
U.S. Department of Health and Human Services
The Supply and Demand of Professional Social Workers Providing Long-Term Care Services: Report to Congress
U.S. Department of Health and Human ServicesOffice of the Assistant Secretary for Planning and Evaluation
March 2006
This report was prepared by the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP), in collaboration with other federal agencies. For additional information about the study, you may visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the ASPE Project Officer, Linda Bergofsky, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, SW, Washington, DC 20201. Her e-mail address is: Linda.Bergofsky@hhs.gov.
This report was prepared by staff from the Department of Health and Human Services' Office of the Assistant Secretary for Planning and Evaluation in consultation with the Centers for Medicare and Medicaid Services, the Administration on Aging, the Department of Veterans Affairs, the Health Resource and Services Administration, and the Department of Labor's Bureau of Labor Statistics.
TABLE OF CONTENTS
- I. INTRODUCTION
- VI. SOURCES OF DATA USED IN DERIVING CURRENT AND FUTURE ESTIMATES
- A. National Industry-Occupation Employment Matrix
- B. Current Population Survey
- C. 1% Public Use Microdata Sample of the 2000 Census
- D. NASW and CSWE
- IX. FACTORS INFLUENCING DEMAND AND SUPPLY OF SOCIAL WORKERS IN LONG-TERM CARE
- A. Job Substitution
- B. Social Worker Training
- C. Wages and Benefits
- D. Changes in the Long-Term Care Environment
- APPENDIX 1. EFFORTS TO INCREASE THE SUPPLY OF PROFESSIONAL SOCIAL WORKERS SERVING OLDER ADULTS
- A. Private Sector Sponsored Activities
- B. Public Sector Sponsored Activities
- APPENDIX 2. PARTICIPANTS IN STAKEHOLDER DISCUSSIONS
- LIST OF FIGURES
- FIGURE 1: Middle Series Projections of US Population age 65 and over, 2005 to 2050
- FIGURE 2: Estimates of Professional Social Workers, All Settings
- FIGURE 3: Estimates of Professional Social Workers in Long-Term Care
- FIGURE 4: Comparative Projections of Social Workers in Long-Term Care
I. INTRODUCTION
In fiscal year 2004, the Senate Labor, Health and Human Services, and Education Appropriations Bill requested that the Department of Health and Human Services (HHS) assess the availability of professional social workers in long-term care settings. Specifically, the Bill directed HHS "to study and quantify the current and future supply and demand for professional social workers serving older adults across the continuum of long-term care services. The Department should report these findings to the Committee and furnish recommendations for addressing any identified future shortage areas, including cooperative strategies involving federal agencies, professional associations, and schools of social work."
This report is a product of work between the Office of the Assistant Secretary for Planning and Evaluation in HHS, other federal agencies in HHS, and the Departments of Labor and Veterans Affairs (VA). Staff at these Departments assisted this effort by sharing information and data on social workers in long-term care settings and reviewing sections of the Report to Congress.
II. OVERVIEW OF DEMOGRAPHIC TRENDS
The aging of the birth cohorts born between 1945 and 1965 (the "baby boom" cohorts) will be the most significant factor increasing the demand for long-term care and supportive services over the next half century. As shown in Figure 1, the number of individuals who are age 65 and older is expected to more than double, increasing from 35 million in 2000 to over 86 million in 2050.1 As a result, nearly 21% of the population will be age 65 and over by the middle of the century.
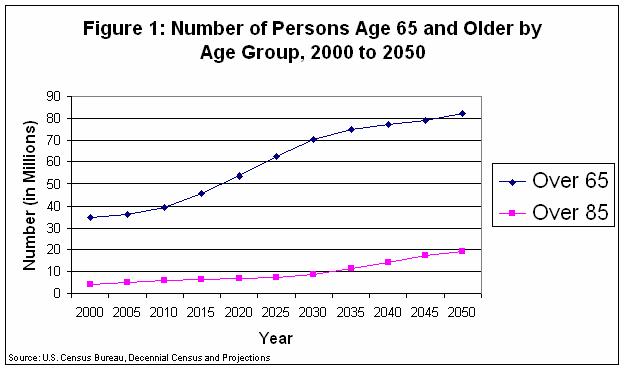
While not all elderly persons will require long-term care services, age is a very strong predictor of the need for both acute health and long-term care services, and the number of persons aged 85 and over is projected to increase five-fold by 2050. If recent trends continue, experts predict that the number of persons requiring long-term care services (i.e., skilled nursing care, alternative residential care, or home and community-based care) could increase from approximately 8 million to 19 million in 2050.2, 3 This will no doubt increase demand for long-term care workers, in general, and for professional social workers specifically, because they provide critical services such as care coordination, case management, mental health services and supports, government program eligibility determination, care giving support and counseling.
