
This report, developed by the Urban Institute and RTI International, examines the characteristics of selected LTC RAPs as part of the effort to determine the feasibility of evaluating the programs. The site descriptions do not constitute full case studies, but they capture key program features relevant to structuring a rigorous evaluation. A final report in this study, to follow this report, will assess and present evaluation design options for the LTC-RAPs. [118 PDF pages]
"Acknowledgments
The authors appreciate the time and information provided by representatives, apprentices, and partners of the long-term care registered apprenticeship programs we visited to conduct this study. We also thank our Co-Project Officers, Marie Squillace in the Office of the Assistant Secretary for Planning and Evaluation of the U.S. Department of Health and Human Services and Laura Ginsburg in the Office of Apprenticeship at the Employment and Training Administration of the U.S. Department of Labor for the invaluable insight and guidance they provided throughout the study.
Glossary
AAI -- Advancing Apprenticeship Initiative, a U.S. Department of Labor (DOL)-led initiative to promote the expansion of registered apprenticeship to high-growth industries that traditionally do not use the apprenticeship model for employer-sponsored training.
CNA -- Certified Nursing Assistant, an occupation in which employees work in free-standing or hospital-affiliated nursing homes caring for persons with clinical needs and/or needing assistance in activities such as eating, bathing, and similar activities.
Competency -- The attainment of manual, mechanical or technical skills and knowledge, as specified by an occupational standard and demonstrated by an appropriate written and/or hands-on proficiency measurement.
Competency-Based Apprenticeship -- An apprenticeship that measures skill acquisition through successful demonstration of acquired skills and knowledge, as verified by the program sponsor. Programs utilizing this approach must still require apprentices to complete an on-the-job training (OJT) component of registered apprenticeship. The program standards must address how OJT will be integrated into the program, describe competencies, and identify an appropriate means of testing and evaluation for such competencies. A competency-based apprenticeship may take a shorter or longer time to complete based on the apprentices ability to learn a skill or acquire knowledge.
DOL -- U.S. Department of Labor.
DSS -- Direct Support Specialist, an occupation in which employees provide care in group homes for persons with intellectual and developmental disabilities needing monitoring and assistance in daily activities.
Enrollment Status -- Whether an apprentice is registered currently in an apprenticeship, has completed an apprenticeship, has cancelled their apprenticeship (or had it cancelled by their employer), or suspended in good standing for an indefinite period of time with the intention of completing it.
GED -- General equivalency degree, which is an alternative credential to a high school diploma when not completed within the secondary education system.
HHA -- Home Health Aide, an occupation in which employees work in home health and hospice agencies providing services to people living in the community having clinical needs and/or needing assistance with eating, bathing, and similar activities.
HHS -- U.S. Department of Health and Human Services.
HSS -- Health Support Specialist, an occupation in which employees work in assisted living facilities and retirement homes providing care for largely elderly persons needing monitoring and assistance with daily tasks.
Hybrid Apprenticeship -- An apprenticeship that measures skill acquisition through a combination of a specified minimum number of hours of OJT and the successful demonstration of competency as described in a work process schedule.
LTC RAP -- Long-Term Care Registered Apprenticeship Programs are developed by employers, employer associations or labor-management organizations to train employees of nursing homes, rehabilitation centers, home health agencies, assisted living facilities, retirement homes, and group homes for people with disabilities using the apprenticeship model. These programs have been registered with the Office of Apprenticeship (OA) or a State Apprenticeship Agency (SAA).
OA -- Office of Apprenticeship, the office designated by DOLs Employment and Training Administration (ETA) to administer the National Apprenticeship System.
Occupation -- A field of work in which employees perform similar roles and responsibilities. Employees in a given occupation may work in a range of different settings. For example, employees working in the occupation of CNA usually work in nursing homes, but may also work in home health agencies and assisted living facilities.
OJT -- On-the-Job Training, training that occurs during the performance of an apprentices regular job responsibilities at their place of employment. OJT is essentially learning that occurs by doing ones actual job responsibilities over the course of their employment.
PHI -- Organization formerly known as the Paraprofessional Healthcare Institute, which works to strengthen the nations long-term care direct care workforce, including nearly 3 million HHAs, certified nurse aides, and personal care attendants.
RAPIDS -- Registered Apprenticeship Partners Information Data System, the administrative database maintained by DOLs OA to manage registered apprenticeship programs. RAPIDS contains apprentice-level (e.g., demographic) and sponsor-level (e.g., types and lengths of apprenticeships offered by the employer) information.
Registered Apprenticeship -- A formal employment relationship designed to promote skill training and learning on-the-job. The National Apprenticeship Act (NAA) of 1937 established the foundation for developing and expanding the nations skilled workforce through registered apprenticeship programs and standards for safeguarding the welfare of apprentices. Often referred to as the Fitzgerald Act, the NAA created a comprehensive system of partnerships among business, labor, education, and government that has shaped skill training through registered apprenticeship for succeeding generations of American workers. Basic components of Registered Apprenticeship include on-the-job (hands-on) learning, related theoretical instruction (often in a classroom setting), progressive wage increases as the apprentice advances in skill attainment and a mentor-apprentice relationship. An apprentice who successfully completes a registered program, which usually requires 1-5 years, is awarded a certificate of completion of apprenticeship. An OA registered program is one in which employers, or groups of employers, and unions design, organize, manage, and finance apprenticeship programs under the standards developed and registered with OA or a DOL ETA-recognized SAA. Employers, or groups of employers, and unions also select apprentices who are trained to meet certain pre-determined occupational standards. For more information, see the OA web site at http://www.doleta.gov/oa/.
SAA -- State Apprenticeship Agency, an agency of state government that has responsibility and accountability for apprenticeship within a state. Only a SAA may seek recognition by the OA as an agency which has been properly constituted under an acceptable law or Executive Order, and authorized by the OA to register and oversee apprenticeship programs and agreements for federal purposes.
Sponsor -- An employer, employer association, or labor-management organization that registers and operates an apprenticeship program. For example, an individual nursing home, a home health agency or an association representing these businesses may host and operate apprenticeships for its employees.
Time-Based Apprenticeship -- An apprenticeship that measures skill acquisition through completion of at least 2,000 hours of OJT as described in a work process schedule.
Executive Summary
Improving the skills of the workforce is often proposed as a strategy for improving the quality of care in long-term care settings (Institute of Medicine, 2008). The long-term care system currently lacks a formal training and career development system that is applicable across different states and long-term care settings. A federal standard requires a minimum of 75 hours of training for certified nursing assistants (CNAs) in skilled nursing facilities and home health aides (HHAs) providing home health care services but the content of this training greatly varies. There are no federal (or sometimes even state) training requirements for personal assistant service workers, personal care attendants, aides in assisted living facilities, or direct care workers serving people with developmental disabilities (Institute of Medicine, 2008).
One strategy for improving the skills of workers in the long-term care system is to expand registered apprenticeship. It combines classroom and experiential learning, wage growth, and job ladders. The goals of the apprenticeship strategy are to raise skill levels, productivity, and organizational efficiency and thereby permit employers to improve the quality of care and pay higher wages. The Long-Term Care Registered Apprenticeship Programs (LTC RAPs) are registered by the U.S. Department of Labors (DOL) Office of Apprenticeship (OA) and developed by employers, employer associations, and labor-management organizations. They provide formal training and work experience for direct care workers in long-term care settings. Although few employers currently operate LTC RAPs, the Federal Government considers this training approach as a potential way of improving job quality and quality of care in the industry as a whole.
As an initial step in testing whether the registered apprenticeship model is an effective approach for training long-term care workers, the U.S. Department of Health and Human Services (HHS) and DOL have funded a study to examine design options for evaluating LTC RAPs. This report, developed by the Urban Institute and RTI International, examines the characteristics of selected LTC RAPs as part of the effort to determine the feasibility of evaluating the programs. The site descriptions do not constitute full case studies, but they capture key program features relevant to structuring a rigorous evaluation. A final report in this study, to follow this report, will assess and present evaluation design options for the LTC RAPs.
The sites selected for this study are among the largest programs in number of apprentices and represent a range of occupations, apprenticeship models (time-based or competency-based), and geographic regions. Apprenticeship programs are on average small with 3-5 active apprentices during a year. But, this study selected large LTC RAPs because of the advantages of scale in developing rigorous evaluation designs. The LTC RAP sponsors selected are Developmental Services, Inc. (Indiana), the Evangelical Lutheran Good Samaritan Society (Idaho), Home Care Associates (Pennsylvania), Air Force Villages, Inc. (Texas), and Agape Senior (South Carolina). Employer sponsors offered a LTC RAP in one of the four occupations -- CNA, developmental support specialist (DSS), health support specialist (HSS), and HHA. Additional details on these programs are available in the site summaries provided in Appendix B.
The study team conducted semi-structured interviews with key sponsor staff involved in the LTC RAPs, apprentices, and partners to obtain information on the goals and structure of the LTC RAPs, the settings in which they operate, recruitment and selection of apprentices, on-the-job training (OJT) and related technical instruction components, wage progression, program data, perspectives on benefits and challenges, and sustainability and replicability of the programs. The following section provides a summary of the findings from the five sites visited.
Implementation of Long-Term Care Registered Apprenticeship Programs in Five Sites
The five sites designed and implement their LTC RAPs in different settings. Each LTC RAP sponsor usually implemented their LTC RAP for only one of the four occupations in this study. Four of the five sponsors are paid principally through Medicaid reimbursements, which all sponsors considered as being too low to support their LTC RAP costs. As a result, each sought supplementary external funding.
The LTC RAP intervention is generally consistent across the sites visited. Most sites (Good Samaritan, Home Care Associates, Air Force Villages, and Agape) used the LTC RAP for advanced training and mentoring of employees who had already received basic training and had leadership or personal qualities for which they were selected into the apprenticeship. Alternatively, one site (Developmental Services) used its LTC RAP for entry-level training of all new employees. The sites visited were among the largest LTC RAPs. Still, the size of even these sites varied widely, ranging from 26 to 1,150 in total number of apprentices registered between January 2005 and May 2011.
Four sites (Good Samaritan, Home Care Associates, Air Force Villages, and Agape) recruit their apprentices from current employees who must apply or be recommended and be selected for an apprenticeship. The fifth site, Developmental Services, places all new hires into its LTC RAP as apprentices are recruited through employment advertising and employment screening processes. Recruitment challenges, particularly associated with finding motivated and qualified apprentices, were problematic for Developmental Services, the one site that required all direct care workers to participate in the apprenticeship program.
The goals of the LTC RAPs, which are roughly consistent across sites, are to improve the long-term care workforce in order to improve quality of care delivered and to create jobs that are more attractive for apprentices who perform caregiving. Sites also noted that reduction in medical errors, receipt of state certification for workers, and improvement of the self-sufficiency of workers were additional goals of the LTC RAP.
One site (Air Force Villages) uses the LTC RAP as part of a formal occupational career ladder, while four additional sites use the program as a way of introducing a career ladder or seniority system within the workforce. All sites use the LTC RAP to improve the quality of care and increase the stature of the job in the eyes of the apprentice. Quality of care could be inferred from data kept by most sponsors on clinical proficiency checks or client satisfaction, or from survey inspection results in facilities, but none of the LTC RAP sponsors currently analyze these data to determine the effectiveness of their programs. Instead, they rely on anecdotal evidence which they believe strongly indicates improvements in worker skills and quality of care. Apprentices in these sites are usually middle-age females with high school degrees or general equivalency degrees (GEDs), which differs somewhat from the national profile of LTC RAP apprentices in each of the occupations of training. Rates of employees actively participating in or having completed an apprenticeship varied greatly across sites (43%-96%).
The programs varied considerably in the total length of the apprenticeships offered. They ranged from 1,680 hours of training with Good Samaritan to 3,232 hours with Air Force Villages. The difference is largely in the length of OJT.
The LTC RAP covers many of the same core competencies provided in basic training to all long-term care workers. However, the LTC RAPs go beyond the basics to provide a more extended period of advanced and specialty training to reinforce learning and improve techniques covered in basic training, as well as to teach more advanced material. The LTC RAPs also widen the scope of training by including some soft skills components such as person-centered care delivery, communication skills, and receipt of mentoring.
Sponsor budgets for patient services and staff development programs such as LTC RAPs are greatly influenced by public payer long-term care reimbursement policies. In the United States, long-term care services are paid out-of-pocket, or seldom, through privately held long-term care insurance policies. Facilities often charge higher rates for private paying patients, who are only a minority of patients receiving care (approximately 22% of patients in nursing homes (AHCA, 2011)). Medicare covers only short-term acute care in nursing homes facilities if the patient had a preceding recent hospital stay and for home health services. Once a person completely exhausts their private assets for long-term care services, state Medicaid programs become the payer of last resort. In fact, Medicaid pays for the services for almost two-thirds (63% (AHCA, 2011)) of all nursing home patients. Because of Medicaids dominant financing role, state Medicaid programs are the key rate setter. Since state governments have competing demands for their resources, Medicaid rates are usually lower than any other payer source.
Under these circumstances, wage progression for apprentices is greatly constrained by public payer reimbursement rates that are widely perceived by the industry to be too low. Wage increases in the sites visited total approximately $1.25 per hour for apprentices by the time they complete the program, although one large sponsor with multiple locations noted that a wage increase does not occur at all of its locations. Wages start off low, around $7-$9 an hour. Apart from wage increases, all sites noted that the pride and distinction of apprentices relative to their co-workers was a major incentive for participating in the program.
The LTC RAPs visited collect a limited amount of outcome data, often because of resource and time constraints, and do not formally monitor the performance of the program. Most of the sites interviewed have data on wages and benefits paid, tenure, and turnover, but these data are not collected in the same form across sites or even regularly.
The primary benefit of the LTC RAPs noted by all sponsors is that they produce a better skilled workforce. Even those sponsors who do not explicitly track apprentice performance or client satisfaction described what they perceive to be an impact on work quality. Many of the apprentices interviewed said that they recognize the improvement in the skills they learned during the LTC RAPs. These workers said that they appreciate having the qualifications to serve their clients effectively. In fact, their perception of performing at a higher quality than non-apprentices was generally viewed as a more important benefit of the program than the wage increases earned in the apprenticeship. Notwithstanding, the emphasis by sponsors and workers on job quality, sponsors were not particularly concerned with tracking or monitoring the outcomes of the LTC RAPs relative to other workers.
Two key issues for the LTC RAP model are the sustainability of the programs and the potential for replication by other sponsors. Regarding sustainability, some site managers highlighted the costs of their LTC RAPs -- namely the cost of wage increases, and the financial and time resources required to prepare training resources and implement the apprenticeship -- as the major barrier to operating the program. These high costs almost always were reported in interviews without detailed documentation. One site, which reported costs of $8,000-$10,000 per apprentice for only the related technical instruction component, has ended its LTC RAP ostensibly because of unsustainable costs. Another site suggested outside funding similar to South Carolinas $1,000 apprenticeship tax credit would help defray costs.
Lack of qualified candidates among staff to participate in apprenticeship was a common theme. Developmental Services noted the availability of qualified recruits as a challenge, although this registered apprenticeship program was unique in training all of its several hundred employees using the registered apprenticeship program. Still, other sites selected only better qualified staff for apprenticeships.
Some sites also noted that buy-in from leadership and a champion for implementing the LTC RAP were important to sustainability. Some sites are still testing whether apprenticeship is the right training approach on a subset of their staff. Some sponsor leadership has not supported full implementation. For example, Good Samaritans program is voluntary for its facilities to offer and for employees to participate.
One concern of apprentices -- the lack of a recognized and portable credential -- may hinder the sustainability of LTC RAPs. For example, staff and apprentices at Home Care Associates noted that while the apprentices are proud of earning their apprenticeship credential, they also find it challenging to communicate the meaning and the value of the credential with other individuals in their field. However, the use of a community or technical college as a training provider may lend credibility to the apprenticeship credential.
The sites visited rarely reported partnerships with the workforce investment system, the educational system, or the long-term care industry, all of which often help sustain training programs. For example, staff seldom identified partnerships with One Stop Career Centers, community colleges, or long-term care industry groups. The lack of such partnerships may greatly hinder sustainability. The initiative for developing such partnerships, if they are to occur, may need to come from the partnering organizations as opposed to from sponsors.
Some sites indicated that their LTC RAPs could easily be replicated, suggesting that the most significant obstacle to replication was that other long-term care providers were not aware of the apprenticeship model as a training option. The staff at Good Samaritan and Air Force Villages suggested that a successful program may be difficult to replicate without a champion. Agape administrators and apprentices credited their local champion with the success of the registered apprenticeship program and suggested that it would not have been implemented without the champions efforts.
Replicability also seems to depend on a variety of local conditions, including the degree to which sites are dependent on Medicaid and Medicare reimbursement for revenue. Sites that were able to identify other funding sources besides Medicaid and Medicare did not cite as many financial constraints to their work. Therefore, while Medicaid and Medicare reimbursement provided a budget constraint on many of the LTC RAPs, it did not appear to be a deciding factor in the success of the programs.
Implications for Policy
The goals of the LTC RAP are to increase the skills and productivity of the workers, raise quality of care, prolong job tenure and reduce turnover, and improve job satisfaction and employee wages. The sponsors interviewed for this study saw these advantages as reasons to operate their LTC RAP. However, other findings in this report present a challenging picture for apprenticeship, or any other advanced training for that matter, in the long-term care industry. A central problem in this field is the inability of employers to achieve and document sufficient cost savings or extract sufficient revenue increases from gains in productivity and quality of care that might result from a more highly skilled workforce. Another problem is a third-party reimbursement system that does not provide higher payments to higher quality providers, which limits the ability of employers to pay wage increases for progressing through and completing an apprenticeship. Other challenges, such as limited knowledge of the approach and limited recognition of credentials, reflect the fact that LTC RAPs are still in their early stages in the industry.
The registered apprenticeship model is intended to be self-sustaining because the sponsor uses its training budget for the LTC RAP in place of the training approach they would use otherwise. Usually, new long-term care workers receive only minimal basic training before they start work. In four of the five sites visited, the LTC RAP provides training that lasts much longer than is typical, far exceeding the usual minimal requirements. As such, apprenticeship does indeed generate more training, but presumably at additional cost to employer sponsors. Therefore, in order for the program to be sustained, the benefits of the LTC RAP need to outweigh the costs.
While these challenges do exist, expanding the number of these programs in the long-term care setting may offer an innovative approach to addressing the workforce shortage. While the number of LTC RAPs is small compared to the universe of registered apprenticeship programs, some ground has been gained through efforts by OA to promote LTC RAPs in the industry and new initiatives such as the Health Professions Opportunity Grants program, which provides health care occupational training to welfare recipients and other low-income individuals, requires partnerships with registered apprenticeship. If evaluated, these combined efforts at expanding LTC RAPs may offer some evidence of their effectiveness and document ways for addressing the challenges. Thus, policymakers potentially could consider registered apprenticeship as a partial means to address the long-term care workforce shortage and the need for better skills, but the need to understand and address the challenges to its success are formidable.
Implications for Evaluation Design
Although the main discussion of evaluation options will appear in a subsequent report, this report provides an overview of the implications for any potential future evaluation drawn from the site visits. Several aspects of the LTC RAPs visited are relevant to a better understanding of how these programs may be evaluated in the future:
-
A key issue is whether the sites program goals are the same and the intervention is generally uniform across sites. The goals across programs need to be relatively similar in order to evaluate the programs as a whole. Although the programs are registered by DOL, sponsors have considerable latitude in deciding their goals and activities. That said, the goals of the LTC RAPs visited are roughly consistent across the programs.
-
The duration of the LTC RAPs is an important issue for any evaluation. An evaluation that involves longitudinal analysis would need to consider how much time is needed to implement an intervention in order to be able to assess its full effect. The programs in this study vary widely in time for completion, ranging from 1,680 hours to 3,232 hours (approximately 1.5 years). Longer interventions can be more expensive than shorter ones, particularly if they involve multiple waves of data collection.
-
The size of the LTC RAPs visited ranged from eight to 183 active apprentices as of May 2011. These sites were the largest sites with active programs, but they were still relatively small for using conventional experimental or quasi-experimental evaluation options. One option would be to pool samples of apprentices across multiple programs but such an approach might complicate efforts to assure that comparison groups are appropriate.
-
Across these sites, limited data on important outcomes are collected. Most sites did obtain data on wages, benefits, tenure, and turnover, but not in a common form across sites. Most sites collect annual turnover but one tracks only monthly turnover. Any future evaluation would involve collecting additional data beyond what sites currently collect.
-
Designing valid comparison groups for those entering apprenticeships may be difficult because of the selection process for entrants into the program. Almost all sites have selection criteria for apprenticeships; employees must typically apply or be recommended and subsequently be assessed and selected for an apprenticeship from a subset of all employees. As a result, regular workers not selected to enter apprenticeships would not be a valid comparison group, since unmeasured differences between them and apprentices would likely bias estimates of the program impact. A randomized control trial effectively addresses such selection issues. However, without random assignment, evaluators must seek other options to distinguish between program effects and effects linked to unmeasured individual differences by identifying natural experiments or quasi-experimental evaluation methods.
-
A final potential complicating factor is that most programs have apprentices who complete the apprenticeship serve as mentors to the remaining non-apprentice staff. This intentional spillover of the intervention to non-intervention employees makes the comparison of apprentice outcomes to non-apprentice outcomes within a site extremely difficult. An evaluation might require a comparison group outside of the sponsors organization, or at least another of the sponsors facilities not subject to the intervention, to address this issue.
-
Evaluating the gains and losses for employers using the LTC RAP model is another option. There are research tools for assessing the employer perspective, but usually not in an experimental or comparison group context.
1. Introduction
The United States lacks a formal training system for long-term care occupations with and few government standards that regulate the qualifications of long-term care workers. However, there is an unprecedented need for skilled long-term care workers with the passage of the Patient Protection and Affordable Care Act (ACA) and the growing health care needs of the aging Baby Boom generation. To address this issue, the U.S. Department of Labor (DOL) has expanded the use of registered apprenticeship, a training approach that combines classroom instruction and work-based learning, to long-term care occupations. This section introduces the use of the registered apprenticeship model for long-term care training and the potential for evaluating the approach.
1.1. The Long-Term Care Industry and Registered Apprenticeship
Improving the skills of the long-term care workforce is often proposed as a strategy to improve the quality of care in long-term care settings (Institute of Medicine, 2008). Long-term care workers include certified nursing assistants (CNAs) in nursing homes, home health aides (HHAs) working for home health agencies, health support specialists (HSSs) in residential care facilities, and direct support specialists (DSSs) in group homes or facilities for persons with intellectual disabilities. These workers assist people with disabilities with daily activities such as bathing, eating, shopping, and housecleaning in private dwellings as well as in various types of group residential care facilities and nursing homes.
With the aging of the population, the need for long-term care workers is increasing. The demand for long-term care services in the United States is projected to roughly double between 2000 and 2030 as the population ages (Johnson, Toomey, and Wiener, 2007). DOL projects that HHAs and home care personal care assistants will be among the fastest growing occupations between 2008 and 2018 (DOL, 2009).
Conversely, the United States faces current long-term care workforce challenges, which will grow larger in the future. Residential care providers and nursing homes already report high turnover rates ranging from 40%-70% (NCAL, 2010; American Health Care Association, 2007) and many vacancies. Low compensation and few options for advancement result in weak incentives for workers to enter or remain in the long-term care field (Khatutsky, Wiener, Anderson, and Squillace, 2011). Moreover, the low-skill levels of many workers in these occupations make it costly for employers to raise job quality through paid training. Employers are also often dependent on reimbursement rates set by state Medicaid programs, further constraining them from raising wages to attract new workers.
The long-term care system lacks a formal training and career development program that is applied across different states and long-term care settings. A federal standard of a minimum of 75 hours of training for CNAs in skilled nursing facilities (SNFs) and HHAs is required, but the content of this training greatly varies. There are no federal (or sometimes even state) training requirements for personal assistant service workers, personal care attendants, aides in assisted living facilities, or direct care workers serving people with developmental disabilities (Institute of Medicine, 2008). One solution to improving the skills of these workers is to use low-cost strategies so that employers can justify higher wages with the promise of a more productive workforce. Another solution is to restructure employment in the long-term care industry so that entry-level work affords the opportunity of career advancement and wage progression.
Apprenticeship, which addresses both of these solutions, is a well-established strategy to train workers by combining classroom and experiential learning and placing workers into careers that offer the opportunity for advancement and wage progression. The apprenticeship model is distinguished by its integration of instruction and work. Apprentices learn occupational competencies in formal classroom settings and while working at a job that directly applies and reinforces those competencies. Structuring training in this way provides apprentices with an income and assurance that the skills they obtain are in demand by employers. In addition, the work-based learning offered by on-the-job training (OJT) helps workers to understand how their classroom instruction is relevant to their work. Evidence suggests that the returns to apprenticeship training exceed the returns to community college instruction (Hollenbeck, 2008).
An essential component of apprenticeship is clear wage and career progression. Wage increases are often tied to the completion of certain occupational competencies, either in their classroom instruction, OJT, or both. Regardless of the specific structure of the wage progression, under all circumstances apprentices who complete their program should continue to work for the employer at a higher wage than when they started the apprenticeship. This advancement opportunity, which is tied to the mastery of competencies, provides an incentive for the apprentices to acquire skills demanded by employers.
Apprenticeships in the United States are sponsored by private employers, jointly by an employer or group of employers and a union, and by the military. They are highly decentralized in terms of decisions by apprenticeship sponsors regarding curriculum and program structure. Most programs operate within the Registered Apprenticeship system, which is supervised by DOLs Office of Apprenticeship (OA), and state apprenticeship agencies (SAAs). The OA certifies program completion, protects the safety and welfare of apprentices, provides guidance and technical assistance to program sponsors, monitors program equal opportunity plans to prevent discrimination against women and minorities, and promotes the expansion of the use of apprenticeship by employers. The OA works with SAAs and its own regional staff to reach out to potential sponsors on the registered apprenticeship model and how they could implement it for training their employees.
In 2001, the OA1 launched its Advancing Apprenticeship Initiative (AAI), which emphasized the expansion of apprenticeship programs in industries were currently growing and did not have a history of using the apprenticeship model. At the time, these high-growth industries included health care, especially in long-term care occupations. This strategy was based on recommendations by a 2001 General Accounting Office report, Registered Apprenticeships: Labor Could Do More to Expand to Other Occupations. The report recommended that the registered apprenticeship model was highly successful in construction and manufacturing industries and should be replicated and expanded into other industries to develop a skilled workforce.
To address the call for expanding registered apprenticeship to the long-term care industry, the OA developed a strategy to reach out to the long-term care industry. Since then, some industry providers have used the registered apprenticeship model to develop a skilled long-term care workforce to help lower a variety of costs, including those associated with retraining costs resulting from high turnover and medical error. More advanced skills earned by apprentices may also provide employers the opportunity to create a natural career ladder that may entice job applicants interested in upward mobility and improve the lives of long-term care workers overall. Moreover, registered apprenticeships involve a wage progression within the program, as occupational competency trainings (short components where a specific job skill or task is mastered) are successively completed. This wage progression, along with the distinction of participating and completing the apprenticeship, introduces the possibility for career advancement as it may improve the skills of the long-term care workforce.
1.2. Evaluating Long-Term Care Registered Apprenticeship
To assess whether the registered apprenticeship model is an effective approach for training long-term care workers, the U.S. Department of Health and Human Services (HHS) and the DOL have funded a study to better understand LTC RAP characteristics to inform possible design options for future evaluations of LTC RAPs. To develop evaluations, HHS and DOL need to understand: how LTC RAPs are structured and implemented, the perspectives of sponsors, apprentices, and partners: and the successes and challenges of operating LTC RAPs. This report examines the characteristics of five LTC RAPs for providing such information to assess potential evaluation design options for evaluating LTC RAPs.
