
Monday, July 27, 2015
Overview of Frontotemporal Degeneration
Carol F. Lippa, M.D.
Professor and Interim Chair
Department of Neurology
Director, Memory and Cognitive Disorders Program
Drexel Neurosciences Institute
Drexel University College of Medicine
Philadelphia, PA 19102
Member, Medical Advisory Council, AFTD
What are the Related Dementias?
- Dementia is the general term used to describe those who lose memory and cognitive abilities to the point where they can not function normally.
- Alzheimer’s disease (AD) is the most common dementia subtype. Over half of those with dementia have AD.
- The more common nonAD dementias include FTD, Lewy body dementia and vascular cognitive impairment. We call these the “related dementias” The cause, symptoms, biology, progression and management of each differ.
FTD and the Related Dementias?
- The importance of the related dementias was acknowledged in May of 2013, when an ADRD workshop addressed special research priorities for the Alzheimer's disease-related dementias.
- Included frontotemporal (FTD), Lewy body (LBD), mixed, and vascular dementia.
- Organized by the NINDS in collaboration with the NIA
- Part of the National Plan to Address Alzheimer's Disease.
What is Frontotemporal Degeneration (FTD)
- FTD is similar to AD in that brain cells in specific brain regions die before they should. They symptoms experienced reflect the region within the brain where the cells die.
- FTD differs from AD in that the areas involved are not the same as those involved in forming new memories. So, their presenting symptom is not memory loss.
- The initial and primary problems are diverse and reflect functions served by the frontal and temporal lobes. This can be very specific.
- Cognitive or behavior change.
- Personality, language or complex reasoning are often involved.
- More often hereditary and younger in onset.
Every Convolution of the Brain Serves a Different Function
 |
RK: Case Report
- RK was employed as a high-powered administrative staff until age 46 when her personality and behavior changed.
- She developed socially inappropriate behavior. This lead to several arrests, and she would attempt to elude and assault the officers. Her change in personality prompted neurological evaluation.
- Delusions: damaged air, drinking water: analyzed samples. “Malevolent environment.”
- Obsessive behavior: collecting garbage in dumpsters.
- Her father, paternal grandfather and brother also developed changed in personality in their 40’s.
- Neuropsychological testing revealed difficulty with naming objects. Poor abstraction and judgment. She had no insight into her personality change
- Over the next few years, she became apathetic and developed severe problems with speech. She
- She died at age 53, after approximately seven years of symptoms.
Overview of Frontotemporal Degeneration
- Once thought rare
- 8% of the DUCOM Memory database
- 12% of DUCOM Brain Bank subjects
- Symptoms
- Language
- Mood changes: depressed, irritable, or euphoric
- Disinhibition
- Planning/organization
- Apathy
- Bizarre behavior
- Criminal behavior
- Carbohydrate craving
- Perseveration
FTD: History
- 1892: Pick described: semantic dementia with left temporal atrophy
- 1906: frontal lobe case described
- 1907: Alzheimer described pick bodies from pick’s original case
- 1990’s: some cases linked to the tau gene on chromosome 17
