
U.S. Department of Health and Human Services
The Home Health Aide Partnering Collaborative: Implementation Manual
Miriam Ryvicker, Ph.D., Theresa Schwartz, B.A., Sally Sobolewski, M.S.N., Terese Acampora, M.A., R.N., Marki Flannery, M.A., Elizabeth Buff, R.N., B.S.N., M.S., Ann Marie Hess, M.S.N., M.S., Robert Rosati, Ph.D., and Penny Feldman, Ph.D.
Visiting Nurse Service of New YorkCenter for Home Care Policy and Research
August 2007
PDF Version: http://aspe.hhs.gov/daltcp/reports/2007/HHAPartmnl.pdf (74 PDF pages)
This report was prepared under contract #HHSP23320044304EC between the U.S. Department of Health and the Center for Home Care Policy and Research. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the ASPE Project Officer, Marie Squillace, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. Her e-mail address is: Marie.Squillace@hhs.gov.
The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
TABLE OF CONTENTS
- FOR SENIOR LEADERS
- Introduction to the Home Health Aide Partnering Collaborative
- FOR MANAGERS IMPLEMENTING THE COLLABORATIVE
- Why We Need to Improve Teamwork in Home Health Care
- How a Collaborative Works
- Overview of Collaborative Goals and Strategies
- The Importance of Gaining Buy-In
- Using the PDSA Cycle to Set Goals, Test Changes, and Adapt Ideas
- Goal 1: Improving Support to Home Health Aides
- Goal 2: Improving Patients' Functional Independence
- FOR SENIOR LEADERS AND MANAGERS
- Celebrating Success and Planning for Spread
- Sustaining the Gains
- LIST OF FIGURES
- FIGURE 1: Who Participates
- FIGURE 2: Learning Collaborative Model
- FIGURE 3: PDSA Cycle
- FIGURE 4: Percentage of Patients Showing Improvement in Bathing at Discharge
- FIGURE 5: Tests of Change
- LIST OF EXHIBITS
- HHA Job Perceptions Survey
- Clinician Survey
- Items for Measuring Patients' Functional Outcomes
- Nurse-Aide Interaction: The Five Promises
- Paraprofessional Manager Tool for Partnering Collaborative Conference Calls
- Paraprofessional Manager Tool for Partnering Collaborative Team Meetings
- Activities of Daily Living (ADL) Tool
- "What I Can Do for Myself" Tool
- Role-Play Script for Introducing the Functional Improvement Tool
- HHA Partnering Collaborative: Tasks and Timeline
ACKNOWLEDGEMENTS
Many individuals and organizations contributed to the development of the Home Health Aide (HHA) Partnering Collaborative and this Implementation Manual.
The HHA Partnering Collaborative adapted the Breakthrough Series model of collaborative learning developed by the Institute for Healthcare Improvement (IHI), including the Plan, Do, Study, Act methodology developed by Associates in Process Improvement.
Under the guidance of Sally Sobolewski and several of the manuals co-authors, the Collaborative Faculty at the Visiting Nurse Service of New York (VNSNY) -- comprised of clinical directors, quality improvement (QI) specialists, and administrators -- worked with managers and field staff throughout the agency to develop the tools and strategies presented in this manual.
The Office of the Assistant Secretary for Planning and Evaluation (ASPE), U.S. Department of Health and Human Services, funded an evaluation of the HHA Partnering Collaborative developed and implemented at VNSNY (Contract No. HHSP23320044304EC). The development of this manual was funded by ASPE as a product of the evaluation. As the federal project officer for the project, Marie Squillace provided direction to and feedback on drafts of the manual as it developed.
Several individuals reviewed a draft of the manual and provided valuable feedback that informed the final set of revisions. The reviewers were: Donna Locurto (Visiting Nurse Association of America), Laura Peterson (independent health care consulting practice), Adele Pike (Visiting Nurse Association of Boston), Maureen Schnider (Partners Home Care in Boston, Massachusetts), Vicky Agramonte and Christine Stegel (both from IPRO, New York States QI Organization).
ABOUT THIS MANUAL
The HHA Partnering Collaborative is a quality improvement (QI) project developed and implemented at the Visiting Nurse Service of New York. The primary purpose of the Collaborative was to enhance the quality of work life for home health aides while improving outcomes for home health patients. This Implementation Manual emerged out of the lessons learned from an evaluation of the agency-wide spread of the Collaboratives tools and strategies. For more information on the results of the evaluation, see HHA Partnering Collaborative Evaluation: Practice/Research Brief at http://aspe.hhs.gov/daltcp/reports/2007/HHAPartrb.htm.
The beginning of the manual includes an introduction to the Collaboratives framework, goals, and methods, geared specifically toward senior leaders in home health agencies, QI organizations, or other settings who wish to adapt the Collaboratives methods and strategies.
The remaining sections of the manual are geared primarily toward managers and other key personnel responsible for implementing the Collaborative within their organizations. These sections describe the purpose of the Collaborative, offer guidelines for implementing and testing the Collaboratives strategies, and provide instructions for carrying out tests of change in the context of this intervention.
The final two sections -- "Celebrating Success and Planning for Spread and Sustaining the Gains -- offer suggestions and resources of use to both managers implementing the Collaborative and senior leaders in home health agencies.
In addition to adopting and adapting the tools presented here, we encourage senior leaders and managers to use any language from the manual that may be helpful for presentations, project materials, and Collaborative activities.
INTRODUCTION TO THE HOME HEALTH AIDE PARTNERING COLLABORATIVE
As leaders in home health care, you almost certainly have grappled with the question of how to get everyone -- patients, nurses, home health aides (HHAs), family members, and therapists -- to work together toward common goals. You probably also have found that, given the complexity of home health services, this is not easy to achieve. The overarching goal of the Home Health Aide (HHA) Partnering Collaborative is to foster positive relationships among patients, families, HHAs, nurses, and other home care clinicians to create an effective care team that works together toward patients well-being. In particular, the HHA Partnering Collaborative aims to create opportunities for both patients and HHAs to become more actively involved in managing the patients care and moving the patient toward greater independence.
You may ask -- how realistic is it to expect that increasing collaboration among HHAs, clinicians and patients will actually lead to measurable improvements in patient outcomes? Two prominent researchers from Yale University found that when clinicians and aides worked with their patients to establish and track functional health goals that were meaningful to the patient, there was a significant, measurable improvement in patients functional outcomes, along with a significant reduction in patient hospitalizations.1
Moreover, an evaluation of the HHA Partnering Collaborative implemented at the Visiting Nurse Service of New York (VNSNY) found that a similar approach yielded a significant improvement in two of three targeted activities of daily living (ADLs) -- transferring and ambulation. The impact was strongest in transferring, where the randomized trial conducted at VNSNY showed that 61% of patients in the intervention group experienced improvement from the start of care to discharge, compared to only 53% in the control group. Smaller, though statistically significant, differences were also found in ambulation.2
An emerging body of literature, including the two home care studies described above, provides evidence that collaboration improves the quality of patients care and the quality of employees work life. This manual offers strategies for achieving a healthy work organization. A healthy workplace is defined as one that integrates the goals of performance improvement with the goal of promoting employee health and well-being.3 Such an organization is one that will employ established principles of quality improvement (QI) to integrate professional and paraprofessional services, establish effective cross-disciplinary learning, and yield positive changes in employee, organizational, and patient outcomes.
Promoting Culture Change and Workforce Sustainability
The HHA Partnering Collaborative addresses two key issues that hinder the capacity of home health providers to deliver the best possible care. First, the Collaborative serves as a catalyst for change in the culture of health services, moving away from a purely professional model of care and toward self-care management. In the traditional, professional model of health services, patients, family members, and paraprofessionals have limited roles in decision-making about important aspects of a patients care. Typically, patients are seen as care recipients, and HHAs as unskilled workers who do for the patient. The self-care management model is centered on patients and informal caregivers as active participants in decision-making and goal-setting, with HHAs playing a key supportive role. The tools introduced in the HHA Partnering Collaborative manual provide an opportunity for moving toward a self-care management model of home health services.
Secondly, the Collaborative offers useful strategies for improving the sustainability of the paraprofessional workforce. In the United States, over 600,000 HHAs provide supportive services and personal assistance to patients receiving home health care. Although aide services are essential to the health and well-being of home care patients who receive them, the nurses and therapists who comprise the professional home care workforce all too often treat HHAs as unskilled workers with little potential to enhance the overall effectiveness of patient care. The devaluing of aide services has, in turn, been cited as a contributor to aide dissatisfaction, aide turnover and less than optimal patient outcomes. The HHA Partnering Collaborative addresses growing public interest in strategies to develop the capacity of the aide workforce and better integrate these paraprofessionals into care delivery.
What Is a Collaborative?
The HHA Partnering Collaborative adapts the Institute for Healthcare Improvement (IHI) Breakthrough Series model of collaborative learning.4 In this model, organizations convene a core team that commits to making continuous and measurable improvement toward a specific goal. The team utilizes the Plan, Do, Study, Act (PDSA) Cycle to make rapid, testable changes that inform each step in the improvement process. Health care providers in a wide range of organizational settings throughout the United States -- including hospitals, home care agencies, primary care practices, nursing homes, and community-based health centers -- have employed the collaborative model and PDSA Cycle to achieve improvement in a variety of areas. These areas include disease-specific clinical practices, patient safety, access to care, efficiency of care, and other organizational issues. (See IHI, 2003, for a sampler of Breakthrough Series Collaboratives and their results.)
Depending on the changes being sought, collaborative teams have been constituted in multiple ways, drawing on participants from across different disciplines, provider settings, and sectors within the health care industry. For example, a collaborative may consist of: clinicians from different disciplines within a hospital; staff from eight home care agencies within a geographic region; or personnel coming together from primary care practices, a local hospital, a home care agency, and a community health center.
The Structure of this Collaborative
The HHA Partnering Collaborative brings together HHAs, nurses, therapists and patients to improve teamwork toward common goals that promote patients well-being. Since the integration of paraprofessional and professional services is a key element of this collaborative, the leadership team consists of personnel who manage both aspects of home health services. In some smaller agencies, managers may be responsible for coordinating the services of HHAs and clinicians simultaneously, whereas larger agencies may rely on separate divisions for managing the two, or they may contract with external agencies for paraprofessional services. Whatever the size or structure of your agency, the tools and strategies of the HHA Partnering Collaborative can be adapted to promote teamwork among all members of the home care team.
Your collaborative may be organized in a variety of ways. You may choose to launch your own internal collaborative, engaging multiple teams or branches within your agency. Alternatively, you may choose to collaborate with leaders of other agencies within your geographic region, or to work with your states QI Organization as part of a wide-scale effort. Working across organizations may be valuable for pooling resources and sharing ideas to promote large-scale change in a cost-effective manner.
The Importance of Buy-In
As in any performance improvement project, change does not happen overnight. As senior leaders, make sure that you provide full support to the project. The more fully you integrate the change objective into the organizations overall goals and strategies, the more effective the Collaborative will be. This includes not only verbal support and endorsement, but also a commitment to protecting the projects resources and staffing needs when other pressing priorities arise within the agency. If you have quantifiable measures that you use for performance more broadly, integrating the Collaboratives measures into that broader set of performance goals can be another powerful indicator of your support.
Moreover, the active participation of field staff and patients throughout the entire change process is key to a successful Collaborative. The PDSA Cycle is integral to this process, as it allows you to gain ongoing feedback from those on the front-line. This is your key to adapting the Collaboratives tools and strategies to best suit the needs of your agency and to gaining buy-in from staff members and patients alike. To guide you through this, we have included a set of tips in each section of this manual to address issues you might encounter related to buy-in. As leaders, the more you listen and adapt to the needs of staff members and patients, the better your chances for creating positive, wide-spread, and sustainable change. More tips on gaining buy-in are included in Setting Aims and Defining Strategies.
What You Will Need to Implement This Collaborative
A successful Collaborative involves the full participation of individuals from a range of disciplines and with a variety of roles throughout your organization. As you begin the initiative, you will need to convene a core Collaborative Leadership group who will provide support and guidance throughout the project. This group includes:
-
A designated chair (or two co-chairs) of the Collaborative responsible for coaching participants and providing ongoing leadership and support.
-
A planning group, consisting of 2-5 individuals who will share the responsibility of planning Collaborative meetings and events.
-
Senior leaders in your organization.
-
QI specialists, staff education personnel, and/or expert consultants, if available.
Make sure you have the support of senior leaders in your organization (e.g., the chief operating officer) who can authorize the allocation of time and resources to the project. The Collaborative chair will need to dedicate time to lead the team in preparing Learning Sessions (described in later sections), reviewing data, and guiding the team through multiple tests of change. Generally, the chair should be able to commit about 12-16 hours per week during the first few months of the Collaborative and then gradually decrease his or her time commitment to about two days per month after the sixth month. Each member of the planning group should be able to commit roughly two days per month to the project, with the greatest time commitment in the beginning of the project.
If your agency has dedicated QI specialists or staff education personnel, their technical support may be valuable throughout the project. Or, if resources allow, you may wish to hire an external consultant who can provide guidance and expertise in QI methods related to the projects goals. You may also choose to allocate some time for an administrative assistant to provide support, including scheduling meetings, creating and copying forms, tabulating data, and creating data displays.
