ADVISORY COUNCIL ON ALZHEIMER'S RESEARCH, CARE, AND SERVICES
Monday, April 29, 2013
Alistair Burns
National Clinical Director for Dementia
Dementia Timeline
- National Dementia Strategy February 2009
- Antipsychotics Report Time for Action November 2009
- Public Accounts Committee January 2010
- National Clinical Director (NCD) appointed February 2010
- General Election May 2010
- Prime Ministers Challenge March 2012
- Reorganisation of the NHS April 2013
Dementia
- National Dementia Strategy: 17 objectives (February 2009)
- Anti-psychotic Report - 11 recommendations (November 2009)
- Public Accounts Committee 10 conclusions (January 2010)
Covers of various reports available at dementiachallenge.dh.gov.uk, including
- Living well with dementia: A National Dementia Strategy
- The use of antipsychotic medication for people with dementia: Time for action
- Improving Dementia Services in England -- an Interim Report
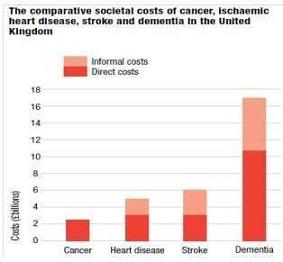
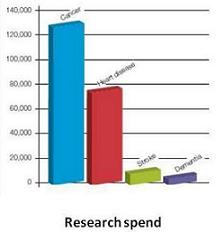
- Dementia 2010: The economic burden of dementia and associated research funding in the United Kingdom
- Dementia 2012: A national challenge
- The Right Prescription: a call to action on the use of antipsychotic drugs for people with dementia
- Handbook: using the Dementia Commissioning Pack
- Using the Commissioning for Quality and Innovation (CQUIN) payment framework
- The Operating Framework for the NHS in England 2012/13
- Innovation Health and Welfare
- Establishment of Memory Services -- Results of a survey of Primary Care Trusts, final figures 2011
- The NHS Atlas of Variation in Healthcare: Reducing unwarranted variation to increase value and improve quality
Change attitudes/raise awareness
- From: Lonely, isolated, people in care homes
- To: Engaged & alive individuals actively involved in life
"Quality outcomes for peole with dementia: building on the work of the National Dementia Strategy"
- Timely diagnosis and support in primary care
- Dementia in the General Hospital
- Dementia in Care homes
- Reduction of antipsychotics
- Support for carers
|  |
Outcomes for people with dementia
| By 2014, all people living with dementia in England should be able to say |
| I was diagnosed in a timely way | I understand, so I make good decisions and provide for future decision making | I get the treatment and support which are best for my dementia, and my life |
| Those around me and looking after me are well supported | I am treated with dignity and respect | I know what I can do to help myself and who else can help me |
| I can enjoy life | I feel part of a community and Im inspired to give something back | I am confident my end of life wishes will be respected. I can expect a good death |
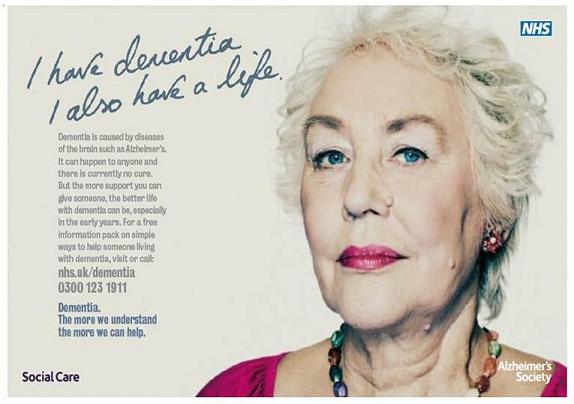
"Unlocking diagnosis: The key to improving the lives of people with dementia"
- Timely diagnosis and support in primary care
- Dementia in the General Hospital
- Dementia in Care homes
- Reduction of antipsychotics
- Support for carers
|  |
