
U.S. Department of Health and Human Services
State Wage Pass-Through Legislation: An Analysis
WORKFORCE ISSUES: No. 1
Institute for the Future of Aging Services
December 20, 2002
This report was prepared under contract #HHS-100-01-0025 between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and the Institute for the Future of Aging Services. For additional information about the study, you may visit the DALTCP home page at http://aspe.hhs.gov/daltcp/home.htm or contact the ASPE Project Officer, Andreas Frank, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, SW, Washington, DC 20201. His e-mail address is: Andreas.Frank@hhs.gov.
Workforce Issues is a series of occasional issue briefs, produced by the Paraprofessional Healthcare Institute and the Institute for the Future of Aging Services, to explore policies that affect the long-term care direct-care workforce. The issue briefs are part of a broader project funded by the U.S. Department of Health and Human Services to support the recruitment and retention of direct-care workers in long-term care.
To learn more about the National Initiative to Improve Recruitment and Retention of the Paraprofessional Workforce in Long-Term Care, contact:
- The Paraprofessional Health Care Institute through its National Clearinghouse of the Direct Care Workforce ate-mail: info@directcareclearinghouse.orgweb: www.directcareclearinghouse.org
- The Institute for the Future of Aging Services ate-mail: ifas@aahsa.orgweb: www.futureofaging.org
Twenty-one states have implemented "wage pass-through" programs with the stated expectation that doing so will help address the shortage of direct-care workers employed by long-term care providers in their states. A wage pass-through is an additional allocation of funds provided through Medicaid reimbursement for the express purpose of increasing compensation for direct-care workers. The purpose of this issue brief is to:
- Describe the structure of wage pass-through programs in selected states;
- Summarize what is known about the impact of these programs on the recruitment and retention of direct-care workers; and
- Identify key design elements that states should consider if they choose to implement a wage pass-through.
THE DIRECT-CARE LABOR MARKET: BACKGROUND
Increasing Demand
The demand for direct-care workers in nursing homes and in home and other community-based long-term care settings is increasing rapidly as the population ages and rising numbers of people with disabilities of all ages need assistance. While the long-term care field has long been characterized by a high rate of worker turnover, in recent years, providers -- home health agencies, nursing homes and assisted living facilities -- and consumers directing services in their own homes have experienced increasing difficulty finding workers to fill the positions at all. A recent General Accounting Office study reported annual turnover rates for nursing home aides ranging from 40 to 100 percent.1 In 2002, 37 states reported that they consider the direct-care shortage a serious workforce issue.2
Below Average Industry Wage
One reason providers find it difficult to recruit and retain direct-care staff is that the prevailing industry wage is below average, while the work is demanding. In 1999, the median wage of direct-care workers was $7.97 per hour, one-third less than the median wage for all workers across all occupations ($11.87 per hour). In 2000, the median wage for direct-care workers increased slightly to $8.21 per hour. As shown in Table 1, these wages fall below federal poverty levels,3 especially for home care aides.

