
U.S. Department of Health and Human Services
The Contribution of Self-Direction to Improving the Quality of Mental Health Services
Vidhya Alakeson
2006/2007 Harkness Fellow Office of the Assistant Secretary for Planning and Evaluation
November 2007
PDF Version (56 PDF pages)
This paper was prepared under a Harkness Fellowship. Funds for this fellowship were provided by the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and the Commonwealth Fund. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the ASPE Project Officer, Vidhya Alakeson, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. Her e-mail address is: Vidhya.Alakeson@hhs.gov.
The opinions and views expressed in this report are those of the author. They do not necessarily reflect the views of the Department of Health and Human Services, the Commonwealth Fund, its directors, officers or staff, or any other funding organization.
TABLE OF CONTENTS
- III. METHODOLOGY
- V. DIFFERENCES IN SELF-DIRECTED CARE BETWEEN STATES
- 1. The Scope of Self-Direction
- 2. Governance
- 3. The Role of Peers
- 4. Level of Consumer Responsibility
- 5. Relationship to the Rest of the System
- VIII. CONSUMER VIEWS OF SELF-DIRECTION
- 1. Support as well as the Budget
- 2. Peer Support
- 3. Greater Flexibility in Meeting Needs
- 4. Recovery Orientation
- 5. Different Relationship with Providers
- IX. IMPACT ON SERVICE USE AND OUTCOMES
- 1. Service Use
- 2. Outcomes
- 3. Costs
- X. ISSUES FOR THE FUTURE
- 1. Working with Medicaid
- 2. The Scope of Self-Direction
- 3. Developing the Peer Movement
- 4. Information and Education
- 5. Budgeting
- 6. Improving Administrative Systems
- 7. Quality Assurance
- 8. Cross-Learning with Other Disability Groups
- XI. CONCLUSIONS
- APPENDICES
- APPENDIX 1: Interview Participants in Case Study States
- APPENDIX 2: Interview Participants
- APPENDIX 3: State Program Descriptions
- APPENDIX 4: Requests for Reimbursement Made by Participants in Floridas Self-Directed Care Program in District 8 Between July 2005 and March 2007
- LIST OF FIGURES
- FIGURE 1: The Scope of Self-Directed Care for Adults with SMI in Different States
- FIGURE 2: Comparing the Characteristics of SDC and Non-SDC Participants Florida
- FIGURE 3: Baseline Consumer Responses for the Current Mental Health System Compared to Fourth Quarter Responses for Empowerment Initiatives
- FIGURE 4: Comparing Personal Outcome Measures for Self-Directed Care and Community Mental Health Services in Florida
- FIGURE 5: Comparing the Utilization Rates for Services of SDC Sample and Matched non-SDC Sample in 2005 - 2006
- LIST OF TABLES
- TABLE 1: Overview of Self-Directed Care Programs for Adults with Serious Mental Illness in Five States
- TABLE 2: Number of Purchases Made by Category in Self-Directed Care in District 8 in Florida, July 2005 - March 2007
- TABLE 3: Amount Spent by Category by Empowerment Initiatives Participants in Multnomah County, Oregon, 2005 - 2006
- TABLE 4: Model Consumer Budget for Kalamazoo County Mental Health Services 2005 - 2006, Michigan
EXECUTIVE SUMMARY
The final report of the Presidents New Freedom Commission on Mental Health identified two principles that should underpin reform of the mental health system: services and treatments must be consumer and family centered; and care must focus on increasing consumers ability to successfully cope with lifes challenges, on facilitating recovery, and on building resilience.1 Self-direction is identified as one possible means by which to achieve these goals.
There are currently five states with self-directed care (SDC) pilots or established programs for adults with serious mental illness (SMI): Florida, Iowa, Maryland, Michigan and Oregon, with a pilot under development in Texas. For the purposes of this report, SDC programs are considered to be ones that include person-centered planning, individual budgeting and provide participants with access to support services. While programs share a philosophical approach and the core components of self-direction, there is significant variation in the design across states.
Self-direction for adults with SMI is in the early stages of development and currently serves a very small number of consumers. Therefore, it is not possible to draw any firm conclusions about its potential to meet the goals of the New Freedom Commission. However, evidence from existing SDC programs indicates that it is a promising approach, worthy of further investigation. Self-direction has been shown to improve consumer satisfaction with services compared to traditional community mental health services. According to interviews with consumers, this is in large part due to the focus on recovery rather than symptoms; the flexibility of the approach in meeting individual needs; and the support provided by counselors and peers in articulating goals and developing spending plans.
Despite fears about the capacity of individuals with SMI to make informed choices about their care, there is no evidence that outcomes are worse under SDC than under professionally-controlled services. On the contrary, early evidence is that outcomes improve, with participants in SDC making less use of crisis stabilization units and crisis support compared to non-participants and greater use of routine care and supported employment. The most significant savings from SDC will be brought about if these early findings indicating a shift to greater prevention and early intervention are sustained over the long term, reducing the need for costly, acute services.
While initial findings from SDC are promising, the report discusses some of the issues that need to be addressed if self-direction is to successfully expand and make a significant contribution to improving the quality and outcomes of the public mental health system. These include: extending the scope of SDC to include traditional mental health services; finding ways of integrating self-direction for adults with SMI with Medicaid regulations and funding streams; and developing an active peer movement as a source of advocacy for self-direction and as a source of alternative services to provide consumers with choice and flexibility.
I. WHAT IS SELF-DIRECTED CARE?
In its final report, the Presidents New Freedom Commission on Mental Health2 identified two principles that should underpin reform of the mental health system. First, services and treatments must be consumer and family centered. Second, care must focus on increasing consumers ability to successfully cope with lifes challenges, on facilitating recovery, and on building resilience.3 The report identified self-directed care (SDC) as one way of delivering services that is in line with these principles and could make an important contribution to improving the quality of mental health services.
Self-direction or SDC is a method of delivering services that is based on giving each consumer control of an individual budget with which to purchase goods and services to meet his or her needs. It is frequently also referred to as consumer-direction but, for the purposes of this report, self-direction or SDC will be used.
By transferring control of financial resources to consumers, self-direction should create greater responsiveness from the public mental health system to the preferences and choices of consumers.4 Under self-direction, consumers can use their individual budget to purchase goods and services of their choice rather than ones that are chosen on their behalf, breaking out of existing service silos to some extent. This shifts money away from services that consumers do not support and away from providers with whom they do not want to work. This has the potential to create a pattern of service provision that is less focused on medical interventions and more recovery-oriented because it harnesses the expertise and experience of consumers in managing their own conditions.
SDC has its roots in the independent living movement. It was identified as one way in which individuals with disabilities could achieve greater self-determination.
Self-determination has five over-arching principles:
- Freedom to decide how a person wants to live his life;
- Authority over a targeted amount of dollars;
- Support to organize resources in ways that are life enhancing and meaningful to the individual;
- Responsibility for the wise use of public dollars and recognition of the contribution that individuals with disabilities can make in their communities;
- Confirmation of the important role that individuals with disabilities must play in a redesigned system.5
SDC is a model of service delivery that supports self-determination. Its core components include:6
- Person-centered planning. This is a comprehensive strategy for putting necessary services and supports in place to help individuals achieve their goals. It is conducted by individuals who identify their own strengths, capacities, preferences, needs and desired outcomes, together with their freely chosen supporters.
- Individual budgeting. Budgets provide a mechanism for people to have control over the money spent on their services along with control over who will provide the services and supports named in their individual plan. The total value of a budget is based on an individuals level of need and the amount of money that the state can provide to meet that need.
- Support services. Programs generally provide access to two types of support service: a counseling and advice service that helps consumers identify their goals, make informed decisions about how best to meet them and develop a spending plan; and a financial management service that handles the administrative, taxation and payroll functions relating to consumer purchases.7
The earliest manifestation of SDC dates back to 1953 when Los Angeles County established a consumer-directed attendant care program to enable polio survivors who used iron lungs to live at home rather than in hospitals. In the 1990s, self-direction was given a major boost through two Robert Wood Johnson Foundation (RWJF) grant programs: the Self-Determination Initiative and the Cash and Counseling Demonstration and Evaluation Program.
The Self-Determination Initiative aimed to give individuals with developmental disabilities and their families greater control over the services they received. It began in New Hampshire in 1993 and was subsequently extended to cover initiatives in eighteen other states. Each state implemented self-determination in a different way but included core elements such as person-centered planning, individual budgets and support brokerages8 in their programs. An evaluation of the impact of the program on the quality of life of participants in five states was conducted by the Center for Outcome Analysis. The evaluation reported a shift in decision-making away from professionals to individuals with developmental disabilities and their families and friends and consistent improvement in perceived quality of life in all five states. Other quality of life indicators, such as respondents productive behavior and progress towards goals, showed inconsistent results from state to state.9
The Cash and Counseling National Demonstration and Evaluation Project began in the mid-1990s with grants from the RWJF and the Office of the Assistant Secretary for Planning and Evaluation at the U.S. Department of Health and Human Services. In 1998, Medicaid approved three Cash and Counseling programs in Arkansas, Florida and New Jersey under the section 1115 Medicaid authority. These programs conducted an experimental trial of consumer-directed services for adults with disabilities, elders and children with developmental disabilities. The services that were eligible for self-direction consisted of personal care and related services under the states Medicaid State plans or their section 1915(c) waivers. All three states eventually submitted amendments to end the randomization of individuals into control or treatment groups, thereby permitting all individuals in the control group and new participants to direct their care.
In an evaluation conducted by Mathematica Policy Research, Inc. and by the University of Maryland, the Cash and Counseling approach was found to significantly reduce unmet personal care needs and significantly improve quality of life for participants and their care givers. Participants did not report poorer health as a result of self-direction and in some cases, they were less at risk than those in the control group.10 Based on the success of the demonstration, the program was extended to include a further 12 states in 2004.
By contrast with other disability groups, SDC has been much slower to develop in mental health. Although isolated programs existed before 2000, the first recognized pilot of SDC for adults with serious mental illness (SMI) began in the Jacksonville area of Florida in 2002.
II. OBJECTIVE OF THE REPORT
This report focuses on adults with SMI served by the public mental health system. It aims to identify and describe the range of SDC programs for this group currently being pursued by states and bring together existing evidence relating to the impact of these programs on individuals and on state resources. In doing so, it attempts to contribute to ongoing debate about effective strategies for improving the quality and outcomes of the public mental health system. It is early in the development of self-direction for individuals with SMI and the number of consumers currently served by these programs remains very small. Therefore, the findings and conclusions presented here are preliminary and further investigation will be required before definite conclusions can be drawn.
The report is aimed primarily at state and local-level policy-makers and individuals in consumer or other advocacy organizations who are interested in self-direction and want to learn from the experiences of other states in shaping their own approach to self-direction. It is hoped that the report will also be of interest to a broader policy audience interested in improving the quality of mental health services, as well as those interested in self-direction across disability groups.