III. DEFINITION OF A PROFESSIONAL SOCIAL WORKER
As noted earlier, the Senate Labor, HHS and Education Appropriations Bill requested that HHS assess the availability of professional social workers in long-term care settings. This report presents our estimates of the current and future number of professional social workers in long-term care settings, using a definition of professional social worker from the National Association of Social Workers (NASW)4 and the Council on Social Work Education (CSWE). Specifically, NASW and CSWE define a professional social worker as one who has graduated from a CSWE accredited program with at least a bachelor's degree in social work.a
Bachelors of Social Work (BSW) programs prepare graduates for direct service positions such as case workers. Programs include courses in social work values and ethics, dealing with a culturally diverse clientele, at-risk populations, promotion of social and economic justice, human behavior and the social environment, social welfare policy and services, social work practice, social research methods, and field education. Accredited BSW programs require a minimum of 400 hours of supervised field experience.4
Masters degree programs in Social Work (MSW) prepare graduates for work in their chosen field of concentration, including health and aging, and continue to develop the skills required to perform clinical assessments, manage large caseloads, and explore new ways of drawing upon social services to meet the needs of clients. MSW programs last two years if pursued on a full-time basis and include a minimum of 900 hours of supervised field instruction, or internship. Entry into a master's program does not require a bachelor's degree in social work, but most master's degree programs offer advanced standing (allowing for acceleration of the master's program) for those with a bachelor's degree from an accredited social work program.5
IV. DEFINITION OF LONG-TERM CARE
Long-term care is generally defined as the array of medical, social, personal care and related services designed to meet the needs of people living with chronic health problems that limit their ability to perform everyday activities. The need for long-term care services is frequently determined by one's need for assistance with activities of daily living (ADLs) and/or instrumental activities of daily living (IADLs). ADLs refer to the basic self-care tasks of everyday life, such as eating, bathing, dressing, toileting, and transferring.6 IADLs refer to more complex tasks associated with independent life such as shopping, housekeeping, doing the laundry and money management. Long-term care may also be defined in terms of the settings associated with care delivery--institutional, residential, community or home--although what specific services or entities are included in each category may vary widely. For the purposes of this report, long-term care settings are comprised of nursing facilities, other residential care (e.g., assisted living, group or congregate living facilities), home health and selected community-based settings (e.g., adult day health and multi-purpose senior centers as specified in the North American Industry Classification System or NAICS).b
V. PROFESSIONAL SOCIAL WORKERS AND THEIR ROLES IN LONG-TERM CARE SETTINGS
Social workers who have completed specific course work and field work in aging (typically at the master's level) represents one of the fastest growing segments of the profession.7 These workers address a broad array of problems uniquely facing elders and their families, including functional impairment, psychological problems or cognitive impairments, grief and loss, legal and ethical issues, and end of life concerns.7
Social workers with a bachelor's degree in social work tend to be employed in long-term care settings at a higher rate than those with an MSW. A 1995 survey of social work practitioners revealed that 1% of respondents with an MSW were employed in nursing homes or hospices and that 3.7% identified services to the aged as their primary practice area.8 In contrast, respondents with a BSW indicated that 11.5% worked in a nursing facility or hospice setting and 16.5% identified services to the aged as their primary practice area.8 Although there is no clear explanation for this differentiation in the literature, it is most likely related to the complex interplay of financing and reimbursement of social work services in general and/or the lack of a statutory distinction between BSW and MSW in fulfilling Medicare and Medicaid Conditions of Participation. In general, MSW-level social workers are specifically trained to provide counseling for complex problems, complete assessments, improve organizational functioning and perform other complex tasks that social workers with a BSW are not trained to do.
Social worker responsibilities vary widely, depending upon the setting, and their role(s) in that setting. Social workers seek to help people across the life span function better in their environments, identify and cope with problems and improve relationships with others.5, 7 Social workers may be distinguished from other "helping professionals," including nurses and psychologists, through their knowledge of community resources, their focus on client strengths (rather than pathology), skills in engaging the client and use of the person-in-environment (P-I-E) frameworkc for assessing and addressing psychosocial, psychological and social problems,9 and their pursuit of social change on behalf of vulnerable populations, such as long-term care residents.
According to standards promulgated by NASW in 2003,10 social workers in long-term care settings should focus on several key areas, including:
- the social and emotional impact of physical or mental illness or disability,
- the preservation and enhancement of physical and social functioning,
- the promotion of the conditions essential to ensure maximum benefits from long-term health care services,
- the prevention of physical and mental illness and increased disability, and
- the promotion and maintenance of physical and mental health and an optimal quality of life.
When bachelors and masters-level social workers are employed in the same long-term care setting, it has been reported that BSWs and MSWs typically have different, yet complementary responsibilities. Barth's 2001 study of BSW and MSW employment markets indicates that these workers rarely compete with one another for jobs.11 For example, a social worker with a BSW in a nursing home might serve as a discharge planner for short-stay residents in a post-acute unit, while a social worker with a MSW might provide clinical supervision of the BSW as well as counseling and other behavioral interventions to long-stay residents and their families.
VI. SOURCES OF DATA USED IN DERIVING CURRENT AND FUTURE ESTIMATES
There are several data sources that are useful for estimating the current and future demand for social workers in long-term care settings:
A. National Industry-Occupation Employment Matrix
The National Industry-Occupational Employment Matrix (OEM) is developed by the Bureau of Labor Statistics (BLS) within the Department of Labor as part of its ongoing Occupational Employment Projections Program. The purpose of the OEM is to determine current and future employment by occupation and industry. The most recent OEM contains employment projections for 725 occupations (including social work) in 284 industries (including long-term care settings such as home health agencies, nursing care facilities, residential care facilities, and community care for the elderly) for 2002 and 2012.
B. Current Population Survey
The CPS is a monthly survey of about 60,000 households conducted by the Bureau of the Census for BLS. The CPS is the primary source of information on the labor force characteristics of the U.S., including estimates of employment/unemployment released every month by BLS. The sample is selected to represent the civilian non-institutionalized population age 16 and older, and respondents are asked detailed socioeconomic questions such as employment status, occupation, industry, earnings, hours of work, and other demographic variables such as education. As a result, the CPS can be used to identify respondents that report that their occupation is social work and who are employed in long-term care settings.