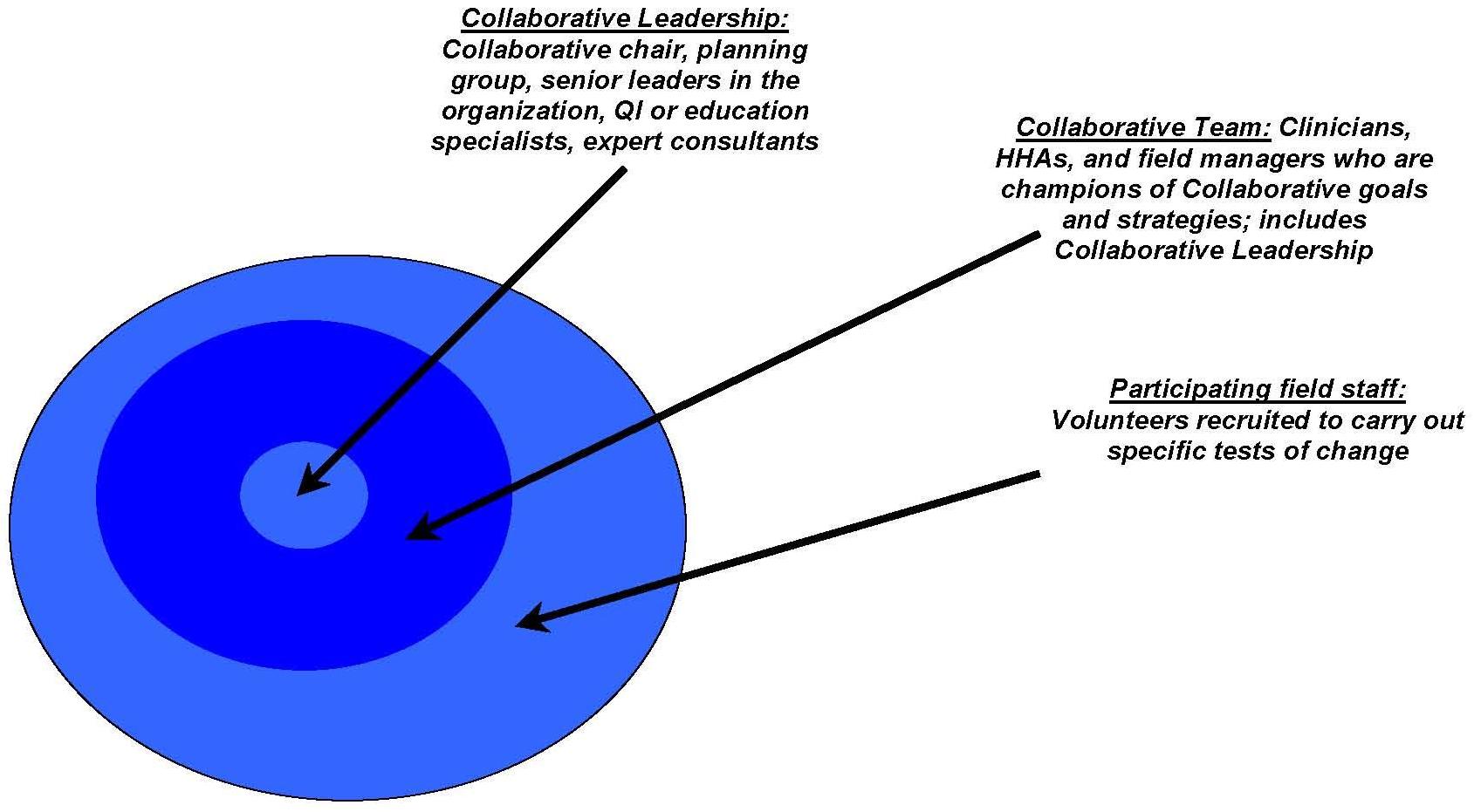
The Collaborative Leadership is at the core of the larger Collaborative Team, which includes clinicians, HHAs, and field managers who can serve as champions of the project and motivate change throughout your organization. All members of the Team will need to devote 6-15 months to the project. Although members of the team may play different roles, it is important that everyone is able to follow the project through to facilitate collaborative learning. The Collaborative will rely on the backing of senior leaders in adjusting the workload expectations of team members, as well as participating field staff who will not always be involved but will devote time to carrying out tests of change. (For an illustration of who is involved in the Collaborative, see Figure 1.)
Finally, you will need to ensure a mechanism for collecting data and feeding back results to team members and field staff who carry out tests of change on the front-line. Reporting back results to front-line staff in an efficient, real-time fashion is key to motivating and sustaining improvement. If such an infrastructure is not already in place, senior leaders should make sure that the team has access to the technical expertise of a QI specialist or consultant who can guide team members in developing a feasible mechanism for data collection and reporting.
A high-level task list for the HHA Partnering Collaborative, including a suggested schedule for the project, is shown as "HHA Partnering Collaborative: Tasks and Timeline." See illustration of the IHIs Learning Collaborative model (Figure 2).
You may also find these references helpful for background on the Learning Collaborative model, the PDSA Cycle, and other aspects of performance improvement:
-
Langley, G.J., Nolan K.M., Nolan T.W., Norman, C.L., Provost, L.P. (1996). The Improvement Guide: A Practical Approach to Enhancing Organizational Performance. San Francisco, CA: Jossey-Bass Publishers.
-
IHI (2003). The Breakthrough Series. IHI's Collaborative Model for Achieving Breakthrough Improvement. Available at http://www.ihi.org.
-
Plsek, P. (2000). Spreading Good Ideas for Better Healthcare: A Practical Toolkit. VHA.
WHY WE NEED TO IMPROVE TEAMWORK IN HOME HEALTH CARE
HHAs play a vital role in the care, therapy, and well-being of home care patients. They work within a service delivery team consisting of nurses, therapists and other professionals, and are typically in the patients home on a more frequent basis than other members of the team. HHAs act as clinicians eyes and ears in evaluating patients progress. However, all too often aide services are not well integrated into the home care team, creating barriers to aide job satisfaction, aide retention, and improvement in patient outcomes.
Enhancing teamwork in home health services is important for aides quality of work life, as well as patient satisfaction and well-being. The following scenarios illustrate some of the dilemmas that arise without a well integrated home care team.
Scenario One: When Jane Brown started receiving assistance with bathing and dressing from Susan Lloyd, a home health aide, she was hoping that Ms. Lloyd would take care of some household chores that had been neglected for quite some time. After Ms. Brown requested several times that Ms. Lloyd dues the shelves and mop the floor, Ms. Lloyd tried to explain that these tasks were not part of her care plan as specified by the nurse, Patricia Albert. Over the course of a few weeks, Ms. Lloyd and Ms. Brown had some tense interactions. Finally, Ms. Brown's son called the nurse manager and complained that Ms. Lloyd was not getting along with his mother, which resulted in Ms. Lloyd being replaced and transferred to a different case.
Similar conflicts arose with the new HHA, followed by a seemingly endless stream of replacements. Each HHA assigned to Ms. Brown grew frustrated, and a couple began to question whether they should continue in this line of work. Both Ms. Albert and the nurse manager started to wonder if there was a better solution. Ms. Brown and her family seemed to have expectations from the very beginning that home health services would include household help. How could this have been avoided?
Scenario Two: Cheryl Green, a home health aide, has been visiting Phillip Anderson five mornings per week ever since he returned home from the hospital. Although Mr. Anderson has been making good progress with his physical therapist, he wishes he could get back to his usual activities more quickly. Ms. Green and Mr. Anderson have developed a good rapport, and Mr. Anderson has spoken openly with Ms. Green about his concerns. He is especially eager to become steady enough to get on and off the bus using his cane so that he can return to his weekly church services.
Ms. Green wants to do more to support Mr. Anderson, but is not sure where to start. She rarely is in Mr. Andersons home at the same time as his physical therapist, Nancy Kim, who usually visits in the afternoon. Helping Mr. Anderson reach his goal does not seem to be spelled out in the care plan that Ms. Kim leaves posted in the kitchen. Ms. Green thinks it is a shame that with all the time she spends with Mr. Anderson, there isnt more she can do to help him improve his mobility.
Scenario Three: After working with Anna Reyes for about four weeks, Rosa Martin, a home health aide, noticed some unexpected changes. Ms. Reyes seemed less focused than usual when making day-to-day decisions and had started sleeping more during the day. Despite her concern, Ms. Martin hesitated to discuss it with Denise Arthur, the nurse who coordinated Ms. Reyes care. In the past, Ms. Martin had shared observations with nurses, but she felt that she was not taken seriously. By the time she was assigned to Ms. Reyes, Ms. Martin was skeptical that her observations could make a difference. Although Ms. Arthur provided two visits per week, she did not notice the changes in Ms. Reyes behavior for several days. At that point, Ms. Arthur realized she should call Ms. Reyes primary care physician to discuss the potentially adverse effects of the change the doctor had made to her medications two weeks before. Ms. Arthur wished that she had noticed the changes sooner.
Do these scenarios sound familiar?
All of these situations could have turned out better with positive communication, support, and common understandings among all members of the home care team.
In this manual you will find a guide to adopting and adapting the tools and practices of the HHA Partnering Collaborative, which was developed by and implemented at the VNSNY. The HHA Partnering Collaborative provides tools and strategies for addressing the issues depicted in the scenes above. Through this effort, your agency can work to improve teamwork so that
- patients are supported in setting goals and moving toward greater independence;
- aides become valued members of the team;
- clinicians are prepared to work effectively with everyone involved in the patient's care;
- patients, aides, family members, and clinicians all feel that their voices are heard.
Take-Home Message
Working toward better collaborative in home health care can help to improve key aspects of both staff satisfaction and patient well-being. The tools and strategies of the HHA Partnering Collaborative are a starting point for improving relationships among clinicians, aides, and patients throughout your agency.
HOW A COLLABORATIVE WORKS
The HHA Partnering Collaborative adapts the IHI Breakthrough Series model of collaborative learning.5 The purpose of a Collaborative is to go beyond traditional educational approaches in order to accelerate improvement. IHIs model provides a structure for learning and action that enables participants to jumpstart improvement by making real, ongoing changes on the front-line.
A successful Collaborative involves the full participation of individuals from a range of disciplines and with a variety of roles throughout your organization. A group of leaders is responsible for developing a framework for change, planning Collaborative meetings and events, and providing ongoing support and guidance to everyone involved in the project. The Collaborative Leadership consists of a designated chair and planning group, senior leaders in your organization, QI or staff education specialists, and, at times, expert consultants. The leadership is at the core of the larger Collaborative Team, which includes clinicians, HHAs, and field managers of both clinical and paraprofessional services who serve as champions of the project and motivate change throughout your organization. The Collaborative Team brings together individuals who can authorize the allocation of resources and staff time to the project, offer clinical and technical expertise, and provide day-to-day leadership.6
In forming the team, be sure to involve field staff and managers who can serve as champions of the Collaborative. Try to identify individuals who are:
-
Opinion-leaders among their peers.
-
Willing to take risks in promoting new ideas.
-
Able to commit to the project for a period of 6-15 months.
With the guidance of the Collaborative leaders, team members commit to making continuous and measurable changes toward a well-defined goal. When planning for specific tests of change, the Collaborative Team also recruits volunteers among the field staff to carry out the tests and provide feedback on their experiences with the Collaborative strategies when implemented on the front-line. Although these volunteers are not formally members of the Collaborative Team, their participation and input are integral to the improvement process. Be sure to recruit willing volunteers who are already motivated to make changes.
Take-Home Message
The IHI's model for collaboration learning brings together a team of individuals from different backgrounds and disciplines who commit to making ongoing improvement toward a specified goal. Be sure to involve champions of change who can provide day-to-day leadership throughout the project and recruit willing volunteers who are motivated to carry out tests of change.
Who Participates in the Collaborative?
The figure below illustrates the different groups that comprise the Collaborative. Clinicians and HHAs full participation -- both as members of the Collaborative Team and as volunteers who implement specific tests of change -- is key to a successful Collaborative.
| FIGURE 1: Who Participates |
 |
The Timeline for Learning and Action
Underlying every successful Collaborative is a clear problem statement, a framework for addressing it, a measurement strategy, and evidence that helps identify relevant change strategies. This is why many organizations consult with an outside organization like IHI, work with an expert consultant, or join with other providers in order to do this pre-work for their Collaboratives.7 In this manual, we provide a general framework outlining goals and strategies that can serve as a starting point for your improvement project.
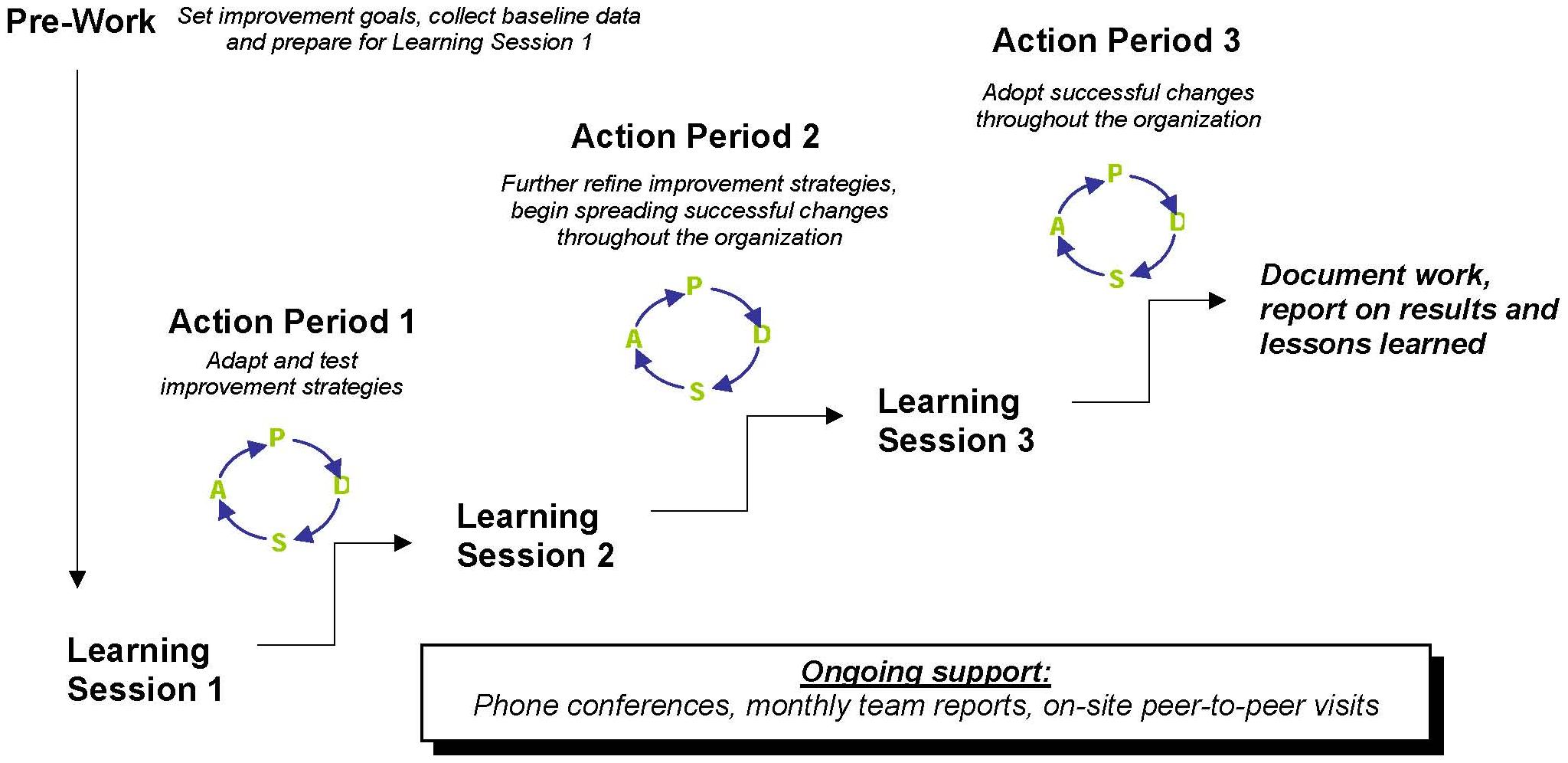
With a framework already established, the Collaborative Team alternates between Learning Sessions and Action Periods."8 The Learning Sessions provide an opportunity for team members to meet face-to-face and discuss improvement strategies with the guidance of senior leaders and experts in the field. Team members engage in dialogue about their methods, results, and lessons learned from their tests of change. A typical Collaborative includes three Learning Sessions, over the course of 6-15 months. These sessions often bring together participants from different sites for a full day of presentations, workshops, and informal dialogue. Depending on how your Collaborative is organized, you may decide to conduct shorter or more frequent sessions.
