
EHR Payment Incentives for Providers Ineligible for Payment Incentives and Other Funding Study
Michelle Dougherty and Margaret WilliamsAHIMA Foundation
Michael MillensonHealth Quality Advisors LLC
Jennie HarvellU.S. Department of Health and Human Services
June 2013
Printer Friendly Version in PDF Format: http://aspe.hhs.gov/daltcp/reports/2013/EHRPI.pdf (88 PDF pages, Main Report)Free PDF Reader: http://get.adobe.com/reader/ 
This report was prepared under contract between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and the AHIMA Foundation. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/office_specific/daltcp.cfm or contact the ASPE Project Officer, Jennie Harvell, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. Her e-mail address is: Jennie.Harvell@hhs.gov.
The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
TABLE OF CONTENTS
- I. BACKGROUND
- A. The HITECH Act, Its Goals and This Study
- B. Increased Importance of This Study
- C. Study Approach
- D. Study Definitions
- II. INELIGIBLE PROVIDERS AND THEIR PRACTICE CHARACTERISTICS
- A. Identifying the Ineligible Providers
- B. Ineligible Provider Characteristics
- III. HEALTH IT ADOPTION AND CLINICAL IMPACT
- A. EHR Adoption Rates for Eligible Providers
- B. Adoption Drivers for Ineligible Providers
- C. EHR Adoption Rates for Ineligible Providers
- D. Ineligible Providers' EHR Use and Clinical Utility
- IV. OPTIONS TO ENCOURAGE USE OF EHR TECHNOLOGY BY INELIGIBLE PROVIDERS
- A. Summary of Options for Incentives, Other Funding, and Support
- B. Other Options -- Guidance from Technical Advisory Group
- V. GUIDANCE FOR EVALUATING OPTIONS
- A. TAG Guidance for Evaluating Options to Support EHR Use by Ineligible Providers
- B. Targeting Technology and Support for Ineligible Providers
- VI. ECONOMIC FACTORS FOR EVALUATING BENEFITS AND COSTS OF NEW INTERVENTIONS
- A. Key Principles of Cost-Benefit Analysis
- B. Assessing Existing Evidence on Effectiveness of EHR and Interoperability
- C. Factors for Evaluating the Costs and Benefits of a Program
- D. EHR Cost-Benefit Considerations for Ineligible Providers -- An Example
- E. Summary of Cost-Benefit Considerations for Making Incentives and/or Other Funding Available to Ineligible Providers
- F. Cost-Benefit Considerations for Making Incentives and/or Other Funding Available to Ineligible Providers
- G. Considerations to Promote Interoperability
- VII. CONCLUSION
- APPENDICES (separate file)
- APPENDIX A: Medicare and Medicaid EHR Incentive Programs
- APPENDIX B: Definitions and Certification of EHR Technology
- APPENDIX C: Public Health Service Act Section 3000(3) as Added by HITECH Section 13101 -- Provider Analysis
- APPENDIX D: Ineligible Provider Characteristics
- APPENDIX E: Long-Term and Post-Acute Care Provider Profiles
- APPENDIX F: Behavioral Health Provider Profiles
- APPENDIX G: Safety Net Provider Profiles
- APPENDIX H: Other Health Care Provider Profiles
- APPENDIX I: Table Summary of Patient Protection and Affordable Care Act Provisions with Relationship to Ineligible Providers and Health IT Use
- APPENDIX J: Behavioral Health Provider Analysis
- APPENDIX K: Grant, Demonstrations and Cooperative Agreement Programs
- APPENDIX L: Loan Programs
- APPENDIX M: Technical Assistance Programs
- APPENDIX N: Administrative Infrastructure Building Programs
- APPENDIX O: Anti-Kickback Statute EHR Safe Harbor Regulation
- APPENDIX P: Private Sector Programs to Advance Certified EHR Technology
- APPENDIX Q: Regulations for Medical Records
- APPENDIX R: Technical Advisory Group Summary
- APPENDIX S: Evaluating Benefits and Costs of New Incentives for EHR Adoption by Ineligible Providers
- APPENDIX T: CIO Consortium EMR Cost Study Data
- APPENDIX U: Abbreviations and Acronyms
- APPENDIX V: References
- LIST OF FIGURES
- FIGURE 1: Providers Identified in HITECH
- FIGURE 2: Number of Ineligible Provider Organizations
- FIGURE 3: Number of Patients Served by Ineligible Provider Type
- FIGURE 4: Total Medicare Expenditures for Services Delivered by Ineligible Provider Type
- FIGURE 5: Medicaid Expenditures for Services Delivered by Ineligible Provider Type
- FIGURE 6: LTPAC Provider Characteristics
- FIGURE 7: Behavioral Health Provider Characteristics
- FIGURE 8: Total Spending for Mental Health and Substance Abuse Treatment
- FIGURE 9: Safety Net Provider Characteristics
- FIGURE 10: Stages of the EHR Incentive Programs in Relationship to National Quality Strategy and Goal of Health System Transformation
- FIGURE 11: EHR Adoption Rates for a Basic EHR by Physicians and Hospitals
- FIGURE 12: Federal Health Information Technology Strategic Plan
- FIGURE 13: Lack of Comparability of EHR Adoption Rates
- FIGURE 14: Factors to Consider for Prioritizing Ineligible Providers
- FIGURE 15: 2012 Study on Importance of Skilled Information Technology Workforce on EHR Costs and Benefits
- FIGURE R1: TAG Priorities for Evaluation Criteria
- LIST OF TABLES
- TABLE 1: Ineligible Providers by Cluster in Alphabetical Order
- TABLE 2: Eligible Professionals and Eligible Hospitals under the Medicare and Medicaid EHR Incentive Payment Programs
- TABLE 3: Ineligible Providers by Cluster in Alphabetical Order
- TABLE 4: HIT/EHR Adoption Rates for Ineligible Providers
- TABLE 5: Current or Proposed Direct Support Programs
- TABLE 6: Current Indirect Support Programs
- TABLE 7: TAG Evaluation Approach for Ineligible Providers
- TABLE 8: EMR*Care Facts and Statistics
- TABLE 9: Five-Year Costs
- TABLE 10: Average Medicare, Medicaid and Other Payments
- TABLE 11: Annual EMR Costs
- TABLE A1: Medicare and Medicaid EHR Incentive Program
- TABLE A2: Stage 2 CMS MU Objectives
- TABLE A3: 2014 Edition Certification Criteria for Base EHR Definition
- TABLE C1: Environmental Scan of Health Care Provider Defined and Providers Eligible/Ineligible for Incentives
- TABLE C2: LTPAC HITECH Provider Analysis
- TABLE C3: Behavioral Health HITECH Provider Analysis
- TABLE C4: Safety Net HITECH Provider Analysis
- TABLE C5: Other Health Care HITECH Provider Analysis
- TABLE J1: Providers Identified in HITECH and Included in This Study
- TABLE J2: Providers Evaluated, but Did Not Meet Study Criteria to be Included in This Study
- TABLE K1: Potential Health IT Enhancements Eligible for ONC HIE Cooperative Agreement Funding
- TABLE O1: Anti-Kickback Statute EHR Safe Harbor 42 CFR Sec. 1001.952(y)
- TABLE S1: EHR Adoption Rates by Ineligible Providers
- TABLE S2: Hospital Adoption of Basic EHR
- TABLE S3: Hospital Adoption of Advanced EHR
- TABLE S4: Subacute Facility Adoption of Basic EHR
- TABLE S5: Subacute Facility Adoption of Advanced EHR
- TABLE S6: Ambulatory Care Provider Adoption of EHR
- TABLE S7: Home Health Care Provider Adoption of EHR
- TABLE S8: Hazard Regression Results -- Adoption of Advanced EHR
- TABLE T1: CIO Consortium Report: Electronic Medical Records Cost Study
ABSTRACT
Background
This study was conducted in response to a requirement in the Health Information Technology for Economic and Clinical Health Act (HITECH Act) of the American Recovery and Reinvestment Act of 2009 (ARRA) (Pub.L. 111-5). Title IV of Division B of ARRA directs the Secretary to conduct several studies including the study described in Section 4104(a):
(B) DETAILS OF STUDY. -- Such study shall include an examination of --
- the adoption rates of certified EHR technology by such health care providers;
- the clinical utility of such technology by such health care providers;
- whether the services furnished by such health care providers are appropriate for or would benefit from the use of such technology;
- the extent to which such health care providers work in settings that might otherwise receive an incentive payment or other funding under this Act, under Title XIII of Division A, under Title XVIII or XIX of the Social Security Act, or other;
- the potential costs and the potential benefits of making payment incentives and other funding available to such health care providers; and
- any other issues the Secretary deems to be appropriate.
The Centers for Medicare and Medicaid Services (CMS) made available ARRA/HITECH funds to the Office of the Assistant Secretary for Planning and Evaluation (ASPE), in the Office of the Secretary within the U.S. Department of Health and Human Services, to conduct the study required in Section 4104(a). The study was directed and managed by ASPE. ASPE awarded a contract to the American Health Information Management Association (AHIMA) to complete the study. The study addresses the questions in Section 4104(a).
Findings and Conclusions of the Study
-
Health care providers not eligible for the Medicare and Medicaid Electronic Health Record (EHR) Incentive Programs (referred to as the EHR Incentive Programs) can be organized into four clusters: Long-Term and Post-Acute Care (LTPAC); Behavioral Health; Safety Net; and Other. Generally, these health care providers provide health care services to some of the most vulnerable and costly individuals in our society, and the care they deliver would often benefit from electronic communication with other providers
-
The funding made available under ARRA/HITECH (e.g., funding for demonstration grants, cooperative agreements, etc.) to health care providers not eligible to participate in the EHR Incentive Programs is not expected to support widespread adoption and use of EHR technologies (including certified EHR technologies) by these ineligible providers. The one exception to this finding pertains to the $1.5 billion made available under the ARRA to Health Resources Services Administration for health centers that include support for the acquisition of health information technology (health IT) systems.
-
Implementation of provisions in the Affordable Care Act may support the use health IT by health care providers not eligible for the EHR Incentive Programs and bring new market pressures on these providers to use such technologies and electronically exchange health information.
-
Implementation rates of EHR technologies, including implementation of certified EHR technologies, by providers not eligible to participate in the EHR Incentive Programs are lagging behind that of health care providers who may participate in the EHR Incentive Programs (i.e., eligible professionals and eligible hospitals).
-
Nonetheless, many health care providers not eligible to participate in the EHR Incentive Programs are adopting some level of technology to meet their clinical and business needs.
-
Providers not eligible to participate in the EHR Incentive Programs generally provide health care to some of the most vulnerable and costly individuals in our society, and the care they deliver would benefit from the use of EHR technology, including the ability to communicate electronically with other providers. The need for health information exchange is particularly important given the multiple providers often involved in caring for these patients, and the number of transitions in care experienced by patients treated by these health care providers.
-
A minority of providers not eligible to participate in the EHR Incentive Programs may be affiliated with health care providers/organizations that are eligible to receive incentive payments under the Medicare and Medicaid EHR Incentive Programs. However, these relationships have not supported widespread use of certified EHR technology by providers not eligible to receive incentive payments, in part, because currently available certified EHR technology does not support the clinical and business needs of providers who are not eligible for EHR incentives.
-
Activities are underway to fill gaps in health IT standards to support the interoperable exchange of documents at times of transitions in care and care plans during transitions in care as well as when care shared across multiple clinicians.
-
Various stakeholders have suggested options that could be considered to support implementation of certified EHR technologies by health care providers who are not eligible to participate in the EHR Incentive Programs. These options include:
-
Direct support such as making available:
- financial assistance (e.g., through incentives, grants (including demonstration grants) or loans) to support the acquisition and use of certified EHR technology; and/or
- technical assistance to support the acquisition and use of this technology.
-
Indirect support such as:
- further development of the nationwide health IT infrastructure to allow for the electronic use and exchange of interoperable information needed to provide services to persons served by these health care providers; and
- extending various Medicare and Medicaid authorities to support implementation of health information technologies, including certified EHR technologies, by health care providers who are not eligible to participate in the EHR Incentive Programs.
-
-
Strategic planning and coordination across programs is needed to identify the most promising policy options, and support successful implementation and use of certified EHR technologies by health care providers who are not eligible to participate in the EHR Incentive Programs. Some of the factors that should be considered in evaluating the costs and benefits of different options include:
-
Built to last: Interventions should support the technology infrastructure needed for the emerging health care delivery and business models envisioned in the Affordable Care Act, the nationwide health IT infrastructure, and EHR Incentive Programs to allow for the interoperable exchange and reuse of health information.
-
Patient-centered: Interventions should promote a patient-centered approach to care delivery and outcomes.
-
Tailored and targeted: The need for interventions should be evaluated in terms of the clinical utility of the technology by a range of health care providers. It is likely that different technology solutions will be required to achieve policy goals.
-
Smartly clustered: Interventions may need to be clustered to accrue the most benefit from the investment.
-
Spend wisely: Consideration should be given to the costs of technology (which are declining) and providers' margins and ability to cover all or some of these costs.
-
Conclusions of the Study
Many of the health care providers not eligible for the Medicare and Medicaid EHR Incentive Programs, such as LTPAC and Behavioral Health providers, have a frequent need to exchange health information on behalf of their patients, who are among the most vulnerable and costly in our society. One of the key benefits of the use of health IT is the ability to exchange information to communicate and coordinate services on behalf of patients, and their physicians and entire care team who are often located in different geographic areas and practice settings. Advancing the adoption of certified EHR technology solutions by providers not eligible for the EHR Incentive Programs may support the realization of the goals associated with implementing a nationwide health IT infrastructure, new models of care delivery and coordination, and the Medicare and Medicaid EHR Incentive Programs.
Filling critical gaps in standards is important to support the interoperable exchange of health information on behalf of vulnerable persons who receive services across the care continuum, including (but not limited to) health care providers who are not eligible for the EHR Incentive Programs. In addition, the specification of standards to support interoperable health information exchange is necessary but may not be sufficient to support the development and implementation of certified EHR technology solutions for these providers. Other actions will likely be needed to support and accelerate the use of certified EHR technology by health care providers not eligible for the EHR Incentive Programs.
EXECUTIVE SUMMARY
The Health Information Technology for Economic and Clinical Health Act (HITECH) includes Title XIII of Division A and Title IV of Division B of the American Recovery and Reinvestment Act of 2009 (Pub.L. 111-5) (ARRA). It is estimated that pursuant to HITECH, over $15 billion1 in incentive payments for the adoption and meaningful use of certified electronic health record technology (CEHRT) will be available between 2014 and 2019 to help certain health care providers improve the quality, safety, and coordination of care while also achieving efficiency gains to help control costs. HITECH-designated hospitals, physicians, and others as eligible for financial incentives for the adoption and meaningful use of CEHRT. Other categories of providers are ineligible. In addition, Title VIII of Division A of the ARRA made available $2 billion to the Office of the National Coordinator for Health Information Technology (ONC) to carry out activities in HITECH, including the development of a nationwide health IT infrastructure that allows for the electronic use and exchange of health information. Through these HITECH provisions, certain providers are eligible for incentive payments and other funding to support their adoption and use of electronic health record (EHR) technology as a part of the emerging nationwide health IT infrastructure.
However, Congress recognized the importance of providers not eligible for EHR incentive payments or other funding to support the implementation of the nationwide health information technology (health IT) infrastructure. Section 4104(a)2 of the HITECH Act required the Secretary of Health and Human Services (HHS) to conduct a study to determine the extent and manner in which payment incentives and other funding for implementing and using certified EHRs should be made available to those providers who received minimal or no HITECH payments. The study is required to address the following factors:
- the extent to which ineligible providers work in settings that might otherwise receive an incentive payment or other federal funding under ARRA, the Social Security Act, or otherwise;
- adoption rates of certified EHR technology (CEHRT) by ineligible providers;
- clinical utility of such technology for ineligible providers;
- whether the services ineligible providers furnish are appropriate for or would benefit from such technology;
- the potential costs and benefits of making payment incentives and other funding available to ineligible providers; and
- any other issues the Secretary deems appropriate. For purposes of this study we identified the extent to which options and incentives had been proposed or implemented to support the use of the technology, including use by ineligibles.
The Secretary is required to submit a report to Congress on the findings and conclusions of this study.
The use of health IT by all health care providers has become increasingly important. Although the Patient Protection and Affordable Care Act of 2010 (Pub.L. 111-148) as amended by the Health Care and Education Reconciliation Act of 2010 (Pub.L. 111-152) (collectively known as the Affordable Care Act)) does not provide funds to support technology acquisition costs, implementing many of its value based purchasing and delivery model provisions as well as other provisions depends heavily upon a health IT/EHR infrastructure.3 In 2011, the National Quality Strategy Report to Congress similarly identified increased use of health IT as one of ten principles to adhere to when designing initiatives to bring about better care, healthy people and healthy communities, and affordable care. In addition, the growing sophistication of health IT applications developed by the private sector underscores the importance of the use of technology to support the health and health care of every American.4
Ineligible Providers
We identified health care providers as those listed in Section 3000(3) of the Public Health Service Act, as added by Section 13101 of HITECH. Those providers identified as ineligible for Medicare and Medicaid EHR incentives and the focus of this report were organized into four clusters: Long-Term and Post-Acute Care (LTPAC); Behavioral Health; Safety Net; and Other, as shown in Table 1 below. As described below, we also considered the extent to which these ineligible provider types received other funding to support their use of EHR technology.
This study identified over 54,000 ineligible provider organizations and 344,000 ineligible professionals delivering services to 51 million individuals across the United States. This summary statistic excludes those ineligible providers clustered in the "Other Provider" category above due to challenges with comparability. Although some of the ineligible providers have an ownership affiliation with eligible providers (and therefore potential access to EHR incentive funds), the majority do not.
| TABLE 1. Ineligible Providers by Cluster in Alphabetical Order | |||
| Long-Term & Post-Acute Care (LTPAC) | Behavioral Health (BH) | Safety Net Providers (FQHC and RHC) | Other |
|
|
|
|
Services delivered by these LTPAC, behavioral health, and FQHC/RHC providers account for $181 billion in combined Medicare and Medicaid expenditures -- over 20 percent of the total Medicare and Medicaid expenditures in health care.5 Safety net providers deliver care to a large number of patients as a primary care provider. Among the LTPAC, Behavioral Health, and Safety Net providers, this study found the provider types accounting for the largest share of Medicare and Medicaid expenditures were: nursing home, home health care, and community mental health providers.
We considered whether the ineligible provider types received other funding under HITECH for purposes of implementing and using EHR technology. With the exception of funds provided to certain safety net providers for their use of health IT, the other funding (e.g., demonstration grants) made available to certain ineligible provider types is not expected to support widespread adoption and use of EHR technology by these ineligible providers.
The Medicare and Medicaid EHR Incentive Programs authorized by HITECH (also referred to as the EHR Incentive Programs) have been successful in accelerating the use of EHR technology by eligible hospitals and professionals. The EHR Incentive Programs increasingly require that providers eligible for incentives engage in health information exchange (HIE). Transitions in care between providers eligible for incentives and providers who are not eligible are common. For example, in 2008, almost 40 percent of all Medicare beneficiaries discharged from acute care hospitals received post-acute care; and of these beneficiaries, more than 15 percent were readmitted to the acute care hospital within 30 days of hospital discharge.6 Instances of shared care are also common between eligible and ineligible providers. For example, Medicare requires that both the physician and HHA sign a home health plan of care. Thus, the normal course of patient care necessitates that eligible providers will exchange health information with ineligible providers. Some providers not eligible for EHR incentives are also adopting EHR technology, but those EHRs are not necessarily compliant with the EHR Incentive Programs criteria used by eligible hospitals and physicians, including requirements that would support interoperable HIE and health information reuse. Effective communication and information sharing across all providers is essential to improving the quality of care, bettering health of communities, and lowering per capita costs. Better alignment of the health IT solutions used by eligible and ineligible providers could promote better HIE and affect health care quality and the ability of eligible providers participating in the EHR Incentive Programs to engage in electronic exchange and care coordination activities with ineligible providers.
In addition to the EHR Incentive Programs, this study identified relationships between ineligible providers and provisions of the Affordable Care Act that could support the use of health IT and/or HIE by these ineligible provider types. We found 40 provisions of the Affordable Care Act that apply to providers not eligible for the EHR Incentive Programs and either require or support the use of health IT and/or HIE with or by these providers. Many of these HIE provisions will advance new care and service delivery models to improve care coordination and quality. Most of these provisions will engage one or more of the ineligible provider types who may not have the health IT infrastructure that could support the reform activity. As these provisions are implemented, new market pressures on ineligible providers to use health IT may increase.