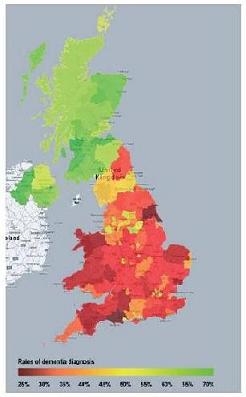
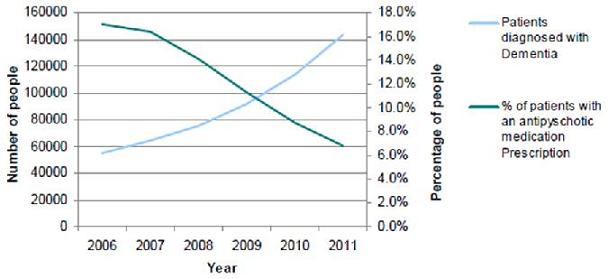
Rates of dementia diagnosis across the UK
Dementia in Primary Care
- Quality Outcomes Framework (QOF)
- Number of people with dementia
- Review every 15 months
- Blood tests
- Care plans for carers of people with dementia
- Directed Enhanced Service (DES)
- Case finding in people attending for a vascular risk check
- In people with Learning Difficulties
- In people with neurological conditions
- ? People over age 75
- Health Check
Advertisement
Three Publications
- Timely diagnosis and support in primary care
- Dementia in the General Hospital
- Dementia in Care homes
- Reduction of antipsychotics
- Support for carers
|  |
 |  |
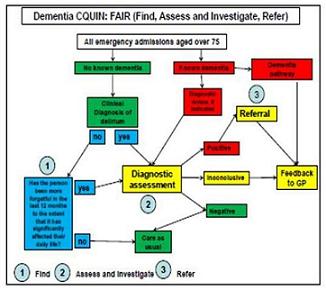
Hospital Care in Dementia
Two Publications
- Early diagnosis and intervention in primary care
- Dementia in the General Hospital
- Dementia in Care homes
- Reduction of antipsychotics
- Support for carers
|  |  |
Antipsychotics in Dementia
- Define the challenge
- Get the evidence
- Talk about it
- Get political support
- Come up with a solution
- Measure the change
|  |  |
 |  |  |
 | | |
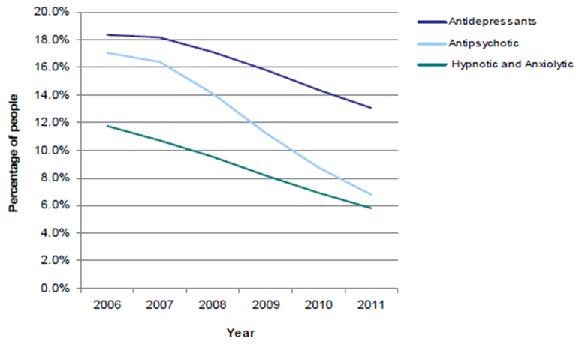
National Audit of Antipsychotics in Dementia 2012
Other Medications Prescribed
Three Publications
- Timely diagnosis and support in primary care
- Dementia in the General Hospital
- Dementia in Care homes
- Reduction of antipsychotics
- Support for carers
|  |
 |  |
Two Publications
- Timely diagnosis and support in primary care
- Dementia in the General Hospital
- Dementia in Care homes
- Reduction of antipsychotics
- Support for carers
|  |  |
Information
Dementia Timeline
- National Dementia Strategy February 2009
- Antipsychotics Report Time for Action November 2009
- Public Accounts Committee January 2010
- National Clinical Director (NCD) appointed February 2010
- General Election May 2010
- Prime Ministers Challenge March 2012
- Reorganisation of the NHS April 2013
Two Publications
Key Challenges
- Improvements in health and care
- Dementia friendly communities
- Better research
The NHS in England Before the Reforms
| Department of Health |
| 10 strategic health authorities (SHAs) |
| 152 primary care trusts (PCTs) |
| Health services: NHS trusts and primary care services |
The NHS in England After the Reforms -- outcomes, commissioning, patients
| Department of Health |
| NHS Commissioning Board |
| 23 commissioning supportive services | 4 regional commissioning sectors |
| 27 local Commissioning Board offices |
| 212 clinical commissioning groups |
| Health services: NHS trusts and primary care services |
Dementia
| D | Diagnosis |
| E | Early identification |
| M | Management of symptoms |
| E | Effective support for carers |
| N | Non drug treatments |
| T | Treatment of medical conditions |
| I | Information |
| A | At, and towards, end of life |
Responding to the Dementia Challenge in England
Yves Joanette, PhD, FCAHS
Scientific Director, CIHR Institute of Aging
Executive Director, ICRSAD
Some Facts...