In between Learning Sessions, the Collaborative Team engages in an Action Period, carrying out multiple tests of change using the PDSA Cycle." The PDSA Cycle is a method for continuously testing changes and adapting them to their environment to obtain better outcomes (described in the sections to follow). During the Action Periods, team members implement and test improvement strategies and collect data to measure their progress. Team members continue to communicate with one another by participating in conference calls, sharing monthly progress reports, peer-to-peer site visits, and other mechanisms. In the collaborative model, peer-to-peer support is key for motivating change, so it is critical to keep communication going during the Action Periods.
At the end of the Collaborative, the team documents the results and lessons learned throughout the project. Team members present their results to non-participants, either within their organization or at external meetings and conferences.
Figure 2 illustrates the IHIs Learning Collaborative model. For more information on the model, visit http://www.ihi.org.
Take-Home Message
Learning Sessions and Action Periods are at the core of the Learning Collaborative model. The Collaborative team may decide to modify this framework, depending on the resources available and the structure of your organization. Whatever your timeline, be sure to maintain the key elements of shared learning and continuous tests of change.
| FIGURE 2: Learning Collaborative Model |
 |
| Adapted from: IHI (2003). The Breakthrough Series. IHI's Collaborative Model for Achieving Breakthrough Improvement. Retrieved February 22, 2007, from http://www.ihi.org/ihi. |
OVERVIEW OF GOALS AND STRATEGIES
Goals
The ultimate goal of the HHA Partnering Collaborative is to (1) improve aide quality of work life and job retention, and (2) improve home care for patients with functional dependencies in bathing, transferring, and ambulation. Participants will adopt and adapt tools and strategies to optimize the role of the aide as a member of the care team. As part of the Partnering Collaborative, participants will focus on the following goals:
Process Goals:
-
Improve teamwork among nurses, aides, therapists, and patients.
-
Identify patients needs and support patients as they gain functional independence.
Outcome Goals:
-
Improve HHA quality of work life and retention.
-
Increase patients functional independence at discharge in ambulation, bathing, and transferring.
Strategies
A core team of approximately 12-15 Collaborative participants, consisting of a chair or two co-chairs to serve as Collaborative leaders, selected clinical managers, field staff and other personnel, will commit to a continuing improvement process over the course of 6-15 months. This team will work together to set goals related to improving collaboration among patients, aides and nurses. The Collaborative Team will initiate small-scale tests of change that will allow you to adopt and adapt the Collaboratives practices to best suit the needs of your agency. Learning sessions will provide a venue for participants to become familiar with the Collaboratives tools and strategies and develop a plan for implementing and testing them on the ground.
The VNSNY Collaborative engaged in four main strategies, bulleted below. Your Collaborative might want to start with adapting or adopting these or experimenting with other strategies through a series of PDSA Cycles.
-
The ADL Tool, a functional health improvement tool that structures common goal-setting among nurses, patients, and aides.
-
The Five Promises, a guideline for communication designed to foster positive interaction between nurses and aides.
-
Phone conferences and in-person meetings between managers of paraprofessional and professional services.
-
Strategies for improving clinical supervision of aides, such as changing documentation in order to make nurses and therapists more aware of their interactions with aides and to hold them accountable for face-to-face supervision
The Collaborative team will track results using the PDSA Cycle, described in more detail in the sections that follow.
Expectations
The Collaborative Leadership will:
-
Convene a core team of participants, including clinicians, aides, field managers, and other personnel.
-
Plan Collaborative learning sessions.
-
Identify team members who can be champions of change.
-
Work with participating team members to develop plans for implementing Collaborative practices on the front-line.
-
Offer coaching to the Collaborative Team.
-
Ensure appropriate mechanisms for collecting, analyzing, and reviewing data through the PDSA Cycle.
-
Ensure mechanisms for ongoing communication among team members, such as listservs, teleconferences, and face-to-face meetings.
-
Provide participants with feedback using data that measure their progress toward well-defined goals
Members of the Collaborative Team will work together to:
-
Develop quantifiable goals for improving performance by adapting Collaborative tools and practices.
-
Plan and implement tests of change using the PDSA Cycle.
-
Designate a scribe to record the teams decisions pertaining to PDSA Cycles and issues discussed during Collaborative meetings and events.
-
Recruit volunteers to help carry out tests of change.
-
Develop and implement a plan for spreading Collaborative practices among all members of the home care team.
-
Measure performance at baseline and monthly.
-
Share information with the Collaborative Leadership, including details of changes made and data to evaluate these changes.
-
Keep communication going within the team to facilitate collaborative learning, using listservs, teleconferences, and/or face-to-face meetings.
Take-Home Message
The Collaborative Team will adapt or adopt key strategies developed by VNSNY's HHA Partnering Collaborative to work toward improving quality of work life for HHAs and the functional health of patients. Team members will plan and implement multiple tests of change using the PDSA Cycle, setting quantifiable goals and measuring progress on an ongoing basis. These tests of change will allow the team to adapt the Collaborative strategies to obtain better outcomes.
THE IMPORTANCE OF GAINING BUY-IN
Positive change does not happen overnight. The challenges of spreading good ideas have driven experts from a variety of disciplines to investigate the many factors that influence the success of a performance improvement effort. Even some of the best ideas do not catch on right away. The more prepared you are to address the challenges of buy-in, the more potential you will have to achieve your goals through the HHA Partnering Collaborative. Throughout this manual you will find a variety of tips and strategies for accelerating progress and getting participants on board.
Here are a few key points to keep in mind, drawing from the research on performance improvement.9
-
Mobilize Opinion-Leaders to be Champions of Change.
In his seminal work on the diffusion of innovation, Everett Rogers10 points out that innovations tend to spread slowly and small, beginning with the efforts of leaders who actively promote the new ideas. A certain proportion of people -- usually between 10% and 20% -- enthusiastically embrace innovation early in the spread process. This group, referred to as early adopters, is essential for generating momentum and making change visible to the rest of the organization. As early adopters begin to achieve their goals, the spread accelerates dramatically, and individuals or groups who are somewhat more risk-averse begin to adopt the change ideas. Finally, the new ideas spread to the laggards, who are generally skeptical of all types of change. Based on this model, it is important that you begin by identifying opinion-leaders throughout your organization who can become early adopters of Collaborative practices. Aim for an initial 10%-20% adoption point, and make sure that others can observe the progress made by the early adopters. Encourage the early adopters to talk to their peers -- they are your champions of change!
-
Be Open to Reinvention.
Experts on performance improvement have underscored the importance of adaptation in creating positive and sustainable change. Since members of any organization are part of a complex social network, a good idea will not always fulfill its potential if implemented in the same exact way from one setting to the next. This is why leaders should be open to reinvention so that the change idea is spread in a way that best fits the environment. It is critical that, as leaders, you send a clear message about the core concept of the change idea, but remain flexible about the details of how it is implemented. Leave some room for experimentation, and encourage participants to offer their input about what works and what does not.11
-
Tailor your Message to Your Audience.
Researchers have pointed out that everyone has a different threshold for change -- some people are more ready for change than others.12 As leaders, make sure you keep the finger on the pulse so that you are aware of your audiences readiness for change.13 You may find that readiness varies from one part of an agency to another, so be sure that your message speaks to the needs of your audience.
Take-Home Message
Be sure the Collaborative Team openly addresses the challenges of buy-in throughout the course of your Collaborative. Mobilize opinion-leaders to be champions of the Collaborative strategies, and allow for adaptation to best suit the needs of your organization. Listening to participants' feedback and understanding your audience are essential to generating enthusiasm for testing and reinventing improvement strategies.
USING THE PDSA CYCLE TO SET GOALS, TEST CHANGES, AND ADAPT IDEAS
As you begin the Collaborative process, you may find yourself asking these questions:
-
How will we experiment with selected strategies and develop useful adaptations?
-
How will we go about getting feedback from participants?
-
How will we know if the change is working?
-
How will we develop useful adaptations?
-
How will we make our progress visible throughout the organization?
-
How will we sustain the changes once we have made them?
To address these concerns, the HHA Partnering Collaborative utilizes the PDSA Cycle, a method for accelerating improvement by continuously testing changes and adapting them to their environment to obtain better outcomes. The PDSA Cycle provides a structured approach to assessing agencies progress toward improvement goals.
The PDSA Cycle was developed by Associates in Process Improvement14 and adapted by the IHI. IHI integrated the PDSA Cycle into their Breakthrough Series model of collaborative learning, in which team members commit to making continuous and measurable improvement toward a specific goal. The HHA Partnering Collaborative adapts this model for improvement. The suggestions and diagrams in the next several pages are adaptations of the IHIs guidelines for using the PDSA method. For further tips, tools, and examples of the PDSA Cycle, visit http://www.ihi.org.
The PDSA Cycle will enable you to:
-
Start small and learn before expanding.
-
Study what has happened.
-
Learn from participants throughout your organization.
-
Act quickly on what you have learned by:
- Adjusting the plan.
- Abandoning the idea.
-
Experiment with adaptations of the idea.
-
Minimize resistance to change by testing new ideas and creating opportunities for adaptation.
What Happens in a PDSA Cycle?
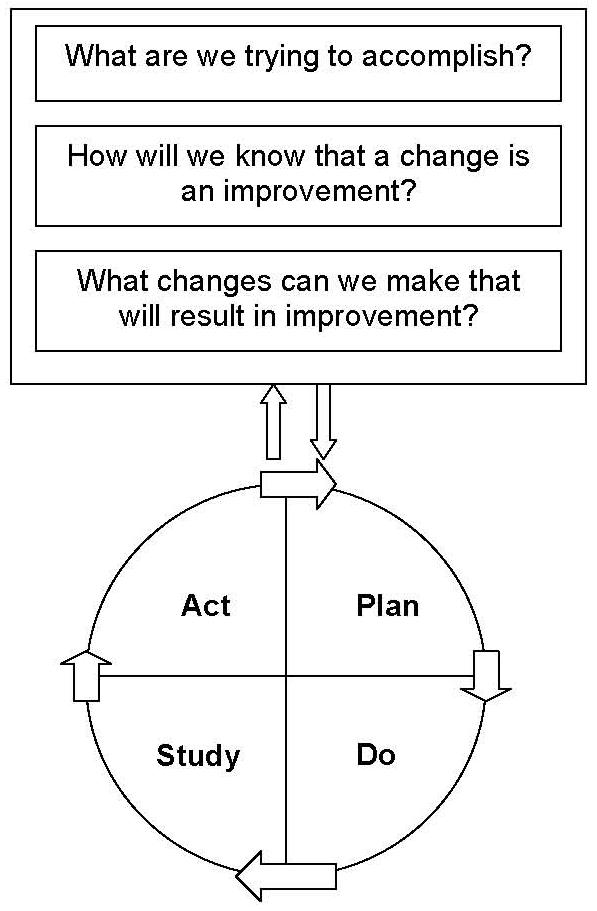
The PDSA Cycle is based on three main questions, as shown in the diagram below.15 These questions are integral to any improvement effort, as they focus our attention toward clearly defining our goals, strategies, and method for testing change.
| FIGURE 3: The PDSA Cycle |
 |
| Diagram adapted from: Langley G.J., Nolan K.M., Nolan T.W., Norman C.L., Provost L.P. (1996). The Improvement Guide. San Francisco, CA: Jossey-Bass Publishers, Inc. |
In any PDSA Cycle, the team sets an objective for a specific, measurable, and feasible change that can be implemented quickly. In the beginning of a performance improvement project, changes are tested on a small scale, allowing participants to measure and study their results over a short period of time -- anywhere from a few days to a few weeks. Through this learning process, team members take stock of the successes and challenges of the change, and decide on how to act on the lessons learned. This leads the team into the planning phase of the next PDSA Cycle, allowing participants to engage in a continuous improvement process.
Below we describe the steps in the PDSA Cycle. In the pages that follow, we provide some examples specific to the HHA Partnering Collaborative.
Step 1: Plan
-
Define the objective of the test cycle.
-
Develop a plan for implementing the change: Who? What? When? Where?
-
Decide on what measures will be collected and how participants will collect the data.
-
Make predictions about the potential successes and challenges of the test.
Step 2: Do
-
Implement the plan on a small scale.
-
Observe and document what did and did not work.
-
Collect and begin to analyze data.
Step 3: Study
-
Finish analyzing the data.
-
Study the results and compare them to your predictions.
-
Summarize and take stock of what was learned.
Step 4: Act
-
Based on what was learned in the test, decide on to do next: Adopt the ideas and expand the scope? Adapt them? Abandon them?
-
Prepare a plan for the next test.
The PDSA Cycle is an essential tool for gaining buy-in among participants. To be clear, you do not need consensus from the beginning -- rather, you can use the PDSA Cycle to gain buy-in over time. Engaging in continuous tests of change will allow you to adapt and modify change ideas to best suit the needs of your environment. As you find out what does and does not work, you can refine the improvement strategies and enhance your potential to achieve better results. Seeing your measures improve can motivate you to try out more, aim higher, and adopt changes we might otherwise have resisted.
Setting Aims and Defining Strategies
At the beginning of your improvement project, it is crucial that the Collaborative Team agrees upon specific, measurable aims. These aims are your overarching goals over the long term. Each PDSA Cycle is based on a shorter-term objective that helps you take steps toward your long-term aims.