To guide the data collection and analysis conducted, the study addresses the following research questions:
-
What are the goals of the LTC RAP?
-
What are the apprenticeship sponsors work settings and characteristics, and how might these influence the outcomes of the registered apprenticeship?
-
What core competency trainings are offered by sponsors?
-
Are apprentices paid to attend training or is it accomplished outside of work hours?
-
What participation incentives are offered? How is the LTC RAPs wage progression or career ladder structured?
-
What are the major recruitment sources for the LTC RAP? How are apprentices selected? What recruitment challenges do these programs face?
-
What are the demographic and educational characteristics of apprentices?
-
What resources are available to the LTC RAP? How many staff are dedicated to the program? Does the sponsor have relationships with partners that provide resources?
-
What are the perceived outcomes of the LTC RAP, and what outcomes does the sponsor currently measure?
-
What are the factors that contribute to a programs sustainability and replicability?
-
What are the implications of the LTC RAPs for the feasibility of evaluating them in the future?
To best answer these questions, information for the analysis is primarily drawn from visits to five LTC RAPs. Each of these sites has a registered apprenticeship program for at least one of the following long-term care occupations:
-
DSSs, who work in group homes or other facilities to assist clients with developmental disabilities.
-
CNAs, who work in nursing homes and SNFs.
-
HHAs, who work for agencies that provide long-term care services to clients in their homes.
-
HSSs, who work in residential care facilities.
After providing an overview of each of the selected sites, this report provides a cross-site analysis of apprentice recruitment and characteristics, the features of the LTC RAPs, the resources necessary to operate the programs including any partnerships, such as with educational entities, the potential impacts of the programs, and the sustainability and replicability of these programs. The report concludes with a discussion of the implications for evaluation of the LTC RAP model. Data collected through the site visits was supplemented by data from the Registered Apprenticeship Partners Information Data System (RAPIDS). The findings from this report will inform the development of the feasible evaluation designs that could be implemented to study the effects of the LTC RAPs. A final report will assess and present these evaluation design options.
1.3. Methodology
The site selection process used four criteria to identify a dozen potential sites to visit. To best inform the most rigorous potential evaluation design options, the size of the program served as the primary site selection criterion, with the sites having the largest numbers of apprentices entering programs making the initial selection list. To obtain diversity in the LTC RAPs selected, secondary criteria included the region of the country, occupation (DSS, CNA, HHA, and HSS), and type of apprenticeship model (time-based or competency-based).
It was originally planned for the study team to visit six LTC RAPs for this study. However, the study team experienced difficulty obtaining commitment to participate from some sites originally recommended for several reasons. Two sites were in the process of ending their LTC RAPs because the program was too expensive to continue running. One site had delayed full implementation of its LTC RAP because of spending cuts. Based on the site selection process and the agreement of sites to participate in the study, the five sites selected are:
-
Developmental Services, Inc. -- a not-for-profit, private direct support services provider to persons with developmental disabilities in southern Indiana, which has sponsored its LTC RAP since 2004.
-
Evangelical Lutheran Good Samaritan Society (Good Samaritan) -- a not-for-profit, private, national nursing home chain headquartered in Sioux Falls, South Dakota, which has sponsored its LTC RAP since 2003.2
-
Home Care Associates -- a not-for-profit, worker-owned home health care provider in Philadelphia, Pennsylvania, which has sponsored its LTC RAP since 2006.3
-
Air Force Villages, Inc. -- a not-for-profit, private retirement community in San Antonio, Texas, which has sponsored its LTC RAP since 2009.
-
Agape Senior -- a faith-based, for-profit umbrella corporation which owns 38 for-profit and not-for-profit companies providing long-term care services in a variety of facilities across South Carolina, which has sponsored its LTC RAP since 2009.
In late 2010 and 2011, the study team sent two-person teams to conduct 2-3 day site visits to each LTC RAP. To systematically examine the five LTC RAPs, semi-structured interviews were held, most often in-person, with staff from apprenticeship sponsors, apprentices, and partners. Questions were designed to elicit information on the implementation and evaluation potential of the programs for the development of evaluation design options for this project (the interview guide is provided in Appendix C).
While staff at the sponsoring organizations were readily available for interviews, accessing apprentices and partners was more challenging. Apprentices, for the most part, were not centrally located because of the varied settings in which they work and train so it was challenging to interview a robust sample of apprentices. The study team also had to rely on sponsor staff to recruit apprentices for interviews so it is possible that only apprentices with more positive experiences were recruited. Representatives from the community college system and the workforce investment system that acted as resources to the LTC RAPs were contacted separately to be interviewed, typically by phone. These partners were usually not highly involved with the implementation of the LTC RAPs, either because they were seen as a competing source of training (in the case of community colleges in many of the states), or because they were seen as a separate DOL program (in the case of the workforce investment system). Perspectives from the workforce investment system are largely absent from this report because it was rarely involved in the operation of the LTC RAPs and was not considered a key partner by the sites.4
After the site visits, the researchers developed five-page summaries of the interviews using any background documents provided by the sites and notes from the site visit interviews. These summaries were sent to the administrators of the LTC RAPs for review to ensure that all information was accurate and to clarify any questions that arose as the reviews were written. These summaries are provided in Appendix B. Cross-site analysis was conducted on the various program design and implementation elements including apprentice recruitment and characteristics, the features of the LTC RAPs, program resources, partnerships, perceived program impacts, and program sustainability and replicability. The next section of this report provides an overview of the five LTC RAPs and compares overall characteristics of the sponsors and the programs.
2. Long-term CARE Registered Apprenticeship Program Sites
The interviews conducted with program staff, apprentices, and partners during the site visits to five LTC RAPs -- Developmental Services, Inc. (Indiana), the Evangelical Lutheran Good Samaritan Society (Idaho), Home Care Associates (Pennsylvania), Air Force Villages, Inc. (Texas), and Agape Senior (South Carolina) -- offered an in-depth understanding of the development and operation of these programs. This section provides summary descriptions of each of the LTC RAPs and compares overall features across sites such as sponsor characteristics, work settings, core competency training, and program characteristics.
2.1. Summaries of Selected Long-Term Care Registered Apprenticeship Program Sites
To provide an understanding of the LTC RAPs selected for study, a short description of each program is provided. More detailed descriptions of the LTC RAPs are provided in Appendix B of this report.
Developmental Services, Inc.
Development Services Incorporated is a private, not-for-profit firm that provides direct support services to clients with developmental disabilities. Its mission is to aid its clients in having fulfilling lives and managing the administration of their basic medical care. Ultimately, Developmental Services plans to move clients towards self-sufficiency, consistent with a plan developed with the client and his or her case manager.
The company receives client referrals from Medicaid state case managers. Developmental Services serves approximately 1,700 clients in group home and independent living settings across 30 counties in southern Indiana. The companys headquarters is located in Columbus, Indiana, approximately 45 miles south of Indianapolis. Apprentice training is conducted at the Columbus facility, while client care occurs throughout the state. Since direct support is by its nature dispersed and not concentrated in a single facility, Developmental Services operations are spread throughout the southern Indiana region. Initially, Developmental Services monopolized direct support service provision in the region, although now it has many competitors. Developmental Services operates 14 program facilities and oversees a large number of group homes across the region.
Developmental Services operates a registered apprenticeship program for DSSs. DSSs are responsible for assisting clients with developmental disabilities with the administration of their medicine, domestic activities in group homes and independent living facilities, transportation, and engagement with the community. They are expected to prevent or intervene in crises that emerge, and assist clients in becoming more self-sufficient. In 2004, Developmental Services sought the highest quality and lowest cost training program available, eventually deciding on registered apprenticeship. The apprenticeship program was formalized and registered with DOL in 2005. Developmental Services based the design of its LTC RAP on a training program it had operated since it was founded in 1975, for which all newly hired DSSs become apprentices. There are currently 700 apprentices at Developmental Services. In 2007, as a result of DOLs decision to increase the hours required for DSS apprenticeships, Developmental Services increased its core competency requirement to 216 hours of related technical instruction and 3,000 total hours, the majority of which is OJT. Initially, Developmental Services had time requirements of 144 hours of related technical instruction and 2,000 total hours.
Since 2007, Developmental Services apprentices who complete their requirements are certified as direct support providers by the State of Indiana. There is no associated promotion or earnings increase for apprentices upon completion of the program, but Developmental Services is interested in implementing a wage increase upon completion.5 Developmental Services cannot charge patients for direct support services; they must accept established Medicaid reimbursements as compensation. Therefore, tightened Medicaid reimbursements from the state have limited the ability of Developmental Services to raise wages for any staff upon completion of the apprenticeship program. While promotion and wage progression are not currently offered at Developmental Services through the apprenticeship program, it is expected to increase retention of apprentices who appreciate a professional and skilled work environment.
Home Care Associates
Home Care Associates is a worker-owned company founded in 1993 and provides home health services to clients in the Philadelphia area. HHAs, trained by Home Care Associates, offer care to clients in their homes to assist them in living independently.
Home Care Associates began its LTC RAP for HHAs in 2006. The company was introduced to the registered apprenticeship model through its affiliate, Cooperative Home Care Associates, and worked with PHI (formerly known as the Paraprofessional Healthcare Institute) to develop its own program. After consulting with the OA representative, Home Care Associates developed core competencies for their HHA position based on its current training program to meet the requirements of the LTC RAP.
HHAs at Home Care Associates provide both heartwork services and home health services. Heartwork services include basic companionship and assistance for clients who are able to live independently, but require companionship or care to live comfortably in their own homes. These services include light housekeeping, meal preparation, running errands, and communicating with and accompanying clients to health care providers. Home health services include assistance with basic medical care, including taking temperature, pulse, and blood pressure, changing non-sterile bandages, assistance with rehabilitative care, and assistance with administration of medicines. The program requires 2,025 total hours of OJT and related technical instruction to master the HHA core competencies. A total of 230 hours of related technical instruction in core competencies is required of apprentices, including 150 hours in basic training, 40 hours in enhanced basic training, and 40 hours of other enhanced training. Aides shadow mentors when they receive basic training. While all aides employed at Home Care Associates participate in basic training, only apprentices go on to take enhanced training.
There are currently approximately 200 aides at Home Care Associates, of which 25 have completed the apprenticeship program.6 Over the course of its history, Home Care Associates has trained and placed over 1,000 aides. The base wage for aides is $8.50 and all employees are guaranteed full-time employment. An HHAs base wage is increased by $0.20 upon the completion of the enhanced training and every specialty competency, which raises his or her hourly wage to at least $9.70.7 While the registered apprenticeship HHA guidelines require completion of two specialties, Home Care Associates requires that its apprentices complete all possible specialties, which are geriatrics, disabilities, mental illness, hospice and palliative care, dementia, and peer-mentoring. After completion of the entire apprenticeship program, aides also receive a $200 bonus, receive an official badge with their apprenticeship credential, and become a mentor for other HHAs. Costs associated with the wage increases have prevented Home Care Associates from continuing the LTC RAP.
Evangelical Lutheran Good Samaritan Society
Evangelical Lutheran Good Samaritan Society, or Good Samaritan, is the largest not-for-profit nursing home chain in the United States with 230 locations, mainly in rural areas. Its central headquarters is located in Sioux Falls, South Dakota. Its average facility size is under 100 beds but it also has some very large campuses in metro areas. The types of facilities range from single-site nursing facilities to sites that provide several types of care including skilled and long-term nursing care, assisted living, and care in independents homes located in neighborhoods.
Good Samaritans LTC RAP for advanced CNAs was started in 2003. The initial rationale to adopt the apprenticeship model for training was the need for better quality of care. National staff fielded a survey that identified a need for advanced CNA training above and beyond 75-hour federal requirement. The national staff routinely publicizethe program in employee newsletters, fliers, articles, and other promotional material as well as on its web site. LTC RAPs are only offered at 25 of the 186 facilities, with each facility operating its LTC RAPs independently. Nationally, 147 apprentices are currently active. Across the two nursing homes visited in Boise and Idaho Falls, Idaho, approximately 32 apprentices are currently registered, the most of any of the 25 sites.
Good Samaritans philosophy is more of a bottom-up approach to building the LTC RAP at its facilities with its national leadership staff serving primarily as a resource for local campuses that want to develop an apprenticeship program. This approach requires that local leadership staff initiate and manage the LTC RAPs and work with human resources and clinical staff to offer the program to selected employees. Even though the Good Samaritan national leadership has developed an infrastructure for the LTC RAPs, local campuses can lack commitment in terms of management time and employee incentives to incorporate the program into their institutions. Turnover among local leadership who championed the program is another problem.
The apprentice must complete the advanced CNA training, mentoring, and one specialty competency with approximately 180 hours of related technical instruction and between 1,500 and 2,500 hours of OJT. Some local sites appear to customize how the program is implemented and how long it takes to complete the apprenticeship. The primary intended outcomes of the LTC RAP are to improve the quality of care, empower CNAs, and improve retention by providing a career lattice to encourage staff development and promotion. The program also produces CNA mentors who are extensively used for training new hires.
Air Force Villages, Inc.
Air Force Villages is a not-for-profit retirement community located on two campuses in San Antonio, Texas. Its clientele includes a large number of retired military personnel. Each campus has large independent living complexes made up of apartment-type and standalone housing units. In addition, both campuses have SNF units. The main campus is certified for 104 SNF beds and 20 new assisted living facility beds coming on line in 2011, with approximately 75 of the SNF beds currently occupied. The second campus is certified for total occupancy of 650 including the 64-bed assisted living, secured Alzheimers disease unit and 35 non-dementia assisted living facility beds. The organization is undergoing a major expansion, building a new neighborhood-like complex to be known as the The Mission with household-type arrangements. Once the expansion is complete, the existing facilities will also be restructured into household-type arrangements.
The organization does not take Medicaid patients because reimbursement is too low for the quality of care it wishes to provide. Consequently, Air Force Villages takes private pay residents for whom staff provide a full continuum of care, some short-term Medicare-reimbursed skilled rehabilitation patients for which the facilities are increasing the number over time. Many residents also have coverage as retired members of the military through the militarys CHAMPUS insurance benefit.
Air Force Villages began its apprenticeship program in 2009 in response to its planned expansion as a means of training CNAs in its skilled nursing units in a new model of care to enact culture change. Current CNAs receive advanced training as HSSs and serve as universal workers, conducting all required tasks (e.g., resident care, housekeeping, cooking, laundry) for a small group of residents residing in one household building. In this new model of care, 2-3 HSSs serve 13-14 skilled nursing residents in a small house-like building. The new model of care could also be applied to residents in existing traditional buildings (e.g., long hallways of rooms), which are also being reorganized into neighborhoods.
Approximately 40 apprentices have been trained in three cohorts of approximately 12-15 CNAs each. The apprenticeship is 3,232 hours in length (232 hours of related technical instruction, and 3,000 hours of OJT). Although the intended purpose of the classes is to train CNAs as universal workers, other outcomes include higher wages, longer tenure, and most importantly, higher quality, person-centered care for residents needing skilled nursing care. After existing CNAs are trained, new employees will also be trained as HSSs.
Agape Senior
Agape Senior is the umbrella corporation for a mix of 38 for-profit and not-for-profit companies that provide coordinated and interrelated long-term care services in a variety of facilities across South Carolina. Founded in 1999 in West Columbia, Agape was the first long-term care provider to sponsor a registered apprenticeship program in South Carolina. Corporate headquarters is located in West Columbia, South Carolina, and facilities exist in Conway, Laurens, Rock Hill, and other sites throughout the state. Across all its facilities, Agape has approximately 800 beds and has been able to maintain high occupancy rates in both assisted living and SNF settings.
Agapes LTC RAP was started in 2009 and offers advanced CNA and palliative care competencies. The LTC RAP is overseen by the Chief Human Capital Office, which orchestrates all educational efforts at the company. The advanced CNA apprenticeship is one of four apprenticeship programs operated at Agape (the others are not associated with direct care occupations and include dietitians and management), and is only one facet of a broader educational mission at the company. Agape executives are dedicated to building an educated workforce and only hire senior staff that can serve as instructors in these educational efforts. These educational initiatives for CNAs, along with other opportunities for more senior staff, are all components of Agape University, the educational arm of the company. In addition to the four apprenticeships, the company has partnered with Goodwill Industries and Midlands Technical College to provide basic CNA training for employees who are not already certified. Agape continues to build relationships with technical colleges in the region to strengthen these educational efforts and provide of instruction for the LTC RAP.
Agape is currently working with its third cohort of apprentices. The first cohort, who was trained in 2009, began with 18 apprentices.8 Sixteen of the apprentices became certified at the end of 2009. The second cohort, trained in 2010, expanded to 35 participants with 21 successful graduates. Agapes third cohort of 59 apprentices began its program in 2011, with 52 still enrolled as of August 2011. With a total of 1,400 employees and a strong teaching staff, the company expects enrollment in the apprenticeship to continue to grow.
An apprentice in the LTC RAP has to participate in 265.5 hours of related technical instruction and 2,000 hours of OJT to complete the basic CNA, advanced CNA, and palliative care certifications registered with DOL. As the LTC RAP only accepts employees who are already certified as CNAs with the basic CNA training, apprentices only have to complete 143.5 hours of related technical instruction (103.5 hours for advanced CNA, and 40 hours for palliative care) and 1,700 hours of OJT. The palliative care competency is certified by the National Palliative Care test. The operation of the LTC RAP is uniform across Agapes facilities because all related technical instruction is conducted simultaneously over a distance learning platform. The primary intended outcomes of the registered apprentice program are to improve the education of the Agape workforce and improve the quality of care. Two additional benefits regularly noted by Agape staff were that the LTC RAP reduces CNA turnover and helps to differentiate and reward high-quality CNAs.
2.2. Apprenticeship Sponsor Characteristics and Work Settings
The five sites visited differ along the site selection criteria discussed -- program size, geographic region, occupational focus, and apprenticeship model (Table 1). Four of the sites are private, not-for-profit providers (Developmental Services, Good Samaritan, Home Care Associates, and Air Force Villages), while Agape is a for-profit provider. Home Care Associates is also a worker-owned firm, so its employees share in the organizations profits every year. The five sites provide a wide range of long-term care services.
Three of the five sites visited (Good Samaritan, Air Force Villages, and Agape) provide nursing care services to clients using CNAs. In all three sites, employees provide long-term care for clients at nursing homes and retirement communities maintained by the sponsor. Good Samaritan has a LTC RAP to train relatively new CNAs, while Air Force Villages is training its current CNA employees to become HSSs, using the registered apprenticeship model to provide more holistic care of medical and personal care needs for its residents. Agapes LTC RAP trains current employees certified as CNAs to become advanced CNAs, with expertise in palliative care.
In contrast, both Developmental Services and Home Care Associates provide services to clients at home and in group home settings. Developmental Services provides support to clients with developmental disabilities living in a network of group homes and independent living facilities. DSSs, who are trained during the first year of employment through the LTC RAP, help their clients progress toward self-sufficiency in accordance with a plan developed by the clients case manager. This includes supervising clients in workshops where they engage in paid work, assisting in money management, and administering medicine. In Philadelphia, Home Care Associates employs HHAs to provide services in the homes of elderly persons and other clients with cognitive deficits across the city, including clients with Alzheimers or dementia, mental illness, and developmental disabilities. The nature of the work of these aides varies with the needs of the client and can include assistance with medications and wound care, nutrition and meals, chores around the house, and errands. All HHAs receive basic training provided by Home Care Associates but only those who demonstrate excellence in their care skills and leadership qualities are selected for the LTC RAP. Employees completing apprenticeships then become designated mentors to less experienced HHAs.
Four of the LTC RAP sponsors (Developmental Services, Good Samaritan, Home Care Associates, and Agape) receive Medicaid reimbursement for services provided. Only Air Force Villages does not accept Medicaid reimbursement because leadership perceives the level of reimbursement to be too low to provide an adequate level of care. Staff from the remaining sites also indicated that Medicaid reimbursement rates are too low for services provided. Both Developmental Services and Home Care Associates staff cited these payment rates as an important constraint on their operations, and both organizations have sought supplemental funding. Agape staff did not feel as constrained by Medicaid reimbursement rates because they have been successful in attracting clients to the assisted living who can pay out-of-pocket or with long-term care insurance. Good Samaritan, Home Care Associates, Air Force Villages, and Agape accept Medicare reimbursement, which has higher reimbursement rates but has narrower service coverage. While these four sites all accept private paying patients, whose payments are higher than Medicaid reimbursements, Developmental Services opts to only serve Medicaid patients as a part of its mission.
2.3. Core Competency Training
All five LTC RAPs provide training in specific core competencies to mark progress and completion of the apprenticeship. The core competency trainings developed for the LTC RAPs are designed to ensure that apprentices learn the skills needed to provide high-quality, long-term care, combining the necessary knowledge and experience in personal care and medical practices. LTC RAPs can also have advanced competencies or specialties that apprentices may have to complete. The personal care medical skill competencies apprentices have to master are occupation-specific. For example, CNA apprentices at Good Samaritan have to complete a set of core competency trainings in advanced CNA skills and an additional training in an advanced competency such as restorative care, care for dementia residents, or medication administration. Similarly, apprentices at Agape complete core competency trainings in advanced CNA, with additional advanced training in palliative care and communicating with dementia patients. Apprentices at all sites felt that the core competency trainings often touched on skills they had already learned on-the-job, but provided information on and practice in the competency or skill in considerably more depth.
These LTC RAPs also have core competency trainings that addresses soft skills such as effective communication with staff and clients, managing stressful situations or difficult clients, and mentoring and leadership skills. For example, DSS apprentices at Developmental Services attend training on and must demonstrate competency in non-violent conflict intervention as clients with developmental disabilities may respond physically toward DSSs when under stress. Home Care Associates has core competency training on mentoring and leadership skills. Information on the core competency trainings for each sites LTC RAP is discussed in Section 4 of this report and a complete listing of the competency trainings is provided by site in Appendix A.
2.4. Registered Apprenticeship Program Characteristics
The different characteristics of the sites influence the design and operation of each of the LTC RAPs. In particular, the sites experience with training prior to creating the LTC RAP, interest in developing career ladders or better quality jobs, the size of the program, and the length of time and experience with the registered apprenticeship model may influence the characteristics of the LTC RAP.
Previous Training
Pre-existing intensive training programs with OJT components at Developmental Services and Home Care Associates facilitated a smooth transition to the use of the registered apprenticeship model for their training. Developmental Services simply augmented its established direct support training program, which had been operating since 1975, to meet the requirements for the DSS LTC RAP. Classroom and OJT hours have been increased since Developmental Services initiated its LTC RAP, and the curriculum for the related technical instruction has been more formalized. Home Care Associates was able to use registered apprenticeship certification as a way to distinguish between staff who had successfully completed the existing enhanced training regimen and those who had not. In transitioning its existing training model to the LTC RAP, Home Care Associates modified its enhanced training to match the HHA core competencies; OJT and mentoring received new emphasis, and a wage progression for apprentices was implemented.
Career Advancement
The potential career ladder is emphasized at Air Force Villages, where the HSS position is a promotion for CNAs, with licensed practical nurses (LPNs) and registered nurses (RNs) as more senior positions to HSSs. There are no articulated career ladders for the DSSs at Developmental Services, the HHAs at Home Care Associates, and the CNAs at Good Samaritan and Agape. Home Care Associates emphasizes that the LTC RAP is not intended to develop a career ladder for HHAs but to create a quality job for the industry, providing stable, full-time HHA employment with benefits and where growth in skill level is rewarded through wage progression and mentor status. Agape staff suggested that while there is no specific career ladder put in place by the LTC RAP, apprentices are known and are considered to be more experienced than other CNAs by both their peers and their supervisors. Staff at Agape and Home Care Associates shared that some of the apprentices have pursued or are considering pursuing nursing degrees. In this sense, the LTC RAP offers a door to advancing the careers of the apprentices, even if it does not provide an explicit career ladder.
Program Size
Nationally, LTC RAPs are relatively small in size, with a mean number of active apprentices of 37 and a median of six, as shown in Figure 1. According to data in the RAPIDS system,9 Developmental Services is the largest of the sponsors visited, with 183 active apprentices at the time of the site visit and a total of 1,150 apprentices enrolled since 2005 (Table 1). Related technical instruction at Developmental Services is conducted by one full-time medical trainer and a human resources staff person. Good Samaritan also has over 100 active apprentices (118) and has enrolled 389 apprentices since 2005. Apprentices at Good Samaritan complete most of their related technical instruction material outside of work using DVDs and workbooks. In-class training at Good Samaritan is conducted outside of work hours for both students and instructors.
Air Force Villages, Home Care Associates, and Agape sponsor smaller LTC RAPs than Developmental Services and Good Samaritan. Air Force Villages has 36 active apprentices and has enrolled 62 apprentices since it began in 2009. While initially started as an on-line course, the Air Force Villages LTC RAP now uses 7-8 managers at the facility who teach related technical instruction in 2-hour increments in-house. Agape has 38 apprentices currently enrolled, with a total of 59 apprentices over the course of its operation. Home Care Associates is the smallest of the LTC RAPs visited with eight registered apprentices at the time of the visit and 26 apprentices enrolled since it started in 2006. This sponsor has two instructors that provide all training, including related technical instruction for the LTC RAP.
Experience with or length of time operating the LTC RAP differed across sites. Developmental Services, Home Care Associates, and Good Samaritan all started their programs at least 5 years ago -- 2005, 2006, and 2003, respectively. Air Force Villages and Agape both began their programs in 2009. However, the length of the programs existence does not necessarily correlate with larger numbers of apprentices. While Developmental Services has a well-established program that trains all new workers and is the largest sponsor visited, Home Care Associates and Good Samaritan have relatively small programs even though they have been existence longer than Air Force Villages and Agape. Both Air Force Villages and Agape have plans to expand their LTC RAPs in the near term.
| FIGURE 1. Number of Registered Long-Term Care Apprentices by Site and National Mean and Median (May 2011) |
|---|
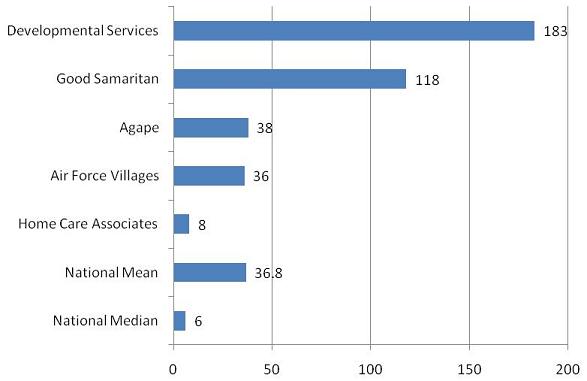 |
| SOURCE: Calculations by authors, RAPIDS data on apprentices from January 2005 to May 2011. |
| TABLE 1. Characteristics of the Selected Long-Term Care Registered Apprenticeship Program Sites | |||||
|---|---|---|---|---|---|
| Program Characteristics | Program Site Indiana Developmental Services | Program Site Idaho Good Samaritan | Program Site Pennsylvania Home Care Associates | Program Site Texas Air Force Villages | Program Site South Carolina Agape Senior |
| Type of sponsor organizations | Private, not-for-profit direct support provider | Private, not-for-profit multi-site nursing facilities | Worker-owned, not-for-profit home health aide provider | Private, not-for-profit retirement community | Private, a combination of for-profit and not-for-profit, skilled nursing facility, Assisted Living consortium |
| Apprenticeship occupation(s) | Direct support specialist | Certified nursing assistant | Home health aide | Health support specialist | Certified nursing assistant |
| Types of services provided | Direct support for clients with developmental disabilities and group home management | Nursing home care | Home health services, primarily for the elderly and those with cognitive deficits | Independent living, skilled nursing care, assisted living, home health | Skilled nursing care, assisted living |
| Revenue sources | Medicaid, United Way, and private donations | Medicare, Medicaid, private insurance and out-of-pocket | Medicare, Medicaid, private insurance and out-of-pocket | Private insurance and out-of-pocket, CHAMPUS, Medicare, | Medicare, Medicaid, private insurance and out-of-pocket |
| Date when program established | 2004 | 2003 | 2006 | 2009 | 2009 |
| Number of active registered apprentices (as of May 2011) | 183 | 118 nationally (32 in Idaho sites visited) | 8 | 36 | 38 |
| Number of apprentices (registered and those completed) currently employed | 497 | 178 | 25 | 59 | 55 |
| SOURCES: Data collected from Interviews at and materials from LTC RAP sites, October 2010-June 2011; and calculations by authors, RAPIDS, January 2005-May 2011. | |||||
3. Program Recruitment, Participation, and Completion
Recruitment of apprentices is a key part of the LTC RAPs visited. Some sites recruit apprentices from the local labor market through traditional hiring methods such as newspaper advertisements and job fairs whereas others select apprentices from employees within the organization. The characteristics of apprentices also vary across the sites visited. This section discusses the recruitment sources, participation incentives, recruitment challenges, characteristics of apprentices, and completion of the LTC RAPs.
