
Accelerating Adoption of Assistive Technology
This report examines and assesses the often overlooked potential of assistive technology (AT) to benefit unpaid family caregivers who assist chronically disabled elders living at home. Although research has identified benefits, only a handful of publicly-funded family caregiver support programs give much attention to enabling caregivers’ access to AT. Strategies for disseminating and encouraging adoption of these programs’ promising practices are discussed. [109 PDF pages]
"Acronyms
| AAA | Area Agency on Aging |
|---|---|
| ABLE | Advancing Better Living for Elders |
| ACT | Advancing Caregiver Training |
| ADL | Activity of Daily Living |
| ADRC | Aging and Disability Resource Center |
| ADSSP | Alzheimers Disease Support Services Program |
| AMP | Adaptive Modification Program |
| AoA | HHS Administration on Aging |
| ASPE | HHS Office of the Assistant Secretary for Planning and Evaluation |
| AT | Assistive Technology |
| ATLAS | Assistive Technology Long-term Advocacy and Support |
| BWC | Bureau of Workers Compensation |
| CAP | Caregiver Advisory Panel |
| CAPABLE | Community Aging in Place, Advancing Better Living for Elders |
| CARES | Caregiver Adaptation to Reduce Environmental Stress |
| CAS | Consumer Assessments Study |
| CAST | Center for Aging Services Technologies |
| CATEA | Center for Assistive Technology and Environmental Access |
| CDC | HHS Centers for Disease Control and Prevention |
| CDPH | California Department of Public Health |
| CIL | Center for Independent Living |
| CM | Case/Care Manager |
| CMS | HHS Centers for Medicare and Medicaid Services |
| DME | Durable Medical Equipment |
| ESP | Environmental Skill-Building Program |
| FCA | Family Caregiver Alliance |
| FIM | Functional Independence Measure |
| FPCE | Fall Prevention Center of Excellence |
| FTE | Full-Time Equivalent |
| HHS | U.S. Department of Health and Human Services |
| HM | Home Modification |
| HSC | Health Sciences Center |
| HUD | U.S. Department of Housing and Urban Development |
| IADL | Instrumental Activity of Daily Living |
| ILRU | Independent Living Research Utilization |
| IMS | In-Home Monitoring System |
| InSTEP | Increasing Stability Through Evaluation and Practice |
| LNA | Licensed Nursing Assistant |
| MDS | Minimum Data Set |
| MFP | Money Follows the Person |
| MSD | Musculoskeletal Disorder |
| MSI | Musculoskeletal Injury |
| NAC | National Alliance for Caregiving |
| NASW | National Association of Social Workers |
| NATTAP | National AT Technical Assistance Partnership |
| NFCA | National Family Caregivers Association |
| NFCSP | National Family Caregiver Support Program |
| NIH | National Institutes of Health |
| NIOSH | National Institute for Occupational Safety and Health |
| NLS | No Lift System |
| NORC | Naturally Occurring Retirement Community |
| NRCSHHM | National Resource Center on Supportive Housing and Home Modification |
| NWTHS | Northwest Texas Healthcare System |
| OARS | Older Americans Resources and Services Instrument |
| ODEP | Office of Disability Employment Policy |
| OT | Occupational Therapy |
| PCP | Primary Care Physician |
| PIAT | Pennsylvanias Initiative on Assistive Technology |
| PT | Physical Therapy |
| RCI | Rosalynn Carter Institute for Caregiving |
| REACH | Resources for Enhancing Alzheimers Caregiver Health |
| RESNA | Rehabilitation Engineering and Assistive Technology Society of North America |
| RN | Registered Nurse |
| SCI | Spinal Cord Injury |
| SHARP | Senior Housing Assistance Repair Program |
| SW | Social Worker |
| TEP | Technical Expert Panel |
| VA | U.S. Department of Veterans Affairs |
| VHA | VA Veterans Health Administration |
Executive Summary
Introduction
Family caregivers -- including relatives, friends, neighbors, and others who provide unpaid support -- perform immensely valuable work, helping older adults with chronic disabilities get the help they need at home, rather than entering a facility. Recently, the Office of the Assistant Secretary for Planning and Evaluation (ASPE) funded a study that combined 2004 National Long Term Care Survey Caregiver Supplement data with Minimum Data Set (MDS) data to examine the impacts of caregiver stress on nursing home use (Spillman & Long, 2009). Results showed that caregiver stress was the most powerful predictor of an extended nursing home stay, accounting for about a quarter of nursing home entries from the community.
Of the dimensions of caregiver stress, physical strain followed by financial hardship, was the most powerful predictor -- higher than emotional stress or social constraints. Nearly a third (31%) of caregivers reported that caregiving is a physical strain. Caregivers interviewed for the survey indicated that physical strain from activities such as lifting and transferring was a big problem for them. In addition, over 50% of the caregivers surveyed were over the age of 65, which raises their risk of physical strain when they provide this assistance.
The problem of caregiver physical strain has received little attention in family caregiver support efforts, with most programs focused on emotional support or respite. The U.S. Department of Health and Human Services' ASPE contracted with the Lewin Group and our consultants, Drs. William Mann and Majd Alwan, for this study to lay the groundwork for accelerating the use of assistive technology (AT) and home modifications (HM) to reduce caregiver physical strain. The study has two components. For the research component, the study team conducted a systematic literature review to assess and synthesize the evidence base that AT/HM reduces family caregiver physical strain. Drawing on findings from the review, in the adoption/dissemination component, we developed user-friendly resources and recommendations to encourage and facilitate the National Family Caregiver Support Program (NFCSP) to include appropriate services to reduce caregivers' physical strain, as part of the range of services they offer. This project is funded through one of several provisions in the American Recovery and Reinvestment Act of 2009 to advance the use of technology to support older people and their caregivers.
The project focused primarily on the NFCSP as a dissemination venue because this large federal program is where many family caregivers go for support. Established in 2000 as part of the reauthorization of the Older Americans Act (Title III E) and administered by the Administration on Aging (AoA), the NFCSP funds services to support family caregivers caring for people age 60 and older and people of any age with Alzheimer's disease or related dementia. The program also supports grandparent/ relative caregivers of children and of adults under age 60 with disabilities. Allowable services include information, assistance with accessing services, counseling, support groups, training, respite, and supplemental services, which include AT/HM, transportation, medical supplies, and other services.
This final report summarizes results from all study activities. Part I is the full literature review report. An annotated bibliography of studies included in the literature review is provided in Appendix A. Part II is the report from the adoption/dissemination stage of the study, and Appendix B and Appendix C are the two guides developed to educate family caregivers and NFCSPs about AT/HM to reduce caregiver physical strain. Results of an online survey conducted by the Family Caregiver Alliance (FCA) are presented in Appendix D.
Methods
For additional details on study methods, see the literature review report (Part I and Appendix A) and the adoption/dissemination report (Part II).
Systematic Review of the Research Literature
The first component of the study was a review of the literature to assess and synthesize the evidence base on the effects of AT/HM on reducing family caregiver physical strain. Much of the research and activity on promoting technologies to reduce caregiver injuries/physical strain has focused on paid caregivers (e.g., nurses, nurse aides, orderlies), particularly those working in nursing facilities and hospitals. Thus, we examined the literature on outcomes among paid caregivers in institutional and home and community-based settings to identify implications for family caregivers. We also examined the literature on the impact of AT/HM on increasing independence of older adults living at home, because any device that increases independence for the care recipient is likely to simultaneously relieve the burden for care providers (Mann, 2001). Finally, we reviewed the small but growing body of literature on AT/HM interventions that focus on family caregivers directly.
To identify relevant published and unpublished studies, we combined a search of the academic literature in PubMed/MEDLINE with a targeted Internet search of websites with information about technology and long-term care. Additional studies surfaced through other sources, including examination of reference lists of included studies, conference proceedings, and discussions with members of the study technical advisory group and caregiver advisory group.
Development of Strategies for Increasing Dissemination of AT/HM
To develop recommendations for increasing the dissemination of AT/HM to reduce caregiver physical strain to a wider audience of family caregivers and service providers, we conducted webinars/teleconferences, site visits, and telephone interviews with experts and stakeholders.
Information about innovative strategies and recommendations for addressing caregiver physical strain were obtained through a combination of webinars/teleconferences, site visits, and telephone interviews with technical experts, family caregivers, and NFCSP staff. In addition, program officers from ASPE and AoA, along with two consultants with expertise in the design and use of AT/HM, provided input throughout the project (e.g., participating in webinar discussions, commenting on report drafts).
First, we recruited a technical expert panel (TEP) of AT/HM experts and a Caregiver Advisory Panel (CAP) of individuals with both personal caregiving experience and knowledge of broad family caregiving issues. The study team met with the TEP by teleconference/webinar in January 2010. This was followed by a teleconference/webinar with the CAP in February 2011. These discussions provided the opportunity to garner input on the draft literature review. We also met with some key experts individually by phone. In December, 2011, we convened a joint meeting of the TEP and CAP, which provided opportunity to elicit input from both groups on drafts of the two guides developed through this project and recommendations for future initiatives.
To learn about strategies for accelerating the use of AT/HM to mitigate caregiver strain through the NFCSP network, we conducted site visits to 11 NFCSP programs in person (Connecticut, Maryland, Pennsylvania, Utah) or by phone (Alabama, California, Hawaii, Illinois, Indiana, Iowa, Wisconsin). The sites represented diverse experiences with AT/HM. They included: programs using advanced/innovative approaches to providing AT/HM to family caregivers; sites that were interested in the area, but not sure how to initiate a program; and sites with no efforts specifically focused on promoting AT/HM. The selected programs also represented diverse geographic regions. We interviewed NFCSP administrators, managers, case managers (CMs), and participants at program offices and in the homes of older adults and family caregivers to gain deeper understanding of caregiver needs related to physical strain as well as effective solutions. The visits took place between June and November 2011. Information gained from the site visits was used to develop the NFCSP strategy guide. Site visit participants were asked to review a draft of this guide and provide feedback through an online tool.
After meeting with the joint TEP/CAP panel and incorporating their input on draft documents, the next step was to convene a panel of 11 NFCSP program representatives. The panel was convened in October 2011. Participants provided input on suggested strategies and resources for NFCSPs that emerged from the site visits, as well as recommendations for additional policy and research activity to accelerate the use of AT/HM to reduce caregiver physical strain. The NFCSP panel was asked to review the guides developed through this project and to provide feedback through an online tool.
Finally, the FCA conducted an online survey of family caregivers on the use of AT, which was fielded over six months. A snowball sampling methodology was used to recruit a convenience sample of family caregivers to complete the survey through the FCA, Aging and Disability Resource Centers (ADRCs), and some Area Agencies on Aging (AAAs). A total of 423 surveys were initiated. The survey inquired about experiences and needs related to AT/HM, training on the use of AT/HM, and caregiver physical strain. The Lewin Group was able to analyze those survey results for this final report.
Key Findings from the Literature Review
Findings from Facility-Based Studies
Most of the research on AT/HM to mitigate caregiver strain has been conducted with caregiving staff in nursing facilities and hospitals, while physical strain among family caregivers has received less attention. Although family caregivers perform many of the same services as caregiving staff in nursing facilities and other settings, caregivers at home are less likely to have access to assistive devices such as mechanical lifts that can help protect them from physical strain associated with caregiving. The studies based in nursing facilities and hospitals examined the effects of mechanical aids for lifting and transferring on caregiver strain. The devices were often provided in combination with other interventions such as training in device use, collaborating with caregiving staff to assess the need for AT, and "zero lift" (avoidance of manual lifting) policies. Significant positive impacts were found on reducing caregiver injuries, resulting in fewer lost workdays and long-term cost savings, and increased feelings of comfort and safety for people receiving care. These studies also reported the danger of increased caregiver injury resulting from lifting a minimal or non-weight-bearing person without a mechanical device. Important factors affecting program success included ensuring sufficient time and training to use the equipment and overcoming caregiver resistance to using new devices.
Findings from Studies with Home Care Workers
A small number of studies examined the use of assistive devices among home care workers who assist older adults living at home. In contrast to facilities, large devices such as mechanical lifts are less available in home settings where home care workers and family caregivers provide care. However, one pilot program in Canada (Craib et al., 2007) used a registry of loaner lifts as an affordable way to provide home care workers with access to ceiling lifts.
Of the few studies with home workers, most focused on the use of back-belts, and the research on the effectiveness of these devices has been mixed. In the TEP panel discussions, an expert indicated that gait belts and slings could be used, but only if the care recipient was partially weight-bearing. Waters (2007) discusses the National Institute for Occupational Safety and Health (NIOSH) lifting equation guidelines and how they relate to safe patient-handling. The guidelines state that caregivers should not lift more than 35 pounds of a patient's weight; therefore, if a patient is non-weight-bearing, they should use AT. In a NIOSH (2009) publication on Safe Patient Handling Training for Schools of Nursing, an algorithm is presented for lifting patients. They suggest that if the patient can partially bear their weight and is cooperative, then the caregiver can use a gait/transfer belt or a power-stand assist lift for the transfer.1
Findings from Studies with Older Adults Living at Home
Several experimental studies tested the benefits of providing older adults living at home with occupational therapy (OT) interventions, including AT/HM. A key element of these interventions is a person-centered approach, in which OTs assess the home and work with the older person to identify solutions to increase their capacity to age in place. All of these studies found positive results, including user satisfaction with the devices, reduced functional decline and improved functioning, reduced depression, reduced need for paid assistance, and lower expenditures for nurse and case management visits. Although this decreased need for assistance would likely reduce physical strain for caregivers (because they would be providing less care), it was not directly measured in any of the studies. Many of the devices used were low-cost, such as hand-held showers, reachers, grab bars, nightlights, and tub mats. These studies highlight the importance of assisting older adults with proper assessment of the need for AT/HM and raising awareness and acceptance of new technologies, because many older adults and family caregivers were unaware of available AT/HM solutions that might assist them. Older adult receptivity to using AT/HM was related to both the characteristics of the device, such as intrusiveness, and the characteristics of the older adult, such as social support. Also important was the capacity of service agencies to provide AT/HM to older adults, including CM and social worker (SW) training on the benefits and uses of AT/HM, and the time allocated for tasks related to these services.
Findings from Studies with Family Caregivers and Dyads
Studies testing the provision of OT services including AT/HM to family caregivers or family caregiver/older adult dyads reported positive results of this approach. Benefits included less need for assistance, reduced caregiver burden, less time spent caregiving, decrease in caregiver depression, enhanced caregiver skills, enhanced caregiver ability to self-care, fewer problem behaviors of people with dementia, and reductions in health care costs. However, none of the studies directly measured impacts on family caregiver physical strain. Similar to the studies with older adults, these studies demonstrated the effectiveness of small, low-cost devices. The most common HMs needed included enhancements to bathroom safety (grab bars, walk-in shower, hand-held showerhead, shower seat); modifications to address the older adult's memory loss (additional lights, signs, and labels); and devices for activity engagement. Family caregivers' ability to implement HM was related to attributes of the modification (e.g., the cost, ease and comfort of use), attributes of the caregiver (skills, personal resources, available supports, younger age, early adopters of technology), and the quality of the caregiver-older adult relationship. Additionally, this research highlights the importance of effective caregiver training on technology use, person-centered approaches that involve both caregivers and care recipients in identifying solutions, and CM/SW knowledge of AT/HM for family caregivers.
Conclusion and Research Gaps
The evidence suggested that a wide range of AT/HM could help prevent strains and other injuries among caregiving staff in facilities,enhance functioning and independence of older adults, reduce the need for assistance, and reduce various aspects of caregiver burden. Many of the programs found to be successful used a person-centered approach that included assessing the care recipient's environment and needs, identifying solutions, training in the use of AT/HM, addressing injuries, and assessing results, in many cases including OT.
However, additional research is needed to directly measure outcomes on physical strain among caregivers in the home. Also, additional research is needed to assess long-term impacts of various types of devices on different aspects of physical strain among family and paid caregivers in the home setting and their cost impacts. Also needed is additional research on how to overcome barriers to more widespread adoption of equipment and safe handling practices that have been found to be effective in reducing physical strain. Finally, more research is needed to develop technologies designed for use by older adults and their caregivers in the home.
Key Findings from Experts and Stakeholders
Findings from the FCA Online Caregiver Survey
The online caregiver survey showed that many caregivers are purchasing AT/HM and find it useful. However, findings also suggested a need to raise awareness of available AT/HM, to address caregivers' concerns about costs, and to offer caregiver training on AT/HM and techniques to minimize physical strain. The Internet, physicians' offices, and AAAs were the top places where caregivers go for information on AT/HM.
Strategies and Resources for Family Caregivers and NFCSPs
The site visits and discussions revealed many tips and resources that can help family caregivers reduce their risk of physical strain, assess their homes, and select, access, and pay for AT/HM. We also identified a number of innovative strategies and resources that the NFCSP network can use to assist family caregivers with AT/HM.
As a first step in disseminating this information, the study team developed a guide for family caregivers and a guide for NFCSPs. Each guide will be made available in both a print handout version and an online version and disseminated through ADRCs and various other channels. In addition, research findings from this study have been or will be presented at three national conference.2 Also, findings were presented in a guest blog on http://www.disability.gov, which is operated by the Office of Disability Employment Policy (ODEP) and has nearly 30,000 followers. Results will also be shared at a retreat of the National Association of Community Health Centers in January 2012 and the Greater Wisconsin Agency on Aging Resources Conference in September 2012.
AT Expert Panel and Caregiver Advisory Group Suggestions for Adoption/Dissemination Strategies
In discussions with experts and stakeholders, consensus emerged that accelerating the use of AT/HM to reduce physical strain among family caregivers will require a comprehensive dissemination strategy. Building on the dissemination of the resource guides developed through this project, additional recommended strategies for dissemination included:
-
Developing multiple informational resources (e.g., videos, brochures, training courses on AT/HM and preventing physical strain).
-
Disseminating the information through multiple channels (e.g., online, physicians' offices, community organizations, the media).
-
Reaching multiple target audiences (e.g., family caregivers, CMs and SWs who work with caregivers, physicians, builders, and contractors).
A suggested next step was to convene a national meeting of a wider group of stakeholders involved in AT/HM for older adults and their caregivers, to develop and carry out a dissemination plan. Panel participants noted that this could provide opportunity for the AoA Aging Network to establish new partnerships.
AT Experts and Family Caregiver Advisory Group Suggestions for Policy
In addition, panel participants agreed that overcoming barriers to family caregiver use of AT/HM will also require changes to several aspects of health, long-term care, and housing policy, including:
-
Challenges to accessing AT/HM should be addressed within programs that offer and/or pay for some AT/HM services (e.g., Medicare, Medicaid, U.S. Department of Housing and Urban Development (HUD) housing assistance programs). Experts and stakeholders recommended expanding coverage to include a comprehensive array of AT/HM, to respond to individual needs for support to retain independence and live at home. In addition, these programs need to be better aligned in support of the common goal of supporting family caregiving and community living for older adults.
-
Another frequently mentioned recommendation was to expand coverage in public programs for OT and physical therapy (PT) services. OTs can provide in-depth assessment of a person's home and suggest specific solutions that could help the person maximize function and retain independence.
-
Another issue raised by several panel participants is the need to modify housing and zoning laws to support aging in place and multi-generational living and to enact policies encouraging universal design in new construction.
Suggestions for Future Research
The discussions indicated two broad areas where additional research is needed:
-
To develop and expand AT/HM efforts, additional research will be needed to identify effective approaches and evaluate their impacts on reducing caregiver strain, increasing independence of the care recipient, and saving costs. These research questions could be addressed through a potential demonstration project.
-
Also needed is additional research to develop and test new AT/HM products designed specifically for family caregivers and older adults living at home. Panel participants discussed that one of the barriers to using AT/HM is that many products are designed for use in institutions, rather than in the home.
Conclusion
The above recommendations suggested by experts and stakeholders are supported by the research literature. Implementing these actions to encourage the use of AT/HM to reduce caregiver physical strain would also support recent federal efforts to promote community living, evidence-based health care, and cost savings.
References
Craib, K., Hackett, G., Back, C., & Cvitkovich, Y. (2007). Injury rates, predictors of workplace injuries, and results of an intervention program among community health workers. Public Health Nursing, 24(2), 121-31.
Mann. W.C. (2001). Potential of Technology to Ease the Care Provider's Burden. Rehabilitation Engineering Research Center on Aging. Report for National Institute on Disability and Rehabilitation Research, U.S. Department of Education.
NIOSH. (2009). Safe Patient Handling Training for Schools of Nursing. NIOSH Publications and Products. Retrieved from: http://www.cdc.gov/niosh/docs/2009-127/.
Spillman, B.C., & Long, S.K. (2009). Does high caregiver stress predict nursing home entry? Inquiry, 46(2), 140-161.
Waters, T. (2007). When is it safe to manually lift a patient? American Journal of Nursing, 107(8), 53-59.
Part I. Literature Review
Introduction
Family caregivers -- including relatives, friends, neighbors, and others who provide unpaid support -- perform immensely valuable work, helping older adults with chronic disabilities get the help they need at home, rather than entering a facility. Recently, ASPE funded a study that combined data from the 2004 National Long Term Care Survey Caregiver Supplement with MDS data to examine the impacts of caregiver stress on nursing home use (Spillman & Long, 2009). Results showed that caregiver stress was the most powerful predictor of an extended nursing home stay, accounting for about a quarter of nursing home entries from the community. Of the dimensions of caregiver stress, physical strain, followed by financial hardship, was the most powerful predictor -- higher than emotional stress or social constraints. Nearly a third (31%) of caregivers reported that caregiving is a physical strain. Caregivers interviewed for the survey indicated that physical strain from activities such as lifting and transferring was a big problem for them.
Common causes of physical strain among all caregivers are transferring/lifting individuals and communication problems with people with dementia (Wångblad, Ekblad, Wijk, & Ivanoff, 2009). Oftentimes people with dementia become confused due to their inability to interpret signals from their bodies or from their surroundings, which contributes to resistance towards caregivers when they attempt to transfer them. In addition, over 50% of the caregivers surveyed were over the age of 65, which raises their risk of physical strain when they provide this assistance.
The problem of physical strain has received little attention in family caregiver support efforts, with most programs focused on emotional support or respite. A recent two-part study sought to identify ways to accelerate the use of AT/HM to reduce physical strain among family caregivers. Part I and Appendix A summarize the research component of the study, which involved a systematic literature review to assess and synthesize the evidence base for AT/HM in reducing family caregiver physical strain. Part II will present findings from the adoption/dissemination component which focused on developing user-friendly resources and suggestions for how to encourage and facilitate the spread of AT/HM to mitigate family caregiver physical strain. Examples of dissemination materials are provided in the Appendices.
Comprehensive Literature Review
To enhance understanding of AT/HM interventions that could benefit family caregivers, we included published and unpublished research on:
-
Technologies and programs designed to reduce physical strain/injuries among caregiving staff in institutions/residential facilities (nursing facilities, hospitals, assisted living facilities). Compared with the scant literature on family caregiver physical strain, more research activity has focused on technologies to reduce injuries among paid caregivers, with most of the focus on caregiving staff in nursing facilities and hospitals. Workers in nursing and residential care facilities experienced the highest injury rates of any occupational setting in 2010, according to data recently released by the U.S. Bureau of Labor Statistics (PHI National, 2011). This literature is relevant to family caregivers, because although paid caregivers and family caregivers have different circumstances, they provide many of the same types of support and have many of the same physical needs (DSW Resource Center, 2011).
-
Technologies and injury prevention programs designed to reduce physical strain/injuries among the home care workforce.
-
AT/HM services designed to promote independence of older adults with disabilities living at home. While the focus of this study is on reducing physical strain for caregivers, any device that increases the level of independence for the care recipient is likely to simultaneously decrease the amount of assistance needed and thereby indirectly relieve burden for care providers (Mann, 2001).
-
Programs providing AT/HM services with a direct focus on family caregivers.
To identify relevant published and unpublished studies, we combined a search of the academic literature in PubMed/MEDLINE with a targeted Internet search of websites with information about technology and long-term care. These websites included the National Rehabilitation Information Center literature database (http://www.naric.com/research/rehab/default.cfm), http://www.techforltc.org, http://www.hcbs.org, http://www.colemaninstitute.org, http://www.abledata.com, http://www.gerontechnology.info, and http://www.caregiver.org. Additional studies surfaced through other sources, including examination of reference lists of studies included in the literature review, conference proceedings, and discussions with members of the study's TEP and CAP.
To address the study objectives, the PubMed search combined statements for five concepts: (1) caregivers/care settings, (2) physical strain, (3) AT, (4) HM, and (5) physical strain prevention efforts (Table A-1). A preliminary search led to many studies touching on the topic of AT and caregiver physical strain, including many laboratory tests of devices. The scope of the review was then refined to exclude laboratory studies and focus on studies examining the use of AT/HM in real-world settings. The review was limited to English language articles involving adult participants, excluding articles about caregivers of children with disabilities because they would likely need different types of technologies. We included studies with any type of design that addressed the research questions.
The final search strategy was executed in PubMed/MEDLINE on October 14, 2010, and resulted in a total of 431 "hits." An updated search was carried out approximately one year later, on October 6, 2011, to identify new studies published during the past year, which yielded an additional 15 hits, for a total of 446 articles.
A data abstraction table (Appendix A) was used to enter detailed information on included studies, including bibliographic information; details on the population, setting, and intervention examined (types of AT/HM, funding); findings (economic impacts, impacts on caregiver injury/strain, other outcomes for caregivers and care recipients, and lessons learned); and recommendations provided by study authors, based on full-text review of the studies. To assess the strength of the evidence, we also extracted details on each study's design, sample, methods, and limitations. Two researchers reviewed each entry.
Results
Overall Search Results
We screened the 446 abstracts and titles resulting from the PubMed searches to identify potentially relevant studies; 409 studies were excluded because they did not meet the inclusion criteria, and 37 were retrieved for closer evaluation (Figure A-1). Upon full-text review, 12 studies were determined not to meet the inclusion criteria, and the remaining 25 articles were included. Although the targeted website search provided some relevant background information, the targeted sites (listed in the 'Methods' section) did not yield any studies that met the inclusion criteria for this study. Twenty-seven relevant studies were identified through other sources (e.g., reference lists of included studies, conference presentations, suggestions from the TEP and CAP), for a total of 52 included articles.
To rate the strength of the evidence provided by each study, we used an adapted version of Moore, McQuay, and Gray's (1995) five-tiered model for rating research design strength (Table A-2). None of the studies achieved the highest level of design: a systematic review of multiple randomized controlled trials. Overall, 17 of the studies were randomized control trials, six were quasi-experiments with a comparison group, 18 used a single group pre/post-design, five were non-experimental (e.g., retrospective studies), and six used qualitative methodologies. To assess the generalizability of the studies, we also examined the participants and settings represented in each study.
Data were not comparable across studies because the included studies varied in design, methods, intervention, study population and setting. Many of the studies focused on interventions targeting workers in nursing facilities and hospitals (21 studies); no relevant studies focused on assisted living. Most of the studies involved a small number of participants and facilities, often limited to a single facility. The research involving the home care workforce was quite limited (four studies). The Centers for Disease Control and Prevention's (CDC) NIOSH (2009) recently recognized this research gap of limited studies addressing AT to reduce physical strain for home care workers, noting "a particular need to address musculoskeletal disorders (MSDs) in the home health setting where interventions such as lifting equipment are generally unavailable." Another noted research gap in the home care field is how to overcome barriers to implementation of equipment and safe handling practices that have been found to be effective (NIOSH, 2009). Sixteen studies focused on AT/HM to promote independence of older adults with disabilities living at home, of which ten were randomized controlled trials. Eleven studies involved family caregivers or the care receiver/family caregiver dyad.
