Castillo).
** More information on Interventions to Reduce Acute Care Transfers (INTERACT) program provided in Section 3.1 and Appendix A.
2.6. Site Visits
Site visits were conducted with three strategically identified providers engaged in cutting edge information exchange to support care coordination for persons receiving LTPAC/LTSS:
-
Chicago's Rush University Medical Center's Bridge Model Care Transition Program, improves care transitions through a patient-centered approach that engages a multidisciplinary health care team to help older adults safely transition back to the community through intensive care coordination that includes HCBS providers and others in the health delivery system.
-
Beechwood Homes, a 272-bed skilled SNF in Western New York, provides a continuum of LTPAC services. Beechwood Homes is one of the first LTPAC providers to participate in HIE through a regional HIEO.
-
Eastern Maine HomeCare (EMHC), part of Eastern Maine Health System (EMHS), an integrated delivery system (IDS), is using HIE to support continuity and cost-effective care across the delivery system, implementing care management practices to support complex/fragile patients, and using telehealth to support service delivery in remote areas.
Interview guides and observation protocols guided the site visits. In-person visits were conducted with the sites and their exchange partners and stakeholders, including clinicians, case and care managers, administration, discharge planners, quality assurance (QA)/Performance Improvement staff, IT staff, and HIEO staff. The site visits provided rich case studies of the state of HIE to support LTPAC/LTSS and opportunities to advance HIE, including interoperable HIE.
3. Findings
The findings from the literature review, environmental scan, and key informant discussions are organized around six areas that address the research questions. The discussion is guided by the study framework, and highlights the themes, trends, barriers, facilitators, lessons learned, leading practices, gaps, and policy implications relevant to the use of HIE to support care coordination for persons receiving LTPAC/LTSS services. The six areas are discussed in the following sections:
-
3.1 Evidence Base for HIE to Support Care Coordination During Transitions and Instances of Shared Care.
-
3.2 Incentives to Support Care Coordination and Transitions in Care on Behalf of Persons Receiving LTPAC/LTSS.
-
3.3 Initiatives to Support the Adoption of Health Information Technology and Electronic HIE.
-
3.4 State of HIE to Support Care Coordination.
-
3.5 Process, Outcome, and Cost Measures and Metrics to Assess HIE Interventions on Care Coordination.
-
3.6 Interventions and Activities to Support Care Coordination for Persons Receiving LTPAC/LTSS.
3.1. Evidence Base for Health Information Exchange to Support Care Coordination During Transitions and Instances of Shared Care
This section examines the evidence base around care coordination to support transitions in care and instances of shared care including the impact of failures of care coordination, and the potential role of HIE interventions and programs to support care coordination and care transitions.
Failures of Care Coordination During Transitions and Shared Care
Failures of care coordination and failure to transfer key information often occur during care transition and handovers.16, 17, 29, 30, 31 Examples include failure to transfer the results of medical tests and important information from the medical record, little or no information from referring primary care providers, and inadequate or missing discharge summaries.32 Failure to make available complete, accurate, and timely information (such as medication-related information) at times of transitions contributes to adverse events, threatens safety and quality of care, and increases costs.14, 17, 18, 25, 26, 33, 34, 35, 36, 37, 38 Some of these errors could likely be avoided with timely and accurate information exchange.
Failures of care coordination also often result in avoidable hospitalizations and readmissions and undermine patient care.35, 39, 40 Hospitals' readmission rates are high and costly, and many of these readmissions are preventable.19, 21, 41, 42, 43 There is a national public policy focus on reducing avoidable hospitalizations and readmissions, and this goal is used for both quality measurement and performance-based incentives for Medicare and other insurance programs.41 Hospital readmission rates vary across types of LTPAC/LTSS providers, with SNFs and home health care agencies typically having the highest rates of inpatient readmissions.13
Adverse events such as medication errors occur frequently during care transfers and during instances of shared care. Many medication errors can be prevented or ameliorated with simple strategies that include exchanging relevant patient information. The lack of communication between doctors, hospitals, and community pharmacies has been found to be the major cause of medication errors.35 To address this increased risk of medication errors during care transfers, the Joint Commission and the Institute for Healthcare Improvement have provided national leadership to support medication reconciliation at each point of transfer. Medication reconciliation refers to the process of reviewing the patient's complete medication schedule at the time of admission, transfer, and discharge and comparing it with the schedule being considered for the new setting of care.30, 44 It also refers to the process of identifying the most accurate list of all medications that the patient is taking, including name, dosage, frequency, and route, by comparing the medical record to an external list of medications obtained from a patient, hospital, or other provider. Medication errors may occur when care is shared by multiple physicians and other providers because these clinicians may be unaware of the patient's complete medication list or health status.45
Evidence Base for HIE to Support Care Coordination
Care coordination is enhanced through expedited patient information flow, which reduces duplication of care services such as tests or procedures and the likelihood of conflicting care plans12, 13, 14, 15, 16, 17, 18 and medical errors,24 and can result in cost savings.39, 46, 47 The exchange of clinical information is especially important during care transition, when patients are transferred from one health setting to another. In addition, HIE improves population health through electronic surveillance, more accurate and timely clinical research, and more effective consumer and patient engagement.48 While no single intervention implemented alone, or bundle of interventions, appears to be associated with reduced risks of rehospitalizations,49 many successful interventions involve a strong information exchange component.41, 50
For example, Ouslander et al. evaluated the INTERACT tool--a quality improvement (QI) intervention that includes a set of tools and strategies designed to assist SNF staff in early identification, assessment, communication, and documentation about changes in resident status (See Appendix A for more information on this program). INTERACT has a number of information exchange components such as transfer documents with a checklist of recommended items. Nursing facilities using INTERACT had lower self-reported hospitalization rates after implementing the tool; however, the investigators were not able to determine which components were most strongly associated with changes in hospitalization rates.51
Many other care transition models, programs, initiatives, and best practices (e.g., ONC Challenge Grants, Partnership for Patients, Medicaid Transformation Grants) have an information exchange component, exchanging key patient information, including information to support care transitions and medication reconciliation and management.7, 36, 52, 53, 54, 55, 56 Some of these programs and initiatives are briefly described below (see Appendix A for more details). Further, some of these models, programs, and initiatives encourage the use of HIT to support HIE across care settings.52, 57, 58
CMS produced a "Roadmap to Better Care Transitions and Fewer Readmissions"36 focusing primarily on discharges from acute care hospitals. The Roadmap identifies elements of good transitions, including some that involve HIE-standardized, accurate, and timely communication and information exchange between the transferring and receiving provider. The Roadmap also identifies the type of information that should be exchanged at times of transitions in care. The conclusions in Section 5 compares these elements to the actual types of HIE information that were found to be exchanged. Other elements of good transitions include collaboration across health and LTPAC providers and other services and supports; patient and/or caregiver training; patient-centered care plans; procurement and timely delivery of durable medical equipment (DME); and ensuring the sending provider maintains responsibility for patient care until the receiving clinician or organization confirms the transfer and assumes responsibility.
Promising components and interventions to reduce hospital readmissions are identified in white papers on care coordination.41, 59 A list of these components and interventions is provided in Appendix D. There are many models for organizing care coordination and the care coordination model used is less significant to success than a close working relationship between providers, care coordinators, and patients, facilitated by communication and sharing of information.59
The promising components are consistent with evidence-based approaches promoted by Medicare's QI organizations, the Institute for Healthcare Improvement, and AHRQ as being areas that can reduce avoidable readmissions. The components include:60
-
Intensive post-discharge followup -- Placing frequent telephone calls, as well as sending encouragement and reminders to keep appointments.
-
Enhancing care coordination at the interfaces between care settings by ameliorating process breakdowns of information -- Seamlessly transferring patient information from inpatient care team to post-discharge care team.
-
Addressing medication discrepancies -- Helping patients understand how to use medications and warning signs that would warrant an emergency call to the physician.
-
Providing coaching and patient education -- Providing patients comprehensive information instructions on self-care and medication management and equipping patients with digital tools to document care and communicate with the care team.
-
Identifying issues, receiving actionable data from the home, and intervening early in the home to decrease acute care visits and exposure to preventable readmissions.
-
LTPAC Health IT Collaborative. A roadmap for health IT in long term and post-acute care, 2010-2012. Available athttp://library.ahima.org/xpedio/groups/public/documents/ahima/bok1_047579.pdf. Accessed July 25, 2013.
-
McDonald K, Schultz E, Albin L, et al. Care coordination measures atlas version 3. Rockville, MD: Prepared by Stanford University under Subcontract to Battelle on Contract No. 290-04-0020 for the AHRQ; 2010. AHRQ Publication No. 11-0023-EF.
-
Singer SJ, Burgers J, Friedberg M, et al. Defining and measuring integrated patient care: Promoting the next frontier in health care delivery. Medical Care Research and Review; 2011; 68(1):112-127.
-
Office of the National Coordinator for Health Information Technology policy framework RFTOP. Solicitation No 12-233-SOL-00615; 2012.
-
Informed Medical Decisions Foundation. What is shared decision making? Available at http://informedmedicaldecisions.org/what-is-shared-decision-making/. Accessed January 12, 2013.
-
Gruneir A, Bronskill S, Bell C, et al. Recent health care transitions and emergency department use by chronic long-term care residents: A population-based cohort study. J Am Med Dir Assoc; 2012; 13(3): 202-206.
-
Mor V, Intrator O, Feng Z, et al. The revolving door of rehospitalization from skilled nursing facilities. Health Aff; 2010; 29(1): 57-64.
-
Naylor MD, Kurtzman ET, Pauly MV. Transitions of elders between long-term care and hospitals. Pol. Polit. Nurs. Pract.; 2009; 10(3): 187-194.
-
Boling PA. Care transitions and home health care. Clin in Geriatr Med; 2009; 25(1): 135-148.
-
Bayley KB, Savitz LA, Rodriguez G, et al. Barriers associated with medication information handoffs. In: Henriksen K, Battles JB, Marks ES, et al., editors. Advances in Patient Safety: From Research to Implementation. Rockville, MD; 2005.
-
Chhabra PT, Rattinger GB, Dutcher SK, et al. Medication reconciliation during the transition to and from long-term care settings: A systemic review. Res Soc Admin Pharm; 2012; 8(1): 60.
-
Forster AJ, Murff HJ, Peterson JF, et al. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med; 2003; 138(3): 161-167.
-
Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med; 2009; 360(14): 1418-1428.
-
Thorpe KE. The Medicare advantage experience: Lessons for reform to original Medicare. Atlanta, GA: Emory University Rollins School of Public Health; 2012.
-
Clancy CM. Commentary: Reducing hospital readmissions: Aligning financial and quality incentives. Am J Med Qual; 2012; 27(5): 441-443.
-
Barnsteiner JH. Medication reconciliation: Transfer of medication information across settings-keeping it free from error. J Infus Nurs; 2005; 28(2 Suppl): 31-36.
-
Sentinel events statistics for 2011. Jt Comm Perspect; 2012; 32(5): 5.
-
Office of the National Coordinator for Health Information Technology. Getting to impact: Harnessing health information technology to support improved care coordination. In State HIE Bright Spots Synthesis: Care Coordination Part 1. Washington, DC: ONC; 2012. Available at http://statehieresources.org/wp-content/uploads/2013/01/Bright-Spots-Synthesis_Care-Coordination-Part-1_Final_010913.pdf.
-
Murray LM, Laditka SB. Care Transitions by older adults from nursing homes to hospitals: Implications for long-term care practice, geriatrics education, and research. J Am Med Dir Assoc; 2010; 11(4): 231-238.
-
LaMantia MA, Scheunemann LP, Viera AJ, et al. Interventions to improve transitional care between nursing homes and hospitals: A systemic review. J Am Geriatr Soc; 2010; 58(4): 777-782.
-
Rippen HE, Pan EC, Russell C, et al. Organizational framework for health information technology. Int J Med Inf; 2013; 82(4): e1-e13.
-
Office of the National Coordinator for Health Information Technology. Update on the adoption of health information technology and related efforts to facilitate the electronic use and exchange of health information. Washington, DC: Office of the National Coordinator for Health Information Technology; 2013.
-
Patterson ES, Roth EM, Woods DD, et al. Handoff strategies in settings with high consequences for failure: Lessons for health care operations. Int J for Qual Health Care; 2004; 16(2): 125-132.
-
Gleason K, Brake H. Medications at transitions and clinical handoffs (MATCH) toolkit for medication reconciliation. Rockville, MD: AHRQ; 2012; 11(12)-0059.
-
Siefferman JW, Lin E, Fine JS. Patient safety at handoff in rehabilitation medicine. Phys Med Rehabil Clin N Am; 2012; 23(2): 241-257.
-
Lucian Leape Institute. Order from chaos: Accelerating care integration. Boston, MA; 2012.
-
Kripalani S. Care transitions. In Perspectives on Safety. AHRQ Web M&M; 2013.
-
Allen J, Ottmann G, Roberts G. Multi-professional communication for older people in transitional care: A review of the literature. Int J Older People Nur; 2012; 7(4).
-
Burton R. Improving care transitions. Health Aff and Robert Wood Johnson Foundation; 2012; 10.1377/hpb2012.17.
-
U.S. Department of Health and Human Services. Roadmap to better care transitions and fewer readmissions. Available at http://www.healthcare.gov/compare/partnership-for-patients/safety/trans…. Accessed August 6, 2012.
-
Terrell KM, Miller DK. Challenges in transitional care between nursing homes and emergency departments. J Am Med Dir Assoc; 2006; 7(8): 499-505.
-
National Transitions of Care Coalition. Improving transitions of care: The vision of the national transitions of care coalition. Washington, DC; 2008.
-
Brown RS, Peikes D, Peterson G, et al. Six features of Medicare coordinated care demonstration programs that cut hospital admissions of high-risk patients. Health Aff; 2012; 31(6): 1156-1166.
-
Bez A. Preventing unnecessary hospitalizations for nursing home residents. Podcast on Internet; 2012.
-
Metzger J. Preventing hospital readmissions: The first test case for continuity of care. Falls Church, VA: Computer Sciences Solutions Global Institute for Emerging Healthcare Practices; 2012; WA12_0155 HCG.
-
Rutherford P. Reducing readmissions -- First, for the patient. Cambridge, MA: Institute for Healthcare Improvement; 2012.
-
Joynt KE, Jha AK. A path forward on Medicare readmissions. N Engl J Med; 2013; 368(13): 1175-1177.
-
Agency for Healthcare Research and Quality. Medication Reconciliation. Available at http://www.psnet.ahrq.gov/primer.aspx?primerID=1. Accessed January 27, 2012.
-
Centers for Medicare and Medicaid Services. Eligible professional meaningful use menu set measures, measure 7 of 10: Medication reconciliation. Available at http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/downloads/7_Medication_Reconciliation.pdf. Accessed August 28, 2013.
-
Frisse ME, Johnson KB, Nian H, et al. The financial impact of health information exchange on emergency department care. J Am Med Inform Assoc; 2012; 19(3): 328-333.
-
Kind A, Jensen L, Barczi S, et al. Low-cost transitional care with nurse managers making mostly phone contact with patients cut rehospitalization at a VA hospital. Health Aff; 2012; 21(12): 2659-2668.
-
Health Information Exchange Roadmap: The landscape and a path forward. ONC Grant #7U24AE000006-02. Washington, DC: National eHealth Collaborative; 2012.
-
Hansen LO, Young RS, Hinami K, et al. Interventions to reduce 30-day rehospitalization: A systematic review. Ann Intern Med; 2011; 155(8): 520-528.
-
Phillips CO, Wright SM, Kern DE, et al. Comprehensive discharge planning with post-discharge support for older patients with congestive heart failure. J Am Med Assoc; 2004; 291(11): 1358-1367.
-
Ouslander JG, Lamb G, Tappen R, et al. Interventions to reduce hospitalizations from nursing homes: Evaluation of the INTERACT II collaborative quality improvement project. J Am Geriatr Soc; 2011; 59(4): 745-753.
-
Coleman EA. The care transitions program. Available at http://www.caretransitions.org/. Accessed August 6, 2012.
-
Boston University. Project RED. Available at http://www.bu.edu/fammed/projectred/presentations.html. Accessed August 6, 2012.
-
Institute for Clinical Systems Improvement, Minnesota Hospital Association and Stratis Health. Reducing avoidable readmissions effectively (RARE). Available at http://www.rarereadmissions.org/resources/collaboratives.html. Accessed November 19, 2012.
-
Boult C, Green AF, Boult LB, et al. Successful models of comprehensive care for older adults with chronic conditions: Evidence for the Institute of Medicine's "retooling for an aging America" report. J Am Geriatr Soc; 2009; 57(12): 2328-2337.
-
Healthcentric Advisors. Safe Transitions Project. Available at http://www.healthcentricadvisors.org/safe-transitions-cp.html. Accessed August 6, 2012.
-
Society of Hospital Medicine. Project BOOST: Better outcomes for older adults through safe transitions. Available athttp://www.hospitalmedicine.org/AM/Template.cfm?Section=Home&CONTENTID=27659&TEMPLATE=/CM/HTMLDisplay.cfm. Accessed August 6, 2012.
-
Centers for Medicare and Medicaid Services. EHR Incentive Programs: Stage 2. Available at http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Stage_2.html. Accessed June 14, 2013.
-
Metzger J. Preparing for accountable care: Coordinated care. Falls Church, VA: Computer Sciences Solutions Global Institute for Emerging Healthcare Practices; 2012; WA12_0280 HCG.
-
eCaring LLC. Preventable readmissions: A prime target for healthcare innovation. Available at http://blog.ecaring.com/preventable-readmissions-a-prime-target-for-healthcare-innovation/. Accessed July 18, 2013.
3.2. Initiatives to Support Care Coordination and Transitions in Care on Behalf of Persons Receiving Long-Term and Post-Acute Care/Long-Term Services and Supports
This section describes some of the funding and programmatic initiatives and incentives that promote care coordination around transitions and shared care including programs that include or expand HIE involving LTPAC/LTSS providers. These include new health care payment and delivery models, and initiatives to reduce LTPAC/LTSS transfers and readmissions to hospitals.
The Federal Government has established a number of incentives and programs designed to reduce the escalating costs of health care in the United States and close well-documented gaps in care and care coordination that occur in the fee-for-service (FFS) reimbursement environments. Many of these programs support implementation of service delivery models intended to improve care and reduce costs. Several of these programs are described below and in more detail in Appendix A.
Accountable Care Organizations
One model of care is the Accountable Care Organization (ACO). ACOs are groups of providers ranging from IDSs and primary care medical groups to hospital-based systems and virtual networks of physicians, who are jointly accountable for achieving measured QIs and reducing the rate of health care spending growth.61
On November 2, 2011, CMS finalized new rules under the Affordable Care Act to help physicians, hospitals, and other health care providers (in some cases including LTPAC/LTSS providers) improve and coordinate care for Medicare patients through the Medicare Shared Savings Program to facilitate coordination and cooperation among providers to improve the quality of care for Medicare FFS beneficiaries and reduce unnecessary costs.
HIE is considered essential for ACO success. In 2012, a majority of HIE initiative stakeholders responding to the annual eHealth Initiative survey indicated that they are either participating in an ACO and/or patient-centered medical home (PCMH) efforts or intend to do so in the near future.6
One of the ACO initiatives relevant to LTPAC/LTSS is the Pioneer ACO Model, a population-based payment initiative for health care organizations and providers experienced in coordinating patient-centered care across care settings.62 At least ten of these Pioneer ACOs include LTPAC/LTSS providers (Table 3-1).
TABLE 3-1. ACOs Identified with LTPAC/LTSS Providers
| ACO Organization | Service Area | Participating LTPAC/LTSS Provider Type |
|---|---|---|
| Beacon, LLC (formerly Eastern Maine Healthcare System, ME) -- IDS | Central, Eastern, & Northern Maine | SNF, HHA, HCBS |
| Fairview Health Services (MN) -- IDS | Minneapolis, Minnesota Metropolitan Area | HHA, Senior services |
| Franciscan Alliance (IN) -- IDS | Indianapolis & Central Indiana | HHA |
| HealthCare Partners of Nevada (NV) -- IPA | Clark & Nye Counties, Nevada | SNF |
| Montefiore ACO (NYC) -- Partnership in an IDS & IPA | New York City (the Bronx) & lower Westchester County, New York | HHA |
| OSF Healthcare System -- IDS | Central Illinois | HHA |
| Partners HealthCare (MA) -- IDS | Eastern Massachusetts | HHA, other LTPAC |
| Plus! (formerly North Texas ACO, TX) -- IPA (recently announced no longer participating in Pioneer program) | Tarrant, Johnson & Parker counties in North Texas | HHA, also participates in an regional HIEO |
| Steward Health Care System (MA) -- IDS | Eastern Massachusetts | Hospice, HHA |
| Trinity Pioneer ACO, LC (formerly TriHealth, Inc) IA -- IDS | Northwest Central Iowa | HHA, Mental Health |
SOURCE: Descriptions of Pioneer ACO projects from CMS Innovations web site: http://innovation.cms.gov/Files/x/Pioneer-ACO-Model-Selectee-Descriptions-document.pdf.
NOTE: Independent physician association (IPA).
Patient-Centered Medical Homes
A PCMH is a team-based model of care led by a physician who provides continuous, coordinated care throughout a patient's lifetime to maximize health outcomes.63 This care model promotes improved access and communication; care coordination and integration; and care quality and safety.
Models for Dual Eligibles
Based on new authority in the Affordable Care Act, CMS is testing capitated and managed FFS financial alignment models to improve care and control costs for the dual eligible population (i.e., persons who are dually eligible for Medicare and Medicaid).64 These demonstrations change the payment approach and financing arrangements among CMS, the state, and providers. The capitated demonstrations will use managed care plans to coordinate services for beneficiaries through a person-centered planning process. Some states require its plans to contract with community-based organizations (CBOs) to provide LTSS coordinators, and may require its plans to contract with Area Agencies on Aging (AAAs) to coordinate with HCBS. These models of care can benefit from effective exchange of information across providers engaged in care coordination.
Community-Based Care Transitions Program
Another initiative is the Community-Based Care Transitions Program (CCTP), designed to improve transitions of high-risk Medicare beneficiaries from inpatient hospitals to home or other care settings, improve quality of care, reduce readmissions, and document measurable savings to the Medicare program. Participating CBOs are paid an all-inclusive rate per eligible discharge based on the cost of care transition services provided at the patient level and implementing systemic changes at the hospital level. According to information from the CMS Innovations web site, at least half of the CCTP recipients were determined to have LTPAC or LTSS participation in their program. Examples of these CBOs identified with participating LTPAC/LTSS providers are provided in Appendix F, based on detailed summaries available for organizations funded in the first two of four funding rounds.
State Innovation Model
The CMS State Innovation Model awards incorporate incentives and funding for HIE and EHR adoption among LTPAC providers, federally qualified health centers (FQHCs) and other safety net providers to enable multi-payer service delivery and payment models.
Medicare-Medicaid Initiatives to Reduce Avoidable Hospitalizations
Other CMS Innovations use bundled care payment models to reduce hospitalizations, one model is targets acute care and post-acute care episodes, and another model targets post-acute care only. These models are designed to lead to higher quality, more coordinated care at a lower cost to Medicare, and may benefit from HIE to support care coordination.
CMS Innovations -- Hospital Readmissions Reduction Program
A CMS Innovations initiative called the Hospital Readmissions Reduction Program focuses on long-stay nursing facility residents who are enrolled in the Medicare and Medicaid programs. The goal of the program is to reduce avoidable inpatient hospitalizations.65, 66 Payments will be reduced for hospitals with high 30-day admission rates for acute myocardial infarction, heart failure, and pneumonia. CMS has proposed expanding the list of conditions in fiscal year 2015.
Changes to Medicare Physician Payment Policy
Medicare Physician Fees for Care Transition
Under the Medicare 2013 Physician Fee Schedule, CMS created a "G" billing code that enables physicians to bill for delivery of care transition services to Medicare beneficiaries in the 30 days following a discharge from a hospital, an SNF, or a community mental health center.
Medicare Physician Fees for Chronic Care Management Services
Under the Medicare 2014 Physician Fee Schedule, CMS proposes to cover physician services to pay for non-face-to-face complex chronic care management services for Medicare beneficiaries who have two or more significant chronic conditions. Complex chronic care management services include regular physician development and revision of a POC, communication with other treating health professionals, and medication management.67
Medicaid Payment Models
Balancing Incentive Program
The Balancing Incentive Program makes grants available to states to increase access to non-institutional LTSS and lower costs through improved systems performance and efficiency, creating tools to help consumers with care planning and assessment, and improving quality measurement and oversight.
Other Care Coordination Interventions and Activities
A number of public and private entities, including AHRQ, the Partnership for Patients, the Society of Hospital Medicine, Medicare QIOs, and Patient Safety Organizations have developed initiatives to reduce hospital readmissions. These initiatives include tools, resources, and technical assistance to help hospitals and communities understand and address the factors that lead to frequent readmissions21 and make it easier to improve care coordination and care transitions.
The Medicare QIO program includes a focus on post-acute care providers, transitions in care, and care coordination/management. One QIO initiative provides technical assistance to LTPAC and other providers in Colorado, Minnesota, and Pennsylvania through the HIT for Post-Acute Care Special Innovation Project. The QIOs help providers optimize their use of HIT to support medication management and care coordination in transitions of care, and advancing HIE. Selected QIO resources related to care transition improvement efforts are available from state QIO sites.68
-
eHealth Initiative. 2012 report on health information exchange: Supporting healthcare reform. Washington, DC: eHealth Initiative; 2012.
-
LTPAC Health IT Collaborative. A roadmap for health IT in long term and post-acute care, 2010-2012. Available athttp://library.ahima.org/xpedio/groups/public/documents/ahima/bok1_047579.pdf. Accessed July 25, 2013.
-
McDonald K, Schultz E, Albin L, et al. Care coordination measures atlas version 3. Rockville, MD: Prepared by Stanford University under Subcontract to Battelle on Contract No. 290-04-0020 for the AHRQ; 2010. AHRQ Publication No. 11-0023-EF.
-
Singer SJ, Burgers J, Friedberg M, et al. Defining and measuring integrated patient care: Promoting the next frontier in health care delivery. Medical Care Research and Review; 2011; 68(1):112-127.
-
Office of the National Coordinator for Health Information Technology policy framework RFTOP. Solicitation No 12-233-SOL-00615; 2012.
-
Informed Medical Decisions Foundation. What is shared decision making? Available at http://informedmedicaldecisions.org/what-is-shared-decision-making/. Accessed January 12, 2013.
-
Gruneir A, Bronskill S, Bell C, et al. Recent health care transitions and emergency department use by chronic long-term care residents: A population-based cohort study. J Am Med Dir Assoc; 2012; 13(3): 202-206.
-
Mor V, Intrator O, Feng Z, et al. The revolving door of rehospitalization from skilled nursing facilities. Health Aff; 2010; 29(1): 57-64.
-
Naylor MD, Kurtzman ET, Pauly MV. Transitions of elders between long-term care and hospitals. Pol. Polit. Nurs. Pract.; 2009; 10(3): 187-194.
-
Boling PA. Care transitions and home health care. Clin in Geriatr Med; 2009; 25(1): 135-148.
-
Bayley KB, Savitz LA, Rodriguez G, et al. Barriers associated with medication information handoffs. In: Henriksen K, Battles JB, Marks ES, et al., editors. Advances in Patient Safety: From Research to Implementation. Rockville, MD; 2005.
-
Chhabra PT, Rattinger GB, Dutcher SK, et al. Medication reconciliation during the transition to and from long-term care settings: A systemic review. Res Soc Admin Pharm; 2012; 8(1): 60.
-
Forster AJ, Murff HJ, Peterson JF, et al. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med; 2003; 138(3): 161-167.
-
Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med; 2009; 360(14): 1418-1428.
-
Thorpe KE. The Medicare advantage experience: Lessons for reform to original Medicare. Atlanta, GA: Emory University Rollins School of Public Health; 2012.
-
Clancy CM. Commentary: Reducing hospital readmissions: Aligning financial and quality incentives. Am J Med Qual; 2012; 27(5): 441-443.
-
Barnsteiner JH. Medication reconciliation: Transfer of medication information across settings-keeping it free from error. J Infus Nurs; 2005; 28(2 Suppl): 31-36.
-
Sentinel events statistics for 2011. Jt Comm Perspect; 2012; 32(5): 5.
-
Office of the National Coordinator for Health Information Technology. Getting to impact: Harnessing health information technology to support improved care coordination. In State HIE Bright Spots Synthesis: Care Coordination Part 1. Washington, DC: ONC; 2012. Available at http://statehieresources.org/wp-content/uploads/2013/01/Bright-Spots-Synthesis_Care-Coordination-Part-1_Final_010913.pdf.
-
Murray LM, Laditka SB. Care Transitions by older adults from nursing homes to hospitals: Implications for long-term care practice, geriatrics education, and research. J Am Med Dir Assoc; 2010; 11(4): 231-238.
-
LaMantia MA, Scheunemann LP, Viera AJ, et al. Interventions to improve transitional care between nursing homes and hospitals: A systemic review. J Am Geriatr Soc; 2010; 58(4): 777-782.
-
Rippen HE, Pan EC, Russell C, et al. Organizational framework for health information technology. Int J Med Inf; 2013; 82(4): e1-e13.
-
Office of the National Coordinator for Health Information Technology. Update on the adoption of health information technology and related efforts to facilitate the electronic use and exchange of health information. Washington, DC: Office of the National Coordinator for Health Information Technology; 2013.
-
Patterson ES, Roth EM, Woods DD, et al. Handoff strategies in settings with high consequences for failure: Lessons for health care operations. Int J for Qual Health Care; 2004; 16(2): 125-132.
-
Gleason K, Brake H. Medications at transitions and clinical handoffs (MATCH) toolkit for medication reconciliation. Rockville, MD: AHRQ; 2012; 11(12)-0059.
-
Siefferman JW, Lin E, Fine JS. Patient safety at handoff in rehabilitation medicine. Phys Med Rehabil Clin N Am; 2012; 23(2): 241-257.
-
Lucian Leape Institute. Order from chaos: Accelerating care integration. Boston, MA; 2012.
-
Kripalani S. Care transitions. In Perspectives on Safety. AHRQ Web M&M; 2013.
-
Allen J, Ottmann G, Roberts G. Multi-professional communication for older people in transitional care: A review of the literature. Int J Older People Nur; 2012; 7(4).
-
Burton R. Improving care transitions. Health Aff and Robert Wood Johnson Foundation; 2012; 10.1377/hpb2012.17.
-
U.S. Department of Health and Human Services. Roadmap to better care transitions and fewer readmissions. Available at http://www.healthcare.gov/compare/partnership-for-patients/safety/trans…. Accessed August 6, 2012.
-
Terrell KM, Miller DK. Challenges in transitional care between nursing homes and emergency departments. J Am Med Dir Assoc; 2006; 7(8): 499-505.
-
National Transitions of Care Coalition. Improving transitions of care: The vision of the national transitions of care coalition. Washington, DC; 2008.
-
Brown RS, Peikes D, Peterson G, et al. Six features of Medicare coordinated care demonstration programs that cut hospital admissions of high-risk patients. Health Aff; 2012; 31(6): 1156-1166.
-
Bez A. Preventing unnecessary hospitalizations for nursing home residents. Podcast on Internet; 2012.
-
Metzger J. Preventing hospital readmissions: The first test case for continuity of care. Falls Church, VA: Computer Sciences Solutions Global Institute for Emerging Healthcare Practices; 2012; WA12_0155 HCG.
-
Rutherford P. Reducing readmissions -- First, for the patient. Cambridge, MA: Institute for Healthcare Improvement; 2012.
-
Joynt KE, Jha AK. A path forward on Medicare readmissions. N Engl J Med; 2013; 368(13): 1175-1177.
-
Agency for Healthcare Research and Quality. Medication Reconciliation. Available at http://www.psnet.ahrq.gov/primer.aspx?primerID=1. Accessed January 27, 2012.
-
Centers for Medicare and Medicaid Services. Eligible professional meaningful use menu set measures, measure 7 of 10: Medication reconciliation. Available at http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/downloads/7_Medication_Reconciliation.pdf. Accessed August 28, 2013.
-
Frisse ME, Johnson KB, Nian H, et al. The financial impact of health information exchange on emergency department care. J Am Med Inform Assoc; 2012; 19(3): 328-333.
-
Kind A, Jensen L, Barczi S, et al. Low-cost transitional care with nurse managers making mostly phone contact with patients cut rehospitalization at a VA hospital. Health Aff; 2012; 21(12): 2659-2668.
-
Health Information Exchange Roadmap: The landscape and a path forward. ONC Grant #7U24AE000006-02. Washington, DC: National eHealth Collaborative; 2012.
-
Hansen LO, Young RS, Hinami K, et al. Interventions to reduce 30-day rehospitalization: A systematic review. Ann Intern Med; 2011; 155(8): 520-528.
-
Phillips CO, Wright SM, Kern DE, et al. Comprehensive discharge planning with post-discharge support for older patients with congestive heart failure. J Am Med Assoc; 2004; 291(11): 1358-1367.
-
Ouslander JG, Lamb G, Tappen R, et al. Interventions to reduce hospitalizations from nursing homes: Evaluation of the INTERACT II collaborative quality improvement project. J Am Geriatr Soc; 2011; 59(4): 745-753.
-
Coleman EA. The care transitions program. Available at http://www.caretransitions.org/. Accessed August 6, 2012.
-
Boston University. Project RED. Available at http://www.bu.edu/fammed/projectred/presentations.html. Accessed August 6, 2012.
-
Institute for Clinical Systems Improvement, Minnesota Hospital Association and Stratis Health. Reducing avoidable readmissions effectively (RARE). Available at http://www.rarereadmissions.org/resources/collaboratives.html. Accessed November 19, 2012.
-
Boult C, Green AF, Boult LB, et al. Successful models of comprehensive care for older adults with chronic conditions: Evidence for the Institute of Medicine's "retooling for an aging America" report. J Am Geriatr Soc; 2009; 57(12): 2328-2337.
-
Healthcentric Advisors. Safe Transitions Project. Available at http://www.healthcentricadvisors.org/safe-transitions-cp.html. Accessed August 6, 2012.
-
Society of Hospital Medicine. Project BOOST: Better outcomes for older adults through safe transitions. Available athttp://www.hospitalmedicine.org/AM/Template.cfm?Section=Home&CONTENTID=27659&TEMPLATE=/CM/HTMLDisplay.cfm. Accessed August 6, 2012.
-
Centers for Medicare and Medicaid Services. EHR Incentive Programs: Stage 2. Available at http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Stage_2.html. Accessed June 14, 2013.
-
Metzger J. Preparing for accountable care: Coordinated care. Falls Church, VA: Computer Sciences Solutions Global Institute for Emerging Healthcare Practices; 2012; WA12_0280 HCG.
-
eCaring LLC. Preventable readmissions: A prime target for healthcare innovation. Available at http://blog.ecaring.com/preventable-readmissions-a-prime-target-for-healthcare-innovation/. Accessed July 18, 2013.
-
McClellan M, McKethan AN, Lewis JL, et al. A national strategy to put accountable care into practice. Health Aff; 2010; 29(5): 982-990.
-
Pioneer Accountable Care Organization Model: General fact sheet. CMS, Center for Medicare and Medicaid Innovation; 2012.
-
American College of Physicians. What is the patient-centered medical home? Available athttp://www.acponline.org/running_practice/delivery_and_payment_models/pcmh/understanding/what.htm. Accessed August 30, 2013.
-
Centers for Medicare and Medicaid Services. State Demonstrations to Integrate Care for Dual Eligible Individuals. Available athttp://www.cms.gov/Medicare-Medicaid-Coordination/Medicare-and-Medicaid-Coordination/Medicare-Medicaid-Coordination-Office/StateDemonstrationstoIntegrateCareforDualEligibleIndividuals.html. Accessed October 28, 2013.
-
Centers for Medicare and Medicaid Services. Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents. Available at http://www.innovations.cms.gov/initiatives/rahnfr/index.html. Accessed November 20, 2013.
-
Centers for Medicare and Medicaid Services. New program to increase quality in nursing facilities. Available athttp://www.cms.gov/apps/media/press/release.asp?Counter=4454&intNumPerPage=10&checkDate=&checkKey=&srchType=1&numDays=3500&srchOpt=0&srchData=&keywordType=All&chkNewsType=1%2C+2%2C+3%2C+4%2C+5&intPage=&showAll=&pYear=&year=&desc=&cboOrder=date. Accessed November 20, 2012.
-
Centers for Medicare and Medicaid Services. Details for Regulation #CMS -1600-P. Available athttp://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched/PFS-Federal-Regulation-Notices-Items/CMS-1600-P.html. Accessed August 8, 2012.
-
Colorado Foundation for Medical Care. Links/resources/tools for providers -- care transitions improvement efforts. Available athttp://www.cfmc.org/integratingcare/provider_resources.htm. Accessed July 14, 2013.
3.3. Initiatives to Support Adoption of Health Information Technology and Electronic Health Information Exchange
Health Information Technology for Economic and Clinical Health (HITECH) Act
There are other facilitators for LTPAC/LTSS providers to engage in HIE, some of which are a result of program initiatives targeting other health care providers that are involved in care coordination for the LTPAC population, such as hospitals and physicians. The HITECH Act,e enacted as part of the American Recovery and Reinvestment Act of 2009, promotes the adoption and meaningful use (MU) of certified EHRs. This legislation was the foundation of the EHR Incentive Programs for eligible professionals (EPs), eligible hospitals (EHs), and critical access hospitals (CAHs); the development of criteria for what constitutes MU of EHRs; and the EHR certification criteria and standards that must be integrated into certified EHR technology (CEHRT) used by eligible providers in the EHR Incentive Programs.
The goal of MU is to support the use of certified EHRs to improve health care in the United States.69 The focus of Stage 1 of the EHR Incentive Programs has been on EP, EHs', and CAHs' adoption of certified EHRs, and the MU of data captured by EHRs. The Stage 2 MU requirements, effective fiscal year 2014, add to this foundation and require electronic exchange of health information and will support electronic coordination of care efforts by EPs, EHs and CAHs. Stage 3 MU requirements are expected to include requirements to support the interoperable exchange of additional content at times of transitions and referrals in care.
LTPAC/LTSS providers such as HHAs, inpatient rehabilitation hospitals, long-term acute care hospitals, and SNFs are not eligible for the Medicare and Medicaid EHR Incentive Programs.70 Nonetheless, the ability of LTPAC providers to exchange health information electronically with EPs, EHs, and CAHs could affect the ability of EPs, EHs and CAHs to qualify for incentive payments, and could impact the success of the EHR Incentive Programs to improve care coordination.1 LTPAC/LTSS providers that want to use EHRs and participate in HIE must either pay for the costs of EHRs or find other sources to offset these costs such as the shared savings ACO programs or the State Innovation Model.
Selected MU Stage 2 criteria related to care coordination and HIE include the following:58
-
Care Transitions. When transitioning a patient to another care setting, the EP, EH, or CAH should provide a summary of care record for each transition of care or referral. The Summary of Care Records is to include, if known, a care plan.
-
Patient Visits. Provide a clinical summary for patients for each office visit.
-
Reminders. Use clinically relevant information to identify patients who should receive reminders for preventive and/or followup care with patients on relevant health information.
-
Communication. Use secure electronic messaging to communicate with patients on relevant health information.
-
Data Use. When a patient transitions from one provider to another, medication reconciliation should be performed. The EP, EH or CAH who receives a patient from another setting of care or provider of care, or who believes an encounter is relevant should perform medication reconciliation.71
-
Data Portability. Patients must be able to view and download their own health information and also be able to transmit that information to a third party.
Stage 2 MU measures that will be required in Stage 2 and are particularly relevant to LTPAC are:
-
EPs, EHs, and CAHs requirement to provide a summary of care document for more than 50% of transitions of care and referrals, with 10% sent electronically across vendor and provider boundaries (i.e., between recipients using different EHR technology vendors for transitions of care and referrals).72, 73
-
Other MU criteria and measures include the capability to generate and transmit permissible prescriptions electronically, submit electronic data to immunization registries or Immunization Information Systems electronic syndromic surveillance data to public health agencies, and identify and report cancer cases to a state cancer registry. For more information see: http://www.healthit.gov/policy-researchers-implementers/meaningful-use-stage-2.
-
As the Healthcare Information Technology Policy Committee74 continues to consider requirements for Stage 3 MU, there will be a greater focus on transitions/referrals of care.
Federal HIT Principles and Strategies
HHS is committed to realizing a patient-centered, value-driven health care system supported by the secure exchange of information across all providers of care. HIT serves as a foundational building block for achieving better health outcomes at lower costs. HHS recently released its HIE Principles and Strategy report, which notes that a "critical part of enabling the secure flow of information across the system is advancing the adoption of HIT standards through voluntary certification of HIT and HIE products and services."75 As part of this strategy, ONC said in a webinar that it will move forward with determining the potential scope and criteria for a HIT certification program and criteria for providers not eligible for the EHR Incentive Programs, starting with LTPAC (and behavioral health). In addition, CMS is considering ways in which Medicare and Medicaid payment policies can advance interoperable HIE by providers not eligible for the EHR Incentive Programs. Policymakers hope that by specifying EHR certification criteria for products needed by LTPAC providers that adoption of certified technology will increase and support interoperable HIE.75, 76
LTPAC providers were included in the 2011-2015 federal HIT Strategic Plan released by the ONC in March 2011. The Strategic Plan describes the need to support HIT adoption and information exchange in LTPAC, behavioral health, and emergency care settings and describes why continued investment is needed to fully support HIE.76
ONC Roadmap
ONC has developed a Standards, Interoperability, and Certification Roadmap that recommends establishing LTPAC (and Behavioral Health) HIT certification; and disseminating open source toolkits for Admission/Discharge/Transfer (ADT) alerts.75
3.3.1. Facilitators of HIE -- HIT Standards, Specifications, and Certification
EHR Certification for LTPAC
Some of the EHR technology certification criteria used for the EHR Incentive Programs are applicable to care transitions and coordination in LTPAC settings.70 The ONC Final Rule for Standards, Implementation Specifications, and Certification Criteria for EHR Technology encourages EHR technology developers of products for providers who are not eligible for the EHR Incentive Programs to certify their projects to: (1) transitions of care module and other appropriate modules; and (2) other certification criteria that make it more efficient for EPs, EHs, and CAHs to electronically exchange health information.77 MU Stage 2 transitions of care certification criteria require that EHR technology: (1) receive, display in human readable format, and incorporate transition of care/referral summaries according to specified standards; and (2) create and transmit transition of care/referral summaries according to the standard adopted. At the time of this report, approximately six LTPAC EHR vendors had products certified by ONC Authorized Testing and Certification Bodies.78
In addition, a private sector organization, Certification Commission for Health Information Technology (CCHIT), has also established LTPAC EHR certification criteria. At the time of this report, six LTPAC EHR vendors have CCHIT certified products.79
To date, LTPAC provider use of these certified EHRs is believed to be low. Nonetheless, some LTPAC providers are reportedly using HIT applications that incorporate ONC-adopted standards that support the Patient Summary Record (i.e., Health Level 7 (HL7) Clinical Document Architecture (CDA)/Continuity of Care Document (CCD)/C32 (MU Stage 1 requirement).
E-Prescribing
Persons receiving LTAC services are often prescribed multiple medications. E-prescribing is complicated for a number of reasons. E-prescribing typically involves multiple parties -- both the prescriber and the pharmacy. However, in certain institutional settings such as SNFs, e-prescribing will involve at least three parties -- the prescriber, facility, and pharmacy -- and may include other entities such as payers. The 2014 MU requirements issued by ONC include a standard for e-prescribing that once adopted will support this three-way information exchange. Use of interoperable e-prescribing technology solutions in SNFs will likely require changes in the current prescribing workflow and technical assistance to support implementation of e-prescribing in SNFs.
Standardizing Interoperability Specifications
There are specific workgroups sponsoring work on HIT and HIE standards that support care for persons receiving LTPAC, including these workgroups managed under the S&I Framework and HL7.80 These HIT and HIE standards include the Consolidated Clinical Data Architecture (CCDA) (exchange standard referenced in MU Stage 2), a more robust, implementable standard.f Relevant workgroups include:
-
S&I Longitudinal Coordination of Care (LCC) Workgroup (http://wiki.siframework.org/Longitudinal+Coordination+of+Care).
-
The S&L LCC Workgroup is advancing the electronic exchange of information at times of referrals and transition of care and exchange of care plans. The LCC Workgroup consists of two active sub-workgroups (SWGs): the Longitudinal Care Plan and LTPAC Transitions in Care SWGs. The Longitudinal Care Plan SWG has developed the Use Case for the interoperable exchange of the care plan, and identified the functional requirements to support its exchange. The LTPAC Care Transition SWG is developing a requirements-driven view of data elements required for information exchange based on a set of user stories related to transitions and referrals in care.
-
The S&I LCC Workgroup is working with HL7 to refine the CCDA Implementation Guide (a requirement in MU Stage 2) to support the exchange of more robust documents for transitions and referrals of care, and care plans. The updated CCDA Implementation Guide (being balloting in Fall 2013) includes new and enhanced document templates for the Transfer Summary, Consultation Note, Referral Note, and Care Plan.
-
The S&L LCC Workgroup is also reviewing the Domain Analysis Model developed by the HL7 Patient Care Workgroup (see HL7 below), providing input around care plan exchange (http://wiki.hl7.org/index.php?title=Domain_Analysis_Model).
-
-
The ONC S&I Electronic Signature for Medical Document Initiative (http://wiki.siframework.org/esMD+Initiative).
-
This CMS initiative will identify a standard for digital signatures for medical documents (such as care plans).
-
Facilitator -- Other ONC HIT Initiatives
As described below, ONC has directed some resources to engage LTPAC providers in state HIE activities and now has some programs and resources for LTPAC providers.
Challenge Grants
The ONC Challenge Grants are engaging LTPAC providers in HIT, EHR, and HIE activities at the federal, state and regional level to improve transitions of care. Federal Challenge grants to support LTPAC are operating in four states -- Oklahoma, Massachusetts, Colorado, and Maryland.81, 82
-
Oklahoma's Challenge Grant program is focused on HIE for care transitions, and is based on real-time Activities of Daily Living (ADL) documentation. The HIE partner is SMRTNET -- Secure Medical Records Transfer Network -- a robust HIE network serving Oklahoma's health care systems. SNFs were provided with access to the Internet and computers and then a clinical documentation tool, a "lite" EHR called CareTracker that allows caregivers to record required resident documentation and scans for changes in resident conditions and provide alerts when the conditions change. CareTracker helps to create a Situation, Background, Assessment, and Recommendation (SBAR, see Appendix A for more information), one tools in the INTERACT program, for communication and the Universal Transfer Form (UTF) if the patient is transferred to the ED or hospital. SMRTNET worked with providers to determine what information should be transferred via the UTF. SMRTNET supports an enhanced version of Direct, a low-cost HIE solution. LTPAC providers can query for patient information and securely send information to providers such as hospitals and physicians. Some of the partner sites with EHRs (e.g., hospitals) can click a link that connects directly to a web-based SMRTNET view, and structured data from the LTPAC providers can be imported to populate a patient's chart.
-
Massachusetts' IMPACT project is "meeting LTPAC providers where they are" by providing the Local Adaptor for Network Distribution (LAND) and Surrogate EHR Environment (SEE). LAND allows organizations with fully implemented EHRs capable of generating the newly specified transition of care and care plan data elements to create, transmit, and receive these new document types. SEE, intended for organizations without an EHR and lacking the ability to create these documents, allows providers to view, edit, and send documents to the receiving facility via Direct message transmission from a web browser. The IMPACT project is working to create tools to generate, translate, and view UTFs via the HIE. At the time of this study, there were 11 LTPAC facilities participating in IMPACT, all in Worcester County, Massachusetts, with plans to continue to expand as the state's HIE structure improves.
-
Colorado's HIE and program participant, the Colorado Regional Health Information Organization (CORHIO), is working in four targeted early adopter communities toward integrating HIE to improve care transitions. CORHIO is working with LTPAC organizations, including home health, hospice, SNFs, assisted living, long-term acute care hospitals and residential care facilities for the developmentally disabled to improve care transitions to and from acute care settings through HIE. The goals of the program are to facilitate adoption of HIE by the LTPAC community, develop a community protocol for information sharing across care transitions, and measure the impact of HIE on quality of patient care and rates of hospital readmissions. HHAs receive resources and training as part of their participation in this program.
-
Maryland and its partner, an operational regional HIEO called the Chesapeake Regional Information System for Our Patients (CRISP) are leveraging Maryland's statewide HIE to electronically share critical pieces of clinical information, including information on advance directives, in near real-time as residents of LTPAC facilities transition from one care setting to another. The project seeks to deploy new scalable technology among LTPAC providers and geographically proximate hospitals that will enable the exchange of care transition data. Three LTPAC facilities have been awarded funds for the adoption and use of HIT to support improved transitions of care for their patients as they transition between hospitals and their facility. These LTPAC providers are or will be able to use CRISP's encounter notification service to alert physicians and care coordinators in real-time when one of their patients has an encounter with a Maryland hospital, such as an ADT. These alerts are sent via a direct secure message or HL7 message to an EHR system.
Beacon Communities
ONC provided funding to 17 selected communities that are considered beacons for their communities in the development of secure, private, and accurate systems of EHR adoption and HIE.83 Some of the Beacon Communities included participation with LTPAC providers such as HHAs and SNFs. Beacon Communities in Rhode Island, Western New York, and Bangor, Maine are connecting HIEOs with LTPAC providers. The Rhode Island Beacon Community has targeted up to 84 nursing facilities across the state and engaged them in CurrentCare, a secure electronic network that gives health care providers access to the patient information. The Keystone Beacon Community in Pennsylvania developed an HIE tool that allows SNFs and HHAs to share a patient's information inexpensively and securely, with or without an EHR. The KeyHIE Transform tool is an all-inclusive, web-based service that transforms the electronic nursing home Minimum Data Sets (MDS) and home health Outcome and Information Assessment Set (OASIS) into an HL7 CCD so that SNFs and HHAs can share this information with other care providers (see Appendix A for more information about KeyHIE).
Community of Practice
ONC initiated a new long-term care community of practice (CoP), supported by the state HIE initiative, which provides opportunities to discuss areas of interest, collaborate, and share knowledge, information, experience, and best practices. This CoP is engaging with policymakers and implementers to identify opportunities to expand HIE in LTPAC and prioritize future advancements such as medication management, lab results integration, and advance directives.
Direct Project
The Direct Project (http://directproject.org/)28 was launched by ONC in 2010 "to support the use of standards-based protocols for an easy-to-use, secure, and scalable method of sending encrypted and authenticated health information over the Internet such as clinical summaries, CCDs, and laboratory results, to other providers who also own a DIRECT address."6, 84 The most basic implementation of the Direct Project is secure e-mail via an e-mail client or web portal, which works just like regular e-mail, but with an added level of security required to transport sensitive health information. The Direct Project can serve as a solution for simple, point-to-point HIE around specific use cases. This tool can help LTPAC/LTSS providers to send and receive secure messages and electronic attachments with others in their network quickly, easily, and at a low cost, and facilitates referrals and transitions of care.33 Limitations of Direct include limited or low uptake, in part due to a lack of a provider registry.
-
Dougherty M, Harvell J. Opportunities for engaging long-term and post-acute care providers in health information exchange activities: Exchanging interoperable patient assessment information. Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Office of Disability, Aging and Long-Term Care Policy; 2011. Available athttp://aspe.hhs.gov/daltcp/reports/2011/StratEng.htm.
-
Affordable Care Act. National pilot program on payment bundling. Public Law 111-148 and Public Law 111-152. 2010: Section 3023.
-
Engquist G, Johnson C, Johnson W. Medicaid funded long-term supports and services: Snapshots of innovation. Center for Health Care Strategies, Inc.; 2010.
-
Woodcock C. Long-term services and supports: Challenges and opportunities for states in difficult budget times. National Governors Association; 2011.
-
National Alliance for Health Information Technology. Report to the Office of National Coordinator for Health Information Technology on defining key health information technology terms. Washington, DC: U.S. Department of Health and Human Services, Office of the National Coordinator of Health IT; 2008.
-
eHealth Initiative. 2012 report on health information exchange: Supporting healthcare reform. Washington, DC: eHealth Initiative; 2012.
-
LTPAC Health IT Collaborative. A roadmap for health IT in long term and post-acute care, 2010-2012. Available athttp://library.ahima.org/xpedio/groups/public/documents/ahima/bok1_047579.pdf. Accessed July 25, 2013.
-
McDonald K, Schultz E, Albin L, et al. Care coordination measures atlas version 3. Rockville, MD: Prepared by Stanford University under Subcontract to Battelle on Contract No. 290-04-0020 for the AHRQ; 2010. AHRQ Publication No. 11-0023-EF.
-
Singer SJ, Burgers J, Friedberg M, et al. Defining and measuring integrated patient care: Promoting the next frontier in health care delivery. Medical Care Research and Review; 2011; 68(1):112-127.
-
Office of the National Coordinator for Health Information Technology policy framework RFTOP. Solicitation No 12-233-SOL-00615; 2012.
-
Informed Medical Decisions Foundation. What is shared decision making? Available at http://informedmedicaldecisions.org/what-is-shared-decision-making/. Accessed January 12, 2013.
-
Gruneir A, Bronskill S, Bell C, et al. Recent health care transitions and emergency department use by chronic long-term care residents: A population-based cohort study. J Am Med Dir Assoc; 2012; 13(3): 202-206.
-
Mor V, Intrator O, Feng Z, et al. The revolving door of rehospitalization from skilled nursing facilities. Health Aff; 2010; 29(1): 57-64.
-
Naylor MD, Kurtzman ET, Pauly MV. Transitions of elders between long-term care and hospitals. Pol. Polit. Nurs. Pract.; 2009; 10(3): 187-194.
-
Boling PA. Care transitions and home health care. Clin in Geriatr Med; 2009; 25(1): 135-148.
-
Bayley KB, Savitz LA, Rodriguez G, et al. Barriers associated with medication information handoffs. In: Henriksen K, Battles JB, Marks ES, et al., editors. Advances in Patient Safety: From Research to Implementation. Rockville, MD; 2005.
-
Chhabra PT, Rattinger GB, Dutcher SK, et al. Medication reconciliation during the transition to and from long-term care settings: A systemic review. Res Soc Admin Pharm; 2012; 8(1): 60.
-
Forster AJ, Murff HJ, Peterson JF, et al. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med; 2003; 138(3): 161-167.
-
Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med; 2009; 360(14): 1418-1428.
-
Thorpe KE. The Medicare advantage experience: Lessons for reform to original Medicare. Atlanta, GA: Emory University Rollins School of Public Health; 2012.
-
Clancy CM. Commentary: Reducing hospital readmissions: Aligning financial and quality incentives. Am J Med Qual; 2012; 27(5): 441-443.
-
Barnsteiner JH. Medication reconciliation: Transfer of medication information across settings-keeping it free from error. J Infus Nurs; 2005; 28(2 Suppl): 31-36.
-
Sentinel events statistics for 2011. Jt Comm Perspect; 2012; 32(5): 5.
-
Office of the National Coordinator for Health Information Technology. Getting to impact: Harnessing health information technology to support improved care coordination. In State HIE Bright Spots Synthesis: Care Coordination Part 1. Washington, DC: ONC; 2012. Available at http://statehieresources.org/wp-content/uploads/2013/01/Bright-Spots-Synthesis_Care-Coordination-Part-1_Final_010913.pdf.
-
Murray LM, Laditka SB. Care Transitions by older adults from nursing homes to hospitals: Implications for long-term care practice, geriatrics education, and research. J Am Med Dir Assoc; 2010; 11(4): 231-238.
-
LaMantia MA, Scheunemann LP, Viera AJ, et al. Interventions to improve transitional care between nursing homes and hospitals: A systemic review. J Am Geriatr Soc; 2010; 58(4): 777-782.
-
Rippen HE, Pan EC, Russell C, et al. Organizational framework for health information technology. Int J Med Inf; 2013; 82(4): e1-e13.
-
Office of the National Coordinator for Health Information Technology. Update on the adoption of health information technology and related efforts to facilitate the electronic use and exchange of health information. Washington, DC: Office of the National Coordinator for Health Information Technology; 2013.
-
Patterson ES, Roth EM, Woods DD, et al. Handoff strategies in settings with high consequences for failure: Lessons for health care operations. Int J for Qual Health Care; 2004; 16(2): 125-132.
-
Gleason K, Brake H. Medications at transitions and clinical handoffs (MATCH) toolkit for medication reconciliation. Rockville, MD: AHRQ; 2012; 11(12)-0059.
-
Siefferman JW, Lin E, Fine JS. Patient safety at handoff in rehabilitation medicine. Phys Med Rehabil Clin N Am; 2012; 23(2): 241-257.
-
Lucian Leape Institute. Order from chaos: Accelerating care integration. Boston, MA; 2012.
-
Kripalani S. Care transitions. In Perspectives on Safety. AHRQ Web M&M; 2013.
-
Allen J, Ottmann G, Roberts G. Multi-professional communication for older people in transitional care: A review of the literature. Int J Older People Nur; 2012; 7(4).
-
Burton R. Improving care transitions. Health Aff and Robert Wood Johnson Foundation; 2012; 10.1377/hpb2012.17.
-
U.S. Department of Health and Human Services. Roadmap to better care transitions and fewer readmissions. Available at http://www.healthcare.gov/compare/partnership-for-patients/safety/trans…. Accessed August 6, 2012.
-
Terrell KM, Miller DK. Challenges in transitional care between nursing homes and emergency departments. J Am Med Dir Assoc; 2006; 7(8): 499-505.
-
National Transitions of Care Coalition. Improving transitions of care: The vision of the national transitions of care coalition. Washington, DC; 2008.
-
Brown RS, Peikes D, Peterson G, et al. Six features of Medicare coordinated care demonstration programs that cut hospital admissions of high-risk patients. Health Aff; 2012; 31(6): 1156-1166.
-
Bez A. Preventing unnecessary hospitalizations for nursing home residents. Podcast on Internet; 2012.
-
Metzger J. Preventing hospital readmissions: The first test case for continuity of care. Falls Church, VA: Computer Sciences Solutions Global Institute for Emerging Healthcare Practices; 2012; WA12_0155 HCG.
-
Rutherford P. Reducing readmissions -- First, for the patient. Cambridge, MA: Institute for Healthcare Improvement; 2012.
-
Joynt KE, Jha AK. A path forward on Medicare readmissions. N Engl J Med; 2013; 368(13): 1175-1177.
-
Agency for Healthcare Research and Quality. Medication Reconciliation. Available at http://www.psnet.ahrq.gov/primer.aspx?primerID=1. Accessed January 27, 2012.
-
Centers for Medicare and Medicaid Services. Eligible professional meaningful use menu set measures, measure 7 of 10: Medication reconciliation. Available at http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/downloads/7_Medication_Reconciliation.pdf. Accessed August 28, 2013.
-
Frisse ME, Johnson KB, Nian H, et al. The financial impact of health information exchange on emergency department care. J Am Med Inform Assoc; 2012; 19(3): 328-333.
-
Kind A, Jensen L, Barczi S, et al. Low-cost transitional care with nurse managers making mostly phone contact with patients cut rehospitalization at a VA hospital. Health Aff; 2012; 21(12): 2659-2668.
-
Health Information Exchange Roadmap: The landscape and a path forward. ONC Grant #7U24AE000006-02. Washington, DC: National eHealth Collaborative; 2012.
-
Hansen LO, Young RS, Hinami K, et al. Interventions to reduce 30-day rehospitalization: A systematic review. Ann Intern Med; 2011; 155(8): 520-528.