| Canadians with Alzheimer's disease or a related dementia |
| Now | 500,000 |
| Within a Generation | 1,100,000 |
| Cost to Canadians for dementia care |
| Now | $15 billion |
| Within a Generation | $153 billion |
| The time Canadians will be providing in informal care |
| Now | 231 million hours |
| Within a Generation | 756 million hours |
| Rising Tide: The Impact of Dementia in Canada, ASC, 2010 |
Global Context
January 2012
NAPA (USA) | February 2012
JPND (Europe) | March
WHO |
 |  |  |
Canada: 10 Provinces & 3 Territories, 13 Provincial Health Systems
Provincial Plans on Dementia
- Quebec
- « Meeting the Challenge of Alzheimers Disease and Related Disorders - A Vision Focused on the Individual, Humanism, and Excellence » May, 2009.
- Bristish-Columbia
- « The Provincial Dementia Action Plan for British ColumBia - Priorities and Actions for Health System and Service Redesign » April 2012
- Ontario
- « 10 by 20 : Ontario action plan for dementia » 2010
- Alberta
- « Strategic directions in healthy aging and contiuning care in Alberta - Alzheimer disease and other dementias » 2002
- Manitoba
- « A strategy for Alzheimer disease and related dementias in Manitoba » 2002
- Newfoundland and Labrador
- « Provincial strategy fo Alzheimer disease and other dementias : a plan of action » 2001
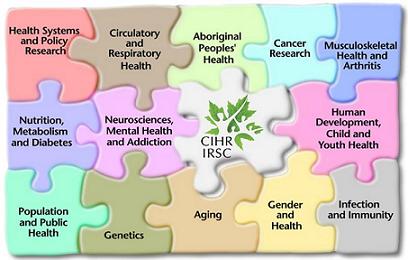
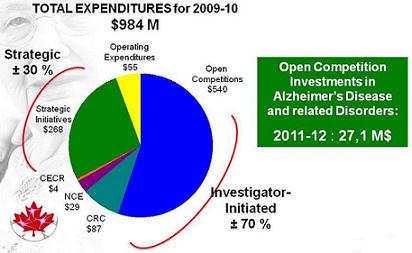
Canadian Institutes of Health Research
CIHR Expenditures 2009-2010
CIHR Strategic Investments Roadmap Signature Initiatives
| Enhance Patient-Oriented Care and Improve Clinical Results through Scientific and Technological Innovations | - Patient-Oriented Research SUPPORT Units (SPOR)
- Personalized Medicine
- Community Based Primary Health-Care
- Pathways to Health Equity for Aboriginal Peoples
- International Collaborative Research Strategy for Alzheimers Disease
- Canadian Epigenetics, Environment and Health Research Consortium
- Inflammation in Chronic Disease
- Evidence Informed Health-Care
|
| Support a High-Quality, Accessible and Sustainable Health-Care System |
| Reduce Health Inequities of Aboriginal Peoples and other Vulnerable Populations |
| Prepare For and Respond To Existing and Emerging Threats to Health |
| Promote Health and Reduce the Burden of Chronic Disease and Mental Illness |
| + Canadian Longitudinal Study on Aging |
Cognitive Impairment in Aging
- Canadian Dementia Knowledge Translation Network
- Cognitive Impairment in Aging partnership (20+ partners)
|
 |
International Collaborative Research Strategy for Alzheimer's Disease
ICRSAD in a Nutshell...