3.1. Recruitment Sources
As shown in Table 2, all sites advertise for new hires through typical job resources such as newspapers and the Internet, and at job fairs. Staff at Developmental Services, Home Care Associates, and Good Samaritan noted that the apprenticeship is a major attraction for job applicants. Apprentices at Home Care Associates suggested that word-of-mouth was particularly important in recruitment of general staff, from among whom apprentices are selected; employees actively spread word about the quality of the training at Home Care Associates. Home Care Associates also recruits entry-level employees from the Philadelphia Workforce Development Corporation, which provides an Industry Specific Partnership Initiative training grant to fund the basic training for new hires who receive Temporary Assistance for Needy Families (TANF) benefits. Agape apprentices also noted word-of-mouth about the quality of Agape training as an important factor, not in attracting general staff to Agape but in fostering interest among the CNAs in the apprenticeship itself. After the first cohort, non-apprentice CNAs learned about the nature of the program and the value that supervisors placed on the training received by apprentices.
Four of the five LTC RAPs visited (Air Force Villages, Good Samaritan, Home Care Associates, and Agape) recruited apprentices from within their existing workforce through a selection process conducted by management (Table 2). Managers often selected staff with positive attitudes, leadership qualities, and experience. At Good Samaritan, one manager indicated that she could determine whether a staff member would succeed as an apprentice immediately after they were hired, on the basis of their enthusiasm for the job. At Air Force Villages, managers emphasized that it was essential to select staff who they believed would succeed in the apprenticeship. Home Care Associates and Air Force Villages both had minimum tenure requirements for apprentices. Staff must be employed at Home Care Associates for 6 months and at Air Force Villages for between 3 and 6 months before entering the LTC RAP. Home Care Associates requires the recommendation of a supervisor before a staff member can enter the apprenticeship. At Air Force Villages, future apprentices also go through the application process and are required to demonstrate motivation and provide reasons for enrolling. Agape uses an employee assessment software tool, called Wingspan, to rank their CNAs and classify them as being in the top 20%, middle 70%, or bottom 10% of its workforce. Apprentices are primarily chosen from the top 20%, with a recommendation from a supervisor. As Developmental Services places all new hires into its LTC RAP, apprentices are recruited through employment advertising and screening processes.
3.2. Participation Incentives
All sites provide a wage progression as a participation incentive for their LTC RAP (Table 2). At Developmental Services, wages for new job entrants begin at $7.25 per hour, and increase by at least $1.25 per hour after the initial apprenticeship training is completed. Developmental Services does not offer a wage increase with the completion of each competency training or with the completion of the program, as several of the other registered apprenticeship programs do. The Good Samaritan facilities in Boise and Idaho Falls offer an incentive of $0.25 and $0.50 wage increase after the completion of each core competency training, respectively, although staff at Good Samaritans national campus stated that not all of its sites offer a wage increase because they cannot afford it. Home Care Associates provides a $0.20 wage increase after the completion of each competency training, for a typical total wage increase of $1.20 from a base hourly wage of $8.50. Home Care Associates also offers apprentices a one-time $200 bonus upon completion of the LTC RAP. Air Force Villages offers either a wage increase and/or a bonus only upon the completion of the program, which is worth up to 8% of salary for employees, who start working at $9.09 per hour. Agapes classroom training lasts approximately 1 year, and it provides a wage increase of a quarter every quarter from a base wage of $9.00-$11.00, depending on experience. This raise was very important to Agape apprentices, but almost all apprentices noted that they had not been informed about the wage progression before starting the apprenticeship. The wage progression for the initial year of the Agape apprenticeship is supported by a $1,000 tax credit for each apprenticeship offered by the state.
Non-pecuniary participation incentives include the pride and value associated with certification of completion of the apprenticeship. In Indiana, registered apprenticeship is one of three methods of earning direct support certification from the state. While certification is not required for developmental support specialists in Indiana at this time, Developmental Services managers anticipate that the state will 1 day mandate certification and believe that their LTC RAP prepares staff for this eventuality. Completing an apprenticeship is also a matter of pride and distinction for the apprentices, particularly at the three sites where apprentices are selected for training out a pool of incumbent workers. Since the long-term care industry typically affords few opportunities for advancement, the additional distinction of being selected for the program provides recognition of apprentice achievements among their peers. Apprentices at Home Care Associates mentioned the pride they took in their status within the organization as a motivating factor in completing the training before they noted the wage incentives. Apprentices at Good Samaritan and Air Force Villages shared this emphasis on the sense of achievement associated with completing the LTC RAP. The pride felt by Agape staff was reinforced by the fact that they were distinguished from their peers by their supervisors as examples to follow. One apprentice kept her certificate of completion at work and was particularly satisfied the certificate is endorsed by Northeastern Technical College. Agape apprentices have also received coverage in local print media.
3.3. Recruitment Challenges
Recruiting qualified apprentices can be challenging for all sites (Table 2). Human resources staff members at Developmental Services noted that while they can consistently hire 25-30 apprentices a month, they never turn away qualified applicants and always have vacancies to fill. Most sites mentioned that the greatest challenge is finding apprentices who have the right personal disposition and dedication to the job to be successful in the long-term care industry. Developmental Services can have difficulty in finding enough qualified applicants as many applicants see direct support work as a babysitting job, and are naïve about the challenges associated with the work.Thus, Developmental Services targets hiring on those applicants who can manage stress and who have a good understanding of the job.Good Samaritan, Home Care Associates, Air Force Villages, and Agape address this problem by only recruiting apprentices from incumbent workers, who are screened for these qualities. The staff at Air Force Villages emphasized the importance of selecting motivated incumbents by highlighting that poorly motivated workers who fail to attend training would lower morale for all apprentices. Agape LTC RAP staff use the apprenticeship as a mark of distinction for CNAs that they want to highlight as particularly productive workers.
Another recurrent obstacle to recruiting new apprentices is the challenge of funding training and wage increases. Most sites are dependent on the adequacy of Medicare and Medicaid reimbursements to finance this essential feature of apprenticeship. Usually, these reimbursement rates are not sufficient to maintain the expenses of a LTC RAP. Each site responded to these pressures differently. Air Force Villages does not accept Medicaid, relying instead on clients with private insurance, Medicare, or out-of-pocket payments. Developmental Services serves only Medicaid patients, but the organization is supported by funding from the United Way and other charitable sources. Home Care Associates is able to support basic training for staff who receive TANF through a local training grant and enhanced training with grants from two foundations. However, it is currently not operating its LTC RAP as the funding for the enhanced training has ended. Agape has been profitable and is not limited to Medicaid reimbursements, so it has not been as concerned about affording the wage progression. However, Agape staff emphasized South Carolinas $1,000 tax credit for each apprentice trained as an important method of defraying the $2,080 per year cost of its $1 wage increase. Agape staff suggested that the CNAs who became apprentices were the most likely to receive wage increases anyway because they were the most productive workers.
3.4. Characteristics of Apprentices
A large majority of the registered apprentices in all five sites who have enrolled since 2005 is women. Eighty-three percent of apprentices are women at Developmental Services, 92% at Home Care Associates, and 100% at Good Samaritan, Air Force Villages, and Agape (Table 3). This distribution reflects the gender composition of the long-term care industry nationally (Khatutsky, Wiener, Anderson, and Squillace, 2011). The racial composition of the registered apprentices enrolled at each site varies more dramatically. According to RAPIDS data, 96% and 87% of the apprentices at Developmental Services and Good Samaritan, respectively, are White. Seventeen percent of apprentices at Agape, less than 15% of apprentices at Air Force Villages, and none at Home Care Associates are White. African-American apprentices who have enrolled in the apprenticeship program make up 85% of the staff at Home Care Associates and 71% of apprentices at Agape, but less than 10% at all other sites. The apprentices at Air Force Villages are predominantly (74%)Hispanic. The racial compositions of the sites apprentices reflect the populations of lower income and lower skill populations in the regions they serve. The mean age of apprentices in all sites is over the age of 35. Developmental Services and Good Samaritan have somewhat younger average workforces (39 and 38 years, respectively) than Home Care Associates and Air Force Village (43 years) or Agape (41 years).
Most apprentices at all sites except for Home Care Associates hold a high school diploma as their highest degree earned, with many of the remaining apprentices holding a general equivalency degree (GED). At Home Care Associates, 42% of apprentices have a diploma and 12% have a GED, leaving 46% with 11 years of high school or less. Few apprentices at the sites have any college experience, although staff at some sites suggested that a few apprentices may leave the sponsoring organization to attend nursing school. The exception was Agape, where 13 apprentices (23% of the apprentices recorded in the RAPIDS data) had at least some college. This was likely due to the fact that the local technical college system was an important recruitment source for Agape.
Demographically, the sites visited differ from the national profile of LTC RAPs. Developmental Services is the only site that closely resembles the wider population of DSS LTC RAPs. However, this is primarily because the majority of registered apprentices in the DSS occupation nationally are employed at Developmental Services. Differences emerge between the other four sites and the wider population of apprentices in the same occupations. The other four sites have older apprentices than is typical in their occupation nationally. Home Care Associates has a considerably higher share of workers that are African-American and high school dropouts than HHA LTC RAPs nationally. In contrast, Good Samaritan has more educated and White apprentices than CNA apprentices nationally. Air Force Villages, like Home Care Associates, has more minorities than other CNA or HSS LTC RAPs nationally (in the case of Air Force Village, more Hispanics). Its apprentices are also more likely to have graduated high school than the typical CNA or HSS apprentices.
3.5. Program Completion
Nationally, about half of long-term care apprentices in LTC RAPs since 2005 have either completed or are still participating in their program. At the two largest sites, the share of active apprentices or those who have completed of all enrollees (43% of all Developmental Services apprentices and 46% of all Good Samaritan apprentices) was less than the national share. Of the three smallest programs, Home Care Associates (96%), Air Force Villages (95%), and Agape (93%) have had greater success with retaining apprentices in the program and having them complete the program. Developmental Services difficulty in determining apprentices work ethic before enrollment may explain its higher dropout rate. The LTC RAPs at Developmental Services and Good Samaritan are also several years older on average than the relatively apprentices at Air Force Villages and Agape. The older programs dropout rates may reflect the fact that their apprentices have a higher exposure over time to the risk of dropping out. While the older programs may be more mature and perhaps even more effective as a result, the enthusiasm of the newer programs may help in retaining apprentices.
| TABLE 2. Recruitment and Selection of Apprentices at Organizations Studied | |||||
|---|---|---|---|---|---|
| Selection Characteristics | Program Site Indiana Developmental Services | Program Site Idaho Good Samaritan | Program Site Pennsylvania Home Care Associates | Program Site Texas Air Force Villages | Program Site South Carolina Agape Senior |
| Characteristics of prospective apprentices | Patient, caring individuals with soft skills who are detail oriented and able to carefully document the care they deliver | Incumbent workers with good attendance, highly rated functional proficiency, and positive personal characteristics | Incumbent workers with dedication to their work and successful performance in basic training | Incumbent workers who are conscientious and have good attendance records | Incumbent workers, most in the top 20% of CNA ranked by performance |
| Recruitment sources | New hires solicited through newspaper ads, job fairs, word-of-mouth | Incumbent workers | Incumbent workers | Incumbent workers | Incumbent workers |
| Entry requirements | Experience, dedication to the job; 75% of applicants are not hired | Approval of manager | Employment for at least 6 months, recommendations from supervisor and chief operating officer | Employment for at least 3 months, approval of manager | Recommendations from supervisor |
| Incentives for participation | All new hires are required to participate in the apprenticeship program; wage increase commensurate with experience (typically a $1.25 per hour increase); receipt of state-recognized credential | $0.25 and $0.50 raise in Boise and Idaho Falls, respectively, per competency training | $0.20 raise per competency training ($1.20 in total), and a $200 bonus upon completion; receipt of state-recognized credential | Increase of up to 8% of base salary upon completion for employees with shorter tenure; up to an 8% bonus for employees with longer tenure. | $0.25 raise every quarter of class enrollment for a total of $1 for four quarters of study |
| Challenges recruiting apprentices | Finding qualified applicants able to manage the stress of direct support work | None | None | Identifying incumbent workers that are likely to complete apprenticeship | None |
| SOURCE: Data collected from Interviews at and materials from LTC RAP sites, October 2010-June 2011. Abbreviations: CNA (certified nursing assistant). | |||||
| TABLE 3. Apprentice Characteristics at Organizations Studied | |||||
|---|---|---|---|---|---|
| Apprentice Characteristics | Program Site Indiana Developmental Services | Program Site Idaho Good Samaritan | Program Site Pennsylvania Home Care Associates | Program Site Texas Air Force Villages | Program Site South Carolina Agape Senior |
| Average age | 38.7 years | 37.8 years | 43.1 years | 42.6 years | 41.1 years |
| Race/ethnicity | African-American: 2.4% White: 96.0% Hispanic: 1.2% Other: 0.4% | African-American: 2.8% White: 87.4% Hispanic: 6.2% Other: 3.6% | African-American: 84.6% White: 0.0% Hispanic: 11.5% Other: 3.9% | African-American: 8.1% White: 14.5% Hispanic: 74.2% Other: 3.2% | African-American: 71.2% White: 17.0% Hispanic: 3.4% Other: 8.5% |
| Gender | Male: 17.3% Female: 82.7% | Male: 8.7% Female: 91.3% | Male: 7.7% Female: 92.3% | Male: 8.1% Female: 91.9% | Male: 0.0% Female: 100.0% |
| Education levels | High school diploma or more: 99.5% Less than a high school diploma: 0.5% | High school diploma or more: 73.4% Less than a high school diploma: 26.6% | High school diploma or more: 42.3% Less than a high school diploma: 57.7% | High school diploma or more: 62.9% Less than a high school diploma: 37.1% | High school diploma or more: 93.0% Less than a high school diploma: 7.0% |
| Levels of training prior to starting apprenticeship | Varied | Varied | Varied | CNA | Basic CNA |
| Barriers to completion of apprenticeship | Low education rates makes teaching medical competencies challenging | Apprenticeship is optional so many complete some competencies without completing the program | None mentioned | None mentioned | None mentioned |
| SOURCES: Data collected from Interviews at and materials from LTC RAP sites, October 2010-June 2011; and calculations by authors, RAPIDS, January 2005-May 2011. Abbreviations: CNA (certified nursing assistant). | |||||
4. Features of the Registered Apprenticeship Programs
The five sites visited varied in their goals, program duration, completion milestones, type of instruction, and wage progression. The following section provides a detailed summary of these program features. While each of the five LTC RAPs shares the goal of improving the skills of their workforce, their program models vary in important ways. Some LTC RAPs are considerably shorter in the duration of training provided by the sponsor than others, because of the accepted practice of crediting prior experience, and several of the programs do not closely monitor OJT.
4.1. Program Goals
As shown in Table 4, the primary goal for each of the LTC RAPs visited is to improve the skills of its long-term care workforce. Apprenticeship is recognized by the sites as a model that reinforces technical skills and fosters the interpersonal skills that are essential to the industry.Air Force Villages staff considered attentiveness and person-centered care for clients to be an important element in the overall care model and established the LTC RAP to strengthen workers in these areas. Similarly, Agape staff indicated that the instruction in communicating with and caring for dementia patients and communicating with client families to be one of the most important components of the LTC RAP. In addition, staff at four of the five sites (Good Samaritan, Home Care Associates, Air Force Villages, and Agape) reported that the LTC RAPs were designed to improve self-sufficiency and career opportunities and reduce worker turnover. Each of the staff at these sites noted that apprenticeship is used to better train and enrich the jobs of the long-term care staff and, making them more attractive and, thus, reducing staff turnover.
Finally, medical errors in the long-term industry can be very expensive, and well-trained staff may help reduce these errors, saving the sponsors money. However, Developmental Services is the only site that specifically connected the apprenticeship program to the goal of reduced costs through reduced medical errors. Staff at both Developmental Services and Home Care Associates identified that meeting state certification requirements was a goal of their apprenticeship training. Good Samaritan and Home Care Associates staff also said that a goal of the program was to improve the self-sufficiency of its staff by providing good jobs in the long-term care industry, contrary to the typical employment opportunities in these occupations.
4.2. Program Models
Four of the five sites visited (Developmental Services, Good Samaritan, Air Force Villages, and Agape) are considered a hybrid registered apprenticeship model of competency-based and time-based requirements for completion of their LTC RAPs. This means that completion of the apprenticeship requirements is tracked by successfully demonstrating proficiency in each competency training associated with the occupation and by spending a specific amount of time on each competency training (see Appendix A for a detailed listing of the competency trainings by occupation). At Agape, the checklist for assuring mastery of competencies on-the-job was developed at the same time that the curriculum for the related technical instruction was developed, and therefore closely reflects the classroom material.
Home Care Associates LTC RAP is considered time-based, in which apprentices are required to spend a designated amount of time mastering each competency training. Four of the sponsors programs (Developmental Services, Good Samaritan, Home Care Associates, and Agape) are designed around participation in related technical instruction and OJT and have longer program durations, with the expectation that apprentices must demonstrate proficiencies on-the-job in the core competencies. All of the programs require substantially more training hours than, for example, the minimum 75 hours required for CNAs under federal regulation 42 CFR 483.152 to improve quality of care and workforce skills.
As shown in Table 4, the program with the most time requirements is Air Force Villages, which requires 232 hours of related technical instruction and 3,000 hours of OJT (3,232 total hours). For its HHA apprentices, Home Care Associates requires slightly more related technical instruction hours (230 hours) but fewer OJT hours (1,795 hours) for completion (2,025 total hours). Developmental Services requires 216 hours of related technical instruction, and 2,784 hours of OJT, for a total of 3,000 program hours. Good Samaritan requires that its apprentices spend 180 hours in related technical instruction and between 1,500-2,000 hours in OJT. Agape requires 265.5 hours of related technical instruction and 2,000 hours of OJT, although these hours are designed for apprentices without basic CNA certification. All Agape apprentices so far have entered the program as CNAs, and have therefore been credited hours associated with the basic CNA training and experience. These CNAs are required to attend 143.5 hours of related instruction and 1,700 hours of OJT, for a total of 1,843.5 hours. DOL allows LTC RAPs to accept past experience in the field as OJT hours. At Air Force Villages, up to 2,000 hours are credited to the apprentices for past experience. Since all Air Force Villages apprentices are CNAs, they have already received basic long-term care training and their performance on-the-job is evaluated as a CNA.
Each LTC RAP requires its apprentices to participate in OJT, which allows apprentices to practice skills and demonstrate proficiency in the core competencies. As discussed, apprentices at all sites must spend a significant amount of time in OJT (1,500-3,000 hours). While the amount of time spent in OJT varies from week to week, apprentices at these sites typically spend 40 hours per week, depending on their work schedule, in OJT (see Table 5).
Air Force Villages apprentices spend about 8 hours per week in related technical instruction when provided at the beginning of the apprenticeship. Four hours of related technical instruction is outside the classroom with management or experienced apprentices providing hands-on instruction related to classroom knowledge so that apprentices practice their newly-acquired skills. Apprentices complete a self-administered skills checklist during OJT. In addition, throughout the entire apprenticeship period, an apprentices work is monitored through the facilitys routine quality assurance protocols for all staff. If apprentices work is found to be less than satisfactory, remedial instruction focused on the skill requiring improvement is provided. Apprentices thereby gain additional time to practice the art of caregiving. For example, if during a routine quality assurance check the food is not served at the right temperature, the food services manager or dietician would provide remedial instruction to an apprentice to improve food preparation skills.
Table 5 shows that few resources other than supervisory time are used for the OJT component of the LTC RAPs, according to the sites. In the sites visited, OJT is monitored by supervisors or nurses, who are responsible for overseeing the apprentices progress. However, the degree of monitoring varies by site because of the work setting. It is easier to provide more consistent monitoring of the apprentices at Developmental Services, Good Samaritan, and Agape because workers in residential settings are more visible to supervisors. Individual home settings make it more difficult to monitor apprentices at Home Care Associates, who often work alone. Home Care Associates staff reported that supervisors and mentors spend time with the apprentices at clients homes on occasion to monitor their progress and assist in mastering a competency.
Related technical instruction in the LTC RAPs visited is divided between basic and enhanced training at Developmental Services and Home Care Associates, and is presented in a series of modules at Good Samaritan, Air Force Villages, and Agape. For each program, related technical instruction covers material from multiple core competencies approved by DOL (Table 6). (Details on these core competency trainings are provided in Appendix B.) All sites teach common competency training, such as training in medical care administration and communications skills, while other training is occupation-specific. For example, Developmental Services requires training in non-violent conflict intervention (a skill with little import in Air Force Villages retirement community), while Air Force Villages, Home Care Associates, and Agapes curriculum includes dementia training for its apprentices, skills that may not be needed in serving Developmental Services younger clientele. The palliative care specialty taught at Agape was also added because of a special interest that Agapes executives had in palliative care as hospice is a major service provided by the organization.
Related technical instruction is administered by trainers at Developmental Services, Home Care Associates, Air Force Villages, and Agape while it is self-administered by apprentices with CDs and workbooks at Good Samaritan. Air Force Villages began the program by teaching its related technical instruction on-line through a community college sponsored course rather than in a traditional classroom. Later, it switched to an in-house classroom instruction model. Time spent in related technical instruction per week varies for Good Samaritan apprentices because it is self-administered. Air Force Villages apprentices receive about 4 hours per week of related technical instruction. Agape apprentices spend 3 hours in related technical instruction every Thursday for a year. Developmental Services and Home Care Associates apprentices spend more of their time in related technical instruction at the beginning of their employment (basic training) but more advanced related technical instruction is provided at regular intervals.
Only Developmental Services pays for all costs associated with related technical instruction while Home Care Associates receives support from grants to operate its related technical instruction. Agape received grant support for training from its local workforce investment board for its first cohort of apprentices and from South Carolinas Department of Employment and Workforce for its second cohort. The third and largest cohort of Agape apprentices is being supported entirely by Agapes own funds. Air Force Villages previously received a DOL grant for related technical instruction but now has staff trainers from its management staff who conduct the related technical instruction. For apprentices at Developmental Services and Home Care Associates, time in related technical instruction takes place during work hours while it occurs during off-hours for apprentices in Good Samaritan, Air Force Villages, and Agape.
Progress in related technical instruction is monitored by the instructors and through tests. Tests measure the progress in related technical instruction for apprentices at all sites but the degree to which trainers oversee this process varies. As Good Samaritan uses self-administered related technical instruction activities, less oversight occurs. Attendance is also a key part of completing the related technical instruction requirements for the trainer-led instruction at Developmental Services, Home Care Associates, Air Force Villages, and Agape. At some sites, basic training is used as a screening tool for becoming apprentices. Developmental Services does not let staff work in group homes with clients until they successfully complete their basic training, and Home Care Associates uses performance in basic training (which all staff receives) to determine who continues on to receive the enhanced training provided through the LTC RAP. Agape instructors use weekly quizzes, hands-on demonstrations, and the palliative care exam to monitor apprentice progress.
4.3. Progression of Apprentices through the Program
Senior staff, including supervisors, more experienced long-term care workers, nurses, and trainers play a role in monitoring and testing apprentices in all five sites, as discussed on Table 4. Shadowing, or following and observing, more senior staff as they perform tasks during early training sessions occurs at both Developmental Services and Home Care Associates. However, because Home Care Associates apprentices often conduct their work alone in clients homes, it is challenging for supervisors to monitor their OJT activities. The OJT portion of the apprenticeship at Air Force Villages is generally supervised. Apprentices at Developmental Services must have their medical knowledge re-tested at regular intervals after completing their apprenticeship. At Agape, supervisors use competency checklists developed at the same time as the curriculum to regularly monitor the performance of apprentices. The apprentices at Developmental Services and Agape had some sense that their OJT activities were being evaluated by supervisors, but they were often unaware of the extent of the supervision, or that checklists based on competencies were being used.
Mentorship is an essential component of registered apprenticeship, because mentors help apprentices understand the material they are expected to learn during OJT. Since long-term care work can be stressful, mentors assist and counsel apprentices in the program. At Home Care Associates, mentors are chosen from among more senior staff. As noted above, Home Care Associates presents a challenge for mentorship because HHAs provide care in the homes of clients. Senior staff at Home Care Associates are aware of this problem and emphasized the importance of mentoring apprentices when they are at the Home Care Associates headquarters. Mentorship is strongly encouraged at Good Samaritan, and apprentices are expected to mentor non-apprentice workers. While this expands the role of mentorship in the traditional apprenticeship model, Good Samaritan includes mentorship as one of its core competency trainings. These lessons are expected to be passed on to others once the training is completed. In addition to mentoring by supervisors, Developmental Services places a premium on the opportunity for peer-mentoring, particularly at monthly meetings held for staff at each group home. Mentors are expected to discuss problems with apprentices that may emerge during the course of direct care work, rather than only providing instruction. Mentorship training is also provided at Agape, and like the program at Good Samaritan, apprentices are expected to serve as mentors to other CNAs. The apprentices at Agape take their mentorship role very seriously because of the respect they receive from their mentees. While not formalized, mentorship is also valued at Air Force Villages where those who completed the apprenticeship program serve in this capacity.
Each LTC RAP recognizes somewhat different milestones for apprentices. Good Samaritan and Home Care Associates both acknowledge the completion of related technical instruction and OJT associated with individual competency trainings as a completed milestone, and reward each completed competency training with a wage increase. At Good Samaritan, this is because limited resources and job openings prevent the LTC RAP from guaranteeing that apprentices will be able to complete all competency trainings so progress is rewarded at completion of each competency training. Apprentices at Good Samaritans Boise and Idaho Falls campuses are awarded wage increases of $0.25 and $0.50 for each competency training completed, respectively. Apprentices at Home Care Associates are awarded a wage increase of $0.20 per competency for a typical total wage increase of $1.20 and a one-time bonus of $200 at completion. Agape provides a $0.25 raise at the end of each calendar quarter (for a total wage increase of $1.00), roughly coinciding with the completion of related technical instruction modules. Agape supervisors often provide special recognition for the apprentices under their supervision upon completion of the program, including gift certificates and celebratory dinners. Developmental Services does not offer a wage progression with every competency, but it does provide a one-time $1.25 per hour wage increase upon the completion of the basic training, which encompasses the first several weeks of the apprenticeship. Upon completion of the apprenticeship, Developmental Services staff are certified as direct service providers in the State of Indiana. Developmental Services also holds graduation ceremonies for their apprentices, and suggested that it is a major event for both apprentices and their families, who also attend. Air Force Villages offers a combination of wage progression and/or bonus of up to 8% of the employees base salary after all related technical instruction is completed.