III. METHODOLOGY
This report is based on case study visits between February and May 2007 to Florida, Michigan and Oregon, three states with self-directed programs for adults with SMI. During each visit, interviews were conducted with consumers, program staff and state officials to address the following issues (see Appendix 1 for a list of interview participants in the case study states):
- the details of the program in each state;
- what consumers value about SDC;
- the nature of the services available to support consumers in making effective choices;
- the goods and services that consumers purchase;
- how the program fits within the states wider approach to system transformation;
- the challenges states face in setting up, maintaining and extending the program.
Information about programs in other states has been obtained through meetings and telephone conversations with state officials and program managers. (See Appendix 1 for a list of contacts in non-case study states).
The case studies were supported by 20 structured interviews with policy-makers, academic experts, consumer advocates and provider representatives in mental health (see Appendix 2 for a list of interview participants). These focused on the potential of self-direction to improve the quality of mental health services, the scope for extending the approach and the barriers to doing so. The report also draws on published and unpublished academic and policy documents.
IV. WHICH STATES HAVE A SELF-DIRECTED CARE PROGRAM FOR SMI?
Several states include some aspects of self-direction within their mental health administrations.11 This report focuses only on those states that have implemented or are piloting a more comprehensive SDC model that includes the use of an individual budget for adults with SMI within the public mental health system. The states in question are listed below. Table 1 presents highlights from the different programs except the pilot in Texas which is still under development. A more detailed description of each program is presented in Appendix 3.
- Florida: Self-Directed Care
- Iowa: Self-Directed Care
- Maryland: Self-Directed Care
- Michigan: Self-Directed Care
- Oregon: Empowerment Initiatives (EI) Brokerage
- Texas: Pilot Under Development
| TABLE 1: Overview of Self-Directed Care Programs for Adults with Serious Mental Illness in Five States | |||||||
| State | Location | Date Started | No. Participants | Size of Individual Budget | Program Management | Funding Source | Scope of Self-Direction |
| Florida | District 4 (Jacksonville area) and District 8 (Fort Myers area). | District 4 in 2002. District 8 in 2005. | District 4 -- 160 as of July 2007 with a goal to recruit an additional 75 under managed care. District 8 -- 90 as of July 2007. | District 4 -- $1,672 for those with Medicaid and $3,192 for the uninsured per year. District 8 -- $1,924 for those with Medicaid and $3,700 for the uninsured per year. | District 4 managed by Renaissance Behavioral Health Care System (RBHS), a large provider of mental health services. District 8 managed by the local National Alliance on Mental Illness (NAMI) which provides no other mental health services. | Medicaid billed for Medicaid allowable expenditures; e.g., recovery coaches billed as case management. Additional budgets funded by state general revenue. | Additional budget used for services not covered by Medicaid, including alternative clinical providers outside the traditional mental health system. |
| Iowa | Consumers receiving services from Hope Havan, a provider of intensive psychiatric rehabilitation services. | Planning began in February 2006. First participant entered in May 2006. | 18 participants to date and 13 active as of July 2007. Goal to serve 25 consumers by the end of 2007. | $2,000 per participant for the duration of the pilot project. | Psychiatric rehabilitation provider, Hope Haven. | Community reinvestment fund created by setting aside 2.5% of capitation fee under Medicaid managed care contract. | Budget used to achieve one rehabilitation goal chosen by consumer. No other new opportunities for changing services are created by the pilot. |
| Maryland | Washington County (Hagerstown and surrounding area). | February 2007. | 9 active as of July 11, 2007. Goal to serve 30 consumers by June 2008. | Approximately $3,000 but no fixed annual cap. Budget amount is determined by services required by the consumer to meet their recovery goals. | Office of Consumer Advocates, a consumer-run organization. | Budgets funded by state general revenue. | Budget used for services not covered by Medicaid and possibility of accessing alternative clinical providers outside the traditional mental health system. |
| Michigan | Kalamazoo and Oakland Counties, although possible statewide. | Self-determination policy developed in 2003. First consumer with a budget in 2006. | Kalamazoo County -- 11. Oakland County -- 1 and 7 on the waiting list. | No set amount. Consumers can choose to redirect any part of the resources being spent on them in the traditional system. | County Mental Health Services. | Medicaid concurrent section 1915(b)/(c) waiver. | Self-determination exists within the Medicaid system. Consumer budgets do not involve additional resources. |
| Oregon | Multnomah County and Clackamas County. | Multnomah County in 2005 under a CMS Real Choice Systems Grant. Clackamas County in 2006. | Multnomah County -- 25. Clackamas County -- 25. | $3,000 per year. | EI, a consumer-run organization. | State general revenue and some Medicaid funds. | Additional budget used to purchase services not covered by Medicaid. In Clackamas County, budget focused on transition from group homes to independent living. Participation in EI does not create additional opportunities to change traditional services. |
V. DIFFERENCES IN SELF-DIRECTED CARE BETWEEN STATES
While the pilots in different states share a similar philosophy and the core features of self-direction, there is no blueprint for self-direction in mental health. There is notable variation between the different states along the dimensions discussed below. However, at this early stage in the development of self-direction, it is not possible to identify which of these dimensions is more or less critical in creating major culture change in state mental health systems.
1. The Scope of Self-Direction
The most important difference between programs is the scope of self-direction permitted. This has two related dimensions. The first is the extent to which consumers are able to direct services provided by the traditional mental health system, for example, psychiatric visits and counseling, as well as recovery support services. Recovery support services in this context refer to alternative and non-traditional services that have the same objectives as traditional mental health services, for example, community-based support groups, as well as goods and services that enhance a persons integration into the community, for example, a fitness membership or household goods. The second dimension is the extent to which individual budgets are separate and additional to Medicaid funding for traditional mental health services or whether consumers are directing Medicaid resources that are already embedded within the system (see Figure 1).
Looking at the first dimension, states can be divided into two groups: those with SDC programs that allow consumers to purchase recovery support services only and those that permit consumers to also purchase services that are provided by the traditional mental health system. The programs in Iowa and Oregon fall into the former category. Both provide consumers with a budget in addition to the services provided by the traditional mental health system, $3,000 in the case of Oregon and $2,000 in Iowa. This budget can be used to purchase recovery supports not provided by the traditional system in order to achieve a specific goal. In Clackamas County in Oregon, this is to transition from group housing to independent living. In Iowa, individuals can choose a goal relating to housing, education, employment or relationships. Self-direction does not give consumers additional opportunities to change the traditional services they receive.
Florida, Maryland and Michigan fall into the latter category. Although these states provide consumers with a budget primarily to purchase services and, in some cases, goods not provided by the traditional system,12 consumers do have the option to use money from their budgets to visit alternative providers of traditional services. For example, if a consumer is unhappy with the service provided by his psychiatrist and is unable to find another psychiatrist who accepts Medicaid reimbursement rates, the consumer would be permitted to use money from his budget to pay for a psychiatrist outside the Medicaid system. Florida Self-Directed Care is particularly significant in this context because it serves uninsured consumers as well as those with access to Medicaid, Medicare and Veterans benefits. Uninsured consumers in the Florida program receive a larger budget than insured consumers, $3,700 compared to $1,924 for a Medicaid consumer in District 8, but have to spend 48% of their budget on traditional mental health services.
| FIGURE 1: The Scope of Self-Directed Care for Adults with SMI in Different States |
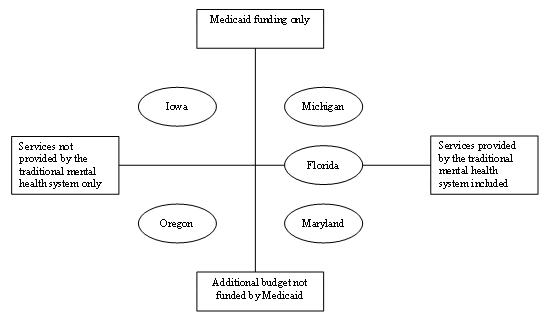 |
The second dimension of variability is the extent to which individual budgets are separate and additional to Medicaid funding for traditional mental health services or whether budgets include Medicaid resources. In this context, existing programs fall into three categories. In the case of Oregon and Maryland, individual budgets are funded by state general revenues and do not include Medicaid resources. They are provided in addition to Medicaid funding for traditional services. By contrast, in Iowa and Michigan, budgets are funded entirely with Medicaid resources. Florida occupies an intermediate position, braiding state general revenue and Medicaid funds. Consumers receive an additional budget funded by state general revenue but all aspects of SDC that are Medicaid eligible are billed to Medicaid, for example, recovery coaches are billed under case management.
Differences in the scope of self-direction across states are largely attributable to the Medicaid regulations in each state. Some states have the flexibility in their existing regulations to pay for some recovery support services using Medicaid dollars. For example, as part of its contract in Iowa, Magellan Behavioral Healthcare must set aside 2.5% of each capitation payment it receives from the state. Money that is set aside forms a community reinvestment fund that is used to support service innovation. Under the pilot phase of SDC, individual budgets in Iowa are paid for through the community reinvestment fund. Although this is a separate fund from the resources used to pay for existing mental health benefits, it consists exclusively of Medicaid dollars. Other states do not have such flexibility, or are choosing not to use it to support self-direction. This means that support services have to be purchased with state general revenue funds that can be used entirely at the states discretion rather than changing the way in which Medicaid funds are spent.
2. Governance
SDC programs have different governance and management structures across states. In Maryland and Oregon, programs are managed by consumer-run organizations under contract with the state or county. In District 8 in Florida, it is run by the local NAMI under contract with the state. In Michigan, however, self-determination is managed by county mental health services.
In Iowa and in District 4 in Florida, SDC is managed by an existing service provider. This can lead to conflicts of interest. For example, the provider could put pressure on the state to use any unspent funds from SDC on other provider activities rather than investing it back into self-direction. While this is not always the case,13 to avoid potential conflicts of interest, it is preferable for SDC to be managed by an organization independent of existing providers.14 In Florida, the Mental Health Program Office is now aware of this issue and is looking to change the management arrangements in the future.
A further development in governance terms is the integration of SDC into managed care in Iowa and in District 4 in Florida. In Iowa, Magellan Behavioral Healthcare began piloting self-direction with 25 consumers receiving intensive psychiatric rehabilitation services through one provider. District 4s community mental health services are in the process of being incorporated into Medicaid managed care run by Healthease and Staywell, subsidiaries of Wellcare that operate in Florida. Wellcare has committed to expand Florida Self-Directed Care to an additional 75 people and, in the initial phase of expansion, to operate the program without making significant changes.15
Managed care has been perceived as a threat to self-direction because the two philosophies seem contradictory. One gives control and decision-making authority to the managed care company and the other to the consumer.16 When interviewed, however, representatives from Magellan and Wellcare presented the introduction of self-direction as an important way of signaling their commitment to providing quality behavioral health care. In fact, there was general agreement among experts interviewed for this report that there could be a good fit between self-direction and managed care, at the very least because of the perceived cost savings from self-direction. Furthermore, the electronic collection of utilization data that is common under managed care also creates potential for a good fit with self-direction because the availability of electronic data makes it easier to develop individual budgets, track expenditures, measure quality and create additional flexibilities.