-
Phillips CO, Wright SM, Kern DE, et al. Comprehensive discharge planning with post-discharge support for older patients with congestive heart failure. J Am Med Assoc; 2004; 291(11): 1358-1367.
-
Ouslander JG, Lamb G, Tappen R, et al. Interventions to reduce hospitalizations from nursing homes: Evaluation of the INTERACT II collaborative quality improvement project. J Am Geriatr Soc; 2011; 59(4): 745-753.
-
Coleman EA. The care transitions program. Available at http://www.caretransitions.org/. Accessed August 6, 2012.
-
Boston University. Project RED. Available at http://www.bu.edu/fammed/projectred/presentations.html. Accessed August 6, 2012.
-
Institute for Clinical Systems Improvement, Minnesota Hospital Association and Stratis Health. Reducing avoidable readmissions effectively (RARE). Available at http://www.rarereadmissions.org/resources/collaboratives.html. Accessed November 19, 2012.
-
Boult C, Green AF, Boult LB, et al. Successful models of comprehensive care for older adults with chronic conditions: Evidence for the Institute of Medicine's "retooling for an aging America" report. J Am Geriatr Soc; 2009; 57(12): 2328-2337.
-
Healthcentric Advisors. Safe Transitions Project. Available at http://www.healthcentricadvisors.org/safe-transitions-cp.html. Accessed August 6, 2012.
-
Society of Hospital Medicine. Project BOOST: Better outcomes for older adults through safe transitions. Available athttp://www.hospitalmedicine.org/AM/Template.cfm?Section=Home&CONTENTID=27659&TEMPLATE=/CM/HTMLDisplay.cfm. Accessed August 6, 2012.
-
Centers for Medicare and Medicaid Services. EHR Incentive Programs: Stage 2. Available at http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Stage_2.html. Accessed June 14, 2013.
-
Metzger J. Preparing for accountable care: Coordinated care. Falls Church, VA: Computer Sciences Solutions Global Institute for Emerging Healthcare Practices; 2012; WA12_0280 HCG.
-
eCaring LLC. Preventable readmissions: A prime target for healthcare innovation. Available at http://blog.ecaring.com/preventable-readmissions-a-prime-target-for-healthcare-innovation/. Accessed July 18, 2013.
-
McClellan M, McKethan AN, Lewis JL, et al. A national strategy to put accountable care into practice. Health Aff; 2010; 29(5): 982-990.
-
Pioneer Accountable Care Organization Model: General fact sheet. CMS, Center for Medicare and Medicaid Innovation; 2012.
-
American College of Physicians. What is the patient-centered medical home? Available athttp://www.acponline.org/running_practice/delivery_and_payment_models/pcmh/understanding/what.htm. Accessed August 30, 2013.
-
Centers for Medicare and Medicaid Services. State Demonstrations to Integrate Care for Dual Eligible Individuals. Available athttp://www.cms.gov/Medicare-Medicaid-Coordination/Medicare-and-Medicaid-Coordination/Medicare-Medicaid-Coordination-Office/StateDemonstrationstoIntegrateCareforDualEligibleIndividuals.html. Accessed October 28, 2013.
-
Centers for Medicare and Medicaid Services. Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents. Available at http://www.innovations.cms.gov/initiatives/rahnfr/index.html. Accessed November 20, 2013.
-
Centers for Medicare and Medicaid Services. New program to increase quality in nursing facilities. Available athttp://www.cms.gov/apps/media/press/release.asp?Counter=4454&intNumPerPage=10&checkDate=&checkKey=&srchType=1&numDays=3500&srchOpt=0&srchData=&keywordType=All&chkNewsType=1%2C+2%2C+3%2C+4%2C+5&intPage=&showAll=&pYear=&year=&desc=&cboOrder=date. Accessed November 20, 2012.
-
Centers for Medicare and Medicaid Services. Details for Regulation #CMS -1600-P. Available athttp://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched/PFS-Federal-Regulation-Notices-Items/CMS-1600-P.html. Accessed August 8, 2012.
-
Colorado Foundation for Medical Care. Links/resources/tools for providers -- care transitions improvement efforts. Available athttp://www.cfmc.org/integratingcare/provider_resources.htm. Accessed July 14, 2013.
-
Office of the National Coordinator for Health Information Technology. Meaningful use -- What is meaningful use? Available athttp://www.healthit.gov/policy-researchers-implementers/meaningful-use. Accessed July 14, 2013.
-
Dougherty M, Williams M, Millenson M, et al. EHR payment incentives for providers ineligible for payment incentives and other funding study. Washington, DC: Prepared for Office of Disability, Aging and Long-Term Care Policy, Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services; 2013. Available athttp://aspe.hhs.gov/daltcp/reports/2013/EHRPI.shtml. Accessed July 14, 2013.
-
LTPAC Collaborative, State HIE Toolkit Module: Vulnerable populations and HIE. 2010.
-
Harvell J, Harr M, Hall EP, et al. Implementing health information exchange in the long-term and post-acute care community -- Perspectives for LTPAC providers and their affiliated organizations. Webinar, December 12, 2012.
-
ECRI Institute and s2a. Crossing the connectivity chasm: Pinpointing gaps in readiness to exchange health information. Plymouth Meeting, PA; 2012.
-
Office of the National Coordinator for Health Information Technology. Health IT Policy Committee. Available athttp://www.healthit.gov/policy-researchers-implementers/health-it-policy-committee. Accessed June 13, 2013.
-
Office of the National Coordinator for Health Information Technology. Principles and strategy for accelerating health information exchange (HIE). Washington, DC: Office of the National Coordinator for Health Information Technology; 2013. Healthcare Information Technology Standards Panel. HITSP enabling healthcare interoperability. Available at http://www.hitsp.org/about_hitsp.aspx. Accessed August 6, 2013.
-
Office of the National Coordinator for Health Information Technology. Federal health information technology strategic plan, 2011-2015. Washington, DC: Office of the National Coordinator for Health Information Technology; 2011.
-
Office of the National Coordinator of Health Information Technology. Initial set of standards, implementation specifications, and certification criteria for electronic health record technology. 2010:45 CFR Part 170.
-
LeadingAge Center for Aging Services Technology. EHR for LTPAC: A primer on planning and vendor section. Washington, DC: LeadingAge Center for Aging Services Technology; 2013.
-
Certification Commission for Health Information Technology. CCHIT certified products. Available at https://www.cchit.org/find-cchit. Accessed June 14, 2013.
-
HL7 International. HL7 EHR system long-term care functional profile, release 1 -- U.S. realm. Available athttp://www.hl7.org/implement/standards/product_brief.cfm?product_id=134. Accessed August 28, 2013.
-
Alwan M. Personal communication about LeadingAge members and participation in health information exchange of electronic medical record data. LeadingAge; 2012.
-
Metz K, Russell W. Improving transitions of care in LTPAC: An update from the theme 2 Challenge Grant awardees. Washington, DC: Office of the National Coordinator for Health Information Technology; 2013.
-
Office of the National Coordinator of Health Information Technology. Beacon Community program. Available athttp://www.healthit.gov/policy-researchers-implementers/beacon-community-program. Accessed December 20, 2012.
-
Smith L. "Direct" your attention to Mass Health Information Exchange (HIE). Massachusetts eHealth Institute (MeHI) Newsletter; 2012.
-
See http://www.hhs.gov/ocr/privacy/hipaa/administrative/enforcementrule/hitechenforcementifr.html.
-
CCDA was developed through the joint efforts of HL7, Integrating the Healthcare Environment, the Health Story Project, and the ONC. CCDA is a more robust, implementable standard, and provides a single source for CDA templates for different document types including the discharge summary and CCD documents and is now the exchange standard referenced in MU Stage 2.
3.4. State of Health Information Exchange to Support Care Coordination
The previous section discussed many drivers of HIE to support care coordination for persons receiving LTPAC services. This section describes factors, facilitators, and barriers that impact the ability of LTPAC/LTSS providers to engage in HIE, and discusses the state of electronic HIE for LTPAC/LTSS providers as it relates to assessments, care plans, and other documents to support transitions in care. While there are many drivers to HIE to support care coordination, there are also important barriers to HIE that will be discussed in this section. These barriers impede care coordination and effective transitions of care; retard improvements in the delivery of quality health care; contribute to higher costs for payers and patients, and poor outcomes; and may eventually stymie EPs', EHs', and CAHs' ability to qualify for incentives for the MU of EHRs.1 Key barriers include continued high costs for technology acquisition, lack of awareness and use of emerging technology solutions, inadequate workforce preparation for IT use, ongoing privacy and security concerns related to HIE, and lack of stakeholder awareness of and use of HIE data standards.
Currently, CMS only requires certain LTPAC providers to complete and electronically transmit assessment information for their residents/patients to state databases for billing under the prospective payment system and QI initiatives.71 Historically, LTPAC providers have focused on technologies that support compliance with federal assessment requirements and billing. These federal requirements do not support interoperable use and exchange of this assessment information.
However, some LTPAC providers are realizing the benefits of moving beyond collecting data solely for billing purposes, and adopting technologies such as EHRs/electronic medical records (EMRs) that support patient care. LTPAC providers are slowly transitioning to software programs that not only support caregiving and their administrative data collection needs for Medicare and Medicaid programs, but also can accept information from and share information with other providers.7, 78
1. Dougherty M, Harvell J. Opportunities for engaging long-term and post-acute care providers in health information exchange activities: Exchanging interoperable patient assessment information. Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Office of Disability, Aging and Long-Term Care Policy; 2011. Available
athttp://aspe.hhs.gov/daltcp/reports/2011/StratEng.htm.
7. LTPAC Health IT Collaborative. A roadmap for health IT in long term and post-acute care, 2010-2012. Available athttp://library.ahima.org/xpedio/groups/public/documents/ahima/bok1_047579.pdf. Accessed July 25, 2013.
71. LTPAC Collaborative, State HIE Toolkit Module: Vulnerable populations and HIE. 2010.
78. LeadingAge Center for Aging Services Technology. EHR for LTPAC: A primer on planning and vendor section. Washington, DC: LeadingAge Center for Aging Services Technology; 2013.
3.4.1. EHR Adoption Rates by Setting
Adoption rates often are reported by levels of EHR functionality. It is important to note that definitions of an EHR differ by type of health care setting and are not comparable across many providers/settings.
EHR Adoption Among Office-Based Physicians
EHR adoption rates are reported to be increasing for two important HIE participants for care coordination -- physicians and short-term acute care hospitals. In 2012, 72% of office-based physicians had adopted an EHR system. Forty percent of physicians have adopted a "basic" EHR with certain advanced capabilities, more than double the adoption rate in 2009.85 For 12 of the 15 EHR Incentive Programs' Stage 1 MU core objectives, physicians achieved at least 50% adoption rates.86
EHR Adoption Among Acute Care Hospitals
The trend in adoption of EHR systems by non-federal acute care hospitals has been steadily increasing since 2008. From 2010 to 2012, EHR adoption of a "basic" EHR sharply increased from 19% to 44%.87 Since 2009, hospital adoption of at least basic and comprehensive EHR systems has more than doubled. The percent of hospitals with CEHRTg increased 18% between 2011 and 2012, rising from 72% to 85%. Hospital adoption rates for each of the 14 EHR Incentive Programs MU Stage 1 Core objectives ranged from 72% to 94%.88
EHR Adoption Among LTPAC Providers
The lack of availability, adoption, and use of interoperable EHRs by LTPAC providers is a major barrier to HIE.89 Based on currently available data, which in some cases is dated, adoption of computerized technology varies among LTPAC providers.70, 88
-
In 2010, the National Survey of Residential Care Facilities (NSRCF), which included residential care facilities, assisted living residences, board and care homes, congregate care; enriched housing programs, homes for the aged, personal care homes, and shared housing establishments, found that 17% were using an EHR system, with 3% using a basic EHR system, and that more than half (55%) of these facilities had one or more of six electronic capabilities associated with a basic EHR.90, 91 A more recent NSRCF was conducted in 2012. However, at the time of this report, results were not available.92 The survey does not include SNFs, HHAs, or hospice providers.
-
Approximately four in ten SNFs (43%) had adopted an electronic information system in 2004.93 There are no national or large-scale surveys of nursing home adoption of EHRs, and estimates from other sources including an expert panel varied widely.94
-
Among home health and hospice care providers, 41% had adopted any EHR, and 10% had a basic EHR system in 2007.95
-
Another study found that certain specialty hospitals that are not eligible for MU incentive payments are less likely to adopt EHR systems. The study was based on the 2009 HIT supplement to the American Hospital Association Survey, which included long-term acute care hospitals, rehabilitation hospitals, and psychiatric hospitals. While 12% of short-term acute care hospitals in 2009 had adopted at least a basic EHR system, only 6% of long-term acute care hospitals, 4% of rehabilitation hospitals, and 2% of psychiatric hospitals had adopted an EHR.96
Because definitions of EHRs vary by survey, the LTPAC adoption rates are not comparable with EHR adoption rates reported for EPs/EHs.
TABLE 3-2. Adoption Rate by Selected LTPAC Provider Types
| LTPAC Provider Setting | EHR Adoption Rate* |
|---|---|
| Skilled Nursing Facilities | 43%** |
| Home and Hospice Care Facilities | 41% |
| Residential Care Facilities | 17% |
| Long-Term Acute Care Hospital | 6% |
* EHR adoption rates are measured differently across provider types and comparisons across provider type is not advised.
** Survey question was adoption of "electronic information systems".
-
Dougherty M, Williams M, Millenson M, et al. EHR payment incentives for providers ineligible for payment incentives and other funding study. Washington, DC: Prepared for Office of Disability, Aging and Long-Term Care Policy, Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services; 2013. Available athttp://aspe.hhs.gov/daltcp/reports/2013/EHRPI.shtml. Accessed July 14, 2013.
-
LTPAC Collaborative, State HIE Toolkit Module: Vulnerable populations and HIE. 2010.
-
Harvell J, Harr M, Hall EP, et al. Implementing health information exchange in the long-term and post-acute care community -- Perspectives for LTPAC providers and their affiliated organizations. Webinar, December 12, 2012.
-
ECRI Institute and s2a. Crossing the connectivity chasm: Pinpointing gaps in readiness to exchange health information. Plymouth Meeting, PA; 2012.
-
Office of the National Coordinator for Health Information Technology. Health IT Policy Committee. Available athttp://www.healthit.gov/policy-researchers-implementers/health-it-policy-committee. Accessed June 13, 2013.
-
Office of the National Coordinator for Health Information Technology. Principles and strategy for accelerating health information exchange (HIE). Washington, DC: Office of the National Coordinator for Health Information Technology; 2013. Healthcare Information Technology Standards Panel. HITSP enabling healthcare interoperability. Available at http://www.hitsp.org/about_hitsp.aspx. Accessed August 6, 2013.
-
Office of the National Coordinator for Health Information Technology. Federal health information technology strategic plan, 2011-2015. Washington, DC: Office of the National Coordinator for Health Information Technology; 2011.
-
Office of the National Coordinator of Health Information Technology. Initial set of standards, implementation specifications, and certification criteria for electronic health record technology. 2010:45 CFR Part 170.
-
LeadingAge Center for Aging Services Technology. EHR for LTPAC: A primer on planning and vendor section. Washington, DC: LeadingAge Center for Aging Services Technology; 2013.
-
Certification Commission for Health Information Technology. CCHIT certified products. Available at https://www.cchit.org/find-cchit. Accessed June 14, 2013.
-
HL7 International. HL7 EHR system long-term care functional profile, release 1 -- U.S. realm. Available athttp://www.hl7.org/implement/standards/product_brief.cfm?product_id=134. Accessed August 28, 2013.
-
Alwan M. Personal communication about LeadingAge members and participation in health information exchange of electronic medical record data. LeadingAge; 2012.
-
Metz K, Russell W. Improving transitions of care in LTPAC: An update from the theme 2 Challenge Grant awardees. Washington, DC: Office of the National Coordinator for Health Information Technology; 2013.
-
Office of the National Coordinator of Health Information Technology. Beacon Community program. Available athttp://www.healthit.gov/policy-researchers-implementers/beacon-community-program. Accessed December 20, 2012.
-
Smith L. "Direct" your attention to Mass Health Information Exchange (HIE). Massachusetts eHealth Institute (MeHI) Newsletter; 2012.
-
Hsiao CJ, Hing E. Use and characteristics of electronic health record systems among office-based physician practices: United States, 2001-2012. NCHS Data Brief No. 111. Hyattsville, MD: National Center for Health Statistics; 2012.
-
King J, Patel V, Furukawa M. Physician adoption of electronic health record technology to meet Meaningful Use objectives: 2009-2012. ONC Data Brief, No. 7. Washington, DC: Office of the National Coordinator for Health Information Technology; 2012.
-
Jha AK, DesRoches CM, Kralovec PD, et al. A progress report on electronic health records in US hospitals. Health Aff; 2010; 29(10): 1951-1957.
-
Charles D, King J, Patel V, et al. Adoption of electronic health record systems among U.S. non-federal acute care hospitals: 2008-2012. ONC Data Brief, No. 9. Washington, DC: Office of the National Coordinator for Health Information Technology; 2013.
-
Coleman EA, Bennett RE, Dorr D, et al. Report on health information exchange in post-acute and long-term care. Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Office of Disability, Aging and Long-Term Care Policy; 2007. Available at http://aspe.hhs.gov/daltcp/reports/2007/HIErpt.htm.
-
Decker SL, Jamoom EW, Sisk JE. Physicians in nonprimary care and small practices and those age 55 and older lag in adopting electronic health record systems. Health Aff; 2012; 31(5): 1108-1114.
-
Caffrey C, Park-Lee E. Use of electronic health records in residential care communities. Hyattsville, MD: National Center for Health Statistics; 2013; No. 128.
-
National Center for Health Statistics. National study for long-term care providers, 2011. Available athttp://www.cdc.gov/nchs/data/nsltcp/NSLTCP_FS.pdf. Accessed August 20, 2013.
-
Hsiao CJ, Hing E. Adoption of health information technology among U.S. ambulatory and long-term care providers. National Conference on Health Statistics. Washington, DC: 2012. Available at http://www.cdc.gov/nchs/ppt/nchs2012/SS-03_HSIAO.pdf. Accessed August 20, 2013.
-
Richard A, Kaehny M, May K, et al. Literature review and synthesis: Existing surveys on health information technology, including surveys on health information technology in nursing homes and home health. Washington, DC: Office of the Assistant Secretary for Planning and Evaluation; 2009. Available at http://aspe.hhs.gov/daltcp/reports/2009/hitlitrev.htm#table2.
-
Resnick HE, Alwan M. Use of health information technology in home health and hospice agencies: United States, 2007. J Am Med Inform Assoc; 2010; 17: 389-395.
-
Wolf L, Harvell J, Jha AK. Hospitals ineligible for federal meaningful use incentives have dismally low rates of adoption of electronic health records. Health Aff; 2012; 31(3): 505-513.
g. Certified EHR is EHR technology that has been certified as meeting federal requirements for some or all of the hospital objectives of MU.
3.4.2. Electronic HIE Capability
While there has been a dramatic increase in the number of United States providers using HIT, expanding interoperability remains challenging, and requires further reducing the cost and complexity of electronic HIE, ensuring trust among the key participants of exchange, and encouraging exchange of information, particularly during transitions of care. ONC is playing a central role in enabling each of these key goals.28
The adoption of EHR/EMRs by LTPAC/LTSS providers could increase the likelihood that these providers will participate in electronic HIE and exchange standardized data to support care coordination. As HIE interoperability standards mature and LTPAC/LTSS and other providers adopt more sophisticated and interoperable HIT including EHRs, the potential for exchanging standardized information and ensure safe, high-quality care, will grow.
-
In 2012, of those hospitals that implemented an EHR, approximately 43% can generate a summary care record for transitions.97
-
Many hospitals are participating in HIE. Exchange between non-affiliated organizations and hospitals with different EHR solutions has recently increased. For example, one study found that in 2009 about 11% of hospitals exchanged data with non-affiliated providers through an HIEO in 2009.98 A more recent study based on a national hospital survey, found that in 2012, 58% of hospitals actively exchanged electronic health information with providers and hospitals outside their organization.93 Another study reported that EHR adoption and HIEO participation were associated with significantly greater hospital exchange activity.99
-
Market research suggests there will be significant investment in HIE in the next few years. A 2012 CapSite report found that 71% United States hospitals plan to purchase HIE tools.100
-
The 2011 National Ambulatory Medical Care Survey found that 29.4% of physicians electronically exchanged a patient clinical summary. Of these physicians, 64.2% used an EMR/EHR vendor, 27.5% used hospital-based systems, 19.5% used secure e-mail attachments, 15.1% used other mechanisms or unknown mechanisms, and 4.6% used HIOs or a state exchange. More than one method of exchange could be reported.93
-
In a recent study by the Bipartisan Policy Center, more than 70% of clinicians surveyed identified lack of interoperability, lack of an information exchange infrastructure, and the cost of setting up and maintaining interfaces and exchanges as a major barrier that prevents information exchange.101
-
The 2010 NSRCF found that of those residential care facilities that had implemented an EHR, nearly 25% of residential care facilities could exchange with pharmacies, and 17% could exchange with physicians.91
-
The 2010 NSRCF is the only national survey on EHR adoption and use by LTPAC providers that asks questions regarding HIE, and reports on the percentage of residential care facilities engaged in electronic HIE with the following health care providers or resources: pharmacies (8.2%), physicians (7.4%), corporate offices (5.6%), hospitals (5.4%), SNFs (4.7%), laboratories (4.4%), other health or long-term care providers (3.7%), resident's personal health records (3.4%), public health reporting (2.9%), and one or more specified providers (15.5%).93
HIEOs and LTPAC Provider Participation
The 2012 eHealth Initiative Annual Survey of HIE surveyed national, state, regional, enterprise, and community-based "initiatives" working on HIE. These initiatives are not specified, but included more than just HIEOs or HIOs. The respondents represented 50% of total known HIE initiative programs. Of the 161 HIEs initiatives that responded to the surveys, 26, or 16%, reported receiving LTPAC providers' data.6 It was not possible to identify the specific number or types of LTPAC providers engaged in HIE initiatives from the survey results. The 2013 and future survey results can track the growth in LTPAC participation in HIE initiatives.
A recent study based on a survey of HIEOs found that there were 119 operational HIEOs in 2012, an increase from 75 in 2010. Operational exchange was defined as the exchange of clinical data between independent entities (e.g., hospitals, laboratories, and payers). The study also found that 1,398 hospitals and 23,341 physician practices were using HIEOs for a variety of functions. Of the 119 operational HIEOs, around 25% reported that LTPAC providers participated by sending data, and 41% by receiving data. Test results (82%) and summary of care records (79%) were the most common exchanged information across all participants. Less than 25% of operational HIEs were found to be financially sustainable, and grants accounted for 52% of HIE efforts. The authors concluded that while more HIEOs are operational, business models do not yet support a viable future.102
6. eHealth Initiative. 2012 report on health information exchange: Supporting healthcare reform. Washington, DC: eHealth Initiative; 2012.
28. Office of the National Coordinator for Health Information Technology. Update on the adoption of health information technology and related efforts to facilitate the electronic use and exchange of health information. Washington, DC: Office of the National Coordinator for Health Information Technology; 2013.
-
Decker SL, Jamoom EW, Sisk JE. Physicians in nonprimary care and small practices and those age 55 and older lag in adopting electronic health record systems. Health Aff; 2012; 31(5): 1108-1114.
-
Caffrey C, Park-Lee E. Use of electronic health records in residential care communities. Hyattsville, MD: National Center for Health Statistics; 2013; No. 128.
-
National Center for Health Statistics. National study for long-term care providers, 2011. Available athttp://www.cdc.gov/nchs/data/nsltcp/NSLTCP_FS.pdf. Accessed August 20, 2013.
-
Hsiao CJ, Hing E. Adoption of health information technology among U.S. ambulatory and long-term care providers. National Conference on Health Statistics. Washington, DC: 2012. Available at http://www.cdc.gov/nchs/ppt/nchs2012/SS-03_HSIAO.pdf. Accessed August 20, 2013.
-
Richard A, Kaehny M, May K, et al. Literature review and synthesis: Existing surveys on health information technology, including surveys on health information technology in nursing homes and home health. Washington, DC: Office of the Assistant Secretary for Planning and Evaluation; 2009. Available at http://aspe.hhs.gov/daltcp/reports/2009/hitlitrev.htm#table2.
-
Resnick HE, Alwan M. Use of health information technology in home health and hospice agencies: United States, 2007. J Am Med Inform Assoc; 2010; 17: 389-395.
-
Wolf L, Harvell J, Jha AK. Hospitals ineligible for federal meaningful use incentives have dismally low rates of adoption of electronic health records. Health Aff; 2012; 31(3): 505-513.
-
Desroches CM, Charles D, Furukawa MF, et al. Adoption of electronic health records grows rapidly, but fewer than half of US hospitals had at least a basic system in 2012. Health Aff (Millwood); 2013; 32(8): 1478-1485.
-
Adler-Milstein J, DesRoches C, Jha A. Health information exchange among US hospitals. Am J Manag Care; 2011; 17: 761-768.
-
Furukawa MF, Patel V, Charles D, et al. Hospital electronic health information exchange grew substantially in 2008-12. Health Aff (Millwood); 2013; 32(8): 1346-1354.
-
CapSite. 2012 U.S. Health information exchange study. CapSite; 2012.
-
Bipartisan Policy Center. Clinician perspectives on electronic health information sharing for transitions of care. Washington, DC: Bipartisan Policy Center; 2012.
-
Adler-Milstein J, Bates DW, Jha AK. Operational health information exchanges show substantial growth, but long-term funding remains a concern. Health Aff (Millwood); 2013; 32(8): 1486-1492.
3.4.3. Facilitators and Barriers to Adoption and Use of HIE to Support Care Coordination
Costs and Workforce Preparation
Key barriers to LTPAC provider participation in HIE activities include lack of funding and/or payment incentives (e.g., no HITECH EHR incentive funding for LTPAC providers), and the workforce that is not well-prepared to implement and use HIT systems (e.g., issues include staff shortages, turnover, and lack of IT skills, and training needs).1, 4, 103, 104, 105, 106
LTPAC providers continue to have lower rates of EHR adoption than other settings such as physician practices and hospitals. LTPAC providers vary widely from small, non-affiliated providers to large networks of facilities. Acquiring and implementing EHRs by smaller providers can be disproportionately expensive. In addition, smaller facilities often lack staff resources to develop, implement, and maintain these systems. Even in larger LTPAC facilities, it can be difficult to attract and retain skilled IT workers to support the necessary systems. High staff turnover rates in LTPAC settings contribute to high staff training costs. Given privacy and security issues when exchanging health information across entities, clinical care providers and IT staff must be well trained to protect personal health information. LTPAC/LTSS providers must train their staff to use EHRs, which can be costly and time intensive.
Data Availability and Standardization
The data exchanged by the HIE initiatives surveyed by the 2012 eHealth Initiative study included inpatient data (discharge list, problem list, inpatient medication list and physician notes); outpatient/ambulatory data (clinical summaries, problem list, ambulatory medication list, physician notes and referrals summary of care record); and public health reports. Clinical summaries, discharge list, outpatient problem list, and ambulatory medication list were the top five types of inpatient and outpatient data reported to be exchanged according to the eHealth Initiative study.6
The Massachusetts IMPACT project identified 483 unique data elements as important for transitions in care. The S&I LCC LTPAC Transition Workgroup worked in collaboration with HL7, to include this data in refinements to the CCDA Implementation Guide. These data elements are available from the S&I LCC Framework.107
A technical expert panel convened by the National Quality Forum (NQF) developed a starter set of data elements based on the concept of a person-centered POC, to support coordinated care and performance measurement of the care process. NQF found that although some clinical data could be derived from EHRs, other starter data elements such as care plan steward, medical equipment, social supports, and task completions would have to come from other information systems such as case management, pharmacy, home care and financial systems.108
The need for health information to support care coordination was an important finding from the study site visits, and is discussed more completely in Section 4. One of the sites that was visited in this study had a care transition program that involved LTSS. This site collected and exchanged a wealth of EHR and other information, mostly as unstructured notes, about the patient and family situation and needs (e.g., medical, psychosocial, and financial data). The site visit discussion provides more detailed information on the types of information exchange to support persons receiving LTSS. In addition, much of the data identified as critical for care transitions and care coordination is presently not electronically exchanged. For example, it was observed during the site visits that most HIT/EHR systems lack the capacity to create, transmit, and incorporate interoperable clinical data such as functional and cognitive status and formal and informal caregiver status. In addition, current, complete medication information was often not available to reconcile medications.
Software and Vendor Issues
Some of the HIE interventions noted that using new software and interfaces with EHRs could be problematic, particularly if these products are first to market, as they may not have been completely tested. Software developers reported needing more time to create "out-of-the-box" capabilities such as discharge summaries or workaround solutions. There was also uncertainty surrounding core EMR vendor HIE interfaces and solutions. For example, vendors may not be willing to develop a customized interface, or they are willing but the cost of such interfaces may be high. There may be no vendor who will develop an interface, for example, in the case of a "home grown" technology solution, or in situations where there is no ongoing maintenance contract.
Even with available standards, interfaces are not easy to implement and smooth implementation of HIE is not guaranteed. There may be significant variability in the interpretation of the standards, for example. Standards such as a CCD do not always have the structure and content to reflect the data needed to support transitions and referrals in care to and from LTPAC/LTSS providers.
Stakeholder and Policymaker Engagement
Stakeholder engagement remains a significant barrier to successful data exchange. The eHealth Initiative survey of organizations that are planning, building, or maintaining technology to help health care entities electronically exchange health data (e.g., HIEOs, state entities, medical groups, hospitals, other types of organizations exchanging data) found that a high percent of those surveyed reported a general lack of stakeholder interest in HIE, and difficulty in engaging stakeholders such as health providers, plans, purchasers, laboratories, and hospitals.6
Another significant challenge reported by HIE initiatives is the multiple and competing programs for advancing HIE. States are coordinating numerous initiatives related to health care system transformation and and controlling rising health care costs. As a result, states have largely focused their HIE efforts on providers eligible for the EHR Incentive Programs, leaving fewer resources for ineligible providers, including LTPAC/LTSS providers and facilities.
Accountability and Incentives for HIE Related to Payment Models
Disincentives to care coordination include payment methods and sources across the care continuum which may not encourage information exchange.109 FFS payment methods, still widely used, create little incentive to coordinate and deliver high-quality care. The new payment and service delivery models (e.g., those listed in Section 3.2 such as ACOs, Medicare and Medicaid Shared Savings Programs, and capitated care models) provide incentives to improve care coordination using HIE.
Privacy, Policy, and Security Issues and Compliance
Many information privacy laws were written before the current digital world was conceptualized. The Health Insurance Portability and Accountability Act provides guidance for the exchange of health information. Many states enacted laws more stringent than HIE guidelines. Some states are adapting current laws to update them for the modern context. State laws vary widely, presenting challenges for developing unified policy solutions or solutions that work across states. This variation creates barriers to technology vendors.
Public trust in HIE is critical to ensuring participation, funding, and policymaker support. Policies that permit (or require) consumers to opt-in vs. opt-out of HIE activities is one of the first of many policy decisions the HIEOs need to make. One of the barriers identified in this study was stringent privacy laws and opt-in requirements that impact patient participation. Consumer and provider participation in HIE is higher in states and other areas that have opt-out policies (e.g., Maine) as compared to opt-in policies. Opt-in policies lower the likelihood that patients will be located when their records are queried through an HIEO. Some states such as Maryland, New York, Rhode Island, and Massachusetts have more stringent privacy laws and opt-in policies.
Maryland's HIE policy, for example, currently restricts the disclosure of protected health information through an HIEO for primary use (treatment). This means that LTPAC providers are not able to gather information from the HIEO about potential patients/residents who may be referred to a LTPAC provider upon hospital discharge, without an existing treatment relationship. The state HIE policy does not allow for HIE in this situation.
Maimonides Hospital and the Brooklyn Health Information Exchange (BHIX) experienced patient consent challenges during implementation. Because of state health privacy policies, if a patient has been admitted to Maimonides Hospital and the hospital has not secured consent from that patient, a policy filter built into the BHIX infrastructure will block an alert from going to the patient's physician(s) and the assigned care coordinator. BHIX estimated that alerts could be sent for an estimated 10,000 additional patients if consent is obtained by the various participating sites.24
Almost half of the surveyed HIE initiatives in 2012 reported that stakeholder concerns about privacy and confidentiality were identified as a moderate or substantial challenge to HIE.6
LTPAC/LTSS Engagement and Interest in HIE
Even though the CMS EHR Incentive Program does not include incentive payments to LTPAC/LTSS providers, these providers report looking forward to participating in HIE with their trading partners -- specifically pharmacies, labs, hospitals and physicians. LTPAC/LTSS providers are looking for assistance in navigating the technology and privacy and security requirements that would allow interoperable HIE with these other health care providers.110
3.4.4. Facilitators -- HIE Tools and Resources
A number of public and private sector activities/tools have been developed that support electronic HIE by LTPAC/LTSS providers.
-
The QIO Program provides technical assistance in three states to Medicare SNFs and HHAs to support their participation in electronic HIE activities.111
-
MDS and OASIS assessments can be transformed into an interoperable LTPAC Summary (into CCD format). The tool developed by KeyHIE and described above enables low-cost, interoperable HIE by nursing facilities and HHAs (http://transform.keyhie.org/).112
-
The Direct Project (discussed in Section 3.3.1) supports low-cost, standards-based exchange for sending encrypted and authenticated health information over the Internet.
-
The Massachusetts statewide HIE incorporated the LAND and SEE developed under Massachusetts' Challenge grant to accelerate LTPAC connectivity. SEE will be available to other states either under open source or through a commercial license from Lantana Consulting Group. LAND is adapter software that organizations can use to convert files or interfaces into "Direct" communications which are compatible with the state's HIE, and vice versa.113 (See Appendix A and Section 3.3.1 for more information.)
-
As described in Section 3.3.1 the SBAR identifies a change in resident condition and communicates patient information in a concise and structured format. Kaiser Permanente and SNFs participating in the Oklahoma State HIE program have implemented an electronic version of SBAR.114
-
The Continuum of Care Improvement through Information New York (CCITI NY) (http://www.ccitiny.org) was established to improve the quality, patient safety, and costs of transferring patients between acute, post-acute, and ambulatory care organizations in the greater New York metropolitan region. The CCITI NY project combines an electronic transfer form process with an automated clinical decision support tool. CCITI NY developed a UTF that provides important patient information to clinicians during transfers, including medications, problems and allergies. Key information is provided to care providers in advance of patient arrival. The UTF also contains clinical decision support functionality by providing alerts for harmful drug-drug and drug-allergy interactions. CCITI NY collects patient information by using the infrastructure and clinical messaging capabilities of participating HIEOs and hospitals.
-
Dougherty M, Harvell J. Opportunities for engaging long-term and post-acute care providers in health information exchange activities: Exchanging interoperable patient assessment information. Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Office of Disability, Aging and Long-Term Care Policy; 2011. Available athttp://aspe.hhs.gov/daltcp/reports/2011/StratEng.htm.
-
Affordable Care Act. National pilot program on payment bundling. Public Law 111-148 and Public Law 111-152. 2010: Section 3023.
-
Engquist G, Johnson C, Johnson W. Medicaid funded long-term supports and services: Snapshots of innovation. Center for Health Care Strategies, Inc.; 2010.
-
Woodcock C. Long-term services and supports: Challenges and opportunities for states in difficult budget times. National Governors Association; 2011.
-
National Alliance for Health Information Technology. Report to the Office of National Coordinator for Health Information Technology on defining key health information technology terms. Washington, DC: U.S. Department of Health and Human Services, Office of the National Coordinator of Health IT; 2008.
-
eHealth Initiative. 2012 report on health information exchange: Supporting healthcare reform. Washington, DC: eHealth Initiative; 2012.
-
LTPAC Health IT Collaborative. A roadmap for health IT in long term and post-acute care, 2010-2012. Available athttp://library.ahima.org/xpedio/groups/public/documents/ahima/bok1_047579.pdf. Accessed July 25, 2013.
-
McDonald K, Schultz E, Albin L, et al. Care coordination measures atlas version 3. Rockville, MD: Prepared by Stanford University under Subcontract to Battelle on Contract No. 290-04-0020 for the AHRQ; 2010. AHRQ Publication No. 11-0023-EF.
-
Singer SJ, Burgers J, Friedberg M, et al. Defining and measuring integrated patient care: Promoting the next frontier in health care delivery. Medical Care Research and Review; 2011; 68(1):112-127.
-
Office of the National Coordinator for Health Information Technology policy framework RFTOP. Solicitation No 12-233-SOL-00615; 2012.
-
Informed Medical Decisions Foundation. What is shared decision making? Available at http://informedmedicaldecisions.org/what-is-shared-decision-making/. Accessed January 12, 2013.
-
Gruneir A, Bronskill S, Bell C, et al. Recent health care transitions and emergency department use by chronic long-term care residents: A population-based cohort study. J Am Med Dir Assoc; 2012; 13(3): 202-206.
-
Mor V, Intrator O, Feng Z, et al. The revolving door of rehospitalization from skilled nursing facilities. Health Aff; 2010; 29(1): 57-64.
-
Naylor MD, Kurtzman ET, Pauly MV. Transitions of elders between long-term care and hospitals. Pol. Polit. Nurs. Pract.; 2009; 10(3): 187-194.
-
Boling PA. Care transitions and home health care. Clin in Geriatr Med; 2009; 25(1): 135-148.
-
Bayley KB, Savitz LA, Rodriguez G, et al. Barriers associated with medication information handoffs. In: Henriksen K, Battles JB, Marks ES, et al., editors. Advances in Patient Safety: From Research to Implementation. Rockville, MD; 2005.
-
Chhabra PT, Rattinger GB, Dutcher SK, et al. Medication reconciliation during the transition to and from long-term care settings: A systemic review. Res Soc Admin Pharm; 2012; 8(1): 60.
-
Forster AJ, Murff HJ, Peterson JF, et al. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med; 2003; 138(3): 161-167.
-
Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med; 2009; 360(14): 1418-1428.
-
Thorpe KE. The Medicare advantage experience: Lessons for reform to original Medicare. Atlanta, GA: Emory University Rollins School of Public Health; 2012.
-
Clancy CM. Commentary: Reducing hospital readmissions: Aligning financial and quality incentives. Am J Med Qual; 2012; 27(5): 441-443.
-
Barnsteiner JH. Medication reconciliation: Transfer of medication information across settings-keeping it free from error. J Infus Nurs; 2005; 28(2 Suppl): 31-36.
-
Sentinel events statistics for 2011. Jt Comm Perspect; 2012; 32(5): 5.
-
Office of the National Coordinator for Health Information Technology. Getting to impact: Harnessing health information technology to support improved care coordination. In State HIE Bright Spots Synthesis: Care Coordination Part 1. Washington, DC: ONC; 2012. Available at http://statehieresources.org/wp-content/uploads/2013/01/Bright-Spots-Synthesis_Care-Coordination-Part-1_Final_010913.pdf.
-
Murray LM, Laditka SB. Care Transitions by older adults from nursing homes to hospitals: Implications for long-term care practice, geriatrics education, and research. J Am Med Dir Assoc; 2010; 11(4): 231-238.
-
LaMantia MA, Scheunemann LP, Viera AJ, et al. Interventions to improve transitional care between nursing homes and hospitals: A systemic review. J Am Geriatr Soc; 2010; 58(4): 777-782.
-
Rippen HE, Pan EC, Russell C, et al. Organizational framework for health information technology. Int J Med Inf; 2013; 82(4): e1-e13.
-
Office of the National Coordinator for Health Information Technology. Update on the adoption of health information technology and related efforts to facilitate the electronic use and exchange of health information. Washington, DC: Office of the National Coordinator for Health Information Technology; 2013.
-
Patterson ES, Roth EM, Woods DD, et al. Handoff strategies in settings with high consequences for failure: Lessons for health care operations. Int J for Qual Health Care; 2004; 16(2): 125-132.
-
Gleason K, Brake H. Medications at transitions and clinical handoffs (MATCH) toolkit for medication reconciliation. Rockville, MD: AHRQ; 2012; 11(12)-0059.
-
Siefferman JW, Lin E, Fine JS. Patient safety at handoff in rehabilitation medicine. Phys Med Rehabil Clin N Am; 2012; 23(2): 241-257.
-
Lucian Leape Institute. Order from chaos: Accelerating care integration. Boston, MA; 2012.
-
Kripalani S. Care transitions. In Perspectives on Safety. AHRQ Web M&M; 2013.
-
Allen J, Ottmann G, Roberts G. Multi-professional communication for older people in transitional care: A review of the literature. Int J Older People Nur; 2012; 7(4).
-
Burton R. Improving care transitions. Health Aff and Robert Wood Johnson Foundation; 2012; 10.1377/hpb2012.17.
-
U.S. Department of Health and Human Services. Roadmap to better care transitions and fewer readmissions. Available at http://www.healthcare.gov/compare/partnership-for-patients/safety/trans…. Accessed August 6, 2012.
-
Terrell KM, Miller DK. Challenges in transitional care between nursing homes and emergency departments. J Am Med Dir Assoc; 2006; 7(8): 499-505.
-
National Transitions of Care Coalition. Improving transitions of care: The vision of the national transitions of care coalition. Washington, DC; 2008.
-
Brown RS, Peikes D, Peterson G, et al. Six features of Medicare coordinated care demonstration programs that cut hospital admissions of high-risk patients. Health Aff; 2012; 31(6): 1156-1166.
-
Bez A. Preventing unnecessary hospitalizations for nursing home residents. Podcast on Internet; 2012.
-
Metzger J. Preventing hospital readmissions: The first test case for continuity of care. Falls Church, VA: Computer Sciences Solutions Global Institute for Emerging Healthcare Practices; 2012; WA12_0155 HCG.
-
Rutherford P. Reducing readmissions -- First, for the patient. Cambridge, MA: Institute for Healthcare Improvement; 2012.
-
Joynt KE, Jha AK. A path forward on Medicare readmissions. N Engl J Med; 2013; 368(13): 1175-1177.
-
Agency for Healthcare Research and Quality. Medication Reconciliation. Available at http://www.psnet.ahrq.gov/primer.aspx?primerID=1. Accessed January 27, 2012.
-
Centers for Medicare and Medicaid Services. Eligible professional meaningful use menu set measures, measure 7 of 10: Medication reconciliation. Available at http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/downloads/7_Medication_Reconciliation.pdf. Accessed August 28, 2013.
-
Frisse ME, Johnson KB, Nian H, et al. The financial impact of health information exchange on emergency department care. J Am Med Inform Assoc; 2012; 19(3): 328-333.
-
Kind A, Jensen L, Barczi S, et al. Low-cost transitional care with nurse managers making mostly phone contact with patients cut rehospitalization at a VA hospital. Health Aff; 2012; 21(12): 2659-2668.
-
Health Information Exchange Roadmap: The landscape and a path forward. ONC Grant #7U24AE000006-02. Washington, DC: National eHealth Collaborative; 2012.
-
Hansen LO, Young RS, Hinami K, et al. Interventions to reduce 30-day rehospitalization: A systematic review. Ann Intern Med; 2011; 155(8): 520-528.
-
Phillips CO, Wright SM, Kern DE, et al. Comprehensive discharge planning with post-discharge support for older patients with congestive heart failure. J Am Med Assoc; 2004; 291(11): 1358-1367.
-
Ouslander JG, Lamb G, Tappen R, et al. Interventions to reduce hospitalizations from nursing homes: Evaluation of the INTERACT II collaborative quality improvement project. J Am Geriatr Soc; 2011; 59(4): 745-753.
-
Coleman EA. The care transitions program. Available at http://www.caretransitions.org/. Accessed August 6, 2012.
-
Boston University. Project RED. Available at http://www.bu.edu/fammed/projectred/presentations.html. Accessed August 6, 2012.
-
Institute for Clinical Systems Improvement, Minnesota Hospital Association and Stratis Health. Reducing avoidable readmissions effectively (RARE). Available at http://www.rarereadmissions.org/resources/collaboratives.html. Accessed November 19, 2012.
-
Boult C, Green AF, Boult LB, et al. Successful models of comprehensive care for older adults with chronic conditions: Evidence for the Institute of Medicine's "retooling for an aging America" report. J Am Geriatr Soc; 2009; 57(12): 2328-2337.
-
Healthcentric Advisors. Safe Transitions Project. Available at http://www.healthcentricadvisors.org/safe-transitions-cp.html. Accessed August 6, 2012.
-
Society of Hospital Medicine. Project BOOST: Better outcomes for older adults through safe transitions. Available athttp://www.hospitalmedicine.org/AM/Template.cfm?Section=Home&CONTENTID=27659&TEMPLATE=/CM/HTMLDisplay.cfm. Accessed August 6, 2012.
-
Centers for Medicare and Medicaid Services. EHR Incentive Programs: Stage 2. Available at http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Stage_2.html. Accessed June 14, 2013.
-
Metzger J. Preparing for accountable care: Coordinated care. Falls Church, VA: Computer Sciences Solutions Global Institute for Emerging Healthcare Practices; 2012; WA12_0280 HCG.
-
eCaring LLC. Preventable readmissions: A prime target for healthcare innovation. Available at http://blog.ecaring.com/preventable-readmissions-a-prime-target-for-healthcare-innovation/. Accessed July 18, 2013.
-
McClellan M, McKethan AN, Lewis JL, et al. A national strategy to put accountable care into practice. Health Aff; 2010; 29(5): 982-990.
-
Pioneer Accountable Care Organization Model: General fact sheet. CMS, Center for Medicare and Medicaid Innovation; 2012.
-
American College of Physicians. What is the patient-centered medical home? Available athttp://www.acponline.org/running_practice/delivery_and_payment_models/pcmh/understanding/what.htm. Accessed August 30, 2013.
-
Centers for Medicare and Medicaid Services. State Demonstrations to Integrate Care for Dual Eligible Individuals. Available athttp://www.cms.gov/Medicare-Medicaid-Coordination/Medicare-and-Medicaid-Coordination/Medicare-Medicaid-Coordination-Office/StateDemonstrationstoIntegrateCareforDualEligibleIndividuals.html. Accessed October 28, 2013.
-
Centers for Medicare and Medicaid Services. Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents. Available at http://www.innovations.cms.gov/initiatives/rahnfr/index.html. Accessed November 20, 2013.
-
Centers for Medicare and Medicaid Services. New program to increase quality in nursing facilities. Available athttp://www.cms.gov/apps/media/press/release.asp?Counter=4454&intNumPerPage=10&checkDate=&checkKey=&srchType=1&numDays=3500&srchOpt=0&srchData=&keywordType=All&chkNewsType=1%2C+2%2C+3%2C+4%2C+5&intPage=&showAll=&pYear=&year=&desc=&cboOrder=date. Accessed November 20, 2012.
-
Centers for Medicare and Medicaid Services. Details for Regulation #CMS -1600-P. Available athttp://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched/PFS-Federal-Regulation-Notices-Items/CMS-1600-P.html. Accessed August 8, 2012.
-
Colorado Foundation for Medical Care. Links/resources/tools for providers -- care transitions improvement efforts. Available athttp://www.cfmc.org/integratingcare/provider_resources.htm. Accessed July 14, 2013.
-
Office of the National Coordinator for Health Information Technology. Meaningful use -- What is meaningful use? Available athttp://www.healthit.gov/policy-researchers-implementers/meaningful-use. Accessed July 14, 2013.
-
Dougherty M, Williams M, Millenson M, et al. EHR payment incentives for providers ineligible for payment incentives and other funding study. Washington, DC: Prepared for Office of Disability, Aging and Long-Term Care Policy, Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services; 2013. Available athttp://aspe.hhs.gov/daltcp/reports/2013/EHRPI.shtml. Accessed July 14, 2013.
-
LTPAC Collaborative, State HIE Toolkit Module: Vulnerable populations and HIE. 2010.
-
Harvell J, Harr M, Hall EP, et al. Implementing health information exchange in the long-term and post-acute care community -- Perspectives for LTPAC providers and their affiliated organizations. Webinar, December 12, 2012.
-
ECRI Institute and s2a. Crossing the connectivity chasm: Pinpointing gaps in readiness to exchange health information. Plymouth Meeting, PA; 2012.
-
Office of the National Coordinator for Health Information Technology. Health IT Policy Committee. Available athttp://www.healthit.gov/policy-researchers-implementers/health-it-policy-committee. Accessed June 13, 2013.
-
Office of the National Coordinator for Health Information Technology. Principles and strategy for accelerating health information exchange (HIE). Washington, DC: Office of the National Coordinator for Health Information Technology; 2013. Healthcare Information Technology Standards Panel. HITSP enabling healthcare interoperability. Available at http://www.hitsp.org/about_hitsp.aspx. Accessed August 6, 2013.
-
Office of the National Coordinator for Health Information Technology. Federal health information technology strategic plan, 2011-2015. Washington, DC: Office of the National Coordinator for Health Information Technology; 2011.
-
Office of the National Coordinator of Health Information Technology. Initial set of standards, implementation specifications, and certification criteria for electronic health record technology. 2010:45 CFR Part 170.
-
LeadingAge Center for Aging Services Technology. EHR for LTPAC: A primer on planning and vendor section. Washington, DC: LeadingAge Center for Aging Services Technology; 2013.
-
Certification Commission for Health Information Technology. CCHIT certified products. Available at https://www.cchit.org/find-cchit. Accessed June 14, 2013.
-
HL7 International. HL7 EHR system long-term care functional profile, release 1 -- U.S. realm. Available athttp://www.hl7.org/implement/standards/product_brief.cfm?product_id=134. Accessed August 28, 2013.
-
Alwan M. Personal communication about LeadingAge members and participation in health information exchange of electronic medical record data. LeadingAge; 2012.
-
Metz K, Russell W. Improving transitions of care in LTPAC: An update from the theme 2 Challenge Grant awardees. Washington, DC: Office of the National Coordinator for Health Information Technology; 2013.
-
Office of the National Coordinator of Health Information Technology. Beacon Community program. Available athttp://www.healthit.gov/policy-researchers-implementers/beacon-community-program. Accessed December 20, 2012.
-
Smith L. "Direct" your attention to Mass Health Information Exchange (HIE). Massachusetts eHealth Institute (MeHI) Newsletter; 2012.
-
Hsiao CJ, Hing E. Use and characteristics of electronic health record systems among office-based physician practices: United States, 2001-2012. NCHS Data Brief No. 111. Hyattsville, MD: National Center for Health Statistics; 2012.
-
King J, Patel V, Furukawa M. Physician adoption of electronic health record technology to meet Meaningful Use objectives: 2009-2012. ONC Data Brief, No. 7. Washington, DC: Office of the National Coordinator for Health Information Technology; 2012.
-
Jha AK, DesRoches CM, Kralovec PD, et al. A progress report on electronic health records in US hospitals. Health Aff; 2010; 29(10): 1951-1957.
-
Charles D, King J, Patel V, et al. Adoption of electronic health record systems among U.S. non-federal acute care hospitals: 2008-2012. ONC Data Brief, No. 9. Washington, DC: Office of the National Coordinator for Health Information Technology; 2013.
-
Coleman EA, Bennett RE, Dorr D, et al. Report on health information exchange in post-acute and long-term care. Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Office of Disability, Aging and Long-Term Care Policy; 2007. Available at http://aspe.hhs.gov/daltcp/reports/2007/HIErpt.htm.
-
Decker SL, Jamoom EW, Sisk JE. Physicians in nonprimary care and small practices and those age 55 and older lag in adopting electronic health record systems. Health Aff; 2012; 31(5): 1108-1114.
-
Caffrey C, Park-Lee E. Use of electronic health records in residential care communities. Hyattsville, MD: National Center for Health Statistics; 2013; No. 128.
-
National Center for Health Statistics. National study for long-term care providers, 2011. Available athttp://www.cdc.gov/nchs/data/nsltcp/NSLTCP_FS.pdf. Accessed August 20, 2013.
-
Hsiao CJ, Hing E. Adoption of health information technology among U.S. ambulatory and long-term care providers. National Conference on Health Statistics. Washington, DC: 2012. Available at http://www.cdc.gov/nchs/ppt/nchs2012/SS-03_HSIAO.pdf. Accessed August 20, 2013.
-
Richard A, Kaehny M, May K, et al. Literature review and synthesis: Existing surveys on health information technology, including surveys on health information technology in nursing homes and home health. Washington, DC: Office of the Assistant Secretary for Planning and Evaluation; 2009. Available at http://aspe.hhs.gov/daltcp/reports/2009/hitlitrev.htm#table2.
-
Resnick HE, Alwan M. Use of health information technology in home health and hospice agencies: United States, 2007. J Am Med Inform Assoc; 2010; 17: 389-395.
-
Wolf L, Harvell J, Jha AK. Hospitals ineligible for federal meaningful use incentives have dismally low rates of adoption of electronic health records. Health Aff; 2012; 31(3): 505-513.
-
Desroches CM, Charles D, Furukawa MF, et al. Adoption of electronic health records grows rapidly, but fewer than half of US hospitals had at least a basic system in 2012. Health Aff (Millwood); 2013; 32(8): 1478-1485.
-
Adler-Milstein J, DesRoches C, Jha A. Health information exchange among US hospitals. Am J Manag Care; 2011; 17: 761-768.
-
Furukawa MF, Patel V, Charles D, et al. Hospital electronic health information exchange grew substantially in 2008-12. Health Aff (Millwood); 2013; 32(8): 1346-1354.
-
CapSite. 2012 U.S. Health information exchange study. CapSite; 2012.
-
Bipartisan Policy Center. Clinician perspectives on electronic health information sharing for transitions of care. Washington, DC: Bipartisan Policy Center; 2012.
-
Adler-Milstein J, Bates DW, Jha AK. Operational health information exchanges show substantial growth, but long-term funding remains a concern. Health Aff (Millwood); 2013; 32(8): 1486-1492.
-
Cagel JG, Rokoske FS, Durham D, et al. Use of electronic documentation for quality improvement in hospice. Am J of Med Qual; 2012; 27(4): 282.
-
Oakes SL, Gillespie SM, Ye Y, et al. Transitional care of the long-term care patient. Clin Geriatr Med; 2011; 27(2): 259-271.
-
Office of the National Coordinator for Health Information Technology. Health IT in long-term and post-acute care. Washington, DC: ONC; 2013.
-
Cherry B, Carter M, Owen D, et al. Factors affecting electronic health record adoption in long-term care facilities. J Healthc Qual; 2008; 30(2): 37-47.
-
S&I Framework. IMPACT transfer of care dataset 20OCT2012. Available at http://wiki.siframework.org/LCC+Long-Term+Post-Acute+Care+(LTPAC)+Transition+SWG. Accessed July 15, 2013.
-
National Quality Forum. Critical paths for creating data platforms: Care coordination. Washington, DC: National Quality Forum; 2012.
-
Folkemer D. Telephone discussion. 2013.
-
Arizona Strategic Enterprise Technology Office. Arizona health information exchange environmental scan: Long-term care. CFDA #93.719. Phoenix, AZ: Arizona Strategic Enterprise Technology; 2012.
-
Centers for Medicare and Medicaid Services. Current work -- what are QIOs doing? Available at http://www.cms.gov/Medicare/Quality-Initiaves-Patient-Assessment-Instru…. Accessed August 28, 2013.
-
Caradigm. Low-cost health IT connectivity for skilled nursing facilities enables clinicians to provide better, more coordinated patient care. Available at http://www.caradigm.com/pages/en-us/press/2012-08-09-data-share-nursing…. Accessed December 2012.
-
Garber L. Massachusetts Technology Park Corporation: Improving long-term and post-acute care transitions. Washington, DC: Office of the National Coordinator for Health IT, State Health Information Exchange Challenge Program; 2012.
-
SaferHealthCare. What is SBAR and what is SBAR communication? Available at http://www.saferhealthcare.com/sbar/what-is-sbar. Accessed December 2012.
3.5. Process, Outcome, and Cost Measures and Metrics to Assess Health Information Exchange Interventions on Care Coordination
This section describes measures of care coordination which may reflect HIE, the conceptual frameworks on which they are based, if applicable, as well as other measures of process, outcomes and costs that may capture the impact of HIE on care coordination. Some of the most common measures to monitor the impact of the HIE interventions on care coordination to support LTPAC are discussed. One of the conclusions from this study is that care transitions and coordination are broadly defined, and measuring the impact of HIE on these care coordination functions is complicated and nascent. More work is needed to define and validate measures that reflect HIE on care transitions and coordination, for both electronic and other means of information exchange.
3.5.1. Care Coordination Measures
This section describes several frameworks that are useful in identifying potential measures of HIE on care transitions and care coordination.
AHRQ Care Coordination Measures
The AHRQ Care Coordination Measures Atlas provides a framework for care coordination measures, and consists of domains that are important to care coordination, informed by a number of care coordination sources.h AHRQ's framework starts with the goal of achieving coordinated care, defined as the means to help achieve care goals by meeting patient needs and preferences, and facilitating delivery of high-quality, high-value care.8 The framework identifies various actions that have been hypothesized or demonstrated to facilitate care coordination and improve the delivery of health care. These actions can guide the selection of relevant measures for HIE interventions that support care transitions and coordination, and can be employed in an improvised or systematic way.
The measures do not gauge the endpoints of care coordination; rather they capture the care coordination processes and activities that may impact those endpoints. Many, but not all of the measures are applicable to HIE in LTPAC/LTSS settings. An example of a care coordination measure relevant to HIE is the percent of patients discharged from an inpatient facility who receive a transition record at discharge, and documentation that all of the specified elements were reviewed with the patient. (See http://www.qualitymeasures.ahrq.gov/content.aspx?id=28140 for information on the care coordination measures rationale and definitions.)
National Quality Forum's Measure Application Partnership
The NQF convened the Measure Application Partnership (MAP), which developed "Measures under Consideration by HHS for 2012 Rulemaking''. These measures include "PostAcute Care/Long-Term Care Performance Measurement Programs".115 The MAP analyzed the quality measurements and the gaps in measurements for LTPAC including shared accountability for care coordination through transitions, functional status, advanced care planning, and mental/behavioral health as they apply to providers and health plans integrating with community organizations. The MAP identified performance measurement for areas with the most opportunity to improve the quality of health care, and examples of core measure concepts are provided in Table 3-3.
TABLE 3-3. LTPAC Highest-Leverage Areas for Performance Improvement and Core Measure Concepts from MAP
| Highest-Leverage Areas for Performance Measurement |
Core Measure Concepts |
|---|---|
| Function |
|
| Goal Attainment |
|
| Patient Engagement |
|
| Care Coordination |
|
| Safety |
|
| Cost/Access |
|
CMS ACO Measures
The ACO measures may serve as another potential source of potential measures related to care coordination, particularly if the HIE intervention is part of the health care delivery under an ACO. The ACO care coordination and patient safety areas being measured are as follows:
- Risk standardized all condition readmissions;
- Ambulatory-sensitive conditions admissions: chronic obstructive pulmonary disease (COPD) or asthma in older adults, heart failure;
- EHR Incentive Programs reporting;
- Medication reconciliation; and
- Falls: screening for future fall risk.
In addition, see the Pioneer ACO measures in Appendix K.
Endpoints of Care Coordination
"Endpoints of care" is another approach to measuring care and reflect the Institute of Medicine goals for quality of care -- safety, timeliness, effectiveness, efficiency, equity, and patient-centeredness.8 Endpoints of care coordination relevant to HIE include rates of ED visits and transfers; hospital admissions/readmissions; disease-specific hospital admissions; mortality and disease; short-term clinical outcomes (e.g., glycated hemoglobin levels for patients with diabetes); functional status (e.g., for telehealth patients); quality of life; and treatment/service adherence.8 The case study sites use endpoints as measures of care coordination supported by HIE.
