
U.S. Department of Health and Human Services
High Service or High Privacy Assisted Living Facilities, Their Residents and Staff: Results from a National Survey
Executive Summary
Catherine Hawes and Charles D. Phillips
Texas A&M University System Health Science Center
Miriam Rose
Myers Research Institute
November 2000
This report was prepared under contracts #HHS-100-94-0024 and HHS-100-98-0013 between the U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Office of Disability, Aging, and Long-Term Care Policy (ASPE) and Research Triangle Institute. Additional funding was provided by American Association of Retired Persons, the Administration on Aging, the National Institute on Aging, and the Alzheimer's Association. For additional information about the study, you may visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the ASPE Project Officer, Gavin Kennedy, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. His e-mail address is: Gavin.Kennedy@hhs.gov
This report was prepared under contracts HHS-100-94-0024 and HHS-100-98-0013 from the Office of Disability, Aging and Long-Term Care Policy, Office of the Assistant Secretary for Planning and Evaluation (ASPE), U.S. Department of Health and Human Services. AARP, the Alzheimer's Association and the National Institute on Aging have also provided support for this project. The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the contractor or any other funding organization.
Background
The most rapidly growing form of senior housing in recent years has been a form of supportive housing or residential long-term care known as assisted living. This growth has been a response to several factors, including the aging of the population, the preferences of the elderly for settings other than nursing homes, the availability of private financing for development and construction of assisted living facilities (ALFs), and public policies aimed at containing use of nursing homes.
| This report presents data on 41% of the ALFs nationwide and on the residents and staff in those facilities. These are the facilities among all ALFs that offer the highest levels of services and privacy. |
The Office of the Assistant Secretary for Planning and Evaluation (ASPE), in the U.S. Department of Health and Human Services, has a long-standing interest in the ability of residential and community-based service providers to meet the needs of the elderly and people with disabilities. As a result, ASPE has funded several studies of residential long-term care, including this first national study of ALFs for the frail elderly. ASPE's interest in assisted living and its ability to meet the needs of the frail elderly has been heightened during the study by a series of reports and a Congressional hearing that raised concerns about quality and consumer protection in assisted living (U.S. General Accounting Office, 1997 & 1999).
The Study
Despite growing interest and a rapidly expanding industry, the knowledge base available to those interested in assisted living is quite limited. Most prior and on-going research has been confined to a relatively small number of facilities and states. However, this study, A National Study of Assisted Living for the Frail Elderly, is based on data collected in a nationally representative sample of ALFs. Several reports based on the data collected about these facilities are available, and each provides data on a sample that is representative of a nationwide universe of ALFs, residents and staff. Those reports include:
-
The results of a telephone survey of approximately 1500 ALFs that describes the universe of ALFs nationwide;
-
A description of the policies and practices, residents, and staff in that segment of the ALF industry that provides the highest level of services and privacy;
-
A description of residents who were discharged from the high service or high privacy ALFs within six months of our initial interview;
-
A report that examines the effect of different environmental and service configurations on such issues as resident satisfaction, the ability of residents to age in place, and the price of assisted living; and
-
A final report that summarizes the findings across all the reports and specifically addresses key study questions, such as the degree to which the current assisted living industry exhibits the philosophy of assisted living and the effect of the mix of services and privacy on residents.
This report is the second of those mentioned above. It reports data on a nationally representative sample of residents and staff in ALFs classified as providing relatively high services or offering a high privacy environment. These facilities, which comprise about two-fifths (41%) of the places calling themselves assisted living, were selected for more extensive and in-depth data collection because they seemed to most effectively exhibit key elements of the philosophy of assisted living.
