
CONTENTS
- The Evaluation of Abstinence Education Programs Funded Under Title V Section 510: Interim Report
- Links Among Different Forms of Adolescent Violence
- The Role of Power and Control in Intimate Partner Violence Perpetration
- National Survey of Homeless Assistance Providers and Clients: Supplemental Analysis
The Evaluation of Abstinence Education Programs
Funded Under Title V Section 510: Interim Report
This report presents interim findings from an independent, federally funded evaluation of the abstinence education programs authorized under PRWORA. This report draws most heavily on four years of implementation experiences in a selected group of abstinence education programs funded under Section 510.
In 1996, Congress authorized $50 million annually for five years to promote abstinence education. This funding was established through a new formula grant program authorized under the Personal Responsibility and Work Opportunity Reconciliation Act (PRWORA) of 1996. Abstinence education programs funded through this new grant program teach an unambiguous abstinence message to youth. Programs receiving these abstinence education funds may not endorse or promote contraceptive use.
Evaluation of Section 510 Abstinence Education Programs
The evaluation addresses three important questions:
- What are the nature and underlying theories of the abstinence education programs?
- What are the implementation and operational experiences of local communities and schools that have received abstinence education funding?
- What are the impacts of abstinence education programs on the attitudes and intentions of youth to remain abstinent, on their sexual activity, and on their risks of pregnancy and sexually transmitted diseases (STDs)?
The first stage of the evaluation entailed selecting programs for study. The evaluation team first visited and observed numerous abstinence education programs across the nation. Eleven of these, representing a range of program models and serving different target populations, were then selected for in-depth analysis. Five of the 11 are referred to as "targeted" programs: they target services to specific, identifiable groups of youth. The remaining six are community-wide, systemic-change initiatives which use the abstinence education funding to increase public awareness of the problems of teen sexual activity, to change community norms and attitudes, to encourage stronger parent-child communications, and to engage youth in abstinence education and support services.
The evaluation includes an extensive implementation and process analysis and an impact analysis. The implementation and process analysis uses program documents, program observations, focus groups with program participants, and parents, along with interviews with program staff and community leaders, to document and understand the abstinence education programs implemented in the 11 sites. The impact analysis uses longitudinal survey data for groups of youth randomly assigned to program and control groups in the 5 targeted program sites. Enrollment in the impact evaluation study samples spanned three school years and was just completed in fall 2001. Therefore, the follow-up data that are necessary for the impact analysis are not available for inclusion in this report.
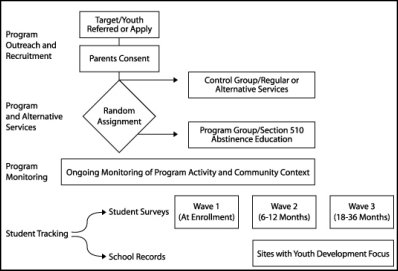 |
| Study Sample Enrollment and Tracking |
Early Implementation and Operational Lessons
The first four years of Section 510 funding for abstinence education have generated a wealth of experience on how local grantees have designed and implemented abstinence education programs. Among the early lessons are the following:
- Section 510 abstinence funds are changing the local landscape of approaches to teenage pregnancy prevention and youth risk avoidance. Despite an initial debate in some states over whether and how to spend abstinence education block grant funds, all states applied for funding at some point, and most are using monies in innovative ways to promote abstinence from sexual activity as the healthiest choice for youth.
- Most abstinence education programs offer more than a single message of abstinence. Examples of curricula and program components from sites participating in the federally funded evaluation indicate the diverse, creative, and often complex nature of many initiatives.
- Most participants report favorable feelings about their program experience. Youth respond especially positively to staff that show strong and unambiguous commitment to the program message. They also like programs that deliver an intensive set of youth development services to enhance and support the abstinence message.
- Abstinence education programs face real challenges addressing peer pressure and the communication gulf between parents and children. Sexual activity often elicits only casual mention among youth, and is tolerated, even promoted, by their peer culture. Many programs attempt to address peer pressure through parents although, engaging parents has proven to be extremely challenging.
- Local schools are valuable program partners, but establishing these partnerships is sometimes difficult. Their broad access to youth makes schools logical and important partners for many programs, but some schools resist collaboration with abstinence programs. Sometimes schools resist because of competing priorities; at other times, resistance stems from debate about health and sex education policies.
Obtaining clear and definitive evidence on the success of abstinence education programs is a difficult task that requires time. The final evaluation report will be completed in summer 2005. During the intervening periods, the study team will prepare a limited number of special-focus reports that address particular questions of interest to Congress or the U.S. Department of Health and Human Services.
