
U.S. Department of Health and Human Services
Coordinating Care in the Fee-for-Service System for Medicaid Beneficiaries with Chronic Conditions
Jennifer Gillespie, Robert Mollica, Jane Horvath andClaudia Williams
National Academy for State Health Policy
May 2005
This report was prepared under contract #HHS-100-03-0025 between the U.S. Department of Health and Human Services (HHS), Office of Disability, Aging and Long-Term Care Policy (DALTCP) and the Research Triangle Institute. For additional information about this subject, you can visit the DALTCP home page at http://aspe.hhs.gov/_/office_specific/daltcp.cfm or contact the ASPE Project Officer, Hunter McKay, at HHS/ASPE/DALTCP, Room 424E, H.H. Humphrey Building, 200 Independence Avenue, S.W., Washington, D.C. 20201. His e-mail address is: Hunter.McKay@hhs.gov.
The opinions and views expressed in this report are those of the authors. They do not necessarily reflect the views of the Department of Health and Human Services, the Research Triangle Institute or any other funding organization.
TABLE OF CONTENTS
OVERVIEW OF FEE-FOR-SERVICE CARE COORDINATION PROGRAMS
Prescription Drug Monitoring Programs
Disease Management Vendor Programs
Health Care Coordination Programs
Health and Long-Term Care Coordination Programs
GEORGIA SERVICE OPTIONS USING RESOURCES IN A COMMUNITY ENVIRONMENT (SOURCE) PROGRAM
Eligibility and Enrollment
SOURCE Sites and Contractors
SOURCE Roles
Services Coordinated
Screening and Assessment
Levels of Care
Carepath
Monitoring
Home and Community-Based Service Provider Accountability
Replication
INDIANA CHRONIC DISEASE MANAGEMENT PROGRAM (ICDMP)
Program Eligibility
Call Center Disease Self-Management Program
Nurse Care Management
Physician Collaboratives
Chronic Disease Management System
Evaluation
Replication
APPENDICES
APPENDIX A. Sources and Selected Readings
APPENDIX B. Georgia SOURCE Carepath
APPENDIX C. ICDMP Care Management Organization Scope of Work
APPENDIX D. ICDMP Nurse Care Manager Performance Expectations
APPENDIX E. ICDMP Sample Letter
LIST OF EXHIBITS AND TABLES
EXHIBIT 1: Level 1 Carepath Goals
EXHIBIT 2: Indiana Chronic Disease Management Program Model
EXHIBIT 3: Call 2 Flow Chart
EXHIBIT 4: Depression Screening from Call 3 Script
EXHIBIT 5: Provider Case Study -- Results of Collaborative
TABLE 1: Examples of Medicaid Managed Care Programs that Integrate Financing for Health and Long-Term Care Services
TABLE 2: Typology of State Medicaid Fee-For-Service Chronic Illness Care Coordination Programs
TABLE 3: Georgia SOURCE/CCSP Comparison
TABLE 4: SOURCE Sites
ACKNOWLEDGEMENTS
The authors wish to thank Hunter McKay, project officer, Office of the Assistant Secretary for Planning and Evaluation within the U.S. Department of Health and Human Services for his guidance and support of this project. We are also grateful to Edith Walsh and Janet O'Keeffe from RTI International for their valuable input, and to Helen Pelletier, of NASHP's staff for her editorial assistance. This report would not have been possible without the assistance of the following individuals.
GEORGIA
- Pat Albritton, co-site coordinator, Diversified Resources, Inc.-SOURCE
- Karen Bacheller, RN, section manager, Community Care Services Program, Division of Aging Services, Georgia Department of Human Resources
- Peter Basler, chief operating officer, Wesley Woods, Emory HealthCare
- Cathie Berger, coordinator of planning, Aging Services Division, Atlanta Regional Commission
- Penny Blackford, care coordination specialist, Community Care Services Program, Division of Aging Services, Georgia Department of Human Resources
- Betsy Boykin, team leader for program development, Georgia Infirmary-SOURCE, St. Joseph/Candler Health System
- Cathy Conrad, case manager supervisor, The Legacy Link, Inc.
- James Cooney, PhD, professor, Institute of Health Administration and Center for Health Services Research, J. Mack Robinson College of Business, Georgia State University
- Dianne Currans, RN, health programs manager, The Legacy Link, Inc.
- Rich Devine, senior planner, Office of Planning and Budget, Georgia Department of Human Resources
- Pat Freeman, executive director, The Legacy Link, Inc.
- Lisa Futrell, RN, site coordinator, Columbus Regional Healthcare System-SOURCE
- Jean Ginn, RN, vice president, SOURCE Care Management
- Virginia Griffin, RN, Albany ARC-SOURCE
- Barbara Hooper, CCSP care coordinator, The Legacy Link, Inc.
- Carrie Hulsey, SOURCE case manager, The Legacy Link, Inc.
- Hunter Hurst, executive director, Georgia Infirmary-SOURCE, St. Joseph/ Candler Health System
- Catherine Ivy, LCSW, director, Care Management Unit, Visiting Nurse Health System
- Doris Jones, LPN, NHA, site coordinator, Blue Ridge SOURCE
- Lauren Jones, RN, Columbus Regional Healthcare System-SOURCE
- Arthur J. Lesesne, Jr., MD, medical director, Wesley Woods Atlanta SOURCE
- Glen Landers, MBA, MHA, senior research associate, Georgia Health Policy Center, Andrew Young School of Policy Studies, Georgia State University
- Norma Jean Morgan, director of aging and community services, Division of Medical Assistance, Georgia Department of Community Health
- Jennifer Schuck, LMSW, director of SOURCE Project, Wesley Woods Center, Emory HealthCare
- Jean Sumner, MD, medical director, SOURCE Care Management, Butler, GA
- Debbie Vansant, site coordinator, Albany ARC-SOURCE
- Sherry Watts, RN, case manager supervisor, SOURCE, Wesley Woods, Emory HealthCare
- Mary Eleanor Wickersham, vice president of corporate development, Home Community Services, Inc.
- Kay Yarbrough, co-site coordinator, Diversified Resources, Inc.-SOURCE
INDIANA
- John Barth, director of managed care, Indiana Family and Social Services Administration
- Melanie Bella, assistant secretary, Indiana Family and Social Services Administration
- Pat Casanova, director of waiver services, Indiana Family and Social Services Administration
- Mike Fowler, Medicaid data director, Indiana Family and Social Services Administration
- Mary Jo Golubski, consultant
- Sherry Gray, director of aging and in-home services, Indiana Family and Social Services Administration
- Emily Hancock, director of long term care, Indiana Family and Social Services Administration
- Pat Miller, senator, Indiana State Senate
- Kathy Moses, director of chronic disease, Indiana Family and Social Services Administration
- Sharon Reynolds, Americhoice (Call Center)
- Marc Rosenman, Regenstrief Institute
- Vi Simpson, senator, Indiana State Senate
- Marcus Washington, Indiana Minority Health Coalition
- Lisa Winternheimer, Indiana Primary Health Care Association
EXECUTIVE SUMMARY
This report describes a range of approaches state Medicaid agencies use to coordinate health services and to coordinate long-term care services with health services for beneficiaries with chronic conditions. It then describes in detail two innovative programs.
Currently, 11 million people with chronic conditions rely on Medicaid for health and long-term care services and utilize a wide range of services from multiple providers in the health and long-term care delivery systems. A lack of service coordination can result in inefficient and unnecessarily costly care. This problem can be compounded when those needing services are dually eligible for Medicaid and Medicare, due to the different financing and reimbursement systems for these programs.
The number of individuals with chronic conditions is estimated to increase from 125 million in 2000 to 157 million by 2020. The projected increase in the number of Medicaid beneficiaries with multiple chronic conditions and complex medical needs has enormous implications for federal and state budgets, as states already devote more than three-quarters of their Medicaid budgets to this population.
In an effort to meet the growing demand for services--and to ensure their quality and improve outcomes while containing costs--states are implementing a range of service coordination approaches and are interested in finding the most effective models. Because the development and implementation of risk-based managed care programs is time consuming and costly, many states are attempting to coordinate services in the traditional fee-for-service setting. Several states have developed fee-for-service approaches to coordinate health care--and in some states both health care and long-term care--for persons with chronic conditions.
We selected two care coordination approaches to highlight in this report. Although many states support care coordination within the Medicaid fee-for-service health system, Georgia's SOURCE program was the only established program we identified that operates in the fee-for-service system, coordinates health and long-term care, and includes dually eligible beneficiaries. This report describes the SOURCE program in depth. We also describe the Indiana Chronic Disease Management Program, an innovative approach to coordinating health care for selected chronic conditions, which serves dually eligible beneficiaries.
Since most dually eligible beneficiaries receive Medicaid in a fee-for-service setting, these programs have the potential to serve a larger number of beneficiaries than risk-based managed care programs. Both programs have two important features that merit attention by other states: (1) they successfully involve primary care physicians in care coordination, and (2) they focus on outcomes.
Both programs have yet to be rigorously evaluated. However, preliminary results suggest that they can be successful in both improving outcomes and containing costs.
BACKGROUND
A chronic condition is one that is likely to last more than a year, limits a person's activities, and may require ongoing health care and long-term care.1 The number of people with one or more chronic conditions is expected to increase between 2000 and 2020 by nearly 26 percent to 157 million, and the number of people with multiple chronic conditions is likely to rise 35 percent to 81 million.
States devote significant resources--more than three-quarters of their Medicaid spending--to provide health and long-term care services for people with chronic conditions.2 These costs are driven in large part by two factors: utilization and lack of coordination in service delivery. Persons with chronic conditions utilize hospital care, physician services, prescription drugs, and home health visits at higher rates than those without such conditions. In addition, people with chronic conditions make extensive use of prescription drugs and services from medical specialists. Finally, many require ongoing long-term care services to address functional needs.3
The provision of a wide range of uncoordinated services from multiple providers in uncoordinated health and long-term care delivery systems is inefficient and costly. The problems can be compounded when those needing services are dually eligible for Medicaid and Medicare--the population more likely than others to have multiple chronic conditions--due to the different financing and reimbursement systems for these programs.
The projected increase in the number of Medicaid beneficiaries with chronic conditions has enormous implications for federal and state budgets. In an effort to meet the growing demand for services--and to both ensure their quality and contain their costs--states are implementing a range of service coordination approaches and are interested in finding the most effective models.
Risk-based managed care is a service approach with the potential to better coordinate care for Medicaid beneficiaries with chronic conditions.4 Several states--Arizona, Florida, New York, Texas and Utah--operate risk-based managed care programs that integrate the financing and management of Medicaid health and long-term care services. These programs generally serve a large number of beneficiaries. Texas serves about 60,000 people and Arizona serves all Medicaid beneficiaries in the state.
Massachusetts, Minnesota, and Wisconsin also operate risk-based managed care programs that integrate Medicaid and Medicare financing and management of health and long-term care services. Programs for the All Inclusive Care for the Elderly (PACE), which also integrate financing and management of Medicare and Medicaid health and long-term care services, operate in many other states as well. However, to date, integrated programs like these have been complex to design and enrollment has been relatively modest. For example, only 8,800 people were enrolled in PACE programs nationwide in 2003.5
Table 1 lists several of these capitated Medicaid health and long-term care managed care programs and the populations they serve, differentiated by the type of Medicare financing they use.