EHR Adoption Rates for Ineligible Providers
This study identified a number of important facts about ineligible providers and their use of EHR technology. Four are particularly salient:
- ineligible providers generally provide health care to individuals who are among the most vulnerable and costly individuals in our society;
- the care they deliver would often benefit from electronic communication with other providers, but that remains uncommon;
- most are adopting some level of technology to meet clinical and business needs, but are not investing in interoperable technology that supports a patient-centered approach; and
- EHR technology products currently used by ineligible providers often are not certified to HHS-adopted standards and criteria, and thus lack interoperability and HIE capabilities, particularly for LTPAC and behavioral health providers.
Collecting information on health IT adoption by the ineligible providers presented significant challenges due to the lack of comparable survey tools, inconsistent definitions and peer-reviewed studies. For ineligible providers, EHR adoption rates ranged from 4 percent to 65 percent. The adoption rates for ineligible providers cannot and should not be compared to adoption rates for eligible hospitals and eligible physicians since they do not measure adoption rates of comparable EHR technology. To illustrate the lack of comparability, the findings from the June 2012 study on health IT adoption for community behavioral health organizations reports that 21 percent of these organizations have EHRs at all of their sites, and 65 percent of survey respondents reported having adopted some form of an EHR at least at some of their sites. Only 2 percent of responding community behavioral health organizations reported adopting technology that could meet the base requirements of the EHR Incentive Program.7
Addressing this technological lag by ineligible providers could support deployment of new models of care delivery and coordination and new payment models for the vulnerable populations most likely to benefit from the service delivery system improvements.
Current and Proposed Initiatives
In this study, more than 30 actions were identified that have been proposed for or implemented in federal or state initiatives that could support (in various amounts, duration, and scope) the use of health IT/EHR technology by ineligible providers.8 The initiatives are categorized in terms of programs that provide "Direct Support" or "Indirect Support" to ineligible providers.
| Direct Support | Indirect Support |
|
|
Evaluating Intervention Options
The 30-plus initiatives mentioned above for advancing health IT for ineligible providers could be coordinated more closely to advance common goals. Based on our analysis and consultation with the Technical Advisory Group (TAG) convened by the contractor for this study, there are some guiding principles that could be considered when evaluating whetheraction is needed for purposes of implementing and using EHR technology by the ineligible providers:
-
Built to last: Interventions should support the development of the emerging health care delivery and business models envisioned in the Affordable Care Act, the nationwide health IT infrastructure, and the EHR Incentive Programs.
-
Patient-centered: Interventions should support improved care delivery and outcomes through the patient-centered approach that technological change is increasingly enabling.
-
Tailored and targeted: Interventions should not be one-size-fits-all, but selected with an understanding of ineligible providers and the technology solution needed to achieve policy goals.
-
Smartly clustered: Interventions should be strategically focused and clustered to get the most benefit from the investment.
-
Spend wisely: In today's fiscally constrained environment careful consideration should be given to the need to support widespread implementation and use of health IT/EHRs by ineligible providers. Such considerations should take into account the ineligible provider's profit margins and ability to pay for some of the technology, and the availability of and need for additional funding to support the acquisition and use of health IT/EHR solutions that will support programmatic and policy goals.
Targeting Ineligible Providers
Not all ineligible providers need CEHRT, nor are all categories of ineligible providers equally critical in achieving overall health system improvements. This study provides guidance and suggested evaluation factors that could be used to determine which providers to prioritize. The TAG considered the factors and prioritized the ineligible providers into following three groupings:
-
Safety net providers: Ineligible safety net providers have already been prioritized for additional support. Safety net providers deliver primary care services to nearly 26 million individuals9 in rural and underserved areas. Congress previously addressed this group of ineligible providers, not through an extension of the HITECH incentive program, but through a $1.5 billion appropriation to Health Resources and Services Administration for health IT grantfunding to support the adoption and use of EHR technology for health centers. This funding, which has not been available to the other ineligible providers, has resulted in a relatively high rate of EHR technology adoption for safety net providers.
-
Long-term and post-acute care and behavioral health providers: Policymakers have directed some attention at advancing the use of health IT/EHRs by the LTPAC providers and behavioral health providers. For example, in 2012 the Substance Abuse and Mental Health Service Administration (SAMHSA) directed $23 million10 in grants and contracts towards the health IT infrastructure and the use of health IT/EHRs by behavioral health providers. In addition, ONC directed $7 million in State Health IT Challenge Grants to advance HIE on behalf of LTPAC providers, and is also supporting HIE on behalf of LTPAC providers in some of the Beacon Community Programs. These providers serve some of the nation's most vulnerable individuals on behalf of whom a significant portion of Medicare and Medicaid expenditures are made. These patients experience frequent transitions in care and require care coordination with eligible hospitals and professionals, and other health care providers. Some of these providers will need interoperable EHR technology to support new care delivery and payment models in the Affordable Care Act (as identified in Appendix I) and in private sector initiatives.
-
Other ineligible health care providers: The use of certain technology interventions could be targeted, as needed, to other ineligible providers to advance policy priorities such as e-prescribing, medication management or lab reporting. These providers are either ancillary service providers that may interface with an EHR or generally have access to CEHRT through their work in other settings. Supporting the use of interoperable interventions through the development of specialized applications would permit efficient HIE between these ancillary providers and health care providers that require the use of certified EHRs, including those providers who are presently eligible for the EHR Incentive Programs.
Economic Factors for Evaluating Options
The decision to implement technology by a provider or implement an incentive or funding program is dependent on understanding the benefits and costs. This section identifies economic factors for evaluating the benefits and costs of programs to accelerate adoption of interoperable EHR technology by ineligible providers. We do this by addressing:
- key principles of cost-benefit analysis;
- findings from evidence on the effectiveness of EHRs;
- criteria for evaluating the costs and benefits of a program; and
- considerations to promote interoperability.
The criteria developed for this report identify several economic factors that could:
- inform the need for and impact of incentives and/or other funding to support the use of EHRs by ineligible provider types; and
- be used to evaluate the need for, and costs and benefits of different incentives and other options to encourage health IT adoption by ineligible providers.
This study considers some of these factors in assessing the potential impact of extending three incentive/funding options and applies the criteria to a private sector study that identifies hypothetical nursing home costs of EHR acquisition and use.
Overall Findings
LTPAC, Behavioral Health, Safety Net, and other providers are not eligible for EHR incentive payments under the Medicare and Medicaid EHR Incentive Programs. Ineligible providers generally provide health care to vulnerable and costly individuals in our society, and the care they deliver would often benefit from electronic communication with other providers. However, such HIE remains uncommon, and addressing this technological lag could support the realization of the goals associated with implementing a nationwide health IT infrastructure and the deployment of new models of care delivery and coordination, and support the HIE goals of the Medicare and Medicaid EHR Incentive Programs.
The ability to address this problem is hindered by data on ineligible providers' health IT use that are unreliable or unavailable, not comparable among ineligible provider types or between any or all of those provider types and the eligible providers involved in the EHR Incentive Program. Despite those barriers, this study addressed the specific questions asked by Congress. This study has:
- provided a rationale for defining health care providers and identified those who are not eligible for the Medicare and Medicaid EHR Incentive Programs, and grouping them into different categories;
- identified other funding made available to these providers who are ineligible for the EHR Incentive Programs and with the exception of certain safety net providers, found that the amount, duration and scope of these other funds will not support widespread use of technology needed to support national policy goals;
- described, to the extent possible, the key characteristics and clinical use of health IT by ineligible providers;
- considered the extent to which ineligible providers work in settings that might otherwise receive EHR incentive payments;
- considered, but could not determine, whether market forces associated with new delivery models such as those encouraged by the Affordable Care Act will be sufficiently widespread to drive adoption of interoperable technologies; and
- identified factors for considering the costs and benefits of making available health IT/EHR incentives/funding for ineligible providers who may be determined to need such support to support national policy goals related to improving health and health care.
I. BACKGROUND
A. The HITECH Act, Its Goals and This Study
There is now widespread agreement that health information technology (health IT) can help providers improve the quality of medical care while also achieving efficiency gains that help control costs. Bipartisan sponsorship for health IT was demonstrated by the inclusion of the Health Information Technology for Economic and Clinical Health Act (HITECH) within the American Recovery and Reinvestment Act of 2009 (ARRA) (Pub.L. 111-5).
HITECH was designed to incentivize Medicare and Medicaid eligible hospitals, critical access hospitals (CAHs), and eligible professionals to use certified electronic health records (EHRs) to collect, store, transmit and use health care information in a meaningful, secure, and timely way. HITECH outlined a number of priorities for the "meaningful use" of EHRs, including e-prescribing, electronic health information exchange (HIE) to improve quality, such as promoting care coordination, and submitting information on clinical quality measures.
HITECH also provided funding for developing a nationwide health IT infrastructure and a framework of privacy, security and other policies and procedures needed to support the electronic use and exchange of health information. HITECH established by statute within the U.S. Department of Health and Human Services (HHS) the Office of the National Coordinator for Health Information Technology (ONC) and tasked it with performing certain duties in a manner consistent with the development of the nationwide health IT infrastructure.11 The goals of the nationwide health IT infrastructure include:
- improve care coordination;
- improve quality, efficiency and patient safety and reduce health disparities;
- promote public and population health;
- engage patients and families; and
- ensure privacy and security.
HITECH also made the Centers for Medicare and Medicaid Services (CMS) responsible for the Medicare and Medicaid EHR Incentive Programs. (For specific timelines and requirements for Medicaid and Medicare incentives, see Appendix A.)
The legislative mandate for this study also originates in HITECH.
To achieve Congress' intended goals and maximize the impact of HITECH funds, incentives focused on physicians, who drive most decisions on care, and on hospitals, where the largest share of health care dollars are spent.12 HITECH-designated specific categories of providers as eligible for incentives under certain specified conditions, while other categories of providers were ineligible, in part because of concern about whether it was possible to establish, in a timely fashion, clear and effective meaningful use standards for them.13 However, Congress recognized those providers' importance in Section 4104(a)14 of the HITECH Act, which requires the Secretary of HHS to conduct a study to determine the extent to which, and manner in which, payment incentives and other funding for implementing and using certified EHR technology (CEHRT) should be made available to those providers who received minimal or no payment incentives or other funding under HITECH. The Secretary is required to submit a report to Congress on the findings, addressing the following factors:
- the extent to which these providers work in settings that might otherwise receive an incentive payment or other federal funding under ARRA, the Social Security Act or otherwise;
- adoption rates of CEHRT;
- clinical utility of such technology for these providers;
- whether the services these providers furnish are appropriate for or would benefit from such technology;
- the potential costs and benefits of making payment incentives and other funding available to these providers; and
- any other issues the Secretary deems appropriate.
B. Increased Importance of This Study
The use of health IT by all providers has become increasingly important since the passage of HITECH in 2009. In particular, the Patient Protection and Affordable Care Act of 2010 (Pub.L. 111-148, as amended by the Health Care and Education Reconciliation Act of 2010 (Pub.L. 111-152) (collectively known as the Affordable Care Act)) contained a long list of provisions addressing access, quality, and cost. Those Affordable Care Act15 provisions included:
- the creation of the Center for Medicare and Medicaid Innovation in CMS to test innovative payment and service delivery models to reduce program expenditures while preserving or enhancing the quality of care;
- improvements in health care coverage, including actions to encourage and expand coverage, and ensure quality coverage;
- improvements in access to Medicaid and enhanced support for the Children's Health Insurance Program (CHIP);
- improvements in the quality and efficiency of health care;
- prevention of chronic disease and improvements in public health;
- support for the current and developing health care workforce;
- improvements in the transparency and integrity of Medicare, Medicaid, and CHIP; and
- improvements in access to innovative medical therapies.
Implementing some of these provisions will depend heavily upon an EHR infrastructure. Those provisions highlight the health and health care implications for the nation of the gap in EHR technology adoption between providers eligible for EHR incentives and providers who are ineligible for such incentives.
For example, health homes are a new model of care intended to link Medicaid enrollees with chronic conditions and providers in a way that enhances coordination and integration of care.16 For that model to be successful, provider types as different as physicians, group practices, rural health clinics (RHCs), community health centers, mental health and substance abuse providers, and home health need to communicate and coordinate.17 Some of these providers are eligible for incentives while some are not. Research has found that providers affiliated with providers eligible for EHR incentives under HITECH may adopt this technology more quickly.18
In a similar vein, the increasing importance of health IT is reflected in the initial National Strategy for Quality Improvement in Health Care (National Quality Strategy), an annual report to Congress mandated by the Affordable Care Act. The initial report in 2011 established three broad aims. They were:19
-
Better Care: Improve overall quality by making health care more patient-centered, reliable, accessible, and safe.
-
Healthy People/Healthy Communities: Improve the health of the United States population by supporting proven interventions to address behavioral, social and environmental determinants of health, in addition to delivering higher-quality care.
-
Affordable Care: Reduce the cost of quality health care for individuals, families, employers, and government.
The National Quality Strategy identifies increased use of health IT as one of ten principles to adhere to when designing specific initiatives to achieve those three aims. The section "Promoting Effective Communication and Coordination of Care" provides specific examples of how "increased adoption of EHRs has the power to cut health care costs, reduce paperwork, improve outcomes, and give patients more control over their health care."20, 21
C. Study Approach
The questions Congress requested that this study examine can be grouped into three categories:
- ineligible providers and their practice characteristics;
- extent of ineligible provider health IT use, its current clinical impact, and the predicted impact of greater use; and
- incentives and other funding options for the use of health IT by these ineligible providers.
To address these questions, this study developed and applied the following approach:
-
Description of United States health care policy goals and the need for health IT, including EHRs: We described key HITECH programs and activities related to this study, including HITECH programs that support the adoption and use (including meaningful use) of certified EHRs, HIE, and criteria and standards for certified EHRs. Key attributes of HITECH were also described within the context of the Affordable Care Act and the National Quality Strategy.
-
Determination of ineligible providers who are the focus of this study: Using the list of health care providers specified in Section 3000(3) of the PHSA, as added by Section 13101 of HITECH, we identified: (i) those provider types eligible to receive incentive payments under current law for the adoption and meaningful use of CEHRT under the Medicare and Medicaid EHR Incentive programs; and (ii) those provider types who are not eligible to receive such incentive payments but could be eligible to participate in the Medicare or Medicaid programs.22 Thus, this report focuses on provider types that: (i) could participate in Medicare or Medicaid; and (ii) are not eligible for EHR incentive payments under the Medicare or Medicaid EHR Incentive Programs. In addition, as described in more detail in the report, we also considered whether any of the provider types ineligible for EHR payment incentives received other funding (e.g., in the form of grants) to support their use of EHR technology.23
-
Identified ineligible provider characteristics: The study provides information, to the extent it is available, on the number of providers in each ineligible provider category and the number of individuals to whom they provide services. The report presents Medicare and/or Medicaid expenditures for services provided by the ineligible provider types.
-
Investigation of the use and utility of health IT, including EHRs implemented by the ineligible providers: To the extent information is available, we examined adoption of EHRs by ineligible providers, their use in practice, and their clinical utility.
-
Identification of current funding, incentive or administrative options to advance use of EHR technology, including CEHRT: We conducted an environmental scan and identified activities undertaken by HHS and others to advance the use of EHRs by providers through incentives or other funding support.
-
Discussion of the study's initial findings with a Technical Advisory Group (TAG): The contractor for this study convened a TAG of experts with expertise in economics, health policy, and Medicare and Medicaid EHR incentive programs and asked them to review the study methodology, initial findings, and other aspects of study design and implementation.
-
Economic factors for evaluating policy options: We engaged a health care economist to identify factors that could be applied to evaluate the cost and benefits of different incentives and other options to encourage health IT adoption by ineligible providers.
D. Study Definitions
Congress requested that this study examine adoption, use and clinical utility of "certified" EHR technology (CEHRT) by ineligible providers. HITECH defines "certified" and "qualified" EHRs. The manner in which those terms were defined in the HITECH and applied in this study is set forth below. Other terms used in the course of this study are also defined and further described in Appendix B.
| FIGURE 1. Providers Identified in HITECH (PHSA 2000(3)) |
|
Adoption of "EHR Technology" Versus "Certified EHR Technology"
For purposes of this study, Congress specifically requested information on ineligible providers' adoption of "certified EHR technology." The certification program in HITECH is currently implemented to support the certification of EHR technology used by hospitals and professionals eligible to participate in the Medicare and Medicaid EHR Incentive Programs. Current EHR technology certification criteria generally support the clinical workflow for eligible providers. While the EHR technology used by ineligible providers can be certified through ONC's EHR certification program, some of the certification criteria do not apply to the technology needed by ineligible providers and also do not include clinical practice and workflow requirements needed by ineligible providers. As a result, few EHR products for ineligible providers, particularly long-term and post-acute care (LTPAC) and behavioral health, are certified.
In September 2012, ONC provided the following guidance on the applicability and certification of EHRs for ineligible providers:
- Secure electronic exchange between all health care settings makes good policy sense;
- EHR technology developers serving ineligible providers are encouraged to certify EHR modules to the transition of care criteria; and
- Acknowledged the role of private certification organizations for these providers.24, 25
HHS has not yet fully assessed the EHR certification criteria needed for technology products used by ineligible providers. For that reason, we could not assess the adoption of CEHRT as defined by the HITECH Act. Instead, we evaluated the adoption of any EHR technology by ineligible providers and looked for evidence of adoption of important features that would be a part of a qualified EHR26 as specified in HITECH. (See Appendix B Definitions and Certification of EHR Technology.)
Qualified EHR Technology
HITECH defined a qualified EHR as: "an electronic record of health-related information on an individual that includes patient demographic and clinical health information, such as medical history and problem lists, has the capacity to provide clinical decision support, support physician order entry, capture and query information relevant to health care quality, and exchange electronic health information with, and integrate such information from other sources."27
Use of EHR Technology
This study requires consideration of the extent to which EHR technology is used by ineligible providers.A definition of "EHR use" was not provided in HITECH requirements for this study. For the purposes of this study, we defined EHR use as how the technology was used in the ineligible provider's practice to support clinical and business operations. To enable comparison among different types of providers, we identified a common set of EHR functionality or modules used in clinical care and operations.
Clinical Utility
A definition of "clinical utility" was not provided in HITECH.28 For the purposes of this study, we defined clinical utility as the ability for the EHR technology to support interoperability and secure information exchange among health care providers by complying with requirements of a "base EHR." To evaluate clinical utility, we considered whether the ineligible provider's EHR technology could meet the requirements of a "base EHR" (which includes transition of care criteria) that will be required, beginning in 2014,for Stage 1 and Stage 2 in the EHR Incentive Programs.29
The Medicare and Medicaid EHR Incentive Programs were intended to increase the adoption and use of CEHRT by eligible professionals and hospitals. However, both the Affordable Care Act and the National Quality Strategy contain a number of provisions and strategies that require the use of EHRs and interoperable health IT technologies across a broad array of health care providers. A new report from the Institute of Medicine, Best Care at Lower Cost: The Path to Continuously Learning Health Care in America, stresses the need for a digital infrastructure to enable providers to deliver better care and generate systems improvement and new knowledge.30 This study will evaluate the providers who are not eligible for the incentive program, yet remain important to the national effort to reform the health care system to improve care and reduce cost.
II. INELIGIBLE PROVIDERS AND THEIR PRACTICE CHARACTERISTICS
A. Identifying the Ineligible Providers
The seemingly simple task of sorting health care providers into different categories (e.g., those eligible and those not eligible for incentives, those who have and use EHR technology and those who do not, etc.) is made complex by both a convoluted system in which overlapping services are provided by different providers and a lack of standardization across provider classifications at the federal and state levels. Thus, for purposes of this study it is imperative to carefully identify who is an ineligible provider. To do that, we applied the following methodology:
-
Determined whichprovider types are listed in HITECH (i.e., PHSA §3000(3)).31
-
Determined which provider types listed in HITECH (i.e., PHSA §3000(3)) are eligible for incentives under HITECH. Table 2 lists those providers who are eligible for either Medicare or Medicaid EHR payment incentive programs, including those whose eligibility for such incentives is dependent upon volume and other thresholds. The providers eligible for either of these payment incentive programs are not the focus of this study (see Table 2).
