
This report provides an overview of Long-Term Care Registered Apprenticeship Programs (LTC RAPs) based on existing administrative data from U.S. Department of Labor. The purpose of this initial review is to support the design of a potential future evaluation of the effects of LTC RAPs on apprentices and the program sponsors that administer or operate them. The report summarizes findings from both apprentice and program-level analyses on how employment and training characteristics vary across different types of apprentices and apprenticeship programs. The report also provides a context for selecting program site visits where more intensive process/implementation analyses will take place and enrich our understanding of the actual operations of LTC RAPs. [59 PDF pages]
"Glossary of Terms
Apprenticeship Agreement -- A written agreement, complying with §29.7, between an apprentice and either the apprentices program sponsor, or an apprenticeship committee acting as agent for the program sponsor(s), which contains the terms and conditions of the employment and training of the apprentice.
Apprenticeship Program -- A plan containing all terms and conditions for the qualification, recruitment, selection, employment and training of apprentices, as required under 29 CFR parts 29 and 30, including such matters as the requirement for a written apprenticeship agreement.
Apprenticeship Standards -- A written agreement between an apprenticeship sponsor and the U.S. Department of Labor (DOL) that outlines all components of the sponsors apprenticeship program including the work processes, related instruction, process for hiring, pledge to affirmative action, responsibilities of apprentices, and maintenance of records.
Certificate of Completion of Apprenticeship -- Acertificate issued by the Registration Agency to those registered apprentices certified and documented as successfully completing the apprentice training requirements outlined in the Standards of Apprenticeship.
Certificate of Training -- A certificate that may be issued by the DOLs Office of Apprenticeship (OA) Administrator to those registered apprentices documented as successfully completing an approved, defined component of the apprentice training requirement as outlined in the Work Process Schedule of the Standards of Apprenticeship.
Certification -- A status conferred based on documentary evidence that:
- The OA has approved a set of National Guidelines for Apprenticeship Standards developed by a national committee or organization, joint or unilateral, for policy or guideline use by local affiliates, as conforming to the standards of apprenticeship set forth in §29.5;
- A Registration Agency has established that an individual is eligible for probationary employment as an apprentice under a registered apprenticeship program;
- A Registration Agency has registered an apprenticeship program as evidenced by a Certificate of Registration or other written indicia;
- A Registration Agency has determined that an apprentice has successfully met the requirements to receive an interim credential; or
- A Registration Agency has determined that an individual has successfully completed an apprenticeship.
CNA -- Certified Nursing Assistant, O*NET-SOC Code 31-1012.00, an occupation in which employees work in free-standing or hospital-affiliated nursing homes caring for persons with clinical needs and/or needing assistance in activities such as eating, bathing, and similar activities.
Competency -- The attainment of manual, mechanical or technical skills and knowledge, as specified by an occupational standard and demonstrated by an appropriate written and/or hands-on proficiency measurement.
Competency-Based Apprenticeship -- An apprenticeship that measures skill acquisition through successful demonstration of acquired skills and knowledge, as verified by the program sponsor. Programs utilizing this approach must still require apprentices to complete an on-the-job training (OJT) component of Registered Apprenticeship. The program standards must address how OJT will be integrated into the program, describe competencies, and identify an appropriate means of testing and evaluation for such competencies. A competency-based apprenticeship may take a shorter or longer time to complete based on the apprentices ability to learn a skill or acquire knowledge.
DSS -- Direct Support Specialist, O*NET-SOC Code 21-1093.00, an occupation in which employees provide care in group homes for persons with intellectual and developmental disabilities needing monitoring and assistance in daily activities.
Enrollment Status -- Whether an apprentice is registered currently in an apprenticeship, has completed an apprenticeship, has cancelled their apprenticeship (or had it cancelled by their employer), or suspended in good standing for an indefinite period of time with the intention of completing it.
HHA -- Home Health Aide, O*NET-SOC Code 31-1011.00,an occupation in which employees work in home health and hospice agencies providing services to people living in the community having clinical needs and/or needing assistance with eating, bathing, and similar activities.
HSS -- Health Support Specialist, O*NET-SOC Code 31-1011.00, an occupation in which employees work in assisted living facilities and retirement homes providing care for largely elderly persons needing monitoring and assistance with daily tasks.
Hybrid Apprenticeship -- An apprenticeship that measures skill acquisition through a combination of a specified minimum number of hours of OJT and the successful demonstration of competency as described in a work process schedule.
Interim Credential -- A credential issued by the Registration Agency, upon request of the appropriate sponsor, as certification of competency attainment by an apprentice. Competency means the attainment of manual or technical skills and knowledge, as specified by an occupational standard and demonstrated by an appropriate written and hands-on proficiency measurement. Programs sponsors shall identify and define all interim credentials and include a list of them in their program standards. Interim credentials can only be issued for recognized components of an apprenticeable occupation as identified by an appropriate job task analysis.
LTC RAP -- Long-Term Care Registered Apprenticeship Programs are developed by employers, employer associations or labor-management organizations to train employees of nursing homes, rehabilitation centers, home health agencies, assisted living facilities, retirement homes, and group homes for people with disabilities using the apprenticeship model. These programs have been registered with the OA or a State Apprenticeship Agency (SAA).
OA -- Office of Apprenticeship, the office designated by the DOLs Employment and Training Administration (ETA) to administer the National Apprenticeship System.
Occupation -- A field of work in which employees perform similar roles and responsibilities. Employees in a given occupation may work in a range of different settings. For example, employees working in the occupation of CNA usually work in nursing homes, but may also work in home health agencies and assisted living facilities.
OJT -- On-the-Job Training, training that occurs during the performance of an apprentices regular job responsibilities at their place of employment. OJT is essentially learning that occurs by doing ones actual job responsibilities over the course of their employment.
RAPIDS -- Registered Apprenticeship Partners Information Data System, the administrative database maintained by the DOLs OA to manage registered apprenticeship programs. RAPIDS contains apprentice-level (e.g., demographic) and sponsor-level (e.g., types and lengths of apprenticeships offered by the employer) information.
Registered Apprenticeship -- A formal employment relationship designed to promote skill training and learning on the job. The National Apprenticeship Act (NAA) of 1937 established the foundation for developing and expanding the nations skilled workforce through registered apprenticeship programs and standards for safeguarding the welfare of apprentices. Often referred to as the Fitzgerald Act, the NAA created a comprehensive system of partnerships among business, labor, education, and government that has shaped skill training through registered apprenticeship for succeeding generations of American workers. Basic components of registered apprenticeship include on-the-job (hands-on) learning, related theoretical instruction (often in a classroom setting), progressive wage increases as the apprentice advances in skill attainment and a mentor-apprentice relationship. An apprentice who successfully completes a registered program, which usually requires 1-5 years, is awarded a certificate of completion of apprenticeship. An OA registered program is one in which employers, or groups of employers, and unions design, organize, manage, and finance apprenticeship programs under the standards developed and registered with OA or a DOL/ETA-recognized SAA. Employers, or groups of employers, and unions also select apprentices who are trained to meet certain pre-determined occupational standards. For more information, see the OA web site at http://www.doleta.gov/oa.
RI -- Related instruction, an organized and systematic form of instruction designed to provide the apprentice with the knowledge of the theoretical and technical subject matter related to the apprentices occupation. Such instruction may be given in a classroom, through occupational or industrial courses, or by correspondence courses, electronic media, or other forms of self-study of equivalent value approved by the Registration Agency.
SAA -- State Apprenticeship Agency, an agency of state government that has responsibility and accountability for apprenticeship within a state. Only a SAA may seek recognition by the OA as an agency which has been properly constituted under an acceptable law or Executive Order, and authorized by the OA to register and oversee apprenticeship programs and agreements for federal purposes.
SOC Code -- Standard Occupational Classification Code, which are used in an Internet-based system (O*NET) for classifying occupations for use by workforce professionals and consumers.
Sponsor -- An employer, employer association, or labor-management organization that registers and operates an apprenticeship program. For example, an individual nursing home, a home health agency or an association representing these businesses may host and operate apprenticeships for its employees.
Term Length -- The sum of hours spent in OJT and related instruction to learn a given occupation. A time-based apprenticeship usually has a single term length (e.g., 2000 hours).
Time-Based Apprenticeship -- An apprenticeship that measures skill acquisition through completion of at least 2,000 hours of OJT as described in a work process schedule.
1. Introduction
The United States faces a critical current and future need for long-term care workers to meet the demands of the aging population. Indeed, the U.S. Department of Labor (DOL) projects that home care personal care assistants and home health aides (HHAs) will be among the fastest growing occupations in coming years (Bureau of Labor Statistics, 2009). Currently, low wages, few fringe benefits, minimal levels of training, and the lack of a career ladder contribute to a chronic workforce shortage. The Institute of Medicine (2008) recently recommended increased training requirements and career development for all direct care workers in order to address this workforce shortage.
Registered apprenticeship is a longstanding approach used in some occupations to provide in-depth training and develop careers. Apprenticeship uses a combination of work-based and formal learning to ensure workers master a specified set of occupational competencies. The National Apprenticeship Act (NAA) of 1937, established the foundation for developing and expanding the nations skilled workforce through registered apprenticeship programs and produces standards for safeguarding the welfare of apprentices. Often referred to as the Fitzgerald Act, the NAA created a comprehensive system of partnerships among business, labor, education, and government that has shaped skill training through registered apprenticeship for succeeding generations of American workers.
Upon completing an apprenticeship, apprentices receive a nationally recognized DOL Office of Apprenticeship (OA) or State Apprenticeship Agency (SAA) certificate of completion recognized by employers and often by state licensing boards. Only an apprenticeship program registered with the OA or a SAA and meeting the minimum requirements for standards of apprenticeship established in 29 CFR 29.5, can receive certification and be recognized across the country.
Registered apprenticeship offers several potential advantages for both long-term care workers and employers. Workers earn salaries while they are learning on the job in the context of actual long-term care settings. Registered apprenticeships may also offer workers incremental pay increases as they earn interim credentials toward recognized steps on a career ladder often by progressing from introductory jobs to acquiring specialized competencies. (http://phinational.org/training/resources/apprenticeships/).
Employers generally gain confidence that trained apprentices have mastered a well-specified set of occupational competencies. A competency-based approach to apprenticeship ensures that learning focuses on practical skills and allows workers to gain credit for skills learned through previous experience. Training occurs at the place of employment and often at a nearby community college, other learning center or on-line. Peer-mentors in some organizations may offer additional support in attaining required skills. An apprenticeship can also help workers gain non-academic skills such as teamwork, communication, and problem-solving.
Long-Term Care Registered Apprenticeship Programs (LTC RAPs), administered by the DOLs OA and developed by employers, employer associations and labor-management organizations, provide formal training and work experience for direct care workers in long-term care settings. The goal of LTC RAPs is to significantly improve worker skill development, job mobility within long-term care settings, organizational productivity, and quality of care. Developing improved job opportunities linked to higher compensation and a career ladder is an important strategy for reducing the long-term care workforce shortage and possibly improving quality of care (Institute of Medicine, 2008). Since the programs inception in 2003, over 100 long-term care employers have offered LTC RAPs employment and training to almost 4,000 apprentices (RTI International/Urban Institute analysis of program data, 2010).
Registered apprenticeship programs are primarily funded directly by employers with some assistance with start-up funding from government (including DOL) or private organization (e.g., foundation) grants. The organizational sponsors of apprenticeship programs register their programs with federal and state government agencies. Sponsors provide on-the-job training (OJT) and academic instruction to apprentices according to their licensing requirements. For example, Certified Nursing Assistants (CNAs) must have a minimum of 75 hours of state-approved training to meet federal requirements, with typical certification courses covering anatomy and physiology, nutrition, body mechanics, infection control, and client rights (OA, DOL Employment and Training Administration [ETA], 2010). A number of additional employers, agencies, and associations have expressed interest in the LTC RAPs model (Office of the Assistant Secretary for Planning and Evaluation [ASPE], 2009).
LTC RAPs include all of the required components of registered apprenticeship. First, OJT occurs at a workers place of employment. Second, related instruction may take place onsite or at technical or community colleges. Related instruction may occur through various modes of instruction (e.g., in-person, web-based, correspondence course). Third, mentoring is often a feature of many apprenticeships, occurring sometimes through mentors who have completed apprenticeships themselves. Mentors provide on-the-job coaching and help apprentices identify and acquire competencies needed to perform their jobs successfully.
Registered apprenticeships are structured to develop increased job competency over time. Apprenticeships can be either competency-based, time-based, or a hybrid of the two, a decision made by sponsors who can shape OJT and curricula previously developed by the OA to suit employer needs. All three types of apprenticeship require apprentices to master a set of competencies, but the time-based approach additionally mandates minimum hours of on-the-job and related instruction.
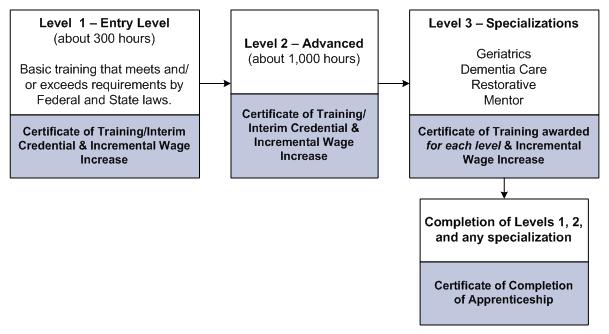
Current LTC RAPs offer apprenticeships in four major occupations: CNAs, Direct Support Specialists (DSSs), Health Support Specialists (HSSs), and HHAs. CNAs, O*NET-SOC Code 31-1012.00, work in free-standing or hospital-affiliated nursing homes caring for persons with clinical needs and/or needing assistance with eating, bathing, and similar activities. The CNA apprenticeship is competency-based and offers two models, one with interim credentials and one without. In the interim credentialed model, apprentices must complete entry-level and advanced level training, which is followed by one or more specialties such as dementia or restorative care (Exhibit 1). After completion of each level and each specialty, apprentices receive a Certificate of Training. Upon completion of Levels 1, 2 and any specialty from Level 3, apprentices receive a Certificate of Completion of Apprenticeship.
| EXHIBIT 1. Certified Nursing Assistant Apprenticeship Model |
| Certified Nursing Assistant Apprenticeship Model O*NET-SOC CODE: 31-1012.00 (Competency-based, interim credentials) |
 |
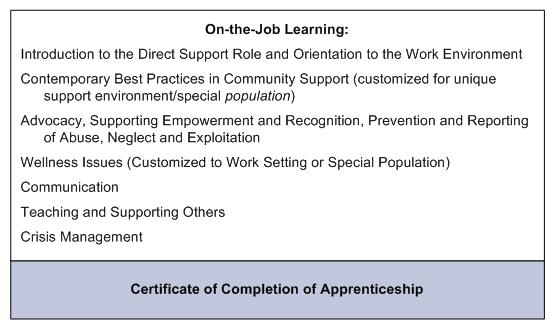
DSSs, O*NET-SOC Code 21-1093.00, provide care most often in group homes for persons with intellectual and developmental disabilities needing monitoring and assistance in daily activities. The DSS apprenticeship currently is a competency-based model with no interim credentials offered, although two organizations, American Network of Community Options and Resources (ANCOR) and the National Association of Direct Support Professionals (NADSP), are developing models offering interim credentials (Exhibit 2). Apprentices who successfully complete all the components of the program receive a Certificate of Completion of Apprenticeship.
| EXHIBIT 2. Direct Support Specialist Apprenticeship Model |
| Direct Support Specialist Apprenticeship Model O*NET-SOC CODE: 21-1093.00 (Competency-based, no interim credentials) (American Network of Community Options and Resources (ANCOR) and the National Association of Direct Support Professionals (NADSP) are developing a model with interim credentials) |
 |
HSSs, O*NET-SOC Code 31-1011.00, work in assisted living facilities and retirement homes providing care for mostly elderly persons needing monitoring and assistance with daily tasks. Assisted living facilities usually do not provide the highly skilled clinical care that is usually provided in nursing homes, thus staff certification requirements for these two settings differ. The HSS apprenticeship currently is a hybrid model (time-based and competency-based) with no interim credentials, although a large national employer has recently developed a model with interim credentials but had not yet registered apprentices using it (Exhibit 3). Apprentices who successfully complete all components of the program receive a Certificate of Completion of Apprenticeship.