C. 1% Public Use Microdata Sample of the 2000 Census
The number of social workers in the U.S. can be estimated from the 1% Public Use Microdata Sample (PUMS) of the 2000 Census. The 2000 1% PUMS data contain records of the characteristics of people from a 1% sample of individuals and housing units from the 2000 Census. The data source for the PUMS files is the 2000 decennial census long-form questionnaire, which includes information on demographic, economic, and housing characteristics of the population. Variables such as occupation, industry (setting), and education are available and can be used to determine if a respondent is a social worker in a long-term care setting.
D. NASW and CSWE Data
Through funding provided by the Center for Substance Abuse Treatment of the Substance Abuse and Mental Health Services Administration, NASW created the Practice Research Network (PRN) in 2000. The PRN collects data from social work practitioners, and uses the data to develop best practices, inform policy, and improve service delivery. NASW has designed and conducted three practice-based research surveys (2000, 2002, and 2004) through the PRN. The surveys collect information on social workers' socioeconomic characteristics such as salary and education, clientele, and practice setting. CSWE collects data annually on the numbers of individuals enrolled in accredited social work programs as well as the number of, and enrollment in, programs that offer an aging specialization (or aging-related field placements).
VII. CURRENT ESTIMATES OF PROFESSIONAL SOCIAL WORKERS IN LONG-TERM CARE SETTINGS
The current BLS estimates and projections of social work employment do not include detail on level of education. However, in describing the education and training needed by most social workers to become fully qualified, BLS notes that, "While a bachelor's degree is the minimum requirement, a master's degree in social work or a related field has become the standard for many positions."12 For the purposes of this report, it was assumed that all BLS employment data on social workers refers to professional social workers. The total number of professional social workers in long-term care settings can therefore be estimated by summing the number of social workers across long-term care industries.
The CPS and the Census 1% PUMS data also do not identify social workers at the level of specificity corresponding to the Congressional request. However, a reasonable estimate of the number of professional social workers in long-term care settings can be constructed by identifying survey respondents who: (1) report their occupations as "social worker," (2) state that they have at least a bachelor's degree (although not necessarily a BSW), and (3) are employed in an industry associated with long-term care (i.e., a home health agency, nursing care facility, residential care facility, or community care for the elderly).
Estimates of the number of professional social workers from the 2002 BLS OEM, the 2004 CPS and the 2000 1% PUMS are presented in Figure 2. The numbers range from a low of 471,075 (2000 1% PUMS) to a high of 522,280 (2004 CPS), with the estimate from the 2002 OEM closer to the low end of the range. Focusing on professional social workers in long-term care settings yields a similarly narrow range of estimates--36,071 to 44,156 (Figure 3). The numbers likely vary due to differences in survey coverage, sampling variations, and differences in how a social worker is defined across the three data sources.


Although there is some variation, these estimates are fairly consistent with other sources. For example, the data presented here indicate that approximately 7.6% to 9.4% of all professional social workers are employed in long-term care settings. Data from a 1999 survey of 19 graduate programs found that just over 6% of graduates worked in the field of aging/gerontology (which includes a range of settings).13 A survey of NASW regular members completed during Summer 2000 found that 5% of respondents identified aging as their primary specialty area and the 2004 NASW PRN survey of licensed professional social workers (NASW members as well as non-members) indicated that 5% of respondents worked in a nursing facility, home health agency or hospice, with 7.8% identifying aging as their primary specialty.14, 15
VIII. PROJECTIONS OF THE NUMBER OF PROFESSIONAL SOCIAL WORKERS IN LONG-TERM CARE
Based on anticipated increases in demand for services and retirements of current practitioners, BLS predicts that total social work employment will increase from approximately 477,000 in 2002 to 604,000 by 2012.16 The industries that are expected to experience the largest increases in social worker employment are ambulatory health care services (health practitioner offices, outpatient care centers and home health care services), social assistance (individual and family services agencies, community services, vocational rehabilitation and child day care services), and nursing and residential care facilities (nursing care facilities, residential care facilities and community care facilities for the elderly).

BLS estimates that the "expanding senior population" will drive growth in employment in home healthcare services, residential care (assisted living, senior living communities and nursing facilities) and hospices. The growth in these industries will affect employment of social workers as well as other occupations, most notably nursing and social and human service assistants.16 As shown in Figure 4, the number of professional social workers employed in long-term care settings is projected by BLS in the Occupational Employment Matrix to increase from approximately 36,000 in 2002 to 55,000 in 2012.
Assuming that the demand for professional social workers in long-term care is driven exclusively by growth in the older population and that all other factors influencing demand and supply of labor remain constant, the number of social workers can be projected for future years. For example, the current proportion of professional social workers in long-term care settings per 1,000 persons age 65 and older in 2012 is 1.29 (55,189 divided by 42,863). Multiplying this proportion by projected increases in the elderly population from 2020 to 2050 results in an approximate doubling of the number of professional social workers in long-term care settings. Using an identical methodology--but basing the proportion on the estimate of professional social workers from the 2000 1% PUMS--yields a similar trend; by 2050, the number of professional social workers in long-term care settings is projected to increase by approximately 65,000 to 109,000.
IX. FACTORS INFLUENCING DEMAND AND SUPPLY OF SOCIAL WORKERS IN LONG-TERM CARE
There are numerous factors--not necessarily unique to social work--that are likely to impact future demand and supply, therefore making it difficult to assess the adequacy of supply relative to demand.