Study Methods
The national population of ALFs sampled for this study included only certain types of residential care settings. The population included all residential care facilities with 11 or more beds that primarily served the frail elderly and that publicly represented themselves as providing assisted living. It also included facilities that did not specifically identify themselves as assisted living but that appeared on some listing of residential care providers and met study criteria for size, mission, privacy and service.1 A telephone survey of a national probability sample of such facilities, representing nearly 11,500 facilities across the nation, formed the basis for our first study report (Hawes, Rose, & Phillips, 1999a and 1999b).
| Distribution of ALFs Nationwide and Those Included in This Report | |||
|---|---|---|---|
| High Services | Low Services | ||
| High Privacy | 11% of all ALFs IN |
18% of all ALFs IN |
|
| Low Privacy | 12% of all ALFs IN |
59% of all ALFs EXCLUDED |
|
As noted, this report focuses on a subset of two-fifths (41%) of the original sample. The facilities in the original sample were divided into groups, based on the level of privacy (i.e., high and low/minimal) and the level of service (i.e., high and low/ minimal) that they provided. An explanation of the way in which these groups were defined is discussed in detail in Section II of the report. Facilities in three of these groups (i.e., high service & high privacy, high service & low privacy, low service & high privacy) were chosen for further study through site visits that included more detailed data collection. The site visits included interviews with facility administrators, staff, residents, and family members, as well as a "walk-through" evaluation of the facility environment. The 300 facilities involved in the site visits represented a population of 4,383 ALFs across the nation -- or all those that met the definition of a facility that offered either high services or high privacy.
The Results
ALF Residents. The residents in the high privacy or high service ALFs were largely white, widowed females, who were quite elderly. More than one-half of the residents were 85 years of age or older. ALF residents were relatively well-educated; 45 percent had completed at least some college. They were also relatively affluent. Most entered assisted living from their own home or apartment (70%) and made the decision with help from someone else (90%), almost always their adult children. However, one-quarter of residents indicated that they had little or no control over the decision to enter a facility.
ALF RESIDENTS
|
Over one-quarter (27%) of the residents suffered from moderate or severe cognitive impairment, one-half of residents (51%) received assistance with bathing, and one-fifth of residents received assistance in some other activity of daily living. The overwhelming majority (77%), however, received help with their medications, and many residents used assistive devices, especially to help with ambulation or locomotion. Almost one-third (32%) experienced urinary incontinence. Two-fifths of the residents considered themselves in only fair or poor health, and, in the year prior to their interview, they used inpatient services at rates much higher than the general population.
Residents were relatively satisfied with the attitudes of staff and how staff treated them (e.g., with respect and affection). Their greatest points of concern about staff were related to inadequate staffing levels and high staff turnover. Residents were split almost evenly in their perceptions of the availability of activities they enjoyed and on the availability of transportation to events they might enjoy. One of the more unsettling findings concerning activities was that almost three-fifths of the residents (59%) indicated that ALF staff never or only sometimes asked them about their activity preferences.
RESIDENTS' PERCEPTIONS
|
Assisted living residents in ALFs classified as providing high services or high privacy were almost equally likely to be found in accommodations consisting of a full apartment or only a bedroom. The majority (81%) had a private living space or shared it with a related individual; however, nearly one-third of the residents did not have a private full bathroom. Most residents (i.e., more than three-quarters) also had other types of autonomy over their environment, such as ability to lock their doors, furnish their apartments and arrange the furniture as they wished, and control the temperature in their room or apartment. Only about half, however, had a refrigerator and only about one-third had space for cooking. Most had access to key supportive devices, such as call buttons and safety railings in the bathroom.
When they needed temporary nursing care, they were most likely to receive it from the facility staff; however, one-third of the residents who needed such care were either discharged to a hospital or nursing home or, with family members, arranged for home health themselves. Finally, fewer than one-third of the residents reported being informed by the facility about the discharge and retention policies. Despite this, the vast majority of residents expected to be able to stay in the facility for as long as they wished.