Because the development and implementation of risk-based managed care programs is time consuming and costly, many states are attempting to coordinate services in the traditional fee-for-service setting. Several states have developed fee-for-service approaches to coordinate health care--and in some states both health care and long-term care--for persons with chronic conditions. The purpose of this study is to examine the literature to identify types of care coordination approaches, and to identify and describe innovative state approaches that other states might be interested in replicating.
| TABLE 1: Examples of Medicaid Managed Care Programs that Integrate Financing for Health and Long-Term Care Services | |||
| State | Program | Medicaid Population Served | Medicare Financing |
| AZ | Arizona Long-Term Care System | Nursing facility eligible older adults and adults with disabilities | Fee-for-service |
| FL | Long-Term Care Community Diversion Program | Nursing facility eligible older adults | Fee-for-service |
| NY | VNS Choice | Nursing facility eligible older adults | Fee-for-service |
| TX | StarPlus | Older adults and adults with disabilities | Fee-for-service |
| UT | Long-Term Care Managed Care Initiative | Nursing facility residents 18 and older | Fee-for-service |
| MA | Senior Care Option | All older adults | Integrated |
| MN | Minnesota Senior Health Options Program | All older adults | Integrated |
| WI | Wisconsin Partnership Program | Nursing facility eligible older adults and adults with disabilities | Integrated |
| Multiple | PACE | Nursing facility eligible older adults (55+) | Integrated |
METHODS
To identify innovative fee-for-service approaches to coordinating health and long-term care services for Medicaid beneficiaries, we reviewed the literature on care coordination. The publications we reviewed are listed in Appendix A.
The literature review and interview with experts revealed that while many states support care coordination within the Medicaid fee-for-service health system, only one state coordinates both health and long-term care services. Georgia's Service Options Using Resources in a Community Environment (SOURCE) program was the only established program we identified that operates in the fee-for-service system, coordinates health care and long-term care, and serves dually eligible beneficiaries.6
To develop the Georgia SOURCE case study, we consulted with Georgia Medicaid officials to develop a list of key informants representing local program sites, providers, and other stakeholders. During a two-day site visit to Georgia, the authors interviewed--individually and in groups--state policy staff, SOURCE program staff, Community Care Services Program (CCSP) staff (a waiver program), physicians, registered nurses, social workers, and Area Agency on Aging (AAA) administrators. Follow-up interviews were conducted by telephone.
The Indiana Chronic Disease Management Program (ICDMP) also operates in the fee-for-service system and includes dually eligibly beneficiaries. The program coordinates health care services for selected chronic conditions, but not--at present--long-term care services. However, program administrators indicate that the program design allows for the coordination of long-term care services in the future. We selected this program for a case study because it provides a model for improving health care coordination for states that are not able to implement more extensive health and long-term care coordination programs.
To develop the Indiana case study, we consulted with Indiana Medicaid officials to develop a list of key informants representing local program sites, providers, and other stakeholders. During a two-day site visit to Indiana, the authors interviewed--individually and in groups--state policy staff, ICDPM program staff, legislators, waiver program staff, physicians, registered nurses, social workers, and staff from the Regenstrief Institute. Follow-up interviews were conducted by telephone. A list of informants for both case studies is included in the acknowledgments section of this report.
OVERVIEW OF FEE-FOR-SERVICE CARE COORDINATION PROGRAMS
States have instituted a range of fee-for-service initiatives to coordinate care for Medicaid beneficiaries with chronic conditions. Based on our review of these initiatives, we identified four primary types of programs:
- Prescription drug monitoring programs,
- Disease management vendor programs,
- Health care coordination programs,
- Health and long-term care coordination programs.
Characteristics of these programs are summarized in Table 2. Although the programs differ substantially, each shares a common goal: to improve or maintain the health of Medicaid beneficiaries with chronic conditions and to control Medicaid expenditures.
With the exception of disease management vendor programs, the programs seek to involve primary care physicians and/or pharmacists in substantive ways. Because lack of physician involvement has been cited as one reason for the failure of many case management/disease management programs to achieve successful results, a number of programs compensate medical providers for their time.7 Each of the programs supplement the physician's role in monitoring a beneficiary's medical status using different approaches.
Prescription Drug Monitoring Programs
Several types of prescription drug monitoring programs are found in Medicaid programs. These programs are designed to reduce inappropriate prescription drug use through a wide range of interventions, from physician education to analysis of Medicaid claims data. Some of these programs include dually eligible beneficiaries because Medicaid pays a significant portion of the prescription drug costs for this population.8 At least three states--Maine, Virginia, and Mississippi--have developed prescription drug monitoring programs.
A Mississippi program reimburses pharmacists for patient counseling and monitoring if the physician refers the patient for this service. Virginia implemented its program by training Medicaid physicians in asthma care and paying pharmacists for beneficiary consultation services if the physician refers the patient. Virginia subsequently replaced this program with a disease management vendor program.
Maine implemented a pilot program called MaineNet to educate physicians about appropriate prescribing practices for dually eligible beneficiaries with certain priority conditions or characteristics, including: diabetes, congestive heart failure (CHF), cardiovascular disease, or receipt of home and community long-term care services. Fifty primary care providers serving 1,100 beneficiaries with priority conditions--5 percent of the beneficiaries with priority conditions statewide--participated in the project.
| TABLE 2: Typology of State Medicaid Fee-For-Service Chronic Illness Care Coordination Programs | ||||
| Program Characteristics | Prescription Drug Monitoring Programs | Disease Management Vendor Programs | Health Care Coordination Programs | Health and Long-Term Care Coordination Programs |
| Scope | Manages polypharmacy | Manages specific conditions | Manages medical care | Manages medical and long-term care |
| Structure | State involvement in program operation and development | State contracts with vendor for program development and operation | State involvement in program operation and development | State involvement in program operation and development |
| Dual eligibles | Included | Excluded | Included | Included |
| Involvement of physicians or pharmacists | Variable involvement | Minimally involved | Moderately involved | Highly involved |
| Care management | Physicians/ pharmacists (not supplemented by an additional case manager) | Call-in centers | Case managers | Case managers |
| Examples of states with programs* | Maine, Mississippi, Virginia | Approximately 17 states | Indiana, North Carolina, Texas | Georgia, Massachusetts |
| * Because states frequently modify their programs or replace them with other programs, those listed here may not be operational at the time of publication. | ||||
The state provided physicians with reports of their prescribing practices based on claims data and the physicians met periodically with a MaineNet health educator to review data and discuss interventions. Physicians received $100 an hour for meeting with the health educator. An evaluation of the program found that the number of potentially inappropriate medications for the elderly declined by 36 percent over the 18-month intervention period. During the same period, the rate of new, potentially inappropriate, prescriptions for the elderly dropped 56 percent, suggesting a change in prescribing behavior.9
Disease Management Vendor Programs
Disease management vendor programs are the most prevalent form of care coordination in state Medicaid programs today. They typically operate independently of physicians in the health care delivery system.10 As of July 2003, 17 states had some form of disease management vendor program in its Medicaid fee-for-service system.11 However, these programs generally exclude beneficiaries who are dually eligible for Medicare and Medicaid.
These disease management programs are characterized by: (1) a contract with a commercial vendor for services related to specific chronic diseases; (2) minimal primary care physician involvement; and (3) a focus on teaching individuals self-management techniques. They also tend to use call-in centers rather than home visits by local case managers as their predominant mode of teaching. At least one state, Washington, requires its vendors to work specifically with beneficiaries who lack social supports and to communicate with the state long-term care system.
Health Care Coordination Programs
Health care coordination programs operate in the existing fee-for-service delivery system. Their purpose is to coordinate care for individuals with specific diseases, including dually eligible beneficiaries. This category includes traditional primary care case management (PCCM) programs, such as North Carolina's ACCESS program. These programs are developed and managed by state agencies with significant involvement by Medicaid providers. They can also include a case manager to assist physicians and to help coordinate health care services and identify needs, typically using targeted case management services.
The Texas Catastrophic Case Management program supplements the services provided in a PCCM program for certain beneficiaries identified using a computer algorithm. They include people with asthma; diabetes; AIDS; high risk pregnancy; complex behavioral health issues; children with special health care needs; and individuals with service costs above $25,000 per year or multiple uses of emergency room services. Dually eligible beneficiaries are excluded.
The ICDMP, an example of a health care coordination program, is described in detail later in this report. The ICDMP promotes self-care for people with asthma, diabetes, and CHF, and engages and supports primary care providers to facilitate changes to the organization and delivery of health care for people with chronic conditions.
Health and Long-Term Care Coordination Programs
A review of published materials and other resources as well as a series of interviews with officials in several states, revealed that although many states support care coordination within the Medicaid fee-for-service health system, they typically do not coordinate both health and long-term care services. Georgia's SOURCE (Service Options Using Resources in a Community Environment) program was the only established program we identified that operates in the fee-for-service system, coordinates health and long-term care, and includes dually eligible beneficiaries.
The strength of the SOURCE program appears to lie in its highly active case management and physician involvement. The program provides a model for improving coordination of health and long-term care services for states that are not able to implement more extensive managed care programs. The model could be used to serve any Medicaid beneficiary with complex conditions including Medicaid-only and dually eligible beneficiaries. The next section presents an in-depth description of the program.
We also identified a pilot project that coordinates health and long-term care services--the Massachusetts Aging Service Access Points Physician Program. The project currently enrolls 50 dual eligible beneficiaries and others at high risk of admission to a nursing facility or hospital. Staff at the state's single entry point agencies work with physicians to coordinate health and long-term care services and physicians are compensated for their participation. The pilot includes a more formalized relationship between the state's health and long-term care systems to support treatment regimens to improve outcomes and increase the likelihood of remaining in the community. However, because it is still in the early implementation stage we do not feature it in this report.
Instead, we chose to highlight the ICDMP, which builds on the PCCM model used in many states. The unique aspects of this program are its emphasis on improving individual primary care provider practices and its focus on a statewide health care delivery system. The ICDMP provides a model for improving health care coordination for states that are not able to implement more extensive health and long-term care coordination programs.
The SOURCE program and ICDMP have two important features that merit attention by other states: (1) they successfully involve primary care physicians in care coordination, and (2) they focus on outcomes.
Physician Involvement. Past effort to coordinate health and long-term care have found it difficult to involve physicians because they operate primarily in the health care system and have little financial incentive to work in or coordinate with the long-term care system.
- Georgia's SOURCE model has been able to overcome these barriers by creating a financial incentive for physicians and then requiring them to perform specific functions, including meeting with case managers.
- Indiana's ICDMP provides practical decision tools and care management services designed to support physicians. Although only a small number of physicians are participating in the program, initial outcomes suggest improvements in provider practices and patient health outcomes.
Focus on Outcomes. Both SOURCE program and ICDMP focus on outcomes. The SOURCE Carepath identifies key outcomes for the participant and the parties responsible for achieving each outcome. ICDMP case management is designed to help individuals with chronic conditions determine their desired outcomes and manage their own care to achieve those outcomes.
