
U.S. Department of Health and Human Services
Ensuring a Qualified Long-Term Care Workforce: From Pre-Employment Screens to On-the-Job Monitoring
The Lewin Group
May 2006
This report was prepared under contract #HHS-100-03-0027 between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and the Lewin Group. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the ASPE Project Officer, Emily Rosenoff, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. Her e-mail address is: Emily.Rosenoff@hhs.gov.
The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
TABLE OF CONTENTS
- I. INTRODUCTION
- A. Overview and Study Purpose
- B. Background
- C. Context and Contribution of this Study
- D. Report Organization
- II. STUDY METHODOLOGY
- A. Research Goal and Objectives
- B. Data Sources
- C. Study Limitations
- III. FINDINGS
- A. Current Practices in Pre-Employment Screening, Background Checks, and On-the-Job Monitoring
- B. Relationship between Past Criminal Background or Incidences of Abuse and Subsequent Abuse, Neglect, and Exploitation
- C. Innovative Screening and Monitoring Strategies
- D. Suggestions by Informants to Improve Processes for Background Checks and On-the-Job Monitoring
- IV. STUDY CONCLUSION AND POLICY CONSIDERATIONS
- A. Conclusion
- B. Policy Considerations
- APPENDICES
- APPENDIX A: References
- APPENDIX B: Process Flow Charts--Screening and Complaint Investigation
- APPENDIX C: State Background Check Requirements and Practices
- APPENDIX D: Key Informants
- APPENDIX E: Data Collection Materials--Data Registry Analytic Plan and Discussion
- APPENDIX F: Screening Mechanisms Used in the Child Care Industry
ACKNOWLEDGMENTS
This report was prepared by The Lewin Group for the Office of the Assistant Secretary for Planning and Evaluation (ASPE), U.S. Department of Health and Human Services (HHS). Charlene Liggins and Emily Rosenoff served as the Government Project Officers at ASPE, providing leadership, guidance and substantive input over the course of the project. We also acknowledge the important guidance and contributions of the Technical Advisory Group (Appendix D). We would like to extend our deepest appreciation to the staff members of the Arizona Board of Nursing and the Kansas Department of Health and Environment, Health Occupations Credentialing Unit for their willingness to share and analyze data from their nurse aide registries. Finally, we sincerely thank all of the individuals who participated in the study, including the national level key informants (Appendix D), stakeholders from the four case study states (Appendix D) and representatives from twelve nursing facilities.
EXECUTIVE SUMMARY
A. Study Overview
In an effort to improve the quality of care provided in long-term care settings, as well as ensure a committed and qualified long-term care workforce, the Office of the Assistant Secretary for Planning and Evaluation, within the U.S. Department of Health and Human Services, contracted with The Lewin Group (Lewin) to study the efficacy of various approaches to pre-employment screening and on-the-job monitoring of nurse assistants to prevent resident abuse in nursing homes. This study is intended to inform policymakers, providers, consumers and other interested parties about the relative contributions and perceived effectiveness of existing federal mandates and state and provider based strategies for preventing or reducing the abuse of vulnerable adults.
Federal and state governments, education and training centers, and employers have created a variety of formal mechanisms aimed at preventing incidences of abuse, neglect and exploitation in nursing homes and other long-term care settings. These mechanisms span a wide spectrum and include certification and licensure of paraprofessional long-term care workers, various pre-employment screening, (e.g., nurse aide registries, criminal background checks and drug tests), and on-the-job training and monitoring.
The two primary methods used for pre-employment screening include checking nurse aide registries and conducting criminal background checks. Federal guidelines require each state to establish and maintain a registry of nurse aides that includes certification information and substantiated findings of abuse, neglect, or financial exploitation in nursing homes. At minimum, these registries must include: (1) the full name of the individual; (2) identifying information, (3) the date of certification; and (4) information regarding substantiated findings of abuse, neglect or misappropriation.1 Federal guidelines require nursing facilities to check their State nurse aide registry to ensure that hired nurse aides are certified to work and meet all state requirements, and that they do not have any substantiated findings of abuse, neglect or misappropriation associated with their license. In addition, long-term care facilities must check other relevant databases they believe will include any information on the potential employee (e.g., criminal background database).2
Some states, either through state law or by choice, collect data beyond the scope mandated through federal requirements for maintaining nurse aide registries. For example, states registries may include data on certified and non-certified health care workers in addition to nurse aides along with additional demographic information such as race/ethnicity, education level or current employer.
Examining the efficacy of screening mechanisms such as state nurse aide registries and criminal background checks comes at a particularly relevant time. Two recent federal studies highlight the urgency for the study from both a long-term care staffing perspective and from a quality perspective. The first study, conducted by the U.S. Health Resources and Services Administration, detailed a widespread shortage of nurse aides and home health aides with a high likelihood of increasingly severe shortages in the future.3 The second study conducted by the Office of the Inspector General (OIG) revealed that nurse aide registries often fail to provide accurate information because of failure to update data or purge outdated data.4
Previous studies have examined rates of abuse in nursing facilities, direct service worker capacity issues, and compliance of states to maintain nurse aide registries. This study looks across all of these issues, by examining the process states go through to collect and maintain information in their registries, state and employer mandated background check procedures, reporting and investigating policies/practices when abuse allegations are made, and the impact of such processes on the direct service workforce, employers and state agencies.
B. Research Goal and Objectives
The goal of this study was to examine current practices at the state and facility levels regarding pre-employment screening and on-the-job monitoring, and how these influence the quality of the long term care workforce. In addition, this study sought to:
- Examine the utility and efficacy of nurse aide registries and criminal background checks as strategies for reducing the incidence of nursing facility resident abuse.
- Determine the relationship (if any) between past criminal background or previous incidences of abuse and the proclivity toward subsequent abuse, neglect or exploitation.5
- Identify, from the perspective of states and nursing facilities, limitations, innovative strategies, and recommendations for improving the current screening and monitoring process for ensuring a qualified long-term care workforce.
C. Key Findings
The efficacy of nurse aide registries and criminal background checks in preventing resident abuse in nursing facilities is difficult to ascertain. Making an accurate assessment regarding the effectiveness of these practices is difficult because every state has a different process for screening and disqualifying potential workers, documenting information in their registries, tracking subsequent employment or complaint data, investigating abuse allegations, reporting relevant findings, and coordinating efforts across state entities. Extensive variation across states affects the ability to make a definitive statement about the efficacy of these strategies to ensure a qualified workforce. The in-depth examination of four states revealed that some aspects of these systems work well, but limitations exist in each state that affects the overall utility of these practices. There is, however, consensus across stakeholders in all four states that criminal background checks are a necessary element of the hiring process. The technology, coordination capabilities and infrastructure exist through on-line registries, fingerprint databases and abuse registries to help employers make the best hiring decisions possible to protect the elderly in their care. States are building on their knowledge, experience, and capabilities to streamline these processes, but there is still room for improvement while balancing the resource intensiveness of making these changes. It is clear that relying on criminal background checks and nurse aide registries are not enough to prevent or reduce abuse in nursing facilities. Ongoing training, education and supervision for workers providing direct care are also key components to maintaining a quality workforce. A summary of our overall project conclusions are provided below.
Criminal background checks are a valuable tool for employers during the hiring process and their use does not limit the pool of potential job applicants. Stakeholders agree that conducting criminal background checks on potential employees is an important aspect of the hiring process to reduce the likelihood of hiring someone who has potential to harm residents in long-term care. There is widespread acceptance throughout the long-term care industry (similar to that of the child care industry), that this practice serves to protect vulnerable adults and ultimately prevent abuse. None of the nursing facilities experienced any negative impact on their applicant pool as a result of this requirement. From the perspective of employers, reducing the amount of time it takes to receive background check results would improve the current system.
A correlation exists between criminal history and incidences of abuse. Based on data we received from Arizona and Kansas, it does appear that nurse aides who had a previous criminal conviction (non-disqualifying offense) had higher rates of substantiated abuse than nurse aides without a criminal history. While this only represents the experience of two states, this analysis does provide evidence to support the rationale for checking the criminal history of potential direct care workers as a screening mechanism for quality.
Criminal background checks are only one component of preventing abuse. Despite a connection between past criminal history and subsequent allegations of abuse, stakeholders consistently reported the following as effective strategies for preventing abuse (many of which are not formal state or industry policy): adequate supervision/monitoring, presence of managers on the floor, decreasing staff burnout, adequate staffing levels, rotating nurse aides on the floor to alleviate pressure of difficult residents, increased education and training, obtaining meaningful employment references (beyond verification of employment dates), valuing and respecting staff, creative recruitment incentives to retain committed staff, instituting a drug-free workplace policy, minimizing temporary hires, and pointing out negative behaviors in the moment and using them as a staff development opportunity.
There are fewer policies in place that support or reinforce post-employment strategies to ensure a qualified workforce. Through this study we have discovered that there is significantly more effort and resources allocated to the pre-employment phase of ensuring a qualified long-term care workforce than the post-employment phase. The policy focus at the state and facility level is on pre-screening applicants before employment and there are structures and regulations in place that support this effort. However, once a worker is hired and working in the field, there is less guidance regarding how best to train, continuously educate and monitor existing employees. As stated before, most states have no process in place to notify employers if an active employee commits a crime that would have prohibited them from working during their background check prior to employment. In the event of employee complaints or allegations of abuse, the effectiveness of state systems often breaks down due to a lack of coordination between multiple state entities involved in the investigation and reporting process. Duplicative efforts waste state resources, prolong investigations and often keep employees out of the workforce unnecessarily.
D. Policy Considerations
National Level Considerations
-
The challenge of individual state registries. Individual state registries and the barriers associated with data sharing across states, limit employer access to useful information about substantiated abuse findings against workers found in other states. Since workers may have been employed in more than one state, a national nurse aide registry has been frequently mentioned as one way to address the issue of long-term care workers with substantiated findings of abuse, neglect, and/or financial exploitation crossing state lines to work in another state. Several issues may pose barriers for the creation of a national nurse aide registry. First, transfer of information across various state and national agencies may be difficult due to state laws and agency ownership of data. Second, the cost of creating and maintaining a national database would require commitment of both staff time and funds from both states and national agencies. Third, certification procedures and requirements vary across states, which further challenge any effort to standardize the process nationwide.
-
Use of disqualifying offenses and waivers. It is important to strike a balance between the need to protect vulnerable citizens from harm and creating unnecessary barriers to employment for qualified individuals, further reducing the potential pool of long-term care workers. There is a paucity of literature examining nurse aides and criminal recidivism and propensity to commit abuse. Criminal recidivism research shows that a history of past criminal convictions may be a possible predictor of future behavior.6 Other research by Cohen (1996) reports that the probability of future dangerous behavior of criminal offenders increases when circumstances are similar to past situations in which criminal behaviors occurred, which has implications for workers who have substantiated findings of resident abuse.7
A review of the Illinois Department of Public Health waiver process for individuals certified to work in hospitals and nursing facilities indicates that many individuals with criminal records can work in the health care field with minimal impact on patient safety. In Illinois, individuals with specific criminal convictions are banned from working in certain health care professions but can apply for waivers. In an examination of waiver applications from 1996 to 2003, 5,706 individuals with convictions applied for waivers. 4,130 (72%) of these individuals were granted waivers. Ninety-seven individuals (or 2.3% of the 4,130 individuals) had their waivers revoked; 38 of these individuals had revoked waivers because of substantiated finding of abuse, neglect, or theft and 59 individuals due to a second disqualifying conviction.8
Additional research in the area of criminal recidivism, specifically in relation to elder abuse, neglect, and financial exploitation is necessary to develop evidence based lists of disqualifying offenses. Justification for the inclusion or exclusion of various crimes that constitute states lists of disqualifying offenses is unclear, and the lack of consensus across states on this issue illustrates the complexity of making a solid connection between past criminal activity and the proclivity to commit abuse in long-term care settings. In the absence of such evidence, policymakers and employers must still balance the need to protect vulnerable populations with the need to maintain an adequate direct care workforce to accommodate a growing older adult population.
-
The screening process requires a significant amount of resources. As states make efforts to improve their screening processes (e.g., expanding the criminal background check to other states or incorporating federal level checks, expediting the turnaround time for results, expanding the screening process to other types of workers), the costs will inevitably increase. States will need additional capacity (staff and financial resources) to meet the demand for quality screens on increased numbers of workers in a timely manner. It is important to balance the financial burden across state agencies, employers and direct service workers in an equitable manner so that screening processes can continue to improve.
State Level Considerations
-
Keeping registry data current to maximize their utility. A recent OIG study revealed that nurse aide registries may not always contain the most up-to-date, or accurate information. In a survey of 200 randomly selected long-term care facility administrators, 44% (87 individuals) surveyed stated that they periodically rechecked nurse aide registries to ensure that substantiated findings had been posted to the registry. Fifteen administrators found that a nurse aide previously listed as registered and free of a substantiated finding of abuse was later listed to be unqualified for work due to a substantiated finding, failure to attain active registration status, or failure to be certified as a nurse aide. The nurse aide registry is only helpful to employers if the information is current.
-
Increasing the utility of the nurse aide registry with public awareness and education. In most states, employers are the only ones who benefit from the information contained in the nurse aide registry. By increasing consumer knowledge and use of the registry, the state can further protect the public by offering additional resources and information on individual long-term care workers.
-
Incorporating alternative screening mechanisms. Nursing home administrators use several practices (not required by federal regulations) to screen potential employees and to monitor current nurse aides. Eighty-five percent of administrators surveyed for a recent OIG report used additional screening procedures such as criminal background checks, and/or personal and employment reference checks.9 Implementing random drug tests and criminal background checks on existing employees may be another way to monitor employees after they have cleared original pre-employment screens. Conducting drug testing may be a more effective method for screening out individuals with a criminal history in drug abuse rather than a comprehensive ban.10 Findings demonstrate the need to use creative and multi-pronged strategies for screening and monitoring direct care paraprofessionals.
-
Examining states practices related to investigating and reporting abuse. Current state practices for investigating and reporting abuse cases appear duplicative and lack adequate coordination across entities. This creates overlap for agencies conducting the investigation, burden for the employers, and a protracted suspension period for the direct service worker involved.
I. INTRODUCTION
A. Overview and Study Purpose
In 2000, there were 35 million people 65 years of age and over in the U.S., an increase of 12% from 1990. When baby boomers (born from 1946 through 1964) reach the age of 65, starting in 2011, the number of individuals 65 years of age and over is expected to rise.11 The rapidly aging long-term care workforce and high turnover rate pose barriers for meeting the long-term care needs of the growing older adult population.
In an effort to improve the quality of care provided in long-term care settings, as well as ensure a committed and qualified long-term care workforce, the Office of the Assistant Secretary for Planning and Evaluation (ASPE), within the U.S. Department of Health and Human Services, contracted with The Lewin Group (Lewin) to study the efficacy of various approaches to pre-employment screening and on-the-job monitoring of nurse assistants to prevent resident abuse in nursing homes. This study is intended to inform policymakers, providers, consumers and other interested parties about the relative contributions and perceived effectiveness of existing federal mandates and state and provider based strategies for preventing or reducing the abuse of vulnerable adults.
B. Background
Vulnerability of older adults in long-term care settings. Examining the value of federal, state and provider strategies for preventing or reducing the incidence of abuse is vital for the protection of residents in long-term care service settings. Long-term care consumers often have physical, cognitive and functional impairments that make defense from and reporting of abuse, neglect, or exploitation difficult. Consumers with long-term care needs may lack strong advocates provided through a spouse or family support network.
While abuse, neglect, and financial exploitation occur in a variety of formal and informal long-term care settings by both paid and unpaid caregivers, the quality of long-term care in nursing facilities is of particular concern because past reports have demonstrated higher incidences of abuse in comparison with other settings. The House Committee on Government Reform, for example, issued a report in 2001 that demonstrated a high rate of abuse in nursing homes. Over a two-year period, nearly one-third of all certified nursing facilities had been cited for some type of abuse violation that had the potential to cause harm or had actually caused harm to a nursing home resident. Ten percent of nursing homes were cited for abuse violations that caused actual harm to residents.12 A 2002 General Accounting Office (GAO) study estimated that almost 30% of the nations 17,000 nursing homes were cited for deficiencies involving actual harm to residents or placing them at risk of death or serious injury.13
Definitions of abuse, neglect and exploitation. According to the National Center on Elder Abuse, abuse, neglect, and exploitation in the context of long-term care are defined as any knowing, intentional, or negligent act by a caregiver or any other person that causes harm or a serious risk of harm to a vulnerable adult. Abuse in nursing homes is defined as the willful infliction of injury, unreasonable confinement, intimidation, or punishment with resulting physical harm, pain, or mental anguish for all residents, even those in a coma (42 CFR § 488.301). This includes physical abuse (inflicting, or threatening to inflict, physical pain or injury on a vulnerable elder, or depriving them of a basic need), emotional abuse (inflicting mental pain, anguish, or distress on an elder person through verbal or nonverbal acts), and sexual abuse (non-consensual sexual contact of any kind). Neglect is generally defined as the intentional or unintentional withholding of food, medication, or other necessities that result in the older persons failure to thrive.14 Federal statute (42 CFR § 488.301) states that neglect in nursing homes is the failure to provide goods and services necessary to avoid physical harm, mental anguish, or mental illness. Exploitation in the context of long-term care is defined as the illegal taking, misuse, or concealment of funds, property, or assets of a vulnerable elder.15 Individual states vary in their definitions of abuse, neglect, and exploitation.
Strategies to improve workforce quality and reduce risk of abuse. Federal and state governments, education and training centers, and employers have created a variety of formal mechanisms aimed at preventing incidences of abuse in nursing homes and other long-term care settings. These mechanisms span a wide spectrum and include certification and licensure of direct paraprofessional long-term care workers, various pre-employment screening, (e.g., nurse aide registries, criminal background checks and drug tests), and on-the-job training and monitoring.
Federal Guidelines for Certified Nurse Aide (CNA) Registries. The two primary methods used for pre-employment screening include checking nurse aide registries and conducting criminal background checks. Federal guidelines require each state to establish and maintain a registry of nurse aides that includes certification information and substantiated findings of abuse, neglect, or financial exploitation in nursing homes. At minimum, these registries must include: (1) the full name of the individual; (2) identifying information; (3) the date of certification; and (4) information regarding substantiated findings of abuse, neglect or misappropriation.16 Federal guidelines require nursing facilities to check their state nurse aide registry to ensure that hired nurse aides are certified to work and meet all state requirements, and that they do not have any substantiated findings of abuse, neglect or misappropriation associated with their license. In addition, long-term care facilities must check other relevant databases they believe will include any information on the potential employee (e.g., criminal background database).17
Requirements beyond Federal Guidelines. Some states, either through state law or by choice, collect data beyond the scope mandated through federal requirements for maintaining nurse aide registries. For example, states registries may include data on certified and non-certified health care workers in addition to nurse aides along with additional demographic information such as race/ethnicity, education level or current employer. See Appendix C for a comprehensive list of state requirements for certification and employment.
Statutes Authorizing Criminal Background Checks. Criminal background checks provide another avenue for screening potential long-term care employees. Two federal statutes enable health care providers to perform criminal background checks on prospective employees. Public law 105-277, Section 124 enables nursing facilities and home health care agencies to request fingerprint based national criminal history checks by the FBI for employees or job applicants seeking positions involving direct patient care. In addition, Public law 103-322 § 320928 enables federal criminal background checks to be performed on individuals employed in long-term care settings other than nursing facilities and home health agencies. This law allows for checks to be conducted on individuals who work for, own, or operate a business that provides care to the elderly or individuals with disabilities.