A 2002 labor market analysis of direct-care workers in California, sponsored by the California Employment Development Department, found caregiver occupations in that state were paid lower wages and benefits than competing occupations and offered fewer opportunities for advancement. For example, when comparing wages for competing occupations in the same geographic area as a nursing facility, researchers found that the hourly wage of nursing assistants at the facility averaged 10 percent less than that of other wage earners in the area.4 These low prevailing wage rates have made it difficult for many long-term care providers to compete for workers with other employers offering less physically and emotionally demanding, low-wage jobs. Even as the economy has slowed, providers have seen little improvement in their ability to recruit and retain direct-care staff.5
Faced with significant shortages of direct-care workers in long-term care, 21 states have enacted wage pass-through provisions as part of their Medicaid programs. These provisions are intended to provide additional state and federal dollars to long-term care providers to fund an increase in direct-care worker wages. Table 2 summarizes recently enacted state wage pass-through legislation.6
| TABLE 2. Summary of State Wage Pass-Through Legislation | |||
| State | TargetPopulation | ProviderParticipation | ImplementationAnalysis |
| Arizona | All workers | ||
| California | Skilled nursing facilities (SNF) only | Mandatory | Audit |
| Colorado | Home care | Voluntary | Survey |
| Illinois | Home care | Mandatory | Annual report |
| Kansas | Started with SNF/extended to home care | Voluntary | |
| Louisiana | SNF only | ||
| Massachusetts | Started with SNF/extended to home care | Mandatory | |
| Maine | All workers | Mandatory | Audit |
| Michigan | SNF only | Mandatory | Audit |
| Minnesota | SNF only | Mandatory | Plan |
| Missouri | SNF only | Mandatory | Survey |
| Montana | SNF and personal care | Voluntary | Plan and audit |
| North Dakota | SNF only | Voluntary | |
| Oklahoma | SNF only | Mandatory | |
| Rhode Island | All workers | Plan and audit | |
| South Carolina | All workers | Expanded cost report | |
| Texas | Home care | Mandatory | |
| Virginia | SNF and personal care | Voluntary | Report |
| Washington | Home care | Mandatory | Audit/other |
| Wisconsin | SNF only | ||
| Wyoming | SNF only | Voluntary | |
Medicaid's Impact on Wages
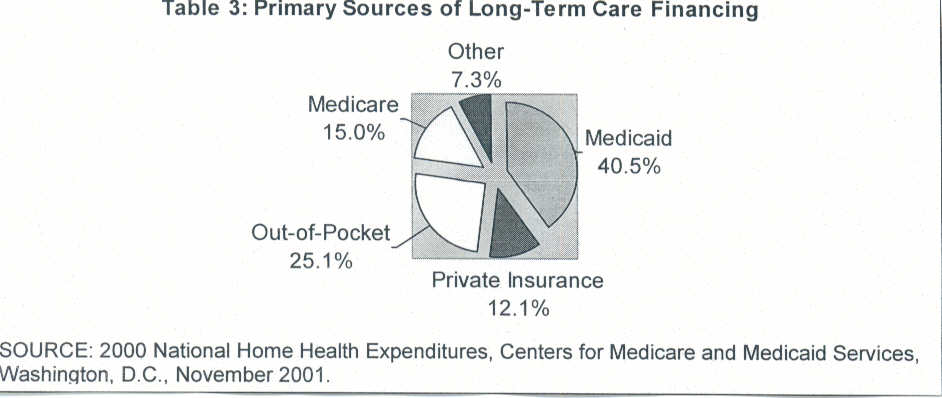
Medicaid, jointly funded by federal and state government and administered by the states, is the largest source of funding for long-term care services (see Table 3). Reimbursement by Medicaid programs creates the framework within which employers set wages for direct-care workers.
Most states establish Medicaid payment rates for nursing homes, Medicaid home- and community-based waiver services, and personal care based on the providers' expenditures in a designated prior year and then make adjustments to account for inflation or other factors that impact costs. For each provider group, states can either establish a single payment rate or set different amounts, determined by size of the facility, acuity of patient mix, ownership, geography, or other criteria. The payment rate contains detailed direction to providers on which costs are allowable, including costs of compensation to workers. Typically, in order to control Medicaid program costs, states set their rates near the average (mean), middle (median), or 70-90th percentile of historic expenditures of all the providers in the payment class.
If either the initial base rate or the annual updates are set too low, the Medicaid payment will be too low to cover provider costs, including the amount spent on wages. In addition, the rate setting mechanism creates incentives for providers to keep all costs, including wages down. These state limits discourage providers from incurring costs beyond the allowable amount; if a provider pays higher wages or hires more workers, or incurs other added costs, these costs will not be reimbursed by the state.
During periods of high competition for labor, wages across the entire workforce begin to rise but direct-care wages cannot keep pace since, by its very nature, a payment system based on historic average expenditures does not reflect current conditions. At such times, the gap between direct-care wages and other wages widens. Turnover and vacancies increase, as direct-care workers are attracted to higher paying jobs and providers experience difficulty attracting new workers. To address this situation, many states make wage adjustments to make the compensation of direct-care workers competitive. Some states elect to increase their Medicaid reimbursement rates permanently and enhance wages by increasing allowable costs for the salaries of workers in caregiving occupations. Other states have implemented a wage pass-through to make this adjustment, providing a one-time additional allocation in Medicaid reimbursement funds for the express purpose of increasing compensation for direct-care workers.