Evidence from Studies with Caregiving Staff in Facilities
Of the 21 studies based in nursing homes and hospitals, 12 focused on the effects of specific technologies and training (Table A-3) such as mechanical lifting devices. Although data are not comparable across studies due to differences in the interventions, study design, outcome measures, and time period examined, a common finding was that many devices lessened physical strain and decreased worker injuries.
In studies incorporating feedback from caregiving staff, the caregivers reported reductions in perceived physical strain. This was measured in terms of perceived exertion (Owen, Keene, & Olson, 2002); perceived risk of injury/discomfort and ease of lifting patients (Engst, Chhokar, Miller, Tate, & Yassi, 2005); perceived force used (Engst, Chhokar, Robinson, Earthy, & Yassi, 2004); perceived physical stress (Owen & Garg, 1994); perceptions of fatigue, comfort with tasks, and safety (Yassi et al., 2001); and reported comfort and ease of using the devices (Hunter, Branson, & Davenport, 2010).
Several studies using quasi-experimental designs found that assistive devices reduced worker injuries, particularly back injuries and musculoskeletal injures (MSIs). Several studies also reported fewer workdays lost as a result of the reductions in injuries (Owen, Keene, & Olsen, 2002; Engst et al., 2004; Alamgir et al., 2008; Chhokar, Engst, Miller, Robinson, & Tate, 2005; Li, Wolf, & Evanoff 2004; Park, Bushnell, Bailer, Collins, & Strayner, 2009). All of the studies examining cost impacts reported savings when AT was consistently used, due to reduced workers' compensation claims costs (Chhokar et al., 2005; Li, Wolf, & Evanoff, 2004; Park et al., 2009). Engst et al. (2005) found a 68% decrease in compensation costs related to transferring and lifting injuries, but a 53% increase in costs related to re-positioning injuries, which may have been because the caregivers were less likely to use AT for re-positioning patients. In several of the studies that examined long-term impacts, direct cost savings were not fully realized until a few years after program inception (Chhokar et al., 2005; Alamgir et al., 2008, Engst et al., 2005).
A few studies identified problems with the design of some commonly used devices, in particular sliding sheets, causing these devices to be ineffective at reducing caregiver physical strain. In a survey of over 1,000 nurses in two states, Trinkoff, Brady, and Nielsen (2003) found that the availability of lifting teams and lifting devices were associated with lower odds of MSD, but transfer boards/sliding sheets and adjustable beds were associated with higher odds of back MSD for those who use the devices. Consistent with these findings, a study by Baptiste, Boda, Nelson, Lloyd, and Lee (2006) found that caregivers preferred the air-assisted devices; caregivers ranked the draw sheet last in comfort, ease of use, perceived injury risk, time efficiency, and patient safety. The study noted that this is important because the draw sheets were one of the most commonly used transferring devices in caregiving institutions.
Nine studies evaluated more comprehensive multi-component injury prevention programs in nursing homes or hospitals (Table A-4). In addition to providing assistive equipment and training, common components of these programs also included: assessment of the need for AT devices through observations or interviews with caregiving staff (Hunter, Branson, & Davenport, 2010; Lynch & Freund, 2000; Owen & Garg, 1994); having patient-handling staff test equipment before purchase/installation (Charney, Simmons, Lary, & Metz, 2006; Engkvist, 2006); involvement of caregiving staff beyond intervention participant role (Brophy, Achimore, & Moore-Dawson, 2001; Nelson et al., 2006); and a more involved approach to handling workers who were injured (Collins, Wolf, Bell, & Evanoff, 2004; Morgan & Chow, 2007). Many of the interventions discussed in these studies also adopted a "no" or "zero lift" policy (i.e., requiring use of assistive devices and prohibiting or minimizing manual assistance).
Most of the studies examining multi-component ergonomic interventions found evidence of significant decreases in workplace injuries. A randomized controlled trial to test the effect of various patient-handling devices did not find a statistically significant change in injury rates over the one-year period of the intervention, although it did find other positive outcomes (Yassi et al., 2001). In a randomized controlled trial corresponding with the Yassi (2001) study, the new AT had mixed effects on different types of physical strain: it reduced peak spinal loading for several patient-handling tasks, but increased cumulative spinal loading, which could present problems for caregivers over the long term (Danyard et al., 2001). In a one-year back injury prevention program, Lynch and Fruend (2000) found that the number of back injuries after implementation of the program was 30% lower than during the prior three years' average. Engkvist (2006) analyzed the effects of a No Lift System (NLS), and found that, in comparison to nurses at two hospitals without the NLS, nurses at the NLS hospital reported fewer injuries, less pain/symptoms, less absence from work due to musculoskeletal pain/symptoms, and less physical tiredness.
Over half of the multi-component facility intervention studies reported economic outcomes and all of these studies found evidence of significant savings due to reduced workers' compensation claims (Hunter, Branson, & Davenport, 2010; Morgan & Chow, 2007; Charney et al., 2006; Nelson et al., 2006; Brophy, Achimore, & Moore-Dawson, 2001; Collins et al., 2004). Nelson et al. (2006) also reported improvements in job satisfaction.
These studies also reported positive results for care recipients. Charney et al. (2006) reported that patients received fewer injuries, like skin tears or falls, when using various AT equipment. In Owen, Keene, and Olson (2002), surveyed patients at an intervention site felt more comfortable and secure being transferred using assistive devices. Similarly, in another study residents at a nursing home felt more comfortable and secure being weighed using a hoist or a wheelchair ramp, in comparison to the manual transfer from wheelchair to scale (Owen & Garg, 1994). Engst et al. (2004) found that patients were less agitated being transferred from bed to toilet using AT, in comparison to the manual transfer or being cleaned in bed. A decrease in agitation was also noted in Collins et al.'s (2004) study, in which violent physical acts by patients decreased upon implementation of a safe patient-handling program. Hunter, Branson, and Davenport (2010) found that patients provided positive feedback about the lifting equipment.
In a few studies, a major barrier to implementing AT such as ceiling lifts or stand-up lifts was the amount of time that it took for caregiving staff to use (Engst et al., 2005; Engst et al., 2004; Li, Wolf, & Evanoff, 2004). Other concerns were that staff felt their jobs were more hectic and were more worried about making mistakes when using assistive devices (Engst et al., 2005), which the authors potentially attribute to the increased training and time needed to use the devices.
Other studies identified barriers related to the facility culture or management practices. Khatutsky, Wiener, and Anderson (2010), using national data sets, found no evidence that lifting device availability reduced the probability of being injured. However, mandatory overtime, poor training, being a new worker, and not having enough time to provide activity of daily living (ADL) help did increase the probability of being injured. In the study by Hunter, Branson, and Davenport (2010), the purpose of the three-year program was to instill a culture change in the institution; however, one of the challenges the program ran into was staff resistance to this change from current practices.
Evidence from Studies with Home Care Workers
Four studies (Table A-5) found that reductions in physical strain for home care workers who used AT, including redesigned clothing for persons in wheelchairs (Nevala, Holopainen, Kinnunen, & Hanninen, 2003) and injury prevention programs involving back-belts (also called back braces) (Kraus, Schaffer, Rice, Maroosis, & Harper, 2002; Leff, Habenback, & Marn, 2000). In the Leff, Habenback, and Marn (2000) study, injury reductions were not realized until about a year into the program, suggesting that persistent use of multiple interventions over time may be needed. Craib, Hackett, Back, and Cvitkovich (2007) found that, although the group receiving interventions including education and access to a lift registry experienced fewer time-loss injuries, reporting of injuries was higher. The authors suggested that this may be because the intervention increased workers' ability to recognize injuries and awareness of how to report them. A limitation of this research is that these studies were conducted with small samples in a single agency.
A 2008 review of the literature on the effectiveness of lumbar supports (not specific to caregivers) found a need for additional research, including randomized controlled trials, to determine their effectiveness for preventing low-back pain (van Duijenbode, Jellema, va Poppel, & Tulder, 2011).
Another finding from the studies on home care workers is that some groups of these workers were more at risk of injury than others. Workers at greater risk for new lower back injury included those with a greater body mass index, those with back problems at entry into the study, and those with a history of back injury (Kraus et al., 2002), as well as full-time workers and those with less than college education (Craib et al., 2007).
Evidence from Studies with Older Adults with Disability Living at Home
All of the studies of AT/HM interventions targeting adults with disabilities living at home found positive effects, primarily enhanced independence (Table A-6). In the Massachusetts low-cost AT demonstration, 90% of clients reported satisfaction with the low-cost devices, 60% found them to be "very helpful," and 70% used them regularly. Petersson, Lilja, Hammel, and Kottorp (2008) found that older adults with disabilities in Sweden who received HM significantly improved in self-reported independence and safety with toileting tasks and transferring tasks such as getting in and out of the home. In a randomized controlled trial study by Mann, Ottenbacher, Fraas, Tomita, and Granger (1999), participants who received a functional assessment, a home environment evaluation, and AT/HM based on their evaluation results experienced less functional decline than the control group. Participants also incurred less expenditures for nurse and case management visits. Liu and Lapane (2009), analyzing data from the Second Longitudinal Study on Aging, found that HM (like railings or bathroom modifications) were associated with reduced risk of decline among community-dwelling adults aged 70 and older. Stark, Landsbaum, Palmer, Somerville, and Morris (2009) found that adults in a suburban naturally occurring retirement community (NORC) improved significantly in their subjective ratings of their daily activity performance after receiving a HM. The improvement was maintained for two years.
In a non-randomized, single group pre/post study, Horowitz, Brennan, Reinhardt, and MacMillan (2006) reviewed the effects of optical and adaptive devices on disability and depression among older adults who had acquired a recent vision impairment and who were applying for vision rehabilitation services. They interviewed the sample (n=138) at pre-service and at 5-month follow-up. Participants were asked about their use of optical devices (including magnifier, telescope, special sunglasses, or other) and adaptive aids related to vision loss (large-print telephone dials, handwriting guides, talking books, other talking items, large-print reading materials, long white cane for mobility, or other aids). Researchers found that use of optical devices was significantly associated with declines in functional disability and depressive symptoms over time. These results were not found with adaptive devices.
Wilson, Mitchell, Kemp, Adkins, and Mann (2009) conducted a randomized controlled study to examine an AT/HM intervention's impact on functional decline of aging individuals with a disability. The study involved 91 participants with a variety of impairments. The intervention group received an evaluation of their home and potential AT/HM needs, which the study provided, paying part or all of the cost. The AT included a variety of devices, such as grab bars and bath benches. HM included ramps, widening doorways, and lighting/electrical changes. The intervention also included adaptive behaviors or changes in task performance to help reduce strain. The control group received health care already available through community resources. Outcomes were tracked through in-home interviews using the Older Americans Resources and Services Instrument (OARS) and the Functional Independence Measure (FIM). Analysis showed slower decline in function in the treatment group over the two-year intervention period. Additionally, that group was found to be more likely to use AT instead of personal assistance to maintain their independence.
Several studies with older adults living at home examined multi-component programs with an OT component for adults with a disability living at home and found positive outcomes. Participants in the Advancing Better Living for Elders (ABLE) program (Gitlin et al., 2006; Rose, Gitlin, & Dennis, 2010), an ongoing clinical trial begun by the National Institutes of Health (NIH) in 2005, experienced less difficulty with ADLs and instrumental activities of daily living (IADLs). ABLE provides five OT visits, a PT visit, and identification and installation of appropriate HM for adults age 70 and older (Gitlin et al., 2006). Average costs per ABLE participant were $439 for equipment and HM and $783 for therapy, for a total of $1,222. Researchers recommended that HMs be reimbursable through Medicare, which is not part of current policy (Gitlin et al., 2006).
Building on the ABLE demonstration, the Community Aging in Place, Advancing Better Living for Elders (CAPABLE) pilot is comprised of the ABLE program, a person-centered nurse intervention, and home safety/modification handyman services (Szanton et al., 2010). The program aims to enhance low-income older adults' ability to age in place and improve the functionality of their homes and was described as: "Each service synergistically builds on the others by increasing the participants' bio-psycho-environmental capacity to function at home." The pilot was theorized to avert costly health utilization by increasing medication management, problem-solving ability, strength, balance, nutrition, and home safety, while decreasing depression and risk of falls. Szanton et al. (2011) performed a prospective randomized controlled pilot trial of the CAPABLE pilot with 40 low-income older adults with one or more ADL difficulties or two or more IADL difficulties in the Baltimore, Maryland area. The intervention group (n=24) received up to six OT visits, up to four nurse visits, and handyman repairs and modifications costing an average of $1,300. The control group (n=16) received the same number of visits, but with a trained research assistant who was not an OT or a registered nurse (RN) and participated in sedentary activities of their choice (like scrapbooking). The OT assessed the home for HM needs, coordinated with the handyman to install the HM, and trained the individual using the HMs, which included grab bars, rails, and raised toilet seats. Nearly all (94%) of the intervention group stated that CAPABLE made their lives easier, compared to 53% of the control group. Szanton et al. (2011) noted that the intervention making their lives easier is theoretically connected to a decrease of functional difficulties. They suggest that future research review the potential effects on long-term outcomes, including nursing home admissions.
Similarly, in the Howard County/Montgomery County (Maryland) Aging in Place/Better Living at Home program OTs, SWs, community health nurses, and older adults collaborate to facilitate independence and aging in place for older adults, using AT/HM (Sheffield, 2011). The OT provides a comprehensive person-centered evaluation of the home, including the physical, psychological, social, and financial strengths and needs of the client. The OT works with the person to prioritize needs and develop appropriate solutions, such as developing emergency response plans, removing environmental hazards, providing adaptive equipment and training in adaptive equipment, and providing education in adaptive strategies for daily activities. The retrofit specialist provides logistical support to implement the identified solutions. Existing community resources and funding sources are used to pay for AT/HM when possible. Frequently prescribed equipment included hand-held shower holders, reachers, tub benches, tub mats, raised toilet seats, grab bars, bedrails, night lights furniture risers, and pill dispensers. Results of a randomized trial indicated that the intervention reduced hours of paid weekly assistance by 43% and cost less than $1,000 per person served (Sheffield, 2011). On average, $150 was spent on equipment for the participants, with the rest of the money going to the OT/SW assessment. The estimated one-year savings per client was $3,133 in Howard County and $4,631 in Montgomery County. The estimated program savings, then, was approximately $7,000 for every $1,000 spent on the intervention. Using funds saved from reduced service needs, the program has expanded to serve more people. This intervention improved functional independence and safety, decreased fear of falling, and showed an increase in quality of life (Becker, 2011).
In the Assistive Technology Long-term Advocacy and Support (ATLAS) intervention, aging individuals with intellectual disabilities and their social support network worked with an OT for four sessions to identify and problem-solve issues through environmental strategies, including AT/HM, using a consumer-directed, collaborative approach (Mirza & Hammel, 2009). The intervention was theoretically based on the Competence-Environmental Press Framework that was applied and adapted by Gitlin. Consistent with findings from similar interventions reported above, ATLAS was associated with higher levels of performance and satisfaction.
The Increasing Stability through Evaluation and Practice (InSTEP) program, conducted by the Fall Prevention Center of Excellence (FPCE), also incorporates an OT component and home assessments (FPCE, 2011). The FPCE is a consortium of the University of Southern California Leonard Davis School of Gerontology; the Veterans Administration Greater Los Angeles Healthcare System Geriatric Research, Education, and Clinical Center; California State University Fullerton's Center for Successful Aging; the California Department of Public Health State and Local Injury Control; and the University of California, Los Angeles School of Medicine. InSTEP, which is offered through community centers, includes an exercise program and assessment of medical and home risks for older adults at risk for falls. The program includes three models, with the high-intensity model including a home evaluation and follow-up by an occupational therapist whoprovides referrals for HM. The InSTEP program is currently being tested, but preliminary data indicate improvements in balance and mobility and improved understanding of risk factors associated with falls.
A case study of Lutheran Homes of Michigan suggests that telehealth devices can help reduce hospital readmissions among older adults (Gehm, 2011). In exploring ways to help older adults remain in their homes, the organization established the Aging Enriched Network, a one-stop model for information and referral to a wide range of services that older adults need to stay at home, including home health care and telehealth and monitoring systems. The services are offered by Lutheran Homes or pre-screened providers. It also features a call center and a shared electronic health referral and record exchange program. The organization receives discharge notices from the local hospital and it connects older adults to home care or subacute care services. In a small study of the telehealth program, 12 of the 15 people who were discharged from the hospital without a telehealth device experienced a readmission or an unexpected revisit to a physician, compared to one or two of the 18 members of the telehealth group.
A few studies examined factors related to the readiness of older adults with disabilities to use AT/HM. In the ABLE study, higher readiness to use technology was associated with: younger age, African Americans with financial difficulties, use of active-oriented compensatory strategies, use of cognitive oriented strategies, and less depression (Rose, Gitlin, & Dennis, 2010). The strongest predictor of change in readiness to utilize compensatory strategies was social support.
Program capacity to provide AT/HM to older adults was another major issue noted in the literature. In the Howard County program, challenges included funding for therapists, equipment, and modifications, and using existing staff resources (Becker-Omvig & Smith, 2010). The Howard County program was able to overcome initial resistance from clients and staff through "logical arguments, emotional arguments, building trust, and concrete reality," as well as enlisting champions and showing efficacy (Becker-Omvig & Smith, 2010).
The Massachusetts demonstration highlighted several challenges related to program capacity, including that CMs need consistent training on the benefits and uses of AT (Gottlieb & Caro, 2001). The authors recommended that an expert on AT equipment be hired, that CMs allocate time for tasks related to AT, and that agencies develop systems to order and deliver equipment to clients and allocate funds for AT.
Demiris, Oliver, Dickey, Skubic, and Rantz (2008) evaluated the implementation of a "smart home" project in the apartments of nine residents of an independent retirement facility through qualitative interviews and observational sessions. This included an In-Home Monitoring System (IMS) which had a set of wireless infrared proximity sensors to detect motion and pressure switch pads. The IMS also included a stove sensor, a cabinet sensor, and a bed sensor. They identified three phases of adoption and acceptance of the sensors: (1) familiarization; (2) adjustment and curiosity; and (3) full integration. The residents reacted positively to the sensor technologies and did not feel that these interrupted their daily activities. Additionally, the residents did not express privacy concerns.
Mann, Marchant, Tomita, Fraas, and Stanton (2002) examined older adults' receptivity to home telehealth care, which they defined as the provision of health care evaluation, medical advice, and the delivery of services to the home through the use of telecommunication technologies, including information, communications, and monitoring technologies. The researchers used the Rehabilitation Engineering Research Center on Aging Consumer Assessments Study (CAS). They developed the "Home Care Monitoring Devices" questionnaire to gauge frail older adults' receptivity to devices including a thermometer, metered dosage inhaler, blood pressure monitor, blood glucose monitor, and medication compliance monitor. Results indicated that the sample strongly accepted the concept of home health monitoring and the different devices. One of the determining factors of perceived intrusiveness of these devices was equipment characteristics. An analysis of subjective comments found that participants thought these devices would be useful for others, but not necessarily for their own personal use.
Anemaet and Trotter (1999) reviewed the literature on home assessments and their effects on the safety and functional independence of older adults living at home. They made the case for home assessments being the first step in ensuring proper AT/HM are brought into the home. The authors described some of the considerations home care providers face in using a home assessment tool:
-
Comprehensive -- covers pertinent details.
-
Format and Time ease of use.
-
Guidance step-by-step.
-
Objectivity some assessments allow for an objective scoring of home safety.
Anemaet and Trotter (1999) suggest that home care providers use home assessment tools3 that include:
-
Safe at Home (Securing a Functional Environment with the Anemaet-Trotter Home Observation and Modification Evaluation). This comes in an objective form, which uses ordinal scales, as well as in a descriptive form, which does not use a scoring mechanism but is similar to the objective form.
-
The Functional Environmental Assessment. This tool takes the assessor through potential hazards in the home that can be scored based on the care recipient's difficulty with those hazards.
-
Home Safety Checklist. This was developed by the U.S. Product Safety Commission. This assessment tool lists the potential hazards in the home and providers' recommendations for addressing those hazards.
Evidence from Studies with Family Caregivers and Dyads
Several demonstration studies tested programs to provide OT services and AT/HM to family caregivers of older adults with dementia or the family caregiver dyad (Table A-7).All found positive effects for caregivers, such as reduced burden and reduced hours spent caregiving, although none of the studies directly measured impacts on caregiver physical strain. Most of the studies focused on caregivers of people with Alzheimer's, but the findings are relevant to all caregivers.
Buettner, Yu and Burgener (2010) conducted a systematic literature review of studies with rigorous research methods related to the effects of technology-based interventions for people with early-stage Alzheimer's disease. Their search yielded ten studies, only one of which focused on the effects for caregivers. That study tested the SAFE House System (Kinney, Kart, Murdoch, & Conley, 2004), which consists of a camera and sensors routed through a controlled unit to a website that is accessed with a broadband-connected computer. Caregivers are alerted through text messages from the website if any potentially unsafe activity is detected. Some of the positive benefits of the system included peace of mind for the caregivers; however, 50% of the caregivers surveyed felt that the system made their lives more difficult because of the technological burden.
NIH established the Resources for Enhancing Alzheimer's Caregiver Health (REACH) Initiative in 1995 to research interventions to support family caregivers of people with Alzheimer's disease and related disorders (Gitlin et al., 2003; Gitlin, Hauck, Dennis, & Winter, 2005; Girlin & Greening, 1997). REACH included an Environmental Skill-Building Program (ESP), which provided family caregivers with education about the disease and strategies for modifying the home to help solve problems with care recipient behaviors. Education was provided through visits with OTs who also provided problem-solving training and adaptive equipment. Caregivers participating in REACH reported being less upset with memory-related behaviors, less need for assistance, better affect, and tended to maintain skills at 12 months. Upon demonstrating that this program was successful in reducing caregiver burden and enhancing caregiver skills in managing care recipients, a recent two-year translational project was conducted by Gitlin, Jacobs, and Earland (2010) to examine the translation of the ESP for home care delivery as a reimbursable Medicare Part B Service. Caregivers received ESP training for patient therapeutic needs, as defined under Medicare Part B Service. Caregivers reported a large increase in knowledge and skills for understanding topics like dementia and home safety. A majority reported enhanced ability to care for and manage the care recipient and enhanced self-care. The translational project for funding the ESP program through Medicare Part B presents a potential future for home caregiver interventions (Gitlin, Jacobs, & Earland, 2010).
REACH VA, part of the REACH II intervention sponsored by the National Institute on Aging and the National Institute on Nursing Research, served stressed caregivers of people with Alzheimer's or related dementia from 24 Veterans' Medical Centers in 15 states (Nichols, Martindale-Adams, Burns, Graney, & Zuber, 2011). Findings at 6 months from the REACH VA initiative found that problematic behaviors of care recipients with dementia decreased (Goy, Freeman, & Kansagara, 2010). Follow-up for REACH VA found that caregiver burden and depression decreased, as did time spent caregiving (Goy, Freeman, & Kansagara, 2010). In addition, early findings from the REACH VA showed declines in inpatient, pharmacy, and outpatient costs (Nichols et al., 2011).
Gitlin, Winter, and Dennis (2010) studied 272 caregiver-patient dyads, with 136 randomized to the intervention group. The implemented intervention was Advancing Caregiver Training (ACT); this included up to eight OT sessions and two nursing sessions. This was followed by a 16-24 week maintenance phase, which included three brief OT contacts through telephone. The OT assessed the need for and willingness of the caregiver to use adaptive equipment, which was purchased and paid for through grant funding. These included devices to help with IADLs (mobility, seating, medication taking, transfers), ADLs (eating, toileting), and safety (monitoring devices). Sixty-three dyads received assistive devices, with an average of three devices per dyad. The average cost was $152.52 for ordering, delivering, and installing the equipment. At 4 months, 87.6% of devices ordered were reported as being in use and ranged from somewhat to very helpful. The most popular/needed devices were for activity engagement (e.g., games, puzzles), followed by bathroom/toileting challenges. The latter included grab bars, raised toilet seats, and tub benches. The least issued devices were for ambulation and transferring, which were also the most expensive. This study demonstrates the effectiveness of small, low-cost AT in helping to reduce caregiver burden, with bathing and toileting devices among those most commonly needed. The reported device use rate (87.6%) was high and Gitlin, Winter, and Dennis (2010) report this may have been due to the client-centered approach in the intervention, which included working with the caregiver to identify the problematic behaviors. AT was provided only when approved by the caregiver. Gitlin, Winter, and Dennis (2010) suggest that caregivers need education on the range of assistive devices and where they can obtain them, exposure to the potential benefits of the assistive devices, and training on how to use them.
A randomized controlled trial by Schulz et al. (2009) tested a program for family caregivers of people aged 35 and older with spinal cord injury (SCI). Although they did not receive AT or HM, the caregivers received in-home and telephone-based sessions to improve their knowledge about how to reduce environmental stress, in addition to how to reduce personal stress and improve health and self-care, access to support, and emotional well-being. A dyad intervention provided the same elements (like improving their own emotional/physical well-being) to care recipients and also taught care recipients ways they could help reduce caregiver burden. The intervention targeting the dyad improved quality of life of the dyad, measured by depressive symptoms, burden, social support and integration, as well as self-care problems and physical health symptoms. No significant effects were obtained for the caregiver-only intervention, raising questions about the efficacy of this approach.
Several studies examined issues affecting the successful dissemination of AT/HM to caregivers. Carswell et al. (2009) reviewed the literature related to AT solutions for people with Alzheimer's disease and examined how those solutions could relate to problems faced by the population at night. Four of the articles were night-specific and related to monitoring and guidance. They did not relate to caregiver physical strain. Fourteen papers related to both night and day AT solutions. These also did not relate to caregiver physical strain, but some of the AT related to alleviating caregiver mental or emotional strain through calming the care receiver and alleviating verbal aggression and agitation. Technologies examined in this literature included "Smart Homes" to better monitor people with Alzheimer's disease, intelligent sensors that could be used for monitoring or as an alarm system, grab bars, bathtubs, and showers. One of the researchers' suggestions for persons with Alzheimer's disease using AT is to ensure user-centered design and acceptance. They stressed the importance of involving stakeholders in all aspects of assessing for and deciding on AT for the home; this helps increase their acceptance of the AT.
As part of an ongoing randomized controlled trial of Maximizing Independence Phase 2, Marquardt et al. (2011) reviewed the barriers to implementing suggested HMs for people with dementia. An architect assessed the home environments of 82 community-dwelling elderly individuals in North/Northwest Baltimore. The assessments included observation, a house plan sketch, and a caregiver questionnaire. Results showed that the entrance and interior stairs were a major obstacle in the homes of study participants, with many lacking safety railings. Bathroom safety was also an identified obstacle, with 57% of the study already having grab bars installed and almost 50% having modifications like a walk-in shower, hand-held showerhead, or a shower seat. Caregivers' reasoning for modifying the home included the care receiver's physical limitations, most commonly for bathroom safety. Another primary reason was the care receiver's memory loss; these modifications include additional lights, signs, and labels.
Messecar (2000) interviewed 24 primary family caregivers to determine the factors affecting the caregivers' ability to implement home environmental modifications. Environmental modifications were defined as "actions taken to organize the home, protect the elderly individual, structure the elderly individual's day, supplement the elderly individual's function with devices and environmental cues, work around the limitations of the environment to provide care, and make the home more pleasing." Factors identified as affecting the caregivers' ability to implement modifications included attributes of the elderly individual, attributes of the modification, quality of the caregiver-elderly relationship, caregivers' skills, personal resources of the caregiver, and the informal and formal supports available. Messecar provides a list of recommended interventions to help strengthen the caregiver's ability to use environmental modifications, including performing an environmental and functional assessment. They also recommended researching and acquiring modifications tailored to the individual older adult, as well as communicating with the care receiver about potential modifications and supplemental existing resources.
In the Marquardt et al. (2011) study, the caregiver's physical strain was not listed as a reason for adding modifications. However, some reasons for not accepting suggested modifications include the price and care recipient acceptance.