3. The Role of Peers
The extent to which peers are involved in self-directed programs varies across states. In consumer-run organizations, peers are responsible for program management and for providing support services, for example, EI in Oregon and SDC in Maryland. In other programs, peers are not responsible for management but provide support services, such as in Michigan. In Iowa, consumers continue to work with certified intensive psychiatric rehabilitation practitioners. Florida continues to have professionals as well as peers providing support services and, in some instances, peer providers are also professionally qualified.
Who provides support and counseling is significant because many consumers express a preference for peer-provided support. In interviews, consumers said that they valued the more equal relationship that they could have with a peer and the unique advice that peers could provide as a result of their lived experience of mental illness (see Section VIII.2 for further discussion).
4. Level of Consumer Responsibility
The level of responsibility expected of consumers varies across programs. Some programs take a more brokered approach to self-direction, where the consumer decides how money is spent but some of the follow up is done by the counselor acting on the consumers behalf or by the consumer with the counselor. In other programs, the consumer is expected to be more autonomous. This variation is significant because of the impact it has on who participates in self-direction and the extent to which the approach is suitable for more vulnerable consumers. Here the contrast between the programs in Florida and Oregon is instructive.
In working with consumers in Clackamas County who are transitioning to independent living, EI in Oregon adopts a hands on approach and provides intensive support. Resource brokers meet consumers weekly and are on call 24 hours a day if consumers need them. Many consumers have daily telephone contact with their resource broker and brokers often accompany individuals to make purchases. This intensity of support is essential to making self-direction work for this population, many of whom are in the early stages of recovery and have not lived independently for a number of years.
By contrast, the Florida program has historically tended to target consumers who were able to take on significant responsibility. Initially, participants were expected to complete a significant amount of paperwork and digest a large number of rules and processes. There was a sense that they had to be able to manage alone if they wanted to self-direct. Some vestiges of this remain, for example, the fact that some enrollment is still conducted by mail rather than face-to-face in District 4.
This focus on autonomy is reflected in the 2007 evaluation of the Florida program which found that participants were better educated than non-participants in the mental health system and less likely to be from a minority group. 86.3% of participants had completed high school compared to 34.4% of non-participants and 24.4% were from a minority compared to 49.6% of non-participants (see Figure 2 below).17 This echoes an earlier independent evaluation which concluded that the program is formally structured to expect both considerable initiative and a high tolerance for independent paperwork on the part of participants. This aspect of program design may limit its applicability; a wider group of individuals could potentially benefit if they were provided more explicit support for developing skills in identifying goals, making decisions and planning recovery.18
Some changes to the initial program design have already been made in response to participant feedback, including a reduction in paperwork, greater self-referral and peer-to-peer recruitment by telephone and face-to-face visits. The most recent Legislative Budget Request submitted by Floridas Mental Health Program Office acknowledges the 2007 evaluation results and re-emphasizes that self-direction should be a viable option for all individuals with SMI. Furthermore, the introduction of managed care participants into the program is likely to change the demographic mix given that the population served by Staywell and Healthease is less affluent and less well educated than the average consumer in Floridas community mental health system. To create a more inclusive program under these circumstances, the state envisages more frequent contacts between consumers and life coaches and a greater level of support for consumers in developing their first life action plan.
5. Relationship to the Rest of the System
All self-directing consumers continue to receive some services from the traditional mental health system. Acute services such as crisis support and stabilization, for example, are not included in individual budgets in any state. However, self-direction is generally perceived as a parallel track to the traditional system and, in some states, consumer who choose to direct some of their own care have to opt out of traditional services. For example, consumers in Florida who are eligible for case management or assertive community treatment and opt for self-direction have to forgo these services. Other states, for example, Michigan, operate a more blended system in which consumer who opt for self-direction maintain a relationship with a chosen case manager.
| FIGURE 2: Comparing the Characteristics of SDC and Non-SDC Participants in Florida |
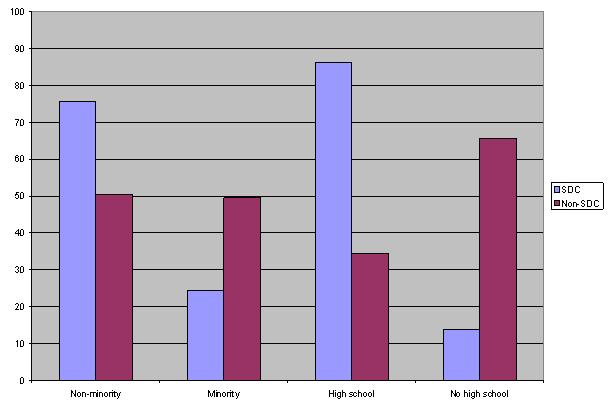 |
| SOURCE: Florida Department of Children and Families, Mental Health Program Office (2007). |
The exception to this view of SDC as a parallel service track is in Oregon. EI is seen as part of the continuum of care rather than a parallel track. Consumers participate for a year, with the possibility of a few additional months under special circumstances. The purpose of EI is to kick start recovery and to move participants in a year to a position where they are able to sustain recovery-focused activities without the support of the brokerage.
The extent to which self-direction is central to a states approach to improving the quality of mental health services also varies. Although embryonic in all states, officials interviewed in some states perceived self-direction to be an important part of achieving the kind of transformation outlined in the Presidents New Freedom Commission on Mental Health and it was integrated into wider activities. In others, it was thought of as more peripheral, with greater emphasis being placed on other strategies, for example, peer specialists or consumer-operated services. Overall, experts interviewed for this report agreed that self-direction will not serve the needs of all consumers and is one of several approaches that together may improve the responsiveness and performance of the mental health system. Others approaches referred to by experts include the development of decision-aides that can support consumers to take an active part in clinical decision-making and the participation of consumers in governance bodies that influence the overall design and implementation of services.19
VI. CONSUMER SPENDING IN SELF-DIRECTED PROGRAMS
Table 2 and Table 3 illustrate how consumers choose to use their budgets in District 8 in Florida and in Multnomah County in Oregon. It is important to note that Table 2 for Florida is based on the number of requests for reimbursement in each spending category, while Table 3 for Oregon derives from actual spending per category. Appendix 4 shows the full range of purchases made by consumers in District 8 in Florida between July 2005 and March 2007. For the purposes of the table below, purchases have been grouped by category.
| TABLE 2: Number of Purchases Made by Category in Self-Directed Care in District 8 in Florida, July 2005 - March 2007 | ||
| Category | No. request for reimbursement | Percentage total requests for reimbursement (%) |
| Medication | 206 | 16 |
| Transportation | 164 | 13 |
| Psychiatrist visits | 147 | 12 |
| Counseling | 96 | 8 |
| Rent and utilities | 91 | 7 |
| Dental services | 83 | 7 |
| Personal appearance | 78 | 6 |
| Information Technology | 76 | 6 |
| Other therapies | 58 | 5 |
| Physical fitness | 53 | 4 |
| Other hobbies | 41 | 3 |
| Vision services | 40 | 3 |
| Education | 40 | 3 |
| Arts and crafts | 24 | 2 |
| Food | 23 | 2 |
| Household items | 17 | 1 |
| Medical other | 17 | 1 |
| Employment-related | 5 | 0.5 |
| SOURCE: Authors analysis based on data from District 8 program office. | ||
The four largest spending categories in District 8 in Florida are medication (16%), transportation (13%), psychiatric services (12%) and counseling (8%). The four largest spending categories in Multnomah County in Oregon are household items such as furniture and cooking utensils (15%), alternative therapies such as massage therapy (14%), information technology (IT) supplies (12%) and goods and services relating to personal appearance such as a haircuts and clothing (10%). The differences in spending between the two states reflect differences in the scope of self-direction described in Section V.1. This explains why there is far greater spending on traditional mental health services in Florida than in Oregon. However, there are many similarities in the spending patterns that illustrate the benefits of SDC to consumers.
| TABLE 3: Amount Spent by Category by Empowerment Initiatives Participants in Multnomah County, Oregon, 2005 - 2006 | ||
| Category | Amount spent by category ($) | Percentage total spent by category (%) |
| Household items | 9,431.70 | 15 |
| Alternative therapies | 8,436.09 | 14 |
| Information Technology | 7,354.86 | 12 |
| Personal appearance | 6,109.49 | 10 |
| Employment-related | 5,197.30 | 9 |
| Personal relationships | 4,386.26 | 7 |
| Transportation | 3,696.50 | 6 |
| Arts and crafts | 3,339.66 | 6 |
| Physical health and nutrition | 2,726.43 | 4 |
| Other hobbies | 2,388.16 | 4 |
| Medical services | 2,236.57 | 4 |
| Animal companions | 1,700.95 | 3 |
| Rent and moving expenses | 1,396.05 | 2 |
| Life planning | 1,087.39 | 2 |
| Other | 1,138.04 | 2 |
| SOURCE: Authors analysis based on data from EI. | ||
Both states report a huge diversity in spending that is partially masked by the spending categories in Table 2 and Table 3. For example, the physical fitness category in Table 2 includes the following purchases: 42 health club memberships; seven bicycle-related purchases; one weight loss program; weighing scales; tai chi classes; and one request for exercise equipment (see Appendix 4 for further detail of individual purchases). This reflects one of the central features of self-direction. It is able to tailor services to the specific needs of individual consumers because they choose what is provided and by whom.
In both states, consumers use their budgets to access goods and services that are not covered by the traditional system. This includes medical care in the form of dental and optical services and some pharmaceuticals. The largest category of items not covered is recovery support services that address other aspects of an individuals life that are affected by mental illness rather the mental illness itself. For example, consumers join weight watchers to help with their physical fitness, put some of their money towards utilities to ensure that they can stay in their apartment or buy a computer to help them develop a micro-enterprise. Addressing these wider issues supports recovery in ways that traditional services are often unable for two reasons.