8. McDonald K, Schultz E, Albin L, et al. Care coordination measures atlas version 3. Rockville, MD: Prepared by Stanford University under Subcontract to Battelle on Contract No. 290-04-0020 for the AHRQ; 2010. AHRQ Publication No. 11-0023-EF.
115. National Quality Forum. MAP pre-rulemaking report: 2013 recommendations on measures under consideration by HHS, final report. ISBN 978-1-933875-47-7. Washington, DC: National Quality Forum; 2013.
h. These include: (1) Antonelli RC, McAllister JW, Popp J. Making care coordination a critical component of the pediatric health system: A multidisciplinary framework. New York, NY: The Commonwealth Fund. May 2009. Publication No. 1277. (2) The CMS Definition of Case Management; (3) Coeira E. Guide to health informatics. 2nd ed. London, England: Hodder Arnold, a member of the Hodder Headline Group; 2003; (4) Mathematica Policy Research Report -- Coordinating care for Medicare beneficiaries: Early experiences of 15 demonstration programs, their patients, and providers: Report to Congress. Princeton, NJ: Mathematica Policy Research, Inc.; May 2004; and (5) NQF -- Endorsed definition and framework for measuring care coordination. Washington, DC: National Quality Forum; 2006.
3.5.2. HIE Impact Measures
The literature review for this study specifically examined the evidence around the impact of electronic HIE. A summary of the literature review is provided in Appendix F. No studies of the impact of HIE in LTPAC/LTSS settings were identified. Further, the evidence of HIE impact remains sparse. Among the measures used to evaluate HIE, health care utilization is the most widely used (e.g., hospital admissions, rates of laboratory tests).116 Only one of the three randomized controlled studies included in this review identified positive HIE outcomes, which was significant cost savings in ED charges per visit at one of the two hospitals involved.117 Moreover, in three studies, HIE use was associated with greater health care services utilization.46, 118, 119
The lack of results supporting HIE to improve cost and clinical outcomes such as quality of care and safety is not surprising due to the nascency of HIE, methodological challenges in assessing outcomes (e.g., sufficient volume of use, complex study designs, short study intervention periods, need for control groups). The studies aggregated costs and other utilization measures, and results may be confounded by factors such as differences in illness severity in the study groups.
Kern et al. developed a framework and with advice of a national expert panel, searched the literature to identify functionalities enabled by EHRs and HIE across three health care settings (ambulatory, inpatient, and ED). Each of 233 functionality-setting combinations were rated on their likelihood of having a positive financial effect; top-scoring functionalities were validated with the expert panel. The most highly rated HIE functionalities driving financial value included sending and receiving imaging and laboratory reports and allergy history, authorizations for procedures; receiving discharge medication lists from ED and inpatient settings; and enabling structured medication reconciliation.120
46. Frisse ME, Johnson KB, Nian H, et al. The financial impact of health information exchange on emergency department care. J Am Med Inform Assoc; 2012; 19(3): 328-333.
-
Hincapie AL, Warholak TL, Murcko AC, et al. Physicians' opinions of a health information exchange. J Am Med Inform Assoc; 2011; 18(1): 60-65.
-
Overhage JM, Dexter PR, Perkins SM, et al. A randomized, controlled trial of clinical information shared from another institution. Ann Emerg Med; 2002; 39(1): 14-23.
-
Vest JR. Health information exchange and healthcare utilization. J Med Syst; 2009; 33(3): 223-231.
-
Vest JR, Jasperson J. What should we measure? Conceptualizing usage in health information exchange. J Am Med Inform Assoc; 2010; 17(3): 302-307.
-
Kern LM, Wilcox A, Shapiro J, et al. Which components of health information technology will drive financial value? Am J Manag Care; 2012; 18(8): 438-445.
3.5.3. Care Transition and Coordination Measures Used by Identified HIE Interventions
Most the identified HIE interventions identified, including the sites visited measure the impact of the care transitions and coordination interventions. Not all of the measures may be directly attributable to the exchange of information nor were they reported to be so. It was also not possible from the environmental scan to separate measures used for electronic HIE interventions from non-electronic HIE, with the exception of a measure of whether transitions of care were accompanied by electronic care of summary. For both electronic and non-electronic HIE, the most common measures reported were the rates of ED visits and walk-in care, and hospital admissions and/or hospital readmissions. Three interventions reported that they monitored discharge disposition and two interventions measured length of hospital stay as a measure of their success. Other areas measured for the HIE interventions were impact on duplication of services; unnecessary tests and treatments; medication reconciliation completion rates; transmission of transition record after discharge; transmission of information within 2 hours of discharge; pending test results followed up after discharge; fall rates; changes in rates of urgent care, if patient self-management of medications goals were met; rates of ADEs; functional outcome measures; customer satisfaction; and efficiency, speed and satisfaction with the transition of care process.
3.6. Health Information Exchange Interventions Identified for Study
This section describes and characterizes the use of HIE to support care coordination for persons receiving LTPAC/LTSS services based on the literature review, environmental scan, key informants, and site visits. Selected HIE interventions and activities to support care coordination are described, guided by the frameworks, including the entities involved (affiliated, non-affiliated, and patients/family members/caregivers) and type of data exchanged, the use of an EHR and any electronic tools to support HIE, interoperability standards, user interfaces, and workflow. Information that LTPAC/LTSS providers have that other providers may find useful is highlighted.
3.6.1. HIE Interventions Identified for Study
HIE "interventions" or activities were identified that support transitions and information for persons receiving LTPAC/LTSS care and described in Appendix G. The interventions described in this section were not confirmed or updated by informants, other than for the three case study sites. The interventions were categorized by: (1) individual LTPAC/LTSS providers; (2) groups of LTPAC/LTSS providers that were part of a national corporation or chain; (3) HIEOs such as regional health information organizations and community HIEOs that support HIE for multiple participating LTPAC/LTSS providers and their exchange partners; and (4) health care provider networks with HIE. There is overlap among these four categories. For example, a HIEO may be helping LTPAC providers participate in HIE, and within that state, a participating LTPAC provider that was actively engaged in HIE may also be identified as another intervention.
HIE interventions that included electronic HIE with LTPAC/LTSS providers were identified in 22 states. This likely does not include all of the states with electronic HIE to support care coordination for persons receiving LTPAC/LTSS services. The type of LTPAC/LTSS provider participating in the intervention is also noted. The most frequent LTPAC/ LTSS provider type reported to be engaged in exchange is HHA, followed by SNFs. Four of the interventions involve senior housing, two with continuing care retirement communities, one with a LTCH, and three with HCBS or other LTSS, including one AAA.
The next section describes some of the more common HIE interventions to support care coordination for persons receiving LTPAC/LTSS services, including the context for HIE, users and workflow, key exchange partners, technology, standards and data. Selected examples are provided. More in-depth information, observations, and insights from the three site visits are discussed in Section 4, and in the individual site visit summaries in Appendix H, Appendix I and Appendix J.
3.6.2. HIE to Support Care Transitions
This section describes some of the uses of HIE supporting care transitions with LTPAC/LTSS providers, specifically: (1) transfers from an LTPAC/LTSS to a hospital; and (2) transfers from a hospital to an LTPAC/LTSS provider. Interventions varied in how HIE was used to support care transitions. This section provides examples of the technology, workflow, data exchanges, and users.
Transition from LTPAC/LTSS to Hospitals (ED, Acute Care, Psychiatric)
Electronic HIE
Electronic exchange from LTPAC/LTSS to ED and hospitals was commonly implemented using directed, peer-to-peer, and query-based technology, with variations across providers.
Peer-to-Peer Exchange
For the small number of LTPAC/LTSS providers that have an EHR, a custom interface sent ADT data using secure HL7 version 2 messaging standards, usually using Direct. ADT messages are sent for specific types of events or use cases, such as inpatient admission. ADT messages typically include key information such as medications, lab test results, demographics, allergies, problems, diagnoses, discharge summaries, vital signs, and clinical notes. The ADT event updates are sent from the HIEO to specific providers through secure messaging, perhaps using a Virtual Provider network connection (e.g., Beechwood Homes, Western New York through HIN, and Cedar Living Nursing Home, Oklahoma through SMRTNET.
Direct exchange is being used to support a variety LTPAC HIE activities such as exchanging CCDs (e.g., CORHIO), sending ADT messages to hospitals supplemented with data from INTERACT and care paths with decision support (i.e., Oklahoma SMRTNET).
-
When a patient is admitted to the ED, the SBAR content is electronically sent to ED staff, and alerts ED doctors if more information is available in the HIEO about the patient (e.g., Golden Living Nursing Home through Indiana HIE).
-
The HIEO may send alerts to specific care providers such as the patient's primary care provider for events such as hospital admission or discharge.
-
More advanced functionality reported by a small number of interventions were real-time alerts upon hospital admission, sent to primary care physicians, mental health providers, and HHA staff.
Query-Based Exchange
Hospital ED admission staff can query for LTPAC patient information via a HIEO upon admission, and retrieve patient information, typically in a CCD format, and distribute to clinical staff.
-
At least one hospital automatically prints the CCD and other information and adds it to the patient chart (Indiana HIE).
-
The HIEO may send alerts to specific care providers such as the patient's primary care provider.
-
Hospital staff at some hospitals can access patient exchange information at the HIEO and import into their hospital EHR (e.g., Norman Regional Hospital, Oklahoma SMRTNET), which was reported to greatly increase physician use of the information.
Non-Electronic HIE
Before electronic HIE was available, information exchange predominately occurred by paper and/or via fax, photocopying, mailing, and telephone calls. Most LTPAC/LTSS sites reported faxing additional information that could not be sent electronically to hospitals, HHAs, and other providers.
At one site, when the SNF sends patients to the hospital, typically through the ED, the SNF also send a packet of information in hard-copy (e.g., demographics, diagnosis, medication list, labs, history and physical [H&P]). However, the SNF found that this information is not accompanying the patient to the medical unit where they are admitted. Another challenge is locating the patient in the hospital and ensuring that the hospital staff know that the patient was admitted from a SNF.
Data Sent from LTPAC Providers at Transitions
The following types of data were found to be transmitted by LTPAC providers at times of transitions in care: INTERACT information (including SBAR), transfer form, face sheet, most recent H&P, recent hospital discharge summary, nurse's progress notes; orders related to acute condition, current medication list or administration record, advance directive, care limiting orders, relevant lab results, relevant x-ray reports, immunization records, and physical therapy notes.
Less frequently sent data from LTPAC providers at transitions included patient assessments including functional and cognitive status (e.g., from MDS, OASIS), wound care and other images, fall and other risks were also sent but less frequently.
HIE Recipients/Users at Hospitals
The types of hospital staff that most often reported to be users of the information sent by LTPAC providers included: hospital admission clerks, ED and hospital clinicians, emergency medical technicians, hospital social workers, and case and care managers. Patient's primary care providers and specialists were also identified as recipients of the information provided by LTPAC providers.
Transition from Hospital to LTPAC/LTSS
This section describes HIE from hospitals to the receiving LTPAC/LTSS provider. The flow of HIE from hospitals to LTPAC/LTSS providers was more common than the reverse direction.
Electronic HIE
Peer-to-Peer Exchange
Point-to-point exchange from the hospital to the LTPAC/LTSS sites using Direct or other means was not commonly reported. One of the case study sites, Rush University Medical Center, does send secure e-mail using their e-referral software to LTPAC/LTSS providers.
Query-Based
To prepare for the return of the patient, the LTPAC/LTSS sites typically are provided with access to web-based portals to query hospital information while the patient is hospitalized. When the patient's name is entered into the portal, data can be accessed from hospitals and other providers. The information is typically available via a community or virtual health repository.
-
Depending on the interface available through the EHR or an HIEO, SNF staff can view and use the hospital information in different ways. At least one site reported that they can view all records for the patient, or select only those from a particular facility. A sidebar provides a menu of types of information from which an authorized provider can choose (e.g., lab results, admission and discharge summaries, radiology notes, and a summary information sheet).
-
Often other data were available from outpatient providers, laboratories, and other LTPAC/LTSS providers.
-
Because this is a portal, information needs to be retrieved and repurposed rather than accessed directly from the LTPAC/LTSS's EHR system.
- Some HIEOs offer sophisticated applications to access and use the HIE information in data repositories.
- PatientCare360 used by CORHIO has the ability to create, view, and print a CCD into a Summarization of Episode Note.
Non-Electronic HIE
There are many examples of non-electronic exchange of information when patients transition from a hospital to a SNF or home care (e.g., using fax and sending hard-copy documents).
-
Some SNFs and post-acute providers report using clinical liaisons (e.g., intake or admission nurses) to gather information and assess patients in the hospital prior to being transferred to the SNF or a rehabilitation center (e.g., Beechwood Homes, Chicago Rush University Medical Center referral SNF).
-
Rush University Medical Center, was working with their EHR vendor to develop standard reports that would be sent to their referral sources (e.g., LTPAC/LTSS providers), but not via electronic HIE as the Rush EHR does not have the capability to generate this standardized report.
-
Hospital discharge planners more often send hard-copy and fax discharge orders to LTPAC/LTSS providers.
HIE Recipients/Users at LTPAC
The LTPAC users of the information sent by hospitals include charge nurses, directors of nursing, care transfer coordinators, wellness nurses, physicians, and pharmacists.
Data Sent to LTPAC at Transitions
The following types of data may be transmitted by hospitals to LTPAC providers at times of transitions in care: updated hospital information; transfer form; medications; nurses notes; H&P; diagnoses; operative report and other relevant clinical data (e.g., functional status, therapy, skilled nursing services, and the hospital discharge summary).
Information that is less frequently sent from hospitals to LTPAC providers included nutrition, fall risk, physical inactivity rates, ADL, instrumental ADL (IADL), fall history, and self-management information collected in relation to conditions such as COPD, heart disease, diabetes, and asthma. In addition, one HIE intervention involved the hospital sending wound care images to the home care provider.
HIE Impact and Care Coordination Measures Used
Many of the identified HIE interventions reported efforts to measure the impact of their care transitions interventions. The most common measure was related to hospital readmission rates. Other measures reflecting care transitions were the rates of ED visits and hospital admissions. Three interventions reported that they monitored discharge disposition and two interventions measured length of hospital stay.
3.6.3. HIE to Support Eligibility and Authorizations
HIE is also being used to send information to the state Medicaid program for eligibility determinations. Currently, all 98 nursing facilities in Utah use the HIEO, Utah Health Information Network (UHIN), to send an electronic request to obtain preauthorization for Medicaid coverage. This exchange provides a low-cost mechanism to securely send electronic documentation to the state to determine whether individuals meet Medicaid eligibility requirements. This exchange helps ensure timely service delivery and accurate information between the SNF and the Utah Medicaid program. An electronic preauthorization form is sent through secure e-mail, with attachments such as the scanned MDS, physical, and history; and eliminates copying and faxing, which the state no longer allows. The application prepopulates the form with provider information, as well as patient information such as name, birth date, and Medicaid number through state databases. The application requires diagnoses and includes a look up function for the ICD-9 diagnosis codes. UHIN is piloting this program with the HHAs.
4. Synthesis of Findings From Case Studies of Health Information Exchange to SUPPORT CARE Coordination for Persons Receiving LTPAC/LTSS
During the literature review and key informant interviews, potential sites were identified for in-depth analysis of HIE activities. Site visits were conducted with three strategically identified providers engaged in HIE to support care coordination for persons receiving LTPAC/LTSS. The purpose of the site visits was to evaluate the information exchange practices for persons receiving LTPAC and/or LTSS related to transitions of care, shared care and other administrative purposes. HIE practices were evaluated regardless of format (telephone, fax, e-mail, exchange network), however, special interest was paid to the current status of electronic exchange including the policy drivers, barriers preventing its use and opportunities for expansion.
The sites provided a snapshot of exchange processes from different types of LTPAC and LTSS providers in different geographic regions: (1) Chicago's Rush University Medical Center's Bridge Model Care Transition Program, which improves care transitions through a patient-centered approach that engages a multidisciplinary health care team through intensive care coordination to help older adults safely transition back to the community that includes LTSS; (2) Beechwood Nursing Home, 272-bed SNF in Western New York, and one of the first LTPAC providers to participate in HIE through a regional HIEO; and (3) EMHC, part of EMHS, an integrated health care delivery system, which is exchanging information with affiliated and non-affiliated partners.
Observation protocols and interview guides guided the site visits. Interviews were conducted with LTPAC provider staff and stakeholders, including clinicians, QA/performance improvement staff, IT staff, administration, referral sources, and HIE network administrators. Key HIE exchange partners were contacted during the site visit including acute care providers who exchange important information during care transitions. The site visits provided rich case studies of best practices and lessons learned around HIE to support care coordination.
Each site visit was two days in length. A summary report was developed for each site that provides the following information: (1) background information on the site; (2) a description of the community HIEO; (3) a summary of grants, other policy initiatives and stakeholders that either supported the advancements in HIE or were key partners; (4) an overview of the site's EHR and HIT systems and development plans related to HIE; (5) findings from discussions on the workflow processes that required HIE; (6) a summary of HIE processes; and (7) identification of barriers and opportunities. Summaries of the site visits are included in Appendix H, Appendix I and Appendix J.
This section synthesizes findings and lessons from the site visits and implications for expanding HIE to support care coordination for persons receiving LTPAC services. The findings are organized as follows:
- Site Visit Summaries and Key Characteristics:
- Rush University Medical Center Transitional Care;
- Beechwood Homes; and
- EMHC.
- Synthesis of HIE findings from the Site Visits:
- HIE at transitions of care, shared care, and other administrative types of HIE;
- Summary of electronic HIE;
- Summary of LTPAC data that could be prioritized for electronic HIE;
- Use of HIT standards by the sites to support HIE; and
- Overall findings, challenges and opportunities to advance HIE.
4.1. Summary of Site Visits
HIE has been a long-standing practice between LTPAC and other health care providers both at transitions of care and in support of shared care. The sites evaluated expressed the importance of timely, complete and accurate information for improved care coordination programs including integration of community services. Currently they use many ways to communicate and/or share information such as face-to-face, telephone, fax/e-fax, e-mail, secure messaging, access to hospital EHR systems and use of a community HIEO. Two of the three sites (Beechwood Homes and EMHC) were participating in HIEOs.
The sites visited identified drivers that helped to advance more efficient, electronic HIE to support new processes, models of care and payment. Specifically, new initiatives resulting from the Affordable Care Act and other government programs were identified as providing either the impetus or funding to improve care coordination and/or some HIT infrastructure improvements. Two sites evaluated (Rush and EMHC which are IDSs) have multiple care manager programs such as hospital discharge planners, primary care managers and community care teams (CCTs). Both sites have care managers supporting coordination of post-hospital care including LTSS community services. They also hold regular care team meetings across multiple provider sites to improve communication, coordination, and care planning.
Summary findings from the three site visits are described below and include an overview of each site, identification of the policy drivers for improved HIE practices, an overview of the HIE and EHR tools used, and a summary of the exchange activities. Detailed site visit summaries are included in Appendix H, Appendix I, and Appendix J.
4.1.1. Rush University Medical Center, Transition of Care Programs
Background
Rush University Medical Center (Rush) is part of the Rush System for Health, an IDS with hospitals and ambulatory care practices. Rush is an urban hospital located in downtown Chicago, Illinois with multiple programs focused on improving care transitions including improving transitions with SNFs and HHAs, and programs focused on reducing hospital readmissions and care coordination with community-based services.
A key components of Rush's Facility Transitions in Care and Bridge Programs is coordination with community-based LTSS. Through a patient-centered approach, Rush works to improve care transitions through intensive care coordination that starts in the hospital and continues into the community. The multidisciplinary health care team is extended beyond the hospital's physicians, nurses, pharmacists, and case managers to include the community resource team (therapists and community providers such as home health, SNFs, and other services). The team identifies and addresses the services and resources needed by the patient and works to eliminate barriers that will prevent them from safely transitioning back to the community and meeting their health care goals.
Grants, Policy Drivers and Other Funding Models Advancing HIE
The transition of care programs at Rush have focused on Medicare beneficiaries only. However, Rush has emerging programs that will extend their transition programs to adults of all ages who have chronic conditions. Rush has worked to improve the care transition process for more than 5 years. More recently, two programs -- the CMS Hospital Readmission Reduction Program and CMS CCTP have spurred initiatives to improve processes, communication and information sharing between the hospital and community partners.
- CMS Hospital Readmission Reduction Programs: In response to the CMS program, Rush implemented the Readmission Reduction Project RED Pilot to reduce the number of readmissions and maintain an overall readmission rate of less than 12.3%. At the time of the site visit in April 2013, they had identified interventions and started their pilot project. Interventions related to LTPAC to reduce hospital readmissions include improved coordination and communication prior to hospital discharge (such as participation of LTPAC providers in discharge planning rounds), better access to hospital EHR data to facilitate transitions, and development of post-discharge protocols. Protocols or processes developed include:
- A home care nurse visit within 24 hours after discharge (same day if possible).
- A physician visit to the SNF within 48 hours after discharge.
- Social work followup with community services within 24-48 hours to ensure services were started.
-
CMS CCTP (3026 Program): Rush is a partner in the Illinois Transitional Care Consortium (ITCC) which is currently participating in the CMS funded CCTP.
The ITCC is deploying the Bridge Program to help manage community-based care transitions. With this program Medicare beneficiaries who have at least one chronic condition requiring followup care and are at risk for rehospitalization are assigned a Bridge care coordinator (BCC). Upon discharge from the hospital, the BCC assists the patient with engaging community services and resources for a 30-day period. Figure 4-1depicts the providers and services targeted for coordination. The BCCs frequently access, share, and exchange health information to coordinate community services to assess the patient's needs, communicate with care managers, and coordinate community services.
FIGURE 4-1. Bridge Program Systems Targeted for Coordination

At the time of the site visit, Rush was not involved in any of the new payment models (such as an ACO or bundled payment), however they are exploring future accountable care arrangements.
Community HIE Organization
The State of Illinois is developing a federated model for their HIEO using a record locator service that will reach out to regions and bundle and route information. The Chicago-area region does not currently have an operational HIEO to facilitate automated, electronic exchange of information. However, Rush staff indicated one is under development with an organizational structure in place and software selected.
Summary of EHR and HIT Systems and Development Plans Related to HIE
Rush University Medical System uses the EPIC EHR system for all patient care documentation in the hospital and ambulatory care sites. EPIC has achieved MU Stage 2 certification for its ambulatory and inpatient applications.i
HIE from hospital to LTPAC/LTSS providers relies on multiple methods to communicate and exchange information including telephone, fax/e-fax, secure e-mail, and the use a proprietary electronic referral application (e.g., Allscripts Care Management application). Some Chicago-area hospitals allow LTPAC providers to access their EHR to facilitate communication and information sharing; however, Rush's policy limits EHR access to only staff and physicians and does not allow access to non-affiliated providers such as LTPAC and LTSS providers.
The Allscripts Care Management application facilitates the electronic exchange of some health information (e.g., unstructured narrative messages as well as medical record document attachments) between Rush and their community partners including LTPAC organizations. The community partners who pay a subscription fee and use the Allscripts application can receive messages and attachments from Rush and pull some of the information into their EHR.
Health Information Routinely Exchanged
Clinical, demographic and service information is communicated by hospital case managers and care coordinators to community providers such as HHAs, SNFs, and/or HCBS providers. They use a number of methods to communicate and share information including face-to-face, telephone, fax/e-fax, e-mail, secure messaging, and Allscripts care management application. The lack of HIE tools and an HIEO are a challenge for Rush and their partners. Rush's exchange of health information with LTPAC providers and other community partners typically occurs during the transition of care and followup process. Section 4.2 in this report and Appendix K provide additional information on information routinely exchanged.
4.1.2. Beechwood Homes, Getzville, New York
Background
Beechwood Continuing Care is a non-profit, long-term care community in the greater Buffalo, Western New York area. The community comprises independent living, assisted living, and rehabilitative/SNF services. The site visit conducted as part of this study focused on Beechwood Homes (Beechwood), a 272-bed nursing and rehabilitation facility with specialty units in early dementia, hospice, and rehabilitation. Its specialty rehabilitation unit, Wesley Rehabilitation Center, is designed specifically for residents with intensive, short-term rehabilitation or complex medical needs. Beechwood has embraced a patient-centered quality of life focus and is undergoing a transformation to a household environment rather than nursing units.
To deliver short and long-term care to its residents, Beechwood coordinates care and services with a number of health care professionals and community partners including physicians, local hospitals, ancillary services providers including pharmacies, labs and radiology, health plans, and other LTPAC providers. Beechwood has begun participating in the Western New York regional HIEO, HEALTHeLINK, which is advancing electronic information exchange capabilities in the area.
Grants, Policy Drivers and Other Funding Models Advancing HIE
Beechwood's payer mix is primarily Medicaid, Medicare, and Medicare managed care. They also have a limited percentage of private pay and insurance in their payer mix. Beechwood is not participating in any of the emerging payment models that could potentially advance HIE capabilities; however, the Western New York Beacon Community did provide grant funding for the interface costs to connect Beechwood to the regional HIEO. Both the Beacon grant and hospital readmission reduction initiatives helped to spearhead a focus on HIE practices including ways to improve practices and information sharing between the hospital and community partners.
-
Reducing Hospital Admissions/Readmissions. Although the CMS Hospital Readmission Reduction Program applies to hospitals, Beechwood continuously monitors their readmission rates and clinical processes to reduce unnecessary hospital transfers. Beechwood uses the INTERACTII program to assess and manage residents' change in condition. Standardized INTERACT protocols include checklists and documentation used by Beechwood to support communication between the attending physician and the receiving hospital should transfer to the hospital be warranted.
- ONC Beacon Grants. Beechwood was selected as one of five LTPAC partners in the Western New York Beacon Community. The Western New York Beacon Community's efforts are focused on improving clinical outcomes and patient safety through HIT and HIE. The Beacon grant supported the interface costs to connect the LTPAC vendors to the regional HIEO to send ADT alerts for a resident. In addition to Beechwood's hospital-SNF transfer initiative described above, the Western New York Beacon Community has identified four long-term care use case priorities for 2013:
- Lab and radiology results delivery from lab and radiology providers to Beechwood's EHR through HIE (currently in process).
- Care planning and regulatory requirements after admission acceptance including current data available, data/forms needed, responsible parties, and training needs (currently in process).
- Access to data needed for admission criteria including trigger mechanisms, data available/needed, responsible parties and training (completed).
- Patient preference notification (future consideration).
Community HIE Organization
As noted above, Beechwood participates in HEALTHeLINK the regional Western New York HIEO. There are more than 2,900 providersj participating in the HIEO with 35 of those providersk submitting clinical data. The data available includes: ADT alerts, radiology reports, radiology images, labs, transcribed reports (such as an H&P, discharge summary, operative report), ED reports, medication history data, and diabetic measures. HEALTHeLINK obtains its medication history from SureScriptsl and recently began receiving medication data from Buffalo Pharmacies (which is Beechwood's long-term care pharmacy). Buffalo Pharmacies is sending data on Beechwood residents including the resident name, drug name and strength, directions for use, quantity dispensed, date dispensed, and the prescriber.
Health care providers including Beechwood access patient information on HEALTHeLINK using the Virtual Health Record (VHR) portal. Any provider in the region who has signed a participation agreement and has Internet access can use the VHR. Providers may choose to get results delivered from HEALTHeLINK. Currently, Beechwood sends ADT alerts and is working on an interface to have lab and radiology reports delivered through HEALTHeLINK directly to their EHR system.
Summary of EHR and HIT systems and Development Plans Related to HIE
Beechwood has an EHR system, Answers on Demand (AOD), to support the clinical, billing, and administrative operations of their organization. AOD has been certified as an EHR module under the ONC Certification Program for MU Stage 1 program.m Consistent with Stage 1 certification, the AOD systems have the capability to create, export, and import a patient summary record (using the HL7 C32 CCD standard). However, at this time, Beechwood does not use this functionality due to workflow issues.
Beechwood has electronic, secure access to area hospital EHR systems (or a special shared drive) to support the information gathering and communication process at transition from the hospital. They also access patient health information electronically through HEALTHeLINK's VHR. The information accessed from the HIEO is used to support the admission assessment and care planning processes such as past medical history and recent hospital reports including the discharge summary. As noted above, Beechwood only sends ADT alerts to the HIEO and is working on receiving lab and radiology report results using a standard interface to their EHR. Beechwood does not send information electronically to hospitals and other community providers.
Beechwood developed a physician portal to their EHR to streamline sending their resident's health information to the physician for signature. Physicians log into the AOD system to access records that require their review and signature. Physicians can also review the resident's medical record and write progress notes and orders (e.g., medication, treatment, others). In 2013, Beechwood plans to automate physician order communication with the pharmacy by entering physician orders into the AOD system which are then transmitted to the pharmacy order entry system.
Health Information Routinely Exchanged
Beechwood regularly exchanges information with non-affiliated community health care partners including local hospitals, physician practices, labs, pharmacies, radiology/imaging, SNFs, HHAs, and hospice providers. They use many ways to communicate and share information such as face-to-face, telephone, fax/e-fax, e-mail, mail. In addition they use secure messaging, access to hospital EHR systems, and use of a community HIEO. Health information is communicated and shared at transitions of care and continuously during a resident's stay. Section 4.2in this report and Appendix K provide additional information on the information routinely exchanged.
-
Epic MU Stage 2 Certification Details: http://www.epic.com/software-certification.php.
-
Health care professionals include physicians, nurse practitioners, physician assistants, chiropractors, nurses, pharmacists, and dentists.
-
Health care providers include hospitals, regional reference labs, regional radiology, telemonitoring sources (home health), long-term care facilities, and medication history sources.
-
SureScripts is a company that operates the nation's largest electronic e-prescribing network, linking pharmacies and healthcare providers to make the prescribing process safer and more efficient.
-
See http://www.aodsoftware.com/content/news/aod-softwares-answers-ehr-recei….
4.1.3. Maine HomeCare, Bangor, Maine
Background
EMHC is the home care and hospice division of the EMHS. The health system is an IDS with hospitals, ambulatory care practices, LTPAC providers (home health, hospice, SNFs, and assisted living) and ancillary services. The home care division includes three agencies and seven offices serving both urban and rural areas covering two-thirds of Maine. EMHC also provides telehealth services to patients in the health system and has been successful in reducing hospital admissions and ED visits.
EMHS is both an innovator and a leader in health care having received grants to test new models of care and payment, and industry awards and recognitions. HIT has been a key factor in supporting their innovative practices and a strategy to manage health care for a population that covers a large urban and rural geography. The State of Maine has an operational statewide HIEO, called HealthInfoNet (HIN). Both the EMHS and EMHC participate in HIN.
Grants, Policy Drivers and Other Funding Models Advancing HIE
Medicare is the primary payer for both the Eastern Maine HHAs and hospice providers (approximately 75% of their payer mix collectively). Medicaid, private insurance and self-pay make up the remainder of the EMHC payer mix. The EMHS has received grants and other funding to test new models of care and payment specifically through improved care coordination and case management including community services. The grants have supported a number of programs and HIT enhancements to facilitate communication and coordination.
As described below, EMHS participates in several grants, new payment models and policy initiatives that have driven improvements in the HIT infrastructure supporting communication and care coordination across providers and services:
-
CMS Hospital Readmission Reduction Programs. The EMHS focuses on reducing hospital readmissions not only to comply with the CMS program requirements, but also as a way to improve quality of care and reduce costs. To reduce hospital readmissions, the hospital and LTPAC providers are improving coordination and communication prior to discharge; access was improved to hospital EHR data to facilitate transitions; case management/care coordination meetings are occurring across health care settings and with community service providers, and the telehealth is used to monitor the clinical status of targeted high-risk populations.
-
ONC Beacon Grants. EMHS received an ONC Beacon Community grants funded by the ONC to build and strengthen local HIT infrastructure and test innovative approaches to make measurable improvements in health, care and costs.
The Bangor Beacon Community's grant helped to support a HIT infrastructure used for testing new accountable care and payment models and manage patient populations. The goals of the Bangor Beacon Community grant were to use HIT effectively to improve the health of people with select chronic diseases, reduce costs associated with hospital admissions and ED visits, reduce variations in care, and improve population health related to immunizations and sharing immunization data.n
The Beacon grant supported the acquisition of a single EHR application across the multiple home care agencies in the EMHC division, which improved information access and sharing. The grant also supported the acquisition of new telehealth equipment to expand the program and its use for monitoring the target population. It also supported expansion of the Maine HIEO, HIN, to include submission of selected home care data to the exchange (ADT alerts and the home care POC).
-
U.S. Department of Agriculture (USDA) Grant to Expand Telehealth. One of EMHC's agencies in rural Maine received a $50,000 federal grant from the USDA's Rural Utilities Service to expand its telehealth program with matching funds. The agency was able to purchase an additional 28 telehealth units.
-
New Care and Payment Model Programs to Advance Care Coordination and Reduce Costs. EMHS is currently participating in two programs to test the development of new care delivery and payment models to improve care coordination and reduce costs.
-
Pioneer ACO:
EMHS was selected as one of 32 ACOs under this Center for Medicare and Medicaid Innovation (CMMI) initiative. Under this 3-year arrangement with CMS, the EMHS ACO shares Medicare savings in year 1 and moves to a capitated rate per beneficiary in years 2 and 3 if they meet the following reporting and/or performance requirement:
- 1st Performance Year. Report 33 measures to share in up to 50% or 60% (depending on their model) of Medicare shavings.
- 2nd Performance Year. Report eight measures and be paid for performance on 25 measures.
- 3rd Performance Year. Paid for performance on 32 measures and paid for reporting on one survey measure related to functional status.
The 33 quality measures used to assess performance have been endorsed by the NQF and are reported across all 32 Pioneer ACOs. Appendix L provides a detailed list of these measures, along with the NQF measure identifier and corresponding data submission requirement. The primary domains for the 33 measures are patient/caregiver experience, care coordination/patient safety, preventive health, and at-risk populations.
EMHS developed its HIT infrastructure over time. The HIT infrastructure provides the ability to manage the health for their population. This includes initiatives to use the same EHR applications across its HHAs, expand Maine's HIEO, and expand home care's use of telehealth. Care coordination initiatives have also been implemented to manage the population's health and reduce costs. The care coordination initiatives include: use of primary care managers through the PCMH, and CCTs to help engage appropriate HCBS for patients in need; and implementing regular care coordination meetings across the sites of care including LTPAC and LTSS.
-
PCMHs:
In addition to being a Pioneer ACO, EMHS also participates in two PCMH projects. The State of Maine established 22 PCMH projects and CMS demonstration project for Multi-Payer Advanced Primary Care Practice.
The PCMHs are reimbursed by three types of payers: Medicare, MaineCare, the state Medicaid Program, and commercial insurers. Medicare and MaineCare pay $7 per member per month for care management in the medical home and $3 per member per month for community-based care management. Maine is projecting it will achieve budget-neutrality by decreasing patient inpatient admissions by 6%-7%, decreasing ED visits by 5%, and decreasing specialty consultations and imaging by 5%.
In EMHS's PCMH, a patient care manager is embedded in the primary care clinic to work directly with individuals and their care team to develop a personalized POC. They partner with applicable care providers and care coordination teams across settings such as inpatient care managers, cardiology care managers, mental health care managers, home care and home health service and palliative care to manage risk, costs and transitions. The personalized POC includes individualized services, custom plans based on patient needs, co-management goals, and self-management plans. The patient care managers also perform outreach to other services and providers such as community-based services and LTPAC providers. Accessing updated electronic information and ADT alerts through the HIEO, sharing information with health care providers and coordinating community-based services are all crucial to the coordination of care efforts of the PCMH.
-
Community HIE Organization
Maine has a statewide HIEO known as HIN, an independent, non-profit organization that was established as the state's HIE in 2006. HIN has been operational exchanging clinical data since June 2009. In 2010, Maine received grants from several sources to expand the technology infrastructure including a state HIE Collaborative grant, an ONC Regional Extension Center (REC) grant (HIN is the REC), and the Beacon Community grant.
All 38 of Maine's acute care hospitals are under contract to connect to the HIEO. HIN has connected 34 of the 38 hospitals, 376 ambulatory provider sites including primary and specialty care practices, all/some FQHCs, 12 mental health agencies, two HHAs (both are part of IDSs) and two long-term care providers. The information available on HIN includes patient demographics, medications, medication history, allergies, lab and test results, vital signs, image reports, transcribed reports, problem lists, and ADT alerts.
EMHC participates in HIN by sending electronic ADT alerts and home care plans of care, and accessing electronic information to support start of care, assessment and care planning activities. A future project is planned to transmit the home health lab results to HIN and medication information from Miller Pharmacy which provides medications to EMHS's SNFs.
Summary of EHR and HIT Systems and Development Plans Related to HIE
EMHS has multiple software applications supporting their operations. The EMHC division does not use the same EHR application as the health system hospitals and physician practices. The hospitals and physicians use the Cerner EHR application. The home care division uses the McKesson Horizon Homecare application. Cerner has an application known as PowerChart that supports organizations with multiple entities. PowerChart provides quick access and viewing of the most frequently used and/or clinically relevant information.
EMHC currently uses Phillips Healthcare Telehealth Solutions as their telehealth vendor. The telehealth tools include in-home devices (a base unit and the measurement device) and a cloud-based software application.o The telehealth data collected includes clinical data, questionnaire responses, and risk screen results. EMHC is currently working on an interface to bring the telehealth data into the agency's EHR system.
EMHC is in the process of developing a physician portal to the HHA's EHR to streamline the process of sending their patient's health information to the physician for signature. Physicians will log into the McKesson EHR system to access the records that require review and signature. Once implemented, physicians will have the capability to review other patient medical record information and write progress notes and orders (medication, treatment or other types).
Health Information Routinely Exchanged
As an IDS, EMHS maintains an IT network that allows affiliated providers to access information in different EHR systems and through PowerChart. EMHC also exchanges information with non-affiliated partners including hospitals, physician practices, community service providers, and other LTPAC providers primarily through telephone, e-fax, and secure e-mail. HIN provides another source of information on patients which is particularly useful for background information at the start of care/assessment process. Health information is routinely be communicated and shared at transition of care process and continuously during a patient's stay. Section 4.2.1 in this report and Appendix J provide additional information on the information routinely exchanged.
n. See http://www.healthit.gov/policy-researchers-implementers/bangor-beacon-community.
o. See http://www.healthcare.philips.com/goto/telemonitoring.
4.2. Synthesis of Health Information Exchange Findings from Site Visits
The exchange of health information is a critical function in the delivery of care to patients in LTPAC organizations. All three site visits identified multiple clinical and administrative processes requiring the exchange of information. LTPAC providers and their partners use many different methods to exchange information -- face-to-face communication, telephone, fax, e-mail, access to EHR systems, and HIEOs.
A number of findings are consistent across the three site visit locations:
-
LTPAC organizations are beginning to use electronic HIE, but in a very limited way.
-
Communication and sharing of information occurs in multiple ways to support transitions and shared care. Increasing the use of electronic HIE methods will improve the timeliness and efficiency of communication, although it cannot completely replace face-to-face and telephone communication between health care providers.
-
While HIEOs have some content that is useful for background information for admission, assessment, and care planning purposes, LTPAC providers require detailed medical record data prior to admission including narrative progress notes, assessments, and current medications that reflect changes. Access to the hospital EHR system often provides more timely and detailed information than what is currently available from HIEOs (as observed at two sites) to support the transfer of care process.
-
The two sites that are IDSs have community care coordination programs to achieve improved health outcomes for specific target populations, and focus on reductions in ED use and hospital readmissions, as well as the costs of care. Community care coordinators and teams work with HCBS providers, with communication primarily by telephone and fax. There may be opportunities for improved efficiency through the use of HIEOs by and other electronic communication with home and community-based providers; however, these types of providers are not currently participants of the HIEOs.
-
Some HIT messaging standards are embedded in LTPAC EHR systems and sometimes used to connect these providers with HIEOs. Further, the interoperability standards in Stage 2 of the EHR Incentive Programs (which will support more robust HIE for transitions in care or shared care with LTPAC/LTSS providers) are not yet used. Many of the standards required through the EHR Incentive Programs could be used to support HIE with and by LTPAC providers, but integration and use of these standards into LTPAC EHR products often requires additional investment of time, financial resources, and organizational awareness. Some standards are still early in their maturity level requiring a significant level of effort to implement.
A synthesis of the HIE findings from the three sites is summarized below using the framework developed for this project. The synthesis describes exchange activities to support transition of care, shared care, and other administrative functions from the perspective of the LTPAC organization. An expanded analysis of 35 identified information exchange workflows is detailed in Appendix K.
4.2.1. Health Information Exchange for Transition of Care
Health information is shared and exchanged to support a number of care processes as a patient transitions between care providers. The type of data shared to support transitions in care and the methods of exchange are summarized below. During transitions, information is typically exchanged face-to-face, by telephone, fax, and on some occasions, electronically.
-
Referral and Preadmission Assessment. The information typically exchanged during referral and for preadmission assessments includes patient demographics, problems/diagnoses, medications, allergies, treatment orders, activity level, diet, isolation precautions, labs, progress notes (e.g., 3 days of narrative notes), recent H&P, operative reports and pertinent assessments/evaluations including cognitive and functional status. The referral and preadmission assessment information is exchanged using multiple methods -- face-to-face meetings potentially including participation in hospital discharge planning rounds, telephone, fax, access to the hospital EHR (depending on hospital policy) and if available access to community HIEOs.
-
Referral for Community Services. The community care coordinators obtain information on patient goals and care plan information, patient demographics, problems/diagnoses, medications, allergies, treatment orders, progress notes, recent history, and physical and pertinent assessments/evaluations such as a cognitive status exam and functional status assessments. Setting up community services requires the exchange of information unique to the service provider. Typical information includes demographic and payer information, services requested, and when relevant, clinical information such as diagnosis and medications.
If the community care coordinator is an employee of the IDS, they access that information from the EHR system (hospital or physician practice) and communicate that information with the HCBS provider, typically by telephone, fax, and sometimes e-mail. If the community care coordinator is not an employee (e.g., they provide community care coordination through an AAA/Aging and Disability Resource Center (ADRC)), they have additional challenges in obtaining the necessary information from the hospital discharge planners by telephone or fax and relaying the information to HCBS providers by telephone, fax, and e-mail at times. In the Rush CCTP funded by CMS (discussed in the Rush Site Visit report in Appendix H), some of the BCCs are employees of organizations like the AAA and ADRC and are able to make special arrangements to access the hospital EHR to obtain necessary information on the patient.
-
Transfer/Admission to LTPAC. The transferring provider (often an acute care hospital) sends a comprehensive set of updated health information at the point of transfer. The information may include an order for discharge to the LTPAC provider, a transfer summary, medication orders, updated medication administration records, treatment orders, key lab results, discharge summary, recent progress notes, special nursing care instructions (e.g., ostomy, wound, catheter care, dressings, IV), fall risk assessments, rehab/restorative progress and treatment plans, infection control/safety precautions, equipment and supplies needed, advanced directives and/or limited treatment orders and followup care contact information. The transferring provider usually communicates this information via paper documents, telephone, and fax. For hospital transfers, some information may be accessed by the LTPAC provider directly from the hospital EHR prior to admission when security measures and protocols have been established between the organizations.
-
Transfer to Hospital or Another Health Care Provider from LTPAC. The LTPAC provider sends a comprehensive set of updated information at the point of transfer with the patient when they go to the hospital or to another health care setting. This information typically includes a transfer summary (which includes diagnosis/problems, medication orders, treatment orders, allergies, vital signs, functional and cognitive assessment data), pertinent recent labs, recent narrative progress notes, copies of current medication administration records, and advanced directive/do not resuscitate (DNR) orders. SNFs may send the items identified in the INTERACTII protocols when sending the patient to the hospital (e.g., transfer form, SBAR/nurses notes, recent physician orders and current medications, advanced directives). When sending to another LTPAC organization, they may also send the latest MDS or OASIS data set. This information is typically sent in paper format.
-
Discharge Information from LTPAC Provider to Patient and Community Service Provider. When patients are discharged from LTPAC they are provided with a detailed discharge POC and instructions including information on discharge medications, self-care instructions, and followup care. As part of the discharge planning process, the LTPAC provider may also assist the patient with identifying and setting up community-based services to support a successful transition. In these circumstances, the discharging LTPAC provider typically communicates this information via telephone, fax, and sometimes e-mail to the community-based service provider.
-
ADT Event Reporting to HIEOs. The two sites that participated in an HIEO electronically transmitted and received ADT events via an electronic interface with the HIE. The events reported included the patient identifier, the event (admission or discharge/transfer), date, and time. HIEOs use the ADT event reports to monitor changes and alert other treatment providers to a change in status.
4.2.2. Health Information Exchange for Shared Care
LTPAC providers frequently coordinate and share care with other health care and service providers. When sharing care, there are related HIE processes to support assessment, care planning, and ongoing monitoring. A summary of HIE activities to support shared care is described below along with the type of data shared. During instances of shared care, information is typically exchanged by telephone, fax/e-fax, or electronically such as via secure e-mail, use of HIEOs, or customized portals/data entry processes when available.
-
Assess Needs and Goals. There are multiple processes related to assessing needs and goals at the start of care that require HIE.
-
Initial assessment and development of admission care plan (such as at times of hospital discharge): To complete the assessment and initial care plan development, nurses, therapists and other interdisciplinary team members require recent hospital information and past medical history information to evaluate the patient. Information needed includes the hospital discharge summary, recent H&P, operative report, recent labs, summary of care records, past assessments, social history, and advanced directives. Typically, LTPAC receives the information needed to help complete the initial assessment and develop the admission POC via paper copies sent with the patient or via fax or telephone. In some cases, LTPAC providers electronically access the hospital EHR (if protocols have been established) and/or the HIEO. Medical record information needed, but not exchanged by the hospital or available from the HIEO must be requested from the hospital (e.g., discharge summary not sent at transfer) and is typically received via mail.
-
Coordination with physician at start of care: The admission transfer summary, physician orders, medications, treatment orders, therapy evaluation, and home care POC content are all reviewed and signed by the physician. For a SNF patient, the physician completes a face-to-face visit, documents a progress note, and reviews and signs the POC and physician orders. Two sites were implementing customized physician portals to the LTPAC EHR to streamline information exchange. The physician logs into the LTPAC EHR portal to access and review patient information and sign their orders. When an HIEO was available with medication history information, it could be accessed electronically to help with the admission medication reconciliation process, although not a guaranteed source of complete medication history information.
-
Communication with pharmacy, lab, and other service providers: The LTPAC provider communicates physician admission orders to the pharmacy, lab and/or other service providers as appropriate. Data exchanged includes demographic and payer information and the detailed orders for medications or services. Typically this is done via telephone, fax or custom web-based portal set up by the pharmacy or lab/radiology service provider. Results received from lab and radiology providers were sent via fax, dedicated printer to LTPAC, or available on the provider's web portal. One HIEO, HIN, was establishing an interface to route results from the lab/radiology provider through the HIE to the SNF's EHR using HL7 results reporting message standards.
-
-
Create, Maintain, Update, and Implement Care Plan. After initial assessment, a care plan is established and maintained over time. The care plan is typically developed by the interdisciplinary team and communicated to the attending physician and the patient/family initially and with updates. The physician may review the POC during routine patient visits to a SNF. In home care, the care plan updates are communicated via the home care POC document. Care plan information and updates are communicated to the family in person, via telephone or through a narrative summary mailed to the representative.
-
Monitor, Followup and Respond to Change. LTPAC providers monitor the ongoing care needs of patients, respond to changes in the patient's condition and followup on care and services required. HIE is required to support multiple care processes.
-
Transmission of telehealth data: Patient's transmit telehealth data from their device and base station in their home to a cloud-based application. The telehealth nurse in home care accesses clinical data including blood pressure, weight, blood sugar, pulse, oxygen saturations, and responses to individualized questions. Home care nurses monitor the telehealth data on the cloud-based telehealth system. The data was not available in the home care EHR (although an interface was being developed at one site). The use of telehealth in an SNF was not observed during the site visits. EMHS had a telepsychiatry pilot program that could not be maintained due to reimbursement issues.
-
Ongoing communication and coordination with physicians: LTPAC providers update the physician with status changes. Information exchanged includes test results, requests for new or revised orders, telephone orders, physician order renewals, home care POC recertification, and physician visit progress notes. These types of updates occur by telephone, fax, and/or secure e-mail. Two sites established physician portals to their LTPAC EHRs to facilitate the review and signature process.
-
Order changes for medications, labs, and radiology tests: When the LTPAC provider communicates change in patient status, the LTPAC provider may obtain from the physician a new order or an order to change a medication (or another intervention). The LTPAC provider typically receives these order changes verbally from the physician via telephone. The physician signs the telephone orders in person, sent via mail, or through the physician portal to the LTPAC EHR.
For SNFs, there is also a communication process in which medication and other order changes are sent to the long-term care pharmacy. The pharmacy receives the physician order information from the SNF, often via telephone or fax. The pharmacy verifies the medication prescription with the ordering physician. The long-term care pharmacy enters the order in the pharmacy's electronic medication order system and dispenses the medications to the SNF.
New or changed orders for labs and radiology tests are communicated via telephone, fax, or through a custom web portal as a requisition to the appropriate ancillary service provider by the LTPAC provider. In home care, the nurse may draw the lab. In a SNF, a facility nurse or lab technician draws the lab or gathers the specimen. Results are returned from the lab and radiology provider to the LTPAC provider often by fax or dedicated printers or custom web portal. In Western New York, the HIEO was in the process of developing and implementing an electronic results delivery process to route results from the lab/radiology service providers through the HIEO to the LTPAC EHR.
-
-
Change of Status and Updates with Patient and Family. When there is a change in status, the patient and/or their family is notified by the LTPAC provider of the change and related care/treatment plans. This is frequently communicated in person, by telephone or e-mail based on preference.
-
Specialist Visits, Evaluations, and Referrals. LTPAC providers may identify and schedule visits with specialists (cardiologist, audiologist, psychologist, etc.) or set up a referral for community services to support the patient in their home. Information is exchanged to set up the service including demographic, payer, and service requirements. When applicable, progress notes or visit summary records are shared with the LTPAC provider.
4.2.3. Other Administrative Health Information Exchange
LTPAC providers exchange health information in support of administrative processes such as billing and required reporting.
-
Quality Measure Reporting. LTAPC sites are collecting and/or submitting quality measure data to support grants and initiatives. EMHS Pioneer ACO is required to report 33 quality or performance measures electronically to CMS (see Appendix L for detailed measures). The data is collected through various mechanisms depending on the data elements -- through the EHR or abstracted from medical records and reported through a defined facility process.
CMS also requires electronic submission of federally mandated data or item sets (MDS, OASIS, inpatient rehabilitation facility-patient assessment instrument [IRF-PAI], Hospice Item Sets,p LTCH Care Data Setq). The CMS electronic transmission requirements for assessments do not leverage available HIT standards. CMS uses assessment data for several purposes including calculating quality measures.
-
Mandatory Reporting. Public health authorities and state agencies may maintain registries or repositories for reportable public health data. The type of data to report varies by community and state. For example, immunization data or influenza and pneumonia data may be reportable information to public health agencies to detect outbreaks. Some states, such as New York, have customized electronic web portals to enter and submit reportable data.
-
Payment. LTPAC providers may exchange electronic health information with payers to support their case management and claims adjudication processes. Payers may request, in electronic formats, relevant medical record documentation to assess continued coverage, validate services billed, or determine medical necessity. Requested documentation may include physician orders, certification/recertifications, progress notes, flow sheets, medication and treatment administration records, assessments, and other relevant data determined by the payer.
4.3. Summary of Electronic Health Information Exchange
Among the site visits (even in the most advanced) the information that is electronically available for exchange is limited and incomplete. LTPAC providers use multiple methods to share and exchange information frequently relying on mail, fax and secure e-mail when data and documents are required to move from one provider to another. While the current state reflects these traditional forms of communication, trends emerged across all three sites where technology supported electronic information exchange.
-
EHR Access and Other Tools. Some hospitals recognize the need of LTPAC providers and social worker/community care coordinators to have access to patient information in the hospital EHR both at preadmission and after admission. They have established agreements and secure protocols to either provide direct access to the hospital EHR or provide electronic data/documents on a dedicated network drive. One organization (Rush) uses a proprietary care management referral application that allows the secure, electronic exchange of unstructured notes and attachments to share information between providers who were subscribers of the service. Users of that application report it is helpful in sharing basic information; however, it does not provide two-way communication and is not as complete as access to the hospital EHR to support the preadmission and transfer or care process.
-
Physician Portals to LTPAC EHR. Two of the sites (Beechwood and EMHC) developed physician portals to their respective EHR applications to streamline the exchange process with the attending physician. In both cases, the physician can log into the SNF or HHA EHR system and access their patient's information to review and sign (e.g., telephone orders, POC, etc.).
-
HIE Organizations. Two of the sites (Beechwood and EMHC) have active HIEOs in their community. While the LTPAC providers can access their patient's information from the HIEO, there is very limited inclusion of LTPAC data on the exchange. LTPAC providers at both sites send and receive electronic ADT event notifications via an HL7 message standard. EMHC transmits to the HIEOs the home care POC via the HL7 results message standard, but the POC content is not standardized. Beechwood is developing an interface using the HL7 results message standard to receive electronic lab results from the lab through the HIEO to their EHR.
The type of information commonly available from the HIEOs includes: ADT events, problem list, prescription/medication history, allergy information, lab and other test results, vital signs, transcribed reports (e.g., hospital H&P and discharge summary), and visit summary records. While this information is useful in understanding the patient's history to support the assessment and care planning function, it does not include the type of information accessed from the hospital EHR on preadmission, which is needed to support the transfer of care/admission process for the LTPAC provider.
4.4. Summary of Long-Term and Post-Acute Care Data That Could be Prioritized for Electronic Health Information Exchange
LTPAC organizations have a frequent and ongoing need to exchange information -- both as a receiver and a sender. As noted, electronic HIE is beginning to occur, but primarily by allowing access by LTPAC providers to hospital and HIEO information. Minimal information has been requested from LTPAC providers for inclusion by the HIEO, or sent electronically from the LTPAC EHR directly to another provider's EHR.
The following list summarizes the type of information frequently provided by LTPAC organizations and exchanged with other health care providers. This health information can provide the basis for expansion of HIEOs' LTPAC content and/or HIT standards development efforts to facilitate interoperable exchange.
-
Current demographic information.
-
Transfer summary and/or discharge POC.
-
Current problems/diagnoses.
-
Medication and treatment orders.
-
Recent medications administration records to show the what and when medications were given (at transition of care).
-
Current allergies.
-
Recent vital signs and trending reports.
-
Telehealth data and trending reports.
-
Recent immunization, lab, radiology, and other specialized test results.
-
Recent narrative progress notes at transfer to assist clinical staff in hand-off of care.
-
POC.
-
Assessments such as cognitive function, physical function, fall risk, MDS, OASIS, etc. (depending on the receiver).
-
Advanced directives and/or DNR order.
-
Referral -- such as to community service/aging services to and/type of service requested and past history data.
-
Immunization data.
-
ADT events for HIEOs.
4.5. Use of Health Information Technology Standards to Support Interoperability and Exchange
Basic HIT and interoperability standards are sometimes used to support electronic HIE at the sites (e.g., use of HL7 version 2 messaging). One of the three sites (Rush) has an EHR vendor that is certified for Stage 2 of the EHR Incentive Programs, but demonstration of HIE with LTPAC providers outside of their network was not observed. None of the sites have implemented standards identified for Stage 2r to support more robust HIE at times of transitions in care and for instances of shared care on behalf of persons receiving LTPAC/LTSS (because Stage 2 HIE requirements were not in effect at the time of the site visits). In addition, the focus has been on the application of these standards to providers eligible for the EHR Incentive Programs and there is a lack of awareness about the extensibility and applicability of these standards by and to LTPAC/LTSS providers.
Generally, HIE using the LTPAC EHR systems does not leverage HIT standards included in either Stage 1 or Stage 2 EHR Incentive Programs. For example, standards used to exchange information from LTPAC EHR systems used HL7 message standards (e.g., HL7 version 2.x) rather than document standards such as the CCD or CCDA. While many of the standards required by the EHR Incentive Programs could be used to support HIE with and by LTPAC providers, integration and use of these standards into LTPAC EHR products often requires additional investment of time, financial resources, and organizational awareness of the availability and applicability to support HIE. Further, some standards are still early in their maturity level requiring a significant level of effort to implement.
4.6. Findings, Challenges, and Opportunities Identified from Site Visits
A number of overall findings and impressions emerged from the three site visits which provide a snapshot of the current state of HIE by LTPAC to support the transition of care, shared care and care coordination processes. In addition, barriers to and opportunities for advancing HIE in LTPAC settings were also identified across the sites visited.
Transitions of care are complicated and require a multipronged approach to communication and information exchange. LTPAC providers receiving the hand-off of care from hospitals or other providers must gather information from multiple sources using multiple communication/exchange methods to accurately start care, assess the patient, and develop an appropriate POC. Electronic HIE can create efficiency in the process and improve the timeliness and availability of health information; however, communication in person and by telephone will continue to be necessary to ensure a safe hand-off in care.
New care delivery and payment models are highlighting the importance of care coordination including community services. Programs and initiatives that focus on improved care coordination across settings are highlighting the importance of a HIT infrastructure and financial support for establishing and implementing such infrastructures. The CMS Hospital Readmission Reduction Initiative, CCTP, Beacon Community grants, PCMH programs, and Pioneer ACO all provided an impetus to support coordination and information exchange processes and some funding to advance HIT infrastructures.
Both Rush and EMHS have programs to extend care management and coordination that include community-based services to improve health outcomes and reduce costs. EMHS leaders indicated that care management services along with a HIT infrastructure were critical strategies for helping reach their QI measures and achieve cost savings as a Pioneer ACO. While community care coordinators are instrumental in the care management process, many of the LTSS service providers (e.g., transportation and meal services) are generally not part of HIE activities. Integration of LTSS and HCBS are important to achieving health care goals and outcomes (and are being tested as part of some CMMI initiatives) for high cost/high-risk populations. However, these HCBS/LTSS providers do not use EHR systems and are not on the radar as potential contributors or users of data from HIEOs. The information systems they do use are not interoperable, which contributes to using time-consuming telephone, paper, and fax.
Electronic HIE in LTPAC may be contingent on additional funding sources or policy initiatives. Initiatives to improve care coordination and breakdown the silos between health care providers through electronic HIE were often driven by new policies and funding models. As noted at the site visits, several types of programs and initiatives spurred care coordination and improved HIE practices. Informants at one of the visited sites indicated that additional funding will be needed to support electronic HIE to improve care coordination.
HIE organizations are evolving and the value proposition for LTPAC providers is just beginning to emerge and has not yet been realized. HIEOs are beginning to collect information from different providers including ancillary service providers and maintain this information in one consolidated location. However, at this time, the observed HIEOs do not provide a complete picture of the patient nor include the level of clinical data needed to support LTPAC processes around care transitions. The information needed by LTPAC providers to support the transition of care/admission process requires detailed medical record data found in hospital EHRs. Timely access to HIEO data may be another limitation. A LTPAC provider's access to needed preadmission data may be delayed until a patient is admitted to LTPAC, a treatment relationship is established, and consent is obtained. Once the treatment relationship is established, information in the HIEO is often useful to LTPAC providers, particularly in terms of past medical history, services and medications. However, the data in the HIEO, while expanding, is currently not comprehensive; thus requiring other information sources to be accessed and information exchange methods to be used.