Despite these two laws, an earlier law passed by Congress in 1972, Public law 92-544, created a barrier for states attempting to conduct background checks. This law stipulated that in order for background checks to occur, states had to first pass a law authorizing health care employers to request such background checks from state and local government officials, and then seek approval of the law from the U.S. Attorney General. However, Public law 105-251 § 222, passed in 1998, remedied some of these barriers by enabling state designated businesses or organizations involved in the licensure or certification of individuals providing care to children, the elderly, or individuals with disabilities to request federal criminal background checks of potential employees even in the absence of a state statute authorizing criminal background checks.18
On-the-Job Monitoring. Long-term care facilities also play a role in maintaining the quality of the long-term care workforce through their employment and monitoring practices. These monitoring practices might include supervision of direct care paraprofessional workers by other personnel, training, and education. Gaining a better understanding of the effectiveness and use by employers of screening mechanisms as well as on-the-job monitoring enables policymakers and relevant stakeholders to understand the balance between the need to protect vulnerable individuals with long-term care needs with the need to ensure that potentially qualified long -term caretakers are not being inappropriately screened out by highly sensitive screening tools.
C. Context and Contribution of this Study
Examining the efficacy of screening mechanisms such as state nurse aide registries and criminal background checks comes at a particularly relevant time. Two recent federal studies highlight the urgency for the study from both a long-term care staffing perspective and from a quality perspective. The first study, conducted by the U.S. Health Resources and Services Administration, detailed a widespread shortage of nurse aides and home health aides with a high likelihood of increasingly severe shortages in the future.19 The second study conducted by the Office of the Inspector General (OIG) revealed that nurse aide registries often fail to provide accurate information because of failure to update data or purge outdated data.20
Previous studies have examined rates of abuse in nursing facilities, direct service worker capacity issues, and compliance of states to maintain nurse aide registries. This study looks across all of these issues, by examining state processes for collecting and maintaining information in their registries, state and employer mandated background check procedures, reporting and investigating policies/practices when abuse allegations are made, and the impact of such processes on the direct service workforce, employers and state agencies.
D. Report Organization
The remainder of this report includes the following sections:
-
Study methodology, including research goals and objectives, data collection methodology, data analysis, study assumptions and limitations.
-
Major findings, including the impact of pre-employment screening mechanisms, training and on-the-job monitoring in reducing the risk of resident abuse. In addition, findings include similarities and differences in pre-employment screening processes across state systems, gaps or limitations of current processes, emerging innovations within the states and recommendations shared by key informants for improving the screening process, improving communication and coordination of information across stakeholders and streamlining the system for employers and direct service workers.
-
Implications and conclusions, including key issues and themes related to major findings, as well as the policy, regulatory and practice implications of the study, and directions for future research.
II. STUDY METHODOLOGY
A. Research Goal and Objectives
The goal of the study was to examine current practices at the state and facility levels regarding pre-employment screening and on-the-job monitoring, and how these influence the quality of the long term care workforce. In addition, this study sought to:
- Examine the utility and efficacy of nurse aide registries and criminal background checks as strategies for reducing the incidence of nursing facility resident abuse.
- Determine the relationship (if any) between past criminal background or previous incidences of abuse and the proclivity toward subsequent abuse, neglect or exploitation.21
- Identify, from the perspective of states and nursing facilities, limitations, innovative strategies, and recommendations for improving the current screening and monitoring process for ensuring a qualified long-term care workforce.
B. Data Sources
For this study, Lewin relied on both primary and secondary data sources. The sources used include key informants at the federal, state, and facility levels, CNA registry data, abuse registry data and relevant literature and reports.
Federal and National Key Informant Interviews. Guided by ASPE and a technical advisory group (TAG), Lewin gathered data from a numerous primary sources to capture a variety of stakeholder perspectives. In the initial stages of the project, Lewin conducted fourteen key informant interviews targeting experts in several key areas related to the project, including: experts in long-term care, elder abuse, law enforcement, federal representatives working on related projects (Centers for Medicare and Medicaid Services (CMS)), and nursing home industry and direct care workforce representatives. Preliminary interviews focused on soliciting input related to project topics, strategies, and contacts for experts in the field. After speaking with key informants, Lewin formed a TAG representing a broad spectrum of stakeholders. TAG members assisted the research team with: (1) developing a work plan focused on eliciting a better understanding of how screening mechanisms are used and interpreted and the practice variation that exists across and within states, (2) clarifying relevant policies and identifying relevant research, and (3) ensuring that the project added to the existing body of research.
State Key Informant Interviews. Arizona, Illinois, Florida, and Washington were selected as case study states based on several relevant characteristics developed in collaboration with ASPE and the TAG. Criteria included:
- Geographic location;
- Mix of urban versus rural populations;
- Diversity of resident population;
- Diversity of direct care worker population;
- Comprehensive nurse aide registry;
- Criminal background check requirement;
- Use of waivers or other sanctions for direct care workers; and
- Size of older adult population.
For each state, Lewin conducted stakeholder discussions via telephone with selected state representatives. Lewin conducted interviews from September 2005 to January 2006 with the following stakeholders:
- Nurse Aide Registry personnel;
- State survey and certification representatives;
- Long Term Care Associations;
- Adult protective service (APS) representatives;
- Law enforcement;
- Ombudsmen;
- Medicaid fraud unit; and
- Workforce development board agency.
Interviews with state stakeholders focused on policies and practices related to the prevention of resident abuse in nursing homes--specifically, the approach to criminal background checks and use of nurse aide and abuse registries. Discussions with state staff provided a better understanding of the different practices imposed by the states and rationale pertaining to the employment of individuals with criminal histories or previous offenses of abuse, neglect or financial exploitation. In addition, stakeholders provided information about current state processes, capacity issues, system structures, and suggested improvements. Information gathered was used to contextualize discussions with employers at the facility level about their practices and perspectives on the value of different strategies for reducing the incidence of resident abuse.
Nursing Facility Site Visits, Interviews, and Surveys. In addition to telephone interviews with state level stakeholders, Lewin conducted in-person site visits or phone interviews with informants in three or four nursing facilities in each state.22 Nursing facilities were selected for the following reasons:
- Diversity: When selecting facilities, Lewin considered the facilities geographic characteristics (e.g., size, resident population, ownership type (chain versus freestanding nursing facility), business model (for profit, non-profit, religious affiliation)).
- History and reputation: Lewin selected facilities (based on state recommendations) that had a history of overcoming staffing/resident challenges, experienced positive/negative management changes that affected performance, or had a reputation of consistency, and positive survey results.
- Labor market: Lewin selected some facilities dealing with a constrained labor market to elicit whether the high demand for employees resulted in different hiring practices.
At each facility, Lewin conducted interviews from November 2005 to March 2006 with the following stakeholders:
- Representatives from management (Administrators and Regional Directors);
- Director of Nursing and Staff Development Nurse;
- Human resources/risk management personnel; and
- CNAs.
Interviews with facility level stakeholders focused on the policies and practices employed by the facility regarding the screening, hiring, training and monitoring of nurse aides. Discussions with facility level stakeholders solicited, from a variety of perspectives, an understanding of the utility and relative contribution of registries and background checks in reducing the incidence of resident abuse and ensuring a qualified long-term care workforce. Discussions also revealed aspects of the process that are most and least useful, strategies employers use to enhance the screening process as part of corporate requirements, suggestions to improve the current system, and insight into effective training and monitoring practices.
Detailed discussion guides for all interviews with TAG members, key informants, and state and facility level stakeholders are included in Appendix E.
Analysis of Registry Data
Originally, ASPE intended to gain access to states registry data and criminal background databases and use this data to ascertain:
- The relationship between direct care workers with criminal background and rates of abuse, neglect, and/or financial exploitation; and
- The relationship between direct care workers with prior history of abuse, neglect, and/or financial exploitation and subsequent findings of abuse, neglect or exploitation.
Lewin worked closely with the Arizona Board of Nursing (AZBN) and the Kansas Department of Health Occupations Credentialing to conduct a secondary data analysis of state nurse aide registries and criminal history databases to explore the relationship, if any, between past criminal convictions or previous incidences of abuse and proclivity towards abuse, neglect and financial exploitation. These two states were selected because they use both nurse aide registries and criminal background checks as screening mechanisms.
Lewin originally requested raw data files of the nurse aide and abuse registries, as well as information on criminal background status, from both Arizona and Kansas. Due to regulations that prohibit the release or sharing of information on individuals criminal history, Lewin then requested Arizona and Kansas to conduct the analyses of state databases and then share aggregated results with the research team. Lewin provided an analysis plan (see Appendix E) for both states to follow that would examine the differences in abuse rates between nurse aides who had a criminal conviction or previous substantiated abuse finding, and nurse aides without such history. The data analysis plan also included demographic characteristics of nurse aides with substantiated findings of abuse, neglect or exploitation.
Each state submitted information on the following:
- The percentage of nurse aides in the abuse registry with past criminal histories (non-disqualifying offenses).
- The percentage of nurse aides in the statewide nurse aide registry with past criminal histories (non-disqualifying offenses).
- Basic demographics and type of abuse allegation.
Document Review
To augment interview and site visit data, relevant documents were reviewed, including federal reports, state statutes, research literature, and literature provided by nursing facilities. Appendix A contains the bibliography of literature reviewed.
C. Study Limitations
Numerous barriers, outlined below, prevented Lewin from analyzing the relationship between criminal background and proclivity for abuse using registry data from multiple states.
Barriers to Accessing Data on Criminal History. Accessing the repository of criminal record data collected by state agencies is prohibited by federal laws and state statutes established to protect individual privacy. Sharing this information is prohibited, even in aggregated form. Similarly, in a limited number of states that follow an open record policy for releasing criminal background information, access to information remains highly restricted. For example, open record states may restrict information sharing on criminal background records to other state offices. Further, if open record states allow a non-state entity to access information, many allow these entities to conduct criminal background checks on a single individual only--using name, date of birth, or social security number.23
Barriers to Accessing Data on Substantiated Abuse. Similar barriers arise when attempting to access nurse aide registry information on substantiated findings of abuse, neglect, and financial exploitation. Due to privacy laws, states contacted could not release the full extent of their databases to entities outside the state agency. For example, despite having a rich database that contains abuse, neglect, misappropriation, and criminal background data, Wyoming could only provide information on whether a person has been disqualified and could only release information for individuals who consented to the release of their information. Approximately 56% of Wyoming nurse aide applicants consent to releasing information to third parties.
Relevant Data Housed in Multiple Registries, Maintained by Multiple Agencies. Access to criminal background data and state nurse aide registry data are not the only obstacles encountered in conducting the quantitative component of this study. For example, few states maintain information on licensure, abuse, neglect, financial exploitation, and criminal history in one registry.24 The majority of states maintain two or more registries containing information on licensure of various health professionals, findings of abuse, neglect, and misappropriation of property, and criminal background.25 Access to needed data would require the approval by multiple entities and these entities would need to release identifying information for each individual in order to match records from each state database. As noted previously, access to comprehensive identifying information is difficult. In addition to the difficulties of correlating data across multiple registries in one state, nurse aide registry data may be of poor quality.
Inconsistent Data Quality. The quality of nurse aide registry and criminal history data impacted our ability to conduct a meaningful analysis. A study by the OIG revealed that nurse aide registries often fail to provide accurate information. Federal law requires that substantiated findings of abuse, neglect, or financial exploitation be recorded within ten days of the substantiated finding. In the national survey, OIG conservatively estimated that one in four records of nurse aides with substantiated findings was not updated within the required ten day period. Of even greater concern was the finding that one in eight nurse aide records were not updated three months later, long after the federally mandated ten day period. Further, many states failed to meet the federal requirement of removing records of inactive nurse aides (defined as failure to practice in 24 consecutive months) therefore enabling uncertified individuals to continue working.26 Several states that were approached to participate in this study expressed resistance because databases were not consistently purged. Interestingly, some states indicated that they have never purged their database. Some states reported that they have several hundred-thousand records in their database, including many inactive workers which would compromise the quality of the data. For these states, conducting the secondary analysis would have required significant resources and data cleaning to produce meaningful results. Due to access barriers, Lewin needed to rely on the willingness of state workers to conduct this analysis. State contacts generally indicated a high level of interest in the study but simply did not have the staffing capacity to conduct the analyses.
III. FINDINGS
To answer the questions posed by this study, it is essential to examine the various components that constitute the systems for pre-employment screening (i.e., use of nurse aide registries and criminal background checks) and post-employment processes (i.e., training, on-the-job monitoring, and complaint investigation and reporting practices). While there are federal requirements to maintain a nurse aide registry and conduct pre-employment background checks, there are no requirements standardizing the implementation practices employed by states and nursing facilities. As such, implementation of these requirements varies considerably across states. The following section presents findings from four states regarding pre- and post-employment practices and innovations. Illustrating the variation in practices across the four states are process flow charts contained in Appendix B depicting: (1) the process for CNAs seeking certification; (2) process for CNAs seeking employment; and (3) process for handling complaints or allegations against CNAs of abuse, neglect, or exploitation.
A. Current Practices in Pre-Employment Screening, Background Checks, and On-the-Job Monitoring
1. Maintenance of the Nurse Aide Registry
To understand the utility and overall effectiveness of the nurse aide registry, it is important to have a clear sense of the structure, content, maintenance and capabilities within the state for sharing relevant information. The department or association responsible for the nurse aide registry varies greatly in each state. There is also significant variety in the content recorded in states registries, as well as the means and timing of updates to the registry. Many states encounter difficulty in keeping the state nurse aide registry up-to-date since there are different entities within each state that keep track of the different aspects of information recorded. Through state level informant interviews in the four study states (Arizona, Florida, Illinois, Washington), the level of variation among responsible entities who maintain the nurse aide registry, the contents, and the ease with which updated information is accessed became evident.
The nurse aide registry is maintained by the AZBN, the Department of Health in Florida, the Department of Public Health in Illinois, and the Department of Social and Health Services in Washington. Though each state entity fulfills the same role, they are different sectors within each state governments structure. Arizona, Florida, Illinois and Washington contain information on CNAs, registered nurses (RNs) and licensed practical nurses in their nurse aide registries. Illinois also includes home health aides, personal care aides, and developmental disability aides in its registry. All four states record most demographic information including social security number, name, address, etc. However, each state varies in keeping record of other relevant information, such as date of competency completion, employment status, criminal background check status and date, substantiated findings, disqualifying offenses, waiver status, and current employer.
The complexity of maintaining the nurse aide registry stems from the need to receive updated information from other state departments handling different types of information that must be recorded in the registry. Criminal background check status, for example, must be gathered from the background check unit in the state, which in many cases is different from the entity that maintains the nurse aide registry. Information about employment (i.e., employer and status) requires updated information from employers or by certified workers themselves. If this is not done regularly, it impedes the ability of the entity maintaining the nurse aide registry to keep current and accurate records. Also, limited staffing capacity to maintain the registry and high nurse aide turnover are additional challenges that states face in updating the nurse aide registries consistently and accurately.
2. Criminal Background Check Processes
a. Disqualifying criminal offenses
Federal guidelines require criminal background checks to be conducted prior to the employment of CNAs. The goal of conducting criminal background checks is to ascertain whether or not applicants have a disqualifying criminal conviction that would prohibit them from working in a long-term care setting. Most states have developed a list of criminal offenses that prohibit an individual from obtaining either state certification/licensure or employment (blanket disqualification). However, there is no consensus across states regarding which crimes should be considered disqualifying offenses. Some states disqualifying offense lists include felonies only, while other states include felonies and select misdemeanor offenses such as driving under the influence and domestic violence convictions. The length of time (number of years) since conviction that would prohibit a person from working in a long-term care setting also varies by state. In some states, any felony conviction, regardless of when it occurred, automatically disqualifies someone from being employed. In other states, only specific felonies committed in the last five years result in blanket disqualification. In some cases, states consider convictions on juvenile records when making a determination of suitability.
To examine the level of variation that exists across states in terms of the types of crimes resulting in blanket disqualification, Lewin compiled a cross-state summary including data from 50 states and the District of Columbia regarding the use of criminal background checks in screening CNAs (see Appendix C). These matrices provide a concise summary regarding the state entities that conduct criminal background checks on nurse aides, laws or regulations that authorize criminal background checks and types of crimes27 that result in disqualification from employment as a CNA.
Matrix 1 (in Appendix C) provides an overview of the criminal background check process by state and shows variability across states at the certification and employment levels. In addition to states cross-checking against lists of different disqualifying offenses, states also vary in their requirements for conducting either a state or federal (Federal Bureau of Investigations (FBI)) level background check. The timing of the background check also varies, with nearly 40% of states (n=20) requiring the criminal background check prior to certification of nurse aides, and 80% (n=4128) requiring the check before employment. One implication of states requiring the background check prior to employment but not prior to certification is that individuals with criminal backgrounds can become certified and listed in the registries, possibly leading to an overstatement of the CNA supply in these states. In addition, this policy can be an issue for nurse aides who can complete their training and education, receive state certification to work, yet are not able to secure a job if they cannot clear the background check.
Matrix 2 (in Appendix C) provides details regarding regulations by state, again illustrating enormous variation in policies and regulations, in terms of types of crime (felonies and misdemeanors) and allowable time period since conviction (five years, ten years, no limit, and inclusion of juvenile record), that constitute the basis for disqualifying a potential worker from employment in the long-term care industry. For example, the allowable time since conviction in Colorado is ten years for certain disqualifying offenses, while for other offenses there is no limit (i.e., any history of violent crime, regardless of when the crime was committed prohibits an individual from employment). The allowable time since conviction in Delaware ranges from 5-10 years depending on the type of offense, and Virginia grants exemptions for offenses committed more than five years prior to application if the individual has only one conviction.
b. Similarities in the criminal background check process across states
Stakeholder discussions and facility site visits and interviews revealed some common criminal background check practices among Arizona, Florida, Illinois, and Washington. These commonalities include the following:
-
State statutes mandate that nursing facilities perform checks on CNA certification/licensure status and criminal history. In each of the four states we examined, nursing facilities are required by law to verify that nurse aides seeking employment have active certification and that criminal background checks are completed before hiring. In addition, state certification entities perform criminal background checks and verify that the nurse aide has no disqualifying offenses on their record.
-
Waivers or exemptions are permitted in all four states. While a waiver or exemption process exists in these states, the procedure for granting waivers or exemptions varies widely. For example, Arizona does not permit exemptions to any individual with a history of a felony in the past five years. Illinois permits waivers for a select number of crimes and with the permission of the Director of Public Health. In Illinois, a waiver application of an individual who has been convicted of an offense and who is typically ineligible for a waiver is still accepted, though far fewer exceptions are granted. Florida permits waivers and Washington permits exemptions if applicants follow certain appeal procedures. In Florida, potential CNAs bear the burden of showing sufficient evidence that they should not be disqualified and can be granted waivers under certain conditions set forth by law. (See Appendix C for Disqualifying Offenses.)
-
Registries contain detailed information that exceeds requirements detailed in federal guidelines. Federal guidelines dictate that registries contain the following information: full name of the individual, identifying information (social security number, address, etc.), the date of certification, and information regarding any substantiated findings of abuse. However, all four states maintain additional information in their registry databases. For example, databases in all four states include some demographic information (e.g., gender, race, education). Databases in Arizona, Florida, and Washington can capture employment status. Illinois collects training information and waiver information. Two states, Illinois and Florida provide information about inactive CNAs. While states reported what their databases have the capacity to collect on all individuals, this level of data is not necessarily collected for each individual in the registry.
c. Background checks variation across states
Despite some commonalities in the process for checking criminal background and disqualifying offenses, there is significant variation in how states approach screening the long-term care workforce. Differences include the following:
-
In contrast to Florida and Washington, Illinois and Arizona perform criminal background checks on a diverse range of workers. Illinois maintains information on home health aides, personal care aides, and developmental disability aides. Arizona performs criminal background checks on all direct care, human services, and supportive services employees working in residential and long-term care facilities.