First, there are limits to what Medicaid will pay for. Medicaid typically does not pay for room and board or for social and recreational activities that are not focused on medical or remedial outcomes to address a particular impairment and functional loss. Second, states can restrict the scope of what can be covered by narrowly defining medical necessity criteria. Medical necessity criteria are developed by states for the purpose of determining who will be eligible for state plan services. They vary by state and have traditionally been driven by the medical needs of the individual. However, in the context of self-directed services under section 1915(c) waiver programs or in section 1115 demonstration programs, the needs assessment typically covers more than an individuals medical needs, creating scope for individuals to receive recovery support services where they can be directly related to a need identified in an individuals service plan.20
Where consumers are permitted to spend their budgets on traditional mental health services, for example, in Florida, some choose to see a private psychiatrist or counselor if they are unable to find a provider they are happy with who also accepts Medicaid reimbursement rates. However, not all choose to use their budget for traditional services. Some are satisfied with their existing Medicaid services and want to maintain a relationship with their current providers. Others want to maximize the amount of money that they have to purchase recovery support services. This in part reflects the high percentage of consumers in the public mental health system who live in poverty and need support with the basics of sustaining a life in the community: food, rent, utilities, transportation and personal hygiene.
In all states, consumers are encouraged to maximize the value of the money they have at their disposal by drawing on resources from other pubic programs and from the community and only using their individual budget as a last resort. For example, if an individual requires transportation and can receive a bus pass through vocational rehabilitation, his self-directed budget should not be used. It should only be used for items that cannot be funded in any other way. One of the important roles that counselors play is to knit together the disparate parts of the public system for consumers and help them access the full range of available resources.
VII. THE IMPACT OF SELF-DIRECTION ON SATISFACTION
By putting individuals in control, self-direction has been shown to lead to significant increases in consumer satisfaction. Findings from EI show a noticeable increase in different dimensions of consumer satisfaction when comparing consumers experiences in the traditional mental health system with experiences at the end of the first year of EI (see Figure 3).
| FIGURE 3: Baseline Consumer Responses for the Current Mental Health System Compared to Fourth Quarter Responses for Empowerment Initiatives |
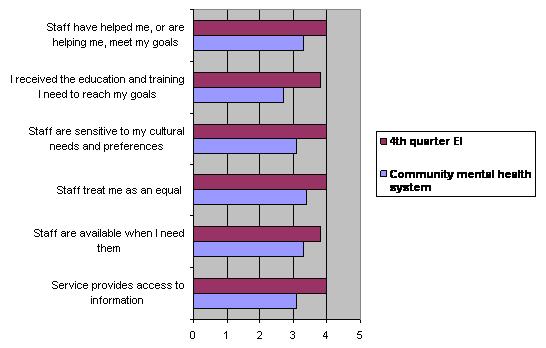 |
| SOURCE: Ami Sullivan (2006) Empowerment Initiatives Brokerage: Service quality and outcome evaluation, Oregon Technical Assistance Corporation. NOTE: Scores based on a four point agreement scale. 4 = strongly agree, 3 = somewhat agree, 2 = somewhat disagree, 1 = strongly disagree. |
Consumers in Iowa report an average satisfaction score of 4.9 for SDC based on a scale of one to five. Satisfaction among providers and case managers is also high, with both groups scoring 4.2 on average.21 Consumers participating in Florida SDC report similar improvements in satisfaction. Figure 4 compares the self-reported experiences of participants in Florida Self-Directed Care with an unmatched sample of participants receiving traditional community mental health services. It uses the personal outcome measures developed by The Council for Quality and Leadership that address quality of life rather than simple satisfaction. It is interesting to note that self-directed consumers are less positive than consumers in the community mental health system only when it comes to issues of abuse and neglect from service providers and security of service provision (bars 24 and 25 in Figure 4). This most probably reflects the fact that self-direction does place greater expectations on consumers and demand additional responsibility. However, the chart reports the perceptions of program participants and does not reflect greater incidence of abuse and neglect in SDC compared to traditional service delivery.
| FIGURE 4: Comparing Personal Outcome Measures for Self-Directed Care and Community Mental Health Services in Florida | ||
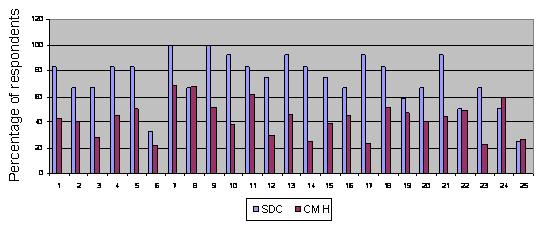 | ||
| 1. People Choose Personal Goals 2. Choose Living Arrangements 3. Choose Where They Work 4. Have Intimate Relationships 5. Are Satisfied With Services 6. Are Satisfied With Life Situation 7. Choose Their Daily Routine 8. Have Privacy As Needed 9. Decide To Share Information | 10. Decide When To Share Info 11. Live In Integrated Environments 12. Participate In Life Of Community 13. Interact With Others In Community 14. Perform Different Social Roles 15. Have Friends 16. Are Respected 17. Choose Services | 14. Perform Different Social Roles 15. Have Friends 16. Are Respected 17. Choose Services18. Realize Personal Goals 19. Are Connected To Natural Supports 20. Are Safe 21. Exercise Rights 22. Are Treated Fairly 23. Have Best Possible Health 24. Are Free From Abuse & Neglect 25. Experience Continuity & Security |
| SOURCE: Florida Peer Network (2007). | ||
These findings are supported by evidence presented in a forthcoming paper by Professor Ce Shen and colleagues at Boston College and the University of Maryland. They compare the experiences of older adults with and without a mental health condition in the Cash and Counseling demonstration in Arkansas. Sixteen percent of the elderly population in the Arkansas demonstration had a diagnosis of mental illness. Of those, 92.1% had a diagnosis in the low cost category. According to the International Classification of Diseases, 9th Revision codes,22 the low cost category includes, but is not limited to the following: neurotic depression, neurasthenia, depersonalization syndrome, hypochondriasis, other unspecified neurotic disorders, adjustment disorders, reaction (adjustment) to chronic stress, affective psychoses, brief depressive reaction, neurotic depression, psychogenic depressive psychosis, conduct disturbance as adjustment reaction, and destructiveness as adjustment reaction.
Prof. Shen and colleagues report that participants with a mental health condition who were in the treatment group and directing their own personal care services were more satisfied with their care arrangements, with the reliability and performance of their caregivers and had greater life satisfaction than those with a mental health condition in the control group. Older adults with a mental health diagnosis directing their own services were no more likely to experience adverse health events, such as falls or injuries, than those receiving agency services. The authors conclude emphatically that if a client is mentally ill, it is better for him or her to be in Cash and Counseling than in traditional treatment.23
VIII. CONSUMER VIEWS OF SELF-DIRECTION
In interviews about their experiences with self-direction, consumers identified specific features of the approach that they valued. These underpin the overall increase in satisfaction reported in Figure 3 and Figure 4.
1. Support as well as the Budget
One of the central messages from consumers interviewed for this report was the importance of the support and advocacy they received alongside the budget. Consumers across programs agreed that, given their financial circumstances, the individual budget was important. However, without the support provided by their counselor, the money alone would not have contributed significantly to their recovery. As one consumer in Oregon put it:
Its not about money, thats what Im trying to say. Its about the healing, the help, the growth that I get from them. The money plays a role . But people arent trying to scam anyone.
An important part of the support consumers felt they received came through the person-centered planning process. Counselors tend to work with consumers for several hours to identify goals and then develop a spending plan. In the case of EI, for example, the planning process has three stages which require separate meetings and involve a consumer and his resource broker spending 6-8 hours together. Furthermore, counselors in SDC are able to provide ongoing support to ensure that consumers make progress in achieving their goals. Consumers commented that creating a person-centered plan was only a starting point and that plans were meaningless without good follow up.
In contrast, the traditional system was seen by consumers to be unsupportive and consumers felt uninformed about their diagnosis and medications. In part, this reflects the heavy case loads of case managers. No case manager could invest as much time as SDC counselors in the planning process. They tend to spend 1-2 hours developing a care plan. But for individuals who have never been asked to articulate objectives and have rarely had the opportunity to express preferences because of poverty and illness, effective planning depends on investing time. This upfront investment in the planning process is critical to making SDC effective.
2. Peer Support
In the majority of SDC programs, counselors are peers. Peers bring additional value to the relationship between consumers and counselors. First, consumers do not perceive the same imbalance of power between themselves and peers as they do with professionals. This facilitates a true partnership that underpins the success of self-direction. As one consumer in Oregon put it:
I relate better to people who can say my life was a little like yours or validate what Im saying. With a case manager, they are all professional. Im perfect and Im not going to show any emotion. Im left feeling that small.
Second, peers act as effective role models for consumers who are seeking to rebuild a life in the community. They have unique knowledge that comes from their personal experience of living with mental illness. This allows them to act as expert guides and to work with consumers to knit together various recovery support services and resources. Peers combine learned knowledge of how to access public support such as vocational rehabilitation and Ticket to Work programs with real life experience of finding housing, cheap haircuts and free food in the community. Many facets of this knowledge are beyond the reach of professionals.
3. Greater Flexibility in Meeting Needs
One of the criticisms that consumers interviewed for this report made of the traditional system is that it treats diagnoses rather than individuals and, therefore, lacks flexibility. Consumers valued the flexibility that SDC gave them to meet their individual needs. This is reflected in the diversity of goods and services purchased under self-direction. Other types of flexibility were also important to consumers, for example, the ability to schedule services when they needed them rather than having to fit around providers. As one consumer in Michigan commented:
The other thing is that peoples needs dont necessarily follow nine to five. If Im looking for something to do on Saturday afternoon, my case manager is not going to leave her family and say, I have to go and help this person develop her social skills at this activity for two hours.
With an individual budget, this consumer in Michigan has been able to hire an assistant to work with her on social skill development at times that meet the consumers need and not vice versa. Overall, the flexibility of SDC comes from giving consumers control over all the dimensions of service provision -- the who, what, where and when.
4. Recovery Orientation
Consumers expressed the view that the public mental health system focused too heavily on illness and did not foster wellness. They valued the fact that SDC was explicitly focused on creating or sustaining a life in the community and on the full range of their needs. As one consumer in Oregon put it:
The traditional system focuses on do you feel suicidal today. Instead of saying, do you feel suicidal today, they should focus on something good. They only talk to my depression. They dont see me as a whole person.
Consumers identified two other important ways in which they felt self-direction was recovery-focused. First, it provided consistent support that helped them stay well and did not mimic the cyclical nature of the traditional system. Consumers reported that traditional services tended to step in at times of crisis and then withdraw once they were stable rather than being provided on an ongoing basis.
Second, they felt that SDC demanded a certain amount of responsibility and active participation from them and this was seen to be a positive aspect of the approach. They felt that the traditional system demanded little of them and made it difficult for them to be involved in their own care, in part reflecting a view that they were incapable of taking control.
5. Different Relationship with Providers
In some cases, consumers reported that self-direction changed their relationship with providers. They felt that the flexibility to change providers gave them a way of putting pressure on providers to improve. A consumer and board member in District 4 in Florida put it as follows:
In the old system, the level of service depended on zip code. Consumers couldnt put pressure on providers to improve. The program now spends a bit more on transportation than it used to because consumers are free to choose.