The International Collaborative Research Strategy for Alzheimers Disease (ICRSAD)
- Is one of CIHRs Major Initiatives (RSI)
- Covers Alzheimers Disease and related neurodegenerative disorders
- Focuses on two complementary objectives:
- Strengthen the Canadian innovative and collaborative research efforts on neurodegenerative diseases through the CCNA
- Support international leadership and the insertion of Canadian research in international collaboration
ICRSAD -- The Concept
Global Opportunity
International Component
- Wellcome Trust Neurodegeneration Program
- Team Grant: Alzheimers Disease (France-Quebec-Canada)
- Centres of Excellence in Neurodegeneration
- Canada-China Team Grants in Alzheimers Disease and Related Disorders
- ADNI Canadian Program
- Canadian ADNI Centers
- ADNI Secondary and Methodological Analyses
Centres of Excellence in Neurodegeneration
Centres of Excellence in Neurodegeneration
- Standards for determining the vascular contribution to neurodegeneration
Joanna Wardiaw (MRC), Martin Dichgans (DZNE), Eric Smith (CIHR) - Integrated approach to identify novel genes for frontotemporal lobar degeneration
MarcCruts (VIB), Christian Haass (DZNE), Dieter Edbauer (DZNE) - Mitochondrial dysfunction and susceptibility to Parkinson's disease: New models of pathogenetic interactions
Donato A. Di Monte (DZNE), David S. Park (CIHR), Fabio Blandini (MDS), Anthony H.V. Schapira (MRC) - Early synaptic plasticity and network dysfunction in transgenic (tg) rat models of Alzheimer's disease (AD)
Michael Rowan (HRB/SFI), Claudio Cuello (CIHR), Martin Fuhrmann (DZNE) - Immune subtype in Parkinson disease
Thomas Gasser (DZNE), Antonio P. Strafella (CIHR) - C. elegans models of mitochondrial deficiency in the nervous system
Daniele Bano (DZNE), Siegfried Hekimi (CIHR), Mario de Bono (MRC) - The GENetic Frontotemporal Dementia Initiative (GENFI): a new multi-centre platform for the study of frontotemporal lobar degeneration
Martin Rossor (MRC), Giovanni B. Frisoni (MDS), Torik Ayoubi (VIB), Mario Masellis (CIHR) - Identification of generic supressors of proteinopathies
David Rubinsztein (MRC), Joerg Gsponer (CIHR)
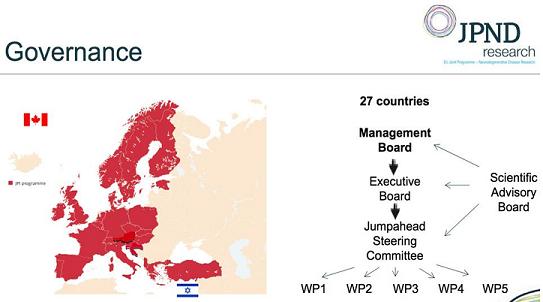
JPND
EU Joint Programme Neurodegenerative Disease Research
4 May 2012
Canada has joined JPND as the first ever Third Country member. Israel joins as full member to bring total number of countries participating in JPND to 27.
At the twelfth JPND Management Board meeting on May 4th, 2012, two countries' applications for membership of JPND were accepted:
Israel becomes the 26th full member country of JPND, following the applications of Austria and Croatia earlier in 2012. Full membership of JPND is open to EU Member States and EU-Associated Countries.
In a first for JPND, Canada's application for Third Country membership of JPND was also accepted. Canada now participates in JPND according to the recently published JPND Policy on Third Country Participation.
This brings the total number of countries participating in JPND to 27.