| EXHIBIT 3. Health Support Specialist Apprenticeship Model |
| Health Support Specialist Apprenticeship Model O*NET-SOC CODE: 31-1011.00 (Hybrid model -- combination of Competency and Time-based, no interim credentials) (Comfort Keepers, a large national employer, developed a model with interim credentials) |
 |
HHAs, O*NET-SOC Code 31-1011.00, work in home health and hospice agencies providing services to people living in the community having clinical needs and/or needing assistance with eating, bathing, and similar activities. The HHA model is a competency-based apprenticeship offering interim credentials or Certificates of Training when apprentices complete various levels of training within the occupation (Exhibit 4). The apprenticeship begins with entry-level (Level 1) training, of which at least 16 hours of classroom training must be completed before beginning the supervised practical training component. Apprentices receive a Certificate of Training upon completion. To receive the Certificate of Completion of Apprenticeship, apprentices need to complete Level 1 and then any two specialties.
| EXHIBIT 4. Home Health Aide Apprenticeship Model |
| Home Health Aide Apprenticeship Model O*NET-SOC CODE: 31-1011.00 (Competency-based, interim credentials) |
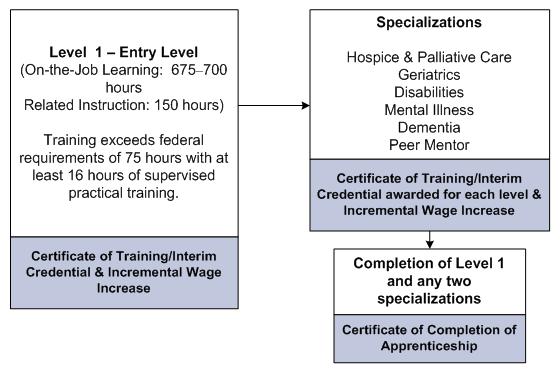 |
Specialty training differs across the three occupations that have such training. CNAs can specialize in dementia care, geriatric care, restorative care, or mentoring. HHAs can specialize in care for people with disabilities, palliative care for patients receiving hospice, care for people with mental illness, dementia care, geriatric care, or mentoring. HSSs can receive specialty training in dining services, environmental services, or as an activity director, certified medication aide, certified nurses aide, HHA, or rehabilitative aide. Following completion of each type of specialty training, apprentices also receive a Certificate of Training.
Generally, competency-based apprenticeship programs emphasize skill mastery without requiring a specified time commitment to training, although OJT ranges from 3-5 months for each level of training with varying hourly ranges of related instruction. In contrast, time-based apprenticeships mandate occupational competencies apprentices must learn for certification within a fixed amount of time at the end of which participants receive a certificate. Time-based apprenticeships generally provide an extended period of entry-level training lasting a minimum of 2,000 hours, with at least 144 hours of related instruction.
Although the number of LTC RAPs is currently small compared to the number of apprenticeship programs in other industries with a deep history with the apprenticeship model, expanding the number of these programs in the long-term care setting offers an innovative approach to addressing the workforce shortage. To assess the potential for the apprenticeship model to improve worker competencies, employer productivity, and quality of care delivered, ASPE in the U.S. Department of Health and Human Services and the DOLs OA and the Office of the Assistant Secretary for Policy have contracted with RTI International, and its subcontractor, the Urban Institute, to develop evaluation design options that could be used to assess LTC RAPs. The tasks involved in developing options for evaluation design include analyzing existing administrative data on LTC RAPs, conducting site visits of selected apprenticeship work sites, and using the information obtained to develop the potential evaluation designs for consideration by ASPE and DOL.
This report provides an overview of LTC RAPs based on existing administrative data from DOL. The purpose of this initial review is to support the design of a potential future evaluation of the effects of LTC RAPs on apprentices and the program sponsors that administer or operate them. The report summarizes findings from both apprentice and program-level analyses on how employment and training characteristics vary across different types of apprentices and apprenticeship programs. The report also provides a context for selecting program site visits where more intensive process/implementation analyses will take place and enrich our understanding of the actual operations of LTC RAPs.
2. Methodology
The findings in this report were developed by analyzing administrative data on apprentices and apprenticeship programs collected by the OA from employers, employer associations and labor-management organizations that sponsor apprenticeship programs. Staff from sponsoring programs enters data into an Oracle relational database system called the Registered Apprenticeship Partners Information Data System (RAPIDS). Data are updated as apprentices begin their apprenticeships and complete competency-level trainings, but may be updated at other times as well (particularly for the time-based apprenticeships). OA staff review and approve the information entered into RAPIDS. For this report, several apprenticeship sponsors provided information on the administrative data entry process to further understanding of the data.
The RAPIDS database contains information on apprenticeship programs of any type (not exclusively LTC RAPs) in 34 states, of which 25 are federally administered and nine are administered by SAAs (Exhibit 5). Twenty-seven of these states did have LTC RAPs in the data analyzed for this report. The remaining SAA/state-administered states (Connecticut, Delaware, District of Columbia, Hawaii, Maine, Maryland, Massachusetts, Minnesota, Montana, New Mexico, New York, North Carolina, Oregon, Puerto Rico, Vermont, Virginia, Virgin Islands, Washington, and Wisconsin) do not provide data to the national RAPIDS database, so the database is not a reflection of LTC RAPs in the nation.
| EXHIBIT 5. States Providing Data to National RAPIDS Database | |||||
|---|---|---|---|---|---|
| OA/Federally Administered States | SSA/State-Administered States | ||||
| Alabama Colorado Indiana Missouri North Dakota Tennessee Wyoming | Alaska Georgia Iowa Nebraska Oklahoma Texas | Arkansas Idaho Michigan New Hampshire South Carolina Utah | California Illinois Mississippi New Jersey South Dakota West Virginia | Arizona Kansas Louisiana Ohio Rhode Island | Florida Kentucky Nevada Pennsylvania |
For this report, OA staff provided an extract from RAPIDS of all apprentices and employer sponsors (hereinafter known as programs) in long-term care occupations over a 5-year period, from 2005-2009. Data provided included information on entry-level, advanced, and specialty training within occupations registered with the DOL as apprenticeable.1 The occupations covered include CNA, DSS, HSS, and HHA. This report examines 3,744 records of individual apprentices who started their apprenticeship between January 2005 and December 2009. These apprentices were in 121 unique programs. The data allow analysis at the apprentice-level as well as the program-level.
The data in this report provide a profile of long-term care apprentices, programs, and employers. The apprentice characteristics include age, sex, race, ethnicity, educational attainment, and the current enrollment status of an apprentice in an apprenticeship (registered currently, completed, cancelled, or suspended). Program characteristics include duration of the on-the-job and related instruction components of the apprenticeship (in hours), the source/mode of related instruction, and whether the apprenticeship was a competency-based program involving no specific time requirement for completion, or a time-based program involving learning of competencies in a fixed number of hours. Although RAPIDS includes data on each training level received, in cases where one person undertakes more than one training (e.g., a competency-based program with an interim credential), the analysis of apprentices includes only the individuals most recent training. Employer information includes workforce size, program size, number of affiliated sites, whether the program is a national program, region of the employer, duration of the program, and the source/mode of related instruction.
These analyses portray the types of workers, mix of programs, and types of employers involved in long-term care apprenticeships. We present findings on counts of apprentices, and proportions or means of these apprentice and program characteristics. As the reports purpose is to present a descriptive overview of the LTC RAP, we do not include tests of statistical significance.
For some items that were available for analysis, there are missing or questionable data. This was an especially severe problem for wage data. Sometimes, instead of entering actual wage rates, sponsors enter wage rates that were specified in an apprentices agreement with their employer, which may not be the true wage the apprentice receives. In addition, the collection of wage and other data is not the sponsors primary concern so obtaining accurate wage data often requires a time commitment that OA and SAA field staff cannot afford. Consequently, the wage data appeared inaccurate or inconsistent upon analysis. For these reasons, we do not present findings from that analysis because the data appears to be unreliable.
To understand the quality of wage and other data as well as the data entry process, we interviewed staff from two program sponsors responsible for the RAPIDS data entry process at their organization. These brief interviews were conducted using a general discussion guide to glean information on the same topics across program sponsors, such as who entered data and how often, problems experienced in doing so, and what improvements were needed in RAPIDS. We present summary findings of these interviews in the next section to inform the presentation of our analyses of RAPIDS data.
DOL previously consolidated information about occupational competencies (e.g., knowledge, skills, and abilities) described in this report in work process schedules. Work process schedules are detailed documents ranging from three to ten pages in length that contain information regarding OJT and related instruction for each competency. Information from these documents is included to illustrate the variety of specific trainings (e.g., advanced CNA training) within the four major occupations.
| EXHIBIT 6. LTC RAP Occupational Competency Trainings and RAPIDS Codes | |||
|---|---|---|---|
| Competency Trainings | RAPIDS Code* | ||
| Certified Nurse Assistant (CNA) | |||
| CNA Entry-Level | 824 | ||
| CNA Entry-Level | 824C or CB | ||
| CNA Advanced | 824A | ||
| CNA Specialty: Restorative | 824R | ||
| CNA Specialty: Dementia | 824D | ||
| CNA Specialty: Geriatrics | 824G | ||
| CNA Specialty: Mentor | 824M | ||
| Home Health Aide (HHA) | |||
| HHA Entry-Level | 1086 | ||
| HHA Entry-Level | 1086CB | ||
| HHA Specialty: Disability | 1086A | ||
| HHA Specialty: Hospice and Palliative Care | 1086B | ||
| HHA Specialty: Dementia Care | 1086D | ||
| HHA Specialty: Mentor | 1086E | ||
| Health Support Specialist (HSS) | |||
| HSS Entry-Level and Specialty Training | 1086AA | ||
| Direct Support Specialist (DSS) | |||
| DSS Entry-Level | 1040 | ||
| DSS Entry-Level | 1040CB | ||
| * Codes without a letter suffix designate time-based apprenticeships. Apprenticeable Long-Term Care Trainings: OA, DOL/ETA. | |||
Each occupation and competency training within an occupation is identified in RAPIDS using a system of codes. Codes containing only numbers are trainings for time-based apprenticeships, while codes with lettered suffixes pertain to competency-based apprenticeship trainings. Exhibit 6 presents the list of RAPIDS training codes for specific competencies for all four LTC occupations . Even though HSSs working in assisted living facilities or retirement homes have seven specialty trainings, RAPIDS contains only one code (1086AA) for any type of training for this occupation. We analyzed RAPIDS data first across all competency trainings within each of the four occupations, and then for each competency training within each occupation.
3. Results
This section of the report presents results of descriptive analyses of the DOL RAPIDS data and sponsor interviews regarding data entry issues. First, we describe the findings from data at the apprentice-level to understand how important apprentice characteristics vary across and within major occupations. We then present results at the program level to understand how programs vary across and within occupational groups. Apprentice-level analyses are presented in Tables 1-5, and program-level analyses in Tables 6-10.
3.1. Apprentice-Level Analyses
Apprentice-level analyses in Tables 1-5 include descriptive results on 3,744 apprentices in the RAPIDS database describing demographic characteristics, enrollment status, and apprenticeship characteristics.
| Highlights of Apprentice-Level Findings
|
The sample derived from the RAPIDS data extract included 3,744 apprentices representing four broad occupational groups. There are 1,695 (45% of the sample) CNAs employed mostly in nursing homes, 1,087 (29%) DSSs employed in group homes/facilities providing housing and supportive services to persons with intellectual disabilities, 567 (15%) HSSs employed in assisted living facilities, and 395 (11%) HHAs employed in home health or hospice agencies.
Table 1 presents the overall distribution of apprentices on selected characteristics and also across the four major occupations. Overall, a majority of apprentices are more than 30 years old. The age distribution varies by major occupational group, with CNAs being younger than DSSs and HSSs. CNAs have the highest proportion of those under the age of 20, with 21% of CNAs under age 20 compared to only between 5% and 9% of apprentices in the other major occupations. Of all occupations, CNAs also have the lowest proportion of those aged 50+ (9%). In comparison, 27% of DSSs and 18% of HSSs are aged 50 and over. In terms of age distribution, HHAs resemble CNAs with 47% under the age of 24 and 9% aged 50 and over.
As expected, most of the apprentices are female. Overall, only 14% of apprentices are males. The proportion of females is similar across occupations.
| TABLE 1. Characteristics of Long-Term Care Apprentices by Occupational Group | ||||||
|---|---|---|---|---|---|---|
| Characteristics | N | Overall | Major Occupational Group: CNA (824) | Major Occupational Group: DSS (1040) | Major Occupational Group: HSS (1086AA) | Major Occupational Group: HHA (1086) |
| Number of Apprentices | --- | 3744 | 1694 | 1087 | 567 | 395 |
| Age (%) | 3,744 | --- | --- | --- | --- | --- |
| Under 20 | --- | 13.0 | 21.1 | 5.4 | 6.5 | 8.9 |
| 2024 | --- | 21.2 | 21.7 | 15.1 | 19.8 | 38.0 |
| 2529 | --- | 12.1 | 12.2 | 9.4 | 13.8 | 16.5 |
| 3039 | --- | 20.3 | 20.8 | 21.4 | 20.6 | 13.9 |
| 4049 | --- | 18.0 | 15.2 | 21.9 | 21.7 | 13.7 |
| 50+ | --- | 15.5 | 9.0 | 26.8 | 17.6 | 9.1 |
| Female (%) | 3,744 | 85.7 | 88.5 | 79.3 | 89.4 | 86.1 |
| Race(%) | 3,744 | --- | --- | --- | --- | --- |
| White | --- | 70.4 | 54.6 | 89.2 | 79.4 | 72.9 |
| African-American | --- | 18.1 | 28.0 | 5.9 | 7.9 | 23.5 |
| Hispanic | --- | 8.0 | 13.8 | 1.8 | 7.1 | 1.8 |
| Unknown Race | --- | 3.6 | 3.6 | 3.0 | 5.6 | 1.8 |
| Education(%) | 3,631 | --- | --- | --- | --- | --- |
| Up to 11 years of schooling | --- | 9.7 | 17.6 | 0.7 | 6.0 | 4.6 |
| GED | --- | 12.7 | 21.9 | 1.7 | 8.5 | 8.1 |
| High School Graduate | --- | 72.9 | 53.3 | 95.3 | 82.7 | 85.1 |
| Some Post-Secondary Education | --- | 4.7 | 7.2 | 2.4 | 2.9 | 2.3 |
| Enrollment Status (Last Event Code)(%) | 3,740 | --- | --- | --- | --- | --- |
| Registered | --- | 38.6 | 33.5 | 33.5 | 73.2 | 25.1 |
| Completed | --- | 27.3 | 34.3 | 33.4 | 4.4 | 13.2 |
| Cancelled | --- | 34.0 | 32.2 | 33.1 | 22.4 | 61.5 |
| Suspended | --- | 0.1 | 0.1 | 0.0 | 0.0 | 0.3 |
| Term Length (hours) | 3,744 | 2,200 | 1,345 | 2,638 | 4,139 | 1,874 |
| Related Instruction Length (hours) | 3,464 | 198 | 112 | 239 | 398 | 125 |
| Related Instruction by Sponsor (%) | 3,744 | 72.7 | 71.3 | 92.1 | 23.6 | 96.0 |
| SOURCE: RTI International/Urban Institute analysis of RAPIDS data. NOTES: Registration after 1/1/2005, most recent training. | ||||||
Apprentice programs recruit a relatively diverse group of people: 70% are White, 18% are African-American, 8% are Hispanic and 4% are identified as other race. There is substantial variation in diversity across occupations: CNAs are the most diverse group of apprentices (28% of CNAs are African-American and 14% are Hispanic, followed by HHAs, who are 24% African-American and 2% Hispanic). In contrast, DSSs and HSSs are the least diverse occupations -- 89% and 79% respectively are White.