-
Determined which of the providers as listed in PHSA §3000(3) are not eligible for incentives and which of these "ineligible" provider types could participate in Medicare and/or Medicaid programs (see Table 3).
(See Appendix C for a description of the: Medicare and Medicaid EHR Incentive Programs, the health care providers listed in §3000(3) of the PHSA, and which of these providers are eligible for or ineligible for incentives under the Medicare or Medicaid EHR Incentive Programs).
-
We also reviewed the other funding made available to the ineligible provider types to support their use of EHR technology (see Section V). With the exception of funds provided to certain safety net providers for their use of health IT, the activities supported by these additional funds do not support widespread adoption and use of EHR technology by these ineligible provider types. Thus, for purposes of this report, these additional funds were considered to be "minimal."
| TABLE 2. Eligible Professionals and Eligible Hospitals under the Medicare and Medicaid EHR Incentive Payment Programs | ||
| Eligible Professionals (EP) | Medicare EHR Incentive Program | Medicaid EHR Incentive Programa |
| Physicians (MD/DO) | X | X |
| Dentists/Oral Surgeons (DDS/DMD) | X | X |
| Podiatrists (DPM) | X | |
| Optometrists (OD)b | X | X |
| Chiropractors (DC) | X | |
| Nurse Practitioners (NP) | X | |
| Certified Nurse Midwives (CNM) | X | |
| Physician Assistants (PA)c | X | |
| Eligible Hospitals (EH) | Medicare EHRIncentive Program | Medicaid EHRIncentive Programd |
| Acute Care Hospital | X | X |
| Critical Access Hospitals (CAHs)e | X | X |
| Indian Health Service Hospitalsf | X | X |
| Children's Hospitalsg | X | |
| Cancer Hospitals | X | |
| Territory Hospitals | X | |
| ||
Those providers identified as "ineligible" for EHR incentives and which are the focus of this report were organized into four clusters: LTPAC; Behavioral Health; Safety Net; and Other. The ineligible provider types in each of these clusters are listed below and presented in Table 3. See Appendix C for the health care provider types listed in PHSA §3000(3), including those identified as ineligible for the EHR Incentive Programs, and the definitions of the providers listed in Section 3000(3).
-
Long-Term and Post-Acute Care: Home health agency (HHA), hospice, freestanding and hospital-based in-patient rehabilitation facilities, intermediate care facilities for individuals with intellectual disabilities (ICFs/IID), long-term acute care hospitals, and freestanding and hospital-based nursing homes.
-
Behavioral Health: Clinical social worker, community mental health center (CMHC), psychiatric hospital/unit including substance abuse, residential treatment centers (facilities for mental health and/or substance abuse) and clinical psychologist. Identifying providers included in the behavioral health cluster was particularly challenging in large part due to the historic blurring of behavioral health providers and the services provided by these entities.
-
Safety Net: Federally qualified health center (FQHC) and RHC.
-
Other: Ambulatory surgical center (ASC), blood center, renal dialysis facility, laboratory, dietician/nutritional professional, pharmacist, pharmacy, and therapist (physical therapist; occupational therapist, speech-language pathology).
| TABLE 3. Ineligible Providers by Cluster in Alphabetical Ordera | |||
| Long-Term & Post-Acute Care (LTPAC) | Behavioral Health (BH) | Safety Net Providers (FQHC & RHC) | Other |
|
|
|
|
| |||
Extent to Which Ineligible Providers Work in Settings that Receive Incentive Funding
It is important to note that some ineligible providers do have access to CEHRT, and Congress requested that this study determine the extent to which ineligible providers work in settings that might be receiving health IT incentive funding. When data were available, we identified the percentage of the ineligible providers affiliated with eligible hospitals or eligible professionals in Appendix D (includes data and references by setting) and summarized the findings below:
-
Long-Term and Post-Acute Care: The American Hospital Association (AHA) surveyed 4,800 hospitals32 of which 24 percent have a skilled nursing unit; 29 percent have a physical rehabilitation unit; 7 percent have a LTCH unit; 27 percent offer home health services; and 20 percent offer hospice services.
-
Behavioral Health: The AHA survey of 4,800 hospitals33 indicated 33 percent have an inpatient psychiatric unit and almost 10 percent offer substance abuse treatment. Twelve percent of clinical psychologists and 31 percent of clinical social workers work in the hospital setting.
-
Safety Net: Fifteen percent of RHCs are owned by hospitals and 49 percent of independent clinics are physician owned.
-
Other: The AHA survey34 reported 24.5 percent of hospitals have an ASC. Sixty-five percent of ASCs are physician owned. Ten percent of renal dialysis facilities are hospital-based. Nine percent of emergency medical service providers are hospital-owned. Ten percent of pharmacies are owned by hospitals and 23 percent of pharmacists work in hospitals. Fifty-five percent of laboratories are hospital-based. Approximately 28 percent of physical and occupational therapists work in hospitals and 13 percent of speech-language therapists work in hospitals. Thirty-two percent of dietician/nutritional professionals work in hospitals.
Reassignment of Incentives
Eligible professionals may practice in more than one setting or exclusively in settings that are ineligible for incentives. Eligible professionals may reassign their incentive payments, in accordance with the Medicare reassignment rules, to entities that are ineligible for the incentive payments. Eligible professionals have a choice of where they reassign their incentive payments. For example, professionals working in FQHCs may reassign their incentive payment to the FQHC; however there is no guarantee that they will reassign their incentive payment if they also have their own practice and chose to use the incentive for their own EHR.
Hospital-based eligible professionals cannot receive EHR incentive payments. Data was not available on the extent to which professionals such as physicians practice exclusively in ineligible provider settings.
Eligible professionals who practice in settings like hospitals, nursing homes, FQHCs, CMHCs, etc. may practice in a diverse number of settings. It may not be a realistic way of subsidizing the EHR cost for an ineligible provider by relying on the reassignment of EHR incentive payments.
B. Ineligible Provider Characteristics
To understand the size of the ineligible provider markets, the number of patients they serve, and their impact on the Medicare and Medicaid programs, this section analyzes the key data below and then summarizes the information and additional provider characteristics for three of the ineligible provider clusters (LTPAC, Behavioral Health, and Safety Net):
- Total number of ineligible provider organizations;
- Total number of patients served by ineligible provider type;
- Total Medicare expenditures by ineligible providers; and
- Total Medicaid expenditures by ineligible providers.
The following section does not present this type of information for the "Other Provider" cluster. These "Other Providers" deliver ancillary services (e.g., pharmacy, laboratory, etc.) to the total population in contrast to the other ineligible provider clusters (in which services are provided by defined provider types or organizations). In addition, the services delivered by many of these "Other" ineligible providers are limited to a single clinical domain (e.g., laboratory work or medication orders). Thus, some of these "Other Providers" may not require the functionality of a complete EHR, but instead may use specific health IT applications. Given the variability of providers in the "Other" cluster, the following summary excludes these providers. Information about these "Other Providers" can be found in Appendix H.
The information and sources of data used to complete the analyses for the LTPAC, Behavioral Health, and Safety Net clusters described in this section are detailed in Appendix D. This appendix also contains the data and sources for the "Other Providers" cluster.
Total Number of Ineligible Providers
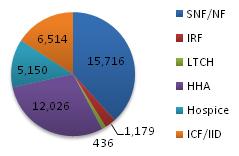
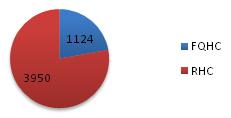
There are almost 55,000 ineligible LTPAC, behavioral health, and safety net provider organizations. Nursing homes (SNF/NFs) have the highest number of providers followed by HHAs. The graph presented in Figure 2 represents provider organizations. Not represented are ineligible professionals. In behavioral health there are 94,000 clinical psychologists and 250,000 clinical social workers.
| FIGURE 2. Number of Ineligible Provider Organizations(not including ineligible professionals) Total = 54,484 | |
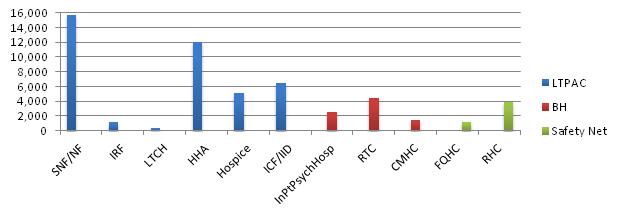 | |
| LTPAC | Total: 41,021; SNF/NF: 15,716; IRF: 1,179;LTCH: 436; HHA: 12,026; Hospice: 5150; ICF/IID: 6414. |
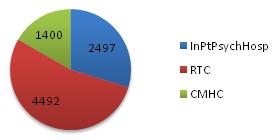
| BH | Total: 8,389; Inpatient Psychiatric Hospital including substance abuse: 2,497; Residential Treatment Center including substance abuse 4,492; CMHC: 1,400. NOTE: Data does not include methadone treatment centers or other outpatient substance abuse treatment facilities. |
| Safety Net | Total: 5,074; FQHC: 1,124(via 9,300 service delivery sites); RHC: 3,950. |
Total Number Patients Served by Ineligible Providers
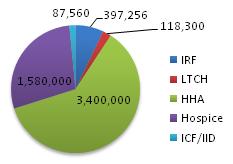
| FIGURE 3. Number of Patients Served by Ineligible Provider TypeTotal = 51.1 million | |
 | |
| LTPAC | Total: 6,969,071; SNF/NF: 1,385,955; IRF: 397,256; LTCH: 118,300; HHA: 3,400,000; Hospice: 1,580,000; ICF/IID: 87,560. |
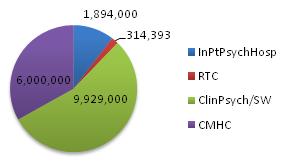
| BH | Total: 18,152,631; Inpatient Psychiatric Hospital including substance abuse: 1,909,238; Residential Treatment Centers including subtance abuse: 314,393; Clinical Psychologist/Social Worker: 9,929,900; Community Mental Health Clinic: 6,000,000. |
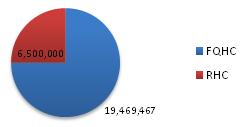
| Safety Net | Total: 25,969,467; FQHC: 19,469,467; RHC: 6,500,000.a |
| |
There are 51.1 million patients served by ineligible providers in LTPAC, behavioral health and safety net organizations. As illustrated in Figure 3, safety net providers, who are primary care providers, treat the largest number of patients (almost 26 million). CMHCs and clinical psychologists and social workers treat the second largest number of patients (almost 16 million).
Total Medicare Expenditures by Ineligible Providers
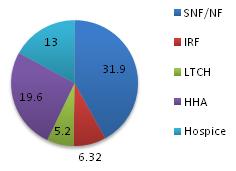
| FIGURE 4. Total Medicare Expenditures for Services Delivered by Ineligible Provider TypeTotal = $83.1 billion | |
 | |
| LTPAC | Total: $76.2B; SNF/NF: $31.9B; IRF: $6.32B; LTCH$5.2B; HHA $19.6B; Hospice $13B. |
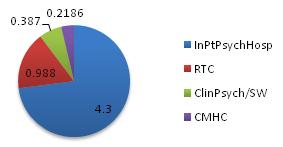
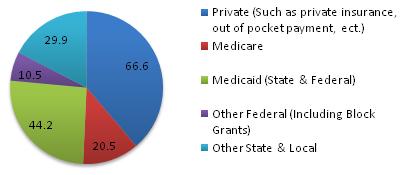
| BH | Total: $6.1B; Inpatient Psychiatric Hospital including substance abuse $4.5B; Residential Treatment Facility: $0.988B; Clinical Psychologist and Social Worker: $0.387B; CMHC: $0.219B; Psychiatric Outpatient: $0.000926B; Outpatient Substance Abuse: $0.51B. NOTE: The bulk of mental health and substance abuse treatment services are not covered by Medicare (or Medicaid), but through Substance Abuse and Mental Health Service Administration (SAMHSA) block grant funding. This report identifies ineligible provider types as those that particpate in and are funded by Medicare or Medicaid. Thus, SAMHSA expenditures are not included. |
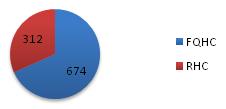
| Safety Net | Total: $0.986B; FQHC : $0.674B; RHC: $0.312B. |
Medicare expenditures for services delivered by ineligible providers account for approximately 15 percent of total Medicare expenditures. Using Medicare expenditure data from different sources and different years, we estimate that annual Medicare expenditures for LTPAC, behavioral health, and safety net ineligible provider types were approximately $83 billion out of $550 billion.35 As outlined in Figure 4, expenditures for services delivered by LTPAC providers account for more than 90 percent ($76 billion) of Medicare expenditures made to this subset of the ineligible providers. (Note: Medicare expenditures were not found for ICF/IID because services by these providers are not covered by Medicare.)
Total Medicaid Expenditures by Ineligible Provider
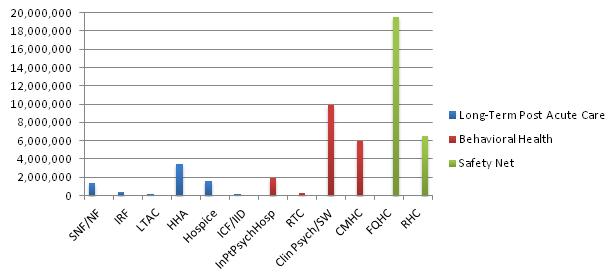
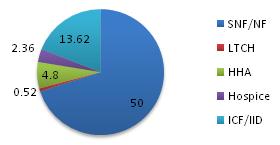
Medicaid payments made for services delivered by ineligible providers account for more than 20 percent of total Medicaid expenditures. Using Medicaid expenditure data from different sources and different years, we estimate that annual Medicaid expenditures for all ineligible provider types were approximately $98 billion out of $400 billion.36 As illustrated in Figure 5, expenditures for three providers, nursing homes, CMHCs and ICF/IIDs, account for more than 80 percent ($79 billion) of Medicaid expenditures made to LTPAC, behavioral health, and safety net ineligible providers. Medicaid expenditures were not found for long-term care and inpatient rehabilitation hospitals that provide Medicare level of care services
| FIGURE 5. Medicaid Expenditures for Services Delivered by Ineligible Provider TypeTotal = $98.1 billion | |
 | |
| LTPAC | Total: $71.3B; SNF: $50.0B; LTCH: $0.540B; HHA: $4.8B: Hospice: $2.36B; ICF/IID: $13.62B. |
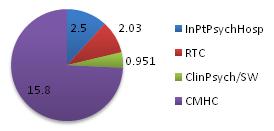
| BH | Total: $21.74B; Inpatient Psychiatric Hospital including substance abuse: $2.96B; Residential Treatment Centers including substance abuse: $2.03B; Clinical Psychologist/Social Worker: $0.951B; Community Mental Health Clinic: $15.8B. NOTE: The bulk of mental health and substance abuse treatment services are not covered by Medicaid (or Medicare), but through SAMHSA block grant funding. This report identifies ineligible provider types as those that particpate in and are funded by Medicare or Medicaid. Thus, SAMHSA expenditures are not included. |
| Safety Net | Total: $5.05B; FQHC: $4.25B; RHC: $0.8B. |
| Long-Term and Post-Acute Care (LTPAC) Characteristics | |
| Number of providers | 41,021 |
| Description | LTPAC facilities provide care over extended periods either in-facility or in-home, to patients with a variety of conditions, including patients suffering from terminal illness. The benefits and services provided typically include: skilled nursing/nursing facility services, rehabilitation services, and assisted living services. Medicare and Medicaid are the predominant payers for several LTPAC provider types. |
| Number of patients | 6,969,071 |
| Medicare revenue | $76.2 billion |
| Medicaid revenue | $71.3 billion |
| Owned by eligible provider | The affiliation of LTPAC providers with providers eligible for incentives varies by LTPAC provider type--ranging from 6.4% of skilled nursing facilities (SNFs) are hospital-based to 80% of IRFs are hospital-based. |
| Medicare profit margin | Medicare margins range from 5.1% for Hospice to 18.5% for nursing homes. |
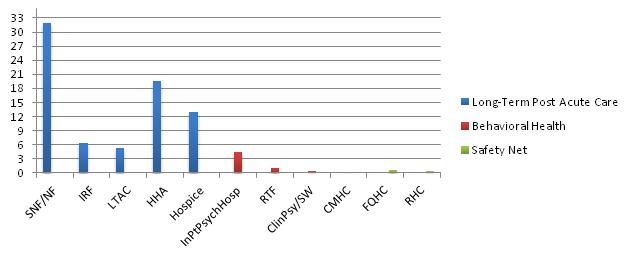
| FIGURE 6. LTPAC Provider Characteristics | |
| Number of LTPAC ProvidersTotal = 41,021 | Number of LTPAC Patientsby Provider TypeTotal = 6,969,071 |
 |  |
| Medicare Expendituresfor LTPAC ProvidersTotal = $76.02 billion | Medicaid Expendituresfor LTPAC ProvidersTotal = $66.4 billion |
 |  |
| Behavioral Health (BH) Characteristics | |
| Number of providers | 8,389 facilities |
| Description | Behavioral Health providers treat clients for a variety of mental health and substance abuse disorders and related illnesses and conditions. Inpatient facilities typically provide a range of institutional/residential services. Partial hospitalization services are provided through hospital outpatient departments, CMHCs, or substance abuse treatment facilities. Clinics are reserved for short-term evaluation, diagnosis, and monitoring of individuals suffering from mental illness or substance abuse. These services use specially trained staff, such as advanced psychiatric practice nurses and aides, as well as psychologists, psychiatrists, clinical social workers, and licensed therapists to manage the often medically complex patients. |
| Number of patients | 18,152,631 |
| Medicare revenue | $6 billion |
| Medicaid revenue | $21.3 billion |
| Owned by eligible provider | 72% of psychiatric inpatient units are hospital-based. |
| Medicare profit margin | We were able to identify reported profit margins for; psychiatric hospitals/units have a Medicare profit margin of 5.92%. |
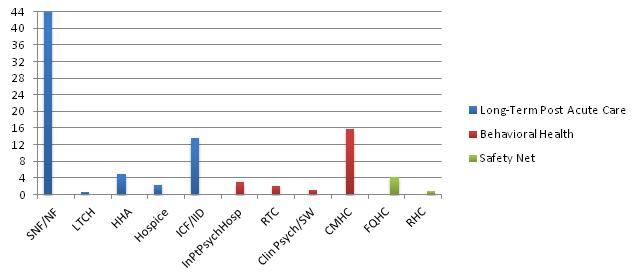
| FIGURE 7. Behavioral Health Provider Characteristics | |
| Number of Behavioral HealthProvider OrganizationsTotal = 8,389 facilities | Number ofBehavioral Health PatientsTotal = 18,137,393 patients |
 |  |
| NOTE: This graph shows provider organizations. There are 343,340 Clinical Psychologists/Clinical Social Workers. | |
| Health Provider OrganizationsTotal = $6 billion | Medicaid Expenditures forBehavioral Health Provider OrganizationsTotal = $21.3 billion |
 |  |
In terms of expenditures made for providers that deliver behavioral health services, for purposes of this study, the focus is limited to Medicare and Medicaid spending for services delivered by those provider types who could participate in the Medicare or Medicaid programs but are not eligible for EHR incentive payments. The graphic below presents total spending for all mental health and substance abuse services. As the graphic suggests, Medicare and Medicaid expenditures account for less than 40 percent of total spending for all mental health and substance abuse services (i.e., approximately 38 percent of the $171 billion in total spending for mental health and substance abuse treatment in 2009). Thus, there are other behavioral health provider types that deliver important mental health and substance abuse services that are not included in this study because they are not covered by Medicare or Medicaid.37
| FIGURE 8. Total Spending for Mental Health and Substance Abuse Treatment 2009 Total = $171.7 billion |
 |
| Safety Net Characteristics | |
| Number of providers | 5,074 (clinic settings) |
| Description | FQHCs provide access to medical care for individuals living in medically underserved areas and to medically underserved populations. They offer on site, or by contract, a wide variety of medical services (e.g., approximately 9,900 physicians see patients at FQHCs). RHCs, by contrast, may be private or non-profit clinics of almost any size. They are located in non-urban medically underserved areas or health professional shortage areas. |
| Number of patients | 25,969,467 |
| Medicare revenue | $986 million |
| Medicaid revenue | $5.05 billion |
| Owned by eligible provider | FQHC ownership is governed by PHSA Section 330 and is limited to entities that are generally not separately eligible for EHR incentive payments. RHCs operate under a variety of corporate structures. Health Resources and Services Administration (HRSA) reports that a majority of RHCs are owned by clinicians or hospitals that are eligible to receive EHR incentive payments. |
| Medicare profit margin | Little information is in the public domain regarding profit margins for Safety Net Providers. RHCs typically operate at a deficit due in large part to the volume of patients without insurance. |
| FIGURE 9. Safety Net Provider Characteristics | |
| Safety Net Providers, by TypeTotal = 5,074 | Safety Net Provider Patient VolumeTotal = 25,969,467 |
 |  |
| Medicare Expenditures by Type ofSafety Net Provider(expenditures in millions)Total = $986 million | Medicaid Expenditures by Type ofSafety Net Provider(expenditures in millions)Total = $5.05 billion |
 |  |
III. HEALTH IT ADOPTION AND CLINICAL IMPACT
The EHR Incentive Programs made available incentives and other funding to eligible providers encouraging their adoption and use of CEHRT. The structure of the program for eligible providers is incremental -- spurring the use of EHRs starting in 2011, increasing access and HIE in 2014, and building towards a transformed health care system after 2016.