JPND
EU Joint Programme Neurodegenerative Disease Research
JPND
EU Joint Programme Neurodegenerative Disease Research
- Improve the scientific understanding of the disease.
- Improve the medical tools available to doctors to identify and treat the disease.
- Improve the social care and structures available to assist patients, their families, and health service providers so that patients can receive optimum care at all stages of their illness.
- To add value to national investments through coordinated action
- To encourage the development of national research strategies in ND
- To engage in partnership to reach the full potential of JPND
Implementation Plan
A first-phase JPND Implementation Plan has been agreed for the period of 2012-2014. The plan has three major action areas:
- Annual Calls for Proposals
- Action Groups to determine research needs and opportunities
- Action Groups to promote engagement, commitment and partnerships
USA Conference
On November 9, 2012, at the headquarters of the American Association for the Advancement of Science (AAAS) in Washington, DC, a conference was held to explore the potential of enhanced transatlantic research collaboration in the area of neurodegenerative diseases. The conference was organized by JPND in close collaboration with the science counselors from the Embassies of France, Poland, Austria, Finland, Germany, Ireland, Italy, Spain, and Sweden, and the American Association for the Advancement of Science.
The aim of the conference was the showcase JPND and to attract the attention of potential American partners in order to achieve their possible future affiliation. The even was well attended, with approximately 40 participants from scientific institutes, universities, industry, NGOs, European embassies, and US government departments and agencies.
ICRSAD -- The Concept
General Framework
CCNA Framework
CCNA -- Bringing Together Canadian Expertise
CCNA -- The Vision
The vision of the CCNA is to bring together the best of Canadian research in the field of neurodegenerative diseases affecting cognition -- supported by CIHR as well as by other partners -- in a collaborative and synergistic space to work on bold, innovative and transformative research that will ultimately impact the quality of life and the quality of services for those having to live with the effects of neurodegenerative diseases affecting cognition and their caregivers
CCNA -- Characteristics
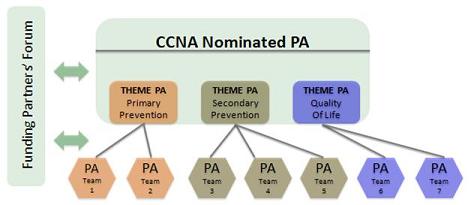
- Excellent governance -- The Nominated Principal Applicant (NPA) and the three Theme Principal Applicants (PA) will together play a crucial role in creating a interactive research space, with the necessary common resources, where interdisciplinarity and distinct perspectives of various neurodegenerative diseases will lead to potential innovative solutions