Regarding educational background, apprentices rarely have a college education and high proportions of some occupations did not complete high school. Overall, most apprentices (86%) are high school graduates or have a GED and almost 5% have some post-secondary education. About 10% have up to 11 years of schooling but have not completed high school or received a GED. Again, some differences are apparent across major occupations. Only 75% of CNAs have either completed high school or a GED. In contrast, over 90% of the other three major occupations completed high school or a GED, with the highest proportion among DSSs (97%).
We compared the findings on demographic characteristics of CNA and HHA apprentices with findings from two national surveys, the 2004 National Nursing Assistant Survey and the 2007 National Home Health Aide Survey to understand how representative apprentices are of the national population of these workers (Exhibit 7). First, compared to CNAs working in nursing homes nationally, CNAs in apprenticeships are younger (50% of CNA apprentices are under the age of 30 compared to 30% of CNAs nationally). There are slightly more male apprentices than among all CNAs (11.5% versus 8%). CNA apprenticeship programs attract a higher proportion of Latinos (15% in programs versus 9% nationally) but fewer African-Americans (31% in programs versus 39% nationally). CNA apprentices have lower educational attainment compared to CNAs nationally: almost 93% of CNA apprentices have a high school or less than a high school education, compared to 75% of CNAs nationally.
Similar patterns hold for HHAs. HHA apprentices on average are younger than HHAs working in home health and hospice agencies across the country: 45% of HHA apprentices are under the age of 30 compared to only 13% of HHAs nationally. Almost twice as many males are apprentices (12% versus 5%). However, it appears that HHA apprenticeship programs enroll fewer minorities: 5% of HHA apprentices are Hispanic and 15% are African-Americans compared to 8% of Hispanics and 35% of African-Americans nationally. Similar to CNA apprentices, HHA apprentices are less educated than HHAs in general: virtually all (97%) of HHA apprentices have high school education or less, compared to 60% of HHAs nationwide.
The apprenticeship enrollment status categories presented in Table 1 are registered, completed, cancelled and suspended. An apprenticeship may be cancelled if an apprentice elects not to complete training, or if their employer cancels their participation for some reason. An apprentice may be granted a suspension if their apprenticeship is interrupted for some reason, but they still plan on returning to complete it at a later date.
Apprenticeship enrollment status pertains to the latest status recorded for the specific training in which each person was registered. For example, CNAs may be in entry-level training, advanced training, or one of the four specialty trainings in which one may enroll after completing advanced training. Therefore, an enrollment status of registered for a given CNA in advanced training means they have already completed entry-level training and are registered for advanced training. Each apprentice appears only once in the data, meaning that their completion status for prior trainings is not shown in the table -- only the status for the training in which they most recently enrolled appears. The proportion of trainings completed would have been only slightly higher had we analyzed the data at the training-level rather than the apprentice-level because relatively few apprentices are in trainings beyond entry-level training.
| EXHIBIT 7. Demographic Characteristics of Apprentices Compared to National Estimates (percent) | ||||
|---|---|---|---|---|
| Characteristics | CNA Apprentices | CNAs Nationally | HHA Apprentices | HHAs Nationally |
| Age | ||||
| Under 30 | 49.7 | 29.8 | 45.4 | 13.2 |
| 30-44 | 29.3 | 35.9 | 27.4 | 30.3 |
| 45+ | 21.0 | 34.3 | 27.1 | 56.5 |
| Gender | ||||
| Male | 11.5 | 8.0 | 11.9 | 5.0 |
| Female | 88.5 | 92.0 | 88.1 | 95.0 |
| Race | ||||
| White only | 68.5 | 53.4 | 83.2 | 53.3 |
| African-American only | 30.8 | 38.7 | 15.2 | 34.9 |
| Other | 0.7 | 7.9 | 1.6 | 11.8 |
| Hispanic or Latino | 15.0 | 9.4 | 5.0 | 8.3 |
| Education | ||||
| <12 years | 17.6 | 12.9 | 5.4 | 7.2 |
| GED | 21.8 | 17.8 | 8.3 | 14.4 |
| HS graduate | 53.2 | 44.6 | 83.7 | 38.2 |
| 13 years college/trade | 0.2 | 19.8 | 0.0 | 34.2 |
| College/post grad | 0.0 | 4.9 | 0.0 | 5.9 |
| Unknown | 7.2 | 0.0 | 2.6 | 0.0 |
| SOURCE: RTI International/Urban Institute analysis of RAPIDS data, the 2004 National Nursing Assistant Survey, and the 2007 National Home Health Aide Survey. | ||||
Of all apprentices enrolled in the database since January 1, 2005, as of December 1, 2009, 39% (1,445 apprentices) were currently registered in a specific training, 27% (1,020 apprentices) had completed a training since 2005, and 34% (1,273 apprentices) had cancelled (e.g., dropped out) their participation since 2005. Only two apprentices had a status of suspended, meaning that they had been granted a leave of absence. The enrollment status results presented are cumulative over time, therefore, the proportions for completed and cancelled are much higher than results from a cross-sectional snapshot of only calendar year 2009, where 75% of apprentices were registered, 7% had completed their training, and 18% had cancelled their participation.
Again, as with other characteristics, enrollment status varies greatly by major occupation. Among CNAs and DSSs, about 33% of apprentices are currently registered (568 and 364 apprentices respectively). The proportion of registrants is much higher for HSSs at 73% (415 apprentices) in part because of recent DOL grants to expand apprenticeships for this occupation. About 25% (99 apprentices) of HHAs are currently registered. The proportion of completed trainings vastly varies depending on major occupation: CNAs have the highest proportion (34%), followed by DSSs (33%). About 13% of HHAs have completed training, and only 4% of HSSs, again because of recently awarded DOL grants for this occupation that led to new registrants who have not had sufficient time to complete their training as of December 2009. As stated earlier, the proportion of cancellations is high and ranges from 62% for HHAs to 22% among HSSs. The proportion of cancellations for CNAs and DSSs is similar (32% and 33% respectively).
Finally, the RAPIDS data provide information on the training aspects of apprenticeships. Term length comprises both the OJT component and the related instruction for a competency training (e.g., entry-level or a single specialty, as opposed to the length of the whole apprenticeship, which may include several trainings across time), with a mean of 2,200 hours. Term length across competency trainings within occupations is lowest for CNAs (1,345 hours) and highest for the HSSs (4,139). Term length for DSSs was 2,638 hours and 1,874 hours for HHAs.
On average, there are 198 hours of related instruction for each competency training. HSSs have the longest related instruction period per competency training (almost 400 hours). DSSs had an average of 239 hours per competency training. Related instruction for HHAs and CNAs is shorter, 125 and 112 hours per competency training, respectively.
Related instruction may be obtained directly at the employer work site, or offsite (e.g., community college, vocational school). Related instruction by sponsor describes whether the employer provided the related instruction onsite or whether it was obtained at an offsite location (e.g., community college). Overall, 73% of apprentices had their related instruction provided onsite. There are significant differences by occupation: most of the HHAs receive this training onsite (96%), followed by DSSs (92%) and CNAs (71%). Only 23.6% of HSSs receive their related instruction at their sponsors location (again, because DOL provided grant funds to these employers to have apprentices receive this training from an external source).
RAPIDS includes data on some very large providers that potentially skew the results, particularly on total workforce size (apprentices plus other employees) and possibly other characteristics examined. Therefore, we re-ran the analyses with four large employers removed. We removed the two largest employers who contribute the largest numbers of apprentices within each of the four occupations (St. Johns Mercy Medical Center, which contributes 644 currently registered CNAs, HSSs, and HHAs, and Developmental Services, Inc. which contributes 924 currently registered DSSs). We also removed the two employers (Gary Job Corps and Womens East Reception Federal Prison with 396 and 297 CNAs respectively) who contributed the largest numbers of apprentices who were not currently registered (had either completed or cancelled their apprenticeships) so that the data would reflect the most recent composition of registered apprentices.
Removing these four programs changed the results on some characteristics substantially:
- Apprentices in all occupations were somewhat older, particularly CNAs and DSSs.
- Substantially more DSSs were female.
- More CNAs were White and fewer DSSs were White.
- CNAs were better educated, and there was more variance in the educational status of DSSs instead of clustering around high school graduates.
- CNAs and DSSs had higher proportions of registered apprentices.
- DSSs and HSSs had notably higher term lengths and related instruction lengths than the full sample.
- Fewer apprentices had related instruction provided by the sponsor across all occupation groups.
Tables 2-5 disaggregate the results by whether the apprenticeships are time-based (requiring the apprentice to complete a certain number of hours of work and related instruction) or competency-based (requiring an apprentice to acquire specific competencies through work and related instruction regardless of the apprenticeship length). Approximately 72% of all apprentices across the four major occupations are in competency-based apprenticeship programs.
Further, two of the major occupations (CNAs and HHAs) have competency-based training beyond entry-level, and these advanced or specialty training programs are grouped together to provide a better understanding of the characteristics of workers who progress beyond entry-level training. About 32% of apprentices (391) in competency-based apprenticeships have participated in advanced or specialty training when available. Detailed information at the apprentice-level on each of the individual advanced or specialty apprenticeship trainings for CNAs and HHAs is provided in Appendix A. Currently, the DSS model does not offer interim credentials or advanced and specialty training, and the HSS model is a hybrid model combining both competency-based and time-based apprenticeships. Although HSSs have specialty trainings, the model does not offer interim credentials so these data did not separately delineate these trainings as such.
Table 2 displays characteristics of apprentices working as CNAs. Among the three categories presented, 416 apprentices are in time-based training (Code 824), 922 apprentices are in entry-level competency-based training (Codes 824C and 824CB), and 356 apprentices are in advanced or specialty trainings. Specialty trainings include a dementia specialty (Code 824D) providing training to care for persons with various levels of dementia, a geriatrics specialty (Code 824G) focusing on care for older nursing home residents, a restorative specialty (Code 824R) focusing on care for persons requiring rehabilitative services after surgery or other similar event, and a mentoring specialty (Code 824M), designed to be completed after one other specialty training has been completed, which provides instruction on how to mentor other apprentices in their job responsibilities. Details on apprentice demographics by individual training can be obtained from Table A-1 in Appendix A.
| TABLE 2. Characteristics of Certified Nursing Assistants | ||||
|---|---|---|---|---|
| Characteristics | N | Time-Based (824) | Entry-Level Competency-Based (824C & 824CB) | Advanced or Specialty (824A, 824R, 824D, 824G & 824M) |
| Number of Apprentices | --- | 416 | 922 | 356 |
| Age (%) | 1,694 | --- | --- | --- |
| Under 20 | --- | 16.1 | 30.6 | 2.3 |
| 2024 | --- | 27.9 | 22.2 | 12.9 |
| 2529 | --- | 16.1 | 10.1 | 12.9 |
| 3039 | --- | 20.9 | 20.3 | 22.2 |
| 4049 | --- | 12.5 | 11.6 | 27.8 |
| 50+ | --- | 6.5 | 5.2 | 21.9 |
| Female (%) | 1,694 | 88.5 | 87.0 | 92.4 |
| Race (%) | 1,694 | --- | --- | --- |
| White | --- | 70.9 | 40.4 | 72.5 |
| African-American | --- | 22.6 | 33.8 | 19.1 |
| Hispanic | --- | 2.2 | 22.6 | 4.8 |
| Unknown Race | --- | 4.3 | 3.3 | 3.7 |
| Education (%) | 1,681 | --- | --- | --- |
| Up to 11 years of schooling | --- | 9.0 | 25.4 | 7.6 |
| GED | --- | 7.3 | 31.5 | 14.1 |
| High School Graduate | --- | 60.1 | 41.4 | 76.1 |
| Some Post-Secondary Education | --- | 23.6 | 1.8 | 2.3 |
| Enrollment Status (Last Event Code) (%) | 1,691 | --- | --- | --- |
| Registered | --- | 59.8 | 21.7 | 33.4 |
| Completed | --- | 18.3 | 43.6 | 28.9 |
| Cancelled | --- | 21.9 | 34.6 | 37.6 |
| Suspended | --- | 0.0 | 0.1 | 0.0 |
| Term Length (hours) | 1,694 | 2,305 | 1,116 | 814 |
| Related Instruction Length (hours) | 1,440 | 193 | 83 | 83 |
| Related Instruction by Sponsor (%) | 1,694 | 72.8 | 88.4 | 25.0 |
| SOURCE: RTI International/Urban Institute analysis of RAPIDS data. NOTES: Registration after 1/1/2005, most recent training | ||||
Compared to advanced or specialty trainings, both time-based and entry-level competency-based trainings enroll younger apprentices: 16% of those in time-based training, and 31% of those in entry-level competency-based training are under the age of 20, compared to only 2% among those in advanced or specialty training. Additionally, 28% of CNAs in time-based training and 22% in entry-level competency-based training are aged 20-24. In comparison, 13% of CNAs in advanced or specialty training belong to this age group. Only 6% of CNAs in time-based training and 5% in entry-level competency-based training are aged 50 and over, and among advanced or specialty trainees this proportion reaches 22%, which might be expected to be higher than entry-level training.
In all CNA trainings, most apprentices are female, but the highest proportion of females is in advanced or specialty trainings (92%). These trainings attract CNAs of different racial composition: 71% of apprentices enrolled in time-based trainings are White, compared to 40% of apprentices in entry-level competency-based training and 72% among those in advanced or specialty trainings. Similarly, entry-level competency-based training attracts the highest proportion of Hispanics -- 23%, which is much higher than 2% for time-based and 5% for advanced or specialty trainings. Seemingly, Hispanics may be more attracted to entry-level competency-based training than time-based training.
In terms of educational attainment, the profiles differ by training type. In time-based and advanced/specialty training, apprentices with 11 years of schooling or less comprise 9% and 8% respectively, while they represent a quarter of apprentices in entry-level competency-based training. On the other hand, 32% of apprentices participating in entry-level competency-based training have a GED and 41% are high school graduates, compared to 7% and 60% among apprentices in time-based training and 14% and 76% of apprentices respectively in advanced/specialty training. Time-based trainings also enroll the highest proportion of those with some post-secondary education (24%).
Regarding enrollment status, almost 60% of apprentices (249) enrolled in time-based training are registered, meaning they were currently participating in training, compared to 22% of apprentices (200) in entry-level competency-based and 33% (118) in advanced or specialty training. Apprentices in entry-level competency-based training exhibit the highest proportion of completed trainings: 44%, followed by those in advanced/specialty trainings (29%), with time-based training last (18%). Almost 22% of CNAs in time-based training are reported as having cancelled their training, followed by 35% among those in entry-level competency-based training and by 38% of those in advanced/specialty training. Only one CNA, in entry-level competency-based training, is reported as having been granted a suspension.
In line with expectations, term length is highest for time-based training with 2,305 hours, followed by 1,116 hours for entry-level competency-based training and 814 hours for advanced/specialty training.
The time-based trainings also have the highest number of hours for related instruction (193), followed by 83 hours for each entry-level competency-based and advanced/specialty training.
Time-based and competency-based trainings are characterized by a high proportion of CNAs receiving related instruction onsite (73% and 88% respectively). Only a quarter of CNAs involved in the advanced/specialty trainings receive such instruction onsite.