A. Job Substitution
The job growth attributable to the aging of the population that will occur in long-term care settings will likely be shared between social workers and several other occupations. Other professionals, such as registered nurses, and paraprofessionals (such as therapists, nurses aides, home health aides, personal care workers and other individuals calling themselves case workers or social workers) provide services and supports that may currently be considered under the purview of social work.12 For example, both registered nurses and social workers can perform hospital discharge planning functions, act as case managers and (with appropriate training and licensure, if required) provide psychotherapy. Similarly, individuals holding a bachelor's degree in a human services field and social workers with a BSW deliver assessment and case management functions in many state and local departments of social services.
While the future demand for services cannot be precisely predicted, it is likely that there will be an increased need for professional and paraprofessional workers, including social workers, to meet the growing demand in long-term care services. Non-social work professionals and paraprofessionals may fulfill some portion of that demand. However, the degree to which other professional workers and paraprofessionals substitute for a professional social worker in a long-term care setting is difficult to predict because it is related to a number of factors. These factors include regulatory requirements, the ability of employers to hire professional social workers, proven efficacy of social work interventions relative to other professionals or paraprofessionals in long-term care settings, and shifts in social service delivery systems and financing systems for long-term care.
With regard to efficacy, Rizzo and Rowe reviewed the literature on social work practices among the elderly to identify the strength of available evidence on the effectiveness of social work interventions.17 Using criteria of the evidence-based practice model, they concluded that the strongest evidence for social work effectiveness exists in health care facilities (i.e., hospitals). While there is some evidence of effectiveness in areas such as caregiving and geriatric evaluation, the literature does not clearly differentiate between social workers and other providers. Moreover, the available research does not differentiate between providers with different levels of social work education (MSW vs. BSW) and the others who do not have specific social work training. In short, while some evidence exists to support the positive impact of social work practices, there is less evidence to set apart social work as a distinct professional role across the long-term care continuum, which impacts demand for the discipline.18
B. Social Worker Training
An important factor influencing the supply of professional social workers in long-term care is the ability to attract students into social work careers in long-term care settings. Research has shown that there are three major barriers to attracting social work students to aging fields/settings: (1) limited numbers of adequately trained faculty to influence students to choose field placements in long-term care (or oversee their long-term care field placement, (2) lack of institutional support for geriatric curricula,19 and (3) absence of financial support and/or incentives for students while in training.
Schools and Departments of Social Work have proportionately few full-time aging/gerontology social work trainees in field placements (practica), primarily due to lack of trainee funding for MSW students, particularly during second-year placements.20
"Despite dramatic increases in the perceived need for social workers trained to work with older adults, the availability of government sponsored training programs has declined. With the exception of the Veterans Administration Geriatric Research Education and Clinical Centers, no significant national resource presently exists for supporting students interested in aging. Historically, an important source of stipends was the Administration on Aging (AoA), which distributed nearly $80 million between 1966 and 1984 to 185 colleges, community colleges, and universities to support the development of aging curricula and training (Peterson, 1987). These funds dramatically increased the numbers of students in aging, many of whom became leaders in the field. A good example of the power of student stipends to attract and train leaders in social work is the use of federal training money under Title IV-E (of the Social Security Act), which is "re-professionalizing" the child welfare system in many states and making graduate level social work education available to many disadvantaged and minority students who might not otherwise be able to attend graduate school."21
Social work educators cite fiscal constraints of their respective universities as a major barrier to recruitment of faculty experts in aging and an obstacle to the development and offering of new courses.22 Researchers have further found that when these barriers are creatively and competently addressed, student interest rises in social work careers working with older adults.23
There are approximately 10,000 social work educators across all program levels.24 The Hartford Foundation Gerontological Faculty Scholars program has funded the training of 53 individuals over the past 3 years; however, there may be a lack of adequate training resources specific to gerontological social work education. Forty-one percent of respondents to the 1994 Council of Geriatric Education Centers' survey cited fiscal constraints as a major barrier to the recruitment of social work faculty with expertise in aging and to the development and offering of new courses. The lack of curricula with a focus on gerontology has been most notable among social work programs at smaller colleges and universities, those in states with lower per capita income, and colleges that did not have any kind of multidisciplinary gerontology center.25
The number of social work students in the aging specialty also has significant implications for the future long-term care social work workforce. Between 1996 and 2001, CSWE reported that the number of students enrolled in MSW programs dropped by 7.4% and the number of students that had selected an aging specialization declined by 15.8%.d A 2005 report from a CSWE survey of social work programs (both BSW and MSW) in seven states that produce just over 11,000 graduates in a year--California, Florida, Illinois, New York, Ohio, Pennsylvania and Texas--found that an average of 5.9% of students (predominantly master's level) are in an aging concentration and that approximately one in ten students was in an aging field placement, including both BSW and MSW programs.26
While the social work programs in the states mentioned above do provide some gerontological training, the majority of BSW and MSW educational programs contain little or no gerontology content. For example, it is estimated that 80% of BSW students graduate without any specific course work in aging.21, 26
C. Wages and Benefits
Wages and benefits also directly influence occupational choices and supply. Practice-based research conducted by NASW showed that, in 1999, annual income among full-time social workers was lowest for those employed in nursing facilities and hospices.27 Specifically, these workers reported median income of $38,500 compared to $51,110 for full-time work in child welfare agencies and $43,330 in schools. BLS also indicated that the mean annual salary in 2002 for social worker positions in nursing care facilities ranged from $30,040 to $33,460, among the lowest of any setting. Although the income differentials may be linked to reimbursement (e.g., social work services in most long-term care settings including hospice, home health and skilled nursing facilities are bundled into the prospective payment rates), the salary difference also results from use of non-professional social workers in nursing facilities such as social service designees.28
D. Changes in the Long-Term Care Environment
In preparing projections of future social work employment, we assumed that the current long-term care environment would remain constant. However, there are changes underway that could influence how care is delivered and by whom. For example, as other forms of residential care and services have become more prevalent, "recent declines in rates of nursing home residence may reflect broader changes in the health care system affecting older Americans."1 Similarly, as the Baby Boom cohorts reach their sixth decade and beyond, there will be large increases in some very vulnerable sub-groups that may require more intensive services, specifically the oldest old, older women, elderly racial minorities and those living in or near poverty.29 However, a priori, it is not possible to determine with any certainty how these changes may alter the demand for social workers in long-term care settings.