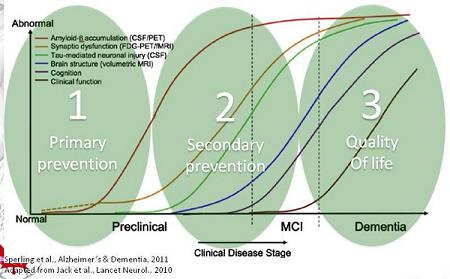
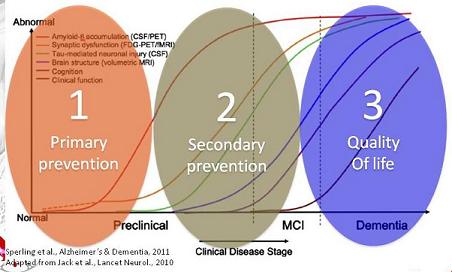
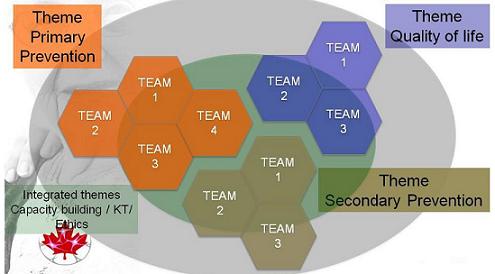
- Excellent research teams within each of the three themes (Primary Prevention, Secondary Prevention and Quality of Life) -- Each of these teams will submit an innovative, out-of-the-box research program for five years meant to have a significant impact
CCNA -- Qualifiers
- CCNA will be
- Comprehensive -- All three themes and cross-cutting topics (Ethics, KT and training)
- Inclusive -- Canadas excellence in this area of research; established and new investigators; knowledge users
- Innovative -- Focus on out-of-the-box high-impact research
- Connected globally -- In synergy with the best groups in the world
CCNA -- Partners
A unique role for CCNA Partners
- Highly interested groups or organizations involved in the transformation of discoveries into impactful solutions
- Partners will not only bring extra resources to the CCNA, but will also:
- Contribute to the shaping of the research program (1st Partners Forum)
- Represent a privileged source of transformation of discoveries into impactful measures
- Be in constant synergy with the CCNA teams and leaders (Yearly Partners Forum)
Canadian Institues of Health Research
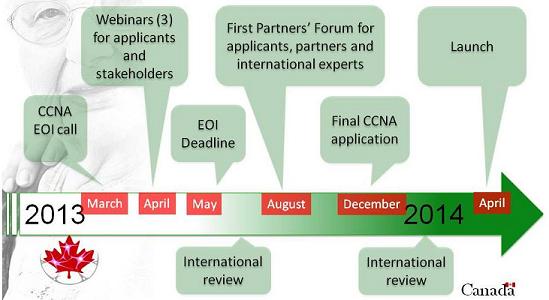
CCNA -- The Timeline
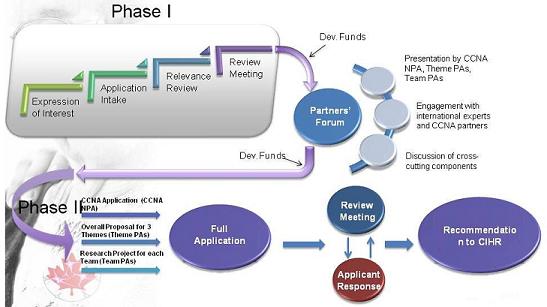
CCNA -- The Process
Canada: A Node of Innovation in a Global Network
Discussion
Break
Richard J. Hodes, M.D.
Chair, Federal Research Subcommittee
Establishing Research Milestones and Tracking Progress
Alzheimer's Disease Research Summit Recommendations
- Session 1: Interdisciplinary Approach to Discovering and Validating the Next Generation of Therapeutic Targets for AD
- Session 2: Challenges in Preclinical Therapy Development
- Session 3: Whom to Treat, When to Treat, and What Outcomes to Measure
- Session 4: Drug Repurposing and Combination Therapy
- Session 5: Nonpharmacological Interventions
- Session 6: New Models of Public Private Partnerships
Research Summit Recommendations
Alzheimer's Research Summit Recommendations May 2012
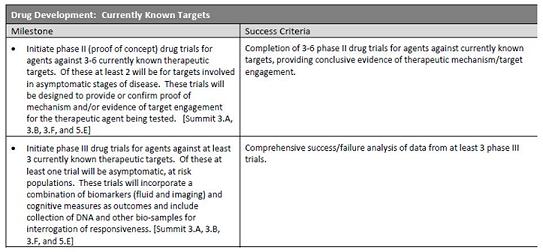
Recommendations related to Drug Trial Milestones
- 3.A. Initiate treatment trials in asymptomatic, at-risk individuals using uniform biomarkers and cognitive outcomes informed by data from Alzheimers disease trials using patients with more advanced disease.
- 3.B. Collect DNA and other biosamples from these studies to enable subsequent interrogation based on treatment response and predictors of decline in the groups receiving placebo.
- 3.F. Develop treatments for patients with symptomatic Alzheimers disease and support proof of concept studies to validate novel targets for cognitive and neuropsychiatric symptoms across all disease stages.