Table 3 displays characteristics of apprentices in the DSS occupation, who are apprentices working in facilities providing housing or services to persons with intellectual disabilities in order to promote independence and community inclusion. There are two types of training for DSSs: entry-level time-based (Code 1040), comprising 565 apprentices and entry-level competency-based (Code 1040CB) comprising 522 apprentices. There are no interim credentials or advanced specialties for DSSs, but ANCOR and NADSP are in the process of revising apprenticeship standards to develop them.
| TABLE 3. Characteristics of Direct Support Specialists | ||||
|---|---|---|---|---|
| Characteristics | N | Overall | Time-Based (1040) | Competency-Based (1040CB) |
| Number of Apprentices | --- | 1,087 | 565 | 522 |
| Age (%) | 1,087 | --- | --- | --- |
| Under 20 | --- | 5.4 | 3.0 | 8.1 |
| 2024 | --- | 15.1 | 13.5 | 16.9 |
| 2529 | --- | 9.4 | 8.5 | 10.3 |
| 3039 | --- | 21.4 | 20.7 | 22.2 |
| 4049 | --- | 21.9 | 21.6 | 22.2 |
| 50+ | --- | 26.8 | 32.7 | 20.3 |
| Female (%) | 1,087 | 79.3 | 87.7 | 74.5 |
| Race (%) | 1,087 | --- | --- | --- |
| White | --- | 89.2 | 96.1 | 81.8 |
| African-American | --- | 5.9 | 2.3 | 9.8 |
| Hispanic | --- | 1.8 | 1.6 | 2.1 |
| Unknown Race | --- | 3.0 | 0.0 | 6.3 |
| Education (%) | 1,033 | --- | --- | --- |
| Up to 11 years of schooling | --- | 0.7 | 0.8 | 0.6 |
| GED | --- | 1.7 | 0.2 | 3.2 |
| High School Graduate | --- | 95.3 | 99.1 | 91.3 |
| Some Post-Secondary Education | --- | 2.4 | 0.0 | 5.0 |
| Enrollment Status (Last Event Code) (%) | 1,086 | --- | --- | --- |
| Registered | --- | 33.5 | 9.2 | 59.9 |
| Completed | --- | 33.4 | 55.9 | 9.0 |
| Cancelled | --- | 33.1 | 34.9 | 31.1 |
| Suspended | --- | 0.0 | 0.0 | 0.0 |
| Term Length (hours) | 1,087 | 2,638 | 2,127 | 3,190 |
| Related Instruction Length (hours) | 1,075 | 239 | 226 | 252 |
| Related Instruction by Sponsor (%) | 1,087 | 92.1 | 100.0 | 83.5 |
| SOURCE: RTI International/Urban Institute analysis of RAPIDS data. NOTES: Registration after 1/1/2005, most recent training | ||||
DSSs in time-based training tend to be older: 25% of them are under the age of 30 compared to 35% among those who are enrolled in competency-based training. Similarly, almost 33% of DSSs in time-based training are aged 50 and over, compared to 20% among those who are enrolled in competency-based training. A higher proportion of apprentices in time-based training are female -- (88% versus 75%) and White (96% versus 82%). Respectively, competency-based training has a more diverse group of apprentices: almost 10% are African-American compared to 2% in time-based training.
While time-based training enrolled more apprentices who are high school graduates (99% versus 91%), competency-based training attracted 25 individuals with post-secondary education while time-based training attracted none.
Enrollment status varies substantially by training type among DSSs: only 9% of apprentices (52) in time-based training are currently registered compared to almost 60% (312) among those in competency-based training. Conversely, 56% of apprentices in time-based training have completed the apprenticeship compared to only 9% among those in competency-based training. The proportion of cancellations is similar between the types of training (35% and 31%). It appears that none of the DSSs were granted a suspension.
For these trainings, competency-based trainings involve even more hours (3,190) than time-based programs (2,127 hours). Similarly, the related instruction length is 226 hours for time-based training and 252 hours for competency-based training. All of the related instruction is conducted onsite for time-based training and 84% of teaching is done onsite for competency-based training.
Table 4 provides details for the apprenticeship program in the HSS occupation (1086AA), which is a hybrid model combining competency-based and time-based training. There are no interim credentials offered for this model (as the research was underway, a large national employer developed an interim credentialed model). Although there is only the single occupational code in the data, DOL has developed work process schedules for various roles in which HSSs may participate depending on their assigned role in an assisted living facility or home. These roles include rehabilitative aide, HHA, environmental services aide, dining services aide, certified nursing aide, certified medication aide, and activity director. It is not clear whether HSSs in these data participate in apprenticeships specifically designed for these various roles. There are 567 HSSs employed in these data.
Almost 7% of HSSs are under 20 years old and 20% are 20-24 years old. About 18% are over 50 years old. Most HSSs are female (89%) and 80% are White. About 8% are African-American. Six percent of HSSs have less than 11 years of schooling and almost 9% have a GED. However, the great majority of HSSs have graduated from high school (83%). About 3% have some post-secondary education.
Among all the major occupations, HSSs have the highest proportion (73%) of apprentices currently registered (415). Slightly over 4% have completed training, and 22% have cancelled their enrollment. Term length for this occupation is 4,139 hours, which is much larger than other occupations. The apprenticeship for HSSs involves about 400 hours of related instruction. Only 24% of programs for this training conduct their teaching onsite.
| TABLE 4. Characteristics of Health Support Specialists | ||
|---|---|---|
| Characteristics | N | 1086AA |
| Number of Apprentices | --- | 567 |
| Age (%) | 567 | --- |
| Under 20 | --- | 6.5 |
| 20-24 | --- | 19.8 |
| 25-29 | --- | 13.8 |
| 30-39 | --- | 20.6 |
| 40-49 | --- | 21.7 |
| 50+ | --- | 17.6 |
| Female (%) | 567 | 89.4 |
| Race (%) | 567 | --- |
| White | --- | 79.4 |
| African-American | --- | 7.9 |
| Hispanic | --- | 7.1 |
| Unknown Race | --- | 5.6 |
| Education (%) | 521 | --- |
| Up to 11 years of schooling | --- | 60 |
| GED | --- | 8.5 |
| High School Graduate | --- | 82.7 |
| Some Post-Secondary Education (%) | --- | 2.9 |
| Percent by Enrollment Status (Last Event Code) (%) | 567 | --- |
| Registered | --- | 73.2 |
| Completed | --- | 4.4 |
| Cancelled | --- | 22.4 |
| Suspended | --- | 0.0 |
| Term Length (hours) | 567 | 4,139 |
| Related Instruction Length (hours) | 553 | 398 |
| Related Instruction by Sponsor (%) | 567 | 23.8 |
| SOURCE: RTI International/Urban Institute analysis of RAPIDS data. NOTES: Registration after 1/1/2005, most recent training | ||
Table 5 provides details on all trainings in the HHA occupation: 71 apprentices are involved in time-based training (Code 1086), 289 apprentices are involved in entry-level competency-based training (Code 1086 CB) and 35 apprentices are involved in various specialty trainings, including disability, hospice and palliative care, dementia, or mentoring (Codes 1068A, 1068B, 1068D and 1068E respectively). Although there are two other specialty trainings for HHAs (mental illness and geriatric occupations), there were no apprentices in the data for them. Data on these specific specialties are presented in Table A-2 in Appendix A.
Age distribution varies by type of HHA training. For example, HHAs in time-based training tend to be older -- none of them are under 20 years of age, with higher proportions concentrated in the top age groups: 15% are aged 30-39, 34% are aged 40-49 and over a quarter are aged 50 and over. In contrast, almost 12% of HHAs in entry-level competency-based training are younger than 20 years old, and 45% of them are between 20 and 24 years old. Less than 4% of HHAs in entry-level competency-based training are aged 50 and over. HHAs enrolled in specialty trainings largely are on the far ends of the age distribution; 38% of them are under the age of 24, 29% are between ages of 40 and 49, and 20% are aged 50 and over.
Time-based training has the highest proportion of females (94%) and minorities (48% African-Americans, 7% Hispanic). In contrast, entry-level competency-based training enrolls 19% African-Americans and less than 1% Hispanics. Eleven percent of HHAs in specialty trainings are African-American.
| TABLE 5. Characteristics of Home Health Aides | |||||
|---|---|---|---|---|---|
| Characteristics | N | Overall | Time-Based (1086) | Entry-Level Competency-Based (1086CB) | All Specialty (1086A, 1086B, 1086D, & 1086E) |
| Number of Apprentices | --- | 395 | 71 | 289 | 35 |
| Age (%) | 395 | --- | --- | --- | --- |
| Under 20 | --- | 8.9 | 0.0 | 11.8 | 2.9 |
| 20-24 | --- | 38.0 | 12.7 | 44.6 | 34.3 |
| 25-29 | --- | 16.5 | 12.7 | 18.3 | 8.6 |
| 30-39 | --- | 13.9 | 15.5 | 14.5 | 5.7 |
| 40-49 | --- | 13.7 | 33.8 | 6.9 | 28.6 |
| 50+ | --- | 9.1 | 25.4 | 3.8 | 20.0 |
| Female (%) | 395 | 88.1 | 94.4 | 85.8 | 71.4 |
| Race (%) | 395 | --- | --- | --- | --- |
| White | --- | 72.9 | 40.9 | 78.9 | 88.6 |
| African-American | --- | 23.5 | 47.9 | 19.0 | 11.4 |
| Hispanic | --- | 1.8 | 7.0 | 0.7 | 0.0 |
| Unknown Race | --- | 1.8 | 4.2 | 1.4 | 0.0 |
| Education (%) | 395 | --- | --- | --- | --- |
| Up to 11 years of schooling | --- | 4.6 | 16.9 | 1.7 | 2.9 |
| GED | --- | 8.1 | 8.5 | 7.3 | 14.3 |
| High School Graduate | --- | 85.1 | 74.7 | 88.6 | 77.1 |
| Some Post-Secondary Education | --- | 2.3 | 0.0 | 2.4 | 5.7 |
| Enrollment Status (Last Event Code) (%) | 395 | --- | --- | --- | --- |
| Registered | --- | 25.1 | 14.1 | 25.3 | 45.7 |
| Completed | --- | 13.2 | 56.3 | 2.1 | 17.1 |
| Cancelled | --- | 61.5 | 28.2 | 72.7 | 37.1 |
| Suspended | --- | 0.3 | 1.4 | 0.0 | 0.0 |
| Term Length (hours) | 395 | 1,874 | 1,656 | 2,000 | 1,281 |
| Related Instruction Length (hours) | 395 | 125 | 184 | 113 | 106 |
| Related Instruction by Sponsor (%) | 395 | 96.0 | 100.0 | 100.0 | 54.3 |
| SOURCE: RTI International/Urban Institute analysis of RAPIDS data. NOTES: Registration after 1/1/2005, most recent training | |||||
Time-based training also seems to attract the highest proportion of workers with 11 years of schooling or less (17%). In comparison, other HHA trainings attract less than 3% of apprentices with 11 years of schooling or less. None of the apprentices in time-based training have any post-secondary education. Educational attainment is higher for those involved in entry-level competency-based training (2.4% have some post-secondary education) and specialty trainings (6% have some post-secondary education).
In terms of enrollment status, time-based training has the lowest proportion (14%) of currently registered apprentices (10) followed by entry-level competency-based training (25%; 73 apprentices) and specialty trainings (46%; 16 apprentices). However, the proportion of trainings completed shows a different trend: HHAs in time-based training have the highest proportion of completion at 56%, followed by specialty trainings at 17% with apprentices in entry-level competency-based training having the lowest proportion of completion of only 2%.
Cancelation rates are high in this group: 28% of apprentices in time-based training, 73% of apprentices in entry-level competency-based training and 37% of apprentices in HHA specialty trainings have cancelled their involvement. One HHA, in time-based training, was granted a suspension.
Regarding the length of apprenticeship, term length is lowest for specialty trainings (1,281 hours) and highest in entry-level competency-based training (2,000). Apprenticeships in time-based training average 1,656 hours.
On average, there are 125 hours of related instruction. Time-based training is characterized by the longest related instruction of 184 hours, followed by the 113 hours in entry-level competency-based training. The mean for related instruction for specialty trainings is 106 hours. For time-based and entry-level competency-based training, all of the instruction is provided onsite by sponsors. Slightly over half of those in specialty training are trained at the sponsors site.
3.2. Program-Level Analyses
Program-level analyses describing program characteristics, geographic location, apprenticeship characteristics and training information on source/mode of related instruction are presented in Tables 6-10 and include descriptive results on 121 apprenticeship programs in the RAPIDS database. The sample size for these program-level analyses can be very small (single digits), so the results should be interpreted with caution.
Table 6 presents data on program-level statistics by the four large occupational groups. Of the 121 programs in the database, 56 programs (46%) enroll CNAs with an average total workforce (defined as apprentices plus all other employees) of 1,803 persons across an average of 16 sites, 18 programs (15%) enroll DSSs with a mean total workforce of 259 apprentices across a mean of 16 sites, 34 programs (28%) enroll HSSs with an average total workforce of 147 apprentices, and 13 programs (11%) enroll HHAs with a mean total workforce of 311 apprentices. The assisted living facilities employing HSSs and the home health agencies employing HHAs each have only an average of one site. Only CNA and DSS programs involve multiple sites (18% and 11% respectively). None of the assisted living facilities or home health agencies operate their apprenticeship programs across more than one site.
There are six nationally-sponsored apprenticeship programs, representing 5% of all programs in the RAPIDS database. Only CNA programs have any national sponsored programs (11% of these programs).
| Highlights of Program-Level Analyses
|
The geographic distribution of all programs is as follows: five programs each are located in Northeast and Mid-Atlantic (4% each), 12 programs are located in Southeast (10%), 16 programs in the Central region (14%), 61 program in the Midwest (53%) and six programs in the West (14%). CNA programs are distributed in every geographic region. Not all programs are represented in each geographic region. For example, there are no DSS programs in the Mid-Atlantic region, no HSS programs in the Northeast and Mid-Atlantic regions and no HHA programs in the Northeast and West regions. The largest concentration of programs by region for each occupation is in the Midwest region (48% for CNA programs, 38% for DSS programs, 68% for HSS programs and 77% for HHA programs).
The overall mean length of apprenticeship program is 2,621 hours across all programs. CNA programs have 1,720 hours on average, compared to 3,296 hours for DSS programs, 4,256 hours for HSS programs, and 1,289 hours for HHA programs. The average length of related instruction of 319 hours is distributed as follows: 330 hours for CNA programs, 349 hours for DSS programs, 361 hours for HSS programs and 122 hours for HHA programs. Related instruction in each of these occupations is longer than the federally required 75 hours of instruction.