A recent online survey examined predictors of family caregivers' receptivity to using various types of AT, defined broadly as including training/mentoring services (National Alliance for Caregiving (NAC), 2011). Overall, caregivers were most receptive to technologies related to delivering, monitoring, tracking, or coordinating the care recipient's medical care. More highly burdened caregivers were more likely to find the following AT potentially helpful: an interactive system for physical, mental, and leisure activities; a passive movement monitoring system; caregiver training simulations; caregiving coaching software; and a caregiver mentor matching service. The following groups of caregivers were more likely to express receptivity to technologies: caregivers under age 50, early adopters of technology4 (vs. late adopters), caregivers of minority race/ethnicity (African American, Hispanic, Asian American, or other) over the age of 50 (vs. European American caregivers over age 50). The most commonly reported obstacle was the belief that the technology would be expensive.
Another major factor affecting caregiver and care recipient receptivity to AT noted in the literature is the level of ease and comfort of using the device for caregivers and care recipients. Mann (2010) found that wheelchairs and lifts, the most frequently used devices for mobility, were both very problematic in a home setting. One of caregivers' main concerns was that transferring a person without a lift seemed easier than using a lift, due to potential and/or actual discomfort of the person being assisted when a lift was used. In addition, family caregivers noted that transferring a person manually was more efficient than using a lift: one caregiver stated that transferring a care recipient manually took 20 seconds, while using an electronic lift took four minutes. Similarly, in a study by Messecar (2002), family caregivers said that environmental modifications had a few negative outcomes, including that it increased their workload.
The National Research Council, Committee on the Role of Human Factors in Home Health Care (2011a) developed a guide to human factors design considerations for health information technology in the home, focusing on computer or sensory and surveillance technology. The authors posited that designers and developers need to consider all factors, including the person with the disability and care provider, the tasks, the equipment and technology, and the environment. A specific guideline was that "devices should require minimal force, repetitive action, and sustained physical effort for operation." They should also be customizable to accommodate differences in individuals' height, reach, and range of motion.
A companion book, Health Care Comes Home: The Human Factors (National Research Council, 2011b), recommended including care recipients and home caregivers in the testing of medical devices that may be used in the home in order to reduce risk and analyze the appropriateness of technologies for the home. The authors noted that devices designed for institutional use come with many enhancements that are not appropriate for the home and suggested that untrained users need devices to be as simple as possible. They suggested that designers develop two versions of devices, for untrained and professional users. A related consideration is assessing the home environment. Many homes are unique and not well-suited for the needs of an aging adult. Home assessments can help caregivers greatly through the introduction of simple AT/HM, like tub benches or grab bars. The authors stated that a good time for a home assessment is prior to hospital discharge, to facilitate a smoother transition to the home. Universal design, which is "intended to create residential settings that work for everyone regardless of size, age, or ability," avoids the needed costs for HM, like ramps and bathroom remodels.
The National Research Council (2011b) also discussed the need for effective caregiver training on the use of technology. Caregiver training effectiveness depends on the timing of the training (if it is a time of stress), the number of sessions (if only one session is provided), and the cultural appropriateness of the training. Because people learn differently, including through pictures, text, word, video, and one-on-one, the authors suggested that multiple training options for caregivers be considered.
Project CARES (Caregiver Adaptations to Reduce Environmental Stress), funded by AoA, was designed to increase NFCSP staff knowledge about AT/HM for family caregivers (Sabata, Liebig, & Pynoos, 2005). Training topics included the basis of HM and AT, analysis of major activities that cause physical burden and their relationship to the environment, identification of solutions to problems, identification of caregivers' needs related to the home environment, different types of caregivers, resource identification, making CARES a reality in a participant's community, and the development of a proposal for an activity that could be completed in six months. Many of the 20 staff participants reported that their agency gained new knowledge about HM and new ways to meet caregiver needs.
The ability of professionals to recognize family caregiver physical strain and be familiar with AT/HM is also addressed in the National Association of Social Workers' (NASW) Standards for Social Work, Practice with Family Caregivers of Older Adults (2010). The Standards note that SWs need to assist family caregivers in preserving their own health through helping them to modify their caregiving roles. The standards also note the need for SWs to know of resources available to caregivers, including respite care and AT, and to assess the household environment for HM needs and the family caregiver's capacity to fulfill their role as caregivers.
Discussion
AT/HM Interventions with Promise for Reducing Physical Strain among Family Caregivers
Lifting/transferring devices. The literature suggests a need for increased access to lifting and transferring devices to support caregiving in the home. The facility-based research has shown the effectiveness of mechanical aids for lifting and transferring combined with other interventions such as training in device use, collaborating with caregiving staff to assess the need for and select AT, and "zero lift" policies. Significant positive impacts were found on reduced caregiver injuries, resulting in fewer lost workdays and long-term cost savings, and increased feelings of comfort and safety for people receiving care. These studies also reported the dangers of increased caregiver injuries of lifting a non-weight-bearing person without a mechanical device.
In contrast, of the few studies with home workers, most focused on back-belts, and the research on the effectiveness of these devices has been mixed. NIOSH guidelines recommend that equipment such as a hoist or mechanical lift be used for a whole body lift of a non-weight-bearing person. Gait belts and slings can help position and provide back-up when assisting a partially weight-bearing person. They can also be used for maneuvering a non-weight-bearing person into a hoist sling.5 One pilot program in Canada (Craib et al., 2007) used a registry of loaner lifts as an affordable way to provide home care workers with access to ceiling lifts.
In the studies with older adults and family caregivers at home, lifting and transferring equipment was one of the least frequently needed types of AT/HM but were used by some families.
Small, low-cost AT/HM. In the home-based studies, many of the devices used were low-cost, such as hand-held showers, reachers, grab bars, nightlights, and tub mats. These studies highlight the importance of assisting older adults with proper assessment of the need for AT/HM and raising awareness and acceptance of new technologies. Older adult receptivity to using AT/HM was related to both characteristics of the device, such as intrusiveness, and characteristics of the older adult, such as social support. Also important was the capacity of service agencies to provide AT/HM to older adults, including CM/SW training on the benefits and uses of AT/HM as well as the time allocated for tasks related to these services. As with the studies with older adults, these studies demonstrated the effectiveness of small, low-cost devices. The most common HMs needed included enhancements to bathroom safety (grab bars, walk-in shower, hand-held showerhead, shower seat); modifications to address the older adult's memory loss, such as additional lights, signs, and labels; and devices for activity engagement.
Electronic technologies. Several studies reported on the usefulness of electronic technologies in the home, such as telehealth care and remote monitoring systems. However, in some cases the technological burden of the devices was a challenge for caregivers. Future research and development may lead to more user-friendly versions of these technologies.
Home assessments, training, and OT. Several experimental studies tested the benefits of providing older adults and/or family caregivers at home with OT interventions, including AT/HM. Benefits included less need for assistance, reduced caregiver burden, less time spent caregiving, decrease in caregiver depression, enhanced caregiver skills, enhanced caregiver ability to self-care, fewer problem behaviors of people with dementia, and reductions in health care costs.
A key element of these interventions is a person-centered approach, in which OTs assess the home and work with the older person to identify solutions to increase their capacity to age in place. The OTs also assisted in ordering the devices and arranging for installation, as well as provided training and conducted follow-up visits. All of these studies found positive results, including user satisfaction with the devices, reduced functional decline and improved functioning, reduced depression, reduced need for paid assistance, and lower expenditures for nurse and case management visits. Although this decreased need for assistance would likely reduce physical strain for caregivers, this was not directly measured in any of the studies.
Implications for Dissemination Efforts
The literature suggests important lessons for efforts to accelerate the dissemination of AT/HM among family caregivers of older adults living at home.
Many studies identified caregiver or older adult resistance to using new AT/HM as a challenge. This suggests a need for efforts to increase awareness and acceptance of AT/HM.
Additionally, studies with family caregivers highlight the importance of CM and SW knowledge of AT/HM for family caregivers. Also important is ensuring that CMs have sufficient time to allocate to AT/HM services. Another suggestion is that CMs use a comprehensive, easy to use, objective tool for assessing home safety and identifying AT/HM needs. Several such tools have been developed.
The perceived cost of the AT/HM was another major barrier to device acceptance. This suggests a need for increased coverage of AT/HM in health care programs, combined with outreach to increase awareness of existing funding sources.
Identified Research Gaps
This review also identified several research gaps that could be addressed in future studies. No studies were found that directly measured outcomes on family caregiver physical strain, and few studies involved home care workers. Additional research is needed to assess long-term impacts of various types of devices on different aspects of physical strain among family and paid caregivers in the home setting and their cost impacts. Also needed is additional research on how to overcome barriers to more widespread adoption of equipment and safe handling practices that have been found to be effective. Attributes of the device, such as ease, comfort of use, time required to use the device, and intrusiveness, were major factors associated with receptivity to AT/HM. Thus, further research is needed to develop technologies designed for use by older adults and their caregivers in the home.
References
Alamgir, H., Yu, S., Fast, C., Hennessy, S., Kidd, C., & Yassi, A. (2008). Efficiency of overhead ceiling lifts in reducing musculoskeletar injury among carers working in long-term care institutions. Injury, 39(5), 570-577.
Anemaet, W.K., & Moffa-Trotter, M.E. (1999). Promoting safety and function through home assessments. Top Geriatr Rehabil, 15(1), 26-55.
Baptiste, A., Boda, S., Nelson, A. Lloyd, J., & Lee, W. (2006).Friction-reducing devices for lateral patient transfers: A Clinical Evaluation.AAOHN Journal, 54(4), 173-80.
Becker, M.B. (2011). Aging in Place Better Living at Home A Person-Environment-Task Framework. HCBS Presentation 2011.
Becker-Omvig, M.B., & Smith, C.A. (2010). Reducing the Costs of Home and Community Based Care: A Person-Environment-Task Framework. GSA Presentation 2010.
Brophy, M.O., Achimore, L., & Moore-Dawson, J. (2001).Reducing incidence of low-back injuries reduces cost. AIJHAJ, 62(4), 508-11.
Buettner, L.L., Yu, F., & Burgener, S.C. (2010). Evidence supporting technology-based interventions for people with early-stage Alzheimer's disease. Journal of Gerontological Nursing, 36(10), 15-19.
Carswell, W., McCullagh, P.J, Augusto, J.C., Martin, S., Mulvenna, M.D., Zheng, H. & Jeffers, W.P. (2009). A review of the role of assistive technology for people with dementia in the hours of darkness. Technology and Health Care, 17, 281-304.
Charney, W., Simmons, B., Lary, M., & Metz, S. (2006). Zero lift programs in small rural hospitals in Washington State: Reducing back injuries among health care workers. AAOHN Journal, 54(8), 355-58.
Chhokar, R., Engst, C., Miller, A., Robinson, D., & Tate, R.B. (2005). The three-year economic benefits of a ceiling lift intervention aimed to reduce healthcare worker injuries. Applied Ergonomics, 36(2), 23-29.
Collins, J., Wolf, L., Bell, J., & Evanoff, B. (2004). An evaluation of a "best practices" musculoskeletal injury prevention program in nursing homes.Injury Prevention, 10(4), 206-11.
Craib, K., Hackett, G., Back, C., & Cvitkovich, Y. (2007).Injury rates, predictors of workplace injuries, and results of an intervention program among community health workers. Public Health Nursing, 24(2), 121-31.
Danyard, D., Yassi, A., Cooper, J.E., Tate, R., Norman, R., & Wells, R. (2001). Biomechanical analysis of peak and cumulative spinal loads during simulated patient-handling activities: A substudy of a randomized controlled trial to prevent lift and transfer injury of health care workers. Applied Ergonomics, 3(2), 199-214.
Demiris, G., Oliver, D.P., Dickey, G., Skubic, M, & Rantz, M. (2008).Findings from a participatory evaluation of a smart home application for older adults. Technology and Health Care, 16, 111-118.
Direct Service Workforce (DSW) Resource Center. (2011). Building Capacity and Coordinating Support for Family Caregivers and the Direct Service Workforce: Common Goals and Policy Recommendations Emerging from the CMS Leadership Summit on the Direct Service Workforce and Family Caregivers. Washington, DC: Author.
Engkvist, I. (2006). Evaluation of an intervention comprosing a no lifting policy in Australian hospitals. Applied Ergonomics, 37(2), 141-48.
Engst, C., Chhokar, R., Miller, A., Tate, RB, & Yassi, A. (2005). Effectiveness of overhead lifting devices in reducing the risk of injury to care staff in extended care facilities. Ergonomics, 48(2), 187-99.
Engst, C., Chhokar, R., Robinson, D., Earthy, A., & Yassi, A. (2004). Implementation of a scheduled toileting program in a long term care facility: Evaluating the impact on injury risk to caregiving staff. AAOHN Journal, 52(10), 427-35.
Fall Prevention Center of Excellence. (2011). InSTEP Brief: Increasing Stability Through Evaluation and Practice. Retrieved from: http://www.stopfalls.org/resources/downloadables/InStep-Brief.pdf.
Gehm, D. (2011). Lutheran Homes of Michigan. Preparing for the Future: Developing Technology-Enabled Long-Term Services and Supports for a New Population of Older Adults.LeadingAge CAST Report.
Gitlin, L.N., & Greening, S.E. (1997). REACH Reaches Philadelphia Through Jefferson's College of Health Professions. Health Policy Newsletter.
Gitlin, L.N., Hauck, W.W., Dennis, M.P., & Winter, L. (2005). Maintenance of Effects of the Home Environmental Skill-Building Program for Family Caregivers and Individuals With Alzheimer's Disease and Related Disorders. Journal of Gerontology, 60A(3), 368-74.
Gitlin, L.N., Jacobs, M., & Earland, T.V. (2010).Translation of a dementia caregiver intervention for delivery in homecare as a reimbursable Medicare service: Outcomes and lessons learned. The Gerontologist, 50(6), 847-54.
Gitlin, L.N., Winter, L., Corcoran, M., Dennis, M.P., Schinfeld, S., & Hauck, W.W. (2003). Effects of the Home Environmental Skill-Building Program on the Caregiver-Care Recipient Dyad: 6-Month Outcomes Fromthe Philadelphia REACH Initiative. The Gerontologist, 43(4), 532-46.
Gitlin, L.N., Winter, L., & Dennis, M.P. (2010). Assistive devices caregivers use and find helpful to manage problem behaviors of dementia. Gerontechnology, 9(3), 408-414.
Gitlin, L.N., Winter, L., Dennis, M.P., Corcoran, M., Schinfeld, S., & Hauck, W.W. (2006). A randomized trial of a multicomponent home intervention to reduce functional difficulties in older adults. JAGS, 54(5), 809-16.
Gottlieb, A.S. & Caro, F.G. (2001). Extending the Effectiveness of Home Care for Elders ThroughLow-Cost Assistive Equipment. New York, NY: Center for Home Care Policy and Research, Visiting Nurse Services of New York.
Goy, E., Freeman, M., & Kansagara, D. (2010). A Systematic Evidence Review of Interventions for Non-professional Caregivers of Individuals with Dementia. VA-ESP Project 05-225.
Horowitz, A., Brennan, M., Reinhardt, J.P., & MacMillan, T. (2006). The impact of assistive device use on disability and depression among older adults with age-related vision impairments. Journal of Gerontology, 61B(5), S274-S280.
Hunter, B., Brandon, M., & Davenport, D. (2010). Saving costs, saving health care providers' backs, and creating a safe patient environment. Nursing Economic$, 28(2), 130-134.
Khatutsky, A., Wiener, J.M., & Anderson, W.L. (2010). Work Related Injuries AmongCertified Nursing Assistants Working in Nursing Homes. Washington, DC: RTI International.
Kinney, J.M., Kart, C.S., Murdoch, L.D., & Conley, C.J. (2004).Striving to provide safety assistance for families of elders: The SAFE House Project. Dementia, 3(3), 351-370.
Kraus, J.F., Schaffer, K.B., Rice, T., Maroosis, J., & Harper, J. (2002). A field trial of back belts to reduce the incidence of acute low back injuries in New York City home attendants. Int J Occup Environ Health, 8(2), 97-104.
Leff, E.W., Habenback, G.L., & Marn, K.K. (2000).Preventing home health nursing assistant back and shoulder injuries. Journal on Quality Improvement, 26(10), 587-600.
Li, J., Wolf, L., & Evanoff, B. (2004). Use of mechanical patient lifts decreased musculoskeletal symptoms and injuries among health care workers. Injury Prevention, 10, 212-16.
Liu, S.Y., & Lapane, K.L. (2009). Residential modifications and decline in physical function among community dwelling older adults. The Gerontologist, 49(3), 344-54.
Lynch, R.M., & Freund, A. (2000). Short-term efficacy of Back Injury Intervention Project for Patient Care Providers at One Hospital. AIHA Journal, 61(2), 290-294.
Mann, W.C. (2001). Potential of Technology to Ease the Care Provider's Burden. Rehabilitation Engineering Research Center on Aging.Report for National Institute on Disability and Rehabilitation Research, Department of Education.
Mann, W.C. (2010). Assistive Technology for Individuals WithDevelopmental Disabilities in Florida: A Feasibility Project. Florida Developmental Disabilities Council, Inc.
Mann, W.C., Marchant, T., Tomita, M., Fraas, L., & Stanton, K. (2002). Elder acceptance of health monitoring devices in the home. Care Management Journals, 3(2), 91-98.
Mann, W.C., Ottenbacher, K.J., Fraas, L., Tomita, M., & Granger, C.V. (1999). Effectiveness of assistive technology and environmental interventions in maintaining independence and reducing home care costs for the frail elderly. Arch FamMed, 8, 210-217.
Marquardt, G., Johnston, D., Black, B.S., Morrison, A., Rosenblatt, A., & Lyketsos, C.G. (2011). A descriptive study of home modifications for people with dementia and barriers to implementation.J Hous Elderly, 25(3), 258-273.
Messecar, D.C., Archbold, P.G., Stewart, B.J., & Kirchling, J. (2002). Home environmental modification strategies used by caregivers of elders. Research in Nursing and Health, 25, 357-370.
Messecar, D.C. (2000). Factors affecting caregivers' ability to make environmental modifications. Journal of Gerontological Nursing, 32-42.
Mirza, M., & Hammel, J. (2009). Consumer-directed goal planning in the delivery of assistive technology services for people who are ageing with intellectual disabilities. Journal of Applied Research in Intellectual Disabilities, 22, 445-457.
Moore, A., McQuay, H., & Gray, J.A.M. (Eds.). (1995). Evidence-based everything. Bandolier, 1(12), 1.
Morgan, A., & Chow, S. (2007). The economic impact of implementing an ergonomic plan. Nursing Economic$, 25(3), 150-156.
National Alliance for Caregiving. (2011). e-Connected Family Caregiver: Bringing Caregiving into the 21st Century.
National Association of Social Workers. (2010). NASW Standards for Social Work Practice with Family Caregivers of Older Adults.
National Research Council. (2011a). Consumer Health Information Technology in the Home: A Guide for Human Factors Design Considerations. Committee on the Role of Human Factors in Home Health Care. Washington, DC: The National Academies Press.
National Research Council. (2011b). Health Care Comes Home: The Human Factors. Committee on the Role of Human Factors in Home Health Care, Board on Human-Systems Integration, Division of Behavioral and Social Sciences and Education.Washington, DC: The National Academies Press.
Nelson, A., Matz, M., Chen, F., Siddhartan, K., Lloyd, J., & Fragala, G. (2006). Development and evaluation of a multifaceted ergonomics program to prevent injuries associated with patient handing tasks. International Journal of Nursing Studies, 43(6), 717-33.
Nevala, N., Holopainen, J., Kinnunen, O., & Hanninen, O. (2003).Reducing the physical work load and strain of personal helpers through clothing redesign. Applied Ergonomics, 34(6), 557-63.
NIOSH. (2009). State of the Sector: Health Care and Social Assistance.
Nichols, L.O., Martindale-Adams, J.L., Burns, R., Graney, M., & Zuber, J. (2011). Translation of a Dementia Caregiver Support Program in a health care system. Arch Intern Med, 171(4), 353-358.
Owen, B.D., & Garg, A. (1994). Reducing back stress through an ergonomic approach: Weighing a patient. Int J Nurs Stud, 31(6), 511-19.
Owen, B.D., Keene, K., & Olson, S. (2002). An ergonomic approach to reducing back/shoulder stress in hospital nursing personnel: A five year follow up. International Journal of Nursing Studies, 39(3), 295-302.
Park, R.M., Bushnell, P.T., Bailer, A.J., Collins, J.W., & Strayner, L.T. (2009). Impact of publicly sponsored interventions on musculoskeletal injury claims in nursing homes. American Journal of Industrial Medicine, 52(9), 683-97.
Petersson, I., Lilja, M., Hammel, J., & Kottorp, A. (2008).Impact of home modification services on everday life for people ageing with disabilities. J Rehabil Med, 40(4), 253-60.
PHI National. (2011). Nursing and Residential Care Workers Suffer Highest Occupational Injury Rates. http://phinational.org/archives/nursing-and-residential-care-workers-suf....
Rose, K.C., Gitlin, L.N., & Dennis, M.P. (2010). Readiness to use compensatory strategies among older adults with functional difficulties. International Psychogeriatrics, 22(8), 1225-39.
Sabata, D., Liebig, P., & Pynoos, J. (2005).Environmental coping strategies for caregivers: Designing and implementing online training for staff of family caregivers support programs. Alzheimer's Care Quarterly, 6(4), 325-31.
Schulz, R., Czaja, S.J., Lustig, A., Zdaniuk, B., Martire, L.M., & Perdomo, D. (2009). Improving the quality of life of caregivers of persons with spinal cord injury: A randomized controlled trial. Rehabil Psychol, 54(1), 1-15.
Sheffield, C. (2011). Aging in Place & Better Living at Home. Howard County Office on Aging.
Spillman, B.C., & Long, S.K. (2009). Does high caregiver stress predict nursing home entry? Inquiry, 46(2), 140-161.
Stark, S., Landsbaum, A., Palmer, J., Somerville, E.K., & Morris, J.C. (2009). Client-Centered Home Modifications Improve Daily Activity Performance of Older Adults. Can J Occup Ther, 76, 235-45.
Szanton, S.L., Tanner, E., Agree, E., Boyd, C., Weiss, C., Guralnik, J., & Gitlin, L.N. (2010). A Multi-Component Pilot to Enhance Aging-in-Place Capacity for Low-Income Older Adults. Program No. 2105-4.2010 Abstract Viewer, The Gerontological Society of America.
Szanton, S.L., Thorpe, R.J., Boyd, C., Tanner, E.K., Leff, B., Agree, E., Xue, Q., Allen, J.K., Seplaki, C.L., Weiss, C.O., Guralnik, J.M., & Gitlin, L.N. (2011). Community Aging in Place, Advancing Better Living for Elders: A bio-behavioral environmental intervention to improve function and health-related quality of life in disabled older adults. JAGS, Brief Report.
Trinkoff, A., Brady, B., & Nielsen, K. (2003). Workplace prevention and musculoskeletal injuries in nurses.The Journal of Nursing Administration, 33(3), 153-58.
van Duijenbode, I., Jellema, P., van Poppel, M., & Tulder, M.W. (2011). Lumbar supports for prevention and treatment of low back pain (review). The Cochrane Library, (2).
Wångblad, C., Ekblad, M., Wijk, H., & Ivanoff, S.D. (2009). Experiences of physical strain during person transfer situations in dementia care units. Scandanavian Journal on Caregiving Sciences, 23(4), 644-50.
Wilson, D., Mitchell, J.M., Kemp, B.J., Adkins, R.H., & Mann, W. (2009). Effects of assistive technology on functional decline in people with a disability. Assistive Technology, 21, 208-217.
Yassi, A., Cooper, J.E., Tate, R.B., Gerlach, S., Muir, M., Trottier, J., & Massey, K. (2001). A randomized controlled trial to prevent patient lift and transfer injuries of health care workers.Spine, 26(16), 1739-46.
Part II. Strategies for Expanding the Use of AT/HM to Reduce Family Caregiver Physical Strain: Results of Expert and Stakeholder Discussions
Introduction
Many family caregivers experience risk of physical strain, which often results from lifting and transferring, communication problems with a person with dementia, and homes that need repair and/or are not designed to support aging in place. However, the problem of caregiver physical strain has received little attention in family caregiver support efforts, with most programs focused on emotional support or respite. A two-stage study sought to identify ways to promote the more widespread use of AT/HM to mitigate physical strain among family caregivers of older adults with chronic conditions living at home.
The first stage (Part I and Appendix A) provided a systematic review of the research literature on the use of AT/HM to reduce physical strain associated with caregiving. The evidence suggested that a wide range of AT/HM could help prevent caregiver back strains and other injuries, enhance functioning and independence of older adults, and reduce the need for hands-on assistance and caregiver burden. Many of the programs found to be successful used a person-centered approach that included assessment of the environment and needs, identifying solutions, training in the use of AT/HM, addressing injuries, and assessing results, in many cases including occupational therapists.
This Part presents findings from the second stage of the study, in which we collected input from experts and stakeholders to identify strategies and recommendations for accelerating the use of AT/HM to reduce family caregiver physical strain. The project focused primarily on NFCSP as a dissemination venue because this large federal program is a source of direct support for many caregivers. Established in 2000 as part of the reauthorization of the Older Americans Act (Title IIIE) and administered by AoA, the NFCSP funds services to support family caregivers caring for people age 60 and older and people of any age with Alzheimer's disease or related dementia (AoA, 2011). The program also supports grandparent/relative caregivers of children and adults under age 60 with disabilities. Allowable services include information, assistance with accessing services, counseling, support groups, training, respite, and supplemental services, which include AT/HM, transportation, medical supplies, and other services.
Methods
To better understand family caregivers' experiences and needs related to AT/HM, training, and physical strain, we analyzed results from an online survey conducted by the FCA of family caregivers on the use of AT, which was fielded over six months (Appendix D). A snowball sampling methodology was used to recruit a convenience sample of family caregivers to complete the survey through FCA, ADRCs, and some AAAs. A total of 423 caregivers responded to the survey.
We also obtained information about innovative strategies and recommendations for addressing caregiver physical strain through a combination of webinars/teleconferences, site visits, and telephone interviews with technical experts, family caregivers, and NFCSP administrators. In addition, staff from ASPE and AoA, within the U.S. Department of Health and Human Services, along with two consultants with expertise in the design and use of AT/HM, provided input throughout the project.
First, we recruited a TEP and a CAP. TEP participants included experts in the design and use of AT/HM for family caregivers and older adults. CAP participants were individuals with both personal caregiving experience and knowledge of broad family caregiving issues. The study team met with the TEP by teleconference/webinar in January 2011. This was followed by a teleconference/webinar with the CAP in February 2011. These discussions provided opportunity to get input on the draft literature review. We also met with some key experts individually by phone. In December 2011, we convened a joint meeting of the TEP and CAP, which provided opportunity to elicit input from both groups on drafts of the two guides developed through this project and recommendations for the future.
To learn about strategies for accelerating the use of AT/HM to mitigate caregiver strain through the NFCSP network, we conducted site visits to 11 NFCSP programs, in person (Connecticut, Maryland, Pennsylvania, Utah) or by phone (Alabama, California, Hawaii, Illinois, Indiana, Iowa, Wisconsin). The sites represented diverse experiences with AT/HM. They included: sites using advanced/innovative approaches to providing AT/HM to family caregivers; sites that were interested in the area, but not sure how to launch an initiative; and sites with no activity in AT/HM. The selected programs also represented diverse geographic regions. We interviewed NFCSP administrators, managers, CMs, and participants at program offices and in the homes of older adults and family caregivers to gain a deeper understanding of caregiver needs related to physical strain and effective solutions. The visits took place between June and November 2011. Information gained from the site visits was used to develop the NFCSP strategy guide. Site visit participants were asked to review a draft of this guide and provide feedback through an online tool.