-
States use a variety of identifying information to perform checks on criminal history and disqualifying offenses. States use a variety of identifying information to perform background checks ranging from more reliable data such as fingerprints to less reliable data such as name and date of birth. For example, Arizona and Florida use fingerprint data for all checks. Illinois uses a combination of name and date of birth to perform an initial check and if this information results in a positive result for criminal history, Illinois runs an additional check using fingerprint data to confirm results. With additional funding received as part of the CMS demonstration, Illinois will move to a fingerprint system in January 2006. Similar to Illinois, Washington uses a combination of name, date of birth, and fingerprint data. In this case, name and date of birth are used to run an initial check and fingerprint data are only used when name and date of birth do not appropriately identify the individual or if a positive result occurs.
-
States use a variety of databases to run background checks. In Arizona, fingerprints are run through both state and national (FBI) databases. At the state level, Arizona relies on the Automated Fingerprint Identification System (AFIS) that houses all criminal prints collected in the state. At the national level, Arizona uses the FBI database. Florida uses fingerprints to check for criminal records in the Florida Department of Law Enforcement database. If this state level check results in a positive identification, fingerprint checks are run a second time against the FBI database. Illinois uses name and date of birth to check the state police database. If state level checks result in a positive identification, Illinois utilizes fingerprint data to check the FBI database. Washington uses identifying information such as name and date of birth to run a criminal background check through the Washington State Patrol database. If name and date of birth do not appropriately identify a person (such is the case when two people have the same name and date of birth), Washington utilizes fingerprint data. In addition, Washington will perform fingerprint checks using the FBI database in particular situations (e.g., when a person has recently moved to the state).
-
In contrast to Florida and Illinois, Arizona and Washington provide information on pending cases of abuse, neglect, or exploitation. In Arizona, entities or individuals submitting background check requests must provide the name, license number, and social security number in order to access whether or not applicants are currently under investigation for abuse, neglect, or exploitation. Washington also includes pending abuse cases filed against workers in their registry. Employers have the discretion to hire, ask the applicant for information regarding the circumstances, or deny employment based on pending charges noted in the registry.
d. System gaps--limitations of existing screening practices
An analysis of background check processes in these four states highlighted gaps in the criminal background check system that may lead to limitations in the effectiveness of these screening mechanisms. Identifying potential limitations to current background check processes may provide ideas for states trying to improve their systems and inform stakeholders about the complexities of this process.
-
Criminal background checks only capture activity prior to employment. One of the biggest gaps in the current system is the single point in time nature of the criminal background check. The underlying assumption for checking an individuals criminal history is that individuals who commit certain types of crimes are not appropriate for working in close proximity with vulnerable populations in long-term care settings. There are additional assumptions about the character of individuals with a criminal history that make them less desirable employees. The current system has no method for tracking criminal activity that occurs after the worker is employed. Unless states require periodic review of criminal history on a regular basis, employers have no knowledge of any criminal behavior their employees may engage in once they are working.
-
Current systems do not effectively capture crimes committed in other states. One of the most common discussions we had with stakeholders centered on states inability to access information about criminal history outside their own state. Privacy protections often prohibit information sharing between states, and information collected in the FBI database relies on states submission--which is often incomplete. Costs of FBI fingerprint checks also prevent some states from checking the national database for every applicant seeking certification or employment.
-
Disqualifying criminal offenses that preclude an individual from obtaining either state certification or employment differ widely across all states. Appendix C details how all 50 states and the District of Columbia approach the criminal background check process and define disqualifying criminal offenses through their state statutes. States are not consistent in their criteria for blanket disqualifications that prohibit potential nurse aides from working in long-term care settings. Drug charges are a particular issue, as many interview respondents indicated that individuals with a history of drug related crimes are less reliable in terms of work attendance and job commitment, yet few states include drug convictions in their list of disqualifying offenses. In reference to their statutes regarding drug offenses, a representative from one state reported You can use drugs and still work with the elderly; you just cant sell them and work. The rationale for which criminal offenses make the list in each state is inconsistent, and the time delimitation of certain offenses varies across states and lacks evidence to support any preference.
-
Information delay of criminal background check can put facilities and residents at risk. Facilities can hire employees while their criminal background check is pending. In some states, the criminal background check process can take several months. This may put both the residents and facility at risk as well as waste labor resources if in fact the background check shows criminal activity. Facilities rely on information they receive from the criminal background check and would like this process expedited so they can avoid hiring, training and investing in employees they may need to terminate based on results of the screen.
-
Inadequate communication and coordination between relevant stakeholders can impede the process. In all four states, multiple entities participate in the background check process. Consequently, communication and coordination of information across state agencies is critical to the criminal background check process. State and federal legislation can pose barriers to communication across agencies. States have tried to address communication issues. For example, Arizona offers a free quarterly newsletter to the public that contains information on verified cases of abuse, neglect, and misappropriation. This regular communication is one way to increase communication across relevant stakeholders.
Once allegations have been made and an investigation takes place, additional communication is necessary to close the loop and ensure substantiated findings make it to the appropriate registry. Multiple entities can investigate abuse allegations in skilled nursing facilities (state surveyor, APS, ombudsman, etc.), with no systematic coordination or communication of findings across investigative entities.
-
Inadequate resources result in gaps in the background check process. Additional financial resources and/or staff would improve the criminal background check process in several ways. Budget limitations and attendant staff allocation issues affect quality, completeness, and timeliness of registry data. For example, understaffing in Washington poses barriers to a comprehensive background check system because state patrol statutes mandate that pending cases must be dropped after 12 months. Inadequate staffing levels lead to unprocessed cases, which result in missed opportunities to review individuals. In addition, states frequently cited the high cost of procuring and processing fingerprint background checks as a barrier within the current system. Many states would rather use fingerprint checks at the state and national level, but simply cannot afford to implement this practice. Due to cost issues, some states are considering shifting the costs of background checks to applicants. However, this may prevent qualified applicants from applying for jobs.
-
Entities performing background checks use data that cannot be easily verified. Applicants can potentially falsify information if entities do not rely on fingerprint data. For example, some states rely on name and date of birth to perform state level background checks, defaulting to more reliable fingerprint data only when name and date of birth result in more than one match or when applicants have recently moved to the state (within three years). Individuals who do not want to submit fingerprint data can easily claim that they have lived in the state for more than three years and thus bypass the more rigorous fingerprint based background check.
-
Inaccurate hits or errors on the criminal background check may falsely exclude qualified workers. Individuals with common names may experience positive hits on their criminal background check when they in fact have not committed a crime. In this situation, some states are able to conduct a fingerprint background check to ensure they are checking the background of the correct individual, but this is not always the case. Individuals often bear the burden for clarifying errors associated with their background check results which is takes time and unnecessarily delays their entry into the workforce.
-
The background check process often fails to account for unlicensed workers in licensed facilities or individuals working outside licensed facilities. Current processes do not account for the criminal history of workers without licenses (e.g., housekeeping and kitchen staff) in licensed care facilities, yet these individuals often have frequent contact with residents. In addition, states do not have statutes requiring background checks on individuals working outside licensed facilities such as individuals providing home health care.
-
Interpretation of pending cases in the abuse registry is difficult for employers during the hiring process. Solid arguments exist on both sides of the issue of whether or not to include pending cases in abuse registries. One the one hand, including abuse cases that are pending in the registry allows employers to learn if there are issues of misconduct associated with someone they may be trying to hire into their organization. From a conservative standpoint, some employers welcome the information to be safe rather than sorry, and they appreciate the option to pursue details of the pending case with potential applicants they have particular interest in hiring. However, pending cases can be detrimental to a worker seeking a new job position before the case has reached resolution. States are required to investigate all allegations that are brought against an employee--whether frivolous in nature or not. While a case is pending, which can be up to several months, workers under investigation due to a false accusation have difficulty finding employment and are placed into a guilty until proven innocent framework until the case is dismissed.
-
Some states have adopted a waiver system for direct service workers to appeal a decision to prohibit employment while other states have no appeal system in place. Some state systems are ironclad and there are few opportunities for workers to appeal the decision made by the state. Issues highlighted previously factor into this scenario. Criminal background checks conducted with name and date of birth can often generate false positives for individuals with common names, for which there is little recourse in some states. Similarly, in states where there is no time delimitation associated with offenses, a potentially qualified and capable person may be prohibited to work because of an assault charge they had 20 years ago--regardless of maturation, rehabilitation or contextual factors associated with the crime.
3. Post-Employment Processes
Compared to pre-employment requirements at the federal, state, and employer levels, monitoring during the post-employment phase is less formal. There are fewer regulations and policies in place to track the criminal activity of nurse aides once they are actively employed. State resources are allocated primarily to pre-screening activities, with fewer resources and requirements focused on training (e.g., in-services, management training), monitoring practices or subsequent follow-up criminal background checks.
a. Training
Discussions with stakeholders at the state and nursing facility levels in the four study states revealed that the requirement states place on nursing facilities for on-the-job training primarily concern health and safety issues under licensure. Many of the facilities interviewed do provide on-going training to nurse aides regarding what constitutes abuse, neglect, and financial exploitation (committed by peers or residents relatives and friends), resident rights, clinical topics, and other related issues. However, the frequency and regularity of trainings specifically focused on preventing abuse and neglect varies by facility. Several nursing supervisors mentioned using potentially problematic behaviors (e.g., raised voices, negative comments about residents, delayed responses to call lights, etc.) as teachable moments to work with staff to better understand the connection between these behaviors and incidents of abuse and neglect.
Directors of nursing and staff development nurses at the facilities interviewed rarely, if ever, receive specialized management training that would assist them in recognizing incidences of abuse and neglect. They rely primarily on their experience in managing potentially difficult scenarios between residents and staff.
b. On-the-job monitoring
On-the-job monitoring is not well-defined, nor are there any state requirements to standardize facility practices. In the absence of any state requirements, independent and chain facilities reported implementing policies such as random drug testing and random criminal background checks to routinely monitor existing employees. In addition, facilities interviewed reported a variety of strategies to facilitate on-the-job monitoring, including locating work spaces for nursing supervisors on the floor, pairing new hires with experienced nurse aides, assigning pairs or teams of staff to residents, and offering ways for staff to report concerns about the behavior of their peers anonymously.
c. Complaint investigation and reporting
All facilities interviewed follow a similar set of procedures for responding to complaints and allegations. Following a complaint, nurse aides are suspended without pay while the facility conducts an internal investigation and notifies the state about the pending complaint. If the complaint is substantiated, the nurse aide is terminated, a report is filed with the state, and the nurse aide registry is notified. If the complaint is not substantiated, the nurse aide is reinstated with back pay and the state and registry are notified.
What complicates this process for employers is the fact that multiple entities (e.g., state licensing agency, ombudsman, attorney general, APS, law enforcement, etc.) can receive and investigate complaints and allegations simultaneously. Process flow charts in Appendix B show the state-specific processes for handling complaints or allegations against CNAs. The quality and level of coordination and communication across agencies varies by state, which further complicates and compromises the timeliness of the investigation process. Nursing facilities reported that the process for complaint investigation and resolution can be time-consuming given the possibility of multiple entities investigating the same complaint. In addition, state entities involved in reporting and investigation indicated that they are under-resourced and lack the staff to respond to cases efficiently and effectively. During the course of a protracted investigative process, a nurse aide under suspension without pay typically seeks other employment. If the allegations are not substantiated, employers can lose qualified workers.
The involvement of multiple entities and lack of role clarity among them also can be confusing for residents and their advocates in terms of which entity or agency to notify regarding a complaint or allegation.
B. Relationship between Past Criminal Background or Incidences of Abuse and Subsequent Abuse, Neglect, and Exploitation
Analyses of nurse aide and abuse registries in Arizona and Kansas suggest that there is a correlation between prior history of criminal conviction and subsequent incidences of abuse, neglect, and exploitation. We were not able to determine which crimes had the strongest association with subsequent findings of abuse, neglect or misconduct due to the privacy issues associated with sharing criminal background data on individuals. We did not have access to the type of crime or date of criminal conviction to further elucidate the relationship between prior criminal history and substantiated findings of abuse post-employment. States can perform this type of analysis on the data in their own administrative files, but the states we partnered with for this study did not have the resources to devote specifically to this effort. Findings from the two states are presented below.
Kansas
The Kansas Department of Health and Environment, Health Occupations Credentialing Unit analyzed their abuse registry from December 1990 to March 2005. Over this period, 710 individuals were entered with a substantiated finding of abuse, neglect or exploitation. Table 1 shows the distribution of individuals by type of substantiated allegation. Kansas calculated the percentage of nurse aides with a substantiated finding of abuse that also had a non-disqualifying criminal conviction prior to employment. Twenty-one percent of the 710 individuals in the abuse registry also had a hit when their criminal background check was conducted prior to employment, compared to 14% in the overall population of nurse aides in the state.
| TABLE 1 | ||||
| Abuse*N (%) | NeglectN (%) | ExploitationN (%) | TotalN (%) | |
| Individuals by Abuse Type | 472 (66) | 190 (27) | 48 (7) | 710 (100) |
| * Abuse = physical, sexual, and verbal | ||||
Arizona
The Arizona Board of Nursing (AZBN) Abuse Registry contains information on RN aides under investigation by the AZBN. The AZBN investigates nurse aides for the following reasons: (1) a complaint is filed against an active nurse aide on-the-job, (2) the criminal background check results in a positive hit, or (3) the nurse aide answers yes to previous criminal conviction on the state application for certification. The registry contains information on pending cases and tracks potential violations, actual violations, substantiated findings and outcomes of all investigative actions (suspension, fines, additional hearing, case dismissal, etc.). As of April 2006, the AZBN Abuse Registry contains data on 4,154 individuals. Of the 4,154 individuals in the Abuse Registry, 1071 (26%) have a prior criminal conviction and 829 (20%) have an incidence of previous misconduct.
As of April 2006, there were a total of 20,764 active CNAs in the AZBN registry database. According to the AZBN, the number of CNA's that have submitted to fingerprints for certification are 13,799 (some nurse aides were certified by the state prior to implementation of the state requirement to conduct fingerprint background checks). From the population of active nurse aides who have submitted fingerprints, 9,426 have had both a state (Department of Public Safety (DPS)) and federal (FBI) fingerprint background check documented in the state database. Of the 9,426 individuals with documented state and federal checks, 6.2% had a positive felon or offender hit on the state background check through the DPS and 10.1% had a positive felon or offender hit on the federal background check conducted by the FBI.
C. Innovative Screening and Monitoring Strategies
Several aspects of the screening and monitoring process were cited by state informants and facilities as innovative practices that contribute to ensuring the employment of a high quality long-term care workforce.
-
Arizona Fingerprint Clearance Card System. The nursing facilities interviewed in Arizona cited the Fingerprint Clearance Card System, implemented in 1999, as an innovative practice for facilitating criminal background checks of employees and monitoring subsequent criminal behavior after they are employed. Arizonas comprehensive Fingerprint Clearance Card System is administered by the DPS to perform background checks on and to track arrest activity of individuals working in positions of direct care and service of potentially vulnerable populations (e.g., nursing facilities, home health agencies, child care agencies, schools etc.). Development of the Fingerprint Clearance Card system occurred through collaborative efforts of five state agencies (Department of Health Services (DHS), Department of Education, Department of Economic Security, Department of Juvenile Corrections, and Administrative Office of the Court) in an effort to improve the quality of the workforce across professional fields. For example, to work in long-term care settings, individuals must obtain a Fingerprint Clearance Card by going through a background check.
It is important to note that technically CNAs are not required by the state to obtain Clearance Cards to work in long-term care settings because they already undergo a criminal background check during the certification process required by law and governed by the AZBN. However, the practice of most nursing facilities is currently to require potential hires to have a Clearance Card and it is common for facilities to require students training to be CNAs to have Clearance Cards before working directly with residents. Because the Fingerprint Clearance Card process was developed collaboratively across five state agencies, the resulting list of disqualifying offenses used is far more expansive than the list specified in the state statute for certifying nurses aides administered by the AZBN.
This Fingerprint Clearance Card system allows law enforcement to identify individuals who are direct care workers serving vulnerable populations when any arrest is made and fingerprints are taken. Upon arrest and booking, fingerprints are entered into a database (AFIS), which sends a flag to the (DPS) for individuals with Fingerprint Clearance Cards. DPS then notifies the appropriate agency representing the field in which the individual is currently employed (in the case of a long-term care employee, DHS would be notified) that the employee has been recently arrested for a crime. Ideally, in the case of a CNA arrest who has a Clearance Card, DHS would contact the AZBN so that employers could be notified of the employees recent conduct. This process gives employers updated information on employee conduct, and addresses the limitation of criminal background checks being performed at a single point in time prior to employment. However, the effectiveness of this notification chain is dependent on the accuracy and currency of the nurse aide registry and breaks down if the registry does not routinely receive updated information regarding changes in employment/employer status.
The Fingerprint Clearance Card is valid for six years and costs $52.00 ($24.00 for the FBI check, $3.00 for the Arizona Bureau, and $25.00 to DPS to support personnel costs and fingerprint technicians).
-
When individuals or entities request background check records, offer detailed information. In Arizona, individuals or entities requesting background check records do not simply receive a yes or no regarding the eligibility of an applicant. Instead, background check requests include detailed information such as the types of crimes the applicant has committed. This information may play a role in hiring decisions. If the applicant has a criminal conviction that does not automatically disqualify them from working, the employer can use their own discretion to assess the context of the crime and make an appropriate hiring decision based on their needs.
-
Illinois Nursing Home Sweep identifies workers with existing and relevant arrest warrants after they have cleared the criminal background check prior to employment. In Illinois, state police within the Medicaid Fraud Unit conduct monthly checks of all staff and residents within long-term care facilities that receive Medicaid financing to ascertain if any of these individuals have outstanding warrants for their arrest. The Medicaid Fraud Unit uses discretion to determine which arrest warrants are relevant to pursue based on contextual factors (e.g., warrants for unpaid parking tickets are bypassed, warrants for assault or theft are pursued). Officers arrive at facilities unannounced to make the appropriate arrest. According to the fraud unit in Illinois, arrests are made each month during these sweeps. When this process was first implemented, facilities were not fully supportive and viewed the process as intrusive. However, over time facilities have become accustomed to the process and recognize its benefit. Now many facilities proactively contact the fraud unit requesting the sweep as a means of quality checking current employees without paying for follow up criminal background checks.
-
Perform background checks a wide variety of individuals that serve people with long-term care needs. Florida performs background checks on any employee that has contact with residents in long-term care facilities. These checks include housekeeping, maintenance and kitchen staff.
Facility Level
-
Facilities with adequate resources contract with private companies to conduct their own pre-employment background checks. For the purposes of expediting the hiring process and minimizing potential liability, some facilities (many of which are part of national chains) contract directly with private firms to conduct background checks of potential employees. They report that the costs incurred are warranted because the background checks are conducted more quickly and cover databases from all 50 states. In addition, the list of disqualifying offenses required by corporate human resources policy typically is more stringent than that specified by the state.
-
Facilities require drug tests on all job applicants. Many facilities cited drug testing as a critical component of the hiring process because of the correlation between drug use and absenteeism, inferior caregiver skills, diminished therapeutic relationships with residents and overall unreliability on the job. Drug testing is considered an asset because of the negative impact drug use can have on the safety of the workplace environment for both staff and residents. The drug testing requirement is also seen as a deterrent for potentially unreliable and problematic staff. Many facilities we interviewed stated that far more applicants are denied employment due to positive drug tests than having a positive hit on their criminal background check.
-
Facilities conduct random criminal background checks and random drug tests annually on existing employees to maintain quality. Some larger chain facilities have corporate requirements to continually check the criminal status and/or drug use of existing employees. In addition to random drug tests for a sample of employees, one corporate chain has implemented random criminal background checks on an employee sample to determine whether existing employees have had relevant criminal convictions after passing the initial screen before hire.
-
Facilities offer financial incentives to employees for referring successful hires. To address the challenge of recruiting, hiring, and retaining qualified staff, several facilities interviewed offer financial incentive programs, such as bonuses and salary increases, to encourage current employees to refer qualified colleagues for open staff positions. These facilities believe that that peer referrals enhance the likelihood of identifying qualified candidates who will meet the hiring requirements, as well as fit successfully into the organizational culture and community.
