
Penny Feldman, Ph.D., Miriam Ryvicker, Ph.D., Robert Rosati, Ph.D., Theresa Schwartz, B.A., and Gil Maduro, Ph.D.
Visiting Nurse Service of New York
Center for Home Care Policy and Research
This report was prepared under contract #HHSP23320044304EC between the U.S. Department of Health and the Center for Home Care Policy and Research. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the ASPE Project Officer, Marie Squillace, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. Her e-mail address is: Marie.Squillace@hhs.gov.
The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
BACKGROUND AND PURPOSE
In the United States, over 600,000 home health aides (HHAs) provide supportive services and personal assistance to patients receiving home health care.1 Although aide services are essential to the health and well being of patients who receive them, the nurses and therapists who comprise the professional home care workforce all too often treat HHAs as “unskilled” workers with little potential to enhance the overall effectiveness of patient care. The devaluing of aide services has, in turn, been cited as a contributor to aide dissatisfaction, aide turnover and less than optimal patient outcomes. Recent years have seen a growing interest in strategies to develop the capacity of the aide workforce and better integrate these paraprofessionals into care delivery. The Visiting Nurse Service of New York (VNSNY) launched such an initiative in 2003.
The VNSNY Home Health Aide (HHA) Partnering Collaborative was designed to better integrate professional and paraprofessional services and employ established principles of quality improvement to achieve two main goals: (1) improving the quality of work life of home care paraprofessionals, and (2) increasing nurses’ and aides’ support for patients’ improvement in key activities of daily living. The Collaborative also aimed to facilitate change in the culture of health services, moving away from a purely professional model and toward self-care management. In the traditional, professional model of health services, patients, family members, and paraprofessionals have limited roles in decision-making about important aspects of a patient’s care. Typically, patients are seen as care “recipients,” and aides as “unskilled” workers who “do for” the patient. The self-care management model is centered on patients and informal caregivers as active participants in decision-making and goal-setting, with HHAs playing a key supportive role.
VNSNY is the largest not-for-profit home care agency in the United States serving an average of 25,500 patients daily throughout New York City, Nassau and Westchester County. Like other home care agencies VNSNY has struggled to integrate aide services into its service delivery teams of nurses, therapists and social workers, who provide frontline care under the leadership of their respective teams’ patient service manager (PSM). The complex structure of home health services -- with a widely dispersed patient population, a widely distributed workforce and heavy reliance on contracted aides -- poses several challenges to integration. First, except for the bi-weekly face-to-face supervision required by Medicare and Medicaid, nurses’ visits often cannot be scheduled to coincide with the aide’s assigned schedule. Second, it is not generally feasible for aides to leave their patients to attend team meetings scheduled at a more central location. Third, most aides report to both an aide coordinator or manager and to a nurse or therapist who is responsible for the patient’s overall care plan. Mixed messages and a lack of coordination between clinical and aide services create barriers to providing high quality care and achieving high levels of satisfaction among nurses, aides, and patients.
In light of this complexity, the Collaborative intervention included four main strategies to address both workforce issues and the need for increasing support for patients’ self-management (see the attached Implementation Manual at http://aspe.hhs.gov/daltcp/reports/2007/HHAPartmnl.htm for more detail on the improvement strategies and the Collaborative model):
-
Implementation of the "Five Promises" -- a set of field supervision practices designed to promote positive and effective communication among all caregivers while in the patient's home.
-
Use of an "Activities of Daily Living (ADL) Tool" -- a functional health improvement tool used to structure common goal-setting among nurses, patients, and aides.
-
Proactive communication between PSMs and Licensed Agency coordinators -- a recommended weekly phone call or fax to cover aide supervision and service delivery issues.
-
Increase in field support and supervision provided to aides, with required documentation.
These strategies emerged from a 12-month learning Collaborative process modeled after the learning Collaboratives developed and widely disseminated by the Institute for Healthcare Improvement (IHI) to promote sustainable change across the health care industry (IHI, 2003). This model has become increasingly prominent across health care settings as a way of jumpstarting improvement, testing new strategies, and adapting them to continuously achieve better results.
After an initial pilot period, the Collaborative’s tools and strategies were tested through a randomized trial conducted between April and September 2005. At the beginning of this period, a total of 45 VNSNY acute and congregate care service teams throughout the Bronx, Brooklyn, Manhattan, and Queens were randomly assigned to control and intervention groups. Following the randomized trial, the strategies were spread to the original control teams between February and July 2006, completing the agency-wide implementation of the Collaborative.
EVALUATION
The project staff at the Center for Home Care Policy and Research conducted a two-phase evaluation, examining the impact of both the randomized trial and the subsequent agency-wide spread on a range of measures, including: (1) HHA job perceptions and retention; (2) case-mix adjusted patient outcomes and discharge dispositions; and (3) patient service use. The evaluation also aimed to identify the successes and challenges of the Collaborative implementation. The two-phase structure of the evaluation allowed us to address the short-term impact of the Collaborative, as well as issues related to the sustainability and effectiveness of the intervention when spread agency-wide.