After meeting with the joint TEP/CAP panel and incorporating their input on draft documents, the next step was to convene a panel of 11 NFCSP program representatives, which took place in October 2011. Participants provided input on suggested strategies and resources for NFCSPs emerging from the site visits, as well as recommendations for additional policy and research activity to accelerate the use of AT/HM to reduce caregiver physical strain. The NFCSP panel was asked to review the guides developed through this project and to provide feedback through an online tool, similar to the one used to elicit feedback from site visit participants.6
Results
Findings from Online Caregiver Survey
Although the survey was not representative of all caregivers, the demographic profile of respondents was similar to that reported in other research (87.4% women, average caregiver age 57, average care recipient age 72).
Nearly 61% said they had used an assistive device, most commonly mobility aids, bathing aids, medication assistance, and toileting aids. In addition, 83.8% had used technology for calling for help in an emergency. In the majority of cases, the caregiver or another family member paid for the AT themselves. Reasons for not using AT included a lack of awareness, not needing it, and costs. A similar portion of respondents (62.8%) had used HMs, which were also paid for primarily by family caregivers. Most respondents said that the AT/HM was very helpful. Although 67% said they experienced moderate or heavy physical strain from caregiving, most (59.4%) had not received training on device use or techniques to minimize the risk of physical strain. The most frequently mentioned source for information on AT/HM was the Internet (67.4%), followed by physicians (47.3%) and AAAs (37.9%).
Strategies and Resources for Family Caregivers and NFCSPs
The site visits and discussions revealed many tips and resources that can help family caregivers reduce their risk of physical strain, assess their homes, and select, access, and pay for AT/HM. We also identified a number of innovative strategies and resources that the NFCSP network can use to assist family caregivers with AT/HM.
As a first step in disseminating information and strategies that emerged from this study, the research team developed a guide for family caregivers (Appendix B) and a guide for NFCSPs (Appendix C). Each guide will be made available in both a print handout version and online version and disseminated through NFCSPs, ADRCs and various other channels. In addition, research findings from this study have been presented at several national conferences. Also, findings were presented in a guest post on http://www.disability.gov, which is operated by ODEP and has nearly 30,000 followers.
Strategies and resources for family caregivers
Major barriers mentioned in both the TEP and CAP discussions, as well as in the literature, included a lack of awareness of safe handling techniques and available AT/HM and fears of technology. As one CAP member discussed, most caregivers are thrust into their roles as caregivers; they lack time to prepare for their caregiving responsibilities, including time to learn about AT/HM. Another member pointed out that, in some instances, it could be a simple matter of introducing the caregiver to the technology. As one TEP member commented, "We could do a lot to improve people's lives by raising consciousness that physical strain does not have to be a part of caregiving and that it is modifiable." Many caregivers do not realize that they can do something to reduce their physical strain.
A related barrier, noted in the TEP discussion, is a tendency of many caregivers towards "over-helping." This suggests that efforts are needed to educate caregivers and care recipients on ways to support the care recipient's independence, which can also be one of the more cost-effective solutions to reducing strain. Training in techniques for communicating with persons with dementia could help reduce physical strain resulting from miscommunication and conflicts when caring for this population.
TEP members commented that renters are more likely than owners to be reluctant to make physical changes to their homes, because they have less control over their settings, and 20% of older people live in rental housing. However, the group noted that under fair housing law, landlords must allow people to make reasonable modifications in their homes. In many cases, after contacting the landlord, renters have installed AT/HM without any problems.
Our research uncovered many resources that can assist families with AT/HM, including guides and checklists for assessing home safety, sources of information on choosing AT/HM, and general caregiver support resources. Other potential sources of assistance include primary care physicians (PCPs), occupational therapists, local aging service providers, Centers for Independent Living (CILs), State Assistive Technology Projects, and AT re-use programs.
Strategies and resources for NFCSPs
The site visits and panel discussions suggested a number of steps that the Aging Network can take to increase access to AT/HM to reduce family caregiver physical strain. Many NFCSPs, in conducting home visits, look for AT/HM that the family may need. Phone assessments may be necessary in difficult to reach, rural areas. A strategy that several programs have found helpful is for CMs or family caregiver specialists to bring along samples of commonly used AT that caregivers can try, such as a shower bench. Some programs use assessment forms or checklists, which can help staff with assessing a caregiver's need for AT/HM. After the initial assessment and selection of AT/HM, program personnel noted the importance of following up with caregivers over time to ensure the usefulness of the equipment and its correct use. In some instances, the NFCSP conducts the initial assessment and then refers to another provider or organization for more in-depth assessment as needed. Many potential partnerships for assessments were suggested, including occupational/physical therapists, RNs, home health agencies, rehabilitation services, vocational rehabilitation agencies, care transitions teams, disability organizations, and state AT projects. Community colleges that provide training programs and continuing education courses for home health aides could be a way to reach this workforce, in addition to online training programs.
To help families find a contractor to complete the HM, NFCSPs can form relationships with local businesses, in order to refer people to providers who others have used and who have a proven record of good results.
To help make AT/HM affordable and accessible, many programs include AT/HM in the array of services provided with NFCSP Supplemental Services funds. Another way to help caregivers access AT is to build or refer to an AT re-use or lending program. Agencies can also leverage some of the many other potential funding sources for AT/HM.
Another recommendation was for programs to conduct outreach to raise awareness of existing resources to address caregiver physical strain among family caregivers, physicians, and other health and human services providers. This could be done by partnering with various community organizations to disseminate information to caregivers or presenting information at events and locations in the community where older adults and family caregivers go such as physicians' offices, places of worship, and senior centers.
Panel Suggestions for a Dissemination Strategy
The expert, caregiver, and NFCSP panels were asked their recommendations for expanding dissemination to reach a wider non-academic audience. Participants discussed general recommendations pertaining to an overall dissemination strategy, as well as specific suggestions for dissemination aimed at distinct target audiences.
Overall dissemination strategy
Panel participants noted that different materials are needed for different purposes. TEP participants recommended providing objective, evidence-based materials to inform caregivers and the public about AT options.
An idea that was discussed was to produce multi-media implementation guides and educational materials for the effective interventions targeted, if applicable, at each of the potential user groups: family as well as professional caregivers. The educational materials and implementation guides could use video and web technology and be disseminated through leveraging existing resources including ADRCs and AoA's Family Caregiver Support Programs, and possibly on AT product databases such as AbleData, TechForLTC, Center for Aging Services Technologies (CAST) Clearinghouse, and caregiving websites such as the FCA.
A frequently mentioned example was the training component of the Aging in Place/Better Living at Home program in Howard and Montgomery Counties, Maryland. The program is developing training programs for three audiences: (1) video-based trainings for professionals including occupational therapists, physical therapists, and SWs; (2) video-based learning for staff at AAAs and other social service agencies, to help with determining the need for a referral to OT; and (3) for the general public, an informational resource providing neutral information on the pros and cons of the various types of AT/HM that are available. A representative of the program noted that it will take a non-academic approach to training; the videos will include real-life caregivers in the context of the home. The videos will be short (about 3-5 minutes) and available online.
Panel participants discussed that partnerships between AAAs and ADRCs and other disability organizations, in particular, could provide a useful opportunity for the aging and disability communities to learn from each other. They noted that, compared with older populations, the younger disability population has tended to be more assertive in advocating for systems change. The disability perspective could be useful for AoA to consider in these areas, and perhaps the groups could collaborate to develop mass education campaigns that could support each other.
Other suggested partners or opportunities include:
-
The U.S. Food and Drug Administration, which is working on an effort to provide consumer information on medical devices (U.S. Food & Drug Administration, 2011).
-
Centers for Medicare and Medicaid Services (CMS) Innovation grants, established through the Patient Protection and Affordable Care Act, which seek to improve costs, quality, and access.
-
The U.S. Department of Agriculture extension services with universities, which work on aging issues. Some AAAs have established connections with these organizations, but in some cases that connection has not been made.
Dissemination to family caregivers
Participants identified four issues that dissemination efforts will need to address, in addition to providing AT/HM, to ensure that the equipment is used and is helpful: (1) assessment of home safety and AT/HM needs, including re-assessment over time; (2) acceptance of AT/HM, including overcoming common concerns such as renter issues, fear of losing benefits, concerns about the look of the devices, and the concern that a device may symbolize disability and desire to maintain a sense of normalcy; (3) training on how to use the AT/HM and training in communication with persons with dementia, as well as retraining as needed; and (4) proper installation -- the group discussed that contractors and handymen vary in their knowledge of how to properly install assistive equipment.
Experts and stakeholders suggested a variety of materials to provide information for family caregivers. Families need repeated exposure to the possibilities of AT. A layering strategy with public health campaigns to normalize the use of these products was mentioned as an important component. The comment was made that these materials could empower families to help themselves.
Panel members also noted the need to make materials available in multiple languages and to ensure that materials are at a reading level that the average person can comprehend.
-
Websites: TEP and CAP participants agreed on the need for better tools and resources to inform families about AT/HM. They commented that although many websites address AT/HM, many of these sites are not very useful to family caregivers. A noted problem is that, although several websites are available that provide caregivers with information about AT products and services, they are often tied to marketing for a company's products. These websites do not provide objective guidance to help caregivers decide what they need or results of rigorous scientific evaluation. The suggestion was made to create a clearinghouse of information that would be a website or single source where caregivers can search by topic and get information on assessments, available AT, and videos.
-
Videos: Panel participants suggested that simple visuals are best to get information across to the public and professionals alike. They noted that people want neutral information without marketing or advertising. The FCA identified over 100 training videos, but most were determined to be poorly presented or low quality production. A comment was made that videos can be powerful and helpful in getting the message across effectively and time-efficiently, as caregivers are likely to be short on time. An example mentioned is an aging services provider that is using its Distance Learning Center to provide free video-based education (http://www.mmlearn.org/). Social media was suggested as a possible mechanism for disseminating the videos.
-
Tools: The suggestion was made, in addition to the videos, to offer a tool such as a decision-making tree as a person-centered way to assist families in decision-making.
Consensus emerged on the need to embed information in different places in order to reach a wide audience of caregivers, including those who are paying privately for AT/HM and who are not connected to AAAs. Many possible venues and strategies for reaching family caregivers were suggested:
-
Existing caregiving and AT/HM websites, blogs, conferences, newsletters, and mailing lists.
-
Home improvement stores (e.g., Home Depot, Lowes) could be asked to provide a display, handouts, and/or videos on aging in place in the stores.
-
Disease-specific websites, such as the MS Society.
-
Health care providers, including orthopedists, chiropractors' offices, and community health centers.
-
HMOs and long-term care insurance providers.
-
Villages and NORCs, which screen service providers and help residents obtain services.
-
Group settings, as in Skills2Care, a home-based OT program to improve the well-being and skills of family caregivers that is available as an individual or group class (Jefferson Elder Care, 2011).
-
PACE programs, which provide more integration of services, and care teams that could include occupational therapists.
-
Mass media was also considered; however, panel participants noted that this is expensive and has a "dissolve effect." However, short 1-minute tips on a cable channel were mentioned as a possible strategy. Television/radio public service announcements were also suggested. Another idea was media outreach targeting specific writers who might be interested in this topic and appearing in op-eds and newspaper articles. Another idea was to convene a Congressional briefing and invite reporters.
Panel participants also suggested going to places where caregivers are, such as houses of worship, barber shops, waiting rooms of doctors' offices, local caregiver associations, and libraries.
Ideas included working with utility companies to include information in utility bills, working with fire departments to give people information when they visit people's homes, working with Chambers of Commerce to reach employed caregivers in the workplace, disseminating information through caregiver coalitions and respite care coalitions, and working with disability organizations, vocational rehabilitation agencies, pharmacies, volunteer organizations like Rebuilding Together, and hospital discharge planners.
Dissemination to CMs, SWs, and NFCSPs
The TEP and CAP panels generally agreed that the focus needs to be on CMs and SWs, because they spend the most time with older adults and family caregivers. As a TEP member noted, CMs work directly with caregivers and see a lot of things; training and resources could help them be comfortable giving referrals. However, AT/HM is not typically taught in schools of nursing or social work. One participant commented that aging services tend to foster a dependency model, with the focus on the need for help, rather than how to maximize capacity. Often, workers do not think of AT/HM as one of the ways they can help a person.
Staff at one of the visited sites recommended that CMs look at the home and educate caregivers about the relationship between the home environment, health, and function, because their job includes supporting people in the home. In addition, they advised reminding staff that they do not need to know it all and can lean on other providers -- to see their job as identifying issues, not performing the services.
The consensus was that advancing the use of AT through the NFCSP must involve more than leaving a brochure or a link to a website. Caregiver acceptance of technology will require raising awareness among the NFCSP network about the value of technology and capacity-building in the Aging Network. Panel participants suggested developing training materials for caregiver program staff and disseminating them in various formats, such as electronic media, webinar, and videos that staff could reference. A few available courses were mentioned as examples. One course is a new Caregiving Certificate Program offered by the Rosalynn Carter Institute for Caregiving (RCI) through Georgia Southwestern State University, which includes course content on AT/HM.7 Many nurses have enrolled. Also, the University of Southern California offers a certificate in HM; most of the students who enroll are nurses, CMs, and social service employees. Four courses are available, with content on falls, sensory, mobility, and cognitive issues.8
Training of CMs, case workers, and other staff in how to assist caregivers with accessing technology was a major issue that arose in the TEP and CAP discussions as well as in the literature review.The TEP discussion emphasized the importance of the issue of training CMs and SWs. Participants noted that, although occupational therapists provided services in many of the interventions examined in the literature, the reality is that CMs/SWs are more often the staff who will be in direct contact with the targeted populations and identifying their AT needs. As such, direct training related to AT/HM should be implemented among this workforce to ensure that they can appropriately assist and refer caregivers. TEP members noted that this component of assessment has not been well integrated into CM/SW training.
Panel members commented that case workers need more training on body mechanics and the kinds of resources and strategies available to help reduce physical strain. For example, in some cases simply having a person sit in a different chair can reduce the need for assistance with transferring. Hence, staff training should also focus on how to help people find information and resources. CAP members suggested that more CM training might also help alleviate caregiver concerns over the cost of some AT/HM. CMs may not be properly informed about the costs of these devices, of which some come very cheaply.
Dr. Gitlin, a renowned scholar on AT/HM interventions, described workshops in Pennsylvania to heighten CMs' awareness of home safety for people with disabilities, which she said has been well received. The training was through the Pennsylvania Care Management Institute, which provides ongoing education for CMs. The program uses a home-grown assessment approach. The CMs asked three questions of families of people with disabilities, which were highly predictive of perceived quality of life, such as, "Do you have assistive devices in your home?" These questions could be included as part of a CM's risk assessment tool. A benefit of using a short set of assessment items (2-3 questions) is that assessing caregivers can take a lot of time and money. Getting that information more quickly can help avoid using limited funds on lengthy comprehensive assessments and having little left for services.
Dissemination to physicians
TEP and CAP participants also discussed the need to teach physicians about AT/HM, noting that physicians are not expected to be experts, but they need to be aware of the issue in order to make appropriate referrals. One CAP member stated that she has found medical professionals to be lacking in AT/HM knowledge. Another member supported this and said that we should target the education of PCPs in order to ensure that they are properly educated about AT/HM for caregivers.
In addition to directly educating physicians, the group discussed reaching audiences in non-traditional ways such as developing materials for the physicians' television network. Another suggestion was to disseminate a list of questions that patients could ask their physicians.
Dissemination to contractors
A suggestion was to reach consumers and give them information on how to select a contractor and what to tell them. Another suggestion was to work with training programs for contractors.
Panel Suggestions for Policy
Expand Coverage for a Comprehensive Range of AT/HM in Public Programs
Funding in health and long-term care programs to cover the costs of AT/HM was a major problem noted in both the literature and discussions with experts and stakeholders. Panel participants discussed the need to better align public programs, including Medicare, Medicaid, and HUD, to work together in supporting access to AT/HM, in addition to addressing challenges within each program.
TEP and CAP panelists discussed that the long-term care financing system will pay for certain solutions, which may not be the best solution. Generally, devices must fit in a medical category and be provided by an authorized provider in order to be covered. Another limitation is that Medicaid covers solutions that benefit the care recipient, but not the caregiver.
In the TEP discussion, the experts agreed that reimbursement for AT/HM and one-on-one work with caregivers in the home is difficult to obtain and that advocacy is needed to increase reimbursement for AT/HM. Additionally, TEP members noted that, for many caregivers, the decision to spend money on AT/HM can be difficult. Many caregivers become caregivers in a crisis situation and are unsure what caregiving expenses they may need to pay in the future, whether the person's condition might change, and how long the person will be able to continue living at home. eCAPmembers also discussed caregiver concern of the AT/HM costs as a barrier to their implementation. In cases where coverage is available through private insurance, many caregivers and care recipients have expressed reluctance to adopt these technologies due to potentially high co-payments.
Although many sources provide some funding for AT or HM, reimbursement varies across states and is typically limited to certain allowable products and services from participating providers. A January 2011, analysis of state payment for aging services technologies by the LeadingAge CAST found that 44 states reimburse for Personal Emergency Response Systems, which was the most commonly reimbursed technology (Peifer, 2011). An increasing number of states also reimbursed for other technologies, such as medication management (16 states), and telemonitoring/home telehealth (seven states). Other sources of funding include Title III of the Older American's Act and Medicaid state plan services (including Programs of All-Inclusive Care for the Elderly). In addition, the U.S. Department of Veterans Affairs (VA) programs in the states operate an extensive telehealth program for veterans.
TEP members discussed that many interventions can be provided relatively inexpensively. On average, the cost of the intervention in Maryland was in the hundreds of dollars. However, some older people may need major modifications or repairs in order to continue living in their homes, such as fixing a roof or installing a first-floor bathroom. Staff at one of the visited sites commented that many homes in their area are in poor condition, and this has significant health impacts, but resources are insufficient to help. Many homes do not have a half-bathroom on the first floor, and many older people with chronic illness are unable to safely walk up and down stairs.
In addition, TEP members commented on the importance of considering home and vehicle modifications and technologies to help people get outside of the home. Although much attention has focused on AT/HM for inside the home, getting in and out of the house and vehicles can be very problematic for someone who needs assistance, indicating the need to think beyond the front door.
Also noted was the importance of home repairs in conjunction with HM to improve accessibility. Dr. Gitlin commented that many provide care in very unsafe home conditions -- an average of eight home hazards, such as a lack of handrails in good repair and slippery floors. The American Occupational Therapy Association states, "Home modifications are used in conjunction with assistive devices and home repairs" (2011). Some HM may not be possible without home repair. A member of the TEP pointed out the importance of considering home repair first, in some instances, before installing HM. For example, installing handrails in a home to help an individual maneuver the stairs may not be as important as first fixing the stairs. Oftentimes, AT may not be possible to use in the home without HM or repairs (e.g., installation of ramps to a home and widening doorways to accommodate a wheelchair).
Increase involvement of occupational therapists and physical therapists
Discussion with one TEP member emphasized that reducing physical strain among family caregivers requires a multi-prong approach, with OT and PT as critically important components. CMs and other staff in the Aging Network can be trained to identify family caregiver risks and home hazards, but identifying specific technologies and training caregivers in specific techniques requires the involvement of trained health professionals. Some very simple techniques, accompanied by assistive devices, could provide family members with better back protection and reduce the strain they experience. Many people with chronic illness/disability and their families also need hands-on training in the use of new technologies, regardless of the size or complexity of the device.
The working group noted that occupational therapists are critical because they are the most skilled at assessing home safety issues, but noted that families can do their own assessments as well. A suggested model was to include communication with occupational therapists about more complicated issues, but not necessarily include them in each assessment. CMs or SWs could conduct assessments, with occupational therapist involvement achieved through telehealth applications, remote interactive videos, or "telepresence," in which a robotic video camera can be remotely controlled via the Internet, to help occupational therapists interact with people remotely.
The issue is not only about cost, but identifying the correct types of AT, which is an area where occupational therapists can help. Staff at one of the visited NFCSP sites noted that CMs can "plant the seed" by identifying issues and making referrals. Occupational therapists can then help increase function and increase community participation.
Panel participants mentioned several studies involving occupational therapists that found evidence of success; these are included in the literature review (Part I).
Encourage housing designs that support aging in place and family caregiving
To support multi-generational housing, "visitability", accessibility, and universal design are integral to ensuring individuals can age in place. In Connecticut, the Hartford area CIL succeeded in the passage of no-cost legislation to encourage "visitability" of new homes; that is, housing designs that are accessible to visitors with disabilities. The Hawaii State Unit on Aging is involved in a task force that is a partnership between the private sector and county and state governments to promote physical structures that support aging in place and multi-generational living (Home for Life Task Force, 2011). One working group is focused on providing information about HM and aging in place through ADRC services, including an educational website, options counseling that includes AT/HM options, intake and assessment forms. The second working group is providing recommendations for zoning legislation and accessory dwelling unit rules.
Montgomery County, Maryland has developed Design for Life Montgomery, a voluntary certification program for Visit-Ability and Live-Ability in single family attached and detached homes in the county. There was a Zoning Text amendment 06-17 approved by the Montgomery County Council establishing this program.9
Suggestions for Future Research
Identify Effective Dissemination Approaches and Evaluate Outcomes
Additional research is needed to evaluate approaches to disseminating AT/HM among family caregivers and to measure impacts on caregiver physical strain, as well as impacts on community living/nursing facility utilization and costs.
While our literature search found many studies documenting the effectiveness of assistive equipment in nursing homes and institutions, research evaluating the use of AT/HM to reduce physical strain among family and paid caregivers in the home was much more limited. In the TEP meeting, participants suggested that a reason for this research gap may be that conducting controlled research in peoples' homes is extremely difficult, due to the logistics of arranging home visits and the challenge of controlling for the variance across home care work settings.
Although a growing number of studies have evaluated outcomes of providing family caregivers with AT/HM services, these studies have not measured caregiver physical strain as a specific outcome. In the TEP discussion, the experts agreed that the majority of caregiver intervention research has focused on reducing caregiver emotional stress or improving care recipient independence, rather than reducing caregiver physical strain.
Other important outcomes to measure include reducing nursing home entry and independence and quality of life for older adults. Any device that increases the level of independence for the care recipient is likely to simultaneously decrease the amount of assistance needed and thereby indirectly relieve burden for care providers (Mann, 2001). The TEP discussion, however, suggested the association between AT and caregiver strain may be more complicated. Traci Galinsky noted that, anecdotally, some caregivers often left care recipients in bed rather than manually lift them, which wasdifficult and put them at risk of injury. Some of these caregivers assisted care recipients in getting out of bed more often after receiving hoists or other devices. Although the effect was an increase in physical exertion among caregivers, this was seen as a positive effect because getting help with transferring improved quality of life for care recipients and the caregivers were using assistive devices to minimize physical strain.
Jon Sanford noted that research is almost always focused on the care recipient and impacts on increasing their independence. This is assumed to correlate with decreased need for assistance, but more outcomes data are needed to show the extent to which AT/HM helps family caregivers and paid home care aides. Outcomes to examine include reducing family caregiver physical strain, increasing function of older people, cost savings, decreased falls, and other benefits to caregivers.
For study design, panel participants suggested case studies paired with quantitative research. A suggestion was to take two comparable communities and use existing resources in one community and compare it to the intervention community, which would receive information dissemination. Case studies with cluster interviews can provide rich and detailed information, while randomized trials can provide evidence of outcomes.
Participants suggested aligning the demonstration with an existing project, such as VA Independence at Home or Medicare Care Transitions. They noted that both outcomes and the process by which information is delivered are important to study.
Develop AT Designed for Family Caregivers
A problem, noted in the TEP discussion, is that many of the available assistive devices are institutional and need to be redesigned so that they can fit into a home. Also, many homes need to be designed to allow the technology to work effectively. While the majority of older people with chronic disabilities strongly prefer to live at home, many homes are not designed or arranged to support safety and independence for people with physical or cognitive impairment, or to support caregiving in the home. A simple solution is to make the AT more adaptable to home environments. TEP members stated that AT needs to be redesigned to become more adaptable to the home and more accommodating to home environments, in addition to training family caregivers on the use and benefits of AT/HM.
Conclusions and Discussion
The FCA online caregiver survey (Appendix C) found that many caregivers are purchasing AT/HM and find it useful. However, findings also suggested a need to raise awareness of available AT/HM, to address caregivers' concerns about costs, and to offer caregiver training on AT/HM and techniques to minimize physical strain. The Internet, physicians' offices, and AAAs were the top places where caregivers go for information on AT/HM.
The site visits and discussions revealed many tips and resources that can help family caregivers reduce their risk of physical strain, assess their homes, and select, access, and pay for AT/HM. We also identified a number of innovative strategies and resources that the NFCSP network can use to assist family caregivers with AT/HM.
Suggestions for a Dissemination Strategy
In discussions with experts and stakeholders, consensus emerged that accelerating the use of AT/HM to reduce physical strain among family caregivers will require a comprehensive dissemination strategy that includes:
-
Developing multiple informational resources (e.g., videos, brochures, training courses on AT/HM and preventing physical strain).
-
Disseminating the information through multiple channels (e.g., online, physicians' offices, community organizations, the media).
-
Reaching multiple target audiences (e.g., family caregivers, CMs and SWs who work with caregivers, physicians, builders, contractors).
A suggested next step was to convene a national meeting of a wider group of stakeholders involved in AT/HM for older adults and their caregivers in order to develop and carry out a dissemination plan. Panel participants noted that this could provide opportunity for the AoA Aging Network to establish new partnerships.
Suggestions for Policy
In addition, panel participants agreed that overcoming barriers to family caregiver use of AT/HM will also require changes to several aspects of health, long-term care, and housing policy.
-
Challenges to accessing AT/HM will need to be addressed within programs that offer some AT/HM services (e.g., Medicare, Medicaid, HUD assistance programs). Experts and stakeholders recommended expanding coverage to include a comprehensive array of AT/HM, to respond to individual needs for support to retain independence and live at home. In addition, these programs need to be better aligned in support of common goals.
-
Another frequently mentioned recommendation was to expand coverage in public programs for OT and PT services. Occupational therapists can provide in-depth assessment of a person's home and suggest specific solutions that could help the person maximize function and retain independence.
-
Another issue raised by several panel participants is the need to modify housing and zoning laws to support aging in place and multi-generational living and to enact policies encouraging universal design in new construction.
Suggestions for Future Research
The discussions indicated two broad areas where additional research is needed:
-
To develop and expand AT/HM efforts, additional research will be needed to identify effective approaches and evaluate their impacts on reducing caregiver strain, increasing independence, and saving costs. These research questions could be addressed through a potential demonstration project.
-
Also needed is additional research is to develop and test new AT/HM products that are designed to meet the needs of family caregivers and older adults living at home. Panel participants discussed that one of the barriers to using AT/HM is that many products are designed for use in institutions, rather than in the home.
The above suggestions experts and stakeholders are supported by the research literature. Implementing these actions to encourage the use of AT/HM to reduce caregiver physical strain would also support recent federal efforts to promote community living, evidence-based health care, and cost savings.
References
Administration on Aging. (2011). National Family Caregiver Support Program (OAA Title IIIE) web page. Accessed December 27, 2011. Retrieved from: http://www.aoa.gov/AoARoot/AoA_Programs/HCLTC/Caregiver/index.aspx.
American Occupational Therapy Association. (2011). Home Modifications and Occupational Therapy. Fact Sheet. Retrieved from: http://www.aota.org/Consumers/professionals/WhatisOT/PA/Facts/39470.aspx.
Home for Life Task Force. (2011). Interim Report to the Twenty Sixth Legislature, State of Hawaii, January 14, 2011. Retrieved from: http://www.capitol.hawaii.gov/session2010/studies/commjlcaip.asp.