Adoption of CEHRT, including interoperable technologies, is lagging among ineligible providers. However, ineligible providers are beginning to adopt health IT that supports their current clinical and business needs. As eligible providers prepare for interoperable HIE in 2014, they will likely need to exchange information with ineligible providers. It is unclear at this time whether market pressures will push ineligible providers and their vendors to implement interoperable HIE needed for health care reform and successful meaningful use implementation.
A. EHR Adoption Rates for Eligible Providers
It is important to understand EHR adoption rates for ineligible providers in the context of EHR adoption rates for eligible providers.
The HITECH Act authorized incentive payments under Medicare and Medicaid for eligible professionals, eligible hospitals, and CAHs that adopt, implement, upgrade, or demonstrate meaningful use of CEHRT, and beginning in 2015, payment adjustments under Medicare for failing to demonstrate meaningful use. The EHR Incentive Programs are being implemented in stages:
-
Stage 1: Beginning in 2011, the first stage of the EHR Incentive Programs focuses on adoption of technology with the capability to collect coded and structured information needed for future stages.
-
Stage 2: Beginning in 2014, the second stage of the EHR Incentive Programs on data exchange, care coordination, and clinical decision-support.
-
The third stage of the EHR Incentive Programs, which may begin in 2016, is expected to focus on improved outcomes and costs shown through robust clinical quality measures.
Figure 10 depicts the stages of the Medicare and Medicaid EHR Incentive Programs and the relationship to the National Quality Strategy and the goal of health system transformation.
| FIGURE 10. Stages of the EHR Incentive Programs in Relationship to National Quality Strategy and Goal of Health System Transformation |
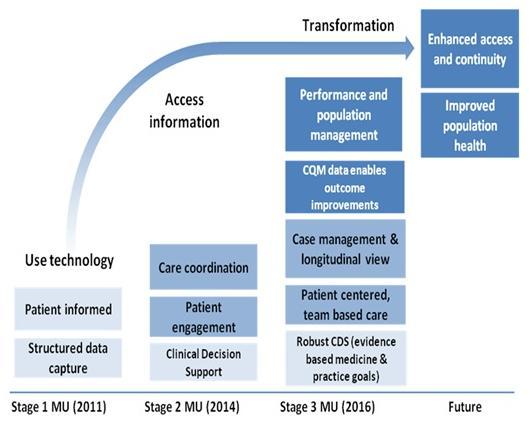 |
| SOURCE: National Quality Strategy--The Future of Quality Measurement. ONC, AHRQ, CMS Presentation. September 14, 2012. |
The Medicare and Medicaid EHR Incentive Programs have been accelerating the use of EHR technology by eligible hospitals and professionals and increasing the requirements to achieve interoperability and exchange.38 An ONC evaluation of the rate of adoption of a basic EHR39 by office-based providers and hospitals shows that EHR incentives have increased adoption in the first year of the program jumping approximately 15 percent between 2010 and 2011. (See Figure 11.)
| FIGURE 11. EHR Adoption Rates for a Basic EHR by Physicians and Hospitals |
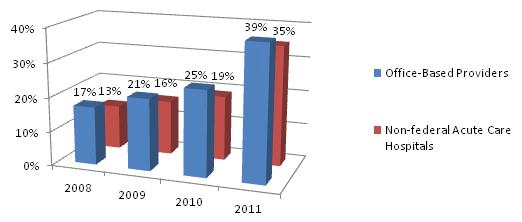 |
|
Another recent study considered two data sources to evaluate EHR adoption by physicians and found that rates rose steadily and doubled from 2005 to 2011, reaching 67.8 percent for family physicians in 2011.40, 41 The researchers attributed this increase to several influences:
- the passage of the HITECH in 2009 with financial incentives for the adoption and meaningful use of EHRs and penalties for lack of engagement;
- the creation of 62 health IT Regional Extension Centers (RECs) across the country to provide technical assistance to support EHR adoption; and
- health IT adoption and use at the state level including the presence of managed care organizations, integrated delivery systems, and large medical practices.42
As eligible hospitals and eligible professionals adopt CEHRT and move to meet Stage 2 requirements in the EHR Incentive Programs, they are beginning to implement more sophisticated technologies to advance data sharing and HIE in 2014. These interoperable technologies will be required to realize the improvement and cost savings goals of the EHR Incentive Programs, National Quality Strategy, and health system transformation.
B. Adoption Drivers for Ineligible Providers
Providers not eligible for EHR incentives are also adopting EHR technology, but their EHRs are not aligned with the requirements for certified EHRs in the stages outlined above for the Medicare and Medicaid Incentive Programs, particularly in the areas of interoperability and HIE (discussed in more detail in Section III.D, Ineligible Providers' EHR Use and Clinical Utility). The ONC's 2011-2014 Federal Health Information Technology Strategic Plan recognized the disconnect between eligible providers' EHRs and ineligible providers, stating that "ensuring health information availability at the point of care would require addressing this difference in health IT use by ineligible providers."43 (See Figure 12.)
| FIGURE 12. Federal Health Information Technology Strategic Plan |
| "HHS plans to propose more rigorous health information exchange requirements which may encourage providers that are not eligible for the incentive programs (e.g., long-term and post-acute care facilities, community mental health centers or substance use disorder treatment providers) to adopt health IT and participate in health information exchange." "For future stages of meaningful use, the plan is to propose health information exchange and interoperability requirements that are more rigorous, so that patient information follows patients to the point of care and informs critical health decisions. This will require overcoming barriers across geographies and stakeholders (i.e., providers, laboratories, hospitals, pharmacies, behavioral health clinics, and patients)." |
In general, most ineligible providers are not adopting technologies to facilitate electronic communication and information sharing directly with other providers or through HIE networks. Many ineligible providers routinely exchange clinical information with other health care partners (often through paper and fax), but electronic HIE is uncommon except for specific use cases (e.g., laboratories to share results and pharmacies for e-prescribing). Uptake of interoperability and HIE has been minimal for ineligible providers for several reasons including:
-
Vendor systems serving the ineligible provider markets generally do not have the functionality to support interoperability and HIE.
-
There is a lack of available CEHRT.
-
Nationally recognized standards are not yet available to support functionalities and interoperable exchange of data needed to support key care processes and contexts that are unique to the various types of ineligible providers.
As previously noted, a number of Affordable Care Act initiatives could use a health IT infrastructure to reduce care fragmentation and improve care coordination as a means of improving quality and reducing cost. In Appendix I, we identified 40 provisions of the Affordable Care Act that apply to ineligible providers within each of the four clusters that either: (i) require or could support the use of health IT; and/or (ii) require or imply the exchange of health information. Some of the HIE provisions require electronic HIE, while other provisions do not specify the method of exchange (e.g., information exchange could electronic or manual). For example:
-
Some of these provisions reference the use of health IT to implement new care coordination models, including medical homes and health homes, and seek to improve care coordination and case management for high-risk, high-cost beneficiaries. These provisions reference the use of health IT/EHRs to support communication, link services, support care over time and across settings, and/or support the reporting of quality measures.
-
Some of these provisions focus on care coordination and imply the exchange of information to: support coordinating care across Medicare and/or Medicaid providers, improve safe and effective care transitions, support hospital discharge planning to ensure appropriate post-acute care placement, secure feedback from beneficiaries and family members, require quality measure reporting, and focus on clinical collaboration by funding clinical education programs.
-
Two provisions included grant programs to support the adoption and use of information technologies or EHRs by long-term care facilities (see Sections 6114 and 6703 of the Affordable Care Act). Funds were not appropriated for either provision and these provisions were not implemented.
It is possible new market pressures will be brought to bear on ineligible providers to use technology as provisions that focus on HIE are implemented. While these provisions are expected to advance the use of technology by at least some of the ineligible providers, it is still unknown how widespread this impact will be.
To understand the state of adoption and use of EHR technology, including interoperable technologies related to the EHR Incentive Programs, the next section describes what is known about each ineligible provider.
C. EHR Adoption Rates for Ineligible Providers
Collecting information on health IT/EHR adoption rates for providers ineligible for meaningful use incentive funding presented significant challenges. The lack of a common definition of an EHR and its functionality severely limits cross-provider comparisons and comparisons with EHR adoption rates by providers participating in the Medicare and Medicaid EHR Incentive Programs (Figure 13). Moreover, there are very few comprehensive, peer-reviewed, published studies on EHR adoption rates by providers not eligible for the EHR Incentive payments. The challenges are summarized in a study conducted by the University of Colorado, Denver44 which evaluated existing surveys on health IT and found:
- Significant variability in breadth and depth of survey content, data item construction, terminology, and definitions (when definitions are provided at all).
- Issues of sample size and representativeness make it difficult to rely on the accuracy of estimates produced by the surveys.
- Respondents from a single state survey limit thegeneralizability of findings to the national picture.
| FIGURE 13. Lack of Comparability of EHR Adoption Rates |
 EHR adoption rates for ineligible providers cannot be compared to eligible providers. EHR adoption rates for ineligible providers cannot be compared to eligible providers.
|
Table 4 summarizes what is known about ineligible providers' full or partial adoption of EHR technology based on the limited information available.
At best, these adoption rates can be used to indicate the need to adopt technology to support some clinical and business processes. However, in general, the adoption rates for ineligible providers cannot and should not be compared to the adoption rates across ineligibles or with adoption rates for eligible hospitals and eligible physicians since they do not measure comparable EHR technology. To illustrate the lack of comparability, the findings from a June 2012 study conducted by the National Council for Community Behavioral Healthcare on health IT adoption for community behavioral health organizations reports that 21 percent of organizations have EHRs at all of their sites; 65 percent of the behavioral health organizations surveyed reported having adopted some form of an EHR at some of their sites. Only 2 percent of responding community behavioral health organizations reported adopting technology that could meet the base meaningful use requirements.45
One agency is addressing the need for comparable national EHR adoption data for certain ineligible providers. The Bureau of Primary Health Care at the HRSA is leveraging the Uniform Data Systems administrative dataset to collect information on the EHR adoption rates in FQHCs. Since 2010 FQHCs have reported EHR information annually.46
| TABLE 4. HIT/EHR Adoption Rates for Ineligible Providers | ||
| Ineligible Provider | Use an EHR? | Adoption Rates of Basic (non-certified)EHRs for Some Clinical Processes |
| Long-Term & Post-Acute Care | ||
| Home Health Agencies (HHAs) | Yes | 43%a |
| Hospice | Yes | 43%a |
| Intermediate Care Facilities for Individuals with Intellectual Disabilities (ICF/IID) | Unknown | |
| Long-Term Care Hospitals (LTCHs) | Yes | 6%b |
| Nursing Homes (SNFs/NFs) | Yes | 43%c |
| Inpatient Rehabilitation Facilities/Units | Yes | 4%b |
| Behavioral Health | ||
| Clinical Social Workers | Yes | Unknown |
| Community Mental Health Centers (CMHCs) | Yes | 21% adopted some form of EHRs at all sites, 65% adopted some form of EHRs at some sites, 2% report adopting a base EHR that can meet Meaningful Used |
| Psychiatric Hospitals/Units | Yes | 2%b |
| Psychologists | Yes | Unknown |
| Residential Treatment Centers (Mental Health and/or Substance Abuse) | Yes | Unknown |
| Safety Net Providers | ||
| Federally Qualified Health Centers | Yes | 79.6%e |
| Rural Health Clinics | Yes | 42%f (limited study n=65 of 3950 providers) |
| Health Care Related | ||
| Ambulatory Surgical Centers | Yes | 18%g |
| End Stage Renal Dialysis Facilities | Yes | Unknown |
| Emergency Medical Service Providers (Ambulance ) | No | Unknown |
| Pharmacies | No | 12%h * |
| Laboratories | No | 24.2%i (can post to an EHR via interface) |
| Blood Centers | No | Unknown |
| Therapists (PT, OT, SLP) | Yes | PT- 28%j |
| Dieticians and/or Nutritional Professionals | Yes | Unknown |
| Pharmacists | No | *See Pharmacy |
NOTE: Technology and thus percentages are not comparable to one another or to rates of adoption for CEHRT used by eligible hospitals and professionals.FOOTNOTES:
| ||
In general, the findings for ineligible providers reflect implementation of EHR functions that support some business and clinical needs for that particular provider type. Even though some providers are fully electronic, most have only partially implemented a system and are maintaining hybrid processes (both paper and electronic). The majority of providers have limited or no capability to electronically exchange information and generally cannot support meaningful use functions related to transition of care. One group of ineligible providers -- pharmacies, laboratories, ambulance services, and blood centers -- appear to maintain specialized health information systems that share information with EHR technology, but these health information systems do not constitute an EHR system themselves. Some of these providers use specific health IT applications rather than the complete functionality of CEHRT. Further, some of these applications may need to support interoperable exchange with certified EHR systems.
D. Ineligible Providers' EHR Use and Clinical Utility
Ineligible providers are adopting technology to support some clinical and business processes, but EHR products used by ineligible providers have generally not supported interoperability. It is not surprising given limited EHR technology to support exchange for eligible providers and almost none that supports interoperable exchange by ineligible providers. Requirements for interoperable exchange for eligible providers are just now being implemented with Stage 2 of the EHR Incentive Programs. To address questions from the ineligible providers regarding EHR certification interoperability, the Federal Government provided guidance in July 2012 recommending voluntary certification to the transitions of care module. It is unclear at this time whether market pressures will push ineligible providers and their vendors to implement interoperable HIE needed for health care reform and successful implementation of the Medicare and Medicaid EHR Incentive Programs.
To understand ineligible providers' use of an EHR, we looked at adoption rates, use in practice, clinical utility as it relates to the base EHR requirements that will apply beginning in 2014 for Stage 1 and Stage 2 of the EHR Incentive Programs, the need for HIE, and barriers to adoption. Findings for each ineligible provider cluster are summarized below with more detailed information by each ineligible provider type detailed in Appendices E-H.
Use of the EHR in Practice
To understand how the EHR was used in patient care and to support daily operations, we evaluated the following categories of EHR functionality:
- Admission, discharge, and transfer (ADT)
- Appointments
- Order entry and management
- Clinical notes
- Assessments
- Care plan
- Condition-specific documentation
- Medication and treatment records
- Pharmacy information system
- Lab information system
- Therapy information system
- Patient portals
- Patient eligibility determinations
- Billing
- Staffing
Clinical Utility
To assess clinical utility and determine the ability of health IT to improve care and patient impact, we examined the base EHR functionality as described in the September 4, 2012 ONC final rule on health IT standards, implementation specifications, and certification criteria for CEHRT that must be met for the Stage 1 or Stage 2 meaningful use requirements by eligible professionals and eligible hospitals under the Medicare and Medicaid EHR Incentive Programs. We considered whether these requirements could be implemented in information systems used by ineligible providers because there was a need for similar functionality in systems used by these providers. This should not be construed as saying the ineligible provider's EHR technology meets the base EHR requirements. The following functions were evaluated:
- Patient demographics, health information, and problem lists
- Clinical decision support
- Physician order entry
- Support clinical quality measures
- Exchange health information (send, receive, and integrate to support transition of care)
- Privacy, security, and integrity features
Barriers to Adoption
To fully understand limitations to adopting EHR technology, we collected information on the barriers that limited or prevented adoption and use of EHR technology by the ineligible providers. We categorized the barriers as follows:
- Lack of capital
- Perceived inequity regarding lack of incentives
- Lack of awareness of the need to implement an EHR
- Lack of demand for an EHR
- Lack of a certified vendor for provider specialty
- EHRs available lack of alignment with meaningful use criteria
- Workforce limitations to implement and maintain an EHR
- Limited decision support for complex clinical condition
- Lagging standards for clinical processes
- Lack of consent management
| Long-Term and Post-Acute Care EHR Use and Clinical Utility | ||
| EHR needed | Yes | |
| Adoption rate | Range from 4% to 43% | |
| Use in practice |
|
|
| Clinical utility |
|
|
| Need for information exchange | High, as patients transition from the LTPAC facility to hospitals and have frequent episodes of care coordination with primary care. | |
| Barriers to adoption |
|
|
| Behavioral Health EHR Use and Clinical Utility | ||
| EHR needed | Yes | |
| Adoption rate | Range from 2% for Psychiatric Units/Hospitals to 21%-65% adoption of some EHR technology by behavioral health providers | |
| Use in practice |
|
|
| Clinical utility |
|
|
| Need for information exchange | Need for exchange is high, but complicated by 42 CFR Part II. Significant efforts through SAMHSA and the National Council for Community Behavioral Healthcare have identified opportunities to advance exchange on behalf of behavioral health providers, and standards have been developed and are currently being piloted for electronic exchange of health information that is subject to these increased privacy protections. | |
| Barriers to adoption |
|
|
| Safety Net EHR Use and Clinical Utility | ||
| EHR needed | Yes | |
| Adoption rate | 42% for RHCs to 68.5% for FQHCs | |
| Use in practice |
|
|
| Clinical utility |
|
|
| Need for information exchange | High, as Safety Net providers are typically required to contract with a wide range of other providers and specialists within their care networks, and patients will travel across this network. | |
| Barriers to adoption |
|
|
Other Provider EHR Use and Clinical Utility
As was the case in presenting information about the Other Providers expenditure and volume information, it is difficult to provide aggregate information about this group's EHR adoption and use. Other Health Care Providers rely on health IT; however, with the exception of ASCs, the Other Providers' need for health IT appears to be limited to a specific ancillary service. Appendix H provides information (to the extent it was available) for each provider identified.
IV. OPTIONS TO ENCOURAGE USE OF EHR TECHNOLOGY BY INELIGIBLE PROVIDERS
The previous sections described the ineligible providers, the patients they serve and their use of EHR technology. From this analysis, we identified a number of important facts about ineligible providers and their use of EHR technology. Three are particularly salient:
- ineligible providers generally provide health care to some of the most vulnerable and costly individuals in our society;
- the care they deliver would often benefit from electronic communication with other providers, but that remains uncommon; and
- most ineligible providers are adopting some level of technology to meet clinical and business needs, but are not investing in interoperable technology that supports an integrated, patient-centered approach.
This technological lag by ineligible providers may have consequences. Advancing the use of EHR technology, particularly to support HIE, could support new models of care delivery and coordination and new payment models for the vulnerable populations most likely to benefit from the goals of Better Care/Healthy People/Healthy Communities and Affordable Care.
Stakeholders have identified a variety of direct and indirect actions that could be used to encourage adoption of EHR technology by ineligible providers. It should be noted that some of these options have been implemented while others have only been proposed. This summary simply lists and does not endorse any of these options. These actions include:
- Proposals to extend the current Medicare and Medicaid EHR Incentive Program;
- Grants, demonstrations, and cooperative agreement programs (federal and state);
- Loan programs (federal and state);
- Technical assistance programs;
- Administrative infrastructure building activities (standards and testing); and
- Other actions (rule changes).
These actions have been advanced by a variety of stakeholders and are described below and in more detail in Appendix A and Appendices K-O.