WAGE PASS-THROUGH ANALYSIS
Effectiveness of Wage Pass-Through Programs
Data on the impact of wage pass-through programs on the recruitment and retention of direct-care workers are limited. A follow-up survey conducted by the North Carolina Division of Facility Services of 12 states that implemented wage pass-through programs found that:
- Three states said their wage pass-through program had no impact on recruitment and retention of direct-care workers;
- Three states could not determine whether wage pass-through programs measurably affected recruitment and retention; and
- Four states reported that their wage pass-through program either had a positive impact on recruitment and retention or "probably had some positive impact" on those issues.7
Within the past three years, formal evaluations of wage pass-through programs have been conducted in only three states: Michigan (2000), Massachusetts (2001), and Kansas (2001). The results of these evaluations are ambiguous.
- Michigan found that, in 13 years of providing annual wage pass-through funds, wages earned by certified nurse assistants increased by 61 percent while turnover rates for that position decreased by 21 percent during that time.8
- A survey of Massachusetts' nursing homes found that the wage pass-through contributed to an overall increase of 8.7 percent in nurse aide wages in the first year. In combination with a broad package of interventions enacted by the legislature, Massachusetts' nursing homes reported improved stabilization in their vacancy rates after several years of escalating vacancies.
- In Kansas, one year after implementing a wage pass-through program, the annualized turnover rates for all positions eligible for wage pass-through funds decreased slightly from 111 to 101 percent. The Kansas program funded less than half of the increase in wages identified as needed by the providers.9
A review of current data does not support the efficacy of wage pass-through programs. There may be a variety of reasons for this, such as the timing of existing legislative efforts, the lack of a common methodology used to measure recruitment or retention, or the difficulty of isolating the effect of a wage pass-through from other recruitment or retention initiatives. Nonetheless, many state legislators are embracing wage pass-throughs as one of a series of potential options. As one state legislative leader said, a wage pass-through is a "down payment" -- the first step toward a more comprehensive effort to sustain a competent and stable long-term care workforce.10
The political process, however, may be too uncertain to guarantee that provider funding will keep up with its actual labor costs and competitive market wages. Medicaid funding is subject to the state budgetary process. State Medicaid budgets for all programs and services are set through annual or bi-annual legislative appropriations. Since both provider rates and pass-through amounts are set within the context of the state budget process, provider payments -- and thus, indirectly, wages to workers -- are dependent on overall budget availability and on the political choices governors and state legislators must make between competing spending priorities within that budget.
Approaches to Structuring a Wage Pass-Through
Two methods are commonly used by states to calculate the amount to be allocated for wage pass-through programs. States can either identify a set dollar amount to increase worker wages "per hour" or "per patient-day" within the Medicaid reimbursement rate, or states can require that providers spend a percentage of a specific rate increase on higher compensation. A survey of states in 1999 found that 10 of 16 states implementing wage pass-throughs used a set dollar figure, with pass-through amounts ranging from 50 cents to $2.14 per hour or up to $4.93 per patient-day. The remaining six states established wage pass-throughs as a percentage of the increased reimbursement rate. For example, 80 percent of Minnesota's 40 percent rate increase was earmarked for wages and benefits.11
These methods determine the amount available for increases in wages. Regardless of how the wage pass-through is calculated, states must also decide whether to give explicit direction to providers about how the money can be used (e.g., exclusively for increases in base hourly wages) or to allow them flexibility to use the funds in a variety of ways -- increasing staffing hours, targeting the increases to hard to fill shifts, or paying retention bonuses.
Designing and Implementing a Wage Pass-Through
States have confronted a number of design issues as they have implemented wage pass-throughs.
- Size of the Wage Increase: At what level should the proposed wage increase be set to attract/retain workers to direct-care jobs?