While all sites acknowledge workers who complete the LTC RAP and recognize the achievement within their organization, Developmental Services and Home Care Associates offer credentials that arerecognized in the long-term care labor market. Developmental Services representatives actively participated in the state-level discussions on DSS credentialing in Indiana in 2007, where they successfully advocated for the inclusion of registered apprenticeship as one of three sources of a DSS credential. Although Indiana does not currently require DSS workers to be certified, Developmental Services anticipates that at some point there will be such a requirement. Home Care Associates representatives were similarly successful in lobbying the state legislature to develop certification requirements for HHAs that were based on the training and skills the company requires for its own apprentices. Despite the fact that these credentials are officially recognized by the state governments of Indiana and Pennsylvania, apprentices and administrators agreed that it was unclear whether other employers understood apprenticeship training or valued the apprenticeship. Apprentices at Agape similarly earn a palliative care certification that is widely recognized. Another advantage of the Agape apprenticeship is that since the diploma provided upon completion is administered by the Northeastern Technical College, it offers a degree of legitimacy with other employers who know and respect the South Carolina technical college system.
| TABLE 4. Features of the Selected Long-Term Care Registered Apprenticeship Program Sites | |||||
|---|---|---|---|---|---|
| Program Features | Program Site Indiana Developmental Services | Program Site Idaho Good Samaritan | Program Site Pennsylvania Home Care Associates | Program Site Texas Air Force Villages | Program Site South Carolina Agape Senior |
| Program Goals | |||||
| Improve the quality of client care | --- | X | --- | X | X |
| Improve and expand skills of workforce | X | X | X | X | X |
| Reduce medical errors and liability risks | X | --- | --- | --- | --- |
| Meet state certification requirements | X | --- | X | --- | --- |
| Improve self-sufficiency and career opportunities | --- | X | X | X | --- |
| Reduce worker turnover | --- | X | X | X | X |
| Total hours required for completing the program | 3,000 | 1,680-2,180 | 2,025 | 3,232, although 2,000 hours may be credited for previous experience | 2,256.5 |
| On-the-job training hours | 2,784 | 1,500-2,000 | 1,795 | 3,000 | 2,000 |
| Related instruction hours | 216 | 180 | 230 | 232 | 265.5 |
| Mentoring or peer support | Supervisors (who have finished the program) mentor-apprentices at all sites. Peer support occurs on-the-job, as well as in monthly meetings. | Peer-mentoring is strongly encouraged by management. One purpose of the apprenticeship is to train CNAs who can mentor non-apprentices. | Mentoring is harder because aides work alone in client homes, but apprentices are mentored at headquarters by their supervisors. | Mentoring occurs in related technical instruction, but apprentices are expected to provide documentation of their progress in OJT to receive credit for the apprenticeship. | Mentoring occurs during OJT but it is not formalized |
| Milestones | Wage increase for completion of initial training; DOL certification of completion | Wage increase for completion of each competency; DOL certificate of training | Wage increase for completion of each competency; DOL certificate of completion | Wage increase or bonus for completion of related technical instruction; DOL certificate of completion | Certification of completion for each training unit; DOL certification of completion for entire program; National Test for Palliative Care Providers |
| Wage progression | After completing basic training, they are given a wage increase commensurate with experience (typically a $1.25 per hour increase), from a base rate of $7.25. | Apprentices receive wage increases upon the completion of a core competency. At the Boise and Idaho Falls facilities, this increase is $0.25 and $0.50, respectively. | Apprentices receive a $0.20 wage increase upon the completion of a core competency, from a base rate of $8.50. | Apprentices receive up to an 8% wage and/or bonus increase after related technical instruction is completed, from a base rate of $9.09. | Apprentices receive a $1 increase upon program completion, from a base rate of $9 to $11. |
| Bonuses for completion (i.e., one-time only) | None | None | $200 bonus upon completion of all competencies | Up to 8% of salary upon program completion if no wage increase | Small gift card as a bonus |
| Additional credential(s) earned beyond DOL interim certificate(s) of training, and certificate of completion at end of apprenticeship | Become registered apprentices, state recognition as certified direct support providers | No credentialing other than becoming a registered apprentice | State certification as a HHA | No credentialing other than becoming a registered apprentice | Become registered apprentices and state certified palliative caregivers |
| SOURCES: Data collected from Interviews at and materials from LTC RAP sites, October 2010-June 2011. Abbreviations: CNA (certified nursing assistant); OJT (on-the-job training); DOL (U.S. Department of Labor); GED (general equivalency degree): HHA (home health aide). | |||||
| TABLE 5. Features of On-the-Job Training (OJT) Components of the Selected Long-Term Care Registered Apprenticeship Program Sites | |||||
|---|---|---|---|---|---|
| On-the-Job Training Features | Program Site Indiana Developmental Services | Program Site Idaho Good Samaritan | Program Site Pennsylvania Home Care Associates | Program Site Texas Air Force Villages | Program Site South Carolina Agape Senior |
| Hours spent in on-the-job training (weekly) | Varies; typically 40 hours a week | 32-40 hours a week | 40 hours a week; Full-time employment guaranteed | 32-40 hours a week | Full-time employment hours |
| Resources used for on-the-job training | Medical sheets to document and coordinate medication of clients | None | None | A small amount of supervisor time | None |
| Monitoring of progress | Monitored by supervisors assigned to a group home, nurses, and trainers; progress reported to human resources | Monitored by supervisors | Monitored by supervisors, usually through follow-up with apprentices at headquarters or observations at client homes | Apprentices expected to provide documentation of their progress based on apprenticeship outline | Tests and quizzes after each training unit OJT monitored by supervisors |
| SOURCES: Data collected for Interviews at and material from LTC RAP sites, October 2010-June 2011. | |||||
| TABLE 6. Features of Related Technical Instruction Component of the Selected Long-Term Care Registered Apprenticeship Program Sites | |||||
|---|---|---|---|---|---|
| Related Technical Instruction Features | Program Site Indiana Developmental Services | Program Site Idaho Good Samaritan | Program Site Pennsylvania Home Care Associates | Program Site Texas Air Force Villages | Program Site South Carolina Agape Senior |
| Hours spent in related technical instruction (weekly) | Varies; 30 hours per week in initial weeks, with training scheduled at regular intervals afterward | Varies | Varies | 8 hours per week | 3 hours weekly |
| Provider of related technical instruction | Training provided by in-house instructors, with curriculum developed by Indiana University | Self-administered training with DVDs and workbooks provided by Good Samaritan | Training provided by two instructors, one of whom was a former apprentice | Initially the training conducted on-line by the North Central Kansas Technical College; now taught by several in-house managers | Training provided by instructors who are mostly in-house experts; hired from outside for one course on dementia |
| Related training built upon pre-existing training at the organization | Yes | No | Yes | No | No |
| Payer of related technical instruction | Developmental Services, supported by funding from the United Way, private donations, fund-raisers, and ARC | Good Samaritan | Home Care Associates, supported by the Philadelphia Workforce Development Corporation and two foundations | DOL grant initially supported training, but now Air Force Villages provides instructors to teach classes during work hours | Agape Senior |
| Related technical instruction takes place during work hours | Yes | No | Yes | Varies | No |
| Required courses | Medical orientation, CPR, core medical training, conflict prevention and resolution | Advanced CNA training, and one additional competency from among mentoring, restorative, dementia, and medication administration | Case management, peer-mentoring, best practices, and communication, working with clients with physical disabilities, hospice care, and mental illness | Medical terminology 1, medical terminology 2, environmental services, restorative, dementia, person-centered care, activity assistance, and soft skills* | Advanced CNA (geriatric and mentoring competencies) and palliative specialty |
| Monitoring or progress | Monitored by the trainer in the classroom, and by competency tests | Must complete a workbook, which is certified by an LPN or RN. A competency checklist is completed with an RN. | Progress monitored by instructors and more senior aides who discuss application of classroom training on-the-job with apprentices. | Weekly quizzes, midterm exams, module tests, homework assignments and attendance requirements | Quizzes, module tests |
| SOURCES: Data collected from Interviews at and materials from LTC RAP sites, October 2010-June 2011. Abbreviations: DOL (U.S. Department of Labor); CNA (certified nursing assistant); LPN (licensed practical nurse); RN (registered nurse); ARC (Appalachian Regional Commission); CPR (cardiopulmonary resuscitation). * NOTE: Soft skills include communication skills with staff and clients, managing stressful situations or difficult clients, anger management. | |||||
5. Resources for Registered Apprenticeship Programs
Ensuring the availability of adequate resources for operating the LTC RAPs that were visited was stated as a challenge for all of the sponsors except for Agape. However, even sponsors who faced financial challenges felt that the LTC RAP was worth the investment. These resources required for successfully operating a LTC RAP include staff for training and supervising apprentices, space and equipment for training, and funding for paid time in related technical instruction, wage progression, and bonuses. This section provides a summary of the resources needed across the sites visited and the challenges that the sponsors experience in providing these resources. Staff and budgets for the LTC RAPs are modest across all five sites, and some sites supplement their resources with assistance from partner organizations.
5.1. Staffing
The sites are restricted in the level of oversight staff they can provide to the LTC RAP, either because of structural constraints (e.g., HHAs usually perform their tasks alone in client homes), or because of resource constraints (e.g., time away from performing reimbursed job tasks with clients). The LTC RAPs visited operate with few, if any, staff dedicated solely to the LTC RAPs (Table 7). Two of the LTC RAPs (Developmental Services and Home Care Associates) employ one or two instructors, although training is also occasionally outsourced to other organizations. Although Agape uses its own staff to teach most modules, it hires outside trainers for teaching the dementia module. Developmental Services initially relied on existing staff to provide in-house training, and eventually hired an LPN to expand their capacity to provide rigorous training in-house, particularly the medical curriculum. Home Care Associates instructor is a graduate of the sponsors training program (although before it became a registered apprenticeship). Good Samaritan also uses LPNs and RNs currently employed as staff to provide training to CNA apprentices. As previously discussed, Air Force Villages has in-house training staff -- 7-8 employees in managerial positions -- that provide related technical instruction and have more senior nursing staff monitor OJT performance.
5.2. Budget and Cost Issues
All sponsors bear the cost of or raise funds to support the related technical instruction component of the program, including wages for staff conducting training, curricula, and class materials (Table 7). One cost that is handled differently across the five LTC RAPs is the payment of apprentices time during training. Two of the LTC RAPs (Developmental Services and Home Care Associates) allow apprentices to complete related technical instruction during work hours, while Good Samaritan, Air Force Villages, and Agape do not. Good Samaritan provides apprentices with curricula and instructional DVDs, but requires them to complete their training off the clock. Air Force Villages and Agape offer 2-hour and 3-hour related technical instruction sessions, respectively, although it is conducted during non-work hours at the facility. Staff at Developmental Services or Home Care Associates, which arelocated in states with occupational certification requirements, indicated that apprentices pay for the fees associated with state certifications.
Completing training during work hours can be an advantage for apprentices as workers who seek training outside of their employer may need to forgo wages they could have earned while in training. All sites pay apprentices wages during their OJT. Both Developmental Services and Home Care Associates apprentices are paid for their time during related technical instruction. However, apprentices at Good Samaritan, Air Force Villages and Agape must complete related technical instruction on their own time. None of the apprentices pay for the training materials.
The most serious budget constraint facing the LTC RAPs is low reimbursement rates for long-term care services. Sponsors that accept Medicaid and Medicare (Developmental Services, Good Samaritan, Home Care Associates, and Agape) often have to raise private funds to cover costs of the LTC RAPs. Providers are explicitly restricted from charging Medicaid clients a supplemental fee. Air Force Villages does not accept Medicaid from clients but receives reimbursement from Medicare, private insurance, and out-of-pocket payments by residents. Reducing training costs was the key outcome for Developmental Services in selecting the registered apprenticeship model over other options such as the local community college, which they found to be more expensive. However, the concern is that low reimbursement rates may prevent long-term care providers from investing in more rigorous training when it is not government mandated, including investment in registered apprenticeship. For example, Home Care Associates has discontinued its program due to its cost, which is estimated to be between $8,000 and $10,000 for an apprentice.10 Staff at Home Care Associates noted that Medicaid reimbursement rates in Philadelphia are lower than most other localities in the state, despite the fact that the cost of living is higher in the city. As a result, the LTC RAP relied on contracts and grants to operate the full apprenticeship program.
The LTC RAPs visited have also been affected by the recent recession. Home Care Associates staff suggested that the home health industry is especially hard hit because families have an incentive to reduce costs by providing informal care for elderly family members rather than paying for home health services. Many states have responded to reduced tax revenue by cutting Medicaid reimbursement rates, further exacerbating sponsors fiscal challenges in operating their LTC RAPs. The sponsors that rely primarily on Medicaid referrals for its clients have felt these cuts and this may challenge the sustainability of their LTC RAP.
It should be noted that few data on specific costs for operating the LTC RAPs are available for this study. While staff were specific on the what the potential costs were for operating the LTC RAP (e.g., related technical instruction, equipment, transportation, management, wage increases), it was difficult to link amounts to each of these costs either because the sites did not want to share proprietary information or did not track costs across time or separately from other training activities. It was especially challenging for sponsors to know what costs could be attributed to the program or to the apprentice. In turn, this made it difficult to quantify the monetary benefits to the apprenticeship programs in each site retrospectively, especially in measuring the marginal benefits of increased productivity or quality of care, without a more in-depth study.
5.3. Partner Roles and Resources
The LTC RAP sponsors work with an array of partners to provide care and to maintain their apprenticeship programs. The roles these partners play fall into three basic categories: funders, referral sources, and training providers (Table 8). The primary role of the partners is funding training and other LTC RAP expenses. Most sites found these partners important to the success of the apprenticeship.
The budget constraints faced by long-term care providers visited create strong incentives to seek external funding for the LTC RAPs. Developmental Services incurs $500,000 in costs for the organization (not only training expenses) that are not covered by Medicaid reimbursement annually, and pays for these expenses through foundation support. Donations and grants are received through the United Way, individual donors, fund-raising events, Appalachian Regional Commission (ARC) funds, and other grants. These funds help to cover apprentice training and wage progressions. Developmental Services longstanding relationship with the United Way has allowed it to consistently provide high-quality direct support services despite reimbursement rates that staff believe are inadequate.
Home Care Associates supports its related technical instruction specifically through two partnerships: one with the Philadelphia Workforce Development Corporation, and one with the Patricia Kind Family Foundation and the Pew Charitable Trusts. The Workforce Development Corporation provides an Industry Specific Partnership Initiative training grant, a state-led effort, to fund basic training of HHAs receiving TANF. The Patricia Kind Family Foundation grant funded enhanced training for all apprentices at Home Care Associates. Good Samaritan has initially received a Council for Adult and Experiential Learning grant to start their LTC RAP. Subsequent funds from National Alzheimers Association assisted Good Samaritan in finishing their dementia care training material.
Other partners have helped more directly with content and provision of the apprenticeship training. For example, while related technical instruction is provided onsite at Developmental Services, the curriculum for the medical training was developed in partnership with Indiana University. Air Force Villages developed their program materials after considering a CNA curriculum developed by faculty at the North Central Kansas Technical College (NCKTC) that was used in the on-line training program first used for the LTC RAP. Partner organizations also play a role in introducing long-term care providers to registered apprentices in the first place. Home Care Associates was introduced to the apprenticeship model through its partnership with the PHI.
Agape has been better able to fund its own training than the other four sites, but it also pursued financial support from the workforce investment system and from the South Carolina Department of Employment and Workforce when it started its RAP. Like Developmental Services, Agape developed its curriculum and competency checklists in cooperation with a local educational institution, Northeastern Technical College. While the college is not currently involved in the registered apprenticeship program training, it continues to supply Agape with new CNAs who graduate from basic CNA training at Northeastern. Finally, Agape does receive state support through a one-time $1,000 apprenticeship tax credit for each registered apprentice.
The OA and SAAs have also been important and active partners for many of the LTC RAPs, especially in their initial stages. The OA in Indiana worked with Developmental Services to convince the State of Indiana to include registered apprenticeship as a valid fulfillment of the requirements for the direct support certification. The Indiana OA also helps to promote the program and find applicants for the LTC RAP at job fairs. Air Force Villages also received a DOL grant to fund the first on-line course taken by apprentices, although this grant has ended. Home Care Associates worked with OA in Philadelphia to start its LTC RAP based on a program in New York developed by PHI. Registered apprenticeships in South Carolina are administered through the state technical college system, which collaborated closely with Agape in designing its LTC RAP and provided technical assistance.
The partnerships with the workforce investment system (the public employment and training system authorized by the Workforce Investment Act of 1998) and unions are minimal. The workforce investment system occasionally refers job applicants to Developmental Services and Home Care Associates but has no involvement in the LTC RAPs. Two reasons for the lack of partnership may be: (1) the program is not considered a primary responsibility of the workforce investment system; and (2) most apprenticeship sponsors do not reach out to the system. Agape Senior had a more substantial relationship with the workforce investment system, which provided a grant to fund related technical instruction for its first cohort of trainees in 2009. Workforce investment funds were not available in subsequent years to support Agapes program, but the workforce system in South Carolina is generally supportive of and receptive to apprentice programs in the state. No relationship exists between the workforce investment system and Good Samaritan or Air Force Villages. A union, the 1199 Service Employees International Union (SEIU) in Philadelphia, occasionally provides some training for Home Care Associates in which apprentices may participate. No unions partner with Developmental Services, Good Samaritan, and Air Force Villages. There are no partnerships with entities within the long-term care infrastructure such as the state Medicaid program, state units on aging, or area agencies on aging that have involvement in the LTC RAPs, because the apprenticeship programs are viewed as an internal, often experimental, training method with no direct relevance to the work of the Medicaid program or other state agencies. These agencies are involved in monitoring and regulating the sponsors delivery of care, but do not oversee training efforts such as the LTC RAPs.
| TABLE 7. Staffing and Resources of the Selected Long-Term Care Registered Apprenticeship Program Sites | |||||
|---|---|---|---|---|---|
| Staffing Characteristics | Program Site Indiana Developmental Services | Program Site Idaho Good Samaritan | Program Site Pennsylvania Home Care Associates | Program Site Texas Air Force Villages | Program Site South Carolina Agape Senior |
| Training and supervisory staff operating LTC RAP | 30 supervisors; 2 instructors | 6-8 shift supervisors (RNs) and some LPNs | 1 instructor | 7-8 instructors | 1 program director, multiple instructors, several RN supervisors |
| Roles of Staff | Supervisors monitor progress of apprentices on site; trainers provide related instruction and document fulfillment of core competencies in related technical instruction and OJT. | Staff administer checklists of skills; other experienced CNAs mentor-apprentices. | Staff instructs and tests apprentices on related technical instruction material. | Develop and customize materials, provide instruction, provide some oversight of OJT. | Supervisors monitor progress of apprentices on site; trainers provide related technical instruction and document fulfillment of core competencies in related technical instruction. |
| Special qualifications for staff | Medical trainer is an LPN; all supervisors completed the program. | Mentors are former or current apprentices. | Instructor is a former apprentice. | Instructors are management staff within organization with direct content experience. | Program director has background in education; instructors are management staff within organization with direct content experience. |
| SOURCES: Data collected from Interviews at and materials from LTC RAP sites, October 2010-June 2011. Abbreviations: OJT (on-the-job training); CNA (certified nursing assistant); LPN (licensed practical nurse); RN (registered nurse). | |||||
| TABLE 8. Role of and Resources Contributed by Partners at the Selected Long-Term Care Apprenticeship Sites | |||||
|---|---|---|---|---|---|
| Partner Types | Program Site Indiana Developmental Services | Program Site Idaho Good Samaritan | Program Site Pennsylvania Home Care Associates | Program Site Texas Air Force Villages | Program Site South Carolina Agape Senior |
| Federal Office of Apprenticeship or state apprenticeship agencies | Indiana Office of Apprenticeship | National Office of Apprenticeship | Philadelphia Office of Apprenticeship | San Antonio Office of Apprenticeship | South Carolina Department of Employment and Workforce; Office of Apprenticeship; U.S. Department of Agricultural Rural Utilities Service |
| Community-based organizations and foundations | United Way provides additional funding | Center for Adult Education and Learning provided an initial program start-up grant | Philadelphia Workforce Development Corporation, Patricia Kind Family Foundation, and the Pew Charitable Trusts provided training grants | --- | Agape Foundation |
| Workforce investment system | Local workforce investment board occasionally refers applicants | --- | Local workforce investment board occasionally refers applicants | --- | South Carolina workforce investment system provides $1,000 tax credits for each apprentice |
| Educational institutions (secondary or post-secondary) | Indiana University developed training curriculum and output measures | --- | --- | Initial curriculum developed by North Central Kansas Technical College | Northeastern Technical College provides related technical instruction |
| Industry groups | Southern Indiana Provider Network provides best practices and promotes the program | --- | PHI provided technical assistance on the establishment of the apprenticeship program | Pioneer Network, Sage Action PACT, PHI resources were used in developing curriculum | --- |
| Unions | --- | --- | 1199 SEIU provides training on occasion | --- | --- |
| SOURCES: Data collected from Interviews at and materials from LTC RAP sites, October 2010-June 2011. Abbreviations: PHI (formerly known as Paraprofessional Healthcare Institute); SEIU (Service Employees International Union). | |||||
6. Potential Impacts of Registered Apprenticeship in Long-term CARE Sites
LTC RAPs are intended to provide apprentices with the skills to retain their employment with the sponsor, and increase worker productivity and the quality of care for patients. While several of the LTC RAP sites noted some tracking of employment tenure and turnover, they collect and use the information sparingly and do not formally monitor the overall performance of their LTC RAP. However, sponsors and apprentices believe there is a value to the LTC RAP model as discussed in the section below.
6.1. Apprenticeship Completion and Employment Outcomes
Apprentice participation and completion varies across the sites visited, with total enrollment since 2005 ranging from 26 in Home Care Associates to 1,150 in Developmental Services (Table 9). Active participation or completion (as opposed to not actively participating and never finishing) at the five LTC RAPs varies considerably across sites. More than half of apprentices drop out at Developmental Services and Good Samaritan (57% and 54%, respectively) but only 4%, 5%, and 7% at Home Care Associates, Air Force Villages, and Agape, respectively, do so. The higher dropout rates at Developmental Services and Good Samaritan are typical of LTC RAPs nationally and may be attributable to the length of the programs operation as apprentices have more exposure to dropping out. A reason for the dropout rate unique to Developmental Services is that all direct support staff are or have been apprentices. To date, 651 apprentices have left Developmental Services and did not completedthe program. Staff indicated that most left in the first several weeks of the program because they were not suited to the occupation.
Developmental Services, Home Care Associates, Air Force Villages, and Agape have much lower dropout rates than other LTC RAPs in the same occupation. Home Care Associates and Air Force Villages were unusually successful in minimizing dropout rates, but the implementation and operation of the LTC RAP was not without challenges in each. Home Care Associates had to discontinue its program because of program costs. Thus, a low dropout rate does not make a LTC RAP immune from challenges.
6.2. Outcomes of the Registered Apprenticeship Programs Measured by Sponsors
The LTC RAPs visited collect a limited amount of outcome data. This was often because of resource and time constraints and no formal monitoring of the performance of the program. Staff at all the sites indicated that they collect data on wages, benefits, promotions, tenure, and turnover (Table 10). Home Care Associates and Air Force Villagesstaff mentioned that they track wage and bonuses given to apprentices for completing the LTC RAP. Developmental Services, Home Care Associates, and Agape staff noted that they have tracked client satisfaction but have not linked the results to the LTC RAP. Anecdotally, supervisors at Agape have observed that clients are more satisfied with apprentices or apprentice completers than they are with other CNAs. No sites reported that they tracked whether the LTC RAP had an effect on worker satisfaction, worker productivity, or quality of care.
Data on apprentice turnover, measured as the number of workers who leave the sponsor that need to be replaced divided by the average number of employees, are not currently collected in all sites. However, all say that turnover can be calculated from employment records. Some sites measure turnover for both their general staff and for apprentices, specifically. For example, Developmental Services has a 49% annual turnover rate for apprentices and Air Force Villages has a 4% monthly turnover rate for all employees. Home Care Associates reported a 57% turnover rate for all employees, although staff indicated that only a few apprentice completers have left its employment with one moving on to become an RN. Good Samaritan experienced a 4% turnover rate in 2010 among active apprentices and those apprentices who enrolled but did not complete the apprenticeship. Agape had a similarly low turnover rate of 7% for its first cohort of apprentices. The site plans on calculating the one-year turnover rate for its second cohort in the fall of 2011, but staff expect the turnover rate to be at 0% (i.e., 100% retention). Since turnover data are not provided in the RAPIDS data, it is unclear how these statistics compare to non-apprentice long-term care staff generally. Anecdotally, Developmental Services staff suggested that its turnover rates were comparable to other direct support providers in southern Indiana. Lower turnover rates for Air Force Villages apprentices may be the result of the selection process that identifies workers that are likely to succeed as a HSS, and the reduction in turnover cannot be attributed to the LTC RAP.
Developmental Services maintains an information system recording client feedback and satisfaction, and staff noted that most other direct support providers in Indiana maintain similar information. Indiana University assisted Developmental Services in collecting these data and ensured that it collects information that is comparable to other client satisfaction databases. The outcome data currently collected are rarely used to monitor the performance of the LTC RAP. Staff at Home Care Associates also indicated that they collect outcome data on apprentices but do not use it for performance monitoring other than for turnover. Air Force Villagesstaff reported that turnover rates appeared to decline after the LTC RAP was established cannot attribute this directly to the LTC RAP. Air Force Villages staff also noted that turnover rates have declined, possibly as a result of the recession. Developmental Services staff noted that its measurement of client satisfaction is difficult to use as an assessment tool of apprentice performance because the situation of every client is different and not easily compared across apprentices. They also indicated that some apprentices leave the sponsor for jobs with other direct support providers but have returned because they prefer the work environment at Developmental Services.
6.3. Sponsor Perspectives on the Registered Apprenticeship Model for Long-Term Care Occupational Training
The primary benefit of the LTC RAPs noted by all sponsors was that the registered apprenticeship program produced a better skilled workforce. While most sponsors visited not explicitly track apprentice performance or client satisfaction, staff noted the positive impact the program had on work quality. For example, the Good Samaritan program at Idaho Falls has had no deficiency citations on CNA issues on state surveys for several years, which they attribute to the training CNAs receive as apprentices. Developmental Services staff saw the increased quality of their workforce as a way to minimize overall costs including the reduction of costly medical errors such as errors in drug dosage. They considered the LTC RAP as a risk management tool. Agape staff reported that two of its SNFs, Conway and Rock Hill, have been awarded five stars on the recent round of health surveys. They believed that the improvement is in part attributable to the apprenticeship program but also the companys other educational efforts, including three other apprenticeships for non-long-term care occupations.
Home Care Associates staff suggested that in addition to having better skills, apprentices are simply more dedicated to the job than other employees because they feel appreciated and respected. Staff at Good Samaritan noted that the program provides positive indirect effects to non-apprentices, who benefit from apprentices mentoring and greater knowledge and skill. This benefit may be relevant to other LTC RAPs where only a portion of the total workforce is enrolled. Another benefit of the apprenticeships highlighted by sponsors is that the possibility of apprenticeship training helped to attract new applicants. Developmental Services human resources representatives noted that the LTC RAP was a major selling point at job fairs, and Home Care Associates apprentices reported that they told colleagues in the long-term care industry about their positive experiences with the LTC RAP.