A. Summary of Options for Incentives, Other Funding, and Support
In this study over 30 actions, plans, proposals, or initiatives were identified that make available or propose federal or state actions to support ineligible providers' use of EHR technology.47 These current or proposed actions focused on advancing the use of health IT; including by modernizing the health care infrastructure to facilitate new models of care delivery or payment, or targeting the use of technology by a particular group of ineligible providers who sometimes are limited to a particular geography. Detailed descriptions of these initiatives are available in Appendix A and Appendices K-O. The initiatives described below are summarized and categorized into two groups: initiatives that provide direct support to ineligible providers and those providing indirect support.
Direct Support Options
There are five types of initiatives that offer direct support to ineligible providers to acquire and use health IT. The initiatives include both current and proposed programs and include providing support through extending the current EHR incentive program, grants paid to providers to purchase technology, loan programs, and administrative rules. Table 5, below, summarizes the direct support options. More detailed information is provided in Appendix A and Appendices K-N.
| TABLE 5. Current or Proposed Direct Support Programs | |
| Initiative | Summary |
| Proposals to extend EHR incentives to providers not eligible for such incentives under current law. | Current law makes available EHR Incentive payments to eligible health care provider types.Several stakeholdersa,b,c,d,e,f,g have stated that there is a need to extend the EHR Incentive Programs under HITECH to include many ineligible provider types, such as long-term and post-acute, and behavioral health providers. These stakeholders describe the lack of incentives as a barrier to achieving needed quality, continuity, and coordination of care improvements; as well as a barrier to enabling needed data analytics to measure, improve, and transforming service delivery. Some of these stakeholders propose extending the same incentive structure as is implemented in the EHR Incentive Programs. Others recommend establishing meaningful use metrics that reflect key clinical and non-clinical measures for the vulnerable populations served by ineligible provider types, and aligning the current meaningful use measures for the EHR Incentive Programs with these metrics. |
| Health IT grants to support health IT acquisition | Grants administered by HRSA were made available to safety net providers to enhance or purchase EHRs and health IT. Separately, the Affordable Care Act authorized grants to long-term care facilities to assist in purchasing EHR technology but funds were not appropriated.Several stakeholder groups have stated that there is a need to extend current and/or create new grant programs to support the acquisition and use of health IT, including interoperable EHRs, by ineligible providers.c,e,g |
| Health IT loan program | Some states, such as North Dakota, Minnesota and Maine, offer health IT loan programs to both eligible and ineligible providers. For example, North Dakota made $5 million available in a revolving loan fund to directly support eligible and ineligible providers in purchasing health IT. Some stakeholder groups have proposed making available various loan programs to support the acquisition and use of EHR technology.a,d,e,gIn addition, Title XIII of HITECH permitted the ONC to establish a grant program to states (and Indian tribes) for a loan program for providers to support the purchase and use of certified EHRs, training of personnel, or secure HIE. |
| Technical assistance programs for EHR technology implementation consulting | CMS is working with Quality Improvement Organizations (QIOs) to provide technical assistance to ineligible Medicare providers, particularly LTPAC providers, in three states to support HIE activities.jIn addition, QIOs are collaborating with RECs to leverage CEHRT for quality improvement purposes through their Learning and Action Networks and expanding their assistance to ineligible health care professionals. CMS anticipates continuing to promote technical assistance to advance health IT across multiple health care settings in the QIO program.Separately, HITECH funded RECs to provide technical assistance to eligible professionals to implement CEHRT. Several stakeholder groups have proposed making available technical assistance to support the acquisition and/or use of health IT/EHRs by ineligible provider types either by extending the RECs or through new grant programs.a,c,e,g |
| Other Subsidies | Broadband connectivity has become increasingly vital to the effective delivery of health care, and it can be uniquely transformative in rural areas, where distance poses a substantial challenge. To increase access and use of this critical communication service, the Federal Communications Commission (FCC) provides support for broadband connectivity to certain qualifying health care providersh (such as CMHCs) in rural areas, and in some cases urban areas. The FCC's Rural Health Care (RHC) Programs include the Healthcare Connect Fund and the Skilled Nursing Facilities Pilot Program.i Through these programs, the FCC makes available broadband connectivity at highly discounted rates (see Appendix N). One state (Minnesota) investigated modifications to the Medicare and/or Medicaid cost report structure to permit as allowable expenses costs for CEHRT acquisition for nursing homes. (Minnesota Medicaid pays cost-based reimbursement.) |
FOOTNOTES:
| |
Indirect Support Options
Other initiatives do not involve directly funding providers. Instead, these options span a wide array of activities. These options:
- have provided funds to states to develop health IT plans and infrastructure, including support to ineligible providers;
- have funded demonstration projects to test new delivery and care coordination models supported by health IT;
- have helped certain ineligible provider types address workforce skill gaps by providing technical assistance such as tools and resources to help in selecting, implementing and using an EHR;
- have and are continuing to advance technical standards that will support needed interoperable health information by ineligible providers; and
- may remove perceived barriers to the adoption of EHR technology.
Table 6 summarizes the options and groups them into five categories. More detailed information is provided in Appendix K and Appendices M-O.
| TABLE 6. Current Indirect Support Programs | |
| Initiative | Summary |
| Health IT grants to states for infrastructure development and outreach | Grants have been provided to state governments to build a health IT infrastructure to: (1) support HIE; (2) develop health IT plans to address vulnerable populations (behavioral health and LTPAC); (3) establish new care delivery models; (4) overcome barriers to exchanging sensitive behavioral health information; and (5) provide education and outreach. |
| Health IT grants to community groups and providers to demonstrate health IT solutions that support new models of care delivery and HIE | As of 2012, SAMHSA had two grant programs available to approximately 100 behavioral health providers to demonstrate health IT solutions. Separately, the Beacon Community Grants were funded by ONC to strengthen the technology infrastructure and exchange capabilities. Seventeen communities across the country were funded, some of which included a focus on certain ineligible providers. One community received additional funding to extend HIE to behavioral health. |
| Technical assistance resources and toolkits for EHR implementation | HRSA funded development of technical assistance materials for safety net providers. It has included toolkits, EHR acquisition guides and training webinars. The QIO Program in Minnesota, with the support of private funding, developed a web-based toolkit to support health IT adoption by nursing homes and HHAs. SAMHSA funded the development of health IT resources for behavioral health. |
| Infrastructure development: policy and health IT standards | The ONC Standards and Interoperability Workgroup Longitudinal Coordination of Care Workgroup and private sector partners are supporting the development and testing of health IT standards to address gaps in standards that create barriers for ineligible providers to implement interoperable EHR systems and participate in HIE. HHS currently supports programs to develop industry policies and standards for HIE and test their effective use. Efforts to date have focused on health IT standards initiatives needed to increase behavioral health and LTPAC providers in HIE activities. For example, work is underway to develop standards that could be integrated into technology solutions used by eligible and ineligible providers for the interoperable exchange of more robust of Summary Documents and Care Plans at times of transitions in care and to support instances of shared care. |
| Anti-Kickback Statute (AKS) EHR Safe Harbora | While not a "program", a regulation established by the Office of the Inspector General created a safe harbor to the AKS for certain arrangements involving the donation of interoperable EHR software or information technology and training services.The safe harbor permits certain individuals and entities to donate (and cover up to 85% of cost) of items and services in the form of software or information technology and training services. The arrangement between the donors and recipients must meet certain conditions in order to receive safe harbor protection. This safe harbor is scheduled to sunset at the end of 2013. (See Appendix O for additional information.) |
FOOTNOTE:
| |
B. Other Options -- Guidance from Technical Advisory Group
In addition to the initiatives above, the TAG convened by the contractor for this study identified other administrative levers that could be used to advance the use of CEHRT by ineligible providers who participate in the Medicare and Medicaid programs. The TAG was comprised of experts on health care policy, economics, financing, and health IT. The descriptions below present suggestions identified by the TAG and is not intended to endorse any of these options, but simply to convey ideas discussed by the TAG.
Program Regulations
The ineligible providers identified in this study participate in the Medicare and/or Medicaid program in which there are program/payment rules and regulations that govern their participation. The TAG suggested that these requirements could reference the use of CEHRT by the ineligible provider. For example, current regulations include requirements for maintaining medical records and some refer to electronic records. The language could be updated to reflect contemporary use of EHR technology aligned with Meaningful Use criteria, while balancing the goal to promote widespread EHR adoption and resources needed to support such adoption. (See Appendix Q for an example of current regulatory language for medical records.)
Condition Grants on Use of Interoperable Health IT
Another option suggested by the TAG to accelerate the use of health IT/EHRs by ineligible providers would include in the use of interoperable health IT (consistent with requirements with the EHR Incentive Programs) in grant program requirements where the use of health IT and HIE is needed. This could ensure that government funds are used to support consistent health IT policy goals and that grants available to ineligible providers increase the adoption and use of CEHRT.
Program Oversight Through Health IT
There are on-going concerns about health care fraud involving both eligible and ineligible provider types. Technology can play a role in program oversight. The 2005 report to ONC on the Use of Health Information Technology to Enhance and Expand Health Care Anti Fraud Activities48 stated that "technology can play a critical role in detecting fraud and abuse and it can help to pave the way toward prevention. While technology cannot eliminate the fraud problem, it can significantly minimize fraud and abuse and ultimately reduce health care fraud losses. The use of advanced analytics software built into the nationwide health information infrastructure is critical to fraud loss reduction."
V. GUIDANCE FOR EVALUATING OPTIONS
A. TAG Guidance for Evaluating Options to Support EHR Use by Ineligible Providers
The HITECH EHR incentive program not only provided direct support to acquire CEHRT, but also a complementary set of programs to ensure eligible hospitals and professionals could be successful in using CEHRT in a meaningful way. In contrast, the more than 30 actions/plans/initiatives mentioned above to advance health IT for ineligible providers have little coordination or common strategic purpose behind them. For that reason, the TAG convened by the contractor for this study provided the following guidance for evaluating and prioritizing different initiatives to support the implementation and use of EHRs by ineligible providers:
-
Built to last: Interventions should support the technology infrastructure needed for development of the emerging health care delivery and business models envisioned in the Affordable Care Act, the development of the nationwide health IT infrastructure, and the Medicare and Medicaid EHR Incentive Programs.
-
Patient-centered: Interventions should support improved care delivery and outcomes through the patient-centered approach to care delivery that technological change is increasingly enabling.
-
Tailored and targeted: Interventions should not be one-size-fits-all, but selected with an understanding of ineligible providers, barriers, costs and benefits for health IT adoption and the costs and benefits to Medicare and Medicaid. Interventions do not need to be directed to an entire provider type, but could be targeted to a subset (e.g., providers of a certain size or in a certain location).
-
Smartly clustered: Investments to support the acquisition and/or use of CEHRT by ineligible providers should be strategically focused, including considerations about what interventions may need to be clustered to get the most benefit from the investment. For example, interventions that provide financial support to acquire and use technology may also need to be clustered with technical assistance programs to ensure the technology is implemented successfully.
-
Spend wisely: Determining the need for incentives and/or other funding to support the use of health IT/EHR technology by ineligible providers should include considerations of the following: the ineligible provider's profit margins; the ability to target investments to ineligible providers who need and could benefit from such technologies; the ability to leverage and align the use of such technology to other program requirements; and the ability to use such technologies to support needed program oversight. In addition, when determining the need for incentives and/or other funding to support widespread use of technology solutions by ineligible provider types, consideration should be given to whether funds have been made available, and if so, the amount, duration, and scope of these funds to support the acquisition and use of CEHRT by targeted ineligible provider type(s). The following section includes information on the other sources of funds that were made available through HITECH and other programs to support the use of health IT/EHRs by some of the ineligible provider types.
B. Targeting Technology and Support for Ineligible Providers
In an era of limited resources, targeting and tailoring interventions takes on a particular importance. Not all ineligible providers need CEHRT, nor are all categories of ineligible providers equally important in achieving overall health system improvement. Figure 14 outlines factors that could be used to determine which providers to prioritize for implementing and using health IT/EHRs. The TAG considered the ineligible providers and suggested three priority groups. Further analysis of the individual provider types within each group is needed, but was out of scope for this study.
-
Safety net providers: Ineligible safety net providers have already been prioritized by HHS for additional support. Safety net providers deliver primary care services to "well over 25 million low-income patients"49 in rural and underserved areas. Congress previously addressed this group of ineligible providers not through an extension of the HITECH incentive program, but through $1.5 billion in health IT grant funding available from HRSA to support the adoption and use of EHR technology. This funding, which has not been available to other ineligible providers, has resulted in a relatively high rate of EHR technology adoption for safety net providers.
-
Long-term and post-acute care and behavioral health providers: Policymakers have directed some attention at advancing the use of health IT/EHRs by LTPAC and behavioral health providers. For example, in 2012 SAMHSA directed $23 million toward health IT infrastructure and the use of health IT/EHRs by behavioral health providers. In addition, ONC directed $7 million in State Health IT Challenge Grants to advance HIE on behalf of LTPAC providers and is also supporting HIE on behalf of LTPAC providers in some of the Beacon Community Programs. In addition, through the CMS QIO, $2.5 million was made available for QIOs in three states (Minnesota, Pennsylvania, and Colorado) to provide technical assistance to Medicare participating SNFs and HHAs to improve the use of health IT by these providers. These efforts aim to improve patient coordination, prioritize transitions of care, reduce medication errors, create key partnerships, and apply effective quality improvement techniques using health IT.
This category of providers serves some of the nation's most vulnerable individuals and use a significant portion of the Medicare and Medicaid budgets. Patients served by these providers experience frequent transitions in care and episodes of care coordination with eligible hospitals and professionals. Some of these providers may need interoperable EHR technology to support new care delivery and payment models in the Affordable Care Act (as identified in Appendix I) and in private sector initiatives.
-
Other ineligible health care providers: The use of certain technology interventions could be targeted, as needed, by other ineligible providers to advance policy priorities such as e-prescribing, medication management, or laboratory results reporting. These providers are either ancillary service providers that may use health IT applications to interface with an EHR or generally have access to CEHRT through their work in other settings. Supporting the use of interoperable interventions through the development of specialized applications would permit efficient HIE between these ancillary providers and health care providers that require the use of certified EHRs, including those providers who are presently eligible for the Medicare and Medicaid EHR incentive payments.
| FIGURE 14. Factors to Consider for Prioritizing Ineligible Providers |
|
The TAG suggested several factors that could be considered to assess the need for supporting the use of health IT/EHRs and whether incentives or other funding options are needed. Table 7 identifies these key factors and suggests questions that could inform a possible course of action. Appendix R provides a summary of the TAG suggestions and includes scenarios considering two ineligible providers and their need for interventions.
| TABLE 7. TAG Evaluation Approach for Ineligible Providers | |
| Goals |
|
| Assess |
|
| Determine Action |
|
If, based on consideration of the preceding factors and questions, a conclusion is reached to encourage the use of EHR technology by certain ineligible provider types through the use of incentives or other options, understanding the benefits and costs of implementing options may be an important factor in decision-making. The next section provides an economic framework that could be applied to conduct such an analysis.
VI. ECONOMIC FACTORS FOR EVALUATING BENEFITS AND COSTS OF NEW INTERVENTIONS
The decision to implement technology by a provider or implement an incentive program or other initiative to support the use of such technology could be informed by an understanding the benefits and costs. This section presents economic factors for estimating the benefits and costs to programs to accelerate adoption of interoperable EHR technology by ineligible providers. We do this by addressing:
- key principles of cost-benefit analysis (CBA);
- findings from evidence on the effectiveness of EHRs;
- criteria for evaluating the costs and benefits of a program; and
- issues associated with promoting interoperability.
Because of the very limited data available on the extent of ineligible providers' use of health IT, and the costs and impact of the use of this technology by these ineligible provider types, this section of the report often found it necessary to draw inferences from the evidence available on eligible providers.50
A. Key Principles of Cost-Benefit Analysis
Incremental Effects
CBA compares the incremental benefits accruing from a policy to its incremental costs. A policy creates incremental benefits or costs only if it causes changes in behaviors. Although the adoption of EHRs by ineligible providers is expected to grow with or without government intervention, the shape of that adoption curve is uncertain. Any program designed to increase adoption will produce benefits only if it accelerates adoption above and beyond the projected natural growth path. The benefits of a policy intervention accrue from incremental adoption above the forecast trend, but since it can be difficult to target a subsidy just towards incremental adopters (that is, those who a subsidy will influence) the cost of such programs can be high relative to the benefits.
Determining Perspective
Considering the benefits and costs of an intervention to increase EHR adoption is dependent on the stakeholder's perspective (e.g., government/payer, provider, patients, EHR vendor). For purposes of this report, we viewed the costs of the intervention as accruing to the government. Benefits may include improvements in the quality of care and reductions in health care spending, including reduced costs of health IT/EHR solutions. Some of these benefits accrue to the recipient of the intervention, and some may ultimately be realized by the government as the payer and to the patient. The following highlights the importance of considering the perspective when describing costs and benefits:
As previously described, CEHRT includes both fully certified and modularly certified EHR solutions. Incentives could support the acquisition costs of a comprehensive (fully) certified EHR or costs of certified EHR modules (e.g., a module that supports the exchange of information to support transitions in care). The costs to the government of supporting the acquisition costs of certified EHR modules would be less than the costs supporting acquisition of a fully certified EHR. At the same time, the provider, patient, and payer would be expected to realize benefits of reduced costs and improved quality through the effective use of a certified EHR module that supports the exchange of information to support transitions in care.
B. Assessing Existing Evidence on Effectiveness of EHR and Interoperability
While there have been numerous studies of the benefits and costs of EHR adoption by hospitals and physicians, there have been very few studies targeting ineligible providers. For the purpose of this report, we assume that there are parallels. Research data shows that EHR technology is expensive. Based on cost estimates reviewed by the Congressional Budget Office for physician and hospital EHR systems,51 Dranove concluded that EHR costs could account for about one percent of total provider costs if adoption costs are amortized over 10 years. (See Appendix S.I.C for a discussion on the Evidence of the Benefits and Costs of EHR Adoption.) Some research has suggested that EHR technology may not pay for itself, let alone generate significant savings. Other research, focusing on systems that target the kind of functionality included in the EHR Incentive Programs, has been more positive.52, 53 Overall, the picture of early EHR effectiveness has been ambiguous. Figure 15 highlights the findings from a recent study54 that takes a more nuanced view of EHR adoption and helps explain the inconsistent findings.
| FIGURE 15. 2012 Study on Importance of Skilled Information Technology Workforce on EHR Costs and Benefitsa |
| A 2012 study viewed the EHR as a business process innovation whose success requires human capital skilled at working with information technology. It noted that hospitals located in more information technology-intensive communities enjoy larger cost savings after adoption of an EHR. In addition, hospitals with more experience with earlier forms of EHRs from the 1990s enjoyed large cost savings after adoption of an advanced EHR.This is potentially important for ineligible providers, who often do not have information technology-proficient staff or information technology support. Return on investment for EHR technology and reduction in costs may be more difficult to achieve in those circumstances. Workforce initiatives and the availability of technical assistance programs for EHRs may be critically important in enabling those providers to achieve cost and quality goals. |
|
The full potential of health IT may not be unleashed until providers routinely use the technology to share clinical information. At present, however, the EHR market is fragmented and exchanging information across different vendor platforms can be difficult. The positive news is that eligible professionals and eligible hospitals will be incrementally adopting more interoperable technology as the latest rules for the Medicare and Medicaid EHR Incentive Programs go into effect.
Still, given the early stages of implementing interoperable technologies, it is difficult to predict the magnitude of the benefits of information exchange or how those benefits may vary across provider types. For that reason, this analysis does not attempt to model or quantify any benefits from information exchange. This is an important limitation of this analysis given the widespread belief, but limited empirical base, that the largest benefits of the use of EHRs will accrue as a result of HIE.55
Evaluating Evidence on Effects of Incentives on Adoption
In Appendix S, we present results of original research by Dranove on the effect of the HITECH Act incentives on hospital adoption of EHRs using data reported to the Healthcare Information and Management Systems Society (HIMSS) Analytics database. The results from the analysis of this database, which provides comparable current and historical data on acute care hospital EHR adoption,56 highlights the powerful potential for incentives to promote EHR adoption.