D. Suggestions by Informants to Improve Processes for Background Checks and On-the-Job Monitoring
Informants offered several suggestions for improving the background check process.
-
Create online registries. Representatives from Washington noted that online registries would enable interested parties to check the registry in real time instead of waiting for registry staff to sort through paper for relevant information.
-
Create a national registry. While cost and administrative issues present barriers to the creation of a national registry, representatives across states noted that a national registry would result in a much improved background check system since individuals would not be able to cross state lines to gain employment if disqualified for employment in another state.
-
Approach allegations of abuse, neglect, and exploitation of elderly as seriously as allegations of abuse, neglect, and exploitation of children. Several respondents noted that similar strategies could be used to prevent abuse, neglect, and exploitation in these two populations. Part of prevention includes the knowledge of substantial consequences when prosecuted for various crimes. Several informants noted that investigation and prosecution of elder abuse cases lacks the level of visibility and urgency that child abuse cases have historically received.
-
Perform background checks prior to training programs. Some interview respondents suggested that training programs clearly detail background check procedures so that individuals who may be potentially ineligible for work do not proceed through training programs without fully understanding what will be required of them to gain employment. In addition to notifying them of the background check requirement, nurse aide training programs should also inform students that waiver processes exist that, under certain circumstances, can enable a person with a disqualifying offense to gain certification.
-
Increase training and monitoring of long-term care staff. Increased training of long-term care staff was often cited as a way to prevent abuse, neglect, and exploitation. Recommendations included increasing the number of on-site trainings offered by state APS. In addition, increasing the presence of full-time paid ombudsmen in facilities may deter criminal activity as well as abuse, neglect, and exploitation.
IV. STUDY CONCLUSION AND POLICY CONSIDERATIONS
A. Conclusion
The efficacy of nurse aide registries and criminal background checks in preventing resident abuse in nursing facilities is difficult to ascertain. Making an accurate assessment regarding the effectiveness of these practices is difficult because every state has a different process for screening and disqualifying potential workers, documenting information in their registries, tracking subsequent employment or complaint data, investigating abuse allegations, reporting relevant findings, and coordinating efforts across state entities. Extensive variation across states affects the ability to make a definitive statement about the efficacy of these strategies to ensure a qualified workforce. The in-depth examination of four states revealed that some aspects of these systems work well, but limitations exist in each state that affect the overall utility of these practices. There is, however, consensus across stakeholders in all four states that criminal background checks are a necessary element of the hiring process. The technology, coordination capabilities and infrastructure exist through on-line registries, fingerprint databases and abuse registries to help employers make the best hiring decisions possible to protect the elderly in their care. States are building on their knowledge, experience, and capabilities to streamline these processes, but there is still room for improvement while balancing the resource intensiveness of making these changes.
It is clear that relying on criminal background checks and nurse aide registries are not enough to prevent or reduce abuse in nursing facilities. Ongoing training, education and supervision for workers providing direct care are also key components to maintaining a quality workforce. A summary of our overall project conclusions are provided below.
Criminal background checks are a valuable tool for employers during the hiring process and their use does not limit the pool of potential job applicants. Stakeholders agree that conducting criminal background checks on potential employees is an important aspect of the hiring process to reduce the likelihood of hiring someone who has potential to harm residents in long-term care. There is widespread acceptance throughout the long-term care industry (similar to that of the child care industry), that this practice serves to protect vulnerable adults and ultimately prevent abuse. By virtue of prohibiting potential workers from certification or employment who have a disqualifying criminal conviction, the pool of individuals entering the long-term care field would theoretically be smaller. However, none of the nursing facilities interviewed experienced any negative impact on their applicant pool as a result of this requirement. According to sources from two state nurse aide registries, the number of CNAs continues to rise each year, further indicating that the criminal background check requirement is not significantly restricting the pool of potential workers entering this field. From the perspective of employers, reducing the amount of time it takes to receive background check results would improve the current system.
A correlation exists between criminal history and incidences of abuse. Based on data we received from Arizona and Kansas, it does appear that nurse aides who had a previous criminal conviction (non-disqualifying offense) had higher rates of substantiated abuse than nurse aides without a criminal history. Due to limitations with access to criminal history data, it is not clear which criminal offenses (if any) have the strongest correlation with subsequent findings of abuse, nor can we determine if the recency of a criminal conviction is a contributable factor in the correlation between criminal history and abuse. However, the analysis of these two states does provide evidence to support the rationale for checking the criminal history of potential direct care workers as a screening mechanism for quality.
Criminal background checks are only one element of preventing abuse. Despite a connection between past criminal history and subsequent allegations of abuse, stakeholders consistently reported the following as effective strategies for preventing abuse, (many of which are not formal state or industry policy): adequate supervision/monitoring, presence of managers on the floor, decreasing staff burnout, adequate staffing levels, rotating nurse aides on the floor to alleviate pressure of difficult residents, increased education and training, obtaining meaningful employment references (beyond verification of employment dates), valuing and respecting staff, creative recruitment incentives to retain committed staff, instituting a drug-free workplace policy, minimizing temporary hires, and pointing out negative behaviors in the moment and using them as a staff development opportunity.
There are fewer policies in place that support or reinforce post-employment strategies than pre-employment to ensure a qualified workforce. This study revealed that there are significantly more resources allocated to the pre-employment phase of ensuring a qualified long-term care workforce than the post-employment phase. The policy focus at the state and facility level is on pre-screening applicants before employment and there are structures and regulations in place that support this effort. However, once a worker is hired and working in the field, there is less guidance regarding how best to train, continuously educate and monitor existing employees. As stated before, most states have no process in place to notify employers if an active employee commits a crime that would have prohibited them from working during their background check prior to employment. In the event of employee complaints or allegations of abuse, the effectiveness of state systems often breaks down due to a lack of coordination between multiple state entities involved in the investigation and reporting process. Duplicative efforts waste state resources, prolong investigations and often keep employees out of the workforce unnecessarily.
B. Policy Considerations
National Level Considerations
-
The challenge of individual state registries. Individual state registries and the barriers associated with data sharing across states, limit employer access to useful information about substantiated abuse findings against workers found in other states. Since workers may have been employed in more than one state, a national nurse aide registry has been frequently mentioned as one way to address the issue of long-term care workers with substantiated findings of abuse, neglect, and/or financial exploitation crossing state lines to work in another state. Several issues may pose barriers for the creation of a national nurse aide registry. First, transfer of information across various state and national agencies may be difficult due to state laws and agency ownership of data. Second, the cost of creating and maintaining a national database would require commitment of both staff time and funds from both states and national agencies. Third, certification procedures and requirements vary across states, which further challenge any effort to standardize the process nationwide.
-
Use of disqualifying offenses and waivers. It is important to strike a balance between the need to protect vulnerable citizens from harm and creating unnecessary barriers to employment for qualified individuals, further reducing the potential pool of long-term care workers. There is a paucity of literature examining nurse aides and criminal recidivism and propensity to commit abuse. Criminal recidivism research shows that a history of past criminal convictions may be a possible predictor of future behavior.29 Other research by Cohen (1996) reports that the probability of future dangerous behavior of criminal offenders increases when circumstances are similar to past situations in which criminal behaviors occurred, which has implications for workers who have substantiated findings of resident abuse.30
A review of Illinoiss Department of Public Health waiver process for individuals certified for work in hospitals and nursing facilities shows that individuals with criminal records can work in the health care field with minimal impact on patient safety. In Illinois, individuals with specific criminal convictions are banned from working in certain health care professions but can apply for waivers. In an examination of waiver applications from 1996 to 2003, 5,706 individuals with convictions applied for waivers. 4,130 (72%) of these individuals were granted waivers. Ninety-seven individuals (or 2.3% of the 4,130 individuals) had their waivers revoked; 38 individuals had revoked waivers because of substantiated finding of abuse, neglect, or theft and 59 individuals due to a second disqualifying conviction.31
Additional research in the area of criminal recidivism, specifically in relation to elder abuse, neglect, and financial exploitation is necessary to develop evidence based lists of disqualifying offenses. Justification for the inclusion or exclusion of various crimes that constitute states lists of disqualifying offenses is unclear, and the lack of consensus across states on this issue illustrates the complexity of making a solid connection between past criminal activity and the proclivity to commit abuse in long-term care settings. In the absence of such evidence, policymakers and employers must still balance the need to protect vulnerable populations with the need to maintain an adequate direct care workforce to accommodate a growing older adult population.
-
The screening process requires a significant amount of resources. As states make efforts to improve their screening processes (e.g., expanding the criminal background check to other states or incorporating federal level checks, expediting the turnaround time for results, expanding the screening process to other types of workers), the costs will inevitably increase. States will need additional capacity (staff and financial resources) to meet the demand for quality screens on increased numbers of workers in a timely manner. It is important to balance the financial burden across state agencies, employers and direct service workers in an equitable manner so that screening processes can continue to improve.
State Level Considerations
-
Keeping registry data current to maximize their utility. A recent OIG study revealed that nurse aide registries may not always contain the most up-to-date, or accurate information. In a survey of 200 randomly selected long-term care facility administrators, 44% (87 individuals) surveyed stated that they periodically rechecked nurse aide registries to ensure that substantiated findings had been posted to the registry. Fifteen administrators found that a nurse aide previously listed as registered and free of a substantiated finding of abuse was later listed to be unqualified for work due to a substantiated finding, failure to attain active registration status, or failure to be certified as a nurse aide. The nurse aide registry is only helpful to employers if the information is current.
-
Increasing the utility of the nurse aide registry with public awareness and education. In most states, employers are the only ones who benefit from the information contained in the nurse aide registry. By increasing consumer knowledge and use of the registry, the state can further protect the public by offering additional resources and information on individual long-term care workers.
-
Incorporating alternative screening mechanisms. Nursing home administrators use several practices (not required by federal regulations) to screen potential employees and to monitor current nurse aides. Eighty-five percent of administrators surveyed for a recent OIG report used additional screening procedures such as criminal background checks, and/or personal and employment reference checks.32 Implementing random drug tests and criminal background checks on existing employees may be another way to monitor employees after they have cleared original pre-employment screens. Conducting drug testing may be a more effective method for screening out individuals with a criminal history in drug abuse rather than a comprehensive ban.33 Findings demonstrate the need to use creative and multi-pronged strategies for screening and monitoring direct care paraprofessionals.
-
Examining states practices related to investigating and reporting abuse. Current state practices for investigating and reporting abuse cases appear duplicative and may lack adequate coordination across entities. This creates overlap for agencies conducting the investigation, burden for the employers, and a protracted suspension period for the direct service worker involved.
V. CONSIDERATIONS FOR ADDITIONAL RESEARCH
There are several areas for future research that may further inform this issue but were beyond the scope of this study.
- Examining the use of screening mechanisms for additional direct care paraprofessional workers such as home health aides, etc.
- Exploring the possibility of conducting criminal background checks for direct care paraprofessional workers through a national and international system.
- Gaining a better understanding of how state appeal processes work for individuals flagged during criminal background checks.
- Exploring the barriers individuals with criminal history (but not disqualifying offenses) experience in gaining employment even when they have appropriate certification or licensure.
- Gaining a better understanding of the reporting and investigations process when a resident brings a case of abuse, neglect, and financial exploitation to the attention of facility staff.
- Gaining a better understanding of post-employment risk factors for abuse.
NOTES
-
42 CFR 483.75 (e)(5); 42 CFR 483.13 (c)(1); 42 CFR 483.13 (C)(1)(ii)(A); 42 CFR 483.75 (e)(6).
-
National Center for Health Workforce Analysis, Bureau of Health Professions, Health Resources and Services Administration. (2004). Nursing Aides, Home Health Aides, and Related Health Care Occupations--National and Local Workforce Shortages and Associated Data Needs. vi-v.
-
Department of Health and Human Services, Office of the Inspector General. (2005). Nurse Aide Registries: State Compliance and Practices (OEI-07-03-00380). 8-13.
-
Lewin experienced multiple barriers to acquiring and linking nurse aide registry and abuse registry data from the states to analyze quantitatively the relationship between criminal history or past findings of abuse and subsequent abuse allegations. These limitations are detailed in the Study Limitations section of this report.
-
Cooper G., and Sheets, V. Criminal Conviction and Nursing Regulation: A Supporting Paper. Paper presented at the 1998 National Council of State Boards of Nursing Annual Meeting, Albuquerque, New Mexico. Cited in Massachusetts Board of Registration in Nursing. (1999). Good Moral Character: Qualification for Initial Nurse Licensure. Boston, MA.
-
Cohen, D. (1996). Notes on the Clinical Assessment of Dangerousness of Offender Populations. Retrieved September 16, 1999, from the World Wide Web: http://www.priory.com/psych/assessin.htm. Cited in Massachusetts Board of Registration in Nursing. (1999). Good Moral Character: Qualification for Initial Nurse Licensure. Boston, MA.
-
Personal communications with Linda Mills, April 27, 2005.
-
Department of Health and Human Services, Office of the Inspector General. (2005). Long Term Care Facility Compliance and Practices (OEI-07-04-00140).
-
Interview with Miriam Aukerman, Western Michigan Legal Services, February 2, 2005.
-
U.S. Census Bureau. (2001). U.S. Census 2000 Brief: The 65 Year and Older Population.
-
Special Investigations Division, Committee on Government Reform. (2001). Abuse of Residents is a Major Problem in U.S. Nursing Homes. 3-4.
-
U.S. General Accounting Office. (2002). Nursing Homes: More can be done to protect residents from abuse. (GAO-02-312); U.S. General Accounting Office. (2002). Nursing Homes: Many shortcomings exist in efforts to protect residents from abuse. (GAO 02-448T)
-
Levine, J. (October 2003). Elder neglect and abuse: A primer for primary care physicians. Geriatrics. Volume 58, Number 10.
-
National Center on Elder Abuse. (2005) Frequently Asked Questions. Retrieved January 8, 2006 from http://www.elderabusecenter.org/default.cfm?p=faqs.cfm#one.
-
42 CFR 483.75 (e)(5); 42 CFR 483.13 (c)(1); 42 CFR 483.13 (C)(1)(ii)(A); 42 CFR 483.75 (e)(6).
-
Federal Statutes Authorizing Criminal Background Checks for Nursing Facility Job Applicants and Employees. (Online), July 19, 2005. http://www.cms.hhs.gov/medicaid/reports/backchks.pdf.
-
National Center for Health Workforce Analysis, Bureau of Health Professions, Health Resources and Services Administration. (2004). Nursing Aides, Home Health Aides, and Related Health Care Occupations--National and Local Workforce Shortages and Associated Data Needs. vi-v.
-
Department of Health and Human Services, Office of the Inspector General. (2005). Nurse Aide Registries: State Compliance and Practices (OEI-07-03-00380). 8-13.
-
Lewin experienced multiple barriers to acquiring and linking nurse aide registry and abuse registry data from the states to analyze quantitatively the relationship between criminal history or past findings of abuse and subsequent abuse allegations. These limitations are detailed in the Study Limitations section of this report.
-
It is important to note that only for profit and non-profit facilities agreed to be interviewed. No public facilities participated in this project.
-
Interview with Hal Sklar, Federal Bureau of Investigations, December 13, 2004.
-
Arizona, Arkansas, California, Kansas, Michigan, and Wyoming maintain one registry for licensure, abuse, neglect, financial exploitation, and criminal history information.
-
Iowa, Washington, and Wisconsin confirmed that they maintain more than one registry for licensure, abuse, neglect, financial exploitation, and criminal history information.
-
Department of Health and Human Services, Office of the Inspector General. (2005). Nurse Aide Registries: State Compliance and Practices (OEI-07-03-00380). 8-13.
-
Because the list of disqualifying offenses in most states is so expansive, we have cited the statute for reference rather than providing a detailed listing of the specific offenses developed by each state.
-
Some states require both pre-certification and pre-employment checks.
-
Cooper, G., and Sheets, V. Criminal Conviction and Nursing Regulation: A Supporting Paper. Paper presented at the 1998 National Council of State Boards of Nursing Annual Meeting, Albuquerque, New Mexico. Cited in Massachusetts Board of Registration in Nursing. (1999). Good Moral Character: Qualification for Initial Nurse Licensure. Boston, MA.
-
Cohen, D. (1996). Notes on the Clinical Assessment of Dangerousness of Offender Populations. Retrieved September 16, 1999, from the World Wide Web: http://www.priory.com/psych/assessin.htm. Cited in Massachusetts Board of Registration in Nursing. (1999). Good Moral Character: Qualification for Initial Nurse Licensure. Boston, MA.
-
Personal communications with Linda Mills, April 27, 2005.
-
Department of Health and Human Services, Office of the Inspector General. (2005). Long Term Care Facility Compliance and Practices (OEI-07-04-00140).
-
Interview with Miriam Aukerman, Western Michigan Legal Services, February 2, 2005.
APPENDIX A: REFERENCES
Alaska HHS Statute, Licensure of Child Care Facilities. (2003). Title 14, Chapter 35. Retrieved from http://nrc.uchsc.edu/STATES/AK/al_47.htm#pgfId-486626.
Alaska Regulations. (2002). Child Care Facilities Licensing. Chapter 62. Retrieved from http://nrc.uchsc.edu/STATES/AK/ak_62.htm#pgfId-709944.
Arizona Department of Economic Security. Certification and Supervision of Family Child Care Home Providers, Section 6 A.A.C.5, Article 52. Retrieved from http://nrc.uchsc.edu/STATES/AZ/az_3TOC.htm.
Arizona Department of Health and Human Services Regulations. Child Care Facilities. Section 9 A.A.C.5. Retrieved from http://nrc.uchsc.edu/STATES/AZ/Az_9TOC.htm.
Braun, K.L., Suzuki, K.M., Cusick, C.E., & Howard-Carhart, K. (1997). Developing and testing training materials on elder abuse and neglect for nurse aides. Journal of Elder Abuse & Neglect 9(1), 1-15.
California Regulations. (2004). Title 22, Division12, Chapter 1--General Licensing Requirements. Retrieved from http://nrc.uchsc.edu/STATES/CA/ca_22_12_1.htm#pgfId-845906.
Cohen, D. (1996). Notes on the Clinical Assessment of Dangerousness of Offender Populations. Retrieved September 16, 1999, from http://www.priory.com/psych/assessin.htm. Cited in Massachusetts Board of Registration in Nursing. (1999). Good Moral Character: Qualification for Initial Nurse Licensure. Boston, MA.
Cooper, G., and Sheets, V. Criminal Conviction and Nursing Regulation: A Supporting Paper. Paper presented at the 1998 National Council of State Boards of Nursing Annual Meeting, Albuquerque, NM. Cited in Massachusetts Board of Registration in Nursing. (1999). Good Moral Character: Qualification for Initial Nurse Licensure. Boston, MA.
Department of Health and Human Services, Office of the Inspector General. (2005). Long Term Care Facility Compliance and Practices (OEI-07-04-00140).
Department of Health and Human Services, Office of the Inspector General. (2005). Nurse Aide Registries: State Compliance and Practices (OEI-07-03-00380). 8-13.
Federal Nursing Homes Laws and Regulations. 42 CFR 483.156.
Federal Nursing Homes Laws and Regulations. 42 CFR 483.75 (e)(5); 42 CFR 483.13 (c)(1); 42 CFR 483.13 (C)(1)(ii)(A); 42 CFR 483.75 (e)(6).
Federal Statutes Authorizing Criminal Background Checks for Nursing Facility Job Applicants and Employees. (2005). Retrieved July 19, 2005 from http://www.cms.hhs.gov/medicaid/reports/backchks.pdf.
Kansas Child Care Licensing And Registration Laws. (2001). Retrieved from http://nrc.uchsc.edu/STATES/KS/ks_newTOC.htm.