For example, you might set an overarching aim in the area of patients self-management of specific ADLs:
Aim: Increase the percentage of patients with improvement in ambulation by 30% within nine months.
Although the teams aim is long-term and wide in scope, within each PDSA Cycle you will set objectives on a smaller scale. Keep these tips in mind when setting the aim of a test cycle:
-
Your aim should be specific and concrete.
-
Set a numerical target with a clearly defined measure and a specific timeframe for achieving your target.
-
Continually remind team members of the aim throughout the improvement process.
-
If necessary, refocus the aim or redefine its scope.
-
Clearly define who is carrying out the test and the role of each team member and volunteer who may be participating in the test cycle.
The team should also clearly define the strategies to be tested, whether you are experimenting with a simple change on a small scale or implementing a change agency-wide. To work toward the example above (improvement in ambulation), the team would plan multiple sequential PDSA Cycles. For example:
Cycle 1: Five nurses pilot the practice of talking with patients about setting ADL goals. Each nurse speaks with two patients (ten patients total) with dependency in ambulation within one week. The nurses report back to the Collaborative Team on the outcomes of their conversations with patients.
Cycle 2: The Collaborative Team develops a tool for setting specific ADL goals and involving HHAs and family members to support patients in working toward their goals.
Cycle 3: Over the course of four weeks, five nurses each test the protocol with two patients (ten patients total) who have dependency in ambulation. Each nurse gives the patients HHA instructions on how to support the patient in using the tool. Each nurse collects data on the patients progress in ambulation and receives feedback from patients, family members, and HHAs. Participating nurses and HHAs report their experiences to the Collaborative Team. The team studies the data on patients progress in ambulation.
Cycle 4: The Collaborative Team revises the tool and expands the test. Within four weeks, 20 nurses each test the tool on two patients (40 patients total). Each nurse collects data on the patients progress in ambulation and receives feedback from patients, family members, and HHAs. Participants report back to the team. The team studies the data on patients outcomes in ambulation.
Cycle 5: The Collaborative Team concludes that the tool is a success and works with the agencys operations staff to implement the protocol throughout the entire agency. In addition, plans are implemented to establish an ongoing monitoring and feedback system to collect data on patients functional outcomes and make the data widely available on a regular basis.
Similarly, the team should plan for a sequence of test cycles to improve aides quality of work life alongside the changes to increase patients functional improvement. For example, the team may set the following aim and plan PDSA Cycles accordingly:
Aim: Increase the percentage of HHAs who agree that they are treated as an important member of the care team by 30%.
Cycle 1: The Collaborative Team administers a brief survey to HHAs about their perceptions on whether or not they are treated as an important member of the care team and on their communication with nurses and patients. The survey may be administered either to all aides in the agency or, if the Collaborative is targeting a particular part of your agency (e.g., a geographic region), to a smaller group of aides. The team analyzes and studies the data to learn about aides perceptions at baseline.
Cycle 2: Five nurses pilot the practice of talking with HHAs about tasks the aide can engage in to support the patients progress toward his or her functional goals. Each nurse speaks with one HHA (five HHAs total) within one week. The nurses report back to the Collaborative Team on their conversations with aides.
Cycle 3: The Collaborative Team develops a guide for nurse-aide communication related to the patients functional progress. The team identifies a small group of nurses (e.g., ten nurses) who volunteer to try the new strategy.
Cycle 4: Over the course of four weeks, ten nurses each implement the communication guide with one HHA (ten HHAs total). Each nurse asks for feedback from the aide on what helps or hinders his or her communication with nurses and feelings of being integrated into the care team. Each nurse invites the aide to share this input at a Collaborative Team meeting. If the aide chooses not to, the nurse reports on the conversation to the Collaborative Team.
Cycle 5: The Team modifies the communication guide based on the feedback received from aides and nurses. The team expands the test, involving 30 nurses who each follow the guide with two aides (60 HHAs total). The test takes place within four weeks. The HHA survey is administered to the 60 aides involved in the test. Participants report back to the team. The team studies the data on aides perceptions of their integration into the care team and their communication with nurses and patients.
Cycle 6: The Collaborative Team concludes that the communication guide is a success and works with the agencys operations staff to implement the guidelines throughout the entire agency. The Team also works with operations staff and senior leaders in the agency to make sure that a long-term plan is in place to regularly collect data on HHAs job perceptions and feed back the data to managers and front-line staff.
Although the test cycles described above incorporate the basic principles of PDSA, they use the PDSA method for different purposes. The PDSA method is designed to be very flexible. Some test cycles may focus on developing a new mode of communication or designing a new tool and getting preliminary feedback from the people who are affected (e.g., patients, aides, clinicians, etc.). Other tests may focus on conducting a baseline survey or record review and studying the data before testing new improvement strategies. The PDSA method can be adapted to the context and realities of your agency and the needs of the Collaborative Team.
Take-Home Message
Every test of change calls for clearly defined objectives, strategies, and measures. Be sure that the Collaborative Team specifies the Who?, What?, Where?, and When? of each test. By carrying out multiple PDSA Cycles, the team will learn through experience how to adapt the change strategies to suit your environment. Always remember: Be clear and firm about your goal, but flexible on how to get there.
Example of a PDSA Cycle
Improving Patient Involvement in Self-Management of Functional Health
Plan
-
Develop an aim statement: Increase patients involvement in setting functional improvement goals (e.g. regain ability to dress lower body).
-
Make predictions: Patients will be receptive to talking about setting goals.
-
Define strategy for improvement: Five nurses will each engage one patient in a conversation about their goals for ADL improvement.
-
Define measure: Number of patients who set functional health goals, as reported by nurses who are assigned to conduct the experiment.
Do
-
Over the course of two weeks, each of the five nurses engages a patient in a conversation about their functional goals.
-
Each nurse documents the conversation and any goals the patient set.
Study
-
Team members and participating volunteers meet to discuss the test.
-
How many patients set a goal? Did the conversations facilitate goal-setting?
-
Were patients receptive to talking about ADL improvement?
-
Did clinicians encounter any barriers?
Act
-
Should we try the change with more patients?
-
Should we modify or further develop the change?
-
Should we address any barriers encountered during the test?
-
These decisions will be the basis of the next PDSA Cycle.
Tips for Testing Change Ideas
-
Start with changes that are easy to implement.
-
Plan for multiple, sequential tests of change.
-
Designate a scribe to document plans for upcoming tests of change, action taken, and feedback from team members and volunteers carrying out tests of change.
-
Test proven or new ideas on a small scale. For example, three nurses, three HHAs, one physical therapist, and five patients on bathing tasks.
-
Move quickly to test changes. Rather than testing changes over a year or quarter, complete tests over the course of a month, week or day.
-
Work with willing volunteers.
-
Listen to feedback from field staff carrying out tests of change and collect data during each test cycle.
Measuring Your Progress
Measuring progress is an integral part of continuous improvement. The PDSA Cycle calls for collecting and analyzing well-defined measures over time, allowing the Collaborative Team to track its progress toward selected goals.
Two types of measures play a role in the improvement process.
-
Outcome measures indicate the results of your teams performance from the patients or staff members perspective. For example, a project aimed at improving integration of HHAs into the care team might administer a survey asking HHAs about the extent to which they feel they are treated as an important member of the team. The survey could be administered at multiple points throughout the Collaborative to track how aides job perceptions change over time.
-
Process measures indicate whether staff practices are being carried out as planned. For example, a team focused on improving communication between nurses and aides might track the percentage of patients with bi-weekly documentation of aide supervision.
It is important to collect both types of measures in any improvement project. When choosing what measures you will collect in a test of change, consider these tips:
-
Make sure your measures directly relate to your goals. Ask yourselves, Will these measures help us understand whether we have achieved our goals?
-
Do not worry about acquiring new resources for data collection. If you do not have the latest technology for collecting and analyzing data, plot your measures with a pencil and paper.
-
Your measures should be easy to analyze. Most of your measures will be analyzed in terms of percentages, such as the percentage of patients who improve in transferring, or the percentage of patients with bi-weekly documentation of HHA supervision.
-
Clearly define your target population. This will determine the denominator in your calculation. For example, when calculating the percentage of patients with improvement in transferring, do you want to know the percentage of all patients, or just the percentage of those who had a dependency in transferring at the start of care?
-
Make sure that you can quickly feed back data to participants. Rapid turnaround is key to keeping up the momentum for continuous improvement.
Example: Plotting Outcomes Over Time
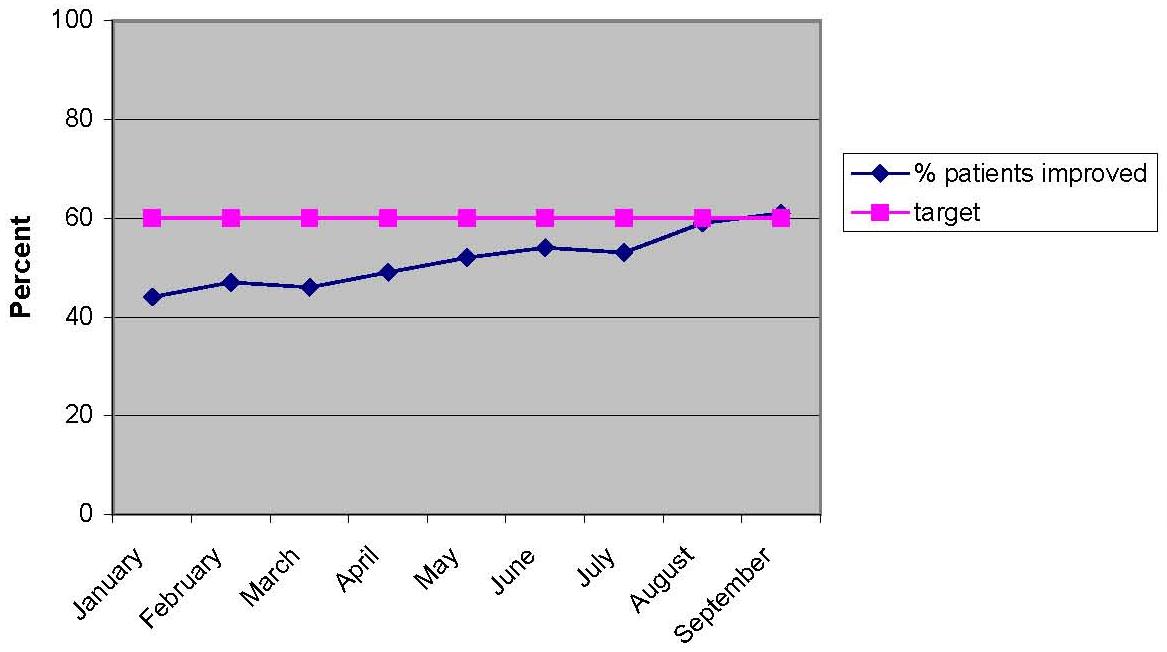
By charting your results over time, you can see how your improvement efforts move you toward your goals. In the example below, the team sets a target of 60% improvement in bathing over a nine-month period among patients needing assistance in bathing at the start of care. Through multiple PDSA Cycles, the team refines its strategies and ultimately reaches its goal. With the target of 60% plotted on the chart during the entire effort, team members are continually reminded of their goals and see how they get closer to it with each test of change.
| FIGURE 4: Percentage of Patients Showing Improvement in Bathing at Discharge |
 |
Take-Home Message
At the center for every successful improvement project are measures that are clearly defined, easy to collect and analyze, and readily accessible to all participants. Be sure to select measures that directly relate to your goals and quickly feed back data to team members and participating volunteers so that everyone involved can learn from the results.
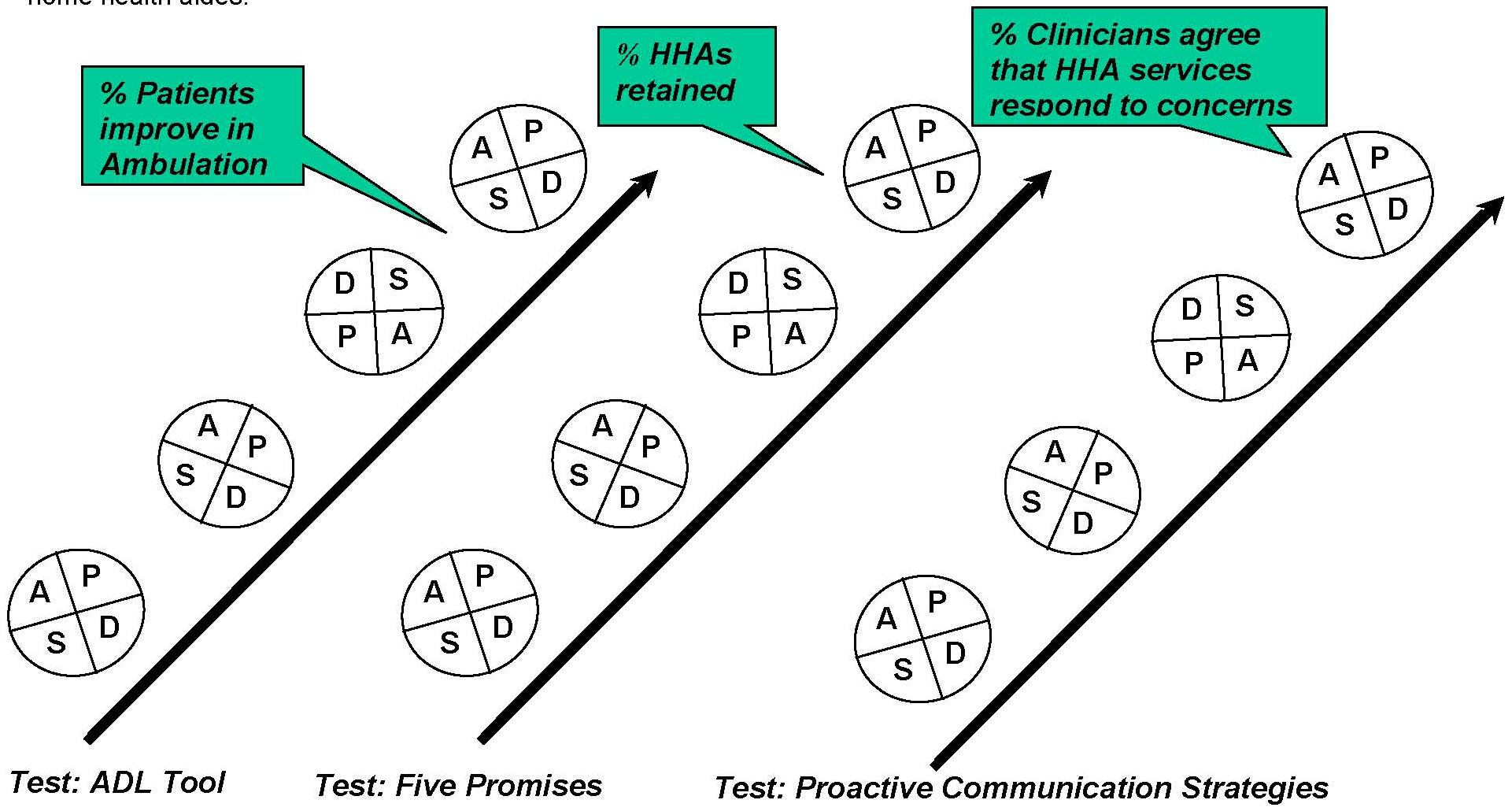
Multiple, Continuous Tests of Change
Tests of change are not only continuous, they also happen alongside other changes simultaneously. For example, the team may choose to focus on improving patients functional self-management, while also focusing on improving field support for HHAs.
| FIGURE 5: Tests of Change |
 |
| Diagram adapted from http://www.ihi.org/ihi. |
Measuring Progress toward HHA Partnering Collaborative Goals
In working toward the goals of the HHA Partnering Collaborative, you will need to collect a variety of measures. The table below suggests several measures and data sources for assessing your progress toward each goal. For some of the measures, participants will need to conduct surveys on staff members opinions about their work relationships. Other measures draw on the Outcomes and Assessment Information Set (OASIS) and information from administrative records. The OASIS is a core set of screening and assessment items, including standardized definitions and coding categories that form the foundation of a comprehensive assessment for all clients of home health agencies certified to participate in Medicare or Medicaid.16
The table also indicates some of the strategies the team may test throughout the Collaborative process. The strategies are meant to be flexible; with an enthusiastic team, you might arrive at new innovations for achieving Collaborative goals.