- 5.E. Develop standard outcome measures to enable data comparisons across studies. These include but are not limited to ecologically valid measures of real world function, quality of life, and physical and cognitive function.
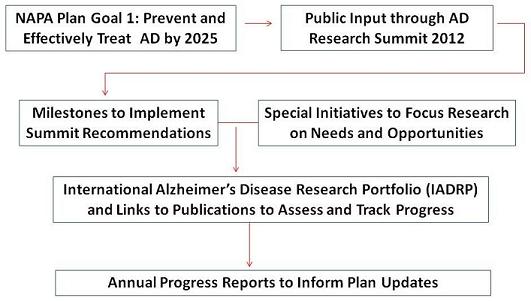
Milestones to Implement Recommendations of the NIH 2012 AD Summit
- Drug Development: Repurposing and Combinations
- Drug Development: Currently Known Targets
- Drug Development: Novel Targets
- Development of Non-Pharmacological Interventions
- Biomarkers of Disease Progression
- Epidemiology
- Research Resources
- Partnerships to Accelerate AD Drug Development
- Infrastructure
- Study Recruitment and Participation
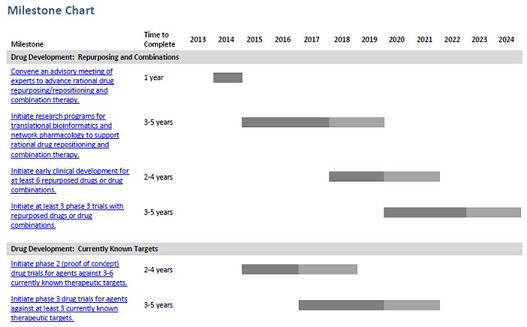
Milestone Chart Example
Milestone Table Example
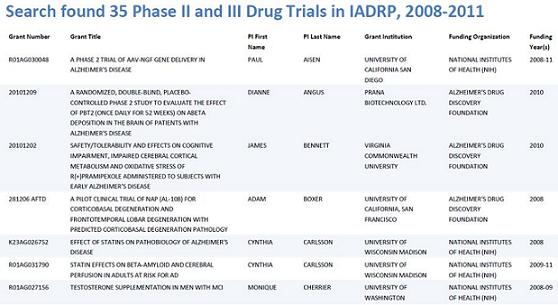
Drug Trials Search Example
International Alzheimer's Disease Research Portfolio -- Participating Funders
| Current Members | Recent Commitments |
- US Federal Agencies -- NIH, CDC, HRSA, AHRQ, AoA, VA, DoD
- Alzheimers Association
- Alzheimers Drug Discovery Foundation
- Alzheimers Research UK
| - Bright Focus
- Alzheimers Society UK
- Alzheimers Australia
- Alzheimers Society Canada
|
|---|
| Actively encouraging submissions from AD funders -- IADRP contacts: Nina Silverberg (silvebergn@mail.nih.gov), Charlene Liggins (ligginsc@mail.nih.gov) and Heather Snyder (hsnyder@alz.org) |
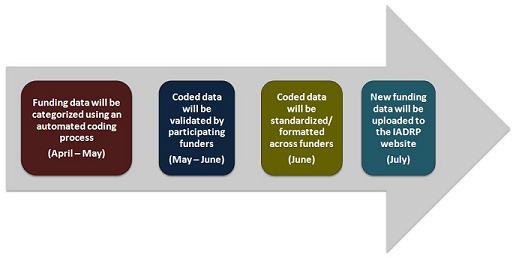
International Alzheimer's Disease Research Portfolio -- Upcoming Coding and Validation Process
FY 2013 Alzheimer's Disease Request for Funding Announcements
| RFAs | $s in 2013 -- up to |
| Interdisciplinary Approach to Identification and Validation of Novel Therapeutic Targets for Alzheimer's Disease (R01) | $23 M |
| Alzheimer's Disease Therapeutics Program (U01) | $1 M |
| Alzheimer's Disease Prevention Trials (R01) | $45 M |
| Alzheimer's Disease Phase I Clinical Trials (R01) | $4 M |
| | Total -- $73 M |
New AD Research Findings -- FY 2013
- Genetics of AD May Vary Among Different Populations: Risk of Late Onset AD in African Americans
- The Monetary Costs of Dementia in the United States
Genetics of AD May Vary Among Different Populations: Risk of Late Onset AD in African Americans
- African Americans have a higher incidence of late-onset AD than Caucasians.