This report was prepared for the Department of Health and Human Services' Office of the Assistant Secretary for Planning and Evaluation's Division of Children and Youth Policy by Mathematica Policy Research, Inc. The Project Officer, Meredith Kelsey, may be reached at (202) 690-6652. A copy of the report may be found on the Internet at http://aspe.hhs.gov/search/hsp/abstinence02/index.htm.
Links Among Different Forms
of Adolescent Violence
An examination of the literature regarding violence among adolescents reveals problems with obtaining reliable estimates of the prevalence of different forms of violence. However, many aspects associated with the family of origin, peer group, and affiliations associated with a source of prior victimization play an integral role in the perpetration of violence. Specifically, the research found that child maltreatment, lack of parental supervision, victimization by peers, perceived social support among peers, and witnessing peer violence was predictive and/or correlated with perpetration of dating and other forms of violence.
This review lays the groundwork to better understand the prevalence, correlates, and consequences of aggressive behaviors such as physical, sexual, verbal, and coercive violence. It also delineates the association between dating violence and other forms of peer violence, and synthesizes how patterns of aggressive behavior vary by sex, developmental stage, and other individual-level factors. In order to address these goals, this analysis provides an operationalized description and theoretical interpretation of adolescent aggression, identifies the predictive factors for dating and other forms of aggression in adolescence, examines the protective and moderating factors for the development of violence in adolescence, and discusses links between perpetration and victimization of dating violence, adolescent aggression, and risk and protective factors.
For this review, adolescent violence was divided according to two broad categories: dating violence and other (non-dating) peer violence. Dating violence encompasses verbal (cursing and threatening), physical (pushing, slapping, punching, kicking, and beating), sexual (coercion), and psychological aggression that takes place between current or former partners in a heterosexual romantic relationship. Peer violence excludes violence between current and former dating partners and refers to a wide spectrum of adolescent peer-on-peer aggressive behaviors including verbal (bullying and threatening) and physical violence (shoving, hitting, gang/group fighting, carrying a weapon), as well as psychological aggression. Issues of rape are not included in this discussion.
Theoretical background
For those studies that adopted a conceptual framework, the theoretical dispositions reflected three categories: 1) psychological theories (attachment, social learning and social control); 2) sociological theories (social disorganization, developmental-ecological, and feminist theories); and 3) hybrid theories (a combination of these theories).
Several theories exist which attempt to find the origins of adolescent aggression. Among these are attachment theory, social learning theory, social control theory, exchange, social disorganization, developmental-ecological theory, and feminist theory. The combination of several theories often builds on the strengths of earlier frameworks and also attempts to address their weaknesses. Integrating elements of biological, psychological, and sociological theories seeks to optimize the explanatory power of this combined, or hybrid theory. It is believed that processes and characteristics related to brain function, family, and social institutions have long-term influences on behavior, which lead to a relatively static potential antisocial behavior. This potential is affected by short-term factors, such as inebriation or boredom, and situational factors such as victim availability.
Prevalence and consequences
The totality of the literature is in singular agreement that violence, including dating violence, is a serious public health issue. However, estimating the extent to which incidences of violence have occurred has not been clearly delineated. There are inherent limitations of prevalence statistics due to reporting differences, varied definitions of violence, and methodological difference in the study. Despite these limitations, the fact remains that violence among adolescents continues to be a serious issue.
Studies estimating the prevalence of violence among adolescents most often focused on both perpetration and victimization most likely due to the high probability of experiencing both.
Discussion
Although the literature examining factors related to perpetration and victimization of various forms of adolescent violence is rather extensive, very few studies approached the question, "What is the association between dating violence and other forms of peer violence?" The literature structured the findings and discussion on shared or unique factors (risk or protective) predictive of both behaviors. Despite the lack of direct evidence, the literature does provide a multiplicity of findings to which inferences can be made regarding links among various forms of adolescent violence.
The majority of the studies examined predictive factors or correlates of adolescent violence from a risk, rather than protective/moderating perspective. They principally included individual level factors rather than community level factors. The literature highlights several factors common to the perpetration of both peer and dating violence. The most predominant factor is the strong association between history of abuse or victimization, future victimization, and concurrent or subsequent perpetration of violence. Many aspects associated with the family of origin, peer group, and affiliations associated with a source of prior victimization play an integral role in the perpetration of violence. Specifically, the research found that child maltreatment, lack of parental supervision, victimization by peers, perceived social support among peers, and witnessing peer violence was predictive and/or correlated with perpetration of dating and other forms of violence. A secondary finding was the association between adolescent violence and involvement in anti-social behaviors, particularly the use of substances such as alcohol and drugs. Additional factors that are common among all forms of violence include accepting attitudes toward use of violence, particularly among males.