ALF Staff. The project investigated facility staff's knowledge of the appropriate response in a variety of situations involving relatively common health problems among frail older persons. In many instances, the vast majority of staff was aware of the proper response to specific situations, including most medication management issues. On the other hand, a significant number of staff members were poorly informed about antipsychotic drugs and some issues related to the care of individuals with dementia. More troubling, the majority of staff members were almost completely unaware of what constitutes normal aging. Given the goal of enabling residents to age in place and the advanced age of current residents, these results are particularly disquieting. Poor training and knowledge in these areas may in the future become more and more troublesome and risky, both for providers and residents, since many of the conditions staff identified as a "normal part of aging" were potentially treatable and reversible.
STAFF
|
Most staff in the high privacy or high service ALFs reported relatively high levels of satisfaction or positive affect toward their working conditions. Two areas, however, were a concern or area of low satisfaction for most staff. The first was their pay level, which usually ranged from between five and nine dollars per hour for personal care attendants. They also expressed dissatisfaction with what they viewed as limited possibilities for advancement.
Personal care staff did not report their workload as overly heavy, and the median number of residents for whom they cared was fourteen.2 In a nursing home this level of staffing would cause concern for some experts. However, as discussed above, the ALF residents were not as impaired as nursing home residents. At the same time, the survey demonstrated that most direct care staff in ALFs also had responsibility for a variety of tasks in addition to direct resident care, including housekeeping, laundry, and meal service. This complicates any attempt to evaluate the adequacy of staffing levels or compare them to those in other settings.
| The median ratio of direct care staff to residents was 1:14; however, these staff, particularly the PCAs typically were responsible for tasks such as laundry, housekeeping, and meal service, in addition to direct resident care. |
Walk-Through Observations. The observers' judgments about the physical plant in assisted living facilities indicated that these settings were largely well-maintained, clean, relatively homelike settings for the frail elderly with a wide range of social and recreational resources. Most were in suburban areas, and nearly half (46%) were single story buildings.
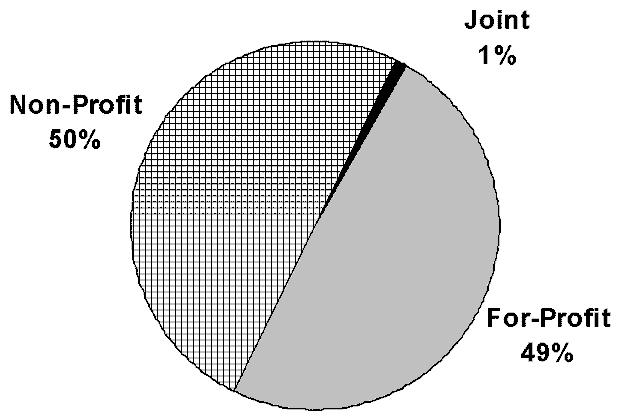
Facilties, Administrators, and Staffing. Assisted living facilities were almost equally likely to be operated by for-profit as by not-for-profit entities. However, the vast majority (79%) of organizations that owned or operated the high service or high privacy ALFs were involved in the operation of other types of supportive housing for the elderly, such as nursing homes and congregate apartments. Almost two-thirds (64%) of the not-for-profit ALFs, for example, were located on a multilevel campus that housed various types of supportive housing for the elderly, including a nursing home. Indeed, nearly half (49%) the owners of all of the high service or high privacy ALFs owned or operated nursing homes, and nearly half (46%) of these ALFs were part of a multi-facility system or "chain" of assisted living facilities.
| Ownership in High Privacy or High Service ALFs |
 |
Facilities showed some variation in the level of functional limitations and cognitive status among their residents. In most ALFs, relatively few residents had significant functional limitations and care needs. In most ALFs, assistance with medications was the only area in which they reported most residents needing and receiving help. However, approximately 15 percent of ALFs seemed to have a substantial proportion of residents with somewhat heavier physical care needs, such as need for help with transfers and other middle-range and late loss ADLs. Administrators also reported fairly high "turnover" rates among residents, with an average annual rate of 41 percent of the residents each year.