The program-level RAPIDS data provide the opportunity to examine where and how the related instruction takes place. However, RAPIDS mixes the source (where) and the mode (how) within the same categorical variable, so it is not possible to completely disentangle the issues of location of training and method of training delivery because only a few programs respond to both issues. Rather than losing one of these characteristics (source and mode) by omitting them from the analysis, we report on both characteristics together as found in the single RAPIDS variable. Over 26% of all related instruction takes place onsite where each sponsor is located. Community colleges provide instruction for 38% of all programs, and vocational schools provide instruction for 23% of all programs. Ten percent of programs are offered on line (web-based), 9% are offered by correspondence course, and slightly less than 2% are located at technical schools.
| TABLE 6. Characteristics of Long-Term Care Programs by Occupational Group | ||||||
|---|---|---|---|---|---|---|
| Characteristics | N | Overall | Major Occupational Group: CNA (824) | Major Occupational Group: DSS (1040) | Major Occupational Group: HSS (1086AA) | Major Occupational Group: HHA (1086) |
| Number of Employers | --- | 121 | 56 | 18 | 34 | 13 |
| Employer Characteristics | ||||||
| Mean Employer Total Workforce | 121 | 948 | 1,803 | 259 | 147 | 311 |
| Mean Number of Affiliated Sites | 121 | 10 | 16 | 16 | 1 | 1 |
| Percent with Multiple Sites | 121 | 9.9 | 17.9 | 11.1 | 0.0 | 0.0 |
| National Program | 6 | 5.0 | 10.7 | 0.0 | 0.0 | 0.0 |
| Geographic Characteristics (%) | 115 | --- | --- | --- | --- | --- |
| Northeast-DOL Region 1 | --- | 4.35 | 6.0 | 11.1 | 0.0 | 0.0 |
| Mid-Atlantic-DOL Region 2 | --- | 4.35 | 8.0 | 0.0 | 0.0 | 7.7 |
| Southeast-DOL Region 3 | --- | 10.43 | 18.0 | 5.6 | 2.9 | 7.7 |
| Central-DOL Region 4 | --- | 13.91 | 10.0 | 22.2 | 17.7 | 7.7 |
| Midwest-DOL Region 5 | --- | 53.0 | 48.0 | 22.2 | 67.7 | 76.9 |
| West-DOL Region 6 | --- | 13.9 | 10.0 | 38.9 | 11.8 | 0.0 |
| Apprenticeship Characteristics | ||||||
| Mean Term Length | 121 | 2,621 | 1,720 | 3,296 | 4,256 | 1,289 |
| Mean Related Instruction Length | 117 | 319 | 331 | 349 | 361 | 122 |
| Source/Mode of RI* | ||||||
| Onsite | 121 | 26.5 | 26.9 | 33.3 | 2.9 | 76.9 |
| Community College | 121 | 38.0 | 19.6 | 44.1 | 73.5 | 15.4 |
| Technical School | 121 | 1.7 | 0.0 | 0.0 | 5.9 | 0.0 |
| Vocational School | 121 | 22.8 | 44.6 | 8.6 | 0.0 | 7.7 |
| Correspondence | 121 | 9.1 | 0.0 | 33.3 | 14.7 | 0.0 |
| Web-based | 121 | 10.0 | 7.1 | 22.2 | 12.1 | 0.0 |
| SOURCE: RTI International/Urban Institute analysis of RAPIDS data. NOTES: Registration after 1/1/2005, most recent training * Source/Mode of Related Instruction -- categories are not mutually exclusive: one program can have instruction from several sources. | ||||||
The source/mode of related instruction varies by program type. Among CNA programs, the most frequent source/mode was a vocational school (45%), followed by onsite sponsor location (27%), and community college (29%). For DSS programs, the most frequent source/mode was a community college (44%), followed by correspondence course and onsite sponsor location (33% each) and web-based programs (22%). For HSS programs, the most frequent source/mode was a community college (73%), followed by correspondence course (15%) and web-based (12%). Among apprenticeship programs for HHAs, most related instruction was conducted onsite (77%), followed by community college (15%) and vocational school (8%).
We also conducted the same sensitivity analyses for these program-level statistics by removing the four large employers noted in the prior section on apprentice-level findings. The change in results though was much less substantial. Only total workforce size for DSSs, HSSs, and HHA employers became smaller after removing the four programs. No other program-level characteristics changed greatly.
| TABLE 7. Characteristics of Certified Nursing Assistant Programs | |||||
|---|---|---|---|---|---|
| Characteristics | N | Overall | Time-Based (824) | Entry-Level Competency-Based (824C & 824CB) | Advanced or Specialty (824A, 824R, 824D, 824G & 824M) |
| Employer Characteristics | --- | --- | --- | --- | --- |
| Number of Employers | --- | 56 | 28 | 13 | 15 |
| Mean Employer Total Workforce | 56 | 1,803 | 232 | 3,109 | 3,604 |
| Mean Number of Affiliated Sites | 56 | 16 | 2 | 24 | 37 |
| Percent with Multiple Sites | 56 | 17.9 | 7.1 | 23.1 | 33.3 |
| National Program | 6 | 10.7 | 0.0 | 15.5 | 26.7 |
| Geographic Characteristics (%) | --- | --- | --- | --- | --- |
| Northeast-DOL Region 1 | 3 | 6.0 | 3.6 | 0.0 | 18.2 |
| Mid-Atlantic-DOL Region 2 | 4 | 8.0 | 7.1 | 0.0 | 18.3 |
| Southeast-DOL Region 3 | 9 | 18.0 | 14.3 | 9.1 | 36.4 |
| Central-DOL Region 4 | 5 | 10.0 | 10.7 | 18.2 | 0.0 |
| Midwest-DOL Region 5 | 24 | 48.0 | 57.1 | 72.7 | 0.0 |
| West-DOL Region 6 | 5 | 10.0 | 7.1 | 0.0 | 27.3 |
| Apprenticeship Characteristics | |||||
| Mean Term Length | 56 | 1,720 | 2,240 | 1,071 | 1,312 |
| Mean Related Instruction Length | 52 | 331 | 525 | 155 | 121 |
| Source/Mode of RI* | |||||
| Onsite | 56 | 26.9 | 17.9 | 38.5 | 33.8 |
| Community College | 56 | 19.6 | 10.7 | 15.4 | 40.0 |
| Technical School | 56 | 0.0 | 0.0 | 0.0 | 0.0 |
| Vocational School | 56 | 44.6 | 60.7 | 38.5 | 20.0 |
| Correspondence | 56 | 0.0 | 0.0 | 0.0 | 0.0 |
| Web-based | 56 | 7.1 | 7.1 | 0.0 | 13.3 |
| SOURCE: RTI International/Urban Institute analysis of RAPIDS data. NOTES: Registration after 1/1/2005, most recent training * Source/Mode of Related Instruction -- categories are not mutually exclusive: one program can have instruction from several sources. | |||||
Table 7 presents the same characteristics as in Table 6, but only for CNA programs, comparing time-based (28 programs), competency-based (13 programs), and specialty programs (15 programs). Most of the time-based programs are concentrated in the Midwest, Southwest and Central regions. No CNA programs are nationally sponsored in the time-based program. In addition to national programs which represent 16%, entry-level competency-based CNA programs are only available in three regions -- the Midwest, Southwest and Central regions. Advanced and specialty programs for CNAs are available in the Southeast, West, Northeast and Mid-Atlantic regions. Twenty-seven percent of advanced and specialty CNA training programs are national.
Regarding term length, time-based CNA programs are on average the longest (2,240 hours), compared to 1,312 hours for advanced/specialty programs and 1,071 hours for entry-level competency-based programs.
| TABLE 8. Characteristics of Direct Support Specialist Programs | ||||
|---|---|---|---|---|
| Characteristics | N | Overall | Time-Based (1040) | Competency-Based (1040CB) |
| Employer Characteristics | ||||
| Number of Employers | --- | 18 | 1 | 17 |
| Mean Employer Total Workforce | 18 | 259 | 700 | 233 |
| Mean Number of Affiliated Sites | 18 | 16 | 1 | 17 |
| Percent with Multiple Sites | 18 | 11.1 | 0.0 | 11.8 |
| National Program | 0.0 | 0.0 | 0.0 | 0.0 |
| Geographic Characteristics (%) | 18 | --- | --- | --- |
| Northeast-DOL Region 1 | --- | 11.1 | 0.0 | 11.8 |
| Mid-Atlantic-DOL Region 2 | --- | 5.6 | 0.0 | 5.9 |
| Southeast-DOL Region 3 | --- | 0.0 | 0.0 | 0.0 |
| Central-DOL Region 4 | --- | 22.2 | 0.0 | 23.5 |
| Midwest-DOL Region 5 | --- | 22.2 | 100.0 | 17.7 |
| West-DOL Region 6 | --- | 38.9 | 0.0 | 41.2 |
| Apprenticeship Characteristics | ||||
| Mean Term Length | 18 | 3,296 | 2,127 | 3,365 |
| Mean Related Instruction Length | 18 | 349 | 226 | 356 |
| Source/Mode of RI* | ||||
| Onsite | 18 | 33.3 | 100.0 | 29.4 |
| Community College | 18 | 44.1 | 0.0 | 46.6 |
| Technical School | 18 | 0.0 | 0.0 | 0.0 |
| Vocational School | 18 | 8.6 | 0.0 | 9.1 |
| Correspondence | 18 | 33.3 | 0.0 | 35.3 |
| Web-based | 18 | 22.2 | 0.0 | 23.5 |
| SOURCE: RTI International/Urban Institute analysis of RAPIDS data. NOTES: Registration after 1/1/2005, most recent training * Source/Mode of Related Instruction -- categories are not mutually exclusive: one program can have instruction from several sources. | ||||
Related instruction length and source/mode also varies by type of training: time-based programs average 525 hours of related instruction and are mostly conducted at vocational schools (61%) and onsite (18%), compared to a mean of 155 hours for entry-level competency-based programs and an average of 121 hours for advanced/specialty programs. About 7% of related instruction for time-based programs is web-based. Entry-level competency-based programs are equally likely to be conducted at vocational schools and onsite (38% each) followed by community colleges. None of the entry-level competency-based programs are conducted via the web or by correspondence, or at technical schools. Related instruction for the advanced/specialty programs is most frequently conducted at community colleges, followed by onsite training and vocational schools. About 13% of related instruction for advanced/specialty programs is web-based. Additional detailed information for each specialty competency for CNAs is shown in Table A-3 in Appendix A.
Table 8 presents the program characteristics for DSS programs comparing the one entry-level time-based program versus the 17 entry-level competency-based programs. In terms of geographic location, the only time-based program is located in the Midwest. There are no national programs. Entry-level competency-based programs are distributed across the country and are located in every region with the exception of the Southwest with the highest concentration in the West and Central regions.
The one time-based program has a term length of 2,127 hours with 266 hours of related instruction which is conducted onsite by its sponsor. On average, the entry-level competency-based DSS programs are 3,365 hours long and have a mean of 356 hours of related instruction. Related instruction for these programs is most commonly conducted at a community college (47%), followed by training by correspondence (35%), onsite training by the sponsor (29%) and web-based training (23%).
| TABLE 9. Characteristics of Health Support Specialist Programs | ||
|---|---|---|
| Characteristics | N | 1040AA |
| Employer Characteristics | --- | --- |
| Number of Employers | --- | 34 |
| Mean Employer Total Workforce | 34 | 147 |
| Mean Number of Affiliated Sites | 34 | 1 |
| Percent with Multiple Sites | 34 | 0.0 |
| National Program | 0 | 0.0 |
| Geographic Characteristics (%) | 34 | --- |
| Northeast-DOL Region 1 | --- | 0.0 |
| Mid-Atlantic-DOL Region 2 | --- | 0.0 |
| Southeast-DOL Region 3 | --- | 2.9 |
| Central-DOL Region 4 | --- | 17.7 |
| Midwest-DOL Region 5 | --- | 67.7 |
| West-DOL Region 6 | --- | 11.8 |
| Apprenticeship Characteristics | ||
| Mean Term Length | 34 | 4,256 |
| Mean Related Instruction Length | 34 | 360 |
| Source/Mode of RI* | ||
| Onsite | 34 | 2.9 |
| Community College | 34 | 73.5 |
| Technical School | 34 | 5.9 |
| Vocational School | 34 | 0.0 |
| Correspondence | 34 | 14.7 |
| Web-based | 34 | 12.1 |
| SOURCE: RTI International/Urban Institute analysis of RAPIDS data. NOTES: Registration after 1/1/2005, most recent training * Source/Mode of Related Instruction -- categories are not mutually exclusive: one program can have instruction from several sources. | ||
Table 9 presents the program-level data for HSS programs. The mean workforce size across the 34 programs was 147 workers. Geographically, 23 of the programs (68%) are in the Midwest, with the remainder spread fairly evenly across the Central and West regions, and only one in the Southeast. The mean term length was 4,256 hours, and the average length of related instruction was 360 hours. Regarding the source/mode of related instruction, community colleges provided 74% of training, 15% was provided through correspondence courses, and 12% was via web-based courses.
Table 10 compares characteristics on the 13 HHA programs across the five time-based programs (38% of the total), the two entry-level competency-based programs (15% of the total) and the six specialty programs (46% of these programs). The mean employer workforce size is largest for the entry-level competency-based programs (840) as compared to the much smaller workforces in the time-based (307) and specialty (137) programs. None of the programs has multiple sites (each program is a standalone program).
| TABLE 10. Characteristics of Home Health Aide Programs | |||||
|---|---|---|---|---|---|
| Characteristics | N | Overall | Time-Based (1086) | Entry-Level Competency-Based (1086CB) | All Specialty (1086A, 1086B, 1086D, & 1086E) |
| Employer Characteristics | |||||
| Number of Employers | --- | 13 | 5 | 2 | 6 |
| Mean Employer Total Workforce | 13 | 311 | 307 | 840 | 137 |
| Mean Number of Affiliated Sites | 13 | 1 | 1 | 1 | 1 |
| Percent with Multiple Sites | 13 | 0.0 | 0.0 | 0.0 | 0.0 |
| National Program | 0 | 0.0 | 0.0 | 0.0 | 0.0 |
| Geographic Characteristics (%) | 13 | --- | --- | --- | --- |
| Northeast-DOL Region 1 | --- | 0.0 | 0.0 | 0.0 | 0.0 |
| Mid-Atlantic-DOL Region 2 | --- | 7.7 | 20.0 | 0.0 | 0.0 |
| Southeast-DOL Region 3 | --- | 7.7 | 0.0 | 50.0 | 0.0 |
| Central-DOL Region 4 | --- | 7.7 | 0.0 | 0.0 | 16.7 |
| Midwest-DOL Region 5 | --- | 76.9 | 80.0 | 50.0 | 83.3 |
| West-DOL Region 6 | --- | 0.0 | 0.0 | 0.0 | 0.0 |
| Apprenticeship Characteristics | |||||
| Mean Term Length | 13 | 1,289 | 1,211 | 2,000 | 1,117 |
| Mean Related Instruction Length | 13 | 122 | 168 | 128 | 82 |
| Source/Mode of RI* | |||||
| Onsite | 13 | 76.9 | 100.0 | 50.0 | 66.7 |
| Community College | 13 | 15.4 | 0.0 | 50.0 | 16.7 |
| Technical School | 13 | 0.0 | 0.0 | 0.0 | 0.0 |
| Vocational School | 13 | 0.0 | 0.0 | 0.0 | 16.7 |
| Correspondence | 13 | 0.0 | 0.0 | 0.0 | 0.0 |
| Web-based | 13 | 0.0 | 0.0 | 0.0 | 0.0 |
| SOURCE: RTI International/Urban Institute analysis of RAPIDS data. NOTES: Registration after 1/1/2005, most recent training * Source/Mode of Related Instruction -- categories are not mutually exclusive: one program can have instruction from several sources. | |||||
Geographically, most of the time-based programs are located in the Midwest (80%), with the others located in the Mid-Atlantic region. The entry-level competency-based programs are in the Southeast and the Midwest. One specialty program is located in the Central region and five are in the Midwest.
Term length in time-based programs averages 1,211 hours with a mean of 168 hours of related instruction which is conducted onsite by employers. The two entry-level competency-based programs average 2,000 hours of instruction and average 128 hours of related instruction with one conducted onsite by the sponsor and one conducted at a community college. Term length in specialty programs averages 1,117 hours with a mean of 82 hours of related instruction, which is mostly conducted onsite (67%), followed by community colleges and vocational schools (17% each). Additional detailed information for each specialty training for HHAs is shown in Table A-4 in Appendix A.
Appendix A Table A-5 and Table A-6 provide a list of the programs contained in the data and the number of apprentices they contribute by major occupation. Table A-5 lists all programs (121) regardless of whether they had currently enrolled (registered) apprentices at the date of the RAPIDS data extract (December 2009). Table A-6 lists only those programs (79) with currently enrolled (registered) apprentices as of December 2009. We discuss results across these two tables to provide sufficient context for understanding.
The most common program is located within a relatively small (100 total employees) nursing home or assisted living center, which may or may not be part of a chain. Several entities operate small group homes for persons with intellectual disabilities with approximately 25 employees in each home. A detailed review of the data provides an understanding of several large programs that skew the results on total workforce size and apprentices upward. Several large hospital systems and large providers of group homes employ substantial numbers of apprentices. For example, St. Johns Mercy Medical Center in St. Louis, Missouri, has employed 644 apprentices over time and now trains 324. Developmental Services, Inc. in Indiana, which services group homes for persons with intellectual disabilities has provided 924 apprenticeships over time and 274 currently. Nearly 400 apprentices have been sponsored by the Gary Job Corps in Texas, but none were currently enrolled as of December 2009.