X. PERSPECTIVES OF STAKEHOLDERS
HHS held a series of informal discussions focusing on the supply and demand for professional social workers in long-term care settings. The topics of these discussions included: (1) overall perspective on social workers in long-term care settings, (2) factors affecting the supply of, and demand for, professional social workers in long-term care, and (3) cooperative strategies between HHS, schools of social work and professional associations that could address the adequate supply of professional social workers in long-term care. Participants of these meetings were all professional social workers representing practitioners, faculty, federal partners, researchers, policy makers, and professional and provider associations. An overview of private and public sector initiatives to train social workers and faculty in gerontology that were identified by stakeholders appears as Appendix 1. A list of stakeholder discussion participants is attached as Appendix 2.
Stakeholders hypothesized that one hurdle to recruiting and training professional social workers--and other staff--into long-term care settings might be pervasive negative attitudes and stereotypes about aging and elders. For example, it was reported that students perceive that all work with the elderly involves caring for demented and bed bound clients, in unpleasant settings, and with all care leading to poor outcomes. Without meaningful exposure to the aging population through didactic or practicum experiences, it was reported that the majority of social work students complete their studies with no knowledge of the many programs and services available for elders and their families, or any understanding of the vast diversity in the aging population. However, the aging of our population dictates that most social workers will be working with elders (or their caregivers) at some point in their professional careers.
The other main themes that mentioned by all the stakeholder groups were as follows:
- While NASW and others have enumerated the wide variety of tasks that social workers perform in long-term care settings and/or working with older adults, there is little documentation about how social workers perform these tasks or what social workers do that other professionals (or para-professionals) do not. In addition, it is not clear how these tasks relate to specific credentials or demonstrated mastery in specific long-term care settings or working with specific sub-populations.
- The perceived lack of financial incentives in the form of stipends, loan forgiveness and wages is viewed as the most pronounced barrier to the recruitment and retention of professional social workers into long-term care careers.
- Professional gerontological social workers in the not-for-profit and public sectors are increasingly being challenged to prove their value to their organizations. Stakeholders further reported that the movement toward filling long-term care jobs with professional social workers is not consistently occurring because the demonstrated cost-effectiveness or efficacy of social work interventions in long-term care settings is not proven.
XI. DATA LIMITATIONS AND METHODOLOGICAL ASSUMPTIONS
Because there are no definitive data on professional social workers in long-term care in the U.S., the estimates presented in this report relied on multiple sources and an approach designed to approximate the definition of professional social worker from the NASW and CSWE. The accuracy of the estimates is therefore dependent on how well our "working" definition of professional social worker in long-term care corresponds to the NASW/CSWE definition, and the quality of the data.
In some cases, the estimates may be too high. For example, the Current Population Survey, 1% Census data, and other occupational surveys rely on self-reported information on occupation. Individuals with a bachelor's degree or higher may report that they are employed as a social worker, but may not have an actual BSW or MSW. In other cases, the estimates may be too low: individuals who meet the educational criteria for professional social worker, but whose primary job responsibilities involve management, supervision or administration, might not identify his/her occupation as social worker. The estimates may also understate the number of professional social workers serving the long-term care needs of the elderly because they work outside the industries identified in the surveys--home health agencies, nursing care facilities, residential care facilities, or community care for the elderly. For example, social workers that do discharge planning for elderly patients in hospitals or other ambulatory care settings are not included in the tabulations. However, despite these data limitations, the estimates are remarkably consistent with NASW survey data on the number of professional social workers employed in nursing facilities, home health agencies, and hospices.
The projections of the number of professional social workers in long-term care were based on the assumption that the demand for, and supply of, social workers in the future would be driven exclusively by growth in the older population. This is a strong assumption, and as discussed in Section IX, there are many factors--job substitution, changes in social worker training, changes in health care reimbursement policies that could in turn affect wages and benefits, and other changes in the long-term care infrastructure--that could influence future demand and supply. However, without any empirical evidence on the likely impact of these factors, some of which are no doubt countervailing, it is impossible to easily incorporate them into projections. The assumption that demand and supply is exclusively a function of the aging of the population was therefore a necessary simplifying assumption to begin modeling efforts. Future projections could incorporate greater complexity once additional data become available and we have a better understanding of the inter-related factors associated with the demand and supply of social workers in long-term care.
XII. CONCLUSIONS AND RECOMMENDATIONS
- Using data from the most recent OEM, the 2004 CPS, and the 1% PUMS from the 2000 Census, approximately 36,100 to 44,200 professional social workers are currently employed in long-term care settings.
- If the ratio of professional social workers to the population age 65 and older remains constant, approximately 110,000 professional social workers will be needed in long-term care settings by 2050.