Even when consumers chose to remain with the same provider, they reported that the ability to go elsewhere meant that providers treated them differently. They were treated with more respect and were more likely to be listened to. They described it as being more like a private insurance client who has the flexibility to take his business elsewhere if he is unhappy with the service and, therefore, providers work harder to keep hold of his custom.
IX. IMPACT ON SERVICE USE AND OUTCOMES
It is early in the development of self-direction for adults with SMI and evidence on service use and outcomes is limited. Findings should, therefore, be treated as tentative.
1. Service Use
Given the flexibility of an individual budget, consumers will direct a greater proportion of spending towards recovery support services that address the other facets of their lives that are affected by mental illness. There is also anecdotal evidence that consumers will purchase more services from peers as well as professionals. Most significantly, evaluation of the Florida program shows that self-directing consumers are more likely to make use of routine and early intervention services that support their ongoing recovery and less use of crisis services compared to a matched sample of non-self-directing consumers (see Figure 5).24
| FIGURE 5: Comparing the Utilization Rates for Services of SDC Sample and Matched non-SDC Sample in 2005 - 2006 |
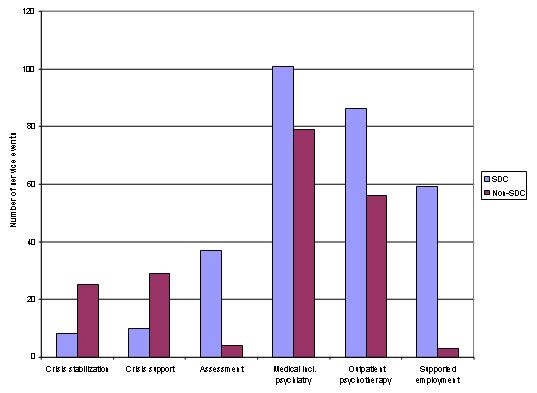 |
| SOURCE: Florida Department of Children and Families, Mental Health Program Office (2007). |
2. Outcomes
Evidence relating to the outcomes of SDC is very scarce. An initial evaluation of the Florida Self-Directed Care program demonstrated improved outcomes compared to traditional service delivery. On average, participants spent a significantly greater number of days in the community after joining the program than they did in the year prior to enrolment, that is to say not in hospital or in prison. Participants also scored significantly higher on the global level of functioning scale in the year following program participation than they did in the year prior to joining the program.25 However, the 2007 evaluation indicates that, having controlled for differences in education, there is no significant difference in employment or housing outcomes between self-directing and non-self-directing consumers.26
Results from the first year of EI are promising. Before the start of the program, only 23% of participants were in employment and 8% were in education. By the end of the first year, this had risen to 47% and 44% respectively, suggesting an improvement in mental health stability as well as social integration.27 EI participants were receiving traditional services only before entering the program which may indicate that EI is more effective at promoting mental health recovery than traditional services. However, a direct comparison between the two service systems was not conducted as part of the evaluation. Furthermore, participants were not followed beyond their year in the program so it is unclear whether the positive effects identified continued.
3. Costs
There is no evidence that improved outcomes are associated with higher costs. For the most part, individuals are good stewards of public money, spending less than their budgeted amount. Programs report few cases of fraud and abuse.28 In fact, it is more common for programs to report that the greater transparency of an individual budget prompts participants to actively seek to improve value for money. For example, consumers who choose self-determination in Michigan often do so because they feel that the traditional system is not providing value for money. As one consumer put it:
I was receiving services through Assertive Community Treatment and I felt like my needs were not being met. I came once a week to them. They came once a week to me. It took them longer to drive from the agency to my house than they spent with me. When I went to them, it was the same. In my case, I need to be weighed weekly so I would get weighed and go on my way. Basically, I felt like they [the Assertive Community Treatment team] were not doing anything and I wanted to get my needs met.
A former participant in EI who is now a staff member described her ability to get more for her money by bargaining with providers in the market place:
I did rolfing and massage. I had thyroid cancer so I was always hunching forward and now I can sit straight without hurting and the massage helped me to not be keyed up all the time. I did that twice a month. I was able to get a really good deal. I went and said, this is what Im trying to do with my life, this is how much money I have, can you help? They did and they helped others in EI too.
Many of the alternative services that participants choose are less expensive and can be as effective as their clinical equivalents. In the State of Georgia, for example, day treatment costs on average $6,491 a year compared to peer support which costs $1,000 a year. Over a 260 day period, adults with schizophrenia, bipolar and severe depression receiving peer support showed a statistically significant improvement in symptoms/behavior, skills and needs/resources compared to those in day treatment.29 While the Georgia certified peer specialists program is not itself a SDC program, peer supports are available to consumers opting for SDC.
In the case of EI in Clackamas County, the savings generated by supporting people to live independently can be relatively easily calculated. It costs the county between $40,000 and $60,000 a year to house an individual with a serious mental health condition in a group home. For $10,000 per person per year, EI has successfully helped 14 people since June 2006 to move into supported independent housing. This figure includes the value of the individual budget, the costs of a resource broker and the administrative costs of the program. The housing itself is paid for by the individual and by rent subsidies but is not funded by mental health services. Freeing up places in group homes has allowed the county to move people out of the state mental hospital, saving in the region of $70,000-$80,000 per person per year.30
The most significant savings from SDC will be brought about if early findings indicating a shift to greater prevention and early intervention are sustained over the long term. If individuals who currently make regular use of acute services, such as crisis stabilization units, can be supported through less costly routine and early intervention services to the extent that their use of acute services significantly reduces, the savings will be significant. Other savings will be generated by participants moving into work and off welfare payments but calculating the full range of possible savings across different funding streams is extremely complex.
X. ISSUES FOR THE FUTURE
Initial findings from SDC pilots are promising. However, there are many issues that need to be addressed if self-direction is to successfully expand and make a significant contribution to improving the quality and outcomes of the public mental health system.
1. Working with Medicaid
The joint federal-state Medicaid program is the single largest source of funding for public mental health services and is expected to account for an increasing share of the resources that underwrite state administered mental health services.31 Therefore, although there are other funding sources that can be used to develop self-direction,32 the extent to which this approach can be supported through Medicaid is highly significant for the future of SDC.
In contrast to other disability groups for whom section 1915(c) home and community-based waiver programs have been an effective vehicle for implementing self-direction, there is no single regulatory framework within which to implement self-direction for adults with a primary diagnosis of mental illness. Provisions introduced by the Deficit Reduction Act of 2005 (Pub.L. 109-171), codified in the Social Security Act as section 1915(i),33 section 1915(j)34 and Benchmark Plans, section 1937 of the Social Security Act,35 create new options for states wanting to implement self-direction for individuals with SMI. However, it remains unclear if and how states will use these new options. Furthermore, the new options do not provide a quick fix. Implementing self-direction will continue to require significant leadership at the state level in order to identify how self-direction can be accommodated within the Medicaid rules in a particular state.
Medicaid rules pose other, significant challenges for self-direction. Perhaps the most important is the fact that self-direction pushes at the limits of what Medicaid will support. Medicaid was designed to fund health care services based on medical necessity criteria and these criteria are being applied more strictly by states to constrain growing costs. However, one of the features of self-direction that consumers value, and that underpins the overall value of the approach, is the ability to purchase recovery support services that contribute to improving mental health without being specifically health services.
States have overcome this issue to date by relying on general revenue funding. But as more general revenue funding is used to match federal Medicaid dollars, states have less available for flexible funding and many competing priorities. In the medium term, there is a need to develop a funding model for self-direction that will ensure sustainability and maintain the flexibility of SDC that consumers value.
As a first step, the sustainability of SDC can be improved by securing Medicaid funding for the support functions that the programs provide, for example, counseling. This is being successfully done in some states, for example, Florida. With the approval of peer specialists as a Medicaid billable service, much of the support provided to consumers can be funded under this category as well as others. Although some states are reluctant to seek Medicaid support for peer services, fearing that this will lead to peer support becoming overly formalized, it does present a good option to improve sustainability.36
There was some agreement among experts interviewed for this report that improving the sustainability of self-direction would also require better coordination between Medicaid and other sources of welfare support. There are two approaches to achieving this: blending and braiding. Blending involves pooling funds from different sources into a single budget, while braiding coordinates funds from different sources but maintains separate lines of accountability for each funding stream. Braiding is the approach currently being used by Florida, for example, to combine Medicaid funding with state general revenue in its SDC program.
This kind of coordinated funding approach has been more successfully developed for children with serious emotional disturbance than it currently has for adults with SMI. For example, Wraparound Milwaukee is a unique type of managed care entity that serves children and adolescents with serious emotional disorders who are identified by the Child Welfare or Juvenile Justice System as being at immediate risk of residential or correctional placement or psychiatric hospitalization. Wraparound Milwaukee pools funds through case rates paid by the child welfare and juvenile justice systems, receives a monthly capitation payment for each Medicaid child enrolled, and coordinates other insurance and Supplemental Security Income payments to form a type of insurance pool.37 Blending or braiding different budgets together would increase the financial support available for SDC, while only using the most appropriate source to fund each particular service.
2. The Scope of Self-Direction
While the separation of Medicaid-funded and non-Medicaid-funded services in SDC in large part reflects the issues discussed above, restricting self-direction to recovery support services limits its capacity to create significant change in the public mental health system. Proponents of SDC, for example, the National Coalition of Mental Health Consumer/Survivor Organizations,38 agree that, if funding issues could be overcome, it would be desirable for consumers to have greater choice over who provides their traditional mental health services and which services they receive. Just as self-direction in developmental disabilities has led to a shift away from behavioral therapy and diet and nutrition services,39 the expectation is that self-direction in mental health would shift resources away from services that are unpopular among consumers and of questionable therapeutic value, for example, day treatment.40
However, by resisting all or nothing approaches to self-direction, programs can develop a continuum that allows individual consumers to choose how much control they want to have. A similar graduated approach is being developed in home and community-based waiver services for other disability groups, with North Carolina, South Carolina and Wisconsin putting in place programs that allow older participants to choose to receive a budget for some of their services but not necessarily all. For example, they can receive a budget to pay for a personal care worker and continue to receive all their other services from an agency. The authors of a recent report looking at this second generation of self-directed programs in long-term care argue that this continuum may make self-direction more manageable for a larger and more diverse population and more appealing to older adults. It also provides a way for states to offer some consumer control without having to implement a comprehensive SDC model.41
3. Developing the Peer Movement
The development of an active peer movement is an important complement to self-direction. First, peers are essential advocates for self-direction. It will be more difficult for states to sustain self-direction without an active base of participants and peers advocating for its maintenance and expansion. The absence, until 2006, of a unified consumer movement for adults with SMI was identified by several interview participants as one reason why self-direction has been slower to develop in mental health than in other disabilities. While there have long been strong advocacy groups, many of these are family rather than consumer-led organizations that have not always been ready to recognize the ability of individuals with mental health conditions to take responsibility for their own lives.