In the Final Rule for Stage 2 of the Medicare and Medicaid EHR Incentive Programs, CMS estimates that approximately 91 percent of acute care hospitals (and 52 percent of eligible professionals) will qualify as meaningful users of CEHRT by 2018.57 Dranove's analysis shows that hospitals and affiliated ineligible providers increased adoption of EHRs after the passage of the HITECH Act. If the adoption curve continues, Dranovepredicts that by 2016 70-85 percent of hospitals will have adopted EHR technology.58
The increase in the adoption rate that occurred at the time that HITECH was enacted is predicted to lead to a 13.4 percentage point increase in the number of hospitals that adopt an EHR by 2016.59 Similarly, physician adoption rates have also been reported to increase since the introduction of the EHR Incentive Programs.60 As discussed in Section III.A of this report, a 2013 analysis of two data sources evaluated EHR adoption by physicians and found that rates doubled from 2005 to 2011 reaching 67.8 percent for family physicians in 2011 (and that family physicians had the highest rate among office-based physicians). Researchers estimated that by the end of 2013, the EHR adoption rate among family physicians will exceed 80 percent.61 The authors of this study attribute increases in EHR adoption rates, in part, due to the availability of incentive payments.
C. Factors for Evaluating the Costs and Benefits of a Program
The goal of government incentive programs is to reduce the costs and/or increase the benefits of EHR adoption. In this section we describe these program costs and benefits in more detail. An effective program needs to change the behavior of the ineligible provider. Appendix S provides a simple example to illustrate the many factors involved in predicting the extent to which providers will adopt EHR technology regardless of incentives, and, more importantly, how incentives may accelerate adoption.
Dranove suggests that the following factors should be considered in estimating EHR adoption rates, benefits, and estimating the incremental impact of incentives:
-
Factors affecting adoption costs in the absence of incentives:
- Provider size: Adoption costs tend to increase with the size of the provider due to the need for greater system capacity and complexity, as well as the need to train additional staff. However, fixed adoption costs increase less than proportionately with size for two reasons. First, there is a substantial fixed component to health IT costs. Second, larger providers will likely have lower financing costs.
- Access to capital independent of size: Providers with superior access to capital can more easily finance the substantial costs of adoption. Thus, for-profit providers, non-profits that enjoy favorable financial performance, and providers that are part of large systems may enjoy greater access to capital.
- Presence of complementary labor inputs: EHR technology is a business process innovation, and successful implementation requires access to labor that is skilled at working with information technology.
-
Factors affecting adoption benefits:
- Size: Adoption benefits are likely to increase proportionately with size.
- System membership: To the extent that information exchange creates spillover benefits, providers in systems (e.g., affiliated with eligible hospitals) will internalize these benefits.
- Patient severity: EHR technology may be more likely to improve outcomes for patients with complex conditions.
- Market competitiveness: To the extent that EHR technology improves quality and this leads to higher demand, then a competitive provider may value EHR technology more than a provider that faces little or no competition.
- Provider objectives: Providers that value quality of care independent of profits may value EHR more highly than a purely profit-driven provider.
-
Factors affecting incremental adoption: Size, ownership, and system membership may predict EHR adoption, but do not necessarily predict incremental adoption from the incentive program. The model suggests that incremental adoption depends on the following:
- The size of the incentives: This will depend upon the specific incentives under consideration. In the example in Appendix S and presented below, the size of the incentive is evaluated in proportion to the provider's total Medicare and Medicaid revenues.
- The size of the provider: Larger providers are likely to perceive larger gaps between benefits and costs, whether positively or negatively, simply because the stakes are higher. Thus, it will take bigger incentives to motivate them.
- Number of fence-sitters: The number of providers for whom the costs of adoption exceed the benefits in the absence of incentives but for whom the benefits exceed the costs with incentives.
- Financial versus clinical: The extent to which the provider's decision to adopt EHR is based on financial rather than clinical considerations.
Most of these factors are supported by an empirical analysis of HITECH (Appendix S). Dranove's analysis of adoption data based on the HIMSS Analytics database shows that smaller hospitals responded more strongly to HITECH incentives, which could indicate that smaller hospitals were more likely to be fence-sitters. For-profits also responded more strongly to incentives, likely because they placed more weight on financial considerations.
The biggest unknown when forecasting incremental adoption is identifying the fence-sitters. Without reliable empirical data, a simple statistical theory about incremental adoption rates could be used to predict an adoption curve. A situation where very few providers have adopted health IT suggests that most are far away from choosing to adopt, and an incentive program may not change many minds. When most have adopted, there are few providers left who need to be influenced. The biggest impact of any incentive program will come when some, but not all, providers have adopted.62
Appendix J lists adoption rates of EHR technology by ineligible providers. There are a few classes of ineligible providers (e.g., rehabilitation hospitals, LTCHs, and psychiatric hospitals), where less than 10 percent have adopted an EHR. On the other hand, about half of providers in other categories (e.g., nursing homes and home health care) have adopted some components of an EHR. The analysis compared by Dranove suggests that in considering the need for and size of incentives to advance EHR adoption it is important to take into account the percentage of providers who have (and have not) adopted this technology.
Comparing Different Approaches to Encouraging Incremental Adoption
When evaluating a specific program to encourage EHR adoption, there are many considerations for the government including:
- Size: How large are the incentives?
- Variability: Are incentives "one-size-fits-all" or tailored (e.g., are incentives larger for some providers than for others)? Which providers get the largest benefits from adoption? Which enjoy the largest cost reductions?
- Benefit size: How large are the benefits to the government relative to the incentives?
- Interventions for fence-sitters: Does the program target fence-sitters?
- Adopters versus non-adopters: Will the program pay for adoption by providers that have already adopted and/or would have adopted in the absence of incentives?
Program Approach Examples
-
EHR Incentives: HITECH creates financial incentives under Medicare and Medicaid for eligible hospitals and other eligible providers that meet a range of criteria for their use of CEHRT. Incentive payments have several advantages. Under the current program, the government can stipulate precisely the certification criteria that EHRs must meet in order to be certified, and how providers must use the CEHRT to qualify for incentive payments. These requirements enable providers to easily understand and compute the financial benefits of compliance. On the other hand, incentives tend to be broad based, so the government may incent providers that would have adopted EHRs and complied with the stipulations even if no incentive payments were forthcoming. Our research suggests that HITECH's incentives have had a powerful effect on EHR adoption.
-
Financing programs: Low-interest loan programs to finance EHR adoption tend to be low-cost programs. In the long run, the cost of these programs to the government is equal to the discount on the interest rate afforded to the providers, plus modest costs for program administration, though they can have a high return because they could target certain types of providers (i.e., those who are small and unaffiliated with larger systems). We are aware of a few states with loan programs to support EHR adoption, including programs that include ineligible providers. We are unaware of any studies documenting whether this program has been effective.
-
Technical Assistance (EHR/Health IT Consulting): Research has shown that the EHR is more effective when adopting providers are in a community rich with information technology expertise. Programs that provide health IT training to ineligible providers that lack a workforce with the expertise to implement interoperable EHR technology might be considered. Such assistance could be usefully coupled with a program to provide financial incentives or other funding. These programs can target health IT-poor communities, both by reducing the costs and increasing the benefits of EHR implementation and use. These programs should be of sufficient duration to ensure that the EHR systems are fully implemented and integrated into the workflow, and that the staff are fully trained.
D. EHR Cost-Benefit Considerations for Ineligible Providers -- An Example
The following is an example of the application of the EHR cost and benefits considerations (as described by Dranove) to a for-profit nursing home chain provider. Dranoveindicates that a health care provider would consider financial factors, such as the cost of acquiring, installing, and maintaining the EHR as well as any potential impact on efficiency. The provider may also consider the impact on quality, both because higher-quality could translate into more demand and higher revenues, and because it might directly care about quality independent of financial considerations.
Nursing Home Case Study
To construct the example, this study leverages and extends data from a cost study completed by the CIO Consortium (CIOC) entitled, "Electronic Medical Records (EMR) Cost Study -- Final Report: Implementing and Operating Electronic Medical Records in Long-Term & Post Acute Care Environment." The CIOC constructed a hypothetical LTPAC chain provider named "EMR*Care." EMR*Care was described as a for-profit, 25 facility chain provider operating in two states. Table 8 describes facts and statistics for EMR*Care.63
| TABLE 8. EMR*Care Facts and Statistics | |||
| Type of Organization | For-Profit | ||
| States of Operation | North Carolina, Florida | ||
| Types of Facilities | Skilled Care | ||
| Number of Facilities | Total 25 (10 in North Carolina and 15 in Florida) | ||
| Range in Bed Size | 80-240 | ||
| North Carolina | Florida | Totals | |
| Average Licensed Bed | 120 | 120 | 120 |
| Average Total Licensed Beds | 1200 | 1800 | 3000 |
| Average Total Patient Days | 1044 | 1566 | 2610 |
| Average Total Occupancy | 87% | 87% | 87% |
| Average Medicare Occupancy | 16% | 20% | 18.40% |
| Average Medicaid Occupancy | 67% | 58% | 61.60% |
| Average Occupancy--All Other | 17% | 22% | 20% |
| Number of Employees (assume 60 overhead) | 1127 | 2270 | 3457 |
| Average Medicare Rate | 463.5 | 420 | 441.75 |
| Average Medicaid Rate | 203.5 | 166.5 | 185 |
| Average Rate--All Other | 197 | 141 | 169 |
| Annual Revenue | $213,919,463 | ||
In addition, the CIOC study estimated reasonable five-year costs for the organization, EMR*Care, to acquire and implement any one of three available technology options (Table 9) using input from "leading EMR solution vendors in October 2010."64
| TABLE 9. Five-Year Costs | |||
| EMR Costsa,b | 5 Year Total EMRCosts Per Facility | 5 Year EMRCosts Per Bed | |
| SaaS Option: EMR*Care contracts with an EMR vendor for a hosted EMR solution. EMR*Care provides its own help desk support. | |||
| Total Costs: | $259,394 | $2,162 | |
| Hosted Option: EMR*Care purchases EMR software and contracts with a 3rd party for helpdesk support. | |||
| Total Costs: | $254,279 | $2,119 | |
| In House Option: EMR*Care purchases EMR software with maintenance from the vendor, then provides their help desk support and hosts their data center using their own equipment. | |||
| Total Costs: | $355,616 | $2,963 | |
| |||
The CIOC EMR cost study made some assumptions regarding the nursing facilities included in this hypothetical, for-profit, two-state chain organization that provides services in 25 nursing facilities.65 Some of these assumptions included:
- Availability of one information technology leader for the organization (before and after implementation);
- Number of computers/devices per facility prior to EMR implementation (16) and number of post-EMR implementation (45);
- Availability of user technical support for the chain organization prior to EMR implementation (four technicians) and number post-EMR implementation (10 technicians);
- The in-place clinical/billing system would need to be updated to support EMR implementation;
- The facilities have the network infrastructure in place to support servers;
- For the "in-house technology option" the needed Data Center (that supports back-up/recovery, shared storage, security, etc.) is assumed to be available; and
- Initial EMR implementation training is assumed to cost $5,000 per facility and subsequent on-going annual training is assumed to cost $2,000 per year per facility.
The CIOC study estimated that annual costs for each EMR option not only varied by offering, but also over time, with higher costs incurred in the first year.
Example Refined
Using the CIOC data, we calculated average Medicare, Medicaid, and other payments per nursing facility per year; and average total nursing facility revenue per facility per year. Table 10 reflects these calculations.
| TABLE 10. Average Medicare, Medicaid and Other Payments | |||||
| EMR*Care--Facts and Statistics | Annual Revenue Per Facility | Average Annual Revenue Per Facility | |||
| North Carolina | Florida | North Carolina | Florida | ||
| Average Medicare Rate | 463.5 | 420 | $2,825,941 | $3,200,904 | |
| Average Medicaid Rate | 203.5 | 166.5 | $5,195,563 | $3,679,896 | |
| Average Rate--All Other | 197 | 141 | $1,276,170 | $1,182,048 | |
| Annual Revenue | $9,297,673 | $8,062,849 | $8,680,261 | ||
For purposes of this example, we assumed that EMR costs were divided equally across each of the five years (in contrast to the CIOC study) and estimated average annual costs for each of the three EMR technology options (see Table 11). Annual EMR costs for each nursing facility for the three technology options range from $50,856 (for the hosted EMR option) to a high of $71,123 (for the in-house EMR option).
| TABLE 11. Annual EMR Costs | ||
| EMR Costs | Annual EMR Costs per Facility | EMR Costs as Percent of Average Annual Facility Revenue ($8,680,261) |
| SaaS Option | ||
| Total Costs | $51,879 | 0.6% |
| Hosted Option | ||
| Total Costs | $50,856 | 0.6% |
| In House Option | ||
| Total Costs | $71,123 | 0.8% |
| Average | $57,953 | 0.7% |
We then calculated EMR costs for each of the three technology options as a percent of average annual nursing facility revenues using the revenue data included for the CIOC hypothetical chain organization. As can be seen in Table 11, the cost of three technology options is less than one percent of average annual facility revenues.
Analysis of Economic Factors Applied to Nursing Home Case Study
Discussion -- Provider Revenues
The example presented above does not include revenues from other lines of business. For example, a review of a few annual reports submitted by organizations that deliver LTPAC services (including nursing facility services) to the Securities Exchange Commission (SEC) for the fiscal year ending in 2011 describes that some of these organizations derive revenues from other sources (i.e., sources of revenue in addition to Medicare Part A SNF payment, Medicaid nursing facility payment, and other sources of payment for nursing home services). For example, the SEC filings indicate that some chain nursing home organizations also receive Medicare Part B payments for: (i) therapy services delivered to their non-Part A covered nursing facility residents and in some cases delivered to non-institutionalized persons; and/or (ii) physician services delivered to Medicare and Medicaid-paid nursing home residents.
In considering the need for financial incentives to support the acquisition and use of health IT, including EHRs, it is important to consider all revenue sources available to the ineligible provider type(s).
Discussion -- EMR Costs
The CIOC study is based on technology solutions and costs for these solutions in 2010. Technology costs are reportedly decreasing. In addition, the range of technology options is also changing, including the introduction of lower cost solutions. For example:
-
ONC has implemented:
- EHR certification programs (as discussed in Section I.D Study Definitions and Appendix B) that make it more effective and efficient to electronically exchange health information between providers. The EHR certification program permits certification of both comprehensive EHRs and EHR modules;66 and
- The ONC Direct Project provides a low-cost approach to support electronic HIE by enabling simple, secure transport of health information between authorized care providers. On average, Direct is available at a cost of $10-$20 per address. In some cases, grant funds allow Direct to be offered at no cost to providers. Technology solutions (such as certified EHRs or certified EHR modules) could use Direct as the mechanism to send documents.67
-
The Geisinger/Keystone Beacon Community in Danville, Pennsylvania has developed a tool that will be available nationally to enable low-cost HIE by nursing homes and HHAs.68 This tool is built on work that ASPE sponsored that transforms the nursing home and HHA assessments (Minimum Data Set (MDS) and Outcome and Assessment Information Set (OASIS)) into interoperable, clinically-relevant LTPAC summary documents. The LTPAC summary document is represented using interoperability standards and is aligned with the standard used to exchange documents in the EHR Incentive Programs. The Geisinger tool will transform the MDS and OASIS assessments upon request from any nursing home or HHA provider and will make the resultant LTPAC Summary available to authorized clinicians and/or HIE organizations. The fee schedule for using the tool is based on the number of resident/patients per provider and is expected to cost less than $1,000 per year.
-
The Massachusetts LTPAC Health Information Exchange Challenge Grant (the IMPACT Project) is developing technology tools know as "LAND"69 and "SEE"70 to facilitate HIE by LTPAC organizations to enable health care providers who do not have EHRs to incrementally and progressively send and receive health information. LAND and SEE will be made publicly available in the summer of 2013. LAND will be purchasable through Orion Health under the name "Rhapsody" at an estimated cost of $2,000-$10,000 per year per organization depending on volume of purchases and size of the organization. The software for SEE will be made available for free, but will likely cost a community or state approximately $20,000-$50,000 per year to install and maintain.71
-
As previously described, some EHR vendors of products for ineligible providers (e.g., LTPAC providers) have had their products certified by ONC-Authorized Testing and Certification Bodies under the temporary certification program established by ONC to support meaningful use Stage 1. Under this program those products were required to demonstrate that they conformed to interoperability standards and certification criteria adopted by HHS through regulation. In addition to or instead of seeking certification through ONC's certification process, some vendors have had their products certified by other entities or to other standards that have not been adopted by HHS (e.g., the CCHIT's proprietary "CCHIT Certified" LTPAC program, which includes an additional certification criteria specific to home health and skilled nursing). Also, as noted, in the ONC 2014 Edition Standards and Certification Criteria final rule issued to support the Medicare and Medicaid EHR Incentive Programs, ONC encouraged vendors of EHR products for ineligible providers to, at a minimum, seek certification of their products as meeting EHR module requirements to support the exchange of information at times of transition in care. It is not yet known what the impact will be on EHR vendors and whether they will seek certification of their products for ineligible providers, nor what the cost impact of such certification will be. While use of interoperability standards, implementation specifications, and certification criteria may reduce some costs of developing products (including reducing the need for a number of customized interfaces), there will still be product development and acquisition costs associated with developing and using technology solutions that support interoperable HIE.
Discussion -- EHR Costs Relative to Profit Margins
Assuming that Medicare margins for SNFs are 18.5 percent (as estimated by MedPAC) and that margins for Medicaid and other revenue sources are zero, annual EMR costs of less than 1 percent for any one of the three technology solutions described in the example above would seem to be affordable to providers that have a similar patient and payer mix. Further, assuming these EMR costs and provider profit margins:
- for those providers that are motivated by quality/clinical considerations in addition to financial considerations, investing in EMR acquisition and use would seem to be a rational business and clinical decision; and
- to the extent that use of the technology improves quality and this leads to higher demand, then a competitive provider may value the EHR technology more than a provider that faces little or no competition.
Understanding the provider's profit margins (across all revenue sources) relative to the costs of needed technology solutions is one important factor when considering the need for incentive payments.
Discussion -- Cost Savings of Using an EHR
To estimate the cost savings that these hypothetical nursing homes might realize as a result of using an EHR, we used Dranove'sestimate of 3 percent cost savings (which includes costs savings of 2 percent of total revenues and 1 percent of monetized quality of care improvements).72 Thus, in our example, the annual cost savings (relative to aggregate annual revenues) for each of the hypothetical nursing homes are, on average, approximately $260,000 per year per facility.
In this example, because estimated annual savings ($260,000) exceed the estimated annual EMR costs (average annual costs -- $57,953), we would expect the nursing home to adopt an EMR. However, as Dranovenotes, "a rational decision maker might not follow this simple go/no-go adoption decision if the benefits appear to outweigh the costs but there is uncertainty about benefits or costs that will be resolved over time. The decision maker may prefer to wait for the uncertainty to be resolved before adopting."73
In circumstances where technology costs are relatively modest and/or cost savings are expected to exceed the technology costs, and health IT adoption by the ineligible providers is believed to be too low or slow, implementation of any one or more incentive/funding options (e.g., financial incentives, technical assistance, etc.) could remove/reduce uncertainty about the benefits of acquiring and using certain technology solutions.
Discussion -- Other Considerations
The above example embeds many assumptions that may not be applicable to the wide array of ineligible provider types and/or to the various types of health IT/EHR technology solutions that may be needed to improve quality and continuity of care. In addition, the example is silent with respect to certain factors that may influence decisions to invest in technology. The following discusses some of these assumptions and factors, their implications, and the applicability to other types of ineligible providers.
-
The preceding hypothetical describes a mid-size, for-profit nursing home chain provider operating in two states; and makes several assumptions including assumptions about the:
- participating providers' annual revenue and profit margins;
- availability of IT leadership and technical support (pre and post-acquisition); and
- hardware and software costs, and costs of initial and on-going maintenance/training (pre and post-acquisition).
It is unlikely that these same assumptions will be applicable across ineligible provider categories. For example, independent and smaller providers (e.g., independent clinical social workers, psychologists, or therapists) will likely not have the same payer mix, revenue streams and amounts, and levels of information technology leadership and technical support as was assumed for this mid-size nursing home chain organization and their provider members.
The cost of EHR implementation may be higher for these providers if information technology leadership and technical support are not available in-house. In addition, Dranoveindicates that providers with favorable financial performance (e.g., for-profit providers) may be able to more easily access financing to support the costs of technology adoption, and that smaller providers may have less access to capital at favorable rates.