One of the emerging uses and potential values of the data maintained by HIEOs is the ability to perform population health analytics, which could support a variety of activities such as understanding health outcomes across populations, providers, service delivery models, advancing clinical decision support tools to support practices found to be effective, and supporting public health and safety. However, the realization of this value proposition was not observed during these site visits. The ability to perform these advanced analytics functions is contingent on several factors including the HIEO's structure and purpose, its technical infrastructure, the quality and comprehensiveness of their data, and the ability to reuse this data to support these analyses.
Adoption of electronic HIE applications by LTPAC providers is beginning, but interoperable exchange is non-existent. The primary mode of exchanging health information by LTPAC providers continues to be traditional methods -- telephone, fax, and secure e-mail with PDF attachments. New processes are emerging to improve the timely and efficient exchange of information including use of: secure access to the hospital EHR, shared network drives to house hospital information, proprietary electronic referral applications for subscribers to exchange information, customized portals for physicians to access LTPAC providers' EHRs, and access to community HIEOs.
When HIEOs are available, some LTPAC providers are participating, primarily by accessing medical history information after admission to assist in the assessment and care planning processes. In some limited instances, information is being sent from LTPAC providers to HIEOs (e.g., ADT messages and the home care POC). Some HIEOs such as HEALTHeLINK anticipate delivering results between ancillary service providers and LTPAC providers.
EHR applications used by LTPAC providers may include some basic HIT messaging standards (e.g., HL7 2.3 or 2.5); however, standards-based document exchange meeting MU Stage 2 requirements, such as the exchange of a patient summary record, was not observed to be sent or received by providers or the HIEO. When electronic exchange was implemented, the cost, complexity and lack of technology solutions that support "standardized", interoperable HIE were identified as barriers.
Quality and performance measure data are being collected. All three sites are collecting and reporting some type of quality/performance measurement data. None of the three sites collected measures specific to HIE activities; however, timely exchange was identified by the sites as a factor that contributes to improved performance. The following list summarizes the focus of pertinent quality measures at the three sites:
-
Number and rates of hospital admissions/readmissions over a period of time (e.g., for a SNF, home care, telehealth program).
-
Hospital readmission rates for target populations related to the CMS Hospital Readmission Reduction program, Beacon Community grant, and/or identified high-risk/high cost populations.
-
Mortality rates.
-
Rates of physician followup completed within 30 days post-discharge.
-
Increased understanding of medications and discharge POC.
-
Decreased patient and caregiver stress.
-
Nursing home placement rates.
-
Clinical data reporting/measurement for target populations (e.g., completion of labs with certain values for diabetes patients).
-
Cost of encounters for a target population.
-
Average cost savings over a period of time for target populations in accountable care payment arrangements.
-
Required CMS quality measurement/reporting data for SNFs, HHAs, and hospice.
As noted, EMHS collects 33 required quality measures as a Pioneer ACO (see Appendix J, Attachment J-1). EMHC also collects quality performance data on their telehealth program to quantify the reduction in ED, hospital admissions and associated costs. EMHS has been able to quantify a significant impact on key performance indicators and costs for the 167 patients in the telehealth program in 2012, reducing hospitalization and ED visits by an average of 65% for target diagnoses, resulting in an estimated $2.1 million in health care savings. EMHC also reports that for every dollar invested in home care during the first year of the pilot, they saved $3 as an ACO.
4.7. Barriers for Challenges to Advancing Health Information Exchange
The findings and observations above begin to highlight a number of barriers or challenges related to HIE and advancing its use by LTPAC providers and the expanded use of electronic HIE. This section describes the barriers or challenges that were identified by the site visit providers.
Medication Reconciliation Challenges at Transitions of Care/Admissions
All three sites identified medication reconciliation as one of their biggest challenges during transition of care. Hospital discharge medications must be reconciled with the patient's pre-hospital regime and post-hospital POC. Exacerbating the problem is often the lack of primary or attending physician's historical knowledge of the patient and their overall POC, and the lack of complete and accurate medication history information, even when a HIEO is available. For example, some HIEOs use SureScripts for filled prescription history data. The prescription information from HIEOs may not reflect all of a patient's prescriptions and whether the patient filled them. In some cases there is a lag time for a pharmacy to report the information to SureScripts. While the information is useful to LTPAC providers, it cannot be considered the complete and accurate trusted source. Because medication reconciliation is critically important for patient safety and continued care, improvements are needed to ensure safe hand-offs at transition from the hospital to the LTPAC provider.
Need for Improved Efficiency in HIE Between LTPAC Provider and Pharmacy
For SNFs, there is also a communication process in which medication and other order changes are sent to the long-term care pharmacy. However, this process is typically not supported through electronic, interoperable transmission. Both Western New York and Maine's HIEOs have begun work to address this gap by connecting a long-term care pharmacy to their exchange.
Lack of Efficient Exchange of Information Between LTPAC and Attending Physicians
During a patient's stay in LTPAC, these provider organizations must frequently exchange information with attending physicians for status changes and updates, order changes, obtaining signatures, POC and certification updates, etc. Typical exchange processes include photocopying, making printouts, or scanning medical record information to mail, fax and send via secure e-mail. However, these methods are labor intensive and highly inefficient for both providers. Two of the LTPAC sites (Beechwood and EMHC) developed physician portals to their EHR applications in lieu of interoperable exchange between the physicians' EHR and the LTPACs' EHR. While this is a first step toward improved efficiency and information access, it does not provide a process for the exchange of information from physician's EHR and the LTPAC provider's EHR. This is an important issue because both the LTPAC provider and physician share responsibility for care and treatment, but the information continues to be maintained in silos, and is not reusable, resulting in data re-entry.
Even with Standards, Interfaces are not Easy to Implement and Must be Customized
As noted a number of times in this report, standards may be available, but they are challenging to use and require significant resources to implement. Barriers include the use of older standards which contributes to the need for vendors to support customized interfaces, the cost of developing the interfaces and the time to test and implement. While newer standards may facilitate exchange of information, one HIEO informant reported that some of the standards lack specificity, which has resulted in variations in implementation and requires that the HIEO transform reportedly "standardized" information into a consistent format. Further, vendors have been slow to adopt these newer standards, for several reasons including that they have not been tailored and tested for LTPAC implementation.
Lack of Awareness of HIE Standards
In general, there is little awareness among providers (including LTPAC providers) and others regarding the upcoming MU Stage 2 standards, or of the standards emerging through the S&I Framework or being balloted through HL7 to support the exchange of health information including on behalf of persons who receive LTPAC/LTSS services. In some cases there is awareness, but limited resources (time and money) to support implementation of these available/emerging standards. Several respondents, including representatives from HIEOs, health systems administrators, and LTPAC and other providers noted the lack of available resources to support various HIE implementations with LTPAC providers. Appendix L provides a table that identifies the standards that are available to support the types of LTPAC data frequently provided to or requested by other health care providers.
The findings from these site visits also informed opportunities to expand HIE to support care coordination for persons receiving LTPAC/LTSS, discussed in the next section.
4.8. Opportunities to Advance Health Information Exchange for Persons Receiving Long-Term and Post-Acute Care/Long-Term Services and Supports
The following opportunities were identified, based on the site visits, to advance the use of current state of information sharing and exchange involving LTPAC/LSSS.
Care Coordination for QIs and Reduced Costs must Engage LTPAC and LTSS
Health system transformation initiatives are placing focus on the need for improved information sharing and exchange capabilities. Findings from the site visits indicate that LTPAC and LTSS are instrumental in care coordination efforts to improve quality and reduce costs particularly for high-risk/high cost patient populations. For example, care coordination services across care settings and community services are important for improving quality of care and a key strategy for EMHS in achieving their needed health savings as an ACO. There are several opportunities that could support care coordination through information exchange related to these care delivery models including:
-
The exchange of a patient-centered care plan can support care coordination across providers and care managers. Using the standard for care plans (being balloted by HL7 in the Fall 2013) could enable the interoperable exchange of care plans across team members and over time. The exchange of care plans can support continuity and quality of care, and align multiple care plans across health care providers. HIEOs can play a critical role in supporting the exchange and alignment of care plans. Further, access to care plans could enable population health analytics by HIEOs.
-
Greater involvement of community-based services in HIE activities will support the care coordination models being developed. Integration of community-based services is identified as a key service to improve quality of care and reduce costs for target populations. Electronic exchange of basic health information (such as demographic, scheduling and messaging) with community-based service providers will improve continuity and coordination of care.
-
The availability of electronic LTPAC assessment data creates an immediate opportunity for HIEOs to access data that is ubiquitous across LTPAC providers. MDS data is available for all patients in Medicare or Medicaid certified SNFs, OASIS data is available for all Medicare patients receiving home health services, and IRF-PAI data is available for Medicare covered patients in inpatient rehab facilities. HIEOs may want to explore how to include federally required patient assessment data in their network particularly if they are performing advanced population analytics to help support new delivery and payment models. The low-cost technology solutions could transform the assessment data into interoperable and reusable summary content.
Explore Expanded Information Sharing and HIE Options for LTPAC
The nature of care delivery by LTPAC providers requires the exchange of health information with clinical partners, the patient, family and other stakeholders. Many of the current HIE processes are labor intensive and inefficient. Over 35 HIE workflows were identified using the frameworks applied in this study to support transitions of care, shared care, and other administrative functions. There are multiple strategies that could be explored to improve the HIE capabilities between LTPAC and other provider organizations such as the following:
-
Exploring partnerships between non-affiliated organizations to allow authorized providers to view data in EHRs, support point-to-point information exchange between EHRs and/or expanded use of Direct secure e-mail messaging of non-interoperable health information.
-
Identifying additional information, methods for obtaining this information, and opportunities to reuse the information to support care giving. For example, HIEOs at two of the sites identified pharmacies as a source of important electronic medication information. HIEOs could make available electronic medication information to LTPAC providers or pharmacies could deliver electronic medication directly to the LTPAC providers. Further, work is needed to explore the feasibility, benefits, and barriers of exchanging electronic medication information from pharmacies, including long-term care pharmacies.
-
Increased emphasis on development and testing of HIT standards would ease the implementation of interoperable HIE across the continuum including by LTPAC/LTSS providers.
5. Conclusion
This report presents study findings from an environmental scan, literature review, key informants, and site visits, and was guided by frameworks to describe the state of HIE to support care coordination for persons receiving LTPAC/LTSS services and fill key information gaps. HIE includes both electronic and non-electronic exchange of health information. The study frameworks captured important use cases for and dimensions of HIE when used to support care coordination for LTPAC/LTSS. These frameworks can be applied to future studies and policy and standards activities to advance the use of HIE for LTPAC/LTSS.
Drivers and facilitators of and barriers to the use of HIE to support care coordination for persons receiving LTPAC/LTSS are identified, along with opportunities to address these barriers and challenges, and accelerate the adoption of HIE, including interoperable HIE.
This study highlights the importance of information exchange in care coordination. While there are many models for care coordination, the care coordination model used was found to be less significant than a close working relationship between providers, care coordinators and patients and the exchange of timely, key information. A key component of programs and interventions identified in this study to support care coordination is the communication of critical information, using electronic and other means.
However, health information is siloed and often not shared, or shared in a timely manner across providers/caregivers or between health information systems. This lack of timely HIE results in poor continuity and coordination of care, safety and quality problems, redundancies in tests and other services, avoidable ED and hospital admissions, and associated avoidable costs.
LTSS Providers as Key Partners in Care Coordination
LTSS providers along with LTPAC providers are important partners in care coordination and transitions from hospitals. LTSS providers have important information that is generally not exchanged, such as functional and cognitive status, potential risks (e.g., fall history), elder abuse reports, use of services such as DME and homemakers, and information about the patient and family/caregivers that may be relevant to care. New delivery and payment models serve as drivers for LTSS to participate in HIE, particularly for HHAs, but barriers exist. There are few incentives for LTSS participation in HIE, low rates of EHR adoption, and disparate non-interoperable systems (e.g., client tracking, elder abuse reporting, and eligibility).
Drivers for and Barriers to HIE
Drivers of HIE are identified including new care delivery and payment models that recognize the importance of effective care coordination between providers, including LTPAC and LTSS providers. State and federal initiatives to support the adoption of HIT, EHRs, and electronic HIE are also described (e.g., standards, certification, programs to encourage adoption).
Many of the drivers as well as barriers addressed in this study relate to the adoption of HIT such as EHRs, including CEHRT, to support electronic HIE. Adoption of electronic HIE by LTPAC/LTSS providers is growing but has been modest and much slower than other health care sectors. This is due in part to limited financial incentives for LTPAC/LTSS EHR adoption. Participation in HIEOs by LTPAC/LTSS providers is also modest, and driven largely by incentives from the HIEOs and other sources (e.g., providing connectivity, hardware, software, training, and tools). There is a lack of information about the value proposition of their participation in HIEOs. LTPAC/LTSS providers currently do not contribute much data to HIEOs.
Interoperability standards are available or being developed that can accelerate HIE around care coordination, including transitions. However, there is little use of current standards by LTPAC providers or embedded in their HIT products. Further, there appears to be low awareness among LTPAC and other providers regarding the upcoming MU Stage 2 requirements and standards, or of the standards emerging through the S&I Framework and being balloted through HL7 to support the exchange of health information including on behalf of persons who receive LTPAC/LTSS services. In some cases there is awareness, but limited resources to support implementation of these available/emerging standards.
Further, when electronic HIE is available to LTPAC providers, use is reported to be modest due to the impact of HIE on workflow, including time involved to use electronic exchange applications; a lack of well-defined use cases for electronic HIE; usability issues related to the technology and display of data; perceived value of the information (e.g., timeliness, completeness, accuracy); the need to train and retrain LTPAC staff due to high turnover; limited resources to implement and support HIE, and privacy and security barriers.
Characteristics of HIE to Support Care Coordination for Persons Receiving LTPAC
An in-depth analysis of the methods for HIE and types of data exchanged was undertaken to understand the state of HIE to support care coordination. HIE around care coordination, particularly transitions, was found to be complex and relies on multiple methods of HIE. The methods of exchanging health information by LTPAC providers continue to be predominantly non-electronic (including telephone and fax) and at times electronic, but generally non-interoperable HIE (using secure e-mail with PDF attachments). Because of the complexity of care transitions, there will always be a need for face-to-face and telephone communication.
Common data exchanged around care transitions and shared care functions are identified, as well as key data gaps, which can inform and help prioritize opportunities for expanding data available through electronic HIE, and associated standards. Data commonly exchanged during transitions and shared care were compared with data identified in the literature as important for transitions and coordination (e.g., CMS Roadmap to Better Care Transitions and Fewer Readmissions) and reported by study informants. Important data but not commonly exchanged include comprehensive care plans with patient goals and preferences, advance directives and power of attorney, a reconciled medication list, the patient's cognitive and functional status, planned interventions, followup appointment schedule with contact information, formal and informal caregiver status and contact information, designated community-based care provider, and social supports.
Medication reconciliation during transitions of care is critical to care coordination and patient safety, and is one of the most highly rated functions of HIE, but significant challenges exist related to the exchange of this information. Determining the pre-hospital medications and reconciling with post-hospital medications to determine ongoing medication orders is challenging. HIE between LTPAC providers and pharmacies is usually inefficient. Exacerbating the problem is physicians' lack of historic knowledge of the patient and the overall POC, and lack of complete and accurate medication history information. Access to medication information remains a challenge even when a HIEO is available.
New processes are emerging to improve timely exchange of information, including secure access to hospital and LTPAC providers' EHRs, shared network drives to house hospital information, proprietary electronic referral applications for subscribers to exchange information, and access to HIEOs. These new processes are generally not advancing interoperable HIE.
Accelerating Interoperable HIE by LTPAC/LTSS Providers
This study identified policy and other opportunities for accelerating electronic HIE by LTPAC/LTSS, including the following:
-
Providing additional incentives to support LTPAC/LTSS use of electronic HIE; without incentives participation by LTPAC/LTSS will likely remain low.
-
Increasing LTPAC/LTSS provider awareness and use of interoperability standards.
-
Better communicating the emerging value proposition and benefits of electronic HIE to LTPAC/LTSS providers.
-
Identifying additional, well-defined use cases relevant to LTPAC/LTSS.
-
Better defining and validating measures that reflect HIE, electronic and other means, on care coordination.
- Conducting further study to better understand:
- LTSS providers' data, data needs, systems, and potential for HIE, and educate HIEOs and other stakeholders about the value of LTSS participation in HIE.
- How HIE is and can be used to engage patients/consumers and their families and caregivers in the coordination of their care (e.g., patient portals and other means).
In summary, advancing HIE to support care coordination for persons receiving LTPAC/LTSS will require a multifaceted approach, including leveraging opportunities in the policy and health service delivery environments; providing financial incentives to accelerate HIE; improving enabling technology such as EHRs and interoperability standards; identifying key HIE use cases and modifying workflows to support electronic HIE; improving measures to monitor the impact of HIE on care coordination processes and outcomes; and widely communicating the value proposition of HIE with and for LTPAC/LTSS providers and patients. This study identifies several opportunities and areas of further study to guide future efforts to address challenges and barriers, and provide more incentives for the use of HIE to support care coordination for persons receiving LTPAC/LTSS.
Appendixes
Appendix A. Selected Programs and Initiatives That SUPPORT CARE Coordination and Information Exchange for Persons Receiving LTPAC/LTSS Services
TABLE A-1. Selected Programs and Initiatives that Support Care Coordination and Information Exchange for Persons Receiving LTPAC/LTSS Services
| Program/ Initiative Name |
Description | Program Office | Initiative Type | Link |
|---|---|---|---|---|
| Initiative to Reduce Avoidable Hospitalizations Among Nursing Facility Residents | Focuses on long-stay nursing facility residents who are enrolled in the Medicare & Medicaid programs, with the goal of reducing avoidable inpatient hospitalizations. CMS will support organizations that partner with nursing facilities to implement evidence-based interventions that improve care & lower costs. | CMS Medicare-Medicaid Coordination Office & CMMI | QI Program | http://innovations.cms.gov/initiatives/rahnfr/ |
| Partnership for Patients | Supports physicians, nurses, & other clinicians working in & out of hospitals to make patient care safer & to support effective transitions of patients from hospitals to other settings. | CMMI | QI Program, involves Hospitals Engagement Networks | http://innovations.cms.gov/initiatives/Partnership-for-Patients/index.html http://partnershipforpatients.cms.gov/ |
| Community-Based Care Transitions Program (CCTP) | The CCTP is designed to improve transitions of high-risk Medicare beneficiaries from hospitals to home or other care settings, improve quality of care, reduce readmissions, & document savings to the Medicare program. CCTP allows community-based health care & social services providers (e.g., CBOs, HCBS) to receive a Medicare FFS benefit payment for care transitions. | CMMI | Incentive Program | http://innovations.cms.gov/initiatives/Partnership-for-Patients/CCTP/index.html |
| Quality Improvement Organization (QIO) Program--Integrating Care for Populations & Communities (ICPC) | ICPC brings together hospitals, SNFs, patient advocacy organizations, & other community stakeholders to implement process improvements related to medication management post-discharge followup, & plans of care for patients who move across health care settings. | CMS/CO Foundation of Medical Care | QI Program | http://www.cfmc.org/integratingcare/Default.htm |
| State Action on Avoidable Rehospitalizations (STAAR) Initiative | STAAR seeks to reduce rehospitalizations in MA, MI, OH & WA, by engaging payers, state & national stakeholders, patients & families, & caregivers at multiple care sites & clinical interfaces. | IHI | QI Program | http://www.ihi.org/offerings/Initiatives/STAAR/Pages/default.aspx |
| Medicaid MLTSS Programs | MLTSS is an arrangement between state Medicaid programs & contractors through which the contractors receive capitated payments for LTSS & are accountable for the delivery of services & supports that meet quality & other standards set in the contracts. | CMS Disabled & Elderly Health Programs Group | Incentive Program | http://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/ Delivery-Systems/Downloads/MLTSSP_White_paper_combined.pdf http://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/ Delivery-Systems/Medicaid-Managed-Long-Term-Services-and-Supports-MLTSS.html |
| Beacon Community Programs | The HIE activities of Beacon Communities are considered to be "beacons" in the development of secure, private, & accurate systems of EHR adoption & HIE. All Beacon communities include HIE between providers, & some include LTPAC providers. | ONC | Grant Program | http://www.healthit.gov/policy-researchers-implementers/beacon-community-program Sample profiles: http://www.healthit.gov/policy-researchers-implementers/western-new-york- beacon-community |
| State HIE Challenge Grants | ONC awarded 4 Challenge Grants to state HIE programs to focus on HIE involving LTPAC providers. | ONC | Grant Program | http://healthit.hhs.gov/portal/server.pt?open=512&mode=2&objID=3378 |
| Accountable Care Organizations (ACOs), including the Pioneer ACO | ACOs are groups of doctors, hospitals, & other health care providers, who come together voluntarily to give coordinated high-quality care to the Medicare patients they serve. The Pioneer ACO Model is an initiative launched by CMS to show how particular ACO payment arrangements can best improve care & generating savings for Medicare; & to test alternative program designs to inform future rulemaking for the Medicare Shared Savings Program. Designed for organizations with experience operating as ACOs or similar arrangements, it provides ACOs successful in achieving shared savings in the first 2 years the opportunity to move into a population-based payment in year 3. | CMS, CMMI | Payment Policy | http://innovation.cms.gov/initiatives/Pioneer-ACO-Model/index.html http://innovations.cms.gov/initiatives/ACO/index.html |
| Hospital Readmissions Reduction Program | The goal of the program is to reduce avoidable inpatient hospitalizations. The Hospital Readmissions Reduction Program was enacted as part of the Affordable Care Act, effective October 1, 2012. Organizations with a high 30-day admission rates for acute myocardial infarction, heart failure, & pneumonia may see their annual hospital Medicare payments reduced by up to 1%. CMS proposed expanding the list of conditions in fiscal year 2015 to include patients admitted for an acute exacerbation of COPD; elective total hip arthroplasty & total knee arthroplasty. | CMS | Payment Policy | http://innovation.cms.gov/initiatives/CCTP/index.html http://www.cms.gov/apps/media/press/release.asp?Counter=4454&intNumPer Page=10&checkDate=&checkKey=&srchType=1&numDays=3500&srchOpt=0& srchData=&keywordType=All&chkNewsType=1%2C+2%2C+3%2C+4%2C+5& intPage=&showAll=&pYear=&year=&desc=&cboOrder=date http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/ AcuteInpatientPPS/Readmissions-Reduction-Program.html |
| Models for Dual Eligibles | Based on the Affordable Care Act, CMS is testing capitated & managed FFS financial alignment models to improve care & control costs for the dual eligible population (persons dually eligible for Medicare & Medicaid). Demonstrations change the payment approach & financing arrangements among CMS, the state, & providers. The capitated demonstrations use managed care plans to coordinate services for beneficiaries through a person-centered planning process. | CMS | Payment Model | http://www.medicaid.gov/affordablecareact/provisions/dual-eligibles.html http://www.cms.gov/Medicare-Medicaid-Coordination/Medicare-and-Medicaid- Coordination/Medicare-Medicaid-Coordination-Office/ http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/ MLNProducts/downloads/Medicare_Beneficiaries_Dual_Eligibles_At_a_Glance.pdf |
| Patient-Centered Medical Home (PCMH) | Several provisions in the Affordable Care Act directed at establishing & promoting the PCMH, which is a team-based model of care led by a personal physician who provides continuous & coordinated care throughout a patient's lifetime to maximize health outcomes. This includes the provision of preventive services; treatment of acute & chronic illness; & assistance with end-of-life issues. This care model promotes improved access & communication; care coordination & integration; & care quality & safety. | Various federal agencies & departments | Payment Model | http://pcmh.ahrq.gov/ http://www.cms.gov/Medicare/Demonstration-Projects/DemoProjectsEvalRpts/ downloads/FQHC_APCP_Demo_FAQsOct2011.pdf |
| Medicare Physician Fee Schedule (MPFS) rule--Transitional care management (TCM) | CMS issued the final 2013 MPFS Rule. CMS is paying for TCM services supporting healthy transitions after hospital stays. It includes a new policy to pay a patient's physician or practitioner to coordinate care in the 30 days following a hospital or SNF stay. This rule recognizes the work of community physicians & practitioners in treating a patient following discharge from a hospital or nursing facility to ensure better continuity of care & help reduce patient readmissions. | CMS | Incentive Program | http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network- MLN/MLNProducts/downloads/MedcrephysFeeSchedfctsht.pdf http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/ PhysicianFeeSched/index.html?redirect=/physicianfeesched |
| Medicare Physician Fee Schedule (MPFS) rule--Complex chronic care management | Under the Medicare 2014 Physician Fee Schedule, CMS proposes to cover physician services to pay for non-face-to-face complex chronic care management services for Medicare beneficiaries who have 2 or more significant chronic conditions. Complex chronic care management services include regular physician development & revision of a POC, communication with other treating health professionals, & medication management. Under the proposal, the physician practice must use & demonstrate MU of an EHR. The practice also must have 1 or more advanced practice RNs or physician assistants whose job descriptions include care for beneficiaries with complex chronic conditions. | http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/ PhysicianFeeSched/index.html?redirect=/PhysicianFeeSched/ | ||
| Balancing Incentive Program | The Balancing Incentive Program was created by the Affordable Care Act & authorizes grants to states to increase access to non-institutional LTSS. The program will help states transform their LTSS by lowering costs through improved systems performance & efficiency, creating tools to help consumers with care planning & assessment, & improving quality measurement & oversight. The program provides new ways to serve more people in HCBS. Federal Matching Assistance allows states to make structural reforms to increase SNF diversions & access to non-institutional LTSS. Enhanced matching payments are tied to the percentage of a state's LTSS spending. | CMS | Incentive Program | http://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/ Long-Term-Services-and-Support/Balancing/Balancing-Incentive-Program.html |
| Picker/ Commonwealth Fund Long-Term Care Quality Improvement | The program seeks to improve the health care delivery system & spur innovation by raising the quality of LTPAC/LTSS, & improving care transitions for patients by integrating these services with the other care that they receive. | Commonwealth Fund | QI Program | http://www.commonwealthfund.org/Program-Areas/Archived-Programs/ Delivery-System-Innovation-and-Improvement/Long-Term-Care-Quality-Improvement.aspx |
| Medicaid Transformation Grants | Funds to states for the adoption of innovative methods to improve effectiveness & efficiency in providing medical assistance under Medicaid. CMS encouraged states to look at how HIT & the exchange of health information could be leveraged to improve Medicaid services (e.g., reduce medical errors through the implementation of EHRs, clinical decision support tools, or eRx). | CMS | Incentive Program | http://www.medicaid.gov/index.html |
| Bridge Model (See Rush University Medical Center site visit summary in Appendix H for more information) |
The Bridge Model (Bridge) is an evidence-based, social work- based transitional care model designed for older adults discharged home from an inpatient hospital stay. Bridge helps older adults to safely transition back to the community through intensive care coordination that starts in the hospital & continues after discharge to the community. | ITCC | Transitional Care Model | http://www.transitionalcare.org/the-bridge-model http://www.naswil.org/news/chapter-news/featured/social-work-and-the-bridge- model-the-key-to-successful-transitional-care/ |
| Minimum Data Set (MDS) & OASIS--Continuity of Care Document (CCD) Transformer, called KeyHIE Transform™ | The software is designed to enable LTPAC providers such as SNFs & HHAs to participate in HIE regardless of whether they use an EHR. KeyHIE Transform™ is an all-inclusive, web-based service that MDS & OASIS into HL7 CCD & ADT registration message, & publishes the CCD & registration message to KeyHIE for direct delivery. | Partnership between Geisinger System Services & BridgeGate International | IT solution for LTPAC, low cost | http://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/ NursingHomeQualityInits http://www.bridgegateintl.com |
| Medicare QIO Technical Assistance (e.g., Health IT for Post-Acute Care Special Innovation Project) | One of the QIO programs provides technical assistance to LTPAC & other providers in CO, MN, & PA through the Health IT for Post-Acute Care Special Innovation Project, to help LTPAC providers optimize their use of HIT to support medication management & care coordination in transitions of care, & advancing HIE. Selected QIO resources related to care transition improvement efforts are available from state QIO sites. | CMS | Evidence-Based Interventions, Education, Data, Networking, Assistance | http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/ AcuteInpatientPPS/Readmissions-Reduction-Program.html http://www.cfmc.org/integratingcare/provider_resources.htm |
| Project Re-Engineered Discharge (RED) Toolkit | The toolkit includes 5 tools that provide step-by-step instructions to provide a springboard for hospitals to proactively address avoidable readmissions. It helps hospitals reduce readmissions rates by replicating a discharge process that resulted in 30% fewer hospital readmissions & ED visits. | Boston University School of Medicine, Department of Family Medicine, funded by AHRQ | Evidence-Based Intervention & Toolkit | http://www.bu.edu/fammed/projectred/presentations.html http://www.bu.edu/fammed/projectred/toolkit.html http://www.ahrq.gov/professionals/systems/hospital/red/toolkit/index.html |
| Interventions to Reduce Acute Care Transfers (INTERACT & INTERACTII) | INTERACT CORlkit is for SNF staff to reduce avoidable hospital admissions. Under the existing licensing agreement, the INTERACT materials cannot be incorporated into software, including EHR systems. An electronic version, eINTERACT, is in the development & testing phase for partners that wish to embed the INTERACT program & tools within their EHR. | INTERACT program, developed by the INTERACT interdisciplinary team, led by Dr. Joseph Ouslander, with input from many direct care providers & national experts in projects based at FL Atlantic University, supported by the Commonwealth Fund. | Evidence-Based Intervention & Toolkit | http://interact2.net http://interact2.net/tools.html |
| Medications at Transitions & Clinical Hand-offs (MATCH) Toolkit | Provides a step-by-step guide to improving medication reconciliation process. | Northwestern Memorial Hospital, Chicago, IL | Evidence-Based Interventions & Tools | http://www.ahrq.gov/qual/match/match.pdf |
| Reducing Avoidable Readmissions Effectively (RARE) Campaign | Participating hospitals in the RARE Campaign can choose to participate in 1 of the 3 different RARE sponsored learning collaborative, focused on making improvements in the 5 key areas known to reduce avoidable readmissions. | Institute for Clinical Systems Improvement, the MN Hospital Association, & Stratis Health | Evidence-Based Interventions & Collaborative | http://www.rarereadmissions.org/ |
| Home Health Quality Improvement (HHQI) National Campaign | Seeks to reduce avoidable hospitalizations & improve medication management for home health patients by uniting home health & other providers across multiple health care settings. | WV Medical Institute | Evidence-Based Interventions, Education, Data, Networking, Assistance | http://www.homehealthquality.org |
| Care Transitions Program | Supports patients & families; increases skills among providers; enhance the ability of HIT to promote HIE across care settings; implements system level interventions to improve quality & safety; develops performance measures & public reporting mechanisms; & influence health policy at the national level. | Division of Health Care & Policy Research, University of CO School of Medicine | Evidence-Based Interventions & Tools | http://www.caretransitions.org |
| Patient Safety Tool: Transitions of Care Checklist | This checklist provides a detailed description of effective patient transfer between practice settings. | National Transitions of Care Coalition Advisory Task Force | Evidence-Based Interventions & Tools | http://www.beckersasc.com/asc-accreditation-and-patient-safety/patient-safety- tool-transitions-of-care-checklist.html |
| Quality Health First Program | Helps physicians to identify, prevent & manage diabetes, heart disease, breast cancer, asthma, & other conditions in their patients; utilizes information from the IN Network for Patient Care to assemble lab results, immunizations, diagnoses, cardiology & radiology reports, procedures & medication information. This information is organized in easy-to-read patient summaries that can be used before, during or after patient visits to make the best use of physicians' time. | IN HIE | QI Program | http://www.ihie.org/Solutions/quality-health-first-program.php |
| Direct | Direct support the use of standards-based protocols for an easy-to-use, secure, & scalable method of sending encrypted & authenticated health information over the Internet such as clinical summaries, CCDs, & laboratory results, to other providers who also own a DIRECT address. Direct supports simple use cases in order to speed adoption, & seeks to replace slow, inconvenient, & expensive methods of exchange & provide a future path to advanced interoperability. | ONC | IT Solution | http://directproject.org |
| Local Adaptor for Network Distribution (LAND) & Surrogate EHR Environment (SEE) | LAND & SEE are available for public use. LAND allows organizations with fully implemented EHRs capable of generating the newly specified transition of care & care plan data elements to create, transmit, & receive these new document types. SEE, intended for organizations without an EHR & lacking the ability to create these documents, allows providers to use their web browser to access their SEE mailbox, & view, edit/update, & send these documents to the receiving facility via Direct message transmission from the browser to the next care provider. | MA IMPACT Project | IT Solution | http://mehi.masstech.org/what-we-do/hie/impact/land-and-see |
| LeadingAge Center for Aging Services Technology (CAST) | EHR for Long-Term & Post-Acute Care: A Primer on Planning & Vendor Selection 2013. | Assist LTPAC in EHR selection. The primer shows which EHR vendors have met ONC certification. | http://www.leadingage.org/uploadedFiles/Content/About/CAST/Resources/ 2013_CAST_EHR_For_LTPAC_A_Primer_on_Planning_and_Vendor_Selection.pdf |
NOTES: This appendix provides selected initiatives, programs, tools and resources and is not intended to represent all of the current initiatives, programs, tools, and resources.
CO = Colorado; FL = Florida; IL = Illinois; IN = Indiana; MA = Massachusetts, MI = Michigan, MN = Minnesota; OH = Ohio; PA = Pennsylvania; WA = Washington; WV = West Virginia
Appendix B. Framework to Characterize Health Information Exchange to SUPPORT CARE Coordination for Persons Receiving LTPAC/LTSS Services
B.1. Care Coordination Model Functions, Care Integration Constructs and Activities
TABLE B-1. Coordination of Care Model Activities by Functions and Integration Constructs
| Care Coordination Model Functions, Integration Constructs, and Examples of Activities | |||
|---|---|---|---|
| Care Coordination Mechanisms/Function1 |
By Care Integration Constructs (information exchange participants)2 |
Examples of Care Coordination Mechanisms and Activities |
Important to Capture for LTPAC HIE |
Coordinated care integration:
|
|||
| Transitions in Care & Hand-offs |
|
|
|
| Shared Care | |||
| Assess Needs & Goals |
|
|
|
| Create a Plan of Care (POC) |
|
|
|
| Monitor, Followup, & Respond to Change |
|
||
| Link to Community Resources |
|
|
|
NOTES: Care coordination functions/mechanisms adapted for HIE and LTPAC/LTSS based on AHRQ Care Coordination Measures Framework;1 Care Constructs adapted from Singer Integration of Care Constructs.2
- McDonald K, Schultz E, Albin L, et al. Care coordination measures atlas version 3. Rockville, MD: Prepared by Stanford University under Subcontract to Battelle on Contract No. 290-04-0020 for the AHRQ; 2010. AHRQ Publication No. 11-0023-EF.
- Singer SJ, Burgers J, Friedberg M, et al. Defining and measuring integrated patient care: Promoting the next frontier in health care delivery. Medical Care Research and Review; 2011; 68(1):112-127.
B.2. Facet: Health Information Exchange Technology Component
The Technology Facet captures information around interoperable HIE in a detailed and uniform manner.
TABLE B-2. Examples of Categories Associated with the Technology Facet
| Category | Characteristics | Examples of Sub-categories and Measures |
Important to Capture for LTPAC/LTSS |
|---|---|---|---|
| Functionality |
|
|
|
| Non-functional Requirements |
|
|
|
| Data Feeds & Interoperability |
|
|
|
| Data Transport |
|
|
|
| User-based IT Design |
|
|
|
| Cost |
|
|
|
| Hardware, software |
|
|
|
B.2.1. Data and Information (See Table B-3 for Details)
The Data category of the Technology Facet describes the characteristics of the data and information exchanged, what type of information, in what format, the mechanisms of exchange, and the senders and receivers of the information.
TABLE B-3. Examples of Categories Associated with the Data Category Within the Technology Facet
| Category | Characteristics | Examples of Sub-categories and Measures |
Important to Capture for LTPAC/LTSS HIE |
|---|---|---|---|
| Data Content |
|
|
|
| Data Coding & Standards |
|
|
|
| Quality, Availability, & Timeliness |
|
|
|
| Data Format |
|
|
|
B.3. Facet: Use and Workflow Related to Health Information Exchange
Categories that are tied to the actual use of exchanged health information, including exchange through more conventional means (e.g., paper print out, fax, in person) are captured under this facet. This facet covers not only the "individual" user but also the "group" user discussed in many of the models that were used to develop the HIT organizational framework. Also included are the individual factors relevant to many of the care coordination models such as type of LTPAC/LTSS provider, clinical disciplines involved in the HIE intervention, "ownership," usability, motivation, workflow, perception of usefulness, adequate training, and comfort with an HIE intervention and related technology.
Capturing details around user attitudes, usability and workflow, ownership, and knowledge provides insights critical to understanding how HIE is used to support care coordination and its impact on care. This information can help to identify user-related barriers and facilitators.
TABLE B-4. Examples of Categories Associated with the Use and Workflow Facet
| Category | Characteristics | Examples of Sub-categories and Measures |
Important to Capture for LTPAC/LTSS HIE |
|---|---|---|---|
| HIE User |
|
|
|
| User Attitudes |
|
|
|
| Workflow |
|
|
|
| Ownership/ Buy-in |
|
|
|
| Knowledge |
|
|
|
B.4. Facet: Environment for Health Information Exchange and Care Coordination
The environment facet captures categories that the contextual factors that can influence HIE care coordination, including which patient population(s), which setting(s) and what timeframe. In addition, care coordination effects may be impacted by facilitators and barriers of care coordination. Examples of factors that may facilitate or impede care coordination and the exchange of health information include the availability of resources, payment structure, patient complexity and capacity, and local culture.
TABLE B-5. Examples of Categories Associated with the Environment Facet
| Category | Characteristics | Examples of Sub-categories and Measures |
Important to Capture for LTPAC/LTSS HIE |
|---|---|---|---|
| Culture/Organizational |
|
|
|
| Business drivers |
|
|
|
| Leadership |
|
|
|
| Setting |
|
|
|
| Resources & Support |
|
|
|
B.5. Facet: Outcomes of Health Information Exchange to Support Care Coordination
The outcomes facet provides the categories of the measures related to HIE approaches and affect care coordination, quality, satisfaction (e.g., with care coordination, care, HIE), efficiency and costs.1, 2, 3, 4, 5, 6, 7, 8, 9, 10
TABLE B-6. Examples of Categories Associated with the Outcomes Facet
| Category | Characteristics | Examples of Sub-categories and Measures |
Important to Capture for LTPAC/LTSS HIE |
|---|---|---|---|
| Clinical |
|
|
|
| Business/Financial |
|
|
|
| Adoption |
|
|
|
| Care Coordination Measures |
|
|
|
NOTES:
- Kern LM Dhopeshwarkar R, Barron Y, et al. Measuring the effects of health information technology on quality of care: A novel set of proposed metrics for electronic quality report. Jt Com J Qual Patient Saf; 2009; 35(7): 359-369.
- Frisse ME, Johnson KB, Nian H, et al. The financial impact of health information exchange on emergency department care. J Am Med Inform Assoc; 2012; 19(3): 328-333.
- Kern LM, Wilcox A, Shapiro J, et al. Which components of health information technology will drive financial value? Am J Manag Care; 2012; 18(8): 438-445.
- Bailey JE, Wan JY, Mabry LM, et al. Does health information exchange reduce unnecessary neuroimaging and improve quality of headache care in the emergency department? J Gen Intern Med; 2013; 28(2): 176-183.
- McDonald K, Schultz E, Albin L, et al. Care coordination measures atlas version 3. Rockville, MD: Prepared by Stanford University under Subcontract to Battelle on Contract No. 290-04-0020 for the AHRQ; 2010. AHRQ Publication No. 11-0023-EF.
- Leath B, Mardon R, Atkinson D, et al. NIH-community care coordination performance measures (NIH-CCCPM) project technical report on project: Standardizing community care coordination measures linked to improvements in quality of life and health outcomes among vulnerable populations. Rockville, MD: Westat; 2012.
-
Forster AJ, Murff HJ, Peterson JF, et al. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med; 2003; 138(3): 161-167.
-
Frisse ME, Johnson KB, Nian H, et al. The financial impact of health information exchange on emergency department care. J Am Med Inform Assoc; 2012; 19(3): 328-333.
-
Society of Hospital Medicine. Project BOOST: Better outcomes for older adults through safe transitions. Available athttp://www.hospitalmedicine.org/AM/Template.cfm?Section=Home&CONTENTID=27659&TEMPLATE=/CM/HTMLDisplay.cfm. Accessed August 6, 2012.
-
Kern LM, Wilcox A, Shapiro J, et al. Which components of health information technology will drive financial value? Am J Manag Care; 2012; 18(8): 438-445.
-
Gordon P, Camhi E, Hesse R, et al. Processes and outcomes of developing a continuity of care document for use as a personal health record by people living with HIV/AIDS in New York City. Int J Med Inf; 2012; 81(10): e63-e73.
-
Leath B, Mardon R, Atkinson D, et al. NIH-community care coordination performance measures (NIH-CCCPM) project technical report on project: Standardizing community care coordination measures linked to improvements in quality of life and health outcomes among vulnerable populations. Rockville, MD: Westat; 2012.
-
Wolf L. National Governor's Association long-term care and health information exchange coordinate care to improve outcomes. Kindred Healthcare; 2011. Available at http://www.nga.org/files/live/sites/NGA/files/pdf/1105HIELARRY.PDF.
-
Bailey JE, Wan JY, Mabry LM, et al. Does health information exchange reduce unnecessary neuroimaging and improve quality of headache care in the emergency department? J Gen Intern Med; 2013; 28(2): 176-183.
-
Kern LM, Dhopeshwarkar R, Barron Y, et al. Measuring the effects of health information technology on quality of care: A novel set of proposed metrics for electronic quality reporting. Jt Comm J Qual Patient Saf; 2009; 35(7): 359-369.
-
Kern LM, Blumenthal D, Pincus H, et al. Quality measures for capturing the effects of health information exchange. AMIA Annu Symp Proc; 2008; 1001.
Appendix C. Environment Scan and Literature Review Sources
The literature review and environmental scan sources included peer-reviewed scientific and academic articles and the grey literature. Sources included trade journals, reports from the public and private sectors, and other identified material relevant to health information technology (HIT) and health information exchange (HIE) in long-term and post-acute care (LTPAC)/long-term services and supports (LTSS) settings, transitions of care, care coordination and longitudinal care plans for persons who receive LTPAC/LTSS services, and interventions to reduce hospital readmissions and medication errors in this population. Care coordination and care transitions literature was also reviewed to identify effective models of care and the role of information sharing and exchange. Sources for published articles were PubMed, Google Scholar, and the International Medical Informatics Association Inventory of HIT Evaluation Studies and Systematic Reviews (http://evaldb.umit.at). The inclusion criteria included studies based in the United States from 2007 and later. References from the most relevant articles were also reviewed to identify any important published articles that were not identified from the targeted search.
Search terms included "Health Information Exchange" plus other terms including, but not limited to: "Care Coordination," "Care Transitions," "Long-Term Care," Long-Term and Post-Acute Care," "Nursing Home," "Post-Acute Care," "Home Health," "Long-Term Support Services," "Hospice," "Care Transitions," "Hospital Readmissions," "Medication Management," "Medication Reconciliation," "Outcomes," and "Measures."
The environmental scan sources included:
-
Web sites of HIE organizations and participating health care systems with participating LTPAC providers such as Utah Health Information Network, HEALTHeLINK (Western New York), Secure Medical Records Transfer Network (Oklahoma), HealtheNet (Maine), Colorado Regional Health Information Organization, Delaware Health Information Network, and Maimonides Health Care System.
-
The Office of the National Coordinator for Health Information Technology (ONC) Theme 2 Challenge Grant Awardees Update Report.1
-
Presentations on HIE and LTPAC providers available from the Internet (e.g., by Challenge grantees, Beacon communities).
-
Materials provided by key informants and expert project advisors, including Michelle Dougherty from the American Health Information Management Association (AHIMA) and Dr. Larry Garber from Reliant Health, a LTPAC provider and a Challenge Grant recipient.
-
The Office of the Assistant Secretary for Planning and Evaluation (ASPE) web site and ASPE-sponsored webinars (with AHIMA) on HIE and LTPAC.
-
The most recent ONC report on adoption of HIT to facilitate the electronic use and exchange of health information.2
-
State, federal, and other web sites of initiatives and programs that support care coordination and transitions, such as the Standards and Interoperability (S&I) framework and workaround exchange to support care transitions and key S&I workgroup reports, models, use cases, and findings.
-
Meaningful use criteria under the electronic health record Incentive Programs to support HIE for care transitions.
-
Accountable care organization (ACO) model descriptions to improve care transitions and descriptions of funded ACOs.
-
Centers for Medicare and Medicaid Services programs, rules, and funding initiatives that support new models of care including LTPAC, such as the Center for Medicare and Medicaid Innovation, Community-Based Care Transitions Program State Demonstrations to Integrate Care for Dual Eligible Individuals, and physician payment incentive programs.
-
The Arizona HIE environmental scan for long-term care.3
-
National Quality Forum reports related to care coordination and measures, including the Critical Paths Care Coordination project.
-
Other federal, state, and community initiatives including the State Action on Avoidable Re-hospitalizations Initiative and initiatives undertaken by Quality Improvement Organizations.
Notes
-
Metz K, Russell W. Improving transitions of care in LTPAC: An update from the Theme 2 Challenge Grant awardees. Washington, DC: ONC; 2013.
-
Office of the National Coordinator for Health Information Technology. Update on the adoption of health information technology and related efforts to facilitate the electronic use and exchange of health information. Washington, DC: ONC; 2013.
-
Arizona Strategic Enterprise Technology Office.Arizona health information exchange environmental scan: Long-term care. CFDA #93.719. Phoenix, AZ: Arizona Strategic Enterprise Technology; 2012.
Appendix D. Promising Components and Interventions to Reduce Readmissions
TABLE D-1. Promising Components and Interventions to Reduce Readmissions
| Comprehensive Discharge Planning | |
| Assess Transition Risks |
|
| Prepare the Patient |
|
| Develop Post-Discharge Plan of Care (POC) |
|
| Post-Discharge Support and Care | |
| Prepare the Next Provider of Care |
|
| Ensure Post-Discharge Followup |
|
| Ensure Post-Discharge Support |
|
SOURCE: Metzger J. Preparing for accountable care: Coordinated care. Falls Church, VA: Computer Sciences Solutions Global Institute for Emerging Healthcare Practices; 2012; WA12_0280 HCG.
Appendix E. Summary of Literature on Health Information Exchange Outcomes and Related Measures
Studies on the impact of electronic health information exchange (HIE) on health care and other outcomes can provide evidence-based measures of HIE impact. Hincapie et al.1 conducted a systematic review of literature to identify and describe evidence of HIE impact on health care outcomes. Of 207 abstracts retrieved, only five articles met the inclusion criteria (e.g., original investigations in English that focused on HIE outcomes, definition of HIE). None of these five studies included long-term and post-acute care/long-term services and supports settings. Of these, three were randomized controlled trials, one involved retrospective review of data, and one was a prospective study. Hincapie found that HIE benefits on health care outcomes are still sparsely evaluated, and that among the measurements used to evaluate HIE, health care utilization is the most widely used.
The few articles that met the inclusion criteria varied significantly in methodology and different measures were used for outcome assessments. The majority of the outcomes measures focused on health care utilization such as number of visits to ED and duplication of services and costs. Only one of the three randomized controlled studies included in this review identified positive HIE outcomes. Overhage et al. found significant cost savings in ED charges per visit at one of the two hospitals involved.2 In comparison, Lang et al. did not find differences in the number of repeated visits to EDs 2 weeks after the initial visit;3 Hansagi did not find findings favoring HIE in any of the outcomes measured.4 Moreover, in Vest's retrospective analysis, HIE use was associated with greater health care services utilization.5
Hincapie noted several reasons for the lack of results supporting HIE to improve cost and clinical outcomes such as improved quality of care and safety. The study intervention periods were relatively short, varying from 6 months to 30 months, which could prevent long-term benefits to become evident. Also, all studies aggregated costs and other utilization measures for analyzing data and results may be confounded by other factors such as illness severity differences in the study groups. Thus, there are few evidence-based measures of HIE impact that can inform HIE intervention impact measures.
A more recent study by Frisse et al. investigated the impact of HIE within the ED setting.6 Frisse studied the impact of HIE on several health services outcomes, including hospital admissions, head and body computed tomography (CT) use, and laboratory test ordering. Two methods of clinician access to HIE were investigated, including direct access to the HIE through a secure web browser. Frisse found that for EDs that provided direct access to HIE information through a portal, patients whose information was accessed when compared to matched patients whose information was not accessed had statistically significant differences in utilization for three outcomes: hospital admissions from the ED were reduced, while use of head CTs and chest x-rays increased.
Bailey et al. also note the dearth of evidence to support HIE to reduce unnecessary testing and improve the quality of ED care, and conducted a recent study, published in 2012, of whether HIE used in EDs reduces potentially unnecessary neuroimaging, increases adherence with evidence-based guidelines, and decreases costs in the ED evaluation of headache. HIE use was associated with decreased diagnostic imaging and increased evidence-based guideline adherence in the emergency evaluation of headache, but was not associated with improvements in overall costs.7
Kern et al. developed a framework and with advisement of a panel of 28 national experts, searched the literature to identify functionalities enabled by EHRs and HIE across three health care settings. They rated each of 233 functionality-setting combinations on their likelihood of having a positive financial effect, and validated the top-scoring functionalities with the national expert panel. The most highly rated HIE functionalities that could drive financial value are:
-
Send and receive images, imaging reports and laboratory results.
-
Receive discharge medication list from ED and inpatient settings.
-
Enable structured medication reconciliation.
-
Send and receive medication history from other providers for unstructured medication reconciliation.
-
Send a query and receive information about formulary compliance.
-
Send and receive allergy history.
-
Facilitate quality improvement reporting to external organizations.
-
Send and receive authorizations for procedures.8
These high-value functionalities can serve as the basis for measures of data exchange functionality and for benchmarking (e.g., to monitor and compare what functionalities are available).
Hincapie recommended that future HIE evaluations with different levels of interoperability should incorporate a framework that allows a detailed examination of HIE outcomes that are likely to positively affect care.
Two existing HIE evaluation frameworks were identified in the literature review for this study. One was developed by Dixon et al.9 for evaluating the costs, effort, and value of nationwide HIE with evaluation domains of five broad categories: implementation, technology, policy, data, and value. Each category enumerates a variety of measures and measure types. For example, the data exchange measures include volume of clinical data exchange activities inside the local HIE, completeness of information in a summary patient record, effort needed to massage the data into a normalized form, times/instances when required data are not available due to any reason, volume of clinical data exchange activities, number of patients registered within the HIE, ability to share data using continuity of care document/clinical document architecture formats, and percent of the data shared within the local HIE available as a clinical result.
These measures can help to better monitor and interpret the impact of care transitions and care coordination. For example, if an HIE intervention is to send secure Direct e-mail and the summary of care record is incomplete (data) because key data are not captured by the EHR or the interfaces with the EHR are not correctly developed (technology) or if only a small percent patients are registered with the HIE (implementation, policy, data) and can have their date retrieved or sent, or if staff are not trained to use the HIE (implementation), then the impact of the HIE intervention on other measures such as hospitalizations and rehospitalizations will be weak.
Another framework, developed by the University of Maryland Center for Health Information and Decision Systems (CHIDS) is called the Evaluation Framework for Sustainable HIE. This framework consists of five interrelated and dimensions that are mutually reinforcing, and adequate performance in each dimension is necessary for the overall success and continued viability of a HIE organization (HIEO): value creation and sustainability; governance; technology; community engagement; and public trust. The CHIDS framework is relevant to measuring success and sustainability of the HIEO, but does not provide a framework to measure care coordination impact and outcomes.10
Notes
-
Hincapie AL, Warholak TL, Murcko AC, et al. Physicians' opinions of a health information exchange. J Am Med Inform Assoc; 2011; 18(1): 60-65.
-
Overhage JM, Dexter PR, Perkins SM, et al. A randomized, controlled trial of clinical information shared from another institution. Ann Emerg Med; 2002; 39(1): 14-23.
-
Lang E, Afilalo M, Vandal A, et al. Impact of an electronic link between the emergency department and family physicians: A randomized controlled trial. Can Med Assoc J; 2006; 174(3): 313-318.
-
Hansagi H, Olsson M, Hussain A, et al. Is information sharing between the emergency department and primary care useful to the care of frequent emergency department users? Eur J Emerg Med; 2008; 15(1): 34-39.
-
Vest JR. Health information exchange and healthcare utilization. J Med Syst; 2009; 33(3): 223-231.
-
Frisse ME, Johnson KB, Nian H, et al. The financial impact of health information exchange on emergency department care. J Am Med Inform Assoc; 2012; 19(3): 328-333.
-
Bailey JE, Wan JY, Mabry LM, et al. Does health information exchange reduce unnecessary neuroimaging and improve quality of headache care in the emergency department? J Gen Intern Med; 2013; 28(2): 176-183.
-
Kern LM,Wilcox A, Shapiro J, et al. Which components of health information technology will drive financial value? Am J Manag Care; 2012; 18(8): 438-445.
-
Dixon B, Zafar A, Overhage JM. A framework for evaluating the costs, effort, and value of nationwide health information exchange. J Am Med Inform Assoc; 2010; 17(3): 295-301.
-
Agarwal R, Crowley PK, Khuntia J, Mithas S. The District of Columbia Regional Health Information Organization (DC RHIO) Current Progress and the Road Ahead -- An Assessment Report based on the CHIDS HIE Evaluation Framework. University of Maryland Center for Health Information and Decision Systems, College Park, MD; 2010. Available at:http://www.rhsmith.umd.edu/files/Documents/Centers/CHIDS/DCRHIOAssessmentReport.pdf.
Appendix F. Examples of Community-based CARE Transition Program with LTPAC/LTSS Participation
TABLE F-1. Examples of Community-Based Care Transition Programs with LTPAC or LTSS Participation
| ACO | Service Area | LTPAC/LTSS Provider Type |
|---|---|---|
| Aging & Long-Term Care of Eastern Washington | Eastern Washington | In-Home Services |
| Southeast Washington Aging & Long-Term Care | Southeast Washington | In-Home Care, ADC, HCRR |
| Eddy Visiting Nurse Association | Upstate New York | HHA |
| Advanced Care Transitions (ACT) | Marin County, California | Long-Term Care Ombudsman, In-Home Support Service |
| Community SeniorServ | Southern California | Meals on Wheels, Senior Lunch Program, Adult Day Services |
| Jewish Home for the Aging Geriatric Services Inc. | San Fernando Valley, California | Rehabilitative Services, Independent Living Facilities, ALF, SNFs, Dining & Nutrition at Home, Hospice Care, Senior Centers |
| Los Angeles Mid-City Integrated Care Collaborative | Los Angeles, California | SNFs, Rehabilitation Centers, CBOs |
| Catholic Health Care Transitions Services, Inc. | Southeast, Florida | HHA, SNF |
| Osceola-St. Cloud Community-Based Care Transitions Coalition | Osceola-St. Cloud, Florida | SNF |
| Elder Options | Mid-Florida | HHA, SNF |
| AgeOptions (with Rush University Medical Center [RUMC] Care Transitions Program) | Cook County, Illinois | LTSS, HHA, SNF |
| Southern Alabama Regional Council on Aging (SARCOA) | Southern Alabama | In-Home Service, Independent Living, ALF, SNFs |
| Top of Alabama Regional Council of Governments (TARCOG) | Northern Alabama | HCBS |
| Community Connections' Aging & Disability Resources | Pierce County, Washington | Long-Term Care Ombudsman, Adult Day Services, In-Home Support Services, Nutrition Services & Senior Centers |
| Eastern Virginia Care Transitions Partnership | Eastern Virginia | ADC, Home Care/Personal Care, Meals on Wheels |
| Appalachian Community Transitions (ACTion) Project | Southwestern Virginia | Adult Day Health Care, SNF, Meal Services, Home Care Services |
| Lower Rio Grande Valley Development Council | Lower Rio Grande Valley, Texas | Long-Term Care Ombudsman Program, Community Assistance |
| El Paso, Texas Aging & Disability Resource Center (ADRC) | Far West Region, Texas | Senior Care Services, Hospice Care |
| Deep East Texas Council of Governments (DETOG) on Aging (AAA) | Eastern Texas | ADC, Home-Delivered Meals |
| Central Texas Aging & Disability Resource Center (ADRC) | Central Texas | Home Services, ADC, Home-Delivered Meals |
| Care Connection Aging & Disability Resource Center (ADRC) (Care Connection) | West of Houston, Texas | Age Well Live Well--Fitness Programs, Fall Prevention, Medication Management, Healthy Living Series, Hospice Care, HHA, Meals on Wheels, Senior Services |
| Area Agency on Aging (AAA) of Southeast Texas | Southeast Texas | Home-Delivered Meals, Transportation Services, Long-Term Care Ombudsman Program, Benefits Counseling Program |
| Chattanooga Regional Medicare Community-Based Care Transitions Program (CCTP) | Southeast Tennessee | CHOICE Program (in-home services), Congregate Meal Programs, Home-Delivered Meal Services, Homemaker Services, Nutrition Transportation, Senior Centers |
| Carelink, Inc. | Providence, Rhode Island | Home Services, SNF |
| Upstate Care Transitions Coalition | Appalachia Area, South Carolina | Counseling & Support Groups, Mobility Assistance Programs, ALF, HHA, NHs, Rehabilitation Centers |
| York County Area Agency on Aging (AAA) | Central Pennsylvania & Northern Maryland | ADC, Nutrition Services, Personal Care Services, Senior Centers, Transportation Services |
| Carondelet Chronic Care Navigation Program | Southern Arizona | Hospice & Palliative Care |
| Area Agency on Aging (AAA), Region One | Maricopa County, Arizona | Home-Delivered Meals, Independent Living Facilities, 24hr Senior Help Line |
| Sun Health | Northwest Area of Maricopa County, Arizona | SNFs, Independent Living Facilities, ALF, Rehabilitation Centers |
| CareLink | Central Arkansas | Meals on Wheels, Home Care, Medication Prescription Drug Counseling, Senior Center |
| San Diego Care Transitions Partnership | San Diego, California | Transportation Services, Personal Assistance, Laundry Services, Protective Support |
SOURCE: Descriptions of CCTP projects from CMS Innovations web site: http://innovation.cms.gov/initiatives/CCTP/CCTP-Site-Summaries.html.