In addition, several large nursing home programs contribute large numbers of apprentices. The Evangelical Lutheran Good Samaritan Society is a chain of nursing homes with 122 branches (nursing homes), each having approximately 100 employees, contributed 254 apprentices overall but only 84 currently. The Georgia Health Care Association program is an association with 55 participating nursing homes averaging 100 employees each, contributed 120 apprentices overall and 69 current apprentices.
The three largest contributors of currently enrolled CNAs are St. Johns Mercy Medical Center in St. Louis (174), the Evangelical Lutheran Good Samaritan Society in South Dakota (84), and the Georgia Health Care Association located in suburban Atlanta (69). The three largest contributors of currently enrolled DSSs are Developmental Services, Inc. in Indiana (274), Macomb Oakland Regional Center in Michigan (22), and Hope Community Resources in Alaska (19). The three largest contributors of currently enrolled HSSs are St. Johns Mercy Medical Center in St. Louis (82), Comfort Keepers in San Diego (43), and Memorial Health System in Kansas (39). The three largest contributors of currently enrolled HHAs are St. Johns Mercy Medical Center in St. Louis (68), Harbor Home Healthcare in Michigan (9), and Home Care Associates of Philadelphia (8).
3.3. Findings from Interviews with Program Sponsors
We conducted interviews with staff from two organizations selected by OA staff to inform our understanding of the quality of RAPIDS data and the data entry process. These organizations were Evangelical Lutheran Good Samaritan Society, a large owner of nursing homes, and the Georgia Health Care Association, an association for nursing homes in Georgia. Topics included the overall data entry process, sources of information for wage data, and problems encountered during RAPIDS data entry and recommendations for improvement. Generally, one person is responsible in these organizations for entering data into RAPIDS from information contained in enrollment forms at the beginning of an apprenticeship. Thereafter, both programs entered data at the completion of trainings or on an as needed basis. On a 10-point scale, with 10 being the best quality and 1 being the worst quality, one program rated information contained in an apprentices application form at a 7, requiring follow-up with an apprentice to obtain or clarify information. After all data were collected though, these programs rated data entry at a 9-10.
Regarding problems entering data, or changes needed in the RAPIDS system, one program experienced problems in transitioning data electronically between the advanced training data fields and specialty training data fields, saying that instead of entering the data into RAPIDS, they sent the data in an e-mail to DOL. Another program said that using RAPIDS was cumbersome and not user friendly. For example, one cannot go back to the previous screen. One program stated that it would be useful to add one more data field to track the entire length of time of ones apprenticeship across all trainings completed.
Wage data entered into RAPIDS are hourly data. Entry and exit wages were the apprentices actual wage at apprenticeship entry and exit. The pre-apprenticeship wages entered are the same as the entry wage. One program granted an automatic 25 cent hourly increase in wages for completing a training, while another program provided a wage increase or bonus only at the discretion of various nursing homes within the larger organization, largely dependent on whether there were budgeted funds at the time to do so.
4. Discussion
LTC RAPs offer a distinctive model for expanding the amount of training and expertise of long-term care workers. If successful, the program will improve the productivity of workers and reduce turnover, thereby making wage increases possible without adding to the costs. Moreover, LTC RAPs will give employers confidence that their trained workers have the appropriate competencies. The descriptive analysis of the RAPIDS data provides a starting point for understanding the nature of the current status of LTC RAPs. This section discusses the relevance of the findings for the current task order.
4.1. Apprentice-Level Findings
Over the 5-year analysis period from January 2005 to December 2009, there were 3,744 apprentices (of which 1,445 apprentices are currently active (registered)) representing four broad occupations -- CNAs, DSSs, HSSs and HHAs. While age distributions varied across occupations, a majority of apprentices were age 30 and older (although a majority of apprentices in the CNA and HHA occupations were under age 30).
In comparison to national data such as the National Nursing Assistant Survey and the National Home Health Aide Survey, RAPIDS data show that apprentices are considerably younger, less educated and include more males than CNAs and HHAs working in the field nationally. Generally, it appears that apprenticeships for these two occupations are functioning as an early/entry career training program for people just starting out rather than for retraining of existing workers. No similar comparison data are available for DSSs and HSSs, both of which lack a clear set of national training requirements. Therefore, apprenticeships for these latter occupations may be serving as a type of credentialing in the absence of formal national training requirements.
Most of the apprentices are female, but there is a higher representation of males among DSSs, perhaps because persons with intellectual disabilities have a higher proportion of male clients, potentially necessitating a larger male presence in facilities serving this population. It may also be related to the fact that direct support work in this occupation involves less hands-on personal care.
Generally, apprentices comprise a group with low educational attainment. Apprentices rarely have college education and high proportions of some occupations did not complete high school, not surprising given that these are low-wage jobs. Again, comparisons to the National Nursing Assistant Survey and the National Home Health Aide Survey demonstrate that apprentices have lower levels of education than CNAs and HHAs working in nursing facilities and home health agencies nationally. In part, apprentices may be participating in apprenticeships to try to compensate for their lack of formal education.
LTC RAPs provide training to many minorities. RAPIDS analyses show that apprenticeship programs manage to recruit a relatively diverse group of people; overall, 30% are non-White or Hispanic. There is substantial variation in terms of diversity across occupations: the CNA occupation attracts the most diverse group of apprentices compared to DSSs that enroll the least diverse group of apprentices.
A key issue for these programs is the proportion of apprentices completing training versus the proportion who has cancelled their participation. Since January 2005, over 27% of workers in the data have completed an apprenticeship, versus 34% who have cancelled their involvement over time. Even in calendar year 2009 alone, more than twice as many apprentices had cancelled their participation (18%) as those who completed their training (7%) although not everyone who may have started in 2009 may have had enough time to potentially complete it by years end.
Among CNAs and DSSs, who together account for the large majority of apprentices in the data, although one-third of apprentices in each occupation have completed their training, one-third in each occupation has cancelled their training. Only 13% of HHAs had completed their training, coupled with a very high proportion of cancelled trainings (62%). It is troubling that the proportion of cancellations is at least as high or higher than the proportion of completions. Long-term care workers have a very high turnover rate, partly because of low wages. The wage rates in LTC RAPs are still low, so it is not surprising that many do not complete training. An issue for a future evaluation is how well apprentices compare to non-apprentices on measures such as turnover.
The apprenticeships average 2,100 hours in length, approximately one year, which includes about 200 hours of related instruction, which is offered by the employer for about three-quarters of participants. This level of related instruction is far beyond the minimum federal training requirements of 75 hours for CNAs and HHAs. Although many states mandate more than 75 hours, they do not reach the 200 hours of related instruction that is required under the LTC RAP.
4.2. Program-Level Findings
Overall, 121 programs are included in the database and described in this analysis. Almost half (46%) of all programs are for CNAs, about one-fourth are for HSSs (28%), 15% are for DSSs, and only 10% are for HHAs. There are only 35 apprentices in the HHA specialty competencies, too few to warrant further refined analyses of those specialty programs at this time.
The mean total workforce size of the CNA programs (1,803) dwarfs the total workforce size for the programs for the remaining major occupations, whose workforces range in the low hundreds, but this is the result of a few large hospital systems with nursing home businesses affiliated with them. Although there is current major demand for CNAs nationally, it is unlikely that nursing homes will be the setting of the biggest growth in long-term care jobs. Only programs with CNA and DSS apprenticeships involve multiple sites, with the remainder having only one location. Only six programs are nationally sponsored (all are for CNAs). Half of the programs (61) are in one DOL region (the Midwest), while the rest are spread fairly uniformly over the remainder of the DOL regions. DSS programs are the only major program type where a majority or plurality of programs is not in the Midwest, but in the West, where seven of the programs (39%) are located.
Although not all programs report data on the length of the overall apprenticeship and its related instruction component, those that do average about 2,000 hours overall and 319 hours for the related instruction component. The largest overall apprenticeship length is for DSSs, which averages 3,267 hours, which is twice as long as that of the next longest apprenticeship overall length (1,783) for CNAs. Potentially, DSSs might have been given more credit for prior time worked than other major occupations.
Regarding related instruction, community colleges and vocational schools provide important contributions in addition to those of program sponsors, who may not be able to provide such training if their organization is relatively small. The most common source of related instruction is community colleges (38% of all programs), followed by the sponsors themselves providing onsite training (27%) and then through vocational schools (23%). This differed by major occupation, with 45% of CNA programs using vocational schools for this component, 44% of DSS programs and 75% of HSS programs favoring community colleges, and 77% of home health agencies providing this instruction onsite at the employer.
4.3. Assessment of RAPIDS Data for Use in Planning for or Conducting a LTC RAPs Evaluation
The RAPIDS data provide insight into many characteristics of apprentices, apprenticeships, and sponsoring programs. Most importantly, given they include the universe of apprentices and programs, counts of each provide a broad measure of entrants at any time or the total number of apprentices or programs over time. As such, these data can be used for program reporting, for monitoring overall enrollment trends, and for showing a range of worker and program characteristics. For example, data on the variety of sources of related instruction (e.g., community college, correspondence course) reveal several ways programs interface with the community when training apprentices.
Of special interest to this project is the use of the data by the RTI/Urban team to help identify programs for site visits and for thinking about what is possible for a large-scale evaluation. Specifically, the list of programs by region and counts of currently enrolled apprentices by major occupational group can be used for helping select sites to visit in the current project. After identifying a subset of possible programs to visit, the RAPIDS data could be used to narrow the subset according to other characteristics in the data. For example, decisions about choices of site visits will be informed by data on programs that have several apprentices in the advanced or specialty occupations or programs that have both a large proportion of cancellations and a large number of currently enrolled apprentices.
Because the RAPIDS data are usually entered by sponsors and not through a centralized data entry function, much of the RAPIDS data lack certain characteristics for use in quantitative analysis for a future evaluation. First, there are large amounts of missing data in many data fields. Second, timeliness of data entry or updates may vary across employers, which would be important for data that is particularly time dependent (e.g., wages, enrollment status). Third, some problems encountered by employers interviewed for this report may prevent employers generally from entering completely reliable data.
Fourth, while some data probably have little or no measurement error in terms of data entry accuracy because they change little over time or are observed without error (e.g., demographic characteristics), other data had obvious problems due to either data entry error or variability in coding the same data fields by different programs. For example, according to DOL staff, the starting wage could be entered as either the actual beginning wage of an apprentice or the wage entered on the apprentice agreement, which may or may not be the actual wage. As a result, our preliminary analysis of the wage data showed that the pre-apprentice wage may be larger than the starting wage, and the ending wage may be less than the starting wage. Because of these issues, for quantitative data that may have a narrow range or are expected to change but only by small amounts over time (e.g., wages), a future evaluation contractor would probably need to collect such data in a centralized fashion and employ a range of data entry quality control measures to reduce potential measurement error.
Fifth, the data lack certain important measures of the effects of apprenticeship over time. For example, because RAPIDS includes no data on whether an apprentice is still employed at the same or another employer, one cannot estimate placement and retention rates. Such data could potentially be acquired from unemployment insurance data records. In addition, the system lacks data on employer costs and benefits because the OA does not have the authority to collect it. Finally, the RAPIDS system does not include data on one of largest future sources of apprenticeships, the expected large-scale implementation of apprenticeships in Washington State. Given the size and scope of that future project (and potential other large projects in various states), any future evaluation will have to obtain data that goes beyond the current RAPIDS database.
The RAPIDS data are useful for monitoring enrollment trends and understanding various characteristics of apprentices and programs. But, additional data sources designed explicitly for any future evaluation effort will be needed to support quantitative analysis, especially key outcomes such as turnover and program costs. Further, at their current scale, most LTC RAP programs are too small and too dispersed geographically to support detailed analyses and separate evaluations. Any future evaluation will depend on having a large enough number of apprentices participating in apprenticeships over time to provide a large enough sample in each occupation for evaluation. As of December 2009, only 1,444 apprentices were currently participating in training (registered), with only approximately 300-600 apprentices in each major occupation, except for HHAs, of which there were only approximately 100 currently registered apprentices.
5. References
ApprenticeableLong-Term Care Occupations. (2009). Office of Apprenticeship, U.S. Department of Labor, Employment and Training Administration.
Code of Federal Regulations, Title 29, Chapter 1, Part 29, Labor Standards for the Registration of Apprenticeship Programs. http://ecfr.gpoaccess.gov/cgi/t/text/text-idx?type=simple;c=ecfr;cc=ecfr;sid=143d19382ea018fb14e80c66aaa9de4e;idno=29;region=DIV1;q1=Labor%20Standards%20for%20the%20Registration%20of%20Apprenticeship%20Programs;rgn=div5;view=text;node=29%3A1.1.1.1.23 accessed on 09/06/11.
Institute of Medicine. (2008). Retoolingfor an aging America: Building the health care workforce. Washington, DC: The National Academies Press.
PHI Training and Organizational Development Services Ladder. http://phinational.org/training/resources/apprenticeships/ accessed on 03/31/10.
RFTO ASPE LTC RAP. (2009). Design Feasibility Study to Evaluate the Long-Term Care Registered Apprenticeship Program.
U.S. Department of Labor, Bureau of Labor Statistics.(2009). Occupational outlook handbook, 2010-11 edition: nursing, psychiatric, and home health aides. http://www.bls.gov/oco/ocos326.htm accessed on 01/29/11.
Notes
-
An apprenticeable occupation is one that is specified by an industry and that must:
- Involve skills that are customarily learned in a practical way through a structured, systematic program of on-the-job supervised learning;
- Be clearly identified and commonly recognized throughout an industry;
- Involve the progressive attainment of manual, mechanical or technical skills and knowledge which, in accordance with the industry standard for the occupation, would require the completion of at least 2,000 hours of OJT to attain; and
- Require related instruction to supplement OJT.