-
The preceding example was silent on whether the hypothetical organization was:
- affiliated with other providers in the health system (e.g., hospital-based nursing homes, nursing homes that are a part of an integrated delivery system or participate in Accountable Care Organizations (ACOs)); and
- motivated to acquire and use technology solutions to support and improve clinical care.
The transformation underway in the health care system is expected to increase collaborations and affiliations across health care providers. Emerging health care reform models (e.g., ACOs, Patient-Centered Medical Homes, etc.) are creating new relationships between health care providers eligible for EHR incentive payments and providers who are ineligible for such payments. Dranove'sanalysis suggests that EHR adoption rates by ineligible providers affiliated with acute care hospitals increased after the passage of the HITECH Act. In addition, Dranove indicates that providers that participate in health systems will realize benefits as a result of such participation, and that such benefits may influence the provider's decision to adopt needed technology.
However, at present, there is limited information about types of providers engaged in the various integrated models, and no evidence concerning the impact of such partnerships on technology adoption. Further, how widespread the trend of increasing provider collaborations will be across the health care delivery system, and the impact of such collaborations on technology adoption by ineligible providers, is unknown.
Dranovenotes that non-profit providers may be more motivated to acquire and use technology solutions if they are more focused on clinical considerations (in contrast to providers that are more focused on financial considerations). However, because of the lack of data on ineligible non-profit providers' revenue sources and amounts, and technology costs; we were unable to analyze the cost savings that different classes of non-profit ineligible providers might realize through the use of different technology solutions.
E. Summary of Cost/Benefit Considerations for Making Incentives and/or Other Funding Available to Ineligible Providers
There is considerable uncertainty regarding future trends of EHR adoption by ineligible providers. This uncertainty is due in part to changes in the health delivery system that are driving increasing collaborations and partnerships across the health care continuum, increasing emphasis on improving quality of care while reducing health care costs, and declining technology costs. These factors may result in ineligible providers choosing to adopt technology solutions at higher frequencies even without the use of financial incentives.
Considering the need for financial incentives and/or other funding to support the costs of acquisition and/or use of technology solutions (to support and/or accelerate adoption) is complex and should take into account the:
- provider's revenues (across all sources);
- availability, including the amount, duration and scope, of other funding to support the use of technology for the targeted provider type(s);
- the type of technology that needs to be encouraged and the costs of such technology; and
- availability of certified technology solutions to support policy objectives.
Technology solutions that support HIE are the types of technology that will most likely focus on the goals of health system transformation to improve the quality and continuity of care.
In addition to considering the ineligible provider's ability to afford technology solutions, the provider's access to and need for specific technology support (e.g., technical assistance) for the initial acquisition and on-going implementation will also require consideration. Making available such assistance could signal support for the use of the technology solution, reduce uncertainty about the benefits of the solution, and thus, accelerate the acquisition and use of the technology.
F. Cost/Benefit Considerations for Making Incentives and/or Other Funding Available to Ineligible Providers
If the assumptions described in the example above are accurate, the hypothetical may suggest that payment incentives are not warranted for this specific class of ineligible provider. If the policy goal is widespread adoption of EHRs, consideration could be given to designing an incentive structure that would target those ineligible providers that lack the financial capacity and/or system relationships that would support the acquisition and use of such technology.
-
Dranove suggests that smaller and unaffiliated providers may face challenges in supporting the acquisition and use of EHR technology. For example, it may be possible to structure a low-cost loan programs and/or other options in such a way to support EHR acquisition and use and target these smaller and unaffiliated providers.
-
Whether or not financial support is needed to support the acquisition and use of health IT hardware and software, EHR users will require on-going information technology support. Again, if the goal is widespread EHR adoption, it may be possible to design interventions (such as technical assistance) that would target those ineligible providers that do not have access to such assistance (either due to the lack financial capacity and/or system relationships).
As implied in the examples above and the discussion of additional factors, the benefits and costs of any incentive or funding option will be a function of the targeted health IT/EHR intervention, and the type, amount, duration, and scope of any incentive/funding option.
G. Considerations to Promote Interoperability
In 2005, two key studies were published providing an analysis of the potential impact and business case for advancing interoperable EHRs in health care. These studies identified the value of interoperable EHRs and predicted cost savings with widespread adoption.
-
The Center for Information Technology Leadership's study74 summarized the business case for national implementation of standardized HIE and stated that fully standardized health information exchange and interoperability (HIEI) could yield a net value of $77.8 billion per year once fully implemented. Non-standardized HIEI offers smaller positive financial returns. The clinical impact of HIEI for which quantitative estimates could not be produced would likely add further value.
-
The RAND's study75 concluded that effective EHR implementation and networking could eventually save more than $81 billion annually -- by improving health care efficiency and safety -- and that health IT-enabled prevention and management of chronic disease could eventually double those savings while increasing health and other social benefits. They noted that these savings may not be fully realized without changes to the health care system.
These studies highlighted two reasons for policymakers to consider widespread adoption of interoperable health IT through the use of incentives and other funding: (1) providers must absorb the costs of EMR systems, but consumers and payers are the most likely to reap the savings;76 and (2) even if EMR systems were widely adopted, the market might fail to develop interoperability and robust information exchange networks.77 The RAND study estimated potential efficiency and safety savings of more than $81 billion per year with widespread adoption (90 percent) of interoperable EHR systems.78
In 2013, RAND published an update to their study noting that the projected savings and adoption rates are significantly less than what had been projected in 2005 for the following reasons:79
- There has been sluggish adoption of health IT systems significantly below the 90 percent threshold specified by the RAND team in 2005 needed to achieve efficiency and savings;
- The choice of systems are neither interoperable nor easy to use; and
- Health care providers and institutions have failed to reengineer care processes to reap the full benefits of health IT.80
The "staged design" of the Medicare and Medicaid EHR Incentive Programs for eligible providers merits attention in terms of the current state of interoperable HIE. The stages of the EHR Incentive Programs envisioned a "building block" approach for implementation -- first acquiring health data, then using standards to exchange data to support care coordination, and reusing data to support health system transformation:
- Stage 1 starting in 2011 focused largely on the use of EHR technology that stores structured health information;
- Stage 2 (to be implemented beginning in 2014) will focus on accessing health information to support care coordination, patient engagement and clinical decision support; and
- Stage 3 (may be implemented beginning in 2016) will focus on health system transformation including the use of health data to improve population health, quality and outcome of care, and case management.
As described earlier in the report, many of the ineligible provider types could benefit from, but are not adopting, interoperable EHR technology solutions that support HIE on behalf of their patients, many of whom experience frequent transitions between care settings and instances where care is shared across unaffiliated care providers. The lack of standards that support interoperable exchange of health information to support the care needs of populations served by providers not eligible for incentive payments has been identified as one barrier to the adoption and use of EHR technology that supports this functionality. Work is underway to partially address this gap through the ONC-sponsored Standards and Interoperability Framework-Longitudinal Coordination of Care Workgroup. This community-led Workgroup is developing standards for the interoperable exchange of more robust of Summary Documents and Care Plans at times of transitions in care and to support instances of shared care.81 It remains to be seen whether these standards, once finalized, will be integrated into technology solutions used by eligible and ineligible providers.
While there are a number of initiatives targeting ineligible providers to advance their use of health IT, only a few programs provide direct support to ineligible providers to acquire EHRs and those programs are focused on narrow group of providers. Further, there are only a few initiatives that are advancing interoperable HIE with and by ineligible providers. As discussed by the TAG, none of the programs for ineligible providers are sufficient to promote widespread adoption of CEHRT, including technology that supports interoperability in the same manner as the EHR incentive program for eligible hospitals and professionals. This should not come as a surprise given the difference in funding for direct support -- the HITECH EHR Incentive Programs is estimated to make available over $15 billion82 in incentive payments available to help eligible hospitals and eligible professionals improve the quality, safety, and coordination of care while also achieving efficiency gains to help control costs.
Given the on-going rise in EHR adoption, policymakers may find it cost effective to focus on promoting adoption and use on interoperable technologies by ineligible providers, which would support the goals of the Affordable Care Act, the National Quality Strategy, and HITECH.
Further, the on-going changes in the provider landscape, specifically the growth of formally integrated provider systems as well as the growth of delivery models such as ACOs, create opportunities to accelerate HIE with ineligible provider types, including interoperable HIE. These new delivery systems may be able to internalize the benefits of HIE in ways that could not be accomplished by individual providers. On-going system growth is likely to further promote EHR adoption and the possibility of interoperability among eligible and ineligible providers; however, it is impossible to predict the impact of market forces.
VII. CONCLUSION
This study provided a rationale for identifying provider types not eligible for EHR incentive payments. The study identified the provider types who may participate in Medicare and Medicaid but are not eligible for the EHR Incentive Programs implemented under HITECH, and identified other funding sources directed to some of these ineligible provider types to support their implementation and use of health IT/EHRs. Providers ineligible for the Medicare and Medicaid EHR Incentive Programs were clustered into four categories: long-term/post-acute care, behavioral health, safety net, and other provider types.
The ineligible provider types described in this report have a frequent need to exchange health information on behalf of their patient populations, many of whom represent the most vulnerable and costly in our society. One of the key benefits of the use of health IT for ineligible providers is the ability to exchange information to communicate and coordinate services with a patient, their physician, and the entire care team who are often located in different geographic areas and practice settings.83 However, such HIE remains uncommon. Closing this technological gap by ineligible providers could support the realization of the goals associated with implementing a nationwide health IT infrastructure, new models of care delivery and coordination, and promote the HIE goals of the EHR Incentive Programs. Policies to address this challenge are hindered by data on ineligible providers' health IT use that are unreliable or unavailable, not comparable among ineligible provider types or between any or all of those provider types and the eligible providers involved in the EHR Incentive Programs. A critical part of enabling the secure flow of information across the system is advancing the adoption of health IT standards through voluntary certification of health IT and HIE products and services. In addition, empirical data demonstrating the business case for investing in interoperable EHRs to improve quality of care and reduce costs is lagging for ineligible providers.
This study described key characteristics of provider types identified as not eligible for EHR incentive payments, and their affiliation with eligible providers and clinical use of health IT to the extent possible.
The study identified (but did not endorse) several actions, programs and initiatives that have been leveraged or proposed to provide "direct support" or "indirect support" to ineligible providers for their acquisition and/or use of health IT/EHRs, including: extending the EHR Incentive Programs, grant and loan programs, technical assistance, developing and implementing a health IT infrastructure to support interoperable HIE with and by ineligible providers, and using other administrative tools (e.g., rulemaking) to support or require the use of health IT by ineligible provider types.
The study also identified several:
-
Economic factors that could inform the need for and impact of incentives and/or other funding to support the use of EHRs by ineligible provider types, including:
- provider size, affiliation with providers eligible for EHR incentives and/or with integrated delivery systems, and financial/quality objectives, and
- overall competiveness of particular markets.
-
Factors that could be considered to evaluate the need for, and costs and benefits of different incentives and other options to encourage health IT adoption by ineligible providers, including consideration of:
- all sources of revenue by ineligible provider type,
- acquisition and implementation costs of needed health IT/EHR solutions (including access to and costs of on-going technical assistance), and
- profit margins for ineligible provider types.
The study noted that there is a lack of strategic planning or coordination with respect to programs and activities that include a focus on the use of health IT/EHRs by some of the ineligible provider types. Such strategic planning could assist in identifying gaps in current activities to advance the use of EHR technology by ineligible providers and support investments that maximally leverage and are aligned with current policy priorities, and are efficiently targeted. This study described the importance of having good, reliable and nationally representative data regarding health IT/EHR adoption rates by ineligible providers in order to assesses the need for and effectiveness of investments that seek to advance the acquisition and/or use of health IT/EHRs by ineligible providers. This study also identified several factors that could be considered in estimating EHR adoption rates.
With the exception of the $1.5 billion in other funding directed to the use of health IT by certain safety net providers, the other funding that has been directed to some of the other ineligible provider types for purposes of implementing and using EHR technology was not considered to be sufficient in amount, duration, and scope to support widespread adoption and use of this technology by these ineligible provider types. However, this observation begs the question as to whether incentives or other funding is needed to support or accelerate the implementation and use of EHRs by the ineligible provider types. There are keyconsiderations that will help inform discussion on the need for incentives and/or other funding to support the use of EHR technology by ineligible providers. These considerations include the extent to which market forces that have emerged in response to the EHR Incentive Programs and new delivery models such as those encouraged by the Affordable Care Act will drive adoption of interoperable EHR technologies across the health care continuum, including use of such technology by ineligible providers.
Should policymakers determine the need for interventions to accelerate or advance the use of CEHRT solutions for certain ineligible provider groups, the following additional factors could be considered.
-
Built to last: Interventions should support the technology infrastructure needed for the emerging health care delivery and business models envisioned in the Affordable Care Act, the nationwide health IT infrastructure, and EHR Incentive Programs to allow for the interoperable exchange and reuse of health information.
-
Patient-centered: Interventions should promote a patient-centered approach to care delivery and outcomes empowering patients and their care support network.
-
Tailored and targeted: Interventions should not be "one-size-fits-all" but must consider the cost of adoption and the provider's need for clinical utility and availability of the technology. It is likely that different technology solutions will be required to achieve policy goals for different ineligible provider types. Finally, the costs and benefits to Medicare and Medicaid should be a factor.
-
Smartly clustered: Interventions may need to be clustered to accrue the most benefit from the investment. Strategically considering and supporting the type of heath IT functionality (including certified EHRs) needed to realize policy goals may help remove some uncertainty in the market. Such support could accelerate adoption by some providers not eligible for EHR incentive payments, and could serve to reduce the amount, duration, and/or scope of incentives/other funding. In addition, direct support to implement health IT/CEHRT may need to include technical assistance and workforce initiatives to ensure implementation of technology is appropriate to achieve quality and cost goals by the targeted ineligible provider.
-
Spend wisely: In today's fiscally constrained environment careful consideration should be given to the ineligible providers' margins and ability to cover all or some of the cost of technology. In addition, consideration should be given to the availability (i.e., amount, duration, and scope) of other funding to support the acquisition and use of CEHRT by the targeted ineligible provider type(s).
In considering the need for incentives and other funding to support EHR use by ineligible providers, policymakers may wish to consider the feasibility of designing programs targeting ineligible providers that lack the financial capacity or system relationships to support the acquisition of CEHRT. Policymakers may also wish to consider technical assistance interventions targeting those ineligible providers who do not have a health IT-proficient workforce or access to health IT support to advance the acquisition and use of EHR technology, and extend to these providers key lessons learned based on an evaluation of the adoption and use experiences of providers who were eligible for incentives.
NOTES
-
HITECH authorized the Medicare and Medicaid EHR Incentive Programs. The Centers for Medicare and Medicaid Services (CMS) estimate that between 2014 and 2019 $15.4 billion will be made available in incentive payments. This estimate: (i) includes net payment adjustments in the amount of $2.1 billion for Medicare providers who do not achieve meaningful use in 2015 and subsequent years; and (ii) does not include estimates of the benefits of participating the Medicare and Medicaid EHR Incentive Programs. (http://www.gpo.gov/fdsys/pkg/FR-2012-09-04/pdf/2012-21050.pdf, p.53971, September 4, 2012.)
-
Section §4104(a): "The Secretary of Health and Human Services shall conduct a study to determine the extent to which and manner in which payment incentives (such as under Title XVIII or XIX of the Social Security Act) and other funding for purposes of implementing and using certified EHR technology (as defined in Section 1848(o)(4) of the Social Security Act, as added by Section 4101(a)) should be made available to health care providers who are receiving minimal or no payment incentives or other funding under this Act, under Title XIII of Division A, under Title XVIII or XIX or such Act, or otherwise, for such purposes."
-
Appendix I identifies some of the ACA provisions that: (i) pertain to some of the providers ineligible for the EHR Incentive programs; and (ii) require or support the use of health IT and/or health information exchange.
-
Report to Congress: National Strategy for Quality Improvement in Health Care, March 2011. http://www.healthcare.gov/news/reports/quality03212011a.htm.
-
National Health Care Expenditure Data for 2009. Centers for Medicare and Medicaid Services. http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/NHE-Fact-Sheet.html.
-
Gage, B. et al. "Post-Acute Care Episodes Expanded Analytic File. Final Report. April 2011." Prepared for the Office of the Assistant Secretary for Planning and Evaluation. http://aspe.hhs.gov/health/reports/2011/pacexpanded/index.shtml#ch1.
-
"HIT Adoption and Readiness for Meaningful Use in Community Behavioral Health." National Council for Community Behavioral Healthcare. http://www.thenationalcouncil.org/galleries/business-practice%20files/HIT%20Survey%20Full%20Report.pdf.
-
The initiatives are described in Appendix A and Appendices K-N. In the course of identifying current federal and state initiatives, we identified some private sector programs and highlighted those in Appendix P.
-
FQHC serve 19.4 million patients. (The Henry J. Kaiser Family Foundation. "Patients Served by Federally-Funded Federally Qualified Health Centers, 2010." http://www.statehealthfacts.org/comparebar.jsp?ind=426&yr=138&typ=1&sort=a&rgnhl=15.)
Using data from 2008, the total number of patients seen in RHCs is estimated to be between 5 and 8 million. For purpose of this report we use the average of this range (i.e., 6.5 million patients per year). (The George Washington University, 2012, p.51, http://www.healthit.gov/sites/default/files/private/pdf/quality-incentives-final-report-1-23-12.pdf.)
-
Total grant and contract funding for 2012 provided by SAMHSA staff. (September 12, 2012.)
-
Section 3001 of the Public Health Service Act (PHSA), as added by Section 13101 of HITECH.
-
Stark, P. (2010). Congressional Intent for the HITECH Act. American Journal of Managed Care, 16: SP24SP28.
-
Ibid Stark.
-
Section §4104(a): "The Secretary of Health and Human Services shall conduct a study to determine the extent to which and manner in which payment incentives (such as under title XVIII or XIX of the Social Security Act) and other funding for purposes of implementing and using certified EHR technology (as defined in Section 1848(o)(4) of the Social Security Act, as added by Section 4101(a)) should be made available to health care providers who are receiving minimal or no payment incentives or other funding under this Act, under title XIII of division A, under title XVIII or XIX or such Act, or otherwise, for such purposes."
-
Patient Protection and Affordable Care Act. The law is available on the HealthCare.gov website. http://www.healthcare.gov/law/full/index.html.
-
Medicaid's New Health Home Option. The Henry J. Kaiser Family Foundation. Publication #8136. Available at: http://www.kff.org/medicaid/upload/8136.pdf.
-
Ibid Kaiser Family Foundation.
-
Findings from an analysis by David Dranove of adoption and use of EHRs by ineligible providers indicate that interoperable technologies are generally not used (Appendix R).
-
Report to Congress: A National Strategy for Quality Improvement in Health care. Report available at: http://www.healthcare.gov/law/resources/reports/quality03212011a.html#na.
-
Ibid Section 3, "Policies and Infrastructure Needed to Support Priorities."
-
Ibid Section 3, Principle 7, "Health Information Technology."
-
In this report, and consistent with section 3000(3) of the PHSA, the term "provider" is intended to refer to various types or categories of health care providers, which is broader than the term "provider" for purposes of Medicare and Medicaid.
-
In general, Section §4104(a) of HITECH requires that this study determine the extent to which and manner in which payment incentives and other funding for implementing and using certified EHR technology should be made available to health care providers who receive: minimal or no payment incentives under HITECH, Medicare, Medicaid, or otherwise for such purposes.
-
ONC Final Rule. Health Information Technology: Standards, Implementation Specifications, and Certification Criteria for Electronic Health Record Technology, 2014 Edition; Revisions to the Permanent Certification Program for Health Information Technology. http://www.gpo.gov/fdsys/pkg/FR-2012-09-04/pdf/2012-20982.pdf.
-
We recognize that private sector entities may establish their own EHR certification program separate from ONC. At the time of this report we are aware of one organization (Certification Commission for Health Information Technology (CCHIT)) that has established criteria applicable to LTPAC and behavioral health providers. For purposes of this study, we did not take into account certification via private sector programs because of their limited scope (range of ineligible providers) and limited uptake/use by those ineligible providers to whom the programs apply.
-
PHSA Section 3000. http://www.hhs.gov/ocr/privacy/hipaa/understanding/coveredentities/hitechact.pdf.
-
PHSA Section 3000(13). http://www.gpo.gov/fdsys/pkg/BILLS-111hr1enr/pdf/BILLS-111hr1enr.pdf.