Appendix G. Health Information Exchange Interventions and Activities Identified That SUPPORT CARE Coordination for Persons Receiving LTPAC/LTSS
TABLE G-1. HIE Interventions and Activities Identified that Support Care Coordination for Persons Receiving LTPAC/LTSS
| Entitles Engaged in HIE to Support Care Coordination for LTPAC/LTSS | HIEO and Any Relevant Initiatives | Types of Exchange Partners with the Entities | LTPAC/LTSS Exchanges Data (y/n) and How | Links |
|---|---|---|---|---|
| RI NHs, 13 trained NHs, more to be trained* | Currentcare Beacon Community |
Hospitals, laboratories, outpatient | Not yet or limited use. | http://www.currentcareri.com/matriarch/default.asp |
| Briody NH & Brothers of Mercy, SNFs, Western NY | HEALTHeLINK/ HealtheNet Western NY Beacon Community |
Hospitals, primary care, laboratories, SNFs | Yes, both have LTPAC EHR software, likely with interfaces to HIE, no additional information available, assume similar to Beechwood, 1 of 3 SNFs participating in HIE in Western NY. | http://wnyhealthelink.com http://www.briody.org/ http://www.brothersofmercy.org/skillednursing.htm |
| Beechwood Homes, a SNF, part of Beechwood Continuing Care, Getzville, NY (also study site visit) | HEALTHeLINK/ HealtheNet Western NY Beacon Community |
Hospitals, primary care, laboratories, other SNFs, HHA | Yes, AOD EHR has interfaces to send an ADT through secure HL7 messaging. Can access data via HEALTHeLINK from portal. | http://www.beechwoodcare.org http://wnyhealthelink.com http://www.wnyhealthenet.org/ |
| Eastern Maine Health Care (EMHC),* a HHA (also study site visit) | HIN Bangor Beacon Community ACO |
Hospitals, primary care, laboratories, CCRC | Yes, HHA have Allscripts & telehealth. Can send self-management information in relation to COPD, heart disease, diabetes, & asthma to HIN. Can access data from HIN via portal. | http://easternmainehomecare.org/home-health-services.aspx?id=68257 http://www.hinfonet.org/ http://www.hinfonet.org/resources/health-information-exchange/hie-participant-list |
| Brookdale Senior Living (BSL) communities (throughout US, including TX & FL) | HIEO depends on community INTERACT, CMS Innovations Grant, Transitions of Care Program in TX & FL |
Hospitals | Yes, for CMS Innovations project some other BSL facilities outside the INTERACT project, a small number of BSL post-acute providers are exchanging with local private or regional HIEOs using Direct. | http://seniorhousingnews.com/2012/08/13/assisted-living-program-for-reducing-rehospitalizations-could-have- national-impact http://www.brookdaleliving.com |
| Cedar Creek Living Center, a SNF, Norman, OK | SMRTNET Challenge Grant |
Hospitals, primary care, laboratories, NHs, Norman, OK Regional Health System | Yes, Direct secure e-mail sends SBAR, UTF using INTERACT for transitions. Staff can access VHR. | http://www.smrtnet.org/home http://www.resourcesystems.net/LongTermCare/CareTracker.aspx |
| Cathedral Square Corporation, housing, services & long-term care (LTSS) needs, VT | VHIE SASH model |
HCBS, LTSS, hospitals, primary care physicians | Scheduled to exchange through VHIE by Fall 2013 so that program will be interoperable with community health teams & the VT hospitals' EHRs. The primary care providers & hospitals that are part of the medical homes are already connected through the Blueprint for Health & a clinical registry. Physicians participating in the Blueprint for Health record data about their patients in a registry or an EHR. Housing services enters data directly into a clinical registry. Health status information that will be sent among the community's SASH exchange partners includes nutrition, fall risk, physical inactivity rates, ADLs, IADLs, fall history, & basic health information. Hospitals use the ADT messages & this will be facilitated with HIE. | http://cathedralsquare.org/future-sash.php http://www.vitl.net/health-information-exchange/blueprint-for-health |
| Montefiore Medical Center,* Integrated Delivery System (IDS), New York, NY | Bronx RHIO, a borough-wide system that supports exchange between Bronx hospitals, health centers, NHs, HHAs, community-based physician practices for patients who have signed consent forms ACO |
Hospitals, primary care, health centers, laboratories, NHs, HHA | Yes, HHA, SNF have integrated EHR links to community-wide system within the IDS, inpatient & outpatient EHRs. They also have access to patient data through Bronx RHIO. | http://www.prnewswire.com/news-releases/montefiores-bronx-accountable-healthcare-network-to-participate-as- medicare-pioneer- accountable-care-organization-135871133.html http://www.innovations.ahrq.gov/content.aspx?id=3651 |
| CO LTPAC providers: 65 SNFs, 3 ALFs, 30 HHAs, 14 hospice organizations, 1 LTPAC | CORHIO Challenge Grant, ACO |
Hospitals, laboratories, primary care physicians, other LTPAC providers | Yes, Viewing community health record from hospitals LIVE on CORHIO. Includes ADT's, Lab Results, Pathology results, Transcription reports, H&P. | http://www.corhio.org/ http://statehieresources.org/wp-content/uploads/2012/05/CORHIO-Challenge-Grant-Summary-Report-April-2012.pdf |
| Complete Home Care, HHA, CO | CORHIO Challenge Grant, ACO |
Hospitals, primary care, laboratories, NHs | No. | http://www.completehhc.com http://www.corhio.org http://www.corhio.org/news/corhio-e-newsletter/patient-care-coordination-improves-after-home-health-providers- connect-to-hie-%281%29.aspx |
| MA IMPACT:* 8 NHs, 2 HHA, 1 Long-term acute care facility, 1 IRF participating | MeHI HIE Challenge Grant |
Hospitals, community health care centers, medical homes, ambulatory care providers, HHA, SNFs | Yes, wide variety of information including functional status. | http://mehi.masstech.org/what-we-do/press-releases/massachusetts-awarded-two-hie-challenge-grant http://wiki.siframework.org/LCC+Long-Term+Post-Acute+Care+(LTPAC)+Transition+SWG |
| Golden Living SNF s & Maria Joseph Continuing Care Community, PA | Keystone HIE ONC Grant to Geisinger, Beacon Community |
Hospitals, physicians, HHA | Yes, Golden Living has EHR with interfaces to HIE. Maria Joseph Continuing Care is an early adopter of the MDS-to-CCD tool & is sending this assessment data to hospitals & other providers. | https://www.keystonebeaconcommunity.org http://www.healthit.gov/policy-researchers-implementers/keystone-beacon-community |
| NY Presbyterian System affiliated LTPAC providers, New York, NY (Beth Israel Medical Center [hospice], Hebrew Home for the Aged [SNF], Village Center for Care [SNF], North Shore Long Island Jewish Health System [SNF], & VNSNY [HHA, see below for separate description] are the LTPAC providers in the NYCLIX) | NYCLIX (RHIO) HRSA Special Projects of National Significance Information Technology Networks of Care Initiative, Supports Select Health--a NYCLIX Medicaid Managed Special Needs Plan for Persons Living with HIV & AIDS | Yes, most providers send & receive information via NYCLIX such as ADT, diagnoses, medications, lab results, radiology reports, allergies, discharge summaries, & other clinical data, query NYCLIX to retrieve information. | http://www.healthix.org | |
| UT: 98 SNFs | UHIN | All SNFs connected for Medicaid eligibility use case | Special use of UHIN for Medicaid authorization for NH services process, now all electronic system, being pilot for HHA. | http://uhin.org |
| Avalon Healthcare throughout UT | UHIN cHIE | Yes, 14 Avalon SNFs in on system have EHR, can push information to HIE. | http://www.avalonhci.com/communities/utah/ | |
| Maimonides Medical Center (Mental Health Home), Brooklyn, NY | BHIX NY State HEAL grant to demonstrate enhanced care coordination |
Mental health providers, hospitals, outpatient care clinics, 13 organizations with which Maimonides works | Yes, BHIX provider portal & messaging system to send & receive information including real-time alerts when patient has inpatient, ED, psychiatric admission or discharge, care coordinators monitor these events. | http://www.bhix.org http://www.maimonidesmed.org/Main/ClinicalServices/Psychiatry_45.aspx http://ehrintelligence.com/2013/04/03/brooklyn-hie-supports-mental-health-patients-coordinates-care/ http://statehieresources.org/wp-content/uploads/2013/01/Bright-Spots-Synthesis_Care-Coordination-Part-I_Final _012813.pdf |
| Kindred Health care, US (Post-acute care hospitals, nursing centers, rehab services) | Varies by location, facilities in IN are exchanging through the IHIE ACO, InteractII Program, MA Challenge Grant |
In a few communities, hospitals in their care markets, & physicians with plans to expand significantly with EHR implementation | Yes, varies by location, 1 provider uses Direct to send UTF** through VPN for transition, Kindred is rolling out PCC EHR, planning for interoperable exchange in all care markets, starting with sending the CCD. | http://www.kindredhealthcare.com |
| Senior Home Health, 22 HHAs, FL | FL HIE Partners with ACOs across FL |
Hospitals, physicians, other providers | HHAs have EHR & can access HIE information including, medications & test results from other physicians, facilities. | http://www.seniorhomecare.net http://www.florida-hie.net/ |
| MD: 4 SNFs awarded funds for adoption of HIT to support improved transitions of care for patients as they transition between hospitals & their facility | CRISP Challenge Grant |
Hospitals, other LTPAC providers | Yes, providers query patients they are treating for information in the HIE. Information obtained through the portal can be printed & incorporated into records. Types of data available: patient demographics, lab results, radiology reports, medication fill history, discharge summaries, H&Ps, operative notes, & consults. ENS notifies providers when 1 of their patients has an encounter at a MD hospital. Alerts are sent via a Direct secure message or HL7 into an EHR system. |
http://crisphealth.org/ http://www.times-news.com/local/x730873032/Nursing-homes-win-tech-grant http://crisphealth.org/FOR-PROVIDERS/Serivces-for-Long-Term-Care |
| Erickson Living Retirement Community, MD | CRISP Challenge Grant Program | Hospitals, physicians & CRISP partners | http://www.crisphealth.org | |
| Golden Living Post-Acute Recovery Centers, Central IN | IN HIE Central IN Beacon Community |
Hospitals, LTPAC providers, community health & behavioral health centers | Yes. | http://www.ihie.org/ http://m.govhealthit.com/news/major-long-term-care-provider-signs-hie-deal http://www.goldenlivingcenters.com/home.aspx |
| Visiting Nurse Service of NY (VNSNY) | NYCLIX (RHIO), Bronx RHIO, BHIX, NYCHHIP, LIPIX | Hospitals, EDs, community health centers, SNFs, pharmacies, clinical labs, diagnostic imaging centers, etc. | VNSNY enrolls physicians to use web portal to: manage their patient list with VNSNY; see current clinical information on their medications & other data; & review, sign or change the POC & modifications. The Web Portal is useful for physicians who have patients in home care, but whose EMRs cannot yet support electronic exchange of data with VNSNY or through RHIOs. VNSNY: accepts eReferrals & face-to-face attestations; display wound images & other data forms; & adapt more tightly to smartphones. A VNSNY allows the physician to: Refer patients electronically from the EMR, automatically drawing patient data from the EMR & adding instructions for home care. Receive the POC electronically, review & approve or change it, return it to VNSNY & file it in the EMR. Send & receive clinical messages electronically to & from VNSNY, & file a copy of the exchange in the EMR. |
http://healthix.org http://www.vnsny.org/why-vnsny/getting-started/health-information-exchange http://www.vnsny.org/system/assets/0000/0548/HIEFactSheet102507-English.original.pdf?1226441761/ |
| Rush University Medical Center (RUMC), Chicago, IL care transitions program, & HRS Home Care & partner SNFs (also study site visit) | Currently no HIE, MetroChicago planned The Bridge Model--EDPP, Project BOOST, HRS has received a CMS/CMMI 3026 (CCTP) Grant, RUMC plans to connect with Chicago MetroChigago HIE Fall 2013 ACO in planning phase |
HHA, SNFs, CBOs, aging services | Rush has an EHR system (EPIC) & provides access to select EHR information to facilitate information sharing particularly during the pre-discharge phase when transition plans are being established. Uses multiple methods of HIE with LTSS, LTPAC providers & other community partners, ranging from phone, fax, mail & e-mail to a referral management system by Allscripts called ECIN which allows messages & attachments to be exchanged in a secure manner. For providers with Allscripts EHR, the information can be pulled into their EHR application. HIE primarily occurs in the transition of care process in the following areas:
|
http://www.transitionalcare.org/the-bridge-model/ http://www.ehcca.com/presentations/readsummit2/golden_pc.pdf |
| Cleveland Clinic, HHA, Cleveland, OH Also small number of HIE initiatives for interfaces with specific LTPAC providers in OH |
Private HIE for EPIC users, plans to join Clinisyc Clinical HIE PCMH pilot |
Other EPIC users affiliated HHAs using Allscripts, & affiliated hospitals, outpatient In 1 Cleveland clinic facility, built interfaces with local SNF using PCC |
SNF PCC Interfaces with EPIC; HHA Allscripts interfaces with EPIC. Will be moving to EPIC home health module soon. | http://www.clinisync.org/ http://www.darkdaily.com/cleveland-clinic-and-university-hosptials-to-join-clinisync-ohios-statewide-health-information- exchange-329#axzz2tAnIEB6Z |
| DE: 48 SNFs connected | DHIN | NA | NA, more information needed. | http://www.dhin.org/ |
| MN LTPAC providers, primarily SNFs | CHIC through HIE-Bridge | NA | No, early in process of getting connected & participating. | http://www.hiebridge.org/ http://www.medinfosystems.org/web_documents/part_c_release_for_website_posting.pdf |
| Litchfield Woods Health Care Center, SNF, CT | Charlotte Hungerford Hospital Connect, Community HIE (Siemens Mobile MD HIE) | Hospitals, HHA | Yes, more information needed. | http://www.athenahealthcare.com/CT_Litchfield_Woods.aspx |
| KS HHAs (3 identified) | KHIN | NA | NA. | http://www.khinonline.org/files/KHIN_Participants_Map/013114_map.pdf |
| Council on Aging of Southwestern OH, an AAA | HealthBridge HIE Greater Cincinnati Beacon Community, ACO |
NA | Receive ADTs through Direct, admission alerts from hospitals, ED, More information NA. | http://www.healthbridge.org/WhoWeServe/OtherProviders.aspx |
| Visiting Nurse Service of Greater Cincinnati, OH & Northern KY | HealthBridge HIE Greater Cincinnati Beacon Community, ACO |
Hospitals, primary care, health centers | Receive ADTs through Direct, admission alerts from hospitals & ED. More information NA. | http://www.healthbridge.org/Portals/0/GC%20Beacon%20Overview%20new%20v2%20final.pdf http://www.healthbridge.org/WhoWeServe/OtherProviders.aspx |
| Central IL Health Information Exchange (CIHIE), connecting 30 LTPAC providers | Hospitals, ambulatory clinics, physician groups | LTPAC providers MDS data converted to CCD format, & pulled into CIHIE, where it becomes part of the patient's longitudinal record that can be accessed by any provider in CIHIE through clinician portal. Organizations with EHR that can consume CCD can pull this MDS information into their system. | http://cihie.org/ http://cihie.org/#/news/4553179412 |
NOTES: This table reflects HIE interventions identified from an environmental scan and literature review and is not intended to represent all HIE interventions and activities. Information regarding these interventions was gathered from a variety of sources, including telephone and e-mail inquiries; web sites, public or requested reports; presentations; webinars; and meeting summaries. All of these interventions have some type of electronic HIE. NA means more information was not readily available at the time of this report.
* AOD is Answers on Demand EHR software; PCC is Point Click Care EHR software.
** The UTF contains medication lists, advance directives, the patient's functional status such as activities of daily living (ADL) and instrumental ADL, treatment plans, and other data elements required by the next provider of care in order to seamless assume responsibility for the patient.
CO=Colorado; CT=Connecticut; DE=Delaware; FL=Florida; IL=Illinois; IN=Indiana; KS=Kansas; KY=Kentucky; MA=Massachusetts; MD=Maryland; ME=Maine; MN=Minnesota; NY=New York; OH=Ohio; OK=Oklahoma; PA=Pennsylvania; RI=Rhode Island; TX=Texas; US=United States; UT=Utah; VT=Vermont.
Appendix H. Site Visit Summary: Rush University Medical Center, CARE Transitions Program, Bridge Program
Executive Summary
Snapshot of Rush University Medical Center LTSS and HIE
-
Organization Type: Hospital (1 of 4 hospitals in Rush System for Health).
-
Size: 664 beds.
-
Transitional Care Programs: Health and Aging Department with Transitional Care Services including the Bridge Program. Approximately 1,800 patients in program annually.
-
Community Engagement: Founder and member of ITCC developer of the Bridge Model/Program.
-
CMS Funding: ITCC is participating in the CMS funded CCTP.
- EHR: Epic Technical Support for Information Sharing:
- Epic Care Anywhere -- HIE only for Epic clients (used primarily by hospitals and ambulatory care practices).
- Allscripts -- Care management application to share information with other subscribers.
- An HIEO is under development in Illinois and the Chicago area, but not operational at the time of the site visit.
A site visit was conducted to Rush University Medical Center (RUMC) to explore what, how, and with whom health information is exchanged including on behalf of persons receiving long-term services and supports (LTSS). RUMC is part of the Rush System for Health, an integrated delivery system with hospitals and ambulatory care practices. Rush is an urban hospital located in downtown Chicago, Illinois, with multiple programs focused on improving care transitions including improving transitions with skilled facilities, home health agencies (HHAs), reducing hospital readmissions and care coordination with community-based services.
A key component of Rush's Facility Transitions in Care and Bridge Programs is coordination with LTSS programs in the community. Through a patient-centered approach, Rush works to improve care transitions through intensive care coordination that starts in the hospital and continues into the community. The multidisciplinary health care team is extended beyond the hospital's physicians, nurses, pharmacists and case managers to also include the community resource team (therapists and community providers such as home health, skilled nursing facilities [SNFs], and other services). The team identifies and addresses the services and resources needed by the patient and works to eliminate barriers that will prevent them from safely transitioning back to the community and meeting their health care goals.
Rush University Medical System uses the Epic electronic health record (EHR) system for all patient care documentation in the hospital and ambulatory care sites. Epic is a Meaningful Use (MU) of Certified EHR Technology having achieved MU Stage 2 certification for its ambulatory and inpatient applications.1
Health information exchange (HIE) from hospital to long-term and post-acute care (LTPAC)/LTSS providers relied on multiple methods to communicate and exchange information including phone, fax/e-fax, secure e-mail, and the use a proprietary electronic referral application (AllscriptsCare Management application). Some Chicago-area hospitals allowed LTPAC providers to access their EHR to facilitate communication and information sharing, however, Rush's policy limits EHR access to only staff and physicians and does not allow access to non-affiliated providers such as LTPAC and LTSS providers.
The Allscripts Care Management application facilitates the electronic exchange of some health information (e.g., unstructured narrative messages as well as medical record document attachments) between Rush and their community partners including LTPAC organizations. The community partners who subscribe to the Allscriptsapplication can receive messages and attachments from Rush and pull some of the information into their EHR if they use an Allscriptsapplication.
LTSS Provider Definition
Long-Term Services and Supports (LTSS) are services and supports used by individuals of all ages with functional limitations and chronic illnesses who need assistance to perform routine daily activities such as bathing, dressing, preparing meals, and administering medications. LTSS include institutional and community-based services such as nursing homes, care management, adult day care, home-delivered meals, transportation providers, and other services.
At Rush, HIE between the transitional care programs and LTSS typically occurs during four phases:
-
Pre-discharge (prior to and at transition).
-
At the point of transition.
-
Immediate post-discharge (within 24-48 hours after transition).
-
30-Day followup after discharge (during shared care).
Clinical, demographic and service information is communicated by hospital case managers and care coordinators to community providers (HHA, nursing facilities, and/or home and community-based services [HCBS] providers). The lack of tools to facilitate exchange, such as a HIE organization (HIEO) is a challenge for Rush and their partners. Staff interviewed during the site visit identified a number of opportunities for improvement including:
-
Identifying the need for a HIEO available to all community partners.
-
Finding the right balance in the amount of information sent versus the information needed between the hospital and their community partners.
-
Developing standardized reports.
-
Integrating LTSS needs in a patient-centered plan of care (POC).
-
Redefining case management and care coordination to achieve a patient-centered, longitudinal care that includes partnerships with community partners.
Because of Rush's ongoing initiatives to improve transitions and coordination, they have pilot projects with HHAs and nursing facilities to improve processes and communication. These projects include ongoing multidisciplinary case management meetings on a regular basis to discuss care and process issues and work in partnership to improve outcomes.
Background on Rush University Medical Center Transitional Care Programs
About Rush System for Health and Rush University Medical Center
Rush System for Health is a not-for-profit academic medical center comprising RUMC (which we also refer to as Rush in this report), Rush University, Rush Oak Park Hospital, and Rush Health. Rush encompasses a 664-bed hospital, serving adults and children, including the Johnston R. Bowman Health Center. The Bowman Center provides acute inpatient and day rehabilitation services for older adults and people with short-term and long-term disabilities,and has apartments for moderate to low-income seniors.
The mission of Rush is to provide the very best care to patients. Their education and research endeavors, community service programs and relationships with other hospitals are dedicated to enhancing excellence in patient care for the diverse communities of the Chicago area now and in the future. The vision is for Rush to be recognized as the medical center of choice in the Chicago area and among the very best in the United States. Rush was named one of the nation's top 50 hospitals in 11 out of 16 specialty areas, including geriatrics in 2012-13 U.S. News & World Report.
Department of Health and Aging and Transitional Care Programs
Rush has a Department of Health and Aging under the direction of Robyn Golden, LCSW. Robyn has an extensive background in health care including acute care, LTPAC, and HCBS. In addition to her health care background, Robyn also has an in-depth understanding of policy issues from her Fellowship on Capitol Hill working for Senator Hillary Clinton and collaborating with agencies such as the Centers for Medicare that Medicaid Services (CMS) and the Office of the Assistant Secretary for Planning and Evaluation. She and her team strive to evolve practice by creating and testing new models of care by merging practice, research, policy and education.
The mission of Rush Health and Aging (RHA) is "to promote wellness by improving access to psychosocial and medical resources for patients, those who care for them and the community." RHA conducts research, develops programs, and provides service to improve healthy aging. RHA services include:
-
Health promotion and disease prevention.
-
Social work services focusing on wellness through assessment and connections to resources.
-
Transitional care for moving from the hospital to home and coordination of services for at-risk seniors.
-
Resource centers with information on program, services and supports (Anne Byron Waud Resource Center for Health and Aging at the Johnston R. Bowman Resource Center and the Tower Resource Center at the Tower Hospital Building).
-
Rush Generations (a membership program for individuals and caregivers who are concerned about aging well that provides tools and resources on healthy aging).
-
Developing and testing new models of care and health care innovations.
Within the Department of Health and Aging is the Transitional Care Team under the management of Madeleine Rooney, MSW, LCSW. The transitions team is comprised of social workers who provide direct services to support the discharge planning process and coordinate services with community caregivers and programs.
Enhanced Discharge Planning Program
The Enhanced Discharge Planning Program (EDPP) was designed by the Rush transitional care team to aid in patients' transitions from the hospital to their home (beyond the typical hospital discharge planning process). The transition services are coordinated by social workers who provide telephone followup and short-term (30 day) care coordination for recently discharged adults. The social workers conduct a bio-psychosocial assessment that includes a review of medical records, discharge plans and participation in pre-discharge interdisciplinary rounds.
The social workers interact, typically by telephone and some e-mail, with patients and caregivers after discharge to identify gaps in care and help address identified needs. The social workers are a resource for patients and caregivers. A randomized control trial showed a decreased in hospital readmission rate at 30, 60, 90, and 120 days post-discharge. Participants were more likely to make and keep followupappointments, had a better understanding of medication management, experienced reduced caregiver burden and had lower mortality rates as a result of the EDPP interventions.
Illinois Transitional Care Consortium
Rush is a member the Illinois Transitional Care Consortium (ITCC).2 Originally convened by Rush, the Consortium was formed in 2008 to bring together leaders from area organizations who were struggling with issues related to care transitions. The stakeholders are described below and cut across the silos of health care to discuss their mutual challenges and strategies to address the problems. Some of the challenges the ITCC set out to tackle included:
-
Improved access to information to support community-based organization (CBO) programs including better longitudinal data on the patient's history, past service utilization and access to relevant medical record information (such as the name of the primary care physician, followup appointments, demographic data, diagnoses, medications, and cognitive and physical function assessments).
-
The need for improved funding models that supported transitions and coordination with community organizations.
-
The need for improved relationships and recognition by hospitals of community providers and organizations to support the transition and care coordination process.
Over time the ITCC developed, tested, and refined concepts to address their mutual challenges. One of those concepts is known as the Bridge Model and was the foundation for a CMS Community-Based Care Transitions Grant (both described below). The Bridge Model concept was inspired by the Rush EDPP and then developed by the merging of best practices identified by the ITCC members.
The ITCC includes partners from CBOs, hospitals and research, evaluation and policy groups. ITCC includes the following partners:
Community-Based Organizations
-
Aging Care Connections.3 Aging Care Connections is a private, not-for-profit organization dedicated to serving older adults and their families through community-based services that promote dignity, self-respect and independence. Aging Care Connections is the suburban Chicago Area Agency on Aging (AAA) and Aging and Disability Resource Center (ADRC) and is the central administrator for ITCC. Services provided by Aging Care Connections include: information and assistance about resources, care coordination, education and training, chore keeping, transportation, home-delivered meals, respite, support groups and more.
-
Shawnee Alliance for Seniors.4 Shawnee Alliance for Older Adults programs serve persons over the age of 60 and their caregivers. Programs provide access to services that enable older adults to maximize their independence and remain in the community, advocating for the rights of older adults and their quality of life in the community and in nursing homes, and protecting older adults from abuse, neglect, and exploitation. They have developed and administer preventive primary health and social services and also provide services such as case management and counseling.
-
Solutions for Care.5 Solutions for Care serves the adult community and the people who for care for them. They work to find the resources that preserve independence and dignity, that lead to greater self-sufficiency and a higher quality of life. They work with individuals to access the resources available to manage their care.
Research, Evaluation and Policy Groups
-
Health and Medicine Policy Research Group.6 The Health and Medicine Research Group is an independent, not-for-profit research and advocacy institute with a focus on Illinois public health and care for the poor and under-served.
-
University of Illinois at Chicago (UIC), School of Public Health.7 The UIC School of Public Health works in partnership with community and governmental organizations to improve the health of the public and provide a learning experience for students and advance innovative research.
Hospitals
-
Rush University Medical Center -- Health and Aging.8
- RHA offers innovative programs and services designed to measurably improve health and quality of life through its program, services, and innovative research. The RHA focuses on adults and caregivers as discussed earlier in this report.
- Other Chicago Area Hospitals include Adventist LaGrange Memorial Hospital, Memorial Hospital of Carbondale, Herrin Hospital, and MacNeal Hospital.
The Bridge Model
The ITCC developed the Bridge Model to improve care coordination. It was originally developed with a focus on older adults, but is merging as a program for adults of all agencies with chronic conditions. Inspired by the EDPP noted earlier in the report, the Bridge Model9 is a social work based approach to transitional care that builds off of the aging network, designed to help older adults with chronic conditions discharged from an inpatient hospital stay to safely transition back to the community through intensive care coordination that starts in the hospital and continues after discharge to the community. The Bridge Transitional Care Program is a hospital and community partnership. There is physical office space at Rush for the Bridge Care Coordinators (BCCs) to receive referrals and access hospital and community records. The BCCs have expertise in geriatrics, strong clinical and advocacy skills, experience working in both community and hospital settings, and knowledge of state, federal and community resources. At Rush, the BCCs are their employees, but at other area hospital sites the Aging Care Connections and Shawnee Alliance for Seniors employ the care coordinators.
The Bridge Model was built and refined based on the experiences of the Consortium members and the challenges their patients' faced at care transition when they transitioned across various health care providers, payers and service delivery models. The ultimate goal was to coordinate existing systems (Figure H-1) to better serve older adults and their caregivers.
FIGURE H-1. Bridge Program Systems Targeted for Coordination

The Bridge Model assesses transition/discharge plans and issues related to home health, medical care, medication management, self-management and psychosocial complications using a proprietary accountability and communication tool called PERFECT (see Attachment H-1) to improve transitions to home care. The PERFECT form defines the mutually agreed upon expectations for care, documents the services identified and communicates problems and resolutions. A pilot project was conducted by the ITCC and anecdotal results found that PERFECT helps to identify risk elements for readmissions.
BCCs work with the discharge planners to screen for and coordinate post-hospital medical and community services for older adult care. BCCs often work out of dedicated Aging Resource Centers (ARCs) inside hospitals. The ARCs provide a dedicated space for older adults and their caregivers to explore community resources, health information and caregiving materials, and to develop community care plans prior to discharge. The Bridge Model is comprised of three phases:
-
Pre-Discharge. BCCs within the hospital identify older adult patients who may be at risk for post-discharge complications. Referrals can originate with hospital discharge planners or be generated through an integrated risk screen in the Epic EHR. The BCCs meet with older adults and/or their caregivers in the hospital room or in the ARC to identify unmet needs and to set up services prior to discharge. BCCs may also prepare individuals for discharge by reviewing medical records or meeting with an interdisciplinary team within the hospital.
-
Post-Discharge. Often new needs are frequently identified soon after an older adult returns home. BCCs call consumers within 24-48 hours after discharge to conduct a secondary assessment and intervene on identified needs. Areas of need include understanding discharge instructions, transportation issues, physician followup, burdened caregivers, problems with home health care, difficulty obtaining and/or understanding medications and others.
-
30-Day Followup. The BCCs followup with patients at 30 days post-discharge to track their progress and address emerging needs and to ensure that people are connected to longer-term support services.
Evidence has shown a positive impact on readmissions, physician followup, understanding of discharge plans, understanding of prescribed medications, access and timeliness of community services, and mortality. Bridge community partners reported improvements in receiving more complete information at the point of transfer and understanding patient more completely before services are started.
Rush University Medical Center Case Management
Rush has case management services lead by Sandy McFolling, Hospital System, Director of Case Management. The director also oversees the utilization review and clinical documentation improvement functions as well as social workers who work in transplant and chemotherapy. The case management strategy is to develop partnerships in the community and build collaboration with the hospital.
The focus of LTSS programs at Rush relates to improving care transitions through a patient-centered approach that engages a multidisciplinary health care team to identify and address barriers in collaboration with community providers. Their multidisciplinary team includes: nursing, physicians, nurse and social work case managers, pharmacists and Bridge social workers.
Rush has multiple departments/business units and five programs focused on improving care transitions:
-
Facility Transitions in Care (July 2008 - Current). The case management department makes a followup phone call within 24 hours to the receiving SNF to determine if pertinent information was received and correct, the patient presented as expected, and the patient/family was satisfied with the plan. The goal is to resolve issues immediately and establish a basis for collaborative problem solving and process improvement between case management, nurses, physicians and facilities. Since the program started, Rush reported readmissions to the hospital within 30 days of discharge decreased from 43.9% in 2007 to 11.9% in 2012.
-
Skilled Facility Rush Coordinated Care -- Rush Physicians and Nurse Practitioners (2012 - Current). A program at four SNFs is aimed to improve coordination of care through engagement of Rush nurse practitioners and physicians. With this program, the patient is seen by the physician or nurse practitioner post-hospital discharge at least twice in the first week and then weekly until they are stable. The nurse practitioner works closely with the nursing home staff through face-to-face discussions, bedside teaching and ongoing availability by cell phone. Quarterly meetings are held with the Rush Coordinated Care Director, each skilled facility owner/administrator, and Case Management Director. Monthly data is tracked to identify areas of success and need for improvement.
-
HHAs Care Transitions (2010 - Current). Since 20% of persons discharged from Rush are discharged to HHA services, this project was initiated to improve coordination. There are a number of initiatives that are underway with HHAs that provide services to Rush patient's to improve the coordination of care, patient quality and safety around the following common goals:
- Increase patient satisfaction;
- Decrease hospital readmissions;
- Provide patient/family centered care;
- Perform accurate and timely medication reconciliation;
- Provide timely referrals;
- Improve hand-offs and provision of discharge services; and
- Decrease frequency of Bridge social work followup calls related to issues.
The HHAs that are part of the CMS Community-Based Care Transitions Program (CCTP) also participate in a pilot project where the care team holds a weekly care conference to monitor the patient's clinical and social status to identify issues and implement timely interventions to prevent readmissions and/or address chronic problems such as poorly controlled pain. The goal is to operationalize the best practices that emerge from the CCTP grant at Rush and with community partners.
-
Inpatient Collaborative Care Model (August 2010 - Current). This pilot project developed and tested a standardized set of interdisciplinary care coordination protocols on one medical unit to promote patient satisfaction, reduce readmissions and decrease fragmented care. The program utilized concepts from the Bridge Program and Project Better Outcomes for Older Adults through Safe Transitions (BOOST).
-
Readmission Reduction Project RED Pilots (October 2012). The goal of this project was to maintain an overall readmission rate of less than 12.32% at Rush. Under this project, Rush is developing and implementing processes and maintenance metrics to achieve a reduction of 20% in the overall readmission rate. At the time of the site visit, Rush completed initial meetings, identified a bundle of 12 reinforcing interventions, and started a pilot. Next they will implement daily risk reports and use a new discharge advocate flow sheet in Epic to analyze results.
-
The Bridge Program. Described above.
The success of Rush's care transition and community engagement programs is dependent on having the right people, processes and information available. The section titled "Health Information Exchange Information Flow" will describe the information needed at key points of transition and shared care. These programs have been recognized for their innovation and success having won awards from the Case Management Society of America and URAC (an organization that promotes health care quality through accreditation, education and measurement programs).
-
Illinois Transition of Care Consortium, Bridge Model. http://www.transitionalcare.org/the-bridge-model.
Policy Drivers for Increased Focus on Transitional Care Programs
There were two Federal Government programs that provided opportunities to expand programs to improve transitional care processes, improve performance, or test new models of delivery and payment that involved LTSS as described above. They include funding under a CMS 3026 Grant for Community-Based Transitions Program and the Hospital Readmission Reduction Program.
CMS Community-Based Care Transitions Program (3026 Program)
The ITCC is currently participating in the CMS funded CCTP. ITCC members -- Aging Care Connections and Health and Medicine Policy Research group -- provide program management support and AgeOptions serves as the central administrator.
The goals of the CCTP are to improve transitions of beneficiaries from the inpatient hospital setting to other care settings, to improve quality of care, to reduce readmissions for high-risk beneficiaries, and to document measurable savings to the Medicare program.10 In the Rush system eligible individuals for the Bridge Program are Medicare beneficiaries who have at least one chronic condition that requires followup care and meet certain risk criteria for rehospitalization (e.g., over 60 years of age, has at least one chronic condition, lives alone and/or goes home with home health or discharged to a SNF participating in the 3026 Program). The Bridge program serves approximately 1,800 patients. The Bridge Model is a core component of the ITCC CMS CCTP contract.
The ITCC plan (separate from the CCTP) is expanding its use and replication the Bridge Model. Expansion and replication of the Bridge Model beyond the Chicago area is also a component of the CCTP. Figure H-2 Identifies the replication sites around the country -- expansion into five sites were related to the CCTP and twelve others were funded by their community or individual hospital resources.
FIGURE H-2. Replication Sites for Bridge Model and Community-Based Care Transition Program Sites
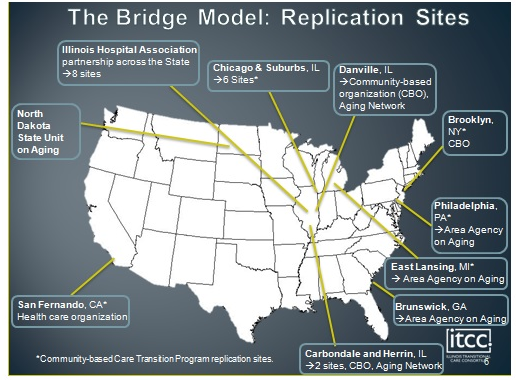
Hospital Remission Reduction Initiatives
Rush has focused on improving the transition of care through various initiatives starting in 2007. As a result of the CMS Hospital Readmission Reduction Initiative,11 Rush began a readmission reduction project in 2012.
Other Emerging Payment Models such as ACOs
Rush is not currently involved in any of the new payment models such as an ACO or bundled payment, however they are exploring new accountable care arrangements. Dr. Julio Silva is a vice president and the CMIO at Rush reported that Rush is applying for a Medicare Shared Savings plan in the Fall 2013. There is a Medical Home Network, the interviews with staff did not indicate that LTSS programs were integrated into the Medical Home Network and services.
-
Readmission Reduction Program. CMS Web site: http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/Readmissions-Reduction-Program.html (accessed May 20, 2013).
Overview of Health Information Exchange to Support Long-Term Care Services and Supports at Rush University Medical Center
The availability, use and exchange of information are crucial to providing LTSS. As noted in the programs above, Rush has been dedicated to improving the transition of care process for a number of years. To accomplish this goal they have engage various departments/staff within the hospital system, affiliated providers such as physician practices owned by Rush, and non-affiliated providers.
This section describes the non-affiliated providers that were interviewed during the site visit, describes the technical infrastructure at Rush including the availability of a community HIEO, and describes the health information exchanged at transition of care and during shared care using a framework designed under this project.
Rush University Medical Center LTSS-Related Non-Affiliated HIE Partners
During the site visit, three community (non-affiliated) partner organizations were interviewed to discuss the types of HIE/sharing that occurs as well as the challenges and opportunities. They are not the only LTSS community partners, but selected for study purposes.
-
Health Resource Solutions (HRS) Home Care.12 HRS, a Medicare-certified HHA, serves the Chicago area (an 11 county region) providing nursing and therapy services including: 24-hour telemonitoring, geriatric care, psychiatric care, neonatal care, pediatric care, pediatric infusions, IV therapy, high tech infusions, physical therapy, occupational therapy, social work, and disease statement management.
Specific to this project and LTSS, HRS is the preferred home care provider for the 3026 Grant (CMS CCTP) and Rush HHA Transitions in Care Program. They actively participate in pre-discharge planning at the hospital with the interdisciplinary team for high-risk Medicare beneficiaries. Under the Bridge Program they utilize the PERFECT tool to improve the success of transitions. In addition, HRS has found that their use of telemonitoring for select cardiology conditions has reduced hospital readmissions resulting in preferred provider status for RUMC and other Chicago-area hospital cardiologists.
An HRS staff member is at the hospital receiving referrals, assessing the patient, and interacting with hospital case management staff. HRS uses Allscripts EHR for home care and receives their referral information through the AllscriptsCare Management tool for sharing relevant information at the point of transfer from the hospital to home with home care services (such as demographics, financials, referral, medication information, equipment needed and clinical information related to care needs). Some of the information in the Allscripts Care Management tool can be integrated into the HRS EHR such as demographics. Other information is printed and scanned into theAllscripts EHR.
-
Warren Barr Pavilion.13 Warren Barr is a SNF that has partnered with Rush in their Skilled Facility Rush Coordinated Care Program. They provide sub-acute rehabilitation services, orthopedic rehabilitation, a specialized chronic heart failure transitional cardiac care program, advanced wound care, IV therapy, and other specialized skilled nursing service.
At the time of the site visit Warren Barr was just in the process of implementing an EHR system -- Point Click Care (PCC). They used Allscripts Care management for referrals from Rush which also provided relevant information (history and physical [H&P], labs, therapy, progress notes, social work notes, durable medical equipment [DME], demographics and financial data). Because information in Allscripts Care management is not interoperable and PCC does not support interoperable information exchange, information from Allscripts Care management cannot be automatically incorporated into the PCC system -- it must be re-entered if it is to be incorporated into Warren Barr's EHR. Warren Barr utilizes the Interact tools including the Situation, Background, Assessment and Recommendation Report (on paper now, but electronic once PCC implemented).
When Warren Barr sends patients to the hospital (typically through the emergency department) they send by hard-copy a packet of information (demographics, diagnosis, medication list, labs, H&P, etc.). Warren Barr does not create an electronic, interoperable transfer form to support the transition. They have found that information often does not make it to the medical unit where the patient eventually stays. Another challenge is finding the patient in the hospital and ensuring that the staff are aware that they are a Warren Barr patient.
A Rush physician and nurse practitioner sees patients at the SNF and will document in the SNF's EHR. For Rush patients these clinicians will also have to document in the Rush EHR system. The physician can access the Rush EHR to obtain any information needed for shared care.
-
Aging Care Connections.14 Aging Care Connections (the suburban Chicago AAA, and ADRC) offers programs and social services to adults age 60 and older and their family members to enhance their ability to remain as independent as possible in their own community. There are over 80 different programs and services available in these categories:
- Information and assistance coordinated point of entry (resources, benefits, assessment, etc.);
- Comprehensive care coordination;
- Homemaker services;
- Transportation;
- Home-delivered meals;
- Community Care Program;
- Respite;
- Elder Abuse (authorized by Illinois Department of Aging and AgeOptions, the AAA in suburban Cook County, to conduct case work services to investigate reports of suspected abuse, neglect or exploitation);
- Benefits assistance;
- Support groups; and
- Caregiver support program.
Aging Care Connections is funded in part by federal and state government agencies, the local AAA, local municipalities and townships as well as private funding like the United Way. They maintain an electronic client management information system (CMIS) and paper-based client records to records (but not an EHR). The information system maintains client records such as demographic records, results of screenings/qualifications for services, limited medical information such as medications and assessments, and service utilization records. The CMIS is not integrated with other community partner information systems/EHRs. In their role to investigate Elder Abuse, they must maintain a specific computer to access the state database to upload reports.
When Bridge social workers and/or case managers identify the need for the HCBS listed above, they share via phone, fax and e-mail demographic information, and other initiation of service information. The social workers spend significant time moving information manually, following up by phone or e-mail to make sure information was received, and following up to make sure services were implemented. Aging Care Connection has data sharing agreements to access medical record information at some area hospitals to support the transition planning process. Where agreements are in place, staff at the Aging Care Connection may access the hospital EHR to review relevant information such as the discharge plans, diagnosis, medications and assessments.
Rush University Medical Center's Technology Infrastructure
To understand the technology infrastructure and future plans, Dr. Julio Silva was interviewed during the site visit. In addition to Dr. Julio Silva being a vice president and the CMIO at Rush, he is also the Medical Director for MetroChicago HIEO which is under development.
Electronic Health Record System
Rush University Medical System has a tag line for the EHR -- "one patient-one record." Both the hospital and ambulatory care practices use Epic EHR system for all patient care documentation in the hospital and ambulatory care sites. There are approximately 1,000 physicians in the Rush system -- 6% are employed by Rush and 40% are affiliates. Rush also extends Epic on a fee-for-services basis to some non-Rush physicians and manages the IT infrastructure for a management fee. Epic supports the Care Transition Program by providing the ability to route information to staff or affiliated provider (e.g., results delivery, routing to an in-box). Rush utilizes Epic's HIE platform Care Anywhere. Care Anywhereis only available to Epic EHR system users, however, and the use of Epic is limited in the LTSS community.
The Patient Care Managers at Rush use a different application document their narrative care management notes. At this time there is not an interface between the care managers' application and the Epic EHR. Rush is working on an electronic Bridge template in the EHR system. This template would enable the electronic incorporation of the BCCs documentation including their assessment of post-discharge risk elements in the Epic EHR and viewable by all authorized users of the system.
Health Information Exchange Organization
The State of Illinois is developing a federated HIE model with a record locator services that will reach out to regions and bundle and route information. One of the regions in Illinois is the Chicago area. There is currently not an operational HIEO in the Chicago area; however, there has been a big push to support HIE in the region since many different EHR systems are deployed -- none of which talk to one another. As a result, a MetroChicago HIEO is under development with Dr. Silva serving as the Medical Director.
A Metropolitan Council comprised of 120 hospitals and communities are working together to establish the HIE. The Council began with addressing governance. In April 2013, they selected a HIE vendor. Dr. Silva indicated during the interview that the MetroChicagoHIE platform will support care coordination efforts. The HIE will have functionality to support Direct messaging, event notification for primary care providers, results routing, referral management, and eventually population management, analytics and case management.
AllscriptsCare Management System and Web Referral
To communicate with LTSS providers, LTPAC providers and some community partners, Rush uses the Allscripts Care Management application for communication/referrals with community partners. The secure communication includes non-structured messages and attachments for information such as demographics, financials, services recommended, medication information, equipment needed and limited clinical information related to care needs. Subscribers have full access to information exchanged while non-subscribers could access some minimal limited amount of information. For providers who have the AllscriptsEHR program, some information such as demographics can be integrated/populatedinto the EHR application. Otherwise information must be printed and scanned or re-entered into the EHR application. Users of the AllscriptsCare Management application find that it has significantly helped with the timely transfer of information to support transition of care. However, communication is not bi-directional. Information is sent only one way from the hospital. Some of the challenges of the system include the limited content exchanged and the cost for community partners to subscribe.
About 80% of patients are not in the Rush network of providers (or preferred partners) who use Epic and/or AllscriptsCare Management, resulting in the majority of communication around transitions occurring by phone, faxing and e-mail.
Health Information Exchange Information Flow
Table H-1 describes the information exchange activities for Rush and their LTSS services as they coordinate transition planning services. The exchange scenarios are not limited to electronic exchange.
HIT Standards Used
It was not possible to determine the level or type of health information technology (HIT) standards used to facilitate exchange. Epic is a certified EHR application and therefore meets the applicable standards required for Stage 1. Allscripts Care Management does not appear to use interoperability standards (such as a continuity of care document or clinical document architecture) since content and attachments could not be incorporated. However, it appears that Health Level 7 v2 messaging standards for demographics are used to move data from Allscripts Care Management into Allscripts EHR.
HIE Related Measures
Rush did not report or discuss any specific HIE measures, but they do collects data in their EHR and other systems to track outcome measures. They have metrics related to outcomes with transition and coordination of care under the case management department, which may be related to their exchange of information:
- Rates of readmission (readmission to any hospital in 30 days over the total number of hospital discharges);
- Increased physician followup(completed visits by 30 days post-discharge);
- Increased understanding of medications and discharge POC;
- Decreased patient and caregiver stress; and
- Nursing home placement.
TABLE H-1. HIE by Care Coordination Function and Partners, Rush University Medical Center Bridge Program
| Transitions of Care | ||||||
|---|---|---|---|---|---|---|
| Care Coordination Function | Across Members of the Care Team Within Affiliated Organization | Between Staff in an Organization and Other Non-Affiliated Care Providers Including Community Services | Between Staff in an Organization and Patient/Family Members | Type of Exchange | Data | Sender and Receiver |
| Assessment/Referral | ||||||
| Referral for Community Services | Patient is assessed for risk factors, discharge plans are being evaluated. A referral for LTSS evaluation is made. |
|
|
Case Managers to Bridge Social Workers | ||
| Case managers make referral to appropriate HHA provider. |
|
Case Manager to HHeA Nurse | ||||
| Case managers make referral to appropriate facility provider (e.g., SNF). |
|
|
Case Manager to SNF Nurse | |||
| BCCs social worker assesses patient to determine services needed. Makes referral to community service provider if need is determined and/or followup to ensure services in place--pharmacy, DME, counseling, etc. |
|
|
BCC to Home & Community Service Provider | |||
| Transitions of Care | ||||||
| Transfer/Admission to LTPAC/LTSS | Obtain physician order or communication for discharge, services, and/or followup. |
|
|
Case Manager and/or BCC to Hospital Attending Physician | ||
| Prior to discharge, a pharmacy student reviews the discharge instructions sheet & completes a pre-discharge medication reconciliation. |
|
|
||||
| Patient transferred to HHA. |
|
|
Hospital nursing staff to HHA Nurse | |||
| Patient transferred to SNF. |
|
|
Hospital nursing staff to facility Nurse | |||
| Discharge from LTPAC to Another Provider | Patient transferred from facility back to hospital. |
|
|
Facility Nurse to hospital | ||
| Followup Post Transfer | ||||||
| LTSS Care Coordinator followup with Community Service Provider & Patient | Case Management makes followup contact within 24-48 hours on all home health & SNF transfers to assist in assuring services started, answer questions, etc. |
|
|
Case Manager to HHA or Facility | ||
| Patient Care Coordinators and/or BCCs followup with referrals made for community services. |
|
|
Care Coordinator to Community Service Provider | |||
TABLE H-2. Shared Care Information Exchange Activities
| Shared Care | ||||||
|---|---|---|---|---|---|---|
| Care Coordination Function | Across Members of the Care Team Within Affiliated Organization | Between Staff in an Organization and Other Non-Affiliated Care Providers Including Community Services | Between Staff in an Organization and Patient/Family Members | Type of Exchange | Data | Sender and Receiver |
| Assess Needs and Goals | ||||||
| Admission Physician Visits/Evaluation (NH) | Rush physician & NP visit SNF patient 2 times during first week after admission & weekly until stable. |
|
|
Rush physician/NP & SNF Nurse | ||
| Create and Maintain Plan of Care | ||||||
| Care Management/ CCT Meetings | Weekly case management meetings between Rush & HHA Provider. |
|
|
Rush Care Coordinators, BCCs, Home Health Care Managers | ||
| Quarterly meeting between Rush & Facility Provider (part of SNF Rush Coordinated Care Program). |
|
Rush Coordinated Care Director, Facility Representative, Case Management Director | ||||
| Monitor, Followup, and Respond to Change | ||||||
| Ongoing physician visits/ evaluation (NH) | Rush MDs & NPs visit SNF patient for regular scheduled visits & as needed to meet medical needs of patient. |
|
|
Rush MD/NP & SNF Nurse | ||
TABLE H-3. Other Information Exchange Activities
| Shared Care | ||||||
|---|---|---|---|---|---|---|
| Care Coordination Function | Across Members of the Care Team Within Affiliated Organization | Between Staff in an Organization and Other Non-Affiliated Care Providers Including Community Services | Between Staff in an Organization and Patient/Family Members | Type of Exchange | Data | Sender and Receiver |
| Mandatory Reporting | ||||||
| Elder Abuse Reporting | Elder Abuse Reporting by Rush Partner Aging Care Connection |
|
|
Aging Care Connections Coordinator to State Agency. | ||
Barriers and Opportunities for Improved Health Information Exchange Practices
Over the course of the two-day site visit, a number of issues were identified related to information exchange in support of care transitions and engagement of LTSS programs. Rush staff and community partners interviewed offered observations on both barriers and opportunities to improvement in improved HIE, communication and coordination practices.
Barriers
-
Need for an HIE Network Available to All Community Partners:
-
The lack of a referral application (that is affordable to all) to share information between the hospital and next care providers is a significant issue since 80% of Rush's discharges do not go to a provider within the system (or a preferred provider). Allscripts Care Management has been very helpful, but its use is limited to certain providers (i.e., those who have chosen to invest/acquire this software). AllscriptsCare Management is also limited because it does not allow bi-directional communication. Clinicians report a need for an electronic system that would allow routing of transition in care/shared care information to additional non-affiliated provider types.
-
The Chicago-area HIE has not considered how to engage community partners such as home and community service providers in the HIE. They are planning for supporting transition of care processes with providers such as HHAs and nursing facilities, but had not identified community service providers as target for the HIEO.
-
Home and community service providers find it a barrier that they cannot electronically access information from other providers EHRs, medical records, or client service records for implementation of services, assessment and care planning activities. Information (such as a mini-mental exam) completed by the various providers, if electronic and available on an HIE, would provide valuable information and reduce duplication.
-
An HIEO could provide the foundation for a longitudinal (community) care plan that would be invaluable for communicating patient goals and coordinating services across multiple care providers. Providers would have important information available reducing the need to "start from scratch" with each encounter, streamlining communication and aligning services.
-
-
Need to Redefine Traditional Case Management and Recognize Care Coordination Roles:
-
The traditional view of case management from a hospital discharge perspective needs to change to achieve a patient-centered approach to coordination and collaboration that extends beyond discharge, engages community partners and helps to support the patient in meeting their health care goals.
-
Rush representatives expressed a concern that current payment models did not cover care coordination/case management roles needed by some patients and include the provision of LTSS programs and HCBS. They saw an opportunity as new care delivery and payment models emerged (such as ACOs).
-
There were concerns expressed about the limited understanding of the importance of partnering and including LTSS and HCBS services in new payment models. Inclusion of LTSS and HCBS is beginning to emerge in some ACOs as a strategy to manage costs and improve outcomes.
-
Opportunities
-
Balancing the Amount of Information Sent Versus Information Needed:
-
Senders and receivers of information are often challenged to get the right information and the right amount of detail to support their clinical purpose. Either too much information is sent creating an overload for the receiving provider ("sleuthing") or too little information is sent -- it is often all-or-nothing. Redundant data is also common. Staff would like to see a portal that would allow a receiver to control the amount and type of information they can access to support the transition and shared care processes. This would be addressed with an HIE if it includes the information needed by receiving providers. Depending on its structure and governance, this request could be accommodated via the forthcoming Chicago-area HIE.
-
-
Development of Standardized Reports:
-
HIE tools such as Allscripts Care Management currently do not have standardized reports that for tracking and trending of data based on clinical content, risk assessment tools or other reporting requirements between Rush and their community partners.
-
Rush Case Management Department is talking to Epic about developing standard reports for their referral sources. Currently the capability is not available.
-
-
Integration of LTSS Needs in a Patient-Centered POC:
-
Early screening and identification of patients who may require LTSS is crucial. The lack of consistent screening across all relevant admissions can be problematic. Hospitals could address this by implementing a screening tool of the psychosocial elements and risk factors to determine early during a hospital stay which patients may need services. Establishing a care plan prior to discharge is crucial to ensuring appropriate services are set up and consistent with the discharge and teaching plans. This is very challenging when the referral is made after discharge. Similarly, implementation of such screening tools and shared care planning mechanism prior to a hospital stay; for example, in emerging service delivery reform models (e.g., ACOs) might also improve care and decrease costs.
-
Community care coordinators/social workers often establish a community care plan, but it is not integrated with a larger plan for the patient. A patient may have many care plans established by various providers that are not coordinated or reconciled with each other.
-
A sustainable vision for aging and disability services is needed that includes improved integration.
-
Conclusion
Rush has developed a number of programs and processes to improve care transitions and coordinate with community providers. Their LTSS programs are integrated into interdisciplinary teams and community providers are engaged in the discharge planning process. Almost all of the participants in the transition process report an opportunity for improved communication and efficiency through technology. Some tools such as AllscriptsCare Management have been helpful in facilitating information exchange, but they are not consistently applied across all community providers and services. Coordination and deployment of services is at the heart of the LTSS programs at Rush. Staff spend a significant time with communication tasks (making calls, followup, sending faxes, verifying receipt) to share information with service providers. Technology and improved tools could be beneficial in supporting the work of LTSS providers.Attachment H-1. PERFECT Form
| PATIENT NAME: _________________________ | DISCHARGE DATE: _________________________ | SOC DATE: _________________________ |
| HOME HEALTH AGENCY: _________________________ HH CASE MANAGER CONTACT # (if different): _________________________ |
SOC RN CONTACT #: _________________________ TELEMONITORING AVAILABLE?: _____ Yes _____ No |
The PERFECT Form is a communication and accountability tool developed to encourage collaboration after hospital discharge between home health partners and the clinical team at RUSH. The information provided by the admitting RN in the field provides a critical snapshot of the patient in their home environment and helps us define care expectations for a successful transition from hospital to home.
How to use the PERFECT form:
- Please check yes or no for each of the care expectations listed
- Utilize the interventions column as a guide for addressing problem areas
- Use the comments section to provide any additional information
- Actions taken to resolve a problem
- Additional information about a situation
- Please contact Madeleine Rooney, MSW at RUSH at 312-942-6995 within 48 hrs. if any issues remain resolved or if any delay in care is present
- Fax completed form to 312-563-6548 within 72 hrs. of admission to the agency
- Attach additional comments on separate pages as neede
Hand off communication is essential to assure quality coordination of care.
| Care Expectations | Interventions | Additional Information | ||
|---|---|---|---|---|
| Plan of Care | ___ Yes ___ No |
Plan of care discussed with pt. & family/ consent for care signed? |
|
Note any special orders: |
| ___ Yes ___ No |
Health literacy issues identified at SOC? | |||
| ___ Yes ___ No |
Barriers to scheduling visits present? | |||
| Equipment/ Supplies | ___ Yes ___ No |
Provided within expected timeframe? |
|
DME Provider #: |
| ___ Yes ___ No |
Additional DME needs? | |||
| ___ Yes ___ No |
Telemonitoring needed? | |||
| Reconciliation of Medications | ___ Yes ___ No |
Pt has dc instructions? |
|
Pharmacy #: |
| ___ Yes ___ No |
D/C list match meds found in home? | |||
| ___ Yes ___ No |
RN contacts patient w/in 24 hrs-missing meds obtained | |||
| ___ Yes ___ No |
Pt. able to obtain meds w/out barriers? | Who fills the pillbox? | ||
| ___ Yes ___ No |
Pillbox in home? | |||
| ___ Yes ___ No |
Are medications adequately managed? | |||
| Follow Up MD | ___ Yes ___ No |
MD appt scheduled within 10 days? |
|
PCP #: MD Appt: MD Appt: MD Appt: |
| ___ Yes ___ No |
Can pt physically get to the appt? | |||
| ___ Yes ___ No |
Is transportation available for f-up appt.? | |||
| Expectations | ___ Yes ___ No |
Is patient satisfied with discharge plan and services provided? | 48 hour quality assurance call completed | |
| Caregiver & Support | ___ Yes ___ No |
Is primary caregiver available? |
|
Caregiver: |
| ___ Yes ___ No |
Community resources needed? | Pt Support: | ||
| ___ Yes ___ No |
Were community resources arranged prior to d/c? | Contact #: | ||
| Therapy | ___ PT ___ OT ___ ST ___ None |
Therapies provided w/in 72 hrs unless otherwise ordered? | Contact MD if additoinal orders needed |
| Was RN visit performed 24 hrs post D/C? ___ Yes ___ No | ||
|---|---|---|
| ___ Patient/family declines care | ___ Unsafe environment | ___ Family refuses out of network co-pay |
| ___ Care exceeds capacity | ___ No skilled need | ___ Patient re-hsopitalized before first visit |
| ___ Unable to local patient | ___ Patient not discharged from hospital | ___ Insurance out of network |
| ___ Cancelled by referral source | ___ Another agency providing services | ___ Referred to another agency |
Appendix I. Site Visit Summary: Beechwood Homes
Executive Summary
Snapshot of Beechwood Continuing Care
-
Organization Type: Long-term care community.
- LTPAC Services:
- Independent Living.
- Assisted Living.
- Rehabilitative and SNF.
- Size:
- Beechwood Homes: 272 skilled beds with a 3 specialty units: 36-bed early stage dementia unit; 27-bed Wesley Rehabilitation Center; 22-bed dedicated hospice unit.
- Blocher Homes: 57 assisted living units.
- Asbury Pointe: 110 independent living apartments.
-
Grant Funding: Beacon Community of Western New York--grant assistance provided to Beechwood for technical interfaces to participate in HIE.
-
EHR: AOD.
-
Regional HIEO: HEALTHeLINKTM (Western New York HIE).
To understand health information exchange (HIE) for long-term and post-acute care (LTPAC) providers, a site visit was conducted at Beechwood Homes (Beechwood). Beechwood is a non-profit long-term care community in the greater Buffalo, New York area. The community is comprised of independent living, assisted living and rehabilitative/skilled nursing services. The site visit conducted at Beechwood Continuing Care focused on Beechwood Homes, a 272-bed skilled nursing and rehabilitation facility with specialty units in early dementia, hospice, and rehabilitation. Its specialty rehabilitation unit, Wesley Rehabilitation Center, is designed specifically for residents with intensive, short-term rehabilitation or complex medical needs. Beechwood has embraced a patient-centered quality of life focus and is undergoing a transformation to a household environment rather than nursing units.
To deliver short-term and long-term care to its residents, Beechwood coordinates care and services with a number of health care professionals and community partners including physicians, local hospitals, ancillary services providers including pharmacies, labs and radiology, health plans and other LTPAC providers. Beechwood has begun participating in the Western New York regional HIE organization (HIEO), which is advancing electronic information exchange capabilities in the area.