Since most dually eligible beneficiaries receive Medicaid in a fee-for-service setting, the care coordination programs discussed in this paper have the potential to serve a larger number of beneficiaries than risk-based managed care programs. Formal evaluations are needed to determine their impact on health and long-term care costs and outcomes.
GEORGIA SERVICE OPTIONS USING RESOURCES IN A COMMUNITY ENVIRONMENT (SOURCE) PROGRAM
Georgia's SOURCE is a voluntary program that operates in a Medicaid fee-for-service delivery system. It coordinates all of the services typically covered in traditional home and community-based services (HCBS) programs, but also coordinates primary health care services for both Medicaid-only beneficiaries and for individuals dually eligible for Medicare and Medicaid. The Governor set a statewide enrollment limit of just over 5,500, and eight SOURCE sites currently serve about 4,100 members. SOURCE staff indicated that they hope to fill all the slots as soon as possible, and are currently negotiating with the Governor's office to increase the number of slots.
The program began in 1997 under Georgia's existing PCCM program. It was developed by the St. Joseph/Candler Health System's Georgia Infirmary with support and encouragement from the state Department of Community Health (DCH) and grew out of an effort to develop a PACE program.12 Today, the SOURCE program is a hybrid, built on components of several different care delivery and coordination models including disease management and Medicaid PCCM.
The primary goals of the Georgia SOURCE program include:
- Reducing the need for long-term institutional placement and increasing community options for Medicaid eligible persons;
- Maintaining health and function and slowing the decline that can result from chronic conditions, and preventing the progression of chronic conditions;
- Eliminating service delivery fragmentation through managed care principles, outcome-based management, and relief from programmatic constraints; and
- Increasing cost-efficiency by reducing inappropriate emergency room use, multiple hospitalizations, and nursing facility placement caused by preventable health complications through the promotion of self-care and informal supports.13
Key components of the SOURCE program include:
- Physician involvement in coordinating health and long-term care services;
- Enhanced case management of health and long-term care services facilitated by smaller case loads and increased flexibility in authorizing and changing services;
- Person centered planning;
- Accountability of HCBS providers; and
- Expedited enrollment in HCBS.
In terms of other programs, SOURCE is most similar to traditional HCBS waiver programs, like Georgia's own long-standing and successful waiver program, the CCSP.14 However, the two programs also differ in important ways. A comparison of the two is presented in Table 3. A key difference is that unlike traditional HCBS programs, SOURCE case managers work directly with primary care physicians to assure that participants' primary health care and long-term care services together promote health and physical functioning. The Georgia DCH pays the SOURCE site contractors a monthly fee for enhanced case management. Contractors receive $150 per month per enrollee for the services of the medical director and primary care physician and for case management services.
All other Medicaid services are reimbursed separately on a fee-for-service basis. The contractor typically pays 10-20 percent of this fee ($15-$30) to the primary care physician to cover additional administrative time required for effective medical case management of SOURCE's chronically ill and generally medically complex participants.15
In many communities, SOURCE operates side by side with the waiver program, and in some areas of the state, the AAA administers both programs. Due to waiting lists for CCSP services, the waiver program is a source of referrals to SOURCE.
Coordinating with Medicare is a central issue for states exploring programs that coordinate medical care for dually eligible beneficiaries. Georgia takes a long-term view of the effect of managing medical costs for Medicare beneficiaries. State officials expect that the timely provision and coordination of primary health care and LTC services can: (1) prevent or delay admission to a nursing facility, and (2) reduce medical spending through reduced emergency room use and fewer hospitalizations for ambulatory care sensitive events. The state also expects Medicaid savings from reductions in its payments for the Medicare inpatient deductible ($800+), co-payments, and emergency room visits.
Eligibility and Enrollment
Eligibility criteria for SOURCE are both broader and narrower than under CCSP, the traditional waiver program. The financial criteria are more stringent because SOURCE enrollees must be eligible for SSI, which has very low income criteria, compared to CCSP which serves individuals with income up to 300 percent of the federal SSI income level.16 On the other hand, SOURCE's service criteria are less stringent because participants do not have to meet nursing home level of care criteria as required by CCSP, as long as they have a chronic condition or disability that requires medical management in order to avoid nursing home placement.
| TABLE 3: Georgia SOURCE/CCSP Comparison | ||
| Program Component | Georgia SOURCE | CCSP |
| Eligibility | (1) Financially eligible for Medicaid at 100% or below of SSI, and (2) meets nursing facility level of care criteria or has a chronic condition or disability that requires medical management to avoid nursing home placement | (1) Financially eligible at 300% or below of SSI, and (2) meets nursing facility level of care criteria |
| Service authorization |
|
|
| Services coordinated |
|
|
| Physician involvement | Participating primary care physicians and the medical director agree to work directly with patient case managers in reviewing medical issues, plan of care, functional status, community care needs | Physicians approve participant plan of care annually and any changes to the plan of care as needed. There is no physician involvement in the delivery of services. |
| Participant/case manager contact | Face-to-face meeting every 3 months and once a month by phone. More frequent contact as needed or as directed by physician | At least every 3 months |
| Participant call line | Emergency response line and 24/7 access to case management agency | Emergency response line |
| Case manager/provider contact | Monthly meetings with HCBS providers, quarterly meetings with primary care physicians, and more frequent meetings as needed | As needed |
| Case manager/medical director contact | Weekly. Every case reviewed monthly | Not Applicable |
| Case manager caseload | Average of 40-50 clients | Average of 70-85 clients |
| Administrative agency | Department of Community Health | Department of Human Resources, Division of Aging Services |
Individuals are referred to the program by AAAs, physicians in the community, hospital discharge planners, and informal sources. The majority of referrals come from primary care physicians. The AAAs, which operate the traditional waiver program, CCSP, refer individuals who would otherwise go on a CCSP waiting list or who do not meet that program's nursing home level of care criteria. Individuals receive an assessment from and may be enrolled by the SOURCE contractor.
SOURCE Sites and Contractors
Eight SOURCE sites administer the SOURCE program in 120 of Georgia's 159 counties. The characteristics of SOURCE sites vary greatly. As shown in Table 4, the eight SOURCE contractors include an AAA, a private for-profit case management agency, two hospitals with outpatient clinics, two nursing facilities, an adult day center for rehabilitation, and a regional council on developmental disabilities. Each operates in a defined geographic area. State officials contend that the variety of SOURCE contractors allows innovation and accommodates local needs and conditions, from urban Atlanta to very rural communities.
The Georgia DCH selects contractors, who must meet its standards. Each is responsible for developing a network of physicians and HCBS providers. The contractor oversees budgeting and quality and, perhaps most importantly, provides health leadership through a medical director. The contractor may or may not directly provide the case management services; however, if case management is subcontracted to a different organization (a case management agency or AAA for example), the SOURCE contractor agency must maintain strong connections to individual case managers, particularly through the medical director.
| TABLE 4: SOURCE Sites | |||
| Contractors | Location | Type of Organization | Enrollment(Feb. 2004) |
| Albany ARC | Albany | Regional Council for DD | 221 |
| Blueridge (UHS-Pruitt) | Blueridge | Nursing facility | 481 |
| Columbus Regional Healthcare System | Columbus | Teaching hospital | 445 |
| Diversified Resources Inc. | Waycross | For-profit case management agency | 394 |
| Ethica | Butler | Nursing facility | 1,056 |
| Georgia Infirmary, St. Joseph/Candler Health System | Savannah | Adult day center for rehabilitation | 721 |
| Legacy Link | Gainesville | Area Agency on Aging | 202 |
| Wesley Woods, Emory Healthcare | Atlanta | Geriatric hospital | 573 |
| Total | 4,093 | ||
Most contractors directly provide case management services, but at least one SOURCE contractor subcontracts with the local AAA to provide case management. This flexibility to provide or subcontract case management services is similar to the way the CCSP program operates. All of the contractors provide enhanced case management and assure the active participation of primary care physicians. In addition, each site has a medical director who provides leadership at the SOURCE agency and works directly with all case managers. The medical director helps to tie the health and long-term care services together for each individual participant and helps case managers interact with the participant's primary care provider as well as other physicians who may provide care.
SOURCE Roles
Medical Director
The role of the SOURCE medical director is a significant and distinguishing feature of the program and cannot be subcontracted to a separate case management agency. Medical directors are employed or contracted by the SOURCE agency for a percentage of their time. Their primary responsibility is to lead the case management team, approve enrollment of new participants, and approve care plans. In addition, they review all issues case managers raise such as concerns with medical treatments, complications, participant non-compliance, and physician relationship issues. The medical director also reviews overall utilization data. A key role of the medical director is to help case managers address health care issues. For example, they may review treatment information provided by the case manager and determine that a conflict exists in the treatment regimens prescribed by a participant's two doctors. In such a case, the medical director then helps the case manager determine how to address these issues or intervenes directly with the physicians. Similarly, a medical director can work in tandem with a SOURCE physician to train case managers in the basics of disease self-management and to identify signs of deterioration or complications.
Primary Care Physicians
SOURCE primary care physicians play a major role in the program. Because SOURCE enrollees must choose one of the 533 SOURCE providers as their primary care physician, some observers have expressed concerns that potential enrollees who have an established relationship with a non-SOURCE primary care physician might be unwilling to enroll. In many cases, however, SOURCE staff indicated that enrollees lacked a regular primary care physician prior to enrollment and used emergency rooms to obtain primary care. Thus, in practice, enrollment in SOURCE has not usually required enrollees to leave their primary care physician. Rural physicians are often the only available provider in an area and feel obligated to care for Medicaid clients.
Physicians must provide a thorough exam or evaluation for new SOURCE participants who were not otherwise part of their practice prior to enrolling in SOURCE.17 In addition, SOURCE physicians must be available to case managers, as needed, outside formal case review meetings. Physicians meet quarterly with the case manager to discuss each SOURCE participant. During these meetings, the care plan, treatment regimens, health and functional status, and long-term care services are reviewed. Physicians are expected to have appropriate medical records and relevant office staff in attendance at these meetings.
Physicians from both urban and rural areas were supportive of the program; several described SOURCE's case management as an extension of their practice. Physicians reported that SOURCE has the ability to improve chronic care and practice among physicians. The medical director of the Ethica site in rural Butler, Georgia, indicated that she participates in SOURCE because it helps her care for her more complex patients, many of them Medicaid beneficiaries. One physician indicated that the program made it easier for physicians to care for people with multiple conditions and that physicians were more confident that enrollees would receive additional, needed services.
Physicians who understand the complexity of treating patients with serious functional, medical, and financial challenges appear to highly value SOURCE. Participating physicians appreciate the highly interactive and assertive case management because it allows them to call on SOURCE to address treatment compliance issues and to provide information about the home environment, and other health-related information that might otherwise be unavailable. At a minimum, they appreciate that participants who have a medical or other problem are likely to call the SOURCE program first. SOURCE staff then assesses the severity of the situation and involve the physician only if necessary.