The pages that follow include additional suggestions on how to collect and analyze your measures.
| Goal | Strategies | Key Measures | Data Source |
| Improve HHA quality of work life and job retention | Five Promises Improve clinical supervision and collaboration between nurses/therapists and aides Proactive communication strategies between managers of professional and paraprofessional services | % of HHAs who strongly agree that they are treated as an important member of the care team | HHA Survey |
| % of clinicians who strongly agree that HHAs are competent in tasks required | Clinician Survey | ||
| % of clinicians who strongly agree that HHA services respond to their concerns | Clinician Survey | ||
| % of HHAs retained on the job | Administrative/Human Resource Records | ||
| Improve patients functional independence | Patient ADL Tool | % of patients improved in: Ambulation, Transferring, Bathing | OASIS |
Suggestions for Data Collection and Measurement
The key to assessing a Collaboratives progress is to collect basic measures that are easily interpreted and understood by everyone involved in the project. Data analyses should remain simple and to the point to assure that results are fed back to all members of the Collaborative Team and participating field staff in a timely manner. The following describes key measures used in the VNSNY Collaborative and different approaches to collecting the data. The measures and methods may be adapted as appropriate for your agency.
HHA Retention
At VNSNY, the evaluation team defined HHA job retention as whether or not an aide provided at least one visit in the pay period following a designated point from the start of the Collaborative. You may decide to measure retention as your Human Resources department defines it. Be sure to choose the measure and timeframe that is most relevant to your agency.
HHA Job Perceptions Survey
To measure HHA job perceptions and quality of work life, you may choose to administer a brief survey. Depending on the size of your agency and resources available, you may decide to create a pen-and-paper, phone or web-based survey. You can calculate simple percentages to determine the distribution of responses to each question. There are sample questions in the HHA Job Perceptions Survey (below) which can be adapted as you find appropriate.
Clinician Survey
The VNSNY Collaborative developed a short survey to learn about clinicians self report of practices related to the Collaboratives goals and strategies. The eight-question survey (below) addresses key themes such as communication between clinicians and aides, and the usefulness of the functional health improvement tool tested during the course of the Collaborative. Field managers administered the survey to clinicians on paper during routine monthly meetings. The survey was kept anonymous to encourage candid responses. As with the HHA Job Perceptions Survey, you may choose a different method of data collection based on the resources available to you. Simple percentages were calculated to determine the distribution of responses to each of the questions.
Patients Functional Outcomes
To measure patients functional outcomes, you may use items from the start of care and discharge in the OASIS. At VNSNY, we compared the Activities of Daily Living Measures for Ambulation (M0700), Transferring (M0690), and Bathing (M0670) from admission to discharge to determine patients progress. If you do not have the OASIS readily available for analyses, functional scores can be collected as you wish during admission and discharge for comparison. The OASIS items are shown below (Items for Measuring Patients Functional Outcomes). You might choose to measure improvement in patient function for a selected period of time in either of two ways: (1) the percentage of patients in categories 1-5 below who reduced their score at least one point between admission and discharge; or (2) the average change in total ADL score (categories 0-5) for all patients between admission and discharge.
| HHA JOB PERCEPTIONS SURVEY | ||||||||
| 1: | How often do the nurses and therapists you work with give you the help you need to do a good job? | |||||||
| Never | Sometimes | Usually | Always | |||||
| 2: | How often do the nurses and therapists you work with treat you as an important member of the care team? | |||||||
| Never | Sometimes | Usually | Always | |||||
| 3: | How often are your opinions about patients heard and appreciated by the nurses and therapists you work with? | |||||||
| Never | Sometimes | Usually | Always | |||||
| 4: | How often do you discuss patients progress walking, bathing, and getting out of bed with the nurses and therapists you work with? | |||||||
| Never | Sometimes | Usually | Always | |||||
| 5: | How often do you talk to patients themselves about the progress they are making walking, bathing, and getting out of bed? | |||||||
| Never | Sometimes | Usually | Always | |||||
| 6: | Do you agree or disagree with the following statement? Overall I am a satisfied employee. | |||||||
| Strongly Disagree | Disagree | Not Sure | Agree | Strongly Agree | ||||
| CLINICIAN SURVEY | ||||||||
| 1: | How often do you talk to HHAs about patients general health? | |||||||
| Never | Seldom | Occasionally | Frequently | Always | ||||
| 2: | How often do you talk to HHAs about their role as supporter rather than doer of care? | |||||||
| Never | Seldom | Occasionally | Frequently | Always | ||||
| 3: | How often do you engage patients and HHAs in a conversation about patients functional progress? | |||||||
| Never | Seldom | Occasionally | Frequently | Always | ||||
| 4: | How useful do you find the functional health improvement tool in facilitating these conversations? | |||||||
| Not Useful | Somewhat Useful | Useful | Very Useful | |||||
| 5: | How often do you talk to HHAs about patients care plans? | |||||||
| Never | Seldom | Occasionally | Frequently | Always | ||||
| 6: | How often do you make changes to patients care plans? | |||||||
| Never | Seldom | Occasionally | Frequently | Always | ||||
| 7: | How often do you taper HHA hours as patients become more independent? | |||||||
| Never | Seldom | Occasionally | Frequently | Always | ||||
| 8: | How often do you let HHAs know when you will be making your next visit? | |||||||
| Never | Seldom | Occasionally | Frequently | Always | ||||
| ITEMS FOR MEASURING PATIENTS' FUNCTIONAL OUTCOMES |
| (M0700) Ambulation/Locomotion: Ability to SAFELY walk, once in a standing position, or use a wheelchair, once in a seated position, on a variety of surfaces. |
| 0 - Able to independently walk on even and uneven surfaces and climb stairs with or without railings (i.e., needs no human assistance or assistive device).1 - Requires use of a device (e.g., cane, walker) to walk alone or requires human supervision or assistance to negotiate stairs or steps or uneven surfaces.2 - Able to walk only with the supervision or assistance of another person at all times.3 - Chairfast, unable to ambulate but is able to wheel self independently.4 - Chairfast, unable to ambulate and is unable to wheel self.5 - Bedfast, unable to ambulate or be up in a chair.UK - Unknown |
| (M0690) Transferring: Ability to move from bed to chair, on and off toilet or commode, into and out of tub or shower, and ability to turn and position self in bed if patient is bedfast. |
| 0 - Able to independently transfer.1 - Transfers with minimal human assistance or with use of an assistive device.2 - Unable to transfer self but is able to bear weight and pivot during the transfer process.3 - Unable to transfer self and is unable to bear weight or pivot when transferred by another person.4 - Bedfast, unable to transfer but is able to turn and position self in bed.5 - Bedfast, unable to transfer and is unable to turn and position self.UK - Unknown |
| (M0670) Bathing: Ability to wash entire body. Excludes grooming (washing face and hands only). |
| 0 - Able to bathe self in shower or tub independently.1 - With the use of devices, is able to bathe self in shower or tub independently.2 - Able to bathe in shower or tub with the assistance of another person: (a) for intermittent supervision or encouragement or reminders, OR (b) to get in and out of the shower or tub, OR (c) for washing difficult to reach areas.3 - Participates in bathing self in shower or tub, but requires presence of another person throughout the bath for assistance or supervision.4 - Unable to use the shower or tub and is bathed in bed or bedside chair.5 - Unable to effectively participate in bathing and is totally bathed by another person.UK - Unknown |
GOAL 1: IMPROVING SUPPORT TO HOME HEALTH AIDES
The scenarios introduced earlier could all have turned out differently with better teamwork. Each of the goals of the HHA Partnering Collaborative addresses an area of improvement that is important for developing positive work relationships among all members of the home care team. The first of these goals is to improve support to aides by focusing on two key areas:
-
Promote positive nurse-aide interactions in the patients home.
-
Strengthen partnering relationships between clinical staff and paraprofessional managers through proactive communication and coordination of services.
With better field support and partnering
Scenario One: Ms. Lloyd, who was replaced by another aide, would have worked with Ms. Albert, the nurse, to develop a common understanding with the patient and her family of the aides role and responsibilities. Ms. Lloyd would have had a better chance of a positive work relationship with her patient, Ms. Brown. Both Ms. Lloyd and Ms. Albert would have had support from their managers to proactively address the problem at hand. Ms. Alberts and Ms. Lloyds managers would have had an ongoing partnership that would have allowed them to find viable solutions to provide Ms. Brown with uninterrupted service and support the aides role as supporter, rather than doer, of care. Both Ms. Lloyd and Ms. Albert might have been more satisfied with their work.
Scenario Three: Ms. Arthur and Ms. Martin, who did not freely share their observations with one another, would have established a sense of trust to allow for more open communication about Ms. Reyes well-being. Ms. Martin would have gained a level of comfort sharing her observations with Ms. Arthur, helping the nurse address potential problems with Ms. Reyes medication before they became serious complications.
The following guidelines offer strategies for improving support to aides so that your agency can achieve the kinds of outcomes illustrated above.
HHA Support -- Part I: Improving Nurse-Aide Interactions in the Field
Rationale: Surveys show that a key predictor of turnover is employees dissatisfaction with their supervisors.17 For this reason, clinical supervisors can have a major impact on HHA retention rates. Positive communication can prevent aides from feeling under-utilized or under-appreciated, which could negatively affect their work and overall patient outcomes. Patient outcomes have been shown to improve when aides serve as the clinicians eyes and ears and clinical and paraprofessional staffs work together to address a patients health care needs.18
Expectation: Clinicians and aides show recognition to one another and actively discuss all aspects of patient care. Clinicians supervise aides at each visit, encouraging them to openly discuss patient progress and goals.
Change Concept: A guideline for interaction between clinicians and aides can promote productive discussion of patients goals and increased staff satisfaction.
Aims:
-
Increase HHA perception of appreciation by their clinical supervisors (nurses/therapists) by x%.
-
Increase clinicians satisfaction with HHA competency in the tasks required to care for patients by x%.
-
Increase HHA job retention by x% or reduce HHA turnover by x%.
Measures:
-
Percentage of HHAs who strongly agree that they are treated as an important member of the care team.
-
Percentage of clinicians who strongly agree that HHAs are competent in tasks required to care for patient.
-
Percentage of patients with bi-weekly documentation of HHA supervision.
-
Percentage of HHAs who continued to work at the agency over a specified period of time.
Changes:
-
Clinicians and aides will integrate a tool called the Five Promises into everyday home care practice. Positive and regular communication will become the standard practice among HHAs and clinicians. (Nurse-Aide Interaction: The Five Promises can be found below).
-
Clinicians will document their supervision of aides through a paper or electronic supervision form, allowing the Collaborative Team to track its progress toward improving nurse-aide interactions.
Promoting Staff Buy-In and Support
Use the PDSA Cycle to overcome resistance: Based on our experiences at VNSNY, you might find that some clinicians resist adapting the Five Promises, while others respond with enthusiasm. Those who resist might feel that the Five Promises reflect what is already being done in the field and simply state the obvious. Although the guidelines may seem straightforward, we discovered at VNSNY that they were not necessarily standard practice before the Collaborative.
The PDSA Cycle is your key to overcoming resistance. Involving field staff with opportunities to give feedback on their experiences with the Five Promises can give clinicians and aides a sense of ownership over the changes being made, which may help to achieve buy-in. Starting out with small tests of change will allow the Collaborative Team to modify aspects of the new strategy that may be a source of resistance. As your measures begin to show improvement, those who have previously resisted adopting the practice may become convinced that it is worthwhile. Alternatively, you may decide to abandon the Five Promises or substitute it with another strategy, depending on what you hear from field staff carrying out tests of change on the front-line.
Raise the bar: You may also find it helpful to remind field staff that even if many staff members already engage in positive, open communication in the patients home, you want to make it the gold standard. Having a guideline that reminds people of this expectation can make a big difference in moving toward your goal. Members of the Collaborative Team -- especially clinicians and aides -- play an important role in motivating their peers to make the Five Promises common practice.
Use friendly reminders: Clinicians are often bogged down with paper work and new tasks being asked of them. Ongoing reinforcement of your goals can prevent the Five Promises from being tossed aside and forgotten. Encourage field staff to carry the Five Promises tool with them at each visit as a reminder that positive communication is now a top priority.
Tips for Testing Changes in HHA Field Support
-
A job perceptions survey for HHAs is an excellent way to assess whether they feel they are appreciated and treated as an important member of the team. See earlier section -- Suggestions for Data Collection and Measurement -- for more information on administering a survey.