(Source: DOL/OA, 2010)
Appendices
Appendix A. Detailed Tables on Certified Nursing Assistants, Home Health Aides, and Apprenticeship Sponsors
| TABLE A-1. Characteristics of Certified Nursing Assistants by Occupational Group | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Characteristics | N | Overall | OC: Time-Based (824) | OC: 824A | OC: 824C | OC: 824D | OC: 824G | OC: 824M | OC: 824R | OC: 824CB | OC: Entry-Level Competency-Based (C and CB) | OC: Advanced or Specialty |
| Apprentices | --- | 1,694 | 416 | 248 | 811 | 20 | 31 | 41 | 16 | 111 | 922 | 356 |
| Age (%) | ||||||||||||
| Under 20 | 357 | 21.1 | 16.1 | 2.4 | 34.4 | 0.0 | 3.2 | 2.4 | 0.0 | 2.7 | 30.6 | 2.3 |
| 2024 | 367 | 21.7 | 27.9 | 14.9 | 22.4 | 15.0 | 9.7 | 7.3 | 0.0 | 20.7 | 22.2 | 12.9 |
| 2529 | 206 | 12.2 | 16.1 | 11.3 | 10.4 | 20.0 | 19.4 | 9.8 | 25.0 | 8.1 | 10.1 | 12.9 |
| 3039 | 353 | 20.8 | 20.9 | 20.6 | 19.0 | 25.0 | 29.0 | 24.4 | 25.0 | 29.7 | 20.3 | 22.2 |
| 4049 | 258 | 15.2 | 12.5 | 26.2 | 10.4 | 25.0 | 25.8 | 36.6 | 37.5 | 20.7 | 11.6 | 27.8 |
| 50+ | 153 | 9.0 | 6.5 | 24.6 | 3.5 | 15.0 | 12.9 | 19.5 | 12.5 | 18.0 | 5.2 | 21.9 |
| Female (%) | 1,694 | 88.5 | 88.5 | 93.6 | 86.7 | 90.0 | 87.1 | 90.2 | 93.8 | 89.2 | 87.0 | 92.4 |
| Race (%) | ||||||||||||
| White | 925 | 54.6 | 70.9 | 74.2 | 36.4 | 55.0 | 58.1 | 82.9 | 68.8 | 69.4 | 40.4 | 72.5 |
| African-American | 474 | 28.0 | 22.6 | 16.5 | 37.1 | 40.0 | 41.9 | 2.4 | 31.3 | 9.9 | 33.8 | 19.1 |
| Hispanic | 234 | 13.8 | 2.2 | 4.8 | 23.4 | 0.0 | 0.0 | 12.2 | 0.0 | 16.2 | 22.6 | 4.8 |
| Unknown Race | 61 | 3.6 | 4.3 | 4.4 | 3.1 | 5.0 | 0.0 | 2.4 | 0.0 | 4.5 | 3.3 | 3.7 |
| Education (%) | ||||||||||||
| Up to 11 years of schooling | 296 | 17.6 | 9.0 | 8.5 | 28.0 | 10.0 | 0.0 | 4.9 | 12.5 | 5.5 | 25.4 | 7.6 |
| GED | 368 | 21.9 | 7.3 | 14.2 | 33.0 | 20.0 | 3.2 | 17.1 | 18.8 | 20.2 | 31.5 | 14.1 |
| High School Graduate | 896 | 53.3 | 60.1 | 75.3 | 38.3 | 55.0 | 96.8 | 78.1 | 68.8 | 64.2 | 41.4 | 76.1 |
| Some Post-Secondary Education | 121 | 7.2 | 23.6 | 2.0 | 0.6 | 15.0 | 0.0 | 0.0 | 0.0 | 10.1 | 1.8 | 2.3 |
| Enrollment Status (Last Event Code) (%) | ||||||||||||
| Registered | 567 | 33.5 | 59.8 | 29.4 | 11.7 | 25.0 | 93.6 | 14.6 | 94.6 | 25.1 | 21.7 | 33.4 |
| Completed | 580 | 34.3 | 18.3 | 22.2 | 49.2 | 45.0 | 3.2 | 70.7 | 2.7 | 13.2 | 43.6 | 28.9 |
| Cancelled | 543 | 32.1 | 21.9 | 48.4 | 38.9 | 30.0 | 3.2 | 14.6 | 2.7 | 61.5 | 34.6 | 37.6 |
| Suspended | 1 | 0.1 | 0.0 | 0.0 | 0.1 | 0.0 | 0.0 | 0.0 | 0.0 | 0.3 | 0.1 | 0.0 |
| Term Length (hours) | 1,694 | 1,345 | 2,305 | 606 | 1,124 | 1,280 | 2,000 | 795 | 1,193 | 1,064 | 1,116 | 814 |
| Related Instruction Length (hours) | 1,440 | 112 | 193 | 72 | 86 | 102 | 197 | 68 | 116 | 62 | 83 | 83 |
| Related Instruction by Sponsor (%) | 1,694 | 71.3 | 72.8 | 5.7 | 86.8 | 100.0 | 6.5 | 100.0 | 75.0 | 100.0 | 88.4 | 25.0 |
| SOURCE: RTI International/Urban Institute analysis of RAPIDS data. NOTES: OC = occupational code. Registration after 1/1/2005. | ||||||||||||
| TABLE A-2. Characteristics of Home Health Aides by Occupational Group | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Characteristics | N | Overall | OC: Time-Based (1086) | OC: Entry-Level Competency-Based (1086CB) | OC: 1086A | OC: 1086B | OC: 1086D | OC: 1086E | OC: All Specialty (1086A, 1086B, 1086D, & 1086E) |
| Apprentices | --- | 395 | 71 | 289 | 16 | 4 | 14 | 1 | 35 |
| Age (%) | |||||||||
| Under 20 | 35 | 8.9 | 0.0 | 11.8 | 6.3 | 0.0 | 0.0 | 0.0 | 2.9 |
| 2024 | 150 | 38.0 | 12.7 | 44.6 | 75.0 | 0.0 | 0.0 | 0.0 | 34.3 |
| 2529 | 65 | 16.5 | 12.7 | 18.3 | 18.8 | 0.0 | 0.0 | 0.0 | 8.6 |
| 3039 | 55 | 13.9 | 15.5 | 14.5 | 0.0 | 0.0 | 14.3 | 0.0 | 5.7 |
| 4049 | 54 | 13.7 | 33.8 | 6.9 | 0.0 | 75.0 | 42.9 | 100.0 | 28.6 |
| 50+ | 36 | 9.1 | 25.4 | 3.8 | 0.0 | 25.0 | 42.9 | 0.0 | 20.0 |
| Female (%) | 395 | 88.1 | 94.4 | 85.8 | 37.5 | 100.0 | 100.0 | 100.0 | 71.4 |
| Race (%) | |||||||||
| White | 288 | 72.9 | 40.9 | 78.9 | 93.8 | 75.0 | 85.7 | 100.0 | 88.6 |
| African-American | 93 | 23.5 | 47.9 | 19.0 | 6.3 | 25.0 | 14.3 | 0.0 | 11.4 |
| Hispanic | 7 | 1.8 | 7.0 | 0.7 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| Unknown Race | 7 | 1.8 | 4.2 | 1.4 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| Education (%) | |||||||||
| Up to 11 years of schooling | 18 | 4.6 | 16.9 | 1.7 | 6.3 | 0.0 | 0.0 | 0.0 | 2.9 |
| GED | 32 | 8.1 | 8.5 | 7.3 | 0.0 | 50.0 | 21.4 | 0.0 | 14.3 |
| High School Graduate | 336 | 85.1 | 74.7 | 88.6 | 81.3 | 50.0 | 78.6 | 100.0 | 77.1 |
| Some Post-Secondary Education | 9 | 2.3 | 0.0 | 2.4 | 12.5 | 0.0 | 0.0 | 0.0 | 5.7 |
| Enrollment Status (Last Event Code) (%) | |||||||||
| Registered | 99 | 25.1 | 14.1 | 25.3 | 18.8 | 50.0 | 71.4 | 100.0 | 45.7 |
| Completed | 52 | 13.2 | 56.3 | 2.1 | 6.3 | 50.0 | 21.4 | 0.0 | 17.1 |
| Cancelled | 243 | 61.5 | 28.2 | 72.7 | 75.0 | 0.0 | 7.1 | 0.0 | 37.1 |
| Suspended | 1 | 0.3 | 1.4 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| Term Length (hours) | 395 | 1,874 | 1,656 | 2,000 | 2,000 | 675 | 675 | 675 | 1,281 |
| Related Instruction Length (hours) | 395 | 125 | 184 | 113 | 185 | 40 | 40 | 40 | 106 |
| Related Instruction by Sponsor (%) | 395 | 96.0 | 100.0 | 100.0 | 0.0 | 100.0 | 100.0 | 100.0 | 54.3 |
| SOURCE: RTI International/Urban Institute analysis of RAPIDS data. NOTES: OC = occupational code. Registration after 1/1/2005. | |||||||||
| TABLE A-3. Characteristics of Certified Nursing Assistant Programs by Occupational Group | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Characteristics | N | Overall | OC: Time-Based (824) | OC: 824A | OC: 824C | OC: 824D | OC: 824G | OC: 824M | OC: 824R | OC: 824CB | OC: Entry-Level Competency-Based (C and CB) | OC: Advanced or Specialty |
| Employer Characteristics | ||||||||||||
| Number of Employers | --- | 56 | 28 | 3 | 10 | 3 | 3 | 4 | 2 | 3 | 13 | 15 |
| Mean Employer Total Workforce | 56 | 1,803 | 232 | 5,724 | 2,307 | 4,032 | 101 | 6,084 | 4,075 | 5,783 | 3,109 | 3,604 |
| Mean Number of Affiliated Sites | 56 | 16 | 2 | 59 | 19 | 41 | 1 | 62 | 41 | 41 | 24 | 37 |
| Percent with Multiple Sites | 56 | 17.9 | 7.1 | 66.7 | 20.0 | 33.3 | 0.0 | 50.0 | 33.3 | 33.3 | 23.1 | 33.3 |
| National Program | 6 | 10.7 | 0.0 | 33.3 | 10.0 | 33.3 | 0.0 | 50.0 | 33.3 | 33.3 | 15.4 | 26.7 |
| Geographic Characteristics | ||||||||||||
| Northeast-DOL Region 1 | 3 | 5.4 | 3.6 | 33.3 | 0.0 | 0.0 | 0.0 | 0.0 | 33.3 | 0.0 | 0.0 | 13.3 |
| Mid-Atlantic-DOL Region 2 | 4 | 7.1 | 7.1 | 0.0 | 0.0 | 0.0 | 25.0 | 0.0 | 33.3 | 0.0 | 0.0 | 13.3 |
| Southeast-DOL Region 3 | 9 | 16.1 | 14.3 | 33.3 | 10.0 | 33.3 | 50.0 | 0.0 | 0.0 | 0.0 | 7.7 | 26.7 |
| Central-DOL Region 4 | 5 | 8.9 | 10.7 | 0.0 | 10.0 | 0.0 | 0.0 | 0.0 | 0.0 | 33.3 | 15.4 | 0.0 |
| Midwest-DOL Region 5 | 24 | 42.9 | 57.1 | 0.0 | 70.0 | 0.0 | 0.0 | 0.0 | 0.0 | 33.3 | 61.5 | 0.0 |
| West-DOL Region 6 | 5 | 8.9 | 7.1 | 0.0 | 0.0 | 33.3 | 25.0 | 50.0 | 0.0 | 0.0 | 0.0 | 20.0 |
| Apprenticeship Characteristics | ||||||||||||
| Mean Term Length | 56 | 1,720 | 2,239 | 627 | 983 | 1,253 | 1,750 | 855 | 1,779 | 1,361 | 1,070 | 1,312 |
| Mean Related Instruction Length | 52 | 331 | 525 | 72 | 171 | 99 | 182 | 68 | 166 6 | 107 | 155 | 121 |
| Source/Mode Related Instruction* | ||||||||||||
| Onsite | 56 | 26.9 | 17.9 | 2.4 | 30.0 | 33.3 | 0.0 | 100.0 | 66.7 | 66.7 | 38.5 | 33.8 |
| Community College | 56 | 19.6 | 10.7 | 66.7 | 20.0 | 66.7 | 50.0 | 0.0 | 0.0 | 0.0 | 15.4 | 40.0 |
| Technical School | 56 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| Vocational School | 56 | 44.6 | 60.7 | 0.0 | 40.0 | 0.0 | 50.0 | 0.0 | 33.3 | 33.3 | 38.5 | 20.0 |
| Correspondence | 56 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| Web-based | 56 | 7.1 | 7.1 | 0.0 | 0.0 | 33.3 | 25.0 | 0.0 | 0.0 | 0.0 | 0.0 | 13.3 |
| SOURCE: RTI International/Urban Institute analysis of RAPIDS data. NOTES: OC = occupational code. Registration after 1/1/2005. * Source/Mode of Related Instruction -- categories are not mutually exclusive: one program can have instruction from several sources. | ||||||||||||
| TABLE A-4. Characteristics of Home Health Aide Programs by Occupational Group | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Characteristics | N | Overall | OC: Time-Based (1086) | OC: Entry-Level Competency-Based (1086CB) | OC: 1086A | OC: 1086B | OC: 1086D | OC: 1086E | OC: All Specialty (1086A, 1086B, 1086D, & 1086E) |
| Employer Characteristics | |||||||||
| Number of Employers | --- | 13 | 5 | 2 | 2 | 1 | 2 | 1 | 6 |
| Mean Employer Total Workforce | 13 | 311 | 307 | 840 | 35 | 250 | 188 | 125 | 137 |
| Mean Number of Affiliated Sites | 13 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Percent with Multiple Sites | 13 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| National Program | 0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| Geographic Characteristics | |||||||||
| Northeast-DOL Region 1 | 0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| Mid-Atlantic-DOL Region 2 | 1 | 7.7 | 20.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| Southeast-DOL Region 3 | 1 | 7.7 | 0.0 | 50.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| Central-DOL Region 4 | 1 | 7.7 | 0.0 | 0.0 | 50.0 | 0.0 | 0.0 | 0.0 | 16.7 |
| Midwest-DOL Region 5 | 10 | 76.9 | 80.0 | 50.0 | 50.0 | 100.0 | 100.0 | 100.0 | 83.3 |
| West-DOL Region 6 | 0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| Apprenticeship Characteristics | |||||||||
| Mean Term Length | 13 | 1,289 | 1,211 | 2,000 | 2,000 | 675 | 675 | 675 | 1,117 |
| Mean Related Instruction Length | 13 | 122 | 168 | 128 | 1,660 | 40 | 40 | 40 | 82 |
| Source/Mode Related Instruction* | |||||||||
| Onsite | 13 | 76.9 | 100.0 | 50.0 | 0.0 | 100.0 | 100.0 | 100.0 | 66.7 |
| Community College | 13 | 15.4 | 0.0 | 50.0 | 50.0 | 0.0 | 0.0 | 0.0 | 16.7 |
| Technical School | 13 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| Vocational School | 13 | 0.0 | 0.0 | 0.0 | 50.0 | 0.0 | 0.0 | 0.0 | 16.7 |
| Correspondence | 13 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| Web-based | 13 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 |
| SOURCE: RTI International/Urban Institute analysis of RAPIDS data. NOTES: OC = occupational code. Registration after 1/1/2005. * Source/Mode of Related Instruction -- categories are not mutually exclusive: one program can have instruction from several sources. | |||||||||
| TABLE A-5. List of Programs by Location and Apprentice Count by Major Occupation (All Apprentices) | |||||||
|---|---|---|---|---|---|---|---|
| Region | State | Program Name | Certified Nursing Assistants 0824 | Direct Support Specialists 1040 | Health Support Specialists 1086AA | Home Health Aides 1086 (excluding 1086AA) | Total |
| 1 | MA | Lifelinks, Inc. | 0 | 20 | 0 | 0 | 20 |
| 1 | NH | Crotched Mountain Foundation | 0 | 17 | 0 | 0 | 17 |
| 1 | NJ | Burnt Tavern Rehabilitation & HCC | 4 | 0 | 0 | 0 | 4 |
| 1 | NJ | Genesis Healthcare -- Phillipsburg Center | 3 | 0 | 0 | 0 | 3 |