SOURCE site staff found that physicians generally became interested in SOURCE participation if they had ten or more likely participants in their caseload and that involvement might not be satisfactory for those with fewer than ten patients enrolled in the program.
Case Managers and Supervisors
The central function of SOURCE is case management. The Case Management Team comprises individual case managers, the supervisor, the SOURCE project manager, and the medical director. The team meets at least weekly to establish, review and revise care plans, monitor participant progress, and resolve issues. Currently 101 case managers work in the SOURCE program.
Case management supervisors oversee the entire case management team and provide oversight and assistance to individual case managers as needed. Supervisors review each case file monthly, provide feedback to case managers, and document the review. Supervisors must have a bachelor's degree in one of a range of areas from an accredited university and at least five years' experience planning and implementing health care and/or human services for elderly persons or persons of all ages with disabilities. They must also be able to demonstrate successful team participation in multi-disciplinary planning and management of healthcare and/or human services. Program staff indicated that most of the case management supervisors are registered nurses or former case managers with experience in a care delivery setting.
Case managers are either employees of the SOURCE agency or employed by a subcontractor. No contractor uses both models. Case managers are required to be highly active in determining and addressing participant needs and are expected to use a range of resources to achieve these objectives. Case managers conduct an initial participant assessment and identify an array of services that would benefit the participant based on that assessment. They then arrange for services and follow-up with participants within two weeks of the start of services to ensure that appropriate care is being provided. Program administrators stated that case managers who are not registered nurses can provide quality case management services. Educational criteria are not established for case managers. The case managers we met with included a registered nurse, social workers, and one with a bachelor's degree but no clinical training. Program administrators believed that that the most effective sites typically employed case managers from a variety of backgrounds.
Caseloads average between 40 and 50 participants. Case managers contact each participant at least monthly and visit the participant at least quarterly. In addition, case managers are expected to accompany participants to medical appointments when needed to support compliance with treatment orders or disease self-management or to help enhance treatment in other ways.
Staff described the program enthusiastically and noted that SOURCE allowed them to make decisions, change the care plan, arrange all necessary services, and hold service providers accountable. Case managers and supervisors involved in both CCSP and SOURCE felt that SOURCE case managers have more flexibility, more responsibility, and more accountability than they do in CCSP. They stated that the flexibility of the SOURCE model allowed them to reduce the need for nursing home placement, maintain health and functional ability, and to slow the decline that can result from chronic conditions. Finally, people familiar with both programs felt that the high quality of care demanded for SOURCE participants benefits CCSP participants by raising the expectations of those involved in their care.
Consumer-Centered Approach to Case Management
The SOURCE approach to case management is grounded in person-centered planning. The SOURCE manual lists the "member centered approach" as one of the program's three major themes. Active participation by the enrollee and his or her family is encouraged. In-home service providers are required to honor the member's expectations for:
- Reliability of service (including timing of visits);
- Competency, compatibility, and consistency of staffing; and
- Responsiveness to member concerns.
Case managers indicated that few quality problems arose because only the higher quality HCBS providers were selected to be SOURCE providers. Additionally, while a consumer cannot fire a provider, the case managers have the authority to stop using providers at their own discretion or when requested by the consumer. Case managers indicated that, in practice, providers tended to improve service delivery in response to criticism and thus avoid termination. Dissatisfaction with services was largely related to individual preferences not being met (e.g., services not being provided at the time consumers wanted).
Services Coordinated
Because the Medicaid service components are fee-for-service, the care plan is based on desired outcomes rather than a set amount of funding. Case managers are required to utilize all services covered by Medicare and Medicaid as well as other publicly and privately funded services necessary to support the participant.18 They also coordinate access to services that supplement the care plan, but do not generally control funding from other programs. For example, the SOURCE case managers can ensure that a participant receives Older American's Act services provided by the AAAs if needed. The most commonly used services are personal care services and meals. Transportation was cited as the most critical service provided.
Although services otherwise available in the community must be utilized, it is expected that some needs will not be covered by traditional third-party payers or generally available as community resources. In these instances, case managers are expected to work creatively to develop ways to address needs that reflect the individual's ability to pay. As a result, case managers often work with community organizations to develop new resources (for example, obtaining clothing, air conditioners, and other needed items through donations). SOURCE case managers we interviewed spoke often about the importance of building strong relationships within the larger community in order to leverage resources to support those most in need.
In addition, each SOURCE agency is required to reserve some SOURCE funds, or secure other resources, for essential items and services that are necessary to keep someone in the community but that are not otherwise covered or available without charge. The SOURCE provider manual lists a number of examples of such items and services, among them nutritional supplements and incontinence supplies. These services or supplies are only provided after review and approval by the medical director and are delivered on a case-by-case basis. The SOURCE sites document all services provided with these funds for review by state officials who periodically consider changes in the program's covered service package.
Local SOURCE contractors did not describe coordination with Medicare as a problem even though dually eligible beneficiaries are not restricted from seeing Medicare providers. Case managers actively discourage beneficiaries from setting up appointments without first notifying their SOURCE physician or case manager. Case managers and SOURCE administrators stressed that due to the high level of case manager involvement, they know when participants are scheduled to see other physicians or providers. Agencies work closely with local hospitals to educate them to recognize SOURCE participants and to notify the SOURCE agency when one of its clients is treated in the emergency room or admitted. SOURCE managers felt that they often had the cooperation of the hospital discharge planners because the coordination efforts of the SOURCE case manager often made the hospital discharge planner's job easier.
SOURCE case managers appear to build strong relationships with participants and their families who keep them informed about health and other important developments. Case managers did not express concerns about the lack of formal coordination with Medicare benefits or formal restrictions on participants' access to any and all providers. They felt it was their job to stay informed about their clients' service use and that it was quite possible to do a good job at this. With the implementation of the Medicare prescription drug benefit, SOURCE case managers will have an additional responsibility to assist participants to enroll in the most appropriate program, and to deal with coverage issues that may arise for their dually eligible participants.
Screening and Assessment
Potential SOURCE participants are screened to determine if they meet financial and service eligibility criteria. Screening for basic eligibility must occur within three days of referral. Case managers then conduct an assessment in the person's home, which must be completed within five days of the screening. As in the traditional waiver program, this assessment captures psychosocial and environmental information, and comprehensive health information. The assessment is used to prepare an initial care plan, which is reviewed with the participant and/or family caregiver. The assessment is also provided to the SOURCE physician with whom the client will enroll. The assessment provides information not always available to physicians, such as the names of other treating providers and a full medication list.
If new participants have no prior relationship with the selected SOURCE physician, they receive a physical exam, the results of which are incorporated into the care plan as appropriate. The program has found that participants have been willing to change physicians in order to receive the enhanced case management and coordination available through SOURCE.
Levels of Care
The case management team assigns a level of care and officially enrolls the individual in the program based on the assessment and recommended services. The levels of care are not directly correlated to specific services; rather the assigned level is used to create a general budget framework and an expected level of service utilization. The program also uses these assignments in the care planning process, as discussed below.
The level of care assignment helps to finalize the service array into a detailed plan of care that is included in a carepath document (described in the next section) that serves as the primary tool for monitoring services. The medical director and the SOURCE primary care physician approve the carepath, which is essentially a standard protocol for case managers and physicians to monitor participant outcomes.
The program has established four levels of care with four corresponding carepaths. Levels one and two include people with substantial cognitive and/or physical impairments who meet nursing home level of care criteria. In 2002, about 70 percent of SOURCE enrollees met the nursing facility level of care criteria. Levels three and four include participants who have at least one chronic condition but do not meet nursing facility level of care criteria. Case managers indicated that Level 4 participants are high functioning and do not require many services. Their focus for this group is generally on education about disease self-management techniques and encouraging participation in wellness activities and programs.
Carepath
The carepath focuses on: (1) identifying key outcomes for the participant, and (2) identifying the parties responsible for achieving each outcome. Each carepath has goals (expected outcomes) and is customized to the unique needs of each participant. It addresses a wide range of health and long-term care issues, such as skin care, medical compliance, availability of informal supports, nutrition/weight, key clinical indicators, ADLs and IADLs, cognitive impairment and problem behaviors.
The carepath documents the participant's goals/outcomes and lists the specific services and the frequency with which they will be delivered as well as the providers who will support the attainment of a participant's goals. Each care path clearly delineates the roles and responsibilities of the participant, the primary care physician, and the case manager. See Appendix B for an example of a carepath form.
The carepath differs from traditional waiver care plans because it links specific levels of care to expected outcomes for that level. These outcomes include such key clinical indicators (depending on the chronic condition) as weight, ADL/IADL functioning,19 and skin condition. The Level 1 carepath contains 13 goals, listed in Exhibit 1, the maximum number of goals in a carepath, and includes all the goals of Levels 2, 3, and 4. Each participant's customized care plan details how the goals will be achieved.
Monitoring
While service delivery is monitored for timeliness, participant satisfaction, and quality, services are also reviewed to assess the extent to which they (or a specific provider) are facilitating attainment of the individual's goals. The carepath facilitates monitoring by specifying the responsibilities of the case manager and the physician as well as any informal or formal supports required to achieve desired outcomes. It also includes a guide for quarterly review and comment on the extent to which goals are, or are not, being met.
| EXHIBIT 1: Level 1 Carepath Goals |
|
Case managers arrange for services and follow-up with clients within two weeks of the start of services to ensure that appropriate care is being provided. To the extent that client goals are not being achieved (carepath variance), the client's case is reviewed and, when necessary, adjusted during the weekly meeting of the case management team. Case managers also meet with HCBS providers monthly.
The case manager meets quarterly with the participant's physician to review the long-term care services care plan and the client's health conditions and treatment plan. During these meetings, they review treatments, services, and outcomes. The carepath document is then revised to reflect the findings of the physician/case manager meeting. The case management team then reviews the carepath changes, which require the approval of the medical director as well as the SOURCE physician.
This process of changing the care plan can occur whenever needed and is not limited to the quarterly review. As a result, SOURCE case managers and medical directors have the flexibility to authorize changes in care plans and to have services provided without state pre-approval. In contrast, changes in a CCSP care plan require that the case manager send paperwork to the beneficiary's primary care provider, who has 60 days to approve the new care plan. After the physician approves the care plan, it must be approved by the state agency and entered into the state payment system before the services can be delivered.
Home and Community-Based Service Provider Accountability
Case managers are responsible for assuring that HCBS providers meet client needs and deliver quality services. When they do not, the case manager is responsible for replacing the provider. This differs from CCSP which, like most traditional waiver programs, utilizes all providers who meet the state standards, and rarely terminates providers because it requires a time-consuming and cumbersome process. While SOURCE must construct its provider list from those already approved for use in the CCSP program, SOURCE can decline to utilize low performers. Each SOURCE site has a process for terminating providers who do not meet performance standards. In practice, SOURCE staff members closely monitor performance and act quickly to terminate providers if their performance is not satisfactory. The SOURCE program staff also conduct scheduled and surprise visits to the member's home to monitor the quality of service delivery.
SOURCE tracks service utilization against authorizations by requiring HCBS providers to report services provided in a monthly report to each case manager. Case managers also use these reports to monitor general spending.