-
A clinician survey can provide the team with feedback on HHA competency and communication in the patients home. See section on data collection for suggestions on administering a clinician survey.
-
Engage staff members in establishing a work plan for documenting HHA supervision. Set a specific target for the frequency of HHA supervision that will motivate clinicians to make it a priority.
-
Use a standardized form for documenting supervision that is easy to complete and use consistently. In addition to noting the aides performance on tasks related to the service plan, you may choose to include a few key questions:
- What is the quality of the aides relationship with the patients family (i.e., good, fair, or poor)?
- Does the aide follow the plan of care?
- Has the plan of care been revised recently?
Take-Home Message
Improving support to aides in the patients home is an integral part of improving the quality of work life for HHAs. The Collaborative Team will test strategies for improving nurse-aide interaction and increasing clinicians awareness of their role in supervising and collaborating with aides to improve patient outcomes. Brief surveys asking field staff about their perspectives on nurse-aide relationships can be valuable for tracking your agencys progress in HHA field support.
HHA Support -- Part II: Improving Communication Among Managers
Rationale: In all home health agencies, a skilled nurse or therapist provides clinical supervision to the aide in the patients home. In addition, most agencies have separate managers who provide general oversight of professional and paraprofessional services. Sometimes these are the same person, while sometimes they are different individuals. No matter how aide services are structured, however, nurses and aides often receive different messages from their managers. Mixed messages and a lack of coordination between clinical and aide services create barriers to providing high quality care and achieving high levels of satisfaction among nurses, aides, and patients. Setting standard expectations for partnering and communication can help solve problems efficiently and reduce confusion about the aides assigned tasks, schedule, and role.
Expectation: The Collaborative Team will work to improve partnering relationships among field staff and their managers, and to make proactive communication standard practice.
Change Concept: Setting an expectation for clear, regular communication between clinical and paraprofessional supervisors and for consistent messages to front-line clinical and paraprofessional staffs will facilitate positive work relationships between clinicians, aides, and patients.
Aims:
-
Increase clinicians satisfaction with HHA competency in the tasks required to care for patients by x%.
-
Increase HHA perception of appreciation by their clinical supervisors (nurses/therapists) by x%.
Measures:
-
Percentage of clinicians who strongly agree that aide services respond to their concerns.
-
Percentage of aides who strongly agree that they are treated as an important member of the care team.
Changes:
-
Managers will participate in monthly phone conferences to discuss issues related to aide services. You can find a tool in this manual for these calls (Paraprofessional Manager Tool for Partnering Collaborative Conference Calls).
-
If management of aides and nurses is divided among different staff in your agency -- or if multiple managers are responsible for aide services -- managers will meet regularly (e.g., bi-weekly or monthly) by phone or in person to discuss issues related to the supervision and delivery of aide services. An additional tool for in-person meetings can be found in this manual (Paraprofessional Manager Tool for Partnering Collaborative Team Meeting).
-
The team will designate a scribe to circulate meeting agendas, summarize issues covered and document agreed upon solutions.
Promoting Staff Buy-In and Support
Remember that proactive communication saves time. Depending on workload and staffing issues, some managers may be resistant to participating in regular conference calls or meetings. However, establishing a regular schedule for communication will eventually save time by preventing problems and reducing more round-about means of communication. As participating managers become accustomed to regular meetings and more comfortable raising issues, they will become more efficient at trouble-shooting. Building managers support for regular communication is an area where use of PDSA Cycles may be an important vehicle for gaining managers buy-in.
Use the PDSA Cycle to figure out what works best. Carrying out continuous PDSA Cycles can help the Collaborative Team figure out how to implement proactive communication strategies in a way that is both feasible for managers and effective at preventing and solving problems. You may wish to experiment with different meeting schedules (e.g., every week, bi-weekly, etc.) or different modes of communication (e.g., face-to-face meeting vs. phone conference). Whatever your approach, be sure to listen to feedback from managers implementing the new strategies.
Tips for Testing Changes in Partnering
-
You may decide to test different kinds of logs and follow-up sheets. You may adapt either of the tools as a guide for conducting phone conferences or in-person meetings. The first tool -- Paraprofessional Manager Tool for Partnering Collaborative Conference Calls -- provides a general guide of how to plan for and organize a conference call, with room to document general issues related to Collaborative practices, aide scheduling, and service problems. The second tool -- Paraprofessional Manager Tool for Partnering Collaborative Team Meeting -- provides a more detailed list of questions that managers may wish to address on a regular basis. Either tool may be modified to address the issues most relevant to your agency.
-
Depending on the structure of your agency, you may find it useful to develop a daily communication log that managers can use (by fax or email) to inform one another about current aide assignments, hours, and any special concerns. Take advantage of the PDSA Cycle to experiment with different approaches to proactive communication.
-
No matter what the mode or frequency, encourage participating managers to use the conference calls or in-person meetings as an opportunity to share information and solve problems.
Take-Home Message
Proactive communication among managers is key to improving support to HHAs. The Collaborative Team will test the strategies developed by VNSNYs Collaborative to set expectations for clear, regular communication among managers of clinician and aide services. Staff surveys can help you track your progress toward improving HHA support by providing insight into clinicians and aides perspectives on HHAs integration into the care team.
| NURSE-AIDE INTERACTION: THE "FIVE PROMISES" | ||
| EVERY TIME you are in a patients home together, take five minutes for the following interaction: | ||
| 1. | Introduce yourself and show your I.D. |  |
| 2. | Discuss the progress the patient is making toward achieving his/her functional health goals. |  |
| 3. | Review together, any changes in the service plan and/or duty sheets. |  |
| 4. | Discuss any observations or concerns about the patient that you have today. |  |
| 5. | Thank each other. Make sure you communicate about the next nursing visit and the ongoing or changing home health aide schedule and/or assignment. Make sure contact phone numbers are in the home. |  |
| PARAPROFESSIONAL MANAGER TOOL FOR PARTNERING COLLABORATIVE CONFERENCE CALLS | |||
| To Schedule The Conference Call Manager of paraprofessional services checks and updates the contact list Manager of paraprofessional services calls manager of clinical services to schedule 30 minute call | |||
| The Day of the Call Manager of paraprofessional services calls manager of clinical services Select a Timekeeper, a Scribe and a Leader Go through the Conference Call Tool Select date and time of next call Select who will be initiating the next call If the Clinical Manager is out or not able to do the call, make sure you call each other and reschedule the call Do not end the week by not doing the call The Scribe must e-mail or fax this tool to ____________________ Fax# ___-___-____ Phone# ___-___-____ | |||
| Paraprofessional Manager: | Date: | Office: | Unit: |
| Are aides and nurses using Five Promises? | |||
| Are there any issues regarding morning/afternoon cases? | |||
| Are any patients and HHAs working with the ADL Tool? | |||
| Are there any service issues that we need to discuss? | |||
| PARAPROFESSIONAL MANAGER TOOL FOR PARTNERING COLLABORATIVE TEAM MEETINGS | |||
| DATE: | WEEK# | ||
| YES | NO | COMMENTS | |
| Are aides and nurses using the Five Promises? | |||
| Are aides following the service plan? | |||
| Are there any special circumstances the manager should know about? | |||
| Is there a service plan for each case? | |||
| Are there any supervision issues? | |||
| Are there any expected schedule changes next week? | |||
| Are there any discharged cases this week? | |||
| Are there any replacement issues? | |||
| Are there any problem patients that we need to know about? | |||
| Are there any problems with aides? | |||
| Are there any areas that lack aide capacity? | |||
| Have any aides attended a training class over the last week? | |||
| Number of AM/PM Cases (Can any patients be changed from AM to PM service?) | |||
| Number of aides working on short-hour cases | |||
| Number of aides working long-hour cases | |||
| Names of patients and aides using ADL Tool | |||
| Are there any other issues or concerns? | |||
GOAL 2: IMPROVING PATIENTS FUNCTIONAL INDEPENDENCE
Working together to improve patients functional capacity is important for both patients well-being and staff satisfaction. The second goal of the Collaborative is to improve patients functional independence. In this section you will find tools and strategies for involving aides in patients care more effectively. With strategies like these, the earlier Scenario Two would have turned out differently
Scenario Two: Ms. Green, who wanted to support Mr. Anderson in his recovery, would have had an opportunity to set common goals with Mr. Anderson and his physical therapist, Ms. Kim. Ms. Green would have engaged in activities that supported Mr. Anderson in taking steps toward his goals on a day-to-day basis. Mr. Anderson would have had a better chance of getting back to his church, and Ms. Green would have felt that her time and skills were being put to better use.
Rationale: When home care staff and caregivers are not present, patients have to engage in ADLs on their own. Patients often will avoid performing a task because they are afraid their attempt will result in a fall or injury. In some cases patients resort to unsafe methods of bathing, walking, or transferring. By setting functional health goals at the start of care, patients can become better prepared to manage their own health care needs and less reliant on home care staff. Working toward specified goals is a team effort that strengthens the relationship between patients, clinicians and HHAs. Two prominent researchers from Yale University found that using this type of collaborative approach to establishing and tracking functional health goals led to a significant improvement in the functional outcomes of home health patients and to a reduction in patient hospitalizations.19
Expectation: Patients and all members of the care team will work together in setting goals and taking steps toward greater functional capacity. Patients, family members, clinicians, and HHAs will share a common understanding of the HHAs role as a supporter, rather than doer, of care. The care team will engage in a self-management model of functional health as standard practice.
Change Concept: A tool for tracking patient goals, especially in areas of functional improvement, will be used to help the nurse, HHA and patient get on the same page regarding home care goals.
Aim:
-
Increase percentage of patients with improvement in ambulation, transferring and bathing (or other specified outcomes) by x%.
Measures:
-
Percentage of patients improved in ambulation, transferring and bathing (or other specified outcomes).
Changes:
-
The Collaborative Team and participating volunteers (clinicians and aides) will carry out small tests of change to try out different versions of the functional health improvement tool. Through the PDSA Cycle, the team will adapt the tool to best suit the agencys needs.
-
Clinicians will keep the tool in the patients home so that patients and HHAs can use it to record patient progress on a weekly basis.
-
Once the team has agreed on an adaptation of the tool, clinical managers will engage field staff in activities to familiarize everyone with the tool and make it standard practice throughout the agency.
Promoting Staff Buy-in and Support
Be clear about who should use the tool. The functional health tool is not appropriate for everyone. Patients with severe cognitive impairment or advanced illness may not be suited to use the tool. The Collaborative Team should establish clear guidelines for determining when the tool is most useful. Recognizing that you have realistic expectations about the tools utility can help minimize staffs resistance to trying it out.
Get field staff involved. Based on our experiences at VNSNY, clinicians may expect patients to resist using the tool and, in turn, resist using it themselves. Training clinicians on how to best introduce the tool can help them get past this barrier. Role-plays between clinicians and HHAs are a great way to prepare field staff to address patient resistance. At one of our learning sessions, team members familiar with the tool acted out a script on the dos and donts of introducing the tool to patients (below). This added some humor and creativity to the discussion and gave those new to the tool a chance to learn from the experiences of early adopters. Video can also be used as an engaging way to present the tool to field staff. Our education staff involved HHAs and clinicians in creating a video in which they shared their experiences with the tool and how their patients benefited from it. The video received a positive response from both clinicians and HHAs as a great way to introduce the tool and get everyone excited about using it.
Reinforce the aides role as supporter of care. To minimize patient resistance, clinicians should be upfront with patients about the aides role in the home. If a patient believes that the HHA is there to perform household tasks, as opposed to helping them become more independent, he or she may be resistant to a change in the aides role.
Keep going! Getting staff buy-in for the functional improvement tool may not be easy, but we encourage you to not give up. Continue to engage field staff in small tests of change and listen to their feedback. By addressing clinicians and aides concerns, you can gain wider support and achieve better results. The tool is not meant to solve all problems in the home, but it can be used to foster positive relationships among the clinician, patient and HHA.
Tips for Testing Changes in Patients Functional Health
Two versions of the functional improvement tool are available for use with patients at their start of care. These tools emerged out of VNSNYs Collaborative process, as the team worked to find a way to promote patients self-management while strengthening collaboration. Although the tools concentrate on bathing, transferring, and ambulation, they can be adapted to set goals in other areas. Both tools aim to promote collaboration among members of the care team, but they are structured and utilized differently. The first version -- the ADL Tool -- was originally designed as a training tool for aides. The nurse or therapist would work with the aide to develop his or her skills in supporting the patients functional progress. The clinician, aide, and patient would first discuss the patients goals together. The aide would then work with the patient over the course of four weeks, documenting the patients functional progress using the tool. The clinician would follow up on these tasks as part of his or her supervision of the aide. The second version of the tool -- the What I Can Do for Myself Tool -- was designed for the patient to fill out with the aides support. (See the Activities of Daily Living (ADL) Tool and the What I Can Do for Myself Tool below.)
You may decide to test either version of the tool and make necessary adjustments to better suit patients unique needs and goals. In the Collaborative at VNSNY, the following guidelines were used for each version of the tool, drawing in part on a patients OASIS information at the start of care:
-
ADL Tool
- At a minimum, the tool was used with all new patients receiving aide services and scoring 1 or higher on their start of care OASIS in questions M0700 (ambulation), M0670 (bathing), or M0690 (transferring).
- The tools wording is directed towards the aide or clinician with language such as can get up from all surfaces safely.
- With 32 items and four goals, it allows for exploration of items within grooming and dressing, as well as for patients to write in their own personal goals.
-
What I Can Do for Myself Tool
- This tool can be used with all patients regardless of their OASIS scores at the start of care.
- The tool is written from the patients perspective, with language such as I can roll over in bed.
- This tool has fewer items to check off on the front page regarding what a patient can or cannot do independently. There is more of an emphasis on goal formation and achievement.
- Patients have the option to select a goal from a series of examples and are encouraged to reach out for support from aides, clinicians, and family members.
If you choose to introduce either version of the tool to your agency, you may wish to adapt the Role-Play Script for Introducing the Functional Improvement Tool to give an example of how to introduce the tool to patients (below).