Kieffer-Andrews, M. (1998). High Risk Behavior vs. Public Protection. Paper presented at the 1998 National Council of State Boards of Nursing Annual Meeting, Albuquerque, NM. Cited in Massachusetts Board of Registration in Nursing. (1999). Good Moral Character: Qualification for Initial Nurse Licensure. Boston, MA.
Levine, J. (October 2003). Elder neglect and abuse: A primer for primary care physicians. Geriatrics. Volume 58, Number 10.
Long Term Care Community Coalition. Certified Nurse Aide Screening and Continuing Education: A National Survey of State Requirements with Recommendations for Improvement. (2004). Retrieved July 20, 2005 from http://www.ltccc.org/publications/documents/CNAReqmtsApril2004.pdf.
Michigan Regulations. Child Care Licensing-Child Care Centers, Department of Consumer and Industry Services Directors Office. (2003). Part I. General Provisions, R 400.5101 Definitions. Retrieved from http://nrc.uchsc.edu/STATES/MI/mi_400.htm#pgfId-629703.
National Center on Elder Abuse. (2005) Frequently Asked Questions. Retrieved January 8, 2006 from http://www.elderabusecenter.org/default.cfm?p=faqs.cfm#one.
National Center for Health Workforce Analysis, Bureau of Health Professions, Health Resources and Services Administration. (2004). Nursing Aides, Home Health Aides, and Related Health Care Occupations--National and Local Workforce Shortages and Associated Data Needs. vi-v.
National Child Care Information Center, Child Care Workforce Qualifications. Retrieved from http://www.nccic.org/poptopics/qualifications.html.
Special Investigations Division, Committee on Government Reform. (2001). Abuse of Residents is a Major Problem in U.S. Nursing Homes. 3-4.
U.S. Census Bureau. (2001). U.S. Census 2000 Brief: The 65 Year and Older Population.
U.S. General Accounting Office. (2002). Nursing Homes: More can be done to protect residents from abuse. (GAO-02-312).
U.S. General Accounting Office. (2002). Nursing Homes: Many shortcomings exist in efforts to protect residents from abuse. (GAO 02-448T).
APPENDIX B: PROCESS FLOW CHARTS--SCREENING AND COMPLAINT INVESTIGATION
Through our interviews with state agencies in the four case study states (Arizona, Florida, Illinois and Washington), we discovered that each state differs in its approach to screening nurse aides before certification and employment. The process for investigating abuse allegations and reporting subsequent findings to appropriate state agencies also differs by state. The following flow charts illustrate the screening and investigative processes for the four states we examined.
ARIZONA
A. Process for CNAs Seeking Certification:

B. Process for CNAs Seeking Employment:
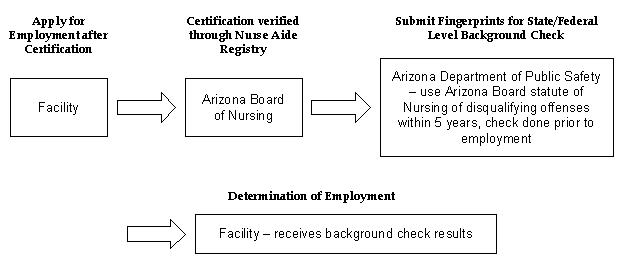
Fingerprint Clearance Card System (FPCC): Process for all direct care, human services, and supportive services workers in licensed long-term care facilities, EXCEPT those certified by the Arizona Board of Nursing, seeking employment, or CNAs in certain training programs with direct care contact:

C. Process for Handling Complaints or Allegations Against CNAs of Abuse, Neglect, Exploitation:

FLORIDA
A. Process for CNAs Seeking Certification:
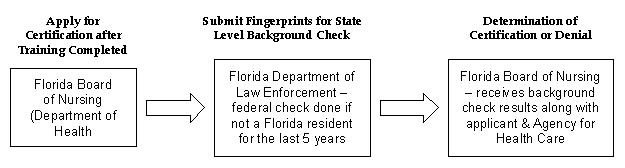
B. Process for CNAs Seeking Employment:

C. Process for Handling Complaints or Allegations Against CNAs of Abuse, Neglect, Exploitation:
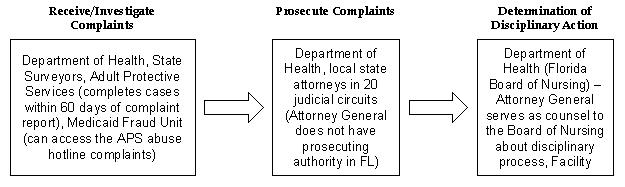
ILLINOIS
A. Process for CNAs Seeking Certification:

B. Process for CNAs Seeking Employment:
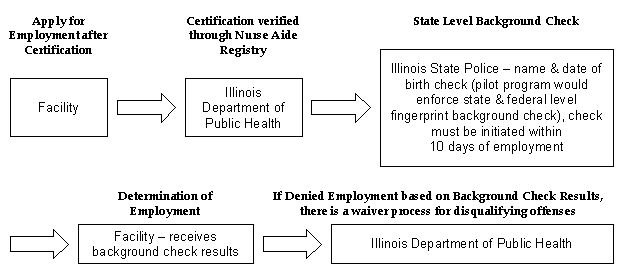
C. Process for Handling Complaints or Allegations Against CNAs of Abuse, Neglect, Exploitation:

WASHINGTON
A. Process for CNAs Seeking Certification:
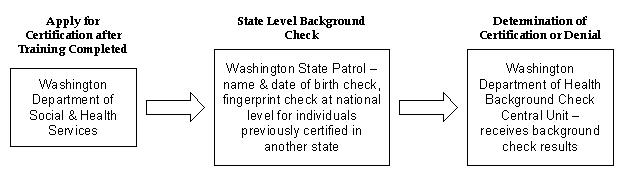
B. Process for CNAs Seeking Employment:
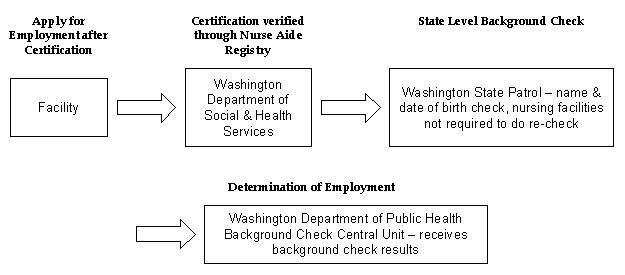
C. Process for Handling Complaints or Allegations Against CNAs of Abuse, Neglect, Exploitation:
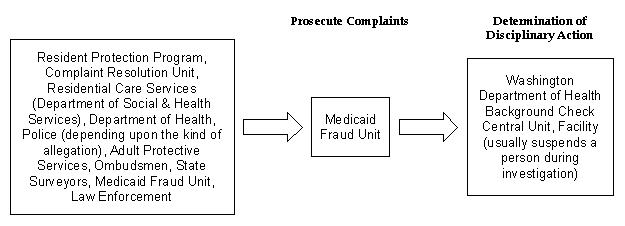
APPENDIX C: STATE BACKGROUND CHECK REQUIREMENTS AND PRACTICES
Matrix 1: Overview Across States
This matrix provides an overview of state requirements and practices for using criminal background checks in the certification and employment of CNAs.1 The process for criminal background checks varies across states at the certification and employment levels in terms of the use of state and/or federal level checks and disqualifying offenses. Twenty states require criminal background checks on CNAs prior to certification (all states reported state level checks with 11 states requiring additional federal level checks). Forty-one states require criminal background checks on CNAs prior to employment (37 states reported state level checks with 22 states requiring additional federal level checks).
| State | State Entity Responsible for Maintenance of Nurse Aide Registry | Criminal Background Check Required by State Law Prior to Licensure/ Certification | Relevant State Statute Requiring Criminal Background Check Prior to Licensure/ Certification | Blanket Disqualification Preventing Licensure/ Certification | State Level Check Prior to Licensure/ Certification | Federal Level Check Prior to Licensure/ Certification | Criminal Background Check Required by State Law Prior to Employment | Relevant State Statute Requiring Criminal Background Check Prior to Employment | Blanket Disqualification Preventing Employment | State Criminal Records Check Prior to Employment | Federal Criminal Records Check Prior to Employment |
| AK | Alaska Board of Nursing | Yes | Regulation 12 AAC 44705 | Yes | Yes | No | Yes | Regulation 20-33-01 | Yes | Yes | Yes |
| AL | Alabama Department of Public Health, Division of Licensing Center | No | n/a | n/a | n/a | n/a | Yes | Statute 22-50-90 | Yes | Yes | Yes |
| AR | Arkansas Department of Human Services, Division of Medical Services | No | n/a | n/a | n/a | n/a | Yes | Law Code 20-33-201 | Yes | Yes | Yes |
| AZ | Arizona State Board of Nursing | Yes | Arizona Revised Statute 32-1648; ARS 36-411 | Yes | Yes | Yes | Yes | Arizona Revised Statute 36-411 | Yes | Yes | Yes |
| CA | California Department of Health Services, Aides & Technician Certification Section (ATCS) | Yes | California Health and Safety Code, Section 1337 | Yes/ No | Yes | No | Yes | California Health & Safety Code 1265.2 | Yes | Yes | No |
| CO | Colorado Department of Regulatory Agencies; Colorado Board of Nursing; Department of Human Services | No | Colorado Revised Statute 12-38.1-104(3)a, 12-38.1-106(1)e, Nurse Aide Practice Act | No | Yes | Yes | Yes | Colorado Statute 27-1-110 | Yes | Yes | Yes |
| CT | Assessment Systems, Inc., now called Promisor | No | n/a | n/a | n/a | n/a | Yes/ No | 1999 Connecticut House Bill 6727 | Yes | Yes | No |
| DC | Assessment Systems, Inc. | No | n/a | n/a | n/a | n/a | Yes | D.C. Code 32-1351 | Yes | Yes | No |
| DE | Assessment Systems, Inc. | No | n/a | n/a | n/a | n/a | Yes/ No | Title 16, Part II, 1141 | Yes | Yes | Yes |
| FL | Florida Department of Health | Yes | n/a | Yes | Yes | Yes | Yes | Florida Statute 435.03 | Yes | Yes | Yes |
| GA | Georgia Health Partnership, Nurse Aide Registry | No | n/a | n/a | n/a | n/a | No | Statute 131E.265 | No | n/a | n/a |
| HI | Hawaii Department of Commerce & Consumer Affairs, Nurse Aide Program | No | n/a | n/a | No | No | No | n/a | n/a | n/a | n/a |
| IA | Iowa Department of Inspection & Appeals, Department of Public Safety Division of Criminal Investigation (criminal background monitored), Department of Human Services (adult abuse monitored) | No | n/a | n/a | n/a | n/a | Yes | Statute 135C.33 | No | Yes | Yes |
| ID | Idaho Board of Nursing | No | n/a | n/a | n/a | n/a | Yes | Section 307 of the Medicare Prescription Drug, Improvement, & Modernization Act (MMA) | Yes | Yes | Yes |
| IL | Illinois State Department of Public Health, Department of Education & Training | Yes | Criminal Background Check Act | No | Yes | No | Yes | Health Care Worker Background Check Act 255.46.15 | No | Yes | No |
| IN | Indiana State Board of Health, Division of Long Term Care | Yes | Indiana Code 16-28-13-3 | Yes | Yes | No | Yes | Statute 16-27-2-5 | Yes | Yes | No |
| KS | Kansas Bureau of Investigation | No | n/a | n/a | n/a | n/a | Yes | Kansas Statute Annotated 39-970 & 65-5117 | Yes | Yes | No |
| KY | Kentucky Board of Nursing, Cabinet for Health Services | Yes | Kentucky Revised Statute Chapter 314.103 | Yes | Yes | Yes | Yes | Kentucky Revised Statute 216.793 | Yes | Yes | No |
| LA | Louisiana Department of Health & Hospitals, Nurse Registry | No | n/a | n/a | n/a | n/a | Yes | n/a | Yes | Yes | No |
| MA | Massachusetts Department of Public Health, Division of Health Quality | No | n/a | n/a | n/a | n/a | Yes | Massachusetts General Law C6, Section 172 C | No | Yes | No |
| MD | Maryland Nurse Aide | No | n/a | n/a | n/a | n/a | Yes | n/a | Yes | Yes | No |
| ME | Maine Department of Human Resources, Certified Nurse Aide Registry | Yes | Maine Regular Session 2003, Chapter 376, H.P. 579-L.D. 780 | Yes | Yes | No | No | n/a | n/a | n/a | n/a |
| MI | Michigan Nursing Home Monitoring Unit | No | n/a | n/a | n/a | n/a | Yes | Michigan Act 303 of the Public Acts of 2002 | Yes | Yes | Yes |
| MN | Minnesota Department of Health, Nurse Assistant Registry | No | n/a | n/a | n/a | n/a | Yes | Statute 245C | Yes | Yes | Yes |
| MO | Missouri Department of Social Services, Division of Aging, Level I Medication Aides & Certified Medication Technicians; Missouri Division of Aging, Central Registry Unit | Yes | Nursing Practice Act 335.011 to 335.096 | Yes | Yes | No | Yes | n/a | Yes | Yes | No |
| MS | Assessment Systems, Inc. | No | n/a | n/a | n/a | n/a | Yes | House Bill 1077 | Yes | Yes | Yes |
| MT | Montana Department of Health, Licensing & Certification Bureau; Department of Public Health & Human Services | No | n/a | n/a | No | No | No | Chapter 37.1.203 | No | No | No |
| NC | North Carolina Department of Health & Human Services, Division of Facility Services, Board of Nursing | Yes | Nursing Practice Act, 90-171.48 | Yes | Yes | Yes | Yes | North Carolina General Statute 131E-265 | No | Yes | Yes |
| ND | North Dakota Department of Health, Emergency Health Services Division, Board of Nursing | No | n/a | n/a | n/a | n/a | No | n/a | n/a | n/a | n/a |
| NE | Nebraska Department of Health & Human Services & Human Services Regulation & Licensure | No | n/a | n/a | n/a | n/a | No | n/a | n/a | n/a | n/a |
| NH | New Hampshire Board of Nursing, Division of Public Health | Yes | Senate Bill 94 (legislated in 2003), Revised Statute Annotated 151 | No | Yes | No | Yes | Senate Bill 94 (legislated in 2003); amended Rehabilitation Services Administration statute 151 | No | Yes | No |
| NJ | Assessment Systems, Inc. | Yes | Chapter 26:2H-83 | Yes | Yes | Yes | Yes | Statute 26.2H.83 | Yes | n/a | n/a |
| NM | New Mexico Department of Health, Licensing & Certification | Yes | Chapter 61, Article 4, 61-3-18, 61-3-28 | Yes | Yes | Yes | Yes | Caregivers Criminal History Screening Act | Yes | Yes | Yes |
| NV | Nevada State Board of Nursing | Yes | Nevada Revised Statutes 632.344 | No | Yes | Yes | Yes | Nevada Revised Statute 499.185 | Yes | Yes | Yes |
| NY | New York Department of Health, Office of Continuing Care, Bureau of Professional Credentialing in the Department of Health; Assessment Systems, Inc. | No | n/a | n/a | n/a | n/a | Yes | Sections 400.23, 763.13, 766.11 of Title 10, Section 505.14 of Title 18 of the New York Codes Rules & Regulations | Yes | Yes | Yes |
| OH | Ohio Department of Health, Nurse Aide Registry | No | n/a | n/a | n/a | n/a | Yes | Statute 3701.881, 3712.09 | n/a | Yes | Yes |
| OK | Oklahoma Department of Health, Nurse Registry | No | n/a | n/a | n/a | n/a | Yes | Title 63-1-1950.1.F.1 | Yes | Yes | Yes |
| OR | Oregon Secretary of State, Board of Nursing | Yes | Oregon Administrative Rule 851-062-0005 | Yes | Yes | Yes | Yes | Oregon Revised Statute 181.537 | Yes | Yes | Yes |
| PA2 | Pennsylvania Nurse Aide Registry, Assessment Systems, Inc. | Yes | Older Adult Protective Services Act, Health & Safety, 35PS, subsection 10225.501 | Yes | Yes | Yes | Yes | Act 13, 10225.103 | n/a | n/a | n/a |
| RI | Rhode Island Department of Health | Yes | State Rules & Regulations for licensing of nursing facilities, Section 13.04 | Yes | Yes | No | Yes | Statute 23.17.34 | Yes | Yes | No |
| SC | South Carolina Department of Health & Environmental Control; ASI Processing Center | No | n/a | n/a | n/a | n/a | No | n/a | n/a | n/a | n/a |
| SD | South Dakota Board of Nursing | No | n/a | n/a | n/a | n/a | Yes/ No | n/a | n/a | n/a | n/a |
| TN | Tennessee Department of Health, Board of Nursing | No | n/a | n/a | n/a | n/a | Yes | Chapter 1200-8-6 | n/a | Yes | Yes |
| TX | Texas Department of Human Services, Texas Department of Public Safety | No | n/a | n/a | n/a | n/a | Yes | Health & Safety Code 250.004, 250.006, 142.004 | Yes | Yes | No |
| UT | Utah Nurse Aide Registry, Health Technician Certification | No | n/a | n/a | n/a | n/a | No | Statute 26.21.9.5 | No | n/a | n/a |
| VA | Virginia Department of Health Professions, Board of Nursing | Yes | Code of Virginia 32.1-126.01 | Yes | Yes | Yes | Yes | Statute 32.1-126.01 | Yes | Yes | Yes |
| VT | Vermont Board of Nursing | No | n/a | n/a | n/a | n/a | Yes/ No | n/a | n/a | n/a | n/a |
| WA | Washington Department of Health (certification level), Department of Social & Health Services (facility level) | Yes | Uniform Disciplinary Act | Yes | Yes | No | Yes | Revised Code of Washington 43.43.830 | Yes | Yes | No |
| WI | Wisconsin Department of Health & Family Services, Department of Regulation & Licensing | Yes | Uniform Licensure Act Chapter 50, 50.065 | Yes | Yes | Yes | Yes | Uniform Licensure Chapter 50, 50.065, 48.685 | Yes | Yes | Yes |
| WV | West Virginia Office of Health Facilities Licensing | No | n/a | n/a | n/a | n/a | No | n/a | n/a | n/a | n/a |
| WY | Wyoming Board of Nursing, Department of Health | No | WS 7-19-201 | No | Yes | Yes | No | n/a | n/a | n/a | n/a |
| NOTE: Information in the table above is current as of December 2005. | |||||||||||
Matrix 2: Details of Regulations Across States
This matrix provides details on regulations for certification and employment of CNAs across states. There are two separate processes and requirements prior to certification and employment of CNAs in terms of criminal background checks, disqualifying offenses, and other consideration made in each process. The states differ in terms of which felonies or offenses are included in their list of disqualifying offenses as well as the look back periods for prohibitive disqualifying offenses. For example, the look back period in Colorado is ten years for certain disqualifying offenses, while for other offenses there is no look back period. The look back period in Delaware ranges from 5-10 years depending on the type of offense, and Virginia grants exemptions for offenses committed more than five years prior if the individual has only one misdemeanor.