Replication
Georgia's experience suggests that agencies operating traditional waiver programs can build stronger outcome-driven case management models, like the SOURCE model, that include primary care physicians. SOURCE was implemented by overlaying a 1915(c) waiver on an existing 1915(b) PCCM arrangement and other states could adopt this approach. An additional coverage option is to use targeted case management under the state plan to contract with an agency to pay for the site coordinator, case managers, medical director, and primary care physician involvement. Information about various Medicaid coverage options for SOURCE and similar programs can be obtained from CMS regional offices.
States interested in replicating this or a similar program need to assure that they have an infrastructure of primary care physicians and case managers who understand how to manage chronic conditions, as well as a range of available HCBS to support individuals with chronic conditions. States with single-entry point systems already have the building blocks in place for forming linkages with primary care providers.
Single entry points that recognize the importance of health care and the need to better coordinate primary health care with long-term care, may be better able to build partnerships with health care professionals. Those that see their role as more limited--to address the functional needs of waiver participants--may have more difficulty arranging partnerships and working with medical providers. Primary care and other health care providers must be willing and able to collaborate with the single entry points as well.
Georgia Medicaid program administrators are confident that the SOURCE program helps delay or prevent nursing home placement, and reduces preventable hospital in-patient and emergency room use. However, sufficient data are not yet available to evaluate program outcomes. A preliminary analysis completed shortly after the program began suggested that SOURCE was slightly more effective than the traditional waiver program in reducing ambulatory care sensitive events and repeated inpatient hospital admissions. A formal evaluation is needed to determine the actual impact of the SOURCE program model on long-term costs and outcomes.
However, given the complex needs of people with chronic conditions and the complicated health and long-term care systems they must navigate, care coordination will always be a critical component of quality care for the growing number of people with chronic conditions.
INDIANA CHRONIC DISEASE MANAGEMENT PROGRAM (ICDMP)
In 2003, the Indiana Department of Family and Social Services Administration in partnership with the Department of Health and other local stakeholders developed the ICDMP. The goal of the program is to improve patient self-management, primary care physician practices, and the health care delivery system infrastructure for people with chronic conditions.
The ICDMP program supplements care management services provided in Indiana's PCCM program for certain Medicaid-only and dually eligible beneficiaries with asthma, diabetes, and CHF. The supplementary services include phone-based care management--a common feature of Medicaid disease management vendor programs--and in-person nurse care management, the primary intervention associated with health care coordination programs.
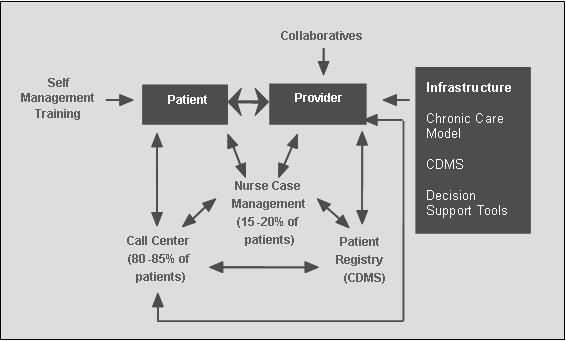
The ICDMP is a health care coordination program with three levels of intervention: the patient, the provider and the delivery system infrastructure. (See Exhibit 2).20
- At the patient level, the program uses call center and nurse care management services to help participants develop self-management goals and skills. For a child with asthma, goals might include knowing and reducing exposure to asthma triggers, knowing how to use peak flow meters and spacers, and knowing when to take asthma management medications.
- At the provider level, the program supports learning collaboratives to help physicians provide better care to patients with chronic disease. A collaborative consists of workshops to help physicians design and implement changes in their practices to promote better chronic care management. Practice level changes could include using a patient registry, developing a system to flag patients' charts, using flow sheets to ensure that preventive services are completed during regular office visits, and scheduling planned visits--a preventive visit analogous to a well-child visit--for patients with chronic conditions.
- At the infrastructure level, the program has developed a Web-based patient registry and promoted decision support tools, which include guidelines for the three target conditions, examples of self-management goals, and patient education materials.21 The tools have been distributed to all primary care providers including non-Medicaid providers.
| EXHIBIT 2: Indiana Chronic Disease Management Program Model |
 |
| SOURCE: ICDMP, 2004. |
Program Eligibility
EDS, the state's Medicaid fiscal agent, identifies Medicaid enrollees with the target diseases (diabetes, CHF (adults only), and asthma) by electronically scanning claims data for evidence of relevant diagnostic codes or related drug utilization. Participants are also identified through self or physician-referral, although referrals are infrequent. Persons who are not eligible for the program are those who are institutionalized; participating in a HCBS waiver; subject to Medicaid spend-down; diagnosed with end-stage renal disease; transplant recipients; or enrolled in risk-based managed care plans. As of March 2005, approximately 30,000 of the 800,000 Medicaid beneficiaries in Indiana were enrolled in the program.
Once eligible beneficiaries are identified, they are stratified into low and high-risk groups based on historical claims data including pharmacy use and inpatient episodes. The state and its partners identified program participants at the start of the program and now conduct quarterly reviews of the data to identify those recently diagnosed with target diseases or newly enrolled in Medicaid. The state forwards the list of eligible members developed by EDS to the call center disease self-management program.
Call Center Disease Self-Management Program
Low-risk participants--approximately 80-85 percent of the total targeted population --are enrolled in the phone-based disease self-management program operated by the call center. High-risk participants receive nurse case management, discussed in the next section.
The call center began operations on July 1, 2003.22 AmeriChoice, the state's Medicaid enrollment broker and PCCM administrator, operates the call center. The state amended its enrollment services contract with AmeriChoice to include the call center services, which are billed at a fixed rate based on volume.
Using computerized scripts, AmeriChoice care coordinators make calls to the low-risk care management participants every three months. The Indiana-based Regenstrief Institute developed the scripts, which are programmed to guide the care coordinator through a series of questions based on the member's responses. Program and call center staff review the scripts to ensure that the language level and concepts are understandable to participants. Scripts have been developed for the first three cycles of calls, covering nine months. Scripts for subsequent calls are under development.
The first three calls cover an initial assessment and basic education on the target disease, medications, and self-care skills. The first phone call is designed to confirm eligibility, complete an initial assessment, and describe the program. Members are encouraged to talk to their physician about issues identified by the assessment (e.g. getting a flu shot, taking aspirin (for CHF), or monitoring blood sugar (for diabetes)). The coordinator educates the member about the disease process and offers educational materials. After this call, the members are sent a letter summarizing their responses and encouraging them to discuss its contents with their doctor during their next visit. A sample letter is provided in Appendix E.
The program is voluntary and most of the members contacted agree to participate. If a member declines to participate, she is called again after a month. Approximately 10-15 percent of eligible members cannot be reached by phone. If a member cannot be reached after three attempts, she is sent the introductory letter but no additional calls are made. By November 2004, all of the high-risk members and 30-40 percent of the low-risk members had been contacted by the program.
| EXHIBIT 3: Call 2 Flow Chart |
 |
| SOURCE: Regenstrief Institute. |
The second call is much more detailed than the first, covering more topics and in greater detail. Respondents are asked questions designed to determine if the member is having problems with medications, doctor visits, or transportation. Education is also provided on (for example, diabetic foot care, self glucose monitoring, and insulin administration). Exhibit 3 on the next page illustrates the topics and sequencing of the second call.
The third call reviews and reinforces the topics addressed in the prior call. For example, if a member received a flu shot after being encouraged to do so during the second call, she would be congratulated and encouraged to continue to get a flu shot annually. This call also addresses smoking cessation and depression in greater depth than the prior calls.
As part of the call, care coordinators administer a depression screen and members are invited to discuss topics from a list that includes diet, exercise/physical activity, and preventing complications (for diabetes only). Afterwards, call center staff submit a report to the member's primary care provider.
| EXHIBIT 4: Depression Screening from Call 3 Script |
We are almost done with our call. I have just a few more questions about how you are feeling, "over all." Many people that I talk to that have chronic health problems feel down or depressed from time to time. This is important to know, because feeling this way can affect your life in many ways and can make it harder for you to take the best care of yourself. In responding to each of these next questions, I would like you to think about how you have been feeling in the last two weeks--just the last two weeks.
A lot of people with [Care Coordinator--say member's condition(s)] feel down or depressed from time to time. Sometimes these feelings come and go. Other times they stay around and can cause big problems. It is important to talk to your doctor about these feelings. She/he can help decide if you need to be treated to help make the symptoms go away. She/he can also help decide if the feelings are affecting how well you are able to take care of yourself. Your doctor might not know about these feelings unless you tell her/him. Be sure to write this down and talk to her/him about these feelings at your next doctor visit. |
In addition to phone care management responsibilities, the call center is also responsible for assembling and mailing the Provider Toolkit (discussed later) to all Medicaid providers statewide, handling provider and self-referrals to the program, reporting program statistics to the state, and maintaining a website.
Call Center Staffing and Training
The call center staff consists of a manager, two supervisors, a trainer, and 26 care coordinators who handle all the calls. The supervisors and trainer must be registered nurses. Most of the care coordinators have call center experience and often an associate or bachelor's degree. Care coordinators receive three weeks of introductory training, which includes pre and post-test components. Physicians from the Regenstrief Institute developed and tested the training curriculum, phone scripts, and the Chronic Disease Management System (CDMS) software used by the call center. The call scripts are highly detailed and designed for use by non-clinical care coordinators.
The training curriculum includes information about the target diseases, Medicaid eligibility, and the enrollment broker software. The call center care coordinators are also trained to identify markers indicating the member might have an acute health care need requiring more intensive and immediate care management or physician intervention. In such cases, one of the registered nurses on staff follows up with the member and has the discretion to elevate the member to the high-risk group. Call center hours are staggered and include Saturday mornings to accommodate the schedules of working families.
Nurse Care Management
In addition to the services provided by Call Center staff, the ICDMP includes a comprehensive nurse care management program for high-risk participants, which provides local, personalized, and intensive care management. The nurse care management component of the program began operating August 1, 2003. High-risk participants are first contacted by care coordinators, who confirm eligibility, complete an initial assessment, and describe the program. Following the call, members are sent a letter indicating that a nurse care manager will make the next contact. Members typically remain in the nurse care management program for 4-6 months before "graduating" to phone-based care management.
Nurse Care Management Organizations
The state contracted with two organizations to provide nurse care management--the Indiana Primary HealthCare Organization and the Indiana Minority Health Coalition. They were selected based on their active engagement in and knowledge of local health care systems and their ability to provide services statewide. Each county in Indiana is assigned to one of the two organizations. Indiana Primary Healthcare--the association of federally qualified health centers--is responsible for the rural counties, while Indiana Minority Health Coalition focuses on urban counties, primarily in central Indiana. The organizations are required to have a program director and a supervisor.
Each organization employs 15 nurse care managers and is paid an annual fee of $100,000 per nurse.23 This fee includes the salary of the nurse, training, mileage, and any other costs incurred by the organizations in fulfilling its scope of work. The program director and supervisors at each of the organizations meet monthly with the nurses, conducting group consultations on some of the more difficult and complex cases. The program director and supervisors from both organizations meet weekly with the state ICDMP staff to discuss progress, issues, and challenges.