Take-Home Message
Working together toward functional health goals has been shown to help increase patients involvement in their care while improving teamwork among clinicians, patients, and aides. The Collaborative Team may adopt or adapt either of the functional health tools described above, depending on the teams goals and your organizations needs. Be sure to get staff involved in testing the tool(s) and continually listen to participants feedback on their experiences with each test of change.
| ACTIVITIES OF DAILY LIVING (ADL) TOOL | ||||||||||
| Patient Name: | Coordinator of Care (Nurse or Physical Therapist): | |||||||||
| PATIENT DIRECTIONS: Check INDEPENDENT in the areas that you feel you can perform ALONE, SAFELY and WITHOUT help. Check NEEDS ASSISTANCE in the areas that you need someone to assist you with OR you feel UNSAFE in performing alone. Once you complete these areas your Nurse &/or Therapist will review these items with you and together we will design a PLAN OF CARE to help promote your independence at home. Your Home Health Aide is an important member of your Home Health Care Team and will be working closely with you, your Nurse and/or Therapist to help you regain your independence. Each week we will reevaluate your progress and identify strategies to help promote your independence at home. | ||||||||||
| Activity of Daily Living Component | Week 1Patient Response Date: ___/___/___ | Week 2 Date: ___/___/___ | Week 3 Date: ___/___/___ | Week 4 Date: ___/___/___ | ||||||
| I can do this alone | I need help to do this | Independent | Needs Assistance | Independent | Needs Assistance | Independent | Needs Assistance | |||
| Bed mobility and transfers | ||||||||||
| 1. | Rolls from side to side | |||||||||
| 2. | Moves from lying to sitting up | |||||||||
| 3. | Can get walker, cane or crutches | |||||||||
| 4. | Can get in and out of bed | |||||||||
| 5. | Sets self up safely to get up | |||||||||
| 6. | Can get up from all surfaces safely | |||||||||
| 7. | Can maintain standing | |||||||||
| Ambulation | ||||||||||
| 1. | Can walk to and from the bathroom | |||||||||
| 2. | Knows safety precautions/techniques | |||||||||
| 3. | Can move walking device | |||||||||
| 4. | Can move legs (to take steps) | |||||||||
| 5. | Can change directions | |||||||||
| Bathing | ||||||||||
| 1. | Can get in and out of tub or shower | |||||||||
| 2. | Washes upper body | |||||||||
| 3. | Washes chest, trunk, and private areas | |||||||||
| 4. | Washes legs | |||||||||
| 5. | Washes hair | |||||||||
| 6. | Adequately dries skin | |||||||||
| Grooming | ||||||||||
| 1. | Can hold a comb/brush | |||||||||
| 2. | Can bring comb to top of head | |||||||||
| 3. | Combs or brushes hair | |||||||||
| Dressing | ||||||||||
| 1. | Gets clothing, shoes, and brace(s) from closets or drawers | |||||||||
| 2. | Can put arms in sleeves | |||||||||
| 3. | Can pull shirt over head | |||||||||
| 4. | Places legs into pants | |||||||||
| 5. | Can pull up pants | |||||||||
| 6. | Can put on brace (if indicated) | |||||||||
| 7. | Can put on shoes and socks | |||||||||
| 8. | Can fasten clothes | |||||||||
| 9. | Can fasten shoes | |||||||||
| 10. | Can take off clothes | |||||||||
| 11. | Can safely put away shoes | |||||||||
| TEAM MEMBERS: | ||||||||||
| Nurse Name: | Home Health Aide Name: | |||||||||
| Physical Therapist Name: | Occupational Therapist Name: | |||||||||
| GOALS WEEK ONE: | GOALS WEEK TWO: | |||||||||
| GOALS WEEK THREE: | GOALS WEEK FOUR: | |||||||||
| WHAT I CAN DO FOR MYSELF TOOL | |||||||||
| Instructions: Describe an activity you used to do and want to do again. I hope to get better at, be more independent in, or accomplish this goal: |  |
Purpose: Patients should use this form to write and watch their progress as they try to reach their goals. Home health aides should use this form to support the patients goals. | |||||||
| My Daily/Personal Routine | Week 1Date: ___________ | Week 2Date: ___________ | Week 3Date: ___________ | Week 4Date: ___________ | |||||
| I can do myself | I need help | I can do myself | I need help | I can do myself | I need help | I can do myself | I need help | ||
| Moving in and out of bed and chairs | |||||||||
| 1. | I can roll over in bed | ||||||||
| 2. | I can move from lying down to sitting up in bed | ||||||||
| 3. | I can get in and out of bed | ||||||||
| 4. | I can reach my walker, cane, or wheelchair from the bed | ||||||||
| 5. | I can stand up from the side of the bed | ||||||||
| 6. | I can get up and stand from any seat or chair | ||||||||
| 7. | I can stay standing on my own once I stand up | ||||||||
| Walking or using a wheelchair | |||||||||
| 8. | I can move my legs forward and take steps | ||||||||
| 9. | I can turn around when I am walking | ||||||||
| 10. | I can move my walker, can or wheelchair myself | ||||||||
| 11. | I can walk or I can wheel my chair to my bathroom | ||||||||
| 12. | I can move around safely because I use proper footwear, have enough lighting, and remove cords and clutter | ||||||||
| 13. | I can use stairs | ||||||||
| 14. | I can walk outside | ||||||||
| Bathing | |||||||||
| 15. | I can get into and out of my tub or shower | ||||||||
| 16. | I can wash my arms and head area | ||||||||
| 17. | I can wash my chest, back, and private areas | ||||||||
| 18. | I can wash my legs | ||||||||
| 19. | I can wash my hair | ||||||||
| 20. | I can dry myself | ||||||||
| How I Can Do More for Myself | |||||||||
| Instructions: Check the boxes for the items you will try to do for yourself. | |||||||||
| Now that I am home, I will: | |||||||||
 |
Talk to my nurse or therapist to help me decide on a goal that I really think I can reach and how long it will take to reach this goal. | ||||||||
|
Ask my nurse or therapist to help me figure out the steps I need to take to get to this goal.
|
||||||||
|
Write what I want to be able to do in my own words. | ||||||||
|
Check off how I am doing every week and talk to my nurse and/or therapist about how I am doing with my plan at least one time a week. | ||||||||
|
Ask everyone helping me at home (family and/or aide) to encourage me to do whatever I can by myself. | ||||||||
|
Talk to my caregivers (family or aide) about reaching my goal.
|
||||||||
|
Plan with my nurse and/or therapist how I can keep taking care of myself and stay as independent as I can after my homecare services end. | ||||||||
| Examples of what I hope to get better at, be more independent in, or accomplish (my goal): | |||||||||
|
Cook dinner |  |
To achieve some of thesegoals, several of the itemson the other side of thispage shoudl be selected. | ||||||
|
Use the toilet by myself | ||||||||
|
Take care of my own home | ||||||||
|
Improve my leg strength | ||||||||
|
Walk in the park | ||||||||
|
Shop at the store | ||||||||
|
Go to church, synagogue, or my place of worship | ||||||||
|
Other (describe): | ||||||||
| ROLE-PLAY SCRIPT FOR INTRODUCING THE FUNCTIONAL IMPROVEMENT TOOL |
| The purpose of the functional improvement tool is to consciously involve patients, aides, and nurses in setting common goals related to patients functional health. Although we often feel rushed and may be tempted to do something just to get it done, the process of setting and making progress toward a patients goals works best when all members of the care team work together. This role-play illustrates a positive way of introducing the functional improvement tool so that everyone is on the same page. |
| Nurse: Ms. Johnson, weve talked about a lot of different areas, including how you are doing with walking and being afraid of falling. I was wondering what goals you have set for yourself, what you would like to be able to do that you arent able to do right now.Patient: Well, you know, I fell before I went into the hospital and I certainly dont want that to happen again.Nurse: Tell me how you fell.Patient: I fell right in the bedroom. I was getting out of bed to go to the bathroom. And next thing you know I was on the floor and couldnt get up. It was a good thing I was wearing my button, you know.Nurse: Were you using your walker when you were getting out of bed?Patient: Now I told you that I only like to use that when I go outside. Its hard to get around in here with that walker. Its such a small space.Nurse: Lets figure out what you can do for yourself right now and what you do need help with. Is that OK with you?Patient: I guess so.Nurse: Great. This piece of paper is for you and its called What I can do for myself. It lists some activities that are important to see what you need help with, what you can do on your own. Lets start with the moving in and out of bed and chairs. Do you have a pen or pencil somewhere?Patient: I dont know where anything is right now. I told you, Im just getting back home. I was in the hospital for almost a week.Nurse: Thats OK. Use my pen for now. Can you read the words with your glasses?Patient: Turn that light on for me.Nurse: What does the first line say?Patient: I can roll over in bed.Nurse: Are you able to do that yourself?Patient: Well, yes, of course.Nurse: OK. So youre putting the check in the "I can do myself" box. What does the next line say?Patient: I can move from lying down to sitting in bed. Well I can do that too. Its the walking that I have problems with, and getting into the shower too.Nurse: OK, so youre putting a check in the "I can do myself box" too. Next?Patient: I can get in and out of bed. Well, I thought I could but thats where I fell, when I was walking to the door.Nurse: I want to see you get up from the bed. So, can you walk into the bedroom with me? I know you dont like to use your walker, but you also said that you were anxious not to fall again. Until the therapist can come and start working with you, can you agree to use your walker so that you will be more secure?Patient: I guess I dont have any choice. But I have such a hard time getting through the doorway to the bedroom and bathroom with this walker that I usually just leave it outside the door.Nurse: Ill work with you on how to turn and go through the door sideways and Ill call to put in the request for the PT. |
| Ms. Johnson walks to the bedroom door. |
| Nurse: You did really well so far in using the walker. You seem steady. How do you feel while you are walking?Patient: Well, I did better than I thought. Im a little tired though. Now here I am at the doorway and getting through here is just such a struggle.Nurse: Let me show you how to turn the walker more easily and take a few steps sideways. Is that OK with you? Nurse addresses the audience: Here is where I show Ms. Johnson a better way to use her walker and have her demonstrate again. When Im done she can get in the doorway with the walker safely. I go through the remaining items in a similar fashion.Nurse: Getting back to the goals. I heard you say that you want to be able to walk safely without falling, and that you want to be able to get back to walking in the hallway and also be able to get a taxi to go to the doctor and see your sister.Patient: Thats right.Nurse: OK, then write those goals down at the top of the paper. Patient writes. Tomorrow, well finish this list and well talk to the HHA: about it. Can you read the rest of the lines before I come tomorrow so you can do the check offs then?Patient: I can do that without you, you know.Nurse: Great, but Ill go over it with you and the HHA: tomorrow so that we all understand the same thing, OK?Patient: Sure. |
| The next day, the HHA: is in the patients home when the nurse arrives at the door. |
| Nurse: Hi, Im Ms. Bradley. Heres my ID. Isnt it a terrible picture?HHA: Hello, Ms. Thomas. Heres my ID. My picture isnt any better!Nurse: Well, Im really happy youre here. Lets go in and talk to Ms. Johnson. I was here yesterday and we started working on filling out the ADL tool -- you know what that is, right?HHA: I think I was taught something about that but I havent used it before. Can you explain it to me?Nurse: Sure because really you are very important in getting Ms. Johnson to be able to do as much as she can for herself safely so she can reach her goals and be more independent.HHA: Well you know I really like to help my patients and do things for them.Nurse: Really helping Ms. Johnson will be getting her to do as much as she can for herself. Because she wont always have you with her, right?HHA: I guess you have a point. |
| The HHA and nurse walk together into the room where Ms. Johnson is sitting. |
| Nurse: Hello, Ms Johnson. I met Ms. Thomas at the door and we were talking about how you are doing, what you can do yourself and what you may need help with. Im going to get the paper we filled out yesterday and go over everything with Ms. Thomas and you. Also I want to go over the service plan with both of you. These two papers fit together you know.Patient: You dont have to go get the paper. I have it here. I knew youd want to put me through more of this. I really want to get this over so my aide can go shopping and help clean up.Nurse: Well its great that you have it here. Ms. Thomas is very important in helping you get to those goals you talked about yesterday -- being able to walk safely, walk longer, and get outside to a taxi when you need to.Nurse (continued): Ms. Thomas, these were the things Ms. Johnson said were important and she wanted to get back to doing. Nurse (continued): Ms. Johnson, lets look at that tool you checked off yesterday. It looks like you did more checking.Patient: Yes, I said I didnt want to spend all day on this so I went ahead and made those checks.Nurse: Ms. Thomas, take a look at this. These are all the areas Ms. Johnson can do by herself using her walker. You may still need to remind her about doing things safely though -- like making sure that she does use her walker whenever she walks -- OK? HHA: Yes.Patient: Yes, I guess, but lets get going with this.Nurse: Lets go over the bathing part so that Ms. Thomas knows what she needs to help you with and what you can do. With Ms. Thomas and the therapist coming, and with you getting stronger, the hope is that these needs help check-offs in the bathing part will change to I can do myself. Ms. Johnson, Ms. Thomas can help you with checking off this paper weekly. If you do it together, you can both talk about what you still need help with and what you can do yourself. Is that OK with both of you? HHA: Yes.Patient: Sure.Nurse: Also the therapist and I will look at what youve checked at least once a week to see how you are coming along with getting to your goals. Ms. Thomas, do you have a clearer idea about this tool and how you and Ms. Johnson are going to use it? Can you tell me what you are going to do?HHA: Well, Im going to make sure Ms. Johnson does whatever she can for herself. Ill be checking to make sure she is doing it right, and if not, Ill remind her -- I think you said to coach her. Ms. Johnson and I will be looking at that paper together at least once a week to see if she can do more for herself. And Ill talk to you and the therapist about what I am doing and what Ms. Johnson is still having problems with or can do really well.Nurse: Thats great. Ms. Johnson, what about you?Patient: Ill give it a try. I really do want to be able to do more things myself you know. |
Take-Home Message
The functional health tool does not make life perfect, but it does provide a framework for common goal-setting and increasing support to patients in managing their self-care. The tool can be a starting point for involving the aide as the patients coach, rather than as a doer of care. Remember that including patients and the entire care team in a conversation about the patients goals may be just as important as documenting the patients goals and progress.