As well as advocacy, the development of strong peer networks ensures that there is a supply of alternative services to support self-direction. Peers can act as counselors and facilitators of person-centered plans. They can also be alternative providers of a range of other services, for example, supported employment, developing Wellness Recovery Action Plans and mentoring and counseling services. If they are trained and certified, peer delivered services are eligible for Medicaid reimbursement. Developing a cadre of trained peer specialists has become central to Michigans approach to self-determination, for example. Although the state mandated person-centered planning in 1996, it discovered that without an alternative workforce to facilitate planning and support consumers, the task was left to case managers whose workloads and established patterns of practice prevented self-determination from flourishing. In many ways, peers perform a similar function to family members in SDC for other disabilities. They expand supply, making choice and flexibility a reality for consumers.
4. Information and Education
Expanding self-direction depends on information and education on several fronts. First, consumers need to be educated about self-direction. The visibility of existing programs remains low. Consumers interviewed for this report were wary of exercising choice, worried that this may lead to services being taken away from them. They were reluctant to ask for a change of case manager, for example, fearing that this would go against them and many claimed to have been dissuaded from making changes by traditional providers and case managers. Peers can play an important role in dispelling fears and supporting consumers to be more active and involved in their own care.
There is also a need for public education to ensure that the sustainability of self-direction programs is not threatened by public misunderstanding. At present SDC is embryonic and the amount of money being spent is relatively small. At this scale, it is relatively easy for these programs to avoid public scrutiny, although this was not the case in Florida. The program received negative media coverage because public dollars were being spent on leisure activities and this was not considered an appropriate use of mental health funds. If programs are expanded, it will not be long before further questions are asked about the way in which public money is being used. It is, therefore, important that the public has a greater understanding of the concept of recovery from SMI and how non-health care purchases such as household furniture and music lessons contribute to mental health and a life in the community.
Finally, there is a need to educate the provider and professional communities. Initially, providers can be resistant to self-direction for fear of losing funding with the introduction of a more competitive environment and of being left to serve consumers with the most complex conditions.42 Provider resistance can easily stop self-direction in its tracks and, therefore, outreach to help providers understand the program and how they can continue to play a part is vital. Involving providers early on will prevent the program being derailed at a later stage. In District 8 in Florida, for example, state officials worked with providers to identify where existing resources could be found to support the creation of a SDC program. This ensured provider buy-in from the outset.
Initial outreach needs to be supported by longer term efforts to educate and inform providers and professionals about recovery and the capacity of consumers to collaborate in their own care. Effort is being directed towards the development of collaborative decision-making models that seek to boost consumers ability to participate on an equal footing in clinical discussions and decisions. For example, Professor Patricia Deegan is working in partnership with the Wyandot Mental Health Clinic in Kansas City and the University of Kansas School of Social Welfare to pilot a new software program called CommonGround that promotes shared decision-making. This and other decision-aides are an important part of changing provider mindsets, as is the introduction of more certified peer specialists into the traditional system. Embedding the concept of recovery into initial clinical training will also be a critical part of changing provider mindsets.
5. Budgeting
At present, most SDC programs offer consumers a flat budget, irrespective of their condition. This partly reflects the fact that the budget often supplements services from the traditional mental health system and is not expected to reflect the full set of needs that the mental health system is expected to meet. As these programs develop, it is important to move towards differentiated budgets that better reflect individual need. If programs select individuals that are further on in their recovery but the budget is based on average per person spending, it is easy for individuals to under-spend their budgets.43 The real test of the effectiveness of the program will come when budgets accurately reflect need.
At the same time, providers also need to be able to breakdown the costs of specific services so that consumers can make effective choices about value for money. This is difficult for services such as day treatment where different elements are bundled together. It is also challenging where services are commissioned under a block contract. However, experience in Michigan shows that these issues are not insurmountable. The Community Mental Health Administration in Kalamazoo County has been able to assign prices to services at an individual level even when they are commissioned through a bulk contract so that it is possible for each consumer to be shown the amount of money being spent on his or her service package. An individual consumers annual budget is included below for illustration.
| TABLE 4: Model Consumer Budget for Kalamazoo County Mental Health Services 2005 - 2006, Michigan | |
| Service | Yearly Cost ($) |
| Pathways Clubhouse | 3,416.88 |
| Psychiatric outpatient evaluation | 339.74 |
| Interact RN service | 248.88 |
| Pathways supported employment | 493.78 |
| Interact support employment | 1,887.00 |
| Rent subsidy -- transitional | 2,172.00 |
| Interact medication review | 135.00 |
| Hope Network -- case management | 272.67 |
| Interact case management | 2,999.37 |
| Interact RN service | 497.76 |
| Annual total | 12,463.08 |
Even within a relatively small budget, individuals can make choices that improve their satisfaction with the services they receive, improve their health and increase value for money. Therefore, an important step in the development of self-direction would be to show consumers how much is being spent on their care and how it is being spent within the traditional system. This is something that few consumers are aware of but is being developed in Michigan as part of its approach to self-direction. Consumers can request to see their budget, even if they choose not to go further and self-direct. So far, approximately 100 consumers have chosen to see their budget in Kalamazoo County.
6. Improving Administrative Systems
As self-direction develops, there is a need to reduce the administrative burden both for consumers and program administrators. Perhaps the biggest administrative burden in some existing programs stems from the use of checks for payment. This approach significantly adds to the administrative costs of running SDC and can act as a barrier to expansion because counties and districts that are not currently participating do not want to take on this burden. Many stores do not accept third party checks which causes problems for consumers and the use of checks can reduce the job of a counselor to that of a walking ATM, as recovery coaches in Florida have described themselves. They have complained about the miles they spend traveling from one consumer to the next simply to deliver the checks consumers have requested.
As these programs grow it will be vital to develop a more efficient financial management system. States that are currently relying on checks already have well developed networks of fiscal intermediaries that administer self-directed programs for other groups. There are significant efficiencies to be made in building on this existing infrastructure.
Further improvements could be made to the administrative process through the adoption of IT-based systems to manage interactions between the state, consumers and fiscal intermediaries. A system called the Consumer Direction Module has been developed by the Cash and Counseling program and is currently being used by Rhode Island and West Virginia, with New Mexico and Alabama looking to be actively using it by the end of 2007. It is popular with consumers and reduces the time required to approve and revise spending plans. Mental health administrations could leapfrog a phase of development by adopting these tools early on.
7. Quality Assurance
Quality assurance raises particular challenges in the context of self-direction for adults with SMI. As with self-direction for other disability groups, there is concern that individuals will make choices that are not supported by evidence and this will compromise their health and welfare. More specifically in the context of mental health, there is concern that, in times of crisis, individuals may not be able to make effective decisions and, therefore, self-direction may place them at additional risk.
There is no evidence from existing programs that self-direction leads to a deterioration in outcomes. On the contrary, satisfaction and outcomes appear to improve. Mental health consumers lack clinical knowledge but they are experts in their own personal, day-to-day experience of living with a condition, particularly a chronic condition such as SMI. There are very few medical situations where there is only one course of action. In most cases, there is a choice to be made and treatment decisions need to take into consideration the consumer experience in order to be effective. For example, a qualitative study of 29 patients diagnosed with psychiatric conditions conducted by Patricia Deegan at the University of Kansas found that all 29 used personal medicine alongside psychiatric medication. Personal medicine was either activities that gave meaning and purpose to life or specific self-care strategies. Patients reported discontinuing psychiatric drugs when they interfered with important personal medicine. Deegan found that few clinicians discussed personal medicine with clients, despite the fact that this would have improved the effectiveness of treatment.44
Furthermore, there is appetite among consumers for better access to evidence. In interviews, one of the complaints consumers made about the traditional system was that it did not provide them with information about their diagnosis and treatment. Rather than limiting the scope of self-direction to protect quality, effort needs to be directed towards educating consumers to make effective choices. This will be an important part of successful models of SDC.
At times of crisis, people do struggle with decision-making but this is not a permanent state and there are ways around it. As well as providing support for decision-making, the use of advance directives in which individuals describe how they want to be treated when they are not in a position to decide for themselves should be encouraged. Participants can also nominate a representative, such as a family member or friend, to make decisions on their behalf when they are unable to do so. This is common in self-direction for other disability groups.
8. Cross-Learning with Other Disability Groups
Self-direction is better established in other disability groups than it is for adults with SMI. Consumers in California have been able to hire personal care attendants since the 1950s and there are more than 370,000 people directing their own personal care attendants through Californias In-Home Supportive Services Program alone compared to a few hundred self-directing consumers across public mental health systems.45 Many of the initial problems that states are facing in implementing SDC in mental health have been faced by other disability groups and, therefore, more could be learned by looking across disabilities.
Conversely, other disability groups could learn from the development of peer supports and peer services in mental health as an important complement to self-direction. For example, programs seeking to transition elders or adults with developmental disabilities out of nursing homes and other institutional settings could learn from the experience of Clackamas County in Oregon where peer support has enabled adults with SMI to move into their own homes.
XI. CONCLUSIONS
SDC for adults with SMI is at a very early stage in its development. Initial findings are positive and indicate that self-direction could play an important part in creating a higher performing public mental health system that responds more effectively to consumer needs.
There are two aspects to SDC in mental health that appear to be critical to its success. The first is that self-direction shifts control over the different dimensions of service delivery -- the who, where, when and what -- to service users. Much attention in health care focuses on being able to choose who provides a service but this has its limits. Experience of mental illness is highly individualized and recovery is a very personal issue. Self-direction gives individuals the opportunity to choose between different types of treatment and develop packages of care that respond to their specific needs. For many people, a personalized package of care involves addressing wider aspects of health such as wellbeing, self esteem, employment and family life. The second critical feature of self-direction is that it provides consumers with support from the outset rather than leaving them to navigate the complex public system alone. In the rest of the health care system, individuals have to seek out their own sources of information and advice, whether that is their doctor, friends or family.
There is a clear need for more rigorous research before firm conclusions can be drawn about the effectiveness of self-direction. This will be greatly aided by the proposed randomized control trial of Texas SDC pilot.46 In the meantime, while giving consumers control of financial resources through an individual budget has attracted attention and controversy, the value of supporting consumers to articulate goals and develop plans to achieve them should not be overlooked as an extremely important component of SDC. States that are hesitant about implementing individual budgets can start to improve existing services by providing peer support to enable consumers to play a more active part in service planning and become more self-determined. In this way, states can begin to reshape mental health services around the needs and preferences of consumers.