- Since then other genes have been identified
FTD v AD
- Younger onset
- More likely hereditary, often autosomal dominant
- Nonmemory presentation
- More legal and safety issues
- Many develop motor problems
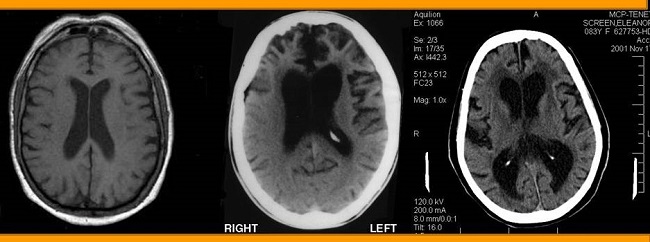
FTD: Imaging
 |
 |
 |
 |
|---|---|---|
 |
 |
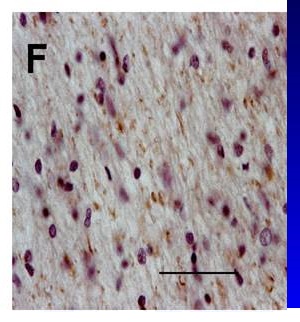 |
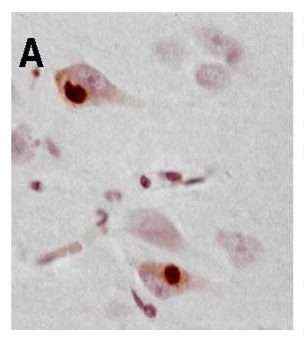
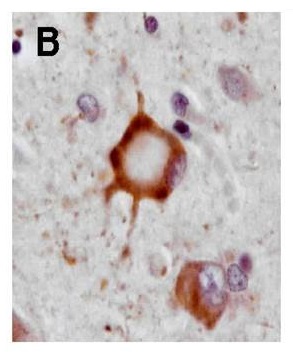
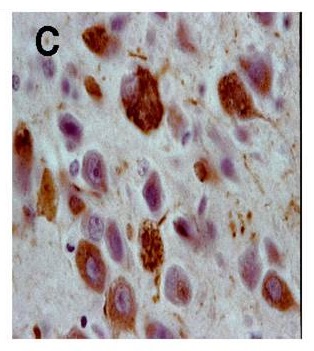
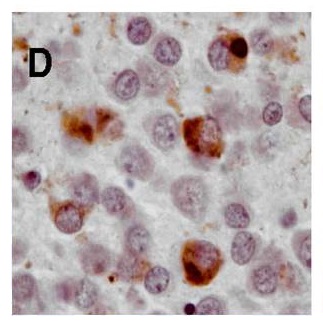
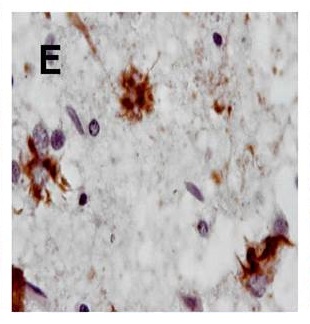
FTD:Tau, TDP-43 or Ubiquitin PathologyNOT AD pathology
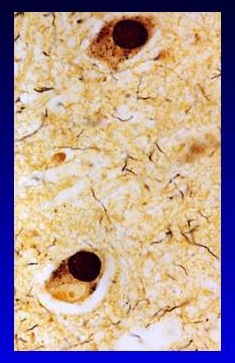 |
 |
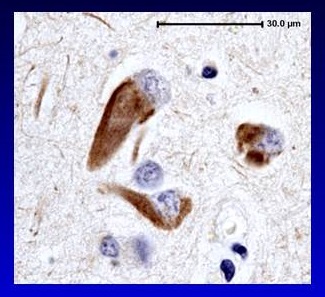 |
|---|
FTD: Genetics
- The majority cases of FTD are sporadic
- A minority have autosomal dominant transmission
- Chromosome 17 - Tau AND progranulin genes
- Chromosome 9 - C9ORF72
- Chromosome 1 - TDP-43
- Chromosome 16 - FUS mutations
- Chromosome 20 - Prion mutations
- MANY Unlinked
- No overlap with AD mutations
- No environmental factors identified
FTD is Associated with Movement Problems
- FTD patients may develop ALS -- weakness and problems swallowing/breathing
- FTD patients may develop problems similar to Parkinson’s disease -- slowness, stiffness, shaking
- FTD patients are at risk for falls -- due to cognitive (impulsive, inattentive, careless, restless) and motor combinations
Interventions
- Problems moving, walking or swallowing
- Physical therapy -- ambulation, assistive devices, bed mobility, gait training, orthotics, spasticity, balance and strengthening exercises
- Occupational therapy -- strategies and devices to improve or maintain basic activities (dressing, bathing, eating)
- Swallow -- articulation therapy, nonverbal communication devices, aspiration assessment and feeding strategies.
- Variable symptoms and progression involving language, behavior and cognition.
- Medications for cognitive, behavioral
- Medications for psychosis, depression, sleep problems
- Assess acute changes -- infection, pain
- Assess for safety -- driving
- Needs Assessment and legal
Resources
 |
AD-Related Dementias Workshop
May 1-2, 2013
FTD Recommendations: Laboratory
- Recommendation #1, #3 and #4.
- Clarify the mechanisms of disease pathogenesis and associated neurodegeneration /toxicity of the FTD variants
- Recommendation #2.
- Develop better FTD in vivo and cell-based model systems
FTD Recommendations: Clinical
- Recommendation #1.
- Identify new genes (genetic causes)
- Recommendation #2.
- Develop FTD biomarkers for diagnosis and disease progression
- Recommendation #3.
- Understand phenotypic heterogeneity and natural history
- Recommendation #4.
- Create an international FTD clinical trial network
FTD: Summary Slide
- The related dementias comprise at least a third of all dementias, and thus are contributing substantially to our evolving trillion dollar health problem.
- FTD symptoms differ from those of AD, and they may require more special services including PT/OT, swallow and communication therapies, and legal planning.
- The underlying biology and genetics differs from AD
- Research working toward a cure lags that of AD
- AD goal -- treat AD by 2025
- Disease visibility, support services, education and care strategies also lag behind those for AD. Need to be developed and monitored.
****THANK YOU***
Files
Document
Mtg17-Slides1.pdf (pdf, 1.75 MB)