| State | Details of Process Before Licensure/Certification | Details of Process Before Employment |
| AK | Criminal checks are conducted via fingerprinting. There are no automatic disqualifying criminal offenses, but there are potentially 20 offenses that warrant disqualification from certification and these offenses are sent to the AK Board of Nursing for a case by case review. Examples include murder, manslaughter, assault, sexual assault, robbery, burglary, etc. | Checks are done on any caregiver, including CNAs, except for professionals. Waivers can be granted depending on certain factors. Blanket disqualifications include murder, kidnapping, rape, sexual abuse, felony, endangering the welfare of an incompetent person, arson. |
| AL | n/a | Checks are done for direct care workers, and the look back period is entirely discretionary. A survey must be completed and if abuse is found, the person may be dismissed but this is at the discretion of the state employer. Certain disqualifying offenses would bar a person from employment. |
| AR | n/a | Exemptions from disqualifying offenses depend upon work history, age, time of crime, threat level, etc. A person with a criminal history may be employed temporarily while the search is being conducted. Certain offenses (not substance abuse) are blanket disqualifiers. |
| AZ | Fingerprints are required for initial or lapsed, suspended, or revoked CNA certification--not renewal which is a potential flaw in the system. If cleared for 2 years, they don't need to submit again, and an appeal is possible. A full set of fingerprints taken by AZ Department of Public Safety for licensure of persons providing direct care, home health or supportive services. Blanket disqualifications for certification include any felony conviction in the past 5 years, and individuals who have a felony conviction must have completed all sentencing and probation prior to the 5 year period. | Criminal background checks do not have to be performed for CNAs, but all residential care institutions, residential care institutions, home health agencies, nursing care institutions, or any person with direct care, home health services or supportive services as a condition of employment, must have a valid fingerprint card for all employees (Section 25-411). Fingerprint check is done by AZ Department of Public Safety and shared with FBI. Substance abuse and assault are included in disqualifying offenses. |
| CA | Criminal checks are conducted via fingerprinting. Even if criminal background check turns up a hit on a discretionary offense, the investigation process may take months--in which case, the nurse aide can work. Blanket disqualification: Several felony offenses result in automatic denial to certification unless the individual has obtained a certificate of rehabilitation or the department has determined in accordance with the law that the offense should not disqualify the individuals form working (as marked with D). Other violations (DUI, prostitution, vandalism) will be considered but there must be evidence of rehabilitation. Investigators review the evidence and make recommendations. | Statute seems to apply only to nursing home administrators, not direct care workers. If a person received certification of rehabilitation and criminal information/accusation is dismissed, it is at the departments discretion to decide whether or not grant an exemption. Blanket disqualifications include most offenses, except misdemeanors to which person pleaded no contest. |
| CO | The background check is a requirement for nurse aides only, not nurses. It is done through checking all addresses the applicant has lived in lifetime. The check done within the U.S. only, not in foreign countries. However, starting July 2005, this law is most probably going to be repealed, and they would no longer require background checks for nurse aides in CO. | Fingerprints required by Department of Human Services for investigation by the CO Bureau on Investigation, and FBI. The look back period is 10 years for some, none for others. This applies to employment contracts entered into or renewed after July 1, 1999. For 10 year offenses, those crimes committed as juveniles can be appealed if 7 years have passed, others can appeal at any time. Applicants only reconsidered based on mistake of fact if convicted of permanently disqualifying offense. Employees of certain health care facilities run by Department of Human Services who provide direct care to person vulnerable b/c of age, health, disability, etc. Any felony relating to sex, domestic violence, or child abuse, other crime of violence, 3rd degree assault, many misdemeanors, substance offense, are disqualifying offenses. |
| CT | No criminal background checks are conducted on CNAs. Facilities do conduct criminal background checks prior to employment, but it is not state regulated. | Background checks are required for caregivers in nursing/residential care homes, home health aides, adult day care centers, etc., with a look back period of 3 years. Applicants with any offenses can request a hearing with Commissioner of Public Health, and can be hired if hearing determines there is no risk of harm to care recipient or that conviction does not bear on fitness for employment. Disqualifying offenses include sexual assault, abuse/assault of elderly, larceny, burglary, robbery. |
| DC | n/a | All employees are required to do background checks. The Health-Care Facility Unlicensed Personnel Criminal Background Check Act of 1998 has been amended to limit the period in which criminal convictions would bar an unlicensed person from employment with a health care facility to the 7 years preceding the criminal background check. |
| DE | They strongly urge all training programs to do background checks during training. This would prevent programs from training individuals who would be ineligible to work. Background checks are not conducted on CNAs prior to certification. Some facilities do conduct criminal background checks, but it is not state regulated. | Fingerprint background checks and mandatory drug tests are required. An applicant is exempt from a background check if qualifying check was performed within the last 5 years. If an individual was convicted of non-listed offense, the employer must evaluate the offense to determine suitability. The look back period is 5-10 years depending on offense. There is no time limit for sex felonies. Nursing home employees, whether or not they are direct care providers, require background checks. Disqualifying offenses include all felonies and Class A misdemeanor or substance related misdemeanors within the last 5 years, all violent felonies within 10 years, and any felony sex offense without time limit. |
| FL | Fingerprinting for background checks is done through FL Department of Law Enforcement and the FBI. Disqualifying offenses include most crimes. | Level 1 check for all employees who have contact with the residents, including housekeeping staff, is required. The check includes Abuse Registry screening and FL Department of Law Enforcement screening. If an individual is a resident of FL for less than 1 year, then full FBI check using fingerprints is done. Disqualifying offenses include sexual misconduct, abuse/neglect/exploitation, murder, manslaughter, vehicular homicide, assault, battery, arson, kidnapping, prostitution, robbery, incest, child abuse/child molestation, mostly felonies or crimes/offenses involving minors/elderly. Only applies to offenses committed on or after October 1, 1995. However, according to state law 435.07, the appropriate licensing agency may grant to any employee otherwise disqualified from employment an exemption for the listed offenses. |
| GA | They encourage trainings to do background checks for individuals who will later work in facilities that will run background checks. | Employer has absolute discretion. No disqualifying offenses on employment. |
| HI | They have a federally mandated CNA registry check, but this is not the same as a background check because it only includes convictions if against a resident while in a nursing home. No other past history is reviewed. | The state does not require background checks, but the employer can require it if they want to pay for it. |
| IA | n/a | Every new hire to a nursing home has background check, along with nurse aide dependent adult abuse, and children abuse registries checks. If criminal record found, facility can choose to either hire or request evaluation from DHS so person can explain why he or she should be hired. Then the facility makes the determination of whether to hire the person. For example, if a person had DWI 10 years ago, they may be approved to work as an aide but not as driver. Each nursing facility employee must have a criminal background check. No disqualifying offenses on employment. |
| ID | They are changing the law very soon to have requirements for background check prior to certification. | Fingerprint background checks are done with the FBI. They are 1 of 7 states to participate in the Background Check Pilot Program. Disqualifying offenses include any conviction of abuse against nursing home residents. |
| IL | Certain federal and state requirements must be met prior to certification of a nurse aide. Fingerprints submitted to state police for background checks. Individuals disqualified from working can get a waiver. | Employees wrongfully suspended based on inaccurate criminal record check are entitled to pay back, including direct care workers. IL created a waiver system, where criminals who apply for jobs in nursing homes are given a waiver form to fill out. 90% of waiver requests are approved, even if a criminal has 11 convictions. No crime is exempt from the waivers. If an individual has committed certain crimes they may not work in facilities unless a waiver is issued by the Department of Public Health. Disqualifying offenses include murder, homicide, manslaughter, kidnapping, indecent solicitation of a child, assault, battery, stalking, theft, robbery, criminal neglect of an elderly or disabled person, forgery, burglary, arson, etc. |
| IN | Background checks are done using date of birth and SSN through the state police. Fingerprints are only used if required by a facility for additional verification. Disqualifying offenses are all offenses listed in the code. | Facilities decide if they want to use fingerprints in addition to DOB, SSN, and also if they want to run FBI check in addition to check done by state police. Disqualifying offenses are listed in code, and include rape, battery, 10 years for theft, murder. |
| KS | n/a | Overall, look back period for disqualifying offenses is forever. However, for certain offenses the look back period is 5 years, while for other offenses the look back period is forever. Disqualifying offenses include most violent and serious crimes, such as murder and sexual assault or child abuse. Offenses result in an indefinite prohibition, a 5 year prohibition, or a length determined by Kansas in relation to the offense. |
| KY | Fingerprints are submitted by all licensure applicants for background checks. Certain disqualifying offenses would bar a person from certification. | Fingerprint background checks are a state law requirement as a condition of employment. |
| LA | Currently updating regulations, so soon it may be law to require background checks prior to certification. | No fingerprint background checks used. Very simple check done at the state level through the state police, but in some areas, just done at the local level through previous records. |
| MA | n/a | The state statute requires all individuals being employed to provide services to elderly or disabled persons must provide criminal record information prior to employment. This includes individuals with any direct or indirect contact with elderly or disabled person such as home health aides, personal care attendants, and meal deliverers. |
| MD | CNAs are asked on the application to disclose any misdemeanors or felonies, but no background check is done. | State level background check is required. Sometimes checks are done at the national level. |
| ME | ME passed a law in November 1, 2003 that prevents individuals from being certified and listed in registries if they have any felony in the past 10 years of a crime resulting in an incarceration of 3 years or more, or a crime of less than 3 years if it involved sexual misconduct, abuse, neglect or exploitation in both health care and non-health care settings. | Facilities are required to check if the individual is registered/ certified. |
| MI | n/a | Fingerprint background checks are conducted. Disqualifying offenses include any felony, regardless of type in last 15 years, which prohibits a person from working in a nursing home, any misdemeanor that involves abuse, neglect, assault, battery, or criminal sexual conduct against anyone or fraud or theft against a vulnerable adult, or a state or federal crime that is substantially similar to such a misdemeanor within the 10 years immediately preceding the date of application for employment or clinical privileges or the date of the date of the independent contract. |
| MN | Even if a misdemeanor is found on record that prevents person from working in facilities, certification is not taken away. | Background checks are done through name and DOB on the state level. If there is reason to believe that other offenses may have occurred, then fingerprints are collected to run the federal check. Individuals also have the right to request reconsideration, and appeals are handled on a case by case basis. Some misdemeanors will prevent individuals from working only at certain facilities, but it varies. Disqualifying offenses include murder, theft, misdemeanor, felony, etc. |
| MO | Fingerprints are sent to state patrol for background checks. Disqualifying offenses include any listed A or B level felony such as arson, assault, burglary, causing a catastrophe, child molestation, domestic abuse, violence, elderly abuse, rape, incest, kidnapping, murder, sexual abuse, rape, manslaughter. | MO requires criminal background checks for all employees hired after a certain date, but not for employees who were already working in the facility when the law passed. The facilities are supposed to call and verify with registry of applicant's certification. The facility is not allowed to hire individuals with certain criminal felony charges, such as adult abuse. |
| MS | Sometimes background checks are done in nursing homes during the training process. Individuals are allowed by the state to train under the supervision of the instructor without having the check done, so some nursing homes do not run background checks before training. | Fingerprints are used for background checks. Disqualifying offenses include felony conviction of possession or sale of drugs, murder, manslaughter, robbery, rape, sexual battery, sex offense, child abuse, arson, larceny, burglary, assault, abuse or battery of a vulnerable adult, etc. |
| MT | n/a | MT does not require background checks. An agency can refuse employment depending on nature of crime, relative to the work. There are no absolute bars on employment in the state. |
| NC | Background checks are required for licensure in NC. Disqualifying offenses include counterfeit, homicide, rape, robbery, prostitution, kidnapping, burglary, assaults, etc. | A nursing home or home care agency shall submit a request to the Department of Justice under G.S. 114-19.3 to conduct a background check within 5 business days of making the conditional offer of employment. No exceptions made, but no automatic bars. Nursing home must run check, but after that, decision not to hire based on criminal background is up to the facility. Nursing home or a home care agency shall not employ an applicant who refuses to consent to a criminal background check. |
| ND | n/a | Background checks are not a requirement in the state. |
| NE | There is no certification process in the state. Individuals are just put on the registry. | Facilities are not required to do background checks by law, but most do checks to make sure those with misdemeanors are not working there. |
| NH | Some CNA training programs conduct background checks, but this is not mandated by law. There is no list of disqualifying offenses. All licensure and employment decisions are made on a case by case basis. | Most facilities do criminal background checks, but there is no legislation currently requiring them to do so. There is no list of disqualifying offenses, so all licensure and employment decisions are made on a case by case basis. |
| NJ | Fingerprint background checks are required. Criminal history records are permanent, so if an individual is disqualified from working in the state, a determination of rehabilitation must be filed. Disqualifying offenses are listed is state statute include murder, homicide, manslaughter, death by auto, aiding suicide, assault, battery, leaving scene of accident, kidnapping, sexual assault, robbery, car jacking, any theft related charge including shoplifting, endangering welfare child, elderly, or incompetent person, and any drug offense other than possession of marijuana or hash less than $5,000. If ever convicted of any crimes, individuals must claim it on their application, or they will be permanently disqualified. | Nurse aides/personal assistants are required to do background checks. The law allows anyone to be rehabilitated, based on nature of crime, time, conduct, etc. Disqualifying offenses are for any disorderly personal offense. |
| NM | Fingerprint background checks are required by law under the Nursing Practice Act. Disqualifying offenses include being guilty of fraud or deceit, convicted of a felony, incompetent, guilt of unprofessional conduct. | Fingerprints, photo ID, and SSN are used for background checks. Disqualifying offenses include homicide, kidnapping, rape, robbery, child abuse, abuse, neglect, financial exploitation, etc. |
| NV | Fingerprints are used by NV Records and the FBI for background checks. There are no barriers on crime, so if a background check shows positive for crimes it is handled on a case by case basis. The individual with certain crimes might have restrictions placed on which types of facilities they are allowed to work depending on the crimes. There are no barriers for certification based on previous crimes, only on where they are allowed to work. | An employee has time to correct the information within a reasonable amount of time if the criminal history is wrong. Information is received from the Central Repository for NV Records of Criminal History about background checks. Criminal background checks are conducted through SSN and date of birth, not through fingerprinting. Termination of employment could result if convicted of certain crimes. |
| NY | n/a | Fingerprint background checks are required prior to employment. Disqualifying offenses include assault, sexual offense, larceny, robbery, bribery, etc. |
| OH | Background checks only done by nursing homes before employment. | Background checks are done on direct care providers. Facilities look at crimes to the degree that they relate to the nature of the work, and they allow rehabilitation. |
| OK | FBI background checks done by the employer. If criminal records show up on an individual, then the certification can be taken away. | Background checks apply to nurse aides. Disqualifying offenses include indecency/immorality, drugs, property, domestic abuse, any criminal act, sexual abuse. |
| OR | The Board of Nursing is the sole judge of eligibility for certification. If an applicant has been arrested, charged, or convicted of any criminal offense, has past, current or pending disciplinary actions in Oregon or another jurisdiction, or falsifies application, the a determination shall be made as to whether it has a demonstrable relationship to the performance of nursing assistant duties, in which case certification may be denied. | Fingerprint background checks are required. Facilities may also obtain Information through child protective services, DMV, court records, and other state data systems. Disqualifying offenses are determined by considering the nature of crimes. |
| PA | Some training programs require background checks in advance of starting the program so they do not have to eliminate people post background check. Background checks are done by Department of Education prior to training. If the individual is a PA state resident for less than 2 years, then a FBI background check is done, but if the individual is a PA resident for more than 2 years, then only a state background check done. Disqualifying offenses include criminal homicide, murder, manslaughter, assault, rape, kidnapping, sexual assault, aiding in drug delivery, indecent exposure, arson, burglary, theft, etc. | If a nurse aide has worked in the same facility for 10 years and then applies at a new facility, the individual would need to have a background check. The only exemption is for employment of 1 year or greater prior to December 1996, and only with the same employer. Act 13 requires background checks for certified/licensed staff hired after October 1997 and for anyone presenting themselves for employment. |
| RI | Individuals have to coordinate with the state attorney general's office to get a letter to include in their licensure application. | All employees are required to do background checks. An individual with any offenses can appeal to the employer who then has final discretion. The background check is not conducted through fingerprinting. Disqualifying offenses include murder, manslaughter, first/second/third assault, felony, drug offenses, etc. |
| SC | Individuals need to work for a specified number of hours during the 2 year certification process to become certified. No background check is required. | No background check is required. The only consideration is how the crime relates to the job, and whether the employer thinks the applicant is unfit or not. |
| SD | No criminal background checks are conducted on CNAs. | A few nursing facilities do conduct background checks, but it is not state regulated. Two years ago there was an attempt to pass legislation to require mandatory criminal background checks for unlicensed staff in assisted living centers. This was defeated by the SD Health Care Association, mainly because of the cost of paying for the criminal background check. |
| TN | n/a | Fingerprints must be submitted for state and federal background checks within 7 days of employment. |
| TX | n/a | The Department of Public Health requires employee identification information to run background checks. The law applies to those direct care workers who are unlicensed or uncertified, and does not include all employees. If the agency receives notice that a person has been convicted of a disqualifying offense, then the agency/facility must determine whether the offense is a contra-indication to employment. Disqualifying offenses include criminal homicide, kidnapping and unlawful restraint, indecency with a child, sexual assault, aggravated assault, injury to a child, elderly individual, or disabled individual, abandoning or endangering child, aiding suicide, agreement to abduct from custody, sale or purchase of a child, arson, robbery, assault, burglary, etc., but not substance abuse. |
| UT | n/a | Discretion is used by the employer to decide on a case-by-case basis according to the nature of the conviction and job sought. Each facility has its own requirements for background checks. |
| VA | Background checks are done using DOB and SSN, not fingerprints. Disqualifying offenses include murder, manslaughter, assault, abuse or crimes against children, and other crimes of violence. | VA requires background checks of all staff employed by a nursing home or adult care residence. The background check is done through the state police, so it does not pick up on any convictions from other states. Exemptions could be given after 5 years if an individual has only 1 misdemeanor. Disqualifying offenses include murder, manslaughter, assault, abuse or crimes against children, and other crimes of violence. |
| VT | No criminal background checks are conducted on CNAs prior to certification. | Some facilities conduct background checks, but it is not state regulated. |
| WA | Applicants are reviewed on a case by case basis. A federal background check is done only if an individual was previously certified in another state, but no fingerprinting is used. Disqualifying offenses are followed according to the uniform disciplinary act. | A WA State Patrol background check is required which only screens for crimes committed in WA. When a nursing home employee moves on to another nursing home the background check must be conducted again by the new employer. No federal background check is required. |
| WI | Any person who is seeking certification requires background check and resident abuse record search. Disqualifying offenses include violent crimes, mot substance abuse. | All employees require background checks and resident abuse record searches. They allow exceptions with proof of rehabilitation, except for homicide, and most sex acts. Disqualifying offenses include most serious crimes, especially "substantially related" to care of the resident. Includes violent crimes, but not substance abuse. |
| WV | n/a | Background checks are not required in WV. A nursing home is required to make an effort to screen out people who may have a history of undesirable conduct. |
| WY | Applicants must pay $60 in addition to the $60 application fee for the fingerprint background check through the Division of Criminal Investigation. WY does not have a limitation on disclosure of past criminal offense. All prior convictions, even if deferred or suspended, must be acknowledged on all applications and renewals. | n/a |
Notes
-
State statutes and policies current through December 2005.
-
On 30, 2003, the Supreme Court of Pennsylvania held the criminal background check prohibitive hire provisions of the Older Adults Protective Services Act (OAPSA) to be unconstitutional for individual plaintiffs. The Pennsylvania Department of Aging expects legislative action in the near future. Until this new legislation goes into effect, protective services will comply with outlined guidelines by the OAPSA. The official notice is available at: http://www.aging.state.pa.us/aging/lib/aging/NIXON-InterimPolicy.pdf.