6.4. Apprentice Perspectives on the Long-Term Care Registered Apprenticeship Program
Almost all interviewed apprentices had very positive feedback for the program. While many commented that learning the material requires substantial effort, almost all considered this effort worthwhile and the unpaid time for classes well spent. Many of the apprentices interviewed said that they recognized the improvement in their skills learned during the LTC RAPs. These apprentices and apprenticeship completers interviewed said that they felt better qualified to help their clients. They were also more likely to cite their higher quality work as a benefit of the program before they mentioned the wage progression they received. Apprentices at Agape were astonished at the depth of the information they received during the related technical instruction. They had been introduced to the material during their basic CNA training but did not know how much else there was to learn. In particular, Agape hospice employees reported great benefits from learning how to support families and their clients through dementia progression, end of life, and dying. These apprentices said that they were eager to apply this knowledge on-the-job. In Air Force Villages, apprentices said that their new role as HSSs allowed them more time with clients and reduced their overall caseload. Apprentices at Good Samaritan mentioned that they learned more specialty skills such as caring for dementia patients.
Apprentices also valued the wage increase related to the program participation. Although most apprentices reported that the wage increase was not their primary reason for participating in the program, it was valued and provided a good incentive for participating in and completing the program. In fact, Agape apprentices reported that they did not know about it until they actually started the program. However, some apprentices commented that the wage increase is relatively small. Apprentices at Home Care Associates indicated that they saw the wage progression as important because HHAs are perceived as being the bottom of the nursing career ladder with less of an opportunity for career advancement and earnings growth. Agape executives also noted that CNAs were the lowest rung of the career ladder, but that they were the most important rung.
Mentoring opportunities were another feature of the program that elicited many positive responses from apprentices. While the mentoring component is not formalized in all the programs visited, apprentices at each of the sites said that they enjoyed serving as mentors. They felt that being seen as more experienced and valued after completing the program helped them be good mentors to other employees. Apprentices at Developmental Services found that the emphasis on mentoring and peer-mentorship in the OJT component of the LTC RAP was more fulfilling than the more isolated work that they had conducted in long-term care facilities. Apprentices at Good Samaritan mentioned that they learned about mentoring skills and considered these skills valuable.
One weakness of the LTC RAPs highlighted by several apprentices across sites is that other employers and community colleges may not recognize a completion of certification from a registered apprenticeship as a meaningful occupational credential. Apprentices noted that it is not a certification from a formal degree program or a training program that is familiar to most employers. Apprentices at Agape disagreed with this perception noted by apprentices from other sites, saying their apprenticeship certification was from Northeastern Technical College, and was therefore considered legitimate to employers. Apprenticeship and the technical college system are recognized as important components of the workforce investment system in South Carolina, which contributes to the portability of the apprenticeship certification in the state. Agape apprentices also participated in the palliative care worker test and received additional national certification that they understood was portable across jobs. In contrast, staff at Developmental Services suggested that the State of Indiana was not deeply invested in apprenticeships, and as a result Developmental Services apprentices doubted their certification would be fully appreciated by other employers. Home Care Associates staff and apprentices noted this challenge to the recognition of the apprenticeship credential with other employers.
6.5. Partner Perspectives on the Long-Term Care Registered Apprenticeship Program
Almost all interviewed apprentices had very positive feedback for the program. While many commented that learning the material requires substantial effort, almost all considered this effort worthwhile and the unpaid time for classes well spent. Many of the apprentices interviewed said that they recognized the improvement in their skills learned during the LTC RAPs. These apprentices and apprenticeship completers interviewed said that they felt better qualified to help their clients. They were also more likely to cite their higher quality work as a benefit of the program before they mentioned the wage progression they received. Apprentices at Agape were astonished at the depth of the information they received during the related technical instruction. They had been introduced to the material during their basic CNA training but did not know how much else there was to learn. In particular, Agape hospice employees reported great benefits from learning how to support families and their clients through dementia progression, end of life, and dying. These apprentices said that they were eager to apply this knowledge on-the-job. In Air Force Villages, apprentices said that their new role as HSSs allowed them more time with clients and reduced their overall caseload. Apprentices at Good Samaritan mentioned that they learned more specialty skills such as caring for dementia patients.
Apprentices also valued the wage increase related to the program participation. Although most apprentices reported that the wage increase was not their primary reason for participating in the program, it was valued and provided a good incentive for participating in and completing the program. In fact, Agape apprentices reported that they did not know about it until they actually started the program. However, some apprentices commented that the wage increase is relatively small. Apprentices at Home Care Associates indicated that they saw the wage progression as important because HHAs are perceived as being the bottom of the nursing career ladder with less of an opportunity for career advancement and earnings growth. Agape executives also noted that CNAs were the lowest rung of the career ladder, but that they were the most important rung.
Mentoring opportunities were another feature of the program that elicited many positive responses from apprentices. While the mentoring component is not formalized in all the programs visited, apprentices at each of the sites said that they enjoyed serving as mentors. They felt that being seen as more experienced and valued after completing the program helped them be good mentors to other employees. Apprentices at Developmental Services found that the emphasis on mentoring and peer-mentorship in the OJT component of the LTC RAP was more fulfilling than the more isolated work that they had conducted in long-term care facilities. Apprentices at Good Samaritan mentioned that they learned about mentoring skills and considered these skills valuable.
One weakness of the LTC RAPs highlighted by several apprentices across sites is that other employers and community colleges may not recognize a completion of certification from a registered apprenticeship as a meaningful occupational credential. Apprentices noted that it is not a certification from a formal degree program or a training program that is familiar to most employers. Apprentices at Agape disagreed with this perception noted by apprentices from other sites, saying their apprenticeship certification was from Northeastern Technical College, and was therefore considered legitimate to employers. Apprenticeship and the technical college system are recognized as important components of the workforce investment system in South Carolina, which contributes to the portability of the apprenticeship certification in the state. Agape apprentices also participated in the palliative care worker test and received additional national certification that they understood was portable across jobs. In contrast, staff at Developmental Services suggested that the State of Indiana was not deeply invested in apprenticeships, and as a result Developmental Services apprentices doubted their certification would be fully appreciated by other employers. Home Care Associates staff and apprentices noted this challenge to the recognition of the apprenticeship credential with other employers.
6.5. Partner Perspectives on the Long-Term Care Registered Apprenticeship Program
LTC RAP partners were indirectly involved in assisting sponsors by providing the programs support through grants or donations or technical assistance at the beginning of the programs. Some organizations, such as PHI, are dedicated to the promotion of successful health care workforce models and thus benefit from the success of organizations like Home Care Associates. Home Care Associates also receives funding from local welfare and workforce agencies to train entry-level HHAs but does not receive funding or support for the registered apprenticeship program. Developmental Services received some short-term foundation support and worked with the state apprenticeship office to get its program off the ground; however, it has no current partners that support its efforts. Likewise, the Center for Adult and Experiential Learning provided funding to Good Samaritan for establishing its program, but the program had not received any additional funding since. All the sites received assistance from their states OA representative or their states apprenticeship agency in developing and registering their programs. Thus, at much of the partnering occurred at the beginning of the programs, the sites had few active partners from which to draw perspectives.
| TABLE 9. Apprentice Participation in the Long-Term Care Programs Studied | |||||
|---|---|---|---|---|---|
| Apprentice Participation, Completion, and Employment Levels | Program Site Indiana Developmental Services | Program Site Idaho Good Samaritan | Program Site Pennsylvania Home Care Associates | Program Site Texas Air Force Villages | Program Site South Carolina Agape Senior |
| Number of apprentices who entered the program | 1,150 | 387 (entire organization) | 26 | 62 | 112 |
| Number of apprentices who completed the program to date | 314 | 60 (entire organization) | 17 | 23 | 37 |
| Number of apprentices currently registered or completed | 497 | 178 (entire organization) | 25 | 59 | 52 |
| Number of apprentices not completing the program | 651 | 211 (entire organization) | 1 | 3 | 25 |
| Reasons for not completing program | Most dropouts left in the first several weeks of the program because they could not handle the stress of direct support work | Restorative, dementia, and medication aide competency trainings taken if interested or if a related position is available | Dropping out is rare | Dropping out is rare | Dropping out is rare |
| SOURCES: Data collected from Interviews at and materials from LTC RAP sites, October 2010-June 2011; and calculations by authors, RAPIDS, January 2005-May 2011. | |||||
| TABLE 10. Outcomes Measured by Selected Long-Term Care Registered Apprenticeship Program Sites | |||||
|---|---|---|---|---|---|
| Outcomes | Program Site Indiana Developmental Services Measured | Program Site Idaho Good Samaritan Measured | Program Site Pennsylvania Home Care Associates Measured | Program Site Texas Air Force Villages Measured | Program Site South Carolina Agape Senior Measured |
| Wages | X | X | X | X | X |
| Benefits | X | X | X | X | X |
| Promotions | X | X | X | X | X |
| Bonuses | --- | --- | X | X | X |
| Tenure | X | X | X | X | X |
| Turnover | X | X | X | X | X |
| Client satisfaction | X | --- | --- | --- | --- |
| SOURCES: Data collected from Interviews at and materials from LTC RAP sites, October 2010-June 2011; and calculations by authors, RAPIDS, January 2005-May 2011. | |||||
7. Sustainability and Replicability of the Registered Apprenticeship Programs
Two key issues for the LTC RAP model are the sustainability and replicability of the programs. The sites visited highlighted the high costs of their LTC RAPs, recruiting challenges, a lack of support from the sponsors leadership, and lack of a recognized credential as potential barriers to sustainability. The sites also indicated that their LTC RAPs could easily be replicated, given the right conditions and the presence of a champion within the organization. The following section provides an overview of the sponsors views on sustainability and replicability.
7.1. Sustainability of the Registered Apprenticeship Model for Long-Term Care Occupational Training
One of the greatest barriers to the sustainability of the LTC RAP is the high cost of training and incentives to participation such as wage increases. These high costs almost always were reported in interviews, but sponsors did not provide the study team with any detailed documentation. Employers by nature are propriety about their business operations and some sponsors may not have wanted to provide details on costs. Some sponsor staff noted that such costs were incurred as part of the sponsors management staff responsibilities and did not record the separate costs for design and implementation of the LTC RAP. Nor were costs for materials development presented. Only one site, Home Care Associates, calculated that the related technical instruction costs for one apprentice as between $8,000 and $10,000. This program appeared to be at the high end of costs because of various more expensive training components involved. Home Care Associates ultimately discontinued its LTC RAP precisely because of the challenge of these costs when its foundation support ended. For Home Care Associates as well as other home health care service sponsors, demand for long-term care services has declined during the recession as some families began providing care themselves. In addition, Medicaid budgets and reimbursement rates have been reduced as state tax revenue declined with the economy. Sponsors attempted to cover costs that could not be covered by normal revenues with grants and other philanthropic donations. Unfortunately, these funds have also been more difficult to obtain because of the recent recession.
The costs of developing sufficient training resources were also a barrier to sustainability. Good Samaritan and Air Force Villages management noted that they prepared much of their materials at considerable costs in management time. Air Force Villages stated that DOL could help sustain LTC RAPs by developing related technical instruction materials and resources so that sponsors could focus on recruitment activities and OJT. The only site that did not cite cost issues as a major barrier to sustainability, Agape, suggested that it expected to expand the size of the program. Agape staff acknowledged the costs in management time required to develop the curriculum, but considered them a one-time cost. Agape staff found the financial assistance provided by South Carolinas $1,000 per person apprenticeship tax credit particularly helpful, and suggested that other LTC RAPs would benefit from other states providing this level of support for apprenticeship.
Recruitment also has the potential to pose problems for sustainability. If qualified and interested applicants are not available, then apprenticeship programs cannot be sustained. However, this did not seem to be a major issue to the LTC RAPs visited. All five registered apprenticeship programs except for Developmental Services only offered apprenticeships to select employees and they thought their employee pool had a sufficient number of qualified individuals. Developmental Services staff reported that they were not worried about recruitment as a threat to its sustainability, although they did note that its applicant pool is not always well-qualified. They suggested that they never receive enough qualified applicants that they would turn anyone away. In a labor market with many low-skilled individuals looking for work, overall recruitment for the sites was not cited as a problem.
Another factor to program sustainability noted by some sites was the need for buy-in by the firms leadership. Developmental Services has dedicated all of its training resources to the LTC RAP and leadership in the organization has supported the use of the program for all employees. Some sites are still testing whether apprenticeship is the right training approach on a subset of their staff and sponsor leadership has not supported full implementation. For example, Good Samaritans program is voluntary for its facilities to offer and for employees to participate. Home Care Associates supports the program only for its top-performing HHAs and the program is offered only when resources are available.
One concern of apprentices -- the lack of a recognized and portable credential -- may hinder the sustainability of LTC RAPs. For example, staff and apprentices at Home Care Associates noted that while the apprentices are proud of earning their apprenticeship credential, they also find it challenging to communicate the meaning and the value of the credential with other individuals in their field. This is especially problematic as the site is working with its state industry association and the state to develop a licensing requirement for HHAs. However, the use of a community or technical college as a training provider may lend credibility to the apprenticeship credential. For Agape apprentices, they saw their apprenticeship credential as legitimate and recognizable because it was from the local technical college where they received related technical instruction.
The sites visited rarely reported partnerships with the workforce investment system, the educational system, or the long-term care industry, all of which often help sustain training programs. For example, staff seldom identified partnerships with One Stop Career Centers, community colleges, or long-term care industry groups. The lack of such partnerships may greatly hinder sustainability. For Developmental Services, the educational system was a competitor for providing training that the sponsor could conduct more cost-effectively in-house. Similarly, long-term care industry groups were not involved as partners other than providing some technical assistance early on in the program development. The impetus for developing such partnerships may need to come from the partnering organizations as opposed to the sponsors to be seen as valuable.
7.2. Replicability of the Registered Apprenticeship Model for Long-Term Care Occupational Training
One of the greatest barriers to the sustainability of the LTC RAP is the high cost of training and incentives to participation such as wage increases. These high costs almost always were reported in interviews, but sponsors did not provide the study team with any detailed documentation. Employers by nature are propriety about their business operations and some sponsors may not have wanted to provide details on costs. Some sponsor staff noted that such costs were incurred as part of the sponsors management staff responsibilities and did not record the separate costs for design and implementation of the LTC RAP. Nor were costs for materials development presented. Only one site, Home Care Associates, calculated that the related technical instruction costs for one apprentice as between $8,000 and $10,000. This program appeared to be at the high end of costs because of various more expensive training components involved. Home Care Associates ultimately discontinued its LTC RAP precisely because of the challenge of these costs when its foundation support ended. For Home Care Associates as well as other home health care service sponsors, demand for long-term care services has declined during the recession as some families began providing care themselves. In addition, Medicaid budgets and reimbursement rates have been reduced as state tax revenue declined with the economy. Sponsors attempted to cover costs that could not be covered by normal revenues with grants and other philanthropic donations. Unfortunately, these funds have also been more difficult to obtain because of the recent recession.
The costs of developing sufficient training resources were also a barrier to sustainability. Good Samaritan and Air Force Villages management noted that they prepared much of their materials at considerable costs in management time. Air Force Villages stated that DOL could help sustain LTC RAPs by developing related technical instruction materials and resources so that sponsors could focus on recruitment activities and OJT. The only site that did not cite cost issues as a major barrier to sustainability, Agape, suggested that it expected to expand the size of the program. Agape staff acknowledged the costs in management time required to develop the curriculum, but considered them a one-time cost. Agape staff found the financial assistance provided by South Carolinas $1,000 per person apprenticeship tax credit particularly helpful, and suggested that other LTC RAPs would benefit from other states providing this level of support for apprenticeship.
Recruitment also has the potential to pose problems for sustainability. If qualified and interested applicants are not available, then apprenticeship programs cannot be sustained. However, this did not seem to be a major issue to the LTC RAPs visited. All five registered apprenticeship programs except for Developmental Services only offered apprenticeships to select employees and they thought their employee pool had a sufficient number of qualified individuals. Developmental Services staff reported that they were not worried about recruitment as a threat to its sustainability, although they did note that its applicant pool is not always well-qualified. They suggested that they never receive enough qualified applicants that they would turn anyone away. In a labor market with many low-skilled individuals looking for work, overall recruitment for the sites was not cited as a problem.
Another factor to program sustainability noted by some sites was the need for buy-in by the firms leadership. Developmental Services has dedicated all of its training resources to the LTC RAP and leadership in the organization has supported the use of the program for all employees. Some sites are still testing whether apprenticeship is the right training approach on a subset of their staff and sponsor leadership has not supported full implementation. For example, Good Samaritans program is voluntary for its facilities to offer and for employees to participate. Home Care Associates supports the program only for its top-performing HHAs and the program is offered only when resources are available.
One concern of apprentices -- the lack of a recognized and portable credential -- may hinder the sustainability of LTC RAPs. For example, staff and apprentices at Home Care Associates noted that while the apprentices are proud of earning their apprenticeship credential, they also find it challenging to communicate the meaning and the value of the credential with other individuals in their field. This is especially problematic as the site is working with its state industry association and the state to develop a licensing requirement for HHAs. However, the use of a community or technical college as a training provider may lend credibility to the apprenticeship credential. For Agape apprentices, they saw their apprenticeship credential as legitimate and recognizable because it was from the local technical college where they received related technical instruction.
The sites visited rarely reported partnerships with the workforce investment system, the educational system, or the long-term care industry, all of which often help sustain training programs. For example, staff seldom identified partnerships with One Stop Career Centers, community colleges, or long-term care industry groups. The lack of such partnerships may greatly hinder sustainability. For Developmental Services, the educational system was a competitor for providing training that the sponsor could conduct more cost-effectively in-house. Similarly, long-term care industry groups were not involved as partners other than providing some technical assistance early on in the program development. The impetus for developing such partnerships may need to come from the partnering organizations as opposed to the sponsors to be seen as valuable.
7.2. Replicability of the Registered Apprenticeship Model for Long-Term Care Occupational Training
Staff interviewed at the LTC RAPs wererelatively certain that other organizations could replicate the LTC RAP and suggested that the most significant obstacle to replication was that long-term care providers were not aware of the apprenticeship model as a training option. A staff person at Developmental Services introduced the organization to registered apprenticeship because she discovered how inexpensive the model was compared to other advanced training options. She thought that other direct support service firms would find Developmental Services registered apprenticeship model cost-effective. One condition that would make apprenticeship a potentially cost-effective training option if states would implement more stringent certification regulations and employers would need a more rigorous training program such as apprenticeship to meet these standards.
Home Care Associates staff saw its registered apprenticeship program as a success because it was built off its current training. The model Home Care Associates used was developed by PHI, in partnership with DOL and had already been tested and implemented in New York. Thus, the LTC RAP was a replication of previous efforts but modified to the needs of the sponsor.
The staff at Good Samaritan and Air Force Villages suggested that a successful program may be difficult to replicate without a champion. Administrators of the Developmental Services and Home Care Associates programs explicitly rejected this suggestion, arguing that anyone could successfully implement the model. However, the apprentices and staff at Developmental Services suggested that their local champion was integral to the performance of the program. Agape administrators and apprentices credited their local champion with the success of the LTC RAP and suggested that it would not have been implemented without his efforts.
Site staffs views on replicabilityalso seems to depend on a variety of local conditions, including the degree to which sites are dependent on Medicaid and Medicare reimbursement for revenue. Sites that were able to identify other funding sources in addition to Medicaid and Medicare did not cite as many financial constraints to their LTC RAP. However, it was not clear that low reimbursement rates were a primary obstacle to the success of these programs. Developmental Services staff reported feeling constrained by Medicaid reimbursement but operated a large and successful LTC RAP, while Home Care Associates had to end its LTC RAP because of these same financial constraints. Neither Agape and Air Force Villages were constrained by Medicaid reimbursement rates because both had additional revenue streams. Therefore, while Medicaid and Medicare reimbursement provided a budget constraint on many of the LTC RAPs, it did not appear to be a major factor in being able to replicate the program.
Another important determinant of replicabilitywas the nature of demand for long-term care services (demand for HHAs seems to be more volatile than demand for CNAs or DSSs). Several sponsor staff cited the recession and reduced demand for long-term care services as a reason for cutting costs. In the case of Home Care Associates, this contributed to the decision to end its LTC RAP for the time-being. The need for state certification and licenses was also a commonly cited constraint on replicability, insofar as staff were not as enthusiastic about the LTC RAP if they did not think their training would be recognized elsewhere. The sponsors that lobbied for state credential recognition and occupational standards, such as Developmental Services and Home Care Associates, had a great sense of pride in the credentials they were providing apprentices. Agape has all of its apprentices take a national palliative care certification test, so this credential is more widely accepted. While most sponsors suggested that broader acceptance of their credential was important, none seemed to be concerned that this would result in apprentices leaving their LTC RAP for other employment or changing careers. The lack of widespread use of registered apprenticeships as a training model also stymies efforts to create awareness about LTC RAPs. While sites already had operating LTC RAPs, some suggested that DOL and others could help to better promote LTC RAPs to other long-term care providers.
As noted earlier, few of these LTC RAPs had any contact with the workforce investment system. Those who did were primarily one-time grant recipients. After further inquiry, none of the sites suggested that lack of involvement with the workforce investment system was a barrier to replicability. With financial constraints as a continuing problem for LTC RAPs, grants for incumbent worker training through the workforce investment system may assist in successful program implementation.
8. Implications for Policy and Evaluation Design
This study of LTC RAPs visited five sites -- Developmental Services (Indiana), Home Care Associates (Pennsylvania), Good Samaritan (Idaho), Air Force Villages (Texas), and Agape (South Carolina) -- to understand their program design and implementation and their evaluation potential for better understanding the effects of the training program on apprentices, sponsors, and industry. The findings from these visits, including the advantages and the challenges of LTC RAPs from the sponsor, apprentice, and partner perspectives, are summarized throughout this report. The implications of these findings for both policy and evaluation are described below.
8.1. Policy Implications
The goals of the LTC RAP are to increase the skills and productivity of the workers, raise quality of care, prolong job tenure and reduce turnover, and improve job satisfaction and employee wages. The sponsors interviewed for this study saw these advantages as reasons to operate their LTC RAP. However, other findings in this report present a challenging picture for apprenticeship, or any other advanced training for that matter, in the long-term care industry. A central problem in this field is the inability of employers to achieve sufficient cost savings or extract sufficient revenue increases from gains in productivity and quality of care that might result from a more highly skilled workforce. Part of the problem revolves around the difficulty to this point of documenting cost savings or productivity gains.
Another problem is a third-party reimbursement system that does not provide higher payments to higher quality providers. These problems limit the ability of employers to pay significant wage increases for progressing through and completing an apprenticeship. Other challenges, such as limited knowledge of the approach and limited recognition of credentials, reflect the fact that LTC RAPs are still in their early stages in the industry. If LTC RAPs were to expand broadly, more employers and workers may begin to recognize the credentials of those completing apprenticeships as reflecting genuinely high professional skills. A key question is whether sufficient outside support or employer interest will generate an expansion of LTC RAPs. A rigorous evaluation of LTC RAPs may affect the outcome. Were an evaluation to show significant net benefits for employers, for quality of care, or for workers, the LTC RAP approach potentially could attract significant support as one way of dealing with the well-recognized and long-term problems of building a well-qualified long-term care workforce.
The registered apprenticeship model is intended to be self-sustaining because the sponsor uses its training budget for the LTC RAP in place of the training approach they would use otherwise. Usually, new long-term care workers receive only minimal basic training (75 hours in the nursing home and home health care occupations) before they begin work. In four of the five sites visited, the LTC RAP provides training that lasts much longer than is typical, far exceeding the usual minimal requirements. As such, apprenticeship does indeed generate more training, but presumably at additional costs to employer sponsors.
In order for the LTC RAPs to be sustained and spread more widely, the benefits of the LTC RAP need to outweigh the costs. Apprenticeship training is intended to increase the skills and productivity of the workers, the quality of care, prolong job tenure, and reduce turnover. How well the program does so is still uncertain. Sponsors typically receive no government or other outside resources for the development and operation of their LTC RAPs, and therefore must dedicate significant internal resources for continuing the LTC RAPs. Medicaid reimbursement, the primary payer in long-term care, is relatively low compared to other payers and does not recognize the need for or existence of direct care workers with training beyond the minimum level. For the sponsors, higher skills therefore may come at significant non-reimbursable costs unless the skills that workers learn result in greater productivity, which is hard to accomplish or prove in a service industry such as long-term care.
While these challenges do exist, expanding the number of these programs in the long-term care setting may offer an innovative approach to addressing the workforce shortage. From January 2005 to December 2009, there were 3,744 individuals who began LTC RAPs in 121 unique programs (Anderson, et al., forthcoming). While this number is small compared to the universe of registered apprenticeship programs, some ground has been gained through efforts by the OA to promote LTC RAPs in the industry. In addition, as part of the landmark ACA of 2010, Congress authorized funds for the Health Professions Opportunity Grants program, which supports the development of health care occupational training programs, including long-term care, for welfare recipients and other low-income individuals. It is required that these programs partner with SAAs to develop registered apprenticeship opportunities for serving participants and engaging health care employers. If evaluated, these combined efforts at expanding LTC RAPs may offer some evidence of their effectiveness and document ways for addressing the challenges. Thus, policymakers potentially could consider registered apprenticeship as a partial means to address the long-term care workforce shortage and the need for better skills, but the need to understand and address the challenges to its success are formidable.
8.2. Evaluation Design Implications
The main purpose of this report is to provide information relevant to assessing designs of any future evaluation of LTC RAPs. Although the analysis of evaluation options will appear in a subsequent deliverable, this section delineates aspects of the LTC RAPs visited that are relevant to future evaluations. Before considering how the site characteristics inform potential evaluations, it is important to recognize the possibly wide scope of evaluations. The outcomes of interest certainly involve workers and employers but could include consideration for client and funder outcomes as well. For workers, the key outcomes are any costs (such as foregone earnings) and how well LTC RAPs improve their skills, wages, job stability, job satisfaction, and long-term earnings. For employers, the key outcomes are the added training costs as compared with the benefits of a more skilled workforce. Were LTC RAPs to increase productivity and quality, clients may be receivea higher quality of care without imposing added costs on taxpayers or other funders. The discussion in this section focuses on worker and employer impacts.
Several characteristics of LTC RAPs are relevant to evaluation designs, including: (1) the goals and activities of the programs; (2) the duration of the programs; (3) the size and scalability of programs; (4) the availability of data; (5) the recruitment and selection of apprentices into the programs; and (6) the implications of sponsors use of apprentices to improve non-apprentice staff performance.
One issue is whether the sites program goals and the intervention are generally uniform across sites. Although the programs are registered through DOL, sponsors have considerable latitude in deciding their goals and activities. That said, the goals of the LTC RAPs visited are roughly consistent across the programs: to improve the skills of the long-term care workforce in order to improve quality of care and to create more attractive jobs for apprentices who perform caregiving. Achieving these goals help sponsors meet state certification requirements, reduce errors in caregiving, reduce turnover, and create career opportunities for apprentices. The activities of LTC RAPs are also generally consistent across the sites visited. Most sites used the LTC RAP for advanced training and mentoring of employees who had already received basic training and had leadership or personal qualities for which they were selected into the apprenticeship. One site used its LTC RAP for entry-level training of all new employees.
The duration of the LTC RAPs is an important issue for any evaluation. An evaluation that involves longitudinal analysis would need to consider how much time is needed to implement an intervention to be able to assess its full effect. The programs visited have a wide range in time for completion, with the shortest program being 1,680 hours and the longest program being 3,232 hours (approximately 1.5 years). The remaining programs were approximately 2,000 hours. Longer interventions can be more expensive to evaluate than shorter ones, particularly if they involve multiple waves of data collection.