Several data sources were used in the evaluation, including: (1) a HHA Job Perceptions Survey; (2) human resource and administrative data; and (3) the Outcomes Assessment and Information Set (OASIS), which is a nationally used, standardized patient assessment instrument collected at the start-of-care, at discharge, and every 60 days, whichever is sooner. We also collected qualitative data on the implementation process, including interviews with field managers and observation of team meetings and training sessions.
RESULTS2
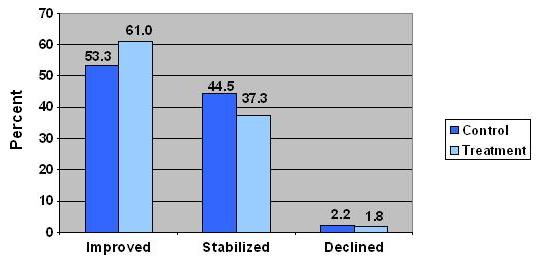
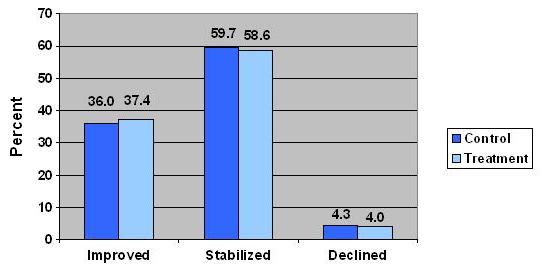
Short-Term Impact: Randomized Trial. The major impact of the Collaborative was on patients’ functional outcomes. During the randomized trial, patients in the intervention group had significantly better case-mix adjusted outcomes on two of three targeted areas of daily living -- transferring and ambulation -- than patients in the control group. In transferring (Figure 1), 61% of patients in the intervention group showed improvement from the start-of-care to discharge, compared to only 53% in the control group.3 Thus, approximately 14% more patients improved in the intervention group than in the control group. Although the differences were smaller in ambulation (Figure 2), they were still statistically significant, with 37% showing improvement in the intervention group, compared to 36% of the control group. The larger impact in transferring is consistent with national data indicating that it is more difficult to generate improvement in ambulation than in transferring.4
The improvements in patients’ functional outcomes were achieved without any major change in service use. Thus, increased focus on communication and common goal-setting yielded better outcomes without the need for more visits. Nevertheless, functional improvements were not associated with a significant reduction in length of stay, nor were they associated with greater likelihood of discharge to the community. Across both treatment and control groups, length of stay was approximately 55 days, while approximately 89% of patients were discharged to the community.
At both baseline and follow-up, aides who responded to short job perceptions surveys reported that they were generally treated as an important member of the team, received necessary help from nurses and therapists to do their job and had their opinions about patients “heard and appreciated.” They reported that they often discussed patients’ progress in walking, bathing and getting out of bed -- both with nurses and therapists and with patients themselves. There were no significant differences between aides working with Collaborative teams and aides in the control group, perhaps because aide respondents might in general have been more satisfied with these aspects of their job than non-respondents, who had shorter job tenure at the agency and worked fewer hours.
Job retention was relatively high across the board. Approximately 72% of aides employed during each phase of the evaluation were still actively employed and serving at least one VNSNY patient seven months after the start of the intervention (or spread period). Of all the factors analyzed, aide work hours proved to be the most powerful predictor of job retention; the more hours an aide worked per week, the more likely she or he was to remain in the workforce. Association with a Collaborative team did not increase an aide’s likelihood of being in the VNSNY aide workforce seven months after the start of the Collaborative.
Long-Term Sustainability: Agency-Wide Spread. Follow-up analyses during the agency-wide spread showed that the original intervention group sustained the improvement in patient ADL outcomes ten months after the randomized trial. This suggests that the Collaborative tools and strategies generated changes in frontline practice that were maintained over the long-term. However, the original control group did not show significant improvement after joining the intervention during the agency-wide spread. The spread also did not show an impact on the other patient outcomes examined (discharge disposition and length of stay), service use measures, aide job perceptions, or aide retention. It is possible that the original control group did not show significant improvement because it was difficult to maintain a certain level of intensity in peer-to-peer communication -- which was a major driver of the Collaborative -- as the initiative expanded (discussed further below).
IMPLEMENTATION: SUCCESSES AND CHALLENGES
Collaborative Tools and Strategies. Interviews with managers and observation of team meetings suggested that some of the Collaborative strategies spread more easily than others. Both professional and paraprofessional staff widely embraced the Five Promises. Licensed Agency personnel credited the Five Promises for improvement in nurse-aide relationships, reporting that aides felt more appreciated on the job and more comfortable communicating directly with nurses.
