
ADVISORY COUNCIL ON ALZHEIMER'S RESEARCH, CARE, AND SERVICES
Monday, December 2, 2013
Alzheimer’s Disease: A Rapid-Learning System
Lynn Etheredge
National Advisory Council on Alzheimer’s Research, Care, and Services
Fundamental Challenge
- Create a rapid learning health system to advance and deliver much better prevention and treatment for each patient
- Health sector: 315 M; 17 % of GDP; complex, variable, dynamic, pluralist & public-private; many therapies that aren’t very effective; underused IT
- Learning (now): limited #s of patients & researchers, data poor, slow, expensive, RCT-focused, with many gaps; slow delivery-system learning/use of best practices
Toward A Rapid-Learning Health System
- HIT-EHRs, big data, and learning networks are starting to change every aspect of healthcare.
- Accelerating biomedical research
- NIH: Biobanks w/EHRs & genomics, 20-30M patient research networks, BD2K. VA: Million veterans biobank
- Learning what works
- FDA: Sentinel (125 M patients). PCORI: national CER system & databases
- Delivering better care
- EHRs national use, CMS $10 B innovation center & ACOs, large health plans
A Rapid Learning Model
- Research: Faster progress in biomedical research, prevention, and treatment requires large-scale databases (millions of patients), data-sharing, and research collaboration
- Cancer research has shifted to genetics, pathways, & “precision medicine”. Most cancers involve 2-8 sequential alterations over 20-30 yrs, a dozen signaling pathways (Vogelstein 2013). Likely similarities for many chronic conditions, e.g. Alzheimer’s
- Recent NIH large data initiatives include: Cancer Genome Atlas, 3 open science “data clouds”, international data-sharing agreement; 20-30M patient data registry network
- An enormous potential for learning much more, much more rapidly -- from national data strategies that are now possible
- Assessment: Much faster learning will be possible about what works best for individual patients
- 1,000 targeted cancer drugs now in development
- For new targeted cancer therapies that show persuasive evidence of effectiveness (e.g. 30%-60%), FDA is considering reducing or eliminating Phase 3 RCTs
- FDA Sentinel system: 24 hour studies (125 M patients) vs. 5 yrs +
- Implementation: A rapid-learning system involves researchers, biotech, physicians, patients, families, delivery systems, and payers
- ASCO’s rapid-learning cancer system (CancerLinQ database for all cancer patients + IBM’s Watson)
- CMS $10B Innovation Center for national rollout of best practices (patient safety (60,000 lives), million hearts, strong start; 40+ models)
Data from 97% of Cancer Care is Lost
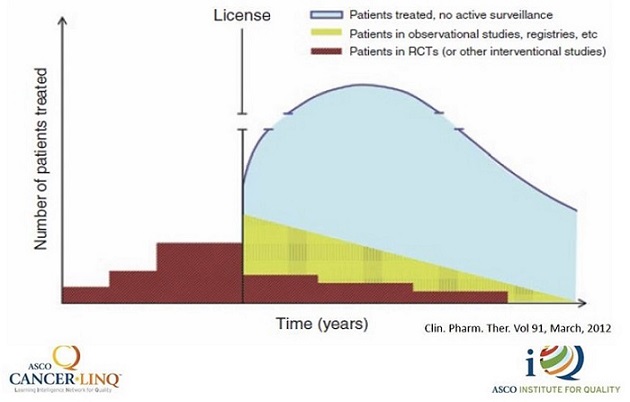 |
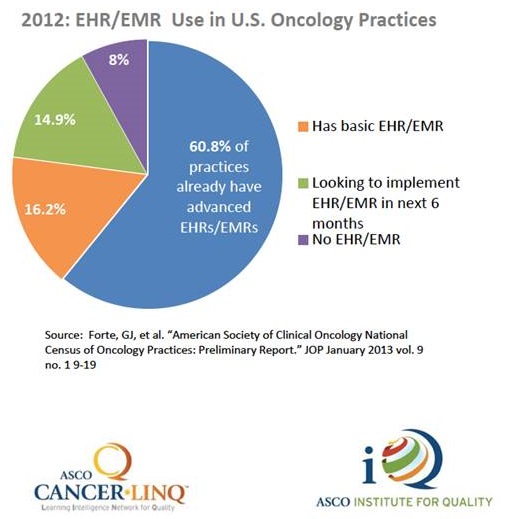
Health Information Technology Revolution
- Widespread adoption of EHRs by physicians and hospitals
- Improved data processing and storage capacities
- Rapid analysis tools
- Advances in natural language processing
 |
#1. Alzheimer’s: Rapid-Learning
- Build an international Alzheimer’s Disease learning network with large research databases.
- US RL data infrastructure (current):
- VA (8 M, age 65+), HMO Research Network (14M); NIH databases & research studies; FDA’s clinical data repository; Medicare Chronic Disease Warehouse (32 M, 1999-2011); United-Optum & Wellpoint (30M+ enrollees each); FDA Sentinel (125M); PCORI registries
- Alzheimer’s registries and networks (e.g. NIA), CAMD pharmaceutical industry initiative
- US RL data infrastructure (current):
- Many technical and policy/administrative issues will need to be identified and resolved. A collaborative effort, with data-sharing.
A Case For Data-Sharing
- If 10 institutions each share 100 cases
- Database = 1,000 cases
- Every institution gets 900 added cases for a contribution of 100 = 9:1
- If 100 institutions each share 1,000 cases
- Database = 100,000 cases
- Every institution gets 99,000 added cases for a contribution of 1,000 = 99:1
- Data-sharing is a high pay-off strategy. More data-sharing multiplies benefits.
#2. Alzheimer’s: Rapid-Learning
- Build the Alzheimer’s data system as part of a national EHR-HIT strategy
- Develop a downloadable EHR “App” (or module) for patients with Alzheimer’s and dementia
- Supports standardized data collection and reporting to national Alzheimer’s research registries
- Supports two-way communications to physicians about best practices, practice guidelines, decision support
- Includes patient & family reported data, information and involvement
- One-click access to key resources, e.g. MedlinePlus, Alzheimer’s Association, support networks for physicians and patients
- Could be used to demonstrate adherence to requirement for test of cognitive impairment, quality reporting & new payment incentives
- Federal requirement: all HHS-supported EHRs accept and work with this App
#3. Alzheimer’s: Rapid Learning
- Develop and advance “best practices” models for Alzheimer’s disease
- Project ECHO (New Mexico)
- Use CMS’s innovation authorities and $10 B funding to roll these out nationwide for Medicare and Medicaid patients
- Home and community-based care
Summary
- #1. A large international learning and data-sharing network
- #2. An EHR-Apps initiative
- #3. National rollout of best practices
“How much faster can we learn?” is now a question to which new answers can evolve for Alzheimer’s Disease.
Return to
National Alzheimer's Project Act Home Page
Advisory Council on Alzheimer's Research, Care, and Services Page
Advisory Council on Alzheimer's Research, Care, and Services Meetings Page
Files
Document
Mtg10-Slides5.pdf (pdf, 1.04 MB)