The size of the LTC RAPs visited ranged from eight to 183 active apprentices as of May 2011. These sites were selected because they were the largest sites with active programs that agreed to participate in the site visit analysis. Studying large-scale programs is especially important for assessing whether experimental evaluation options are feasible in achieving sufficient samples of apprentices to be able to detect small differences in outcomes. For example, if one wants to know the effect of the LTC RAPs on annual turnover, one needs sufficient sample sizes to have the statistical power to detect relatively small differences in the turnover rate of apprentices compared to non-apprentices. Based on national registered apprenticeship data, LTC RAPs have a median size of only six active apprentices, much smaller than all but one of the sites visited. As of May 2011, there were only about seven sites with more than 25 active apprentices. Given that LTC RAPs are typically smaller individual programs than suitable for experimental evaluations, one option would be to pool samples of apprentices across multiple programs, but such an approach might complicate efforts to assure comparison groups are appropriate.
Across these sites, limited data on outcomes are collected. Most sites did obtain data on wages, benefits, tenure, and turnover, but not in a common form across sites. Most sites collect annual turnover but one tracks only monthly turnover. Any future evaluation would involve collecting additional data beyond what sites currently collect.
Designing valid comparison groups for those entering apprenticeships may be difficult because of the selection process for entrants into the program. Almost all sites have selection criteria for apprenticeships; employees must typically apply or be recommended and subsequently be assessed and selected for an apprenticeship from a subset of all employees. As a result, regular workers not selected to enter apprenticeships would not be a valid comparison group, since unmeasured differences between them and apprentices would likely bias estimates of the program impact. A randomized control trial effectively addresses such selection issues. One approach that can control for measured differences in individuals is multivariate analysis, but it cannot capture unmeasured differences in skill level, experience, motivation, and aptitude for service in long-term care. Another approach is to use natural experiments in which a process that is independent of individual characteristics selects who participates and who does not; the resulting assignments can be random from the perspective of unmeasured differences in individual characteristics. The use of quasi-experimental methods for evaluating LTC RAPs may also offer options for drawing appropriate comparison groups, but they do not always do as well at controlling for unmeasured differences between treatment and control groups.
Another factor identified in this report that is relevant to an evaluation is the spillover effects of the LTC RAPs. In most of the sites visited, employers designed the program so that apprentices who complete the apprenticeship serve as mentors to the remaining non-apprentice staff. This intentional spillover of the intervention to non-intervention employees makes comparison of apprentice outcomes to non-apprentice outcomes within a site extremely difficult. An evaluation would need a comparison group outside of the sponsors organization, or at least another of the sponsors facilities not subject to the intervention, to address this issue. Gaining the cooperation of organizations not involved in apprenticeship in a future evaluation may be difficult. At the same time, employers may greatly value any positive impacts of these spillovers of their LTC RAPs.
Because the sponsors bear the costs of investing in and operating LTC RAPs and because their decisions will largely determine the scale of the LTC RAPs, evaluating the gains and losses for employers using the LTC RAP model is critical. There are assessment tools for gauging the employer perspective, but usually not in an experimental or comparison group context. The feasibility of evaluation options involving employers will be examined in a subsequent report.
References
American Health Care Association. 2011. LTC Stats: Nursing Facility Patient Characteristics Report, June 2011. Washington, DC.
American Health Care Association. 2007. Trend in Certified Nursing Facilities, Beds, and Residents, CMS Nursing Facility OSCAR Standard Health Survey Data, December 7, 2007. Washington, DC.
Anderson, W., G. Khatutsky, J.M. Wiener, R.I. Lerman, and D. Kuehn. 2010. A Descriptive Analysis of the U.S. Department of Labors Long-Term Care Registered Apprenticeship Program. Report to the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation. Research Triangle Park, NC: RTI International. http://aspe.hhs.gov/daltcp/reports/2010/LTCappre.shtml.
Eyster, L., B. Barnow, D. Nightingale, J. Trutko, C. OBrien, and D. Kuehn. Forthcoming. Implementation and Early Training Outcomes of the High Growth Job Training Initiative. Report to the U.S. Department of Labor, Employment and Training Administration. Washington, DC: The Urban Institute.
Hollenbeck, K.. 2008. State Use of Workforce System Net Impact Estimates and Rates of Return. Presented at the Association for Public Policy and Management Meetings. Los Angeles, CA.
Institute of Medicine. 2008. Retooling for an Aging America: Building the Health Care Workforce. Washington, DC: The National Academies Press.
Johnson, R.W., D. Toomey, and J.M. Wiener. 2007. Meeting the Long-Term Care Needs of the Baby Boomers: How Changing Families will Affect Paid Helpers and Institutions. Washington, DC: The Urban Institute.
Khatutsky, G., J.M. Wiener, W.L. Anderson, and M.R. Squillace.2011. Understanding Direct Care Workers: A Snapshot of Two of Americas Most Important Jobs. Waltham, MA: RTI International. http://aspe.hhs.gov/daltcp/reports/2011/CNAchart.htm.
Lerman, R., L. Eyster, and K. Chambers. 2009. The Benefits and Challenges of Registered Apprenticeship: A Sponsors Perspective. Report to the U.S. Department of Labor, Employment and Training Administration. Washington, DC: The Urban Institute. http://www.urban.org/publications/411907.html.
Mikelson, K., and D.S. Nightingale.2004. Estimating Public and Private Expenditures on OccupationalTraining in the United States. Report to the U.S. Department of Labor, Employment and Training Administration. Washington, DC: The Urban Institute.
Mueser, P., K. Troske, and A. Gorislavsky.2007. Using state administrative data to measure program performance. Review of Economic and Statistics 89:4, 761-783.
National Center for Assisted Living. 2010. Findings of the NCAL 2009 Assisted Living Staff Vacancy, Retention, and Turnover Survey. Washington, DC. http://www.ahcancal.org/ncal/quality/Documents/2009NCALVacancyRetentionTurnoverSurveyReport.pdf.
U.S. Department of Labor, Employment and Training Administration.2011. Registered Apprenticeship: FAQs. http://www.doleta.gov/oa/faqs.cfm.
U.S. Department of Labor, Bureau of Labor Statistics. 2009. Occupational Outlook Handbook, 2010-11 Edition: Nursing, Psychiatric, and Home Health Aides.
Notes
-
At the time of the launch of the initiative, OA was named the Office of Apprenticeship Training, Employer and Labor Services (OATELS).
-
Locations in Boise and Idaho Falls , Idaho were visited for this study.
-
Home Care Associates is currently not operating its registered apprenticeship program due to a lack of funds, although it currently employs past apprentices and is interested in restarting the program.
-
A survey of registered apprenticeship sponsors showed that only a small portion of sponsors are aware of or use services through the workforce investment system (Lerman, Eyster, and Chambers, 2009) so a lack of active partnerships was not unexpected.
-
While no wage increase is offered after the LTC RAP is completed, there is a small wage increase after basic training is completed. All apprentices start at $7.25 an hour. After basic training, wages are increased depending on experience. Apprentices with no experience typically see their wages increase to $8.50, or by $1.25 from the training wage.
-
RAPIDS data as of December 2009, including apprentices registered since January 2005.
-
Please note that HHAs are considered worker-owners and receive a share of the annual company dividends in addition to their wages.
-
Staff recollection of apprentice enrollment differs modestly from RAPIDS records. Staff estimates are presented here, and the RAPIDS data are discussed below.
-
Reported numbers of active apprentices by sites were found to differ from the RAPIDS system on some occasions. Discrepancies were often because the most recent cohort of apprentices had not all been entered into the system at the time of the visit.
-
The Home Care Associates LTC RAP was particularly expensive because of a generous wage progression ($1.20 per hour), a $200 bonus, a dedicated trainer, and equipped training room (as opposed to using staff volunteer time), holding training during work hours, and hiring additional training staff for specific class sessions.
-
While no wage increase is offered after the LTC RAP is completed, there is a small wage increase after basic training is completed. All apprentices start at $7.25 an hour. After basic training, wages are increased depending on experience. Apprentices with no experience typically see their wages increase to $8.50, or by $1.25 from the training wage.
-
In addition to the competencies described here, apprentices are also expected to be competent in community and service networking, facilitation of services, education, training, and self-development, vocational, educational, and career support, organizational participation, building and maintaining friendships and relationships, provide person-centered support, and supporting health and wellness.
-
Trainees are paid $7.25 an hour, the minimum wage. The wage increase offered upon completion of basic training varies by the experience of the apprentice. Inexperienced apprentices typically receive a wage increase of $1.25 to $8.50.
-
Registered Apprenticeship Partners Information Data System (RAPIDS) data as of December 2009, including apprentices registered since January 2005.
-
RAPIDS data as of December 2009, including apprentices registered since January 2005.
-
Please note that HHAs are considered worker-owners and receive a share of the annual company dividends in addition to their wages.
-
RAPIDS data as of December 2009, including apprentices registered since January 2005.
-
Home Care Associates administrative staff suggested the apprenticeship program had 100% completion and retention, although RAPIDS data indicate that one apprentice had dropped out of the program.
-
Staff recollection of apprentice enrollment differs modestly from RAPIDS records. Staff estimates are presented here, and the RAPIDS data are discussed below.
Appendices
Appendix A. CORE Competencies by LTC RAP
Core competencies taught in the Long-Term Care Registered Apprenticeship Program (LTC RAP) sites are presented below. In some cases, investigators were provided with a list of core competency training by the sites, and in other cases these lists were supplemented with a description of the specific courses in which these courses were taught. For example, a case management course would provide instruction on multiple core competencies relevant to case management. In other cases, this coursework supplements required core competencies with instruction that is considered valuable to the LTC RAP (such as mentorship training). Both core competencies and courses (if they were provided) are presented below.
Developmental Services, Inc.: Direct Support Specialist (DSS)
- Community living skills and supports.
- Communication.
- Documentation.
- Participant empowerment.
- Assessment.
- Community and service networking.
- Facilitation of services.
- Education, training, and self-development.
- Advocacy.
- Vocational, educational, and career support.
- Crisis prevention and intervention.
- Organizational participation.
- Building and maintaining friendships and relationships.
- Provide person-centered supports.
- Supporting health and wellness.
The Evangelical Lutheran Good Samaritan Society: Certified Nursing Assistant (CNA)
- Demonstrates advanced understanding of infection control.
- Demonstrates effective communication.
- Incorporates appropriate interventions to maximize physical functioning and mobility, maintaining proper body mechanics.
- Implements appropriate interventions to maintain continence and minimize problems related to elimination.
- Functions as a member of the health team within the health care facility.
- Demonstrates ethical/professional practices.
- Assists with treatments, procedures, and specimen collection.
- Pain recognition and non-medical interventions implemented.
The training at Evangelical Good Samaritan Society includes:
- Advanced CNA.
- Mentor.
- Restorative.
- Dementia.
- Medication administration.
Home Care Associates: Home Health Aide (HHA)
- Role of the HHA.
- Client rights and confidentiality.
- Communication and problem-solving skills.
- Personal care skills.
- Health-related tasks.
- In-home and nutritional support.
- Infection control.
- Safety.
- Understanding the needs of various client groups.
Enhanced training for apprentices at Home Care Associates includes:
- Case management.
- Peer-mentoring.
- Best practices.
- Communication.
Air Force Village: Certified Nursing Assistant (CNA) and Health Support Specialist (HSS)
Certified Nursing Assistant:
- Demonstrates advanced understanding of infection control.
- Demonstrates effective communication.
- Incorporates appropriate interventions to maximize physical functioning and mobility, maintaining proper body mechanics.
- Implements appropriate interventions to maintain continence and minimize problems related to elimination.
- Functions as a member of the health team within the health care facility.
- Demonstrates ethical/professional practices.
- Assists with treatments, procedures, and specimen collection.
- Pain recognition and non-medical interventions implemented.
Health Support Specialist:
- Communication.
- Resident care.
- Restorative care.
- Resident rights.
- Documentation.
- Infection control.
- Safety
The training at Air Force Village includes:
- Two medical terminology modules.
- Dementia.
- Restorative.
- Activity assistance.
- Person-centered care.
- Soft skills.
- Environmental services.
Agape Senior: Certified Nursing Assistant (CNA)
- Interpersonal and communication skills.
- Health Insurance Portability and Accountability Act (HIPAA) protections.
- Active listening, assertive communication with patients.
- Customer service.
- Psychosocial aspects of aging.
- Body mechanics.
- Cancer.
- Stages of dying.
- Post-mortem care.
- Body systems during the aging process, including the dermatological, respiratory, cardiovascular, and renal systems.
- Dementia care and communication with dementia patients.
Appendix B. Site Summaries
Development Services Incorporated
| Program Sponsor: | Development Services Incorporated |
|---|---|
| Apprenticeship Occupation: | Direct Support Specialist (DSS) |
| Location Visited: | Columbus, Indiana |
| Date of Visit: | December 8-9, 2010 |
Overview of Site: Development Services Incorporated is a private, not-for-profit firm that provides direct support services clients with developmental disabilities. Its mission is to aid its clients in having fulfilling lives and managing the administration of their basic medical care. Ultimately, Developmental Services plans to move clients towards self-sufficiency, consistent with a plan developed with the client and his or her case manager.
The company receives client referrals from Medicaid state case managers. Developmental Services serves approximately 1,700 clients in group home and independent living settings across 30 counties in southern Indiana. The companys headquarters is located in Columbus, Indiana, approximately 45 miles south of Indianapolis. Apprentice training is conducted at the Columbus facility, while client care occurs throughout the state. Since direct support is by its nature dispersed and not concentrated in a single facility, Developmental Services operations are spread throughout the southern Indiana region. Initially, Developmental Services monopolized direct support service provision in the region, although now it has many competitors. Developmental Services operates 14 program facilities and oversees a large number of group homes across the region.
Developmental Services operates a registered apprenticeship program for DSSs. DSSs are responsible for assisting clients with developmental disabilities with the administration of their medicine, domestic activities in group homes and independent living facilities, transportation, and engagement with the community. They are expected to prevent or intervene in crises that emerge, and assist clients in becoming more self-sufficient. In 2004, Developmental Services sought the highest quality and lowest cost training program available, eventually deciding on registered apprenticeship. The apprenticeship program was formalized and registered with the U.S. Department of Labor (DOL) in 2005. Developmental Services based the design of its LTC RAP on a training program it had operated since it was founded in 1975, for which all newly hired DSSs become apprentices. There are currently 700 apprentices at Developmental Services. In 2007, as a result of DOLs decision to increase the hours required for DSS apprenticeships, Developmental Services increased its core competency requirement to 216 hours of related technical instruction and 3,000 total hours. Initially, Developmental Services had time requirements of 144 hours of related technical instruction and 2,000 total hours.
Since 2007, Developmental Services apprentices who complete their requirements are certified as direct support providers by the State of Indiana. There is no associated promotion or earnings increase for apprentices upon completion of the program, but Developmental Services is interested in implementing a wage increase upon completion.11 Developmental Services cannot charge patients for direct support services; they must accept established Medicaid reimbursements as compensation. Therefore, tightened Medicaid reimbursements from the state have limited the ability of Developmental Services to raise wages for any staff upon completion of the apprenticeship program. While promotion and wage progression are not currently offered at Developmental Services through the apprenticeship program, it is expected to increase retention of apprentices who appreciate a professional and skilled work environment.
Program Design: Developmental Services began researching training program options for it staff in an effort to reduce medical error rates in 2004. A cost-effective way to reduce error rates was the primary motivation for adopting the LTC RAP. Recruitment and retention for Developmental Services had always been robust for Developmental Services because of the broad awareness of the quality of their training. Training through the community college was quickly ruled out as too expensive, although the company did consider using the training offered by the College of Direct Support, a regional provider of such training. Developmental Services leadership ultimately determined that the LTC RAP was both cost-effective and easily integrated into its existing training activities, which relied heavily on a combination of related technical instruction and on-the-job training (OJT). To initiate the LTC RAP, Developmental Services first contacted DOLs Office of Apprenticeship (OA), which directed them to Indianas OA. The goal of the LTC RAP was to provide low-cost training that would reduce error and risk in client care.
The DSS registered apprenticeship program occupation has 15 core competencies, which are taught through a combination of related technical instruction and OJT. Many of the competencies, such as community living skills and participant empowerment, revolve around the unique circumstances implicit in the regular social contact maintained with clients by apprentices in this occupation. Unlike many long-term care occupations, DSSs interact socially with their clients for extended periods of time. Other competencies emphasize soft skills such as communication and client advocacy. More technical competencies include documentation and assessment skills. A trainer at Developmental Services emphasized that documentation skills were critical for the success of apprentices, since multiple staff work with the same client and need to stay apprised of incidents and drug administration. Another core competency is crisis prevention and intervention. Since clients can react unpredictably in stressful situations, apprentices spend time in both formal training and OJT learning strategies for diffusing difficult interactions with clients.12
Developmental Services places a high value on job candidates who have soft skills and the capability to manage stress that is inherent to direct support provision. Many applicants are not fully aware of the challenges associated with the work, and instead can view it as a baby sitting job. Developmental Services is therefore interested in applicants with prior direct support experience who are interested because they have the desire and aptitude for the rigorous training provided by the registered apprenticeship program. Developmental Services receives approximately 100 applications a month and extend offers to 25-30 applicants. Applicants almost always accept the job offer. Developmental Services staff indicated that they rarely turn away qualified applicants because Developmental Services usually has open positions to fill. The company advertises in newspapers, on-line, and at job fairs, and is always looking for new venues to seek out more qualified applicants. Applicants often come to Developmental Services with cardiopulmonary resuscitation (CPR) and other certification, but the company is selective in recognizing these certifications, preferring to re-teach its own curriculum during related technical instruction. Currently, only CPR training from the Red Cross and the American Heart Association are accepted; applicants without this certification are required to go through CPR training at Developmental Services.
Apprentices at Developmental Services are primarily White (96%) and female (83%), but range widely in age (the average age for a Developmental Services apprentice is 39; 25% are under 27 years old, while 25% are 51 years old or older). Most are not highly educated, but do have a high school diploma (95% of apprentices has a high school diploma as their highest degree). However, many apprentices have worked as a DSS or were employed in long-term care, and join the company with considerable experience. Developmental Services also employs many students as part-time employees and floaters. The 20-30 floaters move among group homes and Developmental Services facilities as they are needed to fill vacancies. Floaters have higher wages, fewer hours, more flexible schedules, and fewer benefits, making the position more attractive to students. Most apprentices have earnings that qualify them for the earned income tax credit. Apprentice-to-client ratios vary depending on the severity of the clients developmental disabilities.
For the OJT component at Developmental Services, apprentices must demonstrate a wide range of competencies in each work setting. However, apprentices are generally not aware that they are fulfilling specific core competency requirements for the LTC RAP. They understand what they are expected to know, but they do not always understand the structure of the registered apprenticeship model. The supervisors of apprentices, on the other hand, are knowledgeable in the core competency requirements. They confirm with the human resources department that an apprentice has dedicated the requisite hours to each of the core competencies and has mastered them. OJT occurs in the context of performing ongoing job responsibilities. The corecompetencies all come up regularly in the group homes and workshops, and supervisors constantly provide instruction and guidance. Developmental Services supervisors and the trainer providing clinical instruction suggested that work-based learning also occurs through regular team meetings and interactions with nurses on staff.
Related technical instruction starts with a set of basic training courses that are required before apprentices provide services for clients. This basic training includes medical orientation, training in two core medical competencies, CPR, and agency orientation, and can take as little as 10 days, depending on how quickly apprentices work through the on-line instructional material and how successful they are in passing assessments. After the basic training period, additional training is provided on non-violent conflict intervention, additional reviews of medical competencies, and related technical instruction for the 15 core competencies listed above. All tests related to medical core competencies are re-taken annually, and this often involves additional training. Developmental Services requires 3,000 hours dedicated to learning and practicing core competencies. Of the 3,000 hours, 216 are spent in related technical instruction. Most of the training is provided by either a human resources staff member responsible for overall operation of the apprenticeship program, or the medical trainer.
Developmental Services employs approximately 30 supervisors who work with apprentices. All Developmental Services supervisors have completed the Developmental Services LTC RAP. These supervisors meet with staff in group homes on a monthly basis to discuss clients. In addition to the monthly group meetings, the supervisors monitor staff as they do their work on a more regular basis. Each group home also has a nurse responsible for its clients. The nurse supervises apprentice administration of drugs, and is available for medical emergencies or to answer any questions that the apprentice may have. Consultation with the nurse is required before a clients medical regimen can be adjusted. Nurses report to the human resources department on apprentice performance and mastery of the core competencies. Peer-to-peer support occurs on a daily basis, since multiple apprentices work together in the same group home. Peer-to-peer engagement also occurs at monthly group meetings, when a wider circle of apprentices working in the same group home have an opportunity to discuss challenges with each other.
The only scheduled wage progression occurs when the basic training is completed. All apprentices start at $7.25 an hour. After basic training, wages are increased depending on experience. Apprentices with no experience typically see their wages increase to $8.50, or by $1.25 per hour from the training wage. After basic training is completed, no subsequent bonuses or wage increases associated with the completion of the remaining related technical instruction and OJT are offered. However, as of 2007, apprentices who complete the LTC RAP are certified as direct support providers in Indiana. Before then, certified direct support providers had to receive training through the College of Direct Support or Ivy Tech Community College. However, some apprentices expressed skepticism about how many employers would recognize the apprenticeship credential, since they are accustomed to the better established Ivy Tech and College of Direct Support credentials.
Program Resources: All training at Developmental Services is conducted during work hours, although apprentices going through basic training are paid a lower wage than apprentices who have completed this basic training.13 Many of the competency tests can be completed on-line. Thus, if apprentices are renewing their competencies, they are not required to do this during work hours. There are no substantial equipment costs for the LTC RAP. The curriculum and tests for the medical orientation training were developed by Developmental Services, but other curriculum for related technical instruction was developed by Indiana University. Since the State of Indiana recognized persons completing a LTC RAP as certified direct support providers in 2007, there have been no additional licensing costs associated with the program at Developmental Services. Indeed, a major impetus for the LTC RAP at Developmental Services was to avoid the high licensing costs at the College of Direct Support.
Apprentices do not bear the cost of tuition, textbook, or school expenses but they are expected to travel to Columbus for initial related technical instruction. All instruction is conducted during work hours, although apprentices have the option of being tested on-line outside of work hours if it is more convenient for them. Apprentices assisting more self-sufficient clients who do not live in group homes bear the transportation costs of going from their homes to and client appointments and errands.
Developmental Services relies on United Way and other donors and grants to cover expenses in excess of reimbursements provided by Medicaid. Developmental Services also confers with seven other direct support providers in the Southern Indiana Provider Network (SIPN), which acts as a trade association and discusses employment and training issues. They do not receive resources from SIPN but they discuss best practices and promote the LTC RAP model.
Program Outcomes to Date: About 700 apprentices are currently enrolled in the LTC RAP at Developmental Services. As of December 2009, 34% of Developmental Services apprentices had completed the program, 30% were registered but had not yet completed the program, and 36% had dropped out.14 Developmental Services employee turnover rate was 49% in 2009, with 59% of the total turnover occurring within the first year of the apprentices time at Developmental Services. Some separations involve apprentices who have been certified but who had left Developmental Services employment. However, Developmental Services staff reported that most of the separations arise quite early in the training period, usually within a few months after being hired.
Developmental Services has an outcome measurement system that is largely based on client feedback and satisfaction. This measurement system is a way of providing a quantitative work goal. Most direct support providers in Indiana have a similar client-based outcome measurement system, although comparing client outcomes can be challenging because of the variety of client conditions. Indiana University assists Developmental Services in collecting these data. While the client data collected are not strictly an attempt to measure return on investment for the LTC RAP, Developmental Services does consider the LTC RAP as a cost minimization strategy.
Perceived Benefits and Challenges of the Program: Developmental Services staff reported that the primary benefit from the LTC RAP is its role as a risk management tool to reduce the risk of serious medical errors. Well-trained staff make fewer mistakes, which in the direct support industry can be costly. Apprentices at Developmental Services share the view that they receive much better training at Developmental Services as compared to less comprehensive training in non-apprenticeship programs offered by other employers and training organizations. The added training is a primary attraction of working at Developmental Services for the apprentices, who take pride in their skills. The apprentices also noted that the frequent peer interaction and peer learning is more fulfilling than their experience at other agencies, where the management is more hierarchical and less feedback is offered. One shortcoming of registered apprenticeships noted by many of the staff is that few other agencies recognize registered apprenticeship certification, and local community colleges do not accept certification for academic credit.
Sustainability: Developmental Services is not concerned about recruiting individuals to enter its LTC RAP. While staff aresomewhat concerned about the quality of many of the applicants, they are not concerned about program sustainability. The major challenge to sustainability cited by the staff was the cuts made to Medicaid reimbursement in Indiana as a result of the recession, as well as the persistent problem of covering costs that are not reimbursed by the state through grants and donations.
Evaluation Potential: The scale of the Developmental Services LTC RAP may meet the criteria for conducting several of the evaluation designs under consideration. Since Developmental Services requires all applicants to go through the LTC RAP, and since it never receives qualified applications in excess of their needs, a random assignment of the apprenticeship model within Developmental Services would be challenging, and would require substantial changes to its selection policies. A more promising evaluation strategy may incorporate other direct support providers in the SIPN group. These providers have expressed an interest in the apprenticeship model.
Home Care Associates
| Program Sponsor: | Home Care Associates |
|---|---|
| Apprenticeship Occupation: | Home Health Aide (HHA) |
| Location Visited: | Philadelphia, Pennsylvania |
| Date of Visit: | January 20, 2011 |
Overview of Site: Home Care Associates is a worker-owned company founded in 1993 and provides home health services to clients in the Philadelphia area. HHAs, trained by Home Care Associates, offer care to clients in their homes to assist them in living independently.
Home Care Associates began its LTC RAP for HHAs in 2006. The company was introduced to DOLs LTC RAP through its affiliate, Cooperative Home Care Associates, and worked with PHI (formerly known as the Paraprofessional Healthcare Institute) to develop its own LTC RAP. After consulting with the state apprenticeship agency (SAA) representative, Home Care Associates developed core competencies for their HHA position based on its current training program to meet the requirements of the LTC RAP.
HHAs at Home Care Associates provide both heartwork services and home health services. Heartwork services include basic companionship and assistance for clients who are able to live independently but require companionship or care to live comfortably in their own homes. These services include light housekeeping, meal preparation, running errands, and communicating with and accompanying clients to health care providers. Home health services include assistance with basic medical care, including taking temperature, pulse, and blood pressure, changing non-sterile bandages, assistance with rehabilitative care, and assistance with administration of medicines.
There are currently approximately 200 aides at Home Care Associates, of which 25 have completed the apprenticeship program.15 Over the course of its history, Home Care Associates has trained and placed over 1,000 aides. The base wage for aides is $8.50 and all employees are guaranteed full-time employment. An HHAs base wage is increased by $0.20 upon the completion of the enhanced training and every specialty competency, which raises his or her hourly wage to at least $9.70.16 While the registered apprenticeship HHA guidelines require completion of two specialties, Home Care Associates requires that its apprentices complete all possible specialties, which are geriatrics, disabilities, mental illness, hospice and palliative care, dementia, and peer-mentoring. After completion of the entire apprenticeship program, aides also receive a $200 bonus, receive an official badge with their apprenticeship credential, and become a mentor for other HHAs. Costs associated with the wage increases have prevented Home Care Associates from continuing the LTC RAP.
Program Design: The Home Care Associates LTC RAP for HHAs grew out of its established training program. The company provides basic training to all new employees. HHAs who show promise for greater responsibility such as mentoring and supervisory roles are recommended by senior staff to participate in Home Care Associates enhanced training. In this training component, HHAs further develop their leadership skills in home health care and learn specialized skills. It is from this enhancing training that the LTC RAP design has emerged and the competencies for HHAs were developed.