- Equity: Will the wage increase be extended to direct-care workers across all health care settings? Only in long-term care settings? Or only within a subset of long-term care providers?
- Universality: Is provider participation in the wage pass-through to be optional or mandatory?
- Specificity: How flexible or specific should the guidelines be for use of the funds?
- Accountability: What audit and enforcement procedures need to be in place and how do they relate to existing payment and auditing systems?
- Continuity: Will funding for the pass-through be a one-time wage adjustment or will it be built into the rate as a base for subsequent years?
- Notice: How much time and education do providers need to implement the increase as envisioned by the state?
Size of the Wage Increase
The intent of a wage pass-through is to reduce vacancies and turnover among direct-care staff. Therefore, it must be set at a level that is likely to affect the behavior of both potential new applicants and existing workers. Each state determines the size of the wage increase to be proposed, using a variety of factors that can include:
- The current industry wage in the state
- How the current wage compares with the industry wage in surrounding states
- How the current wage compares with competing employment opportunities
- The cost of living and the general economic condition of the state
The state of Wyoming provides an example of how one state calculated the wage rate for its wage pass-through program. In response to a request from the state legislature for an analysis of the salary and benefit levels necessary to attract, retain, and build a skilled direct-care workforce, the Wyoming Department of Health in 2001 recommended increasing entry-level wages of direct-care workers by $3.31 per hour from an average of $6.92 to $10.23 per hour.12 The recommended new wage rate was set at 90 percent of the regional average hourly wage paid to all low-wage workers in similar jobs in 12 western states.13 A statewide survey of former direct-care workers who had left the field also supported the Department of Health's recommendation. The survey found that $10 per hour (more for workers with experience) is the wage at which most former workers reported they would have stayed. In addition, direct-care worker wages in the state were compared with wages of workers with equivalent levels of education and training. The state found that merely matching the local entry-level wage in retail and service industries would not be sufficient given the stress and difficulty of direct-care positions.
Equity
In implementing a wage pass-through, states must decide how to allocate it. Should it include all new and existing direct-care workers in both nursing home and community-based settings or should it be targeted to a subset of workers where the perceived need for workers is the greatest? Most wage pass-through programs have typically been directed toward nursing home workers since state Medicaid spending for long-term care goes primarily to pay for care in nursing homes.14 However, targeting a subset of direct-care workers can have unintended consequences, for example, creating tension between the "haves" and "have-nots" and encouraging workers to move between health care settings in search of higher wages.
Similarly, a wage pass will not impact providers equally. Because nursing homes and other Medicaid providers often have a mix of Medicaid and non-Medicaid recipients, each provider will receive a different amount of money to distribute to their direct-care workforce. Workers in facilities/agencies with larger numbers of Medicaid recipients will receive a higher wage increase than those in facilities/agencies with fewer Medicaid recipients, unless the participating provider or the state supplements the Medicaid wage pass-through with additional, non-Medicaid funding.
Both California and Massachusetts reported confusion among workers as to how big an increase they could expect because of the variation based on providers' Medicaid censuses. As a result, after two years of implementing wage pass-throughs that left workers confused and disappointed, California passed the Wage Adjustment Rate Program (WARP). Under this program, each provider negotiates a specific amount for the wage increase with its workers, which is then funded through the state's Medi-Cal program.15 In Massachusetts, the Coalition to Reform Elder Care (CORE) -- a statewide advocacy coalition of consumers, providers, social workers, and labor unions -- proposed establishing a reimbursement mechanism for the wage pass-through program that bypassed Medicaid altogether, setting up a state appropriated fund which would target wage increases to individual nursing home providers based on the number of nurse aide hours in each facility.16
Universality
In implementing a wage pass-through program, states must choose whether to make provider participation optional or mandatory. In Wyoming, for example, one-fifth of the state's long-term care providers chose not to participate, fearing that raising wages for direct-care workers would increase other compensation-related costs, such as payroll taxes, not funded by the increase.17 A survey of Washington State's nursing homes, conducted shortly after the implementation of that state's wage pass-through program, found that 25 percent of the nursing home providers did not participate in the program. Key reasons cited by providers for not participating included insufficient funding to cover the cost of the increase and fear that funding for the raises would not be sustained over time.18
A wage pass-through raises other issues for providers who have recently increased wages. Unless explicitly noted in a state's legislation, raises that went into effect prior to the start date of the wage pass-through will not be eligible for reimbursement. As a result, providers who already pay more may feel that the legislation penalizes them. The possibility of pass-through legislation can, therefore, serve as a barrier to providers' increasing wages.