APPENDIX D: KEY INFORMANTS
(TAG Members, State & Federal Stakeholders, and Other Informants)
| Name | Organization or Area of Expertise |
| Technical Advisory Group Members | |
| Steve Shields | Nursing Home Administrator, Meadowlark Hills |
| Debbie Deem | Victim Specialist |
| Diane Menio | Center for Advocacy for the Rights and Interests of the Elderly |
| Judy Bontrager | Arizona State Board of Nursing |
| Joanne Marlatt Otto | National Association of Adult Protective Services |
| Lori Porter | National Association of Geriatric Nursing Assistants |
| Steve Irwin | Kansas Department of Health and Environment |
| Brian Whitley | U.S. Department of Health and Human Services, Office of the Inspector General, Office of Evaluation and Inspections |
| Catherine Hawes | Texas A&M University |
| Lisa Nerenberg | Expert in Elder Abuse |
| Paul Greenwood | San Diego Prosecutors Office, Special Unit on Elderly Crime |
| Miriam Aukerman | Western Michigan Legal Services |
| Key Informants--Experts in Temporary Assistance for Needy Families and Re-entry Issues | |
| Roberta Meyers-Peeples | National H.I.R.E. (Helping Individuals with criminal records Reenter through Employment) Network |
| Elizabeth Nevins | Re-entry Policy Council |
| Diane Williams | Safer Foundation |
| Sharon Dietrich | Community Legal Services |
| Hollis Turnham | Paraprofessional Healthcare Institute |
| Jodina Hicks | Safer Foundation for Public Policy and Community Partnerships |
| Key Informants--Content Knowledge in Relevant Federal Projects | |
| Marie-Therese Connolly | U.S. Department of Justice, Coordinator of Nursing Home Initiative |
| Stuart Bernstein | U.S. Health Resources and Services Administration, Project Officer for report on Nursing Aides, Home Health Aides, and Related Health Care Occupations: National and Local Workforce Shortages and Associated Data Needs |
| Donna Rabiner | Research Triangle Institute International, Director of report on Financial Exploitation of Older Persons |
| Amber Wolfe | U.S. Department of Health and Human Services, Centers for Medicare and Medicaid Services, Contact for pilot program for national and state background checks |
| Hal Sklar | Federal Bureau of Investigations, expert on FBI criminal database |
| Linda Mills | Consultant for Annie E Casey Foundation |
| Daniel Sheridan | Johns Hopkins University, expert in elder abuse, helped conduct a survey of nursing homes surveyors |
| Ann Burgess | University of Pennsylvania School of Nursing, expert in sexual abuse |
| State Level Informants | |
| Arizona | |
| Judy Bontrager | Arizona State Board of Nursing |
| Valerie Smith | Arizona State Board of Nursing |
| Theresa Berry | Arizona State Board of Nursing |
| Sylvia Balistreri | Arizona Department of Health Services |
| Tina Dannenfelser | Arizona Department of Economic Security |
| Mike Timmerman | Arizona Department of Public Safety |
| Dennis Seavers | Arizona Board of Fingerprinting |
| Bob Nixon | Arizona State LTC Ombudsman |
| Steve Lacy | Region I Area Agency on Aging - Long Term Care Ombudsman (Phoenix) |
| Kathleen Pagels | Arizona Health Care Association |
| Steve Duplissis | Medicaid Fraud Control Unit of Arizona |
| Florida | |
| Dan Coble | Florida Board of Nursing, Florida Department of Health |
| Chris Shoemaker | Florida Department of Children and Families |
| Lee Ann Gustafson | Florida Office of the Attorney General, Board of Nursing Counsel |
| Terry Bucher | Florida Association of Nurse Assistants |
| Elizabeth Dudek | Florida Agency for Health Care Administration Division of Health Quality Assurance |
| David Lewis | Florida Office of the Attorney General, Medicaid Fraud Unit |
| Lee Ann Griffin | Florida Health Care Association |
| Illinois | |
| Bryan Hutchcraft | Illinois Department of Public Health |
| Debra Bryars | Illinois Department of Public Health |
| Sally Petrone | State LTC Ombudsman, Illinois Department on Aging |
| Connie Jensen | Illinois Department of Public Health |
| Sheila McFadden | Illinois Department of Public Health |
| Terry Sullivan | Illinois Council on Long Term Care |
| Debbie Belt | Illinois Health Care Association |
| Lt. Gordon Fidler | Illinois State Police Medicaid Fraud Unit |
| Cara Smith Pat Keenan Kathleen Quinn | Illinois Attorney Generals Office, Medicaid Fraud Control Unit |
| Washington | |
| Lew Maudsley | Washington Division of Residential Care Services |
| Patricia Bossert | Washington Division of Residential Care Services |
| Lori Melchiori | Adult Protective Services, Washington Department of Social and Health Services |
| Kary Hyre | Washington LTC Ombudsman Program |
| Mike Keller | Washington Office of the Attorney General |
| Lamona Foster | Washington Department of Social and Health Services Background Check Central Unit |
| Vicki McNealley | Washington Health Care Association |
APPENDIX E: DATA COLLECTION MATERIALS--DATA REGISTRY ANALYTIC PLAN AND DISCUSSION GUIDES
DATA REGISTRY ANALYTIC PLAN
A. CNA Registry and Criminal Background/Abuse Data
The following is a list of variables needed on each individual in your registry to complete the secondary data analyses to address the two primary research questions for this study:
- The relationship between potential direct care workers with criminal backgrounds and rates of abuse, neglect, and/or financial exploitation; and
- The relationship between direct care workers with prior history of abuse, neglect, and/or financial exploitation and proclivity towards abuse, neglect, and/or financial exploitation.
B. Registry Variables
Age (18-25, 26-35, 36-45, 46-55, 56-65, 66+) Race/Ethnicity Gender Education Level Employment Status Certification Status Date of Licensure
C. Abuse/Neglect Database
Type of Abuse Case Date of Abuse Case Abuse Case Pending/Substantiated Neglect Case Date of Neglect Case Neglect Case Pending/Substantiated Misappropriation of Property Case Date of Misappropriation of Property Case Misappropriation Case Pending/Substantiated
D. Criminal Background History
Type of Offense Date of Conviction
E.Analyses: Frequencies and Correlations
-
Frequencies on:
Age (18-25, 26-35, 36-45, 46-55, 56-65, 66+) Race/Ethnicity Gender Education Level Employment Status Certification Status Date of Licensure (also include mean, median) Type of Abuse Case Date of Abuse Case Abuse Case Pending/Substantiated Neglect Case Date of Neglect Case Neglect Case Pending/Substantiated Misappropriation of Property Case Date of Misappropriation of Property Case Misappropriation Pending/Substantiated Type of Criminal Offense Date of Criminal Conviction
-
Cross Tabs:
Run each variable in Group A by each variable in Group B.
Variable Group A:
Type of Abuse Case Date of Abuse Case Abuse Case Pending/Substantiated Neglect Case Date of Neglect Case Neglect Case Pending/Substantiated Misappropriation of Property Case Date of Misappropriation of Property Case Misappropriation Case Pending/Substantiated Type of Criminal Offense Date of Criminal Conviction
by
Variable Group B:
Age (18-25, 26-35, 36-45, 46-55, 56-65, 66+) Race/Ethnicity Gender Education Level Employment Status Certification Status Date of Licensure
-
Three-Way Cross Tabs:
Run Type of Criminal Offense by each variable in Group A by each variable in Group B.
Variable Group A:
Type of Abuse Case Abuse Case Pending/Substantiated Neglect Case Neglect Case Pending/Substantiated Misappropriation of Property Case Misappropriation Pending/Substantiated
Variable Group B:
Age (18-25, 26-35, 36-45, 46-55, 56-65, 66+) Race/Ethnicity Gender Education Level Employment Status Certification Status Date of Licensure
KEY STAKEHOLDER/TECHNICAL ADVISORY GROUP PRELIMINARY INTERVIEW DISCUSSION GUIDES
A. General Interview Questions
Introduction:
The Office of the Assistant Secretary for Planning and Evaluation (ASPE) under the U.S. Department of Health and Human Services (HHS) has contracted with The Lewin Group to assist them with a new study examining the use of screening mechanisms and on-the-job monitoring activities by long term care employers in ensuring a qualified long-term care workforce. ASPE is particularly interested in this issue because of the quickly aging long-term care workforce, high turnover rate, and limit on new pools of direct care workers. This project is also intended to inform current work at Centers for Medicare and Medicaid Services (CMS) to conduct pilot projects to experiment with improved ways of conducting background checks and evaluating the effectiveness of various methods for preventing the employment of abusive long-term care workers.
We received your contact information from fill in the name and affiliation of the person who supplied contact information and believe that you may offer a valuable perspective on fill in with relevant expertise area.
Background Questions:
We want to learn a little more about your background and interest in the quality of the long-term care workforce.
Please tell us a little more about your work and interest in the quality of the long-term care workforce.
Issues to Consider:
From your perspective, what are the most important issues for us to consider in terms of quality of the long-term care workforce?
Additional Information:
- Do you have anything else to add?
- Do you have any information regarding these issues that you could pass on?
- Do you have any suggestions for additional key stakeholders that we should speak to?
Wrap Up
Do you have any questions for us?
Thank you for your time and helpful feedback. If you have some more thoughts after our conversation today, please feel free to contact [provide contact name and information]. In the event that we have additional questions, can we contact you in the future [verify their contact information]?
B. Questions for Representatives Familiar with Abuse/Neglect/Misappropriation and/or Criminal Background Registries
Introduction:
ASPE under the HHS has contracted with The Lewin Group to assist them with a new study examining the use of screening mechanisms and on-the-job monitoring activities by long-term care employers in ensuring a qualified long-term care workforce. ASPE is particularly interested in this issue because of the quickly aging long-term care workforce, high turnover rate, and limit on new pools of direct care workers. This project is also intended to inform current work at CMS to conduct pilot projects to experiment with improved ways of conducting background checks and evaluating the effectiveness of various methods for preventing the employment of abusive long-term care workers.
We received your contact information from fill in the name and affiliation of the person who supplied contact information and believe that you may offer a valuable perspective on the use of abuse/neglect/misappropriation and/or criminal background registries in the states.
Background Questions:
We want to learn a little more about your background and interest in the quality of the long-term care workforce.
Please tell us a little more about your work.
Issues to Consider:
Abuse, Neglect, and Misappropriation Registry
- Which agency maintains this abuse, neglect, and misappropriation registry?
- What types of long-term care workers are detailed in your abuse, neglect, and misappropriation registry?
- How often is the registry updated?
- What sort of information is collected in the registry?
- What kinds of cases are recorded in this registry?
- Adjudicated cases only?
- Individuals accused of neglect, abuse, and/or misappropriation?
- Both adjudicated and accused cases?
Criminal Background Registry
Do you have a registry that details the criminal background of long-term care employees?
If the subject answers yes, ask the questions below.
- Which agency maintains this registry?
- How often is the registry updated?
- What sort of information is collected in the registry?
- What types of criminal offenses disqualify an individual from working in the long-term care industry? Can you send us a list of these disqualifying offenses?
- How long are the individuals disqualified for?
- What state statute mandates determine disqualifying criminal offenses?
- When does the criminal background check occur--prior to state CNA certification or prior to employment?
- Does the state require fingerprint background check?
- If yes, are these checks performed at the state or federal level (FBI database) or both?
- Who performs the check--the state bureau of investigation checks using SS#, name, DOB?
- How much do background checks cost and who bears the financial burden?
Communication between Two Registries
If two agencies maintain the registries, ask the following questions.
- If two agencies maintain the registries, do these agencies exchange information in the registries?
- If yes, how does this exchange occur?
Effectiveness of Registries in Screening Long-Term Care Workers
- How effective are registries in capturing individuals with histories of abuse/ neglect/misappropriation and/or criminal background?
- Are there any improvements that could be made to registries so that they capture information more accurately?
Use of Registries in Screening Long-Term Care Workers
- Which agency, entity, or individual uses these registries to screen out individuals from working in the long-term care workforce?
- Do you feel that these registries appropriately screen out individuals from working in the long-term care workforce?
- If no, why not?
- Are there any improvements that could be made to registries so that they screen out individuals more appropriately?
Long-Term Care Workforce Issues
- From your perspective, what are the most important issues for us to consider in terms of quality of the long-term care workforce?
- Do you have any recommendations for reforming policies?
Additional Information:
- Do you have anything else to add?
- Do you have any information regarding these issues that you could pass on?
- Do you have any suggestions for additional key stakeholders that we should speak to?
Wrap Up
- Do you have any questions for us?
Thank you for your time and helpful feedback. If you have some more thoughts after our conversation today, please feel free to contact [provide contact name and information]. In the event that we have additional questions, can we contact you in the future [verify their contact information]?
C. Questions for Representatives Familiar with Elder Abuse Issues
Introduction:
ASPE under HHS has contracted with The Lewin Group to assist them with a new study examining the use of screening mechanisms and on-the-job monitoring activities by long-term care employers in ensuring a qualified long-term care workforce. ASPE is particularly interested in this issue because of the quickly aging long-term care workforce, high turnover rate, and limit on new pools of direct care workers. This project is also intended to inform current work at CMS to conduct pilot projects to experiment with improved ways of conducting background checks and evaluating the effectiveness of various methods for preventing the employment of abusive long-term care workers.
We received your contact information from fill in the name and affiliation of the person who supplied contact information and believe that you may offer a valuable perspective on the effectiveness of employee screening tools currently used to protect vulnerable elders from being subject to abuse, neglect, misappropriation of property and/or being victimized in other ways.
Background Questions:
We want to learn a little more about your background and interest in the quality of the long-term care workforce.
Please tell us a little more about your work.
Issues to Consider:
Abuse, Neglect, and Misappropriation Registry
All states are mandated by federal law to maintain a registry that records incidences of abuse, neglect or misappropriation.
- Are you familiar with abuse, neglect, and misappropriation registries in the states?
- Do you think that these registries are effective tools for screening out applicants for long-term care positions?
- If yes, why?
- If no, why?
Criminal Background Registry
- Are you familiar with the criminal history registries in the states?
- Do you think that these registries are effective tools for screening out applicants for long-term care positions?
- If yes, why?
- If no, why?
Effectiveness of Registries in Screening Long-Term Care Workers
Are there any improvements that could be made to registries so that they capture information more accurately?
Long-Term Care Workforce Issues
- From your perspective, what are the most important issues for us to consider in terms of quality of the long-term care workforce?
- Do you have any recommendations for reforming policies relating to the use of long-term care employee screening tools to protect elders?
Additional Information:
- Do you have anything else to add?
- Do you have any information regarding these issues that you could pass on?
- Do you have any suggestions for additional key stakeholders that we should speak to?
Wrap Up
Do you have any questions for us?
Thank you for your time and helpful feedback. If you have some more thoughts after our conversation today, please feel free to contact [provide contact name and information]. In the event that we have additional questions, can we contact you in the future [verify their contact information]?
TECHNICAL ADVISORY GROUP INITIAL INTERVIEW DISCUSSION GUIDE
Introduction:
Thank you for agreeing to serve on the Office of the Assistant Secreatry for Planning and Evaluations (ASPEs) technical advisory group for ensuring a qualified long-term care workforce. ASPE has contracted with The Lewin Group to assist them with a new study examining the use of screening mechanisms and on-the-job monitoring activities by long-term care employers in ensuring a qualified long-term care workforce. ASPE is particularly interested in this issue because of the quickly aging long-term care workforce, high turnover rate, and limit on new pools of direct care workers. This project is also intended to inform current work at Center for Medicare and Medicaid Services (CMS) to conduct pilot projects to experiment with improved ways of conducting background checks and evaluating the effectiveness of various methods for preventing the employment of abusive long-term care workers.
As a member of the Technical Advisory Group, we are asking you to provide feedback and direction to ASPE and The Lewin Group on key project activities to ensure the project outcomes are field and policy relevant. Today, we hope that you can provide feedback on:
- The work plan; and
- Site selection including:
- states and facilities to visit,
- key stakeholders we should speak to at those sites, and
- important discussion questions for the interviews.
Background Questions (only ask these questions if we have not spoken to them previously):
Before we discuss these specific items, we want to learn a little more about your background and interest in the quality of the long-term care workforce.
- Please tell us a little more about your work and interest in the quality of the long-term care workforce.
- From your perspective, what are the most important issues for us to consider in terms of quality of the long-term care workforce?
Feedback on the Work Plan
You have had the opportunity to review our project work plan which has four major components:
- Secondary data analysis of three selected states CNA and resident abuse registries;
- Stakeholder discussions via four site visits;
- Follow up discussions with several national experts and other stakeholders; and
- A final report.
- Does the work plan adequately address the following study objectives:
- To establish an understanding of the current screening processes for the long-term care workforce;
- To describe the association between direct care workers with certain previous criminal histories and previous incidences of neglect with proclivity towards abuse, neglect and financial exploitation;
- To develop a better understanding of the extent to which employers are limiting an important group of potential direct care paraprofessionals by screening out potentially viable employees with certain criminal histories inappropriately; and
- To describe innovative approaches to hiring and monitoring direct care workers, including the use and interpretation of background checks, and employee training and supervision practices?
- If No to any of the above, what changes to the work plan do you suggest to ensure the study objectives are met?
- Does the work plan reflect research that would add value to the existing research and understanding of:
- Improving the quality of care provided in long-term care settings; and
- Ensuring a committed and qualified long-term care workforce?
Feedback on the Site Visits
The project team plans to conduct site visits to four states. We propose visiting the three states that are currently conducting the registry analysis (Kansas, Arizona, and Alaska) and an additional state. The visits are intended to help us understand:
- How long-term care employers interpret and use criminal background checks in their hiring decision and practices;
- The efficacy of state registries in documenting providers with incidences of abuse, neglect, and/or financial exploitation of residents; and
- The training or supervision of long-term care workers with previous histories of abuse, neglect, and or financial exploitation.
We plan to interview in each state the following individuals:
- State ombudsmen;
- State nursing board representatives;
- Nursing home administrators;
- Front-line supervisors;
- CNAs at each long-term care facility site; and
- Residents or resident representatives from each case study site.
- Do you have any suggestions for how the fourth study state should be selected?
- Who are the key state level informants and local providers we should interview during our site visit (suggestions of names or positions)?
- What questions should we ask during the state level interviews? What questions should we ask during the facility level interviews?
Wrap Up
Our plan is to conduct the site visits and discussions with experts during this spring and summer and then hold a teleconference with you and the rest of the advisory group late summer to discuss our major findings from both the quantitative and qualitative analysis as well as to discuss a proposed outline for the final report.
Those are all the questions we have for you--do you have any questions for us?
Thank you for your time and helpful feedback. If you have some more thoughts after our conversation today, please feel free to contact [provide contact name and information].
KEY INFORMANT INTERVIEW DISCUSSION GUIDE (STATE LEVEL)
Study States
- Arizona, Illinois, Florida, and Washington
Potential State Informants (will depend on state structure and involvement; most state informants will be interviewed by telephone)
- State survey and certification
- AAHSA and AHCA Affiliates
- Adult protective services
- Law enforcement
- Ombudsmen
- Medicaid fraud unit
- Workforce development board agency
- Long-term care worker association
General State Structure Questions
- Which entity is responsible for maintaining the worker registry?
- Which entity runs criminal background checks (is this the same entity that maintains the registry)?
- Does the state require a background check?
- Which entities are involved in determining the states list of disqualifying offenses?
- Does the state allow waivers?
- Which organization is responsible for conducting statewide nurse aide training and placement?
Questions by Informant Group
Certification Personnel
- What type of information is contained in the registry? And what are the main sources of data?
- What types of workers are listed in the registry?
- Does the registry contain individuals with active certifications only?
- Does the registry include adjudicated and/or pending cases of abuse, neglect, or misappropriation of property?
- If pending cases are recorded, what is the system for categorizing complaints? Are facilities and specific CNAs cited?
- Does the registry include information on individuals criminal backgrounds?
- How is criminal background information communicated to registry staff (if different entities)?
- How often is the registry updated? In addition to updates, what steps are taken to ensure the quality of registry information?
- What information is provided to facilities when checking the registry?
- What proportion of nursing homes do you think use the registry to screen out potential and actual perpetrators of abuse, neglect and misappropriation? Why do you think some nursing homes do not use the registry for this purpose?
- How would the registry be made more effective for and user friendly to employers in screening potential employees?
- What does the background check entail (if criminal background checks are required by the state)?
- Who is responsible for conducting background checks?
- Is a federal criminal background check required? Does it check from crimes committed in other states? If not required, why?