The HHA LTC RAP occupation has nine core competencies, which are taught at Home Care Associates through a combination of related technical instruction and OJT. Since HHAs are expected to provide companionship for clients, several of the competencies revolve around understanding this role including the first competency in The Role of the Home Health Aide, as well as Client Rights and Confidentiality, Understanding the Needs of Various Client Groups, and Communication and Problem Solving Skills. Instruction in communication is especially important for HHAs, who often function as an intermediary between clients and health care professionals. Other competencies are more task-oriented, including personal care skills and health-related tasks. Since HHAs are tasked with monitoring clients who may become progressively less capable of living independently, aides require skills in basic household maintenance. The core competencies that fall in this category include in-home nutritional support, infection control, and safety.
The program requires 2,025 total hours of OJT and related technical instruction to master the HHA core competencies. A total of 230 hours of related technical instruction in core competencies is required of apprentices, including 150 hours in basic training, 40 hours in enhanced basic training, and 40 hours of other enhanced training. Aides shadow mentors when they receive basic training. While all aides employed at Home Care Associates participate in basic training, only apprentices go on to take enhanced training. Enhanced training includes additional instruction in case management, peer-mentoring, best practices, and communication. Thus, apprentices not only have a higher level of training in the core competencies taught to all aides, they also develop leadership and mentoring skills. Other enhanced training includes working with clients with physical disabilities, hospice care, and mental illness.
Registered apprenticeship for the HHA occupation is unique in that aides do much of their work alone in private households. This makes OJT challenging to supervise and record as a part of the apprenticeship program. Home Care Associates has addressed this issue by emphasizing the role of more experienced aides as mentors to newer aides. Mentor aides, who receive related technical instruction on mentoring within the apprenticeship program, ensure that learning on-the-job and supervision for the program occur. Mentors are not continuously present with aides but they interact with them regularly to monitor the competencies they are achieving. OJT occurs in the context of performing ongoing job responsibilities and interactions with mentors at the Home Care Associates headquarters. Instances for apprentices to demonstrate the core competencies all arise regularly in the clients homes.
Apprentices at Home Care Associates are primarily African-American (85%) and female (92%). The average age for a Home Care Associates apprentice is 43. While data are only collected by DOL on registered apprentices at Home Care Associates, HHA apprentices had similar demographic characteristics to all Home Care Associates aides. Education levels for the apprentices are low. Only 42% of apprentices even have a high school degree, with only an additional 12% holding general equivalency degrees (GEDs). The remaining 46% of apprentices are high school dropouts. Some aides come to Home Care Associates with prior work experience as HHAs.
Program Resources: Home Care Associates has two grants to help fund training. The Philadelphia Workforce Development Corporation awarded the company an Industry Specific Partnership Initiative training grant that funds basic training for aides receiving Temporary Assistance for Needy Families. The Industry Specific Partnership Initiative grant is a sector-specific grant intending to target high-growth industries. HHAs had the fourth highest projected employment growth rate from 2006 to 2016 of the 181 occupations identified by the Commonwealth of Pennsylvania as high priority occupations for industry partnerships. A grant from the Patricia Kind Family Foundation and the Pew Charitable Trusts funded the enhanced and specialty training beyond the basic training, which apprentices and not all HHAs participate in.
Training for nurses in home health care is also occasionally provided by the 1199 Service Employees International Union (SEIU) Training Fund (the national health workers union). Although Home Care Associates works with the union, its workers are not unionized because they are worker-owners. Home Care Associates closest partners are other members of the PHI network, who introduced the company to new training and corporate models.
Medicare and Medicaid reimbursement rates for home health care vary by county in Pennsylvania. The reimbursement rate for Philadelphia is lower than less urban counties but the costs of care and the levels of sickness are higher in the city. Wages for the aides are also higher in Philadelphia because the citys high cost of living. These factors put a major fiscal pressures on Home Care Associates, which necessitates outside funding such as grants for the apprenticeship training. Home Care Associates is working with its state association to lobbying on these issues with the state legislature.
Recruitment Process: To be eligible to participate in Home Care Associates LTC RAP, aides had to have at least 6 months of experience at Home Care Associates, including the completion of the basic training courses. This instructional time and the time on-the-job over the course of the 6 months of employment are counted towards apprenticeship completion because aides are learning required competencies during this early training period.
In addition to completing their basic training and a tenure requirement, aides are also required to have recommendations from their scheduling supervisors and the Chief Operating Officer at Home Care Associates to become an apprentice. In recruiting apprentices, priority is given to aides who have successfully completed enhanced training courses. Apprenticeship at Home Care Associates is therefore an augmentation or enrichment of a broader instructional regimen already in place. It also offers program completers a credential that demonstrates their expertise in this field.
Aides are recruited through a variety of venues, although most find out about Home Care Associates through word-of-mouth. The company has a good reputation among the areas HHAs because it offers full-time work and company dividends. Aides, and especially apprentices, are an integral part of recruiting other HHAs for Home Care Associates because they believe in the value of the program.
Program Outcomes to Date: As of December 2009, 65% of Home Care Associates apprentices had completed the program, 31% were registered but had not yet completed the program, and 4% had dropped out of the program.17 The turnover rate for all aides recorded by Home Care Associates was 57% in 2010. The turnover rate for apprentices is much lower than other employees.18 Sixty-six percent of aides employed at Home Care Associates have been working there for more than 1 year. The average tenure of an aide is 39 months. Turnover has declined somewhat with the recession, according to Home Care Associate staff. The apprenticeship program is currently not operating but apprentices who completed the program see a wage increase and become mentors within the company to other aides.
Home Care Associates has been recognized for its training program on several occasions. They have been awarded the Governors Achievement Award, the American Society on Aging's Best Practice Award, the Better Business Bureau's Best Health Service Award and the Philadelphia County Assistance Office's Employer Recognition Award. The Home Care Associates training model was specifically cited as a reason for the companys recognition.
Perceived Benefits and Challenges of the Program: The primary benefit of the LTC RAP from the perspective of both apprenticeship completers and administrators at Home Care Associates is the pride that it provides for aides. Aides that complete the apprenticeship have significant stature within Home Care Associates as mentors to others. Their completion of the program entitles them to regular pay increases and bonuses, which is an important incentive in an occupation, which is often perceived as being the bottom of the nursing career ladder. Apprentices receive a badge indicating their completion of the program, which they take great pride in. Apprenticeship completers interviewed also noted that Home Care Associates apprenticeship program helped them to market the company to clients because of the rigorous training of their aides and to recruit new aides.
One of the challenges to Home Care Associates LTC RAP has been earning recognition for certification outside the organization. While apprentices are well respected within Home Care Associates, and aides feel as if Home Care Associates has a good reputation in the wider HHA community, completion of a registered apprenticeship is not always received as the mark of expertise or professionalism outside the company. Senior staff at Home Care Associates noted that they sometimes have difficulty conveying the meaning of the credential to aides, clients, and others in the industry. While this has been a challenge, Home Care Associates was able to work with the Commonwealth of Pennsylvania to develop licensing requirements for HHAs based on the training and skills the company requires. They hope that this state recognition will make apprenticeship more valuable to other employers and expand its in Pennsylvania. However, without increases in Medicaid reimbursement or other outside resources for the program, expansion of the training approach would not seem likely, according to Home Care Associates staff.
Sustainability: Demand for home health services has declined during the recession, and schedulers have faced some challenges guaranteeing full-time employment for current aides. However, Home Care Associates staff does not foresee any long-term problems with the sustainability of their work or the offering of basic training to new hires. However, the apprenticeship program, which includes the enhanced and specialty training, is too expensive for them to sustain currently. Senior staff hope to initiate the LTC RAP again but this will be dependent on the availability of outside resources and demand for home health services. The two major components of the cost of the registered apprenticeship program are the regular raises and bonuses for apprentices and the cost of the related technical instruction for which Home Care Associates needs additional resources. The basic related technical instruction for an apprentice costs between $8,000-$10,000.
Evaluation Potential: Evaluation of Home Care Associates LTC RAP may be challenging because of the criteria used to select apprentices and the current lack of scale appropriate for impact or non-experimental analyses. Apprentices are not randomly selected. Home Care Associates chooses the most qualified and promising aides to be apprentices. Non-apprentice HHAs at Home Care Associates also go through most of the basic training that is counted towards the apprentices related technical instruction. If non-apprentice aides are used as a comparison group, their training could substantially contaminate the impact estimate. Since apprentices are not randomly selected from among the HHAs at Home Care Associates, any comparison between apprentices and non-apprentice aides will overstate the impact of apprenticeship training. With appropriate financial assistance, Home Care Associates could conceivably develop a demonstration program that offers a complete apprenticeship experience to all of its HHAs. These aides could then be compared to a comparison group in another home health services provider that does not provide a comparable training program.
Evangelical Lutheran Good Samaritan Society
| Program Sponsor: | Evangelical Lutheran Good Samaritan Society |
|---|---|
| Apprenticeship Occupation: | Certified Nursing Assistant (CNA) |
| Location Visited: | Conference Call with National Staff; Boise and Idaho Falls Nursing Facilities |
| Date of Visit: | November 30, 2010 for call; January 11-12, 2011 for Idaho visit |
Overview of Site: Evangelical Lutheran Good Samaritan Society, or Good Samaritan, is the largest not-for-profit nursing home chain in the United States with 230 locations, mainly in rural areas. Its central headquarters is located in Sioux Falls, South Dakota. Its average facility size is under 100 beds but it also has some very large campuses in metropolitan areas. The types of facilities range from single-site nursing facilities to sites that provide several types of care including skilled and long-term nursing care, assisted living, and care in independents homes located in neighborhoods.
Good Samaritans LTC RAP for advanced CNAs was started in 2003. The initial rationale to adopt the apprenticeship model for training was the need for better quality of care. National staff fielded a survey that identified a need for advanced CNA training above and beyond 75-hour federal requirement. The national staff routinely publicize the program in employee newsletters, fliers, articles, and other promotional material as well as on its web site. LTC RAPs are only offered at 25 of the 186 facilities, with each facility operating its LTC RAPs independently. Nationally, 147 apprentices are currently active. Across the two nursing homes visited in Boise and Idaho Falls, Idaho that were visited, approximately 32 apprentices are currently registered, the most of any of the 25 sites.
Good Samaritans philosophy is more of a bottom-up approach to building the LTC RAP at its facilities with its national leadership staff serving primarily as a resource for local campuses that want to develop an apprenticeship program. This approach requires that local leadership staff to initiate and manage the LTC RAPs and work with human resources and clinical staff to offer the program to selected employees. Even though the Good Samaritan national leadership has developed an infrastructure for the LTC RAPs, local campuses can lack commitment in terms of management time and employee incentives to incorporate the program into their institutions. Turnover among local leadership who championed the program is another problem.
The apprentice must complete the advanced CNA training, mentoring, and one specialty competency with approximately 180 hours of related technical instruction and between 1,500 and 2,500 hours of OJT. Some local sites appear to customize how the program is implemented and how long it takes to complete the apprenticeship. The primary intended outcomes of the LTC RAP are to improve the quality of care, empower CNAs, and improve retention by providing a career lattice to encourage staff development and promotion. The program also produces CNA mentors who are extensively used for training new hires.
Program Description: The LTC RAP includes five competencies: (1) advanced CNA, (2) mentor, (3) restorative, (4) dementia, and (5) medication administration. The related technical instruction component is a structured curriculum contained in workbooks with accompanying DVDs. The rationale for the DVDs was to provide training that was available at every site, uniform in nature, and not dependent upon the availability of the instructors. Both Idaho sites rely on these materials, with CNAs completing each instructional workbook and competency either over approximately one-quarter (Idaho Falls) or 1 year (Boise). CNAs study on their own or form study groups. Most study at home. Local sites offer selected competency trainings based on facility skill needs. For example, in the two Idaho sites visited, neither site used the medication administration competency training.
Related technical instruction is completed without pay, almost always completed outside of working hours. Apprentices receive pay increases at completion of each competency ($0.25 per hour in Boise, and $0.50 per hour in Idaho Falls) with apprentices receiving interim credentials for doing so. Completion of each workbook requires that supervisors (licensed practical nurses or registered nurses (RNs)) certify that apprentices can perform the required set of skills on the associated checklist, which is different for each competency. The restorative specialty also requires passing a test to successfully demonstrate proficiency.
OJT varies in length as it is based on a CNAs prior knowledge and current abilities. For example, if a CNA has a prior background in caregiving, he or she may need far fewer hours of OJT to demonstrate proficiency than those with no experience in caregiving. Apprentices must demonstrate skills contained in checklists and the workbooks. Mentors work with apprentices and sign off on their checklists as they successfully demonstrate skill proficiency. Good Samaritan staff indicated that mentors can and should teach others. Less experienced CNAs feel safer often when they are working with their peers rather than supervisors, and it is easier for them to ask questions. Mentors will talk with supervisors if there are performance issues that they cannot address. There is no set length of time for completing the OJT component in the Idaho sites, although Idaho Falls staff could feasibly complete the entire apprenticeship of 3-4 competencies in 1 year, while Boise staff could take 3-4 years to complete the program.
The national registered apprenticeship program requirements for gaining approval for a LTC RAP requires completion of an application form containing a section on the number of hours to be spent in the apprenticeship. National Campus staff understood from DOLs OA that total apprenticeship hours had to be approximately 1 year in duration. To meet this requirement, Good Samaritan national staff gave each component a length of time so when all related technical instruction and OJT hours were combined, the various components added up to 1 year. However, National Good Samaritan staff noted that they had reviewed data indicating that less than a year was needed to gain the required skills. National Good Samaritan staff suggested that if a sponsor is running a competency-based program, one should not have to meet any requirement for OJT hours.
Program Resources: Both Idaho sites have a human resources staff member who administers the LTC RAP as part of their job responsibilities. The Idaho Falls site also has one additional staff person involved in scheduling and supervision of clinical issues. There is no onsite instructor for either site as the instructor from its headquarters presents course material on the DVDs. Each site actively encourages mentors who have completed the mentor competency to mentor and support to other CNAs both in and outside of the LTC RAP. Both Idaho sites had at least a dozen mentors each. Supervisors (nurses or care managers) seem to be involved only to review the checklists of care giving issues at the end of each instructional workbook.
In recent years, no partners have contributed to program development or implementation nationally or at either site, although Good Samaritan had received at program inception an initial Council for Adult and Experiential Learning grant sponsored using DOL funding to help establish the program. However, Good Samaritan staff developed the materials themselves. Initially, they received some limited consulting from PHI who provided some guidance and shared some materials that they were allowed to reference. No workforce-related or training partnerships were used locally in the Idaho sites. The Boise DOL office had at one point attempted to work with the facility but did not maintain the effort after the DOL staff member changed jobs. One of the reasons for the lower level of involvement from the Boise DOL office is that Good Samaritan is a national LTC RAP, and therefore does not have direct contacts with all the DOL offices or SAAs in the companys locations.
Recruitment Process: At the Idaho sites, management selects CNAs to participate based on a variety of criteria. More objective criteria include length of employment, work attendance history, and ones rated functional proficiency in performing client care activities. However, personal characteristics that are not easily measured such as interpersonal skills, overall attitude, work ethic, and motivated are used to select apprentices. In one Idaho site, several staff responded that they would know a good apprenticeship candidate almost immediately after the new employee was hired, largely based on personal characteristics. In addition, participation in the apprenticeship program is voluntary.
Program Outcomes to Date: In the national registered apprenticeship data, approximately 387 apprentices have been registered since 2005, although additional apprentices were registered before the inception of the national reporting system. In the Boise site, 46 were enrolled since 2005. Twenty-six apprentices had not completed the entire apprenticeship either because they were no longer employed by the facility (20) or still employed but not actively participating (six). In the Idaho Falls site, approximately 15 CNAs were registered in the program, with 12 still actively participating.
In the two Idaho sites, not all apprentices intend to complete the entire apprenticeship, largely as a result of how the program is implemented. In Boise, apprentices start and complete the mentor competency over the first year, and then take other competencies (advanced, restorative, and dementia) as interested but not more than one each year because the facility cannot afford more than one pay increase per year. It also takes time to learn and implement the skills taught and provides apprentices something to look forward to over time by building more specialized skills and experience within the company. In Idaho Falls, apprentices usually start with the advanced CNA competency training and subsequently take the mentor competency training. Then, unless there is a job opening on the rehabilitation or dementia units, an apprentice may not take the rehabilitation or dementia competency trainings.
Perceived Benefits and Challenges of the Program: According to the companys management staff and staff at both Idaho sites, the primary benefit is improving the quality of care provided by CNAs. They reported that the programs positive spillover effect extends to all CNAs, even those who are never apprentices, via the mentoring process. Both Idaho facilities actively encourage mentors to work with other CNAs on staff to improve caregiving skills because such feedback is almost always better received from peers as opposed to management. The Idaho Falls site has experienced no deficiency citations on CNA issues in state surveys over the last two years, which staff think is largely due to the role of mentors working across all CNAs. Staff suggested that it is possible that there is a positive effect on CNA tenure as only 4% of active or recently completed apprentices left employment in 2010 compared to 49% turnover for all Good Samaritan CNAs. The LTC RAP also serves as an implicit marketing tool for high school and vocational technical school students. These students must satisfy their clinical requirements at the facility for their beginner CNA certification and are able to observe the assistance and positive atmosphere provided by apprentices through their mentoring activities and may want to become employees after certification. Apprentices cited various benefits in roughly the following order: sense of empowerment/pride in their work, the enjoyment of mentoring others, the pay increase, and the desire to be always learning.
With low reimbursement rates and margins in the long-term care industry, it is very difficult to incentivize programs financially through higher wages. Staff reported that when finances are tough, facilities can lose focus, and education is the first thing to be cut. National staff emphasized that the need for better caregivers has not gone away, and that facilities should invest in staff development to achieve better quality of care.
At both Idaho facilities, apprentices receive certificates when completing each competency training as well as the DOL certificate of completion of the apprenticeship. National staff noted that some facilities have awards ceremonies or recognize CNAs in other ways at apprenticeship completion. However, the Idaho sites facility staff reported that the certificates do not hold much meaning to apprentices currently. The certificate is not seen as a universal document as staff in other Idaho facilities do not recognize it. These managers suggested that the apprenticeship program needs to be recognized by other facilities to increase its value to apprentices who receive the certificates. When hiring, other employers only look at years of service when determining pay and do not ask how much training one has received.
Sustainability: National staff indicated that enrollment in the LTC RAPs is stagnating nationally as the program is in only 25 sites after 7 years of implementation. Sometimes a site discontinues the program when the local champion in facility management leaves the organization. In addition, the lack of funds for wage increases potentially removes higher wages as an incentive. Budget constraints at the Boise facility also led to the decision not to pay apprentices for taking related technical instruction as was originally planned. Idaho Falls has never paid for related technical instruction time. Medicaid reimbursement for nursing home care is not increasing, so facilities face leaner budgets over time. Competing demands within facilities also poses problems in new facilities adopting the program. In the two Idaho sites, continued enrollment does not seem to be a problem because new employees are always being hired, providing opportunities for selecting apprentices. Both Idaho facilities have strong champions on staff, who considerthe improvements in quality of care and staff attitudes direct benefits of the program.
Evaluation Potential: The number of apprentices at any one time, both nationally and at any one site, is low for purposes of a rigorous evaluation of outcomes using statistical techniques. Individual facilities are limited by patient bed size in terms of the number of apprentices they could generate. Unless the national staff can encourage other facilities to participate, Good Samaritan could not provide enough apprentices for a national evaluation using multivariate statistical analyses because the analyses would lack sufficient sample sizes of apprentices within the organization.
Selection bias is also an issue for evaluating Good Samaritan in that it is not clear how apprentices are selected. Unless detailed discrete, uniform criteria are used to select apprentices across sites, one could not know whether apprentices differed on unobservable characteristics. The risk of selection bias appears high as management at both Idaho sites effectively select the best CNAs on personal attributes to become apprentices so they provide appropriate role models for non-apprentices.
The varied implementation of the program across sites presents another evaluation challenge in that while the materials are consistent across sites, facilities customize the order of presentation to meet immediate facility needs, and offer the specialty trainings either if desired (Boise) or needed by the facility (Idaho Falls). Both Idaho facilities thought the mentor competency was the most important because of the potential for improving quality of care via peer feedback. Both facilities purposefully encourage apprentices to influence care delivered by non-apprentices, making selection of a within-facility comparison group problematic. Other Good Samaritan facilities without apprenticeship programs could potentially serve as a control group.
Air Force Villages, Inc.
| Program Sponsor: | Air Force Villages, Inc. |
|---|---|
| Apprenticeship Occupation: | Health Support Specialist (HSS) |
| Location Visited: | San Antonio, Texas |
| Date of Visit: | January 25-26, 2011 |
Overview of Site: Air Force Villages is a not-for-profit retirement community located on two campuses in San Antonio, Texas. Its clientele includes a large number of retired military personnel. Each campus has large independent living complexes made up of apartment-type and standalone housing units. In addition, both campuses have skilled nursing facility (SNF) units. The main campus is certified for 104 SNF beds and 20 new assisted living facility beds coming on line in 2011, with approximately 75 of the SNF beds currently occupied. The second campus is certified for total occupancy of 650 including the 64-bed assisted living, secured Alzheimers disease unit and 35 non-dementia assisted living facility beds. The organization is undergoing a major expansion, building a new neighborhood-like complex to be known as the The Mission with household-type arrangements. Once the expansion is complete, the existing facilities will also be restructured into household-type arrangements.
The organization does not take Medicaid patients because reimbursement is too low for the quality of care it wishes to provide. Consequently, Air Force Villages takes private pay residents for whom staff provide a full continuum of care, some short-term Medicare-reimbursed skilled rehabilitation patients for which the facilities are increasing the number over time. Many residents also have coverage as retired members of the military through the militarys CHAMPUS insurance benefit.
Air Force Villages began its apprenticeship program in 2009 in response to its planned expansion as a means of training CNAs in its skilled nursing units in a new model of care to enact culture change. Current CNAs receive advanced training as HSSsand serve as universal workers, conducting all required tasks (e.g., resident care, housekeeping, cooking, laundry) for a small group of residents residing in one household building. In this new model of care, 2-3 HSSs serve 13-14 skilled nursing residents in a small house-like building. The new model of care could also be applied to residents in existing traditional buildings (e.g., long hallways of rooms), which are also being reorganized into neighborhoods.
Approximately 40 apprentices have been trained in three cohorts of approximately 12-15 CNAs each. The apprenticeship is 3,232 hours in length (232 hours of related technical instruction, and 3,000 hours of OJT). Although the intended purpose of the classes is to train CNAs as universal workers, other outcomes include higher wages, longer tenure, and most importantly, higher quality, person-centered care for residents needing skilled nursing care. After existing CNAs are trained, new employees will also be trained as HSSs.
Program Description: The apprenticeship program was originally introduced to Air Force Villages by San Antonio DOL OA staff. When the program was implemented, the first related technical instruction classes were provided by North Central Kansas Technical College (NCKTC) on-line through its modular on-line program for HSS. Twelve CNAs participated in the original apprenticeship training and received college credit for it. Subsequent related technical instruction for the remaining cohorts wereconducted internally, with no college credits given. Instructors are recruited from facility management with in-house expertise. They also modified and tailored the NCKTC curriculum to the needs of the organization. Air Force Villages used materials from several organizations involved in the culture change movement, including the Pioneer Network, Action PACT, and PHI.
The class curriculum lasting 232 hours consists of eight modules: medical terminology (two modules with 45 hours); dementia care (16 hours); restorative care (30 hours); activity assistance (30 hours); environmental services (40 hours); person-centered care (16 hours); and soft skills (15 hours). Each module within the class has a folder, resources, and written materials. Program staff are particularly proud of developing the soft skills module which includes communication, mentoring, anger management, coping strategies, how to take care of themselves emotionally, how to prevent absenteeism, how to properly resign, and many other skills employees need to learn to be a responsible worker. Such skills are often lacking among newly hired employees. Staff reported that it had not been difficult to accommodate language and cultural differences in their instruction.
Each module is taught onsite by management over several weeks in two-hour classroom lectures on Tuesdays and Wednesdays prior to or after CNA apprentice shifts. For example, the director of environmental services will teach the environmental module, the safety director will teach Occupational Safety and Health Administration requirements, and the director of food services will teach dietary requirements. Each instructor designs his or her own class materials and assigns homework, quizzes, and tests, depending on the class content. Air Force Villages used the DOL LTC RAP materials to determine how many hours to devote to the mastery of competencies within the program but developed all the training curricula without relying on the DOL work process schedules. Instructors collect feedback from participants and modify coursework as needed. For example, a sequence of courses was changed after apprentices requested it. Apprentices can do some related technical instruction and OJT activities for a particular competency concurrently. For example, they can participate in OJT for one module and attend the next class at the same time. The organization is strict about class attendance; if apprentices miss more than two classes in one module, they are not allowed to complete the class. However, they may be eligible to participate in future offerings of the class.
There are no costs for apprentices to participate in the LTC RAP. At Air Force Villages, CNAs start at $9.09 per hour. Participating CNAs are unpaid for the programs related instruction, but receive up to an 8% wage increase after completion of the 7-9 month class, or a bonus up to 8% of current salary if they were already topped out in their pay grade. There is a formula based on tenure that program managers use to choose between wage increases or bonuses. The OJT portion for the entire apprenticeship consists of 3,000 hours. RNs, licensed vocational nurses, and/or CNA mentors supervise OJT and ensure that apprentices practice all the skills they learned. Instructors have developed a form that is used for each student to document their OJT.
A graduation ceremony is conducted at the end of the class. Apprentices invite families, friends, and the facilitys residents who are important to them. Each apprentice receives a DOL certificate and a new badge for HSS. Apprenticeship completers no longer receive college credit hours for program participation; however, the certificate of completion is considered a nationally recognized certification. CNAs who have completed the apprenticeship can also become mentors. However, the mentoring is not official and mentors are not formally designated. There is no mentoring module for the LTC RAP at this time but there is a desire to formulate one.
Future plans for the program include the following: (1) participation of all new CNA hires; and (2) development of a career ladder for two levels of HSS with training curriculum for these levels and respective wage increases associated with these steps. Topics considered for these future modules include understanding the budget of the organization and financial statements, role of mentors, conducting an independent project, and grief and dying.
Program Resources: The organization is led by a capable administrator who inspires care and concern for both residents and employees. She espouses a vision of culture change made explicit in the new model of care. In effect, this administrator serves as an effective champion for the LTC RAP and has effectively led the rest of the management team in fulfilling that vision.
In spite of the name of the organization, managers and staff do not necessarily have military backgrounds and come more from mainstream health care. Managers willingly participate as instructors and develop class materials. This involves roughly a 6-12 two-hour sessions for each module taught. The ongoing costs for the program are primarily printing and the instructors use of their time to teach classes. There is administrative support necessary to enroll students into DOLs RAPIDS database and document grades and attendance.
Local DOL staff introduced the registered apprenticeship program to Air Force Villages human resources staff in 2009. The first cohort was provided instruction through on-line courses using an existing curriculum of the NCKTC. Initial DOL grants for CNAs to attend that first class were not renewed because there were no more grants for this type of on-line related technical instruction at the college. The administrator has unsuccessfully sought to obtain funding to offset the costs for operating the related technical instruction.
Recruitment Process: Only certified CNAs are eligible to participate in the LTC RAP. CNAs must be employed in the facility for at least 3-6 months before applying to the registered apprenticeship program so that management can first assess whether they are a good fit. Staff evaluate whether the applicants have enough passion for the job, are conscientious workers, and have a good work attendance record. Some employees quickly see that they are not a good fit for the nature of work involved for the HSS position. Staff noted that if you start to lose people from the program, it affects the morale for the remaining participants. Eventually, all CNAs will be selected for the class, but CNAs will still have to prove themselves as responsible, caring workers prior to participation.