- While their theoretical framework may be unique, social workers in long-term care settings perform tasks, including assessment, psychosocial support, active treatment, and case management that may also be performed by other disciplines.
- There are efforts underway to include additional aging-related content into social work curriculum and to encourage professional social workers to seek employment in long-term care settings. It is unclear at this time whether or not these efforts will have a substantial impact on the future supply of professional social workers in long-term care.
- Because of the uncertainties noted above, it is difficult to determine whether or not the current and future number of professional social workers will be adequate to care for an increasingly older American population; however, the likely increased demand for social work services will no doubt provide a strong impetus for continued job growth in the future.
HHS has identified a set of tasks that could be undertaken in an effort to better understand and assess the future demand for and supply of professional social workers in long-term care settings.
1. Training and Education:
- Continue to encourage innovative state and local programs experimenting with new training curriculum for social workers in geriatrics and long-term care.
- Explore effective ways to ensure continuing educational opportunities for social work faculty specializing in long-term care.
- Continue to support public and private initiatives currently underway intended to improve the availability of social workers with training in gerontology.
2. Linkages to Workforce Development Initiatives:
- Explore partnership opportunities between schools of social work, long-term care employers and state and local workforce development systems (e.g., workforce investment boards and community colleges).
- Develop linkages between federal agencies and existing national strategic planning efforts and partnerships with professional associations, schools and other entities aimed at recruiting new pools of workers and providing training resources for social workers with geriatric training.
3. Data Collection and Research Efforts:
- Continue to support data collection and analysis efforts.
APPENDIX 1: EFFORTS TO INCREASE THE SUPPLY OF PROFESSIONAL SOCIAL WORKERS SERVING OLDER ADULTS
A. Private-Sector Sponsored Activities
In 1999, the Hartford Foundation launched a multi-year effort entitled "Strengthening Geriatric Social Work Initiative". The Initiative consisted of several elements including a Faculty Scholars program of research support to junior faculty, a Practicum Partnership Program (PPP) demonstrating various educational training models, and the Social Work Competencies Project and Clearinghouse at CSWE (SAGE-SW, 2002). In 2001 it added a Geriatric Social Work Pre-Doctoral Fellows program and the Geriatric Social Work Curriculum Enrichment program that has since funded some 80 BSW and MSW programs with specific gerontological content across the U.S. The PPP provided grants to six schools of social work to develop partnerships with consortia of field agencies. The aim of the initiative is to build consortia that provide excellent comprehensive gerontological training to MSW students. Nearly half of the MSW programs in the country expressed interest in this program; 11 received one-year planning grants, and six of these were selected for multiyear implementation grants. To date, over 300 students have graduated from these PPPs. Four months post-graduation, over 80% of these graduates report working with older adults.30, 31 Over 24 million dollars have been expended from the John A. Hartford Foundation to launch this capacity-building investment. Hearst Foundation endowments of over $2,500,000 in geriatric social work education along with $30 million from other private sources have helped to reinforce this workforce development initiative. These private sector funds have shown that social work students do pursue careers in geriatric social work when incentives, training and educational supports are made available.
The Atlantic Philanthropies have funded over $5 million in grants to provide continuing education as well as policy and health services research with the goal of increasing the supply and improving the quality of care provided to older adults by social workers. It is part of a human capital development program targeted to enhancing the geriatric skills of doctors, nurses, social workers and direct care workers. The Atlantic Philanthropies work globally with the overall goal "To bring about lasting change that will improve the lives of disadvantaged and vulnerable."
The Institute for Geriatric Social Work (IGSW), located at Boston University School of Social Work, is dedicated to advancing social work practice with older adults and their families. Established through a five-year grant from the Atlantic Philanthropies, IGSW is committed to improving the quality of gerontological social work practice and to helping practicing social workers effectively address the challenges of our diverse and growing aging population. IGSW offers a range of free or inexpensive, convenient, and accessible training programs to practicing BSW or MSW social workers--the large majority of whom have received little or no training in aging. In 2004, IGSW will train over 6,000 practitioners in over 23 conferences and through a series of internet-based training courses. Also in 2004, IGSW is beginning a large randomized controlled trial to test the effectiveness of a social work intervention in primary care, a project they believe will be the most important social work research project in the country. And, in 2005, IGSW will be making training grants available to community-based organizations serving the elderly.
NASW and the Center for Health Workforce Studies at the University of Albany are analyzing the results of a national workforce study designed to obtain information about the education, job settings (including long-term care) and work activities of licensed social work professionals. "A Study of the Roles and Use of Licensed Social Workers in the United States" is examining issues related to the provision of social work services to older adults. The survey captured information that will increase understanding of the clinical practice of social workers currently involved in the delivery of direct care services. The project has received funding support from Atlantic Philanthropies and the John A. Hartford Foundations.
The American Cancer Society funds a number of grants to support training, research and career development in areas of specific interest to oncology social workers working in both acute and long-term care settings. These grants include stipends to social work students at the master's and doctoral levels, post-doctoral fellowships, research scholarships and faculty research training grants. Awards range from $12,000 for one-year to master's level students to as much as $400,000 per year for five years to research scholars.
B. Public Sector Sponsored Activities
Under Title III-E of the Older Americans Act as reauthorized in 2000, the National Family Caregiver Support Program funded Care PRO, a collaboration between the American Society on Aging, the American Nurses Association, the American Occupational Therapy Association and NASW, to increase the skills and knowledge of professionals providing needed services to family caregivers. The primary goal of the program was to train a minimum of 10,000 professionals from social work, occupational therapy and nursing professions in order to demonstrate increased competence in identifying the needs of family caregivers in their day-to-day practice. A total of $444,000 was provided for the program, which started in 2002 and is scheduled to end in 2005.