- Is the criminal background check conducted through name, social security number, or fingerprint check?
- Are penalties imposed if the facilities do not conduct the checks?
- When is the check conducted and what is the turn-around reporting time for background checks? Can an individual work in a facility before the check is made?
- Who gets verification that the individual does or does not have a criminal record or previous history of abuse, neglect or financial exploitation?
- What type of coordination do you have with law enforcement? With protective services?
- How effective are criminal background checks in screening out potential and actual perpetrators of abuse, neglect and misappropriation?
- What offenses result in a prohibition from working in the long-term care workforce and what is the prohibition (e.g., permanent prohibition, a five-year prohibition)?
- Who makes these decisions and what evidence are decisions about disqualifying offenses based on?
- Has the state become more or less strict over time? Why?
- If your state grants waivers, for what and why do you do so? What proportion of aides on your state nursing aide registry are employed under a waiver (if possible, categorized by: juvenile claims, violent crime, nonviolent crimes, and drug related convictions)?
- Does the state impose special trainings or supervisory provisions when providing alternative waivers or sanctions to direct care workers with previous offenses of abuse, neglect or financial exploitation?
- What legal barriers does the state face in implementing criminal background checks (e.g., ruled unconstitutional in Pennsylvania)?
State Surveyors
- Does your state have statutes that mandate reporting and/or investigation of cases of abuse, etc. in long-term care facilities? What are the most and least effective aspects of the statutes and why?
- Do you use the nurse aide registry (and other registries) in your work? If so, how?
- Do you communicate findings of abuse, neglect and/or misappropriation to the agency that maintains the registry? If so, how and in what timeframe? Do they add your findings to the registry?
- Does the state impose special trainings or supervisory provisions when providing alternative waivers or sanctions to direct care workers with previous offenses of abuse, neglect or financial exploitation?
- Drawing from your survey experience, what are the characteristics and practices that seem to distinguish nursing homes with low or no problems with abuse, neglect or financial exploitation of residents and those that seem to have continuing problems?
Attorney General
- How many cases of abuse, neglect and misappropriation of nursing home residents by staff do you receive annually? How many are actually prosecuted? A conviction obtained? In what proportion of these cases did the defendant have a prior criminal background?
- What are the barriers to reporting incidents to your office and effectively prosecuting them? How might these barriers be reduced or overcome?
- Who is responsible for carrying out criminal background checks on nursing home staff in this state?
- Do you think criminal background checks are effective in screening out potential perpetrators of abuse and neglect in nursing homes?
Prosecutors (in county of facility location)
- How many complaints about alleged abuse, neglect and misappropriation in nursing homes are reported to you annually? Who reports them to you and how?
- What actions do you take as a result of these complaints?
- What proportion of complaints to your office is substantiated? What happens to the perpetrator if complaints are substantiated?
- Do you report substantiated claims to the states nurse aide registry? If so how and in what time frame? If not, why not?
- How is information communicated to the entity maintaining the registry? Do reports make it into the registry?
- What in your opinion would have the greatest impact on reducing the incidents of abuse, neglect and misappropriation by nursing home staff?
Police Chief (in county of facility location)
- How many complaints about alleged abuse, neglect and misappropriation of property in nursing homes are reported to you annually? Who reports them to you and how?
- What actions do you take as a result of these complaints?
- What proportion of complaints to your office is substantiated? What happens to the perpetrator if complaints are substantiated?
- Do you report substantiated claims to the states nurse aide registry? If so how and in what time frame? If not, why not?
- How is information communicated to the entity maintaining the registry? Do reports make it into the registry?
- Have you engaged in any training with facilities to help them understand the magnitude of the problem of elder abuse?
- What in your opinion would have the greatest impact on reducing the incidents of abuse, neglect and misappropriation by nursing home staff?
Adult Protective Services
- How many complaints about alleged abuse, neglect and misappropriation in nursing homes are reported to you annually? Who reports them to you and how? Describe the nature of these reports.
- Does APS have a role in complaint investigation in nursing homes?
- What role, if any, does APS have with nurse aide registries?
- Do you communicate findings of abuse, neglect and/or misappropriation to the agency that maintains the registry? If so, how and in what timeframe? Do they add your findings to the registry and if so, how often is this done?
- How long is it from time of complaint report to determination of substantiated abuse?
- Do state statutes mandate reporting and/or investigation of cases of abuse, etc. in long-term care facilities? Are these state statutes effective in halting abuse and/or preventing future abuse?
- What in your opinion would have the greatest impact on reducing the incidents of abuse, neglect and misappropriation by nursing home staff?
Probation and Parole Officers
- Are individuals reentering the community encouraged to seek jobs in the long-term care sector? Why or why not?
- How successful are parolees in obtaining jobs in the long-term care workforce?
- Do you perceive that some parolees are unfairly denied employment? Why or why not?
- Of your parolees who have returned to the workforce performing direct care work, have you heard about incidences of abuse, neglect or financial exploitation perpetrated by these individuals?
Medicaid Fraud Units
- Does your agency receive reports regarding CNA abuse, neglect, or misappropriation of property? If yes, how many cases about alleged abuse, neglect and misappropriation in nursing homes are reported to you annually? Who reports them to you and how? Describe the nature of these reports.
- When you investigate cases, what sort of information do you find out about the circumstances that wasnt known before you stepped in?
- Do you communicate findings of abuse, neglect and/or misappropriation to the agency that maintains the registry? If so, how and in what timeframe? Do they add your findings to the registry?
Ombudsman
- With whom do you communicate findings of abuse, neglect and/or misappropriation of nursing home residents? Do you communicate directly with the agency that maintains the registry? If so, how and in what timeframe? Do they add your findings to the registry?
- Drawing from your ombudsman experience, what are the characteristics and practices that seem to distinguish nursing homes with low or no problems with abuse, neglect or financial exploitation of residents and those that seem to have continuing problems?
- What in your opinion would have the greatest impact on reducing the incidents of abuse, neglect and misappropriation by nursing home staff?
Waivers and Hearing Process Personnel
- What criteria are used to determine if an applicant can be granted a waiver?
- How was this criteria originally formulated?
- How effective is the current waiver process? To what extent are nurse aides who are employed as a result of the waiver found to abuse, neglect residents or otherwise be poor performers? How does this compare to other employees hired without a waiver? Does the waiver process appropriately balance the needs of individuals who have been inappropriately banned from working in the long-term care workforce with the need to protect older adults?
- Does the state impose special trainings or supervisory provisions when providing alternative waivers or sanctions to direct care workers with previous offenses of abuse, neglect or financial exploitation?
- Is there an appeals process for individuals who have been wrongly identified as having a criminal background or for individuals who have a criminal background but believe that they should still be able to work in the long-term care industry?
- If yes, please describe this appeals process:
- How does someone apply for an appeal?
- How long does the appeals process take?
- What criteria are used to make a decision on the appeal?
- Who makes this decision?
- Does the appeals process appropriately balance the needs of individuals who have been inappropriately banned from working in the long-term care workforce with the need to protect older adults?
- What is the tendency of recurrence in the situations where people with substantiated abuse are reemployed? Do you get many repeat offenders?
Workforce Development Board Agencies
- Do you think particular criminal histories warrant banning an individual working in the long-term care workforce? If no, why? If yes, which criminal histories warrant a ban?
- Do you place individuals with criminal histories into the long-term care workforce?
- Have you encountered barriers in placing individuals into the long-term care workforce? If yes, what barriers?
- Do convicted nurse aides return to the long-term care workforce not functioning as a nurse aide, but in a less skilled job function for which background checks are not conducted?
Long-Term Care Worker Association (e.g., Florida Association of Nurse Assistants)
- Do you think particular criminal histories warrant banning an individual working in the long-term care workforce? If no, why? If yes, which criminal histories warrant a ban?
- Do nurse aides with previous criminal histories or histories of abuse, neglect or exploitation experience any special training or monitoring in the workplace because of that history? If so, how effective is this training or monitoring?
AAHSA and AHCA Affiliates--get their perspective on this issue and how the various parties have been dealing with it.
KEY INFORMANT INTERVIEW DISCUSSION GUIDE (FACILITY LEVEL)
Facility:
Name:
Address:
Facility Informants:
Facility Characteristics:
Questions by Informant Group:
Management
General Hiring and Screening Mechanisms
- What types of screening mechanisms does your facility perform when hiring nurse aides? Which of the mechanisms you have identified do you think are most and least effective in screening out potential perpetrators of abuse, neglect and financial exploitation and who do you think this?
- Are there requirements about nurse aide screening and criminal background checks that are imposed on all of the chains facilities or is this the discretion of individual facilities? (for chain facilities)
- What are your main recruiting sources?
- Does the facility employ uncertified nurse aides? If yes, what level of screening is used for these individuals?
- What proportion of your nurse aide staff are temporary hires from outside agencies?
- What proportion of your nurse aide staff are foreign workers? How are they screened? How do you know if these individuals have a criminal background?
- What are nursing assistant turnover and retention rates at your facility?
- Do you think criminal background checks and other screening mechanisms have an impact on the incidence of abuse, neglect and misappropriation in nursing homes?
- What efforts/strategies have had the most significant impact on rates of abuse/neglect in your opinion?
Nurse Aide Registries
- Do you check the nurse aide registry prior to hiring an aide? If YES, then:
- What information do you obtain from the registry? Do you check for substantiated cases of abuse and neglect?
- Who checks the registry and to whom and how do they report their findings?
- How do you use this information in the hiring process? What proportion of applicants is screened out as a result of your use of the registry?
- Do you check registries of neighboring states if an applicant has worked or lived in other states?
- Is the nurse aide registry a useful tool for screening potential employees with past incidences of abuse, neglect, or misappropriation of property? Why or why not?
- Does the use of registries to identify substantiated incidents of abuse unnecessarily limit the pool of potential applicants?
- How can the nurse aide registry be made more effective for and user friendly to employers in screening potential employees?
- What are the facilitys requirements for reporting abuse to nurse registries? Who does it, how, when?
Criminal Background Checks
- Do you conduct criminal background checks on nurse aides prior to hiring them? If YES, then:
- How are they conducted and who carries them out?
- Do you use the nurse aide registry to obtain criminal background information on prospective employees?
- Who do you receive verification from that the individual does or does not have a criminal record?
- What is the cost of doing background checks? Are checks cost prohibitive?
Director of Nursing & Staff Development Nurse
- What factors do you think may account for higher incidences of abuse, neglect or theft?
- What is your role in preventing abuse, neglect or financial exploitation among nurse aides?
- Do you provide specific in-service training related to abuse, neglect or financial exploitation? About how many hours of this type of training do CNAs receive during the first six months of employment?
- Do you provide specific in-service training related to aides working with residents with cognitive or behavioral problems? About how many hours during the first six months?
- What does it mean to monitor a nurse aide?
- What probationary practices does the facility employ with nurse aides? What happens in terms of training and monitoring nurse aides during probation periods?
- What do you think are the most effective strategies for preventing abuse, neglect or financial exploitation?
- What type of training and continuing education do you provide charge nurses and other front line supervisory staff regarding the detection and prevention of abuse, particularly with respect to recognizing problem nurse aides
- Are there requirements about nurse aide in-service training and monitoring imposed by owner? (for chain facilities)
- Do you know when the facility hires someone with a criminal background or history of abuse?
- Do nurses and/or CNAs or families report allegations of abuse to you? About how many complaints do you receive over a six month period? What actions do you take as a result? What actions does the facility management typically take as a result of your reporting allegations of abuse?
- What has your experience been in using the nurse aide registry and what kind of information do you get from it? What are the benefits of this system and how could the system be improved?
Human Resources/Risk Management Personnel
- What policies does the nursing facility employ to prevent resident abuse, neglect or misappropriation?
- For nurse aides who have criminal histories or prior histories of abuse, neglect or misappropriation, are there any special policies or practices in place to mitigate risk?
- Is information obtained from the nurse aide registry and background checks valuable to the facility in terms of hiring and monitoring practices? Why or why not?
- Does the use of registries to identify substantiated incidents of abuse unnecessarily limit the pool of potential applicants? Are there certain prior histories or offenses that unfairly or unnecessarily disqualify applicants?
- What are the reporting policies regarding abuse, neglect and misappropriation?
- What kinds of actions result in a dismissal of an employee?
- During the course of your internal investigation, do you involve other investigative agencies such as law enforcement, APS, or DHS?
- Who do the residents report allegations/complaints to in this community?
- What improvements to the current system would you like to see?
APPENDIX F: SCREENING MECHANISMS USED IN THE CHILD CARE INDUSTRY
Each state develops unique child care workforce regulations and requirements. To examine individual states rules regarding child care workforce regulations, five states were selected: Michigan, Alaska, California, Arizona, and Kansas. The following information outlines key findings regarding child care workforce regulations for these states.
MICHIGAN
In Michigan, the Department of Consumer and Industry Services lists guidelines for the licensing of child day care centers. The rule states that a licensee must:
- Demonstrate to the department that he or she is of good moral character as defined in the good moral character act.
- Submit to a Michigan department of state police criminal history check and a family independence agency check for a history of abuse and neglect
- Notify and submit new hires credential to the department.
- Develop a written screening policy for all staff and volunteers who have contact with children.
- Have all staff at the time of hire sign a written statement that they are aware that abuse and neglect are against the law, they have been informed of centers policies on child abuse and neglect, and that they are mandated by law to report cases of abuse and neglect.
The department prohibits the presence of staff in a child care center who have been convicted of child abuse or neglect, or have been convicted of a felony involving harm or threatened harm. Records of such acts are placed on the central registry for substantiated abuse or neglect in the state. Further, the state also required the minimum presence of two staff members at any one time in the centers. They have strict rules of discipline prohibited by staff, which includes any physical or emotional forms of punishment.1
ALASKA
Alaskas Department of Health and Social Services has established laws for the licensure of child care facilities. They require evidence that the licensee has sufficient experience, training, or education in fulfilling the care giving duties, and they require each person to submit fingerprints to the Department of Public Safety to conduct state and national criminal background checks from criminal justice information.2 In addition, as a way of monitoring the licensee, the department requires an annual self-monitoring report. The department will not grant licenses or allow individuals to have contact with children in a child care facility if they have a history of:
- domestic violence;
- alcohol or substance abuse;
- within the last ten years, indicted on charges of stalking, assault, arson, reckless endangerment, perjury;
- endangering the welfare of a child in the second degree;
- neglect or abuse of a child; or
- physical, mental health, or behavioral problems that pose a risk to well-being of children.
For licensed child care facilities with one or more employees or regular volunteers, the department mandates that before employment to work with children, employees or volunteers must meet personnel qualifications, must be of reputable character, and have must submit a criminal justice information report with two fingerprints for hiring clearance. They also rule that any employee or volunteer, who has a record of child abuse or has given a child alcohol, tobacco, or a controlled substance, must be removed from the center.3 The child care facility is required to keep written records of all employees, and permit a licensing representative to review records.
CALIFORNIA
The California Department of Social Services has established child care center general licensing requirements. Prior to employment or initial presence in the child care facility, the department conducts criminal record review of any person in the child care facility who has contact with children, in addition to the licensee applicant for the child care facility. Under the California Department of Justice, there is the Child Abuse Central Index which maintains statewide, multi-jurisdictional, centralized index of child abuse investigation reports. Each child protection agency is required to forward reports of every child abuse incident it investigates to the California Department of Justice. Criminal record clearance is necessary for all persons in the child care facility who are also required to submit two fingerprints to the Department of Justice to search FBI criminal history records as well.
If after the criminal background check, a person is found to have convicted of a sex offense against a minor, inflicted any cruel or inhuman corporal punishment or injury upon a child, or have been convicted of a felony or criminal offense specified by the department, this persons employment will be immediately terminated and will be barred from entering the child care facility.4
ARIZONA
In Arizona, the Department of Health Services has guidelines for child care facilities to follow. The department requires that an applicant for a license to run a child care facility must submit all credentials, along with a copy of a two fingerprints and criminal history release form. In addition, the licensee must ensure that each staff member at the facility submit two fingerprints to the Department of Public Safety within seven working days after becoming a staff member.
As part of the licensees responsibilities, they shall ensure that during hours of operation, a parent, or representative from the department, local health department, child protective services, or local fire department, be allowed immediate access to the facilities. Staff members are mandated to report all suspected or alleged child abuse or neglect to Child Protective Services, and within 24-hours must notify the department as well. Licensees must keep staff records and reports on file throughout the period of employment.
Each licensee must provide training to each staff member who provides child care services to children within ten days of the starting date of employment or volunteer service. The training includes: health and nutritional requirements, child guidance and methods of discipline, child abuse or neglect detection, prevention, reporting, and accident and emergency procedures.5 A licensee must ensure that staff members maintain consistent, reasonable rules and limitations for a childs behavior, and must explain to the child why a particular behavior is not allowed. No staff member is permitted to use a method of discipline that could cause harm to the health or welfare of the child, no corporal punishment, no restraints or medications used in disciplines, and no discipline administered to any child by another child. As a disciplinary measure, a provider may place a child in time out.
Complaints about a provider or child care facility may be registered with the department. The department will investigate allegations and shall maintain records of all complaints against a provider. This information will be available to parents and to the general public upon request permitted by law.6 This practice makes past complaints available to employers about prospective providers.
KANSAS
The Kansas Department of Health and Environment established child care licensing and registration laws. They have the power to grant licenses for child care facilities and have access to the premises for inspection. The law states that no person shall work in the child care facility who:
- Has a felony conviction for a crime against persons, or as a juvenile committed an act that would constitute as a felony as an adult.
- Has a felony conviction under the controlled substances act.
- Has committed an act of physical, mental, or emotional abuse or neglect or sexual abuse.
- Has had a child declared, in any state, to have been deprived or in need based on allegations of physical, mental, or emotional abuse or neglect or sexual abuse.
- Has had parental rights terminated.
Under the department, each child care facility must register each employee or volunteer in the facility. Within one week of new hire, the name and birth date of the person must be filed with the department for the purpose of criminal history and child abuse registry information histories. Each person caring for children must also go through a health assessment no later than 30 days after employment and must meet all health testing and safety requirements. There is also a written discipline policy for methods of guidance. It is prohibited to use: corporal punishment (spanking, slapping, etc.), verbal abuse, binding or restricting movement, withholding food, misusing treatments.7
CONCLUSION
Although there are similarities in child care workforce laws among states, this five state examination highlights the significant flexibility states have in determining screening regulations for the child care workforce.
Notes
-
(2003) Michigan Regulations. Child Care Licensing-Child Care Centers, Department of Consumer and Industry Services Directors Office, Part I. General Provisions, R 400.5101 Definitions. Available at: http://nrc.uchsc.edu/STATES/MI/mi_400.htm#pgfId-629703.
-
(2003) HHS Statute, Licensure of Child Care Facilities. Title 14, Chapter 35. Available at: http://nrc.uchsc.edu/STATES/AK/al_47.htm#pgfId-486626.
-
(2002) Alaska Regulations. Child Care Facilities Licensing. Chapter 62. Available at: http://nrc.uchsc.edu/STATES/AK/ak_62.htm#pgfId-709944.
-
(2004) California Regulations. Title 22, Division 12, Chapter 1--General Licensing Requirements. Available at: http://nrc.uchsc.edu/STATES/CA/ca_22_12_1.htm#pgfId-845906.
-
Arizona Regulations, Arizona DHHS, Child Care Facilities. Section 9 A.A.C.5. Available at: http://nrc.uchsc.edu/STATES/AZ/Az_9TOC.htm.
-
Arizona Department of Economic Security, Certification and Supervision of Family Child Care Home Providers, Section 6 A.A.C.5, Article 52. Available at: http://nrc.uchsc.edu/STATES/AZ/az_3TOC.htm.
-
(2001) Kansas Child Care Licensing And Registration Laws. Available at: http://nrc.uchsc.edu/STATES/KS/ks_newTOC.htm.