The proactive communication strategies between PSMs and Licensed Agency Coordinators also spread with relative success. Managers reported that, despite the time commitment required, the conference calls and in-person meetings helped to solve problems more efficiently by strengthening the partnering relationship. The new strategies also set the context for innovation. In particular, one team developed a protocol for the coordinator to send the PSM a daily log of aide-patient assignments, aide schedules, and service issues. Additional teams adopted the new protocol, reporting to the Collaborative faculty that it was a useful tool for preventing miscommunications about aide services.
Spreading the ADL Tool proved more challenging. Although anecdotal evidence suggested that aides were in favor of the tool because it helped them make better use of their skills, clinicians were less open to using it. Some PSMs were not persuaded of the immediate value of the tool and resisted extra work for their field nurses. Others who were more enthusiastic about the tool nevertheless struggled to gain buy-in from the field nurses, who actually would be responsible for initiating its use. During the agency-wide spread, the Collaborative faculty implemented a revised version of the tool, which was designed to be more patient-centered and user-friendly. The faculty continued to meet resistance, however, and decided to pursue a broader initiative to improve both clinician and patient readiness for a self-management approach to care.
That patient outcomes improved even while the Collaborative struggled to spread the ADL Tool suggests that it was not the tool itself that led to better outcomes. Rather, the results may have stemmed from the overall emphasis on functional improvement and on collaboration among the clinician, aide, and patient to motivate and enable patients to achieve concrete improvements.
Moving From “Experiment” to Agency-Wide Spread. Throughout each phase, the Collaborative emphasized peer-to-peer communication as the main driver of the spread. In designing the spread process, the Collaborative faculty recruited frontline staff to be champions of the Collaborative tools and strategies, rather than relying on traditional educational approaches. Discussions with members of the Collaborative faculty suggested that this spread method was more effective during the “early adopter” phase and randomized trial than it was during the agency-wide spread. As the Collaborative grew larger, the messages communicated from peer-to-peer became more “diluted.” This may help to explain why the final spread period did not result in new improvements in patient or aide outcomes.
CONCLUSIONS
The most significant results of the Collaborative were improvements in patients’ ability to perform the basic function of transferring with no additional visit intensity. This outcome may have important implications for patient well being. The lack of impact on HHAs’ job perceptions or retention, however, was a shortcoming of the initiative. These findings suggest four key lessons that should be considered in future efforts to adapt the Collaborative’s tools and strategies.
First, in order to generate improvement in aides’ perceptions of the job and quality of work life, future efforts need to involve aides more directly throughout the improvement process. Although aides were involved in the Collaborative during its pilot period, sustaining aides’ participation in subsequent phases of dissemination proved more challenging. Aides’ work schedules and geographic dispersion make it difficult for aides to attend in-person meetings, where participants provide feedback on their perceptions of the new strategies and share their experiences with implementing and adapting them. Future efforts at replicating and adapting the Collaborative intervention need to address the challenges of involving aides as full participants in the process.
Second, the fact that work hours were the strongest predictor of aide job retention may highlight the need to address structural issues that currently prevent aides from obtaining a full workload. For example, organizations may choose to focus on the scheduling of aide services to minimize travel issues that may make it difficult for aides to take on multiple cases.
Third, although the intervention had a positive and statistically significant effect on both patient transferring and ambulation, only the transferring outcome was substantially improved, while the increased improvement in ambulation was modest. In order to enhance the impact of an evidence-based strategy (such as the ADL Tool) on patient function, the strategy needs to be streamlined into usual practice. Clinicians’ perceptions of the ADL Tool as redundant and time-consuming underscore the importance of allowing for adaptation to achieve better results. Perhaps more important, organizations need to move beyond implementing a specific tool to address larger cultural issues and attitudes about self-care management. Both nurses’ and patients’ expectations of patients’ involvement in their care can pose barriers to improvement. Improving patients’ functional self-management therefore calls for widespread support throughout an organization in promoting a self-management model of care.
Finally, the two-phase evaluation design allowed us to assess the intervention’s sustainability at a ten-month follow-up point. Although we saw sustained improvement in patient outcomes in the original intervention group, it was difficult to achieve these results in the larger spread throughout the rest of the agency. These findings highlight the challenges of spreading and sustaining improvement throughout a large organization. It is therefore critical that leaders not only identify and implement appropriate improvement strategies, but also address the challenge of how to communicate the change message most effectively within the contexts of their organizations.
| FIGURE 1. Patient Outcomes: Transferring (Randomized Trial) |
 |
| FIGURE 2. Patient Outcomes: Ambulation (Randomized Trial) |
 |
-
Occupational Employment, Training, and Earnings Data: Occupation Search. U.S. Department of Labor, Bureau of Labor Statistics. October 4, 2006. http://data.bls.gov. Retrieved July 10, 2007.
-
The methods and results of the evaluation are reported in detail in the Final Report.
-
Stabilization is defined here as having no change from admission to discharge.
-
Granger, Carl V., M.D. (2005). "Quality and Outcome Measures for Rehabilitation Programs." http://www.emedicine.com/pmr/topic155.htm#target9.