- Genome wide association study included 1968 African American AD cases and 3928 African American controls.
- Genotypes with strongest association with risk of LOAD among African Americans were ABCA7 (odds ratio 1.8) and APOE (odds ratio 2.3).
- Association with ABCA7 was 60 percent stronger among African Americans than among individuals of European ancestry.
- Identification of disease associated variants helps identify targets for genetic testing, prevention, and treatment. A variety of detection, treatment and prevention strategies will be needed.
Reitz, C. et al. JAMA. 2013;309(14):1483-1492
The Monetary Costs of Dementia in the U.S.
New England Journal of Medicine, April 4, 2013
M. Hurd, P. Martorell, A. Delavande, K. Mullen, K. Langa
- Used Health and Retirement Study (HRS)
- Diagnosis of dementia in ADAMS sub study
- Estimate of national prevalence: 14.7% in population 71 or older in 2010
- HRS data on use and cost of health care services; amount and type of informal care
- Adjusted for co-morbidities and demographics
- Want cost attributable to dementia
Total (Population) Costs
- In 2010
- Actual spending: Paid health care services, nursing home, in home paid help etc.
- $109 billion = $28,000 per year per individual
- Adding in informal care: $159-$215 billion = $42,000-$56,000 per individual
- In 2040
- Sharply increased fraction of population in their late 80s or early 90s
Baby boom
- Actual spending: $259 billion (in 2010$)
- Adding in informal care: $379-$511 billion (in 2010$)
Down Syndrome Research Update
- On April 16-17, 2013, the Advancing Treatments for Alzheimers Disease in Individuals with Down Syndrome meeting was held.
- Over 40 leading researchers in these fields attended
- Meeting summary and recommendations will be posted soon at: www.nia.nih.gov
- Meeting sponsors included: Eunice Kennedy Shriver National Institute of Child Health and Human Development, the National Institute of Neurological Disorders and Stroke, and the National Institute on Aging, the Down Syndrome Research and Treatment Foundation and Research Down Syndrome
April 2013 Meeting Logo
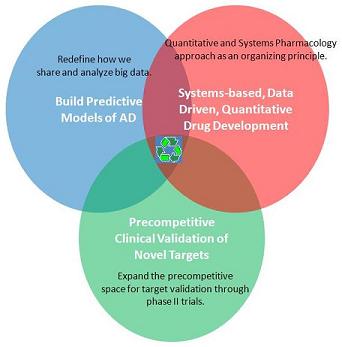
Facilitate Partnership for Open Innovation Engaging all Stakeholders
Alzheimers Disease-Related Dementias Workshop
May 1-2, 2013, Natcher Auditorium, NIH Campus, Bethesda, MD
- NINDS, together with NIA, will host a workshop to solicit input and develop recommendations on research priorities and timelines for AD-Related dementias.
- Outline of Workshop Topics:
- FTD and AD-Related Tauopathies
- Lewy Body Dementias
- Vascular Contributions to AD-Related Dementias
- Mixed Dementias
- Clinically Important Diagnostic Challenges in Dementias
- Health Disparities in AD-Related Dementias
- The workshop will define the state of the science and identify the critical opportunities and barriers in each of the dementias, whether basic, translational, or clinical.
- Register link
Discussion
Public Comments
Return to
National Alzheimer's Project Act Home Page
Advisory Council on Alzheimer's Research, Care, and Services Page
Advisory Council on Alzheimer's Research, Care, and Services Meetings Page