Jefferson Elder Care (JEC). (2011). Professional Training web page. Accessed December 27, 2011. Retrieved from: http://www.jefferson.edu/carah/elder_care/training.cfm.
Mann, W.C. (2001). Potential of Technology to Ease the Care Provider's Burden. Rehabilitation Engineering Research Center on Aging. Report for National Institute on Disability and Rehabilitation Research, Department of Education.
Peifer, S. (2011). CAST Analysis of State Payment for Aging Services Technologies (ASTs). A LeadingAge CAST Report.
U.S. Food and Drug Administration. (2011). Home Use Devices web page. Accessed December 27, 2011.Retrieved from: http://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/HomeHealthandConsumer/HomeUseDevices/default.htm.
Appendices
Appendix A. Annotated Bibliography Figures and Tables
| FIGURE A-1. Literature Review Flow Diagram | ||
|---|---|---|
| PubMed/Medline Database Search (n=446) | ||
| Abstracts/Titles Screened (n=446) | Citations excluded within reason (Irrelevant, laborator studies) (n=409) | |
| Potentially relevant articles retrieved for more detailed evaluation (n=37) | Full-text articles excluded (Irrelevant, laboratory studies) | |
| Relevant Articles (n=25) | ||
| Total articles included in analysis (n=52) | Additional articles identified through review of reference lists of cited studies and other sources (n=27) | |
| TABLE A-1. PubMed/MEDLINE Search Strategy and Results | ||||
|---|---|---|---|---|
| Search | Concept | Search String* | Results (hits): Original Search (10/14/2010) | Results (hits): Search Update (10/6/2011) |
| 1 | Caregivers/ care settings | "Caregivers"[MeSH] OR caregiver*[tiab] OR "Home Health Aides"[MeSH] OR "home health aide*"[tiab] OR "home health worker*"[tiab] OR "home nursing"[MeSH] OR Health Personnel[MeSH] OR "Nurses' Aides"[Mesh] OR "long-term care"[MeSH] OR "Skilled Nursing Facilities"[Mesh] OR "Nursing Staff"[Mesh] OR "Home Care Services"[Mesh] OR "Assisted Living Facilities"[Mesh] | 372,857 | 390,224 |
| 2 | Physical strain | stress[tiab] OR strain[tiab] OR injury[tiab] OR injuries[tiab] OR "low-back pain"[MeSH] OR "back pain"[MeSH] OR "Moving and Lifting Patients/adverse effects"[Mesh] OR "Transportation of Patients/adverse effects"[Mesh] OR "Fatigue"[Mesh] OR "Cumulative Trauma Disorders"[Mesh] OR "Physical Exertion"[Mesh] OR "physical burden" | 1,017,601 | 1,089,348 |
| 3 | Assistive technology | "self-help devices"[MeSH] OR "self-help devices"[tiab] OR "assistive technology"[tiab] OR "assistive technologies"[tiab] OR "Protective devices"[MeSH] OR "adaptive equipment"[tiab] OR "adaptive technology"[tiab] | 34,182 | 35,901 |
| 4 | Home modifications | "Home modifications"[tiab] OR "Environment Design"[Mesh] OR "environmental modification" OR "environmental home modification" OR "home environmental modification" | 2,776 | 3,138 |
| 5 | Physical strain prevention | "Back Injuries/prevention and control"[Mesh] OR "Accidents, Occupational/prevention and control"[Mesh] OR "physical morbidity" | 5,478 | 5,746 |
| 6 | Set 1 AND Set 2 AND Set 3 | 258 | 9 Limits: English, Publication date from 10/1/10 | |
| 7 | Set 1 AND Set 2 AND Set 4 | 7 | 1 Limits: English, Publication date from 10/1/10 | |
| 8 | Set 1 AND Set 5 | 631 | 11 | |
| 9 | Set 6 OR Set 7 OR Set 8 | 864 | 20 | |
| 10 | Set 9 Limits: English, with Abstracts, All Adult (19+ years) | 156 | 7 Limits: with abstracts, All adult (19+ years) | |
| 11 | Alternate | Set 9 Limits: English, with Abstracts | 453 | 17 Limits: with Abstracts |
| 12 | Set 11 NOT "Child"[Mesh] | 410 | 14 | |
| 13 | Set 12 NOT Set 10 | 275 | 8 | |
| 14 | Final search | Set 10 + Set 13 | 431 | 15 |
| * PubMed search tags: [MeSH] = MeSH heading; [tiab] = title and abstract. | ||||
| TABLE A-2. Number of Studies Found, by Study Design and Population* | ||||||
|---|---|---|---|---|---|---|
| Study Design* | Caregiving Staff in Facilities | Home Care Workers | Older Adults with Disabilities at Home | Family Caregivers of Older Adults and Family Caregiver/ Older Adult Dyads** | Total | |
| Specific Devices | Multi-Component Programs | |||||
| I. Systematic review of multiple randomized controlled trials | 0 | 0 | 0 | 0 | 0 | 0 |
| II. Randomized controlled trial | 3 (Danyard et al., 2001; Yassi et al., 2001; Baptiste et al., 2006) | 0 | 1 (Kraus et al., 2002) | 10 (Becker-Omvig & Smith, 2010; Sheffield, 2011; Mirza & Hammel, 2009; Rose et al., 2010; Gitlin et al., 2006; Szanton et al., 2010; Szanton et al., 2011; Mann et al., 1999; Petersson, 2008; Wilson et al., 2009) | 3 (Gitlin et al., 2003; Gitlin et al., 2005; Schulz et al., 2009) | 17 |
| III(a). Quasi-experimental: comparison group | 3 (Owen, Keene, & Olsen, 2002; Engst et al., 2004; Engst et al., 2005) | 2 (Morgan & Chow, 2007; Engkvist, 2006) | 1 (Craib et al., 2007; Engkvist et al., 2006) | 0 | 0 | 6 |
| III(b). Quasi-experimental: single group pre/post | 4 (Li, Wolf, & Evanoff, 2004; Alamgir et al., 2008; Chhokar et al., 2005; Park et al., 2009) | 6 (Hunter, Brandon, & Davenport, 2010; Charney et al., 2006; Nelson et al., 2006; Brophy, Achimore, & Moore-Dawson, 2001; Collins et al., 2004; Lynch & Freund, 2000) | 2 (Nevala et al., 2003; Leff et al., 2000) | 3 (Gottlieb & Caro, 2001; Stark et al., 2009; Horowitz et al., 2006) | 3 (Gitlin, Jacobs, & Earland, 2010; Nichols et al., 2011; Marquardt et al., 2011) | 18 |
| IV. Non-experimental studies (cross-sectional, single group post-test only, retrospective) | 2 (Trinkoff et al., 2003; Khatutsky et al., 2010) | 1 (Owen & Garg, 1994) | 0 | 1 (Liu & Lapane, 2009) | 1 (NAC, 2011) | 5 |
| V. Qualitative (focus groups, individual interviews, observation, literature reviews) | 0 | 0 | 0 | 2 (Demiris et al., 2008; Mann et al., 2002) | 4 (Carswell et al., 2009, Sabata, Liebig, & Pynoos, 2005; Messecar, 2002; Kinney et al., 2004) | 6 |
| Total | 12 | 9 | 4 | 16 | 11 | 52 |
| * Levels I-V are adapted from Moore et al."s (1995) five-tiered model for viewing research design strength. ** One study (Schultz et al., 2009) included care recipients with spinal cord injury age 35 and older and their family caregivers. | ||||||
| TABLE A-3. Studies on Specific Technologies for Caregiving Workforce in Nursing Homes/Hospitals | |||
|---|---|---|---|
| Author/ Publish Date | Study Participants and Sample Size | Intervention/ Study Explanation | Key Findings |
| Alamgiret al., 2008 | 3 long-term care facilities in Vancouver, Canada. | Longitudinal study conducted with analysis of injury trends from 6 years pre-intervention to 4 years post-intervention. Study evaluated the effectiveness of overhead lifts in preventing MSIs. 110 lifts were installed in the 3 facilities. | Injury Prevention The relative risk for MSI and working days lost per bed decreased after installation of the ceiling lifts, compared with the pre-intervention period. Costs/Savings The estimated payback period (recovering costs of the ceiling lifts with savings from decreased injury claims) was around 6.2-6.3 years when just using direct costs, but 2.06-3.2 years factoring in indirect costs. |
| Baptisteet al., 2006 | 77 caregiving staff in the acute care unit of a large Southeastern Veterans Administration hospital. | Every 2 weeks, each of the 8 acute care units received 1 of 8 randomly selected devices. 7 of the 8 devices were commercially available lateral-transfer devices or friction-reducing devices: (1/2) 2 types of air-assisted devices (the AIRPAL and the HoverMatt), (3) a silicone-filled tubular sheet (the Slipp); (4/5) 2 types of twin flat sheet sets with extended pull straps (the Flat Sheet Set and Maxi Slide); (6) a hollow fabric sleeve with straps to assist the transfer (Resident Transfer Assist); (7) a hollow fabric sleeve that requires a push action to perform the transfer (the Maxi Trans). The eighth device was the traditional draw sheet, which served as a baseline measure. Data was collected through caregiver surveys, which measured comfort, ease of use, perceived injury risk, time efficiency, and patient safety through caregiver ratings. 179 transfers were completed using the 8 devices. | Technology Rankings Air-assisted devices were preferred, with the AIRPAL and HoverMatt ranking first and second, respectively. The Resident Transfer Assist ranked third, the Maxi Slide forth and the Slipp fifth. The Flat Sheet Set had an overall rank of sixth, with caregivers reporting that the device was slippery and unmanageable and that they had difficulty keeping the 2 sheets together beneath the patient during the transfer. The draw sheet, which is the traditional lateral-transfer device used in many settings, was the worst method and not recommended. As this is a commonly used device, Baptiste et al., argued against its continued use. |
| Chhokaret al., 2005 | A Canadian-based extended care facility. | Longitudinal study to examine the effects of an overhead ceiling lift in 1 extended care facility. Injury trends 3 years pre and 3 years post-intervention were analyzed, spanning from 1995-2001. Lifts were installed in 1998. 65 ceiling lifts, servicing 125 beds and 3 bathtubs, were installed in the facility. Education on use of the lifts was provided to all patient-handling staff. | Injury Prevention While the number of claims and claim costs had been increasing prior to the intervention, these trends reversed during the intervention period, indicating a decrease in injuries. Costs/Savings An estimated $412,754 was saved during the 3 years post-intervention. Substantial decreases in the number of claims, costs, and time-loss were not observed until 2 years post-intervention. |
| Engstet al., 2004 | A 75-bed unit in a long-term care facility (in Canada) was the intervention group. Another unit in the same hospital served as the comparison group. 50 of the 75 residents in the intervention group participated and 50 of 75 residents in the control unit participated. For the intervention group, selection was based on their continence program and potential benefits to participation. | A new individualized scheduled toileting program for residents with incontinence was implemented. This included 10 mechanical lifts (5 sit-stand lifts and 5 seated lifts) that were purchased for the intervention group's unit to use. Staff were trained on use of these mechanical lifts. Both the intervention and comparison groups received education on recognizing agitation in residents. 32 workers in the intervention unit completed pre and post-intervention questionnaires, with 17 workers in the comparison unit doing the same. | Injury Prevention The use of a mechanical lift to transfer residents to and from a toilet reduced physical risk of MSD/MSI for nursing home workers, in comparison to cleaning residents in beds. The intervention led to decreases in the amount of force necessary to complete the task and the duration and severity of awkward postures (neck, shoulder, lower back) that are typical when cleaning residents. Patient Response In addition, resident agitation significantly decreased in the comparison group, while increasing in the comparison group. |
| Engstet al., 2005 | 34 staff members from a 75-bed extended care unit in Canada that received ceiling lifts served as the intervention group. 16 staff members of a 75-bed extended care unit in the same hospital, which did not receive lifts, served as the comparison group. | Ceiling lifts were installed in the intervention unit, which took 6 months to complete. During this time, staff in the intervention unit were trained on lift use. A pre-intervention questionnaire was administered to both groups. The post-intervention questionnaire was administered a year later, after the intervention period had ended. | Costs/Savings Total costs for the intervention were $284,297, which included purchasing and installing the intervention and hiring a program coordinator. Savings over 1 year for "all resident handling" were $9,835 in MSI claims and for "lifting and transferring tasks" were $14,493 in MSI claims. The payback period was estimated at 9.6 years for resident handling tasks and 6.5 years for lift and transfer tasks, due to savings from reduced compensation costs. Injury Prevention Perceived risk of injury and discomfort to neck, shoulders, upper and lower back, and arms/hands for care staff significantly decreased. All staff in the intervention group felt that the ceiling lifts made lifting residents easier and 96% felt that the lifts made their job easier to perform. |
| Khatutsky et al., 2010 | Data from the 2004 National Nursing Assistant Survey; the 2004 National Nursing Home Survey; Online Survey, Certification, and Reporting; and the Area Resource File. | Retrospective analysis on the effect lifting device availability had on the probability of being injured. | Injury Findings Multi-variate analysis did not find availability of lifting devices reduced probability of being injured. The analysis did find that mandatory overtime, poor training, being a new worker, and not having enough time to provide ADL help increased the probability of injury. The study concluded that injuries are a major issue and possible interventions include more comprehensive training, reducing mandatory overtime, and providing support for certified nurse assistants new to the field. |
| Li, Wolf, & Evanoff, 2004 | 61 staff members were surveyed pre-intervention; 36 completed a follow-up survey. The staff came from 3 nursing units in a small community hospital in a suburb of St. Louis, Missouri. | Mechanical patient lifts were provided and hands-on training sessions in lift usage was conducted by hospital personnel and all staff involved in patient-handling were expected to attend. 1 portable full body sling lift and 2 portable stand-up sling lifts ("E-Z Lift" and "E-Z Stand" by EZ Way Inc, Minneapolis, Minnesota). Friction-reducing sheets (Maxi-slides) were used to position patients in bed in preparation for lift usage. | Injury Prevention Musculoskeletal symptoms and MSIs decreased. Correlating with that, lost workday injury rates also decreased. Costs/Savings Annual workers' compensation costs for nursing personnel on the intervention units declined from an average of $484 per full-time equivalent (FTE) pre-intervention to $151 per FTE post-intervention. |
| Owen, Keene, & Olson, 2002 | The medical-surgical units of two rural hospitals in the Mid-western US. The study included 37 volunteers at the experimental site and 20 volunteers at the control site. All were female nursing personnel staff working in the medical-surgical units. | 5 assistive devices were implemented at the experimental site, including: (1) a mechanical, battery-operated lift for transferring non-weight-bearing patients to and from bed to chair and commode, (2) a battery-operated stand-up lift for transferring weight-bearing patients with the same tasks, (3) a walking belt with handles for transferring weight-bearing patients who need less assistance with the above tasks, (4) a friction-reducing sheet for use in transferring people from bed to stretcher and vice versa and for lifting up in bed, and (5) a toileting device for toileting in bed. | Injury Prevention For all tasks, nursing staff in the experimental site rated perceived exertion significantly lower than the control site study participants for both shoulder and lower back. The number of back injuries, lost work, and restricted days also decreased in the experimental group. At the control hospital, back and shoulder injuries, lost workdays and restricted days remained stable. Patient Response Patients were also surveyed about their feelings of comfort and security. At the experimental site, patients reported higher comfort levels and security levels in the transfer or lift when assistive devices were used. |
| Park et al., 2009 | All nursing homes in Ohio (887 total nursing homes). | In 2000-2001, the Ohio Bureau of Workers' Compensation (BWC) sponsored interventions to reduce injuries in nursing homes, including training, consultation, and grants of up to $40,000 to purchase equipment, including lifts, electric beds, and other devices. This study evaluated the impact of the intervention on back injury claim rates using BWC data on claims, interventions, and employer payroll for all Ohio nursing homes during 1995-2004. | Injury Prevention The greatest impacts were seen with equipment. A $500 equipment purchase per nursing home worker was associated with a 21% reduction in back injury rate. Costs/Savings This injury rate reduction translated to an estimated $768 reduction in claim costs per worker, a present value of $495 with a 5% discount rate applied. |
| Trinkoff, Brady, & Nielsen, 2003 | 1,163 actively licensed RNs in two states, 57% of whom worked in hospitals. These RNs also worked in nursing homes and home health agencies. | Survey asked about the availability of AT (lifting devices, lifting teams, transfer sheets, adjustable beds) and the availability/use of training programs. Data analysis measured the effectiveness of these in lowering odds of neck and back MSDs. | Injury Prevention Both lifting teams and lifting devices were associated with lower odds of back MSI/MSD. In contrast, availability of transfer boards/sliding sheets and adjustable beds were associated with higher odds of back MSD for those using those devices. |
| Danyardet al., 2001 | Winnipeg's Health Sciences Center (HSC) Used the same selection criteria as study (below). Unit Assistants from each ward were selected for participation -- Sample size was 36 UAs, 12 from each arm of the study. | Utilized a quasi-dynamic biomechanical computer model of the lumbar spine (WATBAK) to calculate the magnitude of the compressive and shear forces acting at the L4-L5 level during patient-handling | Injury Prevention This study examined both peak spinal pressure and cumulative spinal loading. Researchers found that education/ technique training and the use of new AT resulted in reduced spinal loading for several tasks. However, the use of AT contributes to an increased cumulative spinal loading. Use of AT takes much longer than manual transfer, in many instances, resulting in prolonged forward flexed trunk postures. Over the course of months or years, this can also cause problems. |
| Yassiet al., 2001 | Winnipeg's HSC 3 wards with the highest risk for MSD were chosen from the Winnipeg HSC, an acute and tertiary care hospital in Canada: medical, surgical, and rehabilitative. Each ward was randomly assigned to 1 arm of the study (resulting in 1 medical, 1 surgical, and 1 rehabilitative unit on each arm -- a total of 9 wards). Only permanent staff to each ward were included, float pool staff were not. | 1 ward used usual practice, while the other 2 wards had various patient-handling devices, including a mechanical total body lift, a transfer belt or sit-stand lift or mechanical total body lift, slide devices, and transfer belts. The devices were used to move patients from floor to bed or chair, from bed to chair or chair to bed, from bed to stretcher or vice versa, moving patient in bed, or walking with patient, respectively. | Injury Prevention The wards with accessible mechanical equipment showed decreased fatigue of workers, improved comfort with patient-handling tasks, and increased perception of safety among staff. |
| Number of Studies: 12. | |||
| TABLE A-4. Studies on AT/Ergonomic Interventions for Caregiving Workforce in Nursing Homes/Hospitals | |||
|---|---|---|---|
| Author/ Publish Date | Study Participants and Sample Size | Intervention/Study Explanation | Key Findings |
| Brophyet al., 2001 | A 525-bed nursing home in upstate New York. | A 5-step ergonomics program consisting of: (1) creation of a resident transfer evaluation team, (2) establishment of an accident review committee, (3) mandatory ergonomics training for new nursing aides, (4) regular maintenance checks for lifting equipment, and (5) direct access to the management and budget process. During the 7-year study period, the facility purchased 8 smooth movers, 10 hydraulic stretchers, 7 Hoyer lifts, 1 Arjo lift, 9 Sarita lifts, and 1 Maxilift. | Injury Prevention Comparing the pre-intervention period (1992-93) and the intervention period (1994-98), significant reductions were seen in low-back injuries (from 15.7 to 11.0 per 100 full-time nursing aids), lost workdays (from 1,476 per year to 625 per year), and lost workdays per full-time nursing assistant (from 7.8 to 3.0). Costs/Savings The yearly cost associated with low-back injuries declined from $201,100 before the intervention to $91,800 during the intervention. |
| Charneyet al., 2006 | Washington Hospital Services, a self-insured workers' compensation program, implemented the zero lift program in 31 of its 38 hospitals. | Zero lift program -- The program replaced manual lifting, transferring, and re-positioning of patients with mechanical lifting or use of other patient assist devices. Equipment "vendor fairs" were held that allowed patient-care staff to have "hands-on" experience with the equipment. A zero lift committee was established which was responsible for implementing the program, including making purchasing decisions. Equipment purchased included vertical lifts, lateral-transfer stretchers, sit-to-stand lifts, ceiling lifts, and non-friction transfer sheets for re-positioning. | Injury Prevention Patient-handling injury claims decreased by 43% in participating hospitals from 2000 to 2004 (from 3.51 to 2.23), and the time lost frequency rate decreased by approximately 50% (from 1.91 to 1.03 per 100 FTEs). Patient Response Patients experienced fewer injuries during lifts (fewer skin tears, falls, less pain). |
| Collins et al., 2004 | 6 nursing homes across 2 states with a total of 1,728 nursing staff. | 6-year study of a "best practices" MSI prevention program from 1995 through 2000. The program included mechanical lifting equipment and re-positioning aids, worker training on the use of the lifts, a medical management program, and a written zero lift policy. The equipment included friction-reducing sheets for re-positioning residents in bed and two types of mechanical lifts, based on the resident's level of physical dependency. | Injury Prevention Resident handling injury claims rates decreased significantly in the post-intervention period. Patient Response Assaults and violent acts by residents towards caregivers declined after the safe resident handling and movement program was implemented. Costs/Savings Expenses to purchase lifting equipment and provide worker training, the initial investment was recovered in slightly less than 3 years. |
| Engkvist, 2006 | 3 hospitals took part. The first included 8 wards in a hospital where a NLS had been introduced earlier (called the NLS hospital). The other 2 hospitals had 11 corresponding wards (control hospitals). The study population consisted of all nursing personal employed in the NLS hospital and control hospitals. A total of 487 persons were included, all belonging to 1 health care network in Melborne. | In the NLS hospital, nurses tested equipment and participated in the equipment purchasing decisions. Equipment was purchased based on each ward's assessed needs: Purchases included: 3 hoists, 2 standing walker hoists, 210 slide sheets, 3 rolling frames, 25 walk-belts, 44 foot-stools, 41 bed-ladder straps. | Injury Prevention Compared with nurses at the control hospitals, those at the NLS hospital reported fewer injuries, had less pain/symptoms, had less absence from work due to musculoskeletal pain/symptoms, and rated physical tiredness lower. |
| Hunter, Branson, & Davenport, 2010 | Northwest Texas Healthcare System (NWTHS). This program was for all clinical staff across all units. | A safe patient-handling program, also known as minimal or no lift practice was implemented in the NWTHS. A vendor, Diligent, was selected for providing lift equipment and assisting in implementing the program. They provided training and education to in-house clinical staff. They also assessed departmental needs for certain devices like ceiling lifts, portable equipment, and support supplies. | Injury Prevention During the 2.5 years of the program, the number of worker injuries reduced from the baseline of 20 per year to 5 injuries in 2007, 5 in 2008, and 1 injury from December 2008 through July 2009. Patient Response Patients and staff provided positive feedback about the lifting equipment used for safe-patient-handling. Costs/Savings Prior to the program, the facility experienced an average of 20 injuries per year, with an average direct cost per injury of $27,402 and average total direct costs per year of $548,040 associated with worker injuries. The total cost of the 3-year program, including equipment, training, and consultation, was $582,081. As a result, the facility nearly recouped the cost of the three-year program within 1 year. |
| Lynch & Fruend, 2000 | Program took place at a 440 bed acute care hospital. Impact evaluation was done for the 374 nurses and other patient-handling staff who completed training. | A 1-year Back Injury Prevention Program was implemented at a 440-bed acute care hospital. This program included the following components: (1) An ergonomic evaluation of patient-handling; (2) Purchase of patient transfer devices, like walking belts, transfer boards, and patient hoists were selected; (3) A train-the-trainer program was implemented before training for staff, and (4) training of 374 nurses and patient-handling staff was conducted. | Injury Prevention The number of back injures was 30% below the prior 3 years average. Immediately following training, reported injuries in the final quarter were 1/7th of the 3 prior quarters. |
| Morgan & Chow, 2007 | Shady Grove Adventist Hospital -- MD community hospital with 269 beds. | A comprehensive ergonomic plan was created in 2001 and implemented in 2003. The plan included patient lifting equipment, as well as establishing policies for no manual lifting and patient-handling, training employees, and other elements. OSHA guidelines were used to determine lifting strategies and equipment, which included the use of gait/transfer belts, full body slings, toileting slings, and bathing mesh slings. It was noted that SGHA would be purchasing ceiling lifts. All new staff were required to complete electronic ergonomic and patient lifting training. A mandatory annual training was implemented for all clinical and non-clinical staff. Case management was also implemented after staff were injured, to insure proper healing time and future prevention of injuries. | Injury Prevention Over 2 years, workers' compensation claims related to MSIs decreased from $0.31/$100 of payroll to $0.17/$100 of payroll, lower than the 4 comparison hospitals. Costs/Savings Over a period of 2 years, workers' compensation costs decreased by $238,330. |
| Nelson et al., 2006 | 19 nursing home units and 4 SCI units in 7 Southeast United States facilities. | A multi-faceted program which included providing patient-handling equipment based on needs identified in an ergonomic assessment, in addition to patient safety leaders and a no lift policy. Several devices were purchased to assist in the handling of patients, including ceiling mounted patient lifts, floor-based full body sling lifts, mechanical lateral-transfer aids, powered stand assist lifts, friction-reducing devices, and gait belts with handles. | Injury Prevention There was a decrease in the rate of MSIs. Technology Rankings Participants ranked the patient-handling equipment as the most effective component of the intervention, with 96% of respondents rating it as "extremely effective." The no lift policy was ranked second (68% said extremely effective), and the peer safety leader was ranked third (66% said extremely effective). Significant increases in 2 job satisfaction subscales (professional status and task requirements) were reported. Costs/Savings A cost/benefit analysis projected that annual costs for the program would be $123,037, and it would result in injury costs savings of $327,636 annually, for projected annualized cost savings per year of $204,599. Over a 10-year period this translates to over $2 million dollars of savings, excluding inflation. The analysis did not include the indirect costs of injury and low morale among workers. |
| Owen & Garg, 1994 | A single nursing home. 6 female nursing students participated in the laboratory study and nursing assistants participated in the intervention part of the study. | 38 nursing assistants volunteered to identify stressful tasks -- weighing a patient was considered to be one of the most stressful tasks. A laboratory study was developed to test differences between ways of weighing patients: (1) currently used manual lifting of patient from wheelchair to scale; (2) transfer via hoist, and (3) a wheelchair ramp scale. 6 female senior nursing students were evaluated performing these tasks. The hoist and wheelchair ramp were then made available to nursing assistants on 2 floors of the facility. A nurse observer discussed the use of this new equipment with nursing assistants to determine their perceived physical stress. | Injury Prevention The laboratory study found that compressive force to L5S1 and shear force were reduced using the hoist and wheelchair ramp. When the equipment was made available to the nursing assistants, nurse assistants reported that perceived physical stress to shoulder, back, and body was reduced using the hoist and wheelchair ramp. Patient Response Resident feelings of comfort and security increased. |
| Number of Studies: 9. | |||
| TABLE A-5. Studies at AT/HM/Ergonomic Interventions for Paid Caregivers in the Home | |||
|---|---|---|---|
| Author/ Publish Date | Study Participants and Sample Size | Intervention/Study Explanation | Key Findings |
| Craibet al., 2007 | 6 home support agencies in British Columbia, Canada. 5 of the agencies adopted 1 or more of the interventions, while 1 agency participated as a control group. | Interventions used in this study were: (1) an education and training module, (2) a risk assessment tool and resource guide to guide supervisors through assessment of the risks to workers in clients' homes and information on precautions, and (3) a lift equipment registry. 2 manufacturers agreed to provide a combined total of 25 lifts (20 ceiling and 5 freestanding lifts) for the registry. For the 1-year study period, the lifts were loaned to clients who would have to arrange to purchase the lifts by the end of the study period. If funds could not be found to purchase the lift, then the manufacturer would consider donating the lift to the client. | Injury Prevention Overexertion and falls were the majority of workplace injuries, both before and after the interventions. Workers at agencies receiving interventions reported significantly more workplace injuries than those from the comparison site, which may indicate increased ability to recognize injuries and/or awareness of injury reporting at intervention sites. Workers at agencies receiving interventions had fewer time-loss injuries compared with members of the comparison site. Workers more at risk of injury were those with a history of work injuries, full-time workers, and workers with less than college education. |
| Kraus et al., 2002 | 12,772 home attendants in 9 agencies in New York City. | This study was organized/supervised by the Citywide Central Insurance Program and its Home Attendant Program of New York City. 9 home care agencies in New York were chosen for a clustered randomized controlled trial. These agencies were randomized into 3 groups: (1) the back-belt group, (2) lifting advice-only group, and (3) control group. Workers in the back-belt group were trained to use the back-belts and were required to utilize them. | Injury Prevention Home care attendants using back-belts experienced a somewhat lower rate of low-back injury than did those in the advice-only and control groups, which was only marginally significant. Subgroups at greater risk for new lower back injury were those with a greater body mass index, back problems at entry into the study, and a history of back injury. These groups may benefit more from the use of back-belts. |
| Leff, Habebach, & Marn,2000 | Franklin County Home Health Agency (St. Albans, Vermont) 32 Licensed Nursing Assistants (LNAs) were evaluated for risk of injury during transfer. This was a part of evaluating the current situation for LNAs at the home health agency before implementing the program. | A Performance Improvement team developed an Injury Prevention program, for which they developed solutions and action plans to address Injury Prevention at the agency. These solutions were grouped into short-term, mid-term, and long-term solutions. The primary short-term solution was safety and health training. Risk management forms were also developed to determine hazardous situations. Another solution included the provision of a gait belt to each LNA for transfer of patients. It was also determined that LNAs would not have more than 7 patients per day. Mid-term solutions included identifying heavy lift patients and planning LNA shifts accordingly. The long-term solution was to conduct a post-offer, pre-hire PT screening for LNAs. The solutions mentioned above began to be implemented in 1996 and efforts were made to standardize the program. | Injury Prevention The program gradually reduced LNA back and shoulder injuries. Employee injuries were reduced from 4-10 per quarter to 0-3 per quarter. Lessons Learned It took at least a year for the program to show evidence of reducing injury rates, so interventions require patience and persistence. Researchers also suggest that multiple interventions may be necessary for a problem that has multiple causes. |
| Nevalaet al., 2003 | 5 personal helpers of people with physical disabilities living at home in Finland. | Clothing design changes for people needing assistance transferring to a wheelchair.1 The five helpers, all women, were measured at their worksites for their physical workload and strain before and after clothing redesign. The measurements for physical workload and strain were carried out before the clothing redesign and 1 year after the design. Workers' movements were videotaped and analyzed, and muscular activity and heart rate were measured using portable devices. | Injury Prevention The redesign of clients' outerwear decreased the physical workload and strain of the personal helpers in some measures including the number of correcting hand motions and grasping motions, fewer forward bent postures, and lower mean muscular activity of the trapezius and of the erector spinae muscle. |
Number of Studies: 4.