Nurse Care Managers
The scope of work for both care mangers and supervisors is outlined in a contract between the state and the care management organizations. (See Appendix C. Appendix D describes minimum qualification for care managers.) The nurses hired by these organizations often know and have worked with members' primary care doctors and are familiar with referral networks and community resources. The program directors and supervisors indicated that many of the most effective nurse care managers have many years of experience and are mature and flexible. Nurse care managers are currently responsible for an average of 70 clients.
Nurse Care Management Process
Once the call center has made the first contact with a member, the member's contact information along with a summary of the initial assessment is forwarded to the appropriate nurse care management organization, and the member is assigned a specific nurse care manager based on the location of his or her primary care provider. (Members with the same provider are assigned to one nurse).
The assigned nurse's first step is to set up a time to visit the primary care provider's office to review the member's chart and to identify conditions, risk factors, and any existing care plan. The nurse also tries to meet with the physician during the visit to discuss any specific issues or barriers the physician would like addressed through the care management process. Once the nurse completes the chart review, she initiates contact with the member by phone to introduce the program and set up a home visit.
Nurse care management is delivered in three ways: in-person home visits, office visits to primary care providers, and phone-based counseling. Home visits are an especially critical component of the program, helping nurse care managers assess the member's environment, resources, and state of mind, and permitting a more tailored and personalized care management approach. While the initial visit is made to the home, many of the subsequent contacts, which occur about once a month, are made by phone. In denser urban areas, where the costs and time required to travel to a member's home are minimal, subsequent visits also frequently occur at the member's home.
The main concern members voice about the program is that it is too short. But the short duration of the intervention--4-6 months--is by design. The program was carefully crafted to help members identify and act on their own care management concerns, not to manage care on their behalf. The care management process teaches members how to be more engaged in their own health and health care, including developing the skills to manage their care, and the knowledge and confidence to discuss concerns with providers or Medicaid staff when the intervention ends.
For example, when members have concerns about their interaction with a physician, if nurses observe the member is not getting appropriate care, or when the member has been incorrectly told that items such as peak flow monitors and spacers (medical devices to treat asthma) are not covered by Medicaid, the nurse does not immediately get on the phone to resolve the issue. Instead, she discusses the issue with the member and encourages him to discuss issues and concerns directly with the provider or Medicaid staff. The nurse follows up with the member or the provider to make sure the member was able to get his concerns addressed and his needs met.
The concept of improving self-care by empowering members is central to the program's design and operation. However, if the program expands to include HCBS waiver participants, traditional care management services may also be required to meet their more complex needs and to assist those who are not able to care for themselves.
Interaction with Primary Care Providers
In addition to working with members on self-care skills and providing education, nurses also help implement care plans developed by providers, highlighting the important relationship between nurses and primary care providers. Nurses make an initial contact with physician practices to review member charts and then schedule one of the care management sessions in conjunction with an office visit to give the care manager, the member, and the provider a chance to jointly discuss chronic care issues. The nurse provides written feedback to the physician after the initial home visit and at the end of the 6 month intervention. Because one care manager is paired with each practice, the nurse has multiple opportunities to interact with physicians and their staff, in order to develop a flexible and collaborative relationship.
The relationship between the care manager and the provider can take many forms. In some cases the nurse care manager communicates mainly with the office manager; at other times, she works directly with the physician. Nurses often remind doctors about the resources included in the Physician Toolkit. Physicians did not immediately embrace these resources, but after the program had been operating for a year, ICDMP has noticed increasing openness and engagement from physicians who are starting to ask more questions about the program.
Co-morbidities
Many members enrolled in ICDMP have multiple chronic conditions. The program officially enrolls a member for only one disease; however, in practice, the nurse care manager will often address both CHF and diabetes. This has worked fairly well for members with both conditions, probably because the behavior change goals are often similar for the two diseases.
Seventy percent of people with diabetes also have depression. Care managers found addressing depression and other mental health co-morbidities more challenging due to the complex nature of mental illness. Nurses and their agencies have developed strategies to address mental health issues. In some cases, the nurse care manager will discuss the member's condition first with the primary care physician or psychiatrist to determine if the member is ready for the ICDMP or if mental health treatment is needed first. If the person is particularly fragile, the nurse care manager will sometimes contact the mental health care manager to see if the first visit can be conducted jointly, lessening the stress for the member. The focus is on effective implementation of the nurse care management intervention not on treating the mental health condition.
Completion of Nurse Care Management
When high-risk participants have completed their 4-6 month participation in the nurse care manager program, they are transferred back to the call center for ongoing care management. The care plan is forwarded to the call center, including notes about the member's care management goals, and suggestions and pointers for how to work with the individual. The call center calls them two weeks after their "discharge" and follows up again a month later. If any issues or complications arise during the transition phase, the member is re-enrolled in the nurse care manager program. After this transition phase, members continue on the regular call center cycle of quarterly calls.
Physician Collaboratives
Physician learning collaboratives are designed to help physicians provide better care to patients with chronic conditions. The use of collaboratives is based on the idea that by working collaboratively, organizations and providers who share similar goals can accelerate change. To date, the state has implemented four collaboratives as part of ICDMP. Each involved 2-3 in-person learning sessions.
The program provides time between sessions to allow for the development and testing of practice level changes, and the final session is focused on sharing lessons learned. To date, 48 practice teams, composed of a physician, a nurse, and an office manager, have participated in collaboratives in different parts of the state. Exhibit 5 summarizes one physician's experience in a collaborative.
The first collaborative included 25 practice teams and focused on CHF and diabetes; the second focused on CHF, diabetes, and asthma; the third on asthma only; and the fourth on CHF, diabetes, and asthma. The state is planning a fifth collaborative in the Fall of 2005.
While collaboratives can addresses all three chronic conditions, each provider team may select one or more conditions as the focus of its efforts, and relays monthly progress reports to ICDMP. These reports track team performance on the state's mandatory measures (one for each condition) and on 3-4 additional goals providers have chosen.
Early participants were enthusiastic about the collaborative; however, the initiative has faced challenges. The original collaborative design called for three, two-day learning sessions and a final meeting over a 12 month period. The period was shortened because physicians said they could not be absent from their practices that long. As an incentive to participate, the program is free and physicians get continuing education credit. Yet, only about half the practice teams make it through the whole process. The initiative is also time and resource intensive for state managers.
| EXHIBIT 5: Provider Case Study--Results of Collaborative |
| Provider profile. The provider is one of the largest safety net providers in Indianapolis with several sites and a previous commitment to care management (asthma coordinators are on staff). Eighty percent of patients are covered by Medicaid. First steps. The provider completed a chart audit to identify all children with asthma. Goals. To get asthma patients on control medications, establish home and school action plans for these patients, and establish care improvement goals. Care delivery changes as a result of participation in the collaborative. The provider added a bright chart label to identify patients with asthma and attached pre-printed post-it notes with questions on severity for the physician to probe. These visual reminders prompt the physician to follow-up with the patient, even if she has visited the office for another reason. The asthma coordinator, who participates in every office visit with asthma patients, conducts post-visit follow-up. Issues. (1) The high-rate of visit no-shows made it hard for the provider to introduce prevention activities and trace progress. (2) The asthma coordinator found that if asthma was under control (the patient did not complain) the physician would not address asthma management in the visit (eroding progress on prevention). (3) The provider cannot bill Medicaid for the asthma coordinator's participation in the well child visit. |
| SOURCE: Adapted from a presentation by Thomas Inui, 2004. |
The mandatory measures are:
- All diseases: Percent of patients with at least one self-management goal.
- Diabetes: Percent of patients with HbA1c level of less than eight.
- CHF: Hospital readmission rate.
- Asthma: Percent of patients with persistent asthma who are treated with anti-inflammatory medications at effective doses for appropriate durations.
The figures reported by the physicians who participated in the first collaborative are promising. Between June 2003 and July 2004, the percentage of diabetes patients with HbA1C less than 8 percent increased from 28-59 percent. The percentage of patients with CHF who had at least one self-management goal increased from 14 percent to 86 percent.
Chronic Disease Management System
All Medicaid providers in Indiana have access to the state's electronic patient record and disease registry, the CDMS. This system is housed at the Department of Health and was developed from a template created by the Montana Quality Improvement Organization. The state downloads claims data into CDMS for all care management participants. The call center and the nurse care managers enter care management summaries into the system.
Physicians can use CDMS to generate alerts, identify subsets of patients, and track their progress toward goals. They can also enter their own care management information to CDMS, making the registry a complete chronic care record. To date, however, few physicians have used CDMS as a tool to document and manage office-based care. The state is launching a physician survey to investigate the reasons and explore examples of when and where physicians are using the system.
Even without formal study, however, it is clear that the burden of data entry is one reason for low provider participation. In addition, the system cannot be used for other office functions such as claims submission or as a complete electronic patient record, as it only includes information related to the patient's chronic condition. A final issue is that providers do not have full access to the CDMS; they can see information entered by nurse care managers but not notes from the call center.
Evaluation
The program is planning a two-part evaluation. The first part is a randomized controlled study that will include analysis of clinical and claims data for providers in the Indianapolis area using the Regenstrief electronic medical record.24 The second part will include analysis of claims data for all members statewide and a phone survey of a random sample of providers and members.
Evaluating this program presents many challenges. Indiana is fortunate to have electronic clinical data available for some of the participants. However, clinical data will not be available for the statewide evaluation, and claims data pose certain limitations.25
The state contracted with the Regenstrief Institute to conduct the evaluation and to design, implement, and provide ongoing quarterly maintenance of the following services for a total cost of $1 million over a two-year period (August 2003-July 2005):
- CDMS software, member selection, and risk stratification;
- Call center scripts; and
- Nurse care manager training materials.26
Replication
ICDMP was implemented under the authority of a 1915(b)(4) waiver of the Social Security Act. The medical state plan services provided by the ICDMP are eligible for federal financial participation at the state's regular federal medical assistance match rate.
The program has required substantial time and attention from the state's Medicaid agency staff, both during the initial design and implementation. Once operational, however, the program only requires one full-time state employee to serve as the program director. Nonetheless, many states may feel they lack the programmatic expertise, management capability, or local partner organizations to make such a program work.
CMS has made available a State Medicaid Director Letter dated February 25, 2004, for guidance on the available approaches to financing disease management and health care coordination programs.27
The ICDMP offers a promising health care coordination approach to address cost and quality issues. However, the outcome of the formal evaluation is needed to determine the actual impact of the model on costs and outcomes.
NOTES
-
Partnership for Solutions. Making the Case for Ongoing Chronic Care--Chartbook (Baltimore, MD: Johns Hopkins University, 2002).
-
'Risk-based' means the provider receives a set (capitated) payment for each enrollee and must provide all contracted services. Depending on the program, providers have varying degrees of financial risk that the funds they receive will not be sufficient to provide all needed services.
-
Care coordination for Medicaid beneficiaries enrolled in Medicare managed care plans may create administrative complications for states interested in coordinating care for dually eligible individuals. (See Walsh and Clark, 2002.)