The HRSA Bureau of Health Professionals supports accredited health professions schools through its Geriatric Education Center (GEC) grants. Since 1985, 375,000 health professionals have received training in geriatrics through the GECs. GECs:
- Improve the training of health professionals in geriatrics, including geriatric residencies, traineeships and fellowships.
- Develop and disseminate curricula on the treatment of health problems in elderly individuals.
- Train and re-train faculty to provide instruction in geriatrics.
- Support continuing education for health professionals who provide geriatric care.
- Provide clinical geriatrics training in nursing facilities, chronic and acute care hospitals, ambulatory care centers and senior centers.
Social workers are one of the most prominent disciplines trained in GECs. In FY2001 HRSA spent $7.6 million funding 36 GECs. That year alone, 5,545 social workers received GEC grants; HRSA has funded grants to between 4,000 and 5,000 social workers under the GEC grant program in each of the subsequent years. [Note: HRSA has not committed funding to GECs beyond FY 2006.]
Indian Health Service (IHS) has a two-part scholarship program for health professionals, including clinical social workers, who must have a master's degree to practice. The preparatory program provides financial support to enrolled members of any federally recognized AI/AN tribe for up to two years of pre-professional training. The recipient of the preparatory scholarship has no obligation to serve. Additionally, the IHS provides up to four years of support during professional training for which the recipient incurs a service obligation. The IHS also offers a loan repayment program that is available to clinical social workers.
Enabling legislation mandates that the Department of Veterans Affairs (VA) assist in the training of health professionals for its own needs and those of the nation. Approximately 45,000 students and trainees in associated health education programs at the undergraduate, graduate and post-graduate levels, receive clinical experience at the VA facilities. The VA is affiliated with over 100 Graduate Schools of Social Work, and operates the largest and most comprehensive clinical training program for social work students--training approximately 600-700 students per year. Student funding support of $38.8 million is provided each year and includes 45 Geriatric Assessment Stipends of 500 hours each, 340 MSW student stipends at VA medical centers annually and 557 stipends for MSW programs at $4,112 each. Moreover, the Veterans Health Administration (VHA) requires that all applicants for the position of social worker must have an MSW from a school of social work accredited by the CSWE and be licensed or certified at the master's level to independently practice social work in a state.e In addition, VHA has developed a core competency requirement for its long-term care social workers, including an annual aging-related competency assessment every year in which each social worker must present a psychosocial assessment and participate in peer review of cases.
APPENDIX 2: PARTICIPANTS IN STAKEHOLDER DISCUSSIONS
The following individuals participated in stakeholder discussions:
Centers for Medicare and Medicaid Services Sonya Bowen Robert Connolly Mary Guy Terry Kay Jeanne Nitsch Anita Panicker Armen Thoumaian Dan Timmel Regina Walker-Wren.
Health Resources and Services Administration Joan Weiss
Veterans' Administration Kristin Day (Central Office) Jill Manske (Central Office) Susan Morse (Stratton Medical Center)
Non-Federal Margaret Adamek, Indiana University/Purdue University-Indianapolis Deidre Arnowitz, Beth Sholom Continuing Care Kathleen Ell, University of Southern California James Callahan, Brandeis University Sue Chandler, University of Hawaii JoAnn Damron-Rodriguez, University of California, Los Angeles Dave Dempsey, NASW Jan Edwards, Sheltering Arms Senior Project Nellie Garcia Kovacs, The Institute for Urban Family Health Robyn Golden, NASW Susan Goodwyn, Greater Cleveland Elder Abuse Domestic Violence Roundtable Roberta Greene, University of Texas Mit Joyner, West Chester University of Pennsylvania Eric Kingson, Syracuse University Jane Isaacs Lowe, Robert Wood Johnson Foundation Diane Long, Caring for Elders Project Jim Lubben, Boston College Ed Mendez Santiago, New York Department of Aging Pam Merkle, Association in Aging with Developmental Disabilities Nancy Morrow-Howell, Washington University Andrew Scharlach, University of California, Berkeley Tazuko Shibusawa, Columbia University Maria Torres, People in Progress Patricia Volland, New York Academy of Medicine Julia Watkins, CSWE Jane Wickencamp, Weinberg Community Council for Jewish Elderly Joan Zlotnick, NASW
REFERENCES
-
Federal Inter-Agency Forum on Aging-Related Statistics (2004). Older Americans 2004: Key Indicators of Well Being. U.S. Government Printing Office: Washington, DC. [http://agingstats.gov]
-
Stone, R. (2000). Long-Term Care for the Elderly with Disabilities: Current Policy, Emerging Trends, and Implications for the Twenty-First Century. Milbank Memorial Fund.
-
Gonyea, J.G., Hudson, R.B., and Curley, A. (2004). The Geriatric Social Work Labor Force: Challenges and Opportunities in responding to an Aging Society. Institute for Geriatric Social Work: Boston, MA.
-
National Association of Social Workers, https://www.socialworkers.org/profession/overview.asp.
-
National Association of Social Workers (2002). Social Work Profession Fact Sheet, Accessed at http://naswdc.org/pressroom/features/general/profession.asp on February 25, 2004.
-
Kane, R.A., and Kane, R.L. (1981). Assessing the Elderly: A Practical Guide to Measurement. Lexington Books: Lexington, MA.