-
Smart, Andrew. A Multi-dimensional Model of Clinical Utility. International Journal for Quality in Health Care, 2006. http://intqhc.oxfordjournals.org/content/early/2006/09/02/intqhc.mzl034.full.pdf.
-
ONC Final Rule. Health Information Technology: Standards, Implementation Specifications, and Certification Criteria for Electronic Health Record Technology, 2014 Edition; Revisions to the Permanent Certification Program for Health Information Technology. http://www.gpo.gov/fdsys/pkg/FR-2012-09-04/pdf/2012-20982.pdf.
-
Smith, Mark et al. Best Care at Lower Cost: The Path to Continuously Learning Health Care in America. Institute of Medicine, Committee on the Learning Health System in America. Washington, DC: The National Academies Press, 2012. http://www.iom.edu/Reports/2012/Best-Care-at-Lower-Cost-The-Path-to-Continuously-Learning-Health-Care-in-America.aspx.
-
HITECH Section 13101 amends the PHSA by adding Section 3000(3) which provides a definition of health care provider. http://www.gpo.gov/fdsys/pkg/BILLS-111hr1enr/pdf/BILLS-111hr1enr.pdf.
-
AHA data on hospital-based specialty units is from American Hospital Association, AHA Hospital Statistics, 2012 Edition.
-
Ibid AHA.
-
Ibid AHA.
-
As described more completely in Appendix D, Medicare expenditure data for each ineligible provider type was identified. This data was aggregated across all ineligible provider types. Available data sources reported annual Medicare expenditures for different years spanning 2009-2011. Using this data, annual Medicare expenditures were identified for each ineligible provider type and then summed to estimate aggregate annual expenditures for all ineligible provider types (i.e., totaling approximately $83.1 billion). Total Medicare expenditure data was obtained from the 2011 CMS National Health Care Expenditure data at http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/downloads/highlights.pdf.
-
As described more completely in Appendix D, Medicaid expenditure data for each ineligible provider type was identified. This data was aggregated across all ineligible provider types. Available data sources reported annual Medicaid expenditures for different years spanning 2008-2011. Using this data, annual Medicaid expenditures were identified for each ineligible provider type and then summed to estimate aggregate annual expenditures for all ineligible provider types (i.e., totaling approximately $98 billion). Total Medicaid expenditure data was obtained from the 2011 CMS National Health Care Expenditure data at http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/downloads/highlights.pdf.
-
Substance Abuse and Mental Health Services Administration. National Expenditures for Mental Health Services and Substance Abuse Treatment, 1986-2009. HHS Publication No. SMA-13-4740. Rockville, MD: Substance Abuse and Mental Health Services Administration, 2013. Table A.2, p.58.
-
ONC Federal Health Information Technology Strategic Plan (2011-2015). http://healthit.hhs.gov/portal/server.pt/gateway/PTARGS_0_0_4318_1211_15583_43/http%3B/wci-pubcontent/publish/onc/public_communities/f_j/onc_website___home/fed_health_strategic_plan/fed_health_it_strategic_plan_home_portlet/files/final_federal_health_it_strategic_plan_0911.pdf.
-
A base EHR is defined by ONC as including: patient demographics, patient problem lists, patient medication histories (EH)/medications taken by the patient (EP), clinical notes, electronicorders for prescriptions, laboratory results viewing, and imaging results viewing. http://www.gpo.gov/fdsys/pkg/FR-2012-09-04/pdf/2012-20982.pdf.
-
Family physicians had the highest rate among office-based physicians.
-
Xierali, I. et al. "The Rise of Electronic Health Record Adoption Among Family Physicians." Annals of Family Medicine. Vol. 11, No. 1, January/February 2013.
-
Ibid Xierali.
-
ONC Federal Health Information Technology Strategic Plan (2011-2015), pp. 12-13. http://www.healthit.gov/sites/default/files/private/utility/final-federal-health-it-strategic-plan-0911.pdf.
-
Richard, A., Kaehny, M., Kramer, A. Literature Review and Synthesis: Existing Surveys on Health Information Technology, Including Surveys on Health Information Technology in Nursing Homes and Home Health. University of Colorado, Denver. Division of Health Care Policy and Research.February 2009. http://aspe.hhs.gov/daltcp/reports/2009/hitlitrev.htm#execsum.
-
"HIT Adoption and Readiness for Meaningful Use in Community Behavioral Health." National Council for Community Behavioral Healthcare. http://www.thenationalcouncil.org/galleries/business-practice%20files/HIT%20Survey%20Full%20Report.pdf.
-
Uniform Data Systems Manual. Bureau of Primary Health Care, HRSA. Appendix D, Page 135. http://bphc.hrsa.gov/healthcenterdatastatistics/reporting/2011manual.pdf.
-
The initiatives are described in Appendix A and Appendices K-P. In the course of identifying current federal and state initiatives we identified some private sector programs and highlighted those in Appendix P.
-
ONC Health Care Anti-Fraud Project Task Order HHSP23320054100EC. September 2005.
-
George Washington University. "Quality Incentives for Federally Qualified Health Centers, Rural Health Clinics and Free Clinics: A Report to Congress." January 23, 2012; p.9. http://www.healthit.gov/sites/default/files/private/pdf/quality-incentives-final-report-1-23-12.pdf. In 2010, FQHCs served 19.4 million in 2010 (http://bphc.hrsa.gov/uds). Estimates of the number of patients seen in RHCs per year are between 5 million and 8 million patients. (George Washington University report, p.8)
-
The material below was prepared for this study by David Dranove, PhD, an economist and the Walter McNerney Professor at the Kellogg School of Management, Northwestern University. See Appendix S for the full report.
-
Congressional Budget Office, 2008, "Evidence on the Costs and Benefits of Health Information Technology" (pp.17-18).http://www.cbo.gov/ftpdocs/91xx/doc9168/05-20-healthit.pdf.
-
Chaudhry, B., Wang, J., Wu, S., Maglione, M., Mojica, W., Roth, E., Morton, S., Shekelle, P.. 2006. Systematic Review: Impact of Health Information Technology on Quality, Efficiency, and Costs of Medical Care. Annals of Internal Medicine 144(10): 742-752.
-
Buntin, M., Burke, M., Hoagline, M., Blumenthal, D. 2011. The Benefits of Health Information Technology: A Review of the Recent Literature Shows Predominately Positive Results. Health Affairs 30(3): 464-471.
-
Dranove, D., Forman, C., Goldfarb, A., Greenstein, S. 2012. "The Trillion Dollar Conundrum: Complementarities and Health Information Technology." NBER Working Paper No. 18281.
-
Walker, J., Pan, E., Johnston, D., Adler-Milstein, J., Bates, D.W., Middleton, B. "The Value of Health Care Information Exchange and Interoperability." Health Affairs (Project Hope) Suppl Web Exclusives (June 2005): W5-10-W5-18. http://content.healthaffairs.org/content/early/2005/01/19/hlthaff.w5.10.long.
-
The HIMSS Analytics Database includes historic EHR information. HIMSS Analytics Database was originally derived from the Dorenfest IHDS+ Database in July 2004. The database is now known as the HIMSS Analytics® Database.
-
Stage 2 Medicare and Medicaid EHR Incentive Programs Final Rule (pp. 54140 and 54142). http://www.gpo.gov/fdsys/pkg/FR-2012-09-04/pdf/2012-21050.pdf.
-
The definition used in our study of what constitutes an "Electronic Medical Record (EMR)" is based on attributes collected in the HIMSS Analytics database and is not comparable to the definition of an EHR in the Incentive Programs.
-
Over time, this gap will decrease as more hospitals would adopt EHR with or without the incentives in HITECH.
-
U.S. Department of Health and Human Services, Office of the National Coordinator for Health IT. Office of Economic Analysis, Evaluation, and Modeling. http://dashboard.healthit.gov/HITAdoption/.
-
Xierali, I., et al. "The Rise of Electronic Health Record Adoption Among Family Physicians." Annals of Family Medicine. Vol. 11, No. 1, January/February 2013.
-
Based on information developed by David Dranove, PhD, an economist and the Walter McNerney Professor at Northwestern University's Kellogg School of Management. Incremental effects where any program designed to increase adoption will produce benefits only if it accelerates adoption above and beyond the projected natural growth path. The benefits of a policy intervention accrue from incremental adoption above the forecast trend.
-
Table 8 facts and statistics are based on Table 1 (p.10) of the CIOC study "Electronic Medical Records (EMR) Cost Study -- Final Report: Implementing and Operating Electronic Medical Records in Long-Term and Post Acute Care Environment." Table 8 modifies the CIOC data to correct an error in the total "Average Total Patient Days" presented for the facilities operating in Florida and corrects the subsequent revenue calculation that is the annualized product of average per diem payment rates and occupancy rates across payers for this hypothetical chain organization. The original CIOC Table 1 is found in Appendix T. Randy Kirk, EVP & CTO Direct Supply, Inc. and Deborah Green (formerly with LaVie Care and now EVP and COO at AHIMA) assisted in modifying the table presented in this report. Both were contributing authors to the CIOC report.
-
CIO Consortium "Electronic Medical Records (EMR) Cost Study -- Final Report: Implementing and Operating Electronic Medical Records in Long-Term and Post Acute Care Environment," p.13.
-
CIO Consortium "Electronic Medical Records (EMR) Cost Study -- Final Report: Implementing and Operating Electronic Medical Records in Long-Term and Post Acute Care Environment," pp.12-17.
-
Health Information Technology: Standards, Implementation Specifications, and Certification Criteria for Electronic Health Record Technology, 2014 Edition; Revisions to the Permanent Certification Program for Health Information Technology. http://www.gpo.gov/fdsys/pkg/FR-2012-03-07/pdf/2012-4430.pdf.
-
The Direct Project.The Direct Project supports cases of pushed communication between providers, hospitals, laboratories, public health, and other health settings of care and permits standards-based exchange of a variety of documents such as: summary care records, referrals, discharge summaries and other clinical documents in support of continuity of care and medication reconciliation, and communication of laboratory results to providers. http://wiki.directproject.org/.
-
Keystone Beacon Community Gobbler Transform Tool. http://transform.keyhie.org/.
-
"LAND" is a computer that connects the Health Information Exchange Organization in the state and the LTPAC provider's EHRs or electronic documents (such as the MDSv3 and OASIS-C assessments). LAND allows electronic clinical information from the LTPAC provider to be transformed into a standard LTPAC summary or other standard electronic summary document and then send it through the HIE Organization to the next provider of care, such as an emergency department or HHA.
-
"SEE" is software for a website that HIE Organizations can host so that LTPAC organizations that lack EHRs can still send and receive electronic health information. Similar to a Gmail or Hotmail website, clinicians in LTPAC organizations can use their computer's web browser to access their SEE mailbox, view an electronic summary document that has been sent to them, update that document with new information such as changes in medications or wound status, and then send the updated summary document electronically through the HIE to the next provider of care for the patient.
-
Personal Communication with: Larry Garber, M.D. Medical Director for Informatics, Reliant Medical Group Principal Investigator, IMPACT Project, 630 Plantation Street, Worcester, Massachusetts, 01605, Lawrence.Garber@ReliantMedicalGroup.org.
-
Appendix S: Evaluating Benefits and Costs of New Incentives for EHR Adoption by Ineligible Providers EHR Payment Incentives for Providers Ineligible for Payment Incentives and Other Funding. Section III.A: A Simple Example.
-
Walker, J., Pan, E., Johnston, D., Adler-Milstein, J., Bates, D., Middleton, B. The Value OfHealth Care Information Exchange And Interoperability. Health Affairs, January 2005.
-
Hillestad, R., Bigelow, J., Bower, A., Girosi, F., Meili, R., Scoville, R., Taylor, R. Can Electronic Medical Record Systems Transform Health Care? Potential Health Benefits, Savings, AndCosts. Health Affairs, 24, no.5 (2005): 1103-1117.
-
Ibid Walker and Hillestad.
-
Ibid Walker and Hillestad.
-
Ibid Hillestad.
-
Kellermann, Aurthur, Jones, Spencer. "What It Will Take To Achieve The As-Yet-Unfulfilled Promises Of Health Information Technology." Health Affairs 32, no.1 (January 2013): 63-68. http://content.healthaffairs.org/content/32/1/63.abstract.
-
Ibid Hillestad.
-
See http://wiki.siframework.org/Longitudinal+Coordination+of+Care+%28LCC%29.
-
HITECH authorized the EHR Meaningful Use incentive Programs. The Medicare and Medicaid Electronic Health Record Incentive Program -- Stage 2 Final Rule. CMS estimates that between 2014 and 2019 $15.4 billion will be made available in incentive payments. This estimate: (i) includes net payment adjustments in the amount of $2.1 billion for Medicare providers who do not achieve meaningful use in 2015 and subsequent years; and (ii) does not include estimates of the benefits of participating the Medicare and Medicaid EHR Incentive Programs. http://www.gpo.gov/fdsys/pkg/FR-2012-09-04/pdf/2012-21050.pdf, p.53971. September 4, 2012.)
-
Kramer, A. Richard, A., Epstein, A. Winn, D. May, K. Understanding the costs and benefits of health information technology in nursing homes and home health agencies: Case Study Findings. University of Colorado, Denver, Division of Health Care Policy and Research. June 2009. http://aspe.hhs.gov/daltcp/reports/2009/HITcsf.htm#summary.
EHR Payment Incentives for Providers Ineligible for Payment Incentives and Other Funding Study
Files Available for This Report
- Main Report
- HTML http://aspe.hhs.gov/daltcp/reports/2013/EHRPI.shtml
- PDF http://aspe.hhs.gov/daltcp/reports/2013/EHRPI.pdf
- APPENDIX A. Medicare and Medicaid EHR Incentive Programs
- HTML http://aspe.hhs.gov/daltcp/reports/2013/EHRPIap.shtml#appendA
- PDF http://aspe.hhs.gov/daltcp/reports/2013/EHRPI-appendA.pdf
- APPENDIX B. Definitions and Certification of EHR Technology
- HTML http://aspe.hhs.gov/daltcp/reports/2013/EHRPIap.shtml#appendB
- PDF http://aspe.hhs.gov/daltcp/reports/2013/EHRPI-appendB.pdf
- APPENDIX C. Public Health Service Act Section 3000(3) as Added by HITECH Section 13101 -- Provider Analysis
- HTML http://aspe.hhs.gov/daltcp/reports/2013/EHRPIap.shtml#appendC
- PDF http://aspe.hhs.gov/daltcp/reports/2013/EHRPI-appendC.pdf
- APPENDIX D. Ineligible Provider Characteristics
- HTML http://aspe.hhs.gov/daltcp/reports/2013/EHRPIap.shtml#appendD
- PDF http://aspe.hhs.gov/daltcp/reports/2013/EHRPI-appendD.pdf
- APPENDIX E. Long-Term and Post-Acute Care Provider Profiles
- HTML http://aspe.hhs.gov/daltcp/reports/2013/EHRPIap.shtml#appendE
- PDF http://aspe.hhs.gov/daltcp/reports/2013/EHRPI-appendE.pdf
- APPENDIX F. Behavioral Health Provider Profiles
- HTML http://aspe.hhs.gov/daltcp/reports/2013/EHRPIap.shtml#appendF
- PDF http://aspe.hhs.gov/daltcp/reports/2013/EHRPI-appendF.pdf
- APPENDIX G. Safety Net Provider Profiles
- HTML http://aspe.hhs.gov/daltcp/reports/2013/EHRPIap.shtml#appendG
- PDF http://aspe.hhs.gov/daltcp/reports/2013/EHRPI-appendG.pdf
- APPENDIX H. Other Health Care Provider Profiles
- HTML http://aspe.hhs.gov/daltcp/reports/2013/EHRPIap.shtml#appendH
- PDF http://aspe.hhs.gov/daltcp/reports/2013/EHRPI-appendH.pdf
- APPENDIX I. Table Summary of Patient Protection and Affordable Care Act Provisions with Relationship to Ineligible Providers and Health IT Use
- HTML http://aspe.hhs.gov/daltcp/reports/2013/EHRPIap.shtml#appendI
- PDF http://aspe.hhs.gov/daltcp/reports/2013/EHRPI-appendI.pdf
- APPENDIX J. Behavioral Health Provider Analysis
- HTML http://aspe.hhs.gov/daltcp/reports/2013/EHRPIap.shtml#appendJ
- PDF http://aspe.hhs.gov/daltcp/reports/2013/EHRPI-appendJ.pdf
- APPENDIX K. Grant, Demonstrations and Cooperative Agreement Programs
- HTML http://aspe.hhs.gov/daltcp/reports/2013/EHRPIap.shtml#appendK
- PDF http://aspe.hhs.gov/daltcp/reports/2013/EHRPI-appendK.pdf
- APPENDIX L. Loan Programs
- HTML http://aspe.hhs.gov/daltcp/reports/2013/EHRPIap.shtml#appendL
- PDF http://aspe.hhs.gov/daltcp/reports/2013/EHRPI-appendL.pdf
- APPENDIX M. Technical Assistance Programs
- HTML http://aspe.hhs.gov/daltcp/reports/2013/EHRPIap.shtml#appendM
- PDF http://aspe.hhs.gov/daltcp/reports/2013/EHRPI-appendM.pdf
- APPENDIX N. Administrative Infrastructure Building Programs
- HTML http://aspe.hhs.gov/daltcp/reports/2013/EHRPIap.shtml#appendN
- PDF http://aspe.hhs.gov/daltcp/reports/2013/EHRPI-appendN.pdf
- APPENDIX O. Anti-Kickback Statute EHR Safe Harbor Regulations
- HTML http://aspe.hhs.gov/daltcp/reports/2013/EHRPIap.shtml#appendO
- PDF http://aspe.hhs.gov/daltcp/reports/2013/EHRPI-appendO.pdf
- APPENDIX P. Private Sector Programs to Advance Certified EHR Technology
- HTML http://aspe.hhs.gov/daltcp/reports/2013/EHRPIap.shtml#appendP
- PDF http://aspe.hhs.gov/daltcp/reports/2013/EHRPI-appendP.pdf
- APPENDIX Q. Regulations for Medical Records
- HTML http://aspe.hhs.gov/daltcp/reports/2013/EHRPIap.shtml#appendQ
- PDF http://aspe.hhs.gov/daltcp/reports/2013/EHRPI-appendQ.pdf
- APPENDIX R. Technical Advisory Group Summary
- HTML http://aspe.hhs.gov/daltcp/reports/2013/EHRPIap.shtml#appendR
- PDF http://aspe.hhs.gov/daltcp/reports/2013/EHRPI-appendR.pdf
- APPENDIX S. Evaluating Benefits and Costs of New Incentives for EHR Adoption by Ineligible Providers
- HTML http://aspe.hhs.gov/daltcp/reports/2013/EHRPIap.shtml#appendS
- PDF http://aspe.hhs.gov/daltcp/reports/2013/EHRPI-appendS.pdf
- APPENDIX T. CIO Consortium EMR Cost Study Data
- HTML http://aspe.hhs.gov/daltcp/reports/2013/EHRPIap.shtml#appendT
- PDF http://aspe.hhs.gov/daltcp/reports/2013/EHRPI-appendT.pdf
- APPENDIX U. Abbreviations and Acronyms
- HTML http://aspe.hhs.gov/daltcp/reports/2013/EHRPIap.shtml#appendU
- PDF http://aspe.hhs.gov/daltcp/reports/2013/EHRPI-appendU.pdf
- APPENDIX V. References
- HTML http://aspe.hhs.gov/daltcp/reports/2013/EHRPIap.shtml#appendV
- PDF http://aspe.hhs.gov/daltcp/reports/2013/EHRPI-appendV.pdf
To obtain a printed copy of this report, send the full report title and your mailing information to:
U.S. Department of Health and Human ServicesOffice of Disability, Aging and Long-Term Care PolicyRoom 424E, H.H. Humphrey Building200 Independence Avenue, S.W.Washington, D.C. 20201FAX: 202-401-7733Email: webmaster.DALTCP@hhs.gov
RETURN TO:
Office of Disability, Aging and Long-Term Care Policy (DALTCP) Home [http://aspe.hhs.gov/office_specific/daltcp.cfm]Assistant Secretary for Planning and Evaluation (ASPE) Home [http://aspe.hhs.gov]U.S. Department of Health and Human Services (HHS) Home [http://www.hhs.gov]
Last Updated: 08/08/2013