| |||
| TABLE A-6. Studies on AT/HM/Ergonomic Interventions to Promote Independence for Older Adults with Disability | |||
|---|---|---|---|
| Author/ Publish Date | Study Participants and Sample Size | Intervention/Study Explanation | Key Findings |
| Becker-Omvig & Smith, 2010 | Older adults living in the community in Howard/ Montgomery County, Maryland. | The Joint Howard County Montgomery County OT Intervention for Older Adults: a pilot program providing older adults in Howard County, Maryland with in-home assessments and OT interventions including HM, AT, consultation, information and referral. OT focuses on the interaction of the person, the environment, and the occupation. | Implementation Issues The program was able to overcome initial resistance from staff and clients through "logical arguments, emotional arguments, building trust, and concrete reality." Lessons learned were the importance of champions, showing efficacy, and training. Challenges included funding for therapists, equipment, and modifications and using existing staff resources (training SWs and others, dissemination). Cost Savings Results of a randomized trial indicated that the intervention reduced hours of paid weekly assistance by 48% and cost less than $1,000 per person served. Promote Independence This intervention improved functional independence and safety, decreased fear of falling, and showed an increase in quality of life. |
| Sheffield, 2011 | The data for 71 participants in Howard and Montgomery Counties; complete data was available for 60 participants. | Howard County/Montgomery County (Maryland) Aging in Place/Better Living at Home program. | Same findings as those listed above |
| Demiriset al., 2008 | 9 older adult residents in apartments. | A participatory evaluation of a "smart home" project implemented in the apartments of nine residents of an independent retirement facility. This included an IMS which had a set of wireless infrared proximity sensors to detect motion and pressure switch pads. The IMS also included a stove sensor, a cabinet sensor, and a bed sensor. The researchers conducted 75 interviews with the 9 residents and conducted observations. | Acceptance of Technology Results indicate that there are three phases of adoption and acceptance of the sensors: (1) familiarization; (2) adjustment and curiosity, and (3) full integration. The residents reacted positively to the sensor technologies and did not feel that these interrupted their daily activities. Additionally, the residents did not express privacy concerns. |
| Gitlinet al., 2006 | 319 community living adults, age 70+, who reported difficulty with 1 or more ADLs. Study participants were recruited from an AAA, media announcements, and posters at senior housing and community settings. 160 were randomly assigned to the experimental group, and 159 were in the control group. | ABLE: This NIH clinical trial is a 6-month home intervention with 5 visits from occupational therapists (4 90-minute visits and one 20-minute telephone contact) to identify functional concerns and compensatory strategies; 1 PT visit (90 minutes). OT and PT sessions involved HM and training in their use; instruction in strategies of problem-solving, energy conservation, safe performance, and fall recovery techniques; and balance and muscle strength training. After the OT contacts, appropriate HM were identified to be installed before the sixth contact. AAAs ordered HMs like grab bars, rails, and raised toilet seats. | Promoting Independence At 6 months, ABLE participants had less difficulty than the control group with IADLs and ADLs. Benefits were sustained at 12 months for most outcomes. Costs Average costs per participant were $439 for equipment and HM and $783 for therapy, for a total of $1,222. Researchers recommended that HMs be reimbursable through Medicare, which is not part of the current policy. |
| Gottlieb & Caro, 2001 | CMs identified 196 home care clients who they believed would be good candidates for assistive equipment. The participant's age ranged from 61 to 101, with a median age of 81. | Massachusetts Assistive Equipment Demonstration: CMs from participating home care agencies worked to increase access to AT by identifying clients who they thought would be good candidates for assistive equipment, informing clients about equipment options, encouraging use of equipment, assisting with acquisition and installation of equipment, following up with clients regarding additional equipment needs, and incorporating equipment-related activities as part of their routine client reassessment visits. A key component of the demonstration was training conducted by occupational therapists for the participating CMs. | Implementation Issues 70% of clients reported using the assistive equipment regularly, 60% found the equipment to be "very helpful", and 90% expressed high overall satisfaction. Researchers suggest that CMs be provided with more consistent training on assistive equipment, be allocated more time to focus on assistive equipment, and more funds should be allocated for it. Costs Despite being encouraged to spend $150 on AT for clients, the average amount expended was $76. About half of the equipment distributed was for meal preparation, with others used for bathing, dressing, and mobility. |
| Horowitz et al., 2006 | The sample consisted of older adults who acquired a recent vision impairment and were applying for vision rehabilitation services. | They interviewed the sample (n=138) at pre-service and at 5-month follow-up. Participants were asked about their use of optical devices (including magnifier, telescope, special sunglasses, or other) and of adaptive aids related to vision loss (large-print telephone dials, handwriting guides, talking books, other talking items, large-print reading materials, long white cane for mobility or other aids). | Reducing Functional Decline A hierarchical regression analysis was conducted and researchers found that the optical device use was significantly associated with functional disability decline and a decline in depressive symptoms over time. These results were not found with adaptive devices. |
| Liu & Lapane, 2009 | Analysis of the Second Longitudinal Study on Aging (National probability sample of community-dwelling adults 70+ in 1994-1995). | The objective of their analysis was to quantify the extent residential modifications reduce the risk of subsequent physical functional decline in older adults | Reducing Functional Decline Results indicate that HM (like railings or bathroom modifications) were associated with reduced risk of decline among community-dwelling adults aged 70+. |
| Mann et al., 1999 | 104 home-based frail elderly persons living in western New York. 52 were assigned to the treatment group and 52 to the control group. | Participants received a functional assessment, a home environment evaluation, and AT/HM based on their evaluation results | Reducing Functional Decline The intervention group experienced less functional decline than the control group. |
| Mann et al., 2002 | A sample drawn from the Rehabilitation Engineering Research Center on Aging CAS, a 10-year longitudinal study of over 1,000 elders with disabilities which began in 1991. Selected subjects from Western New York. Interviewed 71 elders scheduled for their annual CAS interview in 1998. | Reviewed the benefits of home telehealth care, which they define as the provision of health care evaluation, medical advice, and the delivery of services to the home through the use of telecommunication technologies, including information, communications, and monitoring technologies. The researchers used the Rehabilitation Engineering Research Center on Aging CAS. They developed the "Home Care Monitoring Devices" questionnaire to gauge frail older adults' receptivity to devices including a thermometer, metered dosage inhaler, blood pressure monitor, blood glucose monitor, and medication compliance monitor. | Acceptance of Technology The results of the study indicated that the sample strongly accepted the concept of home health monitoring and the different devices. One of the determining factors of perceived intrusiveness of these devices was equipment characteristics. The researchers' analysis of subjective comments found that participants thought these devices would be useful for others, but not necessarily for their own personal use. |
| Mirza & Hammel, 2009 | 75 aging individuals with intellectual disabilities living in the community | In the ATLAS intervention, aging individuals with intellectual disabilities and their social support network worked with an occupational therapist for 4 sessions to identify and problem-solve issues through environmental strategies, including AT/HM, using a consumer-directed, collaborative approach. | Participant Satisfaction ATLAS was associated with higher levels of performance and satisfaction. |
| Peterssonet al., 2008 | 73 subjects recruited from an agency in Sweden providing HM services (intervention group). The intervention group's referrals had been approved and they were scheduled to receive HM. The comparison group consisted of 41 subjects waiting for their applications to be assessed for approval. | The purpose of the study was to examine the impact of HM on older adults with disabilities and their self-rated abilities in completing everyday functions. | Promote Independence Research found that older adults with disabilities in Sweden who received HM significantly improved in self-reported independence and safety including toileting and transferring tasks. |
| Rose, Gitlin, & Dennis, 2010 | This was a follow-up study to Gitlin et al., 2006, using data collected from the experimental group. Of the 160 original participants, data on 148 were used for this study. | ABLE intervention (see Gitlin et al., 2006 explanation). | Implementation Issues Higher readiness was associated with: younger age, African American race with financial difficulty, use of active-oriented compensatory strategies, use of cognitive oriented strategies, and lower levels of depression. However, the strongest predictor of change (from initial to final session) in older adults' readiness to utilize compensatory strategies of the ABLE intervention was social support. This finding supports the literature discussing the positive health benefits of social support. |
| Stark et al., 2009 | NORC. | A client-centered HM program for older adults was implemented. This was a quasi-experimental, single group prospective study, where participants' subjective ratings of daily activity performance were evaluated before and after the intervention (baseline/post/post). | Promote Independence Researchers found that adults in a suburban NORC improved significantly in their subjective ratings of their daily activity performance after receiving a HM. The improvement was maintained for two years. |
| Szantonet al., 2010 | Older adults selected with the help of the Baltimore City Commission on Aging and Retirement, the Baltimore Housing Authority, and Comprehensive Housing Assistance -- they were placed in an intervention and control group. | CAPABLE: Building on the ABLE demonstration, the CAPABLE pilot, is comprised of the ABLE program, a client-centered nurse intervention, and home safety/modification handyman services. The intervention group had their physical, mental, and environmental challenges addressed through 3 services -- OT, nursing, and the assistance of a construction specialist who made necessary home repairs, while the comparison group participated in life-review sessions that have been shown to improve mental activity only. (See study description at http://magazine.nursing.jhu.edu/2010/11/house-calls/) | Cost Savings/ Promoting Independence While findings were not yet available, the pilot is theorized to avert costly health utilization by increasing medication management, problem-solving ability, strength, balance, nutrition, and home safety, while decreasing depression and risk of falls. |
| Szantonet al., 2011 | The study consisted of 40 low-income older adults who have 1 or more ADL difficulties or 2 or more IADLs difficulties in the Baltimore, Maryland area. | CAPABLE. | Promoting Independence The researchers found that the study demonstrated moderate to strong effect sizes for mean change differences between the two groups over the course of the study. They also found that 94% of the intervention group stated that CAPABLE made their life easier in comparison to only 53% of the control group. |
| Wilson et al., 2009 | 91 older adults with disabilities. | The intervention group received an evaluation of their home and potential AT/HM needs which were provided and paid for (in full or in part) by the study. The control group received health care already available through community resources. Outcomes were tracked through in-home interviews using the OARS and the FIM. | Reducing Functional Decline Analysis of this data shows that there was slower decline in function over the 2 year intervention period in the treatment group. Additionally, the group was found to be more likely to use AT instead of personal assistance to maintain their independence. |
| Number of Studies: 16. | |||
| TABLE A-7. Studies on AT/HM/Ergonomic Interventions to Support Family Caregiving and Family Caregiver Data | |||
|---|---|---|---|
| Author/ Publish Date | Study Participants and Sample Size | Intervention/Study Explanation | Key Findings |
| Studies Involving Family Caregivers | |||
| Gitlinet al., 2003 | Primary caregivers who reported at least 1 limitation in ADL or 2 dependencies in IADLs of the care recipient were selected/recruited from the Philadelphia Corporation for Aging. 255 people agreed to participate101 were randomly selected as control and 89 as intervention group participants. | REACH: Tested ESP, which was part of the NIH's REACH. ESP provided family caregivers of people with ADRD with education about the disease process and how the environment can affect care receivers' behaviors and assistance with problem-solving strategies and ways to modify the home, through 5 home contacts and 1 telephone contact by occupational therapists who provided the education, problem-solving training, and adaptive equipment. Strategies for HM included using equipment (grab bars or handrails), removing, rearranging, or relabeling objects; using color contrast; and placing objects in purposeful locations. | Reducing Caregiver Stress The home environmental approach does reduce stress in objective and subjective burdens and enhances select aspects of caregiver well-being. Caregivers reported less upset with memory-related behaviors, less need for assistance, and better affect. |
| Gitlin, Hauck, & Dennis, 2005 | 127 of the 190 participants in the previous study. | REACH: Following the 6 month active phase of the previous study there was a 6 month maintenance phase. This study measures maintenance of effects from the previous study at 12 months. | Reducing Caregiver Stress Caregiver affect improved and there was a trend for maintenance of skills. |
| Nichols, Martindale-Adams, Burns, Graney, & Zuber, 2011 | Stressed caregivers of people with dementia from 24 VA Veterans Health Administration (VHA) medical centers in 15 states. | REACH VA (part of REACH II): The REACH VA initiative provides education, a focus on patient safety, caregiver support, and skill-building for caregivers in dealing with difficult patients. This is an intensive intervention that includes 12 individual home and telephone sessions and 5 telephone support groups over a 6 month period. 24 Home-Based Primary Care programs across the country are participating in the intervention. (See study description at http://aging.senate.gov/award/vet5.pdf.) | Reducing Caregiver Stress Outcomes from baseline to 6-month follow-up included significant improvements in burden, depression, impact of depressive symptoms on daily life, caregiving frustrations, and troubling dementia related patient behaviors. Caregivers also reported per day decreases of 2 hours on caregiving duty. Costs/Benefits Preliminary examination of Veteran health care use showed declines in inpatient, pharmacy, and outpatient costs. VHA costs to deliver the intervention would be $2.93 per day. Participant Response Staff and caregiver satisfaction and perception of benefit were high. |
| Sabata, Liebig, & Pynoos, 2005 | This demonstration project comprised 4 steps, with different samples for each one. (1) Needs assessment: 29 people recruited from the LA Caregiver Resource Center in 4 focus groups to assess the most problematic and physically demanding activities for caregivers, plus 120 randomly selected participants from a list of 300 AAA contacts, for a survey to determine what HM services were available through AAAs. (2) Training: A 10-week course to NFCSP staff, recruited from the NFCSP staff directory. The first 20 registrants from each course offered (there were 2) were offered enrollment, resulting in 40 NFCSP staff participating in training courses. (3) Implementation: Same sample as for Training. (4) Evaluation: Survey sent to training participants. | AoA funded Project CARES (Caregiver Adaptations to Reduce Environmental Stress), which sought to train staff of the NFCSP about AT/HM for caregivers. The findings of the needs assessment contributed to the development of the training. Implementation included proposals or plans of action written by training participants. In the last 2 weeks of the training course, participants were asked to write a proposal or plan of action to identify an activity to be completed within 6 months, identifying resources and partners to complete this activity. Some of these proposals included developing in-service training for caregivers to use HMs and leading a caregiver support group about HMs. A likert scale was used to rate material usefulness and open-ended questions for participant progress/experience. | Needs Assessment The needs assessment found the AT/HM most frequently used by caregivers was "grab bars". Caregivers noted that HMs were also useful for the older adult with mobility problems. The most problematic activities for caregivers of persons with Alzheimer's disease included bathing, toileting, and using steps. The most physically demanding activities were lifting, transferring, and bathing. Caregivers reported that their use of HMs and ATs was limited due to the cost and difficulty in finding someone to make the modifications. Training The evaluation component measured the success of training and implementation. Participants felt that they were more knowledgeable about HMs and had more resources available to them to connect clients to services. |
| Studies Involving Caregiver/Case Recipient Dyad | |||
| Carswellet al., 2009 | Systematic Literature Review. | The authors review the literature available on AT that can assist people with dementia and their caregivers during the night. | Reducing Caregiving Stress Some of the AT helped alleviate caregiver mental or emotional strain through calming the care receiver and alleviating verbal aggression and agitation. |
| Gitlin, Jacobs, & Earland, 2010 | 22 occupational therapists implemented ESP to caregivers. 41 caregivers participated to receive ESP services. | ESP (part of REACH) a two-year translational project was conducted with a home care practice as a reimbursable Medicare Part B Service | Reducing Caregiver Stress Caregivers receiving ESP reported improvements in knowledge, skills, and well-being. 100% of caregivers said they would refer use of ESP to other caregivers. Costs Since ESP sessions were reimbursed through Medicare when integrated with patient-directed therapy, it has potential for being sustained through this mechanism. |
| Kinney et al., 2004 | 19 families who were caring for a relative with dementia. | The authors describe the process of installing a monitoring system in the homes of participating families (The SAFE House), which consisted of a camera and sensors routed through a controlled unit to a website that is accessed with a broadband-connected computer. Caregivers are then alerted through text messages from the website if any potentially unsafe activity is detected. | Reducing Caregiving Stress Some of the positive benefits of this system included peace of mind for the caregivers; however, 50% of the caregivers surveyed felt that the system made their lives more difficult because of the technological burden. |
| Marquardt et al., 2011 | Community-dwelling sample of 82 elderly people with dementia. | The study examined home environmental features, safety issues, and health-related modifications in the each participant's home. Caregiver reasoning for implementation of HM and barriers to implementation were analyzed. | Promoting Independence/ Safety Caregivers' reasoning for modifying the home included the care receiver's physical limitations, most commonly for bathroom safety. Another primary reason was care receiver memory loss these modifications included additional lights, signs and labels. |
| Messecaret al., 2002 | 24 caregivers of community-dwelling elders with a variety of impairments. | Qualitative study of family caregivers' decision to use HM. | Environmental Modification Use The decision to use environmental modifications was determined by a complex evaluation of the benefits and disadvantages for both the caregiver and care receiver. Benefits for care receivers included improved functioning, safety, comfort, energy conservation, and preservation of self-identity. Benefits for caregivers included decreased workload, making monitoring and keeping the elder safe easier, reducing the unpleasantness of tasks, and having their own needs accommodated. Negative outcomes for care receivers included feeling stigmatized by the modification, being disappointed in the amount of improved function, being afraid to use the modification, or being unable to use the modification. Negative outcomes for caregivers included having their workload increased or feeling that the care receiver's functioning was not improved enough to warrant continued use. |
| National Alliance for Caregiving, 2011 | Quantitative online survey of 1,000 technology using family caregivers who were 18+, provided at least 5 hours/ week of unpaid care to an adult relative or friend who needed help due to a physical or mental illness, disability or frailty. | The survey examined family caregiver receptivity to 12 technologies that could help them provide care. The researchers also examined barriers to the use of technology, the factors that influence technology use, and sources caregivers trusted for technology information. | Technology Use Caregivers were most receptive to technologies related to delivering, monitoring, tracking, or coordinating the care recipient's medical care. Caregivers under age 50 were more likely to be receptive to technology use. The most commonly reported obstacle was the belief that the technology would be expensive. |
| Schulz et al., 2009 | 173 caregiver and care receiver (individuals with SCIs) dyads recruited from Pittsburg and Miami. | Participants were randomized into 3 groups: (1) a caregiver/care receiver dyad intervention group, (2) a caregiver-only intervention group, and (3) an information-only control group. This study does not look at the effect of AT/HM, but does include measurements for physical health symptoms. The study measured quality of life outcomes depressive symptoms, burden, social support and integration, self-care problems, and physical health symptoms. The caregiver-only intervention consisted of 5 in-home sessions and 2 telephone sessions (all 60-90 minutes in length) over 6 months. These were designed to provide caregivers with the knowledge to reduce environmental and personal stress, improve upon health and self-care, enhance access to support, and improve emotional well-being. The dual-target intervention utilized the same model as the caregiver-only intervention for the caregiver of the dyad. For the care recipient, the same elements were provided (like improving emotional well-being). In addition to learning about the benefits to their own emotional/physical well-being, care recipients were taught ways in which they may assist in reducing caregiver burden. In addition to the 5 in-home sessions and 2 phone calls, care recipients also participated in 5 telephone support group sessions. The control group received a packet of information about SCI, aging, community resources, and caregiving. 3 check-in calls were also conducted. | Dyad Quality of Life The intervention targeting the caregiver/care receiver dyad improved quality of life of the dyad (measured by depressive symptoms, burden, social support and integration, self-care problems, and physical health symptoms). No significant effects were obtained through the caregiver-only intervention, raising questions about the efficacy of this approach. |
| Number of Studies: 11. | |||
Appendix B. Family Caregiver Guide to Assistive Technologies and Home Modifications
Caregivers give much needed support for older adults with disabilities or illness living at home. But often caregiving can be a physical strain. When you take care of yourself, you can better help your family member or friend. Many assistive technologies (AT) and home modifications (HM) may help make life easier for you and protect your safety and safety of your family member.
Did you know...?
-
Lifting more than 35 pounds by yourself is not safe. Moving a person can greatly increase your risk of injuries like back strain. If a person cannot support any of their weight, lifting them alone is unsafe.10 A hoist or lift can help protect you and your loved one.
-
Caring for a person with dementia can lead to physical strain. The person may get confused and resist help. They may need a lot of care. Making the home better suited for a person with dementia could help.
-
Helping a person do things on their own when they can is best. When a person gets too much help, they may get more dependent. Many kinds of AT/HM can help a person do more on their own and stay safe. This can help them keep their strength and reduce the amount of help they need. That eases the strain on you. Also, using AT/HM to do things on their own may help your family member maintain their dignity and deter depression.
-
Many AT/HM can be useful for people of all ages and health. But many of the changes that older people and caregivers need are things that can be useful for anyone. It could be as simple as a new light or a bath mat. Many people of all abilities use hand rails. Pill boxes can help anyone remember to take meds.
-
Many AT/HM are low or no cost. Some of the most needed items are small and low cost. Many places offer low cost used equipment. Some lend this equipment for free. Some home modifications are free, like clearing clutter.
-
Renters can use AT/HM. Many renters use AT /HM. Under Fair Housing law, you may make reasonable home mods in a rental home. Talking with your landlord first is a good idea.
Assessing your needs and choosing the right AT/HM helps make sure it will work for you. This guide lists many resources that can help. Some also offer other caregiver support. We list where to go for more help with choosing and obtaining AT/HM. The resources are free or low cost.
| Definitions
|
| Example AT/HM Needed by Family Caregivers and Older Adults
|
TOOLS FOR ASSESSING YOUR NEEDS
These are tools to help assess your home safety and needs. They give ideas on home safety, caregiver health and strain, and AT/HM.
AARP
Home Fit Guide
AARP's "Home Fit Guide" gives advice, tips, and checklists to help people make their home safer to live in as they age. Search for "Home Fit Guide" on the AARP homepage. It includes:
-
Do You Have a "Livable" Home? Checklist on whether your home is "livable" and will meet your needs now and in the future. An Occupational Therapist can help with this step.
-
What is Universal Design? Information on features that make a home easier to live in for someone of any age or ability.
-
Home Safety Checklists: Safety checklists for parts of the home--entries and exists, yard, steps and stairs, bathrooms, kitchens, living rooms, and bedrooms.
-
Home Maintenance by Season: Checklists for home maintenance by season to keep the home safe.
-
Home Energy Tips and Projects: Tips for cutting energy use and saving money.
Web: http://www.aarp.org
Mail: 601 E Street, NW, Washington, DC 20049
Toll-Free: 888-OUR-AARP (888-687-2277) / Toll-Free TTY: 877-434-7598
American Medical Association
Caregiver Self-Assessment Questionnaire
This tool helps you assess your risks. With your doctor's help, it helps you decide what's best for you and your family member. Search "Caregiver Self-Assessment".
Web: http://www.ama-assn.org/
Mail: 515 N. State Street, Chicago, IL 60654
Phone: 800-621-8335
South Dakota Caregiver Program
Caregiver Self-Assessment
This tool helps caregivers assess where they need help. It includes help with AT and learning how to safely lift and transfer. Search "Caregiver Self-Assessment".
Web: http://dss.sd.gov/
Phone: 605-773-3656 or 1-866-854-5465
IDEAS Consulting
Environment and Communication Assessment Toolkit
This Toolkit suggests home mods for communicating with a person with dementia. It focuses on people in long-term care settings, but can also help caregivers at home. A webinar is also provided (http://www.alzpossible.org/wordpress-3.1.4/wordpress/webinars-2/833-2/).
Web: http://www.ideasconsultinginc.com/#
Mail: 8055 Chardon Road, Kirtland, Ohio 44094
Phone: 440-256-1880
Centers for Disease Control and Prevention (CDC)
What You Can Do to Prevent Falls
This toolkit tells how to make your home safer and help prevent falls (http://www.cdc.gov/ncipc/pub-res/toolkit/WhatYouCanDoToPreventFalls.htm).
Web: http://www.cdc.gov/homeandrecreational safety/falls/index.html (more about Older Adult Fall Prevention)
Phone: 800-CDC-INFO (800-232-4636) TTY: (888) 232-6348
Fall Prevention Center of Excellence
This center provides many tools with ideas to prevent falls.
Web: http://www.stopfalls.org/
Mail: University of Southern California Andrus Gerontology Center, 3715 McClintock Ave., Room 228, Los Angeles, CA 90089-0191
Phone: 213-740-1364
Promoting Safety and Function Through Home Assessments
This article provides an overview of home safety assessments and three different assessments in the appendix.
Web: http://plaza.ufl.edu/mlwsail/6_promoting%20safety.pdf.
INFORMATION ON CHOOSING AT/HM
These resources can help with choosing the right AT/HM. Some will also connect you to makers and sellers of AT/HM.
AbleData
This site is funded by the federal government as a source of info on AT. It contains many fact sheets and guides on choosing AT by type of impairment. Select "Library", then "AbleData'sPublications".