-
Beers, M.H., and Berkow, R. (Eds.) (2004). The Merck Manual of Geriatrics. Chapter 9: Geriatric Social Work. Accessed online at http://www.merck.com/mrkshared/mmgeriatrics/home.jsp on May 18, 2004.
-
Gibelman, M., and Schervish, P.H. (1997). Who we are: A second look. NASW, Washington, DC.
-
Vitt, L. (Ed.) (2003). Gerontological Social Work in Encyclopedia of Retirement and Finance. Greenwood Press: Westport, CT.
-
National Association of Social Workers (2003). Standards for Social Work Services in Long-Term Care Facilities. Washington, DC.
-
Barth, M.C. (2001). The Labor Market for Social Workers: A First Look. The John A. Hartford Foundation: New York, NY.
-
Bureau of Labor Statistics, U.S. Department of Labor. Occupational Outlook Handbook, 2004-05 Edition, Social Workers. Accessed online at http://www.bls.gov/oco/ocos060.htm on November 16, 2005.
-
Doelling, C., Matz, B., and Kuehne, J. (1999). "Job Market of 1998 MSW Graduates." Paper prepared by the Social Work Career Development Group, Mimeo.
-
National Association of Social Workers (2000). Practice Research Network, 1(3).
-
National Association of Social Workers, Center for Workforce Studies (2005). Survey of Licensed Social Workers in the United States.
-
Bureau of Labor Statistics, U.S. Department of Labor (2003-2004; Winter). Occupational Outlook Quarterly.
-
Rizzo, V.M., and Rowe, J.M. (2003). Studies of the efficacy of social work services in aging with a focus on cost outcomes: Preliminary key points and information. Unpublished manuscript.
-
ASPE Stakeholder listening session #3, June 10, 2004.
-
Strengthening Aging and Gerontology Education for Social Work (2001). A Blueprint for the New Millennium. Council on Social Work Education: Alexandria, VA.
-
Dawson, G.D., and Santos, J.F. (2000). Combating failure: An investigation of funding for education and training of geriatric care personnel. Notre Dame, IN: University of Notre Dame, Gerontology and Geriatrics Education Office.
-
Scharlach, A., Damron-Rodriguez, J., Robinson, B., and Feldman, R. (2000). "Educating social workers for an aging society: A vision for the 21st century." Journal of Social Work Education, 36(3): 521-538.
-
Damron-Rodriguez, J., and Lubben, J. (1997). "The 1995 White House Conference on Aging: An agenda for social work education and training." In C. Saltz (Ed.), Social Work Response to the 1995 White House Conference on Aging: From Issues to Action (pp. 65-77). Haworth Press: New York, NY.
-
Lubben, J.E., Damron-Rodriguez, J., and Beck, J.C. (1992). "A national survey of aging curriculum in schools of social work." Geriatric Social Work Education, 18: 157-171.
-
Watkins, J. (2004). Personal communication.
-
Damron-Rodriguez, J.A., Villa, V., Tseng, H.F., and Lubben, J.E. (1997). "Demographic and organizational influences on the development of gerontological social work curriculum." Gerontology and Geriatrics Education, 17(3): 3-18.
-
Center for Social Work Education, Gero-Ed Center (2005). Annual Progress Report on the Status of Gerontological Social Work Education.
-
National Association of Social Workers (2002). Practice Research Network: Social Work Income 2, 1(6). Washington, DC.
-
Rowell, M.E. Fields, A.S., and Cohen, B. (2002). "Health personnel in the US: 2000-2015." Albany, NY: Center for Health Workforce Studies, State University of New York, unpublished monograph.
-
U.S. Administration on Aging, National Aging Information Center. Accessed online at http://aoa.gov/prof/statistics/future_growth/aging21/program.asp on February 24, 2004.
-
Scharlach, A., Damron-Rodriguez, J., Robinson, B., and Feldman, R. (2003; March/April). "Social work: Building its role to serve an aging nation." Aging Today, 24(2):7-8.
-
Damron-Rodriguez, J., Lawrance, F.P., and Lee, S.E. (2004). Practicum Partnership Program (PPP) Collaborative Evaluation Report II: Outcomes 2000-2003. John A. Hartford Foundation.
NOTES
-
Another common term found in the literature is clinical social worker; these represent a subset of professional social workers that have obtained a master's degree and have completed at least two years of supervised therapeutic social work practice. Employers may also classify jobs as social work regardless of educational requirements; similarly, individuals may self-report their occupation as social worker, again without regard to educational achievement.
-
The NAICS has a five-digit classification structure, with a sixth digit for national industries. With some important exceptions, it provides a set of standard industry codes that describe the industrial structure and composition of the United States. The U.S. Census Bureau produced a cross walk from the industry codes used in the 2000 Census to the NAICS.
-
Generally, P-I-E refers to the core social work practice of "starting from where the client is" (i.e., framing the therapeutic relationship and viewing all issues from the client's perspective). For a more complete description of social work theory and practice with older adults, please refer to A National Agenda for Geriatric Education: White Papers (Chapter 11, The State of the Art of Geriatric Social Work Education and Training) first published by the Health Resource and Services Administration (HRSA) in 1995.
-
Social work programs in the U.S. confer about 15,000 bachelor's degrees and 16,000 master's degrees annually.
-
The VHA has qualification standards for each clinical discipline, which define the standards that someone must meet to qualify. These standards are based on federal law (the most recent version was PL 106-419). The Secretary of Veterans Affairs allows a newly hired social worker up to 3 years to become licensed at the independent level if they begin work without a license (VA can non-competitively direct hire social workers who complete a VA field placement within one year of graduation).