| 1 | NJ | Shady Lane Home & Child Development Center | 20 | 0 | 0 | 0 | 20 |
| 2 | PA | Clepper Manor | 4 | 0 | 0 | 0 | 4 |
| 2 | PA | Home Care Associates of Philadelphia | 0 | 0 | 0 | 26 | 26 |
| 2 | PA | Nugent Convalescent Home, Inc | 2 | 0 | 0 | 0 | 2 |
| 2 | PA | William Penn Care Center | 1 | 0 | 0 | 0 | 1 |
| 3 | GA | Georgia Health Care Association | 120 | 0 | 0 | 0 | 120 |
| 3 | KY | Homestead Nursing & Rehab LLC | 29 | 0 | 0 | 0 | 29 |
| 3 | KY | Pine Meadows Health Care LLC | 35 | 0 | 0 | 0 | 35 |
| 3 | SC | Agape Community Hospice of the Pee Dee | 22 | 0 | 0 | 0 | 22 |
| 3 | SC | Carriage Hills Living Center | 1 | 0 | 0 | 0 | 1 |
| 3 | SC | Georgetown Hospital Systems | 2 | 0 | 0 | 0 | 2 |
| 3 | SC | Hampton Regional Medical Center | 0 | 0 | 7 | 0 | 7 |
| 3 | SC | Right at Home | 8 | 0 | 0 | 5 | 13 |
| 3 | TN | WR Community Services | 0 | 3 | 0 | 0 | 3 |
| 4 | AR | Conway STW Apprenticeship Training Comm | 25 | 0 | 0 | 0 | 25 |
| 4 | CO | Colorado State Veterans Home | 9 | 0 | 0 | 0 | 9 |
| 4 | SD | Comfort Keepers of South Dakota | 0 | 0 | 15 | 0 | 15 |
| 4 | SD | Country Place Living | 0 | 0 | 5 | 0 | 5 |
| 4 | TX | Air Force Village | 10 | 0 | 15 | 0 | 25 |
| 4 | TX | Comal County Senior Citizens | 0 | 0 | 2 | 0 | 2 |
| 4 | TX | Country Place Living | 0 | 0 | 17 | 0 | 17 |
| 4 | TX | FMC Carswell Hospital | 15 | 0 | 0 | 0 | 15 |
| 4 | TX | Gary Job Corps | 396 | 0 | 0 | 0 | 396 |
| 4 | UT | Spine, Orthopedic & Sports Physical Therapy, LLC | 0 | 0 | 0 | 15 | 15 |
| 4 | WY | Ark Regional Services -- Day Habilitation Services | 0 | 6 | 0 | 0 | 6 |
| 4 | WY | Ark Regional Services -- Residential Services | 0 | 5 | 0 | 0 | 5 |
| 5 | IA | Comfort Keepers | 0 | 0 | 16 | 0 | 16 |
| 5 | IA | Comfort Keepers -- Marshalltown/Ames | 0 | 0 | 2 | 0 | 2 |
| 5 | IA | Comfort Keepers -- Ottumwa | 0 | 0 | 3 | 0 | 3 |
| 5 | IN | Developmental Services, Inc. | 0 | 924 | 0 | 0 | 924 |
| 5 | IN | Memorial Home Care | 0 | 0 | 0 | 26 | 26 |
| 5 | KS | Aberdeen Village | 0 | 0 | 20 | 0 | 20 |
| 5 | KS | Bethany Home Association | 0 | 0 | 6 | 0 | 6 |
| 5 | KS | Brewster Place Retirement Community | 1 | 0 | 0 | 0 | 1 |
| 5 | KS | C P Home Plus of Scandia | 0 | 0 | 1 | 0 | 1 |
| 5 | KS | C P Senior Living Clay Center | 0 | 0 | 5 | 0 | 5 |
| 5 | KS | C P Senior Living Belleville | 0 | 0 | 2 | 0 | 2 |
| 5 | KS | C P Senior Living Hoisington | 0 | 0 | 9 | 0 | 9 |
| 5 | KS | C P Senior Living Larned | 0 | 0 | 3 | 0 | 3 |
| 5 | KS | C P Senior Living Marysville | 0 | 0 | 6 | 0 | 6 |
| 5 | KS | C P Senior Living Seneca | 0 | 0 | 4 | 0 | 4 |
| 5 | KS | Cornerstone Village Retirement Community | 9 | 0 | 0 | 0 | 9 |
| 5 | KS | Good Samaritan Society | 0 | 0 | 23 | 0 | 23 |
| 5 | KS | Hilltop Lodge, Inc. | 0 | 0 | 32 | 0 | 32 |
| 5 | KS | Memorial Health System | 0 | 0 | 39 | 0 | 39 |
| 5 | KS | Midland Care Connection | 0 | 0 | 15 | 0 | 15 |
| 5 | KS | Parkside Homes, Inc. | 0 | 0 | 23 | 0 | 23 |
| 5 | KS | Pleasant View Home | 0 | 0 | 19 | 0 | 19 |
| 5 | KS | Rush County Memorial Hospital | 0 | 0 | 7 | 0 | 7 |
| 5 | KS | Rush County Nursing Home | 0 | 0 | 9 | 0 | 9 |
| 5 | KS | The Cedars | 0 | 0 | 14 | 0 | 14 |
| 5 | KS | Villa Maria, Inc. | 0 | 0 | 67 | 0 | 67 |
| 5 | MI | Home Helpers | 1 | 0 | 0 | 0 | 1 |
| 5 | MI | Brahak, Matoshko, Butzin & Assoc; Chiropractic Clinics | 1 | 0 | 0 | 0 | 1 |
| 5 | MI | Fraser Villa Living Center | 11 | 0 | 0 | 0 | 11 |
| 5 | MI | Harbor Home Healthcare | 0 | 0 | 0 | 10 | 10 |
| 5 | MI | Heritage Community of Kalamazoo | 0 | 0 | 0 | 12 | 12 |
| 5 | MI | John S. Demare, D.O. | 1 | 0 | 0 | 0 | 1 |
| 5 | MI | Lutheran Homes of Michigan | 0 | 0 | 0 | 16 | 16 |
| 5 | MI | Macomb Oakland Regional Center Inc | 0 | 43 | 0 | 0 | 43 |
| 5 | MI | Medical Wellness Center | 1 | 0 | 0 | 0 | 1 |
| 5 | MI | Mt. Clemens General Hospital | 1 | 0 | 0 | 0 | 1 |
| 5 | MI | St. John North Shores Hospital | 1 | 0 | 0 | 0 | 1 |
| 5 | MI | St. Josephs Mercy Hospital | 1 | 0 | 0 | 0 | 1 |
| 5 | MI | The Neurosurgery Group, P.C. | 1 | 0 | 0 | 0 | 1 |
| 5 | MI | WadhamsCreek Senior Community | 7 | 0 | 0 | 0 | 7 |
| 5 | MO | St. Johns Mercy Medical Center | 232 | 0 | 128 | 284 | 644 |
| 5 | MO | Womens East Reception, Diagnostic & Correctional Center | 297 | 0 | 0 | 0 | 297 |
| 5 | OH | Hearth & Home Assisted Living | 2 | 0 | 0 | 0 | 2 |
| 5 | OH | Brookfield Personal Retirement Care Center | 1 | 0 | 0 | 0 | 1 |
| 5 | OH | Brookhaven Home Health Care, Inc | 0 | 0 | 0 | 1 | 1 |
| 5 | OH | Covington Care Center | 1 | 0 | 0 | 0 | 1 |
| 5 | OH | Franklin Ridge | 1 | 0 | 0 | 0 | 1 |
| 5 | OH | Grace Brethren Village | 2 | 0 | 0 | 0 | 2 |
| 5 | OH | Humility Of Mary Health Partners | 19 | 0 | 0 | 0 | 19 |
| 5 | OH | Koinonia Homes, Inc | 0 | 11 | 0 | 0 | 11 |
| 5 | OH | Maria-Joseph Living Care Center | 1 | 0 | 0 | 0 | 1 |
| 5 | OH | Pleasant Hill Manor | 3 | 0 | 0 | 0 | 3 |
| 5 | OH | The Brethren Home | 2 | 0 | 0 | 0 | 2 |
| 5 | OH | Trinity Mission New Paris | 2 | 0 | 0 | 0 | 2 |
| 6 | AK | Caring Bridges Assisted Living Home | 3 | 0 | 0 | 0 | 3 |
| 6 | AK | Community Connections, Inc. | 0 | 2 | 0 | 0 | 2 |
| 6 | AK | Focus, Inc. | 0 | 1 | 0 | 0 | 1 |
| 6 | AK | Hope Community Resources | 0 | 24 | 0 | 0 | 24 |
| 6 | AK | Reach, Inc. | 0 | 2 | 0 | 0 | 2 |
| 6 | CA | Catholic Charities | 0 | 2 | 0 | 0 | 2 |
| 6 | CA | Clovis Adult Health Career Committee | 18 | 0 | 0 | 0 | 18 |
| 6 | CA | Comfort Keepers -- Claremont | 0 | 0 | 1 | 0 | 1 |
| 6 | CA | Comfort Keepers -- Coronado | 0 | 0 | 3 | 0 | 3 |
| 6 | CA | Comfort Keepers -- Costa Mesa | 0 | 0 | 3 | 0 | 3 |
| 6 | CA | Comfort Keepers -- San Diego | 0 | 0 | 43 | 0 | 43 |
| 6 | CA | Fresno City College | 0 | 3 | 0 | 0 | 3 |
| 6 | CA | Fresno New Connections | 0 | 1 | 0 | 0 | 1 |
| 6 | ID | Elmore Medical Center Hospital | 20 | 0 | 0 | 0 | 20 |
| 6 | WA | Sunbridge Healthcare -- Washington State | 12 | 0 | 0 | 0 | 12 |
| 11 | SD | The Evangelical Lutheran Good Samaritan Society | 254 | 0 | 0 | 0 | 254 |
| SOURCE: RTI International/Urban Institute analysis of RAPIDS data. | |||||||
| TABLE A-6. List of Programs by Location and Apprentice Count by Major Occupation (Currently Registered Apprentices Only) | |||||||
|---|---|---|---|---|---|---|---|
| Region | State | Program Name | Certified Nursing Assistants 0824 | Direct Support Specialists 1040 | Health Support Specialists 1086AA | Home Health Aides 1086 (excluding 1086AA) | Total |
| 1 | MA | Lifelinks, Inc. | 0 | 13 | 0 | 0 | 13 |
| 1 | NH | Crotched Mountain Foundation | 0 | 7 | 0 | 0 | 7 |
| 1 | NJ | Burnt Tavern Rehabilitation & HCC | 2 | 0 | 0 | 0 | 2 |
| 2 | PA | Clepper Manor | 4 | 0 | 0 | 0 | 4 |
| 2 | PA | Home Care Associates of Philadelphia | 0 | 0 | 0 | 8 | 8 |
| 2 | PA | Nugent Convalescent Home, Inc | 2 | 0 | 0 | 0 | 2 |
| 2 | PA | William Penn Care Center | 1 | 0 | 0 | 0 | 1 |
| 3 | GA | Georgia Health Care Association | 69 | 0 | 0 | 0 | 69 |
| 3 | KY | Homestead Nursing & Rehab LLC | 27 | 0 | 0 | 0 | 27 |
| 3 | KY | Pine Meadows Health Care LLC | 35 | 0 | 0 | 0 | 35 |
| 3 | SC | Agape Community Hospice of the Pee Dee | 22 | 0 | 0 | 0 | 22 |
| 3 | SC | Georgetown Hospital Systems | 2 | 0 | 0 | 0 | 2 |
| 3 | SC | Hampton Regional Medical Center | 0 | 0 | 5 | 0 | 5 |
| 3 | SC | Right at Home | 3 | 0 | 0 | 5 | 8 |
| 3 | TN | WR Community Services | 0 | 3 | 0 | 0 | 3 |
| 4 | CO | Colorado State Veterans Home | 3 | 0 | 0 | 0 | 3 |
| 4 | SD | Comfort Keepers of South Dakota | 0 | 0 | 15 | 0 | 15 |
| 4 | SD | Country Place Living | 0 | 0 | 2 | 0 | 2 |
| 4 | SD | Yankton Federal Prison Camp | 0 | 10 | 0 | 0 | 10 |
| 4 | TX | Air Force Village | 10 | 0 | 15 | 0 | 25 |
| 4 | TX | Comal County Senior Citizens | 0 | 0 | 2 | 0 | 2 |
| 4 | TX | Country Place Living | 0 | 0 | 1 | 0 | 1 |
| 4 | TX | FMC Carswell Hospital | 1 | 0 | 0 | 0 | 1 |
| 4 | UT | Spine, Orthopedic & Sports Physical Therapy, LLC | 0 | 0 | 0 | 2 | 2 |
| 4 | WY | Ark Regional Services -- Day Habilitation Services | 0 | 1 | 0 | 0 | 1 |
| 5 | IA | Comfort Keepers | 0 | 0 | 9 | 0 | 9 |
| 5 | IA | Comfort Keepers -- Marshalltown/Ames | 0 | 0 | 1 | 0 | 1 |
| 5 | IA | Comfort Keepers -- Ottumwa | 0 | 0 | 1 | 0 | 1 |
| 5 | IN | Developmental Services, Inc. | 0 | 274 | 0 | 0 | 274 |
| 5 | IN | Memorial Home Care | 0 | 0 | 0 | 2 | 2 |
| 5 | KS | Aberdeen Village | 0 | 0 | 13 | 0 | 13 |
| 5 | KS | Bethany Home Association | 0 | 0 | 6 | 0 | 6 |
| 5 | KS | C P Senior Living Clay Center | 0 | 0 | 4 | 0 | 4 |
| 5 | KS | C P Senior Living Belleville | 0 | 0 | 1 | 0 | 1 |
| 5 | KS | C P Senior Living Hoisington | 0 | 0 | 5 | 0 | 5 |
| 5 | KS | C P Senior Living Larned | 0 | 0 | 3 | 0 | 3 |
| 5 | KS | C P Senior Living Marysville | 0 | 0 | 4 | 0 | 4 |
| 5 | KS | C P Senior Living Seneca | 0 | 0 | 3 | 0 | 3 |
| 5 | KS | Good Samaritan Society | 0 | 0 | 23 | 0 | 23 |
| 5 | KS | Hilltop Lodge, Inc. | 0 | 0 | 29 | 0 | 29 |
| 5 | KS | Memorial Health System | 0 | 0 | 39 | 0 | 39 |
| 5 | KS | Midland Care Connection | 0 | 0 | 15 | 0 | 15 |
| 5 | KS | Parkside Homes, Inc. | 0 | 0 | 13 | 0 | 13 |
| 5 | KS | Pleasant View Home | 0 | 0 | 8 | 0 | 8 |
| 5 | KS | Rush County Memorial Hospital | 0 | 0 | 7 | 0 | 7 |
| 5 | KS | Rush County Nursing Home | 0 | 0 | 7 | 0 | 7 |
| 5 | KS | The Cedars | 0 | 0 | 14 | 0 | 14 |
| 5 | KS | Villa Maria, Inc. | 0 | 0 | 36 | 0 | 36 |
| 5 | MI | Home Helpers | 1 | 0 | 0 | 0 | 1 |
| 5 | MI | Harbor Home Healthcare | 0 | 0 | 0 | 9 | 9 |
| 5 | MI | Lutheran Homes of Michigan | 0 | 0 | 0 | 4 | 4 |
| 5 | MI | Macomb Oakland Regional Center, Inc | 0 | 22 | 0 | 0 | 22 |
| 5 | MI | WadhamsCreek Senior Community | 2 | 0 | 0 | 0 | 2 |
| 5 | MO | St. Johns Mercy Medical Center | 174 | 0 | 82 | 68 | 324 |
| 5 | MO | Womens East Reception, Diagnostic & Correctional Center | 24 | 0 | 0 | 0 | 24 |
| 5 | OH | Hearth & Home Assisted Living | 2 | 0 | 0 | 0 | 2 |
| 5 | OH | Brookhaven Home Health Care, Inc | 0 | 0 | 0 | 1 | 1 |
| 5 | OH | Brookfield Personal Retirement Care Center | 1 | 0 | 0 | 0 | 1 |
| 5 | OH | Franklin Ridge | 1 | 0 | 0 | 0 | 1 |
| 5 | OH | Grace Brethren Village | 2 | 0 | 0 | 0 | 2 |
| 5 | OH | Humility of Mary Health Partners | 14 | 0 | 0 | 0 | 14 |
| 5 | OH | Koinonia Homes, Inc | 0 | 4 | 0 | 0 | 4 |
| 6 | AK | Community Connections, Inc. | 0 | 2 | 0 | 0 | 2 |
| 6 | AK | Focus, Inc. | 0 | 1 | 0 | 0 | 1 |
| 6 | AK | Hope Community Resources | 0 | 19 | 0 | 0 | 19 |
| 6 | AK | Reach, Inc. | 0 | 2 | 0 | 0 | 2 |
| 6 | CA | Catholic Charities | 0 | 2 | 0 | 0 | 2 |
| 6 | CA | Comfort Keepers -- Claremont | 0 | 0 | 1 | 0 | 1 |
| 6 | CA | Comfort Keeper -- Coronado | 0 | 0 | 3 | 0 | 3 |
| 6 | CA | Comfort Keepers -- Costa Mesa | 0 | 0 | 3 | 0 | 3 |
| 6 | CA | Comfort Keepers -- San Diego | 0 | 0 | 43 | 0 | 43 |
| 6 | CA | Fresno City College | 0 | 3 | 0 | 0 | 3 |
| 6 | CA | Fresno New Connections | 0 | 1 | 0 | 0 | 1 |
| 11 | SD | The Evangelical Lutheran Good Samaritan Society | 84 | 0 | 0 | 0 | 84 |
| SOURCE: RTI International/Urban Institute analysis of RAPIDS data. | |||||||