| Administrators reported an annual turnover rate for residents of 41%. |
Staffing varied considerably across facilities. According to administrators, on first shift, one-quarter of the ALFs had direct care staff to resident ratios of 8-to-1 or lower, and another quarter had ratios of 16-to-1 or greater. (In evaluating these reports, it is important to remember that the personal care attendants (PCAs) reported very different staffing ratios, with a median of 1-to-14 and one-quarter of the PCAs reporting that they cared for 23 or more residents). While staffing ratios varied considerably, there was some consistency across ALFs in the types of staff used. For example, the sampled ALFs that were site visited almost universally utilized some licensed nursing services. Staff turnover was lowest among licensed nursing staff, but administrators estimated that roughly one-quarter of all direct care staff turned over during the course of a year.
FACILITIES
|
The most common basic monthly charge in the high privacy or high service ALFs was between $1,735 per month and $19,990 -- or an average of about $1,800. However, because of the diversity among ALFs in the number and types of services included in that base rate, one is not quite sure what that sum purchased. For example, relatively few facilities (36%) provided temporary nursing care as part of their base monthly rate, while a substantial majority (80%) provided planned recreational activities. For those residents who exhausted their funds paying at this level, many facilities were willing to accept payments from alternative sources if they were available (e.g., charity, SSI, Medicaid). However, policy in a substantial proportion of facilities (45%) required the discharge of those who exhausted their private financial resources.
Conclusions
There are a number of policy issues surrounding the emergence and growth of assisted living and its ability to help meet the long-term care needs of the elderly and disabled. This report begins to address some of these by focusing on only those facilities that seem to most closely embody the philosophical tenets of "assisted living." Thus, the report describes the facilities that offer either high privacy or high services -- or both -- and their policies and practices, particularly with respect to services, policies on autonomy and resident control, and staffing. Further, this report describes the characteristics of the residents and their perceptions about the care they receive and the environment of the facilities in which they live. In providing this descriptive data, we begin to address questions about the role and performance of assisted living facilities and their place in the constellation of long-term care services. We also attempt to relate the descriptive data to the central study questions about whether ALFs embody the principles of assisted living and whether the needs of residents are being met. These issues are discussed at length in Section VII on conclusions. Finally, it is important to note that even in this special subgroup of ALFs, there was tremendous variability in ownership, size, staffing, policies, and performance along key dimensions.
In conclusion, assisted living appears to offer an important type of residential long-term care setting for persons with mild or moderate disabilities who cannot safely or securely live alone but do not need the level of care provided in a nursing home. Further, the high privacy or high service ALFs provide this care in a setting that has many components valued by consumers, particularly in terms of privacy and environmental autonomy. In addition, most high service or high privacy ALFs offered a wide array of services. The issue of whether such services can meet residents' unscheduled needs is more complex. Moreover, the degree to which such facilities enable residents to age in place is clearly mixed unless one limits the concept to one of "aging in place without significant decline in physical or cognitive functioning." Finally, assisted living is still a largely private-pay sector and, among the high service or high privacy ALFs, one that is largely unaffordable for most moderate and low income older persons unless they spend down their assets or receive help from relatives.
NOTES
-
Facilities that did not call themselves "assisted living" had to have at least 11 beds, primarily serve the frail elderly, house no more than two unrelated individuals in a room, provide at least two meals a day, 24-hour supervision, housekeeping services, and assistance with at least two activities of daily living (ADL) or one ADL and assistance with medications.
-
These data come from the staff interviews, and the staff interviewed almost exclusively worked the day shift. Information on staffing by shift appears in Section VI of the report.
| The Full Report is also available from the DALTCP website (http://aspe.hhs.gov/_/office_specific/daltcp.cfm) or directly at http://aspe.hhs.gov/daltcp/reports/. [The Full Report is in the Portable Document Format (PDF). You will need a copy of the Acrobat Reader in order to view it.] |