Program Outcomes to Date: Approximately 40 apprentices have been enrolled at the time of the site visit. Almost all apprentices have completed the apprenticeship, with language being an issue for one CNA, and class attendance issues with another half dozen CNAs. The program is in its third cohort with about 12 enrollees who are scheduled to complete it in summer 2011. Management now perceives the class as an essential part of its staff development program.
According to LTC RAP managers, the completion rates are high. Program managers could think of only one person who dropped out because of moving to another job. One of the reasons that completion rates are high is that management provides a lot of support and work with apprentices to help them complete the program. As the most common problem is child care, on occasion, they will allow apprentices to bring their children to class.
Anecdotally, Air Force Villages managers observe that their monthly turnover rate is lower since the programs inception but the measure would require refinement for use in a future evaluation. No data on quality of care have been developed. The administrator suggested that the best outcome measures for understanding whether the facility is providing good quality of care would be patient and staff satisfaction measures. They quantify quality by measuring feedback from residents and staff by conducting staff and resident/satisfaction surveys every other year. They also collect data on falls, infection rates and are now engaging in a new study called Interact II to measure and reduce re-hospitalization rates.
Air Force Villages collects data on tenure, turnover, and wage increases, although it has not sought to evaluate it to understand how the LTC RAP contributes to these outcomes. Turnover calculations exclude temporary employees. Their turnover rates are calculated separately for each facility. Monthly turnover rates range between zero and about 10% of CNA staff, with the average monthly turnover rate between 1% and 5%. Staff suggested that some of the organizations lower turnover rate may be attributable to the bad economy as there are fewer job openings in the industry.
Perceived Benefits and Challenges of the Program: The perceived main benefits of the program are higher quality of care for residents and building relationships among staff. The goal is to train CNAs so they can provide all services needed so that residents can build bonds with caregivers and CNAs can spend more time with residents. Apprentices expressed high satisfaction with the new model of care in that it increases their perceived value of their role. Many apprentices interviewed spoke of being empowered and respected for their care contributions. The LTC RAPs biggest challenge is financial stability. Management is assessing the need to partner with DOL given the lack of ongoing financial support. It would appear that Air Force Villages can operate the class less frequently once all current CNAs are trained. An additional challenge comes from CNAs sometimes being resistant to doing all tasks in addition to personal care activities. They may be worried about time constraints and feeling overwhelmed with its new model of care.
Evaluation Potential: The site does not appear to provide enough apprentices for a future experimental or quasi-experimental evaluation. Some data such as tenure and wages exist that potentially could be used for a future evaluation. However, the organization does not routinely compare wages and other outcomes between LTC RAP participants and non-participants.
Agape Senior
| Program Sponsor: | Agape Senior |
|---|---|
| Apprenticeship Occupation: | Certified Nursing Assistant (CNA) |
| Location Visited: | West Columbia (corporate headquarters, assisted living, assisted living dementia unit, and SNFs) and Conway (assisted living, including a dementia care assisted living unit, and SNF), South Carolina; Phone calls with Northeastern Technical College and South Carolina Workforce Investment Board |
| Date of Visit: | August 3-4, 2011 for South Carolina visit; August 8, 2011 for calls |
Overview of Site: Agape Senior is the umbrella corporation for a mix of 38 for-profit and not-for-profit companies that provide coordinated and interrelated long-term care services in a variety of facilities across South Carolina. Founded in 1999 in West Columbia, Agape was the first long-term care provider to sponsor a registered apprenticeship program in South Carolina. Corporate headquarters is located in West Columbia, South Carolina, and facilities exist in Conway, Laurens, Rock Hill, and other sites throughout the state. Across all its facilities, Agape has approximately 800 beds and has been able to maintain high occupancy rates in both assisted living and SNF settings.
Agapes LTC RAP was started in 2009 and offers advanced CNA and palliative care competencies. The LTC RAP is overseen by the Chief Human Capital Office, which orchestrates all educational efforts at the company. The advanced CNA apprenticeship is one of four apprenticeship programs operated at Agape (the others are not associated with direct care occupations and include dietitians and management), and is only one facet of a broader educational mission at the company. Agape executives are dedicated to building an educated workforce and only hire senior staff that can serve as instructors in these educational efforts. These educational initiatives for CNAs, along with other opportunities for more senior staff, are all components of Agape University, the educational arm of the company. In addition to the four apprenticeships, the company has partnered with Goodwill Industries and Midlands Technical College to provide basic CNA training for employees who are not already certified. Agape continues to build relationships with technical colleges in the region to strengthen these educational efforts and provide instruction for the LTC RAP.
Agape is currently working with its third cohort of apprentices. The first cohort, who was trained in 2009, began with 18 apprentices.19 Sixteen of the apprentices became certified at the end of 2009. The second cohort, trained in 2010, expanded to 35 participants with 21 successful graduates. Agapes third cohort of 59 apprentices began its program in 2011, with 52 still enrolled as of August 2011. With a total of 1,400 employees and a strong teaching staff, the company expects enrollment in the apprenticeship to continue to grow.
An apprentice in the LTC RAP has to participate in 265.5 hours of related technical instruction and 2,000 hours of OJT to complete the basic CNA, advanced CNA, and palliative care certifications registered with DOLs OA. As the LTC RAP only accepts employees who are already certified as CNAs with the basic CNA training, apprentices only have to complete 143.5 hours of related technical instruction (103.5 hours for advanced CNA, and 40 hours for palliative care) and 1,700 hours of OJT. The palliative care competency is certified by the National Palliative Care test. The operation of the LTC RAP is uniform across Agapes facilities because all related technical instruction is conducted simultaneously over a distance learning platform. The primary intended outcomes of the RAP are to improve the education of the Agape workforce and improve the quality of care. Two additional benefits regularly noted by Agape staff were that the LTC RAP reduces CNA turnover and helps to differentiate and reward high-quality CNAs.
Program Description: Aside from the basic CNA certification (identified as level one, which currently all apprentices have had upon entering the LTC RAP), the program has three competencies that apprentices must demonstrate mastery of: (1) geriatric, (2) mentor, and (3) palliative care. The first two competencies are part of the Advanced CNA (level two) portion of the LTC RAP. The third palliative care competency is optional for apprentices but all apprentices to date have completed the competency. While there is no distinct module for mentorship training, the curriculum adopted by Agape incorporates mentorship training in all other modules.
Related technical instruction is conducted uniformly across all Agape sites through the use of distance learning technology. Most instruction is conducted in person at either the West Columbia or the Conway facility, but apprentices at all facilities participate in class over a two-way video feed. Classes are held every Thursday, from 3:00 to 6:00 p.m., and are conducted on the apprentices own time. Different instructors are used for each module, and all instructors are senior staff members at Agape, with the exception of the courses on dementia, which utilize an outside instructor. Instructors produce their own course curriculum and material to hand out to apprentices. Classes typically include some lecturing, a substantial amount of hands-on activities, and a quiz. Notes are provided to the apprentices, and most apprentices maintain their notes together for future reference. One apprentice from an earlier cohort suggested that she still refers back to her course notes on-the-job, even after graduating. The apprentices said that while they do not receive homework, they all studied the material on their own time at home. They noted that it would be hard to get certified if they did not study on their own time.
Course content for the related technical instruction was designed to deepen the CNAs understanding of the material they learned in basic CNA training, with a special emphasis on geriatrics and palliative care. Apprentices are trained in a variety of interpersonal and communication skills, including coursework on the HIPAA protections, active listening, assertive communication with patients, and customer service. After these initial sessions, apprentices learn more medically substantive material, including the psychosocial aspects of aging, body mechanics, cancer, the stages of dying, and post-mortem care. Subsequent classes cover the changes that occur in a variety of body systems during the aging process, including the dermatological, respiratory, cardiovascular, and renal systems. At the end of the related technical instruction, apprentices spend several weeks learning about dementia, specifically how to communicate with those experiencing dementia.
Related technical instruction is completed on apprentices own time and without pay. Apprentices receive pay increases of a quarter every quarter. Thus, for every quarter of the class completed (somewhat less than a calendar quarter), each apprentice gets a $0.25 per hour raise in pay, from a starting wage of $9.00 to $11.00, depending on prior experience. Those who complete the entire related technical instruction therefore receive a $1 per hour raise. No interim credentials are earned, but at the end of the LTC RAP, apprentices receive a certificate of completion. If they pass a state examination, they become certified palliative care providers.
In addition to quizzes taken in class and the state palliative care certification test, supervisors of apprentices confirm that apprentices can practice their skills on-the-job. A competency checklist was developed with the related technical instruction, and this checklist is used by senior staff to monitor apprentices on-the-job. OJT is facilitated by many of the instructors for the Agape LTC RAP, who are also supervisors who work with the CNAs on a regular basis (except apprentices providing hospice care in client homes). In addition to the LTC RAP competency checklist, ongoing monitoring of all CNAs (both apprentices and non-apprentices) is conducted through compliance rounds, as well as annual clinical skills checks. Standard check-off sheets are used for both apprentice and non-apprentice CNAs for compliance rounds, so their performance can theoretically be compared in future evaluation efforts. Both the related technical instruction and the OJT components are typically completed in 1 year.
Program Resources: Ten percent of the Agape Chief Human Capital Officers time is dedicated to the LTC RAP, as well as 60% of his assistants time. A third person spends a small amount of time entering data into the national registered apprenticeship reporting system, RAPIDS. In addition to this dedicated staff, many senior staff volunteertheir time to plan curriculum for and teach related technical instruction. OJT is provided by supervisory staff that monitor and mentor all CNAs as a normal part of their job but specially tailor their oversight with apprentices to the LTC RAP competencies. The checklist used to monitor apprentices (as opposed to regular Agape employees) was developed at the same time as the curriculum and reflects each competency trainingreceived in the classroom. Agape Senior has also purchased three distance learning units and an $80,000 bridge unit for the distance learning system. These were used in combination with the three distance learning units received from Northeastern Technical College to deliver related technical instruction. The college paid for these units using a grant from Apprenticeship Carolina.
Agape Senior has internally covered its training costs for the third cohort of apprentices. In the first cohort, training was funded by a workforce investment board training grant to Northeastern Technical College, and in the second cohort, by a South Carolina Department of Employment and Workforce grant (which was funded by federal stimulus money). These resources for training were helpful for initiating the LTC RAP but Agape staff anticipate that they can continue training without outside financial support. Currently, financial resources for apprentice wage increases is provided by a one-time apprenticeship tax credit from the state worth $1,000 per apprentice. Agape continues to pursue grants to support its educational efforts, including a U.S. Department of Agricultural Rural Utilities Service grant to purchase additional distance learning equipment to expand the LTC RAP to rural Agape locations. Grant-seeking by Agape is facilitated by its unique corporate structure; while most of the long-term care provider companies owned by Agape Senior are for-profit, it also owns not-for-profit companies and a foundation that are free to apply for grants. Agape maintains close partnerships with South Carolinas technical college system and with the workforce investment system but does not rely on partnerships with unions or trade associations.
Recruitment Process: Apprentices are recruited from incumbent Agape employees with basic CNA certification, although the program registered with DOL can be completed by those who are not certified (certified apprentices are simply credited with the hours associated with basic CNA competencies). For each of the three cohorts, the LTC RAP has been advertised on a bulletin board but most have been recruited through supervisors. Agape supervisors assess and rank their employees so that each is placed in either thetop (20%), middle (70%), or bottom (10%) of the staff. Apprentices are typically selected from the top 20% group, although some are drawn from the middle 70% group. While some of these assessments are subjective, Agape attempts to be rigorous in its differentiation of employees and is currently using assessment software called Wingspan. The LTC RAP is advertised to CNAs as an advanced training program that will make them better caregivers. Few of the apprentices were told about the associated wage increase initially, and only found out about it after starting the program. Apprentices from earlier cohorts play an important role in the recruitment process. Other CNAs are encouraged to participate by previous graduates, and these graduates set a standard in the quality of their caregiving that all employees are expected to follow.
Program Outcomes to Date: According to the national registered apprenticeship data, 59 apprentices have registered since the program began in 2009, although additional apprentices entering the program in 2011 have not been entered into the RAPIDS system. RAPIDS reports that apprentices were distributed across four Agape facilities but two additional sites have been added to the program during the third cohort in 2011. Although Agape staff recalled that 18 apprentices were registered in the first cohort, RAPIDS data indicate 20 registered. Both sources agree that 16 apprentices completed the program. RAPIDS data suggest that 39 apprentices were registered in the second cohort, and Agape staff indicated that 21 graduated (again, Agape staff recollection of initial enrollment is 35, diverging somewhat from RAPIDS records). Retention of apprentices is high; 93% of apprenticeship completers in the first cohort were still employed with Agape the following year. The retention rate for the larger second cohort of apprentices will be calculated in the fall of 2011, but it is expected to be 100%. Anecdotally, the quality of apprentices is thought to have improved tremendously. Quality improvements can be tracked empirically using supervisor checklists and data from Wingspan rankings and clinical rounds, although this comparison has not been made yet. Agape staff suggested that their recent good survey results (no citations for quality of care issues) can be attributed to better trained CNAs who have undergone the LTC RAP training. Wage data are not tracked by apprenticeship status but are available for all employees.
Perceived Benefits and Challenges of the Program: Most of Agapes staff agreed that the primary benefit of the LTC RAP is to improve the skill level, and therefore the quality of care, of the CNAs. Agape has a strong educational mission and the LTC RAP is considered to be an integral part of its strategy for developing a skilled workforce. The LTC RAP has been a useful vehicle for promoting knowledge of specific topics that are considered important by Agape executives, such as the proper practices to care for patients with dementia. Staff also suggested that the apprenticeship has reduced turnover and given workers a new sense of pride in their work. Supervisors make it clear to all of their CNAs that they consider apprentices to be exemplary workers. Management suggested that because the apprentices were their best CNAs, it was likely that they would have received a raise anyway, so they are happy to pay for a wage progression that is tied to additional investment in the workers human capital. Most apprentices share managements enthusiasm for the higher skill levels imparted by the LTC RAP. For Agape apprentices, the pay increase is highly valued but of secondary importance. They deeply appreciate the sense of pride they get from being recognized for their achievements. Apprentices felt that their certification would be recognized by other employers, especially since the palliative care test that they took was a statewide certification test. Nevertheless, few apprentices sought jobs elsewhere. Finally, both management and apprentices noted how much patients families appreciated the additional care and expertise furnished by apprentices relative to non-apprentices. The primary challenge associated with the program has been the cost of the wage progression, although this cost is not prohibitive for Agape. Staff indicated that a great deal of confidence in his instructors and in the operation of the distance learning equipment.
Sustainability: Agape staff believed the LTC RAP is not only sustainable but that it will expand over the next several years. South Carolinas tax credit for apprenticeship programs is viewed as an additional incentive that has helped to win the support of Agape executives, but even this benefit is not considered to be essential to the sustainability of the program. The companys executives and the LTC RAP instructors are committed to the program and in the third cohort (which is the largest class yet) the program is being operated successfully without any outside support except for the state tax credit. For many long-term care providers, reimbursement that is perceived to be inadequate threatens the sustainability of LTC RAPs. However, Agape has been profitable enough to feed several million dollars worth of profits back into indigent care and charitable contributions to local colleges through the Agape Foundation. The staff felt that additional apprenticeship promotional materials from DOL would help them to expand their apprenticeship.
Evaluation Potential: Agapes registered apprenticeship program population is small but sufficient for rigorous evaluation, particularly if cohorts are pooled across time and the size of the registered apprenticeship program continues to increase. While there are many Agape facilities, their concentration in South Carolina, the predominance of a few particularly large facilities, and the continuity in management and approach to caregiving across sites should help in the evaluation process.
Selection bias in the recruitment of apprentices at Agape poses problems for evaluation. While the selection process is somewhat subjective, it is clear that the highest quality apprentices are chosen for the program, and there may also be a certain degree of self-selection. Certain employee assessment techniques, such as the ranking of employees, could be very helpful in modeling the apprentice selection process and therefore eliminating the selection bias from any evaluation. Another obstacle related to selection processes is that any comparison group selected from among Agape employees may benefit from spillovers of the apprenticeship. Apprentices regularly share what they learn with other CNAs and provide an example to follow. Such spillover into a comparison group could distort the estimated impact of the program.
In addition to employment records kept by Agape (which could be verified by researchers using unemployment insurance wage records), the company keeps employee quality records that could be used in an evaluation. All CNAs, including apprentices and non-apprentices, are ranked according to job performance. Each CNA is also monitored during regular compliance rounds.
Appendix C. Semi-structured Interview Guide for LTC RAP Site Visits
Development of Potential Research Designs to Evaluate the Long-Term Care Registered Apprenticeship Program
Site Visit Interview Guide
Introduction
I am (we are) researchers from [RTI International and/or the Urban Institute]. We are conducting a research study of Long-Term Care Registered Apprenticeship Programs (LTC RAPs) for the U.S. Department of Health and Human Services and U.S. Department of Labor (DOL). The goal of the study is to provide the Federal Government with feedback regarding how a future evaluation of these programs could be designed.
Our visit here today is a part of the study to learn about how these programs are implemented. We are conducting a total of six 3-day site visits to selected programs to talk with [apprentices, LTC RAP directors and staff; employer staff (if different from the LTC RAP director and staff), related instruction providers (either onsite or offsite); state workforce agency liaisons; state and local workforce investment board (WIB) staff; and DOL Office of Apprenticeship (OA) state and regional directors]. Our aim is to learn from your experiences, not audit or judge your programs.
Confidentiality Statement: Before beginning the interview, I (we) want to thank you for agreeing to participate in the study. I (we) know that you are busy and we will try to be as focused as possible. We have many questions and are going to talk to many different people, so please do not feel as though we expect you to be able to answer every question. Your participation in this discussion is voluntary and you may choose to not answer questions you do not wish to.
In addition, before we start, I want to let you know that though we take notes at these interviews, information provided will not be linked with the name of the person who provided the information in our report about the site visits. When we write about our findings, information from all interviews is organized and presented so that no one person can be identified.
With your permission, we would like to tape record the interview so that as we review our notes, if anything is unclear, we would review that part of the tape to clarify what was said. After the interview, we will send you our written notes regarding the interview to receive any comments you may have for us. Do we have your permission to tape record the interview?
Yes No
Do you have any questions before we begin?
Will you participate?
Background Information and Program Context
- Before we begin, wed like to get some general information on you and verify some information about your Registered Apprenticeship Program. [Ask for a card.]
- Name and Title
- Organization name
- Contact information (address, telephone, fax, e-mail)
- Web site address
- Role in Registered Apprenticeship Program and how long involved in program
- We learned a little about your organization from public sources. (Tell them 2-3 things). Would you provide some additional background about your organization and its workforce needs? How does the local labor market affect your hiring and retaining of long-term care staff? [Look up information on company/organizational information, occupations and skills needed for organization, and local labor market conditions prior to visit.]
- What are your reasons for participating in a Registered Apprenticeship Program? How was it decided to use registered apprenticeship rather than other training options?
- What were the main goals/purposes of yourRegistered Apprenticeship Program?
Design and Early Implementation
- Please describe how your Registered Apprenticeship Program is designed and how these features compare to other training options.
- Occupation(s) of focus [CNA, DSS, HSS, and/or HHA]
- Skills/competencies to be learned [consult work process documents from DOL]
- Length of the program
- Number of apprentices active at this time and over the course of the year.
- Selection process for apprentices
- Time spent in structured on-the-job training (OJT) per week and over the course of the program
- Time spent in classroom or on-line receiving related instruction per week and over the course of the program
- Milestones (such as interim credentialing, advanced training) and testing
- Scheduled salary increases through the program (wage progression)
- Mentoring or informal peer-to-peer support
- Intended outcomes such as licensure, retention, or promotion
- How did the start-up and early implementation of your Registered Apprenticeship Program proceed (e.g., on-time, slow, etc.)? What financial resources or materials, or additional personnel or organizational relationships, did you need to begin the program? What factors facilitated project start-up? What factors hindered project start-up? How were they resolved?
Recruitment of Apprentices
- How do you recruit participants? What incentives (if any) are used to encourage participation? How does recruitment into your Registered Apprenticeship Program differ from recruitment activities for other training programs you offer?
- Is there an application process or test for employees or individuals to be accepted into your Registered Apprenticeship Program?
- Has it been easy or difficult to recruit participants into your Registered Apprenticeship Program? If there are difficulties in recruiting enough apprentices, what factors make recruitment difficult?
Training
- What does the training curriculum contain? May we view/have copies of any materials used?
- How is the time spent in OJT structured (e.g., duration, frequency, content)?
- Who is providing instruction, supervision, and mentorship? What qualifications do they have?
- What other resources are needed for the OJT (e.g., equipment)?
- What skills are apprentices learning and how are they learning them?
- How is the time spent in related instruction structured (e.g., duration, frequency, content)?
- Where is the related instruction provided -- onsite or at a separate training provider (e.g., community college, vocational/tech school, WIBs, in-house, other)?
- What are the qualifications of the instructors (e.g., nursing degree)? If in-house, what challenges, if any, have there been in hiring and retaining instructors?
- Who pays for the related instruction?
- Do apprentices receive any funds from the local One-Stop or WIB for related instruction? Does your state provide tuition subsidies for apprentices?
- Is the time spent in related instruction paid by the employer (i.e., is this time spent in the classroom during work hours)?
- What costs does an apprentice incur for participating in your Registered Apprenticeship Program (e.g., tuition, books, equipment)?
- How is the apprentices overall progress monitored? Who is responsible for the apprentice? How does coordination occur between the onsite mentor or supervisor and classroom instructors?
- How does your training program compare to other training programs for this occupation?
Partnering (where relevant, questions are also asked of employers and other types of co-sponsoring organizations including unions, associations, and government agencies)
- Please describe the key partnership(s) with other organizations for your Apprenticeship Program, including the role and responsibilities of each partner:
- Federal/state/regional apprenticeship organizations
- Education/training organizations (e.g., community colleges, universities/colleges, technical schools, state boards of nursing)
- One-Stop Career Centers/WIBs
- Employer or industry associations
- Labor-management organizations
- Others?
- How are employers recruited?
- Do one or more partners operate in multiple states?
- How were partnerships formed? Evolved over time?
- How do partners work together and communicate?
- How do partners ensure quality of training?
- Were there any organizations that you wanted to be more involved but were not? What were the reasons for their lack of involvement?
Staffing and Resources
- Please describe your Registered Apprenticeship Programs management and staffing structure:
- Type and number of project staff
- Their roles in the program (e.g., clinical experience, mentors, classroom/related instruction)
- Employed versus contracted staff and oversight
- Location of staff
- Experience and/or credentials
- Frequency of turnover and recruitment process for new staff
- What are the major ongoing costs/expenditures for your Registered Apprenticeship Program? [If available, obtain budget document.]
Apprentice Participation and Characteristics
- How many apprentices are currently enrolled in your Registered Apprenticeship Program? How many apprentices have been enrolled over the life of the program regardless of whether they completed their apprenticeship? How many apprentices are enrolled over the course of a year?
- What are the important characteristics of your apprentices? [Review data in RAPIDS prior to the site visit.] Are there challenges with particular groups of apprentices (e.g., English as 2nd language, literacy, cultural/ethnic differences)?
- How many apprentices have completed your Registered Apprenticeship Program? Of those that completed the program, how many are still working at your company/organization? Are they still working in the same role, or have they changed jobs/been promoted in the organization? What challenges have apprentices experienced in completing the program? Have you been able to take any action to help apprentices complete the program?
- Have any apprentices dropped out of your Registered Apprenticeship Program? What have been the reasons for leaving the program?
- How far did they make it in the program before leaving? Do you know what any of them are doing now?
Apprenticeship Outcomes
- What measures do you use to assess the benefits of apprenticeship to participating apprentices (e.g., length of employment or promotions or increased wages)?
- How do the apprentices outcomes compare to the outcomes of employees or similar groups of individuals who do not participate in the program?
- Is your company tracking the changes in retention, productivity, quality of work, skill level of employees, or your overall return on investment related to costs? What have been the outcomes to date?
- How do you collect this information and how often? Do you have a database that you use?
- What are the advantages and disadvantages of the program to the employer? What have been the advantages and disadvantages of the program to the apprentices? Overall, what were the greatest impacts of your Registered Apprenticeship Program?
- Within the Registered Apprenticeship Program, are there other approaches, strategies, or services that you believe would contribute to better outcomes for the apprentices or the company/organization?
Sustainability, Replicability and Lessons Learned
- Has your Registered Apprenticeship Program become a regular activity in your company/organization? Are you seeing a return on investment? What resources are needed to better implement and sustain the program?
- To what extent would you recommend the Registered Apprenticeship Program to employers or organizations thinking about sponsoring a Registered Apprenticeship Program?
- What features of your Registered Apprenticeship Program would you recommend to other employers or organizations in designing their program?
- What features of the project would be difficult for other employers or organizations to use in designing their program?
- Looking back, what do you consider your most important accomplishments for your Registered Apprenticeship Program?
- What do you believe to be the main lessons learned from your Registered Apprenticeship Program?
- Is there anything that we have not asked but you will like to tell us about your program?
Supplemental Questions for Other LTC RAP Respondents
Trainers/Supervisors at Apprentices Employer (if not Program Sponsor) and Related Instruction Providers
- What is your role in designing and oversight of apprentice training activities?
- What do you teach them?
- How has the training for apprentices differed from training provided to other employees/students in this occupation?
- How do you test their mastery of a particular skill or subject area?
- What resources would you need as a supervisor/trainer/classroom instructor to bring more apprentices into the program?
LTC Apprentices (Note: The team will attempt to talk to apprentices in different phases of the program -- new enrollee, middle of training, completed training, and dropouts if available)
- How did you become an apprentice? How did you find out about the program? Why did you decide to become an apprentice? How is the program different from the regular training provided by the employer to other employees?
- How does the apprenticeship program differ from other training opportunities you may have had for this or a similar job?
- What does your typical week as an apprentice look like (e.g., general schedule during the week; time in OJT versus related instruction)? What kinds of skills are you learning?
- What do you think of the overall apprenticeship program? What did you think of the training you receive while on-the-job? In the classroom? What parts of the program worked best in your opinion (e.g., mentoring, skills learned, wage increases)? What parts of the program need improvement in your opinion? How does the apprenticeship program compare to other training or education experiences you have had? How has this training helped you do your job?
- Have there been any costs to you in participating in the apprenticeship program? Is your time spent in the classroom or in on-line training on the clock, or do you have to spend your own unpaid time to complete classroom or on-line training?
- What credential(s) will you have when you complete the program? Do you earn any credentials as you progress through the program? What position or title will you have when you complete the program?
- What have been the advantages to being in the apprenticeship program? What have been the disadvantages? Would you become an apprentice again, or encourage other people to become apprentices here? What are your career goals and does this apprenticeship move you toward achieving these goals (e.g., career advancement/career lattice, intent to stay in field, commitment to job/field)?
DOL OA State or Regional Directors/State Workforce Agency Liaisons/State and Local WIB or One-Stop Career Center Staff
- What has been your involvement with the LTC RAP in your area generally? What involvement specifically have you had with this LTC RAP we are interviewing here?
- How difficult or easy is it to market the Registered Apprenticeship model to long-term care providers? What have been some of the successes and challenges in marketing Registered Apprenticeship to long-term care employers?
- How did this LTC -RAP get started?
- What have been this LTC -RAPs accomplishments to date? What are any ongoing challenges?
- In your opinion, does the LTC -RAP have the capacity to increase the number of apprentices they have? What resources do you think the program would need to do so?
Checklist of Items to Collect/Review Ahead of or During Site Visit
- Background information about the local economic conditions, local labor market data, and information on industry in the area.
- Background information about the organization.
- Additional documentation/reports detailing major program components.
- Evaluation reports that may have been prepared on the program.
- Blank set of forms used in the apprentice file.
- Diagram showing how apprentices flow through the program (if they have it).
- Organizational chart for the company/organization (if they have it).