NOTES
-
President's New Freedom Commission (2003). Achieving the Promise: Transforming Mental Health Care in America: Final Report.
-
The Presidents New Freedom Commission on Mental Health was established in April 2002. With a membership of 22 commissioners, the Commissions objective was to identify policies that could be implemented by federal, state and local governments to maximize the utility of existing resources, improve coordination of treatments and services, and promote successful community integration for adults with a serious mental illness and children with a serious emotional disturbance. The Commissions final report was published in May 2003.
-
President's New Freedom Commission (2003). Achieving the Promise: Transforming Mental Health Care in America: Final Report.
-
Albert O. Hirschman (1970). Exit, Voice, and Loyalty: Responses to Decline in Firms, Organizations, and States. Cambridge, MA: Harvard University Press.
-
Center for Self-Determination (2005). Crafting the Instruments of Freedom: Tools of Self-Determination.
-
It is worth noting that the definition of self-direction provided by the Centers for Medicare and Medicaid Services (CMS) includes a quality management strategy as a fourth component.
-
Judith Cook, Shawn Terrell and Jessica Jonikas (2004). Promoting Self-Determination for Individuals with Psychiatric Disabilities Through Self-Directed Services: A Look at Federal, State and Public Systems as Sources of Cash-outs and Other Fiscal Expansion Opportunities. Substance Abuse and Mental Health Services Administration (SAMHSA).
-
A support brokerage is an agency that arranges for the specific services a consumer and/or family needs. Support brokers work with consumers to define their needs and goals, provide them with information about resources and identify potential providers. Brokers then act as personal agents of the consumer, implementing choices made by the consumer.
-
RWJF. Self-Determination for People With Developmental Disabilities. http://www.rwjf.org/reports/nypreports/sdpdd.htm [Accessed July 17, 2007].
-
RWJF. Choosing Independence: An Overview of the Cash and Counseling Model of Self-Directed Personal Assistance Services.
-
More information about state programs that include elements of self-direction can be found in a forthcoming report on self-direction in mental health produced by the Bazelon Center for Mental Health Law with support from SAMHSA.
-
Self-direction in Michigan operates within the Medicaid system and does not use additional state general revenues. Therefore, consumers are able to purchase alternative services but the purchase of goods is strictly limited in order to comply with Medicaid regulations.
-
The provider in Iowa does not have the ability to put pressure on the state to redirect unused funds. Funds are set aside for self-direction and unspent money is used to bring additional participants into the program.
-
Steve Dowson (2004). Independence and the Support Sroker Role. NDT.
-
Interview with Bill Kale, Vice President, Wellcare Behavioural Health, May 2007.
-
Simon-Rusinowitz et al. (2000). Implementation issues for consumer-directed programs: Views from policy experts. Ethics, Law and Aging Review, 6, 107-130.
-
Florida Department of Children and Families, Mental Health Program Office (2007). Report on the Effectiveness of the Self-Directed Care Community Mental Health Treatment Program as Required by s.394.9084. F.S.
-
Gregory B. Teague and Timothy L. Boaz (2003). Evaluation of Adult Mental Health Self-Directed Care Project. Florida Department of Children and Families, Mental Health Program Office.
-
Judith Cook (2005). Patient Centered and Consumer Directed Mental Health Services. Prepared for the Institute of Medicine, Committee of Crossing the Quality Chasm -- Adaptation to Mental Health and Addictive Disorders.
-
CMS advises that the following process should be followed for service planning. States must assess individuals needs, strengths and preferences for services. Assessment information supports the development of the service plan and budget. The service planning process must be person-centered and directed and identify the individuals needs, preferences, choices and abilities and strategies to address those preferences, choices and abilities. Once the service plan is developed, a service budget is developed that accounts for how the funds in the budget will be used to purchase the services and supports that are identified in the service plan. The budget is also developed using a person-centered and directed process. Therefore, the service budget can and often does encompass services and supports that are linked to a need identified in the service plan and is not limited to only medical needs.
-
Joan Discher (2007). Presentation made at the National Home and Community-Based Waiver Conference, Albuquerque, NM, October 1, 2007.
-
Available at: http://www.cdc.gov/nchs/about/otheract/icd9/abticd9.htm.
-
Shen et al. (2007). Does Mental Illness Affect Consumer Direction of Community-Based Care? Lessons from the Arkansas Cash and Counseling Program. The Gerontologist, forthcoming.
-
Florida Department of Children and Families, Mental Health Program Office (2007). Report on the Effectiveness of the Self-Directed Care Community Mental Health Treatment Program as Required by s.392.9084. F.S.
-
Florida Department of Children and Families, Mental Health Program Office (2007). Report on the Effectiveness of the Self-Directed Care Community Mental Health Treatment Program as Required by s.394.9084. F.S.
-
Ami Sullivan (2006). Empowerment Initiatives Brokerage: Service Quality and Outcome Evaluation. Oregon Technical Assistance Corporation.
-
RWJF. (2006). Choosing Independence: An Overview of the Cash and Counseling Model of Self-Directed Personal Assistance Services.
-
Larry Fricks. Recovery and Systems Transformation for Schizophrenia. Unpublished.
-
Clackamas County reports the annual cost per person of a state mental hospital as $160,000. Although the absolute difference in costs between the state hospital and a group home is $100,000, health services and Social Security income are provided to individuals in group homes but these additional costs are included within the annual cost of the state hospital. Clackamas County estimates the annual cost of services covered under the Oregon Health Plan for individuals with serious mental illness as $13,500 per person and minimum annual Social Security income as $7,500 per person. Therefore, the real per person saving in transferring individuals from the state hospital into a group home can be no greater than $80,000 per year.
-
Smith et al. (2005). Using Medicaid to Support Working Age Adults with Serious Mental Illnesses in the Community: A Handbook. Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services. http://aspe.hhs.gov/daltcp/reports/handbook.htm.
-
Judith Cook, Shawn Terrell and Jessica Jonikas (2004). Promoting Self-Determination for Individuals with Psychiatric Disabilities Through Self-Directed Services: A Look at Federal, State and Public Systems as Sources of Cash-outs and Other Fiscal Expansion Opportunities. SAMHSA.
-
CMS is in the process of developing a state Medicaid Directors letter and a preprinted application for this state plan option. States interested in pursuing a 1915(i) should consult their CMS regional office representative.
-
Further information and guidance for states can be found at: http://www.cms.hhs.gov/SMDL/SMD/itemdetail.asp?filterType=none&filterByD....
-
Further information and guidance for states can be found at: http://www.cms.hhs.gov/SMDL/SMD/itemdetail.asp?filterType=none&filterByD....
-
A copy of the letter issued by CMS to state Medicaid Directors on August 17, 2007 regarding Medicaid reimbursement for peer support services can be found at: http://www.cms.hhs.gov/SMDL/downloads/SMD081507A.pdf.
-
Bruce Kamradt (2000). Wraparound Milwaukee: Aiding Youth With Mental Health Needs. Juvenile Justice Journal, 7(1), 14-23.
-
The National Coalition of Mental Health Consumer/Survivor Organizations was created in 2006, bringing together individuals who were previously identified as consumer, ex-patients and psychiatric survivors respectively.
-
Interview of Tom Nerney, Center for Self-Determination, December 2006.
-
Interview with Daniel Fisher, psychiatrist and Director, National Empowerment Center. In certain states where it operates, Magellan Behavioral Healthcare has already stopped offering day treatment to clients and is investing in a range of alternative psychiatric rehabilitation services.
-
Brenda Spillman, Kirsten Black and Barbara Ormond (2007). Beyond Cash and Counseling: The Second Generation of Individual Budget-based Community Long-Term Care Programs for the Elderly. Kaiser Family Foundation.
-
Views expressed by providers in Maryland during stakeholder consultations regarding the development of a self-directed care pilot in the state.
-
This is the approach used to calculate the individual budget in Florida.
-
Patricia E. Deegan and Robert E. Drake (2006). Shared decision making and medication management in the recovery process. Psychiatric Services, 57(11).
-
Center for Personal Assistance Services (2004). Californias In-Home Supportive Services Program: Who is Served? California Healthcare Foundation.
-
For further information on the proposed experimental evaluation of the Texas pilot of self-directed care, see http://www.cmhsrp.uic.edu/nrtc/sdc.asp.
APPENDIX 1: INTERVIEW PARTICIPANTS IN CASE STUDY STATES
Florida
| Letty Ballard | Transformation Coordinator Mental Health Program Office Department of Children and Families |
| Roxanne Campbell | SDC Contract Manager (District 4) Mental Health Resource Center, Inc. |
| Gene Costlow | Human Services Program Director, District 4 Drug Abuse and Mental Health Program |
| Mark Engelhardt | Associate in Technical Assistance Department of Mental Health Law and Policy Louis de la Parte Florida Mental Health Institute University of South Florida |
| Roderick Hall | Director for Mental Health Department of Children and Families |
| Patrick Hendry | Executive Director Florida Peer Network |
| Clint Rayner | Mental Health Advocate and Educator in Chief Office of Consumer and Family Affairs Department of Children and Families |
| Gregory Teague | Associate Professor Department of Mental Health Law and Policy Louis de la Parte Florida Mental Health Institute University of South Florida |
+ Florida self-directed care consumers.
Michigan
| Patrick Barrie | Deputy Director Mental Health and Substance Abuse AdministrationDepartment of Community Health |
| Kendra Binkley | Contracts Manager Department of Community Health |
| Jean Dukarski | Director Justice in Mental Health Organization |
| K. Cody Fitzpatrick | Kalamazoo County Community Mental Health and Substance Abuse Services |
| Irene Kazieczko | Director Bureau of Community Mental Health Services Department of Community Health |
| Tina Lauer | Peer Kalamazoo Self-Determination Program |
| Joe Mockbee | Peer Kalamazoo Self-Determination Program |
| Pamela Werner | Person-Centered Planning Specialist Department of Community Health |
| Kim Zimmerman | Consumer Empowerment Specialist |
+ Consumers with self-determined arrangements.
Oregon
| Rob Ingram | (former) Executive Director Empowerment Initiatives, Inc. |
| Dianne Duerscheidt | Executive Director Oregon Technical Assistance Corporation |
| R. Drake Ewbank | Board Chair Empowerment Initiatives, Inc. |
| Gina Hahn | Brokerage Administrative Specialist Empowerment Initiatives, Inc. |
| Michael Hlebechuk | Residential Supports Coordinator Office of Mental Health and Addiction Services Department of Human Services |
| Jessica Leitner | Behavioral Health and Developmental Disabilities Services Manager Clackamas County |
| Bob Nikkel | Assistant Administrator Office of Mental Health and Addiction Services Department of Human Services |
| Joan Rice | Multnomah County Behavioral Health Services |
| Amy Zulich | Program Manager and Resource Broker Empowerment Initiatives, Inc. |
+ Consumers of Empowerment Initiatives, Inc.
