
Tuesday, April 29, 2014
Clinical Services Update
Shari M. Ling M.D.
Deputy Chief Medical Officer
Centers for Medicare & Medicaid Services (CMS)
Center for Clinical Standards & Quality
Road Map
- Innovative Models
- Care Transitions
- Patient and Family Engagement Campaign
- Workforce Education
- Technical Solutions
Implementation Milestones
| February 2013 | September 2014 | July 2015 |
|---|---|---|
| Patient and Family Engagement Campaign (PFEC) (12-18 months) |
|
|
Health Care Innovation AwardsRound 2
- In May 2013, the Innovation Center announced a 2nd round of Health Care Innovation Awards, specifically soliciting proposals in 4 specific categories of care:
- One of the four categories, “improve care for populations with specialized needs,” designates proposals that target care for persons with AD as a priority population for funding.
- Awards are expected to be announced by the Spring/Summer 2014.
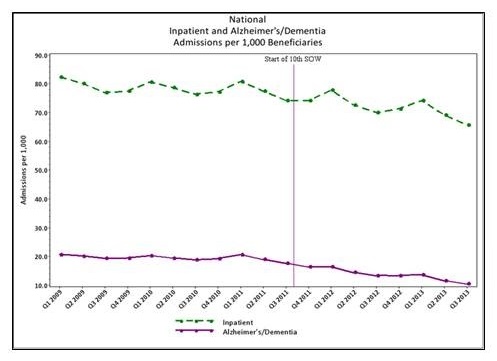
Care Transitions: National Inpatient and Alzheimer’s/DementiaAnnual Admissions per 1,000 Beneficiaries
| Start Date | End Date | Eligible Beneficiaries |
Inpatient Hospitalizations | Alzheimer's/Dementia Hospitalizations |
||
|---|---|---|---|---|---|---|
| Admissions | Admissions per 1,000 Benes |
Admissions | Admissions per 1,000 Benes |
|||
| 01/01/2009 | 12/31/2009 | 34,943,557 | 11,073,504 | 316.90 | 2,784,616 | 79.69 |
| 01/01/2010 | 12/31/2010 | 35,482,297 | 11,100,183 | 312.84 | 2,761,930 | 77.84 |
| 01/01/2011 | 12/31/2011 | 36,022,892 | 11,042,902 | 306.55 | 2,653,296 | 73.66 |
| 01/01/2012 | 12/31/2012 | 36,685,228 | 10,699,398 | 291.65 | 2,116,603 | 57.70 |
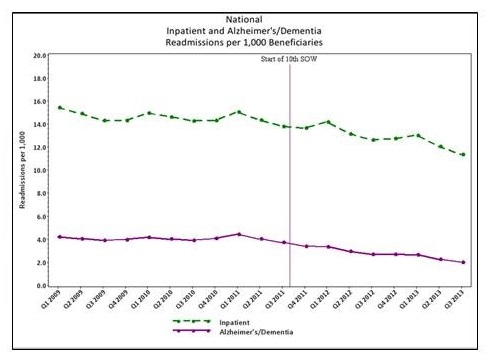
Alzheimer’s Events 2009 - 2013
| Admissions | Re-Admissions |
|---|---|
 |
 |
Patient & Family Engagement Campaign (PFEC)
- Focus: The QIO shall design its PFEC work to target behaviors among beneficiaries that address Care for Individuals Diagnosed with Dementia
- Generate processes designed to increase awareness and engagement by providing decisive tools, so patients and families make better decisions related to health care services they receive;
- Enable patients, their families, care givers and the public in general to interact among themselves and obtain information related to health care services they receive related to Dementia / Alzheimer’s Disease.