CELEBRATING SUCCESS AND PLANNING FOR THE SPREAD
As you take stock of your achievements and the lessons you have learned, you should begin to plan for spreading the Collaborative strategies throughout your entire agency. Spreading good ideas is not always easy. This is why the Collaborative Team needs to stay actively engaged in planning for and managing the spread process. Team members need to work together to develop a plan for communicating the key messages throughout the agency and continuing to motivate change. You should also work with operations staff in your agency to identify opportunities for hardwiring changes into your agencys standard operating procedures. Below are a few tips on planning and managing the spread process.20
-
Disseminate the Evidence Throughout Your Agency. You may wish to create a story board demonstrating the improvements achieved and lessons learned throughout the Collaborative. A story-board is a catalogue of evidence in support of the project, including graphs and other visuals illustrating your results, as well as key points summarizing the benefits of the new strategies. You may also choose to include quotations from field staff who participated in tests of change and had positive things to say about the Collaborative practices. The story-board can either be posted in a highly visible, physical location or publicized electronically. Whatever the mechanism, be sure to make the evidence widely accessible to field staff and managers throughout your agency.
-
Expand the Network of Support. Just as you did in the beginning of your Collaborative, be sure to identify opinion-leaders who will communicate with their peers about the benefits of adopting the Collaborative practices. This time, however, the network will reach beyond the Collaborative Team itself. You may wish to recruit field staff who volunteered to participate in tests of change throughout the Collaborative and encourage them to become spokespersons for the spread effort.
-
Plan a Series of Kick-Off Sessions. Like the earlier Learning Sessions, you may wish to plan one or more kick-off sessions to jumpstart the spread process and bring together field staff and managers in a discussion about the Collaborative practices. These sessions are an opportunity for those not previously involved in the Collaborative to learn from their peers about the strategies tested and their successes. Most of all, the kick-off sessions should be fun and informal, generating excitement about spreading the changes agency-wide.
-
Ensure a Mechanism for Getting the Message Out Day-to-Day. Whether you are spreading the ADL Tool or promoting the Five Promises, make sure you have a mechanism in place for communicating about the new strategies on a day-to-day basis. Field managers play a key role in making field staff aware of the new strategies and integrating the strategies into everyday practice. You may wish to use bulletin boards, email, fliers, or other means of communication as regular reminders that keep the spread moving forward.
-
Continue to Measure Your Progress. Collecting data and reporting back results to managers and field staff is just as important during the spread process as it is during the Collaborative. Continue to use measures that are easy to analyze and interpret and feed back results quickly. You may wish to create updated story-boards on a quarterly basis and post them in a central location. Remember, regular measurement is central to continuous improvement and helps to send the message to everyone on the front-line that improvement is an ongoing process, rather than a one-time event.
-
Integrate Collaborative Strategies Into Usual Practice. The ultimate goal of the spread process is to make the Collaborative strategies common practice. The team should identify ways in which the new practices can be hardwired into your agencys systems of documentation, reporting, and patient assessment. For example, if you are spreading the ADL Tool agency-wide, the patients functional assessment upon admission may be linked to a set of criteria that will trigger the use of the tool for eligible patients. Moreover, the discharge assessment may include a follow-up item pertaining to the tool. Streamlining the new strategies into the information and documentation systems already in place will facilitate the spread. You may also work with field managers to develop a system for documenting field staffs use of the Collaborative tools and strategies. This will help the team keep track of the progress of the spread, as well as create a mechanism for keeping field staff aware of their role in implementing the new practices. Also, be sure to incorporate the new strategies into your agencys in-service training and orientation materials so that newcomers are fully onboard.
-
Plan for Additional PDSA Cycles. Early on in the Collaborative, your tests of change will start on a small scale. As you expand the effort to an agency-wide spread, you should expand the scope of your tests accordingly. Continuing with ongoing tests of change will help to identify potential barriers to a wide-scale spread and further adapt the strategies so that they can be integrated into usual practice.
As discussed throughout this manual, addressing the challenge of gaining buy-in should be an integral part of the Collaborative. This is no less the case during the spread effort. This is why it is important to adapt your improvement strategies so that they are likely to spread successfully, especially among later adopters, or individuals who are less motivated to try out new ideas. In his seminal work on the diffusion of innovation, Everett Rogers identified five attributes of a change idea that affect the likelihood of it being adopted and its chances for spreading widely and quickly.21 Based on these attributes, you may wish to consider the following while planning for the spread effort:
-
Make sure that managers and field staff can see the advantages of the new strategies over the old way of doing things. For example, they will be more likely to adopt a new strategy -- such as the Five Promises or a regular managers phone conference -- if they see that it can lead to better performance outcomes without adding too much extra work.
-
Make sure that the new strategy is compatible with the needs and values of potential adopters and the environments in which they work. For example, a functional health improvement tool may be more likely to spread if clinicians agree with the basic principles of a self-management model.
-
You may wish to streamline or simplify a particular strategy to enhance its potential to spread successfully. The simpler the idea, the better.
-
You may find it useful to engage field staff in small-scale tests for a limited period before hardwiring it into usual practice. Potential adopters are more likely to buy in to the new strategy if it is trialable -- that is, if they can test it out first on a limited basis.
-
Disseminate the evidence in favor of the new strategies as widely as possible, and encourage early adopters to discuss the strategies informally with their peers. The more observable the evidence in favor of the change idea, the more likely field staff and managers will be to adopt it.
For further insights on how to plan for and achieve a successful spread, refer to Paul Plseks Spreading Good Ideas for Better Healthcare: A Practical Toolkit. VHA (2000). You may also visit http://www.ihi.org for additional resources.
SUSTAINING THE GAINS
As the Collaborative practices become widespread throughout your agency, the Collaborative Team needs to proactively address the challenge of sustainability. Not only do you need to make sure the new strategies become common practice, but you also need to work toward sustaining your agencys improvements over the long-term. The Collaborative Leadership -- and, in particular, senior leaders of your agency involved in the initiative -- play an important role in ensuring access to the resources needed for sustaining your achievements.
Senior leaders can help sustain the gains of the Collaborative in the following ways:
-
Make sure the agencys infrastructure for data collection and reporting is maintained over the long-term and is made widely accessible throughout the agency (e.g., field managers should have access to data pertaining to their staffs performance).
-
Help managers gain access to a network of individuals who can provide ongoing support and guidance on QI methods and issues related to the Collaboratives goals. This network may consist of QI and staff development or education specialists internal to your agency, as well as experts from QI organizations, the IHI, or other organizations.
-
Most importantly, ensure that all senior leaders in your agency continue to support the sustaining effort and make it a priority among the agencys strategic goals.
For further insights on the factors that facilitate the spread and sustainability of new practices, refer to: NHS Modernisation Agency, Spreading and sustaining new practices: sharing the learning from the Cancer Services Collaborative (CSC) (2002).
Take-Home Message
Spreading and sustaining new improvement strategies is not easy. However, with the continuing engagement of the whole Collaborative Team, the involvement of opinion-leaders on the front-line, and the full support of your agencys senior leaders, you can successfully spread the Collaborative practices throughout your agency and sustain the gains over the long-term. Continue to use the PDSA Cycle as a way of making the Collaboratives goals and strategies part of everyday practice, as well as making shared learning and ongoing improvement the norm throughout your agency.
| HHA PARTNERING COLLABORATIVE: TASKS AND TIMELINE | |
| Below is a suggested timeline and list of the major tasks that will take place throughout the Collaborative. More detailed guidelines and tips for implementing the Collaborative's methods, tools, and strategies are included throughout the manual. The timeline adapts the Institute for Healthcare Improvement's Breakthrough Series Model for Collaborative Learning, including the Learning Sessions and Action Periods. You will need to develop your own Learning Sessions to best meet the needs of the Collaborative Team. | |
| MONTH 1 | |
| Senior Leaders | Form the Collaborative Team
|
| Senior Leaders and Collaborative Leadership | Convene for an introductory meeting Suggested agenda items:
|
| Collaborative Leadership | Establish mechanisms of communication among team members
|
| MONTHS 2-3 | |
| Entire Team | Collect baseline data on key Collaborative measures |
| Planning Group | Prepare for Learning Session 1 (LS1)
|
| BEGINNING OF MONTH 4 | |
| Entire Team | Hold Learning Session 1 |
| MONTHS 4-7 | |
| Entire Team | Action Period 1 (AP1)
|
| Planning Group | Prepare for Learning Session 2 (LS2)
|
| BEGINNING OF MONTH 8 | |
| Entire Team | Hold Learning Session 2 |
| MONTHS 8-11 | |
| Entire Team | Action Period 2 (AP2)
|
| Planning Group | Prepare for Learning Session 3 (LS3)
|
| BEGINNING OF MONTH 12 | |
| Entire Team | Hold Learning Session 3 |
| Entire Team | Action Period 3 (AP3)
|
| MONTHS 12-15 | |
| Planning Group | Prepare for wrap-up session
|
| END OF MONTH 15 | |
| Entire Team | Convene for wrap-up session At the end of your Collaborative, be sure to bring together the entire Collaborative Team to synthesize your results and celebrate your success. You may wish to plan a meeting -- or a series of meetings -- involving all team members, as well as any field staff who volunteered to carry out tests of change. Use these meetings to:
|
| MONTH 16 AND BEYOND | |
| Entire Team | Document and disseminate the evidence for spread
|
NOTES
-
Tinetti M.E., Baker D., Gallo W.T., Nanda A., Charpentier P., O'Leary J. (2002). Evaluation of resorative care vs. usual care for older adults receiving an acute episode of home care. JAMA 287(16):2098-2105; Baker D.I., Gottschalk M., Eng C., Weber S., Tinetti M.E. (2001). The design and implementation of a restorative care model for home care. Gerontologist 41(2):257-63.
-
For more detail on the results of the evaluation, see HHA Partnering Collaborative Evaluation: Practice/Research Brief at http://aspe.hhs.gov/daltcp/reports/2007/HHAPartrb.htm.
-
Sainfort F., Karsh B., Booske B.C., Smith M.J. (2001). Applying Quality Improvement Principles to Achieve Healthy Work Organizations. The Joint Commission Journal on Quality Improvement 27(9):469-483.
-
IHI (2003). The Breakthrough Series. IHI's Collaborative Model for Achieving Breakthrough Improvement. Retrieved February 22, 2007, from http://www.ihi.org/ihi.
-
IHI (2003). The Breakthrough Series. IHI's Collaborative Model for Achieving Breakthrough Improvement. Retrieved February 22, 2007, from http://www.ihi.org/ihi.
-
For more information, see "Forming the Team" at http://www.ihi.org.
-
IHI (2003). The Breakthrough Series. IHI's Collaborative Model for Achieving Breakthrough Improvement. Retrieved February 22, 2007, from http://www.ihi.org/ihi.
-
IHI (2003). The Breakthrough Series. IHI's Collaborative Model for Achieving Breakthrough Improvement. Retrieved February 22, 2007, from http://www.ihi.org/ihi.
-
For a more extensive review and further insights on spreading change ideas, refer to: Pisek P. (2000). Spreading Good Ideas for Better Healthcare: A Practical Toolkit. VHA.
-
Rogers E.M. (1995). Diffusion of Innovations. Fourth Edition. New York, NY: Free Press.
-
Brown S.L., Eisenhardt K.M. (1998). Competing on the Edge: Strategy as Structured Chaos. Cambridge, MA: Harvard Business School Press; Lewin R., Regine B. (2000). The Soul at Work: Embracing Complexity Science for Business Success. New York, NY: Simon & Schuster; Zimmerman B.J., Lindberg C., Plsek P.E. (1998). Edgeware: Complexity Resources for Healthcare Leaders. Dallas, TX: VHA Publishing.
-
Backhard R., Harris R.T. (1987). Organizational Transitions: Managing Complex Change, Second Edition. Reading, MA: Addison-Wesley; Bridges, W. (1991). Managing Transitions: Making the Most of Change. San Francisco, CA: Perseus Press; DiClemente C.C., Prochaska J.O. (1982). Self-change and therapy change in smoking behavior: A comparison of processes of change in cessation and maintenance. Addictive Behaviors 7(2):133-142.
-
Plsek P. (2000). Spreading Good Ideas for Better Healthcare: A Practical Toolkit. VHA.
-
For an in-depth look at the PDSA Cycles and many examples of how it has been applied, see: Langley G.J., Nolan K.M., Nolan T.W., Norman C.L., Provost L.P. (1996). The Improvement Guide. San Francisco, CA: Jossey-Bass Publishers, Inc.
-
Langley G.J., Nolan K.M., Nolan T.W., Norman C.L., Provost L.P. (1996). The Improvement Guide. San Francisco, CA: Jossey-Bass Publishers, Inc. http://www.ihi.org.
-
For more information on the OASIS, go to http://www.cms.hhs.gov/PrivProtectedData/13_OASIS.asp.
-
Feldman P.H. (1994). Dead-end work or motivating job? Prospects for frontline paraprofessional workers in long-term care. Generations 18(3):5-10; Mickus M. (2007). Voice From the Front: Recruitment and Retention of Direct Care Workers in Long-Term Care. Poster Presentation, AcademyHealth Annual Research Meeting.
-
Tinetti M.E., Baker D., Gallo W.T., Nanda A., Charpentier P., OLeary J. (2002). Evaluation of restorative care vs. usual care for older adults receiving an acute episode of home care. JAMA 287(16):2098-2105; Baker D.I., Gottschalk M., Eng C., Weber S., Tinetti M.E. (2001). The design and implementation of a restorative care model for home care. Gerontologist 41(2):257-263.
-
Tinetti M.E., Baker D., Gallo W.T., Nanda A., Charpentier P., O'Leary J. (2002). Evaluation of restorative care vs. usual care for older adults receiving an acute episode of home care. JAMA 287(16):2098-2105; Baker D.I., Gottschalk M., Eng C., Weber S., Tinetti M.E. (2001). The design and implementation of a restorative care model for home care. Gerontologist 41(2):257-263.
-
Tips adapted from NHS Modernisation Agency, Spreading and Sustaining New Practices: Sharing the Learning from the Cancer Services Collaborative (CSC), (2002); http://www.ihi.org.
-
Rogers E.M. (1995). Diffusion of Innovations, Fourth Edition. New York, NY: Free Press.
To obtain a printed copy of this report, send the full report title and your mailing information to:
U.S. Department of Health and Human ServicesOffice of Disability, Aging and Long-Term Care PolicyRoom 424E, H.H. Humphrey Building200 Independence Avenue, S.W.Washington, D.C. 20201FAX: 202-401-7733Email: webmaster.DALTCP@hhs.gov
RETURN TO:
Office of Disability, Aging and Long-Term Care Policy (DALTCP) Home [http://aspe.hhs.gov/_/office_specific/daltcp.cfm]Assistant Secretary for Planning and Evaluation (ASPE) Home [http://aspe.hhs.gov]U.S. Department of Health and Human Services Home [http://www.hhs.gov]