Iowa
| Joan Discher | General Manager Iowa and Nebraska Care Management Centers Magellan Health Services |
| Chris Simms | Manager, Program Innovation Magellan Health Services |
| Jennifer Tripp | Vice President Magellan Behavioral Healthcare |
Maryland
| Lissa Abrams | Director Office of Adult Services Mental Hygiene Administration |
| Paula Lafferty | Consumer Liaison, Mental Health Transformation Mental Hygiene Administration |
| Tom Merrick | Mental Health Transformation Mental Hygiene Administration |
| Ethel Nemcek | Director Office of Consumer Advocates |
NOTE: In-person or telephone meetings held in non-case study states.
APPENDIX 2: INTERVIEW PARTICIPANTS
| Judi Chamberlain | Director of Education and Training National Empowerment Center |
| Judith Cook | Director Mental Health Services Research Program University of Illinois, Chicago |
| Mark Covall | Executive Director National Association of Psychiatric Health Systems |
| Patricia Deegan | Co-Founder Institute for the Study of Human Resilience Boston University |
| Paolo Del Vecchio | Associate Director of Consumer Affairs Center for Mental Health Services Substance Abuse and Mental Health Services Administration |
| Robert Drake | Professor of Psychiatry, and Community and Family Medicine Dartmouth Medical School |
| Daniel Fisher | Executive Director National Empowerment Center |
| Michael Fitzpatrick | Executive Director National Alliance on Mental Illness |
| Larry Fricks | Co-Founder Appalachian Consulting (former) Director Office of Consumer Relations Georgia Department of Mental Health |
| Robert Gettings | (former) Executive Director National Association of State Directors of Developmental Disabilities Services |
| Robert Glover | Executive Director National Association of State Mental Health Program Directors |
| Bill Kale | Vice President WellCare Behavioral Health |
| Ron Manderscheid | Director of Mental Health and Substance Use Program Constella Group |
| Tom Nerney | Director and Co-Founder Center for Self-Determination |
| Terry Pratt | Deputy Director Disability and Elderly Health Programs Group Centers for Medicare and Medicaid Services* |
| Michael Schoenbaum | Senior Advisor for Mental Health Services, Epidemiology, and EconomicsNational Institute of Mental Health |
| David Shern | President and CEO Mental Health America |
| Gary Smith | Human Services Research Institute |
| Patricia Taylor | Executive Director Faces and Voices of Recovery |
| Jennifer Tripp | Vice President Magellan Behavioral Healthcare |
* Other staff in the Disability and Elderly Health Programs Group were also interviewed.
APPENDIX 3: STATE PROGRAM DESCRIPTIONS
Florida: Self-Directed Care
Florida currently has SDC programs in two Districts: District 4 which is the Jacksonville area and District 8 which is the Fort Myers area. In both cases, the program is funded by state general revenues and Medicaid where purchases are eligible, for example, clinical services. The total cost of SDC in both Districts is $930,000 per year. The programs vary to some degree and will be described separately.
District 4
The program in District 4 began in 2002 and is now managed by RBHS, one of the largest mental health providers in the state. There are currently 160 participants, 60% of whom are insured and 40% of whom are uninsured. Insured participants receive an annual budget of $1,672, with insurance picking up the remaining costs of care. The uninsured have an annual budget of $3,192 but must spend 48% of it on clinical services.
The program has five professionally qualified recovery coaches who work as sub-contractors. Providers of clinical, dental and optical services have to be part of the SDC provider network for purchases to be approved. This allows them to bill RBHS directly.
District 4 is in the process of integrating its community mental health services into managed care. The managed care organizations Healthease and Staywell, subsidiaries of Wellcare, have committed initially to maintain SDC as it currently operates and to enroll an additional 75 consumers.
District 8
The program in District 8 began in 2005. District 8 was chosen as an expansion site because its mental health services already had a strong recovery focus. In contrast to District 4 that received additional money to set up its program, District 8 was largely funded with existing money already in the system.
The program is run by the local NAMI and currently has 90 active consumers, 60% of whom are insured. Insured consumers receive $1,924 if they are Medicaid or VA eligible and $2,811 if they are Medicare eligible. The uninsured receive $3,700 but, again, must spend 48% of it on clinical services. Life coaches are qualified peers and are employed directly by NAMI and there is no approved provider network for clinical, optical and dental care as in District 4. In expanding the program to District 8, program managers felt that this imposed an unnecessary constraint on consumer choice.
Iowa: Self-Directed Care
The pilot program in Iowa is run under Magellan Behavioral Healthcares Medicaid managed care contract. Program planning began in February 2006 and the first participant entered the program in May 2006. The program aims to serve 25 consumers who are already receiving intensive psychiatric rehabilitation services through one particular provider. Each consumer has to identify one rehabilitation goal relating to housing, education, employment or relationships and can use a budget of $2,000 to work towards that goal.
Under Magellans managed care contract with the State of Iowa, Magellan is required to set aside 2.5% of its capitation fee as a community reinvestment fund. The purpose of the fund is to support innovation and the development of best practice. The fund is being used to support the pilot and pay for the individual budgets.
Maryland: Self-Directed Care
In March 2005, the Mental Hygiene Administration and the Department of Disabilities convened a task force to investigate self-direction approaches. One of the task forces recommendations was a self-direction pilot that began in February 2007. The pilot and its individual budgets are supported with state general funds. Additional costs for training, program evaluation and other related technical assistance are funded by the states SAMHSA Mental Health Transformation State Incentive Grant.
The initial pilot in Washington County aims to have 30 consumers with a self-directed budget by June 2008. As of July 11, 2007, the program had nine active consumers. The pilot is managed by a consumer-run organization, the Office of Consumer Advocates, although the financial transactions are managed by the local Core Services Agency, an arm of county government. The Core Services Agency operates as a local mental health authority that does not provide services. One full-time and two part-time peer advocates (two FTE) have been hired by the Office of Consumer Advocates to support consumers with self-direction.
The program is budgeted at a level that each consumer could, on average, manage a budget of approximately $3,000 but there is no cap on the amount allotted to each individual. Instead, budgets vary from consumer to consumer based on the services that the consumer identifies as necessary to support his or her ongoing progress in recovery. The program places a high value on finding community resources within natural support networks wherever possible. Once the services that need to be purchased to support a consumers recovery have been identified, an application for resources is made by the Office of Consumer Advocates to the Core Services Agency.
Michigan: Self-Determination
Policy guidance issued by Michigan Department of Community Health in 2003 states that each Community Mental Health Services Program shall develop and make available a set of methods that provide opportunities for the consumer to direct their specialty mental health services and support arrangements.
The development of self-determination has been stimulated by the award of state grants to Kalamazoo and Oakland Counties in 2005 to develop individual budget arrangements for consumers who choose self-determination. Consumers who opt for self-determination are presented with a cost breakdown of the services they receive and can choose to use all or part of that money to purchase alternative goods and services. Under the medical necessity criteria in Michigans 1915b/c waiver, there is adequate flexibility to support self-determination within Medicaid.
Self-determination is managed by county mental health service providers but peers are employed to support consumers through the process. There are currently eleven individuals in Kalamazoo County with an individual budget and one in Oakland County, with a further seven who are in the process of developing a budget.
Oregon: Empowerment Initiatives (EI) Brokerage
EI Brokerage was initiated under a CMS Real Choice Systems Grant that was awarded in 2001. The grant ended in September 2005 but EI continues to work under contract with Multnomah and Clackamas Counties. EI is a consumer-run organization and has three peers who are employed as resource brokers. It provides a one year program that uses person-centered planning and an individual budget of $3,000 to kick start the recovery process. Its total annual cost is $10,000 per consumer served.
In Clackamas County, EI has a specific focus of supporting individuals in group homes to move into independent living facilities. When approached by the state to build more group homes, Clackamas County proposed to work with EI instead. The objective is to free up spaces in group homes that can then be used for people moving out of the state hospital. Since June 2006, EI has successfully supported 14 people to transition to independent living. The housing brokerage is state funded but overseen by Clackamas County.
The brokerage in Multnomah County is more similar to SDC programs in other states. It is funded by a mixture of Medicaid dollars and state general revenue. It aims to support individuals to progress in their mental health recovery. EI currently serves 25 consumers in Multnomah County.
Texas
The details of the Texas pilot are currently unavailable as the pilot is still in development.
APPENDIX 4: REQUESTS FOR REIMBURSEMENT MADE BY PARTICIPANTS IN FLORIDAS SELF-DIRECTED CARE PROGRAM IN DISTRICT 8 BETWEEN JULY 2005 AND MARCH 2007
| Category | No. Requests for Reimbursement |
| Medicine | 206 |
| Psychiatrist | 147 |
| Transportation | 105 |
| Counseling | 96 |
| Dental services | 83 |
| Clothing | 63 |
| Rent | 63 |
| Health club | 42 |
| Vision services | 40 |
| Car repair | 38 |
| Internet | 30 |
| School | 27 |
| Art and craft supplies | 24 |
| Food | 23 |
| Car insurance | 18 |
| Utilities | 15 |
| Social club | 15 |
| Computer supply | 14 |
| Computer | 13 |
| Haircut | 12 |
| Software | 11 |
| Telephone | 9 |
| Furniture | 9 |
| Psychosocial rehabilitation | 9 |
| Books | 6 |
| Bedding | 5 |
| Music lessons | 5 |
| Bicycle | 5 |
| Medicare premium | 5 |
| Printer ink | 5 |
| Smoking cessation | 5 |
| Hearing aids | 4 |
| Occupational license | 4 |
| Magazine subscription | 4 |
| Camera supplies | 4 |
| Writers club | 3 |
| CDs | 3 |
| Massage therapy | 3 |
| Personal hygiene | 2 |
| Moving expense | 2 |
| Vitamins | 2 |
| Bicycle accessories | 2 |
| Musical instruments | 2 |
| Language learning | 2 |
| Copier | 2 |
| Household supplies | 2 |
| Stamps | 2 |
| Car registration | 2 |
| NAMI convention | 2 |
| Home insurance | 2 |
| Typewriter | 1 |
| Supportive employment | 1 |
| Weight loss program | 1 |
| Security box | 1 |
| Tai Chi classes | 1 |
| Dog training | 1 |
| AARP membership | 1 |
| Aquarium | 1 |
| Sound studio time | 1 |
| Drivers license | 1 |
| Computer repair | 1 |
| NAMI membership | 1 |
| Fishing equipment | 1 |
| Weighing scales | 1 |
| Cosmetics | 1 |
| Nutritionist | 1 |
| Sewing machine | 1 |
| Pet fee | 1 |
| Self-help materials | 1 |
| Exercise equipment | 1 |