Of the studies that focused on individual level risk factors relating to perpetration of adolescent violence, the focus was almost exclusively on gender and on identifying the differences in the types of violence perpetrated by males versus females. The literature notes that it appears females are more likely to perpetrate milder forms of dating violence (pushing, shoving, slapping), but males are more likely to rape or conduct a seriously violent act (including sexual assault). It is also apparent that being a female puts an individual at greater risk of being a victim of all forms of violence.
The current research primarily focuses on individual level factors while excluding the influence of community level factors. The exclusion of community level factors not only limits the knowledge of their influence, but also confounds the influence of individual level factors. Likewise, studies that addressed community level factors did so at the exclusion of individual level factors.
However, there is also a lack of research examining protective factors or factors that moderate against the perpetration of various forms of adolescent violence. Not only is there a significant lack of research, the little research that does exist is split among various definitions of protective factors. Specifically, studies commonly examined factors that moderate against victimization rather than examining factors that would buffer against an adolescent engaging in the perpetration of violence. As mentioned previously, the main reason for the current status of research is most likely due to the overwhelming multiplicity, complexity, and integration (overlap) of individual, developmental, community, and school factors within an open system, presenting methodological difficulties that have limited the ability to conduct a large scale comprehensive study of
adolescent violence.
This report was prepared for the Centers for Disease Control and Prevention by Battelle International. The Project Officer, Joyce McCurdy, may be reached at (770) 488-4410. A copy of the report may also be obtained from the Policy Information Center by referring to PIC ID# 7698.
The Role of Power and Control in
Intimate Partner Violence Perpetration
A review of the literature and the available measurement instruments concerning Intimate Partner Violence was undertaken to identify psychological and sociological factors that might be amenable to modification in a case-control study.
The purpose of this study was to assist the Centers for Disease Control and Prevention (CDC) in developing an understanding of psychological and sociological factors that are potentially modifiable causes of Intimate Partner Violence (IPV) perpetration by men. Some of these include substance abuse, poor impulse control, depression, patriarchal attitudes toward women, victim blaming, and socioeconomic status. Three theoretical orientations to examine IPV were considered: attachment theory, feminist-informed theory, and resource theory. Also examined were the links between IPV and power and control, risk and protective factors that mediate IPV by men, and research on programs that address power and control with perpetrators of IPV.
Major Findings and Recommendations
The literature review focused on three theoretical orientations commonly used to examine intimate partner violence. While these are not the only theories reflected in the literature, they are the dominant ones reflected in most research on IPV perpetration. They are Attachment theory, Feminist-informed theories, and Resource theory.
Attachment theory is when poor childhood attachment by the male to a parent due to separation, deprivation, and bereavement creates a frustrated emotional dependency in which the child's needs are never fulfilled. During adulthood, the individual replicates the parent-child relationship, creating the same emotional dependency and subsequent frustration with his current intimate partner. As a result of the insecure attachment experienced during childhood, batterers are particularly sensitive to rejection from their intimate partners. This frustration may drive the individual to abuse or batter his intimate partner.
Feminist-informed theories regard intimate partner violence as a consequence of a patriarchal society that promotes male coercive power and domination over females. Males engage in intimate partner violence because they believe it is a right associated with being a man, reflective of the endorsement of the use of aggression and violence by men to denote power and control in the greater society.
Resource theory postulates that marital power results from the control of resources and that violence is a mechanism through which an individual attempts to compensate for deficient resources and gain control over these resources. When resources are scarce, aggression and violence are employed to increase an individual's marital control. A man who perceives that he has lost control in an intimate relationship and who also views the costs for engaging in abuse as being less than the rewards is likely to use IPV to restore his power.
Summary of the Research Protocol
The case-control study protocol was structured around three logic models that link perpetration of intimate partner violence by men against women to risk and protective factors for IPV as derived from the literature review. Logic models were developed to test attachment theory, feminist-informed theory, and resource theory. The following six hypotheses were derived to test these logic models:
- Hypothesis 1. Men who batter are more likely than men who do not batter to report attachment problems in childhood that have contributed to problematic attachment styles in adult relationships. This may in turn lead to poor emotional regulation, which may set the stage for a battering event (Attachment theory).
- Hypothesis 2. Men who batter are more likely than men who do not batter to report a history of violence in their family of origin and to exhibit psychopathology and personality traits that increase the likelihood of severe battering either directly or indirectly as a result of a poor ability to regulate their emotions (Attachment theory).
- Hypothesis 3. When randomly selected from the community, batters are more likely than non-battering males randomly selected from the community to report that they know how to be violent, expect use of violence to correct any loss of control or other imbalance in their intimate relationships, and value violent approaches to correcting such imbalances over other options based on mutual respect (Feminist-informed theory).
- Hypothesis 4. Men who witnessed IPV or other forms of domestic violence as children and who, as adults, expect use of violence to correct imbalances in their intimate relationships, are more likely than men without a comparable history and a similar set of expectations to perpetrate IPV if they perceive a threat to their dominance in an intimate relationship (Feminist-informed theory).