Beechwood strives to be a leader/innovator in their area. Beechwood has embraced technology and looks for opportunities to expand its use of health information technology (HIT) to support their clinical and business operations, and identified regional HIE activities as important for their organization. They were selected as one of five LTPAC partners for the Western New York Beacon Community. As one of 17 Beacon Communities nationwide, Western New York is building and strengthening local HIT infrastructure and testing innovative approaches to make measurable improvements in health, care, and cost. Funded by the Office of the National Coordinator for Health Information Technology (ONC), the Western New York Beacon Community's efforts are focused on improving clinical outcomes and patient safety, through HIT and HIE.
The regional HIEO, HEALTHeLINK, is leading efforts to transform Western New York health care through the Beacon grant. Beechwood joins other community service providers (such as hospitals, physicians, labs, pharmacies, radiology centers, home health care, hospice, and payers) in participating in the regional HIE network. Beechwood is currently sending admission/discharge/ transfer (ADT) messages to the HIE and is working on receiving lab and radiology results through HEALTHeLINK.
Beechwood has the electronic health record (EHR) application Answers on Demand (AOD). They are using many modules in the system with ongoing plans to expand its use to support clinical and facility operations.
Health information is exchanged in many different ways (phone, fax, e-mail, mail, secure electronic exchange, portals, etc.) during key clinical and administrative processes. The flow of exchanged health information occurs in three categories: (1) hand-offs in care; (2) shared care; and (3) other administrative. Beechwood routinely exchanges information to complete preadmission assessments, at transfer and discharge, when assessing the patient in the development of their initial plan of care (POC), for ongoing maintenance of the patient's POC, and with status changes. Health information is also exchanged for administrative purposes to support billing and reporting.
A number of opportunities were identified over the course of the two-day site visit to expand HIE in support of clinical and/or business processes, or to address barriers. The opportunities and/or barriers include:
-
Opportunities to improve care delivery with better availability of information.
-
Need for clarified and/or implementable standards to support interoperability and HIE.
-
Ideas for expanding participation in HIE by LTPAC facilities by increasing the value proposition.
-
Beechwood with their community partners the Western New York Beacon Community and HEALTHeLINK, continue to explore new ways to improve care transition and coordination activities for their patients and the community they serve.
Background on Beechwood Homes
Beechwood Continuing Care1 is a non-profit, long-term care community in the greater Buffalo, New York area. The community is comprised of independent living, assisted living and rehabilitative/skilled nursing services. The site visit conducted at Beechwood Continuing Care focused on Beechwood Homes (Beechwood), a 272-bed skilled nursing facility (SNF) and rehabilitation facility with specialty units in early dementia, hospice, and rehabilitation. The Wesley Rehabilitation Center is designed specifically for residents with intensive, short-term rehabilitation or complex medical needs. Beechwood has embraced a patient-centered quality of life focus and is undergoing a transformation to a household environment rather than nursing units.
In addition to Beechwood Homes, there are independent living apartments at Asbury Pointe and assisted living units at Blocher Homes.
To understand the HIE processes at Beechwood, interviews were completed with facility staff in administration, nursing, admissions, rehab, information technology, and health information management (HIM). In addition, discussions were completed with the following community partners who exchange information with Beechwood:
- HEALTHeLINK (regional HIEO);
- Kaleida Hospitals and Lab;
- Catholic Health System;
- Buffalo Pharmacies, Inc.;
- Buffalo Ultrasound (radiology);
- Family Choice Health Plan;
- Amedysis Home Health; and
- Hospice Buffalo Palliative Care.
Beechwood has an EHR system and is a participant in the Western New York HIE HEALTHeLINK. Information exchange occurs in many different forms with these community partners -- traditional methods including phone, fax and e-mail as well as look access to hospital EHRs or shared drives, web portals, and through HEALTHeLINK.
1. See http://www.beechwoodcare.org/.
Western New York Beacon Community
The Western New York Beacon Community is one of 17 Beacon Communities funded by the ONC to build and strengthen local HIT infrastructure and test innovative approaches to make measurable improvements in health, care, and cost. The Western New York Beacon Community's efforts focus on improving clinical outcomes and patient safety by using HIT and HIE in diabetes care management. The Western New York Beacon is using technology to achieve its goals, which include:2
Improving the care of patients with diabetes in primary care practices and demonstrating progress toward meaningful use (MU) requirements through the use of registries, electronic diabetes guidelines (EHR prompts and alerts), and medication histories.
Reducing emergency department (ED) visits, hospitalizations for ambulatory care sensitive conditions, and 30-day readmissions rates for individuals with diabetes, and for a subset of diabetics with co-morbid congestive heart failure.
Strengthening HEALTHeLINK by adding new data sources and expanding the number of data feeds contributing to the HIE (i.e., adding discharge medications from hospital data sources).
The Western New York Beacon Community has engaged multiple types of health care providers to achieve these goals. In addition to hospitals, physician practices, they have also engaged LTPAC providers, specifically five SNFs and five home health agencies. Nursing home partners were selected if they were willing and able to set up an EHR interface to HEALTHeLINK. To assist Beechwood in being an active participant in the Western New York Beacon initiatives, the Beacon grant covered the cost to develop an interface from the nursing home EHR (AOD) to HEALTHeLINK.
One of the initiatives that the Western New York Beacon Community is focused on is hospital discharge then admission to a SNF to determine how HEALTHeLINK can improve efficiency, improve the patient transfer process and reduce adverse outcomes (For more information seehttp://www.healthit.gov/sites/default/files/private/beaconfactsheet_westernny.pdf). It should be noted that the Western New York Beacon Community is monitoring the efforts of the ONC Standards and Interoperability (S&I) Longitudinal Coordination of Care (LCC) workgroup specifically on emerging standards to support transfer of care information and in MU Stage 2 of the EHR Incentive Program.
In addition to the hospital-SNF transfer initiative, the Western New York Beacon Community has identified four long-term care use case priorities for 2013 (Attachment I-1):
- Lab and radiology results delivery from lab and radiology providers through HIE to Beechwood's EHR;
- Care planning and regulatory requirements after admission acceptance;
- Access to data needed for admission criteria; and
- Patient preference notification (future consideration).
Work has begun on the first use case priority to deliver lab and radiology results and on the second use case. Access to data for admission criteria is operational.
2. Western New York Beacon Community Fact Sheet. http://www.healthit.gov/sites/default/files/private/beaconfactsheet_westernny.pdf (also available in Appendix A).
HEALTHeLINK Western New York Regional Health Information Exchange
As noted above, Beechwood participates in HEALTHeLINK,3 which is a Regional Health Information Organization (RHIO) in Western New York. The operating costs for the HIE are currently covered by three major health plans and four hospital systems. HEALTHeLINK is also one of 13 communities selected to collaborate with the U.S. Department of Veteran Affairs in the Virtual Lifetime Electronic Record (VLER). At this time, the HIE does not conduct significant data analytics functions on Western New York population data except some basic trending and graphing of tele-monitoring data (e.g., blood sugars). Providers access this information using the virtual health record (VHR). Any provider who has signed a participation agreement and has Internet access can utilize the VHR. Providers may choose to get results delivery from HEALTHeLINK directly into their connected (eligible) EHRs. HEALTHeLINK is also part of the statewide network to collect childhood immunizations as well as syndromic surveillance.
3. See http://wnyhealthelink.com/.
Overview of HEALTHeLINK Providers and Health Information Exchange
HEALTHeLINK has prioritized eight types of health information to be available on the exchange network to providers and payers. The HIE also identifies the status of which providers are submitting the clinical data.4 Based on information reported on the HEALTHeLINK web site, there are currently 35 providers submitting clinical data and over 2,900 professionals accessing the data in the exchange network in the Table I-1 categories.
The professionals participating in the HIE include physicians, nurse practitioners, physician assistants, chiropractors, nurses, pharmacists, and dentists. HEALTHeLINK identifies on their web site the participating professionals5 and their ability to complete EHR-to-EHR exchange with a continuity of care document (CCD) and results delivery.
To have information exchanged on the HIE, a patient must give consent (see consent form at:http://wnyhealthelink.com/files/consent_form_12-20-10.pdf). Currently there are almost 450,000 individual patient consent forms signed in Western New York, and New York State has stringent patient consent policies requiring a patient to consent before their information can be shared through HEALTHeLINK. Patients have several options: They can give consent to all care providers in the HEALTHeLINK network on the date of their signature who provide their care; they can specifically identify providers who can access their information; patients can exclude a single provider or group, they can opt to consent for emergency care access only, and finally a patient can choose to never have their information accessed under any circumstances. Beechwood only needs to obtain patient consent to access their information on the HIE, if there is no valid consent in the system. At this time, the patient does not have the ability to access their information on HEALTHeLINK, however, a patient portal is being considered.
TABLE I-1. Provider Types and Health Information Available on HEALTHeLINK HIE
| Provider Type | No. of Providers Connected | ADTs | Radiology Reports | Radiology Images | Lab | Transcribed Reports History* | ED Reports | Medication History Data | Diabetic Measures |
|---|---|---|---|---|---|---|---|---|---|
| Hospital | 13 | X | X | X | X | X | X | X | |
| Regional Reference Labs | 3 | ||||||||
| Regional Radiology | 8 | X | X | X | |||||
| Tele-Monitoring Sources (Home Care) | 4 | X | |||||||
| Long-Term Care Facilities | 3 | X | |||||||
| Medication History Sources | 3 | X | |||||||
| Professionals | 2,943 |
* The type of transcribed reports varies based on health care provider. HEALTHeLINK's specifies the content sent by each provider on the webpage Providers of clinical Data (http://wnyhealthelink.com/Patients/Participants/ProvidersofClinicalData…).
HEALTHeLINK works with health care providers and their vendors to establish interfaces to the exchange organization. They meet with the vendor to determine the information that can be sent and received and the format. Some of that content can be sent and received using HIT standards depending on the vendor's capabilities. Regardless of whether standards are available, HEALTHeLINK is able to work with providers to establish interfaces the exchange organization. HEALTHeLINK monitors the efforts of the ONC S&I LCC workgroup specifically on emerging standards to support transfer of care information and care plans and will leveraging the standards identified in MU Stage 2 of the EHR Incentive Program.
Facilitating medication reconciliation at the point of transfer was an important aspect of the Western New York Beacon grant. HEALTHeLINK has been working with pharmacies and providers to receive medication information. Currently HEALTHeLINK receives medication history information from SureScripts and Buffalo Pharmacies, Inc. and are currently working with area hospitals to receive medication information upon discharge. While the sources provide a majority of medications, it is missing over-the-counter medications, medications prescribed where the patient paid cash instead of an insurance payer, or medications filled by pharmacies not reporting to SureScripts.
See http://wnyhealthelink.com/Patients/Participants/ProvidersofClinicalData….
See http://wnyhealthelink.com/Physicians/Participants/ParticipatingHEALTHeL….
Beechwood Engagement with HEALTHeLINK
Beechwood is one of five long-term care facilities currently participating in HEALTHeLINK. The other providers are Briody Healthcare Facility; Brothers of Mercy Nursing and Rehab, Heritage Centers, and Schofield Residence. Buffalo Pharmacies, Inc., an institutional pharmacy that serves LTPAC providers in Western New York, is also exchanging information.
Technology
To access information on HEALTHeLINK, providers only need an Internet connection. To exchange data with the HIE, Beechwood (and the other LTPAC providers) must have an EHR that has a custom interface to send and data using HIT standards whenever possible. For receiving data Beechwood and other LTPAC providers access the VHR portal. The VHR allows a clinician with patient consent, to query on a patient's name to see all clinical results available from sources connected to HEALTHeLINK. Some EHRs are capable of receiving patient information directly into the patient's electronic medical record while others have the added capacity to receive "pushed data" from the VHR.
Data Sent by Beechwood
In October 2012, Beechwood completed the first phase of engagement with the HIE which was sending ADT messages when a patient leaves the nursing facility. ADT event updates are sent from HEALTHeLINK to a provider through secure messaging using a Virtual Provider Network (VPN) connection. ADT messages are sent by the following standard categories of events:
- ED visit to inpatient;
- Inpatient admission;
- Outpatient visit; and
- Outpatient to inpatient admission.
At this time, Beechwood is not sending any other data to HEALTHeLINK beside the ADT event update. Area hospital staff has indicated that they would like nursing notes from long-term care providers, however, that use case has not been developed at this time.
Data Received by Beechwood
Beechwood primarily uses HEALTHeLINK to access information from the VHR portal and see the data that the patient has consented to be shared (limited to the data types listed in Table I-1). Beechwood users have an established security profile and login with two factor authentication. The exchange also has the capability to graph lab values for trending purposes.
Beechwood is currently working on having the Electronic Lab and Radiology Results Delivery functionality enabled. The first priority is to route lab and radiology results from the facility's lab and radiology providers though HEALTHeLINK and then into Beechwood's EHR system.
Additional Opportunities for Beechwood to Provide Information to the HIE
Beyond ADT events, Beechwood does not submit other health information to the HIE at this time; however they do have information generated during a patient stay that would be valuable to other providers/payers who use HEALTHeLINK. Potential information types include:
- Immunizations and tuberculosis (TB) test results;
- Advance directives;
- Skin assessments;
- Minimum data set (MDS) and assessment summary;
- SNF admission History and Physical (H&P);
- Nursing notes (e.g., three days prior to transfer to inform hospital nursing staff);
- SNF transfer form;
- SNF discharge summary; and
- Scanned image of consent form(s).
Access and Security
Beechwood staff may access the VHR portal once a patient is identified for admission consideration (as long as patient consent has been obtained for data to be shared on the exchange). HEALTHeLINK has established strict policies for access and authentication. To access information, users log into the HIE portal. The login process prompts a phone call or text message from HEALTHeLINK with a unique pass code to enter the site. The system only calls the predetermined phone number for the user. Providers may also use a security fob. As an additional security feature, Beechwood receives a report weekly which identifies the facility users who have accessed HEALTHeLINK to verify that access is appropriate and to remove terminated users.
Users and Clinical Processes
The admissions and nursing staff are the primary users of HEALTHeLINK, but other facility staff use the HIE network including social work, therapy, and the attending physicians. The primary clinical workflow supported by the HIE is the admission/transition of care process. The nurse manager in the Wesley Rehabilitation Center is the most frequent user of the exchange due to the volume of admissions and discharges to the unit. The other disciplines using the exchange are frequently accessing information to support their assessment and care planning functions post-admission.
Overview of Technology and Electronic Health Records at Beechwood Continuing Care
Beechwood has an Information Technology department that plans and deploys the technology infrastructure across the organization
Beechwood's Technology Infrastructure
Beechwood's technical infrastructure is built on a virtual environment with thin client and virtual desktops. The campus sites are connected via a fiber backbone. They deploy multiple types of hardware and devices including desktops, laptops, mobile devices, bar code scanners and printers.
Beechwood has multiple software applications for their business units including:
- Medical Record -- AOD Clinical (described below);
- Billing -- AOD;
- HIE -- HEALTHeLINK;
- Maintenance application;
- Purchasing application;
- ADP with scheduling and human resources module;
- Therapy scheduling and billing -- Aris (hosted module; data manually imported/exported to MDS and billing application);
- Recreation: Linked Senior Application;
- Staff Development -- Silver Chair Learning; and
- Administrative -- Microsoft Suite and Office Logic for e-mail.
In addition to hardware and server upgrades and replacements, Beechwood plans on adding DocuWare document management software that is a document imaging and indexing software for paper-based medical records or PDF documents that should be included. A "file cabinet" will be set up for AOD to allow scanning of medical record documents by patient ID. AOD software has the capability of pulling records from the document management system while in the application.
Electronic Health Record System
As noted above, Beechwood's clinical or EHR application is AOD. Beechwood was one of the first users of AOD in New York. They are frequently a reference site and helped start an AOD User Group in Western New York area. To understand how Beechwood uses the AOD application, Table I-2 describes the modules used and any related notes that emerged during interviews.
TABLE I-2. AOD Modules Used
| AOD Clinical Module | Notes |
|---|---|
| Admissions | Admission coordinator uses laptops to enter data into AOD directly from hospital site. Hospital data will be scanned & available in the AOD system. Once admitted change of status & workflow routing messages will be sent to relevant staff from the AOD system. |
| Face Sheet & Census | |
| MDS | |
| Care Plan | |
| Interdisciplinary Notes | Beechwood uses templates & unstructured narrative notes. |
| User Defined Assessments | Include initial assessments by disciplines & quarterly updates. |
| Incident Tracking | |
| Immunization & TB Testing | Includes both input & reporting to the State of New York through the state HCS for outbreaks, immunizations, other reportable infections & required disaster plan reporting. This portal also provides messages to Beechwood such as emergency notifications. |
| Point-of-Care | Nursing assistant ADL charting documentation at point-of-care (kiosk touch pads). Beechwood was a beta test site for AOD on this application. Homemakers (special types of nursing assistants who work on the nursing units which are called households at Beechwood) will also use this for activity tracking such as laundry, housekeeping, activities, dining, meal & fluid intake. |
| Alerts & Messaging | AOD has developed alerts & messages. Beechwood can chose to turn on or off the messages. They can be sent in AOD application or to a person's e-mail in Office Logic. Examples of clinical alerts include completion of vitals & assessments such as ADT, falls, skin, etc. |
| Physician Orders, Medication & Treatment Records | Currently a manual process. Beechwood faxes all physician orders (including medications) to Buffalo Pharmacies, Inc. Medication & treatment records are provided by the pharmacy. The goal is to have all order entered into AOD & pushed to the pharmacy. |
Beechwood's Work List and Future Plans with Answers on Demand (AOD)
Immediate Projects
Lab and Radiology Result Routing. Beechwood was working with HEALTHeLINK and AOD to have lab and radiology results routed from their lab and radiology providers into the AOD software using Health Level 7 (HL7) messaging.
Automate Interventions to Reduce Acute Care Transfers II (INTERACTII)6 and Situation, Background, Assessment, and Recommendation (SBAR)7 Process. Currently Beechwood is completing the INTERACTII process manually at the point of transfer to the hospital (INTERACTII includes transfer of care protocols and documentation). Beechwood is working with AOD to use automation and the clinical application to complete the information. Beechwood administration would like to see the nursing staff use the SBAR tools because it provides useful information for analysis of data and communication with physicians.
Physician Order Entry. Currently the long-term care pharmacy handles the medication orders and related reports (physician order summary, medication and treatment administration records). In 2013, Beechwood would like to begin their project to move physician ordering through the AOD system. Automate the physician order process to have orders entered into AOD and pushed to pharmacy. A VPN link has been established with Buffalo Pharmacies and data transfer issues will be addressed next. AOD currently uses HL7 messages to send ADT information and medication order information to pharmacy with basic elements. AOD will migrate to National Council for the Prescription Drug Programs 11.x once the standard is completed. AOD has the capability of incorporating admission orders from the hospital if medications are sent in a CCD format, however, at this time the hospital does not send the information in an electronic, standardized format.
Future Projects
Beechwood has identified projects they would like to address in the future. They include:
Train more users on report capabilities of the application to better optimize the use of information to support clinical and business decision-making. AOD has many reports built into all areas of the program including daily and weekly census, clinical reports such as falls, infections and skin condition, daily charting reviews, activity of daily living (ADL) reports, missed charting report, case mix index reports, quality measures report, multiple financial and billing reports.
Improve workflow and in-box messaging to notify pertinent staff that something is late or has been missed.
Work with Medicare liaisons to streamline their process and use of AOD. Implement ongoing evaluation of documentation processes to identify opportunities to complete in AOD application and move away from manual processes.
INTERACT II is a quality improvement program to manage acute changes in condition and provide tools for assessment and communication when sending the patient from the nursing home to the hospital. http://interact2.net.
SBAR documentation tool that prompts the nurse to collect comprehensive information prior to calling the doctor to report a change in condition.
Continuity of Care Document (CCD)
The AOD system has the capability to create, export and import a C32 CCD through the admission and census module. Currently trigger events are tied to census events which have been identified as problematic for two reasons: (1) the delayed nature of the census in which events are not entered into AOD until after midnight/next day;8 and (2) the census is not accessible by nursing. AOD is identifying alternate methods for nursing to generate a CCD.
8. The census event process is (entering admission, transfer and discharge events into ADO) are tied to billing. For that reason, recording the census events in AOD are held for up to 24 hours so it can be verified to ensure accuracy since the events are linked to the billing system.
Health Information Exchange at Beechwood
The availability, use, and exchange of information capabilities are crucial for a Beechwood to begin care and coordinate care with other service providers. Information exchange occurs in multiple different methods -- via phone, photocopies, fax and e-mail as well as through access to the hospital EHR, customized portals and the HIE.
This section describes the providers that were interviewed during the site visit, describes both the internal Beechwood view of HIE activities and the point of view from Beechwood's community partners. HIE information flows are summarized in a matrix at the end of this section.
Health Information Exchange -- Perspectives from Beechwood Business Units
During the site visit, interviews were conducted with Beechwood staff to discuss key processes/workflows that require the exchange of information. Interviews were conducted with the department representatives from admissions, nursing, social service, rehab, Medicare liaisons and billing, and HIM. Based on the interviews Table I-3 summarizes discussions by workflow process, highlights the information exchange process, and shares other notes/insights.
TABLE I-3. Skilled Nursing Facility (SNF) Workflow Processes
| Process | Information Collected and/or Exchanged | Additional Notes from Discussions |
|---|---|---|
| Preadmission/ Admissions | Admission provides daily updates to the area hospitals with the number of beds open. Currently this information is relayed by telephone to hospital discharge planners to facilitate relationship-building & enhanced communication. Beechwood reviews & obtains hospital information to assist in the preadmission assessment & admission/transition of care. They use multiple mechanisms to collect & review the information including on-site visits, hospital EHR access, secure e-mail/e-fax with attachments, telephone. The hospital information needed includes:
| The admissions department has the ability to log into 1 of the area hospitals EHRs through portals to assist in the admission process. This is useful for updates during a patient's stay. Another area hospital does not have the capability for remote access to the EHR through a portal (must be on-site). In this second hospital discharge planners must use extra steps to make information available remotely to support the transfer/preadmission process. Frequently the information is not updated & there have been delays with the decision-making & discharge process. At times the hospital discharge summary is not available at the time of transfer from the hospital & admission to Beechwood. Sometimes the hospital will fax the discharge summary after admission to Beechwood or the HIM department will request the missing information from the hospital. This process requires Beechwood to complete a written request for information from the hospital & may take significant time to receive. HIM will begin using HEALTHeLINK to check for availability first & then use the written request process if the information is not available. |
| Nursing Admission/ Start of Care | Nursing receives information from hospital prior to admission (see Admissions above for type). The nurse manager accesses HEALTHeLINK for additional patient information including past history particularly after admission during the assessment & care planning process. | The admission process has opportunity for improved efficiency. Beechwood had a meeting with their area hospitals to identify the type of information needed from the hospital:
|
| Physician Order process including Medications | The nurse manager contacts the physician typically by phone to review admission orders from the hospital & obtain new verbal orders. The orders including medications are written out & sent by fax to pharmacy. HIM manages the physician order signature process by sending the orders to physicians & tracking for their timely return. This includes verbal/telephone orders initiative by nursing & therapy as well as regular orders. The physician is mailed the order to obtain his/her signature or kept in a folder at the Beechwood front desk that the physician picks up & signs when he/she is at the facility. | Beechwood is working on a project to communicate physician orders including medications to the pharmacy electronically through AOD. Beechwood is looking into the use of a physician portal to AOD to provide a mechanism for physicians to log into Beechwood's EHR to sign orders & complete documentation. |
| Status updates to the physician | Nursing communicates status updates to the physician via multiple routes--phone updates, folder for followup during routine physician visit. The status updates are communicated for many reasons such as change in the patient's condition or communication of a lab or test result. | |
| Physician visits | HIM maintains the regulatory required physician visit schedule & communicates with the physician by mail notifying them when their patients are due for a visit. | |
| Lab & Special Tests | Lab & radiology/ultrasound physician orders are communicated to the providers by telephone. Results are delivered in multiple ways depending on the service provider--by fax, by mail, via a dedicated printer sent from the provider to Beechwood, access to results on the provider's web portal, or through HEALTHeLINK. An interface is under development to delivery results through HEALTHeLINK directly into AOD. | |
| Nursing Patient Referral to Specialist | A referral document is completed by nursing in paper format & sent with the patient when scheduled for a specialist visits. The specialist returns a refer/consult visit (either a paper form that comes with the patient or mails the consult report to Beechwood after completion). | |
| Transfer to the Hospital | At transfer to the hospital from Beechwood, nursing completes the INTERACTII envelope of information & sends information to hospital with the patient. (This is a paper-based process at this time). The INTERACTII envelope includes the following information: transfer form, face sheet, recent H&P, recent physician orders, current MAR, advanced directives & care limiting orders, relevant lab/radiology reports, & personal belongings sent. | INTERACTII is used; however, nursing is not using the SBAR because of the amount of time to complete the information. Administration has identified this process for re-evaluation & completion in AOD (the capabilities are available in AOD, but Beechwood has not begun using this functionality yet). |
| Rehab Services | Rehab staff complete an admission assessment which requires the following hospital information:
| It is important for therapy to have an accurate picture of the patient, their condition, & their goals before they begin treatment. At times they do not have all of the information they need to assess the patient's status at admission if hospital records were not sent or available at transfer. Therapy has not been using HEALTHeLINK, but will be trained. When information is needed they ask the HIM department to request the information from the hospital (often it is the operative report). Paper copies are returned by mail. |
| Medicare Coverage Determinations & Communication with Family | The Medicare nurse evaluates the patient for coverage, makes coverage decisions & communicates with the interdisciplinary team by e-mail. They monitor the patient's status over time & make continued coverage decisions. The Medicare nurse verifies insurance coverage & related coverage criteria, they communicates by e-mail coverage & clinical criteria to interdisciplinary team. The Medicare nurse develops monitoring tools for nursing such as clinical flow sheets & documentation guidelines for nurse's progress notes (this information is not in AOD). The Admissions Coordinator sends an update to pharmacy, ultrasound/radiology & lab via fax regarding Medicare coverage. When lab & test results are returned, they receive a paper copy from the unit coordinator (the information not in the AOD system at this time). The Medicare nurse monitors the patient's status for continued coverage. They review the Nursing 24-Hour Reports are maintained in AOD & alerts/messages sent designated staff. The Medicare nurse communicates with patient/representative at end of coverage by telephone & with a written letter that specifies the end of coverage date & appeal information. The Medicare nurse communicates with Medicare HMO case manager sending status updates & continued coverage information (e.g., the type of skilled nursing or rehab services the patient is receiving). These updates are by phone & fax. The HIM department mails the Medicare Certification/Recertification form to the physician for signature according to the required schedule while the patient is on Medicare. The physician signs & returns the certification by mail. Some physicians who see patients at Beechwood routinely have a folder at the front desk that holds the orders & forms that require their signature to eliminate the mailing process. | Monitoring tools/guidelines are developed & kept in a notebook at the nursing station. This process has been identified for evaluation by the IT team to determine opportunities to utilize AOD more fully for incorporation of customized flow sheets & documentation guidelines related to Medicare cover. Beechwood reported an increase in the number of patients with Medicare HMOs (e.g., Medicare Advantage). These plans have different coverage criteria & 2 no longer require a 3-day hospital stay. Medicare nurses communicate with coverage & change of status updates. They use the nursing 24-hour report & therapy reports as tools to identify patients with new conditions that would affect coverage. |
| Care Planning & Communication with Family | Social service communicates with the family on admission & during multiple times during the patient's stay--this communication is typically by phone, mail & sometimes e-mail based on family preference. They provide written information mailed to the family on care conference dates & provide an update of the care plan team's recommendations if they were not present at the conference. | The social service department uses the AOD system for their documentation including progress notes & assessments. They also use HEALTHeLINK for additional supporting documentation in conducting their initial assessment & care plan. |
| Discharge Planning & Discharge Process | They also work with the family in planning for discharge. The communication is primarily by phone & mail. They review teaching & instructions with patient & family at the time of discharge & provide a paper copy of the information. Discharge instructions are developed for the patient by nursing, therapy, social service & other members of the interdisciplinary team. The instructions are reviewed with the patient & family/caregiver prior to discharge. A copy of the discharge instructions are sent with the patient. Social services may assist with the transition home by identifying HCBS. They may also initiate services on behalf of the patient/family. Typically they communicate via telephone & fax with the community service provider. | |
| Census/ADT Events | HIM enters the census/ADT events in the AOD systems each morning for the prior day ending at midnight (e.g., ADTs, room changes). Certain ADT events used by the HIE are electronically communicated from AOD to HEALTHeLINK. | |
| Billing | HIM prints and/or copies medical record documentation for billing. Request for medical record documentation is mailed in following situations:
| All claims are electronically billed except a select few. Some insurance companies require medical documentation (e.g., workman's compensation or no fault insurance)--documentation is copied & mailed with claim. Request for medical records via e-remittance has been problematic as there are concerns with missing a request (e.g., e-mail printout cuts off information). |
Health Information Exchange Partners -- Perspectives From Non-Affiliated Community Partners
During the site visit, interviews were conducted with Beechwood's HIE community partners -- non-affiliated organizations that provide health care and/or services. Table I-4 summarizes the key organizations that Beechwood shares information with, identifies the type of information exchanged with each organization, and summarizes discussions on the exchange process and information sent/received.
TABLE I-4. Perspectives from Non-Affiliated Community Partners
| Organization | Information Exchanged Between Beechwood & Organization | Additional Notes from Discussions |
|---|---|---|
Hospital Systems:
| For a transfer from the hospital to Beechwood, the following information is provided. The information is typically in an electronic format such as PDF or JPG. Transfer form. Transcribed reports:
| During discussions challenges were identified with the availability of the discharge summary at the point of transfer to Beechwood. Hospital policy may result in delayed submission of the discharge summary to HEALTHeLINK until after discharge (once physician signature is obtained). When this happens the information on the discharge summary is not available to Beechwood staff at transition of care when it is needed. Significant challenges were identified & discussed related to the availability of accurate medication information at discharge including the ability to reconcile pre-hospital medications with the post-hospital medications. The lack of MAR data was another challenge identified when not provided at transition of care from the hospital to Beechwood. Beechwood staff uses the MARs to evaluate the medications the patient received in the hospital & the time. Update: Discharge meds are now available from the Catholic Health System & will be available from Kaleida by late 2013. Therapy information is not currently received by Beechwood & is an opportunity for HIE. |
Pharmacy:
| Physician orders including medications are written out by nursing & sent by fax to pharmacy. Buffalo Pharmacies sends the following paper-based records to Beechwood at the end of each month:
| Beechwood would like to move toward physician orders being generated in AOD & prefers that physicians enter the orders through their system. This would enable the use of electronic medication administration & treatment records (currently these are paper-based & manually completed). Beechwood believe that this would be the safest approach rather than trying to interface AOD to the physician's EHR. MU may be a challenge since physicians must prescribe a percentage of medications through their system. As noted above obtaining an accurate medication history is a challenge. SureScripts (which supplies information to HEALTHeLINK) does provide a medication history, however not all pharmacies use SureScripts, so the information may not be complete. AOD does not use SureScripts. |
Laboratory:
| Lab orders. Lab results. | Lab results are being routed through HEALTHeLINK to the physician practice. Beechwood can access results through the HIE, but there is currently not a direct link to AOD. A custom interface is under development to allow lab results to be electronically delivered into the AOD system. Currently Beechwood maintains lab results in paper medical record. There is potential in the future to order labs through HEALTHeLINK, currently it is a manual process of calling the lab to set up the draw when a physician order is received. |
Radiology/ Ultrasound:
| Radiology orders. Radiology reports. Radiology images. | To obtain radiology/ultrasound services, Beechwood accesses Buffalo Ultrasound online system or calls in an order. The results are phoned to the facility to provide a verbal update & then the final reports are available online for access. Buffalo Ultrasound maintains a portal for Beechwood to order the test & access the results. Buffalo Ultrasound is currently working on automating the results delivery process through HEALTHeLINK. The order/requisition process will continue as is--Beechwood will either call Buffalo Ultrasound to request the test or submit the request through their portal. Buffalo Ultrasound does not plan on processing requests for tests through HEALTHeLINK due to patient identification issues. |
Home Health & Hospice:
| When Beechwood discharges a patient to Home Health or Hospice they provide the following medical records in paper format:
| The home health & hospice providers were interested in having the information available on HEALTHeLINK if it was feasible for the HIE & for AOD. The Home Health & Hospice providers discussed their HIE needs at transition of care from the hospital. They also need an up-to-date, timely discharge summary at the time of hospital transfer & reported that it was 1 of their biggest challenges in the transition of care process. |
Health Information Exchange Information Flow
Table I-5 describes the information exchange activities for Beechwood in three areas: (1) hand-offs in care; (2) shared care; and (3) other administrative exchange. The exchange scenarios are not limited to electronic exchange of information, but encompass any exchange workflow. The summary table provides a synopsis of the HIE activities from the perspective of a nursing home/SNF using the framework established by Westat.
TABLE I-5. HIE by Care Coordination Function and Partners, Beechwood Homes
| Transitions of Care | ||||||
|---|---|---|---|---|---|---|
| Care Coordination Function | Across Members of the Care Team Within Affiliated Organization | Between Staff in an Organization and Other Non-Affiliated Care Providers Including Community Services | Between Staff in an Organization and Patient/Family Members | Type of Exchange | Data | Sender and Receiver |
| Referral/Assessment | ||||||
| Preadmission assessment | Hospital Stay: Patient is assessed by Beechwood staff while at the hospital to determine appropriateness of placement. |
|
| Hospital nurse to Admissions in Beechwood. | ||
| NH to NH: Patient is assessed by Beechwood while at another NH to determine appropriateness of placement. This may occur when a patient or family desires a change in facility. |
|
| Beechwood admissions & NH admissions. | |||
| Home to NH: Patient is assessed by Beechwood for appropriateness of placement. |
|
| Attending Physician & to Beechwood Admissions. Patient representative to facility admissions. | |||
| Transition of Care (transfer or discharge) | ||||||
| Transfer/Admission to LTPAC | Transfer from hospital to Beechwood |
| Updated hospital information:
| Hospital nurse to Beechwood admissions | ||
| Transfer from home to Beechwood |
|
| Physician to Beechwood | |||
| Discharge from LTPAC to Another Provider | Transfer from another NH to Beechwood |
|
| NH to Beechwood | ||
| Discharge from Beechwood to another NH |
|
| Beechwood to NH | |||
| Discharge home from Beechwood Facility (with home health services) |
|
| Beechwood nurse to home health nurse | |||
| Transfer to Hospital from LTPAC | Transfer Beechwood to hospital |
| INTERACTII Envelope:
| Beechwood Nurse to Hospital (ED or receiving unit) | ||
| Discharge Information from LTPAC to Patient | Discharge home from Beechwood facility (without home health services) |
|
| Beechwood social service, therapy, nursing to patient (or family or representative) | ||
| Discharge from LTPAC to Community Service Provider(s) | Social service assists with setting up community services to assist a patient with successful transition |
|
| Social service to community service provider | ||
| ADT Event Data to HIE Network | ADT message to HIE to communicate admissions & discharge information |
|
| Beechwood to HIE | ||
| Followup Post Transfer/Discharge | ||||||
| Generally Not Applicable--Followup is addressed in Shared Care Section | ||||||
TABLE I-6. Shared Care Information Exchange Activities
| Transitions of Care | ||||||
|---|---|---|---|---|---|---|
| Care Coordination Function | Across Members of the Care Team Within Affiliated Organization | Between Staff in an Organization and Other Non-Affiliated Care Providers Including Community Services | Between Staff in an Organization and Patient/Family Members | Type of Exchange | Data | Sender and Receiver |
| Assess Needs and Goals | ||||||
| Coordination with physician at Start of Care including Medication Reconciliation & Orders, Evaluation/ Certification & Plan of Care | Admission orders & medication reconciliation --review transfer form & hospital information to reconcile medications & establish Beechwood facility orders & initial physician POC. |
|
| Beechwood nurse to Attending Physician | ||
| Therapy order, evaluation & certification communicated with physician & mailed for signature. |
| Beechwood Therapist to Attending Physician | ||||
| Communicate Physician Orders & medications to Pharmacy | Communicate admission orders & medications to pharmacy. |
|
| Beechwood Nurse to Pharmacy | ||
| Communicate orders for labs, radiology & special tests to service provider & return test results | Communicate lab orders to lab provider. |
|
| Beechwood Nurse or Unit Coordinator to Lab | ||
| Communicate Radiology orders to lab provider, |
|
| Beechwood Nurse or Unit Coordinator to Radiology/ Ultrasound | |||
| Request additional medical record information from hospital to assist with admission assessment & care planning process | Beechwood Interdisciplinary Team request additional information from hospital to complete an assessment, |
|
| HIM to hospital | ||
| Communicate with patient and/or family/ caregiver for additional information & advanced directive | Beechwood Interdisciplinary Team interview patient/family for information to complete initial assessment. |
|
| Interdisciplinary team to Patient and/or family | ||
| Create and Maintain Plan of Care | ||||||
| Create & Maintain Patient's Plan of Care & Orders | Regular review & update of physician orders. |
|
| Nursing/Unit Coordinator to Physician | ||
| Care Plan Update with Patient/Family | Beechwood Interdisciplinary Team updates to patient & family POC. |
|
| Social service to patient and/or Family | ||
| Monitor, Followup, and Respond to Change | ||||||
| Ongoing Physician Visits/Evaluation | Routine physician visit. |
|
| Nursing (for status updates) & HIM (for scheduling) to Physician | ||
| Change in condition/status update and/or order change request to the attending physician | Change in condition, status updates & order changes. |
|
| Nursing to Physician | ||
| Change in Condition/Status update to Patient/ Family/Caregiver | Change in condition, status updates & order changes. |
|
| Depending on topic: Nursing, social service or interdisciplinary team member to patient/ family | ||
| Specialist Visit/ Evaluation | Specialist visit (surgeon, neurologist, dentist, psychologist, etc.). |
|
| Nursing/Unit Coordinator to Specialist | ||
| Communicate physician order changes to pharmacy & order medications | Communicate physician order (including medication) changes to the pharmacy & order medications. |
|
| Beechwood Nurse to Pharmacy | ||
| Order changes for lab, radiology & special tests & return of results | Request new Lab or Radiology/Ultrasound or other specialized test. |
|
| Nursing or Unit Coordinator | ||
| Routine physician order review & recertification | Medicare/Medicaid certification/recertification forms sent to physician for signature. |
|
| HIM to Attending Physician | ||
TABLE I-7. Other Information Exchange Activities
| Other Exchange Activities | ||||||
|---|---|---|---|---|---|---|
| Care Coordination Function | Across Members of the Care Team Within Affiliated Organization | Between Staff in an Organization and Other Non-Affiliated Care Providers Including Community Services | Between Staff in an Organization and Patient/Family Members | Type of Exchange | Data | Sender and Receiver |
| Quality Measures | ||||||
| Electronic submission of mandatory data sets which includes quality measures | Electronic submission of mandatory data set which includes quality measure data. |
|
| Beechwood to CMS | ||
| Public Health | ||||||
| Public health & state registries for reportable conditions | Report required data to the State of New York through the state's Health Commerce System for & including required disaster preparedness reporting. This portal also provides messages to from the state such as emergency notifications. |
|
| Beechwood to State of New York for required reporting. Emergency notifications & other requests for data & communication are sent from the state through HCS to Beechwood. | ||
| Payment | ||||||
| Communication with Payer Case Manager | Billing/Medicare Nurse updates to payers regarding initial & continued coverage. |
|
| Medicare nurse to payer case manager | ||
| Communication with Ancillary Service Providers for Billing | Relay billing information & Medicare/Medicaid coverage status to community providers--pharmacy, lab, radiology/ultrasound. |
|
| Admissions to ancillary service providers | ||
| Communicate with Patient/Family for Payer Coverage | Medicare nurse to family to relay Medicare coverage start & stop, |
|
| Medicare nurse to family/rep | ||
| Payer Medical Record Requests | Remittance, medical review, or RAC request for medical records. |
|
| HIM & Billing to Payer | ||
Barriers and Opportunities for Improved Health Information Exchange Practices
Over the course of the two-day site visit, a number of issues were identified related to information exchange in support of care transitions and ongoing shared care. Beechwood staff and community partners interviewed offered observations on barriers and opportunities for improvement to advance HIE, communication, and coordination of care.
Barriers
Availability of information for preadmission assessment and decision-making. Consistent and timely availability of hospital information was identified as a challenge/barrier by Beechwood. Some hospitals do not provide information to the HIE which makes the preadmission assessment and discharge planning processes challenging and fraught with potential delays. Some hospitals allow portal access to the EHR application, which allows access to data from the current stay for evaluation; however, it is inconsistent across area hospitals. Problems and delays occur in assessment and discharge planning when there is not a strategy to allow remote access to hospital data.
Medication reconciliation challenges on admission. Beechwood's medical director and nursing staff expressed significant concerns with the quality and accuracy of the medication information they are receiving on discharge from the hospital to determine the correct medication plan to implement at the nursing home. Each hospital communicates medication information differently and on different forms. The medication information received from the discharging hospital is not reconciled with the patient's pre-hospital medication regime. Obtaining a complete and accurate medication history (prior to hospital stay) to reconcile with the hospital medication orders is very difficult. To ensure accuracy and patient safety, a strategy is needed to improve the medication reconciliation process for episodes of care that span prior to, during, and following discharge from hospital stays.
Standardized discharge summary content. The hospital discharge summary is a crucial document in establishing a POC by Beechwood and supporting Medicare coverage for the patient. The discharge summary may not be available upon discharge. Each hospital has different information on their discharge summary -- standardization of content would be highly beneficial to the LTPAC facility.
Need for customized interfaces may be a barrier. When the Western New York Beacon was trying to recruit long-term care providers one of the obstacles they encountered was not the lack of technology (EHRs and/or clinical systems were in use by LTPAC facilities, but the inability to get their vendor to develop a customized interface, the cost of the customized interface or the lack of a vendor to complete an interface (e.g., home grown, or no ongoing maintenance contract) were barriers.
Even with standards, interfaces are not easy to implement. Beechwood and their vendor identified the application of standards as a challenge/barrier. The identification of standards to facilitate exchange of information does not guarantee easy implementation of data exchange. A standard may be identified, but there is significant variability in the format (e.g., HL7 message formats to make ADT feeds work). The lack of standard definitions for ADT messages is also a challenge -- most organizations have internally generated ADT events making implementation across a community challenging. Standards such as a CCD do not necessarily have the right structure to accurately reflect the LTPAC facility summaries such as the nursing home summary at discharge/transfer.
Opportunities
Expand type of information available on the HIE. As noted above, Beechwood reported challenges with obtaining consistent hospital information to support the transition of care process. They identified the potential of HEALTHeLINK as being a source of data, but the type of information they require is not always available. As noted during discussions with the community providers and Western New York HIEO, the HIE could evaluate the type of information the long-term care facilities use and/or request and develop plans to have the information available on the HIE. Beechwood routinely submits a written request for information from the hospital, which may take a significant amount of time to obtain (a written request is required and medical records are mailed to the facility).
POC developments should include long-term care. HEALTHeLINK has begun early discussions around a patient-centered POC particularly in the context of a Medicaid health home. Input from LTPAC providers like Beechwood, should be considered in the process given the providers' role in coordinating and implementing a comprehensive POC that is health and wellness driven and involves multiple providers. Beechwood staff indicated during interviews that having access to a longitudinal POC would be very helpful in understanding and aligning with the overall goals for the patient.
Conclusion
To serve their patients, Beechwood routinely exchanges health information at transition of care and coordination of ongoing care. There are a number of opportunities to further expand the use of the HIE to support the care delivery process and with their community partners. Beechwood's current EHR vendor is engaged with their initiatives and working to support their advancements with HEALTHeLINK. Sending ADT messages to the HIE and viewing information through the portal are important first steps, however, expansion of the type of information available on the HIE and the inclusion of LTPAC data is needed to increase the use and value to communities like Beechwood.
Additional References
Coleman EA. Falling through the cracks: Challenges and opportunities for improving transitional care for persons with continuous complex care needs. Journal of American Geriatrics Society 51:549-555, 2003.
Gilikin, J. Job Description for a Discharge Planner. eHOW.com.
Herndon L, Bones C, Kurapati S, Rutherford P, Vecchioni N. How-to Guide: Improving Transitions from the Hospital to Skilled Nursing Facilities to Reduce Avoidable Rehospitalizations. Cambridge, MA: Institute for Healthcare Improvement; June 2012.
Kaleida Health Corporate Policy and Procedure: # GDL.12 Guidelines for Completing the Adult Patient- Resident Discharge Form (KH00505). Reviewed February 2, 2012.
Kolus, K. Hospital discharge summaries often delayed; may affect nursing home re-hospitalizations. Long Term Living, 2011.
NYAHSA. Advisor -- First Quarter 2011 -- LeadingAge New York article about a LTC patient transfer http://www.leadingageny.org/home/index.cfm/linkservid/94A335A9.../0/.
Attachment I-1. Western New York Beacon Community Long-Term Care Use Case Priorities and Hospital-SNF Transfer Use Case Summary
Long-Term Care Use Cases -- February 11, 2013
Results Delivery
- Data Availability
- Next Steps/Timing
- Responsible Parties
- Training Needs
Care Planning and Regulatory Requirements after Admission Acceptance
- Current Data Available
- Data/Forms Needed
- Next Steps/Timing
- Responsible Parties
- Training Needs
Access to Data Needed for Admission Criteria
- Trigger Mechanism
- Data Available
- Data Needed
- Next Steps/Timing
- Responsible Parties f. Training Needs
Patient Preference Notification (future considerations)
Hospital Discharge and Admission to Long-Term Care Facility
Overview
Western New York Beacon is reviewing the hospital discharge and admission to long-term care facility process in order to determine how HEALTHeLINK, as the RHIO, can improve the efficiency, innovate patient transfer and reduce adverse outcomes. The e-Health Network of Long Island currently has long-term care facilities as part of their HIE.9 Three states (Colorado, Massachusetts and Oklahoma) have ONC funded pilots to connect long-term care facilities to RHIOs. There is a national Coordination of Care Workgroup that is developing standards for transfer of information.10
Background
The Centers for Medicare and Medicaid Services (CMS) requires that all hospitals participating in Medicare/Medicaid services provide a "discharge planning evaluation (that) must include an evaluation of the likelihood of a patient needing post-hospital services and the availability of the services."11 The hospital is also responsible for arranging for the initial implementation of the discharge plan, once developed. A listing of community-based services, long-term care, sub-acute care, home care and other services and levels of care must be maintained by the hospital. Discharge plans for patients in need of skilled nursing typically include the following elements:
- Demographics;
- Primary language;
- Family members/notification of discharge;
- Primary diagnoses;
- Allergies;
- Medications (including immunizations and reconciliation review);
- Diet;
- Advance directives;
- Mental status;
- History of falls;
- Skin integrity;
- Assistive/protective devices (i.e., hearing aids, glasses, walkers, etc.);
- ADL status;
- Special instructions;
- Belongings sent; and
- Followup care.
Additional information that is often included is:
- Pain score;
- Last vital signs (BP, pulse, respiration, temperature);
- Time of last medication(s); and
- Patient/Family preferences for care.
While all of these elements would be useful, and some vital to the ongoing care of the patient, there is currently no national standards or requirements for hospitals as to what is essential to be included in the discharge plan.12
According to a study done in 2000, American adults aged 65 and older experience 200 hospital admissions and 46 nursing home admissions per 1,000 persons annually.13 Recent Medicare studies show that of those Medicare patients hospitalized, close to 20% will be rehospitalized within 30 days, often due to lack of communication and missing information at the time of discharge to another facility.14
Process
Currently, the hospital discharge process starts as early as date of admission. Hospitals receiving Medicare/Medicaid payments or Joint Commission accredited are required to provide discharge plans for each patient. Almost all hospitals have a dedicated department for discharge planning/patient care management, usually staffed by nurses and/or medical social workers. This staff works closely with the doctors and other members of the care team, to facilitate patient discharge. Responsibilities include:
Assuring all patient assessments are completed prior to discharge, including psycho/social assessments, ADLs, patient ongoing needs.
Finding appropriate followup care, including LTPAC and home care.
Interviewing patients/family members for preferences.
Problem lists, medications (including reconciliation), immunizations, allergies.
Communication with the patient and family members of what to expect, warning symptoms, contact information.
Summary of care provided by the hospital.
Compilation of all required documents to be provided to the receiving facility.
The receiving facility needs to evaluate patients to be transferred in order to identify areas of concern and assure discharge care plan will meet the patients' needs and can be implemented in a timely manner. Once the need for LTPAC has been made, the discharge planner will meet with the patient and family members to describe this need and determine preferences. The discharge planner must then try and determine if there is care available at preferred sites and if not, discuss alternatives with the patient and family. This marks the beginning of shared patient information between the hospital and long-term care facility. The long-term care facility needs several key elements in order to determine bed availability for a patient (gender, problem list, ADL status, cognitive status, psycho/social status, assistive devices, IV needs, etc.). Once the long-term care facility has enough information to determine bed availability, they can accept the referral and the discharge planner can proceed with final discharge arrangements. Currently, this process takes place by phone and paper.
Access
The Health Insurance Portability and Accountability Act (HIPAA) allows for access to information on a "need to know" basis, allowing for transitions of care to qualify as need. HEALTHeLINK' s current consent policy provides for level 1 and level 2 access; level 1 for treatment, quality improvement, care management and insurance coverage (preauthorization) reviews. Care Management is defined as:
"(i) assisting a patient in obtaining appropriate medical care, (ii) improving the quality of health care services provided to a patient, (iii) coordinating the provision of multiple health care services to a patient or (iv) supporting a patient in following a plan of medical care. Care Management does not include utilization review or other activities carried out by a Payer Organization to determine whether coverage should be extended or payment should be made for a health care service."15
The discharge of a patient from a hospital to a long-term care setting qualifies on all four of these counts.
Other Communities
Several Beacon projects are already automating the discharge process from hospital to long-term care settings and meeting with great success. The Colorado RHIO is already reporting a reduction in the amount of time for discharge processing from an average of 35 hours 21 minutes, pre-HIE, to 25 minutes average time post-HIE, a savings of almost 35 hours in the process. In addition, they report that 70% of the care transitions data is exchanged electronically and 70% is exchanged within the targeted number of hours.16 Massachusetts and Oklahoma are also reporting early successes using HIE for the exchange of needed data between hospitals and long-term care facilities. The process is similar:
- Hospital (Data Sender) records required pt. data elements in HIE or Community Health record;
- Hospital sends electronic referral notice to skilled nursing or long-term care facility;
- SNF admissions gets referral and accesses patient data on HIE to review and accept referral; and
- Information now available electronically for core users and Doctor at SNF.
There is precedence in New York State for long-term care facilities to be connected to a RHIO that include hospitals. The following long-term care facilities share information through e-Health Network of Long Island: Bellhaven Center for Rehabilitation and Nursing Care; Cedar Lodge Nursing Home; Eastern Long Island Hospital; Grace Plaza Nursing and Rehabilitation Center; Hilaire Rehab and Nursing; Long Island State Veterans Home; Nassau Extended Care Facility; Nesconset Nursing Center; Peconic Bay Medical Center; Peconic Bay Skilled Nursing and Rehabilitation Center; Physician Offices in Suffolk and Nassau Counties; San Simeon by the Sound Center for Nursing and Rehabilitation; Southampton Hospital; St. James Healthcare Center; Stony Brook University Medical Center; Suffolk County Department of Health Services; Winthrop University Hospital; Woodhaven Adult Home; and Woodhaven Nursing Home.
Next Steps for HEALTHeLINK
In order for HEALTHeLINK to achieve similar successes, the following would be needed:
- Assess hospital capabilities to transmit electronic discharge data elements;
- Assure interfaces are set up to send to HIE;
- Provide assistance on HIE access and training to hospital discharge planning staff;
- Set up electronic referral process (could be done later in the process and continue current notification process); and
- Set up admissions coordinator for HIE access and provide assistance and training.
Working with several state HIEs, ONC is studying "ways in which HIE can improve care coordination and transitions of care with LTPAC providers and the patients and caregivers they serve." With the goals of "Increasing the ability of providers, patients and caregivers to view/download/transmit timely, accurate information through HIE during transitions (and) reducing adverse events -- hospital readmissions, medication errors." These goals align with HEALTHeLINK's own mission and vision and are the logical next steps for the organization.
Longitudinal Coordination of Care (LCC) Workgroup, http://wiki.siframework.org/Longitudinal+Coordination+of+Care+WG.
CMS Code of Federal Regulations (CFR), 482.43 (b)(3).
National Citizens' Coalition for Nursing Home Reform: Annual Meeting notes October 23, 2009.
Gabrel CS, Jones A. The National Nursing Home Survey. Vital Health Statistics 13, 2000; 147: 1-121.
Rau, J. Medicare to Penalize 2,217 Hospitals for Excess Readmissions. Kaiser Health News. October 12, 2012.
HEALHeLINK Policy #P04 Patient Consent -- current revision August 23, 2010, and HEALTHeLINK Glossary of Terms -- Care Management.
Office of the National Coordinator. Inaugural Meeting: Long-Term and Post-Acute Care Community of Practice (COP). January 23, 2013.
Appendix J. Site Visit Summary: Eastern Maine Health System, Eastern Maine Homecare
Executive Summary
Snapshot of Eastern Maine HomeCare
Organization Type: Home care and hospice division of the EMHS.
LTPAC Services: Home Health Care and Hospice with Telehealth.
- Size:
- EMHS covers 2/3 of the geography of Maine.
- 8,000 Employees.
- 7 Hospitals.
- Physician Practices.
- Home Care & Hospice (EMHC)
- 3 Agencies with 4 Offices.
- 68,323 Visits.
- 3,300 Patients Serviced.
- 7 Nursing Facilities.
- 1 CCRC.
- Emergency Transportation (Ground & Air).
- Pharmacy, DME, Medical Supply Vendors.
- Grant Funding:
- Bangor Beacon Community Grant, Funded by ONC.
- Patient-Centered Medical.
- Home Demonstration Project.
- Maine's Pioneer ACO.
- EHR (Home Care & Hospice):
- McKesson Horizon Home Care and Phillips Telehealth.
HIE Network:HealthInfoNet serving Maine.
To understand health information exchange (HIE) for long-term and post-acute care (LTPAC) providers, a site visit was conducted at Eastern Maine HomeCare (EMHC). EMHC is the home care and hospice division of the Eastern Maine Health System (EMHS). The health system is an integrated delivery network (IDN) with hospitals, ambulatory care practices, LTPAC providers (home health, hospice, nursing homes and assisted living) and ancillary services. The home care division includes three agencies and seven offices, serving both urban and rural areas covering two-thirds of Maine. EMHC also provides telehealth services to patients in the health system, and has been successful in reducing hospital admissions and emergency department (ED) visits.
EMHS is both an innovator and a leader in health care having received grants to test new models of care and payment, and industry awards and recognitions. Health information technology (HIT) has been a key factor in supporting their innovative practices and a strategy to manage health care for a population that covers a large urban and rural geography.
EMHS received an Office of the National Coordinator for Health Information Technology (ONC) Beacon Community Grant in 2010 to support improvements in the health of people with chronic conditions and reduce costs. The Bangor Beacon Community achieved these improvements through a care coordination program that was facilitated by HIT. LTPAC providers were an integral component of the grant particularly the use of home care services and telehealth technology. The grant provided an opportunity for EMHC to upgrade its electronic health record (EHR) platform to a single solution across all of their agencies and sites and increase the number of telehealth units available for use. To illustrate the effectiveness of the program, outcomes for patients on telehealth were tracked. In 2012 hospital and ED visits dropped from over 70% before telehealth to 8% while in the telehealth program. This drop in hospitalization and ED visits resulted in savings of over $2 million.
Maine has a statewide HIE called HealthInfoNet® (HIN). HIN was operational in 2009, but expanded its technology infrastructure in 2010 with the ONC Beacon Community Grant, ONC Regional Extension Center (REC) Grant and State HIE Cooperative Agreement Program funding. All of Maine's acute care hospitals are under contract to connect to the statewide HIE along with ambulatory providers, federally qualified health centers (FQHCs), mental health agencies, home health agencies (HHAs) and two nursing homes. HIN has select types of information available including medication history, allergies, lab and test results, vital signs, image reports, transcribed reports and a problem list. HIN also provides tracking for six admission/discharge/transfer (ADT) events and sends notifications to HIE participating organizations when they have a treatment relationship with the patient. EMHC utilizes HIN as part of the admission process to gather information on new patients and assist with the start of care assessment process. The agency also submits the patient's home care plan to HIN.
EMHS has been an incubator for testing new health care delivery and payment models participating in both Maine and Centers for Medicare and Medicaid Services (CMS) Patient-Centered Medical Home (PCMH) projects and launching one of 32 Pioneer Accountable Care Organizations (ACOs) in the United States. EMHS Pioneer ACO has 14,000 attributed Medicare participants. EMHC is an integral part of both programs working closely with patient care coordinators and community care teams (CCTs) to improve the health and outcomes for high-risk patients and reduce their costs. The use of telehealth for homebound patients has been an important tool for daily monitoring and interventions when clinical measures require attention. As noted above, the use of telehealth has resulted in dramatic reductions in hospital and ED visits for the 167 patients using the service in 2012.
EMHS maintains the technical infrastructure for the IDN including EMHC. The home care division has its own EHR application -- McKesson Horizon Homecare -- used by all of the home care and hospice agencies and sites. The hospitals and ambulatory sites use the Cerner Millennium EHR system. Cerner has a tool for known as PowerChart for multi-entity organizations. PowerChart pulls the most relevant patient information from the various entities together in one view and provides a link to HIN. EMHS physician practices use Centricity.
EMHC uses Phillips Healthcare Solutions for its telehealth program. Units in the home transmit data to a cloud-based clinical software application where it is recorded for monitoring, tracking and trending. Currently the telehealth data does not connect with the EMHC EHR, but an interface is under development.
Health information is exchanged in multiple ways (phone, fax, e-mail, customized portals, and HIN during clinical and administrative processes. HIE information flows occur in three categories: (1) transitions of care; (2) shared care; and (3) administrative processes. EMHC routinely exchanges information during preadmission assessment, at transfer and discharge, at start of care when assessing the patient and developing their plan of care (POC), with ongoing monitoring and maintenance of the patient's POC and recertification, and with status changes. EMHC developed a physician portal to their EHR to improve the exchange of information with physicians for reviewing and signing the patient's POC and orders.
A number of barriers and opportunities for improvements in HIE were identified over the course of the two-day site visit. The opportunities and/or barriers identified by EMHC representatives include:
Barriers
Cost/reimbursement barriers to expand the telehealth program.
Policy barriers for engagement of LTPAC in new delivery models related to homebound status for home care patients and three-day hospital stay for skilled nursing facility (SNF) Medicare beneficiaries.
Opportunities
Use of a consolidated (community) patient-centered care and treatment plan to enhance care coordination.
Opportunities for improvements in medication reconciliation process after hospital discharge.
EMHS is an innovative organization that is demonstrating how LTPAC providers and technology can and should be integrated into new care delivery and payment models. Their patient-centered approach to care coordination embraces the spectrum of providers and integration of community services to provide the high-quality care in the most cost-effective setting. Technology plays an important role in supporting their coordination of care infrastructure and is viewed as a critical tool for future enhancements in their delivery and payment models.
Background on Eastern Maine HomeCare and Eastern Maine Health Systems
EMHC1 is the home care and hospice division of EMHS2 based in Bangor, Maine. The mission of EMHS is to maintain and improve the health and well-being of the people of Maine through a well-organized network of local health care providers who together offer high-quality, cost-effective services to their communities.
1. See http://easternmainehomecare.org/.
Eastern Maine Health System
The EMHS is a non-profit organization comprised of:
Acute care inpatient hospitals including a psychiatric hospital and tertiary trauma center.