Web: http://www.abledata.com/
Mail: 8630 Fenton Street, Suite 930, Silver Spring, MD 20910
Phone: 800-227-0216 or 301-608-8998 / TT: 301-608-8912
HomeMods.org
HomeMods.org offers guides to independent living at home for older adults and people with disabilities. Some relate to HM and housing repair. Go to the "Resources" Page and click "Library".
Web: http://www.homemods.org
Mail: Andrus Gerontology Center, University of Southern CA, 3715 McClintock Avenue, Los Angeles, CA 90089-0191
Phone: 213-740-1364
Center for Assistive Technology and Environmental Access (CATEA)
National Public Website on Assistive Technology
Here, you and your family member can learn about AT and other help for people with disabilities.
Web: http://assistivetech.net/
Mail: 490 Tenth Street, Atlanta, GA 30332-0156
Phone: 404-894-4960 (V/TTY)
This Caring Home
This project of Weill Cornell Medical College tells ways caregivers can make the home safer for people with dementia. It can be useful for all family caregivers. Caregivers can learn many things from this site. They can learn how to assess home safety and find out about products to help with giving care. These products could help ease stress for you and your family.
Web: http://www.thiscaringhome.org
Technology for Long-Term Care
This site provides pictures and descriptions of over 1,200 products for long-term care. This includes devices for bathing, memory, dressing, eating, falling, wound care, and much more. The site also includes articles and questions to ask sellers about the devices.
Web: http://www.techforltc.org/
Mail: 8055 Chardon Road, Kirtland, Ohio 44094
North Dakota Family Caregiver Project, ND State University
Assistive Technology and Older Adults: The Journey Through Caregiving
This is a useful guide for family caregivers of older adults at home. It answers many questions about AT, home safety, and HM.
Web: http://www.ndsu.edu/ndsu/aging/caregiver/pdf/assistive/manual.pdf
Mail: EML Room 277F, Fargo, ND 58105
Phone: 701-231-7391
National Association of Home Builders
Directory of Certified Aging in Place Specialists
This directory lists remodelers11 who are trained in the needs of older adults. They are also trained in HMs for aging in place, remodeling projects, and solving common problems. Search for "Find a Certified Aging in Place Specialist".
Web: http://www.nahb.org
Mail: 1201 15th Street NW, Washington, D.C. 20005
Phone: 1-800-368-5242
GENERAL CAREGIVER SUPPORT
These resources and websites can help you find caregiver support. Some also tell about home safety, AT, and HM.
AARP Caregiver Site
This website provides caregiver support and info on many topics.
Web: http://www.aarp.org/relationships/caregiving/
Mail: 601 E Street, NW, Washington, DC 20049
Toll-Free Nationwide: 888-OUR-AARP (888-687-2277) / Toll-Free TTY: 877-434-7598
Family Caregiver Alliance (FCA)
FCA offers many useful resources for family caregivers. A fact sheet tells about types of AT that may help you and your family member. It also tells how to find AT, how to pay for it, and how to decide what you might need. Go to "Fact Sheets", "Caregiving Issues and Strategies", "Assistive Technology". It is free online, or $2 a copy. (To order, go to "Fact Sheets", "Order Publications".)
Web: http://www.caregiver.org
Mail: 180 Montgomery St, Ste 900, San Francisco, CA 94104
Phone: (415) 434.3388; (800) 445.8106
National Alliance for Caregiving (NAC)
NAC offers many materials for family caregivers, such as booklets, tip sheets, webcasts, and meeting materials. These are in the "Resources" section of their website. You can also find your state caregiving coalition ("Coalitions", "Coalitions by State"). These coalitions help caregivers meet their social, health, financial, and emotional needs.
Web: http://www.caregiving.org/
Mail: 4720 Montgomery Lane, 2nd Floor, Bethesda, MD 20814
Phone: 301-718-8444
National Family Caregivers Association (NFCA)
NFCA's website offers many caregiving resources ("Caregiving Resources"). They also provide ways for caregivers to connect with each other ("Connecting Caregivers"). NCFA also offers free support through its Family Caregiver Community.
Web: http://thefamilycaregiver.org/
Mail: 10400 Connecticut Avenue, Suite 500, Kensington, MD 20895-3944
Toll Free: 1-800-896-3650, Phone: 301-942-6430
Rosalynn Carter Institute for Caregiving (RCI)
RCI works to improve supports for caregivers. This site offers links to many caregiver resources, including reports and tools on helping caregivers in the home. It includes a home safety assessment checklist, connections to sites for HM, and other resources helpful to family caregivers. Go to "Caregiver Resources."
Web: http://rci.gsw.edu/
Mail: 800 GSW Drive, Georgia Southwestern State University, Americus, GA 31709-4379
Phone: (229) 928-1234
Alzheimer's Association
The Alzheimer's Association offers a 24-hour helpline, local offices, and info for caregivers.
Web: http://www.alz.org/
Mail: Address: 225 N. Michigan Ave., Fl. 17, Chicago, IL 60601
24-hour helpline: 1.800.272.3900
Department of Veterans Affairs (VA) Caregiver Support
The VA offers many services to help caregivers of veterans. This website tells about these services. The "Caregiver Tool Box" can help you find tools that work for you. The VA's Caregiver Support Line gives info on the help offered and helps with getting services. They can also connect you with your local Caregiver Support Coordinator, or just listen.
Web: http://www.caregiver.va.gov/
VA Caregiver Support Line: 1-855-260-3274
WHERE TO GO FOR MORE HELP WITH AT/HM
The people and programs below may be able to give you more help with AT/HM. Contact them if you have questions or concerns about your home's safety. Some may be able to help you choose, access, and pay for AT/HM.
Your local aging services provider
This could be a National Family Caregiver Support Program, Area Agency on Aging, Aging and Disability Resource Center, or other program in your area.
These programs can help you get the services you need to care for yourself and your loved one. They can also refer you to other programs that might be able to help.
These can be found in the Eldercare Locator: http://www.eldercare.gov/eldercare.net/public/resources/topic/Caregiver.aspx
Phone: 1-800-677-1116
For more information about the National Family Caregiver Support Program, see http://www.aoa.gov/AoARoot/AoA_Programs/HCLTC/Caregiver/index.aspx.
Your primary care doctor
When you meet with your or your family member's doctor, tell them that you are a family caregiver. Tell them about any problems that your family member is having with daily activities, falling, or driving. Consider asking for a referral to an occupational therapist or someone else who can help you assess your needs and find out about AT/HM that might help. You could also ask where you can go for other support with caregiving. With a doctor's order, Medicare may pay for some or all of the cost of certain medical devices (http://www.medicare.gov)
Phone: 1-800-MEDICARE
An occupational therapist (OT)
OTs can help people do things they want or need to do.
They may visit your home and suggest changes to help you or your loved ones create a safer environment.
To learn more about how an OT might help you, visit the American OT Association.
Web: http://www.aota.org/About.aspx
Mail: 4720 Montgomery Lane, PO Box 31220, Bethesda, MD 20824-1220
Phone: 301-652-2682 / TDD: -800-377-8555
Your local Center for Independent Living (CIL)
CILs can help you by helping the person with a disability get the supports they need. This may include access to AT/HM.
These can be found in the ILRU Directory: http://www.ilru.org/html/publications/directory/index.html
Phone: 713-520-0232 ext. 130 (Voice/TTY)
Your nearest State AT project
These projects help people with disabilities to live independently through the use of AT. They serve people of all ages.
A state listing is offered at the State AT Projects Information Center, http://www.abledata.com/abledata.cfm?pageid=113573&top=16050&ksectionid=19326&stateorganizations=1
You can contact AbleData for more information at 800-227-0216 or 301-608-8998.
Pass It On Center
This center helps people with disabilities get affordable used AT.
Web: http://www.passitoncenter.org/
Phone: Toll Free 1-800-497-8665 or TDD: 1-866-373-7778
Non-Profit Resources
Below is a listing of just a few additional national nonprofit resources that provide assistance to family caregivers with AT/HM.
Easter Seals is a nonprofit, community-based health agency that assists children and adults with disabilities attain greater independence. Their resources include information on accessible homes, transportation, and workplaces. You can go to their webpage to locate an Easter Seals near you.
Web: http://www.easterseals.com
Mail: 233 South WackerDrive, Suite 2400, Chicago, IL 60606
Phone: 800-221-6827
Rebuilding Together is a national nonprofit that works to preserve affordable homeownership and revitalize communities. Some of their work includes a national Safe at Home initiative, helping to address home repair and maintenance issues.
Web: http://www.rebuildingtogether.org/
Mail: 1899 L Street NW, Suite 1000 Washington D.C. 20036
Phone: 800-473-4229.
The National MS Society has state chapters that can help people with MS and their families receive resources and services they need, including accessing assistive technology.
Web: http://www.nationalmssociety.org/index.aspx
Mail: 733 Third Ave, 3rd Floor New York, NY 10017
Phone: 800-344-4867
The Muscular Dystrophy Association is a nonprofit health agency dedicated to curing muscular dystrophy. They have over 200 offices around the country, some of which have partnered with family caregiver programs to help bring assistive technology to the homes of individuals living with muscular dystrophy.
Web: http://www.mda.org/
Mail: 3300 E. Sunrise Drive Tucson, AZ 85718
Phone: 800-572-1717
Appendix C. Helping to Reduce Caregiving Physical Strain: Guide for National Family Caregiver SUPPORT Programs
The National Family Caregiver Support Program (NFCSP), Area Agencies on Aging (AAAs) and partnering organizations provide an array of services to meet the needs of family caregivers. However, a frequently overlooked problem for many caregivers is the physical strain of caregiving. In fact, caregivers of older adults who experience physical strain are more likely than those with financial, emotional, or social strains to say that they are highly stressed. By helping reduce the physical strain of caregiving, NFCSPs and other aging and disability organizations can help decrease the chances that an older person ends up in a nursing home for a long stay.12
Background
A major source of physical strain such as back injuries among family caregivers is lifting and transferring. Many nursing homes and hospitals have rules against manual lifting and provide mechanical lifting aids for caregiving staff to use. Family caregivers, however, are less likely to be aware of safe lifting techniques or to have access to devices like ceiling lifts. Safe handling guidelines state that 35 pounds is the most a person can safely lift.13
Whenever possible, equipment such as a hoist or mechanical lift should be used for a whole body lift of a non-weight bearing person. Gait belts and slings can help position and provide back-up when assisting a partially weight-bearing person. They can also be used for maneuvering a non-weight-bearing person into a hoist sling.14 NFCSPs should consult with nurses, occupational therapists, and/or physical therapists to learn more about caregiver training on safe handling.
Another source of physical strain is communication problems in caring for a person with dementia. Oftentimes people with dementia become confused due to their inability to interpret signals from their bodies or from their surroundings. This contributes to resistance towards caregivers when they attempt to transfer them, which increases caregivers' risk for physical strain. Training on communicating with people with dementia can help address physical strain from caring for a person with dementia. AT/HM for cognitive impairment--such as activities/games, devices for memory and communication, additional lighting, labels, and signs--can also help in this area.
| Definitions
|
Homes that are in need of repairs or are not designed to meet the needs of older adults with functional impairments also contribute to increased physical strain. In addition, many family caregivers are themselves over age 60, which raises their risk of physical strain. Home repairs and modifications that may be needed range from removing clutter or repairing a handrail to major renovations like installing a wheelchair ramp, downstairs bathroom, or stair lift.
In addition to increasing safety for family caregivers, a wide range of AT/HM can assist older adults increase their functioning and independence (for examples, see the Text Box to the right). These range from complex technologies, such as telehealth and remote monitoring systems, to simple tools like grab bars and pill boxes. This can reduce the amount of help they need and ease the strain on family caregivers.
This guide presents several strategies NFCSPs can use to include assistive technologies and home modifications (AT/HM) to reduce caregiver physical strain as part of the range of services they offer.15
A Resource List at the end provides resources for additional information and assistance with addressing caregiver physical strain and connecting caregivers to AT/HM.
| Example AT/HM Needed by Family Caregivers and Older Adults
|
ASSESSING HOME SAFETY AND THE NEED FOR AT/HM
Many NFCSPs, in conducting home visits, look for AT/HM that the family may need. In difficult to reach, rural areas, programs sometimes use phone assessments. A strategy that several programs have found helpful is for case managers to bring along samples of commonly used AT that caregivers can try, such as a shower bench.
Case study: Wisconsin ADRCs
In Wisconsin, Aging and Disability Resource Centers (ADRC) Options Counselors bring "AT Kits" with them on home visits. The Wisconsin AT Resource Center (http://www.atresourcecenter.org) worked with the Independent Living Center to develop the AT Kits and provided tools and training for ADRCs on how to introduce AT to caregivers. The kit includes about 90 assistive devices, with some of the smaller items available to test and photos and descriptions of larger items provided in a manual. These include devices for hearing, vision, personal care, cooking, driving, recreation, and more, ranging from pill boxes to electronic lifts.
Some programs use assessment forms or checklists that include questions about AT/HM needs. These tools can help case managers or family caregiver specialists with assessing a caregiver's need for AT/HM. Some relate to home safety and design. Others address caregiver overall health, including physical strain and the need for AT/HM. A list of assessment forms and checklists is provided in the Resource List.
| Home Assessment Tips
|
After the initial assessment and selection of AT/HM, programs noted the importance of follow-up with caregivers over time to ensure the usefulness of the equipment and its correct use. This can help ensure that the AT is used and that people have the AT/HM that is right for them. As an individual ages, or their condition progresses, certain AT may no longer be of use to them and/or they may need different types of AT/HM.
Some caregiver programs partner with other providers to assist with assessments. In some instances, the NFCSP conducts the initial assessment and then refers to another provider for more in-depth assessment as needed. Providers and organizations that may be able to assist with caregiver assessments are listed in the Resource List.
HELPING FAMILIES FIND A CONTRACTOR
NFCSPs can form relationships with local businesses to build a network of local contractors that provide HM services. Through these relationships, NFCSPs can refer people to providers who others have used before and who have a proven record of good results. At the Howard County Office on Aging, staff include a retrofit specialist who can install modifications recommended and paid for by the agency. The specialist also knows reliable contractors in the area and can refer clients to them for services not covered by the agency.
| Tips for Helping Make AT Affordable and Available
|
HELPING MAKE AT/HM AFFORDABLE AND AVAILABLE
Often, family caregivers know what AT/HM they need, but do not know where to find affordable devices and services. NFCSPs can help by including AT/HM in services covered with NFCSP funds. They can also provide access to an AT reuse program and help with accessing other funding sources.
NFCSP supplemental services funds can be used for AT/HM
The federal government sets no specific restrictions on the use of these funds for AT and HM. The Older Americans Act states that supplemental services are to be provided "on a limited basis." Administration on Aging guidance to states suggested defining this as no more than 20% of spending. Although this is a general guideline and not a rule, most states limit their supplemental services to 20% or less. In states we spoke with, the per person limit for all supplemental services ranged from $250-$750 a month, or $1,500 a year. Some states allow caps to be waived if funds are available. In other states, services are approved on an individual basis. Many programs use NFCSP funds to help pay for AT/HM. Some also help pay for installation and maintenance of equipment.
Case Study: Philadelphia AAA
In Philadelphia, Title III-E provides a one-time $2,000 benefit for HM, plus $250 a month that can be used for respite, services, and/or supplies. When a caregiver applies for services, the case manager visits the home, discusses the NFCSP and entitlement benefits, and asks if the client is interested in services. Legislation has been proposed to increase the one-time benefit but has not passed.
Another way to help caregivers access AT is to build or refer to an AT reuse or lending program. AT reuse programs can help people get the AT they need at lower cost, if not free. Lending programs are useful for individuals who want to try out a device before buying it or who need a device to use for a short period of time. Agencies can educate families about donation of their used equipment. In Connecticut, the assessments inquire about AT/HM or medical equipment the family has and no longer uses. If the family has unused equipment, they are asked if they would be willing to donate it. Numerous organizations throughout the country are involved in AT reuse or loan programs, including State Assistive Technology Projects, Centers for Independent Living, hospitals, churches, Washington Area Wheelchair Society, Easter Seals, American Cancer Society, and Craigslist.
Case Study: Illinois NFCSPs
In Illinois, NFCSPs have formed many partnerships on AT/HM, including with Centers for Independence Living (CILs), State AT Projects, and Easter Seals programs. One of the CILs publishes a statewide newsletter that includes a section on used AT/HM that can be purchased at a low cost. The Springfield CIL provides access to used AT equipment. It also has a statewide newsletter of equipment for sale or giveaway. Most of the Illinois senior centers will accept walkers, benches, canes, and sometimes wheelchairs.
Case Study: Indiana AAAs
In Indiana, one of the AAAs operates a "lending library" of equipment that caregivers may borrow for a period of time. The library primarily includes sensory or monitoring technology to assist family caregivers of older adults with Alzheimer's disease or other dementia. The equipment library was created as part of the Alzheimer's Disease Support Services Program (ADSSP) grant. Some of the sensory technology requires families to pay the provider a monthly fee. Some families have been able to pay the fee through private pay; others had the equipment uninstalled. Another Indiana AAA partners with a church that has a lending library.
Although supplemental service can help, these funds are limited and usually insufficient to pay for high cost AT/HM that many caregivers need. Agencies can overcome this challenge by leveraging other sources of funding for AT/HM. To purchase large, expensive items (e.g., installation of a ramp) often requires patching together support from multiple sources. A case manager or "funding specialist" can help with coordinating funding sources. The Resource List lists some of the many potential AT/HM funding sources available. Some of the funding sources can assist caregivers. Others focus on AT/HM for the care receiver, which can also benefit the caregiver.
PUBLIC OUTREACH TO RAISE AWARENESS OF CAREGIVER PHYSICAL STRAIN AND AVAILABLE SOLUTIONS
Many caregivers, including many who pay privately for services, are not connected to Aging Network services and may not know about AT/HM that may help reduce their physical strain. The Resource List describes various resources and approaches for raising awareness among family caregivers and professionals who work with caregivers. These strategies include working with physicians and other health care providers to bring information to family caregivers and presenting at events and places where older adults and caregivers go.
RESOURCE LIST
Resources for Additional Information on AT/HM
Below are resources that provide information about AT/HM and can help NFCSPs with assessing the need for and choosing AT/HM and with finding ways to obtain and pay for it.
The Administration on Aging
This resource connects you to a number of different resources on services for older adults and their family members. They also have a page on the history and purpose of the National Family Caregiver Support Program.
Web: http://www.aoa.gov/AoA_programs/HCLTC/Caregiver/index.aspx.
Phone: 202-619-0724
AbleData
AbleData provides information on AT and rehab equipment. Their website contains many fact sheets and consumer guides to help with selecting AT for various impairments. On the "Library" page, choose "AbleData's Publications".
Web: http://www.abledata.com/
Phone: 800-227-0216 or 301-608-8998 / TT: 301-608-8912
HomeMods.org
This website contains information on aging in place and independent living for older adults and people with disabilities. Some of the resources are specific to HM and home repair. The site also offers a Home Modification Resource Guide. The guide covers general information, assessment, financing, product/program, program development and implementation, and research/education. For these resources, go to the "Resources" Page and click on the "Library" link.
Web: http://www.homemods.org/
Phone: 213-740-1364
The Center for Assistive Technology and Environmental Access (CATEA)
CATEA operates a National Public Website on Assistive Technology. Here, NFCSPs and caregivers can learn about AT and other community resources for people with disabilities.
Web: http://assistivetech.net/
Phone: 404-894-4960
Rehabilitation Engineering and Assistive Technology Society of North America (RESNA)
RESNA operates the National AT Technical Assistance Partnership (NATTAP) website. This project assists state and territory AT projects. The website provides state-specific info on device loan, re-use, and demonstration projects.
Web: http://resnaprojects.org/nattap/RESNA.html
Phone: 703-524-6686 / TTY: 703-524-6639
Technology for Long-Term Care
Tech for Long-Term Care provides info on over 1,200 products that can help with long-term care needs. These include devices for assistance call, bathing, communication and memory, dressing, eating, fall management, and incontinence. It also includes products for leisure, lifting and transferring, medication management, mobility, wander management, and wound care.
Web: http://www.techforltc.org/
National Institute for Occupational Safety and Health (NIOSH)
Family caregivers perform many of the same tasks as home health care workers. NIOSH suggests guidelines for the safe practices among this workforce, which also apply to family caregivers. NIOSH's science blog on physical strain among home health care workers (http://www.cdc.gov/niosh/blog/nsb041610_nurse-erg.html) suggests devices that can increase safety in home care. This blog links to resources to learn more about ergonomics in home care. One resource is the NIOSH Hazard Review: Occupational Hazards in Home Healthcare. Another is an article by Parsons, Galinsky, and Waters on Preventing Musculoskeletal Disorders in Home Healthcare Workers. A second NIOSH blog focuses on safe patient handling in healthcare settings (http://www.cdc.gov/niosh/blog/nsb092208_lifting.html).
Web: http://www.cdc.gov/niosh/
Phone: 800-CDC-INFO (800-232-4636) or TTY: 888-232-6348
Fall Prevention Center of Excellence
Fall Prevention Center of Excellence information for individuals and families as well as information for service providers on falls prevention. The information for service providers includes videos, tools, articles, and a database of continuing education courses for nurses, social workers, care managers, physicians, and other professionals.
Web: http://www.stopfalls.org/individuals_families/if_bm.shtml
Phone: 213-740-1364
The Center for Healthy Aging
The Center for Healthy Aging assists aging service providers to implement healthy aging programs. Resources provided include manuals, toolkits, research, examples of model health programs, and links to websites on health topics. It includes resources on fall prevent and home safety.
Web: http://www.healthyagingprograms.org/
Phone: 202-479-1200
This Caring Home
This website provides useful info for programs and caregivers on home safety for people with dementia. It also applies to older adults and people with disabilities. The site also assists with finding products to ease the burden of caregiving. Case managers and family caregiver specialists can use this website and/or refer caregivers to it.
Web: http://www.thiscaringhome.org
North Dakota State University. Assistive Technology and Older Adults: The Journey Through Caregiving.
This guide is useful for both caregivers and NFCSPs. It helps organizations prepare family caregivers to care for an older person with a chronic disease or disability (http://www.ndsu.edu/ndsu/aging/caregiver/pdf/assistive/manual.pdf).
ASSESSMENT FORMS AND CHECKLISTS
-
Rebuilding Together Home Safety Checklist: This checklist was developed with the Administration on Aging. Search "Home Safety Checklist" on the Rebuilding Together homepage.
Web: http://www.rebuildingtogether.org/
Phone: 1-800-473-4229 -
CaregiverNJ Home Safety Assessment Checklist: The New Jersey Institute on Technology developed this checklist with the NJ Department of Health and Senior Services. It provides home safety guidelines and a specific checklist for people with Alzheimer's disease and other dementias. Search "Home Safety Assessment Checklist" on the CaregiverNJ homepage.
-
AARP Home Fit Guide and brochure: AARP provides many resources that could help NFCSPs assist caregivers with AT/HM. This includes a Home Fit Guide and a brochure on No-Cost/Low-Cost Home Improvements for a More Comfortable Safer, and Easy-to-Live-In Home.
Web: http://www.aarp.org/
Phone: 888-687-2277 or (TTY) 877-434-7598 -
IDEAS Consulting Environment and Communication Assessment Toolkit: This Toolkit and corresponding webinar focuses on people with dementia in long-term care settings, but can also help with family caregiving at home. The Toolkit and corresponding webinar focus on identifying environmental barriers to communication and changing the environment to facilitate communication.
Website: http://www.alzpossible.org/wordpress-3.1.4/wordpress/webinars-2/833-2/
-
Centers for Disease Control and Prevention (CDC), Toolkit on "What You Can Do to Prevent Falls." This toolkit describes what families can do to prevent senior falls and increase home safety.
Web: http://www.cdc.gov/homeandrecreationalsafety/falls/index.html
Phone: 800-CDC-INFO (800-232-4636) TTY: 888-232-6348 -
Promoting Safety and Function Through Home Assessments
This article provides an overview of home safety assessments and three different home assessments in the appendix.
POTENTIAL SOURCES OF ASSISTANCE WITH ASSESSMENTS
-
Occupational therapists (OTs), physical therapists (PTs), or registered nurses (RNs): Several caregiver programs provide referrals to OTs, PTs, or RNs (either on staff or an outside provider) when a need for AT/HM is identified, or encourage the family to contact their family doctor for an OT referral. These professionals can provide more in-depth assessments, identify issues, make additional referrals, and OTs can help older people increase function and community participation. In some instances, as in the Philadelphia AAA, OT services are paid for with NFCSP funds. In Connecticut, the Home Care Program for Elders provides global assessments, refers to an OT if AT is deemed necessary, and pays for the OT or physical therapist services. Communication between the case manager and the OT is very important. The OT should also conduct a follow-up visit if possible.
To learn more about the benefits of occupational therapy, visit the American Occupational Therapy Association.
Web: http://www.aota.org/About.aspx
Phone: 301-652-2682 / TDD: 800-377-8555 -
Direct service workers, such as home health aides and personal care aides, could informally assess and help identify AT/HM needs. AAA staff could reach out to service agencies about the available AT, so that they can train aides going into homes on AT and HM. These workers have hands-on experience assisting the person and could suggest AT/HM that would be helpful. The Salt Lake County Office on Aging has a partnership with their local home health agency. Case managers speak with home health aide supervisors to determine if the people they serve may need AT/HM.
-
Non-profit community service organizations: In California, the Area 4 Agency on Aging stated that they contract with various organizations that offer AT/HM to conduct assessments. A case manager provides in-depth assessments for services in the home. Certified nursing assistants conduct assessments for in-home services, such as personal care and homemaker services. Agencies that provide HM services conduct home assessments. Home Delivered Meals Assessors conduct assessments and they review a home safety checklist with the potential client and/or family member. These contracted providers must educate clients regarding fall prevention and complete a simple Home Safety checklist. Programs in both California and Iowa have worked with the non-profit organization Rebuilding Together, to assess for and recommend/install HM in the home. The Honolulu Office on Aging works with Project Donna in Oahu County, Hawaii, a faith-based volunteer organization that provides home assessments and other services.
-
Departments of Rehabilitation Services/Vocational Rehabilitation often will conduct home assessments.
-
Care transitions teams can conduct assessments prior to hospital discharge. Agencies noted the importance of reaching people during transitions from a hospital. This is a chance to provide equipment that can help with independent living and prevent nursing home entry. Some of the AAAs in Illinois havebegun to work with hospitals and discharge planners on education and outreach.
-
Disability organizations, including Centers for Independent Living (CILs) and disability specific organizations, such as the MS Society, offer another resource for assessments. In Utah, the CILs can conduct home evaluations. The AAAs send a case worker to conduct an in home assessment. If there is a need for a more intensive assessment, a referral to a CIL is given.
-
AT/HM companies. Some companies provide free in-home assessments. However, AAAs we spoke with noted a need for protections to avoid conflict of interest. Agency staff need to offer choice, remain neutral, and not recommend any particular company's products.
-
Fire departments: The Springfield, Illinois NFCSP has a partnership with the fire department. The fire department goes into the home and assesses for fall prevention. They also provide and install free smoke detectors. Illinois AAAs also refers caregivers to the Illinois AT program and the caregiver resource center.
POTENTIAL RESOURCES FOR MAKING AT/HM AFFORDABLE AND ACCESSIBLE
-
The Pass It On Center the National Assistive Technology Reuse Center offers a directory of reuse locations and additional information about and assistance with AT reuse.