PFEC -- Dementia/Alzheimer’s
- Five (5) QIOs are involved with PFEC targeting clinical diagnosis of dementia/Alzheimer’s disease
- Participating QIOs
- California (HSAG)
- Kentucky (HCE)
- Michigan (MPRO)
- Missouri (Primaris)
- New York (IPRO)
- The QIOs have established their tactics for achieving success
- End: July 2014
Persons Impacted
| State/QIO | # Directly Reached | # Indirectly Reached |
|---|---|---|
| California (HSAG) | 1250 | n/a |
| Kentucky (HCE) | 630 | n/a |
| Michigan (MPRO) | 560 | n/a |
| Missouri (Primaris) | 339 | 29,704 |
| New York (IPRO) | 160 (80 beneficiaries w/ 80 graduate caregivers) | 882 |
Lessons Learned
- Beneficiaries are receptive to using technology and knowledge to actively engage in their healthcare;
- For some of the target audience the QIOs have learned that Hispanic communities have providers of care but many have English as a second language and are located in a high crime area;
- Identified that many have limited knowledge of dementia-care best practices, resources; and that many may be unaware, due to recent diagnosis of dementia or Alzheimer’s disease, of evidence-based practices for quality of life practices;
- Learned that dementia-care resources exist, but beneficiaries have limited understanding of how helpful these resource can be to caregivers;
- Recognized that beneficiaries and families require education regarding the need, and ability, of being responsible for their healthcare decisions;
- Acknowledged that care is poorly coordinated between hospitals and community resources;
Health Resources and Services Administration (HRSA) ADRD Activities
- Reviewing 45 Geriatric Education Centers applications for continued funding for ADRD education and training
- Writing statement of work for contract for unified curricula
- GEC grantees are working with the National Task Group on Intellectual Disabilities and Dementia Practices to develop an ADRD curricula focused on individuals with intellectual disabilities
- HRSA geriatrics grantees are currently participating in monthly conference calls with representatives of other Federal agencies to learn about those agencies’ dementia programs.
- Partnering with ACL to provide training to the ADRC network
Technical Solutions in the Clinical Environment
- Physicians and hospitals are eligible for incentive payments for their meaningful use of certified EHR technology. As of April 2013:
- more than 291,000 professionals, representing more than 50% of the nation’s eligible professionals, received EHR incentive payments; and
- over 3,800 hospitals, representing about 80 % of eligible hospitals (including Critical Access Hospitals) received EHR incentive payments1.
- Certified EHR technology must use certain specified health IT standards.
- Health IT standards support health information exchange and reuse.
- Update on the Adoption of Health Information Technology and Related Efforts to Facilitate the Electronic Use and Exchange of Health Information: A Report to Congress. Prepared by: ONC. June 2013.
Clinical Workflowin Caring for Persons with ADRD
- Detection
- Diagnosis
- Care Planning
Opportunities to Apply Health IT Solutions to Clinical Workflow: Some Examples
- Detection
- Detection Workflow: Primary Care Providers may detect cognitive impairment using 1 of 8 Brief Cognitive Tools recommended by CMS and NIH
- Example of HIT Activity: Identify health IT content standards needed for items in the Brief Cognitive Tools to enable interoperable exchange and re-use of this information in EHRs/health IT applications .
- Diagnosis
- Diagnosis Workflow: Primary Care Providers or Specialists may make a diagnosis of ADRD by conducting a dementia work-up: history, cognitive exam, and laboratory
- Example of HIT Activity: Identify health IT content and exchange standards needed for a dementia work-up to enable:
- bi-directional and interoperable exchange of consultation requests and results between PCP and specialist, and
- re-use of dementia work-up information.
- Care Planning
- Care Planning Workflow: Care planning for persons diagnosed with ADRD would:
- engage individual/family members/other care team members; and
- address: all health concerns; individual/family member/caregiver preferences, availability and needed supports; I&R to community supports; and need for advance care planning.
- Example of HIT Activity: Identify and fill gaps in Health IT standards to allow for the interoperable exchange of care plans and content needed on behalf of persons with ADRD.
- Care Planning Workflow: Care planning for persons diagnosed with ADRD would:
Files
Document
Mtg12-Slides2.pdf (pdf, 1.19 MB)