Physician practices.
LTPAC providers including home care agencies and hospice providers, nursing facilities, a continued care retirement center, and assisted living facilities.
Ancillary services including emergency transport companies (ground and air), pharmacy, durable medical equipment (DME) and medical supply vendors.
The largest hospital in the EMHS is Eastern Maine Medical Center (EMMC) -- a 411-bed medical center located in Bangor, Maine. EMMC's service area is comprised of approximately two-thirds of the state. The hospital is the hub referral hospital for 21 hospitals in rural Maine. EMMC and its medical staff of nearly 400 providers and more than 3,000 clinical and support staff provide three-quarters of the primary care hospital services offered in the greater Bangor area, as well as specialty and intensive care services.
EMHS has embraced technology as a key factor in supporting both the health care delivery needs of a population that covers a very large, often rural geography and new innovative models of care they are implementing. As an organization they embrace a culture of technology and innovation having achieved the following industry recognition and key implementation milestones:3
- EMMC "Top 100 Most Wired Hospitals" Hospital and Health Networks Magazine;
- HIMSS Davies Award Recognition;
- EMHS CIO of the Year recognition by HIMSS;
- Telemedicine including ICU, ED, Radiology, Pediatrics, Psychiatry, Home Care Telehealth, electronic medical record (EMR) infrastructure at all sites of care (acute and community);
- System-wide Hospital EMR Infrastructure;
- PowerChart access to support care delivery across all providers; and
- Founding member of HIN, Maine's HIE.
EMHS provides and supports the information technology needs of EMHC.
3. Remington Technology Summit. "Integrating Technology the Platform for a Shared Savings Model." March 2013.
Eastern Maine HomeCare
EMHC is an affiliate and the home care and hospice division of EMHS. In 2012, the EMHC covered nearly 1.37 million miles to make 68,323 home care, hospice, and telehealth visits to 3,300 patients.4 Lisa Harvey-McPherson, RN, MBA, MPPM is the President and CEO of EMHC and Vice President of Continuum of Care for EMHS. During interviews, EMHS CEO Michelle Hood, noted the importance of having a Vice President in the health system dedicated to integrating the continuum of care into the health system's strategies.
EMHC is comprised of three agencies with four different sites in northern, eastern, and central Maine serving urban, suburban and rural areas (see Figure J-1). The division was created as hospital systems merged resulting in one home care agency in 2006. The agencies/sites include:
- Visiting Nurses of Aroostook
- Caribou (home office for corporation); and
- Houlton.
- Hancock County HomeCare and Hospice
- Ellsworth.
- Bangor Area Visiting Nurses
- Bangor.
FIGURE J-1. EMHC Service Areas
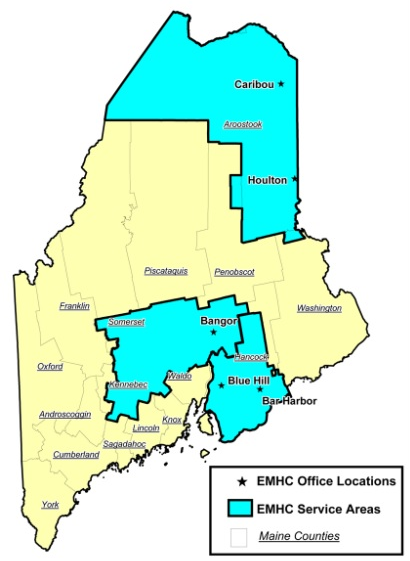
The EMHC division has 230 staff and a multidisciplinary team professional team consisting of physicians, nurses, social workers, aids, care managers/coordinators, physical and occupation therapists and quality/performance improvement staff. They provide home care and hospice services primarily to older Medicare recipients for circulatory, respiratory, injuries, and cancer diagnoses. (Summarized in Table J-1.)
TABLE J-1. EMHC Summary -- Age, Diagnosis and Payers
| Average Age | Top Diagnoses | Medicare | Medicaid | Blue Cross | Other Private Insurance | |
|---|---|---|---|---|---|---|
| Home Care | 66% are 65 or older | Circulatory System Respiratory System Injuries | 62% | 9% | 8% | 21% |
| Hospice | 81% are 65 or older | Neoplasms Circulatory System Signs & Symptoms | 88% | 4.5% | 3% | 4.3% |
Telehealth
EMHC has delivered telehealth services for over 10 years and has integrated it into both home care and primary care with the Bangor Beacon Project. Due to the large geographic area covered by EMHC (approximately 6,000 square miles), telehealth has been an important technology in delivering care to individuals in both urban and rural areas. It is also an important strategy in the care delivery and payment projects that EMHS and the Bangor Beacon Community have deployed. To further understand the telehealth program at EMHC, this section discusses the costs, process and outcome measures tracked.
4. See http://easternmainehomecare.org/.
Telehealth Cost Considerations
The cost of implementing and expanding the telehealth program was identified by EMHC CFO as a challenge. The home care agency invests a significant amount in the equipment (for example, the general cost of an in-home telehealth unit is approximately $3,500). Currently the EMHC has 79 units with an average of 65 deployed in a patient's home at any one time.
In general the EMHC finance staff reported that the home health care reimbursement structure does not have a mechanism to pay for the expense of telehealth equipment which is a limitation for program expansion. This is exacerbated by the payer mix and rural cost structure for some of the EMHC agencies. For example, services provided to patients in Hancock County are reimbursed under the rural cost structure where the state reimburses the agency 50% of the cost of delivering services. As a result, EMHC has had to rely on grant funding and philanthropic support to purchase telehealth devices.
The Beacon Community tested the application of tele-psychiatry between nursing homes and a geriatric psychiatric nurse, but they could not sustain the program under the current reimbursement structure.5 A final report on this project was under development at the time of the site visit.
There have been overall financial gains as a result of telehealth. EMHC has had an overall reduction in the cost of care per episode with telehealth. The visit utilization drops from 15-16 visits/episode to 13-14 visits/episode. To understand the impact, the cost difference between an in-home visit and telehealth encounter is $120.
Telehealth is also a strategy utilized in the Pioneer ACO, however, the cost-benefit ratio and overall financial impact was not addressed during the site visit. EMHS Pioneer ACO is working with EMHC to develop a congestive heart failure (CHF) telehealth program to serve patients who are not eligible for home health under Medicare because they are not homebound. The CHF telehealth program would make available telehealth equipment, daily telehealth monitoring and in-home nursing visits for medication adjustments. EMHC are pursuing this model because it had been effective in reducing ED use and hospital readmission rates during the Beacon project.
Technology
EMHC currently uses Phillips Healthcare Telehealth Solutions6 as their telehealth vendor. With the Phillips system, EMHC collects clinical data, questionnaire responses, and risk screen results. EMHC previously used video telehealth monitoring, but found it was not as effective except for monitoring particularly with behavioral health issues. With video telehealth, the lack of clinical data (such as vital signs) to track and trend status and changes proved more useful.
The telehealth tools provided by Phillips include both in-home devices and a cloud-based software application:
TeleStation. The base unit is placed in the patient's home to enable secure, two-way flow of information between the remote telehealth nurse (via the web-based clinical review software) and the patient.
Measurement Device. In addition to the base station, the patient may use in-home monitoring wireless devices to collect clinical measure data. Data is sent to the base TeleStation.
Web-based Clinical Review Software. The base station sends telehealth data to a cloud web-based software application where the patient's clinical measure data is stored. The home care agency/telehealth nurse accesses this program to review the patient data and determine clinical interventions.
The Phillips telehealth devices collects clinical measure data (described below in Telehealth Clinical Process) and can prompt the patient to submit responses to basic questions such as how they are feeling. The system also has the capability of providing education to the patient. The telehealth nurse evaluates the patient's clinical measure data daily in the Phillips web-based clinical software. The software displays current, past and trending data.
The telehealth software also provides validated patient surveys or screening tools to assess for risk and display current status (See Figure J-2 Patient Risk Summary). EMHC's telehealth system provides risk screenings, status, and evaluation tools are available for the following areas:
- Probability of Readmission;
- Medication Adherence;
- Depression Scoring;
- Nutritional Screening; and
- Activities of Daily Living/Instrumental Activities of Daily Living.
FIGURE J-2. Patient Risk Summary
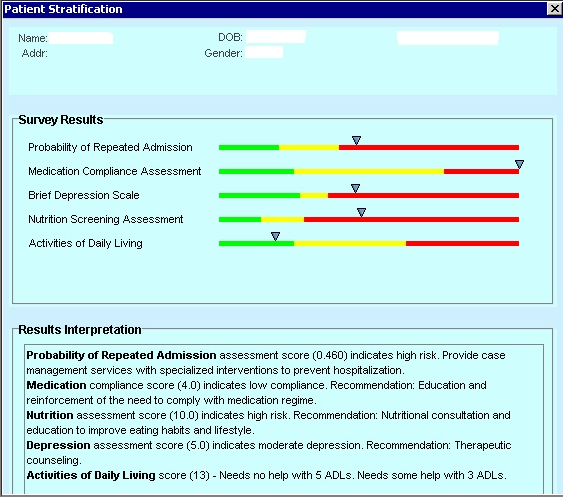
Clinical Data and Clinical Process
Patients selected for the telehealth program enter data each day into their device and respond to questions and prompts. The data reported by the patient can include any of the following clinical data depending on their condition:
Blood pressure.
Weight.
Blood sugar.
Pulse.
O2 saturations.
- Patient responses to individualized questions such as their
- Shortness of breath symptoms;
- Dietary compliance; and
- Endurance level.
The telehealth nurse reviews the patient data every day. Physician orders for telehealth identify the parameters for appropriate data ranges. When the patient's telehealth data is outside of the range, the system triggers a "red flag," and the telehealth nurse calls the patient and provides consultation over the phone to determine the next level intervention (such as a home visit or physician notification). Most of the issues can be handled by the telehealth nurse over the phone, who also communicates with the home care nurse, particularly when a concern requires followup and a nurse visit is scheduled.
Telehealth Outcomes
To understand the impact that telehealth has on EMHS programs, EMHC measures key performance indicators and outcomes related to the Beacon Community, Pioneer ACO and PCMH programs. EMHC collects the following data on telehealth patients to track outcomes.
- Patient identifier;
- Primary telemedicine diagnosis;
- Patient age;
- Secondary diagnosis;
- Payment source;
- Number of hospitalizations for telemedicine diagnosis in previous 6 months;
- Average cost of hospitalization;
- Prior ED visits for primary telemedicine diagnosis in previous 6 months;
- Average cost of ED visit;
- Number of hospitalizations for telemedicine diagnosis while on program;
- Home health/hospice in home nurse (RN) visit;
- Average cost of in-home nurse (RN) visit;
- Number of telemedicine encounters;
- Average cost of telemedicine encounter; and
- Health system cost savings.
TABLE J-2. Telehealth Patient Outcomes Results by Diagnosis in 2012
| Diagnosis | # of Patients | Percentage Hospitalized 6 mo. Prior to Telemed* | Percentage Hospitalized While on Telemed** | Percentage ED Visits 6 mo. Prior to Telemed* | Percentage ED Visits While on Telemed** |
|---|---|---|---|---|---|
| CHF | 57 | 86% | 14% | 84% | 14% |
| COPD | 36 | 83% | 6% | 83% | 6% |
| Diabetes | 15 | 53% | 9% | 53% | 9% |
| Cardiac | 54 | 56% | 4% | 56% | 4% |
| Other | 5 | 80% | 0% | 80% | 0% |
* Data obtained from patient interviews at time of admission to telehealth program. Patients admitted to hospital were admitted for their chronic diagnosis (CHF, COPD, etc.).
** Data represents actual hospitalizations/ED visits occurring during patient's length of stay on home health program for their telehealth diagnosis.
EMHS uses the telehealth data to calculate outcomes such as reduced hospitalizations and ED visits (Table J-2) as well as costs savings based on priority diagnoses (Table J-3). Overall EMHS has been able to quantify a significant impact on key performance indicators and costs for the 167 patients in the telehealth program in 2012, reducing hospitalization and ED visits be an average of 65% for target diagnoses resulting in an estimated $2.1 million in health care savings.
TABLE J-3. Estimated Health Care Cost Savings Results by Diagnosis
| Diagnosis | No. of Pts | Savings |
|---|---|---|
| CHF | 57 | $490,049 |
| COPD | 36 | $373,365 |
| Diabetes | 15 | $118,386 |
| Cardiac | 54 | $992,267 |
| Other | 5 | $84,482 |
NOTE: The estimated savings is net after accounting for the cost of telehealth visits and technology.
CMS prohibits payment for telemedicine services in Metropolitan Statistical Areas (MSAs). Despite a shortage of geriatric psychiatry services Medicare will not fund the geriatric tele-psychiatry service.
See http://www.healthcare.philips.com/main/products/telehealth/.
Bangor Beacon Community
The Bangor Beacon Community was one of 17 Beacon Communities building and strengthening local HIT infrastructure and testing innovative approaches to make measurable improvements in health care and cost. The Beacon Community received a three year (April 2010 - March 2013), $12.75 million grant from the ONC. Using HIT as a foundation, Bangor Beacon improved the health of patients with chronic conditions including diabetes, chronic obstructive pulmonary disease (COPD), CHF, and asthma. HIT allowed the Bangor community of providers to connect health record information and care management to improve the quality of care and reduce unnecessary utilization. The Bangor Beacon community work is the foundation of the EMHS Pioneer ACO. Bangor Beacon Community's work focused on the following five priority areas:7
Improving the health of people with chronic conditions such as diabetes, COPD, CHF, and asthma.
Reducing costs associated with hospital admissions and ED visits by increasing the quality of care for high-risk patients.
Improving population health through proper immunization and sharing of immunization data among providers.
Reducing variation in the delivery of evidence-based medicine and improving care quality across the community.
Bringing community leaders and organizations together to use health information effectively, improve efficiency, and improve care and quality.
The Bangor Beacon Community was comprised of 12 partners led by EMHS. The partners represent multiple types of health care providers. In addition to hospitals, physician practices, they also engaged LTPAC providers specifically the home care providers noted below and a SNF.
Bangor Beacon Participants (* = Home Care Providers)
- Acadia Hospital;
- Community Health and Counseling Services*;
- Eastern Maine Community College (EMCC);
- EMHS;
- EMHC*;
- EMMC;
- EMMC Clinical Research Center;
- HIN;
- Maine Primary Care Association;
- Penobscot Community Health Care;
- Ross Manor (rehabilitation and SNF);
- St. Joseph Healthcare*; and
- Stillwater Health Care (rehabilitation and SNF).
FIGURE J-3. Illustration of Bangor Beacon Community
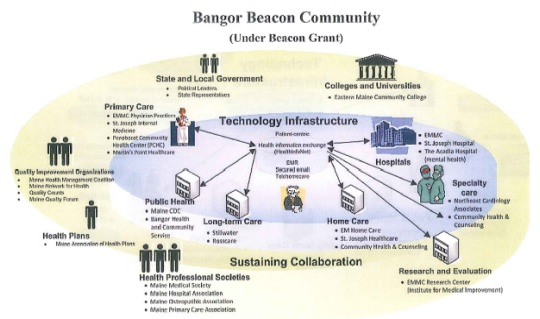
The Bangor Beacon Community worked to improve the health of chronically ill people in the Bangor region by developing a sustainable care coordination model that was facilitated by HIT (Figure J-3) the Bangor Beacon Community). The Bangor Beacon Community strove not only to improve the health of chronically ill through improved care coordination, but also to demonstrate reduce costs and improved population health.8 Integration of LTPAC providers, home care, and telehealth was an essential component of the strategy to deliver high-quality health care in the most cost-effective setting.
See http://www.healthit.gov/policy-researchers-implementers/bangor-beacon-community.
2012 Annual Report Bangor Beacon Community .
HealthInfoNet® Health Information Exchange Network
As noted above, HIT and HIE provides an infrastructure for the Bangor Beacon Community (and Pioneer ACO) to meet its goals -- the ability to exchange information is instrumental for improving care coordination. At the heart of the technical infrastructure of the Bangor Beacon Community (Figure J-3) is the HIN.9 HIN is an independent, non-profit organization that was established as the HIE for the State of Maine in 2006.
HIN has been operational exchanging clinical data since June 2009. In 2010, they received grant funding to expand the technology infrastructure including a state HIE Collaborative Grant, an ONC REC grant (HIN is the REC), and the Beacon Community grant. Today HIN is funded by many sources including charitable foundations, subscription fees from Maine health care providers, and the state and Federal Government.10 EMHS was a founding member of HIN and also served as the beta site for the interoperability demonstration project. HIN is one of only a few HIEs in the country that was operational prior to 2010 before the passage of the Health Information Technology for Economic and Clinical Health (HITECH) Act.11
2012 Annual Report Bangor Beacon Community.
Overview of HealthInfoNet Providers and Health Information Exchanged
All 38 of Maine's acute care hospitals are under contract to connect to the HIE. HIN has 34 of the 38 hospitals connected, 376 ambulatory provider sites including primary and specialty care practices, FQHCs, mental health agencies, home health and two long-term care providers. Throughout 2013, HIN will work to establish connections with the four remaining hospitals and expand the types of data shared by hospitals that are already connected. It will also continue to connect new ambulatory sites.
HIN maintains medical information on more than 1.1 million patients or 76% of all of the residents in the State of Maine. Maine is an opt-out, consent model state meaning patient information is automatically included in the HIE unless the patient opts-out of participation in the exchange. During interviews, HIN Executive Director, Dev Culver, reported that 70% of the patients who participate in the statewide exchange have health information posted from one or more non-affiliated providers.
HIN provides a consolidated view of specific types of health record information organized around the patient. The information available on HIN includes the following:
- ADT event tracking and notification;
- Patient Demographics (name, birth date, address, sex, phone number, social security number and insurance);
- Medication (prescriptions) and medication history (through SureScripts);
- Allergies;
- Lab and test results (including graphing of results);
- Vital signs (including graphing of results);
- Image reports;
- Transcribed reports (e.g., summary records); and
- Problem list (conditions, diagnosis and/or health problems from participating providers).
Certain classes of information are not included on the HIE including information from substance abuse or mental health providers and HIV diagnoses and results of HIV tests.
HIN supports public health by reporting certain illnesses (like Influenza and Lyme Disease) to public health experts at the Maine Center for Disease Control and Prevention (Maine CDC).12
12. About HealthInfoNet Better. Easier.Safer pamphlet.
Health Information Exchange Technology and Standards
HIN allows providers to identify with or link to a patient. Once they are linked HIN is able to push event and documentation notifications to the provider. There are currently six "notifiable" events and this list is expected to grow. There is a near real-time monitoring that can occur which has the potential to improve communication, efficiency and effectiveness particularly for care management.
HIN is also emerging as middleware allowing a provider or a user to specify information they would like to receive on a patient. HIN routes (or pushes) the information to a reconciliation cue at which point the receiver reviews and decides whether to incorporate the data/document into their EHR. Issues are emerging with this practice including the potential to overwhelm the user with too much information to review and reconcile.
Figure J-4 provides an illustration of HIN's technical architecture. Information is exchanged using a variety of standards including Health Level 7 (HL7) version 2.x for messaging and clinical document architecture (CDA) and continuity of care document (CCD) for document exchange. Table J-4 summarizes the information exchanged and HIT standard used by HIN and EMHS's ability to support the standards.
FIGURE J-4. HealthInfoNet HIE Technical Architecture
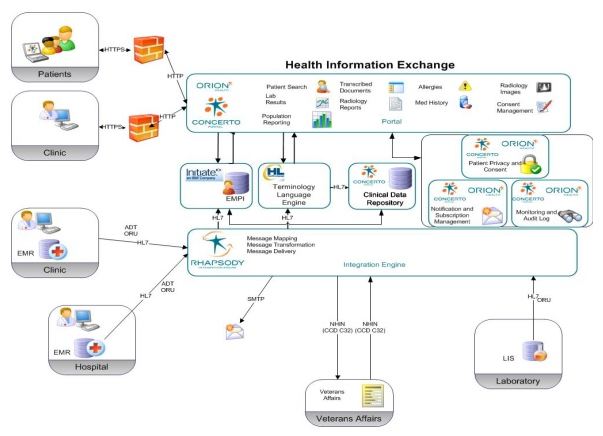
TABLE J-4. HIT Standards Used by HIN and EMHS Capabilites
| Information Type | HIT Standard and HIN Use/Findings | EMHS Standards-Based Exchange Capability |
|---|---|---|
| Messaging | HL7 Version 2.x. | Supporting ADT messages. |
| Labs | HL7 Version 2.7 (may receive in other HL7 versions, but converts to 2.7). | Supporting lab standards. |
| Documents | HL7 2.3x to 2.5x--HIN may receive document data. HL7 CDA--The content sent in the wrapper is good, but data in the document requires clean up because it is not standardized. HL7 CCD--HIN is experiencing problems with this standard. Every vendor has implemented it differently. HIN will take the CCD if they can parse out the data. | The home care POC & other documents are sent using HL7 a results message. The content of sent as a text blob. Application versions used by EMHS currently do not have the capability to support a CDA. Next version of EMHC EHR may include CCD, but it has not been installed at this time. |
| Medications | RxNorm or NDC codes. NCPDP used for communication standard. | Not applicable. As a user requests a look up of the medication history, HIN queries the medication database from SureScripts & the Maine Medicaid database for the latest information. |
Data Received (Retrieved) by Eastern Maine HomeCare
EMHC approved users access HIN and view patient information through the community view in the Cerner PowerChart. The primary users at EMHC are the intake coordinators who handle the admission process to EMHC and hospice, nurse managers, and community coordinators (see PCMH). They access the following types of information:
- ADT information -- particularly to monitor transfers to the hospital for patients receiving services. Key triggers are:
- Inpatient Admission/Admission; and ED
- Admission/Discharge.
Summary of care documents (e.g., hospital discharge summary).
Vital signs.
Laboratory tests and results.
Medications.
Data Sent to HealthInfoNet by Eastern Maine HomeCare
HIN has a Home Care and Hospice Data View, which presents summary of care document information sent by the EMHC EHR. The summary of care document includes medication and laboratory data from the home care POC.
There are two other HHAs and two SNFs participating on HIN. They have access to HIN data and send ADT alerts and diagnoses for the problem list.
Additional Opportunities for EMHC to Provide Information to HIN
During interviews with HIN, opportunities for submitting other home care information were discussed including submitting the Outcome and Information Assessment Set (OASIS) and minimum data set (MDS) patient assessment summary. Information was provided on Keystone HIE pilot study in Danville, Pennsylvania and references available on the standards and interoperability (S&I) Framework Longitudinal Coordination of Care (LCC) wiki. Tools are available for a HIE organization and LTPAC provider to send the OASIS and MDS in the CMS format, have it transformed into a CCD and sent to HIN. Also discussed was a new opportunity to test the S&I Framework LCC initiative to exchange a home care POC using the HL7 Consolidated CDA standard.
User Access and Security
HIN creates and manages all user accounts for providers/caregivers who have access to the exchange. The exchange maintains five roles for use access that define the scope and nature of an individual user's access to patient identified clinical data. Employers, insurance companies, and the government cannot access patient information at this time.
After a user has been "authorized" by HIN, they are sent a secure login and required to change their password immediately. Passwords must be unique and can only be reset by authorized personnel who can verify the user's identity.13 HIN maintains audit reports to keep track of who views the records in the exchange.
At the time of the site visit, patients did not yet have online access to their health information on HIN. However, they may request a printed or CCD copy of their HIN record through their provider and/or request an audit from HIN on who has accessed their medical information through the exchange.
HIN Support for Care Management
HIN provides EMHS with the technical tools to coordinate care using HIE and secure e-mail messaging.
HIN has a care management portal view which provides pertinent data for the various care managers in the system (such as primary care managers, inpatient care managers, cardiology care managers, mental health care managers, home care nurse managers, and palliative care nurse managers). This portal view reduces the care manager's search time when accessing patient data and allows selected information to be viewed on one screen. Data elements incorporated into this portal view include:
- Patient demographics;
- Insurance coverage;
- Primary care provider information;
- Allergies;
- Medications (including prescription);
- Immunizations;
- Diagnoses;
- Encounter/Visit History;
- Diagnostic and imaging test results; and
- Vital sign records.
The availability of technical tools to support care management across different types of provider organizations and health systems is instrumental for EMHS to test and deploy new care and payment models in accountable care and medical homes.
13. See http://www.hinfonet.org/about-us/privacy-and-security.
Participation in New Care and Payment Models and Grants to Advance Care Coordination
Bangor Beacon Community has built an integrated organization to test new payment and care delivery models through grant and other funding. As a result, CMS selected EMHS, the lead agency for the Bangor Beacon Community, to be one of 32 Pioneer ACOs in the United States. Figure J-5 illustrates the building blocks for EMHS's progression from an integrated health system to an ACO. Having an IT infrastructure and focus on quality improvement were instrumental building blocks in the migration.
FIGURE J-5. Progression to an ACO
This section describes in more depth two care coordination and payment models -- the EMHS Pioneer ACO program and PCMH initiative -- and how home care and telehealth are engaged. It also discusses two other grant programs that have supported care transitions.
Eastern Maine Health System Pioneer Accountable Care Organization
EMHS was selected as one of 32 ACOs under the Center for Medicare and Medicaid Innovation Pioneer ACO initiative,14 which started in January 2012. Under this five-year arrangement with CMS the EMHS ACO bills Medicare under existing fee-for-service (FFS) rules for their attributed patients during the first two years of the project and then transitions into capitated payment in year 3 of the pilot. The ACO shares Medicare savings in year 1 and then move to a shared savings/shared loss mode in year 2. In year 3 the Pioneer ACOs will chose a portion of the Medicare spend for per member per month payment, and continue with shared savings/losses for the remaining Medicare revenue. Throughout the pilot shared savings are based upon financial performance and 33 quality measures reported to CMS.
-
1st Performance Year: Report 33 measures to receive up to 50% or 60% (depending on their model) of Medicare shavings.
-
2nd Performance Year: Report eight measures and paid for performance on 25 measures.
-
3rd Performance Year: Pay for performance on 32 measures and pay for reporting on one survey measure related to functional status.
The 33 quality measures used to assess performance have been endorsed by the National Quality Forum (NQF) and reported across all 32 Pioneer ACOs. Attachment J-1 provides a detailed list of measures, NQF measure ID, method of submission and reporting or performance requirement. The following list summarizes the primary domains that the 33 measures fall under:
-
Patient/Caregiver Experience such as timely appointments, education, access to specialists. There are seven measures in this domain that are submitted via a survey.
-
Care Coordination/Patient Safety such as medication reconciliation after discharge from an inpatient facility, hospital readmissions, falls screening. There are six measures in this domain that are submitted by EHR Incentive Program Reporting or a special web interface.
-
Preventive Health such as influenza immunizations, pneumococcal vaccination, certain screenings. There are eight measures in this domain submitted through the GPRO web interface.
-
At-Risk Populations (Diabetes, Hypertension, Ischemic Vascular Disease, Heart Failure, Coronary Artery Disease) such as specific clinical measures. There are 12 measures in this domain all submitted through the GPRO web interface.
The EMHS ACO has begun to look at home care pathways based on disease process and how to integrate community services and supports for non-homebound patients (such as the CHF telehealth program described above). They are also evaluating the value added contribution of the CCTs (related to PCMH), home care and hospice to the ACO. EMHC reports that for every dollar invested in home care during the first year of the pilot, they save $3 as an ACO.
EMHS utilizes a system called Arcadia to manage and report quality measurement data. The ACO quality measure data is pulled into the Arcadia system through direct interface from either the EHR or other import mechanism. All provider organizations that are part of the ACO are required to collect and report quality measure data. For those organizations that are not part of the EMHS technical infrastructure are required to report quality measures in a spreadsheet format for importing. Arcadia is also used for other quality reporting processes including Meaningful Use (MU) required reporting.
14. CMS Pioneer Accountable Care Organization (ACO) Model Program Frequently Asked Questions. See http://innovation.cms.gov/Files/x/Pioneer-ACO-Model-Frequently-Asked-Questions-doc.pdf.
Patient-Centered Medical Home
In 2009, Maine established 22 PCMH projects state including the EMHS Primary Care Medical Home Demonstration Project. One year later in 2010 CMS issued a demonstration project -- Multi-Payer Advanced Primary Care (MAPCP) -- in which Maine was selected as one of eight states to have Medicare participate as a payer.
The PCMH's are reimbursed by three types of payers: Medicare, MaineCare (state Medicaid Program) and commercial insurers. Medicare pays $7/member/month for PCMH services and $3/member/month for CCT. Maine is projecting to achieve budget-neutrality by decreasing patient inpatient admissions by 6%-7%, decreasing ED visits by 5%, and decreasing specialty consultations and imaging by 5%.
In addition to PCMHs, MaineCare developed health homes that serve individuals with:
Two or more chronic conditions.
One chronic condition and who are at-risk for another.
- Serious mental illness (SMI) including:
- Adults with SMI; and
- Children with severe emotional disturbance (SED).
The care management infrastructure in the PCMH includes at a minimum a nurse patient care manager embedded in each primary care practice who works with high-risk/high cost patients in the four priority diagnoses established under the Beacon project: diabetes mellitus, chronic heart failure, COPD, and asthma. The primary care managers also target patients who are in risk corridor populations identified under the ACO program as well as high cost patients. If they cannot be effectively managed in the primary care practice, then a referral is made to the CCT to address the patient's need in the community.
Referrals for the PCMH care management come from a variety of sources including:
- Provider referrals;
- Hospital discharge referral;
- Predictive modeling reports from payers;
- Specialized queries and reports that target patients in the four priority diagnoses and look for clinical measures such as certain lab values; and
- Registry data.
The patient care managers work directly with individuals to develop a personalized POC. They collaborate with other relevant care coordination teams such as inpatient care managers, cardiology care managers, mental health care managers, home care and home health service, and palliative care to manage risk, costs and transitions. The personalized POC includes individualized services, custom plans based on patient needs, co-management goals and self-management plans. The patient care managers also perform outreach to other services and providers such as community-based services and LTPAC providers. They share information through various tools such as Cerner's PowerChart, e-fax, etc.
PCMH care managers utilize the Centricity EHR system used by all EMHS primary care providers. The patient care managers utilize a number of standardized protocols and have other embedded tools and templates in the EHR. The care managers have developed a care management visit template for documenting in the EHR and have customized the templates based on the patient's condition.
The patient care managers tracking quality and performance improvement indicators for both primary care practices and for care managed patients in the areas of:
- Clinical outcomes;
- Preventive measure outcomes;
- Health care utilization; and
- Patient reported outcomes.
As noted above, EMHS PCMH may receive reimbursement for community-based care management. Phase II of their medical home program included the development of CCTs. The CCTs manage "super users" (high-risk/high cost patients) with frequent hospitalizations and/or ED visits. Overall health care savings are expected to be realized through reductions in these types of visits.
Eastern Maine HomeCare Patient-Centered Health Home Project -- Community Care Teams
CCTs are multidisciplinary, community-based care teams that provide support for the most complex, high-risk, high-need and/or high cost patients served by the PCMH Pilot Sites. The CCT assists patients overcome barriers to care, improve health compliance and outcomes, and reduce avoidable ED use and hospital admissions. The CCT managers are Licensed Clinical Social Workers, the teams include MSWs, RNs, and pharmacy students who work out of the EMHC office. They are actively engaged with community partners including the Area Agency on Aging, Local Healthy Maine Partnerships, and Bangor Public Health.
There are approximately 800 EMHS patients in this CCT program with a variety of challenges that impact their health outcomes and utilization such as mental health conditions, substance abuse, frequent ED use, medication compliance, or psychosocial concerns (e.g., senior housing issues, transportation issues). While dedicated to specific PCMHs, the CCT receives referrals from various sources including care managers at the PCMH, EMHC and hospital. They also identify potential patients be regularly analyzing data from the hospital EHR and HIN looking for individuals who have been in the ED and had multiple ED visits, individuals with complex conditions (medical and/or behavioral health co-morbidities) and targeting based and payer.
The following list provides an example of the type of criteria used to identify potential patients for the program:
- Two or more ED visits for chief complaint that is readily identified as non-emergent;
- Transitions of care;
- History of medication non-compliance; and
- Two or more chronic illnesses or one chronic illness with a co-morbid behavioral health diagnosis.
CCTs use the document remotely to the primary care setting EHR. The CCTs develop an individualized treatment plan and are working on getting the plan on HIN. One of the challenges for the CCT is the lack of a centralized record -- they must log into multiple systems to conduct their work, which is time consuming. A project is in development to allow the CCT information to flow into HIN.
Transitional Care Project (No Longer Funded)
The Beacon grant helped in supporting a transitional care project providing telehealth for patients who were not homebound and did not qualify for home care. Currently there is no funding to sustain the transitional program for patients who do not qualify for home care. When patients do meet home health qualification (i.e., homebound, skilled need) then EMHC uses telehealth partnered with nursing care managers to support home care services, with the goal of reducing ED visits and rehospitalizations.
U.S. Department of Agriculture (USDA) Grant to Expand Telehealth
Hancock County HomeCare and Hospice received $50,000 in federal grant funds (USDA's Rural Utilities Service) to expand its telehealth program and with matching funds. The agency was able to purchase an additional 28 units.
Overview of Technology at Eastern Maine HomeCare
The Information Services (IS) department supports many of the strategic priorities and centralizes the management of the technical infrastructure for of the EMHS. The IS strategic plan is a piece of the overall EMHS strategic plan. Prior to 2005 the organizations that comprised the health system maintained their own technical infrastructure and applications. Since 2005, the IS department has begun to consolidate the infrastructure bringing together all of the EMHS hospitals onto the same EHR, PACS, billing, human resources, payroll, coding and abstracting applications. The top priorities for the IS department at the time of the interview were: implementing the MU Program requirements, transitioning to ICD-10, addressing the infrastructure needs to support the ACO, and merge a new hospital and home care into the EMHS.
EMHS eligible providers have attested for MU Stage 1 and are aggressively working on Stage 2. Based on interview discussions, IS leaders are finding MU Stage 2 requirements much more complete than Stage 1 and fit into the organization's interoperability platform.
For budgetary reasons, EMHS was not able to move to a single EHR application for all of the HHAs in the division until the Beacon grant. The grant provided the extra funding to bring together all of the home care and hospice agencies onto a single set of applications (McKesson).
Eastern Maine HomeCare Technology Infrastructure
TABLE J-5. EMHC Software Applications
| Application | Vendor | HIE Notes |
|---|---|---|
| Home Care | McKesson Horizon Homecare (http://www.mckesson.com/providers/home-care/agency-management/mckesson-homecare/) | See section below with modules used. Physician portal to McKesson EHR under development. |
| Telehealth | Phillips Healthcare Solutions (http://www.healthcare.philips.com/main/products/telehealth/) | Cloud-based system, currently does not interface with McKesson EHR or HIE; however, plans underway for EHR integration (both home care & primary care). Telehealth nurse can set up the primary care physician as a user in the Phillips system. |
| Health Information Exchange | HealthInfoNet (http://www.hinfonet.org/) | Physician POC sent from the McKesson EHR to HIN. Working on sending lab results. |
| Quality Monitoring & Risk Management | HomeCare Gold (http://www.homehealthgold.com/index.php) | Data scrubbing & analytics application. Interfaced with McKesson Horizon EHR. |
| Hospice Pharmacy | Hospice Pharmacia (https://www.hospicepharmacia.com/index.aspx) | Interfaces with McKesson EHR. |
| Staffing | McKesson Horizon Homecare (http://www.mckesson.com/providers/home-care/agency-management/mckesson-homecare/) | |
| Patient Accounting/ Billing/ Financial System | HomeCare Accounting Solutions (http://has-software.com/) |
EMHC has multiple software applications supporting their operations. Table J-5 provides a summary of the applications that support the home care and hospice operations. The EMHC division does not use the same EHR application as the EMHS hospitals and physician practices. The hospitals use the Cerner EHR application and the physician practices use GE Centricity. Cerner also has an application known as PowerChart (referenced earlier in the report). PowerChart supports organizations that have multiple entities by providing quick access and viewing of the most frequently used and/or clinically relevant information. The hospital provides access to its LTPAC partners to PowerChart to facilitate HIE at transition and during shared care.
Electronic Health Record Systems
Moving toward one EHR vendor has been a significant project for EMHC. As hospitals and home care agencies merged, each agency had their own EHR application. The Beacon Community Grant provided the financial resources to invest in a single EHR infrastructure across all home care and hospice sites. This allowed the organization to build interfaces to the hospital HIT systems, HIN and other service providers such as pharmacies and labs. The interfaces could be leveraged to connect other LTPAC organizations to EMHS and/or HIN.
As noted above, EMHC has McKesson Horizon Homecare EHR application and utilizes various clinical modules including:
- Inquiry/referral tracking;
- Face Sheet and Census;
- Comprehensive Assessment and OASIS;
- POC;
- Physician Orders including Medications;
- Interdisciplinary Notes;
- User Defined Assessments;
- Clinical Decision Support; and
- Physician Orders, Medication and Treatment Records.
Eastern Maine HomeCare's Work List for Electronic Health Record, Telehealth and Health Information Exchange
The EMHS's IS department in collaboration with EMHC have identified three priority projects currently under development. The following projects, once complete, will improve EMHC's interoperability and HIE capabilities:
Interface between Phillips Telehealth and McKesson Horizon EHR: EMHC is working on an interface between Phillips telehealth and the McKesson EHR so staff can access the patient's clinical information from a single source rather than two separate systems. Currently having issues with the different segments of HL7 being transmitted between systems. Once the interface is complete, staff will have access to the telehealth data transmitted from the patient home in the EMHC EHR.
Physician Portal to McKesson Horizon HomeCare: EMHC is completing a project to set up a physician portal so physicians, medical assistants, or care managers can log into the Home Care EHR. In May 2013, this project was in the demonstration phase. Primary care clinicians will have access to telehealth data (including results and trending), other clinical data in the home care record, and perform functions like write and sign the home care POC as well as other orders.
Home Health Lab Data to HIE: The IT department is working on an interface to send home health care lab results to HIN.
Data Analytics
EMHS utilizes a number of data analytics approaches to leverage their information in support of decision-making. Interviews with various staff and stakeholders illustrated how data analytics tools and query/report processes were used to pinpoint patients that required additional attention, identify risk, or measure improvement. This section highlights two areas where data analytics tools are used: (1) EMHC uses the tool Home Health Gold for quality assurance and performance improvement, and (2) HIN is leveraging its data to support population health in support of the ACO.
Home Health Gold
EMHC division utilizes a tool called Home Health Gold, which is a data scrubber, and analytics tool that is interfaced with the home health EHR. The Home Care Quality Assurance/Performance Assurance director uses the information to regularly assess clinical, operational and financial data.
Figure J-6 shows the Home Health Gold Dashboard. The tool can analyze, report, and trend various types of data including:
- OASIS outcomes (before being updated on the CMS Home Health Compare web site);
- Clinical and quality outcomes based on OASIS data;
- Utilization of therapy services;
- Case mix level;
- Hospitalization and ED rates;
- Risk factors;
- Inconsistency in documentation between the clinical record and OASIS; and
- Related financial data.
The Home Health Gold data can be viewed by home care/hospice site or in aggregate for the division. The analysis is reviewed and discussed weekly with the EMHC care management team. Monthly and quarterly reports are reviewed, changes monitored and data reported on a score card.
FIGURE J-6. Home Health Gold Dashboard
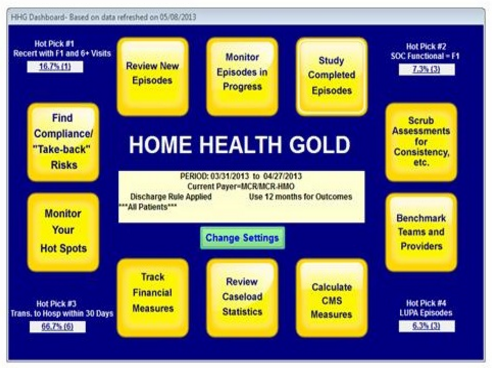
HealthInfoNet Population Analytics
HIN is moving toward population health management including support for the Northern New England ACO Collaborative (multi-state and multi-provider) and their need for analytics at a broader community/population level. HIN is focusing on data analytics to drive changes in care. For examples, HIN is analyzing data in such areas as:
Services utilization -- e.g., ADT events allow HIN to track hospital/ED utilization and rehospitalization rates).
Patterns of care -- advanced analytic techniques are used to find patterns and predict behavior.
Comparisons -- compare doctors, their outcomes and ordering patterns to determine.
Risk monitoring -- track patient risk scores and the impact of new clinical data on the score which could support emerging programs in patient risk score profiles.
The potential for leveraging the data of standardized assessments used by LTPAC providers to support population analytics was discussed during the site visit. For example, the OASIS and MDS have provided LTPAC organizations a wealth of data for analytics programs. LTPAC organizations large and small have been harvesting the data to assess quality, performance and risk. As HIN continues to move into big data analytics for population health inclusion of the OASIS and MDS data and the patient assessment summary could provide a rich source of information.
Health Information Exchange at Eastern Maine HomeCare
The availability, use and exchange of information is crucial for an EMHC to begin care and coordinate care with other service providers. Information exchange occurs through multiple different methods -- via phone, photocopies, fax and e-mail as well as through access to the hospital EHR, customized portals and the HIE. This section describes HIE in two ways:
Home health care processes and workflows.
HIE information flows around hand-offs in case, shared care, and administrative processes.
Home Health Care Processes
EMHC staff described the clinical workflow processes for care and how information is used and exchanged. Table J-6 describes the process, information collected and/or exchanged and observations by staff.
TABLE J-6. Home Health Care Workflow Processes
| Process | Information Collected and/or Exchanged | Notes |
|---|---|---|
| Referral/Intake | Collect clinical, demographic & payment information on potential admissions. Enter patient demographic into EMHS EHR to create a patient identifier which creates a record in Horizon Home Care for the patient. Perform an additional level of screening of patients to ensure appropriateness of care. Verify insurance coverage. | Hospital nurse managers work with the post-acute care liaisons on the hospital unit to determine discharge plans. When the decision to admit to EMHC is made, central intake collects information on a patient & communicates with the relevant agency/sites. They maintain patient information on Cerner PowerChart & on a shared network drive for the home care nurse manager to access during their assessment at the start of care. |
| Start of Care | Nurse or therapist assesses the patient & develops a POC. They admit the patient & call the physician from the patient's home. Meds are verified from the discharge summary & the attending called when there are discrepancies. If there is a certain type of medication interaction alert EMHC requires a call to the physician. The OASIS Start of Care & comprehensive assessment are completed. | The nurses & therapists have laptops & document at the point-of-care in the patient's home. The ACO is beginning a new pilot program where the pharmacist sends pharmacy students with the physical or speech therapist to assist with medication reconciliation when they are completing the start of care visit. |
| Home Care Plan of Care (Certification & Recertifications) | The POC includes demographic, insurance, medications, diagnoses, physician orders & visit schedule, care plan goals, & specific assessments. The Comprehensive Assessment & OASIS Start of Care data flows into the Home Care POC (485). The POC is available for physician review & signature. Recertifications are completed based on the required schedule based on an update of a subset of information the comprehensive assessment. | EMHC has developed a physician portal to their McKesson EHR system. Physicians using the portal log in to access the health record documents & orders requiring their review & signature. The physician has the option to annotate, sign or reject. In the portal the physicians can view:
|
| Home Health Visits | Home health staff (nurses, therapists, aids) document at the patient's home using laptops and/or telephony. Aide documentation is completed via telephony. Nurses complete their documentation on their laptop including their clinical notes & plan for the next visit. The clinical notes reflect the nursing care plan. | Aides call in & an automated care plan is read to the aides who use buttons on their phone to identify if a task was complete or not. A telephony report is created for the record & the visit shows up as completed. If there are incidents or concerns, staff complete documentation at the agency not from the patient's home. |
| Order & Medication Changes | The physician is called for new order requests. The nurse/therapist enters the orders into the EHR. Physicians using the portal can sign in the EMHC EHR. Assistants print out the orders for non-portal physicians. The orders are printed out & faxed to the physician. | Orders not signed in the portal, but faxed & maintained in the paper-based medical record. |
| Lab, Radiology & Other Tests | Orders for labs are tracked & when required are drawn & brought to the lab. Lab results are currently in paper format & maintained in the paper-based medical record. Electronic lab results are available on HIN (the lab provider reports results directly to HIN). | Discussed the use of document imaging, but there is not a plan to use scanning to include the lab results in the electronic record. |
| Telehealth | Patients upload data daily to telehealth nurse in Caribou Maine. Data collected is based on patient condition & may include:
| Information is accessed on the Phillips cloud-based application. An interface is currently under development to make telehealth data available in the McKesson EHR. |
| Multidisciplinary Care Plan | Currently EMHC has a care plan (separate from the POC (485)). Each discipline maintains a separate care plan based on the discipline & problem. The hospice care plan is multidisciplinary. | EMHC is starting a new multidisciplinary care plan based on the OMAHA system. The care plan will flow from the comprehensive assessment & OASIS to identify preliminary care plan problems, goals & interventions. |
| Discharge | A discharge POC is developed for the patient. A discharge order is obtained from the physician & a discharge summary completed if requested. EMHC may coordinate with community services as needed to assist with care transitions. | |
| Hospice-Specific Functions | An interface has been created with Hospice Pharmacia. Demographic & medication information is exchanged with Hospice Pharmacia. | Hospice Pharmacia is a national company that provides hospice medications & pharmacy management. They cover the cost for some meds. |
Health Information Exchange Information Flow
Table J-7, Table J-8, and Table J-9 describe the information exchange activities for EMHC in three categories: (1) hand-offs in care; (2) shared care; and (3) other administrative exchange. The exchange scenarios are not limited to electronic exchange of information, but encompass any exchange workflow. The summary tables provide a synopsis of the HIE activities from the perspective of a HHA.
Health Information Exchange Related Measures
TABLE J-7. HIE by Care Coordination Function and Partners, Eastern Maine HomeCare
EMHC does not report or identify any specific HIE measures. They report the 33 required quality measures as a Pioneer ACO. These measures are detailed in Attachment J-1.
| Transitions of Care | ||||||
|---|---|---|---|---|---|---|
| Care Coordination Function | Across Members of the Care Team Within Affiliated Organization | Between Staff in an Organization and Other Non-Affiliated Care Providers Including Community Services | Between Staff in an Organization and Patient/Family Members | Type of Exchange | Data | Sender and Receiver |
| Assessment/Referral | ||||||
| Preadmission Assessment | Hospital care manager to post-acute care provider liaison for assessment & discharge planning |
|
| Hospital care manager to post-acute care liaison & central intake | ||
| Home Care intake gathers relevant information from multiple sources for use by EMHC |
|
| Hospital, physician office & home care intake | |||
| Referral for Community Services | Hospital care manager to community services when patient does not qualify for home health or SNF services |
|
| Hospital care manager to community coordinator | ||
| Patient input on Community Services | Hospital Care Managers with Patient & Family to build the discharge POC. |
|
| Patient care manager & patient/family | ||
| Transition of Care (transfer or discharge) | ||||||
| Transfer/Admission to LTPAC | Order for Home Care |
|
| Hospital to EMHC Central Intake | ||
| Discharge Information from LTPAC Provider to Patient | Discharge POC developed by home care for patient. |
|
| Home care to patient and/or caregiver | ||
| ADT Event Data to HIE Network | Home Care ADT feeds to HIN (2 way). |
|
| Home care EHR to HIE | ||
TABLE J-8. Shared Care Information Exchange Activities
| Shared Care | ||||||
|---|---|---|---|---|---|---|
| Care Coordination Function | Across Members of the Care Team Within Affiliated Organization | Between Staff in an Organization and Other Non-Affiliated Care Providers Including Community Services | Between Staff in an Organization and Patient/Family Members | Type of Exchange | Data | Sender and Receiver |
| Assess Needs and Goals | ||||||
| Initial Assessment & Development of Admission Plan | Nurse and/or therapist assesses patient & develops POC. |
|
| Central Intake & Nurse Manager and/or Therapist | ||
| Coordination with physician at Start of Care including Medication Reconciliation & Orders, Evaluation/ Certification & Plan of Care | Medication reconciliation upon admission to home health care with Primary Care Manager. |
|
| Home care nurse & Patient Care Manager in PCMH | ||
| Start of care, orders & plan coordinated with physician. (Nurse calls the physician from the patient's home) |
|
| Home care nurse calls the attending physician | |||
| Pilot Pharmacy Student for Medication Reconciliation: Start of care, orders & plan--when therapist completes the start of care in a patient's home, a pharmacy student assists with medication reconciliation |
| Pharmacy Student & Therapist & Physician | ||||
| Physician reviews & signs 485 POC |
|
| Home care to Physician | |||
| Data to HIE Network | Physician POC sent to HIN for inclusion on HIE. |
|
| Home care EHR to HIN | ||
| Create and Maintain Plan of Care | ||||||
| Care Management/ Community Care Team Meetings | Coordinate care management functions with Patient Care Manager in the PCMH |
|
| Home Care Nurse Manager & PCMH Patient Care Manager | ||
| Monitor, Followup, and Respond to Change | ||||||
| Transmission of telehealth data from patient | Patient submits telehealth data via devices for monitoring by EMHC telehealth nurse. |
|
| Patient to telehealth home care nurse | ||
| Change in condition/ status update and/or order change request to attending physician | Physician order changes & signature on new orders |
|
| Home care to Physician | ||
| Referral to Community Care Team | Referral to CCT if patient is not meeting goals & additional services are needed |
|
| Home care nurse to manager to CCT care manager | ||
| Participate in CCT meetings when patient is also in PCMH and/or utilizing services of CCT |
|
| Home care to CCT | |||
| Coordination with physician for ongoing Orders, Evaluation/ Certification & Plan of Care | Physician recertification |
|
| Home care to Physician | ||
TABLE J-9. Other Information Exchange Activities
| Other Exchange Activities | ||||||
| Care Coordination Function | Across Members of the Care Team Within Affiliated Organization | Between Staff in an Organization and Other Non-Affiliated Care Providers Including Community Services | Between Staff in an Organization and Patient/Family Members | Type of Exchange | Data | Sender and Receiver |
|---|---|---|---|---|---|---|
| Quality Measure | ||||||
| Electronic submission of mandatory data sets which includes quality measures | Submission of OASIS data which includes CMS required quality measure data. |
|
| Home care to CMS | ||
| Submission of Hospice quality measures. |
|
| Hospice to CMS | |||
| ACO Measures | Pioneer ACO Measures (EMHS) | Pioneer ACO Measures (EMHS ACO Partners). |
|
| Home care to ACO data repository | |
| Public Health | ||||||
| Unknown | ||||||
| Payment | ||||||
| Payer Medical Records Requests | Remittance, medical review, or RAC request for medical records. |
|
| HIM & Billing to Payer | ||
Barriers and Opportunities for Improved Health Information Exchange Practices
Over the course of the two-day site visit, a number of issues were identified related to information exchange in support of care transitions and ongoing shared care. EMHC and EMHS staff interviewed offered the following insights on both barriers and opportunities for improvement in using HIE to improve communicating and coordinating care.
Barriers
Barriers to Expansion of Telehealth. The use of telehealth has shown promise for improving patient care management, outcomes and cost, but EMHC identified challenges with the reimbursement structure coupled with high cost of the equipment create challenges for expanding the technologies use across a broader population with a large, rural geographic area.
Policy Barriers in New Delivery Models Related to LTPAC. Staff at EMHC identified three policies that have limited their ability to implement innovative service delivery under their Pioneer ACO model. The policies are based on long-standing Medicare FFS coverage rules. These rules and their implications for service delivery and cost savings are described below:
One of the FFS rules requires that home health recipients be "homebound" in order to qualify for Medicare coverage of home health services. EMHC indicates that this rule will continue to be applied even when, beginning in 2014, the EMHS ACO will enter its third year as an Pioneer ACO program and e-paid: (i) for Medicare Part A covered services using a payment method that shares savings with Medicare for cost of Part A covered services; and (ii) a per member/per month capitated payment rate for Part B covered services.15
As previously described in this report, EMHC determined that delivery of telehealth health services to target population patients who are not homebound (e.g., CHF telehealth program) would reduce costs by reducing avoidable hospitalizations and ED visits. EMHC staff identified the continued application of the requirement that patients must be homebound to qualify for home health services even when services are delivered under its ACO program will limit their ability to deliver cost-effective, high-quality care.
The second Medicare FFS coverage rule stems from the Medicare Part A program Medicare coverage for SNF beneficiaries. They must have had a qualifying three day prior hospital stay to qualify for Medicare Part A coverage. EMHC staff indicated that CMS has determined that beginning in 2014 it will waive the three-day prior hospitalization requirement for the Pioneer ACO attributed patients. EMHC reports that once this waiver goes into effect it anticipates that the EMHS ACO will increase its ability to deliver cost-effective quality care by eliminating unnecessary prior hospital stays or reducing the number days an individual stays in a hospital prior to SNF admission. EMHS is working with nursing homes in the Bangor region to prepare for direct admissions to SNF from the EMMC ED. The three-day stay barrier, will be removed when, as described above, the EMHS ACO enters its third year as an Pioneer ACO program and will be paid: (i) for Medicare Part A covered services using a payment method that shares savings with Medicare, and (ii) a capitated rate for Part B covered services.
The Bangor Beacon geriatric tele-psychiatry project for nursing facilities also identified CMS regulatory barriers to providing services to nursing facilities in Penobscot County. CMS prohibits reimbursement for telemedicine services for patients residing in a MSA designated location. While the Beacon tele-psychiatry project successfully expanded access to geriatric psychiatry, the program was discontinued due to CMS payment prohibition. Nursing facility patients needing geriatric psychiatry consultation are now transported via ambulance to Acadia Hospital the EMHS affiliated psychiatry hospital.
15. For eligible beneficiaries who are enrolled in Part A and Part B, Part A finances post-institutional home health services furnished during a home health spell of illness for up to 100 visits during a spell of illness. Part A finances up to 100 visits furnished during a home health spell of illness if the following criteria are met: Beneficiaries are enrolled in Part A and Part B and qualify to receive the Medicare home health benefit; Beneficiaries must have at least a three consecutive day stay in a hospital or rural primary care hospital; and home health services must be initiated and the first covered home health visit must be rendered within 14 days of discharge from a three consecutive day stay in a hospital or rural primary care hospital or within 14 days of discharge from a SNF in which the individual was provided post-hospital extended care services. If the first home health visit is not initiated within 14 days of discharge, then home health services are financed under Part B. After an individual exhausts 100 visits of Part A post-institutional home health services, Part B finances the balance of the home health spell of illness. Basically, if an eligible beneficiary has Part A and Part B, Part B will cover and finance home health if the above criteria isnot met. If an eligible beneficiary has Part A only -- all home health is covered and paid for under Part A. If an eligible beneficiary has Part B only -- all home health is covered and paid for under Part B. The requirements that beneficiaries need skilled services and be homebound applies to all eligible beneficiaries regardless of whether it is paid for under Part A or B.
For Eligible Beneficiaries Who are Enrolled in Part a and Part B, Part a Finances Post-institutional Home Health Services Furnished During a Home Health Spell of Illness for up to 100 Visits During a Spell of Illness. Part a Finances up to 100 Visits Furn
Advancement of a Consolidated, Patient-Centered Care and Treatment Plan. EMHS has a number of care managers and care management programs particularly for high-risk/high cost patients. Each establish individual treatment plans and frequently coordinate with other program managers. There could be significant value to a comprehensive patient-centered POC that is maintained on a community site (like HIN) when population care management and payment models are used (e.g., accountable care). The care coordinators are trying to get the individualized treatment plans on HIN which could be a first step toward a patient-centered community care plan.
Focusing on Medication Reconciliation Challenges. Reconciling medications on admission is a challenge for EMHC. It is a labor-intensive process for the home health nurse to determine what medications a person was on prior to hospitalization and what they should be on after their hospitalization. Engagement of the Primary Care Manager has been helpful, but only applies to limited cases when they are a participant in the PCMH. As HIN and EMHS evaluates processes for continued improvements in efficiency, medication reconciliation could be prioritized.
Conclusion
EMHS is an innovative organization providing industry leadership on how LTPAC providers and technology can be integrated into new care delivery and payment models. Their patient-centered approach to care coordination embraces the spectrum of providers and integration of community services. Technology plays an important role in coordination of care programs for priority populations who are high-risk/high cost. EMHC has been able to demonstrate improved outcomes and reduced costs through their telehealth program.
EMHS is advancing their HIT infrastructure in step with new health care innovation grant programs including the Beacon Community Grant, which along with the PCMH and Pioneer ACO have helped to spearhead additional support for the organization's technical infrastructure including expansion of the statewide HIE, deploying the PowerChart cross-enterprise patient EHR, and prioritizing interfaces between systems that improve access and efficiency of clinical users. EMHC exchanges health information in multiple ways with clinical partners during transition of care and when delivering home care services. There is still greater potential to expand the use of technology to increase electronic HIE, but it will take time to allow for systems and HIT standards to mature.
Attachment J-1. Eastern Maine Health System Pioneer Accountable Care Organization Quality Measures
Description of ACO Measures: Excerpts and Table from CMS "Accountable Care Organization 2013 Program Analysis--Quality Performance Standards Narrative Measure Specifications" Report
On November 2, 2011, the CMS finalized new rules under the Patient Protection and Affordable Care Act (Affordable Care Act) to help doctors, hospitals, and other health care providers better coordinate care for Medicare patients through ACOs. ACOs create incentives for health care providers to work together to treat an individual patient across care settings -- including doctor's offices, hospitals, and long-term care facilities. The Medicare Shared Savings Program (Shared Savings Program) will reward ACOs that lower their growth in health care costs while meeting performance standards on quality of care and putting patients first. Participation in an ACO is purely voluntary. (ACO Provider Fact sheet: http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/sharedsavingsprogram/Downloads/ACO_Summary_Factsheet_ICN907404.pdf.)
To participate in the Shared Savings Program, ACOs must meet all eligibility and program requirements, must serve at least 5,000 Medicare FFS patients and agree to participate in the program for at least 3 years. Providers and suppliers who are already participating in another shared savings program or demonstration under FFS Medicare, such as the Independence at Home Medical Practice pilot program, will not be eligible to participate in a Shared Savings Program ACO.
Medicare providers who participate in an ACO in the Shared Savings Program will continue to receive payment under Medicare FFS rules. That is, Medicare will continue to pay individual providers and suppliers for specific items and services as it currently does under the Medicare FFS payment systems. However, CMS will also develop a benchmark for each ACO against which ACO performance is measured to assess whether it qualifies to receive shared savings, or for ACO's that have elected to accept responsibility for losses, potentially be held accountable for losses. The benchmark is an estimate of what the total Medicare FFS Parts A and B expenditures for ACO beneficiaries would otherwise have been in the absence of the ACO, even if all of those services were not provided by providers in the ACO. The benchmark will take into account beneficiary characteristics and other factors that may affect the need for health care services. This benchmark will be updated for each performance year within the agreement period.
CMS is implementing both a one-sided model (sharing savings, but not losses, for the entire term of the first agreement) and a two-sided model (sharing both savings and losses for the entire term of the agreement), allowing the ACO to opt for one or the other model for their first agreement period. CMS believes this approach will have the advantage of providing an entry point for organizations with less experience with risk models, such as some physician-driven organizations or smaller ACOs, to gain experience with population management before transitioning to a shared losses model, while also providing an opportunity for more experienced ACOs that are ready to share in losses to enter a sharing arrangement that provides a greater share of savings, but with the responsibility of repaying Medicare a portion of any losses.