Specificity
States must also decide how much flexibility or specificity to build into their rules for use of wage pass-through funds. Providers generally advocate for flexibility in the distribution of funds to allow them to use the funds to meet their most pressing financial needs. Workers and consumer advocates typically seek detailed instructions on use of funds to ensure that funds intended to increase the wages and benefits of direct-care workers are used exclusively for that purpose.
While states often require audits or expanded cost reports for wage pass-through funds,19 they usually determine compliance with the requirements of the legislation by monitoring total direct-care compensation expenditures. This practice allows providers discretion in using wage pass-through funds to meet what they perceive as their most crucial staff needs. For example, rather than directing the money to increase base wages, providers might choose to provide shift differentials, longevity increases, overtime bonuses, benefits, or end-of year bonuses.
It is also possible, depending on the language of the enabling legislation, for providers to use pass-throughs to pay for staffing costs that are not related to increasing the wages of direct-care workers. For example, a survey of Washington State nursing homes found, of 79 respondents, 19 did not provide new salary increases. Of these 19 providers, two-thirds used wage pass-through funds to defray the cost of raises granted in the recent past. Other providers were found to have used a portion of the money to increase the salaries of registered and licensed practical nurses rather than low-wage direct-care staff as intended by the legislation.20
Accountability
States that intend to evaluate the impact of the wage pass-through on provider expenditures must examine their current auditing and enforcement procedures. States implementing wage pass-throughs have employed a number of accountability systems including:
- Requiring providers to submit a plan describing how they intend to institute the increase;
- Conducting a survey of providers after the implementation of the pass-through to determine whether and how they participated;
- Requiring providers to submit expanded cost reports; or
- Conducting a full state audit.21
If the goal of the wage pass-through is to ensure that direct-care workers receive wage increases, the state must go beyond measuring direct-care spending in aggregate. Aggregate spending can increase or decrease independently of wage levels, because of changes in the number of staff hours over the year, a shift in staff composition to a greater number of new hires starting at low entry-level wages, a change in the mix of pool and overtime use, and other staffing pattern changes.
If the wage pass-through is implemented as a supplement to their Medicaid budgets, states may be required to set up a separate auditing system to monitor these funds. This can be cumbersome and expensive for both providers and the state.
Continuity
Many employers are hesitant to increase the base pay of direct-care workers with wage pass-through funds because most states finance these initiatives with annual or biannual appropriations. Providers fear that these programs will not be reauthorized; creating a funding "cliff" that will result in an unsustainable labor-cost structure in future years. Given this uncertainty, some states, for example California, structured their wage pass-through to offer direct-care workers a bonus or other "one-time" compensation increase. To avoid creating such a funding "cliff," states can also consider integrating their wage pass-through into their regular rate structure or they can establish a permanent salary reserve. Louisiana completed an incremental step toward the latter strategy by establishing a permanent trust fund within the state treasury using state and federal Medicaid funds. The interest generated by the fund was dedicated to increasing compensation of direct-care personnel employed by Medicaid-certified nursing homes. This mechanism, however, is unlikely to generate sufficient revenue to significantly increase the wages or benefits of the state's direct-care workforce.22
Notice
Providers need clear, timely information on the structure of the proposed wage pass-through to implement it effectively. Legislative appropriations and Medicaid rate setting, provider fiscal years, and labor contracts can work on different calendars: For example, legislatures may set a state budget that governs program funds from July 1 through June 30, while the rate setting process may work on a regular calendar year, January to December. Therefore, effective dates for legislative action should be set to allow state agencies to develop rules in time for provider implementation. Thinking through the implementation issues ahead of time and addressing them clearly will allow all parties to be aware of what is expected. Start dates of wage pass-through legislation need to build in enough time for administrating agencies to develop implementation policies and notify providers.