Web: http://www.passitoncenter.org
Phone: Toll Free 1-800-497-8665 or TDD: 1-866-373-7778 -
Medicaid and state funded home and community based services programs: In many states, Medicaid and/or state funded home and community based services programs cover some AT/HM. However, this funding is often limited and used for other needed services. The Philadelphia AAA noted that many caregivers do not use Medicaid waivers for AT/HM due to estate recovery. Iowa's Medicaid waiver provides help with purchasing AT/HM for the care recipient. Maryland uses a state-funded Senior Care program to fill gaps in HM and OT services. It provides a recommended cap of $500 per person per month. The funds can be used for flexible services including an in-home aide, respite, and other services. Building relationships with Money Follows the Person (MFP) demonstration programs can also be helpful. These programs are working to increase the use of person-centered, home and community based services. A list of grantees is available here: http://www.mfp-tac.com/Grantees.aspx.
-
Medicare provides limited coverage of occupational therapy and medical equipment.
-
State Assistive Technology Projects: The Assistive Technology Act funds a statewide AT program in each of the 50 states and six territories; the majority of these programs support AT device reuse activities, and many operate device loan closets.16 They can help NFCSPs leverage community resources and expand their network. Although some State AT Projects focus on younger adults with disabilities, some aging organizations have found them a useful source for AT for older persons and their caregivers. Illinois AAAs refer caregivers to the Illinois AT Program, which helps people obtain many different types of AT to remain as independent as possible. A state listing is available at the State AT Projects Information Center. State AT Projects may be another resource for conducting home assessments and/or supplying AT/HM. Illinois NFCSPs partner with their State AT Project for these purposes. The Utah Center for Assistive Technology (http://ucat.usor.utah.gov/) provides a loan program, device design and modification, home assessment, assessment of aptitude for using technologies, and other services.
Web: http://www.abledata.com/abledata.cfm? pageid=113573&top=16050&ksectionid=19326&stateorganizations=1
Phone: You can contact AbleData for more information at 800-227-0216 or 301-608-8998. -
Centers for Independent Living (CILs): These can be found in the ILRU Directory.
Web: http://www.ilru.org/html/publications/directory/index.html
Phone: 713-520-0232 ext. 130 (Voice/TTY) -
State and federal veterans assistance programs: The Philadelphia Corporation on Aging refers caregivers to Veterans Administration funds, in addition to other sources of assistance with purchasing AT/HM.
-
Home repair assistance programs: The U.S. Department of Housing and Urban Development (HUD) provides loans for home improvement and repair and a rural home improvement and repair loan/grant program. The Philadelphia AAA, using state and city funds, has a minor home repair program called SHARP (Senior Housing Assistance Repair Program) which provides services to low income senior homeowners who reside in Philadelphia. The Philadelphia AAA also provides referrals to the Adaptive Modification Program (AMP) which is administered by the Philadelphia Housing Development Corporation. AMP can provide up to $25,000 of home modifications for Philadelphians with disabilities of all ages.
-
USDA: The USDA provides grant funding and low-interest forgivable loans for people in rural areas. Iowa uses USDA funds for their more rural counties.
-
Private non-profit organizations (disability organizations, CILs, faith-based): In Alabama, the AAAs typically work with agencies, such as Catholic Charities, other faith-based organizations, and Alzheimer's associations, as a resource for donated products.
-
Companies: Some companies may offer discount programs for purchasing AT. In Indiana, some AAAs havenegotiated a reduced price with Lifeline or First Alert. These companies provide systems for automatically alerting 911 and the caregiver in an emergency. When the AAAs refer a client, the person can purchase the AT for a negotiated rate. Local construction companies may donate materials. When partnering with an AT company, agencies should make sure to give families a choice and not recommend any particular product.
-
Self-pay: NFCSPs should encourage and assist private pay individuals to thoroughly review their options for AT/HM. These options could include private insurance, home equity loan, and volunteer help from family and friends. Caregivers may be able to find equipment for sale online (e.g., Google and Amazon) for lower cost than through durable medical equipment (DMEs) companies.
-
Other: Other possible funding sources for AT/HM include: telecommunications equipment purchase programs, Developmental Disabilities Administration, and Division of Rehabilitative Services. Other sources are high school/community college building trade department, local demonstration projects, and National Institutes for Health Demonstration Grants. In Iowa, the Des Moines school system had a program in their building trades department to assist with AT. One funding stream paid a stipend to students, while other funding streams paid for teachers and equipment to make AT available to older homeowners. Another suggestion was to partner with community colleges.
RESOURCES FOR PUBLIC OUTREACH TO RAISE AWARENESS
-
Work with primary care physicians (PCPs) and Accountable Care Organizations, on providing information to family caregivers. PCPs are a very important resource for family caregivers. NFCSPs can suggest that family caregivers talk with their doctor about AT/HM. NFCSPs might also partner with PCPs in the community to spread information about supports for caregivers. Other contacts may include chiropractors, orthopedists offices, community health agencies, and pharmacies. NFCSPs may also suggest that family caregivers inform their primary care providers that they are a family caregiver and ask the doctor questions about AT or HM. Their physician may be able to give them information about devices that may make their job easier. They may also be able to suggest what training is available to family caregivers on proper lifting/transferring techniques.
-
Cornell University runs an Environmental Geriatrics website with helpful information on home safety, HM, housing options, and related resources. The site provides an animated course on "Environmental Geriatrics: Improving Function & Safety". This course may be a good tool to share with primary physicians in the community.
-
Another resource for physician partners is the American Medical Association guide on Guidelines for the Use of Assistive Technology: Evaluation, Referral, Prescription
Web: http://www.ama-assn.org/ama1/pub/upload/mm/433/assistivetechnology.pdf
-
Partner with other organizations to disseminate information to caregivers. Possible partners to consider include ADRCs, universities, peer support, online caregiver training programs, CILs, caregiver coalitions, or veteran's assistance programs. ADRCs provide a useful way for the disability and aging communities to learn from each other. Illinois AAAs have worked with veterans' health centers, which refer clients to the AAA. They noted that the veteran's independence program offers a benefit guide for veterans in the state that could be useful for caregivers of veterans. An Illinois AAA has also organized an expo geared toward veterans and caregivers age 50 and over. They offer free information and health screens at the expo.
-
Provide information about AT/HM at events (fairs, expos, caregiver conferences)--In California, the San Diego County Aging & Independence Services holds caregiver conferences and offers live online workshops. These events include information on AT/HM.
-
Present about AT/HM in the community--In Wisconsin, the Eau Claire ADRC presents information on AT when requested. Many of the requests for presentations come from senior centers and senior apartment complexes. Other potential places to present are community centers and churches.
-
Present to large employers--In Connecticut, the North Central AAA presented information about caregiving to employees of a large Connecticut and Massachusetts employer. They set up a booth of information including content about AT/HM. Chambers of Commerce are a potential partner for reaching employed caregivers in the workforce.
-
Reach out to the media--Newspaper articles have reported on Connecticut's Money Follows the Person Program. The program provides AT/HM for care recipients that are also helpful for their caregivers.
-
Use State Assistive Technology Projects as a resource: State AT projects assist people with disabilities of all ages in obtaining technology that fits their lives to help them be more independent. The Philadelphia AAA uses Pennsylvania's Initiative on Assistive Technology (PIAT), the state's AT center, as a resource for educating caregivers and older adults.
-
Work with long-term care insurance agencies or HMOs: These organizations are interested in maintaining the health of family caregivers and their loved ones. They may be willing to disseminate information about NFCSP services as they relate to AT/HM.
-
Connecting with home builders associations or local home improvement stores: NCSFPs may consider asking these locations if they can disseminate some information about AT/HM in their stores. This can increase awareness in both home builders and family caregivers about AT/HM.
Appendix D. Family Caregiver SUPPORT Program Survey
The FCA developed a brief survey that was disseminated to family caregivers of older adults and people with disabilities. Responses included both multiple choice options and open-ended fields.
The survey was fielded online for six months, through the ADRCs, some AAAs, and the FCA's National Center on Caregiving. Responses from the survey can help NFCSPs and other organizations to offer family caregivers with services that reduce physical strain through the use of AT/HM.
The Lewin Group examined the survey results. The survey results provide an overview of:
- Kinds of AT/HM caregivers have used and reimbursement mechanisms;
- Benefits of AT/HM to caregivers;
- Training and information needs of caregivers; and
- Additional information needs.
Respondents
A total of 423 individuals responded to the survey. A majority of the caregivers were women (87.4%). Their average age was 57, and the average age of the care recipient was 72. These demographics are in line with research which shows that caregivers are predominantly women and middle-age or older.17
Use of Assistive Technology
Almost 61% of respondents stated that they used assistive devices to make it easier to provide care for their loved one or to help their loved one maintain independence. Of those using assistive devices, the most commonly reported items were: mobility aids (92.7%), bathing aids (88.6%), medication assistance (75.5%), toileting aids (72.7%), dressing aids (48.2%), transfer aids (40.0%), and food preparation devices (34.5%). The findings are illustrated in Figure D-1 below. When asked about other assistive devices used, responses included: communication devices (large telephones, speech software), devices for hearing/vision loss, monitoring devices, and some lifts.
| FIGURE D-1. Assistive Devices Used by Respondents |
|---|
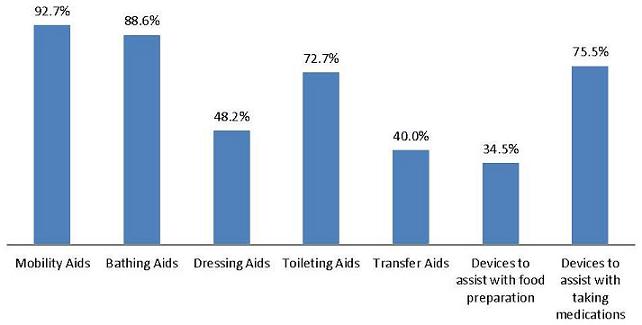 |
When asked what electronic technologies the caregiver or the person they cared for had ever used, the most common response was technology that called for help in an emergency (83.8%). This was followed by online communication tools to facilitate the caregiving process (31.2%), health technology (29.2%), and smart home technology (5.2%).
The majority of respondents paid for the AT on their own or another family member paid for it (62.3%). Private pay was followed by the family member who used or benefited from the AT (49.1%), Medicare (44.3%), private insurance (25.0%), other community service organization (15.6%), Medicaid (14.6%), and VA (6.6%).
Among the remaining respondents who had never used AT, the most common reason for not using it was that they were not aware of options (62.6%). This was followed by not having a special reason/never thought about it (26.6%), never having a need for the AT (25.2%), and the cost/not being able to afford it (24.5%).
Impact of Assistive Technology
A question on the survey ascertained the extent to which AT had helped the respondent as a caregiver. Over three-quarters (75.1%) of respondents said the AT had helped a lot, followed by 24.4% who said it helped a little. One respondent said it did not help, and no respondents said it made things worse. This is illustrated in Figure D-2 below.
| FIGURE D-2. How Assistive Technology has Helped Caregivers |
|---|
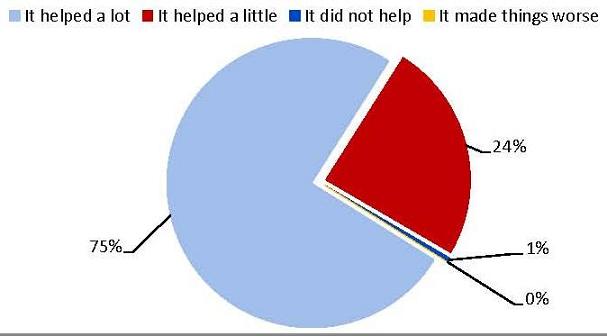 |
Forty-six survey respondents provided comments on how AT had helped them as caregivers. Common themes are reported below:
-
Increased independence and safety of the care recipient (15 respondents): Caregivers remarked that their family members were no longer completely reliant on them and that they were able to maintain independence with the help of AT. Most responses related to mobility, autonomy, and improving quality of life. One caregiver stated, "My husband is bedridden now; it's unlikely he'll be able to stand or walk in the future. The lift has made it possible for him to move from one room to another, use his wheelchair, [and] have meals with the family."
-
Needed to use the technology/was very helpful/made life easier (15 respondents): Many caregivers mentioned the usefulness of specific technologies, particularly monitoring systems (mentioned by 8 respondents). One caregiver stated, "I don't have the time to describe what a living hell it would be for us without these devices."
-
Well-being of caregiver (9 respondents): Some caregivers noted how much more relaxed they were due to AT. It was helpful to know that their loved one could be more independent. In the case of monitoring systems, caregivers were also more able to go about their daily tasks without worrying about the care recipient as much. Caregivers did not specifically mention their physical well-being; rather, they brought up their mental/emotional well-being and less time spent caregiving, which would likely decrease their physical strain. One caregiver stated, "Having the assistive devices we use has enabled my husband to maintain as much independence as possible, so he doesn't have to rely on me for everything he wants to do. This alone has helped me because I work full time in a very stressful job, so to come home to stressful situations doesn't help me to maintain my sanity."
-
Resistance of care recipient (4 respondents): Some caregivers mentioned that their loved ones were resistant to the technologies. One mentioned her mother's resistance to the pill organizer, which helps the caregiverknow if she has taken her pills for the day. One caregiver stated, "In some cases it was very helpful. In most cases, because of the reluctance or resistance of the person I've cared for to use the equipment, it wasn't helpful at all."
-
Avoided institution (2 respondents): Two caregivers mentioned the importance of AT in keeping their loved one in the home, with one stating that her "husband would have been in a residential facility well before now, or I would have broken."
-
More assistive technology is necessary (2 respondents): Two caregivers also suggested that more AT is needed. One caregiver, whose father has since passed, stated that so much more could have been done, like providing a lift for the caregiver's father. The other caregiver noted that they have had a lot of success with AT; however, they currently need an electric air pressure changing mattress to top his hospital bed to prevent pressure sores, but Medicare requires that the patient needs to have two sores to be eligible for the item.
-
Training/assistance is necessary (4 respondents): A few caregivers mentioned the need for more training in using the AT. One respondent commented that the care receiver had difficulty learning some of the more complicated technical devices. One caregiver mentioned the need to self-educate: "I practically turned into an occupational therapist trying to find ways to accomplish all the various ADLs which changed, and changed, and changed again throughout my mother's decline. I did a great deal of research online to educate myself and come up with practical solutions." Another caregiver stated, "getting training for use of things like wheelchairs, doing transfers (safely) with gait belt, etc. would be MOST USEFUL to avoid injury for us -- the caregivers."
Use of Home Modifications/Home Repair/Vehicle Modification
The majority of respondents (62.8%) had HM (e.g., wheelchair ramps, handrails, grab bars), over a third (37.8%) reported home repair/maintenance (37.8%), and a smaller amount (9.1%) reported having had a vehicle modification. This is illustrated in Figure D-3 below.
The most common payment source for modifications and repairs was payment by the caregiver or another family member (64.0%). This was followed by payment by the family member who used or benefited from the HM (43.9%). The other payment sources included Medicare, Medicaid, VA, community/service organizations, private insurance and do not know, which were reported by 1.7%-7.9% of respondents.
| FIGURE D-3. Modification Use by Respondents |
|---|
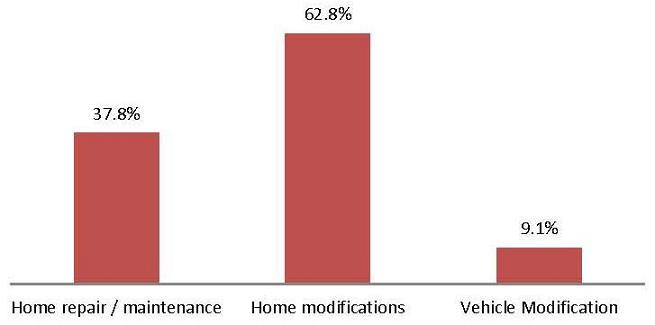 |
Of the respondents who indicated they or the person they care for had never had a HM, the most common reason was lack of need (38.0%). This was followed by cost (30.4%), not being aware of HM options (19.6%) and not owning the home (16.3%).
Impact of Home Modifications
| FIGURE D-4. How Home Modifications have Helped Caregivers |
|---|
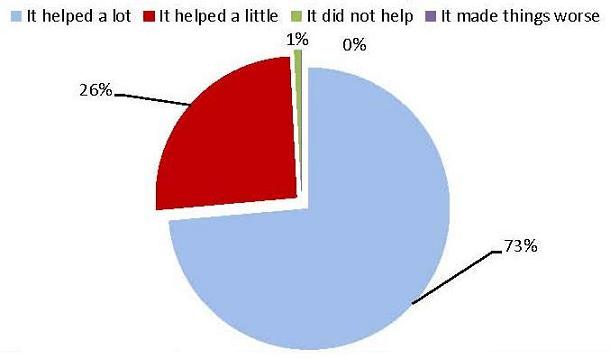 |
When asked the extent to which the HM had helped the caregiver, responses were similar to the parallel question about AT: 73.6% of respondents claimed that it helped a lot, followed by 25.6% who said it helped a little. Two respondents said it did not help, and none said it made things worse. This is illustrated in Figure D-4 above.
Forty-three respondents provided comments on the extent to which HM has helped them, and a number of themes arose.
-
Increased independence and safety of the care recipient (12 respondents): As with AT, caregivers felt that HM allowed their loved one to be safe and independent. One caregiver pointed out the importance of modifications that allowed her husband to just get in and out of the house: "The modifications enabled my husband to leave the house with me, as the caregiver. This enabled us to remain active in the community." Another pointed out the psychological benefit of giving "the care recipient some feeling of control and independence in the home."
-
The HM was very helpful/made life easier (19 respondents): Many of the open-ended responses were more general comments on how the modifications have been helpful overall. One caregiver highlighted the importance and usefulness of very simple HM: "Simple ramps and grab rails were invaluable." Many of these responses related to how the HM helped the care recipient get in/out of the house, take showers independently or with the help of the caregiver, and prevent falls.
-
Well-being of caregiver (4 respondents): One caregiver pointed out the helpfulness of the HM for her own well-being: "The ramp we installed in the garage has been a lifesaver for me as a 73-year-old female caregiver for my husband." Another caregiver mentioned living with a disability herself, stating, "for one thing, showers are much easier with fold down seat, grab bars and hand-held shower for the handicapped [care recipient] and the handicapped caregiver (me)."
-
Resistance of care recipient (2 respondents): Two caregivers pointed out their loved one's resistance to use of the HM. One stated that there were "more things I could use to help my husband but he doesn't want to, so I do a lot for him, in fact I do everything for him."
-
More HM is necessary (8 respondents): A few caregivers pointed out that they needed more HM. One stated that the modifications were not good enough to help the recipient maneuver in and out of small places. Another stated that they were not enough to allow her to leave her mother, who has Alzheimer's, to be by herself. Two of the caregivers who mentioned that more modifications were needed also mentioned cost. One stated that they wanted a zero step shower, but it was too expensive. Another stated that "there are many more modifications that would be useful but unfortunately they are not in our budget."
-
Specific types of HMs used (9 respondents): Some of the respondents used the open-ended field to list the specific HM they received/completed; however, they did not provide any more details beyond that.
Training and Information
When asked whether they or the person they care for has ever had training in device use, simplifying self-care tasks,or techniques to minimize the risk of physical strain/injury from caregiving, the majority (59.4%) said they had not received training. This is important to note given that a majority (67%) of respondents also stated that they experienced moderate or heavy physical strain while caring for their family member. This is illustrated in Figure D-5 below.
| FIGURE D-5. Caregiver Physical Strain Levels |
|---|
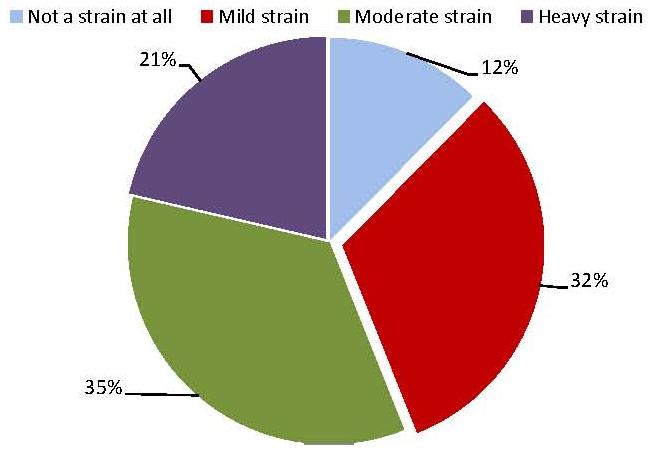 |
Respondents were also asked where they would go if they needed information or training about technologies or HM. The most common response was the Internet (67.4%), followed by a physician (47.3%), an AAA (37.9%), a family member/friend (27.9%), or another community/service organization (23.2%). Other options included a CIL, VA, church, or senior center, which ranged from 3.7% to 11.4% of caregiver responses. Sixty-two respondents provided other responses, including: other agencies such as Assistive Technology Centers, associations, and family caregiver programs. Notably, 12 individuals indicated that they were not sure/just did not know where to go for information or training, or that the resources were not available in their area. One individual wrote, "That's just it -- I don't know where to go." Another stated "never thought about it, no money."
In addition to AT/HM, caregivers reported a need for more help or information with a number of other issues, most commonly managing their emotional stress (72.6%) and finding time for themselves (70.7%). Nearly half said they needed help managing their physical stress (46.8%). Response categories and percentages are in Table D-1 below.
| TABLE D-1. Additional Needs of Caregivers | ||
|---|---|---|
| In addition to technology and HM, do you feel a need for more help or information with any of these other issues? (Check all that apply) | ||
| Answer Options | Response Percent | Response Count |
| Managing your emotional stress | 72.6% | 228 |
| Finding time for yourself | 70.7% | 222 |
| Keeping the person you care for safe at home | 56.4% | 177 |
| Balancing your work and family responsibilities | 52.5% | 165 |
| Help in dealing with agencies or providers (bureaucracies) to get services | 47.5% | 149 |
| Managing your physical stress | 46.8% | 147 |
| Information about financial help | 42.4% | 133 |
| Managing incontinence or toileting problem | 41.7% | 131 |
| Overnight respite services | 35.0% | 110 |
| Managing challenging behaviors, such as wandering | 33.4% | 105 |
| Counseling or support groups | 30.3% | 95 |
| Adult day services | 22.0% | 69 |
| Transportation | 21.3% | 67 |
| Choosing an assisted living or nursing home | 18.2% | 57 |
| Information about my family member's condition or disability | 17.8% | 56 |
| answered question | 314 | |
| skipped question | 109 | |
Survey Conclusion
Results of this survey indicate that many caregivers have used AT/HM and found them helpful. However, findings highlight the need for more outreach and education about AT/HM. A majority of respondents said they turn to the Internet for this information, highlighting the need for reliable and accurate information on the web. Other frequently mentioned information sources were physicians, AAAs, and community organizations. Databases of AT do exist online; however, they are often difficult for the family caregiver to navigate. For example, AbleData, sponsored by the National Institute on Disability and Rehabilitation Research, provides information on almost 40,000 assistive products. However, in some cases, caregivers may give up on searching unless they already know what they are looking for in advance of visiting the website. Additionally, better linkage between the problems identified and possible technology solutions is critical.
Another gap identified by this survey is training on device use, simplifying care tasks, or techniques to minimize physical strain. Other frequently mentioned areas where caregivers said they need more information or help include managing their emotional stress and finding time for themselves.
Funding for AT/HM is another concern mentioned by caregivers in this survey. AT/HM is largely purchased by the family caregiver or by the care recipient with disabilities. Some caregivers specifically mentioned not having enough money -- that the cost was a barrier to purchasing AT or installing HM. More information needs to be disseminated to caregivers about potential funding sources for AT/HM and sources for low-cost or no-cost devices; expanding coverage of AT/HM in public programs would also help. In the open-ended fields, many caregivers indicated a need for help obtaining needed AT/HM. Many of these caregivers have experienced moderate and sometimes heavy physical strain as a result of caregivingor are concerned about the possibility of future injury as a result of caregiving. One caregiver stated, "A shower that has dispensers, safety bars, and a stool is a wonderful thing. Now that I have injured myself caring for Mom, I need them!"
Notes
-
These are for transfers to and from: Bed to Chair, Chair to Toilet, Chair to Chair, or Car to Chair. These are transfers that family caregivers are more likely to perform.
-
Pam Doty, Lisa Alecxih, Vice President, Greg Link, Kathleen Kelly, Margaret Campbell-Kotler, and Mary Becker. "Expanding the Use of Assistive Technologies and Home Modifications." National Home and Community-Based Services Conference. Washington, DC: September 13, 2011.
"Recent Efforts Supporting Assistive Technology and Home Modifications to Reduce Family Caregivers' Strain." Symposium.The Gerontological Society of America 64th Annual Meeting. Boston, MA: November 19, 2011.
Majd Alwan, Molly Gavin, Cindy Gruman, Susan I. Klein, and Greg Link. "Promoting and Using Technology to Reduce Family Caregiver Strain and Foster Independence."Aging in America, the 2012 Annual Conference of the American Society on Aging. Washington, DC: March 30, 2012 (accepted).
-
These assessments are included in the appendix of the article, which can be accessed at http://plaza.ufl.edu/mlwsail/6_promoting%20safety.pdf.
-
Early adopters of technology are those who are more likely to report trying a technology when it is relatively new and untested. Late adopters wait until the technology is widely tested and used before adopting the technology.
-
The Safe Patient Handling Training for Schools of Nursing guide, developed by NIOSH provides helpful information for family caregivers on how to handle or transfer their family members. http://www.cdc.gov/niosh/docs/2009-127/pds/2009-127.pdf.
-
The Lewin Group originally developed three resource guides for dissemination: (1) a Family Caregiver Resource Guide; (2) a NFCSP Resource Guide, and (3) a NFCSP Strategy Guide. The NFCSP guides were combined into one.
-
Information on the program is available on the RCI website at http://www.rosalynncarter.org/academic_programs/.
-
Information on the University of Southern California certificate can be found at http://www.homemods.org/.
-
Information received in email correspondence with Meg Campbell-Kotler, VA Caregiver Support Program.
-
CDC/NIOSH Lifting Equation. In Waters, T. 2007. When is it safe to manually lift a patient? American Journal of Nursing, 107[8], 53-59.
-
Fees are associated with this service.
-
Spillman, BC and Long, SK. 2009. "Does High Caregiver Stress Predict Nursing Home Entry?" Inquiry 46(2):140-161.
-
CDC/NIOSH Lifting Equation. In Waters, T. 2007. When is it safe to manually lift a patient? American Journal of Nursing, 107[8], 53-59.
-
The Safe Patient Handling Training for Schools of Nursing guide, developed by NIOSH provides helpful information for family caregivers on how to handle or transfer their loved ones. http://www.cdc.gov/niosh/docs/2009-127/pdfs/2009-127.pdf
-
For additional information on the study that led to this guide, see The Lewin Group, January 2012. Accelerating Adoption of Assistive Technology to Reduce Physical Strain among Family Caregivers of Older Adults with Chronic Illness Living at Home: Final Report.
-
U.S. Department of Education, "Reuse Your Assistive Technology," http://ed.gov/programs/atsg/at-reuse.html
-
By comparison, in the 2009 Caregiving in the U.S. survey, 66% of caregivers were women and their average age was 48. National Alliance for Caregiving in collaboration with AARP. November 2009. Caregiving in the U.S. 2009. http://www.caregiving.org/pdf/research/Caregiving_in_the_US_2009_full_report.pdf.
To obtain a printed copy of this report, send the full report title and your mailing information to:
U.S. Department of Health and Human Services
Office of Disability, Aging and Long-Term Care Policy
Room 424E, H.H. Humphrey Building
200 Independence Avenue, S.W.
Washington, D.C. 20201
FAX: 202-401-7733
Email: webmaster.DALTCP@hhs.gov
RETURN TO:
Office of Disability, Aging and Long-Term Care Policy (DALTCP) Home [http://aspe.hhs.gov/office_specific/daltcp.cfm]
Assistant Secretary for Planning and Evaluation (ASPE) Home [http://aspe.hhs.gov]
U.S. Department of Health and Human Services (HHS) Home [http://www.hhs.gov]