-
One other state, Massachusetts, had a pilot program for 50 beneficiaries that met all three of these criteria. However, when NASHP began work on this project, the program had just begun and did not have enough operating experience to report.
-
A. Chen et al., Best Practices in Coordinated Care (Princeton, NJ: Mathematica Policy Research, Inc., 2000).
-
The new Medicare drug benefit created under the Medicare Modernization Act is likely to reduce incentives for states to include the dually eligible in prescription drug monitoring programs. While the states will retain some financial responsibility for prescription drug costs for the dually eligible, they may not have access to the prescription drug utilization data necessary to monitor use.
-
Muskie School of Public Service, Institute for Health Policy. MaineNet Project Description. Retrieved April 14, 2005. http://muskie.usm.maine.edu/projectbriefs/MaineNET.jsp.
-
See Williams, 2004 for a discussion of Medicaid disease management vendor programs.
-
Medicaid Disease Management & Health Outcomes. Retrieved February 8, 2005. http://www.DMNOW.org. The site lists about 23 states with disease management vendor programs. Not all are included in our count because a few of the states have DM contracting only within their MCO programs, and two states seem only to have pharmacist-based programs.
-
SOURCE is a trademarked name of the St. Joseph/Candler Health System in Savannah, GA. The St. Joseph/Candler staff provides technical assistance to the Department of Community Health (DCH) to develop best practices. Its contract with DCH includes development and refinement of the SOURCE program.
-
Georgia SOURCE provider manual.
-
SOURCE is administered by the DCH, the state's Medicaid Agency. CCSP, the state's traditional waiver program, is managed by the Department of Human Resources' Division of Aging Services, through AAA single entry points.
-
This compensation is considerably more than physicians receive for participating in the regular PCCM program. Physicians in hospital-based SOURCE sites typically do not receive this compensation because they are on salary. Payment arrangements vary by site.
-
To receive SSI, a person must have an income level of about 74 percent of the federal poverty level or less and resources of $2,000 or less. In addition, he or she must be age 65 or older or have a disability if under age 65.
-
Payment for this clinical exam or evaluation differs by physician and SOURCE contractor. In some cases, the clinical evaluation might be considered covered by the monthly administrative fees. In others, Medicaid or Medicare might be billed.
-
This includes both Medicaid state plan services and waiver services including personal care, adult day health, personal emergency response, and homemaker services.
-
ADLs include bathing, dressing, eating, toileting, and mobility. IADLs include preparing meals, doing housework, using the telephone, managing medications, paying bills, and getting around outside the home.
-
This program approach mirrors the Chronic Care Model developed by Dr. Ed Wagner, Director of Improving Chronic Illness Care, a national program of The Robert Wood Johnson Foundation. For more information, go to http://www.improvingchroniccare.org/change/index.html.
-
Prior to the implementation of the ICDMP, the Indiana Department of Health worked with physicians throughout the state to develop consensus based guidelines for asthma, diabetes and CHF. All of the provider materials are available at http://www.indianacdmprogram.com/.
-
Call Center costs are billed as Medicaid services at 62 percent FFP.
-
The state receives 75 percent federal financial participation for this fee.
-
The providers of about 15 percent of Medicaid members in central Indiana use the Regenstrief electronic medical record.
-
E. Walsh, D. Osber, C. Nason, et al., "Quality Improvement in a Primary Care Case Management Program," Health Care Finance Review Vol. 23, No. 4 (Summer 2002): 71-84.
-
The Regenstrief Institute is a 25-year-old research foundation located on the Indiana University School of Medicine campus, and is dedicated to the study and improvement of health and health care delivery. For additional information about the Institute, see: http://www.regenstrief.org/.
-
Available at: http://www.cms.hhs.gov/states/letters/smd022504.pdf.
APPENDIX A. SOURCES AND SELECTED READINGS
Agency for Healthcare Research and Quality, 2002. Prevention Quality Indicators, Version 2.1. Rockville, MD.
Anderson G., Knickman J., 2001. "Changing the Chronic Care System to Meet People's Needs." Health Affairs. Volume 20, Number 6.
Anthony S., et al, 2001. "Medicaid Managed Care for Dual Eligibles: Case Studies of Programs in Georgia, Minnesota, and Pennsylvania." Kaiser Commission on Medicaid and the Uninsured.
Casalino L., et al., 2003. "External Incentives, Information Technology, and Organized Processes to Improve Health Care Quality for Patients With Chronic Diseases" Journal of the American Medical Association. 289:434-441.
Chen A., Brown R., Archibald N., Aliotta S., Fox P., 2000. "Best Practices in Coordinated Care." Mathematica Policy Research, Inc. Princeton, NJ.
Commission on Affordable Housing and Health Facility Needs for Seniors in the 21st Century, 2002. "A Quiet Crisis in America." A Report to Congress. Washington, DC.
Cyphers G., 2002. "Findings from the 2002 Quick Survey on State Human Service Agencies' Responses to Budget Shortfalls." American Public Human Services Association (APHSA).
Department of Community Health, Division of Medical Assistance, State of Georgia, 2001. "SOURCE CarePath Training Guide."
DMNow.org. Retrieved 9 January 2003. "Operational Structures for Implementation of Disease/Case Management." [http://www.DMNow.org]
Feder J., Komisar H., Niefeld M., 2000. "Long-term Care in the United States: An Overview." Health Affairs. Volume 19, Number 3.
Folkemer D., 1994. "State Use of Home and community-based services for the Aged Under Medicaid: Waiver Programs, Personal Care, Frail Elderly Services and Home Health Services." AARP, Public Policy Institute.
Foote S., 2003. "Population-Based Disease Management Under Fee-For-Service Medicare." Health Affairs, Web Exclusive, July 30, 2003
Gillespie J., Rossiter L., 2003. "Medicaid Disease Management Programs: Findings from Three Leading U.S. State Programs." Disease Management Health Outcomes 2003: 11(6): 345-361.
Henry D., Mendelson D., Fallieras A., 2003. "Clinical Pharmacy Management Initiative: Integrating Quality into Medicaid Cost Containment." Center for Health Care Strategies.
Holahan J., Wiener J., Lutzky A., 2002. "Health Policy for Low-Income People: States' Responses to New Challenges." Health Affairs, Web Exclusive, May 22, 2002.
Institute of Medicine, Committee on Identifying Priority Areas for Quality Improvement, 2003. Priority Areas for National Action: Transforming Health Care Quality. National Academy Press, Washington, DC.
Institute of Medicine, Committee on Quality of Health Care in America, 2001. Crossing the Quality Chasm: A New Health System for the 21st Century. National Academy Press, Washington, DC.
Institute of Medicine, Committee on Rapid Advance Demonstration Projects: Health Care Finance and Delivery Systems, 2003. Fostering Rapid Advances in Health Care: Learning for System Demonstrations. National Academy Press, Washington, DC.
Justice D., 1991. "The Integral Role of Case Management in Authorizing Services Under State Community Based Care Programs." National Association of State Units on Aging. Washington, DC.
Kaiser Commission on Medicaid and the Uninsured, 2003. "Medicaid Spending Growth: A 50-State Update for Fiscal Year 2003." Washington, DC.
Kozak L., Hall M., Owings M., 2001. "Trends in Avoidable Hospitalizations: 1980-1998." Health Affairs, March/April 2001; 20(2): 225-232.
Landers G., 2004. Final Report: The Georgia Long-term Care Partnership 2001-2004 (Atlanta, GA: Georgia Health Policy Center, Georgia State University).
Lawrence D., 2002. From Chaos to Care. Perseus Publishing, Cambridge MA.
Lerch S., 2002. "Avoidable Hospitalizations Among Medicaid Recipients in Washington State." Washington State Institute for Public Policy.
McNickle L., 2000. "Breakthrough in Elder Care." Health Progress. Volume 81, Number 3.
Mollica R., Saucier P., Riley T., Booth M., 1997. "Protecting Low Income Beneficiaries of Medicare and Medicaid in Managed Care, Volume II: Coordination of Benefits, Payment Mechanisms and Quality Management." National Academy for State Health Policy. Portland, ME.
National Chronic Care Consortium, 1997. "Case Management for the Frail Elderly: A Literature Review on Selected Topics." Bloomington, MN.
National Chronic Care Consortium, 2000. "Case Management: Methods and Issues." University of Maryland Center on Aging, The Robert Wood Johnson Foundation Medicare/Medicaid Integration Program. College Park, MD.
National Conference of State Legislatures, 2003. "Disease Management Programs."
National Governor's Association, 2002. "State Efforts to Prevent and Manage Diabetes." Washington, DC.
National Pharmaceutical Council, 2003. "State Medicaid Resource Kit: Maintaining Quality and Patient Access to Innovative Pharmaceuticals in Challenging Economic Times. Washington, DC.
North Carolina Department of Health and Human Services, Division of Medical Assistance, 2002. Report to the Senate Appropriations Committee on Health and Human Services, the House Appropriations subcommittee on Health and Human Services and the Fiscal Research Division on Medicaid.
Partnership for Solutions, 2002. "Chronic Conditions: Making the Case for On-going Care." Johns Hopkins University. Baltimore, MD.
Partnership for Solutions, 2002. "Alzheimer's Disease: The Impact of Multiple Chronic Conditions." Johns Hopkins University. Baltimore, MD.
Partnership for Solutions, 2002. "Multiple Chronic Conditions: Complications in Care and Treatment." Johns Hopkins University. Baltimore, MD.
Partnership for Solutions, 2002. "Physician Concerns: Care for People with Chronic Conditions." Johns Hopkins University. Baltimore, MD.
Partnership for Solutions, 2002. "Public Concerns: Caring for People with Chronic Conditions." Johns Hopkins University. Baltimore, MD.
Rawlings-Sekunda J., Curtis D., Kaye N., 2001. Emerging Practices in Medicaid Primary Care Case Management Programs. National Academy for State Health Policy. Portland, ME.
Rosenbach M., Young C., 2000. "Care Coordination in Medicaid Managed Care: A Primer for States, Managed Care Organizations, Providers, and Advocates." Center for Health Care Strategies, Inc. Washington, DC.
Seniors and People with Disabilities, Department of Human Services, State of Oregon, 2002. "Contract RN Service Policy and Procedure Manual."
Smith V., Kramer S. and Guyer J., 2003. "Coordinating Medicaid and Medicare Prescription Drug Coverage: Findings form a focus group discussion with Medicaid Directors." Kaiser Commission on Medicaid and the Uninsured. Washington, DC.
Strunk B., Ginsburg P., and Gabel J., 2002. "Tracking Health Care Costs: Growth Accelerates Again In 2001: Hospital costs have secured their place as the leading driver of health care cost increases, for the second straight year." Health Affairs, Web Exclusive, September 25, 2002.
Sprague L., 2003. "Disease Management to Population-Based Health. Steps in the Right Direction?" National Health Policy Forum, The George Washington University, Washington, DC.