Under both models, if an ACO meets quality standards and achieves savings and also meets or exceeds a Minimum Savings Rate (MSR), the ACO will share in savings, based on the quality score of the ACO. ACOs will share in all savings, not just the amount of savings that exceeds the MSR, up to a performance payment limit. Similarly, ACOs with expenditures meeting or exceeding the Minimum Loss Rate (MLR) will share in all losses, up to a loss sharing limit. To provide a greater incentive for ACOs to adopt the two-sided approach, the maximum sharing percentage based on quality performance is higher for the two-sided model. ACOs adopting this model will be eligible for a sharing rate of up to 60%, while ACOs in the one-sided model will be eligible for a sharing rate of up to 50%. Under both models, CMS will base the actual savings percentage for the individual ACO (up to the maximum for that model) on its performance score for the quality measures. As with shared savings, the amount of shared losses will be based in part on the ACO's quality performance score.
Medicare offers several ACO initiatives including:
Medicare Shared Savings Program (https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/sharedsavingsprogram/index.html?redirect=/sharedsavingsprogram/) -- a FFS program.
Advance Payment Initiative (http://innovation.cms.gov/initiatives/Advance-Payment-ACO-Model/index.html) -- for certain eligible participants in the Shared Savings Program.
Pioneer ACO Model (http://innovation.cms.gov/initiatives/Pioneer-ACO-Model/) -- population-based payment initiative for health care organizations and providers already experienced in coordinating care for patients across care settings
ACO Quality Measures
Under the CMS ACO initiatives, before an ACO can share in any savings created, it must demonstrate that it met the quality performance standard for that year. CMS will measure quality of care using nationally recognized measures in four key domains:
Patient/caregiver experience (7 measures).
Care coordination/patient safety (6 measures).
Preventive health (8 measures).
- At-risk population:
- Diabetes (1 measure and 1 composite consisting of five measures);
- Hypertension (1 measure);
- Ischemic Vascular Disease (2 measures);
- Heart Failure (1 measure); and
- Coronary Artery Disease (1 composite consisting of 2 measures).
The 33 quality measures are provided at-a-glance in Table J-10 below. For each measure, the table includes (1) the ACO measure number, (2) its domain of care, (3) the title of the measure, (4) its measure steward and NQF number (if applicable), (5) the method of data submission, and (6) when the measure is subject to pay for reporting versus pay for performance. Note that for the diabetes-related measures, five of the six measures are grouped into one "all-or-nothing" composite performance rate. Similarly, the two coronary artery disease measures are also grouped into one "all-or-nothing" composite rate for reporting purpose. In addition, six of the Consumer Assessment of Healthcare Providers and Systems (CAHPS) measures are scored together as one measure and one of the CAHPS measures is treated separately.
The ACO quality measures align with those used in other CMS quality programs, such as the Physician Quality Reporting System (PQRS) and the EHR Incentive Programs. The ACO quality measures also align with the National Quality Strategy and other U.S. Department of Health and Human Services priorities, such as the Million Hearts Initiative. In developing the final rule, CMS listened to industry concerns about focusing more on outcomes and considered a broad array of measures that would help to assess an ACO's success in delivering high-quality health care at both the individual and population levels. CMS also sought to address comments that supported adopting fewer total measures that reflect processes and outcomes, and aligning the measures with those used in other quality reporting programs, such as the PQRS.
TABLE J-10. Measures for Use in Establishing Quality Performance Standards that ACOs Must Meet for Shared Savings
| ACO # | Domain | Measure Title | NQF Measure #/ Measure Steward | Method of Data Submission | P4P Phase-in PY1 | P4P Phase-in PY2 | P4P Phase-in PY3 |
|---|---|---|---|---|---|---|---|
| AIM: Better Care for Individuals | |||||||
| 1. | Patient/Caregiver Experience | CAHPS: Getting Timely Care, Appointments, & Information | NQF #5, AHRQ | Survey | R | P | P |
| 2. | Patient/Caregiver Experience | CAHPS: How Well Your Providers Communicate | NQF #5 AHRQ | Survey | R | P | P |
| 3. | Patient/Caregiver Experience | CAHPS: Patients' Rating of Provider | NQF #5 AHRQ | Survey | R | P | P |
| 4. | Patient/Caregiver Experience | CAHPS: Access to Specialists | NQF #5 AHRQ | Survey | R | P | P |
| 5. | Patient/Caregiver Experience | CAHPS: Health Promotion & Education | NQF #5 AHRQ | Survey | R | P | P |
| 6. | Patient/Caregiver Experience | CAHPS: SDM | NQF #5 AHRQ | Survey | R | P | P |
| 7. | Patient/Caregiver Experience | CAHPS: Health Status/Functional Status | NQF #6 AHRQ | Survey | R | R | R |
| 8. | Care Coordination/ Patient Safety | Risk Standardized All Condition Readmission | CMS; NQF #1789 (adapted) | Claims | R | R | P |
| 9. | Care Coordination/ Patient Safety | Ambulatory-Sensitive Conditions Admissions: COPD or Asthma in Older Adults (ACO version 1.0) | NQF #275 AHRQ PQI #5 | Claims | R | P | P |
| 10. | Care Coordination/ Patient Safety | Ambulatory-Sensitive Conditions Admissions: Heart Failure (HF) (ACO version 1.0) | NQF #277 AHRQ PQI #8 | Claims | R | P | P |
| 11. | Care Coordination/ Patient Safety | Percent of Primary Care Physicians who Successfully Qualify for an EHR Program Incentive Payment | CMS | EHR Incentive Program Reporting | R | P | P |
| 12. | Care Coordination/ Patient Safety | Medication Reconciliation | NQF #97 AMA- PCPI/NCQA | GPRO Web Interface | R | P | P |
| 13. | Care Coordination/ Patient Safety | Falls: Screening for Future Fall Risk | NQF #101 NCQA | GPRO Web Interface | R | P | P |
| AIM: Better Health for Populations | |||||||
| 14. | Preventive Health | Influenza Immunization | NQF #41 AMA-PCPI | GPRO Web Interface | R | P | P |
| 15. | Preventive Health | Pneumococcal Vaccination for Patients 65 Years & Older | NQF #43 NCQA | GPRO Web Interface | R | P | P |
| 16. | Preventive Health | BMI Screening & Followup | NQF #421 CMS | GPRO Web Interface | R | P | P |
| 17. | Preventive Health | Tobacco Use: Screening & Cessation Intervention | NQF #28 AMA-PCPI | GPRO Web Interface | R | P | P |
| 18. | Preventive Health | Screening for Clinical Depression & Followup Plan | NQF #418 CMS | GPRO Web Interface | R | P | P |
| 19. | Preventive Health | Colorectal Cancer Screening | NQF #34 NCQA | GPRO Web Interface | R | R | P |
| 20. | Preventive Health | Breast Cancer Screening | NQF #31 NCQA | GPRO Web Interface | R | R | P |
| 21. | Preventive Health | Screening for High Blood Pressure & Followup Documented | CMS | GPRO Web Interface | R | R | P |
| 22. | At-Risk Population--Diabetes | Diabetes Composite (All-or-Nothing Scoring): Diabetes Mellitus: Hemoglobin A1c Control (8%) | NQF #729 MN Community Measurement | GPRO Web Interface | R | P | P |
| 23. | At-Risk Population--Diabetes | Diabetes Composite (All-or-Nothing Scoring): Diabetes Mellitus: Low Density Lipoprotein Control | NQF #729 MN Community Measurement | GPRO Web Interface | R | P | P |
| 24. | At-Risk Population--Diabetes | Diabetes Composite (All-or-Nothing Scoring): Diabetes Mellitus: High Blood Pressure Control | NQF #729 MN Community Measurement | GPRO Web Interface | R | P | P |
| 25. | At-Risk Population--Diabetes | Diabetes Composite (All-or-Nothing Scoring): Tobacco Non-Use | NQF #729 MN Community Measurement | GPRO Web Interface | R | P | P |
| 26. | At-Risk Population--Diabetes | Diabetes Composite (All-or-Nothing Scoring): Diabetes Mellitus: Daily Aspirin or Antiplatelet Medication Use for Patients with Diabetes & Ischemic Vascular Disease | NQF #729 MN Community Measurement | GPRO Web Interface | R | P | P |
| 27. | At-Risk Population--Diabetes | Diabetes Mellitus: Hemoglobin A1c Poor Control | NQF #59 NCQA | GPRO Web Interface | R | P | P |
| 28. | At-Risk Population--Hypertension | Hypertension (HTN): Controlling High Blood Pressure | NQF #18 NCQA | GPRO Web Interface | R | P | P |
| 29. | At-Risk Population--Ischemic Vascular Disease | Ischemic Vascular Disease (IVD): Complete Lipid Panel & LDL Control (100mg/dL) | NQF #75 NCQA | GPRO Web Interface | R | P | P |
| 30. | At-Risk Population--Ischemic Vascular Disease | Ischemic Vascular Disease (IVD): Use of Aspirin or Another Antithrombotic | NQF #68 NCQA | GPRO Web Interface | R | P | P |
| 31. | At-Risk Population--Heart Failure | Heart Failure: Beta-Blocker Therapy for Left Ventricular Systolic Dysfunction (LVSD) | NQF #83 AMA-PCPI | GPRO Web Interface | R | R | P |
| 32. | At-Risk Population--Coronary Artery Disease | Coronary Artery Disease (CAD) Composite (All-or-Nothing Scoring): Lipid Control | NQF #74 CMS (composite)/ AMA-PCPI (individual component) | GPRO Web Interface | R | R | P |
| 33. | At-Risk Population--Coronary Artery Disease | Coronary Artery Disease (CAD) Composite (All-or-Nothing Scoring): Angiotensin-Converting Enzyme (ACE) Inhibitor or Angiotensin Receptor Blocker (ARB) Therapy--Diabetes or Left Ventricular Systolic Dysfunction (LVEF 40%) | NQF #66 CMS (composite)/ AMA-PCPI (individual component) | GPRO Web Interface | R | R | P |
SOURCE: Accountable Care Organization 2013 Program Analysis -- Quality Performance Standards Narrative Measure Specifications, prepared for Quality Measurement and Health Assessment Group, Center for Clinical Standards and Quality, Centers for Medicare and Medicaid Services, by RTI International, Waltham, and Telligen West Des Moines, IA.
NOTE: ACO = accountable care organization; NQF = National Quality Forum; P4P = pay for performance; P= performance; R = reporting. For more information see: http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/sharedsavingsprogram/Downloads/ACO-NarrativeMeasures-Specs.pdf.
Appendix K. Summary of Information Routinely Exchanged by the Three Sites Visited, by CARE Coordination Function
TABLE K-1. HIE Activities for Transitions of Care
| Transitions of Care | |||||
|---|---|---|---|---|---|
| Care Coordination Function | Between Members of a Care or Service Team Within or Across Non-Affiliated or Affiliated Organization | Between Staff in an Organization and Patient/Family Members | Type of Exchange | Data | Sender and Receiver |
| Assessment/Referral | |||||
| Preadmission Assessment | Preadmission assessment process to gather information to evaluate the patient for appropriateness of admission & obtain clinical, demographic & financial information for communication with care team. |
|
| Discharge planner/case manager hospital nurse manager exchanges information with LTPAC Admission Coordinator/ Liaison | |
| Referral for Community Services | LTSS Care Coordinators assess patient needs, work with hospital discharge team, & identify HCBS that would assist the patient in a successful transition. |
|
| LTSS Care Coordinator to community service provider | |
| Patient input on Community Services | LTSS Care Coordinator obtains information from the patient on their discharge & HCBS plan/ preferences as well as past services utilized & successes. |
|
| Patient/representative & LTSS care coordinator | |
| Transition of Care (transfer or discharge) | |||||
| Transfer/ Admission to LTPAC | Hospital or discharging organization provides information to transfer care to the LTPAC provider. |
|
| Transferring provider (e.g., hospital) to LTPAC provider (admission/intake coordinator and/or nursing staff) | |
| Transfer to Hospital from LTPAC | LTPAC organization transfers patient to hospital. |
|
| LTPAC provider (nursing staff) to hospital ED (typically sent with ambulance provider) | |
| Discharge from LTPAC to Another Provider | LTPAC organization discharges patient to another health care provider (e.g., another LTPAC provider). |
|
| LTPAC provider (nursing staff) to other provider (typically nursing staff) | |
| Discharge Information from LTPAC Provider to Patient | When patient is discharging home or discontinuing home health services, the LTPAC provider develops a POC & instructions for the patient. |
|
| LTPAC provider to patient/caregiver | |
| Discharge from LTPAC with Referral to Community Service Provider(s) | For patients discharging from LTPAC who requires community services, the LTPAC provider may followup. |
|
| LTPAC provider to community service provider | |
| ADT Event Data to HIE Network | ADT message to HIE to communicate admissions & discharge information. HIEs may use these messages to notifying other treatment providers of an ADT. |
|
| LTPAC to HIE | |
| Followup Post Transfer/Discharge | |||||
| LTSS Care Coordinator followup with Community Service Provider & Patient | LTSS care coordinator follows up with community provider to ensure services were started & assess progress. | LTSS care coordinator follows up with patient/ caregiver to ensure services were delivered, assess progress, & determine if changes are required. |
|
| Care coordinator to community service provider & patient |
TABLE K-2. HIE Activities for Shared Care
| Shared Care | |||||
|---|---|---|---|---|---|
| Care Coordination Function | Between Members of a Care or Service Team in Either an Non-Affiliated or Affiliated Organization | Between Staff in an Organization and Patient/Family Members | Type of Exchange | Data | Sender and Receiver |
| Assess Needs and Goals | |||||
| Initial Assessments & Development of Admission Plan | Nurse, therapist & other interdisciplinary team members assesses patient & develops & admission POC. |
|
| Nurse, therapist and/or other members of interdisciplinary team to Hospital/physician nurse or care managers. | |
| Coordination with physician at Start of Care including Medication Reconciliation & Orders, Evaluation/ Certification & Plan of Care | Review admission transfer form & identify physician orders. Complete medications reconciliation of pre-hospital medication regime with post-hospital medications with attending physician to determine LTPAC plan. Develop POC (home care) & therapy evaluation/certification (SNF). |
|
| LTPAC Nurse and/or therapist to Attending physician for review & signature | |
| Communicate Physician Orders & Medications to Pharmacy (SNF & hospice) | Communicate admission orders & medications to pharmacy. |
|
| LTPAC nurse to pharmacy | |
| Communicate orders for labs, radiology & special tests to service provider & return of test results | Communicate lab, radiology & other specialized test orders to provider & return of results. |
|
| LTPAC nurse or to service provider Results returned to LTPAC nurse from service provider | |
| Admission Physician Visits/ Evaluation (SNF) | Attending physician and/or NP visit nursing facility patient after admission (within 3o days or more frequently as determined by organization protocol & patient condition). |
|
| LTPAC Facility Nurse & attending physician/NP | |
| Request for additional medical record information from hospital to assist with admission assessment & care planning process | LTPAC interdisciplinary team request additional information from hospital to complete an assessment. |
|
| LTPAC HIM to hospital | |
| Communication with patient and/or family/caregiver for additional information & advanced directives | LTPAC interdisciplinary team interview patient/ family for information to complete initial assessment & determine goals for the development of the care plan |
|
| LTPAC interdisciplinary team to patient and/or family/caregiver | |
| Create and Maintain Plan of Care | |||||
| Create & Maintain Patient's Plan of Care & Orders | Develop & maintain patient's interdisciplinary POC & physician orders. Reviewed by physician & signed if required. |
|
| Nursing to attending physician | |
| Care Plan Update with Patient/Family | LTPAC interdisciplinary team updates to patient & family POC. |
|
| LTPAC representative (e.g., nurse, therapist, social worker to patient and/or family | |
| Care Management/ Community Care Team Meetings | Regularly scheduled care management meetings between all care managers including LTPAC providers (e.g., primary care managers for PCMH, hospital case managers, CCT managers, LTPAC care managers). |
|
| Care managers from different organizations within affiliated organization | |
| Monitor, Followup, and Respond to Change | |||||
| Transmission of telehealth data from patient | Transmit telehealth data each day from patient home to telehealth nurse for monitoring and/or followup. |
|
| Patient Telehealth Nurse | |
| Routine physician order review & recertification | Regular review & update of physician orders, home care POC/recertification, and/or therapy recertification. |
|
| LTPAC nursing and/or therapist to attending physician review & signature | |
| Change in condition/status update and/or order change request to attending physician | Change in condition, status updates with or without order changes. |
|
| Nursing and/or therapist to physician. Physician signature for order changes. | |
| Communicate Physician Orders changes to pharmacy & order medications (SNF & hospice) | Communicate order changes & medications to pharmacy as applicable to setting. |
|
| LTPAC nurse to pharmacy | |
| Pharmacy printing & delivery of monthly physician order recap, medication & treatment administration records | When pharmacy provides the patient's monthly physician order recap, MAR & treatment record forms to LTPAC providers (e.g., SNFs), the forms are sent at the end of each month for the next month. |
|
| Long-term care Pharmacy to LTPAC provider where applicable (e.g., some SNFs that use the pharmacy to provide this information) | |
| Change in Condition/Status update to Patient/ Family/Caregiver | Change in condition, status updates & order changes communicated to patient and/or family/ caregiver. |
|
| Depending on topic: nursing, therapy, social service or other interdisciplinary team member to patient/family | |
| Ongoing physician visits/evaluation (SNF) | MD/NP visit facility patient for regular scheduled visits & as needed to meet medical needs of patient. |
|
| MD/NP & LTPAC nurse | |
| Specialist visit/evaluation (SNF) | Specialist visit (surgeon, neurologist, dentist, psychologist, etc.). |
|
| LTPAC nurse to Specialist | |
| Order changes for lab, radiology & special tests & return of test results | Request new lab or radiology/ ultrasound or other specialized test & return of results. |
|
| LTPAC nurse or to service provider. Results returned to LTPAC nurse from service provider | |
| Referral to Community Care Team (home care if available) | Referral to CCT if patient is not meeting goals & additional services are needed. |
|
| Home care nurse to manager to CCT manager | |
TABLE K-3. Other Health Information Exchange Activities
| Other | |||||
|---|---|---|---|---|---|
| Care Coordination Function | Between Members of a Care or Service Team in Either an Non-Affiliated or Affiliated Organization | Between Staff in an Organization and Patient/Family Members | Type of Exchange | Data | Sender and Receiver |
| Quality Measure Reporting | |||||
| Electronic submission of mandatory data sets which includes quality measures | Submission of mandatory assessment data sets which includes CMS required quality measure data. |
|
| LTPAC provider to CMS | |
| ACO Measures | ACO required measure reporting from all ACO partner organization whether (both affiliated & non-affiliated organizations). |
|
| LTPAC provider to ACO data repository | |
| Mandatory Reporting | |||||
| Public health & state registries for reportable conditions | Reportable event data such as immunization data to public health authority as required. |
| Examples:
| LTPAC provider to public health authority and/or state registries | |
| Elder Abuse Reporting | Required elder abuse reporting if concerns identified. |
|
| LTPAC/LTSS representative to state agency | |
| Payment | |||||
| Eligibility Determinations with Payer | Eligibility determinations & utilization review for Medicaid through HIEO, accesses state Medicaid provider database & patient database. | Portals. MMIS. |
|
| LTPAC contacts payer to verify eligibility when required Medicaid officials LTSS provider |
| Communication with Payer Case Manager | LTPAC clinical liaison provides updates to payers regarding initial & continued coverage. |
|
| LTPAC clinical liaison to payer case manager | |
| Communication with Patient/ Representative of Medicare Coverage Ending | LTPAC provider liaison notifies the patient/ representative in writing with the Medicare end of coverage date & reason along with their appeal options. Telephone and/or in-person discussions may occur to understand the coverage decisions. |
|
| LTPAC liaison (e.g., Medicare Nurse) to Patient/Representative notifying them of coverage ending date & reason. | |
| Payer Medical Record Requests | Remittance, medical review, or RAC request for medical records. |
|
| LTPAC HIM & billing to payer | |
Appendix L. Standards Available to SUPPORT Health Information Exchange of Long-term and Post-acute CARE Data
TABLE L-1. Standards Available to Support HIE of LTPAC Data
| LTPAC Data Frequently Provided to or Requested by Other Health Care Providers | Available Standards | Included in CCDA Ballot (Fall 2013)* |
|---|---|---|
| Demographic information | In 2014 Edition: Race & Ethnicity. OMB Standards for Maintaining, Collecting, & Presenting Federal Data on Race & Ethnicity, Statistical Policy Directive No. 15, October 30, 1997. Administrative Gender: HL7 V3. Preferred language: ISO 639-2 | The following refinements to the CCDA were being balloted Fall 2013: 1.1 US Realm Header (V2) This template defines constraints that represent common administrative & demographic concepts for US Realm CDA documents. Further specification, such as documentCode, are provided in document templates that conform to this template. |
| Discharge Summary | In 2014 Edition: CCDA & several vocabulary standards. (Note: CCD/C32 & CCR are only referenced for receipt to accommodate legacy systems. CCDA is required for send & receive.) | The following refinements to the CCDA were being balloted Fall 2013: 1.1.10 Discharge Summary (V2) The Discharge Summary is a document that is a synopsis of a patient's admission to a hospital; it provides pertinent information for the continuation of care following discharge. The Joint Commission requires the following information to be included in the Discharge Summary:
The CCD represents a core data set of the most relevant administrative, demographic, & clinical information facts about a patient's health care, covering 1 or more health care encounters. It provides a means for 1 health care practitioner, system, or setting to aggregate all of the pertinent data about a patient & forward it to another to support the continuity of care. The primary use case for the CCD is to provide a snapshot in time containing the germane clinical, demographic, & administrative data for a specific patient. More specific use cases, such as a Discharge Summary or Progress Note, are available as alternative documents in this guide. |
| Transfer Summary | In 2014 Edition: Patient Summary Record. CCDA & several vocabulary standards. | The following refinements to the CCDA were being balloted Fall 2013: 1.1.22 Transfer Summary (New) This document describes constraints on the CDA header & body elements for a Transfer Summary. The Transfer summary standardizes critical information for exchange of information between providers of care when a patient moves between health care settings. Standardization of information used in this form will promote interoperability; create information suitable for reuse in quality measurement, public health, research, & for reimbursement. |
| Consultation Note/ Referral Note | In 2014 Edition: Patient Summary Record. CCDA & several vocabulary standards. | The following refinements to the CCDA were being balloted Fall 2013: 1.14 Consultation Note (V2) Consultation Note is generated as a result of a request from a clinician for an opinion or advice from another clinician. Consultations involve face-to-face time with the patient or may fall under the guidelines for tele-medicine visits. A consultation note includes the reason for the referral, history of present illness, physical examination, & decision-making component (Assessment & Plan). 1.1.6 Continuity of Care Document (V2) See above. 1.1.20 Referral Note (New) This clinical document communicates pertinent patient information to the consulting provider from a referring provider. The information in this document would include the reason for the referral & additional medical information that would augment care delivery. Examples of referral situations are when a patient is referred from a family physician to a cardiologist for followup for a cardiac condition or a when patient is sent by a primary care provider to an ED. |
| Progress Note | CCDA & several vocabulary standards. | The following refinements to the CCDA were being balloted Fall 2013: 1.1.6 Continuity of Care Document (V2) See above. 1.1.18 Progress Note (V2) This template represents a patient's clinical status during a hospitalization or outpatient visit; thus, it is associated with an encounter. Taber's medical dictionary defines a Progress Note as "An ongoing record of a patient's illness & treatment. Physicians, nurses, consultants, & therapists record their notes concerning the progress or lack of progress made by the patient between the time of the previous note & the most recent note." Mosby's medical dictionary defines a Progress Note as "Notes made by a nurse, physician, social worker, physical therapist, & other health care professionals that describe the patient's condition & the treatment given or planned." A Progress Note is not a re-evaluation note. A Progress Note is not intended to be a Progress Report for Medicare. Medicare B Section 1833(e) defines the requirements of a Medicare Progress Report. |
| Care Plan | In 2014 Edition: Patient Summary record may include care plan fields, including: goals & instructions. In addition, the 2014 rule requires that the following information be exchanged (if known) as part of transitions & referrals in care: care team, including primary care provider of record & any additional known care team members beyond the referring & transitioning provider. | The following refinements to the CCDA were being balloted Fall 2013: 1.1.2 Care Plan (New) CARE PLAN FRAMEWORK A Care Plan is a consensus-driven dynamic plan that represents all of a patient's & Care Team Members' prioritized concerns, goals, & planned interventions. It serves as a blueprint shared by all Care Team Members, including the patient, to guide the Care Team Members (including Patients, their caregivers, providers & patient's care. A Care Plan integrates multiple interventions proposed by multiple providers & disciplines for multiple conditions. A Care Plan represents 1 or more POC(s) & serves to reconcile & resolve conflicts between the various POCs developed for a specific patient by different providers. While both a POC & a care plan include the patient's life goals & require Care Team Members (including patients) to prioritize goals & interventions, the reconciliation process becomes more complex as the number of POCs increases. The Care Plan also serves to enable LCC. The CDA Care Plan represents an instance of this dynamic Care Plan at a point in time. The CDA document itself is NOT dynamic. Key differentiators between a Care Plan CDA & CCD (another "snapshot in time" document):
|
| Unstructured Document | NOTE: 2014 Edition: Certification prohibits use of the "unstructured document" document-level template (in the CCDA). | The following refinements to the CCDA were being balloted Fall 2013: 1.1.24 Unstructured Document (V2) A UD type can: (1) include unstructured content, such as a graphic, directly in a text element with a mediaType attribute; or (2) reference a single document file, such as a word-processing document, using a text/reference element. … |
| Procedures: Note | In 2014 Edition: Procedures: SNOMED-CT or Use CPT-4 & HCPS for physician services & other health care services. These services include, but are not limited to, the following:
| The following refinements to the CCDA were being balloted Fall 2013: 1.1.16 Procedure Note (V2) Procedure Note encompasses many types of non-operative procedures including interventional cardiology, gastrointestinal endoscopy, osteopathic manipulation, & many other specialty fields. Procedure Notes are differentiated from Operative Notes because they do not involve incision or excision as the primary act. The Procedure Note is created immediately following a non-operative procedure & records the indications for the procedure &, when applicable, post-procedure diagnosis, pertinent events of the procedure, & the patient's tolerance of the procedure. The document should be sufficiently detailed to justify the procedure, describe the course of the procedure, & provide continuity of care. |
| Procedures: Section | The following refinements to the CCDA were being balloted Fall 2013: 2.62 Procedures Section (entries optional) (V2) This section describes all interventional, surgical, diagnostic, or therapeutic procedures or treatments pertinent to the patient historically at the time the document is generated. The section should include notable procedures, but can contain all procedures for the period of time being summarized. The common notion of "procedure" is broader than that specified by the HL7 Version 3 RIM, therefore this section contains procedure templates represented with 3 RIM classes: Act, Observation, & Procedure. Procedure act is for procedures that alter the physical condition of a patient (e.g., splenectomy). Observation act is for procedures that result in new information about a patient but do not cause physical alteration (e.g., EEG). Act is for all other types of procedures (e.g., dressing change). The length of an encounter is documented in the documentationOf/encompassingEncounter/ effectiveTime & length of service in documentationOf/ ServiceEvent/effectiveTime. 2.62 .1 Procedures Section (entries required) (V2) This section describes all interventional, surgical, diagnostic, or therapeutic procedures or treatments pertinent to the patient historically at the time the document is generated. The section should include notable procedures, but can contain all procedures for the period of time being summarized. The common notion of "procedure" is broader than that specified by the HL7 Version 3 RIM, therefore this section contains procedure templates represented with 3 RIM classes: Act, Observation, & Procedure. Procedure act is for procedures that alter the physical condition of a patient (e.g., splenectomy). Observation act is for procedures that result in new information about a patient but do not cause physical alteration (e.g., EEG). Act is for all other types of procedures (e.g., dressing change). | |
| Results: Lab results; Imaging results; Procedure results | In 2014 Edition: Other standards available. LOINC SNOMED-CT CPT-4 DICOM: Imaging Results Applicable HIPAA code set (i.e., ICD-9-CM or CPT 4) (Procedures) | The following refinements to the CCDA were being balloted Fall 2013: 2.65 (Results Section (Entries optional)) This section contains the results of observations generated by laboratories, imaging & other procedures. The scope includes observations of hematology, chemistry, serology, virology, toxicology, microbiology, plain x-ray, ultrasound, CT, MRI, angiography, echocardiography, nuclear medicine, pathology, & procedure observations. This section often includes notable results such as abnormal values or relevant trends. It can contain all results for the period of time being documented. Laboratory results are typically generated by laboratories providing analytic services in areas such as chemistry, hematology, serology, histology, cytology, anatomic pathology, microbiology, and/or virology. These observations are based on analysis of specimens obtained from the patient & submitted to the laboratory. Imaging results are typically generated by a clinician reviewing the output of an imaging procedure, such as where a cardiologist reports the left ventricular ejection fraction based on the review of a cardiac echocardiogram. Procedure results are typically generated by a clinician to provide more granular information about component observations made during a procedure, such as where a gastroenterologist reports the size of a polyp observed during a colonoscopy. 2.65.1 (Results Section (Entries required)) The Results section contains observations of results generated by laboratories, imaging procedures, & other procedures. These coded result observations are contained within a Results Organizer in the Results Section. The scope includes observations such as hematology, chemistry, serology, virology, toxicology, microbiology, plain x-ray, ultrasound, CT, MRI, angiography, echocardiography, nuclear medicine, pathology, & procedure observations. The section often includes notable results such as abnormal values or relevant trends, & could contain all results for the period of time being documented. |
| Current problems/diagnoses | In 2014 Edition: Problems. §170.207 (a)(2) SNOMED CT Use SNOMED CT for:
| The following refinements to the CCDA were being balloted Fall 2013: 2.19 Health Concerns Section (New) The Health Concerns section contains data that describes an interest or worry about a health state or process that has the potential to require attention, intervention or management. |
| Recent Vital Signs & Trending Reports | LOINC (e.g., body temp, BP, heart rate, height, weight) U CUM (for units of measure) SNOMED-CT Note: The 2014 Edition does not require use of any specific vocabulary set, but ONC has previously considered comments recommending the 3 vocabularies above. | The following refinements to the CCDA were being balloted Fall 2013: 2.71 Vital Signs Section (entries optional) (V2) The Vital Signs section contains relevant vital signs for the context & use case of the document type, such as blood pressure, heart rate, respiratory rate, height, weight, BMI, head circumference, pulse oximetry, temperature, & body surface area. The section should include notable vital signs such as the most recent, maximum and/or minimum, baseline, or relevant trends. Vital signs are represented in the same way as other results, but are aggregated into their own section to follow clinical conventions. 2.71.1Vital Signs Section (entries required) (V2) The Vital Signs Section contains relevant vital signs for the context & use case of the document type, such as blood pressure, heart rate, respiratory rate, height, weight, BMI, head circumference, pulse oximetry, temperature, & body surface area. The section should include notable vital signs such as the most recent, maximum and/or minimum, baseline, or relevant trends. Vital signs are represented in the same way as other results, but are aggregated into their own section to follow clinical conventions. |
| Advanced Directives and/or DNR Order | SNOMED-CT (e.g., Intubation, tube feedings, life support, CPR, antibiotics) | The following refinements to the CCDA were being balloted Fall 2013: 2.1 Advance Directives Section (entries optional) (V2) This section contains data defining the patient's advance directives & any reference to supporting documentation, including living wills, health care proxies, & CPR & resuscitation status. If the referenced documents are available, they can be included in the CCD exchange package. The most recent directives are required, if known, & should be listed in as much detail as possible. This section differentiates between "advance directives" & "advance directive documents". The former is the directions to be followed whereas the latter refers to a legal document containing those directions. 2.1.1 Advance Directives Section (entries required) (V2) This section contains data defining the patient's advance directives & any reference to supporting documentation. The most recent & up-to-date directives are required, if known, & should be listed in as much detail as possible. This section contains data such as the existence of living wills, health care proxies, & CPR & resuscitation status. If referenced documents are available, they can be included in the CCD exchange package. Structured Advance Directives including but not limited to, Intubation & Ventilation, Medications, Antibiotics treatment are represented using Advance Directive Observation template(s). Advance Directive Organizers are used to group the observations for each type of Advance Directive by type (e.g., 1 Organizer for Medications, & 1 for Resuscitation). NOTE: The descriptions in this section differentiate between "advance directives" & "advance directive documents". The former are the directions whereas the latter are legal documents containing those directions. Thus, an advance directive might be "no cardiopulmonary resuscitation", & this directive might be stated in a legal advance directive document. |
| Allergies | In 2014 Edition: RxNorm for medication allergies. SNOMED CT for Allergy/Adverse Event Type Value Set (e.g., allergies to: substance, drug, food, dander, propensity to adverse reactions). | The following refinements to the CCDA were being balloted Fall 2013: 2.2 Allergies Section (entries optional) (V2) This section lists & describes any medication allergies, adverse reactions, idiosyncratic reactions, anaphylaxis/anaphylactoid reactions to food items, & metabolic variations or adverse reactions/allergies to other substances (such as latex, iodine, tape adhesives). At a minimum, it should list currently active & any relevant historical allergies & adverse reactions. 2.2.1 Allergies Section (Entries required) (V2) This section lists & describes any medication allergies, adverse reactions, idiosyncratic reactions, anaphylaxis/anaphylactoid reactions to food items, & metabolic variations or adverse reactions/allergies to other substances (such as latex, iodine, tape adhesives). At a minimum, it should list currently active & any relevant historical allergies & adverse reactions. Both Sections 2.2 & 2.2.1 contain "Allergy Concern Act" |
| Cognitive Status | In 2014 Edition: Patient Summary Record to include cognitive status if known. CCDA includes standards to represent cognitive & functional status using LOINC/SNOMED-CT/ICF. | The following refinements to the CCDA were being balloted Fall 2013: 2.40 Mental Status Section (New) The Mental Status Section contains observation & evaluations related to patient's psychological & mental competency & deficits including cognitive functioning (e.g., mood, anxiety, perceptual disturbances) & cognitive ability (e.g., concentration, intellect, visual-spatial perception). |
| Functional Status & Assessments Service Utilization; Case Management/Care Coordination Notes | In 2014 Edition: Patient Summary Record to include functional status if known. CCDA includes standards to represent cognitive & functional status (ADL & IADL) using LOINC/ SNOMED-CT/ ICF. | The following refinements to the CCDA were being balloted Fall 2013: 2.16 Functional Status Section (V2) The Functional Status Section contains observations & assessments of a patient's physical abilities. A patient's functional status may include information regarding the patient's general function such as ambulation, ability to perform ADLs (e.g., bathing, dressing, feeding, grooming) or IADLs (e.g., shopping, using a telephone, balancing a check book). Problems that impact function (e.g., dyspnea, dysphagia) can be contained in the section. |
| Recent Medications Administration Records (at transition of care) | In 2014 Edition: For meds: use RxNorm [ADDED INFO--RxNorm includes First Databank, Micromedex, MediSpan, Gold Standard Alchemy, & Multum] For immunizations use HL7 Standard Code Set CVX--Vaccines Administered | The following refinements to the CCDA were being balloted Fall 2013: 2.39 Medications Section (entries optional) (V2) The Medications Section contains a patient's current medications & pertinent medication history. At a minimum, the currently active medications are listed. An entire medication history is an option. The section can describe a patient's prescription & dispense history & information about intended drug monitoring. 2.39.1 Medications Section (entries required) (V2) The Medications Section contains a patient's current medications & pertinent medication history. At a minimum, the currently active medications are listed. An entire medication history is an option. The section can describe a patient's prescription & dispense history & information about intended drug monitoring. This section requires either an entry indicating the subject is not known to be on any medications or entries summarizing the subject's medications. |
| Immunization, Syndromic Surveillance, & Cancer Reporting | In 2014 Edition: Electronic submission to immunization registries. HL7 2.5.1 & HL7 2.5.1 Implementation Guide for Immunization Messaging Release 1.4. Electronic submission to public health agencies for surveillance or reporting. HL7 2.5.1 §170.205 (d)(3) PHIN Messaging Guide for Syndromic Surveillance (incorporated by reference in §170.299) & Conformance Clarification for EHR Certification of Electronic Syndromic Surveillance, Addendum to PHIN Messaging Guide for Syndromic Surveillance (incorporated by reference in §170.299). Electronic submission of lab results to public health agencies. HL7 2.5.1 Implementation specifications. HL7 Version 2.5.1 Implementation Guide: Electronic Laboratory Reporting to Public Health, Release 1 (US Realm) | The following refinements to the CCDA were being balloted Fall 2013: Public health reporting/surveillance 2.32 Immunizations Section (entries optional) (V2) The Immunizations section defines a patient's current immunization status & pertinent immunization history. The primary use case for the Immunization section is to enable communication of a patient's immunization status. The section should include current immunization status, & may contain the entire immunization history that is relevant to the period of time being summarized. 2.32.1 Immunizations Section (entries required) (V2) The Immunizations section defines a patient's current immunization status & pertinent immunization history. The primary use case for the Immunization section is to enable communication of a patient's immunization status. The section should include current immunization status, & may contain the entire immunization history that is relevant to the period of time being summarized. |
| Medication & Treatment Orders | In 2014 Edition: Electronic prescribing. NCPDP SCRIPT Standard, Implementation Guide, Version 10.6, & RxNorm. For meds: use RxNorm. [ADDED INFO--RxNorm includes First Databank, Micromedex, MediSpan, Gold Standard Alchemy, & Multum] For immunizations use: HL7 Standard Code Set CVX--Vaccines Administered. | The following refinements to the CCDA were being balloted Fall 2013: 3.50 Medication Activity (V2) A medication activity describes substance administrations that have actually occurred (e.g., pills ingested or injections given) or are intended to occur (e.g., "take 2 tablets twice a day for the next 10 days"). Medication activities in "INT" mood are reflections of what a clinician intends a patient to be taking. For example, a clinician may intend for a patient to be administered Lisinopril 20mg PO for blood pressure control. However, what was actually administered was Lisinopril 10mg. In the latter case, the Medication activities in the "EVN" mood would reflect actual use. 3.51 Medication Dispense (V2) This template records the act of supplying medications (i.e., dispensing). 3.52 Medication Information (V2) A medication should be recorded as a pre-coordinated ingredient + strength + dose form (e.g., "metoprolol 25mg tablet", "amoxicillin 400mg/ 5mL suspension") where possible. This includes RxNorm codes whose Term Type is SCD, SBD, GPCK, BPCK. NOTE: The dose (doseQuantity) represents how many of the consumables are to be administered at each administration event. As a result, the dose is always relative to the consumable. Thus, a patient consuming a single "metoprolol 25mg tablet" per administration will have a doseQuantity of "1", whereas a patient consuming "metoprolol" will have a dose of "25mg". Value Set: Medication Clinical Drug 2.16.840.1.113762.1.4.1010.4 All prescribable medication formulations represented using either a "generic" or "brand-specific" concept. This includes RxNorm codes whose Term Type is SCD, SBD, GPCK, BPCK, SCDG, SBDG, SCDF, or SBDF. Value set intentionally defined as a GROUPING made up of: Value Set: Medication Clinical General Drug (2.16.840.1.113883.3.88.12.80.17) (RxNorm Generic Drugs); Value Set: Medication Clinical Brand-specific Drug (2.16.840.1.113762.1.4.1010.5) (RxNorm Branded Drugs). |
| Advance Directive Observation (V2) | SNOMED-CT (e.g., Intubation, tube feedings, life support, CPR, antibiotics.) | The following refinements to the CCDA were being balloted Fall 2013: 3.3. Advance Directive Observation (V2) This clinical statement represents Advance Directive Observation findings (e.g., "resuscitation status is Full Code") rather than orders. It should not be considered a legal document. The related legal documents are referenced using the reference/externalReference element. The Advance Directive Observation describes the patient's directives, including but not limited to:
|
| Cognitive status & Assessments | In 2014 Edition: Patient Summary Record to include cognitive status if known. Other standards: SNOMED-CT. | The following refinements to the CCDA were being balloted Fall 2013: Cognitive Status: 3.15 Cognitive Abilities Observation (New) The Cognitive Abilities Observation represents a patient's ability to perform specific cognitive tasks (e.g., ability to plan, logical sequencing ability, ability to think abstractly). Value Set: Mental & Functional Status Response Value Set 2.16.840.1.113883.11.20.9.44 A value set containing 2 SNOMED-CT qualifier codes that are common responses to mental & functional ability queries. Specific URL Pending Valueset Source: http://vtsl.vetmed.vt.edu/. 3.16 Cognitive Status Observation (V2) This template represents a patient's cognitive status (e.g., mood, memory, ability to make decisions) & problems that limit cognition (e.g., amnesia, dementia, aggressive behavior). The template may include assessment scale observations, identify supporting caregivers, & provide information about non-medicinal supplies. 3.17 Cognitive Status Organizer (V2) This template groups related cognitive status observations into categories. This organizer template may be used to group questions in a PHQ. |
| Functional Status | SNOMED-CT, ICF, LOINC | The following refinements to the CCDA were being balloted Fall 2013: 3.34 Functional Status Observation (V2) This template represents the patient's physical function (e.g., mobility status, ADLs, self-care status) & problems that limit function (dyspnea, dysphagia). The template may include assessment scale observations, identify supporting caregivers, & provide information about non-medicinal supplies. This template is used to represent physical or developmental function of all patient populations & is not limited to the long-term care population. |
| Assessment Scale | The following refinements to the CCDA were being balloted Fall 2013: 3.8 Assessment Scale Observation An assessment scale is a collection of observations that together yield a summary evaluation of a particular condition. Examples include the Braden Scale (assesses pressure ulcer risk), APACHE Score (estimates mortality in critically ill patients), Mini-Mental Status Exam (assesses cognitive function), APGAR Score (assesses the health of a newborn), & Glasgow Coma Scale (assesses coma & impaired consciousness). | |
| Assessments Instruments such as MDS, OASIS | CDA (but Not included in CCDA) | |
| Assessment Summary Documents | Represented using CCD. | The following refinements to the CCDA were being balloted Fall 2013: 1.1.6 Continuity of Care Document (V2) See above. |
| Other-Privacy/Security | In 2014 Edition: (a) Encryption & decryption of electronic health information--(1) General. Any encryption algorithm identified by the NIST as an approved security function in Annex A of the FIPS Publication 140-2, (January 27, 2010) (incorporated by reference in §170.299). (b) Record actions related to electronic health information. The date, time, patient identification, & user identification must be recorded when electronic health information is created, modified, accessed, or deleted; & an indication of which action(s) occurred & by whom must also be recorded. (c) Verification that electronic health information has not been altered in transit. Standard. A hashing algorithm with a security strength equal to or greater than SHA-1 (as specified by the NIST in FIPS PUB 180-4 (March 2012)) must be used to verify that electronic health information has not been altered. (d) Record treatment, payment, & health care operations disclosures. The date, time, patient identification, user identification, & a description of the disclosure must be recorded for disclosures for treatment, payment, & health care operations, as these terms are defined at 45 CFR 164.501. (e) Record actions related to electronic health information, audit log status, & encryption of end-user devices. (1)(i) The audit log must record the information specified in sections 7.2 through 7.4, 7.6, & 7.7 of the standard specified at §170.210(h) when EHR technology is in use. (ii) The date & time must be recorded in accordance with the standard specified at §170.210(g). (2)(i) The audit log must record the information specified in sections 7.2 & 7.4 of the standard specified at §170.210(h) when the audit log status is changed. (ii) The date & time each action occurs in accordance with the standard specified at §170.210(g). (3) The audit log must record the information specified in sections 7.2 & 7.4 of the standard specified at §170.210(h) when the encryption status of electronic health information locally stored by EHR technology on end-user devices is changed. The date & time each action occurs in accordance with the standard specified at §170.210(g). (f) Encryption & hashing of electronic health information. Any encryption & hashing algorithm identified by the NIST as an approved security function in Annex A of the FIPS Publication 140-2 (incorporated by reference in §170.299). (g) Synchronized clocks. The date & time recorded utilize a system clock that has been synchronized following (RFC 1305) Network Time Protocol, (incorporated by reference in §170.299) or (RFC 5905) Network Time Protocol Version 4, (incorporated by reference in §170.299). (h) Audit log content. ASTM E2147-01(Reapproved 2009), (incorporated by reference in §170.299). Treatment means the provision, coordination, or management of health care & related services by 1 or more health care providers, including the coordination or management of health care by a health care provider with a third party; consultation between health care providers relating to a patient; or the referral of a patient for health care from 1 health care provider to another. [65 FR 82802, Dec. 28, 2000, as amended at 67 FR 53266, August 14, 2002; 68 FR 8381, February 20, 2003] |
NOTE: Some of the standards described will change as a result of ballot reconciliation.
Appendix M. Glossary
Accountable Care Organization (ACO)
An ACO is a type of payment and delivery reform model that ties provider reimbursements to quality metrics and reductions in the total cost of care for an assigned population of patients. A group of coordinated health care providers form an ACO, which then provides care to a group of patients. The ACO may use a range of different payment models, which include capitation or fee-for-service. The ACO is accountable to the patients and the third-party payer for the quality, appropriateness, and efficiency of the health care provided.1
Basic Activities of Daily Living (ADLs)
Basic ADLs are those skills needed in typical daily self-care, such as bathing, dressing, feeding, and toileting.2
Center for Medicare and Medicaid Innovation (Innovation Center)
The Innovation Center identifies, creates, tests, and evaluates new payment and service delivery models to reduce program expenditures while preserving or enhancing the quality of care furnished to Medicare, Medicaid, and Children's Health Insurance Program beneficiaries. Several of the Innovation Center's models are testing the use of HIT in payment and payment and service delivery models, including the Health Care Innovation Awards and Pioneer Accountable Care Organization models.
Continuity of Care Document (CCD)
The CCD specification is an XML-based markup standard intended to specify the encoding, structure and semantics of a patient summary clinical document for exchange. The CCD specification is a constraint on the Health Level 7 Clinical Document Architecture standard. The patient summary contains a core data set of the most relevant administrative, demographic, and clinical information facts about a patient's health care, covering one or more health care encounters. It provides a means for one health care practitioner, system, or setting to aggregate all of the pertinent data about a patient and forward it to another practitioner, system, or setting to support the continuity of care. Its primary use case is to provide a snapshot in time containing the pertinent clinical, demographic, and administrative data for a specific patient.3
Clinical Document Architecture (CDA)
The CDA is a document markup standard that specifies the structure and semantics of clinical documents. A CDA document is a defined and complete information object that can include text, images, sounds, and other multimedia content. The document can be sent inside a Health Level 7 message and can exist independently, outside a transferring message. The first release of the standard filled an important gap by addressing common and largely narrative clinical notes. It left out certain advanced and complex semantics, both to foster broad implementation and to give time for these complex semantics to be fleshed out within Health Level 7. Being a part of the emerging Health Level 7 version 3 familyof standards, the CDA derives its semantic content from the shared Health Level 7 Reference Information Model and is implemented in Extensible Markup Language. The Health Level 7 mission is to develop standards that enable semantic interoperability across all platforms.4
Consolidated Clinical Document Architecture (CCDA)
CCDA is a consolidated library of reusable Clinical Document Architecture templates for nine common document types, including the Continuity of Care Document based on a consistent framework of document sections and representation of different types of structured clinical data.5 A conceptual view is available at: http://blogs.gartner.com/wes_rishel/2012/03/19/a-new-approach-to-clinical-interop-in-stage-2-meaningful-use/.
Direct Project
The Direct Project specifies a simple, secure, scalable, standards-based way for participants to send authenticated, encrypted health information directly to known, trusted recipients over the Internet. The Direct Project allows secure communication of health data among health care participants who already know and trust each other and thus is bound by a set of simplifying assumptions. The Direct Project assumes that the sender is responsible for several minimum requirements before sending data, including the collection of patient consent where appropriate.6
Electronic Health Record (EHR)
An electronic record of health-related information on an individual that conforms to nationally recognized interoperability standards and that can be created, managed, and consulted by authorized clinicians and staff across more than one health care organization.7
Electronic Medical Record (EMR)
An electronic record of health-related information on an individual that can be created, gathered, managed, and consulted by authorized clinicians and staff within one health care organization.8
Health Information Exchange (HIE)
The electronic movement of health-related information among organizations according to nationally recognized standards.9
Health Information Organization (HIEO)
An organization that oversees and governs the exchange of health-related information among organizations according to nationally recognized standards.10
Health Insurance Portability and Accountability Act (HIPAA)
Provides federal protections for personal health information held by covered entities and gives patients an array of rights with respect to that information.11
Instrumental Activities of Daily Living (IADLs)
IADLs refer to skills beyond basic self-care that evaluate how individuals function within their homes, workplaces, and social environments. IADLs may include typical domestic tasks, such as driving, cleaning, cooking, and shopping, as well as other less physically demanding tasks such as operating electronic appliances and handling budgets.12
Interoperability
Interoperability in health care is the ability of different information technology systems and software applications to communicate, to exchange data accurately, effectively and consistently, and to use the information that has been exchanged.13
Long-Term and Post-Acute Care (LTPAC)
LTPAC has been used to describe services across the spectrum of care such as including skilled nursing facilities, home care, hospice, long-term acute care hospitals, inpatient rehabilitation facilities, assisted living facilities, medication management, and independent care. There is no standard definition of LTPAC. Some LTPAC services include Long-Term Services and Supports (see below).14
Long-Term Services and Supports (LTSS)
LTSS are services and supports used by individuals of all ages with functional limitations and chronic illnesses who need assistance to perform routine daily activities such as bathing, dressing, preparing meals, and administering medications. LTSS include institutional and community-based services such as skilled nursing facilities, care management, adult day care, home-delivered meals, transportation providers, and other services.
Master Patient Index (MPI)
Individual providers and organizations that treat patients maintain an index of their patients, called a MPI. It contains the patient identifiers and the patient's identifying personal and demographic information. The MPI maintained by organizations are unique only within the organization. It serves as a directory of patients for ready reference, verification, and identification of the patient and patient information.15
Nationwide Health Information Network (NwHIN)
The NwHIN is the portfolio of nationally recognized services, standards and policies that enable secure Health Information Exchange over the Internet. Often also used as an umbrella term to describe the result of standards harmonization and pilot testing activities led by the U.S. Department of Health and Human Services, Office of the National Coordinator for Health Information Technology.16
Patient-Centered Care
Patient-centered care is health care that establishes a partnership among practitioners, patients, and their families (when appropriate) to ensure that decisions respect patients' wants, needs, and preferences and that patients have the education and support they need to make decisions and participate in their own care.17
Patient and Consumer Engagement
Patient and consumer engagement is defined as "actions individuals must take to obtain the greatest benefit from the health care services available to them."18
Personal Health Record (PHR)
An electronic record of health-related information on an individual that conforms to nationally recognized interoperability standards and that can be drawn from multiple sources while being managed, shared, and controlled by the individual.19
Regional Health Information Organization (RHIO)
A health information organization that brings together health care stakeholders within a defined geographic area and governs Health Information Exchange among them for the purpose of improving health and care in that community.20
Self-Management
Self-management is defined as consumer/patient initiative and responsibility for actions to maintain or improve health or manage a condition irrespective of specific clinical relationships.
Shared Care
Also referred to as "shared management of care," is defined as the patient and the health care provider(s) working as a team, which may also include family/friend/lay caregivers designated by the patient, guided by the preferences and expectations of the patient.
Shared Decision-Making (SDM)
SDM is a collaborative process that allows patients and their providers to make health care decisions together, taking into account the best scientific evidence available, as well as the patient's values and preferences.21
Standards
Published statement on a topic specifying the characteristics, usually measurable, that must be satisfied or achieved to comply with the standard; technical, functional, or performance-based, in this context.22
Standards and Interoperability (S&I) Framework
The S&I Framework was adopted by the Office of the National Coordinator for Health Information Technology to harmonize interoperability specifications that support national health priorities. It is a robust network of providers, vendors, and experts from both the public and private sectors with a focus on providing tools, services, and guidance to facilitate the exchange of health information.
Virtual Health Record (VHR)
The Health Information Exchange interventions identified in this study referred to a VHR as a comprehensive electronic health record that was accessed using a secure browser.
Accountable Care Organizations (ACOs). See http://www.acofp.org/Practice_Management/ACO/Medical_Home/, accessed March 2013.
Encyclopedia of Nursing and Allied Health, ©2002 Gale Cengage.All Rights Reserved. Full copyright.
Continuity of Care Document. See http://en.wikipedia.org/wiki/Continuity_of_Care_Document.
Dolin, RH, L Alschuler, C Beebe, PVBiron, SL Boyer, D Essin, and JE Mattison. (2001). The HL7 clinical document architecture.Journal of the American Medical Informatics Association, 8(6): 552-569. The National Alliance for Health Information Technology. Available at: U.S. Department of Health and Human Services. Report to the Office of the National Coordinator for Health Information Technology on Defining Key Health Information Technology Terms. http://healthit.hhs.gov/defining_key_hit_terms, accessed June 4, 2012.
What is Consolidated CDA? See http://www.hl7standards.com/blog/2012/03/22/consolidated-cda/, accessed March 2013.
NwHIN Direct page. See http://www.nhindirect.org/.
Continuity of Care Document. See http://en.wikipedia.org/wiki/Continuity_of_Care_Document.
The National Alliance for Health Information Technology.Available at: Department of Health and Human Services. Report to the Office of the National Coordinator for Health Information Technology on Defining Key Health Information Technology Terms. Seehttp://healthit.hhs.gov/defining_key_hit_terms, accessed June 4, 2012.
Ibid.
Ibid.
Ibid.
Encyclopedia of Nursing and Allied Health, ©2002 Gale Cengage.All Rights Reserved. Full copyright.
Informed Medical Decisions Foundation. What is Shared Decision Making? See http://informedmedicaldecisions.org/what-is-shared-decision-making/.
LTPAC Health IT Collaborative. See http://www.ltpachealthit.org/content/about-long-term-and-post-acute-care.
Appavu, SI. Analysis of Unique Patient Identifier Options. Part 3: Unique Patient Identifier. Available athttp://www.ncvhs.hhs.gov/app3.htm, accessed April 24, 2012.
National eHealth Collaborative.2012. Information Exchange Roadmap: The Landscape and a Path Forward.
Hurtado, MP, EK Swift, and J Corrigan. 2001. Envisioning the National Health Care Quality Report. National Academies Press.
A New Definition for Patient Engagement: What is Engagement and Why is it Important? Washington, DC: Center for Advancing Health; 2010.
The National Alliance for Health Information Technology.Available at: Department of Health and Human Services. Report to the Office of the National Coordinator for Health Information Technology on Defining Key Health Information Technology Terms. Seehttp://healthit.hhs.gov/defining_key_hit_terms, accessed June 4, 2012.
Ibid.
Informed Medical Decisions Foundation. What is Shared Decision Making? See http://informedmedicaldecisions.org/what-is-shared-decision-making/.
The National Alliance for Health Information Technology.Available at: Department of Health and Human Services. Report to the Office of the National Coordinator for Health Information Technology on Defining Key Health Information Technology Terms. Seehttp://healthit.hhs.gov/defining_key_hit_terms, accessed June 4, 2012.
Files Available for This Report
- Main Report
- HTML http://aspe.hhs.gov/daltcp/reports/2013/HIEengage.shtml
- PDF http://aspe.hhs.gov/daltcp/reports/2013/HIEengage.pdf
- APPENDIX A. SELECTED PROGRAMS AND INITIATIVES THAT SUPPORT CARE COORDINATION AND INFORMATION EXCHANGE FOR PERSONS RECEIVING LTPAC/LTSS SERVICES
- HTML http://aspe.hhs.gov/daltcp/reports/2013/HIEengage.shtml#appendA
- PDF http://aspe.hhs.gov/daltcp/reports/2013/HIEengageA.pdf
- APPENDIX B. FRAMEWORK TO CHARACTERIZE HEALTH INFORMATION EXCHANGE TO SUPPORT CARE COORDINATION FOR PERSONS RECEIVING LTPAC/LTSS SERVICES
- HTML http://aspe.hhs.gov/daltcp/reports/2013/HIEengage.shtml#appendB
- PDF http://aspe.hhs.gov/daltcp/reports/2013/HIEengageB.pdf
- APPENDIX C. ENVIRONMENT SCAN AND LITERATURE REVIEW SOURCES
- HTML http://aspe.hhs.gov/daltcp/reports/2013/HIEengage.shtml#appendC
- PDF http://aspe.hhs.gov/daltcp/reports/2013/HIEengageC.pdf
- APPENDIX D. PROMISING COMPONENTS AND INTERVENTIONS TO REDUCE READMISSIONS
- HTML http://aspe.hhs.gov/daltcp/reports/2013/HIEengage.shtml#appendD
- PDF http://aspe.hhs.gov/daltcp/reports/2013/HIEengageD.pdf
- APPENDIX E. SUMMARY OF LITERATURE ON HEALTH INFORMATION EXCHANGE OUTCOMES AND RELATED MEASURES
- HTML http://aspe.hhs.gov/daltcp/reports/2013/HIEengage.shtml#appendE
- PDF http://aspe.hhs.gov/daltcp/reports/2013/HIEengageE.pdf
- APPENDIX F. EXAMPLES OF COMMUNITY-BASED CARE TRANSITION PROGRAM WITH LTPAC/LTSS PARTICIPATION
- HTML http://aspe.hhs.gov/daltcp/reports/2013/HIEengage.shtml#appendF
- PDF http://aspe.hhs.gov/daltcp/reports/2013/HIEengageF.pdf
- APPENDIX G. HEALTH INFORMATION EXCHANGE INTERVENTIONS AND ACTIVITIES IDENTIFIED THAT SUPPORT CARE COORDINATION FOR PERSONS RECEIVING LTPAC/LTSS
- HTML http://aspe.hhs.gov/daltcp/reports/2013/HIEengage.shtml#appendG
- PDF http://aspe.hhs.gov/daltcp/reports/2013/HIEengageG.pdf
- APPENDIX H. SITE VISIT SUMMARY: RUSH UNIVERSITY MEDICAL CENTER, CARE TRANSITIONS PROGRAM, BRIDGE PROGRAM
- HTML http://aspe.hhs.gov/daltcp/reports/2013/HIEengage.shtml#appendH
- PDF http://aspe.hhs.gov/daltcp/reports/2013/HIEengageH.pdf
- APPENDIX I. SITE VISIT SUMMARY: BEECHWOOD HOMES
- HTML http://aspe.hhs.gov/daltcp/reports/2013/HIEengage.shtml#appendI
- PDF http://aspe.hhs.gov/daltcp/reports/2013/HIEengageI.pdf
- APPENDIX J. SITE VISIT SUMMARY: EASTERN MAINE HEALTH SYSTEM, EASTERN MAINE HOMECARE
- HTML http://aspe.hhs.gov/daltcp/reports/2013/HIEengage.shtml#appendJ
- PDF http://aspe.hhs.gov/daltcp/reports/2013/HIEengageJ.pdf
- APPENDIX K. SUMMARY OF INFORMATION ROUTINELY EXCHANGED BY THE THREE SITES VISITED, BY CARE COORDINATION FUNCTION
- HTML http://aspe.hhs.gov/daltcp/reports/2013/HIEengage.shtml#appendK
- PDF http://aspe.hhs.gov/daltcp/reports/2013/HIEengageK.pdf
- APPENDIX L. STANDARDS AVAILABLE TO SUPPORT HEALTH INFORMATION EXCHANGE OF LONG-TERM AND POST-ACUTE CARE DATA
- HTML http://aspe.hhs.gov/daltcp/reports/2013/HIEengage.shtml#appendL
- PDF http://aspe.hhs.gov/daltcp/reports/2013/HIEengageL.pdf