- Hypothesis 5. Men who batter are more likely than men who do not to report a history of battering to indicate that a power imbalance in their relationship leads them to believe that they have lost control of important resources that they must regain through the use of violence (Resource theory).
- Hypothesis 6. The relationship between power, perceived loss of control, and battering is stronger among men who have a high need for power in their intimate relationships (Resource theory).
The literature review and instrument review deliverables for this project were designed to inform development of a research protocol for a case-control study. The new insights gained from the proposed case-control study provide a valuable opportunity to enhance understanding of factors that contribute to IPV perpetration and are amenable to early intervention.
This report was prepared for the Centers for Disease Control and Prevention by Battelle Memorial Institute. The Project Officer, Joyce McCurdy, may be reached at (770) 488-4266. A copy of the report may also be obtained from the Policy Information Center by referring to PIC ID# 7697.
National Survey of Homeless Assistance Providers and Clients:
Supplemental Analysis
A secondary analysis of data from the National Survey of Homeless Providers and Clients (NSHAPC) attempts to help local, State, and Federal policymakers, research directors, and service providers better understand the characteristics, service use, and unmet needs of homeless people living with co-occurring conditions that can be grouped into selected problem categories.
The National Survey of Homeless Providers and Clients (NSHAPC), conducted by the U.S. Census Bureau on behalf of 12 sponsoring Federal agencies, was designed to provide the kind of data that can support policy development and research initiatives. During the first part of this survey, the Census Bureau drew a representative sample of all known providers of homeless services in the United States. During the second part, it randomly selected clients from that sample. More than 4,000 clients of the selected service providers were interviewed. That sample of clients is substantial enough to support analyses of subgroups of interest to the sponsoring agencies (e.g., clients living with mental health problems). The findings and methods of the initial NSHAPC study are described in the technical report Homeless Programs and the People They Serve.
Although the NSHAPC study yielded rich data, those data do have limitations. Nevertheless, the NSHAPC data do allow analysts to make reasonable estimates of problem prevalence among a broad population of homeless people. Analysts can also use client reports of current symptoms to identify factors associated with problems among homeless individuals.
People who become homeless face many problems, including unemployment, a lack of stable relationships, mental illness, substance abuse, domestic violence, experiences as runaway or throwaway youth, and experiences with readjustment after release from hospitals and jails. The size and breadth of the NSHAPC dataset make it ideal for exploring selected problems in the context of homelessness or risk for homelessness and for producing generalized results that better support policy development.
Major Research Questions and Conceptual Framework
Although others have studied the causes and correlates of homelessness, little is known about the interplay among risk and protective factors, service needs (e.g., substance abuse and mental health treatment; vocational rehabilitation), and homeless experiences. A secondary analysis of the NSHAPC dataset was undertaken to help local, State, and Federal policymakers, research directors, and service providers better understand the characteristics, service use, and unmet needs of homeless people living with co-occurring conditions that can be grouped into selected problem categories. The focus was particularly on problems that may represent risk or protective factors for homelessness. Also, examining six subgroups of interest to the sponsoring agencies expanded the initial NSHAPC analyses, which concentrated on describing the characteristics of clients in the dataset. These characteristics are as follows:
- Clients with mental health problems
- Clients with drug and alcohol problems
- Clients with multiple health problems
- Clients with co-occurring mental health and substance abuse problems
- Number of homeless episodes
For each of these sub-populations, five major questions in the research were addressed:
- What are the demographic characteristics associated with problem severity?
- What risk and protective factors are associated with problem severity?
- What are the current situations and issues of clients living with problems?
- What services do clients with problems use?
- What unmet needs do clients with problems report?
This report was prepared for the Office of the Assistant Secretary for Planning and Evaluation by Westat. The Project Officer, Walt Leginski, may be reached at (202) 260-0384. A copy of the report may also be obtained from the Policy Information Center by referring to PIC ID# 7250.
About the Policy Information Center
The Policy Information Center (PIC) at the Department of Health and Human Services (HHS), is a centralized source of information on policy research and program evaluation studies, completed as well as in progress, that are supported by HHS agencies or staff offices. PIC also includes studies on HHS programs that are conducted by other organizations. The PIC on-line database at http://aspe.hhs.gov/pic provides project descriptions of these studies. Inquiries about PIC services should be directed to (202) 690-6445 or webmaster.pic@hhs.gov.
The ASPE Highlighter is now available as an electronic newsletter. If you wish to sign up to receive the ASPE Highlighter newsletter, please email listserv@list.nih.gov with “SUBSCRIBE ASPE-HIGHLIGHTER” as the message, or sign up here.