Thornton C., et al., 2002. "Constrained Innovation in Managing Care for High-Risk Seniors in Medicare + Choice Risk Plans." Mathematica Policy Research, Inc., Princeton, NJ. [http://aspe.hhs.gov/daltcp/reports/constrai.htm]
Wagner E., et al., 2001. "Improving Chronic Illness Care: Translating Evidence Into Action." Health Affairs. Volume 20, Number 6.
Walsh E., Clark W., 2002. "Managed Care and Dually Eligible Beneficiaries: Challenges in Coordination." Health Care Financing Review. Fall 2002/Volume 24, Number 1, 63-82.
Walsh E., Osber D., Nason C., et al. "Quality Improvement in a Primary Care Case Management Program," Health Care Finance Review Volume 23, Number 4 (Summer 2002): 71-84.
Weissman J., Gatsonis C., Epstein A., 2002. "Rates of Avoidable Hospitalizations by Insurance Status in Massachusetts and Maryland," Journal of the American Medical Association, November 1992; 268: 2388-2394.
Wheatley B., 2001. "Medicaid Disease Management: Seeking to Reduce Spending by Promoting Health." State Coverage Initiatives, Washington, DC.
Williams C., 2004. "Medicaid Disease Management: Issues and Promises." Kaiser Commission on Medicaid and the Uninsured, Kaiser Family Foundation, Washington, DC.
Zhan C., Sandl J., Biermand AS., et al., 2001. "Potentially Inappropriate Medication Use in the Community-Dwelling Elderly. Findings from the 1996 Medical Expenditure Panel Survey." Journal of the American Medical Association. December 12, 2001. Volume 286(22):2823-2829.
APPENDIX B. GEORGIA SOURCE CAREPATH
[This appendix is currently available only in Portable Document Format (PDF); a copy of the Acrobat Reader is needed to view it. It can be viewed as part of the full PDF file (link at top of this document) or separately at http://aspe.hhs.gov/daltcp/reports/ccMedbenB.pdf. ]
APPENDIX C. INDIANA CHRONIC DISEASE MANAGEMENT PROGRAM (ICDMP) CARE MANAGEMENT ORGANIZATION SCOPE OF WORK
Nurse Care Management Organization Contractor(s) shall:
- Hire, train, and maintain qualified nurse care managers in numbers sufficient to manage caseloads with up to 150 participants actively in Intervention Phase, participants are followed through the Reinforcement Phase. Contractor shall require a Bachelor's Degree in Nursing and 1 year experience in Community Health setting or Chronic Disease management; or Bachelor's work equivalent of formal nursing certificate and 3-5 years in Community Health setting or Chronic Disease management preferred. OMPP will provide initial training to Contractor on program components. Contractor shall provide ongoing training to nurse care managers on program components. Contractor shall utilize OMPP Nurse Care Manager Performance Expectations (Exhibit B) for description of Position Summary, Key Responsibilities, Critical Skill, Knowledge and Behaviors, Education and Experience, and Special Licenses or Transportation Demands to fulfill the terms of this contract.
- Train nurse care managers in the use of the chronic disease data management system (CDMS). OMPP will provide initial training to Contractor, further training will be the responsibility of the Contractor.
- Establish and maintain relationships with participating doctor offices and coordinate participant care information.
- Make appropriate case assignments to nurse care managers, based on caseloads assigned by the call center.
- Initiate care management with participants as quickly as possible after assignment to the network has been made by the call center.
- Provide a computer with Internet access to each nurse care manager.
- Prepare monthly monitoring reports, as directed by OMPP and meet OMPP performance measurement standards.
- Coordinate activities with other Chronic Disease Management Program partners.
- Meet semi-weekly with OMPP or more often at the sole discretion of OMPP.
- Maintain an appropriate number of supervisors consistent to assure compliance with performance expectations of the contract. Supervisory duties are not separately reimbursable under this contract and considered inclusive within the nurse care manager payment.
- Provide one program director who serves as a representative for the Contractor. Program director will act as liaison to OMPP. Program director duties are not separately reimbursable under this contract and are considered inclusive within the nurse care manager payment.
- Any travel necessary to perform the duties of this contract is not separately reimbursable.
Reporting requirements shall include but not be limited to the following:
- Contactor shall provide monthly reports on the number of disease management participants in the network as well as the number served by each nurse care manager. The participants shall be counted in either the intervention phase or reinforcement phase. Any request to increase nurse care manager staffing must be included in this report on current caseloads.
- Contractor shall submit a monthly roster for each nurse care manager, detailing progress on their individual caseload. The Contractor's operating efficiency will be measured and reported monthly, including but not limited to the following criteria:
- Nurse care managers will successfully complete 100% of calls/visits with program participants, as detailed in Exhibit B--Nurse Care Manager Performance Expectations,
- Nurse care managers will successfully complete 100% of calls/visits with the participant's PMP as detailed in Exhibit B--Nurse Care Manager Performance Expectations,
- Nurse care managers will record all contacts with participants and providers in CDMS, including participant's clinical data.
- Nurse care managers will complete participants' care plans within the required time frame,
- Nurse care managers will respond to inquiries/contacts from program participants and providers within one business day.
- Contractor shall provide written quarterly assessments of operating efficiency, including proposed strategies for improving efficiency.
APPENDIX D. INDIANA CHRONIC DISEASE MANAGEMENT PROGRAM (ICDMP) NURSE CARE MANAGER PERFORMANCE EXPECTATIONS
Position Summary. The primary responsibility of this position is the day-to-day management of the more severely classified participants of the Chronic Disease Management Program. This includes face-to-face encounters and telephonic encounters with these participants. Care Management is defined as on-going self-management support, referrals/reminders for appropriate testing and physician visits, on-going assessment of participant status, and working with Primary Medical Providers of the participants to ensure proper management during and after the nurse care manager intervention.
Performance Expectations
- Manage caseload of up to 150 participants actively in Intervention Phase and follow those participants through the Reinforcement Phase.
- Intervention Phase is defined as lasting 4-5 months and includes the following activities:
- Participant assessment--face to face encounter in the home, physician office, care management vendor location, or community location;
- Nurse Care Manager contact with Primary Medical Provider (PMP);
- Plan development/clarification--face to face encounter preferably done in conjunction with a PMP visit;
- Home assessment if first assessment was done outside of the home;
- Education/Training--telephonic contact with participant at a minimum;
- Problem Identification/Problem Solving--telephonic contact with participant at a minimum to provide self-management support training at point of first contact which includes problem identification, collaborative goal-setting, problem solving and regularly scheduled follow-up to assure goal attainment and setting of new goals;
- PMP contact by Nurse Care Manager to transition participant to Reinforcement Phase.
- Reinforcement Phase is defined as lasting up to 2 months and includes the following telephonic activities to check on participant's self-management activities, problem-solving barriers, and set new goals as appropriate.
- Follow up calls--minimum of one call a month for two months;
- Transition to Call Center Management.
- Intervention Phase is defined as lasting 4-5 months and includes the following activities:
- Prepare care plan with participants and their families based on clinical guidelines endorsed by the Indiana Chronic Disease Management Program.
- Establish and maintain in-depth knowledge of the chronic disease data management system (CDMS).
- Enter participant data in CDMS within one business day of every contact with participant.
- Work with Call Center staff to receive messages, new participants to be case managed, and utilize Call Center staff for appropriate out-going calls as needed.
- Conduct health assessment of participants based on a tool provided by OMPP.
- Encourage participants to follow care plan by addressing any identified barriers. This would include information on Community Support Resources that may be needed.
- Assist participants to understand their condition and set goals and achieve self-selected outcomes through education, counseling, and on-going support.
- Coordinate activity with the participant's PMP through regular contact with the PMP.
- Develop an action plan in concert with the PMP for use upon release from care management.
- Work to develop and maintain relationship with primary care practices consistent with the goal of obtaining a systemic change of caring for the chronically ill:
- Assist in building care management into primary care,
- Communicate with PMP offices for updates of relevant lab tests and values, procedures, medications, etc. and update CDMS with this information,
- Assist PMP office staff with working in CDMS as necessary,
- Do case list review for each primary care physician,
- Build trust based on one-on-one case review and planning, participant supports by care manager to alleviate work for practices,
- Support guidelines by identifying medication change needs and communicate to participants' physicians,
- Serve as resource for Primary Medical Provider in managing Medicaid participants with chronic disease.
Critical Skill, Knowledge and Behaviors
Success in this position requires that the Contractor's employee will:
- Exhibit in-depth knowledge of the consensus guidelines developed by the Chronic Disease Management Program.
- Possess strong communication, teaching/education, patient-centered counseling skills to create collaborative relationships with participants and physicians.
- Encourage patient empowerment that allows participants to help themselves and display respect for participant choice and preference.
- Demonstrate excellent verbal and interpersonal communication skills.
- Be capable of working within a highly matrixed environment.
Education and Experience
- High school diploma; Bachelor's Degree in Nursing and 1 year experience in Community Health setting or Chronic Disease management; or Bachelor's work equivalent of formal nursing certificate and 3-5 years in Community Health setting or Chronic Disease management.
- Case management experience with chronically ill patients, one year preferred.
Special Licenses or Transportation Demands
- Current State of Indiana licensure as Registered Nurse.
- Individual will cover territory as determined by Chronic Disease Management Program criteria.
APPENDIX E. INDIANA CHRONIC DISEASE MANAGEMENT PROGRAM (ICDMP) SAMPLE LETTER
Here is a list of topics that we discussed during our recent call. Some were areas that caused you some difficulty. Others you wanted to learn more about. Please take this list with you to your next doctor's visit and show it to your doctor. This list may help you and your doctor talk about questions or concerns you may have.
We talked about these areas: [Only those items discussed on the previous call would be listed.]
- Sometimes having difficulty with medicines.
- Sometimes having difficulty taking your medicines on schedule.
- Keeping track of your weight.
- Talking with your doctor about what the best weight for you would be.
- Cutting down on salt in foods.
- You are not very likely to start doing more physical activity in the next 6 months.
- Likely to start doing more physical activity in the next 6 months.
- You would like to learn more about physical activity.
- Sometimes having difficulty testing your blood sugar every day.
- Sometimes your blood sugar is above 300.
- Sometimes having difficulty checking your feet every day.
- It's time for your check-up this year at the eye doctor.
- Sometimes eating sweets.
- Sometimes drinking sodas, lemonade, fruit juices, or coffee with sugar.
- Wanting help with food choices--more fruits and vegetables.
- Wanting help cutting down on fat when cooking.
- Wanting help cutting down on fast foods.
- Trying to do more physical activities, but finding it hard to do them regularly.
- Thinking about trying to start regular physical activities in the next 6 months.
- Wanting to know more about regular physical activities.
- You would like help to quit smoking.
If you have any questions about this list, you can call us at the toll-free number above.
Thank you again for taking the time to talk with us and to answer our questions. Remember: We will be calling you again in about three months to check on you and find out how you are doing. If you have questions before then, call the toll-free number. There is someone at this number Monday through Friday from 8 A.M. to 7 P.M. and on Saturdays from 8 A.M. to 1 P.M. To get more information about the program and your health, you can also visit our website at http://www.indianacdmprogram.com.
Sincerely, Care Coordination Services, Indiana Chronic Disease Management Program