In Massachusetts, the state rate-setting agency provided a $20 million wage pass-through for calendar year 2001 beginning on January 1. During that year, the state budget appropriated an additional $15 million wage for increases for the fiscal year beginning on October 1, 2001, but subject to different rules. This mid-year change led to a lot of confusion among providers as to how the funds could be spent.23 In California, a wage pass-through was passed in August 1999. The money to fund the wage increases began to flow to providers in mid-October of that year; however, the state did not publish any instructions for providers on how they could spend the funds until April 2000. This led to reluctance on the part of some providers to implement the wage increases and contributed to findings of poor compliance in the state audit.24
CONCLUSION
Through wage pass-through initiatives, states have enacted interim interventions to allocate, for a single budget year, new resources to address significant shortages of direct-care workers. To date, supporting data are lacking to demonstrate the efficacy of the wage pass-through as a tool to reduce worker vacancies and turnover. In analyzing implementation of wage pass-throughs in 21 states, however, it appears that several key design choices can affect the overall impact of the wage pass-through on direct-care worker salaries. These design choices include determining:
- The size of the salary increase;
- To whom it will be targeted;
- The amount of flexibility providers have in its implementation;
- Whether provider participation will be optional or mandatory;
- The type of accountability to be required;
- Whether the wage pass-through will be integrated into the on-going wage structure; and
- How and when to educate providers about the program.
States considering wage pass-through initiatives also should recognize that low wages, by themselves, are not the sole cause of high vacancy and turnover among the direct-care workforce. Adequate wage levels are important in recruiting and retaining committed and high-quality workers for direct-care jobs; however, an increase in wages cannot, by itself, resolve recruitment and retention problems. Numerous research studies, conducted in a variety of states and spanning all care settings, indicate that factors other than wages and benefits are also important for job satisfaction.25 Of particular importance is that people in caregiver occupations feel they are not respected or valued by the administrators and nurse supervisors who manage their work environments.26 Policymakers and providers also need to look at the clinical and life skills education and training provided to workers to help them prepare for the job, and the supports -- including on-going education, mentoring and linkages to social services -- that may be needed to retain them. In short, solving today's workforce shortages and meeting future demands will require policymakers and providers to examine not merely workers wages and benefits but also how they are educated, trained, supervised, and managed.
For more information on wage pass-throughs and other direct-care workforce policy issues, visit the website of the National Clearinghouse on the Direct Care Workforce, www.directcareclearinghouse.org.
ENDNOTES
-
United States General Accounting Office, Nursing Workforce: Recruitment and Retention of Nurses and Nurse Aides Is a Growing Problem (Washington, DC, May 2001).
-
Paraprofessional Healthcare Institute and the North Carolina Department of Health and Human Services, Office of Long Term Care, Results of the 2002 National Survey of State Initiatives on the Long-Term Care Direct Care Workforce (Raleigh, NC, May 2002) [hereafter cited as 2002 State Survey].
-
The General Accounting Office determined median earnings were $12,265 for home health aides and $13,287 for nursing home aides in 1999. Home health aides, thus, are earning annual salaries that are 27 percent below the poverty line for a family of four and only 11 percent above that line for a family of two. Nursing home aide earnings are 25 percent below poverty for a family of four and 16 percent above for a family of two.
-
California Employment Development Department, California Caregivers: Final Labor Market Analysis (Sacramento, September 2002).
-
According to the 2002 State Survey, only four states reported that the shortage of direct-care workers was not currently a problem while seven states reported slight improvement in the stability of the workforce.
-
Data Compiled from: Paraprofessional Healthcare Institute and the North Carolina Department of Health and Human Services, Office of Long Term Care, Results of the 2002 National Survey of State Initiatives on the Long-Term Care Direct Care Workforce (Raleigh, NC, May 2002); North Carolina Division of Facility Services, Results of a Follow-Up Survey to States on Career Ladder and Other Initiatives to Address Aide Recruitment and Retention in Long-Term Care Settings (Raleigh, NC, September 2001); North Carolina Division of Facility Services, Results of a Follow-Up Survey to States on Wage Supplements for Medicaid and Other Public Funding to Address Aide Recruitment and Retention in Long-Term Care Settings (Raleigh, NC, November 2000); and North Carolina Division of Facility Services, Comparing State Efforts to Address Recruitment and Retention of Nurse Aide and Other Paraprofessional Aide Workers (Raleigh, NC, September 1999).
-
In the remaining two states, one had implemented its wage pass-through too close to the publication of the survey to have had an impact, and the other did not respond. North Carolina Division of Facility Services, Results of a Follow-Up Survey to States on Wage Supplements for Medicaid and Other Public Funding to Address Aide Recruitment and Retention in Long-Term Care Settings (Raleigh, NC, November 2000) [hereafter cited as State Follow-Up Survey 2000].
-
By comparison, per capita income in the state rose 55 percent over the same period.
-
Kansas allocated a fixed amount of $4.3 million to finance its wage pass-through program but since nursing homes requested $9 million in funding for enhancing compensation, the state reduced each facility's requested allocation by approximately 47 percent. This prompted ten facilities to drop out of the program.
-
Senator Mark Montigny, Chair of the Senate Ways and Means Committee for the Massachusetts Legislature, in announcing his Nursing Home Quality Initiative for FY 2000.
-
North Carolina Division of Facility Services, Comparing State Efforts to Address Recruitment and Retention of Nurse Aide and Other Paraprofessional Aide Workers (Raleigh, NC, September 1999) [hereafter cited as 1999 State Survey].
-
State of Wyoming Department of Health, Report to the Joint Appropriations Committee on Study of Nonprofessional Direct Care Staff Recruitment, Retention and Wages (Cheyenne, December 2001).
-
The regional average was $11.37 per hour. They also found that the average in the states bordering Wyoming was even higher, $11.81 per hour.
-
According to the State Surveys (1999-2002) cited above, 8 of 20 states implemented wage pass-throughs for nursing homes only. Two additional states began as initiatives for nursing home workers only and were extended to other workers in subsequent years. Additionally, Arkansas passed a wage pass-through for nursing home workers that was never funded.
-
Darryl Nixon, Director of Public Policy, California Association of Health Facilities, interview, September 9, 2002.
-
Deborah Thomson, "Issues in the Development of a Wage Pass-Through for Certified Nurse Aides," Unpublished memo submitted to the Alzheimer's Association of Massachusetts.
-
In response to a survey assessment of the state's wage pass-through programs, 21 percent of Wyoming nursing homes reported that they did not accept these funds due to the impact on the employer share of fringe benefits paid to staff receiving increased wages. Wyoming, however, is atypical in this respect; most states consider payroll-related expenses permissible uses for wage pass-through funds. State Follow-Up Survey 2000.
-
Washington Department of Social and Health Services, Aging and Adult Services Administration, Management Services Division, Office of Rates, Report to the Legislature: Wage Increases for Nursing Home Low-Wage Direct Care Workers (Seattle, February 2002).
-
The State Follow-up Survey 2000 found that all but one state (Missouri) felt satisfied with the accountability process used to verify wage pass-through program spending.
-
Washington Department of Social and Health Services, Aging and Adult Services Administration, Management Services Division, Office of Rates, Report to the Legislature: Wage Increases for Nursing Home Low-Wage Direct Care Workers (Seattle, February 2002).
-
State Follow-Up Survey 2000.
-
State Follow-Up Survey 2000.
-
Deborah Thomson, op. cit.
-
Darryl Nixon, Director of Public Policy, California Association of Health Facilities, interview, September 9, 2002.
-
See Pennsylvania Department of Aging, In Their Own Words, A Report to the Pennsylvania Intra-Governmental Council on Long-Term Care (Harrisburg, February 2001). Also Kathleen Kopiec, The Work Experiences of Certified Nursing Assistants in New Hampshire (Concord: The New Hampshire Community Loan Fund, October 2000).